RF_M_5_SUDHA.pdf
Media
- extracted text
-
RF_M_5_SUDHA
HINDU
THE
Me
Hospital or hell hole?
It was nearly midnight on May 30 this
year. Sudhadevi, a middle-aged woman living
in Koramangala, suffered burns all over her
body. Moaning and writhing in agony, she
was rushed to St. John's Hospital where she
was given emergency treatment. But she was
refused admission on the ground that no bed
was available. The desperate relatives went
from one hospital to another seeking further
treatment for Sudhadevi. but in vain.
Finally, around 3 a.m., they brought her to
the burns centre of the Victoria Hospital.
They were aghast to find that not one doctor
was on duty. By the time the junior doctor
arrived and gave her a pain killer, it was 8.30
a.m. He told the family that the senior doctor
would attend on her, that he was
participating in a meeting right then. It was
noon when the senior doctor arrived and
began treatment. But he need not have
bothered: a few minutes later, she breathed
her last.
This is an account given by Vimochana, a
forum' for women’s rights that is making
efforts to draw attention to what it says the
poor conditions in the only State-run burns
centre in the city, which is the only refuge for
people who cannot afford private medical
care. "Not only is the environs detrimental to
the recovery of the patient, being situated in
the midst of noise and squalor, absolute
apathy, callousness, but the indifference of all
the staff is distressing." says Vimochana.
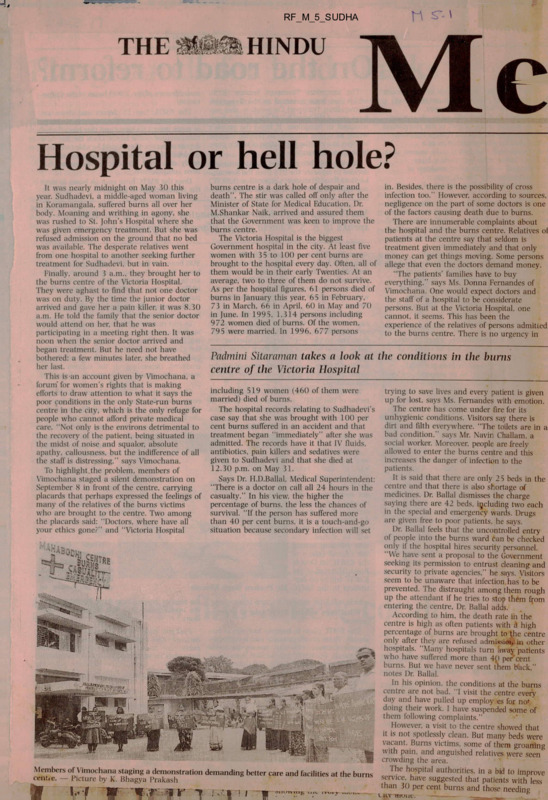
To highlight.the problem, members of
Vimochana staged a silent demonstration on
September 8 in front of the centre, carrying
placards that perhaps expressed the feelings of
many of the relatives of the burns victims
who are brought to the centre. Two among
the placards said: "Doctors, where have all
your ethics gone?” and "Victoria Hospital
burns centre is a dark hole of despair and
death". The stir was called oil’ only after the
Minister of State for Medical Education. Dr.
M.Shankar Naik. arrived and assured them
that the Government was keen to improve the
burns centre.
The Victoria Hospital is the biggest
Government hospital in the city. At least five
women with 35 to 100 per cent burns are
brought to the hospital every day. Often, all of
them would be in their early Twenties. At an
average, two to three of them do not survive.
As per the hospital figures, 61 persons died of
burns in January this year. 65 in February.
73 in March, 66 in April, 60 in May and 70
in June. In 1995. 1.314 persons including
972 women died of burns. Of the women.
795 were married. In 1996. 677 persons
in. Besides, there is the possibility of cross
infection too." However, according to sources,
negligence on the part of some doctors is one
of the factors causing death due to burns.
There are innumerable complaints about
the hospital and the burns centre. Relatives ol
patients at the centre say that seldom is
treatment given immediately and that only
money can get things moving. Some persons
allege that even the doctors demand money.
"The patients' families have to buy
everything." says Ms. Donna Fernandes of
Vimochana. One would expect doctors and
the staff of a hospital to be considerate
persons. But at the Victoria Hospital, one
cannot, it seems. This has been the
experience of the relatives of persons admitted
to the burns centre. There is no urgency in
Padmini Sitaraman takes a look at the conditions in the burns
centre of the Victoria Hospital
including 519 women (460 of them were
married) died of burns.
The hospital records relating to Sudhadevi's
case say that she was brought with 100 per
cent burns suffered in an accident and that
treatment began ‘‘immediately" after she was
admitted. The records have it that IV fluids,
antibiotics, pain killers and sedatives were
given to Sudhadevi and that, she died at
12.30 p.m. on May 31.
Says Dr. H.D.Ballal, Medical Superintendent:
"There is a doctor on call all 24 hours in the
casualty." In his view, the higher the
percentage of burns, the less the chances of
survival. "If the person has suffered more
than 40 per cent burns, it is a touch-and-go
situation because secondary infection will set
trying to save lives and every patient is given
up for lost, says Ms. Fernandes with emotion.
The centre has come under fire for its
unhygienic conditions. Visitors say there is
dirt and filth everywhere. "The toilets are in a
bad condition." says Mr. Navin Challam. a
social worker. Moreover, people are freely
allowed to enter the burns centre and this
increases the danger of infection to the
patients.
It is said that there are only 25 beds in the
centre and that there is also shortage of
medicines. Dr. Ballal dismisses the charge
saying there arc 42 beds, including two each
in the special and emergency wards. Drugs
are given free to poor patients, he says.
Dr. Ballal feels that the uncontrolled entry
of people into the burns ward can be checked
only if the hospital hires security personnel.
"We have sent a proposal to the Government
seeking its permission to entrust cleaning and
security to private agencies," he says. Visitors
seem to be unaware that infection has to be
prevented. The distraught among them rough
up the attendant if he tries to stop them from
entering the centre. Dr. Ballal adds.
According to him, the death rate in the
centre is high as often patients with d high
percentage of burns are brought to the centre
only after they are refused admission in other
hospitals. "Many hospitals turn away patients
who have suffered more than 4() per’cent
burns. But we have never sent them back."
notes Dr. Ballal.
In his opinion, the conditions at the burns
centre are not bad. "I visit the centre every
day and have pulled up employ es for nof
doing their work. I have suspended some of
them following complaints."
oHowever, a visit to the centre showed that
it is not spotlessly clean. But many beds were
vacant. Burns victims, some of them groaning
with pain, and anguished relatives' were seen
crowding the area.
The hospital authorities, in a bid to improve
Members of Vimochana staging a demonstration demanding better care and facilities at the burns
centte. — Picture by K. Bhagya Prakash
service, have suggested that patients with less
than 30 per cent burns and those needing
x ; '.. „
.
I
11 l v a i < j j i c.
— .- . -
--_____
tro
Monday, September 15, 1997 1
Bangalore
> I':
11
I
'F-
iBi
.1
f
-
<
'
:
'
■
'Mi
■
iV Bl v
j
I
W-
ll
ih
■
»•,
4^-
.. j
y
A view of the burns ward in the Victoria Hospital. — Picture by K. Bhagya Prakash
intensive care should be kept in separate
wards. Patients with infections should be
isolated. “This can be done provided we are
given men, material and space. There is no
Intensive Care Unit in this hospital although
a proposal was made five years ago and the
space earmarked,” says Dr. Ballal, adding that
six ventilators will be installed at the Victoria
Hospital soon.
The Minister, Dr. Naik, admits that there
may be one or two black sheep among the
hospital staff. The charges against the hospital
arc vague, according to him. “I have asked
Vimochana to give me in writing specific
complaints about the staff and also about
corruption in the hospital.” He says it is
planned to shift the burns ward to the
building that will be vacated when the
Jayadeva Institute of Cardiology is moved to
its new building in Bannerghatta.
Vimochana has made suggestions for the
better functioning of the burns centre. It has
suggested that an ambulance with facility for
providing first aid should be kept ready; that
a classification of burn be made; that burn
centres be set up in difi’erent parts of the city;
and that higher salaries be given to the
doctors and staff considering that their jobs
are highly stressful and emotionally
exhausting. Vimochana feels that better pay
will help end corruption.
Some private hospitals do extend medicare
to burns victims but the cost of treatment is
high. The Mallya Hospital, which has been
given an ISO 9002 certificate, opened a burns
centre earlier this year with plastic surgeons
offering specialised care. Says Dr.
Nandakumar Jairam. Medical Director of the
Hospital; "We have two beds. The unit was
set up as we felt the need to provide better
facilities.” No patient is turned away whatever
the percentage of burns. Emergency treatment
begins as soon as the burns victim is
admitted. It is up to the patient's relatives to
decide whether treatment should be
continued at the hospital or the patient taken
to another hospital, he says.
“The cost depends on the extent of burns,
the degree of burns, the complications and
plastic surgery. We try to give the maximum
possible concessions. It is not only treatment
of burns. Skin grafting has to be done later,”
observes Dr. Jairam. Among the hospitals that
treat burns victims are the M. S.Ramaiah and
St. John's Hospitals. The Manipal Hospital has
so far treated one victim of bums, it is learnt.
What prompted Vimochana to take up the
issue of burns victims? “In the process of
following up cases of dowry death, our
attention was drawn to the medicare available
for the women who manage to survive —
particularly those who suffer burns. We found
that even if they survive the torture inflicted
on them by their own people, the callousness
of the State medical establishment, which is
the only hope of the majority of those who
cannot afford private medical care, drives the
women to painful death," says Vimochana.
“As it is, women are suffering. And when
they come to the burns centre, the staff treat
them cruelly. Why should they come there to
die?” asks Ms. Fernandes.
For the last 18 years. Vimochana has been
working on issues relating to domestic
violence. A study of cases of unnatural deaths
of married women in the city was taken up
by the team consisting of Ms. Fernandes, Ms.
A. Ragini. Ms. N.Shanti. Ms. K.Satya and Ms.
Gouramma.
Many of these are not accidental deaths:
they are cases of murder, feels Vimochana.
“We want a special cell for such cases set up
as the guilty are not being charged. Such a
cell should investigate cases of burns
sustained accidentally and prove that these
are not cases of murder,” says Ms. Fernandes.
The study has found that many of the burns
victims were from the Tannery Road and
Magadi Road areas, D.J.Halli and
Mahalakshmi Layout.
Dowry deaths are investigated by the Anti
Dowry Cell (ADC) in the CoD located in
Cauvery Bhavan. The Cell probes death of
women occurring within seven years of
marriage following harassment for dowry. It
takes over the investigation only after a case
is registered. In a year, 230 to 240 cases are
investigated of which between 20 and 25 per
cent are from the city and a majority from
the economically weaker sections of society.
After investigation, the ADC gives the final
report. “The chargesheet is filed if there is
enough evidence against the alleged party. A
‘B ’report is prepared if it is found during
investigation that death was accidental. A ‘C’
report is filed if we cannot detect a case,” says
Mr. A.R.Infant, DIG (CID).
Mr. Infant says that this year, the ADC has
filed chargesheets in 27 dowry death cases
out of the 39 cases reported. In 1996, 61
dowry deaths were reported in the city and
58 persons chargesheeted.
There are allegations that policemen have
been found to take the thumb impression of
the burns victim on a blank paper, for
preparing the statement. Mr. Infant denies the
charges against policemen including that they
demand money during investigations. “These
(the allegations) are vague. I am ready to
take action provided I get specific petitions. A
written complaint was handed over recently
and it is being investigated.'' In his view, the
statement of the police officers should be
given credence and summary trials made in
some cases.
31
HEALTH CARE WASTE DISPOSAL
= An exjploijratiion
: Problem definition <& Probable Solutions
^Extract from the executive summary)
Department of Community Medicine
M S Ramaiah Medical College
Bangalore - 5G0 054 INDIA
HEALTH CARE WASTE DISPOSAL - AN EXPLORATION
PROBLEM DEFINITION :
Health Care Waste is casually dealt with both by Health Care settings and
the Civic bodies. This is dangerous to Health care Personnel, Waste handlers
and the Community. Reasons for this appears to be :
1
Lack of awareness
among doctors, nurses, administrators
about hazards of improper Health Care
Waste management; options available
for its proper management; lack of
awareness among Waste handlers (
Ayahs, personnel near incinerator and
land filling sites, rag pickers) regarding
hazards of Health Care Waste.
2
Lack of Information support
for doctors, administrators, nurses.
Waste handlers
3
Lack of practices like
ffi
4
- segregation of infected Waste and
sharps
- disinfection of infected waste
- Sanitary landfilling
- Recycling of recyclable items
- use of protective devices
- periodic medical examination
- Immunisation of Personnel
- Precautions for prevention of HIVAIDS
- Incineration facilities meeting
Central Pollution Control Standards.
bodies of Health Care settings and
Lack of effective organisational
Lack of coordination between civic bodies and Health Care settings.
EXECUTIVE SUMMARY
9
HEALTH CARE WASTE DISPOSAL - AN EXPLORATION
PROBABLE SOLUTIONS
CAPACITY BUILDING
of Doctors, Administrators^ Nurses,
Waste handlers on hazards of Health
Care Waste; available options for its
management; available cooperation
from the civic body - through training
and information support. Segregation
of Infected Waste promoted as a culture
in Health Care settings.
STRENGTHENING FACILITIES FOR FINAL DISPOSAL OF HEALTH CARE
WASTE
a) It is suggested that 500 acres of land
outside the city limits be earmarked,
developed and managed for Solid
Waste disposal - of which a portion
be earmarked for Health Care Waste
disposal.
b) Sanitary Landfilling taken up
I
c) Cooperative common incinerators
meeting central Pollution Control
Standards for Health Care Waste
which is infected are commissioned
and their function is supervised and
monitored.
I
d) Small industries are set up for
recycling plastic items, metal sharps
(and ? Bandage cloth after
decontamina tion)
i
e) Better transportation vehicles covered and automatic are procured
and a parallel system is practiced for
the transportation of General Solid
Wastes and Health Care Waste
separately by the civic bodies.
EXECUTIVE SUMMARY
i
10
i
HEALTH CAREv>VASTEpiSPpSAL^^DdRLO^TOPfe>
f) All Health Care settings - big and
small are registered at the 12 Sub
health Offices of the city. The Sub
health Offices can be focal points of
support to respective Health Care
settings located in their jurisdictional
areas. Periodic returns related to
Waste generation to be submitted to
Sub-health Offices by the respective
Health Care settings. Based on
these calculations, logistics of
transportation is jointly arranged
and managed by joint contributions
and participation by both the
management of Health Care settings
and Gvic bodies.
AWARENESS ACTIVITIES
a) Health education materials like
posters, pamphlets, booklets, flip
charts on Health Care Waste
management in local language is
developed and consciousness is
created among Waste handlers and
the community
b) Community's involvement is to be
sought in identifying areas for
Sanitary land fill and hygienic
practices of Waste collection and
transport - of both General Waste
and Health Care Waste.
c) There is a need to start a resource
centre in the City which can provide
information support in the form of
periodic news letters and other
means to all Health Care settings,
NGO's, etc.
An NGO can be
supported to take up this role with
the back up of a Medical college
resource.
EXECUTIVE SUMMARY
11
HEALTH CARE WASTE DISPOSAL - AN EXPLORATION
INFECTION CONTROL COMMITTEES
It is suggested that infection control committees be established in all
Health Care settings where bed strength is more than 100 ; and the committee
to supervise Health Care Waste Management, Hospital Acquired Infections and
General Infection Control.
RESEARCH ACTIVITIES
- The investigators suggest that the State Government shall encourage the
Civic bodies to take up the following research activities in collaboration with
Medical Colleges and Engineering Colleges on priority;
a) developing curriculum for training doctors, nurses, administrators, waste
handlers in the area of health care waste management
b) Feasibility studies to recycle metal sharps , plastic items in safe ways
c) techno-economic assessments of solid waste/health care waste in different
cities, towns, etc.
d) conducting waste surveys in different Health Care settings including
measurement of quantity of such generated waste
e) feasibility studies for efficient establishment and running of common
incinerators/ sanitary land filling/ composting etc.
f)
sentinel surveillance of hazards due to Health Care Waste management in
selected ranges of the City
g) studying sickness absent^H^m and causes for the same among waste
handlers
h) maintenance and period)
personnel
XLCUTIVE SUMMARY
v of morbidity registers of health care
12
HEALTH CARE WASTE DISPOSAL - AN EXPLORATION
RECORDING AND REPORTING
The investigators suggest that systems of recording and reporting o the
following events are developed and submitted periodically to the infection
control committee of the city/ civic body by health care settings.
- Quantity and type of waste generated
- Illness/ injuries noted among waste handlers
- Difficulties faced and solutions adopted to solve the same by Health
Care settings in Health Care Waste management
- Immunization status of staff regarding tetanus, typhoid and hepati :is B
- Training status of staff on Health Care Waste management.
The investigators feel that legislative control is to be exercised only after
capacity building and strenghtening of facilities is taken up for two to three
years
Till sanitary land filling/ common incineration facilities/ individual
incineration facilities/ safe recycling methods of some of the items of Health
Care Wastes become available or other methods of treatment and disposalI are
to be the options available for
accessible and adopted the following appear
<
immediate action;
1) Disinfection of waste before disposal
2) Segregation of infected waste and metal sharps
3) Safe practices within Health Care settings
4) Practice of universal precautions for preventing HIV-AIDS
5) Capacity building of Health Care personnel and waste handlers
6) Document quantity of waste generated
7) Document hazards due to Health Care Waste
The investigators have made an attempt to draft a manual for training
doctors, nurses, house keeping officers, administrators and educational
material for waste handlers (ayahs, pourakaarmikas etc,, ) It is being planned
to field test and subject it for wider consultation before being put for practical
use.
EXECUTIVE SUMMARY
13
BURNS CARE IN INDIA:
For professionals dealing with burns care in India, the
high mortality, morbidity, unknown
epidemiology and socio
economic problems remain areas of great concern.
ROW DO WE COMPARE WITH DEVELOPED COUNTRIES?
1. We do not have a single centre dedicated to burns
care.
A
2. Our 50% mortality is in the 30-40% BSA Burn group.
In the west and east this is in the 60-80% range depending on age.
3. The morbidity is very high.
THE CHANGES THAT NEED TO BE MADE:
1. We need to start burns centres dedicated to the care
of burns, at least one in each State.
2. The prevailing centres and District hospitals need
upgrading.
3. Intensive care facilities should be provided.
4. Well trained & motivated multidisciplinary burns
teams should be introduced and the number of Staff
1
should be adequate.
5. Barrier nursing and rigid environmental bacterial
control are absolutely essential.
WHY IS IT SO DIFFICULT TO CHANGE?
1. LACK OF AWARENESS:
The majority of Policy makers, administrators,
doctors and the public are probably unaware of how
an ideal burns centre should run?
Cotd. .2
2
2. FINANCES:
The inability to mobilise funds to upgrade these
units appears to be a major deterrent to change.
3. LACK OF MOTIVATED PERSONNEL:
As of now, very few professionals take up burns care
exclusively- It is essential to have full time, mo
tivated personnel for an y long term improvements to
be felt.
THE SOCIO ECONOMIC PRCSLEM:
A large percentage of major burns occurs in the lower
socio-economic
group.
Illiteracy,
over-crowding,
marital disharmony and poverty all contribute to the
etiology, morbidity and mortality of burns.
BOW CAN CHANGES COME ABOUT?
The existing system needs complete overhauling if we
are to make any major impact. This can only come about
if the Government, Policy makers. Administrators,
Doctors, Industry, previous patients and concerned
Social groups all put their heads together to solve the
issues previously mentioned. One start would be to
bring together all concerned persons in A BURNS
FOUNDATION.
A more detailed report is available with:
DR.RAVI NARAYAN,
Society For Community Health Awareness, Research & Action,
326, 5th Main, 1st Block,
Koramangala, Bangalore.95.
Ph: 553 1518.
<
}
Phone : 5531518
Fax
: (080) q5 333 58
Attn. QHC
COMMUNITY HEALTH CELL
Nc. 367, ‘Srinivasa Nilaya’, Jakkasandra, 1st Main, 1st Block, Koramangala, BANGALORE - 560 034.
Workshop : “Citizens Participation in the management of Public
Hospitals”
Venue : Victoria Hospital, Bangalore (New Kitchen near Reception).
Date : 1st September, 1997
Time : 9 a.m - 4.30 p.m.
Organised by : CAG / PAC / Victoria Hospital / Bowring Hospital / CHC
BACKGROUND / OBJECTIVES
*
A Workshop on the theme “Citizens Participation in the Management of Public Hospitals”
is being organised by Citizens Action Group, Public Affairs Centre, Victoria Hospital,
Bowring Hospital, and Community Health Cell, on 1st September 1997 from 9 a.m. to 4.30
p.m. at Victoria Hospital.
*
The objectives of the Workshop are to explore some practical ways and means by which
citizens groups can support the management and improvement of services / facilities in
Public Hospitals in the city.
*
The Workshop will consider a Citizen Action Group study on Public Hospitals and case
studies on Public hospital experiences and will reflect on some broad principles and
framework to enhance citizen participation in responding to the situation.
*
Two specific areas of need will be focussed upon in depth through group discussion^ as
specific examples in which some focussed action can be initiated after the Workshop.
These are: (a) Waste Management practices in Hospitals' (b) Burns Care - Problems &
Solutions.
■
*
The
The Workshop
Workshop will
will be
be an initiative primarily to enhance the interactive dialogue between
citizens groups, public hospitals and health training and policy research centres in the city.
The workshop is being hosted by the Medical Superintendent of Victoria Hospital (br.
Ballal) and his team. Participants will be primarily staff from both Victoria and Bowring
hospitals but a representative team from all the public and private hospitals in the city vVill
also be invited to participate.
26th August, 1997
Dr. Ravi Narayan,
Coordinator, CHC
Society for Community Health Awareness, Research and Action
Registered under the Karnataka Societies Registration Act 17 of 1960, S. No. 44/91-92
Registered Office: No. 326, Sth Main, 1st Block, Koramangala, Bangalore - 560 034.
Workshop : “Citizens Participation in the Management of Public Hospitals*’
Time
9.00 am - 9.30 am
Resource persons
Tentative Programme
Breakfast
9.30 am - 11.00 am
Session I
9.30 am - 9.50 am
9.50 am - 10.00 am
10.00 am - 10.15 a.m.
10.15 am - 11.00 a.m.
11.00 am - 11.15 am
11.15 am- 11.45 am
11.45 am - 12.30 pm
12.30 pm - 1.00 p.m.
1.00 pm - 1.15 p.m.
1.15 - 2.00 p..m.
Welcome
Introduction by participants
Background and Objectives of Workshop
Public Hospitals and Citizens participation An overview
CAG
Report
on
Public
Hospitals
incorporating case studies
TEA
11.15 a.m. - 1.15 p.m.
Session II
Reflections on CAG Report
Questions / Answers
Experiences / Suggestions
Insight into waste management practices in
Hospitals
Bums Ward Management (Presentations)
LUNCH
2.00 p.m. - 3.00 p.m.
Dr. Ballal (Victoria Hospital)
Ms. Nomita Chandy (CAG)
RN (CHC)
Ms. Anjana Iyer (PAC)
Dr. S. Ganapathi (CAG)
Moderator:
Dr.
Saraswathy
Ganapathy
Dr. Ballal (Victoria Hospital)
Dr.
Chandramma
(Bowring
Hospital)
Participants
M.S. Ramaiah Medical College
team
St.John’s Medical College team
Session III
2.00 p.m - 3.00 p.m
3.00 - 3.45 p.m.
3.45 - 4.00 p.m.
4.00 - 4.30 p.m.
Group discussions:
Themes
I - Hospital Waste Management
ii. Bums Ward Management
(Number of groups discussing themes will
depend on number of participants opting for
the specific theme)
3.00 p.m. - 4.00 p.m.
Session IV
Plenary: Reports of Group Discussions Suggestions
_________________ TEA_________________
Plan of Action and Key Recommendations of
Workshop; Summing up.
Chairperson: Rapporteurs
resource persons.
(separate list)
and
Chairperson: Ms. Pramila Nesargi
Background Papers
1) Summary of CAG Report; 2) Public Hospitals and Citizens’ Participation ;
3) Rogi Kalyan Samiti - A Report ; 4) Health Care Waste management - A Report;
5) Burns Care - The problems - some solutions
Special Guests
1. Minister of Health ; 2. Minister of Medical Education ; 3. Bangalore City Corporation Commissioner;
4. Director of Health Services ; 5. Ms. Pramila Nesargi, Chairman, Visitors' Board, Victoria Hospital ;
6. Sri Rajanna, Chairman, Visitors' Board, Bowring Hospital.
Bangalore Hospitals and the Urban Poor
A Report Card
- Anjana Iyer & Suresh Balakrishnan
(PUBLIC AFFAIRS CENTRE, Bangalore).
A Summary
The quality of hospital services is an important element in the package of services th^t
citizens rely on, during periods of physical disorder and trauma. While medical services
have seen many a technical advance, it has been accompanied by increases in costs and
complexity, there has been a growing concern over the deteriorating quality of health
care provided by public hospitals. These problems become more visible when it comes to
the question of health services to the poor.
How do citizens, especially the poor experience these services? What is their feedback to
the health care system? where are the improvements required? In order to examine these
issues, the Public Affairs Centre, Bangalore, recently designed and carried out a study.
The study assesses difficulties encountered by the poor while making use of hospitals, the
quality of specific components of service, and the different types of action for improving
services, the findings of this study are expected to provide a framework for public
interest groups and administrators of health care design systems for improving access to
health care for the poor and the quality of service that they receive.
The study of hospital services in Bangalore was conducted by the Public Affairs Centre, a
non-profit organisation based in Bangalore, in collaboration with the Citizens’ Action
Group. This study attempted to generate feedback from the urban poor on the quality of
hospital services they receive. Three categories of hospitals were surveyed - Government
or “Public” hospitals, hospitals run by the Bangalore City Corporation (BCC) and
missionary' / charitable trust hospitals.
The study was carried out in three parts;
* Forty one case studies on the experiences of the poor with hospital services
* A field survey using a structured questionnaire on different aspects of feedback from
sections of the urban poor on hospital services, and
* A series of interviews with hospital administrators on their perceptions of problems
that affect the quality of hospital services.
*
Conclusions
♦
The urban poor in Bangalore have been using a variety of options for health care.
While Government hospitals play a major role, other hospitals, including Mission and
Private hospitals contribute to health care for the poor. Any strategy for health care
for the poor has to envisage appropriate inputs for all the institutions involved in this
sector.
♦
In terms of costs, Government hospitals come out as the cheapest source of health
care for the poor. This is not only in terms of percentage of patients enjoying free
treatment, but also of total costs incurred by an overwhelming majority of the
patients. The unfortunate part of this otherwise positive phenomenon is that a major
part of the costs incurred by the poor are towards illegitimate side-payments often
extorted by different participants in the health care system.
♦
♦
But the most significant problems seem to be in the quality of medical care that the
poor receive. To start with, the waiting time they have to go through before receiving
medical attention and treatment seems to be quite high. Second, injections and
medicines, presumably free or subsidised, are often not available at Government
hospitals. But the more important problem seems to be the total absence of standards
or the lack of awareness among patients about what they can expect at hospitals. It is
form this point of view that Mission and Private hospitals seem to be serving the poor
in a much better manner.
♦
♦
The manner in which activities are managed in the Government hospitals also merit
attention. The seriousness of this problem can be seen from a simple area like
cleanliness of hospitals, although there was no major difference in the frequency with
which cleaning was earned out across different types of hospitals, the level of
cleanliness at Government hospitals were rated in much poorer terms. Similarly, the
poor need to run form pillar to post, to find medicines, sometimes in life and death
situations, while being treated in Government hospitals - whereas, dispensaries of
Mission hospitals are rated to be far more efficient in this regard.
♦
♦
One approach to seeking better quality of medical services and facilities that the poor
are compelled to seek, is by resorting to speed money payment. This approach seems
to apply to all levels of medical personnel (from doctors to sweepers), and for all
types of sendees (from operations to entry into wards without authorisation).
Although there is wide variation in the quantum of payments, the problem seems to
be most acute in Corporation Maternity Hospitals, which are used primarily by the
poor. Designing interventions to reduce the instances of extortion could certainly
begin there.
(In collaboration with CITIZENS' ACTION GROUP, Bangalore).
itI S' - b
Efficacy in Administration of Hospitals
A Case Study of Private & Government Hospitals in Bangalore
Flush Anthony
Doctoral Fellow
ISEC, Bangalore
Suggestions^ecommendations
1. Hospital management and organisational structure needs a complete overhaul in the
case of government hospitals. The work load of doctors and other staff is an area of
concern which needs attention. The first step can be filling the vacant posts and
deleting/reshuffling the posts that non-functioning and unspecified.
2. The practise of doctors being appointed as administrators in government hospitals
seems to be a problem as far as the poor management of human as well as other
resources are concerned, since they are not trained in administrative/management
skills. The relatively superior management systems observed in private hospitals can
be attributed to the fact that these are managed by ‘administrators’, trained or
experienced.
3. The efficiency of the hospital lies in the nursing care provided. Better nursing care is
assured through division of labour and continuous monitoring created through
different categories of nursing staff. For example, supervisory level staff at
ward/floor levels, who ensure efficient management in private hospitals. This is one
area government hospitals need to reform their organizational structure.
4. Greater devolution of power to the senior officials is necessary in the case of
government hospitals which ensures effective handling of complaints from patients
thereby ensuring efficient management and customer satisfaction.
5. It is clear from the analysis that government hospitals has high occupancy rate. This
can be translated into efficient income improving mechanisms if there are systems
introduced, which will ensure identification of income levels of patients without
giving way for leakages. This will to some extent arrest corruption in government
hospitals.
