SDA-RF-CH-1A.14.pdf
Media
- extracted text
-
) Pergamon
1222
SDA-RF-CH-1A.14
Soc. Set. Med. Vol. 47. No. 9. pp. 1223-1230. 1998
I. H. Burnley
Mathers, C. (1994) Health Differentials Among Adult
Australians Aged 25-64 Years. Health Monitoring Series
No. I. Australian Institute of Health and Welfare,
Australian Government Publishing Service, Canberra.
Omran, A. R. (1972) The epidemiologic transition: a the
ory of the epidemiology of population change. Milbank
Memorial Fund Quarterly 49, 509-538.
Omran, A. R. (1983) Epidemiologic Transitions in
International Encydopeadiu of Population, cd. J. Ross,
pp. 172-175. Free Press, New York.
Phillips, D , Kawachi. I.. Marshall, S. and Purdie,
G. (1991) No evidence for social class inequalities in
intervention for coronary heart disease in Otago 19871989. New Zealand Medical Journal 104, 507-510.
Powlcs, J. and Salzbcrg, M, (1989) Work, class or lifestyle?
Explaining inequalities in health, in Sociology of Health
and Illness, cd G Lupton. J. Najman. MacMillan.
• l: S0277-9536(98)00135-X
Saunders. R. (1996) Poverty^Income Dis/rifa.,„ IH.
Health: an Australian Study, SPRC RepoJ’"**
Proceedings. University of New South Wales. — jW
Shepherd, J. (1995) Whither rural practice.
Journal of Australia 162, 232.
;Sf.
Shryock. H. S. and Siegel. J. (1973) The Meth^f^.
Materials of Demography. Vol. 2. US Depan^f^J
Commerce, Washington DC.
Tesh, S. N. (1988) Hidden Arguments, Political
and Disease Prevention Policy. Rutgers University
New Brunswick,
Thompson, P.. Hobbs. M and Martin. C. (1988) The’Xand fall of ischaemic heart disease in AustiJ*
Australian and New Zealand Journal of Mcdicb^ft
327-337.
• :
Tolhurst, H. M.. Ireland, M. C. and Dickensdjr'.r'
A. (1990) Emergency and after-hours work performed
in country hospitals. Medical Journal of Australia
458-465.
Triin. A. (1994) Extending epidemiologic transition th^*South Melbourne.
Riley, J. C and Alter, G. (1996) The sick and the well:
m Social Dimensions of Health and Disease
adult health in Britain during the health transition
Zealand Perspectives, cd. J Spicer, A. Triin and J, a
Walton, pp. 144-160. The Dunmore Press. Palntcntot
Health Transition Review Supplement 6, 19-44.
Rogers, R. G. and Hackcnbcrg, R. (1987) Extending epi
North.
.
Umbcrson, D (1992) Gender, marital status and focii’
demiologic transition theory: a new stage Social
control of health behaviour. Social Science and Medici*'
Biology 34, 234-243.
34, 907-917.
•••??$&•.
Rollcy, F. (1995) Enough to make you sick? Geographical
Wykc, S. and Ford, G. (1992) competing explanations ^'
perspectives on health and health care in rural
associations
between
marital
status
and
health.
Scrfol
Australia, unpublished PhD Thesis, Department of
‘ Science and Medicine 34, 523-532
'
Geography, University of New England. Armidale.
'('> 1998 Elsevier Science Ltd. All rights reserved
Printed»" Great Britain
0277-9536/98 SI9.00 + 0.00
CH - I#TOWARDS QUALITY OF CARE IN CHILD HEALTH
PROGRAMMES: A CHALLENGE FOR THE PARTNERSHIP
IN HEALTH AND SOCIAL SCIENCES*
SHUBHADA KANANI
Department of Foods and Nutrition, M.S. University of Baroda. Baroda, India
Abstract—Several child health care programmes, though often well conceived, are poorly implemented
al field level and focus primarily on quantitative achievements to the neglect of quality of care. This
paper presents a quality of care (QOC) framework for child health programmes from the perspectives
of the management system of an organization and the provider-client interface at point of service deliv
ery. The paper subsequently describes the application of qualitative and quantitative research tools
drawn from the social sciences and health sciences for planning and evaluating quality of care. An inte
grated and complementary use of these tools is recommended. It is suggested that minimum standards.
which are region specific, be articulated for quality maintenance in child health programmes. These
standards may be upgraded as quality improves. Finally, the challenges which a partnership of the
health and social sciences may have to take up are discussed. These include advocacy for prioritization
of QOC in child health programmes, facilitating an environment which supports quality of car£ pro
moting inter-disciplinary action research, training students in social science research in universities and
research organizations, documenting success stories. (( J) 1998 Elsevier Science Ltd. All rights reserved
Key words—quality of care, child health programmes. developing countries
INTRODUCTION
I several developing countries of the world, matraal mortality rate (MMR), infant mortality rate
MR) and rates of malnutrition continue to be
tpressingly high. About 99% of maternal deaths
k to complications of pregnancy take place in
[doping countries. The region with the largest
rrcpancy between births and infant deaths is
Inca, which has 20% of births and 29% of
aths. In South Asia, the corresponding figures arc
*/• and 61% respectively (Maine and Allman,
90) Several child health care programmes,
Nigh often well conceived, are poorly impnented at field level and focus primarily on
■ntitativc achievements, such as number of beneBries covered, and neglect the important area of
of care. For example, programmatic
torch n India has revealed that maternal and
M health (MCH) services suffer from several selfcdue to insufficient planning, inadequate train
ed supervision of manpower, lack of
^unication with intended beneficiaries and sub
mit poor utilization of services, culturally inapJPriatc services and socio-economic constraints
Jas inferior status of women (Dutta. 1993).
