Content of Training of Non-Literate CHW and Fever related training material
Item
- Title
- Content of Training of Non-Literate CHW and Fever related training material
- Creator
- Anant Phadke
- Abhay Shukla
- PHC Cell
- Date
- 1998
- extracted text
-
t *
Medico Friends Circle
PHC Cell Meet, 7th July, 1998
Dear Friend,
Greetings from Pune!
Dt: 15 June ‘98
We wish to share during the forthcoming PHC Cell meet, some aspects of the content of our
training of semi-literate/non-literate CHWs. It is hoped that MFC friends would give their critical
feedback on it.
Enclosed is:
1. A note 'Content of Training of Non-Literate CHWs’
This outlines in a pointwise form the curriculum of the first two modules of our training
programme. This was first prepared by us for the PHC Cell meeting at Nasik (Sep.’96) and later
on improved through a series of meetings in Pune in which apart from the two of us, Deepti
Chirmule, Mira Sadgopal. Amita Godbole also participated.
Out of this curriculum for the first two modules, in the coming PHC Cell meeting, given
the time constraint we would share the pedagogy of only the diagnosis and treatment of fever as
an illustrative example. The curriculum outline of this is given in Module II of this note.
2. Fever related training material
This includes a. English translation of our pictorial diagnostic chart for fever. Dr. Sham Ashtekar's chart is
included for reference.
< •
b. Summary table of our diagnostic card game. Each cell in this table represents one card, and
each row represents a set of cards corresponding to one 'patient'. We will be bringing the actual
cards for the meet.
c. A note - 'Preparing fever diagnostic chart'.
We hope that this material will give an idea about our method of training on this topic. We
have used this material for four different groups of CHWs . including Primary educated and semi
literate health workers. The experience has been quite positive. Plbase go through the material and
give your critical comments during the PHC Cell meet on 7th Julv.
Looking forward to meeting you.
With Regards,
-■
Anant Phadke
Abhay Shukla
50, L.I.C. Quarters,
992/993 -23,
University Road
Rajendranagar.
Pune - 411 016
Pune-411 030
Jt.
$
•1i
1
CONTENT OF TRAINING OF NON-LITERATE CHW
(Prepared by the Pune Collective by considerably modifying the earlier note prepared
by Abhay Shukla and Anant Phadke for the Nasik meeting in September ‘96.)
1
The Objective
The objective of the training of CHWs is to enable them to
i.
provide First Contact Care in case of some common ailments which can be easily diagnosed
and treated locally without sacrificing the minimum quality of care or safety of the patient,
u..
timely refer cases with dangerous symptoms and signs.
1U.
foster preventive, promotive health action at community level.
do health education required to the first three activities.
II
Limited Scope of the Training
A training programme for non-litcratc I semi-literate, (man)' are more or less at the same level of
conceptualization as the non-literate) would have to be limited in its breadth and depth. This is because of
the fact that even though the non-educatcd do use some abstract concepts in their daily life, their ability- to
grasp and retain a large number of abstract concepts is limited. The content of the training programme for
the non-educated CHW would be tailored to the limited clinical (symptomatic / curative) and non-clinical
(preventive, promotive) tasks to be performed by them and the methodology would also be shaped by their
inability to read, write and their shorter attention span for didactic teaching.
III
The tasks to be performed by CHWs
a.
Clinical Tasks
These would include diagnosis and treatment of some common ailments and timely advice about
referral when needed. The list of conditions to be treated would depend upon prevalence, seriousness,
ease of diagnosis, case of treatment find scope for timely intervention .
1
1.
Based on these criteria, following symptoms / ailments would to be taught in that order of priority,
diarrhoea, fever, cough, minor miurics. After completing the training about these ailments, during
first two or three modules . the following symptoms / ailments would be taken up in a year's time
in the follow-up shibirs and monthly meetings :
weakness, pain in abdomen, back-ache, joint -pains, car-discharge, white discharge, ring-worm,
scabies, conjunctivitis, first-aid in emergencies.
b.
Non-Clinical Tasks
Participation in various preventive, promorivc health programmes at the community level in the
capacity of a frontline health worker c.g. immunization, drinking water - purification, ante-natal
care, malaria control etc.
Health education as regards all the above activities and on socially sensitive issues like stigma
around menstruation, infertility, begetting only girl-children. Health -education would be aimed at
demystifting medical science and stopping exploitative medical practices.