6. There is a need to ensure provision of medical social workers in government hospitals
to support and help poor patients. They can provide guidelines and information to
patients in meeting their demands as rights and also can act as a mediator between the
administration and the patients.
I
7. There is a need to develop systems of supervision and vigilance in government
hospitals to ensure that corruption is arrested, which will help a long way in building
the image of government hospitals. This is very important as it can initiate positive
changes in the work culture/environment of the government hospitals.
8. It is also essential to build systematic awareness among the people on the role of
efficient public health care system, which ensures demand for public health sendees
as it is obligatory on the part of the government to provide health services to the
people and the poor cannot be in a position to access private services. The present
day duality in health care access is denying the opportunity of improving government
hospital management as only the poor are accessing it, who tend to be less articulate
about the problems and who will have limited access or information about the
redressal machineries.'
9. A greater role for medical professionals and their associations have to be recognised
in this regard to influence the authorities in revamping the hospitals with better
facilities and more human resources. The medical fraternity has to take a pro-active
role in ensuring that poor people get their due share of efficient health care from the
public system.
10. For the implementation of any of the above suggestions, it is imperative to build
vigilant citizens’ action on this front. Herein emerges the role of NGOs in initiating
and campaigning for such a move. It should be in the direction of creating awareness
among the people about health care as their right, through various mechanisms which
are effective in reaching the lower rungs of the economic ladder, they can also take
initiative in campaigning for incorporating minimum health care as fundamental right
in the constitution as such, perhaps as part of the ‘right to Life (Article 21). This will
provide the people a legal mechanism to seek redressal when this right is denied,
also, bringing the medical profession under the CPA should also be taken up, for it
would confer certain beneficial results such as: medical records will be maintained
more rigorously, the patient’s right to information will be respected, greater
standardization will become necessary, standards of nursing homes will have to
improve and corruptive practices will be checked. To begin with, they can even
sponsor medical social workers to government hospitals. Implementation of health
tax for certain categories of income should also be put forward as outlay for health
expenditure tend to decrease. Any effort for greater privatization of health care
should be prevented on the grounds that poor will dispossessed and discriminated.
'
r\
*
1
This section introduces creative and innovative
experiments that reflect proactive efforts of
administrators, citizens and NGOs in producing
models that needs to be disseminated and shared.
The initiatives covered in this would attempt to
highlight the need for creating mechanisms for
people's participation that hinges around
replicability and adaptability. We welcome
contributions to this section.
Rogi Kalyan Samiti, Indore :
People’s Participation in Managing
Public Hospitals
A /Taharaja Yashwantrao Hospital in Indore,
-LVXMadhya Pradesh is today operationalising a
Samiti is also empowered to receive donations in cash
or kind from the public. These funds can be used for
improving hospital administration, upgradation of
facilities and to provide medical care to the poor and
needy, free of cost or at extremely subsidised rates as
compared to private hospitals.
Today, Rogi Kalyan Samitis have been set up in
all the 45 districts of the State. Though most of the
innovations like systemic improvements and
introduction of user charges are confined to district
hospitals, similar efforts are seeping to the sub-district
level hospitals also. Perhaps, the most heartening
experience has been the highly interactive role played
by people’s representatives, local body officials and
citizens in bringing about this change. This innovative
experiment has brought about many tangible and
indirect benefits. A total of Rs. 8 crores has been
collected by the Samitis in various districts; daily
collections range between Rs. 1,000 and Rs 15,000
in each hospital depending on the location. The
scheme also attracts considerable allocation from the
MP’s and MLA’s discretionary funds. The District Red
Cross Societies which are working in tandqm vith
Rogi Kalyan Samitis have become quite active.
The experience of the Rogi Kalyan Samitis
highlights certain valuable ‘learnings’:
unique and innovative programme which is fast
setting new standards in hospital management. For
people who are familiar to the hospital, the
turnaround is nothing short of a miracle! The
hospital, which at one point of time was considered
to be a premier institution for providing medical
services in the country, had over the years
deteriorated to abysmal levels. Newspaper reports
• For one, it is important not only to create
carried horror stories on the appalling conditions,
institutions for the public welfare but equally so
especially the existence of thousands of rats and
or more to ensure regular maintenance and
rodents!
upkeep, provision for improved facilities, regular
It was the plague scare in 1994 that catalysed
review of performance and also to ensure that - —
the district administration to clean up the hospital
the morale of the work force remains at optimum
imum
by embarking on a Programme called Kayakalp
level of motivation.
Abhiyan - or operation metamorphosis/rejuvenation.
• It is essential to involve citizens to fund and
The District Red Cross Society was identified to
manage various projects taken up to improve
undertake this task. The mammoth 730 beds hospital
civic life; this would force the system to be,more
along with five other supporting hospitals were
accountable to the general public.
evacuated and all the patients shifted to 12 hospitals
• The idea to introduce some amount of user
situated in different parts of the town. The entire
charges in public institutions generates a demand
complex was cleaned and disinfected; some 150
from the beneficiaries to be given better services
truck loads of garbage and junk was removed from
the hospital.
and professional attention. This also prevents any
misuse of the highly subsidised government
The whole exercise was participatory in nature
facilities by people who have easy access to them.
and involved the people of the town in drawing up
the policy framework for every stage of the
Source : Rogi Kalyan Samiti: People's Participation
operation. Further to this, it was decided to put in
in the Management of Public Health Institutions by
place a committee to act as a group of Trustees for
S.R. Mohanty, Rajiv Gandhi Missions Occasional
the hospital, called the Rogi Kalyan Samiti or the
Papers - Document 002/96
Patient Welfare Committee and another executive'
committee to manage the day to day functions of
the hospital. The Rogi Kalyan Samiti, registered as
an NGO, was given complete control over the
functioning of the hospital. The Executive
Committee meets every week and deliberates on
changes and improvements that could be affected on
a continuous basis.
To improve the financial position of the
hospital, it was decided to introduce user charges
subject to certain criteria; funds received are
deposited with the Rogi Kalyan Samiti. Apart from
funds received from imposition of user charges, the
♦ Public Eye ♦ Vol. 2 No.l Jan-Mar. 1997
.
.
J
■-
WORLD HEALTH ORGANIZATION
CH - 1211 GENEVA 27 - SWITZERLAND
.
•
■
TcL: (41 22) 791 21 11 Telex: 415416
FACSIMILE: (41 22) 791 07 46
Direct Facsimile:
n ^-3
FACSIMILE Message No.
Page. lif of .
pages
To: Dr R. Narayan, CHC, Society for Community Health and
Awareness, Research & Action, No. 326, 5th Main, 1st Block,
Koramangala, Bangalore 560 034, India
From: Director, ARA
Your ref'
Our ref: P9/181/113
...... .3.2.Q45
Subject;
Fax No.; 80 5533358
Date; 20 August 19^7
MEETING ON POLICY-ORIENTED MONITORING OF
EQUITY IN HEALTH AND HEALTH CARE - Geneva, 29
September - 3 October 1997
I am delighted that you will be able to participate in the above meeting and am pleased to advise you that
WHO will cover your costs.
In view of your extensive experience in India in the use of existing data sources and your concern for
objective analysis of the health inequities at community level, I am pleased to invite you to serve as Moderator
of Panel #2. The subject for this panel is “Using existing data sources to assess equity in health and health care
at the national, provincial, and district levels in developing countries. Please see the attached draft Programme
for details of the issues to be covered by panellists. In order to prepare for this task I would be grateful if you
would familiarize yourself with these issues. Your own comments and observations during the session will be
a welcome addition to the proceedings.
For the duration of the meeting you will serve as a WHO Temporary Adviser and I am attaching a note
containing information about financial and travel arrangements as well as on insurance, visas and vaccinations.
Please read this note carefully. A travel authorization has been prepared for you and you will shortly receive
instructions from The World Health Organization, Indraprastha Estate, Mahatma Gandhi Road, New Delhi
110002, telephone: 11 331 78 04 or fax 11 331 86 07. In the meantime, you may make your reservations through
WHO.
Hotel accommodation has been reserved for you at the Hotel Moderne, rue de Berne, Telephone 732 81
00 or Fax 738 26 58. Should you be arriving after 18.00 hours on 28 September please advise the hotel direct.
We are very much looking forward to your participation in this meeting and should you require any further
information you can either contact me or Ms Marianne Jensen who is the focal point for Equity in this Division
and is also coordinating the meeting.
E. Tar&S).
3i°1s
cc: SEAROFax 91 11 331 8607
TOO®
VAaX39/0HAi
moieizm xvj io:ot nsr zk
80 -T"
t
PUBLIC HOSPITALS AND CITIZENS PARTICIPATION
Some Reflections
I. Citizens participation in the Management of Public Hospitals
0 Public Hospital Management and staff - Victoria / Bowring
0 Government Health Policy makers - DHS/KHSDP/IMA
0 Technical Resource Groups - CHC, MSRMC, SJMC, etc.
0 Citizens Groups
0 Others
II. Citizens Participation : The potential
0
0
0
0
0
Feedback to improve services
Watchdog Role - Surveys/reviews
Financial support to improve services
Complimentary/supplementary/facilitatory services
Representative participation in Management
IILCitizens participation : some Models.
0
0
0
0
0
Hospital Volunteers / Auxiliaries
Visitors / Boards / committees
Rogi Kalyan Samitis
Citizens/NGOs providing complementary services on contract
Others???
IV.Case Studies
1. Hospital Auxiliary
0
0
0
Visiting patients
providing food and medicine and reading material
facilitating use/access of facilities at OPD
2. Rogi Kalyan Samitis (M.P.)
A. Cleanliness
B. User charges
C. Collect Donations - used for
• improving Hospital administration;
• upgradation of facilities
• provide medical care to poor (free or extremely subsidised)
V. Citizens Participation : Some issues
•
Need for change in Management / professional attitudes
(Patient as Beneficiary - - to Patient as participant)
•
•
Opportunities for feedback / interactive dialogue to be created
Focus on what is wrong? and not who is to blame?
(fault finding - - to problem solving)
•
Focus on the poor and marginalised
(the most dispossessed / discriminated)
VI.The Future of‘Participation’
1. Can we manage cleanliness and Hospital waste management?
2. Can we improve specific services
=> Burns Ward
=> Mortuary
=> Canteen
=> Others
3. Can we provide ‘social workers/volunteers’ to facilitate access and use of
OPD services?
4. Can we be watchdog to check unhealthy and corrupt practices?
VILWorkshop Framework:
1. Watchdog Role : CAG / PAC Studies
2. Complementary Strategies
3. Improving Waste Management Hospital {Public Health}
4. Improving Burns Care {Clinical}
5. Interactive Dialogue
6. Any other Action?
Dr. Ravi Narayan, Community Health Cell, Bangalore.
For further details or follow-up please contact:
Community Health Cell,
No.367, ‘Srinivasa Nilaya’, Jakkasandra I Main, I Block, Koramangala,
Bangalore - 560 034.
Phone : 553 15 18
Fax : 080 - 553 33 58.
I
Aug / Sep '97
(A NEWS LETTER OF Banjara GROUP OF COMPANIES)
F°r Private Circulation Only
CHILDREN OF UNHAPPY PARENTS
Sangeeta complains bitterly to her dearest friend about her
matrimonial problems. The crying sessions
inevitably end with “If it were not
for my daughter, I would have
) left him long ago.”
nside
//
<
. I Sangeeta is not alone in her
I lament. Innumerable couples
//
Crash
I from various backgrounds are
I facing a similar situation. Highly
I
Qowinjws
I incompatible, their lives have
I
'ifnokws
'ifll become long bouts ofviolent fights
. I or miserable sulking. They have no
'111,1 only to blame? I doubts that their marriage is over,
I and that reconciliation is not possible.
of oil time I Yet they continue to live under one
/ roof - only for the sake of the children.
Lifl1
v
Many a time parents are blissfully unaware that their late night
fights have woken up their child in the next room, and she is
cowering in fear in the dark, listening intently to the venom in
their tones even though she is not
comprehending the words.
Since parents arc the absolute symbols
of security and safety to the child, their
bickerings leave the child totally
confused about its identity.
Traditional Indian values have always frowned upon divorce.
Even living away from the spouse is not generally accepted by
society. Even women who find their marriages intolerable, and
have living parents willing to look after them and the
grandchildren, do not move away from their husbands, only
because they are scared of gossiping tongues, and the stranglehold
of society’s traditions.
Such children are very prone to develop
feelings of insecurity, and may grow up
as adults who are not sure of
themselves, having chronic relationship
problems. They some times lose ||||
the capacity to form and maintain ||||
lasting relationships.
||||
Often one hears the threat “Who will marry
your daughter if you separate from your spouse?” Many stories
are told in hushed tones about children of single parents
developing behavior problems, turning into drug addicts, and
finally starting to hate the very parent who brought them up.
Psychiatrists have found that I®
problems such as bedwetting, truancy, lying, stealing, and even
deterioration in academic performance can be correlated to the
disturbances caused in their innocent minds due to tension in
the house.
Our culture does not allow us free expression of love. Very few
parents hug, cuddle or kiss each other in front of their children.
Their best and most loving moods are spent behind closed doors.
But their bickering, their differences and their fights filter out
and wrench the children’s little hearts.
With the changing social system, and with pressures mounting
on marital life, it is time to do an indepth introspection of what
is good for die children and what is not.
>
James Baldwin said “Children have never been good at listening
to their elders, but they have never failed to imitate them”. Their
observation capacity is very acute, and most children observe
body language, a communication which does not tell lies. Parents
who stop shouting at each other when their child walks into the
room, cannot hide from her the resentment or anger their bodies
are expressing towards each other.
Psychologists have been doing studies and pointing out that
children with a single but contented parent grow up more happily
than those with two quarrelling parents. Many parents are under
the misconception that if they do not shout and fight in front of
their children, diey are shielding the little ones from the tensions.
Even this myth has been proven wrong.
N--------------------------- /J-
It is even worse when one parent tries to complain about the
other to a little child. This confuses the child even more, whose
innocent mind refuses to acknowledge that loving daddy or
in any contest between power ana patience, bet on
alienee
I
I
the twenty first century. They can contribute
to their child’s overall development and
compensate for the lacunas in our memorizingoriented educational system.
mummy can actually be a villain. Value
systems are shattered, and the child starts
confusing all rights and wrongs.
Very few children can take sides — to them
both parents are valuable. When they express
so much anger and hatred towards each other,
the child starts doubting whether it is capable
of getting any love from either of them.
I
On the other hand, a single parent who is at
peace with himself or herself, may at least
partially fill the vacuum due to the absence of 4
the other parent, and give a much better
upbringing and enjoyable childhood, enabling the child to
redevelop its sense of security.
Women are more educated, assertive and independent in the
current generation. They will not be satisfied accepting the
subservience to their “lord and master” as their mothers and
grandmothers did. They have ambitions and aspirations. They
are also most likely to be living in nuclear families with no other
surrogate mother for their children.
Similarly, fathers have become more aware of the growing
competition and challenges their children will have to face in
All goes well if there is an understanding
between the father and mother. Even if they
are no longer deeply in love with each other,
2 they can maintain a peaceful household if they
J agree to disagree. However, if they are not
being able to control their tempers, or if they
are prone to unending bouts of sulking and
' coldness, they should understand the impact
their behavior is having on their growing children. There is nb
use in their sacrificing their personal desires “for the sake of the
children.” Maybe they are doing more harm than good in these
circumstances.
There arc many family counsellors available, at least in the larger
cities. Child psychologists can guide parents on the needs of
their children. It is far more pragmatic to understand with the
help of specialists or well meaning friends, as to what is best for
the child. This can lead to rational decisions, which can lessen
the hurt and pain that incompatibility or separation brings.
CAN NEITHER LIVE WITH HER NOR WITHOUT HER!
In the beginning Brahma created man, but then he came to the
fashioning of woman, he found he had no more solid materials
left. So Brahma took:
The clustering of rows of beeds, joyous gaiety of sunbeam,
weeping of clouds, fickleness of winds, the timidity of the hare,
the vanity of the peacock, hardness of adamant, the sweetness
of honey the cruelty of the tiger, the warm glow of fire, the coldness
of snow, the chattering of jays, the cooing of the kokila, the
hyporcisy of the crane, compounding all these together, Brahma
made woman and gave her to man.
Eight days later the man return to Brahma "My Lord, the creature
you gave me poisons my existence. She chatters without rest,
she takes all my time, she laments for nothing at all and is always
alway:
ill, take her back" and Brahma took the woman back.
'dz>D'f2& ^ric-LAri&fZY WlTM A^z
AP6N'T You, HgU<&A ?
WUAT&J&R.
&A\/& YOU
$
cMfib
But eight days later the man came again to God and said "My
Lord, my life is very solitary since I return this creature. I remember
she danced before me, singing, I recall how she glanced at me
from the corner of her eye, how she played with me, clung to
me. Give her back to me" and Brahma returned the woman to
him again. Three days only passed and Brahma saw the man
coming to him again "My lord" said he "I do not understand
exactly how it is, out I am sure that the woman causes me more
annoyance than pleasure. I beg you to relieve me of her".
But Brahma cried "Go away and do the best you can" and the
man
cried
"I
cannot
live
with
her"!
"Neither can you live without her!" replied Brahma.
And the man went away sorrowful murmuring "Woe is me, I
can neither live with her nor wiithout her:!
You
FO(2
MV &=>UP
<
r
If you risk
NOTHING,
THEN YOU
I
RISK
y I
r
EVERYTHING
i
- Geenei Dams
£
O
V
J
t
WHEN REAL ESTATE PRICES CRASH 'i
z
installments, say up to 50 months?
The investors who were putting in their mor^ey with
great expectations of multiplying it manifold, now start
shying away from the market. The greedy sellers who
did not let go even when they received offers far above
their expectations, are left wondering what to do.
Then comes a phase when no one is interested in
investing in real estate. Investors look for greener
pastures elsewhere, those who had given token advance
for properties are not willing to give the balance
amounts, and even genuine buyers are apprehensive
"Buy One Flat and
whether
they should buy or wait till prices crash further.
take one Toilet Free."
Large builders and idle landlords decide to just hold
never stop.
on, construction activity slows down, and everyone
Power cuts have become the order of the day, and starts talking about vague things like “tight money
we are all used to them. Periodically our lights, fans,
market”, whatever that is supposed to mean.
and all other gadgets come to a halt. So is it with real
This
situation
estate. Just when the merry
persists until someone
>x
go round seems to be
PLEASE HEAR WHAT I’M NOT SAYING
notices that prices have
moving merrily along,
started creeping upwards
I
wear
a
mask,
a
thousand
masks,
everything grinds to a halt.
masks that I'm afraid to take off,
again. Vague people ring
and none of them is me.
The person who had
up landlords to enquire
expected to get 1,000
I give you the impression that I'm secure,
whether they are still
that confidence is my name and coolness is my game,
rupees rate for his property,
interested in selling their
that the water's calm and I'm in command,
and had subsequently
and that I need no one.
property. New schemes
become greedy when he
are announced and
But don't believe me.
received offers of 1,200 and
My surface may seem smooth by my surface
people are surprised to
is my mask, ever-varying and ever-concealing.
1,400, was quoting 2,000 of
note
that a significant
Beneath lies no complacence.
late. He was thinking it is
number of units pre
Beneath lies confusion and fear and aloneness.
just a matter of time before
But I hide this. I don't want anybody to know it.
actually sold.
he gets it. Suddenly he
I panic at the thought of my weakness and fear being
Those who were
realizes that his phone has
exposed.
keeping
their money ijdle
That's why I frantically create a mask to hide behind,
stopped ringing. The agents
to shield me from the glance that knows.
get
the
uncanny
feeljng
and buyers are no longer
But such a glance is precisely my salvation.
that
they
are
missing
put
My only hope, and I know it.
clamouring for his property.
on something. A sens^ of
Reluctantly he agrees
That is, if it's followed by acceptance,
insecurity creeps in, that
If it's followed by love.
to bring his price down to
prices may go out of their
It's the only thing that can liberate me from myself,
1,800. Still no takers. He
from my own self-built prison walls,
reach. Phones start
from the barriers I so painstakingly erect.
tries 1,600, and then in
ringing more often. New
exasperation he calls up the
It's the only thing that will assure me
offices of real estate
of what I can't assure myself,
person who had made a
agents crop up at every
that I'm really worth something.
firm offer of 1,400. The
I want you to hold out your hand
street corner; and every
latter is now too busy to
even when that's the last thing I seem to want.
other xerox shop, t^a
come on the line. The
stall, and autorickshaw
Each time you're kind and gentle and encouraging ,
gentleman who had made
each time you try to understand because you really care,
driver starts offering
Iwant you to know that.
an offer of 1,200 and was
properties.
pleading desperately, is now
Who am I, you may wonder.
This
cycle
I am someone you know very well.
claiming that he does not
For I am every man you meet,
continues with distinct
have the money, and would
and I am every woman you meet.
regularity in every major
the seller agree to
Arthur Ashe
~“i
Every large city
has seen it happening —
repeatedly. Real estate
prices spiral upwards,
there is a euphoria of
investments multiplying
dizzily and more and
more people pouring
money into high profile
real estate ventures.
With speculation rife all
round, people think that
the merry go round will
—<7
city of the country. The only
variation is the number of
years of the boom and ebb,
which may increase or
decrease. Yet every time it
happens there are armchair
experts who lament — “Our
„
city is becoming prohibitively
expensive, prices are going up every week, no one can
afford to buy a house any more” and on the other side
of the cycle “There is a saturation, nobody is interested
in buying, too many projects have come up.”
The fact is that it is the wise person who buys
LIFE
An Experience of a lifetime...... College.
Passing out from a elite school, college meant an
atmosphere vibrant with fun and frolic, a mixture of gals
and guys, a paradise of glitz and glamour and the group
of the guns and roses. But my opinion it seemed, was a
far cry from reality. The prevalent situation compelled me
to join an Evening College, a decision I considered the
best as far as graduation was concerned. The crowd
predominantly comprised of students from economically
and financially unsound family backgrounds. The students
were an epitome of determination, grit and hard work,
most of whom were employed in physically fatiguing
occupations and trades, displayed sneer enthusiasm and
resolve towards education, by making themselves present
for the evening classes. Despite the tiredness and fatigue
of the day gone by, education to them was more than just
studying, if was an experience, the rich experience of
college life. Cutting across barriers of caste, creed, colour,
status and position we assembled as one to attain a
common objective - a graduation. It sometimes, was a
sorry sight to see students nod, and fall asleep in the class
- a result of the sternuous job. Nevertheless, every hurdle
was braved and every bridge crossed, to attain ones goal.
The friendliness that existed despite the differences
especially in terms of status or position was a clear
indication to the world that a little brotherhood and love
could do wonders.
In conclusion, apart from the gaining considerably with
regard to education and passing out as graduates, I have
to say I have gained more as a person. It has made me a
person responsible towards my commitments, caring-for
the needs of the deprived, independent-in nature,
diplomatic-in dealing and more importantly a person who
gives patriotism more prominence to religion. As the adage
"More of We, and Less of Me" was never meant truer.
Mark Noronha
St. Joseph's Evening College
|| when there is a lull in
jl sales and in price rise.
P The buyer has a wide
Ilir * choice, he is not under
tl ■
pressure of prices going
up every day, and the
sellers need his money.
.-/- w
_____________________ Even though it may
appear that there is no appreciation of his investment
in the near future, he stands to benefit greatly in an
extended period of time if he is patient. As someone
wisecracked “By real estate and you cannot be a loser,
after all God stopped manufacturing it long ago.”
/tig
SOME RANDOM THOUGHTS AND
MANY UNANSWERED QUESTIONS
Does humanity mean just being a'jood to others? One look at the
face of the man whose little chna'was stricken with blood cancer
was as though a lifetime was not enough to understand1 our roles
Religion,
beliefs,
values
— all structures getting
as a human.
I
" '
'
'
demolished by a stout question "Why me?" How does one explain
iit: Karma,, destiny,
' ”
~
God
in heaven? Is it not deeper conditioning
of a mind that is thoroughly conditioned
conditioned .... live for you must, be
good for you should, believe or else you'll stray.
How about peeling off layers of conditioning by questioning — to
begin with? Question your own existence did I choose to be born?
Is this life mine? Why should it be a gift of God I've been told
exists; I've never felt or seen. Do I then believe rhetoric or should
I explore with what I have — my senses?
Why should Gandhi's monkeys shut themselves from experience?
Why so much talk on walking the treaded path? Why is man's
impermanence always be seen in spiritual religious context? Why
can't the body that we day in and day out live with, be part of a
fulfilling experience? Why so much relevance to sex? Why can't
genitals be treated as the hand that touches, eyes that see, ears
that hear? Why can't love be easy instead of oeing frivolous or
an awesome feeling?
,
Signs from the soul
come silently, as silently as the sun
enters the darkned world.
- Tibetan proverb
(
GREATEST OF ALL TIME
In a converted barn at the lower end of a circular driveway in
Michigan, USA, is the headquarters of GOAT, an acronym of
"Greatest Of All Time, Inc". If the proverb rings a bell, yes, it is
the office of Muhammed Ali, the world boxing champion of
the sixties who was more famous for declaring himself the
greatest.
In his heyday the world had ridiculed him for his boasting.
Today Olympic participants are encouraged to keep on
repeating to themselves that they are the greatest, the fastest,
the best — and it works!
Ali is now 55, his mouth and body slowed by Parkinson's
disease, yet arguably the best known and one of the most
beloved figures in the world. He shot back into limelight last
summer in Atlanta when he stood alone in the spotlight, the
world watching, his hands trembling, as he lit the Olympic
flame.
.ociay he travels all over the globe doing good deeds. He visits
schools, campaigns against child abuse, and for peace and
tolerance. He is teaching and preaching a new poetry, slower,
without rhymes, with a stream of consciousness, and a deeper
meaning.
Ali receives letters from all over the world. Disabled people.
Old sixties activists. Republican. Black. White. Christian. Jewish.
Muslim. A little boy from Germany, a boxing fan from England,
a radiologist from Sudan, a secretary from Saudi Arabia — the
multitudes thank him for giving them hope.
He has shown to the world that when illness strikes
you down from being the greatest boxer to one
who cannot even walk properly, one can still be the greatest.
He may well be saying to the world "I have the greatest heart."
GOOD NEWS TO ALL SMOKERS
HELPING HAND
on its 14th Anniversary
wishes all smokers of all ages to join our
BIGGEST
ANNIVERSARY SWEEPSTAKES
DRAW
Where every smoker is a sure winner, all
smokers have a chance to win our major
prizes
1st Prize:
A brand new CANCER,
Gingivitis Goiter & Asthma
2nd Prize:
Hepatitis, Hypertension & Cerebral
Tumour
3rd Prize:
Rheumatic Heart Disease
Smokers also have a chance to win our
consolation prizes such as
Tartar Deposit, Bad Breath,
ATTITUDE
Stained Teeth, Loss of Appetitte
There was a man, as pitiable as one could be, who had
spent his whole life in drunken brawls, petty crimes and generally
being the grime of the earth.
This man begat two sons — strong young men full of life.
One took to a life of crime, became an antisocial and merrily
Allowed in his father’s footsteps. The other studiously avoided
nis father, burnt the midnight oil, and became a learned and
respected person.
When these two youngsters were accosted by a curious
acquaintance and asked why they chose such a life, surprisingly
they had the same answer to give... "With a father like that,
what else did you expect me to be?”
& Swollen Gums
REMEMBER,
the more sticks you puff the g
more chances of winning, our fab^
prizes are waiting,
SEE YOUR
RESULTSEC R
E
^DETA
WINNER ■!!
• The famous shoe company wanted to have outlets in every
town of the country. They sent two marketing executives, one to
Lakshadweep and one to the Andamans, since these were the
two territories of India where they had not reached out yet.
The man sent to Andamans returned within a week. He gave
a terse report “No one in the Andamans wears shoes, their
lifestyle is totally different. Let us not waste our time there.” The
man sent to Lakshadweep sent a frantic telegram asking for
stocks to be dispatched immediately. “No one in Lakshadweep
wears shoes,” he wrote “every person is a potential customer.
What an opportunity!”
CLAIM YOUR PRIZES
AT YOUR NEAREST FUNERAL HOMES!
HURRY !!!
Deposit your Grand Prizes
at the nearest CEMETERY.
composed by S. RAM
FEEDBACK ----------------------------------------------Season’s greetings to you and your band of dedicated people in
your team. Thank you so much for sharing with us your Banjara
News. I shall be grateful if you could please include us in your mailing
list, so that we have something to read that is so very thought
provoking.
Mrs. Sunanda Naganand, Principal
Sishu Griha High School, HAL III Stg
Banjara News happened to land on my table, and I just enjoyed
reading its contents. It is thoughtfully and interestingly arranged.
Congrats. Please put my name on your circulation list.
Narayan Prasad, Manager (HRD)
Haheja Group, Bangalore
am dashing off these few lines in grateful acknowledgement of your
April/May issue of Banjara News. The articles are highly informative
and in particular I like the one on “Laughter” the best. Please let me
know if there is scope to start a similar newsletter at Hyderabad.
Pratap Singh, IPS (retd)
Gen Secy, Forum for Street Children
Greetings to you from Africa. How are you and your project of helping
people. I would like to tell you that I really appreciate the help that
you have given me during those days. It is very very useful to me in
my priestly ministry. Thank you.
I would be happy if you could from time to time keep me upto date
with your publication.
Fr Luke Mulayinbal, SDB
Dar-es-Salaam, Tanzania
appreciate the human touch in your behavior.
S. Srinivas, B Com
Srinagar, Bangalore
Thank you very much for Banjara News. It has a fine article on
“Laughter”. Congrats.
The world is in need of peace. Our country is moving through a narrow
gate. It needs enlightenment, spiritual values, moral discipline and
sincere seekers of Truth. Let us take up the brooms or brushes to
clear the country. “Go beyond”.
Swami P Vincent,
Spirituality Centre, Kanyakumari
It is a pleasure reading your in-house magazine, which is informative,
educative and humorous. The same is displayed in our Association
Reading room for benefit of the general public.
