Family Planning Programe: Women as 'Targets'
Item
- Title
- Family Planning Programe: Women as 'Targets'
- Creator
- Padma Prakash
- Date
- 1987
- extracted text
-
61]
'
vA.-.
r
I
commonh '.'
.
:: clu.
47/1,(First Floorjb.. t’arks i'.oari
F P PROGRAMMEWOMEN AS 'TARGETS'
BArJGALOaE-560 001
This discussion note addresses the following:
1.
Women have been the focus of the family planning programme
not just in the last decade but ever since its inception. In the
last decade this emphasis has been intensified. Whatever the
changes in the policy over the years women have remained the
'target population' for the family planning programme.
2.
This focus on women has had several consequences for
women - on the one hand while it has made contraception available
and legal, it has placed a heavy burden on them of having to deal
with the coercive practices incorporated in the programme, and of
the high load of morbidity associated with the unsafe methods and
practices being promoted. And it is highly debatable whether
the mere availability of contraception has given them any control
over their reproduction.
2.
What do we do about this situation? Should we oppose the
programme for its large ideological fundamental ideological
reasons and in so doing also accept that we would not then may
not then have access to contraception at all? Or do we seek to
make it less coercive and more relevant to our needs?
Women as focus of programme.
India was one of the first countries to promote family
planning as a national programme, Even before the formal process
of planning began, it had been recognised by the health committees
that were set up that in order to ensure the health of the mother,
it was necessary to bring down the number of pregnancies she
underwent. Towards that end contraceptive advice was one of the
components of the maternal and child health programmes. In the
50s family planning was made an integral part of the MCH programmes.
In the early years when the family planning unit and its several
clinics were set up the only method promoted was the rhythm
methods but soon the FPU began to test contraceptives for effacacy,
safety and acceptability and to undertake work to develop newer
contraceptives. Between 1958 and 1962 the clinics of the FPU
tested a variety of foam tablets, spermicidal jellies and
diaphramgms. The emphasis right from the beginning was on getting
women as acceptors. So much so that at the end of the first plan
when an evaluation study was carried out it was found that the
clinical approach which had been adopted had 'medical, feminine
and middleclass bias'.
...2....
2 By the third, plan family planning was a more serious issue
and. became more firmly integrated, into the national programmes
with an allocation of forty times that of the previous plan.
The approach also changed - on the advice of the Ford
Foundation. It was during this time that sterilisation was
adopted as part of the programme and Lippe's loop, which had
already been discarded in the west, was introduced with
manufacturing facilities set,up with the help of the Population
Council. The changes in approach also included the starting
of the post partum family planning programme,5 funded by the
Council and put into action around 1968. The programme was
launched with the intention of using the hospital base to
promote direct fp assistance to women either after child birth
or after MTP. Inevitably this reinforced the female bias of
the programme. At the same time it brought with it an element
of coercion - services could be and were withheld if women
did not accept sterilisation.
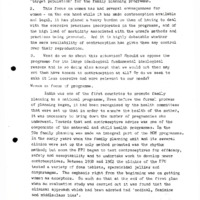
The accompanying table shows these various trends in this
period. After an large increase in the number of IUD acceptors,
the device fell into disrepute and even the incentive schemes
could not revive it. From a record number of over 910,000 IUDs
acceptors, in 1966-67 it fell to about ^-59,000 by 1968-69.
The initial emphasis on sterilisations showed up as a sharp
increase in the number of vasectomies which constituted
55 per cent of all methods. By 1969 a combination of factors
served to push the only other female method (other than IUD)
female sterilisations - which constituted 26 per cent of all
sterilisations. In 1967-68 with the USAID supplying condoms
for the Nirodh marketing programme the number of condom users
went up comprising >+0 per cent of all acceptors. At the same
time, the introduction of the newer methods & so meant a
deemphasis of. the diaphragm (the diaphragm- jelly combination
had shown good results in the FPU tirals). From combination
had shewn geed .
onwards the device almost disappeared from the scene although
on paper at least, it is one of the methods offered in the
'cafeteria' approach of the programme. The last half of the
60s thus saw the introduction of two new contraceptive methods
for women neither of which really took off at this stage; at
the same time it also saw the demise of the then, but the stage
was set for a tremendous expansion of the fp services.
