RF_DR_11 _SUDHA.pdf
Media
- extracted text
-
RF_DR_11 _SUDHA
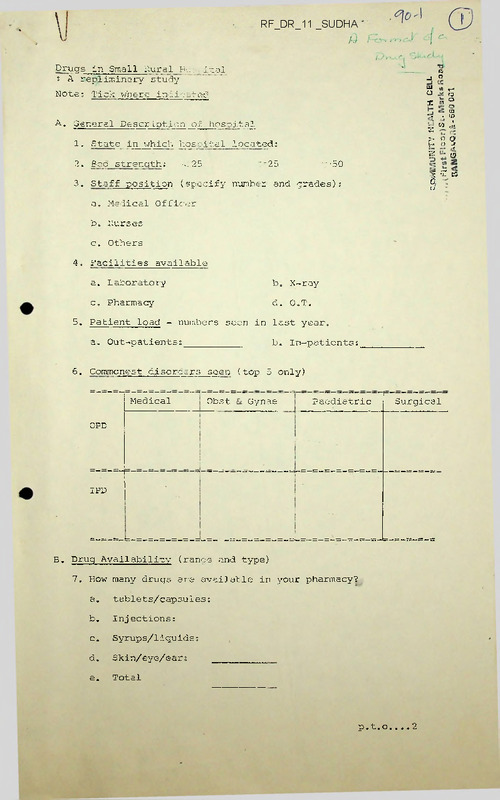
Drugs in Small Rural Ho-.... j-cal
s A repliminary study
'
«
J ”
1x1
Notes Tick where indicated
tn rw
o
°
x « S
03
co J.
‘r
General Description
of hospital
.
-
A.
„
1.
• in
x
> o 0?
n
State in which hospita 1 1 ocateds
h o -j
(5
2
2.
Bg° strength;
3.
Staff position (specify number and grades) s
<25
•<50
”25
S •’£ ts
a.
Medical Officer
b.
Nurses
c.
Others
0
4’ Facilities available
5.
a.
Laboratory
b. X-ray
c.
Pharmacy
d. O.T.
Patient load - numbers seen in last year.
a.
6.
b. In-patients:
Out-patientss
Commonest disorders seen (top 5 only)
Medical
Obst
Gynae
Paediatric
■
Surgical
OPD
________________
IPD
B.
Drug Availability (range and type)
7.
How many drugs are available in your pharmacy?
a.
tablets/capsules:
b.
Injections;
c.
Syrups/liquidss
d.
Skin/eye/ear:
e.
Total
p.t.o....2
2
8.
9.
What are the brands you stock in the following categories?
(Mention brane names (company names in brackets) eg.,
Beralgan (Hoechst))
a.
Antibiotics
b.
Ana1gesic/antipyretic
c.
Anti-inflammatory
d.
Antidiarrhoeals
e.
Steroids
f.
Ho rmonal preparations
g.
Psychotropic drugs
h.
Anti-histaminics
i.
Cough syrups
j.
Tonics/Vitamins
k.
Skin preparations
1
Non-allopathic drugs
(or combinations)
m.
Food substitutes
n.
Eye/ear preparations
What fixed-drug combination drugs do you.stock in the
following categories?
a.
Antibiotics
b.
Vitamins with other drugs
c.
Steroids with other drugs
d.
Antihistaminics with others
3
C.
Drug selection/Purchase/Pricino
10.
Who selects drugs in your hospital?
11.
What are all the criteria for selection?
12. Do you purchase -
a.
whole sale;
b.
by generic names
retail
or
through medical representative
brand names?
13.
Do you purchase any drugs in bulk? Specify.
14.
Do you prepare any medicines/mixtures/ointments in
the hospital? Specify.
15.
Do you get drugs donated from abroad?
(Mention names and sources).
16. How do you price your medicines?
(What percentage formula over wholesale-retail price)'
a. Injections;
b. Tablets/capsules;
c. Vaccines;
d. Samples;
e. Foreign drugs;
D. Dispensing/Prescribing
17. ’What categories of staff in your hospital -
a. prescri: :?
. b.
incense?
4
18.Do you have a trained pharmacist?
Does -y°ur hospital dispense drugs in any of the following
situation? If so, in each one (a) who prescribes? (b) who
dispenses?
(c) is there a standardised list for each level?
19.
a.
Mobile clinics
(b)
(c)
b.
Village Health Centre/Sub-Centre
(a)
(b)
(c)
c.
School/Hostel/infirmary
(a)
(b)
(c)
d.
Rehabilitation Centre
(a)
(b)
(c)
What is the regime you follow in your hospital for the
treatment of (specify brand names of drugs) -
20.
a.
Malaria
b.
Tuberculosis
c.
Diarrhoea in children
aDo
21.
b.
you have any policy about use of expired, drugs?
If you use.
some beyond the expiry date, which are these?
ci.For how long beyond expiry date do you use them?
5
Do you use any drugs as Placebos?
22.
Yes/No
If yes, which are the commonest and
for what situation?
Are you aware of the drugs banned by the Government in
July 1983?
23.
Do you have a banned brand list?
Have you weeded these drugs out of your hospital?
E.Drug information
How do you/your staff get information on drug indications/
doses/side effects.
24.
a.
Product literature
- Yes/No
b.
Drug company handouts
- Yes/No
c.
Any other sources
25.
F.
a.
formulary;
b.
list of minimum/essential drugs; and
c.
standardised drug regimes?
Adverse Reactions
26.
G.
Do you have in your hospital -
Have you had any adverse reactions with drugs in your
practice in the last one year?
YES/NO
If yes, specify;
Drug Budget
26.1
What is the annual expenditure on drugs in the last
financial year?
26.2
Did the pharmacy run at a loss or a profit?
If so, how much during that year?
LOSS/PROFIT
6
H.
Additional Information
27.
Have you taken any initiatives in recent times to
rationalise the prescribing/dispensing practices
in your institution?
What are they?
How successful have you been?
28.
If there are any other problems/issues that you
have come across with your hospital, please
mention them here.
29.
Have you identified any forms of irrational prescribing,
over-prescribing, under-prescribing or wrong prescribing
of the medical practitioners in your area through
prescriptions your patients may have brought with them?
Give details.
.... .7
7
30. Are there any pressing drugs issues on which you would
like reliable information?
31. Do you have any suggestions for issues/problems that
should be discussed/considercd at the workshop? Mention.
V R G E N T
yourprompt attentionplease
GD Ravindran
LT Menezes
Jose Joseph
St John's Medical College Hospital
Bangalore 5( 0034
24 OCT 1984
Dear
The Catholic Hospital Association of India (CHAI) are holding
a Workshop on 'Drug Prescribing and Drug Policy' as part of
their annual meeting this year. The announcements and details
have been given in the July/August issues of MEDICAL SERVICE.
If we can move towards a rational and low cost drug policy in
our hospitals, we can reduce the burden of our patients, the
community and our institutions. This aim is in keeping with the
CHAI's 'New Vision'.
As a preliminary to the Workshop, we are undertaking a survey
on certain drug issues in our hospital. We would like you to
give us frank feed back so that we can catalyse more relevant
policy decisions.
The enclosed questionnaire should be filled in by you and sent
back to :
COMMUNITY HEALTH CELL
326 V Main I Block Koramangala
Bangalore 560034
by the 10th of November 1984, latest.
The short notice is
regretted. However, keeping in mind the importance of the problem
and the need for action, we are sure you will respond positively.
The objective is to highlight common problems and issues not
specific institutional problems.
In case you have instituted certain changes in policy during
your work in the hospital, please refer to the earlier Situation
while answering the questions and mention changes brought about
by you in Q.27.
Remember we are trying to determine what the situation is and
not what it could be. Also none of the questions are a test
of your knowledge!!
or an evaluation of your institution!!
It is just a study to stimulate action in the CHAI network.
For your information, the MEDICAL SERVICE—Oct-Nov 1984 issue
will give useful background information on drugs. Write to
Fr John Vattamattom, Editor, MEDICAL SERVICE, CBCI Centre,
Goldakkhana, New Delhi 110001, for your copy.
Looking forward to an early reply and hoping to meet you
during the Workshop,
Yours sincerely.
GD Ravindran
enclosure
LT Menezes
Jose Joseph
Drucs in Sma11 Hural Hos..-ita 1
; A( repliminary study
Note; Tick where indicated
A. General Description on hospital
1.
State in which bos Ital located?
2.
Bed strength;
3.
Staff position ( .pecify number and grades):
<.2~
a.
Medical Of fir :r
b.
Nurses
c.
Others
25
*
-50
4• Facilities available
5.
a.
Laboratory
b. X-ray
c.
Pharmacy
d. 0„T.
Patient load - numbers seen in last year.
a.
6.
Out-patients;b. In-patients.
Commonest disorders seen (top 5 only)
------ Medical
—
Obst Si Gynae
Paediatric
Surgical
OPD
..
IPD
•
1
B. Drug Availability (range and type)
7.
*■
How many drugs are available in your pharmacy?
a.
tablets/capsules:
b.‘
Injections;
c.
Syrups/liquids?
d.
Skin/eye/ear;
e.
Total
p. t. o.. .. 2
2
8.
9.
What are the brands you stock in the following categories?
(Mention brand names (company names in brackets) eg.,
Beralgan (Hoechst))
a.
Antibiotics
b.
Analccsi c/arJripy r c sic
c.
Anti-ir.:r 1 ~.mr etor
d.
Antidi arrhoeals
e.
Steroids
f.
Horm onal preparations
g.
Psychotropic drugs
h.
Anti-histaminics
i.
Cough syrups
j.
Tonics/Vitamins
k.
Skin preparations
1.
Non-allopathic drugs
Tor combination's)
m.
Food substitutes
n•
Eye/ear preparations
What fixed-drug combination drugs do you stock in the
following categories?
a.
Antibiotj.es
b.
Vitamins with other drugs
c.
Steroids with other drugs
d.
Antihistaminics with others
3
3
C.
D.
Drug selection/, u rchase/Pri ci no
10.
Who selects .Irugs in your hospital?
11.
What
12.
Do you purchase -
criteria for reliction?
a.
whole sale;
b.
by generic names
retail;
or
through medical representative
brand names?
13.
Do you purchase any drugs in bulk? Specify.
14.
Do you prepare any medicines/mixtures/ointments in
the hospital? Specify.
15.
Do you get drugs donated from abroad?
(Mention names and sources).
16.
How do you price your medicines?
(What percentage formula over wholesale-retail price)
a.
Injections:
b.
Tablets/capsules:
c.
Vaccines:
d.
Samples:
e.
Foreign drugs:
Dispensing/Prescribing
17.
What categories of staff in your hospital -
a.
prescribe?
b. dispense?
18.Do you have a trained pharmacist?
Does your hospital dispense drugs in any of the following
situation? If so, in each one (a) who prescribes? (b) who
dispenses?
(c) is there a standardised list for each level?
19.
a.
Mobile clinics
(a)
(b)
(c)
b.
Village Health Ccntre/Sub-Centre
(a)
(b)
(c)
c.
School/Hostel/infirmary
(a)
(b)
(c)
d.
Rehabilitation Centre
(a)
(b)
(c)
What is the regime you follow in your hospital for the
treatment of (specify brand names of drugs) -
20.
a.
Malaria
b.
Tuberculosis
c.
Diarrhoea in children
aDo
21.
b.
you have any policy about use of expired drugs?
If you use
some beyond the expiry date, which are these?
c_ For how long beyond expiry date do you use them?
5
22.
Do you use any drugs as Placebos?
Yes/No
If yes, which are the commonest and
for what situation?
23.
Are you aware of the drugs banned by the Government in
July 1983?
Do you have a banned brand list?
Have you weeded these drugs out of your hospital?
E.Drug information
24.
25.
How do you/your staff get information on drug indications/
doses/side effects. L
a.
Product literature
- Yes/No
b.
Drug company handouts
- Yes/No
c.
Any other sources
Do you have in your hospital -
a.
F.
<
b.
list of minimurn/essential drugs; and
c.
standardised drug regimes?
Adverse Reactions
26.
G.
formulary;
Have you had any adverse reactions with drugs in your
practice in the last one year?
YES/NO
If yes, specify;
Drug Budget
26.1
What is the annual expenditure on drugs in the last
financial year?
26.2
Did the pharmacy run at a loss or a profit?
If so, how much during that year?
LOSS/PROFIT
6
H.
Additional Information
27.
Have you taken any initiatives in recent times to
rationalise the prescribing/dispensing practices
in your institution?
What are they?
How successful have you been?
28.
If there are any other problems/issues that you
have come across with your hospital, please
mention them here.
29.
Have you identified any forms of irrational prescribing,
over-prescribing, under-prescribing or wrong prescribing
of the medical practitioners in your area through
prescriptions your patients may have brought with them?
Give details.
7
30.
Are there any pr.s.ing drugs issues on which you would
like reliable information?
31.
Do you have any suggestions for issues/problems that
should be discussed/considered at the workshop? Mention.
41st ANNUAL CONVENTION
CATHOLIC HOSPITAL ASSOCIATION OF INDIA
23-26 NOVEMBER 1984
WORKSHOP THEMEs
towards a people-orJ.ented drug policy
'Eternal vigilance is required to
ensure that the health system
does not get medicalised, that the
doctor-drug producer axis does
not exploit the people and that
the abundance of drugs does not
become a vested interest in ill-health'
----- ICI-iR/ICSSR Health for All Report.
Venue: ST JOHN'S MEDICAL COLLEGE, BANGALORE 560034
SIGNIFICANCE OF THE THEME
2
THE Workshop is to help participants understand the
issues relevant to drug prescribing, drug distribution
and pharmacy policy in our institutions in the context
of the ICMR/ICSSR warning and to challenge them to
participate in the growing national response to
the problem.
WHAT does the 'abundance of drugs' mean to the millions
of the poor in our country who struggle in life to
make both ends meet? Can they ever have access to the
modern health care system which has become a business
today, rather than remaining at the service of humanity
at large? Do they have essential and life saving drugs
at their reach within a price range they can afford?
IS our drug policy today more profession-oriented, drug
industry-oriented rather than patient-oriented? Whose
interests are we serving in our institutions?
HOW can we move towards a more people and patient-oriented
drug policy?
THESE are some of the QUESTIONS which we shall respond to
in our Workshop.
OOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOO
"Community Health is a process
of enabling people- to exercise
collectively their responsibi
lities to maintain their health
and to demand' health as their
right. Thus it is beyond mere
distribution of medicines,
prevention of sickness, and
income generating programmes".
—CHAI new vision
OOOOOOOO GOO Ci OOOO „ OOOOOOOOOO 0 OOOOOOO
OBJECTIVES
1.
3
TO CREATE AM AWARENESS Of 3 -
the health situation in India, the role of drugs
in health care, the pattern of drug production
in India vis-a-vis the people's health needs, the
dynamics of the drug industry, the pattern of drug
distribution and -availability in the health system,
the national drug policies and laws.
2.
TO CREATE AN AWARENESS OFs=
irrational use, over use and misuse of drugs by
health personnel.
3.
TO DISCOVER.
the social, economic, political, cultural and
other factors responsible for this problem.
4.
TO DISCOVER
how all of us are part of the problem at a
personal level.
5.
TO CONSIDER
the various responses at national/regional levels
in the areas of s-- consumer awareness and people's
movements," continuing professional education;
pressure group on policy makers; search for low cost
alternatives; individual/group action; institutional
policy changes.
6.
TO DIECOVER
ways and means by which we can respond to this
situation at individual, institutional and
r-gional/national levels.
4
PROGRAimJ-ie highlights
^Sessions on:
Understanding the problem
Drugs and the dealing ministry
Towards rational therapeutics
What to do to tackle the problem
Seme initiatives in the country
The people's medicine
jnGroUp discussions ons
What/why the problem in our health institutions?
What can we do to tackle this problem?
jjjLiturqy
Reflecting on our calling and the faith dimension
of our response
;i^Exhibition on;
Socio-political dimensions of Health and Drugs
Rational Drug Therapy
Home remedies and Herbal medicines
:;^Studies on•.
Drugs for a Community Health Center
Understanding the iniection/tonic culture
Use/misuse of drugs in surgery
Drug situation in small rural hospitals
Cost of treatment
:i;Cultural Programme
Understanding the problem from the poor man's
point of view.
f
5
SYNOPSIS OF PAPERS
Drugs for Primary Health Care (c M Francis)
An integral part of our commitment to primary health care is
the provision of essential drugs to all those who need
them, in adequate quantity and quality and at affordable
prices wherever the person is. The various aspects of
the drug problem needing our attention include production,
what drugs are required, choice of drugs, National Drug
Policy, selection of drugs, drug production and procurement,
logistics of supply, quality control, regulating the drug
trade, drugs for immunization, drugs for cure, drugs for
symptomatic relief, search for new drugs, drug information
and the need for evaluation of the efficacy of primary
health care including drugs.
The Ten Commandments of the Drug Industry (Augustine Veliath)
1.
Thou shalt have tens of thousands of drugs
2.
Thou shalt not question the price of a drug
3.
Thou shalt not tamper with nature's garden
4.
Thou shalt respect they doctor more than thyself
5.
Thou shalt betray thy people and thy nation for petty rewards
6.
Thou shalt not covet, court, or subscribe to any other
system of medicine
7.
Thou shalt never reveal company secrets
8.
Thou shall first seek remedies for fashionable ailments
9.
Thou shalt be a dumping ground for banned drugs
10.Thou shalt be a guinea pig for new and untried drugs.
6
The Ethics of Prescribing (George Lobo, sj)
Discusses reasons for the unfortunate situation related to
drugs prevalent today, viz., technological model of
health care leading to manipulation of the patient,
search and demand for instantaneous cure of symptoms,
mystification of medicine, profit motive and 'free
enterprise' of the pharmaceutical industry, a deep
rooted cultural alienation from the people, exploitation
of dependent developing countries, decreasing emphasis
being given to preventive medicine and other systems
of medicine.
The use of drugs should be regulated by the principles of
totality (overall good of the pati-fent) and of double
effect (the good effect overriding any harmful effect).
It suggests remedies for the development of a personcentred and holistic approach to health care.
Professionals in the Church - an introspection. (George Joseph)
Serious questions have been raised about the institutional
witness of the church in India, particularly its
relevance in the social context of today. In the case of
the Healing Ministry there is urgent 'need to critically
look at our priorities and commitment and our style of
functioning in the light of the gospel. The role of the
professionals have to be reassessed as part of ah
overall effort to bring back the true spirit of 'Diakonia'
into this ministry.
The whole issue regarding the need for evolving a 'rational
drug policy' has to be seen in this perspective.
7
What is Rational Drug Therapy? (Mira Shiva)
Rational drug therapy means practice of socially
conscious, relevant, concerned and yet scientifically
sound medicine. It recognizes the non-role of drugs
in certain conditions, the role of alternative systems
of medicine and recognizes the limitations of Western
Medicine n our social context.
It emphasises selective use of drugs based on essentiality,
efficacy, safety, easy availability, easy administration,
quality drugs preferably of indigenous production.
Rational Drug Therapy recognizes the concept of essential
drugs and the concept of graded essential drug lists for
different levels of health personnel. It recognizes the
right of health personnel and consumers to drug information
and its effective communication.
It is taking of a conscious decision to boycott certain
drugs and use others only when needed. It means
prescription with awareness, to avoid as far as possible
— iatrogenesis (drug induced problems, drug interactions,
adverse drug reactions and emerging drug resistance).
It is understanding the role of drugs and rational drug
therapy in the emerging health movement.
"What can be done at a pharmacy level (Alan Cranmer)
(a)
Management of Pharmacy Services include involving the
users of the service; the Pharmacy Committee - its
constitution and functions, viz., implementation of
hospital policy, selection of medicines, sources of
medicines, cost versus quality, basic drugs and formula
tions, medicines banned in India and abroad, medicines
from other systems; stock control;, prescribing
discipline and pharmacy discipline.
(b)
Good dispensing services involve need for good
professional- service to patients, proper presentation
of patient's medicines, preparation of medicines in.
the pharmacy compared to purchase, medicines in the
pharmacy and at clinic level.
contd.
8
(c)
Relationships with suppliers, ie., with representatives
in the pharmacy and an assessment of products offered
and their.sources.
(d)
Educational requirements - basic courses., legal
requirements, course content, continuing education for
pharmacists.
(e)
Relationships with hospital colleagues.
9
INITIATIVE IN THE COUNTRY
(1)
Arogya Dakshata Mandal, Pune has been raising awareness
about drug related issues among medical professionals
and the lay public since the past 8 years. They publish
a monthly—'Pun.. Journal of Continuing Health Education' —
on drug issues and are also bringing out a book •.
'Rational Drug Therapy' in December 1984.
They launched a movement called 'Operation Medicine' in
1977 against irrational prescription of vitamins, tonics
and tinned foods.
(2)
All India .Drug Action Networks A number of groups have
been working in the field of drug related issues at
various levels during the past 3-4 years. They have
been in contact with each other and have been working
informally together sharing information, putting forward
a memorandum (demanding a Rational Drug Policy),
participating in campaigns, lobbying with government etc.
In August 1984, they felt the need to have a more organized
base and have formed the All India Drug Action Network.
CHAI is also a member of the Network.
(3)
Lok Vigyan Sanghatana, Maharashtra, or the People's Science
Movement have launched campaigns about anaemia and
irrational anti-anaemia drug preparations and also about
over the counter drugs. They organize jathas, hold district/
town seminars, write in the mass media etc.
(4)
Kerala Sastra Sahitya Perished is a voluntary non-government
organization consisting of scientists, doctors, engineers,
social scientists, teachers, students, workers, peasants,
technicians who arc committed to popularising science and
channelising it for social revolution. The KSSP has recently
decided to cake up the Drug issue and initiate a big campaign
to expose the anti-people and exploitative tactics of tho
Multinational Drug Companies. The questions of essential
versus non-essential and dangerous drugs, the inadequacy
of drug safety control measures, the rising prices of
life saving drugs and the non-implementation of the Hathi
Committee recommendations are the highlights of the
programme.
10
(5)
LOCOST or Low Cost Standard Therapeutics is a collective
voluntary enterprise for rational therapeutics. LOCOST
aims to promote low cost, scientifically tested medicine
under generic names. LOCOST is a response to a growing
demand and challenge of the voluntary health sector to
meet the needs of the deprived sectors of the society
for not only low priced but also good quality medicine.
LOCOST includes procurement, quality testing and control,
distribution and educational efforts, and is located in Gujarat.
(6)
Sangarapet Mission Tablet Industry in Karnataka is a
successful small scale venture providing low cost, good
quality formulations to some mission hospitals in the
country.
(7)
Low Cost drugs and Rational Therapeutics Cell of the
Voluntary Health Association of India, New Delhi, has
been instrumental in bringing together various groups in
India on the issue of drugs. They have been providing
informational backing to these groups, organizing meetings,
informally coordinating some actions etc.
(8)
medico friends circle is a group of socially conscious
individuals, interested in the health problems of our
people. Through their monthly bulletin, they discuss
drug issues among others. They have formed a Rational
Drug Policy Cell and have launched a campaign on antidiarrhoeal s.
(9)
The Kurji Holy Family Hospital Formulary is the result
of the accumulated experience of the hospital over the
last 10 years. It gives a comprehensive, list of drugs
to treat 98% of the hospital admissions. It also gives the
generic name, dosage, indications, contra-indications
and side effects of these drugs. Information about
comparative cost of treatment is also provided.
11
(10)
State Fcrums: During the past year drug action forums
have been active in Andhra Pradesh and West Bengal.
Drug Action forums are also being initiated in Gujarat
and Orissa.
(11)
The Pharmacology Department of the Post-Graduate Institute
of Medical Education and Research, Chandigarh, provide
unbiased' technical information on drugs and therapeutics
through a monthly publication 'The Drugs Bulletin'.
(12)
Othersz
The following organizations have also been
involved in drug related, issues and are part of the
All India Drug Action Network;
•
Consumer guidance Society of India, Bombay
Consumer Education Research Centre, Ahmedabad
Federation of Medical Representatives
Association of India
Health Services Association, Calcutta
Delhi Science Forum, New Delhi
People's Participation in Science and Technology,
Madras/Bangalore
Centre for Science and Environment, Delhi
Centre of Social Medicine and Community Health,
J N University, Nev/ Delhi
W hat w e
c a n
d o ?
— Support them
— Join them
— Keep them informed about what you are doing
12
RESOURCE MATERIALS
: People, Pills and Prescriptions, column in MEDICAL
SERVICE since May-June 1984.
; Objectives of the Workshop, a handout.
; Understand:.ng the Drug situation in our Hospitals,
a check list.
: Towards a People-Oriented Drug Policy, Special
Convention Issue of MEDICAL SERVICE (October-November
1984) and a supplement to this issue will be
distributed during the Workshop.
i
Drugs awareness and Action, mfc BULLETIN Special Issue
No.107 November 1984.
i DECCAN HERALD Supplement on the 'Workshop.
"What people really need, first
and foremost is clean drinking
water
school and
land, not urban hospitals with
their wonder drugs".
— Planning Commission
AN INSPIRATION
13
Reading
The story of the sickman
at the pool of Bethsaida
John 5?
1-9
Reflection
The action of Jesus in bypassing the pool is an
invitation to us to look more critically at
our own health care system. Thanks to our
emphasis on curative health care, we have grown
accustomed to thinking solely in terms of the
health needs of the individual rather than addressing
ourselves to the community as a whole. While
concentrating on the symptoms, we have failed
to take into account the environment and other
social factors. Poor sanitation, polluted water
supply, the superstitious beliefs and taboos
of the community are also related to sickness and
disease.
Further, the miraculous pool in its ineffectiveness is
a symbol of our own ineffective health care system
despite the highly qualified doctors and nurses,
well equipped private arid public hospitals, medical
research centres and multinational drug industry.
The poor man in the gospel story lived very close to
the pool, yet he was helpless because of his
poverty. In like manner the poop in our midst
remain helpless in the shadow' of an expensive,
curative health care system that is geared
exclusively to the service of the rich.
Source; The Bible; Aspirin or Dynamite
by Cedric. Rebello s.j.
GIVE YOUR BABY THE BEST
START IN LIFE
1. Should I breastfeed my baby?
Yes, every mother should breastfeed her baby.
Breast milk is nature’s first gift to your baby, and
there is no other substitute for it. For the first 4 to 6
months, breast milk is your baby’s best and
complete food. Do not be misled by people who
suggest powdered milk ‘in case you think you do
not have enough milk’. It has been found that
almost all mothers are capable of producing more
than enough milk for their baby’s need.
Nature in all its wisdom has ensured that you can
breastfeed successfully. All you need is the deter
mination to breastfeed, and faith in your own ability
to breastfeed successfully. Remember that breast
milk has many qualities which make it unique from
all other artificial milks available.
2.
Will I be able to breastfeed successfully?
A common reason mothers give for stopping
breastfeeding is the fear that they do not have
enough milk, and so they introduce their babies to
artificial feeds in the first few days after birth.
Research shows that in practice, almost every
mother can breastfeed successfully. Rarely is there
any physical reason for being unable to feed the
baby naturally. The most important thing to
remember is that the mother must want to breast
feed, have confidence in her ability to breastfeed
successfully and must not lose hope.
Further, studies have shown that women who want
to breastfeed actually produce more milk than
those who don’t want to. or are indifferent about
breastfeeding their babies. Many women fail to
breastfeed successfully, even though they want to,
because they believe, incorrectly, that they do not
have enough milk for their baby’s need. The truth is
that almost all mothers are capable of producing
more than enough milk for their baby’s need.
J.
What is Colostrum? Is it important for my
baby?
For the first day or two, the milk that flows from the
breast is called colostrum. This first milk is extreme
ly nourishing for the newborn. What makes
colostrum even more special is the fact that this
first milk is full of antibodies produced by the
mother. These antibodies protect the newborn
against some diseases and infections at a time when
the baby is particularly vulnerable. Later milk also
contains these antibodies, but not as much as the
first milk. In addition, colostrum also has certain
properties that prevent allergic diseases like
asthama and eczema which are more common in
bottlefed babies.
Traditionally, in many Indian homes, colostrum is
thrown away. Today we have learnt that in actual
fact, colostrum is extremely valuable to the new
born. Throwing away the colostrum deprives the
newborn of the best possible nourishment avail
able, as well as the protection that it offers against
disease. Colostrum is very rich in proteins,
minerals and vitamins. In fact, colostrum is just
what the newborn needs soon after its birth.
No matter where a mother delivers her baby, at
home, hospital or the nursing home, she should
COMMUNi.Y iUALTH CELL
47/1,(FirstFloor)St. Marks ftoad
BANGALORE - 560 G01
insist that the baby is kept with her in the same
room. This way she can ensure that her baby gets
the benefits of colostrum. Put the baby to the breast
soon after birth. The sooner the baby starts suckl
ing the breast, the sooner and better the milk will
flow. In addition, it will receive the benefits of
colostrum which flows only for the first day or two.
According to many doctors, colostrum has life-long
health preserving benefits.
4.
How often should a baby be breastfed in a
day?
Babies usually cry when they are hungry. Put your
baby to the breast each time it cries for a feed. This
demand feeding is a better way to feed your baby
instead of fixed schedules.
Babies could also cry for some other reasons, such
as if their nappy is wet or if the clothes are too tight.
Having checked that none of these is the source of
trouble, you should interpret the baby’s cry as its
demand to be breastfed.
Your baby is a special person, an individual unlike
other babies. It is not just a hungry stomach to be
filled at regular intervals. Once you accept that the
baby may ask for a feed at different times, depend
ing on when it is-hungry, you are well on your way
towards breastfeeding successfully. If you worry
each time it cries for a feed too soon, you are more
likely to lose your milk. This happens because
worry can interfere with the ‘let down’ of the milk
from your breasts.
While some babies setde down to a routine of
demand feeding after a few weeks, others don’t. So
do not compare your baby with other babies. Just
breastfeed your baby when it cries for a feed.
As the baby grows it may ask for fewer feeds and
may setde down to a regular demand routine, every
two, three or four hours. Sometimes your baby may
demand a feed more often than other times. This
could be for many reasons: the baby may be extra
hungry, growing rapidly, teething or is just upset. If
the baby needs extra feeds, your own milk supply
will adjust to its needs if you let the baby suckle as
much as it wants to and whenever it demands a
feed.
5.
How long should each breastfeed last?
Let your baby tell you how long it needs to suckle
2
your breasts to get its fill. A hungry baby will cry for
milk. The old rule of 10 minutes on each breast was
created because that was roughly the average time
diat a baby takes to feed. But each baby is different.
So while some babies take less than 10 minutes to a
side to get their fill, others may take longer.
During the first few months, you may find that your
baby wants a feed very frequendy. This is not un
usual and is the baby’s way of increasing your milk
supply to suit its growing needs. People may tell
you that a baby gets all the milk that it needs in the
first few minutes at each breast. But all babies are
not alike. A lot will depend on how vigorously the
baby suckles, the strength of your ‘let down’ reflex
and the time taken for the ‘let down’ or start of the
milk flow.
Remember that some babies enjoy suckling even if
they have had their fill. There is no reason to stop
this unless you have some other work to do, or if
you have sore nipples. This ‘comfort suckling’ is
considered by many experts to be an important
factor in the child’s emotional development.
When your baby has had its fill on one breast, in
other words, when it loses interest in feeding,
change it to the other side. Let the baby continue
feeding on the other breast as long as it wants to.
There are times when the baby will feel less hungry,
is sleepy or just tired and may not want to suckle
very long. Don’t worry about this, and don’t force
the b.aby to feed. Just offer your breast after a litde
while.
6.
How does a mother know if her baby is getting
enough milk?
It is true that when you breastfeed you cannot
actually see how much milk the baby drinks.
However, if your baby sleeps well, is healthy, active
and playful when awake and gains weight steadily
each mondi, then you can be sure that your baby is
getting enough milk for its nourishment and
growth.
7.
How can I increase the flow of milk in my
breasts?
The baby’s suckling is the best way to start and
increase the flow of milk in your breasts, and the
sooner the baby is put to the breast, the sooner and
better will be the flow of milk. Let the baby suckle as
frequently as possible because the more often a
baby suckles the breast, the better it stimulates the
breast to produce more milk. This is Nature’s secret
to start and increase the flow of milk to meet your
baby’s growing needs.
Sometimes emotions like embarrassment, tension,
or fatigue can also interfere with the ‘let down’ of
the milk. A mother should therefore, relax and sit
comfortably when she feeds her baby.
"When the baby suckles, it stimulates two hormones
which are released into the mother’s bloodstream.
One of these hormones stimulates a strong flow of
blood through the breasts and activates the milk
making tissue. The other hormone causes the
breasts to push out or ‘let down’ the milk from the
breasts. This is generally felt as a ‘pins and needles’
sensation or a frill feeling in the breasts. If the milk
doesn’t ‘let down’, your baby will not get all the
milk that is available in the breasts. Fortunately
Nature has ensured that when the baby suckles
frequendy, the ‘let down’ reflex works well.
8.
What should I eat to increase the flow of milk in
my breasts? Are there medicines to increase this
flow?
There are no special foods or medicines to improve
the quality and quantity of breast milk. To breast
feed successfully and to maintain her own health, a
nursing mother should eat slightly more of the food
she normally eats. There is no need to eat anything
special. An extra helping of rice or chapati, dal,
green leafy vegetables and fresh fruits will give the
nursing mother all the nourishment she needs to
produce enough milk for her baby and to maintain
her own health. Eggs, fish and meat are also good.
What is important is to eat slighdy more of every
thing that she normally eats, rather than eating
anything special while nursing her baby.
Finally be assured, you can increase your milk
supply. Nature has made sure that when the baby
suckles the breast frequendy, the milk will flow
well. All you need is the confidence in your natural
ability to breastfeed successfully. Eat and rest well.
These early months can be a challenge, demanding
much patience and determination on your part. So
do relax and enjoy your baby. Remember that not
only is your baby receiving the best food available,
but also both your baby and you are building a
happy and secure relationship during this period.
9.
How should a mother hold the baby while breast
feeding?
There is no ideal position to hold the baby while
breastfeeding. The main thing is to make yourself
comfortable because you will be in that position for
some time, and try to make the baby comfortable.
Pain and discomfort can reduce the ‘let down’ of
milk.
Support the baby’s weight with a pillow on your
lap. Another pillow under the arm supporting the
baby will also help.If you are sitting, it is easier to
feed if you sit upright and lean slightly forward.
Hold the baby with its chest and stomach against
you, so that it doesn’t have to turn its head around
and can feed comfortably. Some babies like to have
something to hold on to while feeding—give the
baby your finger to hold onto. At night, lie on your
side and breastfeed the baby.
Don’t push the baby’s mouth onto your nipple.
This could frighten the baby. Instead, stroke the
side of its mouth with your nipple. If your breast is
very full, you may have to hold it back so that the
baby’s nose is not smothered. But don’t bother to
hold your nipple or breast once the baby starts
suckling. Expressing a little milk from a full breast
will soften it enough to enable the baby to hold on.
When breastfeeding, part of the areola (the dark
area around the nipple) should go into the baby’s
mouth as the milk reservoirs are under the areola
and need to be emptied by the baby’s suckling. If
only the nipple goes into the baby’s mouth, not
enough milk will flow out. The baby would have to
suckle extra hard and this could lead to sore
nipples. If you have an extra large areola, hold it
between the finger and thumb and squeeze them
together. This will make the areola flatter and easier
for the baby to take in its mouth.
You may notice that at times your baby stops
suckling and looks around. This happens because
the ‘let down’ causes the milk to be spurted in an
uneven flow. Several spurts of milk come out, and
then there is a short pause before the milk flows
again. Your baby is adapting to the flow of your
milk and its breathing pattern is also altered to fit in
with this drinking pattern.
3
10.
How should a mother stop a feed?
Some babies simply let the nipple go when they
have had enough to drink, while others have to be
gently removed from the breast. Some babies also
like to suckle even after they have had their fill. This
is called ‘comfort suckling.’ According to many
doctors, this should be encouraged because it helps
the emotional development of the baby.
Do not abruptly pull the baby’s mouth away from
your breast while it is feeding. The force could
damage the nipple and the areola, apart from
frightening the baby. Instead, put the tip of your
little finger in the corner of the baby’s mouth and
gently draw the baby away.
11.
How can I tell when the baby has had enough
milk?
Babies often show they have had enough milk
simply by falling asleep. But before they go to sleep,
they may unclench their fists, smile, refuse to drink
anymore or just arch their back. Don’t force the
baby to feed any more if it doesn’t want to. Learn to
accept your baby’s judgement about when and how
much it wants to feed.
12.
Can a woman with small breasts produce enough
milk?
Some women with small breasts worry about their
capacity to produce enough milk for their baby’s
need. The size of the breasts have no relation to their
capacity to produce milk. Women with small
breasts can and do produce more than enough milk
for their babies. Worry will only reduce the flow
of milk. What is important is not the size of your
breasts, but allowing your baby to suckle frequently.
Frequent suckling will stimulate your breasts to
produce more milk. This is the secret to successful
breastfeeding.
13.
Can a mother breastfeed while having her
periods?
There is no reason why a mother should not breast
feed during her periods, since this will not harm
her or the baby. Some mothers say that their babies
are temperamental when they have their periods.
This is quite likely due to the mother's own
menstrual tension being communicated to the
baby. There is no difference in the mother’s milk,
during her periods.
14.
Can a mother breastfeed even when she is
ill?
Yes, a mother can continue breastfeeding her baby
even while she is ill, without harming the baby. In
most cases, the baby will get the protection against
the mother’s illness from the antibodies present in
breast milk.
Most medicines taken for illnesses do pass into the
breast milk but in such small quantities, that they
are unlikely to harm your baby. Consult a doctor
who will prescribe medicines which are less likely to
harm the baby. The doctor will also advise the
mother to continue breastfeeding.
However if the mother has high temperature,
jaundice or septacaemia, the doctor will advise her
to discontinue breastfeeding until she recovers. A
mother who has been advised to stop breastfeeding
during an illness should however, express her milk
regularly and throw it away until she has fully
recovered from the illness. This practice will ensure
that her flow of milk is not reduced. On recovery
she should resume breastfeeding die baby.
During the period when she has been advised to
discontinue breastfeeding, the mother can give the
baby fresh cow, goat or buffalo milk or even milk
from the local dairy centre. Do not dilute this milk.
Generally speaking in most common illnesses, a
mother can continue breastfeeding without any ill
effects on the baby.
15.
Should
ill?
a
baby
be
breastfed
even
when
Yes, your baby can certainly be breastfed even when
it is ill. In fact it is very important that you continue
breastfeeding while the baby is ill because your milk
will provide the baby with antibodies to protect it
fiom other illnesses which can set in when it is
already weak. Breast milk will also give the baby the
nourishment and strength to recover from the
illness.
Do not stop breastfeeding when the baby is ill,
unless your doctor advises you to stop. But this is
rare. Unless your baby is so ill that it is not allowed
milk, the baby will do better drinking breast milk
than any other milk. Breast milk is much easier for
the baby to digest. Besides, the baby will recover
faster from vomiting, diarrhoea and dysentry if it is
given breast milk.
16.
Can a
pregnant?
mother
breastfeed
when
she
is
Yes, a mother can certainly continue to breast
feed her baby all through her pregnancy without
any ill effects on either the breastfed baby, the baby
in the womb or herself. However, a pregnant
woman who is breastfeeding her earlier child
should eat slightly more for the sake of the breast
fed baby and herself as well as for the baby growing
in her womb. All three require good nourishment
during this period.
17.
Is it possible that breastmilk may not suit my
baby?
Babies are rarely allergic to breast milk. Nothing
could be more suitable than what Nature intended
to feed your baby. In fact animal milk and powder
milk are unnatural for the baby’s system. It has
been found that bottle fed babies are more likely to
suffer from allergies like asthama and eczema.
Bottle fed babies are also more prone to diarrhoea.
Do breastfeed your baby. Breast milk is the safest
and most nourishing food available for your baby.
18.
What should a mother do about breastfeeding
if she has had a caesarian operation?
Except in rare cases, there is no reason why a
woman who has had a caesarian operation cannot
breastfeed as successfully as the woman who has
had a normal delivery. However, after a caesarian
operation you are bound to be in pain. If you are
determined to breastfeed, then you would have to
put your pain and discomfort aside and insist that
your baby be brought to you as soon as you are
awake. As a bonus, breastfeeding your baby will
help to compensate for some of .the disappoint
ment you may feel not having experienced a
normal childbirth.
Unlike a mother who has had a normal delivery,‘
you will not be able to breastfeed immediately after
childbirth as you will be under the effect of
general anaesthesia. However, insist that your baby
be brought to you as soon as you are awake and
kept with you. Also you should insist that you do
not want your baby to be bottle fed. Put the baby to
the breast whenever it cries for a feed, instead of
feeding it at fixed schedules. It is vital that you put
the baby to the breast as soon as you are awake, so
that your baby is not deprived colostrum. Frequent
suckling will stimulate your breasts to produce
more milk. In a day or so, your milk supply will
settle down to suit your baby’s need.
At first you may face a problem deciding on a com
fortable position to breastfeed. Sitting up after a
caesarian operation can be painful. However, don’t
let this problem put you off breastfeeding. Lie on
your side and let the baby suckle your breasts. After
the baby has had its fill.on one side, ask.someone to
help you turn to the other side and continue
breastfeeding from the odter breast.
Remember breast milk is the best and complete
food for your baby, besides being the safest and
most hygienic. For your baby’s sake, put your pain
and discomfort aside and insist oh breastfeeding
your baby as soon as you are awake. Do not let
people discourage you from breastfeeding. After
all, as a mother, you would not like to deprive your
newborn of the best food available.
19.
Should a baby be kept with the mother while
she is still in the hospital or nursing home?
Every mother should insist that her newborn is kept
with her in the same room, no matter where she
is—at home, hospital or the nursinghome. This is
called ‘rooming in’.
Many hospitals and nursing homes keep the
newborn separately for the first few days. Al
though a nurse will bring the baby to the mother
in the course of the day, she may give the baby an
occasional ‘top’ or bottle feed. Even a single botde
feed of milk powder can disrupt the formation of
the normal suckling habit and reduce the mother’s
milk supply.
This happens because suckling the mother’s nipple
requires greater effort on the baby’s part. Nature
intended it to be this way. This extra effort by the
baby helps to stimulate the breasts to start and
increase the flow of milk. On the other hand,
suckling the feeding bottle is much easier. If your
baby gets used to suckling from a feeding bottle, it
5
will not exert much pressure while suckling your
breast. If the baby doesn’t suckle hard enough, it
will not stimulate the breasts enough to produce
more milk. This can reduce the flow of milk from
your breasts. Therefore it is vital that ever}' mother
insists that her baby is kept with her soon afterbirth
and is exclusively breastfed. Not only would the
baby get colostrum that flows for the first day or
two, but frequent suckling whenever the baby cries
for a feed will ensure a good flow of milk.
20.
How can a working mother continue breast
feeding after she returns to work?
Most working mothers are entitled to three months
maternity leave. A mother who is keen to breastfeed
her baby should take as much of this leave after
delivery. This will ensure that at least for the first
diree months of life, her baby is exclusively breast
fed while she is at home. During this period, do not
make die mistake of getting your baby used to
bottle feeds before you return to work. Just because
you have to return to work, does not mean that
botde feeding is the only answer to feeding your
baby.
The problem of breastfeeding arises during the
working hours when the mother is away at work.
However, if she is determined to breastfeed, she
can hand express her breasts in the morning before
leaving for work. Store this expressed milk in a
clean covered container which has already been
properly sterilized in boiling water. This pre
caution would ensure that no germs enter the
baby’s body. Breast milk can be stored in the
refrigerator for a few hours, and reused while the
mother is away. Do not warm expressed milk
directly over the fire. To warm this milk put the
container in a bowl of hot water. A family member
who stays at home with the baby can give the feed,
using a clean spoon.
Once the mother returns home, she can breastfeed
her baby. A working mother who wishes to breast
feed should follow this practice: breastfeed the
baby before leaving for work; hand express your
milk and store this milk which can be reused in
your absence, and resume breastfeeding when you
return. This will ensure that your baby is not
deprived of your milk during these crucial months
of life. Expressing your milk everyday before leav
ing for work acts as a double bonus. Besides
providing the baby with the best nourishment
available, it also prevents your milk flow from
reducing.
Some mothers may complain that expressing
breast milk every' morning would involve much
time and effort, just when sheliasso many other
household chores to finish. But if you balance the
benefits of continuing breastfeeding with this extra
effort and time, you will be convinced to make
the right decision—to continue breastfeeding. You
will also have the satisfaction that your baby is getting
the' best possible nourishment. After all, breast
milk is the best and. complete food for the baby
during the first 4 to 6 months of life. Remember,
there can be no other substitute for it.
21.
How do I express milk from my breast?
Wash your hands before you express the milk. Use
both hands to squeeze gently from the base of the
breast towards the areola (the dark area around the
nipple) and the nipple. Then squeeze the breast
and the areola between the fingers and the thumb
till the milk flows out.