S H Zaheer, Zaheer Welfare Association
I appreciate the quality of your magazine. It is very helpful ar^d
informative. I would like to receive it regularly.
Nawaz Ahmed, Bharathi Ns§i
We are highly indebted to you for having conducted a workshop for
our teachers on “Counselling”. According to our teachers it was very
enlightening, informative and interesting. It would help the teachers
to go beyond classroom teaching into the intricacies of the human
mind and in particular the child. It provided various skills and ideas
to understand, help, listen, analyse and empathize with people around
us. We wish to keep close contact with your organisation.
Mrs A Manimala, Principal, ASC School
Thank you for sending Banjara News regularly. “Laughter” was
interesting. Recently a club has been formed in Bombay where a
group of senior executives indulge in about 20 minutes of hearty
laughter before lunch —it acts as an appetizer. Anyway, keep up the
variety in your newsletter.
Jagmohan Singh, Mumbai
On behalf of the Rotaract Club of Bangalore Cantonment South I
would like to thank you for the excellent workshop on Inter-Personal
relationships that you conducted for our members.
Thanks a lot for sending me the newsletter. It is very educative reading
it. Besides giving an insight into social life and society, it also focuses
on ways and means of leading a more meaningful life, in this so very
commercialized society of ours, especially in the wake of
liberalization.
Mark Noronha, Bangalore 38
Rajesh Bhatia, President, RCBCS
I was very happy to have attended your course, especially because
I could interact with people like you. Your sessions were enriching,
enlightening and practical as well.
Thank you for including my name on your mailing list. I find the articles
and certain quotes in “Banjara News” very interesting. I very much
J Britto, Baruipur, W Bengal
HUMAN DEVELOPMENT INDEX
A new concept has been developed to measure the
development of a society or country. The earlier concept of GNP
(Gross National Product) relied only on economic growth. The
new parameter relies on overall development of the society and
is called the Human Development Index (HDI).
HDI is a composite of three variables — longevity,
knowledge and standard of living. Longevity, measured in terms
of life expectancy is a proxy for good health. Knowledge
represents education and technical know-how. Standard of living
indicates level of consumption.
The HDI provides an alternative to GNP for measuring the
relative socio-economic progress of a nation. Analysis of the three
components of HDI helps in identifying areas which demand
policy attention. The HDI also reveals existing disparities within
the country even more strikingly. Though it is a recent tool, HDI
has already had a major impact on the policy making on
economic development.
We found the workshop very helpful and hope that you will follow it
up with a more detailed workshop in the near future.
I am greatly appreciative of your service to people in need. I am very
interested in your newsletter, please add my name to your list.
FRIENDSHIP
Friendships are not mere juvenile fancies but a
continous pursuit enveloping all human
relationships in all spheres of Society. Friendhsips
precipatating into love produce the usual debris
of sonnets, carbon monoxide sighs, oxygen short
nights, letters longer than your telephone bill,
jealous fits of ammonia and supercharged
dreams that can put Shakespeare to shame.
Friendship moves the stars that you cannot see. It
moves the birds which you do not have, to song.
Fascinating as to how the brief mechanical event
can generate such giant expenditures of neural
energy. Our spaceships, our skyscrapers, our
stock markets are but deflection of this basic
drive.
-
IS HE ONLY TO BLflME?--------------Almost every marriage vow is made with true sincerity.
Every young man has stars in his eyes when he ties the knot
binding him “for life” to his charming and blushing bride.
i
Yet every marriage runs into stormy weather sometime
or the other As soon as the honeymoon phase is over, the
couple gets down to the business of running the household.
Arguments take place, there are fights and shouts, sulking
and crying. There are also tender moments of making up,
torrid hours of passionate love making. There are shareddays
of joy, and lonely days of disharmony.
But marriages go on nevertheless. At least most Indian
marriages do. Somewhere along the line, children come
around, and a happy threesome or foursome evolves. There
are joyous family outings, and tense days of illness. Father’s
nromotion becomes an event of celebration for all at home,
nd the death of a puppy throws a pall of gloom over the
entire household.
One would presume that in this scenario, everyone would
be contented and they would live happily ever after. But
sometimes that does not happen. On a catastrophic day, when
she felt that her entire world collapsed, the wife learns that
her husband has been having an affair!
The home is no longer the same. Every celebration
becomes hollow, every family occasion a tense day to be
tolerated and got over with as soon as possible. The wife is
shattered. She cannot believe that it is happening to her. She
has always been faithful to her husband, never so much as
looked at another man—and this is the reward for her loyalty
and drudgery.
The wife’s parents are taken into confidence. Their wrath
against their son-in-law is uncontrollable. Other relatives
caution against hasty confrontation. Well meaning friends
talk about the “future of the children.” The wife sobs on the
shoulder of anyone who is willing to listen to her.
Many cannot believe that this particular husband is doing
such a filthy act. He seemed to be such a gentleman, they
eminiscence. Always a sober and quiet man, he rarely even
looked at other women. And he has such a charming and
beautiful wife who is still young and vivacious. Such sweet
children, a cozy home, and everything else that he could have
asked for. And yet he goes and does such a dastardly act. The
condemnation is universal, and all sympathy goes to the wife.
If one were to take the trouble of looking a little deeper
into the problem, a different picture would emerge. The
problem started not when the other woman came into the
life of the husband — it started much earlier. Years ago, the
marriage was already losing its lustre. The magic of the
relationship was gone. The wife had taken the husband for
granted, and the husband was sure that there is something
missing in his life.
Young and vivacious, yes. But the wife would present her
worst side to the husband. She would be lounging around in
a baggy housecoat or decrepit sari when he came nome from
a tiring day. She would
present a contrasting picture
to the prim and attractive 1
women he would accost
outside.
She would be caring and
look to his daily needs, yes.
But that even a housekeeper
could do. When he woke up
in the morning, she would
either be already in the
kitchen, or getting impatient
to be there. At night, she
would still have a number of
chores left when he was
feeling romantic and wanting to get into bed.
When on outings, she would shrug uncomfortably i ?he
even puts his arm around her shoulder. In company she would
never come and sit next to him. They had nothing in cornu ion
to talk about. On the other hand, she would never fai to
express her disapproval when he so much as talked pleasantly
to another woman.
Despite all this the marriage was just rolling on. The
husband was too straightforward to think of other women.
He did not have affairs before his marriage (at least not too
many or too involved), and he was not inclined to having
them now. He generally kept away from the flashy and pu »hy
women, and tried to occupy himself with his work.
But the emotional vacuum was nevertheless there. While
his wife fulfilled her needs by getting more and more invoked
with children and family, he had no one to exchange his love
with. His men friends were no solace. Work only made him
more lonely. And he hated getting into any form of addiction.
That was the point at which a very homely but caring
woman met him. She also was not looking for an affair and
certainly not with a married man. She found so many gc od
qualities in him, that she gravitated more and more towards
him. There was a pain and loneliness that touched her healrt.
She genuinely wanted to befriend him, and enjoy the pleasure
of his intellectual company.
The chemistry of man-woman relationship being what
it is, on a quiet secluded evening they found themselves
pouring their hearts out, and before the evening ended, th ey
were in each others’ arms. It was too late to retract, and tf ey
both realised that they do not want to keep away from each
other. They found a pleasure which had been denied to th( m
since many years, a warmth and comfort that both wc re
longing for very deeply.
The progress from the first embrace to sex was smooth,
without any words, and with equal enthusiasm. They were
lovers. And very happy being so. The husband found a new
meaning to his life. He did not love his wife any less, his
commitment to his children was still complete. But his lo^e
4^-
'J
/
affair was the lifeline which gave him motivation.
J
Innumerable loving husbands and fathers
L find diemselves in this predicament. Their affairs
*' I-J ' V cannot be hidden forever. Sometime or the other,
r the cat is out of the bag. The reaction of wives
^>1/
:varies from wailing and chest beating to anger
\ and walkouts. They curse the “other woman” as
r’ evil, degraded and cunning. They try to fool
" themselves that if the other woman nad not come
into their husbands’ lives, the marriage would
have gone on wonderfully.
In all such situations, it is impractical to blame the
husband alone. In fact there is no point in trying to pinpoint
Nothing lasts for ever; not even your troubles
- Arnold Glasgow
depressed,
7ere is someone wh„
HELPING hand
forfree, confidential
c°unsilling
y >>
on‘individual basis
<
Ono« working days
be,ween4.7pm
(about us)
WHAT’S NEW AT Banjara
Banjara RESIDENCY:
Another phase of the residential layout Banjara RESIDENCY is being
offered off flennur Road, a pleasant twenty minute drive from Cantonment.
Plots of different sizes have been laid out to form a well planned little colony
in calm and green surroundings, very close to HBR layout of BDA.
This project was launched after the spectacular success of Banjara Orchards
which extended itself into twelve phases, and has now become a landmark in
that area. Banjara Residency is much closer to the main road and is in an
area likely to develop very fast into a posh suburb of the city.
I The titles of the area are perfect, and immediate registrations are being carried
1I out, transferring complete title to the purchasers. It is a matter of pride to
I Banjara that the buyers include defence personnel, professionals, senior
executives and highly respectable people from different walks of life.
Comefo
and unbiased
blame at all. What is needed is to build emotional bridges,
show that extra care which every human needs, and responds
to.
Love is a very pure and basic human emotion. It
transcends barriers of social restrictions and norms. If true
love exists between a husband and wife, there would definitely
be more understanding. There would be more concern of
each other? desires and wants. And regardless of how many
“odier women” accost the husband, he will always come back
to his wife. And a truly loving wife will welcome him back to
begin another honeymoon that will increase their love for
each other many fold.
We require
^/7
more volunteers for our4^
extension services at
/
various hospitals,
children's homes etc.
If you are willing to spare
y^three hours once a week, we
/
provide free training.
’xs==j Just give us a ring
You do not need an an ■
an appointment
to:
QueensRoad
F
° Bon *iay Can,onment Stat
^galore 560052
5,at'on)
PIK"«^U2S
r
COMFORT Banjara
In continuation of our desire to provide affordable housing in good localities,
we are shortly launching our forty fourth project in Sultanpalya, an extension
of the posh R T Nagar. One, two and three bedroom apartments designed to
suit every budget, have been planned in an airy and well ventilated building
a stone’s throw from shopping, bus stops and schools. Clearances have t
obtained, and a few flats are being offered at pre-construction prices to the
lucky ones who wish to control inflation by ensuring that their home is reserved
for them.
THE ACADEMY
Banjara Academy continues to be a beehive of activity, with counselling,
interpersonal relationships, managerial skills, and family betterment
workshops being organized for the general public as well as for in-house
participants. Conducted by a team of highly qualified and dedicated resource
persons, the Academy’s programmes are very interactive and applicable to
day to day ife.
The Academy is also conducting lectures every alternate Thursday at 5:30
pm, covering various aspects of improving quality of life. These lectures are
open to all.
Banjara Academy has recently held workshops and lectures for Christ
College, Rotary Clubs, CPR1, St. Ann’s College, ITI Limited, Inter Religious
Harmony Movement, Chinmaya Mission School at Hubli, Kirloskar Electric
Company at Bangalore and Hubli, and MYRADA at Gokak.
“Edited, (Printed andTuMisfied (forprivate circulation only) 6y (Dr. Ali “Khwaja, (Banjara group, (Darus Salam, Queens (Kgad,
(Bangalore - 5G0 0S2. (Phone : 2260674,2265628
r
HOW DOES ONE BRING UP A HEALTHY BUOYANT
CHILD SINGLEHANDEDLY?
CAN ONE MANAGE A CAREER AND CHILD, AND
DO GOOD JUSTICE TO BOTH?
LET US EXPLORE THE ANSWERS IN AN
INTERACTIVE WORKSHOP ON
SINGLE PARENTING |
Responsibilities of a single parent increase by more than double
since he or she has to take on the additional burden of an alien
role, which one is neither trained for nor tuned into.
Many people scare single parents about the ill effects on children
brought up without a father or a mother. Innumerable questions
and doubts arise which make a single parent feel confused, guilty
or inadequate.
This workshop aims towards understanding the role of a single
parent, provide insights in developing better skills for effective
parenting, try and fill the void due to the absence of one parent,
and to share individual experiences.
MEANT FOR THOSE WHO ARE:
★ Single parents due to death or separation from spouse,
★ Managing children alone in long absences of spouse,
★ Unable to take the vital decision of taking the plunge
towards single parenthood,
★ Desiring to help single parent families, as teachers,
relatives or friends.
LOOKING AHEAD:
We hope this would be a stepping stone to a continuous learning
and evolving process, perhaps also in the form of a self help
support group.
A workshop jointly organized by
Banjara ACADEMY and
SHRISTI SPECIAL ACADEMY
DATE
: Saturday, 20th September 97
9:30 am to 3 pm
VENUE
Banjara Academy,
Queens Road, Bangalore - 560 052,
Phone: 2265628 2260674
FEE
: Rs. 180/- including lunch,
tea and course material.
SHRISTI SPECIAL ACADEMY
Shristi is 'a venture of young and dedicated professionals who
desire to bring sunshine into the lives of special children. It caters of
children of all a’ges who have different needs or disabilities, and who
belong to all strata of society. Shristi provides a new environment to
build up healthy bodies and minds, giving personalized attention and
unlimited tender loving care.
Shristi also has programmes and supportive services for children
with varied developmental disabilities, specific learning disabilities,
mothers with risk pregnancies, offspringofAIDS patients and terminally
ill children. It offers consultancy to regular and special schools, and
counselling and guidance to parents in understanding children better.
Shristi’s centre at 58 MIG, 3rd Main Road, KHB Colony I Stage,
Magadi Road, Bangalore 560 079 (Phone: 3488538) is open to visitors
who wish to be rainbows bringing sunshine into the lives of special
children.
BANJARA ACADEMY
Banjara Academy is an institution dedicated to the improvement
of quality of life. Jt aims to being together experts and professionals, to
share their knowledge and experiences in various fields ranging from
HRD, counselling, family life, parenting, matrimony, leadership,
personal development, social decision making, to professional
excellence.
Short term interactive workshops are conducted year round for
small groups of general public as well as for people with specific needs.
APTITUDE TESTING AND CAREER GUIDANCE is
offered on all w’brking days through psychological tests, exhaustive
career information, and counselling. CORRESPONDENCE
COURSES are also offered year round, in Counselling and
Personality' Development.
Banjara ACADEMY
Banjara Academy is an institution dedicated to the improvement
of quality of life. It aims to bring together experts and
professionals, to share their knowledge and experiences in
various fields ranging from HAD, counselling, family life, personal
development, social decision making, to professional excellence.
The Academy lays stress on practical aspects of betterment,
and the workshops are designed to be brief but comprehensive.
A pioneer in this field, the Academy’s uniqueness lies in focussing
on practical aspects of finding solutions to day to day problems
of individuals.
Besides conducting high profile executive development and
management programmes, the Academy offers very affordable
interaction workshops in meaningful subjects like counselling,
self-development etc. It offers unique workshops for children,
to make the study process an exciting experience.
Banjara Academy has planned ongoing programmes ranging
from half day workshops to exhaustive training modules, in the
following areas:
* Counselling Skills
* Preparing for a Career, Career Counselling
* Communication and Effective Speaking
★ Leadership and Assertiveness
★ Self Development Programmes
★ Parent Training Programmes
★ Beginning a retired life
* Caring and Sharing
★ Improving Matrimonial Harmony
★ Children’s workshops for study skills
APTITUDE TESTING AND CAREER GUIDANCE is offered
round the year through psychological tests, exhaustive career
information, and counselling. Fee Rs. 100/- only.
CORRESPONDENCE COURSES are also offered year round,
in Counselling, Personality Development, and Understanding
Computers for a fee of Rs.500/- and Rs. 250/-.
For enquiries, details of programmes, and registrations, please contact:
Mr Ali Khwaja
Wg Cdr K M Vijayan (Rtd)
BTech(IIT) MIE
Chairman
M Sc B Com PGDPM PGDFM
President
Banjara ACADEMY
Queens Road, Bangalore -560 052
Phones: 2265628 / 2260674
Fax: 080-2260674
THREE DAY WORKSHOP IN
CAREER GUIDANCE
ANDYOUTH COUNSELLING
THE WORKSHOP:
Opportunities for students have widened
considerably in the past tew years. There are innumerable
avenues where lucrative careers can be pursued. This also
creates confusion regarding which direction one should
head for. Many students blindly ape others in joining up
with so-called lucrative courses, ending up paying large
sums of money for careers they may not have aptitude
for. This interactive and practical workshop aims to train
people in understanding, guiding and channeling youth
to a better future.
WHAT IT PROVIDES:
* Understanding children and adolescents
* Understanding their interests and aptitudes
* Developing and conducting psychometric tests
* Relating to emotions, aspirations and dreams
* Tackling parent-child conflicts
* Gathering and disseminating career information
WHOM IT IS MEANT FOR:
□ Teachers who want to give a little more
.□ Parents interested in guiding children
j Others interested in the future of youth
DATES : Tue 30th Sep, Wed 1st and Thu 2nd October
9:30 am to 4:30 pm
VENUE
Banjara Academy, Queens Road,
Bangalore 560052 Phones : 2265628, 2260674
(on the way to Cantonment Station)
FEES
Rs. 450/- (inclusive of lunch, tea and course
materials)
Working paper 120
BANGALORE HOSPITALS AND THE URBAN POOR:
A REPORT CARD*
SURESH BALAKRISHNAN
ANJANA IYER
*
PUBLIC AFFAIRS CENTRE
BANGALORE
The Project was carried out in collaboration with the Citizen Action Group,
Bangalore. It has benefited from the advice and guidance of a group consisting
of Ms. Nomlta Chandy, Dr. Nlrmala Murthy, Dr. Saraswathl Ganapathy, Ms.
Surya Vaz, and Dr. Samuel Paul. The project was initiated by Dr. Samuel Paul;
the design and conduct of the study was carried out by MBA, Bangalore.
BANGALORE HOSPITALS AND THE URBAN POOR:
A REPORT CARD*
SURESH BALAKRISHNAN
ANJANA IYER
PUBLIC AFFAIRS CENTRE
BANGALORE
The Project was carried out in collaboration with the Citizen Action Group,
Bangalore. It has benefited from the advice and guidance of a group consisting of
Ms. Nomita Chandy, Dr. Nirmala Murthy, Dr. Saraswathi Ganapathy, Ms. Surya
Vaz, and Dr. Samuel Paul. The project was initiated by Dr. Samuel Paul; the design
and conduct of the study was carried out by MBA, Bangalore.
Contents
Executive summary
1.0
Introduction
2.0
Profile of respondents
3.0
Usage of hospitals
9
4.0
Cost of treatment
12
5.0
Quality of service
17
6.0
Medical care
22
7.0
Speed money
26
8.0
Overall impressions that patients hold
30
9.0
Conclusions
33
3
7
x
Public Affairs Centre, Bangalore
2
BANGALORE HOSPITALS AND THE URBAN POOR:
A REPORT CARD
1.0
1.1
Introduction
The quality of hospital services is an important element in the package of services
that the poor rely upon, during periods of physical disorder and trauma. While these
services have seen many a technical advance, it has been accompanied by
increases in costs and complexity. There has been a growing concern over the
deteriorating quality of health care provided by public hospitals. These problems
become more visible when it comes to the question of the service to the poor.
The lack of awareness and education, and difficulty to pay open market rates for
health services compounds the problems associated with quality of public health
care.
1.2
How do citizens, particularly the poor, experience these services? What is their
feedback to the health care system?
Where are the improvements required? In
order to examine these issues, the Public Affairs Centre and the Citizens Action
Group have designed and carried out this study, so as to assess difficulties
encountered by the poor while making use of hospitals, perceived quality of specific
components of service, and their ratings of different areas of action for improving
services. The findings from this study are expected to provide a framework for
public interest groups and administrators of health care systems to design system^
for improving access to health care for the poor, quality of service they receive, and
improve satisfaction from services provided.
7
1.3
The city of Bangalore has a population of four and a half million, of which 20% are
estimated to be slum dwellers. The facilities for health care of citizens in the public
domain consist of three large public hospitals run by the state health department,
three speciality hospitals under the central government, a large number of maternity
and child care hospitals run by the City Corporation, as well as other hospitals run by
Public Affairs Centre, Bangalore
3
I
charitable trusts and Missions. A large number of Private clinics and nursing homes
are spread over the city, which also provide services to the urban poor.
These
hospitals provide treatment on in-patient and out-patient basis, depending on the
• nature of the health problem.
1.4
The Report Card on health care services is based on a study of user perceptions
and ratings from four types of hospitals: large Public hospitals, small City Corporation
run Maternity hospitals, Mission & Charity hospitals, and Private hospitals. This was
followed with a series of interviews with hospital administrators to identify systems
and processes that explain some of the phenomena described by users. The first
two stages of the study were carried out in association with Marketing & Business
Associates (MBA) during January, 1996 and April, 1996. The third stage of the
study was carried out with the help of Ms. Piush Antony, Doctoral Fellow, ISEC,
Bangalore.
1.5
Short cases were written up on the basis of a series of in-depth interviews. >
These interviews covered:
Patients’ access to service and availability of the service
Cost of services
Reliability of services including diagnostic services (X-rays etc.)
Satisfaction - cleanliness, politeness, waiting time, the treatment itself
Timely availability of drugs
Patient information systems - providing records to patients etc.
Speed money paid
Perceptions of patients on out-patient, critical and general surgical care
Satisfaction with post surgical / long term care
1.6
The field survey was designed using inputs from the case studies. It covered a
sample of 361 citizens drawn from 12,896 economically weaker households
scattered across 65 locations in and around Bangalore city. Households with
incomes below Rs. 3500/- per month were considered for the sample. Separate
Public Affairs Centre, Bangalore
4
questionnaires were administered for in-patients and out-patients (See Annexe 1
and 2). The survey focused on themes such as :
Usage profile of different types of health care services
Quality of medical care and facilities
Cost of services
Behaviour of doctors and hospital staff
Dynamics of speed money
Overall satisfaction
1.7
The in-patient sample covered 108 users of Government hospitals, 46 users of
Corporation hospitals, 63 users of Mission and charity hospitals and 63 users of
Private hospitals. Of the 81 out-patients covered in the study, 47 were users of
Government hospitals, and 34 used Mission and charity hospitals.
1.8
The study of hospital administration used a purposive selection of three
government run and three private hospitals preceded the data collection. All thd
government hospitals selected, are attached to nursing schools and medica
colleges which send students for training and house surgency. The three
hospitals selected constitute prominent government hospitals in the city in terms
of bed strength. These are K. C. General hospital, Malleswaram, Lady Curson
and Bowring, Shivaji Nagar, Victoria hospital, Kalasipalayam.
Of the three
private hospitals, one is a full fledged medical institution with various medical and
paramedical courses and another with only nursing and paramedical courses.
The third in this category, when compared to others is of the status of a nursing
home with only 80 beds. The hospitals chosen are located in different parts of the
city and provide representativeness in the selection of the sample. These are St:
Martha’s hospital, St: John’s hospital and P.D. Hinduja hospital.
1.9
The interviews of hospital administrators went into processes in hospitals, that
would explain some of the systems and constraints under which the health care
system operates. It dwelt on themes such as :
Public Affairs Centre, Bangalore
5
t
Facilities available at the hospital
Cost of providing services
' Operating and administrative procedures -staffing, availability of medical and
para-medical personnel, patient information systems
Staff salaries and motivation
Waste management
Quality standards (or standards of service) available
Hospital policies
1.10
The findings from these stages is presented in separate sections that follow, and
the concluding section outlines the recommendations for further action to
improve the quality of services for the poor in public hospitals.
Public Affairs Centre, Bangalore
6
Profile of respondents
2.0
2.1
The sample survey covered a wide spectrum of the poor from different parts of
Bangalore. The scope was restricted to include individuals who had made use of
hospital care during the last six months, in order to ensure quality of data.
2.2
Over sixty percent of the sample of in-patients was female. The heads of
households in this sample were mainly skilled workers (57%), and
(18%)
unskilled workers; the rest included petty traders, salesmen, etc. While nineteen
percent of the sample were illiterate, thirty two percent had some schooling, and
forty four percent had SSC or higher level of education. Fifty one percent of them
used a common tap, fourteen percent used municipal pumps, and thirty four
percent had taps at home.
Chart 2.1 : Respondent profile (in-patients) by occupation
25%
18%
□unskilled
□ SKILLED
□ OTHERS
57%
2.3
In case of out-patients, fifty four percent of the sample were males. Twenty five
per cent were literate, forty eight per cent had some school education, and
twenty seven had studied up to or higher than the SSC level. Fifty one per cent
of them used common taps for drinking water, ten percent used municipal
pumps, and thirty eight percent had taps at home.
Public Affairs Centre, Bangalore
I
Chart 2.2 : Respondent profile (out-patients) by source of drinking water
38%^ o
O
O
O O
9
□COMMON
TAP
Q o o a*
O O C o/
/Oo © o O o o
/o O O o o 0 O/'
□ MUNCIPAL
PUMP
DO O O G O X
o b
O o Qj/
□ OWN TAP
w
»
* * a/
IO0/
52%
Public Affairs Centre, Bangalore
8
3.0
3.1
Usage of hospitals
The study did not explicitly seek to assess the extent to which different types of
hospitals are being used by the urban poor. Given the purposive sampling to
cover all types of medi-care used by the poor, the profile of the sample does not
reflect the actual extent of usage of public hospitals.
But the sample does
indicate that education, income, occupation or locality do not have a significant
bearing on type of hospital used.
Chart 3.1: Profile of users occupation across different types of hospitals
100%
90% -
-IB
-25-
-26-39-
80% 70% -
□ Others
60% -
59
50% -
□ Skilled
57
40% -
63
□ Unskilled
51
30% 20% -
10% -
^26*
v13v
0% --
Govt,
hospital
3.2
Corpn.
hospital
Mission
hospital
Private
hospital
"Offen, poverty drives people to use Government hospitals. Here,
sometimes, experiences during treatment are so bad that they force
patients to visit Private hospitals. Kasturiamma, who has had the
experience of being treated at a Government hospital and has escorted
other patients as well, is one such person. Raju, on the other hand, is
willing to go back to the Victoria hospital in spite of his unpleasant
experiences, for he simply cannot afford Private care. ”
Public Affairs Centre, Bangalore
9
Chart 3.3 : Time taken before seeking treatment
100% -|
32
6
80% -
60% -
19
25
63
40% -
□ > 15 days
□ 5 -15 days
□ 3-4 days
^1-2 days
32
29
24
20% 0%
Govt.
3.5
✓
Corpn.
Mission
Private
Given the economic status of the poor, it was presumed that “free” treatment
would be a very important reason for using Government hospitals. Low cost was
the main reason for choice by thirty percent of the respondents using
Government Hospitals and Corpn. Owned maternity hospitals. But cost was pot
the only concern in making choice. The choice of hospital is largely influenced by
the urgency of treatment as well as the sequence of events that preceded
hospitalisation - proximity is a major explanation for maternity cases - quality and
familiarity seem to be equally important. The chart that follows gives a profile of
reasons given for choice of hospitals.
Chart 3.4: Principal reason for selecting hospital
(given by % of respondents using the type of hospital)
Govt.
Corpn.
Mission
Private
Proximity
22
72
24
63
Acquaintances
28
17
31
30
Good treatment
21
17
34
22
Recommended
27
2
27
26
Inexpensive
30
30
10
2
Others
6
14
8
2
Public Affairs Centre, Bangalore
11
4.0
4.1
Cost of treatment
As mentioned earlier, the basic premise in setting up public hospitals was to
provide free or cheap medi-care for the poor. While it is subsidised to a large
extent in the government hospitals, there also appears to be some diversity in
the extent of subsidy. Government hospitals have elaborate rules about rates for
services like provision of bed, medicines, operation costs, tests and food, which
depends on the income levels of the patients. Government employees and
pensioners are charged differently, based on their salary drawn.
4.2
Differential rates are adopted mainly based on the income of the patient and as
laid down by the government of Karnataka; a profile from one of the Government
hospitals covered in the third part of the study revealed the following. There are
two types of wards : general ward and special ward. General ward follows three
categories of income : below Rs. 600, above Rs. 600 and above Rs. 1200. No
charges, are taken for beds from any of the above for general ward category
The payments for other wards and services are given in Chart 4.1.
Chart 4.1 : Norms for charges at Government hospitals
4.3
Gen. ward I Operation
Income category
Norm
Below Rs. 600 pm
Free
Free
Free
Free
Rs. 600 -1200 pm
Half
Free
Half
Half
Above Rs. 1200 pm
Full
Free
Full
Full
Others
Food is free for everyone, expect for government servants whose basic pay is
above Rs. 1640. Ward charge reductions for the government servants are also
made based on the basic pay up to Rs. 1000 of Rs. 2/-, from Rs. 1000-1500 of
Rs. 5/-, from Rs. 1500-2500 of Rs. 8/-, and from Rs. 2500-3000 of Rs. 10)-.
Food is not free for those drawing pension above Rs. 500, but are exempted
from paying ward charges. Subsidies on lab services are made similarly.
Public Affairs Centre, Bangalore
L2
4.4
In the case of Mission hospitals, on an average, the charges for services are
high compared to government hospitals. But, as the sample hospitals studied
work on a principle of charity, the administration has discretionary powers to write
off the bills in the case of poor deserving patients. There is wide variation across
the Mission hospitals studied in case of charges for various services. For
example, bed charges vary between Rs. 15 for a general ward bed in the case of
Mission hospital I to Rs. 400 for deluxe ward bed in the case of hospital III.
Within a hospital, there are various types of wards which will have different
*
charges, based on the services provided. In Mission hospital III, differential
charges are applicable to the kind of ward that are chosen by the patient. There
are three kinds of wards : general, semi-private and private. In the general ward
a bed is charged Rs. 15. Semi-private wards contain rooms with 2-6 beds
ranging from Rs. 45-110. private wards are single bedded rooms. The rent for
these rooms are Rs. 200-235. While medicine charges are not under any kind of
reduction, food, lab services and operation charges vary according to the wards
chosen by the patient. For example, the operation charges for a caesarean
delivery is Rs. 1600 in general ward, in semi-private ward, Rs. 3000 and in
private it is Rs. 4000.