- 3 By the Fourth Plan population control became an integral and.
important component of development programmes. The government
policy set definite goals - bringing down the birth rate to
2.5 per eelOOO in 10-12 years. The fp programme from this point
has made no pretensions of being anything other than a means
of reducing numbers - since goals have to be achieved in
specified periods ' targets.' had to be set and the evaluations
were in terms of 'births averted'. The objective of providing
birth control measures is thus a far cry from the current fp
objectives directed at controlling population growth.
The 70s was the decade of the camp approach introduced to
get quick results. In the early 70s the technique of conducting
tubectomies by the vaginal method which did not require more
complicated surgical procedures was only just being introduced,
and most tubectomies were conducted at hospitals on part of the
past partum service. The sterilisation camps therefore were
for vasectomies. While the first such camp was in Maharashtra
in the early 60s, it was the 1971 vasectomy camp in Kerala which
was spectacular - 15,000 vasectomies in a one-month period.
The fact that it was during the lean period and that higher
compensations and extra rations were given had not a little to
do with these numbers. Several other states organised such
camps until 1972 when in one such camp, 11 people died of
tetanus, and the camps were promptly discontinued. In the two
years between 1971-72 and 1972-73 the number of vasectomies
jumped by 197 per cent. But as a backlash of the vamp-associated
deaths there was a drastic drop in vasectomies and the programme
only 'recovered' during the emergency. Tubectomies constituted
only 16 per cent of all sterilisations in 1971-72 although in
the following two years they made up about half not because
there was any major increase in their humbers but because of
the reduced total of sterilisations.
The early 70s also saw the introduction of the MTP act which
was aimed at reducing the number of illegal abortions. It
resulted in servere problems including death. It allowed for
abortions not only for therapeutic reasons but also for 'social'
reasons - contraceptive failure. However, the committee which
was constituted to formulate the Act categorically stated that
this was not being mooted as a family planning measure. It is
possible that because of the non availability of safe and
effective contraceptive methods MTPs are being resorted to as
an fp measure.
- h- The impact of the emergency on the fp effort is too well
known to need elaboration. It must be mentioned that during the
period 1975-77 there was, of course, a fantastic increase in
vasectomies, but also an increase in tubectomies and condom users
while the number of IUD users actually dropped in 1977 after a
>+0 per cent increase in 1975 and 76, probably because the pill
which was introduced in 1975—75 was being pushed vigorously then.
The post -emergency period brought a drop in all acceptors and
the fp programme was on a low key for a while. In 1976 a National
Population Policy was formulated. It advocated a set of incentives
and disincentives and also stipulated that for grant© allocation
to the states the 1971 population figures would be taken into
consideration and some proportion of the aid would be linked to
fp performance. This led to all kinds of atrocities in achieving
1 targets' and Maharashtra even tabled a Bill to make sterilisation
after two children compulsory.
The fp programme in the Sixth Plan was directed at aspects
other than merely the control of population. However it also set
the target of achieving Net Repreductive Rate (NRR) of unity; in
order to achieve this the birth rate had to be brought down to 21.
Other components of the programme included other targets- death
rate to 9, infant mortality to 60. FP targets were set as
sterilisations 22 million, IUD 7.9 million acceptors.
The Sixth plan targets have been over achieved in the case of
IUDs and very nearly fulfilled for sterilisations. The new
policy for the seventh plan has set more fantastic targets
especially for oral contraceptives and IUDs.
Since the 1980s the fp programme is being pursued, with a new
intensity and has finally 'recovered from the emergency excesses.
There has been an 129 pen cent increase in all acceptors since
1980; a 239 per cent increase of IUD users; 15-0 per cent increase
in tubectomies; and a 365 per cent increase in equivalent pill
users as against a mere 50 per cent increase in vasectomies and
106 per cent increase in condom users. There is every reason to
believed that of late the emphasis has shifted from terminal
methods to specing methods such as IUDs and oral contraceptives.