V
Content of Training
This would be tailored to the clinical and non-climcal tasks mentioned above. Moreover some basic
information Sbout the structure and functioning of human body as well as the structure and function of our
health care service system will have to be taught, with a view to enable CHWs to build liaison with the rest
of the system in the form of referral etc.
A list of the detailed topics is attached.
CONTENT OF CHW TRAINING
MODULE-I
1.1
Rationale for CHV> s and their Role
a
Rationale of CHW - where doctor is not needed.
b
Specific advantages of CHWs - availability, physical and cultural accessibility, demystification,
low-cost
What CHW can do a treatment of minor ailments
b suspect high-risk cases
c. refer early enough to higher level care for other ailments .
d to work as a catalytic worker in community health for preventive programmes e g
immunization. ANC etc.
e. health education
1.2
CHW Functioning
a.
Difficulties faced by CHW especially in the initial period
b.
Why user charges ? sustainability, accountability, value for service.
Dealing with patients : Non-rivedical aspects.
d.
1.3
Storage and Handling of Medicines, record keeping
Concept of Health and Disease
a.
Participants’ concept of health, disease and disease causation: matching with trainer's concept of health
and disease
b. Discussion and Analysis of disease causative agents into components of epidemiological triangle agent, host, environment
Agents : toxins, smoke, germs;
d.
Concept (broad) of infection and immunity
e.
Portal of entry : nose, mouth (GI tract), skin etc.
3
f.
Host : e.g. malnounshmcnt. role of diet
fi
Environment : e.g. lack of sanitation.
ll.
Concept of Epidemiological triangle: social causes of disease
How to prevent diseases
1.4
Structure and function of Body
a.
Participants' knowledge of bodv / organs
b.
Body is made up of systems and specialized organs e.g. gastrointestinal system, respiratory ; other
systems for other functions
c.
Gastro-intestinal system, its organs and the process of digestion and absorption.
d.
Explanation of some phenomena like hunger, heartburn, vomiting, diarrhoea, intestinal colic,
in terms of type of disturbances of normal bodily functions.
*
5
Diarrhoea
a.
Diseases commonly seen in the area as per trainees' perceptions
b.
What is diarrhoea ? Why diarrhoea occurs, patho-physiology of diarrhoea:
Uncomplicated diarrhoea and bloods- diarrhoea;
d.
Dehydration-signs. significance:
Treatment of dehydration - 'household saline' - how to prepare it how much to give. Difference between
'oral-saline' and intravenous saline;
f.
Five danger-signs in diarrhoea
unconsciousness/' listlcssncss. conunuous vomiting not responding to ORS. inability to breast
feed / suck, convulsions, not passed urine for more than 8 hours
g.
Clinical approach to diagnosis: key questions to be asked regarding every diarrhea patient:
* Diarrhea since how many days'?
*Any blood in stools'?
*Any vomiting accompanying diarrhea?
For children below 4 years, additional questions;
‘Is the child feeding/drinking?
‘When did the child pass urine?
h.
Drug treatment
i.
Prevention of diarrhoea-measures at personal and social level. Household chlorination.
4
b.
Treatment
i.
Supportive care - washing. hair removal, removal of pus. scab,
necrotic tissue.
n.
Treatment of infection with local application : GV lotion, antibiotic cream or herbal
medicine ?
I. 9
Boils
Common sites for boils - legs, scalp.
Diagnosis - Local pain, swelling, pus formation, often bmphademus
The treatment ft.r boils :
Local treatment for boils - salt, paste, fomentation If no relief in 2-.~ days antibionc is needed.
NOTE : Systemic antibiotics tn advanced module. )
6
(NOTE : Advanced module on diarrhoea will deal with treatment of bloody diarrhoea, cholera and medicines tike
cotrimoxazole and metronidazole. Treatment of associated vomiting. Method of well-chlorination to be taught in the
advanced module.)
1.6
Treatment of cuts, wounds and minor pyodermas
a.
Wounds heal on their own if they arc not infected.
b.
How docs wound get infected ? By soiling. Germs from soil,
contaminated applications. Not by dietary indiscretion.
c.
Tetanus is caused by contamination with tetanus spores present in dung and soil.
d.
Technique
arresting bleeding by local pressure: apply sustained pressure at the proper site for at least five
minutes. Bleeding generally stops.
