RF_NUT_5_A_SUDHA.pdf
Media
- extracted text
-
... ..
.
r Sb :
- - X.RF_NUT_5_A_SUDHA
....... .
di
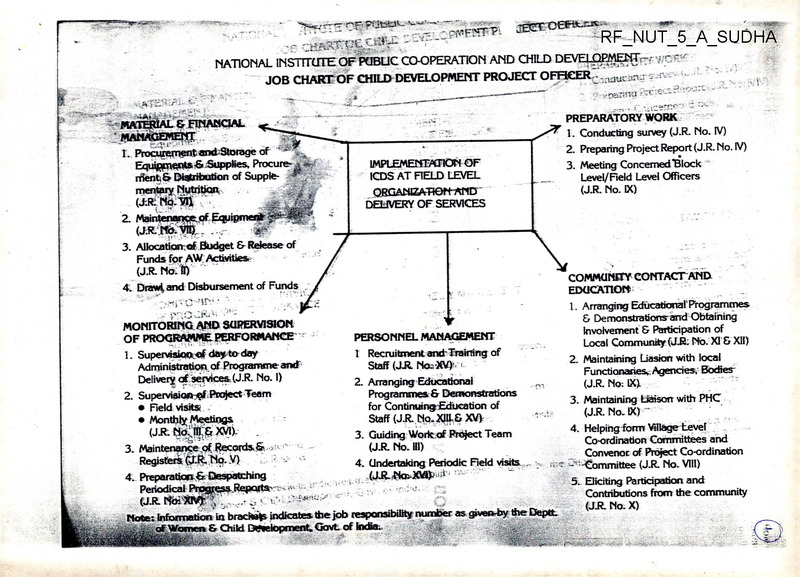
NATIONAL INSTITUTE OF PUBLIC CO-OPERATION AND CHILD DEVEipP^NT^z v T, ■'
JOB CHARTOF CHILD DEVELOPMENT PROJECT OFHCER7 0 ;_ _ —--------- - :yganua rTCX'-..^
4
? ,r.a*TkF,'’3
PREPARATORY WORK
r 1. Conducting survey (J.R. No. IV)
-‘5- ■
—• *
-r
' MMWOEWEftT
I. Procurement and Sorage of
Equipm^rts -& Supplies, Procurerrient;& Distribution of Supple
mentary Nutrition
(J;R:Nb.Vll
2. Preparing Project Report (J.R. No. IV)
--
IMPLEMEHmFJON OF
ICDS AT FIELD LEVEL
ORGANIZATION-AND
DELIVERY OF SERVICES
3. Meeting Concerned "Block
Level/Field Level Officers
(J.R. No. IX)
2. Maintenancnof Equi|
(J.R..M&.VI1J,.
3. Allocation of Budget & Release of
Funds for AW Activities.
(J R. No:!)
COMMUNITY CONTACTAND
EDUCATION
1. Arranging Educational' Programmes
& Demonstrationyand Obtaining
Involvement & Participation of
Local Community (J.R. Mb. XI & XII)
4. Drawl, and Disbursement of Funds
-
c-'ir-’ • - -
:.!r:
■
MONITORING AND SUPERVISION
OF PROGRAMME PERFORMANCE
1. Supervision®! day to day
Administration, of Programme and
Delivery of services (J.R. No. I)
2. Supervision^.Project Team
• Field visits
• Monthly Meetings
• /
-
PERSONNEL MANAGEMENT
1 Recruitment and'Training of
Staff (JR. Nos'XV)4 1
2. Arranging Educational
Programmes & Demonstrations
for Continuing Education of
Staff (J.R NQ.XJIL& XV>
3. Guiding Woric of Project Team
(JR. No. HI)
2. Maintaining Liasion with local
Functionaries, Agencies, Bodies
(J.R. No: IX).
3. Maintaining Liaison with PHC
(J.R. No.lX) ~
4. Helping form Village Level
Co-ordination Committees and
Convenor of Project Co-ordination
4. Undertaking Periodic Field visits .. s {S-e S‘-^ommittee (JJt No. VIII)
4. PreparatiopfeDespatching
5. Eliciting Participation and
-Contributions from the community
UJt NoiXlVfc v
< v ....
■
(J.R.N0. X)
Note : Information in bracIMs indicates the job ^responsib.lrty number as grver^ the Deptt
of Women & Child D^elopment, GovL of Incfia.
(jjty«&xyik
F5C..i5l'- .r '
3. Maintenance of Records & .
Registers (JIR.N0. V)
.. ;
L
•
--T
'
< . , .
■ .
JOB RESPONSIBILITIES OF CDPOs
SKILLS
PREPARATORY____TASKS/SUB-TASKS
(F”
(D___________
WORK
1. Conducting a survey
(J.R. No. IV)
y
1. Identification of villages/
wards/families/beneficiaries for setting up AWs
1. Collecting information
about villages, analysing
and compiling information
2. Creating community
awareness about the
1CDS programme parti
cularly among the
Panchayats, Mahila
Mandals, BDO, MO,
Block Samiti and other
voluntary organisations etc.
2. Communication and
public speaking with
different categories
of persons
3. Obtain concurrence for
location of AWs
3. Elicting support from the
community
4. Help and supervise
AWWs/Supervisors in
i. conducting a survey
ii. filling up survey register
iii. compiling survey
information
iv. selection of benefi
ciaries
v. updating survey data
vi. compiling vital statistics
4. Talking to people to elicit
information, taking inter
views recording informal
interpreting information
r
•:;5
I
5. Writing project report
6. Interpreting survey data
7. Planning follow up actio
■
W
2. Preparation of project
report with necess
ary base-line infor
mation
5. Compile survey infor
mation collected by
AWWs/Supervisors, Prepar
ing project report (profile),
submitting to Programme
Officer
3
.
■ v
-
6
(3)
(2)
(1)
I
‘ti
a
I
Community Contact and
Education
1. Contact local people, local
bodies, different agencies and
organisations
1. Obtain inuoluement
and participation of
local community in
the ICDS
programme and
arrange educational
programmes and
demonstrations.
- BDO
— Panchayat
— Mahila Mandals
— Youth Groups
— Voluntary Organisations
— Primary School
— Rural Development
Programme functionaries
— Public Health Engineering
(water & sanitation)
— District Extension and
<»
Media Officer
(JR No. XI & XIII)
2. Maintaining liasion
with local
functionaries/ agencies/bodies.
1. Talking to local people,
addressing larger
gatherings, communicating
correct messages
2. Establishing linkage with
different people/
organisations agencies
etc.
I
3. Organising educational
publicity programmes,
melas etc. for community
Explain the programme
to them
'I
2. Discuss with local community
their expectation from the
ICDS project.
(JR No. IX)
.•jfB
3. Identify and suggest areas for
people's participation, discuss
with local people the help
they can render in the ICDS
programme.
4. Encourage people to
participate in the ICDS
programme and to contribute
towards its successful
implementation by
i.
ii.
4
s -al
availing services
providing shelter, food
supplements, waste
material etc.
n
5. Arrange educational
programmes/ publicity
meetings/exhibitions/meals
etc. for encouraging
involvement of local people
and for creating awareness,
utilizing the funds available
under IEC for this purpose.
4
■■
■
'^9
II
<n
.........
(3)
(2)
_________
■ . .................. ..
■
I
6. Mobilize community
resources for strengthening
services.
I.
— mothers,
artisans
— local groups
— adolescent girls
primary school teachers
— material resources
■
7. Work out Indicators for
monitoring people’s
participation in ICDS.
8. Make periodic visits to AW
centres to assess the
participation of the
community.
I
3. Maintain functional
liaison with Primary
Health Centre
(JR No. IX)
I
i
f.
9. Contact MO for
M-
— health check ups
— immunization
— timely supply of medicine
kit and training of AWWs in
Its use
— joint visits to project area
10. Work out an action plan for
effective delivery of health
services.
*0
:1
11. Identification of ‘at risk’
children and mothers
I
12. Attend meeting of district
medical adviser/CMO
i
1
4. Convene project
coordination
committee
(JR No. VIII)
13. Form the project
coordination committee
14. Brief members about their
role and responsibilities.
1. Conducting meeting.
■
2. Recording minutes of
meeting.
' ■ ^9
15. Prepare agenda items, fix
date of meeting, convene
meeting, help to conduct
meeting and prepare the
minutes.
§
I-'.
I
5
■••yk
1 SB
vs?
' 'Mil
(3)
(2)
(1)
«
16. Take follow up action on the
decisions, orient
Supervisors/ CDPOs/ AWWs
about decisions taken.
5. Help in formation of
village level
coordination
committees
(JR No. XII)
17. Identify local influential
persons for co-opting in the
village coordination
committee.
18. Brief members about ICDS
purpose of committee and
their role
19. Orient supervisors, ACDPOs,
AWWs about the method of
conducting the meeting
20. Organise the first 1-2
meetings of the coordination
committee
1. Collecting information about
people who can be made
members of the committee
2. Convening meeting of the
committee
‘•w
3. Recording minutes of
meeting.
4. Communicating with people
n
■■■
21. Help wherever necessary to
fix dates of further meetings,
convene meeting and record
minutes
r
i
V;
1
22. Plan follow up action on
decisions taken
23. Involve committee members
in the activities of AW Centre
6. Obtain contribution
of local community
for
bullding/materials
(JR No. XI)
Personnel Management
1. Recruitment and
training of staff
(JR No. XV)
24. Help AWW to obtain
accomodation for the AW
centre
1. Identify and prepare a list of
eligible AWWs/Helpers as per
the prescribed qualifications
2. Arrange for selection of
AWWs/Helpers
i
v
J
■’I
1. Preparing statements of
eligible AWWs/Helpers, their
qualifications and
experience, untrained/
trained workers etc.
Form Selection Committee,
hold interviews for selection.
6
,’usS
'll
(3)
(2)
(1)
3. Issue appointment orders to
AWWs/Helpers
2. Conducting interviews for
selection of AWWs/Helpers
4. Make a list of untrained
ACDPOs/ Supervisors/AWWs/
Helpers and send
requirements of training to
the programme officer
3. Drafting appointment
orders, deputation orders
etc.
4. Conduct sessions during
orientation training of
AWWs/Helpers/Supervisors
S ACDPOs
«
5. Depute untrained
functionaries for training and
trained functionaries for
refresher courses.
6. Organise short term
orientation training at project
level for newly recruited
ACDPQs/Supervisors/AWWs/
Helpers in case a job training
course In not due
immediately.
7. Intimate number of vacancies
of AWWs/Supervisors/
ACDPOs to Programme
Officer.
f
s
■
■
■■
■
’ ■ -fi'-ri:/
■..-'WtJ!
?
■<
8i Fill up vacancies/make
; •
arrangements In case of long
leave by project Staff
I
♦
9. Provide advance to
AWWs/Helpers before they
proceed for training
10. Take session in training
courses for Supervisors/
AWWs/Helpers*
1
2. Arrange educational
programmes and
demonstrations for
staff development
(JR No. XIII & XV)
11. Identify areas/services which
require to be strengthened In
the block on the basis of
I. visits
ii. performance in the field
iii. scrutiny of records and
registers
iv. information from
MPRs/QPRs
1. Demonstrate appropriate
methods of organising
activities, growth monitoring,
conducting meetings etc.
,z
2. Scrutinizing MPR data for
planning follow up action
3. Motivating functionaries for
service delivery
.. « J
• Circular No. 15-3/85 CD dated 23 February 1989
7
1
I
i.
__Jl_
!
e
I
i ■
(3)
(2)
111
-
4. Supervising delivery of
services by field
functionaries
&
F
■
12. Demonstrate/arrange
demonstrations, Invite
resource persons, local
artisans etc. to build skills of
AWWs/Supervisors/ACDPOs
In conducting pre school
activities, growth monitoring,
community meetings, home
visits, mahila mandal
meetings etc.
•
■I
1
g1
13. Develop the office of the
CDPO as a resource centre*
H
14. Obtain material like picture
books, teaching aids, play
material, reference material
for the resource centre
'W
15. Ensure the utilisation of
material by ACDPOs/
Supervisors/ AWWs
■I
16. Circulate material from the
resource centre among
different AW Centres to
Introduce variety in the
programme
f'
i
17. Motivate AWWs/Supervisors
and ACDPOs to fulfil their job
responsibilities utilizing
competent/experienced
workers as resource persons
X
r
' ..•>
'’S'
19. Identification of gaps/lacunae
for strengthening service
delivery
•4
-
18. Make a list of AW Centres
according to their
'
performance
■'
* National Policy of Education, 1985 POA
4
■■
11
■
i—4
8
■
-
■
■<.
■
.
;r
V-
..
/■
■■
\
«
(3)
(2)
(1)
■
s
20. Identification of difficulties in
supervision
'
3. Supervision of
project team
through project
meetings
21. Arrange project meetings at
the project office
(JR No. Ill)
■
I. strengthening delivery of
services
H. enhancing skills
iii. improving supervision
24. Set goals/targets for
achievement in consultation
with project functionaries
25. Plan a monthly tour
*
programme and submit to
programme officer
4. Guide the work of
the project team
1
(JR No. Ill)
26. Make periodic field visits to
AW Centres. Use the
following to observe the work
of AWWs
‘
.
. :• - -V
23. Plan follow up action based
on the reports of field visits
for
■
■■
■
22. Plan the content for
discussion during the
meeting
-'■'1
■ -■ wa
■
if
•1
1. Prepare a tour programme
2. Demonstration of correct
method for delivery of
different services
■
3. Conducting a review
meeting
1
J
5. Undertake periodic
field visits
(JR No. XVI)
i. records and registers
ii. discussions with AWWs
iii. monitoring check list
lv. discussions with
f beneficiaries and
community
■
27. Monitor achievements against
set targets
fl
28. Appraise performance of
ACDPOs/Supervisors/AWWs
for filling up ACRs
I
. at
29. Conduct a monthly review
meeting
9
i
k.
-
i
I
F
.4
. ..
ife...
■/ft
30. Make arrangements for field
placement of trainee
AWWs/Supervisors/CDPOs/
ACDPOs*
I
Monitoring and
Supervision of
Programme
performance
.
1. Principal Executive
Functionary for
supervision of dayto-day
Implementation of
programme/services
(JR No. I)
4’
¥
2. Supervision of
project team
through field visits
(JR No. II and XVI)
•.J.:
i
1. Mapping AW Centres and
working out circles for
supervision
1. Know the
ACDPOs/ Supervisors/AWWs/
Helpers, their qualifications
and abilities
2. Observation and monitoring
delivery of services by
project staff
2. Prepare an annual action plan
for the project
- ’Ml
3. Skill In using checklist for
monitoring
3. Check the location of AW
Centres in the project and
distance/mode of travel to
different Anganwadi Centres
4. Discussion with project staff
for supervision during
project meeting
4. Distribute circles to
Supervisors/ACDPOs, making
them coterminus with the
circles of LHV
> . • iFw
5. Organizing project level
meetings, recording minutes^
of the meeting
5. Discuss with
supervisors/ACDPOs and
prepare a plan of supervision
of AW Centres including;
I. frequency of visits of
CDPOs/ ACDPOs/
Supervisors
IL time to be spent at each
AW Centre
lii. joint visits with medical
staff
II'
6. Discuss with
Supervisors/ACDPOs,
check lists for monitoring AW
Centres: pre school activities,
Nutrition and Health activities,
community activities**
*
1 Ir. '
6. Identification of
lacunae/gaps in delivery
of services
•.'S
• Circular No. 44/85 AT dated 7 March 1986
*• Checklist for monitoring AW* has been developed by NIPCCD
I. •
10
■i
i
(2)
(1)
(3)
7. Discuss with
Supervisors/ ACDPOs
information recprded |n
supervisors diary or check-list
1.
8. Make available records and
registers to AWWs/
Supervisors/ACDPOs as per
the requirement of the State
Govt./MlS Manual. Ensure
timely replenishment of
registers to AWWs/
Supervisors
3. Maintenance of
Registers and
records
(JR No. V)
i
9. Open all records/registers at
project office prescribed by
State Govt/MIS Manual
t
‘■S
1. Filling up different
records/registers, MPRs,
APRs and checking those
filled by the project staff
‘ ’S/
2. Compiling Information
in MPRs
'•O
3. Interpreting data from MPRs JO
4. Preparing a list of action
points for follow up work
10. Ensure maintenance of
reglster/records at the AW
level/project office
11. Maintain files as per
requirement
J
12. Check records maintained by
AWWs/Supervisors/ ACDPOs
and office staff
■
*
13. Guide AWWs/Supervisors/
ACDPOs to fill-up-records/
registers correctly
.<■
■
t
II
1
I
'1
4* Preparation of and
despatching
periodical progress i
reports
;
(JR No. XIV)
i
I
1
a
i
• ‘ ; f’ f; t
J
.i
1 I
17. Ensure filling up MPR of
AWWs, corripiling of
information by supervisors for
their circles
,
11
I
■ ■
16. Prepare a compilation of
circulars issued by the State
Government
/■o;>
v
■k.
15. Make arrangements for filling*
Up records/registers in case
of illiterate/semi literate
AWWs and orient them to fill
records correctly.
4
'
i"- ' ’ ' 'aia.
14. Ensure updating of
information in
records/ registers
»
.a.
I
■’'1
? •, r-?
■ w ;
■AJl.
(2)
(1)
t
18. Compile information from
MPRs and timely submission
to State Programme Officer
and Central Government
every month
I
19. Fill up APR and send to
Programme Officer and
Central Government
■
*r
(3)
■
£
!
I
s
20. Prepare list of action points
on the basis of MPRs for
strengthening service delivery
I
i:
■r
-
21. Maintain appropriate
discipline In office
i"
w
■-
22. Build a team of ICDS project
staff for effective
implementation of the
scheme. Maintain good
Interpersonal relationships
f
w-
I
■
I
Material and Financial
Management
t-..
I
I
!
|
L Procurement,
transportation
storage and
distribution of
equipment and
supplies and SNP
•
(JR No. VI)
2. Accounting for and
maintenance of
equipment
V
4
(JR Ho. VII)
’.V'Jt
i
;
'
1. Prepare a list of equipment
required for
— project office
— anganwadi centres
2. Send requisition for
procurement of equipment to
the Programme Officer
3. Make arrangements for*
procurement, storing
supplementary nutrition*
other equipment to AWC
4. Ensure uninterrupted supply
of SN to AW Centres
-
1. Working out the
requirements of the project
preparing lists and writing to
the programme office
2. Writing letters making
notings, draftings
3. Maintaining files, making
stock entries
4. Preparing accounts
statements.
5. Buidling a team spirit
6. Filling up ACRs
•z
■
5. Replenishment of medicines
in AW Centre**
t
6. Ensure entries are made in
the respective stock registers
• Circular No. 15 - 2/89-90 dated 19 May, 1989
Circular No. 15 - 3/85-CD dated 23 February, 1989
■
I
I
L.J
1
(1)
(2)
(3)
—
7. Make arrangements for
replenishing stocks/
maintenance of equipments.
3. Drawing and
Disbursing Officer to
allocate budget and
release of funds for
AW activities
(JR No. II & X)
■
: :
8. Send requisition for release of
funds for ICDS project
9.
Draw money for incurring
expenditure on salaries,
supplementary nutrition,
material etc
10. Incur expenditure from
contingency allocation for
material/articles for AWCs
<*
i
■
11. Ensure proper utilization of
funds and maintenance of
accounts of the project
12. To get prepared an audited
statement of accounts at the
completion of the financial ‘
year
13. Plan activities as part of the
IEC activities. Request for
release of IEC funds and
arrange for organising
activities
'W
■
-W
r-
I
••
■
4
I
Z
; fig-
/
fell
13
_ __ _
10.
FOR REPORTING
formats
—
—
Incidence as compared
format -I
to last month
4
AWW-S MONTHLY MONITORING RETORT FORM
1. Month
.
Other important events: (Pl. Tick)
-- -----
2. Year-------
Name of the Village where AW is located
Diarrhoea
b)
Live births
c)
Still births
d)
Total deaths
i)
0 to <1 year
ii)
1 to <3 year
(b) Total Population of Children 0 to 6 years---------------
iii)
3 to <6 years
Supplementary Nutrition was distributed at AW:
iv)
Pregnant Women
during delivery
(a) Total Population of the AW Area—- ----------------- -
5
6.
Previous month
a)
4. S.No. of AW
Number
(b) Moderately regular (c) Irregular
(a) Very Regular
(15-21 days)
(21+days)
e)
(<15 days)
7. Quality of Supplementary Nutrition:—
Good/Acceptable/Poor.
No. previous month
11.
No reporting month j
Pregnant Women
ii)
Lactating Women
Date
Reviewed by
Signature
ii) Sector
MO/LHV/HA (F)
—Grade III/IV
Immunisation carried out in the month. (Please Tick)
Note:
9.
Yes/No
i)
i) ANM/MPHW(F)
—Grade 11
BCG
Total No. of:
O.R.T. advised Yes/No.
8. NumberofmalnourishedchildrenO-6yrs,ascomparedtolastmonth.
Grade
Reporting month
DPT
IBSEiS
Yes/No
T.T.
Polio
Measles
DT
Yes/No
Yes/No
Yes/No Yes/No |
-i
-
102
i) The report is for the whole months (1 st to the last day).
The report should be discussd with ANM & LHV and
finally submitted to the sector MO at the sectoral meeting.
Jr
ii) Information on item S-6-7-8 and 10 (d) & (e) are same
as AWW is providing to CDPO for MPR.
••• •
Si
10S
MR.
-
FORMAT-2
'J.;1
State
Pincode
SECTOR MEDICAL OFFICER’S MONTHLY
REPORT ON SECTORAL MONITORING AND CON
TINUING EDUCATION FOR MONTH OF
Note:
1. Name of the PHC/CHC __________________________
2. The report is to be submitted to the project adviser (MO
I/C-PHC/CHC) on the 1st working day of the following
month.
2. Sector No. I/II/III/IV (Circle your sector No.)
3. Total Population of:
(i) your sector
1. Reference month Ist-last day of the month under
report.
________
3. All the MMRs received from AWWs in your sector till
last day each month should be submitted to MO I/C PHC
alongwith your report.
(Meeting must be held between 26th and last day of each month)
4. Please indicate the address in full including PINCODE
at which the quarterly check for your honorarium may be
sent.
(ii) Reported AWs in your sector
4. Sectoral meeting held on
at village
i
5. Topic discussed for continuing education
6.
Staff Position
No.
Sanctioned
No. in
Position
-
No. Attended
Meeting
) LHV/HA(F)
-t
ii) ANMs/MPHWs(F)
ii) AWWs
7. Did MS participate in the meeting Yes/No
a*
8. ^4o. of AWs visited by you during the month
9. Remarks, if any
Date
Signature
Name of MO
Designation
Sector/PHC
Town/Village P.O.
District
104
105
INTEGRATED CHILD DEVELOPMENT SERVICES
FORMAT-3 (A)
(MMR Proforma for Rural & Tribal Project Adviser)
Monthly Monitoring Report of Project Adviser (MO-I/C
Block PHC for the month of
19 (From 1st day to
last day of the month under report).
3. Name of the Block PHC/CHC
4. Name of the ICDS Project
_______________
6. No. of AWs in the PHC/CHC: Sanctioned
Reported
Functional
7. Population: (i) Total in PHC/CHC
(ii) Reported AWs (All Sectors)
a
Number of Sectoral Level Trg. courses organised by
9.
I ■
-
No of participants (All sectors)
Staff Position
i) Medical Officers
ii) LHVs/HAs(F)
iii) ANMs/MPW(F)
iv) AWWs
L
Grade II
12.
Quality of supplementary nutrition food:(Pl. Tick)
Good/Acceptable/Poor.
No. in
No.
Sanctioned Position
Total No.
DPT
BCG
POLIO
Mea Tetanus
Immunised
sles
Toxiod
in the PHC
1st 2nd 3rd 1st 2nd 3rd
(Reg.Women)
/CHC
1st 2nd
i) In the repor
ting month
ii) Total since
s
1st .April
14. Incidence of other important events:-______
Event
No. Previous month
all MOs.
b
No.Reporting month
13.
Immunisation performance figure (To be filled in from
available information at the Block PHC/CHC).
5. Total Number of Sectors in the PHC/CHC area
8
No. Previous month
________________________
Type ofProject(Rural/Tribai/U rban)
Sector Reported
Grade
Grade III & IV
I. Name of the State
2. District
10.
No. ofAWs where supplementary nutrition was distributed
(a) Very Regular(b) Moderately(c) Irregular
Regular
(2 l~days)
(15-21 days),
(< 15 days)
11.
Malnourished children 0-6 yr as compared to last month
No. Attended
Meeting
Not applicable
Not applicable
(a) Diarrhoea*
(b) Total Births
(c) Total Deaths
i) 0 to <1 year
ii) 1 to <3 years
iii) 3 to <6 years
iv) Preg. women
during delivery.
107
No. Reporting month
INTEGRATED CHILD DEVELOPMENT SERVICES
Yes/No
♦ ORT Advised
15 Supply Position:
Occasionally
Available
Regularly
Available
Supply Position
Not
Available
FORMAT-3 (B)
I
11
(MMR Proforma for Urban Project Adviser)
of
Monthly Monitoring Report of Project Adviser for the month
19. (from 1st day to last day of the monnth under report).
Iron & Folic Acid
1
Name of the State
Tablets_________________ _
2
(a) Name of the City(b) Urban Project
Medical Kits
he
Vit. ‘A’
Administrative3Deptt.: Corporation/Municipality/State Health
Deptt.
_ ______________________
16 (a) PHC Meeting held on
(b) DA Present Yes/No
Date_______________
■«
4
Signature
_
No. of AWs in the Project: Sanctioned
Reported
Functionnal
Name
5
CHC old PHC
Population: (i) Total in Project
Address
(ii) Reported AWs
(All Sectors)
Pincode
5
* Pl. indicate the address with pincode to send you the
quarterly cheque/Information foryour honorarium.
Staff Position
.No.
Sanctioned
No. in
Position
No.
Trained
Medical Officers
LHVs/HAs (F)
Note:
L
ANMs or MPHW (F)
Despatch the report to the Central Cell within eight
days after the end of each month.
AWWs
•
2.
Copy of MMR should be sent to the State Co-ofdinator
and Chief District Adviser within 8 days after the end
of each month.
7
is
biLM
108
No. of AWs wher supplementary nutrition was distributed:
a) Very Regular
(b) Moderately Regular
(c) Irregular
(21+Days)
(15-21 Days)
(<15 Days)
109
-
iI
Malnourished children 0-6 yr as-compared to last month
12 Supply Position:
.^ade________ No.Previous Month________ No.Reporting month
Supply Position
____________
■"•cade II
_ iTadelll & IV
Quality of supplementary nutrition food:
Good/Acceptable/Poor.
» Immunisation performance figure (To be filled in from avail-
ISotalNo.
DPT
13. Sectoral Training conducted
DA Present:
POLIO
.nnmunised
the PHC
Mea
sles
1st 2nd 3rd 1st 2nd 3rd
Tetanus
Toxiod
(Preg. Women)
1st 2nd
Name
PHC
Address
Total since
1st April
Pincode
Incidence of other important events:-
No. Previous month
No. Reporting month
^a) Diarrhoea*
<b) Total Births
uc) Total Deaths
0 to <1 year
ii)
?ii) I to <3 years
mi) 3 to <6 years
av) Preg. women
_____ during delivery.
* ORT Advised
Yes/No
Signature
Date
Intherepor
ting month
Event
Not
Available
Medical Kits
______
Vit. ‘A’
Iron & Folic Acid
Tablets___________*_____________
information at the PHC).
BCG
Occasionally
Available
Regularly
Available
* Pl. indicate the address with pincode to send you the
quarterly cheque/Information for your honorarium.
Note:
1.
Despatch the report to the Central Cell within eight
days after the end of each month.
Copy of MMR should be sent to the State Co-ordinator
and Chief District Adviser within 8 days after the end
of each month.
Yes/No
Il 1
< .^1
■
INTEGRATED CHILD DEVELOPMENT SERVICES
FORMAT-4
District Adviser’s Monthly Monitoring Report for the month of.
1. Name ofthe State
District
tW
Remarks about the following events as compared to last month:
al
Event ______ No. Previous Month No. Reporting Month
(a) Malnourished
Children 0-6 Yrs
Grade II
Grade III & IV
(b) Diarrhoea*
(c) Total Births
(d) Total Deaths
i) 0 to <1 year
ii) 1 to <3 years
iii) 3 to <6 years
iv) Preg. women
during delivery.
_________________
7. Remarks about the (a) Co-ordination with CDPO and (b)
Mr
I
2. Number of Sanctioned ICDS Projects in the district
3. Number of Operational ICDS Project under your charge
4. Number of Project Advisers under your charge
5. Details of Monthly Monitoring Reports received from the PHC
_
of Operational CDS Projects under your charge. *
No. of
Date of PHC Topics
Name of Name of Date of
Participants
Level Meet Dis
MMR
PHC
ICDS
cussed MO/LHV/
ing and
Checked
Projects
(Title CDPO/MS/
Continuing
and
Others
only)
despatched Education
Food Quality at AW centre:
Good/Acceptable/Poor
Signature
Name (in block letters)
Full Address
j
*w
Pincode_________ _________ _
Date-------- ------------------ -----Please do indicate Pincode in the address.
Note:
1.
2.
3.
The Monthly meeting in all ICDS projects under your
charge should be completed within 7 days after the end
of each month.
z
This MMR should be submitted to Central Cell within
11 days, after the end of each month;
Copy of MMR should be sent to the State Coordinator
within 11 days, after the end of each month.
113
112
£
INTETGRATED CHILD DEVELOPMENT SERVICES
FORMAT-5
Chief District Adviser’s Monthly Review Report for the month
of
19.
District
1. Name of the State
Population
2. Date of District Level Meeting (including ICDS)
6. Immunisation performance in the district (These figures are to
be filled from the available informatidn for children below 1 years
under UIP at the District Headquarters)____________________
TTto
No.
Pregnent
Measles
Polio
doses
immunised BCG D.P.T. Doses
women
1st 2nd 3rd 1st 2nd 3rd
in the distt
1st dose/
2nd dose
i) During
the month
3. Number of ICDS Projects in the District:-
(a) Sanctioned•
ii) Total Since
1st April
(b) Operational.•
4. Number of ICDS health functonaries in the District:-
(a) District Advisers
I
(b) Project Advisers
7. Remarks about the following events as compared to last month
No. Reporting
I No. Previous
EVENTS__________ month
(a) Malnourished Children
5.
Name of
District Adviser
No. of Proj
ect Adviser
reports
Name of
Name of.
Project Projects/PHCs despatched
Under his charge. by PAs in
the district to
Central Cell.
Grade II
GUI & IV
(b) Diarrhoea
(c) Total Births
(d) Total Deaths
i) 0 to <1 year
ii) 1 to <3 year
iii) 3 to <6 years
iv) Preg. women
during delievery.
i)
ii)
iii)
iv)
8. Remarks regarding food quality at AW centers: (Plase Tick)
Good/Acceptable/Poor
114
is
115
[g
..
..
9 . Number of participants in Distt Level Meeting.
< (a) District Adviser(b) Project Advisers
W:
INTEGRATED CHILD DEVELOPMENT SERVICES
FORMAT-6
(c) CDPOs (d), Distt. Social welfare
officers (e)
QUARTERLY REPORT OF THE DIVISIONAL ADVISOR
Others-------------- -—
10. Quarterly remuneration of ReceivedNot received
the District for MMRs
1. Name of the Divisional Adviser
Date
Distributed/Not distributed
Division
State
2. Report for the Quarter ending 31 st March/3 Oth June/3 Oth Sept?
31st Dec. 1994
Date
(Pl. Tick)
11. No. of Lectures taken for Social Welfare functionaries during
3. Date of Divisional Level Monitoring Conference
the month•
4. No. of districts in the division
Remarks if any
___________
5. No. of Chief District Advisors in the division
Signature
6.____________
Name of CDA District
Name (in block letters)
Designation
i-2?-’
Full Address
Date
Pincode
it
No. of Projects/PHC’s No. of CDA
Report sent
under his charge
in quarter
under
Review
yh;r: -
Please do indicate Pincode in the address.
Note:
1.
The District level review meeting of ICDS should be
combined with the routine monthly meeting at the
District Headquartef.
2.
This monthly Review Report must be submitted to
Central Cell within 21 days after the end of each month.
3.
Copy of MMR should be sent to State Coordinator
w ithin 21 days after the end of each month.
;'r----------;
’ -----------------
7. Participants in the Meeting:
(a) No. of CDA’s
______________
(b) No. of Programme officers
(c) State Level functionary
116
(If yes, write name & Designation)
117
INTEGRATED CHILD DEVELOPMENT SERVICES
(d) Senior Consultant
(Yes/No)
FORMAT-7
(e) Cbnsultant
QUARTERLY REPORT OF THE SENIOR ADVISER
If Yes, write names
1. Name of the Senior Adviser
8. District not Represented in the meeting
2. Report for the quarter ending 31 st March/3 Oth June /3 Oth Sept/
31st Dec. 199 (PL Tick)
9. Monthly Review of ICDS activities at divisional level done
regularly/irregularly
10. Lecture taken by consultant during the meeting (Yes/No)
11. Last Quarterly Meeting
3. (a) District Level meetings attended (Places and dates):
Held/Not Held
If held, date
12. Remarks if any
Name (block letters)
Designation
NOTE:
The Divisional Adviser is also supposed to review the
ICDS Programs with District Level functionaries dur
ing routine monthly meeting at the division.
2.
This report prepared for special ICDS session as "Quar
terly Divisional Level Monitoring Conference must
be submitted to central cell within in I month after the
Name of Distt
Date
Name of Distt
Date
Distt.
Date
Distt.
Date
Distt.
Date
Distt.
Date
Distt.
Date
Distt.
Date
(d) If you have attended any other ICDS meeting, please give
date and place:
4. No. of lectures for Social welfare functionaries delivered
during the reported Quarter
_______________________
5. Date when Expenditure Statement dispatched
end of each quarter.
A copv of the report should be sent to the State
Coordinator as well.
118
Date
(c) Field visits to PHC with ICDS projects in the quarter (Place
and Date):
Full Address
1.
Name of Distt
(b) Project level meetings attended (place and date):
Signature
Date
State
6. Specific recommendations if any
119
■■
1
!
4
■
Date
Signature
Name
INTEGRATED CHILD DEVELOPMENT SERVICES
-
ft
FORMAT-8
QUARTERLY REPORT OF THE STATE COORDINATOR
Full Address
1. Name of the sate coordinator
2. State/U.T.
Note:
1.
At least one meeting or visit is expected each month.
2.
A brief report on 3 (a), (b) and (c) above should be sent
to Central Cell and State Coordinator.
3.
The quartertv report should be submitted to Central
Cell within 30 days, after the end of each quarter.
____________
3. Report for the quarter ending: 31 st Mar/30th June/30th Sept
31st Oct. 199 (PL tick)
4. Project Status (At the end of the reporting quarter).
Sector No. Sanctioned No. Functioning No. allotted for
monitoring
Central
State
Total
5. a) No. of functionaries in position at the end of the quarter
i)
Chief District Advisers (CDAs)
ii) District Advisers (DAs)
___________________
I
b) MMRs receipt position (at the end of reporting quarter)
!f
f-W
Month
in the
reporting
Quarter
CD As Report
DAs report
Expected I Received Expected Received Expected Received
1st Month
2nd Month
3rd Month
I
TOTAL
I
120
/ -
PAs(MOl/C PHC)!
Report
121
6. Consultants performance (at the end of the reporting quarter)
Participants
Training Course
No. of No.
3 day No. of MOs CDPOs Othen
2 day
1 day
Consul of
Regu courses
Refesher| Intro
ants at Qtly
held
the end Repts. Seminar ductory lar
of quarter Recd.______
Quarterly report of senior Adviser: Received/Not received
7.
8. No. of Lecture hours devoted for social welfare functionaries
during the quarter by:i) State Coordinator ii) Sr. Advisor
11. Specific problems/points (if any) related to above may be
mentioned below.
12. Paper cutting/'/assembly questions if any on ICDS the quarser
(Please attach copies thereof).
Signature of State Coordinator
Signature of ODA
Name
Name
Date
Date
Note: Quarterly report should be submitted to central cell within 45
days after the end of each quarter.
iii)ODA
iv) Consultants
v) CDAs
vi)DAs
9. Quarterly Expenditure Statement submitted to the Central Cell
by (Blease tick).
i) State Coordinator............ Yes/No
10. Monitoring Feedback from Central Cell, received for the
month of
in the quarter.
Action taken
by State Coordinator
Comments on
a)
b)
c)
d)
e)
f)
Shortfall in MMRs
Staff Position
Sector Level
Supplies
Vital Statistics
Immunisation
122
-
123
^4? '
-
sw
I*
ii
i
<<
CL
& E
co >
E
u
u
z
S
co
UQ
O
>
w
co
o'
O
k.
E
o
I S
2 2□
_
>
w
Q
Q
u
5C
o
Q
Q-
ai
23
U
Os
i
H
<
ss:
o
E
c
5
c
V
o:
ta
c.
us
.£
£
•o
8
co
Q
X '
c.
H
O
•o'
s
•o
t»
Cl
£ 8
g
o
eg
a.
Almost at the very outset of ICDS in 1975, it was decided that
the academic community of the medical colleges of India would
constitute the ‘external investigator’ component for evaluation and
research. In this endeavour, as manias 29 senior faculty members
from 27 medical colleges, located within a reasonable distance to 33
experimental ICDS projects, unanimously resolved at a meeting
held at the All India Institute of Medical Sciences (AIIMS), New
Delhi in November, 1975, to act as its honorary' consultants with
twin role of (i) evaluation and research; and (ii) orientation and
training of the functionaries.
E"
o
d
3
Fl
55
00
t*-
o
o .E
4>
b>
4
8 $O
Z co
w
2
’8
i
u
s
k.
o
•8u.£
•o
o
Z
Qi
Q
U
sJp
2
EVALUATION AND RESEARCH SYSTEM
o
>
E
I
O
§ E
§ >
<
oi
k]
OD
V>
•E
£<
cc
Chapter in
‘i
O
co
Z
<z
SE To------
>
5
cn
z
o *
fl
•E
to
H
O
C
o
•o
o
QC
Vi
c/i
<
C-
.2
U
52
<
co
<Z)
5
-Si
o-
v
o
s
T
[
©
£fi s
J g
3
c
u
■g
These consultants agreed to work under the overall guidance
of the Central Technical Committee (CTC) of ICDS. The group
unanimously laid down following guidelines to achieve various
goals of ICDS:
■ r 'O ■
(a)
The evaluation and research methodology should be
updated from time to time through meetings of the
consultants and the academic staff of the CTC;
(b)
The evaluation and research should involve minimum
possible resources with active participation of the
postgraduate students and faculty members belonging
to the respective departments ofthe ICDS Consultants;
•5
>
o
Q
CH.
*Qi *Z Zs
it
•o’
c2
125
124
4
INAUGURAL
S^KEBttMML^^INAIiDNmNOWmDNSmCCCD
KEYNOTE ADDRESS
Early Childhood Care for Child Survival, Growth and Development in India
Patrice Engle, Section Chief, CD&N, UNICEF
In her keynote address, Ms Engle clarified basic concepts of the ECC-SGD framework. She answered 3 basic
questions - the what, why and how of this framework.
I.
WHAT characterizes a programme in ECCSGD?
Any programmatic effort that simultaneously addresses the three goals for children: survival, growth, and
development.
1.
Definition of the letters :
E : Early, prior to age of school entry, up to age 8;
C: Child, person from conception to age 18 (CRC definition);
C : Care, what family members and other members of society do for a child to facilitate the
processes of growth and development;
S : Survival, absence of mortality, and including health;
G : Growth, or an increase in size, which requires good nutrition particularly under the age of
two, and for women, during adolescence, and during pregnancy and lactation. Good nutrition
requires not only sufficient energy for growth, but also specific micronutrients such as iron,
zinc or iodine;
D : Development refers to an orderly process along a continuous path, in which a child learns to
handle more complicated levels of moving, thinking, speaking, feeling and relating to others.
Children vary enormously in their rates of development, but all cover essentially the same
sequence of developmental changes.
Developmental domains
Motor
The ability to move and to coordinate muscles
Cognitive
The ability to think, reason, and solve problems
Linguistic
The ability to communicate
Social
The ability to relate to other people
Emotional
The ability to feel and recognize emotions
2.
Characteristics of ECC-SGD programmes
It must include attention to nutrition, early childhood development, and health.
May have different entry points - e.g., health care, nutrition (not only food but also information),
growth monitoring, parenting classes, day care for children of employed women, special needs
children, community development, women’s empowerment groups, and care for children in special
circumstances (e.g., refugees).
UNICEF, Chennai & Hyderabad
November 24-26, 1999
14
SUSRBSIONAILSEMINAFgaNt INNOVATIONS Ir^ECCq
3.
Examples of programmes from India : Do they meet these criteria? Are these examples of ECCSGD programmes?
Midday meals
Public distribution systems
Pulse polio and vitamin A
Growth monitoring and promotion programmes
Balby Friendly hospitals
Preschools
Women’s thrift and credit groups
Parent support groups
Day care center for children of working mothers
that provides food and nutrition education as well as an
educational program
II.
Studies show that
a.
Nutrition is important for development. Even from the *IQ’ perspective, it has been seen that ♦
♦
♦
early nutritional supplementation in a nutritionally at risk population will result in significant
increases in cognitive development and IQ through adolescence.
a number of other nutritional interventions have resulted in long-term benefits of
approximately 10 IQ points such as •
Iodine : absence can lead to deficits in IQ or, if extreme, to cretinism
•
Iron affects cognitive functioning and increased attention.
•
Breastfeeding can result in higher IQ scores
•
Low Birth Weight without excellent family support is associated with lower levels of
physical and mental development.
India has one of the highest rates of malnutrition among children under 5; as many as 53%
of children are classified as mildly or moderately malnourished.
2.
Combined nutrition and early childcare programs have a greater impact on development
than either alone.
3.
A second reason for these combined programmes is that they may work better than the
individual programmes
a.
Increased motivation : A parent may be more likely to adhere to nutritional recommendations
that take time and effort if they believe that their child will become brighter because of feeding.
b.
Overlap of skills: A parent who learns to help the child develop better may also become more
attentive to the changes in the child, and identify children’s hunger cues or danger signs for illness.
HOW can ECCSGD programs be made most effective?
1.
Interventions should start early, and continue late
♦
♦
Any intervention to affect children’s nutritional status (as measured by height) must occur in the
first two years of life, preferably including the prenatal period.
Children who are born at term and weigh less than 2500 grams have a greater risk of being
shorter, and mentally delayed and are less likely to achieve in school than those born with a
higher weight. They are also more vulnerable to other risks.
Interventions for poor children from infancy onward show significantly greater effects at
adulthood than interventions that begin at ages 3 and 4.
UNICEF, Chennai & Hyderabad
November 24-26, 1999
J
yes
WHY do we think that ECCSGD is important for helping children develop
1.
III.
no
no
no
no
no
usually not
usually not
- depends on what they do
~
-
15
INAUGURAL
SUB^REBIONALSEMINAR GN INNOVATIONS1N£CCD
Newsweek, Nov. 1: Results from a carefully controlled study of early day care in North Carolina,
USA, showed that “poor children enrolled in high-quality day care from infancy do much better
academically and economically than low-income kids who don’t get that initial boost. As adults,
children who received the intervention were more than twice as likely to attend college and be
employed. “Craig Ramey, who did the study, concludes, “ It has become crystal clear that if you
wait until age 3 or 4, you are going to be dealing with a series of delays and deficits.”
Combining cognitive enhancement and food supplementation has a significantly greater effect
on children’s development than either one alone among children less than 24 months.
Grantham-McGregor in Jamaica found that home visiting to increase cognitive skills plus
supplementary feeding among 12-24 month old stunted children in Jamaica resulted in greater
effects than either home visiting or supplementary feeding alone. But the greatest long-term
effect was seen for the group who received the educational stimulation.
2.
Interventions should be culturally appropriate and be consistent with what families want for
their children.
Families’ values for their children often depend on how they earn their living and what they think that
their children’s chances of survival are. Based on these values, parents have investment strategies
fortheir children that make sense to them. We must understand them in order to build on them.
The way those families must support themselves, and children’s chances of survival influences what
parents want from their child. These conditions also affect parents' investment strategies with their
children, or their child-rearing patterns.
Many families are in transition - they move to urban areas, begin to change their desires for their children,
begin to replace farming with wage labor. Schooling may be much more important than before. As their goals
for children change, parents may need help in learning how to achieve the new goals. They also need support
to keep valuable child-rearing traditions that may disappear. So, we should be aware of where in this transition
families are as we design programs. We should respect parents’ goals for their children, and assist those
whose goals are not in agreement with their behavior (e.g., valuing obedience and quiet, while wanting children
to do well in school).
IV.
Where do we go from here?
A.
Develop ECC-SGD perspective in
Growth monitoring and promotion programmes - incorporate assessment and recommendations
for psychosocial care ((Indonesia)
Baby Friendly hospitals - improve newborn care for development , such as touch for LBW
babies, contact with mothers including those with c-sections, showing mothers the abilities that
children already have at birth (USA)
Preschools - provide information for children and mothers on appropriate foods (helps with
inappropriate food choices)
Day care for working mothers - Provide information regarding how to prepare foods, provide
health services, and, if needed, supply supplementary foods (e.g., Philippines, SEWA centers,
ICDS centres).
Parent support groups - Information on growth and development as well as health or income
earning.
B.
Develop innovative models for addressing these aspects of child development
India and USA both developed similar programs during the 1960s and 1970s to address the problems
of children in poverty. Both have changed and matured over time; both have been criticized as
ineffective, and both have shown that there are clear evidences of positive impacts at a broad
national level. Both have also recognized the importance of beginning to intervene in the earliest
UNICEF, Chennai & Hyderabad
November 24-26, 1999
16
' I
F'
L
r
INAUGURAL.
SUB REGIONAL SEMINAB ON INNOVATIONS IN ECCO *
■
years. Comparing the resources used for each can make us aware of how much is done in India by
ICDS with so few resources. For example in ICDS, an AWW and assistant may handle up to 83
children, whereas in the Head Start program in USA, the same pair handles about 15 children.
i
I
The experience of both programs has led to the recognition that it is essential to begin
earlier, and to develop different models for care. Head Start now has an Early Start program
with home visiting and nutritional support. They have also designed specific programs for
children of migrant parents who work in changing areas.
There is no one right way; we need to be aware of the multiple needs of the child for
survival, for growth, and for development, as well as for protection and participation. We
need to take the parents’ investment strategies, and the reality of their lives, into account.
We need to recognize that investing in children is a very cost-effective use of public and
private funds, particularly for children under three years of age. But the cost is high, because
the efforts that parents have been putting into child rearing has never been paid for. As we
move forward, to the next millennium, we will find more families transitioning into the new
model of child rearing, and we must be ready to meet the challenge of addressing their
needs and assisting parents to support children.
UNICEF. Chennai & Hyderabad
November 24-26. 1999
17
9
W s
r
SUBREGIONA^SEMINARO^INNawnONSINECCIl
NATIONAL PERSPECTIVES
THE YOUNG CHILD IN THE 21st CENTURY IN INDIA : IDEAS FOR TODAY AND TOMORROW
MrSK Mutto, Director, NIPCCD, New Delhi
VISION STATEMENT
Balika Samariddhi Yojana - starting early
•
Ensure child survival
DPEP
•
Facilitate growth of the child
RCH
•
Promote development of the child with the
element of participation
STRATEGIES FOR MAXIMIZATION
•
Home visits, NHED, enhancing capabilities
among caregivers
•
Maternal nutrition and for 0-2 child
•
complementary feeding
•
Hygiene
•
Institutional deliveries/ante natal care
•
Contraception and spacing
•
FLE for adolescent girls; anaemia
•
Creativity in pre school and making schools fun
GOALS AND OBJECTIVES
•
Reduce infant mortality to half of the present
level by 2020
•
Eliminate Grade III and IV malnutrition by 2010
•
Eliminate vaccine preventable disease by 2010
•
Get all children into school by 2020
TODAY’S SITUATION
•
Infant mortality is 71
•
30% babies have low birth weight
•
Most babies are delivered at home, causing
deaths as well as congenital defects
•
Over 50% children are malnourished
•
100 million children are out of school
GOVERNMENT INITIATIVES
•
ICDS - a holistic approach to child development
•
IMY and RWDEP - empowering women
UNICEF, Chennai & Hyderabad
November 24-26, 1999
LOOKING INTO THE FUTURE
Survival will improve; development requires
attention
AIDS is a potential killer of children
Education deserves further attention
Rise in demand for child care services
Support mechanisms for and early detection of
disabilities important
23
i
snuEF^ispBznvE
SUB REGIONAL SEMINAR ON INNOVATIONS IM ECCO
a
STATE PERSPECTIVES
department of social welfare, tamilnadu
Mr. Sakthikanta Das, Secretary
Innovations in ECCD in Tamil Nadu
Started new facilities and new inputs like 1 egg a day for each child
Numerous number of Anganwadi Centres, Health centres, help centres, mid day meal centres exist and
serves as focal point for community mixing and exchanging ideas and needs.
Importance of Education
Need to educate youth to develop both technically and economically
Software a high source of employment for youth
Tamil Nadu at the forefront of technological advancement
Anganwadi centres to help shape and develop children with a view to sending them to Primary school
Child to be given all facilities regardless of gender
Work for 0 percent drop outs.
Importance of ECCD
Early childhood care and development crucial and essential in shaping the future, nature and character
of the child
The family, community, anganwadi centres, etc., needs to have an integrated and comprehensive approach
towards ECCD.
Anganwadi centres not merely feeding centres but plays an integral part in creating awareness on the
importance of development of the child, nutrition, education, health, etc.
They bring other social groups into the programme
Training programmes are regularly held for women and children in rural areas. Attractive reading material
and innovative pictures, etc.
Much importance given to the micro level situation where family is the focal point for improvement in
ECCD
Realising the gaps in the implementation of various programmes, the Govt, of Tamil Nadu has tried to
improve.
DIRECTORATE OF SOCIAL WELFARE, GOVTERNMENT OF KERALA
Ms Ishita Roy, Director
Objectives of ECD
•
•
®
•
•
Recognise that the child’s right to survival, development, protection and participation is universal and with
no discrimination whatsoever,
Ensure that every child is healthy, well nourished and cared for and able to achieve full development
potential and active learning capacity, so as to give the best possible start to life for the young child.
Develop and mainstream community-based approaches to ECD for children under three years of age.
Enhance the capabilities of care-givers
Increase family and community participation
UNICEF, Chennai & Hyderabad
November 24-26, 1999
25
I J
I I •
1
k
••
’ ‘ -a .S'
- SraTEFERSFBOTVE
SUBREGIONAL. SEMINAFFON INNOVATIONS IN ECCa
Effective training programmes for various levels
Orientation to the community through the resource group consisting of AWW, Teacher, HM, Opinion Leader
Periodical reviews with field staff - CDPOs and PDs
Training
Ongoing training programmes at various levels involving MLTCs, AWTC instructors, Supervisors, AWWs,
RDDs, PDs and CDPOs
Strategies to ensure girls’ education
Improve literacy among adolescent girls, through bridge course
Improve vocational skills through training programmes
Information & Communication
Publication of Newsletter in Telugu for supply to all the AWCs to create awareness of Mothers Committees
as well as brochures on their role and responsibilities
Press tours/exposure visits to various Projects, Anganwadi centres
Organisation of photo exhibition
Production of TV /Ad. Film documentaries on various programmes
UNicef, Chennai & Hyderabad
November 24-26, 1999
29
I
•4
*
STATE PERSPECTIVE ON ICDS, 1999- 2000
Mr. B.3. Kanti, Department of Women and Child, Government of Karnataka
In Karnataka ICDS programme was launched on 2nd Oct
1975 at T Narasipura of Mysore District with 100 centres.
The scheme expanded gradually and has emerged as the
most effective child survival scheme of the state. The
present project and Anganwadi profile is as follows :
Rural
Urban
Tribal
Total
166
166
10
10
9
9
185
185
(100%)
Anganwadi Centres
Sanctioned 35856
Operational 35846
1120
3194
3047
40170
40013
(99.6%)
ICDS Projects:
Sanctioned
Operational
1120
ICDS scheme has spread over in ail the 175 taluks and
10 urban areas of the state. Rest are being covered under
World Bank assistance. Added to this, all the 27districts
are sanctioned with District ICDS Monitoring Ceils
entrusted with reviewing of ICDS programme.
The six package of services under the scheme are being
effectively implemented in the state by the Zilla
Panchayats. The Dept is monitoring and guiding the
implementation of the scheme based on the guidelines
issued by the State Government and the Government of
India from time to time.
Supplementary Nutrition Programme
In Karnataka, supplementary feeding is being carried on
in all the 185 projects in 6 days, a week. Ablend of Energy
Food and locally prepared food out of rice is given on
different days. At present, apart from children below 6
years, pregnant and nursing mothers, adolescent girls in
the age group of 11-18 and Anganwadi workers and
helpers are also enrolled for supplementary feeding. An
average of_24 days of feeding is registered in the state.
The state government is bearing a cost of 52% from the
central government. The state government releases funds
to ZPs_periodically under both feeding and administrative
components.
Preschool activities
Pre school activities in AWCs are made more attractive
and innovative by developing and introducing integrated
approach - a blend of COPPC and thematic Approach.
This new approach which is being practiced in the centres
successfully since 1991 is well accepted by the
beneficiaries. 5.86 lakh boys and 5.71 lakh girls are
attending pre school activities. Special efforts are made
for enrolment of girls.
DSERT in collaboration with the Dept and Unicef has
conducted workshop on the development of ECE curriculum,
activity bank and activity kit. ICDS functionaries like
Sub Regional Seminar on Innovations in ECCD,
Chennai - November 24-26,1999
CDPOs, Supervisors and Aws were actively involved in
the workshop.
District Primary Education Project
It is proposed to strengthen Anganwadi centres providing
pre school equipment in some of the selected districts
under DPEP programme with the coordination of Director,
District Primary Education Project in the state. This project
was started in the yeaM9Q4 - 95. The main purpose of
the scheme is to see that girls who are engaged in looking
after siblings in the houses thus depriving themselves of
school going, are made to attend schools by keeping
AWCs open upto 5 pm; This programme aims at the
increase in the attendance of girls in schools. The AWWs
and AWHs who have to work in the AWCs up to 5 pm will
be paid an additional honorarium of Rs. 300 for AWWs
and Rs. 250 per month under DPEP. An amount of Rs.
2000 one time grant will be released to AWCs for
purchasing pre school equipment and toys. At present,
2405 AWCs in 28 ICDS blocks of 11 districts are covered
under this programme.
Health Services
Immunization and Health check up are being conducted
in the AWCs with the coordination of the Health
Department. JpinlLVisits of medical officers and CDPOs
and middle level functionaries of both departments are
being conducted. Referral services are given to the
severely malnourished children who are suffering from
chronic diseases. Of the total children 20.55 lakh children
are weighed and of this 12.50 (61%) lakh constitute
malnourished children. Stringent action is taken to reduce
the percentage of malnourished children by gearing up
health checkup and referral services.
Two days joint Training course has been organised by
the Dept of Health and FW services to AWWs and lady
junior health assistants during 1996-97 in Kolar and
Chitradurga districts on pilot basis. Jt is proposed to
conduct these training courses in other districts of the
state in phased manner.
Translation of Training materials
The department had developed six types of traininq
materials in Kannada to enable the AW worker to
understand the concept of ICDS programme. This was
done with the assistance of Unicef.
Staff and Training Position of ICDS Functionaries
sanctioned
filled
185
219
183
144
663
38928
CDPO
ACDPO
Supervisor 2036
AWWs
40170
vacant
trained untrained
2
157
124
75
Cj3732)
663
659 27993
25
20
11518
89
Decentralised Training
Anganwadi Workers
Programme
for
The Department of Women and Child Development in
Karnataka has taken up an innovative decentralised and
revised programme of Refresher Training of Anganwadi
workers of 6 days during at the district level with the
financial assistance from UNICEF with a view to clear the
heavy backlog. As a pilot project this programme was
taken up in four districts in Gul ba rga, DK. Bellary and
Shimoga Districts during 1993 - 94. Evaluation of the
pilot project was conducted by the NIPCCD, Bangalore
which indicated the success of the training programme.
Therefore, the Refresher Training was extended to the
remaining districts during 1994 - 95 and continued up to
1996-97. For this purpose, Core Teams at district level
Involving District Assistant Director of Women and Child
Development, CDPO, supervisors, Medical officers, and
instructors of AWTCs were constituted. £5250 Anganwadi
workers have been trained under this programme. Final
concurrent Evaluation of the programme was again
conducted by NIPCCD, Bangalore during 1996 which
indicated success of the programme. Based on the
previous experience it is proposed to continue the training
programme under UDISHA during..2000.
The ATI was specifically entrusted with responsibility of
facilitating training at_district training instituteJDIIs) by
setting up necessary dish antennae, making available TV
sets and STD phone lines and providing space for
conducting training programme. The department of W &
C undertook responsibility for developing software for the
workshops in collaboration with NIPCCD, Bangalore and
other NGOs.
The programme was transmitted from the Earth Station
at Bangalore to all the districts. The training included
issues relating to ICDS such as techniques in pre school
activities, growth monitoring and other new schemes of
the department. In the first phase, the training was
imparted to ADS, CDPOs, ACDPOs, Pos, Supervisors
and principals of AWTCs. The total No^of functionaries
under this training was 718.
In the subsequent phase, under UDISHA, it is proposed
to conduct four satellite tele-workshops each year on the
subject stated below :
—————
1.
Community participation and convergence of
services of ICDS at AWCs.
2.
Impact of Nutrition on Pregnant and Nursing Mothers
and children below 6 years.
3.
Importance of health education to the community
4.
Importance of pre school activities in AWCs.
Satellite-Based Interactive Training Programme
The first innovative satellite based interactive training
programme was organised in the state of Karnataka at
Bangalore during Feb 1995. Based on the previous
experience the Department has organised training
programme for all the district officers and ICDS
functionaries through satellite based interactive Network
in May 1997 in collaboration with ATI, Mysore at ISRO
Bangalore.
The department is coordinating with other departments
for implementing ICDS activities. Theleading NGOs like
Sumangali Sevashram, Sutradhar, Promise Foundation.
Guild of Service, Jindal, Prerana, Sumaha,Lords, Myrada,
etc., have also been involved in the implementation of
ICDS programme in the state.
v . /
EARLY CHILDHOOD DEVELOPMENT
Ms. Ishita Roy, Secretary, Directorate of Social Welfare, Government of Kerala
Early children development is a time of opportunity and
learning. It is a process when the child unfolds behavioural
patterns from immature to mature, which enables the child
to emerge from a dependent entity to an independent adult.
The more a child receives, better his intelligence, his
personality and his growth and development. Therefore
the need for more protection, care, affection, interaction,
stimulation and learning. These are the rights of the child
and not mere concessions.
The efforts, therefore, should lie in advocating a rightsbased strategy which should respond to a vision of children
in the 21” century who are respected, protected and loved.
In order to ensure the best interest of the child it is essential
to guarantee his economic, social, cultural and civil rights.
More importantly every single child ought to be guaranteed
equality of opportunities without any distinction and this
could perhaps come from the creation of a caring
Sub Regional Seminar on innovations in ECCD,
Chennai - November 24-26,1999
i
community, right from the parents to guardians, to care
providers, to neighbours, to peer groups, to policy-makers
and implementors.
We are all aware of the fact that India has been a signatory
to CRC. The ratification of the CRC implies obligation on
the State Governments to respect, protect, facilitate and
fulfil rights as embodied in CRC. It also implies that the
unreached should be reached, specially those belonging
to SCs, STs, those disadvantaged due to socio-economic
and socio-cultural factors, the neglected and all the juvenile
delinquents, etc. It also implies moral obligation on the
family and community to provide care and protection
because many of the violations of child rights take place
within the household, and sometimes with the knowledge
of the community. This is particularly with regard to issues
of protection such as child suicides, child abuse and their
sexual exploitation.
90
Kerala, as the entire nation is aware of, has gone for a
massive decentralisation of democratic authority, where
40% of the State's Plan funds have been given to the
local bodies for implementation at the local level. The
objective is that through local initiative, the effort should
aim at effective delivery of services, increased
accountability and openness and transparency in decision
making. Towards achieving this end, monitoring by
People’s Committees as in the case of Panchayath
committees should be strengthened which act as watch
dogs in Kerala.
While talking of ECD, one might not forget that malnutrition
among young children remains as one of the most difficult
and complex goals. The effort, therefore, should be on
reducing malnourishment by reaching out to children in
the most curcial age group of under three years and
focusing on caring practices in the household, improving
access to health care and a safe environment, reducing
gender discrimination and enhancing the nutritional status
of the adolescent girls.
Recognise that the child's right to survival,
development, protection and participation i»
universal and with no discrimination whatsoever,
Ensure that every child is healthy, well nourished
and cared for and able to achieve full development
potential and active learning capacity, so as to
give the best possible start to life for the young
child.
Develop and mainstream community-based
approaches to ECD for children under three years
of age.
Enhance the capabilities of care-givers
Increase family and community participation
Strengthen ‘joyful learning' in anganwadis
Strengthen linkages between the anganwadi, the
primary school and the health care system
In Kerala, low birth weight among infants is an important
indicator of the risk of malnutrition. It is also emerging as
a major cause of chronic illness later in life, as well as a
factor in mental retardation. Therefore, better care of
adolescent girls and women, especially during pregnancy,
would be vital in improving the nutritional status of both
women and children. These pre-birth factors have to be
addressed to within child development and nutrition
programming of the State.
A child rights framework would, therefore, include a
strong networking between Governments and the civil
society, specially the women, the youth and local Govts.
And enabling and empowering them to identify their
own opportunities and design specific interventions that
are best suited to local realities.
Sub Regional Seminar on Innovations in ECCD,
Chennai - November 24-26,1999
Psycho-Social stimulation and child parent interaction has
a very significant implication for physical and cognitive
development of the child. Neglect of children, specially at
the age less than 3 years, has serious implications in terms
of over all development, readiness for schooling and
learning capacity in the child. Therefore, the right of all
women to be informed and counselled on appropriate
infant and young child feeding practices needs to be
recognised and implemented. This task should not be
difficult because in Kerala, as Primary-data based studies
reveal, there are already higher levels of health awareness
and information among women, higher level of maternal
utilisation of the health system and greater decision
making roles of women in the households compared to
their counter parts in the rest of the country. What would
be important, therefore, is to channel their interest towards
encouraging a parent-child interaction and psycho-social
stimulation for the child, especially the under-twos.
Early childhood development should therefore have the
following objectives :
In order to achieve these objectives, the tasks would
include developing and testing community based
approaches for children under three years, strengthening
the decentralised planning that is already in place,
encouraging action research, facilitating networks of civil
society partners, to articulate, establish and demonstrate
quality standards for ECD, promoting scaling up of early
joyful learning activities with the help of DPEP, developing
communications strategy and concentrating on training
of functionaries and assuring the right of every child to
safe water and a clean environment. One must also realise
that a strategy to fulfil child development and nutrition
rights needs to be inter-sectoral and therefore there is a
need to focus efforts to address 'pre-birth' causes of
malnutrition by focussing on adolescent girls as stated
earlier.
It may not be out of place to submit that State level task
forces on Nutrition, Adolescence and Information,
Education, Communicaton have been established in
Kerala for effective formulation and implementation of
strategies. A state level ECD task force is also in the offing.
Not to sound pompous, it is important to repeat that
Kerala has the lowest birth and death rates in India
and has more hospital beds relative to the population
than any other state. The rate of immunisation is among
the highest in India, and the current date indicate that
girls are immunised at the same rate as boys. The rate
of literacy among persons in the state who are 7 years
old and above is more than 90%. One of the most
radical implementation of land reforms in India has
taken place in Kerala. There have been important
achievements with respect to the abolition of
untouchability. Women in Kerala have made
outstanding gains in the sphere of health and education.
We have the best public food-distribution system
among Indian states. The circulation of newspapers is
more widespread in Kerala than elsewhere in India.
91
SlALh&ERSPECTNE
But amongst all this exclusiveness Kerala is faced with
an insecure adolescent, an extremely high rate of suicides
including family suicides, an abominable rate of
consumption of liquor and drugs and tranquilisers and a
high rate of child morbidity. The rapid growth of
consumerism fosters exaggerated notions and
hypertrophied aspirations about domestic comforts, and
standard of living, etc. Increasing alcoholism and a
stressing education system are also responsible for the
increasing suicidal behaviour. Here lies the need for
building up partnership with families, neighbourhood
groups, NGOs, corporate sectors, trade unions, the police,
legal bodies, academic institutions, line departments of
Governments, local bodies and the media for effective
dissemination of key messages for the development of
the child. Addressing the inter-related needs of the whole
child in an integrated manner through such a partnership
would help in prioritising programme intervention from
the child's perspective.
are time bound and cannot remain unattended. The
prevailing situation certainly exemplifies the challenges
before us to promote early childhood development, as in
the development of children lies the strength of a nation.
The vision therefore, would be an environment where no
child would be deprived of childhood and where the child
would grow in a healthy, discrimination and crime free
and a safe and hygienic environment in the next
millennium. Fortunately, thanks to policy makers, Kerala
is already undergoing a renaissance in terms of
empowerment of the community and the people at the
grassroots.
“Janakeeya Asootharanam’ or People’s Planning
would surely safeguard the child’s rights and reach
the unreached.
In the next millennium Kerala would epitomise light
and hope for every civil society to follow, as it has
already set standards in the present times
The tasks of realising the goals and objectives associated
with multi-dimensional and inter-linked needs of children
SPMU, WORLD BANK 1CDS PROJECT
Mr. G. Srinivasan, I.A.S., Women & Child Welfare Department, Government of Andhra Pradesh
ICDS Services
Situation Analysis of ICDS
Health
Indicators
Immunization for children and pregnant mothers
Start of
ICDS I
in 1991
End of
ICDS I
1997
End of
APER
2003
5
82
24
62
<3
100
18
40
50
65
16.87
4.87
12.00
29.60
6.35
15.00
Nil
1.16
Health checkup
Nutritional Status
Grade III & IV
10
Grade I & Normal
61
Low Birth Weight Incidence 33
Infant Mortality Rate
71
Enrolment of Girls
in School
s 42
Referral services
Treatment
Nutrition
Supplementary feeding
Growth monitoring and promotion
Indicators (In lakhs)
Nutrition and health education
Safe drinking water
Children receiving SNR 12.8
Women receiving SNR
2.3
Early Childhood Education 8.0
Adolescent girls
Empowerment
Nil
Environmental sanitation
Project Coverage
Women's empowerment programmes
■
Establishing ICDS Projects in 143 New Blocks within
the project period of 1998-2003
■
Quality improvement of ICDS schemes of 108 (79
rural + 29 tribal blocks) existing projects.
Supportive Services
Early childhood care and pre-school education
Non-formal education and adult literacy.
Objectives of ICDS - APER in ECE
Quality improvement of ECE in 32960 AWC centres
Curriculum
Sub Regional Seminar on Innovations in ECCD,
Chennai - November 24-26,1999
92
snmsPEf^eEOimB -
|
j
Orientation to the community through the resource
group consisting of AWW, Teacher, HM, Opinion Leader
Monitoring system
Training teams at District level
Periodical reviews with field staff - CDPOs and PDs
Improve school enrollment and retention
Relieve older siblings (mostly girls) from the burden
of child care and enable them to attend school
Prepare children adjust to formal schooling
Increase community participation in pre-schooling
by setting up Mothers’ Committee
Ensure universal reach of the deprived groups
Strategies to link pre and primary school
Ensure birth registration
Ensure all 4+ children attend AWC
Establish AWC adjacent to primary school
Share list of eligible students with primary school
Ensure children admitted in the school through AWW
Certificate of attendance and date of birth for school
admission
Ensure all 5+ children move from AWC to class 1
Participation of DPEP staff and teachers in ECE
/ WOO
Training
■
Ongoing training programmes at various levels
involving MLTCs, AWTC instructors, Supervisors,
A’WWs, RDDs, PDs and CDPOs
Strategies to ensure girls' education
Improve literacy among adolescent girls, through
bridge course
Improve vocational skills through training programmes
Information fir Communication
Publication of Newsletter in Telugu for supply to all
the AWCs to create awareness of Mothers
Committees as well as brochures on their role and
responsibilities
Press tours/exposure visits to various Projects,
Anganwadi centres
Organisation of photo exhibition
Production of TV /Ad. Film documentaries on various
programmes
Effective training programmes for vanous levels
CHILDHOOD CARE
Mr. Sakthikanta Das, Department of Social Welfare, Government of Tamilnadu
Thanked UNICEF for inviting him to the Seminar. Stated
Now as we are in the 20,h Century, there has come about
that last year in August a Workshop was held and all the
a refining of the changes taken place in the previous
issues have been carried forward for completion and
centuries. A major change has come about in the financing
implementation. As we enter into a new millennium it is
systems, new modes of keeping a track and accounting.
time to come to a conclusion of the
There has also come about a great
plan of actions put forth from this
change towards human resources
Seminar. Tamilnadu has a History
development and much importance
Right from the birth of a
in Early Childhood Care and
and focus has been given to it in
child whether a boy or a girl, early
Development and is a model for
the mid 80’s. Software has gained
childhood care and development
other States and Countries. Over
a high place in South India and is a
starts which is very crucial and
the years the Government has
high source of employment to the
essential in shaping the future
come up with new facilities and new
youth. Industrial and Technological
and nature and character
inputs like 1 egg a day given to each
changes have taken place
of the child.
child etc.
massively. And it is important to
educate and develop the human
Numerous number of Anganwadi
mind both technically and
Centres, Health centres, help centres, mid day meal
economically so that they can be used as valuable
centres exist and is a focal point for community mixing
resources in various fields of work.
and exchanging ideas and needs. There is a need for
people to take part in this kind of mixing so that more
Tamilnadu has achieved a certain degree of development
awareness will be created. The 18th & 19th Centuries
more than other States of India especially in the field of
witnessed a number of changes in the development of
Software Technology. Human capital is very important in
mankind both socially and economically. An industrial
the coming millennium and more focus is given to the
revolution came about and production systems changed.
development of the human mind in Tamilnadu. Right from
Sub Regional Seminar on Innovations in ECCD,
Chennai - November 24-26,1999
93
'3
STAi±:W=RSPECTIVE
the birth of a child whether a boy or a girl, early childhood
care and development starts which is very crucial and
essential in shaping the future and nature and character
of the child. It is important and imperative that the same
should be started at home under the watchful eye of the
parent. Which is why this Workshop is important to
reiterate the importance of ECCD.
It is important to have an integrated and comprehensive
approach towards this — The family, community,
anganwadi centres etc. all have a comprehensive
integrated role to play. Anganwadi centre is just known as
a feeding centre - it is not only that but also the anganwadi
volunteers and workers are there to create an awareness
on the importance of development of the child, nutrition,
education, health etc and they are there to educate the
parents on how to look after the child, how to go about
shaping the child s future etc. They also bring social groups
into the programs. The family also has a role to play and
also the community. All these forces joined together should
concentrate on one thing THE CHILD.
A Symposium was held in August 1998 for this concept.
Training programs were held for women and children in
rural areas. Attractive reading material and innovative
pictures etc were used. A lot of importance was given to
the MICRO LEVEL SITUATION. To create a socio economic background it has to be evolved around families,
the plans should be specific, it should be district specific,
program specific and they should have a clear perspective
on the programs and monitoring of the same. Over the
years the Government of Tamilnadu has realized the gaps
in the implementation of its programs and it has tried to
improve. 100% attention is tried to be given to the
Anganwadi centres. Centres are to educate children and
to shape them and develop them to attend primary
schools.
To meet the growing changes in the coming age and to
attain the employment level in various industries and
organizations, it is important for the child to be educated
and develop his mind power regardless of gender. There
should be 0 drop outs. Plans for the next century should
be specific and importance should be given to the
anganwadi centres which are the hub of activity for Child
hood care and Development. Therefore our main thought
and aim and focus should be THE CHILD ONLY AND
ONLY CHILD.
METHODOLOGY IN TEACHER TRAINING
STORY TELLING WORKSHOP
Prema Daniel, S C S Kothari Academy for Women
INTRODUCTION
6.
To prepare aids for story telling
Story telling is a wonderful language development activity.
It can help children to develop listening skills, speaking
skills, interest in stories, imagination, self confidence, and
social skills. Children, who find it difficult to sit still to listen
to story being read from a book, will be attentive to the
active, animated, participatory style of story telling.
7.
To enjoy and have fun telling stories
Story telling as an art form is older than stories written in
books. History and legends have been passed on from
generation to generation by story tellers all over the world.
Some people have a gift for telling stories, whereas others
may have to practice to develop the skill.
Children can also be encouraged to tell stories. They can
repeat stories that have been read or told by the teacher,
or create original stories based on pictures or real life
experiences.
OBJECTIVES
1.
To learn to tell stories
2.
To select stories for children
3.
To develop language and communication skills
4.
To develop imagination and creativity
5.
To participate and share ideas
Sub Regional Seminar on innovations in ECCD,
Chennai - November 24-26,1999
DURATION OF THE WORKSHOP
The workshop should be five hours, and can be split into
two sessions of two and half-hour each.
WHAT, WHY AND HOW
(The what, why and how of story telling can be done in
small group discussions and brainstorming. The outcome
of the discussion can be written on the blackboard. The
following paragraphs are some of the likely points that
may rise out of the discussion).
Choosing a Story
A good story for story telling will be similar to a good
story book for reading. It will be appropriate for the age
and level of language development of your group of
children. A good story will have the following
characteristics :
>
A simple plot
>
Only one or two main characters (minor characters
have small, simple parts)
>
5 to 15 minutes in length depending on age of
children
94
SUB GROUP^PRESENTATIONS
(e)
method of making
(f)
the trainees views of the experience in terms
of the learning denved from it
L
Ask each trainee to select the toy he or she is going
to make. Being able to make a choice encourages
the creativity of the individual trainee
The trainee next provides a written descnption of the
toy in the format developed in the preparatory stage
Steps
Discussion with the group of trainees of the ways in
which the child develops at the stages under
consideration (eg.) Baby, infant, toddler, preschooler
It is up to the trainer to ensure that the toys will
cover a variety of dimensions of child development
across the group
Make a list of the developmental changes occurnng
at that stage in all dimensions. Physical, social
emotional, intellectual and language.
Brainstorm a list of types of toys that would promote
the different dimensions of development at the
specific stages.
Each trainees makes a toy, using natural matenals
found in the local environment or from waste matenal
■
The trainees should have an opportunity to play with
the toys at some point and give feed back.
■
It is important that there is a practice situation - a
home, school, or child care centre where children
can be observed playing with the toys
Examples
■
Soft toys (allowing for expressions of both positive
and negative emotions)
■
Toys that make a noise (heanng development and
fine motor co-ordination)
■
Toys that develop language (puppets)
■
Toys that encourage social interaction (card games)
Give some thought to the next developmental stage
so that toys can be made to extend the child
Draw on the creativity of the trainees. Ask them to
come up with specific ideas for toys which can be
made for a particular age group.
Before this observation the trainer, trainees need to
develop a checklist
1.
What to observe in the way the child plays with the toy
2.
How trainees should interact with the child to
facilitate learning from playing with toy
3.
How can the trainee extend the child's learning
beyond the particular toy
4.
How can the trainee use the opportunity to educate
other care givers, including parents, in the value of play
5.
Follow up the practice situation - discussion in the
group on the value of toy making as a learning
experience
Toys should be safe, well made and strong.
They should also be colourful and if possible of different textures.
NUTRITIONAL STATUS, PHYSICAL DEVELOPMENT AND EDUCATION
Indian Council for Child Welfare, Tamil Nadu
Middle Level Training Centre for ICDS Funcitionaries
Children reflect the developmental potential and
prospect ofa country. India being a developing country
needs healthy children with better brain power.
Education plays a vital role mostly in all aspects of
development of a country.
INTRODUCTION
One of the most important resources of any community
is its children. Children are the citizens of tomorrow who
would substantially contribute to the social, economic and
an all round development of the country. Invariably the
parents and society would desire that their children should
possess healthy body and mind.
Sub Regional Seminar on Innovations in ECCD,
Chennai - November 24-26,1999
Poor nutritional status of children reflects poor
development potential and prospect. Nutrition plays an
important role in national development. People with
malnutrition contribute little to national progress and
become a big burden. Malnourished children who grow
into adulthood have poor stamina, poor mental and
psychomotor competencies.
The quality and quantity of the child's food always reflect
the rate of his physical and mental development. It has
been well recognised that protein deficiency is one of the
commonest deficiencies seriously affecting the physical
and mental health of children and this deficiency not only
affects growth but also leads to retardation of mental
118
suaGRauRPREs^mTaNs
♦
development of growing children. Brain development is
also influenced by food (qualitative and quantitative) like
other organs. It is truly said that a sound mind is in a
sound body because for either of them to be sound good
nutrition is very essential.
Disturbances in growth occur most commonly in the
period immediately after weaning. A child may not
be able to attain his full potentials in height and
weight if food at any time during childhood is
insufficient for a significant penod.
WHAT IS NUTRITION
The term nutrition refers to the nutritional status of the
individual whose body utilise essential nutrients properly
according to the body requirements. According to E N
Tod hunter a well known nutritionist, Nutrition deals with
all that makes a man healthy, functioning, creative human
being through a well chosen diet.
Nutrients are constituents of food that must be
supplied to the body in suitable amounts for
maintenance of normal health with functioning
capacity. The nutrients include water, protein,
carbohydrates, fats, vitamins and minerals.