Collect this milk in a clean cup or container which
has been boiled previously. Cover the container
and store the milk in the refrigerator. Expressed
milk can be stored in the refrigerator and reused
within a few hours. If there is no refrigerator in your
home, store the expressed milk in a cool place. Milk
which is kept outside a refrigerator must be used
within 2 to 3 hours after being expressed.
To warm the milk, put the container in a bowl of
hot water. Do not warm expressed milk direcdy
over die fire. Use a clean spoon to feed die baby.
22.
What should every nursing mother know
about cleanliness and care of her nipples and
breasts?
Every morning while having a bath, wash your
nipples and breasts with plain water. Avoid using
soap on your breasts and nipples as this would
remove the natural oils secreted by your breasts to
keep them from cracking. While you do not have
to wash your breasts and nipples before a feed, do
remember to wash them after and dry' them well.
This precaution will prevent your nipples from
cracking. Cracked or sore nipples can be painful.
The important thing to remember is to wash vour
breasts and nipples with water and keep them dry
between feeds.
23.
What should a nursing mother eat to maintain
a good flow of milk?
There is no evidence that any food, drink or
vitamins will increase or decrease the flow of milk,
as long as you eat enough of a variety of foods.
However to produce enough milk for the baby and
to maintain your own health, you should eat a little
extra of whatever you eat normally. An extra
he.ping of rice or chapati, dal, fresh green leafy
v egetaoles, fish, eggs, meat and fresh frdits will give
you all the nourishment that you need to produce
more than enough milk for your baby and will help
you maintain your own health.
It is sensible to eat according to your appetite and
try not to lose weight—die fat stored in your body
during pregnancy' will slowly be lost when you
breastfeed. Avoid overeating. A mother who eats
sensibly will not only provide her baby with plenty
of milk, but will also ensure that her own body isn’t
being drained of food resources to meet her baby’s
need.
Even poorly nourished mothers manage to breast
feed their babies adequately for the first 4 to 6
months before extra food is required for the
normal growth and development of the baby.
However, these mothers breastfeed at the cost of
their own bodies—their bodies lose calcium and
proteins. The more babies these women bear and
feed, the poorer their health becomes.
How much extra should you eat while nursing?
You should eat slighdy more than you do when you
are not pregnant. Is there anything you should eat
more of when feeding the baby? No. Assuming that
you are eatinga variety of food in your normal daily
diet, just eat slightly more of everything. This will
provide enough nourishment both for your baby
and you.
24.
Is it true that vegetarian mothers cannot
produce enough milk and so should not breast
feed?
No, this is not true. A vegetarian mother can
breastfeed successfully and produce enough milk
for her baby. Traditionally in most Indian homes
people eat a vegetarian diet, and women through
the ages have lived and reared their children while
eating a vegetarian diet. As long as the nursing
mother eats slightly more than what she eats
normally when she is not pregnant, she will
produce more than enough milk for her baby.
There is absolutely no reason to fear that a woman
eating a vegetarian diet will deprive her baby of
adequate nourishment. A vegetarian diet which
contains a variety of foods like rice or chapati, dal,
fresh green leafy vegetables, ‘paneer’, curd and
fresh fruits will provide enough nourishment both
to produce enough milk and to maintain the
mother’s own health.
2b. Should a nursing mother drink extra water so
that her milk is not too thick and is easy for
the baby to digest?
The amount of water that a mother drinks has no
relation to the consistency of breast milk, which
differs from person to person. Some mothers fear
that their milk is too watery, while others feel their
milk is too thick for the baby to digest. The truth is
that the consistency of breast milk has nothing to
do with its quality. Breast milk, whether thin or
thick is perfect for your baby.
In summer, a nursing mother finds herself very
thirsty. This is hardly surprising, considering that
the baby is taking a great deal of milk from you
everyday. Don’t force yourself to drink extra water,
just drink as much as you want to.
26.
Will breastfeeding spoil my figure?
No, breastfeeding will not spoil your figure. On the
contrary, breastfeeding is Nature’s way of restoring
your figure. During pregnancy a woman’s body
stores up fat in preparation for nursing the baby.
This extra fat is used up when the mother starts
breastfeeding. In fact, breastfeeding helps the
mother lose the extra weight she gains during
pregnancy. In addition, the womb which has
stretched to hold the growing baby, also regains its
normal size when a hormone is released during
breastfeeding.
Is breastfeeding effective in delaying the next
pregnancy?
It has been found that frequent and regular breast
feeding may help to delay the next pregnancy.
Breastfeeding alone, however, will not provide
27.
7
complete protection. A mother who breastfeeds
should also take some other precaution to avoid
pregnancy.
28.
When should a breastfed baby start eating
softfoods? What should it eat and how do I start
my baby on these foods?
For the first 4 to 6 months, breast milk is your
baby’s best and complete nourishment. After this,
its growing body needs additional nourishment.
You don’t need to buy special foods for your baby.
You can prepare them at home inexpensively from
the same things you use for the family meal.
However, your baby still needs breast tnilk in
addition to its new diet, so continue breastfeeding
as long as you can.
After the first 4 to 6 months, your baby must also
get a share of the family foods. Give the baby one
type of food at a time until it learns to enjoy a variety
of foods. Start with small quantities and gradually
increase them to suit its age and appetite. Feed the
baby frequently.
Your baby will grow well on foods like kichari,
dalia, dal mixed with rice or chapati, lightly cooked
fresh green leafy vegetables, half boiled eggs and
fish. Fresh fruits like papaya and banana along with
fresh orange, musami or lime juice are also good
for the growing baby.
Mash the food well to make it easy for the baby to
swallow and digest. Add a little ghee, butter or oil.
This makes the food tastier amd gives extra
energy'.
Soft foods should be given between breastfeeds.
Encourage the baby to feed itself with its fingers.
This is part of its growing and learning experience.
By one year, your baby is ready to eat the food you
prepare for the rest of the family.
29.
Should a breastfed baby also -be given extra
vitamins and juices? At what age should these
be given?
As long as the nursing mother is healthy and eats
enough ofa variety of foods, there is no need to give
extra vitamins and juices to a breastfed baby for the
first 4 to 6 months of life. Breast milk will give the
baby all that it needs during this period.
Once the baby is 4 to 6 months old, its growing
B
body needs additional nourishment. Your baby is
now ready to eat soft foods. You can also give the
baby fresh orange, musami or lime juice.
30.
What precautions should I take when preparing
a meal or feeding my baby?
Most mothers know the importance of hygiene. But
often a busy mother may overlook some details of
cleanliness. Can any mother afford to take this risk?
The hidden dangers—germs that you cannot seecan lead to illnesses in the family. A baby is more
likely to fall ill. You need to be extra careful if there
is a baby at home.
Keep your home and surroundings clean. Germs
breed in dirt and contaminated food and water,
causing diarrhoea, and spreading diseases like
cholera, dysentry and gastroenteritis. Drinking
water must be strained through a clean cloth,
boiled and cooled. Store this water in a clean
covered container. Give your baby food which is
freshly prepared. Wash your hands before you
cook the meal or feed the baby. Keep utensils clean.
Wash them well before and after use, and rinse
under running water.
31.
Are special baby foods available in the
market better than soft foods prepared at
home?
Special foods for babies available in the market are
based on a mixture of powdered milk with some
carbohydrates like wheat and rice. These foods
which are cereal and milk based are expensive. On
the other hand, a wise mother can provide her
growing baby with all the nourishment it needs
with die same things she uses to make the family
meal. Instead of spending large sums of money on
tins of baby foods, she can buy good wholesome
food for the entire family, including the baby. Soft
foods prepared at home give the baby a better
variety of foods, in addition to providing all the
nourishment it needs.
32.
Should I give soft foods before or after a breast
feed?
Soft foods should be given between breastfeeds,
preferably a couple of hours after abreastfeed This
is advised because a baby will not make an extra
♦V)
effort to eat soft foods when it is very hungry. This is
because suckling the mother’s breast comes naturally
to a baby, whereas it has to learn to eat soft foods. A
hungry baby will be less interested in eating soft
foods on an empty stomach. Having had a breast
feed a couple of hours earlier, the baby will not be
too hungry when offered soft food and may show
more interest in this food than otherwise.
On the other hand, if you offer the breast im
mediately after it has been fed soft food, the baby
will not suckle the mother’s breast strongly since it
is not hungry at that moment. When the baby fails
to suckle strongly, it will not stimulate the breasts to
produce more milk. Eventually the flow of milk
may reduce. Therefore, breastfeed your baby and
offer it soft foods a couple of hours later. Give the
next breastfeed a couple of hours after its last meal
of soft foods. In this manner the baby will continue
to get the double benefits of its mother’s milk as
well as soft foods.
33.
Should a mother continue soft foods when the
baby is ill?
It is incorrect to stop feeding a baby when it is ill. In
fact the baby needs nourishment even more so
to recover from its illness. Food will give it the
strength to fight other illnesses which can set in
when the body is already weak.
Soft foods like kichari, dalia, rice or chapati mixed
with lightly cooked dal and vegetables will not harm
the baby. Sometimes when the baby is ill, it does
not feel hungry or may prefer to eat food other than
what it normally eats. While recovering from its
illness, the baby’s appetite will improve. Give the
baby slightly more than what it normally eats
because it needs additional nourishment to regain
its health.
34.
Why does my baby have diarrhoea while teething?
Is it because it is teething or the fact that I have
started giving it soft foods?
Often mothers tend to associate teething with
diarrhoea. This is incorrect. Diarrhoea occurs
when the baby eats contaminated food or drinks
water which is contaminated. Moreover when a
baby is teething, it tends to pick up things lying
around the house and chew on it. These objects
can carry germs into its body and cause diarrhoea.
If you prepare soft foods hygienically, there is no
reason why the baby should have diarrhoea.
Introducing soft foods will not cause diarrhoea, as
long as they are well prepared. Wash your hands
before you make the meal or feed the baby. Use
fresh food. Use clean drinking water. Keep the
utensils clean. These precautions will help to
prevent diarrhoea.
35.
What is diarrhoea?
Diarrhoea is not a single disease. It is a symptom
that accompanies intestinal disorders. When a baby
has diarrhoea, it passes frequent watery stools
which may be foul smelling. Diarrhoea causes loss
of vital body fluids and salts. In somes cases, the
stools may also have blood and mucus.
36.
Is diarrhoea dangerous?
Yes, diarrhoea can be dangerous especially for
babies and young children below two years. If you
fail to replace the fluids and salts that a baby loses
during diarrhoea, it can lead to a dangerous
situation called ‘dehydration
.
*
Remember pro
longed diarrhoea can lead to dehydration and even
death. Do not take diarrhoea lightly. Unfortunately
some mothers think diarrhoea is not serious. This is
not true. Diarrhoea can become very serious if you
neglect it.
37.
Is it true that breastfed babies have less chance
of getting diarrhoea?
Yes, it is true that babies who are breastfed
exclusively rarely have diarrhoea. Breast milk is not
only free of germs but also helps to prevent the
growth of those germs that cause diarrhoea. It has
been found that bottle fed babies have diarrhoea
six times more often than breastfed babies. This is
because the feed is not prepared hygienically. For
a bottle feed to be safe, you need to take many pre
cautions, like sterilizing the feeding bottle and
nipple and boiling the water to make the feed.
Breastfeeding takes care of all this trouble. Breast
milk is the safest and most hygienic way to feed
your baby. Breastfeed as long as you can, even
when the baby has diarrhoea. Breast milk will give
the baby all die nourishment it needs to recover,
besides being easier for die baby to digest. In
9
addition, antibodies in your milk will protect the
baby from other illness which can set in when the
baby is already weak from diarrhoea.
38.
What should I do when my baby has diar
rhoea?
There is a simple and inexpensive treatment that
every parent can administer at home. Start the
treatment at the first signs of diarrhoea.
In aglassful of boiled and cooled water, add a pinch
of salt (14 teaspoon). Make sure this solution is not
saltier than your tears. Then add two teaspoons of
sugar or ‘guf and dissolve it well. The baby may
refuse to drink this solution, but insist on giving the
solution frequently in small quantities.
It is important that the baby drinks a glassful of this
solution ever}' time it passes a watery stool. This is
approximately the amount of liquid it loses every
time it passes a watery stool. So make sure that you
replace the fluids it has lost. Continue giving this
solution until die baby stops passing water}' stools.
Plain water which is boiled and cooled, rice kanji or
coconut water can also be given in addition to the
salt and sugar solution. Remember to continue
breastfeeding and normal feeding during diar
rhoea. If the baby’s condition doesn’t improve
within two days, contact your doctor immediately.
39.
What is ORS?
ORS stands for oral rehydration salts. These salts
are specially prepared to deal with the loss of vital
salts from the body. Mixed with boiled and cooled
water, this ORS soludon becomes a good rehydra
tion fluid. They come in packets and are available at
a chemist. Follow the instructions on the packet to
make the solution.
Give the home prepared salt and sugar solution or
the ORS solution every time it passes a water stool.
Continue giving this solution until it passes normal
stools. Some mothers simply stop feeding their
babies during diarrhoea. This is not good for the
baby for it needs nourishment. Give the baby
lightly prepared foods like kichri, dalia or rice and
curd.
41.
Diarrhoea is caused by germs which breed in
contaminated food and water, dust and unsanitary
surroundings. These germs enter the baby’s body
through contaminated food or water.
There are simple measures that you can' take to
prevent diarrhoea. Keep your home and sur
roundings clean. Drinking water must be strained
through a clean cloth, then boiled and cooled.
Store this water in a clean covered container. Keep
your utensils clean. Wash them before and after use
and rinse under running water. Give your baby
freshly cooked food. Wash your hands before you
cook the meal or feed the baby. All clothes includ
ing undergarments and bed linen must be clean
and fresh. Finally continue to breastfeed your baby
as long as you can, even when the baby has
diarrhoea. Breast milk is the safest and most
hygienic way to feed your baby.
42.
Should I give tonics or special foods when the
baby has diarrhoea?
You don’t have to give a tonic or any special kind of
food when the baby has diarrhoea. Just make sure
that it drinks plenty of liquids and eats well when it
has diarrhoea. When the baby has diarrhoea, you
need to replace the fluids it loses. It also needs
good nourishment to regain its strength both to
recover and to fight against other illnesses which
can set in when it is already weak.
10
Would a breastfed baby catch a cold ifthe mother
drinks cold water?
No, this is not true. Breast milk comes at the right
temperature to suit the baby, irrespective of the
cold or hot drinks the mother consumes.
43.
40.
What should I do to prevent my babyfrom getting
diarrhoea?
Since breast milk contains antibodies, does this
mean that a breastfed baby does not require
immunization against common childhood
diseases?
Although antibodies present in the mother’s milk
o give immunities to some common childhood
diseases, every baby should be immunized
regularly to completely eliminate the risk of these
diseases Table 1 gives the immunization schedule.
Remember that immunization is effective only
w en a regular and complete dose is given. The
baby should not be ill at the time of immunization.
Breastmilk contains mother’s natural immunities to
protect the baby against illness. Breastfeed your
baby as long as you can. In addition follow the
immunization schedule to completely eliminate
the risk of common childhood diseases like tuber
culosis, diphtheria, whooping cough, tetanus,
poliomyelitis and measles.
TABLE 1 IMMUNIZATION SCHEDULE
WHAT
WHY
3-9 months
BCG vaccine
protect against tuberculosis
3-9 months
3 doses of DPT and Polio vaccine protect against diphtheria, whooping
cough, tetanus & poliomyelitis
at intervals of 4-6 weeks each
protect against measles
Measles vaccine
WHEN
9-12 months
1 Ha-2 years
1st booster for DPT and Polio
5-6 years
DT booster
protect against diphtheria & tetanus
UNITED NATIONS CHILDREN'S FUND
73 LODI ESTATE, NEW DELHI - 110003
INDIAN NATIONAL CODE
™oreCT
BREAST-FEEDINg
■u
<3
MINISTRYRO^SOC!AIF 1ND1A
NEW^^ WELFARE
■5-r
[Copy of Ministry of Social Welfare,
Government of India,
Resolution No. 18-11/81-NT
dated 19 December 1983]
Indian National Code for Protection and
Promotion of Breast-feeding
The Government of India affirms the right of every child
to be adequately nourished as a means of attaining and
maintaining health. Infant malnutrition is a major contri
butory cause of high incidence of infant mortality and
physical and mental handicaps. The health of infants and
young children cannot be isolated from the health and
nutrition of women. The mother and her infant form a bio
logical unit. Breast-feeding is an integral part of the
reproductive process. It is the natural and ideal way of feeding
the infant and provides a unique biological and emotional
basis for healthy child development. The anti-infective
properties of breast-milk protect infants against disease. The
effect of breast-feeding on child-spacing, on the health and
well-being of the mother, on family health, on family and
national economy and on food production is well-recognised.
Breast-feeding is, therefore, a key aspect of self-reliance and
primary' health care. It is the nation’s responsibility to
encourage and protect breast-feeding, and to protect pregnant
women and lactating mothers from any influence that could
disrupt it. Inappropriate feeding practices lead to infant
malnutrition, morbidity and mortality in our children.
Promotion of breast-milk substitutes and related products like
feeding bottles and teats do constitute a health hazard.
Promotion of breast-milk substitutes and related products has
been more extensive and pervasive than the promotion of
information concerning the advantages of breast-milk and
breast-feeding, and contributes to decline in breast-feeding. In
the absence of strong interventions designed to protect,
promote and support breast-feeding, it can be anticipated that
this decline will continue, and that even larger numbers of
infants and young children will be placed at risk of infections,
malnutrition and death. Only when young infants cannot be
breast-fed, and when other sources of human milk are
unavailable, other food becomes necessary. It is important for
infants to receive appropriate complementary foods, usually
when the infant reaches four to six months of age, and the
emphasis should be placed on local foods and traditional
practices, complemented only when necessary, and under
proper guidance, by industrially processed products. Govern
ment appreciates that, guided by the highest considerations
for the proper nutrition and health of the World's children,
the World Health Assembly adopted in May 1981, an
International Code of Marketing of Breast-Milk Substitutes.
Government recognises that this code, although an important
measure to regulate production and marketing of products
which interfere with breast-feeding, is only one aspect of the
measures government should undertake to protect and
promote the healthy growth and development of infants and
young children.
Educational systems, social services, families, commu
nities, women’s organisations and other non-governmental
organisations should be involved in the protection and
promotion of breast-feeding and other activities aimed at the
improvement of maternal, infant and young child health and
nutrition. In the light of the foregoing considerations, and in
view of the vulnerability of infants in the early months of life
and the risks involved in the inappropriate feeding practices,
including the unnecessary and improper use of breast-milk
substitutes and feeding accessories, it is necessaty to regulate
the marketing of such products. Government, therefore,
resolves to adopt the following Code:
Article 1. Aim of the Code
The aim of this Code is to contribute to the provision of
safe and adequate nutrition for infants, by the protection and
promotion of breast-feeding, and by ensuring the proper use
of breast-milk substitutes, when these are necessary, on the
basis of adequate information and through appropriate
marketing and distribution.
Article 2. Scope of the Code
The Code applies to the marketing, and practices related
thereto, of the following products: breast-milk substitutes,
including infant formula; other milk products, foods and
beverages, including bottlefed complementary foods, when
marketed or otherwise represented to be suitable, with or
without modification, for use as a partial or total replacement
of breast milk; feeding bottles and teats. It also applies to their
quality and availability, and to information concerning their
use.
Article 3- Definitions
For the purposes of this Code:
“Breast-milk
substitute”
means
any food being marketed or other
wise represented as a partial or
total replacement for breast-milk,
whether or not suitable for that
purpose.
“Complemen
tary food”
means
any food, whether manufactured
or locally prepared, suitable as a
complement to breast-milk or to
infant formula, when either be
comes insufficient to satisfy the
nutritional requirements of the
infant. Such food is also com
monly called “weaning food” or
“breast-milk supplement”.
3
“Container”
means
any form of packaging of products
for sale as a normal retail unit,
including wrappers.
“Distributor”
means
a person, corporation or any
other entity in the public or pri
vate sectorengagedinthebusiness
(whether directly or indirectly) of
marketing at the wholesale or
retail level a product within the
scope of this Code. A “primary
distributer” is a manufacturer’s
sales
agent,
representative,
national distributor or broker.
“Health
care system”
means
governmental, non governmental
or private institutions or organi
sations engaged, directly or
indirectly, in health care for
mothers, infants and pregnant
women; and nurseries or child
care institutions. It also includes
health workers in private practice.
For the purpose of this Code, the
health care system does not
include pharmacies or other
established sales outlets.
“Health worker” means
a person working in a component
of such a health care system,
whether professional or non
professional, including voluntary,
unpaid workers.
“Infant formula” means
a breast-milk substitute formu
lated industrially in accordance
with applicable ISI standards, to
satisfy the normal nutritional
4
requirements of infants up to
between four and six months of
age, and adapted to their physio
logical characteristics.
Infant
formula may also be prepared at
home, in which case it is
described as “home prepared”.
“Label”
means
any tag, brand, mark, pictorial or
other descriptive matter, written,
printed, stencilled, marked, em
bossed or impressed on, or
attached to, a container (see
above) of any products within the
scope of this Code.
“Manufacturer”
means
“Marketing”
means
“Marketing
personnel”
means
a corporation or other entity in
the public or private sector
engaged in the business or
function (whether directly or
through an agent or through an
entity controlled by or under
contract with it) of manufacturing
a product within the scope of this
Code.
product promotion, distribution,
selling, advertising, product pub
lic relations, and information
sendees.
Any persons whose functions
involve the marketing of a
product or products coming
within the scope of this Code.
“Samples”
means
single or small quantities of a
product provided without cost.
“Supplies”
means
quantities of a product provided
for use over an extended period,
free or at a low price, for special
purposes, including those pro
vided to families in need.
Article 4. Information and education
4.1
Government shall ensure that objective and
consistent information is provided on infant and young child
feeding for use by families and those involved in the field of
infant and young child nutrition. This responsibility shall
cover the planning, provision, design and dissemination of
information and their control.
4.2
Informational and educational materials, whether
written, audio, or visual, dealing with the feeding of infants
and intended to reach pregnant women and mothers of
infants and young children, should include clear information
on all the following points: (a) the benefits and superiority of
breast-feeding; (b) maternal nutrition, and the preparation for
and maintenance of breast-feeding; (c) the negative effect on
breast-feeding of introducing partial bottle-feeding; (d) the
difficulty of reversing the decision not to breast-feed; and (e)
where needed, the proper use of infant formula, whether
manufactured industrially or home-prepared. When such
materials contain information about the use of infant formula,
they should include the social and financial implications of its
use; the health hazards of inappropriate foods or feeding
methods; and, in particular, the health hazards of unnecessary
or improper use of infant formula and other breast-milk
substitutes. Such materials should not use any pictures or text
which may idealize the use of breast-milk substitutes.
4.3
Donations of informational or educational equipment
or materials by manufacturers or distributors should be made
only at the request and with the written approval of the
appropriate government authority or within guidelines given
by government for this purpose. Such equipment or materials
may bear the donating company’s name or logo, but should
not refer to a proprietary product that is within the scope of
this Code, and should be distributed only through the health
care system.
6
Article 5. The general public and mothers
5.1
There shall be no advertising or other form of
promotion to the general public of products within the
scope of this Code.
5.2 Manufacturers and distributors should not provide,
directly or indirectly, to anybody, samples of products within
the scope of this Code.
5.3
In conformity with paragraphs 1 and 2 of this Article,
there should be no point-of-sale advertising, giving of samples,
or any other promotion device to induce sales directly to the
consumer at the retail level, such as special displays, discount
coupons, premiums, special sales, loss-leaders and tie-in-sales,
for products within the scope of this Code. This provision
should not restrict the establishment of pricing policies and
practices intended to provide products at lower prices on a
long-term basis.
5.4
Manufacturers and distributors should not distribute
to pregnant women or mothers of infants and young children
any gifts of articles or utensils which may promote the use of
breast-milk substitutes or bottle-feeding.
5.5
Marketing personnel, in their business capacity,
should not seek direct or indirect contact of any kind
with pregnant women or with mothers of infants and young
children.
Article 6. Health care systems
6.1
The health authorities in the country should take
appropriate measures to encourage and protect breast-feeding
and promote the principles of this Code, and should give
appropriate information and advice to health workers in
regard to their responsibilities, including the information
specified in Article 4.2.
7
6.2
No facility of a health care system should be used for
the purpose of promoting infant formula or other products
within the scope of this Code. This Code does not, however,
preclude the dissemination of information to health
professionals as provided in Article 7.2.
6.3
Facilities of health care systems should not be used for
the display of products within the scope of this Code, for
placards or posters concerning such products, or for the
distribution of material provided by a manufacturer or
distributor other than that specified in Article 4.3.
6.4
The use by the health care system of “professional
service representatives”, “mothercraft nurses” or similar
personnel, provided or paid for by manufacturers or dis
tributors, should not be permitted.
6.5
Feeding with infant formula, whether manufactured
or home-prepared, should be demonstrated only by health
workers, or other community workers if necessary; and only
to the mothers or family members who need to use it; and the
information given should include a clear explanation of the
hazards of improper use.
6.6
Donations or low-price sales to institutions or
organizations of supplies of infant formula or other products
within the scope of this Code, whether for use in the
institutions or for distribution outside them intended for the
recuperation of malnourished children and other medical
reasons or for the infants of mothers who cannot breast-feed
and who cannot afford to purchase adequate amounts, may be
made. If these supplies are distributed for use outside the
institutions, this should be done only by the institutions or
organisations concerned. Such donations or low-price sales
should not be used by manufacturers or distributors as a sales
inducement.
6.7
Where donated supplies of infant formula or other
products within the scope of this Code are distributed outside
8
an institution, the institution or organization should take steps
to ensure that supplies can be continued as long as the infants
concerned need them. Donors, as well as institutions or
organizations concerned, should bear in mind this res
ponsibility.
6.8
Equipment and materials, in addition to those
referred to in Article 4.3, donated to a health care system may
bear a company’s name or logo, but should not refer to any
proprietary product within the scope of this Code.
Article 7. Health workers
7.1
Health workers should encourage and protect breast
feeding; and those who are concerned in particular with
maternal and infant nutrition should make themselves
familiar with their responsibilities under this Code, including
the information specified in Article 4.2.
7.2
Information provided by manufacturers and dis
tributors to health professionals regarding products within
the scope of this Code should be restricted to scientific and
factual matters, and such information should not imply or
create a belief that bottle-feeding is equivalent or superior to
breast-feeding. It should also include the information specified
in Article 4.2.
7.3
No financial or material inducements to promote
products within the scope of this Code should be offered by
manufacturers or distributors to health workers or members of
their families, nor should these be accepted by health workers
or members of their families.
7.4
Manufacturers and distributors of products within the
scope of this Code should disclose to the institution to which a
recipient health worker is affiliated any contribution made to
him or on his behalf for fellowships, study tours, research
grants, attendance at professional conferences, or the like.
Similar disclosures should be made by the recipient.
9
Article 8. Persons employed by
manufacturers and distributors
8.1
In systems of sales incentives for marketing personnel,
the volume of sales of products within the scope of this Code
should not be included in the calculation of bonuses, nor
should quotas be set specifically for sales of these products.
This should not be understood to prevent the payment of
bonuses based on the overall sales by a company of other
products marketed by it.
8.2
Personnel employed in marketing products within
the scope of this Code should not, as part of their job
responsibilities, perform educational functions in relation to
pregnant women or mothers of infants and young children.
This should not be understood as preventing such personnel
from being used for other functions by the health care system
at the request and with the written approval of the appropriate
authority of the government concerned.
Article 9. Labelling
9.1
Labels should be designed to provide the necessary
information about the appropriate use of the product, and so
as not to discourage breast-feeding.
9.2
Manufacturers and distrubtors of infant formula
should ensure that each container has a clear, conspicuous,
and easily readable and understandable message printed on it,
or on a label which cannot readily become separated from it,
in an appropriate language, which includes all the following
points:
(a)
the words “Important Notice” or their equivalent;
(b)
a statement of the superiority of breast-feeding;
(c) a statement that the product should be used only on the
advice of a health worker as to the need for its use and the
proper method of use;
10
(d)
instructions for appropriate preparation, and a warning
against the health hazards of inappropriate preparation.
Neither the container nor the label should have pictures of
infants, nor should they have other pictures or text which may
idealize the use of infant forumla. They may, however, have
graphics for illustrating methods of preparation. The terms
“humanized”, “maternalized” or similar terms should not be
used. Inserts giving additional information about the product
and its proper use, subject to the above conditions, may be
included in the package or retail unit. When labels give
instructions for modifying a product into infant formula, the
above should apply.
9-3 Food products within the scope of this Code,
marketed for infant feeding, which do not meet all the
requirements of an infant formula, but which can be modified
to do so, should carry on the label a warning that the
unmodified product should not be the sole source of
nourishment of an infant. Since sweetened condensed milk is
not suitable for infant feeding, nor for use as a main ingredient
of infant formula, its label should not contain purported
instructions on how to modify it for that purpose.
9.4
The label of food products within the scope of this
Code should also state all the following points: (a) the
ingredients used; (b) the composition/analysis of the product;
(c) the storage conditions required; and (d) the batch number
and the date before which the product is to be consumed,
taking into account the climatic and storage conditions of the
country.
Article 10. Quality
10.1
The quality of products is an essential element for
the protection of the health of infants and therefore should be
of a high recognized standard.
10.2
Food products within the scope of this Code should,
11
when sold or otherwise distributed, meet applicable ISI
standards.
Article 11. Implementation and monitoring
11.1
Government shall give effect to the principles and
aim of this Code through legislation and other suitable
measures. National policies and measures, including laws,
which are adopted to give effect to the principles and aim of
this Code, shall be publicly stated, and shall apply on the same
basis to all those involved in the manufacture and marketing
of products within the scope of this Code.
11.2
The manufacturers and distributors of products
within the scope of this Code, and appropriate non
governmental organizations, professional groups, and
consumer organisations are expected to collaborate with
government in the implementation of this Code.
11.3
Independently of any other measures taken for
implementation of this Code, manufacturers and distributors
of products within the scope of this Code should regard
themselves as responsible for monitoring their marketing
practices according to the principles and aim of this Code, and
for taking steps to ensure that their conduct at every level
conforms to them.
11.4
Non-governmental
organizations,
professional
groups, institutions, and individuals concerned should draw
the attention of manufacturers or distributors to activities
which are incompatible with the principles and aim of this
Code, so that appropriate action can be taken. The appropriate
governmental authority should also be informed.
11.5
Manufacturers and primary distributors of products
within the scope of this Code should apprise each member of
their marketing personnel of the Code and of their res
ponsibilities under it.
12
COMMUNITY !■ UALTH CELL
St. Marks Road
47/1. (First F!oor)
8ANGALOR £. 550 001
41st Annual Convention of the Catholic Hospital Association of India
Workshop on; TOWARDS A PEOPLE-ORIENTED DRUG POLICY
23-25 November 1984 ; St John's Medical College and Hospital
Objectives
WHAT IS THE PROBLEM
1.
To create an awareness of
a. the health situation in India
b.
the role of drugs in health care
c.
the pattern of drug production in India vis a vis the
d.
the dynamics of the drug industry
e.
the patterns of drug distribution/availability in the
f.
the national drug policies and laws.
s
*
people
health needs
health system
2.
To create an awareness of the -^growing -
a. irrational use
3.
b.
over use
c.
misuse of drugs by health personnel
To look at the above issues within the context of the
CHURCH HEALTH SERVICES
4.
To try and understand the problem from the people's point
of view.
HOWAJHY the problem?
5.
At the broader level to discover the social, economic,
political, cultural and other factors responsible for
this problem.
6.
At personal level to discover how all of us are part of the p
problem atthe individual and the institutional levels.
WHAT TO DO TO TACKLE THE PROBLEM?
7.
To consider the various responses at the national/international
levels by groups/institutions/governments in the areas of -
a. consumer awareness and people's movements
b.
continuing professional education
c.
pressure groups on policy makers
p.t.o...2
2
8.
d.
search for low cost alternatives
e.
individual/group action
f.
institutional policy changes
To discuss ways and means by which participants can
respond to this problem at-
a. individual
b.
institutional and
c.
regional/national levels
and identify ways and means by which follow up action
will be taken in this growing commitment.
PROGRAM
Preparatory Workshop for Faciliatiqn Team
11.00 am
17th November 1984
St John's Medical College, Bangalore
11.00 am
Introduction of team/theme and details of
the programme
11.20 am
Group d:ccussion:
a. What are the different dimensions of
the drug policy and prescribing issues
in India?
b. What information would we like to have
to further understand and analyse this problem?
12.40 p.m.
Plenary session;
Listing out what we would like to know
1.00 plm.
LUNCH
2.00 p.m.
Information check list
3.30 p.m.
Tea
4.00 p.m.
Planning the group discussion and the
5.00 p.m.
Video presentation on the theme.
facilitation
•5
3
DRUG ISSUES
Information check list
A. Drug Industry
Output
Profits
Type
Pattern of production
Structure
Drug Policy
Prices
Quality control
Research and Development
Consumption of :Drugs
B. Drug Policy Issues (Problems)
Plethora of formulations
Mark up
Brand names
Net worth returns
Fixed drug combinations
Transfer pricing
Bio-availability argument
Sales promotion
Dumping
Samples
Me-too drugs
Advertising
Drug controls
C. ptug Policy Issues (solving Problems)
Essential drug list
Formulary (level of use)
Generic prescribing
Bulk Drug formulation
Price control
Bulk purchasing
Labelling
Quality control
Low cost production
Cooperatives
Herbal gardens
Pharmaceutical code
Physicians code
Counter advertising
Consumer Awareness
D. Drug Laws/Policies/Reports
Drugs and cosmetics Act
Drugs & Magic Remedies Art
The Pharmacy Act
Hathic Committee Report
p.t^o.
4-
E.
National Drug Policy
Drug Price Control Orders
Health for All Report
Govt. Ban of 22 drugs
Irrational Drug use/prescribinq types
Types
Extravagant
Overprescribing
Incorrect
Multiple
Under-prescribing
Causes
Inadequate basic training
Lack of continuing education
Lack of supervision
Inappropriate desire for p
prestige
Drug company sales
promotion
Drug company misinformation
Heavy patient load
F.
<
Patient presssure
Panic/fear inc. ••
_
induced prescription
Incorrect generalisations
Lack of patient
awareness
Doctor-Drug producer axis
Problem Drugs
Specific
Analgin
Amidopyrin
Ancdloxin.
Bromides >
Chloral hydrate
Cloquinols
Dipyrone
E-P Forte
Ergot
Gripe water
Kaolin
Lomotil
Methapyrilene
-
Nialamide
Oxyphenbutazone
Phenylbutazone
Phenacetin
Practolol
Penicillin
Quinine
Sulphonamides
Strychnine
Yohembine
f^o $
Groups
G.
H.
Antibiotic combinations
Anabolic steroids
Analgesics
Antidiarrhoeals
Enzymes
Fixed dose combinations
Placebos
Steroids
OTC Drugs
Unani/Ayurvedic drugs
Church Health Services (context)
Institutional response
New vision/option
Community response
Humanisation
Holistic healing
Issues of social justice
People's Point of view
Availability
Cost
I.
Accessibility
Cross-cultural conflicts
Mystique of injections
Communication failures
Self prescribing
Low cost home remedies
Initiatives
Meetings and workshops
Newsletters/bulletins
Books/j ournals
Professional awareness
Continuing education
Consumer awareness
Signature campaign
Memorandum to policy makers
Public interest litigation
Low cost drug production
Bulk/central purchasing
Cooperatives
Herbal gardens
Formularies
Codes
J. Case studies
Bangladesh Ban
Operation Medicine
VHAI cell
Drug Action Network
IOCU HAI
Social Audit
mfc Rational Drug Policy
Cell
Vincents Case
Ankuran
KSSP
Lok Vidnyan Sanghatana
LOCOST
Bangarapet Tablet Industry
Kurji formulary
State Forum (AP/WB)
•soOd a&oa^ gyaartso duou^, ootgadorttfu •
e’daw
fidUjUUd
dUddd
GrodO
0030^ GdjOdUddndUj •
rttfu,
rtfia firedort^
<SdO
.* fidOde)I’fifiUq
dOSUj ZS^rttf dOfJOjj esde.fi ■£ fid rtd •
ojSTSn d^fiUZJOfi
d,
d^u^dft axTaoddOdOdU
dddcj3rts?ui
ZJfiUvOvUdG)
e>3 (A)wk>$ fiartua ©3 d^d^ood daodrtou dudd ddvurtvymj
dfibjodu-
fireUo
fiOdUU
fiuaod fiartu aue.durtFu
^du
aau^ifiCLraoOrt
fiUdfidd rtUO
©0
23dUrta$ Ufid^dci
rtfirtdom ozs^oduddu^
osoacstfac.n d<3dd rouaoaudym fiasuduuuu^dsj'u &jz3u
fiadu fia^yrt'5'uaofirt
fiuacrafi odd dOfiOr>dym esde.® o<3odo rtaodorttfo (A)otradd_> • rodaduadfidm cAjouafi
zyjuad^rwu odd de. fid d^duae-^dradofiuo^ doraadu ae.Odu • rtudurtu —dauu rts?u
odd dfiJOp,.dJUcj rfaodorttfdu^ duaudu- -sodfi S0dp3oduum odd
tfackj
30e.«dem (AJouradJ^jdo duae.d_y oodoaarttfu
od duadad3u< Bdoodu zjfin z3O3du
doS duraudu- a/z^sodot^d ■ydd duam ddo^rttfu duaddd avdcxVae.rtS
*
d^^io
dUdG)d"aQoi •
dOd
dUZ)® OdOOfp
oduoddd od dexadd TSsSJi-u
*
rwv„i
*
ciUU7)Ud<2
UficiLivU
'ST.-.' OdU^xJ
d_;t-^30JJd<i odooudd ridritf ddri9Om
5e.ddo
d_>
330dUd
c6udrwum eraouu
iiojrivy^, eddu ‘ad^rSVdu< sosu&ajoj • da^rsud dxxaoddudam ^xjaaodyudrn
©adj dodfxraSM52um zSdpoJj ood ■scsod^JdJci ddJdddduha doyay^rju a^odude^d^o:—
Zuocio dj"ae.ri$j. fioJje. dd, fiu^e. roJdd^ Zuo3<
;?aoou o^dd fioau Soft da^fiad^S uj-adudjJo ■goOrVa fiudd noajdd dj3$TJwm
djdaddom gdud TSd^dv ?jAn 3<?000.0dart ddort uzsaodoFddrtejs5JJo•
&wdo(
rtpF dOoacddrt^dSrt atram d&^rWrto-a
OJO7)h
rjO3d
*
5
iiidrJOoXa^
dufi)cje.fi OOZJ
rt^ro a><i3rts?od
nd duodyert^do^. doddj odoasd
*
dOfiadO”aOOdOdO cZ OciirtliJjjUO
vOfi)e.da^0ed
coE'jadOe^ cUdoF doafi zrao co_>odu~ae.rtrt\?dJcz ao^u~ae.fi<xirtvidUc£ d<3d doao ccxxadrt ddOd
■j9d3rts?oj do duds d 3coJu„ <roowartud ae.dcs dOrradurts'du^ rtdod.odart no duoay#
rts?dOct aududoae.rtdud rtoajdo duuuO oauoduortJ odudu zrad^^ou 3C3hndS<^o •
duaoaoo ddFrttfud ejadooduo ^dufiuum ■aoud ^odfi fe duuau-jrttf ufin aoSoa^d
duduu od^odud duaduu d.3e.drt^t-»d zjdod &idOdUc^ doae.uuart pjaduodudau dad_^
<Sdu £,dG><3e_^u •
d>i:^3oduom lAJuMartudJo doSwcj^rt^u doaddd. 00<dJ«r, doroadu z3e.uu3jdOQ
fi^/fi^dGdu
droSo ^iOduoddad
dudd^dc^ eyao^^ 3‘v^.oS ududadJa
aodart
*
Cozart d_jdu dfiudou Juu)udu<3e.oO?j djOtt
*
o>jdc>uduo duaddu
*
u^uduud-afiQrt
ovuuaodudu• odu dudO£q$ddu^ codyrt
&e.rt duniu&^^d ooe.0
^25Uada_a
zjuOu*
&u5 .oduaQj.fiadcya ZjU.jU CLrae.rtu^, s5uda_5rtu3_j-fij dudosj'SS)^ ©de.® ddae-rtrt^u
Zu^fi
zjOoo aodudaooudu •
C0WMJN1TY ESAI.TW CfLL.
2
■z3iqi2iri'i?(xkJ 4 U>5(. KiS5JGjJ.JOm So2Jzj S3Js®3 3jJC.d
-e<L SOjJZJr
o6'J-a^0a6'<a'ac\Xj30 • *dv.
0^.3 6)630 600
*1U<^E3 kcj^ JC. *c2gJO 6O"a 60CiOO 3_«> CO 3 ^OfiCj
Bi4cJn'X>(
-:^QjrWm fidaosOvritf cvadJUm ^osOoJjj^Jq BiqurW
a<ant1om
sj^gJjs
aa^JaCo aaojdan djaaFts^S
*
zSitarW 3joj^ eSuS^j
—'---------------------------3030 oudOO6$_F3^
ti&artev„
e>^<3 COoJo afida^ 3,3j(W ■sujj araOoJju^ gJocva
o
:—
GUOaGoO^
(Xxja(L3OGk5ua^.cod *<?q$
3_jm©3aJ Hi3 <5'J'J~c)O> rlV <jjo6\ja<r1m) 2J5xJ
odjjdaa a^jjucuj s^aao?
*
Gv^Oj
okJOacU
sjgsj •
cdixOSC.F 30dOk/pj
wj a
*c) 0 JUm J •
cbOOJOO JtXJa
ooJoo3e.FJ ddoatS-S
‘sa^&oetxja
<9o£J<J
3aOOO.J
djjae.0ju3oat33
2J^U)3O •
dOdOO GLa^ea^^
OOGUO5CF3
cJ’cldciy •
3JU
cjGUdGG
J aparin^aa aoaoaFrt sodaaotf 3^3'30 a&o^ &rajvaJi3 araoojjy^a •
O_jOcd0
0(i_<jG0O
OdOa^coOGiO O<,3 >600 3 3 33 J 3 CS cGxj3"
*
eoaxrtf
og3jo3gf'J
Soad-S doaufiA’ u.&3(jodoao(i fMod 5>3o3
eSiqcaris?^ <Ja 3&33F3 uuguj 3oraci3 esyirttf&J << aaaa.J doa3Jym
600oo3<Fj •
3G.A3oae.83 oo3tJusa/
S^urivjj
3z(ao3orteoz
aoa^rtvo
akraroFrteo dodo.,
ooasjom s^^oae.hckrarkiS-sS• 3o$e.oQjOJorw 3<x.633o< ve>arai3ja 3s3
0p)a0%,ym vvouaius t)0j3e.ojrt§e. euse-rtS
*
sjutju
ot^o^o 5>aje.?Gfa5e_- <5j-an ziso^j aow
3^_FJ
3otd< a>tfzWckJ5 ass?)^
g’gJjj
:5UugUU ocJ^d •
cJG.JvJ
oo Gknjosasi a^s3§
*
o?k)?3003ah ‘asjj a<£a3Jewam 3tf3rtfio<vaoju3j • ausockjj
St^cW iaj?5<3 aajO33J< arac^cjjck)
rSJ scraps c^sn^ojjjr!