fortunately, even al the highest policy making
nition that a conscious effort is needed to opera
tionally define quality of care in the context of child
health programmes, its indicators and standards:
and that a satisfactory level of quality cannot be
automatically ensured. For example, the recently
formulated National Nutrition Policy (1993) of the
Government of India, articulates several important
measures to improve child health, describes admin
istrative and monitoring procedures, but does not
elaborate on how quality maintenance can be
ensured, nor on the role of research in this regard
(Government of India, 1993).
In this paper, the evolution of the concept of
quality of care (QOC) for health care systems.
family planning programmes and women's health
programmes is described. This is followed by an
elaboration of a QOC framework for child health
programmes. The importance of a partnership
between the social sciences and health sciences for
operationalizing a QOC framework is then high
lighted. followed by suggestions of some research
tools for planning and evaluating QOC. Examples
from the author's research experience on process
evaluation of selected child health programmes arc
given in the appropriate sections.
there docs not appear to be adequate rccog.torlicr version of this paper was presented at the
Asia and Pacific Social Sciences and Medicine
inference (February 11 -16. 1996) at Perth. Australia.
QUALITY OF CARE: EVOLUTION OF THE CONCEPT
According to Mensch, in the years following the
Alma Ata conference, the concern of medical
anthropologists regarding culturally appropriate
1223
122-1
Quality ol care ill child hcahli programmes
S Kimani
care and community involvement in primary health
care laid the ground work for much of the ensuing
work on quality of existing services (Mensch. 1993).
Elaborating on the concept of ’continuous quality
development' proposed in 1993 by the WHO
Regional Office for Europe and the Danish health
authorities, Racoveanu and Johansen have stated
that, in essence, continuous quality development
involves setting and achieving goals for quality on a
continuous basis (Raceveanu and Johansen. 1995).
Health care of good quality encompasses the three
areas of:
• structure (organizational settings of care).
• process (skills deployed in delivery of ser
vices).
• outcome (effects of care given on health and
well-being of patients).
According to the authors, medical technology
impinges on all these three components and has a
profound effect on continuous quality development
with particular reference to utilization, appropriate
ness and cost-benefit of technologies.
Saturno has highlighted the importance of volun
tary (as opposed to mandatory) commitment to
quality, especially in situations where the state owns
anil provides most health care and where health
personnel arc salaried employees. Professionals deli
vering health care should be motivated and
involved in qualitative assurance on a voluntary
basis as a part of a clearly defined strategy
(Saturno, 1995). Describing the Iberian Programme
of Training and Implementation of Quality
Assurance Activities in Primary Health Care, the
author reports that training was the most important
strategic factor for success, along with implemen
tation of principles of planned change, including
building on strengths, analyzing systems, identifying
influential persons and fostering a sense of the need
for quality assurance. Bruce operationalized a qual
ity of care framework for family planning pro
grammes and emphasized that improvement in
quality of care is an important determinant of con
traceptive acceptance and sustained use (Bruce.
1990).
Defining quality in terms of the way individuals
arc treated by the system providing services, Bruce
and Jain have emphasized that client knowledge
and satisfaction with the care received should not
be viewed simply as bridges to continued use, but
also as valued end products of conscientious man
agement and caring service (Bruce and Jain. 1990).
Building on Bruce’s family planning framework,
Mensch has suggested a list of four elements for a
women's health care QOC framework (Mensch,
1993):
(I) provider-woman information exchange: conwomen regarding diagnosis.
veying information to
treatment options, side effects, and listening to and
understanding women;
1225
;lrd 10 kno,,.
(3) interpersonal relations: sensitive treatment of •
women including privacy, respectful behaviour, gjv
ing adequate time:
■ i
(4) mechanisms to encourage continuity of careinformation about follow-up visits, referrals, other
available services.
Child health care programmes, unfortunately
Administration &
have received scant attention with regard to sy^
Management
tematic development of a comprehensive QQq
Inadequate
' humanpower
framework and its field level application. What ft
development
documented in literature are examples of proce&i
k-Poor in fraand/or impact evaluations of child health pro.
; stucture &
'"resource
grammes.