NUTRITION AND EDUCATIONAL ACHIEVEMENTS
The scientific evidences show that nutritional depreciation
in infants and children is a risk factor in the formal
educational system. Children who are undernourished
show slow learning capacity and difficulties in mastering
school materials and so among these children most of
them are drop outs from school.
>
As per Mohanty et al no. of studies conducted in
India and abroad have revealed a great relationship
between academic achievement and socio
economic status on the otherhand determines the
nutritional status of a child. So there is a direct
relationship between the educational achievement
and nutrition.
>
Good health is necessary for sound body and mind.
A hungry child can never be expected to think and
act well, the physical damage can be remedied later
with the supplementation of good diet but the
damage done to the brain during the pre-school year
is most irreversible and permanent.
>
Nutritional deprivation interferes with child's
motivation, power of concentration and learning
capacity and these children are handicapped and
learning some of the academic skills whichever is
very essential for learning. The hazards of
malnutrition and undernutrition are serious obstacles
to the promotion of physical and mental health of
children. Poorer the nutrition the more difficult for
the child to learn and cope up with the school life,
hence for children to learn
>
effectively good health is essential. Malnourished
child is weak, lathargic and cannot concentrate.
>
In developing countries like India among the low
income segment of population infections and
malnutrition are often endemic. Among them
prevalence of PEM and micronutrient deficiencies
are generally extremely high (Pellet 1983 P. 115-125)
>
Early malnutrition is more harmful in influencing later
behaviour which may include absence from school,
apathy while in school or reduced potential (Srikantia
1979 P.30-33, Smar 1972)
>
The brain at birth is closer to its adult size than any
other organs in the body. It composes 10 percent
of the body weight at birth by six months of age the
brain is 50% of its weight in adulthood at 1 year of
age it is 60% and at 5 years 90% and at 10 years of
Good nutritional status is very essential for the
normal development and the growth of the organs
of the body.
Nutritional status in our children at present is in
jeopardy due to poverty, unemployment, diseases,
illiteracy, rapid population growth, rapid urbanisation,
environmental degradation, superstitions, beliefs
and taboos present in the society.
The national monitory Bureau provides some valuable
insights into this problem. Its analysis reveals that the
significant declines in moderate to severe malnutrition
achieved over the 70's and 80*s have entered a phase of
stagnation, while earlier 77.5 % of the 1 - 5 year children
had moderate to severe malnutrition, by the end of the
80's the level came down to 52.5 % over the 90’s however
this proportion has lingered on and around much the
same level. These degrees of severe and moderate
malnutrition are no doubt concentrated among the poorest
sections while the rest of the mild cases malnutrition get
distributed into other household as well.
NUTRITION AND PHYSICAL DEVELOPMENT
The word development denotes to increase in skill and
function, whereas growth denotes to increase in physical
size of the body which can be measured in terms of kgms
for weight and centimeters for the length of the body. Hence
growth and development are considered together because
the child grows and develops as a whole. So growth and
development not only imply physical aspect but also
intellectual emotional and social aspects (Park and Park
1983 P.465)
Growth is the function of nutrition-undernourished
children are shorter and lighter than fed ones (Tigard
1974). Insufficiency of energy and protein are the
commonest cause of failure in growth of human
beings. In growth there are always two basic activities
♦
increase in size
♦
malnutrition
Sub Regional Seminar on Innovations in ECCD,
Chennai - November 24r26,1999
Full maturity stops growth. Current
malnutrition retards malnutrition as well as
increase in size, That is height.
119
si^jmoijpmESEfmn'ioNs
'
age it is 95% of the total brain weight at adulthood
(Sen 1985 P.37). The head circumference of a child
at birth is 63% of the adult circumference of head
(Robinson 1975).
>
■■■
have permanent damage (Cravioto and co-workers 1963
,1965 P.449-69). Studies indicate that iron deficiency with
or without anemia interferes with cognitive functioning.
Usually young children with anemia appear to show
decreased attentiveness and ability to focus on and
sustained interest in learning a task.,
According to Winich and Rosso 1968 the reduction
in brain weight appears to be permanent due to poor
nutritional condition and reduction in brain size will
likely lead to future functional impairment of the brain.
>
Study conducted by Losoft and co-workers
demonstrated that iron deficient infants were
hesistant and fearful, less active and responsive,
had shorter attention spans and were less persistent
at certain tasks.
>
Malnutrition may produce structural and metabolic
derangement in the central nervous system that
can limit its capabilities and performance (Coursin
1972 P. 177-202)
>
Malnutrition as a risk factor of the educational future
of infants and children should be a major concern
for health, nutrition and educational policies.
>
With programmes like ICDS being actively
implemented in the region changes are possible.
While imparting training to all those functionaries
dealing with ICDS and other NGOs working with
the community the following participatory exercises
can be adopted. (Annexure I & II refer)
NUTRITIONAL DEPRIVATION
Nutritional deprivation during early childhood has been
found to be associated with smaller head circumference,
lower brain weights and altered biochemistry of the brain.
Protein calorie inadequacy during childhood can lead to
irreversible impairment of mental functions in later life.
Severe malnutrition will lead to disturbances in learning
ability memory and behaviour. Severe deficiencies for a
prolonged period of time could never be made up
particularly with the size of the head. If short term deficit
occurs in the 1“ year, the permanent effects can be
prevented by a good diet (Robinson 1978 P.476). If
malnutrition has persisted for 4 months or more in early
months of life nutritional rehabilitation may not fully correct
the retardation On the other hand , the infant who has
had the benefit of reasonably good nutrition during the 1"
year of life who then develops kwashiorkor is not likely to
'■
COMMUNICATION AND CHILD DEVELOPMENT
Indian Council for Child Welfare, Tamil Nadu
Middle Level Training Centre for ICDS Funcitionaries
Communication is a process of sharing ideas,
information, attitudes, values or instructions with
individuals or with groups to facilitate progressive
change in knowledge, attitudes and practices. It
involves both giving and receiving information.
INTRODUCTION
Communication may be verbal or non verbal. Verbal
communication implies use of words in non-verbal
communication we use gestures, facial expressions,
postures etc.
PURPOSES OF COMMUNICATION
Some of the important purpose of communication are;
-
giving and receiving information
instructing and educating
persuading others to change
strengthening beliefs
entertaining
improving human relationships
satisfactory wants
The primary method of giving and receiving
information is speaking and listening.
Sub Regiona' Seminar on innovations in ECCD,
Chennai - November 24-26,1999
Language is a form of communication. Recently language
has been known as a means of ‘thinking, feeling and
reacting to things"particularly in childhood, language plays
a formative role in the development of the child's personality
and abilities. Language is not merely a medium of
expressions but it means feeling, thinking and perceiving.
Every child in this world, whatever his or her mother tongue
uses language to fulfill certain objectives. Language is
thus an excellent tool to realise our purposes and its
influence in a child's life is multifaceted and multidimensional.
IMPORTANCE OF
DEVELOPMENT
LANGUAGE
IN
CHILD'S
Most of child's learning depends on language which is
the basis of all social communication. The acquisition of
words is essential for abstraction and concept formation
and in almost all higher learning and higher mental
processes- such as thinking, planning, reasoning, paying
attention, remembering and judging. Failure to become
skillful in communication — speaking, writing, reading,
greatly impairs a child's general mental or cognitive
development.
>
Speech is a kind a behaviour that helps the child to
move from a world of egocentrism to a world of
120
?
I
f SU3GRaUE»PR^QfmnONS
I
®
conversation, play, etc. Likewise, ail lessons in all
subjects could be taught in blissful mood. Walls
have been painted at the bottom so as to enable the
children to scribe/write/draw whichever they like.
During this process, the teachers should know the
teaching techniques well and no commands should
be used. Awarding punishments is avoided. The
teacher should not sit in a chair and she should
mingle with the children. It is very ideal that the
teacher sit in the middle of the children. The Teacher
friendly relationship should be established.
Evaluation of the programme activities
A study has been made on some Anganwadi centrs in
DPEP districts in Tamil Nadu which focussed on some
specific areas, such as, daily duration of the PSE
component, content, facilities available, age range and
involvement of the children, attitudes and skills of the
workers and so on.
Duration of Ere-school Education (PSE)
The Anganwadi centres function from 8.30 am to 4.00
pm. The children come to the centre at about 9.30 a.
The duration allotted for the pre school component is two
hours in the forenoon (i.e. 10.00 am to 12.00 noon) and
one hour in the afternoon which is allotted exclusively for
outdoor games after lunch and rest. More indoor and
outdoor games should be included in the syllabus.
Regarding the availability of equipment, it is disheartening
to note that enough equipment are not available in all the
centres.
The teaching learning materials which facilitate learning
are not sufficient in many centres. The AWWs/CWOs
themselves prepare some materials and the Dept, supplied
some which are not quite enough and not in proper
condition to use.
Regarding toilet facilities, it is really disgusting to mention
that there is no toilet facility in all the AW centres. In
some urban areas, proper drinking water is found available
whereas protected water is being kept in earthen pots in
the rural areas.
The AWWs have expressed their views while interviewing
about the facilities that they require more teaching learning
materials, a cupboard to preserve those materials and
furniture.
Anganwadi children
In some of the centres visited, attendance of girl children
is higher than the boys. On the whole 50% of the children
were present at the centre on the day of observation.
Involvement of the children is not upto the expectation
The DPEP is giving various training for capacity building.
Conclusion
The Anganwadi centres can function efficiently and the
all round development of all the children can be achieved
and the AW centres can be strengthened if more facilities
in terms of equipment, teaching learning materials,
refresher course to AWWs are given from time to time.
Necessary steps may be taken for the enrichment of the
AW centres so that the future citizens who are the Nation's
asset can be shaped well in the AW centres.
COMBATTING MALNUTRITION IN ICDS, DEPT OF SOCIAL WELFARE
D NGO and ICDS partnership in promoting ICDS activities
Planning & Coordination among ICDS Functionaries in implementing Case Study Method at Household Level
Chennai (Projects 1-12)
Salem (Projects 1-2)
Chennai District: In Chennai district, an attempt
was made to rope in NGO support to conduct atrisk camps for mal-nourished children in all the 12
ICDS projects.
INTRODUCTION
1.
Child care
Childcare should be the sole responsibility of the
state which may engage in partnership with
parents, employers, community and NGOs. With
the 73rd Amendment to the Constitution the subject
of women and child development is to come under
the local bodies. In this context ‘participation’
2.
Birth of Valarmadi (growing moon)
The initiation for NGO cooperation was made when
the CDPO of the 8,h project met and had discussion
with Ms. Sujatha, member of Lion’s Club of Madras
assumes a renewed significance requiring the NGOs
Airport. Further discussions were held between the
to play a major role. So far there has not been any
concrete proposal for collaboration between NGOs
and the ICDS. In future there are avenues for NGOs
to be active collaborators in addressing key issues
of children.
Project Officer, Programme Officer and the NGO
and finally a solution was reached (as stated by the
NGO). The NGO committed itself to do the
necessary for all the children who are ’at risk’ in all
the 12 projects and she named this proposal as
‘VALAR MADT or the growing phase of the moon.
Sub Regional Seminar on Innovations in ECCD,
Chennai - November 24-26, 1999
127
SimGROUP^PRESENTATIONS
The first pilot programme was scheduled for the 23rd,
Friday of July, 1999 at 2 p.m. The complete agenda
was charted out by the NGO.
3.
persons who could help. The other names were kept in
store so as to approach them during subsequent functions
like National Nutrition Week Celebrations, World Breast
feeding week, etc.
Planning
1.
During the subsequent review meetings this proposal
was discussed by the PO and CDPOs in order to
mobilise optimum support for the camps.
Elected Representatives and local Councillor Ward
members were not approached as it was a period
of hectic canvassing for elections.
Initially there was doubt and ambiguity regarding
the materialising of such efforts.
2.
As planned the first pilot programme took place and
all the CDPOs attended the camp keeping aside their
other busy schedules. The project officers were
introduced to club members. The 2nd project in line
to conduct the next camp was having its agenda
finalised with the NGO. The list of resourceful
persons was handed over and the process of
contacting people went on smoothly.
In Vyarsarpati slums the supervisors and ANWs said
that since the community was from the lower
economic strata they had very little to contribute.
However a local NGO came forward to allow at-risk
children in that area to attend their clinic free of cost
during the follow up phase.
NEED POR EFFECTIVE COMMUNICATON
The programme officer and the CDPO contacted and
appraised each other of the latest developments made.
The PO was always ready to help, guide and disseminate
information on list of resource persons in the city. The
Mobile team instructor bridged the communication like
between the Project Office and District Office
(geographically set apart by 25 Kms)
The Project Officers in turn constantly interacted with the
subordinate staff to implement the decisions.
CONSTRAINTS
The only limitation in contacting resource persons by the
AWW was that she had no identity card as an ICDS
functionary. Through letters of introduction provided by
the PO and CDPO the process of contacting people and
mobilising resources continued further.
Clear identification of day to day tasks in harmony with
the set goals and district delegation of responsibility to
one or more persons/ teams and allocation of tasks (in
case the person entrusted is unable to proceed) made
the work easy.
SNOW BALL EFFECT & NETWORKING
The resource person's list was initially drawn from the thrust
given in the pilot programme. Thereafter it was the act of
moving from one person to another, identifying others and
adding more to list of people willing to sponsor ICDS activities.
Though some of them were not ready to sponsor at that
time due to various reasons, they provided names of other
Sub Regional Seminar on Innovations in ECCD,
Chennai - November 24-26,1999
Local Community Support & Goodwill
The resourcefulness of the ANW workers were used
to tap the local community. It is a positive step to
envisage local community contribution, however
meager the amount may be
PREPARATORY PHASE
Before each camp, the communication network between
the ICDS functionaries strengthened to make the camp
successful Each and every stage of the process was
plannea and discussed by District and Project Officers,
consulted, communicated and executed by the field staff.
Constraints
GOOD WORKING RELATIONSHIP AMONG ICDS
FUNCTIONARIES AND CONGENIAL WORK CLIMATE
Easy Accessibility and openness of the top executive to
the field workers, children and organisers to share their
expenences and constraints (whether at work or in mobilising
support) helped to find alternative solutions and strategies
Among the child care organisers the CDPO and PO were
looked upon respectfully and very often affectionately
addressed as 'Amma' and they would abide by the tasks
set by the supervisors. Motivating these workers and
recognising their inherent talents and commitment was
always a boost to bring success to this 'at-risk' camp.
The workers always strove to do their very best and this
was possible through the excellent organising capacity
and effective communication and feed back and also
decentralisation in planning of activities by workers themselves.
FOLLOW UP
Presently follow up is going on in all the projects. Special
attention to these children has been mandatory and
exclusive involvement and personal intervention in the
follow up is assured from CDPO to worker level. Close
reviewing and rechecking by supervisory staff has paved
way for undivided attention at all levels.
OUTCOME
The impact of the programme would be available only
after evaluation camp is held in December, 1999.
LESSONS TO LEARN FOR ICDS
•
Replenishing ability of ICDS functionaries to mobilise
community support through new contacts.
•
Forming a network of interested individuals to work
for children.
128
Attempt towards professionalism and scientific
management in child care services
mothers who were not satisfied at the referral
Hospitals. Since 75% of the ’at-risk’ children could
be improved from dietary patterns and practice and
improving environmental sanitation, the ICDS project
team wanted to promote its Extension Services.
Thus they decided to use the Case Study Method at
the Household level.
Changing concepts from welfare to development
Introduction of short term need-based strategic
planning to promote long term planning.
INDIVIDUAL CASE STUDY
AT THE HOUSEHOLD LEVEL
THE SIGNIFICANCE OF CASE STUDY
SALEM DISTRICT
The in depth Case Study of ‘at-risk’ children is three
pronged with emphasis on:
The ‘at-risk’ children weigh camps in Salem District
Projects commenced in January, 1999. The Salem district
programme officer conducted monthly review meeting for
CDPO (Project Officers) to give special attention to
malnourished children.
1.
2.
l
-I
3.
Prevention
Extension of existing health and nutrition services
to the doorstep
Adoption of ‘at-risk’ children jointly by supervisors,
ANWs, Anganwadi workers and helpers with helpers
as link workers and their joint counselling with
mothers of ‘at-risk’ children.
Search Meeting for identifying areas with ’at-risk’
children
It was observed by the PO, Statistical Investigators
and Medical Officers that malnourished children
were more in particular projects. To rule out doubts,
it was jointly decided to conduct re-survey of all areas
with a new checklist by Anganwadi workers.
There has been proper infiltration of goals and objectives
from top to bottom level and the desired results has been
internalised ana executed at all levels.
Designing a new *at- risk’ format
FOLLOW UP
Monthly Progress Reports were reviewed at each
meeting but did not give a clear picture on
Malnutrition. A new comprehensive format was
jointly designed at the review meeting.
The follow up and reporting and constant reviewing and
developing alternate strategies have been the major
strength of this programme.
Intermediary Phase
In June, 1999 when the magnitude of at-risk’
children was manageable and when the follow up
had to be speeded up, the District and Project team
thought of embarking on a new method/approach.
This was also due to low clinical attendance of
EXECUTION OF THE WORK
The key person is the Anganwadi worker who keeps track
of weight gained by ’at-risk’ children and studies the whole
gamut of social, economic, demographic and ecological
factors. The worker and helper provide a good feed back
report to supervisors, which in turn is converted into a
comprehensive analytical report which is thoroughly
reviewed at the District level review meeting.
i
CHILD TO CHILD SOUTH INDIAN RESOURCE GROUP
Dr. Indu Balagopal, Overview of the Child-to-Child Approach
The Child-to-Child philosophy and approach has the
following components :
It empowers, is non-discriminatory and nonexploitative.
It is a holistic approach that deals with all the aspects
of a child’s growth and development. This includes
life skills education, intellectual and psychosocial
development and health education.
It focuses on the joy of learning through need-based,
activity-oriented and fun-filled learning approaches.
. It seeks to instill a positive attitude to learning and
acquiring knowledge.
It is based on the observation that children have a
great influence on other children, their own families,
and the community.
It utilizes conducive learning atmospheres, rather
than intensive training programs.
It recognizes the fact that children can act as change
agents to bring about increased awareness and
implementation of better health, inter-personal, civic,
communal and environmental practices.
Thus the scope of C-to-C includes providing knowledge,
instilling life-skills and civic consciousness, developing
responsible behaviour and interpersonal skills and
sensitization to bringing about a harmonious life in existing
socio-political conditions.
Sub Regional Seminar on Innovations in ECCD,
Chennai - November 24-26,1999
129
SUBSRDUPSPRESENTAnONS
Children can be seen as learners, communicators and
doers. When children learn about health and social issues
and life skills and internalize this knowledge, they help
better themselves. When they share this knowledge with
other children, their own families, and significant others
in the community, they communicate their new found
values. Through such Communication they can gradually
influence other children, their own families and the
community, thereby serving as agents of change.
Providing knowledge is only one form of empowering
children. They have to be given life skills in the form of
decision making and problem-solving abilities, and
leadership qualities, thereby developing self-esteem and
selfconfidence. Responsible behaviour and civic
consciousness are important components But, most
important, this has to be done through appropriate learning
environments, and facilitated through good interpersonal
relations, love, care and compassion. Children have to
be made conscious of safe environments and have to
learn to live in harmony with their surroundings.
2.
Children can act as change agents in the community
to bring about increased awareness on personal
hygiene, environmental hygiene and nutrition.
3.
C-to-C is a holistic approach and deals with all
aspects of children's growth and development. This
includes physical health, intellectual enhancement
and psychosocial development.
4.
Children can influence their families and the
community, to improve their life skills and contribute
to a healthy society.
5.
The C-to-C programme includes all children, is nondiscriminatory and non-exploitative. This auto
matically takes care of not only children with special
needs, but also eliminates exclusion of children due
to caste, creed, culture, language or economic
status. It creates the right environment for positive
acceptance of differences.
6.
The strong underlying sense of joy and happiness
should not be forgotten. This is best achieved
through need- based, activity- oriented and fun- filled
approaches to learning.
7.
Children should develop a positive attitude to learning
and acquiring knowledge. This can be achieved
through creating conducive learning atmospheres,
rather than through intensive training programmes.
(We don’t “train" children for peer education)
The entire approach should be participatory as far as
possible.
Wherever possible the children must be involved right from
the phase of inception. The project/activities must be chalked
out with the participants, taking care to see that they are
fully involved in brainstorming the project. It may be
surpnsing to find how sensible and down-to-earth the children
can be when it comes to trouble - shooting and sorting
out practical difficulties in implementing the program.
THE CHILD-TO-CHILD APPROACH
The C-to-C programme was introduced in the early
eighties, in response to a given situation where older
children were left in charge of their younger siblings while
their mothers went to work. It was recognized that children
had great potential, and given the knowledge they could
serve a useful role in the well being of the younger children.
Thus the idea of child-to-child, or older child caring for or
teaching a younger child - was born.
Over the years the practice of C-to-C has under gone
tremendous change. The basic approach of empowering
children with information and instilling confidence, was
much misunderstood and misused. Children were paired
off to interpret child-to-child, and were mostly used as
messengers who followed instructions. They hardly
understood the implications of the messages they
conveyed in the classroom, or in the community. Being
activity- based, children became performing artistes
without internalizing the knowledge they had gained. In
many programmes, children are still used as teacher
representatives who mechanically report what they have
been taught.
Based on the enthusiasm for learning, with a sense of
involvement, children are seen as learners, doers and
communicators. In other words, when children learn about
health issues and internalize them, they help themselves.
When they use their knowledge to influence other children,
their families and their society, they are seen as doers.
In service delivery like personal hygiene and environmental
cleanliness, at home, individual children can act. But action
in the community is usually more effective through groups
of children. As communicators, children can influence their
peers, younger children, and society, taking on social
problems and dealing with them. Bringing about social
change is best effected through collective action.
The child-to-child philosophy and approach has the
following components:
Thus the scope of “Child-to-Child" or "Children in charge"
has expanded. Providing knowledge is only a part of
empowering children. They have to be given living skills
in the form of decision-making and problem solving
abilities, leadership qualities and developing self esteem
and self confidence. Responsible behavior and civic
consciousness are important components. And most
important of all, interpersonal relationships with love, care
and compassion and teamwork have to be nurtured
through appropriate learning environments and facilitation.
Children have to be made conscious of safe environments
and have to learn to live in harmony with their surroundings.
And with peace and consideration for others, comes happiness.
1.
METHODOLOGY
Children can be given health education which they
can apply to themselves, their peer groups and
younger children.
Sub Regional Seminar on innovations in ECCD,
Chennai - November 24-26,1999
To simplify practice and apply the concept, the C-to-C
approach is best implemented through sequential steps.
130
I
SUBGROUPPRESEMmON^
1.
Identifying the problem or issue
2.
Finding out all about it
3.
Planning action
4.
Implementing action
5.
Review of action and impact
6.
Redesign activity or plan of action.
theatre etc. Messages have to be clear and simple
so that children learn the basic facts, and convey
them to others. Songs and plays should not be so
complicated that the message is lost in the
performance.
While planning activities, the time factor has to be
considered. While some topics may be easily
understood and put in practice, some others especially those needing social change, or attitudinal
adjustments, may take much longer. In some
communities, even accepting children as
messengers will need major cultural change.
Children can and should be involved at every one of
these steps.
1.
Identify Problem :
These could be health related issues like an
epidemic, environmental issues, lack of civic
amenities, social or cultural issues, discrimination,
unacceptable life styles or any other problem. Or
even simple child care.
At this stage, it is important that children fully
comprehend the messages they are conveying and
have internalized them.
4.
This is the easiest and most enjoyable part of the
process. Children should be actively involved in
every action but at the same time should not feel
that it is a burden or additional chore. The time and
place have to be carefully planned before
implementation.
The children and the community should be nelped
to identify the pressing problem and how it affects
them and society.
This could be done through group discussions, essay
writing, poster competition or even role plays. Once
everyone agrees on the topic to be pursued, we go
to the next step.
This is the stage at which children develop a sense
of responsibility, and refine their critical thinking
skills. With development of self-esteem and self
confidence, they take initiative and show leadership
qualities. Their creative and productive skills are
used to achieve the objectives.
It is important that in the initial stages, adults are
involved in guiding and facilitating children's
discussions. In the classroom situation the teacher
is the anchor, while in other situations youth who
have been sensitized to issues can act as moderators.
The second step is to find out about the issue
concerned regarding the cause, effect and action to
be taken.
2.
This step could be a continuous process, as the
messages may need constant reinforcement.
Different approaches and strategies could be used
to strengthen the concept.
5.
Finding out more :
More information can be gathered through books or
films, and where necessary, civic authorities could
be requested to provide relevant inputs.
This is the beginning of the process of empowering
children. It is crucial that at this stage, norms are set
and children's responsibilities are clearly spelt out.
Planning action :
In the third step, children by themselves, or in
groups, or with the help of adults, plan the action
necessary to deal with the problem. They plan the
action they will take in the school, home or
community. Action could be through multifarious
activities like campaigns, poster exhibitions, street
plays, indoor and outdoor games, songs, puppet
Sub Regional Seminar on Innovations in ECCD,
Chennai - November 24-26,1999
Review :
At this stage, children with or without the help of
adults, learn to analyze their activities and the effect
or impact they had. These could be subjective or
objective, through discussions, physical indicators
or interviews with target groups. This is the stage of
monitoring their actions and evaluating the process,
as well as impact of action. This step trains the
children for critical review of their actions and honest
reporting. Objectivity and analytical skills enable the
children to develop maturity.
This is the process of increasing the knowledge base.
Children could be involved in surveys, identifying
causes and understanding the need for intervention.
If the topic involves technical or specialized inputs,
resource persons could be called in.
3.
Implementation :
This step is very important, and critical and children
have to be guided with sensitivity and care.
6.
Reorganize :
In this last step, the mistakes and problems are
understood, and action plans are redesigned to
ensure success.
If the problem was one of non-acceptance of
children's abilities, more ground work with the
community to help them understand children and
their potential will have to be done. Or children
131
I
SmSGRDUP^PRESEfmnONS
-
themselves may have problems with each other. This
may need adult intervention.
AGE GROUP OF CHILDREN
I
•
•
»
►
Children of all ages can be part of the child-to-child
programme. From infancy children have to be given
knowledge and guidance for healthy habits and
wholesome living. At this stage they learn by
facilitation from conducive environments as well as
by example.
As they get older, children get more interactive and
naturally exchange information and ideas. Creating
positive learning environments and providing enough
opportunities will kindle the enthusiasm of the
children for active inquiry based learning. If learning
through fun and creativity are encouraged, children
are stimulated to think for themselves and be more
productive.
This approach is most commonly used in the school
age group, as children of this age are enthusiastic
leaders. They are willing to be substitute teachers,
health workers or even inspectors! It is also very
effective with adolescents as they are mostly
dropouts from the mainstream, and are looking for
some recognition and some outlet for their energies.
Thus it is evident that the child-to-child approach
has wide ramifications and can be used in many
imaginative ways. The underlying principle is that
the children should understand and enjoy the actions
they take, so that the impact is sustainable.
The guidelines provided to children could include a
whole range of issues, but they should be dealt with
in an ethically and morally acceptable way.
Children's sensibilities should not be challenged and
it should be understood that children are sensitive
Sub Regional Seminar on Innovations in ECCD,
Chennai - November 24-26,1999
..............................
'
'
'■
beings. Children as a source of information about
issues that are pertinent to them has to be
recognized and actions planned have to respect
children’s opinions.
PARTICIPATION
This is the general outline of children’s participation at
every step. Different problems or topics will involve the
participation of children to different extents. From following
instructions, conveying messages, action in the home or
community, taking part in planning to initiating action and
bringing on social change or policy decisions, children
can be involved at every stage. If they are part of the process
there is more likelihood of action and sustained impact.
■
Ultimately, it is hoped that children's involvement in
issues concerning them, their families and society
will serve to empower them and assist their
development into useful and productive individuals
who will contribute to a harmonious and peaceful
world
LINKAGES
This approach is comprehensive and can be incorporated
in any programmes dealing with children. The main
linkages with other programmes are:
1.
Children’s rights, emphasizing on education,
nutrition, right to family, right to expression and most
of all, Right to Happiness.
2.
Equality and inclusive patterns with non
discrimination - this covers gender equality,
acceptance of individual differences, inclusion of
disability, tolerance of economic or social
deprivation, lagging in scholastic abilities, as well
as equal opportunities for all castes & creeds.
3.
Activity based and enquiry oriented learning methods
are similar to the innovative educational
methodologies of DEEP and DIET.
4.
The Gandhian ideals of empowerment through
knowledge vital to sensible living and optimisation
of resources. Head, Hand & Heart should be given
importance in education. Dignity of labour should
be taught. This is seen in the C-to-C concept of
learning by doing
5.
Awareness programmes and self-help groups community centred.
6.
Good parenting skills and family life education.
7.
Leadership training and value education.
8.
Disaster intervention through living and coping skills.
9.
Technical training & skills empowerment, prevocational skills encouraged through activity based
action plans and sequential methodology.
132
O co
S’ &
Child to Child Resource Group - SPECIFIC EXAMPLES OF APPLICATION
if
Tried and tested in Mobile Creches, Mumbai
bi
?i
is
f- o
KNOWLEDGE
I. Provision of Daily Care
KJ
Healthy habits relating to ■
1. Feeding - How, when and
what
CO O
sI
o
5
m
o
o
o
SKILLS
1. Infant feeding - response to cues, during
feeding
2 Toilet
2 Helping the child by sensitive responses
to cues for elimination etc.
3. Washing, clothing
3 Habit formation
4 Sleep
4
Bathing and dressing
STRETEGIES
1. Instructional
IMPLEMENTATION
I
2. Discussions in the classroom set-up
3. Following a set routine for habit formation
4. Experiential learning - by doing
5. Theme projects on personal hygiene
5 Care of hair, nails, eyes and ears
6 Soothing and nurturing techniques
II. Nutritional Needs
1
Nutritive and balanced diets
2. Illnesses and apathy due to
malnutrition
3. Diet in illness
1 Age-related diets and proper cooking of
food
2 Components of a balanced diet, and diet
for sick children
3 Recognition of under-nourishment and
mal-nourishment
1. Theme projects on teeth, vitamins etc.
2. Participation in preparation of healthy
foods
3. Health education to mothers directly and
through children to reinforce healthy
cooking practices
4. Care of sick children by other children
III. Growth and Development
Motor Development
Principles 1
Milestones and related
activities
Organising activities according to the needs,
characteristics and interests of children.
Integrated curriculum consisting of fun
activities, desk games and field games.
Encouragement of verbal and non-verbal
Communication
1. Group games for lateral as well as
vertical grouping of children
2. Play and stimulation activities
III. Growth & Development
Socio-emotional
Development
2. Special needs of the
handicapped
III. Growth & Development
Cognitive Development
Basic concepts and general
knowledge
III. Growth & Development
Literacy and Numeracy
Literacy and Numeracy
III. Growth & Development
Value-based education
Value-based education - The
moral aspect of life
1. Need for communication
2. Games to increase awareness regarding
Handicaps.
Creative problem - solving and decisionMaking Critical thinking abilities
Classroom activities, Self-evaluation
exercises Group games
1. Reading and writing skills
2 Mathematics
Non-formal approach with integrated
teaching material
1. Communication skills to reach out to
Community
Non-formal approach with integrated
teaching material
Ba
2 Good manners and civic sense as a habit
GJ
GJ
r
-i
KNOWLEDGE
o cn
®
E.
CT
if
IV. Health Education
tr
=■
Concept of good health
1. Recognition of good health
1. Common
childhood
illnesses, diseases and
disabilities
2. Recognition of illnesses, their causes
and consequences.
2. Preventive and promotive
measures for Good health
S’
3. Immunisations
co O
SKILLS
3. Good habits and practices for prevention
of illness and spread of diseases
4. Ensuring
immunisation
against
preventable childhood illnesses.
STRETEGIES
IMPLEMENTATION
1. Theme projects on common illnesses like
diarrhoea and worm infestations, disease
spread through water - jaundice polio etc.,
diseases from droplet infections like
mumps, measles and chicken-pox, diseases
spread through vectors like malaria etc.
Most topics easily understood
and implemented Better
compliance of treatment, and
hospital referrals. Some topics
like tuberculosis and leprosy
too complicated for children.
§
2. All aspects to ensure minimal spread of
disease - good personal habits, environments
sanitation and timely treatment
s oi
cn
3. Project on immunisation - Mothers'
meetings and arranging for immunisation
of all children.
m
o
o
o
V. Safe & Healthy
Environment
Concept of healthy environment
in the home and outside
1. Proper disposal of waste
1. Instructions and discussions followed by
actual practice
2. Cleanliness inside and outside the house
3. Planting kitchen gardens
Very successful
2. Reinforced by songs, desk games and
puppet shows
3. Home visits by teacher to support
children's role
V. Safe & Healthy
Environment
Common hazards in the
surroundings
1. Avoiding risk factors like loose electrical
connections, open water storage tanks.,
rusty nails, mad stray dogs etc.
2. Making the home safe for children
1. Theme project on accidents dealing with
the cause and consequences
2. Appointment of child leaders to act as
watchdogs
Children were helpless in
altering environment, but were
more aware of risk factors.
Homes became safe.
3. Avoiding accident risk factors in the
home and creche.
V. Safe & Healthy
Environment: Water
1. Clean water for drinking,
cooking and washing
2. Importance of clean potable
water
3. Prevention of disease
spread through water, and
consequences of diarrhoea
and dehydration
V. Safe & Healthy
Environment
Food : Cooking and
Preserving
£
Food: Cooking and Preserving
1. Maintaining sanitary conditions
2. Checking source of water
3. Making water potable
4. Disposal of waste water
5. Providing liquids to sick children, and oral
rehydration therapy.
1. Project on water - properties, uses
Sources of water
Partially
implemented
successful
-
2 Boiling and filtering water to make it
potable
3. Care of the sick child - providing drinking
water, cold compress, making ORS etc.
if
4. Project on diseases and infestations
spread through water.
1. Proper cleaning of raw materials before
cutting and cooking
2. Covering of cooked food and hygienic
preservation
7
1
Songs and other activities
2. Theme projects on flies, vitamins, and on
diseases spread through food.
3. Disposal of garbage
3. Demonstration and supervision of
hygienic practices during home visits.
4. Protection from flies, ants and rats.
4. Ensuring proper garbage disposal
1
Very effective. Reduced
morbidity in children.
2. Planning and development
of material was done with
participation of the children.
3. Programmes are best imple
mented if activities are decided
by the children themselves.
s
i
■I
!
MOBILISING SUPPORT FOR ENABLING CARE OF YOUNG CHILDREN, GIRLS AND WOMEN
C Radhakrishnan, Kerala State Social Welfare Board
By the word children we mean those below 14 years of
age. 41% of the population of India are children as per
the census of 1971. If you try to study a nation, first you
have to understand the condition and status of the children
in that country. They are the main factor to determine the
future of the country. Their health, their education, their
individuality, their mannerisms, their behavioural attitudes
towards the society etc., are to be attributed to the future
development of a nation. Children are the most precious
nature's gift to humankind.
The child is a developing person and is in continuous need
of care, stimulation and nurturing. These should be
provided by parents, the family and the society at large.
But with the collapse of traditional social security
arrangements more and more children are deprived of
parental and family care. As a result, millions of children
are thrown away to the streets or to the cold cradles of
some charitable institutions. Now there are more than 30
million children in our country who have been disowned
by their parents because of destitution or poverty, out of
marriage birth, death or desertion of one or both parents.
Of the 30.80 million children in need of care and protection,
only 3 percent are in about 1500 statutory and 3000 nonstatutory children's institutions in the country. In addition,
roughly 20,000 children and young persons below 18 years
are in jail along with adult prisoners in the country. Of all
these children and young persons, 80 per cent are boys.
Of all the children and young persons in need of care and
protection, 40 per cent are destitute and 25 per cent are
orphaned without any adult protection or care. And
contrary to common preconceptions, of all the children in
need of care and protection, only 30,000 are delinquents
and among the delinquents, only 8 per cent are girls. As
their parents are unable to adequately fulfill their parental
responsibilities, these children become the responsibility
of the society and the state.
In every town and city, in our country amidst opulence
and plenty there are a large number of street and working
children. They are robbed of their childhood pleasures
and adult protection and are prone to crime, misery, abuse
and exploitation. Deprived of life, affection and sympathy
of a family and subjected to exploitation, abuse and
unhealthy living conditions, these children develop a strong
sense of inferiority and insecurity, which create in them,
fear, anxiety and guilt which in turn affect their mental
health and well-being.
The children on the streets, obviously are also deprived
of the educational and intellectual development Even if
they have received some education, they lapse in to
illiteracy, since circumstances have made them dropouts
from the schools over a long period of time. This is the
case when the most important direction in the chapter on
the directive principle of the State policy, in the Indian
constitution being that the State will endeavour to give
free and compulsory education to every child in the age
group of 6 to 14.
Sub Regionai Seminar on Innovations in ECCD,
Chennai - November 24-26,1999
Most often street children fall victims to social evils like
drug addiction and are used by the drug mafias for
smuggling drugs. They fall victims of organised mafia
who force the children in to begging and the children some
times are made handicapped for forced begging.
The Supreme Court of India has declared that definition
of right to life, which is given in the Article 21 is the
backbone of Indian constitution, that the right to life means
the right to live with dignity and the right to privacy. But
the street children of India have neither dignity nor privacy
in their lives. They are subjected to life of extreme
humiliation, miseries and darkness.
Article 3 of the Universal Declaration of Human Rights
provides :
Everyone has the right to life, liberty and security.
Article 5 of the Declaration provides :
No one shall be subjected to torture or to cruel,
inhuman or degrading treatment or punishment.
Article 6 (1) of the International Covenant on Civil and
Political Rights provides :
Every human being has the inherent right to life.
This right shall be protected by law. No one shall
be arbitrarily deprived of his life.
But with all these statutes and legal protection, in practice,
the street children are deprived of their dignified and secure
life.
All children in the streets work to survive. A survey
conducted in Bombay shows that 71% of street children
were found to be simply looking for income to support
themselves and their families. Some came to the city to
support their families. Some came to the city to support
their impoverished families in the country side. Most street
and working children were found to be law abiding, but
there was no protection against extortion, physical abuse
and subjection to indignity and brutality by police and other
authorities, which for them was part of their way of life.
As we have seen all children of the streets work to survive,
there are a large number of children living with their
families are sent to labour in farms and factories or the
streets instead of schools. This is not a phenomenon
existing only in a poverty ridden country like India. The
World Development Report 92-93 of ILO states that
millions of child labourers are there, even in developed
countries like USA, UK, Italy, Spain and Belgium. After
the collapse of Soviet Union and after the resurgence of
capitalisation in that country. Child labour is increasing
in alarming dimension there also.
Millions of children are there in India who are deprived of
all their rights and compelled to work for their and their
families livelihood. The largest number of child workers
135
SUB ERDUPPRESENTATIONS
■
'"if
are in India. The reason can be attributed to the prevailing
poverty and illiteracy The inadequate agricultural reform
laws and ever increasing unemployment may be some
other reasons.
Learning and play are the essential ingredients for the
balanced development of a growing human being. When
work is imposed upon the child against his or her wishes,
at the cost of learning and play it becomes exploitive in
nature.
The miseries of working children have been listed below
as per the findings of a study conducted by national labour
Institute, Child Labour Cell. 1992
Working and Street Children of Delhi :
1.
Starting full time work at too early an age
2.
Too many hours spent at work which prevent the
child from attending school because of lack of time
and excessive fatigue.
3.
Work that results in excessive physical, social and
psychological strain up on the child.
4.
Work and life on the streets or in factories in
unhealthy and dangerous conditions.
5.
Inadequate remuneration for work.
6.
Inhibition of Child’s self confidence and self esteem.
According to the 1981 Census 13.6 million children are in
the labour force. 11.2 million are main workers and 2.4
million are marginal workers. In 1983, National Planning
Commission had projected the number of child workers
at 17.36 million. The finding of a sample survey conducted
by the Operation Research Group in 80-81 was that the
working children in India are 44 million. But the unofficial
figure amounts to more than a 100 million.
A clear understanding of the problem at various levels in
the society is the first step in the elimination of child labour.
In the process of the formulation of any programme or
action plan, one should have a thorough understanding
of the existing reality.
The most important issue is whether the society is really
aware of the seriousness of the problem and whether it
has a will to solve the problem.
In Indian culture, the woman is considered as Sakthi, the
Goddess. In ancient India, women had a respectable
position in the social setup. Gradually due to the male
domination of the society the woman was degraded and
her position in the society was that of a slave. Even after
all the so called women’s liberation movements her
position, more or less remains the same. Even though
one half of the population in our country is women they
form the largest vulnerable group in the country, suffering
life long discrimination at home, the work place and in
the community and their marginalisation is further
aggravated if they belong to lower caste and class, rural
or minority groups.
Sub Regiona1 Seminar on Innovations in ECCD,
Chennai - November 24-26,1999
It is not denying that the women in India today has
achieved or is struggling to achieve new freedoms and a
new place in society. Many doors are opening to her: she
can work in many fields, her vote can sway elections,
education is expanding her universe. She is exhilarated
by the new freedom but not yet secure in it.
Many married women are trapped in dehumanising
personal situations in the family. They persist in tolerating
battering, humiliation and physical and mental cruelty. She
is compelled to continue to suffer this torment, as most
often she will not be accepted by her parents. She remains
vulnerable to continued violence or degraded status at
home or exploitation and social prejudice. Battering of
younger married women in families by spouses or in-laws
may be linked to the horrific circumstances of dowry
extortion A tragic toll of 5817 dowry deaths was officially
reported in 1993. Most often the culprits could not be
booked due to the illicit nexus between the police and the
husbands or in-laws. Most women suffer in silence
because they know that they are powerless, as most of
the indignities and deprivations are perpetuated by the
very institutions and authorities meant to protect their
rights. Other marginalised group are the victims of rape
and sexual harassment. The number of rape cases
reported in 1993 was as high as 11,242 along with 20985
cases of molestation and 12.009 cases of eve-teasing.
Victims of rape, instead of getting sympathy, support and
justice are usually being socially ostracised and confront
unspeakable prejudice from the police and judiciary.
Another most vulnerable group are the commercial sex
workers. The girls and women who are economically and
socially the most marginalised are often forced or duped
to adopt the profession to escape destitution caused by
desertion, abuse, neglect or poverty. A Umcef report
estimates that 30% of all prostitutes in Six major cities in
India were below the age of 20 and also 40% of these
prostitutes entered the profession before 18 years of age.
Child prostitution are also not uncommon in India. As
per the report published in 'Times of India *, there are
about 4 lakh child prostitutes in India, who are mostly
destitute and even the abducted children who are sold to
flesh traders where they are forced to entertain 2 or 3 or
more clients per day. These prostitutes get infected with
STD and even HIV, as they most often have no access to
health care facilities.
The following interventions may be arranged to mobilise
support for enabling care for the children and women:
1.
Sensitisation of police officials at all levels about
the rights of children and women.
2.
Issuance of identity cards to street children and sex
workers.
3
Ensure strict police action in complaints of physical
or sexual abuse
4.
Providing professionally managed night shelters
preferably run by NGOs with at least minimum basic
facilities to the street children.
136
5.
Organising evening informal education courses to
the street and working children
14.
Effective intervention of the women's wing of political
parties in matters of women in distress.
6.
Providing mobile health teams and clinics in areas
of high concentration of street children.
15.
Establishing financial and employment assistance
16.
7.
Organising vocational training with high employment
potential to older street children and women.
Effective implementation of family counselling
services.
8.
Laws related to minimum age of employment of
children, medical examination, maximum hour of
work, ban on children working on hazardous
industries, payment of wages, etc., should be strictly
enforced.
9.
Implementation of women's empowerment
programmes and legal literacy programmes.
10.
Sensitisation of police for prompt and severe action
in cases of domestic violence against women.
11.
Establishing family courts in each districts.
12.
Implementation mechanism of various laws such
as that a woman cannot be arrested at night and that
a police officer’s refusal to register a complaint of
rage be treated an offence etc., may be strengthened.
13.
Establishing short stay homes preferably by NGOs
or women's groups with imagination and creative
power, for women in distress to go with children in
safety.
I
It is high time that the India Government, the largest
democracy in the world, should do something about to
solve all these problems with the cooperation of non
governmental organisations and with the assistance of
the International bodies like Unicef. We have a number
of juvenile correction centres, remand homes, short stay
homes, Govt, orphanages, etc. We should remember
that the child of today will be the future citizen of our
country. So the investment made on children will be an
investment in the future of our country. As in China we
can make it mandatory for children up to the age of 14
years to attend schools.
It is not that the government cannot do anything but the
Government does not want to do anything sincerely. Let
us solve all our problems with a sense of commitment,
bring quality of life to all our citizens through persistent
efforts.
As Swami Vivekananda said :
‘ Arise, Awake and stop not till the goal is achieved’
*
NETWORK FOR INFORMATION ON PARENTING
(A TAMIL NADU INITIATIVE)
Maya Gaitonde, Bala Mandir
The Indian philosophical and cultural traditions states :
Matru Devo Bhava : first
the Mother as Primary care giver
Pitru Devo Bhava . then
the Father as the primary care supporter
Acharya Devo Bhava . next
the Teacher as the care enhancer
Athithi Devo Bhava : and.
all the 'others' as the care influencers
INTRODUCTION
The wisdom of India's traditionally child friendly parenting
practices are deeply embedded in its cultural patterns,
beliefs and norms and today there is an increasing
understanding that these are in accordance with well
researched universally accepted critical inputs of child
development.
Sub Regional Seminar on Innovations in ECCD,
Chennai - November 24-26.1999
Despite childcare services gaining great deal of
importance, very large number of children in their early
years are still living in the family setting. Hence there is a
need to advocate the Family as the First Learning Site for
the child and acknowledge the significant influence family
has on the care and development of the child. In effect
the parenting responsibilities in the earlier years are of
critical significance
NEED FOR NETWORKING
The need for a Network for Information on
Parenting emerged at a meeting on 2nd March 1999,
during which a peer group review was being made of a
new Parent Education tool. This tool, a flip chart for larger
audiences in Tamil Nadu, had emerged from the process
of a partnership between Bala Mandir and UNICEF,
Chennai (Oct 98 - Mar 99) for the indegenisation and
conversion into a flip chart of the Hincks Dellcrest, Toronto,
Canada. Parent Education - 'Learning through Play'
calendar (Birth - 3 years).
137
SUBBROUP^RESEmmmNS
Participants at that meeting and subsequent one's
facilitated by UNICEF were from among NGOs and
professionals in ECCD, Educational and Research
Organisations, and Government Department of Social
Welfare and Education. What emerged from the highly
interactive and contributory discussions were shared
concerns that:
In the past few years, joint family norms are being
forsaken and the nuclear family system has made
several comprehensive demands on the skills of
family members, depriving children the opportunity
to understand extended family and older generation
who can give care and emotional support. One
aspect of life affected by these trends is the inability
of the family to provide optimal child rearing
environments in the context of widespread changes
in the social fabric of families, neighborhoods and
communities.
There are very few institutions and programmes for
children below 3 years.
The significance of Parenting in ECCD had been
ignored and a new initiative
■
Post-Independent generation in India believes that
they are educated while the older generations were
not. Due to the indifference towards the first hand
wisdom of the earlier generations and its non
availability under one roof due to nuclear family
system, the younger generation has feeble access
to it and added to this, is the lack of scientific
knowledge of child development.
■
Rapid economic changes have not only led to
marginalization with consequent changes in the
social structures of urban and rural communities,
but also changing life styles that cut across all
sections of society. In their struggle for survival the
knowledge of communities with respect to child
rearing is not only being eroded but also more
alarmingly, being replaced by undesirable practices.
■
Safety nets of health and nutrition have been set up
by Government, attempting to ensure basic
minimum standards of survival and growth of
children of the deprived communities. However,
much more still needs to be done in these areas, as
well as, in areas of the psychosocial inputs, so
essential for the integrated and holistic development
of children as human beings.
■
The educated woman either for economic reasons
or aspiration is, for most part of the day, unavailable
for her child and is dependent on institutional care/
family support thus deflecting/diluting her role as
mother and primary care giver.
■
The commercial myopic focus of schools has
necessitated a redefinition of early child rearing.
to address it in an organised way is needed.
For a better understanding of parenting and child
rearing and child development, there is a need to
create a platform to facilitate exchange of ideas and
experiences, discussions and debate on issues
regarding child development.
To prevent possible paralleling of efforts, there was
a need to converge, consolidate and strengthen
existing efforts and expertise in ECCD, to promote
the best interest of the child.
•
There should be a concerted effort to reach the
unreached and create an awareness on support
programmes that enhance parenting capabilities.
•
A need of a child is a statement, but a right implies
that society has to work towards its being made
available and there was a need to advocate respect,
dignity and realisation of the right s of young children
as per the Constitution of India and the UN
Convention on the Rights of the Child (CRC).
PARENTING PROGRAMME
There are several reasons that warrant a massive
Parenting Programme.
■
■
It has now been adequately shown through research
that the way children respond to their environment
and develop their learning capabilities are
consequences of the nature of nurture, nourishment
and stimulation received from the foetal stage
through their early years. The maximum process of
the brain development of the child occurs during
the first three years of life. The need for children to
receive appropriate stimulation, emotional security
and fulfillment of their basic physical needs of
nutrition, health and protection form the very
beginning cannot be underestimated.
Family structures all over the world continue to
change in response to industrialization, urbanization,
population growth, increasing longevity and
migration. While these changes have created new
opportunities, they have also disrupted familiar
cultural practices and survival patterns that families
have developed over the years to cope with their
multiple responsibilities.
Sub Regional Seminar on Innovations in ECCD,
Chennai - November 24-26,1999
THE NETWORK WOULD WORK
To increase knowledge base
■
gather, synthesize and disseminate information on
child development
■
draw from field experience, traditional wisdom and
scientific research
I
Identify communication channels
I
keep up to date with the latest research worldwide
on ECCD.
■
interactive stimulation process so vital to holistic
child development
138
g SUaGfKIUPPRESENTATIONS
'
■
'-‘‘.W*
that the life cycle approach of interventions at each
stage of the child’s
trauma of rejection based on gender, disability,
colour, ordinal position etc.
development is essential for accelerating and
building on earlier positive actions.
equalising gender opportunity
To serve as a catalyst to
increase awareness of issues affecting children
develop material/ messages for propagation of
positive parenting practices
identify strategies to help move communities,
organisations and government from rhetoric to
practice, policy to program implementation.
To build bridges
Foster networking with those with common concerns
and interests
Work across sectoral divisions
Put people in touch with the work of others, with
organising meetings, working forums, publications
etc.
PARENTING IS TRUSTEESHIP NOT OWNERSHIP
All parents want the best for their children. They are in a
position to be the best observer of and, consequently, are
best able to provide for the physical and psychological
needs of their children. Children need to be exposed to
certain environmental experiences/mteractions for optimal
development to take place and Parents and caregivers
will provide these experiences if they know how to and
why they are important. Since there is no one way to rear
children, each culture has developed its own method of
parenting.
To enhance the quality of parenting parents and those in
a parenting role must have some knowledge of the basic
child rearing tools.
1.
KNOWLEDGE ABOUT CHILD DEVELOPMENT
children's normative patterns
stages in physical, social and language development
serving as a communication point
nutritional and health needs at vanous stages.
To serve as a sounding board
emotional needs and typical early social-emotional
behaviour
dialogue with funders and decision makers about
issues of parenting
to forestall inappropriate parental responses to
their emotions and behd^tour.
for policy formulation, programming planning and
implementation
2.
To support efforts
OBSERVATION SKILLS FOR MORE EFFECTIVE
PARENTING ARE
strengthening capacities of child rearing in parents
and communities
a basic need of all parents, regardless of socio
economic status or educational level
for creating a positive nurturing environment for all
children and especially from deprived and unreached
communities.
necessary to help them discover the match between
a child’s ability to readiness
a means to help the child reach given developmental
goal.
To propagate on
culture specific and holistic child rearing practices
necessary to help a parent to enhance
development
developmentally appropriate stimuli
3.
rights of the child
ALTERNATE STRATEGIES FOR PROBLEM
PREVENTION AND DISCIPLINE - PARENTS
NEED
coping capabilities of caregivers
insights on managing child behaviours.
community based child care services as
complimentary rather than alternate to parenting
knowledge and skills regarding alternate method of
discipline
impact of positive and negative parenting
To focus on
stages of parenting - parental readiness, planning
for parenthood-pregnancy, preparing for safe
delivery, early years of the child
Sub Regions Seminar on Innovations in ECCD,
Chennai - November 24-26,1999
the understanding of techniques for problem
avoidance
these basic child rearing tools to handle a
child/parent’s frustrations more skillfully.
139
I
*
3
SUB GROUP^PRESENTATIONS
4.
USING
THE
EXPERIENCES
HOME
FOR
LEARNING
to the actions a child carnes out,
to the feelings a child experiences
how to take advantage of settings, routines, and
activities in the home to create learning and problem
solving opportunities.
for enhancing the child’s language skills.
6.
turn household objects into learning material for
children’s exploration.
the tremendous impact they have on their children’s
lives.
and enjoy child interaction and rearing.
5.
PARENTS NEED LANGUAGE
LEARNING TO GIVE NAMES
TOOLS
PARENTS NEED SUPPORT - TO UNDERSTAND
that through their attention, expressed pleasures,
listening and interest, they are nourishing the child's
growing sense of self.
-
to the things a child notices
and to make parenting a joyful experience.
BABY FRIENDLY TOILETS A NOVEL EXPERIENCE IN ERODE DISTRICT
P. Amudha, Additional Collector, Erode District, Tamil Nadu
CHILD HEALTH- AN INTRODUCTION
Over the past few decades children are fortunately being
recognized as people in their own right with their special
requirements. Quality survival of the human race depends
on provision of adept care to its vulnerable population in
their formative and developmental life years. Health
services for children should therefore be aimed at
improving the future quality of human resources of the
nation by enabling as many children as possible to reach
adulthood with their potential uncompromised by illness
environmental hazards, or unhealthy lifestyle.
Availability of child health services is must at all levels of
healthcare. The organisation of total care of children
involves the integration of many disciplines including social
services and education apart from the health sector. Ideal
child health services should be need based,
comprehensive and delivered at the doorsteps as far as
possible. The nature of services to be provided should be
preventive, promotive, curative as well as rehabilitative.
At the same time, constant efforts must be simultaneously
initiated to plan need based research related to child health
problems in the community and utilise their outcome for
upliftment of the existing standards of care.
The aims of the services should be to save life, restore
health, and rehabilitate children through timely care by
competent health care providers. Parents should be
enlisted as partners in the children’s health. They should
understand ways of promoting good health, recognizing
illness, and taking appropriate actions, wherever essential.
Most importantly, child health services should be provided
in a cordial, compassionate, and caring manner. Those
providing these services must be aware of children's rights
and protect them genuinely.
The constitution has time and again, reiterated the
importance of improving child health. Article 39 stressed
that children should be given opportunities and facilities
Sub Regional Seminar on Innovations in ECCD,
Chennai - November 24-26,1999
to develop in a healthy manner and they should not be
abused. In 1974, India reaffirmed its constitutional
obligations to children in the ‘National policy for children’.
The policy states that “It shall be the policy of the state to
provide adequate services to the children, both before and
after birth and through period of growth, to ensure their
full physical and mental and social development. The state
shall progressively increase the scope of such services
so that, within a reasonable time, all children in the country
enjoy optimum conditions for their balanced growth."
In 1990 the Government of India endorsed all the 27
survival and development goals for the year 2000, agreed
on at the world summit for children. The summit also drew
attention to four sets of rights of children, namely: Right
to survival; Right to protection; Right to development and
Right to participation. In 1992, India ratified the convention
on the rights of the child and adopted the “National plan
of action: A commitment to the child". This plan has now
been translated into state programmes of action for
children and further into district plans.
The plan is guided by the principle of 'First call for children',
i.e., the essential needs of children should be given highest
priority in the allocation of resources at all times.
SCHOOL HEALTH
Health care of children should be closely integrated with
education, play activities, sports and social welfare, so
that children grow into healthy, physically fit emotionally
stable, mentally alert, well informed adults who can
effectively advance their own growth and development,
families welfare, and national enrichment. A child spends
good amount of time in the school. The school should
provide the child with a healthy environment to ensure
best physical, social and emotional health.
Integrated Child Development Services (ICDS) scheme
is a multi departmental and inter sectoral programme
140
i
EK
SUB GROUP PRESENTATIONS
COMMUNITY PARTICIPATION PROCESS IN ICDS
MAHALIR MANDRAMS - in CHEVAL TRICHY, VIRUDHANAGAR, DIHDIGAL - VADAMADURAI
DIRECTORATE OF SOCIAL WELFARE, TAMIL NADU
INTRODUCTION
OBJECTIVES OF CPF
Keeping the major objectives of the scheme in mind, the
Integrated Child Development Services was planned and
implemented with the view that at one point people
themselves will own the ICDS Programme.
Broad objectives of the Community Participation
Programme are :
1.
To make a community realise its basic needs and
find ways and means of fulfilling them by itself
2.
To sensitize women about Government Welfare
programmes and empowerment of women.
In order to effectively realise the goals and objectives of
the scheme, the functionaries of ICDS are expected to
give further inputs so that there will be a high involvement
of the community.
3.
To prepare a community to work hand in hand with
the Government by effectively participating in the
ICDS Services and ultimately to let it own the
programmes.
The Community Participation Programme to reach the
community was developed in order to make the objectives
of the scheme a reality. As the name itself suggests, the
community as a whole is considered important for the
programme's success.
4.
Assuming ownership, women's participation in all
ICDS activities is expected to become a reality. By
making use of the available resources in the
immediate environment, these groups will also be
economically self-reliant and independent.
However, even after many years of implementation the
community has still not thought of owning the ICDS. It is
still at the receiving end.
CHANNELISING THE CPP
VISION of CPP
The Community Participation Programme can be
channelised in two ways: One way is by forming
Mahalir Mandrams through which the objectives
of ICDS can be fulfilled. Formation of groups
through services rendered is the other way.
The main vision of the programme is to form a
village level mandram in all the villages followed
by the formation of a sectoral level mandram.
Formation of a federation at the project level is
expected to proceed this.
CONTENTS OF CPP TRAINING
1.
Self Exploration :
To explore oneself so as to realise one’s actual identity
2.
Understanding
To understand one’s uniqueness, respecting one’s own experiences as important.
3.
Communication :
Skills
To facilitate and strengthen communication between the ICDS functionaries and the mothers
so as to aid in the formation of a cohesive group
4.
Respect
To highlight the significance of listening, understanding and trust.
5.
Values
To explore the values of ICDS imbibing the same among the mothers.
6
Social Systems
To understand, experience and explore the social systems, thereby tapping the resources,
more effectively.
7.
Formation of
Mahalir Mandram
To emphasise unity and its strength and hence the need for groups.
8.
Functioning of
Mahalir Mandrami
To understand the five different levels of individual functioning in a group (Observer, detractor,
participant, contributor and leader)
9.
Evaluation of
Mahalir Mandram
To enable the participants to evaluate the involvement of Mahila Mandram in ICDS services
and to draw an action plan for future implementation of ICDS Services
Sub Regional Seminar on Innovations in ECCD,
Chennai - November 24-26, 1999
-SUBGRaUPPRESENTWnONS
SELF
EXPLORATION
VALUES
UNDERSTANDING
SOCIAL
SYSTEMS
COMMUNICATION
SKILLS
FORMATION
OF MAHALIR
MANDRAMS
STEPS IN MOBILISING MOTHERS TO FORM
GROUPS
After completion of initial training at the grassroots level,
the next step was to meet the mothers. The beneficiaries
of the scheme were the first to be met, since rapport had
already been established with them. The next step was to
concentrate on door to door meet in order to motivate the
mothers who were not contacting the AWW. This was
followed by street to street contact which paved the way
for further contact. These ultimately facilitated meeting
of mothers at large and thus aided them to form groups.
Groups which thus emerged were sensitized on the need
for formation of Mahalir Mandram, objectives behind it,
significance of the office bearers and effective ways of
the functioning of Mahalir Mandram. (Groups so formed
could function as a Mandram by electing its office-bearers.)
RESPECT
FUNCTIONING
OF MAHALIR
MANDRAM
EVALUATION
OF MAHALIR
MANDRAM
TRAINIiNG
Training forms the solid base to reach the desired goal.
So, by and large, all the project functionaries undergo
training in a phased manner. Training of trainers means
that persons will take up the role of trainers wherever they
impart training.
The main features in training are content and curriculum,
which are uniform for all the functionaries. The module
for supervisors, ANMs AWWs and helpers were designed
by the Trainers themselves. This was done through a
process of experimental learning wherein norms of
training were followed at all times.
TRAINER
CDPO
HELPER
SUPERVISOR.
ANM, AWW
VARIOUS STAGES IN THE FORMING AND STRENGTHENING OF MMS
The AWWs have been able to mobilise the
mothers and form groups only in some areas.
Therefore intervention by trainers became
necessary and required action was taken by
them. A district level team was formed
composing of Project Officers, trainers, Child
Development Project Officers, Superintendents
and Auxiliary Nurse Mid-wives. This team rose
to the occasion and stood by the AWWs to find
ways to strengthen the Mahalir Mandram.
Clusters were formed and village level
workshops were conducted by the trainers,
exclusively at the weaker centres. Similar
workshops were conducted covering all the
centres by Sup. and AWW.
Frequent review meetings at all levels also
helped in a very significant way.
Sub Regionai Seminar on Innovations in ECCD,
Chennai - November 24-26.1999
Yet there was a long way to go and the strategy had to be
changed to let the AWWs also get refreshed and
motivated.
A need based workshop proved to be the most important
password to pave the way for the emergence of another
Mobile Trainers Team.
It was a pleasant surprise that the AWW and mothers
had formed this team on their own and worked for the
betterment of the weaker areas of Mahalir Mandrams.
Meanwhile there was a significant and simultaneous
concentration of district team at various levels. At this
juncture there was an intervention by Agencies, other than
the Government sectors which also strengthened the
Mahalir Mandrams.
These interventions paved way for the formation of all
Mahalir Mandrams.
J
90% groups
formed
Growth of Mandram in the ICDS Projects in and around Chennai
Intervention - Chennai Councillors. Lions Club. Guild of Service
* Sectoral meet
* Formation of mobile team of AWW and Mothers
70% groups
formed
Need based workshop for Anganwadi Workers
Review Meet of PO, CDPO, Trainers
Cluster workshop at village level
Mobilisation of mothers
30% groups
formed
20% groups
fo lined
Training of AWWs and
<.
Leaders
,
THUMB RULES FOR OUR SUCCESS
❖
Many hurdles were faced but in due course the
process of building up of Mahalir Mandrams
continued.
❖
For any programme to be a success a strong
foundation has to be laid and in this activity, the first
step to lead towards the goal is proper planning and
scheduling at various levels.
❖
The next one was the actual execution of the plan.
The other rules which guided the programme to the
path of success were that the Dictrict Team was
available at all the crucial moments. The members
had a very clear understanding of their roles and
were present at all crucial junctures.
❖
Regularly conducting review meeting at different
levels also helped in the process of building Mahalir
Mandrams.
❖
Formats were designed with regard to the workshops
and meetings which gave the actual position of the
progress made.
Sub Regional Seminar on Innovations in ECCD.
Chennai - November 24-26. 1999
❖
Having realised the role of TEAM, coordination was
the foremost thought in everyone’s mind.
❖
Another significant factor in the process of formation
of MM was the emergence of a Mobile Trainers
Team, comprising of AWW and the mothers
themselves which surprised even the district team.
The aim of this team was to concentrate on the
weaker Mandrams and to strengthen them. Local
leaders posed a big problem but this was solved by
the timely intervention of the functionaries. They
actually established a link between Mandrams,
leaders and functionaries.
❖
Another interesting factor was that continuing
education on health and nutrition became an
important tool in the formation of mothers groups.
❖
The success story was documented at every stage
because this can become a reference for others.
Real success lies when the community is no more
dependent on others and slowly there has been a
withdrawal at many levels as the Mahalir Mandrams
have started to establish themselves.
SUB GROUP mESENTAHONS
o.
Planning at
all levels
I
Execution
District Team
at Crucial
i
\ Review
6^^
0
Simultaneous
' Designing of ;
\ Formats /
\ Moment
.0
0
'
Withdrawal
Approach
COrOlNUING EDUCATION
from going to the factory and also led to sending then, to
school. The MM had even facilitated in giving books and
clothes to the children.
The other way in which the groups started forming was
through the continuing education on health and nutrition.
The initial planning for training was done at the district
level. This team consists of PO and MTI. Curriculum
was planned according to the needs of the community.
This team trained the project level functionaries at District
l^vel who in turn concentrated on functionaries at the
sectoral level. Then the grass root level team focussed
its attention on the targeted group, the mothers. Though
at the initial stage the attendance of mothers was
negligible, later the sessions started attracting them and
this led to formation of groups.
The MMs have started to function on their own and the
impact by them is remarkable. They are very independent
and can decide for themselves. Their self esteem has
been boosted and now they are working towards the
concept of equality. They have become self-sufficient and
are actively participating in the activities in and around
the centre. They have been solving the problems faced
by the community and have now become Role Models.
TACKLING CHILD LABOUR BY MM
PARTICIFATION AND CONTRIBUTION
The other strategy which helped in strengthening the
Mahalir Mandrams was the process by which the problem
of child labour was dealt with.
The CPP has played a vital role in enhancing the AWW
and motor interactions and in formation of Mahalir
Mandrams which hiked the ICBS services both
qualitatively and quantitatively.
The Mahalir Mandrams were motivated by AWW to meet
the Labour officer in the Match factory to free the bonded
labourers. Later the members of the Mandram stopped
their own children who had been working in the match
factory and decided to campaign against this problem in
the village. They also went on a hunger strike which
triggered the minds of the villagers to stop their children
The percentage of enrollment in pre-school has increased
. Supplementary nutrition and active participation in
weighing has become a reality. The MMs also extend
their help in bringing children to the centre. They shoulder
responsibilities and share their work in the on-going
activities and special programmes.
Sub Regional Seminar on Innovations in ECCD,
Chennai - November 24-26,1999
STRENGTH OF MM
HOW TO USE:
SPECIAL WEANING FOODS:
For children below 1 year:- Add Energy Food to boiling water, stir well for a minute,
cool ■rid spoon feed the gruel.
Besides Energy Food, with the
technical collaboration of C.F.T.R.I..
Mysore. KSACP Ltd. is also
manufacturing Special Weaning
foods having a high calorie density
per unit volume. By feeding this food,
an infant can consume a larger
amount of t rue food in one sitting and
will have adequate nutrition also. The
special weaning food is
recommended for infants at about 46 months of age. This food is also in
powder form and will have to be
reconstituted in pre-boiled warm
water, see it thin and to spoon feed.
Special weaning food formulations
are being produced by the Company
at present having certain percentages
enzyme rich cereal flours with or
without skimmed milk powder.
For •
or Wc.
Energ;
iren above one year:- MLx Energy Food with pre-boiled and cooled water
• ater. roll into balls and serve.
xi can be consumed directly too.
HOW TO STORE:
Store Energy Food only in clean, dry rooms free from insects and rats. Do not store
in damp rooms, or with moist materials. Avoid keeping the material directly on the
floor. (Use polythene sheet/Bamboo mat or wooden planks as dunnage). Energy
Food should also be stored away from infested materials and non-food items. If
stored under hygienic conditions, it can be preserved for 3 months from the date
of manufacture. The room in which the material is stored should be maintained
very clean. If possible, at intervals of 2 months, spray the walls of the room with
2% Malathion after emptying the room completely.
tfoar Babiff prowi/ty
fiood.
I
In the absence of suitable storage rooms, commercially available metallic bins may
also be used.
Do not open the packets till the time of actual use. If the left over material is to be
preserved for a short time, store in a clean tin container with a tight fitting lid. Do
not use food from opened or damaged packets that are exposed to unhygienic
conditions.
PROXIMATE COMPOSITION AND NUTRITIONAL VALUE OF
ENERGY FOOD
G/lOOg
Moisture_____
Protein (N.x6. 25)
Fat__________
Minerals______
Fibre________
Carbohydrate
Calories______
Calcium
Phosphorous
Iron
Vitamin A_____
Vitamin B|
Vitamin Bo
Niacin________
Folic Acid
5-7
14-15______
2- 4_______
3- 4_______
1-2______
68-72
370-380
1 gm______
0.5-1.0 gm
40 mg - 60 mg
1500 lu ~
0.6 mg
0.8 mg
5 mg
0.01 mg
•4^
AGRO Educational Material presented with the Compliments of
CORN Karnataka State Agro Com Products Ltd
LlK??
ri (A Govt, of Karnataka I aidertaking)
Sj
*3;
'“5
I’.B. No. 2479. Bcllary Road. Hebbal.
Bangalore-560 024.
I
FOOD FOR THOUGHT:
■
Protein Caloric malnutrition is a predominant nutritional deficiency among the
children ol the vulnerable group in developing countries. Due to inadequate intake
of basic supplements such as pulses, milk and vegetables, vitamin deficiency
disorders also set in. thus impairing the physical and mental growth at such a
crucial and sensitive stage of their lives.
In developir rnergy Food as a diet supplement, considerable thought has been
devoted to the selection of suitable raw materials conducive to growth in children.
The major raw materials required for the manufacture of Energv Food are Wheat/
Maize Grits. Bengal gramdhai. Jaggerv and edible Groundnut cakc/Sova*
Flour/Soya Dhal which are easy to procure and arc cosi-clteciive loo.
PROCESS OF PRODUCTION:
One of the various activities that the Karnataka State Agro Corn Products Limited
i> engaged in currently includes the manufacture of this ready-to-eat. processed
weaning food namely Energy Food tor Nutritional Intervention Programme
undertaken by the various Departments of the Government of Karnataka. The
weaning food manufacturing Units have been set up at Mysore. Belgaum.
Chitradurga Raichur and DoddabaLajxir with the tcehnical collaboration of
C.F.T.R.L. a pioneer Food Research Institute of Government of India. These Five
Units have an installed capacity of 90 metric tonnes of weaning lood per davTTHe
weaning food is being supplied currently (bTfie Education DepartnyentJoF'
distribution to Prc-primary and Primary children7 under Mid-day Meals Scheme.
It is also being supplied to the Social Welfare and Women & Children UWare
Departments for distribution to various beneficiaries namclv pre-primaiy children.
Tegnant Mothers, lactating women, severely malnourished children and others.
DXICEF has also assisted this project by way of supplying plant and machinery
Rigorous quality control is necessary in the manufacture of Energv Food at al!
stages ol production. This is done by AGRO CORN with the consultancv back up
arrangements with C.F.T.R.I.. Mysore. Raw materials confirm to the PFA standards
wherever they are applicable or to other specifications laid down.
PACKING:
The Indian Council of Medical Research has estimated the protein-calorie
requirement of pre-school children (I -6 years) at 17-22 gms of proteins and 12001500 calorics per day whereas the school going children need 33-41 gms of proteins
and 1800-2100 calories per day.
Keeping in view the above factors. Central Food Technological Research Institute.
(CFTRII Mysore, has designed and developed Energv Food so as to proride in a single
ration atieast hall uic content oi proteins and 1/3 of calories vital tor a chiicTs ’
growth. Practically a ready to sen-e food, this diet cnricherwasextcnsivelv tried out
in the nutrition programme of the Indian Population Project of Karnataka.
QUALITY CONTROL:
Energv Food manufactured under expert technical supervision is machine packed
in flexible pouches ol 1-5 Kgs capacity. Further protection is provided bv the
secondary p/ck used for every 25 units for convenient distribution.
W I
i
'"
I * Si:'feO
g-J
xJ • -
DISTRIBUTION STRATEGY:
INGREDIENTS:
To ensure that this health food reaches the under and malnourished segment of
the target population, it is now utilised for the school feeding programmes of the
Gon. of Karnataka and_Nuirition Intervention Programmes of other states.
By adopting proper developmental market straie^v. Agro Com is also popularising
Energv Food as a consumer item as io give an indication of the quantity of
Weaning Food to be given to children. 55 gms of this Energy Food can substitute at
a cheaper cost. 2 slices of Standard Bread loaf and 112 ML of Milk.
I
(011?
7/
The process consists mainly of pre-clcaning all the raw materials, roasting them
under optimal conditions, powdering them to the required mesh size and mixing
them ultimately.
Energv Food is a sweet powder with a pleasant natural flavour. 100 gms of Energv
Food provides 14 gms of protein and 380 calories of energv. which is about 40%
of the protein requirement and 18'of the energv needs of a 6 vear old child. This
quantity of Energv Food provides upto 50 ol the required essential Vitamins A.
B;. B2. Niacin. Folic Acid as well as minerals like Calcium and Iron. Thus Energv
Food is a wholesome food supplying substantial pan of the dailv nutritional
requirement of a growing child.
The mix has a good acceptability. It can be consumed as such and docs not need
any pre-rooking as imhe case of other-high protein supplements, if desired iLcan
be mixed with water or milk to make a porridge or paste. It can also be used in
preparing Halwa. Pancake (Sweet Dosa). Chappathi etc.
Results of National (valuation of ICDS (Various studies)
Nutrition :
•
•
•
•
•
•
•
•
•
•
•
Adequate intake of all nutrients except Vit. A(1981, Singhal)
Intake of protein was low (Joshi 1977)
Caloric gap of 400-500 (Jyoti Kumari 1985)
Improvement in severe malnutrition but not much impact on mild and
moderate malnutrition.
Rapid decline in Xerophthalmia over a period of two years in Tamil Nadu
(Chandra 1984) due to ICDS.
Malnutrition was attributed to various factors like poor socio-economic
conditions, inadequate health & nutrition education, faulty weaning
practices, lack of ante-natal care, low birth weight, repeated pregnancies,
superstitions and beliefs, large sized families and insanitation (Bapat
1983)
90% had very poor home stimulation in terms of availability of toys,
games and reading materials and provision of affection and warmth
(Jyothi Kumari 1985)
Taste important factor in quality of supplement consumed.
The nutritional status of pre-school children improved and their level of
Hb increased after deworming and or introducing suppl. Nutrition and iron
therapy (Soundarajan 1985)
Breast feeding, weaning at an early age and complete immunization
identified as important determinants of nutritional status (Kamala 1985) &
protection against diseases, IMR in every breast-fed and weaned infant
was low (Mathur 1983).
Anthropometric measurements indicated chronic malnutrition among the
expectant mothers. 75% showed nutritional deficiency and 93% anemic
and had inadequate intake of mineral and vitamins.
Immunization
• Only 52% mothers adhered to the immunization schedules. Reasons were
ignorance, indifferent attitude, lack of awareness regarding schedule, non
availability of vaccines, fear of side effects, inconvenient timings (& fixed
days) and long distances to be travelled (Khanna 1983)
• Not much studies on TT coverage of women.
Health And Nutrition Education (HNE)
•
•
It was reported that HNE rarely conducted by AWW and only small
percentage of AWWs were rated satisfactory on skills in planmlag and_
implementation of HNE (Sharma 1986).
Treatment by mothers of diarrhea improved where ORS was used or home
based fluids.
Community Participation
•
•
•
•
Low or marginal community participation.
ICDS functionaries also did not perceive the importance of community
participation.
Low level of community participation was attributed to lack of awareness
and knowledge of ICDS scheme, ignorance, poverty, lack of time on the
part of villagers, inadequate training of AWW, lack of transport facilities,
etc (Ramdev 1982).
Factors considered critical for strengthening and promoting community
participation were, skills of the worker in eliciting community
participation, exUtenc.e__.of-Coordination- committees, frequency of their
meetings and involvement of local organizations. (Sharma A. 1986)
Source : Preventing Maternal Mortality Evidence, Resources, Leadership, Action.
Safe Motherhood Initiatives, RH Matters 1999.
Maternal Mortality
International conference on Population and Development in Cairo 1994, ICPD + 5 in
1999 at New York decided that Governments agree to reduce MMR by year 2000 of half
of 1990 levels and at 2015 by a further half.
Eoc-essential obs care
•
Basic EOC - Parenteral antibiotics, parenteral oxytocic drugs, parenteral anti
convulsants, manual removal of placeMent&,?removal of related products and assisted
ragijnal delivery, (could be provided at community level also).
•
Comprehensive EOC above and surgery (caesarian) and blood transfusion.
Reasons for decline in Developed countries.
1 Levels of poverty
T Living conditions
Better nutrition
Greater autonomy of women
T Standards of OBG.
Aseptic practices in assisting deliveries.
Drugs to combat sepsis, eclampsia & Haemorrhage
Lower fertility rates by birth control
Improvement in safety of caesarians
Legalization of abortions and provision of safe services.
Leadership of midwives and obg. Specialists for better training and services.
Maternal deaths audits.
Tackle the following issues :
•
•
•
•
Women’s low status and lack of decision making power —> Empowerment.
Information to recognize the signs of complications
Health education.
Able to access care when complications develop
referral.
Resources to reach an appropriate care facility in time -> transportation.
Key lessons ofpast decade.
• Risk approach does not help to predict which women will develop
complications and which women will not.
• Use of family planning methods does reduce unwanted pregnancies.
• Training of TBA’s has not reduced MMR as they cannot handle
emergencies/complications.
• The limited procedures carried out in the name of ANC and PNC have had
little impact in lowering Maternal Mortality and morbidity. These services
are more for the infants than for women, (paradigm shift to avoid turning
two sets of distinct and legitimate needs into competing demands for
appropriate care.
• More resources on ANC than into delivery and immediate post partum
care, emergency obs. care and safe abortions.
Making every maternal death count:
•
•
•
•
•
•
Improving / upgrading emergency obs. services.
Training of professionally recognized community and facility based
midwives, (including post partum care).