Cleaning of wound with soap and clean water: (ordinary soap water or savlon solution), drying.
e.
Application of medicine (gentian violet or herbal medicine - like aloe. - leaves of Indian gooseberry).
f. .
Bandaging - when possibility of contamination exists -aloe as bandage: and to protect from repeated
injury
Change bandage when it gets soiled.
g
Signs of w ound healing.
h.
bites.
Tetanus prophylaxis - deep penetrating or grossly contaminated wound! or animal
S'
When to refer :
a.
b.
d.
c.
t
When bleeding doesn't stop.
When muscle, or bone is exposed: when the wound gapes
Suspicion of nerve injury or fracture
Spreading infection not responding to routine management
Signs of spreading infection - cellulitis, hmphadenitis. fever with
rigors.
(Note : Acianccd module contains treatment with cotrimoxazote: scabies and infected scabies, sccondarv
complications of wound infection - septicaemia, mag., ts: reasons for non-healing.)
1.7
Pyoderma
a.
Brief Description: Common sites, causation - role of hygiene and
prevention.
5
I
MODULE - II
FEVER
2.1
Fever
a.
Concepts :
I.
ii
iii.
Fever is a symptom due to protective mechanism.
Causes of fever - commonly infective
Treatment is of 2 types :
treatment of fever
treatment of cause
n
b.
Role of antibiotics in Bacterial infection only.
Skills:
it.
iii.
.Assessing degree of fever
Sponging
Deciding dose of Paracetamol. Chloroqum
Categories of Causes :
i.
ii.
iii.
d.
Viral infection e.g. Flu
Pyogenic infection e.g. Boils
Parasitic infection e.g Malaria
Diagnosis of serious Fevers for immediate referral :
1.
ii.
iii.
iv.
Enteric
Meningitis
Pneumonia;
Cerebral Malaria
Ominous looking fever (When immediate referral to hospital is needed)
i.
ii.
iii.
iv.
v.
Continuous high fever for more than 7 days
Unconsciousness
Convulsions;
Neck-rigidity (suspect brain-involvement)
Breathlessness (suspect pneumonia)
7
e.
Diagnosis of cause of fever : Six key questions to.be asked to every patient
i.
iii.
iv.
vi.
f.
Supportive treatment of fever
n.
g.
Sponging and general measures
Oral Fluids
Symptomatic Treatment
1.
.2
Fever for how many days ?
Continuous or periodic ?
Is there cold, sneezing ?
Is there cough ?
Pain anywhere ?
Any other trouble ? (diarrhoea, urinary complaint etc.)
Paracetamol: indications and dosage :
( repeat dose of Paracetamol if necessary)
Malaria :
ii.
iii.
iv
VI.
Participants' experiences of Malaria
What causes Malaria
Spread - Cycle
Complications - Cerebral Malaria
RBC destruction, spleen involvement
Clinical picture - diagnosis
Fever - alternate day or recurring at the same tune daily, with rigors subsides with sweating.
Vomiting common, no localizing symptoms like cold and cough, normal between fever episodes.
VII.
Blood examination diagnosis
How and why a blood smear is taken. What is seen on examination of the slide
vni.
(Demonstration'!
Management - Treatment, prevention. NMEP
Treatment - Treatment of fever, dose of Chloroquine.
How to administer Chloroquine - First treat fever with Paracetamol allow the fever to come
down, give food, give Chloroquine about an hour after food.
No need for injections / IV unless complications
Chloroquine is bitter in taste, causes gastric irritation
Concept! need for radical treatment
8
Prevention of Malaria :
Prevention of bleeding - filling up of ditches, guppy fish in water bodies. Anti-adult measures spraving of houses, burning ncem leaves in the houses. Prevention of infective bites - use of
mosquito nets. Early diagnosis and adequate treatment.
2.3
Viral Fever :
Fever due to common cold and flue like fet er. clinical features, self-limiting nature (5 days) diagnosis,
treatment with I aracctamol. home remedies, no use of antibiotics and no need for any injection.
2.4
Fever due to pus-forming organism
Boils, abscess, infected wounds.
High fever with rigors, local pain, swelling, often lymphadenitis
Treatment of cause and treatment of fever.
(Other topics to be outlined include pharx-ngitis/tonsillitis; unitary tract infection, fever with dysentery)
Each topic will be taught using the following structure :
a.
b.
d.
e.
f.