. ‘management
In India, a recent process evaluation study oo
C.Monitoring : focus
integrated child development services (1CDS) in the
.•on quantile not
State of Gujarat (India) had a client-centred focus ■ ’/quality
(Kanani and Zararia. 1996). It sought to elicit pef^j ■'ion some services
1
1
ceptions and service utilization patterns of ICDS9
beneficiaries, as well as beneficiaries contribution fo.j
ICDS. through the use of a mix of qualitative and.’
participatory research methods. Data gathered from!
in children's education.
nutrition'health status
iroup
beneficiary groups
adequate manner
Service
Utilization
* Poor by
women
* Better by
children
Variable
Quality
of Care
’ Good quality
of care leads
to increased
com num ity
participation
Empowerment of Women
through Nutrition Health
Education (NHE)
iot all services
Health' & ‘Non-health
components not well
integrated
‘ Neglect of communication
f
* Inadequate home visits
by functionaries
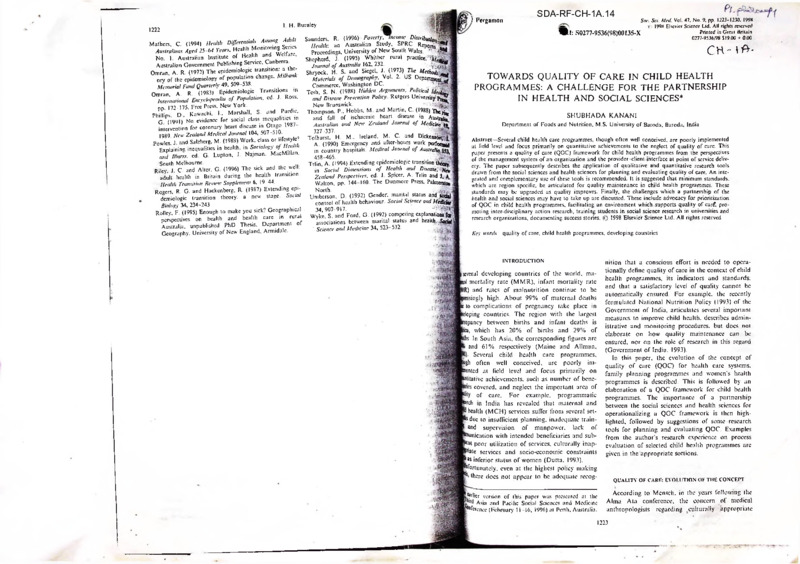
five regions in Gujarat (Fig. I) revealed that:
j
• Though the ICDS is conceptualized as an into-;
Fig. I. Current status of ICDS tn Gujarat, a snapshot picture of the findings of a social assessment
grated scheme, it was not implemented as such at ■
study (Kanani and Zararia. 1996)
field level Selected senices receive more emphasil^
while others are neglected.
Ft
• Utilization by intended beneficiaries depended* ^medical oflicers at the PHC centres in urban
developing countries is needed, which will help
on factors such as regular availability and access-' SSrural areas revealed that functionaries al all
focus attention on this issue and provide some
bility of senice. quality of implementation, rappoflj Was devoted a major portion of their time in plandirection towards this end This paper elaborates on
of ICDS worker with community members,, pcr< gfcfand implementation of the family planning
such a framework in the subsequent sections. The
ccived benefit of service by people
^immunization programmes, as they considered
QOC framework is client-centred and focuses on
• In ICDS centres where the field functionaries:
more important than other programmes
process and outcome indicators which are likely to
were motivated and gave 'good' quality care as per*, Wing anemia control and vitamin A deficiency
reflect QOC. Finally, a list of qualitative and quan
ccived by the people, the beneficiaries tended to
?®Uol programmes. Material and financial
titative research tools is suggested to help design
the services. Further, in such centres, the comm*d Sources, monitoring and supervision, and commuand evaluate QOC in child health programmes.
nity. especially local NGOs, did contribute to ICDS
SfcContacts were all geared towards family plan
in varying degrees, by way of voluntary time, 1W»; band immunization.
or space, or materials to run the ccnfie. Poor
THE QUALITY OF CARE FRAMEWORK FOR CHILD
rfgOr quality implementation of nutrition pro
agemen t and inadequate administrative support *] dines was reflected in irregular and inadequate
HEALTH PROGRAMMES
government authorities were key factors obstructmf ■ Tolies of vitamin A and iron, poor record mainIn the context of caring for the health of chil
quality of care. These included lack of skill-w^l
nce, infrequent supervision and training. Not dren, QOC may be viewed from two perspectives*:
and hands-on training, acute shortage of basic*^
^singly, there was a high prevalence of vitamin
(1) The overall services and management system
terials to run ICDS centres, cursory supervi^^
jficiency (Bitot’s spots) and anemia (Hb levels)
of an organization;
mechanical monitoring with little attention to q [School children and pregnant women in the
(2) The point of service delivery, that is, the pro
ity of service and overburdened field funC!*5L"ik
fcareas. The authors stated that unless strong
vider-client interaction and outcome.
who had virtually no access to transport facilfo
&Cy efforts arc made to convince policy
Tables I and 2 present the components of a
From the study, the importance of developing p? of the importance of controlling maternal
suggested QOC framework for child health pro
‘human resource’ in ICDS. the functionaries a :[wild undernutrition, it is unlikely that the
grammes, and indicators which will help measure
levels, became evident.
of national nutrition programme will
these components.
An investigation was carried out on the nvJ
ment of national nutrition programmes wi
primary health care (PHC) system in the
Madhya Pradesh, India (Kanani and
1995). It was evident from the extensive ,n
and observation data that low priority
component of the PHC programme
affected the quality of its implement^
example, one-year long observations of 1
P1 the foregoing it is evident that a quality of
Framework for child health programmes in
'jv;
Pkd from a session conducted by the author as part
| training workshop organized by Women’s Health
Sbcacy Cell of the Women’s Studies Research
(WSRC). Baroda, entitled. Action Linked
prch for Women’s Health. April 1994.
