RF_NUT_4_SUDHA.pdf
Media
- extracted text
-
RF_NUT_4_SUDHA
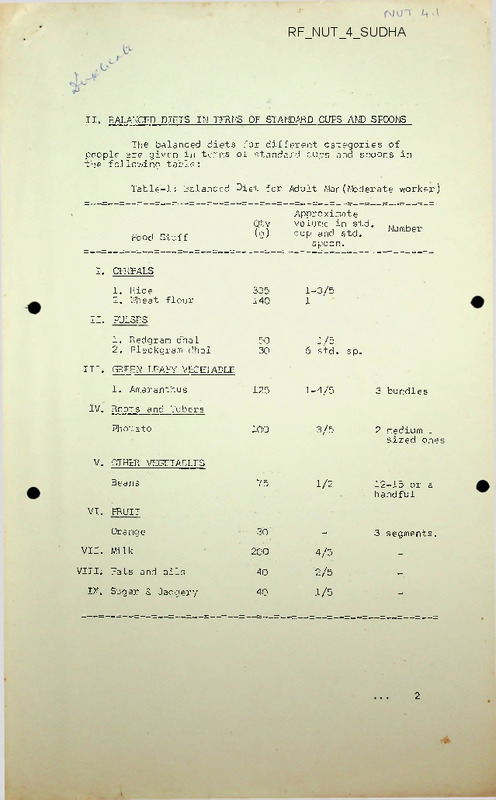
II. BALANCED DIETS IN TERMS OF STANDARD CUPS AND SPOONS
The balanced diets for different categories of
people are given in terms of standard cups and spoons in
the following table:
Table-1: Balanced Diet for Adult Mar(Moderate worker)
Food Stuff
Qtv
(9)
Approximate
volume in std •
cup and std.
spoon.
Number
I. CEREALS
1. Rice
2. Wheat flour
335
140
1-3/5
1
50
30
1/5
6 std. sp.
125
1-4/5
3 bundles
100
3/5
2 medium ~
sized one
75
1/2
12-15 or a
handful
3 segments.
II. PULSES
1. Redgram dhal
2, Elackgram dhal
III. GREEN LEAFY VEGETABLE
1. Amaranthus
IV. Roots and Tubers
Photato
V. OTHER VEGETABLES
Beans
VI. FRUIT
■ 30'
-
VII. Milk
200
4/5
-
VIII; Fats and oils
40
2/5
-
40
1/5
-
Orange
IX. Sugar 8. Jaggery
2
= 2 =
Table-II: Balanced “ let for an Adult Women (Moderate Worker)
(1]
_ 14)-” = - =
(2)
(3)
230
120
1
■ -4/5
45
25
-1/5
5 std. sp.
125
1-4/5
I, CEREAL
1. Rice
2. Wheat
II. PULSES
1. Rcdgram dhal
2. Blackgram dhal
III. GREEN LEAFY ’T’GrT/ ’JJE
Amaranth
3 bundles.
IV. ROOTS AND TUtERS
Potato
:
75
1/2
1
V. OTHER VEGETABLES - Beans
75
1/2
12-155or a
handful.
VI. FRUITS - Orange
30
-
3 segments
or a quarter
fruit.
VII. Milk
200
4/5
-
VIII. Fats and Oils
35
1/5
-
30
6 Std. sp. -
IX. Sugar and Jaggery
Table-Ill: Additional Al. .owance for Pregnancy and Lactation
I-actation
Pr.ignancy
Food Stuff
)
Ippx.Vol.
- .n std.cup.
50
1/5
Appx.Vol.
in std.cup
N0,
I. CEREALS:
Rice
Wheat
II. PULSES:
Redgram dhal
III. GREEN LEAFY
VEGETABLE
25
2/5
VI. Milk
V. Fats & Oils
125
i
40
60
1/5
2/5
20
2 std.sp.
3/4 bun-25
dies
- 125
15
2/5
3/4bundl-
1/2
4 std.sp.
4
= 3 =
Table - IV: Balanced Diet for a Child between the Age
3-6 years (Ref. - 6 year s qld child)
Food Stuff
Qty
(g)
Appx.Vol.in
std, cup
(1)
(2)
(3)
140
60
3/5
2/5
30
15
15
6 std. sp.
3 "
3 "
75
1-1/5 std.cup
No.’
I. CEREALS <
1. Rice )
2. Wheat -flour
-
II. PULSES
1. Redgram dhal
2. Blackgram dhal
3. Other grams
III. GREEN LFAFY VEGO ABLE:
Amaranth
1-i bundles
IV. ROOTS AID TUBERS
Potato
"
50
2/5
50
2/5 std.sp.
8-10 in no.
5 segments.
1 medium size
V. OTHER VEGETABLES
Beans'
VI. FRUITS
Orange
50
2/5- std.cup.
VII. Milk
250,
1
"
VIII. Fats and Oils
25
7
std.sp.
40
'8 std. sp.
IX. Sugar and Jaggery
plV'T^TIorS
HEALTH<NUTRITION AND AGRICULTURAL DEVELOPMENT
(an exploration focusing on Karnataka State)
This exploratory report, is the first step, towards the
initiation of a participator dialogue, between researchers
from various academic disciplines, health and development
action initiators, non-formal educators and others in
Karnataka state, on an area of increasing concern and
importance, with a view, to identify areas of interactive
and participator research, forcusing on agricultural workers
and rural communities.
(The report forms part of a larger, sabbatical assignment
undertaken by me at the London School of Hygiene and
Tropical Medicine from October 1986 to September 1987.
The assignment was an exploration of the relationships
between Health and Agricultural Development.
It included
a review of the health effects of Agricultural development
policies and the occupational health of Agricultural
workers.)
Ravi Narayan
Community
Health
Cell
Centre for Non-formal and continuing Education
Bangalore
(August 1987
)
HEALTH, NUTRITION AND AGRICULTURAL DEVELOPMENT
(an exploration focusing on Karnataka State
CONTENTS
Page
Introduction
Section I
1.
Karnataka State - a profile
2.
Agricultural Development in Karnataka - an overview
3.
The State of Food and Nutrition in Karnataka
4.
The Health Status in Karnataka - some indicators
Section II
5.
Drought - natural or man-made
6.
Kyasanur Forest Disease
7.
Irrigation and Malaria
8,
Japanese Encephalitis
9.
Handigodu Syndrome
10.
Endemic Genu Valgum
11.
Hazards of Sericulture
12.
Food toxins and contaminants
13.
The Eucalyptus Debate
14.
Tribal Health and Nutrition and the impact of
Development
15.
The environmental impact of Agroforestry
Section III
16.
Issues and research priorities
17.
A plan of Action
18.
A bibliography and resource list
)
11.
HAZARDS OF SERICULTURE
The sericulture agro-industry is a rapidly expanding, high priority
development programme which has seen a 300% increase in the context of land
being brought under mulberry cultivation in the last 30 years.
Mulberry
leaves are eaten by the caterpillar Bombyx mori to form its cocoon of
protein silk. The rearing and feeding of caterpillars, the supervision and
'sunning', important processes during cocoon, formation are family based
rural cottage industries spread throughout the rain fed and irrigated
Southern, interior Karnataka.
The cocoons are sold in special markets and the silk thread is removed in
special reeling and spinning units which are also rurally based but not
always home based.
The silk thread is then wove'n into silk of various grades with both
traditional hand looms and electrically operated power looms which are also
part of rural industry.
Studies undertaken by the Ross Unit of occupational health based at St.
Johns Medical College, Bangalore, in Mallur and neighbouring villages of
Kolar district established that many sericulture workers in both homes and
reeling units, who handle the silk cocoons, have skin and respiratory
ailments, an atopic/allergic reaction to certain antigenic products related
to the silk protein.
These were demonstrated in small pilot studies but
larger surveys are required to establish the extent of this problem and
magnitude or morbidity across the agro-industry.
The weaving units have been inadequately assessed from an occupational
health point of view but the noise levels are in the hazardous range and
noise induced deafness could well be a significant problem. The problem of
child labour is however a more important problem in this aspect of the
industry.
This is partly because of the fact that weaving is a family
based industry and all members of the family are inducted into service.
However with the increase of power looms the situation is rapidly changing
and workers other than family members need to be employed.
These
additional workers include children, often under very exploitative wage
conditions and school dropout rates are usually high in villages with
sericulture development especially weaving units. The health problems that
these child workers face during their work in noisy, crowded, poorly lit
loom sheds need immediate assessment.
With the rapid growth of sericulture, the magnitude of the above hazards
especially in terms of population at risk, will increase greatly in the
years to come.
A larger issue of importance will be the increasing
diversion of land, normally used for food and fodder, to an export oriented
cash crop, which could have serious repercussions for the community.
In
many areas where sericulture development has taken place, there is
additionally diversions of land for eucalyptus as well.
Together, this
diversion would mean decrease in local food grain production.
There is
already increasing evidence that this is taking place in some regions like
Kolar district in Karnataka and the long term health and nutrition
consequences are obvious.
31
N_g.TR I 7 1 0 N __ Z^c^-ccxl
JL
Milk: It is an ides’.1 food for infants and children and a good supplementary
food for adults. It is nearly a complete food existing in nature. It contains
all the nutrients.
Composition:
Protein
Fat
Lactose
Calories
Rich:
(hrs, per 100 gms
*
Cow1s milk'
Buffalo's milk
Human milk
3.2
4.1
4.4
67
4.3
8.8'
5.0
117
1.1
3.4
7.4
65
in calcium
Deficient:
1^. is deficient in iron and vitamin C
Daily rt-cuirement:
Adults
Children
Expectant mothers
10 oz or 284 gms (non—vegetarian
requirement - 20 oz or 568 gms)
20 oz
40 6z
Milk borne infections: from the animal - Bovine tuberculoses, (Brucellosis)
anthrax, achinomycosis, Q. Fever
from the human - typhoid, paratyphoid, dyssntries,
handler &
cholera, diphtheria, infective
environment
hepatitis.
Preventjon:
Pasteurization -if effectively done - phosphatase tost will be
Boiling
negative
Sice: Kain cereal consumed in south India, cheapest source of energy and
contributes 70-80% of calories. Main source of thiamine add nicotinic acid.
By virtue of its quantity it provides nearly 50% of protein requirements.
Proteins of rice is of better quality than wheat although the protein content
cf wheat is more-.
--Composition:
Gms, pe r 100 grs
Protein
Raw rice(mld)6.8
Parboiled-. .
rice Vmld)
6.4
mgm
mgm
CHO
Fat
Thiamine
Nicotinic
78.2
0.5
0.06
1.9
79.0
0.4
0..21
3.6
Parboiled rice is superior in nutritive value to raw rice as regards the
thiamine and nicotinic acid are concerned.
Daily requirements: 14.$zs or 400 gms Ir milled raw rice is being consumed,
it cm bo partially substituted by wheat, jowar or ragi. Thic improves <he
nutritive value of the diet (N.B. 100 gms or rice contains more pre reins than
in 100 gms of milk).
Wheat: Next to rice, wheat is the most important cereal
Daily requirements:
14 oz or 400 gms
Composition: (whole wheat)
Per 100 uns
iMMa
11-S
Fat
1.5 gms
CHO
71.2 gms
Thiamine
0.45mgms
Niacin
5.60mgms
Though it has protein to the extent of 11.8% it lacks in lysine» l| is a good
source of thiamine and niacin.
Millets: Jowar and Ragi : - Jowar is deficient in lysine and has an excess
of leucine. The consumption of jowar is occasionally found to be issociated
with pellagra.
?agi is a popular millet in South India. It is very rich in calcium, and is
a''ir source of iron, phosphorous and thiamine.
-2-
Vily requirements:
Ip combination with cereals daily requirement is 14 oz
or 400 gms.
Jowar
Ragi
Prdrin
gm
CHO
gm
10.4
7.3
72.6
72.0
Calcium
gm
25.0
344.0
Pulses: Pulses are next in importance to cereals as an article of diet in
India. The common pulses ased are red gram, green gram, bl..ck gram dhal, Bengal
gram, dry beans, and dried peas.
Pulses are rich in protein containing about 20-25 g of protein per' 100 gms. In
vegeterian diets, pulse1 are the main source of protein. Pulse ■ ar? good sour-ns
cf B group vitamins, especially thiamine and riboflavins. Sprouted pulses a?e
good sources of vitamin C.
Daily requirements:
3 oz or 85 gms
Proteins $
Bengal gram
Black gram
Reg gram
Green gram
17.1
24.0
22.3
24.0
Mgn t>er 100 gms
mgm
mgm
m<Tn
Ribofirvine
Thiamine
Niacin
0.3
0.42
0.45
0.47
0.15
0.37
0.19
0.39
2. 9
2.0
2. 9
2.1
iron
10.2
9.1
5.8
7.3
Groundnuts: Groundnuts or Peanuts are ex:tensively ,grown in Indi,a. It is
rich in fat, protein is equal to pulses. It is also rich in nico tinic acid.
thiamine and riboflavine.
Composition;
Per 100 gms
Protein
Fat
OHO
Thiamine
Riboflavine.
Nicotinic acid
Ic-ily requirements:
25.3$
40,1$
26,1$
0,9 mg®
O.'IS mgm
19/9 mgm
5
jj
j
jj
h
J
Groundnuts after
extraction of fat is a cheap
and rich source of proteins
1^ combination with pulses 3 oz
Green leafy vegetables: Eg. spinach, amaranth, fenu greek, cabbage are cheapest
protective foods. These are excellent source of carotene and vitamin C.
They are also good sources of calcium, iron, riboflavine and fo,ic acid. They
provide cellulose which acts as roughage. It plays an important role in persons
who go on diet to cut down calories.
Daily requirements:
4 oz or 114 gms.
Oil: Eg. groundnut oil, gingelly oil etc. vegetable fat. It is 100$ fat,
yields 900 calories per 100 gms. Contains no vitamin, contains more of
polyunsaturated fatty acids. Lowers the serum cholestrol.
Daily requirements:
2 oz or 57 gms
Ghee: Animal. Except for little moisture it nearly cent per cent fat. Yields
between 820 to 895 calories. Good source of vitamin A (200 i.u./lOO gms)
contains more of saturated fatty acid and hence tries to raise serum cholestrol.
Dail^ requirements:
In combination with other fa^,.like-oil 2 oz (n.B.
vegetable fats usually do not cont'i n vitamin A)
7anaepathi: Popular cooking media in our country. It is manufactured by
hydrogenation of vegetable oils. 0n hydrogenation saturated fatty acid content
increases.*
Gives about 7)0 i;u. of A and 150 i.u. of 'D' per 100 gms. It is
.00$ fat and yields 900 calories.
-:_lv requirement: In combination with other fats 2 oz.
’c added by manufacturers accordin." to gover-im-'.^t
-5■ & Jaggery: These are carbohydrate foods. Sugar is a pure ca fh-hyd
end contains no proteins, fats or minerals. 400 cal./lCO gm<
<.aggery: Is used in place of sugar. 383 cal./lOO gms. It is also rich
source of iron 11.4 mgm/100 g.
Daily requirement:
Sugar/and/or jaggery - 2 oz or 5'i < ac.
/feu: It is an important source of animal protein. It contains also the
nutrients except CHO.lt contains protein, "at, calciinr, all the vitamin
except C. It is a complete protein containing all essential amino acids.
Composition:
Protein
Fat
Minerals
K Cals
Dally requirement:
Hoot and tubers:
13.3P
13.3G‘’
1+3
1 egg (ly oz)
Generally used as vegetables.
Potatoes, tap'iooa, carrot, onion, raddish. These especially potatoes are
rich in CHO. Poor source of fac and protein. Good source of calcium and
phosphorous.
Carrot rich in carotene
Potatoes rich in vitamin C
Daily requirement:
3 ozs or 85 gms.
IIHtlWtl!
Assessment of Protein-energy Malnutrition (PEN)
a)
Biochemical tests
Changes in the body's composition in malnutrition are most readily
assessed in general terms by anthropometric techniques which measure the mass
of tissue in the body or arm etc. Many biochemical tests are indirect
measures of the processes which are in progress during the course of
developing malnutrition. Biochemical tests may therefore be more sensitive
to recent dietary experience and may revert rapidly towards normal when a
malnourished child has only just started to recover.
Tests can be categorised into measurements on i) blood and ii) urine.
Blood tests are not always acceptable in population studies but provide the
opportunity for other useful tests eg. Hb.
Blood tests
1.
Circulating proteins of liver origin
a) Albumin: insensitive but important when low
b)
c)
d)
e)
Transferrin: studied only in severe PEM
Lipoproteins: no more sensitive than albumin
Thyroxine binding pre-albumin: preliminary studies only
Pseudocholinesterase and other liver enzymes: insensitive
Liver-produced proteins are particularly sensitive to a fall in the
dietary protein intake but the concentration in the blood depends not just
on the rate of synthesis but also on the breakdown rate of each protein.
The breakdown rate of albumin adjusts as the synthesis rate falls thus
minimising the effect of the reduced intake of protein. Transferrin does
not show this phenomenon - nor probably does T.B.P.A. but little wprk on
this protein so far. Both proteins may prove more sensitive than albumin
which is often near normal in marasmus * Transferrin and T.B.P.A. show
greater falls than albumin in kwashiorkor but their levels have not been
reported in marasmus. Both tests are time consuming and expensive.
Lipoproteins behave rather like albumin: although both are rather insensitive
any fall is important. At albumin levels below 3-0 gm/100 ml a whole range
of other disorders of hormonal and amino acid concentration are evident and
reflect impaired hepatic function.
Albumin is the simplest and most useful blood test for PEM but is still
of no value_in_demonstrating the extent of growth failure or wasting jn
marasmic children.
2.
Indices of recent absorption: urea, cholesterol.
3. Amino acid levels a) valine reduced particularly in kwashiorkor
b) alanine low in starvation states eg. marasmus
but too variable. Tends to rise in protein
deficiency.
Non-essential amino acids
c) Ratio essential amino acids
. Low in
kwashiorkor, normal in marasmus. Ljkel^vo
change within 2-3 days of altering the diet.
- 2 -
Urinary tests
1. Creatinine excretion. Creatinine is spontaneously formed by the
cyclization of creatine phosphate (C.P.) present as a high-energy compound
in muscle. Creatinine is excreted unchanged in the trine, the rate reflecting
the mass of C.P. in the body. Since the concentration of C.P. is constant
in muscle, its exclusive site, the excretion rate of creatinine reflects
muscle mass. Creatinine excretion is, however, somewhat variable, and in field
studies accurate urine collections for long times are impracticable. Three
hour collections have been tried - coefficient of variation 25%; 24 hour
collections - 10% coefficient. Most meaningful method is to express the
creatinine in terms of the child's height in cm. since this will indicate
the amount of muscle that a child has for his size. Muscle mass in Kg =
creatinine excretion in mgm. » 50. Creatinine is theoretically one of the
best indices of malnutrition since it■ does reflect the pvtent of-muscle.
atrophy - a key featurfi—of-the whole spectrum of PEM from kwashiorkor to
marasmusCreatinine excretion is increased for a short time during stress
eg. trauma or infection.
2.
Urinary tests indicating recent dietary intake.
a) Total Urinary N
. x Urea N
bl —-----
,
.....
% falls on a low protein diet
> Urea N ms
*
mg creatinine1" suitable for single urine but limited usefulness..
d) Urinary SO^/creatinine: ? reflects intake of S-amino acids.
Limited usefulness;,
3.
a) Urinary Hydroxyproline 24 hr excretion: reflects the rate of
growth and related to the turnover of collagen. Increased
excretion in infection; not easy to measure.
b) Hydroxyproline index (OHPs x body wt)
creatinine
Disadvantage of two variables each of which may affect index.
Useful for single urine. Index age dependent and thought to
reflect growth.
Significance of biochemical values
Deficit
<2.8
At risk
2.8 - 3.5
Amino acid ratio
> 3.0
2.0 - 3.0
Acceptable
> 3.5
< 2.0
Other index
< 2
-
> 2
Urea N/creatinine
< 10
Serum albumin
> 10
Serum albumin is the most commonly used biochemical index but it reflects
the extent of liver synthesis which appears well maintained in starvation
states and the index.although simpler, is less sensitive than the T.B.P.A. and
transferrin blood concentrations. Urinary creatinine is the biochemical test
of choice for showing the extent of the nutritional deficit but it is impracti
cable to obtain an accurate estimate of muscle mass by this technique.
W.P.T. James,
February, 1973
Skinfolds
Anthropometric Assessment (Cont.)
Use Harpenden calipers. If other types of caliper are used
the standards for these calipers must be used as calipers with
different pressures and area of cross section at jaws give
different results.
The standard measurements are:
1. Biceps: over the mid-point of the muscle belly with the arm
resting supinated on the subject's thigh.
2. Triceps: over the mid-point of the muscle belly, mid-way between
the olecranon and the tip of the acromion, with the upper arm
hanging vertically (Edwards, Hammond, Healy, Tanner and Whitehouse,
1955 , Brit.J.Nutr. volume 9, p.133, 1955.)
3.
4.
Subscapular: just below the tip of the inferior angle of the
scapula, at an angle of about 45 to the vertical.
Suprailiac: just above the iliac crest in the mid-axillary line.
At these four sites, the skinfold is pinched up firmly between the
thumb and forefinger and pulled away slightly from the underlying
tissues before applying the calipers for the measurement.
If only a single measurement is taken, the triceps skinfold is
the most useful.
If several measurements are made an estimate of
total body fat can be made from the total of four skinfolds (Dumin
and Rahaman. Br.J.Nutr. 1967, vol.21, p.681).
The differences in fat percentages become progressively smaller
for each 5 cm. difference in skinfold as the skinfolds increase in
size.
Percentages of fat corresponding to the total value of
skinfolds at four sites (biceps, triceps, subscapular
and suprailiac)
Total
skinfold
(mm)
15
20
25
50
55
40
45
50
55
60
65
70
75
80
85
90
95
___ Fat
Men
5.5
9.0
11.5
13.5
15.5
17.0
I8.5
20.0
21.0
22.0
23.0
24.0
25.0
26.0
26.5
■ 27.5
28.0
(% body weight) ___________
Women
Boys
Girls
15.5
I8.5
21.0
23.0
24.5
26.0
27.5
29.0
30.0
31.0
52.5
55.5
54-0
55.0
36.0
56.5
9.0
12.5
15.5
17-5
19.5
21.5
23.0
24.O
25.5
26.5
27.5
28.5
29.5
—
-
12.5
16.0
19.0
2i^°MMUNJTy HEALTH CELL
(First Floo.-JSt. Marks Road
25.O BANGALORE-560 001
27.0
28.5
29.5
30.5
32.0
55-0
34.0
-
—
—
-
(Rounding off in the percentages of fat accounts for the differences
between adjoining values not being uniform^
The following measurements of triceps skinfold thickness are those
which can be considered as including the ran.'.e of "normal" values for
French-Canadian schoolchildren measured in 1970.
Lower limit
3rd percentile
6
7
8
9
10
11
12
13
14
15
16
Upper limit
97th percentile
Boys
Girls
Boys
Girls
5.6
5-5
5.4
5-3
5-3
5-A
5.5
5.6
5.5
5.3
5.1
6.4
6.1
6.3
6.5
6.7
6.8
6.9
7.0
7-3
7-9
8.5
12.6
11.9
12.9
14.5
16.4
18.0
19.0
19.8
19.8
19.0
18.0
15.0
16.0
17.5
19.5
21.0
21.5
22.0
22.J
22.8
23.3
23.8
Read from grapsh of Jenicek and Demirjan, Amer. 1I. Clin. Nutr,
1972, 25, 576.
L
Robson et al (Amer. J. Clin. Nutr. 1971, 24, 864) have found that
Black children in Dominica have much thinner triceps skinfolds than
London White schoolchildren although the std^fficapular measurements of the
two groups are the same. A racial difference in triceps skinfolds has
therefore been suggested and would certainly explain the very high
proportion of West Indian Black children with thin triceps values.
However, American Black and White children chow no differences in their
response in triceps or subscapular skinfolds to changes in weight, and
this suggests that the differences in West Indian children's subcutaneous
layer of fat may be determined by environmental rather tnan ethnic
factored
Differences in other skinfolds have been found e.g. subscapular
skin thickness is different in French-Canadian and London children but
the triceps measurements are approximately equal.
Changes in skinfold thickness have been observed over the years
e.g. secular changes in triceps measurements have been very marked in
Canadian children with an increase from 6 to 10mm average in boys'
values in the last 17 years. Nutritional factors rather than genetic
control therefore may be more important.
Most London and Canadian children are weaned early onto diets
containing very high quantities of protein and energy. This will produce
faster growth rates with an increased likelihood of childhood obesity.
Many young obese adults were obese in childhood and have an excessive
number of fat cells in their bodies. This excess, which is probably
determined in the first six to 24 months of life, "programmes" the body
for life-long obesity and perhaps an earlier death. Present values for
skinfold measurements although "normal" may not be "ideal", and we cannot
be certain of the significance of thin triceps skinfold measurements in
community surveys. Sequential changes in an individual's measurements
will be significant, however, and the finding of a low percentage of
body weight as fat means that a subject's energy reserves are limited.
W.P.T. James
VITAMIN AND MINERALS
Daily Requirement for an adult
Vitamin A
5000 I.U.
1. Xeropthalmia. Blindness
2. Decrease Resistance to UR VI
5. Inner Ear Deafness
4. Acne
Vitamin D
400 I.U.
1. Rickets in children
2. Osteomalacia in adults
Thiamine
1.5 mgms
1. Beri Beri
2. Neuritis
Riboflavine
1.5 mgms
. Angular Stomatitis
. Photoph
Glossitis
Nicotinic Acid
15 mgms
Cyanocobalamine
1 mcg.
Pathothemic Acid
5 mgms
Choline Parent substance
acetylcholine
and a constituent
of Lecithin
2 gms
Deposition of fat i.1 liver and
Haemorrhagic degen 'ration of
liver and kidney
Ascorbic acid
50 gms
1. Scurvy
2. Decrease resistance to infection
Pellcgara
Anaemia
1. Chick Pellagara
2, Hair growth
Anaemia
Folic acid
1.5 mgms.
Vitamin E & K
Not known
1. Vitamin E_- sterility in male
?, Vitamin K - Bypoprothromhinaemia
Ca.
1 gm.
1. Borne defects
2. Hair
5. Blood disease
Iron
15 mgms.
Anaemia
Fluoride, Ion
in water
1-2 ppm
Dental caries
‘
Essential Fatty acids nutritionally important and. necessary tor growth
They are Linoleic, Linolenic and Arachidonic acids. They cinnot be synthesised
in the body and have to be supplied in the diet. Linoleic- -nd Linoenic acid
are of veritable origin and present in cotton seed, groundnut and linsee o_ls
while Arachidonic acid is of fish and animal origin. E..F.A. regulate
cholesterol metabolism.
DAILY BALANCED DIET FOR AN ADULT
Gms
Cereals (rice chiefly milled)
Dhal (red gram)
Green vegetable (cabbage)
Potatoes
Cauliflower
Banana
Oils ft fats
Sugar (in tea, coffee & sweets)
Milk (cow)
Mutton
Egg
Agathi
<;ais
500 (540x~) 1020
5.55
100
2"
100
T
100
51
100
15C
150
45C
50
40C
100
6"
100
200 (194x2) 52£
85
50
45
50 ■
J1U
COMMUNITY ^^harksRoad
47n.(F
^
*
t
Floor) - 56o()O1
Food System and Society
b ft N G'A u °
Interface between the Socio-economic Status and the
Health and Nutritional Status of Women and pre-School
Children of the Rural and Urban Poor in Eastern India.
(Abstract)
Dr. B. Chattopadhyay, D.Litt.(Econ)
Consultant, UNRISD, Geneva.
I.
Introduction. This project sponsored by a number of U.N. Agencies such as
the UN Research Institute for Social Development, Geneva, UN University,
Tokyo, and the UNICEF, Nev/ Delhi, has grown out of a proposal before the UN
System, mooted after the World Food Conference, for a global study of famine
risk in the modern world.
It was felt that the study of famine
risk would be
too narrow because of various definitional problems of identyfying famine.
Famine Codes and Scarcity Manuals in different parts of Hie world use different
definitions.
Moreover, nothwithstanding the prevalence of the Famine Code in
India, the Bengal famine of 1943 was never declared to be a famine, although
perhaps three million people had died.
It was also felt that famine risk is
endemic in large parts of the Third V/orld because of the extreme vulnerability
of certain segments of the population, during certain seasons, almost every
year, to conditions of food shortage percipitated by lack of purchasing power
and employment.
It was felt that such vulnerability exposing segments of the
population to acute distress conditions even at the slightest fluctuation of
food production, caused by drought or flood, is a consequence of an essentially
multi-faceted structure of determination involving a large number of variables -
ecological, physiographic, socio-economic, technological and cultural.
It was
consequently felt that a System Approach in the proper sense of the term would
be the-best methodological standpoint for the analysis of food systems and
society in all their interaction.
Famine, or acute distress, would then
represent breakdown points of the system through which the system reproduces
itself.— the breakdown points acting more like safety valves.
II.The Components . Food System and Society is then considered to be a
generalised system like any other system.
sub-systems.
It would be composed of a set of
Notionally, w£ think of the main sub-systems of the general
system called "Food Systems and Society" envisaged in terms of information and
output flows and feed-backs.
The Sub-System, which is relatively stable
over the relevant time -span, is the Ecological and Physiographic’ Sub-System,
changes in which can be observed only over the relatively-long run.
The
Ecological and Physiographic Sub-System can be represented and measured, in
terms of parameters such as those relating to the.water regime(rain fall, sub
soil water, surface run off etc.), relief, forest-cover, basic soil properties
etc.
In some cases fluctuations, such as those in rainfall, can also be
parametrised whereby short run changes can be impounded into long run parameters
2
The Ecological - Physiographic Sub-System thus, represented by a set of
parameters, provide, so to speak, the stage for the inter-play of socio
economic forces including property relations, quality and quantity of the
labour force, technology and culture.
It is through the interaction of the
Ecological - Physiographic Sub-System and the Socio-economic Sub-System that
specified configurations of the food system arise.
The Socio-economic Sub-System can be represented by a whole range of
parameters such as pattern of land holdings, cropping pattern and intensities,
incidence of Scheduled Castes and Scheduled Tribes, incidence of landless
Agricultural labour, interaction with the Urban Metropolitan centres,
availability of controlled irrigation, technology, particularly agricultural
technology, etc.
A whole range of data is available to enable us to express
these parameters in terms of suitable magnitudes on different scales.
The
Physiographic - Ecological Sub-System provides a range of information inputs
into the Socio-economic Sub-System which digests these inputs generating a
structure of production and distribution of food with different social forces
exercising different degrees of control over access to food
.
*
It is possible,.
then, to think of methods of subsuming the entire range of variables -and
parameters in a Composite Index of Food Insecurity to which specified segments
of the population, such as, Scheduled Castes, and.Scheduled Tribes or landless
labourers, are exposed.
The net output of the interaction'of the first two
sub-systems is, then, this composite index of food insecurity, which in turn
becomes the information-input for the Nutritional and Health Sub-System.
It is
possible that the Ecological —Physiographic■ Sub-System also provides certain
direct information inputs of an epidemiological character to the Health and
Nutritional Sub-System.
For instance, data show that in eastern India
incidence of Gastro-Enteritis has a certain seasonal profile, which may be the
consequence of environmental hazards compounded with food insecurity.
The Nutritional and Health Sub-System can also be represented by a
range of parameters relating to Nutritional levels,'deficiency signs, morbidity
and mortality .profiles, access to Health Care delivery system of, particularly,
the segments who suffer from Food Insecurity etc.
factors
practices
There may be other associational
such as Health Culture and Health Habits, Community Habits and Taboos,
of pre-Natal and post-Natal care. etc.
The purpose of the project being reported here is to identify the
interaction among the three major sub-systems in terms of a.whole range of
parameters to arrive at a composite measure of the entire system of interactions
* For instance, .the interaction between the two.sub-systems is such im
Eastern India that tribals and semi-tribals have been driven to the
low-productive, arid plateau regions.
3
anong the variables, and, finally to arrive at a multifactor index of
vulnerability.
The idea is to use techniques of estimation of a Multi-Variate
System model methods of cluster analysis, factor analysis etc. to arrive at a
composite measure of vulnerability in regard to Food, Nutrition
and Health.
Such an index of vulnerability will, as far as can be envisaged at the present
state of our research, be in the nature of a Mahalanobis Distance measure in
multi-dimensional spa®..
It can provide important guidelines for resource
allocation between regions and communities, and a method of evaluation
&
monitoring.
III.
The Survey .
Ehe foregoing analytical scheme, largely quantitative in
nature, will be based on an extensive compilation of available secondary and
primary data from various agencies in Eastern India, Governmental ani otherwise.
It is expected that the Multi-Variate analytical techniques used in course of
arriving ax the composite Distance Measure will also tell us quite a bit about
the relative weights of the various components of the system represented by the
whole range of parameters,which we propose to estimate for each of the 46 districts
in the three states of Eastern India, West Bengal, Bihar and Orissa.
However,
since there is no a priori general theoretical framework in the revived body of
knowledge for identyfing the linkages among the variables and the sub systems,
it is proposed to identify some of the linkages by examining the situation at the
micro-level, in clusters of villages in a set of sample districts : four rural
districts and two urban areas in each of .the three, states of West Bengal, Bihar
and Orissa, including the Calcutta Metropolitan Development area.
These micro-
surveys are designed to capture.the linkages among the three sub systems for
specified communities, households and individuals, including women and pre-school
children.
The survey is purposive and is aimed at catching the typologies of
vulnerability under different Ecological and Demographic contexts in the three
states of Eastern India.
It may be possible to evolve certain norms specific to
given connuni.ties — norms which are not based on studies on communities in the
U.S.A, or such other Western countries.- The physiology ' of the tribal nan in,
say, Phulbani in Orissa is not likely to be the same as that of a Toxas peanut
farmer, for example.
The survey will also attempt diagnostic- studies of disease
profiles and access to health care delivery; it will not use any inputs such as
drugs, pills, special feeding pi-ogramneR etc. to elicit information from the
community.
Instead, an attempt will be made to report back to the community sone
of the more easily comprehensive findings through Audio-Visual techniques readily
understood by indigent segments of the inhabitants in the target areas, so that
the community gains a degree of understanding about its human predicament, and
may think of doing something at its own initiative to rectify the perceived
inadequacies.
IV.
The Team. Inevitably, the team is composed of a wide rarge of disciplines —
Medical Scientists, Statisticians, Economists, Geographers, Anthropologists,
Agricultural Scientists etc. At the moment we have a team of about 20 professionals
engaged in this work, supported by a number of computing hands and investigators.
Our main problem at the current phase of our research is the challenge of ihe
massive compilation and processing of the secondary data, and the challenge of
Rett~ing up the logisties of the survey which will begin in West Bengal and Orissa
by the middle of this year.
^■<S
/
C- l<-
C^
y^t^7tf.(_uCx7
^cbCc^l,
Ci-^dAa-YL'iu al
JZx^a/tLe
4>-^<
dLel'a^
<<?
Au?..-J /A
rx/uT
INTEGRATION OF A NUTRITION PROGRAMME WITH HEALTH AND
----AGRIOULTURE
*
--COMMuNHV
-
^-8.
w
c-tL
Vt i kS
"''•^HGAtOTE-MOOOtJolken
In the Indian Social Institute Training Centre
from which I come, we are trying to help fulltimers in rural development from South East Asian countries to
critically evaluate the work their organisation is doing. This
requires first a critical understanding-of their own society:
What is the prevailing concept of under-development and
development which is at the base of all development policies of
their government? This sort of approach has made us all increasingly
aware of the deeper causes which lay behind a process of change we
call ’development’, yet in reality is the development of certain
strata in society only. In an unjust distribution of development
gains we find the basic answer'to the questions Why can the masses
not be mobilised (blocking of motivation), why can the local
resources not be tapped?
Introduction:
1.
The issue of Justice
It is relevant to mention this in the introduction to our theme:
Integration of a Nutrition Programme with Health and Agriculture.
It is meaningful to link these three sectors together? but to be
so more fully, these have to be placed into the totality of social
reality of a country.. I am very much impressed that this Seminar
has been guided by a paper of high quality, indicating that those
developing countries which have brought about a radical transforma
tion of inegalitarian structures have been most successful in
meeting the basic needs of the people despite scarcity of resources.
Only in the context of this total transformation was it possible
to create a new system of Agriculture and a new health system. An
equitable distribution of increased food production and the
priorities of the health-care-system eliminated basically the
problem of malnutrition. The question is then raised: Where this
re-structuring of society has not occurred: "Is it the fate of
nutrition planners to be 1 patient revolutionaries1 biding his time
with pilot projects and marginal influence". For us in India this
question has a very realistic ring. What to say about the apparent
new commitment of Governments to Nutrition Programmes which
excludes however, the more decisive commitment to transforming
unjust and oppressive social structures responsible for the
constant widening gap between rich and poor? I’ll tell you
frankly my opinion: Within oppressive and unjust social structures
creative participation of the people can never be what it should.
The proof is the constantly increasing percentage of the people
who are forced to live below the subsistance level.
In such a situation what real hope can integration of nutrition
programmes with health and agriculture give? I believe the honest
answer is in the saying: Better light a candle than curse the
darkness. Symbolic islands can be created through this approach,
provided it is based on a philosophy of immense trust in the
...2/.
2
capacity of the people. Where this real love of the people
- animates nutrition^-programme-planners an approach which integrates
nutrition with health arid agriculture can make a great difference.
2.
Example of a comprehensive rural health programme
I wish to give this example because it constitutes quite a
sizeable island, covering a population of 40,000. It was
initiated in 1970 by a doctor couple (Dr. Arole) in Jamked,
Maharashtra, and covers about 30 villages. The project demonstrates
it seems to me how best the Chinese model of comprehensive
health-care can be implemented in a feudal society..
This comprehensive rural health project is guided by the three
basic concepts of a) participation of the community
b) delegation of responsibility to lesser
trained personnel
c) mobile health' teams
Under Five Clinics are central to the activities of the project..
as one of the goals of the project is to reduce mortality rate
of the under five by 50% within four years. Through these Clinics
supplimentary feeding is carried out in most villages. The
community takes the responsibility of providing fuel and utensils,
they do the actual cooking. The stress of health education and
the actual experience of improved health among the children has
motivated the community to work for better water supply, and to
set apart some land to grow food for this programme. The project
is collaborating with agencies involved in agricultural development.
But in comparison with another major project in this state, in
Kanakapura Taluka, where the thrust has been in agricultiral
extension for small farmers, more than on nutritional programmes,
the impact of increased agricultural production seemed to have
remained small. Care of minor illnesses, health and nutrition
education of the mothers, and immunisation programmes arranged by
the villagers themselves, are other activities of these under
Five Clinics. I do not think it necessary to give more details
about the various other goals and activities of this project.
Instead I wish to point out some of its characteristics which have
impressed me most and which are relevant for our purpose.
Emphasis on the educational aspect of the programme
Not only the mothers but the whole community is exposed to
continuous nutrition and health education. Not only the explanations
given by health workers, but also the actual results of a programme
in which many take an active part, achieve this result. I was
much impressed by the villager, who has been trained as health
educator, and wanders from village to village. He had a session
in the village I visited. In a dramatic way he explained his
charts to the villagers seated on the ground around him. Since
I knew the local language, I myself got fascinated by his way of
communicating, pointing out concrete examples of his reference among
the audience. I understood that the best communicators are
’found among the people themselves.
a)
3 -
b) The people are made to understand that food-supply from outside
was only meant as a starter. They would have to grow the food
required for feeding programmes. Some, members of the community
did get motivated to donate some of their land.
c) The nutrition programme being part of a comprehensive health
programme meeting the basic health needs of the people, supported
by locaH resources (primary health workers, collaborators and
material supplies),- has a very strong demonstration effect. As
child mortality declined, motivation for planning the family
became effective.
d) The educational impact of the programme is very much
strengthened by the central role of the local permanent workers
who are fully identified with the community. Much of the training
of other health and nutrition workers is also given locally. They
escape thus getting alienated from the people through a sophisticated
training in a city. Experience has shown that team-members trained
in city-conditions, tend to leave this rural areas soon agafcu
Evaluation; The Jamked project shows the possibility of creating
health through a comprehensive approach in which community teams,
inspired by dedicated animators (the Aroles) are able to bring to
life the participation of the village communities. The remarkable
success of the project and the spirit which animates it, has
encouraged many other groups in India to launch similar ventures..
Just now a new team of medical mission sisters is reaching out
into the area bordering on Jamked. Dr. at ole told the sisters:
"Do not imitate the Jamked project, you can do better; be creative."
Provided success does not blind the groups involved to the fact
that they are still up against formidable obstacles, rooted in the
unjust structures of ownership of land and concentration of
political power in the hands of a minority, they are doing a
highly meaningful service to the people. Though they have to work
within the constraints of the prevailing structures, reflected in
the caste-system, they are instrumental in expanding the educational
processes in a direction which will make people more critically
aware of the still deep rooted elements of a highly inegalitarian
society. It might be worthwhile to discuss whether or not such a
comprehensive approach can and should evolve further into genuine
conscientization leading ultimately to the emancipation of the
masses.
3.
Food for Work
I
had the, opportunity to listen -to your first reports on
programming concrete projects. In all of these food for work
had an important place.
What is surprising about food for work programmes is that
some lock.upon them as a curse, others as a great blessing. When
visiting in Maharashtra, a massive food for work project, I was
much impressed by hundreds of men and women constructing
percolation tanks that would greatly increase the agricultural
production. A few critical questions, however, brought out a
..4/-
- 4 -
a number of serious drawbacks of the programme. Nutrition
education was totally- absent; more serious: the land below the
percolation tanks belonged to the richer farmers of the villages.
And an accident of lorries with grain having been diverted to the
market of a nearby township, still further darkened the picture.
As I wish to elicite discussion, on what the conditions for a good
Food for Work Programme are, I cite another case. Over thousand
men and women have been involved in a programme which lasted
several years. It was greatly effective in increasing agricultural
production in the area. A network of channels were dug which
would bring the water from the main canal into the fields of the
farmers: fields were levelled and bunded. All excellent on
first inspection. But there were non-intended effects. The
earning capacity of the farmers was increased permanently through
the labour of this army of workers. These, however, after
completion of the project were back where they were initially:
in poverty, unemployment and helplessness. The inequality gap
between them and the farmers had been widened as a result of the
project. This case demonstrated how linking of Food for Work and
agricultural development needs a good deal of political wisdom to
be really contributing towards genuine development. The question
as to what impact such programmes have on the social structures of
society cannot be ignored. I am sure that many of you have been
connected with such projects which really improved the productive
capacity and the income of the beneficiaries themselves. I too,
know many such projects.
A friend of mine visited' recently some region of Andhra Pradesh.
On his return he wrote to me: "I was shocked to see how priests
and sisters have become corrupt in handling development projects.
He was not referring explicitly to Food for Work Projects. But
the problem is common to all development work. If our preoccupation
is only in terms of efficiency, of effective programming etc.,
there will be a missing link. Development programmes, however
well conceived, do not automatically bear fruits of justice,
integrity and responsibility. It is strage that so many organisa
tions which go under a spiritual name pay so little attention to
this. I am Including the organisation to which I belong. We
expose a host of people to responsible work, supply them with lots
of material inputs, and expect them to be good and honest without
helping them to discover motives to be so. Exposed to a host of
pressures it is not easy to swim against the stream, especially
with the increasing shortage of food-stuffs and constantly rising
prices. Food For Work programmes are to a high degree vulnerable
and expose the persons handling them to the pressures mentioned,
in an atmosphere of wide-spread corruption and of 'let me get up'
philosophy.
4.