4.5
The study went into a detailed investigation of different types of costs that are
borne by patients using different options for medi-care - in terms of formal
payments made, and informal side payments or expenses that took place. Ten
percent of the patients using Government hospitals succeeded in obtaining
totally free treatment, another seven percent had to spend on speed money only.
At an aggregate level, the cost of treatment is, as expected, the highest in
Private, followed by Mission hospitals; Corporation hospitals which by and largp
catered to a specific aspect of health are reported the lowest cost per
hospitalisation. The profile is given in Chart 4.2.
Chart 4.2 : Average expenses on treatment at different hospitals
Public Affairs Centre, Bangalore
13
4000 -!
3500
331
2500
2000
1500
252
G3 Speedmoney
3 535 □ Legitimate
Ha
2T32
1000
1626
500 -
211
J___ l34j5 _____ T_____
0
Govt.
4.6
HH 229
■i
3000
Corpn.
Mission
Private
The profile of costs suggests that Government hospitals are still the cheape:
source of medi-care for the poor. But for a minuscule minority who may get free
treatment, the cost at a Mission or Private hospital is no less than Rs. 500/-.
n
contrast, forty four percent of the users of Government hospitals have spent less
than Rs. 500/-. The details of a classified profile are given in the chart below.
Chart 4.3: Total Expense on treatment across different types of hospitals
Govt.
Corpn.
Mission
Private
2
3
No expense
10
Up to Rs. 100
8
2
Rs. 101 to 200
10
15
Rs. 201 to 400
11
41
3
2
Rs. 401 to 500
15
9
2
6
Rs. 501 to 800
7
13
11
8
Rs. 801 to 1000
11
13
21
10
Rs. 1001 to 1500
4
2
8
13
Rs. 1501 to 2000
8
2
13
11
Rs. 2001 to 3000
4
2
14
10
Above Rs. 3000
12
27
37
Public Affairs Centre, Bangalore
1
14
4.7
But the hardships that the poor face in accessing this “free” treatment needs to
be examined by relating it to the purpose for which their scarce resources are
drained. Over fifty percent of the patients using Government hospitals had to pay
speed money, and eighty seven percent in maternity hospitals.
In contrast
around twenty-nine percent made such payments in Mission hospitals, anc
twenty four percent in Private hospitals. The most important element is speed
money that the poor have to pay; about 25% of the respondents reported that
around 50% of their expense was on speed money.
Chart 4.4: Percentage of cost expended on speed money
100%
24
80% -
34
□ 95 to 100%
60% -
□ 30 to 50%
9 Up to 30%
40% -
□ Nil
20% -
0%
[Will _
Private
4.8
“Often, cost of services at the so-called free Government hospital was
more than what it would cost to go to a Private hospital. The experience of
Shahtaz Banu is a pointer to this state of affairs. In her own words, “it is
wiser to go to a Private hospital, pay the heavy fees and be looked after
well rather than go to a Government hospital get treated badly, and still end
up paying for every aspect of the service”.
4.9
The moot question is whether the staff in Government and Corporation hospitals
are so poorly paid in comparison to the mission and private hospitals that they
need to depend on speed money for making ends meet. Data collected on pay
scales across hospitals is given below in Chart 4.4.
Chart 4.5: Salary scales for hospital staff
Public Affairs Centre, Bangalore
15
!
Govt. (3)
Mission 1
Mission 2
Mission 3
Nurse - SN
1520-2900
1490-2350
1570-3611
2000 cons
Nurse - SSN
1720-3300
1750-2650
1770-4071
Nurse - WS/Sup.
1830-2770
1910-4393
Nurse - 8WS
2150- 3030
Ayahs/ Wardboys
4.10
840 - 1340
910- 1350
850- 1955
1658/1469
The Government hospitals have a standard package of pay scales for different
grades of nurses and other support staff. In these hospitals appointments are
made by the government health department after going through a process of
selection. Mission hospitals follow different pay scales and there is no uniformity
in terms of grades within a job type and the compensation package. While all the
hospitals follow a package of basic pay and dearness allowance, which is linked
to cost of living index, Mission III follows a method of basic and variable dearness
allowance based on minimum wages act and arrives at a consolidated pay or
various grades of staff. A comparison of government and private hospital staff in
terms of pay reveal that except in the case of Mission II, other two Mission
hospitals have relatively low salaries for the nursing and other support staff. It
therefore seems that government hospital staff are paid competitive salaries
when compared to mission hospitals, and that there is no special reason on that
account for medical staff to be chasing speed money.
Public Affairs Centre, Bangalore
16
5.0
5.1
Quality of service
The first aspect of service that the study went into was waiting time before
doctors would examine the patient after reaching the hospital.
It is often, in
extreme distress that a patient reaches the hospital - delay in medical response
not only prolongs the agony but could also lead to further deterioration and
complications in the patients condition. The data on waiting time for doctor's
examination and commencement of treatment in emergency cases tends to be
very ominous, across all types of hospitals; the smallest average waiting time of
38 minutes was reported by those using Private hospitals. A closer examination
of disaggregated data suggests that a small set of cases where the waiting
period was reported as over three hours made it look so extreme. Of the 179
patients who felt that they had gone to the hospital in emergency conditions, forty
seven percent had to wait more than ten minutes to get a doctor’s attention,
while twenty three percent had to wait more than forty minutes. A profile of the
delay in examining a patient is given below in Chart 5.1.
Chart 5.1 : Time elapsed before receiving attention of doctor
100%
90% -
>5
28
80% -
70% -
24
60% -
50% 28
□ above 30 mins
25
2
X
40% -
S’
□ 10 to 30 mins
26
29
□ Immediate
14
2- 2
Supto 10 mms
30% -
20% 25
10% -
32
31
33
0% Govt.
Public Affairs Centre, Bangalore
Corpn.
Mission
Private
1
!
5.2
“Kasturiamma’s mother is not alive to tell us the tale of her experience at
the emergency ward of a Government hospital. At 5.00 a.m. there is not a
soul at the so-called emergency ward who is awake to provide the
assistance. After much cajoling, a doctor is summoned by a reluctant
nurse and ward boy. There is no sense of urgency in the trainee doctor's
movements. The patient continues to be critical. Medicines are prescribed,
but the pharmacy is shut. The patient, a victim of apathy, finally succumbs
to her illness.”
5.3
Private hospitals tend to be much better in starting treatment once the
examination has been completed - forty nine percent report that treatment
commenced within ten minutes of reaching the hospital. The Mission & Charity
hospitals seem to fare relatively badly in this critical area, with only thirty percent
reporting that treatment commenced within ten minutes - perhaps they are
overstretched for doctors, or their para-medics do so good a job that doctors can
take their time. But the situation is much worse in Government hospitals, where
over fifty percent of the patients report having to wait fifteen minutes to three
hours for treatment to commence. Details are given below in the chart below.
Chart 5.2 : Time before treatment commenced for emergency patients
100%
9
90% -
35
80% -
39
36
42
70% -
□ above 30 mins
60% 26
50% -
□ 10 to 30 mins
18
□ upto 10 mins
31
40% -
7
14
28
30% -
□ Immediate
8
20% -
32
32
10% -
22
21
0% -
Govt.
Public Affairs Centre, Bangalore
Corpn.
Mission
Private
18
Chart 6.5: Areas calling for improvement
100%
90%
-S-S-S
is
sss
80% -
s ss
ss
i S5
Ss
4U
3S
s*s
70% -
□ Cleanliness
60% -
□ Information from staff
50% -
40% -
□ Availability of facilities
30% -
□ Quality of treatment
20% -
□ Staff behaviour
10% 0%
Govt.
Public Affairs Centre, Bangalore
Corpn.
Mission
Private
25
7.0
7.1
Speed money
The non-formal payments for hospital services have been clubbed under the
label “speed money”.
There seems to be little difference across different
hospitals, when one looks at the average amount paid. The profile is given in
Chart 7.1.
Chart 7.1: Quantum of speed money payments by in-patients
(in Rs.)
350
300 250 -
200 150 100 50 0Govt.
7.2
Corpn.
Mission
Private
A closer look at the quantity of payment made by different patients indicate that
the phenomenon is at its peak in Corporation hospitals, even though it is the
smallest in terms of the average amount. Almost 87% of patients using
Corporation hospitals are paying speed money. The case studies suggest that
maternity cases have, traditionally, evoked a sort of celebration rather than
pathos of illness - yet, it does not explain why speed money had to be paid to get
hot water, or to get the baby examined. The study also indicates that Mission
and Private hospitals are not free of this malaise. Since less than 30% of users of
Mission and Private hospitals pay speed money, it could be assumed that the
problem is limited to Government hospitals.
Public Affairs Centre, Bangalore
26
7.3
"Many mothers like Sushiiakumari, face the problem of having to cough up
money to see their new-born babies. Rates - 150 rupees for a female baby
and 200 rupees for a male baby. To add insult to injury, it is clearly a
perverse form of gender discrimination. And the peculiar market forces
that seem to have pegged the rates uniformly all over Bangalore.
Sometimes, fact can be stranger than fiction.ff
Chart 7.2 : Profile of speed money payments in different hospitals
(given by % of respondents using the type of hospital)
7.4
Govt.
Corpn.
Mission
Private
No money paid
49
11
71
76
Upto Rs. 100
14
29
19
7
Rs 100 to Rs. 400
23
50
5
5
Above Rs. 400
13
11
5
13
Many of the reasons for payment have something to do with particular services
which may have been part of the package of services to be provided free of cost
in Government and corporation hospitals. But a sizeable amount seems to be
paid as a token of appreciation or consideration for services/flexibility in these
hospitals - to what extent they are extorted is a question.
Public Affairs Centre, Bangalore
27
Chart 7.3 : Purpose of speed money payment
(given by % of respondents using the type of hospital)
Govt.
Corpn.
Mission
Private
To ensure good treatment
25
12
6
80
Pay for services
19
19
17
0
Have patient cleaned
8
12
28
20
Flexibility of watchmen
4
2
6
7
Ayahs/nurses etc.
21
17
22
0
Token of gratitude
10
17
33
7
On discharge
8
29
0
0
Others
36
26
6
0
demanded money
7.5
“Staff rarely made a move unless money was paid for every chore. Be it a
case of providing a wheel- chair or of giving the daily dose of medicines.
Many patients, who had visited Bowring hospital had this story to tell.
What is more horrifying is the fact the even surgeries would be scheduled
only when the doctors were “taken care of”. Even a leg that would have to
be amputated if immediate treatment was not given did not merit the due
care.”
7.6
A closer analysis of whether patients who paid speed money experienced
positive results suggests that they were perhaps cheated in the bargain.
A
scrutiny of waiting periods, availability of medicines, etc., when related to speed
money paid, did not indicate any definite pattern. In other words, many of the
patients who reported “not having paid speed money” also indicated that
treatment time was low or that medicines and injections were available to them at
Government hospitals. While it is heartening to see such instances of positive
behaviour in hospitals, it also reflects the agony that many would have gone
Public Affairs Centre, Bangalore
28
through after paying through their nose for services that were supposed to theirs
for the asking.
7.7
“Basha, a 30 year old, was told at the Bowring hospital that he needed to
undergo surgery for his ulcer condition. He waited patiently for almost a
month for his operation to be scheduled. Not being able to take the wait
any longer, he paid Rs. 500 to the doctors. His operation was scheduled
within two days. His post-operative experiences were far from pleasant. In
his own words - “only a wretched person should step inside these
hospitals. ”
Public Affairs Centre, Bangalore
29
t
8.0
8.1
Overall impressions that patients hold about hospitals
The most important factor in creating an impression on the patient is the
perception about the extent to which cure was achieved through the treatment.
Around 83% of patients overall, reported successful treatment, of which 40%
visited the same hospital again after discharge. The overall ratings that patients
gave different types of hospitals, presented below in Chart 8.1 suggests that
treatment at Mission and Private hospitals is seen in more positive light.
Chart 8.1: Overall ratings of hospitals by patients
100%
90% 80% 70% -
60% 50% -
67
58
40% 30% 20% 10% 0% --
8.2
11
13
Govt.
Corpn.
II
35
38
~6~
~~5~
Mission
Private
■ Very good
□ Okay
□ Very bad
The analysis of reasons advanced for overall rating clearly highlights the
importance attached to perceived quality of treatment over aspects such as cost
and staff behaviour. While poor quality of treatment explains over half the ratings
of Government and Corporation hospitals as very bad, around 80% of the ratings
of Mission and Private hospitals as Very Good come from patients who felt that
the treatment was very good. On the contrary, Very Good ratings on account of
Less expensive/Free treatment was highlighted by 21% of the in-patients who
rated the Government hospitals positively.
Public Affairs Centre, Bangalore
30
8.3
The case studies on hospital administration indicated that there are variations
across hospitals in terms of attending to complaints from patients and public.
While all hospitals have a complaint book/box, most grievances are conveyed
orally to doctors/RMO during their daily rounds in the case of government
hospitals and to the ward supervisor/nursing superintendent in the case
private hospitals. The usual complaints in government hospitals are with regard
to cleanliness of the wards and against individual members of the staff.
8.4
In government hospitals there seems to be no mechanism to attend to the
complaints as action on erring nurses or ward staff due to strong political
affiliations of the respective unions. In the case of senior officials, most often
informal channels are used to address any complaints, as senior medical officers
do not exercise their powers to take action on any complaint against
doctors/senior staff. A related difficulty faced by the senior officials is that, certain
complaints like water shortage etc. often falls beyond their capacity to address,
which makes the services short of satisfaction.
8.5
At the same time, another official revealed that they usually get fewer complaints
when compared to private hospitals mainly due to three reasons. First, the kind
of patients they have are from the low income group and tend to be less
demanding - they are less articulate about the extent to which they are eligible for
‘free’ services, and are often ‘private patients’ of a government doctor. In such
cases, they manage to get the same services by bribing the concerned
personnel. Third, the expectations of patients on services and their demanding
capacity are low, since they do not pay for it.
8.6
In the case of private hospitals, complaints are often related to maintenance,
which tend to be addressed immediately by the concerned senior officials and
the redressal mechanisms are in place and work effectively to the satisfaction of
the patients. This stems from the fact that in private hospitals management
bestows greater degree of autonomy to the senior officials who take decisions as
and when the need arises.
Public Affairs Centre, Bangalore
31
8.7
There is no record of patient satisfaction surveys in the hospitals studied, except
in case of two Mission hospitals, conducted two years ago. Of these, two
. hospitals are planning to have a survey in the coming year. In these two
hospitals, based on the previous survey findings, improvements were made as
per the demands of the patients. Issues like timings of diet, visitors, and
ingredients of the diet were attended to based on the patient satisfaction surveys.
(
Public Affairs Centre, Bangalore
32
9.0
9.1
Conclusions
The urban poor in Bangalore have been using a variety of options for health
care. While Government hospitals play a major role, other hospitals, including
Mission and Private hospitals contribute to health care for the poor. Any strategy
for health care for the poor has to envisage appropriate inputs for all the
institutions involved in this sector.
9.2
In terms of costs, Government hospitals come out as the cheapest source of
health care for the poor.
This is not only in terms of percentage of patients
enjoying free treatment, but also of total costs incurred by an overwhelming
majority of the patients. The unfortunate part of this otherwise positive
phenomenon is that a major part of the costs incurred by the poor are towards
illegitimate side-payments, often extorted by different participants in the health
care system.
9.3
But the most significant problems seem to be in the quality of medical care that
the poor receive. To start with, the waiting time they have to go through before
receiving medical attention and treatment seems to be quite high.
Second,
injections and medicines, presumably free or subsidised, are often not available |
at Government hospitals. But the more important problem seems to be the total
absence of standards or the lack of awareness among patients about what they
can expect at hospitals.
It is from this point of view that Mission and Private
hospitals seem to be serving the poor in a much better manner.
9.4
The manner in which activities are managed in the Government hospitals also
merit attention. The seriousness of this problem can be seen from a simple area
like cleanliness of hospitals.
Although there was no major difference in the
frequency with which cleaning was carried out across different types of hospitals,
the level of cleanliness at Government hospitals were rated in much poorer
terms.
Similarly, the poor need to run from pillar to post, to find medicines,
Public Affairs Centre, Bangalore
33
sometimes in life and death situations, while being treated in Government
hospitals - whereas, dispensaries of Mission hospitals are rated to be far more
efficient in this regard.
4
9.5
One approach to seeking better quality of medical services and facilities that he
poor are compelled to seek, is by resorting to speed money payment.
Tpis
approach seems to apply to all levels of medical personnel (from doctors to
sweepers), and for all types of services (from operations to entry into wards
without authorisation).
Although there is wide variation in the quantum of
payments, the problem seems to be most acute in Corporation Maternity
Hospitals, which are used primarily by the poor.
Designing interventions to
reduce the instances of extortion could certainly begin there.
9.6
Patients who have been in-patients at Government hospitals seem to be less
likely to follow up their treatment with subsequent visits. While part of thiL
phenomenon can be explained in terms of the tendency to avoid hospitals as far
as possible, the poor quality of instructions that patients receive is also an
important factor. This is a major area of concern, since improper follow up may
not only lead to poor recovery and dissatisfaction, but also to a waste of all the;
efforts that have already been put in.
9.7
The feedback from patients have also highlighted the serious misgivings they
have on the quality of treatment. Notwithstanding the poor ratings for helpfulness
and courtesy from nursing and other hospital staff, and the speed money paid,
they have highlighted quality of treatment as the major issue.
4
This feedback
highlights the distress that the poor encounter in hospitals, and the urgent need
to create mechanisms for improving quality and creating confidence.
9.8
The willingness of a large sample from the poor to make use of Private and
Mission hospitals, and the average cost of treatment
they have reported,
suggest that “free” treatment is not always preferred at the cost of quality.
It is
true that this does not explain the situation of the destitute and the absolute poor
Public Affairs Centre, Bangalore
34
- but it forcefully presents the fact that “reasonably” priced services which
guarantee quality are the need of the day. The cost profile also suggests that
many of the hidden or illegitimate costs can be recovered as legitimate fees,
4
4
provided hospitals can specify them as services to be paid for - implicit in his
sort of situation is the pressure to bring quality into these services.
t
Public Affairs Centre, Bangalore
35
BANGALORE HOSPITALS AND THE URBAN POOR:
A REPORT CARD
- EXTRACT OIF THE SUMMARY AND CONCLUSIONS
SURESH BALAKRHSHNAN
ANAJAN KYER
PUBLIC AFFAIRS CENTRE
BANGALORE
( UN COLLABORATION WITH CITIZENS ACTION GROUP, BANGALORE )
I
I
I
/U b ckl G-
.• • hjnhfi j
. ibHoi? irn bm
ODH) noftfcioqiG
I
zh )
rb
slbhqeori
Bangalore Hospitals and the Urban Poor
A Report Card
fib ►
;ehr>q
ni
'mIT
A Summary
^ji ri'ff! Ibii^pod rlli 7 iGfxj ndt io w >n • ii
zo
i nrj
»<>•>
The quality of hospital services is an important element in the package of
•xr. M
tmid juda fe gnidu
h
:
services that citizens rely on, during periods of physical disorder and trauma.
While medical services have seen many a technical advance, it has been
accompanied by increases m costs and complexity. There has been a growing
concern over the deteriorating quality of health care provided by public
hospitals. These problems become more visible when it comes to the question of
health services to the poor.
How do citizens, especially the poor experience these services ? What is their feedback
to the health care system ? Where are the improvements required ? In order to
examine these issues, the Public Affairs Centre, Bangalore, recently designed a|nd
carried out a study. The study assesses difficulties encountered by the poor
while making use of hospitals, the quality of specific components of service, and
the different types of action for improving services. The findings of this study are
expected to provide a framework for public interest groups and administrators
of health care to design systems for improving access to health care for the pbor
and the quality of service that they receive.
The study of hospital services in Bangalore was conducted by the Public Affairs
Centre, a non-profit organisation based in Bangalore, in collaboration with the
Citizens Action Group. This study attempted to
generate feedback from he
urban poor on the quality of hospital services they receive. Three categories of
hospitals were surveyed - Government or "Public" hospitals, hospitals run by
Public Affairs Centre, Bangalore
93OlB\ iv>8 «ntn90
the Bangalore City Corporation (BCC), and missionary /charitable trust
hospitals.
100*1 'IfcrliiJI
1 bnt» <lb)lqt*oH oiol
bit' J tioqoH /■
The study was carried out in three parts:
7 1 MOIqur A
•
>
Forty one case studies on the experiences of the poor with hospital services
•
hfllLhl
d-*'
.................................
. -
9 •
•
f|» 7/01
jod‘4
to •ftJ/-up of!1
jfi
■•
i
A field survey using a structured questionnaire on different aspects of
feedback from sections of the urban poor on hospital services, and
fj^bf* ifijirifi
• vfifim imr pvfiri £9>rr
wnW
A series iof interviews with hospital administrators on their perceptions of
problems that affect the quality of hospital services.
- ■
bsbi91f>
• nod
riili
»
rij
to
Ji n
OJ
3H
rtflhLJp .cuILhoji
i '/to!
11
OHIO /‘Xi £
1
rI
ste A\v
«W) »s\ UMh M W
111
yMH
I'
il
MlltJ m
lOifLLIO
io ?in9no<
Loh
If. . ,f ! >7‘ H I-* dilbHp'/di
9fiJ 701 )Tf»> rtJlh^f OJ
l-HJ <lfU4hffl
noil jl K
i brtf ^qu-jio )?<n
Jildir
A
q d In
rnai*^L ol
fliihbfi ;.•
»
9fii bn5
iwfi Oji-n
/noil 4
^dbool
6 iOP'Jf/
<*bJi
nhhj-1
Public Affairs Centre, Bangalore
,. •
J Hot
:i
4ntrn
v >i
ribdru
non
/Ju
kJ
but? oriT
•iI t<.*
n.i ^‘or/i*
oj boiqm
?‘>no,99)h j
ut
»ji
9iolbf nj>H rd t ?hd noidj uu^
th
Mi
. •>
j mb
7bi7
ly/onifiit >
?9 > >b <#ni /OTcrrni io!
Mf[! /d botjuLno > <*f»
infrfu.
/ b'HTlh ■
Jj? i
>Ui
rl oriT «HHf
Jr’ #rt
up
b'J '
HI n
Tf':
\V\30 ' ’
i
r
-1;
Efficacy in Administration of Hospitals:in Bangel ore
A Case Study of Private a :■ i d G o v e r r«me nt Hospitals
Piush Antony
Doctor al Fellow
ISEC, Bangalore
I ntroduct.i on
>
)
Like any nther areas or
of socio-economic reality ideologica'
underpinnings influence our understanding of matters related to
time and space
health. The concept of health care has changed over
the relative
regard!ng
and these changes have occurec, most 1y
the
production
and
efficiency of the state versus market in market versus state
______ The
distribution of health care services.
of
the
cornmod i ty 'health co i e an.d no c
di-bate focuses on the nature
bi 1 ty of
r
grod health.To put it in other words, is the responsi
Tn s
individual°
distribution of health care social rather than
the
from
system of health care existing in a country evolves
Accordi
ng
1y
definition of health care as social or individual.
n
domi riant patterris
patter r=> ~f health care, One envisages
there are two domiriant
soci
•?.!
i tern of
where
•e u 11 a b 1 e ssystem
'•/ stem w
h c* r e ?h; *—
- - - 1th
» ! -f ’• is seen as an
but
yocd tea i in as hot on iy a nasic • ;
ronsurnpt i«v.
ecoriom
ic
a i and
.-. so as a basic precondition for enjoying socj .■■ "C PC4 ;
■d
c
• • ••
equality. rhe ether cone i eves fie^itli as aAt
r.f'.
1
i
7
’.
i
C^'
I
the level of
and hence p r • i v c I i s a t i c c i s e n c o u r a g c d . three schools of thought:
d r senu rse , this gets transferred as
<t
a private good and is
c o n s»? r v a t i s for whom health c?re is
y
left t.o the market to t?o di str i bu i,ed and pr i ced accord: n j to - ‘.-t■ a
h a t heal
t h c a r e i s J .' o t ■: i
-nd HMma.-.d; 1
1 i feralc
bar al 3 hold the view tthat
heaith
there is a role fo.- rhe
private ewe; a social
therefore there
soc ia 1 good and therefore
tl
’
-.e
concept
welfare stat^;
covernmerit to play, which is akiii to
as
a
social
good and as a
and the marxi^t recognise health care
the
state
and
demands
1ed by
right which should ne control
controlled
tn1ons
understanding of c'ass relat
rela.ions
in s r«cie t• y to a • ■ a1y s e
i’,- i v? r ?■ i t y sn d disparity of health care.
The neo-classical school of economics■: is divided over the relati ‘/C
and state
in oachieving the objectives of
merits of market and
state in
ser v i C£-‘S . Flut cue to
the
allocation
of
health care services.
efficiency ir.
of
1930s
and
the
of Great Depression
1 930s
tiie inr iuetsue of
'fvifsian' economics, many
capitalist
countries
made
coin
;tr
i
es
many capitalist countries made >ar^
:arg;= scaic
period
in
refitments
pcst-war
t ne
;
i
?fitments in th.- oost~war
De
•?jcial services. State i ntc rven t i on was advoca ugg L’'
e ity with
market forcer, in achieving a high level of eccnomi;;: c-l c t i
prod’.• c11 ve . However,
full emp 1 oyinerit by making iibera; marKe^o more
r.._
with the arrival of stagflation all over the western capitalist
^orld in ISVds Kernesian economics and welfare- state lost its
Re ce s s ion and co n c o mm11 a nf.
ider» logical as well as mater-1 a 1 basis,
resulted in mounting budgetary
decrease in the gov-rrment revenues
r.
rl.at.o to reduce public e-n.-.r.n • • uro or
deficits ferring i.hv
the skate
monotar
welfare acti t i.
1rhe
ne revival cf neo-class ion 1
ir, pup i
spending responsible for i 1 advedsr
cccounted the • f
i! i 3
c d or; p r i v a t i s a r i o
cconorfii c d -'- e ! cp^cr •.r.
•:
i
->m wires in.c luding ’w
into the prov i r i cn <•: ■
1
det>ri;.e ove r th•=■• s t
capi tai i st*
..t.’ r i" ■
bar.r'.d
on the nature
in health
me’sly
fr<.mi
the very
health care, but
it ^r.nnGCPh
(*api “■ aTi st. eccn•?roe -.
'? ■■
In India,
In
India health planning was declared an integral part of socio
economic planning before independence, and after independence > the
proi vded by the Bhore
blue print for national- health poli cy ---heal th care
commi ttee had recommended the free provision of fol 1 owed the
The successive five year plans also
serv i ces.
recommendations of the report.
)
)
regard i ng our health
i nherent problems regarding
But there are some mnerent
This
is
nattern
and
utilisation.
crucial
in
expend!ture
’„X5:;s;:ndTn9Ptbe present state of our puPHe health system and the
The sectoral prirotiqs
i ncreasi ng trend towards privatisation,
health policies were skewed towards
implemented in the national
i
___
___
curative medicine and certain categories of health personnel ahd
towZrdrce"rtaTn'reg'i'o “ns7About 55 per cent of public expenditure i s
, a <and medical education while majority
spent on curative health care
to
suffer from a host of infectious and
of the population continue
communicable diseases and the share of public health services,
.auo to the health needs is just one third of
which are more relevant
In medical education also, the actual emphasis
total expenditure. 1
has been on producing the well trained
t-^"^ but
hut. highly
hiahlv specialised
soecialised man
j
the
health
policy
documents ke(pt
power in curative services while
in
social and
,g the
physicians
on repeating
the need
need for
for creating
c.
As
a
result we
preventive medicines
i..« — . — . • • — and
.para medical personnel.^
havi ng servaal
have more than one doctor per nurse instead
Similarly
nurses per
per doctor.
doctor.
Similarly we
we have one doctor for about ev^ry
there
is
only on mid-wife or health visitor
3381 population, while
per 13977 population.
fpct
of having basic health facilities. Ihis is evident from the f^t
ve ,
cent
of
population
li
that in rural areas where more than 70 per
are
per
cent
of
beds
only about 30 per cent of doctors and 17
care
heal
th
located.
The problem of rural urban disparities in
services is further aggrevated by the disparities in the regional
rural-urban
distribution.
If we super impose regional an
disparities, there emerges the real extent of inequalities in the
distribution of health care
between various parts or the study.
The gross disparities
of health care . wi th . no
pa i t u i co in
iii the
01.^ distribution
~ ----- ------health
needs of people, has taken place in spite
relevance to 'the
-- -of the fact that government owns about 75 per cent of total
hospitals and dispanceray beds.
1
Moreover, most policy initiatives concentrate on the ii nstrumerta
He^lth
role of health, rather than on its intrinsic importance.
has been looked upon as c\ means to increase product, i v i ty and not. on
its own sake.4 As a result the national health policy (1983) is
basically concerned with demographic details to be achieved by the
productive rate. It does not
year 2000 AD and issues such as net
r
such as
as equitable
deal with broader philosophical questions such
depri
vati or of
on
the
current
provision of health services and
certain sections.
So we see the genesis of the crisis as the paucity of public f uf.ds,
low priority given to health budget and the demand for health
do not match and this has given rise to financial crisis ir. t h e
system. The latest available data show that only 75 per cens of
population has access to health care. The ratio of population per
hospital bed is 1371 which is lower than the ratio for South <\s i a
but htgh when compared to other low income countries and middle
->3BI
The per capita health expenditure by the
income countries,
govenment is a dismal amount of Rs.40 per man,woman,and children
per year.'Of this Rs. 24 is spent for the urban areas and the
remaining
16 in the rural areas.
On the other hand, studies
remai ni ng Rs.