**
^aO-JQCkJ •
&<■>,
oigrsv 30o<kra’J
*
s^ora
flG) 3JJrc)U:C'rfc?OZ3 0a i J ^§3^)000003 3n$J^0~c)3 nV 030 el a^rj j CkJtti3>ScJ^0
aagrw *<5
0a^rt j
0jgF)OJj3<&j•
rdco ESan^o as^rtao a)c\)o3u"ac.f'saJiSU'J
33jA 5<53JSjEtaf) nj&jyCJ cj^r^Spj ^^
03330^
*
g^.30 cJ^3goOg.JO
r5Sj3jny0m
2J3U3J
^sTaGOUFCkJ
iiVCJ'JoCXJ •
3c5"3,S00
Ckja<hri§3a&3^uJjaJeta<au3w
ujjpcraSt.^ iejG(n3 afiakJiSj-jj "0tL
j
'30Utjpl • oJukJS&JJUp, rT^oa cJdp<a 3c5g a
t’f&ack-)o
o)02J
coaOaOp, aaickjrVaj
^ofs^Sg.jj 3<^iaCj3_>3J-’5Gj aoa 3.jp7)3
zjg'oJCkj
'eJcJU V’'tj(xj^ Coro f5ocj"dJ3 au.Jo
SGT) FiF 3a (loUt)^, •
0<3'j~a(^3'3:—
aooockjtxxj
3
0d<j“a<3a £jgSj JauJOvj) CkraC-M^ adeS^udJokAi R>?.33 <5j-a?.rlG1y
a<cj\j3_3,j *
s-<3 TtJtfciCjrVj1 cSj
*ao<\)
3u0o
ct 0<i)ao3vjc$&j<a3»j3 a^3c3a 3<cj
uo~aa.jO^ xraa v 3j~a
SJQflFS 30033^303^.03e)A
rlv3j
^x-rat^ri^^
v\_racJo• ao 3j
*
3eOS)J3UO
3JO3)SO3d 30e.dJ
ayr>3 ara^jjdnvsk)4 ?;odj(l.a Jj 33^ s_ju3oodJ 3jjarau3c> es^riV^M axradS^odjjgJJ
66 orfajrwaj < &jraoGj?5UJ 3«_93s.J -d<. asds^ aiuwj JaudJv
*
■gvjj aj (g^ja 3_>3c)U3umdj3 asda^j 3^3^
oJuoda^S-
odus?.55 Oujj 36
oh6- 3Uu30 3ao'
wjoxkjj^nrivskj^ afiajdjUja -dt dssi-aj^ 3ymodJ366 flvas^oJosriJdjJ aojj
ttfspt 3sft3»
p03e.odJ 3G3ac-03i eii5e.3 6<6 Se.6 6t3J3<W<i
6?_6
d35F3J«i»JiiraoOrt
jSodot S^j^zraa^Jym 3am) rwacua ^pa<5300^0^4 ■936 crajjtursvj
■-'a)J^g3j3-3 jf)-?•
3
uoJ3do7„ 330^, 3<0 J iodoo 3e_F3
33o& **
33
*
h
*
a5o7<Jt7
h
*
37$3s037
35 37,0 33p333J< OdOcOdOdkJO^, 3< O35)Cddd7O<3O (507<i J0O • 07^,
e>Ji-v ddo7<337M0oom • add aXbododo S^d^z^d-aj?
*
5^3^0
*
333
3753 SocjS PsjoiW
370 iJ ZJU 3 c)£37Od 3aO_5 35?7f) 3O737FcJ7d3) ’ 0303 , <jO 3ojO_-(3cJ73 13<4^u3$dO ?). 0330
30f3 3o7w tf7d/htfo;
aooooJSo oworitfo <60705 zjoJ^r!'asfCJrlV rioradou^
3o7Sjtivo
W(33oodo7rL>i$j3o7uG)(’S 3700300 a Sdodoo -o37aado3o*7-7 a’3o 30 .-^ vOSOcoCuodO
3j OdOtJaJ
obcJJd
3_> adO7?.ncjO3 3 d 0007?. 3~O>) S?.O
33(j mo3:'.om c,rto3 a»SF3 SoddS 0037^3303 Ooddodo crs^jo, Se.036 ojo 3j>5 So^o#
pdodo d033v.>. JJdSjOuJ 3J700 007)33oddriv 365 fidodorsogji-
33acj 3ojj 003 rkjraqj ■?tOOQjcj<ym •
edo7 <9OmS
<s>jo oo„J donredo SjSjoJfi kvrraj 03330^0^0
3>-35_,OdOrtJ7 Cj7<h. 5000d075037_93- eSiJJ kodO 37^3^0 30ZJ 35ad30et dtfSO7O3
37$37O OaddridO
kO7u5
3003 ’aiJjjrSVJ 3ddO^ 30<0JUm (ft)0130307)305 ejfJcJffiOSfitfO
^330 afjood07 OOcJ3 2u3dO3 ®d07?_ai9odo0ni 3~
o07)yfOdd
*
33Oc>OO3Op1j ~>.jO33
I
3O3Oiqi>3
2J.jO&3
1
O3UO3,j3dQ(J•
1
fl&oO < 3030700 3070'00
OCO ■•-'O^0^3
3O7)cjOO 330 ..UO 30^,3 ^7)00 ZJOCJOvjy o<^D 3uco3o37rKJ3
todd3 pj 3-j d3330
373^00 Sc.3
O3_y udO3vJ^_:c7)OdO 30 •
337)3303 &gjjO
’
" '
So7)<hodo3o;i 303000303
OoTxthi’i 307)33?? &333OeiUt)O 3O7)gSO3jO5•
aOcJcJS
ujJyadO.j. vOOO 13 iq003030c^ cJd.u
.'47Odd 307)oUO 307)
Zti^Jf •|0)1V3O 7 too Sod 5&J_j> OadO
J £OOO30
*3.
3o.j^
•053F^vLO0O373 OC^OdO
p_y$o 6a7)3o7
a3<t3odo03o< o3o5o3O3
d3<aOdOo 3<d3 Si_j<o £133304 3O3tfO 307)03-
330 3j5<33l?y tfcira03
37)307)00 ti>«qp <SOd(33VO CodriOT) 303^0 3<jStr 3530 3 33fOff a>07)<o3tfO
T3<^3 £50'30 -37^3037373 "ztitqodtf £15^ 3073^30^
--/3cjd_j 30^0^
37)307
6-03 3373O0_r>Oo3
'g7dtJ3o3VO a5o On^dtf (ft)3a3odo SiS^OdOO 5«.03o5 33>§3V 53a3 p33330ct 255^30
<x)3 •
3~0_) CD' ;0 30 cO • c73_^) 330
09u3
3 dy 3d33p00
*330
tdixScTJ^
3O7dO37_3^> 30 JO
oT’Ory. 37;.^3Om-
.c,adOO3?.fJ<JcjJ ddO7<3«55 5>0odOO3_sd0 3 -St 3_>37SJ &0j ^30< d3?.d 3303^
3'73-
-.dO7.jja2_ 30730 c 30^0000^5 333^'33_D3O
373307003) 300 J <?Oc_cr
(030070.8373 nd 3O03VO 37)33733'-. '9003)330^ 3od_,&3 303
0300
*
&»3 373073^05 2J7U37odOO-
3e_S'o3 9JSOF
37(’-^003'? 033o3o07o35 3§3<gCkJd(? 37p33O73r1^O
33aj37OdOd • eij307o0A' 3^>3^3) SC3307?.37^0037 3 3O737F37CdO3O • &OO3 .J73OF73
37tL3J0m 37a.-SrSaioa0jdO37)3 C9.)Uj <-3 3U7„
370030^3^3^3) 0373 j E>7(JcOo30
duo^OdO fj735.c ^307
cDd7<aoodO7g.3Q:—
3ow3^O 3e_(j&J7o&'0 &<xd3
&&OO3O • t’f)O7C_57) 3^3^00 3>5<33i ^OdOoSoFO
jO 37 Ora37OdO30 •
dd07<30 3737^) 5^3^073 &_>?. 7533073'030 (3e.pF 0703 30?.^
30<4^)30 pO37h cod7aood07<30 300 3537,0 3o3_^.370d0^ <U7d5
Zo7d
*
ud7riv
Ddo,0OdO30
(&J73U0<3O7?.33o000
30733
2Jo(j3o •
dodoo5e.F33
5o7?.M5 355^03030 ^ 307o03 0^.73330t?
’O3O73u3O3ja •
13 MCjrStfdOci .>dd7
*e.a)7O3o
m <i)3<33O 3OG)a<5?C)3 3030^330^ «k.a3 0o7CfW
3od 3_>01307<ndo<yJo • -0< ■zStfyrtVo Oo7<hodo 3o<d de.35 doers3o33o ^000 30730
3_^a •
3OO2J7 1)£)OF OciSoodO 0537,0 3^3_> 3703037MJO o cft)3iX5O7?.nt?7OOdO7n.3 •
-...jd 7Jo
.073 rLTSO^Op,330 U7p-3O700
0>dO7?_3 jGdO O<) dj cjODoj) *330
o33o5
*
35
37337O0d_03Oo o.Jd7 00^3 o
573ra37nS4
4
J
-et
■s^rfert xal Su3,j
zso^aajci;—
ajsjoEj
sajvuFTdcWWp, skjozja Sj^aoa5«
■ao:’-*
ukJT) <J4
uoScotSjvcsjn^jd
~
aoju $8oJjj<ft)_sS- ae.ojsom
<S2;jiJ aoCTc)^
aOJcljv,
a j"c)c5r1VO •
<SjJOa<r
-
rf>uzjao u9cuum ?J
*
4 praosjy^ wjarau
"~
cdjj”d dd) -^.rf dU dUUd^OdUU
2JUd ■Fk dcda^
dUdU q
ho^’F-'J o^eJad
**
doOdUU $_<, U •
d/))UdU d
0(5U”aQ.d3
UOdUU <5)'<FvJ)j
d)£)U~aF^dU duUpj •
cbai^ri'i/ cJof cJrJG
•
zrarfcjaf\5«
i
j
'3JU ZjuJj
sk^araorWo 5
sutxdj
q
5\J s5^ aOfOnolJcZ d^dScXJafcjy)^
aozjjauj
2FkJ~c)fOE" f I5FAJnkJ 4 COFjc) yfl tAJcbO^G'dQ.f'lrJO 3 d_s3
*
pJcJ^nVO^
zJSS^oJJFSJci &£.&->£ a
sjt)G
(ajvj&j,
aju3J7)<.^^^Oo<Vc>b.J5-
* 5^ jOVU J
ZJ"
Sjc^T’CaJ •
auc-OJ aj^FrftW.z
a^rai&ji
>jc>u;jc)hajd?sja^ck) a>&5rf skzcxjucs a^i) F^rahS
*
CuU7ck)O\5U-aC.tb'3d$dU c£ cjOOCkrak^d
d$ck)d •^tj.23^^c)fj dJadd) 198 lCUm CoddCTaEJaOdU^ da_j uuUdaOUUdU • ckrdkd ddUd
eoarVa uua^rt ddaU(W upA)§ududu< -S-uadud x< ddadd» &d daduad^OA #&3u
T&tyrkw < opduduS du"adudi3 ^JO duuaj-s rk)O
*
nc ajjrg^risD
sj7)g;
oOaorSJ
a^sJcjas
?'-o^u;5'fl
Xn)ud SjtjJuj Sudo d>d)J
hti
rDuadjjrarrt
a^a^asu4
gj
gj
Sctiaan ew^Xjisg'w^c.
I3s/^tiia> 03 3oa3FSodj?dJ4 du7)Cj5 aj3FrarttfKO <:'
neaoGcioeriv a3<^3coy Ok3vJ"c)
Se.3 Se.3 djTJtnrwrt
(xTd^JT) Ur/'cD d ('j
•
M(J a5U'J”c)O’C;nV
cJ'Jvj'J’c)^O.jU
Zoy OuU”c)^.rir^?3)
co_j 'Q<2
oTd 1
J^U7)25F
eSz^gjjOfrj
GJcJrVj'c)
gJ<_ ex)
oOc’uUJ
S^cf-K)
ukJ~c) Ck)c^l X.)
■bkckTdck)
od. Cn
r$V7)
2)OJJ
nJ
J
c3ck)«.q$
d' c)U
ve)U j
-36)&j
cJgSOoOO o5(\J c^
*$
0
cjU ^_9'- J •
<5u<^
2)c3Ufi>OCk)6k)
C9(\k) <\)c) Ude) A ck)UO
■tzkri <^n)fk) Ek, .5 •
23^.j
(S</c) rkJ&^^QCK-Tc)
3d^fkJFk) 4 codV'J
0.JUCJ'J'c)"Z^wqOri^? cbiq'jCk) JOm
cJo-5 2Tc)( )“j •
3^ J-S^l 6k)£)c\)JOm
t^K)u:CjCk)fi^U
ZJ^.jGJ •
0c5Ck)
'<\lk)c3 (kTOricJ)
cbuEoauv'Ck)
grap^Jo^ 2J"dc)rt &6SUJ ak^^va ,joj•
.,;
ii3drtoju 6,
*ap
65.30^ SjS'^V &j“ad<ck>rW aSJts^S'JTJOd^-
cdkj&j tS^kcJu
okejj.kyodurVJu.J
ae^oJLrak adaS^S- auk j^.rari &oj£
*
uTa^rjjU duo
£kra<_Muck)
vdaad6kGrv5ahd.-. u likraocjA
*
C0<yOd dU fOU«q^ U f)dtJUdU
(\k)cb) 2jak)
.jUTjo' coy.uckraco
d<ra<h
ckra^)
ck)p<§
auufi Skrdkddar) ^jjo Bajp kujj da^ESad
duEJOyl cofoiuakryd-^-d
djkd-ddra^dr^u -<du da^daUJ dk^dvahS
*
^"kdU
Z&'J'd&t'
u'U^j 23c^9 •
ai<tfa)CuJ k) •
toOcJ^O
2TE)f) Ek)Uo )J25..O )jckTd
2)U. k)
caJZJc)
cd^jc)pjr1^
^''jy
( ICj
ajj^xJTXnri^U
^CkJt1j)>.jOo.J
25^pg3o^Om
^GA-Tdo^F
• EkjSrttfo^ skJurk)^ Ju) (VahrW <3rOForf dkraur&fi drtaF-^jtfu^w^dj •
rtjtfrt *2Jo
da()J •
*i3UU<^G)U fn •
oJOc6^
COT), J $
^JquJT)
cVafvlVFk)^ 5ozoC0?k)
^d-j'S
o^>c3
t-VJ) r\yOpr}^^ e>OihUJ25 hU
OgJ U ^fk) <k>-^
Ck)o2J0
0\3cJ\5atc)HoUa5
_jUO<JU gJQ_F J jOm
•
OOU^c^.J^,
J'i.2) J^rrj SuUdjjU i’njLk)ZJIaJ<3 23dck)^
cJck)^
^cdk
£)^Q_iq
sgbsj
coy <JOvJ~c)C.^r<xJ ZS <9o52^-§ Cr<) <22UO<4iCJUfr) • cbO&kJ lJO
gXJ <9kJ"c) cJO
cj_>
Ebj^p/)Om
'OxJ"c)t3Gj j-
EkKraoSrttfj -^rtex/a
du^adj
Ckra^WJ
dcoadu&krad
0ck)<L'Od
uua^dJudu dup^
ddd^o d>k8 azra^drW d^ddanu- daduF^Soduu
dU7) dU dV7)^ )c
*) “
5
2J"c)c6§ -53 d.
cO vJ
O cxhJ
cJ
cXJ-fJeJoj
U"c) Ok?O oC5U
2JU5) oXJ
AAuA cx5«qjjcTdAoUc$J5xJ <^ coUc5 •
c5j~d Uj
coiSoU'JUU 557)^5-3 •
63#$^
cJU”c)coF<$355 (Jdc5U"355$OA N^U^jcCTdijUU"?)
*cOc)A
jJfe3v'
AU7) Ac g5c5U c^_ uuCaJc6cj jkjU'JctKJU
5jAUcJ'§<,O"U-c) AU*
a5UUeU$
AOcoAUpj
rJj 3s?JU-5'U"c)OC5d
3^3$
AUUU^ "ScqyJ
7tdUj(Um
(Oau^rro^ u"d&j.jc)uJj^ £o-jJu auQoSuojj^h AJ5)3^)FWc)AUjd
2* j(JuU
2J(JOU
_jU
AUtJUA
AJ"dG'U^6U7)UoA bSS^OCkXJ u^yJd^STdd^OCk) ^OSoJJ,
JUQaSuoJu
ocjT)cUcJOUUo5Ue£ A^AUcJ
coOco^U c5J~d AF A^AU <^_
SvA vu^a^S-
s^areSjao tfwj daaiUoritfo ^aojom
okuae^------- aoa-gpa^d
^da
*
O^a
£ rJcJrSO
2J< Ip,
cJOCfijAodO
cjo5 •
eJOadOoS
cd't/da 00 dj'JO^j
codFy-jOdd(y,
(ia_jOOQ_EO
rJjjQ.OoSrtoadrjOc j)JO
d_J SddOcjdJO
S5iJJSiO3|
—
<3u<^_d
CAj~cj(^r1
v?jUS$O<i
^2330^0 c£
Ox^JoSh^/iJO
£3^3^000 050^ OiSoOoOq^.d^YyOO uuo_^cdo
OOOOJOo 30c)<C50^JO tfU3j>50«
ocdc) Of55j
oiOTKpri^OoOci vcisrauo^.jo •
O-JuOTJ^.
-'-^n 030^1 oSOOdiJcjOO
<Ud&VS'u0fn Uj..O
?Jb3 SouSnjuCiOdSOci wSoJoO^'JO • #?£Ug5O4 3O3JO o7)O00< 3O7)§OdOO
T.,Oc><jOOOO)oOf
c^OcdO
->rtdat_rt$
uO<5_jd cocJpoOdO <JO
oSOO-uO acSdl *
td 7 jUo~c)<^u
Joa'ch
6o"d£.ri ZJ'JO
o coO$
-:>oOa£j5$\J
cJUViO) <xjOu J0-7jl 09 j
wjCScSFFSrt^oSO c^ ^coFajo5<jkJO
rdcdSSOd
OOa6>Jo~z)<i j 0 V cdc)rt
23^3^)
Odd<gOdOO
0O7)rJ
3Ojp;5c)J
0"c) $ oOO~c)cdO
rfclti'oJO
OO^ciCjOijkjO
ScaJ po^>3r5§tram a^osdjOcJhooOBr!
OSO^ MDOOpFsJ
Odo„i C3;-5O ripen aaaocXio
cJvi,OoJ^
?fsojo
oot)3>
S5O7)0'!5<.?raJOj3<Uc)m
2»OcJO<aaJO(30<i OOoO
•—
ZSOJpiJSj
c3O”c)oC/c) Jcji
;5oooarar0)$ 5>5or5^o ■sJoUo'a
0Oc)G£)<
*'O
w&sjU^
•
SSOo^idOei
&J3.nriVofi)4h oo^uoSji- S^S^ooOoy^, (Ajotrenod sjoers^nvo wjv^OoJoe^N
;
dpr)^o
*
^o
sP^ojv oeiDoJ 3o7)U3 ^riS'e. QJ-?
*
aooffi$£J33 tfc)ora- ^wFvjJSh Oom
cbOYjO^CJOOa 00^007) yOoOU OLftjOJOo w£3a0 OOZiOcdO .-£ zSifyri'.?(Vstf*
0
c)h
*-307>o2)t>
'So-JO ai^OF
oUosjJwuuJo scoo aaSnjucSofdo^ do’odJC -t^j. a<-rsm So^oJdrttfoJuoT)
■cdBU^riejao 5o •
j6 ixram 3oc>e.rtr5S,r5o-c> oo^cOt) S)ao3Oc)f) as3^oJor30ei 0S0O0 usojo
'■sJd eJ-;F0om' ES-ijS^rVawe.o ho oo^rao^^oo^^ o25_>odos5o^)Jo fdoupsBii
ooejooo
oOahF •
dTuhOT)
Uc)p JaodOdOc) J
DUm jZudOOOT)
<JO~c)flF
wuoJooso.io• ■suod 3ooJoori3) doo^ atraodooriv
*
oX-Tc) JOO
(\XJ~dcooJ JOO
&»oSoJOaTc)rjOa^DcJ
tJOcoc)
^d&^^'-jdOiJO^
*>3o5J
cJc
S.
OdOOdOO
zra?jjj^Ofi t>3 sdJ-ado/'iooo^ •
so„’ atajtorS'jKJoot tfockJiLOodoyo
jjjuvo.’,
dO2J
oJ^jOd
oouyodj^odo aujo 3e.tfocdoao
o5- hddoo7)y3ri$?oj sratxJBUd atssu a<ddo5J<
OOdd~c)35i^
^jjdoj
srauuSo^
i3'9c5r5D,jr50c3c3cra m fJOortah cdojos^doudd ootoa S^J^ojajS" d-^joJo — odo^c-rJoa oj
3<duo ZuOjoao;Jo .Vciojadrkra z3zipriias5Jci hd3oo"ay3rw ckras> Jo„ Kionj&^acj.Jaoixi-v'
Scjih^cJotjortuft oodoa doas.n&j. d -.j.o3 uoo^-do-a^fidod o.’j^oOOoiJe^ oSa3uam
*
50odoS<sfc>h
• -e<L oJ,^odoo ouotjof- So assort ao'agj 3$;'wcOo^d
*
cJoarSO araa .-do Zu^orJah *tzc.
au^rtvsso^
<Jj$r5VrSo<^ croa5^>3da(LhsiOa5 sSoarSc eJfJo.^ da^
£uio&-j..Jo£)(;:-?ah.j • urt aoasj uaaS-oaxU woortortvo ddo^Ja/iori)voa-_cjuod
sJaocado asiu s<tos5dsso^ uut'^oo fjaJaOartosSj, j*
—Jod-. c-)o'Oi'iom cjjcjcjss woau'rt duOyjjdOoS rtoasj rtoasj aSo“au<£cJa s 13<qpd5?
dosjjjOEasorts’o artn aoddS
rtouadodahdod 'soosS attfrtodo cSezSArd^ ,u
s5ocj .
hoa Uc^y jjocjot>oa<.jO<d) so ‘ j osSort «Jo<Joa^o3odoo50c^ SoacsoS^ <Ja JoalSart
c5o oj
oScSo^ <(O0 3c^j
ooa--3Fodoa<*50
zh.dS •
.- 6
6
AU UOO7)Ovd9 U>OuO7)<dd'i?d 3^.
&TaBdUOd ddCLFdddtfdOeZ eSdOdOddtfyJOj
:—
kudo dodudoym Zuoaiua jujt). Ad dooTJU^w stra^ d>odo7)e.ddv zjAn Sda^A
1«
.39 JoSot)oau^e/Jo• 3uj<5 CuravdSraFodO ®J$
*
djGdOa^.AdOd 7U? dO
d£.??aJ Bsjo oJdo^ dd3«in
cJO^^ad^OdS_$ J • O.jU c!07) jA uyjOtOij ZJoUT)^ cJ-.^adj
dd07)dda j ZuOadtj) OUJoyjO.J •
2*
JO dOdOdOOOT)^
U_>
doa(Ld dOZJ S.JOdd d J7) jGS J ^07)oA' Zu J jO dEry.
Ad dOOTJOvd^ J>O7)<iJEja ^0<$:-'^JO7>o (ft)Jc) :— SOtfd 2SOO& &OAcJ OZ50i852JVv4
y ■_9l O(\)c)ddj ydOf Ck/SUdurtj dv>^)4 ?rcb^)<<^)4 Go do a uO7)€.d,yj "Fa jodoymA( ■cUrad.^o&JO
dow<d riou7)d;
dym
axcL-l, oTJUdatf,
<5<u§(
wd§ — oda^a
*
oort <yraddvdo.z otfodoo^ju 8ot>3A ftraed CdrxdJ oMradtfo dodo^ d^S^odo
3-
ajfin zjSouod d^oUdVdOci tuJodiJo dosoj SyudoodfUo Zu^odojo-
4*
oaJSS
<Jj j -', jdddv? d_>uau<JGj daauauo odauaoyodVdOez dudaudod dadaF
do7> j^dodi'y^ d^o^ arariddo^ A.; doo^ySd^ dyodyatrw ?jAn Ude.doc>A
qd^5.y )Oo •
5
6-
•
Joy 4*jOO kf cj^j~aara$ jJ SotjgA osj^fb^do zjAq do>)^iv0n oOddo^ doo~aGcjOc.^.jo •
odooDo^dciJ doa<ad &ra<uddJei £)§doo ydd^daJ JUdEoSoJoddOci d-yardo))
u-\J~d GO cJ) jU •
1 >■
3o<0 ajc?.j dotrudiltfcoo .-z yaodoFdo'au^^ dvoo cSjSodkjazjjjCtra odddoA
*)\_,od
o9c
Ad dooTjyo djudo7)^.ddv
3VdOu..,».5o • daooood v"ao ojOjO
zjA^
ajodooooT) ddoA Aoacjjood Ad doo
ay
*
Ujodoja(tdd<Jocz d?o 5 dzs^AoJo z3\Z.eU
u ^OdOOU ddO^, v ^Odoy^ ZJ.j_j JoA d?(.J.jOuO7)OtJUOd Oj^.uGdO<Z v7)f02JdjOdo •
co a A'odo ocodadd^o Gyatj djo^ u‘^odoyfndou 5oddOcZ odooau-g tJcoudo cdaA
zjj_jdaA '-<13^ j"a jo•
jd.jya^ dor\>cuj zjcoo ajdU d^j^Jo^ djdau JUro rad
Jo7)<zy i/Otoudo-atcddadou “
Ad dooTfyS-dvuo.z djodo'ae.doo
I*
2-
joo-
duam yauooddorkjra ortod A doo'aySWo rwm ddejoddo^ dod dyaci.5 ■Jjdd^yjoj
(Xra<d ftofudoji u_>.radda.5 ooa- yjo dOodoTiA ds5,Jo’-jO7)oddoe.d Ad uoot)u£
UdOrOOcZ cO_J od07)KZ( Io)UG.;. JO )‘
odo zjdn i)9 JUS
3-
u5t.9Uod gjdod^do.z 3$?oddi
o.jOdu J j 2)7) d_q_J j) ‘Uv uOuyAvy d'JOOd ocJrj
jo
dddod nJ dooTidSWo :5jodoym ■gjjUor) duo jn dUdjudoy^
djiiudorxLAd
57 y JO J •
4-
t
odO7)ij
*
yauodoTJy uO7ie.r)d9do< UjOdoTxjddfA’ doOdiudS-oTJUJo• ^SdododOoJ
oodtJo.z d9duo d^ododciduoddivi dOodoD.j
doCudoarau jo ■
odd dau^o' oozj cS^Udo^
dd^ do7>srt ao&u d_>odo7)<duum5o Jo 39JoSoatf^araUdo •
7
coejfu rwa
.
aJSjCJrtJfiJ<
fiorae.^J aljjofijjojj fijfiofiJUJJm
rjfiftjOAj ”Z2t3i-A_><j).1J JfiF orafiJJfi^ • ^JJJ^
*
3(5 fijj e.0^
0,
*
8
fie.CJ(
'ajjftVcraft ficiaj)
■aa^Jjfi ‘a^prtVJ fiofijJj <jfiriVym eHJ 3ortVJftVym jujufijrafi?^ araufi 'aoJ„
0U/Ckjvj uvjofijrae.ci jjrafi^ araftjj-a j*
?ra> raeir.araft fifij^, jjfiojjy^ aojfijfifi
(motraftjfi firajcscsvaj^ rtjrajtdsiuj ofig^araft fie. era J 73qcj ftjrtvjj^ fiftaj^jfijraoafi
yjjsraclaraft oJeiJci vUwofiJJftJajcoJ jj ? a>o.jj fijfifl ofizs^araft fie.erartjJ
*
fi^jj^^uJa
ftjjjjjeSrtVfij< jjfiooj co3juym
3jtfa
jraCJfi acram s, 5e.z>nve?m 3JyjjfiB>ftfi§ujjjfi
"ajj 3jv&. 3JVr6oJJOm
12 gusrW3« ■s.JO0m
o<5jje.ftJ3#,<jJo» ©dorae.
:—
jjjjjoj
JjvjoJjjj^ ta&$
Xrae.'/ jjzj ’a^j auoSj
*
So &j&3,jojjum oe.vjjQi.ra 16 ^joym
ojraoj J&) JUcjp, 73cq<jcjj<91 iCjj^.j •
yju
*
gju apJ fie.co
ajtoftc?) ouu jjdo u< jjtj(3 \>jo.jJ
Jura
u®5 jjooojjraft Surae.rraK>j ara.5ojjj zsoe.ujjj<£ g^?jjq)’Jj« oores jjjJc)J
(jJ"c) ftftVcJJ c£
jjSj
JclCXjj JJ-o.J •
SujjjU^
0'300
<JJJu3c)J<J
T^ljfij OjJ3 C$J J_^fi •
fiajj fifia.ju fiun^^civ araucjoJ o'^fi afi'ojjzjeojuj •
rOc)?5 'JJ3>LjJQ) 560"c) .. C)ft arauJOO JclJ
■aJu (be.o'jj<
ftocJoftvft ‘ariu
oju fijjfift oouu<5oraciftVJj<
Joaraylsra 1 acra„ fikraeci 3j7>uJfiriVJ aara^fioJjjrtoJjj
■'ujje.fiJ
*
7 aficivfijci <rajfi rizjFeraofij
erao ftajF^jjQj 02000^,
*
‘aynvj(n fi(j<x)j *a. >j jo aojj
Oo’J Jfifto
*
JO fio JO
OOJp JU^JCJJQJJvJ^. CAJJoJJJt^j) JdftJ3_sO •
cbofiJo a^ckjJ_^J• ajj ajjju 6o"oeft
jjfie.&ojjJ erayjw^ fivftss eras
^zfitj jfiojjj^ ofiJc^fifijjjj
zsjjf
30 Vo)
.sjjujrac>j323jj
aoaj jjzraJQi arao^^JJ™ j*
fifiJV 'aa^jfis^o^ <a.,jj oajj^cjj*
...
fi^fijje.^
K
T E VILLAGE
Miguel was worrie.
this time. His two year old
son, Juanito, had never been this sick before: he
had a cough that would not quit, he felt hot and had
a dull, faraway look so different from his usual
A serious problem, not
responding to home
remedies
happy laugh. For a week, his wife, Maria, had tried
everyt ing in the house she could think of, yet
nothing worked. Her neighbors cautioned ag:inst
"hot" foods, but Juanito was not hungry anyway and
hardly ate or drank.
THE ' ILL.ACE KAL '
ORF ER
Maria took the boy across the valley to sec Ramon
who kep a small shop in . is farmhouse. Ramon had been
A good diagnosis, but inadequate
selected the year before by th: village for training
treatment due to drug supply
at the health center. From his training, he know that
shortage
prolonged fever and coug;
could be pneumonia. His
stock of medicines no longer included packets of
penicillin tablets: ther: had been a lot of chest colds
around and now only one packet was left. He broke it
open and took out three tablets, embarrassed that he
Disappointment and skepticism
could not give the packet and explaining tha
from the patient
at last
month’s resupply meeting no stock was available. Ramon
was angry too, behind his words of instruction, thinking
of what he’d say to the Health Center Supervisor the
next time. Why bother to go to the meetings at all if
there . ere no drugs? He was ashamed to be trying to
A loss of credibility for the
satisfy the village’s needs with advice alone - it
health worker
wouldnot do, that’s all.
2
IK THE TO'.-.-N
Miguel had walked the burro half the night to get
to the market early. He sold his load of carrots quickly
and took the money to the pharmacy, where he described
1
L
J
Juanito's fever and cough. A young boy was tending the
.
, ,,
Untraineo dispenser,
.
,
.
inaccurate prescribing
shop for his uncle, who was away buying drugs in the
city. He remembered people coming in for fever and his
uncle giving them pills from a bottle lebeled
chloroquine: he could easily reach it. Miguel was
glad to buy the pills and hurried off.
At home Miguel found Juanito no better. Maria had
given him the three penicillin tablets at noon yesterday
when she got home, which he had swallowed with difficulty.
Inappropriate dosage
He smiled weakly as his father attempted to give him
schedule
a chloroquine tablet, but screamed and spit it out with its
bitter taste, his cough and tearless cry sending Miguel and
Maria into deeper despair.
the health center
At the Health Center, one ana a half day’s walk from
the village, Peter, the Supervisor, was not eager to
face the village Health Workers again without enough
Maldistribution of
supplies. It was even worse knowing that the next
limited supplies
region had surplus stocks accumulating from two years
of deliveries, though village workers had only recently
3
3
begun work. His o\ n credibility was at stake; their
enthusiasm for continuing education was dissolving into
discontent and declining attendance, fragmenting the
Declining participation
program which had been so enthusiastically received by
in village health
the villages the year before. He knew he would have to
program
get the Regional Health Office to respond soon, or all
momentum would be lost in yet another example of
government failure.
THE .REGIONAL OFFICE
Jose was perplexed. As Regional Health Officer, the
hospital was his constant concern (as the central
Inadequate salaries contributing
health facility on which two million people depended),
to illegal activities
yet he had the rural health centers, too. Mow both
were complaining about drugs. He knew, as did everyone
else, that drugs, theoretically
ree, were sold by
seme staff members to supplement salaries and income
from unofficial private practice. There was never
Competing demands for inadequate
enough to go around, and he could no longer reallocate
supplies
health center supplies to the hospital - too much demand
in the rural areas now. On top of that he was beginning
to wonder about his administrator, whose latest story
of shipments lost or arriving undercounted only compli
Incomplete record keeping hinders
cated the problem. If he only knew what was used last
planning
year in each center, he’d be able to juggle demands a
bit better, at least until the decision on his own
transfer was made, and he was out of the mess.
4
4
At the hospital, the pharmacist reached high on
the shelf for the last tin of penicillin tablets that
was left. The tcp clattered to the floor as she looked
Poor packing
first at the label, not quite outdated, and breathed a
sigh of relief - until she looked inside at the
crystallised mass of tablets, decomposed after the top
had been loosened in transit. She had nothing to give
the man with the prescription and the woman with the
swaddled child gasping in her arms. They turned away,
wondering what to do next.
Carlos, the hospital administrator, took pride in
his efforts to juggle the region’s inadequate health
resources. His years of service balanced a lack of training
and made him a respected official. He could not, however,
Untrained administrative staff
figure out how to handle the drug mess, which got worse
every year as demand outstripped supply and more health
facilities were opened. A few facilities had overstocks
while others were always out. It all seemed so unpredictable
Rumors of corruption bothered him most of all, a man •SKQft
whose pride in his work at a difficult job had always been
Supply of new health workers
so important. Now, with health workers beginning to provide
rapidly outgrowing the supply
some simple health services in almost every village, the
of drugs
resupply and financial problems were overwhelming. Carlos
understood how tempting valuable drugs were to many staff
trying to get by on the small government salary - but for
people to insinuate that he was involved was the most
unpleasant thing he had to live with. Now if only he could
5
5
get the requisitions and the records together, he could
be able to justify his position to Central Medical Stores
Inadequate management information
and get them to release the emergency request he had
for stock control and financial
placed tv;o weeks earlier.
planning
CENTRAL MEDICAL f-TORES
As Juanito’s parents managed to get the seemingly
lifeless child admitted to the paediatric ward of the
hospital, Enrique, the Chief of Central Medical Stores,
searched into the evening to find the intravenous
Warehouse disorganized
penicillin required. His anger at the disorganization of
the warehouse exhausted him more than the search.
Enrique was responsible, he knew, but how crald he^it
all?
The stock reports were disorganized and he never
Untrained staff
had found time to train the clerks. The late arrival of
shipments cleared from customs after sitting on the
wharf in the rain had compounded the mess, with crates
Mis-estimated lead times,
and cardboard a soggy stew all over the floor. And the
pilferage, spoilage, port
stock count suggested more losses on the docks or in
clearing problems
transit than just to rats and rain.
At <| last he found the penicillin and sent it off
with the pharmacy aide and frightened farmer. He was
too tired to think about the endless emergency requests
Transportation confusion
and vehicle breakdown
from the regions which always seemed to pile in, especially
when vehicles were down, awaiting parts. Even worse.
6
tomorrow the would have to try to get approval
for an air freight purchase of penicillin tablets
Expensive emergency purch
since the lowest bidder had defaulted on the
supplier default
shipment. It would cost a fortune on such short notice....
On a truck heading back towards the village,
Miguel was a mixture of emotions. He was relieved
that the doctors had taken Juanito into the big
hospital and that Maria could stay at his side. But
Continuing hardship
he was frightened by the plastic tubes he had had to
and uncertainty
buy at the pharmacy, which were now connected to
s
*
Juanito
arm. And he was fearful for the future.
Life would be very hard again, now that he would
have to sell seme of his animals to pay for medicines.
But he thanked God that Juanito still had a chance.
CONSUMER ,'LERT—CONSUMER ACTION
*
ravi narayan
The problem
The Indian Council of Medical Research (ICMR) and the Indian
Council of Social Science Research (ICSSR) have, in a joint study
group report entitled 'Health for All - An alternative Strategy'
warned that 'eternal vigilance is required to ensure that the
health care system does not get medicalised, that the doctor-drug
producer axis does not exploit the people and that the
abundance of drug does not become a vested interest in illhealth' . This warning is a serious indictment of the drug
industry and the medical profession in the country. It
confirms the growing evidence that drugs are being pushed
on an unsuspecting public by devious methods which masquerade
as 'sales promotion' of drug companies and 'professional
prescribing practice' by doctors.
A spate of reports have been appearing in our newspapers
and periodicals of late, on drug-related issues and a review
of these highlight that m~ny of the following practices are
not at all uncommon in India:
i)
Sale of drugs banned in other countries eg: Lomotil
and Clioquinol preparations.
ii)
Sale of irrational combinations and formulations
eg., Hathi Committee has suggested weeding out of
atlcast 23 such preparations.
iii)
Sale of drugs without adequate precautionary
product information
iv)
Sale of drugs at highly inflated costs eg: it is
reported that Analgin is being sold at 20 to 30
times the cost of production.
v)
Promotion of drugs for indications that are not
clinically proved and are often potentially dangerous
eg: Promotion of EP forte combinations for pregnancy
testing and induction of abortion. There is well
documented scientific evidence that the risk of
foetal deformity is increased by the use of those
hormonal preparations.
vi)
Sale of spurious,adulterated or po r quality drugs
eg: Turmeric powder in tetracycline capsules and
poor quality and reaction producing intravenous
fluid preparations have been reported.
vii)
Sale of old, expired and unused drugs. There is
the double danger of effects of denatured drugs
as also of inadequate dosage.
viii)
Over-prescription and misuse of tonics, high-protein
foods, hormonal preparations and baby f.cds that are
both superfluous and a drain on the family economy.
ix)
Sale of drugs over the counter without doctor's
prescriptions or the necessary statutory checks.
. x) Production of drugs for profits rather than health
needs of people - eg: The ICMR/ICSSR report highlights
that drugs for diseases like leprosy and tuberculosis
which affect millions arc produced at one-third
Bull. Scs. Vcl.l No.2 Dec83—Jan84
page 11-15.
r-j
: 2:
and one-fourth of the actual requirements while tonics,
vitamins and high protein substitutes are being
produced in wasteful abundance.
It is evident then, that what is needed in the country today
is a c'nsum^r awakening and awareness building process that
will sensitise people to the realities of the drug industry,
mobilise public opinion, sensitise policy makers, confront
the medical establishment and challenge the drug industry.
This process will have to lead to the initiation, promotion
and sustenance cf consumer action to ensure that the drug
policy in India is more ‘people’ and ‘health1 oriented. Is
there any evidence of such an awareness?
Consumer "lort and action
Beginning in the late seventies, there is an increasing
number of organisations, associations, projects and action
groups who have begun to create an awareness cf drug-related
policy issues. These groups arc predominantly if net exclusively
urban-based, consisting cf young professionals and intellectuals
from different ideological backgrounds.
Since the Medical Profession is the ‘instrumental consumer1
ie., they’ prescribe the drugs, many cf these groups have directed
their efforts particularly towards them. Many ethers are health
or development associations, science popularising movements
and consumer associations who are increasingly taking up drug
issues ns one cf their many activities. The list of groups
which makes interesting reading are -
- Voluntary Health Association of India (VHAI), New Delhi
- medico friend circle (mfc) Pune
- Arogya Dakshata Mandal (AIM), Pune
- Delhi Science Forum (DSF), New Delhi
- Society of Yeung Scientists (SYS), New Delhi
- Lok Vignyan Sangathana (PSM), Maharashtra
- Kerala Sastra Sahitya Parishad (KSSP)
- Concern for Correct Medicine (CCM), New Delhi
- Consumer Action Front (CAF), New Delhi
- Consumer Education and Research Centro (CERC), Ahmedabad
- Centre for Education Development (CED), Bombay
- Federation of Medical Representatives Association of
India (FMRA) , Patna.
All India Women's Conference (AIWC) and so on. It is
impossible to document all the efforts of these groups but
the main typos of action they have been involved in ares-
1.
Publications
mfc published two anthologies of their bulletin articles
'In Search cf Diagnosis
*
(1977) and 'Health Care Which Way
to go' (1982) which included many articles on drug policy
. .3
related issues. VHZ.I's special issue of the bi-monthly
'Health f r the Millions' was entitled 'Medicines, as if
people mattered' (1981). It covered many aspects of drug use
nd abuse and tried to stimulate voluntary initiatives from
the public and the medical profession. CED published an
exhaustive, well-researched report on "Aspects of Drug Industry
in India" (1932) to stimulate further interest.
2.
Meetings
These were organised by many of the groups to bring together
people interested in the problem to share views and discuss
action plans. The Drug Industry and the Indian People (DSF,
SYS, FMRA and others, November 1981), Drug Issues and Feasible
Alternatives (VHAI, Pune, Jan ’82), Drug use and Abuse (mfc,
Tara, Jan '82) were three such meetings. The Seminar on
National Health Policy (New Delhi, VHAI, AIWC, CCM, April 1983)
also discussed drug issues and stressed the need for information
dissemination and consumer action.
3.
Educational Campaign through letters and media
AIM launched a movement called 'Operation Medicine' in July
1977 with letters to medical practitioners and articles in the
press requesting for a stop in prescription of forte vitamin
preparations, irrational B-complex formulations, tonics and
tinned foods and boycotting of certain drugs being sold at
inflated costs.
VHAI launched a campaign in March 1982 (international Women's
Day) against the misuse of hormonal preparations for pregnancy
testing. Letters were sent to doctors and chemists informing
them about the dangers and requesting them not to misuse these
•j?r.o<iu.c.t.s^,Ar.tXG.Lsls_w.cce .published in leading newspapers . and
periodicals. The. movement snowballed and the government decided
to ban EP forte combinations. The movement continues to challenge
government action which has given a lag period of six months
to drug companies to move stock before ban becomes effective.
mfc launched a campaign early this year about the rational
management qf diarrhoeas in children with a hope to prevent
misuse-of various available pr..parapions that-do not have
much therapeutic value. .Press releases, informative articles
and ..letters to drug controllers have bqen major constituents
of this campaign.
. ■
. ■-■•■■■■
■■ - ? ?
•
4.
Newsletters/Bulletins
One of the best examples of continuing education of doctors
on drug issues is the Pune Journal ’of Continuing Health Education
published by AIM. This bulletin sensitises its subscribers to
the half-truths of medical advertising apart from- providing
.reliable information on latest drugs. The Drugs Bulletin of
Pharmac logy Department of. Post-Graduate Institute, Chandigarh,
is another example, mfc bulletins have also regularly featured
articles on drug issues.
5■ Information net-work among voluntary
'action groups
T.- maintain this growing interest, VHAI has set up a
special cell on 'Low Cost Drugs and rational Therapeutics'.
This .Cell, has been keeping groups all over India informed about
now problems and follow up action of campaigns. Other groups
have also- initiated informal network exchanges.
4
6. Lev/ Co 3 J -Drue- Ventures
.,.r.
..................... ................................... -...... ■■■--■-
....
;
The- B .nrapot Medical Mission, [Tablet; Industry has been a
very succbisful small, > scale venturis ...in . prcvi&ipg low ebst,
good Quality formulations tc r. limited group of mission hospitals
in the country. Recently in Gujarat ~a ne^'projact-callth.LOCOST.
has been initiatsii This, is, a colleqtiye.' voluntary. ehdbavoUr • for
rational therapeutics through promotion of?low' costp quality,
generic -n-emod medicines.- An important dimension of the project
will bo an educational effort addressed to the voluntary sector
for minimum use of drugs and. the socio-economic implications of
irrational therapeutics. -
7.
Drug Issues in Science Movements
' With’ the growing'-interest on .drug related issues Well-known
science movements in the country like KSSP and- PSM have also
decided to coordinate with other .agencies in joint campaigns.
At the All India convention of the Peop-le^JS'cdjbncfe Mbyement
at Trivandrum ..convened by KSSP .in February 1983, a health group
was formed. which; grew; up, ’a-j pint.- actic n programme, having the .
following'.f our components.
‘r
■ •
a.
Ban on E.P Forte combinations
.. To oppose the wrong arguments, of drug Companies being .used to pressurise government to lift ban order on these
combinations.
b.
Campaign about Anemia in Women and Irrational anti-anaemic
drug preparations in the market. PSM-Maharashtra included
•it as a topic for their yatra in May 1983.
c.
Campaign against irrational Diarrhoea Management in
Children.. mfc, would initiate campaigning frem'June 1983.
d.
Campaign against multinational in Indian Drug Industry.
A campaign by FMRA would be organised in October 1983, to
coincide with the annual Jatha of KSSP and -to make people
aware of the role .of multinational corporations in India.
Towards a people1s movement
All the above efforts are small steps towards a much more
wide based consumer movement against drug use and abuse and
profit oriented drug policies. However, it must be remembered
that in a country like ours when a very large percentage of
people are below the poverty line and when moreXthan 75 percent of
the people have little access to basic health science a consumer
action programmeonly oh drug matters will continue to be -cut
off from the.needs and aspirations of the majority.
