RF_DIS_11_SUDHA.pdf
Media
- extracted text
-
Patient
Guide
RF_DIS_11_SUDHA
fSlABETIC FOOT
l^«:B<»kaaiag aafi'dc&B-
y©anB°
□Dsn nil
Most people pay no particular attention to
Examine your feet every day for blisters, cuts and
loot care. As a diabetic, however, you must
scratches. If you find a change in the condition of your
foot
take special care of your feet to keep them
feet report it to your doctor immediately. If you have
in good condition. If you do not look after
problems seeing the soles of your feet because of arthri
your feet properly, ulcers may form; these
tis or obesity, use a mirror to help you, or ask a friend
could become infected. In serious cases,
or relative to check your feet. Go to the clinic iinmedi-
gangrene can develop and amputation of
ately if you notice any of the following danger signs:
Swelling.
toes, the fool or lower leg may be neces
*
sary. The chances of such problems can be
*
Colour change of a nail, toe, or part of a foot.
minimised with a simple routine of daily
Pain or throbbing.
fool care. Following the guidelines in this
Thick hard skin or corns.
leaflet can help you stay mobile without re
Breaks in the skin, including cracks or blisters.
lying on others for help.
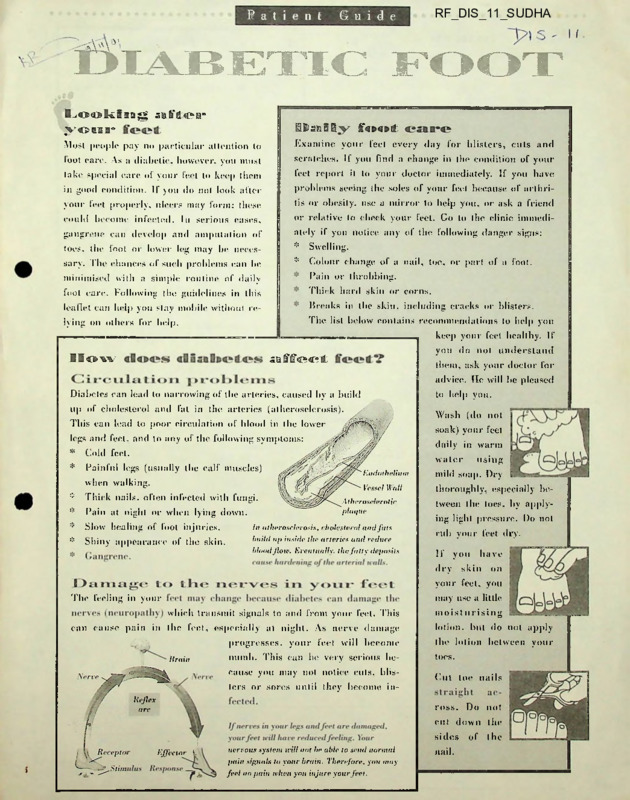
The list below contains recommendations to help you
keep your feet healthy. If
you do not understand
affect
How
them, ask your doctor for
advice. He will be pleased
Diabetes can lead to narrowing of the arteries, caused by a build
lo help you.
up of cholesterol and fat in the arteries (atherosclerosis).
Wash (do not
This can lead to poor circulation of blood in the lower
soak) your feet
legs and feet, and to any of the following symptoms:
*
Cold feet.
*
Painful legs (usually the calf muscles)
daily in warm
using
waler
when walking.
*
Thick nails, often infected with fungi.
*
Pain at night or when lying down.
*
Slow healing of foot injuries.
*
Shiny appearance of the skin.
Endothelium
mild soap. Dry
Vessel Wall
thoroughly, especially be
Atherosclerotic
plaque
In atherosclerosis, cholesterol and fats
build up inside the arteries and reduce
blood Jloiv. Eventually, the fatty deposits
tween the toes, by apply
ing light pressure. Do not
rub your feet dry.
If you
dry
have
skin
on
your feel, you
may use a little
The feeling in your
whieh transmit signals to and from your feel. This
moist u rising
can cause pain in the feel, especially al night. As nerve damage
lotion, but do not apply
progresses, your feel will become
the lotion between your
numb. This can be very serious be
Iocs.