Rs.16
show that in 20001 AD, government will have to spend about Rs.77 to
an out 1lay
ay
is an increasing demand to raise the pl
plan
81 . Hence,
K
, there
.
for public health expenditure.
Also, there are studies to prove that
mat the
tne prouiem
ullc health
problem oi
of the
sector in India is non-fulfilment of the targets especially in R'C
for which 3.7 per
or cent is provided. Because, by and large, they
argue that the existing patten of expenditure still follows tie
colonial pattern.
Literature health economics also reveals that
the economic constraints of present day hospitals in India are the
product of their past legacy. Many of the hospitals were set up by
foreign missionaries who provided all financial assistance. As a
result, they did not find reason to mobilise the financial
resources on their own. Even today, hospitals are not run on
economic principles. At the same time hospital industry operates in
an oligopolistic market. Therefore, the industry has many
many sick
units.
Inspite of these short comings India fares well i n hea 1 th serv i ces
Within India the
compared to most other low income countries.
southern states record a better health status than rest of the
country.
Among the four southern states, Andhra Pradesh spends
least on health and next to it is Karnataka.
Privatisition of health care
In India, till the 1980s, largely government controlled the health
care system. Due to the factors discussed above,which happened at
the macro level, India also opened up its health sector slowly for
pri vati sati on.
Privatisation of health care is based on the following assumptions.
1. helath care is an economic commodity and can be purchased like
any other good.
2-
.
.
...
health care providers have profit seeking and maximising concerns
3. If health care is purely on market mechanism, then prices wil
be reasonable and
4.Government intervention should be limited to correct markec
failures and accomplishing social goals outside the ambit of marks
forces.
Each of these can be debated and are linked to the basic question
of whether health is seen as a social or private good. Supporters
Supporter
of privatisation are of the view that it widens choices to the
consumers and it takes the pressure off the government health car ?
system and offers an alternative.
It is argued that economi p
efficiency gains are likely to occur if governments of the thir d
world begin to cooperate with the private sector.
Critics of privatisation are of the view that, lirUi y hospiialr i n
the third world will widen disparities in health care and they
claim that improvements in health indicates the benefits of a
strong public helath care system, Another assumption that market
efficient than non market is also
based health care is more
dismissed by comparing the National Health Service with the
American private health care.
A significant development in this regard that
Aj
983, with
thA first medical industrial complex which was set up in 11983,
ion
iin hncnifai in Madras. This followed a radical transformat
transformation
in°urban
health
care
system
with
corporate
secotr
making
inroads
health
care
system
withby setting up ^ig hosprtais pith
intourban
prov?:?o
“of
beam
care
health care t
latest equipment
equipment and
and technology. Jhis was possibie because
government support iinn the form of subsidies and its policies
towards
and drug industry.
ds private hospitals
hospital
■'Back ground to the study
/
in the wake of liberalization there is an increasing demand for
privatisation for better services and effTCiency
In the ^se
kaouh
alqn the trend is not different and this is more
noticeable in the’urban centres of India. There are various factors
responsible for this, of which the important ones are an overloaded
public health care system, technological developments of expens
diagnostic and medical equipment and the growing) standario, < v,n|
found in these large metropolis. Moreover, demand for pri a ~
health care is most often artificially created by posing it a9ainst
f-e relative -inefficiency in terms of the quality and quantum of
lerv^cel in public healthcare system; to be precise, the services
rendered by the government hospitals.
hospitals The main accusations raise_
of
against the government
nrivornmAnt. hospitals
hosoitals are corruption,
cor, uotion,
inhuman nursing care and unhygenii c
faci1i ti es, lack
'--- of experts
Indian
health
care system, at least in the urban
environment. Thus.
areas are slowly changing in favour of private capital accumulaticn
-- - of the health
and high technology medicare^for^a few at the cost
of the population. At the same time, the cost qf
needs of ma/orTty
r
ca-e has outgrown the average Indian s capacity and thi s
med i cal
■ > have state sponsored health care. Theref orfe
makes it imperative to
it is necessary to find a way out for the disi1lusionment with the
ex i sti ng public health delivery systems and ensure that it shoulds
not lead to a two tier health care system where a minority
privileged with access to extensive high technology and specialised
high purchasing capacity and governmental
care merely due to their
posed
as inferior, for the rest of the
i s often
care which is
attempts a
population. With
Wi th this in view, the present study systems i n
comparison of the public and private health care
issues of concern to them
Bangalore to raise some pertinent
i
The study probes into both public and private health care in the
city of Bangalore and examine the performance of each sector ,
private in this study refers to hospi tai s owned by individuals and
institutions and government and public are used interchangeably.
Object!ves
Methodology and Sample Selection
/V
y
The study followed case study method, This included un structured
key
questionnaire schedule,
in
depth interviews with the
administrative
officials and perusal of operational manuals and
„ . .
documentation procedures of each hospital.
Some of the main issues addressed in the study included staffs,
customer service, standards and
strength, training and motivation,
- ----- --- , —
procedures of service, hyiegene and waste management and hospital
policies.
A purposive selection of three government run and three private^
Al 1 the government
hospitals preceeded the data collection.
All
hospitals selected, are attached to nursing schools and medical
colleges which send students for training and house surgency. The
three hospitals selected constitute prominent government hospitais
in the city in terms of bed strength. These are K.C.General
hospital,Maileswaram ( case I), Lady Curson and Bowring Shivaj
Nagar ( casell), Victoria hospital, Kaiasippalayam (case III).
Of the three private hospitals, one is a full fledged medical
institution with various medical and paramedical courses ano
another with only nursing and paramedical courses
courses..
The third in
is
of
the
this category, when compared to others
status 01 a
nursing home with only Su beds. The hospitals chosen are locaue~
in different parts of the city thus providing a representativenes=
to the selection of the sample. These are StiMartha’s hospita
(caselV ), St:John
St:John’’ss hospital
hospital (caseV) and P.D.Hmduja hospital
(case VI)
Analysis and findings
This section covers analysis related to various pararreters tha|t
determine efficiency and effectiveness of health care across
government and private hospitals.
Staff and Capacity Utilisation
Tables 1&2 provide the data related to number of beds available;,
doctors, paramedical and other support staff, average Oct Patients
(per day) and average bed occupancy rate (per month).
Table No.1
Profile of Hospitals Studied
Bed
Strength
Avg.Occc.
/Month.
Avg.
CP/Day .
Government
Case I
Case II
Case III
453
686
764
340 (75)
480 (70)
691 (91 )
700
1000
1 240
Private
Case IV
Case V
Case VI
575
800
80
4 n (?n)
7!’O (94)
46 (65)
7 6/1
772
50
Note: Avg.Occ: Average Occupancy , OP:Out Patients
Figures in bracketts a^e per cent
5
Table No:2
Detai 1s of Staff
Doctors
Per. Con. Std. Tot.
Govt.
30 40
Case I
62
Case II 65
75
Case III 32
Private
5
Case IV 58 6
173
Case V 146
14 43
Case VI
Nurses
Others
Per. Std. Tot. N.Aid Help. Para
20
27
35
70
1 27
107
79
123
181
800
140
180
87 9
263
361
45
29
40
1 25
90
115
69
319
54
1 76
408
25
240
299
416
707
25
50
191
18
90 45
175 331
4 28
Note:
Per : permanant,Con:Consultants, Tot:Total,Std:Students,
N.Aid:Nursing aids/Ayahs,Help:Helpers/ward boys/sanitary workers
Para:Paramedical staffs
From the above two tables it is evident that there i s no
substantial difference in occupancy rate across hospitals. On an
to get more out patients per day
average, government hospitals ten'd
\
In terms of number of doctors and
compared to private hospitals,
discernable
trend in government and private
nurses there is no
is
variation
in their numbers
Trainee
hospitals, though there
staff (medical & nursing students) also varied across the hospitals
studied as per the bed strength of the hospital. Since there are
no norms available to comment on absolute numbers, we need to
resort to comparisons across the hospitals in terms of certain
ratios like bed strength to personnel and occupancy rate to
personnel (Tables 3,4 & 5).
Table No.3 Comparison of Personnel & Occupancy against Bed Stength
of Hospitals
Avg.Oc.Rate
Govt.
Case I
Case II
Case III
Private
Case IV
Case V
Case VI
Bed Strength to
Doctors
Nurses
Per. Tot.
Per. Tot
N.Ai ds Hel. P .Med
.75
. 70
. 90
.07
. 10
.04
. 15
.19
. 14
.17
. 18
. 24
1 .95*
. 40
.50
. 10
.04
.05
. 28
.13
. 15
. 04
. 04
.05
. 70
. 94
.65
. 10
. 18
. 18
.12
.40
. 80
. 31
.51
.31
. 80
. 90
.31
.09
. 24
. 23
. 16
. 22
.05
.08
.41
. 35
.Help -.Helpers ,
Note:Per : permanant,Tot:Total, N.Aid:Nursing aid
P.Med:Para Medical staff.
* 800 nursing students get apprenticeship in this hospital.
not vary
The ratio of bed strength to occupancy rate does In both the
and government
hospitals.
substantially across private
p. . _
cases it is well above 70 per cent except case IV, which shows a
relatively high capacity utilisation in terms of beds, In terms of
personnel to bed strength, there is a clear case of private
This essentially means
hospitals ahead of government hospitals,
have
to provide services
to
that personnel in government hospitals h._
•
more number of patients on the average, when compared to
hospitals.
Does this mean workload in the case of government
hospital personnel is relatively high ? In order to answer th. s,
we need to look at'personnel against average occupancy rate.
Table No.4 Comparison of Average Bed Occupancy Rate to Personnel
Avg.Occ.Rate to
Doctors
Nurses
Per. Tot.
Per. Tot
Govt.
Case I
Case II
Case III
Pri vate
Case IV
Case V
Case VI
N.Ai ds
Hel .
P. Med
.09
. 14
. 05
. 20
. 30
. 20
.23
. 30
. 30
2.6
. 55
. 52
.13
.06
. 06
. 37
.19
.17
. 06
.06
. 06
. 14
. 19
. 30
. 20
. 40
. 17
.43
. 54
. 50
1 . 03
. 90
. 54
.12
. 25
. 40
. 22
. 23
.09
.11
. 44
. 60
Note:Per : permanant,Tot:Total ,
P.MedrPara Medical staff.
N.Aid:Nursing aid
, He 1p:He 1pers,
Taking occupancy rate for comparison, we can see that pri vate
hospitals have higher permanant doctors per occupancy compared to
government hospitals. This ratio narrows down to a 1. iimmi ted extent
Stir
if we add consultants and house surgeons to this categroy.
on
an
average,
government
hospita
one can safely conclude that on an average,
doctors service more number of
of patients
patients compared to private
Coming''"to
other
staffs,
there is clear evidenci
hospital doctors. C_
of
occupancy
rate is high in
that the staff work load in terms
to
private
hospitals.
Glaring
government hospitals compared
para medical staff an d
differences can be seen in the case of
1
nursing aids.
Table No.5
Out Patients
Comparison of Personnel Against
Out Patients to
Doctors
Nurses
Per. Tot.
Per■
Govt.
. Case I
Case II
Case III
• private
Case IV
Case V
Case VI
N.Aids
P.Med
.04
.07
.03
. 10
.13
.09
.11
.12
.15
1 .3
. 30
. 30
.06
.03
.03
.03
.03
.03
.08
. 19
.30
.08
.40
1 .08
.23
.53
. 50
.50
.90
.50
.07
. 25
. 36
.06
.43
. 60
, Help:Helpens,
N ,Aid:Nursing aid
:
permanant
,
Tot
:
Total
,
Note:Per
P . Med:Para Medi cal staff.
AS these hospitais need to
1
?'"n
in
to look at the work load with resp
e g tpat
,„.der to get a
.be- a
well . The
Zb^f" doe^sAttend!ng9per out patent is high in the case o f
•■
.
a -•uniformly
) government hospitals^
.
private hospitals compared to <
reveal
that
private
other personnel ro/cc
.
thpir
high ratios with respect to load
of out patients compared to thei
hospital staff has less work
ce.
counterparts in government servi
;
is high
as the above analysis indicates,
indicates there
there is
high level of «erk load
1 personnel compared to
in the case of government hospitaj
and
to bed strength, occupancy al 1
in private hospitals with respect
it has to be recognised that, in
_:
• .
Besides
this,
out patients.
■' ; there exists more beds than what i s
hospitals
the
the government
l
For example, in case iy> w 1 ® this
I
/
sanctioned,
actual 1y
764, there exists 961 beds.
To this
sanctioned bed strength is
workload of government hospital sta.+ is an
extent the recorded \— •• ■ under estimate.
the
of government hospitals,
case
norm
It can aslo be seen that in the patient
+.^^4- i
below the standard f
number of permanant nurses per
.
this norm.
It can
of i-3 Private
private hospitals
hospitals seen to be fo lowing tn
the case of
also be seen
seen that
that this
this ratio is maintained in students f rom
•government hospitals with the help of^sing
government as
as private
private nursing schools.
as well
well as
" like nursing aids and helpers/ward boyb, we
Coming to support staffsubstantial disparity across government and
see that there is no t
two
is/the^aX
ornuJs
’
in?
aids
andXlpers
against
private hospitals,
government hospital
hospi tais
noy rate ,is
very low.
bed strendth, and ddcupancy
’^^8°.
”'the c1ty”° located at
onesfact
in that there are
Viz. , case II & 111, are the
or> prominent
>
1 ess
the most populous areas of the city.
city.
qenerai maintenance of
ect in the genera,
nursing aids and helpers refl
reflect
"leanness and
end hvaiene
hygiene of the
th. hsopitals
hsoditais as «e shal i s^e in
subsequent analysis.
■
; with the officials that, in the
It was revealed in our discussions
the
sanctioned
251 positions of group D/
case- of Case 11 , against 1--- -
(Nursing aids & helpers), the effective strength is only
class IV
’
209, which ’leaves caa gap of 42 positions to be filled in. Similarly
in Case *11,
III, of
c. the
-- 343 sanctioned positions, there are only 301
group D working staff, which leaves again a gap of 42 positions,
It was mentioned by the officials that, for the past three years,
■ ■ ; were freezed by the government
appointments for group D positions
that these -these posts were
for lack of funds. It is to be noticed
i—.
this vacant positions,, those staffs
fixed 40 years back. Besides
-- —
agai nst
thei r
and
postings
are
done
i,
whose
transfers
choices/priorities tend to go on long leaves.
Analysis of Pay Scales
As we are aware that in any professional service, monetory
compensation becomes a crucial incentive for the personnel to
deliver services efficiently, This is the case with health sector
as well. A comparison of pay scales of different grades of staff
’ i order
to see whether any disparities exist
is attempted below in
c.
government and private hospitals and any linkages of that
between c
Table 6 provide 5
to the performance and work load of the staff.
of staff in th 5
data on compensation package for each grade
hospitals studied.
Rs. )
Table No, 6 Pay Scales of Nurses, Ward Boys, and Ayahs (in
Ayahs/Wardboys
Nurses
SSN
SN
Cases I,II & III
840-i340
1720-3300
1520-2900
Pay Scale
Nurses
WS
SSN
SN
Case IV
1750-2650
1830-2770
1490-2350
Scale
V
SN
Case
1 570-361 1
Scale
. Nurses
SSN
1770-4071
Ayahs/Wardboys
SWS
2150-3030
910-1350
Ayahs/V/ardboys
Sup.Nurse
1910-4393
850-1955
Wardboys
Ayahs
Nurses
1469
1
658
2000
Consolidated
Case VI
(821 basic + 900 VDA) (758 basic+900 VDA) (569basic+
900 VDA)
Government hospitals have a standard package of pay scales for
different grades of nurses and other support staff.
In these
hospitals appointments are made by the government health department
after going through a process of selection.
Private hospitals follow different pay scales and there is no
uniformity in terms of grades within a job type and the
compensation package. While all the hospitals follow a package pf
basic pay and dearness allowance, which is linked to cost of living
index, Case VI, follows a method of basic and variable dearness
allowance based on minimum wages act and arrives at a consolidated
pay for various grades of staff. A compariswn of government and
private hospital staff in terms of pay reveal that except in the
case of Case V, other two private hospitals have relatively low
salaries for the nursing and other support staff.
....
. . - the
data that government hospital staff ^re
It can be inferred
from
paid coinpetet i ve salaries when compared to private hospitals.
r •
Along with monetary compensation, training and motivation of staff
nlavs a crucial
crucial role in
in determining
determining the
the efficiencey of the servic
plays a cruuia_ role
_
_ _
--- availability of such incentives
delivery. Table 7 provides data on a. — ,
in the hospitals studied.
s
Table No.7 Training and Motivation for Nurses, Ayahs &_Ward Bo>
Moti vati on/Reward
Evaluation
Trai ni ng
Ni 1
Ni 1
Ni 1
Case I
Nil
Ni 1
Nil
Case II
Ni 1
Ni 1
Ni 1
Case III
Case IV
Case V
Case VI
Probation
Probati on
Ni 1
Ni 1
Yes
Yes
Ni 1
Yes
Ni 1
It can be seen that government hospitalIs are completely devoid of
schemes operational.
any training, motivation and evaluation
c. — . — have
In government hospitals doctors and nurses appoi nted will
is
such
training
thei r appointment,
appointment, and no
training prior to their
our
during
available for rest of the staff. It was revealed
discussions that these trainings for doctors and nurses are
irregu1 ar1y held, which according to some officials amount to non
of evaluation,
existence of any such training. There
.— - is
•- ,no system
.
incentives for motivation for the staff in government hospita11 s.
'Promotions are given based on the seniority following state
government rules.
Some of them h ave
This is not the case with private ;hospitalIs.
probation
and
evaluation
systems,infornal
training in the form of
as well as formal are in place. Incentives are also operational in
...
the case of Case V, which also has an excellent system of traim ng ,
a
and evaluation systems for group D staff.
In Case V hospital
process of four evaluations during the probationary period preceede
ar
confirmation of a temporary staff nurse who has to under go simi 1.....
staff nurse
I evaluation process to reach the confirmed staff
nurse st^ge.
for
ward
boys
which is of
. Similarly there is a training programme
has
a
reward
system
wb i ch
\1 one year duration.
This hospital
awards
.
’
best
department
’
'operates through 'best w^d’ and
Customer Service:
On this front, there are variations across hospitals in termq -.of
All the
attending to complaints from the patients and public.
hospitals have reported having complaint book/box which are
But most often, complaints are
supposed to be checked every-day.
' > doctors/RMO during their■ dai1y rounds i n the
conveyed orally to
hospitals and to the
t.. ward supervisor/nursing
case of government
<
The us jsa 1
superintendent in the case of private hospi tais.
related
to
cleanliness
of
complaints in government hospitals are
the wards and against individuals.
In government hospitals there seems to be no mechanism to attend to
the complaints as rfiany officials reported that they will not be
able to take any action on erring nurses or ward staff due to
’ strong political affliations of the respective unions. In the case
of senior officials, most often informal channels are used to
address any complaints, as senior medical officers do not exercise
their powers to take action on any complaint against doctors/senior
staff. A related difficulty faced by the senior officers is that,
certain complaints like water shortage etc often falls beyond their
capacity
to address,
which
makes
the services s or
sati sfacti on.
At the same time, another official revealed that they usually ge
fewer complaints when compared-to private hospitals mainly due to
three reasons. One, the kind of patients they get are usually from
the low income group and tend to be less demanding and less
articulative about the ’free’ treatment they recieve, second, those
from other income groups, most often government servants, who also
recieve it almost free, will either be a 'private patient of a
doctor in which case he/she sees to that the patient recieves
better care, or manage to get the same services by bribing the
concerned personnel, and the third, the expectations of patients on
services and their demanding capacity are low, since they do not
pay for it.
In the case of private hospitals, complaints are often related tc
maintenance, which will be addressed immeaditely by the concernec
senior officials and the redressal mechani sms are in place and work
effectively to the satisfaction of the patients. This stems from
the fact that in private hospitals
management bestows greater
degree of autonomy to the senior officials who take decisions as
and when the need arises.
___ ' " ’ *
There is no record of patient satisfaction
surveys> i n the thre^
Except
in
case
VI, other two privat^
government hospitals studied. I
hospitals had conducted patient satisfaction surveys two years ago
These two hospitals are planning to havej one more survey in the
coming year. In these two hospitals, based on the previous survey
findings,
improvements were made as per the demands of the
patients. Issues like timings of diet, visitors,, and ingredients of
the diet were attended to based on the patient satisfaction
surveys.
Standards of service/Operational Procedures
■
■
- ’ All the three government hospitals
follow
ant administrative manual
published
by
the
directorate
of
health
Thi s
which is |-- - ----,
. .services.
-•
■'
re
-]
a
t,ion
manual provides rules to be followed by the officials
____ t c.
of the
staff —
and considerations and categories that
to management
-- --are applicable to patients. These hospitals have to produce month 1y
financial reports along with basic statistics of admissions,
discharges, operations and out patients (department wise) to the
directorate of health services.
In the case of private hospitals, respective managements set the
rules and regulations.
In this sense there is no standard
operational manuals for private hospitals. But they follow servic e
manuals prepared by their managements in the case, of
human resource management.
hospitals studied have expressed strongly for the need for
a standard operational manual for different categories of hospita
irrespective of the type of management viz.,private or government,.
They support this for the following expectations.
•
1 .
It
ensures
bas i c
-
‘
-
necess i ties,
re 1 event
upgradati on
-
Q
and
n
the cohere,a, attitude
and corruption which has crept into the medical field.
3. Ensures good quality of health service to the poores
4*. Ensures that health care is a service and not a profit making
i ndustry.
On implementation of such standards, some officials interviewed
have opined that it will not come about by building more number of
big hospitals in the urban areas but by upgrading the existing ones
with more specialisations and facilities and by building smal
hospitals with primary health care so that population in a
particular geographical area can be serviced. Some other officials
were sceptic about the implementation of such standards and opine
that such an action needs tremendous political will.
Similarly, their opinion regarding arriving at and adopting a
system of health care services such as the one in U.K (NHS) , weite
divided.
Some officials welcomed such a proposal but were verpy
n
them, we have to go a long way
pessimistic. According to them,
n
an
implementation
and
overcoming the hindrances for such
Issues
like
un
affordability
creating awareness among the people.
.
of primary, secondary and teritory services, varying education
levels., lack of transport facilities were seen as areas o. concern
by many in adopting a national health service system.
Hospital Policies:
All the hospitals have elaborate systems of documentations as far
as the admisisons, treatment, discharge and other records of the
There are prescribed, printed formats (in some cases
patients.
files) for admission record, doctor’s note, nurse’s note , billing,
progress record, medication record, daily record, 1 ab reporjt,
graphic charts and discharge summary (See the enclosed file for a
sample of forms prescribed). In this case , government and privste
hospitals exhibit no disparity. But in government hospitals there
ntained or
Mis
maintained
c.
i s no
no mechanism to check whether these records are mai
\\not.
Rates of Services Provided:
, i , differs between
____ type of hospitals.. Government hospitals have
This
elaborate rules which govern the rates charged for various services
like provision of bed, medicines, operation costs, tests and food.
tIt
+ mairniw
pvpIs of the patients.
mainly HononriQ
depends nn
on thp
the incnmp
income Ilevels
patients, Government
employees and pensioners are charged differently, based on thei r
salary drawn.
For example, in Case I, the following are phe
charges for various services.
Differential rates are adopted mainly based on the income of the
patient and as laid down by the government of Karnataka. There are
two types of wards: general ward and special ward. General w&rd
follows three categoriesof income: below 600, above 600 and above
1200. No charges are taken for beds from any of the general ward
category. For the first category all the services and other things
are absolutely free. This includes food and operations. Second
category has to pay half the charges and the third category full
charges. In the special ward, three types of beds are there: qeds
which costs Rs.7.50 (40 in number), Rs.12 (10) and Rs.15 (2). Food
is fre^ for everyone, except for government servants whose basic
12
• : at times due to water
wards twice aa day
day also
a! 5° becomes
D®c°mes problematic
YTToYfYciVl
the officialss’ iinn thi
‘---s regard is
scarcity. A major complaint
complawt from
This
seems
to
be
case,
as
This seems to be the
the
case,
lack of sufficient number-of staff • ™
many
posts
government hospitals on an average has less heipe
At the
of that grade have» not
been filled for
1 «
government
not been
sametime, there exists
certain
types
of
groyp^
jpbs_i_|_,
exists certain
be un
hsopitals which seems to
to.be
relevance and proper job
functioning of the hospital
hospital .
Lack of reiev^
description for many group IV j
nt-il-itv of certain staff
efficient. Officials could not explain
are
who are recruited against group
seargent cycle orderly,
no clear job descriptions for jobs like seargen ,
q +" r*
kit boy, literate attendant etc.
Motchi (cobbler), street bearer,
work on an adhoc manner.
Officers tend to give them
t-- some
--
Table No.8 System of Management of Waste
I
II
III
IV
V
VI
—>
2
2
2
2
3
2
Cleanining (No.times
a day)
Yes
No
Yes
No
No
No
Water Scarcity
Yes
Yes
Yes
No
No
No
Power Shortage
Yes
Yes
Yes
Yes
Yes
Yes
Supervi sion
No
No
Yes
Yes
Yes
No
Inc inerator
Yes
Yes
Yes
Yes
Yes
Yes
Pit
2
on
demand
on
demand
1
1
1
Collection of waste
(intervals- months)
pri vate
pr ivate
private BCC
BCC
BCC
Cases
Hyqei ne
Waste Management
Waste Collection
agents
Note: BCC; Bangalore City Coroporation staff
record in waste management,
Private hospitals seems to have better
facilities
as they do not face
They also have better hygiene
problems of water scarcity and power shortage.
have functional
In government hospitals, onl y- one of them
incinerator
which is
the
incinerator.
In the case of Case II >
power'
lack
of
50
KV
installed is not functioning, due to the
i
nci
nerator
.
have
• supply. Two out of the three private hospitalssize,
manages
waste
The third hospital under study, being small Jn l
disposal by resorting to 1the
-- services of city corporation
staff.
14
pay is above Rs.1640. Ward charge reductions for the government
servants are also made based on the basic pay. These reductions are
as follows: basic pay upto Rs.1000-2/-, Rs.1000-1500-5/-, Rs.15002500-8/-, Rs . 2500-3000-1 0/-. For government pensioners, food is not
free for those whose pension exceeds Rs.500, but ward charges are
free. For Rs.500-750 category, ward reduction is'Rs.5, for Rs.7501250-8/- and for Rs.1250-1500-10/-. Reductions in the lab services
are also done in the same way.
In the case of CASE II and III hospitals, categories of beds differ
while the rest remain the same.
For example, in Case II, in the
special ward, there are five types of beds. The cost varies from
Rs.7.50 (20 in number), Rs 15 (10), Rs.30 (6), Rs.100 (6) and
Rs.225 (VVIP rooms 2 in number).
In the case of private hospitals, on an average, the charges for
services are high compared to government hospitals. But, as the
sample hospitals studied work on a principle of charity, the
administration have discretionary powers to write off the bills in
the case of poor and deserving patients.
There is wide variation across the private hospitals studied in
For example, bed charges
case of charges for various services.
vary between Rs.15 for a general ward bed in the case of hospital
IV to to Rs.400 for deluxe ward bed in the case of hospital VI.
Within a hospital, there are various types of wards which will have
different charges, based on the services provided.
In Case IV, differential charges are applicable to the kind of ward
that are chosen by the patient. There are three kinds of wards:
general, semi-private and private. In the general ward a bed is
charged Rs.15. Semi-private wards contain rooms with 2-6 beds
ranging from Rs.45-110. Private wards are single bedded rooms. The
rent for these rooms are Rs.200-235. Whille medicine charges are
not under any kind of reduction, food, lab services and operation
charges vary according to the wards chosen by the patient. For
example, the operation charges for a ceaserian delivery is Rs.1600
in general ward, in semi-private ward, Rs.3000 and in private it is
Rs.4000.
In the case of CASE V & VI hospitals the charges are of similar
In
nature with minor variations, based on the services provided,
the case of hospital V, a medical social worker intervenes i n
matters of rates which are not affordable to the patients.
Hygiene and Waste Management
The efficiency with which a hospital provides services is reflected
in their systems of hygiene and waste management, On this front,
there is a marked difference between government and private
While certain operations like cleaning the
hospitals (Table 8).
is
mandatory in all hospitals .certain
premises and wards
the
government hospitals result in sub
difficulties faced by
the
hospital management in maintaining
optimum performance by
hyg i ene. For example, water scarcity, irregular power supply lack
of incinerator to burn the waste - absense of which leads tc
dumping of all the wastes into a pit in the hospital premises- anc
are collected by the private agents at irregular intervals- lead tc
poor hygiene management in government hospitals. CCleaning of the
I
‘ , waste
It is reported by the government hospital officials that,
corporati on
col lection is given to private agents because
endeavours in this regard turned out to be unreliable in the past.
the same work
<----- hospitals
---- ---- get
But as seen in the table above, private
•j.j corporation staff effectively a^nd at regular• interval s.
done by the
It is not clear, why the
This needs attention and clarification,
get
the services of the
government hospitals are unable to
a
deliberate attempt on
corporation ? or do we have to see it as
the part of hospital administration to give waste disposal
contracts to private agents.
Most of the officials hold the view that 50 per cent of complain ts
regarding the hygiene and cleanliness of government hospitals a re
'imaginary’. They account for the rest as, the kind of patier ts
they get come from low income categories with unhygienic
practices,and additional beds they provide on obligatory basis on •
emergencies make the existing system iinefficient. In this regard,
an official used the analogy of the claims of convent/pub1ic
schools on their better results when compared to government
hospitals. The same is true regarding the performance of hospitals
on records,like mortality rate. For a private hospital, there is no
obligation to attend to all the cases they recieve where as this i s
not the case with government hospitals.
There is no infection control audit in none of the government
hospitals. According to them, 'every thing is made infection free’
Tn stark
and claim to have been using disposable syringes alone;
In
j
’
have
infection
audit
committees,
contrast, private hospitals I.