Provision of safe, legal abortion services, (reason fori in 6 global maternal
deaths).
Strengthening of private care to improve women’s general health,
beneficial ANC, PPC, FP, HE on pregnancy and its complications.
Gradually replace TBA’s with trained midwives n the community.
Chronic maternal morbidity also to be tackled (poor repair of episiotomy
and perineal tears, vesico-vaginal fistula and utero-vaginal prolapse)
Measuring Maternal Mortality (impact indicator)
•
•
•
•
•
Sisterhood method/surveys (asking respondent about sister’s birth histories,
number reaching adulthood, number who have died, age at death, year in
which death occurred, and years since the death, etc)
Verbal autopsy.
RAMOS (Reproductive age Mortality study)
Confidential enquiries (ideal)
Maternal Death Review (recommended by WHO for selected health
facilities).
1
Impact indicators difficult to measure. So process indicators, which provide information
on the actions to be taken to improve the situation. They are affordable and reflect
changes immediately (responsiveness).
Table 1 (pg 26)
Q
JMEWSIDN
SUB^GIONALSEMINARI)N1NNOVffnONS9N£CCD
calling for integrated and life cycle approaches in ECD. It recommended decentralised, flexible, local
models recognising the role of parents as primary care givers in promoting ECD and called for family and
community based interventions.
The launching of the World Bank assisted Women and Child Development project including its nationwide
training component Udisha which embodies much of the recommendations of that workshop.
A meeting of key partners held, at the national level to discuss the ‘vision for young children in India in the
2151 century’. The deliberations called for a transition from welfare to a child rights perspective in defining
such a vision. It emphsised the study of tackling the needs of young children through holistic approaches,
promoting inter-relationships between health, nutritional well-being and psycho-social development in
early childhood as a major challenge that needed to be met through innovative strategies. It also went a
step further in recommending new partnerships for ‘bringing together different sectors and partners at all
levels - parents, families, communities, childcare functionaries and service providers of all sectors, elected
people’s representatives, local self governments, NGOs, professional bodies, media, training/resource
institutions and policy makers’ to reinforce the priority to early childhood development.
Two state level workshops were organised in Early 1998 by UNICEF, Chennai, for the NGO sector in
Tamil Nadu, wherein the strengths and weaknesses in reaching out ECD services to children in the 0-6
age group in the non-govemmental sector were identified followed by an orientation workshop on ECD
held for the non-govemmental sector in August 1998 in Vellore.
A state level symposium on ECCD was organised by UNICEF, Chennai in August, 1998. It brought
together stakeholders from both governmental and non governmental sectors to share their perceptions
on status of early childhood care and development in Tamil Nadu and identify critical gaps and issues. The
recommendations emerging from the symposium also called for preparation of policy on ECD for the state.
The ECD Framework
This framework essentially addresses the age groups below 3 and 3-6 years. Early childhood development is
not preparation of the child in formal school skills. What children need at this stage is health care, nutrition,
love, feeling of security and guided play activities to stimulate their physical and mental growth processes. It is
important to understand that the pre-natal to 3 years is the most critical in terms of growth and development
patterns of physical and mental faculties of the child. The period from 0-6 years is when almost all of the
emotional, cognitive and psycho-social development and patterns of socialization i.e. learning from the
environment occurs It is only in the 6-8 age group that the child is ready for full time schooling, when the child’s
physical and mental avenues are sufficiently developed to make that critical transition to schooling. The ECD
framework then in its broader perspective entails Early Childhood Care for Survival Growth and Development
(ECC-SGD). It propagates:
>
Family focus enabling families to care for children
>
Gender sensitivity to ensure realization of the rights of girls and women
>
An enabling environment for the physical, cognitive, language, social and emotional development of
the child
>
It has a child-centered approach, driven by “the best interests of the child”
>
A rights perspective through new partnerships of parents, communities, civil societies and governments
to meet their obligations to children.
>
Community based interventions in managing and sustaining ECD
I
Early Child Development: A Vision for Young Children in India in the 2131 Century, Meeting of Key Partners
comprising the Departments of Women and Child Development and Education-MHRD, NIPCCD, NCERT,
ICCW, BPNI, World Bank, UNESCO, WFP, CARE and UNICEF, held on June 10, 1999 at New Delhi.
UNICEF, Chennai & Hyaeraoad
November 24-26, 1999
6
1
Twewsww
^BREGiaNALSEMINAKaNINNQVATiaNSINECCa
>
Respect for cultural diversity to encourage locally based and relevant child rearing practices.
>
Reaffirms Commitment to FIRST CALL for Children
>
Best possible start to life of the young child
>
It is an entry point for India’s human development strategy
>
Focus on the crucial and vulnerable age group - prenatal to under three years
The ECC-SGD Framework calls for a transition from welfare to :
•
a child rights perspective
•
addressing the needs of young children
•
designing holistic approaches
•
working out synergistic relationships between health, nutritional well-being and psycho-social
development
•
build new partnerships for “bringing together different sectors and partners at all levels - comprising
of parents, families, communities, childcare functionaries and service providers of all sectors, elected
peoples representatives, local self governments, NGOs, professional bodies, media, training/resource
institutions and policy makers”
•
prioritise early childhood development
Rationale of the Regional Seminar
The southern region of India represented by the states of Tamil Nadu, Andhra Pradesh, Karnataka and Kerala,
has been in the forefront in terms of designing and implementing innovative strategies in ECCD. The progressive
growth in child health, nutrition and child development indicators as compared to the rest of the country, are
testimony to this. It is therefore expected that the sub region would provide leadership in playing a catalytic and
innovative role in promoting the rights of the young child, and that through commitment, participation, networking
and strengthening of resources at this level, it will set an example for the rest of the country in reaching the
goals of early child development. At the same time both the Directorate of Social Welfare and the WBA ICDS
III (formerly TINP) in Tamil Nadu felt the need to network with sister states in the southern region, to create a
platform for mutual sharing of innovative practices in ECCD, and to move on towards defining strategies for
the development of an ECCD policy.
The rationale of the seminar emerged from the need to highlight at the regional level:
•
best practices in ECD
significant achievements in the sub region
consolidate the lessons learnt
At the same time it sought to :
>
Broaden the perspective of child care to focus on early childhood for care, survival, growth and development
Emphasize the need for partnerships with parents, families and communities that highlight their role as
primary care givers
Identify strategies to promote intersectorality in ECCD programmes and linkages pertaining to mothers’
reproductive health and nutrition, children's basic need for care and development, nutrition, water and
sanitation, protection and education
UNICEF, Chennai & Hyderabad
November 24-26, 1999
7
THEMSIDN
SUB REGIONAL SEMINAR VN INNOVATIONS tN£CCD
Promote the establishment of interdepartmental committees (composing Social Welfare, Health, Education
and Rural Development) on ECCD for designing a comprehensive and multi-disciplinary approach to tne
achievement of rights of young children
Forge a sub regional alliance and networking forum that will lead to the development of integrated and
state specific policies on ECCD
Objectives of the Seminar
•
To identify innovations and initiatives in government and non governmental sectors on early childhood
development in the sub-region.
•
To identify existing resources on innovative strategies for purposes of exchange of experiences and
consultation at sub-regional level.
•
To provide a platform for sub-regional networking and forging alliances in shaping the vision for the young
child in the 21st century.
•
To initiate a process of documentation and dissemination of information in the sub-region on initiatives in
critical challenge areas of early child development especially in reaching disadvantaged groups.
Seminar Outcomes
□
Sub regional interface on exchange of best childcare practices for survival, growth and development of the
young child
□
□
□
Recommendations and follow-up action proposed by working groups
Key decisions on the tasks to be initiated at the sub regional level
Consensus on vision for the young child in the 21st century
As we stand on the threshold of the 21st century, reaching all children and women especially from the most
difficult to reach groups is the major challenge. Increasing pauperization and marginalization of communities,
the accompanying instabilities in family and household structures, increased burden of women’s work as a
result of their participation in the labour market along with growth in domestic violence - all have a direct
bearing on the development pattern of the young child.
The Seminar not only provided an opportunity for a large participation from the subregion but was able to bring
a consensus on the vision for the young child in the 21st century. It called for meeting the obligations and
responsibilities of all committed stakeholders in working towards key issues for realizing that vision. It also
provided a platform for significant decisions. It is hoped that both the Consensus Statement and Decisions will
now provide the framework and guideline for further action in the sub region and leadership to the rest of the
country in child care and development
Unless the life of the child in the family and community improves, all development efforts
would be meaningless. There is, therefore, a need to raise awareness and create an ethos
of respect for the rights of the child in society to meet his or her basic developmental
needs. Advocacy and social mobilization areTwo crucial processes which are being
emphasized to achieve this end. With India's ratification of the UN Convention on the
Rights of the Child, the Tights approach to child development is gradually gaining
importance and will henceforth form the basis of Governments strategy towards child
development
• India Country Report on the Convention on
the Rights of the Child (1S97)
UNICEF, Chennai A Hyderabad
November 24-26, 1999
8
Q
SUB REGIONAL SEMINAR ON INNOVATIONS IN
EARLY CHILDHOOD CARE & DEVELOPMENT
November 24-26, 1999, Chennai
MONITORING GROWTH AND DEVELOPMENT
IN ICDS : CHANGE IN PARADIGM
DR. USHA ABROL, REGIONAL DIRECTOR
NIPCCD
Organised by UNICEF - CHENNAJ & HYDERABAD
/
1 vyfxiivo unvifr/n
v
i h*
.
CHANGE IN PARADIGM
*Dr. Usha Abrol
Integrated Child Development Scheme (ICDS) is one of the biggest and well conceived
intervention programme of the world. The programme is based on scientific principles of child
development and is targette3 at overall development of children between 0-6 in an integrated and
comprehensive manner. The programme started in 1975 with 33 projects, expanded to include
3,907 projects (1995), covering three fourth of community development blocks of the country
(Govt, of India, 1995).
The programme can also boast of a very comprehensive monitoring and reporting system.
Growth Monitoring is one of the important activities of the programme which aims at close
supervision of and remedial action for growth faltering and malnutrition..
The field functionaries of ICDS programme are expected to provide a number of services
to promote healthy overall development of the child; care of pregnant women, immunisation,
supplementary nutrition, health check-up etc are all directed towards this ‘goal’ i.e. healthy over
all development of children. The activities of growth monitoring are planned to prevent growth
faltering and promote healthy growth of children. The skills of growth monitoring include
correct assessment of age, proper weighing of children, plotting of weight on growth chart,
interpreting growth curve in terms of nutritional status of the child, and use of growth chart as a
tool to educate the mothers for promoting growth and health of their children.
Over the years, growth monitoring has become a mechanical activity not yielding its
ultimate goal. Some of the problems in growth monitoring are;
i.
The focus is on negative aspects, i.e. only children who are in grade III or IV are
discussed and attention is paid. The effort to prevent growth faltering from normal to one
and one to second grade are few.
ii.
Most of the States are showing significant decrease in number of children in Grade III
and IV and stagnation in Grade II and I malnutrition is large. Only about 50% of the
children come in the ‘normal category’.
iii.
Nutritional status is regarded as an isolated phenomenon . The interactive effect of health
and other aspects of development are not considered.
iv.
Education of mothers about the growth of child using growth chart is very rare.
Dr. Usha Abrol, Regional Director, NIPCCD Regional Centre, Bangalore
1
Now that the programme is almost three decade.; old there is a need to review and
examine the strategies adopted vis-d-vis benefits achieved.
The recent research and thinking in Child Development has recognised that growth is a
complex and multidimensional phenomenon. Growth means increase in size and weight. We
compare the children with standard or average weight for age to know whether the child is
growing properly or not. Thus growth is a process of steadily and continuously growing and any
failure to growth calls for remedial action (therapeutic feeding, medical attention etc). Growth
also depends not only on quantity and quality of food but also on how the body assimilates and
uses the food, which in turn depends on health of the child. The combined effect of nutrition and
health is very well known now. However in ICDS unfortunately nutritional status is taken as an
isolated incidence.
Understanding of the process of growth has also indicated that feeding is a social process
and all component of this social process affect the growth of the child. Mere nutritional intake
will not affect the child’s nutritional status much. The research studies show that parenting style,
psycho-somatic health of mother and family dynamics affect the nutritional status of the child
(Tripathi, 92, Vazir, 1994)
It is now high time that in ICDS we appreciate the fact that development is more than
growth. Growth is increase in size, weight and height in quantitative terms whereas development
is more qualitative and complex such as developing eye-hand coordination for “grasp”.
Similarly learning to sit, crawl and walk are childs progression towards independence and
control of its environment. Thus development means progression of psycho-motor activities,
use and increasing perfection of sense organs - eyes, ears, nose etc, ability to communicate with
adults by developing signals, symbols and language. Child herself is an active agent in the
process of development.
The child development research and empirical evidence has also established the fact that
various aspects of development of child, viz, physical, psycho-motor, cognitive, socio emotion
^etc., are closely inter-linked and affect each other in a synergic manner. Physical growth is
affected by socio-emotional and cognitive development of the child and all other aspects are
affected by physical health of the child. As shown by various studies the family environment
and parenting style also affect the nutritional status of the child.
It is therefore suggested that a more comprehensive and holistic view of growth
monitoring should be adopted in ICDS. Good health does not only mean good weight and height
1 it is also means normal development of cognitive, language and psycho social abilities.
There are three basic components of holistic development;
1. Self motivation - which urges the child to move, walk, manipulate and explore the
environment and become an active partner in her own development. Researches show that
right from birth the child is actively involved in exploration and play leading to learning and
development. For this physical health and normal nutritional status and freedom from
diseases is necessary.
2
K
2. Encouragement and facilitating by adult care giver make the task of the child easier.
Parents/mothers/caregivers are partners in development. Caring means respondine to the
needs of the child or helping her to meet her basic needs. Basic needs go beyond food,
clothing and shelter. Love, affection, stimulation and interaction are also basic needs of the
child which can only be met with the help of care-giver and family.
3. Facilitative environment-which provides the child with various opportunities to play and
learn. Such an environment should includes consistency, predictibility and facilities for
movement for exploration, manipulation and discovery.
Development is a continuous process starting from conception itself during which a child
passes through various stages. Successful passing through one stage is necessary for reaching
the next one. For example co-ordination of lower limbs is necessary before walking,
development of small muscles is necessary before the child could hold a pencil. Every stage of
development requires the child to perfect some tasks. In infancy the child must learn to sit and
crawl, between 1 -2 years the child starts developing language Once the tasks of one stage are
successfully completed the child smoothly moves over to the second one. If the child foils at one
stage, the whole sequence gets delayed. The childs inability to complete certain tasks of a
particular age specific stage is indicative of developmental delays.
The tasks the child performs at various age points are more or less universal They are
usually refered to as milestones of development. These milestones are the approximate aees at
which the children are expected to do certain things. For example children are expected to hold
neck at certain age. For successful completion of these tasks and to proceed on the path of
normal development the child requires the following:
- All body parts and sense organs should be normal; No brain damage disability
- Good physical health;
No chronic, disease disability
- Normal body weight
- Presence of loving and
Stimulating adult care giver;
Both parents alive closeness with
mother in early infancy
- Safe, clean and stimulating
Environment
All the above are <essential ingredients of development. If any one is missing it affects
the development adversely.
For being normal the child has to be bom normal. Stimulation helps to make more neuro
connections and pathways in the brain and thus makes stronger base for development The role
of parents and family becomes important for children below 3 years because they require more
stimulus which can be provided only in the family.
3
Thus the new approach to monitoring should be more holistic and development oriented’
It should start from the time of conceptions, it should include psycho-social development also
and not only physical health and nutritional status. It should recognise the parents as essential
partners in development and should emphasize on providing, safe and stimulating environment
to the child.
In this context, the main goals of new development monitoring would be;
1.
2.
3.
4.
5.
6.
7.
Close monitoring of low birth weight babies
Identification of growth faltering.
Identification of Grade I, II, HI and IV children and remedial action
Ensuring healthy psycho-social development by monitoring milestones in the first two
years
Early identification of developmental delays and disabilities
Achievement of pre-school children in areas of motor development, personal, social,
emotional development; cognitive development and language development
Assess the school readiness in children 4+.
First three are already there in the service package, 4-7 need to be included to achieve
the goals of‘overall development’ laid down in ICDS.
The Strategies
1.
It is felt that there is a need to have a more positive approach to the entire concept of
growth monitoring. In other words it means that the message that 6 your child is healthy
and his weight is normal/good for her age should also be communicated to reinforce child
care practices and mothers should realise that they are doing some things which are good
for their children and they should keep them up and maintain good health of the child.
2.
In order to promote over-all development of the child it is suggested that the milestones
should be indicated in the growth chart along with the age of the child. Thus while
weighing the child the worker can also check whether the child has achieved the
milestone for that age. For example a six month old child should be able to sit, if an eight
or nine month child is not able to sit, he needs to be referred to the health personnel.
3.
Parents should be made partners in the monitoring activities. When the mothers come for
weighing the child it can be discussed with them what their child is doing i.e. sitting,
turning, smiling etc.. This would help in developing a good rapport with AWWs and the
mother.
4.
It is also be proposed that the AWW can organise weighing of children in such a manner
that mothers of same age come together on one day eg.
4
Monday
T uesday
Wednesday
Thursday
Friday
Saturday
Mothers of babies below 6 months
6 months + to 1 year
1 - 2 years
2+3
3+4
5+
These sessions then can become meaningful educational meets where development of the
child in terms of weight, nutritional status, milestones etc., can also be held.
5.
Early identification of disabilities and its advantages are well known. Standardisation of
a tool for early identification of disabilities to be adopted in ICDS universally is required.
This should be an essential part of development monitoring.
6.
Training of functionaries at all levels
6.
Training material, manual, guidebook etc illustrating holistic approach to development
monitoring.
The new tool for development monitoring should therefore include, in addition to the
nutritional grades. The psycho social milestones of development checklist for early detection of
disabilities. A prototype of such a tool is enclosed. The details of the format and modalities
need to be worked out.
Empirical Information
The need for a shift of focus from health to development is being felt for quite some time
(Innocenti Technical Workshop, UNICEF, New York, 1990) However the translation of these
ideas in the programmatic terms is yet to be accomplished mainly due to following reasons;
1.
Relatively inadequate data on developmental aspects of Indian child which is culture and
context specific. Most of the Indian tools and devices are adaptation of Western instruments.
2.
Translation of technical information on psycho-social development in simple non
technical terms.
3.
Inadequate field trials of psycho-social indicators to demonstrate their viability.
However of late a number of efforts have been made to over come above mentioned
problems. These are;
A multicentric cross -sectional collaborative study was undertaken by NIN (1991) in 3
centres in India to develop simple and reliable indicators for early detection of developmental
disabilities in children under six years. This screening test can be used by grass roots
functionaries also.
A similar effort has also been made by NIPCCD wherein age specific norms for children
in the areas of motor, cognitive and psycho -social development for children between 2 - 6 years
have been developed (Usha Abrol, 1994)
5
A
i
1 rivandrum Developmental Screening chart 1 DSC: is a simple developmental screening
chart designed and validated at Child Development Centre Trivandrum for children below 2
years in age. The screening programme has been extensively used by AWWs. There are 17
items in the chart (Dr MKC Nair, IAP, Test Book of Paediatrics)
The normative data on psycho-social development is also available in a number of studies
but the above mentioned are most comphrensive of the lot and have been used in ICDS areas.
Thus the standard information is now available against which the psycho-social
development of Indian children can be monitored. This information however needs to be
examined, consolidated and finalized in terms of a standard set of items which can be used for
monitoring of children in ICDS.
As regarding monitoring the development of children in pre-school i.e 3 - 6 years, a
simple instrument for assessment of progress of children in the areas of motor, cognitive,
language and person social development needs to be developed in simple and non-technical
language which the grass roots level functionaries can easily use. The indicators for “school
readiness” of the child also need to be developed so that the AWW can monitor the progress of
pre-school child.
Thus an improved monitoring tools for development monitoring would help in achieving
the “over-dll development of the child” in the true sense.
6
•H
REFERENCES
1. Abrol Usha, et al, 1994
A Cross Sectional Study of Psycho-social Development of
Children 3 -6 years., unpublished, NIPCCD, Bangalore.
2. Ary a Saroj,
Developmental Screening of Pre-school children. An
Overview, Indian Journal of Disability and Rehabilitation,
July - Dec, 1987
1987
3. NairMKC,
IAP, Text Book of Pediatrics, Child Development Centre,
Thiruvananthapuram.
4. Tripathi,S.K, 1992
Socio Cultural Correlates of Malnutrition in Early
Childhood, NIPCCD, unpublished.
5. Vazir Shahnaz ct al, 1992
Screening Test Battery for Assessment of Psycho-social
Development, Indian Paediatrics, Dec. 1994 Vol.. 31
7
Ml
*^>\T(OnjAL
Z-^JA
»V
©P
Nirc^ tj
CLxiL-g)
Iw /
b£LHI.
^E>£ \? e. l- o 1°
__________ ____ _________ _
K 7a. . Fd.k, (Z
6.
Conclusions and Recommendations
Lt7 7 both, in content and magnitude. It was perhaps
(ceding chapters, therefore, cover ojfr~ai,able- The ^-gs presented in Jhe pre-
Lt the valuable empirical information to its maT 6 d3ta tOctake °Ut S‘ate leVel reports on status °f ICDS to
Lecific to each project and for the State as a who™01
attempt wil1 su99est follow up actions
l SoX'sXTh 'h,P"r °'d°CUn’"', =“■ “ ““
L
bA X "rnXo™ 91 " "“mP'
“» ««-
b"'’
'■ XSXXXXXXX “Par’d' lh'
|
I
j
A
and prevent wastage of ration through spoilage Sem?-ne
ava,lab,l,ty of space for otber activities
placed by permanent and pucca building p9
rmanent structures need to be progressively religible and efforts are required to mobili 9
ornrnunlty s contribution towards this aspect has been negwithin the premises of AWs wherever poslbteTis dXlorab^h1'^5
handpurnps should be installed
able in over eighty per cent of tZe sZmpfe AWs 11 ,
f
°r tOl'et faCilities were ava«Development had issued guidelines to tie Sfcte Govemm t
h
Dkepartment °f Women a"d Child
CW dated 16th April. 198|) If someZ ta^b °n T
9
1986 (Na ,6'9/85
number of AWs would have atleast had some type of toiteUaal'ities^Stat^Go35'
structed once again to provide these facilities in AWs
Governments need to be in
upper cas^ popular,
I
by upper class and
*■
->
XTd,“be
1XXXXXXX
partment of Women and Child DevelopminiU990 totoX t
by 016 DeHowever, a substantial backlog for refresher trainina of fnn
S eaml,na ^'"‘ng of ICDS functionaries,
is imperative for functionaries to receive refresher trainina n °naneS at al1 levels 13 a matter of concern. It
felt that we need to experiment with some new fnnova
£ 7 Y
Upgradin9 tbeir skil>3-is also
possibility of involving academic and technical institutiobVemethods for 'mpart,n9 refresher training. The
peripatetic training in the field needs to be explored The feed'S
9| C°ntinUing educad°" through
framing health functionaries of ICDS has been quite encouraging and'^sidv™"1
CO"e9eS
“XLS xr T
eligibility criteria lor recruitment ot AWWs may be raised fe'iw ’ I
promotion „e„u„
tb.X,™’ X SaSruX
™
«•
15 cha"9'n9 trend suggests that
M
CDPOs has gone through a revolutionary chanqe and has element h
‘ dy' The tralning syllabus of
continuing education to AWWs. It shouto be mandatoMo: ” e^Offic^^omaT f 10
133
SS?5^^y.T^r .•■••-■••
6. Supervisors in the study were found to have more than 30 AWs under their charge. It is too large a number
to provide guidance and support to the functionaries at the grass roots level in a participatory way during
their visits to AWs. The double or additional charge is detrimental for the supportive role she is expected
to perform. There is need to create a post of a substitute Supervisor in every project to manage this prob
lem and also strengthen supervision.
7. Though coordination with health functionaries was reported to be satisfactory by a majority of CDPOs, par
ticipation of ANMs in referral services, health check-up, home visits and in NHE.was foundjp.be marginal
AWWs and AFSMs should work in close collaboration. Ways and means need to be worked out to make
them join hands for taking care of the health needs of women and children. In order to improve accoun
tability, work assessment report of ANMs working in ICDS areas may include evaluation comments of the
CDPO incharge of the project as well.
spent
two h
ascer
plem(
strain
tivities
of col
activit
14. Fund
a ma
needs
tion, i
stage
strear
8. The study revealed that in most cases, eligible beneficiaries were being registered for various services as
per the prescribed criteria. The coverage also showed considerable improvement as compared to earlier
evaluations. However, short falls in tribal areas require appropriate measures, both, to extend outreach and
rnake beneficiaries aware of the services. The positive role played by ICDS functionaries in promoting 15. In line
coverage of health services, namely, immunization, antenatal, post-natal, health check-up and referral ser
tation
vices, could be contrasted with the poor utilization of these services by target population in non-ICDS areas.
?rs f
In tribal projects, differences were considerably larger between ICDS and non-ICDS samples. Therefore, it
never
is recommended that implementation of health services needs to be improved in non- ICDS areas and par
reaso
ticularly in tribal areas.
resen
to the
9. The positive impact of supplementary nutntign and growth monitoring on nutritional status of children
divide
could be seen clearly. The supportive role played by NHE towards this, was also reflected in the results ob
Hope
tained. In non-ICDS areas, semi-solids were introduced to children as late as two years, and less number
the c<
of women were using Appropriate weaning practices. This contributed towards poorer nutritional status of
elude
children as compared to their counterparts in ICDS areas. Efforts should be made to further improve the
indivi
coverage of underthrees for receiving supplementary food by exhaustive door-to-door surveys, encourag
evolv
ing consumption of food at the anganwadi and enhancing mothers’ awareness about appropriate weaning
Supe
practices and supplementary foods for underthrees.
16. It was
10. Despite these differences, it was felt that delivery of NHE was far below the desired level. It is suggested that
the tc
Supervisorsjyhould be given the responsibility of holding formal NHE sessions regularly in AWs under their
the si
charge. Rigorous monitoring by CDPOs and active participation of health functionaries can further im
situat
prove the implementation of this component. For group formation and collecting women at one place for
NHE sessions, locally popular social/recreationalevents may be organised. (Jtiiization of folk media such as
The s
nautanki, kathputli, etc. need to be included in the training curricula of functionaries to strengthen their n^ciaries
skills in imparting NHE effectively.
n diff
to sugge.
11. The positive impact of health and nutrition services also emerged with respect to indicators, namely /Al/?
deavour v
and DDR. These indicators registered lower values for ICDS areas as compared to the latest available SRS
tential of'
estimates at the national level. Further, a declining trend was observed in ICDS areas for IMR when com developrr
pared to the figures available for the years 1987 and 1989 (Source : Department of Women and Child De
ramme s<
velopment). These results make an excellent case for further expansion of ICDS to progressively cover dis
advantaged families by integrated services to ensure survival and development of children and women.
12. The study confirmed that ICDS perhaps, is the only major plank which can make pre-school education available to disadvantaged children. The differences in coverage of children by PSEu were exceptionally large
between ICDS and non-lCDS samples, and particularly so for tribal areas. The findings.further established
the role of PSE in promoting enrolment in elementary school, reducing dropout rate and enhancing reten
tion in school. The status of education of children (6-14 years) collected from household survey for both
samples substantiated these claims.
f
13. Further, ICDS children were found to perform fairly well on tasks associated with learning of numbers and
manipulative skills which are required for formal learning. Mothers also reported that their children were
134
number
y during
xpected
lis prob’Os, parlarginal.
to make
accoun
ts of the
■vices as
o earlier
iach and
omoting
srral ser)S ar
refore, it
and par-
children
suits obnumber
status of
jrove the
icouragweaning
spending 2-3 hours at AWs and were attending pre-school. AWWs were also found to be spending about
two hours per day in PSE activities. The quality of the delivery of this component, however, could not be
ascertained. The informal feedback indicates that there is a tremendous scope for improvement in the im
plementation of PSE component. Non-availability of material for play and learning is one of the major con
straints. Efforts must be made to provide a minimum set of material appropriate for play and learning ac
tivities at every AW. Children of the study were not able to perform certain activities well like identification
of colours and other cognitive tasks. It emphasizes the need for introducing more creative and cognitive
activities.
14. Functionaries, at ail levels reported that irregular supply of food, equipment, material and medicine kits is
a major problem in implementation of ICDS. The efficiency of the concerned administrative machinery
needs to be improved. Whencfistribution of supplementary nutrition is interrupted, besides causing irrita
tion, it has other implications, such as, poor attendance, low enrolment, reversal of children to the earlier
stage of malnutrition and mistrust in AWWs. State Governments should take appropriate measures to
streamline supplies for smoother implemention of the programme.
15. In line with earlier researches, community participation revealed itself as a very weak link in the implementation of ICDS in the present study. Participation of the community was negligible and community mem
bers had low awareness about ICDS programme. The complaint of the community leaders that they were
never consulted at the initial stage of programme implementation, unfolded an important clue to the
reasons for the lack of community participation and~involvement. FtlTimperative to involve community rep
resentatives during the preparatory phase of initiating a project. This generates a feeling of belongingness
to the programme and serves as an effective strategy to augment participation of local agencies and in
dividuals. The feasibility of involving adolescentgirls received some support from the findings of the study.
Hopefully, the new experiment initiated in ICDS to cover adolescent girls would take roots and strengthen
the community participation component as well. All functionaries indicated that it was difficult for them to
elude the pressures exerted by local politics. Hence discretion should be exercised in the involvement of
individuals with political alliances. Effective ways of augmenting community participation need to be
evolved. AWWs apparently do not have the requisite skills for promoting participation. Thus. CDPOs and
Supervisors should take appropriate initiatives in this regard.
16. It was observed that coverage and outreach of services need to be improved in tribal areas, keeping in view
sted that
the topographical factors. It was observed that in urban areas also, the services provided were minimal and
ider their
the situation was worse than that in tribal and rural areas. Steps need to be taken urgently to improve the
rther im
situation in urban slums.
place for
a such as
The study has provided substantial empirical information with respect to implementation of ICDS, its be
hen t**
neficiaries and the impact of various services on the target population. The attempt to study rural, tribal and
urban differences has portrayed unique features of all three types of projects. An attempt has also been made
to suggest recommendations to strengthen the implemention of the programme. It is hoped that this en
•nely /A!/?
deavour will add to our understanding of ICDS and would lead to important policy decisions. ICDS has the po
able SRS
tential of bringing about a silent revolution and becoming a profound instrument of community based human
len comdevelopment programme of our country. We must take concerted steps at all levels to strengthen ICDS prog
Child Deramme so that every child’s^nght to develop to his full potentials and grow optimally can be realized.
zover diswomen.
zation avally large
tablished
ng reten1 for both
bers and
jren were
135
Post Script
The completion of the study on National Evaluation of ICDS in 1992 marked a watershed
in the implementation of ICDS and its philosophy. The findings of the study triggered a series
of actions at various levels. The release of the report of the study by the then Minister of Human
Resource Development in a ceremonial function organised by the Department of Women and
Child Development on 27th July, 1992 gave the document the desired publicity, recognition and
sanctity. The report was disseminated to a mix of over 1500 professional organizations, institutions
and individuals concerned with ICDS. It was well received by one and all and a very positive
feed back was received by the Institute from several quarters.
The academic community has acclaimed the study as a single comprehensive macro level
evaluation carried out systematically and scientifically, covering crucial aspects related to
implementation and impact_otlCDS. The planners and administrators indicated that the empirical
evidence would facilitate several decisions regarding further expansion of the scheme, introduction
of modifications in implementation and in strengthening of ICDS. The training Institutions and
officials of ICDS have shown eagerness in forging effective training strategies and reframing of
administrative structures based on the relationships reported in the findings between skills of
the functionaries and discharge of their roles and responsibilities.
The Department of Women and Child Development, Government of India has been extremely
responsive in implementing the recommendations and suggestions of the study. The information
and insights provided by the report have been used in diverse ways to improve ICDS and its
profile. International Agencies such as C1N1CEF, CARE, WFP, NORAD and World Bank showed
great interest in the review of ICDS presented in the evaluation report. Several of their documents
in the context of proposed interventions and inputs in ICDS were based on the facts and data
of the study.
1995 was celebrated with fervour as 20 years of ICDS. It was an important land mark,
Indian Government committed itself to universalize ICDS to reach out to every corner of the
country. It was reaffirmation of the faith in ICDS as a programme having potential of laying
sound foundation for national human resource development. Between the release of the National
Evaluation of ICDS in 1992 and its reprint in 1997 several changes have taken place in the
policy, thrust and implementation of ICDS Scheme. These years have witnessed a host of new
initiatives aimed at improving the effectiveness of the scheme. It will not be out of place here
to give a brief account of the same.
Extending Out Reach of Children under Three Years of Age
In recent years, particularly after the ICDS 20 years theme dedicated to “Promoting
Complementary Feeding B ORT” (1994-95), there has been heightened awareness of the need
to improve caring practices for the younger child (under 3 years of age), in the family and
community—as distinct from only increasing the “enrolment" of under 3s for the food supplement
at the AWC.
The need for an integrated approach for health, nutritional well-being and psycho-social
development, through strengthened family and community based interventions-reaching out to
younger children (under 3 years) has clearly emerged in recent years. The programme is now
trying to focus adequately on improving the quality of child care in the family-by educating and
136
er
ar
ill
a
fa
di
h(
re
al
u
ir
a
D
B
s
R
k
l<
r
e
v
i
2
C
t
i
c
<
enabling caregivers, for early child development. This includes, for example care of pregnant
and lactating women, breastfeeding and other feeding behaviours, preventing and attending to
illness or health care seeking, hygiene practices, engaging a child in social interaction, providing
a stimulating and safe environment for play and exploration, shelter and supervision. In the
face of the heavy workload of the AWW, this has given rise to issues related to prioritising
different components/services of ICDS and balancing between centre-based and community/
home based activities.
Different strategic options for promoting early child development are being worked out with
related implications for work organisation, training of AWWs and supportive supervision. In the
above context, ejyeixlhe_PQSsibilitv of having an additional child care worker/volunteer is also
under consideration The issue outlined above was addressed in state specific contexts—through
innovative strategies, flexibly responding to local needs, coupled with different training
approaches, processes and content in a National Workshop organised on Early Childhood
Development by the Department of Women and Child Development with UNICEF and the World
Bank on 28-29 August, 1996 in Delhi. The recommendations made during this workshop have
several implications for early childhood care and development components of ICDS (Refer
Report for details).
Improving Nutritional Levels
Implementation experience over the years has revealed that centre based components of
ICDS have been receiving attention with varied results e.g. immunization, health check ups,
referrals, growth monitoring and promotion, supplementary feeding and centre based preschool
education for 3-6 years old children. The need for an integrated approach for health, nutritional
well being and psychological development, through strengthened family and community based
interventions-reaching out to younger children (under 3 years) has clearly emerged. This would
also focus on preventing malnutrition-as early as possible, rather than dealing with it after it
has gccgrred. to address one of the major risks, threatening to limit the development potential
of the young child.
To plan effectively towards this goal the monthly monitoring formats have been amended
to include frequency aspect of delivery of supplementary nutrition and gender and~age specific
information. This has helped in timely detection of interruptions in the nutrition supplements
and in taking early corrective actions. The cost norms of nutrition have been revised upwards.
To enable the community assess the nutritional status of their children on a regular basis,
Community Growth Charts have been designed and supplied to all the States for use in the
Anganwadi Centres. In addition, Food and Nutrition Board (F&NB) with its 43 Community Food
and Nutrition Extension Units (CFNEU) located in 27 States/UTs is being effectively used for
dissemination of vital nutrition and health education to ICDS functionaries/beneficiaries. Further,
these CFNEUs are also being used in monitoring the quality and delivery of supplementary
nutrition in the Anganwadi Centres.
Several initiatives have been made since the 20th year of ICDS (1994-95), denoting a
strategic shift in the programme strategy-to focus on reaching the younger child and to adopt
a preventive, rather than curative approach to malnutrition. The 20th year theme Promoting
Complementary Feeding and Diarrhoea Management focussed on malnutrition prevention and
joint planning, mobilization and orientation activities of ICDS/Health at national/state/district/
project levels using immunization contact points of CSSM with pregnant women and mothers
of infants, to reach this crucial group. The theme symbolised not only the strategic shift to
focus on the younger child, but also on the importance of family based interventions and caring
practices for early child development.
136 A
Early Childhood Development for 3-6 year olds
Early childhood care and education activities (for the 3-6 years age) have emerged as the
most visible daily activity at the anganwadi, sustained for three hours a day. Experience shows
that play way activities when conducted well by a trained and motivated AWW, bring and keep
young children at the AWC. This also motivates both parents and communities, even changing
the perceptions/expectations of parents/communities from preschool centres. Feedback from
AWWs during training programmes, suggests that AWWs feel that this activity wins them credibility
wilh^e^onrrn^t^upport^and recognition. It is also one activity for which they are not
dependent upon external factors e.g. supplies reaching, other sector inputs etc.
In order to strengthen the component field based ECCE enrichment training of AWWs in
selected ICDS projects/districts in 12 states is provided under the NCERT/UNICEF/SCERT/
ECCE project and is geared to promote a child centred, development oriented, interactive,
playway, activity-based approach to promote physlcal/motor development, cognitive
development, communication & language development, social and personality developmenToF
the__young child. The enrichment training uses team training approaches participatory
methodologies and includes hands on experience, demonstration and facilitates observation, as
well as the preparation of local low cost play and support materials during the training.
The involvement of CDPOs/supervisors; in addition to Anganwadi Training Centres Instructors,
and ECCE personnel from District Institutes of Education and Training (DIETS) in training
teams, helps provide effective support for on the job follow up after the training. The enrichment
training intervention also enables the AWW, supported by other project functionaries and
community groups to counteract the pressures for formal and rote learning emanating from the
private sector and primary education.
Pre-school Education
Resource Centres have been located in the CDPO's Offices and the necessary^tie up has
been done with NCERT and SCERTs for development of pre-school material in the local languages
for use in the anganwadi centres. In addition, instructions have been issued for coordinating the
timings between the primary schools and anganwadi centres and for regular visits of primary
school teachers to the anganwadi centres. This has been done to ensure enrichment of pre
school component and better enrolment and retention in the primary schools.
Further, it is pertinent here to review some of the major recommendations made during
National Workshop on ECD held in August 1996 in the context of ICDS which are under
consideration of the Department of Women and Child Development.
(i)
Strengthen joyful play/learning, for 3-6 year olds, based on existing initiatives and
experience, alongwith health and nutrition related interventions.
(ii)
Extend school readiness interventions—making school ready for child and not just child
ready for school.
(m)
Strengthen operational linkages with primary education, also to release girls from sibling
care and promote girls education. Another major step forward has been the strengthened
partnership with primary education, symbolised by the National ECD Workshop (Aug
1996) and its follow up by the education sector, in organising an orientation programme
for State Directors of DPEP, (18-19 September 1996) to facilitate inclusion of ECD in
State DPEP Plans of Action. The conference of State Chief Ministers (July 1996) on
Basic Minimum Services, which, endorsed the significance of ICDS and called for
strengthening its linkages with Universal Primary Education has further accelerated this
process.
1363
a
Focus on Backward Areas
With a view to ensure that the benefits under the Scheme reach, on priority, to the most
disadvantaged sections and the most backward areas, the Department has identified 180 focal
districts on the basis of percentage of population living below poverty line, SC/ST population,
crude birth rate, etc. New projects are sanctioned in the blocks having highest percentage of
SC population (ST population in North East States). Even in the new World Bank-assisted
ICDS-II Project in Bihar and Madhya Pradesh, only blocks having highest percentage of SC/ST
population in these States have been identified for coverage. An additional criteria of adverse
female-male ratio was adopted in identifying districts and blocks for sanctioning new ICDS
Projects.
Strengthening of Infrastructure
The additional funds provided under Social Safety Net (SSN) have been effectively used in
improving basic infrastructure facilities in the anganwadi centres and for providing storage
facilities for supplementary food. Adequate provision of basic infrastructure such as anganwadi
buildings, godowns, equipment and utensils will facilitate improved in the delivery of services
under the scheme.
Convergence of Inter-Sectoral Services
For ensuring cost effective and efficient utilisation of resources in the Social Sector,
instructions have been issued to all the States for ensuring convergence of inter-sectoral services
in the identified thrust areas in the anganwadi centres. The States have been requested to
ensure monitoring of status of convergence at the State level in the District Collectors’ Conference
and at the District level in the monthly meetings chaired by the Collectors.
Involvement of Non-Governmental Organisations (NGOs) under the ICDS Scheme
Greater and effective involvement of NGOs has been attempted by exclusively earmarking
new ICDS projects for implementation by the NGOs. 66 new ICDS projects sanctioned during
1992-94 were earmarked for NGOs. It has been further decided that attempts be made to
handover 10 percents projects in every State to NGOs. Presently around 150 voluntary
organizations are implementing the scheme in selected Anganwadi Centres in various projects.
In addition, all the States have been instructed to involve Mahila Mandals/Women's Cooperatives
in preparing Ready to Eat (RTE) foods for supply to the ICDS beneficiaries with the use _pf
locally available inexpensive and acceptable ingredients. Decision has also been taken to
organise the training of Mahila Mandal Pradhans for sensitizing them to the basic needs of the
programme and for using them more effectively in the implementation of the ICDS Scheme.
Further, the networking of the voluntary organisations/NGOs working in the field of women and
child welfare has been attempted by collecting and collating of the relevant information for
making their effective use in the implementation process.
•Community Based Monitoring Mechanism
The Community Based Monitoring Mechanism (CBMM) which envisages setting up of Bal
Vikas Mahila Samities with elected lady Panchayat Members at the Village, Block and District
levels has been introduced for ensuring monitoring and evaluation of the schemes relating to
women and child welfare at the grassroot level by the members of the community themselves.
The CBMM will provide powerful stimulus to the community to effectively participate in all the
stages of implementation.
136C
Community Partnership
The 73rd and the 74th constitutional amendments have created vibrant and new partnerships
to reach, the most disadvantaged and undeserved and the most vulnerable young children. In
some States, devolution of powers to panchayati raj institution has also involved the transfer
of some functions for managing and monitoring ICDS to district zila parishads, block panchayat
samitis and gram panchayats. This constituted a major opportunity for rooting development
programmes more firmly in the community with the active participation of women.
The Department has recently initiated steps for the constitution of Bal Vikas Mahiia Samitis
at village, block and district levels, with representations from women panchayat members,
NGOs and ICDS functionaries. This is for integrated community based monitoring of all
programmes for women and children, especially for ICDS.
With the recently launched Indira Mahiia Yojana (IMY), new possibilities are unfolding for
ICDS to promote the process of women's empowerment. The Indira Mahiia Yojana has three
components-convergence of intersectoral services; awareness creation; and income generation
activities. It has been initiated in 200 ICDS blocks during year 1996-97.
Plan for Introduction of Services (PIS)
The importance of community preparation and consultation in ICDS, was recognised right
from the beginning, in local situation and needs assessment, identification of disadvantaged
groups and AWC site locations. This resulted in the formulation of Plan for introduction of
Services (PIS), through which new ICDS projects are to be initiated. This is aimed at improving
the participation of communities—especially women, and, improving intersectoral coordination,
right from the beginning.
PIS is a management tool to facilitate effective planning, scheduling and organising of pre
project activities for initiating ICDS. It emphasises that two phases of activities have to precede
operationalisation of new ICDS projects. First, administrative and community preparation, and
secondly, training of frontline workers.
The World Bank Assisted ICDS Project
A Centrally Sponsored Scheme sanctioned during 1991 is under implementation in pre
dominantly tribal and drought-prone rural areas of Andhra Pradesh, Orissa, Bihar and Madhya
°radesh.
In addition to normal ICDS services, the Project provides for additional inputs in the following
areas :
a.
Construction of Anganwadi buildings at village level and CDPO’s office-cum-godown
building at block level, selectively and in the most needed areas.
Experimentation with Nutritional Rehabilitation Centres.
Income Generation Activities for Women.
Women’s Integrated Learning for Life (WILL).
Experimentation with therapeutic food.
f.
Strengthening health and nutrition, awareness generation, community participation,
communications, training, supervision, operations research, monitoring and evaluation
components.
136D
Strengthening the Training Component
Tmining has been perceived as a key instrument for ensuring quality services, creating and
mob l
/"9 TiV ™°tlVatlon and improvement in their communications and community
mobilisation skill. To strengthen the training component, the syllabi for job, refresher and
orientation training for all the ICDS functionaries have been modified, tribal modules for training
Saidwich I
•
functionaries working in the tribal areas have been developed. The
Sandwich Job Trammg course for AWWs has been introduced under the project in order to
strengthen the training of AWWs.
The methodologies and curricula for training/orientation/continued education have been
carefully developed and are continuously reviewed in the light of field experiences of NIPCCD
the apex body of ICDS training. The emphasis on field-based training has increased. Major
modifications have been carried out in the syllabus for the training of functionaries at all levels.
oKill training of trainers has also been emphasised.
The effort is to make training an experiential, two-way process, thus making it more effective
lively and enjoyable. Different training methodologies in use include - brainstorming buzz
sessions group discussions, role play, mock demonstrations, field assignments, quiz and culture
specific forms of creative expression. A variety of training aids such as charts, flannel boards,
graphs, flip books and slide stones/film strips and video films have been developed to support
such processes.
K
Systematic efforts have been made by the Department
towards improving the training of
ICDS functionaries which includes :
i)
Appointment of a “ Modal Officer” for ICDS Training Programme by every StateAssessment of Training Requirement of the State before the commencement of the
financial year.
i
Regular inspection of AWTCs by State Government Officers
ii)
Considering the problems faced by Anganwadi Workers while away on training for a
period of 3 months at a stretch, the Sandwich Pattern of Training for Anganwadi
orkers has been introduced from 1995-96. Under this pattern, the job training has
been divided into three phases of shorter durations. However, it has been observed that
there are some practical problems faced by State Governments as they are finding it
difficult to depute the same batch for third phase of training. Though instructions have
been issued by this Department to State Governments for ensuring that the same batch
is deputed for the third phase, the drop out rate in the third phase is reportedly very
high which needs to be looked into.
iii)
in order to
huge backlog
tu clear the
me nuge
oacKiog of
or untrained
untrained functionaries,
functionaries, an innovative model of
mobile refresher training was experimented on pilot basis in the State of Karnataka
Under this, the workers received refresher training in their
r
T
o
—■ own districts by District Level
C------ Traini?9 Teams 5ons.ilting of one Assistant Director, one Medical Officer, one
CDPO, one Instructor of AWTC and one Supervisor. The main features of this innovative
training programme include :
•
- •
•
Condensed course
Field level staff as trainers
Decentralised training
136E
■
•
Focus on field problems
•
Development of training material
iv)
MLTcTh10 StTn9then trai"ing Of ICDS functionaries, exchange visits among trainers of
trS^r^V2'
“nd*rtaken~ The elective of such visits was to provide exposure
o the instructors to the functioning of different MLTCs/AWTCs; and to provide an
aDoroach
°m the
thC exPer’ence, expertise aS iSovativ"
opportunity to them for learnin9
learning 7r
from
approaches of different training institutions and project functionaries.
v)
A National Review Meeting with State ICDS Directors and NGOs i
involved in ICDS
I raining Programme was held on 30 October 1995 in New Delhi’
The major
recommendations that emerged were :
a.
Need
b.
Non-institutional field based approaches should be adopted for training,
c.
Distance education approaches could be
d.
In order to motivate the functionaries, pro
good work done by workers/trainers by introducing
e.
Software for monitoring training be developed.
to revise the financial norms of AWTCs and MLTCs.
tried out on pilot basis.
awards.
Efforts are being made to implement these suggestions.
Looking Ahead : The Vision
Emerging from two decades of rich experience, today the task ahead is i
‘
'
not only that of
hS ih9h
?
malnutrition - but of promoting every child’s right to development'ICDS
onnn t
PrOmiSe °f Serving aS a Powerful instrument for ensuring equality of
opportunity to present and future generations of disadvantaged groups.
9
V
nro™?35
reaChed 3 Sta9e where il is esscntial to harmonise the expansion of the
Hterv t
3nd,
6Ont6nt enrichment. The spectrum of ICDS services has broadened with the
seX ? nS re a -rl10 the emP°werment of women and communities and convergence of
dZXpmXT'^Xe foXedmtr9in9fPh0file °f 'CDS rededicateS itself t0 Promoting early child
eveiopment — the foundation of human resource development — the vision.
136F
Executive Summary
Integrated Child Deuelopment Seruices (ICDS) is the most comprehensive scheme of the Government
of India for early childhood care and development. It aims at enhancing survival and development of
children from the vulnerable sections of society. Launched in 1975 with 33 projects on an experimental
basis, ICDS has expanded considerably in subsequent years and at present has 5614 sanctioned projects
•of the country comprising 4571 rural, 733 tribal and 310 urban projects. It is perhaps the only country*
wide programme in the world functioning on a large scale, requiring multi-sectoral operations and
intersectoral linkages for its implementation.
ICDS is a unique programme, it encompasses the main components of human resource development
namely - health, nutrition and education. Under ICDS, a package of services, including supplementary nutrition,
immunization, health check-up and referral services, is provided to children below six years of age and expec
tant and nursing mothers. Non-formal pre-school education is imparted to children in the age group 3-6 years
and nutrition and health education to women (15-45 years). It takes a holistic viewi of the development of the
child and attempts to improve both his pre-natal and post-natal environment.
ICDS serves the target group through a network of anganwadis. The anganwadi. literally meaning a courtyard^lay^entre. is the focal point for delivery of services at the community level. Efforts are also made for the
convergence of related schemes/programmes in ICDS project areas such as Safe Drinking Water Supply.
Functional Literacy for Adult Women, and Mobile Food and Nutrition Extension Units (MEU).
Research on ICDS
Since its inception, the programme has generated considerable interest among academicians, planners,
administrators and those responsible for implementing the programme. Consequently, a large number of re
search studies have been conducted to evaluate and assess the impact of the programme on the beneficiaries.
A review of these research studies indicates that ICDS has had a positive impact on beneficiaries and has
the potential of enhancing the child survival rate. Definite improvement has be n reported on major indicators
of health and nutrition like IMR. nutritional status, morbidity pattern, immunization coverage and utilization of
health services. In primary schools, children from ICDS areas were having better competencies on language,
cognitive, conceptual development and behaviour parameters as compared to their counterparts in non-ICDS
areas. Improvement in enrolment and scholastic performance further indicated a positive impact of pre-school
education component of ICDS.
The above mentioned research efforts have contributed considerably to the understanding of the prog
ramme and have helped in identifying bottlenecks and lacunae in the implementation of the scheme. Nonethe
less, the studies have provided only piecemeal information and have not taken systematic stock of the delivery
of inputs vis-a-vis the outputs; nor have these investigated the impact of services on the target groups in a com
prehensive manner. The need for a comprehensive investigation to assess ICDS at the national level has been
felt for long.
The Study
The Department of Women and Child Development. Ministry of Human Resource Development of the
Government of India, which is the nodal Department for the implementation of ICDS, proposed to undertake a
comprehensive review of the scheme and its status at the national level in 1990. With the hindsight of a decade
and a half, such an exercise was considered essential in improving delivery system, its optimal outreach and
m taking decisions regarding its expansion during the Eighth Plan. The National Institute of Public Cooperation
and Child Development (NIPCCDLwas entrusted with the task to undertake an evaluation of ICDS at the na
tional level Accordingly, the Institute planned and carried out the present study during the years 1990-92.
(xxiii)
i
Objectives
ing
oth
The objectives of the study were to :
Op
’)
ascertain the benefits of the scheme on selected outcome indicators related to various services pro
vided to children and women under ICDS;
if)
find out the differences in implementation and utilization of services in rural, urban and tribal areas;
Hl)
identify problems and bottlenecks in the implementation of ICDS; and
iv)
find out the perception of the community about ICDS and the extent of support provided by them in
implementation of the programme.
spr
res
coc
cor
me
gu«
En
Methodology
Ac
tra
an
ttu
to
en
an
Be
de
Sampling Procedure
It was decided that the sanctioning year 1984-85 would be the cut-off point for determining the universe for
selecting the sample. In all, 1.126 ICDS projects (672 rural. 141 urban and 313 tribal) located in 387 districts
of the country met the above criteria. A sample of 100 ICDS projects drawn for the study comprised approx
imately nine per cent of the total ICDS projects identified for sampling. The sample so selected covered 98 dis
tricts in all 25 States and one GT. The sample drawn comprised 54 rural, 28 tribal and 18 urban projects. A
multi-stage random sampling technique was used to select seven anganwadis from each of the projects in
cluded in the study.
Gc
rar
an
Respondents
For indepth information, a sample of the following categories of target groups were selected within the anganwadi area.
pn
Children
0-3 years
3-6 years
Women
Expectant mothers
Nursing mothers
Other women (15-45 years)
Hi
10
10
10
5
5
i)
40
Total
For each ICDS project area, a similar target population sample categorized as above was selected from a
non-ICDS area, located in the neighbourhood of any one of the seven AWs to serve as a control group.
ii)
The team of ICDS functionaries namely AUWs, Supervisors and CDPOs comprised an important set of re
spondents. The concerned functionaries from the selected projects included 698 AWWs, 328 Supervisors and
91 CDPOs. Two community leaders available were interviewed from each of the selected AWs out of
pradhan/sarpanch'lambardar. secretary of youth club, school headmaster/teacher. president of mahila mandal,
councillor of municipality, and reputed/recognised community leader. In all, 1,311 community representatives
were interviewed for the study.
Hi)
Tools
vi)
iv)
v)
Ten proformae schedules were devised to collect information. These were administered in local language
to facilitate communication with respondents. Besides interview, observation method was also used for collect-
I
(xxiv)
ing information pertaining to delivery of services at AW level. The available reports, records, guidelines and
other documents formed an additional source of information.
Operational Details
pro-
Twenty research teams consisting of four members each, were deployed to collect data from 100 blocks
spread over 25 States and one UT. In each team there was one regular faculty member of NIPCCD and three
research rnvestigators recruited locally at the project level. Senior faculty members were assigned the task of
coordinating work of the teams, monitoring and supervision of data collection, and maintaining liaison with the
concerned State Governments for smooth completion of data collection within the stipulated time of one
gust 199T Pr°JeCt F°r co,,ectln9 data* 3,1 teams worked simultaneously in different projects from April to Au-
eas;
n in
Ensuring Data Quality
’ for
nets
roxdiss. A
► in-
an-
The design, scope of the study and tools were planned in consultation with members of the Research
Aduisory Committee. All members of the research team concerned with data collection were given
training in procedures of implementing the design, with a focus and emphasis on filling up the schedules
and its coding frame. The team leaders checked and countersigned euery schedule administered bu
the Inuestigators. Superuisors (senior faculty members of HIPCCD) visited various data collection sites
to oversee the work in progress. Rigorous editing was carried out to detect errors and omissions in
entries of the schedules. It aimed at ensuring accuracy, reliability, internal and external consistency
and uniformity in the recording of data, and improving the fitness of data for feeding and tabulation.
Besides manual checking, the data was further revalidated at the time of data entry by using a specially
developed software to check range/consistency of every coded response of all schedules.
Computer facilities for the study were provided by the National Informatics Centre (NIC) of the
Government of India. Simple statistical measures such as frequencies, percentages, averages and
ranges were used for interpretation. The analysis was done separately for rural, tribal and urban projects
and data was collated for providing a national level picture.
This report has been prepared on selected indicators considered crucial for appraisal of the
programme. The main findings are given below.
Findings
Implementation of ICDS
i)
Over 80 per cent AWs were easily accessible and were located within 3 km distance from beneficiaries'
habitat As compared to PEO study (1976), there was considerable improvement regarding this aspect
A large majority of AWs (60%) were found to have clean surroundings and were located in an environ
ment considered safe, posing little or no danger to children from traffic, pollution, etc. In around 75 per
cent AWs, taps and handpumps were the source of water supply. Further, over 80 per cent AWs had
no toilet facilities available and 78.8 per cent AWs had unsatisfactory drainage system.
n a
H)
Around 67 per cent AWs of rural and urban projects were housed in pucca buildings, whereas 50 per
cent AWs in tribal areas were being run in kutcha and semi-permanent structures.
rend
of
lai.
'es
Hi)
Separate storage facilities for ration were available in 67 per cent AWs.
iv)
Indoor and^outdoor space was rated adequate for conducting pre-school and play activities in only 50
v)
About 20 per cent sanctioned posts of ACDPOs and 28 per cent of Supervisors were not filled up
whereas over 95 per cent AWWs and Helpers were in position.
vi)
The backlog in job training was 20 per cent, 16 per cent and 25 per cent for AWWs, Supervisors and
CDPOs respectively. The backlog for refresher training was around 30 per cent for all categories of
functionaries.
ge
(xxv)
vii)
As compared to earlier national level evaluations (PEO, 1976; Ministry of Welfare, 1981 ], there was a
definite improvement in the educational qualifications of women appointed as AWWs. In the present
study approximately 50 per cent AWWs were matriculates and 13 per cent were above matric.
riii)
With respect to time allocation, it was found that AWWs were devoting one to two hours in a day in con
ducting pre-schdol education activities (60%), another one hour in distributing supplementary nutrition
(79.2%) and an hour in maintenance of records (80%). About 50 per cent AWWs were spending one
hour on home visits which is too short a duration to visit even one household and achieve any mean
ingful results.
ix)
About 74 per cent CDPOs had undergone job training and a majority had job experience of over 5
years.
x)
Fifty per cent CDPOs were able to visit less than 20 AWs in a month due to too much administrative
work, non-accessibility of AWs, inadequate transport, holding additional charge, etc. Therefore, a
CDPO visited an anganwadi once in three months, which is too infrequent to bring about any improve
ment.
xi)
The kind of support provided by CDPO was limited to inspectjon, and verification of stocks and re
cords. Educational and training support like demonstrations, discussion of problems, participation in
activities and holding meetings was carried out by a very small number of CDPOs.
Mi)
Five major problems faced by CDPOs were political interference, lack of community participation, too
much administrative work, non-accessibility of AWs and inadequate training of functionaries.
xiii)
Steps taken by a few CDPOs to strengthen ICDS programme were holding frequent meetings with
functionaries and parents, training AWWs and improving coordination with health functionaries.
xiv)
In case of 40 per cent Supervisors each of them was looking after over 30 AWs. As a result, only 29
per cent were able to meet the prescribed schedule of visiting all AWs once in a month. A majority of
the Supervisors were aware of their supportive role and reported to have conducted both, educational
and skill building activities, during their visits to AWs.
It was found that ANMs extended support to AWWs in health check-up (57%), immunization (80%) and
referral services (35%). However, for other aspects like identification of children at risk, growth monitor
ing and NHE. only a small percentage of workers received assistance.
xvi>
At the anganwadi level, support services from other departments were found to be adequate. The
average number of elementary/primary schools were 135, 150 and 154 in rural, tribal and urban areas
respectively. Early Childhood Care and Education Centres were less in number in urban projects as
compared to tribal and rural. All AWs of the study were covered under the jurisdiction of
PHC/CHC/sub-centre. However, it is a matter of concern that only 40 per cent of AWs had this facility
available in the particular village/ward where AWs were situated.
Beneficiaries
i)
The profile of the households was in line with the guidelines prescribed in ICDS scheme for selection
of beneficiaries. Both ICDS and non-ICDS samples matched to near perfection on socio-economic in
dicators. namely, caste, land ownership and income. Thus, these were considered statistically compat
ible for ascertaining the impact. Around 50 per cent households were marginal and landless labourers.
A large majority (75%) were Scheduled Castes and Scheduled Tribes in the tribal areas. However, in
rural and urban areas, 60 per cent belonged to other caste groups. In all projects, 45 per cent families
were having monthly income less than Rs. 500/- and a small fraction (5%) was in the income group
of Rs. 2,000/ and above. Almost all households were nuclear which was an unusual finding from
sociological point of vieVv and only 2 per cent households had family size of more than ten members.
ii)
In ICDS areas, expectant mothers were utilizing, services of health check-up (50%), immunization
(46%/ NHE (33%) and supplementary nutrition (47%). In non-ICDS areas, the health services provided
(xxvi)
vas a
esent
by PHCs/sub-centres were being utilized only by around 30 per cent expectant mothers. The differ
ences in 1CDS and non-lCDS samples were maximum in case of tribal projects, pointing to the effec
tive role played by ICDS in mobilizing the health system in making health services available at the
»con
trition
g one
nean-
doorsteps of the beneficiaries.
iii)
In the tribal areas, there was short fall of about 20-25 per cent in coverage of nursing mothers under
various services of ICDS. Women in non-ICDS areas nad no access to supplemcritaiy nutrition under
any development/social scheme posing threat to their well being. A case is made for further expansion
to cover this vulnerable beneficiary category under supplementary nutrition.
>ver 5
iv)
Children (0-6 years) were being adequately covered in both, rural and urban areas by ICDS. Hdwever,
there was a shortfall of about 20 per cent in tribal areas. Efforts are required to improve the outreach
of the programme. The contrast between ICDS and non-ICDS areas was reflected particularly in poor
utilization of health services, for both, health check-up and immunization, as only 26 and 30 per cent
children respectively were being covered under these services. Further, both supplementary nutrition
and pre-school education coverage was negligible due to non-availability of pre-schools, thereby de
lative
Dre, a
irove-
priving a large number of children of its benefits.
id re
ion in
v)
Only 8.2 per cent households rendered some support for implementation of services. Across projects,
higher percentage of families in tribal areas came forward to participate in ICDS. Community partici
pation was non-existent in non-ICDS areas due to non-availability of community based programmes.
n, too
s with
DeUvery and Impact of Services
5.
nly 29
)rity of
Hional
A. Nutrition
i)
and
jnitor-
e. The
i area:
cts as
on of
facility
The extent of coverage of the target population, both of children and women, for supplementary nut
rition in the present study showed an improvement when compared to the findings of earlier national
level studies (PEO, 1978; NF1, 1988). A large majority of the registered beneficiaries were availing
supplementary nutrition. Comparatively, a smaller percentage of expectant motherajL3gJMJfaan nurs
ing mothers (50 %) were enlisted at AWs for receiving supplementary food. The coverage of children
(0-6 years), both for rural and urban areas, was above the prescribed norm of 40 per cent of the total
target population. However, enlisting of children In the tribal areas fell short by 10-18 per cent of the
norm of 75 per cent coverage for supplementary nutrition.
ii)
The distribution of supplementary food was reported to be d/srupted for over nintydays in about 27 per
cent AWs in a period of one year. The average number of days for disruption in a year worked out to
be 63.7~~days per AW. Higher percentage of AWs in the tribal and rural areas reported disruption as
compared to AWs in the urban areas. The main problems enlisted by functionaries were non-availa
bility of fuel, insufficient utensils, children taking food home, poor quality of food items, community’s
interference and poorly maintained records.
ection
n/c inmpatjurers.
ver, in
milies
group
; from
ers.
ization
Dvided
iii)
About 38 per cent urban, 29 per cent rural and 19 per cent tribal AWWs reported that the food items
normally served as supplementary nutrition in AWs were not acceptable to the community. The*
reasons reported were being difficult to digest, causing diarrhoea, not tasty and not fit for consumption.
iv)
Fifty seven per cent’ nursing mothers perceived supplementary food as a supplement to their diet and
a large majority reported to have liked the taste. About 50 per cent felt that food items had variety.
v)
The prophylaxis programmes, both for vitamin A and iron deficiency, had better coverage of women
and children in ICDS areas as compared to non-ICDS areas. The predominant role played by AWW in
the coverage emerged clearly as 60 per cent of the beneficiaries reported that these supplements were
distributed by AWWs.
(xxvii)
I
vi)
It was found that 78 per cent AWWs have reported conducting NHE sessions atieast once in the last
three months. In all types of ICDS projects, oalY_about 50 per cent of the enlisted women in the, age
group 15-45 years were receiving NHE. The methods used were mainly discussions (65%-84%) and
demostrations (40%-44%). Almost all of them found it useful. AWWs and Supervisors indicated several
constraints faced by them in conducting NHE sessions; major one being the apathy and disinterest of
the target population to cooperate in assembling at one place at a specified time to attend the session.
vii)
Higher percentage of babies had low birth weight in non-ICDS areas as compared to ICDS areas. In
tribal areas, the difference was double (ICDS-43.3% ; Non-ICDS-80%).
viii)
The difference in the average weights of children from ICDS and non-ICDS areas were negligible for
children in both 0-3 years and 3-6 years age groups. In fact, prevalence of PEM became apparent due
to average weights being lower than the prescribed norms.
ix)
The nutritional status of children in ICDS areas was better than that of children in non-ICDS areas. The
percentage of normal children was 35 in ICDS areas and 31 in non-ICDS areas. Non-ICDS areas also
recorded three per cent more children in Grade III and IV malnutrition as compared to ICDS areas
(ICDS-10.8%; Non-ICDS-13.11%). The differences were found to be more prominent in urban pro
jects.
x)
About 36 lPer cent AWWs were not able monitor growth of children. The reasons given were non-availability ofgrowth charts Jack of skills in filling growth charts, weighing scales not in working condition,
xi)
Twenty five per cent nmsin^roQtbers in ICDS areas against 19 in non-ICDS areas had introduced
s^22.l:soJlds to their jri[agts. The proportion was too small and reflected lack of impact of NHE in profff^
otmg positive feeding practices. This possibly was the contributing factor for higher percentage of mal
nourished children in the age group 0-3 years in ICDS areas.
B. Hea th
i)
Health check-up was carried out, both for women and children, in 85 per cent of the sample AWs at
ieast once during the last three months of the reporting period. In 56 per cent cases, AW was used as
3
hea,tb check'up- The Percentage of health check-up performed by MOs was higher in
urban AWs as compared to AWs in rural and tribal areas. A small percentage (17%-28%) of AWWs
enlisted various constraints in conducting health check-up such as belief in traditional system of
medicine, lack of awareness, reluctance to come for check-up, and shortage and unwillingness of
medical staff to visit AW for conducting health check-ups.
ii)
Fifty per cent mothers in ICDS areas got their children (0-3 years) medically examined as against 38 3
per cent of their counterparts in non-ICDS areas.
iii)
ThC ir°nQa9e Of/h^rZn f°r immunizadon was fou"d to be higher in ICDS areas as compared to
non-ICDS areas for BCG. measles, polio and DPT. The maximum percentage of children immunized
was in urban areas, followed by rural and tribal areas. Immunization coverage as reported by mothers
Rrr -.o a 9reat
With tKe reC°rdS aVailab,e at AWs' The covera9e figures were 50 per cent for
BCG; 32.6 per cent for measles; 47.26 per cent for DPT, and 37.5 per cent for polio for children in the
age group below one y^rJhe coverage for this age group was better than that reported in the study
conductea by NIHFU (1988). In around 47 per cent AWs, immunization could not be carried out as
scheduled due to non-cooperation of health staff and superstitions of parents.
iv)
Fifty two per cent expectant mothers in ICDS areas received tetanus toxoid vaccine against 45 per cent
women in non-ICDS areas. Difference was largest between the two samples in the tribal areas. In
non-ICDS sample, tribal mothers were not even aware of the need to be vaccinated.
(xxviii)
V)
Referral services were provided in 84 per cent AWs of the sample. One third of the workers faced prob
lems like parents did not pursue further treatment, non-availability of transport and hospital located far
off, which adversely affected the delivery of referral services in all types of projects.
vi)
Both in ICDS and non-ICDS areas, the most prevalent practice was to have the delivery performed at
home and in 38 per cent cases, the birth attendants were untrained. However, such cases were more
common in non-ICDS areas. Higher percentage of mothers in ICDS areas received post-natal care as
compared to their counterparts in non-ICDS areas. A lower percentage of tribal women, both in ICDS
and non-ICDS areas, received post-natal care as compared to women in rural and urban areas.
Further, a majority of tribal women from ICDS and non-ICDS areas felt that health services played no
significant role in maintaining the health status of their children (0-3 years).
vii)
IMR recorded for ICDS samples were 81.4; 74.0 and 66.6 for urban, tribal and rural projects respec
tively. These figures were lower than the national SRS estimates for the year 1989. In ICDS areas, DDR
was also found to be less. These two indicators reflect better utilization of health services during an
tenatal and post-natal period and better immunization coverage in ICDS areas.
C. Pre-school Education
i)
The coverage of children 3-6 years old under pre-school was above the norm of 40 per cent for both,
rural and urban projects (around 56%), but was short by 5 per cent in tribal areas. On an average, out
of 77 preschoolers per anganwadi, 43 were enrolled and around 31 were attending pre-school.
ii)
Mothers reported that a large majority of these children (61%) stayed in the anganwadi for its full du
ration and participated in all its activities.
iii)
Comparison between ICDS and non-ICDS areas indicated that relatively a very small number of chil
dren (23.5%) in the age group 3-6 years in non-ICDS areas were receiving pre-school education, the
number being smallest in tribal projects. The coverage of children in ICDS areas under PSE in all types
of projects was about 85 per cent with no specific sex differences.
iv)
About 50-60 per cent children were able to count numbers upto 50 and could count five objects. Com
paratively, a smaller number was able to recognize colours and label them. Almost half the children
exhibited manipulative skills of holding a crayon and colouring a circle.
v)
Of all the children (6-14 years) currently in primary school, 85 per cent in ICDS and 15 per cent in
non-ICDS areas were with pre-school experience respectively. This points towards better school enrol
ment in ICDS areas compared to non-ICDS areas and the role played by PSE in retention at school.
vi)
Disaggregation of information about children in the age group 5-14 years, both in ICDS and non-ICDS
areas, indicated that 89 per cent children with PSE experience were found to be continuing their edu
cation in primary school as compared to 52-60 per cent without PSE in both ICDS and non-ICDS
areas. Lesser percentage of children with PSE were found in the never enrolled category, both in ICDS
and non-ICDS samples. The findings clearly indicated the positive role played by PSE in promoting en
rolment in elementary school, reduction in dropout rate and greater retention in primary school.
D. Community Participation
i)
AWWs reported that it was mainly women (55%), followed by community leader (47%) and adolescent
girls (33%) who offered help in conducting AW activities. Contribution made in kind was negligible and
restricted only to providing site, building and firewood/fuel. Tribal and rural community members pro
vided support to higher percentage of AWWs as compared to their counterparts in urban areas.
ii)
Mahiia mandals were operational only in 49 per cent AWs. Help rendered was restricted to collecting
children for immunization (47%), organising camps (38%) and preparing supplementary food (35%).
(xxix)
■
iii)
Out of 1.311 community representatives included in the sample, only around 60 per cent of them had
rendered some kind of support to ICDS programme. A majority of them had solicited support for
AWW, motivated the community and provided space for the centre. Participation of tribal community
leaders was much more compared to their counterparts from rural and urban areas.
Ten to thirty per cent community representatives informed that they were consulted by ICDS
functionaries at the initial stages of project planning for decisions regarding selection of site, identifi
cation of AWWs and Helpers, etc.
iv)
v)
ICDS functionaries did not approach community representatives for any help in most cases. Eighty per
cent community representatives indicated their lack of awareness about ways and means by which
they could make contributions to the programme. The findings indicate the need to educate the com
munity about their role and also the need for evolving effective strategies to augment community par
ticipation in more feasible ways.
1
In 39 per cent AWs of the study, adolescent girls were being involved in various activities of the anganwadi. There is scope for involving a larger number of girls in the programme. The new scheme envis
aged for adolescent girls seems viable. If implemented effectively, it could result in tapping this re
source of the community for strengthening ICDS.
Conclusions and Recommendations
The data and information collected for the study was rich, both, in content and magnitude. Exhaustivt
analysis could not be carried out for this report due to constraints of time. Only those crucial aspects, whicl
were in accordance with the scope and objectives of the study were analysed. However, it is possible to dis
aggregate data to take out State level reports on status of ICDS and put the valuable empirical data t<
maximum use. Such an attempt would suggest follow up actions specific to each project as well as for the Stab
as a whole.
Important recommendations having policy implications are summarized below :
(0
There is a need to upgrade the physical infrastructural facilities of AWs. A separate storage space fc
ration should be made available. Semi-permanent anganwadi structures need to be progressively re
placed by permanent and pucca buildings. Community’s contribution towards this aspect needs to b
mobilized. Taps and handpumps should be installed within the premises of AWs wherever possibk
Categorical instructions may be issued not to locate AWs in the areas predominantly inhabited b
upper class and upper caste population, as it restricts and hinders utilization of services by the lowf
castes and poor beneficiaries.
(ii)
There is a need to experiment with some innovative methods of imparting refresher training. The po;
sibility of involving academic and technical institutions in strengthening continuing education, throug
peripatetic training in the field needs to be explored. The feedback on involvement of medical college
in training health functionaries of ICDS has been encouraging and positive. Continuing education o
similar lines may be given to ICDS functionaries.
(iii)
It should be mandatory for the Project Officers to organise frequent training workshops at the projelevel. The concept of establishing a resource centre at CDPO’s office also requires serious conside
ation and policy decision.
(iv)
Supervision should be strengthened through appropriate measures. No Supervisor should have moi
than 20 AWs under her charge. A double or additional charge is detrimental for the supportive rol
There is need therefore, to create a post of a substitute Supervisor in every project.
(v)
Participation of ANNs in providing referral services, health check-up, home visits and NHE sessior
needs to be promoted further. Both AWW and ANM should work in close collaboration. Ways ar
means need to be worked out to make them join hands for taking care of health needs of women ar
children. In order to improve accountability, work assessment report of ANMs working in ICDS are.
may include evaluation comments of CDPO in charge of the project as well.
(xxx)
(vi)
Coverage of children under supplementary nutrition, and particularly that of underthrees, should be
improved through exhaustive door-to-door surveys, encouraging consumption of food at the anganwadi and enhancing mothers’ awareness about appropriate weaning practices and supplementary
foods for underthrees.
(vii)
Implementation of NHE was found to be far below the desired level. It is suggested that Supervisors
should be given the responsibility to hold formal NHE sessions regularly in AWs under their charge.
Rigorous monitoring by CDPOs and active participation of health functionaries can improve im
plementation of this component For group formation and collecting women at one place for NHE ses
sions, locally popular sociai/recreational events may be organised. Utilization of folk media such as
nautanki, kathputli, etc. need to be included in the training curricula of functionaries to strengthen their
skills in imparting NHE effectively.
I (viii)
There is tremendous scope for improving the implementation of PSE component Non-availability of
material for play and learning is one of the major constraints. Efforts are needed to provide a minimum
set of appropriate educational aids and material at every AW. Children of the study did not perform well
on identification of colours and other cognitive tasks. This emphasizes the need for conducting crea
tive and cognitive activities as an integral part of PSE.
(ix)
Irregular supply of equipment food items, play material and medicine kits is one of the major problems
in implementation of ICDS. The State Governments should take appropriate measures to streamline
supplies for smoother implementation of the programme.
(x)
In line with earlier researches, community participation revealed itself as a very weak link of ICDS prog
ramme in the present study as well. It is imperative that community representatives should be involved
right from the preparatory stage of initiating a project The feasibility of involving adolescent girls in
ICDS received some support from findings of the study. Hopefully, the new experiment initiated in
ICDS to cover adolescent girls, would take roots and strengthen community participation component
as well. All functionaries reported that it was difficult for them to elude the pressure imposed by local
politics. Some discretion should be exercised in the involvement of individuals/agencies with political
alliances. Effective ways of augmenting participation need to be evolved. A^Ws apparently do^not have
the requisite skills for promoting participation. CDPOs and Supervisors should take appropriate initia
tive in this regard.
(xi)
It was observed that coverage and outreach of services need to be improved in tribal areas, keeping
in view the topographical factors. It was felt that in urban areas also, the services provided were minimal
and the situation was worse than that in tribal and rural areas. Steps need to be taken urgently to im
prove the situation in urban slums.
(xii)
The positive impact of ICDS on health, nutrition and education of children and women makes an ex
cellent case for further expansion of ICDS to progressively cover disadvantaged families by integrated
services to ensure survival and development of children and women.
The study has provided substantial empirical information with respect to implementation of ICDS, its be
neficiaries and the impact of various services on the target population. It is hoped that this endeavour will add
to our understanding of ICDS and would result in important policy decisions. We must take concerted steps at
all levels to strengthen ICDS programme so that every child’s right to develop to his full potential and grow op
timally is realized.
(xxxi)
ANNEXURE-y
Statement showing th e position of Anganuad® Buildings as on 31.3.2000
SI.
No,
1
: Name of the
01 st.
__ 2
: No.of :No.of
AUCs
A'JCs
san»
fun.
3
Anganwadi Centres functioning in
Mahila: Youth
: Commu
Man dal
Asso clnity
bl d.
at 5 on
bld.
4
5
1) Bangalore(U)
1192
1192
2) Bangalor e(R)
1891
1888
3) Bijapur
1301
1301
12
7
6
47
:0 un
8
: Ran
ch a ya t
bld.
:Rented
bl d.