The Educational Dimension
The linking of nutrition, health and agriculture has the advantage
that all three sectors demand primary emphasis on educational
processes if they have to build up new people with new ways of
...5/-
- 5 -
feeling, thinking and acting. You know much more about the nature
and methods of extension education related to these three sectors
than I do. But the best extension education can still miss the
ultimate worthwhile goal of building a community, a horizontal
solidarity, of helping a new spirit of collaboration and sharing
to be born. Mere achievement motivation which results from
successful experience in 'keeping my child health, producing more
on my fields' risks to be infected with striving for egoistic
social advance, which is the root-cause of underdevelopment
understood in depth. Everywhere we see that the same processes
which push up some, keep others down.
The following happened in North India
*
Under the guidance of a
priest the Santals had transformed a jungle area into fertile fields.
They had built, with Food For Work an earthen dam in a valley close
to their settlement. The monsoon broke in. Heavy rains poured
down incessantly. Suddenly in the ‘middle of the night shouts
resounded: "The dam is bursting", men and women ran out of their
houses in the direction of the dam. They worked the whole night,
filling bags with sand to strengthen the dam. The priest was with
them and all got wet to their skin. In the morning the dam still
stood. They had made it together. "During this night the community
was born"', commented the priest in narrating the story. How can
such community experiences become educational processes within
programmes of nutrition, health and agriculture? This seems to be a
critical question if our long-term goal is the creation of a new
society, in which dignity and equality and participation is deeply
experienced within human organisations and institutions. It is
my personal conviction that any organised intervention risks
unconsciously to serve the interests of those who have control
over societal institutions, unless it is clearly guided by long-term
goals of a more just and more human society. Every intervention,
however small it may be, affects the process of change in society.
It either is supporting a process leading to increasing-inequality,
or it belongs to the counter-forces inspired by counter-values,
and which do have a relevance for a change towards greater social
justice.
You may remember the .passage from Solzhenitsyn's novel 'The Inner
Circle1.,., about the sheep producing more wool because of being
better fed. In explicit terms it means: mere extension education,
however Important it is, not accompanied by 'political education'
gained by people organising themselves, establishing their own
institutions, e.g., for credit, marketing, etc.,(reflooting on the
causes of their having little say in policy formulation of
political bodies at various levels), risks to support the existing
power structure. Social workers are easily 'used' by politicians.
And the greatest illusion would be to think that Nutrition
Programmes are neutral, having no political consequences.
Politicians may be interested in Nutrition Programmes (nationally
and internationally) for "political reasons"., which in plain
language means: for the purpose of "feeding" rather than for the
purpose of emancipation and liberation, which really would serve
the interests of the people.
pu-y Lf.-
4
WHO Chronicle, 31: 143-149 (1977)
KEEPINS FOOv SAFE FROM
HARMFUL GERA'S
COMMUNITY HEALTH CELL
47/1,(FirstHoor)St. Marks Road
BANGALORE-560 001
The health of people depends to a large extent on the
fbod they eat. Keeping food safe from harmful germs
and their toxic products is therefore an important
problem, which over the years has engaged the
attention of various WHO expert committees concerned
with different aspects of food hygiene. The latest
report of the WHO Expert Committee on microbiological
aspects of food hygiene, which met in Geneva in March
1976 (with the participation of FAO), has recently
been published-1 and it describes the microbiological
agents of food-borne disease and the microbiological
hazards in relation to foods. The article below, which
is adapted from the secotr part of the report, describes
*
th
Microbiological hazard;
handling and storage.*
etc., as well a;
""
'elated to food processing,
>n movements, tourism,
•
*
t
Centre^ them.
Hazards related to food -'reparation
The largest proportion of food-borne disease is
probably caused not by commercially processed foods but
by food prepared at home, in institutions, or in food
catering establishments. Food-processing plants were
implicated in 6% of food-borne disease outbreaks in the
USA during the period 1968-73 and in nearly 25% of
outbreaks in Denmark during 1954-63. The commonest
causes of disease resulting from food prepared in
kitchens of private homes or institutions in the USA
arc unexpected contamination of the raw food material
and faulty preparationtochniques. One study of disease
outbreaks that could be attributed to food processing
plants suggested that most of the outbreaks were due to
contaminated raw materials (for products not given a
terminal heat process) and to faulty applications of
processing and packaging techniques.
2
Common faults in the handling and processing of
food in homes, restaurants, and other food catering
establishments, which led to disease outbreaks, are
given in Table 1. In some cases several faults were
found without the possibility of identifying the
importance of each one. Several outbreaks of food
poisoning, usually caused by salmonellae, were found
to he due to the transfer of organisms from conta
minated raw food to cooked food by hands, utensils,
and unclean surfaces.
Table-1. Factors contributing to 493 outbreaks of disease
caused by foods processed in homes or in food catering
establishments3
Factor
No. of outbreaks
Inadequate refrigeration
Food preparation far in advance of serving
Infected persons and poor personal hygiene
Inadequate cooking or heating
Food kept “warm" at a wrong temperature
Contaminated raw materials in uncooked foods
Inadequate reheating
Cross-contamination
Inadequate cleaning of equipment
Other conditions
336
156
151
140
114
34
66
53
52
160
° Adapted from BRYAN, F.L. Microbiological food hazards
today-based on epidemiological information. Food technology,
23(9): 52(1974)
Hazards related to storage
Hazards related to the storage of food are determined
by various combinations of factors-length of storage, type
of food, methods of processing and preservation, types and
relative proportions of organisms present, PH, water activity,
and temperature.
1 VW Technical Report Series, Nj.593, 1976 (Microbiological
aspects of food hygiene). Report of a VJl-10 Expert Committee
with the participation of FAO), 103 pages, Price; Sw. fr. 9.-.
3
3
Temperature control is of major importance in
reducing hazards from pathogenic bacteria, limiting spoilage,
and keeping food safe. In countries where refrigeration
facilities are available perishable foods should be stored
at temperatures that inhibit the growth of pathogenic bacteria,
e.,
i.
less than 4°C (or alternatively above 50°C). The law
temperatures must be achieved quickly after processing in
order to obtain the greatest benefit from refrigeration.
Slot; cooling may allow heat-injured spores to recover and
subsequently to grow before the temperature reaches an
inhibiting level.
At low temperatures, particularly under chilled
storage, changes may occur in food usually as a result of
the growth of psychrophilic bacteria such as Pseudomonas,
Achromobacter, Flavobacterium, and Alcaligenes and certain
yeasts and moulds.
Hazards related to food habits
Food habits vary from one country to another and even
within a country, but these habits are subject to change. In
countries where environmental sanitary conditions are poor,
gastroenteric diseases are one of the most important causes of
morbidity and mortality. Food and water are important channels of
transmission of these diseases.
The following factors tend to increase food-borne
diseases:
(1) Intensive production of livestock and the use
of contaminated feeds.
(2) Consumption of raw or undercooked meat or poultry.
This increases the risk of parasitic diseases and bacterial
infections and intoxications, e.g., salmonellosis, toxoplasmosis,
human linguatulosis, Taenia saginata and T. solium infestations,
and trichinosis. Even in countries where meet is thoroughly
inspected to prevent transmission, mild infections of carcases can
still be missed. The habit of cooking large cuts of meats into
which heat cannot adequately penetrate may sometimes be
responsible for these infections.
(3) Consumption of raw milk, either from choice or for
economic reasons.
4
4
(4) Consumption of raw or undercooked fish. Infections
due to Vibrio parahaemolytlcus, biphyllobothrium latum or
other cestodes, trematodes, and nematodes may result.
(5) Consumption of wild animal meat. Out-breaks of
trichinosis have occurred through consumption of wild boar
and bear meat.
(6) Improper home canning of foods. In the USA
the majority of outbreaks of botulism occur as a result of
home canning of vegetables end fruits where adequate processing
has not been carried out.
(7) Preparation of ready-to-eat foods in bulk and
mass feeding, where under certain conditions normal habits of
food hygiene are relaxed.
(3) Consumption of traditional food delicacies. Utijak,
an Eskimo delicacy prepared by' keeping seal flippers soaking
in oil until rotten, has been responsible for whole families
dying from botulism.
Hazards related to population movements end travel
With improvements in the speed and safety of travel,
more and more people now visit other countries; in the case
of "package” tours, organized to attract tourists, a considerable
number of people are exposed to Environmental hazards which
they would not experience in their own countries or homes.
Outbreaks of food-borne disease cue to Staphylococcus
aureus, Clostridium perfringens, salmonellae, V. parahaemolytlcus
cholera and non-cholera international air travel. Strict control
of food hygiene in flight kitchens, as well as on board aircraft
is essential.
JJumerous outbreaks of enteric infection have been recorded
on passenger ships; several of these have been reported on
cruise ships. Replenishment of ships’ water supplies during
a voyage has always presented a particular hazard since many
opportunities exist for contamination of water between ship
and shore. An additional hazard is cross contamination of
drinking-water with bilge or waste water. Several outbreaks
of V. parahaemolytlcus gastroenteritis were reported on cruise
ships sailing from ports in the USA in 1975. In one of these
outbreaks V. parahaemolytlcus serotype OgjK^ was isolated
5
5
from sick passengers and seafood cocktail was implicated. It
was thought that the food was contaminated vdth polluted sea
water. In another investigation of the incidence of gastroente
ritis on a passenger ship, Escherichia coli 027 was. the’
predominant organism isolated from patients with diarrhoea.
In addition to the specific hazards of well-known
enteric infections and. intoxications, travellers and holidaymakers are exposed to other infections usually classed as
"travellers’ diarrhoea"; such infections are of limited
duration. There is evidence that travellers’ diarrhoea is
associated with strains of enterotoxigenic E. coli new to the
individual and acquired through the medium of food and water.
Amoebiasis and giardiasis may also be involved in tourists'
gastroenteritis originating from food and water.
Owing to the influx of large numbers of people to sites
of pilgrimages and refugee camps, the threat of cholera and
other enteric diseases in these places is very real. Camping
and Caravan sites, fairs, and festivals can also present
hazards of food-borne disease outbreaks if the sanitary arrange
ments are not satisfactory.
Hazards related to imnortec foods
Large quantities of foods for human consumption and for
feeding animals are transported from one country, or from one
cart of the world, to another. The exporting country may have
no knowledge of the ways in which their products are used in
importing countries, and foods that are considered safe in the
country of originmay provoke disease in the importing country
as a consequence of different food habits. The importing
country, on the other hand, often has insufficient knowledge
about the production and processing of the food, and public
health authorities are concerned about the unknown risks. This
has led to the setting up of control systems or requests for
guarantees on wholesomeness, absence of pathogens, etc., which
information many exporting countries are generally unable to
give. Import control based only on sampling and testing of lots
is often ineffective and has not been able to prevent several
outbreaks of disease due to imported foods in various countries.
6
6
Eliminating harmful germs
Eifferent processing methods, e.g., heat treatment,
refrigeration; etc., arc available for combating food-borne
disease agents such as bacteria, parasites, and viruses.
The effects of such treatment on these agents or on toxins
produced by them are summarized below.
Effect of heat processing
(1) ton-spore-forming bacteria. Officially approved
heat treatment of moist foods for the purpose of eliminating
non-spore-forming bacteria, notably salmonellae, ranges from
3.5 minutes at 61.1°C for liquid whole egg to 1 second at
132.2®C or over for ultra-high temperature treatment of milk.
Foods with low water activity or high fat content require more
intense heat treatment than foods with high water activity or
low fat content. Such treatment can he expected to effectively
eliminate salmonellae, staphylococci, pathogenic streptococci,
brucellae, etc. Studies of the heat resistance of V. parahaemolyticus have shown that this organism is killed as easily as
other non-spore-forming bacteria,
(2) Spore-forming bacteria. The heat resistance of
spores of C,botulinum type A has been the basis for calculating
minimum heat processes for low-acid canned food for half a
century. Spores of C. botulinum types B and F may have a
heat resistance approaching that of type A; spores of most
type E strains are destroyed at temperatures below 1OO°C
and strains C and D barely survive heating to 100°C. 7he
spores of type G seem to be as resistant as types C and. D.
The heat resistance of C. perfringens type A spores may
approach that of C. botulinum type A, which means that they are
not killed by normal cooking (boiling) of food. The resistance
of spores of non-heemolytic strains is generally higher than
that of B»haemolytic strains. Heat-shocked C. perfringens
spores, when ingested, germinate in the intestine. Later
sporulation of these vegetative forms gives a greater yield
of snores and therefore more toxin.
(3) Parasites. Trichina and several other parasites
are killed by exposure to a temperature of 53°C and all
food-borne parasites seem to be destroyed by boiling (1OO°C)
for a short time.
7
(4) Viruses. Oncogenic viruses in ice-cream mixes
were effectively destroyed by Stannard pasteurization
(63.3°C for 30 minutes or 79.4°C for 25 seconds). Pasteurization
of liquid whole egg at 60°C for 3.5 minutes resulted in a
million-fold or tenthousand-folcl decrease in poliovirus and
echoviruses, respectively. Studies of survival of poliovirus
and Coxsackie viruses during broiling of hamburgers showed
that 4 minutes at u71°C and 76.7°C respectively were required
for 90% reduction. For complete destruction of some viruses
it may be necessary to boil the food.
(5) Microbial toxins, Most fungal toxins, including
the aflatoxins, are not destroyed by boiling or ® autoclaving.
Staphylococcal enterotoxins are also very heat-resistant; more
than 9 minutes at 121.1°C may be required for 90% destruc tion.
Foiling readily destroys botulinal toxins as well as C.perfringens
toxin, but the latter is never or only rarely present in foods.
(6) Microwave heating. Microwave heating of food has
become widespread in recent years. Frequencies of 915 or 1450
MHz are most often used. Microwaves generate heat in foods and
it has been suggested that their effect is solely due to the
generated heat. There are indications of additional modes of
action when vegetative cells are killed by microwave. However,
microwaves do not effectively kill spores at temperatures
below 100°C.
Effects of irradiation
Resistance of food-borne pathogens to ionizing radiation
might be a problem in irradidation preservation of foods. Low
doses of irradiation have been suggested as a means of prolonging
the shelf-life of food and eliminating radiation-sensitive
disease agents such as salmonellae. Large doses (4J3 x 10^ Qy
(gray) 4.8 megarad) or more) have been recommended for
sterilizing canned foods.
(1) Non-spore-forming bacteria. Irradiation of food
with doses of up to 1 x 10^ Gy(l megarad) will effectively
eliminate bacteria such as salmonellae, staphylococci, vibrio,
and others.
(2) Spores. Spores of C. botulinum are among the most
radiation-resistant microbial forms. The dose required to
-3
destroy 90% of spores is a little more than 3 x 10 Gy
(0.3 megarad) for the most resistant strains of types £ and b
and more than 6 x 103 Gy (0.6 megarad) for proteolytic type
F. In the USA, 4.8 x 104 Gy (4.8 megarad) has become the
accepted sterilizing dose for food.
a
(3) Parasites, viruses, toxins. Parasites are rather
sensitive to irradiation. Larvae of Trichlnella spiralis
may survive as much as 1 x 104 Gy (1 megarad) but 1 x 102 Gy
(0.01 megarad) suffices to sterilize the female larvae and
thus interrupt the infection cycle. Viruses are quite resistant
but it is believed that a sterilizing dose (4.8 x 104 Gy or
4.8 megarad) will inactive viruses naturally present in food.
Toxins in food cannot be inactivated by irradiation.
Refrigeration:
(1) rbn-spore—forming bacteria. The growth of
salmonellae is arrested at temperatures below 5.2°C and above
44—47®C. ’ he th er they will actually grow at these temperature
extremes depends on other factors; low pH or water activity
narrows the range of growth. Staphylococci can grow at
temperatures between 6.7°C. and 45.4°C and enterotoxin
production can occur at temperatures ranging from 10°C to 46°C.
The lowest reported temperature permitting growth of
V. parahaemolyticus is 3°C and the riiaximum 44°C.
(2) Spore-forming bacteria. While the growth of
proteolytic strains of C. botulinum is arrested at temperatures
below 10°C it has repeatedly been confirmed that non-proteolytic
E and F strains grow and produce toxins at temperatures down
to 3.3°C. The minimum growth temperature for C. perfringens is
6.5°C but growth is slowed down considerably at temperatures ’
below 20°C. No clostridia have been found to multiply at
temperatures, higher than 50°C. Bacillus cereus can multiply
in the temperature range 7-49°C. Pathogenic bacteria may
remain viable, hut without growth, for a long time in refrigera
ted foods.
(3) Parasites, viruses, toxins. These agents co not
multiply in foot’s but may remain active indefinitely at
refrigeration temperatures.
(4) Moulds. The majority of fungal toxins may be pro
duced in food kept at temperatures between 4°C and 40°C, but
fungi that produce alimentary toxic aleukia can grow and
produce toxin in the range of —2°C to - 10®C with an optimum
temperature for toxin production of 1,5-4°C.
9
Freezing
(1) Nbn-spore-forming bacteria. Freezing not only
results in arrest of growth but also in destruction of some
cells. However, like salmonellae and staphylococci,
V. parahaemolyticus shows better survival at low freezing
temperatures. At - 3O°C, they may survive for longer than
4 months.
(2) Spore-forming bacteria. While the vegetative cells
of bacilli and Clostridia are not much more resistant to
freezing than non-spore-forming organisms, their spores are
highly resistant.
(3) Parasites. Protozoa are generally destroyed by
freezing. Trichinella spiralis, Anisakis, and Toxoplasma
cysts Can be killed by exposure to freezing temperatures for
long enough periods of time. The same is true for intermediate
stages of Taenia ano' Diphyllobothrium latum in fish.
(4) Viruses, toxins, moulds.
very resistant to freezing.
These agents are generally
Water activity, nil, and other factors
Different types of microorganism have characteristic
ranges of growth with respect to the water activity in foods.
The latter is reduced by increasing the concentration of solutes
which can be accomplished by drying and/or the .addition of
agents such as sodium chloride, sucrose, glucose, glycerol,
and propylene glycol. The type of agent used influences the
response of microorganisms to variations in water activity.
Values that are inhibitory to the growth of microorganisms
do hot necessarily destroy them or viruses or toxins. However,
trichina and possibly other parasites die in heavily salted
foods. Minimum and optimum levels of water activity that favour
the growth of different bacteria and moulds may be found in the
report on which this article is based.
The effect of the acidity (or pH) of food on the
growth of different organisms, etc., may be summarized as
follows s
(1) bion-spore-forming bacteria. Staphylococci can
grow under aerobic conditions in food within the pH range
4.3-3,0 or higher, but enterotoxin production (with the possible
exception of type C enterotoxin) does not occur at pH values
below 4.5. The limiting acidity for anaerobic enterotoxin
production is pH 5.3,
10
Salmonellae can grow in the pH range 4.1-9.0 and V.parahaemolyticus in the range pH 4.3-11.0. Values below pH 4 are lethal to
most vegetative cells of pathogenic food-borne bacteria. The
lethal effect and the growth inhibitory effect depend on
temperature, pH, and on the acids used.
(?) Spore-forming bacteria. Growth of C. botulinum in
foods does not occur at pH values below 4.6. At this pH value
the growth of C. perfringens and B. cereus is also inhibited
although the- latter may grow slowly at pH 4.4. in certain
types of food, bacterial spores die out slowly in foods
with pH levels too low to permit growth.
(
(3) Parasites, viruses, toxins. Little or no information
seems to be available about the effect of acids on parasites
in foods. Some viruses are sensitive to acids but others are
very resistant. Most toxins are quite resistant.
(4) Moulds. Aflatoxins can be produced in grapefruit
juice (pH 3.3) and at even lower pH values in laboratory media.
The fungi neutralize (metabolize) the organic acids during
growth.
Fermentation, often combined with other means
(especially salt), is used for preserving many types of food.
The main preserving effect of fermentation is due to acid
production, but other compounds inhibitory to food-borne
pathogens may be formed by fermenting organisms. The growth
of pathogens may be inhibited through competition for essential
nutrients. The only effect of fermentation that can fairly
accurately be predicted is the one based on acidity; the other
effects are still not well understood.
Other factors in food processing or preservation,
e.g., oxidation/reduction potential or the presence of carbon
dioxide, exert small but important effects on pathogenic
organisms in foods. The widespread use of plastic materials
(with low oxygen permeability) for packaging has been discussed
ir recent years. Vacuum packaging prolongs-the shelf-life
of various products but does not offer protection against
growth of all food-borne pathogens.
11
Combined effect of nrcservation methods
The preserving effect of high and low temperatures, low
pH, low water activity, irradiation, and curing salts is increased
when these act together, as is very often the case in food
preservation. The combined effect may be additive or there
may be interaction producing a greater than additive total
effect. These combined effects are difficult to predict
quantitatively because of the complexity of the required
experiments. Even in the case of cured moats where the
combined effect of different treatments (each used at a
sutinhibitory level) is crucial, it is not possible to
predict accurately the minimum changes required to ensure
safety if any part of the treatment is reduced.
Influence of food habits
Microbiological hazards tend to he reduced by certain
food habits, such as:
(I) Pasteurization or boiling of milk. In many tropical
anc subtropical countries, milk is boiled before consumption, thus
reducing the risk of milk-borne disease. V.here pasteurization
can be enforced, the effectiveness of the treatment must be
carefully and continuously controlled. For small and fural
communities, vat pasteurization is recommended in the initial
stages. Modern methods of pasteurization (HTST, high temperature,
short time; and UHT, ultra-high temperature) should he used
in urban areas.
(2) Use of fermented milk. Fermented milk is a common
food, in certain parts of Asia and in central and southern Europe.
The concentration of lactic acid in fermented milks is
sufficiently high to kill or inhibit the growth of salmonellae,
shigellas, and other food-poisoning organisms.
(3) Prolonged cooking of foods. Except when a heat
stable toxin is present, food that is adequately cooked and
eaten while hot is safe. After cooking, prolonged storage with
out refrigeration must be avoided because heat-activated spores
of C. perfringens end B. cercus may germinate and multiply.
(4) Vegetarianism. As meat, meat products, fish,
and eggs are important media for food-poisoning organisms, the
omission of these products from diets diminishes the risk of
food-borne disease. However, the risk of infection with
shigellae, E. coli, parasites, and other intestinal pathos
"
*
originating from vegetable foods remains.
12
Importance of health education in foot; hygiene
Preventive measures in all countries should include
health education to discourage unhygienic food habits. Health
education should start in the schools. Adult education may
be provided in maternal ant4 child health centres and teacher
training colleges, as well as by mobile teams, radio and
television broadcasting, and other means of mass communication.
Travellers, particularly those going to countries
with a low standard of hygiene, should be given information
on the precautions to be taken. The inclusion of such
information in travel brochures and similar literature, as
is done by some travel agencies, should be standard practice;
this information could be combined with details about
vacination requirements. This matter is discussed with
special reference to air travel in the second edition of
Guide to hygiene and sanitation in aviation.
*
General measures for controlling food-borne microbiologi
cal hazards include the sanitary production of raw materials,
cleaning and disinfection of food processing plants, and
hygienic practices by personnel, especially when handling
food. These measures are described in most reference works
on food hygiene and in the Joint FAO/WHO Food Starr arcs
Programme code of practice in food hygiene, which is now under
revision.0
2BAILEY, J. Guide to hygiene and sanitation in aviation.
Second edition. Geneva, World Health Organization (in press).
3CO)?EX ALIMENTARBJS COMMISSION. Be commended international
code of practice: General principles of food hygine. Home,
FAO and WHO, 1969 (Ref. Nt>. CAC/RCP 1-1969).
LIO
COMMUNITY HEALTH CELL
47/1,(First Floor)St. Marks noad
BANGALORE - 560 001
^C’^criaa/
dj <UeA>t^Xz<:
/^n^ceb/c^o
7ct.Q^-i^-a.
ZSa/ar) Kch'c^>u>.
Kcj
C) W&Sffa T /pi-wk
l~G&y t'-Larv .
£'/?/~cLe/r>r<- cbx^>&^
SPapy Zczocca!
<— r^cri^KAr
Fa.cJ'cf-'S
X.
cxA <a)/
Z?e_
g
e) pr&t£~
C-)
*->xar-3
Z&_c
L>
z-Atrt&Zf
M\£^>C_
dj 7 cszxJL
7
^22^2^2^^
p^t^ct^ckI
hcxhi^.
• P»c^-P ^ohs-r-<X<^ ■
ecn')^
4.
/
hex^cXlc^^rr^cL:^o.\
-
T^Acn.-d
pLjp/keXAtX.
~j
I
/Pice.h'c Py>.
759-
oHK'6
rneaLt^
"“I
t-AJO-e^, <>^9
/
drife-cl'Pm
J
|
I
~~"‘
<a.//trux»,X ujtn'k
W xu)u>
•) /3<
7yph crj-<^,
■'['
c.e //no <_-
c h lita-nc,
polio,
eLvkruOnlie.ruh.
-naehicLV m , 6i'e<>'cL< c,z
/ H
13 —
&fa<.phy /er.
Z^/Xy
Mj. fk
Gen. Pre
&Cl
Yc.or>r~> L-
/~excHjr.S
^d^L.i-,~>c^r>L-j, hdle i.
Odankih',
LUcifer Supply
<sd)
S an' /aA
d C~r> ^e>-L>i&ny).
Koxh.
I
/A>-
ts£x<? c t-ixn> e»«
penK&m>
C- C-C-r^iJv? —
iy.
5.
6 .
d—1A k&^-> <-> Ag.
&
t^'fofes-i
&
/P/ooHer-j.
blctt),
Will)
X>iJ
CcZ>HecHCTn
ix-^^-^Acz^f !l)-,
'Dcbfy^cd
hy
C^^)cfLe.nz^ze cf
ex') UOC+t'&^cMa-rz,
^ )
C<^>-^-)
)>-C'&t f^r^ce^) !e
a) /?~nfe
Pcr>r,
^->i-iz7Ci/£ di
—
! ><■■)
YeA
s>7
^~i£--.->h j u^~> cStejXjrrTJ2
'J
lt\
><2
cl%>
/'tJ'-lkri^'i
to
— So
ZCx/laX2
r>^
Lxji-uzr-)
">')
be
fb?
L^eck
tzbeo t>z_ecA-
/Tlvua ■^^i'Z-n^)^
Co”
■p rcjcC.K'CiL^
C-l^>dru^
IY) y
i^lojny
^DC^e-^y
AcXy^.
C-CTL^-j br-i_eo
h>y fb&d-
b<2-
(ZCcnOYnJ ccJly ^<Z.o^o i lets,
/heJf cirC.
^~S-
bvzXLXc^bl''
CXt^Ll^^e.
bo
)~S<^Lo]Cf-M<-TO
M e^-
Ao
,^g
prc-^>
^y>a->e
•gpi'CJ^,
.faKcr” .
‘
^C-iccr> e
•v'Co-PcjC^ , hcrr-LJ^J/'■>cy?5
lc a'b o / x ^yO c>71 ^s-
jyrefjpcry Krc>~>^> J
~LL
/3
c>^
207’cl
^{yjhj-uicrx^,
r^i Le^
~>-
S oi Ii'
C^e 4 <r>^
<^<kII.
cs-ne p-rd-vk> > ^C(f
^SerJ) . y' poh^c-^n
e bo Sp^c^e^
,,
O)<>Ki<rr,
Me/)t
hiy&iE^E
PR£ - A&0 TTolfl
l-i-eoJtL'
/--
£) dg
Cot> k-£n q
/yz^£s^r
C(_ k
O
eruYb -rC-c>- ko
(jQ 6 Z-3
/?-
Vl^cJ -r
/Zt ^AeZ^g/ c</
^rrfe-eKcrt^o
r'&oj'
fajz.fycJ'lf'ca,
P'rc>)'cr&CSCjJ
DtftJx>yIlc^o/hv°>CL<3uo
Z3-
/So/^A
CJfeyOAy/crz SZCjOl. /
Z>-
C>L^.I'Jo7~&C^i<-
>d
rf
ckjZ'I'eelfeck
e>A
cj^3
/exA? •
ep<exx>i
Cr-> -^-e^> K" cj cJ^cnrf)
; ^-err) i c> !e^t 'Co-!
t>7 yex?/z^-Ct/^rz7-S
v'o/vCci.
iij
C^^cenc-.ci^^ceifeei erf Ci
■
^/^^eu'^r'c
O'
>1
$
I
(
£
0
(A
^3' P
0 D^f^;
F)^!S
..
.
ic^
-
&vnc^to'’C^<*
-
c
c
cL^i^
2
footnotes co the Table on Daily Allowances of Nutrirnnma
for Indans (i.e. fable I)
1.
-
Calories:
■
./
(a); Calorie -allowance .Jfor. heavy’'worm does'noc ;include worn Sunder.
special ‘conditions like Tiigli al Ci-cade-r. - ■
2.
Proieins:,
(a)
\
J
:
Adult hllowande .corresponds co- igm/kg; of diecary protein-of •
- N . p •U.. S3 •
'
.
-.
; ■ i
(b)
Inf an t: allowance during"Or-S months is' in terms of ,milk! pro teins
Luring 7-12' indn-tns
part,' of prqcein in cake will be in; cne' fork
of milk-, and s.-uppieinehcar J. feeding will' be derived from veratable.
proteins. i‘ocal
dail
*
’y protein allowance is calculated from cne
ideal weight. Protein allowances daring infancy will be:•'■0 -- 3mori‘ths . _ ,
3-6 months
'
-6 - 3 months
9 - 12 months
'
1
- <
2.3 gm./Ag.
1.3. gm/ig,:
1
8
*
gm./kg.
1.5 gm./kg.
.?
: ....
x. ••.....
•-
(c)
Allowances for children and .ad descents have beencompuced
using body-weights as.-obtained in the we 11-nourished ' groups and..---—
assuming N'.P.U. of 50 for' the' dietary proteins..-
3.
. l;.
Calcium'-:
rd. the absence of precise informa tion on calcium requirement '
of different Ofoups-,,-aTange-of ^llovhnce has'lfeen suggested.
(a) Calcium- allowance;-fern,,-infopts Q-r6 months will be for-—-.
artificially fed infants. Calcium intake f ronf breds t.milk wll-lyi:.“howevjr,, satisfy die needs of breas c-fed infants up co 6 month's .--, a
4.
Iron:-.
-
i.
-,...
<.
(a), xhis.-allipwa&ce-. of 30 mg. iron is for adult woman during her
premenopausal period', 'For ihe pos t-menopausal, woman, iron .allowance
is cne same as for mani,
’■
,-./7
,< G' tJ.-\
.
(b)
ihis allowance-for. pregnant woman will/be throughout,
pregnancy.
'• • •
'7'\ .... .',
/"
j '<• • . "
(c)
This allowance ’is. fb'r j$(c eating woman who is not menstrua t-f
ing. If a woman is -lactating and'; also menstruating, her iron al-low-;'
ance will be 35mg./day.‘ ' '
;(
.
■ ■■
5.
Vitamin a;
uietary allowance for' vi<Eamin a is'-given in term's o'f 'recinol (Vitamin
alcohol) ana B-carotene.- Dither ;p.f .those is used,
detenuing upon the dietary’source of vitamin,. . -.The .factor tb be ifs'-ed
co convert B-carotene -to retinol-.fs:
...
ug. of B-Cam-tene
“
“
-
0.25 ug. .of retinol;--
-
-.
_
■<
G'-
f'A
" " - • ■ - - - - f ._..."3;--_
- ----- . —
1
*' '
. ...
........ --................................ * ...
.e.
....._..oq; <j.•-.v< r t ■”( f
-t.-e- .’?£&?■.-£+•
’
.. .
■_ "J •'
• diet con tains, ^both Vitamin a.ana B-carotene, its content .
Da. eceses s ed-as retinol,--using cae following formulae;. •
1) Retinol content 'ng. + 'u6. retinol + ug. B-carotene x 0.25
.If the retinol-and
carotene content of foods are given as •
ug. in the food compos’ition tables.
ii)
Retinol content (ug:.) + vitamin a(I.CJ) x 0.3 + B-carotene (IU)
x 0.15 if the vitamin a and"’carotene values, are given' in terms of . ’
internatio'nal; units.
i
; -g.
6,7,8. . fhiamine, Riboflavin and Nicotinic acid:
;-
fhe daily allowances of these three vitamins are related co
calorie intake.
the., basic--allowances p;er 1000;.Calories- are:
nn;..."?.:
fhiamine %~0.5mg., Riboflavin + 0.55 mg.1 and Niacin + 6.6mg.>~li~
.niacin^e;,ui'yalents.__________ 2_______ ___ ______ _..1'2_. 2?
-.--Niacin allowance includes. contribution from dietary tryptophan,
60 mgs tryptophan being eqaalh-.co 1 mg
*
of-niacin.-L-Niacin equivalents in a diet
*
are computed as" follows:'
Niacin equivalents (mg.) + Niacin conteht■(mg;) + fryptophan
concent Crng.)
„> u
.. -
O.-kol-ic-Acid:-
_ _ _ _ . _ J _ _ _ _
_ ... 2 ...
..'“a - ..
_ - ..
I>.ietary:allowance of folic acid will be in terms of free folic
ac-id-<b-.casei-.ac.ti..vi.cy) ..preSi3nt_ln_fQods. ... . ...... .
<■ (.a) Folic'acid. requirement appe_rb ..to be_.cdhsid.era.bly increased
during. pregn_nc/- 3 ince “the. exact requirement is not known, a range .
rather^tahn. a single figure, ^ias been-suggestdd• for the^daily allowance
o f-felic- me id daring- pregnane y.^ t _ - .... ....
(b). Vitamin B12;
Vitamin:B12 is.tderi-yed entirely .from foods-of anifeial origin.
11. Vi-camJnD:-d -.
<-T ’ ' ’gY
-a.'j.j -.-z. ■. v a
S-ince.the exact requirement of Vitamin ^.--^s not known, ah
.
•arbitrary allpwanie^ of 200 l.U/day is-.made.. ijM allowance is in
addition to .(some-amount of Vitamin D -._£Kat might be derived fr expos'lre to.’^-unlight.
>•
■•V. , '
■' >....
.. . . -i
12. Fat:
.- --
:2
Since-, human requirement, of .fat is not ^now^, no
allowance-, is recQmme.nded... * ,dQSitabfe .range for. fut in the diet is.
howev-r, indicated, biot should contain 7&t leas l.15 gm. xatderiy
alls 11ko seasama,
get
also desirable that calories aerivta.from fat in tha daily diet
should'’not exceed 30$ of total calories.,- '
- ■
:
4
-
1
-
Ta B. L E 2 .
. ■
Balanced Diets for-'Adult Man. ■
Cereals
Pulses
Green leafy
Vegetables.
Other vegetables
Sedentary work
. ■ Modera te work .
Heavy work
Vege Non-veg
tarian tar ian
(gm)
(gm)
Vege- Non-vege"
. tarian tar ian. .
(gm) '
(gm)
Vege- Non-vegetar ian tar ian
(gm)
(gm)
400 ..
70
400
..
55 -
.475
&)
475
35 ■ ■ •
.650
.65 .
' ' 650
80
!• 1. .:i ' ’ '!
’"'100
100
125' 125.;.
125
125
75
■■ -.1C0 ' ipo
75 ..
75.. -75
' ,.:75.'-. 1
■ -Boots ana '■'tubers
*
100"
75
ioo 100
loo
Bruits
30 +
,30..
30,
'-30" ' 30 "
30
Milk- ■
100
200
200
100
. -200- , 1°°
Bats andj.pils..
- -35- - "40 ..
40'
40 •
30'
‘ '50 ‘
3°
:
H 30 ’
Meat and fish
30.
/.’SOI
, 1 .^oS
*
:
1 30 . . - a- -- ■ ‘ 30 ■ ■ u.
40 '
S ugat' and j_ggery
30
30
■ 40
■ 'Pp. : .P5
bi,... iiiviz
’ 50
*
Groundnuts
*
50
; 31 0"
ji*”' -An additional 30 gin. of fats ana oils caii,Jbe.‘ -included in
the diet in .plape: ofxgroundnutsi
.. ..
* *
.-.
® * MX
fl *
'--•
*
<•
K .r .
TABLE 3. .
...tr Balanced,,P ie.ts ;f or-Adalt-.Wpmaii-i'
'
• "-"Br'o'don tary workMederap_e ..work -.-Hea'tfyswork lidil. aIIowy
' '
■ ( •.. ■
........ '' ":anc'e during
r.-.
"
;
.;..
Vege- Non-veg- Vege- NonVege- Nop- Pregv, Lactatarian etarian, tarian Vege- tarian Ve-gv- handy tion,'
tarian
tarian
(gm)
(gm) , ,jyl^m)--.,..(gm) - ’ -(-gm)- - (gm)1 ~ <gn) (gm)
-------- -----
-
-
-
”1 -
r .“
7 <-•_
-
—
—
-
Cereals.
300
■300 ..
350 - . 36Q
475 ". - 475- . -50 . 100
- • *•- -■ 10
Paises: .i. . ........ ■iegQU 0-.. 45. 7.' ' -70 '' . 55.
.70
' - 55- - '...\125;<
Gr;e.en leafy-- -125
.1125
..-■ 125-• . 25 ; • /25
;125..
'..125?
Vegetables.'" , .
...
' 75
' 100
other vegetables
75
7-5
100
Roots & tubers. * 50
50
75
10.0..
75
--100
30
Bruits
30
30
30
30
30
Milk
..20pi-. 7 100- J -.: 200
■ 200 .
. 100
■ -loon- 125'
125
E-ts. ana- -oils :;1-'-• 30 - " • " 35 - A 35- •■ - - 40
40
45
15'
; .30
Sugar de Jaggery
30
30
- 30
40
■40 - 1..'1Q: • ■ 20
—
.J • —
30
Meat & fish
30
30
•Ci £S
1.
•- 30;
. aO'
. : ..30 .! :
U. ..
.
\: .40
-..
*
. ■ ■ 40
*
Groundnuts;-;../.
: ?.i v '-x
.-1 -... -• ■ wi —'
- - -■ —:s --- .
-*----• - - ----- yC.-. r r
------■
- -r- ■—vv '-TT
-■i “-“
au-1 additional 25 gm. of f^ts and oils Ccn b-, included-in the
diet in place of groundnuts,
■
Ta B LE 4.
Balanced Diets for Children
Pre-school children
1-3 years
4-6 years
"School children
150
50
150
40
200
60
200
50
250
70
250
60
320
70
320
60
50
30
50
30
75
50
75
50
75
50
75
50
100
75
100
75
50
300
20 ,
-
50
200
20
50
250
25
-
50
200
50
250
30
50
200
30
30
50
250
35
50
200
35
30
30
30 .
40
40
50
50
50
50
7-9 years
10-12yrs
VegeNonVege NonVege Non^ege- Nontarian.’ vege- tarian vege- tarian,.veoe- tarianvegetarian.
tarian.
tarian •
tarian
(gm)
(gm)
(gm)
(gm)
(gm)
(gm) (gm) (gm)
Cereals
Pulses
Green leafy vege
tables .
Other vegetables J
.Roots and tubers!
Fruits
Milk
F_ts and oils
Meat & fish I
Bggs.
I
Sugar & Jaggery
3°
.
30
TABLE__ 5.
Balanced Diets for "doles cent Boys & Girls
Girls
Boys
16-18 years .
13-15 years
13-18 years
Vege . Non-Vege Vege Non-Vege'- Vege Non-vegetarian tarian
tarian tarian.
tarian tarian
(gm)
(gm)
(gm)
J gm)
(gm)
(gm)
. 430
oereals.
70
Pulses
Green leafy vegeta'- 100
bles.
75
Other vegetables
430
50
1Q0
75
75
30
250
35
30
-
75
30
150
4Q
30
30
30
-
Roots & tubers
Fruits ■
■Milk
Fats &. Oils
Meat and fish
Eggs
Sugar & Jaggery
Groundnuts.
450
50
100
350
70
150
350
SO
150
75
75
.75
75
100
30
250
45
’’’
40
*
50
100
30
150
50
30
30
40
*
50
75
30
250
35
75
30
150
40
30
30
30
450
70
100
30
-
* An additional 30 gm of fats and oils can be included in the diet
in place of groundnuts.
rv\jT tf i;
C0MtA'j:J'V/ \'stw8tksfiOad
nutrition
Nutrition is a dynamic process in which food is consumed and
utilised for growth and repair of the body.
Growth implies increases in physical measures.
Development implies increase of intellectual and emotional
faculties.
Adequate nutrition which is vital for attaining optimum health
is ensured by providing every individual with a balanced diet.
This diet
contains proteins, fats, carbohydrates, minerals, vitamins and water in
proportionate amounts to provide adequate energy for growth and repair of
tissues.
Proteins (derived from the Greek work "protos" meaning to
come first), are complex organic nitrogenous substances containing carbon,
hydrogen, oxygen, nitrogen and sulphur in varying amounts. Some proteins
also contain phosphorus and iron, and occasionally other
elements.
Protein rich foods are milk, meat, fish and eggs from animal sources and
pulses, nuts and beans from vegetable sources.
The recommended daily allowance for the Indian adult is one
gram per kg. of body weight.
This is increased in infancy, adolescence,
pregnancy and lactation.
Lack of protein and vitamin A can cause serious and permanent
defects in children especially.
These range from impaired mental develop
ment and blindness to death.
■ The reasons for lack of protein in the Indian diet are numerous:
1.
Lack of knowledge of the importance of proteins
2,
Lack of utilisation of locally available proteins
3.
Dietary restrictions
4.
Superstitions and some traditionally harmful customs.
(For example - In some rural areas pregnant women
do not eat green leafy vegetables or drink milk).
5.
Poverty
It was estimated that 10 - 15$ of the people in the world,
or roughly 20$ of the people in the developing countries, did not meet
their energy needs during the decade 1950 - I960, (they were undernourished).
The study was extended to estimate the incidence of protein deficiency as
data became available; this estimate was placed at between 25 and 33$
(Sukhatme 1966).
What has since become clear is that protein deficiency is for
the most part the indirect result of inadequate energy intake.
In other
. .2
2
words, what diets lack is energy foods to avoid the body katabolizing
the protein people do eat.
(Gopalan 1968).
This finding is the opposite
of what has been reported in various studies of the subject, notably the
study on Protein Gap by the U.N. Committee on Application of Science and
Technology to Development (u.N. .1968) which has formed the basis for
international action.
The finding
that protein deficiency is indirectly caused by
low calorie intake is gradually being confirmed by a number of workers
and is also reflected in the recent writings of F.A.O. (1971).
Based on F.A.O. and W.H.O. Studies (1957 to 1965) and the
recommendation of the I.C.M.R. (1968).
Recommended
Levels of Nutrient
Intake for the Pre-Social
Child and Adult in India (Approximations only):
% Prot./Cal
Concentration
% Protein/
Cal Concentration
when NPU relative
to Eggs is 67
Age
Calories
Protein as
Egg in G
*
1-3 years
1,000
12.0
4.8
7.2
Adult Male
2,700
33.0
4.8
7.2
* Defined as average + 20%
Current evidence shows that if a diet has 5% of its calories from
good quality protein, such as in egg or milk, the individual's needs for
protein will be met regardless of whether he is a pre-school child or an
adult man, provided he eats enough to meet his' energy needs.
TABLE
IV
Distribution of households surveyed in India (Maharashtra
State) 1958 by calorie supplies per day per reference man.
CALORIES/per day/per reference man
Upto.1,300
% Frequency
6.8
1,300 - 1,700
9.7
1,700 - 2,100
14.7
2,100 - 2,500
16.3
2,500 - 2,900
16.6
2,900 - 3,300
12.9
3,300 - 5,700
9.0
3,700 - 4,100
5..5
4,100 - 4,500
3.5
4,500 - and over
5.0
100
by National Sample Survey 862 households.