Sh.
j-
vi
Participant's knowledge, perceptions, traditional health practices, sharing common experiences of '
the disease / symptom
Causation.-patho-ph}sioiogy of disease
Cluneal features - symptoms, signs
Diagnosis, differential diagnosis
Referral - need for immediate treatment
Treatment including traditional medicine
Prevention - Personal, social / community
Misconceptions
Nauonal programs
Skills - practice
t
9
i /c<t
J. 11
Prep aring FEVER DIAGNOSIS CHART
Fever is; one of the most common symptoms at the
VHW-level. Fever-diagnosis (i.e. its cause) is however,
the most difficult topic for a non-literate VHW. Since
fever can be due to a serious, life-threatening or
complicated disease, its quite essential that- the VHW
suspects early enough any case that requires referral
to a hospital. Degree of fever is not a reliable
indicator of the seriousness of the underlying disease.
Fever can be high in simple viral infection and is
generally high in malaria, though both these diseases
can be treated by a VHW. Secondly given varied
aetiology, it is necessary for the VHW to detect the
underlying cause of fever correctly. This is not a
simple task.
We think that the best way to overcome the diffi
culty in diagnosis of fever by non-literate VHW is to
give and teach them a pictorial diagnosis-flow-chart.
Sham Ashtekar in his book t Bharat Vaidyak, has given
such a chart for fever-diagnosis in adults, for educated
VHWs. (Appendix-II). W^, found that it was not merely a
question of simply converting this chart into pictorial
form for the benefit of the non-literate VHWs. There are
some problems with this flow-chart.
The main problem with such a purely linear flow
chart is that on the one hand, it has to be followed
meticulously for every fever-case, but on the other hand,
it is not very practical to do so. The VHW can neither
remember the whole flow-chart containing so many questions,
nor can s/he keeps referring to it step by step in every
case of fever.
Another disa Wantage of a purely linear flow-chart
which proceeds downwards through a process of exclusion,
is that though some of the symptoms in a case of fever
are not mutually exclusive, they appear to be so. For
Jexample, cough and cold co-exist many a times; but appear
mutually^ in the ” Bharat Vaidyak " chart .
Keeping these problems in mini, we prepared six key
questions needed for diagnosis of fever
to be asked by
VHW to every case of fever, and then wo organized our chart
(Appendix-III) arounl these six key-questions by subdividing
-2
the flow-chart into six sub-sections.
It is easier for
the VHWs to remember these six key questions than the
whole flow-chart. Once these key-questions are inter
nalized, other questions flow more easily from answers to
these questions.
Sccori lly, we indicated Live nLtuntlonn in tile
diagnostic flow-chart where immediate referral to a
hospital is required. Once these key questions and . '
situations for immediate referral are properly grasped,
there is less likelihood of a VHW making a gross mistake
in diagnosing the cause of an average case of fever.
While indicating the possible diseases necessitating
immediate referral to a hospital, we avoided burdening
the VHW with any diagnostic details of these conditions
( typhoid, meningitis etc.)
To familarize the VHW with this process of asking
key-questions, a 'card-game' was prepared, with a picto
rial set of cards for each of six common conditions
( malaria, common-cold, pyogenic infection, fever with
diarrhoea, UTI, typhoid). The game consisted of the VHW
asking key-guestions one by onn, and receiving the typical
answers by opening the relevant card. If all questions
were correctly asked, all ,the cards would have been opened
giving the respective information, and the VHW would be
able to state the diagnosis. With the help of this card
game, the VHWs were able to internalize the key-questions,
learn subsidiary questions, and follow the reasoning
process to reach the diagnosis. The process was both
challenging and exciting; and was a simulation of reallife diagnostic situations.
Apart frcm this main modification, we made some
minor modifications in Ashtekar's chart. V>e deleted
from his chart, pverperial fever and filariasis for being
rarer conditions and infective hepatitis since patients
themselves diagnose this condition as jaundice. Secondly
we added Sinusitis for being common, specific ailment
and concretized the category of 'pyogenic infection' in
Ashtekar's chart, into Infected wound, boils, purulent
t qnsilit is.
We are aware that any such over-simplified chart
has its own limitations. It glosses over different
clinical presentations of the same disease e.g. malariawill not always present with rigors or with periodic fever
though this seems to be the pattern in Oahanu area.