J
Tempies
9
10
11
:Schools: Make
shi ft
a r r an g emen t
13
12
I Tot al
T4~
123
387
153
158
69
126
117
1 192
236
29
1S9
435
120
1888
94
79
3 28
85
40
1301
21
4 72
416
15
50
293
31 7
17
1 21
733
39
228
107
94
32
1372
258
63 7
787
299
462
36 73
143
46
107
117
1100
4) Bell ary
1372
1372
1
5) Belgaum
36 73
3673
29
19
44 8
734
6) Bidar
1151
1100
7
7
162
458
53
7) Bagalko te
1366
1360
18
22
26 7
31 7
92
50
403
102
89
1360
8) Chikmagalur
1 213
1179
31
16
79
5 84
61
31
52
178
147
1179
9) Chamaraj an agar
1085
1085
3
8
63
491
51
85
26
69
289
1085
973
78
84
49
53
9
1336
86
1262
10) Chitradurga
1336
1336
_2
26
62
11) Da vang ere
126 2
1262
3
10
63
776
70
93
58
103
1 2) Dharuad
806
806
23
19
71
312
46
29
282
24
13) Gulbarga
2350
2350
15
20
194
1126
101
3 20
226
204
10
14
111
298
21
244
888
23
126
44 2
14) Gadag
826
826
15) Hassan
1594
1594
1249
14
806
144
2350
330
40
2
826
41
18
160
243
1594
55
47
449
92
01
1249
263
2356
16) Haveri
1 249
17) Kolar
2361
2356
01
07
310
771
3 84
90
211
319
1 8)Karwar
120 2
1 202
26
38
196
6 20
84
32
63
143
19) Koppala
893
893
12
19
158
357
40
39
152
91
20) Mysore
1930
1930
3
4
380
795
172
120
103
21) Mangalore
1775
1732
13
40
166
1010
60
60
12
22) Mandy a
1655
1655
12
13
354
500
92
144
153
208
1202
15
893
25 7
96
1930
3 24
47
1732
1 79
1655
23) Madikeri
692
692
42
2
144
380
31
28
8
49
8
692
24) Ralchur
1308
1308
01
09
123
609
146
167
115
100
38
1308
25) Shimoga
13 23
1322
9
20
184
677
86
70
96
133
47
1322
26) Tutnkur
233 7
2336
4
8
191
1365
124
129
88
3 26
101
2336
27) Udupi
1027
1027
9
23
184
54 7
35
15
198
16
1027
To t al
40170
40026
315
502
5289
16883
266 2
,’‘4415
4319
2708'
40026
2933
Io
0*
»
REPORT ON DISCUSSIONS HELD WITH SHRI B.V. KANTHI, Dy.
Dir. (ICDS) OF Dept, of WC D, Karnataka on 11.08.2000
1. Functioning ofAnganwadis :
Out of 40,170 Anganwadis sanctioned in the state 40,012 are functional. Though no.
of AWWs are less (39469 Anganwadi workers, 39926 helpers) still the others are
functional by making someone incharge by adjustments locally.
(Appendix A).
2. Shortage of Staff:
There is an acute shortage of supervisors with only 660 in position out of the
sanctioned 1862 (shortfall of 1202). (Though Govt, sanction for recruitment exists
technical ban due to indecision regarding rural pass marks, the posts cannot be
immediately filled up). Shortages in other staff is minimal (Appendix A).
3. Training:
CDPO's and ACDPO's are trained for 2 months at NIPCCD Bangalore. Supervisors
are trained at MLTC (Middle Level Training Centre) Ujire (DK district). Anganwadi
workers are trained for 3 months at 26 training centres (list attached Appx ’B').
training has been intensified as UDISHA (World Bank assisted scheme, all over
India) (Document attached, Appendix 'A') An innovative training programme was
carried out in 1995 for 6 days through UNICEF to clear the backlog of training.
Every 2 years refresher training is carried out for AWWs.
1
Minimum qualification for AWW is 7th std for rural, X std for urban, graduate for
supervisor, MSW or Master in Home Science for ACDPO's & CDPO's.
4. Buildings :
Only 30% of Anganwadis have own buildings. (Appendix C). recently it was felt that
loans could be taken from HUDCO for constructing new buildings but the interest
rate was too high. Finance department is seriously considering sanctioning funds in a
phased manner (Rs. 30 Cr. For 2000-01 may be sanctioned). Cost of each building
works out to slightly above Rs. 1 lakh.
5. Central Funding :
ICDS is 100 percent centrally sponsored scheme (CSS). Administrative and
establishment expenses are totally borne by centre. During 1999-2000 Rs. 7813 lakhs
sanctioned by GOI under CSS. Funds released were Rs. 5111.35 lakhs, against
amount spent by Zilla Parishads Rs. 6424.15 lakhs (Appendix 'D'). This year 20002001 Rs. 7788 lakhs has been sanctioned.
6. State Expenditure:
The state govt, only funds the nutrition supplement through the Zilla Parishads. (Cost
per child/day is Rs. 1.25 and for malnourished child grade III & IX is Rs. 2.50).
During 2000-2001 the state spent Rs. 3634 lakhs under planned expenditure,
Rs. 6022.7£8fe® lakhs under non-planned expenditure, Rs. 962 lakhs under SCP
\\P450\d\Dr. SKK\REPORT ON DISCUSSIONS HELD WITH SHR1 B.doc
,
.
•
:h
(Special Component Plan - Scheduled casts, etc) and Rs. 289 lakhs on TSP (Tribal
Special Plan). Every month 1/12th of the annual amount is released to the ZP’s
Expenditure during 1999-2000 is given in Appendix ’E’ i.e. Rs. 7741.06 lakhs.
7. Vehicles and Equipment
Vehicles are supplied by UNICEF at the scale of one per project (usually one block).
There are a total of 185 projects (99 tribal,10 urban and 176 rural). If a block has
more than 200 Anganwadis then an additional ACDPO is authorised and hence an
additional vehicle is provided. POL is also paid by centre.
Weighing scales (Salter scales) were supplied initially by UNICEF for all the 40,000
Anganwadis. There is an acute shortage of 700 scales and these are likely to be
procured within a month. However many of the original scales supplied by UNICEF
have become faulty and require replacement. (Qty is being assessed.).
8. Medical Kits:
Earlier central government was supplying the kit annually. This year sanction has
been accorded to the state government to purchase locally. Earlier kit used to cost
Rs.300/- now cost estimated at Rs. 600/-. This will be provided locally at district
level through ZP.
9. Other activities ofAIVIV:
The ICDS has viewed seriously the increasing involvement of AWW in pulse polio
programme, census, census of livestock, leprosy, and RCH. Hence they have taken
measures to reduce this and remuneration of Rs. 0.25 per house visited or Rs. 250/per month etc. to act as a deterrent.
10. Relationship with PHC, SC, ANM, etc.
The AWW has no problem working with the ANM’s now. Earlier conflicts used to
arise due to FP targets. Also, all cases of malnutrition taken to PHC’s. Monthly
meetings at Division and Dist. Level with PHC doctors and DHO’s etc.
11. Shortage ofgrowth charts.
This was initially supplied by UNICEF. Now some shortage. Also plan to print new
growth chart based on NIPCCD recommendations to include developmental
milestones also (sample attached) and a copy will be given to the mother also.
12. Teaching aids and toys.
Earlier these were given only one time. Now Rs. 500/- per year per Anganwadi. This
will be provided locally by ZP. Also Rs. 5 crores sanctioned by government for
improving Anganwadis for purchase of durries, fans, utensils etc.
13. Procurement ofNutrition supplement:
Nutrition supplement is given by energy food twice a week in 21 districts and thrice a
week in 11 districts (Based on location of Agro products) Food is based on CFTRI
formula' (see attached composition), prepared by Karnataka State Agro Coi#.
\\P450\d\Dr SKK\REPORT ON DISCUSSIONS HELD WITH SHRI B.doc
5^^ n .
Products. 1 kg packets in 25kg container, ^months shelf life. Other days rice
(through PDS) CDPO at Taluk level procures and distributes through contractor
directly to the Anganwadis (monthly). Firewood or k’oil Rs. 75/- per month to be
given through gram Panchayat. Now directly deducted from ZP and given in
Anganwadi account. Problem still in urban area.
14. Sthree Shakti - Project for empowerment of women being launched. 1 lakh SHG’s
(i.e. 2-3 per Anganwadi) each will have a revolvmgjund_of Rs^ 5000/-, Rs. JO Cr.
being sanctioned. (Budgeted for Rs. 72.67 crores ). Details will be collected later
on launch of programme.
15. Integrated nutrition project (INP) Being launched shortly as pilot project in
Gulbarga, Raichur, Tumkur and Chikmaglur. For children below 2 years of age.
Consultant Tara Gopal Das. (Jt. Secy. Nutrition ^Veena Siva Ram Rao from
Karnataka, so interested in Karnataka first). Details will be made available later.
16. Malnourished children : Totally 11,683 children in grade III & IV in Karnataka.
Immunization status dealt by Health Dept, so no disparity in figures.
17. Mode evaluation : Evaluation done by MODE commissioned by UNICEF on ICDS
functioning in Karnataka in Dec 97 - Feb 98 is also perused, (copy available).
\\P450\d\Dr SKK\REPORT ON DISCUSSIONS HELD WITH SHR1 B.doc
Appendix 'D'
Information ofAnganwadis and budget of Karnataka (1999-2000)
No. of Anganwadi Sanctioned
: 40,170.
No. of Anganwadi functioning
: 40,012.
No. of Anganwadi workers in position
: 39,469
No. of Anganwadi helpers in position
: 39,926
Total budget allocation under CSS for 1999-2000 in lakhs : Rs. 7,813.00
Total Grants released by G.O.I during 1999-2000 in lakhs : Rs. 5,111.35
Total amount spend by the ZP's during 1999-2000 in lakhs : Rs. 6,424.15
Supplementary Nutrition Programme
Total allocation for the year 1999-2000 in lakhs
: Rs. 8,672.75
Expenditure in lakhs
: Rs. 7,741.06
6o I
ScMnsCo"
Anganwadis Training centres in
Karnataka
SI
No.
District
1.
Bangalore
Bangalore (U)
2.
Anekal
Bangalore (U)
3.
Kadur
Chickmagalur
4.
Madekeri
Kodagu
5.
Gulbarga
Gulbarga
6.
Mysore
Mysore
7.
Dharwar
Dharwar
8.
Ankola
Utthara Kannada
9.
Yellapura
Utthara Kannada
10.
Guledgudda
Bagalkote
11.
Amingad
Bagalkote
12.
Kukkanoor
Kopp al
13.
Belgaum
Bel gaum
14.
Ullal
Dakshina Kannada
15.
Ujire - MLTC
Dakshina Kannada
16.
Manipal
Udupi
17.
Hassan
Hassan
18.
Arasikere
Hassan
19.
Bethamangala
Kolar
20.
Sirigere
Chitradurga
21.
Mandya
Mandya
22.
Harapanahally
Davangere
23.
Davangere
Davangere
24.
Shimoga
Shimoga
25.
Tumkur
Tumkur
26.
Kanakpura
Bangalore (R)
*
Government —
«■
common disabling diseases in children
)urse
extent of malnourished children, blind children,
anaemic children
i
causes of mortality and morbidity among children (01 year, 1 -3 years, 3-6 years)
r
Low birth weight, unimmunized mothers, disabling,
killer diseases, poor health care of female infants
I
I
I
Educational Status
Creating awareness in the AWW about
number of children in the 3-6 years age group who
are enrolled for preschool education in the
baiwadis/anganwadis vis-a-vis the total child
population!
number of children enrolled in primary schools; low
enrolment among girls
number of children who drop out by class II
Reasons for children not going to school
need for children to supplement household income
household chores and looking after younger siblings
boys given preference for schooling
Reasons for children dropping out of school
economic
poor quality of education
educational content boring and not related to their
requirements
State)
lack of clothes, books etc.
3. Status of Women in India
□iciting information from AWWs about the educational,
employment, social status of women in their villages*
AWW will be able to
Discussion on low status of women in the society
the
J g. — describe the health, nutrition,
education and economic status
wl
°f toomen
nd
’ ‘NB:
I■
I.
low priority assigned to their health
double burden of economic activity and household work;
Discussion must highlight the problems of women and children in different project areas; urban,
urban slums, rural, tribal to which the trainees belong.
■n
41
■
■ • ■
J
• *
s
I
4
I
— understand and be sensitiue
to the problems of toomen in
the country
i
1:1
|i y
participation in agriculture, animal husbandry activitie
no decision making powers
low education and lack of awareness of their rights
both in the area of work and at home
limitation of activities to the home and family
no control over her income
sexual exploitation
early age of marriage
—- understand the need to improve Health and Nutrition
the status of women
Poor or no antenatal care or medical care
jlj
Eating last in the family, consuming only left-overs afte
the men have finished their meals
liffi'Hd'
’rr
Repeated pregnancies causing malnutrition,
deterioration in health, maternal mortality and low birth
weight babies
llll
U
■' I
j
ii
I
S.
— compare and contrast situation
of women from their areas with
the situation of women in
the country
I , I
II'
Continued hard physical labour through pregnancy*
Employment
Lower wages for the same job
Poor job opportunities
Poor working conditions
Problems of daycare facilities
Only undertake certain vocations deemed appropriate fc
women
I;
it
I;
II i'l'■! ■'
w
■
■Ii
I
■
Factors leading to low status
Economic dependence
Dowry system, desirability for a male child resulting in
female infanticide
Self sacrificing attitude
I
Cycle perpetuated when girls are taught to imitate mother.
Heed to raise status of women
I
educating a woman, educates a family
creating awareness among women so that they can
demand their rights
J
42
I
I
I
activities
Raise status by education and social awareness
programmes and raising age of marriage
r
■ rights
4. Heed for Child Development
Programmes
/
AWW will be able to
■— recall previous sessions to
state the need for programmes
for child development
Perspective on Social Problems
Major problems concerning women and children
(recall from 2/3)
Large population, poverty, malnutrition, disease, high
infant mortality rates, ignorance, poor housing
conditions, unsanitary conditions, lack of potable water,
illiteracy, poverty cycle
Importance of early childhood years as foundations for
future
srs after
Heed for health, nutrition and educational services for
children
w birth
Emergence of ICDS
icy
Starting of ICDS the major child development
programme in India
5. An Introduction to ICDS
AWW will be able to
riate for
ng in
lothers
can
— list the objectives,
package of services,
target group, scope of
the ICDS scheme
Cri-
ICDS
Lv i.1
i I t i
1
1. Philosophy
Scope
Objectives
Package of services
Beneficiaries
Coverage of population, geographical area
2. Staffing pattern
Anganwadi as the focal point in the delivery of
services
AWW as the key grassroot functionary
3. Observational visit to an ICDS project to see the
anganwadi centre, project office, office of the BDO,
PHC or sub-centre, office of the Panchayat, meeting
with CDPO, Medical Officer, BDO, AHM, LHV
community leaders, mahila mandals
Discussion on the field visit
4. Role of local bodies/voluntary organisation in ICDS
(in brief)
43
-,
„ .J. '<
WW***
; ffl
s
1 rainees perception of their role as AWW
..
AWW will be able to
Development of the anganwadi centre as a focal
point in delivery of services
Jref
— understand her role and
responsibilities in the ICDS
Job responsibilities and tasks of an AWW
i
1
!•:" "l it'
B \i
h i'f
J ■
JiI it
a 'i
.J.I
I 11
— understand her role in relation
to other functionaries of ICDS
7. Survey
AWW will be able to
— explain the importance
of undertaking a survey
i!
I ' I I1'
I ■■
■
I.fc
a
'J i
hl.
I
rmIJ
I!
j
Responsibilities of CDPOs, Supervisors and medical staff
as they relate to those of the AWW
'll!
Need for a survey to
identify beneficiaries
build rapport
enlist community participation
introduce the scheme to the community
8. Community Participation:
Concept and Importance
AWW will be able to
What is a community — the people in thefi'rea, voluntary
and other organisations, local bodies
What is meant by community participation
Why is it critical in the context of ICDS
— define what is a community
— understand the importance
of knowing the community
Knowing the community conditions, living conditions,
local customs, practices, values, traditions, caste
structure, power structure, social status, political influence,
exploitative forces, mythological values, resistance to
new ideas, acceptance of certain ideas, possible trouble
makers and rival groups, problems in the area of health,
nutrition and education.
Important leaders, people with whom to work
(Discussion must relate to the communities in which
the trainees work)
Need for creating awareness among people, increasing
consciousness, developing critical understanding of
society and awakening a sense of social responsibility
44
l
I
I
I
I
A
First preparatory task of the AWW
ii
Ii
).C
p
Need for updating survey data
(Note : Method of conducting survey has been dealt
with later in the course)
— explain the concept of
community participation
in the context of ICDS
I,
•
b. Role and Responsibilities
of AWWs in ICDS
10
I'
w.
Heed for -mobilising and motivating people for change,
creating a demand for the services
xzal
eschool Education
^dical staff
. Organisation of Hon-formal
Preschool Activities
Importance of early childhood years for overall
development of children
AWW will be able to
Heed and importance of early childhood stimulation
and preschool education
.
I
enumerate the importance
|i of early years for the child s
|
I
development
■— state why preschool
I education has been
I included in the ICDS
I
;l
I
and the role of play in
the overall development
of children
dealt
□luntary
Reasons for including PSE in the ICDS package
(recall session 4, need for child development
programmes and observational visit to AWC)
J
poverty
illiteracy
lack of home stimulation
universalisation of primary education
nutritional deprivation
occupation of mothers and consequent
lack of time for home stimulation
inadequate skills of parents for
stimulating children
r
Role of play in promoting overall
development in children
ions,
uence,
Use of non formal play way approach in
organising preschool activities
I
I
Readiness of children for school — role of
preschool activities
i to
vouble
lealth,
I
10. Development of Children
(0-6 years)
What is meant by growth and development
Stages of development
AWW will be able to
— explain how children
ch
grow from conception to
six years
sing
f
^ity
— differentiate between
normal and children who are
\different from normal
prenatal
infancy
preschool
Development of children during pregnancy
How children grow
i
Individual differences in children
I
45
it
i
■Rf’-iwii
— understand hoto children learn
through play way activities
~
.ro/f-in °r^riising
preschool activities through
xi_
, the
play-way approach
I
1
s 'lift
if
V-
r
biormai development — milestones in development
How children learn through
immitation
<■
repitition
modelling
■
i ■iil|
Heeds of children as they grow
Need for providing stimulation for child’s developmenl
|5‘
from the infancy period (recall)
11 IrI
Need to organise a variety of activities, songs, games
stones, exercises etc. for promoting the overall
development of children
!
I
■-
■
All activities promote all aspects of development, some!
activities promote some aspects more than others
I
i1
ii
1I
11
!;i
11
ii
»Ilk ft
I
rI ■' i
i il i |
Role of AWWs/mothers in satisfying the needs of
children
S
Recall traditional songs/stories AWWs are familiar with
i-/
11. Activities for PhysicalMotor Development
Activities that promote physical motor development
games; outdoor and indoor
guided and free play, action songs
AWW will be able to
— organise a variety of
activities to promote the
physical-motor development
of children
F''
activities like, threading, sorting, tearing,
clay modelling, folding, plaiting etc.
1
dramatisation of stories, creative movements
Him is
Il
— prepare aids and play
materials for organising
activities for physical
motor development
irF
!
hi
I
fr
IBB
'
iF'/i
f' ■’) i'l
il
ill
ill I
i 'IJ
ML
-1
organising activities in the anganwadi according tc
the age of children, activities for older and
younger children
Outdoor Games
(for large muscle development)
i
running, I sent a letter to my friend, In the pond u..
on the I''
bank, High and low, Oranges and lemons, jumping
from a low wall, hopping, skipping, pushing at an
I '
imaginary rope etc.
I
46
______ .
*
' wacs^snasjJwwxiL' - ■. sjt---- -
ZZZSS^S.
I _
■ '■ ■
**
I
•pment I:.
Points to be kept in mind while organising outdoor play
■'
keeping an eye on children while they play
play in space free from hazards
Indoor Games
Walking on a straight/curved line, walking on a rope,
crawling under the rope, jumping over a rope, rolling
the ball etc.
lopment
Action Songs
When you’re happy and you know it clap your hands,
games,
STFlt t HFTt,
it, some I?
ers
I
I
of
Fine muscle activities
I
ar with I
Threading beads, rolling beads from paper or mud,
sorting of grains, tearing paper, drawing on the floor,
folding paper or cloth, plaiting hair, kneeding clay etc.
ent
Dramatization of Stories
Creative movements/drama
Moving like a tree in the breeze, small seeds growing
into large trees
Preparation of aids for physical and motor development;
ball, beads of clay, sweet wrapper or paper; threading
frames, doll with hair made of wool for plaiting etc.
l
■
o
I
12. Activities for Language
Development
Skills needed for language development:
listening and speaking
a
II
I
n the
g
AWWs will be able to
— organise a variety of activities
to promote language develop
ment in children
— prepare aids and play material
for organising actiuities for
language development
Listening skills
•I
Organisation of activities to promote listening skills:
discriminating sounds made by different objects or mouth,
closing the eye and listening to sounds in the environment,
listening to the beat of different musical instruments
(dhapli, jhun-jhuna, etc.) listening to songs and
imitating these, singing the same song faster or slower
47
I •
--
ir
4III i I
/
i , I I?
■
,
Free Conversation
?haJ9co0nvhlldren USin9 90 °bject’ event’ a Picture
■
■
"i
1p I
oongs and rhymes
III 1
3i'i I
ii I I
Ii i
7:rTH
Singing songs with actions
su
i te d™'
Language games, riddles, question-answers
11.
3. Ac
fe, / De
Story Telling
■
ililli
If
II
!l
:
r j, I
i*
Points to be kept in mind for telling stories
II I
M I
jI
I.1,
I
Ii
I
!?'1
■'j
f
Activities for reading readiness
Sill
■ I1
-pre
for
co
seating of children
eye to eye contact
responding to children’s statements
asking questions about the story
making children think of different
ways to end the story
■'i
ii1'
— orc
ac.
co*
in
I=Xno's,ories'son9s'^^er^io™l
Ij
iiI
A'
™ste'
.
visual discrimination cards, charts, pictures
SSSE?=-'="“
P'‘
L\ ' •
-
through’pte^rrS'd'lng3™™Orieiltalio"
Bi
,
48
-. •;
r
5
W.
L
-‘i-''.•4^41%.
’•
picture reading, description of objects, events
ture
:a!
conversation among children
Writing readiness activities
I'
I
free drawing with chalk or pencil, malting patterns,
copying patterns, joining dots, drawing, writing names
of children, writing alphabet
fl^'
•Pi''
Preparation of aids for language development; flannel
board and flannel story figures, picture cards, picture
books, story charts, puppets — glove, finger, stick,
match box, flexiflans, maxiflans, masks, drums from
tin, sound boxes, rattles with cold drink caps,
ghungroos etc.
Jm,
/
13. Activities for Cognitive
Development
Activities for cognitive development
matching objects, pictures, patterns
mel
:ks,
I
s
j
i
AWW will be able to
| ■
— organise a variety of
activities to promote
cognitive development
in children
I
II
I - — prepare aids and play material
I
for organising activities for
J
cognitive development
I
I
tracing objects, pictures and making
patterns
discriminating between different pictures,
alphabets, objects etc.
serialisation, arranging things in a serial
order, from long to short, heavy to light etc.
grouping of items according to colour, shape, size, use etc
direction of left, right, front, back, above,
below etc.
■
I
Tte'
IH
■
| fl
ids
;on
number concepts like in and out, up and
down, thick and thin, one-to-one matching
counting the number of objects etc.
19
20^
Bl
Ii
environmental awareness, birds, animals,
flowers, trees etc.
I
Developing concepts of colour, texture, shape, size,
weight, smell, taste, time etc.
I
fli’
II
1I
Using the body to develop different concepts and
conducting preschool activities
49
If
I
■~i't
< M■
I life i'i
I
k|
S'' I
h
!
I
Organisation of games, songs, stories for cognitive
development activities, like names of vegetables, fruits
etc.
’JiHi
i
III
rnp-TTTp-rTTp f
fW'TT
■’" bn [‘I
ill
||
■
ft. il I' II
E
sft Hmr ^ft Tfrf ^n'sft’t
3ft r^t mpft nm
fmrh rrtp
#7,
Tpr
qff a^pft
Points to be kept in mind while organising activities in
the anganwadi
|
making children work in groups, providing activities
for both older and younger children, the same
activities in a simple form for younger children and
more complex for older children
I?
‘
variety in activities
I
keeping an eye on children
preparation of aids for cognitive development;
cardboard cards for number and colour matching,
cardboard shapes, colour mixers, smelling bottles,
touch cards, sticks of different sizes for arranging in
order, weight boxes, pictures of animals, birds etc.
Ml 1
i ll Ij
I Il I I
•Ii
H|
III
I'ls'.
p' ■'
ybi;
! ilti
it
14. Activities for Personal, Social
and Emotional Development
AWW will be able to
!
j
I
E;
j
|
Activities for personal, social and emotional development like; I
songs, group games, creative activities, dramatic activities’ B'
puppet plays, doll play, sand and water activities, celebration I
of festivals etc.
IBfi
I
— organise a variety of
activities to promote
personal, social and emotional
development of children
— prepare aids and play material
for organising activities for
personal, social and emotional
development
Songs
This is the way we wash our face, where is thumbkin etc.
B-: ■
■:A- ■
I
Group Games
Chain, tipee-tipee-tap
1
Creative activities
drawing on paper, floor or mud with chalk, stick brick
I
water or paints, clay modelling, collage, papier machie’,
complete the picture drawing
j
Sand and water activities, pouring, sifting, mixing with
|
i
■
colours, taste, smell etc.
Creative Drama
using puppets, masks, dressing up with paper
necklaces, bangles etc.
[ 'I
50
I
I
ft: •.
Mi'
if
f; >
e
ruits
Doll play activities, doll comer with stuffed toys
Celebration of festivals
Narrating stories, songs about local festivals like Diwali,
Raksha Bandhan, etc. Arranging a small celebration at
the AW, inviting parents to the celebration
j
''
Preparation of aids for personal, social-emotional
development
s in
ties
Puppets; glove, finger, paper bag, stick; stuffed toys;
dolls, animals; masks, dressing up items like paper
necklaces, bangles etc.
i-
nd
Points to be kept in mind while preparing aids for all
four sessions
;’y ■
Preparation of aids from low cost/waste
material/locally available material
II
I
multipurpose use of aids
I
II
ft
durability of aids prepared
not to prepare decoration pieces like
fancy dolls, flower vases, embroideries
etc.
t like;
■
ities, w
I:
ation ft
storage of aids
Taking help from the community in making
aids
Involvement of Helpers and parents in collecting low
cost/waste material, preparation and repair of aids
etc.
Making a collection of throw away material in the
Anganwadi
II
:k,
ie,
1
Involvement of Helper and parents in organising
preschool activities using the aids
15. Use of Environmental
Resources in Organising
Preschool Activities
AWW will be able to
Water, sand, fences, trees, animal sheds, bird nests and
cages, parks, flowrs, human body etc. Identification of
available resources in the environment
identify and use things
in her enuironment for
organising preschool activities
Exercises for use of these resources in teaching-learning
of children, eg. tree trunk for climbing, jumping, texture,
colour.
i
I
■
*
What are environmental resources?
51
I
■
'■i.
f fc'! jri
I ...
■
I
■
;I
a ■
Ml
til
»l i
hII
16. Mature Walk as an
Activity to Promote
Overall Development
AWW will be able to
— plan and take children
for a nature walk
■
I . ■
y,
What is meant by nature walk?
Importance of nature walk for creating awareness among'
children, for taking the children out of the AW, for
breaking the montony of the AW activities, for developing
an empathy with the natural surroundings and for learning
from the environment
Planning the nature walk
— use this experience for prom
oting learning in children
Talking to children about the nature walk
Points to be kept in mind while taking children for a
nature walk
f■
11
organising children in lines or groups
walking with them
keeping an eye on them
talking to them
helping them to observe tilings as they walk
collecting material during the walk
J
Enlisting the help of parents while taking children for
the walk
Using material collected for preparing toys, aids and for
creative activities at the anganwadi
Discussion about the walk after returning to the
anganwadi
IIIii
P
Taking trainees for a nature walk
I
[ gr
1
1
ifeil
;1: i . '
fa
KIt
I
!
In urban <areas walks can be arranged to nearby parks,
market, zoo etc. Children can be taken in separate
groups where enough parent volunteers are not
available
17. Use of Theme (or project)
Approach in Organising
Preschool Activities
Theme approach as one method of organising
preschool activities
Why theme approach
■
F I
h i
W
I1 '
I
I
I
selection of theme
planning activities for the theme
time allocation for theme
52
■TJHII^mmTOMjTwniiijqiiiIIIM.IIBMJ..'PI' MU' I I.J4I^SSE.",'1------------
I
AWW will be able to
* — plan activities in the
'
among1
r
dopingi
arning
providing resources for the theme
involving parents/Helper in organising
activities for the theme
arranging an exhibition of children’s
work for parents
AIV based on a theme
or topic
•
'
i
I
I
Some themes to be planned during training,
air, water, rain, weather, trees, animals, birds etc.
I 18. Planning the Preschool
Need to plan a preschool programme
Programme
I | ~ understand the need
Planning a daily programme
a weekly programme based
on different activities or a specific theme
a monthly programme covering different activities or
specific themes
for planning the preschool
k; programme
Points to be kept in mind while planning
■
'^5
■
a
I•
AWW will be able to
I
g— plan a day’s, week’s or a month’s
programme for preschool
education in the AW
-
for
id for
l
need for variety
flexibility
balance in active and passive activities
balance in outdoor and indoor activities
balance in group and individual play
activities promote all aspects of development
management of time
activities for older and younger children
H
Exercise in planning programmes
;{
Using the programme plans during field placement for
organising activities
a
19. Use of Aids in
Preschool set up
AWW will be able to
rks,
: — correctly manipulate the
fc aids and play material
prepared for preschool
activities
1■
I]
20. Likely Problems Faced in the
Field and Tackling these
Selection of aids from those prepared for conducting
activities
Using the aids in a preschool set up
Observation of childrens’ reactions to the activities
Discussing multipurpose use of aids developed for
promoting overall development
Some problems AWWs are likely to Come across in the
field
lack of equipment
lack of sufficient space
53
I
W r '"H V- -
1
=!
•
■I
; ri
■ llill 1
11
'
IT
AWW will be able co
— enumerate likelg problems
in the field in organising
preschool activities and
suggest mays of tackling these
i)
Organisation of Activities
without Equipment
fl
' ill
1
i
■
I
IW
r bh
IfI
II I
I rE:‘4
■ - -• • • - r v
•..'
little time available for planning
not enough guidance from Supervisor/CDPO
lack of awareness among parents about
the importance of play in learning
I
Games and activities that do not require any equipment]
jumping between squares drawn on the floor, hopping or]
one leg, moving to rhythmic clapping, drawing on the
ground with a stick, counting games like fire in the
mountain etc. singing of action songs, creating and
dramatising stories
I
j
Making a collection of waste materials and using these
for
organising activities
.....................................
ii) Management of Space, Time
and People for Conducting
Preschool Activities
Equipment available in the anganwadi
Storage and arrangement of equipment to make the
maximum space available for activities
!
Grouping children for activities, involving half of them
in outdoor activities and the rest inside the anganwadi
and then changing over
Keeping the anganwadi neat and clean, singing songs
like bits of paper lying on tlie ground etc.
Use of outside space for conducting activities
■■
1
Safety outside the anganwadi
Seating arrangement for different activities
illi i'!
..'J
■■wl
Hi
I
p i iiij’i!
11
r
il
Seating of Anganwadi Worker during the activities
Making maximum use of the time available for
organising preschool activities
■
Taking attendance and maintaining attendance register
Organising play activities in the morning to attract
children to the anganwadi
I
B-
Serving meal at the anganwadi towards the end of the
preschool programme
Using meal time for social learning activities
54
I
■
■
—I III IIIIHI'ni'f’"
Using the helper, parents and older children, if they are
around with younger brothers and sisters, youth groups,
adolescent boys and girls for organising preschool
activities specially during the visit of the medical staff
3
■fuipment; r:.
•pping on I
on the I
the
I
and
|
ig these
Use of the available free time for finishing other tasks
Use of the Helper/older children/parents
for collecting waste material and preparation of
teaching aids
II
looking after the hygiene of children
keeping the anganwadi clean
establishing contact with the mothers and
community
I
II
<e the
arranging meeting of mothers/
community
accompanying children for a nature walk
them
anwadi
I Hi) Creating Awareness among
I
songs
Parents and Community about
Preschool Education and
Early Infant Stimulation
I
dS
r
Heed to establish contact with parents/community
through home visits
when parents come to leave/pick up children from
the anganwadi
when AWW meets them in the bazar,
atjdrtans, jagrans, festivals or katha programmes
when AWW organises celebration of festivals at the
anganwadi,
arranging of exhibitions of children’s work,
sports meet,
at a display of newaids and material prepared by the AWW
by inviting parents to see children in activity
r
Discussion with parents about the importance of early
childhood stimulation and preschool education
egister
Ct
of the
i
!
Id) Approaching CDPO/
Superuisor/Primary
School Teacher for Help in
Preschool Education Actiuities
Role of the CDPO, supervisor in preschool education
(Recall from job responsibilities)
supervision
demonstration
arranging outside resource persons
supplying equipment for activities
selecting the anganwadi centre
f
55
•i
■I
iff!*"- »■
®
■
I
Availability of budget with the CDPO for contingent
expenditure
... (;i
e.ibj
Requesting help from the supervisor/ CDPO in
organising preschool activities, obtaining material
■
Si
Mf
Enlisting the support of primary school teacher in
■ ■ I
suggesting new activities for children
use of school space for play, exhibitions,
sports, competitions etc.
admitting children from the AWC into
the primary school
follow up of the progress of children
g- i ;
..
ifti
I
III
BIp
fe-’-
Bl
H 4
S' IM
IW
Jffl
i’i
fl
!
21. Common Behavioural
Problems in Children
AWW will be able to
— identify common behavioural
problems in children and
suggest ways to handle these
■
Some common behavioural problem in children
aggression
withdraw!/ shyness
wetting day time/night time
hyperactivity
fears
truancy
nail biting/thumb sucking
stammering
delayed language development
dependency
Ifi i
1!
Identifying children who appear to be different from
others, don't mix up with .others, refuse to follow the
routine of the AW, don’t take part in group activities or
games, are very shy and withdrawn, always clinging to
the Worker, Helper or another adult, indulging in
destructive activities like breaking things and beating
other children, behaving like very small children,
sucking thumb
M il bn
pI
tBi1
I p'l
/■
Handling these children by paying individual attention;
organising special activities for them
l| i
I
■
I’1
Distinguishing developmental problems from those that
have deeper psychological base, e.g. stammering
between 3 and 5 years vis-a vis stammering after 5
years
1 • if
•i
Referral of acute cases to the PHC/psychologist
56
f 5
iii
..... .
--- ---------
■
i
*=
Hi
-1;':
’ll
p’
I
-T
Discussion with parents of problem children
f'
•
Education of parents in recognising and handling these
problems
.
Nutrition and Health
Nutrition and health services in the ICDS package (recall)
22. Nutrition and Health Services
in the Anganwadi
■
I'
IH
i-
Job responsibilities of an AWW in the area of nutrition and
health (recall)
AWW will be able to
— define her role in the delivery
c health and nutrition
service in the AW
What is growth?
23. Good nutrition for
children and mothers
Recall how a child grows between 0-6 years from Session 10
AWW will be able to
Functions of food for growth and maintenance
of good health
— understand the importance
j of eating a mixed diet
Need to eat a mixed diet/family diet which includes
pulses
cereals
vegetables and fruits
green leafy vegetables and yellow vegetables
and if possible milk and its products
meat, fish and eggs for non-vegetarians and
oil to provide energy, build the body muscles
and protect from diseases
Including as many of these foods as possible in the
diet
■
■
— state reasons tuhy
pregnant and nursing
mothers need more food
!
■■
— explain tvhy infants need
food in modified form
Need for additional family food during pregnancy and
lactation
Eating more green leafy vegetables during pregnancy
to prevent anaemia
Infants at the weaning stage (4 9 months) can eat
properly modified family food e.g. well mashed
vegetables, bananas etc.
Infants need to be given family food to make up the
short fall in the breast milk from 4 to 6 months
57
-jr—j
•_
i
*.11
“ 1 ‘
’ "H
LJ
I■
I
II
_______
j
Small children need to eat more frequently because
they have small stomachs
|r
I
K- I
Small children need more meals because they grow
very fast
!
II I
•/ I'
j
n
■
Ml
■f?
Diets for mothers, infants and children must be
planned keeping in mind cost, availability etc.
Fads, fallacies and good practices associated with
pregnancy and lactation and feeding of infants and
children
24. Feeding and Weaning practices
Ip ihI
it,
th'
" fl :
..
AWW will be able to
i
— understand the importance
of breast feeding
Importance of breast feeding infants for their healthy
growth. Feeding of clostrum to create immunity in-infants
and for stimulating lactation
Mother s diet during breast feeding
(Recall previous session)
— explain the need for introducing Breast feeding on a demand schedule
meaning foods in the child's
diet
Having a bath daily and wearing clean clothes
ip ’Mi
I; fl
■I
fsih*
— describe the methods of
modifying family food for
infants and frequency of
feeds
bleed for timely introduction of weaning foods in the
child’s diet
— discuss urith mothers about
breast feeding and meaning
Giving mixed food to children in modified form for
their growth (Recall previous session)
Fads related to breast feeding (Recall)
*
l'
J 51
p I
II
fl
Jfl.
i-fl
Clse of buffallo’s/cow’s milk, if available, when breast
milk becomes less
Top milk should not be a substitute to introductn
of
well mashed foods for children between 4-6 months
Addition of semi solids makes up the short fall in
breast milk, and the energy deficiency as a result of
this shortfall
fl f'
fl
< I
Frequency of feeding, amount of feed, consistency of
food being served to the infant
r
i
I
I
Discouraging use of powder milk
A-- ij h
F h Ii
flip
I
I
58
J
t
Dilution of top milk related to the age of the child in
the first two months of birth, if and when necessary or
during failure of lactation
Use of spoon or cup with spouts for feeding top milk,
avoiding use of bottle because of difficulty in
sterilisation
A-
Education of mothers about breast feeding, weaning,
top milk preparation, feeding child from the family pot
in a modified form, continuation of feeding even during
sickness of both child and mother, role play exercises
Educating parents to mash/modify family food for
children, hygiene in preparation of weaning foods, fads
related to weaning
'i
it1.
iid
tfli ■
|Li5
• ■'|,i
J
■■■"
J
lib
il
iHl
I >id
Malnourished children are more succeptible to
diarrhoea and other childhood diseases
11
25. Personal and Environmental
hygiene
AWW will be able to
Fleed and importance of keeping self and environment
clean for maintaining good health and prevention of illness
Methods of keeping the surroundings clean
-
I
A!
■
llI ■I
Ii
— understand the importance of
personal and environmental
hggiene
— suggest mays for sanitaiy
disposal of cvastes
— educate mothers about
keeping themselves and
the environment clean
Sanitary methods for disposal of wastes, human and animal
Assistance of community/voluntary organisations in
Preparation of a bore laterine
Preparation of a compost pit
(observational visit)
Planting trees and plants near the Anganwadi
Keeping nose, ears, eyes, hair, body etc. clean, having
a bath, keeping the body clean, wearing clean clothes
Education of mothers about personal and
environmental hygiene (role play)
. Use of Safe Water Supply
I
What is safe and unsafe water?
Sources of safe water
Likely infections as a result of drinking unsafe water;
diarrhoea, polio, jaundice
59
A
? I' 1
. IIMl 1
'i
II
■
..
Il
I!i 'R-i
AWW will be able to
Use of dirty hands to draw out water making it unsafe for
drinking and causing infection
— explain the need for
drinking safe water
— make unsafe mater safe
11
Method of making water safe for drinking
boiling and cooling
chlorine tablets
local methods of purifying water
Alteration by the four pot method
use of filter (Practical session)
Management of diarrhoea
(to be dealt in detail in session 29)
Storing safe water
covering the pot
using a clean container/mug to draw out water
separate washing/drinking water
• Ij
! •'!
27. Immunisation of Children
AWW will be able to
— state the schedule for
immunization of children
.
— make arrangements for
immunization of
children
— discuss with the mothers
the importance of complete
immunization for children
■
.i
1
Importance of immunisation
Immunisation schedule, when to immunize
Diseases against which it is possible to immunize
children
Tuberculosis
Diptheria
Pertussis
Tetanus
Polio
Measles
Protection of new boms from tetanus by immunizing the
pregnant women with two doses of TT
Importance of completing the course of immunisation,
preferably by one year of age
Recording date of birth of new bom and follow up for
immunization and growth monitoring
Identify other children who need to be immunized
1
60
—
t
Making arrangements for immunization
! ..
informing CDPO/Supervisor about number of
children unimmunized/time for immunization
t! *
inform LHV/AJNM
sterilizing equipment (practical)
layout of equipment
"■
I
assistance to the Doctor/ANM
contacting parents
is
I1
Encouraging mothers to bring children to the AW
centre for immunization on their own
Discussing with parents that these diseases can be
serious, the importance of immunization, possible after
effects of immunization and how to handle these,
frequency of immunization and completion of all 3
doses of DPT and Polio for proper immunization, not
to feed for half an hour after polio drops to avoid
negation of effect
if
I l Il i l
I
Instructing Helper/older child/mother to carry on
preschool activities in the Anganwadi Centre while
immunization is going on
28. Malnutrition: the Major
^/ Problem among Children
AWW will be able to
— discuss the causes and
consequences of
malnutrition
I
*
Maintenance of immunization register (exercises)
If
Follow up of children immunized for complete
immunization
•
! -
When children/pregnant women do not get good
nutrition it leads to
low birth weight babies
malnutrition (under weight)
I
Recall health and nutritional status of mother and
children (Sessions 2 & 3)
Malnourished children are more succeptible to
diarrhoea and other childhood infections
deficiency diseases, anaemia, night
blindness, goitre (to be discussed
in detail later)
61
■
•
/■
i
-
infections are more severe in
malnourished children
20. Diarrhoea and its Management
AWW will be able to
— identify the symptoms of
diarrhoea
— discuss how diarrhoea
causes dehydration
— prepare an oral rehydration
solution by the household
method
Causes of diarrhoea
unhygienic environment
unhygienic food preparation
preparing food without washing hands
improper bottle feeding
picking food off the ground and eating without washing.
use of unsafe drinking water.
improper disposal of human faeces
eating stale food during hot weather
Signs and symptoms of diarrhoea
Oral rehydration therapy
I
— explain to mothers about oral
rehydration therapy and
management of diarrhoea
Preparation of the oral rehydration solution for
preventing dehydration due to diarrhoea by the
household method (Practical) •
Preparation of ORS from commercial packets
(Practical)
Need to continue fluid intake/breast milk during
diarrhoea in infants/children
Increased frequency of feeding, feeding small amounts
at shorter intervals
Diet during diarrhoea
Well cooked/mashed foods initially followed by the
usual household food
^0. Nutritional Deficiency Diseases
Early signs of malnutrition; weight faltering, later loss of
weight, child becoming thin, lack of energy
AWW will be able to
— list the common nutritional
deficiency diseases, ailments
and other diseases in
children
— suggest strategies for
combating these
Identification of early signs through regular growth
monitoring (to be'done later)
Continued intake of inadequate diet results in deficiency
diseases
protein energy malnutrition, vitamin A deficiency
(night blindness)
62
*
— refer children with severe
problems to the Health Centre
— use the first aid kit for
administering medicines/
vitamins to beneficiaries
— educate parents for looking
after children suffering from
these diseases
Absence of specific nutrients in the diet like iron or iodine
can cause anaemia and goitre
1
Preventing deficiency diseases
giving vitamin A drops to prevent blindness
giving iron and folic acid tablets to prevent anaemia
Education of parents to look after the food needs of their
children (role play) -----
giving adequate family food to the child
feeding several times a day in quantities sufficient to
satisfy the child
Referral of severely malnourished children to the PHC
Follow up of children at home
■
I
II
Rehabilitation of children after treatment
!
Ji
proper diet
maintaining proper hygiene
31, Common Ailments and
/ Diseases in Children and
how to Handle these »
I
Common health problems in children; cold,sore throat,
cough, fever, sore eyes, tracoma, ear and skin infections,
boils, worms, body ache, acute respiratory infections like
pneumonia
I
OB*
II-
Identification of pneumonia by noting the fast rate of
breathing in children
II
Signs and symptoms of whooping cough, measles,
malaria, typhoid, diptheria, tetanus, TB, polio
■I
i i
is
Diseases preventable by immunization (Recall)
TV
Handling these diseases
Diet during these diseases
continue to feed as much as possible
frequent feeding of semi solids
adequate water intake to prevent dehydration
fads related to eating during illness (Recall)
II
Tl,';
I
Repeated infections/fevers leading to malnutrition
Health problems common in specific regions; urban
slums, hilly areas etc.
\
63
i?
i1 IP
i-
Familiarity with the health kit available at the
anganwadi centres; various medicines, eye drops,
antiseptic lotion, bandages, cotton, scissors
Common medicines from the kit to be administered to
children in case of various ailments
Integrating local remedies for treating common
ailments
Discarding medicines without labels and expired
medicines, reading labels before administering the
medicines
I
Contacting supervisors/ANM to replenish medicines
consumed
Education of mothers about diet during these illnesses
and rehabilitation of children after illness (role play)
Referring to the doctor in case of serious problems
32. Growth Monitoring
What is meant by growth monitoring
AWW will be able to
Need for monitoring growth from birth
i
— monitor the growth of
children by weighing
Frequency of monitoring children 0-3 years and 3-6 years
How to monitor growth
— demonstrate the correct use of
weighing scales
— assess the correct age
and nutritional status ‘
of children
— plot the weights of children
on growth cards and interpret
the trend of the growth curve
*Note
Use of salter/bar weighing scale* for weighing
balancing scale
making zero adjustment
placing the child in the weighing bag
reading weight
recording weight
removing the child from the bag
Points to be kept in mind while weighing
weighing right from birth
weighing at the same time while
Wherever bar scales are not available in AWTCs they should borrow them from the field for training
purposes.
64
J
'•W
"
: ’I
t
■
discuss u)ith mothers reasons
for weight loss and additional
family food for malnourished
children
recording every reading
weighing before food/water intake
whenever possible
1 ■
Exercises in weighing and recording
!:
1
■.!*
Maintenance and repair of weighing scales
Checking birth register/home visit register for the aoe
of the child
Assessment of age where age is unknown
•"ii-l I
H
■Hi !
Preparing a local events calendar for assessing age
-
II • ■■
Plotting weights on growth cards
Describing healthy, faltering and declining growth
curves
Determining the direction of a child's growth line
■
i i1
Exercises in plotting and interpreting growth cards
I I
Interpreting growth trend to identify children ‘at risk’.
(Factors to be done later)
Probing into possible causes for inadequate or no
weight gain even when the child is in the healthy zones
on the cards to prevent malnutrition
iI 1i
i.;
III!
i
Identifying children who require extra food supplements
Maintenance of growth cards
k ■'
|
Use of growth monitoring as a tool for education of
parents
letting parents see growth of child
through gain in weight
early identification of faltering
Listening to and discussing with parents reasons for
weight loss, addition of semi-solids as soon as growth
faltering is observed, introducing softened and mashed
household foods
65
I
Bi
1
ra1 •
Advising parents about proper food for the growing
child, frequency of feeding and blending with family
food patterns
Making home visits to educate parents and discussing
with them the importance of good health,
immunization, safe water, sanitation, hygiene for
promoting good health (method of home visiting to be
introduced in later session)
Role play sessions on discussion with mothers
Convincing mothers to let their children be
weighed/bringing children regularly for weighing
>
Referral of children
i) whose growth is faltering consecutively for 2 3 montlis
ii) severly malnourished children
CJse of tricolour strip only in the absence of salter or
bar weighing scales to screen well nourished from
moderately or severely malnourished children
Points to be kept in mind while using the strip
placing for measurement
overlapping or twisting of tape
Interpreting the tape colour
Explaining the difference between growth monitoring
and nutritional surveilance
(task to be done during field placement)
33. Organisation of Supplementary
Nutrition in the Anganwadi
Recall growth monitoring and selection of beneficiaries for
supplementary nutrition from previous session
AWW will be able to
Identification of children ‘at risk'
— identify mothers and
children at risk
— explain the need for
organising SNP in the AWs
children upto 5 years with weight below 50 percent of the
reference standard
difficulty in breast feeding, introduction of bottle feeding
before six months and delay in giving weaning foods
failure to gain weight for three successive months
birth weight less than 2.5 kgs
66
W
— prepare a variety of
supplementary foods
— ensure proper hygiene
during cooking
— store the SNP correctly
“I jls *
x.
. •
11 11
twin births history of death of more than two siblings
below the age of 12 months
death of either or both of the parents
severe acute infections like measles or whooping cough
birth order 4 or more
spacing of children less than 2 years
only child after a long married life
■
j
I hl
|| Ik; |
! 'ihPl1
Identification of mothers ‘at risk’
I
’I
pre-pregnancy weight 38 kgs or less
weight 40 kgs or less at the 20th week of pregnancy
height of 145 cms or below
twin pregnancy
previous history of still births/abortions/antipartum/
postpartum heammorages/eclapsia
previous history of early neonatal deaths
history of previous ceassarian or forceps delivery
mother’s age above 35 or below 18
mother suffering from TB, severe anaemia, heart
diseases, diabetes
conception after treatment for infertility
four or more pregnancies
fh
Iill
(‘Illi
■''
i
!<
al
r I ’ ' ■'
Need to identify children “at risk” and mothers “at risk”
to prevent such children slipping into malnutrition,
to reduce mortality and morbidity by closely
monitoring the "at risk” category
Ihli
ill
1
i
t
■ a
i
Special attention to children below three years, giving
them their ration in two sittings as they cannot eat all at
one time
J
Ji
Discouraging taking food home to eat as it would then
be used as a substitute for home food
Supervising the helper in preparing children for
supplementary nutrition
fpI
1! i1:
'I
I'
H
67
/ i
wr
■ I'
I
Need to provide supplementary nutrition at the
anganwadi (Recall)
gap between what should be eaten and what is eaten
AWWs role in planning supplementary nutrition
Explaining to mothers that food given at the AW is a
supplement and not a substitute
■.i
■
Distribution of SNP to children and mothers
Maintaining the food stock register
a) Methods of Cooking
and Hygiene in Cooking
Measuring the amount to be cooked according to the
number of children and pregnant and nursing mothers
Different methods of cooking to prevent loss of
nutrients
Hygiene in cooking
Variety of recipes to be prepared at the anganwadi
depending upon the supply of supplementary nutrition
(practical)
Soaking of food grains before cooking for improving
the quality of food
Mixing grains and cooking
Need for variation in the preparation
Introduction of locally grown foods in the preparations
like vegetables etc.
Food habits and food fallacies of the local people to be
kept in mind in preparation of supplementary foods
Amount of food to be served to
children 6 months-3 years
children 3-6 years
pregnant women
nursing mothers
(Recall)
Consistency of food to be served to different age
groups (Recall)
v
WFP/CARE foods served at the Anganwadi
ration for one child, 65 gms wheat, 8 gms oil
(80 gms wheat and 10 gms oil for WFP food)
•1
for preparation of food; soak for two hours, add fresh
vegetables, if possible
store food in dry place, keep the bag closed with
rope, change bag if tom
l
68
£
'•-*1**%•? U
f
MIK
Type of food to be served, processing the food to
make it suitable for small children, not to give very
watery foods to the child, addition of oil wherever
possible
Supplementary nutrition for small children to be given
in two meals during the day
■ r.)
i ' Il i
iihl
KJ
Feeding of the severely malnourished
double the quantity
education of mothers to provide
food at shorter intervals
feeding the under threes also at the
anganwadi
ij ■
II
11 I
I
Importance of making beneficiaries eat at the
anganwadi (Recall)
b) Storage of Food
Proper storage of foods at the Anganwadi for prevention
of infestation
Sunning of grains/cereals
>j] .1
I
id
i
• K
’ ' 'ii
(Jse of local structures for storage e.g. clay granneries, use
Ml
of neem leaves, tightly covered boxes etc.
34. Nutrition and Health Education
Need to educate community on health and nutrition
AWW will be able to
Recall from earlier sessions areas on which to educate
mothers/community about health and nutrition
— explain the need for nutrition
and health education
— make a list of some themes
for education of mothers about
health and nutrition
I
Ki
|ji h:'
'/■I
Methods of educating mothers/community
(to be done later)
individual/home visits
group meetings
35. Ante and post natal care
What is conception, the process of conception
AWW will be able to
Development of the foetus in the womb (recall session 9)
— explain hoiu conception
takes place
Appropriate age for marriage and child bearing, problems
in pregnancy at the adolescent age or after the age of 35 years
(recall mothers at risk’)
— understand horn babies grom
in the tuomb
f
Advantages of a small family
69
■■ fi
1
•'
w
■
fi
I!
L
■z
. i
— understand the need for planfHeed tor spacing births for producing healthy children,
ning families and spacing births for the mother’stealth
— know the carious methods
of contraception
fSMplain the problems of poor
nourishment during pregnancy
Possible side effects of contraception
Heed to eat more family food during pregnancy to produce
healthy babies (Recall)
Heed for iron during pregnancy, deficiency of iron (Recall)
explain the need to educate
mothers about family planning,
ante and post natal care
Dispensing of iron and folic acid tablets for prevention of
anaemia during pregnancy
Administration of injections for tetanus toxide (Recall)
Lack of enough food during pregnancy especially the
last three months leads to low birth weight babies
(Recall)
Low birth weight babies, if not looked after properly,
are more succeptible to fevers and diseases resulting
in malnutrition (Recall)
Other causes of low birth weight
age of the mother, frequent
pregnancies, closely spaced births,
hard physical work during pregnancy,
infections like measles, aneamia in
mothers, use of drugs and alcohol
I
Home visits for giving individual attention to pregnant
women
Role of the health staff in looking after pregnant
women
Ensuring that mothers go to PHC for delivery or
delivery by trained dai
Advising mothers on breast feeding (Recall)
Education of parents to be dealt in a later session
»6. Early Detection of Disabilities
Importance of early detection of disabilities
Identification of some symptoms of the following
childhood disabilities
70
AWW will be able to
— make an early identification
of disabilities in children
visual handicaps
speech impairments
mental retardation
orthopaedic and locomotor handicaps
hearing problems
I'I
1
Ii
— refer cases to the PHC
— integrate disabled children
with normal children in
the AW
-
ii
Referral of these cases to the PHC or District
Rehabilitation Centre
I
Awareness about how to deal with children with
handicaps
Integrating these children with other normal children in
the anganwadi
II
Creating an awareness among normal children about
mixing with and helping children with disabilities
37. Health Infrastructure in a Project
Primary' Health Centre (PHC)
AWW will be able to
Sub centre
— enumerate the health facilities
available near the AW
Services offered in these centres
explain the need for tvorking
in close collaboration
with the health staff
!.
If
I
I: iH1
(In
Role of the ANM/LHV vis-a-vis the AWW (Recall)
I
Linkage between the community. Health Guide and the
AWW
I
Sectoral meetings with the MO for collection of MMRs
and continuing education
■
71
•■'••4 -
•
JI
Male and female health functionaries
Medical Officer
ANM
LHV/Male Supervisor
Dai
Multipurpose Male and Female Health
Workers
(Recall visit)
Submitting report to MO/LHV/ANM
hl;
w
Discussing with parents about ways of handling
children with handicaps
i
J
...
blearest Government hospital/MCH/clinic/dispensaiy in
urban areas
. Treatment of Minor Accidents
and Injuries
ill
'll
-
AWW will be able to
— administer first aid in cases
of emergency
— refer serious cases to the PHC
First aid for children for following accidents
drowning
shock
bums
cuts/ scrapes
heat stroke
bleeding
snake/dog bites
stings
1
Identification of medicines available in the first aid kit
for the above emergencies (recall session 31)
Clse of the first aid kit (Practical)
Referral to the doctor in case of serious emergencies
Community Participation
39. Role of Anganwadi Workers
in Community Participation
AWWs role in creating conducive conditions for
community participation
AWW will be able to
AWW is the link between the ICDS programme and
the community
— enumerate her role in involving
the community in the AW
programme
setting an example of her own behaviour
maintaining contact with the people
keeping them aware of her activities
— explain the need for
community participation
interacting with the community both
formally and informally
creating awareness among the community of their
needs within the perview of the ICDS scheme
vli;.
S'
■
creating awareness among the community about
their roles and responsibilities in the ICDS
40. Areas of Community
Participation
A
General
selecting the location of the Anganwadi and helping in
providing/obtaining accommodation
*■
72
■
'■
, — r—laiimi
II
f
AWW will be able to
— identify the areas in which
community can be involved
— recognise the participation
of the community in the AW
programme
Making the Anganwadi safe for children by constructing a
fence or clearing the space outside, maintenance of the AW
I
making space available for outdoor activities
allowing use of water and toilet facilities
making a compost pit, toilets for the Anganwadi
-
keeping the Anganwadi premises clean
inviting community members to visit the AW and see
what is happening
. introduction of the new AWW to the people and
helping to develop contacts with panchayat, mahila
mandal etc.
1
< ■
using their services in organising bal melas, sports
competitions, exhibitions, festivals, functions etc.
Preschool Education (recall)
organising preschool activities
narrating stories to children, singing songs,
organising puppet plays
:ll
I
"i
looking after children in the absence of Worker
S’
accompanying children for a nature walk
IMh' '
collecting waste material
preparation and repair of aids
, J
keeping the children clean
J
sending children regularly to the AW
assistance in arranging exhibition and display of
children’s work
providing material for different activities of children
I
If
’ll
hr.
’
73
Whs
K-'f
■
................................................
;
______________________________________________________________________ -
.<■
.
..-
____________________________
.
:i.^’ ,h„.
i
“'al
I 5
Health and Nutrition
J.'J
contacting parents to send children for immunisation
helping to organise the immunisation camp
Sf.;:
sterilisation of equipment
I
I■
supplying some vegetables/foods for providing
variety in supplementary nutrition; fuel, spices
II ■
I "
help in cooking and serving food
identification of malnourished children/mothers
■
accompanying them to the PHC, providing transport
in emergencies
-
providing equipment for health and nutrition
education
helping in arranging/attending mahila mandal
meetings
■
Recognising Community Participation
Participation of community may not be in physical
terms alone
i
■W
Community contributes by sending children regularly to
the AW, utilising the services at the AW, locating a
place for the AW, mobilising other people and
clarifying their misconceptions, trying not to create
problem situations for the AWW, willingness to listen to
■
the AWW
Exercises in listing areas of community participation
Cautions in community participation
mobilising community is a slow process
people cannot be rushed into participating
41. Mobilising Community
Participation in ICDS
-Identifying people/agencies/social groups and
organisations who are likely to help in the ICDS programme
74
J
'■i
;fl *3
’
...... 4 -
........
M-
?
11
AWW will be able to
<i
z mahila mandal
youth group
' panchayat
x voluntary organisations
— identify people/agencies/
supportive services that can
be of help in the AW
programme
'I
i !■
L
- Important individuals who are likely to be of help
— enumerate mays of mobilising
groups in the AW programme
Head of the family, men, husbands, the mother and
mother-in-law, wife of the pradhan, village dai, elderly
women, primary school teacher, his/her spouse, social
leader, young boys and girls
I •
5
_ Supportive services available at local and block levels
In the rural areas
Rural development programmes;
lii
..
IRDP, DWCRA, NREP, RLEGP, PHE
(Water supply and sanitation)
. 11
In the urban areas mainly
I ■ ■■■
child guidance clinics
educational institutions
homes for the disabled
. Mobilising community from the initial stages
.
before setting up the AW
after setting up the AW
■i
wli
i
Introducing the scheme to the community, seeking
their approval
I!
Talking to the community about the training
undergone by AWW
Keeping them informed of the new plans and
development
: i|
Taking feedback about the services being provided
from time to time
Communicating with individuals and groups (method
of doing so to be introduced in a later session)
-
ft
75
i
- /
i
^/Ways of utilising social groups, organisations and
individuals in the programmes e.g.
I
family planning education through mahila mandals
II -
repair and maintenance of centres
II
i
preschool activities
survey work, literacy programme, economic activities
etc. through youth groups
z directing older children for education to primary
schools (Recall Role of parents)
Utilising the supportive services in promoting the
Anganwadi programme e.g.
referral of children with problems, disabilities to
child guidance clinics, homes for the disabled
/ enlisting help for water supply/sanitation, RHE and
other developmental programmes
v 42. Coordinating and Working
with Functionaries
AWW will be able to
I
— coordinate ivit/i different
functionaries in the
scheme for effective
implementation of ICDS
Need for AWW to coordinate and work with different
functionaries, groups and individuals in the community
a) Health functionaries
coordinating with them in ensuring provision of
health services; health check up, immunisation,
referral services, health education, family planning
activities, ante and post natal care (recall from
earlier sessions)
I
i
— decide when and where to
contact the different individuals,
agencies, social groups etc.
b) Panchayats
for ensuring registration of births and deaths, water
supply and sanitation, help in filling up of records etc.
c) Other Social Groups
Recall from earlier session role of social groups like
mahila mandals, youth clubs, voluntary
organisations etc.
d) Individuals
Recall from earlier session individuals with whom to
coordinate
»■»
76
*
SSL
—
Tm
III
Decide on whether to contact group or individual,
depending on the issue
J
Approach in contacting these individuals
groups/ organisations
-
informal
formal
• ■
I
When and where should the AWW contact them
at home
at their work place
at the local market/fair
in the morning/evening
i
p
I4
What are the various occasions at which the
Anganwadi Worker can make contact
village fair
functions/festivals or marriages
meetings organised by the local leaders,
CDPOs, Supervisors
i I®
'.Id
Communication
43. Forms of Communication:
Principles, Methods and Barriers
AWW will be able to
— understand the different
forms by which she
communicates
— use a variety of methods
and aids for communicating
Lvith people
with
J
An AWW is communicating all the time with
children
family members
community members
local leaders
different agencies
medical personnel
i
■
I
Different forms by which she communicates
gestures
conversation
written word
aids
‘ i!
I
Caution while communicating with people
careful not to antagonise people
• 1 ..
a
use local dialect
dress neatly but not differently
4
■
not adopt a condescending attitude or talk down to
people
77
'l
■ hi •
■ -1
i
■J
status should not pose a barrier in communication
(
speech should not be hesitant
speech should be clear
not to rush with ideas
Methods of communication
group discussions
problem analysis
talks
role play .
demonstrations
case studies
(Recall methods used in different sessions)
identification of appropriate method for communication
(Jsing a combination of methods for communication
Aids that can be used for communication purposes
aids help trainees understand better
aids help in making learning more effective
aids help in capturing attention of listeners
decide on the kind of aids to be used
Review aids available
check if they are communicating the message,
check for unnecessary details which can distract
people
effectiveness of the aid with the kind of group
4
v44. Conducting Home Visits
AWW will be able to
Need to visit homes
to establish contact with people
— plan and undertake a home visit for educating families
to educate a family, make a
for follow-up of families after group meetings
survey and enlist beneficiaries
for mobilizing community to avail the services
for mobilizing community participation in the
programme
78
I
for guidance at home on different aspects of a
child’s development
"•'t
for observation of the community’s habits/practices
for observing if the people have adopted new
practices suggested
I'I1
hl
for follow up of children at risk’
Planning for a home visit
I
drawing up a monthly/weekly plan of the houses to
be visited
■
deciding on whom to visit first or altering plan in >
case of an emergency
III
ii
reason for visiting a particular home, identifying the
problem of the family to be visited
possibility of collecting a small group from the
neighbourhood for discussion
>
identifying individuals who she may need to take
along during the visits;
ANM, dai, Supervisor, CDPO, local leader, neighbour
Identification of things which she needs to carry with
her for discussion
health card
child’s work
aids
first aid kit
waste material for making play materials/
teaching aids
r 4
45. Role of AWW in Forming
and Activating Mahila
Mandals
How to greet and talk to people, whom to address at
home to best convey the message (Recall from earlier
lesson)
(Task for field placement)
'?•
i
AMhat is a mahila mandal?
-Need for mahila mandal in the village
AWW will be able to
— form and activate a mahila
mandal in her area
I
to sensitize women about their role in the society and
their rights
I.]
II
79
jr
■W
— organise a meeting of
mahila mandal
— inuolue the mahila mandal
in the AW programme
to provide an opportunity for women to socialize with
others and share their problems and experiences
to increase their participation in social life
to build up their confidence
to help solve problems of women
to train women to undertake meaningful activities,
economic and social for themselves and the community
Making use of the existing mahila mandal in the above
activities
Initiating a mahila mandal
r Forming a mahila mandal in a village where there is
none
facilities available for setting up a mahila mandal
composition of a mahila mandal
selection of office bearers and committee members
registration of mahila mandal, role of AWW
management of mahila mandal
- finances
= day-to-day administration
opening account (refer later)
' keeping records
Arranging meetings of mahila mandal
Making physical arrangements for a meeting of the
mahila mandal
fixing date and venue for meeting
drawing up an agenda for the meeting
conducting the meeting
recording the main decision in the meeting
follow up of the suggestions of the meeting
80
1
II
* Linkages between the mahila mandal and the AW
programme
_ Establishing lrr!;ages between the mahila mandal and
the AW programme
1
pl
I
111
Motivating mahila mandals into doing some activities
p
Involving mahila mandals into starting income ,
generating activities like kitchen gardens, preservation
of foods etc. and to involve mothers of the ICDS
scheme
■
I
- Clsing mahila mandal meetings for analysing the
problems of women, education of parents and
mobilizing their participation, discussing problems at*
the AWC and ways in which the mahila mandals can
help solve these problems (Recall)
il
I
Other activities which the mahila mandals can
organise; demonstration during education of parents of
food preservation, enhancing of nutrients etc.
46. Organisation of Balmelas,
Children’s Exhibitions,
Festivals •
Use of balrtnelas, exhibitions, festivals to establish and
maintain contact and impart education to the
community
AWW will be able to
Planning the balmela that could include an exhibition and
display of aids, children’s work, hobby collection work,
well baby show, sports meet, puppet play etc.
— plan and organise community
based functions for
promoting people's involvement
in the programme
I
I
illI
Seeking help from voluntary agencies; mahila mandals, t
youth groups, parents, supervisors, CDPOs, individuals in
the organisation and setting up of these activities and
for funds if needed
¥
Sending invitations to people
Inviting local leaders for inaugurating/talking to people
Themes tor exhibitions
children’s work/games
mother’s work
material available at the AW
ii
health education
nutrition education
81
*
■
'Sc"
------r - ayw-w
■ 1 ..t
illf
:■
r
‘.7.-I’
.
(
47. Parent and Community
Education
AWW will be able to
— define her role in education
of the community, specially
parents
— spell out the areas in
which she needs to
educate the community
— plan and conduct a parent
education meeting
(4$. Areas in which the
AWW needs to educate
community
heed for educating community and parents
»
to create an awareness about the services in the
ICDS programme and its usefulness for the community
to improve their living conditions e.g. using smokeless
chulah, bore laterines
to enlist their participation in the ICDS
Role of AWW in creating awareness and educating parents
and the community
Different settings in which parent and community education
can take place
During home visits, formal meetings, informal
meetings, in the bazar, at the well, at the Anganwadi,
during festivals, community gatherings, meetings of the
mahila mandals, immunization camps etc.
Recall themes from earlier sessions for education of the
community
health and nutrition, care of pregnant and nursing
mothers
needs of children
early childhood stimulation
play and its importance in preschool education and
overall child development
population education
participation of the community in the anganwadi
programmes, their roles and responsibilities
49. Planning and Organising
Programmes for Parent
and Community Education
Points to be kept in mind while arranging a meeting with
parents/community
purpose of the meeting
selection of message to be communicated
avoiding too many themes in one meeting
using the same theme in more than one meeting for
registering impact
using a mixture of aids/communication methods in
different meetings
82
J*
...........
1
- -A
audience for the meeting
time and venue of the meeting
informing about meeting
reminder about the meeting on the day it is
scheduled, assigning tasks to different people for
making seating arrangements etc.
-I
Reviewing aids available/required for the meeting
i, I
Preparation of new aids, if needed
Making seating arrangements
i
Seating of AWW during the meeting
Methods of addressing the group, language to be used,
informal style of speech
Introduction to the topic of the meeting
Ustening to parents/people’s comments
Resolving problems and answering questions of
parents on related or unrelated issues
.-J
Feedback from the group .
about relevance of the theme
for further information on the topic
fortdeciding the topic of the next meeting
I
9
fixing the date for the next meeting
Follow up after the meeting
through home visits
/
informal discussions
50. Education of Mothers to
Promote the Development
of Children Under
Three Years
Care of infants, health and nutrition (Recall)
Heed and importance of early childhood
stimulation (Recall)
Ways of stimulating infants
1
■I
I
83
*
ii -i u
■q
'
__ JI
!
I!
AWW win oe abie to
I
■■i
— describe the need and
importance of stimulating
infants
r
— educate mothers on hocu to
stimulate infants
i
— recall the importance of
growth monitoring and
immunization for children
51. Some more Themes for
Community Education
a) Socio-Economic
Programmes for Women
4
infant games and songs, tickling games,
peek-a-boo games
Educating mothers about talking and playing with
infants
'
Methods of encouraging mothers to bring younger children
to the AWs for supplementary nutrition
Complete immunization of children during this period
(Recall)
Growth monitoring and growth promotion (Recall),
Socio-economic programmes by the government going
on in the area
Who to approach for baining/initialing the activity in
the village
b) Operating Small Savings
1
Account in Post offices/Banks
Help of the Supervisor/CDPO, mahila mandal in helping
women avail such facilities
Need to open a savings account;
inculcating the saving habit
generating interest on tfie money saved
A
Who to approach for opening the account
1. I
Filling in forms for opening the account, deposit and
withdrawl slips, money Cider forms
Saving schemes at the post offices
1
Role of AWW in helping people to open accounts
giving an introduction in the bank/post office
accompanying them to the bank
'I■t
filling up slips — deposits and withdrawal
I
approaching bank/PO officials for help in tilling up forms
I
I
I
I
"T""1 •
84
, ibl■
•US
c) Hou) to Manage a Home
more Efficiently
!
Discussion among trainees about their methods of
managing homes
. Ii
li ■
I
Heed to organize work to save time, energy
(human and material) and money
I 1
!
1
use of fuel saving devices, gobar gas, solar cookers
or smokeless chulhas, arranging demonstrations by
mahila mandals for the community
availability of these equipment and their cost
I -iil
!1
proper storage to avoid wastage through infestation
(recall)
4
i
I 1
enhancement of nutritive value of foods (Recall)
i.
Ideas suggested should keep in mind
needs of the community
practicality of the suggestions
availability of the materials etc.
d) Cleanliness and Sanitation
•
of the Environment and
,
the Home
!
V
1
Keeping the home/outside clean
Growing trees around the house
T;
Covering excreta (recall)
Compost pit (recall)
II
Sanitary laterines (recall)
i
Protecting water sources
. ..
Ventilation
e) Role of Community in
Creating a Healthful
Environment for Children
Recall keeping the home and surroundings clean, safe
making sanitary toilets
infant stimulation
play and learning in children for promoting the overall
development of children
f) Role of father in
decision making
As head of the household father should ensure
immunization of children
■ I
sending children, specially girls for PSE
spacing births and family planning
health of the women/girl child
V
-
■
respect of women
85
I
I. -
■Jfi,
trnwwwai-." > ■
52. Population Education
Need for population education
Who are the people to be educated; women/mothers/
4
fathers-in law/fathers/opinion leaders
it
Methods which people can adopt for
family planning (Recall)
Role of the Primary Health Centre, ANM, LHV in
population education and family planning
Role of the AWW in arranging meetings with the
community in coordination with the PHC
■i
-
Role of AWW in
motivating people to accept family planning methods
clarifying doubts of the community
follow up of people who accept family planning
methods
referral work
review of aids prepared for their use in population
education
preparation and use of aids to educate the
community during the meetings
■
53. Conducting a Survey
Ways of contacting/approaching the community for
eliciting information
AWW will be able to
How to interview
— make a survey of the area
— enlist beneficiaries of the
scheme
■jsa
^■4
— fill in a survey register and
update it regularly
Skills of observation during survey to obtain additional
information
Introduction to the survey register, exercises in making a
survey/recording
Points to be kept in mind while recording
Making the monthly summary in the survey register
Interpreting data to identify children (0-6 years) children
at risk, pregnant women and nursing mothers (Recall)
86
"■ -s
r
—
■
<r
Use of data collected for delivery of services in the
anganwadi
nutrition
immunization
referral
preschool
I
>1
Assistance from CDPO/Supervisor in making a survey
and filling up the register
Assistance of the panchayat, mahila mandal, local
school, yuvak mandal in making the survey and filling
up the register
Updating the survey register
J
I
Updating the survey register every 3 months
■
«
Importance of keeping the survey register up-to-date
Recall using survey as a means of creating awareness
among the community about ICDS and its services,
building rapport and enlisting community participation
(task to be done during field placement)
54. Location of the Anganwadi.
Role of AWW in Making the
Anganwadi Adequate for
Delivery of Services
AWW will be able to
- recognize the hazards and
inadequacies around the
AW in delivery of services
— seek assistance in making
the AW safe
Adequacy of the anganwadi for preschool activities in
terms of
indoor and outdoor play
hazards in the neighbourhood
equipment supply and replenishment
need to make AW safe for preschool activities;
I
fencing a pond or covering a ditch, proper
ventilation and light
Adequacy for community education in terms of
*
accessibility by the community
location in the caste dominated area
distance from beneficiary household
space for conducting community/parent education
meetings
r
S
■
!■
-
Adequacy for health and nutrition services in terms of
space for storage, cooking, washing,
area for disposal of garbage
^4 ' H
I
87
' ' J
____ >
•..X ft
ventilation for smoke to go out
drainage for dirty water
equipment for cooking
availability of toilet/tap/well facility
treatment for pests and insects in the
anganwadi to prevent infection and disease
I ‘
— r
€
c
—/
Role of AWWs in making the anganwadi suitable for
delivery of services
c
Use of community’s space and services for play,
meetings
r
Fixing of windows compost pit, drainage, for making
the AW premises suitable
57
Procurement of equipment from the CDPO/Supervisor
for the anganwadi
55. Planning the Anganwadi
Programme
AWW will be able to
h
<
— plan the programme at the
AW and her schedule
including home visits,
community education,
mahila mandal meetings etc.
I-I
I
I<
p
I'V
Recall planning programme for preschool activities
Heed to plan the programme for the week/month to
include
health and nutrition education
immunization
corTimunity education
adult literacy classes
meetings of the mahila mandals etc.
circle meetings
visits of functionaries/health workers/local leaders/
voluntary workers/officials
filling records
survey work
growth monitoring
.preparation of aids
exhibitions, balmelas, etc.
5
Exercises in planning programmes
T ■
I vi
I J
I
Using the services of the Helper/mothers while AWW is
busy in the above activities
56. Procurement and Storage
of Stocks and Supplies
for the AW
Basic equipment that is supplied to an anganwadi worker for
conducting the programme
88
—— oieb
1
AWW will be able to
— make a list of stocks and
equipment available for
an AW
— procure and store stocks
and supplies for the AW
/
(
/
J
Procuring the material from the CDPO’s office
Some other equipment/materials for preparing aids/play
materials for preschool activities that an AWW can obtain
from the CDPO from the contingency allocation
li<
Equipment for storage of stocks/material (Recall)
Need to maintain a regular flow of food stocks at the
anganwadi
-. I
Availability of records/registers/growth cards/
immunization cards
57. Maintaining Correspondence
z and Contact
AWW Lvill be able to
— curite a letter to
different people
— keep a file of the letters
sent/receiued
How to write a letter to the
Supervisor
CDPO
local leader
voluntary organisation
parent
training centre
LHV/ANM
■ III
Ife,
■ ’ I1
I
Maintaining a file of the letters sent
Reply to a letter received
58. Maintenance of Registers
and Records
Kinds of records an anganwadi worker has to maintain1
(recall those done earlier)
j
■
AWW will be able to
— make a list of the different
records and registers
to be maintained in an AW
— maintain these records
and registers
stock register
attendance register
growth cards
immunization cards
survey register
Heed to maintain the various records
Filling up the various records/registers
Seeking help from community people/parents in
completing records (Recall)
Seeking help/guidance from Supervisors in
maintaining records, requesting Supervisors to make
•
■
■
■'-a
■ 11
' id
'S d’
■
Jl'?i
- I
■
•
d
is
■
i
' “IS!
■■
I
j
J
89
.! 'd '
iii
- /d' •-d r
• ■ dlrejm
°S!""ntS f°r obttlinlng h,!lP in rr"-,rd keeping
Keeping registers covered, neatly stacked
Maintaining a daily diary by the AWW
Information to be recorded in the diary
Need for recording this information
■
■■
1
Use of such information in filling up the monthly
progress report
y
Information that needs to be
entered in the various
columns in the MPR form (Use
of daily diary recordings
from introductory session)
Organisation of time so as t_ f
to fill up the MPR and
submit to Supervisors on time
Information flow from the AWWs MPR.
!s to the Centre
MPR^r f°r.feedback from the Supervisor regarding
1
MPRs to help improve the ICDS programme
59. The Integrated Approach
to Child Development
AWW will be able to
' y ■
— uieiv the child in a holistic
manner
— recall all that has been
done during the training
— deuelop a perspectiue of her
role and responsibilities
in the AW
i
Recall what has been taught during the course
how is a child conceived
process of development in the womb
need for eating extra family food by the mother
need for iron/folic acid during pregnancy
need for tetanus toxide vaccination
delivery by trained dai/PHC doctor
who are at risk’ mothers and children
need for spacing births, permanent and
temporary methods of family planning
Early Childhood Care and Stimulation
Breast feeding babies
I
Weaning of infants and providing them will) mix- u
family food
Immunization of children
90
I
>
Healthful environment for promoting the development
of children
i
personal and environmental hygiene
safe drinking water
Infant stimulation for cognitive, language, socialemotional and physical development
Monitoring growth of children
Non-formal preschool education for children
Problems in children
health related
nutritional
diarrhoea
disabilities
behavioural
igs
■■ j
Handling these problems
I
•S
Referral of cases to PHC
Provision of supplementary nutrition at the anganwadi
Storage of foods at the centre
i
Methods of cooking
Distribution of SNP to children
Supervision of Helper s activity
Education of parents about the health, nutrition and
educational needs of their children, population
education
■
Creating awareness among people about the
programme and their participation in it
Methods of mobilizing community participation
Coordinating with variety of people, agencies groups
for involvement in the anganwadi
\
■
91
■
i"
1
’
•>:
w
i
Methods of communicating with people
Use of home visits, bal melas, mahila mandals,
exhibitions for creating awareness among the
community
Role and responsibilities of the worker in the
Anganwadi
vis-a-vis the CDPO/Supervisor
vis-a-vis the health staff
Conducting a survey of the area
i
Location of the AW centre
Planning the AW programme
!