Dr Norman Bethune, favour for his work in China wrote, "The
best form of providing health care and health protection -would be
to change the economic system which produces ill health to
liquidate ignorance, poverty and unemployment".
One hopes that eventually drug-related issues will become part
of a much wider people's campaign for health development and.socio
political change because at the root of the entire problem cf
drug production and availability lies what Ivan Illich has
aptly described as "Socialiatrogenesis - ie., health policies
reinforcing an industrial organisation which, generates ill-health1.
DRUG PUSHERS OR HEALERS?
"The greatest danger to health in India is the over
mcdicalising of dur health care system. Eternal vigilance
is required that the doctor-drug producer axis does not
exploit the people and that the ‘abundance1 of drugs does
not become a vested interest in health".
- ICMR/ICSSR study on ’Health for All1
—An alternative Strategy.
The problem of Drug policy and low cost drugs encompasses
a very wide spectrum of issues—multinationalism, industrial
policy, medical advertising, research, drug production,
medical education, price control and so on. The recent
upsurge in interest in this important area of health policy
has led to the publication of numerous reports, bocks and
papers and many seminars and workshops have and are being
organised. In the final analysis any collective action in
the form of-policy, analysis, research or education can only
result from an individual understanding of the related issues
translated into a prescribing policy to be accepted vrlunarily
by doctors, nurses, para-professionals and others in
their attempt to contribute to a solution of the problem.
Readers of this note are requested to. th'ink over the
following facts, observations, conclusions taken from WHO,
ICMR, ICSSR, Earthscan, VHAI, Govt, of India and other
source of information. Can we collectively accept as many
of these 9 points.as possible?
(1) 15000 branded drugs are on sale in India but a
Government Cc-mmittee^bclieves that health needs would be met
by only 116 drugs. '
There is now an overproduction of drugs (often very costly)
meant f^r the rich and well to do, while the drugs needed by
the poor people (and these must be cheap) are not adequately
available!
WHO in its report on selection of essential drugs^has
prepared a list cf 200 drugs needed for health care.
d
tu „
The real purpose of an essential drug list must be seen
as taking drugs to those2whc need them most, not as
reducing the drugs bill.
CouId we accept an eseential drug list for cur practice
in which cost would be an important criteria in selection
in addition to efficacy, safety and quality? .... ..
'
0
p
?
.
?
(2) All UN agencies, and governments involved in preparing.'- I).
a list of essential drugs are c nvinced that prescriptions
should be threugh the generic names of drugs only.
Jr
Generic name is not chemical name but official, international
non-p^oprietary name eg., not Acetylsalicylic acid but
Aspirin.
Bran.led named products cost higher because they include
promotional costs and cost of claims cf additional ingredients
. emulation eg., Librium by Roche is available for Rs.16/f.
per 100 tablets but generic equivalents are available for
Rs.1.50.
A study of UNCT >D has shown that bio-availability
argument for branded drugs ie., therapeutic difference^
based on formulation is not very valid for most drugs.
: 2:
Could we accept generic prescribing? ie., Ry Aspirin
not Plusprin, Disprin etc.
(3) In India 60 firms with foreign shares accounted for
70% of the country's total drug sales in 1973-74. The remaining
30% was shared by 116 large and 2,500 small manufacturing
companies.
Drug industry in India is an offshoot of development of
the industry in the Western World and is in private hands which
produces mainly for profit.
ICMR/ICSSR and the Hathi Commission have recommended that
the small scale sector, cooperative sector should be encouraged.
Hospital and dispensary based formulations should be promoted.
Can we prescribe drugs which are Indian rather than foreign,
Government rather than private industry, small scale and
cooperative sector rather than large Isector?
(4) "One of the most distressing aspects of the present
health situation in India is the habit of doctors to prescribe
glamorous and costly drugs with limited medical potential." 1
"The drugs required by the poor are not produced on the
main grounds that there is no profitable market and adequate
demand for them, while the country continues to be flooded
by plethora of costly and wasteful drugs meant for the minor
illnesses of the rich and well to do." 1
"Multiple drug combinations often containing drugs in
amounts far in excess of what is required are presently
marketed: ih .India. There is a collosal^national wastage
of drugs because of such combinations.
Packaging increases the cost of drugs very greatly
because the trend is to make it attractive and highly^elegant
and to add cosmetic embellishments to promote sales!.
The drugs Consultative Committee examined 34 categories
of fixed dose combinations and concluded that in the case of
23 categories cf these formulations, there was no therapeutic
rationale for their marketing.
The Government of India
issued a notification in July 1983, banning 22 fixed drug
combinations.
Cculd we step prescribing drugs whose only additional
advertised values are -
a.
c.
e.
cosmetic embellishment; b. elegant packing;
irrational combination;
d. imitative drugs;
inadequate evidence of greater value?
Do we know which are these banned drugs?
banned? Can we stop prescribing them?
Why were they
(5) 25% of a total production of Rs.700 crores in 1976
as analysed by a Task force cf the Planning Commission was on
vitamins, tonics, health restoratives and digestive enzymes!
An ICMR/ICSSR study observed that production of INH and
Dapsonc are a third and a quarter respectively, of the minimal
requirements of the country. On the other hand, tonics and
vitamins which are mostly alcoholic^preparation and spin money
are produced in wasteful abundance!
3
A NIN study on tonics has shown that most of the high potency
or 'Forte' preparations of multi-vitamins are a sheer economic
waste.q These are not only a drain on the patients' purse but
als; help only to vitaminise our sewage systems.
Can we stop this 'tonic' and 'vitamin' practice?
(6) A WHO report notes that drug advertising and contacts with
representatives of pharmaceutical firms are often the main source
of informe.ticn for a physician on drugs and sometimes theonly
one. Such,information is largely influenced by commercial
interest.
Drugs are often being prescribed by doctors not because
they think a particular one is best suited for the situation but
because the company which produced it gives the maximum monetary
and material advantages and inducements to them. These range
from free samples (often, sold in practice), pens, calendars,
diaries, teas, lunches, travel and conference attendance costs.
Medical training in colleges dees not train future physicians
to judge a preparati n critically ....... nor does it include
conscious immunization against the half truths of persuasive
industrial advertising.
CAN WE STOP ACCEPTING PHYSICIANS
S.AMPLES AND OTHER FORMS OF INDUCEMENT FROM MEDICAL COMPANIES?
(7) Many medicinal herbs and roots that are used by
grandmothers, local dais and village medicine mon have been
scientifically tested and researched and known to have therapeutic
value. Their,descriptions in journals collect dust in reference
libraries. '
Herbal medicines and home remedies are not only low cost
and easily available but their popularisation will help in
breaking the doctor-drug producer axis for over 80% of the
common minor ailments which are new being overtreated.
China has integrated over 50 herbal medicine and home
remedies in their armamentariums not only as a drug policy 2 g
but as an expression of local participation in health care.
Can we propagate simple home remedies and locally available
herbal medicine after studying their efficacy?
(8) A very large number of techniques of healing arc being
researched today in which diseases are tackled and cured without
drugs. Non-drug therapies include Yoga, Pranayama, Meditati-' n,
Accupuncture, Acupressure and Chiropracticc among others.
Traditional systems of Medicine such as Ayurveda, Unani,
Homeopathy which use drugs but of a different sort arc being
researched in various places and the therapeutic effectiveness
of many of their products are being discovered and documented.
Can wc adopt a more open policy of enquiry and introduce
use of tiaditicnal medicine and non-drug therapies in our
practice after.scientific enquiry?
(9) Health Care is becoming increasingly a quest for
priorities, "clean water before anti-biotics, feed before
vitamin pills, vaccination before kidney machines, mothers
milk before powdered baby foods mixed with dirty water, health
for villagers and slums before more„hospitals for the
affluent suburbs of capital cities..
; 4:
In spite of our preoccupation with Drug Prescribing
policy, cc.ul'l we commit ourselves to ether more important
Health Core Priorities?
- ravi narayan
background paper, mfc Annual Meet 1982
References
1. Health for all - an alternative strategy - ICMR/ICSSR
' Report (1980) Chapter on Drugs and Pharmaceuticals
2.
Drugs and, the Third World, Anil Aggarwal, Earthscan
publication, 10 Percy Street, London WIPODR (1978)
3.
Hathi Committee; Report of the Committee on Drugs and
Pharmaceutical Industry, Ministry of Petroleum and
Chemicals, Govt, of India (1975)
4.
In Search of nPiagncsis, an mfc book containing reprints
' from its bulletin
5.
The Selection of Essential Drugs, WHO Expert Committee,
WHO TRS No.615 (1977) and 641 (1979).
6.
Medicines as if people mattered - Health for the Millions
(VHAI Bimonthly) Vol.VII No.283, April-June 1981.
WHAT IS
CONSUMER INTERPOL.?
Consumer Interpol - If you think the name
refers to a force assembled by consumers
to fight international corporate crime,
you are right.
Rampant dumping of hazard
ous products, dangerous technologies and
toxic wastes; countless victims (many of
them disabled, dying or dead); the absence
of any comprehensive effort to bring about
a solution.... These have given rise to
an acute sense of impatience among consumer
groups and prompted action against the un
conscionable deeds of some transnational
corporations and 'aid' agencies.
Consumer
Interpol, set up by the International
Organization of Consumers Unions (IOCU), is
a dynamic entity incorporating an alert
system, safety campaigns, advocacy for re
gulations, research and training.
It aims
to organize citizen action against an
intolerable problem.
HOW DOES IT WORK?
IT'S GLOBAL. Consumer Interpol, as the
name suggests, is global.
At the core of
the network are members of the IOCU group
numbering more than 120 organizations
located in some 50 countries and represent
ing every continent. The Consumer Interpol
is developing regional centres to support
THETHIReT
FORCE
"The Lack of controls on the exports of
toxic, substances that are banned or
restricted poses an undue burden on the
'inner limits ' of man; it poses an undue
burden on the 'outer limits ' of our en
vironment; it poses an undue burden on
developing countries that have not yet
the skills and resources to deal with
the problem adequately. The '3rd system,'
the citizens' groups in developing and
developed countries, must act together
because we cannot rely on the '1st
system, ' the governmental system or the
'2nd systemf the commercial network, to
deal adequately with this problem,
lie
are concerned here with a major health
issue, we are concerned with a human
rights issue, and we are concerned with
the protection of the environment."
— Anwar Fazal, President of IOCU,
Keynote address to an NGO Seminar on
the Export of Toxic Substances, New York,
November 20, 1981.
activities in every part of the world.
Each of these centres wil_ have a wide net
work of correspondents; the aim is to have
at least one in every country. Correspond
ents are drawn from consumer, health and
environmental groups and a wide range of
knowledgeable people including journalists
and scholars.
IT'S PARTICIPATORY. This information-and
-action network encourages participation;
it calls for a cooperative response to a
shared problem. All components of the
Consumer Interpol are two-way systems they GIVE help and they TAKE help. The
'alert' system, for example, welcomes in
formation on hazards from all quarters.
Whatever vital information it receives will
be channelled out as warnings to those who
need it. Regional centres, the collection
and dissemination points, will assess in
formation received with the help of some
experts.
IT'S AN advocacy NETWORK. The Consumer
Interpol does not stop at issuing 'alerts.'
It also takes action from time to time to
ensure that the hazards are removed through
legislation and other means. What the
network will do is flexible and it depends
on the issue at hand. A localised problem
may only need a localised response with
help from a few other organizations. For
a global problem. Consumer Interpol may
mount a campaign involving every concerned
group that wishes to combat the problem.
IOCU is not new to such international cam
paigns.
It is playing a key part in those
involving infant formula and pharmaceuti
cals through the International Baby Food
Action Network (IBFAN) and Health Action
International (HAI).
IT'S SUPPORTIVE. The supportive arm of
Consumer Interpol is aimed at making sure
the action-information balance, vital to
any international campaign, is wellmaintained. Research will feed the system
with detailed information while training
ensures that gathered information is well
stored and efficiently used. A data bank
with links to other documentation centres
will be maintained. There will also be
active links with programmes like: • the
International Register of Potentially Toxic
Chemicals (IRPTC) of UNEP; • the Inter
national Programme on Chemical Safety of
ILO, UNEP and WHO; • the ILO International
Occupational Safety and- Health Hazard Alert
System and • UNEP's Global Environmental
Monitoring System (GEMS).
©0© ©o©
©?
'1:
o At least 25t of US pesticide exports
in 1380 were products that were banned,
heavily restricted, or have never been
registered for use in the United States.
s About 1,5 million people are being
poisoned by pesticides every year, with
half of the cases in poor countries.
Some 30,000 deaths a year - three quar
ters of them in the Third World - are
believed to be due to pesticide poison
s Several million children's garments
treated with a cancer-causin g fire
retardant called Tris were shipped
overseas after being forced off the US
market by the Consumer Product Safety
Commission.
o Many pharmaceutical companies fail to
label their products adequately regard
ing proper use and dosage. Often even
doctors are deprived of crucial infor
mation like potential side effects.
Should you receive information on any of
the following...
© marketing of dangerous consumer goods
like toxic fcods .and dangerous toys
o export of hazardous wastes
o plants that expose workers to serious
health hazards
c adoption in exporting countries of new
bans or strict controls over hazard
ous consumer goods, drugs, -esticides
or industrial chemicals (this is to
alert the network to the possibility
of dumping)
® In. India, the subsidiaries of major
British and American asbestos companies
operate facilities that are 50 years
behind the, standard of practice the
firms observe in their home countries.
® The US Environmental Protection Agency
estimated that in 1980 at least 57
million tons of hazardous waste was
produced in the United States. There
are not enough safe, secure disposal
sites to handle a fraction of it.
o newly reported outbreak^ of Illness or
death due co previously known
hazardous agents
...inform the International Organization
of Consumers Unions (IOCU) and we will
take the appropriate action...
(Our
addresses are on the back oage.)
SanaaTw
tV
Catholic Hospital Association of India
CBCI Centre, Goldakkhana
Mew Delhi 110001
Date: 20.6.1984
Dear Friends,
One of the problems our health services face is that of ever increasing price of drugs. Our
poor people cannot afford to buy drugs for them. The situation will g"o on getting worse unless
corrective measures are taken in time. Drugs that are banned by our government are still
manufactured and sold in our country. The following is an attempt to work towards a more
permanent solution. It is necessary that we all join hands to fight against this evil in the health care
field. If you are convinced of it, all what you have to do is to take a sheet of paper give some
particulars of the health care personnel in your institution (doctors, nurses etc) together with their
signature and send it
Dr. Mira Shiva
Co-ordinator
Law cost drugs & rational therapeutic
Voluntary Health Association of India
C-14 Community Centre
SDA, New Delhi 110016
at your earliest convenience. She will collect all the signatures and send them to the concerned
authorities. Please put the seal of your institution also on the paper.
Requesting your cooperation in this great task and with personal regards,
Yours in the Divine Word,
(FR. JOHN V ATTA MATTOM SVD)
Executive Director
MEMORANDUM
We, the health personnel and citizens of India recognize health as a fundamental right of the
people in this, our welfare state. We recognize and strongly believe that the health status of our
people is more dependent on their access to adequate food, safe and adequate water, proper
sanitation and clean environment.
.lta’.th cell
COWlf’'-;
* 1*
Roai
While we support the over all perspective and approach of the new National Health Policy
Statement and demand its proper implementation, we believe that a 'Rational Drug Policy’ is an
integral part of a good National Health Policy.
We therefore, demand the following :
1.
We have a right to safe, essential, quality drugs which are in keeping with the health needs
of the people, at costs which the majority can afford.
2.
We urge our government to accept and implement the Hath! Committee Recommendations
which are also in keeping with the WHO Guidelines for a Rational Drug Policy.
3.
Further the national drug formulary should be revised and compiled by an expert multi
disciplinary committee keeping the following criteria in mind;
Essentiality
Efficacy
Safety
Cost
Ease of administration
Availability
Potential for misuse.
Such evaluation of the drugs in the market and revision of the lists should be done periodically.
4.
The Essential Drugs Policy should be adopted for all health services government and private,
and priority in production, distribution and dispensing should be given to these essential
drugs.
5.
The public sector should produce essential and life saving drugs on a priority basis at the
national level.
6.
Drug production by multinationals and private manufacturers in India should also be aligned
with national health priorities.
7.
Bulk procurement of essential and needed drugs should be through world-wide competitive
tenders and rationalization of drug purchases should govern both the public sector as well as
private health sector.
8.
Imports and production of non essential, specially hazardous drugs, should be strictly curtailed.
9.
Drugs which have been banned from sale after being marketed for some time in one country
may not be submitted for clinical trial or marketing in India. The onus of proving why a
non-essential drug should be introduced or allowed to continue on the market should be
with the manufacturer and such introduction should be proceeded by adequate trials and
evaluation by Drug Control Authorities.
2
10.
Comprehensive drug legislation which covers areas such as price control at different levels,
patents, and marketing practices should be incorporated to serve the objectives of the national
drug policy and there should be no levies, sales tax or excise duty on any pharmaceutical
product in the essential drugs list by the Central or State governments.
11.
No technology transfer agreement shall be legal and binding which contains restrictive
practices, disproportionate and unnecessary use of imported intermediaries or obselete
technologies or unfair arrangements with respect to prices, payments or repatriation of profits.
12.
The National Drug Policy should state clearly the steps towards a complete abolition of brand
names and as a first step use of generic names should be made compulsory in medical
education, prescribing and labelling of drugs. Generic names should appear more pominently
on all packagings.
1 3.
It shall be the primary responsibility of the manufacturer to ensure the quality of drug products.
However, it shall be the statutory responsibility of the Drug Control Authorities to moniter the
standards and ensure a minimum uniform level of government control. Consequently, the
government shall take all necessary measures to enable the Drug Control Authorities to
function in an effective manner and discharge the statutory duties cast upon them.
14.
It shall be the statutory duty of the drug control authorities to inform health personnel and
consumers of the essential drugs lists, policies, categories or brands of drugs banned for
manufacture or sale, through publication in the national newspapers, magazines, medical
journals with adequate explanations and details.
15.
Availability of drugs required in the Governments National Programmes should be ensured on a
priority basis to the government as well as voluntary and private health institutions. Quotas
for anti TB, anti leprosy, anti malarial drugs, iodized salt etc. should be made easily available
with regularity of supply to the voluntary health institutions wherever possible, specially when
their performance, in health care delivery is known to be effective.
16.
In all review committees, statutory bodies and other such bodies, there should be adequate
representation of consumer groups and voluntary health sector.
17.
Drug companies should follow ethical marketing practices, and this should be ensured by their
own organizations like OPPI, I DMA, IFPMA. We deplore the tendency of these companies
and associations to get around every progressive measure of the government through recourse
to technicalities of the law and through the courts.
18.
The marketing code drawn up by HAI (Health Action International) should form the basis for a
National Code for Marketing Practices. This should be accepted by our government and
should be suitably implemented through legislation.
19.
The government of India should take a lead and endeavour to influence the WHA and WHO
to adopt the Code in the interests of the other developing countries and their peoples.
(IFPMA and HAL Code attached)
— Voluntary Health Association of India
— Centre for Science and Environment
3
— Centre of Social Medicine and Community Health—Jawaharlal Nehru University.
— Catholic Hospital Association of India
— Kerala Sahitya Shastra Parishad
— Medico Friends Circle
— Arogya Dakshata Mandal
— Lok Vigyan Sanghatana
— Consumer Guidance Health Services
— Consumer Education Research Centre
— Federation of Medical Representative Association of India
— Health Services Association, Calcutta
— Drug Action Forum, Calcutta
— West Bengal VHA
— Andhra Pradesh VHA
— Drug Action Forum, Hyderabad
— People's Participation in Science & Technology Madras, Bangalore.
4
Tel: 310694, 322064
Catholic Hospital Association of India
CBCI Centre, Goldakkhana, New Delhi 110001
SECOND ANNOUNCEMENT
41st Annual Convention of CHAI and Workshop on Drug Issues.
I.
Programme
23 (Friday) to 25 (Sunday) November 1984 : Meeting on —
“TOWARDS A PEOPLE ORIENTED DRUG POLICY”
26 (Monday) November 1984 : Annual General Body Meeting.
2.
Venue
St John's Medical College, Bangalore 560 034.
3.
Participants
Members of CHAI and special invitees.
4.
Theme
The Indian Council of Medical Research and the Indian Council of Social Science Research have warned in their
“Health for All” report that “Eternal vigilance is required to ensure that the health care system does not get
medicalised, that the doctor-drug producer axis does not exploit the people and that the abundance of drugs does not
become a vested interest in ill-health”. This meeting is to understand the issues relevant to drug prescribing, drug
distribution'and pharmacy policy in our institutions in the context of the above warning.
5.
General Objectives
5.1.
To inform and make aware the CHAI members of the background to the above problem highlighted by the
Indian Council of Medical Research/Indian Council of Social Science Research.
5.2.
To challenge them to participate in the growing national response to the problem through a —
a) continuing study of the problem;
b)
5.3.
6.
commitment to action at an individual, institutional, regional and national level.
To do this in the light of CHAI’s new vision and in keeping with the Church’s option for the poor.
Specific Objectives
WHAT IS THE PROBLEM ?
6.1. To create an awareness of —
a)
the health situation in India
b)
the role of drugs in health care
c)
the pattern of drug production in India vis a vis the people’s health needs
d)
the dynamics of the drug industry
e)
the patterns of drug distribution/availability in the health system
f)
the national drug policies and laws.
6.2. To create an awareness of the growing —
a)
irrational use
b)
over use
c)
misuse of drugs by health personnel
6.3.
To look at the above issues within the context of the CHURCH HEALTH SERVICES.
-!.
6.
To try and understand the problem from the people's point of view.
HOW/WHY THE PROBLEM ?
6.5.
At the broader level to discover the social, economic, political, cultural and other factors responsible for this
problem.
6.6.
At a personal level to discover how all of us are part of the problem at the individual and the institutional
levels.
WHAT TO DO TO TACKLE THE PROBLEM ?
6.7.
6.8.
To consider the various responses at nationai/international levels by groups/institutions/governments in the
areas of —
a)
consumer awareness and people’s movements
b)
continuing professional education
c)
pressure groups on policy makers
d)
search for low cost alternatives
e)
individual/group action
f)
institutional policy changes
To discuss ways and means by which participants can respond to this problem at
a)
individual,
b)
institutional, and
c)
reeional/national levels
and identify ways and means by which follow up action will be taken on this growing commitment.
AN APPEAL
We request all member hospitals and dispensaries to send representatives who are involved with drug
prescribing and or pharmacy policy in their institutions. These may be doctors/nurses/pharmacists or policy makers.
A preparatory check list of how to study the drug situation in your institution will be featured in the special
issue of MEDICAL SERVICE—October-November 1984. Participants should use it to study their local situation
so that their participation will be more meaningful. The special thematic issue will also give adequate background
material for the meeting.
— EXECUTIVE DIRECTOR
Catholic Hospital Association of India
* For further information/suggestions on the theme, write to :
Drs Ravi & Thelma Narayan
Community Health Cell
326, 5th Main I Block
Koramangala, Bangalore 560 034.
* For further information on registration/accommodation/ticket arrangements etc., write to :
Sr. Anna Maria
Secretary
CHAI Annual Convention Committee 1984
St. Martha’s Hospital, Nrupathunga Road
Bangalore - 560 009.
Group Discussion on Prescribing Policy - Groups Bl & 01
Questions to be pondered about
1.
Can a Hospital devise a formulary of good quality,
cost medicines?
low
Can this be common for all Voluntary Hospitals?
2.
Hou can prescribers' compliance be ensured or is freedom.
of prescribing likely to make this impossible?
Can we ensure Health Workers' compliance with their
formulary (medicine list)?
Will doctors also prescribe from this list?
Is it possible to prevent prescriptions to medical shops
being given?
3.
Where simple low cost drugs will not be sufficient, how do u
we subsidise to all or those who need help most?
Should all patients contribute to the cost of medicines?
-------- If s.o,_ h-ou?
4.
Will a Pharmacy Committee, including Doctors, Administrators
and Pharmacists help in implementing cost control or
quality control policy? (in most Hospitals medicines arc
the second largest item of expenditure'„)
5.
Have we asked our pharmacists to research costs?
does he know how to do so?
Have we provided tools for the job?
If so,
If so,
what tools?
6.
Are bulk drugs purchases possible on a group of Hospitals-base?
What methods can we devise for obtaining low cost drugs
either for one or many Hospitals?
7.
Do we consider proper stock control, record keeping and
auditing of medicines, purchase and distribution:
a)
unnecessary expenditure
b) essential?
What are our reasons for our attitudes?
8.
In many Hospitals the Pharmacy is an important income
producing section.
Will a switch to low cost drugs raise
cost or make it instead a burden on the Institution?
9.
Is the production of medicines in the Pharmacy :
a)
too time consuming
b)
too costly in terms of personnel or equipment
c)
uneconomic?
(Broadly thinking of two types: non sterile prescriptions
and sterile prescriptions)
How would you advise your
Hospital Management?
^4
Primary Health Care
In the game of life and death many people in the world
ore playing against the odds:
f
O 1 In 2 never 3©o a trained health worker
O 1 in 3 ar© without°cl0an drinking water
G 1 in 4 have an inadequate diet
Every year diarrhoea kills 5 million under-fives; malaria k.’ls one million people in
Africa alone. These and other killer diseases are preventable. Doctors and
hospitals offer cures for some. But what can really change the survival odds is a
package known as Primary Health Care (PHC).
DISEASE
CONTROL
WATER AMD
SAE3ITATIO8
surmnoa
O Around two-thirds of
under fivas in the poor
world are rmalnourished
PhC rroana ensuring an
oooiurte affordable food
suppiv and a bolancod
j
0 80% of the world's
disease is related to lock
of safe water and
sanitation.
PHC morns providing
everyone with claan
water and basic
sanitation
<
CHILD
"ULTh
o Some 5 million
children die and another
5 million are disabled
yea/ly from 6 common
childhood diseases.
° O*" half
'"“III.,,
ch"«b,nh
PHC moans
Immunisation against
childhood diseases
and combatting
others like malaria.
iP.ADITIONAl
'■"MEDICINE
HEALTH
EDUCATION
j
bodgets are spent on
drugs.
frugt to 200 essentials,
preferably locally menufactored, and made
a cost they can afford
, 000 n-.'
,boe»
.,ch vea'
,Bop'e ,n lb
un33°^ ol l>‘
odd ■n’«'ed
ol acu'e
hook'«o"r
o Traditional btnh
attendants deliver 60% 80% ol babies m the
developing world.
PHC means enlisting
traditional healers,
giving additional
training and using tradi
tional ^medicines.
nea^d
dtagnos®
Preventing ill
health depends on
changing personal
and social hab«ts
PHC means
educating people in
understanding the
causes of ill health
end promoting their
common
THE WINNING HAND
The eight elements of Primary Health Cara give
everyone - ydung children and poor people
especially - the beat chance of winning the fight
for life.
The coat of putting PHC into practice world
wide is an extra S50 billion a year less than twothirds of what the world spends on cigarettes,
and only one-fifteenth of world military
expenditure
► 000 B ■UTRlTlOa
from: WHO prass kit, •Prograw In primary haalth cara: ravlaw of a atutfy’,
10.10.83
ESSENTIAL DRUGS NEEDED AT THE COMMUNITY LEVEL
NAME OF DRUG
USE
1.
Aspirin
As analgesic, as antipyretic, in rheumatic
arthritis, etc.
2.
Chloroquine
In malaria, amoebiasis, giardiasis, taeniasis
(tape worm infestation), in the acute manifestations of lepra reaction, etc.
3-
Sulphonamides
In bacillary dysentery, urinary tract infection,
meningococcal meningitis, chancroid, trachoma
and inclusion conjunctivitis, etc.
4-
Streptomycin
In tuberculosis, urinary tract infections,meaningitis, bacteriemia and bacterial endocarditis,
respiratory tract infection.
9
Penicillin
In respiratory tract infection,, rheumatic fever.
meningitis, osteomyeelitis, otitis media etc.
6.
Isoniazid
In tuberculosis.
7-
Thiacetazone
In tuberculosis.
8.
Dapsone(DDS)
In leprosy, P.Falciparum (malaria )
9-
Piperazine
In roundworm infestation, also in threadworm
infestation.
1 0.
Mebandazole
Anti-helminthic
1 1.
Diodohydr oxyquinoline
In amoebiasis.
1 2.
Metronidaz ole
In intestinal and hepatic amoebiasis, trichomoni
asis, giardiasis, etc.
w
Ferrous sulphate
In iron r.ficier.cy. anemia.
1 4-
Vitamin A
In Vitamin A deficiency, prophylaxis, etc.
1 5-
Vitamin B Complex
In generalised avitaminosis B, or deficiency
of any vitamin of B-Complex group as in prophylaxi:
1 6.
Thiocarbamazine
Filariasis.
17.
Sulphur ointment
In scabies, psoriasis, ring worm infestation,
lupus erythematosus, etc.
1 8.
Oral rehydration salts
In dehydration
These essential drugs are in keeping with the present disease pattern
in the country hut are available in very limited quantities, There is no
official study estimating the actual requirement of these for the country
as a whole.
Source: Health for All an alternative strategy.
326, V Main, I Block
Koramangala
Bangalore 560034
To ?
The Members of the Faciliation Team
26 OCT 1984
Dear
Further to our letter of 12th September 1984, we had the
first meeting of the facilitation team (for the CHAI Annual
Meeting on 'TOWARDS A PEOPLE-ORIENTED DRUG POLICY12), on
6 October 1984 at St John's Medical College. There were
some interesting preliminary discussions and it was decided
that a short Workshop would be held on 3 Nov 1984 for the
members of the facilitation team to bring them up-to-date
on all the information relevant to the theme of the Workshop
and also to decide together further details of the dynamics
of the CHAI annual meeting on 24-25 November 1984.
I.
Details of the meeting
Date?
Saturday, 3rd November 1984
Time?
11.00 am to 6.00 pm
Venue? Rooms 116-117, Ground Floor, St John's Medical
College, Bangalore
Programme
To identify as a team?
(al What is the problem
i.
ii.
Drug Policy in India Vs. Health Situation.
Irrational use, overuse, misuse of drugs
(b) Why/how the problem
Social, economic, political and cultural factors
responsible for the situation at i» broader level - national
ii. personal level - institutional/professional
(c) What has been done,to tackle the problem
?consider various responses at regional/national/
international levels in the areas of—-
/
/
1. consumer awareness and ©people4s movements
2. continuing professional education
3. pressure groups on policy makers
4. search for low cost alternatives
5. individual/group action
6. institutional policy changes
/II.». P rep a r a.t ion/Background
(a)
You must have received the following background
papers?
1. I>rug Pushers or Healers
2. Consumer Alert—Consumer Action
2
2
3.
Towards a People-Oriented Health Policy
(a Bangladesh Case Study)
4. Community Health Programme ; The new vision of CHAI
5. CHAI Annual Convention ; Second Announcement,
giving details of general/specific objectives of
Workshop
6. MEDICAL SERVICE (CHAI monthly)—MAY-JUNE, JULY, AUG
issues (refer People, Pills and Prescription column).
The
(b)
following eight papers will reach you hopefully
before the 3rd Nov 84 from the Voluntary Health
Association of India, New Delhi;
1.
2.
3.
4.
5.
6.
7.
8.
Our concern about drugs
Hazardous, banned, bannable and dumped drugs
Rationality in banning fixed dose combinations
Essential drugs - a demand for prioritization
Scientific scrutiny of some' over the counter drugs
Memorandum
Criteria of a Rational Drug
Drug Pricing and Pricing Policy
Threejournals
(c)
1.
3,
(d)
which highlight the problem recently -
World Health, July 1984; 2. The Herald Review, 7-14 Oct
The Journal of CMAI, September 1983
Copies of all the above materials and some other key
papers and publications of World Health Organization
and Drug Action Network (India) have also been kept
aside at a counter in the St John's Medical College
Library. You can contact Mr K N Kittur, the Librarian,
to refer to them.
Do find time to JLOok through as much of the material
as possible. Even a cursory perusal would be a helpful
preparation for the Workshop of the 3rd Oct 84.
For any further questions/suggestions, kindly contact us
(Phone 565484). Please intimate your participation or otherwise.
Looking forward to meeting you on the 3rd,
Yours sincerely,
Ravi and Thelma
PS; Lunch and tea will be provided
Copy to; 1. Fr Percival Fernandez, Secretary, CBCI Society
for Medical Education, St John's Medical College
2. Dr GM Mascarenhas, Dean, St John's Medical College
3. Fr Bernard Moras, Administrator, SJMCH
4. Dr AFA Mascarenhas, Medical Superintendent, SJMCH
5. Br Vincent, Administrative Officer, SJMC
•
6. Fr Claude D'Souza, Rector, St Joseph^, Bangalore
7. Fr John Vattamattom, Executive Director, CHAI
8. Sr Anna Maria, St Martha's Hospital, Bangalore
THE DRUG SELECTION PROCESS
*
How many different drugs are available?
What is the range of
drugs currently available? Are there 'duplicate drugs' — many
different drugs all of which serve the same purpose? Are there combinat.
-ion drugs for problems which could readily be treated with single
drugs?
*
How are the drugs selected?
Is there a formalized process or
is it informal? What criteria are used?
*
Is cost a factor?
Who selects the drugs and other pharmaceutical products for
public health programs? The indi idual practitioner? Local health
districts? Hospital pharmacists or therapeutic committees?
A procurement clerk at the national level'
A physician?
*
A national committee?
A pharmacist?
Are drugs bought by their medical(generic) name or by their
commercial (brand) name?
Do pharmacists and medical practitioners
understand the difference be ween generically-named drugs
and brand name drugs?
*
Are traditional medicines and local remedies available
in goernment health programs?
If so, how are they selected
for inclusion?
*
What kinds of drug information are available?
up to date and unbiased?
Is the information
Do pharmacists and medical practitioners
know where to look for information about drugs?
Sources Managing Drug Supply: Management Sciences for Health, pp.52
DISPENSING POLICIES AND PRACTICES
*
What conditions exist at dispensing points?
How are drugs
handled? How accurately and cleanly are drugs dispensed?
How concerned are health officials and health workers about the
quality of compounding and dispensing practices?
*
How often are patients improperly or infeffectively treated
because their medicines have been improperly compounded
or dispensed, or because drugs have deteriorated in inadequate
packaging?
*
At each level in the health care system, whois responsible
for the compounding and dispensing of drugs?
What training
do these individuals have in the principles and practices
of drugs compounding and dispensing?
How much supervision
do these indivudlas receive?
*
What types of pharmaceutical training are available in the
country? Are there standardized education curricula for
pharmacy personnel? Are experience requirements for dispensers
spelled out and reasonable, given the numbers and geographical
distribution of individuals meeting, or eligible for
meeting, these requirements?
*
What resources exist to attract sufficiently educated
individuals to pursue dispenser training and to what extent
can these individuals expect satisfactory remuneration for
the services they provide after completing their training?
*
Are wages and salaries adequate to effectively dissuade
dispensers from engaging in the illegal sale and distribution
of pharmacueitcals?
*
What kinds of packaging are used to dispense drugs to patients?
Is there any mechanized repackaging into course-of-therapy
packets?
In light of losses from poor packaging and the costs
of proper packaging, are there cost-effective alternatives
to present packaging methods?
Could more expensive containers
be recycled?
Source: Managing Drug Sup ly: Management Sciences for Health, p.430
DISPENSING POLICIES AND PRACTICES
*
What conditions exist at dispensing points?
How are drugs
handled? How accurately and cleanly are drugs dispensed?
How concerned are health officials and health workers about the
quality of compounding and dispensing practices?
*
How often are patients improperly or infeffectively treated
because their medicines have been improperly compounded
or dispensed, or because drugs have deteriorated in inadequate
packaging?
*
At each level in the health care system, whois responsible
for the compounding and dispensing of drugs?
What training
do these individuals have in the principles and practises
of drugs compounding and dispensing?
How much supervision
do these indivudlas receive?
*
What types of pharmaceutical training are available in the
country? Are there standardized education curricula for
pharmacy personnel? Are experience requirements for dispensers
spelled out and reasonable, given the numbers and geographical
distribution of individuals meeting, or eligible for
meeting, these requirements?
*
What resources exist to attract sufficiently educated
individuals to pursue dispenser training and to what extent
can these individuals expect satisfactory remuneration for
the services they provide after completing their training?
*
Are wages and salaries adequate to effectively dissuade
dispensers from engaging in the illegal sale and distribution
of pharmacueitcals?
*
What kinds of packaging are used to dispense drugs to patients?
Is there any mechanized repackaging into course-of-therapy
packets?
In light of losses from poor packaging and the costs
of proper packaging, are there cost-effective alternatives
to present packaging methods?
Could more expensive containers
be recycled?
Sources Managing Drug Sup ly: Management Sciences for Health, p.430
PRESCRIBING PRLCTICES OF MEDICAL PRACTITIONERS
*
What are the prescribing habits of health workers like? Are
expensive or brand name drugs used when less expensive drugs would
provide comparable efficacy and safety? Are drugs dispensed for
conditions on which they have no therapeutic effect (such as antibiotics
for the common cold)?
would do the job?
indications?
*
Are two or more drugs used when one drug
Are drugs generally used for the correct
In the correct dosages?
What training do physicians, community health workers, and other
medical practitioners receive in pharmacology and therapeutics?
Is this training adequate in terms of its content and length?
Is
this training reinforced in practice?
*
Are there local treatments of choice or standard norms for
treatment?
If not, would such norms help improve drug use? If
treatment norms exist, howwere
such norms established?
What sources
of information and advice were used to determine the norms?
Are
the treatment norms followed?
*
What materials are available to practitioners for reference on
therapeutic indications, dosages, or side effects? Are these materials
published by drug companies?
By scientific bodies?
Are there any
locally written therapeutics manuals?
*
How do medical practitioners learn about new drugs?
company representatives?
Through drug
Through local drug news periodicals?
Through specialists, colleagues, or superiors?
*
Are physicians, community health workers, and other medical
practitioners aware of drug costs? Is cost a consideration in
prescribing decisions? Is drug cost mentioned in medical and
auxiliary training?
*
Are prescribing privileges limited by the prescriber's level
of training or by the type of health facility dispensing the drugs?
If not, would such limitations Improve drug use?
these limitations reasonable?
If so, are
Do they allow practitioners to
function within their levels of expertise, without exceeding the
limits of their training or ability?
*
Are there local hospital, district, or regional drug committees
which review drug selections and drug use patterns at various health
facilities?
If so, what are the responsibilities and duties of
these commi tees?
How active are they in promoting judicious
economical drug use? Who serves on the committees?
Are there limits on the amount of medication that can be
dispensed at any one time?
Are- these limits reasonable
or do they result in suboptimal treatment or potentially
serious diseases?
Sources Managing Drug Supply: Management Science for Health,
.402
DRUG ACTION FORUM, WEST BENGAL
S/3/5, Srabani, Sector-Ill, Salt lake, Calcutta: 700 064.
ANNOUNCEMENT
Dear Doctor.
................................
Of the drugs that are being marketed in our country, approxi
mately 60%
are either unscientific, harmful, substandard or banned.
Doctors have to depend mainly on the drug companies for information
about drugs.
Tall claims (often false) are made by drug companies
about these drugs while all the harmful side effects and constrain-
dications are not placed before the doctors.
Drugs Action Forum, West Bengal is going to publish a quarterly
journal on Drugs and Rational Therapy which will also contain infor
mations on harmful, banned and unscientific drugs.
The journal will
function under the guidance of an advisory body comparising of some
members of All India Drug Action Network (AIDAN) and other noted
doctors of the country.
Doctors and health personnel are likely to
be benefited.
Annual Subscription Rs. 12.00 (Four issues).
Bank drafts in favour of Drug Action Fonam, West Bengal or
Money orders for subscription may kindly be sent to the following
address:
(Please do not forget to mention your name and address in
M.O. coupon).
Dr. P.K. Sarkar, Editor
JOURNAL OF DRUG ACTION FORUM, W.B
254, Block-B,
Lake Town, Calcutta: 700 089.
are you harming
r
h^ll •'
?
BRAIN TR. ST ON HEALTH Ija^ES.
It is the responsibility of the canaunnx
*
to lee
*r»
the haxerd'
*
of dcugs end chemicals used in daily life, not only to enfegaard
themselves but to work collectively to • • to free policy makers
and manufacturers to remove definitely harmful drugs and cheAieala
from the market or to devise an effective warning ayatam so that
these substance are not *
misused
The message was strongly conveyed
□y the members of panel of Brain Trust Society of India at Indian
Merchants Chambers, Committee room on 10th March 1904. Membersaof
□ anel included Dr.Pawan Sureka,Chairman of Medical Committee of
Consumer Guidance Society of Indie, Dr.T.R.Motwanx a Senior
isxxxSurgeon at Jaslok M Hospital, Dr.S.Adranwala .President of
Bombay opthaImologiat’s Society, Dr.Dinesh Daftary, a dantal
surgeon and Honorary oral pathologist at Tata Institute of Fun
damental Research, Dr.W.S.Rane Joint Honorary Secretary of Bombay
Arogya Dakshata M->ndal, Dr
*
G.S.Hsthi, a Child Specialist and
Ir, N.G.Wagle, Consultant
eh&mioal Tochnologiat.
JAIN KILLER DR'.'GS,
Analgin, a.n pain killer drug (Novalgin, Baralgan,Ultragin,
h'eurolicn etc.) can cause damage to bone marrow causing deficiency
of ±hite blood cells, "Agranulocytosis," a potentially fatal condi
tion.
A doctor who had himself taken just two tablets containing
analgin, developed a.;r.,<nulocytosia and could survive with difficult
after a fight of nearly six months under intensive medical care
*
Analgin has been banned in number of countries including Bangla-
Desh but continues tc be mnr.ufactored even by public pharmaceutical
companies and is freely available in the market without any warning
syatrm to consumers. Pain ia a subjective phenomenon and certain
natural methods like taking rest, message with gentle hands, going
out for a walk 'diversion of mind ate., are preferably to taking
drugs.
Similaraly sponging of the body with witsr or ice cold packs
are better for symptone relief of fever and shoyld be used as a
primary measure. Fever i-d basically body’s defense mechanism and
straps should be on proper diagnosis of cause of fever and specific
treatment of that causo.Paracetamol( ‘me tacin , Crocin, Pyrigesic etc)
is relatively sag® drug and can be usad for relief of pain er fever .
Aspurin another drug( e.g. Disprin) when taken should be consumed wit;-.
t
glass f«i 1 of water or milk and preferably aflter food.
Unfm
the .market is being flaoddd by drug eombinaxions of either use
sr ■ •r:nful
OcrurC-e. '
6 6S/
medicines and it.may sometimes difficult to get sinq
. mats
s
The World Health Organization says:
r j
number ©ff medicines, which are off
ira© vaBsui© and are even dangerous, are often given
to treat diarrhoea. Money and time are
wasted in their use. 99 So...
r '
WKO SSVS UBOTL
has Ndvows?
LOMOTIL (diphenoxylate/atropine) is made by the US
multinational drug company, G.D. Searle; and
promoted to physicians all over the world in terms
such as "established success”, “good tolerance”,
"excellent value” and "ideal for every situation”. This
leaflet — prepared and published by Social Audit Ltd.,
and friends
*
— calls into question these claims.
LOMOTIL may be of value in giving symptomatic relief
for non-specific "travellers’ diarrhoea” in adults. But
experts say Lomotil — and other products like it2 —
have little or no place in the treatment of young
children — especially in developing countries, where
Infective diarrhoeas are the major cause of death in
children aged under three.' Lomotil's limitations
include:
[DOO Ol)0 000108
Lomotil
POTENTIAL DANGERS
QUESTIONABLE USEFULNESS
“Lomotil, which is widely used In the
treatment of diarrhoea in the paediatric ago
group, is dangerous and unwarranted . . .
we urge that all physicians treating Infants
and children avoid the potentially dangerous
use of Lomotil for the treatment off
diarrhoea.”
“The use of Lomotil as an antidiarrhoeal
agent in children is difficult to justify . . . wo
doubt If it has any place in the treatment of
diarrhoea in children.”
(Clinical Notes [1974])1
“Lomotil can relieve the symptoms of acute
gastroenteritis in children, but It can also
mask the signs of dehydration and cause
fatal toxic reactions . . . use of this
combination for treatment of diarrhoea In
children Is hazardous.”
(The Medical Letter [1980])4
(Arch, of Dis. in Child. [1979])6
“A diarrhoea that needs 4 such tablets to be
cured would probably have been cured
without it too. A more prolonged diarrhoea
needs proper Investigation and specific
therapy rather than a blindly harmful
stopcock.”
(Leb.Med. J. [1974])’
ECONOMIC WASTE
Lomotil costs up to 25 times more than other
widely-used symptomatic treatments for
diarrhoea.
“Lomotil is a dangerous combination of
drugs contra-indicated for children under 2
years of age and probably never indicated in
childhood diarrhoea.”