Brain
cause you may not notice cuts, blis
(’ut loe nails
ters or sores until they become inKeflex
art-
ross. Do not
cut down the
sides
Effector
I
nervous system will not be able to send normal
pain signals to your brain. Therefore, you may
feel no pain when you injure your feet.
nail.
of t he
!>li
iiijia
Vootwca f OOs
If vou wear ill-fitting shot's, or shoes which have
*
rough edges inside them, corns and calluses may de
velop. Commercial corn preparations contain mild
*
acid and are loo harsh for your fed. To remove corns
and calluses soak your feet in lukewarm water for 10
Purchase shoes which fit properly. Do not
expert your shoes to stretch.
Carefully check lhe insides of shoes for rough
edges.
*
Leather shoes are best, but all shoes which
minutes and then gently rub off excess tissue with a
let your feet breathe, such as sports shoes,
towel or file. Avoid 'bathroom surgery’ — do not rut
are good for your feel.
off coi ns ami calluses.
*
Prevention is always the best option: wearing com
fortable shoes is most important, but exercises such
as curling and stretching tin* Iocs several times a day
can help prevent callus formation. When walking, ad
justing your gait so that you finish each step on
vour toes, not on the balls of your feet, will also help
to prevent callus formation.
Wear cotton or woollen socks which allow
your feel Io breathe.
8<\x > L wea t-
doist’Ts
*
Do not walk barefoot, even inside your home.
*
Avoid open-toed shoes.
*
Do not wear plastic shoes.
*
Do not wear shoes without socks/stockings.
Athletes foot, which causes itching and skin peel
ing between tin* toes or thickening of the toenails.
should be treated immediately by your doctor.
Proper first aid is important, even for apparently
minor injuries to the feet. Avoid strong antiseptics (e.g.
tincture of iodine), which may irritate the skin. Cover
injuries with sterile gauze, using paper tape if neces
sary. Do not apply adhesive tape to the skin. From
the lime of injury until recovei y. affected feel should
he raised for as long as possible; i.e. sil with your
C'odQciD
feet
As well as delivering oxygen and essential nutrients
around tin* body, blood keeps the body warm. W hen
the circulation of blood is restricted. the amount ol
heat transported around lhe body is also limited. This
means that extremities, such as your feel, will quickly
feel cold. To ensure maximum blood flow lo your feel,
adhere lo the following rides:
Keep warm — wear warm socks/stockings.
feel resting on a foolstool.
Blood vessels conlracl when they gel cold, and
blood flow is therefore reduced.
|D 18*0BUS
As a diabolic you should be in regular contact with
your doctor, who will closely monitor lhe condition of
Avoid smoking — tobacco contracts the blood
vessels and reduces blood circulation.
your feel. Notify your doctor immediately if there is
Do not sil loo close lo a fire or radiator —
any change in the state of your feel.
because of reduced feeling in your feel you
Careful control of your blood sugar level with diet.
may not realise when your feel are adequately
exercise and medication (as prescribed by your phy
warmed: and may damage your feel with too
sician) will keep your diabetes in check. You should
much heal.
also use a strict daily foot care routine. This will mini
Il is not advisable lo sil with crossed legs. This
mise your risk of developing serious Idol and leg prob
compresses arteries in lhe leg and reduces
lems in the future.
blood supply lo the feel.
My instructions and recommendations are:
I HEALTH ISSUES
by auto-immune T-cells, are stimulated
by the oral tablets to secrete more insulin.
This makes them work harder and ulti
mately exhausts them.
But studies on LADA patients in Japan
(Kobayashi etal, Diabetes, 1996) show that
had they been treated with insulin instead
of oral tablets, they would have become
auto-antibody negative, attained euglycemia and become normal within five
ASHA KR1SHN AKUMAR
months to two years (called the ‘honey years compared to patients treated in con
moon’ period) to show up. The cause of ventional ways. Administering insulin to
IABETES is a silent killer. It does not die other, rarer, form, Type 1(b) diabetes, LADA patients allows their beta cells to
kill di reedy but weakens the body sur is nor yet known. Its progression is slow. rest and recover. These patients, however,
reptitiously and leaves it susceptible to a The diagnosis ofType 1(a) diabetes is made may continue to receive very low doses of
insulin, to suppress die immune response
variety of complications. A diabetic is two by estimating the auto-antibody markers.
in countries such as India, where the to a beta cell attack.
to four times more prone to heart disease
and stroke than others. Seventy per cent of fecilit; ft;.’ the estimation of acto-am. iAccording to Dr. C.B. Sanjeevi,
diabetics suffer mild to severe nerve dam
Associate Professor, Department of
Molecular
Medicine,
Karolinska
age, often leading to limb ampur.