Maintaining stocks, registers, correspondence
60. Facilities Available for
the AWW and Helper
Job Training
Honorarium/TA/DA during job training
AWW will be able to
Money available for food transport, fuel
•i
z
''
■
/
1
I
— enumerate the facilities
available to her and
the Helper in the AW
Provision of Refresher Training
Leave facility
— describe ways to maintain
a good relationship with
the Helper, Supervisor
and CDPO
Honorarium as a village Health Guide, for adult education
classes
Further prospects for educated AWWs/Helpers
61. Relationship with Helper
bleed to maintain good relationship with Helper
1
Recognising their contribution in the AW work
Helping to solve her problems
•I
Speaking politely and encouraging her to participate in
the AW programmes
Using her as a contact with local people in case AWW
is not a local person, to understand the local customs,
traditions, values etc.
,1
92
---- .,r..
I
/ 62. Relationship with
Supervisor/CDPO
Approaching supervisor for counselling in personal
problems, disputes with community
I
I
Requesting her help in
improving preschool education activities, enhancing
community participation, community education, arranging
competitions, bal melas etc.
Share her experiences of other AWC and new ideas
Number of visits of a Supervisor and CDPO to the
centre
Continued guidance from Supervisor/CDPO
Availability of CDPO’s office as a resource centre
■ i
■
i
-I
i
^51
'■.^5
■
■
' ■ w
i
93
iWK'fcr i*4
iMaS.S'JIOEKji’O*-:-
■■
II
|
ivyb
SYLLABUS FOR JOB TRAINING OF ANGANWADI WORKERS
OF ICDS PROGRAMME
Februaiy, 1989
!
n[E •H*
NATIONAL INSTITUTE OF PUBLIC COOPERATION & CHILD DEVELOPMENT
5, Siri Institutional Area, Hauz Khas, New Delhi-110 016
I
( ilkf Insirucror
AfigLnv.'udi lie
g Centra
buaijalora
CONTENTS
Pages
Section I
j
\''
onal
Job Responsibilities and Tasks of
Anganwadi Workers
1
Section II
Syllabus and Programme Schedule
13
Section III
Contents of Training
35
■■
■
J
i
Zj
y
SECTION I
JOB RESPONSIBILITIES, TASKS AND SKILLS
!? I
1
R
>1
1
1
-
-
f'-ZTOB
i
.
CHART OF ANGANWADl
-■■
-
«S^^S=!
WORKERS
i
JOB RESPONSIBILITIES of
ANGANWADI WORKERS
I
r
4
PREPARATORY WORK |
_______ i__________ _
SERVICE DELIVERY |
| MANAGEMENT j ADMINISTRATION |
I
MAINTENANCE OF RECORDS
SURVEY TO ENLIST BENEFICIARIES
CHILDREN 0-6 YRS
CHILDREN lAT RISK'
COMMUNITY CONTACT I
A EDUCATION
I
PREGNANT!NURSING MOTHERS
I
ORGANISATION OF
UPDATING
SURVEY DATA
NON FORMAL
PRESCHOOL ACTIVITIES
4
it
REPORT OF CDP0/SUPERVI50R
MOBILIZE COMMUNITY
PARTICIPATION
I
MAINTAIN UASION WITH
-PANCHAYAT
-PRIMARY SCHOOL
- MAH1LA MAN DAL
-DAI
HOME VISITS TO
EDUCATE MOTHERS
-HEALTH Zr
NUTRITION
- PROMOTING
CHILD DEVELOPMENT
I
HOME VISIT TO
IDENTIFY CHILDREN
‘AT RISK'
.........1______
y______________________
;
j PREPARATION & DISTRIBUTION OF
I I supplementary nutrition
I
CHILDREN 6MTHS- 6 YRS
PREGNANT t, NURSING MOTHERS
MOTHERS *AT RISK'
ASSISTING PHC
- IMMUNISATION
- HEALTH CHECK-UP
-REFERRAL SERVICES
- HEALTH EDUCATION
I
FIRST AID
■
BIRTHS i DEATHS
REGISTRATION
GROWTH MONITORING
’
-
Z..
______ _ .
tasks and skills of an anganwadi worker
Job Responsibility
of an AWW
Tasks of an AWW
(1)
_____________ (2)
Survey
1. Contact community,
take interviews,
record data
(i)
/
Skills required in
doing the Tasks
(3)_____________
Talking to different
members of the household
to tell them about the
purpose of the survey
!
Ability to ask questions to
obtain the desired
responses
/
Filling up the survey forms
/
I
4
2. Interpret data to
identify beneficiaries,
at risk" children and
mothers
|
I
3. Update survey data
Adding new information
and deleting irrelevant
information from the
survey forms
4. Register births and
deaths
Keeping track of new
births and deaths and
recording them
1. Organise activities
for physical motor
development,
language develop
ment, cognitive
development, social
development
Conducting games,
narrating stories, singing
songs, organising creative
and cognitive development
activities for children
(U) Service Delivery
I.
Organising nonformal pre
school
education
Communicating with
children
Organising children in
circles and groups
Note: Separate skill has not been listed wherever the skill required to do the task has been built into the task itself.
I
■
3
I
P)
(3)
n.
Introducing variety in the
preschool activities
2. Prepare and use aids
for preschool
activities
Skill in making aids like
puppets, masks, story
figures, puzzles, etc.
Identifying low cost
material which can be used
in organising preschool
activities
3. Replenish aids
Repairing aids
Substituting tom aids by
using alternate material
4. Plan the preschool
programme
Skill in planning different
activities to be organised
in the AW to ensure variety,
keeping in mind time as
well as age of children
111.
Skill in introducing
changes as and when
needed
5. Educate parents
about the import
ance of preschool
education for over
all development of
children
Conducting meetings of
mothers
Talking to mothers during
heme visits and at different
meetings
i
6. Helping in the
admission of older
children in the
primary school
Contacting the parents,
primary school teacher
Finding out requirements
of admission
Helping parents in com
pleting the formalities
of admission
4
(1)
II.
(2)
Growth
Monitoring
1. Weigh the children
2. Assess the age
(3)
Taking weights and read
ing the weights accurately
Calculating the age of the
child
o
3. Plot weight on
growth cards
Plotting weight on growth
cards
■
4. Interpret growth
trend
Interpreting the direction
of the curve
5. Educate parents
about the growth
pattern of their
children and
management of
malnourished children
Talking to mothers about
the growth pattern and
feeding of children
6. Involve mothers in
the process of
growth monitoring
Persuading mothers to
monitor the growth of
their children
I. Assess and
measure the amount
to be cooked
Calculating and measuring
the amount of SNP to be
prepared daily
2. Supervise cooking
by Helper
Observing the cooking by
Helper
i
s
III.
Organisation
of supple
mentary
Nutrition
■
Guiding Helper in correct
method of cooking
3. Help and supervise
the Helper in
preparing children
for supplementary
nutrition
o
4. Distribute
supplementary
nutrition
5
Supervising washing
hands of children
Organising children to sit
and receive supplementary
nutrition
Measuring the amount to
be served to one child
1
a
1
(2)
J;
Supervising distribution
of SNP in an organised
manner
Li
Ensuring that children eat
in the Anganwadi
5. Provide extra
amounts to “at risk”
children
Identification of “at risk”
children
Ensuring supply of extra
ration to such children
I
6. Storage of 3NP
food items
Storing the food items
correctly to prevent spoiling
Checking for spoilage
before cooking
1
7. Educate mothers
about
i) nutrition for
children at home
Preparation and use of
aids for mother’s meetings
ii) their requirements
during pregnancy
ll'1 1
IV.
Providing
support to
Primary
Health Centres
1. Prepare and update
lists of children and
pregnant women for
immunisation
i:’1
2. Prepare parents
q
for immunisation
of children
I
3. Make arrangements
■M
Talking to mothers
for immunisation
4
6
r
mV
Listing children for
immunisation including
the new borns indicating
type of immunisation and
dosage
Talking to parents about
the need for immunisation,
ability to give specific
information related to the
place, specific number of
dosages and possible
immunisation side effects
Sterilisation of equipment
for immunisation
■
(1)
(2)
(3)
Laying out equipment
for the Doctor
■
4. Maintenance of
immunisation
registers
Filling up immunisation
register
5. Follow up through
home visits of new
bom children for
immunisation
purposes
Making home visits and
talking to mothers about
the expected date of
delivery and the
immunisation schedule
6. Demonstrate and
prepare an oral
rehydration solution
to educate mothers
about diarrhoea
management
Preparation of oral
rehydration solution
through the household
method and preferably
demonstrate it to mothers
with children suffering
from diarrhoea
L
r
|
L
j
I
J
Guiding mothers in pre
paration of ORS
7. Follow up through
home visits,
< children suffering
from diarrhoea
Making home visits and
talking to mothers
8. Encourage all preg
nant women to go
for check up to the
PHC or sub centre
Talking to mothers about
the importance of health
check up and anan jc I
the same in consuhniion
with LHV/ANM
I
I
Keeping a record of tlie
number of tablets given
periodically
9. Dispense iron, folic
acid tablets to
pregnant women
IE
i
Dispensing the correct
dosage of iron and folic
acid to pregnant women
f
I ■
I'
I
7
|i
pl)
(2)
J—
. I
■
I'
o;
10. Give vitamin ‘A’
drops to children
Giving correct dosage of
Vitamin ‘A’ drops to
children
11. Refer cases for
health check up to
the PHC
Identifying cases for
health check-up, filling
up a referral slip with
requisite details
12. Provide first aid for
minor ailments and
injuries
Administering first aid
in case of emergencies
13. Early identification
of disabilities
Identifying symptoms of
disabilities in children —
auditory, visual, orthopae
dic, mental for preventive
action
14. Educate people on
health care of
women and children
and family planning
Talking to mahila mandal
members, organising
community meetings
II.
Making arrangements,
preparing talking points
for discussion
Public speaking
(iii) Community
.
. „
i
contact and
education
I.
Community
participation
1. Establish contact
with community
Maintaining continuous
contact with people
Ability to talk to men and
women of different ages
and backgrounds and
establishing rapport with
them
2. Involve community
in various activities
of the Anganwadi
8
■
'
:-.3
B
i
(1)
(2)
3. Encourage mothers
to bring children by
turns, to the AWC
II.
Community
education
(3)
Periodic discussions with
mothers to persude them
to send/accompany
children to the AW
Health & Nutrition
Education
1. Educate parents
about health and
nutrition needs
Planning and organising
meetings of parents for
nutrition and health
education (NHEd)
2. Educate parents
for growth monitoring,
feeding children,
food requirements
during pregnancy and
lactation, man
agement of diarrhoea
Talking to parents
Preparation and use of
aids in the meeting
Preschool Education
1. Educate parents to
create awareness
about early infant
stimulation, import
ance of preschool
education and play
way method of
learning
Planning and organising
meetings of parents about
early childhood
stimulation
Discussion with parents,
preparation and use of
aids in the meeting
Population Education
r
1. Educate parents,
particularly women
about prenatal
development and
methods of family
planning
Talking to people, parti
cularly mothers about
family planning, prenatal
development and care
during pregnancy
2. Motivate commun
ity for family
planning
Planning and organising
meetings of mothers
Contacting LHV/MPW
9
IJ ; ;k
• I
I
I
y
f'
(2)
(1)
III.
Communi
cation
:! li.
iij:
1. Establish contact
with other functionaries/individuals/agencies/
voluntary organisa
tions in tine area
(3)
Identifying important
people, formal and
informal leaders
II.
2. Enlist their support
in the AW programme
I;
3. Make home visits for
educational purposes
4. Form and activate
mahila mandals
I
(v)
Identifying women for
setting up a mahila
mandal
Organising meeting of
mahila manda!
Encouraging participation
of mahila mandal in the
AW programme
5. Organise bal melas,
exhibitions, com
petitions etc.
’ l| I
ir
Arranging a bal mela,
exhibitions, competitions
in the AW
Enlisting support of
supervisors/CDPO for
organising these
(iv) Management
and
Administration
1
I.
II
I
i
I
Maintenance
of Records
1. Fill records
2. Keep records neat
and up-to-date
10
i
■
—
• -
I
SECTION II
SYLLABUS AND PROGRAMME SCHEDULE
I
I
i
;... I
n
(1)
(3)
3. Maintain correspon
dence with indivi
duals, groups and
functionaries
II.
Reporting to
CDPO, Super
visor, Medical
1. Fill monthly/quarterly
Officer
2. Send reports to
Supervisors, CDPOs
and Medical Officers
(2)
Writing letters to different
people
Filing letters neatly
progress reports
J/
(v) Utilisation of
the Services
of the Helpers
1. Supervise and guide
Helpers’ tasks
preparing the
anganwadi for
conducting
activities
cleaning the premises
filling up of drinking
water
putting things back in
place
locking up the AWC
preparing supple
mentary nutrition
2. Involve Helper in
the Anganwadi
activities
11
Encouraging participation
of Helper in other activities
of the Anganwadi and
assigning specific activity
to them
SYLLABUS FOR THREE MONTH JOB TRAINING OF AWWs
A. TRAINING SYLLABUS
In-service job training course has been designed for Anganwadi Workers inorder to equip them
with requisite knowledge and skills needed to discharge their job responsibilities effectively. The
various components of training and the syllabus are given below:—
3 months
72
432
Duration of the course
No. of working days
No. of working hours
Subject
Classroom
instruction
Field
work1
Library
& Audio
visual
Total2
1. General Orientation
13>/2
19'/2
3
36
2. Preschool education
15
66
l'/2
83
3. Nutrition & Health;
Nutrition & Health
Education3
34
54
5'/2
93!/2
4. Community participation,
community education
and communication
56
67
4
127V6
5. Population education
9
3
12
6. Management
23'/2
35'/2
59
7. Holistic approach to
child & wrap up
12
12
8. Evaluation
9
9
172
246
14
4324
'Field loork Includes
i) Class room practical
ii) Observational visits
iii) Field work placement in ICDS project
137 Hrs.
13 Hrs.
96 Hrs.
TOTAL
246 Hrs.
Hhe total hours are inclusive of the time spent on exercises, games, songs, hobby work, that have been included in the
programme schedule to break the monotony.
3Some of the topics from the Health and Nutrition Education component are included in the area of Community
Education.
H'he total number of hours provided are exclusive of the time used for physical exercises, prayers or feedback
sessions, which would start at 9.30 a m.
15
s
I
1
I
The main objective of the general orientation is to familiarise the Anganwadi Worker with the j
existing status of women and children in the country/region and the need for organising
programmes, particularly the ICDS, for their development. It also introduces the Worker to the
objectives, services, scope, beneficiaries, staffing pattern of the ICDS programme and their own
roles and responsibilities vis-a-vis that of the Supervisor, CDRO, MO, LHV and the ANM.
Or
six ye
prorr
non-f
in he
Instr
Instructional Goals
Aft
After the training the AWW should be able to:
i) describe the status of women and children in India
ii:
ii) explain the need for programmes for child development
iii) list the objectives, package of services, target group, scope of the ICDS scheme
iii)
iv) define her role and responsibilities as an Anganwadi Worker
v) explain the need for conducting a survey
iv;
vi) define the term community and the concept of community participation
v;
:!|
vj:
I
I'-ii
vii;
Curriculum Contents
Theory/
discussion
(Hours)
i)
Status of children and women in India;
health, nutrition and educational
6
ii)
Need for child development programmes
3
iii)
ICDS, its philosophy, scope, objectives,
package, beneficiaries, coverage and
staffing pattern
2
iv)
Role and responsibilities of an Anganwadi
Worker
3
V)
Need for conducting a survey
l'/2
vi)
Community participation; concept and
importance
3
1
(Library and audio visual is for a minimum
period of 2,/2 hours)
Field
tvork*
viii;
Curr
3
i)
ii)
iii)
iv)
v)
* Hours do not include field work placement in ICDS project.
!
16
1
T
PRESCHOOL EDUCATION
ith the
One of the services of ICDS is to cater to the developmental needs of children between three and
six years of age and to prepare them for formal schooling. The Anganwadi Worker is expected to
promote the all-round development of children (physical, social, emotional and cognitive) through
non-formal play activities. She must organise a variety of activities and utilise the natural resources
in her environment to structure learning at the Anganwadi.
nising
to the
rown
Instructional Goals
After the training the AWW should be able to:
i) explain the need and importance of preschool education
") deXnm!
9rOWth °f Chi'dren fr°m birth tO SiX yearS’their needs’and milestones in their
dCVCIULJI i icl II
iii)
*e physi“'',anw
”dai
IV) collect waste and throw away material and prepare aids and play material out of these
v) correctly manipulate the aids and play material prepared
vi) utilise the resources available in the environment for teaching-learning activities
vii) draw up a daily/weekly thematic programme schedule for organising preschool activities in
me Anganwadi
viii) discuss the behavioural problems of children.
Curriculum Contents
Theory/
discussion
(Hours)
Fidd
work
i)
Heed and importance of organising
non-formal preschool activities
3
ii)
Development of children from birth
to six years; milestones in development
and needs of children
3
iii)
Activities for physical-motor, language
cognitive, personal, social and emotional
development; preparation and use of aids and
play material for organising these activities
iv)
Clse of environmental resources in
organising preschool activities
5
v)
Theme approach in organising preschool
activities
6
17
24
c
’■
III
til h
lit
I
It
6
vi)
Nature walk as an activity to promote
overall development in children
vii)
Planning the preschool programme
viii)
Problems faced in the field in organising
preschool education
3
ix)
Common behavioural problems in children
3
x)
Use oi aids in a preschool set up
■
*
3
3
L --
(Library and audio visual is for a minimum
’ period of 1 hour)
NUTRITION AND HEA1-TH
The nutrltior. and health components of the ICDS scheme alm al reducllon
morbidity and malnutrition among children and to bring about an improvement in the health and
nutritional status of mothers and children.
Instructional Goals
After the training the AWW should be able to:
i) explain the need for eating mixed family food
ii) discuss the importance of breast feeding and weaning in promoting the health of children
cards, interpret growth trend to mothers and counsel them for care of the chrld
iv) enumerate the schedule for immunization of children and her role in this regard
v) list the common nutritional deficiency diseases communicable disease^and ailments that
cause malnutrition among children; suggest strategies for combating these
vi) identify the signs and symptoms of dehydration, prepare an oral rehydration solution and
I
iF
state the ways of diarrhoea management
Vii) organise and prepare a variety of recipes for supplementary nutrition in the anganwad.
ensuring proper hygiene, enrichment and storage of supplementary nutrition
viii) make a list of the health facilities available near her anganwadi
ix) identify some common ailments in children and pregnant women
■
and administer simple
medicines for these
I
11
1
j^ll
x) render first aid for minor injuries and accidents
xi) detect disabilities in children and refer these to the health centre
xii) organise health, nutrition and population education for mothers
18
i;! ■ihi!
i
Curriculum Contents
Theory/
discussion
Field
work
(Hours)
ortality,
Jth and
i)
Hutrition and health services in the
anganwadi
V/2
ii)
Good nutrition for children and mothers
3
ii>)
Feeding and weaning practices
iv)
Personal and environmental hygiene
v)
Safe water supply
vi)
Immunization of children
vii)
Malnutrition, the major problem among
children
viii)
Diarrhoea and its management
6
ts that :
simple
f/2
l'/2
V/2
l'/2
3
l'/2
ix)
Nutritional deficiency diseases
3
x)
Common ailments and other diseases in
children and how to handle these
3
2
xi)
Growth monitoring
2
11
xii)
Organisation of supplementary nutrition,
methods of cooking, preparation of
simple recipes
l'/2
4/2
xiii)
Nutrition and health education of mothers
xiv)
Ante and post natal care
xv)
Early detection of disabilities
xvi)
Health infrastructure in the area
>n and
nwadi
2
l'/2
lildren
jss the
jrovv
1
3
3
4’/2
3
xvii) Treatment of minor accidents and injuries
(Audio visual and library is for a minimum
period of b1/? hours)
19
1/2
IBi
■ ji
I bii
ii
COMMGrSlTY PARTICIPATION AND COMMUNITY EDUCATION
The (CDS scheme has been conceived as a people’s programme. The AWW therefore, needs to
develop skills in contacting the community, mobilising community participation and educating the
community about the needs of children, objectives and services of the 1CDS programme, proper 4''
■ B;.
child care practices etc.
i
IIit
is I
F” ■
' ||
Instructional Goals
After the training the AWW should be able to:
---i) carry out a simple survey to enlist beneficiaries; children 0-6 years, pregnant and nursing
j
■.
sf
.i ______
_i_!u______
u___
miiha
trt/^v/P^niQtAr
and pxnlain
theand
need
to
mothers
andi children
and
mothers
“atQi
risk
”, fill in the Survey
Register
explain
the need to
■
IS
■
update survey data
ii) explain the concept and importance of community participation in the context of ICDS
i.
i
■
|
iii) identify areas of community participation
■
iv) recognise different forms of community participation in the anganwadi activities
■
I£
v) mobilise community participation in ICDS
vi) identify individuals, groups and agencies for community participation
vii) list ways of utilising groups and individuals in the ICDS programme
viii) form and activate a mahila mandal, arrange and conduct its meetings
ix) locate and mobilise the supportive services available in her area, maintain liaison with
different functionaries, approach individuals, groups and organisations for community
Sil
8
participation
x) define her role in community education and spell out the areas in which she needs to
educate the community
xi) list different topics/messages for community education
■
xii) plan, organise and conduct a meeting for parent education
f
xiii) prepare aids for community education
■■
xiv) undertake home visits to educate the community
F' J N
di
I
xv) organise community based functions; bal-melas, well baby shows, sports meets, exhibition?
competitions etc.
Curriculum Contents
Theory/
discussion
(Hours)
f’i
I
i)
Field
tvork
■.
!• •
1672
Community participation
Role of AWW, areas of community participation,
recognising community participation, methods of
i
Pl’ ’
20
£•
tt-t-
■
Ki'ffWM'*■»••• -
.
-it
mobihsmg community participation, ways of utilising
individuals, groups and agencies in the programme,
coordinating and working with different functionaries
ds to
3 the
□per
ii)
Communication
Forms of communication; principles,
methods and barriers
Conducting a home visit
j
I'
sing
Forming and activating a mahila mandal,
arranging and conducting a meeting of
mahila mandal
?dto
iii)
Parent and community education
Settings and areas in which community
education takes place, planning and
organising parent education programmes
f
lity
l'/2
3
3
6
6
V/i
16'/2
12
3
•
! ”> '
Health and Nutrition Education, role of the
community and fathers in creating healthy
environment for children, management of
home, cleanliness and sanitation of the
environment and home
/ith
4'^
I-
Organisation of bal melas, exhibitions, sports
meet, competitions, festivals, well baby shows
to create community awareness and mobilise
participation
)S
14
3
9
3
Education of mothers to promote overall
development of children under three years,
socio-economic programmes for women,
operating savings bank account
Population education
to
ns,
.
.
I
I
Preparation and use of aids for community
education
iv)
Need for and methods of conducting
a survey
J
6
(Audio visual and library is for a minimum
period of 4 hours)
MANAGEMEMT
rep^ olan^hpOAbnreSPOnHSibilitieS’
Worker has
maintain records, fill progress
lunges. It ,s.
| Instructional Goals
After the training the AWW should be able to:
21
-
I
.| •
s
“I
i
Im
i) plan the anganwadi programme and her own schedule including home visits, community
and adult education classes and meetings of mahila mandals etc.
-
ii) list ways of making the AW centre safe and adequate
Iii
1
iii) produce and store stocks and supplies for the AW
iv) maintain registers and records and a daily events diary
v) fill monthly and quarterly progress reports
If
vi) write letters to different people
?■
Cu
'
vii) enumerate the facilities available for the AWW and Helper
-
viii) describe ways to maintain a good relationship with the Helper, Supervisor and CDPO
I ■
-
;t • •
i)
Curriculum Contents
Theory/
Field
discussion
work
(Hours)
II!
I
I.
I
•
■
■
3
i)
Location of the AW in terms of its adequacy
for delivery of services
3
ii)
Procurement and storage of stocks and
supplies for the AW
3
iii)
Maintaining correspondence with
functionaries, voluntary organisations,
individuals and agencies
3
iv)
Maintenance of registers and records,
filling up monthly and quarterly progress
reports
12
V)
Facilities available for the AWW and Helper
vi)
Planning the AW programme
vii)
Maintaining good relationship with Helper,
Supervisor and CDPO
3
viii)
Problems in field situation and handling
these
3
fl l‘f
■
3
3
Sir;
a
WRAP UP
At the end of the three month training the AWW will spend two days in viewing the child in a
holistic manner, recalling all that has been done during the training and her roles and
responsibilities in this regard.
■
t
■
3MR
. -
ti i .
imunity
•/£■
r-.:?>. ... .. !•
Instructional Goals
After the training the AWW should be able to:
i) explain how a child is viewed in a holistic manner
■
ii) recall the contents of her training
iii) enumerate her role and responsibility in the integrated development
of the child
Curriculum Contents
Theory/
Held
discussion
(work
(Hours)
)P0
i)
id
Integrated Development of the child
12
'
-
’w
rk
••r
H
.J
1
F"
'
■■■
-■
I
I
T
I' '
■f'■
lild in a
es and
;
1
*
? ■ |i
$
B. PROGRAMME SCHEDULE
1
2
10.00-113Q
1130-1.00
3^
4
1.00-2.00 2.00-330
5
GENERAL ORIENTATION____________
Day 1
(J
Introduction to the training centre
ui
f)
N
Day 3
Physical
exercise
(9.30-10.00)
Status of children
in India <-
C
Game
Session
(11.15-1130) (contd.)
Visit to the town
Introduction to
the training
programme
Screening of film/
audio visual/audio
programme
(i I
— health
Need for child
development programmes
Discussion
I,
Activities related to
hobby development,
maintaining a daily
events diary
I
Status of women in India
Im
— education
— social and economic
Discussion on salient themes and role play
(Theory: 2 hrs/Role play: 1 hr.)
— education
— discussion
Theme song
for the course/
group
(9.30-10.00)
Rapport building
(contd.)
— health and nutrition
— nutrition
Day 4
_7 x.
7,
f
(\j
\Q
6
L
Introduction and rapport
building through songs and games
Day 2
330-5.00
Game
Session
(11.15-11.30) (contd.)
H
An introduction
to 1CDS
Film on ICDS
* 31 ' •.
Q-.
J
e
■
-
_____
------------------------ .
1
19
Day 5
Day 6
,---------------------------- :
—
,,
2
Physical
exercise
(9.30-10.00)
■
--------------------
----------------------- -.-zx'.-
■
■
■
■
•
— -----------------
4
5
6
7
Visit to an ICDS project
— Project office
— PHC/Sub centre
— AW
— Block office
Discussion on major points of observation
L
Role and responsi
bilities of an
AWW in ICDS
Theme
Session
song for
(contd.)
the course
(3.15-3.30)
Visit to the
library
a
3
t
■
Conducting
a survey
■ --.i*-
Community parti
cipation: concept
and importance
Game
Session
(3.15-3.30) (contd.)
Development of
children 0-6 yrs.
Session
Hobby
time
(contd.)
(3.15-3.30)
<3.A |1 |
PRESCHOOL EDUCATION
Day 7
^^Organisation of nonformal preschool activities
J;
— need and importance
— activities for promoting overall development
. participatory play and discussion
N
ro
^7 ' I >
.
— growth
— milestones
— needs
I
Day 8
-■ s;
IS
-I
q
-I
C
— outdoor and indoor
— free and guided
— games
— action songs
— creative activities
(Introduction: 20 mins.)
■
1® -
Activities for physical development
i
I
Day 9
Activities tor language development
— listening skills
— free conversation
1
—“songs and rhymes
— stories
— language games
(Introduction: 20 mins.)
Starting preparation of aids and play
material for physical development; ball,
threading frames, beads etc.
H
Starting preparation of aids and j>lay material for
language development, puppets, flannel board,
picture cards, musical instruments etc.
i
(Introduction: 20 mins.)
..................... —■
■m—iwir--- -
1
2
3
’
\
4
5
6
L
Starting preparation of aids and play material for
cognitive development; dominoes, matching,
seritation, colour/touch cards, puzzles etc.
-
7
■
Day 10
Activities for cognitive development
— number
— direction
— time
— environmental awareness
— games, songs, stories
(Introduction: 20 mins.)
i
Day 11
Day 12
-Activities for personal, social and
emotional development
— songs
—puppet play
— group games
— doll play
— creative activities
— sand and water play
a
Use of environmental resources in organising
preschool activities;
water, nests, trees, birds, etc
(Theory: 30 mins.)
N
puppets, stuffed toys, masks etc.
■i
Day 13
Use of theme (project) approach in
organising preschool activities
(Theory: 1 hour)
Day 14
Mature walk as an activity to
promote overall development
(Introduction: 20 mins.)
nwr-rir
Starting preparation of aids and play material
for personal, social and emotional development,
c
H
Exercises and
worksheets for use of
environmental
resources
Audio visual presentation
(4.00-5.00 pm.)
Development of themes
Discussion on themes developed
Use of items collected during nature walk
in preparation of materials/aids
5|Q
|
...
*
I
.-
1 _
......
1
r Day 15
h
2
3
4
Recall
salient
features of
PSE
component
in ICDS
(9.30-10.00)
Common behavioural
problems
Hobby
Session
time
(contd.)
(11.15-1130)
Day 16
5
6
L
a
Use of aids prepared in a preschool/
AW set up or simulated situations
7
I
Exercises in planning
the preschool programme
Likely problems faced in the field in
organising preschool activities and ta ' ’
hese
Discussion
Day 17
hJ
co
k
Physical
exercises
(9.30-10.00)
Day 18
NUTRITION AND HEALTH
Nutrition and health
Reading in the
services in the
Library
Anganwadi
N
Feeding and weaning practices
C
— importance of breast feeding
— need and time for weaning
— fads and fallacies
— planning and preparation of
weaning foods
(Theory: 116 hrs.)
Good nutrition for
children and mothers
Theme
song
(3.15-3.30)
Education of mothers about breast
feeding and weaning
Discussion, role play, case studies
(Theory: 1 hr.)
(■
U
-i/a
8^
"I
i
V
Day 19
y
1
Planting
trees and
plants in
the training
centre (9.30-10.00)
Personal and environ
mental hygiene .
(Theory: 1 hr.)
Observational visit to
see compost pit, sanitary
toilets
~
■
H
I—
Gse of safe water
supply
Theme or
ion
group song (c . d.)
(3.15^3f30)
it hi
JWHh laaF*;
.73'
1
2
3
Day 20j, Fe
:k
session of
previous
week
(930-10.00)
Immunisation of
children
(Theory: 116 hrs.)
Physical
exercises
and prayer
(930-10.00)
Diarrhoea and its
management
Day 21
<
4
5
L
Hobby
Session
time
(contd.)
(11.15-11.30:
Preparation of an ORS
Practical
(930-10.00)
w
Day 23
Day 24
■
Common ailments and Game
Session
diseases in children
(11.15-11.30) (contd.)
Malnutrition: the major
Song and play
problem among children, materials competition
Jon |
causes of malnutrition
a
Nutritional deficiency
diseases
Early signs of
— protein-energy
malnutrition
— anaemia
— blindness
— goitre
N
i i
Introduction to growth monitoring
(9.30-11.30)
Exercises in plotting and
interpreting growth curve
(9.30-11.30)
, 7
L
rxj
Day 22 Group pre\ /\
sentation
\j
at prayer
6
■ I
Hobby
Session
time
(contd.)
(3.15-3.30)
13;^
Education of mothers
about causes,
prevention and
management of
diseases and ailments
Discussion on material \ i
read in the Library
(4.00-5.00)
Plotting weight and
interpretation of growth
curve
H
*
Demonstration weighing
on salter/bar scale;
classroom practical on
weighing inanimate objects
C
Assessment of correct
birth month and year
'
Practical on
weighing children at
AWC/balwadp<,
H
Discussing growth curve with the mothers
Exercises and role play
: £>'! h
3<
I
j
•
------ r \
•
1
2
3
Day 25
Physical
exercises
and prayer
(930-10.00)
Methods of cooking
Organisation of
supplementary nutrition and hygiene in
in the AW
cooking
\y
Day 26
4
6
L
Preparation of simple recipes for
supplementary nutrition
'8
\
Practical
Ante and post natal
care
Nutrition and health education of mothers
1U
I
7
5
Song
(3.15-3.30)
I-
Session
(contd.)
Discussion on themes, exposure to methods
through role play
Hobby
Session
time
(contd.)
(11.15-11.30)
Day 27
Early detection of
disabilities, visual,
speech, mental,
orthopaedic, hearing
Day 28
Health infrastructure. Field visit to
primary health centre or sub-centre
a
Session
(contd.)
Creative activities
competition
UJ
o
i
N
Q
Film/audio visual, library reading/
case study presentations
J (
Discussion on film/audio visual
i ■.
-2. "
-
Treatment of minor
Use of first aid kit
accidents and injuries;
cuts, scrapes, bleeding,
bites, shock etc.
Day 29
\5'
Day 30
Feedback
session
(930-10.00)
COMMUNITY PARTICIPATION & EDUCATION
Role of AWW in
Game
Session
community
H 1.15-1130) (contd.)
participation
C
H
Storage of food
in the anganwadi
Areas of community
participation
— preschool education
— health
— nutrition
Puppet play
competition
Community Session
song
(contd.)
(3.15-3.30)
— health
b
— nutrition
h-;
□ ss'ra
1
2
Day 31
Physical
exercises
and prayer
(930-10.00)
3
4
5
6
7
*
Day 32
i
Day 33
c
2
Physical
exercises
and prayer
(930-10.00)
Day 34
I
Mobilising community
participation in ICDS
Hobby
Session
time
(contd.)
(11.15-1130)
Coordination and
working with different
functionaries
Game
Session
(11.15-11.30) (contd.)
a
Session
(contd.)
Sports meet
Forms of
communication:
principles, methods
and barriers
Song
Session
(11.15-11.30) (contd.)
N
Methods of
communication
Aids for
communication
Conducting a home
visit
Group
Session
game
(contd.)
Hl.15-11.30)
C
Field
L
Ways of utilising
groups/individuals in
the programme
visit
to
Song
Session
(3.15-330) (contd.)
the
homes
.
.
" b IvV- j
V
1
Day 35
4
c-
J|
\
—
Physical
exercise
and prayer
(9.30-10.00)
Role of AWW in
forming/activiti ng
mahila mandals
Folk
Session
song
(contd.)
(11.15-11.30)
H
Initiating a mahila mandal
Discussion
I
— --
1
2
3
6
7
Day 36
Arranging meeting of mahila mandal
Discussion & Role play
L
Organising meeting of mahila mandal
Role Play
Day 37
Discussion on methods Planning of a
of enhancing commun balmela/exhibition of
ity awareness and
aids prepared by AWW/
participation through
festjval/exhibition of
bal melas. well
hobby collection to be
baby shows, sports
held on day 47
meets, exhibition
/
of aids etc.
Cl
Parent and
community
education
~J
I
5
4
Hobby
time
(3.15-3.30)
Session
(contd.)
ro
Day 38
Physical
exercises
(9.30-10.00)
Settings in which parent Community Session
and community educa- singing
(contd.)
tion can take place
(11.15-11.30)
N
Areas in which the AWW needs to educate
the community: health, nutrition, early childhood
care, play, population education, participation etc.
Day 39
Feedback
session
(9.30-10.00)
9
Planning and organising programmes for
parent and community education
C
Conducting a parent education meeting
Education of mothers to promote the
development of children under three years
(Theory: 2 hours)
H
Audio-visual/film/presentation of case studies
Day 40 Feedback
" "---- session
(9.30-10.00)
R v
1
2
3
4
5
6
7
3
Day 41
Physical
exercise
(930-10.00)
Some themes for
community
education
Preparation of messages
for community
education
L
Socio-economic
programmes for
women
Film
(4.00-5.00)
I
Day 42
U
How to manage the home effectively
Operating small savings Visit to bank/
post office
account in banks and
post offices
*
I
Demonstrateon-cum-disetission (Theory: 114 hrs.)
U)
UJ
Day 43
b
Cleanliness
(contd.)
Cleaning the Cleanliness and sanitraining
tation of the home
centre
environment
(9.30-10.00) (Theory: 1 */2 hours)
Song on
cleanlines
(11.15-1130)
’
Game
Session
(11.00-11.15) (contd.)
N
Role of the community Song
Role of
in creating a healthful
(3.15-330) the father
environment for children
in decision
making for
the family
C
Preparation of messages and aids for population
education
H
Dramatic activities competition
4
D?y 44
Population education
c
Day 45
. - T
Use of aids to educate the community
about family planning
Role play
R-
-7-
1 yX y
1
2
Day 46
V
Day 47 ' ' j
3
2
4
How to conduct a survey
7
5
6
L
Exercises in filling up survey data and
interpreting it
Conducting a Bal Mela
Bai Mela (contd.)
I
MANAGEMENT
Day 48
Feedback
(9.30-10.00)
Location of the AW:
Role of AWW in
making the AW
adequate for
organising activities
Song
Session
(11.15-11.30) (contd.)
a
Exercises in making the anganwadi safe
-
Case studies
N
;4.
£
Day 49
Day 50
5
■
I
\
Physical
exercises
(9.30-10.00)
Procurement and
storage of stock and
supplies
Physical
Exercises
(11.15-11.30)
Session
(contd.)
Maintenance of
registers and records
at the anganwadi
Song
(11.15-11.30)
1130)
Registers
(contd.)
— survey
— immunisation
— services for pregnant
and lactating women
— services for children
C
H
Maintaining correspondence
Exercises in letter writing
Exchange of addresses among participants
Exercises in filling up registers and records
I
t
1
I
— food stock
— visitors book
— stock
II
I
Day 51
Day 52. '■. <
Day 53 C \
to 66
5
4
3
2
1
7
Exercises in filling up MPRs,
MMRs and quarterly report
Using the daily diary for
filling a monthly progress
report, quarterly report
(Theory. 30 mins.)
L
Guidelines for field piecement
U
/ - ' "."'i -
6
(Theory: 30 mins.)
Block Field Placement
i
Preparatory work for field placement;
selection and packaging of aids
In the Anganwadi s
• /<?
Day 67
Q
Integrated approach
to child development
Theme
song
(3.15-3.30)
Session
(contd.)
N
Session
(contd.)
Physical
exercises
(3.153.30)
Session
(contd.)
C
Facilities available for the AWWs and helpers
in ICDS
Feedback of the field visit
Learning experiences
- | C'.
ui
Day 68
Integrated approach
(contd.)
Community
singing
(11.151130)
Session
(contd.)
i
Day 69
Integrated approach
(contd.)
■
Day 70
Game
(11.151130)
I
Session
(contd.)
i
Planning the AW
Programme’
Relationship with
H
Helper
Group
song
(3.15330)
Relationship
with
Supervisor/
CDPO
!
Day 71
Likely problems in field situation'
Evaluation of the training programme
Day 72
Evaluation of the trainees
Conclusion of the course
I
I
I
SECTION III
CONTENTS OF TRAINING
1
I
i
r
T
CONTENTS OF TRAINING
1. Defreezing
(a) Introductory session
Instructional Goals
AWW will
— become familiar tuith each
other
Games like zip-zap, name building
— establish rapport tuith trainer
Triadic interviews/group interviews/dyadic interviews
— knoiv about the training
centre, its geography
and rules
Exchange of information with AWWs about the family,
the homes, village etc.
(for details refer to Organising Job Training
of AWWs: Guidelines for Trainers)
1
— understand the objectives
of the course
—relax and get prepared for
training
(b) Introduction to the training
centre
Games and activities to familiarise trainees with
the training centre
make a map of the training centre
describe the route to the dining room/toilet/kitchen
find out about the people working in the Institute
go and find out from a ‘Chowkidaf the name of the
Principal
treasure hunt game
Arrangements made and facilities available for the course
Stipend, TA, mess
Rules and regulations of the training centre
Facilities in and around the training centre
medical, market, entertainment
(c) Introduction to the training
course
Explaining about the course and its objectives
39
(
[
tjcpectadcns c-: trainers
and each other
nc
rainees from the course
Instructing trainees to maintain a daily diary
i
Recording information in the diaiy
H !■
experiences during the course
observations
achievements
'
attitudes/emotions
information that will be needed for
filling up the MPRs
npfj ill■ !
■
Recreational activities that trainees will undertake
during the training period
hobbies
newspaper reading etc.
!'■' Ri'Mi
a-- n!:
lili
J
Ia
' '1ui
ii
Iliff
i ill •:,,
T'l
i
I
iq
I I
LiI
if
i I1 i
■
r
2. Status of Children in India
AWW will be able to
— describe the health, nutrition
and education status of children
in their area
Eliciting from the participants situation of children
in their villages
number of children born in the past one year
number of children who died
number of pregnant women
general health of children
— compare the children in their
area with those of the country
Equating these figures with those expected in a
population of 1.000 people
— understand and be sensitive to
the problems of children in the
country
• health
• nutrition
< education
Comparing the population of the bloc k with the
population of the country and the State
Population of children In the age group 0-6 years (State)
Comparing the child population of the village/block
with that in the country and the State
Health and Nutritional Status of Children
Creating awareness in the AWW about
infant mortality rate in the Stale, comparing it to tlie
national rate
infant and early childhood mortality rale by age and
sex
40
I Ra
i
4
Page 1 of 1
Community Health Cell
From:
To:
Cc:
Sent:
Attach:
Subject:
"umesh kapil" <kapilumesh@hotmail.com>
<secy.wcd@sb.nic.in>
<kapilumesh@hotmail.com >
Saturday, July 28, 2001 11:34 AM
ICDSWS-IP.doc
Minutes: National Consultation on ICDS
Kindly see the attachment
(jet your FREE download of MSN Explorer at http://explorer.msn.com/intl.asp
7/30/01
{PRIVATE} Recommendations
Indian Pediatrics 2001; 38: 721-731
National Consultation to Review the Existing Guidelines in ICDS Scheme in the Field of Health
and Nutrition
This National . Consultation, was. conducted Jo . review Jhe,.e
Development Services (ICDS) Scheme in the field of health and nutrition and recommend
operationally feasible and scienti-fically sound guidelines for more efficient implementation of this
program. The National Consultation was organized in New Delhi on 16th and 17th March 2001, by
Human Nutrition Unit, All India Institute of Medical Sciences, New Delhi and was sponsored by the
Department of Women and Child Development, Government of India. The list of invited participants
is enclosed as Appendix I.
1. Issue
Strengths and Weaknesses of ICDS Scheme
1.1 Introduction
Integrated Child Development Services scheme is the symbol of Government of India’s commitment
to the holistic develop-ment of children. Specific areas of strengths and weaknesses have been
identified which require to be addressed (Table I).
1.2 Recommendations
(/) ICDS is a long-term development program and is not an emergency relief operation. It should be
implemented as a development program for the community. This focus should not be diluted.
(//■) All efforts should be continued to strengthen the ICDS scheme to make it more successful.
2. Issue
Utility of Growth Monitoring in Prevention of PEM and Promotion of Child Health in ICDS
Program
2.1 Introduction
Growth monitoring is a good theoretical concept. It has been tried in several projects with limited
success. It is an operational strategy for the promotion of child health, which enables mothers to
"visualize" growth or the lack of it in their children and to obtain specific practical and relevant
guidance to ensure regular growth and health of their off-spring. This activity provides an opportunity
to improve the interaction between mothers/care givers and health workers. The ultimate objective
of growth monitoring is to ensure that the mothers/care givers behavior pro-motes normal growth
and development of her child.
The manner in which growth monitoring is being implemented in ICDS is serving no useful purpose.
Strong linkages need to be developed in growth monitoring activities for Nutrition and Health
Education for behavior change.
TABLE I - Specific Areas of Strengths and Weaknesses of ICDS Scheme.
Strengths
(/) ICDS program serves as an excellent platform for several development initiatives
in India.
(//) It is a holistic approach to child development involving the active participation of
the family, particularly mothers.
(/'//) It serves the extreme underprivileged communities of the backward and remote
areas of the country.
(/v) It delivers services right at the doorsteps of the beneficiaries to ensure their
maximum participation.
(v) ICDS has largest number of front line functionaries amongst all the development
programs. It utilizes local women as honorary village level workers for the delivery
of the package of services.
(v/) The implementation of ICDS program has made it possible for the health
services to reach the most remote and difficult areas of the country.
Weaknesses
(/) Inadequate emphasis on Nutrition and Health Education (NHE) activities for
behavior change
(Ji) The focus and coverage of children in 0-3 years of age is inadequate.
(///) Lack of effective co-ordination between Health and ICDS functionaries.
(/v) Irregular supply of Supplementary Food due to administrative reasons.
(v) Programmatic emphasis on Community participation is poor.
(v/) The quality of training of Anganwadi workers needs improvement.
(v/7) The referral system is weak.
(v/7/) Home visits by AWWs are infrequent. Malnourished children who cannot come
to Anganwadis due to different reasons remain largely uncovered.
(/x) There is inadequate decentralization; the same guidelines of Government of
India are followed all over the country. (Representative of the Department of
Women and Child Development, GOI stated that some of the recent guidelines
issued are extremely flexible and State friendly).
(x) AWW has not been accorded the dignity and prestige as a voluntary worker.
She is not being treated as an honorary worker.
(x/) Failure to promote effective community leadership and participation.
(x/7) The role of supervisor is marginal and the CDPO s skills require improvement.
2.2 Recommendations
(/) The frequency of weighing for each child should be reduced to every three months. The growth
monitoring activity may be replaced by "Nutritional Assessment and Nutritional Counseling" (NANC)
sessions. These sessions should be organized in such a manner that each child is covered every
three months. The emphasis in NANC sessions should be on Nutritional and Health Counseling of
mothers with objective of changing their behavior for adopting good practices in the field of nutrition
and health. NANC sessions will also provide data on nutritional grades of children for their selection
for the supplementary feeding program.
(/7) The existing growth chart should be simplified to a simple family held Child Card, which should
include parameters on the child (including developmental milestones) and key messages related to
child caring and feeding. The Departments of Family Welfare and Women and Child Development
with the help of eminent scientists in the country should jointly develop and review the new card. It
should be made of durable material and should be kept with the mother. Cognizance should also be
given to state variations. This card should replace all the cards that currently exist, including
immunization card and center based growth charts.
(/77) The community growth chart should be discontinued. (Representatives from Micro-nutrient
Initiative and World Food Programme stated that the community growth chart should not be
discontinued).
(/v) Growth monitoring data should not be viewed as a replacement for national nutritional surveys
and surveillance, which are being conducted in a specialized manner by other institutions/agencies.
3. Issue
Impact of Supplementary Food Provided in ICDS Scheme: Current Status and Future
Recommendations
3.1 Introduction
Supplementary food alone cannot elimi-nate Under nutrition in the community. Hence,
supplementary food provided under ICDS program should not be viewed as an inter-vention to
improve nutritional status of the children. For a meaningful impact, supple-mentary food
administration should be supported with a strong component of Nutrition and Health Education
(NHE) activities to change behavior of community in general and specifically of the mothers. These
two activities should be further supported by strengthening of all other services in the ICDS
package.
3.2 Recommendations
(/) Supplementary food should be viewed and used only as a magnet/ vehicle for provid-ing other
services under the ICDS scheme.
(ji) Supplementary food should be essentially cereal based, palatable and of good quality. It should
be suitable for use in child-ren below 1 year of age (for complementary feeding).
(/77) A randomized controlled trial should be conducted to assess whether and how the
supplementary food component supports the other services provided under ICDS.
4. Issue
Fortification of ICDS Food with Micro-nutrients
4.1 Introduction
Theoretical considerations suggest that there are four problem micronutrients whose intake is likely
to be low in traditional vege-tarian diets during complementary feeding in infancy. These are Iron,
Zinc, Vitamin A and Iodine. Based on performance of relevant national programs and available
scientific evidence in young children, particularly in relation to the magnitude of the problem,
functional benefit from efficacy trials and safety issue, there may be a case for consider-ing
fortification of ICDS supplementary food with Iron only.
4.2 Recommendations
(/) Fortification of ICDS supplementary food may be considered with iron only. The level of
fortification should be decided on scientific evidence.
(//) Policy guidelines of Ministry of Health for management of micronutrient deficiency disorders like
Iron deficiency anemia, Iodine deficiency disorders, Vitamin A deficiency, etc. should also be
followed in ICDS program. This would ensure that ICDS and health peripheral functionaries at the
district, block and village level advocate and implement same/similar messages/ strategies for
preven-tion of micronutrient malnutrition.
5. Issue
Precautions for Distribution of Genetically Modified (GM) Foods as Supplementary Nutrition
in ICDS Program
5.1 Introduction
Rapid globalization has led to increased movement of food commodities in interna-tional trade. GM
foods are subjected to an extensive range of analytical tests for food safety evaluation like chemical
analysis, allergen tests and nutritive composition. The long-term consequences of GM food are still
unknown. Presently, there are more than 800 ICDS projects in which GM food is provided as
supplementary food. (Representative of the Department of Women and Child Development, GOI
stated that this is not factually correct since there is no labelling of GM/non GM food when it is
imported).
5.2 Recommendation
(/) The guidelines for import and use of GM foods as approved by Nodal Ministry of GOI should also
be followed for ICDS supplementary food.
6. Issue
Nutrition Counseling of Mothers through ICDS Scheme for Promotion of Nutrition and Health
of Children
6.1 Introduction
Nutritional counseling of mothers of children 0-2 years is effective in positive behavioral
modification. This is irrespective of the nutritional supplementation provided. Nutritional counseling
improves the know-ledge of the mothers about child feeding practices and counseling skills of
providers. Home visits by AWWs are feasible. Partici-pation of NGO’s is helpful in facilitating
community participation and effective ICDS implementation. Active participation of district health
authorities can improve the ICDS program performance.
6.2 Recommendation
(/) Nutritional counseling of mothers of children 0-2 years is effective in positive behavioral
modification and should be actively incorporated and emphasized in the ICDS program
implementation.
7. Issue
Community Based Rehabilitation of Severely Malnourished Children through Integrated
Health and Nutrition Interventions
7.1 Introduction
Nearly half of under three children in India are moderately or severely malnourished. In the present
form, supplementary feeding of severely malnourished children in the absence of complementary
health services has marginal effect on the nutrition status. An integrated nutrition-health care
approach with continuous monitoring of severely mal-nourished children is more beneficial for
immediate management and their subsequent rehabilitation.
7. 2. Recommendation
(/) For community-based rehabilitation of severely malnourished children, participation of health
workers for management of infec-tions with other supportive interventions is critical.
8. Issue
Realistic Expectations that can be Achieved in the Field of Nutrition and Maternal and Child
Health by Implementation ofICDS Scheme
8.1 Introduction
There is a need to bring about change in the child caring practices in communities. The children
need to be fed more. This can be achieved by counseling of mothers by AWW and ANM. The
nutritional impact is age related; maximum impact is seen in 6-12 months age group. Nutritional
impact can be evaluated in 5 yearly cycles. There is a need for identification and close monitoring of
process indicators for evaluation of ICDS program in this context.
8.2 Recommendations
(/) Nutritional counseling is effective in behavioral modification and hence it should be made a key
component of the nutritional services rendered by ICDS program.
(//) Proactive efforts to encourage parti-cipation of community, community leaders, NGOs and
Community Based Organizations (CBOs) will facilitate and hasten the behavioral change.
(/77) While judging the ICDS program performance, the focus should be on the process indicators
rather than on the final impact (/.e., anthropometry). The decline in the prevalence of malnutrition in
the community is a slow process and the reduction following nutritional interventions are in the
range of 1-6% only.
9. Issue
Strategies for Convergence between Reproductive and Child health (RCH) and ICDS
Programs for Promotion of Maternal and Child Health (MCH), Activities like Immunization,
Antenatal Care (ANC), Post Natal Care (PNC), Vitamin A and IFA Distribution, etc. at Village
Level
9.1 Introduction
The objectives of ICDS and health sector are overlapping to a great extent except for the
components of supplementary feeding pro-gram and non-formal pre-school education, which are
unique to ICDS. Most of the components related to health care are common to both Reproductive
and Child Health program and ICDS. At present there are gaps and overlaps in the coverage of
beneficiaries, i.e., children below 6 years and pregnant and lactating mothers.
For effective convergence, it is essential to outline the activities and specific areas for convergence
between ICDS and health func-tionaries, which can yield maximum benefit for mother and child
dyad. There is also a need to identify the key elements in this process.
Nutrition and related activities can be the primary responsibility of the ICDS function-aries. In areas
that require health input such as care of pregnant and lactating women, immu-nization,
management of minor ailments, management of severely malnourished children and Reproductive
Tract Infections/Sexually Transmitted Diseases services, speci-fic responsibilities of the partners
namely AWW and ANM need to be made clear.
Social mobilization and community participation are critical for the success of any public health
program. In this pursuit, AWW can play an active role with the cooperation of ANM. The minimum
essential home based records of AWW and ANM may be common.
There is a need of developing an implementation framework for convergence of activities of ICDS
and health departments. This would involve revisiting the roles and responsibilities of AWW and
ANM with suitable modification of their training/reorien-tation programs. The process of convergence
will involve political and administrative will at the highest level. Development of coordina-tion
mechanism at various administrative levels i.e., State, District, Block and Village and evolving a joint
mechanism for monitoring and supervision of the program with an inbuilt provision for accountability
is important.
9.2 Recommendations
(/) There should be harmony in the skills and knowledge of functionaries from both the Health and
ICDS departments in the areas that require convergence.
(//) Roles and responsibilities of the health and ICDS functionaries should be specified for better
accountability.
(/77) Implementation framework for convergence at all levels i.e., State, District, Block and Village,
should be clearly stated.
(/V) Success of convergence will require active community participation, and involve-ment of
panchayats, NGOs/ Community Based Organisations (CBOs) and hence there is need for
institutional mechanisms fortheir involvement.
(v) Political and administrative will is critical for working together of Health and ICDS functionaries. It
will also involve developing coordination mechanisms at various levels and streamlining logistics
and supplies in ICDS and health sector.
(v/) Academic institutions like Medical and Home Science Colleges should be assigned important
functions in improving the program quality and performance.
(v/7) Convergence between health and ICDS sector will be possible only if the functionaries from
these two departments are given respect..and.recognition for. their
and considered
equal partners.
(v/77) Policy guidelines of Ministry of Health for prevention and management of common childhood
ailments, breastfeeding, complementary feeding, etc. should also be followed in ICDS program. This
would ensure consistency in the implementation of various activities/similar messages/strategies by
ICDS and health peripheral functionaries at the district, block and village level. It would avoid
delivery of different messages by the peripheral functionaries.
10. Issue
Home Based Care of Newborns by Anganwadi Workers
10.1 Introduction
About 67% of the infants deaths occur in the neonatal period. To bring reduction in the IMP there is
need to provide care to the newborn. AWW can take care of normal neonates. Possibly she can
also provide care to LBW neonates. AWW would require suppor-tive supervision and training for
providing newborn care.
10.2 Recommendation
(z) Operational research is required in selected regions of the country before AWW can be given the
responsibility of care of normal neonates and LBW newborns in the ICDS program in the country.
11. Issue
Multiple Job Responsibilities Assigned to AWWs
11.1 Introduction
The workload of AWW requires to be reassessed. All types of tasks are given to AWWs, which
makes it difficult for her to do the ICDS work. She is already burdened with current responsibilities.
11.2 Recommendation
(/) There is a need of prioritizing the work responsibilities of AWWs keeping in view the educational
status, time available, hono-rarium paid and records to be maintained.
12. Issue
Early Childhood Care for Survival, Growth and Development of Children in ICDS Scheme
12.1 Introduction
Optimal care practices result in overall development of the child including improved nutrient intake
and growth. There is need to define key care messages that should be used to improve children’s
survival, growth and development in ICDS programs as part of the NHE component.
12.2 Recommendations
(/) There is a need for shift in emphasis from Nutrition and Health Education (NHE) to
communication for behavior change through comprehensive communication strategy.
(//) There is a need to develop optimal communication strategy in ICDS scheme using local
adaptation and formative research for behavior change.
(/77) There is a need to incorporate psychosocial care in NHE activities carried out under
ICDS Scheme.
Compiled by: Dr. Umesh Kapil, Additional Professor, Public Health Nutrition, Department of Human
Nutrition, All India Institute of Medical Sciences, New Delhi 110 029, India, Email: kapilumesh©
hotmail.com and Dr. HPS Sachdev, Professor and Incharge, Division of Clinical Epidemiology,
Depart-ment of Pediatrics. Maulana Azad Medical College, New Delhi 110 002, India. E-mail:
drhpssachdev ©yahoo.com
Correspondence to: Dr. Umesh Kapil, Additional Professor, Public Health Nutrition, Department of
Human Nutrition, All India Institute of Medical Sciences, New Delhi 110 029, India. E-mail: kapil
umesh@hotmail.com
Appendix I.
List of Participants
[PRJVATE}Representatives from Government of
India
1. Mr. B. K. Chaturvedi
Secretary,
Government of India,
Ministry of Human Resource Development,
Department of Women and Child Development,
Shastri Bhavan, New Delhi 110 001.
*34. Dr. Subhadra Seshadri,
Head,
Department of Food and Nutrition,
MS University,
Baroda-390 002.
Tel No. 0265-794136 (R), 795526 (O).
Tel. 3389434 (O)
2. Dr. Rekha Bhargava,
Joint Secretary
Government of India,
Ministry of Human Resource Development,
Department of Women and Child Development,
Shastri Bhavan, New Delhi 110 001.
3. Ms. V.S. Rao,
Joint Secretary
Government of India,
Ministry of Human Resource Development,
Department of Women and Child Development,
Shastri Bhavan, New Delhi 110 001.
4. Dr. Gopal Krishna.
Director,
Government of India,
Ministry of Human Resource Development,
Department of Women and Child Development,
Shastri Bhavan, New Delhi-110 001.
Tel. 3385192 (O), 6254613 (R), Fax 3381800.
35. Dr. B.S. Narsingha Rao,
1-2-62/3, M Block,
11/4, Kakaleeya Nagar,
Habsiguda,
Hyderabad-500 007.
Andhra Pradesh.
36. Dr. Maya Chaudhary,
Prof and Head,
Department of Foods and Nutrition,
College of Home Science,
Agricultural University,
Udaipur-313 003.
37. Dr. Kumud Khanna,
Director,
Institute of Home Economics,
J-Block, South Extension, Part-1,
New Delhi.
5. Dr. Padam Singh
Additional Director General,
Indian Council of Medical Research,
New Delhi. Tel. 6856713 (O).
38. Dr. Asha Pratinidhi,
Head,
Department of Preventive and
Social Medicine,
B.J. Medical College,
Pune 411001.
Tel: 0212-4320127 (R) 6128000 Ext. 310
(O).
*6. Dr. Prema Ramachandran
Adviser Health
Planning Commission.
Yojana Bhawan, Parliament Street,
New Delhi. Tel. 3714058 (O).
*39. Dr. Arun Gupta,
Coordinator,
Breast Feeding Promotion Network of India,
BP-33, Pitampura, Delhi 110 034.
Tel: (O) 7443445.
7. Dr. Sudhansh Malhotra,
Assistant Commissioner,
Ministry of Health and Family Welfare
405-D, Nirman Bhavan, New Delhi.
Tel. 3019993 (O), 6417542, 6417547 (R).
40. Dr. Jagdish Sobti,
Coordinator,
Breast Feeding Promotion Network of India,
BP-33, Pitampura,
Delhi 110 034.
Tel. (O) 7443445.
*8. Dr. Ambujam Nair,
Deputy Adviser Health,
Planning Commission, Yojana Bhawan,
Parliament Street, New Delhi.
Tel. 3711104 (O), 5080976 (R).
*9. Dr. B. K. Tiwari,
Adviser Nutrition,
R. No. 355,
DGHS, Nirman Bhawan,
New Delhi.
Tel. 3018113 (O), 3620595 (R).
*10. Dr. T.N. Dwivedi,
Under Secretary,
Department of Women and Child Development,
Shastri Bhavan, New Delhi-110 001.
Tel. 3389984(0), 91380002 (R).
11. Mrs. Vasudha Gupta,
Deputy Secretary,
41. Dr. S. K. Bhasin,
Reader,
Department of Community Medicine,
UCMS and GTB Hospital,
New Delhi.
Representatives from National
Institutions
42. Dr. Kamla Krishnaswamy,
Director,
National Institute of Nutrition,
Jamai-Osmania PO, Hyderabad 500 007.
Tel. 7018909.43.
43. Dr. P. Haridas Rao,
Head, Flour Milling,
Baking and Confectionery Technology,
Central Food Technological Research
Institute,
Mysore 570016.
Government of India,
Ministry of Human Resource Development,
Department of Women and Child Development,
Shastri Bhavan, New Delhi-110 001.
Tel. 3389434 (O).
12. Dr. G.S. Toteja,
Assistant Director General,
ICMR Headquarters,
Ansari Nagar,
New Delhi.
13. Dr. Shashi Prabha Gupta,
Technical Adviser,
Food and Nutrition Board,
Department of Women and Child Development,
Krishi Bhavan, New Delhi.
Ph: 3383823 (O), 686 3063 (R).
Eminent Scientists
14. Dr. B.N. Tandon,
House Number A-2,
Sector 26, NOIDA-201 301,
District Gautam Budh Nagar (UP).
Tel. 4550538.
15. Dr. C. Gopalan,
Director,
Nutrition Foundation of India,
C-13, Qutab Institutional Area,
New Delhi-110 016.
Tel. 6962615, 6965410 (O), 6868126 (R).
16. Dr. Shanti Ghosh,
Consultant MCH,
5, Aurbindo Marg, New Delhi.
Tel. 6851088 (O), 6851088 (R).
17. Dr. K. N. Aggarwal,
Department of Pediatrics,
UCMSand GTB Hospital,
New Delhi 110055.
Tel. 4570175 (R), 2286262 Extn. 502 (O).
18. Dr. Suneeta Mittal,
Department of Gynecology and Obstetrics,
AllMS, New Delhi
Tel. 6197910 (R), 6593378 (O).
*19. Dr. Meena Swaminathan,
11, Rathna Nagar,
Teynam Pet,
Chennai-600 018.
Tel. 254 2790 (O).
20. Lt. Gen. Y. Sachdeva,
G-204, Som Vihar Apartments,
R.K. Puram, New Delhi- 110 022.
Tel. 6194012.
21. Dr. Sushma Sharma,
Vice President,
Tel. 0821-517760 (O).
44. Dr. Dinesh Paul,
Joint Director,
National Institute of Cooperation,
and Child Development,
Opposite Hauz Khas Police Station,
5, Siri Fort Institutional Area,
New Delhi.
Tel. 6963383 (O), 6876110 (R).
45. Dr. Adarsh Sharma,
Additional Director,
National Institute of Cooperation
and Child Development,
Opposite Hauz Khas Police Station,
5, Siri Fort Institutional Area,
New Delhi.
Tel. 6387118 (R), 6962447, 6534014 (O).
*46. Dr. Shahnaz Vazir,
Field Division,
National Institute of Nutrition,
Jamai-Osmania PO, Hyderabad 500 007,
Andhra Pradesh.
Tel. 7018909 Extn. 274 (O), 7018050.
47. Dr. Hanumantha Rao,
Consultant,
National Institute of Nutrition,
Jamai Osmania PO,
Hyderabad 500 007.
48. Dr. Ramesh Bhatt,
Senior Grade Scientist,
National Institute of Nutrition,
Jamai-Osmania PO,
Hyderabad 500 007,
Andhra Pradesh.
Special Invitees
49. Dr. K.K. Rattan,
Block Medical Officer,
CHC Jwalamukhi-176031,
Dist. Kangra,
Himachal Pradesh.
50. Dr. R.C. Agarwal,
Family Welfare Officer,
B.K. Hospital, Dist. Faridabad,
Faridabad-124001 .
Tel. 915415623 (O), 915297896 (R).
Representatives from International and
Bilateral Organisations
51. Dr. Patrice Engle,
Chief,
Child Development and Nutrition Section,
73, Lodi Estate,
UNICEF, New Delhi.
Tel. 4690401.
Nutrition Society of India,
Department of Foods and Nutrition,
Lady Irwin College, 1, Sikandara Road,
New Delhi.
Tel. 6143187, 614 3673 (R), 3358777 (O).
52. Dr. Sheila Vir,
Project Officer (Nutrition),
UNICEF Field Office,
Lucknow.
22. Dr. M. K. Bhan,
Department of Pediatrics,
AllMS. New Delhi.
*53. Dr. Cristine Van Nieuwenhuyse,
World Food Program,
53, Jor Bagh, New Delhi.
Tel. 4694381.
23. Dr. Shinjini Bhatnagar,
Senior Grade I Scientist,
Department of Pediatrics,
AllMS, New Delhi.
Tel. 6594792 Ext. 3290 (O), 6190529 (R).
54. Ms. Deepti Gulati,
Programme Officer,
World Food Programme,
53, Jor Bagh, New Delhi 110 003.
24. Dr. H.P.S. Sachdev,
Professor, Department of Pediatrics,
Maulana Azad Medical College,
New Delhi 110 002.
Tel. 3236031 (O), 6141730 (R).
*55. Dr. Teresa Beemans,
Director, Ml South Asia,
Mocronutrient Initiative,
208 Jor Bagh, Lodhi Road, New Delhi-110
003.
Tel. 4619411.
25. Dr. D.C.S. Reddy,
Professor, Department of PSM,
IMS, BHU, Varanasi-221 005.
Ph: 301506 (O), 0542-316305, 360390 (R).
26. Dr. Rajiv Bahl,
Senior Grade I Scientist,
Department of Pediatrics,
AllMS. New Delhi.
Tel No. 6520275, 6866061 (O), 6318577 (R).
*27. Dr. Deokinandan,
Head, Department of SPM,
S.N. Medical College,
Agra-282002.
Tel:267965/ Ext.113 (O), 215111 (R).
Mobile: 9837094064.
28. Dr. Umesh Kapil,
Additional Professor,
Department of Human Nutrition,
AllMS, New Delhi.
Tel No. 6593383 (O), 6195105 (R).
29. Dr. V. K. Srivastava,
Head, Department of PSM,
KGMC, Lucknow, UP.
Tel. 0522-222204 (R), 266971 (O).
30. Dr. Nita Bhandari,
Senior Grade I Scientist,
Department of Pediatrics,
AllMS, New Delhi. Tel No. 6013098 (R),
6014136 (O).
31. Dr. N.K.Arora,
Additional Professor,
Department of Paediatrics,
AllMS, New Delhi,
Tel No. 6853125 (O), 6493485 (R).
*56. Dr. Sultana Khanum,
Regional Adviser Nutrition,
WHO, SEARO, Indraprastha Estate,
New Delhi.
Tel. 3317804 to 7823 Extn. 26413 (O).
57. Dr. Usha Kiran,
Assistant Country Director, CARE,
27, Hauz Khas Village,
New Delhi 110 016.
Tel. 6564101,6969770.
58. Dr. S.B. Saha,
Project Director,
CARE- Orissa,
372, Shahid Nagar,
Bhubhaneshwar 751 007.
59. Dr. Venkatesh Mannar,
Executive Director,
Micronutrient Initiative,
C/o Micronutrient Initiative,
208, Jor Bagh,
New Delhi.
60. Dr. S. Bulusu,
National Programme Officer,
Micronutrient Initiative
208, Jor Bagh,
New Delhi.
* Invited participants who could not attend.
32. Dr. V. K. Paul,
Additional Professor,
Department of Pediatrics,
AllMS, New Delhi.
Tel. No. 6594372 (O), 6868849 (R).
33. Dr. Amar Jit Singh,
Additional Professor,
Department of Community Medicine,
PGIMER, Sector 12,
Chandigarh-160012.
Tel No. 541031-39, Ext. 277 (O).
AssGGn as you see any of these
anger signs in a pregnant woman
rush her to a hospital
o 30
g CD
g CO
§
3
=_■
CD
£D
o
i
i
co
Bleeding during
pregnancy or delivery
Severe Anaemia with o
without breathlessness
0)
CD
Z5
CQ
CO
I
CD
"C
CO
CD
ZJ
CL
O
CZ
CL
CL
CD
o
nq:
o
o
cz
Z5
15
*<
O
CZ
High fever during
pregnancy or within
one month of delivery
Convulsions or fits,
blurring of vision or
severe vomitting
m
O
o
c
s
CQ
CD
CD
CD
O
°B CD<cd
zr o
o =r D3
O (Q
CD
ST. CD
X °
3-
2o
co o
2
c
=k
c_
CD
Absent movements of
the baby or abnormal
presentations oblique or breech
Bursting of water bag
without any pain
B
co
o
—K
S;
CD
=: Z5
Q_ Q_
co
co
O
CD
3 CD —
CD
7T 3 S
CD
CO 52.
O o o
CD
Care During Pregnancy
o
c
I
CL
i
Take more than usual
amounts of food, plenty
of green leafy vegetables
and us only iodised salt
Take at least two hours of
rest during the day
cz
Z5
_
CD
ZT -s
O
CO
CD
G-
Q) Q.
Z5 CD
CL CD
Z co
=5
CD
CP
o
CD
r—+■
r—4"
C —
CD co
CD
c/)-
3 zr
o
<Q 00
<£Z5 £
z*. CD c
Mother-Child
Protection
Card
'5'7,
CL
R
CT
CD
O ? CD CD CD
O ? Z5 Q. CD
3 w CD §
0 CD
5 O 5
3
o
□
I
CL
CL < 3
CD CD =i.
CO
co X
v<
cr cr 2- c (Q
*< *< 0^ o I
-l CD g:
CD
ro -j cd
2, Z
’•U 2^,
-5 3 cd
CD _
CL
=5’
CD
°
Z =5 Z5
2. =£
zr q CD‘
zr cd
fn o o
—
CD
CD
CD
CL
3
CD ■*
CD
CD CD
Z5 CD
CL
CO
Bic
A
CD
■O o
o :3x 3
CD
DO CD
cn cd
CD
Mother's Education: illiterate/primary/middle/school final/graduate
Girl
Birth Registration: Yes/ No
Birth
Weight
oO
OO
O.IT
Boy ||
Birth order: primi/not a primary
Address
Z
Anganwadi
SHC / Clinic
] Date [
hO
3
o
□
cd
C
□
(Q
O
5
5
CD
*<
Z3
CD
CD
Q.
3
o
CD
O
CD
CD
CD
n'
IT
CD CD
O
o
CD
CT QCD
Z3‘
? CO
o
CD
IT D
CD
Q.
•
a
Q.
C
CD
-•CD
C
_k
15
£ *5 o5'
L°
2.
'hO
'<’
O
CD
3
4-
ZJ
CD
CD
CD
CD
Q- 3
c
_
o_ zr
- zr
■—?
O
? 2 OCD’
CQ
CQ
PHC / Town
I
Z5
o
3
Q.
CD
O
o
CD
cl
CD CD
CD X
(A
O
CD
CD
gms
V)
CD
O
CD
CD
CD
/
Child’s Name
Registration No. f
3'
3
<
/
zr
1
cn
-Q
CZ
CD
=5
e-:
/
3
0
□
§
CD 2.
CO 3 o
CD o
CD
CD
CT - >$
CZ
O
CD
CD
Husband’s Name
/
O
CD
Q.
CD
&
o
o
CD
CD
CD
Age
O
CD
*
CD
3 3
Date of birth
tlMH
CD
o ° ’
zr
o ZT
2.
■S 2
/
>
—
o
°
3 o _ 3 cr
I
ted date of delivery
J
CD
3
z
CD Z5
2- D-
=t: O Q.
=S
Ex,
cr
o
c
r*
5 S
o o
=5 z q. o
O N>
=!.CD
(qCT
/
CD
CD
— O
1
Date of the first day of the last Menstrual period
o
. § ? IT O
CD -< CD (Tx
ICPS
Name of pregnant woman
03
TJ
=!■. O
O
o O
o 2 “
3 Z5
CD
CD CD
O JD
=r c
— JD
Q- o
CD
CD
Z5
o 5-
CD
CD
° On
& CZ
_
3
CD
CD
''->X
'
*
■r
Suman Bhatia
Consultant
Department of Women and Child Development
Shastri Bhawan
New Delhi
27 Dec, 2000
Dear Mrs Saxena,
Enclosed please find a copy of revised proposal of Integrated Nutrition
Project for Karnataka..
Regards, q
(Suman Bhatia)
Mrs Mcera Saxena
Secretary
Department of Women and Child Development
Multi Storeyed Building
Anibcdkar Road, Bangalore-560001
■
•1‘' '■
Integrated Nutrition Project — Karnataka
1.0 Purpose
The purpose of this project is to support and strengthen the Government of
Karnataka’s on-going programs for improving the nutritional status of tlie
community by reducing all forms of micronutrient malnutrition among vulnerable
population.
2.0 Objectives
The objectives of the project are:
• To improve tlie quality, coverage and use of nutrition related services
namely, provision of supplementary nutrition and nutrition education
at AWCs in collaboration with and support from tlie health sub-centre
• To create awareness education to tlie community for development of
proper nutrition habits with the use of low cost Jocally__availablc
resources.
• To empower women through participation in Self-Help Groups. Tliis
is intended to increase ownership of tlie project, and improve
knowledge and practices regarding health, nutrition and infant care.
• To establish Nutrition Rehabilitation Units for management of severe z
malnutrition
3.0 Background
Malnutrition and morbidity are twin problems affecting a major part of the
country’s population - especially' womeni and children. They are undoubtedly tlie
most crucial segment of the population, due not only to their sheer numbers, but
also tlieir special physiological demands. Malnutrition is often associated with
morbidity and mortality thus adversely affecting life expectancy. Additionally, it
causes growth retardation and leads to functional impainnent, disabihty,
diminished productivity and reduced resistance to diseases.
■'
s-T-
An individual’s nutrition is determined by a number of factors acting
directly or indirectly. The causes of malnutrition are complex and include
• Inadequate child caring practices, often governed by cultural and religious
beliefs and status of women in the families
• Poverty and household food insecurity
• Inadequate access to health care services and poor sanitation
• Constraints to the physical and social development of the girl during
childhood and adolescence
• Heavy workloads, social and economic barriers compounded by gender
discrimination in the community and within the family that influence
access to healthcare, intra-household food distribution and access to
information.
Malnutrition is transmitted across generations. LBW infants bom to severely
malnourished women, remain malnourished in tire childhood and adolescence.
These effects are especially devastating in the case of girls who are neglected
during infancy and. childhood. Clironically malnourished girls are therefore, even
more likely to remain malnourished during adolescence and adulthood, and when
pregnant, to deliver low birth weight babies. Early marriage and teenage pregnancy
further deteriorate her nutritional and heal th status.
Household food insecurity also perpetuates across generations. Diminished work
capacity and work output result in low family income and household food
insecurity, dws perpetuating die cycle of household food insecurity and
malnutrition. Therefore, protection and promotion of healdi and nutrition c
women can be achieved dirough a combination of strategies involving concerted
actions by various sectors at different levels.
s
A depressing child nutrition and health scenario is common feature for most of the
states in die country. In Karnataka, it is estimated dial 54 % of children below 4
years of age are underweight and 48 % are stunted or short for their age. Wasting,
which is die most serious nutritional problem, affects 19% of die children in
Karnataka. According to NFHS I (92-93) about 22 % of the children in the state
were low birth, weighing less than 2500 grams at the time of birth. This clearly
indicates die poor nutritional status of modiers. Over 40 % of women suffer from
anaemia due to iron deficiency and close to 30 % women are suffering from severe
and moderate grades of CED. The degree of iron deficiency anaemia is highest in
12-23 mondis old children (78 %) in Karnataka (NFHS II)
Some of the contributing practices to this dismal-situation in Karnataka are:
Intake of dietary energy, proteins, calcium, iron, vitamin A by children are
well below the Recommended Dietary Allowances (RDA).
• Cereals constitute die bulk of diets of women and children. Type of cereal or
millet varies with die region.
• Diets of women and adolescent girls are also deficient in most of nutrients especially iron and vitamin A. Tin's is mainly due to die reason diat average
intake of GLV by women (15 grams) is far below die RD A, which is 100
grams.
• Only 27 /o of rural women in Karnataka initiate breastfeeding on die first
day. About 60 % of modiers discard colostrum and 85 % women give
prelactael feeds to infants. Tills practice which deprives die newborns from
getting benefits of colostrum, exposing diem to dangers of infection.
22% of urban women introduce complementary food before 2 mondis of a<’e
and 84% introduce it above 6 mondis of age.
Integrated Child Development services (ICDS) Scheme is implemented in all of
ic States of India including Karnataka to improve nutrition, hcaldi and
psychosocial status of young children and women. Services provided to local
popu ation under ICDS are: distribution of supplementary nutrition to vulnerable
groups, immunization, health check ups, pre-school education and referral services.
He local point of delivery of services is the Anganwadi Centre (AWC) - childcare
center in the village or urban slum. The centers are run by local conununity based
women childcare workers - die Anganwadi workers.