COMPONENTS AND INDICATORS OF QOC FROM AN
OVERALL PROGRAMME PERSPECTIVE
Client 5 needs
Meeting client needs in a culturally appropriate
manner is imperative to ensure utilization of ser
vices by child caregivers. Service providers also
e
Quality of care in child health programmes
■
S. Kanani
1226
Tabic 2. Quality of u..» al point of service delivery in child health programmes
Table I. The emponems and indict of quali.y of care (QOC> io child health pr^ramnax pr..^..n,ne perspeciy^
ptMients
illustrative indicators
Components
Client needs
(a) Services meet client needs in a timely manner
(a need fulfilled loo late is a need unfulfilled);
• Proportion of needs met by the child health programme and to what
particular, fell needs expressed by clients
»Change in services over time
^prialcncss of (he physical infrastructure to deliver good
iy Giro
—
*
(b) Services respond to the changing needs of clients » Relative extent of focus on girl child in the services
Services arc culturally appropriate, seek to reduce
» Rates of utilization of services for girls and boys
»Gender disaggregated research data and outcome indicators
gender bias against girls
» Proportion of beneficiaries belonging to deprived groups according to social •
Services focus on the marginalized and socio
economic criteria defined according to regional situation
economically deprived sections of the population
• In the child health programme, list services which meet
(a) Short-term goals (c.g. oral rehydration therapy for diarrhoea management!’ '■
There is balance between short-term and long-term
(b) Long-term goals (c.g. environmental sanitation improvement)
.
• Training of health functionaries, extent of focus on QOC
’•
Money, humanpower and material resources arc
• Essential supplies:
'
efficiently managed with a focus on human
(a) Good quality.
resource development
(b) Adequate.
'
(c) Timely
'
• (a)
Monitoring
supervision.
Inclusionand
of QOC
indicators in the management information system• (rt&Iffi
reports, meetings).
.
;
(b) Focus of supervision on the quality of care provided by field functionaries (4 •
• Financial resources:
There is adequate coverage of children and
adolescents (0-18 years) and mothers, i.e.
(a)
Ail ‘severely affected” and ’at risk” children
are provided the ‘complete package*’ of services.
(b)
All children (below 3 years of age) are
provided a minimum package of services.
(c)
Mothers or other caregivers are covered
through mass media and interpersonal
communication
There exists a mechanism for health service
provider-client partnership
There is reduction in childhood mortality.
morbidity and malnutrition, especially in girls
;•
(a) Adequate.
Need based
allocation
• (b)
Proportion
of eligible
children, adolescents and child caregivers covered with
80-100% of specified services, that is,
'
(a) Severely affected,
(b) At risk.
(c)
below caregivers
3 years of age.
(d) Children
Mothers,Other
•
i&BjM
• Improvement in knowledge and skills of caregivers regarding child health airf
nutrition
• Community level health committees for child health programmes—their.
structure and function
™
• Cost sharing proportion of total cost met (in cash or kind) by community’
child health programmes
' n®
• Specific use of participatory approaches and techniques by health function*!
for programme planning, implementation and evaluation
. .. Ja
• Reduction in:
(a) Infant Mortality Rate and Under Five Mortality Rate,
'' ‘}~
(b) Proportion of children in grade I II and grade III malnutrition,
(c) Number and duration of episodes of critical childhood illnesses (e.g.
diarrhoea, upper respiratory tract infection, malaria).
(d) Reduction in micronutrient malnutrition (iron, vitamin A and iodine) and
improvement in growth in school children and adolescents
- 'jj-
Si
valuable and feasible recommendations, ajl
need to respond to client needs in a timely manner;
often services take so long to materialize that they
become irrelevant. Examples abound in the litera
ture of research conducted under short-term pro
jects whose findings rarely find their way to timely
and sustainable programmes. On the other hand,
building quality takes lime; a hurriedly implemented
programme may in fact be counter productive. A
balanced approach, wherein services arc reasonably
timely without sacrifice of minimal quality stan
dards. is called for.
Three years ago. a team from our department
was involved in a process evaluation of the mid-day
meal (MDM) programme in Baroda on the invita
tion of the government officials who wanted a
qualitative improvement
in
the programme
(Kanani, 1994). The participatory evaluation of the
programme, which primarily used qualitative
research tools such as observations, preference
ranking and focus group discussions, yielded several
which were immediately implemented. An eri
is the change brought about in the food item
the cyclic menu to cater to the likes and disliK?
children. Several recommendations emerged^
expressed needs of the parents of children pa
paling in the school feeding programme. ..
Child health services should have in-built;-bilily to respond to the changing needs of;<j
over time In particular, they should actively
to reduce gender bias against girls as regard^]
Illustrative indicators
• Space is adequate lo permit child and caregiver to be comfortable
• Environment is clean
• Facilities and supplies (essential drugs, vaccines, nutrient
supplements) arc adequate
^..provider Interaction
• Empathy and complete attention of provider towards clients
• Technical competence of providers regarding diagnosis, training.
referral and education of clients
,w-up care
• Number of home visits by service providers especially for care of
‘high risk' clients
• Return visits by clients for follow-up care
themselves. Hence there was evidently a need
increase self-esteem among girls and sensitize
:nts to the special needs of their daughters.