Institute, Stockholm, who was in
Diabetes is the main cause of end
Chennai in mid-February to chair the
renal failure and blindness. Yet die caus<
Fifth International Congress of the
of diabetes is not fully understood.
Immunology of Diabetes Society, while
1D DM, 7 i vie the slowly progress! ng form
According to the International
Diabetes Federation, India has nearly 33 (otherwise called the latent amo-immune 30-35 per cent of diabetics in India are of
million diabetics, the largest number for diabetes of the adult or LADA) gets diag Type I (who are classified as cases of
any country. This figure is expected to nosed as NIDDM. The preferred treat NIDDM and test positive for auto-anti
double in the next 10 years. According to ment for auto-immune diabetes (die acute bodies), only 2 per cent get classified as
the WHO, diabetes is a chronic disease or the slowly progressing one) is the insulin-dependent by the still widely fol
in which the body either does not pro administration of insulin. But when the lowed IDDM/NIDDM classification (95
duce or properly use insulin, a hormone diabetes is diagnosed as NIDDM, the ten per cent of the cases are classified as Type
that is needed to convert sugar, starch and dency is to treat it with orally adminis II and 3 percent, malnutrition-induced).
other carbohydrates in food into energy.
tered tablets, and rhe patient usually ends (That 30-35 per cent of NIDDM cases
Until 1997, diabetes was classified as up requiring insulin within three to five test positive for auto-antibodies is borne
insulin-dependent diabetes mellitus years. The beta cells, sick due to the attack out, according to Dr. Sanjeevi, by two
Indian studies - “The
(IDDM) and non-insulin
| Prevalence of auto-antidependent diabetes melli
9 body markers in patients
tus (NIDDM), based on
< with young onset diabetes
the kind of treatment. In
in North India”, Singh
1998, the World Health
A.K. et al, Diabetic
Organisation
recom
Medicine, April 17, 2000,
mended the re-classifica
pages 275-280; and “HLA
tion of diabetes as Type I
and antibody studies on
(a and b) and Type II,
based on etiology (the ori
Diabetics in Eastern India,
Sanjeevi C.B. et al, Tissue
gin and cause) of the dis
Antigens, July 1999, pages
ease.
83-87.)
There are two forms of
The onset ofType I dia
Type I diabetes. In Type
betes is usually in child
1(a), diabetes is caused by an
hood; in fact, the risk of
auto-immune process, that
developing it is higher than
is, a process in which the
that of any other severe
body’s immune system
chronic disease, and is rhe
attacks and destroys the
highest during puberty insulin-producing cells of
between 10 and 12 years for
the pancreas. With glucose Vice-Chancellor of Dr. M.G.R. Medical University M. Anandakannan,
girls and between 12 and 14
unable to enter the cells, it Prof. Hans Wlgznell, Chairman, Committee for the Nobel Prize for
years for boys. It is geneti
builds up in the blood, and Medicine and Physiology, Prof. Rolf Zinkernagel, the 1996 Nobel
cally transmitted too and
the cells starve to death. laureate for Medicine and Physiology and Dr. C.B. Sanjeevi,
among children the symp
Typically, Type I acute Associate Professor, Department of Molecular Medicine, Karolinska
toms can mimic influenza.
onset diabetes takes two Institute, Stockholm.
New light on diabetes
A conference in Chennai emphasises the need for governments to
allocate more funds and resources for research on a vaccine for
diabetes and other treatment methods.
D
86
FRONTLINE, MARCH 30, 2001
The sodium system and the steam water
system have operated satisfactorily.
Coming to full power, the designated
rating is 40MWt or 13MWe. The power
that we can generate from the core
depends on the size of the core. The pre
sent core is of small size and so the core
itself limits the power. Although we did
not have any data on how the fuel will
behave, it has, to our pleasant surprise,
behaved very well. We have raised the
power from 10 MWt to 14MWt.
The question is why we have not gone
up to 40 MWt. The core has behaved well
and the fuel burn-up today is 60,000 MW
days per tonne compared to 25,000 which
was targeted in the preliminary calcula
tions. This itself has shown that the core
can be used for a longer duration - once
the second large core is installed the power
can be raised to 40 MWt.
► But there were technicalproblems in f- ci
handling systems...
After we take the fuel burn-up 'e
100,000 MW days per tonne, we will d: ;•
charge the fuel core and receive a new one
Once the new core comes, the size will k
bigger and the quantity will be more.