V
,
the"committee
meets
occasionally
and
in
Case
cases of IV & VI, t..~
—
may
or
more
frequently
as
the
case
it meets once in three months
be.
On Corruption in Health Care Services
As part of the survey, we attempted to address this issue through
informal interviews with some officials of the hospitals.
It is popularly assumed by many that there is wide spread demand
for speed money (bribe) in
i n government hospitals at almost al 1
levels.
This was answered affirmatively by both government and
private hospital officials.
At the lower levels bribe is so
rampant that, in one of the government hospitals, as reported by ■
the officials themselves, to reveal
the sex of the new born baby,
r
the attendants demand bribe from the patient’s relatives.
It was
reported by the officials that they can do very little to stop such
happenings due to the presence of strong unions of staff. Bes i des
this, it is felt by the authorities that_patients take initiative
in giving tips to get the services done instead of complaining.
At the higher levels, patients are favoured with specialised care,
for
once the doctors
are
'met at their private clinics
consul tati on’ .
" > opine
But as already mentioned,many government hospital officials
cent
of
the
complaints
on
government
hospitals
that about 50 per c--are imaginary.
And they strongly feel that ’ anything that is
given free is not valued’ and recommend a nominal admission fed and
some mechanisms by which income levels (of the patients) can be
checked, which will improve income of the hospitals and ar rest
corruption to some extent, In the present system, anybody who is
not in government sector can claim to have income below 600 or 1000
to avail of the facilities given to these income categories. Many
officials
account
for
corruption
as
''corruption
breeds
corrpution".
For example, according to some • offici als , bribing
concerned officials to obtain tranfers and postings in government
hospitals is a common feature.
Summary and suggestions
’ > understand various dimensions of urban
This study attempted to
in
te7ms
of
the nuances in the performance of private
health care
and government hospitals. The study looked at indicators related to
occupancy, professional personnel, support staff, their management,
patient satisfaction,
hospital policies (including personnel
policies) to understand the linkages between quality of service
provision and management.
It is argued that there is increasing demand for private health
care for its efficient delivery system.
This argument is ofter
posed against the inefficiency of government hospitals. Our study
reveals that the occupancy rate in government hospitals is as high
as that of private ones.
This indicates that, there is greater
demand for public health care system which needs to be revamped to
meet the demand. This also indicates that privatisation is not the
alternative but, improving the delivery of public helath care is
the need of the hour.
It can be seen from the data that there is substantial difference
in the work load for doctors, nurses and paramedical staff in terms
of bed strength, occupancy rate and out-patients. There is a clear
evidence that government hospitals have to attend to far morb
number of patients compared to private hospitals.
While there is higher work load, it is also observed that in
government hospitals, the number of nurses employed are far below
the norms set for serving the patients.
It is also observed that \
at group D level, there are quite a few vacant posts (staff like
nursing aids/ayahs and ward boys/ helpers) which would have
increased the work load of these sections who are responsible fo,_
maintaining the hygiene of hospitals.
In contrast we see that
hospitals,
private hospitals have sufficient number of staff to attend to
hygiene and waste management.
Corruption practices and work load seem to have high corre 1 ation:
when there are more work to be attended, they try to be choosy
based on the monetary tips that is offered. The popular notion
about the services of government hospitals are supportive of this,
as patients offer money as though it is mandatory.
Coming to monetary compensation to the staff, there is no /
appreciable difference between government and private hospitals
especially related to jobs like nurses, nursing aids and helpers
But there are differences in various categories within a posi tion
For example, in private hospitals, there are various position s
within a job type of 'nurse’
where promotions in terms df
I (=,
KU.
responsi bi 1 i ties and pay scale are more easy
floor supervisor, ward in charge etc.).
(ward
supervisor,
While all the hospitals have complaint redressal mechanisms, there
is a clear disparity on actions taken on complaints.
Private
hospitals are far ahead on this front, as the decision making power
is completely left to the senior officials and there is certain
amount of decentralisation.
In contrast government hospital
officials seem to be hesitant to exercise the powers bestowed on
them for they encounter the following situations.
a.
On colleagues of equal rank, they cannot take any action but
refer the complaints to higher ups
b. On group D staff, they would not like to take action as that
would create unrest due to the interference of unions which got
strong political affiliations.
the i r
beyond
be
wou 1 d
c. On
some
occassions
complaints
administrative powers to handle.
i
,
seems to have better hygiene and waste
Private hospitals
management. This~ stems from the fact that there are clear division
of labour among the staff and the line of command is clearly spelt
Added
out. The
ihe same was not the case with government hsopitals.
hsopital
Tess person power and l o, r' I-'
to this, government hospitals have less
In
facilites like adequate water supply. 1.. some cases power shortages |
often result in lack of cleanliness, Absence of supervisory
positions with adequate power of management make it even more
difficult to manage with the existing staffs.
The most important differnce in terms of the quality of services
rendered by private and government hospitals stems from the work
environment and the work culture existing in both, the cases. There
is no continuous monitoring or Jcasqional evaluation and a sense of
commitment is totally lacking in government hospitals as they do
not share the ownership.
This is equally applicable to the
patients also. For the staffs, salary is assured irrespective of
the quality and amount of services they attend to and. for the
patients, it is the cheapest service available than a basic right.
In private hospitals this is maintained through 'role models.’
Suggest i ons/Recommendati ons:
organi sati onal structure needs a
1. Hospital management and organisational
The
mmen u nospi
ua 1.
irie work
wurn
complete overhaul in the case of government
hospitals,
area
of
concern
which
needs
load of doctors and other staffs is an u. _
attention. The first step can be filling the vacant posts and
and
non-functi on i ng
that
posts
the
deleting/reshuffling
unspeci f i ed.
2 . The practise of doctors being appointed as administrators in
government hospitals seems to be a problem as far as the poor
management of human as well as other resources are concerned, since
they are not trained in administrative/management skills. The
relatively superior management systems observed in private
to the fact that these are managed by
hospitals can be attributed
a— .
'administrators,’trained or experienced.
3. The efficiency of the hospital lies in the nursing care
provided. Better nursing care is assured through divison of labour
and continuous monitoring created through different categories of
I1
For example, superviory level staff at ward/floor
nursing staff..
who ensure
efficient management in private hospitals. This
1evels, \
.
the i r
hospitals
need
to
reform
is
one
area
government
organisational
structure.
4.
Greater devolution of power to the senior off i ci als i s
necessary in the case of government hospitals which ensures
effective handling of complaints from patients thereby ensuring
efficient management and customer satisfaction.
5. It is clear from the analysis that government hospitals has high
occupancy rate.
This can be translated into efficient income
improving mechanisms if there are systems introduced, which wi 1 i
ensure identification of income levels of patients without giving
way for leakages.
This will to some extent arrest corruption in
government hospitals.
6. There is a need to ensure provision of medical social workers in
government hospitals to support and help poor patients. They can
provide guidelines and informations to patients in meeting the i r
demands as rights and also can act as a mediator between the
administration and the patients.
7 . There is a need to develop systems of supervision and vigilence
in government hospitals to ensure that corruption is arrested,
which will help a long way in building the image of government
hospitals. This is very important as it can initiate positive
'changes in the work cu1ture/environment of the government
hospitals.
8.
It is also essential to build systematic awareness among the
people on the role of efficient public helath care system, wh i ch
ensures demand for public helath services as it is obligatory on
the part of the government to provide health services to the people
and the poor cannot be in a position to access private services.
The presnent day duality in health care access is denying the
oppurtunity of improving government hospital management as only the
poor are accessing, it, who tend to be less articulative about the
problems and who will have limited access or information about the
redressal machi enari es.
A greater role for medical professionals and their associations
have to be recognised in this regard to influence the authorties in
revamping the hospitals with better facilities and more human
resources.
The medical fraternity has to take a pro active role
in ensuring that poor people get their due share of efficient
health care from the public system.
For the implementation of any of the above suggestions, it is
imperative to build vigilant citizens action on this front, Here i r
gcs the role of -------NGOs in initiating and campaigning for such
emerges
move7. It should be in the direction of creating awareness among the
9.
people about health care as their right, through various mechanisms,
which are effective in reaching the lower rungs of the economic
ladder.
They can .also take initiative
in campaigning for
incorporating minimum health care as fundamental right in the
constitution as such, perhaps as part of the Right to Life (Article?
21). This will provide the people a legal mechanism to seek
redressal when this right is denied. Also, bringing the medica
profession under the CPA should also be taken up, for it would
IS
J
confer certain beneficial results such as: medical records will be
maintained more rigorously, the patient’s right to information will
be respected, greater standardisation will become necessary,
. standards of nursing homes will have to improve and corruptive
practices will be checked. To begin with they can even sponsor
medical social workers to government hospitals. Implementation of
health tax for certain categories of income should also be put
forward as
outlay for health expediture tend to decrease. Any
effort for greater privatisation of health care should be prevented
on the grounds that poor will be dispossessed and discriminated.
***************
n
ROG I KALYAN SAMITI: PEOPLE’S PARTICIPATION
IN HIE MANAGEMENT OF PUBLIC
HEALTH INSTITUTIONS
I
S.R. MOHANTY
RAJIV GANDHI MISSIONS
OCCASIONAL PAPERS
DOCUMENT-002/ 96
PREFACE
/■-
In a recent report of the World Bank the dilemma of developing countries in
the field of public health has been expressed in die following manner
“Most developing countries have achieved remarkable gains in the field of
public health in the last few decades. However, to reinforce this, the deliver}'
system must ensure provision of basic services to households that arc often poor
and dispersed. Along with rising incomes, aging population and increasing
urbanisation, the demand for better hospitals and improved health services arc
rising at a time when public spending in general cannot be increased and in many
eases it is being reduced While financing increasing expectations for health care
facilities is certainly a concern for the policy makers, it is becoming increasingly
clear that people’s participation in maintenance of institutions in the field of public
health is absolutely imperative in order to ensure their smooth functioning’’
It was ironicallx the plague epidemic towards the end of 1994 in the town of
Surat that provided the impetus for an experiment to improve the public health
delivery system in Indore district situated on the Western part of Madhya Pradesh.
The steps taken by the District administration with the help of the people of Indore
to clean up the mammoth Maharaja Yeswantrao hospital which was net only
infested will) thousands of rodents but whose level of hygiene, maintenance and
patient care was appalling, provided the starting point of a project to completely
revamp die public health care machinery by bringing in public participation. The
Chief Minister of Madhya Pradesh Shri Digvijay Singh after personally reviewing
the project, directed that the system be replicated in all the hospitals of die State of
Madhya Pradesh. As a result substantial improvements in die institutions and
improved efficiency in patient care in the public hcaldi delivery system is being
effected in many parts of die state underscoring the need for greater community
control of our public health institutons.
Chapter-1
THE BEGINNING : THE INDORE EXPERIMENT
Maharaja Yashwantrao Hospital which is attached to the Mahatma Gandhi
Memorial Medical College at Indore is an institution which at one point of time
was considered to be a premier institution for providing medical services in the
country. Ever since it was established in its present form in the year 1955, while
there have been occasional moments of glory, the deterioration in the stardard and
condition of the hospital had been gradual but definite. It was the plague scare in
in
Surat in the month of 1994 that attracted the attention of a terrified city to the need
to clean-up the M.Y. Hospital In response to the plague scare a meeting was
organised by the District Administration with important opinion leaders of the
town to discuss the strategy to light the crisis. While most people stressed the need
io improve the cleanliness/civic amenities of the town, several persons drew
attention to the appaling conditions of hygiene in the M.Y. Hospital. The fact that
the hospital has become home to thousands of rats, main of whom had become
enormous in size, added a degree of urgency to the need to eradicate the rodents
and clean-up M.Y Hospital; repair the building; carry out scientific alloLnt of
space and to improve the ovu.-uil administration or the hospital as pan of a
comprehensive package to ensure a kind of metamorphosis to this premier
institution of the Statq, Hie district administration took up the task. It was called KAYAKALP ABHIYAN - or operation metamorphosis/ rejuvenation. For doing
the job quickly while maintaining people's participation and a kind of social audit,
it was decided to do it through the District Red Cross Society. In response to an
appeal made to the people of Indore, donations started pouring in. In die first week
itself, more than Rs. Ten Lacs were collected.
The mammoth 730 beds hospital alongwith five other supporting hospitals
was stripped bare and all of its patients were shifted to 12 hospitals situa ted all
over the town. The entire complex was cleaned, thus removing hundred of tons of
rubbish and killing thousands of rodents; pests and insects. Some 150 truck loads
of garbage and junk was removed from the hospital which covered a mini stadium.
I
* Ui
After this, all the physical facilities were restored and the hospital renovated to a
state better than ever before. Throughout the entire process, the team persisted
with the system of involving the people of the town in drawing up the policy
frame-work for ever}' stage of the operation. A group of citizens numbering over
100 persons and including members of the press, M Ps, M L.As, representatives
of political parties, office bearers of several associations, medical community,
district officials etc. met regularly to give appropriate advice at every' stage
In
one meeting, there was a general apprehension that unless a system was evolved
for ensuring a degree of permanency to these changes then despite our best efforts
the hospital may lapse back into its old state of decadence in no time. As a fallout
of these discussions it was decided to take the following measures at the earliest
1.
2. Introduce user charges in the hospital
3.
Initiate redefinition of administrative responsibilities
The following chapter deals at length with the introduction of user charges
redefinition of administrative responsibilities as well as the emergence of the
concept of the Rogi Kalyan Samiti.
.As is the ease with most major institutions, scientific reallocation of space
was vital to ensure smooth functioning of the hospital . As expected , this also was
the task which proved the most difficult and required immense amount of
coordination and several days of discussions . Tlic following were some of the
important results of the reallocation :
I. All the OPDs of the various departments were to be put in a single wing of the
hospital,
2. The operation theatre complexes were cleared of offices,
3. An emergency ward of 100 beds was created and set aside for unespcctcd
accidcnts/calamitics.
2
4. All the private wards being used as Doctor s consultation rooms were cleared.
5. Some 40 old rooms reclaimed after the cleaning process were used as special*
ist clinics.
6.
Doctors, specialists, wards, and rooms of para-medical staff
every
department were restricted to the wing earmarked for that department only.
7.
Pathological tests of the various departments was centralised
All the above and several other measures to rationalise the use of the
available space not only improved hygiene and eiTcicncy of the hospital but also
immensely enhanced the user’s convenience.
3
CHAPTER-11
ROG I KALYAN SAM1TI - THE CONCEPT
In most government hospitals, not enough attention is paid towards the
problems of General Administration, Coordination, Problem solving and day-
to-day management. As a result, it is left to a handful of officials headed by a
Superintendent and constrained by stringent regulations to manage the
hospitals. After effecting extensive physical improvements, on the basis of
considerable discussions it was decided to put in place a committee to act as a
!
group of Trustees for the hospital and another executive committee to manage
the day to day running of the hospital. The former group was called the ROG I
KALYAN SAMITI or the patient welfare committee. This was to be
registered as an NGO and given complete control oxer the functioning of the
hospital. The cxecutwe comnnttee was to meet even week and go into even
aspect of the running of the hospital, deliberate on changes and improvements
that could be effected on a continuous basis. While L Rog. Kalyan Samiti
had over-all control over the finances available with it. the executivecommittee was to use the finances made available to lt by the Rog. Kalvan
Samiti. Extensive duties and responsibihties were chalked-eut for each
member of the executive committee and this was reviewed in the weeklv
meetings as well as in the sittings of the Rogi Kalyan Samiti.
bi an cflon io improve the financial strength of the institution, it was
decided to introduce user charges in the hospital as it was believed that
excellent health care on a continuous basis cannot be ensured without adequate
financial provision. At the same time it was also felt that free health care was
not perceived as the best kind of health care by the patients themselves. A
'/
committee was set up to determine the modalities for introduction of user
charges.
t
The following broad guidelines were drawn up for the system of
levying user charges :
4
1.
Charges must be levied for all facilities provided in the hospital including
the outdoor patient ticket, pathological tests, indoor beds, specialised
treatment, operation etc.
2.
Tlte poor section of the society and other groups as determined by the
government (for example persons below the poverty lines, freedom fighters
etc.) would be exempted from the levy.
3.
The charges for the general wards would be nominal, while those for
patients in the private wards could be higher. However, in no ease should
be charges in the private wards be higher than 50% of the charges for
similar sen ices in the private sector.
I
4.
Funds received from this would be deposited with the "‘Rogi Kalyan
Samiti” (patient welfare committee).
User charges were introduced in December 1994 for the first time in
the M.Y hospital The charges were extremely nominal and were restricted to
a few items initially. They were expanded and made more comprehensive after
two months. Die progress oi the project was reviewed on a regular basis by
the State Govt. In one such review at Bhopal, under the express directive of
the Chief Minister, the State Government took a policy decision to ensure that
Rogi Kalyan Samitis be set up all over the State of Madhva Pradesh. The
basic characteristic of the Rogi Kalyan Samitis would be as follows :
1.
Rogi Kalyan Samitis (RKS) would be set up in all medical colleges,
district hospitals, community health centre levels.
2. The RKS would have people’s representative, health officials, local
district officials. Panchayat Raj representative as well as leading donors as
their members
3
Hie RKS for its functioning shall be deemed not as a government aucncy
but almost as an N.G.O.
4.
The RKS could utilise all government assets and services to impose the
charges. It would be free to determine the quantum of charges on the basis
of the local circumstances.
5
5. The funds thus received will not be deposited in
- bo a^aaMe „ bo !pa„,
tlic state exchequer but
lk
K.K.S.
Apo,, fro,„ fund!
„pos. ion of
bos b» a
I
argc. The RKS. can use these funds for
1.
Ensuring cleaning, security and other sen tees of the
hospital through
private agencies.
2
Providing unproved facilities by addmon
or upgradation of O.T.
complexes; bum unit; ICCU
paedtatric (ICU); CAT-scan units;
centralised pathological set up etc.
Purchase of equipment, chemicals, furniture
ctncicnt running of the hospitals.
4
P».rt,„s
™d other necessities for
t.d
r
“7' 'l"“Sh
trom financial institutions.
5.
.bra,Bh ,rans
^ovuling a better atmosphere, proving thehiues
for attendants and
■■osur.ng hppro^j lncd|ca|
6.
Endeavour to provide medical
extremely subsidised rates as
care to the poor and needy free of cost or
compared to private hospitals.
6
CHAPTER - III
ROGI KALYAN SAMITI - THE RESULTS
In the last year or so Rogi Kalyan Samitis have been set-up in all the
45 districts of the State. While in some districts the registration has been done
of the committee at all the three levels, in a handfill of districts the process is
being completed. Most of the district hospitals have introduced user charges
' »i
and most improvements have been concentrated in these hospitals, but several
enterprising officers posted at subdivisional levels have also carried out similar
exercises at sub district level hospitals..
One of the most heartening experience has been that MP's. MLA’s.
Office Bearers of Panchayati Raj institutions as well as people at large have
i
been enthused into taking active part in this process. The following have been
some of the highlights of this experiment in the past two years:I
I.
A total of over Rs X.00 Crores has been collected by the various districts
through donations and introduction of user charges
2.
MP’s and MLA's have earmarked funds out of their discretionary MP and
MLA funds for improvements of health institutions.
3. The District Red Cross Society have been functioning in tandem with Rogi
Kalyan Samiti and they have in turn become more active of late.
4.
In most hospitals after the introduction of user charges, privatisation of
various ancillary services viz maintaining cleanliness, security and canteen
services etc. arc being introduced in phased manner.
5.
Daily collection by the Rogi Kalyan Samiti range between Rs 1,000 to Rs
15,000 in each hospital depending on location. A conservative estimate
would put the monthly collection at around Rs 50.00 Lacs.
In
most hospitals the
initial
improvement
effected
includes
improvements in the building, furniture, upgradation of equipment, electrical
fittings, toilets and drainage systems and introduction of privatisation. In
districts where ambitious plans have been put into
<
7
effect such steps as
t
construction of burn units, ICCU, Operation Theatres, hi tech equipment like
MRI s and CAT Scans, centralised pathological umts paediatr.c ICU's
sonography and endoscopy facilities have been provided or arc in the process
of being implemented.
While there has been wide spread appreciation in the improvement in
most of the hospitals the number of patients has increased after the
introduction of user charges. The availability of a large amount of untied funds
brought about the following visiblc/invisiblc benefits as delineated below :
1.
Introduction of a certain amount of privatisation reduced the pressure on
the existing staff and also improved efficiency.
2.
As the RKS was free to function as an NGO it could make Funds
available to the heads of the department to carry out maintenance and
improvements in the.r departments without being constrained by stringent
Govt, regulations.
3.
Availability of funds on a da> to-day contingent expenditure and regular
maintenance ensured better working conditions for the doctors & staff
4
Payment of a certain charges by the panent established the patient s right
io better professional medical attention and therefore he insisted on proper
service from the ofncials concerned.
>
The Doctor and the para-.ned.cal staff also felt a sense of responsibility
and moral pressure to improve their performance and v.e believe that
\vu
have witnessed a definite and positive improvement i
in [he work ethics in
the Govt. Hospitals in the last year half.
8
r
i
CHAPTER - IV
i
1
CONCLUSIONS
In a welfare State like ours, while several institutions have been created to
provide facilities and services to the people at large, very often adequate planning
and care has not gone into maintaining these institutions. As a result of inadequate
funding, lack of proper administration and even a certin degree of callousness on
I
the part of the authorities concerned, the deterioration in the condition of these
institutions and the services they provide is so marked that it often raises
fundamental questions about the abilities, bonafides and
sincerity of the
administrators concerned.
Over the past few decades the surge in population, rising expectations and
cost of health care along with a chronic shortage of vital resources has
unfortunately resulted in a dechne of hygiene, cleanliness and patient care in most
of om public health institutions
Added to this has been the alluicment of
handsome income in the private sector also resuhmg in decline in the smeentv.
motivation and dedication ot doctors and para-medic staff in the public health
institutions
From the experience of Indore and subsequent experience from other
distiicts of Madhya Pradesh, where this institutional arrangement was rcp.’icntcd.
the following conclusions can be made
I
!
-
It is important not onlx to create institutions for the public welfare but it is
also essential to ensure regular maintenance and up-keep, provision for
improved facilities, regular review of their performance and ensuring •hat the
morale of the work force remains at optimum level of motivation.
It is essential to invoke members of the society to fund and managv various
projects taken up to improve civic life and provide for better civic facilities.
While ..iis facilitates easy availability of scarce resources
on the one hand,
it also guarantees the participation of the society at large in the functioning of
public institutions on the other This forces the Government officials manauing
these institutions to be more accountable to the people at lart’e
9
-r
3.
It become clear that it is a good idea to introduce some amount of user charges
in public institutions like hospitals, schools, etc. as this generates a demand
from the beneficiaries to be given dicir due right-thus preventing callous or
irresponsible behaviour by the Government servants in discharge of their
duties.
At the same time, this also prevents unnecessary usc/misuse of die
highly subsidised government facilities by people who have easy access to
them.
As expected the experiment outlined in this report had a few detractors and
some critics but reports of unccascd confidence and satisfaction of patients coming
to the government hospital after these improvements, vastly improved the working
conditions,
improved
hygiene and cleanliness,
upgradation of equipments,
involvement of the society and increased overall efficiency that is
being
institutionalised throughout State provides the inspiration to continue with die
system, streamline it and improve it even birther
There has been an ctfort to create a system which shall be self-sustaining,
where motivation of the staff and the involvement of the public would be pan of a
system designed to guarantee functioning of the hospitals better than ever before.
These arc early days yet. How the new institutional mechanism of Rogi Kalyam
Samitis shape up to take greater control ot the health needs of the community will
depend on how much confidence is reposed by the decision makers in area of
public health.
10
io
ri
A
I
Health Care Waste Disposal
- An exploration
EXECUTIVE SUMMARY
Department of Community Medicine,
M S Ramaiah Medical College,
Bangalore - 560 054 INDIA
* 1997 *
K.
I
ACKNOWLEDGMENT
Bangalore Mahanagara Palike; Centre for Environment Education,
Bangalore; Department of Ecology, Environment and Forests, Government of
Karnataka; All the experts consulted, All Health Care Settings; Departments of
Community Medicine of BMC - Bangalore, MMC - Mysore, KMC - Mangalore,
JJMC - Davanagere; Staff of Bangalore Mahanagara Palike; Rag pickers; are
greatly acknowledged for their Co-operation, and inputs for this endeavour.
The investigators specially acknowledge the help and co-operation received
from the different Departments of M S Ramaiah Medical College; The Dean,
Nursing Superintendent and Personnel Officer of M S Ramaiah Medical
Teaching Hospital; and their colleagues in the Department of Community
Medicine, M S Ramaiah Medical College.
Interested readers are referred to the complete document for details.
T
r-
■
U02PITAL WASTE MANAGEMENT IS AN IMPORTANT
SUBJECT TWAT NEEDS URGENT ATTENTION. IN MOST
CIRCUMSTANCES IT IS APPROPRIATE TO CONSIDER AN
INCREMENTAL APPROACH REALISING TWAT AN
IMPROVEMENT IS OF GREAT VALUE EVEN IF
RESOURCES DO NOT ALLOW ACHIEVEMENT OF
HIGHEST STANDARDS IMMEDIATELY
- REPORT OF A CONSULTATION ON MEDICAL
WASTES MANAGEMENT IN DEVELOPING
COUNTRIES, WHO, GENEVA, 1992.
• /
HEALTH CARE WASTE DISPOSAL - AN EXPLORATION
Health Care Waste, if not handled properly, has the potential t<|> be
hazardous - Hazards may be because of Soil/ Water Pollution to> the
community or to the Health Care Personnel like the doctor. Nurses, Nursing
aides. Helpers, Ayahs, within the health Care Settings. It can also be hazardous
to the Pourakarmikas, personnel of Private contractors. Lorry drivers,
drivers.
personnel at incineration/ land filling sites. Rag pickers.
Hepatitis B, Hepatitis C (not in our country), HIV, Tetanus; and
Staphylococcal infections appear to be the diseases that may be
L~ transmitted.
L—— .
Enteric related infections can affect large communities.
Health Care Waste is being handled very casually in the Developing
Countries. Clear delineation of the problem and measures and methods to
solve the same needs to be modified and adapted to our needs and situations
in Developing Countries.
This was discussed by all the Medical Colleges and Health Officers o the
Bangalore Mahanagara Palike (BMP) in an endeavour organised by the Centre
for Environment Education and Bangalore Mahanagara Palike under the
Chairmanship of Mr. Yelappa Reddy, Retired Secretary II, Government of
Karnataka. Formation of an Infection Control Committee for the City and
Development of a Training/ Reference Manual to meet the requirements of
information support were the two important recommendations, which were
presented to the then Administrator of Bangalore Mahanagara Palike, Dr. A
Ravindra. Both the recommendations were accepted and M S Ramaiah Medical
College was entrusted with the task of supporting the endeavour by
developing the manual.
Department of Ecology, Environment and Forests of Government of
Karnataka came forward to support the endeavour in entirety. Following is
‘ a
brief report of the exploration done to facilitate the development of the
manual.
As the literature available which is useful to the Developing Countries is
meager, informal Consultations were held in different Health Care settings. It
was thought that with insights gained from this, one can proceed further in
developing the Manual.
EXECUTIVE SUMMARY
3
> '
HEALTH CARE WASTE DISPOSAL - AN EXPLORATION
OBJECTIVES
1 To develop a practical working manual for Health Care Waste disposal and
General infection Control in different Health Care settings.
2 To develop such a manual by a process of continued consultation and
interaction with people of different categories who are involved in Waste
Disposal and Infection Control.
This report is a documentation of efforts put in to achieve Objective number 2
Methodology
Apart from literature search and discussion within the Department of
Community Medicine, M S Ramaiah Medical College (MSRMC), two specific
activities were undertaken :
I
Visit to different Health Care settings and Informal Consultation with the
Personnel - 10 dispensaries, 8 Maternity Homes, 10 Private Hospitals and
Nursing Homes and 31 General Practitioners - were held.
Also, information was collected from 4 Medical College Hospitals and 5
Primary Health Centres by Correspondence. [Total 68 Health Care Settings
covered]
II
Interaction and Consultation with a) Experts in Community Health and
Environmental Engineering b) Junior and Senior Health Inspectors of
Bangalore Mahanagara Palike c) Pourakarmikas d) Rag pickers.
Information for the first activity was collected by using a Predesigned
Open ended Questionnaire developed for the purpose in consultation with M S
Ramaiah Teaching Hospital; finalised in consultation with Centre for
Environment Education, CEE, Bangalore Mahanagara Palike, BMP; after field
testing at M S Ramaiah Hospital.
The team which consisted of members from MSRMC, Bangalore
Mahanagara Palike and CEE collected the information.
EXECUTIVE SUMMARY
4
>
■
.—.
■■
-
■
-
■
■
HEALTH CAKE WASTE D.SP
IMPRESSIONS AND MAJOR FINDINGS
I
OUTCOME OF INTERACTIONS WITH PERSONNEL OUTSIDE Tf^E
HEALTH CARE SETTING
Six thousand seven hundred Pourakarmikas and four thousand fojrr
hundred labourers of Private Contractors take the responsibility of Solid Waste
Disposal at grass root level in Bangalore City.
Pourakarmikas find the following Health Care Waste mixed with solid
waste : syringes, needles, cotton, bandage cloth, drip sets, packing materials,
ampoules, vials, glass bottles.
Pourakarmikas appear to be unaware of the diseases transmitted by the
improper management of Health Care Waste.
Pourakarmikas like to use Gloves, masks, boots, if supplied to them.
About 10,000 rag pickers are at work in the City of Bangalore.
Pourakarmikas, labourers of Private contractors and Rag pickers a|e
exposed to the risk of Health Care Waste apart from personnel like Ayahs,
Helpers, Nurses, Nursing aides. Laboratory Technicians and Doctors within the
Health are setting.