(jflscqucntly, sessions were designed to increase
(confidence and participation of girls; simuljeously our interaction with their parents also
u deliberately increased. These self-esteem develtnent sessions greatly enhanced receptivity and
rolvement of girls in the nutrition-education scs-
os.
Acceptance of the programme by the truly needy
>ups, especially in a multi-ethnic society as in
lia, is crucial for its success. The process cvalujq study of 1CDS in Gujarat (Kanani and
aria, 1996) revealed that in order to gain accepce from both the higher caste and lower caste
leficiarics, some child development project offi5(project in-charge) ensured that one of the pair
passrool level functionaries (Anganwadi worker
1 helper) was from the higher caste and the other
sfrom the lower caste.
From the point of view of clients, child health
rammes are likely lo be achieving good quality
if clients express that their needs are met, they
m to avail themselves of services, or bring
is to the programme. Also, a positive feedback
i child caregivers, indicating that they arc more
ible and confident of promoting the health of
’ children and that they have noticed a visible
rovement in the health or nutritional status of
children, is also an indicator of quality of care
Q the perspective of meeting client needs.
wee between short-term and long-term goals
ages was not enough, as the girls were notg
paling and expressing their needs (Agarwal
Kanani. 1994). The focus group discussions,^
revealed that they had a poor sense of sdftlj
hild health programmes in developing countries
e to resolve conflicts arising from ground realilln the field: conflicts between gaining acceptance
immunity members by meeting their immediate
s and the long-term goals of a programme. For
3Ple. a mother may want her child to obtain
relief from symptoms of diarrhoea and may
really be willing lo spare lime for health edu1 aimed at improving personal and environ*1 hygiene practices. Sometimes, health service
ders themselves are pre-occupied with short-
and considered their brothers to be more imp0
Boals to the neglect of (he more important
feeding, health care and education.
recently conducted a nutrition education^
gramme for school girls in which we found
merely communicating health and nutrition^
1227
long-term ones, perhaps because they give visible
returns and are less difficult to achieve. Thus, oral
rehydralion therapy for diarrhoea management may
take up considerable resources of the health system
and scant attention may be paid towards measures
to improve health and hygiene behaviours of child
caregivers.
This was evident in a study we conducted on the
ICDS programme in urban Baroda to assess the
quality of field level implementation of selected
ICDS services using the observation method
together with semi-structured interviews (Kanani
and Patel, 1994). The Anganwadi workers were
more concerned about the number of children
weighed monthly than with educating mothers
about their children’s growth and feeding practices.
Similarly, short-term programmes, such as immu
nization and food supplementation to severely mal
nourished children, received more emphasis than
nutrition health education to mothers, because
these were the ones m focus in the supervision,
monitoring and evaluation system.
Effective management of services
It is essential that human, financial and material
resources are efficiently managed in child health
programmes with particular focus on empowering
the health service providers at all levels.
Empowerment of mothers and other child care
givers can take place to the extent that health ser
vice
providers
themselves
are
empowered.
Empowerment in this context is viewed as a con
tinuous process in which knowledge and skills of
health care providers are enhanced, attitudes are
changed and administrative support is provided for
delivering good quality care. Quality of care should
be the focus in all aspects of management such as
training, logistics of supplies, monitoring and super
vision. Equally important, adequate financial
resources should be available to make it possible to
deliver good quality care. This was highlighted al a
state level workshop on alternative strategies for
improving woman and child nutrition in the State
of Gujarat in India (Kanani and Saiyed, 1995)
which particularly emphasized the need to focus on
‘software’ (human resource development) vis-d-vis
1228
Quality of care in child health programmes
S. Kanani
■------------- Qualitative and quantitative research methods for planning and evaluating QOC in child health programmes
Indicators of Quality of Care
Suggested methods from the health sciences and social sciences
Client needs are understood and met
Services arc culturally appropriate, reduce gender
bias against girls
Services focus on marginalized sections of the
population
• Free listing of needs as expressed by clients
• Proportion of planned needs met by the child health programme: semi
structured interviews and focus group discussions (FGDs)
• FGDs in community
• Matrix ranking of services
• Analysis of difference: access to care for girls and boys. e.g.. gender
discrimination through role plays
• Direct observations of health service providers and child c-aregivers
• Scrutiny of the routine recording system for gender disaggregated service
delivery and service utilization data
• Direct observations of clients receiving services
• FGDs with deprived population groups
• Review of records for service delivery and use data
Services meet
(a) short-term goals
(b) long-term goals
Efficient management ol* human power financial
and material resources
• Direct observations of service implementation
• Review of secondary data monthly reports
• Scrutiny of training curriculum for focus on QOC
• Semi-structured interviews with trainers and recent trainees
• Direct observations of meetings and supervisory visits
• Spot observations. FGDs and in-depth interviews of field functionaries
• Review of secondary data scrutiny of management information system (
reports and circulars) for indicators of QOC
• Budget: allocation of funds for good quality care
• Case studies of ‘well managed' and ‘poorly managed' centres
• Surveys through structured interviews with health service providers and
Adequate coverage of children, adolescents, and
proportion of eligible beneficiaries receiving above 80% of specified
child caregivers
• Direct observations of delivery of services
• Scrutiny of records and monthly reports
• FGDs with and direct observations of child caregivers to assess childcare
knowledge and skills
Existence of health service provider-client partnership • Key informant interviews with representatives of community level ec:—:
and health service providers at all levels
• Direct observations of functionaries of above committees
• FGDs with clients and health service providers
• Epidemiological survey
Reduction in mortality, morbidity and malnutrition
• Analysis of secondary data. e.g. growth charls.case papers at health t
in children and adolescents
schools
• Gender based analysis of impact data
• Case studies of families with children below 3 years of age in ‘poor I
■good health'
‘hardware’ (physical infrastructure). For example, it
was suggested that training of health functionaries
should be field-based and related to operational
aspects of their job functions, with two-way mech
anisms between the trainers and the trainees in
order to make the training more relevant.