Is a megajumpfrom the 13MWe FB1R
to 500MWe Prototype Fast Breeder (PFBR)
realistic?
It is a big step. There is no doubt about
it. Various considerations had gone into
such a decision taken 10 years ago. We are
nor the first to build such large capacity
breeder reactors. The biggest breeder was
Superphenix of 1,200 MWe in France.
The second reason is we have 500
MWe coal-fired thermal power stations in
our country. So experience is available on
the conventional side of500 MWe: design
capability', manufacturing ability, site
installation, and so on. Besides, for 500
MWe reactors, we are already building on
the conventional side the turbines, con
densers, transformers, switchyards, circu
lating water systems, and so on. Similarly,
for the 500 MWe PHWR, we are build
ing the steam generators, calandria, end
shield and so forth for the third and the
fourth units at Tarapur. So our industry
has the capability. There are good indus
tries such as Larsen and Toubro, BHEL,
MTAR and Walchandnagar. We have a
programme to develop manufacturing
technology and we are spending Rs.50
crores on it.
The third reason is when we go for a
higher size reactor, the unit energy cost
comes down and we can be economically
competitive with other sources of energy.
When a decision was made to go for
breeder reactors, we had a collaboration
FRONTLINE, MARCH 30, 2001
agreement with France. For political rea
sons, France discontinued it. Though that
help dried out, we decided to go in a big
way for R&D. In the R&D, we have
placed a large number of contracts with
educational institutions, CSIR (Council
of Industrial and Scientific Research) lab
oratories and others. The in-house R&D,
BARC R&D, and outside R&D give us
the confidence to go for 500 MWe breed
er reactors. The design and rhe R&D
remain practically the same for 250 MWe
or 500 MWe reactor.
> What is the status ofthe PFBR now?
The design of the PFBR nuclear steam
supply systems is the responsibility' of the
IGCA.R. This is being done for the past 10
years. The most challenging task so far is
building the capability to analyse die con
ditions during the normal operations of the
reactor arid under ac.Uent conditions.
Tids includes developing. die computer
codes, safety crite’ia, arid Acuments.
An iinyrrtant point k designing such
a '.op-pL.y high technology project is rhe
ab’i’.ry
rake decisions. We have made a
.
.’mentation oi various thingsand
-.vr -oi; ectnident that we will take the right
'.ikcI.'?-.cis in dais centre.
We have now prepared a preliminary
safety' analysis report and submitted it to
the Atomic Energy Regulatory Board
(AERB) for review which is in progress.
On the design side, preparation of manu
facturing specifications and drawings for
the nuclear steam supply system have also
been done.
For the balance of the plant, which
consists of civil structure, steam water sup
ply system, electrical systems and conven
tional auxiliaries, we have appointed two
consultants - Development Consultant
Limited, Calcutta for the power island, and
Tata Consultants Limited for the nuclear
island. The design work is in frill swing.
The site evaluation including its seis
micity, rainfall, groundwater movement,
flooding level during cyclones and geot
echnology has been completed. Experts
did these studies and data has been pre
sented to the AERB. The AERB has
cleared the site (Kalpakkam).
► So everything isgetting ready andyou are
on coursefor building the PFBR
Safety analysis has been completed
with a high level of confidence. We have
done all the plant dynamic studies for the
PFBR. We are half-way through the reli
ability analysis of the critical system, we
have done the core-distributed accident
study analysis, and accidents due to exter
nal events such as flooding and cyclones.
We are now submitting the final docu
ments to the AERB and we are confident
of getting the AERB’s clearance by March
2001. We have the AERB clearance for
the site. We have prepared the
Environment Impact Assessment report
and it is now ready for submission to the
Tamil Nadu Pollution Control Board. It
will then go to the Union Ministry of
Environment and Forests. In six months,
both these clearance will come.
Coming to the R&D, all our facili
ties hear are operational in various aspects
of materials development. We have test
facilities for hydraulics, sodium, compo
nents
and
structural
mechanics.
Laboratories for non-destructive testing,
post-irradiation, fuel chemistry, sodium
and reprocessing are all operational.
We have also identified R&D insti
tutions outside: the Indian Institutes of
Technology at Chennai, Mumbai and
New Delhi; Structural Engineering
. t jc ■.'< < entre (SERC), Chennai; and
CTF ' .!■? acories (TBRJL, Chandigarh;
Ft ’.■••.a <■ .itrol Research Institute,
Palak!. 'I a defence laboratory. All
this
co.ik: tG a fruition by the middle
of 200[.