Child healdi is also addressed by Reproductive and Child Healdi Programme
winch arm to reduce IMR, CMR & MMR. Tins programme is an extension of
Chlld HeaIth (MCH) 30(1 Chjld Survival
Safe Modierhood
(CSSM.) Programme. However, die improvement is not of die intended level
which is quite apparent from the data discussed earlier.
An individual’s nutrition is determined by a number of factors acting
directly or indirectly. Tlie causes of malnutrition are complex and include
• Inadequate cliild caring practices, often governed by cultural and religious
beliefs and status of women in tire families
• Poverty and household food insecurity
• Inadequate access to health care services and poor sanitation
• Constraints to the physical and social development of the girl during
childhood and adolescence
• Heavy workloads, social and economic barriers compounded by gender
discrimination in the community and within the family that influence
access to healthcare, intra-household food distribution and access to
information.
Malnutrition is transmitted across generations. LBW infants bom to severely
malnourished women, remam malnourished in the childhood and adolescence.
These effects are especially devastating in the case of girls who are neglected
during infancy and childhood. Chronically malnourished girls are therefore, even
more likely to remain malnourished during adolescence and adulthood, and when
pregnant, to deliver low birtli weight babies. Early marriage and teenage pregnancy
further deteriorate her nutritional and health status.
Household food insecurity also perpetuates across generations. Diminished work
capacity and work output result in low family income and household oo
insecurity, thus perpetuating tlie cycle of household food insecurity and
malnutrition Therefore, protection and promotion of health and nutrition ot
women can be achieved through a combination of strategies involving concerts
actions by various sectors at different levels.
A depressing child nutrition and health scenario is common feature for most of tlie
states in tlie country. In Karnataka, it is estimated that 54 % of children below 4
years of age are underweight and 48 % are stunted or short for their age Wasting,
which is the most serious nutritional problem, affects 19% of the children in
Karnataka. According lo NrHS I (92-93) about 22 % of the children m the state
were tow birtli, weighing less than 2500 grams at tlie time of birth. Tills clearly
indicates the poor nutritional status of mothers. Over 40 % of women suffer from
■
■
■
4.0 Summary Project Description
Concerned about tlie grim malnutrition situation in Karnataka amongst all the
southern states and to ameliorate the nutritional level of population, the Govt of
Karnataka has planned to initiate an Integrated_Nutrition Project (INP) in four
districts namely, Raichur, Gulbarga, Tumkur and Chikmagalur. The project will
address tire problems of malnutrition including micronutrient malnutrition by
adopting intergenerational life cycle approach to reduce morbidity and mortahty
due to malnutrition amongst the most vulnerable groups of the population namely:
children 0-2 years, adolescent girls and pregnant and lactating women.
An analysis of the causes of malnutrition reveals tliat die problem is tire result of
multiple factors and no single sectoral programme input can address it effectively.
The programme, therefore envisages bringing in better intersectoral coordination
of various ongoing activities at all levels.
Tlie total cost of the project will be Rs. 565 crores ( approx ) over five years. The
project will consist of seven components, organized as follows:
a) Information, Education and Communication(IEC)
support to women’s SHGs who will be educated and trained on (a)
promotion of child care at family level; (b) preparation of supplementary
food for infants, pre school children, adolescent girls, pregnant and nursing
mothers; nutrition and health education; (c) growing fruits and vegetable
plants,(d) preservation and drying of .fruits and vegetables in peak season’
and (e) monitoring of nutrition situation in the village.
1EC and nutrition counseling, including nutrition-related topics in school
curricula
‘
joint training of local Government and non-govenuncntal functionaries
b) Food Fortification
distribution of fortified supplementary food to vulnerable groups
•
fortification of local cereals
—
c) Supplementation
distribution of Iron Folic Acid supplements to under-threes, adolescent girls,
pregnant and lactating mothers
*
Vitamin A supplementation to children from 9 months to the age of 6 years
|L|» 2
4/
it/
d) Dietary Diversification
•
intervention on micronutrient-rich horticulture produces
e) Health Services
:
•
strengthening linkages with the health sector
establishing Nutrition Rehabilitation Units in each district for management
of severely malnourished cases
o—
-
. w
A
f) Project Management
establishment of a Project Management Unit and its efficient operation
establishment of a Project Steering Committee and support for its activities
g) Monitoring and Evaluation
on-going performance monitoring and feedback, and periodic external
evaluation
community-based monitoring and feedback, using the triple-A approach
5.0 Project Strategy
The strategies of tlic project will be on the lines of National Nutrition Mission,
that is,
~
•
a) Vigorous awareness campaign on malnutrition to reach all sections of the
society
b) Direct interventions for preventing onset of malnutrition among 0-2
years, adolescent girls, and reduce LBW and micronutrient malnutrition
c) Nu tritionJMapping and Surveillance for monitoring the nutrition situation
regularly.
The project has been designed based on assumption that it will support and
strengthen government’s ongoing programmes for improving nutritional
status of the community. Local women of the Self Help Groups will be the
key players in the project. Techmeal support will be provided to SHGs to
build up their own capacity to perform the required tasks. The project also
envisages to strengthen abilities of ICDS and health functionaries working at
field level as well as their trainers to actively support and assist SHGs.
6.0 Project Interventions
6.1 Information, Education and Communication
6.1.1 Support Women’s Self Help Groups (SHGs)
Experiences have shown tliat when_a community is fully involved in design
implementationi and monitoring of nutrition and oilier development projerts’
using a tnple-^process (asscssment-analysis-action), these arc likely to be
T"! SUStain,able- Such Participatory efforts more often meet
die real needs of the people and achieve results ftiat can be continued widi
'I’lnimuin external inputs. The presents project also envisages organizing
SHGs of women from die community and improving dieir knowledge and
AZ v6S
iealth’ nUtnL1°n and Ulfant care
reduce die load of
AWWs. These women will play a critical role in carrying out die main
nutrition activities including:
(a) Setting up self-sustainable_nutritious food production units and
Production of fortified supplementary food. Food produced in tliese units
will be distributed amongst beneficiaries of ICDS scheme.
( ) Educating community about raising vegetables and fruits even in
landless households and die mcdiods of home based preservation and
drying of vegetables and fruits.
(c) Nutrition and health educatiom Acquired knowledge and skills related to
nutrition and infant care will empower them to solve the local problems
and provide support to women and families. They will be able to identify
and optimize existing resources and solutions widiin the community to
solve community problems.
(d) Supervision of regular GMP sessions.These groups will also regularly
monitor die nutrition situation of Hie community.Tliis will include home
visits for momtoring G-I and II malnourished children and counselling
care givers to prevent G-UI and IV malnutrition.
;
Karnataka government has declared a programme called stree shakti for
rura women with a view to give special impetus to die empowennent of
rural women through SHGs. Under the programme each AWW will form
SHGs in die limits of her centre. Each AWW will be given an
mpCpntlnVnn?f—50/’ p m- f°r each 8roup fonnation and supervisors an FTA
ot Rs 200/- pm under die project. For production of supplementary foodand
nursery development women can be selected from diese SHGs. The
Based on community needs assessment and decentralized planning process, *
it will lead to simultaneous improvement through these groups.
The project will be implemented through the development of community
level teams of SHGs, AWW, ANM and school teacher for improved
outreach to ensure that beneficiaries of all the groups are receiving
counseling about appropriate nutrition, health and care.
SHGs formed in tlie Stree Shakti project will be established to produce
appropriate supplementary food, generate awareness and disseminate
messages to the community for developing healthy habits and monitoring.
The women panchayat members at village as well as taluk level will be used
as resource persons for advocacy and community mobilization.
The AWW, supervisors and ACDPOs will extend their help and cooperation
to tlie groups and liaise with them. At taluk level the programme will be
coordinated and monitored by CDPOs.
A District Nutrition Committee headed by C.E.O./ District Collector and
consisting of district level officers of tlie concerned departments, would
implement and monitor tlie progress of implementation every month.
A Programme Management Unit (PMU) at State level headed by Secretary
WCD and assisted by a Consultancy firm will have die responsibility of
management of the project.
It is very important to mention here that tlie project will require
strengthening, initiation and coordination activities including DWCD, Health
and Family Welfare, PR1, Rural Development, Food and Civil Supplies,
Education, Horticulture, Agriculture and Forestry.. This can be handled best
at District Level. This project can also very well complement tlie Border
District Cluster Strategy in Gulbarga and Raichur districts in terms of
nutrition and childcare at family level.
tools (e.g. counselling cards) to help diem conduct IEC sessions more
effectively. IEC strategies in die project can be creative and can help in
taking advantage of all opportunities diat present themselves to integrate key
messages into, ongoing events, '.including everyday unprogrammed
(opportunistic) encounters in the villages. These can be weekly markets,
health melas, specific healdi education days, religious functions, maliila
mandal meetings, home visits, baby shows, literacy programmes etc.
All the field level workers, formal and informal service providers can be
closely involved for enlightening the community and bringing out
behavioural change. Joint training programmes will be organized for
AWWs, ANMs, school teachers, rural development workers, SHGs,
members of VECs and TBAs. Additionally AWWs and ANMs will be
provided training in development of counseling skills so that fiicy will help
tire mothers to adopt nutrition friendly behaviour. They will also receive
training in PEA techniques which can help in moulding people’s behaviour
in participatory manner.
Aiiotlier strategy for establishing good nutritional .practices is to promote
sound nutritional practices in the young children. Nutrition topics will be
included in school syllabus after reviewing the existing one. Young cliildrcn
can also become very responsible message carriers to the families and
community.
Interpersonal as well as mass media channels will be used for 1EC. It is also
proposed that the roles of Supervisors lioin 1CDS and health sectors be
further strengthened in interpersonal communication to support the efforts of
AWWs, ANMs, TBAs. For all communication themes to be addressed
interpersonal aids will be developed or selected from the already existing
ones and translated in kannada. These will include a set of counseling cards,
meant to be used for one to one communication, a set of demo teaching aids.
Short messages for radio broadcasting will be developed to communicate
key behavioral issues to people. Cassettes of these massages can be
distributed at the block level also. Metal stencils with pictorial nutritior
messages will be prepared at District level and distributed to all CDPOs fo:
painting messages on die walls of villages.
strategies for working of SHGs can be worked out at Distt level as the
strategy cannot be the same for the entire district and would depend on a
number of factors including geographical location of villages.
Each group can be provided a seed capital of Rs.15,000 for establishing tire
units. Recurring expenditure needed is expected to be raised from sale
proceeds of products processed.
x
Women of SHGs will be provided training in purchase of quality raw
ingredients, economy of wholesale purchase, safe storage, food processing
and fortification, hygiene and sanitation control and packaging. They will
also be oriented towards nutrition and health needs of vulnerable groups and
good child care practices. Hands on skill training for raising of annual and
perennial vegetable and fruit plants will also be provided. They will also be
provided skill based training in preservation and drying of fruits and
vegetables.
6.1.2 Information Education and Communication (IEC)
Many good practices are operationally simple and do not require heavy
expenditure or extra labour, but require change in behaviour of people. For
example, initiation of breastfeeding immediately after birth, feeding of
colostrum, timely introduction of complementary feeding, for infants, minor
changes in food preparation methods and addition of some locally available
greens in the daily diets and care of girl clrild can bring about observable
changes in nutritional status of people.
Desirable behavioral changes related to nutrition and child caring practices
at household level and in the community can be initiated and sustained only
through effective communication support and demonstration of some
positive results of good practices adopted by lire community. This broadly
aims to stimulate demand for the services, improve feeding and child caring
practices, encourage pregnant women for early registration and for availing
MCH services, prepare adolescent girls for safe motherhood and promote
community participation.
At present most of the programmes emphasize on awareness generation or
providing information only. Most of the field level workers are lacking
counseling skills and have weak communication skills; they also lack IEC
A consultant will be hired for preparation of IEC material specific for
Karnataka.
6.1.3 Training: Key to the implementation of strategies of the project is
AWW and support to them is augmented through SHGs plus ICDS
supervisors CDPOs and District level officials will be a major component of
the project’s early stages. It is expected that ICDS functionaries, even
though have knowledge, will need to be introduced to community based
participatory activities. They also need to develop counseling skills.
Therefore, along with orientation to project interventions focused on tire life
cycle approach they will also be provided training to develop counseling
skills. Other influential change agents who are in contact with women and
their families are ANMs, TBAs, primary school teachers, NGOs, PRI
members, and rural development workers. Empowered with the correct
information and communication skills, these change agents can play an
important role in changing tlie nutrition situation. Teachers have tire oilier
special role of influencing tlie young minds. Therefore combined training of
all key personnel will ensure transmission of tlie same information to the
target group, reinforcement of advice being given and mminial
contradiction.
The following training programmes will be organized for tlie different
categories:
(i) Two days training of trainers for CDPOs, AWTCs, MLTCs,
DPOs, MOs, ICDS and health supervisors.NGOs
(ii) Joint training for 3 half days for AWWs, ANMs, MPWs,
school teachers, TBAs rural development workers, and NCOS
(iii) 5 days training of women of self help groups
Characteristics of training: All training should be participatory; on-going,
process oriented; skill oriented and practical; community-based and multi
targeted.
Four CFNEUs of FNB placed in Karnataka and Hyderabad will provide
training at block level. Training to grassroot level workers and SHGs will be
provided by 23 AWTCs of Karnataka and NGOs in the State and nearby
places.
I
k
I
I
6.2 Food Fortification
Gro'ups-Diriig^’te last 'tae^'d' ®l'l’l''c,"c,,'n,J' |r"“d >" .. .... ....
r,s "s-.“ tt.sHTz“" “•
proved, or sharing and ^Xof^ 4
planned to overcome enm^
.t
L.
beneficiaries get the adyantage of s^Xn"
5°°'
lanuiy. it has been
U,e
S“PP etnenta^ food will be distributed to all lite beneficiaries of 1CDS
pr='X^"d
b^Z toX
adopting the life-cycle Zr"),,^
nticronutrients
P
pre-sch°o1
tl’e year As U,e PraJcct *
0,"C 5,316 of sl^.ion for both macro and
^f^r
be: e^:rXpp±en^^^'t"
f00d8 10'." beV’etbslributed
p™j->
density, taste prcfcraice
"' d'e rCquired nutrilion
precooked foXd X ha erf o„ '
Ready to „sc
~"£jHH»= -
diffZreTage XpsTifferemrec’ °U aC“[ding 10 locaI pS'eren'c^for
.0 the foo8d fcr Taf^Td ST eM
acceptabtiity by n.otbers and adotescent 8ir,s food ^.VsupZddi:
&
form of eitlier laddoos or bars. Food will be enriched with vitamin and
mineral premix. 100 grams of this food will provide 400 calories. For
infants tire mixture can be reconstituted in warm water before feeding and
would not require any cooking. Acceptability trials of food will be done on
the local community before taking a final decision on the type of food. One
kilogram of food can be purchased from SHGs for Rs 15, which includes the
transportation cost also.
Since it will be logistically appropriate to provide the entire monthly quota
once a month as take home ration, tlic food mix may be packed in one kg
packets. Severely malnourished children will be fed at the site. Non
compliance can be checked to some extent by strengthening IEC to mothers
and families
Production of food by locally placed SHGs will be cost effective due to
reduction in transportation cost of locally available raw food and distribution
of processed food. Tire food production units managed by SHGs will be
established in the accommodation provided by village panchayat. Except for
grinding of food, all other processing of food will be done by women of
SHGs. Grinding will be done at village flour mill which will have the
provision of mixing the vitamin and mineral premix also ( wherever possible
chakkis will be modified for mixing vitamin and mineral premixes to four.
Otherwise women will be trained to mix the premix manually). Extra food
produced in the food-producing units can be sold out in the market at an
agreed rate. This will be helpful in improving tlie economic situation of the ....
SHGs.
(ihe value of anything given free is not adequately appreciated. Therefore it
will be considered whether a nominal cost, say 2.00 p per kg for
supplementary food may be recovered. Having paid for the food, it will
directly ensure consumption by the beneficiaries. The funds so collected can
be utilized as additional working capital for the SHGs. However, this
decision may be taken at the forthcoming meeting of Secretary WCD, GOK,
UNICEF and MI.)
6.2.2 Fortification of Local Cereals: The rationale of fortifreation of flour
( cereals and millet flour ) is tliat it is widely consumed, in fairly large
amount everyday. It can be fortified with lower levels of micronutrients
'
discolouration or quality
problem.';As’’80%'of^yaIlages^m'project Districts have electricity operated
flour’mills and most of the villagers get grinding of the cereal done from
those mills; this will be- a cheap and effective method for preventing
micronutrient malnutrition. It will also not require any change in food habits
of the people. The premix' ( containing iron, folic acid and vit A ) will be
mixed with,the flour at the end of milling process by a specially designed
mixer. Fortification of flour in the initial phase will be supervised by an
official designated by the Zila Parishad C.E.O, and later this responsibility
can be overtaken by SHGs.The consumer will be made aware of the
fortification and acceptability trials will be carried out.
6.3 Supplementation
6.3.1 Distribution of IFA supplements to under threes, adolescent girls,
pregnant and lactating women: IFA tablets are distributed to infants and
pregnant and lactating women under die govt programmes, hi order to
improve the health status of girls even before they are pregnant, diis project
envisages to include adolescent girls also in the beneficiaries of tills service.
Tliis also plans to improve efficiency and effectiveness of existing delivery
meebanism and counseling of women for better compliance. Pregnant
women will get IFA tablets for 180 days instead of 100 days.
6.3.2 Strengthening and support of the coverage of the current Vitamin
A supplementation programme for children upto the age of 6 years: The
present coverage wiiich is about 80% at die first dose is not sustained later
particularly because the later doses are not linked to immunization. It is
therefore planned to strengdien IEC and educate SHGs to extend the
coverage and sustain die later doses.
6.4 Dietary Diversification
Intervention on Micronutrient-rich Horticulture Produces: A long term
and sustainable solution to combat micronutrient deficiencies is regular
intake of foods rich in diese nutrients. Efforts aimed at dietary
diversification can be sustainable only when the food sources of iron and
vitamin A are locally available. Food and agriculture policies thus need to
accord higher priority to improving production, preservation and distribution
of vegetables and fruits. It has been observed in different parts of the country
&
that horticultural interventions can motivate families to produce some
vegetables and consume them too. Large scale production of vegetables and
fruits in Karnataka also makes it imperative to take simple techniques of
food processing, especially drying, to people so that vegetables can be dried
and preserved when are in glut. Tliis will reduce post harvest losses as well
as ensure consumption of vegetables during off-season. Cash return may
also be obtained from the sale of surplus produce, which would make
horticulture a sustainable enterprise. Therefore the objectives of horticultural
intervention in tlie project are: (i) to develop nurseries in a cluster of villages
(ii) to supply saplings and seeds to SHGs at subsidized rates (iii) to
encourage growing of at least one perennial and one seasonal crop in the
homes, community, AWCs, schools (iv) to ensure consumption of fruits and
vegetables by community using nutrition counselling, and (v) to generate
awareness about home based food processing and use of low cost cool
chambers for preventing spoilage of food
Methodology: (i) SHGs and AWWs will be provided training in raising
fruits and vegetable plants suited to the taste and climate of different project
districts and in preservation of vegetables and fruits with the help of District
agriculture and horticulture extension centers in collaboration with
Horticulture Research Institute, Bangalore (ii) Seeds and saplings of plants
will be distributed to the community free of cost, (iii) Awareness generation
among community about preservation of fruits and vegetables in season and
use of low cost cool chambers. This responsibility can also be given to
SHGs which can work under the supervision of AWWs and Supervisors.
6.5 Health Services
6.5.1 Strengthening Linkages with Health System: Health and nutrition
arc strongly interlinked. Hence it is necessary that intervention for
prevention and management of tire two sectors be delivered as a combined
package at the community level. To do tliis, it is essential that functionaries
of health and ICDS work together as a team. They can work together to
empower families and the communities to choose appropriate practices to
meet their health and nutritional needs at home and use appropriate facibties
when required.
The Border Cluster Strategy-Under GOl,0NICEF MPO has tire objective of
strengthening RCH services in clusters of 4-5 districts located on the inter
state borders of 16 States with the goal to demonstrate a significant impact in
the reduction of
and malnutrition. It is envisaged that clustering
will enhance tlie impact and cost effectiveness of activities that- address
common problems in these districts. Gulbarga and Raichur districts of
Karnataka which are the project districts also have been identified for
implementation of this strategy. The following mechanism will be adopted
for building and strengthening teams:
-joint training of AWWs, ANMs, TBAs and SHGs
-joint communication drives
-AWW as depot holder for ORS, IFA tablets
-joint household visits for problem cases
-joint updating of records, immunization register or weight
records
- support of ANM in GMP sessions
-joint meetings with MSS or SHGs
-joint review meetings at block district and state level
Some more mnovative activities can be identified at district level.
6.5.2 Setting up Nutrition Rehabilitation Units: In Karnataka 2.6% of
children suffer from severe malnutrition^ -3 sd weight for height criterion)
The presence of oedema or wasting indicates severe malnutrition. The
cliildrcn may or may not have conditions like dehydration, severe anaemia,
life threatening infections, hypoglycemia, hypothermia, severe vitamin A
deficiency, apathy and anorexia. Malnourished infants under 12 months of
age have a greater risk of dying than older malnourished children.
Residential care is essential for initial treatment and for the beginning of
rehabilitation of a child with severe malnutrition. The cliild should be
admitted to the hospital (CHC) with facilities for special nutrition care.
When child starts eating satisfactorily ;uid gaining weight he or she can
usually be nianagcd_at non-rcsidcntial rehabilitation centre_which can be set
uPJlLaJ’HC. Close cooperation between hospital and centre is neccFsary to
ensure continuity of the care. It may be relevant to point out here that it is
better to prevent severe malnutrition than., drain precious resources on
management.
Services to tackle severe malnutrition will be initiated at CHC/PHC level as
^PilSLPfPj-^dt-in one block of each district. After a minimum stay-in tlie
health centre, die mother will be taught about appropriate feeding, how to
adapt family foods , give frequent .feeds, continue breastfeeding to provide
enough energy and nutrition for rapid catch up growth. After tlie discharge,
‘
■'
'■
•
•’
•
’■
'’i
the child and child’s family would be paid follow up visits by die Lady
Icaldi Visitor to prevent relapse.. She will monitor (lie progress of the child
and give practical advice. She will weigh and examine the child clinically
and refer tlie child back to the unit if necessary, using specific referral
entena. She will be assisted by ANM/AWW during the visit
6.6 Monitoring and Evaluation: Monitoring and evaluation of any
intervention programme is necessary to assess the progress and impact of the
project, to check if tlie objectives are realistic and appropriate or if they need
be revised, whether the interventions being implemented as expected and
accepted by target population and having no undesirable side effects.
If the monitoring and evaluation is done together with the community it will
serve two purposes : Firstly, it is a management tool tliat helps people
improve their efficiency and effectiveness. Secondly, it is also an
educational process that helps participants increase their awareness and
understanding of tlie various factors that affect tlieir lives. In so doing it
increases people s control over die developmental process.
Proposed strategies: i) Baseline survey to assess tlie nutrition situation botli
quantitative as -well as qualitative, ii) mid term and end evaluation to
measure tlie acluevement. iii) regular monitoring of tlie process and tlie
achievements. Tlie existing monitoring formats of ICDS may be reviewed
and modified if required for making them result oriented. A small number of
-cy indicators may be identified to help monitoring and management at each
Iv VCl.
iv) A system of collating tlie information received from tlie grass root area at
the district and state level for taking corrective actions
v) Introduction of community based momtoring.
Active community members can be part of. the monitoring teams ( This
responsibility can also be given to SHGs ) In participatory monitoring
methods and indicators are sunpie and are designed to provide timely
i ormation required for taking action at community as well as government
level. CDPO /supervisor can organize a monthly monitoring meeting where
problems and tlieir possible solutions can be discussed. Tliis information can
also comp ement the data collected by ICDS fimetionaries for MPRs and
will be collated at District level
t
7.0 Project Management
a)
Responsibility for the project within the Government of Karnataka will lie
with the Department of Women’s and Child Development (DWCD/SW).
The Secretary DWCD will be assisted by the PMU to ensure that the project
receives the necessary resources and facilities etc., authorizations, and
cooperation of tlie Karnataka government agencies.
b)
Overall direction of the project will be provided by a Project Steering
Committee (PSC) headed by tlie Secretary, DWCD (GO1) and consisting of
Secretary DWCD (Karnataka Government); Director WCD GOK; the MJ
Director/South Asia Region; Chief, CDN UNICEF-India; tire Project
Manager; representatives of tire four District Councils. The PSC will meet
every six months to consider and approve the strategies and work plans for
the project, review and accept tire regular reports of tlie Project Manager,
approve reports to the Government of Karnataka and tlie funding agencies,
and resolve issues that can not be settled at tlie working level.
c)
The project will be managed by an independent Project Management Unit
(PMU) established within /outside ???? DWCD/Kamataka and headed by a
Project Manager reporting directly to tlie PSC. The Project Manager will be
accountable for tlie implementation of the Management Strategy and
Workplan of tlie project, for the smooth functioning of tlie PMU and tlie
efficient administration of project resources, and for tlie preparation and
timely submission of narrative and financial reports to tlie PSC.
d)
Upon approval of tlie project and engagement of tlie Project Manager, tlie
Project Manager will prepare a detailed Management Strategy and a Project
Workplan for consideration and approval of the PSC. The Management
Strategy will set out tlie specific roles and responsibilities of all project
stakeholders, tlie management and decision-making systems, and a Work
Breakdown Structure for the various project components. The Workplan will
be reviewed and updated at each meeting of the PSC.
e)
The Project Manager will submit to the PSC quarterly financial reports,
semi-annual narrative reports, and a comprehensive annual report.
The project will be audited annually by an external auditor. The audit reports
will be reviewed by the PSC.
8, Anticipated Results
Expected results at the impact level and indicators of progress towards
these results are in table-1
Expected Results (Impact)
* 30% reduction in LBW rate________
deduction
in
malnutrition
in
children between 0-3 years within 5
years
deduction in anaemia by 50% within 5
years
Impact Indicators
LBW rate
~
~~~
* Infant mortality rate
•% of underweight children
*% of stunted children
*% of wasted children
*% of children with anaemia
*% of pregnant women with night
blindness
* % of IDD cases_________________
•% of anaemia in pregnant and lactating
women
•% of adolescent girls (11-19 yrs.) with
anaemia
Project Purpose and Outcomes
The purpose of this project is to support and strengthen Govenunent’s on going
programmes for improving nutritional status of tlic community by contributing a
substantial input in tenns of community support tlirough. SHGs of local women
and voluntary organizations and strengthen linkages widi tire health services.
Expected outcomes
1. Improved package of services provided to
mothers and children at the district level, based
on community needs
Outcome Indicators
LIncrease in appropriate use of nutrition and
health services such as:
- % of mother bringing children for GMP every
month
- % of children getting fully immunized before
one year.
2_% of women getting .health and nutrition
a
counseling
%
of children
taking
Vitamin A
supplementation
-% of pregnant and lactating women getting IFA.
2. Women become empowered to demand and
1. No. of SHGs formed and operational.
provide improved nutrition to the children and
2. Good feeding practices (breastfeeding,
themselves.
complementary feeding use of new foods in
children’s diet, increase in the number, of times a
child is fed, active feeding etc.)
3. Good caring practices.
4. Good health seeking practices.
5. % of mothers with children under 2 years who
can interpret growth chart information.
6. % of mothers washing hands after use of toilet
and before handling food.
7. % of . adolescent girls consuming IFA
supplements
8. % of families consuming iodized salt
3. Improvement in knowledge
1
and skills of field - % of field functionaries trained
level workers and their supervisors’ training
- % of mothers counselled
- % of training sessions that allowed participants
to put new knowledge and skills into practice
during training
4. Improvement in 1knowledge,
behaviour of women of SHGs
skills
and
- No. of SHGs providing fortified supplementary
food to ICDS
- No. of nutrition and health education sessions
conducted by SHGs
- No. of home visits conducted by SHGs
5. Provide facility for fortification of local cereal
- No. or % of families eating fortified atta
6. Establishing NRUs to manage severely
No. of severely malnourished children (whor~
malnourished cases.
condition has improved ) ,
7. Strengthen community capacity to participate
-Proportion of community receiving technical
jn and monitor the progress of the project.
assistance to promote participation.
8. Strengthen the capacity at State, District and
-Proportion of functionaries provided training.
Clock level to provide high quality support and
- Number of institutions developed and
training to functionaries of the project.
strengthened.
Annex 1
PROJECT COST
1. Cost of Supplementary Nutrition
Total number of beneficiaries 19,42,321
(includes 0-2 infants, preschool cliildrcn, adolescent girls, pregnant and lactating
women )
Cost of supplementary nutrition @ Rs 1.50/ ben/day for 365 days
Rs.l06,34,20,747/year(for 5 yrs)
(break up for supplementary nutrition for one kg energy and nutrition dense food
in the form ofpanjiri or bar will be -rice/ragi/jowar- 500 gin
gins
Rs 3.00
pulse
-150 gms
Rs 3.00
nuts
50 gms
Ils 1.50
( cost will reduce with
the
bulk
purchase)
sugar
250gms
Rs 4.00
oil
50 gms
Ils 2.50
fuel
Ils 0.50
grin ding +premix
Rs 0.50
Total
1000 gms • Rs 15.00
(food will be sold to each beneficiary at the rate of Rs 2.00/ kg)
2. Support to SHGs
(a) Setting up supplementary food units @ Rs 15000 per unit
Rs 2,16,00,000
(for total of 7200 AlTCs, one unit for a cluster of 5 AWCs will '
I
therefore 1440 units)
(b) For nutrition education, demonstration for preservation, d nydration and cool
chambers @ Rs 2000 per unit one time grant and Rs 1000 pur year
Rs 28,80,000
Rs 14,40,000/ycar x 5
( for 5 yrs)
3.Training
(a) 4 District workshops @ Rs 1 lakh/ workshop
Rs 4,00,000
(b) 8 two days Block level workshops @ Rs 10,000/day/workshop
Rs 1,60,000 x 3 (includes 2 refresher trainings also)
(c) 3 day joint training of grass root level functionaries from
each sector @ Rs 1500/day/programme
t
1 ■
9. Risks
x.x~,"r
“. a
complex and
cultural,
health and illiteracy. The p
b)
^nlnnE11
has many accomplishments to its credit, its own
■n"" t
, ?Ve PT
°Ut lnany pr0blems 11131 need policy and
stitutional reform to be overcome. These might have repercussions on tlie
performance of die project.
unions on me
c)
Failure to obtain die inecessary
------approvals and clearances on timely bar’
from DEA and Ministry of Finance may result in delays in
project
implementation.
d)
The first three risks will best be managed by ensuring die active support and
involvement of the Government of Kamalkka a^d^Zilt P^rishad
aiiu uic xLiia ransiiads, and by close
and
on harmonious
,
WOrkln8 reIafi°nships between DWCD and MOFHW widi odier
££ :ay to e r hTen is’“
evaluation Th. fn wt ? h l
coinPoncnt and careful monitoring ar^
participation of lo^ '
h
managed by encouraging conununication ai^
participation of local panchayat and community. Enabling die district core tmouns
rn tee "tlOn COn]mittccs ta’develop and manage dicir own strategics and activities
to meet their local needs will also be helpful. However, die
¥631*“ Wise cost of the project.
Month#
time schedule has been shown for year I only and likely to change )
Actin’ty
Year 1______
Year 2
Cost
Year 3
Year 4
Year 5
CXi-Dcc
2000
District levd.wotkshopi
4,00,000
Jan-Feb
2001
8 Block Icvd
workshopt___________
1,60,000
1,60,000
1.60,000
Jin-Jun
2001
Feb-Dec
2001
Jan-Jun
2001
Jin-Jun
2001
929 grass root Inrl
training programmes
7200 training
progratonies for SHGs
Baiclincoad line uincy
41,80,500
41,80.500
41.80,500
3,60,00,000
3,60,00.000
3.60,00.000
10,00,000
Devdoptnent and
printing of (EC nutenal.
prepiratior of radio and
TV apoti, includes
hiring of erm iu hint too
22,00,000
Ed>Jul
2001
Operationaliiing
Chakkia for fortification
of aaa________________
To be doddod
Jan-Apr
2001
Sating up ITogramnw
Management Unit
(PMU) at Slate Icvd
Non recurring ocMt
Recurring oo-<_________
EiXablidnng SHGa food
production units________
Nutntion and health
education hy SHGs_____
bi ill al in g production of
aupplcmaitary food_____
bi dialing distribution of
IFAlablcU to ado I.
GirU and to pregnant
women for extra 90
daya(al present go\t ii
giving (FA to pregnant
womoi for 90 days
only)__________________
biilialing monitoring
including community
based monitoring in
ph asci________________
I
Due
2001
Icb-Due
2001
Fd) 2001
onvrardi
Aug 2001
Jul 20001
Ju I-Dec
2001
Distribution of seeds_____
Establishing NRUa at
PllCa_________________
Sub Total
Total
MI
5.00,000
20.00.000
20.00.000
20.00.000
20.00.000
28,80,000
14.40.000
14.40.000
14.40.000
14.40.000
14.40.000
IO6J4.2O,747
106.34.20.747
106.34 20.747
106.34.20.747
106.34.20.747
2J5.OO.OQO
2 J 5.00,000
36,00,000
2 J 5,00 000
2 J 5,00.000
2.35.OO.OOO
36,00,000
36,00,000
36,00,000
36,00,000
Proposed Source
UNICEF
(0,00,000Mini
10,00,000
40,00,000
20.00.000
2,16.00,000
Government
I
2.83,00,000
4,38,500
119 50,79,247
40.000
109,49.00.747
40 000
1 13.52.41.247
______ 40 000
109.49 00.747
______ 40,000
1 13.62,41.247
(total no offunctionarics-27860, total no of training programmes
for 30 participants/progranime-929)
Rs 41,80,500x3
(d) 5 day training of SHGs @ Rs 5000/programine
(216000 members, 30 women from each AWC, 30 women in each
programme, therefore one programme for each AWC, therefore 7200
programmes)
Rs 3,60,00,000 x 3
3. Cost of IF A to adolescent girls @ Rs 15/year/girl
for 14,48,700 girls
Rs 2,27,30,500/year
Cost of IF A to pregnant women for extra 90 days/year
(33465 women)
Rs 7,69,595/year
5 (a) Hiring a consultant for preparation of EC material.
(b)Translation and adaptation and reproduction of EC
material,TV and radio spots
Rs37,00,000
6 Fortification of flour 'x
fto be decided)
7(f) Base line and end line surveys
Rs 20,00,000
(b)Monitoring and Evaluation for 7200 AWCs @ Rs 500/centrc
Rs 36,00,000 x 5
8 Cost of seeds and saplings to be distributed to conununity @
Rs 2,83,00,000
Rs 50/family ( Rs 5000/ village)
9 Establishing 4 NRUs , one in each district at PHC level
training to LHVs - Rs 1500
cost of medicine and diet (Rs 5+15) /day for 15 children
Rs 20x15x30x12x4= Rs 4,38,000+ 1,60,000 (40,000x4 years)
10. Cost of setting up and running PMU at State level
Rs 40,00,000 + 1,00,00,000 (@ Rs 20,00,000/year)
11. Cost of Vitamin A supplementation ( if not provided under RCH)
Logical Framework Analysis
Sl^rrative Summary
Expected Results
Project goal
Reduce
all
form of
malnutrition
through
life
cycle
Impact
-Reduction in LBW rate
-Reduction in malnutriuon in
children between 0-3 years
-Reduction
in
anacmia/mal n u tri ti o n
among
adolescent girls
-Reduction in anaemia in women
and children
Prctccj_______ PurposeTo
To»|rovc
the
quality
Coverage and the use of
>ud3tion related services at
Ah/ Cs in collaboration
iViriv and support from
htUlh sector
Outcomes
- Improved package of service
based on community needs,
provided to mothers , adolescent
girls and children
-To empower women so
VAjI* they arc able to
c/x^tind improved health
anZ nutrition services for
/Mmselvcs
and
their
eA-Idrcn
-Number of SHGs formed and
operational
Performance
Measurement________ .
Indicators
-LBW rate
-% of underweight children
-% of stunted children
-% of wasted children
-IMR
-% of children with anaemia
-% of adolescent girls with
anaemia
-% of pregnant women with
night blindness
-% of women with goiter
Means of Verification
-Establish baseline. Follow up
with implementation reports and
community monitoring, mid
term survey and final end line
survey _____
Indicators
-% of mothers bringing children
for growth monitoring every
month
•% of mothers taking and
feeding supplementary nutrition
-% of women who made three or
more antenatal visits
-number of contacts with health
and
nutrition
teams
for
counselling
-intake of IFA tablets by
pregnant and lactating women
and adolescent girls
-% of children gelling Vitamin A
supplementation
-% of families consuming
iodized salt
-number
of
functional
supplementary food producing
units
-good feeding practices in the
families
-good child caring practices
-good health seeking practices .
-number of specific actions
taken at community level to
imprm-e health and nutrition of
\wmcn girls and children
Assumptions and Risk
Indicators______
-Poli ti cal/sociai/economic
conditions continue to favour
of INP
-Sustained
community
interest
- Magnitude of the problem
and inadequacy of existing
interventions
-Districts continue to allocate
high priority to improvement 3
of services
-Funding agencies provide
timely funds required for
implementation
-Local support for change is
received and maintained
-SHGs arc able to sustain in
terms of production and
economic management
V
Risk Management
-encourage
linkages,
communication
and
collaboration between the
key stakeholders
-encourage districts/ blocks /
villages to have their own
best strategies
-District core group /
nutrition committee will
develop
and
manage
activities
-Strengthen community capacity
to participate Ln and monitor the
progress of the project
-proportion
of
community
receiving technical assistance to
promote participation
Means of verification
-
fyo jcct Resources
■
Technical
Assistance
r
I
!
■
■
Training
Equipment
■
Materials
■
Management
-WCD, GOK. continues to
Indicators
Outputs
capacities of key -Extent of knowledge and skill implement current project
-Improved
-Full participation of key
of functionaries
functionaries
stakeholders
including
-Improved planning, monitoring - Timelines and quality of plans
-Quality of training materials community
and reporting
- Timely approvals and
-Development of Improved need and modules
clearances from DEA and
mills
-proportion of flour
based training material
DFA
modified
to
fortify
flour
-Food production units
-Use of local expertise
-Quality
of
local
specific
EC
-Local specific EEC material
-use of flexible approach to
material
produced
and
used
- Provision for food fortification
-Effectiveness
of
school adapt to changing needs and
-Revision of school curriculum
for
nutrition circumstances
-SHGs able lo participate in curriculum
education
GMP
sessions,
conduct
counseling sessions, and monitor -% of SHGs participating in
GMP. Nutrition counseling and
the nutrition situation
- Community has the knowledge monitoring
about low cost local nutritious -% of functionaries received
training
foods and their benefits
- Community is able to grow and -% of women of SHGs received
training
preserve fruits and vegetables
-Regular supply of IFA tablets -% of training sessions that
allowed participants to learn in
and Vitamin A
participatory manner and apply
into practice during training
- % of community members who
have the knowledge of good
child caring practices
-% of severely malnourished
children treated
-% of field workers who keep
track of G-l and II children and
provided help
-% of mothers who can interpret
growth chart
-% of families received seeds
and provided training in
production and preservation of
fruits and vegetables
% of children adolescent girls
and women who receiver
supplements
■
*'
Continuous assessment
Monthly monitoring by
SHGs
i5
C 4^,
_-
I
« ' -
CURREisT M-TRITION SITUATION IN KARNATAKA.
a. WTRITIOX PROI 'ILE
/. PROTF.IX:L'XLRGVM. ILXLTRIT/OX:
Protein energy malnutrition among children is the most common and serious nutritional
problem.
1 he NNMB Surveys (Rural) over the past two decades have indicated that though the
percentage of children suffering from severe malnutrition has come down from 14.3% to6.4%
and that of normal children increased from 4.6% to 9.5% as shown in the following table, major
pioportion of children still fall under mild and moderate ipalnutrition which is alarming.
TABLE-1
Percentage distribution of children 1-5 years according to nutritional grade. Gomez
classification pooled (.XNMB Surveys).
Period
1975-79
1988-90
1996
Nonna 1 °o
Mild°o
31.1
38.1
"38.6
4.6
4.8
9.5
Malnutrition
Moderate0 o
___ 50,0
48.8
*45.5"
Severe %
__ 14?3~
08.3
06.4
J
N1 IIS survey 1992-93 also revealed that among preschool children, malnutrition is al its
peak during the age of two years, thus indicating the need lor planning clear cut strategics to
combat the problem bef ore the child reaches 2 years of ace.
NNMB Tribal survey 1985-87 revealed that the prevalence of severe and moderate
malnutrition among under five years is 32.9°o and 49.7% respectively, thus indicating that severe
malnutiilion in tribal areas is much higher when compared to rural and urban areas and
emphasising the need for specific strategies to tackle the malnutrition in tribal areas.
TABLE-2
N’XMB report of the Tribal survey 1985-87.
Percent distribution of preschool children (1-5 years) according to nutritional grades:
Boys and Girls pooled.
Nonna I
Mild
15.1
Moderate
49.7
Severe
~32?F
/
TABLE-3
SbvXA'1
Report of urban survey slums. Bangalore 1993-94.
Mild %
37.7
Nonna 1 °o
2.5
I
Moderate °o
53.5’
i
Severe oo
6’3
1
J
The reduction of malnutrition’has therefore been spelt out as a clear stale goaJ and forms
lhe pari of the programme of action for child in Karnataka.
2. 3 HCRONUTRlEyr \ [ALXCITUTIOX.
a) l uamui *71” Deficiency.
The NNM13 reports over the years show that lhe Vitamin A deficiency (Bitot’s spot) is
high in Urban Slums and lower in tribal children, compared to rural counterparts. However, the
trends over the years also show significant decline in percent prevalence of Vitamin A deficiency
from 2.31% (75-79) lo0.5°n (1996) in rural areas, from 7.1% to 1.1% in urban slums and 1.4% to
0.7% in tribal community. Still lhe prevalence is above lhe W’.H.O. criterion of Public Health
Significance i.e.. 0.5%
TABLE-4
Vitamin .A deficiency trends (Rural) XXMB (Karnataka) Rural Repeat survey 1988-90
r
I
r
Year
i Percent Prevalence i
1975-76
1988-90
1996-97
2.3
1.1
!
0.5’
TABLE-5
Vitamin A Deficiency T rends (Urban Slums) NNMB Reports (Karnataka)
1984 and 1993-94.
i
Ii
Year
1975-82
1993-94
i Percent Prevalence i
\1
i
1.1
I
TABLE-6
\ itamin A Deficiency among Tribal Pre-school Child ren (Karnataka)
Survey
J Percent Prevalence
‘------------------------------------------------------------------------------------------------
_____ NNND) Tribal Survey 1985-87
.NTX Jenu Kuruba Tribal Survey 1989
com. ar 1?
compaieu to Kerala.
1.4
'
0.7
t0 nciSllbou^g states like .Yndhra Pradesh and Tamil Nadu, but higher
&
TABLE-7
National sun ey of Blindness 1986-89
Prevalence Rate of Vitamin A Deficiency in 0-6 years population
( Slate
p Karnataka
()!her_Soulhcm_Sla_tes
I Andhra Pradesh
• Tamil N’adu
Kerala
; India (Pooled)
b.
. Rural Piexalencc Rate | Urban Prevalence Rate [
L57
4.9
/
2.78
2.03
0.49
1.36
10.10
1.45
6.544.77
I
i
Io clui e D eficL en cr
Goitre or the enlargement of the thyroid eland is the most c
and visible
manifestation ot iodine deficiency and Goitre Prevalence Survey, is common
used
1 as community
diagnostic tool for identifying iodine deficiency areas.
Surveys conducted in Karnataka state during 1988-91 revealed
that four districts of
Karnataka namely. ChikkaniagaJuR Dakshinakannada.
.
.
---------- Tttarakannada and Kodagu have
prcsiilencc ol niore Ilian l()°o <°!r
' ~’>°llr'; ll’____
US ,om,inS ,Iie '■•ndemic districts of the stale. 1 lowcvcr
the surveys revealed that none of the districts is
free from Goitre though not from Public Health
Significant point of view.
The prevalence is more among females and in the aee uroup of 12 to 18 wananlirm
sTl'l Im all131’0"
10 "C Det'cienC-V Disor(lcrs Con,ro1 Programme by the provision of Iodised
Table-8
Percent Prevalence of Goitre in dilTerent districts in Karnataka 1988-91.
I SI No. |
I-t:
Districts
---------- I
—
i No. of Goiter Cases
1 Chikkamaglur
i
I 2.
| Kodagu________
I D. K. Manga lore
i 3.
I__ 4.____ U. KJJva rwar)
r 5.
I SIliinoga________
_ 7,
__ 8.
__ 9_.
' Bidar___________
I Gulbarga
' Bijapur_________
I Kolar__________
L±
LlZ._ LHeiBiuip.______
i—LI.__ ;_T u mk ur_________
12
I
! Hassan_________
I Raichur_______
: | Banga 1 orc(Rural)
j . ! B a ng a I orejJJ rban)
I N lysore_________
i
17 .___ D ha rwar________
i Mandy a________
:__ 18
I
19'.
; Bel Ianr-2o■. I Chi tradurga
P-L 5
Ml
21
t
Prevalence
I
i
-------------- ------
noFal:
7
4JJ2
_13_ld_
1.069
465
23.12
14.18
U1.67
_6l90
53 7~
_4.85_
244
3^6
2.219
I. 611
_13'25_
473
__ 61__
__ 41_1_
__3«8_
441
151
284
93
234
374
11 36
101
156
II. 650
2.53
----- {
zi
J
izT
"2.6'4
J .94
_L-Z9_
1.73
1.62
i
J.-57
1 20
1.00
6.99
n •
4.91
NIN study on Jcnkuruba tribals-Nutritional status in 1989. revealed The prevalence of
goitre of 4% in school age children and 10°o among adolescents in Mysore and Kodagu districts.
c. Iron Deficiency
'Fhc most common cause of ‘.Anaemia* is Iron Deficiency, which is due to inadequate
intake of uon in our diet.
Studies conducted by National Institute of Nutrition have shown that .63“o of India's
children of below 3 years and 45% between 3 to 5 years suffer from iron deficiency anaemia *
with moderate to severe forms in 10 to 15 percent of cases.
Problem m Kurnutakii
i)
>
The Bidar Integrated Rural Development study estimated that more than 90% of
preschool children suffered from anaemia (Hb% less than 1 IG/dl) and 13.4% from severe
anaemia with haemoglobin level less lhan_.7g._d_l.
ti)
India population project 1 studies in Chitradurga district in 1978 showed that nearly 54%
of preschool children were suffering from anaemia in the areas covered.
TABLE-9
Percent distribution of children according to their haemoglobin levels (1PP)
r
r
r
i_
ili)
Hbg. / dl
Percent, of Children
<7
7-9
9-11
11 or more
2.4
LL8
37.0
47.8
I
I
National Institute of Nutrition study on Jenkuruba tribals in Mysore and Kodagu districts
1989 has revealed that 99°o of preschool children and 100°o of pregnant women among
this tribal population are suffering from anaemia.
TABLE-10
Percentage Frequency Distribution Of Jenkuruba 11B Le\els(g/dl)
|
.Age Group
| Pie School Children (1-5 Years)
I■______
Preonant
Women
___ ___________________________________________________________
_7_
16.3
66.7
'
Haemoglobin Levels
7-9 !
9-11
I
if
57.5
25.0
I
1.2'
33.3 ;
0.0
i
0.0
I
Mean
8.2
6.1
i---------------------- i
The study conducted by University of Mysore in Liban slum reported lhat.^25 to 90% of
o iris are sulTerine from .Anaemia.
i
Document of
a
The World Bank
FOR OFFICIAL USE ONLY
Report No.
IMPLEMENTATION COMPLETION REPORT
I
INDIA
SECOND TAMIL NADU INTEGRATED NUTRITION PROJECT
(CREDIT 2158-IN)
1
February 13,1998
Health, Population and Nutrition Unit
South Asia Region
This document has a restricted distribution and may be used by recipients only in performance
of their official duties. Its contents may not otherwise be disclosed without World Bank
authorization.
/
/
r
CURRENCY EQUIVALENTS
. (as of January 23. 1998)
Currency Unit
Rupee 1
US$1.00
=
Indian Rupee (Rs.)
=
=
US$0,025
Rupee 39.50
government fiscal year
April 1 - March 31
abbreviations and acronyms
APER.P
ANM
CDPO
Andhra Pradesh Economic Restructuring Project
Auxiliary Nurse-Midwife
Child Development Project OIT Icer
CNC
Community Nutrition Center
CNS
CNW •
Community Nutrition Supervisor
Community Nutrition Worker
CNI
Community Nutrition Instructress
CSSM
Child Survival and Safe Motherhood Project
CTC
Communications and Training Center
CWO
Community Welfare Organizers
DEA
GOI
Department of Economic Affairs
Department of Women and Child Development
Developing Women and Children in Rural Areas
Government of India
GOTN
Government of Tamil Nadu\
DWCD
dwcka
ICDS
Integrated Child Development Services
IDA
International Development Association
Information Education and Communication
Infant Mortality Rate
IEC
IMR
.
LBW
Low Birth Weight
MTS'
Mid Term Survey
NFHS
National Family Health Survey
NGO
Non-Governmental Organization
NMP
Nutritious Meals Program
NMC
Nutritious Meals Center
National Nutrition Monitoring B ureau
MNMB
PMU
SAR
Project Management Unit
Staff Appraisal Report
SRS
Sample Registration System
TINP
Tamil Nadu Integrated Nutrition Project
VHN
Village Health Nurse
WCDP
Women and Child Development Project
Vice President
Director
Sector Manager
Team Leader
Mieko Nishimizu
Edwin Lim
Richard Skolnik
Anthony Measham
!
IMPLEMENTATION COMPLETION REPORT
INDIA
SECOND TAMIL NADU INTEGRATED NUTRITION PROJECT
(CREDIT 2158-IN)
CONTENTS
PREFACE
EVALUATION SUMMARY
PART I: PROJECT IMPLEMENTATION ASSESSMENT
A.
B.
C.
D.
E.
F.
G.
H.
I.
Project Objectives
Achievement of Project Objectives
Major Factors Affecting Project Implementation
Project Sustainability
Bank Performance
Borrower Performance
Assessment of Outcome
Future Operation
Lessons Learned
PART II: STATISTICAL TABLES
Table 1:
Table 2:
Table 3:
Table 4:
Table 5:
Table 6:
Table 7A:
Table 7B:
Table 8:
Table 9:
Table 10:
Table,! 1:
Summary of Assessments
Related Bank Credits
Project Timetable
Credit Disbursements: Cumulative Estimated and Actual
Key Indicators for Project Implementation
Studies Included in the Project
Project Costs
Project Financing
Status of Legal Covenants
Compliance with Operational Manual Statements
Bank Resources: Staff Inputs
Bank Resources: Missions
APPENDICES
A.
B.
The ICR Mission’s Aide-Memoire
Borrower’s Contribution to the ICR
I
IMPLEMENTATION COMPLETION REPORT
INDIA
SECOND TAMIL NADU INTEGRATED NUTRITION PROJECT
(CREDIT 2158-IN)
PREFACE
This is the Implementation Completion Report (ICR) for the Second Tamil Nadu
Integrated Nutrition Project in India (Credit No. 2158-IN). A total IDA credit of US$95.8 million
(SDR 73.5 million equivalent) was approved on June 14, 1990 and made effective on December
5, 1990. This amount was subsequently reduced to US$65.99 million.
The credit closed on the original closing date of December 31, 1997. The credit amount
was fully disbursed, with the last disbursement taking place in January 1998.
This ICR was prepared by Anthony Mcasham (Task Manager) and Stuart Gillespie
(Consultant), with technical assistance from Kathleen Finn/P. Subramaniyam, Alaka Singh,
Meera Priyadarshi, R. Sethuraman and Krishna D. Rao. Nira Singh provided office technology
assistance. The ICR was reviewed by Richard Skolnik (Sector Manager, SASHP) and Kazuko
Uchimura (Project Advisor, SARRJ).
Preparation of this ICR began during the October 1997 supervision mission. It is based on
material in the project files, field visits, and discussions with beneficiaries, project staff,
Government officials and Bank staff. The Borrower, Government of India (GOI), contributed to
the preparation of the ICR by preparing its own evaluation of the project’s preparation and
execution, with the assistance of the State Government of Tamil Nadu (GOTN). Comments on
> the report drafts were received from the Borrower and taken into account in the final version.
The cooperation and assistance of GO! and the Government of Tamil Nadu is gratefully
acknowledged.
■H3HSL-L -
•»
r
'
’
■
3k
fc
iq q \
0ClKjcwC
.
roj-eV
IV) c
<3 18 2) \.o^
Ota-V cJK^
[<s os
dA.
CoV
b.
h z\
€ io A .
^e.
<2 tv,
A V
K
0
^5 V o
CZ’''
Go
\riA^
I
H UVcV
9
zi
ex
nr
fl
bs£o\
5'CxaV
\ff2^^
k>
u>-e<^
<X^CaX^
L
,o u
r^z, fa- it>
t^o >*
, Wo
^p^CLCv^ VxA^
I
I
I
I
I
I
I
I
Rt
I
I
’
\VV5
<_ t
\V,C
O - 3b
fc
\flo
II
■ I
IMPLEMENTATION COMPLETION REPORT
!
INDIA
SECOND TAMIL NADU INTEGRATED NUTRITION PROJECT
(CREDIT 2158-IN)
EVALUATION SUMMARY
Introduction
1.
The Second Tamil Nadu Integrated Nutrition Project (TINP II), launched in 1991, was
the second nutrition operation supported by the World Bank in India. Its predecessor, TINP I,
became well-known in international nutrition circles during the 1980s as a "success story",
having achieved a highly significant reduction in severe early childhood malnutrition.
Implementation of TINP II largely overlapped with that of two other IDA-supported Integrated
Child Development Services (ICDS) projects. ICDS I, approved in 1990, covered the states of
Andhra Pradesh and Orissa, while ICDS II, approved in 1993, covered the states of Bihar and
Madhya Pradesh.
Project Objectives
The overall goal of TINP II was to improve the nutrition and health status of children
2.
0-72 months of age, with particular emphasis on 0-36 month olds, and pregnant and lactating
women. Specifically, the project aimed to (i) reduce severe malnutrition among 6-36 month old
children by 50% and 25% in new and existing project areas, respectively; (ii) increase the
propprtion of 6-36 month old children in normal and Grade 1 nutritional status by 50% and 35%
in new and existing project areas, respectively; and (iii) to contribute towards a reduction in
infant mortality rate from 84 to 55 per 1,000 live births and to a 50% reduction in the incidence
oflow
birth weight.
The project covered a total of 318 of Tamil Nadu's 385 rural blocks in 19 of 23 districts,
3.
including the strengthening of activities in 122 existing (i.e.. T1NP I) blocks and expansion to
194 additional blocks. The remaining rural blocks were covered by the ICDS program.
4.
The core strategies intended to realize these objectives were regular growth monitoring
and health checks for all children, with therapeutic supplementary feeding of moderately and
severely malnourished and growth-faltering children, and high-risk pregnant and lactating
women.
5.
Loaming from TINP I, several new or strengthened strategics were proposed for TINP II,
including (i)) the inclusion of moderately malnourished children in the supplementary feeding
program; (ii) improved coverage and quality of antenatal services aimed at improving maternal
'Af.-j
1
^KaIISHh
ata##?
■
K^c
Cd=n^
VAAZ.^
lro 0
CZ^x-\p V-OT’
i To 1
3.
-m
A.V fin
<-
A
Om
C Glz> o <-^
\j>^
f-0
Y
\n C'sJ
(yoo’
iCLaa**-^-
IXz,
V=—-ri-er ■IVu-Xj
a
6Xxx-cd
11 1
X;
Dec • 1^
e>wV
nr-*—-<ryy |/V\^
?
’f
OU
A &•
‘A
J
C^' 'Z- 3
ZJ'&i <■
T57 ( 3^-z)
v-^\ >\ C d -i
. s \. ^3'/,
h
,vv^^<aA>Zv;ok/ e^-o^
W eV t
c^~ tl
o-aTVS
cV%
-AA-
l-x wv<nA^ •
O
v
A
CcV
^■
/
% 11rJA
)
<^xaIo
I
cVJ-£^
°v
S3Zy
£-€IZ Q A^rcv-
Go
o^L
>
S'? I ■•
K
V
<G •’
ce
vv.
3
CT
(Aa-O
/\-
UVO
bO
vu
t\
Oi
Ikzo
13_ 2. 4-
/Sc-Z A>vU*o
'YOU.^
I E C
CA>>
A, r^x c
u>
NC
ACe-^.
fo
V
>
S^gZ)
tkz.
Ho C Vd.
U7
^A
C C^rycl
v^v <l-«X' >w
>v\j
.
3
JocpccV'
' : 1 • x-/
• -i
iii
nulrition and reducing low birth weight incidence; (iii) improved coverage of smalfhamlets and
outlying habitations through appropriate coverage strategies; (iv) strengthening of health referral
i
services for diagnosis and treatment of severely malnourished children and hitth-risk pregnant
mothers; (v) improved child feeding and care practices through effective communications- (vi)
improved co-ordination between nutrition and health personnel through
effective joint training and supervision; and (vii) community education including the formation
of new, and strengthening of existing, women’s groups.
Implementation Experience and Results
6.
The project was successful in achieving its severe malnutrition reduction objective.
Progress towards the reduction of moderate malnutrition was also made, though this proved to be
y. a more intractable problem, and a renewed emphasis on this will be required in the forthcoming
Woman and Child Development Project in the stale. The project contributed to a significant
deduction in the infant mortality rate, as would be expected by its impact on severe malnutrition.
The impact on low birth weight incidence was hard to judge due to the paucity of reliable data
but the data that do exist point to improvement. The persistence of a gender imbalance in child
I
nutritional status, whereby higher proportions of girls are malnourished in the most vulnerable
12-23 month age group, should be addressed in future.
7.
Service delivery and communications were generally well implemented and resulted in
the achievement of most process objectives for women and children. Decentralized, block-level
training worked well, although there was a significant backlog in refresher training which
compromised quality to some extent. The existence of significant inter-district variations in
service delivery performance and communications outcomes suggests the need for a modular, X
site-specific approach to training and communications. While much useful mass media material
was produced and distributed, too little attention was paid to improving the inter-personal
communication skills of Community Nutrition Workers which are vital for catalyzing sustained
behavioral change.
8.
After a slow start, community mobilization, and women's group formation and training in
particular, worked well and contributed to long-term sustainability and active ownership of the
project. Secure linkages to other government-supported income-generation schemes for women
now need emphasis.
9.
The qualitjcof monitoring.was one of the great strengths of TINP II. as it was with TINP
I. The system of tracking key process and outcome data, with built-in data quality checks and a
streamliped set of registers, is efficient and action-oriented. Progress towards impact objectives is
highly visible, building accountability and motivation. Evaluation is overseen bv an expert
committee, although the actual implementation of the mid-term review was poor,
10.
Overall, the timeliness, quality and utility of operational research was unsatisfactory.
X*
Improved assessment criteria for bidding agencies and better monitoring of progress is required
to ensure timely, high quality work and results which can be used to improve the program during x
its lifetime.
iv
11.
Tamil Nadu is one of the five stales involved in the forthcoming Woman and Child
Development Project, From January 1998, all the 318 TINP II b,locks were incorporated into the
ICDS program, wluch is bemg universalized throughout India.
Key Lessons Learned
12.
The main lesson learned from T1NP II is that the adopted strategies were broadly
appropria e, but there is a continuing need to intensify the’focus on localized capacity-building >
community mobihzat.on and targeted, inter-personal communications. Severe malnutrition is
now minimal but moderate malnutrition, with all its detrimental consequences, remains
X
f 8d- ‘Can Thcre needs t0 be a Brcater emphasis in future on improving home-based care and x
feedmg of the youngest children, particular^ girls, to prevent them from becoming
*
malnourished. Geographically, targeting to remote hamlets needs to bejrrioritized for example
through the establishment of mini-centers.
y.
example.
|
r
Community ownership should remain a priority goal. The experience in the latter half of
project with social mobilization should be drawn upon to facilitate active involvement of
more oi the community.
• >’
13.
1
Lth n OveraJ1’SUpP°r,lvc counselling of caregivers and high-quality service delivery, allied
nillars off^ d Tv t0WardS S°C,al mobllization and Participatory planning, should be the /
pillars of future nutation tmprovement strategy. Decentralization, quality and ownership are key
overriding concerns. For the most part, these lessons have alreadv been woven into the proiect
of the forthcoming Woman and Child Development Project in Tamil Nadu, and indeed
other states, though they will need to be vigilantly monitored during its implementation.
Assessment of Outcome
I
i-
• ,15.
rl -
F’J Pr°j'C' °1U'OTme
“'isroclory in tl,ot II,e development objectives were lamely
» tai^lle
8
eai"ST* by TINP ' "'hils'
'I" S-ottndwork for a
sustainable nutrition improvement in the state.
1
IMPLEMENTATION COMPLETION REPORT
INDIA
SECOND TAMIL NADU INTEGRATED NUTRITION PROJECT
(CREDIT 2158-IN)
PART I: PROJECT IMPLEMENTATION ASSESSMENT
1.
Tamil Nadu has had a rich experience with nutrition programming in the last two
decades. The first IDA-supported nutrition project in India was the Tamil Nadu Integrated
Nutrition Project (TINP I) which had a well-documented and highly significant impact on early
childhood malnutrition between 1980-89. In 1982, the stale-funded Nutritious Meals Program
(NMP) was introduced. This program provides a noon meal to children aged 2-14 years and
functions through a state-wide network of feeding centers (NMCs) run by a cadre of Child
Welfare Organizers (CWOs). The Second Tamil Nadu Integrated Nutrition Project (TINP II) was
launched in Tamil Nadu in 19 of 23 districts in January 1991. in a series of five phases over a
period of three years.
2.
Implementation of TINP II largely overlapped with that of two IDA-supported Integrated
Child Development Services (ICDS) projects.JCDS I (approved in 1990) covered the states of
Andhra Pradesh and Orissa, while ICDS II (approved in 1993) covered the states of Bihar and
Madhya Pradesh. In addition, the Bank appraised two new projects in 1997/98: the ICDS
component of the Andhra Pradesh Economic Restructuring Project (A PERP) which is scheduled
to become effective by July 1998, and the Woman and Child Development Project (WCD) in
Kerala, Maharashtra, Rajasthan, Tamil Nadu and Uttar Pradesh, which is scheduled for the Board
in May 1998. The WCD project aims to improve the nutrition and health of pre-school-aged
children and women. Other related Bank-assisted projects in India include seven population
projects and the Child Survival and Safe Motherhood operation, which aimed at improving
family health and reducing maternal and child morbidity and mortality.
A.
PROJECT OBJECTIVES
3.
The overall goal of TINP II was to improve the nutrition and health status of children 072 months of age, with particular emphasis on 0-36 month olds, and pregnant and lactating
women.
4.
Project Coverage. TINP II was intended to cover a total of 3 16 of Tamil Nadu's 385 rural
. blocks, .including the strengthening of activities in 122 existing (i.e., TINP I) blocks and
expansion to 194 additional blocks. The remaining rural blocks are covered by the ICDS
program. In existing TINP blocks, about 6,400 Community Nutrition Centers (CNCs) were to be
amalgamated with the existing NMCs. In new blocks and 20% of villages in existing blocks
where there existed significant coverage gaps, a total of 12,000 NMCs were to be strengthened
by the addition of a new worker who would provide TINP services to under-three year-old
2
children. Finally, in 2,200 villages in new and existing blocks which were not covered by either
TINP dr the NMP, new centers were to be established with two workers and a helper.
5.
Specific Objectives- The impact objectives of TINP II were:
to reduce severe malnutrition (Grade III and IV) among children 6-36 months by 50%
and 25% in new and existing project areas, respectively:
to increase the proportion of children 6-36 months of age in normal and Grade I
nutritional status by 50% and 35% in new and existing project areas, respectively; and
•
to contribute towards a reduction in infant mortality rate from 84 to 55 per 1,000 live
births and to a 50% reduction in the incidence of low birth weight.
Key process objectives, as per the 1990 Staff Appraisal Report, are summarized in Annex
Tabic 5.
6.
Project Strategy. The core strategics intended to realize bhese objectives were:
•
regular growth monitoring and health check-up of all children; and
•
therapeutic supplementary feeding of moderately and severely malnourished and
growth-faltering children and high-risk pregnant and lactating women;
7.
On the basis of lessons learnt from TINP I, several new or strengthened strategies were
proposed for TINP II, including:
•
inclusion of moderately malnourished children in the supplementary feeding program
in order to reduce levels of moderate malnutrition;
•
improved coverage and quality of antenatal services aimed at improving maternal
nutrition and reducing low birth weight incidence;
•
improved coverage of smaller hamlets and outlying habitations through appropriate
coverage strategies including use of women's working groups, adolescent girls, etc.
•
strengthening of health referral services for diagnosis and treatment of severely
malnourished children and high-risk pregnant mothers through existing health
facilities;
•
improved child feeding and care practices through effective communications
requiring the development of communication strategics and strengthening
communication activities through use of print and other media;
J
•
improved co-ordination between nutrilion and health personnel through effective joint
training and supervision, thereby improving the coverage and
quality of health
interventions; and
•
community education including formation of new, and strengthening of existing,
women’s groups.
B.
ACHIEVEMENT OF PROJECT OBJECTIVES
A definitive assessment of the project's impact will await the findings of the final survey
8.
which has recently been completed and is currently being analyzed.
9.
To place the impact objectives in context, they can be compared with the secular trend of
a 5.6% annual reduction in the prevalence of severe malnutrition in Tamil Nadu during the
T78Usfaccording to National Nutrition Monitoring Bureau data. This improvement occurred
during the time that TINP I was underway in approximately half of the rural blocks of the state.
'INP II sought to reduce severe malnutrition by 50% in seven years in new blocks - an annual
decline of just over 7% and an achievable goal. Given the progress already achieved with TINP I,
the other target of 25% severe malnutrition reduction in existing (ex-TINP 1) blocks was also
realistic. Importantly though, TINP II placed particular emphasis on reducing moderate
malnutrition, thus increasing the proportions of children in Grade I and Normal categories.
J
10.
Although available monitoring data have not been differentiated by new and old project
areas, they show that, for the project as a whole, severe malnutrition among under-three year-olds
dropped from 4.9% at the 1992-93 baseline to 1.1% in December 1996 - a 78% aggregate
decline over this period. This suggests that the severe malnutrition objective has easily been
achieved.
11.
Given the "baseline percentage of 76.3% in the combined Grade I and Normal category,
the second impact objective can be seen in hindsight to be statistically impossible (implying, as it
docs, greater than 100% in these categories by project close).1 Between the 1992-3 baseline and
December 1996, on average, there was an increase in the proportion in these categories of 12%.
This represents some progress, although one child in seven in Tamil Nadu remains moderately
malnourished.
12.
All currently available nutritional status data are presented in Table 1. As expected, there
is a strong similarity between the TINP-II baseline and the National Family Health Survey
(NFHS) data collected during 1992-93. The Phase IV and V baseline carried out in 1995 shows a
. better nutritional situation than either of these latter surveys, implying appropriate early^targeting
of TINP II in its first phases to blocks with high proportions of child malnutrition. Monitoring
data suggest the nutrition situation is improving steadily over lime, and significantly better than
1 However this objective had originally been set on the basis of lhe 1939 TINP I terminal evaluation figure of 30%
moderate malnutrition, not the 1992-93 baseline figure of 18 S% Limitations with the MTS preclude an assessment
of the percentage decline in moderate malnutrition since 1989 in old TINP I blocks.
/
<
I
?
i
0-
Kf
%
1^6
£
c\
.Li
r? oox u <-<j
t* < c to
!■
H7E
w&bi y
I
I
I
I
O. CC-C”
3t
bo [to
VJUa (yLVYVO o\
WUX
\J=C^A^- ^^Lk/g
rvxc
S’
CL/v^-^
C-C-LaZk^
b a-’TyV/^’
3
■
4
the picture painted by independent survey data. The one significant outlier dalapoint comes from
the 1996 mid-term evaluation survey which shows particularly high levels of severe malnutrition,
although doubts have been expressed concerning the validity of these data.
'--■
Table 1: Comparison of 0-36 Month Child Nutritional Status (%)
Between Various Surveys and Monitoring Data2
Data source and date
Baseline survey (I992-93)*
National Family Health Survey (1992-93)
Phase IV and V Baseline survey (1995)
Monitoring data (December 1995)
Mid-term Survey (April/May 1996)
Monitoring data (April 1996)
Monitoring data (September 1996)
Monitoring data (December 1996)
P ec.
.
Normal
41.4
43.8
54.6
40.0
44.7
43.8
44.5
45.4
Grade I | Grade II . Grade 111
34.9
1 &~
33.0
29.6
39.4
26.5
40.7
40,2
40,0
I
;
j
|
• i
&iv
18.8
19.1
13.1
16.8
19.0
14.3
14.1
4.9
4.1
2.8
:
3.8
|
9.8
ic- 1.2
i
1.2
13.5
J
!
!
LI
j
i
il-o
i o 7.
• the age group al 1992-93 baseline survey was 6-36 months, which would be expected Io give slightly higher /f
figures than the 0-36 month aggregate.
•
r
13.
With regard to age and gender differentials in nutrition outcomes, malnutrition prevalence
in the project area peaks in the 12-23 month age group. This also happens to be when the gender
difference is most pronounced. In the 1992-93 NFHS, 50% of girls were classified as
underweight as compared to 43% of boys, one of the largest gender differences seen among
states in India. A similar picture was seen at the Mid-Term Survey (MTS), particularly in the 1223 month age group with 12 of 15 districts showing higher proportions of girls being
malnourished than boys.
i
14.
Areas which were not covered by TFNP II at the time of the MTS in 1996 had
significantly higher levels of malnutrition. The two districts with by far the lowest project
coverage were among the worst-performing districts, namely Tiruvannamalai and Dharmapuri.^
No significant difference was found between the situation in main villages and in smaller
ha. 3ts, which implies that where the project docs succeed in reaching hamlets, it is as effective
as in larger villages. In mid-1996 however a significant proportion of these hamlets remained
unrcached (see paragraph 19).
15.
The situation regarding the ambitious objective of halving low birth weight incidence is
unclear owing to a lack of reliable data. 1992-93 NEUS data provide a figure of 23% low birth
weight incidence in Tamil Nadu, almost identical to the 23.5% figure arrived al in the 1996 MTS
from a limited sample of institutional data. Birth weight recording in general is not well carried "K
out and data arc usually both scarce and unreliable. Although it is not possible to judge the '
2 ’
\
All anthropometric data unless otherwise specified arc classified according io the Indian Academy of Paediatrics
(IAP) system which grades children with respect to (he percentage deficit in weight, al a given age. from a reference
standard. In the IAP system, "normal” is 80% or above. Grade I is 70-80%. Grade II. 60-70%. Grade 111. 50-60%
and Grade IV below 50% of the reference median.
!
7
5
degree of improvement, it is clear that low birth
weight tncidence has declined from its baseline
level of about 30%.
rl“C.Mnn';r8Tb“" "hi"cd-
&*£££XSX
<?
•»
S.be
slalus Whereby higher proportions ergiris
Ze Zrr0U'’'
ilh rCEard 10 8e0Bra',hi“l
"
"»
co™ ed
projee, performance was as effective as in larger, more accessible villages
Service Delivery Objectives
►
C0°f ™P " diS,"'1S
'
usually residing in small oullying.hamlels. which do no, have rend.
m TdNPlfscrviccs’
According ,o ,he MTS, ,his "nmeached” popola.ion varies from ■ % in ,hc diXo" Ztad
haml^s oXctts'ih ™hmhPrOgr'SS
bC'"
“V":'S' I’rl’il"er,‘> i"»»«sible
mtets, outreach is still patchy in some districts and needs improvement. \
■ | |
objectives. The latest available project monitoring data (October 1997) noint to
ngl. l*ds ofserv.ee ddivey coverage and .he aehicvemen. ofmany of .he process obkc.w
O/o of pregnant women were registered before 16 weeks (target: 50%), all of whom were
Xget ofVoy Lnlik
"d'rr31
TC‘anUS ,OX°id immUnization covera ge has achieved P\
0-^u f 8°f°
fol'c acid supplement coverage which is 53% versus a target of
J3^''
Scord
i
supplcmentat.on to pregnant and lactating women is virtually'^^l
i
I
r 'ng 0 monitoring data (compared to targets of 60% and 90% for pregnant’and
actating women respectively).
pregnant and
o.
With regard to children, most targets have been
or nre closc 10 being, met. Complete
•nmunization is at 96% (target: I
lUU/o), regular growth monitorinu at 94% (target- 90%) and
Jpplementation of those eligible.
apta'w
,cey
■ i
1
I
6
Ir
21
Data from the 1996 MTS gave lower figures for most of these service delivery factors,
- with the main discrepancy relating to the proportion ofiligible women and children who
received supplementary foods. While the latest monitoring data provide figures of between 9499% the MTS suggested only 40-47%. However, this was reportedly due to a temporary
cessation mTbod distribution that coincided with the mid-term survey in mid-1 996.
22
Health service coverage. TINP has a clearly defined organizational structure with a builtin platform for coordination with the health sector through matching workers at different levels.
In. addition to nutrition-related services, the CNC was intended to be the focal point for key
health services such as immunization, ante-natal and post-natal care. The CNW liaised with the
Village Health Nurse (VHN) to organize immunization sessions every Wednesday, ante-natal
and post-natal care services on Mondays and joint home visits every Thursday,
23.
According to the MTS, home visits by the CNW were regulviy. undertaken, with more
than 85% of mothers on average reporting that cither the CNW or Village Health Nurse (VHN)
.ted them as follow-up following referral. Joint CNW/VHN visits too were occurring
frequently in most districts. Tire MTS however reported the existence of problems wjth
coordination at block level between health and nutrition officjals, and irregular participation in
joint review meetings.
24
Training. The intensive block-level approach to decentralized training of village-based
functionaries has largely been successful. Tire Communications and Training Center (CTC) has
effectively undertaken training of supervisors and other lugher-leve workers, although there
remained a heavy backlog of refresher training towards the end of the project, related to GOTN
funding constraints at that time.
25.
Decentralized joint training of health functionaries along with the Community Nutrition
XVorkers has been successful in laying great emphasis on communications for behavioral change x
particularly with regard to issues such as home-based care and feeding practices for children
and women, complementary feeding strategics, early pregnancy rcgistrafion and ante-natal care.
However, there have been gaps. The CNWs’ own awareness of the different tasks they
ar°e required
the time
required to
to undertak7was
undertake was“ found
found to
to be
be limited
limited in
in certain
certain districts
districts al
al the
time of
of the
the MTS.
MTS. In
In
general, most CNWs knew the'pufpoSe of"weighing
weighing and the criteria for selection into
.
were significant inter-district variations. Such differences
supplementary feeding, although there
pproach to training to enable appropriate skills and knowledge to
suggest the need for a modular a]
be linked to local problems.
27
Pre-school Education. TINP II included pre-school education as a service delivery
component, vfhis component did well, but the objective of increased attendance (> 80/» of
working days) was not monitored regularly/The project also provided orientation trammg on
pre-school educati^o’Child Welfare Officers (CWOs) and tcaching/lcarmng materials to
CNCs.
I
z
7
28. • Conclusions. In sum, service delivery was well implemented and resulted in the
achievement of most process objectives for women and children. There was a hiatus in the
distribution of supplementary food in mid-1996, though this was temporary, and rectified after a
few months. Block-level training worked well, though there was a significant backlog in
refresher training which would have compromised quality to some extent. The existence of
significant inter-district variations in some aspects of service delivery performance suggests the
need for a modular, site-specific approach to training.
r
I
Communications Objectives
29.
The TINP II communications strategies derived from formative research, the findings of
the baseline survey and a communications needs assessment study conducted in 13 districts by
District Communication Officers. During the early years of TINP 11. theemphasis was on state
wide mass media communications on selected themes. A considerable amount of printed
materials, including a newsletter, was produced, widely disseminated and undoubtedly had a
positive eff^efon popular awareness of malnutrition and its causes.
i
I
i
I
30.
The MTS assessed the degree of maternal knowlcdge*of various aspects of nutrition as a
proxy for the impact of the communications component, findings were mixed. Most women
were found to be aware of the existence of growth monitoring within TINP II but the majority
did not know that growth monitoring was intended to be carried out monthly. The great majority
of women believed that supplementary feeding of malnourished children was intended either to
improve weight or improve health or both. Only 25% of children receive complementary foods
from the age of six months. Maternal knowledge of at least one cause of diarrhea ranged from
25-93% between districts. In fact, the pronounced inter-district variation was one of the main
findings. This calls for a more decentralized topic-specific, area-focused strategy of
communication, not one biased towards mass media campaigns.
••
31.
A situation-specific, “mini-campaign" approach to targeted communications was adopted
in recent years, focusing on such areas as growth monitoring, on-site feeding, antc-nalal care,
micronutrient supplementation, breastfeeding and complementary feeding, and the prevention
and management of diarrhea and acute respiratory infections. In addition. IEC efforts directed at
the community resulted in an increase in the weighing of newborn babies soon after birth, v
I
s
32.
Certain innovations such as special sensitization workshops for newly married couples,
village priests and village barbers were important contributions. Traditional practitioners of
Siddha, Unani and homeopathic medicine were oriented and involved in supporting IEC.
Participatory planning workshops for NGOs were convened, and traditional media also used for
communicating project messages. On the other hand, there has been little attempt to
systematically monitor behavioral change, though this is planned lor the future. Also there is a
need to expand successful small-scale IEC-rcla(cd pilots.