Coverage
Though considerable variability exists in coverage
data available in child health programmes, records
maintained by functionaries usually contain infor
mation regarding the number and percentage of eli
gible beneficiaries receiving various services.
However, the important question is: are priority
groups covered, and if so, by which services and to
what extent? In the Indore (Madya Pradesh) study
referred to earlier (Kanani and Khanna, 1995), we
observed that with respect to iron supplementation
of children and women, functionaries focused on
registering new beneficiaries to show achievement of
targets and not on completion of the course of 100
tablets for a given number of beneficiaries.
Compliance of beneficiaries in terms of tablets con
sumed by beneficiaries was rarely monitored.
Further, the problem with supplies was more to do
^nutrition of children. It can guard against im*-n of limited, vertical programmes which have
’
to the socio-economic situation of
l^regio'1
iytiuciion in childhood mortality, morbidity and mallotion
j above components indicative of good qualj are assured, one may expect favourable outin terms of decrease in infant mortality and
mortality rates, morbidity and malnuchildren However, in an environment
O’on among
a
;|/$ocio___ \z deprivation, even reasonably well
I services may not succeed in achieving
___ Thus, as is often said, programmes
„J health have to move beyond the health
'.'.ktor and build bridges with other sectors, cs■' education.
•--y organizations in India have recorded
Missive gains in reduction of child mortality and
....cr) as evidenced in the ‘Anubhav’ series of
(the Ford Foundation. 1987-1988). These
1 experiences have highlighted features
_J sector which contribute to quality of
i as integrating health care activities with
’
I programmes for better health
I to fulfill fell needs of people, recruiting
local women and men as community
*■". or change agents, rationalization of
—j’ workload and assigning manageable
i to them, close monitoring and supervi‘““y management, collaboration with
: and academic institutions, and flexi'3“.r.r.2 design and implementation.
with disproportionate allocation to various <
rather than shortage per se.
Another issue concerning 'eligible L—
vulnerjl
the need to expand the definition of
groups’ to cover school children and c_well, and not restrict our efforts only to ]
children. Malnutrition and chronic r"
widespread in this group as several of our 1
have indicated (Kanani, 1996). A majority of
vantaged adolescent girls suffer from cr/
(>80%) and anemia (>60%). Further, J
looming threat of HIV and AIDS, I*
becomes particularly important in child I
grammes for reproductive health rJ
selling and services, and for f
healthy family life.
■QOC AT THE POINT OF SERVICE DELIVERY
to good quality care is the health service
interaction at the point of service
This htfs been mentioned in the QOC frafor women's health programmes and for
:-3 programmes referred to earlier.
i which can facilitate such interaction
, 'zz.zzj of physical infrastructure so
■ parents and children feel comfortable,
v *?3 of the health service providers
support, listening attentively, as
• technical competence of the health ser'■‘."3. Equally important is quality of fol- or referral services provided by the
Health service provider-client partnership
If mechanisms are developed to e
health service providers and community
lives are partners in child health p
is likely to be greater accountability <tionaries towards their clients and L
of good quality care. Such a partner
central role in empowering child < areg*1
essential knowledge and skills to i
i of research tools from the social sciences
sciences for planning and evaluating qualchild health programmes
purpose of this paper, social science
.23 the predominantly qualitative
-I paradigm of research, while health
-1 represents the predominantly quanJ epidemiological paradigm of research;
though it is realized that there is much overlap
between these two paradigms, and that one may
often include elements of the other. An integrated
approach, which synthesizes research tools from
both the social sciences and the health sciences, not
only yields maximal, usable data al less cost, it is
also a pragmatic approach. Alter all, social change
in communities and behavioural change in individ
uals are important goals of most health care pro
grammes.
In the context of child health programmes, such
a partnership between the health sciences and social
sciences is even more crucial as there is considerable
divergence in conceptual orientation between tra
ditional or modernizing communities on one hand,
and ‘health experts' or health care providers on the
other, with regard to desirable child feeding and
health care practices.
Further, when used in a complementary fashion,
quantitative methods help determine estimates of
phenomena like childhood diseases, prevalence and
rates of health care service utilization, while quali
tative methods yield a better understanding of cul
tural perceptions regarding child care, feeding
practices and childhood illnesses: and the social
determinants of treatment-seeking behaviour among
child care givers in households.
For ensuring quality of care (QOC) in child
health programmes, a blend of research methods in
the social sciences and health sciences is critical.