Preplacement/ Periodic Medical Examination; Immunisation against
Typhoid, Tetanus and Hepatitis B does not exist as a system.
On an average, one Junior Health Inspector supervises the work of 7b
Pourakarmikas in one ward. Each ward, in residential area covers 10 sq. Knji;
About 50,000 population live in each ward.
Approximately 250 Kg of Solid Waste is collected by one Pourakarmika
per day through street scavenging. Approximately 45 street bins will be there
in each ward.
Health education materials on safe methods of handling and disposal df
Solid/ Health Care Waste is scarcely available and used.
About 2100 metric tonnes of Solid Waste is generated in Bangalore CitV
every day.
EXECUTIVE SUMMARY
5
HEALTH CARE WASTE DISPOSAL - AN EXPLORATION
Health Care Waste is likely to be 5 kg per day for a hospital with 15 beds
according to Junior and Senior Health Inspectors of Bangalore Mahanagara
Palike.
Health Care Waste generated in Hospitals is about 600 gm per bed per
day In Clinics/ Dispensaries, waste generated is about 200 gm per day if 30-40
persons are seen on outpatient basis. ( These are based on observations and eye
estimates during the informal consultations)
One hundred lorries belonging to Bangalore Mahanagara Palike and One
hundred and twenty lorries belonging to private contractors carry 6-7 tonnes of
general solid waste twice a day to the outskirts of the city. The lorries are open
and spillage of Waste on the roads is a common feature.
Health Care Waste is casually managed and thrown to the dustbins in the
streets often. Health Care Waste, this way gets mixed with general waste and is
collected together
Gloves and masks were not found to be used by the Pourakarmikas.
Many were found using chappals.
Disposable syringes are sold at rate of Rs. 10 per Kg and Glass bottles are
sold at the rate of Re. 1 to Rs. 2 per bottle depending on the size of the bottle.
A large amount (major portion) of general Solid Waste generated in the
City is simply dumped insanitarily a few kilometers away from the city. A
large amount of Health Care Waste finds its way out getting mixed with this
solid waste.
EXECUTIVE SUMMARY
6
I
__________________ ______________ L
HEALTH CARE WASTE DISPOSAL - AN EXPLORATION
II
OUTCOME OF INTERACTIONS WITH PERSONNEL WITHIN THE
HEALTH CARE SETTING
Segregation of Health Care Waste into Infected Waste and Domestic Waste
is rarely done in the different Health Care settings. Among the 14 Hospitals
visited, in 7 segregation of one or the other item was noticed. In one hospital, a
specific attempt was found to have been made to segregate infected waste.
Plastic dustbins in private Health Care settings and Galvanised Iron bins
in government Health Care settings are the common type of Dustbins found..
Only 22 (32.33%) health Care settings had bins with lids. And onlf 4
(5.88%) Health Care settings had bins with foot operated lids.
Frequency of emptying the bins was done once daily in 43 (63.23/o) and
twice daily in 14(20.58%) Health Care settings.
Using trolley was inoticed in 2 (2.94) Health Care settings for the
transportation of Health Care Waste.
In 54 (79.41%) Health Care settings visited, waste sharps are casually
thrown in the dust bins along with other solid waste.
Common method of disposal of Laboratory specimens - Urine/ stools and
Blood was into the underground drainage system. Only in 3 (4.41%) Health
Care settings visited, blood remains were decontaminated before disposal.
Gloves and Aprons were used by Laboratory technicians in 11 £16.17%)
Health Care settings.
Bombay broom in 36 (52.94%) and native broom in 30 (44.11%) Health
Care settings constituted the type of brooms used in Health Care settings for
sweepings.
Mopping with a Mop cloth was the method of mopping the floor in 55
(80.88%) Health Care settings, whereas Sofa stick with a cloth was used in 6
(8.82%) institutions.
In 52 (76.47%) Health Care settings, no protective devices were usqd by
the waste handlers.
EXECUTIVE SUMMARY
7
HEALTH CARE WASTE DISPOSAL - AN EXPLORATION
In 26 (38.23%) Health Care settings, in house laundry was the rule. In 14
(45.16%) of the General Practitioner's clinics visited, it was reported that linen
was washed in the Ayah's or the Doctor's house. In 19 (27.94%) Health Care
settings, services of outside laundry was utilised.
In 25 (36.76%) Health care settings, contaminated
separately and disinfected before sending to the laundry.
linen was washed
In 57 (83.82%) of the Health Care settings, no facility was available for
waste disposal.
In 26 (38.23%) Health Care settings, contaminated linen was washed
separately.
Out of the 68 Health Care settings visited, 51 (75.00%) felt that it is good
to have a common incinerator.
No Medical examination - Preplacement or Periodic, was in vogue in 60
(88.23%) Health Care settings visited.
Practice of Immunisation against Hepatitis was noticed in only 6 (8.82%)
Health Care settings.
In 40 (61.76%) Health Care settings, attitude of the respondents towards
this informal consultation was encouraging.
In 42 (61.76%) Health Care settings, willingness was forthcoming for
quantification of Health Care Waste and in 44 (64.70%) willingness was
forthcoming to take up field testing of the manual.
EXECUTIVE SUMMARY
8
r'
' *
HEALTH CARE WASTE DISPOSAL - AN EXPLORATION
- ---------------------------- - ------------------------------- ----------------------------
PROBLEM DEFINITION :
Health Care Waste is casually dealt with both by Health Care settings and
the Civic bodies. This is dangerous to Health care Personnel, Waste handlers
and the Community. Reasons for this appears to be :
1
Lack of awareness
among doctors, nurses, administrators
about hazards of improper Health Care
Waste management; options available
for its proper management; lack of
awareness among Waste handlers (
Ayahs, personnel near incinerator and
land filling sites, rag pickers) regarding
hazards of Health Care Waste.
2
Lack of Information support
for doctors, administrators, nurses.
Waste handlers
3
Lack of practices like
4
bodies of Health Care settings and
Lack of effective organisational
Lack of coordination between civic bodies and Health Care settings,.
- segregation of infected Waste and
sharps
- disinfection of infected waste
- Sanitary landfilling
- Recycling of recyclable items
- use of protective devices
- periodic medical examination
- Immunisation of Personnel
- Precautions for prevention of HIVAIDS
- Incineration facilities
meeting
Central Pollution Control Standard^.
EXECUTIVE SUMMARY
9
'*1
HEALTH CARE WASTE DISPOSAL - AN EXPLORATION
PROBABLE SOLUTIONS
CAPACITY BUILDING
of Doctors, Administrators^ Nurses,
Waste handlers on hazards of Health
Care Waste; available options for its
management; available cooperation
from the civic body - through training
and information support. Segregation
of Infected Waste promoted as a culture
in Health Care settings.
STRENGTHENING FACILITIES FOR FINAL DISPOSAL OF HEALTH CARE
WASTE
a) It is suggested that 500 acres of land
outside the city limits be earmarked,
developed and managed for Solid
Waste disposal - of which a portion
be earmarked for Health Care Waste
disposal.
b) Sanitary Landfilling taken up
c) Cooperative common incinerators
meeting central Pollution Control
Standards for Health Care Waste
which is infected are commissioned
and their function is supervised and
monitored.
d) Small industries are set up for
recycling plastic items, metal sharps
(and ? Bandage cloth after
decontamination)
e) Better transportation vehicles covered and automatic are procured
and a_ parallel system is practiced for
the transportation of General Solid
Wastes and Health Care Waste
separately by the civic bodies.
EXECUTIVE SUMMARY
10
. ...................
HEALTH CARE WASH
-
f) All Health Care settings - big and
small are registered at the 12 Sub
health Offices of the city. The Stibhealth Offices can be focal points of
support to respective Health Care
settings located in their jurisdictional
areas. Periodic returns related to
Waste generation to be submitted to
Sub-health Offices by the respective
Health Care settings. Based on
these calculations, logistics of
transportation is jointly arranged
and managed by joint contributions
and participation by both the
management of Health Care settings
and Civic bodies.
AWARENESS ACTIVITIES
a) Health education materials like
posters, pamphlets, booklets, flip
charts on Health Care Wast^
management in local language is
developed and consciousness is
created among Waste handlers and
the community
b) Community's involvement is to be
sought in identifying areas for
Sanitary land fill and hygienic
practices of Waste collection and
transport - of both General Waste
and Health Care Waste.
c) There is a need to start a resource
centre in the City which can provide
information support in the form of
periodic news letters and other
means to all Health Care settings,
NGO's, etc.
An NGO can be
supported to take up this role with
the back up of a Medical college
resource.
EXECUTIVE SUMMARY
TF|
*
HEALTH CARE WASTE DISPOSAL J AN EXPLORATION
INFECTION CONTROL COMMITTEES
It is suggested that infection control committees be established in all
Health Care settings where bed strength is more than 100 ; and the committee
to supervise Health Care Waste Management, Hospital Acquired Infections and
General Infection Control.
RESEARCH ACTIVITIES
The investigators suggest that the State Government shall encourage the
Civic bodies to take up the following research activities in collaboration with
Medical Colleges and Engineering Colleges on priority;
a) developing curriculum for training doctors, nurses, administrators, waste
handlers in the area of health care waste management
b) Feasibility studies to recycle metal sharps , plastic items in safe ways
c) techno-economic assessments of solid waste/health care waste in different
cities, towns, etc.
d) conducting waste surveys in different Health Care settings including
measurement of quantity of such generated waste
e) feasibility studies for efficient establishment and running of common
incinerators/ sanitary land filling/ composting etc.
f)
sentinel surveillance of hazards due to Health Care Waste management in
selected ranges of the City
g) studying sickness absenteeism and causes for the same among waste
handlers
h) maintenance and periodic review of morbidity registers of health care
personnel
EXECUTIVE SUMMARY
12
HEALTH CARE WASTE DISPOSAL - AN EXPLORATION
RECORDING AND REPORTING
The investigators suggest that systems of recording and reporting of the
following events are developed and submitted periodically to the infection
control committee of the city/ civic body by health care settings:
- Quantity and type of waste generated
- Illness/ injuries noted among waste handlers
- Difficulties faced and solutions adopted to solve the same by Health
Care settings in Health Care Waste management
- Immunization status of staff regarding tetanus, typhoid and hepatitis B
- Training status of staff on Health Care Waste management.
The investigators feel that legislative control is to be exercised only after
capacity building and strenghtening of facilities is taken up for two to three
years
Till sanitary land filling/ common incineration facilities/ individual
incineration facilities/ safe recycling methods of some of the items of Health
Care Wastes become available or other methods of treatment and disposal are
accessible and adopted the following appear to be the options available for
immediate action;
1) Disinfection of waste before disposal
2) Segregation of infected waste and metal sharps
3) Safe practices within Health Care settings
4) Practice of universal precautions for preventing HIV-AIDS
5) Capacity building of Health Care personnel and waste handlers
6) Document quantity of waste generated
7) Document hazards due to Health Care Waste
The investigators have made an attempt to draft a manual for training
doctors, nurses, house keeping officers, administrators and educational
material
.. ...... ....... for waste handlers (ayahs, pourakaarmikas etc.,) It is being planned
to field test and subject it for wider consultation before being put for practical
use.
EXECUTIVE SUMMARY
13
___ L
H V-li
BURNS CARE
THE PROBLEM
some sourriONS
FEW THOUGHTS
FROM: THE DEPARTMENT OF PLASTIC & RECONSTRUCTIVE SURGERY
ST.JOHN’S NATIONAL ACADEMY OF MEDICAL SCIENCES
BANGALORE.
Organ!sing burns care continues to be a major problem in
our country with the large numbers of burns and few centres
worki ng in this field. A rough estimate is that there are ap
proximately 6 million cases of which J million require admission
every year. Most minor burns over 15 to 20% of body surface
area or with other associated problems need hospitalisation.
Our centre alone admits approximately 100 to 150 patients
every year.
So the major areas of concern would be to identify the
actual epidemiology of burns in our country and to work to
wards preventing them and simultaneously create more specialised
centres, fully equipped and staffed to give adequate care.
PREVIOUS MORTALITY:
A few years ago, when we reviewed our statistics, we
were alarmed to find a fairly high mortality rate. Most of our
patients succumbed to infections, some due to respiratory
bums and occasionally early acute renal failures. In the
30-40% burns group, we had a 50% mortality rate which meant
that of every 100 admitted in that group only 50 would survive.
At that time, we had a separate ward but two patients
to a room, with nurses common to the entire ward and no iso
lation of instruments or waste of each patient.
Cotd..2
-:2:-
CHANGES MADE:
In consultation with our administrators & microbiologists,
we brought about the following changes:
1. A separate batch of sisters were posted to the burns
ward, who were to wear gowns, caps & masks at all
times and not to move to other wards, in a ratio of
1 nurse:3 patients.
2. The entry of visitors was restricted preferably to
one or two care-givers who are instructed on basic
hygiene and provided with gowns, caps & masks.
3. Each patient was given a single room.
4. Each patient was given a separate BP apparatus, thermo
meter, stethescope, bed pan & waste bucket,etc.
5. Fumigation and cleaning techniques were reviewed.
6. Dressings were shifted from a common area to indi
vidual rooms and separate sterile packs were intro
duced for each dressing. However, bi ns continue to
be used, as well.
At this point, we noticed that frequent change of Senior
Staff Nurses was continuing to be a major handicap
in improving our quality of care.
7. A Senior Staff Nurse, motivated to care for burns
was identified and sent for training and has since
been working in the burns unit. This has helped con
siderably to improve the quality of care.
8. At this point, our medical colleagues agreed to
provide us a cubicle in the Medical Intensive Care
and any patient requiring either ventilatory care or
intensive care could be treated here. This has helpec
to save a few very sick patients.
Cotd..3
-:3:-
9. When possible, in situations hither to unsalvageable,
we started excising the burns early and grafting.
PRESENT SITUATION:
A review of our last year’s work shows;
a. Our mortality rate has come down from 50% to 20%..
b. The 50% mortality had shifted from 30-40% to 50-60%.
In the 40-50%, we had almost 70% survival but this
drastically come down above 50% burns.
c . The few who survived deep burns above 50% underwent
excision of the burns and some had relation homograft.
d. Early excisions helped considerably even in the 30-50% group.
e. Above 50% deep burns the mortality and morbidity
is still very high.
f. Sepsis accounted for more than 60% of the deaths
while respiratory burns was the other major killer.
FUTURE POSSIBILITIES:
It appears at this point that if we need to further
improve the mortality and morbidity of major burns, as
well as the care, we would have to consider major changes
in the organisation and management protocols:
1. Starting a burns centre dedicated to the treatment
of burns. This means full time staff and a ward only
for burns.
2. A burns centre would include intensive care for acute
and sick patients, graded care as well as general
care with all the necessary equipment.
Cotd..4
-:4:-
3. Methods of keeping environmental bacterial count
very low like laminar air flow, air curtains, air con
ditioning, etc., will have to be incorporated.
4. Periodic surveillance protocols and rigid isolation
techniques must be practiced.
5. Early excision and grafting of the bum wound is 1 i kel y
to contribute significantly to reducing hospitalisa
tion, costs, mortality and morbidity.
This however will entail
a. More early operating time on an emergency rather
than scheduled basis.
b. Very good blood bank facilities.
c. Intensive care facilities.
d. More manpower.
6. All the above will require a large team including
intensivists, plastic surgeons, nurses, residents,
microbiologists, nutritionists,
nephrologists, phy
siotherapists and social workers.
MOTIVATING PERSONNEL:
It is no easy task to find personnel to work whole time
in burns. It is labour intensive, involves long hours and
the big dressings can be exhausting. The poor pain con
trol, high mortality and morbidity and i nadeguate monitoring and resusciation equipment probably contribute
to affecting the morale of burn care-givers. Some ways of
overcoming this would include
1. Adequate monitoring facilities including cardiac mo
nitors, pulse oximeters, etc.
Cotd..5
-:5:-
2. Intensive care facilities including ventilators.
3. Adequate staff including dressers, physiotherapists,
social workers, clinical physiologists.
4. Shorter shifts probably six to eight hours.
5. Very good pain control preferably a full time
anaesthetist.
6. Adequate remuneration.
CHOOSING THE DIRECTOR:
A major question at this point is who should head a
burns unit? The acute phase and the numerous medical
complications associated with burns are best managed by
an intensive care specialist with a special interest in
burns. A surgeon really comes into the picture for exci
sions and resurfacing and later reconstructions.
TRAINING THE BURNS SURGEON:
After training in Craniofacial Surgery, Microvascular
Surgery, Hand Surgery and General Reconstructive Surgery,
it would be a retrogressive step to limit onceself en
tirely to burns. But the only way the burns care can
change dramatically is if we have full time doctors
working only in burns. Improving working conditions
would definitely help to draw manpower into burns. The
Shriners Burns Centres and Army
Burns Centres in America
are standing examples of this. The other option is to
introduce a new speciality of burns with a different
curriculum.
DECENTRALISATION OF CARE:
Another thought is the decentralisation of burns care.
All minor and most moderate burns upto 25-30% can be
treated at the periphery. A burns network can be formed.
Cotd..6
I
-:6:-
Centres identified. Personnel could periodically be
trained and basic facilities to care for moderate burns
could be improved at these centres.
EDUCATION & PREVENTION:
Scalds in the kitchen, floor level cooking, the pump stove
appear to be major contributors to burns. We probably
do not have correct statistics regarding suicidal & homi
cidal burns related to marital disharmony. Identifying
the exact etiology, educating through the media, bring
ing in legislations and trying to diffuse marital dis
harmony, alcoholism and dowry harassment
would be re
levant social areas of work to prevent & reduce the
incidence of burns.
THE BOTTOM LINE:
Finances remain a major constraint in establishing
modern centres & running them.
1. To upgrade the major centres to include intensive
care units, good bacterial control, adequate operating
facilities.
2. To upgrade peripheral centres to treat moderate burns.
3. To employ adequate staff and pay them well.
4. To provide for care of poorer patients including
a. Medicines
b. Blood
c. Food
d. Rehabiliation.
5. To provide for regular training facilities at different levels
of burns care-givers both in India and abroad and to
have exchange programmes.
Cotd..7
7
A POSSIBLE START:
One thought is the establishment of a Burns Foundation
which could identify local & international donors and
help with the upgrading of facilities and sponsoring of
individual patients, burn units or beds in a unit, as
well as work towards social change. It could act as a
necleus to bring together people from different walks
of society, concernedabout the problems and keen on
caring for these unfortunate victims. The problems are
multidimensional and it is only by concentrated and
unselfish efforts that we can make any impact. The quali
of burns care in a country is a good reflection of
society’s concern for human life and suffering and I
sincerely wish we could start somewhere to upgrade our
care.
T
X’
5,
wit cbc'MIui TlFHld
r;
<4^4IciHIc4<l -Wi vi<r TfcTR
I
I
I
Iktelftyh M<bbJ Qifr IQ^JIr
jyiklyte
’9
Pnfi
Q
yyrp/i>i^tyte PiAjibSP
1M2
9
>
l£±b
iPh
i£ Ik 41b
jj£iPi>H>
PJ^I^k IM5 N^tell 1X143h[^ frlblktjpte
£
liik^ injky
4iip 'i^myte h^ik^j£te
3
b^teix JXIfotyte bljdk.bjPte
‘ I
(frtefrki i>i4>r?l<b
Mate
E
• % ^Jj-^^l
kl^y-JJXUA
Iftiift
3
I
klk
<klk^
kk Jk±k lisk l^h ,klpv^upj
|k!4> <£
|fr|r ihij-X
Pjiy^x >
t
I^lL^ iate Pty w £ iKocfrjty
!Mh& Jt kte^h ^iPh^te
llia£i?tF ktelfr .4>afejy (ft ^Mhyh <kii <£
^iPb^te |cj> ihiybP c£ |bi>
Inlkir,
Jj
Ikl^ lli^J J£ W^/lteWi
*9
>
'£
‘ I
\2c:
“•
iiid^
U4£
pjkj^ *£
IQ^J
........................... kQJhltb I4> PJkJ^ *3
toMfc*
tmit» suyikfiin hip 10 pjkj^ ‘ 1
(£ hiiy h^)
Kh.-khl£
bbl^h 0
L-<j3|k45 h^lK
’/•
V
........ IHh
....... klk
'L ,
‘9
*9
>
’£
'Z
’ I
£
Z
I
|£b jd£ £ ^klh
IHi £1£1 £ &L
-: Hrbl0 £ IhlW £
' L
P^j^JPi£J !Pfr*£& £> 11^£ : PjIHP Ifo IPIAb£ ■8
' v y
!£ 1P10 k-Mhtek
■£
l£ 10 I^PJFi £i P^lh <£ £iLy <£
|£ 0^£lk M£>lk
|£ k k0 £ £> 8 i Bns
c
■ I
: IPhtir? yi ££b_£
'L
Pjlft ^2 lPr^b£
■9
2in£l<LUlh£i
’0 I
r?4W
Hljdk^de
hlH^l In^M
‘6
<pjrr> <£ Pjiu\pu\ Phjfrufc ^>lb
!>>W
Mb s^pe ££ 000'1
cpj.no cb Pj;^
'8
Q!Ph&£
^Ib. ££
'L
£ /000'S^ £h£ 1^2. ^lPb£fe
■9
£l<£Qite IPUMh^Jh RlS^J
w^'
k^lhUl^
£10^p£ hiblkbjfcfc Pi^|p£
8
r?4>^
mate m^ih Mik P£££
’v
l7>b^
0klh£ PkJ0£J £ k£ Mk
£
r?4>^ .
t£k£ lk£ 01Q Phj££J £ K£ k£.
Z
male
tetafe Pl?l£h khkte P^Jb£
'I
ItaP (£1^
-
s
hk W££
’V
|JLLt£ l^Ktak
......................... IQMJ
"• K££Bk hk lt^£
------ klk I4>
’£
.. .................................... k k ■ " ■■
....frQlfrlfo
10 IfoW
y
T
............ hlk 10 lh££
'I
kkkR 0 I'nte PfolQ'
IM0 h^fc P^jb£ £
*9
IW& £ kkktS Q!Pb£fc
>
lltaikin kkJ£ 0^fk:£J £k 0Mk^|h 0h <£ ££.
’£
Ilh^bho 10 k>2P £ >£^Jh Q!Pb£fe £k
££.
■3
’I
I4.IQ 11^0]£] 10 £?<^sxa/|feK39jk ]c£ £U£jh b££)&. <£ k£ lalplk
(IPX^J |j0 P0£> £ kh khll^ £1)
C*'k)
^PblkhM Itb pjkjfr Inlt?^^ ^t\X
^0
cbkjfriK r?i^p^ £El n4a>!jj/^cb *
- k>£!4
Ij\N?Qlr£ Ib.^b?>jh
pfcjl-r ckkk
Q|p i<^9jir
'9
l^dc^jhj g-n^
■9
ms Miy ipii*
1^ 1H ISA
i?|i>ik.bjPn>
ms
rmL>
mu chi^ij 1 >kt>i<t>
IfcIPISklS
’£
'Jj-lfofyte hllHk.bjElg
Idk^ lnll;!J
l^l^t^le b^dk^Eie
’ I
-w tmm PE^jHi-j c^miy ’iw nmy j^ir im
Z I
1 mm2. k&QtPfe m um (a) iu><b p
1^ j^h nm-nm |k?ii»w pojidp ims
iid^ (n) j£ uSiA ms nmy i^m i^ urns
ih im tj
um (n) urns nyEy j£
WJ^a ia^ a^j <4 km i^iw (u) ums imms
jajap- a
£ita£ iq, mm (a) itmn
migy <uyu> 1^
<£ mm (<s}-n^ s
m umma
• I I
1114&
us
i^s i3j^u mu gm
igm lAggj mmsm g m gs
iiggm
mig <g kgj v 1 g mggj <b mi» 19
uyih mw im mnij-h gps gs hmm m gm ig uyih mom hggj 1 imm
<w gtmm
immm tggj g gm
m mgj gm gm ig gm mg mgm Sg gmg <img g tm
mgg) ms gmm e/s g (m gm ig gmsm m£) mm ai£ m g m gg-hggj (&)
igg a gm £ig ig img ggj gmy jggi m g :t£ kgj gm m umi gm mm ig
pggm ggy g gm <sa <mg g mg gm gh img m mg gg iikg m [msu s/1 mig
g mg igtg imsne mu- gg ig tmm ingm g rrngj gm g& kg| i>ii> g muy <bpg
imi& mu imgA us smg mu ggi sm stgm smg ig hmy 'im-Litm yi t?mg| ib.ii> (t)
IllrbllA Ih>|><£>
m±E
hk WWLkh to kftpyife
^1PW n^iaj
^ik lih^iik iMy kkj^y bki^j hk i^jiakMikh
£ skikiy kkj^h ikkkih> m 1^
1£ Ik^biip J£
ik^k kk£ Hilbun
111^ kk j^>k Eyjt
^Lk kl^
1^
Hbbim j£ jy,
kkkk Mkh ^21 kk^y 9 I Ik kky^J IMS Uk^ jyi^Jlk j?lk lkk&: y> kkk b kilcki Ik <bPb
ikk Slk Ik 4k3i£ IkkM {kbyte kkij Mk kh k
Ikkj kklklk Ugg kl^lkb> kikk k lyite £kk
Ek^h Jj/^k Lte§ MkSmkkAblte kPb Ik
g k^y h4k kklkUk-lkkL hiMkkK (te)
‘0 I
1£2 J^i|lk^ !Ph4W
1UzL Lk^y
'£
Uk lpk>k hkPJ
££>
klk.brp l£3k IPh-klu I4> iikkk 4>!?3K
ilih
~: It^Uk
t ihi- mEie
s
>U>5
j£
’ I
h&uj
lb 1 •■l£k----kkkk
-gllk ypk
g kQklk Ik-lk ‘6
1^'
t
’£
II^ w
1112 141411 Inlh^ 141> iQjtn hl^ I lit(?1V>. 1« gl± 114a
QIPh»te l> lh?cpjtr>
11^
144
F113^ J£
UllUUlit jiEfelifeIhWslll?jltjjllH 14^IS
|lkla 4141? Uj ifefefi 1414
■
^Ikfe Ihfej'fr Jefe lbOAjho l>h P^tlMe IjfflU^lh >llt^ h^feUllfe 114^
W1
IM9
lh 41^5 4-lfefeA '212 fffrlK? ££ “ ^4^ l^lfe ^llfe 1^ hlfefe 4 feHHhiK (£)
III>19 MtfehJIg life ^ilfe P^JIhlk 14141415
Sfeb 14 Jla-ili llllfeklfe
II>19 h4M> l?b> Kfelfe
felfe UhUJho llfe^lfei £ JPfe-lfeU l^fe
ljltjl> ^f> £ Ulb ifel^le £ aiQ. 14 ■£ l<b QlPh>te
41911
IlaP
cfefe •£ Icb QIPK»K> 1014 1 >11^9 Plfeh ■&. 145 ^>1PS»£
IteiR IfetaK fe^iE life (2)
lijllfe 1M4
fe klfe £ IhU^ho <4 IC^M
|£lk> J<£ klfe Ihlb l^fefekllk J^fe ^Jlife fe^fc-£lll 4
llllfeklfe Q9h £ k>0 >ia>lfe> klfe :W
bIM-K l<b bb IPI?»PI> 1£ l^kjfr J^fe IP1PHP.
ifejihfe 111 >19 kik ii?^ $ ifp^- kik i^ii 1? iJiiia i<fe 141411. feisfe^K life ybfife >1^1414£
IP ^IU Ibb kl2 b£»b lute Ibtste I^IXPte
J£ QlPhAte 041?? life hlteill J£t life (I)
—: liaifeln feiP-bj
1 iptfeP1 $4 bin4 4 life tPfefe 4 tsfeib <4 .y?iife.
iil^Jlak feh b£fe hl^llafe '14 14>!4 £ 1>^ t^lhlft life PhJfete 14 45414 1414 44 &fe4
(te)
I lhfi> PhJIHvX hfe±k!fe 4 Pj^JP- Inlh^tb J44I l<nitj ibPl^IhlP- IfelU^lfe life ^klPbfete
I a?l» Q|J IPhl9P 4 >p> IQUJ 4fe IQIPh»K? 114141 441 14 14 fekfe
4[h Cb) <3 14 x IP> Jefe. hQj|>^ itefefete. 21z I t^ltlfe P14& 2fe 14 I4PI4J
4 l£ l^iPhfete
414 lute 14 9mj i^ifetii iyp^ 14 Pig? 14 tzifenaS IQ1-4 414111- ininfeife 1414 &41J1
blhhP KbPP 144 Slj QIPM-te IPP IN9 IhUS l^lfekli life fefej 4 WlPfefete fefej IfePfe'llilll (U)
iii.hiiA ig>> mEte <4
Jik b£e
liaH pjik |<b ijixbft 114 |ii.(?lte 1MJ Uldfete $ 14414 14 uikfej kfefe tMz> life l^lfekl*
U4 llbhlb' IE?? 4 PIE? hlfete <4 IJlJfe l^lfekh 22 1% IPfefe 14 1M2 felfefel Inlttfesfe Jfefefefel
Qih bh iQ9Jlt l^lhkli feh i?kl?-tzfa& Pittite lb Ihtelft IJlsSlte 14 41411 InliPife tell (in)
III>!?r^ Ihtfel Ifelb It? JIcfeiJK
nyjikiit im5 hi^pj imi> <b pjpjp mp-£ic <4 14414.14 41411 fe^ikii i<h 4a ith ni
I Pith ^l> 9ll>Q ?h l^lfcljr? £li ^Ifelfe
« CfelUblte 1112 Erlllb (2)
ityiikh ndb •£ iteipibup. (1)
-: 1414 Iklfe
IhlHPUlk mPlP-rlJ |,PUJ 11,19 ?h hQlhoF,
414H lUlS Sfel’ IfehlC Uh QJ^jH IMUblfe 144 (£)
l£ k tnib. kife^ibk feh !4feii 412
44 4 .41411 4 54
ih-chj 112144 ia> hlk^ inikij <1114 114t?ite. 14 <hJ4 14 Itefehb?. 4? inlihn 114
<bio 4 fem 14 414 ini.hij mis 1 nite it?4) tefe pjpim.a 14 bik4 14414 te^fe 44)
’PL
lahiHli kkit nyy
>h ^19 inf,
Pleliiill sy hl£ l^k kkF
X'ykkms
IhlHt £ kilty InW
y^tz^Ji^RmSltlkeJlnJky ^IkW^
11
y. yiK khk 1.
a?/
<£ uyhB.. » hibmc lWK e ^£* 12
a
«K
(I
1W1^ W1*
<2
ik >h M5>} -e» £ Qimfc pjm^ $ iyiikn
w w6 “XXil
iJj^
2W£
ZZS -
eSm !2 1“
>2 HE 1S M- te
«
I
* «*» S'1
.