!■
z
8
.echniques such as Participatory Rapid Appraisal (PRA)
materials production, and use of
communication skills training for field staffonly came' in late in the project’.
and internal-persona!
j4.
.Conclusions. To conclude, the communications component, which was based on sound
formative research, was effective, albeit to some extent limited by its bias towards X Zia
pproaches. More attention is required to the development of the CN W's inter-personal
V
counselling skiI s^Tlre geographical variation, as with service delivery, again suggests that
ra egies should be flexible, decentralized and problem-focused. This has been recognized by
project management in the last two years and the balance has shifted towards participatory
skdl3'! t reVCa COmmunlcatlon Priorities, and (he development of the CNW's communication
haveZlsZ
7- COmrnUn"y-based innovations, taking advantage of localized opportunities
also been tried out with some success, providing lessons for wide? replication
Community Mobilization Objectives
‘s ' I
k-r flr fCW rarS °f the Pr°jecl’ there was limited.active community participation
Social mobilization really only took off during the second haff of (he project when NGOs
opinion-leaders and newly-elected village panchayat members were oriented
towards
thehas
goals
o the project and moUvated to generate further grassroots support. From this time
there
been active involvement of panchayats in TINP II as reflected in both cash and kind
contributions for CNCs. Repa.r and maintenance of CNCs was undertaken by panchayats
e\T±d fZ IEC a^^ h Ft bCC°me
PanChayal mCmberS- A"
000 has
raised for IEC and facility maintenance by community contributions. One example of an I
novative approach, Rinded by panchayats,^as a campaign to improve birth weight recordinn'
by providing every mother with a birthday card for her newborn child.
36.
recording
Special training and orientation sessions
were organized for women’s working group
members in group dynamics, self-confidence,
formation of self-help groups and thrift and credit
activities. 4430 thrift and credit societies were
formed and, by project close, savings were
ported to be close to the level of 5400,000.
linkaEes^uechlewttid WC"
rOr'na,i°n
,raini"- Howcvc''- ^stainable
in
D'V"°Pi"S W°'™"
Broun fSjST^d ’r° SUrnmarizc’.aftcra slow start, community mobilization, and women's
XnhT
7
5 10 part,Cular’ worked we" and is contributing to long-term
stainabdity and active ownership of the project. Opportunities were realized to orientate
newly-elcctedpanchayat members who themselves became advocates for the project One
nutation, however, was the fadure to secure linkages of these women's groups to other
government-supported income generation schemes for women.
( j
/
(
9
Monitoring and Evaluation Objectives
lag with respect to any particular indicator Dan^HT t'
were identified and replaced.
lollowing up Wlth blocks which
afrcc"finr”7
in iTO7 y
bCen ,rreSL,lar|y Procured. These
8 1108
40.
TINPII’s management
' *
information
system is effective because it is streamlined and
action-focused - information for action not <’
datajor spreadsheets. Thcnumber of registers to be
regularly
CNWsS w„ ^aineanUy reduced Io seven
repularly updated
upda.ed by CNW
,„e
’ during the project in order to
1 to four registers/ x
2ti„„ ™P 11 h“ an “P'rl commillce O" moniloring and cvalualion which oversees Hie
valuanon process, preparing rerros of reference for surveys and reviewing draft reports
Xo-ne dX^ '"6 mid-™
-c ft^iu'X X
ilXs vShTOdpT The" system of trac^T0'10”02 'S °'7 °HllC grCal.Slrc,^,lls of TINP !>• as
oiwlifv k c
u'
7stem of ,rachmg key process and outcome data, with built-in data
q hty checks and a streamhned set of registers, is efficient and action-oriented Blocks that are
although the actual impRmenlZn oXmXn^iew
3,1
Operational Research Objectives
were condud'ed"
’
"“’rn''
'"’d';r,;,k-rn d"ri"E TINP.II and all bur two
ere Concluded. Several among rhem wore only ftnished in I Odd and rhe findings will be used m
Ze 1 'mplen’'n“l»" °<
forthcoming Woman and Child Developmem Proicc, ' e are
Thus rudres me uded a comparison of child sronrmg in projec. and non-proicet area "a s'udv „
^qelaleseverc c|" d malnulrmon will, household level food sccuriry risk, and a rapid
l’""'weisl’' re”"'i"s 0,(’" s'l,t'i's ’F; <ie,i,il'd
of the Appendix, along with (he action taken on the basis of their results. As
3
10
mentioned, the mid-term review, apart from being delayed by about three years, was of a
generally low quality rendering an assessment of impact impossible.
45.
As with the ICDS I project, the timeliness, quality and utility ofloperational research
Appear somewhat limited. Only the study of child stunting was completed in the First three'years ?
of the projectr^mproved assessment criteria for agencies to carry out operational research and
better monitoring of progress is required lolnsurc timely, high quality work and results which
can be used to improve the program during its lifetime.
Physical Targets yq
46.
18,500 centers were functioning at project close, each staffed by two nutrition workers
and a helper. 483 of planned 500 CNCs were constructed out of a targeted number of 500. To
meet increasing demand for hostel facilities for trainees, a second floor'was constructed in the
hostel wing of the Communications and Training Center. Under this project. Maternal and Child
ealth Annexes in 9 Primary Health Centers in four districts, and 10 Primary Health Centers
were constructed at a cost of Rs. 16 million. A computer center was installed in the Project
Management Unit.
, '* M
Procurement
1
47.
During the project there were [argc-scalc irregularities in the procurement of drugs and
supplementary foods Financed by GOTN. Bank staff investigated a complaint in March 1995
that a pharmaceutical company had been prevented from bidding to supply drugs to the project.
It was also discovered that the selected bidder had not met the qualifying criteria. Mis
procurement of drugs was subsequently declared and USS 1.8 million of the credit proceeds were,
cancelled. With respect to procurement of food, Bank insistence that samples be checked by an
. independent laboratory remedied the situation. The project coordinator at the time was
subsequently transferred, reportedly as a result of the mis-procurcmcnt.
In another investigation during 1996; supplementary food supplied by one company was (
round to be of a particularly low protein concentration after a Bank review mission requested that
samples be tested. Payment for the food supplied by this company between December 1995 and
February 1996 has not been made, pending a Final decision by the GOTN. There were also
in^gularities with regard to the procurement of weighing scales, cups and furniture which were J
found to be defective or sub-standard. These problems were rcclilied.
C.
MAJOR FACTORS AFFECTING PROJECT IMPLEMENTATION
49.
Both positive and negative factors affected the implementation of TINP II. On the
positive side, the use of nutritional status criteria to select children for feeding, as opposed to
only poverty criteria, resulted in better targeting to those children who most required extra food.
The focus on growth faltering placed an important emphasis on the prevention of malnutrition as
opposed to merely a therapeutic post-hoc strategy. Another positive factor was the built-in
]
11
3
structural coordination between the health system and TINP II at all levels, with a well-defined
systems of information flow, management and supervision.
50.
Several factors negatively affected project implementation. One of these was the
exhaustion of project funds in May 1997 caused by cancellation of a total of USS30.53 million
(US$20.2 million because of exchange rate savings and USS 10.3 million because of noncompliance with project conditions). This led lo refresher training and communications activities
being stalled for approximately five months. Another was the fact’that a significant proportion of
CNWs were_discovered to be resident outside the village they worked in, contrary to their terms
of employment. This was likely to have compromised community mobilization and service
delivery. There were also problems with the training and supervision of a significant proportion
of Community Welfare Organizers (CWOs) who were promoted lo Community Nutrition
Supervisors and then to the block-level position of Community Nutrition Instructress (CNI),
despite their not meeting the educational qualifications for (he CNI po^Simullaneously, many
of the original TINP I CNIs who were excellent trainers were transferred elsewhere,
elsewhere. y
51.
Overall, during the mid-projccl period, there was a significant fall-off in commitment,
integrity and supervision from project management which percolated down to all levels adversely
I affecting morale and motivation. This fall-off reflected majon.polilical and social developments
which affected every sector during the period from 1991-1996. These problems were addressed
in 1996 by a new project team which successfully set about revitalizing the project. Quality ^7
improvement planning, an open, action-oriented management style and supportive supervision
were all institutionalized to this end. Given the turbulent environment in which the project
operated, it continued to function surprisingly well.
D.
PROJECT SUSTAIN/XBILITY
52.
The prospect for sustainability is good and the state is poised lo take up the Woman and
Child Development Project (WCD) during 1998. The capacity built during TINP II, particularly
human skills and capabilities through training, will certainly benefit WCD, as will the
infrastructure already created..Although the stale has since opted for a one-worker model, the rale
of attrition of tlic second worker (in the existing two-worker model) is low and most of the
second workers will remain for at least 10 years or so.
53.
The Government of Tamil Nadu approached the GO1 in mid-1997 to lake over the
recurrent costs of TINP II as part of universalization of the ICDS program. The slate government
is meeting the recurrent costs of TINP II until they arc assumed by GOI and is financing the food
costs. GOTN has pledged to sustain the women’s groups established under TINP II and
strengthen linkages with ongoing income-generation programs in the slate.
V
12
E.
BANK PERFORMANCE
54.
The performance of the Bank was satisfactory. Bank supervision missions (of which there
were 1 1 during the project) were particularly useful in supporting the intejiializalion of training
needs assessments, more focused use of traditional media for communications, and monitoring
operational research undertaken by the Project Management Unit (PMU) in several areas. Bank
staff brought the procurement problems to the attention of management promptly, and the Bank
acted decisively in dealing with these problems with minimal disruption to project
implementation.
F.
BORROWER PERFORMANCE
55.
Despite certain incidents and an overall weakening of project management in mid-project,
the performance of the borrower was satisfactory. The changes made in project management
during 1996 resulted in irregularities in procurement being rectified and the morale of project
staff being lifted. Clear signals were sent to field staff to emphasise a new openness in project
management and the need to focus on quality improvement and supportive supervision.
* >
56.
The Government of India complied with all of the covenants in the Development Credit
Agreement while the Government of Tamil Nadu complied with all covenants of the Project
Agreement, except the requirement to complete the mid-term review by the end of 1993. The 1/
review finally took place in 1996.
G.
ASSESSMENT OF OUTCOME
. 57.
The project outcome was satisfactory in that it achieved its development objectives,
consolidated the gains made by TfNP I and provided the groundwork for sustainable nutrition
• improvement in the state. In addition, the lessons learned from TINP I and TINP II were
valuable in the design and preparation of the WCD project in which Tamil Nadu and four other
States will participate.
H.
FUTURE OPERATION
58.
Tamil Nadu is one of the five stales involved in the forthcoming Woman and Child
Development Project. From January 1998, all the 318 TINP II blocks were incorporated into the
ICDS program, which is to be universalized throughout India. The TINP II blocks are now under
the general ICDS program and the PMU has merged with the ICDS Directorate. In keeping with
this, TINP II blocks will convert from a two-worker to a one-worker model to be in line with
ICDS. -
I.
LESSONS LEARNED
59.
TINP I had a marked impact on the prevalence of severe malnutrition in Tamil Nadu
during the 1980s. This success was founded on several factors including selective feedimz, I
favourable worker-supervisor ratios, clear job descriptions and a well-focused monitoring
A
I
13
• ,i
system, used to improve project management and implementation. The NFHS in 1992-93
showed that the gap in Tamil Nadu between the severe and moderate malnutrition prevalences
was higher than in any other state.
60.
TINT II sought to move beyond reducing severe malnutrition to also make a significant
dent in the high prevalence of moderate malnutrition. The entry criteria for the feeding
component were broadened to include, moderately malnourished children and growth faltercrs.
Stronger coordination with the health sector, improved coverage of outlying hamlets, better
communications and strengthened community participation through the use of women’s groups,
were other means to this end.
61.
The main lesson learned from TINP II is that these strategies are broadly appropriate, but
there is a continuing need to intensify the focus on localized capacity-building, community
mobilization and targeted, inter-personal communications. Severe nSalnutrition is now minimal
but moderate malnutrition remains significant not only in terms of prevalence but also with
regard to its detrimental consequences. While severe malnutrition can be reduced with center
based therapeutic feeding (providing the child comes to the center), such a strategy in itself will
not sustainably reduce moderate malnutrition. For this to haf^en. the emphasis needs to be on
improving home-based care and feeding of the youngest children to prevent them from becoming
malnourished.
I
62.
Community ownership should remain a priority. The increasing involvement of
panchayats in the latter stages of TINP II is promising, though more of the community should
become more actively involved. Community self-monitoring is just one example, wherby a core
set of key indicators could be tracked by community organizations to increase the visibility of
progress.
/ 63.
One significant factor behind the generally high-quality training within TINP is the
/ presence of a block-level officer - the Community Nutrition Instructress (CNI) - who is herself
/ assisted by Community Nutrition Supervisors (CNS) al a ratio of 1 per 1'5 CNWs. This ratio
between facilitators and mobilizers has been found to exist in several other successful nutrition
\ y programs worldwide, such as Thailand. One lesson learned in TINP II is that the qualifications
for the CNI post can not be compromised if the quality of training and supervision i? to be
maintained.
64.
The TfNP II management information system is just that - a system of using information
. for management - which is essential to identify necessary mid-course modifications. This
effective MIS was not matched by high-quality independent evaluations. The quality control and
data validation checks of child age and weight estimation procedures in future baselines and
evaluations, and the methods of training and supervising field workers in anthropometry in
particular, require greater scrutiny in future.
65.
Other lessons follow. Particular attention needs to be paid to reaching the youngest
children, particularly the girl children, who arc al greatest risk. With regard to area-targeting,
many remote hamlets, with high proportions of scheduled caste groups, still need to be reached
I
t
14
through the establishment of mini-CNCs. The phenomenon of lagging districts, particularly in
the north of the state, has been known for some time. The recommendation of supervision
missions of joint action-planning with district staff and block-level problem mapping, is still
valid.
66.
In sum, for Tamil Nadu, supportive counselling of caregivers and high-quality service
delivery, allied with a concerted move towards social mobilization and participatory planning
shouldJbe the pillars of a future nutrition improvement strategy. Decentralization, quality and
■ o^ership ^e key overriding concerns. For the most part, these lessons have already been woven
’ into the project strategies of the forthcoming Woman and Child Development Project in Tamil
Nadu, though they will need to be vigilantly monitored durihg its actual implementation.
67
Most of these lessons are relevant beyond Tamil Nadu. Nutrition interventions which are
targeted using nutritional criteria, integrated within a broader health system, and effectively
supervised and managed can significantly reduce severe malnutrition. TINP has shown this It
has also shown that to go further and prevent children from becoming moderately malnourished
is in many ways a harder task and one (hat takes longer. The evolution during the last 17 years m
Tamil Nadu towards an approach which stresses human capacity-building, a pro-active
integration with the health system, and the mobilization of eommunitieg to sustain the process
beyond the project, has laid the foundation for sustainable, long-term nutritional improvement.
I
15
implementation completion report
I
INDIA - SECOND TAMIL NADU INTEGRATED NUTRITION PROJECT (Cr.2I5S.lN)
U
Tabic 1: Summary of Asscssmcjits
1
A- Achievement of Objectives
SubiLanhal
Partial
Nellie ible
(^)
(<)
(y)
□
Macro Policies
Sector Policies
Financial Objectives
1
□
□
□
□
□ •->
Institutional Development
Physical Objectives
Poverty Reduction
Gender Issues
NoLcipplicable
X
X
□
Other Social Objectives
Environmental Objectives
□
Public Sector Management
X
Private Sector Development
X
Other (specify)
X
B- Project Sustainability
Likc.lv
X
(Continued)
Unlikely
(^)
□
UocgHilhl
(z)
16
C.
Bank Pcrfomance
Highly
satisfactory
Satisfactory
Deficient
(z)
(z)
C^)
Identification
□
Preparation Assistance
Appraisal
Supervision
D.
X
□
□
Borrower performance
Highly
satisfactory
Satisfactory
Deficient
(z)
(z)
(^)
□
Preparation
•
Implementation
X
Covenant Compliance
Assessment of Outcome
□
X
□
Operation (if applicable)
E.
>
Highly
satisfactory
□
X
Satisfactory
Unsatisfactory
Highly
unsatisfactory
(z)
(^)
(z)
X
□
17
IMPLEMENTATION COMPLETION REPORT
INDIA - SECOND TAMIL NADU INTEGRATED NUTRITION PROJECT (Cr. 2158-IN)
Table?: Related Bank Loans/Credits
Loan/credit title
Purpose
Status
Year of
approval
1. First Population Project
CR312-fN
To support the family welfare program in Five
districts of Mysore (now Karnataka) and six
districts of Uttar Pradesh.
1972
Credit closed June
30. 1980
Project Completion
Report (PCR) 6/81;
PAR 1/82
___________________
2. Second Population
Project
To support the family welfare program in six
districts of Uttar Pradesh and three districts of
1980
Credit closed March
31, 1988
Andhra Pradesh
PCR 1/90; PPAR
8/90
*
3. Tamil Nadu Integrated
Nutrition Project I
(TINP 1)CR 1003-IN
To improve the nutrition and health status of
1980
preschool children ard pregnant and nursing
women
Credit closed March
31. 1989
PCR 1/91; Impact
Evaluation Report
12/94
4. Third Population
To support the family welfare program in six
Project CR 1426-fN
districts of Karnataka and four districts of
1984
Credit closed March
31, 1992
Kerala
PCR 8/93
5. Fourth Population
To support the family welfare program in four
Project CR 1623-IN
districts of West Bengal
1985
Credit closed March
31.1994
PCR. 12/94
6. Fifth (Bombay and
To reduce infant, child and maternal
Madras) Population
morbidity and mortality and to moderate
Project CR 1931-FN
fertility in the cities of Bombay. Madras and
1988
Credit Closed March
31. 1996
other urban areas of Tamil Nadu, and to assist
Implementation
the Municipal Authorities in designing and
Completion Report
implementing improved health and family
10/96
welfare programs.
IS
7. Sixth (First National
To support the family welfare program in the
Family Welfare Training
states of Uttar Pradesh. Andhra Pradesh, and
and Systems
Development) Population
Madhya Pradesh
1989
Credit closed May
31,1997
Project CR 2057-IN
8. Second Tamil Nadu
To improve the nutritional status of children
Nutrition Project (TN1P 11)
aged 6 to 36 months and contribute to a
reduction in infant mortality rate and
CR2158-fN
1990
Credit scheduled to
close December 3 I,
1997
incidence of low birth weight.
9. Seventh (Training)
Population Project CR
2133-IN
To support lower-income women in the rural
areas of Bihar, Gujarat. Haryana. Jannu.
Kashmir and Punjab, through the training of
1990
Credit is scheduled
to close June 30.
1998
1991
Credit scheduled to
close June 30, 2001
1991
Credit closed on
new and existing health workers and non
Health Department personnel
10. Eighth (Family
Welfare Urban Slums)
Population Project CR
2394-IN
To help the Government of India increase the
supply of family welfare services in the slum
populations of Andhra Pradesh. Kamalaka.
West Bengal and Delhi
--------------------------------------------------------------------------- •------- ►
1 1. Child Survival and
Safe Motherhood Project
To increase child survival and promote safe
motherhood, including establishing first
CR 2300-IN
referral units for secondary-level care of
September 30, 1996
ICR 3/97
mothers and their newborns
12. Second Integrated
To improve the nutrition and health status of
Child Development
pre-school children and (heir mothers by
close September 30,
Services Project'll (ICDS
strengthening and increasing the outreach of
2000
II) CR 2470-IN
the 1CDS program in Bihar and Madya
1993
Credit scheduled to
Pradesh.
13. Ninth (Family
To support the family welfare program in the
Welfare Assam, Rajasthan
states of Assam, Rajasthan and Karnataka
1994
Credit scheduled to
close December 3 I,
and Karnataka) Population
2001
Project CR 2630-fN
1994
14. Andhra Pradesh First
To (i) improve efficiency in the allocation
Referral Health System
and use of health resources through policy
close March 3 I,
Project CR 2663-IN
and institutional development: and (ii)
improve system performance of health care
2002-
through improvements in quality,
effectiveness and coverage of health services
at the first referral or secondary level to
better serve the neediest sections of society.
Credit scheduled to
19
1 5. Second State Health
Systems Development
Project CR.2833-[N
To (i) improve efficiency in the allocation
and use of health resources through policy
1997
and institutional development; and (ii)
Credit scheduled to
close March 31,
2002
improve performance of the health care
system through improvements in the quality,
effectiveness and coverage of health services
at the first referral level and selective
coverage at the primary level to better serve
the neediest sections of society.
16. TB Control Project
CR 2936-IN
To reduce mortality, morbidity and disability
due to TB and to reduce the incidence of
infectious TB by focusing on the cure of
1997
2002
infectious patients
17. Malaria Control
Project CR 2964-IN
To reduce death, morbidity and social and
economic losses from malaria through and
improved malaria control program
Credit scheduled to
close December 3 I,
'1997
Credit scheduled to
close March 31,
2003
including: (i) using a belter mix of effective
malaria control interventions responsible to
local needs; and (ii) strengthening the
Directorate of the National Malaria Prouram *
(NMP) and modifying its orientation
18. Reproductive Health
Project CRNOlSO-fN
To improve quality, coverage and
effectiveness of existing Family Welfare
1997
Credit scheduled to
(FW) services and expand their scope to
close March 3 I,
include more elements of a dcFincd package
of reproductive and child health (RCH)
2003
services
19. Rural Women’s
Development Project
CR 2942-IN
To strengthen processes that promote the
economic development of women and create
an environment for social change, including
improving access to better health care
1997
Credit scheduled to
close June 30, 2002
20
IMPLEMENTATION COMPLETION REPORT
INDIA - SECOND TAMIL NADU INTEGRATED NUTRITION PROJECT (Cr. 2158-IN)
Tabic 3: Project Timetable
Steps in Project Cycle
Dale
Identification (Executive Project Summary)
April 26, 1988
Preparation
November 1, 1 989
Appraisal
January 12, 1990
Negotiations
May 4, 1990
Board Presentation
June 14,1990
Signing
September 14, 1990
Effectiveness
December 5. 1 990
Midterm review (if applicable)
October 29, 1996
Loan Closing
December 31,1997
21
nsiPLEMENTATION COMPLETION REPORT
INDIA - SECOND TAMIL NADU INTEGRATED NUTRITION PROJECT (Cr. 2158-IN)
Tabic 4: Credit Disbursements: Cumulative Estimated and Actual
(CASS millions')
r
Appraisal Estimate
Formally Revised **
Actual
Actual as % of Estimate
Date of Final Disbursement
FY9I
FY92
FY93
FY94
4.00
6.00
15.30
31.40
FY95
FY96
FY97
FY98
57.40
4 1.73
‘77.90
51.90
53.58
93.20
63.90
69.39
95.80
65.82
72.80
I 13
103
108
36.93
6.24
8.48
14.73
141
156
96
January 28, 1998
• The Credit disbursed US$72.R0 million in total.
•• Credit in the amount of USS32.3 equivalent was cancelled.
25.70
82
\
\
s
75
2
£
00
To
o
s
£
CM
O
5
O
O'
I—<
m
O
x©
00
O'
O
00
co
vo
£
£
00
£
oc
£
£
\o
m
£
£
■CO'
£
O'
O'
O'
O'
vn
O'
O'
O'
•aO'
£
o
£
O
ii
O
£
o
o
o
o
o
o
o
o
00
CM
z~>.
-O
L>
o
L°
U
F
U
W
H
£
O
Cm
U
z.
o
F
C-
S
(N
ri
o
z
o
b
<
e
w
J
cu
t-1
o
O
V-,
c
CL
c
c
<
co
UJ
CJ
z
s
‘l
<
F
§
o
u
w
GO
Q
s
£
OOOO
«/“J
OO
OQ
t©
\D
O'
o
£
o
i
,E
r
cn
o
Q.
U
O
_co
\D
to
72
’ Co
GJ
£
O
45
o'
<
GO
J2o
5
>
2
75
w
CD
c
O
o
c
c
E
tn
.2
>
O
E
fx©?
u
-o
E
c
c
o
H
CO
I ,tJ
'B
C
©
C
—
nJ
E
E
■1
c
g
a
<v
2
t
cs
c
JJ
_
CD
22
•© ,E
>5?
I
I
6J
J=
C3
“ ‘o'
o
o
v>
Q.
CO
C
O •<_> tn
I _■ g
*
I ■J
o
•- £
<D
3u Cc:
•—
S 5
*-*
E
o
J
c
>
r
□
o
cL
u
d
r.
t2
CO
c
zh
o
•o
o
CJ
7.
zh
u
o
v>
,1
a
c
tn s
>
c
w
C
u
u
VO
E
o
*
E
o
CX
•-<
O
c
rt
rt
c
•S £
i
tn
u
CD
_
•-
ex
.E
£ .E
g- 3
c
£ •£?
feu .2 .2o
u.
■3 «
rv* -n
c: "o
“O
o c
u
1
5
x>
x©
45
-O
rt
CM
E
t2
o
5
-C
r:
o
o
C.
-O
CO
in
zh
o
O
f?
u
">
U
*©
GJ
£
o
00
o
I
I
.2
CU
<
z
o
G>
Z
G
12
F
<
£
O
u
§
o
C
f? —
32 m
O
>
o
F
d
F
Q
<
Z
25
O
2
G-
i
I
g o° sF
J
a
z
o
O
CN
(’.
.2
_
C
-Q. § ra
E o
c
E :C
o
12 .5 .2
o
o
£
■h:
X__
.2
3 .10
m
Q.
’cj). ‘cD 2
-O
<u
ttJ
c
E
uo
5
«
§
C
co
c 6J
o
o
co
OULX)
F F O E
O
o
oZ — r4
F £
O
O
R
£
O I
a
H
h
_u
EX
CX
.1
S
o
o
U-
o
i
\6
>
J
2
I oc
•5
V
I
w
o
f
CJ
8z>
1—
2©
fl
©
O
CO
o
c
o c
2 C
CN
CD
("S
co
V
C5
\6 E
OQ
■2
X©
7*
X©
VO
y
e
2§ *O
c
V
C
rt
O
"O
ro
■g
VO
s
o
E
o
E
o
c
o
t
t
3
CJ)
CL
*0
C
O
c
o
2
U .O
CX •-
ex h
©
GO
O
co
E
E
th
c
‘5
ZJ
E
Z
O'
o
vn
>O
75 o
3 c
o
c
D..2
«-a
<0
xj
bD
ex t c
ex di ’-e
aj
3
CL. o
bQ
CN - E
c c
u —
n
on
cn
c
o
tn
5
E
o
>
u
<
_ ■
I
CL
I
o
O
E
e
o 2
E <
rt
5 ■siao
JU
.2
I
> >
2
I
GO
c
u.
tn
o 5
co E c
-
J
5
©
t-
1
^■
o G.
r1 111
£
>
c
c .2 E
D.
tx
g 33 <
D_
S •“ C .E
-o
g E
o ‘2
© E 5
O _Cf- c •>
o
E
E
E
.
co
E
- "S
1
O
O
£ o_o
F
O
o
"□
E
O
E
o'
a
c
o
3
o,
c §
X©
3 ■o£
o
<—
o
<—»
o'
cz>
.E
o
5 >tn
E
o
c
o
c
C
1
e'
ch
■O
2
I
c
I
tn
’C
0
O'
*u
c
£
o
<J
£
u
c
c
ro
O
»!!•? :
%
I
23
I
IMPLEMENTATION COMPLETION REPORT
INDIA - SECOND TAMIL NADU INTEGRATED NUTRITION PROJECT (Cr. 2158-IN)
Table 6: Studies Included in Project
Study
Purpose as De Fined
at Appraisal/RcdcFincd
1. Base line survey for TFNP II
To collect base line survey data in
(Phase 1 to III districts).
the project area.
2. Base Line Survey for TFNP II
Status
Completed
Impact of Study
Used to measure project
achievements.
— do —
Completed
— do —
While reviewing all project
activities, special attention would
Completed
provided nutritional status
and
be paid to:
a) the new supplementation
reanalyzed by
Bank
of 6-36 months age group
and status of all project
approaches being adopted under
consultant
(Phase IV and V districts).
3. Mid-term review and
Evaluation of TINP II (Phase I
to 111 districts).
the Project;
b) the revised referral procedures
activities, guided follow
up measures to reduce
severe malnutrition.
and the Maternal and Child Health
annex system being tested in
Madurai district and;
c) the new arrangements for
health/nutrition coordination
4. Social assessment study for
To identify the different social and
improving health and nutritional
economic groups in the project
Study identified
immediate needs of the
status in Tamil Nadu
areas and describe their numbers,
communities, and
distribution and relevant
characteristics for (he proposed
recommended broader
Woman and Child Development
program orientation. Main
Completed
issues of strategy and
recommendations utilized
(WCD) project-
for WCD project.
Completed
Study helped develop IEC
5. Study of child stunting in
To measure the prevalence of
program and non-program
stunting (height for age) in 10
project districts and compare with
strategy for promoting
non-project areas.
safe birth intervals.
project areas.
6. Formative research and
strategy design for
communication component.
Aid in the design and conception
colostrum feeding and
Completed
Findings used in mid
of materials and pre-testing for
course corrections and to
Fine-tuning of (he materials.
modify existing IEC
strategies and develop
new strategies for
proposed WCD project.
7. Condition report on bar scales
To assess the working condition of
by monitoring wing, TFNP.
________ I________________ _______
bar-scales in different districts.
Completed
Findings used in assessing
scale requirements.
24
1
Purpose as Defined
at Appraisal/Rcdefincd
Status
8. Rapid assessment survey on
To assess the effectiveness of
Completed
the effectiveness of training on
birth-weight recording before
CNW’s improved their
training and after training of
hnd attitude.
Study
birth weight recording.
Impact of Study
Periodic training of
CNWs.
9. Study on severely
malnourished children in selected
CNCs to observe if they belong
to at-risk families and correlation
to income and literacy.
To assess the percentage of
10. Survey to assess effectiveness
of functioning of one-worker
To identify the most effective
Completed
severely malnourished children
0-36 months in at-risk families.
Study enabled the project
to better combat
malnutrition.
Completed
model for service delivery
model vs. two-worker model and
Study showed that resident
worker and two-worker
I
model work better.
resident vs. non-resident worker
model.
1 1. Study on the extent of
To find out the reason for low
Completed
migration and ante-natal / post
registration of ante-natal mothers;
•
natal mothers, by monitoring
wheather it is due to mothers
migrating at lime of delivery..
wing, TfNP.
*
No significant difference
between actual number of
ante-natal women and
number registered.
Migration was only 7%.
12. Study on the effectiveness of
Laddu vs. Payasam to children of
To find out effectiveness of
supplementation in the form of
7-12 months
Laddu or Payasam.
13. Terminal Evaluation ofTINP
To assess achievements and
impact of TfNP on nutritional
II and base line survey for WCD.
status of children .
Ongoing
Ongoing
25
9
IMPLEMENTATION COMPLETION REPORT
INDIA - SECOND TAMIL NADU INTEGRATED NUTRITION PROJECT (Cr. 2158-IN)
Tabic 7A: Project Costs
Appraisal Estimate (USSM)
Item
Local
Foreign
Costs
Costs
Total
Actual/Latest Estimatc(US$Mj '
Local
Foreign
Costs
CoSis
Total*
Service Delivery
1. Nutrition
89.08
1.93
91.09
103.29
2. Health
26.05
4.07
30.12
9.07
3. Training
6.28
0.33
6.61
NA
Communications
3.25
0.28
3.53
3.93
4.95
0.04
4.99
5.39
1.01
0.06
1.07
NA
1.33
0.05
1.38
1.74
131.95
6.76
138.71
NA
0.38
NA
139.09”
139.54
Project Management
1. Project
Coordination Office
2. Communication/
Training Center
3. Monitoring and
Evaluation
Total Base Costs
Contingencies
Total Project Costs
• GOI maintains records only in Rupees; a blended rate of Rs.31 per USS was used to convert actual GOI llnancing into USS
** including taxes and duties of USS5.0 million
*I
26
I
IMPLEMENTATION COMPLETION REPORT
INDIA - SECOND TAMIL NADU INTEGRATED NUTRITION PROJECT (Cr. 2158-IN)
Tabic 7B: Project Financing
Appraisal Estimate (USSM)
Source
J
' o .
Foreign
Costs
Local
Costs
Actual/Latest Estimate(USSM)
Total
Local
Costs
Foreign
Costs
Total
IDA
87.4
8.4
95.8
96.28
GOTN
43.3
0.0
43.3
43.26
Total
130.7
8.4
139.1
139.54
I
Nutritional Status of Indian Children: Recent Trends and Current Status
H.P.S. Sachdev*
and
Dheeraj Shah
From the Division of Clinical Epidemiology, Department of Pediatrics, Maulana Azad
Medical College, New Delhi 110 002, India.
^Correspondence to: Dr. H.P.S.Sachdev, Professor and Incharge, Division of Clinical
Epidemiology, Department of Pediatrics, Maulana Azad Medical College, New Delhi
110 002, India. E-mail:drhpssachdev&yahoo.com
1
India has made substantial progress in human development since independence
in terms of improvement in life expectancy and fall in under-five, neonatal and
infant mortality rate. Although, nutritional status has also improved, the
improvement in nutritional status has not always kept pace with progress in other
areas of human development. Malnutrition plagues a disproportionately large
number of children in India as compared to most other countries, with prevalence
of wasting being 8 times and severe wasting about 25 times the prevalence in
the International reference population^). The major nutritional problems that
elude solution despite the increase in food availability and implementation of
control programs are protein energy malnutrition (PEM), vitamin A deficiency
(VAD), iron deficiency anemia (IDA) and iodine deficiency disorders (IDD). This
chapter focuses on recent epidemiological trends and the current scenario in
relation to the nutritional status of children in India.
Data on trends in the nutritional profile of children in India is lacking in
several areas of interest. The two major sources of information are the national
surveys, which provide data related to nutrition and cover large segments of
India's population: (i) the periodic surveys carried out by the NNMB(2-5), of the
National Institute of Nutrition, Hyderabad, and (ii) the National Family Health
Surveys 1 and 2 (NFHS 1 and 2) initiated by the Ministry of Health and Family
Welfare, Government of lndia(6,7).The NFHS-1 survey conducted in 1992(6)
covered 24 states, and was designed to be representative of 99% of the young
child population. However, the focus was on reproductive health and data related
to nutrition was secondary and somewhat limited. In NFHS-2 survey, conducted
2
in 1998-99, the data on the nutritional status of children included hemoglobin
levels in addition to the measurement of their height and weight(7). In
comparison, the NNMB surveys covered only eight states with a primary focus on
the rural population, and the preschool age data relates to the 1-5 year age
group. The repeat (1989-90) surveys(2) are particularly valuable as these were
conducted in the areas evaluated earlier (1975-79)(5) with a specific purpose of
eliciting nutritional trends.
Protein Energy Malnutrition
PEM is the most widely prevalent form of malnutrition among children.
Severe PEM, often associated with infection contributes to high child mortality in
underprivileged communities. Further, early malnutrition can have lasting effects
on growth and functional status. Evidence from many sources(2-7) demonstrates
that malnutrition, while still unacceptably high, has declined substantially in the
past few decades. The most outstanding achievement in this front has been the
virtual banishment of acute large-scale famines, of the type that used to decimate
sizable section of the country's population with distressing regularity (once in
seven years) for centuries(8).
Improvement in agricultural production, development of transportation
systems and improvement in water and sanitation are largely responsible for this
change. This is not to deny that pockets of acute hunger still exist in some parts
of the nation in some sections and in times of disasters like droughts and floods,
but these are now dealt with more efficiently.
3
Kwashiorkor and Marasmus
There has been a significant decline in severe protein energy malnutrition
(classical kwashiorkor and extreme forms of marasmus). Classical kwashiorkor
has virtually disappeared from numerous regions. This change in the spectrum
has been occasionally quantified(9). Reliable community based data generated
by the National Nutrition Monitoring Bureau (NNMB) from eight central and
southern states (Andhra Pradesh, Gujarat, Karnataka, Kerala, Madhya Pradesh,
Maharashtra, Orissa and Tamil Nadu) also confirms a decline in clinical
deficiency signs in preschool children (1 to 5 years old) from 1975-79 to 1988-90
in rural areas(2). The overall prevalence of marasmus decreased from 1.3 to
0.6% and Kwashiorkor from 0.4 to 0.1%. Amongst the 12,000 children evaluated
in the "Repeat Surveys", Gujarat showed the highest prevalence of both the
forms (1.1% kwashiorkor and 4.9% marasmus), while in the other states, their
prevalence was below 1%. In the NNMB and National Council for Applied
Economic Research (NCAER) linked survey conducted in 1994 in the same 8
states but in different sampled areas(3), among 1828 preschool children the
overall prevalences of kwashiorkor and marasmus were 0.2 and 0.4%,
respectively. In fact, cases of kwashiorkor were seen only in Madhya Pradesh,
where the prevalence was about 1.4%. However, marasmus was observed in 4
states, the prevalences ranged from 0.4% in Tamil Nadu and Andhra Pradesh to
about 1.4% in Madhya Pradesh and Orissa. Fortunately, a similar declining trend
was documented in the underprivileged urban slums of these 6 states(4) (cities
4
included Ahmedabad, Bangalore, Bhubenashwar, Cuttack, Hyderabad, Nagpur
and Trivandrum). The overall prevalence of marasmus diminished from 3.7% in
1975-79 (n=519) to 0.2% in 1993-94 (n=334). No case of kwashiorkor was
observed.
Nutritional Anthropometry
Anthropometry, despite its inherent limitations, is the most useful
parameter to evaluate nutritional status of children. Table I compares the
estimated prevalences of various indices of malnutrition in these surveys as per
the current international recommendation and nomenclature(10,11). A distinct im
provement in the prevalences of underweight and stunting (including severe
category, namely, below 3 SD) is evident from the NNMB data at an average rate
of 1% per annum. The NFHS(6,12,13) estimates were still lower than the NNMB
- NCAER(3) prevalences at comparable time periods. This could be primarily due
to differences in sampling design, areas surveyed (whole country versus 8 states
and urban plus rural versus rural) and the age groups analyzed (0-4 yrs versus 1-
5 yrs). Malnutrition in these two indices is lower in the first year of life(14), urban
areas(13) and the northern part of the country(12,13,15,16). Fortunately, a
similar overall declining trend was documented in the underprivileged urban
slums of 6 states(4) between the periods 1975-79 to 1993-94 for weight for age
(Gomez classification based on National Center for Health Statistics reference).
It must be carefully noted that there is virtually no change in the profile of
wasting in this period and the NNMB and NFHS estimates are also identical
5
(Table I), indicating thereby that the improvement in weight for age index is
predominantly due to an increase in the height.
In the recently published NFHS-2 survey report(7), almost half of children
under three years of age (47 percent) were underweight, and a similar
percentage (46 percent) were stunted. The proportion of children who wee
severely undernourished was also notable-18 percent according to weight for
age and 23 percent according to height for age. Wasting was less prevalent
affecting 16 percent of children under three years of age. The proportion of
children under three years of age who were underweight decreased from 53
percent in NFHS-1 to 47 percent in NFHS-2 (Fig.1), and the proportion of
severely underweight decreased from 20 percent to 18 percent. Similarly,
prevalence of stunting and severe stunting decreased from 52% and 29% in
NFHS-1 to 45% and 23% in NFHS-2. However, height data in two surveys is not
strictly comparable because children's height was not measured in five states in
NFHS-1.
Malnutrition varies widely across region, states, age, gender and social
groups, being worst in children under two, in the populous northern states, in
rural areas, and among tribal populations and scheduled castes. Among the
states, Madhya Pradesh and Sikkim have the highest and lowest prevalence of
malnutrition, respectively^). In the NFHS-2 data, the prevalence of underweight
ranged from <25% in Sikkim, Nagaland and Arunachal Pradesh to 55% in
Madhya Pradesh and 54% in Bihar and Orissa; severe malnutrition likewise
ranged from around 4% in Sikkim and 5% in Kerala, Mizoram, Goa and Manipur
6
I
to near 25% - again in Bihar and Madhya Pradesh. Regional variations were also
observed for stunting and wasting. In comparison to the urban areas, in rural
areas the overall prevalences of underweight (38.4% vs. 49.6%) and stunting
(35.6% vs. 48.5%) were higher while interestingly wasting (13.1% vs. 16.2%)
was comparable(7). Overall, girls and boys were about equally undernourished,
but girls were slightly more likely to be underweight and stunted, whereas boys
were slightly more likely to be wasted. In the NFHS-1 survey also, there was no
gender differential - in approximately half the states, girls had higher underweight
prevalences, while boys fared worse in the other half. However, on examining
severe malnutrition only, a gender differential became apparent with a higher
proportion of girls being severely malnourished in 11 of the 14 large states(13).
A multivariate analysis from the NFHS-1 survey(1), of the effects of
selected demographic and socioeconomic factors on child malnutrition indicated
that the strongest predictors of child nutrition in India were child's age, child's
birth order, mother's education, and household standard of living. Older children
and children of higher birth order were more likely to be malnourished. Children
whose mothers had little or no education tended to have a lower nutritional
status, even after controlling for a number of other potentially confounding
demographic and socioeconomic variables(17). Children who lived in households
with a relatively high standard of living tended to be better nourished than other
children(1).
Dietary Intake
7
Feeding practices play a pivotal role in determining the nutritional status,
morbidity and survival of children, particularly in the neonatal period and infancy.
Proper infant feeding, starting from the time of birth is important for the physical
and mental development of the child. The timing and type of supplementary
foods introduced in an infant's diet also have significant effects on the child's
nutritional status.
Infant Feeding Practices: NFHS surveys provide nationally representative
data on breastfeeding and supplementation. In NFHS-2 survey, this data were
obtained from a series of questions pertaining to 32,393 births in the three years
preceding the survey(7). Fortunately, breastfeeding is still nearly universal in
India, with more than 95% of all children having been breastfed. However, only
one tenth of infants surveyed in NFHS-1 began breastfeeding within one hour of
birth and a quarter within one day of birth. These figures improved to 16% and
37%
in
NFHS-2,
indicating
improvement
in
breastfeeding
initiation
practices(Tab/e II). A majority of women (64% and 63%) squeezed the first milk
from the breast before commencing breastfeeding. Favorable practices were
more evident in rural areas, educated, scheduled tribes and assisted births by
health professionals.
Exclusive breastfeeding was quite common for young infants, but even at
age 0-1 months more than one third of babies were given water or other
supplements. Overall, 51-55% of infants under four months were given only
breast milk, while 73-77% received predominant breastfeeding (only additional
plain water allowed). The overall median durations of exclusive and predominant
8
breastfeeding were 1.4 mo and 1.9 mo, and 4.7 mo and 5.3 mo, in NFHS-1 and
NFHS-2 surveys respectively.
The use of infant formula was fortunately rare (1% below 1 mo; maximum
9-11% at 8-11 mo). Similarly, the use of bottles with nipples was relatively rare
for breastfeeding children, increasing from 4% in the first month after birth to a
high of 15-17% for children aged 5-6 mo, after which it declined slowly to near
5% for children approaching three years.
Unfortunately, supplementation by solid or mushy food was grossly
inadequate, showing a rise from only 17-24% at 6 mo of age to 68-72% by age
12 mo and a slower rise thereafter to more than 90% for children who were three
years old (Table II). Even though 95% of infants aged 6-9 months were breastfed,
only about one-third received complementary semi-solid foods as recommended.
Supplementation of breast milk by other milk rose steadily with age to 43-46% at
age 8-9 mo and remained fairly constant (at 45-55%) in most of older age
groups. Breastfeeding typically continued for long durations (Table II). The
overall median length of breastfeeding was slightly over two years (24.4 mo-
NFHS-1; 25.2 mo-NFHS-2)(6,7).
Interesting regional differentials emerged. Goa had extraordinarily high
usage of feeding bottles (almost twice as high as any other region) and very poor
achievement of the goals for exclusive breastfeeding and a long duration of
breastfeeding. Punjab, Jammu, Meghalya (NFHS-1); and Delhi, Himachal
Pradesh and Sikkim (NFHS-2) also had an exceptionally low proportion of
children under age of four months who were exclusively breastfed. Rajasthan,
9
Bihar and Uttar Pradesh were consistently the poorest performers for receiving
complementary foods at the appropriate age in both surveys. Some feeding
problems were universal, however no state came even close to achieving the
recommendations for exclusive breastfeeding of children under 4 months of age
or the supplementation of breastmilk with semi-solids at age 6-9 months(6,7).
Both these factors, particularly the latter, are believed to be important factors
contributing to the high prevalence of malnutrition.
General Dietary Intake: Comparative data on this aspect is mostly available from
the NNMB 1975-79 and 1988-90 surveys(2) and National Sample Survey (NSS)
Organization's 1972-73, 1983 and 1993-94 surveys(18). In NNMB surveys, the
nutrient intake was quantified in a proportion of sampled households by 24-hour
recall and weighing. During this period, the household food security situation
hardly changed(19). Similarly, there was little alteration in the overall intake of
quantified nutrients during these 10-15 years(20). However, the disaggregated
data revealed that the energy intake of landless laborers belonging to the lowest
income bracket had increased by 1.36 kcal per consumption unit (CPU) during
this period. Further, the dietaries of preschool children also showed some
improvement, resulting in enhanced energy intake; about 75 kcal in children
between 1 to 3 years (from 834 to 908 kcal; RDI 1240 kcal) and 140 kcal in the
case of children in the 4 to 6 years age group (from 1118 to 1260; RDI 1690
kcal).
10
On the contrary, the data from NSS surveys from India's 17 most populous
states revealed that, at all-lndia level, average calorie intake declined steadily in
both rural and urban areas between 1972-73 and 1993-94. In rural India, average
calorie intake fell from 2,266 Kcal in 1972-73 to 2,221 in 1983 and to 2,153 in
1993-94. In urban India, intake went down from 2,107 Kcals in 1972-73 to 2,089
in 1983 and 2071 in 1993-94(18).
According to the latest overall estimates, the diets provided adequate
amounts of protein (62g/CU/day vs 60g/CU/day), calcium, iron and thiamine, but
the intake of other quantified nutrients (energy, vitamins A and C and riboflavin)
was below the recommended dietary intake (RDI) as laid out by the ICMR.
Energy intake (228 kcal/CU) showed a marginal deficit while the maximum deficit
was seen in vitamin A (350 vs 600 mcg/CU)(19,20). There was a direct
relationship between the level of energy consumption and protein consumption.
This was expected considering that the main source of calories and of protein in
the habitual diets of the poor is nearly the same - consisting of a single staple
cereal with insignificant amount of fat (calorie-rich) and protein-rich food like
pulses or meat(12). Wide variations in nutrient intake were apparent with the
region and socio-economic status. The urban poor had the least intake followed
by rural and urban better off population, respectively(2,20).
A striking finding of both NNMB and NSS surveys was the lack of
parallelism between the average household calorie and protein consumption in a
given state on the one hand, and the prevalence of undernutrition in its children
on the other. Thus the state that showed the best record (lowest prevalence) with
11
respect to undernutrition in children, namely Kerala, was the poorest with respect
to household food consumption. The state with a fairly poor record (Madhya
Pradesh) showed the best figures for household food consumption. There have
been different attempts to explain this apparent paradox between low intakes and
relatively favorable nutritional outcomes. It is possible that in Kerala, nutrients are
better utilized, quite possibly because of the positive interaction between health
care and nutrition(12,18). In addition, high levels of education enhanced health
seeking behavior and nutrition information among the people may have been
responsible for the favorable results. There could be other explanations as well.
One is that the paradox may, in fact, be an illusion. Questionnaires may
underestimate consumption in Kerala because they do not capture adequately
the very diverse components of diets in the State. Another explanation is that the
allocation of food within the household can be assumed to be less inequitable in
in
Kerala than elsewhere. Nutritional outcomes may thus be better than average
intake data suggest.
Analysis of dietary data to assess intra-family distribution of food revealed
that in 50% of the households surveyed, levels of energy adequacy did not differ
between preschool children, adult men and women. Either all of them were
consuming adequate amounts (31% of households) or inadequate amounts (19%
of households). In a quarter of households, the intake was adequate in adults but
inadequate in children. Calorie inadequacy was documented in a greater
proportion of children (60%) than adults (44%)(20). Further, no obvious gender
bias was documented. When the intakes were corrected for requirements, the
12
average calorie intake levels of women were close to 94% of their RDI as against
85% in men. This is contrary to the general belief that women get least.
In conclusion, malnutrition is still a significant problem in the country
despite the observed decline. India and South Asia as a whole have higher rates
of malnutrition than any other region of the world. Among large countries, India
ranks second only to Bangladesh in the proportion of young children
affected(21).
Intrauterine Growth
Birth Weight
In the context of developing countries, intrauterine growth has been
invariably assessed by birth weight. In India, even today a majority of the
deliveries are conducted in the community. Logistic difficulties in recording birth
weight at home preclude accurate national estimates of the magnitude and
trends of Low Birth Weight (LBW). A large volume of data on birth weight from
the 1950s is available from individual studies, mostly hospital based, and this
information has been exhaustively compiled and reviewed(22-26). Regional,
urban - rural and socio-economic differentials, in the same direction as nutritional
anthropometry, are evident. The usual estimates of mean birth weight and LBW
have ranged between 2.5 to 3 kg and 24 to 40%, respectively. In the community
based ICMR multicentric study(27), the urban slum computations of LBW were
27% for Madras, 38% for Delhi and 56% for Calcutta. The oft-cited nationally
13
representative figure for LBW is 30%(19). It is felt that there have been no
differences in the reported mean birth weights and the proportion of newborns
with LBW in the three decades between late 1960s and late 1980s(22,19). These
inferences were based on comparison of data from disparate settings at various
time points. Given the expected marginal magnitude of change in birth weight in
two to three decades in a nation commencing epidemiologic transition, these
inferences from such a research design are not surprising. It would however, be
more valid to analyze data from the same area at different time points.
On analysis of this nature (Table III), a positive time trend for birth weight
is evident in most of hospital based data and the solitary community study(2834). The mean magnitude of improvement is marginal (52 to 126g). However,
this has resulted in a greater reduction of LBW prevalence (by 8 to 12% usually
and 22% in one report). These calculated mean improvements in birth weight are
probably underestimates(32) since concomitant changes in other important
associates have been ignored. With time, the mean birth order has also
decreased and correction for this factor alone(32) enhanced the magnitude of
change in the community study (rural and urban areas combined) from 70g to
100g (the first born newborns have lower weights than later births). The absent
time trend in the two Delhi hospitals may be related to the relatively short gap in
one report(34) and the fact that these institutions primarily care to the
underprivileged population in whom the transition is expected to commence last
of all. In one of these studies(29), the higher percentage of term births could be
14
regarded as the beginning, since term newborns have the best intrauterine
growth as a group.
The slender improvement in birth weight is probably contributed to by
increases in both gestation and birth weight at different gestations (intrauterine
growth curves). The mean improvement in gestation was again marginal (0.3 to
0.8 weeks) and was not uniformly observed. However, these marginal changes in
mean gestations resulted in greater improvement in prematurity rates (4 to 5%).
Recently efforts have been made to collect nationally representative
estimates of birth weights from institutional(35) and community(36). The reliable
institution based National Neonatology Forum (NNF) data(35) for the year 1995
on 30632 births (0.1% births in the country) from 14 participating centers
(Ahmedabad, Bangalore (3 centers), Baroda, Calcutta, Chandigarh, Delhi,
Indore, Ludhiana, Madras, Mumbai, Pondicherry and Shimla) yielded a LBW
prevalence of 31.2% in 29412 live births(35). Only 35% of the LBW infants were
preterm. The Child Survival Safe Motherhood (CSSM) Programme linked District
based data (Center based delivery in 14 Districts in 10 States - Assam, Gujarat,
Madhya Pradesh, Karnataka, Maharashtra, Orissa, Punjab, Rajasthan, Tamil
Nadu and West Bengal) on 27069 births estimated the LBW prevalence to be
much lower at 18.4%(36). Wide regional variations were apparent with values
ranging from a low of 2.7% (Madhya Pradesh) and 5.1% (Assam) to a high of
24.7% (Tamil Nadu) and 40% (Orissa). The strikingly low figures in comparison
to earlier published literature, especially for the poor performing states (Madhya
Pradesh and Rajasthan- 12.8%) in other nutritional parameters including protein
15
energy malnutrition, questions the reliability of the integrated data. Reliable
recording of birth weight in a community requires meticulous training and an
accurate and sensitive instrument.
Gestation
In contrast to the developed countries, the process of labor appears to be
initiated at an earlier period of gestation in a larger proportion of pregnant
women. The incidence of premature birth (<37 weeks gestation) ranges from
7.1% to 22.3%, in contrast to about 5% in the developed countries. The latest
NNF data provides a national estimate of 12.8%. Only 2% of births occur at 36
weeks in western countries, while 3-12% of infants are born at this gestational
age in India. In the Indian setting, the maximum number of births occur at 39-40
weeks gestation, whereas in the West the corresponding figure is 40-41
weeks(25).
Apart from inter-regional difference, there is a marked variation in the
gestational distribution in privileged versus under privileged segments of
population in the same area. The contrast from the developed countries is very
striking in the low socio-economic population, but the difference is considerably
narrowed and even disappears in the privileged class(25).
Birth Weight and Gestation
A two distribution of birth weight and gestation shows that in the birth
weight group of 1501-2000g, only 30-45% of infants are preterm, the majority
16
being full term or post term. For the birth weight group 2001-2500g, 85% or more
are term or post term and only 13-15% are preterm. These findings are
consistent for hospital and community births(25) and have a bearing on the
identification of high risk neonates and defining criteria for LBW in the Indian
setting(27).
Intrauterine Fetal Growth Curves
A comparison of fetal growth curves shows disparity between regions and
socio-economic classes. The economically privileged population has higher
mean birth weights at different gestations, the difference becoming pronounced
after 34 weeks(25).
A classification for infants at birth based on the hospital derived
intrauterine growth curves has been proposed(37). The suggested definitions for
any gestation are: large for date (LFD): birth weight above +2 SD; appropriate for
gestational age (AGA): birth weight between -1 SD and +2 SD; intrauterine
growth retarded (IUGR): birth weight between -1 SD and +2 SD; and small for
date (SFD): birth weight below -2 SD. This classification has support in
observations on distribution of live births, morbidity and mortality in different
groups(25). The percentage distribution for all gestations for LFD, AGA, IUGR
and SFD in the same hospital and draining urban cohort births were 3, 85, 10.5
and 1.5%, respectively. The distribution of AGA, IUGR and SFD in term infants
with birth weight of 2001-2500g was 13%, 85% and 1-2%, respectively. This
17
observation needs to be investigated further as this is the group which
contributes maximally to LBW in lndia(25).
Iron Deficiency Anemia
Iron deficiency anemia (IDA) is the most widespread micronutrient
deficiency in the world affecting more than a billion people. Anemia is a serious
concern for young children because it can result in impaired cognitive
performance,
behavioral and motor development,
coordination,
language
development and scholastic achievement, as well as association with increased
morbidity from infectious diseases(38-40).
The NFHS-2 survey conducted in 1998-99 provided for the first time
information on the prevalence of anemia throughout India(7). Children below the
age of three years had their hemoglobin estimated by Hemocue instrument.
All over the country, about 70.8% of children up to the age of three in
urban areas and 75.3% in rural areas had anemia. Nagaland had the lowest
prevalence (43.7%), Kerala ranked second (43.9%) followed by Manipur (45.2%).
Haryana had the highest prevalence (83.9%) followed closely by Rajasthan
(82.3%) and Bihar (81.3%). These figures suggest that a great majority of young
children (<3 years) are anemic; and in a considerable proportion the anemia is of
a moderate to severe degree(7) (Table IV).
Nationally representative estimates for older children are not available.
Estimates suggest that a great majority (nearly two-thirds, according to some
18
data) of young adolescent girls of 6-14 years are anemic; and in a considerable
proportion the anemia is of a moderate or severe degree(41). In NFHS-2 report,
56% of ever-married girls in the age group of 15-19 years were anemic; and in
20% the anemia was of moderate or severe degree(7). The ICMR multicentric
"High Risk" study(27) on ever married eligible women (13-49 years) recorded an
anemia (hemoglobin <12 g/dl) prevalence of 82% in rural areas (n=5929) and
85% in urban slums (n=7371).
The results of NFHS-2 surveys from most of the states suggest the
highest prevalence of anemia in the age group of 12-23 months(7). The sharp
increase in iron-deficiency anemia among children of age 12-23 months may
partly be attributed to the initiation of weaning-infection coupled with poor
nutritional supplementation. It was also seen that children bom to mothers who
were illiterate or who belonged to scheduled castes/tribes were more likely to be
anemic than their counterparts. Further, children born to moderately and severely
anemic mothers were more anemic themselves, reflecting the consequences of
poor maternal health status on the health of the children(7).
Recent evidence(42,43) suggests that severe iron deficiency anemia
during the first two years of life, when the brain is still developing, may cause
permanent neurologic damage. These new findings add a further sense of
urgency to the current efforts to prevent iron deficiency anemia in children.
Vitamin A Deficiency
19
The National Program for Prevention of Nutritional Blindness has been
functioning for the last 25 years in India. There is unambiguous evidence of
appreciable secular decline in clinical vitamin A deficiency in under five children
in the country. Recently, vitamin A has generated considerable interest and
controversy because of pressure by International agencies for periodic massive
dose vitamin A prophylaxis as a cost-effective strategy for improving child
survival. Biological indicators, both clinical and biochemical are widely used to
assess prevalence and severity of VAD and to evaluate the effectiveness of VAD
control programs.
The classification of xerophthalmia and the prevalence rates suggested by
WHO(44) for assessing public health significance of the problem are XN - Night
blindness>1%, Xib- Bitot spots>0.5%, X2/X3 -Corneal xerosis/ulceration>0.01%,
Xs- Corneal scar>0.05%. Conjunctival xerosis (Xia) is not used, as it is not a
reliable sign.
Night Blindness and Bitot Spots
Night blindness and conjunctival xerosis are the early manifestations of
VAD. Prevalence of Bitot spots has reduced in preschool children between 1960s
and 1990s(2-4,45-47). NNMB repeat surveys(2) in India have revealed a marked
overall decline from 2% in 1976 to less than 0.7% in 1990. However, wide
regional variations are evident and in some areas no child with Bitot spots was
seen. In the NNMB 1994 rural survey(3), none of the children in Kerala, Andhra
Pradesh and Gujarat had Bitot spots while the prevalence ranged from 0.4% in
Karnataka and Orissa to 5.6% in Madhya Pradesh. The prevalence was more
20
than 0.5%, a level suggestive of public health problem, according to WHO
criterion, in the States of Tamil Nadu (0.8%), Maharashtra (1.5%) and Madhya
Pradesh (5.6%).
In the NNMB 1994 rural survey(4), overall 0.9% of adolescent girls (12-18
years old) had Bitot spots; the range being 0.6 to 2.7%. In 4 states no case of
Bitot spot was observed in this age group. The overall prevalence in adult
females was 0.7% (range 0% in Gujarat to 3.3% in Tamil Nadu). Only in 2 States
(Tamil Nadu-3.3% and
Madhya
Pradesh-1 %) values above 0.3% were
documented.
The NNMB 1992-93 rural survey in 10 States was conducted on a much
larger sample size of 26,760 preschool children to specifically address the issue
of linking periodic dosing of vitamin A with universal immunization program(46).
The prevalence of Bitot spots ranged from 0.3% in Kerala and 0.4% in Tamil
Nadu to 3.2% in Gujarat and 3.6% in Madhya Pradesh. The prevalence was
above 0.5% in 8 of the 10 States. Interestingly and paradoxically, the overall
prevalence of night blindness (1.1%) was lower than Bitot spots (1.9%) in 1-5
years old children. A noteworthy observation was the absence of Bitot spots in
infancy, even in slums, in the surveys conducted in the 1990s.
According to the latest countrywide data(47) from Department of Women
and Child Development (DWCD), the overall prevalence of bitot's spots and thus
vitamin A deficiency further declined to 0.2% in the country (Table V). The
prevalence ranged from <0.1% in states of Haryana and Himachal Pradesh to
3% in Mizoram. The prevalence was more than 0.5% in the states of Orissa
21
(0.9%), Mizoram (3%), Maharashtra (0.7%), Karnataka (0.8%), Tamil Nadu
(3.1%), Andhra Pradesh (0.8%) and Madhya Pradesh (2.6%). A noteworthy
finding was that vitamin A deficiency was more prevalent in most southern states
which may be related to the dietary factors.
Keratomalacia
A nationwide survey conducted by the ICMR during 1971-74 showed that
2% cases of blindness were attributable to corneal disease caused by vitamin A
deficiency(19). In the subsequent (1985) national survey of blindness, carried out
under the auspices of the Government of India and the World Health Organiza
tion (WHO), this figure declined to 0.04%(19,26). Data from the School of
Tropical Medicine, Calcutta, once the hotbed of keratomalacia, and from the
Christian Medical College, Vellore(26) are also suggestive of a sharp reduction in
the documentation of keratomalacia (0 to 0.008% in late 1980s). A careful
scrutiny of the hospital data from Calcutta in fact suggests that the decline in the
incidence of keratomalacia had started even before the massive dosage
prophylaxis programme had been instituted(26).
Dietary Intake
The frequency of consumption of vitamin A rich foods has also been
suggested as an indirect measure of assessing VAD in population. Evidence
from Delhi urban slums(48) showed that nearly 73% of children in the age group
12-71 months consumed vitamin A rich foods less than three times per week- a
level suggestive of public health problem, according to WHO criteria. The
frequency of consumption of vitamin A rich food by the families was significantly
22
higher during winters as compared to summers and rainy season and this could
be due to comparatively high cost of dark green leafy vegetables in summers and
rainy season.
Iodine Deficiency Disorders
Iodine deficiency is one of the widespread nutritional deficiencies prevalent
in the developing world and it continues to be significant public health problem. A
spectrum of disorders, besides goiter, collectively referred to as iodine deficiency
disorders (IDD) are caused by environmental iodine deficiency. Children in their
growing period are especially vulnerable to adverse effects of iodine deficiency.
A variety of indicators have been recently recommended by the international
agencies(49) to quantify the magnitude of IDD including goiter, thyroid volume by
ultrasound, urinary iodine excretion and thyroid stimulating hormone (TSH) in
newborn blood. Children in the age group of 8-10 years (excluding TSH) are the
recommended target population because of their combined high vulnerability,
representativeness of community and easy accessibility(49). However, nationally
representative information in the country is primarily based on goiter prevalence
surveys in the entire population and occasionally on clinical evidence of cretinism
which may be unreliable.
In India, not even a single state or Union Territory is free from the problem
of iodine deficiency disorders(50). Out of 275 districts surveyed by various
Government of India Institutions and Central Goiter Survey Teams in 25 states
and 4 Union Territories, 235 were endemic for IDD(50). It is estimated that nearly
23
167 million people in India are exposed to the risk of IDD of which 54 million have
goiter, 2.2 million are cretins and 6.6 million have mild neurological disorders(51).
An early intervention study initiated in 1954 showed an appreciable
decline in the goiter prevalence rate following 6 years of Iodization of salt in
Kangra Valley, Himachal Pradesh(52). In view of the magnitude of the problem
as well as considering the technical, administrative, financial and operational
feasibility, the Government of India took a decision in 1984 to iodize all edible salt
in the country, i.e. Universal Salt Iodization (USI). During recent years, research
surveys have been conducted to evaluate the success of universal salt
iodization. Table VI depicts the status of iodine deficiency in the selected
states(53). The goiter prevalence was documented to be as high as 20.5% in
district Bikaner, Rajasthan to as low as 0.8% in district Pauri, Uttar Pradesh.
However, when the median urinary iodine excretion cut off of >10 mcg/dl was
used as a criterion for assessing iodine deficiency in a population no state
included in the study was deficient. It was found that 68 to 100% population in
the study area was consuming iodized salt(53). In Delhi, the goiter prevalence
rate in school children declined from 55.2% in 1980(54) to 8.6% in 1996(55).
Repeat data revealed a marked reduction in the incidence of neonatal chemical
hypothyroidism (NCH) in highly endemic areas of Uttar Pradesh following salt
iodization(56,57). The observed NCH rates in 1992-96 following salt Iodization
are much lower than earlier projections in other areas also(57).
In the NNMB 1994 rural survey(3), the goiter prevalence rate (mostly
grade I) in adolescent girls was 3.9% (documented in only 3/8 states).
24
The
corresponding figure for adult females was 2.8% and was mostly seen in States
of Kerala, Karnataka, Madhya Pradesh and Orissa. As per the latest estimates of
the sample surveys conducted by the Directorate General of Health Services,
228 of the 367 surveyed Districts in the country are IDD endemic (goiter
prevalence > 10%). The reported rates of NCH from the few available studies
prior to massive input of salt iodization ranged from 6 to 133 per thousand births
(Uttar Pradesh, Delhi, Mumbai and Vishakapatnam). There was a strong
correlation with goiter prevalence rates(56).
Conclusions
There is increasing awareness about the importance of nutritional status,
an important index of the quality of life. Although, there is an overall positive
trend in nutritional outcome during the past few decades, the gain is modest and
predominantly in terms of reduction of more severe varieties of malnutrition. A
favorable transition appears to have been initiated in the less severe varieties of
undernutrition also, notably illustrated by slender improvements even amongst
the poor. These encouraging observations in poor women and children, despite a
steep increase in population and continued social and economic inequity, are
inspiring indications that at long last India may be at the turning point with respect
to nutrition.
Despite the apparent gain, current magnitude of deficiencies in virtually all
nutritional public health indicators is nowhere near the International standards.
25
There is an urgent need to intensify efforts to improve the nutritional profile of
children to optimize human resource development.
I
I
I
26
Table I: Trends in childhood malnutrition in India.
NNMB
Nutritional
Parameter
NNMB
NNMB
1975-79
1988-90
1988-90
(n=6,428) (n=13,422)
Survey
NNMB
1994
(n=1,832)
NFHS-I
NFHS-2
1992-93
1998-99
(n=25,578) * (n=24,600)
Weight for age
Underweight
<2 SD
<3 SD (severe)
77.5
38.0
68.6
26.6
63.6
24.7
53.4
20.6
47.0
18.0
Height for Age
Stunting
<2 SD
<3 SD (severe)
78.6
53.3
65.1
36.8
63.0
35.8
52.0
28.9
45.5
23.0
Weight for
height
Wasting
<2 SD
<3 SD (severe)
18.1
2.9
19.9
2.4
16.7
2.6
17.5
15.5
2.8
3.2
* For weight for age assessment only. The sample size for other two indices was lower.
Adapted from Sachdev HPS. Epidemiological Trends in Nutritional Status of Children and Women
in India. In: Improving Newborn Infant Health in Developing Countries. Eds. A Costello, D
Manadhar, London, Imperial College Press, 2000; pp 99-128.
27
Table II; Breast Feeding and Supplementation Indicators
Indicator
NFHS-1 Data
(1992-93)
NFHS-2 Data
(1998-99)
(%)
(%)
Breastfeeding within one hour of birth
10
16
Breastfeeding within one day of birth
26
37
Discarding first milk
64f
63
Exclusive breastfeeding in infants<4 months
51
55
Breastfed (any amount) at ages
6 months
12 months
24 months
88
57
96
92
59
Median duration of breastfeeding (months)
Exclusive breastfeeding
Predominant breastfeeding
Any breastfeeding
1.4
4.7
24.4
5.3
25.2
Solid/mushy food in breastfed children at ages
6 months
12 months
24 months
17
68
89
24
71
88
+ Among last-born children only.
28
1.9
TABLE III - Trends in Intrauterine Growth.
Comparison
period
(Mean gap in yr)
Observed Changes
Weight
Gestation
Industrial
Hospital
1963 & 1986
MBW +74g
LBW: 34vs25%
NA
NA
Delhi
Hospital
(Poor)
1969 & 1989
(20)
NA
Term* +
0
30
Delhi
Hospital
(Better off)
73-74 & 85-87
(12.5)
NA
NA
+
31
North Arcot
(Tamil
Nadu)
Rural
69-73 & 89-93
(20)
69-73 & 89-93
(20)
MBW +78g
LBW: 27vs16%
MBW +52g
LBW: 19vs11%
M +0.7W
PT: 21vs16%
M +0.8W
PT: 20vs15%
32
Vellore
Hospital
1969 & 1994
(25)
MBW+126g
LBW: 27vs15%
Me +0.3W
PT: 14vs10%
NA
33
Mumbai
Hospital
(Poor)
1988 & 1995
(8)
LBW: 60vs38%
0
NA
34
Delhi
Hospital
(Poor)
1986 & 1996
____ (11)
0
0
NA
Ref.
Area
Setting
28
Rourkela
(Orissa)
29
Urban
(23)
+ indicates significant increase; +p indicates significant at some gestations;
- indicates significant decline; 0 indicates no significant change;
IUGC - Intrauterine growth curves; M - Mean; Me - Median; MBW - Mean birth weight; NA - Not
available; Ref. - Reference number; W - Gestation in weeks;
‘Calculated by comparison with earlier study values cited in Reference 25.
Adapted from Sachdev HRS. Epidemiological Trends in Nutritional Status of Children and Women
in India. In: Improving Newborn Infant Health in Developing Countries. Eds. A Costello, D
Manadhar, London, Imperial College Press, 2000; pp 99-128.
29
IUGC
+P
+P
Table IV: State wise Prevalence of Anemia* (NFHS-2 Data)_________
Anemia Prevalence Rate (%)
State
None
(>Hg/di)
Mild
(10-10.9g/dl)
Moderate
(7-9.9g/dl)
Severe
(<7g/dl)
Andhra Pradesh
28
23
45
4
Arunachal Pradesh
Assam
Bihar
Delhi
Madhya Pradesh
45
27
19
31
16
47
25
30
29
29
56
20
29
31
27
22
18
23
24
29
29
20
24
17
25
32
50
43
59
28
44
39
38
43
19
57
1
0
4
4
7
2
7
2
4
8
1
6
Manipur
Meghalaya
Mizoram
Nagaland
Orissa
Punjab
Rajasthan
Sikkim
Tamil Nadu
Uttar Pradesh
West Bengal
55
32
43
56
28
20
18
23
31
26
22
23
23
32
22
26
17
20
28
22
19
27
22
40
23
19
43
57
53
41
40
48
46
1
4
2
3
3
6
9
8
7
7
5
India
26
23
46
5
Goa
Gujarat
Haryana
Himachal Pradesh
Jammu & Kashmir
Karnataka
Kerala
* Hemoglobin levels are adjusted to altitude when calculating the degree of anemia.
Adapted from reference 7.
30
»
Table V: State wise Prevalence of Vitamin A Deficiency Signs
State/UT
Bitot's Spots
%
Haryana
Himachal Pradesh
Punjab
Rajasthan
Chandigarh
Delhi
Bihar
Sikkim
Orissa
Arunachal Pradesh
Assam
Manipur
Meghalaya
Mizoram
Nagaland
Tripura
Dadra Nagar Haveli
Daman & Diu
Goa
Gujarat
Maharashtra
Kerala
Karnataka
Tamil Nadu
Andhra Pradesh
Madhya Pradesh
0.04
0.01
0.12
0.22
0.00
0.05
0.14
0.19
0.86
0.34
0.45
0.14
0.18
2.97
0.35
0.02
0.38
0.05
0.00
0.20
0.72
0.25
0.77
3.11
0.79
2.62
Pooled
0.21
Adapted from Reference 47.
31
4
Table VI: Status of Iodine Deficiency in Selected States of India
(%)
Age
group
(yrs)
Year
of
Survey
Andaman
(n=622)
9.5
6-12
1997
Median
urinary
iodine
excretion
(mcg/dl)
20.0
Bihar
East
Champaran
XWest
Champaran
(n=1328)
11.6
6-12
1997
10.0
100.0
Delhi
Entire State
(n=7475)
8.6
8-10
1996
17.0
98.6
Himachal
Pradesh
Kangra
(n=1358)
Hamirpur
(n=1413)
Kinnaur
(n=1094)
Solan
(n=6724)
5.7
8-10
1996
16.5
97.9
8.8
8-10
1996
13.5
97.5
6.1
6-10
1996
19.5
99.2
11.4
8-10
1997
15.0
98.1
Name of the
district
selected
Prevalence
of goiter
Andaman
& Nicobar
State
Percentage
of
population
consuming
iodized salt
99.5
Kerala
Ernakulam
(n=1254)
1.0
6-12
1998
20.0
97.4
Pondi
cherry
Entire UT
(n=2065)
2.6
6-11
1997
14.5
100.0
Rajasthan
Bikaner
(n=623)
20.5
6-12
1996
15.5
68.1
Uttar
Pradesh
Uttarkashi
(n=216)
Pauri
(n=604)
Pithoragarh
(n=740)
2.8
6-12
1998
20.0
98.4
0.8
6-12
1998
17.5
97.3
1.5
6-12
1998
20.0
98.9
Adapted from Reference 53.
32
REFERENCES
1. Mishra VK, Lahiri S, Luther NY. Child Nutrition in India. National Family
Health Survey Subject Report No. 14, 1999.
2. National Nutrition Monitoring Bureau. Report of Repeat Surveys (198890). Hyderabad, National Institute of Nutrition, 1991.
3. Nutritional Status of Rural Population: Report of NNMB Surveys.
Hyderabad, National Nutrition Monitoring Bureau, National Institute of
Nutrition, 1996.
4. National Nutrition Monitoring Bureau. Report of Urban Survey- Slums
(1993-94). Hyderabad, National Institute of Nutrition, 1994.
5. National Nutrition Monitoring Bureau. Report for the Year 1979.
Hyderabad, National Institute of Nutrition, 1980.
6. National Family Health Survey: Maternal and Child Health and Family
Planning. India 1992-93. Bombay, International Institute for Population
Sciences, 1995; pp 269-287.
7. National Family Health Survey (NFHS-2), India, 1998-99. Mumbai,
International Institute for Population Sciences (Unpublished)
8. Gopalan C. The changing profile of undernutrition in India. Nutrition
Foundation of India Bulletin 1991; 12: 1-5.
9. Bhattacharya AK, Chattopadhyay PS, Roy Paladhi PK, Ganguli S,
Bhattacharyya N. Kwashiorkor and marasmus: Changing hospital
incidence of syndromic presentation (1957-88). Indian Pediatr 1990' 27'
1191-1198.
10. WHO Working Group. Use and interpretation of anthropometric indicators
of nutritional status. Bull WHO 1986, 64:929-941.
H.Sachdev HPS. Assessing child malnutrition: Some basic issues. Nutrition
Foundation of India Bulletin 1995; 16: 1-5.
12. Rai MK, Vailaya J. The national nutrition scene: An analysis of the results
of two national surveys. Indian Pediatr 1996; 33: 305-312.
13. Gillespie S. Child nutrition in India: Findings from the National Family
Health Survey (1992-93). Nutrition Foundation of India Bulletin 1996' 17'
6-8.
14. Carlson BA, Wardlaw TM. A Global, Regional and Country Assessment of
Child Malnutrition. United Nations Children's Fund Staff Working Papers
Number 7. New York, UNICEF, 1990.
15. Agarwal DK, Agarwal KN. Physical growth in Indian affluent children (birth6 years). Indian Pediatr 1994; 31: 377-413.
16. Kumar R, Aggarwal AK, Iyengar SD. Nutritional status of children: Validity
of mid-upper arm circumference for screening undernutrition. Indian
Pediatr 1996; 33: 189-196.
17. Mishra VK, Retherford RD. Women's Education Can Improve Child
Nutrition in India. National Family Health Survey Bulletin No. 15, 2000.
18. A Note on Nutritional Intake in India: NSS- 50th Round (July 1993 to June
1994). Sarvekshna (The Journal of the NSS Organization) 1997; 21(2):73.
33
19. Reddy V, Shekar M, Rao P, Gillespie S. Nutrition in India. Hyderabad
National Institute of Nutrition, 1992.
20. Reddy V, Pralhad Rao N, Gowrinath Sastry J, Kashinath K. Nutrition
Trends in India. Hyderabad, National Institute of Nutrition, 1993.
21. pA/orld
Bank India Wasting Away: The Crisis of Malnutrition in India.
World Bank.
Report No. 18667-1N, Washington DC, The World Bank: Health, Nutrition
and Population Unit, South Asia Region, 1998.
22.Srikantia
SG.Pattern
P
----------------of growth and development of Indian girls and body
—1.— women. In:
,
...
size of adult 1Indian
Women and Nutrjtjon jn |ncjja Eds
Gopalan C, Kaur S. New Delhi, Nutrition Foundation of India, Special
Publication Series 5, 1989; pp 108-152.
23. Gopalan C, Vijayaraghavan K. Nutrition Atlas of India. Hyderabad,
National Institute of Nutrition, 1969.
24. Gopalan C, Vijayaraghavan K. Nutrition Atlas of India. Hyderabad,
National Institute of Nutrition, 1971.
25. Bhargava SK, Sachdev HPS, Iyer PU, Ramji S. Current status of infant
growth measurements in the perinatal period in India. Acta Pediatr Scand
1985; 319 (Suppl): 103-110,
26. Gopalan C. Nutrition Research in South-East Asia: The Emerging Agenda
for the Future. New Delhi, World Health Organization - Regional Office for
South East Asia, 1994.
27. Bhargava SK, Singh KK, Saxena BN. A National Collaborative Study of
Identification of High Risk Families, Mothers and Outcome of Their
Offsprings With Particular Reference to the Problem of Maternal Nutrition
Low Birth Weight, Perinatal and Infant Morbidity and Mortality in Rural and
Urban Slum Communities. A Task Force Study. New Delhi, Indian Council
of Medical Research, 1990.
28,Satpathy R, Das DB, Bhuyan BK, Pant KC, Santhanam S. Secular trend in
birth weight in an industrial hospital in India. Ann Trap Pediatr 1990' 10’
21-25.