Table 3 describes the potential use of specific
methods to gather qualitative and quantitative data
for the QOC indicators presented earlier in Tables 1
and 2. The qualitative and quantitative methods
suggested are only illustrative of what is possible
and arc by no means exhaustive, or the most desir
able methods. The final basket of methods for a
given program should be region specific, and should
evolve over time.
STANDARDS FOR QOC
As Mensch has staled, the first step in improving
QOC is an articulation of minimum standards that
are acceptable and affordable (Mensch, 1993).
‘Gold standards’ might be impractical to achieve,
given the severe constraints on health services in
developing countries. Further, health services are
likely to be at different levels in terms of years of
implementation, reach and variety of services pro
vided. Hence, policy makers must clearly articulate
at least the minimum acceptable standards that ser
vices will adhere to, which should include all el
ements of care: interpersonal, informational and
clinical.
Secondly, standards should be region or pro
gramme specific, depending ‘on the existing level of
quality in the programme. Also, standards should
evolve and become more stringent so that QOC is
upgraded over the years.
Pergamon
S. Kanani
1230
THE CHALLENGE
In our journey towards quality of care for child
health, what arc the challenges we have to address?
It appears that the health science-social science
partnership will need to commit itself to the follow
ing.
• Advocate for prioritization of QOC in child
health services among policy makers among both
the government and non-govcrnmcnl sectors.
Approaches will have to be found to address the
issue of lack of conviction and commitment in these
sectors for setting up and enforcing QOC standards
for child health care.
• Facilitate the creation of a supportive environ
ment and adequate infrastructure in the health sys
tem which promotes good quality care. In our
process evaluations of national programmes such as
(for the most common problems, refer the
hospital if needed, and oiler the right advice
how to prevent and manage illness in the i.
(UNICEF. 1996).
REFERENCES
Agarwal. V and Kanani. S. (1994) Use of qualiutS^P?*
and behaviour analysis lo design a nutrition co'
cation strategy for disadvantaged school going
•
lesccnt girls in Baroda. Paper presented at the Nut* - 1
Society of India Annual Meeting.
.
Bruce. J. (1990) Fundamental elements of quality of
a simple framework. Studies in Family Planning Jlpi*
S0277-9536(98)00180-4
Soc. Sei. Med. Vol. 47. No. 9. pp. 1231-1246. 1998
'O 1998 Elsevier Science Ltd. All rights reserved
Printed in Great Britain
0277-9536/98 $19.00 + 0.00
CHILDHOOD CONDITIONS THAT PREDICT SURVIVAL TO
ADVANCED AGES AMONG AFRICAN-AMERICANS
SAMUEL H. PRESTON*, MARK E. HILL and GREG L. DREVENSTEDT
Population Studies Center, University of Pennsylvania, 3718 Locust Walk. Philadelphia,
PA 19104-6298, U.S.A.
Abstract—This paper investigates the social and economic circumstances of childhood that predict the
probability of survival to age 85 among African-Americans. It uses a unique study design in which sur
vivors arc linked to their records in U.S. Censuses of 1900 and 1910. A control group of age and race
matched children is drawn from Public Use Samples for these censuses. It concludes that the factors
most predictive of survival arc farm background, having literate parents, and living in a two-parent
household. Results support the interpretation that death risks arc positively correlated over the life
cycle,
1998 Elsevier Science Ltd. All rights reserved
Bruce. J, and Jam, A. K. (1990) Improving quality of
through operations research. Paper presented
TVT/MORE Conference on Operations Rescairh u
Family Planning, Arlington. VA.
Dutta. P K. (1993) Scope of health systems research * ’' ’
ICDS and nutrient supplementation programmes
child survival and safe motherhood programme.
s
referred to earlier (Kanani and Khanna, 1995,
flctor"'°oltelCold°r' m°rlali,y' '°"gCVi,)'- African-A"'eri«‘"*- socio-economic factors, geograph,c
Journal of Maternal and Child Health 4(2), 38-41.
Kanani and Zararia, 1996). we have observed that
Ford Foundation (1987-1988) Anubhav: Experienced'la
community health. New Delhi.
,,.7*^
often, functionaries are well aware of the lacunae in
Government of India (1993) National Nutrition Policy '
field level implementation of programmes. Yet they
Department
of
Women
and
Child
Development/
do not have either the motivation or the knowledge
Ministry of Human Resource Development, New Delhi
and skills to bring about a qualitative improvement
INTRODUCTION
Kanani. S. (1994) Feeding the hungry school child: proceti ;
of more vulnerable members of a cohort has
in their functioning because the- health care system
evaluation of the mid-day-meal program in Baroda city,‘i
sdies of social and economic differentials in morresulted in an unusually healthy group of older
Department
of
Foods
and
Nutrition.
M.S.
University
of'
does not support such efforts
blacks whose robustness is manifest in unusually
Baroda. Urban Basic Services, Baroda Municipal 5ty typically relate circumstances at one moment
• Forge links between the disciplines of the
Corporation and MDM Collcctoratc. Baroda,
low death rates. An alternative explanation is that
time to contemporary mortality risks. Literally
health sciences and social sciences for promoting
Kanani. S (1996) The apartheid of gender: A profiie tM
data on older blacks are flawed by age misreporting
ndreds of studies that date back more than a ccnQOC. For example, interdisciplinary action research
programmes for the girl child in India. Women’s Stitdfo
and that correction of these inaccuracies would
Research Centre, M.S. University of Baroda, Vadht^g ty show that, with rare exception, socially and
can be carried out by the health science-social
eliminate the crossover (Preston et al., 1996).
womically disadvantaged groups suffer elevated
science partnership for testing the feasibility and
India.