(AMREFJ1980D8
(Pediatrics [1980])5
“Lomotil (no value).” (WHO [1976])'
TV <2. VASe
LovaoVlI
SLX
is
Lomotil
HOW USEFUL . . .
“The management of acute diarrhoea In
childhood is essentially dietary . . .
Unnecessary drug prescription fortheso
chldren should be vigorously opposed.”
(The Lancet [1976])9
. . . Against Dehydration?
“The cause of death In diarrhoea Is
DEHYDRATION . . . Diarrhoea is the most
common cause of death in children under
throe years of ago . .
(WHO [1976]) ‘
LOMOTIL is not a treatment for dehydration. It
may reduce the loss of fluid from the body but
can also allow fluids to accumulate in the
paralysed gut.
“LOMOTIL can mask fluid losses without
diminishing them, and the drug itself can
cause fatal adverse effects . . . there is no
evidence that reduced motility diminishes
the loss of fluid and electrolytes into tho
lumen of an Inflamed intestine.”
(The Medical Letter [1975D4
The accumulation of the body’s vital fluids within
the intestine can be just as dangerous as the
more obvious dehydration:
“In diarrhoea, Hfe-threatenlng situations
are reached ... so long as fluid and
electrolytes are excessively lost into the
lumen whether they are expelled from the
lumen to the outside of the body or not. . .”
(J. of Singapore Ped. Soc. [1976])'0
Small feeds of water (or a weak electrolyte
solution) given frequently by mouth is the only
first-line treatment against serious childhood
diarrhoea. If this fails after 24 hours, intravenous
therapy and hospitalisation may be needed.
... Against Infection?
“Acuta diarrhoea In children is usually
Infective, but antibiotics and anti-diarrhoeal
drugs rarely help.”
(Drug and Ther. Bulletin [1978])'1
LOMOTIL Is widely and often successfully used
by adults as a symptomatic treatment of
bothersome, non-specific ‘‘travellers’ diarrhoea"
(which is rarely serious). But in children infective
diarrhoea is serious. LOMOTIL prevents the child
from getting rid of the infective agent and may
prolong the period of infection.'2
“In patients with Infective diarrhoea, the
use of constipating agents make tho carrier
state last longer by stopping the organism
from being excreted.”
(AMREF[1980D8
A comparison between LOMOTIL and a placebo
in treatment of an infective diarrhoea reported
that:
“Febrile volunteers receiving Lomotil
alone experienced over a day more fever
than those In other treatment groups,”
suggesting that “drugs that retard gut
motility may facilitate Intestinal
Infection...”
(JAMA [1973])’3
HOW SAFE?
“Because of Its depressant effects it Is no
longer recommended for children.”
(Brit Med. J. [1976])'4
LOMOTIL poisoning in children can include
atropinism, respiratory depression, coma, and
even death. Symptoms can appear even at near
therapeutic doses:
“Lomotil Ingestion is a cause of serious
poisoning In young children, especially those
aged under five. It Is always hard to assess
the dose In patients suffering from
poisoning, but it seems that young children
may develop pronounced symptoms after
taking only one to five tablets.”
(Brit Med. J. [1977])'5
The difference between therapeutic and toxic
dose is unpredictable:
“We were unable to find a correlation
between the severity of symptoms and the
dose Ingested. Because of this It Is not
possible to predict what dose will be toxic In
children, and while some may have only the
mildest symptoms with relatively large
dosos, others develop sovoro toxicity on
ingesting an amount noar the normal doso.”
(Arch, of Dis. in Child. [19790s
“Thero Is a very narrow range botweon
allegedly therapeutic and toxic dosagos, and
many cases of toxicity In children have been
"/oportod.”
(Pediatrics [1980])s
“Tho narrow margin between therapeutic
and toxic doses, and tho high Incidence of
atropine hypersensitivity, make Lomotil a
potentially dangerous therapeutic agent.”
(Clinical Notes [1974])3
“Tho dangers off this drug to children havo
not boon well recognised. Tho narrow range
between therapeutic and toxic doses, and
also tho possibility of a child being
abnormally sensitive ... may account for tho
severo toxicity sometlmos soon with low
dosage.”
(Clinical Pediatrics [1973])'6
DESPITE THE DANGEROUSLY VARIABLE
RESPONSE, SEARLE’S RECOMMENDED DOSES
FOR INFANTS AND CHILDREN AND THE
PACKAGE WARNING INFORMATION VARY
AROUND THE WORLD.
In the US, LOMOTIL is contra-indicated for
children under two years old.
“This warning by tho manufacturer Is not
because there has been inadequate
paediatric testing of the drug but rather
because severe hfe-threatening reactions
(which are not rare) occur In this age group.”
(Am. Fam. Phys. [1976])'’
In Britain, however, the makers recommend it for
one-year-olds; and in Hong-Kong, Thailand, and
the Philippines it is offered for infants of three
months old.
• typically, no adverse reaction reporting systems
exist; and
• drugs such as LOMOTIL (available only on
prescription in the West) are in practice freely
available over the counter.
HOW EXPENSIVE?
The cost of the smallest available size of
LOMOTIL would for many people in developing
countries be equivalent to at least one day’s
income. Other effective preparations for
symptomatic treatment of diarrhoea' ■•'9 cost
much less.
According to the African Medical and Research
Foundation (AMREF), the cost of treatment with
LOMOTIL is about twice the cost of treatment
with codeine syrup orcodeine phosphate.
Treatment with a kaolin mixture, which may also
give relief20, costs about 25 times less.
*
LOMOTIL WITH NEOMYCIN (an antibiotic)
is recommended by Searle for the treatment
of “diarrhoea of bacterial origin." This is
unacceptable:
“Antibiotic and sulphonamide
preparations should be avoided for the
treatment of diarrhoea even when a
bacterial cause is suspected because
they may prolong rather than shorten
the time taken to control diarrhoea and
carrier states.”
(BNF[1981])2'
“Neomycin not only can cause renal
damage, but also it makes diarrhoea,
dehydration, and nutritional losses
worse and could interfere with oral
rehydration therapy.”
(Population Report , 1980)22
Special circumstances in developing countries
compound the potential danger of treating
Infants with Lomotil in this way. In developing
countries:
children are relatively lighter than those of the
same age elswhere;
the amount of medical supervision is greatly
lower,
“Medicines which should not be used
In the treatment of diarrhoea:...
Neomycin...”
(WHO (1976D9
Treatment with LOMOTIL plus NEOMYCIN
costs about three times more than
treatment with LOMOTIL alone.
REFERENCES:
World Health Organization: Treatment and Prevention of Dehydration in Diarrhoeal Diseases (A Guide for
Use at the Primary Level) (Geneva: WHO, 1976). LOMOTIL is one of 9 treatments not recommended.
The same preparation is sold by Janssen Pharmaceutical Ltd. and known as “Reasec". Other proprietary
names: Diarsed (Fr.); Retardin (Swed.). (Source: Martindale’s Extra Pharmacopoeia, 27th Edition).
3
Drake M E, & Drake M E Jr.: "Lomotil Intoxication in Pediatric Patients" (in) Clinical Notes (June 1974)
pp. 501-2.
4
"Lomotil for Diarrhoea in Children” (in) The Medical Letter (iss. 25,1975) p. 104.
5
"Delayed Cardiopulminary Arrest after Lomotil Ingestion" (in) Pediatrics (Jan 1980) pp. 157-8.
6
Curtis J A, & Goei K M: “Lomotil Poisoning in Children" (in) Archives of Disease in Childhood (iss. 54,
1979) pp 222-5.
7
Uthman S M’ “Some Complications of Diphenoxylate Hydrochloride with Atropine" (in) Lebanese
Medical Journal (iss. 27/5,1974) pp. 521-2.
3 Upunda G, Yudkin J, and Brown G: Therapeutic Guidelines (A manual to assist in the rational purchase
and prescription of drugs) (Nairobi: African Medical and Research Foundation, 1980) p. 96.
9 "Drugs for Acute Diarrhoea in Childhood" (in) The Lancet (Nov. 20,1976) p. 112.
•10 Wong Hock Boon & Michael Toh Ho Sing: "Lomotil Poisoning” (in) The Journal of the Singapore
Pediatric Society (April 1976) pp. 34-7.
11
“Diarrhoea in Children" (in) Drug and Then Bulletin (Jan 6,1978) p. 2.
12
Pittman F E, “Adverse Effects of Lomotil” (letter to editor in) Gastroenterology (Iss. 67/2,1974) pp. 408-9.
13
Dupont H L. & Hornick R B: "Adverse Effect of Lomotil Therapy in Shigellosis" (In) Journal of the
American Med. Assoc. (Dec 24-31,1973) pp 1525-8.
14
Bell D R; "Diseases of the Alimentary System” (in) British Med. J. (Nov 20.1976) p. 1240.
15
Penfold D, and Volans G N. "Overdose from Lomotil" (in) British Med. J. (Nov 26,1977) pp. 1401-2.
16
Snyder R, Mofenson H C, & Greensher J: "Toxicity from Lomotil” (in) Clinical Pediatrics (Jan 1973)
pp. 47-9.
17
Wasserman G S: "Lomotil Ingestions" (letter to editor in) Am. Fam. Physician (Oct 1976) pp. 27-8.
18
Smits B J. "The Irritable Bowel Syndrome” (in) Practitioner (July 1974) p. 43
19
Collins C D: “Lomotil in Treatment of Post-Vagotomy Diarrhoea" (in) British Med. J. (Sept 3,1966)
pp. 560-1
20
Portnoy B L, et al. "Antidiarrhoeal Agents in the Treatment of Acute Diarrhoea in Children" (in) Journal of
the American Med. Assoc. (Aut 16, 1976) pp. 844-6.
21
Bntish Medical Assoc. &The Pharmaceutical Soc. of G.B., British National Formulary 1981, No. 1,
(London: The Pharmaceutical Press and the BMA, 1981) p. 40.
22
The Johns Hopkins University, "Oral Rehydration Therapy (ORT) for Childhood Diarrhoea" (in) Population
Reports (Issues in World Health) (Nov/Dec 1980) p. 54.
1
2
* SOCIAL AUDIT AND FRIENDS
SOCIAL AUDIT Ltd is an independent non-profit making action-research unit, concerned with
improving government and corporate responsiveness to the public generally. Its concern applies to all
corporations and to any government, whatever its politics. Social Audit has reported and campaigned
on a wide variety of public interest issues. Its interest in multinational drug companies and in
development is reflected in this leaflet — with hopefully others to follow — and also in the
publication of Insult or Injury? (An enquiry into the promotion of British food and drug products in the
third world, 1979); and Drug Disinformation (What British and other multinationals tell doctors about
their products at home and abroad, 1980).
This leaflet — for which Social Audit is wholly responsible — could not have been prepared and
published without the generous support given by:
War on Want, 467 Caledonian Rd., London N7 9BE, and Tho International Organisation of
Consumers Unions, Regional Office for Asia and the Pacific, PO Box 1045, Penang, Malaysia.
SOCIAL AUDIT LIMITED 9 POLAND STREET LONDON W1V 3DG
© Social Audit Limited 1981
Gxyvkx
j
L\oq ool .
O|0
The Crazy World of Tonics
Waterbury's Yellow Label Tonic, a brand leader in the Indian
tonics market, contains only 3 milligrams of iron per teaspoon
just 1/10 of which may be absorbed by the body. The Indian Council
of Medical Research (ICMR) recommends atleast 10 milligrams for women.
The producer claims that this tonic stimulates appetites and builds
bodies. But chemical analysis has revealed that it has 10% alcohol
I
content which is the real appetite-stimulant!
“The real culprits behind the 'tonic craze
*
are the manufacturers
of such formulations. The principal reason for their hard selling
of such products is the fact that the tonics and vitamins fall in
'category four' of the Drugs Price Control Act, which means that
there, is no limit on profits made on these preparations —. With
easy pickings and a readymade market, no wonder then that every
new company entering the pharmaceutical world wants to market its
own brand of tonic rather than any life-saving drug!
2
"The first part of the plan was the mounting of an intensive
sales campaign to influence doctors on the need for tonics in their
day to day practice. This was followed by free sampling
"
' -TH CELL
Explaining how the 'tonic craze' is the result of systematic
2
campaigns of the large companies, he says:
"The other part of the marketing gimmickry in selling tonics was
by directly advertising in the mass media, to catch the public eye.
Slogans like "Do you feel tired at the end of the day?
You need.\
Or "A woman needs iron every day" gradually made a deep impact on the
people until many were psyched into believing that they could not
do without a tonic."
We have noted that these tonics are not consumed by the poor but
2
0
2
mainly by the relatively rich whose ordinary diet adequately
meets their vitamin and other requirements. In recent years, evidence
has grown that the excessive vitamins may not simply be discharged
by the body but may even cause severe disorders. Prolonged
consumption of excessive vitamin C may form kidney stones, excessive
vitamin A may cause diseases of the hair, skin and liver and
vitamin D in excess may cause disorders of the kidneys and bones.
2
Take this further example from South East Asia. In the U.K.,
Sanatogen is marketed as a 'nerve tonic'
for old women who believe
in its doubtful ability to tranquillise. But Sanatogen Powder is
marketed to students in Malaysia who believe in its ability to
stimulate their minds. "Worried about exams?" says the advertisement.
Sanatogen will give you "greater energy and concentration". Can a
3
drug both stimulate and sedate?
Thus the sheer irrationality and deliberate exploitation of
consumers through this sinister "tonic racket" is obvious. The fact
that many such 'rackets' continue unabated is a measure of the
enormous influence and power of the large pharmaceutical corporations
not only in India but in many other countries, particularly the
developing ones.
"The incidence of disease cannot be manipulated and so increased
sales volume must depend atleast in part on the use of drugs
unrelated to their utility or need, or in other words, improperly
prescribed. Human frailty can be manipulated and exploited and
this is fertile ground for any one who wishes to increase profits.
The enormous sales of so-called tranquillisers are only a small
part of the crop reaped from this ground. The pharmaceutical industry
is unique in that it can make exploitation appear a noble purpose.
.3
References
1.
Health for the Millions, VHAI, April-June 1981.
2.
Manohar S. Kamath: Some Boost and at what Price?
The Daily Magazine, 7 May 1981.
3.
"The Impact of Multinational Corporations on Health in
Developing countries" by Charles Medawat. Seminar on Health
Food and Nutrition, Consumers' Association of Penang,
Malaysia, 15-20 September 1979.
4.
Drugs and the Common Man: Science Today, November 1970.
THE cost of modern drugs is invariably so high that
an overwhelming majority of the Third world »s
population cannot afford to purchase them.
IN developed countries drug costs represent only 10-20#
of the total health care expenditure. IN MANY DEVELOPING
COUNTRIES PHARMACEUTICAL COSTo REPRESENT 40-60#, It is,
therefore, importer.t that ways and means be found to reduce
the cost of drugs in developing countries
*
THE first thing for any country to do, according to WHO,
is to prepare a list of essential drugs
which they can
afford and which art. needed to met the basic health needs of
the majority of the population
*
But by restricting imports
to these drugs which m<et most of the health needs, and
abolishing the use of brand names for drugs in favour of
generic non-proprietary names, countries can obtain large
savings in drug costs
*
WHO’s Basic Drugs List contains about
200 drugs, subject co modification for national needs, and
according' to the Mahler-Labouisse report to Alma-Ata, “the
number needed for primary health care may be loi.er chan 2-0".
UNCTAD (UN Conference on Trede and Development) has proposed
that developing countries should increase their purchasing
power against the large drug companies. They should centralise
their drug imports via a single state-controlled Drug Buying
Agency, wherever possible, UNCTAD proposes that Third world
countries should also try to join one another and combine
their drug purchases. This will give them further bargaining
power.
*
•source
2
PRIMARY HEALTH CAREl Earthscan Press
Briefing Docyment No 9, July 197b pp 33-34.
2
SRI LANKA has tried such a strategy and obtained
considerable savings
*
SUCH regional purchasing agencies will take time to
set up. In the meantime, UNICEF, which has a substantial
drug purchasing programme of its own, offers to buy drugs
on behalf of developing countries.
UNIDO (UN Industrial Development Organization) is
meanwhile
trying to help developing countries set up
their own basic drug industries, at least for formulation
(tabletting, capsuling, etc) and packa ing drugs.
BOTH UNIDO and WHO feel that many druj needs can now be
met by the judicious use and production of tr editionally**
used herbs.
Many locally available medicinal plants
can also become the source for local production of drugs.
WHERE possible, the UN agencies also propose that developing
countries should cooperate to
>et up Cooperative Pharmaceu-
tical Production and Technology centr< s to produce drugs
for regional markets and help in pooled procurement of
drugs.
THESE ideas indicate the emergence of composite UN
strategy to m. et the pharmaceutical needs of developing
countric-s.
THIS strategy is clearly in conformity with the Nev.International Economic Order. It will also advance appropriate
technology, and the process of technological cooperation
among developing councri< s (TCDC)•
COUNTRY PROFILES
yietnai.i
Growth of plant-based pharmaceuticals.
Herbal gardens in villages.
State farms for medicinal plants.
40 new drugs from local herbs.
Sri Lanka
Bulk purchasing through state Pharmaceutical
Corporation (1372).
Adopted limited list of drugs (60u).
Restricted prescribing to generic names.
(Multi-National Corporations (MNCs)
blew up plan - 1978).
Pakistan
Generic prescribing (failed).
Bang 1 ad esh
1707 drugs banned
(June 1982) in three schedules
Schedule I
: 305 banned immediately.
Schedule II
4 1?4 banned after 6 months.
Schedule III 41268 to be manufactured locally
(Modifications on pressures from MNCs through
U.S.,British, Dutch, German embassies).
Mozambique
Restricted Drugs in Market.
China
Traditional Medicine and Horbal remedies
promoted as part of drug policy.
50 herbal medicines included in policy
Accupuncture promoted.
Bare-foot doctors.
quotes
1
"As commodities, prescription drugs behave
differently from most other items; they are products
that the ultimate consumer rarely selects for himself.
The producer’s sales effort are directed at the
"instrumental consumer", the doctor who prescribes butdoes
not pay for the product.....Physicians receive their
most intensive in-service from agents of the Chemical
Industry."
— Ivan Illich in ’Limits to Medicine'.
2.
"In 1973, the entire drug industry spent an average of
$4500 on each practising physician (in U.S.A.) for
advertising and promotion".
— Ivan Illich in ’Limits to Medicine'.
3.
Many developing countries have found that only 1 to 2%
of the drugs on their markets are essential for meeting
the basic needs of their people. The Joint Mission
Hospitals Equipment Board Ltd (ECHO), which supplied
essential drugs to Christian mission hospitals around the
world, found that about 25 generic drugs were adequate for most
patients in some 98 hospitals all over the thirld world.
— "Drugs and the Third World" Anil Agarwal
An Earthscan publication, 1978.
2
2
4.
As far as sub-standard drugs are concerned, there
is an urgent need to tighten up the drug control
machinery of the states. This will require larger
resources in the form of trained personnel and fully
equipped testing laboratories being made available
to the states. The Food and Drug administration of the
states need to be made more effective. It is well known
that sub-standard and spurious drugs originate largely
in those states where the drug control administration is
ineffective.
— Aspects of the Drug Industry in India
Mukaram Bhagat, 1982.
According to some estimates upto 80% of the present
output of many foreign drug companies comprises of
simple household remedies and inessential formulations.
Essential drugs like insulin, anti-leprosy drugs,
anti—TB drugs, vaccines etc., account for only 30%
of the value of formulations sold by many large firms.
— Drugs on the Market by Jug Suraiya
The Statesman, 8 December 1980.
3
3
On a world-wide scale, an estimated $2 billion are
spent annually on Research and Development in drugs
Of this, less than $70 million or 3.5% is spent
on tropical diseases. At the same time, over 1 billion
poor people or about 30% of the world’s population
are extremely vulnerable to these diseases.
— Drugs and the Thirld World, Anil Agarwal
7
In India, at present, some 20,000 branded medicines
are on the market, a large number of which are
considered irrational. The basic bulk drugs used for
their formulation number only 400. The Hathi Committee
considered just 117 generic drugs (0.6% of the number
of drugs currently marketed) sufficient for satisfying
the basic requirements of the country.
— Aspects of the Drug Industry in India,
Mukanram Bhagat
The Lavraj Kumar Committee, which investigated the profitability
of multinational drug firms during the 1970's found that
their research and development outlays accounted for only 0.83%
of their total costs, with the exception of only 2 companies,
against this, sales promotion, administrative overhead
expenses accounted for 33% of their total costs.
—Foreign Drug Firms Spend Too little on R & D,
The Hindu, 12 March 1980.
4
4
9
/A peculiar feature of the drug industry is that
the consumer is ’captive
.
*
He normally does not
possess sufficient knowledge to make his choice from
a bewildering array of branded products available on
the market. It is his physician who makes this choice
for him. However, the confusion is no less for the
pr scribing physician too: it isvirtually impossible
for him to make a rational evaluation of the thousands
of price and quality alternatives the market is flooded
with.
Further, most doctors can hardly find enough time to
keep abreast of all the latest pharmacological
developments in their respective fields through the
scientific journals. Thus the doctors mainly depend
on information provided by the large manufacturers
as part of their promotional campaign. As.one would expect
much of this information transmitted through beautiful
pamphlets and company medical representatives (the
ubiquitous salesman of the drug industry), is of doubtful
objectivity. In the enthusiasm to promote their products,
many 'ifs
*
and *
buts'
of vital importance are simply
left out in the promotional literature.
— Aspects of the Drug Industry in India,
Mukarram Bhagat.
"The physician who sets about to treat a disease without
knowing anything about it is to be punished even if he
is a qualified physician; if he does not give proper treatment
he is to be punished more severely; and if by his treatment
the vital functions of the patient are impaired, he must be
punished most severely."
— Koutilya Arthashastra
"There are two types of physicians:- those who promote
life and attack diseases:
those who promote diseases and
attack life.
-— Charaka Samhita
One West African study showed that more appropriate
prescribing could cut the drug bill by 70 percent. Most
of this money could be spent on generic drugs, but this
is resisted by the international drug companies who recruit
leading doctors to their cause with little difficulty. These
specialists, heavily involved in private practice, unite
with the pharmaceutical companies under a banner of 'clinical
freedom'.
— David Morley, Professor of Tropical Child Health,
University of London
Reporting in 1956 on the excessive amount of space taken
up by advertisements in Indian newspapers, the Indian Press
Commission commented:
"The largest field of
..Objectionable advertising
which we feel should be put down by law is of drugs and
proprietary medicines
The volume of advertising of
such commodities ranks next only to the volume of advertising
of cosmetics."
— Use and Misuse of the Media
Sumanta Banerjee, World Health, Feb-March 1983
"Because of the great differences between countries, the
preparation of a drug list of uniform, general applicability
and acceptability is not feasible or possible. Therefore,
each country has the direct responsibility of evaluating and
adopting a list of essential drugs, according to its own
policy in the field of health."
— WHO Technical Report Series No.615
Criteria for selection of essential drugs.
V i s u a 1 s
SI No
Theme
Source
Suggested positioning
1.
The World's Best Medicine
UNICEF
After editorial
2.
Living in two Worlds
Church & Social
With CHD team's
Justice (CSA)
article
3.
Dumping
Helping Health
With article
Worker Learn
Misuse/overuse of
medicines
4.
Rare Himalayan herb
Laxman cartoon
With article
and multi-national
Health Care
Misuse/overuse of
pill for headache
Which way to
medicines
Go
5.
Vicious cycle of
With medication as
medicine overuse
Helping Health
a substitute for
Workers Learn
caring
Laxman Cartoon
Health Care
Which Way to Go
_(mfc) _
With or before Drug
Not to be taken
HAI News
With "If there are no—
worthless
June 1982
6. Expensive yes
7.
(mfc)
misuse in our hospital:s
side effects this must
be Argentina"
8.
Who says lomotil has
Social Audit
Before "Crazy world
no value
Handout
of tonics"
(first page
only)
=—=
cs
S3 — 5= »S _ S3.—S3_S3_S3—
L&uiC/'.l ;'j;- 5CQ C
£3—
2
Sl_No
9.
Theme
Source
Suggested Positioning
Doctor, I have taken
Health Care
With "Crazy world of
the tonic
Which Way to
tonics"
Go? (mfc)
10.
11.
A person who eats
Health for the
With "Crazy world of
well does not need
Millions
tonics"
extra vitamins
April-June 1981
What is so new about
Health Care
With 'ORT - what are
sugar-salt solution?
Which Way to Go
the options"
(mfc)
12.
Judge with
The Herald
pharmacology book
Review, Oct 14,
With legal education
1984
13.
Bad information means
Social Audit
With or before "Consumer
bad medicine
(Health for the
Alert—Consumer Action"
Millions, AprilJune 1981)
14.
Remember medicines
Helping Health
With "Towards a Rational
can kill
Worker Learn
therapeutics".
ews from oxfam • news from oxfam • news fro
rom oxfam • news from oxfam • news from o>
m • news from oxfam • news from oxfam • nev
~■— —»-
Press Office • 274 Banbury Road • Oxford 0X2 7DZ
— -—__
Telephone (0865) 56777 • Telex 83610
EMBARGO 11.00 am THURSDAY, 25 NOVEMBER 1982
THE POOR SUFFER THROUGH MULTINATIONAL DRUG COMPANIES' MARKETING PROFITABLE BUT
INESSENTIAL DRUGS IN THE THIRD WORLD, ARGUES NEW BOOK FROM OXFAM
The uncontrolled sale and promotion of drugs in most poor countries means that they
often do little good and can be positively harmful.
Major manufacturers are acting
irresponsibly in the Third World by ignoring the needs of the majority and not taking
responsibility for the safe use of their products.
Dangerous double standards have resulted in anabolic steriods being promoted as
appetite stimulants for malnourished children; an antidiarrhoeal drug banned in
Britain, because of possible crippling side-effects, is freely marketed in the
Third World and sold without warnings.
Antibiotics are sold on market stalls like
loose sweets, encouraging misuse and drug resistance.
For the Third World poor, the cost of basic life-saving medicines is astronomical.
The price of just twenty tablets of the top-selling antibacterial drug in Mexico
would provide a family of four with their basic diet for two weeks.
A small bottle
of an antibiotic syrup costs a poor Bangladeshi family the equivalent of £35 to a
British family earning £135 a week.
In Bitter Pills, Medicines and the Third World Poor, published by Oxfam on
November 25, Dianna Melrose investigates these alarming facts from the perspective
of the poor, drawing on her own field research, evidence from the manufacturers
involved and Oxfam's wide experience of poverty and ill-health in the Third World.
The poor suffer disproportionately from ill-health.
A few dozen essential
'generic' drugs could be used to save millions in the poorest countries from
unnecessary suffering and death.
The know-how to make these key generic drugs
has been available for decades.
We take them for granted in Britain, but the
majority of the Third World poor are denied them because drugs are produced and
sold for profit rather than on the basis of real need.
The rich world dominates
2
drug production.
Aggressive promotion means that the most expensive brand-name
drugs usually sell best.
The poor are therefore forced to pay unnecessarily high
prices and subsidise new drugs for the rich.
Bitter Pills documents the abuses caused by weak controls and reveals that some
manufacturers - including some based in Britain - are not as scrupulous as they
should be in ensuring that Third World patients and prescribers get full information
on their products.
Some even resist moves to introduce tougher controls in the
Third World that they must comply with in Britain.
The book describes some of the positive initiatives taken at local, national and
international levels to rationalise the use of drugs as part of a broader strategy
for better health - recognising that disease which is rooted in poverty can only be
combatted by an onslaught on poverty itself.
It documents the major obstacles that
Third World governments face in trying to crack down on the drug market.
Rich
world manufacturers and their governments have lobbied to block changes that
would benefit the poor.
Practical suggestions for change are addressed to three groups:
Firstly, if the
poor are to benefit, Third World governments must give priority to preventive
and primary health care rather than to costly hospital services.
The private
drug market should be controlled to safeguard health and priority given to purchase
and manufacture of essential drugs.
Rich world governments should actively encourage Third World governments to adopt
the WHO recommendations which, in theory, they have supported.
They could help
Third World governments make informed choices about drug risks and benefits by making
more information available at little cost, and introducing controls to discourage
exports of dangerous and inessential drugs.
Official health aid should not be tied
to purchases of expensive products and high-technology medical services; and
voluntary agencies should strengthen community health projects which do not rely
on imported drugs.
Manufacturers should take full responsibility for ensuring that their products are
used safely and effectively in the Third World and respond to the real health needs
of the poor by marketing low-priced essential drugs.
- 3 -
Dianna Melrose, 30, the author of Bitter Pills, was born in Zimbabwe and grew up
in Latin America.
She holds an MA in Latin American studies from the London
School of Economics and worked as a translator for banking and insurance firms
in the City before becoming an administrator for the British Council.
She joined
Oxfam's Public Affairs Unit in January 1980 and has carried out field research
in Bangladesh, India and the Middle East.
She conducted research for a film on the
marketing of baby milk and medicines in North Yemen and is the author of the
associated book, The Great Health Robbery.
Bitter Pills - Medicines and the Third World Poor, by Dianna Melrose, is
published by Oxfam on November 25 at £4.95.
Distributed by Third World Publications.
Review copies are available on request from the Press Office, Oxfam,
274 Banbury Road, Oxford.
Tel:
Oxford (0865) 56777.
For more information contact Derek Warren, Oxfam Press Office on Oxford
(0865) 56777.
8th November, 1982
BITTER PILLS
MEDICINES AND THE THIRD WORLD POOR
by Dianna Melrose
Published by Oxfam on 25th November, 1982
Distributed by Third World Publications
151 Stratford Road, Birmingham, Bll 1RD
INTRODUCTION
Throughout the Third World millions of the poorest have no access to life-saving
drugs, while drugs are wasted and misused worldwide.
In poor countries those
that are most needed are often the hardest to obtain, at least at prices the
poor can afford.
Through their uncontrolled sale and promotion in most poor
countries, medicines often do little good and can be positively harmful.
1.
A PILL FOR ALL ILLS?
The poor in the Third World - as in Britain - suffer disproportionately from
ill-health.
Disease that is rooted in poverty can only be attacked by an
onslaught on poverty itself.
But a small number of essential drugs could be
used to save millions of the poor from unnecessary suffering and death.
2.
UNEQUAL DISTRIBUTION
The Third World has three-quarters of the world's population but accounts for
little more than 20% of total drug sales.
In the poorest countries, annual drug
expenditure averages only 50p per capita, compared with £35 in the rich world.
Yet this money may represent a crucial proportion of a poor family's income.
Moreover, the distribution of health services is often grossly weighted in favour
of the rich town-dwellers at the expense of the majority of people living in rural
areas.
The poor are therefore forced to rely on untrained drug-sellers offering
potentially dangerous drugs at extortionate prices.
3.
PRODUCER'S MARKET
Throughout the world, drugs are largely produced and sold by private businesses
whose interests are primarily commercial rather than medical or social.
Third
World countries are almost totally reliant on importing finished drugs and so are
subiect to the dramatic price increases which follow inflation.
Inappropriate
patterns of drug consumption are adopted, thanks to the producers' aggressive
promotion tactics.
In North Yemen, non-essential drugs, tonics and vitamin pills
account for an estimated 65? of total pharmaceutical imports.
Only 1.3? of
imports are of drugs to combat the prevelant and crippling diseases of malaria,
bilharzia and TB.
4.
POOR VALUE FOR THE POOR?
DRUG PRICES
In Third World countries, the cost of drugs in real terms is anything up to 20
times higher than in the producing nations.
Expensive brand name drugs are
marketed instead of far cheaper generics.
Hefty overheads for promotion and
research and development into new drugs are passed on to the poor.
Meanwhile
only a fraction of total research spending (equivalent to half the cost of
developing one new drug) is allocated to poor world diseases.
Poor people are
therefore subsidising new drugs for the rich.
5.
INFORMATION OR DISINFORMATION?
DRUG PROMOTION
Drug promotion helps to ensure that 90? of drugs prescribed by GP's in Britain are
brand-name products.
But at least, in drug-producing countries, advertising is
monitored and doctors are supplied with objective information about cost-effectiveness.
Over-the-counter sales are also strictly controlled.
Such restrictions rarely
apply in poor countries, where misleading or inaccurate promotional literature
goes unchecked and where company salesmen may offer free samples and other sales
inducements to doctors and nurses on a lavish scale.
very intense:
Commercial pressure can be
in Nepal, Brazil and several Central American countries, there is
one doctor to every three salesmen (compared to eighteen doctors for every one
salesman in the UK).
6.
BUYERS BEWARE - UNCONTROLLED SALES AND PROBLEM DRUGS
All too often there is a cruel contrast between advertising claims and the reality
of drug use in developing countries.
Powerful drugs with toxic side-effects
are dispensed by illiterate traders - even by children.
accentuated by irresponsible marketing practices.
The dangers are
Amabolic steriods have been
promoted as appetite stimulants for malnourished children.
have been marketed to treat infants with "common diarrhoea."
Powerful antibiotics
Uncontrolled
marketing and sales has already led to epidemics of drug-resistant disease.
3
7.
TRADITIONAL MEDICINE
Traditional medicine is still the major source of health care for three-quarters
of the Third World population.
ancient herbal remedies.
Some important modern drugs are derived from
WHO has urged Third World governments to plan their
health systems so that modern health-workers work alongside traditional healers with each learning from the other, encouraging patients to visit the health
centres more readily.
8.
TRAIL-BLAZERS - SMALL-SCALE SOLUTIONS
A number of pioneering projects have attempted to tackle ill-health in poor
communities with paramedics providing preventative and curative care.
The
People's Health Centre in rural Bangladesh goes beyond the confines of health
care to try to solve the underlying problems of landlessness, inequality and
powerlessness.
Other projects in a range of developing countries are specifically
aimed at finding imaginative solutions to the problems of lack of vital drugs and
misuse of medicines.
9.
HEALTHY SOLUTIONS - THIRD WORLD NATIONAL AND REGIONAL POLICIES
Sri Lanka, Mozambique, China and other developing countries have adopted national
drug policies to cater for the health needs of the majorities.
A wide range of
policy options are open to Third World governments to improve the use and
availability of drugs.
I
The key element needed is political will.
Increasingly
developing countries are exploring the advantages of strength in numbers and
pursuing joint pharmaceutical policies to improve their bargaining power with the
rich world producers.
10.
HELP OR HINDRANCE? - THE RICH WORLD'S RESPONSE
Drug-producing nations have a controlling interest in UN agencies such as WHO
that could do more to assist developing countries.
The British and other rich
world governments adopt different standards for drugs for export and give little
active support to Third World governments attempting to implement bold new drug
policies.
They back home-based manufacturers' interests - sometimes at the expense
of the poor.
Leading drug manufacturers have made concessions to the special needs
of developing countries, but they also bring powerful pressure to bear (even
involving their governments) in blocking positive new controls on the drug market
- 4 -
in developing countries.
This concerted industry lobby is active now in
Bangladesh trying to get the government's new drug policy reversed.
11.
HEALTH NOW - ACTION FOR CHANGE
The principal recommendations are addressed to three groups:
Firstly, if the
poor are to benefit, Third World governments must give priority to primary
health care rather than to costly hospital building projects.
Drug imports
and sales should be brought under central control, and purchases made in
accordance with health needs.
Training for health workers should concentrate
on methods appropriate to their countries' needs and resources
Rich world governments should take steps to ensure that the WHO recommendations
with which they have, in theory, agreed are implemented.
They should
reappraise the need for export controls and publish all available information
on drugs and their safe use.
Official health aid should not be tied to purchases
of expensive products and high-technology medical services; and voluntary
agencies should strengthen community health projects which do not rely on
imported drugs.
Manufacturers should be consistent in the standards they apply worldwide and
adopt higher ethical procedures in disclosing full information and marketing drugs
that are essential to the needs of the poor.
7
LoeosT •
LOCOST ( Low Cost Standard Therapeautics )
is a collective voluntary enterprise for rationa'|
therapeutics. LOCOST aims to promote low
cost, scientifically
generic
names.
tested
medicines
under
LOCOST is a response to a
growing demand and challenge of the volun
tary health sector to meet the needs of the
deprived sectors of society for not only low
priced, but also good quality medicines.
Why LOCOST ?
History of LOCOST
In the last few years, voluntary agencies have
been sensing an urgent need for a rational
drug therapy structure. Some of the main
reasons that led to this sense of urgency
were: widespread irrational prescription pract
ices with no social accountability; the unethical
practices of the drug industry; the lack of a
formal structure and network for low cost and
quality medicines.
Despite seminars, commissions,
researcii
studies and journalistic expose's, there was
no adequate implementation as a response
compared to the magnitude of the problem.
Interested members of the Gujarat Voluntary
Health Association and the Medico Friend’s
Circle discussed the issue and finally sowed
the first seeds of LOCOST in a nebulous form.
In 1982, a team of experienced professionals
in the field of community health got together
and drew up a list of the essential drugs
based on the Hathi Commission, the W.H.O.
recommendations and other such documents.
A search for competent and dedicated person
nel finally led to a modest infrastructure for
>LOCOST.
LOCOST was registered as a public trust at
Baroda in November 1983. The first supply
of LOCOST drugs was despatched in October
1983. Subsequent visits to health institutions
only underscored the need for rational thera
peutics. LOCOST is now well on its way to
establishing a small step, but in the right
direction, in the field of social justice in health.
Several independent studies have revealed the
following facts ;
1.
1.
There are approximately 30,000 formu
lations going on in the market under
various brand names. Most of these are
unscientific.
2.
All these formulations can be reduced to
about 200 in number. Their compositions
can be simplified thus enhancing the
relevance for rational drug therapy.
3.
Marketing them under generic names can
further reduce their costs to the consumer.
4.
Granting a reasonable profit margin, the
present on going rate of profits can be
lowered considerably.
5.
How LOCOST functions.
Procurement : LOCOST has
contacted
a number of reliable low cost drug ma
nufacturers on the
Bombay-Thane
and
Ahmedabad-Baroda-Surat regions whose
integrity and credibility have not
doubted.
2.
been
Some of these manufacturers supply the
drugs specifically ordered by LOCOST.
3.
It is possible to ensure a high quality of
drugs at low costs.
Quality testing and control: LOCOST'S
responsibility is to ensure
a rigourous
of these
drugs before
quality control
despatch.
4
All the drugs distributed by LOCOST are
under generic names and adhere to the
principles of
rational
drug
therapy
as
chartered by the World Health Organization,
the Hathi commission and
other
authe
ntic studies.
5.
It Was widely bSlieved that quality drugs
cannot be made available at low costs. Yet
there was a pressing need from health profe
ssionals working with the poor and margina
lized sections of society for low cost quality
medicines.
Educational efforts : LOCOST creates
an awareness about the
irrational practices
unethical and
of both the health
professionals and the drug industry through
visits, literature, seminars, etc. This enha
nces the scope for rational drug therapy.
An invitation
The LOCOST Organization
LOCOST is governed and managed by
These are,
in short,
objectives,
methodologies
some
of
and
our
aims,
strategy
to
* A board of trustees
evolve and ensure a more "Just Order" in the
* An executive committee
field
* A member secretary
Therapeutics in particular.
* A coordinator and his team
If your
* An advisory board
orientation, philosophy and values, and would
of
Health
in
general,
and Rational
Institution agrees with our
basic
like to collaborate in our collective effort,
— The
Board
of Trustees and Executive
please write to us at the address given below.
Committee frame policies and procedures,
adopt methods and strategies to promote
the objectives of LOCOST.
Postal address : The Coordinator
LOCOST
G P.O. Box No. 134
— The Member Secretary, who is a member
Vadodara 390 001
of the Executive Committee, supervises
and ensures that the LOCOST ideology
and
framework is implemented in the
action wing.
Office address : LOCOST
Arunodaya Building
floor)
(top
Opp. Lakdi Pool
— The Coordinator looks after the day to
Shivaji Road
day administration, arranging the procure
Dandia Bazaar
ment, testing and despatch of quality
Vadodara 390 001
drugs to the various Partners of LOCOST.
Phone : 58481
— The advisory board consists of persons
Involved in developmental activities and
concerned professionals. LOCOST submits
its reports, accounts, budgets and future
plans to the advisory board to ensure its
social accountability.
COMMUNITY HEALTH CELL
47/1,(First FloorlSi. Marks RoStf
SANGAlOHc - I5du 001
Registered with the Assistant Chaiity Commissioner,
Vadodara.
Registration No. E-3329/VADODARA
TO
ft®
SuMey. August 23, 5K5.
"5 Gen. Zlsur Rahman. Although Dr. Chowdhury’S
•Ji nominee failed to win the electoral battle,
'
successfully projected hfs political
,
throughout the country. With this direct in
* ■
volvdment in politics, Dr. Chowdhury, who until
Crusader against
drug=biiip@ri©lsm
R. ZAFRULLAH Chowdhury, who won
A man of serious conviction and action. Dr.
this year's Ramon Magsaysay award for Chowdhury came to Indie in the midst of the
community leadership, sad ho would continue war and started a field-hospital, near the Indo-'
his struggd against multi-national and other pro- ----Bangladesh
——------------border-----------------------------to treat the .wounded freefit-mongering international drug companies, . dem fighters. After the independence of the
“who exploit the developing Third World coun- country in December 1971,
1071 he shifted his small
.—it
tries like Bangladesh by pursuing their policy war-time hospital at Savar and began his work
by constructing a smJI bulldino after getting
Dr. Chowdhury, tne 43-year energetic Bangla a donation of an acre of land from two local
desh physician, who in 1972 founded the "Gano philanthropists.
-Sasthya Kendra" (Peoples Health Centre), a
Within 13 years, the energetic Chowdhury
medical service complex mainly for the rural spread his projects over 40 acres of land and
poor. at Savar. some 35 km off the capital city, his "Gano-Sasthya Trust" has been expanded
fold this correspondent in an exclusive inter- to a great extent At present Dr. Chowdhury
, view in Dhaka that he was "happy" with the has 23 self-reliant units where over one
nev.s of the Magsaysay award.
thousand people work. He employs over 65
*1 am particularly happy that tt-e cause for per cent women, mostly from the poorer sec
which we in Bangladesh are fighting has been tions of society, in his projects, including the
recognised by the tniemational forum. This is "Gano-Sasthya Pharmaceutical Ltd”—which
a recognition of our war against multi-national has become one of the leading medicine pro
exploiters who trade on the ignorance of the ducing industries in the country within few
millions of suffering humanity," Dr. Chowdhury years. His philosophy to recruit a higher per
*d
sa
adding, "but we still have to go a long centage of women in his projects was that the
women, who constitute half of the country's
v/ay to materialise our dream”.
A fieedom f-htcr in 1971s wor of liberation. population, are the, most exploited and they
Dr. ZafrpUah Chowdhury, who had become should get proper support to stand on their
one of the me st debatable men In Bangladesh own feet
One of the specialities of Dr. Chowdhury’s
projects is that all these are designed and run
of any political party) was given the prestigious on a self-reliant basis. The "Gano-Sasthya
Ramon Magsaysay awa<d worth U S $20,000 Trust", among others, has health magazine publiord a gold medal in recogni
---- ’J- on for
- engineering
- o
cabons. printing, agriculture, confectionary,
cloth, shoe and
i new
r’“” pouev on
03 pharmaceutical ^vui.
uriu furniture
lurnuure producing
prooucinp units.
units. The
I he
d-ug a^
cor-pecnenswe medical care people who work arc all treated equal. There
available
a/a-!2wle to ordinary people.
erooie.
• is no bureaucratic structure. All workers, includ
Rettiess
ard
mobile.
Zafrullah ing Dr. Chowdhury, eat the same food and cel
Je same standard of accommodation. "Ganowat> an aci'viT’ against Field Marshal Ayub Sasthya Kendra’ is a ’socialist’ complex where
reg hi e. and tafcx known In live country Dr. Zafrullah Chowdhury is teaching his “self-de
signed socialism . in the very functioning of
the complex.
U.K. along with
There
is another speciality of
Dr.
Chowdhury, In that the people who intend to
D
•hen v/89 known mainly as a "Ousader" aga-n
*
st the multi-nationals in the pharmaceutical sof
ter. also became known in the political arena.
While explaining his past political role, the?
Magsaysay winner told this correspondent
.
i was trying to establish a cause—a uct-co,that is, cheaper and easier health care to the
poorest section of ^ur society. Out peer and
simple hearted people had been exploited by
the multi-nationa! giants for many years, i couid
not succeed earlier because there was no politi
cal support Well. I am not at all out of potties '
as I believe that without political backing it
would be very difficult to implement my ideas.
So. I supported and worked for Gen. Atauf
Ghani Osmany in the Presidential electicna.."
The Magsaysay award winner, however,
thanked President Lt Gen. Hussain Mohammad •
Ershad for his government’s "sincere will” to
frame and implement the much debatable Na
tional Drug Policy. With the new drug policy
the military regime of Gen. Ershad has drastical
ly banned over 300 drug items overnight des
cribing them as “useless and injurious to
health.