..3
3
"Since malnutrition (or the lack of a balanced, diet) is the
outcome of several factors - social,' economic, cultural and psychological
the problem can be solved only by taking action simultaneously at various
levels - individual family, community, national and international levels.
Other measures to ensure people adequate nutrition are:
1)
Increasing food production
2)
Price control
3)
Prevention of food adulteration
4)
Fortification and enrichment of foods
5)
Food aditives
6)
Inventing cheap supplementary foods (e.g. High Protein Foods)
7)
Irradiated Food
8)
Nutrition education, and
9)
Population control
The Government of India is attempting to solve the problem of
malnutrition by implementing the following programmes on a national scale:1)
Applied Nutrition Programme
2)
School, Mid-day, Meal Programme
3)
National Government Control Programme
4)
Crash Programmes in Nutrition (For 0-3 years)
5)
Vitamin'A supplement to facilitate growth and prevent
blindness.
Studies from the United States and the developing countries
reveal the not surprising fact that as family size increases,
spending for food goes down.
per capita
As a result, corresponding diet inadequacies
and nutritional deficits are common.
FOOD CONSUMPTION PATTERNS BY STUDIES OF F.A.O.
Major Parts of India
Rice, Millets and other Cereals
Moderately High
Pulses, Fats and Oils
Moderate
Milk
Low
Meat, Fish and Eggs
Very Low
India (Punjab) and Pakistan
Wheat, Rice
. High
Milk and Pulses
Moderate
Meat, Fish and Eggs.
Low
Cereals constitute upto 80% Calorie Supplies
and upto 70% Protein Supplies
Pulses constitute upto 10% Calorie Supplies
and upto 20% Protein Supplies
Food of Animal Origin constitute upto' 4% Calorie Supplies
Meat, Fish and Milk - 10% Proteins
4
Malnutrition, especially protein calorie malnutrition, is
widespread and is to be feared not only because of its general debilitating
effect but especially because of the irreversible brain damage that
inadequate proteins cause.
Lata from 24 countries indicate that the
prevalence of severe PCM (Protein Calorie Malnutrition) ranges from
0.5$ to 5$ and the prevalence of moderate PCM from 4$ to 43$.
"The human brain reaches-. 90$ of its normal structural develop
ment in the first four years of life.
We now know that during the
critical period of growth, the brain is highly vulnerable to nutritional
deficiences, deficiencies that can cause as much as 25$ impairment of
normal mental ability.
Even a deterioration of 10$ in the diet is
sufficient to cause a serious handicap to productive life.
irreversible brain damage.
This is
What is particularly tragic in all of this is,
that when such mentally deprived children reach adulthood, they are
likely to repeat the whole depressing sequence in their own families.
They perpetuate mental deficiency, not through genetic inheritance, but
simply because as parents they are ill-equipped mentally to understand
and hence to avoid the very nu ritional deprivation in their own children
that they themselves suffered.
In low income countries the high mortality rates among children
in large families and in families with close birth intervals, are in
part due to malnutrition.
The greater the sibling number, the greater
the likelihood of malnutrition among poor families.
Studies of pre
school children in Colombia, for example show that 52$ of the children
in families in which there were -five or more pre-school children were
seriously malnourished, whereas only 34$ of children in families with
only one pre-school child were malnourished.
In Thailand, of the children whose next youngest sibling was
born within 24 months 70$ were malnourished; of those in families
without a younger sibling, only 37$.
Height and weight being affected directly by nutrition showed
variation in children according to family size. Even in high income
countries the children of the poorer families are larger'at any given
age when the number of children in the family is small.
For example,
of 2,169 London day-school students, 11.25 years old, children from
one child families were about 3$ taller and 17 - 18$ heavier than children
from families with five or more children.
The difference in physical growth between children of small
and large families in Great Britain seems to affect mainly the poorer
social classes.
In the higher income classes boys in families with
3 or more children are taller at all ages than boys in small families;
the reverse is true for girls.. In the upper and lower manual working
..5
5
classes children in small families average 3-4$ taller than those in large
families at 7 and 11 years of age and 114 to 2.8$ taller at 15 years.
Diet surveys carried out in India have shown that the average
Indian diet is ill-balanced with an excess of Carbohydrates and very little
protective foods like milk, meat, fish, eggs, fruit and leafy vegetables.
The Nutrition Advisory Committee has designed a diet from the
resources available required to give a total caloric value of 2,400.
Such a diet would cost, in I960 Rs.35 per month per adult.
Only 20$ of
our people in India can afford this.
Indian rural economy is not balanced, for while rural earnings
give only Rs.16 per individual per month, the same individual spends
Rs.20 in that month.
Only 70 crores of the total outlay of 361 crores of rupees is
provided for rural hospitals and health care in our 4th Jive Year Plan.
The .top priorities of the health tasks are not always properly chosen.
The Green Revolution in India has lulled many into a state of
complacency.
While it is true that great progress has oeen made in
increasing food production, the increasing population has almost nullified
this increase, so that the per capita availability of food is only 446 gms.
(cereals and pulses) per day and a per capita availability of 120 ml. of
milk per day.
Yet India has the largest cattle population in the world -
most of the cattle being of poor quality, yielding little milk and serving
no useful purpose, yet consuming much fodder.
The economic advantages
would be considerable if these animals were permitted to be slaughtered
and much needed meat be made available for consumption and more leather
for foreign trade.
About 1/3 of the people have no objection to eating
beef.
Whereas.the proportion of staple cereals and starchy roots in
the North American diet is estimated to be only 25$, and in the British
diet only 31$, in Latin America it is 54$, in Africa 66$, in the Near
East 71$ and in the Ear East over 73$.
Conversely, while the'proportion
of animals products - milk, meat, eggs and fish-- in the typical North
American diet reaches the exceptionally high figure of 40$ and in the
British diet can be as high as 27$, the figure for Europe as a whole is
estimated as 21$. for Latin America 17$, for Africa 11$. for the Near East
9$ and for the Far East 5$.
In only a few regions of the world are there adequate food
supplies.
These are the United States and Canada, Australia, New Zealand,
Western Europe,,parts of Argentina and parts of South East Asia,
regions have already utilized the means of increasing agricultural
.6
These
6
productivity, but only ten centuries in the world today produc j more food
than they consume.
The "dhals" which have a high protein content (vegetarian meat!)
take the place of animals foods in communities where it is consumed
(though in insufficient amounts). However, the body utilises only 40 - 60%
of the vegetable protein which forms the chief kind of protein (in contrast
to nr.i'mwl protein) that is consumed.
Certain essential amino acids like
. Lysine and Methionine are also present in insufficient amounts in this
diet pulses.
According to a National Survey the average d?;’y intake of
calories in India was 1890 calories with a daily protein intake of 53 grams.
Pregnant women, nursing mothers and growing children, ie» ;a
group constituting 60% of the population, lack adequate calories,
proteins, vitamins and minerals.
The result of this is seen in the high
incidence of low birth weight babies, still-births and fairly high
morbidity and mortality rates in children.
Health education for adequate nutrition
and balanced diet
needs to be given to all parents, teachers and health personnel. Many
foods are freely available at reasonable prices and can be used to supplement
the diet.
These (greens and fruits especially) are often locally
available or easily grown in the kitchen gardens, and found both in cities
or in rural areas.
The C.F.T.R.I. has also developed multipurpose food - which is
a blended
flour of groundnuts and Bengal gram.
It is cheap, extremely
nutritious and can be used in a variety or ways. For children especially,
C.F.T.R.I. has a prepared mixture of wheat, groundnuts, arid soya bean or
Bengal gram flour with skimmed milk powder.
More recently, using a machine, C.F.T.R.I. has extracted protein
from leaves and grass.
This process is still in the research stage.
It is interesting to note the view of Dr. P.V. Sukhatme "An insufficient amount of protein in the diet is held to be at the heart
of the problem of persistent and widespread malnutrition in the developing
countries.
However, when one examines the available data, the conclusion
is clear that what diets lack is not protein but energy foods to enable
the body to utilize the protein people actually do eat.
There is no
evidence that the quality and concentration of protein in cereal-legume diets
normally eaten in the developing countries is inadequate to meet protein
needs, provided energy intake is adequate.
essentially a socio-economic problem.
The protein problem is therefore
Production of semi-conventional
cheap, protein-rich foods using modern technology and distribution of
factory foods so produced through special feeding programmes as recommended
...7
7
by
the international bodies, will be a costly and inefficient method of
solving the problem".
Much can be continued to be said on the subject of nutrition, but
at the present time given the familiar family situation of providing
adequate nutrition two things must be emphasised:
1.
The use of locally available foods like green leafy
vegetables in the diet.
2.
Early recognition of nu ritional deficiencies and their
remedy by sound dietary practices and use"of food
supplements prepared by C.F.T.R.I.
A recent report says "Nearly one million Indian toddlers die
every year because they do not get enough to eat-. Although these hapless
toddlers constitute 16.5$ of the population, they account for 40$ of
the total deaths.
One-fifth of the babies born in India never live
beyond the age of five years".
In a paper on Nutrition and Development, Gopalan points out that
apart from the one million small children
who annually fall victim to
malnutrition, many more die of diseases they would have either escaped
or survived if they had been better nourished.
The children would stand
a better chanco if they were more sensibly fed from even the available
foodstuffs.
In a countrywide survey, the severely undernourished pre-school
children (17 - 18$
of the number surveyed) were 40$ lighter in weight than
they should be for their age.
About 14$ were 10 - 25$ lighter than normal
and 65$ were 26 - 40$ lighter than they should be.
Only 5$ were the
right weight for their age.
The question of wants also means that the use of resources may
go far beyond what someone from another social background might consider
quite adequate for survival or even for a good life.
1^ has been-
calculated, for instance, that a child born in the United States is likely
to consume in the course of a lifetime 28 times as much as a child in
India.
TABLE
Estimated consumption per head in I960 in various countries
(U.K. = 100)
U.S.A.
Sweden
West Germany
Mexico
Taiwan
Ceylon
India
■ 140
125
86
' 22
12
9
5
8
Since nutrition is closely bound up with Agriculture, it is imperative
that.the problem of malnutrition which is so serious in India be confront:4.
at "grass-roots" lev'e'l'. • Thtee’possible- avenues ■apjel^.p.en: .. - . y
1.
The growing of'food crops to be-ericourd^ed/ ekpahded'fiftd'
2.
The storage, distribution and allotment 6f food topriority
' I ' ■
given1-positive incentives.,
...
v
-3.
groups (e.g. the vulnerable population)-.'given drie 'attention.
Increased; res'earch and. explo.ratipn; of. food from a)- the sea and
' use
b) of the protein containing vegetable-foods like
groundnuts and. spy.a'bean;' ,
■
: ’r r .f l
-The-oxact -fidhing-'-p'otential- xxf the -ocean- -remains unknown.,-indeed
Ifdrifting • as :a’.‘seiridUs."ind'usffy ds.still <in>jkij^nc.yitin.^gs|Jr.^rts of
*-®i^h
•'•
the 'tftfrid ? ■ Thb-.'Northern-t^ertispher^,'.-is; .Gl^Wate^.andf.iproj^es.-^^^ the
world's fish supplies..-vTiie, §p.uthern- Hpmisphe.r.e. ,^ts 81$jWp.^ep-.bu.fei^ffiSupplies
The fisheries--;6f ■;thei.wo,rl4 j-oould yipld-fa^ mope food -
only 2% of the fish.
.> . and of a particularly valuable type - being of good protein: content.
''
'
‘ if iis of; importance and interest, to look ,t.o, fuiipne tpq.nds„in .food
cultivation for both dhe -rich,-and - the poor j countries. ,1'
i-'.
..
.... ■
..;
■ •
' 1
...
.
The rich countries, with'no greater rate-'q£1.jg£cpHh' inif'~:.-.. yo
but most of it coming from increases in productivity and with only half
the rate of growth in population compared to the developing- countries..
improved their per caput availability of food and were able to export
increasing quantities..
-
As a consequence,: trends in the food supplies of’ the developing
countries have been somewhat more favourable1 than those in production
but this has taken place at the expense of the trading pattern between
•the two groups of countries.
The. Far East and Near East, which were
exporters- of food before the War, are now importing 6; and .7$ respectively
of.their supplies.
Africa- and Latin America are still exporting but on
a much reduced scale.
This unfavourable development, has tended
to increase balance of payment problems and to accentuate the difficulties
resulting from the -almost continuous decline since the Korean boom.in
world prices of primary commodities;. The situation is illustrated by the
example of cereals; the less developed countries (excluding Mainland China)
which exported ten million tons of cereals before the War are now actual]y
importing nearly 20 million tons, and this largely to maintain their
current unsatisfactory level of diet.
Judged by these'trends, the prospects
of stepping up the rates of growth to 3% in total foods and 3.5% in animal
foods over the years 1965 - 2000 seem bleak indeed.
Sine
we cannot take comfort from the past trends, we should
find out what are the possible sources of food supply, what resources we
-9'
9
have and. how we can exploit them to meet our future food needs. Never before
the planning of resources use and land use in particular has assumed so much
importance as at present under the heavy pressure of demographic growth.
TABLE
Rate of Growth (1958-63)
Population
Growth
Per Capita Gross
Domestic Product
(per cent per year compound)
Developed Regions
1.5
5.4
Developing Regions
2.5
1.8
Gross National Product is the value of total annual production of
goods and services supplied by all 'normally resident' individuals,
firms and government bodies.
If 'income' is restricted to income
derived from participation in production GNP also equals the annual
sum of their incomes, including net incomes from abroad.
Gross Domestic Product
Equals GNP minus net income from abroad.
"S H e>
kkP C J<2. /Z/e^c^cnj/'
Nayrie
k
Ld&k
C>j
N /a-j
MycAj^cxhex^
Vr
yi <a.) kkjK^'
TcxAcU-e^
T>&'/ -
/^Ahie^o
I
7k^ impt^^cA. cf R)-rC
£tO/7o
cyyjo)o)^
Da-g
l°!7^
3&.
Pep cx/ctx/'/'ct^
3/.
&h &->~‘'i->'7~J
3x .
‘Sc^'r'ie
Z) c<-i
M M . Mc<o Cr^^GZA
OtAC^
d>.kccr>y
^/ihji
MjnmoA-
^li>75
3k
35'
DHvFP
(Lppl.eA
Ha^~> d
Pk Vall^p
^-r. DO • Cu< >Kiy
3<J.
->
C^/€A-^-i’/'
riLy^'^
(_7ke.<=^yj)
■■
VITAMIN ANP MINERALS
COMMUNITY HEALTH CELL
47/1. (First FloorJSt. Marks Hoatl
8ANGALORE-GGG001
Daily Requirement for an adult
Deficiency
Vitamin A
3000 I.U.
1.
2.
3.
4.
Vitamin D
400 I.U.
1. Rickets in children
2. Osteomalacia in adults
Thiamine
1.5 mgms
1. Beri Beri
2. Neuritis
Riboflavine
1.5 mgms
Nicotinic Acid
15 mgms
Pellegara
Cyanocobalamine
1 mcg.
Anaemia
Pathothemic Acid
3 mgms
Choline Parent substance
acetylcholine
and a constituent
of Lecithin
2 gms
Deposition of fat in liver and
Haemorrhagic degeneration of
liver and kidney
Ascorbic acid
50v^jms
1. Scurvy
2. Decrease resistance to infection
Xeropthalmia. Blindness
Decrease Resistance to URTI
Inner Ear DGafness
Acne
Angular Stomatitis
Photoph $ Vl &
Glossitis
1. Chick Pcllagara
2. Hair growth
Folic acid
1.5 mgms.
Vitamin E & K
Not known
Ca.
1 gm.
Iron
15 mgms.
Anaemia
Fluoride, Ion
in water .
1-2 ppm
Dental caries
Anaemia
1. Vitamin E - sterility in male
2. Vitamin K - Hypoprothrombinaemia
1. BoVne defects
2. Hai\
3. Blood disease
Essential Fatty acids nutritionally important and necessary for growth.
They are Linoleic, Linolenic and Arachidonic acids. They cannot be synthesised
in the body and have to be supplied in the diet. Linoleic and Linoenic acid
are of veritable origin and present in cotton seed, groundnut and linseed oils
while Arachidonic acid is of fish and animal origin. E.F.A. regulate
cholesterol metabolism.
DAILY BALANCED DIET FOR AN ADULT
Cereals (rice chiefly milled)
Dhal (red gram)
Green vegetable (cabbage)
Potatoes
Cauliflower
Banana
Oils & fats
Sugar (in tea, coffee & sweets)
Milk (cow)
Mutton
Eg? .
Agatbi
Gms
Cals
300
100
100
100
100
150
50
100
100
200
50
50
(340x3) 1020
355
27
97
30
150
450
400
67
(194x2) 388
85
45
3114
/;^T/
N e^rng a-'l-
2.5
C /<£. /i
/luth cn~
J cn-t^/A/d/e
k-CoK c^ fZc^c^Le^-> az^> -
2.C>
O d<x^
n^
5f
Tcvn
cly-^ Aon\
^-71
72^^
^9
/KjZ-
Day 'paf>£A)
/^7«.
3d
3/.
32.
>°hh5
M'e^>
3 3.
34.
DH-y
35
j=> Vhlfa-'J
'jD'Y'
Cfep^
3^1.
C^e=^)
/\[ K
d
LO ■ Cw H^-ij ,
)^^adr
VITAMIN AND MINERALS
community health cell
fl7/1. (First FloorJSt. Marks Roafa
BANGALORE - 5GQ 001
Daily Requirement for an adult
Deficiency
Vitamin A
3000 I.U.
1. Xeropthalmia. Blindness
2. Decrease Resistance to URTI
3. Inner Ear Doafness
4. Acne
Vitamin D
400 I.U.
1. Rickets in children
2. Osteomalacia in adults
Thiamine
1.5 mgms
1. Beri Beri
2. Neuritis
Riboflavine
1.5 mgms
Nicotinic Acid
15 mgms
Cyanocobalamine
1 mcg.
Pathothemic Acid
3 mgms
Choline Parent substance
acetylcholine
and a constituent
of Lecithin
2 gms
Deposition of fat in liver and
Haemorrhagic degeneration of
1iver and kidney
Ascorbic acid
50»rgms
1. Scurvy
2. Decrease resistance to infection
. Angular Stomatitis
Photoph d V|o
Glossitis
Pellegara
Anaemia
1. Chick Pellagara
2. Hair growth
Folic acid
1.5 mgms.
Vitamin E & K
Not known
1. Vitamin E - sterility in male
2. Vitamin K - Hypoprothrombinaemia
Ca.
1 gm.
1. BoYne defects
2. Hai\
3- Blood disease
Iron
15 mgms.
Anaemia
Fluoride, Ion
in water
1-2 ppm
Dental caries
Anaemia
Essential Fatty acids nutritionally important and necessary for growth.
They are Linoleic, Linolenic and Arachidonic acids. They cannot be synthesised
in the body and have to be supplied in the diet. Linoleic and Linoenic acid
are of vegitable origin and present in cotton seed, groundnut and linseed oils
while Arachidonic acid is of fish and animal origin. E.F.A. regulate
cholesterol metabolism.
DAILY BALANCED DIET FOR AN ADULT
Gms
Cereals (rice chiefly milled)
Dhal (red gram)
Green vegetable (cabbage)
Potatoes
Cauliflower
Banana
Oils & fats
Sugar (in tea, coffee & sweets)
Milk (cow)
Mutton
Egg
Agatbi
Cals
300 (340x3) 1020
100 '
355
27
100
100
97
30
100
150
150
450
50
400
100
100
67
200 (194x2) 388
85
50
45
50
3114
Breakfast
Calojrie_ Value
1 Puri
Potato Pallaiyam
Br<rc - 1 slice
thick
Erg - 1 med.
1 pat butter
1 cup coffee - jaggery
Milk 3.5 gms
50x4 =
<5x4 =
54x4 =
Total Calorie Value =
200
2§
130
50
216
16
697
Pried Fish & Fish curry
200
Total Calorie Value =
22.6
108
' 2C
•200
Pull Kulambu
Payasam
Total Calorie Value =
Total Calorie Value
for Friday:
SUNDAY
Breakfast
2 sausages
1 egg
5 slices bread & butter
Coffee
Total Calorie Value =
Lunch
Mutton. ■ Biriy.ani
SaZ.ad
Pudding
Chicken
630
■>20
9T
Total Calorie Value =
Tea
Sweet-Jangri
1 cup tea
-
Total Calorie Value = .
150
____ 26
17b~~~
Dinner
Beef roast
Plantain
Sambar Veg.
Curd
216
■414
150
25 .
6-7_
>•
Total Calorie' Val-ue =
Total Calorie Value for Sunday
=
2815
/VUT k'lS"
■ - DIET S'
diet is one that contains the nutrients necessary
A balanced
to maintain good health in the right proportion's.
In planning a diet the following points must be taken into
• consideration,
1)
Total
2)
Proportion of Pt.F. OHO. Min, Vit and H^O
chloric value
■Calories’must provide the energy to maintain B.M. plus extra
energy required'varies -
3)
5)
•
•
Age
Sex
4)
Occupation & condition
a)
•: pregnancy
b)
sickness
c)
convalescent
• ■
.
Average adult - 72,C/hr.
•
.
■
"
72 x 24 * 1728/Day
Sedentary 800 - 900 C
1400 0
bight"work ('ProfT-Business) 900
Moderate work (Mechanic) 14 - 1800C
Heavy labourers/Atheletes 1800C
Diet P - varies
1/2 Veg. P
1/2 Animal
1/3 calories (45 - 50 gms)
Fat
1/4
OHO
Bulk. (Normal adult 400 - 500 gms)
ICMR recommends the daily allowance of Protein as follows
Hen
55 kg./l20 lbs,
Women .45 kg./lOO -lbs
55
55
55
Sedentary work
Moderate work
Very hard, work
Pregnancy
Lactation
45
45
CCx'cuA-
CLcb
u
•
XA.<s>
>. cr
*re,
V (Vo-i
P/Am
Light or sedentary work 2400
Moderate work
'
• ' 2800
Very hard work
•
3600
1 A• n i.
• Co
< 9 • k >
\^<ro
2000
2300
3,500
3>2ki
100
110
.ITEMS
Proteins
Fats
Cho
gms
gms
Cals
value
Ca
P Fg
mg mgs
Vit.A Thiamine
I:.u.
mgs
RibcFlavin
mgs
Nico
7it.C;
tinic
mgs.
Acrnd
..... .
|
L6olf
1
RICE
6.8
.5
78,2 345
10
5.1
0
.09 i
.03
(milled)
RICE
6.4
.4
79
348
.09
9 AL43 0
.21
1
(Par
boiled)
RAGI
7.5
1.3
72
328 544 ’83 :17.4 70
.42
.1
3.6
MAIZE
11.1
66.2 342
.42
10 528 :2
.1
JL502
1.5
WHEAT
11.8
71.2 346
41 506 ‘4.9
108
.12
.45
WHEAT FLOUR 12.1
1.7
69.4 341
48 423 :11.5
49
.29
.49
RED GRAM
22.3
57.6 355
1.7
73 304 .5.8
.45
.51
220
(Dhal)
BENGAL GRAM 20.8
5.6
56 331 9.1
59.8 372
216
.48
.18
(Dhal)
BLACK GRAM 24
1.4
59.6 347 154 385 9.1
.42
64 .
.37
(Dhal)
GREEN GRAM 24.5
1.2
59.9 351
75 405 8.5
83
.72
,15
(Dhal)
AGATHI ' - 8.4
1.4
.21
7.8
93 1130 80 3.9 <9000
.09
46 397 83 25.5 ’9200
BEANS
4
6.3
.1
.03
q 2000
.1
4./^
CABBAGE
1.8
4? 6'
.06
.03
.6
CORIANDER
3.3
7.5
48 184 62' 18^5, 11530
.06
.05
BEETROOT
1.7
8.8
43 203 55 1
•1
.04
.09
CARROTS
.9
.2
10.6
47
80 30 212 3.50^ >.04
.02
71
ONIONS
1.2
49 180; 50
.7
0
.01
0
POTATO
1.6
22.6
10 40
.1' >X,01
97
.7
40
-1
RADDISH
.7
,06 1 • .02^
.1
3.4
17
50 22
.4
5
_a
SWEET POTATO 1.2
.08
28.2 120
20 50 1 -8
10
11^
o
x
.07
YAM
1,4
.1
26
60 20 1.3 130
DOUBLE BEANS 8.3
0
12.3
85
0
.3
40 140 2,3 220
.11
.04
BRINJAIS
1.4
24.5
18 47
4
.9 124
4
.04
.1
C -'ULIFIDWER 2.6
•4
51
30
33 57 1,5
.03
.01
CUCUMBER
.4
.1
2.5
13
0
10 25 1.5
DRUMSTICKS
2.5
.07
.05
.1
26
3.7
30 no 5.3 184
.09
KNOL-KOL
1.1
,05
36
.2
27
.4
3.8
20 35
.01
GOOSE-BEHR IS 0.5
5.5
50 20 1.2
15
.1 13.7
58
.01
TOMATOES
1.9
.07_
.1
3.6
23
20 36 1.8 320
COCONUTS
6.8 62.3 80.4
661 400 210 2.7
0 ■ .08
.3
GROUNDNUTS 26.7 40.1 20.3
.9
50 390 1.6
549
63
.04
.17
banana
1.1
.1 24.7
104
10 30 .25 124
0
1 10.9
0
0
69
.3
LIME
1.5
90 20i
1000
.1
bGG
13•3 13.3 0
60 220i 2.1 1200
173
.27
.18
51
194 115. 150
MUTTON
18.5 13.3 0
0
0
SH-R.K
21.6
.4 0
0
90 143 175. 1.3
0
2500
0
81
BUTTER
0
0
729
CI
CI 0
0
0
LOO
OIL
0
0
0
900
C)
cI 0
.05
150 15
COWS MILK
5.2
4.1 4r4
67 14S1 9E>
.>2
.04
160
.2
BUFFALO MILK 4.3
8.8 5.1
118 21G). 13C)
0
.07
0
1].
51.9
245
C) 1.1
BREAD
7.8
0
900 900
LOO
0
C)
0 900
900
GHEE
0
0
0
0
0
, 0
398
C)
c)
SAGAR
0
LOO '
0
.02
280
JAGGARY
.4
95
383 .Of3 .04 pi.^I
■
0
0
160
118 21£)1 Oi .21
BUTTERMILK
4.3i ■ 8^8 5.1
.6«0L
> C>
*oV
(
I
1.9
0
3.8
0
1.1
1.4
5
4.3
2.6
0
0
0
0
0
2.4
1
2
0
2.4
0
169
99
124
135
88
5
11
17
.5
15
24
.7
!■»
■ .7
22
x$<. ... 12
1
■56
. 2
7 ’
120
. 2
85
, 5
600
.02
31
. 4
. 6
7
__ 0
6"
. 3
26
0
0
. 1
6. 8
0
0
2. 5
0
0
0
0
.1
.18
o
0
.7
0
0
1.2
1
.4
.8
•4
.6
A
i.2
9
7i
o-u
1 o
I 3
ITEMS/
100 gm
1Protein
gms
Fats
gms
Cho
gms
Cals
value
'milled)
Pich ins
6.8
.5
78.2
345
Phoe?horus
(parboiled) 6.4
RAGI
7.3
4
34’9
328
Thiamine
1 „3
79.0
72.0
MAIZE
WHEAT
RED GRAM
11.1
11.8
22.3
3.6
1.5
1.7
66.2
71.2
57.6
342
346
335
BENGAL
GRAM
PhoB";'.sorus, _ iron, Thi ami-ie,
Calcium, Riboflavine,
Phos horus, Thiamine, Vit. A
Phosphorus, thiamine Nicotine
Phosphorus, Thiamine Riboflavine
Nicot-he.
20.8
5.6
59.8
36Q..
black GRAM 24.0
1.4
59.6
347
GREEN GRAM 24.5
AGAl HI
8.4
BE. NS
4.0
C ABB AGE
1.8
GOURIANDER 3.3
;9
CARROTS
C OOSE
BERRIES
0.5
COCONUTS
6.8
GROUND NUT 26.7
EGG
13.3
18.5
HUTTON
SHARK
21.6
BUTTER
0
GHEE
0
4 ■ AMARANTH
1.2
1.4
.5
.1
.6
.2
59.9
6.3
4.6
6.310.6
3481
93
46
27
44
47
Phosphorus, Thiamine, Iron,
Nicot i
Phosphorus, Thiamine, Iron
Reb of lav ine
Phosphorus , h:.: ami r_e, Nicotine
Calcium, Vita ml ■. 4 4 C
Vitamin A
Vitamin C
Vitamin A & 0
Iron
13.7
80.4
20.3
0
0
0
0
0
6.3
58
661
549
173
194
90
729
900
47
Vitamin C, Thiamine
Phcsuhorus, Calcium
Phospl -rus, '
Phosphorus,
’.atin^. Vi t, A
Nicotine
Phosphorus
Vitamin A
Thiamine, Vitamin A, Iron
Vit. C, Vit. A
.1
62.3
40.1
13.3
13.3
.4
3 81.0
100.0
11 iff
NVT L|.|s~
D I E T S'
A balanced
diet is one that contains the nutrients necessary
to maintain good health in the right proportions.
In planning a diet the ..following points must be. taken into
consideration.
1) Total
caloric value
.2) Proportion of-P.F. CHO. Min, Vit and HgO
Calories must provide the energy to maintain B.M. plus extra
■ ,
energy required varies 5) Age
.
. ■
4) Sex
5) Occupation & condition
a) pregnancy
ca|.
b) sickness
c). ponvalescent
-5S0 001
*
Average
adult. - 72 C/hr.
.
72 x 24 = 1728/Day
■
Sedentary 800 - 900 C
__ si—■_—Mght7'work'i'Profl^usi-nes's') 900 - 1400 C*
Moderate work (Mechanic) 14 - 1800C ■
Heavy. labourers/Athcletes 1800C -■
Diet P - varies'
'
.
1/2 Animal
1/2 Veg. P
.
Fat
1/4 - 1/5' calories' (45- 50 gms)
CHO
Bulk. (Normal adult 400
i’
500 gms)
ICMR recommends■the daily allowance of Protein as follows
Men
Women
-IhckuAU
55 kg,/l20' lbs.
45 kg./lOO lbs
-
' p/a
|
j
}
Light or sedentary work 2400 .
Moderate work
2800
Very hard work
5600
55
55
55
5
5
5
J
L.
Sedentary work
Moderate work
Very hard work
Pregnancy
Lactation
45
45
WaV
2_U.se
6
, (q
->
XKCO
u
h_Cj<re>
100
110’
-
k^cro
x
, .5 x
. kv
• 2000 •
‘ ■ 2500
Z<500
X'Kfts
x
\e>Q?>
ITEMS
fl
Prot-
Fats
Cho
eins
gms
gms
gms
Cals
value
Ca
P 'Fe
Fit. A Thiamine
rng mgs
I.U.
mgs
mgs
RiboFlavin
mgs
Nicotinic
Acid
' Fit.C-
mgs.
1.9
6.8
.03
0
.5
78,2 345
10 160 3.1
.09
RICE
0
(milled)
3.8
.09
0
6.4
.21
.4
348
RICE
79
9 143 4
0
(parboiled)
1.1
0
.42
.1
7.3
1.3
328 344 283 17.4 70
72
RAGI
1.4
0
.42
11.1
3.6
66.2 342
.1
1502
MAIZE
10 328 2
.12
5
1.5
0
11.8
71.2 346
41 306 4.9
108
.45
WHEAT
ZL
.29
0
1.7
69.4 341
48 423 11.5
49
.49
WHEAT FLOUR 12.1
2.6
0
22.3
57.6 355
.51
1.7
73 301 5.8
220
.45
RED GRAM
(Th al)
2.4
1
56 331 9.1 ' 216
.18
5.6
59.8 372
.48
BENGAL GRAM 20.8
(Dhal)
2
0
1.4
59.6 347 154 385 9.1
.42
.37
BLACK GRAM 24
64 .
(Dhal)
0
1.2
2.4
.72
.15
GREEN GRAM 24.5
59.9 351
75 405 8-5
83
(Dhal)
169 "
.21
1.2
8.4
1.4
93 1130 80 3.9 9000
.09
7.8
AG1THI
4
99 ■
1
46 397 83 25.5 9200
beans
.. 6.3
.03
.1
124
.4
.03
1.8
476 -27- r-394 -<44
.8 2.000
.06
CABBAGE
.1
3.3
.6
48 184 62 18^5 11530
CORIANDER
7.5
.06
.8
155
.05
1.7
BEETROOT
8.8
43 200 55 1
88
.4
.09
•1
.04
CARROTS
•9
.2
10.6
80 30 212 3.50 "
47
.6
3
.02
zl
.7
0
ONIONS
0
49 180 50
11
1.2
11
.01
.1' \.O1
1.6
.7
40
POTATO
22.6
10 4P
.1
97
1.2
17
no
.06
.1
5
RADDISH
.7
3.4
17
50 22
.4
15
.5
.08
SWEET POTATO 1.2
20 50
.8
10
.3
28.2 120
24
.7
.07
o’’
60 20 1.3 130
1,4
26
111
.1
YAM
0
.7
0
0
DOUBLE BEANS 8.3
.3
12.3 ■ 85
40 14S 2.3 220
22
■Q-\9- . , 12
.11
.04
BRIICALS
24
18 47
1.4
.5
4
.9 124
.1
1
.04
51
CULIFIDWER 2.6
.4
4
50
33 57 1.5
<6
zt
7
'
. 2
.01
.03
0
.1
2.5
13
CUCUMBER
10 25 1.5
5
*
2
120
.07
.05
DRUMSTICKS
26
.1
3.7
30 no 5.3 184
. 5
85
...09 I
36
.05
KNOL-KOL
.2
3.8
.4
27
1.1
20 35
600
,02
.01
5.3
goose-berk:ISO.5
50 20 1.2
15
58
.1 13.7
514
. 4
.01
TOMATOiS
.07.
3.6.
1.9
.1
23
20 36 1.8 320
• 0
7
COCONUTS
6.8 62.3 80.1
661 400 210 2.7
0 • .06
0
"14—1__
63
.9
GROUNDNUTS 26.7 40.1 20.3
549
50 390 1.6
6"
1- 0
.17
.04
banana
104
10 30 .25 124
.1 24.7
1.1
26
0
0
0
*3
0
lime
69
1.5
10.9
90 20
0
.1
1000
EGG
13.3 13.3 0
173
60 220 2.1 1200
0
6. 8
.18
.27
MUTTON
31
18.5 13.3 0
194 115 150 1
. A.
0
2. 5
0
0
21.6
0
SH^RK
0
90 143 175 ! 1.3
n
0
0
0
2500
BUTTER
0
81
0 ! .0
0
729
0
0
0
0
0
LOO
0
OIL
0
0
0 0
0
900
.1
.05
.18
15
150
COWS MILK
4.1
96
3.2
4.4
67 149
..2
p
.*)
.1
.04
.1
160
buffalo muk 4.3
8.8 5.1
118 210 130
'
1.1
0
.07
0
.7
bread
7.8
.7 51.9
245
11
0
0
0
0
900 DO
0
GHEE
LOO
0
0 I 0 900
900
0
0
0
0
0
0
SAGAR
0
0
398
0 1 0
LOO
0
1 95
0
0
1
.02
383 .08 .04 11.4
280
JAGGARY
*
8
1
.1
3
0
BUTTERM HR
.2
0
5.1
118 210 ! 0
160.
4.3
V?
o-\
l> .b
•?
Atco
6 -o t ■ 6-6%
o-V
n/U 7 U-
• DIETS
A balanced diet is one that contains the nutrients necessary to main
tain good health in the right proportions.
In planning a di'et the following points must be taker 'into
consideration.
1)
2)
Total calorie value
Proportion .of P.F. CHO. Min, Vit a:,d HgO
Calories must provide the energy to maintain B.M. plus extra
energy required varies
5) Age
4) Sex .
5) Occupation & condition
■
a)
pregnancy
b)
sickness
c)
convalescent
Average adult - 72C/hr;
72 x 24 = 1728/Day
Sedentary 800 - 900 C
Light work (Prof. Business) 900 - 1400 C
Moderate work (Mechanic) 14 - 1800 0
Heavy labourers/Atheletes 1800 C
Diet P - varies
-J- Veg. P
Fat
CHO
animal
x - 1/3 calories (45 - 50 gms)
Bulk. (Normal adult 400 - 500 gms)
ICMR recommends the daily allowance of Protein as follows:
P/Ams
Men 55 kg./120 lbs.
5 Light or sedentary work 2400
2800
I Moderate work
3600
5 Very hard work
55
55
55
2000
2300
300
45
'-5
45
100
110
1 Sedentary work
5 Moderate work
Women 45 kg./lOO lbs
Very hard work
Pregnancy
Lactation
CTEMS
Prot
eins
gms
RICE
(milled)
6.8
RICE
(parboiled)
6.4
RAM
7.5
MAIZE
11.1
WHEAT
11.8
WHEAT FLOUR 12.1
RED GRAM
22.5
BENGAL GRAM 20.8
BLACK GRAM
24
GREEN GRAM
24.5
AGATHI
8.4
BEANS
4
CABBAGE
1.8
CORIANDER
5.5
BEETROOT
1.7
CARROTS
.9
ONIONS
1.2
POTATO
1.6
RADDISH
.7
SWEET POTATO 1.2
YAM
1.4
DOUBLE BEANS 8.5
BRINJALS
1.4
2.6
CAULIFLOWER
CUCUMBER ■
.4
DRUMSTICKS
2.5
KNOL-KOL
1.1
GOOSE-BERRIES 0.5
TOMATOES
1.9
COCONUTS
6.8
GROUNDNUTS
26.7
1.1
BANANA
LIME
1.5
EGG
15.5
MUTTON
18.5
SHARK
21.6
BUTTER
0
GIL
0
COWS MILK
5.2
BUFFALO MILK 4.5
BREAD
7.8
GHEE
0
SUGAR
0
JAGGARY
.4
BUTTERMILK
4.5
Fe
Fats
Cho
gms
Cals
val
ue
Ca
gms
.5
78.2
545
10 160 5.1
.4
1.5
5.6
1.5
548
79
•528
72
66.2 542
71.2 546
69.4 541
57.6 555
59.8 572
59.6 547
59.9 551
7.8
95
46
6.5
4.6
27
7.5. 48
8.8
45
10.6
47
11
49
22.6
97
5.4
17
28.2 120
26
111
12.5 . 85
4
24
50
4
2.5 • 15
26
5.7
5.8
27
58
15-7
5.6
25
661
80.4
20.5
549
24.7
104
10.9
69
0
. 175
0
194
0
90
0
729
' 0
90067
4.4
118
5.1
51.9
245
0
900
100
598
585
95
118
5.1
1.1
1.7
5.6
1.4
1.2
1.4
.5
.1
.6
.1
.2
0
.1
.1
.5
.1
.5
.5
.4
.1
.1
.2
.1
.1
62.5
40.1
.1
1
15.5
15.5
. .4
81
100
4.1
8.8
.7
100
0
.1
8.8
P
Vit.
A
I.U.
Thi
ami
ne
mgs
Ribo Nico
fla tinic
vi n acid
mgs
0
.09
'.05
Vit.C
mgs
1.9
0
Q 145 4
0
..21
.09 5.8
1.1
.1
5>4 285 17.4 70 ..42
.1
107528 2 1502 .,42
1.4
*12 5
41 506 4.9 108 ..45
48 425 11.5 49 ..49
.29 4.5
.51 2.6
75 504 5.8 220 ..45
.18 2.4
56 551 9.1 216 ..48
154 585 9.1 64 ..42
.57 2
75 405 8.5 85 ..72
.15 2.4
1150 80 5.9 9009 ..21
.09 1.2 .
1
.1
597 85 25.5 9230 ..05
.4
.8 2000 .,06
.05
59 44
.8
184 62 18.5 11550 .05 .06
200 55 1
0 .04 .09
.6
80 50 212 5.50 .04 .02
.4
180 50 .7
0 .08 • :.oi
40
10 40 .7
.01 1.2
.5
50 22 .4
5 .06 .02
20 50 .8
10 ‘.os -.04
.7
60 20 1.5
150 .07
.7
40 140 2.5
220 0
0
0
18 47 • 9
124 ;04 ' .11
.9
.1
51
1
1.5
.04
51
55
0 .05 .01
10 25 1.5
.2
50 110 5.5
.2
184 .05 .07
20 55 .4
56 .05 .09
.5
50 20 1.2
15 5.5 .01 .02
520 .07 .01
20 56 1.8
.4
0 .08 .06
400 210 2.7
.6
50 590 1.6
.65 .9 .5 :14.1
10 50 .25
124 .04 .17
.5
90 20 .5
0 0
0
0
60 220 2.1 :1200 1000 .1
.1
115 150 —
51 .18 .27 6.8
0
0
0 2.5
145 175 1.5
0
0 o
:2500
0
0 - 0
0 0
0
0
0
0
0
150
149 96 .2
15
.05 .18
210 150 .2
160
.04 .1
.1
11 0 1.1
0
0
.07
.7
0 900 900
0
900
0
0
o
0
0
0
0
0
0
.08 .04 11.4 280
.02
0
1
210
0
.2 160
0
0
.1
0
0
0
0
0
0
1
0
0
169
99
124
155
88
5
11
17
15
24
0
22
12
56
Y
120
85
60051
7
0
6
26
0
C
0
0
0
.1
5
0
0
0
0
5
r\
N<J-V Lj-
3
DIETS
A balanced diet is one that contains the nutrients necessary to ma-in-
tain good health in the right proportions.
In planning a diet the following points must be taker into
consideration.
1) Total calorie value
2) Proportion of P.F. CHO. Min, Vit ai.d HgO
Calories must provide the energy th maintain B.M., plus extra
energy required varies
3)
Age
4)
Sex
5)
Occupation & condition
a)
pregnancy
b)
sickness
c)
convalescent
Average adult - 72 c/hr.
72 x 24 = 1728/Day
'
Sedentary 800 - 900 0
Eight work (Prof. Business) 900 - 1400 C
' Moderate work (Mechanic) 14 - 1800 C
Heavy labourers/Atheletes 1800 0
Diet P - varies
■2 Veg. P -y animal
Fat CHO
4" - 1/3 calories (45 - 50 gms)
Bulk. (Normal adult 400 - 500 gms)
ICMR recommends .the daily allowance of Protein as follows:
P/Ams
Men 55 kg./120 lbs.
5
Light or sedentary work 2400
2800
( Moderate work
3600
Very
hard work
5
i
Sedentary work
5 Moderate work
Women 45 kg./lOO lbs 5 Very hard work
A Pregnancy
Lactation
pl,- r ue- 'n 1'
C’le’X
—--------------
2000
2300
300 c
33<so
/
55
55
55
45
45
45
100
110
ITEMS
/vr
Pro
eins
gms
Fats
Cho
gms
gms
Cals3
val
ue
Ca
P
Fe
Vit.
A'
I.U.
Thi
ami
ne
mgs
Ribo Nico
fla tinic
vin acid
mgs
—
78.2 | 545
RICE
(milled)
6.8
.5
. 10 160 5.1 0
09
’.03 1.9
RICE
a 145 4
(parboiled)
548
6.4
.4
,21
79
0
.09 3.8
RAGZ
72
7.5
528 {344/283 17.4 70 .,42
1.5
.1
1.1
MAIZE
11.1
5.6
66.2. 542
107328 2 (1502 ..42
.1
1.4
WHEAT
11.8
71.2 546
1.5
.12 5
41 506 4.9 108 ..45
WAT FLOUR 12.1
1.7
69.4 541 •• 48 425 11.5 49 ..49.29 4.3
BEL GRAM
22.31 1.7
57.6 555
75 504 5.8 220 ..45
.51 2.6
BEIR5AL GRAM 20.8
5.6
59.8 572
56 551 9.1 216 ..48
.18 .2.4
SLACK GRAM
.57 1,2
59.6' 547 ’ 154 585 9.1 64 ..42
24
1.4
GREEN GRAM
24.5, 1.2
59.9 551 ..... 75,[405? 8i5 ' 83 ..72
.15 2.4
AGATHI
7.8
8.4
1.4
95 [11501 80 5.9 9C0G).21
.09 1.2
BEANS
46
4
6.5
.1
1
85 k£al?ao 1.05
CABBAGE
1.8
.1
4.6
.8 2000 .06
27
44
.03
.4
CORIANDER
.6.