Iiky£
te W
Esmfc
14 IWH
3W2HEMS1^
2 to
?1W1
lElBia
E» W'
ih urn <£ yik W W^
Hl,him
wy Iky ^11^ W4^
“ ““
<?
£k J^l£ Ik k^te ikktte in ms
W
Sri
lijim y£ lb hk^kkR IMS IkR » 1£
Iiu>m mpi.R
yii£ Bb yib
Skkiklte kttetk)
ih W
J£
Itekik likMi hikitR ishyite yit Ite£
'
puxb pg^ri jj .biy ly
laM'-iihi yyy kui
^E^^OteSikiykWi^) w^iilE'w?^^l|lx
(k)
trv)
5? i>iim J<£ Jkk^£
_: ^ k W
kW ^llk
•£ I
1
000'03
<a kptpnpe rMh
fo i?fr>
incite l<t>
I lb9> k
itbi9 $
<£ frjijg ij^n
2k!£ Ik 4>b
l^j l^y P4hk
Ikkk
?
-: IP1E> <kj^
I lltlp <Wlt?lnlJ
IhhlaJ ^IMtxbJ Ph I4>
IJIfohlfo
litUBk 1£ IMS kL0_y Iklifr PJ^lj4 10 kin
1^10l?10
10
*6 I
hbPb 10 I?I0!J I^IR (£)
i^lk iki^ (WS 11141 J^k
PJ<£\j>^ 10 kk? 0P 0 0 0 0 3 I?h0 Jt kkki 0h 1?Q] <£ £10 J00y (3)
llii^k iP15iaie
109% iff r?i0ij iffhe 01k
ffi0£i0 (l)
-: M0k)0 0 cblfe^kj 1£L0£10
* R L
10X0 kin pj-lk> IMS 01^Ij |j>10£|0 IkP 0E» blk9J InA 10 l^JIM-k Iff i^£Jk (k)
llk£ 10 k!0y JffU£ 0h& Jff0P kb £10
l7lh IPPkJI?kJ0 h 0X0 lnh?IXlj I0PP |lk0X0 Ukk lkl0 Nkk iff 0101 r 10 £10 ff
10X0 P&XK ExfctP
(£)
1001101010 ^r0 klhi3 bi0P|K 000h Ifi^ 10 kk>-kl0 10 Pjhjk (3)
10X0 P&MS 'j^ PhIK Iff blff&
100 0brkk£ll£ 1000 biff 010g 2h kk0-kk0 091^ Iff kl0kj Ifflk hh lk-0 lnMkl0 ( I)
—: XI0kj0 0 bhj0
'L L
1114g 0101t4n£J £ ffh£J ftlMbbJ 0k 10 0h^0 | II>I?0X0 k01 kite 10 109b Iff
lk01001010 0JJS £140 kX00 liak 11^0 lP0hrate Iff IffPb PXh0 Iff 0.0 lnMkl0 0trate
-:
ff ^bate
'9 L
llfflg £00. kkk ff Jffff ff kb0 Iff 14140 0lff Pfijite lllfflte Ihffj
01S 101£h0. iyy I? IP I h0 Pfijlte 10 Ifrxy 0 14 ix pjfi iff 1414k | IP bite 1£
|>|>3 k010
1£J0 Iff k£klk Illi£lte IkffJ 01b k!0l4
k£kj I00£ Jg IkPffJ r?£klk Ilh00 Ite
lk£J ff klff Jffte k£klk
01b lff40 Iff ff41k£0
£X0 £10 Qi^te bk llhfflte
1000 0000 Jff ffpjfflte 1130 ff£jl0I4te ff hlk£J fr?0lbx \b4i0r4te tpj>l4te 01b
0k3K01j4khl±0bk01Jff llfflte IkXX kPh^te b%0 !5>y incite Ifrff] h IffhK P^jlffk] I XIS
l£1014te 0X£X ff Ldhffj 000X. Iff £1010 InXlkff lEXff I llrhlte Ihffj htralk ff ffhte
klhpk ff klk£J k^XlbX k<k>lff0 £10 ln\0 10
11142 IgU MfrhjtP lit g>cb d41N>-
I
kin Jffkite kffk Jkiate £.X0 P j>lbx kh kffk £iff hoj ff k0iff0 £10 khte iff 14140
—: uxihjx ibxff 100 kteih.0 £10 10 14140
’S 1
th Libipaie LH2. ntalti ’ii’ii
$6/COOC/S6£ h
»IM2 J£
21S2£J2 XKbfyte 14> ££ hlnlj hPJfc 2h £g Etefi 21^ £ £££2 kkk IkklD >lfe£| £ /
££lltl2 P£jlb-£ 111 >12 k±k£12 k kPj£ 1?^ Ik2lS£|21££121££ ££J£ kl!n£l£klkb)
2££ Ik 2122£^2 2b IP 'g k hlP£ Ik l^h £. t?ln£] Ik kkA£j 12k £Jk 11kg. Mk£££ Ik
g P|kPK> 1£ lkl2 In21kll2 Ik UizaiB 2h £g
kkg Ik Mkfi £2.£J £ lk212
-: blb£|
•93
£ kP£ 2k g Elk
llk£12 >k Ph-^JPJ bhb|
HI>12 Mk^JK> Ik PIq£ kPP Ik hlia212 bh lEtk kkgk 2h £g kkhbli^ g 21kk kk£
Ik 2h £lk £K2§. L kPP kb]lb 1212 jk^JIk^jlbh >112^lg £ ^blkkk] Pkglh J£ 1E212
—: IMPS kPfr IM2 kbljph
•S3
IIP22 glk lk££ 1£ £Qlky k £2k
Ikk Ek 2h kk!2-klil2 1^2 £ 2 kJ IE E2I£ Ik k£ l£i£k£ 1££J lj£J 1221112 1£ 1E212
—: IP!F> kb
in^y> ]]£ j* gk
1k
£
>1^15 IfeMJ Ik 1212 klk '1212 k<P.^ Ikty <£ il^Eie 2^1 !£> hlk2k kb £±ih M$2P^2
(2klk2) iPJh^
J<£ Ikbkt 11^42 £ klk <£ Ikbk P}hj2 <2ki£ Ikk £2k PMtl2
bk2k
‘£3
I Ibblk^ 14>
IlbbllA 1^ hlj2 l<k
<£ jUlkbiK t£ ki?£jhjfe glk£l<k P2hk <k£
IQIb ir?£kF^ 211112
l^lhk Qkfc Ikk Ok £2 lk2J2 PlkAh
<£ PPkfrj IlhbllA lk_£J k£Uh £ Ph S/E £ lk22R
U Utk ln21kl& 2?kb] hk lk2J2
—: PPkbj
I lb!9 k±lk »£ khk!2 4>yfi 1£ 1kg 1£ bik2k
kkh
cbh?lj£h 2143kjl^ Bk ^>4* Pkl.^12 £ tdk£J P^lj^h £.2£ k
lk212li£§ <kk2M€ £jk
111 >12 P Jlh ]£ IPk £/ 3 £ It?2bl2 Q<? £ Q>9£ 1£ 1212 lahiklk kkl£k h Elk bj £ lk212
-: PklEE
• vz
I UrMiA I^H. 1W Piyi£n lib
Ih94> P>1 rpufc <£8 2 121k Ikk Hrb|^ I4> o^l<h
V I £ cblkbj c£ M2 lkl2klie
klsky IkliA 2h 12212 k^lky 2k£t
ikbk P1222e
-:
LZ 121k V£ lik£Jk.li£
£21k
l££t £b sbkl^lh
• oz
PPJlKh 1^ wr.
/
•c\
•^^^ppiilppih?
”3
mblnl
J
•S
(
2J1£
‘X
•t
hit lite PJh
hit isfe
I ££ 21^ 1£
lip IPblgft
-/oo t
lEJ^k 2^^ Q>Fj>?h h|ftl>
•k
lhhj>
PMfrh Ihh/l^PJIhVlth/hltPJ >lrP
‘QlfohJK* IfoPjlhMrh h3&/PpfclK>
Phl^h hilt I>I3
Pblfrh bhk^
Ol^njH> k(pihj?lib
Jth hi£H£ 2$ iagy^ W2^
’k
................ h^ma
h-^lb^TK
Pblh-h hili
'11H2
ia
HsKHbi^ I
i^W
WagH
I
hlk l£k£ £
I ^lb
im= kwi^ ££
i^IFQe )myb r-KEE I
tm
Pjh
mb
•* ipn^
i
mm iik£j Pinjibh
(Uhtt Vtttlb)
Kb - lolilb
t
•
ijn hhEk
tm hi V-itfrHfr Sir |mi2 lbi£ yy^ Ighh Unblja IE £
.........
IPshJFPft........
W‘JJ
iyb
(hlHl& Vb&tf)
Kb - llnblft
I
/
f.l
I
|~H>>
1 A>
kd^-b E
5
(Kin>
1 PlRv IP^tj
I
iikllLif
U rrl bl KI
yrt L±
PlL^PL^ yrt
yeix.
.. I
5' Pl tT_pt>
i
!.H p^Ft
r?! ^hA 1 trtbrz> LtT I *b friih.
L£
Kt 1,A> |hAfr
1^ Ltrtei?? yt
i
LH^. RH4
Iv-SjJ 21Mx£
L2^J i_2L^
2Lhh£
I S^PP 2b
1_±
ItfUPlll
IP
bl s
>
H^rr 1J ktPlj± P^SJfr/frPl FP4>Jhj
^HP. 2b
H_2 142
P^JP
2b ^IV* ULb P^rtt 142 LhP
HE
LHUH HitHi£ Pl^PlE
I5 1P1 p 1E»S>Jhil^pb
y>u-
5
Snb>
(_KL£i Ifc Q£1_PB2
I?HbA
JAC
b
ln£?ph
ial^pib
| pip
1P1P
rzHb4
,Snl>> Hl 4>PJ
A>|Pb
iZHfcPt L± |_KL2> L2L2.
J2 1^
? 1P1^ IfrlHg >5nP-fr rfriyite
PAlrH PlrPK ± ppj > hHI PM
£
Ib^pb.
InUyh (Zrtlb^ >1E»
IPIU r?^
L± I Hesjj?
£ frt>
LttlqJiiC
i
l
I IP>4> >lhh£ 2
1_± IK1°>
RAtfPr
Pl £>
£
•*»
A
I
i
I
V*
♦
ANNEXURE - //
A.NNEXURE - HI
Questionnaire for Doctors (Senior, Junior & Residents)
Questionnaire for Outdoor Patients:
Name of the Hospital
Name of Patient
Address
Address
Category of Hospital
Gen.
Maternity
Eye
Diagnosis
TB
1.
2.
What are the common problems
faced by you in the OPD ?
Do you have to wait for a
long time ?
3.
How is the behaviour of doctors ?
4.
How is the behaviour of staff
nurses,ward boys,doctors,etc.?
5.
6.
Are the prescribed medicines
easily available ?
Please give the following details pertaining to you- Dept, only:
1.
Name of your unit
2.
Years of service in
this hospital
: Yes/No
: Good/Bad
3.
Your designation (full-time,
part-time/honorary)
: Good/Bad
4.
Total number of beds
attached to your unit
: Yes/No
i)
Do the doctors on duty ask you
to come to their private
clinics ?
Yes/No
If no, then how many
do you suggest ?
Have you suffered due to
wrong diagnosis by the
doctor ?
Are the number of beds
sufficient ?
: Yes/No
ii)
7.
Others
iii) How many beds were full
: Yes/No
on last OPD/Emergency
8.
day ? Any patient on floor
Have you noticed favouritism,
or pro-relative jumping in
the queue ?
: Yes/No
5.
(s) Total number of actual
hours spent by you per
d -y in treating patients
51
ANNEXURE III
WHAT AILS PUBLIC HOSPITALS ?
On OPD day
On ward day
On operation day
8.
The five most common diseases
seen by you during the last
two years in your unit ?
:
OPD
(b) Average number of patients
treated in OPD per day
in your unit (new + old cases)
(c)
In-patients
How many doctors are there
in your unit?
D
2)
3)
4)
5)
1)
2)
3)
4)
5)
Senior
Junior
6.
(a)
: To a large extent/somewhat/
Are you satisfied with
the competence of your
not at all
9.
Which are the five most
common diseases responsible
for death in your Dept. ?
4)
5)
nursing staff?
(b) Are you satisfied with
the competence of your
: To a large extent/somewhat/
not at all
10. Are all essential medicines
Yes/No
available in your hospital
for indoor and OPD patients ?
resident doctors?
7.
1)
2)
3)
Whether the staff is sufficient
:
Yes/No
List seven essential drugs which are most commonly preserved but are not
for your unit
available in the hospital ?
If no, what type of staff is
not sufficient ?
1)
2)
For what functions ?
3)
4)
Give details of posts lying
5)
6)
7)
vacant in your Dept.
Name of Post
Why?
For How Long ?
Lying Vacant
11. What problems do you face in
the operation room with
—Terence totheavailability—
of equipment, power, staff
support ? Please elaborate.
3
1
WHAT AILS PUBLIC HOSPITALS ?
ANNEXURE III
12. Give frequency of breakdowns
17. (a)
of essential equipment used
by you
Name
Are you satisfied with
the reports available
from other Depts. ?
Yes/No
No. of breakdowns per month
(b) If no, then
Name of Dept.
Reasons for breakdown (Please tick)
Unknown
Mechanical
( )
( )
( )
( )
( )
( )
Negligence
Careless operation
Lack of maintenance
Long use
Reason
18. Under what circumstances do you
refer the patient to other
institutions ?
19. (a) What are cleanliness standards in your wards, operation theatre, OPD ?
13. Please give list of important (must) equipment which you feel that your
OPD
Department should have.
Name of equipment
No. required
Function of equipment
14. Please give details of machines lying unused
Name of machine
lying unused
No. of machines
lying unused
1)
2)
3)
4)
5)
Ward
Operation
theatre
Sanitary
facilities
Excellent
Good
Acceptable
Quite dirty
Extremely dirty
Since when ?
(b) What can be done to improve this ?
Reason for machines lying unused (Please tick)
Uninstalled
Obsolete
20. Are you satisfied with the facilities available in your unit? Please give rating
to the following:
( )
( )
( )
Malfunctioning constantly
Very satisfactory
15. Please give details of machines installed but lying unused due to lack of trained
operators
54
Name of machine
Its use
Since when ?
16. What is the frequency of power failure in your Dept, per month ?
Moderately
Low
Not
Staff
Equipment
Medicine,
dressing
4) Support
service
5) Ward service
6) Operation
theatre
1)
2)
3)
I
I
WHAT AILS PUBLIC HOSPITALS ?
ANNfXURE III
21. What are the phenomena
26. What steps do you take to overenmo
medical instruments, etc ?
non-availability of drugs/
endangering patient care ?
22. Are you satisfied with the
equipment sterilisation
facility of the hospital ?
Yes/No
Please tick:
(a) You report to authoriti,
les
(b) You feel there is no use of
If no, please explain
23. Do you see hospital-acquired
infection ?
reporting
(c) Any other, please specify
Yes/No
7’ ^onsf^you^inton6"’
How common is it?
Very Common
(>50% of patients)
Uncommon
(10-29%)
Very rare
(<2%)
24. Are you facing any dif
ficulties in the Casualty
Dept./Emergency Ward/
Intensive Care ?
If yes, specify
25. Are you satisfied with the
Action is taken
No action is taken
Frequent
(30-50%)
Rare
(2-9%)
‘'"P'0''6'' " de,eriofa,ed ? Pte^e give
28. Do you think there is interference from politicians ?
Yes/No
Does ft affect health services to patients ?
Yes/No
Please elaborate
Yes/No
29. On an average what proportion of your time in the hospital do you devote to :
Patient care
Teaching
Administrative work
Other work
Total
quality of drugs, dressings
100%
etc. supplied by the hospitals ?
30. Does adequate academic interaction with other doctors take place ? Give
If not, specify
rating to the following:
for example:
Regularly
1)
MR
I
Occasionally
Never
Drugs are substandard
2) Irregular supply
3) Quc^.a insufficient—
4) Any other
31. Have you any cornments
on inter-departmental co-operation ?
32. Is immediate action taken on your complaints by the Administration ? Yes/ No
WHAT AILS PUBLIC HOSPITALS ?
33. What administrative steps do you suggest so that no patient becomes a victim
of negSgence ?
34. What kind of statistical information is maintained and available with regard to
your department ?
Satisfactory
I
Unsatisfactory
35. How satisfied are you with other supporting departments ?
Satisfied
Nc< satisfied
X-ray, pathology, anasthesiology
(only for clinical dept, which use these services)
I"
36. Any other instructions/suggestions you would like to give :
I
CO
w
r
i
i
■ i
I /
^Cx/vVyt I
H-C^AA^
Cca^^atxaAAx^
VaTcX ^-TkzyX
P
fXLtreK VmxA
?
c-
^-AyJLc^)
\- M
Tl- 0 v^x^y^lGv’
I *vV 1a/<< - - —
"5 . W/A^^ l\xc^
VA-
013^
A ^Aa °i'^ '•~‘- 7 / '• W . ~ C.
V-^-<U=^PVY^ lo^st Lmo 'f7~^XL3)t’
V ^V-Ja
I qlAi A-k UjJ A«o
(gb-^ ■s
hXp W
jw et^ Pk. 7vM^Xv4-
vWd -k HtjxM
!s-
5 '
'pU^o vva^m^
*
pR^cU^J, P^ct^L
r
L '
P.
Paa
V-al/v
„
■'V^
Ks
r t
H* (k<j
o
6 c%Wbpz?
(V4a43 S Vlccfl^
U<&Jv>
^S "Xs
'i-
.
fi^TTVxA SC|Sr 6>t<rvK cUX-^ IaajuVX.
r-.
^^VZa^a
[ C? cn? f—
^^Vvzv
ft VcA< MUa-^
I
c • ^V
J?' •
,
k^v, kI>
&) I^iJIa. JaTaaAaa
'
^^VtAA/Vt^
'■
i
tk<AA»
\
Ci L\
_ Crlvt^ t^)
S drvJv^l
g- Mlaa^zU<.v xvk^p
iv,
—
Iff
"^7^CLa^Z tt^c
cK^v^A^to^
^v^)
Vvov\
x. YLvtc/
A-^t^vv-LCg
l^v
T'VM
tcz^x (V\ a(3VAAX-
>
’]
’
^>6>A^£xAy?A to C7^^i^ry>V^V^
• Ha?y
c
V-
l^v vQz Mb ‘T
/K
‘^dvoc
0^.
NV^v taw-
V-^^aaxX\
VX/aj^A^xV/ vAaaX) IaxW) V-Cca>\
I
\o •
<
*
w
s
1
I
BURNS CARE IN INDIA:
For professionals dealing with burns care in India, the
high mortality, morbidity, unknown epidemiology and socio
economic problems remain areas of great concern.
HOW DO WE COMPARE WITH DEVELOPED COUNTRIES?
1. We do not have a single centre dedicated to burns
care.
2. Our 50% mortality is in the 30-40% BSA Burn group.
In the west and east this is in the 60-80% range de
pending on age.
3. The morbidity is very high.
THE CHANGES THAT NEED TO BE MADE:
1. We need to start burns centres dedicated to the care
of burns, at least one in each State.
2. The prevailing centres and District hospitals need
upgrading.
3. Intensive care facilities should be provided.
4. Well trained & motivated multidisciplinary burns
teams should be introduced and the number of Staff
should be adequate.
5. Barrier nursing and rigid environmental bacterial
control are absolutely essential.
WHY IS IT SO DIFFICULT TO CHANGE?
1. LACK OF AWARENESS:
The majority of Policy makers, administrators,
doctors and the public are probably unaware of how
an ideal burns centre should run?
Cotd..2
2
2. FINANCES:
The inability to mobilise funds to upgrade these
units appears to be a major deterrent to change.
3. LACK OF MOTIVATED PERSONNEL:
As of now, very few professionals take up burns care
exclusively. It is essential to have full time, mo
tivated personnel for an y long term improvements to
be felt.
THE SOCIO ECONOMIC PROBLEM:
A large percentage of major burns occurs in the lower
socio-economic
group.
Illiteracy,
over-crowding,
marital disharmony and poverty all contribute to the
etiology, morbidity and mortality of burns.
HOW CAN CHANGES COME ABOUT?
The existing system needs complete overhauling if we
are to make any major impact. This can only come about
if the Government, Policy makers. Administrators,
Doctors, Industry, previous patients and concerned
Social groups all put their heads together to solve the
issues previously mentioned. One start would be to
bring together all concerned persons in A BURNS
FOUNDATION.
A more detailed report is available with:
DR.RAVI NARAYAN,
Society For Conmunity Health Awareness, Research & Action,
326, 5th Main, 1st Block,
Koramangala, Bangalore.95.
Ph: 553 1518.
Efficacy in Administration of Hospitals
A Case Study of Private & Government Hospitals in Bangalore
Piush Anthony
Doctoral Fellow
ISEC, Bangalore
Suggestions/Recommendations
1. Hospital management and organisational structure needs a complete overhaul in the
case of government hospitals. The work load of doctors and other staff is an area of
concern which needs attention. The first step can be filling the vacant posts and
deleting/reshuffling the posts that non-functioning and unspecified.
2. The practise of doctors being appointed as administrators in government hospitals
seems to be a problem as far as the poor management of human as well as other
resources are concerned, since they are not trained in admini strative/managemen
skills. The relatively superior management systems observed in private hospitals car
be attributed to the fact that these are managed by ‘administrators’, trained or
experienced.
3. The efficiency of the hospital lies in the nursing care provided. Better nursing care is
assured through division of labour and continuous monitoring created through
different categories of nursing staff. For example, supervisory level staff at
ward/floor levels, who ensure efficient management in private hospitals. This is one
area government hospitals need to reform their organizational structure.
4. Greater devolution of power to the senior officials is necessary in the case of
government hospitals which ensures effective handling of complaints from patients
thereby ensuring efficient management and customer satisfaction.
5. It is clear from the analysis that government hospitals has high occupancy rate. This
can be translated into efficient income improving mechanisms if there are systems
introduced, which will ensure identification of income levels of patients without
giving way for leakages. This will to some extent arrest corruption in government
hospitals.
6. There is a need to ensure provision of medical social workers in government hospitals
to support and help poor patients. They can provide guidelines and information to
patients in meeting their demands as rights and also can act as a mediator between the
administration and the patients.
7. There is a need to develop systems of supervision and vigilance in government
hospitals to ensure that corruption is arrested, which will help a long way in building
the image of government hospitals. This is very important as it can initiate positive
changes in the work culture/environment of the government hospitals.
8. It is also essential to build systematic awareness among the people on the role of
efficient public health care system, which ensures demand for public health services
as it is obligatory on the part of the government to provide health services to th|e
people and the poor cannot be in a position to access private services. The present
day duality in health care access is denying the opportunity of improving government
hospital management as only the poor are accessing it, who tend to be less articulate
about the problems and who will have limited access or information about the
redressal machineries.
9. A greater role for medical professionals and their associations have to be recognised
in this regard to influence the authorities in revamping the hospitals with better
facilities and more human resources. The medical fraternity has to take a pro-active
role in ensuring that poor people get their due share of efficient health care from the
public system.
10. For the implementation of any of the above suggestions, it is imperative to build
vigilant citizens’ action on this front. Herein emerges the role of NGOs in initiating
and campaigning for such a move. It should be in the direction of creating awareness
among the people about health care as their right, through various mechanisms which
are effective in reaching the lower rungs of the economic ladder, they can also take
initiative in campaigning for incorporating minimum health care as fundamental right
in the constitution as such, perhaps as part of the ‘right to Life (Article 21). This will
provide the people a legal mechanism to seek redressal when this right is denied,
also, bringing the medical profession under the CPA should also be taken up, for it
would confer certain beneficial results such as: medical records will be maintained
more rigorously, the patient’s right to information will be respected, greater
standardization will become necessary, standards of nursing homes will have to
improve and corruptive practices will be checked. To begin with, they can even
sponsor medical social workers to government hospitals. Implementation of healtl|
tax for certain categories of income should also be put forward as outlay for health
expenditure tend to decrease. Any effort for greater privatization of health care
should be prevented on the grounds that poor will dispossessed and discriminated.
Bangalore Hospitals and the Urban Poor
A Report Card
- Anjana Iyer & Suresh Balakrishnan
(PUBLIC AFFAIRS CENTRE, Bangalore).
A Summary
The quality of hospital services is an important element in the package of services that
citizens rely on, during periods of physical disorder and trauma. While medical services
have seen many a technical advance, it has been accompanied by increases in costs and
complexity, there has been a growing concern over the deteriorating quality of hea th
care provided by public hospitals. These problems become more visible when it comes to
the question of health services to the poor.
How do citizens, especially the poor experience these services? What is their feedback to
the health care system? where are the improvements required? In order to examine these
issues, the Public Affairs Centre, Bangalore, recently designed and carried out a study.
The study assesses difficulties encountered by the poor while making use of hospitals, the
quality of specific components of service, and the different types of action for improving
services. the findings of this study are expected to provide a framework for public
interest groups and administrators of health care design systems for improving access to
health care for the poor and the quality of service that they receive.
The study of hospital services in Bangalore was conducted by the Public Affairs Centre, a
non-profit organisation based in Bangalore, in collaboration with the Citizens’ Action
Group. This study attempted to generate feedback from the urban poor on the quality of
hospital services they receive. Three categories of hospitals were surveyed - Government
or “Public” hospitals, hospitals run by the Bangalore City Corporation (BCC) and
missionary / charitable trust hospitals.
The study was carried out in three parts;
* Forty one case studies on the experiences of the poor with hospital services
* A field survey using a structured questionnaire on different aspects of feedback from
sections of the urban poor on hospital services, and
* A series of interviews with hospital administrators on their perceptions of problems
that affect the quality of hospital services.
Conclusions
♦ The urban poor in Bangalore have been using a variety of options for health care.
While Government hospitals play a major role, other hospitals, including Mission and
Private hospitals contribute to health care for the poor. Any strategy for health care
for the poor has to envisage appropriate inputs for all the institutions involved in this
sector.
♦
♦ In terms of costs, Government hospitals come out as the cheapest source of health
care for the poor. This is not only in terms of percentage of patients enjoying free
treatment, but also of total costs incurred by an overwhelming majority of the
patients. The unfortunate part of this otherwise positive phenomenon is that a major
part of the costs incurred by the poor are towards illegitimate side-payments often
extorted by different participants in the health care system.
♦
♦ But the most significant problems seem to be in the quality of medical care that the
poor receive. To start with, the waiting time they have to go through before receiving
medical attention and treatment seems to be quite high. Second, injections and
medicines, presumably free or subsidised, are often not available at Government
hospitals. But the more important problem seems to be the total absence of standards
or the lack of awareness among patients about what they can expect at hospitals. It is
form this point of view that Mission and Private hospitals seem to be serving the poor
in a much better manner.
♦ The manner in which activities are managed in the Government hospitals also merit
attention. The seriousness of this problem can be seen from a simple area like
cleanliness of hospitals, although there was no major difference in the frequency with
which cleaning was carried out across different types of hospitals, the level of
cleanliness at Government hospitals were rated in much poorer terms. Similarly, the
poor need to run form pillar to post, to find medicines, sometimes in life and death
situations, while being treated in Government hospitals - whereas, dispensaries of
Mission hospitals are rated to be far more efficient in this regard.
♦
♦ One approach to seeking better quality of medical services and facilities that the poor
are compelled to seek, is by resorting to speed money payment. This approach seems
to apply to all levels of medical personnel (from doctors to sweepers), and for all
types of services (from operations to entry into wards without authorisation).
Although there is wide variation in the quantum of payments, the problem seems to
be most acute in Corporation Maternity Hospitals, which are used primarily by the
poor. Designing interventions to reduce the instances of extortion could certainly
begin there.
(In collaboration with CITIZENS’ ACTION GROUP, Bangalore).
HEALTH CARE WASTE DISPOSAL - AN EXPLORATION
INFECTION CONTROL COMMITTEES
It is suggested that infection control committees be established in all
Health Care settings where bed strength is more than 100 ; and the committee
to supervise Health Care Waste Management, Hospital Acquired Infections and
General Infection Control.
.
RESEARCH ACTIVITIES
- The investigators suggest that the State Government shall encourage the
with
Civic bodies to take up the following research activities in collaboration
<
Medical Colleges and Engineering Colleges on priority;
a) developing curriculum for training doctors, nurses, administrators, waste
handlers in the area of health care waste management
b) Feasibility studies to recycle metal sharps , plastic items in safe ways
c)
techno-economic assessments of solid waste/health care waste in different
cities, towns, etc.
d) conducting waste surveys in different Health Care settings including
measurement of quantity of such generated waste
e) feasibility studies for efficient establishment and running of common
incinerators/ sanitary land filling/ composting etc.
f)
sentinel surveillance of hazards due to Health Care Waste management in
selected ranges of the City
waste'
g) studying sickness absenteeism and causes for the same among
handlers
h) maintenance and periodic review of morbidity registers of health care
personnel
EXECUTIVE SUMMARY
12
Position: 729 (21 views)