Dr. Zafrullah Chowdhury, who was in tha
work with “Gano-Sasthya Projects" should be
eight-member committee to frame the new
non-smokers All the workers must get up in drug policy said. "1. We also tried persistently
the morning and work in the field for a specific to frame and imp^ment such a drug policy
time before going to their respective units. All
during the time of the former government, but
the women workers in the project must know failed I must thank President Ershad for h?s
how to ride a bicycle. They must move from sincere will in this regard and. of course, his
door to door in the villages to motivate people government's courage to implement it despite
about the primary health care. In the initial days, repeated threats from very powerful external
Dr. Chowdhury's plan to send women into the quarters”. If I do not praise Ershad it wou
*d
villages on bicycles was vehemently opposed be a distortion of historical facts".
by many people. But now they have realised
.The debatable drug policy of Bangladesh
the usefulness of the women "Gano-Sasthya
" workers, who educate the villagers not only which was approved by the’ Council of Ad
in matters of health but also helps them to in visors of Gen. Ershad on May 29. 1982 and
acclaimed in many quarers was still under pres
crease their farm output
sure. Dr. Zafrullah Chowdhury was not just a
Dr. Chowdhury's "Gano Sasthya Pharma member of the committee, but p
*ayed
a vital
ceuticals", during the last two years, has been role in its framing and implementation. He said
producing almost every essential drug and has that the now drug policy was not only an
become a competitor of the big multi-national "achievement" of the present government but
companies. “I have been a target of the medic also "a step forward" in providing cheaper medi
ine-imperialist because I wanted to help my cal service to millions of people who suffer
people by supplying them with cheaper and from malnutrition and d»e of su-.zrL' d-seases
more useful medicine." he said.
for want of medicine. "The meo
j industry
In 1978‘s Presidential elections. Dr. Zafrullah should not bo compared with the industry
Chowdhury played a oioneering tola in nominat which produces warheads. !l sb-Tu'd Lo a >cring General Ataul Ghani Osmany. a ret. ed vice-oriented industry and the companies
on
General and the Commander-in-Chief of the which are if'-VcI'.-cd should stop
Bangladesh liberation forces in 1971. as the human miseries." Dr. Ciowdhtury rt-m.;. xe<j.
Dr. Zafrullah Chowdhury m;u
a Gcman
principal candidate agalnstjhe President, Ll
end has o daughter. His wife, who is a Ph.D.
'ond later became a doctor is now a partner
of her adventurous husband in the "Gano-Sas
thya Kendra". Chowdhury said that he did not
consider the Magsaysay award as a personal
rcward.."lt Is a recognition of our joint venture
which aimed at changing an age-old pattern
!n our society," he said. Dr. Chowdhury con
siders the people in the "Gano-Sasthya Trust"
co his "partners In the challenging job". They
(the workers of Gano-Sasthya Trust) have all
the rights to decide whether I should take the
award, or how to spend the money for our
projects on receipt of the amount".
Altnough Dr. Zafrullah Chowdhury is known
for his "crusade" against multi-nauonal
pharmaceutical companies, he is a target of
severe attack from many quarters for his "sec
ret understanding with some other multi-na
tionals" The critics used to say that Dr.
Chowdhury was trying to drive out some multlnationair” with the objective of establishing
other multi-nationals business". When asked to
■comment on this point, he said. "This sort of
■ attack >urfaced only after the new drug policy
was announced. Yes, I used to get donations
from International voluntary organisations., but
they give donations because of their progres
sive attitudes. They are net multi-nat’onal com
panies. they want to help us in our fight against
the profit-mongers". In this context, he pointed
out the names of NODIA of Netherlands and
WAR ON WANT of London, who provide help
for the Gano-Sasthya projects.
Dr. Chowdhury said that the Gano-Sasthya
Trust is not a profit-earning organisation. Tne
main objective of the trust is to ensure adequ
ate medicare to rural people and with minimum
cost.
Explaining how big multi-national companies
were out to make profit, mostly by supplying
useless medicines, he said that the Gano-Sas
thya Pharmaceuticals which started production
only recently has already become a profitable
organisation despite the most minimum prices
for the items. "Our medicines are produced ac
cording to the requirements of our people, and
are 40 to 60 per cent cheaper than the items
produced by the multi-national medicine compa
nies," Dr. Chowdhury said.
Haropn Habib
ECONOMIC AND POLITICAL WEEKLY
Some Recent Articles in Health and-Related Subjects
Health and Medicine
i
Status o,f the Drug Industry in India; Haseeb a Drabu,
January 25, 1986
The Drug Charade; S Srinivasan, January 18,
Controlling Tuberculosis; N H Antia, January
1986
.<1986
An Alternative Strategy for Health Care? The Mandwa Project;
N H Antia, December 21-28, 1985
Maternal and Infant Mortality; Malini Karkal, October 26,
1985
How the Other Half Dies in Bombay; Malini Karkal, August 24,
1985
Infant Mortality in India; Levels, Trends and Determinants;
Leela Visaria, August 10, 17 and 24, 1985
Mortality Toll.of Cities: Emerging Patterns of Disease in
Bombay; Radhika Rarnasubban and Nigel Crook, June 8, 1985
.Treatment Failure in Indian National TB Pra gramme; Kashyap
Mankadi and Klass van der 7een, May 25, 1985
Famine, Epidemics and Mortality in India; A Reappraisal of
the Demographic Crisis of 1876-78; RonaTd Lardinois,
March 16, 1985
Health Hazards of Cotton Textile Workers; Bharat Dogra;
February 16, 1985
Breast Feeding: Collage of Danger Signals; Vimal Balasubrahmanyan, August 25, 1984
Breakdown of Public Health System; D Banerji, June 2-9,
1984
Family Size, Levels of Living and Differential Mortality
in Rural Areas; Some Paradoxes; N Krishnaji, February 11,
1984
Ban on Dangerous Pain-Killers; Padma Prakash, June 25,
1985
Drug Trials: Charade of 'Informed Consent'; Vimal Balasubrahmanyan, June 18, 1983
Impact of Social and Economic Development on Mortality:
Comparative Study of Kerala and West Bengal; Moni Nag,
Annual-Number, 1983
community i-talth cell
47/1, (First i ieo. iU.. Marks .load
BANGALOKE - 660 001
2
National Health Policy and Its Implementation; D Bgnerji,
January 22, 1983
New Patterns in Health Sector Aid; Roger Jeffery, Septem
ber 11, 1982
Little Girls and Death in India; Pranab Bardhan, September
1982
,
Bangladesh's New Drug Policy; John' Cunnington, August 21,
1982
Health for All: A Review and Critique of Two Reports; Malini
Karkal, February 13, 1982
Leprosy Control and Eradication; Padma Prakash, November 28,
1982
Choice of Best or Cheapest Drugs? A Note on Regulating Drug
Supplies; Mahesh S Patel, August 22, 1981
Health for All: A Reaffirmation; N H Antia, August 15, 1981
Nutrition
Protein and Energy Requirements; P V Sukhatme, November 2,
1985
Bashing Nutritionists: The Small-but-Healthy Hypothesis;
Sol Chafkin, May 18, 1985
Ideology and the Poverty-Line Debate; Sheila Zurbrigg,
December 3, 1983
'
■
Jndqrnutrition, Energy Requirement and Adaptation: A Physio
logist's Point of View; L Garby, November 26, 1982
Estimation of Nutritional Intake; Rajaram Dasgupta, July 9,
. 1982
RDAs: Their Limitations and Applications; i< T Achaya,
April. 9, 1983
Measurement of Undemutrition: Biological Considerations;
C Gopalan, April 9, 1983
Malnutrition of Rural Children and Sex Bias; Amartya Sen
and Sunil Sengupta, Annual Number, 1983 ■
We Are Eating Better; K T Achaya, January 1-8, 1983
Measurement of Undernutrition; PV Sukhatme, December 11,
1982
Poverty and iJndernutrition■ in Rural India: A Cross-Sectional
Analysis; Rajaram Dasgupta, September,25, 1982
■
3
Nutritional Norms and Measurement of Malnourishment and
Poverty; Jaya Mehta, August 1^, 1982
■The'Poor as a Social Stratum: Some Economic Criteria for
Studying Poverty; V M Rao and M Vivekananda, July 3, 1982
Administrative Constraints on Rural Development: A Field
View of the Applied Nutrition Programme; Amal Roy and
Vanita Venkatasubbaiah, Review of Agriculture, June 26, 1982
Some Nutritional Puzzles; C Ashok and Mahdav Kulkarni,
April 2A, 1982
Rural Energy Scarcity and Nutrition: A New Perspective;
Srilata Batliwala, February 27, 1982
Calorie Norm Controversy; V M Rao and M Vivekananda,
February 13, 1982
On Measurement of Undernutrition; V M Dandekar, February 6,
1982
Measurement of Poverty and Undernutrition; D Banerji,
September 26, 1981
On Measurement of Incidence of Undernutrition; What is a
Consumer Unit?; N Krishnaji, September 12, 1?81
Measurement of Poverty; V K R V Rao-, August 29,
1981
- On Measurement of Poverty; P V Sukhatme, August 8, 1981
Measurement of Incidence of Undernutrition; Santi K Chakrabarti and Manoj K Panda, August 1, 1981
On Measurement of Poverty; V M Dandekar, July 25, 1981
Some Nutritional Puzzles; V K R V Rao, July 11-18, 1981
On Measuring the Incidence of Undernutrition; P V Sukhatme,
June 6, 1981
On Measuring the Incidence of Undernutrition; N Krishnaji,
May 30, 1981
Family Planning
Towards a Women's Perspective of Family Planning; Vimal
Balasubrahmanyan, January T1.,'. 1986
Two Decades of Sterilisation, Modernisation and Population
Growth in a Rural Context; Stanley A Freed and Ruth S
Freed,. December 7, 1985
Case for Injectible Contraceptives?; Sujit K Das and Pijus
Kanti Sarkar, October 5, 1985
4
Case f"'r Injectible Contraceptives; Iris Kapil, May 11,
1985
Family Planning and the Emergency: ^n Unanticipated
'Consequence; »laka M Basu, March 9, 1985
Retreat on DepoPrlvera; Padma Prakash, December 8, 1984
Problems Concerning Tubectomy Operations in the Rural Areas
of Punjab; Joyce Pettigrew, June 50, 198^
Fertility Decline in Kerala: The Social Justice Hypothesis;
P G K Panikar, March 51, 1984
Use of Laparoscopy for Sterlisation; Padma Prakash, March 17,
198^1
Excess Female Mortality in India; Tim Dyson, March 10, 198^
Mass Use of Injectible Contraceptives; Vimal Balasubrahmanyan,
March 5, 1984
Fertility Differentials in Kerala and West Bengal: The EquityFertility Hypothesis as Explanation; Moni Nag, January 1,
198^4
Breast-Fqp'ding and Family Planning Policy ; Vimal Balasubrahmanyan, December 10, 1985
Amniocentesis: The Debate Continues; Leela Dubey; Septem
ber 17, 1985
Amniocentesis Again; Dharma Kumar, June 11,
1985
Female Infanticide and Amniocentesis; Roger Jeffery and
Patricia Jeffery, April 16-25, 1985
Fresh Focus on 'Natural
*
manyan, “^pril 2, 1985
Family Planning; Vimal Balasubrah
Misadventures in Amniocentesis; L S Vishwanath, March 12,
1982
Misadventures in Amniocentesis; Leela, Dubey, February 19,
1985
Male Utopia or Nightmares?; Dharma Kumar, January 1$, 1985
Hormonal Pregnancy Tests: One More Year's Havoc; Padma
Prakash, August 28, 1982
Where Have .the ‘Women Gone? Insights from Bangladesh on Low
Sex Ratio of India's Populatiorij-Lincoln C Chen, March 6,
1982
Preliminary Demography of 1981 Census; Tim Dyson, August 15,
1981
«
5
Environment
■•Environmental. Conflicts and Public Interest Science;
Vandana Shiva and J Bandyopadhyay, January 11, 1986
Bhopal: The 'dorse Aftermath; Sujit K Das, December 14,
1985-/'
Bhopal: Neglect of Women’s Health Issues; Padma Prakash,
December' 1:4, 1985
Bhopal: a -’orker's Perspective; Rohini Banaji, December
14, 1985
Bhopal: Farce of Rehabilitation; Jagdish and Vijay,
• December 14, 1985
Eucalyptus in Rain-Fed Farm Forestry: Prescription for
Desertification; J Bandyopadhyay and Vandana Shiva,
October 5, 1985
From the Dam to the Chetto.es: Victims of the Rihand
Dam; Satyajit Kumar Singh,"October 5, 1985
Bhopal Gas Disaster: Mockery of Relief andRehabilitation;
Sujit K Das, October 5, 1985V
Project Tiger and People: A Report on Similipal,
August 17, 1985
Population and Environment; Anil Aggarwal, June 15, 1985
Bhopal Tragedy: A Middle Word; Pushpa M Bhargava,
J une 1, 1985
Anti-People Development: Case of Inchampalli Project,
J une 1, 1985
Bhopal Tragedy: Failure of Scientific Community; Padma
Prakash, May 25, 1985
Facade a.nd. Reality of Environmental Protection; Bharat
Dogra, May 18, i985
Bhopal Gas Didaster: Continuing Nightmare; Padma Prakash,
April 6, 1985
Ecology and Social Movements; Gail Omvedt, November 3,
1984
'Women and People’s Ecological Movement: A Case Study
of .'/omen's Role in the Chipko Movement; Shobita
Jain, October 31, 1984
Narmada Valley Project: Development or Disaster?; Ashish
Kothari and Rajiv Bhartari, -June 2-9, 1984-
Forestry in British and Fast-British India: A Historical
Analysis; Ramachandra Guha, October 29 and November 5,
1983
Energy in a Stratified Society: A Case Study of Firewood
in Bangalore; a K N Reddy and V Sudharkar Reddy,
October 3, 1983
Meeting Basic Needs through Micro Planning: Central Role
of Essential Forestry; Vinod K Huria and K T Achaya
august 20 and 27, 1983
Eucalyptus: Why?; Mahasveta Devi, August 6, 1983
.Singhbhum: A Countryside Slowly Dying, Mahasveta Devi,
March 5, 1983
Ecological Crisis andEcological Movements; A Bourgeois
Deviation?; Ramachandra Guha, December 25, 1982
Political Economy of Technological Polarisation; Vandana
Shiva and J Bandyopadhyay, November 6, 1982
Ecology as Science and Science Fiction; Subrata Kumar
Mitra, January 30, 1982 .
Encroachment on Forests: .Government versus People; Sharad
D Kulkarni, January 16, 1982
Industrial Hazards Exported to India; Barry I Castleman,
Rakesh Madan and-Robert Mayer, June 13, 1981
ECONOMIC AND POLITICAL WEEKLY
A Journal of Current affairs and the Social Sciences
Subscription Rates
Institutions: 1 year Rs 250, 2 years Ps ^75, 3 years 700
Individuals:
1 year Rs 200, 2 years Rs 375, 3 years Rs 550
Special Rates
For teachers and researchers: 1 year Rs 150
For students: 1 year Rs 100
Single back issues can be supplied, when available in
stock, at Rs 5 per copy, inclusive) of. postage
Please write to The Manager, Economic and Political
Weekly, 1 Skylark1, .28^ Shahid-Bhagatsingh Road,
Bombay A00038.
.r.
■h CENTRE FOR
■ EDUCATION AND
iP DOCUMENTATION
'
>
A POSTAL DOCUMENTATION SERVICE
SPECIAL FEATURES
• Culled from 150 newspapers
& magazines
• Over 500 information sources
• At your doorstep
• Lowcost
• Adaptable to your specific
needs
COMMUNITY HEALTH CELL
£7/1, (First FioorjSt. Marks Hoad
3 A (m GL O. i c ■ 5 U J Uv 1
WHY DOCPOST ?
CENTRE FOR
EDUCATION AND
DOCUMENTATION
Ten years of rigorous docu
mentation has taught us that
documentation is very expensive,
tedious and lime consuming Yet
it is indispensable to any social or
political work Most groups and
institutions have made efforts to
bridge this information gap, but
have been unable to pursue it
either due to financial, organisa
tional or infrastructural con
st rain is.
CED on the other hand has
concentrated exclusively on docu
mentation. The Centre collects
and classifies a wide spectrum of
information including news clip
pings, analytical articles, back
grounders and data reports culled
from newspapers, magazines and
a host of publications from India
and abroad. Some of these arc
not easily available to those work
ing on specific issues such as the
environment,
occupational
hazards, women, workers and
peasants struggles and nuclear
disarmament.
CED now Iccls confident to oiler
you a viable and alternative postal
documentation service —
DOCPOST.
CED's new service is called
DOCPOST, an alternative and vi
able postal Documentation Ser
vice, which will make available to
you xeroxed material to meet
your
particular
information
needs.
You have three options:
DOCPOST (Regular) where
every fortnight we will post a
packet of material covering the
topics of your interest, for a
period specified^)} you.
DOCT0ST(Spot)where you will
receive bulk material from out
past files, as and when you need
it,
DOCPOST (Selective) where
you need some specific docu
ments or data from out files.
DOCPOST is addressed to
those groups, institutions and in
dividuals who have a need loi in
formation which they cannot
meet due to budgetary or other
constraints. 'Che service has been
organised to cater to the needs of
researchers, journalists, develop
ment and political activists as well
as social science institutions and
documentation or reference cen
tres who may want to enhance
their information base without
creating procedural overloads
So, for those who need infoi ma
tion but find themselves unable to
organise if, DOCPOST is the
. answer.
DOCPOST offers you the op
tion of identifying your areas of
interest from a classification
series that comprises more than
450 heads covering a wide range
of current issues in India and the
world in the field of politics, eco
nomics, development, women,
communication, labour, health,
the environment, social pioblems, and so on.
Once you have identified the
issues on which you need in
formation you can subscribe to
any of the three DOCPOSI catagorics.
WHAT IS DOCPOST ?
It is basically a clippings and
documentation service by post.
which will preside xerox copies of
the documents you need from our
Centre
We have formulated
three catagorics of DOC POSl,
ami you can choose which meets
your needs best.
DOCPOSI (Regular) will enable
you to subscribe to a particular in
dex nunibci ol our classification
system and every fortnight you
will receive all (he matciial we
mark during a stipulated period of
al least three months lioni the
date of subscription I or instance
you may be interested in monitor
ing the implications of all the
aspects ol the Bhopal gas disaster:
legal, medical, political, aeitalional.etc. With DOCPOSI (Reg
ular) you can ensure getting every
important clipping, report, and
article relating to those heads,
whether through press coverage
oi m the loi m ol rcpoi is issued by
groups ami individuals who are
working in the Held. Each month
you can expect to receive al least
2(1 important clippings ami arti
cles as well as the papers and
pamphlets which will enter our
Ides during lhe period.
l oi this, all you have to do is
i) identity the classificati^H
no./.s oi out index ili.it coi;~
icspunds lo the issiic/s ol
\oui choice (like "UC" toi
Bliop.il gas dis.isici)
li) till in the enclosed torin
in) speeds the slatting date and
lhe
umc
period
(ihice
months or more)
iv) and semi us the deposit.
brom that specified dale, you will
receive a set ol material from us
every fortnight period specified.
DOCPOS’! (Regular) also oilers
you the advantage ol having ac
cess to back rclci cnees al favour
able rates, lot winch you would
otherwise pay moic In addition.
a subscription io DOCPOSI
APPLICATION FORM FOR DOCPOST FACILITY
NAME OF PERSON OR INSTITUTION AVAILING OF DOCPOST FACILITY
ADDRESS (TO WHICH DOCPOST SHOULD BE SENT)
TEL. NO
IF INSTITUTION, NAME OF PERSON WHO WILL BE DEALING WITH DOCPOST
FOR INSTITUTIONS/ORGANISATIONS
(Please tick (/) where relevant)
1. GOVERNMENT DEPARTMENT
Ministry of
Nature of Activities
2. NEWSPAPER/MACAZ1NE
GRADING AS PER PALEKAR CRITERIA
*
(Pul A, B, or C)
CIRCULATION
NO OF PUBLICATIONS OWNED BY HOUSE
J. OCCUPATION :
2. MONTHLY INCOME (Please tick)
i)
Below Rs. 7G0
n)
7G1-12OO
in)
12G1-I80G
iv)
Above 1800
I
"I
3.
3. NATURE OF WORK
OFFICE ADDREbS
NON-PROFIT ORGANISATION
NATURE OF ORGANISATION:
ACTIVITIES:
ANNUAL BUDGET 1985:
OTHERS
NATURE OF ORGANISATION
I. ACCEPTED/REJECTED
2. CATEGORY
3. SP. REMARKS
ACTIVITIES
ANNUAL BUDGET (1985)
1/We wish to Avail of the DOCPOST Facility, under DOCPOST REGULAR/DOCPOST SPOT/DOCPOST
SELECTIVE.
Right npw, 1 wish to have material from the following classification Nos.
OOOZ 1
To
Period: From
2- Oil.
To
Period: From
’• fill J
Period: From
To
Period: From
To
<-■ 0-1 1 J
1 am enclosing a deposit of Rs.________________. (Please refer to the rate-chart arid write the deposit
of the category in which you consider yourself).
Designation :
Date :
(Rcgulai) will entitle you to dis
counts of 10% on DOCPOST
(Spot) and 20% on DOCPOST
(Selective) for material outside
your subscribed classification. In
addition you are entitled to a dis
count on CED/CITE publica
tions. Payment for DOCPOST
(Regular) will be periodical and
deposit will have to be made
while subscribing.(l or rales see
chart at the end).
A DOCPOS'I (Spot) subscrip-
H >n entillcsyou to obtain file clip-
PF/ngs during a selected (mini
mum 30 daysjpenod (in the past)
or a loialol 50 consecutive clip
pings l or example,you may be
interested in developments relat
ing to Bhopal during the specific
period between say December 3
and December 31. 198-1 We will
photocopy all the material in our
file between these two dates and
send it to you DOCPOS’I (Spot)
will facilitate time-specific rcler-
In DOCPOS'I' (Selective), you.
can cither come and select your
material, or specify accurately
what material you want to re
ceive. For example, you may
want material only on the medical
aspects of treatment of victims in
Bhopal. Oi more specifically you
may be interested only in the con
troversy regarding the adniimstra^^tion of sodium thiosulphate iniec^Mons
DOCPOS'I' (Selective)
• allows you to meet your specific
need without having to receive
other material, which may be im
port.mt but not of particular use
to you. While there are no sti
pulations of duration or bulk in
this category, the rates ot the:
DOCPOST (Selective) are the
highest.
Important Note.
While making
requests for any DOCPOST
category please keep in mind that
while a large number oi news'
items, articles and booklets arc
placed in out files, certain jour
nals such as Economic and Poli
tical Weekly, and Monthly Re
view arc bound,i.c. their articles
arc not filed along with the rest
So if your request is for articles in
these journals, please mention
this. A comprehensive list of
periodicals which are cut and kept
in the clippings files and those
that are bound separately is pro
vided in Appendices A and B. re
spectively.
OTHER
SERVICES
The CED also houses an array
of books and booklets. These loo
can be replicated for you. If you
want to xerox an entire publica
tion. this can be done at the
DOCPOS'I (Spot) rate Replica
tion of portions of books/
booklets can be done .it the
DOCPOS'I
(Selective) rates
DOCPOST (Regular) subscribers
will avail of concessional rates
here loo.
COSTS
The three DOCPOS’I catego
ries have been conceived with a
positive bias towards making a
subscription to DOCPOST (Reg
ular) the most attractive.
Several considerations have gone
into evohing a differential rate
structure lor DOCPOS'I. Primary
amongst these was our aim to en
sure that groups and individuals
working on small budgets arc
not deprived of DOCPOS'I" facili
ties. Similarly the three categories
of DOCPOS'I — Regular. Spot
and Selective — have been func
tionally oriented because we rec
ognise that information require
ments can vary.
The rates tied below are per
page'(usually size A 4). . Each
copy will come to you with details
of date, publication and our clas
sification number While the rates
may appear expensive al first
glance, il you calculate your re
quirement. keeping in mind the
frequency and coverage,you will
find that DOCPOST offers you a
very cheap alternative. For exarnple-.let us assume that you tall in
our accounting category no.3 (re
fer rate-chart) and have sub
scribed to DOCPOST ( Regular)
And say you arc working on all
aspects of the Bhopal gas disaster.
Assuming that in a month you re
ceive 30 xeroxed pages from us
(i.e. 20 clipping and a ftve-page
special report from a group) al
Re.0.60 each, you will only spend
Rs 18 in a month. And according
to our categorization the max
imum monthly charge (i e. for
no. 1) is Rs. 24 while the minimum
(i e for no.5) comes to a bare Rs
12 for which you will have the
complete documentation on the
issue of your interest al your
door-step.
Now isn't this what most people
have been looking for?
Rate structure for DOCPOST
DOCPOST Deposit
(Regular)
per clas
sificat
ion no.
l.-Govt. organizations (economic, administra
tive depts.)
Newspapers & periodicals (A&B grade)
DOuPOST DOCPOST
(Selective)
(Spot)
.80
160/-
1.00
1.50
C grade newspapers but not those belonging
to houses owning more than 2 publications
Individuals like lawyers, doctors, social
media workers in TV, Radio, Film, Stage etc.
(not being through Advertising/Marketing
agencies)
.70
140/-
.90
1.25
3. - Journalists, teachers, students, social resear
chers
Non-profit institutions with budgets less than
Rs 3 lakhs.
.60
60/-
.70
1.00
4. - Activists organisations, progressive organisa
tions (budget less than Rs 1.5 lakhs per year)
.45
40/-
.55
.70
2. - Govt social organizations, like environment
depts., social welfare depts., labour depts.
Non-profit inslilulions/educational projects
with budgets over Rs 3 lakhs annually
5. - Activists not working elsewhere (i.c. income
less than Rs 700) and non-funded activists
progressive organisations (budget less than
rRsJ 40,000 per year)
.40
25/-
50
.60
6. - Others (i.e those not specified above)
1.50
400/-
2.1X1
10(H)
Nott: Postage will be charged on actuals.
All rales are in Rs per A4 page
Deposit only applies to DOCPOST (Regular).
CH
CENTRE FOR
EDUCATION
AND DOCUMENTATION
3. Suleman Chambers. 4. Battery Street. Behind Regal Cinema. Bombay 400 039 India Telephone 202 0019.
a
SERVICE CENTRE LIBRARY
Latest Awareness Service (Books and Occasional Papers)
_______________ Month ; OCTOBER & NOVEMBER, 1 985.______________
DEVELOPMENT RESEARCH COMMUNICATION AND SERVICES CENTRE.
18B, Gariahat Road, Calcutta - 700 031 .
CHILDREN
b|
pandit barooah, pramila.
Working children in urban Delhi.
(A socio-economic study, which is an enquiry into the
working and living condition of working children in Delhi
urban area. The methodological issues in this book are as
important as the findings themselves.)
Indian Council For Child Welfare, 1977.
1 70p
0|
BANERJEE, RITA.
Child labour - walls of silence.
Frontier, 9th November, 19B5.
DOCUMENTAT ION
B|
SOCIAL SCIENCE DOCUMENTATION CENTRE, ICSSR.
Bibliography of Bibliographies - supplement-3.
(This supplement no. 3 brings under bibliographical control
approximately 180 bibliographies compiled and bibliograph
ies acquired by SSDC during July - August 1984, which
includes cumulative lists of short bibliographies on Agriculture, Education, Scheduled Castes and Scheduled Tribes,
and W oi.,en .)
ICSSR, New Delhi.
36p viii, xiii.
B|
PRINT AND PUBLICATION SALES CONCERN.
Calcutta (in 43 sections).
(Contains maps of 100 dissected zones of the metropolitan
city of Calcutta. Link has been maintained, with the help
of numbers, between a particular ward and its surroundings,
and lanes and by-lanes have been included. A useful hand
book for sales promotion, surveys, market research, and
exact location for public activities.)
Print And Publication Sales Concern, Calcutta.
Un-numbered page.
Rs. 15.00
B|
CHAUDHURI, M. R.
EEL (INDIAN ECONOMIC AND GEOGRAPHIC
STUDIES. COMP)
India in Statistics.
(The volume which has been compiled by the Indian Economic
and Geographic Studies, contains most of the basic statis
tics necessary for socio-economic studies. The statistical
tables have been arranged in.different chapters for conven
ience of use.)
Oxford and IBH Publishing, Calcutta.
1 08p
b|
social science DOCUMENTATION CENTRE, ICSSR.
Periodicals in SSDC current list.
(The present revised list (1985) of periodicals in SSDC
records the availability of 1187 periodical titles current
ly received, which afe either Indian or foreign, including
abstracting, indexing and bibliographical periodicals,
primary journals and news letters.)
ICSSR. New Delhi.
n
■ '
2
ECONOMY
B|
JACKSON, TONY AND EADE, DEBORAH.
Against the .grain - The Dilemma of Project Food Aid.
..(This .book shows that food aid is an ineffective and even
damaging form of assistance which is often given to devel
oping countries. It competes with local crops for customers
and handling and storage facilities, often it does not
reatsh those most in need and does more harm than good.)
Oxfam, Oxford.
132p
£4.50
B|
:
GUPTA, RAN JIT KUMAR.
-Agrarian West Bengal - three field studies.
(Studies were undertaken in three significant areas of West
Bengal : Garbeta and Moyna Police Stations in the district
of Midnapore, and Manteswar Police Station in the district
of Burdwan. The period extends from the beginning of 1975
to the middle of- 1 976 . The publication tries to demonstrate
that the-lack of agrarian breakthrough in West Bengal is tA
be attributed more to motives of power than to motives of
profit.)
Ajanta Publishers, Calcutta.
199p
•
B|
CENTRE FOR RURAL DEVELOPMENT AND RESEARCH.
Calm after the storm - a study report of the oxfam sponsored
crop loan scheme ... in Andhra Pradesh following the 1977
cyclone.
(The report of a study that examined the effectiveness of
the crop loan scheme which was implemented in Andhra Pradesh
-by OXFAM through four Development Groups and by involving
the banks, as a measure of rehabilitation of small and
marginal farmers, after the cyclone of November, 1977.)
CRDR, Madras, 1984.
98p
B|
NAKAMURA, TAKAFUSA AND GRACE, BERNARD R
*
G.
Economic Development of Modern Japan. What has made thi's
sustained growth possible ?
(The present book is an attempt to analyse and focus upon
the salient points of Japan's economic development, in
terms easily understandable to the general student and
reader.)
• Ministry of Foreign Affairs, Japan.
99p
B |
THIRLWAL, A . P .
Growth and development with special reference to developing
economies.
(The book takes a detached economic view of the development
process and demonstrates the relevance of economics to an
understanding of, and solution to, the development obstac
les- of developing countries.)
Macmillan press, London.
398p
B|
DAS, ARUN KUMAR.
(A) Guide to West Bengal land reforms act with rules and
forms.
(The Land Reforms Act with all up to date amendments and
comentary has been presented in this volume to make it
highly useful for this branch of laws, - that aims at
redistributing available lands equitably among landless
peasants from land collected out of surplus holdings.)
Law Book Cooperation., Calcutta, 1980.
I68p
Rs. 25.00
3
B|
JAISWAL, P. L.
cd.
Hand book of animal husbandry.
(A useful book for students and extension workers, which
contains authentic information on various aspects of anim
al husbandry. In the context of significant progress in
research in all the fields of animal sciences, the present
revised edition of the book has been equipped with additi
onal chapters which did net find place in the earlier
edition ,)
ICAR, New DeIhi.
788p
B|
UFPAL, J. S.
ed.
India's economic problems - an analytical approach.
(A collection of essays on Indian economy. Chapters in this
revised editions have been re-written to take into consid
eration that during 1975-77 events in the Indian economy
have changed very fast due to the imposition and removal
of the Emergency Topics like Gandhian Economics and black
money have been given their due importance.)
Tata Mcgrowhill Publishing Company, New Delhi.
409p
B|
WHITTEMORE, CLAIRE.
Land for people : land tenure and the very poor.
(A report prepared by OXFAM which describes the prevailing
land tenure systems in Africa, Asia and Latin America, in
order to help the rural poor to build up an awareness of
those parts of the system that take advantage of them. It
also examines international policies and aid programmes to
judge whether they are really helping the poorest of the
poor or infact further impoverishing them.)
OXFAM, OXFORD, 1981.
55p
B|
MEIER, GERALD
M.
Leading issues in economic development.
(The book emphasizes strategic policy issues in accalerating ths development of poor countries. The 'Leading Issues'
in this new third edition of the book are the policies to
eradicate poverty, reduce inequality and to deal with
problems of unemployment.)
Oxford University Press, New York.
862p
B|
THOMAS, HARFORD.
cd.
(A) Picture of poverty : The 1979 Oxfam report.
(This book is an attempt to document what poverty actually
means for the people who daily have to endure its curse.
It is also an attempt to come to grips with some of its
issues and concepts, to cHart the progress, if any, that
has been.-made to .eliminate it, and to look at some of the
ways poverty may be tackled.)
OXFAM, OXFORD’', 1 979 .
1 1 7p
£
1.50
B| •
WEST BENGAL, GOVT.
. ’
/
Report of the officers' committee on land use in West Bengal.
(This first report on the land use in West .Bengal seeks tn
present a survey on various problems associated with erosion
and conservation hazards in North pnd South. .Bengal', high
lights the critical issues which require urgent attention
and suggests^ an operational programme with the necessary
organisational set up.)
. .
‘
■ ’
Department of Land Utilisation and Reforms and Land and
Land Revenue, West Bengal.
'■
22p + Annex. I-V,
•,
4
B|
BHATTACHARYA, DE3ESH .
(The) Role of technological progress in Indian Economic
Development.
(The book presents the analysis and results of an empirical
study of the role of technological progress in Indian eco
nomic development. It explains why growth has been faster
in certain sector or group of Industries than in others nf
the Indian economy, since the inception of the national
plans .)
The World Press Private Ltd., Calcutta; 1972.
276p
Rs. 20.00
b|
ARROW, KENNETH J.
Social choice and individual values.
(The book provides a basis for a critical evaluation of
democratic theory in general as well as the theory of
economic policy and welfare economices.)
Yale University Press, Haven and London.
124p
0|
ANONYMOUS.
India : Sugar production.
Anonymous.
0|
.
GUHA, RAMACHANDRA.
.
; ;•
Forestry and Social protest in British kumauh; 1893-1921.
(This paper examines the trajectory of social protest in
British Kumaun during the early decades of this century.)
Centre For Studies In Social Sciences, Calcutta, 1935.
EDUCATION
Bj
SENGUPTA, SUMIT
ed.
Bayaska Shikkha 0 Gramonnayan.
(Discussion on different aspects' of Adult Education as it
is being pursued as an important issue by the West Bengal
Govt., specially as the' basis, for rural development.)
'West Bengal Comprehensive Area Development Corporation.
69p
□|
LEGAL EDUCATION AND AID SOCIETY.
Constitutional dynamics of the reservation policy.
Legal Education And Aid Society, Madras, 1985.
I6p
"
GUPTA, K. C.
.
Criminalisation of Campus politics.
.';( Lt is description of what is happening on the campus of
'•:':'our Universities, with increased frequency.)
j.T;
ISI Documentation’-Ccntre , Bangalore. (Reprinted from The
’' £
Radical,.Humanist. March 1 85 .
■
...
0|
ENVIRONMENT
B|
‘. "
•• '
CENTRE FOR ENVIRONMENT CONCERNS - HYDERABAD.
Hyderabad : The State of Art of Physical Environment, A
Citizens' Report, 1985.
(A report on the present state of environment in Hyderabad
city with all its ailments, like unplanned growth, lack of
drainage, swarage and negotiable roads, and supply of scanty
water which is not fit for human consumption. This effort
of a handful of Hyderabad citizens is an effort aimed at
stopping further decay of the city, and making a healthy
Hyderabad. Each issue discussed has a social dimension toe.)
CEC, Secunderabad.
73 p
5
b|
-
AGARWAL, ANIL AND NARAIN, SUNITA
cd.
(The) State of India’s Environment 1 984-85 . The second
citizens' report.
(This report supplements the information provided in The
State of India's Environment, 1932. It is not merely an
update of the emerging environmental activities and concer
ns
in India.
It provides additional information on a
number of subjects not dealt with last time. Thus the infor
mation on nomads and grazing lands, on the occupational
health problems, on the distinct relationship between women
and their environment and on significance of firewood
consumption in cities and town with .its impact on forests Have opened up unexplored vast areas of study.)
Centre For Science And Environment, New Delhi.
-.393p
Rs. 320.00
HEALTH
B|
REYES, DIWATA
A.
ed.
(The) Philippine health situation and the transnational
drug companies.
(The book describes how in the context of a shocking picture
or ill-health in the Philippines the transnational drug
companies are remitting huge profits, and creating high cost
of medical care and medicines.)
AKAP Research, Quezon city, 1982.
44p
POLITY
b|
SNOW EDGAR.
Red star over China.
Penouin books.
621 p
0|
NAGARKAR, V . V .
Crime and politics in India.
ISI, Documentation Centre, Bangalore.
radical humanist, March ’85.)
(Reprinted from the
0|
SHAKIR, MOIN.
Lumpen elements in our politics.
(The author brings out how politicians find in some of our
slums the material they need for their politics of intimi
dation . )
ISI, Documentation Centre, Bangalore. (Reprinted from The
radical humanist, March '85.
□|
KUMAR.
Towards alternative political models.
(This paper originally conceived of as a response to the
debate on non-party political formations (NPPF); as a
response to the papers on the same by Prakash Karat (CPI-M),;
Harsh Sethi (Lokayan) and Young India Project (YIP).)
Young India Project.
SOCIETY
B|
SEN, AMARTYA.
Employment, Technology and Development.
(An informative book for practicing planners and students
of development economics which focuses on the inter relati
onship between institutions, employment and technology, and
the author investigates the institutional factors which
affect policy - making,).
Clarendon Press, London.
1 93p
6
b|
GRIFFIN, KEITH B. AND ENOS, JOHN L.
Planning development.
(The author is concerned with the practical problems if
planning and economic policy in undcrdevelopad countries.
A part is devoted to explaining the characteristics and
uses of planning models and this serious limitations,
specific policies in the four strategic sectors of Agricul
ture, Industry, Education and Population planning - and
the problems of their implementation have been exemplified
by the experience of five selected countries.)
Addison - Wesley Publishing, London.
262p
'
£
4.25.
B|
LITTLE, I.M.D. AND MIRLEES, J.A.
Project appraisal and planning for developing countries.
(The chief purpose of the book is to provide detailed
procedures - and short cults that can be used by those that
develop projects or take decisions ab.ou't them, - and to
explain the economic arguments for these procedures.)
OXFAM, OXFORD, 1979.
'
'
1 1 7p
£1.50
b|
bhatnagar, s.
' - 1
•
rRural .local government in India.
(The book presents an integrated account of the highly
diverse patterns of the Panchayeti Raj as these have been
in force in various states of, the Indian union. Attempt
has bean made to analyse the issues and problems emerging
out of the functioniing of the system, and to suggest
remedial measures at relevant places.)
Light and Life, New Delhi.
278p
•
Rs. 50.00
B|
BETEILLE, ANDRE.
ed .
Social inequality.
(The book offers a selection of contemporary writings on
various aspects of social inequality. All the pieces were
published after 1950.)
Penguin books, Harmonds Worth.
397p
0|
MATHEW, BABU.
An introduction to the Indian Legal System.
(This booklet draws a brief ou.tlinc. of the background
leading to the. development cf the Indian Legal System.)
Legal Education and Aid Society, Madras, August ’1985.
1 Op
‘
D|
ALAM, JAVEED.
Class, Community and Nationality formation : A theoretical
exploration through two case studies.
(In this paper the author is chiefly concerned with analy
sing some of the problematic theoretical aspects centred
around the breakup and separation or crystallisation of
people with similar national composition or make up.)
Centre Fcr Studies In Social Sciences, Calcutta, July *
1985.
68p
□|
BHASIN, KAMALA.
Participatory self-evaluation, practical guide lines. part-I.
(This document bears □ framework for participatory self
evaluation for Voluntary Agencies and Action Groups. The
framework presents a broad spectrum of activities usually
undertaken by Voluntary Agencies and Action Groups, and
provides guide lines for their evaluation.)
ISI, Documentation Centre, Bangalore, 1985. (Reprinted from
Ideas And Action 1985/1; 160, Kamala Bhasin.
7
□|
BHASIN, KAMA LA.
Some suggestions for conducting self-evaluation. Part - II.
ISI, Documentation Centre, Bangal’ore. (Reprinted from :
"Ideos And /Action". Kamala Bhasin. "Are wo on the right
way", 1985/2 - 161.
□|
BHATTACHARJEE , ABHIJIT.
Voluntary Agencies : Identity Crisis.
(This article traces the evolution of voluntary agencies
as they encounter successive disappointment with various
development programmes sponsored by Govt, and other autho
rities.)
ISI, Documentation Centre, Bangalore. (Reprinted from
Mainstream, July 27th '1985.
WOMEN
b|
mukhopadhyay, maitrayee.
Silver shackles - Women and Development in India.
(In the UN Decade for Women, the author, an Indian Sociolo
gist has examined the deteriorating status of Women in
India, how they remain shackled by increasing unemployment,
lack of access to education and health care and the defi
ciencies of their legal status.)
OXFAM, OXFORD, 1934.
100p
Rs. 45.00
0|
VIMOCHANA.
Festivals of films on women.
Vimochana, Bangalore, 1984.
WORKER
b|
PRIA.
Audyogic Swasthya Evang Suraksha.
(Hindi).
(A study and description of the occupational diseases and
the conditions that create them for different types of
workers. Necessary safety measures have been pointed out.)
PRIA, New Delhi.
137p
B|
PRIA.
Worker awareness and occupational health - study report
submitted to ICSSR, New Delhi.
(The adverse effects of Industrialization, in the forms
of occupational health hazards and safety issues including
environmental pollution have been studied, classified and
discussed at length.)
PRIA, New Delhi, 1985.
97p
B|
Books
0|
Occasional Paper.
££vflOP>»£/VT RESEARCH
ANO SERVICES CENTRE
18 2>xG&%}hat Rom CS\CaKi/tta-700 037
/WmiA of DEc'SS&kI JAN '86
Dear friends,
January,
1986.
Over the past two years we have been trying to develop
the Awareness Service«• And from this issue onwards we’ll be giving
you extracts of interesting articles from some of the journals we
receive at the Centre o.» that is in addition to the regular ite"e.
Our subject category is mentioned below. If you need photocopy of
any of the documents listed please write to us. Copies can be made
at 0.75 paise per page + postage. The documents marked * are
available from us on cost + postage basis.
You’ll be noticing that we’re also starting a section
on training workshop informations. If you organise any workshop
please let us know the details beforehand so that we can inform
our readers/members.
Special news section will highlight useful information
from Service Centre and other organizations.
As you see our Awareness list is gradually turning
into a bi-monthly newsletter. Any of your suggestions for making
the service more relevant to your needs are most welcome.
Best wishes for a very happy ’06.
SERVICE CENTRE
Our subject areas
:
Children (specially working
ch ildre n)
Economy (specially International
Aid &. Trade, Multinational)
Ethnic Minorities
Other Minority Groups,
Refugees, Migrants
,
Women (specially working
women )
Workers
sector)
(specially in informal
Communication
Polity (specially Human Rights
&. Civil Liberties)
Society (specially people’s
organisations and grassroot
groups)
Education (specially non-formal
and action-reflection oriented)
Health (specially occupational
and Community health)
Disarmament (including biolo
gical and nuclear warfare)
' Environment
Appropriate &. Alternative
Technologies
Documentation (Participatory
Research &. Training)
COMltfUfy........
«7^(Hr3;>7
BAAlGAlO-—:
7!i C
-2-
CHILDREN
Occasional Papers :
VOLUNTARY HEALTH ASSOCIATION OP INDIA.
-2\re
(i)
hormonal pregnancy tests safe ?
(ii)
The case against ep forte ?
(iii)
Brief review of the present situation of the
oestrogen - progestogen (Ep) drug campaign.
VHAI, New Delhi.
BANERJEE, RITA.
Life in Garbage.
Point counterpoint,
10th October,
1 905 .
COMMUNICATION
Occasional Papers :
WOMEN AND MEDIA GROUP.
Press and Social Movements.
Women and Media■Group,.Bombay,
1 905 .
Articles 5
BENNETT, W. LANCE &.GRESSETT, LYNNE. A.&-HALTOM, WILLIAM.
Repairing the Newt : A case study of the News Paradigm.
(A case study of how the news media "repaired" an
ambiguous story that slipped through the journalistic
,.--gat'es reveals the boundaries of -"what is news &. what is
not" and illustrates an underlying logic about how the
world should be reported.)
PP 50 - 68,Journal of Communication, Vol. 35, No. 2.
Weaver, David. H &. others.