48
5-5
7.5
184 62 18.5 fcL53O|.O5 .06
.8
BEETROOT
.1
8.8
1.7
200 55 1-.
0 .04 .09
45
•4
CARROTS
.2
10.6
80 50 1212! 3-50 .04 .02
• .9
.6
47
ONIONS
1.2
0
11
180 50 .7
0 .08 .01
49
.4
POTATO
1.6
.1
22.6
10 40 .7
40 .1
97
.01 1.2
RADDISH
.1
50 22 .4
.7
17
5.4
5 .06 .02
.5
SWEET POTATO 1.2
28.2 120
20 50 .8
10 .08 .04
.7
YAH
.1
26
1.4
111
■ 60 20 1.3
150 .07 c
.7
DOUBLE BEANS 8.5
220 0
.5
0
12.5
85
40 140 2.5
0
BRINJALS
1.4
18 47 .9
.5
4
24
124 .04 .11
.9
.4
CAULIFLOWER
2.6
50
4
' 1
55 57 1.5
51 .04 .1
CUCUMBER
.1
10 25 1.5.4
0 .03 .01
2.5
15
.2
DRUMSTICKS
26
.1
2.5
50 110 5-5
5.7
184 .05 .07
.2
KNOL-KOL
1.1
.2
5.8
20 55 -.4
27
36 .05 .09
.5
GOOSE-BERRIES 0.5
.1 15.7
58
•50 20 1.2
15 5.3 .01 .02
TOMATOES
20 56 1.8
320 .07 .01
1.9 . .1 ; 5.6
,25
.4
1661 ] ® 210 2.7
COCONUTS
6.8 7^1 80.4
0 .08 .06
.6
|
50
GROUNDNUTS J26.7' |(40.1J 20.5
590. 1.6
|549
‘ 63 .9 .3 14.1J
BANANA
i.r
.1 24.7
.10 50 .25
104
124 .04 .17 ' .3
LIME
1 10.9
1.5
90 20 .3 _0 0
0
0
69
K G’ r
0
60 .220 2.1 (12o67 1000 .1
15.5 15.5
175
.1
MUTTON
0
18.5 13.3
.18 .27 6.8
194
115 150
shah;
21.6
0
90
.4
0 :
0 2.5
145 175 1.3 . -a.
(lOo]
BUTTER
0
0
'1729!
0
0 0 I2500]
0
0
0
' 0
(9001
0
0
GIL
0 0
0
o
0
0
COWS MILK
5.2
4.1
150
4.4
149 96 .2
67
15
.05 .18
BUFFALO MILK 4.5
8.8
118
210 150 .2
160
.04 .1
5.1
.1
BREAD
7.8
11 0 1.1'
0
.7
0
51.9
245
.07
.7
£00]
GHEE
0
0
1'9051
0
0 (90Q) 900
900
0
0
SUGAR
0
100
598
0
0
0
0
0
0
0
JAGC-ARY
.1
.4
.08 .04 11.4 280
..02 z0
95
585
1
BUTTERMILK
8.8
210
0
4.5
118
.2 160
0
5.1
0
.1
—
0-/
6
, Li 7
<5^^
6-6-3 0-
Vit.C
mgs
0
0
0
0
0'
0
0
1
0
0
[169?
99
112/?]
11351
88
rz.
11
17
15
24
0
22
12
56
7
11267
85
/ 6(351
31
7
0
6
26
0
0
0
0
0
.1
3
0
0
0
0
3
/VUT U-16
LONDON
SCHOOL
OF
HYGIENE
AND
TROPICAL MEDICINE
Lectures on Nutrition
to
SA^GALOHlT S MarI<5 i,Oa^
- Sou 001
Diploma in Tropical Public Health
Diploma in Tropical Medicine and Hygiene
Diploma in Clinical Medicine of the Tropics
GENERAL OUTLINE
The subject of nutrition has a wide range and cannot be
dealt with in detail in 12 hours of lectures. Inevitably those
with special interests, e.g. in clinical medicine, paediatrics,
public health, child and maternal health, food production,
economic and social conditions, etc., will find the lectures
inadequate from their point of view.
A reading list is
provided which may do something to fill these gaps.
A further difficulty is that nutritional conditions are
not the same in all parts of the world, and they obviously
differ in urban and rural communities.
There are similarities,
but there are also differences.
We can only teach general
principles, which each student must apply for himself in his
own particular situation.
Both courses are oriented towards the problems of
developing countries.
Since in these countries some 50%
of the population are children under the age of 15, and since
children from a nutritional point of view are more vulnerable
than adults (except for pregnant and lactating women), it is
logical that this set of lectures should be closely related
to those by Dr David Morley on child health.
A list follows of the lectures proposed. We have
tried to choose the subjects which are most important and
interesting.
J.C. Waterlow
February 1975
LONDON SCHOOL OF HYGIENE AND TROPICAL MEDICINE
1975 SESSION
Lectures on nutrition to DTPH, DTM & H and DCTM Courses
(All lectures start at 2.00 p.m.)
27 February
Introductory lecture
Professor J.C. Waterlow
27 February
Assessment of nutritional
status (1)
Professor J.C. Waterlow
1 March
Marasmus and kwashiorkor:
history, classification
and clinical features.
Professor J.C. Waterlow
4.
2 March
Marasmus and kwashiorkor:
pathology and biochemistry
Dr W.P.T. James
5.
6 March
Vitamin A: requirements,
biochemistry, effects of
deficiency
Dr D.I. Thurnham
6.
8 March
Iron absorption and iron
requirements
Professor J.C. Waterlow
7.
9 March
Protein and energy
requirements
Professor J.C. Waterlow
13 March
Long-term effects of
malnutrition
Professor J.C. Waterlow
9.
16 March
Assessment of nutritional
status (2)
Dr W.P.T. James
10.
16 March
(3.00 p.m.)
Dietary surveys
Mrs J. Doughty
11.)
12.)
20 March
(Prevention of malnutrition
(Panel discussion
Professor J.C. Waterlow
Dr T.P. Eddy
Dr W.P.T. James
Mr P.R. Payne
1.
2.
'
ANAEMIA
Def:
cO^^o0’^^000'
A state in which the R.B. Cell Values are less than
normal
Normal Blood Values:
*S
RBC
M
F
5
4.5/cu mm
Hb.
15
14.5 gms/100 cc
PCV
47
42 %
RBC life
-
120 days.
Classification.
I
Principally caused by Impaired production.
A Deficiency of substances essential for Erythropoiesis
1.
Iron
2.
Vit. B12
3.
Folic Acid
4.
Protein
B Endocrine Deficiency
C Physical / Chemical / Other
Injury to Bone Marrow - eg. Benzol^ Radiation pU
Leukaemias.
D Infections
E Failure of Bone marrow
II
Loss of blood - Haemorrhage,
a
serious infestation of
Hook-worm can rofc|its victim of half a pint of blood^one
Day Haemorroids.
Ill
Excessive Destruction of RBC
1.
Fe
D.R. 20-30 mg. Adult.
10-30 mgs. Children.
30 mgms as FeS04 for approx. 8 mg. of
elemental iron.
Source
Meat, B-rinja.ls, tomatoes, green veg. dried
fruits,^milk is poor in Fel The iron of
vegetables is more easily absorbed than the Fe. 6f meat.
Fe may be provided
adequately but may not be absorbed
therefore Utilised.
2
and
2
Deficiency
2.
Typical Microcytic Hypochromic kma&fWt ■
Vit. B12 or Cyanocobalamin - necessary ®>maturation 'of
RBC is know &s Extrinsic Factor interacts with Intrinsic
Factor found in Gastric FMKfcHExintffiXSKkK fundus.
F.
I.
1 mcg / day.
R.
D.
Source
F.
E.
When
is deficient result is Pe mic i ous Ana emi a.
Liver, beef, milk, rice.
+ I.F. Anti Pernicious A Factor
Def: results in Macrocytic anaemia.
3.
Folic Acifl
D.R. 1.5 mg/day
Source green leafy vegetable, liver, kidney, milk.
Deficiency of Vit B12 & Folic Acid together Cause Megaloblastic
Anaemia.
4.
Vit. C
or Ascorbic Acid.
Use discovered by Sir Richard Hawkins in 1593.
D.R. 25-50 mg, Increased in Infection - 2,000 mg. Excess
to be stored.
Source
Fresh fruit, vegetables, and potatoes, GuaVaS Amla
Deficiency - Nutritional anaemia., helps in folic
acid metabolism.
Vitamin 0. ctd.
Synthetically manufactured and know a.s
Ascorbic Acid. Destroyed by prolonged heat and in process of
fruit canning.
Essential for 1) capillary Integrity,
2) Formation of
Intercellular substance and 3) R.B.C. Maturation.
Deficiency
leads to scurvy, anaemia, halitosis, spongy
gums and delayed healing of wounds and haemorrhages.
Vitamin P occ-urs with Vit. C. in fresh fruits especially
lemons. Helps in preventing capillary permeability.
Deff&icy leads to purpura and ca.pilla.ry Haemorrhages.
5.
Traces of Cu, Co and Nicotinamide a.s Catalysts for
Hb synthesis
ANAEMIA IN MEDICAL STUDENTS
DR. MARIE M. MASC/’RENHAS M.B.B.S . (Bombay)
R.I.P.H.
F.
D.P.H(London)
INTRODUCTION
Medical students in the city of Bombay represent a cross section of
population of varied habits and nutrition, belonging to the middle class
and touching the upper strata of society.
This would lead one to believe
that anaemia would be very uncommon, if not rare, amongst such a class of
people, whose profession will later demand guidance of the masses in respect
of their hell th.
But is this really the true state of affairs? Can one safely think of
a medical student as a young and healthy individual consuming an average
nourishing diet?
MATERIAL AHD METHODS
A Student Health Service was started by the Department of Preventive and
Social Medicine of the Grant Medical College, Bombay, in 1961, when students
in the first and third year of their medical cotirse were examined.
In 1962, most of the students volunteered to donate blood for the
national emergency.
A fair number were rejected for having haemoglobin(Hb)
levels below the acceptable limit.
This experience, together with the findings
of Dr.R.S .Sharma who in his survey of 592 University students found a high
percentage of anaemia, pointed out the necessity of including haemoglobin
estimation in the routine examination of medical students at the Student
Health Centre.
From July to December 1963, 175 medical students have been examined at
the Student Health Centre.
Blood was obtained by the finger prick method
and the haemoglobin level estimated by Sahli's method.
Based on the results of Parekh et al.
o
and R.S .Sharma,
3
those students
whose haemoglobin level was 12 (kn.% or more were considered as normal. Those
whose haemoglobin level was below 12 GSu.% were further investigated at the
Haematology Clinic and a full blood count, stool examination and details of
their diet were also done.
Anaemic students were treated and follwed at
the Student Health Centre and their haemoglobin level at the end of 3 months •
treatment was recorded.
FINDINGS
Out of 175 students examined since July 1963, 98 were males and 77 were
females.
Their age group was from 17 to 25 years. Out of 98 male students,
80 had a Hb.level above 12 gm.% and 18 were below 12 Gmi.
In females, however,
out of 77 students, 37 had a Hb. level below 12 Gm% and 40 above 12 Gn$.
These figures are comparable with those of Greendyke1 and
3
R.S. Sharma . The latter found that 47.6$ out of 592 students had
A simpler clinical survey held in
a Hb. level below 12 Gm$.
Gujerat Uhiversity, found 3.5$ of University students anaemic as
judged by "pallor" (personal communication).
Thus anaemia is much more common in females (48.05$) than in
males (18.17$).
The reason for this seems to be the menstrual loss
and greater demand not supplied by an inadequate diet.
More than
two-thirds of the female students were vegetarian, whose diet
was insufficient to supply necessary calories and hematinic
factors (see Table 3), besides being inadequate in proteins.
In
short their diet falls very short of a good and balanced diet,
adequate in calories, proteins and hematinic factors (see Table 4).
TABLE 4_ - A surp-ested balanced diei;
Cereals
Pulses
Green Veg.
Roots & Tubers
Other Veg.
Fruits
Sugar & Gur
Oils & Fats
Milk
Groundnuts
Ozs.
Total calorific
Value
14
3
4
3
3
3
2
2
10
1
1372
288
40
66
30
30
220
460
250
122
Total Veg.
2876
Non. Veg.
Misc.
120
100
Total Non.
Veg.
3096
...
...
...
...
...
...
...
...
...
...
That poor nutrition was the main cause of anaemia is corraborated by the fact that haemogram studies showed hypochromic micro
cytic anaemia which in almost all cases responded to correction in
the diet and iron by mouth.
A vegetarian diet per se should not
be the cause of anaemia, but an ill-balanced diet such as that
taken by the females in this study group especially when associated
These firures are comparable with those of Greendyke1 end
R.S. Sharma .
The letter found that 47.6$ out of 592 students had
A simpler clinical survey held in
a Hb. level below 12 Gm$.
Gujerat Uhivorsity, found 3.5$ of Uhiversity students anaemic as
judged by "pallor" (personal communication).
Thus anaemia is much more common in females (48.05$) than in
males (18.17$),
The reason for this seems to be the menstrual loss
and rreater demand not supplied by an inadequate diet.
More than
two-thirds of the female students were vegetarian, whose diet
was insufficient to supply necessary calories and hematinic
factors (see Table 3), besides being inadequate in proteins.
In
short their diet falls very short of a good and balanced diet,
adequate in calories, proteins and hematinic factors (see Table 4).
Cereals
Pulses
Green Veg.
Roots & Tubers
Other Veg.
Fruits
Sugar & Gur
Oils & F«ts
Milk
Groundnuts
Ozs.
Total calorific
Value
14
3
4
3
3
3
2
2
10
1
1372
288
40
66
30
30
220
460
250
122
Total Veg.
2876
Mon. Veg.
Misc.
*120
100
Total Non.
Veg.
3096
.
.
.
. .
.
. .
.
.
.
.
That poor nutrition was the main cause of anaemia is corrab-
orated by the fact that haemogran studies showed hypochromic micro
cytic anaemia which in almost all cases responded to correction in
the diet and iron by mouth.
A vegetarian diet per se should not
be the cause of anaemia, but an ill-balanced diet such as that
taken by the females in this study group especially when associated
Enquiry into the diet of these student
*
revelled that those students
whose haemoglobin level was less than 12 Gm.% were taking inadequate
calories (raring from 2000 to 2200 cals), insufficient in proteins. Twothirds of these were vegetarians whose diet composition was not enough to
maintain their health (see Table 3),
Those students whose haemoglobin was be ow 12 Gm.% were given iron
sulphate and instructions about their diet.
They were followed up and
all except three responded to this treatment, their haemoglobin level rising
to about 12 Gm.% in three months.
CISCUSSION
A survey of the Hb.estimation in 175 medical students shows that their
Hb.level on an average is far from satisfactory.
30.18% of these students
had a Hb.level less than 12 Gm.% which would perhaps go undetected by a check
up which did not include the Hb.estimation.
with increased menstrual loss can certainly lead to hypocromic micro
cytic anaemia.
This preliminary study conducted at the Student Health Centre has
pointed out the need for a continued check-up on the health of all
University students.
A simple haemoplobin estimation included in the
routine examination, entails very little extra effort and brings the
important fact of anaemia into the limelight.
No effort should be
spared to establish such centres in all the colleges and
instruct
*
the
students about their diet which should maintain their Hb. level high
and keep them fit for their ardous duties.
SUMMARY
At the Student Health Centre run by the Department of Preventive
and Social Medicine of the Grant Medical College, 175 medical students
were examined from July to December 1963 and their haemoglobin level
estimated.
30.18$ of these students had a Hb. level than 12 Gm$j of these,
the majority were females.
The main causative factor of this anaemia was probably an in
adequate and ill-balanced diet, especially in vegetarians.
Treatment of anaemic students with a corrected diet and iron
sulphate yielded good results.
ACKNOWLEDGEMENTS
My thanks are due to the Dean, Grant Medical College and J.J.
Group of Hospitals, Bombay, for permission to publish this paper and
to Dr.A.F.Heredia, Hon. Lecturer, Department of Preventive and Social
Medicine, for 'his valuable help and guidance.
REFERENCES
1.
Greendyke,R.M.,Meriwether,W.A., Thomas, E.T.,Flintjar,J.D. and
Bayliss,M.W.: A suggested revision of normal values for Haemoglobin,
Hematocrit, and Erythrocyte count in healthy adult men.
Amer. J. Clin. Path., 37:429, 1962.
2.
Parekh,J.G., Desai,R.G. and Jhala,H.I.: Professional blood donors,
J.J. Hospital Journal, 1: 97, 1956.
3.
Sharma, R.S.: Status of University students as blood donors,
J.J. Hospital Journal. 8:4, 1963.
***************
community health cell
47/1, (First FIootJSc. Marks Road
VITAMIN E
BANGALORE ■ 560 001
Vitamin E also called antisterility vitamin.
Deficiency in rats causes irreparable damage in germinal epithel
ium of male rats while in female rats full term pregnancy is impossible
resulting into resorption of factus.
In case of female rats, changes
are reversible.
.Characteristics i-
Vitanin E is chemically related to sex hormones.
It is stable to
heat, acid, alkalles, but oxidation takes place in presence of lead
and iron salts and also in rancid fats and ultra violet rays. Vit. E
of related chemical structure,
activity is exhibitedl by four or more compounds^ namely ultra violet
rays$ beta, rand of tocopherol.
Measurementg;Activity is expressed in mgms where alpha tocopherol is used
standard to prevent resorption or factus in pregnant rats under
standard conditions.
P-h.YSiplory: Vitamin E, unlike other fat soluble vitamins is not stored in
liver.
Fatty tissues store small amounts.
Defective absorption of fats also decreases tissue level of vit. E
Functions:-
In human being^ are not yet established.
1.
As an antioxidant i.e., by acce oxygen it is able to minimize
oxidation of carotene.
2.
Therefore synerglzes effect of vit. A.
It has ability to protect R.B.C.S. from haemolysis by such
agents as H202.
3.
In rats, vitamin E promotes efficiency of linoleic acid and
even cure E.F.A. deficiency.
4.
In cows, liberal intake of and tocjiophe'sol leads to increased
milk and butter fat production.
5.
It is necessary for utilisation of sex hormones, cholesterol
and vitamin- D.
P?Uy allowaac.fts:-
.2
2
Pally. allowances5 Is not known for human beings.
Consumption is about 14 mgms/day.
SfluX-CSSJ -
Wheat germ oil, oil of cotton seed and rice germ, germs of
other seeds.
Green leafy vegetables, hats, legumes, egg and meat.
Deficiency;-
Is not known in man.
*
mm
fMUT
BAA/G/i
*
,.<
ir1’’
t_^a'-ksftcad
LOUDON SCHOOL OF HYGIEtiE AND TROPICAL MEDreilSoO OOf
DTPH, DIM & H and MOMT COURSES
fUTRITIOM LECTURES
Protein and Caloric Requirements
A.
Protein requirements
1.
Protein needed for maintenance and growth.
Growth includes weight gain in childhood
formation of foetus and adnexa in pregnancy
production of milk in lactation
2.
Maintenance requirement determined in two ways:
1
from sum of obligatory losses (FAO/wHO 1965)
from minimum emount of good quality protein
(a)
,^s<.z-j7s
needed to maintain I! balance (F;lO/hHO 1971)
Growth requirements calculated from amounts of protein
laid down in new tissue or secreted in milk.
5.
'■S’
Except in young infants and lactating women, requirement
for maintenance greatly overshadows’that for growth.
In infants the safest method of estimating requirements
is from observed intakes of breast-fc-d children growing
normally. See Table I.
4.
In other age groups, requirement calculated in three stages-:
(a) add minimum requirements for maintenance and growth
as in para 2.
(b)
the experimentally determined^results are averages .
Individuals vary with SD'AlC^o of mean. Mean + 2SD
will cover 95^ of individuals. Therefore add 2O7> 3°
for individual variation. Results shown in Table II.
(c)
Above results are in terms of top quality protein,
assumed to be 100$> utilized. Correct for lover
protein quality (NPU) in actual foods. -In UK diet,
NPU A.- 70. In poor’ tropical diets NPU 50-60.
•ytrzni
—------
TABLE I.
Protein requirements of infants estimated from
observed intakes which maintain normal growth
(g/kg/day)
Age (months)
Human milk
Cows' milk1
o -
3
2.6
2.2
3 6 -
6
9
K9
1.5
1.8
9 - 12
1.5
1.25
Values are averages + 2SD
♦Cows' milk formula with protein content
similar to human milk
(Data from: Fomo:i(19CO); Femen and Eay(1958);
Chan and Uaterlow( 19,66) )
<rf rL'Ik
3 a m Ifere not
.2. /-At UTVX/n
Table II - Safe level of protein in terms of diets of protein
qualities of 60, 7° and 8(^6 relative to milk or eggs
Body
weight
kg
Age group
Infants
6-12 months
9.0
Children
1-4 years
Safe level of egg or
_______ milk protein________
g protein
g protein
/kg/day
/person/day
1.53
fl 4
Safe level of food
proteins g/nerson/dav
Score 1 Score
*
Score
80
60
rfeak
14
17
20
23
27
13.4
1.19
16
20
23
4-7
"
20.2
1.01
20
26
29
34
7-10
"
28.1
0.88
25
31
35
41
50
Male adolescents
10 - IJ years
56.9
0.81
30
37
3
15 - 16
"
51.5
0.72
37
4-6
53
62
16 - 20
"
62.9
0.60
38
47
54
63
Female adolescents
10 - IJ years
38.0
0.76
29
36
41
48
15 - 16
"
49.9
0.63
31
39
45
52
16 - 20
"
54.4
0.55
30
37
43
50
37
**
46
*53
62
29
**
36
**
41
48
add 9
add 11
add 13
add 15
add 17
add 21
add 24
add 28
Adult man
65.O
0.57
Adult woman
55-0
0.52
Pregnant woman,
latter half
Lactating woman,
first six months
l
1
*Scores are estimates of the quality of the protein usually consumed relative
to that of egg or milk.
The safe level of protein intake is adjusted by
multiplying the intake of egg or milk protein by 100/score. For example,
100/60 = 1.6? and for a child of 1-4 years the safe level of protein intake
would be 16 x I.67 or 27 g of protein having a relative quality of 60.
The
:*
correction may over-estimate adult protein requirements
COMMUM;TY urn
B.
Enci’gy requirements
1.
New units:
1000 kilocalories (kcals)
=
2.
Q
2.4 megajoules (MJ)
For energy, requirement estimated as average intake
of healthy people.
There is very wide variation
between individuals. Some will need less energy
for the same level of activity, others more. By
contrast, for other nutrients, e.g. protein,
the 'requirement' or safe allowance is the average
+‘a safety margin.
I.
Why the difference?
With other nutrients, if an individual gets more
than his requirement, it does no harm; with energy
an excess intake causes obesity.
I
lj
!
5.
In principle, energy requirement made up of two
components - maintenance and physical activity.
(+ growth in children).
In practice separation
not possible because of difficulty of measuring
expenditure on activity over 24 hours.
Maintenance requirement = about 1,5 x basal metabolic
( Mi n,rr,al acYi rtf y )
ratG
Except in very active people, it makes up the major
part of energy needs. Average needs at different
levels of activity shown in Table III.
4.
Other factors:
Energy needs per kg decrease from infancy
to old age (Table IV)
i)
Age
ii)
Body weight
Small people need less energy than
large ones.
Therefore, for people in normal
nutritional state, requirement should be
calculated per kg body weight.
But for undernourished or overnourished
(weight for height too low or high)
requirement should be related to ideal
weight.
iii) used to be recommended that energy needs reduced
lt
in hot climates.
Latest FAO/WHO Expert Group
abandoned this idea.
5.
Pregnancy
Add 150 kcal/day in 1st trimester
350 kcal/day in 2nd and 3rd trimester
Lactation
Add 500 kcal/day
TABLE
]TI
Energy needs of aycrage man (6$ kg) or woman (55 kg)
according to activity
(kcals/day)
Man
Woman
Maintenance
2600
1900
Light activity
2700
2000
Moderate
5000
2200
High
3500
2600
Very high
4000
2950
Types of activity
office and shop workers, professional men, housewives
(mechanized)
Light:
Moderate: light industry, many farm workers, housewives
(unmechanized)
High:
Some farm workers, forestry, mines, steel, dancers,
athletes
Very
high:
limberjacks, blacksmiths, rickshaw pullers
TABLE
IV
Energy needs at different --.ges
Age
(moderate activity)
kcals/kg
kcals/hcad
0-3/12
Weight
kg
4.6
120
750
3-6/12
6.6
760
6-9/12
8.3
9.6
115
110
105
112
1000
850
101
1350
91
78
2190
71
57
49
46
2600
2900
3070
3000
62
50
43
40
2350
2490
2310
2200
9-12/12
Average 1st year
1-4 years
4-7 "
7-10 "
13.4
20
28
10-13 years
13-16 "
16-20 "
' Adult
37
51
63
65
W0M.’E
10-lJ years
15-16 "
16-20 "
Adult
38
50
54
55
.
910
1830
fVUT U -2-0
(
)F,G
LONDON SCHOOL OF HYGIENE AND TROPICAL MEDICINE
DTPH, DIM & H and DCMT COURSES
NUTRITION - Introductory lecture
General view of world nutritional problems
1.
Nutritional problems divided into four categories:
A.
The major, almost world-wide, problems:
.
-r
e>F
<*■)
brrttf-u.6
B.
protein-calorie malnutrition in children — Mosr
inadequate energy intakes in adults
-vitamin A deficiency
r
in Ae
nutritional anaemias /y
The classical avitaminoses - more localized,
less common:
beri-beri- re
pellagra
o~r>y
Conditions which may have a nutritional cause
in part or whole:
endemic goitre and cretinism
^jA^-peripheral neuropathy
stenosing pyloric ulcer
,.bladder stones
?certain forms of cancer
«/
2
Q L.£>o_
/7Z'_Z'
Often difficult to separate deficiencies from '
effects of toxins, e.g. lathyrism
Z7
>£ u >fty rcru^--> cA rvci / S
— A<»-O
Regional^dif'?'erenc!es1 In distribution of disease
ischaemic heart diease
A look-back at the past
If protein-calorie malnutrition is one of the commonest
diseases in the world, why was it not recognized until
40 years ago?
Possible reasons, from which lessons may be drawn:
A.
Preoccupation with infectious diseases in the tropics^
B.
Scientific fashion: preoccupation with vitamins
and their biochemistry
C.
Preoccupation with problems of developed countries
cic.-n i c *z,c
ndU>/r>f’c
Page 2
J.
Complicating factors:
Malnutrition usually associated with poverty, bad hygiene,
infections, social deprivation, etc.
In considering the end results - inertia, retarded physics,!
and mental development, premature death - difficult, if not
impossible, to separate these factors. Therefore nutrition
should not be regarded as a separate subject, but as an
integral part of public health.
4.
5.
Measures of nutritional state of a country:
A.
Vital statistics, e.g. 1-4 year mortality rate.
Though malnutrition may not be primary cause, it is
usually an associated cause at this age.
Defects of present classification of causes of
death.
B»
Growth of infants and children.
/jh-r- uJP" <aP<THis raises problems: genetic versus environmental
factors;
the question of appropriate standards.
C.
Clinical and biochemical surveys.
D.
Dietary surveys
V/hat can medicine and public health do?
If the problem is shortage of food, the solution lies with
agriculture, economics, transport, education, etc.
The contribution of medicine:
A.
Treatment and rehabilitation of individuals
B..
Defining the extent of the problem - nature of
„ .
deficiency, groups affected, prevalence.-- o-7-iZ'■
C.
Advice on best method of breaking the vicious circle,
e.g. more food versus better water supply
■
Th
Maintaining awareness of the problem, so that account
is taken of nutritional needs by all relevant branches
of government and other agencies.
1"
J.C. Waterloo
February 1973
WT L^|
LONDON SCHOOL OF HYGIENE AND TROPICAL MEDICINE
Department of Human Nutrition
List of Books for Reading and Reference
Recommendations for Courses for DTPH, DTM & H and DCMT
*
UAftO®
1
.-TV
GENERAL NUTRITION
----------------------------------------
HUMAN NUTRITION AND DIETETICS
Davidson, Sir Stanley and Passmore, R.
5th edition. E, & S. Livingstone.
597pp.1972.
£6.00
'This is one of the most important books to be reviewed in these columns
for some time, and must be regarded as a major addition to textbooks of
medical science. It is beautifully written. It is not only a book of
great scholarship but it is extremely readable and it contains some apt
quotations.' - British Medical Journal
'This textbook needs no recommendation to the specialist worker in
nutrition or dietetics, but it is not a book written exclusively for
the specialist: it would be of the greatest interest and value to
doctors engaged in any form of clinical practice or to anybody who has
a responsibility for the feeding and nutrition of a group of people.' Tropical Diseases Bulletin
THE ASSESSMENT OF THE NUTRITIONAL STATUS OF THE COMMUNITY (with special
reference to field surveys in developing regions in the world)
Jelliffe, D.B. fflO Monograph Series No. 55. 271 pp. 1966 £1.80
The standard guide for the planning and conduct of nutrition surveys
and their interpretation. 'This textbook will be an indispensable
guide to nutrition work in developing countries whilst much of the
information in it, particularly that concerning the interpretation of
clinical signs, biological tests and standard anthropometric methods
should also be useful to medical officers in Great Britain.' - Public Health
FOOD FOR MAN
Aykroyd, W.R.
Pergamon Press, London
93pp.
1964
45p
A straightforward non-technical account of nutrients and deficiency
diseases aimed at the intelligent layman with some scientific background.
CONQUEST OF DEFICIENCY DISEASES - Achievements and Prospects
Aykroyd, W.R.
1970 90p
Freedom from Hunger Campaign Basic Study No. 24.
98 pp.
This book describes the advances that have been made in the last 60 years
in elucidating the epidemiology of deficiency diseases and the considerable
progress that has been made towards the elimination of some of them.
HUMAN NUTRITION IN TROPICAL AFRICA
Latham, M.C.
FAO, Rome
268 pp.
1965
£1.00
'A textbook for health workers with special reference to community
health problems in East Africa.' A book at the elementary level, very
well produced, with excellent photographs.
/Cont'd.
2
- 2 GENERAL NUTRITION (cont'd)
JOINT FAO/WHO EXPERT COMMITTEE ON NUTRITION
Eighth Report.
FAO Nutrition Meetings Report Series No. 49
(also WHO Technical Report Series No. 4-77)
80 pp.
1971
40p
This is a report on the latest meeting of the Joint FAO/WHO
Expert Committee on Nutrition held in November 1970. The
meeting concentrated on two main subjects of international
importance - food fortification and protein-calorie malnutrition.
SPECIAL ASPECTS OF NUTRITION
Experimental malnutrition:
MAMMALIAN PROTEIN METABOLISM
Vol. II.
ed. H.N. Munro and
J.B. Allison.
Academic Press, New York and London
642 pp.
1964
£7.50
Chapter 21:
Experimental protein-calorie deficiency
Platt, B.S., Heard, C.R.C. and Stewart, R.J.C.
This chapter describes, in detail, the results obtained
in animals by feeding deficient diets and the methods of
measuring protein values.
Economics:
ECONOMICS OF SUBSISTENCE AGRICULTURE
Clark, C and Haswell, M.
MacMillan Students Edition
250 pp.
1964
£1.25
This is a useful book for anyone interested in the problems
of economics related to food production, unemployment and
poverty.
Food hygiene:
FOOD POISONING /.ND FOOD HYGIENE
Hobbs, B.
2nd Edition.
1968
£2.50
Arnold, London.
252 pp.
A simple account of the subject, useful for anyone
interested in institutional feeding or needing to draw
up regulations about food handling, etc.
Infection:
INTERACTIONS OF NUTRITION nND INFECTION
Scrimshaw, N.S.,
Taylor, C.E. and Gordon, J.E.
WHO Monograph Series
No. 57Geneva.
529 pp.
1968
£2.70
Prepared in consultation with seventeen specialists in
various count rie s.
Pregnancy:
NUTRITION IN PREGNANCY AND DICTATION
WHO Technical Report Series No. 502.
A report of a WHO Expert Committee.
54 pp.
1965
50p
- 3 -
SPECIAL ASPECTS OF NUTRITION (cont'd)
Infant nutrition:
INFANT NUTRITION IN THE SUB-TROPICS .AND TROPICS
Jeliffe, D.B.
WHO Monograph Series No. 29Geneva.
335 pp.
1968
£2.70
2nd Edition.
A standard work on child nutrition in the developing
countries.
Protein-calorie malnutrition:
ADVANCES IN PROTEIN CHEMISTRY
Volume 25.
1971.
ed. C.B. Anfinsen, J.T. Edsall
and F.M. Richards
Chapter:
Protein malnutrition in children
Advances in knowledge in the last ten years
Waterlow, J.C. and Alleyne, G.A.O. p. 117-241
Psychological and social aspects:
DISADVANTAGED CHILDREN
Health, Nutrition and School Failure
Birch, H.G. and Gussow, J.D.
Grune and Stratton Inc.
322 pp.
1970
£4.30
A scientific assessment of the effect of poverty on the
intellectual potential of children.
REQUIREMENTS
CALORIE REQUIREMENTS
Report of the Second Committee on Calorie requirements
FAO Nutritional Studies No. 15.
Rome.
64 pp.
1957
30p
PROTEIN REQUIREMENTS
Report of a Joint FAQ/WHO Expert Group.
FAO Nutrition Meetings
Report Series No. 37Rome.
(also WHO Technical Report Series
No. 301)
71 pp.
1965
50p
REQUIREMENTS OF VITAMIN A, THIAMINE, RIBOFLAVINE AND NIACIN
Report of a Joint FAO/WHO Expert Group. FAO Nutrition Meetings
Report Series No. 41.
Rome.
(also WHO Technical Report
Series No. 362)
86 pp.
1967
40p
REQUIREMENTS OF ASCORBIC ACID, VITAMIN D, VITAMIN B12, FOLATE AND IRON
Report of a Joint FAO/WHO Expert Group. FAO Nutrition Meetings
Report Series No. 47.
Rome.
(also WHO Technical Report
Series No. 452)
75 pp.
1970
40p
FOOD COMPOSITION TABLES
TABLES OF REPRESENTATIVE VALUES OF FOODS COMMONLY USED IN TROPICAL
COUNTRIES
Platt, B.S.
H.M.S.O.
Medical Research Council
Special Report Series No. 302.
46 pp.
1962
70p
LONDON SCHOOL OF HYGIENE AND TROPICAL MEDICINE
COMMUNITY health cell
«/1.(FirStF(oor)S\
Professor J.C. Waterion
February, 1975
BANGALORE-560 007
Protein-energy malnutrition of children
1.
General
Two forms, of PEM can be distinguished - marasmus and kwashiorkor
Marasmus:
(mT“
-
Kwashiorkor:
growth failure
).
,
,
„ „ ,
,
. <i.e. semi-starvation
gro-ss loss of fat and muscle)
growth failure, beginning after weaning
less severe loss of fat than in M
oedema
—
enlarged fatty liver
changes in hair, mucous membranes, skin.
These are the extreme forms.
Intermediate forms (marasmic
kwashiorkor - MK - ) are common.
M has always been known, although different names have been given
to it, e.g. dystrophy. Frequently accompanies gastro-enteritis.
A condition very like K described in Central Europe in the last
century under the name 'flour-feeding injury'.
Other descriptions in the 1920s, especially from Latin America
(distrofia pluricarencial).
The name kwashiorkor introduced by C.D. Williams in Ghana, 1933.
Controversy then about cause ?thiamine deficiency, because of oedema
?infantile pellagra, because of skin lesions
P-C
— rr-L.i^<ccr3a.l
Lcoi o->'v->
By 1945 accepted that the main cause of K is protein deficiency,
although there may be associated vitamin deficiencies.
BrocK produced 'initiation of cure' (loss of oedema) by treatment
with pure amino acids.
Because most of the early descriptions came from Africa and
Central America, Trowell (1945) suggested that K was a disease
of people of African stock. This soon shown to be untrue. In
the late 1940s K described in Chile, Brazil, Mexico, India,
Indonesia. Also in Greece and Italy after World War II.
Page
2
Now recognized that K occurs in almost all developing countries.
The rather dramatic features of K - oedema, red hair, etc have tended, until recently, to obscure the less dramatic
condition marasmus.
The balance is now being redressed.
J.
Nomenclature
Since M and K grade into each other, we need an umbrella name to
cover the whole spectrum.
It is accepted that in both the
underlying deficiencies are of protein and energy, and not of
vitamins.
Hence the name protein-calorie malnutrition - PCM now changed to PEM since the abolition of the calorie.
Note that K and M are descriptive names, whereas PEM is a
causal name.
c.f. distinction between beri-beri and thiamine deficiency.
For public health purposes, PEM is the more useful name.
From a clinical point of view K and M are still useful because
they distinguish different clinical pictures.
4.
Causes
(i)
The classical theory
M = combined, more or less uniform, deficiency of
energy and protein, i.e. quality adequate,
quantity inadequate
e.g. 7/ protein cals, 50 kcals/kg
K = specific deficiency of protein:
quality inadequate, quantity adequate
e.g. 3% protein cals, 100 kcals/kg
MK - intermediate
e.g. 4% protein cals, 70 kcals/kg.
Evidence; in animal experiments, especially pigs, diets
such as those above do produce different conditions
resembling M and K.
in man, the preservation of body fat in K but
not in M shows that there must have been a higher
energy intake.
However, dietary studies in man have never shown
clearly the expected difference in energy intake.
(ii)
The Gopalan theory
Prospective dietary studies in India showed no difference
(quantitative or qualitative) in intakes of children who
developed K or M. Therefore suggested that the difference
lies in the child, not in the food. M represents an
adaptation, K a failure of adaptation.
Page
J
Other factors which may affect the outcome:
Infection may precipitate K
Individual differences in energy requirements.
5.
Classification
Accounts from different countries suggest that in some the most
frequent form of PEM is kwashiorkor, in others marasmus, in others
mixed forms. If accurate comparisons are to be made, there has
to be some accepted system of classification.
A number of different
features have been proposed as essential parts of the kwashiorkor
syndrome without which the diagnosis should not be made,
e.g. dyspigmented hair (Brock and Autret)
skin lesions
(Trowell)
fatty liver
(Waterlow).
However, the importance of these varies from one country to another,
and none of them can be accepted as essential features of kwashiorkor.
The one feature which is regarded by all workers as essential is
oedema.
This is the basis of the very simple Wellcome classification
'of seve're PEM.
““
- -------------- ———
Oedema
Weight 80-60$
Weight less than 60$
of standard weight
for age (Harvard)
Notes:
(i)
0
Under-nutrition
Marasmus
Oedema +
Kwashiorkor
Marasmic
kwashiorkor
Body weight expressed as % of standard
weight for age (Harvard 50th percentile)
(ii) This classification is only intended for
severe PEM, e.g. as in hospitals.
For
less severe PEM, as in community studies,
we have to use a different system.
Therefore a limit has to be set, at
which the classification begins. A
child is not classified at all unless
body weight is less than 80$ of standard
weight for age.
(iii)
The fact that only one clinical feature oedema - is included does not mean that others
are neglected. Once cases have been divided
according to the classification, it becomes
easier to analyze and compare other features,
e.g. tabulate as follows:
Undernutrition
Marasmus
page
4
Kwashiorkor
MK
Clinical
Age, months
% frequency of:
hair changes
skin changes
etc
Biochemical
Hb, g/1
Total protein
g/1
etc
Anthropometric
% Weight for age
% Height for age
etc.
(iv)
When comparisons are made in this way, it is usually
found that cases of M are more severely retarded in
height than cases of K. This suggests a more recent
onset for K.
( v)
If it is true that the different clinical pictures
of K and M reflect different dietary backgrounds
(see para 4), then proper classification is important
for diagnosing the prevailing deficiency, and hence
for prevention.
(vi)
It is often said that M occurs at an earlier age than
K, and that M is becoming more frequent. Both these
statements are probably true, but there is at present
(1972) no hard evidence to support them.
A proper
classification will make it much easier to substantiate
statements of this kind.
Further lectures will deal with:
Nature and cause of the specific features of kwashiorkor
(listed in para 1)
Classification of mild-moderate PEN in prevalence studies
LONDON SCHOOL OF HYGIENE AND TROPICAL MEDICINE
MSc and Diploma in Human Nutrition
Professor J.C.Waterlow
January 197$
Pathological and biochemical characteristics of
kwashiorkor (PEM)
COMMUNITY HEALTH CELL
<7/1,(First FloorJSt. Marks
Superficial signs
BANGAlORE-5€OOU1
Hair changes - Hair is dyspigmented, sparse, thin
and brittle,.
In people of African stock, hair is
often reddish.
In the East and Latin America it is
often white.
In straight hair a white band may
indicate the period of malnutrition.
Mechanism of the dyspigmentation is not
known. S-amino-acid deficiency has been
suggested.
Severe K can occur without any dyspigmentation.
The other changes are due to atrophy of the
hair follicles (see Bradfield^
The hair follicles are part of the epidermal
layer of the skin, which is also atrophic and
thinned.
i S h-y
aJ' gJ (Hfc)Skin
Z3; C C. h
lesions - The typical skin lesion in kwashiorkor has
been called 'crazy pavement dermatosis' and
has some resemblance to the skin lesions of
pellagra.
My impression is that it is
commoner in countries where maize is the
staple. It heals on treatment with protein,
without additional nicotinic acid. ?Role
of tryptophan deficiency
Many cases of kwashiorkor have no skin lesions.
■\ ti
A)
J
_
i
4
/yrcotzuS
. X
p y & Lw
I
"■
'
.
-■ V
»')
<
- Glossitis, cheilosis, angular stomatitis.
These are common, but not always present.
They are probably caused by associated
riboflavin deficiency.
-------- ------
,
J
=
N.B.
Kwashiorkor may be associated with other vitamin
deficiencies, notably of vitamin A and of folic
acid
page
2.
2
Oedema
This is the hall-mark of kwashiorkor.
It is accompanied by
l>w concentrations of total protein and albumin in plasma
(albumin_l=2—g%, compared with normar about 4 g%)l
Total body water is increased; the excess fluid is mainly
extracellular, but in some cases there may also be an
increase in intracellular water as well (not proven).
Note that the clinical test of oedema (pitting on pressure)
is not easily elicited unless some subcutaneous fat is present
(Frenk,
Mexico).
In marasmus there may be some increase
in total body water (Hansen ),
but because there is
less subcutaneous fat oedema is less apparent.
Causes of oedema
-i
Low plasma albumin (Starling's hypothesis); but
no strict correlation between severity of oedema
and extent of reduction of albumin.
-ii
Increased levels of anti-diuretic hormone (ADH) because
of failure of the liver to inactivate the hormone (theory
of the Hyderabad School). Unlikely, because ADH
*
should
cause hypertonic urine, whereas urine always hypotonic.
-iii
Impaired renal excretion of water and sodium, caused by
decreased glomerular filtration rate, which in turn is
caused by a reduction in cardiac output (theory of Alleyne).
-iv
Potassium deficiency, experimentally, causes oedema by a
mechanism which is not entirely clear : probably by in
creasing the reabsorption #f sodium in the renal tubule.