1
-3
Secondly, many uncommon conditions are excluded from this
chart. Thirdly, it deals with fever only in adults. A
separate chart to enable the VHW to diagnose paediatric
fevers such as measles, chicken-pox, mumps, pneumonia
(by counting respiratory rate) is needed. We plan to
make and teach such a chart in the next Shlbir.
(r
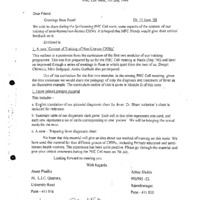
FEVER : DIAGNOSTIC FLOW CHART (For use in adults and children above 6 yrs.)
B 1.2
FEVER
Ask
Painful, lender lower
abdomen or
foul vaginal discharge?
Abortion or childbirth in Yes
last 2 weeks ?
Ask/
Check
No
Ousel acute ?
Yes
Ask/Check
Running nose ?
Yes
Congested throat or
tonsils ?
Ask/
Check
Ask
No
Septic abortion * * ★
Purpere^epsk
No
Ask/Check
Cough >
Yes
No
No
Yes
No
No
Ask/Check
Yellow eyes or
yellow urine froth ?
No
No
No
Refer to
Doctor
Yes
Refer Io Doctor if no
relic! with treatment
Abscess or septic
infection etc.. * *
? Chronic
bronchitis or
tuberculosis lungs
Yes
Meningitis,
encephalitis ***
* **
<
Yes
-
. Ask/,
? Rheumatic fever | Check
rheumatoid arthritis
Lymph node
swelling?
No
zYsk/Chcck
Fever with chills ?
No
Bronchitis * *
Ask/Check
Jointswelling,
migrating joint pains ?
No
Yes
No
Ask/Check
Neck stillness,
altered behaviour ?
Pneumonia
(plague ?) * * *
Hepatitis * *
Ask/Check
Swelling or pus
with throbbing pain ?
_____________ 2________ i
Yes
Ask/Check
Dry cough,
pain in midchest ?
Yes
Pharyngitis or
tonsillitis * *
| Ask/Check
Breathlessness and
chest pain ?
Commoncold*
Yes
? Filariasis
(plague ?) *
Yes
Urinary tract
infection * *
Ask/Check
Burning,
frequency,
turbidity
in urine ?
Yes
Yes
Check
Relatively slow pulse in Yes
continues lever ?
c
Enteric fever ■* **
No
? Any other disease
★ ★ *
No
Yes
Malaria * *
Treat with
chloroquine and
wail for two days 7
Refer to Doctor if no relief
with treatment
★
- Treat, it is a simp, mailer.
* ★ - Treat, bin lake, care and lollow up.
***- Serious illness, refer to health renler/hospilal.
|
| - Suggests serious disease, watch out lor these conditions.
15
o
£
o> P°
B<r
B
p_
o'
I
cr»
L*J
<-/»
B
£L
FT
o
o
I >
I )
B'Si
B-
B-
B-
tn
tA
s &■
§3 Fq
£. I|
M
CD
CD
JJ
(§ g
n
o
i
.0
W*
13
s
i/i
z
§-< CDr
11
H. a
.71
£
o
r
>
<13
P
■ cn
Z
5' §
8 g
•nd
F3
*•
«r<
i!
CD
n>
B-
g
£
co'
Co
S.
I
n
o_
°5
CO
■z
o
z
cd'
o
CO
O
o
<
c
2
2
ai
o
£■ £
CT ET Cn
'K O
S'
~ ~
p K1
.8.
§ o
B- <6G> 2 £
B" B<0 o B- 3
888n>
c» .<»
o>
S D.
O
i-
CT* ET in
£
g
B.
CD
&■
B
-
Er
P
-o
cu
I
*
h
co
</>
CD
" I; K
cd
r/»
■'3
£
cu
R
B.
f? “
C1
- g -39 o.I8-?■§.