29. Man Mohan, Shiv Prasad SR, Chellani HK, Kapani V. Intrauterine growth
curves in north Indian babies: Weight, length, head circumference and
ponderal index. Indian Pediatr 1990; 27: 43-51.
SO.Singhal PK, Paul VK, Deorari AK, Singh M, Sundaram KR. Changing
trends in intrauterine growth curves. Indian Pediatr 1991; 28: 281-283.
31. Trends in Intrauterine Growth of Single Live Borns During 1969-73 and
1989-93 Among Rural and Urban Communities of North Arcot Ambedkar
District, Tamil Nadu, India. Longitudinal Studies in Growth and
Development: Monograph No. 21. Department of Biostatistics Christian
Medical College, Vellore.
32. Mathai M. Changes in health status and birthweight in Vellore over 25
years (1969-1994). Paper presented at Workshop on "Health in
Transition" in Norway, May 1995 (Personal Communication, 1995).
33. Fernandez AR. Changes in birthweight and gestation patterns in Sion
Mumbai. Personal Communication, 1996.
34
34. Ramji S. Changes in birthweight and gestation patterns Delhi. Personal
Communication, 1997.
35. National neonatal perinatal database: Report for the year 1995. National
Neonatology Forum Secretariat and National neonatal Perinatal Database
Nodal Centre, Department of Pediatrics, All India Institute of Medical
Sciences, New Delhi, 1996.
36. Ramji S. Birth weight in Child Survival and Safe Motherhood Programme
Districts. Personal Communication, 1997.
37. Bhargava SK, Ghosh S. Nomenclature for newborns. Indian Pediatr 1974;
11: 445-447.
38. Pollitt E, Viteri F, Saco-Pollitt C, Liebel RE. Behavioral effects of iron
deficiency anemia in children. In: Iron Deficiency: Brain Biochemistry and
Behavior. Eds. Pollitt E, Liebel R. New York, Raven Press, 1982; pp 195208.
39. Agarwal KN. Functional consequences of nutritional anemia. Proc Nutr
Soc India 1991; 37: 127-132.
40. Lozoff B, Jimenez E, Wolf AW. Long term developmental outcome of
infants with iron deficiency. N Eng J Med 1991; 325: 687-694.
41. Gopalan C. Nutrition in Developmental Transition in South-East Asia.
World Health Organization, Regional Office for South East Asia, Regional
Health Paper, South East Asia Regional Office, No. 21, 1992.
42. Hurtado EK, Claussen AH, Scott KG. Early childhood anemia and mild or
moderate mental retardation. Am J Clin Nutr 1999; 69: 115-119.
43. Pollitt E. Early iron deficiency anemia and later mental retardation. Am J
Clin Nutr 1999; 69: 4-5.
44. World Health Organization. Control of Vitamin A Deficiency and
Xerophthalmia. WHO Tech Rep Series NO. 672, 1982.
45. Studies on Preschool Children. Report of the Working Group of Indian
Council of Medical Research. New Delhi, ICMR Technical Report Series
No. 26, 1977.
46. Vijayaraghavan K, Brahmam GNV, Reddy G, Reddy V. Linking Periodic
Dosing of Vitamin A With Universal Immunization Programme - An
Evaluation. Hyderabad, National Institute of Nutrition, 1996.
47. India Nutition Profile. Department of Women and Child Development,
Ministry of Human Resource Development, Government of India, 1998.
48. Kapil U, Saxena N, Srivastava M, Jailkhani L, Nayyar B, Chitkara P, et al.
Assessment of vitamin A deficiency indicators in urban slum communities
of National Capital Territory of Delhi. Asia Pacific J Clin Nutr 1996; 5' 170172.
49. Indicators for Assessing Iodine Deficiency Disorders and their Control
Through Salt Iodization. WHO-UNICEF-ICCIDD. Geneva, World Health
Organization, 1994.
50. Elimination of Iodine Deficiency Disorders in South East Asia, World
Health Organization, Regional Office for South East Asia, SEA/NUT/138
1997; pp 1-8.
35
51. Status Report on the National Iodine Deficiency Disorders Control
Program, Policy and Advocacy Meeting on IDD, New Delhi, 1994.
52.Sooch SS, Deo MG, Karmarkar MG, Kochupillai N, Ramachandran K,
Ramalingaswami V. Prevention of endemic goiter with iodized salt. Bull
WHO 1993; 49: 307-312.
53. Kapil U. Current status of iodine deficiency disorders control program.
Indian Pediatr 1998; 35: 831-836.
54. Pandav CS, Kochupillai N, Karmarkar MG, Ramachandran K, Gopinath
PG, Nath LM. Endemic goiter in Delhi. Indian J Med Res 1980; 72: 81-82.
55. Kapil U, Saxena N, Ramachandran S, Balamurugan A, Nayar D, Prakash
S. Assessment of iodine deficiency disorders using the 30 cluster
approach in the National Capital Territory of Delhi. Indian Pediatr 1996;
33: 1013-1017.
56. Kochupillai N. Neonatal chemical hypothyroidism of nutritional origin: A
major public health problem that impairs growth in developing countries.
Iit. Recent Trends in Nutrition. Ed. Gopalan C. Delhi, Oxford University
Press, 1993; pp 181-193.
57. Kochupillai N. Micronutrient deficiency and human health and
development. Srikantia Memorial Lecture at the XXIX Annual Meeting of
the Nutrition Society of India, November 21-22, 1996, Hyderabad
(unpublished data).
36
Fig. 1: Comparison of Nutritional Parameters in two NFHS surveys
60
u■
50
■
ENFHS-1
40
|
I
% 30
■ NFHS-2
d-
ft
20
Ss
r-
10
■
0
Wt.for age
Wt. for Age
< 2 S.D.
< 3 S.D.
Underweight
Ht. for Age Ht. for Age
<2 S.D.
<3 S.D.
Wasting
37
Wt. for Ht. Wt.forHt.
<2 S.D.
<3 S.D.
Stunting
LOW BIRTH WEIGHT
H.P.S. Sachdev, Professor and Incharge, Division of Clinical Epidemiology, Department of
Pediatrics. Maulana Azad Medical College, New Delhi 110 002.
Intrauterine growth and development is one of the most vulnerable process in the human
life cycle and it's aberrations can result in lasting profound influence in later life. In the context
of developing countries, intrauterine growth has been invariably assessed by birth weight.
Although it may be reasonable to inter that fetuses who have experienced growth restriction in
utero will be lighter and smaller, it must be understood that size at birth does not completely
reflect growth (Gulmezoglu et al. 1997). The suitability of utilizing only birth weight as an
indicator of fetal growth has been debated and criticized (Wilcox 1983. WHO 1995); however, it
is sometimes the only measure available, especially in developing countries (Gulmezoglu et al.
1997;.
The World Health Organization (WHO), on the basis of world wide data had
recommended that newborns with birth weights less than 2500 g may be considered to fall in the
low birth weight (LBW) category - carrying relatively greater risks of perinatal and neonatal
morbidity and mortality and substandard growth and development in later life. The validity of
this definition and the "cut off point" of 2500 g has been occasionally challenged: but has by and
large now gained general acceptance (Gopalan 1994). The latest WHO recommendation (WHO
1995. de Onis and Habicht 1996) has retained this "cut off point" of 2500 g to define LBW and
recommended an additional demarcation of 1500 g to define very low birth weight (VLBW)
babies.
LBW infants encompass a heterogeneous population of newborns. Broadly, the birth
weights may be low because the baby is born small for gestational age (SGA) as a result of
intrauterine growth retardation {synonym intrauterine malnutrition) (IUGR) or because birth is
preterm. In the developed countries, the overwhelming majority of LBW infants are preterms
whereas in the developing nations, including South Asia, the reverse is the case; the great
majority of newborns with LBW are full term infants who are SGA (Gopalan 1994, Gillespie
SI 997).
Attempts have also been made to further classify IUGR as disproportionate or
proportionate on the basis of Ponderal index (weight/length3) (Kramer 1987, Villar et al. 1990).
Disproportionate IUGR infants have a low ponderal index whereas proportionate IUGR babies
have a normal ponderal index (all body dimensions proportionately small).
On the basis of available evidence, the ensuing sections will examine the nature,
consequences and causes of LBW in the South Asian sub-continent and evaluate the various
options for action to address this major public health problem in the region.
1. Nature Of The Problem
1.1.
Magnitude of the Problem
In South Asia (excluding Sri Lanka), even today a majority of the deliveries are
conducted in the community. Logistic difficulties in recording birth weight at home preclude
accurate national estimates of the magnitude and trends of LBW. However, a large volume of
data on birth weight is available from individual studies, most of which are hospital based.
Table 1 compares the LBW prevalence estimates from different countries in South Asia with
other selected regions. The oft cited national estimates for South Asia should only be construed
as broad indicators as these have not been derived on the basis of sound epidemiological
methodology. South Asia has the highest prevalence of LBW and the disparity in comparison to
developed countries and
some developing regions (Africa) is obvious. In fact, the latest
2
projections indicate that more than half of the world's LBW babies are bom in South Asia
(UNICEF 1996).
Table 1. LBW Prevalence (%) in South Asia and Other Regions.
Usual range
in studies
Oft cited
estimate
Major sources
SOUTH ASIA
Bangladesh
23-60
50
Bhutan
India
35-44
24-40
33
UNDP 1996, UNICEF 1996 & 1997.
Nahar 1997. Roy 1997.
UNICEF 1996
Srikantia 1989. UNDP 1996. NNF
1997, Sachdev 1997. UNICEF 1997
UNICEF 1996
UNICEF 1996. Manandhar 1997
Arif 1985, UNDP 1996. UNICEF
1996 & 1997. Bhutta 1997. Zaman
1997
UNDP 1996, UNICEF 1996 & 1997
Region
Maldives
Nepal
Pakistan
25
25-50
18-34
25
Sri Lanka
25
Asia
Africa
Latin America
North America
Europe
Oceania
USSR
Developing countries
Developed countries
Global
21
15
11
7
6
20
7
19
7
17
WHO 1992
WHO 1992
WHO 1992
WHO 1992
WHO 1992
WHO 1992
WHO 1992
WHO 1992
WHO 1992
WHO 1992
Excluding Japan. Australia. New Zealand.
In India, recently efforts have been made to collect nationally representative estimates of
birth weights from institutional (NNF 1997) and community (Ramji 1997) deliveries. The
reliable institution based National Neonatology Forum (NNF 1997) data for the year 1995 on
37082 live births (nearly 0.1% births in the country) from 15 participating centers (Ahmedabad.
Bangalore (3 centers), Baroda. Calcutta. Chandigarh. Delhi (2 centers), Indore, Ludhiana.
Madras. Mumbai. Pondicherry and Shimla) yielded a LBW prevalence of 32.8%. Only 33% of
the LBW infants were preterm. The Child Survival Safe Motherhood (CSSM) Programme linked
District based data (Center based delivery in 14 Districts in 10 States - Assam, Gujarat. Madhya
Pradesh. Karnataka, Maharashtra, Orissa, Punjab, Rajasthan, Tamil Nadu and West Bengal) on
27069 births estimated the LBW prevalence to be much lower at 18.4% (Ramji 1997). Wide
regional variations were apparent with values ranging from a low of 2.7% (Madhya Pradesh) and
5.1% (Assam) to a high of 24.7% (Tamil Nadu) and 40% (Orissa). The strikingly low figures in
comparison to earlier published literature, especially for the poor performing states (Madhya
Pradesh and Rajasthan- 12.8%) in other nutritional parameters including protein energy
malnutrition, however, questions the reliability of this integrated data. Reliable recording of birth
weight in a community requires meticulous training and an accurate and sensitive instrument.
1.1.1. Variation in LBW Prevalence
Apart from manifest inter-country variations in South Asia (Table 1), there is a
considerable variation in the prevalence of LBW within a country. Wide inter-regional, socio
economic and urban versus rural differences in the prevalence of LBW have been recorded
(Bhargava et al. 1985, Bhargava SK 1997, Nahar 1997, Roy SK 1997). In India, the disparity has
ranged from a prevalence of 10% (for the privileged high socio-economic class) to 56% (for the
poor urban slum community) (Bhargava SK et al. 1990, Bhargava SK 1997). Rural and urban
slum deprived populations have consistently recorded the highest prevalence of
LBW.
Interestingly, even in the same region, the underprivileged population has a significantly higher
proportion of LBW (Bhargava SK et al. 1985).
4
1.2.
Low Birth Weight - Relation to Gestation and Intrauterine Growth
The general consensus is that in developing countries, particularly South Asia, an
overwhelming majority of LBW infants have adequate gestation (are term) but are growth
retarded (IUGR) (Gopalan 1994, Gillespie 1997).
It would be of interest to examine some
pertinent data from the region in this context. The recent multicentric data from India (NNF
1997) on over 37,000 live births reveals that one-third (32.8%) of LBW babies are born preterm'.
a proportion which certainly can not be totally ignored. An earlier analysis of hospital and
community births in Delhi (India) had revealed that in the birth weight group of 1501-2000 g,
30-45% were preterm while the corresponding figure was 13-15% in the 2001-2500 g category
(Bhargava et al. 1987). In the NNF study the prevalence of babies with birth weight <2000 g was
10.2%, <1500 g was 3.3% and < 1000g was 0.7% (NNF 1997). On the basis of this data, it would
be justifiable to analyze the gestational distribution and intrauterine growth in the region in
greater detail.
1.2.1. Gestation
Accurate assessment of gestational age is difficult, particularly in the context of
community births. Table 2 , from the available data, compares the distribution of singleton live
births according to different gestational ages from the various regions of India with similar
studies from the developed countries. The depicted ICMR data refers to the multicentric studies
of the Indian Council of Medical Research in rural areas and urban slums (Bhargava et al. 1990).
Some of the important features are also highlighted in Figure 1.
5
Table 2. Comparison ofgestation distributi^ToTIiCe birtWsfmpdr cent).
Author
Place
Data
Base
Sample
size
Sheth
1972
Bombay
Hospital
Low SE
5336
Bhatia 1981
Ghosh 1971
Varanasi
Hospital
Delhi
Hospital
5321
5031
Ghosh
1979
Delhi
Urban
comm
6023
Mittal
1976
Punjab
Hospital
High SE
3163
Singh
1974
Delhi
Hospital
High SE
3550
Sheth
1972
Bombay
Hospital
High SE
1242
Babson
1970
USA
Hospital
0.19
0.10
0.20
0.17
0.26
0.32
0.57
0.79
2.10
3.75
9.40
16.52
39.23
15.12
7.86
2.20
0.57
84.02
5.35
10.63
Gestation
(wk)
<29
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
>43
0.22
0.16
0.34
0.64
1.09
1.89
2.34
4.05
11.60
37.01
26.26
9.48
4.87
0.00
0.00
0.00
0.00
1.28
0.58
0.92
0.94
1.33
1.64
2.84
3.68
6.18
12.31
18.14
22.40
18.23
6.24
2.03
0.70
0.32
0.58
0.16
0.60
0.36
0.89
1.29
1.63
2.50
5.11
8.45
17.37
22.72
22.06
10.00
4.53
1.21
0.48
0.12
0.02
0.08
0.10
0.32
0.86
1.78
2.62
4.10
7.90
15.11
22.55
21.07
11.26
5.08
2.82
4.22
0.38
0.35
0.44
0.73
0.70
0.76
1.17
1.68
4.11
8.98
19.46
22.59
24.30
10.91
2.69
0.76
0.00
1.04
1.24
1.18
3.32
5.18
14.37
18.08
38.56
10.20
4.37
1.46
0.48
0.24
0.32
0.32
0.32
0.64
1.21
1.37
2.42
8.37
16.59
41.87
25.76
0.00
0.00
0.00
0.00
37-41
<37
>41
77.67
22.33
0.00
77.56
19.39
3.05
80.66
13.12
6.22
77.88
10.00
12.12
86.23
10.32
3.45
86.80
7.37
5.83
92.90
7.10
0.00
6
0.59
40000
Bjerkedahl
1973
Norway
Institution
comm
125485
ICMR
1984
India
Rural
3630
ICMR
1984
India
Urban
slum
2534
0.55
0.31
0.42
0.65
1.19
1.91
3.61
8.54
19.70
28.27
20.72
9.50
2.75
1.88
1.50
0.10
0.40
0.20
1.20
0.40
1.20
0.90
6.80
6.50
21.70
13.90
31.10
6.30
5.90
1.80
1.10
0.50
0.10
0.20
0.40
1.50
0.70
1.60
2.50
6.90
5.60
11.00
12.40
34.80
8.30
6.90
2.30
4.30
80.84
5.03
14.13
78.50
12.70
8.80
72.10
14.40
13.50
Figure 1. Comparison of gestation distribution.
45.00
.
•
-
■
_
40.00
4 aL"
11
35.00
Al
30.00
25.00
o
Bi .=
<u
o.
20.00
15.00
10.00
5.00
0.00
29
30
31
32
33
35
34
36
37
38
39
40
41
42
43
>43
Gestation (weeks)
In contrast to the developed countries, the process of labor appears to be initiated at an
earlier period of gestation in a larger proportion of pregnant women. The incidence of premature
birth (<37 weeks gestation) ranges from 7.1% to 22.3%, in comparison to about 5% in the
developed countries. The latest NNF data from India provides a national estimate of 12.3%
(NNF 1997) and a recent study from Kathmandu suggests a figure of at least 15% (Manandhar
1997). Only 2% of births occur at 36 weeks in western countries, while 3-12% of infants are
7
bom at this gestational age in India. In the Indian setting, the maximum number of births occur at
39-40 weeks gestation, whereas in the West the corresponding figure is 40-41 weeks (Table 2.).
Apart from inter-regional difference, there is a marked variation in the gestational distribution in
privileged versus under privileged segments of population in the same area. The contrast from
the developed countries is very striking in the low socio-economic population, but the difference
is considerably narrowed and even disappears in the privileged class. The gestational distribution
in the region is therefore shifted to the left (about 1-2 weeks), more so in the underprivileged
segments of the population.
From the foregoing, it would be logical to conclude that prematurity
(especially
borderline preterm births at around 36 weeks of gestation) too is a significant problem in the
region and that it's contribution to LBW can not be totally ignored.
1.2.2. Intrauterine Fetal Growth
A comparison of fetal growth based on distance curves, reveals disparity from the
developed countries and between regions and socio-economic classes. The socio-economically
privileged population has higher mean birth weights at different gestations, the difference
becoming pronounced after 34 weeks (Figure 2). The limited information on ultrasonography
also reveals that the mean biparietal diameters values are lower than those from the developed
nations in the third trimester and more so near term (Buckshee et al. 198S'). It is evident that the
rhagnitude of intrauterine growth retardation is maximal in the third trimester of pregnancy.
8
4 ooor
3500 -
3000 -
£ 2500 •
A---- A 9ABS0N (USA)
------- URBAN COHORT (HIGH INCOME)
T
X—X URBAN COHORT
•—• HOSPITAL
------ SLUMS
o—o SHETH (HIGH INCOME )
e 3 000 ui
1
1500 •
1000 -
5 001—
28
30
32
34
36
GESTATION
38
40
(WEEKS)
42
44
Figure 2. Comparison of intrauterine growth curves.
1.3.
Recent Trends
An evaluation of the recent trends in the prevalence of LBW in the region may aid in the
formulation oi feasible strategies to tackle this public health problem. In recent years, an
improvement in LBW prevalence has been reported from Sri Lanka (FHB 1992). An up-to-date
analysis of this nature from India has yielded interesting information (Sachdev 1997a).
9
It is felt that there have been no differences in the reported mean birth weights and the
proportion of newborns with LBW in the three decades between late 1960s and late 1980s
(Srikantia 1989. Reddy et al. 1992). These inferences were based on comparison of data from
disparate settings at various time points. Given the expected marginal magnitude of change in
birth weight in two to three decades in a nation commencing epidemiological transition, these
inferences from such a research design are not surprising. It would however, be more valid to
analyze data from the same area at different time points.
On analysis of this nature (Table 3), a positive time trend for birth weight is evident in
most of hospital based data and the solitary community study. The mean magnitude of improve
ment is marginal (52 to 126g). However, this has resulted in a greater reduction of LBW
prevalence (by 8 to 12% usually and 22% in one report). These calculated mean improvements in
birth weight are probably underestimates (Mathai 1995) since concomitant changes in other
important associates have been ignored. With time, the mean birth order has also decreased and
correction for this factor alone (Mathai 1995) enhanced the magnitude of change in the
community study (rural and urban areas combined) from 70g to 100g (the first bom newborns
h^ve lower weights than later births). The absent time trend in the two Delhi hospitals may be
lelated to the relatively short gap in one report (Ramji 1996) and the fact that these institutions
primarily care to the underprivileged population in whom the transition is expected to commence
last of all. In one of these studies (Man Mohan et al. 1990), the higher percentage of term births
could be regarded as the beginning, since term newborns have the best intrauterine growth as a
group.
10
Table 3. Recent trends in prevalence of LBW in India.
Source
Area
Setting
Comparison
period
(Mean gap
in years)
Change in birth
weight
Change in
gestation
Change
in IUG
Satpathy
1990
Rourkela
(Orissa)
Industrial
hospital
1963 & 1986
(23)
MBW + 74g
LBW -34 vs 25%
NA
NA
Man Mohan
1990
Delhi
Hospital
(poor)
1969 & -1989
(20)
NA
Term
0
Singhal
1991
Delhi
Hospital
(better off)
1973-4
&
1985-7 (13)
NA
NA
CMC
1995
North Arcot
(TamilNadu)
Rural
1969-73
&
1989-93 (20)
MBW + 78g
LBW -27 vs 16%
M + 0.7W
PT -21 vs 16%
+P
Urban
1969-73
&
1989-93 (20)
MBW + 52g
LBW-19 vs 11%
M +0.8W
PT -20 vs 15%
+P
Mathai
1995
Vellore
Hospital
1969 & 1994
(25)
MBW+ 126g
LBW -27 vs 15%
Me + 0.3W
PT -14 vs 10%
NA
Fernandez
1996
Mumbai
Hospital
(poor)
1988 & 1995
(8)
LBW -60 vs 38%
0
NA
Ramji
1996
Delhi
Hospital
(poor)
1986 & 1996
(10)
0
0
NA
+: significant increase; +p: significant at some gestations;
significant decline; 0: no significant change;
IUG: intrauterine growth: M: mean: Me: median: MBW: mean birth weight; NA: not available: W:
gestation in weeks; *: calculated in comparison with earlier study values cited by Bhargava et al. (1985).
Fhe slender improvement in birth weight is probably contributed to by increases in both
gestation and birth weight at different gestations (intrauterine growth). The mean improvement
in gestation was again marginal (0.3 to 0.8 weeks) and was not uniformly observed. However.
these marginal changes in mean gestations resulted in greater improvement in prematurity rates
(by 4 to 5%).
11
These improvements in the prevalence of LBW in the absence of any specifically
targeted effective functional program have important managerial implications: (a) betterment in
the LBW prevalence is possible even with the prevailing development scenario of the region; (b)
both intrauterine growth and gestation are significant for enhancing birth weight; and (c) an all
round. integrated approach is likely to yield dividends rather than a narrow (food
supplementation based) strategy.
2. Consequences Of LBW
LBW newborns represent a heterogeneous group of term and preterm infants with
varying risks in subsequent life. The adverse consequences of LBW, including the different
types, have been extensively documented in the literature. This section is restricted to a brief
delineation of those consequences of important public health significance in the context of
developing countries, particularly South Asia to highlight the need for institution of remedial
measures. In this context, the distinction between growth retarded and preterm infants has
usually not been resorted to in the relevant literature.
2.1.
Survival
In consonance with reports from the developed world, the early neonatal mortality in
large birth weight cum gestational age blocks has a curvilinear appearance, increasing in all
directions from a low central range (Bharagava 1985). The striking inverse relationship between
birth weight and infant morbidity and mortality has been documented by several studies from the
region (Bhargava 1985 a, Tabib 1987, Bhutta 1990; FHB 1992, Bhutta 1997). The recent NNF
multicentric data on over 30,000 births confirms this even in a secondary and tertiary level care
12
setting (NNF 1997). In Delhi, a community based longitudinal study of infants with birth
weights of 2000g or less, revealed that over a six year period two-thirds of them had died.
mortality being especially high in the neonatal period and decreasing progressively till 3 years
of age (Bhargava 1984).
2.2.
Growth
LBW survivors demonstrate significant growth retardation, as reflected by lower body
weights, heights and head circumferences, in comparison to normal weight peers (Bhargava
1976. Bhargava 1983. Kalra 1983. Bhargava 1985b. Bavdekar 1994. Bhargava 1995). Although
there is some tendency for catch up growth, the deficits persist even up till 14 years of age
(Bhargava 1995). The catch up is more for the preterm births in contrast to the growth retarded
subjects. There is evidence of delayed skeletal growth and maturation in children aged between 6
to 10 years (Bhargava 1980). While delayed puberty has been reported in LBW children
(Fledelius 1953, Bhargava 1980b). an earlier onset of menarche (preterms - 6 mo and growth
retarded - 1 year) was documented in a longitudinal follow up study (Bhargava 1995). A similar
observation has been made from the developed world setting also (Westwood 1983). This raises
the possibility of an additional handicap for the continuing growth retardation in LBW infants an earlier fusion of epiphysis resulting in a greater adult height handicap.
The above observations pertain to Indian LBW infants who were largely drawn from
relatively poor Indian communities and continued to grow and develop during their childhood in
the same sub-optimal socio-economic conditions. It may, therefore, be argued that these children
continued to labor under the same conditions of relative deprivation that were operative at the
time of their birth, and which in the first instance were responsible for their LBW. These studies
13
do not. therefore, provide an adequate answer to the question as to whether the effects of the
initial handicap of LBW in relatively poor communities can be reversed by and overcome in a
\astly improved (postnatal) physical environment totally free from socio-economic and
nutritional constraints on growth and development (Gopalan 1994).
To seek an answer to this question, we need to look at growth performance of LBW
children under optimal conditions. In a study of this nature (Proos 1992). the effects of adoption
soon after birth of poor Indian infants (81% LBW) into wealthy Swedish families were
evaluated. While marked catch up growth was seen in childhood (mean stunting prevalence
reduced from 62% to 20% after 2 years), inter-individual height and weight differences that
existed at birth persisted in these children. The mean attained adult height (154 cm) of the
adopted Indian girls was just 1cm higher than the mean height of poor adult women living in
India and significantly lower than that for more affluent women in India (159 cm). Girls who
were stunted at infancy when they were adopted were also significantly shorter in adulthood than
their non stunted peers. The improved early childhood growth in these adopted girls had
hastened the onset of menarche and thus cut short the period of rapid pre-menarcheal growth.
Similar inference emerge from review of four other studies (Martorell 1994) in which
undernourished children from poor families were adopted by age five into middle class families;
the adoptees did catch up to some extent, but not all the height deficit suffered was made up.
From the foregoing, it would be reasonable to conclude that LBW suffer growth
retardation in later life which persists till adulthood and that effects of IUGR cannot be entirely
reversed by even ideal environment and nutritional inputs in postnatal life. These growth
retarded adult women (stunted and undenveight) are likely to give birth to LBW babies thereby
perpetuating a vicious cycle through generations.
14
2.3.
Development
Longitudinal studies from this region reveal that LBW infants demonstrate retardation in
motor, adaptive, personal, social
and language development in the first five years of life
(Bhargava 1982, Bhargava 1984). A report suggests that uncomplicated preterms as a group can
demonstrate catch up with normal peers in the motor and mental scales by 18-24 months age
(Choudhari 1991). Some of the developmental retardation can be argued to be a result of the
continued socio-environmental deprivation.
2.4.
Adult Diseases
Recent studies have brought to fore even more sinister possible late effects of LBW
which may become manifest only in late adult life. These observations, briefly outlined below.
lend an ominous new dimension to the traditionally accepted consequences of LBW.
Coronary heart disease (CHD) is common in the Indian sub-continent and the rates are
rising (Chadha 1990, Fall 1997). These high rates, which rise further in migrants (Singh 1995),
are not explained
by known risk factors including obesity, hypertension, smoking and raised
cholestrol. Recent evidence indicates that CHD in the Indian sub-continent is associated with a
particular metabolic profile, the insulin resistance syndrome, which includes impaired glucose
tolerance or non insulin dependent diabetes, insulin resistance, raised serum triglyceride and low
HDL cholestrol concentrations, abnormal plasma clotting factors and central obesity (McKeigue
1991).
Following Barker's initial report from Hertfordshire, England (Barker 1989), several
subsequent global studies have confirmed the association between LBW, especially SFD (Barker
15
199j). and CHD (Rich-Edwards 1995. Fall 1997). The trends in cardiovascular disease with
birthweight parallel similar trends in cerebral stroke (Martyn 1996) other major risk factors for
CHD. including non insulin dependent diabetes mellitus, hypertension (meta-analysis of 32
studies by Law 1996). and disordered lipid metabolism and blood coagulation (Barker 1995).
The "fetal origins hypothesis" has been proposed as an explanation for these associations.
namely, that undemutrition in utero
leads to fetal adaptations that permanently alter the
physiology and metabolism of the body that lead to cardiovascular disease in adult life.
It is tempting to postulate this "fetal origins hypothesis" as the alternative explanation for
the epidemic of CHD and non insulin dependent diabetes in India. Concrete evidence of a similar
association between CHD and LBW has recently been reported from South India (Stein 1996). A
report from Pune suggests that components of the insulin resistance syndrome may be apparent
in early childhood (Yajnik 1995). Among 201 four-year old children, those with lower
birthweight had higher plasma glucose and insulin concentrations after an oral glucose load,
independently of their current size.
The fetal origins hypothesis" is based on epidemiological evidence of associations and a
cause and effect relationship can not be automatically implied. The hypothesis has been
criticized on this and other epidemiological reasoning. Nevertheless, the suggestive evidence
linking LBW and adult disease adds a new dismal dimension to the possible consequences of
LBW.
3. Etiology of LBW
From the preceding sections, it is obvious that LBW is a major public health problem in
South Asia which needs to be addressed on an urgent basis. In order to plan and institute
16
meaningful interventions, it is pertinent to review the various factors which have been reported
to be a cause of LBW. The literature is replete with various studies which have attempted to
answer this question and several exhaustive reviews on the topic have also been published
including from the region (Kramer 1987, Srikantia 1989. Institute of Medicine 1990. Bhargava
1990. Sethi 1991. Kramer 1993, Gopalan 1994 & 1994a, Hirve 1994. WHO 1995a. Gillespie
1997, Gulmezoglu 1997, Deshmukh 1998 ). Before drawing any valid conclusions from such
literature, it would be useful to briefly consider the pertinent methodological issues.
3.1.
Methodological Considerations
The important methodological issues involved in inferring a cause and effect relationship
for LBW on the basis of available studies have been elegantly summarized by Kramer (1987). It
is generally recognized that the etiology of LBW is multifactorial since many factors can
influence the length of gestation or the rate of intrauterine growth. Nevertheless there is
considerable confusion and controversy about the factors that have independent effects on LBW
as well as the quantitative importance of these effects. The various reasons for this include: (i)
Failure to distinguish between IUGR and prematurity as different causes of LBW; (ii) A given
factor might affect the middle or upper range of the birth weight or gestational age distribution
but not those infants identified by the conventional cut-off points as SFD or prematures; (iii)
"Failure to distinguish markers or associated factors from true causal determinants. Many of the
potential determinants are highly associated and their effects are thus mutually confounded.
Failure to control for the confounding variables can lead to erroneous associations between a
factor and IUGR or prematurity. For example, anemia is highly associated with under nutrition,
and if insufficient caloric intake is a true cause of IUGR, failure to control for such intake will
17
produce an association between anemia and IUGR. Anemia, however, may merely be a marker
of poor maternal nutrition, and not a true causal determinant of IUGR. Thus if anemia has no
independent effect on intrauterine growth, routine use of iron supplementation during pregnancy
will have no impact on the rate of IUGR" (Kramer 1987); (iv) Failure to perform a "path
analysis" on the identified factors resulting in lumping together of underlying or indirect
determinants (for example, literacy or age at marriage) with direct or immediate determinants
(for example, maternal anthropometry or food intake); (v) The large number of factors that
could theoretically influence birth weight indicates that each one of them may have a rather
small individual impact. Unequivocal demonstration of statistical significance for small effects
requires the use of large sample sizes as well as control for confounding and other non-random
sources of variation.
Majority of the research in relation to causation of LBW has relied on observational
methods. It is only recently that well designed experimental methods have been utilized to
unambiguously demonstrate a cause and effect relationship. These randomized clinical trials
have enabled the impact of the factors that are amenable to experimental intervention to be also
quantified for their effect. However, not all possible factors can be subjected to an experimental
design (for example, race/ethnicity, socio-economic status or age of child bearing).
3 2.
Intervention Based Causes of LBW
It is generally believed that the solution to LBW in the region lies in improvement of
intrauterine growth. Consequently, majority of relevant research and suggested interventions
have focussed on this aspect only. However, from the preceding sections it is apparent that for
maximum benefit, efforts should also be directed at gestational duration because: (i) Nearly one
18
third of LBW newborns are bom preterm; (ii) The gestational distribution reveals a shift to the
left in comparison to developed nations; and (iii) Positive time trends in prevalence of LBW in
India have been associated with improvements in both intrauterine growth and gestation. In this
context, improvement should be envisaged as a shift of the gestational distribution to the right
(say by one week) even among term newborns (37 to 41 weeks gestation), rather than a classical
decline in preterm births. It is conceivable that the factors affecting intrauterine growth and
gestation are different and should, therefore be searched for separately.
LBW is multifactorial in etiology - nearly 50 individual factors have been evaluated for
their role in causing prematurity and IUGR with statistically significant associations having been
documented for several of them. In order to formulate a meaningful public health intervention
policy, it would be useful to group the factors (Kramer 1987) by the: (i) strength of available
evidence; (ii) potential for public health impact, which depends on both the magnitude of the
effect, e.g., the number of grams of birth weight attributable to it or the relative risk of IUGR.
and its prevalence in the population; and (iii) modifiability. An analysis of this nature (as
suggested by Kramer 1987) is summarized in Table 4. This analysis represents a synthesis of
the currently available evidence, which is largely based on exhaustive meta-analyses or
overviews including unpublished electronic database information on randomized controlled trials
(RCTs) from the Cochrane Library (Kramer 1987. Kramer 1993, WHO 1995 and 1995a, Kelly
1996, Gulmezoglu 1997, Cochrane 1997). The analysis is restricted to factors of importance in
the developing countries, particularly this region, and also excludes those factors related to
medical complications during pregnancy or evaluated in selected groups of suspected fetal
growth retardation. In case of conflicting conclusions arising from observational or experimental
study designs, the latter inference was selected. It should be borne in mind that no matter how
19
convincing the evidence that a given factor is causally related to intrauterine growth or
gestational duration, there is no guarantee that its elimination or reduction will lead to lower
infant mortality or childhood morbidity (Kramer 1987) since there is hardly any data exploring
this possibility.
Table 4. Intervention based assessment of factors evaluated for their effects on gestation
duration and intrauterine growth in developing countries.
Intervention based
assessment
Intrauterine growth
Causal effect ruled out with a
high probability
Protein status/intake
•
•
•
•
Infant sex
Paternal height and weight
Parity
Protein status/intake
•
•
•
•
•
•
•
Marital status
Maternal psychological
factors
Sexual activity
Prior spontaneous abortions
Prior induced abortion
Prior still birth or neonatal
death
Prior infertility
In utero exposure to
diethylstilbestrol
Vitamin B12
Zinc and copper
Calcium, phosphorous and
Vitamin D
Vitamin B6
Urinary tract infection
Genital tract infection
Caffeine and coffee
consumption
Use of marijuana
Racial/ethnic origin
Maternal height
Maternal hemodynamics
Marital status
Sexual activity
Prior still birth or neonatal
death
Prior infertility
Gestational weight gain
Vitamin B12
Zinc and copper
Calcium, phosphorous and
Vitamin D
Other vitamins and trace
elements
Urinary tract infection
Alcohol consumption
Caffeine and coffee
consumption
Use of marijuana
Narcotic addiction
•
•
•
Birth or pregnancy interval
Heavy alcohol consumption
Narcotic addiction
Causal effect unlikely, but
evidence insufficient to rule
out totally
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Causal effect uncertain, but
importance unlikely owing to
small effect magnitude or low
prevalence
Gestation duration
20
•
•
•
•
•
•
•
•
•
•
•
In utero exposure to
diethylstilbestrol
Birth or pregnancy interval
Prior induced abortion
Vitamin B6
Intervention based
assessment______________
Causal effect established, but
importance unlikely, owing to
small effect magnitude or low
prevalence
Intrauterine growth
Gestation duration
•
•
Antiplatelet agents (Aspirin)
Causal effect established and
important, but unmodifiable
Antiplatelet agents (Aspirin)
Infant sex
Parity
Causal effect established and
important, but modifiable over
long term
•
•
•
Maternal height
Socio-economic conditions*
General morbidity, episodic
illness
•
Socio-economic conditions*
Causal effect established,
important, and modifiable over
short or intermediate term
•
•
•
•
•
•
•
Pre-pregnancy weight
Very young maternal age*
Maternal education*
Gestational weight gain
Caloric intake
Malaria1
Tobacco chewing
•
•
•
Pre-pregnancy weight
Very young maternal age*
Maternal education*
Causal effect uncertain, but
potentially important and
modifiable
•
•
•
•
•
Maternal hemodynamics
Strenuous maternal work
Folic acid
Iron and anemia
Other vitamins and trace
elements
Magnesium
Cigarette smoking and indoor
smoke
First antenatal care visit
Number of antenatal care
visits
Quality of antenatal care
•
Stress and anxiety
Maternal work
Caloric intake
Other vitamins and trace
elements
Iron and anemia
Folic acid
General morbidity, episodic
illness
Malaria1
Genital tract infection
Cigarette smoking and indoor
smoke
Tobacco chewing,
environmental toxins
First antenatal care visit
Number of antenatal care
visits
Quality of antenatal care
•
•
•
•
•
•
•
•
•
•
•
These factors have indirect causal influences, z'.e., they affect direct determinants but have no independent
causal impacts of their own. Socio-economic status has been subdivided into maternal education and socio
economic conditions because of the temporal differences required for their modification.
For endemic areas.
21
Pertinent aspects of some of the important factors are briefly outlined below:
3.2.1. Adolescent Pregnancy
Maternal age does not appear to be an important independent determinant of intrauterine
growth or gestational duration (Kramer 1987). However, a very young age exerts indirect effects
by influencing maternal height, weight and nutrition. In a recent report on 242 adolescent
pregnancies (10-18 years) from Gorakhpur in Uttar Pradesh, India (Kushwaha 1993), the LBW
and prematurity rates were 67% and 33%, respectively. The corresponding figures for mothers
below 17 years of age were 83% and 33%, respectively. The indirect causal effects of a very
young maternal age are important, because interventions aimed at delaying pregnancy in young
adolescents might be more effective or more practicable than attempting to influence their
height, weight or gestational nutrition (Kramer 1987, Gopalan 1994). Although the average
female age of first marriage in the region has
steadily increased in the past few decades
(VNICEF 1996), there is still considerable scope for improvement as illustrated in Table 5.
Table 5. Average age (years) offirst marriage in females.
Country
Average age (yrs)
Source
Bangladesh
Bhutan
India
<15
>20
UNICEF 1996
UNICEF 1996
UNICEF 1996
SRS 1993
UNICEF 1996
UNICEF 1996
Pradhan 1997
UNICEF 1996
UNICEF 1996
Maldives
Nepal
Pakistan
Sri Lanka
15-17.5 (most states)
19.6 (20.3% < 18)*
17.5-20
15-17.5
16.4
17.5-20
>20
Refers to female age at "effective marriage".
22
3.2.2. Nutrient Supplementation
The "true" potential of this intervention, which can be modified over a relatively short
term, needs a critical analysis. Meta-analyses (Kramer 1993. Cochrane 1997, Gulmezoglu 1997)
of randomized trials of balanced energy/protein supplementation (<25% protein/ daily
consumption) reveal "only a modest increase in maternal weight gain and fetal growth, even in
undernourished women, and no long term benefits to the child in terms of growth or
neurocognitive development". The weighted mean benefit in birth weight was calculated as 30g
(95% CI 1g to 58g) with, at best, a "clinically trivial effect on mean gestational age", which
though statistically non-significant, resulted in a highly consistent reduced risk of prematurity
(Kramer 1993). Another optimistic estimate of the "modest" increase in birth weight is about
100g (Gulmezoglu 1997). Three recently completed but unpublished trials from rural areas of
India are nearer the former (Kramer 1993) lower benefit estimate. Surprisingly, there was no
evidence of a larger effect in undernourished women; indeed the effect was actually smaller
(weighted mean 24g vs 45g) (Kramer 1993). The "modest" benefits of such supplementation
have been explained by the rather "modest" net increases in energy intake achieved. The average
documented net increases were 200-250 kcal/day and in the trials recording relevant data, non
compliance was substantial (Kramer 1993). The magnitude of non-compliance reported from
research settings is likely to be magnified in the true operational setting of large scale programs.
In a recent study in 174 pregnant beneficiaries of food supplementation (500 kcal/day protocol)
in the Integrated Child Development Services (ICDS) Program, oniy 24% of those registered
actually collected or received supplementary nutrition. Of those who collected, only 11%
consumed 75-100%, and 36% less than 50% of the supplementary nutrition. All of them shared
the supplementary nutrition; about 42% of them shared more than 75% of the food with their
23
family members (Nayar 1997).
Neither balanced isoenergetic protein supplementation nor high protein supplementation
have proved beneficial to either mother or infant and there is a suggestion that these may even
impair fetal growth (Kramer 1993, Cochrane 1997, Gulmezoglu 1997). Similarly, isolated
micronutrient supplementation with either Zinc, Vitamin D. Pyridoxine or Iron has not resulted
in clinically important or statistically
significant positive effects on birth weight. Routine
magnesium supplementation seems to have decreased the incidence of term LBW but the trials
included in this systematic review have either a high number of exclusions or weaknesses in
randomization procedures which makes the results inconclusive. Although, routine iron
supplementation increased serum ferritin and hemoglobin levels, there were no differences on
clinical outcomes of the fetus. The systematic review on routine folate supplementation shows a
reduction in the incidence of term LBW. However, most of the trials defined their populations
poorly and did not give details of the randomization procedures (all of these trials were
performed in populations where iron supplementation was routine). Unfortunately, there is
inadequate data from populations where these micronutrient deficiencies are more common; and
relevant research in this context has been recommended for Zinc, Iron, Folate and Magnesium
(Cochrane 1997, Gulmezoglu 1997).
In a systematic review of relevant studies (Cochrane 1997), nutritional advice, either on
one-to-one basis or to groups of women, proved effective in increasing the pregnant women's
energy and protein intakes but the increases were lower than those reported in trials of actual
protein/energy supplementation. It was felt that the implications for the fetal, infant or maternal
health cannot be judged from the available trials. A recent study from Canada reported an
axerage benefit of 55g in birth weight in adolescent pregnancy with nutrition intervention
24
individualized as a function of diagnosed risk (Dubois 1997). Imparting relevant nutrition advice
assumes significance in the context of developing countries since dietary intake in pregnancy is
strongly influenced by cultural beliefs and practices. Data from 18 different cultures documents
that food restriction is practiced during pregnancy, in order to facilitate an easier labor and
delivery, by lowering birth weights (Brems 1988). Quantitative data from rural South India
demonstrates reduced intake in pregnancy, particularly between 5-7 months and months 8/9; the
average caloric intake being 1700 kcal (Hutter 1996).
From the foregoing, it is evident that routine nutrient supplementation instituted through
large scale programs will, at best, result in marginal benefits in birth weight. Considering the
various aspects of food supplementation programs, particularly the financial perspective in the
region, it may be pragmatic to resort to sound nutritional advice as an alternative economic
intervention.
3.2.3. Energy Expenditure, Work and Physical Activity
Cross sectional data from Ethiopia indicates that among poor women subsisting on a
calorie intake of less than 70% of the recommended intake, birth weights of offspring and weight
gains in pregnancy of women who were actively engaged in heavy labor were significantly lower
than the corresponding values for women who were not so engaged [mean (SD) birth weights
j068g (355) vs 3270g (368)] (Tafari 1980). However, the effect of energy expenditure, work and
physical activity on intrauterine growth is uncertain from a systematic review of the available
data in developing countries (Kramer 1987). Nevertheless, such an effect would be consistent
with biological principles, at least for work involving high energy expenditure. Increased effects,
if confirmed, would identify a factor of major importance in developing countries, where women
often continue strenuous physical work through pregnancy (Kramer 1987, Gopalan 1994).
25
3.2.4. Maternal Anthropometry
Various maternal anthropometric criteria (pre-pregnancy weight, height, weight gain
during pregnancy, attained weight at mid pregnancy and body mass index) have been
significantly associated with intrauterine growth or prematurity. These parameters should be
viewed as "predictors" of LBW to be used for risk detection and intervention targeting, rather
than as representing direct factors amenable to intervention. In the WHO multicentric study
(WHO 1995a), pre-pregnancy weight (OR 2.55, 95% CI 2.3-2.7), attained weight at 20 weeks
(OR 2.77, 95% CI 2.3 - 3.2) and attained weight at 36 weeks (OR 3.09, 95% CI 2.7-3.4)
were
the best predictors for delivering SGA babies while pre-pregnancy weight (OR 1.42. 95% CI 1.3-
1.5) and pre-pregnancy body mass index (OR 1.33, 95% CI 1.1-1.4) were the best predictors for
a preterm delivery. Obviously, attained weight at 36 weeks of pregnancy does not represent a
useful indicator for preventing LBW as it would be too late to implement effective intervention.
3.2.5. Maternal Infections
Amongst the various researched maternal infections in pregnancy, systematic reviews
indicate a beneficial effect with malaria chemoprophylaxis in endemic areas (Cochrane 1997,
Gulmezoglu 1997). Overall, malaria chemoprophylaxis was associated with higher maternal
hemoglobin levels and birth weights. These effects were also more prominent in primigravidae,
who are known to be more susceptible, showing an increase in mean birth weight of 112g (95%
CI 41-183g). (Gulmezoglu 1997). The current incidence of malaria is high in Chittagong
Division of Bangladesh, Southern Bhutan and regions of Sri Lanka (UNICEF 1996).
26
3.2.6. Other Factors
The comprehensive meta-analysis by Kramer (1987) suggests that maternal socio
economic status {including maternal education) have no independent effect on intrauterine
growth. "It is nevertheless, likely that low socioeconomic status may well be a social "cause" of
other nutritional, toxic, anthropometric, or infectious factors that may themselves be causal
determinants. As with maternal age, indirect causal effects may be important for intervention.
The most easily modifiable aspect of socio-economic status is maternal education, although, in
the long term, family income could also be influenced" (Kramer 1987).
There is scarce well controlled data from the developing world evaluating the impact of
antenatal care on LBW (Kramer 1987). Nevertheless, organizing access to quality antenatal care
should be viewed as potentially important since it also offers opportunities for counseling and
risk detection apart from its necessity for maternal health.
Data from developed countries indicates that strategies to reduce smoking during
pregnancy are associated with increased birth weight and lower rate of term LBW (OR 0.80,
95/o CI 0.65-0.98) (Gulmezoglu 1997). Smoking and tobacco chewing during pregnancy does
occur in the region; the precise magnitude, however, is uncertain.
4.
Possible Public Health Interventions To Reduce LBW
It is obvious that the suggested public health interventions to reduce LBW should be
specific for the targeted population and directed at the quantitatively important modifiable
determinants of intrauterine growth and gestation. The quantitative importance of a factor is
dependent on its individual effect magnitude and prevalence; however, issues such as cost
effectiveness, cultural acceptability, and political feasibility are also important determinants of
27
any intervention program (Kramer 1987). On the basis of the focused review in the preceding
sections, the suggested public health interventions are summarized in Table 6. Some
interventions (for example, nutrient supplementation) could be preferentially targeted towards
"at risk" women identified by anthropometry. Over the long term, general improvements in
nutrition, living conditions, water supply and sanitation should increase maternal height and
reduce communicable diseases during pregnancy. It should also be borne in mind that no matter
how convincing the evidence that a given factor is causally related to intrauterine growth or
gestational duration, there is no guarantee that its elimination or reduction will lead to
amelioration of all adverse consequences of LBW including lower infant mortality and childhood
morbidity (Kramer 1987).
Table 6. Suggested public health interventions to reduce LBW.
______________________Interventions_____ _______________
• Delaying child bearing in adolescents
• Efforts to improve nutrition of women, particularly in pregnancy
Options for pregnant women:
■ Nutrition advice
■ Food supplementation
• Access to antenatal care
• Advice on adequate rest in pregnancy, especially in
undernourished women
• Malaria prophylaxis or treatment in endemic areas
• Efforts to stop smoking and reduce tobacco chewing (places
where common practice)
• Improve female education, especially maternal
• General improvements in nutrition
• General improvements in socio-economic conditions
• Improve sanitation and water supplies
The expected benefit with each solitary intervention is small. Further, multiple
pathologies coexist in the region which often adversely interact with each other making their
combined effect greater than the simple additive effect of each condition. It has been
appropriately questioned whether a single intervention is likely to reduce, in a population, the
28
overall rate of a multicausal outcome like LBW which is so dependent on socio-economic
disparities accumulated over generations (Gulmezoglu 1997). The maximum benefit is, therefore
likely to accrue from institution of a combination of interventions.
Wherever possible, the suggested interventions should be amalgamated with the
beneficial customs. For example, it is a common practice in India to deliver the child.
particularly the firstborn at the parental home which offers benefits in term of adequate rest and
nutritional intake in the pregnancy.
5.
Future Perspectives
5.1. Are The Targets Realistic?
The World Summit for Children had set a goal of reduction of the LBW prevalence to
less than 10% (Sachdev 1994). This translates into a prevalence reduction of 15% to 40% (or by
60% to 80% of the current estimates in Table 1) in the available 3 years till 2000 A.D. In order
to ascertain if these targets are achievable by even 2010 A.D. (gap of 13 years), apart from the
regional experience, it would be useful to look at the changes in developed countries (Table 7).
Table 7. Changes in birth weight in developed countries.
Source
Lee 1980
Kessel 1984
Place/Country
Period
Improvements in
Johar1988
USA National
USA National
(States with both weight
& gestation data)
Omaha (USA)
1935 to 1985
Evans 1989
ICE Countries*
1970 to 1984
Chike-Obi 1996
Illinois (USA)
1950 to 1990
1950 to 1975
1970 to 1980
Birth weight
LBW prevalence
Median 60g
No change
7.39% to 6.31%
(14% reduction)
No change
(term newborns)
40 - 100g (in most;
derived from graph)
33g (Black male) to
74g (White female)
No change
(term newborns)
-7% to 6% (White)
-13 to 14% (Black)
^Derived from graph)
The International Collaborative Effort (ICE) countries are USA, England and Wales, Denmark, Bavaria and
North Rhine Westphalia of the Federal Republic of Germany, Israel, Japan, Norway, Scotland and Sweden.
29
In this context, it would be pertinent to examine the birth weight changes in the
developed countries for the preceding few decades to account for the developmental gap between
the industrialized and developing countries. Even in the developed nations, a few decades earlier,
there was no consistent increase in birth weight or reduction in LBW prevalence (Table 7). In
certain regions, no changes could be demonstrated over 25 or 50 years. Wherever evident, the
increases in average birth weight were modest, ranging from 33 to 100g in 10 to 40 years, with a
corresponding decrease in LBW prevalence of about 1% (nearly 14%
reduction from the
original value). In the USA, the decade of 1970s was a period of rapid growth of the number and
scope of federal state and local health prog];rams emphasizing maternal and child health including
nutrition programs (Special Supplemental Food for Women, Infants and Children [WIC
Program] and the Department of Health and Human Services sponsored programs providing such
services as prenatal care, family planning, care of high risk pregnant women and newborns,
regional perinatal care, health supervision and care of infants and children, care of pregnant
adolescents, and genetic diagnostic and counseling services; yet, the median increase in birth
weight was only 60g with a resultant decline in LBW prevalence of 1% (Kessel 1984). Another
noteworthy aspect is the difference in level between the median birth weights for different
countries or states or even amongst races in the same region (blacks and whites), and the way the
relative positions tend to remain steady over the years (Evans 1989, Chike-Obi 1996).
The secular changes in birth weight from India (Table 3) compare favorably with those
from the developed nations (Table 7). However, almost similar improvements in average birth
weights resulted in vastly different changes in LBW prevalence (8 to 12% vs 1%); indicating the
importance of efforts to achieve even modest changes in the region. This difference is a
30
reflection of the comparative birth weight distribution below the cut-off point of 2500g in these
settings.
Considering the earlier time trends from the developed countries and India, it is evident
that it would be virtually impossible to achieve the stated targets by even 2010 A.D. An
optimistic target in this period would be an average increase in birth weight of about 100g with
a corresponding reduction in LBW prevalence of 10-12%.
5.2.
Public Health Interventions
Although there is no specifically instituted program for control of LBW in India.
Bangladesh and Pakistan, majority of the suggested public health interventions (Table 6) are
being addressed through the ongoing programs for population control, maternal and child health,
nutrition and literacy. In India, the important relevant programs include the Reproductive and
Child Health Program (Child Survival and Safe Motherhood Program) focussing on providing
access to antenatal care and family planning including delaying pregnancy in adolescents; the
Integrated Child Development Services Program where apart from new initiatives focussed on
adolescent girls, pregnant mothers are given a nutritional supplement of 500 kcal; and Literacy
Mission. In Bangladesh also, the nation wide Maternal Child Health Program has provision for
antenatal care and family planning whereas the recently instituted Bangladesh Integrated
Nutrition Project (BINP) focuses on family planning advice to newly wed couples and nutrition
education and supplementary nutrition (600 kcal) to pregnant women. The BINP, a World Bank
assisted project, currently covers only 6 thanas (sub districts) and will be extended to 40 thanas
(out of 460) by the end of 1998 and the entire country by 2000 AD. In addition, NGOs like
Bangladesh Rural Advancement Committee also provide supplementation and counseling to
31
pregnant women in their operational areas (Roy 1997, Islam 1997). Similarly, in Pakistan the
maternal care programs, population planning initiatives and nutritional supplementation in
pregnancy (part of safe motherhood initiative) have components addressing the problem of LBW
(Bhutta 1997). In addition, in these countries the ongoing initiatives for general improvements in
socio-economic development, nutrition, literacy and water supply and sanitation are expected to
have a beneficial effect on birth weight in the long term.
It is apparent that in a multi-dimension problem like LBW, no specific vertical program
can be formulated to address the issue on a war footing. The ongoing initiatives in these
countries are in the right direction but may need operational strengthening and convergence to
y ield the maximum benefit. An examination of the specific components of nutrition and other
advice in pregnancy may lead to improvements like specific dietary advice, adequate rest and
stopping smoking and tobacco chewing (in areas where these habits are prevalent). Initiatives to
provide maternity leave for women in unorganized sector are worth considering. Provision of
malaria chemoprophylaxis and treatment for pregnant women in hyperendemic areas deserves
exploration. The relative cost effectiveness of providing nutritional supplementation to all
pregnant women in preference to nutritional advice in pregnancy must be scientifically explored
in a true program setting and the results should determine the need for investing a large
proportion of the available health budget for the former option on a routine basis.
32
REFERENCES
Arif MA, Nizami SQ. A study of 1056 newborn babies. Pakistan Pediatr J 1985; 9: 20-5.
Babson SG, Behrman E, Lessel R. Live bom birth weights for gestational age of white middle
class infants. Pediatrics 1970; 45: 937-42.
Bavdekar AR, Vaidya UV, Bhave SA, Pandit AN. Catch up growth and its determinants in low
birth weight babies: A study using Z scores. Indian Pediatr 1994; 31: 1483-90.
Barker DJP, Winter PD, Osmond C, et al. Weight in infancy and death from ischemic heart
disease. Lancet 1989; ii: 577-80.
Barker DJP, Osmond C, Simmonds SJ, Wield GA. The relation of small head circumference and
thinness at birth to death from cardiovascular disease in adult life. BMJ 1993; 306: 422-6.
Barker DJP. Fetal origins of coronary heart disease. BMJ 1995; 311: 171-4.
Bhargava SK. Bhargava V, Kumari S, Madhavan S, Ghosh S. Babies with severe intrauterine
growth retardation: Linear physical growth from 0-24 months. Indian J Med Res 1976; 64: 14805.
Bhargava SK, Kumari S, Baijal VN, Bhan MK, Taneja S, Choudhury P. Skeletal maturation in
children with birth weight of 2000g or less. Indian J Med Res 1980; 71: 268-72.
Bhargava SK, Duggal S, Ramanujacharyulu TKTS, Choudhury P. Patterns of pubertal changes
and their interrelationships in girls. Indian Pediatr 1980; 17: 657-65.
Bhargava SK, Datta I, Kumari S. A longitudinal study of language development in small for date
children from birth to five years. Indian Pediatr 1982; 19: 123-9.
Bhargava SK. Kumari S, Choudhury P, Ghosh S, Butani R, Bhargava V. A longitudinal study of
linear physical growth of infants with birth weight of 1500g or less from birth to 6 years. Indian J
Med Res 1983; 71: 78-82.
Bhargava SK, Kumari S, Choudhury P. Outcome of low birth weight infants. Acta Pediatr
Scand 1984; 73:406-7.
Bhargava SK, Sachdev HPS, Iyer PU, Ramji S. Current status of infant growth measurements in
the perinatal period in India. Acta Paediatr Scand 1985; 319 (Suppl): 103-10.
Bhargava SK, Iyer PU, Dutta V, Nafde S, Ramji S, Sachdev HPS. Perspectives in low birth
weight- survival and outcome. Proceeding III, IV and V Annual Convention of National
Neonatology Fomm. Indore, Naidunia Printery, 1985a; pp 44-52.
Bhargava SK, Kumari S, Choudhury P, Butani R, Sachdev HPS. A longitudinal study of physical
growth of small for date infants from birth to six years. Nutr Res 1985b; 5: 707-13.
33
Bhargava SK, Sachdev HPS, Ramji S, Iyer PU. Low birth weight: Etiology and prevention in
India. Ann Trop Paediatr 1987; 7: 59-65.
Bhargava SK, Singh KK. Saxena BN. A National Collaborative Study of Identification of High
Risk Families, Mothers and Outcome of Their Offsprings With Particular Reference to the
Problem of Maternal Nutrition, Low Birth Weight, Perinatal and Infant Morbidity and Mortality
in Rural and Urban Slum Communities. A Task Force Study. New Delhi, Indian Council of
Medical Research, 1990.
Bhargava SK. Recent trends in perinatal health in South Asia. 2. India. In: Improving Health of
the Newborn Infant in Developing Countries. Ed. Costello A, 1997 (in press).
Bhargava SK, Ramji S, Srivastava U, Sachdev HPS, Kapani V, Datta V, Satyanarayana L.
Growth and sexual maturation of low birth weight children: A 14 year follow up Indian Pediatr
1995;32:963-70.
Bhatia BD. Bhargava V, Chatterjee M. Koto VLN, Singh LI, Jain NP. Intrauterine growth
percentiles of singleton live bom babies. Indian Pediatr 1981; 18: 647-53.
Bhutta ZA. Neonatal care in Pakistan: Current status and prospects for the future Pakistan
Pediatr J 1990; 14: 11-22.
Bhutta ZA, Rehman S. Perinatal care in Pakistan: A situational analysis. J Perinatol 1997' 1754-9.
Bhutta ZA. Initiatives for control of Low Birth Weight in Pakistan, 1997 (personal
communication).
Bjerkedahl T, Bakketeig L, Lehmann EH. Percentiles of birth weights of single live births at
different gestation periods. Acta Paediatr Scan 1973; 62: 449-54.
Brems S, Berg A. Eating down during pregnancy: Nutrition, obstetric and cultural considerations
in the third world. Discussion Paper prepared for the ACC/SCN. Washington DC World Bank
1988.
Buckshee K, Arora V, Hingorani V. Evaluation of fetal development by real time sonar
cephalometry in Indian pregnant women. J Obstet Gynecol India 1983; 33: 284-8.
CMC. Trends in Intrauterine Growth of Single Live Boms During 1969-73 and 1989-93 Among
Rural and Urban Communities of North Arcot Ambedkar District, Tamil Nadu, India. Longitudi
nal Studies in Growth and Development: Monograph No. 21. Department of Biostatistics,
Christian Medical College, Vellore, 1995.
Chike-Obi O, David RJ, Coutinho R, Wu S-Y. Birth weight has increased over a generation. Am
J Epidemiol 1996; 563-9.
34
Cochrane Library Electronic Database on Randomized Controlled Trials, 1997.
" Gulmezoglu AM, Gamer P. Interventions to prevent malaria during pregnancy in endemic
malarious areas. Date of most recent substantive amendment: 27/02/1997
(http://som.flinders.edu.au/fusa/cochrane/cochrane/revabstr/ab000031.htm).
■ Hodnett ED. Support from caregivers during childbirth. Date of most recent substantive
amendment:
05/12/1994
(http://som.flinders.edu.au/fusa/cochrane/cochrane/revabsti7
ab000156.htm).
■ Kramer MS. High protein supplementation in pregnancy. Date of most recent substantive
amendment:
23/08/1996
(http://som.flinders.edu.au/fusa/cochrane/cochrane/revabstr/
ab000105.htm).
■ Kramer MS. Isocaloric balanced protein supplementation in pregnancy. Date of most recent
substantive amendment: 23/08/1996 (http://som.tlinders.edu.au/fusa/cochrane/cochrane/
revabstr/abOOO 119.htm).
■ Kramer MS. Nutritional advice in pregnancy. Date of most recent substantive amendment:
29/04/1996 (http://som.flinders.edu.au/fusa/cochrane/cochrane/revabstr/abOOO 132.htm).
■ Mahomed K, Gulmezoglu AM. Pyridoxine in pregnancy. Date of most recent substantive
amendment:
21/10/1996
(http://som.flinders.edu.au/fiisa/cochrane/cochrane/revabstr
/abOOO 148.htm).
■ Mahomed K. Routine folate supplementation in pregnancy. Date of most recent substantive
amendment:
21/05/1997
(http://som.flinders.edu.au/fusa/cochrane/cochrane/revabstr/
ab000150.htm).
■ Mahomed K. Routine iron supplementation during pregnancy. Date of most recent
substantive amendment: 20/11/1996 (http://som.flinders.edu.au/fusa/cochrane/cochrane/
revabstr/abOOO 151 .htm).
■ Mahomed K, Gulmezoglu AM. Vitamin D supplementation in pregnancy. Date of most
recent substantive amendment: 16/05/1996 (http://som.flinders.edu.au/fusa/cochrane/
cochrane/revabstr/ ab000168.htm).
■ Mahomed K. Zinc supplementation in pregnancy. Date of most recent substantive
amendment:
21/05/1997
(http://som.flinders.edu.au/fusa/cochrane/cochrane/revabstr/
ab000170.htm).
Chadha SL, Radhakrishnan S, Ramachandran K, Kaul U, Gopinath N. Epidemiological study of
coronary heart disease in urban population of Delhi. Indian J Med Res 1990; 92(B): 424-30.
Choudhari S, Kulkami S, Pajnigar F, Pandit AN, Deshmukh S. A longitudinal follow-up of
development of preterm infants. Indian Pediatr 1991; 28: 873-80.
de Onis M, Habicht JP. Anthropometric reference data for international use: Recommendations
from a World Health Organization Expert Committee. Am J Clin Nutr 1996; 64: 650-8.
Deshmukh JS, Motghare DD, Zodpey SP, Wadhva SK. A study of low birth weight and
associated maternal factors in urban area. Indian Pediatr 1998; 35: (in press).
35
Dubois S. Coulombe C, Pencharz P. Pinsonneault O, Duquette MP. Ability of Higgins Nutrition
Intervention Program to improve adolescent pregnancy outcome. J Am Diet Assoc 1997- 97871-8.
Evans S, Alberman E, Pashley J, Hampton B. International Collaborative Effort (ICE) on birth
weight, plurality, and perinatal and infant mortality. II. Comparisons between birthweight
distributions of birth in member countries from 1970 to 1984. Acta Obstet Gynecol Scand 198968:11-7.
FHB (Family Health Bureau). Study on Low Birth Weight, Neonatal Morbidity and Mortality.
Family Health Bureau, Ministry of Health and Women's Affairs, Colombo. Sri Lanka, 1992.
Fall CHD, Barker DIP. The fetal origins of coronary heart disease and non insulin dependent
diabetes in India. Indian Pediatr 1997; 34: 5-8.
Fernandez AR. Changes in birthweight and gestation patterns in Sion, Mumbai. Personal
Communication, 1996.
Fledelius HC. The long term prognosis for prematurely bom children. A follow up study of 999
premature boys bom in wedlock and 1002 controls. Acta Pediatr Scand 1953; 94 (Suppl): 1-116.
Ghosh S, Bhargava SK, Madhavan S, Taskar AD, Bhargava V, Nigam SK. Intrauterine growth
of North Indian babies. Pediatrics 1971; 47: 826-30.
Ghosh S, Bhargava SK, Moriyama IM. Longitudinal Study of the Survival and Outcome of a
Birth Cohort. Report of Phase I of the Research Project of 01-658-2; Funded by the National
Center for Health Statistics, 3700 East West Highway, Hyattsville, Maryland 20782, USA, 1979.
Gillespie S. Improving Adolescent and Maternal Nutrition: An Overview of Benefits and
Options. UNICEF Staff Working Papers, Nutrition Series, Number 97-002. New York, United
Nations Children's Fund, 1997.
Gopalan C. Low birth weights: Significance and implications. In: Nutrition in Children:
Developing Country Concerns. Eds. Sachdev HPS, Choudhury P. New Delhi, National Update
on Nutrition, 1994; pp 1-33.
Gopalan C. Low birth weight. In: Nutrition Research in South East Asia: The Emerging Agenda
of the Future. World Health Organization, Regional Office for South East Asia, New Delhi
1994a; pp 13-31.
Gulmezoglu M, de Onis M, Villar J. Effectiveness of interventions to prevent or treat impaired
fetal growth. Obstet Gynecol Surv 1997; 52: 139-49.
Hirve SS, Ganatra BR. Determinants of low birth weight: A community based prospective cohort
study. Indian Pediatr 1994; 31: 1221-5.
36
4
Hutter I. Reduction of food intake during pregnancy in rural south India. Prop Med Int Health
1996:1:399-405.
Institute of Medicine. Nutrition in Pregnancy. Washington DC, National Academy Press, 1990.
Islam S. Initiatives for control of Low Birth Weight in Bangladesh, 1997 (personal
communication).
Johar R, Raybum W, Weir D, Eggert L. Birth weight in term infants. A 50-year perspective. J
Reprod Med 1988; 33: 813-6.
Kalra SK, Sarkar P, Vatwani D, De NS. A longitudinal study of low birth weight babies. Indian J
Pediatr 1983; 50: 279-83.
Kelly A, Kevany J, deOnis M, Shah PM. A WHO collaborative study of
anthropometry and pregnancy outcomes. Int J Gynaecol Obstet 1996; 53: 219-33.
maternal
Kessel SS, Villar J, Berendes HW, Nugent RP. The changing pattern of low birth weight in the
United States: 1970 to 1980. JAMA 1984; 251: 1978-82.
Kramer MS. Determinants of low birth weight: Methodological assessment and meta-analysis
Bull World Health Organ 1987; 65: 663-737.
Kramer MS. Effects of protein and energy intakes on pregnancy outcome: An overview of the
research evidence from controlled clinical trials. Am J Clin Nutr 1993; 58: 627-35.
Kramer MS, Coates AL, Michoud MC, Dagenais S, Hamilton EF, Papageorgiou A. Maternal
anthropometry and idiopathic preterm labor. Obstet Gynecol 1995; 86: 744-8.
Kushwaha KP, Rai AK. Rathi AK, Singh YD, Sirohi R. Pregnancies in adolescents: Fetal,
neonatal and maternal outcome. Indian Pediatr 1993; 30: 501-5.
Law CM, Shiell AW. Is blood pressure inversely related to birthweight? The strength of
evidence from a systematic review of the literature. J Hypertension 1996; 14: 935-41.
Lee K-S, Paneth N, Gartner LM, Pearlman MA, Gruss L. Neonatal mortality: An analysis of the
recent improvements in the United States. Am J Pub Health 1980; 70: 15-21.
Man Mohan, Shiv Prasad SR, Chellani HK, Kapani V. Intrauterine growth curves in north Indian
babies: Weight, length, head circumference and ponderal index. Indian Pediatr 1990; 27: 43-51.
Manandhar DS. Recent trends in perinatal health in South Asia. 3. Nepal. In: Improving Health
of the Newborn Infant in Developing Countries. Ed. Costello A, 1997 (in press).
Martorell R, Kettel Khan L, Schroeder DG. Reversibility of stunting: Epidemiological findings
in children from developing countries. Eur J Clin Nutr 1994; 48(Suppl 1): S45-S57.
37
Martyn CN. Barker DIP, Osmond C. Mother's pelvic size, fetal growth, and death from stroke
and coronary heart disease in men in the UK. Lancet 1996; 348: 1264-9.
Mathai M. Changes in health status and birthweight in Vellore over 25 years (1969-1994) Paner
c™»ic/ao„Wr9“OP °n “H“1,h in Tr“siti“" in N™y> May 1995 <Personal
McKeigue PM Shah B, Marmot MG. Relation of central obesity and insulin resistance with high
diabetes prevalence and cardiovascular risk in South Asians. Lancet 1991; 337: 382-6.
S.Td SlnphdPA'5ta,?C' ^trauterine growth and low birth weight criteria in Punjabi
inrants. Indian Pediatr 1976; 13: 679-82.
J
NNP (National Neonatology Forum). Neonatal morbidity and mortality - Report of the National
Neonatal - Perinatal Database. Indian Pediatr 1997; 34: (in press).
N, Recer“ trends in perinatal health in South Asia. 1. Bangladesh. In: Improving Health of
the Newborn Infant in Developing Countries. Ed. Costello A, 1997 (in press).
Nayar D, Kapil U, Saxena N. Nutrient intake and consumption of supplementary nutrition bv
pregnant mothers in ICDS and non-ICDS areas - A pilot study. Indian Pediatr 1997 (in press).
Pradhan A, Aryal RH, Regmi G, Ban B, Govindasamy P. Nepal Family Health Survey 1996
Family Health Division, Department of Health Services, Ministry of Health, His Majesty's
Government, Kathmandu, Nepal, 1997; pp 82-3.
J
Proos LA. Growth and development of Indian children adopted in
Sweden. Acta Universitalis
Upsaliensis, Uppsala University, 1992.
Ramji S. Changes in birthweight and gestation patterns
in Delhi. Personal Communication, 1996.
Ramji S. Birth weight in Child Survival and Safe Motherhood Programme Districts. Personal
Communication, 1997.
Rich-Edwards J, Stampfer M, Manson J, et al. Birthweight, breastfeeding and risk of coronary
heart disease in the nurses' health study. Am J Epidemiol 1995; 141: S78.
Y
Nmrition,’
Hyderabad’ Natio^l Institute of
P’ GiUeSPie S'
Roy SK. Prevalence of low birth weight and factors associated with low birth weight in
Scations) 997 (
- no^dexed
publications), 1997 (personal communication).
38
SRS 1993. Sample Registration System. Fertility and Mortality Indicators 1993. Registrar
General India, New Delhi. 1995.
Sachdev HPS. Indicators for monitoring health goals for the World Summit for Children. In:
Current Concepts in Pediatrics. Eds. Pun RK, Sachdev HPS, Choudhury P. Verma IC. New
Delhi, Jaypee Brothers, 1994; pp 169-75.
Sachdev HPS. Epidemiological trends in nutritional status of women and children in India. In:
Improving Health of the Newborn Infant in Developing Countries. Ed. Costello A, 1997 (in
press).
Sachdev HPS. Nutritional status of children and women in India: Recent trends. NFI Bull 1997a;
18(3): 1-5.
Satpathy R. Das DB, Bhuyan BK, Pant KC, Santhanam S. Secular trend in birth weight in an
industrial hospital in India. Ann Trop Pediatr 1990; 10: 21-25.
Sethi GR, Sachdev HPS, Puri RK. Women’s health and fetal outcome. Indian Pediatr 1991- 281379-93.
’ ’
Sheth P, Merchant SM. Fetal growth in two socio-economic groups. Indian Pediatr 1972; 9: 650-
Singh MB, Giri SK, Ramachandran K. Intrauterine growth curves of live bom single babies.
Indian Pediatr 1974; 11: 475-9.
Singh RB, Niaz MA. Coronary risk factors in Indians. Lancet 1995; 346: 778-9.
Singhal PK, Paul VK, Deorari AK, Singh M, Sundaram KR. Changing trends in intrauterine
growth curves. Indian Pediatr 1991; 28: 281-283.
Snkantia SG. Pattern of growth and development of Indian girls and body size of adult Indian
women. In: Women and Nutrition in India. Eds. Gopalan C, Kaur S. New Delhi, Nutrition
Foundation of India. Special Publication Series 5, 1989; pp 108-152.
Stein CE, Fall CHD, Kumaran K, Osmond C, Cox V, Barker DJP. Fetal growth and coronary
heart disease in South India. Lancet 1996; 348: 1269-73.
Tabib SMSB, Nahar NN, Khan MR. Clinical profile of low birth weight babies. Bangladesh J
Child Hlth 1987; 11: 114-20.
Taiari A, Naeye RL, Gobezie A. Effects of maternal undemutrition and heavy physical work
during pregnancy on birth weight. Brit J Obstet Gynecol 1980; 87: 222-6.
UNDP. Human Development Report 1996. Published for the United Nations Development
Programme, Oxford University Press, 1996.
39
4T
UNICEF Regional Office for South Asia. Atlas of South Asian Women and Children
Kathmandu. United Nations Children's Fund, 1996.
UNICEF. The Progress of Nations. New York, United Nations Children's Fund, 1997.
villar J, de Onis M, Kestler E, Bolanos F, Cerezo R, Bemeded H. The differential neonatal
morbidity or the intrauterine growth retardation syndrome. Am J Obstet Gynecol 1990; 163:
Westwood M, Kramer MS, Murz D, Lovett JM, Watters GV. Growth and development of full
term non-asphyxiated small for gestational age newborns: Follow-up through adolescence
Pediatrics 1983; 71: 376-82.
y?onX AJ’ Intrauterine growth retardation: Beyond birth weight criteria. Early Hum Dev 1983;
8: 189-93.
World Health Organization. Physical Status: The Use and Interpretation of Anthropometry.
Report of a WHO Expert Committee. Technical Report Series No. 854. Geneva, World Health
Organization, 1995.
World Health Organization. Maternal anthropometry and pregnancy outcomes: A WHO
collaborative study. Bull World Health Organ 1995a; 73 (Suppl): 1-98.
Yajmk CS, Fal! CHD, Vaidya U, et al. Fetal growth and glucose and insulin metabolism in four
year old Indian children. Diab Med 1995; 12: 330-6.
Zaman S. Recent trends iin perinatal health in South Asia. 4. Pakistan. In: Improving Newborn
Infant Health in Developing Countries. Eds. Costello A, Manandhar D. London, Imperial
College Press, 2000.
40
Public Health Interventions To Reduce LBW In India
H.P.S. Sachdev, Professor and Incharge, Division of Clinical Epidemiology,
Department of Pediatrics, Maulana Azad Medical College, New Delhi 110 002.
It is obvious that the suggested public health interventions to reduce LBW
should be specific for the targeted population and directed at the quantitatively
important modifiable determinants of intrauterine growth and gestation. The
quantitative importance of a factor is dependent on its individual effect magnitude and
prevalence; however, issues such as cost-effectiveness, cultural acceptability, and
political feasibility are also important determinants of any intervention program (Kramer
1987). On the basis of the focused review in the preceding sections, the suggested
public health interventions are summarized in Table. Some interventions (for example,
nutrient supplementation) could be preferentially targeted towards "at risk" women
identified by anthropometry. Over the long term, general improvements in nutrition,
living conditions, water supply and sanitation should increase maternal height and
reduce communicable diseases during pregnancy. It should also be borne in mind that
no matter how convincing the evidence that a given factor is causally related to
intrauterine growth or gestational duration, there is no guarantee that its elimination or
reduction will lead to amelioration of all adverse consequences of LBW including lower
infant mortality and childhood morbidity (Kramer 1987).
Table: Suggested public health interventions to reduce LBW.
Interventions
Delaying child bearing in adolescents
Efforts to improve nutrition of women, particularly in pregnancy
Options for pregnant women:
<
Nutrition advice
Food supplementation
Access to antenatal care
Advice
on
adequate
rest
in
pregnancy,
especially
in
undernourished women
Malaria prophylaxis or treatment in endemic areas
Efforts to stop smoking and reduce tobacco chewing (places
where common practice)
Improve female education, especially maternal
General improvements in nutrition
General improvements in socio-economic conditions
Improve sanitation and water supplies
The expected benefit with each solitary intervention is small. Further, multiple
pathologies coexist in the region which often adversely interact with each other making
their combined effect greater than the simple additive effect of each condition. It has
been appropriately questioned whether a single intervention is likely to reduce, in a
population, the overall rate of a multicausal outcome like LBW which is so dependent
on socio-economic disparities accumulated over generations (Gulmezoglu 1997). The
maximum benefit is, therefore likely to accrue from institution of a combination of
interventions.
Wherever possible, the suggested interventions should be amalgamated with
the beneficial customs. For example, it is a common practice in India to deliver the
child, particularly the firstborn at the parental home, which offers benefits in term of
adequate rest and nutritional intake in the pregnancy.
Position: 107 (87 views)