K deficiency is very common in kwashiorkor (see below).
It is possible that all these factors may play some part.
3.
Fatty liver
Fatty liver rather variable in different parts of the world, but
comparative figures not available.
Amount of fat may be up to 50% of wet weight - far more than in
any experimental models of PEM.
Very high fat content may cause liver failure (bilirubin
*
,
)]
*
transaminases
increases mortality rate?"
Cause
Decreased synthesis of the protein part of the
lipoprotein which transports triglycerides
"
from liver to fat depots, i.e. failure of'removal
of fat from'the liver.------'
”
page
4.
5
Anaemia
In PEM anaemia characteristically not severe, e.g. Hb 9g/100ml.
It is doubtful if there is truly an anaemia caused by protein
deficiency.
More severe degrees of anaemia caused by deficiency of Fe
or folic_acid.
The claim made for vitamin E deficiency as cause of anaemia
has not been substantiated.
5.
Potassium deficiency
Very common in severe PEM.
loss of K in stool.
Caused mainly by diarrhoea and
K deficiency probably contributes to apathy and weakness,
low cardiac—eut-put, oedema.
Serum K level is a poor guide to existence or degree of
K deficiency.
Diagnosis can only be made by whole body counting, muscle
biopsy or K balance. All difficult and possible only in
best conditions.
Therefore in general, assume that
patients K deficient.
The same applies to magnesium.
(see treatment)
Treatment of severe PEM
A.
Acute stage:
1.
Correction of disturbances of water and electrolyte balance.
If'dehydration, i.v. fluids. M.B. Danger of giving too much;
cardiac failure, pulmonary oedema, death.
Not more than 140 ml/kg/day - 5% glucose in ?/& isotonic
NaCl + K + bicarbonate if acidosis.
2.
3.
4.
Aptibittics: controversy about whether these should be
given routinely, even when no overt infection.
Folic acid
1 mg
5 x daily
Oral feeds: at first weak milk mixtures, in small amounts
at frequent intervals. Nasogastric tube may be necessary.
Work gradually up to stronger mixtures.
If lactose intolerance, use a soya preparation.
page
(Treatment of severe PEN)
B.
Recovery stage:
If possible, child should not be discharged until it has
reached expected weight for height (2-3 months). This
reduces recurrence rate.
The quicker the weight gain (provided it is not fat)
and the shorter the stay in hospital, the better.
Weight gain is more likely to be limited by intake of
energy than of protein. Aim at 150-175 kcals and 3~4 g
protein/1 g.
This calorie content can only be achieved
by adding fat, usually as vegetable oil.
Typical formula shown in table.
Vitamins A and D, organge juice, ferrous sulphate.
4
"’ABIE
milk
sugar
oil
water
milk
sugar
oil
M ... -■
water
oz
oz
fl .oz
fl.oz
g
g
ml
ml
u
16
100
90
85
1000
1
7
500
30
70
500
1
1
16
120
50
80
1000
-
1
16
190
-
60
1000
Dried skimmed milk
2
Evaporated milk
8
Half cream milk
Full cream milk
3i
2
One should aim to provide at least 75 calories/lb body weight/day
(165 calories/kg body weight/day). For any of the formulae in the
above table, this is approximately equivalent to 2 oz feed/lb body
weight/day (125 ml/kg body weight/day).
ULONDON SCHOOL OF HYGIENE AND TROPICAL MEDICINE
j
°
DTPH, DIM & H and DCMT COURSES
Professor J.C.Waterlow
NUTRITION LECTURES
COMMUNITY HEALTH CELL
—— ^13
47/1,(First Floor)St. Marks Road
BANGALORE-5t>0 001
Assessment of nutritional state (IEM) (1)
In community surveys severe PEM (kwashiorkor or marasmus)
found in only 1-4% of children.
Mild or moderate PEM much more
common, and the problem is to assess incidence and severity.
1.
Mortality data
1-4 mortality rate considered a better indicator of
malnutrition than infant mortality rate
Big.
Infant mortality
per 1000 live births
1-4 mortality
per 1000 in age group
0.8
UK
19
Jamaica
55
4.7
Guatemala
91
29.5
In study of causes of death below 5 years in 18 areas of
Latin America, in more than 50% of cases malnutrition
was an underlying or associated cause (Pan American
Health Organization)
2.
Clinical examination
This is necessary to rule out vitamin deficiencies, infection,
parasitism, etc, but is of relatively little value for quantitative
estimates of prevalence or severity of moderate PEM.
Hair changes (dyspigmentation, thinning) and skin changes (dry,
atrophic, glazed appearance) are common, and perhaps reflect
reduced availability of protein for rapidly turning over
epidermal cells.
Quantitatively:
hair diameter reduced - measured microscopically;
increased frequency of atrophic hair bulbs.
(see Nammacher et al. Am.J.Clin.Nutr.
22, 871, 1972
Bradfield, Lancet 2, 1169, 1968)
The practical value of these measurements remains to be determined,
Kr<r-r->a. I
S/c^/laS
page
J.
2
Anthropometry
This is the major tool for community surveys.
The basic data
on age, weight, height.
Subsidiary data are arm, chest and
head circumference, and skin-fold.
It is convenient to express results as per cent of a reference
standard. The most widely used standards are the 'Harvard
Standards' of Stuart and Stevenson (see Jelliffe, 1966 TOO monograph)
-i
Weight for age (weight of child as per cent of weight of
standard child of same age)
The earliest classification was that of Gomez (Mexic&)
based on Harvard Standards:
90-75$
=
grade 1 FEM
75-60$
=
grade 2 PEN
< 6Cf/>
=
grade 3 PEN.
MW
Height for age (height of child as per cent of height
of standard child of same age)
A malnourished child can lose weight, but it cannot lose
height. A low height/age (retardation) may be regarded
as evidence of past malnutrition, leading to growth failure.
Retardation in height is accompanied by retardation in
ossification, and by reduced head circumference.
-iii Weight for height (weight of child as per cent of weight of
standard child of same height)
A low weight/height is evidence of present malnutrition,
in children as in adults.
Note that the Gomez classification (weight/age) does not
distinguish between two quite different situations:
A
B
1 year
1 year
Weight, kg
7
7
Standard
weight, kg
10
10
Weight/age %
70
70
Height, cms
75
64.5
75
100
75
Height/age, %
Weight/height %
10
100
Malnutrition:
Present
Past
Age
Standard
height, cms
92
page
Physiologically these two children are probably quite
different»
Naturally there will be many children who
show both present and past malnutrition.
Arm circumference is a measure of thinness or fatness.
Arm-circumference/head circumference, as suggested by
Kanawati and McLaren (Nature, 228, 573, 1970) gives
essentially the same information as weight/height, but
probably less accurately.
Skin-folds and biochemical measurements will be
considered in the second lecture on assessment.
5
ftcrr~> c\ I
r) Aia/Tiy^d/
Cs~)
ex
^/cczo<^
C erm m u->-» Vy
sA^aeA.
COMMUNITY HEALTH CEL(A '
47/1,(First FloorJSt. Marks Doaq
Treatment of Malnutrition
BAWG&
*-OaE
- 560 001
Treatment involves both public health measures as well as standard
medical therapy of the acutely ill child or adult:
A few facts must always be remembered:
1.
Age distribution of population. About 25$ of the population
is under 5 and 50$ under 15. Child health is a major problem.
2.
Susceptibility to malnutrition: particularly the under 5s and
pregnant women because of the extra food needs for growth of
the foetus or child.
J.
"Malnutrition is the iceberg disease". If 1$ of children
under 5 have classical kwashiorkor or marasmus, it is probable
that ^0 - 60$ of the child population is underweight
and
malnourished.
k.
Malnutrition is part of a vicious circle. Economic and social
factors are important factors in the development of malnutri
tion which itself leads to apathy and inability to work.
Malnourished mothers produce smaller babies who may be
permanently affected mentally despite adequate postnatal care.
5.
In many countries energy deficiency is the major deficit not protein deficiency, eg. Ethiopian adults exist on diets
which seem barely adequate for the known basal metabolic
rates. Marasmus is the great problem in Asian, South American
and Ethiopian children - not kwashiorkor.
In.East Africa protein deficiency is important although
children with kwashiorkor seem to ingest too few calories also.
6.
Vitamin A deficiency and, in Asia, Thiamine deficiency, are
important deficiencies which arise mainly because of social
customs and taboos on particular foods eg. vegetables.
Despite the low calcium intakes in many countries rickets
occurs mainly in areas where skin exposure to sunlight is
limited by social customs.
Treatment must be based on a knowledge of an individual's needs
(requirements), his normal food habits and the"nutritional value o~f~
individual foods. All treatment must be simplg~_an^ practical_with a
strong educational element.
Individual's needs or requirement
A person's requirement for protein or energy is a definite figure.
Allowances given in books refer to expert committees' agreed amounts
which are useful when thinking in community terms and take into account
the variability in requirements from person to person.
- 2 -
Table 1 gives the allowances at different ages for a series of
nutrients: the protein value is increased to take into account the
relative deficiency of some essential amino acids in vegetable proteins
and assumes that only the equivalent of 70% of the protein ingested can
be used efficiently. Thus, for example, a year old child should be
allowed JO grams of protein which is over 2 grams per kilo when the
requirement for growth is only 1.2 grams/kilo of "perfect protein".
Foods
It is simplest to think of the main foods in three categories:
a) the staple foods - cereals, b) the staple roots, tubers and fruits
and c) legumes. Animal protein is not an important constituent of many
communities' diets; it is not worth encouraging its consumption since
it is too expensive. Cereals are important sources of protein as well
as energy. Table 2 shows the nutrient content of a variety of cereals.
The protein is not completely used because of a relative deficiency of
lysine but this can be counteracted either by eating pulses also, or
just eating more staple and using the extra amino acids for energy.
Encouraging the fortification of cereals with amino acids is a waste
of money and irrelevant to the needs of a community.
The cereals are usually milled and used as flour or grain and are
prepared as bread and porridges, or eaten in the grain form. The
quantities listed in Table 2 are for uncooked cereals: cooking leads
to a great increase in the water content of foods eg. maize. A child
cannot eat enough in only two meals/day to satisfy his energy needs
because his stomach is not big enough. If enough cereal can be eaten
to satisfy the energy requirements then his protein requirements will
automatically be met.
Roots and tubers:
In many countries especially in Africa root crops are consumed
largely as staple foods. It is very easy to grow these foods without
much effort. In contrast to the cereal group, the protein content of
roots is very low. When cooked in their fresh state, they contain a
large percentage of water and cellulose. In concentrated flour form,
the energy value improves. In comparison to cereals and legumes the
nutrient value of roots and tubers is poor.
- 5 -
Average protein calorie and other nutrient value of roots per
100 gm. (uncooked)
Protein
gm.
Calories
Ca.
mgm.
Fe.
mgm.
Vit. A
I.U.
Thian.
mgm.
Ribofn.
mgm.
Nico
tinic
mgm.
Vit.C
mgm.
Cassava
(fresh)
0.7
153
20.0
1.5
-
0.07
0.03
0.7
30
Cassava
(flour)
1.5
342
55
2.0
-
Snsete
1-5
190
140
5.0
^^Bread
fruit
1.5
113
25
1.0
-
Plantain
1.0
128
7
0.5
Sweet
Potato
1.5
114
25
1.0
Irish
Potato
2.0
75
10
0.7
Taro
2.0
113
25
Yam
(fresh)
2.0
104
10
Yam
(flour)
3.5
317
20
Food
0.04
0.04
0.8
0
0.02
0.05
0.2
0
0.10
0.06
1.2
20
100
0.05
0.05
0.7
20
100
0.01
0.00
2
*
0
0
-
0.10
0.03
1.5
15
1.0
-
0.10
0.03
1.0
5
1.2
20
0.10
0.03
0.4
10
10.0
-
0.15
0.10
1.0
-
- 4 The Nutrient Value of Legumes
Food
Prot.
gm._
Ca
mgm.
Calories
___________
Groundnut
(Fresh)
15.0
332
Groundnut
(dry)
27.0
579
Pea
25.0
Pigeon Pea
20.0
^^Lima Bean
20.0
Feo
Vit. A
mgm. |
I.U.
Thiam
mgmo
Ribofl.
mgm.
Niaco
mgm.
Vit. C
mgm.
0.5
0.1
10.0
10
0.15
17.0
-
r-
x,5
50
2.5
-
0.9
337
70
5.0
100
0.8
0.2
2.5
328
100
5.0
50
0.5
0.15
2.3
-
326
90
6.0
-
0.5
0.14
1.5
-
Soya Bean
55.0
382
200
7.0
-
1.1
0.30
2.0
-
Soya Bean
milk
3-4
32
12
0.6
-
0.09
0.04
0.2
-
Cow Pea
22.0
340
90
5-0
20
0.90
0.15
2.0
-
Pumpkin Seed JO.O
610
40
10.0
30
0.20
0.20
2.0
-
|
Note that the above foods contain very little Vitamin A - this is
best obtained from eating green vegetables or yellow fruits and vegetables
eg. mangoes, carrots and other greens which contain carotene.
Despite the reasonable iron content of many foods, iron from
vegetable foods is poorly absorbed and anaemia is very common.
Fortification has not answered the problem.
Practical problems:-
Therapy of the acutely ill malnourished subject
The immediate problems are infection, dehydration and diarrhoea.
In malnourished children dehydration is difficult to assess. For
general treatment of gastroenteritis see J. Biddulph, Tropical Doctor
July 1972 2 p. 114 and M. A. Church (same issue) p. 119. A child is
better wit IT oral fluids if he can take them than I.V. There is a
danger of overhydration if staff problems exist. Glucose in oral
fluids encourages absorption of fluid. Lactose intolerance is exceptionally
common in most countries. Feed early and frequently in small .amounts.
Most children with gastroenteritis are malnourished - therefore treating
dehydration without rehabilitation is a waste of time. Organise
rehabilitation with mothers fully involved and treating each other avoid emphasis on drips and drugs as cures. Use .local fo'o3s~encouraging
■
- 5 -
the use of pulses and cereals for protein content: more meals per day,
and special priorities for children in family ration to get in energy.
Community problems
Avoid glamorous projects connected with animal proteins. Go for
good storage conditions for food - 25% of food may be lost by deterioratiorFand pests. If roots are staples encourage legume consumption. If
cereals are staples encourage more frequent meals and higher intakes for
infants and pregnant and lactating mothers? Vegetable consumption needed
in areas with Vitamin A deficiency.
Under-five-clinics very useful with cards for each child - kept by
mother at home and understood as a record of health. Use acute medicine
as introduction to prevention and community efforts.
Malnutrition occurs particularly in the weanling period; after
5-6 months, breast feeding alone is not enough. Infection, poor hygiene
and-inadequate food lead to weanling diarrhoea. Treatment must include
the encouragement of suitable foods for infants. Prolonged breast
feeding on its own may be as harmful as early weaning onto advertised
commercial milk preparatinns.
References
1.
Jelliffe E.F.P. "A new look at multimixes
for the Caribbean"Journal of Environmental Health, September 1971, 17, 1J6-15O
2.
Protein - Calorie Malnutrition
Joint FAO/V.'HO Expert Committee on Nutrition.
W.H.O. Technical Report Series No. ^77, 1971
3.
Infant nutrition in the Subtrrpics and Tropics.
D.B. Jelliffe, W.H.O. Monograph No. 29, 1968
P. T. James
Recommended Daily Intakes of Energy and Nutrients
TABLE 1
Age Range
Infants
0-1
Average
Body
Weight
kg
Energy
(Kcal)
Protein
(gm)
Thiamine
mg
Riboflavine
mg
Nicotinic
Acid
rag
equivalents
Ascorbic
Acid
mg
Vit. A
Vit. D
Calci,’im
mg
PS
PS
retinol cholecaequivalents Iciferol
Fe
mg
7-3
800
20
0-3
0.4
5
15
*
45
10
600
6
1-2
11.4
1200
30
0-5
0.6
7
20
300
10
500
7
3-5
16.5
1600
40
0.6
0.3
9
2®-
300
10
500
8
5-9
22.8
1950
49
0.7
1.0
10
20T
350
2.5
500
10
Boys
9-18
31-61
2800
63-75
1.1
1.4
14-19
25-30
725
2.5
700
13-15
Girls
9-18
33-56
2300
58
0.9
1.4
16
25
725
2.5
700
13-15
Men
65
3000
75
1.2
1.7
18
^
*
3
750 .
2.5
500
10
Women
55
2500
63
1.0
1.3
15
3«s- ;
750
2.5
500
12
2nd & Jrd
trimester
pregnancy
2400
60
1.0
1.6
18
60
750
10.0
1200
15
Lactation
2700
68
1.1
1.8
21
60
1200
10.0
1200
15
Report No. 120.
HMSO.
Based on
Recommended Intakes of Nutrients for UK.Department of Health & Social Security.
Table 2
Average ■protein calorie and other nutrient content of cereals per 100 gm. grain (uncooked)
Food
Protein
Calories
Ca
mgm.
Fe
■ gm.
Vit. A
I.U.
Thiamine
mgm.
Riboflavin
mgm.
Wheat
13-1
353
15.1
2.27
-
0.30
0.08
2.C
0
Rice
6.2
361
3.7
0.45
-
0.06
0.05
1.0
0
Maize
8.0
354
9.0
2.0
-
0.05
0.05
0.6
0
Millet
6.0
332
350
5.0
-
0.50
0.10
1.4
0
Ricotinamide
"'I UU
Vit. 0
mgm.
Sorghum
10.4
355
52.0
4.5
-
0.50
0.12
3-5
0
Oats
12.0
588
60.0
5.0
-
0.50
0.15
1.0
0
Barley
12.0
339
35.0
4.0
-
0.50
0.20
7.0
0
Rye
8.0
350
25.0
3.5
-
0.27
0.10
1.2
0
Teff
8.5
345
110.0
90.0
-
0.50
0.10
2.0
0
47/r,r/iu'jirY HrA,-TH ecu
,(BANGA°Of>Sf'Ma^‘iOad
^7
BA^GAj.o.iE-560 001
BETTER FOOD FOR A HEALTHIER WORLD
WORLD HEALTH DAY 7 APRIL 1974
THE IMPORTANCE OF BREAST-FEEDING
by
Dr Adewale Omololu
Professor of Nutrition
University of Ibadan, Nigeria
Just a few months ago, a mother from a village was sent to my clinic because
her child was not growing as it should.
The child was two months old but weighed
only 2 kilos (5-1/2 lbs).
It was tiny, wrinkled, only skin and bones, and
screaming all the time.
The mother said that the child was bigger at birth but
I felt that he was not getting enough
had been losing weight for the past month.
to eat and so examined her breasts - they were full of milk.
She told me that the
child was not being fed from the breast but with a bottle, but could not tell me
the type of artificial milk product she used.
I then saw the husband and asked him what type of milk he bought for his
child.
He informed me that the child had been doing well and gaining weight on
breast milk but that, on his wife's insistence, he had bought the feeding-bottle
the previous month with all the money he had and was now saving up to buy a tin of
powdered milk.
Thus, the child had had nothing but water from the feeding-bottle
for a month, while the mother's breast‘milk had been expressed and thrown awayl
Luckily, the child had no infection and we were able to get him back on breast
milk.
WHD.74/3
THE IMPORTANCE OF BREAST-FEEDING
2
Before we blame this mother for nearly killing her child, let me say that
before she came to the clinic she was sure she was doing the best thing for him.
She had heard over the radio that powdered milk was the best food for infants.
She had learnt that educated and "upper-class" women used feeding-bottles.
She
had seen posters and advertisements at health centres and on hoardings in town
showing big bouncing babies being fed with bottles.
She too wanted the best for
her child.
Thus, though the child was growing well and was satisfied with her
breast milk, she forced her poor husband to spend all his money on a feedingbottle.
She had no idea that it was not the feeding-bottle but what you put in
it that makes the child grow.
Mothers all over the world want the best for their children - whether they
be in Colombia, Kenya or Japan.
It is unfortunate that they do not all know that
breast milk is the best food for infants.
Over millions of years, the composi
tion of breast milk has been modified and adapted by nature so that it is fully
digested by the baby and gives a good rate of growth.
Cow’s milk is, at best,
an expensive substitute.
It is true that manufacturers have tried to modify cow's milk by steriliza
tion, dilution and supplementation so as to give it a similar composition to human
milk.
However, modified cow's milk as sold in tins - whether powdered or fluid is only a substitute for the real thing.
"Humanized" or homogenized cow's milk
cannot be so completely digested and absorbed by the baby as breast milk - thus,
children have to be fed a lot more of these modified cow's milks to grow well.
In developed countries, where mothers generally feed their infants on modi
fied cow's milk rather than their own breast milk, it has become common practice
for writers to compare breast milk with cow's milk.
Perhaps it is a form of
unconscious justification.
The facts should, however, always be stated - breast
milk is food for infants; cow's milk is food for calves.
If we use cow's milk
to feed human infants, we are using a substitute.
The ideal is breast feeding;
only those who cannot attain this ideal should fall back on cow's milk.
Within the past ten years educated women in developed countries have
realized that by using cow's milk they are giving their children a "second
best".
In most universities in America, Britain and Europe, wives of teachers
WHO.74/3
and professors as well as women graduates have gone back to breast-feeding.
Clubs, like the La Leche League, have sprung up in many countries and towns,
formed by highly educated women.
Their main aim has been to convince and edu
cate other women about the importance of breast-feeding.
The medical profession has confirmed that breast milk, apart from being
fully digested and absorbed by the baby, transfers to him some of the immune
bodies of the mother and makes him less liable to infection.
Breast-fed chil
dren get fewer attacks of diarrhoea, vomiting and' stomach upsets than bottle
fed children.
Mothers who breast-feed develop a closer attachment to and love for their
children.
The children too are more relaxed, contented and happier.
There is
some evidence that this closeness may have far-reaching effects on the future of
the child.
There is also a statistical relationship between cancer of the breast and
women who do not breast-feed.
Breast cancer was found to be more frequent
among women who do not breast-feed.
But the interpretation of this relationship
is not as simple as it may seem because other factors have been shown to play a
role.
In developed countries, where the standard of living is high, where money is
available, where health services are well developed and where social services
like water and sewerage are taken for granted, mothers may be allowed to choose the
second best in feeding their infants.
In most developing countries of the world,
choosing not to breast-feed will have many repercussions not only on the baby but
also on the family and the country.
There are many factors in developed countries that help mothers who decide
to use the feeding-bottle.
Clear, good water is always available - all they have
to do is turn on a tap.
Most homes have storage facilities and refrigerators
where foods and milk can be kept.
These mothers can read and follow the direc
tions about mixing milk powders written on the tins and bottles.
The concept of
germs causing infection is well understood, and cleaning and sterilization of
feeding-bottles are willingly performed.
WHD.74/3
Mothers' in developing countries are not so well provided for.
In most rural
areas in these countries, where over 80% of the population live, water is avai
lable only from streams and springs.
Women may have to walk five to 10 kilo
metres to get a bucket of muddy water for use in the house.
This precious water,
full of germs and particles, is usually the only liquid available for mixing
baby's food.
To boil and filter it is not easy - fuel has to be collected and
this may mean another journey into the forest.
The huts in which most of the rural population live have no storage facili
ties - no cupboards, refrigerators or shelves.
Foods and tins of milk have to
be kept on the floors and under the roofs.
Being without the advantage of formal
education, most women cannot read or understand the directions for mixing the milk
powders or diluting the fluid milk.
Baby scales and nurses may be available at
the clinics and health centres, but these may be 10 kilometres or more away!
The concept of germs causing illness is very difficult to grasp for people
who have been brought up to believe that illness and death are caused be evil
doers, anger of the gods, witch-doctors and the "evil eye".
After being taught
how to sterilize feeding-bottles at welfare clinics, mothers arrive home and
sterilize the bottle and mixtures as they have been taught at the clinic, then
put the bottles in handbags or wrap them up in their head-ties!
They often
believe that once the bottles have been sterilized, they will remain sterile and
fit for use whatever is done to them.
The result is that bottle-fed children in the developing countries get
frequent attacks of gastroenteritis with vomiting, diarrhoea and dehydration.
Doctors and nurses in hospitals spend a lot of their time putting water back into
these babies and most hospitals have special wards for rehydration.
In areas
where these facilities do not exist or where babies are not brought to the hos
pitals early enough, many of them die.
Doctors in developing countries often
believe that putting a child on artificial feeding is like sentencing him to
death.
The cost of the powdered milk takes a large percentage of the family's
earnings in most developing countries.
The example given at the beginning of
this article, where the father had to save for a month to buy a tin of powdered
WHD.74/3
milk for the baby, is very common.
In most developing countries, the price of a
tin of powdered milk may be more than the father's wages for a full day's work.
In the rural areas, he has to sell some of his produce or a farm animal.
The effect of this relatively high cost of baby's food is that the tin of
milk is made to last for as long as possible.
The child, instead of receiving
a proper formula, is given a highly diluted milk which is mostly water and cannot
support growth.
He cries all the time from hunger.
The family has no rest and
the parents become worried, since they cannot understand this situation in which
they are striving to give the best to their child and the child is not happy and
contented.
Very few developing countries have dairy herds to supply cow’s milk.
Milk
powders and evaporated milk have to be imported from developed countries with
foreign currency.
As the number of mothers who stop breast-feeding increases in
these countries, so their governments will have to find more and more foreign
currency to import milk for the children.
The governments of developing coun
tries therefore have an obligation to their people to support the dissemination of
the truth - that the ideal food for babies is breast milk and that cow's milk is
only a second best.
Every facility must be given to mothers to breast-feed their
children for as long as possible.
The factors that make more and more women start giving cow's milk instead
of breast milk are many.
They include:
the increasing tendency for women to go out to work in offices and shops;
the effect of high-powered salesmanship by the baby-food firms;
the tendency to think of bottle-feeding as part of "western civilization",
which must be "better” than the local breast-feeding.
This belief is
strengthened when illiterate rural mothers see sophisticated, educated
"elite" women giving up breast-feeding for bottle-feeding.
If no concerted action is taken, the time will soon come when the female
breast will lose its function of feeding the young and become only a sex symbol.
WHD.74/3
rvu-T i-f.xc|
(?
BETTER FOOD FOR A HEALTHIER WORLD
WORLD HEALTH DAY 7APRIL1974
FOODS FOR BABIES AND TODDLERS
by
Dr E. M. DeMaeyer
Mother's milk is the best food for babies, and meets all their requirements
for the first few months of their lives if they have enough of it.
Breast-feeding is traditionally practised in most countries, but is steadily
becoming less common.
In all countries there is already a significant difference
in the frequency of breast-feeding among rural and urban populations.
For
example, in Guatemala, 98% of babies in rural areas are breast-fed, until the
twelfth month, whereas in the towns this applies to only 57%.
In Taiwan, 97% of
babies of six months are breast-fed against 61% in the towns.
And in certain
rural communities of Mexico there has been in 10 years a reduction of 20% in the
number of breast-fed infants of under six months.
In industrialized countries
with high living standards, relatively few mothers breast-feed their babies, but
the disadvantages of artificial feeding from birth are few in such conditions, as
is demonstrated by the low infant mortality.
The duration of breast-feeding varies from a few weeks to several months, and
may even be prolonged to two or three years, according to circumstances and accep
ted customs in particular countries.
The secretion of milk is usually abundant
during the first year, but tends to diminish afterwards.
Nevertheless, it
provides even then a precious source of high-quality proteins for the baby.
This
is of particular importance in countries where infant diets are very monotonous,
usually consisting of a single cereal or tuber - such as manioc - supplemented by
small quantities of other foodstuffs.
As a consequence, the content of protein,
vitamins and minerals in the diet is inadequate.
In view of the high cellulose
content of some of these foods, the diet, while satisfying the child's hunger, has
little nutritional value and does not provide enough calories.
If the meals are
not evenly spaced and frequent, i.e. five to six a day, it is likely that the
dietary intake of the child will be deficient in terms of calories and other
essential nutrients.
WHD.74/7
FOODS FOR BABIES AND TODDLERS
- 2 -
Let us now look at the problem of dietetic foods for babies and toddlers.
Babies of less than six months
If for some reason - such as a breast abcess or an infectious disease - the
mother cannot nurse her baby, or if her supply of milk is insufficient, the child
must have an adequate substitute for mother's milk for the first six months or so
of his life.
The most usual substitute is cow's milk in one form or another.
It may be fresh or in powdered form - either whole, skimmed or partly skimmed,
acidified, or "humanized".
Preparations of soya milk are also used.
If given
in sufficient quantities and according to the instructions of the manufacturers,
these breast milk substitutes are usually adequate as long as they are given with
due regard to hygiene.
While in countries with clean abundant water supplies the
problem of hygiene can be managed easily enough, it is very serious in countries
where such a supply is not readily available and mothers are likely to have only
rudimentary notions of hygiene.
However, in many countries it has been shown by growth-curves and mortality
rates of artificially fed infants that it is perfectly possible to obtain excellent
results by the use of these substitutes.
Babies of more than six months
Mother's milk or its substitutes meet all the needs of the baby for its first
four to six months of life, although some paediatricians believe that "mixed
feeding" - in the form of fruit or vegetable juices and mashed fruits or
vegetables, or even small quantities of egg or meat - should begin before this
age.
But after six months, such supplementary feeding becomes essential.
The
mother can either prepare supplementary foods herself from fresh produce or,
depending on circumstances, make use of preserved purees of vegetables and meat or
baby foods made of cereals, industrially processed and commercialized on a large
scale.
The latter usually contain flour from one or several cereals, sugar, and
a vitamin and mineral mixture, and they are intended to be prepared with milk.
For this reason they do not need to contain protein either in significant quanti
ties or of high quality, for the milk provides all the first-class proteins
necessary to assure the baby's adequate nutrition.
Often, however, the mother does not know how to feed her baby adequately with
the foodstuffs at her disposal.
Nutritional education can remedy this situation,
and many formulas of very adequate nutritive quality, based on locally available
foods, have been developed.
A combination of a cereal, a leguminous seed (peas,
beans, lentils), a green vegetable and - in some cases - meat, eggs, or milk
provides a mixture that is perfect from the nutritive point of view.
On the
other hand, it is unfortunately often the case that traditional foods, if not
WHD.74/7
- 3 -
properly processed, are ill suited to the needs of babies because of their low
calorie value.
As a result, and because the child is usually not fed more than
twice a day, his nutritional needs are not met.
Were he to be fed often enough,
say six times daily, his nutritional needs might perhaps be satisfied, but such a
solution is rarely feasible or adopted.
In developing countries, the baby foods based on cereals of the type used in
industrialized countries are usually imported and costly.
Moreover, the milk with
which they have to be mixed often has to be imported too, and is therefore also
costly.
As a result, these products are often mixed with water and provide a
diet that is unbalanced because of its deficiency in protein.
A classic example
is to be found in certain Latin American countries, where maize is the staple food
and where a practically pure maize starch, containing no protein, is mixed with
water to form a gruel which is the food commonly used for weaning infants.
In
other regions, rice or wheat starch may be used, with equally disastrous results
for the health of the child.
What can international aid do to provide babies and toddlers with the nut
rients they need?
The international action programme hinges on two measures:
the development of milk production and the development of weaning foods.
Development of milk production on a national scale
The development of the dairying industry is a relatively slow process, as
has been shown by the experience of the United Nations Food and Agriculture
Organization (FAO) and the United Nations Children's Fund (UNICEF) during the past
20 years.
Moreover, ecologic and climatic conditions are not always favourable
for the raising of cattle.
Thus, even in countries where it has been possible to
develop a dairying industry, milk remains an expensive food, the price of which
is beyond the reach of members of the less privileged social classes.
The para
doxical result is that some countries in which the internal demand is fully
saturated from the economic point of view have become exporters of milk, although
their real needs expressed in nutritional terms are only fractionally covered.
Nevertheless, in certain regions of the world the development of the dairying
industry has without any doubt contributed to the improvement of the nutritional
status of children.
Development of weaning foods
As has already been indicated, baby foods based on cereals, whether imported
or locally produced, are in general unsuitable when consumed alone because of
their low protein content.
It is only by mixing them with milk that it is
possible to obtain a food of good nutritive value.
The solution is to produce
and market locally highly nutritive weaning foods that do not require the addition
of milk but meet protein and energy requirements and are designed to supplement
WHD.74/7
the traditional diet of infants and young children.
Such products should be
attractively presented and marketed at as low a price as possible.
This is the policy that FAO, WHO, and UNICEF have applied with growing success
during the past 15 years in developing an international programme of weaning foods.
The first product of this kind, which was not originally developed as a weaning
food but as a beverage to supplement the diet both of adults and children, was
Incaparina, placed on the market with varying degrees of success in the 1960s in
Guatemala and other Central American countries.
Its ingredients included maize
flour and a cottonseed protein concentrate.
In Colombia a modified formula of
Incaparina incorporating maize and defatted soya has been introduced with a view
to producing a more adequate weaning food.
Incaparina and two similar products
are now competing in Colombia with various imported or locally produced weaning
foods, and their introduction has been facilitated by the tax exemptions that the
government has accorded within the fr: ■ ■ >rk of its social policy.
In the last five years other weaning foods have been developed in Algeria
(Superamine), Tunisia, Morocco, Egypt (Su iramine), Turkey (Sekmama) and in Iran
(Shadamin), and are already marketed comirircially in some of these countries.
Typically, they contain a cereal, a mixti e of pulses (chick-peas, lentils), with
the addition in certain cases of soya, si
and sometimes a small percentage of
skimmed milk, a vitamin and mineral mixture, and a flavouring agent.
These food
mixtures are in the form of white or slightly yellowish flours;
they are in some
instances partially pre-cooked, in which case the time required to cook them before
feeding is reduced to three or four iii:r ' is..
This short cooking time is advan
tageous by comparison with instant foods /hen the quality of the water used in the
preparation is doubtful.
In other cases the flour is of the instant type and can
be used at once after mixture with warm water without any additional cooking.
For
such preparations enzymes (amylase) are s Ided during the industrial processing, or
an extrusion process is used.
In both cases, good digestibility without further
cooking is ensured by the transformation of starch into dextrin.
Both these pro
cesses are slightly more costly and are intended to meet the needs of sophisticated
customers.
Packaging varies according to the market but should in principle be
as simple as possible, in the form of polythene bags, for example, containing
300 grams of the product.
This amount is sufficient to supplement the ration of
a young child for three days.
The polythene may be re-inforced by aluminium foil
to offer greater protection against deterioration and also a better presentation.
In Egypt, plastic containers are used.
What is important is to keep the price as
low as possible.
It should not be overlooked that packaging not only can increase the
commercial appeal of a product but also protect its quality.
And the public
should be educated to understand that a locally produced weaning food, although
inexpensive, is not an inferior substitut-/ but can be a product of high quality.
WHD.74/7
Experience shows that in the industrial manufacture of weaning foods the cost of
raw materials usually represents less than half the retail price.
The rest is
accounted for by manufacturing cost, packaging, amortization of equipment,
marketing costs (including advertising), and the retailer's commission.
The retail price of weaning foods that have been developed within the frame
work of the FAo/who/uNICEF programme varies from one country to another, but is
substantially less than that of comparable imported products.
Nevertheless, this
price is beyond the means of the less privileged classes of the population, who can
only benefit from such foods if the social policy of the government is such as to
allow them to be sold at an artificially low price or distributed free of charge.
The main objective, however, remains the introduction into the normal commercial
channels of distribution of a highly nutritive weaning food, which is at the same
time fully adequate for the infant's needs, produced from locally available
resources, and sold at a low price.
This objective seems about to be achieved
in certain countries such as Guatemala, Colombia, Algeria, Egypt, Tunisia, Turkey,
Morocco, and Ethiopia.
It is as yet too early to make a final judgement, but
there are many reasons for believing that this international programme represents
an important contribution to the improvement of the nutritional state and health
of the world's children.
WHD.74/7
NuT <v3°
COMMUNITY health cell
<7/1,(First FloorlSt. Marks Soad
BANGAi.OrtE - 5u0 001
JANUARY 17, 1971
susmhustaw OlflGHZIlli 5ECU0I1
Malnatvition in India
INDIA’S foremost social
problem is lack of pro
per nutrition for millions
of people.
This is the greatest challenge
to the nation’s scientists and ad
ministrators in the 1970s,
savs
pr. C. Gopalan, Director of tho
National Institute of Nutrition,
Hyderabad.
Nutritional deficiency
diseases
account for a large number
of
hospital cases throughout
the
country.
Sample surveys show that many
Infants and school children suf
fer from disorders caused bv an
unbalanced diet, some of them so
serious as to inflict permanent da
mage on body and mind.
The most important end wide
spread nutritional problem is the
inadequate intake of calories and
proteins.
Nearly two per cent of all chil
dren between one and five years
show unmistakable signs of this
deficiency.
But tills is a great underestimate
of the serious ill effects of an
inadequate diet, says Dr. Goplan.i•
The chief deficiency diseases■
Been in India, kwashiorkor and1
marasmus, account for only
a
email fraction of the damage caus
ed to the growing child.
Kwashiorkor, the result of a diet
with very little protein, is evidenc
ed’by swelling of the body, potbel
ly and changes in the colour of
©nt’s skin.
Anaemia
Needless finnmis
Trevor Ilrieherg
also see them at work among ca
sual labour in the ‘ slums of our
towns and cities.
This continuing human tragedy
need not take place at all, for
India has the natural resources to
prevent them — and at little ex-
•prises reconstituted skim
milk,
3 bread, bananas and sugar.
I These nutrients are given
as
■liquids at first. Later, rice and
Ichapatis and other normal articles
■of diet are substituted.
4 Kwashiorkor strikes
children
•between one and five years be
longing to large families.
| Dr. Reddy pointed to the cuts
ion the sick child’s Ups and said
■this was angular stomatitis, the
(result of lack of vitamin B.
The
girl’s bulging forehead
showed lack of vitamin D. DeflXciencies in food delayed the mile
stones
in a child’s growth —
■teething, walking and talking.
A low-nutrition diet was not
.necessarily a sign of poverty, I
llearnt. Often, even the chihhen
High-priced milk and meat, patent foods and medicines are not
needed to beat down calorie-protein-vitamin deficiency.
Research at the laboratories of
the Institute of Nutrition shows
that a simple diet of vegetable
foods — groundnut, pulses and
cereals — in the right proportion
is the answer.
Recipes based on vegetable-protein foods and suitable for feed
ing infants have been tried out
in field studies in villages around
Hyderabad.
'deficiency diseases because their
.parents do not know what makes
Marasmus Is a gradual loss of
Hundreds of children have been
a healthy diet.
flesh and strength. It occurs main Involved in these tests, and the
| Dr. Leela Iyengar, a researcher
ly in Infants.
results demonstrate that even the
’
.of
the institute who works
in
The most widespread deficiency most serious forms of deficiency
the hospital’s outpatient depart
disease of both children and adults can be controlled.
ment, told me she gives her pa
Is anaemia caused by lack of iron.
Keratomalacia, the commonest
tients supplementary
foodstuffs
This is common among preg eye disease of children, can be
and advice on nutrition
besides
nant women, and the cause of combated
by green leafy vege
riiedical attention.
many deaths at childbirth.
tables. But this requires an in
Lack of vitamins is also a po tense, long-term programme
of
tent
destroyer of young lives. teaching the facts about nutrition,
Nearly 10 per cent of school chil and the institute sought a short
dren from poor families do not cut to curb immediately the havoc
it causes.
get enough vitamin A.
A multipurpose powder ’s nreTests revealed that a single oral
But
pre-school children bet
ffiobked and packaged in the hos
ween one and three suffer even dose of 300,000 international units
pital kitchen. Each packet con
more from this lack, which im- of^ vitamin A given to children
tains 70 grams of material, which
pairs sight and ultimately brings £etween one and three, yearly for
Is eaten like gruel with water or
on total blindness.
four years was effective.
tnilk.
This was a very important dis
This packet costs 12 palse to
Rickets, another scourge of the
because trained
public
prepare but .goes free to patients.
Infant, softens the bones. Its cause covery
Taken with one multivitamin and
is
a shortage of vitamin D or health officers are not available
A child being fed liquid vitamin A under a pilot
one iron tablet daily it produces
calcium, and may result in de in sufficient numbers to givp daily
or
weekly
treatment.
Japid improvement in the run
formity.
study project.
down.
Pain in the joints and paraly
The institute now recommends
I The Institute has a clinic in
sis of hands and feet, swelling two doses of 200,000 units each at
the outpatient’s department for
or wasting away are the symptoms intervals of six months, and a merit and applied nutrition block vitamin D on growth.
pregnant women and those with
of beri berl, a nervous disease national programme of treatment on the outskirts of Hyderabad
Vitamin D is fed to children
newborn children. The main procaused by a poor intake of vita on these lines has been included to see feeding trials with pre-school between one and four years in
min B.
children.
groundnut oil from a dropper, and .
in the Fourth Plan.
they also get calcium in liquid 1
Visit any village, particularly
______ by .......
............ .......
Escorted
Miss Thlmmayamthe quarter inhabited by land- ma, a researcher of the institute’s
A 12-month experiment started form. Treatment was given under I
i[
less labour, and you will see the field unit. I recently visited
the early this year is designed
lo a tamarind tree. .
havoc of these diseases. You will Hyatnagar community
develop- gauge the effect of calcium and
It was around midday na w; I
travelled by jeep over dusty ooun- ,1
try roods from one
•viJViS'1 to I
another to see the programme |
The sun was blazing overhead, the i|
landscape was bleak.
Bare scrubland was Interspers- I
ed with solid granite boulders. I
Lines of palmyra palms,
babul I
and an occasional neem
tree I
relieved the monotony of barren |
earth.
j
Height and weight checks made I
every two months had failed to I
show any Improvement in growth, I
Miss Thimmayamma said.
their
was not surprising, since
V41CX1 I
ordinary diet was rice or jo war
with tamarind chutney.
A little dal is added to
this
proteinless, low-calorie diet once
or twice a week.
Most of the children participat- |
ing in this and other experiments
belong to families of landless la
bourers, whose constant conipa- |
Advice
tlem encountered among
them
Is different kinds of anemia.
Dr. Iyengar said 50 to 60 percent
of her patients in the last stages
of pregnancy were anemic, and
tests were being made to find out
how much nutrition women
in
this condition needed.
To maintain the level of hemog
lobin. the protein colouring mat
ter of the red blood corpuscles,
the least iron needed is 30 milli
grams a day.
A deficiency of folic acid can be
met by giving 500
micrograins
daily in the stage preceding deli
very. This also Helps the growth
of the unborn child.
A deficiency of vitamin B be
comes evident when the infant
feeds on its mother’s milk. The
clinic is conducting tests to find
out how much of this vitamin
should be given mothers to prevent
this.
Growth
A daily dose of three migrograms appear to suffice. Patent
medicines contain a much higher
dosage, which goes waste.
Tests are being carried out on
the effects of oral contraceptives
on women. Dr. Iyengar said many
women, especially members
of
poor families, developed a ting
ling numbness in their limbs and
ulcers at the corners of
their
mouths and on their tongues when
they used such pills.
Many cases of vitamin defici
ency were noted in women two
or tliree months after taking the
pills, but their symptoms disap
peared with doses of vitamin B-12
complex.
Married women who used oral
contraceptives ran into strong so
cial- and family pressures to dis
suade them from doing so. The
strongest opposition came
from
mothers-in-law, and the rate of
dropout was about 50 per cent in
general, and higher among the
lower classes.
One problem the Institute
Is
tackling is the .effect of poor nu
trition for a woman on her un
born child. Is it possible to de
vise methods of preventing such
malnutrition from retarding
an
infant's growth in the womb?
Dr. Iyengar treats women Rix
weeks before they are due to de
liver with 50 grams of protein
and 2.300 calories daily in addi
tion to a home diet of about 38
grams of protein and 1,800 calo
ries.