&
Ip
CD
cn
M
t)
o
o
G’
3
CD
CZ)
B'
O
i
B'
R
o>
tzi
10
r■ (
.2
- t
tx
n>
tz>
3 W
§ §
Q
W
tn
to
rf
B S
g3.§■
B
I
8 §
</! • b*
it D'
8
CD
tn
z
o
£
O
o
o
nz
S
tn
o
S'
IQ
3
O
V)
I </>'
(n
z g.Q mH
o
.o
C3 ’Q
o
o
e
CD
3.
o
<
CD
hd
>■
§
I
8
o
B.
n>
r> o
9
| •
Ir
p
r'f
■n
Bp
(»
8 P
“•I
!
o
S-
c5
I
q
B- B:
8
aB a
“
CD
&
O
rzi
Tl
B
P
o
B
"0
P
B
n
HZ
o
3
u
I2
i
3
3
U.
Ph
,■
° SC3
g
o
§
g
H
1a
Ph
■Q
I
5
ft
U<
P on
9
o
Hl J £
ft c <J
d'
rt
ft
I
I
9 a g
ti £ 8 <3
Pi ft
cd
ft
grs
tt"
« e
d o
O O
w
ill
M .S
73 'S)
•C
U
££
Sj
s
o
Pi
o
"C
c§
75
73
£
H
a
o
Z
o
Z
73
CT
i
tn
s
o
•d
E
_o
CX
g.
1
cn
4
g
I3
H
<S
Q)
a>
g .a
•S 8
<D
ci
w
•sift
1
o
pi
a
1
.s
th
QI 8
p
r*.
05 ft
3o
1/5
1 S-5
2
<z
1 ’
■§
§
pq
g» §
11 £
Z
<u
•s JL>
■s
73
■T?
.g
■5a
1
Jg
on 32
ol
JD
11
■I
o
<z>
E -3'
< s
o 5
cn 42
i '
O
o
zo
z
o
<n
<D
o
Z
o
Z
zo
a .-S'
o
Z
o
Z
o
Z
o
Z
ft
fi
i>
is
S s
2.
-g
■g
I’
m
oo
e-j
•5
o
c
<□
a.
•S y
e <s
£<3
g
is
d
Z
11
II
i §
5 a
S
</)
■i
•g
><7
CD
73
r-l §
\D
g
11
<D
Uh
o
.g
E
o
<_)
V)
>»
<D
<D
<D
73
21
2" 1
!$-11 al
oo
o\
<D
o
w
ۥ
a
• e
$ 2. rd
=■ x 5
2Sq
<
<
n ■
VI
*-s
U1
S’
(Ki
3
C
<
n
v.
!Z2
>—•
(z:
t§”
w
2'?
55
§ I’
5 c
/
v>
V
>4
c’e’\ •' )-]
9- n> 2
II
2
§■?'
s.
■
£
*!.
S
n
j
(A
CZ!
I
v
Sr
= rt1
z njkj!
o
i
v
1
f! “V
£ o
I
Z £
c j»
* O
2
=»”
=.
??
C’
H
« =• 3 =.
= &■
S
e »
0 0
n"
CA
c- co
o
«
= 3
a. n
1g <§.° '
5" o-i ’
O
tn
C
c _
I
2
2
5A
- = n
2 g '
_ O (JO
giyi
(!
21
Q;
8 S.S P
= ?s. o-cr
g.
c/s
*-*
* 2.?
o
c
n
r>
o 2- Sc a- •--
q=
I
■=
p 2
2 2(Z
(Z
o
c—- •
(Z
H
n =•
§ ?
5 £
§
!
•••
« •
U1
!
aw
*--• w
S'?
±s-
*Ss- §
aa
Cl
o' 5 § *■0
til r
S'
C. ix.
2 q 2.
VI
<
C/3
V
I
I
p
K.
V
is-
f
r
S2.
S'-
«•
I
7
n= X
Ci
H‘
P
-= c
?=
p
?
T*<p
po
=■» s s
5 =■
? J ••■«3 ?h
“ CR
n
© 0 ®
aee
4
2
o
i
Cj
o’
■I S 3
3S
z g" o
O g. gS
S'S 2
g-2Q
2i
■■O
r
c=
<
n
v.
<
r»
CZl
•tr
h
V
I
£
6
§
><
n
vi
<
2
1
.J
ijr
2. 5
C3
V2
s §
8.S
Q.
.
S’
!r
g
•<2
■—-
<-*■
o
s
!
i
£J
-U
23
2£
' a
. 3>
(hJ
n o
2. r
sf e
§C
'/'■
3
I?
25
5=
l
1
1
a ?=2
i
»
n 2
2 o
3 *
=’?
25
=■
Position: 1383 (15 views)