An important development is that we
are starting the testing of the control rod
drive mechanism, which has been
received at the sire. M. Rajan (Head,
Sodium
Technology
Division,
Engineering
Development
Group,
IGCAR) has completed the work on the
heat and mass transfer: a big sodium facil
ity is there.
On the manufacturing technology
side, we have placed orders with BHEL,
Tiruchi; L&T; MTAR Technologies
Private Limited, Hyderabad; and
Kirloskar Brothers Limited, Pune, for
doing developmental work. We have
given them each a package. All these will
come to a fruition by the middle of2001.
Many industries were involved in build
ing the FBTR, 80 per cent of the work
was done in India. So people are experi
enced in the preparation of specifica
tions,
procurement of materials,
manufacturing and so on. For the PFBR,
we are doing the same components on a
larger scale.
The Union government is enthusias
tic about starting the construction work
on the PFBR. Its importance has been
realised. The Department of Atomic
Energy is enthusiastic. We will start the
construction by December 2001 in the
Ninth Plan itself. The government has
provided Rs. 100 crores for 2001-2002.
Everything depends on us now and we
will push everybody. ■
85
Diabetes in Asia
increases, the patient tends to get easily
injured. These ulcers do not heal quick
ly; often they become gangrenous, neces
ASHA KRISHNAKUMAR
system addresses the complications aris sitating the amputation of the toe, the
ing from diabetes,” he says.
feet, or even the leg.
NDIA has the largest number of dia
Although it is not fatal by itself, dia
According
to
Dr.
Vijay
betics in the world and, according to betes leaves the body open to various Viswanathan, conference secretary and
die World Health Organisation (WHO), complications - neuropathy and vascu Joint Director of M.V.Hospital for
soon one out ofevery four diabetics in the lar problems being the most common.
Diabetes and Diabetes Research
world will be an Indian. The number of
Centre, diabetic foot occurs frequently
diabetics in the country is expected to
- usually within three years of the first
double in the next 10 years.
infection. Thus, early diagnosis is cru
According to the first national Urban
cial. For early diagnosis and treatment
DiabetcsStudy conducted recently by the
there are devices to detect loss of sensa
Di .betes Epidemiology Said;.- Group in
tion (neuropathy), such as monofila
?. population of 11,216 in six cities, die
ments (which determine the protective
ncidence of diabetes is 13.2 per cen • ;.nd
sensation in the feet) and biothesiomediat ot impaired glucose tolerance, ’
•:
ter (an electronic device to determine
cent, fhere has also been an alan.f!
the vibration perception threshold).
increase in the incidence ofdiabekin
Both can be used even by general prac
! .>r. lew y, rs which trend, accord:
titioners and offer reliable prognosis.
esnidy, would continue. Thus ci? i
According to Dr. Vijay Viswanathan,
proven tio -and management is crnuJ Tr
the detection of pressure points under
i idia, as also odier Asian
rhe feet helps predict the
countries where malnu
chances of ulcers.
trition, infection, chang
There
are
also
ing lifestyles and so on are
devices to detect the
major issues.
reduction in the blood
To understand die
circulation in the legs, or
disease in the context of
peripheral vascular dis
die socio-economic and
eases, such as Doppler
cultural aspects of devel
test and Duplex scan
oping countries, the
ning. Foot Scan, anoth
Chennai-based Diabetic
er computerised device
Research Centre and
to detect high pressure
M.V.
Hospital
for
areas under the feet, is
Diabetes, in collabora
useful in taking precau
tion with several national
tionary' measures.
diabetes associations in
Precautionary mea
Asia,
conducted
in
sures are best taken by
Chennai
in
mid Precautionary measures against diabetic foot include the use of
using
appropriate
February a two-day inter appropriate footwear. (Top) The scan of a patient’s foot showing the footwear.
M.V.
national conference on pressure points; (above left) foot pressure with patient’s own
Diabetic Centre, along
“Diabetes in Asia”. The footwear and (above right) wearing footwear developed by the
with the Central Leather
conference, attended by M.V. Diabetic Centre and the Central Leather Research Institute.
Research
Institute
600 diabetologists and
(CLRI), has developed
health-care providers from Asia and Diabetes affects the body’s healing abil special footwear, made of customised
Africa, as also by experts from the United ity. The most common vascular prob moulded insoles.