With this supplementary
diet
the weight of babies at birth is
Miss Thimmayamma, a researcher of the National
Institute of Nutrition, Hyderabad, and Mr. Achari,
the village schoolmaster, with products of the
school garden at Kuntloor.
found to Increase by 300 crams.
At the same time the mother's
health and production of milk and
the infant's production of serum
improve.
According to a survey made by
the Indian Council of Medical Re
search in 1968. a woman's needs
of calories in pregnancy are: se
dentary worker 1,900; moderate
worker 2,200; and heavy worker
3,000.
In the second half of preg
nancy this intake should increase
by 300 calories, and for breast
feeding up to one year the extra
calorie need is 700. .
The daily Intake of Proteins
should be 45 grams, with
an
additional 10 grams for the se
cond half of pregnancy and 20
grams for the period of lactation.
The ma hi need of pregnant wo
men is calories. These should be
ideally available from early pre
gnancy, hut this is not practicable
for most families because of their
low earnings.
But special feeding in the last
six to eight weeks can make a
significant
difference, although
babies will still not reach
em standards in height
weight.
and
Giving mothers additional p?
*tein without
carbohydrates fa
increase the consumption of ca
lories is a waste. Calories and
proteins must tjo together.
and
if folic acid iron are added they
Better nutrition ensures a heal
thier more vigorous and therefore
more productive nation. This goal
is within our grasp if only
we
can educate people on the need
to change their eating habits.
Cheap vegetable foods which
are readily available in the vil
lage, or which can be cultivated
easily, can provide all the calo
ries. proteins, vitamins and other
protective elements the human
body needs.
What Is lacking Is a campaign
■of mass education to carry the
message of better nutrition
to
these in most need of it. Malnu
trition is a problem of public
health and must be overcome
through the joint efforts of re
searchers and administrators.
The time for doing it is right
now.
Malnutrition in Inilia
INDIA’S foremost social
problem is lack of pro
per nutrition for millions
of people.
This is the greatest challenge
to the nation's scientists and ad
ministrators in the 1970s,
says
IDr. C. Gopalan, Director of the
National Institute of Nutrition,
Hyderabad.
Nutritional deficiency
diseases
acconnt for a large number
of
hospital cases throughout
the
country.
Sample surveys show that many
Infants and school children suf
fer from disorders caused by an
unbalanced diet, some of them so
serious as to inflict permanent da
mage on body and mind.
The most important and wide
spread nutritional problem 1$ the
Inadequate Intake of calories and
proteins.
Nearly two per cent of all chil
dren between one and five years
show unmistakable signs of this
deficiency.
But this is a great underestimate
tf the serious ill effects of an
inadequate diet, says Dr. Goplan.
The chief deficiency diseases
Been in India, kwashiorkor and
marasmus, account for only
a
email fraction of the damage caus
ed to the growing child.
Kwashiorkor, the result of a diet
with very little protein, is evidenc
ed’by swelling of the body, potbel
ly and changes in the colour of
Anaennin
Marasmus Is a gradual loss of
flesh and strength. It occurs main
ly in Infants.
The most widespread deficiency
disease of both children and adults
is anaemia caused by lack of iron.
This is common among preg
nant women, and the cause of
many deaths at childbirth.
Lack of vitamins is also a po
tent
destroyer of young lives.
Nearly 10 per cent of school chil
dren from poor families do not
get enough vitamin A.
But
pre-school children bet
ween one and three suffer even
more from this lack, which im
pairs sight and ultimately brings
on total blindness.
Rickets, another scourge of the
Infant, softens the bones. Its cause
is a shortage of vitamin D or
calcium, and may result in de
formity.
Pain in the joints and paraly
sis of hands and feet, swelling
or wasting away are the symptoms
of beri beri, a nervous disease
caused by a poor intake of vita
min B.
Visit any village, particularly
the quarter Inhabited by
land
less labour, and y’ou will see the
havoc of these diseases. You will
Needless hunt an
Tragedy
also see them at work among ca
sual labour in the slums of our
towns and cities.
This continuing human tragedy
need not take place at all, for
India has the natural resources to
prevent them — and at little ex
tra cost.
High-priced milk and meat,, pa
tent. foods and medicines are not
needed to beat down calorie-pro
tein-vita min deficiency.
Research at the laboratories of
the Institute of Nutrition shows
that a simple diet of vegetable
foods — groundnut, pulses and
cereals — in the right proportion
is the answer.
Recipes based on vegetable-pro
tein foods and suitable for feed
ing Infants have been tried out
in field studies in villages around
Hyderabad.
Hundreds of children have been
Involved in these tests, and the
results demonstrate that even the
most, serious forms of deficiency
can be controlled.
Keratomalacia, the commonest
eye disease of children, can bo
combated
by green leafy vege
tables. But this requires an in
tense, long-term programme
of
teaching the facts about- nutrition.
and the institute sought a short
cut to curb immediately the havoc
it causes.
Tests revealed that a single oral
dose of 300,000 international units
of vitamin A given to children
between one and three, yearly for
four years was effective.
This was a very important dis
covery
because trained
public
health officers are not available
in sufficient numbers to glvp daily
or weekly treatment.
The. institute now recommends
two doses of 200,000 units each at
intervals of- six months, and
a
national programme of treatment
on these lines has been included
in the Fourth Plan.
Escorted by Miss Thlmmayamma, a researcher of the institute’s
field unit.. I recently visited
the
Hyatnagar community develop-
Trevor Hfieherg
prises reconstituted skim
milk
bread, bananas and su-v.These nutrients are given
as
liquids at first. Later, rice and
chapatis and other normal articles
of diet are substituted.
Kwashiorkor strikes
children
between one and five years be
longing to large families.
Dr. Reddy pointed to the cuts
on the sick child's lips and said
this was angular stomatitis, the
result of lack of vitamin B.
The
girl’s bulging forehead
.showed lack of vitamin D. Defi
ciencies in food delayed the mile
stones
in a child's growth —
teething, walking and talking.
A low-nutrition diet was not
necessarily a sign of poverty. I
learnt. Often, even flic ciiilihen
of the fairly well to do develop
deficiency diseases because their
parents do not know what makes
a healthy diet.
Dr. Leela Iyengar, a researcher
nt the institute who works
in
the hospital's outpatient depart
ment. told me she gives her pa■ients supplementary
foodstuffs
and advice on nutrition
besides
medical attention.
Advice
A child being fed liquid vitamin A under a pilot
study project.
ment and applied nutrition block
on the outskirts of Hyderabad
to see feeding trials with pre-school
children.
A 12-month experiment started
early this year is designed
to
gauge the effect of calcium and
vitamin D on growth.
Vitamin D is fed to children
between one and four years in
groundnut oil from a dropper, and
they also get calcium in liquid !
form. Treatment was given under
a tamarind tree. .
It was around midday -.*•
*
w
travelled by jeep over dusty coun
try roads from one
vjjlng-: to
another to see fhe programme.;
The sun was blazing overhead, the >
landscape was bleak.
Bare scrubland was Interspers- ■
ed with solid granite boulders. ,
Lines of palmyra palms,
babul ;
and an occasional neem
tree
relieved the monotony of barren
earth.
Height and weight checks macle
every two months had failed to
show any Improvement in growth,
Miss Thimmayamma said. This |
was not surprising, since
tlieir
ordinary diet was rice or jowar
with tamarind chutney.
A little dal is added to
this
proteinless, low-calorie diet once j
or twice a week.
Most of the children participat
ing in this and other experiments
belong to families of landless la
bourers, whose constant compa
nions are hunger and undernou
rishment.
Getting parents to send their
children for treatment is a big.
problem. There are many dropouts,
and when children fall sick their
parents blame the feeding
pro
gramme.
Garden
Pre-school age children in Kuntloor, Andhra Pradesh, are given laddus
three days a week. Each laddu contains 30 gins, of wheat, 20 of green grain,
eight of groundnut and 20 of sugar or gur. It lias a protein value of 10.59
gm. and costs 10 paise to prepare.
At the villages of Kuntloor and
Kohada nutrition is provided to
children of pre-school age in the
form of laddus three days a week.
Each laddu contains 30 grams of
wheat. 20 of green gram, eight
of groundnut and -20 of sugar cr I
gur.
J
Its protein value is 10.59 grams. I
It gives 300 calories of energy I
and costs 10 paise.
a
These nutrients are also turned I
into biscuits, a "prestigious” form I
of food in the village, but this I
is more difficult to prepare.
A keen supporter of the
Im
proved nutrition programme
is
Ramallnga Achari,
the village
schoolmaster.
I
The school has a large, welltended garden, watered by an onrn
well with an electric pump. The
75-foot-deep well cost Rs. 45,000
to dig and cement.
Mr. Achari grows a variety of I
crops, and his poultry yield eggs fl
which he sells in Kuntloor and
the neighbouring villages.
The institute manages a chil
dren’s nutrition ward at Princess
Niloufer Hospital for Women and
•Children In Hyderabad. It> has a
dozen beds.
Dr. Vinodlnl Reddy, the
re- I
searcher in charge of the ward. ]
told me the commonest ailment I
among children brought to her for I
treatment
was edemas of kwa- I
shiorkor. Next came kerotamala- I
cia, rickets and anemias.
I
Ailment
A two-year-old patient from a
distant village was blind
and
showed signs of edema. Her pa
rents had taken her to a local
vald when she developed eye trou
ble, and this quack's "treatment"
had worsened her plight.
One eye was completely
lost,
Dr. Reddy said, as the corena was
damaged beyond repair, but the
other could be partially cured.
If the child had come two days
later she would have lost even this
eye, Dr. Reddy added.
I
Dally, one case of severe rteticlency came to the hospital's
out patient department, and
It
generally turned
out to be the
child of » landless peasant.
The diet Riven In the ward to ,
victims of kwashiorkor Is
high
in proteins and calories and com-
A multipurpose powder .is
cooked and packaged in the
pital kitchen. Each packet
tains 70 grams of material, which
Is eaten like gruel with water or
milk.
This packet costs 12 paise to
prepare but .goes free to patients.
Taken with one multivitamin and
one iron tablet daily it produces
rapid improvement in the run
down.
| The institute has a clinic in
(he outpatient’s department for
pregnant women and those with
newborn children. The main pro-
felem encountered smonflf
is different kinds of
Dr. Iyengar said 50 to £®.pgt(iges
ot her patients In the last » ,inc|
of pregnancy were anemic.
oUt.
tests were being made to
jn
how much nutrition women
this condition needed.
v,»moX"
To maintain the level of
lobln. the protein coIourL”„u«cl
ter of the red blood /°rpujnilli the least iron needed 1» 30
grams a day.
.. -j
*n
A deficiency of folic
met bv giving 500
<lchdaily in the stage Prec®?2 JroWth
very. This also helps the P
of the unborn child.
„ pcA deficiency of vita"?’„ uifant
comes evident when tn"]k. Tlif
mothers wil
finCj
feeds on its mother's
mu • (int
clinic is conducting tests ',tanun
out how much of tnis
'.event
should be given mothers to P
Growth
A daily dose of three bjatent
grams appear to sunice.
. ner
medicines contain a much hlS"
dosage, which goes waste.
Tests are being carri&f?Stlvi‘S
the effects of oral <on^eXanV
on women. Dr. Iyengar said m of
women, especially ^mbers
poor families, developed
and
ling numbness in their lina [heir
ulcers at the cornei
*
mouths and on their tongue
they used such plus.
deflclMany cases of vitamin J tw0
ency were ™ted.iA..w,°akmg the
or three months after taxinv
pllls, but their symptoms «
2
pcared with doses of vitamin D
complex.
Married women who used
contraceptives ran into str<”^ dlscitil and family pressures to Tbe
suade them from doing so. from
strongest opposition came
mothers-ln-law, and the rate jn
dropout was about 50 P<
*J
thc
general, and higher among
lower classes.
One problem the Institute
s
e eneev
trition for a woman on her im
born child. I s it possible to
vise methods ui
an
malnutrition from retarding
a
infant’s growth in the worn! .
Dr. lyenqar treats women alX
weeks before they are due to TO
liver with 50 grams of procm
and 2.300 calories dally In adJJ
tlon to a home diet of about. . «
grains ot protein and 1,300 ca o
ries.
With this supplementary
diet
the weight of babies at birta is
Thimmayamma.
of Nutrition
village school
**
1,
school ga
to Increase by 300 R
time the
m°
of fflHs
of £
to a survey niaj
Council of Medics
1968, a womans
in pregnancy arworker 1.900; moj
2,200; and heavy v
in the second half 01
nancy this intake should in
by 300 calories, and for feeding up to one year the
calorie need is 700.
The daily Intake ot ™
should be 45 grams, v/itn
additional 10 grams for u
Cond halt ot pregnancy a
grams for the period of lac
The main need of pregnai
jnen is calories. These sno
ideally available from early
Miancy, but this Is not pr;»<
tor most families because o
low earnings.
But special feeding in tl
Six to eight weeks can n
significant
difference, al
rvvT
UIoMd R
^3)
Below is presented a figure which attempts to describe
the relation of Kwashiorkor in a community to some of
the factors which are responsible for it and to give some
idea of their intricate relation to one anothor.
THREE PLQhlK
Pfix>Tf=ri
13RIO&G.
2/
if the child is not to fall into the river of
Kwashiorkor in its second or third year, it must
cross from breast feeding alone to a full diet on the
throe planks of prolonged breast feeding animal
protein and xezs vegetable protoln^/lo make the
discussion more complete I would like to briefly
mention the causes and the measures of prevention
of ?rotein calorie Malnutrition in India.
PCM is mainly due to inadequate Intake of
proteins though it can also be due to many pathological
states leading to defective absorption, defective six
digestion, defective utilization or loss of proteins
from the body.
Inadequate Intake is due tOJ
Due to poverty most families
1/ jACLC-noalc. J->iait;.tio^;
in India cannot afford protein rich foods vhichaare
relatively more expansive.
2)
luiPJ^J3g.e.-Q£..Uia,JulXLUApJial-needs,Q£ ..thft, .Child:
Children are weaned from breast or bottle milk to
starchy solids like rice and plantains.
3)
»
11
*
too often the childs
malnutrition begins in the womb with the mothers own
anemia oneU protein calorie defficiency.
i’heso lead//
to birth cf low birth weight and premature babies who
are more susceptil/e to PCM.
4)
CulturaLd£actoga,; inhere arc number of taboos and
superstitions attached to food in India, a large
majority of the population are vegetarians and there-
fox'e eggs and meat are not eaten.
Also though pulses
(Dulj is high in protein value, it is rarely fed to the
weaning infant because of the ;ujfoundod fears that it
will cause digestive problems and eventual death.
3
5)
i>ocial Factors} i’he classical example of social
factor affnctini^ tne diet is that that of the shift
with creator income,
£roa rough rice to aesthetically
more pleasing but nutritionally less valuable polished
rice.
another factor is the recent acceptance of powdered
milk as a peestige of status symbol.
The modern
media of advertising have overplayed the value of
milk powder,
The successful use of bottle feeding
by the well to do make the underprivileged feel that
they are being denied the rights of modern living if
they too cannot follow suit.
This leads to *•
i) darly weaning of babies from breast to bottle feeds.
ii)
since commercial milk powders are relatively more
costly for a lower middle class budget, mothors have
a tendency to stretch a tin to last for longer than
the required time
*
Thus the children get diluted milk.
In the hospital on questioning it was found that some
were giving their eliildren upto 1/loth dilution.
iii)
The lower middle class mother has neighbor the
money, the education, nor the kitchen facilities to
prepare a safe sterile bottle feeds.
The children
therefore receive a dilute, contaminated mixture, low
in nutrients and teeming with bacteria.
The resulting
triad of infective diarrhouey nutritional marasmus
and oral moniliasis is often fatal.
I&I PndV ^VTluK?
I
.1) educational programmes in Nutrition at every level.
1)%&) antenatal clinics
2) ik Maternal and Child welfare centres
3; £k School teachers
4) £1 Health centres
5)
Guncaunity development centres
d)
agricultural agencies
7)
social workers, health visitors and public health
nurses.
... 4 /
II
Introduction of improved farMming methods so that
the food production is good and the protein require
*
sent
of the population are more easily met
*
III
Development of food Industries whereby protective
foods may be made available at a reasonable non
cost to consumers - from local crops.
A good example
of such a product is MPF (Multipurpose food) a protein
rich powder introduced by the CFTKI (Mysore) which
consists of groundnut, flour and roasted .Bengal gram.
IV
Popularization of use of other foodstuffs rich
in protein content like groundnuts, ragl and
*
soyabeans
Muss screening for early detection of cases of
V
ill 30 that adequate nutrition and treatment nay
ba started early and a complete follow up done.
VI
Provision of I-wurnj^ent sponsored n.i d-day souls
in all educational institutions, orphanages,
hospitals, which would supplement the homo diet and
provide other nutrients usually lacking in it.
VII
Family rlatming would be another indirect step
in the prevention of PCM.
smaller families and
better spacing would ensure a regular and good protein
supply to each child without any strain on the family
budget.
Vlll
aesoarcfa work in the discovery of better and
more easily available sources of protein food -
especially for use in the underdeveloped countries
I
LONDON SCHOOL OF HYGIENE AND TROPICAL MEDICINE
Department of Human Nutrition
NUTRITION LECTURES
COMMUNITY HEALTH CELL
Iron metabolism and requiremen4Z/'l«(^‘rst f'loor>Sc- Marks Hoad
BANGALO.iE - 560 001
_
1.
Amounts of Fe in body
2400 mg
350 mg
Haemoglobin
Tissue Fe
Reserve Fe
(ferritin and
haemosiderin)
Normal adult male:
(typical figures)
750 mg
5500 mg
= about 50 mg/kg
Infant at birth
Total Fe
content
300 mg
= about 80 mg/kg
Growth requires
2.
25-50 mg/kg weight gain
Losses
Measured directly or by tracer methods
Normal adult::
0.9 mg/day (12°v per year)
(faeces 0.6, skin 0.2, urine 0.1)
<>>
p'^->
Child
(C5n^) 0.5 mg/day
— Menstruation
Pregnancy, 1st half
2nd half
Lactation
3-
2.8 mg/day (averaged over the month)
(A/nyn?
0.8 mg/day
3.0 mg/day
2.4 mg/day
Absorption of Fe:
Depends on
a) iron status of subject. Anaemic subjects absorb more.
Subjects with iron overload less.
b) nature of food
c) infection reduces absorption
Factors in food which affect absorption:
/c—
Haem Fe (in animal foods) better absorbed than non-haem Fe .
Inorganic Fe only absorbed in reduced form (j~
)
- -rpfco-n
v'./'c , gAJ'A/A/car
Inorganic Fe may form insoluble compounds, e.g. phytates
.
^->
fishier hye^te-
L^>
Is? c-i
Protein enhances absorption of Fe, probably through
binding with S-amino acids
In general, therefore, absorption better with a 'ffood'
diet.
Animal protein in diet
Efficiency of
°/q of calories___________ Fe absorption
4.
A
<10%
10%
B
10 - 25%
15%
C
>25%
20%
^5 V’eae.rcxMie'
,
•'
2x>.. c
etc ic
Requirements calculated by combining figures in
paragraphs 2 and J:
e.g. adult male on type A diet needs
0.9 x 10
=
9 mg/day
References:
WHO Technical Report Series no.405 (1968)
Nutritional Anaemias
WHO Technical Report Series no.452 (1970)
Requirements of ascorbic acid, vitrnnin
D, B12, folate and iron
J.C. Waterlow
■
ruu~r
LONDON SCHOOL OF HYGIENE AND TROPICAL MEDICINE
DTPH, DIM 8c H
k.33
ir
and DCMT COURSES
CH3
clf3
NUTRITION LECTURES
.
Yt ^rnCn fll
Vitamin A
Vitamin A is the name used to include all biologically active
forms of the vitamin.
Sources
Retinol, vitamin A-^, is found in animal tissues.
Dehydroretinol, vitamin Ag, is found mainly in the livers of
freshwater fish; it is much less common than retinol and less
efficiently utilised.
^-Carotene is a yellow pigment occurring in green leafy vegetables
and some fruits. It is an important dietary source of vitamin A,
particularly amongst lower socio-economic groups in developing
countries, J--tp ex to s
to e” <rQ.
'X o/-7 /Acx/'
.
of
zz-eno/e-'u'.
^0^7
Retinol equivalents
1 pg 'retinol equivalent' is equal to 1 Pg retinol in the diet
OR
CH3
CH3
OR
C«3
1 pg retinol is equivalent to
OR
Recommended Intakes
6 Pg p-Carotene in the diet
12 Pg other biologically
active carotenoids in
the diet.
J.33 international units of retinol
10 i.u. p-carotene
(WHO tech. rep. ser. no. 362, 1967)
Age
Recommended Intake pg retinol per day
0 - 6 months
6 - 12 months
Breast milk of well-nourished mother (450 pg)
300
1 -
3 years
250
4 -
6 years
300
7 -
9 years
400
10 - 12 years
575
12 - 15 years
725
16 - 19 years
750
Adults
kind, pregnant women)
750
Lactation
1200
COMMUNITY HEALTH CELL
^7/1,(First Floo.) j .Mark- ■ □ x
BANG.'uG
Absorption of Vitamin A
Retinol and esters (ie organic salts) of retinol are the most
efficiently absorbed in healthy persons with normal fat absorption.
Carotenes are water soluble and poorly absorbed. Raw, finely divided
preparations and the presence of fat in the diet favour a better
absorption of p-carotene. TA
ne^d.
Sa //s . <£)
—>
A6 &e*-hc?A
ft Cc.
Pcictidrarpi i.o
Ktr>Clfec
*
&ift<xlce
oen.
Zq/&4t
erf
Cn
fiyee^rfeck
<yf 3
rf
7
^3
^0
Ay jd )
PZ
■^nc-^'Cy
V- 7
/$7
Qo
6 1
>ei
3c
_ _
hj'He
fo
(>6
/\-CKcd
Ay Ay M
!c
t=—ffi <- !" <^f C-CZZl /C iei Cj
I. Hcr->C.
fc^-iy cheppeA
p . Hoi' r^ ici~> l&n erf y,}' k) errO'
nerrm^.] eero^c^^ K<-^&
/Qp& pep-n )foa.y
fte cet^m^-r-)
3 ^n
<5 m /i.;,
rt<"
66 ^.‘jmlA.
G e5 pcjmjd
- /a/,yW/4
2.
Metabolic function of vitamin A
1.
Vision
(Beaton & McHenry, 1964)
The aldehyde form of retinol
is bound to the protein opsin forming rhodopsin in the rods in
the eye. Light splits the combination, possibly exposing
sulphydryl groups which may stimulate visual excitation.
2.
Control of cell differentiation
(Amer.J.clin.Nutr. 22 (1969) 1081)
Vitamin A may control cell differentiation, possibly by regulation
of protein synthesis, particularly (1) in those tissues where a
rapid turnover of cell numbers occurs, and (2) those tissues
involved in the synthesis of mucopolysaccharides.
Assessment of vitamin A status
1.
Serum measurements
serum vitamin A:
deficient
<10 pg/100 ml I Xeial'e^Aliuco
low
10 - 20
Ipz/fe/' spots
acceptable 20 - 50
^3-carotene:
deficient
<20 pg/100 ml
low
20 - 40
acceptable 40 - 100
These parameters are applicable to all age groups but
2.
(i)
they are affected by dietary intake
(ii)
they do not indicate the size of the liver reserves of
.
vitamin A (90% in healthy person) . Ne
c f v-e- /<-
(iii)
serum vitamin A may be affected by impaired blood transport
of the vitamin. — iriyo I
>rvc-
Dietary enquiry
Should be carried out where avitaminosis A is suspected.
Suggested Reading
Symposium
'Metabolic Function of vitamin A'
(1969) 975-1135.
Nutrition
Vol. II
Amer. J. clin. Nutr. 22
Vitamins, nutrient requirements and food selection
(1964). Eds. G.H. Beaton & E.W. McHenry.
Acad. Press, London.
Nutrition Reviews (1971), 29(1), J.
D.I. Thurnham
fo~rc\ chncnd
n> > flu-
INTEGRATION OF A NUTRITION PROGRAMME WITH HEALTH AND
AGRISULTURE
H. Volken
In the Indian Social Institute Training Centre
from which I come, we are trying to help fulltimers in rural development from South East Asian courtries to
critically evaluate the work their organisation is doing. This
requires first a critical understanding-of their own society:
What is the prevailing concept of under-development and
development which is at the base of all development policies of
their government? This sort of approach has made us all increasingly
aware of the deeper causes which lay behind a process of change we
call 'development’, yet in reality is the development of certain
strata in society only. In an unjust distribution of development
gains we find the basic answer to the question; Why can the masses
not be mobilised (blocking of motivation), why can the local
resources not be tapped?
Introduction:
1,
The issue of Justice
It is relevant to mention this in the introduction to our theme:
Integration of a Nutrition Programme with Health and Agriculture.
It is meaningful to link these three sectors together; but to be
so more fully, these have to be placed into the totality of social
reality of a country,. I am very much impressed that this Seminar
has been guided by a paper of high quality, indicating that those
developing countries which have brought about a radical transforma
tion of inegalitarian structures have been.most successful in
meeting the basic needs of the people despite scarcity of resources.
Only in the context of this total transformation was it possible
to create a new system of Agriculture and a new health system. An
equitable distribution of increased food production and the
priorities of the health-care-system eliminated basically the
problem of malnutrition. The question is then raised: Where this
re-structuring of society has not oc.curred: "Is it the fate of
nutrition planners to be 1 patient revolutionaries1 biding his time
with pilot projects and marginal influence". For us in India this
question has a very realistic ring, 'What to say about the apparent
new commitment of Governments to Nutrition Programmes which
excludes however, the more decisive commitment to transforming
unjust and oppressive social structures responsible for the
constant widening gap between rich and poor? I'll tell you
frankly my opinion: Within oppressive and unjust social structures
creative participation of the people can never be what it should.
The proof is the constantly increasing percentage of the people
who are forced to live below the subsistance level.
In such a situation what real hope can integration of nutrition
programmes with health and agriculture give? I believe the honest
answer is in the saying: Better light a candle than curse the
darkness. Symbolic islands can.be created through this approach,
provided it is based on a philosophy of immense trust in the
...2/
COMMUNITY HEALTH CELL
47/1, (First Floor)Sc. Marks Road
\C .~-W
001
*
2
capacity of the people. Where this real love of the people
animates nutrition-programme-planners an approach which integrates
nutrition with health and agriculture can make a great difference.
2.
Example of a comprehensive rural health programme
I wish to give this example because it constitutes quite a
sizeable island, covering a population of 40,000. It was
initiated in 1970 by a doctor couple (Dr. Arole) in Jamked,
Maharashtra, and covers about 30 villages. The project demonstrates
it seems to me how best the Chines® model of comprehensive
health-care can be implemented in a feudal society..
This comprehensive rural health project is guided by the three
basic concepts of a) participation of the community
b) delegation of responsibility to lesser
trained personnel
c) mobile health teams
Under Five Clinics are central to the activities of the project,.
as one of the goals of the project is to reduce mortality rate
of the under five by 50$ within four years. Through these Clinics
supplimentary feeding is carried out in most villages. The
community takes the responsibility of providing fuel and utensils,
they do the actual cooking. The stress of health education and
the actual experience of improved health among the children has
motivated the community to work for better water supply, and to
set apart some land to grow food for this programme. The project
is collaborating with agencies involved in agricultural development.
But in comparison with another major project in this state, in
Kanakapura Taluka, where the thrust has been in agricultiral
extension for small farmers, more than on nutritional programmes,
the impact of increased agricultural production seemed to have
remained small. Care of minor illnesses, health and nutrition
education of the mothers, and immunisation programmes arranged by
the villagers themselves, are other activities of these under
Five Clinics. I do not think it necessary to give more details
about the various other goals and activities of this project.
Instead I wish to point out some of its characteristics which have
impressed me most and which are relevant for our purpose.
Emphasis on the educational aspect of the programme
Not only the mothers but the whole community is exposed to
continuous nutrition and health education. Not only the explanations
given by health workers, but also the actual results of a programme
in which many take an active part, achieve this result. I was
much impressed by the villager, who has been trained as health
educator, and wanders from village to village. He had a session
in the village I visited. In a dramatic way he explained his
charts to the villagers seated on the ground around him. Since
I knew the local language, I myself got fascinated by his way of
communicating, pointing out concrete examples of his reference among
the audience. I understood that the best communicators are
'found among the people themselves.
a)
- 3 b) The people are made to understand that food-supply from outside
was only meant as a starter. They would have to grow the food
required for feeding programmes. Some members of the community
did get motivated to donate some of their land.
c) The nutrition programme being part of a comprehensive health
programme meeting the basic health needs of the people, supported
by locaZL resources (primary health workers, collaborators and
material supplies), has a very strong demonstration effect. As
child mortality declined, motivation for planning the family
became effective.
d) The educational impact of the programme is very much
strengthened by the central role of the local permanent workers
who are fully identified with the community. Much of the training
of other health and nutrition workers is also given locally. They
escape thus getting alienated from the people through a sophisticated
training in a city. Experience has shown that team-members trained
in city-conditions, tend to leave this rural areas soon agah.
Evaluation; The Jamked project shows the possibility of creating
health through a comprehensive approach in which community teams,
inspired by dedicated animators (the Aroles) are able to bring to
life the participation of the village communities. The remarkable
success of the project and the spirit which animates it, has
encouraged many other groups in India to launch similar ventures..
Just now a new team of medical mission sisters is reaching out
into the area bordering on Jamked. Dr. Arole told the sisters:
"Do not imitate the Jamked project, you can do better? be creative,"
Provided success does not blind the groups involved to the fact
that they are still up against formidable obstacles, rooted in the
unjust structures of ownership of land and concentration of
political power in the hands of a minority, they are doing a
highly meaningful service to the people. Though they have to work
within the constraints of the prevailing structures, reflected in
the caste-system, they are instrumental in expanding the educational
processes in a direction which will make people more critically
aware of the still deep rooted elements of a highly inegalitarian
society. It might be worthwhile to discuss whether or not such a
comprehensive approach can and should evolve further into genuine
conscientization leading ultimately to the emancipation of the
masses.
3.
Food for Work
I had the opportunity to listen to your first reports on
programming concrete projects. In all of these food for work
had an important place.
What is surprising about food for work programmes is that
some look upon them as a curse, others as a great blessing. When
visiting in Maharashtra, a massive food for work project, I was
much impressed by hundreds of men and women constructing
percolation tanks that would greatly increase the agricultural
production. A few critical questions, however, brought out a
..4/-
- 4 -
a number of serious drawbacks of the programme. Nutrition
education was totally absent; more serious! the land below the
percolation tanks belonged to the ■■••icher farmers of the villages.
And an accident of lorries with grain having been diverted to the
market of a nearby township, still further darkened the picture.
As I wish to ellcite discussion, on what the conditions for a good
Food for Work Programme are, I cite another case. Over thousand
men and women have been involved in a programme which lasted
several years. It was greatly effective in increasing agricultural
production in the area. A network of channels were dug which
would bring the water from the main canal into the fields of the
farmers: fields were levelled and bunded. All excellent on
first inspection. But there were non-intended effects. The
earning capacity of the farmers was increased permanently through
the labour of this army of workers. These, however, after
completion of the project were back where they were initially!
in poverty, unemployment and helplessness. The inequality gap
between them and the farmers had been widened as a result of the
project. This case demonstrated how linking of Food for Work and
agricultural development needs a good deal of political wisdom to
be really contributing towards genuine development. The question
as to what impact such programmes have on the social structures of
society cannot be ignored. I am sure that many of you have been
connected with such projects which really improved the productive
capacity and the income of the beneficiaries themselves. I too,
know many such projects.
A friend of mine visited recently some region of Andhra Pradesh.
On his return he wrote to mes "I was shocked to see how priests
and sisters have become corrupt in handling development projects.
He was not referring explicitly to Food for Work Projects. But
the problem is common to all development work. If our preoccupation
is only in terms of efficiency, of effective programming etc.,
there will be a missing link. Development programmes, however
well conceived, do not automatically bear fruits of justice,
integrity and responsibility. It is strage that so many organisa
tions which go under a spiritual name pay so little attention to
this. I am including the organisation to which I belong. We
expose a host of people to responsible work, supply them with lots
of material inputs, and expect them to be good and honest without
helping them to discover motives to be so. Exposed to a host of
pressures it is not easy to swim against the stream, especially
with the increasing shortage of food-stuffs and constantly rising
prices. Food For Work programmes are to a high degree vulnerable
and expose the persons handling them to the pressures mentioned,
in an atmosphere of wide-spread corruption and of 'let me get up'
philosophy.
4.
The Educational Dimension
The linking of nutrition, health and agriculture has the advantage
that all three sectors demand primary emphasis on educational
processes if they have to build up new people with new ways of
...5/-
- 5 -
feeling, thinking and acting. You know much more about the nature
and methods of extension education related to these three sectors
than I do. But the best extension education canstill miss the
ultimate worthwhile goal of building a community, a horizontal
solidarity, of helping a new spirit of collaboration and sharing
to be born. Mei’e achievement motivation which results from
successful experience in ’keeping my child health, producing more
on my fields' risks to be.infected with striving for egoistic
social advance, which is the root-cause of underdevelopment
understood in depth. Everywhere we see that the same processes
which push up some, keep others down.
/
The following happened in North India; Under the guidance of a
priest the Santals had transformed a jungle area into fertile fields
*
They had built, with Food For Work an earthen dam in a valley close
to their settlement. The monsoon broke in. Heavy rains poured
down incessantly. Suddenly in the middle of the night shouts
resounded: "The dam is bursting", men and women ran out of their
houses in the direction of the dam. They worked the whole night.
filling bags with sand to strengthen the dam. The priest was with
them and all got wet to their skin. In the morning the dam still
stood. They had made it together, "During this night the community
was born", commented the priest in narrating the story. How can
such community experiences become educational processes within
programmes of nutrition, health and agriculture? This seems to be a
critical question if our long-term goal is the creation of a new
society, in which dignity and equality and participation is deeply
experienced within human organisations and institutions. It is
my personal conviction that any organised intervention risks
unconsciously to serve the interests of those who have control •“
over societal institutions, unless it is clearly guided by long-term
goals of a more just and more human society. Every intervention,
however small it may be, affects the process of change in society.
It either is supporting a process leading to increasing-inequality,
or it belongs to the counter-forces inspired by counter-values,
and which do have a relevance for a change towards greater social
justice.
You may remember the passage from Solzhenitsyn's novel 'The Inner
Circle'.... about the sheep producing more wool because of being
better fed. In explicit terms it means; mere extension education,
however important it is, not accompanied by 'political education'
gained by people organising themselves, establishing their own
institutions, e.g., for credit, marketing, etc.,Creflecting on the
causes of their having little say in policy formulation of
political bodies at various levels), risks to support the existing
power structure. Social workers-are easily 'used1 by politicians.
And the greatest illusion would be to think that Nutrition
Programmes are neutral, having no political consequences.
Politicians may be interested in Nutrition Programmes (nationally
and internationally) for "political reasons".. which in plain
language means: for the purpose of "feeding" rather than for the
purpose of emancipation and liberation, which really would serve
the interests of the people.
•
•
APPLIED NUTRITION PROGRAMME
It is time we bestow a little attention on Scientific
knowledge that is now available about “ FOOD ” with
fresh concepts and applications, and if only this knowledge
is ‘ applied it is certain that ‘ MALNUTRITION ’ and
‘UNDERNUTRITION’ shall be things of the past. The
right types of highly nutritious-—and cheap foods have got
to be produced, preserved and consumed—-more especially
by children, pregnant and nursing mothers, which
should ultimately become everlasting habits with the
individuals in particular and the community in general.
In a broad sense, it is just this that the much used term
“Applied Nutrition Programme ” envisages, and with the
effective implementation of this programme almost all over
the nation, such serious effects of malnutrition and
undernutrition like blindness amongst children, permanent
crippling and other preventable tragedies could turn
out to be only unpleasant memories of tW past.
Objectives :
_
(i)
To develop progressively a co-ordinated and
comprehensive National Programme of Edu
cation and Training in Applied Nutrition
Programme and related subjects with the
object of stabilizing effective field service to
improve the local diet through production,
preservation and use of protective foods,
(ii)
To ensure effective utilization of these protec
tive foods by the vulnerable group of popu
lation like, pregnant and nursing mothers
and pre-school children,
(iii)
To promote through demonstration and educa
tion among the village communities sound
and hygienic practices for production, pre
servation and use of protective foods, and
one
(iv)
To provide facilities for training in Nutrition
of various personnel involved in the imple
mentation of the programme.
At this stage it would he necessary to know at least
in brief, the various consequences of nutritional defi
ciencies to appreciate better the various aspects of ‘ Applied
Nutrition Programme
DEFICIENCY DISEASES
MALNUTRITION AND UNDER-NUTRITION
Lack offoods
Deficiency
Disease conditions
Milk, Pulses (Grams) Egg,
Pish and Meat.
Proteins
Green leafy vegetables like
amaranth,
drumstick
leaver etc., Fruits like
Gauva, pappaya, Milk
and its products.
Un - polished Rioe, Vegeta
bles, Meat products, pulses,
etc.
Vitamin
‘A’
Vitamin
B’
complex
Fruits like Oranges, Tomato,
Amla. Guava, etc.
Vitamin
‘O’
Milk, Eggs, Cod liver oil,
Butter, etc.
Vitamin
‘D
*
Milk, Green leafy Vegeta
bles and other Vegetables. ~
Minerals
like
Calcium k
Iron.
1 Kwashiorkor ’, - growth
failure
oedema
anemia, Skin and hair
disorders
and
liver
diseases.
Eye disorders
- Night
blindness - ultimately
even
total blindness
tooth troubles - Skin
diseases, etc.,
Beri Beri - stomach and
intestinal
upsets sore
mouth — Diarrhoea —
impaired digestion, etc.
Bleeding Gums, Scurvy.
extreme weakness,
lassitude, anaemia, etc.
Bone
Diseases -' spe
cially in children, and
pregnant mothers (Rick
ets and Osteomalacia,
Tooth troubles, etc)
Poor formation of Bones
and Teeth, anaemia,
General weakness.
Two
The diseases mentioned above are few of the main
important conditions and for every frank nutritional
deficiency, there will be many more who will be suffering
from other minor ailmeaits due to undernutrition and
malnutrition. Accordingly the Applied Nutrition Pro
gramme will enable every concerned village community
to appreciate the needs of various types of nutritious foodsparticularly for the vulnerable group like children, preg
nant and nursing mothers, and how best to produce and
consume each one of them locally.
HOW THEY HAVE DEVELOPED
The various activities unuer \ne ..Applied nutrition
Programme ’ are being started under a phased programme in
many parts of the country specially in selected commu
nity Development Blocks involving hundreds of villages
and lakhs of people and Mysore State has been no
exception to this ; already the various activities have
reached definite stages and are progressing well in a total of
24 C. D. Blocks, selected till now in Mysoie State for all
types of activities like poultry, fisheries, school gardens,
community orchards, etc., apart from establishing supple
mentary feeding Centres. The programme is also assisted
by UNICEF, WHO and FAO.
The Taluk Board will be responsible for carrying out
the programme and the Block Development Officer through
his technical staff will be responsible to provide technical
advice and assistance to the village Communities asso
ciated with this programme and will be responsible for
implementing this programme in all its stages. The staff
of the Primary Health Centres and M..C.H. centres in
various blocks will help to identify the important Nutri
tional deficiencies, advise on Nutrition and Diet problems,
and take part in training programmes.
Three
L
Food Production :
Vegetables and fruit production are
through the establishment of School
gardens, community gardens and
Orchards, home or kitchen gardens
in villages. The above will get
assistance from the Government in
the form of seeds, etc., till they be
come self contained. The produce
will be used for supplementary feeds in Feeding Centres.
Poultry and Hgg Production :
The Villages are assistedto start
poultry units with advanced poul
try farming practices—(1)60 hens
and 6 cocks are supplied initially
by the Governmental agency.
(2) Subsidies for specially built
Poultry houses in the Village Panchayat and Taluk
Board. (3) Free balanced rations to feed these birds for
one year are also given by Government.
A portion of the eggs produced will have to be used for
supplementary feeding in the local Mahila Mandal or
Balawadi Feeding Centre and the rest can be sold with the
ultimate object of being self contained.
Fish Production :
Village Fish ponds are established
with the Governmental assistance
in the form of cash loans, finger
lings, and technical guidance to the
Panchayat. In
addition. the
UNICEF’ is providing ‘ Nylon
Webbing’ ana other supplies with
equipment. The village panchayats
should use a certain quantity of fish for supplementary
feeds to children, pregnant and nursing mothers and the
balance may be sold to reimburse the finances of the
Village Panchayat.
Four
Milk Production :
For purposes of increased Milk Production bv the
farmers themselves in each village, establishment of
intensive pilot pi'ojects under ‘Applied Nutrition Pro
gramme’ are envisaged. At present UNICEF have been
supplying Milk Powder to be used in feeding Centres with
Eggs, Fish, Vegetables and Fruits.
II
Consumption :
n
Consumption of the foods produced
above in the Mid-day meals, in
feeding Centres of Mahila Mandais
and Balawadies in different villages
thus becomes a practical possibility
with the ultimate aim of educating
the community at large.
Training :
The training camps are arranged on Applied/Nutrition
Programme for all categories of personnel (both official
and non-official) who are involved at different levelsState, District, Taluka and village level.
Ill
IV
Education :
All methods and media are used for Nutrition education.
Printed Educational materials are to be sent to various
agencies with a view to educate both staff' and the
community at large, as to the various aspects of
‘Nutrition’.
Such a co-ordinated, comprehensive .National pro
gramme needs a close liaison between various Depart ments.
The ‘Applied Nutrition Programme’ is the peoples,
programme and with their co-operation its object will be
achieved for promoting health, happiness and prosperity of
the individual, family, community, village and the country
as a whole with Mal-nutrition and undernutrition turning
out to be things of the ‘PAST’.
WD P4699—GPB-25.000—23-11-67
Five
■ ,.4
'r
Introduction:
NUTRITION’PROGRAMI-E'FOR CHILDREN. COM
*
’,„fi......
6?''0UU 001
Malnutrition and. under-nutrition constitute serious hazards to the growth and
Development of children in our country, particularly infants and pre-school ace children.
decent surveys indicate that nearly two thirds of expectant mothers and pre-school age
children belonging to poor sections of the community residing in backward areas suffer
from serious malnutrition. Along with the unsatisfactory conditions of hygiene, environ
mental sanitation and control of communicable diseases,- malnutrition and under nutrition
rank as major secondary causes of the high mortality and morbidity which still continue to
prevail among children. The Government of India have, therefore, decided to give high
priority to the problem of nutrition among children in the Fourth plan. This considered
as is,basic to the programme of welfare for children.
v
2. Infants and pre-school children are, from the point of view of nutritional
deficiencies, the most vulnerable segments of our population. During this period in an
individual's life, the foundations of health for the adult age are laid and, therefore,
any serious damage sustained during this period quite often produces irrevocable effects.
Unfortunately, malnutrition is widely prevalent among the vulnerable sections of the
. population in the country, specially among the age group 1-5 years. The mortality and
mordbidity rates among this section are exceedingly high. Mortality in this age group
is 40 percent of total mortality in the country as against 6 to 8 percent in development
countries.
3.
Besides the problem of under-nutrition among children belonging to the lower
socio-economic groups of families, the problem of malnutrition manifests itself in the
form of proteincalorie malnutrition, anaemia and Vitamin A deficiencies. Rec"nt Surveys
carried out in different part' of the country under the auspices of the Indian Council of
Medical Research and the State Nutrition Divisions indicate that out of about 100 million
children in the age group of 1-5 years, about 50 percent suffer from protein-calorie
malnutrition in one form or other. Blindness not caused by Vitamin 'A' deficiency is also
common in the southern and eastern parts of the country. The social cost of such malnu
trition is heavy because the State has to incur large expenditures for the rehabilitation
of the handicapped children in later life. It is therefore necessary to have a supplemen
tary feeding programme for pre-school children, especially those belonging to the vulnerable
sections of the population.