The IUD has found new acceptors for the first time after its
70s debacle. This has become necessary partly because of the
changing age structure whereby a larger number of younger women
- 5 are making up the eligible age group where terminal methods are
not acceptable. Another reason is perhaps the realisation that
despite the increasing numbers of sterilisations this has not
made much of an impact on numbers mainly due to the fact that
acceptors have already had more than the 'right' number of
children.
There can be no doubt that women have been the targets of
the family planning programme - as acceptors and as gunguinea
pigs for a variety of testing programmes involving contraceptives
ahormonal and devices. But strangely there has been very little
interest in investigating simple barrier methods such as
diaphragms - there seem to be no evaluation on whether the
device is in fact, as inconvenient to all sections of women.
Moreover, there has been little research on male methods.
However, not withstanding all this the total number of
acceptors of female methods comprise only about 44 per cent in
1983-84 of all acceptors and in fact have never been more than
that since 1965. In some years as in 1971-72 proportion has been
as low as 15 per cent. But this however, is not so much because
there was a deemphasis on female methods as because there was a
tremendous increase in vasectomies during the 'camp' phase.
Similarly it may be argued that tubectomies although they
comprise 0 per cent of all sterilisations only make up 26 percent
of all acceptors. Are we then justified in stating that women
are the major focus of the family planning programme?
Here we must go beyond the numbers on apaper.
Firstly, it is generally known that of all fp statistics on
acceptors those for sterilisations are the most reliable. The
figures for condom users is based on number of piece distributed
and not on any feedback on usage. It is also well known that the
targets for condoms is the easiest to achieve because all the
officers have to do is dispose of them. The statistics on IUD
users too is something of a myth. In 1984 - for these numbers
include a large number of women who have had the device removed.
In 1984 an Indian Express report revealed that the number of
acceptors of Copper T was much larger than thq number of eligible
couples in the state; and there are innumerable accounts of how
the numbers have been fudged. Oral contraceptives users again
are based on numbers distributed. Effectively therefore, it is
the number of sterilisations which are indicative of what is
really happening.
...6....
- 6 -
Secondly we see from the table that there has been a steady
and almost consistent increase in the number of tubectomies
(ignoring the aberration of the emergency years 75-78). No such
trend is seen in the number of vasectomies which has been exwith
sudden and large increases when it was being vigorously promoted
followed by sharp decreases in the aftermath. In other words
it is not unreasonable infer that regardless of other features
of the policy, female methods sterilisations have been
consistently promoted. Interestingly also the introduction of
the laporoscopic method and the camp approach in 1980 has not
resulted in the kind of increases which occurred for casectomies
in say, I97I-73. This, probably indicates that the steady
increase in tubectomies is not really a result of the camp
approach.
In evaluating the. impact of fp on women, we must take into'
consideration the risk associated with each method. Apart from
vasectomy the only other male method being offered is the condom
which has no risk whatsoever. Vasectomies too cause fewer
problems than do tubectomies. And it is significant that
vasectomies camps were promptly given up when there were deaths
in one such camp in 1972, whereas tubectomies camps are being
actively promoted despite the increasing incidence of morbidity
and mortality associated with these camps. >Since early 80s the
introduction the simpler and shorter procedure of laparoscopic
sterilisation has parodoxically contributed to the increasing
risk involved. According to surveys the infection rates in these
camps is as much as per cent when the theoretical incidence
rate is only about
. Sathyamale' s papaer describes the
incidence of risk associated with each of these methods. In
short all the methods being offered in the mass programme add to
the women's burden of ill health. Even if they comprise only
W per cent of all acceptors the fact remains that women face.is
far greater risk than men in using the available means of
contraception. And the irony is that it is some extent avoidable
risk. For instance, with proper checks for contraindictaions
and good supportive health care some of the IUDs may be very
effective. Similarly, tubectomies particularly laparoscopies,
can be safe and effective (although they do not do away with the
other problems of sterilisation) provided enough attention is
given to the women during and after the operation.
i
Tables Family
(Numbers in Th<
Sear
iO
Insert
ions
£
Total
Accep
tors.
sterilisations
Vasectomies
>!£**
ifo
"no
iote
lubectoaies
Narch
1965
Jan.