.
Kanani. S and Khanna, P. (1995) Studies on the manage* is of death (Williams. 1990, Feinstein, 1993).
This paper investigates the association between
cost of operationalizing the QOC framework pre
ment of vitamin A deficiency and anemia contrdf'pri>>.‘ Ji results are hardly surprising. Healthiness and
social and economic conditions in childhood and
sented in this paper This framework will need to
grammes in urban and rural Indore. Unpublished
the probability of surviving to age 85 among
document. Department of Foods and Nutrition,.MXl aevily arc nearly universal goals, and groups
be modified to suit regional conditions.
h more economic and social resources are better African-Americans. It uses a unique case-control
• Train students in universities and research in
University of Baroda. Baroda.
Kanani. S. and Patel. S. (1994) Process evaluation;of thfl nipped to achieve these goals.
approach in which blacks who survived to age 854stitutions so that personnel, who have an orien
integrated child development services in urban BarodtfJ Recently, studies have begun to investigate the re
in 1985 are (raced to their records from the censuses
tation to both socio-cultural and bio-medical
Unpublished document. Department of Foods'and
ionship between social and economic features of of 1900 or 1910, when they were children. They are
dimensions of health, are available to manage pro
Nutrition. M.S University of Baroda, Baroda.
then matched to a set of black children enumerated
Kanani. S and Saiyed, F. (1995) Report of a M orfahiyjj Mhood and adult health and mortality.
grammes for children and adolescents.
Sviduals and cohorts exposed to disadvantaged
Alternative strategies for improvement of child
al the same age and census in order to identify
• Document and disseminate success stories.
women
nutrition
in
Gujarat.
Organizedyggji mmstanccs in childhood arc typically found to
childhood characteristics predictive of survival to
There is already available a considerable body of
Commissionerate of Health and Medical-; ServfcCK
whence increased levels of morbidity, disability,
age 85. Special attention is paid to whether factors
anecdotal evidence and rich experience in organiz
Government of Gujarat and UNICEF. Gandhinagar./j
Kanani. S. and Zararia, V. (1996) ICDS as people view-® • mortality when they are older adults (see Elo
associated with higher levels of child mortality are
ations who have provided quality care to children
a social assessment of ICDS in Gujarat. blnp^bl^M I Preston. 1992 and Mosley and Gray. 1993 for
positively or negatively associated with survival to
and their families in deprived communities. These
document Department of Foods and Nutrition,
Jews).
age 85.
success stories need to be shared with others such
University of Baroda. Baroda.
‘
tfrican-Americans are sometimes said to repas the ‘Anubhav* series of Ford Foundation and
Maine. D. and Allman. J. (1990) The demography of nW
an exception to the prevailing positive corre
voluntary
health
association
of
India.
ternal and child health in developing countries,
RELATIONS AMONG DEATH PROBABILITIES ACROSS
Health care of women and children in devdop^t ct among death risks across different stages of
Unfortunately, in resource poor situations, many
THE LIFE CYCLE
countries, cd. H M. Wallace and K. Giri. Third.
• Recorded death rates among Africanorganizations do not consider n necessary to spare
Publishing Company, Oakland.
* ‘ .<3 *ricans have "crossed over" those of white
Will children who have been exposed to harsher
precious time or money to document and dissemi
Mensch. B~(I993) Quality of Care: A neglected ding
health environments in childhood be more or less
*hcans throughout the twentieth century.
nate success stories, especially the ‘process'.
sion. In The health of women - A global perspeettv^
l.ikely to survive from childhood to advanced ages?
M. Koblinsky. J Timyan, and J. Gay. Wcstview-W^ ^spitc much higher mortality at younger ages,
Creating this need and making available the necess
^n-Americans have had lower recorded death There arc at least four mechanisms linking child
Oxford. Boulder and San Fransisco.
ary resources is a major challenge.
Raceveanu. N. T. and Johansen. K. S. (1995) TecnnorJ 15 than whites beginning al some age between 70
hood conditions with adult mortality that would
To conclude. UNICEF has stated: “the great
for the continuous improvement of the quality 0 . .
85 (Elo and Preston. 199-1). A common e.xplasuggest an answer to this question. They fall con
challenge of the years ahead is to ensure that any
care. World Health Forum 16, 138-144.
*’ ’
veniently into the typology shown in Table 1. Two
Saturno. P. J. (1995) Towards evaluation of the
jj 0,1 of this crossover is that only the hardiest
family taking a child to a clinic or health centre
mechanisms would suggest that harsher health con
have survived to older ages, the weeding out
care
in
health
centres.
World
Health
Forum
16,
anywhere in the developing world will find a health
ditions in childhood would be associated with
United Nations Children's Fund (UNICEF)
worker who can examine and diagnose, make a de
progress of nations. UNICEF'. New York.
‘
higher adult mortality and two with lower. Within
cision on appropriate treatment, give basic drugs
Or for correspondence.
each direction of influence, one mechanism is direct.
Position: 2675 (4 views)