The Fourth Plan;
4.
The Fourth Ppan provides for an integrated nutrition programme. Where so many are
under nourished, more food is the first step towards better nutrition. The nation wide
endeavour to developsiEKt agriculture along with animal husbandry and fisheries should be
regarded as the base of all effort in nutrition. While this is so, the important problem
remains of widerspread malnutrition among certain vulnerable categories of the population
specially children in the pre-school ages and among school children. This problem needs to
be specifically tackled.
5. The Fourth Plan includes the following schemes under different Ministries/
Departments, for promoting nutrition among children.
Programme
Out lay
( Rs. Crores)
Beneficiaries
( In Lakhs)
6.00
21.5
19.18
150
(a) Prophylaxis against nutritional
aneamia in mothers and children.
4.05
40
(b) Control of blindness in children
caused by Vitamin A Deficiency
( Department of health & Family
Planning)
1.02
160
i) Nutrition programme for pre
school children ( Department of
social welfare.)
ii) School feeding programmes
Ministry of Education &
Youth Services)
iv)(a) Applied Nutrition
(b) Composite programme for Women and
children
'Department of Community Development)
10.00
( To cover 450 CD.Blocks)
6.00
( To cover 1200 CD.Blocks}
=2=
iv) (a) Production of Balahar &
low-cost protein food.
7.70
(bJ Production of weaning food
( 2.5 to 3 lakh tonnes)
0.20
(c) Pilot plan for protein isolate
SKdxjsxBXXXK toned milk
(dept, of food.)
0.40
Total..
53.55
-’WvJ'
‘ k' -
"‘''-"'Oud
U07
1970-71 Budget:
6. The year 1970-71 will mark an important begining in providing nutritional
services to pre-school children belonging to the vulnerable groups of families in the
country. In addition to the Fourth Five Year Plan Programmes for nutrition, a special
programme of nutrition to cover 20 lakh children in the age group 0-3 years in tribal
blocks- and in slum areas of cities will be intiated in the 1970-71 budget.
The Special Programme:
7It has been decided to introduce a special programme to cover 10 lakh children in
tribal areas and 10 lakh children in the slum areas of metropolitan cities. There are
489 tribal development blocks in the country, besides a number of concernrated pockets
of tribal population in very backward rural areas. The Maternity Child Health Centres
and Family Planning Welfare centres Situated in these areas will be made use of for
supplying the nutrition to children. Smmilarly ten lakh children in the age group
0; to 3, residing in the slum areas of metropolitan cities, who are in most urgent need
of supplementary nutrition to ensure normal growth and development, will be supplied with
nutritive food.
8. As children in the age 0-3 years require different types of food as well as different
levels of nutrition, it is proposed to provide the following by way of supplement to the
food they get in their homes.
For children between
0 to 1 year.
Twelve of skimmed milk powder re-constituted, providing
120 calories and 12 grams of protein per day for 250
days in a year.
For children between
1 to 2 years.
One unit of skimmed milk powder reconstituted, plus
one unit of processed or prepared food, giving 300
calories and 12 grams of protein per day, for 250
days in a year.
For children between
2 to 3 years.
One unit of processed or prepared food giving 300
calories and 13 grams of protein per day, for 250
days in a year.
9. It is sestimated that one unit of nutritious food given in different forms per child
per day would cost Rs. 40 per year ( of 250) days per child including administrative and
transport costs, ^t would require Rs.4 crores to cover 10 lakhs children in tribal areas
and another Rs.4 crores to cover 10 lakhs in urban slums. As it will take some time for
the expenditures to come up to this level in 1970-71 an initial provisions of Rs. 4 crores
has been included in the budget.
nutrition programmes for children in the age group 3 to 3 years through Balwadis:
10. The Programme of Nutrition for children in the age group 3 to 5 years, which has
already been included in the Fourth Plan, is being initiated during 1970-71 with the help
of existing Balwadis run by voluntary organisations as well as by Tribal Welfare and
Harijan Welfare Departments in different States. The nutritional contents of the Pro
gramme would provide 300 calories and 15 grams of protein per day per child for 250 days
in a year. On an average the contents of food would have two ounces of cereals and one
ounce of pulses costing 15 paise per day per child. Supervision costs will amount to
1 paise per child per day. Whereever local food is available efforts will be made to
encourage local voluntary organisations to look after the preparation and supply of food
to children. In areas where local food is not easily available, it is proposed to supply
processed food in the form of Balahar; the raw material for preparation of Balahar is likely
to be supplied free of charge of CARE with the cost of preparation and administrative
charges being met from the budget.
11
It has boon decided to provide Rs-. 20 lakhs for this programme in 1970-71 by way of a
^gining. This provision will benefit about 68,600 children in the age group 3 to 5. Thc
xisting Balwadis in Family and child welfare projects and those run by voluntary social
elfare organisations receiving grants from the Central Social Welfare Board and those
romoted in tribal Welfare and Harijan Welfare, will be made use of in supplying nutritional
ervices to children
*
12.
School feeding programme:
The programme of mid-day school feeding programme to provide free meals to children in
the elementary stage of education was initiated in 1962-63 as a Centrally sponsored programme
by the Ministry of Education. The programme was initially started in five states, viz.,
Andhra Pradesh, Kerala, Tamil Nadu, Puhjab and Rajastan. By now all States except Jamy &
Kashmir and Nagaland are operating this programme. In the Fourth plan these programmes
are being implemented in the State sector and Central assistance to the States for the
purpose is included in the plan assistance for develbpmental purposes. It is estimated
that 98.7 lakh school children in the age group 5 to 11 years and 21-3 lakh children in the
age group 3 to 5 years received the benefit of mid-day meals at Primary Schools during
969-70. The State-wise distribution of children covered in this programme is furnished
below for 1969-70.
( in lakhs)
State.
School
children,
‘ - Tamil Nadu
2- Kerala
3 Andhra Pradesh
4= Mysore
5= Orissa
6. Madhya Pradesh
7. Uttar Pradesh
8. Rajasthan
9= Punjab
10- Gujarat
11. Bihar
12. Maharashtra
13. West Bengal
14. Haryana
16.00
16.00,
6.00
8.00
5.95
2.25
6.50
3.50
3.00
2.40
. 5.00
6.00
15.60
2.50
Total...
98-70
Pre-school
children.
Total.
1.00
3.00
0.05
4.00
0.02 ‘
4.50
0.050
0.75
0.95
0.75
5.00
0.75
17.00
19-00
6.05
12.00
5.97
6.75
6.50
4.00
3.75
3.35
5.00
6.75
20.60
3.25
21.27
119.97
The Programme will be continued in the Fourth plan.
Nutrition Programme for children under the Ministry of Health, Family Planning & Urban
Development:
13.
Ihe Programme of nutrition for children under the Ministry of Health, Family Planning
and Urban Development covers three major schemes viz (a) Skimmed milk feeding through
Maternity and Child Health Centres, (b) Prophylaxix against Nutritional Anaemia and (c)
Prophylaxis against Blindne s through Vitamin 'A' Deficiency. The details of the services
provided in these schemes are the following:
okin milk feeding programme through health agencies:
In the last 15 years, UNICEF has been supplying skim milk powder for supplementary
feeding programme of infants, children, pregnant and lactating mothers through health
agencies. The States bear the expenses for transport and distribution. At the present
time about 5,000 tonnes of skim milk powder are distributed annually to about 5 lakh
beneficiaries, through primary health centre' . Care is expected to continue this assistance
with the withdrawal of UNICEF.
a)
During the year >970—71, 5 lakh children in the age group 0.3 years will continue to
get t' e benefit of this service.
Prophylaxis against Nutritional Anaemia for Mothers and Children:
b)
The scheme seeks to provide preventive measures against nutritional aneamia in
mothers and children by administering ferrous sulphate (iron) and folic acid through
maternity and child Health and Family Planning centres.
During the year 1970-71 it is proposed to provide Rs. 40 lakhs to cover JO lakh
children with this service.
c)
Prophylaxis against, blindness in children caused by Vitamin 'A' Deficiency:
A scheme for controlling blindness in children caused by Vitamin 'A' Deficiency is
being implemented by the Department of Family Planning Ministry of Health during the foruth
Five year plan. During the 1969-70 16 lakh children are proposed to be covered by this
scheme. Vitamin 'A' capsules of high dosage would be administered to the children
through M.C.H. and F.P. Centres. The Plan outlay for the scheme is Rs. 40 lakhs.
During 1970-71 ks. 8 lakhs will be provided to cover 16 lakh children with concen
trated doses of vitamin 'A' in the form of capsules.
Programmes. _for the, production of Nutritive Foods under Foods under the Department
Food.
14.
Balahar:
a)
In the Balahar programme the Wheat required for the manufacture of Balahar is
supplied by Care while the cost of edible groundnut flour and an equivalent quantity of
milo or other food grains is met by USAID.
The uovt. of India incur the expenditure on
progessing the raw matterials and the cost of vitamins and minerals and flavouring agents.
The fourth plan includes a provision of Rs. 6.7 crores to produce 2.5 to 3 lakh tonnes
of Balahar to benefit 17 million children. The 1970-71 budget includes a provision of
Rs.50/- lakhs for this programme.
_____ Weaning Food:
b)
The weaning food is comparable to Balahar in nutritional qualities but has the
advantage that it is pre-cooked and has a long storage life, At will fill the need for
low cost protein rich food for commercial marketing. One suit has been developed in
collaboration with Kaira District Milk Procedure co-operative Union Anand with the
assistance of UNICEF and USAID for the production of nutritious low cost pre-cooked
weaning food utilising largely vegetable protein foods. The production of this food has
started r.-cently on a piolt scale and the marketability of this product has been assessed
and it is found that it has great potentiality.
Protein Isolated Toned M^lk:
c)
The object of this project is to encourage the use of oil-seed protein isolate in
toning milk thereby significantly stretching the country's milk supply and lowering the
cost of milk to the consumer. The Department of Food have already taken up two piolt
projects at Bangalore and Madras Dairies with the co-operation of CFTRI, Mysore, respective
State Governments and the United Nations Children fund. The two units are producing 1000
litres of vegetable toned milk per day which are mainly used in the school feeding pro
gramme.
Conclusion:
15.
To sum up, the Nutrition Programme for children, under different heads, will have
the following coverage in 1970-71 .
1. Special programme of
nutrition under Department
of Social Welfare.
20 lakh children in the age 0 to 3 years.
Rs. 40 laksh.
2. Nutrition programme for preSchool children unaer Department of
Social Welfare.
fe.2O
children ±n
years.
Qf , tQ
Mi nia-fexy of Education.
21, 27,000 children in the age of 4 to 5
years.
4. Skin M^lk feeding Programme
under the Department of food.
5 lakh children in the age of 0 to 3
years.
School feeding Under Tlw
fe- 297 laktsh .
5.
Prophylaxis under nutritional anaemia underthe M
Ministzy Bsf Health.
Rs. 40 lakhs.
50 lakh children.
6.
Prophylaxis against blindness
caused by Vitamin A Deficiency
in children under the Ministry
of Health.
16 lakh children.
q
laksh.
16.
The Nutrition Programme will thus cover 20 lakh children in the age group 0 to 3 years.
21.94 lakh children in the age group 3 to 5 years and 98.7 lakh children in the age
group 6 to 12 years during 1970-71. This will provide a sound foundation covering a
sizable population of children on which an extensive programme of nutrition could be built
up in the remaining years of the Fourth plan.
f\)JT M--33-
I
4----------------
f II FOOD
!. ¥0p ARE BEBRG
^JOSOMEA
|
immAT
adulteration
You are being slowly poisoned
fmiifMAT
u investigates
Report by Najmi A. Ajmerwala
’J* OGETHER
with
smuggling,
hoarding and the like, food
adulteration is a flourishing, illegal
business in India. With a small in
vestment, the food adulterator makes
huge profits. For example, if an oil
merchant uses even one per cent of
argemone oil to adulterate edible oil,
his yearly profits could be nearly Rs
50,000. In India, food adulterators
reap a yearly profit of over Rs 500
crores.
A third of all the food marketed
in India is adulterated, says a Health
Ministry survey. It could be even
more.
Art of adulteration
With the growth of knowledge and
advancement of science, adulteration,
which is as old as commerce itself,
has developed from a crude form into
almost a branch of applied science.
The adulterator is no longer the
simple milk seller adding water to
milk (or vice versa). The modern
adulterator has at his command a
vast variety of adulterants with which
to adulterate innumerable foodstuffs;
and he uses them with such skill and
finesse that adulteration has almost
become a fine art too—a very profit
able one at that.
Prohibited dyes, poisonous subs
tances like argemone oil and white
oil in edible oil, washing soda in
powdered sugar and prohibited arti
ficial sweeteners in soft drinks are
but a few of the dangerous adul
terants
used
by
unscrupulous
traders out to make a fast buck.
Spices and masalas are among the
foodstuffs most commonly found
adulterated. The list of adulterants
ranges from comparatively harmless
powdered husk in coriander powder
to lethal lead chromate in tur
meric (type of ginger). Some
times metanil yellow and other prohi
bited dyes, suspected to cause cancer,
are used to colour turmeric and chilli
powder. Besan, which is used exten
sively in cooking, is often adulterated
with kesaridal which contains toxic
matter that can cause paralysis of
the limbs.
Other common adulterants in use
are: ground stone particles in food
grains, vanaspati in ghee, iron filings
in rawa, chicory in coffee and metanil
yellow in sweetmeats.
The list of adulterated foodstuffs
is endless; be they in the form of
whole grains, powdered spices or
liquids such as milk, juices and
squashes. In fact, nothing is spared.
This tribe of adulterators is cer
tainly an ingenious lot. Rumour has
it that there is a factory in South
India which produces pebbles especi
ally designed to resemble rice grains.
Such ingenuity can be, and is, applied
to other articles also. For example,
papaya seeds are often mixed with
pepper corns, which they resemble in
shape, size and colour.
Only a
minute scrutiny can detect such
deception.
Even if the adulterants used are
harmless, they still serve to lower the
nutritional value of the food consum
ed to a level far below that required
for normal health. The health of the
masses, already rendered poor by
nutritional deficiencies, is thereby
further harmed by the cumulative
effect of adulterated food. Also, the
consumer pays prices which are out
Drive for more prosecutions in Maharashtra
No of food sample analysed
No of food samples found
adulterated
Percentage of adulteration
No of prosecutions launched
No of convictions
Fines realised
1972
1973
1974
(up to Sept.)
24,540
20,006
17,625
4032
16%
2530
1164
—
4693
23.46%
1918
304
Rs 153,251
2376
13.55%
2049
982
Rs 573,728
Source: Food and Drugs Administration, Maharashtra
12
HELP the Food and Drug
Authority in checking food
adulteration. The FDA acts
swiftly on consumers’ com
plaints. Readers in Greater
Bombay who suspect food adul
teration can just drop a line to
the FDA office at Griha Nirman
Bhavan, Opposite Kala Nagar,
Bandra, Bombay 400 051, or
dial 536321 and lodge a tele
phone complaint. You need not
give your name. Let your
charges be genuine and addresses
of the shops complete.
of proportion to the production costs
and to the weights and measures he
receives.
When the adulterants used are
harmful (as they often are), they can
cause serious diseases and even death.
In 1969, adulteration of edible oil
with argemone oil resulted in the
deaths of two people in Poona besides
making 60 seriously ill. In 1972, in
a district near Calcutta, nearly 400
people were afflicted with paralysis
after consuming mustard oil adul
terated with white engine oil.
Loopholes in Law
As long ago as 1954, the Preven
tion of Food Adulteration Act was
enacted in Parliament with the hope
that the Act would deter adultera
tors. But it was not to be so. The
loopholes in the Act are so wide
that they have often enabled guilty
offenders to go scot-free. To this
day no punishment has been meted
out to those responsible for the
Poona tragedy. As a matter of fact,
the maximum sentence of six years
rigorous imprisonment with a fine is
not known to have been given even
once.
In Maharashtra, a bill was intro
duced recently in the state Legisla
tive Council which proposes to
change over administration of the Act
itself from the local authorities to
the Food and Drug Administration
(FDA).
At present, the FDA has 200 food
inspectors on its rolls. They go
around the state inspecting shops
and collecting samples from manu
facturers, wholesalers and retailers.
Samples are also being taken from
inter-district check-posts, hospitals,
schools and other institutions. The
Assistant Commissioner of the FDA,
Bombay Circle, told me that the em
phasis of the FDA is on the manu
facturers and the wholesalers rather
than on the retailers. The FDA main
tains seven other circles in Maha
rashtra. It works in close collabora
tion with social service organisations,
notably the Consumer Guidance
Society of India.
The Act gives wide powers to the
food inspectors. They can enter any
shop to inspect any food articles sus
pected to be adulterated or wrongly
branded. They may even exercise
the powers of a police officer in as
certaining details. But all these
powers are of no avail when they are
expected to produce witnesses to
prove their case. Prosecutions launch
ed often fail because of the lack of
reliable witnesses whose evidence
will carry conviction in court. Often
the food inspectors are themselves
not careful enough in preparing the
prosecution case. In a recent case,
the Supreme Court set free an alleged
offender just because the inspector
did not send the stipulated quantities
of samples for testing to the public
analyst.
Delaying procedure
Delays occur when the food sam
ples are sent to the laboratories for
analysis because the laboratories are
short of staff and equipment. For
example, the laboratory in Bombay
which examines around 12,000 to
13,000 cases every month has only 27
analysts, while it needs at least 15
more. Furthermore, the laboratories
lack even basic equipment. For
example, the one in Bombay needs a
short and long-wave ultra-violet lamp
which can detect a wide range of
adulterants like colours and sweeten
ing agents.
In one case regarding adulterated
butter, the interval between the date
when the sample of butter was taken
and the date of filing of the complaint
was six months. But butter remains
in a condition fit for analysis for
three to four months at the most.
Consequently the Bombay High
Court held that the accused could
not be penalised since the sample of
butter had gone bad by the time the
complaint was filed.
Besides the PFA Act, 1954, the
Prevention of Food Adulteration
Rules, 1955 (Central), and various
The modern adulterator
In the absence of more district state rules have been framed to arm
Before prosecuting a defaulter an
elaborate procedure has to be observ level laboratories, the six city-level the Government with adequate power
laboratories in Maharashtra have to to check food adulteration. In accor
ed.
On raiding a shop, the food ins analyse samples from all over the dance with the PFA Act and the
pector has to divide the article of state. Samples picked up at Nasik, related rules, samples are being
food into three separate portions in Sangli, Kolhapur and Thana are sent drawn and analysed and offenders
the presence of at least one indepen to Poona. Each laboratory is thus so hauled into court.
-In Maharashtra alone, 17,652 sam
dent witness. One portion is given to overloaded with work that it is not
the shopkeeper, another is sent to the able to deal with cases as speedily ples were taken from various places
in the first nine months of 1974. Of
public analyst and the third is retain as it should.
Delays also occur while filing a these, 2376 samples (13.55 per cent)
ed by the inspector. The public
analyst is obliged .to send his report case. As the PFA Act, 1954, does were found to be adulterated. All
within sixty days of the receipt of not provide a time limit for filing a over the state, 2049 prosecutions were
case,
complaints are filed as much as launched, but more than 50 per cent
the sample. Once this report' is re
ceived, the food inspector files the a year after the sample is taken. The of the accused were acquitted. Of
resulting delay also affects the pro the 982 convicted, 899 were awarded
case in court.
During this procedure delays occur secution case in favour of the accus
CONTINUED ON PAGE 18
ed.
at the various stages involved.
Himmat January 10, 1975
13
FOOD ADULTERATION — from page 13
punishments and fines amounting to
Rs 5/3,728 were realised.
The figure of the fines realised in
the first nine months of 1974 in com
parison to those of the years from
1966 onwards shows that of late
there is a distinct trend in the judi
ciary not to treat offences lightly.
Statistically, the percentage of food
adulteration in Maharashtra has
come down from 30 per cent in 1966
to .13.55 per cent up to the last
quarter of 1974. This position is very
much better than that obtaining in
other states like Bihar, Orissa, Hima
chal Pradesh and Madhya Pradesh,
where more than 60 per cent of the
food samples tested by official ins
pection agencies were found to have
been adulterated.
This disparity indicates the lack of
uniformity in enforcing the PFA Act
throughout the country. Some states
do try to be sincere about the whole
affair of adulteration, while others
tend to be lukewarm. And even with
in a state, anti-adulteration efforts
are by no means uniform.
The administration of justice also
18
needs to be speeded up. Thousands
of cases are pending with the courts
all over India — some of them for
years. From 1968 to 1971 only about
2600 cases were disposed of out of
more than 25,000 pending against
food adulterators at the beginning of
1968. In Mahrashtra alone, at the
end of 1972, 8669 food adulteration
cases were pending with the courts.
These figures underline the need for
setting up special courts to deal with
food adulteration cases.
The Union Government is propos
ing to amend the PFA Act, 1954, to
increase the sentences on food adul
terators. The technical committee of
Parliament is presently studying the
amendments.
However, as a former Chief Justice
of India pointed out in a recent semi
nar on food adulteration, “very
severe sentences did not always pre
vent breaches of the law." What was
required, he said, was honest and
rigorous administration, continuous
inspection of factories producing
food, warehouses storing it, and other
places from where food was distri
buted. And, finally, what was most
important was greater public co
operation with the authorities to
check this criminal business of food
adulteration.
To sum up, certain essential steps
must be taken to check the spread
of food adulteration :
1)
The Central Government and the
Maharashtra Government are giving
grants for setting up new laboratories
for food testing. The laboratories
should be equipped with modern
equipment, the tests should be
modernised and done as micro-tests
to save time and ■money and should
be uniform all over the country.
2)
Training of personnel should be
immediately taken in hand and a
central institute for training public
analysts should be set up.
3)
To dispose quickly of milk adul
teration cases, a mobile court fitted
with milk testing equipment should
be set uo and in all cases of food
adulteration it is essential that sepa
rate courts should be established to
speed up the judicial process.
(Shortly HIMMAT investigates
Bombay hospitals.)
Himmat January 10, 1075
HIM1V1
FOOD ADULTERATION
16% Food samples ADULTERATED
A'O’
Adulterators make Rs 500 crores a year,f
50% Culprits Acquitted
Poisonous Argemone
mixed with edible oil
rCojSftwu/v/Tv,,
first F/oor)eCA^ Cgfi£
lHMMAT
investigates
t
FOOD ADULTERATION
Adulterators make its 500 crs. every l$ear
WHILE there is frequent uproar in the Indian Parliament caused by the
extent of food adulteration, the actual machinery of bringing to book the
food adulterators is moving more slowly than before.
In Maharashtra alone, one of the best administered states, 16 per cent of
food samples taken were found adulterated. Of those charged, 50 per cent
were acquitted often on flimsy grounds and the rest were given ridiculously
low sentences or charged small fines. HIMMAT’s investigation reveals that
if the Government is serious about dealing with adulteration, both the public,
the law courts and the legislators will' have to think again.
NE-THIRD of all food marketed
in India is adulterated, says a
Health Ministry survey. It could be
more.
. With the growth of knowledge and
advance of science, adulteration,
which is as old as commerce itself,
^as developed from a crude form
■no almost a branch of applied
science. The adulterator is no more
the simple milk seller adding water
to milk (or vice versa). The modern
adulterator breaks ice cubes into
pieces and drops them into milk-cans
as a “preservative”. He has at his
command innumerable prohibited
colouring materials and sweeteners
to work out combinations that would
baffle the smartest of housewives.
What is worse, greedy to make
quick money, he does not hesitate to
adulterate food articles with foreign
materials of proven ill-effects.
In
India, where the adulterators reap a
profit of over Rs 500 crores every
year, highly poisonous argemone oil
which
causes
epidemic
dropsy
(accumulation of watery fluid in any
part of the body) is freely mixed with
ible oil. Mineral oils which can
wash away the intestinal layers. are
added to coconut oil.
Non-permitted dyes such as metanil yellow (used for dyeing cloth) are
added to edible oils. Besan, which
is used extensively in cooking, is
often adulterated with kesari dal
which contains toxic matter that can
cause paralysis of the limbs. Prohi
bited artificial sweeteners such as
dulcin, cyclamate and saccharine,
which are suspected to cause cancer,
are indiscriminately made use of in
the preparation of supari.
Other common adulterants in use
are: ground stone particles in food
grains, vanaspati in ghee, iron filings
in rawa, talcum powder in cardamom,
chicory in coffee, and corn and beans
in chicory.
Some of these adulterants are slow
and poisons; some have proved to
be lethal instantaneously. In 1969,
adulteration of edible oil resulted in
the death of two people in Poona
besides making 60 severely ill. Even
when not poisonous, being foreign
materials, most adulterants are bound
to create health problems in the long
run. Worse still, the half-fed people
of this country are deprived of the
small amount of nutrients that they
so badly need. They are forced to
live . without even knowing the real
taste of food. In children, the de
privation of nutrients may lead to
diseases and stunted growth.
As long ago as 1954, the Preven
tion of Food Adulteration Act was
enacted in Parliament with the hope
that the Act would deter adulterators.
But it was not to be so. The loop
holes in the Act were so wide and
the .punishments to be imposed so
light (a fine of less than Rs 1000 and/
or imprisonment for less than six
months) that the Act, if anything,
boosted the morale of fraudulent
traders and encouraged them to prac
tise their craft even more advantage
ously.
by Bhojan Krishnan
All the same, samples are being
drawn and analysed for possible
adulteration. Shops are being, raid
ed. Goods are seized and suits are
filed almost as a routine. They bring
to book a few adulterators here and
there, while the rest, who are in
numerable, go scot free.
In Maharashtra, where the Preven
tion of Food Adulteration Act is
being enforced fairly strictly, the
Food and Drug Authority’s 200 food
inspectors go around the state inspec
ting shops. They draw samples from
wholesalers, manufacturers and re
tailers. Samples are also being taken
at: inter-district check-posts, hospi
tals, schools and other institutions.
Besides the food inspectors of the
Food and Drug Authority, the iocal
bodies, too, have their own food in
spectors.
There’s a limit to adulteration, here’s a cross-breed between beetroot and nails.”
i
j
Fewer culprits punished
In Maharashtra alone, 24,540 sam
ples were taken from various places
in 1972. Of these, 4032 samples
(16.43 per cent) were found to be
adulterated. Milk tops the list of
adulterated items. All over the state,
2530 prosecutions were launched in
1972, but about 50 per cent of the
accused were acquitted. Of the 887
convicted 600 were sentenced to jail,
and fines amounting to Rs 2,37,862
were extracted from the offenders.
Compared with the figures of five
years ago, that is of 1967, when 4907
prosecutions were launched, last
year only 2530 prosecutions were
launched. As against 1959 imprison
ed that year, only 600 were jailed in
1972. The fines realised also came
down from Rs 5,29,474 in 1967 to
Rs 2,37,862 in 1972.
Statistically, the percentage of
adulteration found in Maharashtra
has come down from 30 per cent in
1966 to 16.43 per cent in 1972. But
these statistics prove nothing, for the
samples which are taken at random
are by no means representative.
FDA officials admit that the action
taken has been so sporadic that for
every adulterator caught there must
be half a dozen more who are making
a fortune by mixing adulterants with
tood articles.
Ttie courts in India are overwhelm
ed with food adulteration cases.
Unlike drugs, where the source of
adulteration can easily be traced to
the manufacturer or certain spurious
firms, food articles can be adulterat
ed at many points, and fixing the
responsibility becomes much more
difficult. The retailers are always
prone to blame the wholesalers for
any adulteration found, and the latter
the former. In foodgrains, there is
scope for adulteration right at the
procurement stage.
In many cases, however, food
adulteration is not deliberate. The
lack of scientific storage systems.
proper containers and packaging
often causes bacterial growth and in
sect infestation. The Government
considers spoiled food articles or
insect-infested items, too, as adulter
ated. But the shopkeeper is helpless.
One wonders , how far the shopkeep
ers can be held responsible for such
adulteration. Stocks with the retail
ers last for only a few days, and if in
those few days the food articles de
teriorate, it means that no proper
care has been taken earlier at the
godowns of the Food Corporation of
India or of the State Trading Corpo
ration or of the wholesalers.
The retailer is not qualified to
spray insecticides or to fumigate the
stock.
indiscriminate use of such
sprays can endanger life. At best,
such articles can be salvaged as far
as possible and the portion unfit for
human consumption disposed of.
There are instances where the Gov
ernment agencies are involved in
distributing adulterated food articles
to the retailers, as in the recent case
of datura seeds found in American
milo. Hundreds of women had to
be employed to handpick datura
seeds, thereby preventing possible
food poisoning.
Over 8000 cases pending
A good many cases are pending
with the courts all over India. Some
of them have been pending for years.
At the end of December 1972, in
Maharashtra alone, 8669 food adult
eration cases were pending with the
courts. This has been a point of re
gret for the Food and Drug officials
as well as the Municipal Corpora
tions, who complain that delays in
the courts hamper their work of en
forcing the Food Adulteration Act.
The Bombay Municipal Corporation
and the Food and Drug Authorityare contemplating the need for spe
cial courts to deal with food adulter
ation cases.
Profiteering doubtless is the main
objective of the adulterators. Social
CONTINUED ON PAGE 15
Implementation of the Prevention of Food Adulteration Act in Maharashtra State
Loopholes in the Law
12
j,
to sign as witnesses. When some of
them do, they try to please the in
spectors and traders equally by fur
nishing false names and addresses.
Besides the PFA Act, 1954, the
Prevention of Food Adulteration
Rules, 1955 (Central), and various
State rules have been framed to arm
the Government with adequate power
to check food adulteration. In
accordance with the PEA Act and
the related rules, samples are being
drawn and analysed and food offend
ers hauled into court.
The PFA Act, 1954, gives wide
powers to the food inspectors. They
can enter any shop to inspect any
food articles suspected to be adulter
ated or wrongly branded. They may
■ even exercise the powers of a police
officer in ascertaining details. But
all these powers are of no avail when
the food inspectors are expected to
produce witnesses to prove their case.
Unwilling , to get involved in court
affairs, very few people come forward
No. of food samples analysed
No. of food samples found adulterated
Percentage of adulteration
No. of prosecutions launched
'No. of persons convicted
No. of persons sentenced to jail
■Fines realised (in Rs)
Himmat, September 28, 1973
1966
1967
1968
1969
21,023
7,623
30
4,924
4,560
1.759
4,09,628
20,099
5,412
27
4,907
3,511
1,959
5,29,474
19,659
4,754
24
4,399
3,007
1,365
5,03,603
16,610
2,852
17.17
2,595
1,385
1,078
5,44,254
1970
1971
1972
19,354
20.250
24,540
2.869
3,789
4,032
14.82
20
16
1,021
2,062
2,530
2,063
1,135
1,164
781 (not available) 600
3,08,419
do
2,37,862
Source : Food and Drugs Administration, Maharashtra State.
FOOD ADULTERATION — from page 13
scientists may put forth many more
reasons, such as ignorance of the
traders about the harmful character
istics of certain adulterants, ignor
ance of the standards prescribed by
the Government, and a general lack
of knowledge of what does and does
not constitute adulteration.
The lack of- uniformity in enforcing
the Prevention of Food Adulteration
Act throughout the country has also
been abetting the spread of adultera
tion. Some states do try to be sin
cere about the whole affair, of food
adulteration, while others tend to be
lukewarm. And even within .a state,
anti-adulteration efforts are • by • no
means uniform.
Some of the local bodies enforce
the Act vigorously, while others, for
want of funds (they can always raise
^fcugh funds by ' way ' of licensing
M^i establishments and by realisa
tion of fines) ignore the Act altoge
ther. Those states. and districts
RING 536321 FOR ADUL
TERATION COMPLAINTS
which are seriously engaged in curb
ing food adulteration are at a‘ dis
advantage. When food articles are
imported from other states or dis
tricts, there is always a chance of
adulterated food
articles being
bought for which the importing
state or district has to bear the brunt
of public wrath. All that a sufferer
state can do .is to draw samples at
the check-posts and Send them for
analysis. By the time the results are
known, the consignment has proba
bly been consumed.
Help the Food and Drug
Authority in checking food
adulteration. The FDA acts
swiftly on consumers’ com
plaints. Readers in Greater
Bombay who suspect food adul
teration can just drop a line to
the FDA office at Griha Nirman
Bhavan, Opposite Kala Nagar,
Bandra (East), Bombay-400 051,
or dial 536321 and lodge a tele
phone complaint. You need not
give your name. Let your
charges
be
genuine,
and
addresses of the shops com
plete.
Mandate Laboratories
Want of adequate laboratory faci
lities perhaps cause no less delay in
the analysis' of food articles. In
Maharashtra, there are only six
moderately equipped laboratories to
carry out tests on- .food ■ samples four Government public- health labo
ratories, one each at Poona, Nagpur,
Amravati and Aurangabad, and two
In Biebrich, on the Rhine, a wine falsifier was condemned to drink six quarts
of his own wine: from this he died. That was in 1482, but it is by no means
the earliest known instance of punishment meted out to food adulterators.
In 1390, an Augsburg wine seller was sentenced to be led out of the city
with his hands bound and a rope round his neck. In Frankfurt, casks in
which false wine had been found were placed with a red flag on the knac
ker’s cart. “The jailer marched before, the rabble after, and when they
came to the river they broke the casks and tumbled the stuff into the
stream.”
But here in India, the food adulterator or illicit liquor-brewer has always
been treated kindly. Despite our MPs’ demand that this species of trader
be sentenced to death, the Government and courts continue to have a soft
spot for the adulterator ■— a fine which seldom exceeds Rs 100 and/or a jail
term of one day.
In Bombay, a milk seller, who was charged with stockpiling blotting paper
with the intent of mixing it with milk products, was acquitted on the ground
that the adulterant was no health hazard!
In many cases, the adulterators are let off with a warning, or a jail term
rich lasts till the rising of the court!
municipal laboratories at Bombay
and Nagpur.
More laboratories alone will not
solve the problem. Facilities for re
search are essential, too, for finding
out new ways of detecting adultera
tion. For example, in the case of
adulteration of colophony in hing
(compounded asafoetida) and artifi
cial sugar in honey, there is no
scientific way of ascertaining the
adulteration. Research is also need
ed to improve the standards of food
articles.
Greater effort is needed in detect
ing adulteration in hotels and restau
rants as also at pavement stalls. All
over the country, adulterated illicit
liquor has been taking a toll of valu
able human lives almost every year.
Treating the adulterators as they are
being treated now in India (see left)
is no answer to the problem. Only
stringent punishment and more pub
lic co-operation can help reduce this
nefarious practice.
BUY BEST
BUY CROWN BRAND |||) THERMIC JUG DELUXE
IDEAL AND ATTRACTIVE
Keeps drinks hot or cold for hours
JEEWANLAL (1929) LIMITED
Crown Aluminium House, 23, Brabourne Road, Calcutta-!.
j Office
t
( Show Room:
Liberty Buildings, Marine Lines, Bombay-20 BR
Phone No. 291156
Kansara Chawl, Kalbadevi Road, Bombay-2.
Phone No. 334859
CALCUTTA • MADRAS •
Himmat, September 28, 1973
HYDERABAD • DELHI • MADURAI • ERANAKULA&
15
"SHARING SOME THOUGHTS ON FOOD"
CuMMuNi'iY HEALTH ~~«-L
47/1, (First Floor )St. Marks Hoad
BANGALORE-560 001
"The most widely shared concern about the “present growth .of world population
is th^—fear that it will outrun the growth of food supplies and bring the
world, or at least the more unfortunate in the developing countries closer
to starvation",
•
GORAN'OHLIN
Throughout human history starvation has seldom been far away for some large
part of humankind. Even when western man was most bemused by the wonders
of science and technology and constantly rising productivity, hunger was
abroad in other parts of the planet..
The inherent and practical limits that soil and fresh water resources
particularly place upon the world's ability to feed its growing populations
are now compounded by energy and fertilizer supply problems, and by
inflation which has put prices of even minimal sustainance beyond the reach
of untold millions. The practical prospects for increasing world food
production in the short term may be in dispute. But there are some very
basic conditions which are not in dispute.
1. Arable and accessible land for additional cultivation of food by existing
methods and known technology is physically limited and economically
expensive to exploit.
2. The use of tractors over a continued period and even the use of fertilizers
is now being found detrimental to the soil in which fragile monocultures
exist.
3- A very large part of the world's potential pasture land is now already
in use.
4. Most of the world Is river systems .readily available for irrigation have
been tapped.
5. Lastly underground water is becoming scarce in many regions. Water
shortages are expected to prevail in about 60 countries within another
decade.
Since time immemorial there has always been a food problem in India, but it
was ignored. 1^ is only in the last 2 decades that serious attempts have
been made to tackle this problem and put the spotlight on food.
A food problem is also present in many other Asian and Latin American
countries but India's is the most urgent and biggest.
Not only does she not grow enough food for herself, but she also cannot
afford to buy food for herself.
The average Indian has 2.25 acres of land (per capita basis). But of the
arable land there is only 0.6 acre. Whereas it is estimated that even to
meet his own food needs the minimum acreage a farmer should have is 1.8.acres.
40$ of the total land is- cultivated and of the cultivated' land only 1/7 is
irrigated.Large areas of land are not cultivated and some must be reserved.
for pasture.
Fertilizer consumption .is 0.5 kg, per hectare. This should increase by
33$. But fertilizer costs are prohibitive to the average farmer.
Coming to the effect on diet and calorie supply, it was estimated that
10-15$ of the people in the world, or roughly 20$ of the people in the
developming world did not -meet their energy requirements in the decade
1950-60.
The estimate of protein deficiency was between 25-33$Diets lack energy foods and ■’’Wte^bod^’then catabolizes the protein (Gopalan 68).
This finding of protein deficiency indirectly caused by low calorie intake,
though opposite of the protein gap theory of U-N. is confirmed by the
F.A.O. (1971).
If a diet has ONLY 5$ of its calories from good quality protein such as in
egg, milk the individuals need for ptotein will.be met regardless of whether
he is a pre-school child or adult man provided he eats enough to meet his
energy, needs.
-:2:«
When- we -know—further-that—the-human bre-in-reaehes"9O0 of its normal structural
development in the first 4 years of life and that even a deterioration of
100 in the diet can cause a serious- handicap to producti’H<-,4ife it is
imperative that food items, in- the-’barly years sup-ly th.-, maximum utilisable
protein. ---This brings us to certain facts of Indian dietary habits which are responsible
in a great extent to the degree of malnutrition found. Cereals which constitute
upto 800 of calorie supplies and 700 proteins in India can be reduced and
if pulses which constitute only 100’calories and 200 protein can be increased
a great leap in nutritional status can be registered.
It is not practical in view of the costs to increase to any great extent
•the food'.of’animal origin though efforts to promote eating of beef to which
1/3 of the Indian people have no objection should be made. Also fish products
from fresh waters is particularly low.
Milk of which the per capita availability is only 6 ozr should be- increased.
Ghee production and the use of milk for sweets should be controlled. It is
estimated that approx. 600 of milk produced in India goes for the making
of these 2 items which only a fraction of Indians, can afford.,
The average Indian gets 1890 calories per day (ideal is 2400 cals) and 53 gms
protein of which a large portion cannot be utilised and so 1 million malnourished
children exist. Toddlers who account for 16.50 population but contribu+e to
400 of all deaths and when millions of mentally deprived children reach
adulthood, and are likely to repeat the whole depressing sequence in their
own families, we know that concrete and practical steps must be immediately ,
taken and these can be summed up in Health Education and Education in Nutrition
and a change in food habits.
Thoug wheat is the.staple diet of Gujarat, Rajasthan and Panjab, rice is
■the staple diet of 2/3 of the population. The rice crop which depends largely
on the monsoon rains is an expensive commodity throughout the.world.
Therefore, more and more- people starting with children must be educated into
eating wheat and othercereals like ragi and millets which are less expensive
to cultivate and more .nutritious to eat.
A change in food habits a breaking down of centuries old tradition and the education of the positive bad effects of certain dietcry supersitions and
beliefs can do much more good than trying to improve .methods of cultivation
and production.
• The use of egg which has' a high ratio of net protein utilised and which in
its unfertilized vegetarian form is acceptable to •’’he most orthodox vegetaria^
must be popularised.
.
An egg a day keeps sickness away is a slogan that CHS can spraad so that with
energy CRS aided meal one egg is contributed by the family themselves to
provide the protective food so necessary to a growing,child.
1-f. is imperative in my opinion that any programme of nutritional aid like
that of your reputed organization be linked with a programme of progressive
health' and nutrition education of the families and children who actually
receive your foods.
The existenoec of tlie balanced diet which is an entirely new concept to
rural’Indians, the use of locally available foods in providing one’s majop'
■needs. The use of pulses or dhals for children esuooially, the popularization
of kitchen gardens and community market's the keeping of poultry and the rearing
of goats are subjects which demand our urgent attention. Goats rearing is
extremely profitable. Goats subsist on minimal fodder ani provide milk, hair
for weaving by the womenfolk into rugs and blankets and ultimately meat for
eating. Fish breeding and eating must be popularized. All waste water must
be utilised in maintaining fruiT'and.-fc^e table trees. Only multiple efforts
on a small scale that amount to a gigantic effort can change the picture of
malnutrition in India. I+ is said give a man- a fish and you feed him for a
day. Teach a man to fish arid he will feed himself for a lifetime.
The villagers problems cannot be attacked piecemeal. Hg cannot have higher
production without education to know how to get it and health to do the
necessary work.
In Ind ia high ideals and responsibility as in the west are lacking but
norals and sacrifice are traditionally present. For the welfare of their
children parents are prepared to go to great lengths of sacrifice. We should
capitalise on this attitude and enlist the active participation of teachers,
parents and elders into our programmes of aid. This will increase their self
pride and dignity and this motivation towards a better life is half the
battle won.
I conclude with the words of THOMAS JEFFERSON, who said, "I know no safe
depositing of the ultimate power of society but the people themselves; and
if we think them not enlightened enough to exercise their control with a
wholesome discretion, the remedy is not to take it frc’’ them, but to inform
their discretion by education"
THANK YOU
fin eh on to cl
the.
731975
I r>
Cflj
ctlnitctviy
7 $—
/2>av^^a.Coi^e
¥'
^9/VvJT
COMMUNITY HEALTH C ..L
POPULATION
AND FOOD
47/1,(First FloorlSt. Marks Road
BANGAlQuE-560 001
"The most widely shared concern about the present growth of world
population is the fear that it will outrun the growth of food supplies
and bring the world, or at least the mor1 unfortunate of the under
developed countries, closer to starvation".
Goran Ohlin
It was Malthus, an English parson born in 1766 and known for his
essay on the "Principles of Population" who sounded the first warning
between growing populations and food production.
<. With an estimated population of 5 million in England in 1700
and the First Census of 1801 giving a figure of 9.2 million, there was
a relative worsening of the nutritional situation for which the enclosure
of the land for pasture (instead of for crop's) was chiefly responsible.
Malthus began by pointing out the disparity between the possible
growth of the population on the one hand and the means of subsistence
on the other:
the population may grow by geometrical progression
whereas the means of subsistence -can grow only by arithmetical progression.
However, as Don Arthur in his book "Survival" says, "The inadequacy
of food and natural resources has hat proved to be limiting in the
determination of the size of
either populations or of families.
the reverse'appears tO'be often true.
Indeed,
In such countries as India, near
famine conditions do not control numbers and frequently it is the unskilled
and the underfed who have the largest families.