1966
813
39
577
28
91*
5
671
1966-67
910
>*O
5
669
22
192
6
837
181*0
1968-69
1969- 70
»*79
1333
282
9
1665
1*59
15
11*
35
55
»*5
102 '
1967- 68
785
1<&8
1056
31
366
U
11*22
1970-71
W
1*51
12
1330
1*88
879
1620
23
1571-72
13
10
32
567
11
2187
1972-73
355
6
2613
1*1*
509
9
3122
1973-7**
372
9
»*03
539
13
197^-75
10
612
71*2
17
1975-76
1*33
607
9
11*
11*38
21
5m
50
17
8261
1977-78
326
7
6199
138
1230
2062
IB
1976- 77
9
5
135*+
2668
i*
1761
17
1978-79
1979-80
552
10
391
7
1093
20
11*81*
12
1*73
9
1778
10
»*39
7
1305
1611*
2k-
1980-31
635
623
25
1931-32
751
5
2219
3398
27
1097
2131
573
585
7
1982-83
1933-8U
9
10
2053
2792
11*
661
1*
3871
31
26
3993
**532
Souroes Compiled From*
Family Welfare Programme Tear Book 1983-al*,
and Annual Reports of the -^apartment.
NoUs Figures for Condoms, biaphrapns and Oral Rm* are is
For Condoms and diaphragms Equivalent user, is derive
•ejtors - By An Methcds
isaixls )
Diaphragm
ORAL
PILLS
Total
Accep
tors
(TA)
Total FA as
Female percent
Aocep of TA
tors
(FA)
-'fo.
>TA
33
$82
28
2066
907
Uk
39
k65
21
1012
62
16
861
k5
29
9*
k75
822
2262
298U
310?
778
25
L2
1366
3390
837
25
35
18U6
3769
5029
93k
1060
25
21
5875
k32k
869
916
15
Jlfo
^£A
So
>SA
>TA
27
kO
53
2321
*5
Mo
22
2kU9
68
31
39
66
2h9G
5&
17
7
5
5
5
3
3k79
51
2
32
0.5
680k
1872
23
3623
316^
29
1
58
0.5
1253k
22
70
61
1
73
0.7
k528
2702
1166
26
1
82
1.5
1723
31
0.5
82
57
0.5
91
1.5
1A
5505
5MS2
2023
233k
37
36
0*5
0.5
120
1*5
3091
183
0.5
555
2262
w
t»k
32
3371
2976
3707
M*28
36
5757
55
52
31
7652
51
a
26
0.6
U308
1206
28
terns of Lquivalont Users.
dividing off take toy 72 and 2 reap.
6U90
1.7
8102
11028
U679
38
L2
3.7
1U876
6557
U4
k
- 7 -
J
Another factor which must be considered is the fact that
the newer methods being introduced - such as injectables or
implants - are not only harmful potentially but are also methods
which a woman has little control over. What do we then do about
this? There is no gainsaying the fact that women need contra
ception and it is our right to demand that the Government make
safe and effective contraceptZon available on demand. In that
sense, that the government is making available a choice - at least
theoretically - of methods for women is not objectionable. What
is to be criticised and condemned is that women today are coerced,
overtly and covertly, to accept certain method irrespective of
their personal and specific needs both in respect to the size of
Jheir family and the choice of method. And then again can a mass
programme in a country like ours can only be useful, effective
and safe if supported by an efficient public health system?
Should there must be a greater emphasis on encouraging men to
accept and use birth control measures? Would this necessarily
tilt the balance the other way so that there are fewer
contraceptive choices for women. And most importantly, the
introduction of long acting hormonal contraceptives, which are
known to be a health burden on the women, must not be allowed.
The note has drawn on data,5 ideas arguments from the following?
1.
2.
3.
Socialist Health Review Issue on Politics of Population
Control, March 198b-.
Vimal ^alasubrahmanyan? Contraception as if women mattered
and Towards £ a woman's perspective on F.P.E.PW. Jan.11, 1986.
Alaka Basu- Family Planning Leacy of the Emergency E P W.
March 9,
1985.
All these are available for sale or are on display at the Meet.
Padma Prakash.
/Chavan/
Npn.
Position: 698 (34 views)