Press Freedom, Media and Development.
1950 - 1979 : A study of 134 Nations.
PP 104 - 1.17, Journal of Communication, Vol. 35, No. 2.
STRODTHOFF,-GLENN
G &. OTHERS.
Media Roles in a Social Movement : A Model of Ideology
Diffusion.
PP 134 - 153, Journal of Communication, Vol. 35, No. 2.
ECONOMY
Books
:
VILLEGAS, EDBERTO
M.
Studies in Philippine political economy.
(In this book the author has dealt with five of the most
critical areas of Philippine Society : labour, oil, foreign
investments, World Bank and IMF control, and the so-called
reforms of the Society. His meticulous research and close
reasoning lead to the conclusion that Philipino consumers
and workers are being exploited and abused for the benefit
of foreign interests and their partners.)
Silengan publishers, Manila.
2
26p
Occasional Papers :
ANONYMOUS.
Negros Sugar Industry situationer.
(The Sugar industry in Negros was started during'the Spanish
colonial period. Today, the biggest sugar corporation have
American equity and in vestment-.. This paper deals with the
present situation in the sugar industry of Negros.)
Anonymous.
-7OMVEDT GAIL AND OTHERS.
Women's Liberation Movement - A collection of documents.
Information Centre, SMD, Pune.
KAUR, JIWAN JOT-.
Women's Movement,
Shackles And Women,
Punjab.
SACHET;ANA.
.
_orc_
Women's Organisations.
'
Sachetana, 1935.(The National Women's Conference, Bombay).
NARI NIRJATAN PRATTRODH MANCHA.
Women's Organisations.
Nari Nirjatan Pratirodh Mancha, Ca,lcu tta . (T he N .W .C.,B’bay).
RAPP, RAYNA.
Women, Religion And Archaic Civilizations : An Introductioni
Feminist Studies, Vol. 4, No. 3, October, 1978.
Articles :
MACEDA - VILLANUEVA, MARION.
Women And Water,
Balai, Asian Journal, No. 10,
1984,
PP 21
- 23.
WORKER
Books
:
WEST BENGAL. LABOUR DEPARTMENT.
(The) Calcutta Gazette, Extra - ordinary. December Sth,1932.
(Elaborate Notification of the rules made by the Governor
in exercise of the power conferred by Section 35 of the
Inter state Migrant Workmen Act, 1979. Published after
previous publication as required by Sub-section(1) of the
mentioned Section I 35f .)
Govt. Printing. West Bengal, Calcutta.
31 p
Articles :
ASIANS ALL OVER THE WORLD.
(A collection of articles look into the Asian immigrant
experience that spans across continents and cross cultures.)
Balai, Asian Journal, No. 12,
PP 14-’24<
EVANGELISTA, SUSAN.
The Pinay As Migrant
States In The 1930S.
Balai, Asian Journal
*
: Filipina Immigration To The United
No.
12,
PP 6 - 9.
PEOPLE'S RIGHTS : SOME ASIAN CASES.
(Priority targets for investigation are economic and
political rights of the majority sectors of Asians Society :
peasants and workers.)
Balai, Asian Journal, No. 9,1984,
PP 8 - 10,
YOSHIO, YOKOYAr,'A.
The Japanese Labour Movement - Gasping for Refreshment.
AMPO, Jaor n - Asia Quarterly Review, Vol. 17, No. 2, 1985.
PP 36 - 48.
-BCentres1
Photo Feature Service
:
We're developing a photobank to help the researchers,
journalists, students, development agencies and others interes
ted. Following subject areas are covered :
PEOPLE
- Informal sector (urban &. rural) working
condition &. living condition.
ECONOMY
- Agriculture, Animal Husbandry, Cottage
Industry, Markets &. Distribution Net Work.
ENVIRONMENT
Right now we have black &. white collection on women sellers
1 child workers. We'll let you know of future additions.
The cost of prints are 8" X 6" - Rs.15.00 & 12" X 10" -Rs.25.00
smaller sizes than these are not possible to make. You can order
the prints by post and in that case you have to pay the postage.
For details please write to
Photo Feature Service,
. SERVICE CENTRE,
1BB Gariahat Road(S),
Calcutta 700 031.
Poster Design
:
We.'ve started designing posters for various organizations.
If interested please contact us.
News of N F S - INDIA
:
NFS - News from Fields and Slums. This news feature service
was started by Bharat Dogra in November 1985. Bharat Dogra
himself hardly needs any introduction with over 800 articles
to his credit on development and human rights issues.
This monthly package of ten articles, about 50 cyclostyled^
pages, is based on field-reports, perspective articles and
news. It is available in both Hindi and English. "It is a
service for supplying articles and news relating to the impact
of development processes on the poor and oppressed people in
India."
We have received two packages so far and find the material
useful and informative. We will be making summaries/extracts
from these articles and carry them in our quarterly journal
DEBACLE.,
..
Subscription
:
a)
For Hindi &, English newspaper &. magazines wanting full
publication rights - Rs., 300/- per month (Rs. 450/- for
getting the service in both languages).
b)
For newspaper &. magazines who will have to translate the
material on their own, full publication rights to NFS is
available at Rs. 200/- per month.
c)
A concessional rate of Rs. 150/- is available for voluantary
agencies,'educational &. research institutes, libraries,
training centres, trade unions, private individuals, and
-5-
FERNANDES, WALTER.
Social Activists And People's Movements.
(The role of social activists or Action Groups have been
discusse.d in- this book, as part of the topics of people's
movements, social change and political alliances.)
Indian Social Institute, New Delhi.
1 86p
■
Rs.
30.00
ICSSR.
Sociology And Social Anthropology. ICSSR Journal of Abstra
cts And Reviews. Volume 14, No, 1, January - June, 1985.
(The present issue of the journal has been based on a
revised classification of themes of Sociology and Social
Anthropology in India, so that it may be representative of
the major trends and concerns in these fields.)
ICSSR, New Delhi.
1 88p
Occasional Papers :
KARGUPPIKAR, LEELAVATI.
Resolution On Personal Law.
Mahila Anyay Nivarana Samiti, Belgaum,
1905.
CACP.
The Citizen's Alliance For Consumer Protection. An Over view.
(The formation of CACP in March 1979 was an attempt to
answer the need of the time : a militant, united and people oriented movement responsive to the interests of the majority
of Filipino consumers.)
CACP .
Articles :
KOHEI HANASAKI.
Grass-roots Movements In The Japanese Archipelago : Ideas
And Experiences.
AMPO, Japan - Asia Quarterly Review, Vol. 17, No. 1, 1985,
PP 34 - 41 .
LABRADOR, VIRGILIO
S .
Over population Or Surplus Labour ?
The part played by labour in the population question.
Balai, Asian Journal, No. 11 ,
PP 7 - 11 .
PAEK-SAN, CHANG.
The Phoenix Of 1984 : A Vibrant Democratic Mass Movement
Erupts In South Korea.
AMPO, Japan - Asia Quarterly Review, Vol. 17, No. 1, 1985,
PP 2 - 25.
TOLEDO, RAYMOND LIM.
Population In The Asian Scene : Hard Questions With No Fast
Answers.
(What are the theories about population control and
national development ? How do they apply to Asia ? The two
questions have answers with shades of life and death for
millions of poverty striken Asians .................. ).
Balai, Asian Journal, No. 11,
PP 2 - 6.
YU, MIZUSHIMA.
A Close Encounter With The Korean Democratic Movement.
AMPQ, Japan - Asia Quarterly Review, Vol. 17, No. 1, 1985,
PP 26 - 33.
-6-
WOMEN
Books
:
SHARMA, KUMUD AND OTHERS.
Women In Focus. A community in search of equal roles.
(The book is based on data collected from two small districts
of Uttar Prad-esh, and unfolds the broader aspects of sex
role differentiation in Indian Society. For Development
planning, it provides grounds for questioning the attitudes
and perceptions of bureaucrats, professionals and others
who formulate policies and programmes.)
Sangam Books, Hyderabad.
1 1 7p
Occasional Papers :
WOMEN’S CENTRE.
.
.
Building Alternate Support Structures For Women - A process
of personal growth and consciousness raising.
(In this paper, whether and to what extent individual help’
is consciousness raising activity, is being examined.)
Women's Centre, Bombay, 1 985 .(The N. W. C., Bombay).
STREE JAGRUTI SAMITI.
- .
------Perspectives And Tasks For The Women's Movement in India.
Stree Jagruti Samiti, Bombay, 1 985 .(The N.W.C., Bombay).
GABRIEL, ANDREA.
Participation of Latin American Women in. Social &• Political
Organisation : Reflections of Salvadoran Women.
Monthly Review, No, Vol - 34, June 1982.
STR I KRITI SAMITI.
Participation Of Women's Organisations
Organisations.
Stri Kriti Samiti, Bombay, 1985.
In Mass And Other
FORUM AGAINST OPPRESSION OF WOMEN. ( The N. W. C., Bombay)
Perspective For Women's Liberation Movement In India.
(This paper aims to discuss some of the very important
problems that the Forum against Oppression of Women have
faced in the course of its existence for nearly 6 years,
between January 1980 to December 1985.)
FAOW, Bombay.
SAHELI.
Relationship Between Consciousness Raising And Helping
Individual Women.
5aheli, New Delhi, 1985.
SAHELI.
Religion And Women.
Saheli, Delhi.
NARI SAMTA MANCH, BOMBAY 1985.
The Role Of Autonomous Women's Organisations.
Nari Samta Man ch, 1 985 .
DUTTA GUPTA, ISHANI AND SEN,SIMONTI.
The Women's Question.
Nari Nirjatan Pratirodh Mancha, Calcutta,
1985.
PRAKASH, PADMA.
Women, Health And Environment.
(This paper is a collection of ideas and information put
together with the intention of arriving at a focus for
discussion of health and environment issues in the Women's
Movement.)
Forum Against Oppression of Women, Bombay, 1985,
(The National Women's Conference, Bombay).
-7-
OMVEDT GAIL AND OTHERS..
Women's Liberation Movement - A collection of documents.
Information Centre, SMD, Pune.
KAUR, JIWAN JOT.
Women's Movement.
Shackles And Women,
Punjab.
SACHETANA.
••
Women's Organisations.
Sachetana, 1 985., (The National Women’s Conference, Bombay).
NARI NIRJATAN PRATTRODH MANCHA.
Women's Organisations.
Nari Nirjotan Pratirodh Mancha, Calcu tta . (T he N.W.C.,B* bay)
*
RAPP, RAYNA.
Women, Religion And Archaic Civilizations : An Introduction
Feminist Studies, Vol. 4, No, 3, October, 1978.
Articles :
MACEDA - VILLANUEVA, MARION.
Women And Water„
Balai, Asian Journal, No. 10,
1984,
PP 21
- 23.
WORKER
Books
:
WEST BENGAL. LABOUR DEPARTMENT.
(The) Calcutta Gazette, Extra - ordinary. December Sth,1982.
(Elaborate Notification of the rules made by the Governor
in exercise of the power conferred by Section 35 of the
Inter state Migrant Workmen Act, 1979. Published after
previous publication as required by Sub-section(1) of the
mentioned Sectionl35j.)
Govt. Printing, West Bengal, Calcutta.
31 p
Articles :
ASIANS ALL OVER THE WORLD.
(A collection of articles look into the Asian immigrant
experience that spans across continents and cross cultures.)
Balai, Asian Journal, No. 12,
PP 14-24,
EVANGELISTA, SUSAN.
The Pinay As Migrant : Filipina Immigration To The United
States In The 19305.
Balai, Asian Journal, No. 12,
PP 6 - 9.
PEOPLE'S RIGHTS : SOME ASIAN CASES.
(Priority targets for investigation are economic and
political rights of the majority sectors of Asians Society :
peasants and workers.)
Balai, Asian Journal, No. 9,1984,
PP 8 - 10.
YOSHIO, YDKOYAMA.
The Japanese Labour Movement - Gasping for Refreshment.
AMPO, Japan - Asia Quarterly Review, Vol. 17, No. 2, 1985.
PP 36 - 48.
-8-
Centres1
Photo Feature Service
:
We're developing, a. photobank to help the researchers,
journalists, students, development agencies and others interes
ted. Following subject areas are covered :
working
PEOPLE
- Informal sector (urban &. rural)
condition &. living condition.
ECONOMY
- Agriculture, Animal Husbandry, Cottage
Industry, Markets &. Distribution Net Work.
ENVIRONMENT
Right now we have black &. white collection on women selie rs
child workers. We'll letyou know of future additions
The cost of prints are 0" X 6" - Rs.15.00 &. 12" X 10" -Rs.25.00
smaller sizes than these are not possible to make. You can order
the prints by post and in that case you have to pay the postage.
For details please write to
■Photo Feature Service,
SERVICE CENTRE,
1 SB Gariahat Road(S),
Calcutta 700 031.
Poster Design
We've started designing posters for various organizations.
If interested please contact us.
News of N F S - INDIA
:
NFS - News from Fields and Slums. This news feature service
was started by Bharat Dogra in November 1985. Bharat Dogra
himself hardly needs any introduction with over 800 articles
to his credit on development and human rights issues.
This monthly package of ten articles, about 50 cyclostyled^
pages, is based on field-reports, perspective articles and
news. It is available.in both Hindi and English. "It is a
service for supplying articles and news relating to the impact
of development processes on the poor and oppressed people in
India."
We have received two packages so far and find the material
useful and informative. We will be making summaries/extracts
from these articles and carry them in our quarterly journal
DEBACLE .
Subscription
:
a)
For Hindi &. English newspaper &. magazines wanting full
publication rights - Rs. 300/- per month (Rs. 450/- for
getting the service in both languages).
b)
For newspaper &. magazines who will have to translate the
material on their own, full publication rights to NFS is
available at Rs. 200/- per month.
c)
A concessional rate of Rs. 150/- is available for voluantary
agencies, educational &. research institutes, libraries,
training centres, trade unions, private individuals, and
-9-
newspaper &. magazines not ■wanting publication rights «■
d)
Send your cheques or information queries to :
BHARAT DOGRA,
D-7 RAKSHA KUNJ,
PA5CHIM VIHAR,
NEW DELHI - 1 1 0 063 .
Centre's Training Activitiesi
Over the past two years we have been engaged in training
activities. We have been concentrating on imparting skills to
development workers, organizers &. social activists in the field
of communications, documentations &. non—formal education.
Most of these workshops were conducted for village level
activists in M ,P ., Bihar &. West Bengal. So far we find that our
followup systems need to be tightened some what and we are working
at that.
In. future issues of our Awarsiisas List -we -will bo gluing
you more details of our experiences in this field. And in the
meanwhile we invite any kind of feed back, ideas &. programmes
from those -of you who are interested or involved with work in
this field.
Please, write to our training c-o-M-di-Qatctt- Top.a
t
*
at the Centre's address.
X.X44-*******
Naerkar
CJO'
LIST
PF BD0K5/0CCUPATIONAL PAPER ON DRUG .
1. 3HAGAT, MU KARRAH.
Aspects of the Drug Industry in India.
Centre for Education and Documentation, Bombay - 39.
1 982, Rs. 15.00,
’
pp 11 9.
2. BAM INTERNATIONAL,
Medicines and Third World, A great invasion.
BAM International.
Rs. 15.00
p. 40
3.. WAR ON WANT.
A dangerous prescription.
War 0n Want (The Health Unit),
4.
5.
6.
London,
U.K. 1984.
INTERNATIONAL TRADE.
BAM International .
BAM International, Manila, Philippines,
DRUGS.
Insaan Ke Liye Dowa Ye Dawa Ke Liye
Drug Action Forum.
1984.
Insaan.
CERC.
Beware of Hazasdous Drugs and Pesticides.
CERC, Allahabad, March’81.
p.40
p.10
7.
CHAUDHURI SUDIP.
The Foreion Controlled Firms in the Production of
Bulk Drugs in India.
8.
WORLD HEALTH ORGANIZATION.
(The) use of essential drugs
committee.
WHO, Geneva, 1983.
Rs. 10/(N)
9.
: Report of a who expert
p.46
DEPARTMENT OF HEALTH, MINISTRY OF HEALTH &. FAMILY PLANNING.
The Ayurvedic Formulary of India, Part- I.
Govt, of India, 1978.
Rs. 11.55
pp324
1 0. CHOWDHRY , Z
&. S .
Essential drugs for the poor :
Bangladesh. (1980-1982).
Gonoshasthya Kendra, Dacca.
Myth and Reality in
p.58
11. MAHFUZULLAH AND FAROOQUE, A.B.M.
Jatiya Oshudh Niti.
ShabarJanyaShwasthya, Dhaka.
p.23
I5LAM, NURUL AND OTHERS
ed.
Nishiddha Oshudher Abhidhan.
Shabar Janya Shwasthya, Dhaka.
TK : 5.00 “
p.50
12.
13.
14.
REYES, DIWATA A.
ed.
(The) Philippine Health Situation and The
Drug Companies.
Original entry under public health.
REY/15.04.01 .
Iransnational
WORLD HEALTH ORGANIZATION.
Prayojoniyo Oshudh; Report of a who expert committee.
Sana Prakashani, Dhaka.
TAK. 12.00
p.101
Pro
. . .
2/
DEVELOPMENT RESEARCH COMMUNICATION AND SERVICES CENTRE
1 8B , Gariahat Road (South), Calcutta 700 031.
Service Centre Awareness list
From this month the awareness list will be produced
bi-monthly.. Annual contribution towards it’s cost will be
Rs. 10.00 for Non-members and Rs. 5.00 for Associate members.
To other documentation centres &, research groups we send it
on an exchange basis.
If you need photocopy of any of the documents listed
please write to us. Copies can be made at ^"Op/page + postage.
A few copies of documents marked with * are available from
us on cost + postage basis.
As you know,
into our library,
areas.
here we list books and documents coming
if they cover any of the following
subject
In future we’ve thinking of listing important articles
published in periodicals as well.. Any of your suggestions
for making the service more relevant to your^ needs are most
weItome.
Documentation Group
Service Centre
SERVICE CENTRE, .,(.13RABY 'u:;;a *
”
...
■ ••
-. s.
a
■■
.n~n-3 a
Latest Awareness Service (Books and Occasional Papers)
Months: August - September, 19B5.
DEVELOPMENT RESEARCH COMMUNICATION AND SERVICES CENTRE.
1BB, Gariahat Road(South), Calcutta - 700 031.
APPROPRIATE TECHNOLOGY
B|
FOLEY, GERALD AND MOSS, PATRICIA.
Improved cooking stoves in developing countries.(Techni
cal Report no. 2, Earthscan Energy Information Programme)
(This Report gives a detailed appraisal of the role of
improved cooking stoves in the wood-scarce areas of the
developing world. Reliable and practically oriented
information is presented, intended both for policy makers
and the scientific and technical community.)
International Institute for Environment and Development,
London.
1 77p
B|
FOLEY, GERALD AND OTHERS.
Gasifiers: Fuel for siege economics.
(A study of the different aspects of gasification, by
which alternative energy called '''producer gases”,
from biomass are being used in place of gasoline or
d.ie.se,! to drive standard engines .of -vehicles, irrigation
pumps and other machinery in mapy coilhtries.-of \the world
today.) ,
.. ..
a
International Institute for Environment and Development,
London, 1963,
5 Bp
B|
MEAUSLAN, PATRICK.
Urban land and shelter for the poor,
(The afifefthtfr has focused on the plight of hundreds of
millions of people in the third world without any real
homes, - while 1987, has been declared by UN as the
international year of Shelter for the HomeletJs.)
International Institute for Environment and Development,
'London, 1 9 85.
140p
CHILDREN
B|
\
0|
INDIA. MINISTRY OF LABOUR.
Report of the committee on child labour.
(Report of the sixteen-me’mbers committee apointed by the
Ministry of Labour, Govt, of India in 1979, - to examine
the state of wide-spread existence of child-labour in
the country and the problems arisg^ng out of that situa
tion. The report measures the dimensioOs of working
children in the light of the legislative frame work in
India for the issue and suggests welfare measures whiah
include health, nutrition, minimum wage and other points.)
Govt, of India, 1979.
106p
"
...
Rs. t| 0.00
THE CONCERNED FOR WORKING CHILDREN.
The Child Labour: Employment, Regulation, Training and
Development Bill 1985.
(Draft of a Bill, presented by CFWC for consideration by
legislators, which seeks to recognise the rights of a
child worker and gives him some protection and opportunity
for growth.)
CFWC, Bangalore, 1985.
34p
2 VHA1 (Sathyamala C.etal)
The under five booklet,
(The .Booklet explains the need for and procedure of
maintaining growth-charts to monitor the health of child
ren in 0-5 age group.)
VHAI, DELHI.
0|
COMMUNICATION
COUSINS, WILLIAM
J. (Tr. Utpal' Basta) .
"-Alochana - sabha" . (Bengali )
(The publication deals with different aspects of Groupdiscussions and small meetings as a communication medium).
CHITRABANI. Calcutta '85.
0|
DOCUMENTAT ION
SSDC, ICSSR.
Library and information science literature - SSDC
- resource list.
(The Social Science Documentation Centre under the Indian
Council of Social Science Research, has presented in this
volume a list of its holdings on library and Information
Science consisting of books, thesegs, periodicals and
standards, intending it to be a forerunner of a union
catalogu e.)
ICSSR, New Delhi.
1 82p
B|
ENVIRONMENT
B|
TIMBERLAKE, LLOYD.
Africa in crisis - the causes, the cures of Environmental
Bankruptcy.
(In the context of famines and hunger which have swept
across Africa, this important new book argues tjnat famine^
are the direct results of unsound economic, agricultural
and environmental strategic^., The natural resources of
Africa, the forests, soils and rivers have been exploited
byrthe poor desperate peasants in a way which is bankrup
ting African Environment. This bankruptcy has been
responsible for many social evils and political issues.)
International Institute for Environment and Development,
9
London .
232p
B|
SAHABAT ALAM MALAYSIA (SAM).
Environment, development and natural resources crisis in
Asia and the pacific (Proceedings: symposium: SAM, 22 - 25 Oct, 1983.)
?
(The volume contains papers submitted for seminar organised
by Sahabat Alam at Penang from 22 - 25 Oct, 1983. The papers
are grouped into sections covering an overview of the
situation, forestry, wild life, mineral and non-mineral
resources, food and agriculture, human settlements, the
working environment and toxic wastes and NGOS.)
SAM PENANG, 1984.
422p
Rs, 85.00
.
B|
GHOSH, R.C. and others.
Environmental effects of forests in India, Indian Forest
Bulletin - 275.
(The paper reviews the .present status of research on
environmental effects of forests -in India. The subject
matter has been divided into the broad fields of Forests
□nd Climate, Forests and Water and Forests and Soil.)
Controller of publications, Delhi, 1982.
20p
Rs.
3.10
3
B|
B|
BULL, DAVID.
(A) Growing problem - Pesticides and The Third World.
(The book investigates the alarming facts about pesticides
from the perspective of the poor, - that they threaten
the health and livelihood of the rural people, though
they bring a promise of higher yields and more food for
the hungry. It suggests how to make the most of pesticides
while minimising their dangers, and concludes with a
series of practical proposals for action by governments,
industry and international oroanisations.)
OXFAM, OXFORD, 1962.
1 92p
AGARWAL, ANIL AMD OTHERS.
* No place to run, Local realities and global issues of
the Bhopal disaster.
(This report is a joint product of three organisations,
The Highlander Research and Education Centre, PRIA and
CSE. It describes the events at Bhopal, exposes the
record of Union Carbide world wide, and analyzes issues
that emerge from this disaster.)
Highlander Centre and SOPRIA., 1985.
40p
Rs. 15.00
B|
SAHABAT,ALAM., MALAYSIA.'
Papan radioactive waste dump controversy.
(The book is an indepth report of the events that led
to the controversy over the siting of a dumjbsite in Papan
to store radioactive materials. It is the story of a peo
ple fighting for their rights to good health, to a safe
environment, and to decide on matters affecting their
future.)
B|
SAHABAT, ALAM., MALAYSIA.
Pesticide dilemma in the Third World - a case study of .
Malaysia.
(A study of the ecological and health hazards of indiscri
minate pesticide application in agriculture, the book
also exposes the inadequate policies pursued by the autho
rities in this respect. SAM has taken a bold attempt to
marshall public opinions on the subject, so that the
public’s interests cannbe made to outweigh those of manu
facturers, agency houses and politicians that often work
hand in.glove with business, to the detriment of common
good.)
Sahabat Alam.. Malaysia, Penang
1 984 .
77P
B|
CH ATT OPADHYAY, K.
(A) Preliminary report of a pilot enquiry on the socal
ecology of Sunderban.
(A work of Social Ecology which informs about the environ
ment of Sundarban area, about the social groups and the
exploitation or utilisation of the environment by them.)
Indian Statistical Institute, Calcutta, 1983.
29p + Tables.
B|
SAHABAT, ALAM., MALAYSIA.
(The) State of. Malaysian Environment 1983 - 84 : Towards
greater environmental awareness.
(The report reveals environmental problems of Malaysia, for
example the discharge of toxic waste into the environment,
effects of misuse of pesticides;, the reduction of potential
for productive forestry and wild liffe, depletion of fishing
resources and wuban environmental impacts like acid rain,
haze occupational health etc.)
SAM, PENANG, 1983.
95p
Rs. 23.00
4
0|
ISI, BANGALORE (Seminar).
Conquering space ?
(The article highlights socio-economic &. cultural dimen
sions of our conquest of space.)
ISI, B’lore - Reprinted from seminar, June *
1905.
□|
EARTHSDAN (Hobson, Sarah).
Dam the river, Damn the peasant.
(The article highlights the low cost effectiveness and
negative social impacts of large scale dams, taking th§
case of two large dams scheduled to be cofapleted by 1908
in Senegal, Africa.)
Earthscan Feature, London, 1985.
2 + 1p
ETHNIC MINORITIES,
MARGINAL GROUPS.
0|
PRATAP ANITA (Sunday) .
Tamil Militants Unite.
(Unity among 'Eelam1 groups and it's implications are
the subject for this article.)
ISI, Bangalore. Reprinted from SUNDAY, 28th Apr. - 4th May
pp 46-49.
7p.
0|
SAMPRADAYIKTA, VIRODHI ARDOLAN .
VIKALP (Vol. 1 , No. 1 ) .
(The publication analytically examines communal violence
and it's impact on society.)
Bulletin of Sampradayikta Virodhi Andolan, Jan -Mar. 1985.
44p
Rs. 3.00
HEALTH
b|
CHAUHAN, SUMI KRISHNA &. GOPALAKR ISHHNAN , K.
(A) Million villages, a million decades, - The world wa.ter
and sanitation decade — from two South Indian Villages.
(While weeare passing through UN's International Drinking
Water Supply and Sanitation Decade (1981—90), this back
IBooks at the roots of the Decade in rural India, concentra
ting on two South Indian Villages and studying how water,
sanitation and health issues affect women, men and children
in the villages,)
International Institute for Environment and Development.
58p.
B|
AGARWAL, ANIL AND OTHERS.
Water, Sanitation, Health - for all, prospects for the
International Drinking Water Supply and Sanitation Decade
1901-90. .
(In view of the UN's .launching of the international Drink
ing Water Supply and Sanitation Decade in 1980, this book
examines the Decade's aims, describes the position globally
and in Kenya, Eilumbia and India.)
International Institute for Environment and Development,
London., 1983.
1 4 5p
0|
DRUG ACTION FORUM, W.B.
"Insaan ke liye dawa.ya dawa ke liye insaan". ( Hindi )
(A booklet underlining problems related to drugs and their
implication on people's health. It talks about shortage
of essential drugs, profiteering by drug companies and
dangerous drugs, among othe^ things.)
Sarvangeen Gram Vikas Kendra
Bihar &. DAF, W ,B .,
April '85.
(trans : M.K.Kedia)
42p
Rs.
3.00
- 5 0|
o
B |
B/
D'SOUZA
A.L.
Guinea worm prevention - Major target of WaterdDecadei
( The article explains the infection cycle of guniea
&. its extent in India... explains its impacts on
9.1pin S. measures for prevention.)
UNDP, Delhi,1905.
7
P*
GHOSH 5 .N .
Census of India 1901.Series 23.West Bengal.Paper 1 of
19S2.Final population totals.
( Contains final population totals of Sbheduled caste
population and scheduled tribe population.)
Govt.of West Bengal,Calcutta.
123 p
Rs. 10.40.
ECKHOLM,ERIK AND OTHERS
fuel wood : The energy cirsis that won't go away.
( The author, has drown surprising new conclusions
about fire wood,loss of sell, population pressure and
poverty.The third world poor need for more fuel than
village 'woodlets can ever provide.lt has been, pointed
out that much more must be done to plant trees on farmers
and to promote energy alternatives.)
International Institute For Environment and Development.
London.
107 p.
HTUNG.NAY AND HUISMANS,JAN W ed.
Industrial hazardous waste management.Industry and
Environment,Special issue,Nov.1903.
( The articles Narrate how the problems posed by production
transpSrtation,stroge and disposal of the hazardous wastes
of various industries are being handled by different coun
tries of the world.Aspects of identification of such wastes
and ignorance as to the exact location of old hazardous
waste dumps have been discussed.)
United Nations Industry and Environment Office.
U.S.
79 P.
b|
pria
Occupational Helth and safety- a manual for activists.
( Provides detailed and minute information regarding
the gretest evil of industrialization in India,- Which
is called occupational health hazard.Different types of
diseases that the wufkers suffer from have been described.
Nature of accidents have been discussed.)
PRIA
New Delhi
91 p.
B|
MOLLISON,BILL AND HOLMGREN,DAVID.
*
( The book synthesizes knowledge about a multitude of
economically useful plants and animals, with land use
ideas from a multitude of desciplines : Ecological
Theory,Econamic Botaney,Anthropology,Horticulture,
Landscape Architecture and Hydrology.
International Tree Corp Institute.
U.S.A.
g
* Perma-Culture one.A perennial Agriculture for human
Settlements
6
MULL IS ON,0 ILL.
Perma culture two.Practical design for town and country
in parmanent agriculture.
( The book attempts to make practical suggestions as to
how the best of benefits may be obtained frorp permanent
agriculture centred on human settlements and'community,
by evolving new approaches and solutions for'.different
climates and occasious so that minimal energy is needed
and more calories may be produced.)
T ag ari.
Australia
1 979 .
144 p.
DOGRA,BHARAT.
*• Poverty development and poverty:
India 1947-84.
( An assessment of the oversale performance of post-indep
endence India in fightings hunger and thirst,in the utili
sation of natural resources,in attempts to introduce land.
reformes and modern agriculture technology etc,which in
totality present a dismal picture only to ex-pose a persiste
nce of wide spread poverty inhs'itteld front colonrial rule in
1 947.These are detailed chapters on the role, of foreign aid
and struggles of the poor for a letter life.)
Bharat Dogra.
New Delhi.
327 p
Rs. 45.00.
B|
3
1
□|
B '
I
SAHA3AT ALAM MALAYSIA.
Seeds and food security: a. .-.seeds '.stydy report.
(A report on one aspect of-the green revolution or the process
of scientific and technological development in the third
world's agriculture.The report sounds an alarm bell on the
situation by analizing the profile of the seed industry and
documenting how the local farmers of Malaysia are responding
..to-high yielding varieties and their problems).
.Bam
Penang
85 p
Rs. 18.00.
HEGDE VIJAY N .
’C
*
&. ’ D1 lands as a resource to rural life - A case.study
+ survey of C &. D lands in sagar,Shimoga,Chikkmagalur B Ka
ppa forest divisions.
( Whats relationship of people to *C ’ & ’D’ classes of land
(unsuitable for agriculture- public land) in selected distr
icts of karnataka and how its being jeppardised by present
Govt.policy of alloting such lands to private companies is
the subject of these
articles.)
z
Arogya Vikasa Prakalpa,
Shimog a
.5 + Vii p.
HUMAN RIGHTS
MASUD ,SYED S .A .
'
, ...
Report of the sub commission on prevention of discrimination
and protection of minorities^'
( Report of sub commission under the commission on human
rights on its thirty sixth session held in geneva between
15 August and 9 September ,198-3.)
United Nations
Economic and Social Council,
Geneva.
1 983 .
P : Vii,III + Annex.
7
@I
COBO,J,R,MARTINEZ
Study of the problem of discrimination against indigen
ous populations.-Final report on thirty sixth session:commission on human rights.
( Last part of the final report,submitted by special reporteur,of the sub commission on prevention of discrimination
and protection of minorities.I tern 11 of the provisional agenda)
Economic and social council,U.N.Geneva.
1 06 p.
UNNAYAN
The 1905 supreme courts view of the eviction rights of
pavement end 'slum’-dwnliers
( The document is a collation of extracts from judgement
delivered by supreme court on 100785 on the 1901 writ pet
ition by olga telh's and others and by the PUCL-CPDR and
others regarding the summary evictions of pavements and slum
dwellers of Bombay.)
Unnayan,Calcutta,July '85 ( extract from supreme court
judoement on july 10'85 )
18 p.
D|
TARKUNDE.Vv.r,.
The terrorist and disruptive activities ( prevention)
act 1985.
( An article highlighting the dangerous elements of this
new act and calling all people to support the demand of
ir's withdrawal/cancellation.)
151 3'Lore.Reprinted from radical humanist june '85.
CHACKO.FR P.A.
The BANJHI massacre some searching questions + supplement.
( Deiailancilfiittaa.liBqa^BnibitigaBgnjlii'’'vill^ga^iaahib^arii js of
ttlistitic±$ibil1iar on april 1 985 in ex janata party MP artony
.The articale highlights the background of the inc
ident and examines it's implications.
POLITY
3/
151 ( Radical Humanist)
Role of black money in party politics.
( The article exposes the role of- black money in Indian
politics.)
151 B'lovfe reprinted from raddical humanist jan '85
PP 6-9
p.
3.
SOCIETY
§|
DESROCHERS , JOHN
Classes in India today.
( The booklet looks at social stretification from the class
view point.A painful contrast is exposed,through idtentification of the various socio-economic and political groups,
between our country's noble ideals and its social realities.
Centre for social action,Bangalore.
125 P’
'
Rs.
4.00.
PREMI,MAHENDRA K. AND TOM,JUDY ,ANN L.
City typology,Migration and Development in India
( Describes the pattern of migration to cities in India,
as also the characteristiiss of migrants and the de terminan ts
of Migration flow.The Govt.of India's urban development
policies have been examined.
East West Population Institute.Honolulu,1983.
153 p.
B
g|
ICSSR .
Sociology and social anthropology,ICSSR.journal of
abstracts and peviews.Vol.13.no.2.July-December.1984.
( A collection of scholarly reviews and valuable abstr
acts, of publication on the varied fields of human soci
ety , including culture,environment,politics religion and
e thnology. I ndex has been provided for the names of the
authors of articles abstracted,as also for authors of
the hooks reviewed.)
ICSSR,New Delhi.
377.p.
Rs. 10.00.
3HAIA,ABHA AND BH AS IN , KAMA-'i&A ed.
Vikas Ke Ayam ; Kuchh Samasyaen,Kuchh Samadhan.
( Intended for development activists who will find this
book to be a guide in the various fields of development,
that provides analysis of facts,project reports and case
studies on adult education,ethnic movements,rural socio
logy and other important issues.)
Fao,New Delhi,1984.
195 p.
B|
UH Bl A® AMOVE (MONTHLY REVIEW ).
She i pub lids
po r iommo n of ipiaanmn^hfofutba’euoDr^aihiee America.
( This set of documents exposes the various dimfifeions of
public policy while dealing with urban-informal sector
( Hawkers,Rickshawpuliers,slurn dwellers) through reproduc
tion of news items,extracts from policy meetings etc.
Contex : July '85 supreme court ruling on encroachments.)
Unnayan,Calcutta,July 185.( BTV bulletin spl.no.250785 .
B|
ISI ® 'UOfS/EllK-YMBSVHE’Y REVIEW )
Basic Christian' communities and the future of Latin America.
(The article explores the interxRPlation between religion
and radical politics/ideas and movements.)
151 B'LCRfE ( Reprinted from monthly review,July-Augst'84 .
Jtl
ISI /HA INSTREAM.
Rajiv Gandhi's policy projection ( an interview)
( Prime Minister's thoughts on policy issues and national
priorities as revealed through interview to financial
Times (London) on Aprifli 4'35.)
ISI B'LO'rE ( Rep ; from Mainstrem april’85 pp 60-62
originally published in Financial Times (London)
WOMEN
|
gb|
3HAIA,ABHA AND 3H AS IN , l< AMLA .
Mahila vikas ke ayam.
( Hindi)
( Study and disetjssious on women's position in society
which is generally male-dominated.Women 1s problems,
sufferings as well as solutions and improvements of
situations have been dealt with at length.)
Fao,New Delhi,
122 p.
MITRA,MANOSHI.
Mata aur go mata; The woman and the sacred cow- A study
of women in dairy.production.
( The data generated by survey has been analysed in order
to answer the basic question of different patterns of
involvement of women in dairying,- constraints,labour
rmputs,gains,participation and the intervention to inten
sify this.Chief areas taken into account are,Nalgonda,
chittoor and Krishna districts of the south.)
9
0I
CENTRE FDR WOMEN'5 DEV E L DP ME NT _S TO DI E S .
Tables on women's co operatives in India.
( A set of tables prepared fumm the particulars received
from the registrars of coppcrotive societies,and from the
individual women's coperatives in the country.
date base
to be used by planners , administratiness , researchers and others.
CWDS.New Delhi,1983.
127 p.
81
2HAS IN ,!<AMLA .
Towards empowerment.
( Report of a south Asian re'agional Training workshop
organized by FFHC/AD at the end of 1983,for women develop
ment workers from 8angladesh,I ndia,No pal,Pakistan, and
Srilanka.)
FAO,Mew Delhi,
237 p.
B|
ACHARYA.SARATHI.
Women and rural development in the third world.
( A study and analysis in thepggspective of the third world
of women’s participation in agriculture,nature of their work,
and of women's role in rural economey together with reccomm
endations on policies.)
Tata Institute Of Social sciences ,Bombay.
146 ; p.
MINISTRY OF RURAL DEVELOPMENT., GOVERNMENT OF INDIA.
Development of women and ahildren in-rural areas( DVJCRA)
( The booklet describes the different aspects of DWCRA
scheme of the central govt.Which aims at enabling women to
make greater use of services offered by IRDP,since presently
only 10% of IRDP benificiaries are women.)
MRD,Govt.of . I ndia and UNICEF ( text by Pria),Delhi, 1 985 .
@|
PRIA ( TANDON R AiJESH et al.)
How to communicate effectivelk/y with grass-roots women ?
( Didactic Bulletin Noz2in the serves:Women's participation
in development deals with ideas about and methods of
commonication in the context of women's organisations.
PRIA + UNICEF New Delhi, 1 985.
S|
PRIA ( TANDON RAJESH ET AL )
How to conduct participatory research among women?
( Didactic bulletin no 1 in the scry'ics women's part
icipation in development- explains the basic principles
of participatory research and it's sole in the context
of organising women.)
PRIA + UNICEF,Delhi, 1 905 .
28 p.
0|
PRIA AND UNICEF ( Khot,seemantini et al)
How to organise women's groups.
(Didactic bulletin no 3 in the seryios: Women's participa
tion in development
dealing with problems and possibities
forming women's group.)
Pria &. Uniccf ,Delhi ,
28 p.
0|
PRIA
Invisible hands : Towards empowerment.
( The re ports narrates the proceedings of a national
workshop held in Udaipur Mar 25-29 '85 and it's major
conclusions regarding income generating projects as a
means of organising women.
Pria,DeIhi,1985 ( Report of national workshop on women's
income generating activities,UDAIPUR,Mar 25-29,85.)
31 ,PB| - Books,
0|
- Occasional Paper.
Part III
~
Dr. Raj-il Desai
Dr. Sagan Desai
Preparations of commenly used Haematinics
Sr.
No.
Compound (Name)
Formulat ion
1.
Aktivakid
£Syrap
(Each 5 Ml.
contains...
Liver fraction
Ferric glycerophosph
Yeast Extract
lysine mono - JtScfcHCL
Vit B-12
125 mg
60 mg
15 mg
25 mg
1.0 mgg
Ingrediants and their quantity
Company
German
Remedies
Cost
Rs.
M.D(rharamacology)
M.D(Pharmacology )
Dose
10.12/
100 ML.
5-15 ml.thrice
daily before or
after meals
2.
Anemadox
Capsules
(Each cap.
cont ains..
Ferrous Fumerate
Folic Acid
Vit B-12
Cal.Carbonate
Vit-D
Vit-C
560 mg
1.5 mg
15 Mcg
200 mg
400 IU
75 mg
Merck
11.51/
28 Cap.
1 Cap. daily
5.
Dumasules
Capsules
(Each Cap.
contains..
Ferrous Fumerate
Vit-B-1
Vit-B-6
Niacinamide
Folic acid
Vit B12
Vit-C
500 mg
5 mg
1.5 mg
50 mg
O.75mg
7.5 mcg
75 mg
Pfizer
R29.52/
100
2 Cap.daily, 1 each
after breakfast
and dinner.
4.
Nori-A
Tablets
(Each tab.
contains..
Ferrous Fumerate
200.00 mg
Wellcome
18.69/
500
Adults & Children
Over 12 yrs.: 1 Tab.
thrice daily and
children 6-12 yrs.
tab.thrice daily
after food
2
Sr.
No.
Com-pound (Name)
5.
Eisocal
6.
Fefol Spansules
Formulation
Ingrediants and their quantity
Company
Tablets
(Each tab.
contains..
550 mg
1000 IU
200 IU
1 mg
0.5 mg
0.5 mg
1 mcg
25 mg
7.5 mg
0.5 mg
0.1 mg
0.05 mg
0.05 mg
1 50 mg
Cipla
Gel. Capsules
(Each cap.
contains,.
Iron Calc. Complex
Vit-A
Vit-D-2
Vit
Vit-B-2
Vit B6
Vit B12
Vit-c
Niacinamide
Folic acid
Copper Citrate
Molybdenum trioxide
Mang, citrate
Dried Ferrous Sulphate
Folic acid
0.5 mg
7.
Folvron-F
Capsules
(Each capo
contains. .
Folic acid
Ferrous Fumerate
(64 mg.of metallic iron)
1.7 mg
194 mg
8.
Ferradd
' Liquid
(Each 5 ml.
contains
Vit-A
Vit-DJ
Vit B1
Vit B@
Iron and ammonium citrate
Nicot inamide
Vit-C
Vit B2
Vit B1
Nicot inamide
Vit B6
Pantothenic aid
Dried Ferrous sulph.__
2500 IU
200 IU
1 mg
1 mg
45 mg
16 mg
50 mg
2 mg
2 mg
15 mg
1 mg
2.5 mg
150 mg
9.
Fesovit
Spansules
Capsules
(Each cap.
contains..
Cost
_____
50
Dose
1 to 2 tab .thrice
daily preferably
after meals
Eskay
Lab.
8.47
15
1 Cap. daily
throughout
pregnancy & lac
tation
Cy'anamid
4.23
50
3 capsules daily
43.47
1.25 Kg
Adults: 10 ml.
thrice daily
Children: 2.5 ml,5ml
thrice daily
8.47
15
1 -2 Cap.daily
children: 1 cap.
daily
Parke-Dav is
Eskay Lab
5
Sr.
No.
Compound (Name)
10.
Folinate B-12
11 .
Formulation
Ingredients and their quantity
Company
Cost
Dose
Rs
Hematrine
12.
Heptaglobin
15.
Higlobin
(a) Capsules
(Each
cap.con
tains. .
Ferrous Fumerate
Folic acid
Vit B12
Vit C
(b) Liquid
(each
10 ml.
contains.
Alembic
Ferrous Numerate
Folic acid
Vit B12
,
250 mg
2.5 mg
0.25 mg
75 mg
250 mg
4-0 fpg
50 .mgn - q
Capsules
(Each cap.
contains..
Ferrous succinate
Succinic Acid
Folic acid i
Vit C
Vit B12
Nicot inamide
1 OOmg
110 mg
0.5 mg
25 mg
2.5 mcg
15 mg
Sandoz
Liquid(Each
15 ml.
contains..
Proteolysed liver
Qxyhae moglob in
Reptene
'
Iron & ammon.pitrate
Nicotinic Acid
Vit B12
Alcohol
1.2 gm
250 mg
750 mg
200 mg
3 mg
6 mcg
0.30 ml.
!jte
Ferrous Fumere
Vit B12
Vit B2
I
Vit B1
^olic acid
V
Nicot inamide
Vit c
300 mg
10 mcg
2 mg
10 mg
2 mg
25 mg
75 mg
Vit B1
Nicotinamide
nsFolic Acid
Vit B12
litrkte
Ferric ammon.c
Vit B2
5 mg
10 mg
0.5 mg
5 mcg
225 mg
2.74 mg
(a) Capsules
(Each Cap.
contains..