Onaa world scale, the inadequacy of food is not related to its
decreasing production, for although it was reduced much more than
population during the II' World War, production per head had overtaken
pre-war rates by 1952/53'.
From 1950 to 1968 world cereal production was increased by 70$.
Subsequently, world production of food has increased by 3$ while
the average population has increased by 1.7$.
And, Gunning
argues that -
"To many the doubling of world population as predicted for the
year 2000, will seem an unsurvivable disaster. Some experts, however,
see it as one necessary condition for the development of world economics
because, in their view, a similar demographic explositon
will be the
only sufficiently strong incentive to force humanity into action. We
have seen the draining of the Dutch Zuiderzee as the result of a strong
demographic pressure.
One can look at a great desert like the Sahara,
a huge economic barrier for the development of Africa.
No attempt at
....2
*
k-M
2
cultivating this desert will be made as long as the present "lack of
world population" continues.
In Khartoum I was told by a Government Official that his ministry
has ready plans for the irrigation of the whole Sudan, for which only
10% of the Nile water appeared to be needed.
actually seen realised!)
(Part of these plans I have
There were only two great obstacles.
One, lack
of money, could certainly be overcome, but the second, lack of population
seemed hopeless because in order to cultivate the soil made available by
the plan, a population of 150 million would be the minimum required. The
Sudan has no more than 15 million inhabitants.
With a stagnant and intermittently diminishing population for many
decades, India in 1921 was unspeakably poor compared to India in 1961.
For quite 40 years before 1921, India's' population did not grow at all.
If anything, it was decimated by pestilence, and even more by recurrent
famines.
But between 1921 and 1961, the annual rate of growth of India's
population accelerated to 2.3% per year.
In 1959, India was even richer
than she was in 1961, despite a still higher annual growth of around
2.5%.
A small population alone is no guarantee of prosperity. On the
other hand, history -has proved that a rapidly increasing population
at certain crucial stages - either by migration or natural increase,
has been a pre-condition of prosperity.
India for proof.
We d.o not have to travel beyond
Ample proof is available in Assam, Rajasthan, Haryana,
Malnad and Bandakaranya.
A steady rate of economic and cultural growth is mor? vital for a
nation's prosperity than a small or diminishing rate of population growth.
The ideal is reached when the two trend lines begin to diverge away from
each other, particularly when the economic growth line continues to show
a comfortably steady upward trend, while the population growth line
shown first a steeply descending followed by an almost level trend.
George Hanar, 36 stated, "I personally haven't the remotest doubt
that if we could mobilize our technology, our man-power, our efforts,
provide the back-up and accelerators that are necessary, we can gradually
"invade" the tropics, convert the better agricultural areas initially
to usefullness in the production of plant materials or the production
of animal materials.
It would-be no problem, in my judgement, to double
or triple world food supplies in terms of the potentials which exist. The
problem is not in terms of potential.
People just haven't really been
able to bring together the consortium of effort which is necessary".
About agriculture, Colin Clark says, "Wo must bear in mind two
very different concepts, namely the amount of land per head required by
a farming community to keep itself fed, and the quite different concept
....3
5
of the amount of land required to keep itself-fully occupied.
These are
based on the two very different concepts of subsistence farming and
commercial farming.
■’.
Neither of these terms is precise or absolute.
Clark has classified the cultivable land in several'categories according- ■
~ rn
’
r- •/ - j v ,?d.i
ryr I ■
r-'\ OV
.M.h ni./V
...
to climatological factors (temperature and rainfall)..^
‘-’ill
fix
■-> - i
One square ''kilbmet'3r’'i'h',Eurbpec (moderate temperature')'' suffaciefit ,e
rainfall^
p.np, pr.ppy^.-ypfir-).-; is.^palledi- onp uni-);. .©fd^stapdardf .lapd”-i,l' hj; fl
ExinjassMolni'Wits^ bfJ®'b?t^h'd^’d:* 1-ahd'"’-',
* the 'phte-htT^l-Iy' c'difivaftio''' •
surfapeiiofl'the^wor-ido isC'75.8’ million'■ km' a'cbo-ird'ih^ ttr' Wb -mbst
f~
estimateq'tand->107J -kmsJ'ta6bbi'di?i<^) tbi.h-moi'e0 optimistic Caibulat'ib^?"’* ' ' mono
.'to-eSiooows -edi do n<tWrV-Js.’.:-I t • fj.rco (■(>■:■ b rt.*• rxs e
'■
The"cultivable surface of the world can feed and clothe, according
f -.i ■ : ■■“■I"'■ ■
.j!o •?: i. 5ii:-‘0nq i ■ •ij. .•••; • •fz-'ie'S bfi. •■.oon'i
to European standards 34.57 billion people (narrow estimate) or 47
billion' tmore optimistic estimate)- -According to Japanese standards -
wher-? '.thei?subsist6ne'>0'un'itcpdr ^efbon-'pSi? yBdr^is'-mueh lower;' th'Sse’'5 -''1'"'
figureS.-Efre-'lEO-^bil-tibribaha i570b'ill£bh?'hl Jc -1'
*•■
•'•••
Vy.(-:Z0-.'
- ai a-aototin^m el it (.-'I.G.oj iowrl phi^umod
'
Fritz Baade (Director of the Institute for World Economics, Kiel
Germany) re'porte1 ffia^ll^ of the^viorld's surface that is now used for
agriculture'could produde mor? than 10 times the present output with the
help of indderri techniques and feed 40 billion people.
The. area Sf Hi ch an average Indian has is 2.25 acres of land (per
capita basis),' as compared to 13.45 acres available to the world citizen-. .
Moreover, the:per capita arable land for an average Inilian is only 0.6
acres.
It is estimated that an individual.requires 1.8 acres of arable
land as the minimum for serving, his food needs.
Charles Kellog, an American authority on soil problems, has demonstrated
that if ’ we brought' into' use only 20$' of the unused area in the tropical
zone tfe would'add over one billion acres, or 40$-of the total to the world's
cultivable land.
Land for grazing, economically productive forestry and for grass
cropping could be developed without much expense.
■India has an area of 1,262,275 square miles or 808 m. acres and
an average density of 370 people per square mile.
Total geographical area in 1,000 acres
Net area, according to village returns
Forests
r
Net area irrigated
Net area sown
Fallow lands
807,856
720,970
126,099
55,682
322,460
58,490
|
5
Not available for cultivation
166,201
|
97,720
(
Other uncultivated land
(including permanent pasture,
grazing)
cultivated
uncultivated
4
That is, about 40$ land is cultivated of which 1/7 is irrigated.
the demands on these lands for crops is very great.
Hence,
Several ways may be
adopted for improving the quantity and quality of food.
I.
Increasing the land under cultivation
It is important that land should be brought under cultivation, and
that wherever possible the farmer has a land holding that is productive
enough to meet his own needs first, and then gain him profit which is
put back into purchasing hybrid seeds, and amenities to improve the farm's
yields.
Agricultural land should be safeguarded by law.
Moreover, reclamation
of land from marshes or swamps, and deserts undertaken.
The cultivation of sorghun, a cereal rich in lysine, and needing
minimal water, should be encouraged in drier areas.
McCormack says, "It is true that large-scale reclamation often
intolves large investment, and it may well be judged that it is more
economic to use other methods of food production.
But the fact that
opportunities exist for extending the area of cultivation should offset a
certain amount of pessimism, especially as concerns the longer term."
In a speech to scientists from all over Europe in 1968, Pope Paul VI
said, "It is perhaps unnecessary to point out that the most terrible calamities,
capable of destroying all the inhabited earth, come from precisely the best
equipped’labbfatofies of modern physical science.
to renounce these things.
May you have the courage
Rather make the earth,fertile, make it produce
bread for all; fight against the sterility of desert zones, intensify farm
production everywhere, make possible victory, your art, your mission and your
glory."
In the same, vein N.M.■ Zhavoronkov summed up the view of technological
optimists with the words that "as long as the sun shone and people were
capable of creative thinking, they had no need to fear the future".
It is still disputed whether there is a possibility of cultivating the
vast areas of humid tropical forest around the equator in these continents.
If more research were undertaken into the problems of tropical agriculture,
however, it would seem that tropicdl food crops (on which little research
has so far been expanded) could at least approach the success of cash crops
such as cocoa and.sugar and other tropical products on which a great deal
of research has been done so that crop-yields have been greatly increased.
Because of the inter-dependence that exists among food needs, food
demands, overall income, agricultural product, total output Gross National
Product (G.N.P.) or Gross Domestic Product (G.D.P.) it is meaningless to
consider a nation’s demand and supply of foodstuffs independently from
5
overall economic progress".
Perhaps now that-men have landed on the moon,
by investing billions of dollars and using a huge reservoir of scientific
brainpower, it would not seem too extravegant to turn to the development
of some of the earth's possibilities for feeding ite people; the relative
cost would be very much less."
Small holdings are not productive enough and more and more farmers
are forced to become labourers on other holdings or become landless.
In "India and Pakistan cultivation is carried on mainly by means of
ox-pl iughs.
It is possible to make reasonable estimates of the amount
of land required to keep the plough team fully occupied during the■cultivating
season, but not to over-strain its capacity.
A method devised in 1945 by
Tarlok Singh can still be regarded as satisfactory.
For most regions of
India this gave a result of 5-5 hectares per adult man as the amount of
land required for full employment during the cultivating season.
It is indeed the shortness of the monsoon which makes draught
animals necessary in India and Pakistan, even when farmers are so poor
that they have great difficulty in feeding them.
Where rainfall is more
abundant in India hand cultivation may be preferable, particularly for some
of the higher value crops such as jute and pepper and the amount of land
required to keep a man full?/ occupied is lower.
In Japan where hand cultivation still prevails (though supplemented
by abundant use of fertilisers, insecticides etc.) careful planning and
diversification of crops make possible the full employment of 2.8 man
equivalents of labour on a farm of only 1.9 hectares".
II.
Irrigation
The rice production, even though inadequate, needs much water
and though the new strains of rice do not need more water they benefit
from more water.
Nearly seventyfive percent of Indian farming is dry farming.
Therefore irrigation projects and methods to utilise water of rivers,
lakes, tanks and wells should take high priority.
Gunning asserts that the actual irrigated surface (15$ of the total
agricultural surface of the world) produces 25$ of the total food output.
Even so at least 5/5 of this surface is not irrigated in the best possible
way.
Expanding the irrigated land even on a world-wide basis is
important.
It is estimated that not yet 5$ of the world's
is used for irrigation.
river water
By sprinkling instead of flooding almost twice
the surface can be irrigated.
Moreover, the newly cultivated land does
not have to be flattened and less salt loss results.
..6
6
Ancient gravity methods are used to dra" water requiring animal
or manpower and thus increasing the economic burden on the farmer.
However, increased irrigation also brings problems of malaria and
schistosomiasis by providing the vector or carriers of these diseases
with suitable conditions for breeding and development and this must be
kept in’iaindA - The provision of pump- sets ■to’1-fiarmers?is,,also of prime
importance.
III.
Regeneration of the land by the use of Fertilisers
Multiple cropping and lack of appreciation of the "rape of the land'
has made imperative that fertilisers be provided and used increasingly
in India.
Incomplete nitrogen cycle due to non-return of faecal products as
sanitary facilities increase and sewage is disposed of and therefore lost
to the land, make it necessary to let the land lie fallow for one or two
years before a new crop can be produced.
Soil erosion is a matter for
serious concern as land can be lost for cultivation.
McCormack says, "I-t seems reasonable to assume that through research
ways can be found to make the infertile but otherwise favourable tropical
soils acceptably productive.
It was through research that the infertile
sandy soils of Florida and, for that matter, many soils in the' South
Eastern United States, were made productive.
Fifty years ago they
were
as low in fertility as many of the soils of the humid tropics.
The Belgians, for example, before suspending their research in the
Congo, had developed an oil palm which when properly grown yielded about
4,000 kilograms of palm kernels per hectare whereas the ordinarly palm
yielded approximately 500 kgs. per hectare.
Fertilizer
Of the actual irrigated surface, three quarters receives an
insufficient amount of fertilizer, i.e. an average of 2 kg. nitrogen per
hectare per year instead of an "optimum" average of 50 kg. per hectare.
Experiments of the FAO jn Ghana gave a tripling of the output per hectare
when sufficient fertilizer was used: 1070 kg per hectare without, 3486 kg.
rice using 40 kg. nitrogen, potassium and phosphorus per hectare, giving
an increase of net income from fl 47 per acre to $ 172 per acre.^^
To give a few figures for comparison:
India
in 1950 had an average fertilizer consumption of 0.5 kg.
per hectare and an average cereal production of 0.65 ton per hectare.
In I960 these figures were 2.5 kg. fertilizer per hectare and 0.83 tons
of cereal per hectare, i.e. an increase of 180 kg. cereal per hectare.
....7
7
Japan increased her average fertilizer consumption between 1950
and I960 from 153 kg. per hectare to 304 kg. per hectare.
Her. cereal
yield went, up from 2.9 tons per'hectare to 4.1 tons per hectare, ,i.e. an
increase of 1200 kg. per hectare.
Holland in I960 used an average of 456 kg. fertilizer per hectare.
Dr. Pauley of the FAO has estimated that: in
i) the years immediately ahead India and Pakistan would need to increase
their consumption of fertilizer at the fantastic rate of 33$ per year.
Also improved strains of rice and wheat now increasingly used in
India, respond more to heavier doses of fertilizers than ordinary strains.
Indian yields for crops other than wheat are quite low by international
standards.
"It has been argued that with better varieties, pest control and
application of fertiliser on the Japanese scale, Indian rice yields'could
be raised to almost 2^ times their present levels".
"Domestic Production as a percentage of -the total supply of food
'’in selected countries..
•
Country
Wheat & Rye
' Rica
Potatoes
Sugar..
Meat
Australia
536$
319
102
353 •
145
India
56
100
106 ■
100
U.K.
46
97
-
37
65
95
•
Inspite of massive investiments since 1950 in the urban and
industrial sectors and inspite of the massive absolute increase in the
urban and industrial population which has broken away from agriculture,
the proportions of populations dependent on agriculture, has stood almost
constant, around 70$, significantly, inspite of the rising share of
industries in the Gross Domestic Product, the percentage share of agriculture
in the G.D.P. in India has also stood fairly constant, around 47$."
IV
Food supplies from the sea-inland waters
Land is limited in supply.
The largest section of the population
live in countries in which .the scope for the extension of arable land
is extremely small.
At the same time, practically the entire supplies
of food care, raised from lands, either directly or indirectly.
For the world as a whole, 87$ of the total supplies of calories
and 70$ of total proteins are derived from "arable lands".
If we include
foods of animal origin excluding fish, we find that the world draws 99$
of calories and 96$ of proteins from lands in general.
With fish as a
food acceptable to large sections of the population, and its vast coastline,
it is surprising that fish farming has not been undertaken more extensively
in India.
....8
8
The foods of sea and inland water origin consist mainly of fish;
seaweeds and other plants growing in water are eaten in negligible
quantities.
Fishery makes very little claim on lands and marine fishery none
0f the total eatch of 53.3 million tons estimated for 1965,
at all.
7.6 millions were from fresh waters.
Though relatively a less important
source for the world as a whole, fr-sh water fish contribute a third of
the total catch in the Far East.
In this region, which is, as we have
seen, so poorly endowed with land resources to feed adequately its large
population, the development of inland fisheries
importance.
The region has large water surfaces.
is of particular
There are, it is
roughly estimated, 37 million hectares of cultivable inland waters in
the Indo-Pacific region.
By far the larger supply of fish, as said before, comes from the
seas and oceans, and the total catc’- from this source has been increased
at 7% a year.
Inspite of their larger population and vast accessibility
to the seas, the present annual catch of marine fish of the developing
countries together is a fifth less than that of the developed regions.
In fact the latter draw practically their entire supply of fish from marine
sources.
In the far East, Japan alone lands 6.6 million tons a year
while the rest of the region only 9.3 million tons. More remarkable
however is the achievement of Peru: annual catch has been expanding by
40$ a year.
This fantastic growth, which has put Peru in the lead
among fishing .nations of the world, is largely due to the growing demand
for fish meal in North America.
such favourable conditions.
Other developing countries may not find
0n the contrary, they would confront
considerable difficulties, largely because of their technological
backwardness.
,khty health cell
CoMMONn
MarksB°arf
N U T R I HOU
1.
How would, you conduct a nutrition survey in a boarding school of 100
students between 5-8 years of age. Suggest measures to improve the
nutritional status of these students.
?! As a medical officer of a Primary Health Centre what would you do in the
following circumstances - Vitamin A deficiency conditions among many
members of a family.
3.
In your practice, as a family physician you encounter nutritional deficiency
cases in a family. What investigations would you conduct to determine that
it i's due to lack of proper diet? Give the composition with quantity of a
balanced diet in a family consisting of a father 40 years, mother 35 years,
one sone 15 years, 2 daughters of 10 and 6 years respectively.
4.
What is kwashiorkor? What are the causes? By what measures can the
prevalence of kwashiokor be reduced in a community.
5.
How would you investigate an outbreak of food poisoning.
6.
Discuss the nutrition value of.milk. Write notes on (i) Composition of a
balanced diet (ii) Role and requirement of Iron and Calcium in the diet
(iii) Diseases associated with faulty diet. .
7.
Vijay an 18 year old employed in heavy labour has the following daily diet.
Point out the omissions and defects in quality and quantity and suggest a
balanced diet fox- him. Rice 8 oz. Pulses lOz
Milk 1 oz Groundnuts 1 oz
Vegetables 2 Oz. Hydrocarbons 4- oz.
8.
What are the various causes of malnutrition in India?
you would recommend to overcome them?
9.
Describe the role of proteins in thehuman diet. State how the requirement
of protein are satisfied in the South Indian diet. Explain how the methods
of cooking and preparation of food may affect the,value of food articles.
10.
What are the measures
Explain the role of proteins in the human diet.
.11.- What is an adequate diet. Mention the food articles (with quantities of
each) which will constitute an adequate diet for a day for a medical student
who weighs 60 kg. and plays tennis for ah hour a day.
12.
Describe the diseases that may be conveyed to man through meat.
the life cycle of I. solium.
13.
Discuss the important of green leafy vegetables in himan diet.
Describe
14’. What is a nutritional survey? State the specific noints to which you will
pay attention mentioning the uses you will make of the data gathered, with
a view to prevention and correction of -dietary defects.
15- Protein deficiency is one of the major public health problems in India.
Discuss this statement.
Name the diseases that
16.
Discuss the value of milk as an article of food.
may be conveyed through milk.
17.
What is meant by Balanced diet. What are the. nutritional deficiency
diseases encountered by our people. Discuss the role of vitamin C in
the diet. Comment on its source in a South Indian diet.
18.
Discuss the role of vitamin C in the human diet. What are the sources
of vitamin C available for people belonging to the low income group.
,19. Discuss the importance of nutrition in'the maintenance of promotion of
health.
2
20.
Short notes on
Protein calorie malnutrition ; Pasteurization of milk
Minimum standards for a good slaughter house ; Boiling of milk ; Meat
borne diseases : Essential unsaturated fatty acids ; Protective foods ;
Eens egg ; Diet survey ; Kwashiokor ; Measly beef ; Pickets •,
Essential amino acids ; Nutritional antropometry ; Botulism ; Relative
merits of mothers milk and. artificial feeding for infants ; Pellagra in
India ; Fortified foods ;
21.
Rice contains greater % of equal proteins than milk ( Yes).
( No )
2.Ghee is richer in fat than groundnut oil ( Yes ) ( No )
3.Proximate principles ar = vegetables, fruits and milk ( Yes )
( No )
4.Kwashiokor is a - Syndrome
5.Vegetable oils are better than animal fats for old people
Yes ) ( No )
Correct figures wherever necessary :Daily requiresent of
’’
n
u
>1
n
•I
H
1!
II
1!
22.
’’
II
n
n
11
I
n
I’
Vitamin
is
"
D is
Thiamine
Riboflavine
Nicotinic acid
Cyanocoblamine
Ascorbic acid•
Calcium
Iron
Floride ■ ion
1000 I.U,
2000 I.U.
20 mgm.
1.5 mgm.
2 mgm.
1 mo 4
80 mgm.
5 gms.
10 mgm.
1-2 ppm.
What is kwashiokor? What are the causes? Bv what measures can the
prevalence of kwashiokor be reduced in a community?
23/ Prescribe a balanced daily.menu for a.family of 5 members, the father,
mother and 3 children aged 16, 9, and 3 years. The family income is
Rs. 150/- a month and the father is a stenogranher.
24.
What are the deficiencies in the- South Indian diet?
suggest to remedy these defects ?
25.
What is an.adequate diet?. Give an example. Explain how the diet taken
bymost of the people in Mysore State differ from this diet. How can the
' defects if any, be rectified?
26.
What steps would you
What type of daily diet would you recommend for a labourer weighing 65 kg
27.
What is meant by a 'Diet survey' and 'Nutrition survey'. Describe in
detail how you would conduct a nutrition survey in a school of 200 pupils
of low income group.
28.
What is the difference between ghee and groundnut oil and their relation
ship to health and disease.
29.
Discuss the advantages and disadvantages of vegetable proteins, even
animal proteins. Describe a balanced diet.
30.
What .is an adequate diet. Prescribe an adequate diet for a moderately
active male medical student weighing 65 kg.
31.
Write short notes on : Mutual supplementation of dietary proteins
Essential unsaturated fatty acids.
Deficiency of Iron in the diet.
nutrition
------------“.
Comment on the following:
I
.
COMMUNITY HEALTH CELL
47/1,(First Ffoor)St. Marks Hoad
BANGALORE - 560 001
a) Milk is an ideal food for adult
requirement depends upon the calories supplied by the
b) Vit
carbohydrates in the diet.
c) Mixed cereals is desirable than a single cereal in our diet.
d)
Phosphatase test protein in a sample of milk states to have been
e)
Ghee is good for health as it is rich in the saturated fatty acids
f)
Louis Pasteur discovered pasteurising method for milk.
pasteurised.
Each person in a central prison is given the following daily dietary
II
allowance:
Bice - 300 G
Pulses 500 G
Hydrogenated vegitable oils 25 fi
Green leafy vegitables 25 g.
Comment on the quality of the above diet.
III.
As a Medical Officer in a Health Centre, what would you do if
you come across Vit. A deficiency
IV.
among many members of the family?
Comment on the following daily diet.
Rat rice (polished)
16 os
Pulses
1 oz
Green leafy Vegitables
T oz
Bringals
2" oz
Butter milk
4 oz
i oz
Sugar
Suggest improvements without increasing the cost of the diet very much.
V
Describe a balanced diet for a family tith an income of Rs.200 per month
consisting of 5 members - one male 45 frears; 1 female (pregnant) 35 years;
and 3 children aged 10 & 6’respectively.
VI.
A family consisting
a)
1 adult male weighing 55 kgs
b)
1 adult female weighing 45 kgs
c)
1 adolescent boy weighing 45 kgs
d)
1 adolescent girl weighing 35 kgs
Calculate the dail$ requirement of protein for the family.
VII.
On analysis of daily diet taken by a family consisting of
1 adult male
(sedentary) 55 kg
1 adult female (
"
) 45 kg
3 children of 5 years
12 kg
8 years
20 kg
It was foun^ toaC?i^yin
nutrients."Comment on the
quality/of the diet.
Protein
100 G
Carbohydrates
1000 G
Fats
55 G
5000 ill (900 mcg of Retinonol)
Vit. A
Vit. B
5 mg
Vite C
1000 mg
Vit. D
2000 IU
Fe
55 mg
Ca
2.5 G
How will you improve?
VIII
What type of daily diet would you recommend for a labourer
weighing 65 kg?
Explain in detail the dietary requirements of the following:
IX
a)
Pregnant mother
b)
Labourer (adult male)
c)
child aged 8 years
Write short notes on:
X.
XII.
a)
First class proteins
b)
Measly pork/beef
c)
Food preservation
d)
Phosphatase test
e)
Milk borne infections
■ ■
A family consists of the following members:
a)
Old lady of 60 years (40 kg)
b)
An adult male going to office (55 kg)
c)
An adult female (45 kg)
d)
Two sons and two daughters of 15, 15, 11 and 7 years of ag
Give a schedule of balanced diet for this family in
germs of rice, pulses, green leafy vegetables, root vegetables,
other vegetables, milk sugar, fish, meat, egg and oil.
3
XIII
A family consists of an adult mele (55 kg) and adult female (45 kg)
and' a child of 5 years weighing 15 kgs. 0n a diet survey of this
family, it was observed that the consumption per day in terms of the
proximate principles and nutrients was as follows:
Proteins
0o
CHO
Pats
a)
b)
••
150 gms.
Vit. A
2000 gms
Vit. B
10 mgm
100 gms
Vit. C
150 mgm
1000 IU
Comment on the quantity and quality of the diet.
Suggest improvements confining your attention to the above
nutrients only.
XIV
A mother with an infant of 6 months old wants to start her chi 14
with artificial feeding with buffalo's milk. What is the quqntity
of the buffalo’s milk and the number of feeds per day that you
would advise? What other advise you would like to give to the mother
about the feeding with the Buffalo's milk? Considering the deficiencies
in the milk, what supplements would you advise?
/vut A A3
DEPARTMENT OF PREVENTIVE & SOCIAL MEDICIDE
ST. JOHN'S MEDICAL COLLEGE, BANGALORE 560034
EXERCISES IN NUTRITION AND DIETETICS
A family consists of the following members:
C.
a) Old lady of 60 years (40 kg.)
f
b) An adult male going to office (55 kg.)
c)
An adult female (45 kg)
d)
Two sons and two daughters of 15, 13, 11 and 7 years of age.
Give a schedule of balanced diet for this family in terms of Rice, Pulses,
Greenleafy vegetables, Root vegetables, othor vegetables, milk, sugar, fish,
meat, egg and-oil.
Coefficient value of the family:
ANSWER:
a
b
c
d
e
f
•
Old lady
Adult male
Adult female
Son, 15 years
Son, 13 years
...
Daughter, 11 years ..
) Daughter, 7 years
0.9
1.0
0.9
1.0
1.0
0.8
0.7
Total
6.3'
•
Requirement of Balanced Diet for the family =
gms
•
1.
Rice
400 x 6.3
2.
Pulses
85 x 6.3
3.
4.
Oz.
=
2520
gms
14
..
88.2 Oz.
=
535.5
gms
3
..
18.9 oz.
G.L. Vegetables 114 x 6.3
=
718.2
gms
4
..
25.2 oz.
Root vegetables
=
535.5
gms
3
..
18.9 oz.
85 x 6.3
5.
Other vegetables 85 x 6.3
=
535.5
gms
3
..
18.9 oz.
6.
Fruits
85 x 6.3
.=
535.5
gms
3.
..
18.9 oz.
7.
Milk
284 x 6.3
=
1789.2
gms
10
..
63.0 oz.
8.
Sugar
57 x 6.3
359.1
gms
2
..
12.6 oz.
9. ’ Fish & meat
85 x 6.3
535.5
gms
10. Eggs
7 eggs
11. Oil
57 x,6.3
359.1
gms
=
... 18.9 oz.
3
1
..
7 eggs
2
...
12.6 oz.
We require for the above family 2400 x 6.3 = 15,120 calories. The above
diet yields approximately 3000 x 6.3 calories. Hence, it is sufficient for the
family.
Q - II.
A family consists of an adult male (55 kg.), and adult female (45 kg.)
and a child of 5 years weighing 15 kgs. On a diet survey of this
family, it was observed that the consumption per day in terns of the
proximate principles and nutrients was as follows
Proteins
CHO
Fats
150 gms.
2000 gms.
100 gms.
Vit. A.
Vit. B.
Vit. C.
1000 I.U.
10 ragm.
150 ragra.
a) Comment on the quantityt and quality of the diet.
b) Suggest improvements confining your attention to the above
(
nutrients only.
-2-
ANSWER:-
: eguirements
■ Male
Chi Id
Female
1.
Proteins
55 gra.
+
45 gms.
+
52.5 gras.
-
152.5 He.
2.
CHC
450 gm.
+
450 gms.
+
180.0 gras.
=
1080.0 gras.
+
40.0 gras.
-
160.0 gr.-.s.
+
35CO.O IU
-
10,500.00 TJ.
3.
Fats
4.
Vit. 'A1
60 gm.
+
3500 IU
+
40 gms.
3500 IU
In terras of Retinol and daily requirement will be 750 miprograms for the
adult and for the child of, 5 years 300 micrograms. It conus to 750 + 750 +
300 = 1800 micrograms. One I.U. of Vit. 'A' = 0.3 rag. So, 10,500 I.U. dill
be 3,150 micrograms.
5.
Vit. *B'
(Thiamine)
..2+2+1
=
5 gras.
6.
Vit. 'C'
..
.. 50. +50
=
140 ragra
Quantity:
Calories requirement 1 + 0.9 + 0.5 = 2.4 coefficient
= 5,760 calories.’
i. COMMENTS:
+40
The above diet will provide Proteins 150 x 4
CHO
,2000x4
Fats
100 x 9
Total
= 600 calorics
=8000
-do= 900
-do-
= 9400 calories
It is more than ample.
QUALITY
:-
:
:
:
Proteins
Fats
Vit. B
Just short:
Short
Sufficient:
CHO - none than ample
Vit. A - very much short
Vit. C - sufficient.
iii. IMPROVEMENT: Cut out CHO (Cereals) and increase the pulses, milk or include
egg. Fat requirement can be met by increasing oil or ghee (60 gras). Vit.A
or Retinol is very rauch short of requirements and leafy vegetables like
araaranath, drum stick leaves and other vegetables like carrot; fruits like
papaya should be included in-the diet. lit. B & C are sufficient.
Q - HI., A mother with an infant of 6 months old wants to start her child
with artificial feeding with buf “'aid's milk. What is the quantity
of the buffalo's milk and the number .of feeds per day that you
would advise? What ether advise you would 1 -ike- to give to the
mother about the feeding with the buffalo's milk? Considering the
deficiencies in the railk, what supplements would you advise? '
ANSWER:.
Buffalo milk yields 118 calories/100 gras. A child of 6 months
(normal), weighing 6.7 kg. will require 600 calories. The child
therefore, requires 600/118 = 5 or 500 gras, of railk or 16 to 17 oz.
of milk. This railk must be diluted with water to reduce the fact
concent and sugar must be added to increase the CHO content.
Coaposition: Buffalo milk
Huraan railk
■
= Fat
8.8
= Fat ” 3.4
sugar 5.1
sugar 7.4
i.e. the railk must be humanised.
Thus, 16 to 17 ozs. of diluted milk must be'given in 4 feeds (8 hrs. once)
during day and one feed before going to bed! Milk is deficient in Iron
and Vit. C. Hence, fruit juices and green leafy vegetables mashed should
be given as supplements.
Nutrition Education Unit
AND
Community Health Project
SUPPORTED BY OXFAM
Project
OCTOBER
1970
—
Report
SEPTEMBER
1971
C. S. I. Campbell Hospital
JAMMALAMADUGU
Cuddapah District, A. P.
SOUTH INDIA.
1. Introduction - Community Health Care.
"Many people are writing symphonies about Community
Health Care, but who is playing the music ?"
In Jammalamadugu
we have a small amateur orchestra and there is music of a sort.
Sometimes we are confused by different scores, and at others
we are uncertain that the audience appreciates the tune.
This
report is a record of discord as well as melody - the Jamma
lamadugu sound" I
•
A Clinical Approach.
"Community Health Care" has become a cliche.
Initi
ally it may only mean a concern on the part of medical and
nursing personnel for the important extra-institutional factors
related to health and disease.
At its best it implies the
involvement of the community in improving its own health.
In an under-privileged society where the dominating
factor is poverty, the majority are so involved in the stru
ggle for survival, that the response to any "felt need" survey
is ciroumsoxibod, and the community involvement in health
care can only be rudimentary.
In our situation the community
health work is really at the initial stage of the definition
given above, and we are conscious that education of the co
mmunity to its health needs and possibilities is a primary
task.
Most people in the villages around here only appear
to appreciate health by its absence.
Consequently it is
important to utilise the management of disease as a fertile
opportunity for teaching about health.
When one member is
ill, the family is a captive, attentive and often receptive
audience.
This clinical or disease-orientated approach
carries the dangers of over involvement in therapeutic care,
but it has the distinct advantage of being related to the
immediate needs of the people.
A health talk about immunisation
C.H.C.
2
or clean ■ delivery may not provoke much interest, but it is
strikingly relevant in a ward where there are children with
neo-natal tetanus.
It is not uncommon in a single clinic
to find two pregnant mothers each with a younger child su
ffering from gross malnutrition of the Kwashkorkor type.
In this context a talk about the relation between family
planning and nutrition is immediately obviou's to all.
.
*
1.2
Components in the Programme .
The different elements in our clinical approach to
community health include; analysis, pilot schemes, service,
teaching and evaluation.
There is a considerable overlap
of these facets in the programme.
1. Analysis - assessment of the health status of the
community and the problems with which people present at clinic
and hospital.
2.
Pilot Schemes - testing out what methods are
acceptable and effective in stimulating the public and prcu
viding health care.
3.
Service - the promotion of health with the preven
tion and treatment of disease.
4.
Teaching and training - an essential part of
health care and integrated with the service component.
It
includes teaching patients and their relatives, and training
members of staff .
5.
Evaluation-i an attempt to answer the questions
“how effective and how economic is any part of the service
in providing health- care for the individual and the community.
ii an opportunity to feed-back information to modify the
vaT.tov.o aspects of the work.
C .H .C.. 3.
In this report there are examples of these various
components as they overlap and complement each other in our
community health programme.
1.3.
Co-ordination in the Hospital Services.
Those of us associated with the OXFAM project at
Jammalamadugu would like to see the community health work
more closely integrated with that of the hospital.- This would
mean several things; the increasing acceptance on the part.
■of all hospital staff of a concern for the health of our
community beyond the confines of the institution, and a closer
physical and financial link between the hospital and the
project.
Already there has been a fruitful co-operation;
a number of the staff financed by OXFAM perform part of
their work within the hospital, for example the Public Health
Tutor besides supervising various aspects of the community
health work, draws on this experience in training the student
*
nurses
In various ways members of the hospital staff assist
with different aspects of the project.
The Nutrition Unit
can only function because parents bring their sick children
to the hospital for help, yet the hospital would not be able
to give these children the care they most need if there was
no Nutrition Unit.
.The dilema before this and other Christian hospitals
is on the' one hand, the need for the institutions to remain
as financially independent as possible, and the challenge.
on the other'hand to pioneer in new ways of community health
care which are essentially unremunerative.
We have made
a useful start in some aspects of community health .care, but
..continued progress will depend on
1. Simplication of techniques to bring sown basie-- ’
costs to a minimum
C.H.C. 4.
2.
Acceptance on the part of the hospital that it
has some financial responsibility for community health care.
3.
Continuing help from OXFAM for much of the out
reach work, especially the rehabilitation of the malnourished
who are usually very poor.
4.
Training programmes in whi.ch to will share our experience
and help us to maintain high standards of care.
5.
Co-operation with the government wherever possible.
Besides orienting our efforts to the national health planning,
our programme should be benefited by a supply of free vaccines
0
and remuneration for family planning services.
1.4.
C-'o-operation with the Government,
The hospital is fortunate to have quite good rapport
with the government on account of thb^fine record of family
'planning work.
In January 1971 the State Health Minister
opened the hew 20-bed tubectomy ward, which is probably the
largest granted to any Christian institution.
In two con
secutive years the hospital has been awarded the shield
for the best family planning effort by a voluntary institution in the state.
The community health project has a happy relation
ship with the state Maternal and Child Health (MCH). Depart
ment, and the Director, Dr. B. Vigg, visited the work here
in November 1971. ’We are now receiving Triple, Polio and
Tetanus Toxoid vaccines directly from this department.
At the District level, we are receiving B.C.G. vaccine
regularly from the District Tuberculosis Officer, and a mem
ber .-of the local health department visits the hospital every
week and vaccinates all the newborn babies in the maternity
and tubectomy wards.aganist smallpox.
9
C.H.C. 5.
We are grateful to the Director, Dr. C. Gopalan, and
Assistant Director, Dr. S.G. Srikantia, of the National
Institute of Nutrition in Hyderabad for their help.
One of
our staff was sent there for training in I.Q. testing as
we plan to try to
correlate the intelligence of the mothers
along with other factors when we evaluate the progress of
children.
With the help of the artists at the N.I.N., we
have developedanumber of village picture sequences that will
be valuable when testing the rural mothers in this are.
1.5.
Training.
This project which started as a service, is beginning
to have an important training function.
All the project
team have learnt a great deal during the development of the
work and attempts have been’ made to try and share this ex
perience with the rest of the hospital staff.
All the student nurses have the opportunity of working
in the different parts of the project.
This gives some realism
to the community health nursing that is integrated in their
course.
The Director of the Christian Medical Association
of India’s Family Planning Project (CMAI,FPP) has asked us
to run a months training programme for nurses from 4 hospitals
in different parts of South India who will be taking part
in a family Health Assurance'Plan.
The scheme is to develop
the concept of the "small family norm" by improving basic
health services with an emphasis on children under 5, and,
having demonstrated the survival effect, encouraging planned
conception.
Although this hospital did not opt to join thier
plan, the CMAI,FPP feel that we have practical experience
in many matters directly relevant to the scheme, and requested
C.H.'C.' 6.
Dr. Ratnaraj, the Medical Superintendent, to let them site
the training here.
We hope the course will' be a practical
joint effort of those working in the CMAI, FPP, the hospital
and the OXFAM project.
Inevitably a major burden will fall
on the community health project.team, but we'
expect
*
to learn
a great'dfeai and accept this as a milestone in our development.
1.6.
Child Weight Cards.
The benefits of home-based health record systems
are now recognised.
The Under-Fives Weight Card developed
by Dr. David Morley was a pioneer in this field.
Our Telugu
card is now used for children in one Government and many
Christian hospitals, and we hope that the technique will be
increasingly accepted in the coming years.
Already the Andhra
Pradesh state Government has produced a card based on the
Morley pattern, even though they have not been bold enough
yet to give it to the parents to keep.
We have already
the value of the cards when counselling parents
stressed
about contraception, and believe the section on Family Planning
is a particularly valuable addition to the card for India.
We are developing a new card which will bear a basic
weight-for-age graph and figures, and on this it should be
possible to print other information locally in the regional
language.
A further modification included is the addition
of two more growth curve lines.
Reference to these lines
will make it possible to classify any child immediately accord
ing to the degrees of malnutrition defined by the Nutrition
Sub-committee of the Indian Academy of Pediatrics.
We hope
that these features will make the card more widely accepta
ble thoughout India.
C.H.C, 7
1.7.
Staff.
W.A.M. Cutting. M.B., M.R.C.P., D.C.H., D.Obst. R.C.O.G.
Mrs. Margot Cutting. M.B«, Ch.B. (Part-time,' Honorary).
Miss. Nirmala Paul. M.Sc. (Nutritionist).
Mrs. M. Margaret Prasad. R.N., R.M., S.T. (Tutor).
Miss. V. Karuna John. R.R., R.M., Public Health Certificate.
Miss. L.S. Deevanamma. R.N., R.M.
Mrs. Surya Bai. R.N,., R.M.
Mrs. Alice Pushparaj. (Family Planning Nurse).
Mr. K. John Kumar. (Higher Grade Typist and Clerk).
Miss. M. Sarala. (Clerk).
Mrs. V. Sugunamma. (Health Demonstrator).
Mrs. B. Rajamma. (Health Demonstrator).
During 1971 Miss. Karunamma successfully completed
her Public Health training at the Lady Reading Health School
in New Delhi, and we were very glad to welcome her back.
Dr. G. Arthur Samuel has commenced his specialist pediatric
training at the Christian Medical College, Vellore, and
he will return in 1973.
The Medical Superintendent has
approved the appointment of a part-time Administrator for
the project from April 1972, and we hope OXFAM will also
support us in this.
Her functions will be partly to handle
the correspondence and finances, and generally supervise
and co-ordinate with the hospital and other services and
also help plan training programmes.
Thus, the foundations
are laid for the continuation of the project after the
gradual withdrawal of Dr. and Mrs. Cutting.
The five nurses are accepted as full members of
the hospital staff in terms of confirmation of service
and provident fund.
The others on the project team would
naturally like -these privileges, but they have not yet been
C.H.C. 8
accepted by the Medical Superintendent.
cial implications are being studied
*
The legal and-finan
and if they cannot
be accepted as actual hospital staff, it is hoped that some
award in lieu of provident fund, and some security of tenure
can be offered to these hard-working people.
1.8. ■ Thanks and Acknowledgements.-
Without the help; support and encouragement of many
people this work would not go on.
to thank OXFAM.
In particular we wish
Dr. John Staley and Mrs. Ausma Ackworth,
the South India Secretaries, have always been ready with-
help, and their faith in what we are trying- to do has been
a real encouragement.
The Area Secretaries Mrs. Reid and
Mrs. Davie, from London and Glasgow, have-written to us
often after their visit to Jammalamadugu.
Though they
have a rather rosy picture of our work, we try to live up
to their expectations 1
We wish to thank Dr. Ratnaraj,
the Medical Superintendent, who has given us wise counsel
and permitted the development of the work in association
with the hospital.
We are grateful to many members of the
public, and patients, young and old, from whom we have
learnt much about the beliefs concerning health and disease
which are essential when trying to run a community health
The cover picture is by Sandoz Limited, India.
project.
Last but not least, I would personally like to
thank all the members of.the staff.
Often their efforts
to help others have been difficult, and sometimes rudely
rejected.
hours.
They.usually work long-and sometimes irregular
They have accepted their delegated responsibilities
and are a cheerful group of people with whom it has been
a pleasure to work.
William A.M. Cutting
iq
.,
—.
od'
IS"
n
--
(Tld^
IU
•'
—
"_
-
"
/f
47/1, (Fir^x
r..-;.,O01
ST. JOHN'S MEDICAL COLLEGE HOSPITAL
BANGALORE-560 034
Telephones:
42061 - 68 ( 8 Lines )
Telegrams: SAINJOHNS
ST. JOHN'S MEDICAL COLLEGE, BANGALORE
DEPARTMENT OF FRI VENTICE & SOCIAL MEDICINE
s_y_l_l_a_b_u_s
Subject : Preventive & Social Pediatrics
Session I
“ Child Growth and Development
i)
Why knowledge needed
ii)
Place of children in Indian Society
iii)
Methods of study
iv)
Principles of Development.
Session II
- Genetics and Health & Genetics Counselling
Session III
— i) Preventive Pediatrics - Divisions
ii) Antenatal Pediatrics
iii)
iv)
Session IV
Prenatal development factors
Neonatal period & Infancis - Delivery,
Registeration, postnatal care, feeding
naming, supplementary feeding and weaning
bathing, clothes, sleep, teething, mile
stones, emotional and social development.
- Milestones in growth and development
i) Weight & Height
ii) Head measurcments/fontanellos
iii) Dentition
iv)
Mental, Physical, Social development.
Well baby clinic - Why? and functions.
Session V
- Visit to well baby clinic
Session VI
- Toddlerhood, Preschool Child Physical Development
Play, Feeding, Toilet training, Sleep
Health Protection - care of ear, nose, throat,
worms - prevention of ill health and accidents.
Motor development, handedness.
Session VII
- Intellectual/Emotional/Social Development of the
Preschool child Nursery School as a Laboratory
Session VIII - Social pediatrics
- Behaviour problems
- Jurenile Delinquency
- Handicapped children
- Mental Retardation
- Maternal deprivation
- Pattered V'aby syndrome
— Child Guidance Clinic
- Social Legislation.
Session IX
- Visit to Child Guidance Centre
Session
- Mortality in children, Rates, cause
preventive and Social measures.
Position: 1046 (15 views)