(b) Liquid(Each
(5ml r-n+i
*
21.58
100
1 Cap. daily
13.07
450 ml.
*ml
Adults? 10 ml.daily
Childrens 1.25 ml.
- 2.5
/day
*
1 ml. daily
500
1 cap. thrice
daily or as
required
Raptakos
19.12
300 ml
15 ml. two or
three times daily
IDPL
28.33
100
One Cap. daily
8.22
5^10 ml. daily
110 ml
4
Sr.
No.
Compound (Name)
14.
Iberol
Formulat ion
Ingredients and their quantity
Company
Cost
Dose
Rs
(a) Film tablets
(Each tab.
contains..
Ferrous sulphate
Vit B12
Liver desiccated
Vit C
Folic Acid
Vit B1
Vit B2
Nicolinamide
Vit B6
Cal.Pantothenate
(b) Liquid (Each
5ml.contains
Ferrous sulph.
Vit C
Vit B12
Vit B1
Vit B2
Nicot inamide
Vit B6
Pant he no 1
Alcohol
Ferrous Sulphate
(c) Iberol-500
Liquid(Each
Vit C
5 ml.contains Vit Bl 2
Vit B1
Vit B2
Nicot inamide
Vit B6
Pant he no 1
Alcohol
!
;
(
•
i
\
;
i
525 mg
12.5 mcg
1 00 mg
75 mg
1 mg
3 mg
3 mg
15 mg
1.5 mg
3 mg
Abbot
18x5-6
100
1 -2 t ab. daily
151 mg
57.5 mg
6.25 mcg
1.5 mg
1.5 mg
7.5 mg
1.25 mg
2.5 mg
0.5 ml.
Abbot
s/oo
240 ml.
10 ml. twice daily
131 mg
125 mg
6.25 mcg
1.5 mg
1.5 mg
7.5 mg
1.25 mg
2.5 mg
0.5 ml
Abbot
14-.24
10 ml. twice daily
24O ml.
Sr.
No.
Compound( Name )
15.
Livibren.
16.
Livogen
Formulation
Elixir (Each
10 ml.
contains...
Capsules
(Each Cap.
cont ains...
*V' 4 B 75 mg
16.
S^nabhinn
Capsules
(Each cap.
cont ains..
Company
Cost
Dose
Parke-Dav is
10.05
228” ml
10 ml. before
food, twice
daily
Liver concentrate Powder
0.1 gm
Dried Yeast
25 mg
Vit B1
5 mg
Vit B2
5 mg
Nicotinamide
45 mg
Cal. Pantothenate
5 mg
Folic Acid
1.5 mg
Vit B6
1 .5 mg
1 0 Mcg
,.Vit B12
Ferrous Fumerate
. 15.0 mg
Alleriburys
10.26
50
1 Cap. daily
after meals
Ferrous Gluco
250 mg
Mang. Sulph
0.155 mg
Copper Sulph
0.2
mg
Vit C
50
%
Vit B12
7.5 mcg
Folic acid
i
1 mg
.Sorbitol________________________ 25__mg.
Merck
9.61
Initially 2 cap,
thrice daily
after meals,
followed by
1 cap.thrice
daily.
Ingredients and their quantity
Liver concentrate
Vit B1
Vit B2
Vit B12
Ferrous Sulphate
Mang.Citrate Soluble
Alcohol (l2$ V/U)
•
I
i
116.25 mg
2.5
mg
2.5
mg
5
mcg
275.74 mg
5.7
mg
1.25 ml
30
6
Sr.
No.
Compound. ( Name )
Fnrmulat ion
Ingredients and their quantity
Company
Cost
Bose
18.
Phosfomin Iron
Elixir
(Each 1 5 ml
contains..
Cal. Glyce rophos.
Sod. Glycero. phos.
Pot. Glycero. phos.
Mang. Glycerophos
Ferric ammonium Cit
Vit B1
Vit B2
Vit B6
Niacinamide
>11. Panthenol
Vit B12
Aocohol
(11$ by volume)
110 mg
80 mg
20 mg
10 mg
46.5 mg
2.0 mg
1 .0 mg
5 mg
15 mg
1 mg
15 mcg
1.7 ml
Sarabhai
13.57
480 ml.
15 ml. thrice
daily or as
required.
19.
Tonoferon
(a) Syrup
(Each 5 ml.
contains. . )
Colloidal Ferric Hydrox
Folic acid
Vit B-J2
Ethyl alcohol (V/V)
500 mg
1.75 mg
7 mcg
. '2.^
East
India
22.00
450 ml.
2.5 - 7.5 ml.
twice daily
(b) Drops(Each
1 ml.
contains..
Colloidal Ferric Hydrox
L-Lysine mono-hd
Vit B12
Folic Acid
Ethyl Alcohol (V/V)
50 mg
200 mg
1 0 mcg
5 mg
. 2-2
East
India
_2
15 ml.
5-10 drops with
milk, two-tliree
times daily.
20.
Siderfol
Capsules
(Each scap.
contains..
Ferrous Fumerate
Vit C
Folic Acid
Vit B12
500 mg
100 mg
5 mg
50 mcg
Raplakos
11.85
50
1 Cap.daily after
meals or more as
needed
21.
Rubragan H.P.
Capsules
(Each
Cap.contains.
Ferrous Fumerate
Vit C
Vit B6
Folic Acid
Vit B12 j
300 mg
100 mg
10 mg
2.5 mg
50 mcg
Sarabhai
5.?6
14
One Cap, twice
daily.
7
7
C o .npojtnd. (Name )
for .lulat ion
Ingredients -nd their quantity
Company
Cost
Dose
22.
Rubraple?:
Elixir (Each
5 ml.
"ant? ins..
Elemental iron,as ferric
anm.cit. and. colloidal iron 58 mg
Vit B1
1 mg
Vit B2
1 mg
Niacinamide
5 mg
V it Bl 2
4 mcg
Vit B6
0.5 mg
rLl.panthenol
1 .5 mg
Alcohol
12 Jo
Sarabhai
1J...22.
480 ml.
5 - 10 ml. ’.tH-fice
daily
25.
Rub rat one
Elixir (Each
5 ml.contains)
Ferric amm. Cit.
Vit B12
Folic acid
Alcohol
SarabSai
1J..69
480 ml.
10 ml. thrice
daily
Sr.
^0.
220 mg
4.17 mcg
0.28 mg
12 %
February, 1985
Source:
MH'S India,
Note
d'he above formulations are simply presented, without comments.
You are requested, to interprets them in the light of Scientific ibtes.
:
. REPORT OF; 'RATIONAL THERAPEUTICS.CELL' ,
MEETING HELD ON23-6-1985
.
. ' All tho.se- pre’senV were
'■■ ■■
:
. < -■ J
,.-.c
. Drs,-. > Arun: Phataky Ani.-jta Srivastava.,' Lakhani
• ft
L.K’.' Chauhan,' Sagun. Desaiy- Ap'hwin Patel,.and
. i.l . -.1 As,shaya..Up.adhyaya3. Tushap.-Sha|i 2. Nimit.ta Bhatt,
. . S. Hriniyasan.. -.-i
j-j/
< •
Our friends from Bombay could not attend the meeting
because of the rioteering'.
'" ' '
•
. :
:
7f-
Agenda of the .meeting- was
X ‘‘
■'
i ''
'
, 1) Disc.ussioh . on Haeniatinics
2) Package Incert Material
. . 3/ Plan of Action of-' the Cell
4)-. Ne,xt Meeting.-:
L^L£TINi(^A-^l V-3;"' Sl’$
■
—---- //ru;. yj^,
-- • -■ • ,oJ Background- papelE3.--.ons Haematinics: yrp.re; prepared .--by, gag-nil Desai,
Anita Srivastava, ■ Rajul Desai andL.N.- Chauhan. ■•
The papers were discussed and following points were' made :
Need of Pe
-
'supplement.
'
.
- The bio availability of iron in vegetables is . very flow . So
if-one has to: take his/her requirement of iron, from vegetables
•only, then it becomes too bulky and expensive. . Then it was pointed
out that the iron is also present in'cereals, jaggery and other
•-pour06,3' which'..also fforms :a ;part of his/her-daily food. "...
:
;
The iron'.content, of breast-;mxlk is low- and -so it was practised
till how that iron ' supplement, should be started at 6-12 weeks
of age. -But now recent studiesJshow that the bio availability of
- iron'in breast milk is very high. So the child does not need Fesupplement at early age, say upto six months.
Premature babies hp.ve poor iron store. In pre-mature-' \'
babies if iron is' given as supplement it interferes with body
mechanism. So it becomes difficult to decide when and'how much
iron- may be £iven' to such babies.
Though the group was concerned about blackening of teeth
due to liquid iron preparations. This concern.is uncalled for
since the staining is transient (Goodman Gilman P.1324)
A variety of substances designed to enhance the absorption
of iron have been marketed, including surface-acting agents,
carbohydrates, inorganic salts, amino acids and vitamins. - One
of the more popplar. of these is' ascorbic acid. When present in
our amount of 200 mg or. more, ascorbic, acid increases the absorption
of medicinal iron by at least 30%. However, the increased uptake
is associated with a significant increase in the incidence of
side effects and therefore the addition of ascorbic acid seems
to have little advantage over increasing the amount of iron
administered.
There is no practical benefit in employing those
compounded preparations.
It is particularly undesirable to use
preparations that contain other compounds with therapeutic
action of their own, such as Vitamin B 12, folate- or cobalt,
since the patient's response to the .combination cannot be easily
interpreted. Despite the highly specific response of iron
deficiency to the element and the straight forward nature of
therapy with iron, it is discouraging to see the frequency with
which expensive preparations with worthless additives ap’e prescribed
(Goodman Gilman).
.<;'v .-,bJ
-2-
Folic acid deficiency is not uncommon specially during
frequency and lactation. Dimorphic anemia is also often found.
So combination of Ferrous sulphate and Folic acid as advocated
by WHO should be made available.
In our country where most women are anemic, we should be
giving iron and folic acid supplements to all pregnant women from
early frequency. The supplements should be made available through
CHV's and other a paramedical health functionaries.
Though
much depends on the national priority some limitations of this
system should also be kept in mind, like early detection of
■“pr^gifftncies is difficult, however effective the CHV is. After
knowing the pregnancy, compliance of women to take the tablets is
often very poor not only due to psychological factors but also due
to untoward effects of Ferrous sulphate like gastro intestinal
upsets. Question of enough resources with the PHC's is also
very important. Again 90% of their energy is diverted to achieve
the family planning targets.
It was also felt that only a Government is not responsible for
'.this negligence of MCE programmes. Medical bodies are also
■ equally responsible for not pressing the
need for effective
MCE programmes.
It was pointed out that the normal standards of Eb
level
of western population may not be applicable for our population.
Then the methodological problem of how to determine normal Hb level
in our population, most of which is iron deficient was raised.
Dr. Aggarwal has suggested that iron supplement may be given till
maximum Hb level is reached. This level may be considered as normal.
Earlier studies suggested that most side effects associated
with the oral administration of iron were of psychic origin.
However more recent studies have established beyond doubt that
physical intolerance does occur. Higher the dose given more
rapid is the response but greater is likelihood that side effects
may be produced. A good policy is to initiate therapy at small
doses in order to demonstrate freedom from side effects at that level
and then gradually to increase the dose upto desired level.
It was <j.lso felt by one of the group members that Ferrous
sulphate is easily oxidised to Ferric salts which are not readily
absorbed. So ferrous fumerate which does not get oxidised very
fast may be preferred. It was quite forcefully said that this
is not necessary. Proper care for prevention of ferrous to ferric
salts can be taken by improving the coating on the tablets. The
anhydrous ferrous sulphate can also be used. A pharmaceutics expert may be consulted+in this regard.
The enteric coated (delayed release) tablets are virtually
worthless since iron is usually absorbed in. upper p-art of small
intestine. The capsule forms of iron preparations are available
in the market but are very costly with no extra benefit. So they
should be avoided.
2 Parentaral administration is indicated only in conditions
mentioned in Paper I. Local reactions including long continued
discomfort at the site of i.m. injection, local discolouration
of skin, and concern about malignant change at the site of
injection make the i.m. route inappropriate except when i.v. route
is inaccessible. Proper care must be taken to avoid any double
therapy and the patient must be informed accordingly.
-5-
- 3 -
Liver extracts are not indicated in any condition.
Common
Vit. B 12 source for vegetarians in India is said to be conta
minated water and legumes.
Formulations of most haematinics in the market are ma
irrational. Very high quantity of one component and insignificant
amount of other nutrients like iron reduces them to mere
economic waste. Rational multivit preparations should be made
available in the market.
In geriatic complaints enzymes are prescribed. The group
unanimously discarded this practice.
Line of Action of RTC
(
I.
i) LOCOST should try to supply the rational combination
of iron and folic acid as recommended in WHO formula.
( ii) Rational multivit formulations - according to recommended
daily allowances both tablets and liquids should be
made available^ through LOCOST.
II.
We must write articles in vernacular press regarding haematinics
Sunil Dosai and Sagun Desai took up responsibilities of
writing such articles.
The first of the series will be
prepared by Sunil Desai before 15th July 1985.
Akshaya and Tushar would help to collect statistics to make
the articles more catchy.
Sagun Desai to guide them to collect
these statistics.
After we have 4-5 articles ready with us we could also think
of having a regular health column in any newspaper.
..
Press releases on various topics like Haematinics, use of
analgesics, antispasmodics etc. should be given. At a time
only one group of drugs should be covered so as to focus
the issue and avoid misrepresentation in the press. The release
would be followed up by articles on the same topic.
III.
RTC would try to create awarenesg among general practitioners
by holding monthly discussions on rational therapeutics of
various diseases. Dr. Lakhani to explore the logistics and
with the help of Chauhan and Sagun will arrange for the first
meeting in the first week of August 1985The information
£bout the meeting will be given as a news item in Baroda
Medical Union Newsletter.
Two days workshop for fresh interns would be arranged to
develop their concious opinion about rational therapeutics.
Sagun Desai and Lakhani to take care of this.
IV.
Letters should be written to drug authorities, questioning
the rationality of many haematinic preparations in the
market. S. Srinivasan to follow up.
V.
We should develop a few posters for each topic for general
education purposes. For this first step would be to jot
down precisely the message. Artist may be contacted afterwards.
Sagun Desai to contact Dr. Palan, who has interest in this
sort of activities.
Package Incerts
The package incert material for ampicillin, mebendazole,
paracetamol and atropine sulphate was prepared gnd circulated to
all our partners before. Their responses were invited stating the
usefulness of such a material for other drugs.
They were also
requested to state five drugs of priority on which they would
like to have- similar material.
- 4 -
We had received 10 responses.Salient features of their
comments were discussed and some of their suggestions will be
incorporated while preparing other material. Their priority
drugs for such material were co-trimoxazole, Metronidazole,
Chlorpromazine, DHQ and Phenylbutazone. All of them found the
information useful, adequate, clear and easy to understand.
NEXT MEETING
Next Meeting of the Cell will take place in the last week
of August, 1985, - tentatively on 25th August at Baroda.
Topics for discussion will be essential drugs and antacids
and enzymatic preparations. The background papers would be
prepared by Sagun Desai and Lakhani respectively.
Bombay group of the Cell would select their topic and
prepare background material for it. Some of those suggested
were Antitusive drugs, Expectorants and Anti-amoebic drugs.
HAEMATIMCS
PART II :
(A)
Dr.Anita Srivastava
M.D.(Paed.)
SOME CLINICAL ASPECTS
Eaematinics in children
IRON s Since dietary iron in children rarely provides
sufficient replacement a supplement is required.
Oral therapy is always preferred unless the patient
is unable to tolerate it or the family is not considered
sufficiently dependable to administer the dose regularly.
The regular response of iron deficiency anaemia to
adequate amounts of iron is an important diagnostic as
well as therapeutic feature.
Oral Therapy
Oral administration of simple ferrous salts (sulfate,
gluconate, frumerate) provides inexpensive and satisfactory
therapy).
The recommended therapeutic dose is 4-6 mg/kg/day
of elemental iron given in 3 daily doses.
Ferrous sulfate is probably the most effective and
least expensive iron containing drug. Since it consists of
20% e£ elemental iron by weight the usual daily dose is
30 mg/kg. Doses of elemental if’on in excess of 6 mg/kg/day
do not result in a more rapid haematological response.
Ingestion of large amounts on milk may significantly
decrease absorption of iron.
Intolerance to oral iron is extremely rare, mal
absorption of oral iron is more frequently invoked than
demonstrated.
While adequqte iron medication is given the family
must be educated about the patient's diet and consumption
of milk should be limited to a reasonable quantity
preferably 500 ml/day or less.
Folic Acid Deficiency
A dose of 1-5 mg orally daily for 4-5 weeks is usually
adequqte to replenish the body stores even in patients with
malabsorption. Patients with simple dietary deficiency can
usually step therapy at this point, if they are on a
proper diet, while patients with malabsorption or increased
need for folate may kk<jhxxe require therapy indefinitely.
Vit,B12 deficiency
a)
Therapeutic trials Give 1-3 mcg Vit.B 12 daily i.m.
for 10 days. If the pt. is B-12 deficient, the response will
be as follows :
Within 24-48 hrs. the marrow will convert from megalo
blastic to normoblastic morphology. Reticulocytosis should
appear within 3 days and peak around the fifth day.Haemaglobin
should return to normal level within 4-8 weeks.(Although
folate deficient patients may respond to very high doses of
B-12 they will not respond to this very low dose).
b)
Subsequently 100 mcg/day i.m. for 2 weeks should be
given to replenish body stores.Then 100-1000 mcg i.m. once
monthly for the rest of life or until underlying disorder
is cured.
c)
Life threatening hypokatenia may occur during early
treatment and serum K+ values should be carefully monitored.
I
- 2
P&rt_II
.a ri < <=• in - crum ’rir - id frpm.i,-n'1y ec-tma-nipthe rrcti-ulocvto■■ u-u-lly reaching it- ne-\ ?t about
Hip four'h d-y -o-e- +-he -t-rt. of treatment Th?- may
ore-’-n^.-d h *
llo->urinoT
r1)
i
M-nnual of paediatric therapeutics
Ed John W. Gr-~ef Thomas E Cone Jr,
2nd Edition
2
Nel pon’s Textbook of Paediatrics
12’h edition.
(B)
HAEMATINICS IN OBSTETRICS
Dr L N chauhan
M.D. (Ob. & §yn. )
B'Ckojqund
Anaemia may anted-to concretion j.t i- often aggr~vated
by orr n«nc” and 4 he ac-ident- of labour may neroetuate it.
Th- me»n m'nimum ®C'pnt'ble Hb 1-vel f the WHO is
11.'1 mi 'dl (WHO- 1Q72)
Adn-nt.in'~ f'l om% of HB the incidence of anaemia. in India
r-nner f• nm ',/'b'qo% in eho -’ev-looed countries the incid-nce
-nges fo-nm '>'1-2'1%.
Anaemia accounts from 15 to'2'1% of all
mntorn-l d.-rt’ s in thi- country mostly’contributeing to
rather than brincr directly re-->->nslblef for maternal de~ths.
In nreenrn-y the -"’emand for hnenp+i nics mostly iron ^nd
Folic A-id -nd 1-s- commonly Vi+.B.12 i- increased to meet
tty riervAa oc 4-hp «pc-> anting r'd cell maso (maximum) and
rrmii>■-mentr or 4ha developing f-tus placenta and uterine
t>vnrrtronhv,
IRON
Tot^i rc-uimment of iron r-noes from 700 to 1400 "mg
during ■nregorncy Overall to-uir-ment for iron i- 4 mazdey and
6.6 mgzd-y in Irrt 4 weeks of pregnancy.
This can be met only
by mob.ili-inc iron -tore- in --’-’ition to achieving maximum
ab-orntion of di.-trry iron, bec-u-e a normal mixed diet
supplier -bout 14 mo of i-on each d-y of which only 1-2 mg
(5-15%) i° p^-orbed.
DieJ--ry ’ rpn ’-ould ’still n^t provide enouoh iron for the
n-eds a47 preon-n-v pur-o.-rium an<i the 1-ct-eion for a woman
on a normal mix-d ^iet. It ’'Ouia b- still ler- in vegetarian
diet. S’no- many ’-’omen -nter—'.reonancy with depleted stores.
Ttr commancst h-em-toloaic?! problem in pregnancy is anaemia
resultino from iron -letlc’-ncy.
over the ye-rs there have been many studies -’hich have
proved w-j-hout doubt th~t iron suonl-ments prevent the
-’eve1 oom-at of -na.-mia »n-i that even in ”omen on a good diet
"ho -re no’ a’Toarently anaemic st l>ookino. the mean Hb level
can b6 rais-d by oral iron therapy throughout preanancy,.
A rrs’uction of Hb is preceded by a depletion of iron
rtor-es, it i- tho-e women who enter preanancy in precarious
i-on Ta-i-nce ’-ith normal Hb who present the m’st difficult
•’iaono-ti^ problems.
3
The UN-8 recommended the supplements of 30-60 mg/day
to those pregnant women who have normal iron stores and
120-240 mg with none.
Whether all pregnant women need iron is controversial
But if it is accepted that iron is necessary a bewildering
number of preparations of varying expenses are available for use.
In those women to whom additional iron cannot be given
by the oral route either because of non compliance or because
of unacceptable side effects parenteral route, can be used.
There is no haematological benefit in giving parenteral
as opposed to oral iron but the failure rate of some women
to take oral preparations is high and the sole advantage is
that the physician can be sure that they have relieved
adequate supplementation.
The majority of women tolerate the cheaper preparations
with no significant side effects and in the interests of
economy z. these should be tried first.
FOLIC ACID
OOer and above pregnancy problem lactation provides an
added folate stress. A folate content of 5 mcg/1 00 ml of human
milk and a yield of 400 to A 500 ml daily implies a loss of
20 to 25 mcg folate daily in breast milk.
The cause of megaloblastic anaemia in pregnancy is
nearly always folate deficiency. Vita 8.12 is only rately
implicated.
Requirement according to MHO recommendations _£1 972)
800 mcg during ante natal period
600 mcg during lactation period
400 mcg
non pregnant adult.
;
The incidence of megoloblastic anaemia in the developing
world is considerably greater and is thought to reflect the
nutritional standards of the population - to the poor socio
economic status of their patients. Food folates are only
partially available and the amount of folate supplied in the
diet is difficult to quantify.
The main point at issue over recent years however is
whether the apparently intrinsic folate deficiency of
pregnancy can predispose the mother to a wide variety of other
obstetric abnormalities and complications in particular
abortion, fetal deformity, prematurity and ante partum
haemorrhage. The extensive literature would seem to be almost
equally divided in its opinion however a more recent report
(Smithells at al 1980) suggests that this supplementation may
prevent Neural tubal defects.
FDLIC. ACID
should never be given without supplemental iron.
A wide variety"of preparations supplying both iron and folate are
available and provided that the folate is not less than 1 00 mcg
daily, all arc aatisfactory for prophylaxis in pregnancy.
Vitamin B 12 : Pregnancy does not make a groat impact on
maternal Vit. B 1'2 stores. Addisonian pernicious anaemia does not
usually occur during the reproductive years. However severe
Vit. B 12 deficiency may be present without morphological changes
in haemopoietic and other tissues. Pregnancy in such patients
may be followed by death in utero or may proceed uneventfully
(Chanarian 1979) . It may be associated with chronic tropical
sprue.
- 4 -
The megaloblastic anaemia which developes is
due to long standing Vit. 8 12 deficiency and super
added folate deficiency.
The recommended intake
of Vit. B 12 is 2.0 mcg/day
in me non pregnant and 3.0 mcg/day during pregnancy
(WHO 1972).
This will be .met by almost any diet which contains
animal products.
Strict vegans who will not eat any
animal derived substances may have a deficient intake
of Vit. B 12 and their diet should be supplemented during
pregnancy,
HAEMATINICS
PART
I
; Pharmacological Aspects
Dr Sagun Desai
Dr. Rajul Desai
INTRODUCTION
Anaemia is a common problem in India, which may be
due to several causes but nutritional deficiency especially of iron and folic acid - contribute to this
to a large extent.
A dec/rease in the oxygen carrying■
capacity of the blood is termed 'anaemia1.
A reduction
in the blood haemoglobin level and in the number of
circulating red blood cells are the characteristics of
anamemia
Drugs to correct aaame anaemia are called
'Haematinics'.
A large number of such preparations afte
marketed in India which vary not only in their ingredients
but also in their cost.
And most often they are
irrational combinations.
Dr. Pierre Blaud, early in 19th century recognised
many of the principles of iron therapy.
He said that
iron should be given at first and increased gradually.
He introduced his pills, containing ferrous carbonate and
sulfate.
Unfortunately, a number of eminent physicians
towards the end of the last century considered for purely
theoretical re"sons that inorganic iron could not be
absorbed, so th-t many expensive and relatively ineffective
iron preparations were developed (Unfortunately the
practice is continued in modern era, wggr even with
knowledge, a paradox.') Modern research has shown that
Dr. Blaud w~s right.
SOME FASTS ABOUT IRON METABOLISM IN BODM
.
- The to^al\body iron is about 2 to 6 gms.
- M^ies - 50 mg./kg. of body wt,
X Females
35 mg./kg. of body wt.
- Of the V’tal iron nearly 2/3rd is present in
the form of haemoglobin and rest is storage iron.
- Approximate daily requirement of elemental iron
is ‘
8 - ‘18 mg. in children
15 - 20 mg. in menstruating women *
10-15 mg. in adult males
20 - 25 mg. in pregnant and lactating women **
Note : Of the available elemental iron about 5-10%
is absorbed in health, this increases upto 30% in
anaemic subjects.
*
Monthly blood loss during menstruation roughly Is
50 ml. which is equivalent to 25 mg. of elemental
iron. This works out to be a loss of 0.3 to 0.6
mg./day, sometimes upto 1.5 mg./day.
**
Fetus accumulates'200-400 mg, of iron, mainly
in the last timGRtds.trimester. Further, iron is
lost during child birth nnd later during lactation.
- 2 -
- Sources of iron :
Milk and milk products are a poor source of iron.
Use f iron cooking utensils increases the iron
content of f 'od.
- IRON eAntent of various foods
High iron content
(more than 5 mg/
100g.)
.....................
NonVeg. '
Vegetarian
Liver
Wheat germ
Intermediate iron
content
1 to '5 mg./lOO g.
Non'Veg.
Vegetarian
-
Muscle
Me^t
Certain
Fish
dri<_d beans
Egg Y ■>lk and fruits
Heart
Low iron content
(less than 1 mg./
100 g.)
Non
Veg.
Vegetarian
Most green
Milk and
vegetables-.
cefieals
milk pro
ducts
Non-green
vegetables
Iron is absorbed from the food throughout the gut,
but chiefly in upper part of small intestine where the
acid medium enhances solubility.
Most iron in food is present in ferric form.
Ferrous iron is more rapidly absorbed rese than ferric,
iron, therefore a reducing agent such as ascorbic acid
(Vitamin C)' greatly increases the amount of ferrous form.
However substantial doses (200 mg 8 hourly with the iron)
are ne.-.ded to produce clinical effect and combined formula
tions often do not contain enough.
When iron is given in large doses, the control
mechanism for bbsorption fails, resulting in excess absorp
tion and,eventually haemosiderosis.
Abnormalities of small intestine may interefere with
cither the absorption of iron -~s in the malabsorption
syndroms on T.c?teTji>c disease or possibly with the conversion
of iron into a soluble and reduced form. Partial
gastrectomy often leads to decreased iron absorption.
In alkaline medium of most of the small intestine iron
is converted into insoluble iron salts (phyt-tes and
■nh^s^hates) • THf-S- leads to inabsorption of most of the
orally taken iron .ven in severe iron deficiency.
When iron is given alongwith tetrac -cline it gets
bound leading to inabsorption of both to a clinically
significant dgteee degree. Therefore the doses of both
should be separate® by at least three hours.
IRON THERAPY
Iron is indicated only for the prevention or cure
of iron deficiency.
25 mg. of elemental iron/day must be available to
the b">ne marrow if an iron deficiency anaemia is to
respond with a rise of 1% of Hb (0.15 g Hb)/day.
Iron therapy is not indicated in anaemia of chronic
disease like rheumatoid
arthritis as there is failure
of utilising stored iron and not the lack of iron.
-3-
3
When oral thereby is used, it is reasonable to
assume that about 30% o f the iron’will be absorbed and
to give about 180 mg. of elemental iron daily. However
calculations are not necessary except when iron is
given by injection.
Total iron (i.v.
=
required in mg
4.4 x body weight in kg.x Hb deficit
in g / 100 ml blood.
This formula allows about 0.5 g to replenish stores.
It is important to remember that with iron dextran (i.v.)
all the iron is biologically available but with i.m. iron
dextr-n about 30% of iron remains bound to muscle and
with iron sorbitol i.m. about 30% is lost by renal
excretion. This is token into adcount when calculating
an i.m.
**
course
of iron 40 mg. i.m. = 30 m.g. i.v.
In pregnancy it is usual to add 0.5 g for needs of placenta,
fetus and blood loss at delivery.
Iron stores are less easily replenished by oral
ther-py than by injection and oral therapy should, be
continued for at le~st two months after the haemoglobin
concentration has returned to normal.
It is illogical to give iron in haemolytic anaemias
unless there is also haemoglobinuria f^r the iron from the
lysed cells remains in the body and haemosiderosis may
ultimately occur.
Indications for Iron Therapy
1.
In iron deficiency anaemia due to chronic blood loss.
2.
In pregnancy - The foetus t-ken upto 600 mg. of
iron from the mother even if she is iron deficient, but the
iron st 'res of a baby b^m to an iron deficient mother mpy
be abnormally low. Dietary iron is seldom adequate and iron
should b<2 given from the fourth month to pregnant women.
3.
i.
e.
In various abnormalities of the gastro intestinal tract
mal absorotion sydromes.
4.
Premature babies and babies
weaned late.
5.
During the treatment of pernicious anaemia alongwith
hydroxocobalamin.
Oral Ir^n Preparations
There is an enormous variety of official and
proprietary iron preparations. For each mg of elemental
ir-^n t~ken by m-uth, ferrous sulphate is as effective and
nn more toxic than more expensive preparations.
Iron given in mixtures may combine with sulphide
ions in the mouth and the resultant black iron sulphide
c-uses blackening of the teeth. Besides liquid prepara
tions are more costly.
-4-
4 It is particularly important to avoid initial
overdosage with iron as the resulting symptoms may cause
the patient to abandon therapy. A small dose is given
initially and increased after a few days.
If given on a£ full stomach iron causes less gastro
'intestin
*
!
upsets but less is absorbed than if it is
given between the meals.
'Common preparations
Preparations
Ferrous sulphate
Strength
Elemtal iron
Dose
1-3 t-bs/day
200 mg.
60 mg.
Ferrous gluconatie 300 mg.
35 mg.
1-4 tabs/day
Ferrous fumarate
65 mg.
1-3 tabs/day.
200 mg.
Choice of oral iron preparations
The evidence as to which preparation provides best
iron absorption with least adverse effects is conflicting.
Unfortunately many of the studies on which claims for
rival^ preparations are made are found on close inspection
to be inadequate . There is little doubt that valid
comparisons c-n only be made with doses of preparations
containing equal amount of elemental iron and under strict
double blind conditions. It has been shown that
gastro intestinal upsets can be greatly influenced by
expectation.
The widespread use of iron prepar_'tions has stimulated
many attempts to find formulations that may provide better
therapy. This is a good thing. Unfortunately it has also
stimulated some to make claims for their products that go
beyond the evifiemze e.ij, ignoring unfavourable and quoting
only f-vourhble evidence regardless of its scientific
quality.
A suggested esw course for iron therapy ;
- Start a patient on ferrous sulphate
- If gastro intestinal upsets, try ferrous gluconate/
succinate/furmerate.
- Addition of Vitin, C increases the amount of iron
absorbed. Therefore lesser dose enn be given which would
decrease gastro intestinal upsets.
If simple preparations fail (this is unlikely) then
oharmaceutically sophisticated and expensive preparations
(slow release forms, enteric coated etc.) may be tried.
From these preparations iron is slowly released resulting in
decreased absorption. A similar result can be- had at less
cost by reducing the dose of conventional preparations.
Duration of ther~py
In general a full dose as,described earlier should
be given until haemoglobin level comes to normal and
then continued at reduced dose for two months to replenish
the stores.
-5-
5 -
Parentaral iron administration
Indications 1.
Ineffective absorption from gut.
2.
If a certain response is essential in a severe iron
deficiency anaemia as in late pregnancy (a blood transfusion
preferred)
3.
Failure of oral iron for unknown reasons.
4.
Poor patient compliance.
Imp : The speed of response is not quicker
(as would
be believed") than that with full doses of oral iron reliably
token and normally absorbed, for both provide as much
iron as an active marrow can use.
Intr-'muscular iron sorbitol is satisfactory, but some
prefer iron dextran.
Intravenous iron dextran is used. Total dose infusion
(TDI ) is preferred over intermitent injections.
Folic acid deficiency may be unmarked by effective iron
therapy. This is liable to happen in pregnancy and so folic ■
acid is commonly given to all pregnant women having anaemia.
A similar thing happens in malabsorption syndrome.
Adverse reactions ;
Mild gastro intestinal disturbances like nausea,
abdominal pain constipation 6r diarrhoea. These can be
minimised by giving it after g food and initial small
amounts which can then be gradually increased.
Adjuvants■ ■ to iron therapy s
Various substances claimed to enhance the efficacy of
iron are Vitamin C. cobalt, copper and manganese. Vit. C
may increase the iron b absorption but it is not necessary
to use costly iron preparations incorporating Vit.C to
achieve this effect. Copper is said to mobilize iron from
storage, while cobalt is claimed to stimulate erythropoietin
production. Cobalt is potentially toxic. Angina., goitre and
congrestive cardiac failure are some of the adverse
effects reported with the use of cobaltous chloride. The
therapeutic value of these agents in the treatment of iron
deficiency anaemia is doubtful..
In the treatment of pure iron deficiency anaemia, the
use of 'shotgun
*
therapy containing a wide variety of
expensive minerals and vitamins alongwith iron is unnecessary
and wasteful.
Vitamin B 12 (cyanocobalamin)
For clinical use hydroxocobalamin is preferred.
DEficiency of vitamin B 12 in the body leads to
( J) pernicious anaemia (A megaloblastic anaemia)
( ii ) •, subacute combined degeneration (degeneration of
brain, spinal cord and peripheral sever nerves)
(iii) Abnormalities of epithetial tissues, particularly
of the alimentary tract (e.g. sore tongue and
mal absorption) .
- 6' -
Function of Vit.B 12 and cause of megaloblastosis s
Uncertain. Vit.B 12 is a conenzyme for an essential stage
in folate metabolism and may affect folate transport into
cells.
Daily requirement s 1 mcg. absorption mainly from ileum.
Several years' supply are normally stored throughout
the bodyj mainly in the liver and its half life is about
a year.
Man gets most of his cobalamin from meat. Cobalamin
does not occur in plants (except in legumes in which it is
made by bacteria in root nodules). Dietary deficiency can
occur in strict vegetarians.
Indications for Vitamin B.12 =
Prevention and cure of conditions due to its
deficiency.
1.
2.
J.
4.
Pernicious (Addisonian) anaemia
Malabsorption szndromes
Tobacco amblyopia (hydroxocobalamin used)
Empirically in variety of neurological conditions peripheral neuritis (esp. diabetic)
Note : As the daily Vit.B 12 requirement is very small
nutritional deficiency is uncommon even among the vegetarians
in India. Majority of nutritional megaloblastic anaemias
observed in India are due to folic acid deficiency.
Folic Acid (Pteroylmonoglutamic acid)
One of the B group of vitamins.
Functions :
- By itself it is inactive
- It is converted into biologically active coenzyme
tetrahydrofolinic acid which is important in the biosynthesis
of aminoacids and nucleic acids.
Deficiency of folic acid leads to megaloblastic
anaemia probably because it is necessary for the production
of purines and pyrimidines which are essential precursors
of DNA.
Sources and requirements
Folic acid is widely distributed especially in green
vegetables yeast and liver.
Daily requirement - about 50 mcg. A diet containing
400 mcg poly glutamates will provide this. Body stores aro
adequqte for a? several months only.
Indications : prevention and cure of the megaloblastic
anaemia due to deficiency at folic acid.
1.
Dietary deficiency - more common in the economically
kaziegw backward areas of the world.
2.
Malabsorption syndromes
5.
Pregnancy - requirement of folate increases from
400 mcg / day to 800 mcg/day. Mild deficiency is
common with a few cases developing severe megaloblastic
anaemia. For this reason many now consider that
routine folic acid administration shojld be added
to routine iron administration. The dose needed
is about 300 mcg/day vigorous iron therapy in preg
nancy may unmask a folic acid deficiency.
4.
In chronic haemolytic states folic acid requirement
is increased.
- 7 -
5.
Drug induced folate deficiency - anticonvulsants
like phenytoin primidone phenobarhitone, antimalarials
like pyrimethamine and urinary antiseptics like
nitrofurantoin cause folate deficiency in the body.
Motes
1.
If Vit.B 12 is injected only the amount necessary
for the saturation of binding sites is retained. The
remaining excess is excreted in the'urine. It is calculated
that 80—95% of a 50 mcg dose of injected Vit.B 12 is retained.
As the dose exceeds 100 mcg large proportions (50-90%) of the
injected dose may appear in the urine within 48 hrs. in
healthy individuals.
2.
Prolonged boiling of food during cooking destroys
practically most of the folate in the food.
Liver Preparations
Crude liver extract owes its activity to the presence
of both Vit. B 12 and folic acid. Being a biological
product liver extract is not very stable, its effect is
less prompt and it is costly. The injection is painful and
can give rise to allergic reactions which could be severe.
Orally these preparations are not so effective and often
not palatable.
Because of their lower efficiency and other
disadvantages, liver preparations are no more advocated in
the treatment of folic acid and Vit. B 12 deficiency
anaemias. In fact liver preparations have become obsolete
since folic acid and Vit. B 12 are available in the pure form.
'Shotgun1 antianaemia preparations
:
The use of antianaemic preparations containing multiple
incredients like liver, iron, folic acid, Vitamin B 12
copper cobalt and manganese must be deplored for various
reasons.
Some of these incredients are unnecessary, wasteful
and only increase the cost of therapy. Mixed therapy can
also cloud the clinical picture and may delay the accurate
diagnosis of the underlying disease.
Thus a favourable
response to Vitamin B 12 in a case of megalablastic anaemia
secondary to gastro intestinal pathology may foster false
and thus abscure the correct diagnosis.
The danger of Jiving
folic acid with inadequate Vitamin B 12 in case of undiagnosed
pernicious anaemia is well known. Patients with pure iron
deficiency anaemia respond to simple iron administration and
an addition of Vitamin B 12 or folic acid is not justifiable.
Moreover it should be noted that whenever a commercial
preparation contains multiple ingredients in a mixture
(combination) most of these ingredients are usually present
in a inadequqte amounts.
These 'shotgun
*
formulations are promoted to preserve
the aged in,health, for anaemia and as tornics. Both their
indiscriminate promotion by commercial interests and their
use by physicians in undiagnosed cases shows a disregard for
patients' interests that is inconsiderate at best and
callous at worst.
References :
1.
Goodman and Gilmhn's 'The Pharmacological Basis of
Therapeutics' 6th Edition (1980)
2.
Clinical Pharmacology by D.R. Laurence 5th Edn.(l980)
5.
Pharmacology and Pharmacotherapeutics by
R.S. Satoskar and S.D. Bhandarkar,8th Edn.(l98j)
a,
HAEMATINICS
PART IV
A SURVEY OF HAEMATINICS (IRON CONTAINING FORMULATIONS)
AVAILABLE IN INDIA
Dr.Sagun Desai, M.D.
Dr.Rajul Desai, M.D.
63
1.
Total No. of Formulations
2.
Number of companies marketing them 37
3.
Formulations
Sr. No .
Numbei?
Formulation Type
Percentage
(fi)
Tablets
6.35
4
Capsules
46.03
29
39.68
Liquids
25
Injections
1
1.59
Special forms drops
6.39
4
spansules etc.
«
------------------------------------------------------------------- 0------------------------------------4.
Number of ingredients
1.
2.
3.
4.
5-
No. of ingredients
No.of formulations
One
Two
Three
Four
Five
Six
Seven
Eight
Nine
Ten
Eleven
Twelve
Thirteen
3
5
3
14
8
6
7
4.76
7.94
4.76
22.22
12.70
9.52
11.11
6.35
7-94
3.17
4.76
3.17
1.59
4
5
2
3
2
1
5.
Various ingredients present
Sr.No .
Name of the ingredient
Percentage (%)
Number
Percentage($)
61.90
82.54
41.27
46.05
15.87
23.81
14-29.
56.00
9.52
4-76?
4.76
1.
2.
3.
4.
5.
6.
78.
910,
11.
Folic Acid
39
Vitamin B12
§5 52
Vitamin C (Ascorbic acia)
26
Other B Complex vitamins
29
Liver Extract
10
Enzymes/amino acids
15
Trace metals
91
141
Alcohol
Other vitamins/minerals
6
Haemoglobin
52
32
Miscellaneous
1.
Expressed as percentage of liquid preparations, since
only liquids contained alcohol.
2.
Include ingredients like dioctyl sodium sulphosuccinate
(laxative) and calcium carbonate.
.r’’
.. ■ ■
c;
- -»&•
* 4
. i--2-
2
Indications (in order of frequency)
6.
a)
b)
c)
d)
e)
f)
g)
h)
i)
:
Anaemia due to nutritional deficiency )for treatment
Anaemia of varied aetiology
(and prophylaxis
Pregnancy and lactation
Convalescence
Lack of appetite
Old age
Loss of vitality
Growth promotion
General - like bleeding disorders,threatened
and habitual abortion, protein deficiency,
post operative, pica, adolescence etc.
7.
Specific contra indications and special precautions
mentioned only for four ( 6.35 % ) formulations.
8.
Form of iron used
Sr. No .
Form of iron
Number
Percentage (%)
1.
2.
3.
45.
Ferrous sulphate
Ferrous fumarate
Ferrous gluconate
Haemoglobin
Others
11
22
2
3
25
17.46
34.92
3.17
4.76
39.68
Cost of the therapy per day
9.
Sr.No.
1.
2.
3.
4.
5.
6.
78.
Range of cost/day
Less than 20 paisa
*
Ji 21 - 25 paisa
26 - 50 paisa
51 - 75 paisa
76 - 100 paisa
1 .01 - 1.50 Rs.
1.51 - 2.00 Rs.
More than 2 Rs.
Number
1
3
14
13
11
10
3
5
Percentage (^)
1.59
4.76
22.22
20.63
17.46
15-87
4.76
7-94
Note : Drop formulations (3) omitted.
* 11 paisa / day.
10.
Comparative cost of Rational Therapy :
Prescribed treatment :
Tab. ferrous sulphate
Tab. Folic Acid
200 mg x 3 times / day.
5 mg x 2 times / day.
2.1 paisa for ferrous sulphate
5.0 paisa for folic acid
7.1 paisa per day.
* based on availability at Sheth Khushalchand Charitable
Medical Centre, as on 17-6-85
*Cost =
1. Tab ferrous sulphate
Rup Pharma/LOCOST
?0 paisa per 100
2. Tab. folic acid
Mercury / LOCOST
Rs.2.50 per 100
-3-
- 5 Alternatively :
Tab. Macrafolin-Iron (Glaxo) 1 tab. thrice a day
each contains ferrous fumerate 200 mg, folic acid 750 mcg
and Vitamin B 12 7«5 mcg. The cost per day works out to
be 15 paisa (Rs.5/ for 100).
*
Issues :
1.
Capsules and liquids form nearly 86% of formulations.
Tablets, only 6%
2.
8J% of formulations have four or more ingredients most of them being unnecessary.
r
"Despito the highly specific response of iron
deficiency to the element and the straight forward
nature of therapy with iron it is discouraging to
see the frequency with which expensive preparations
with worthless additives are prescribed" (Goodman
and Gilman, 6th edition, page 1525) •
5.
It is painful to see that nearly 58% formulations
missed folic acid as one of the ingredients whereas
more than 80% contained Vitamin B 12 and 40% Vitamin C
and B Complex. What is the place of liver extract,
enzymes/amino acids and trace metals, not to talk of
haomoglobin in these formulations ?
4.
Are all tho indications justified ?
5-
Only 6% formulations mention of specific contra indications
and special precautions. Does it mean that 'haematinics'
can be taken safely in any situation since they are
considered to be 'tonics' ?
6.
Though ferrous sulfate is the most effective and least
expensive compound with no more toxic effects, only 17%
formulations contain it whereas ferrous fumerate
and other forms of iron share 557° and 40% respectively.
7.
No comment is required on 'cost'. It speaks of itself.
SOURCE : MIMS India, February 1985
Position: 1267 (12 views)