Kingdom, the United States, and die lem in Asia is the diabetic foot, which
These footwear, which use light
WHO, focussed on early diagnosis, pre accounts for over 50 per cent of all non- weight polyurethane foam, are three
vention of acute and chronic complica traumatic amputations. The Diabetic layered - a tough insole for cushioning,
tions, and die management ofthe disease,
Research Centre is one of the few insti a midsole to absorb shocks and distrib
particularly in the developing countries.
tutions in India that specialise in the ute the load evenly, and an outsole to
According to conference chairman early diagnosis and treatment of the dia give good grip. According to B.N. Das,
Dr. A. Ramachandran, managing direc betic foot.
Assistant Director and Head of the Shoe
tor of the Diabetes Research Centre and
Prolonged diabetes affects the blood Design and Development Centre,
M.V. Hospital for Diabetes, the disease vessels and nerves in the feet, leading to CLRI, the footwear distributes rhe pres
does not receive the attention it deserves loss of sensation. This causes high pres sure in the feet and reduces substantial
in public health policy. “The morbidity sure points or “callus” on the feet, which ly the friction between the shoe and the
and mortality due to diabetes is only thicken the skin and ultimately result in feet. Studies are on to see if these spe
bound to worsen unless the health-care ulcers. When the pressure on the feet cial footwear also reduce ulcers. B
I
FRONTLINE. MARCH 30. 2001
87
‘A cure, or prevention,
appears possible’
Interview with Dr. C.B. Sanjeevi.
“Diabetes is nor fatal by itself, but it
leads to severe complications,” says Dr.
C.B. Sanjeevi, Associate Professor,
Department of Molecular Medicine,
Karolinska Institute, Stockholm, and
the
Chairman
of the
Fifth
International Conference of the
Immunology of Diabetes Society.
Dr. Sanjeevi, who has published
over 70 papers in major international
journals, is on the review panel of sev
eral major journals on diabetes sue'- .
Diabetes,
Diahetologiti,
l '-:
■
Medicine and Diab’tic G.
from a number < f
.:immunology. He is a men .
• r,-.
Scientific and Abstract \tv; v.
Committee
of
the
.• c >.■•;. n
Association for the Study o Diabetes
(EASD), the largest body of diabetes
researchers in the world. He has won
international awards, including from
the EASD and Juvenile Diabetes
Foundation International. At present
he works on the immunology and
genetics of auto-immune diseases,
with special reference to the predic
tion strategy in respect of and vaccine
approach to Type I diabetes.
In Chennai, Dr. Sanjeevi spoke to
Asha Krishnakumar on the disease, its
treatment and the research efforts.
Excerpts:
► What are the symptoms of diabetes
and, clinically, what happens to people
who have the disease!
Type I diabetes is immune-mediated and treated with insulin. The
immune system cells contain antibod
ies produced from B- and T-cells.
There are cell- and antibody-mediated
immune systems. The immune system
primarily protects the body from
invading
organisms,
such
as
pathogens, bacteria, viruses, toxic
chemicals and so on, that enter it
through food and air or through an
injury (in this case the pathogens can
enter the body directly through the
blood stream).
The immune system is present
throughout the body - in the blood
vessels, tissues and cells (primarily the
88
T- and the B-cells). Whatever agents
enter the body first react with the
immune system. On identifying a for
eign matter, the T-cells send signals for
reinforcements and all of them attack
and destroy the invading pathogen.
The immune cells ‘are educated’ to
know what belongs to the body and
what does not.
The T-cells identify some of the
proteins in the beta ceils’which they do
not 'know’, and attack them. But these
proteins are generally covered and not
easily 'seen’ by the T-ceils They are
identified only whet th
a-. e foi some
• .sen tcovewhen
Laetcria or virus t.it.T.- ■■ body and
attacks specific tissue.’,.
I he identification of ;re protein in
the beta cells by the T-ce'i- happens
because of genetic factors and infec
tion. Some genes make the body sus
ceptible to the disease. If a person gets
a viral infection, the virus destroys the
growth ofsome insulin-producing beta
cells, the contents of which are then
released. The T-cells see them as for
eign bodies and get activated after
interacting with the susceptible genes
and send signals for more T-cells to
attack the contents of the cells released
because of the viral infection. In this
attack, the healthy beta cells also get
killed. This process continues till all
the beta cells ultimately get killed. The
speed of the destruction of the beta
cells is determined by the presence of
the number of genes that contribute to
the disease.
If the process happens rapidly from a few months to within a year or
two - it is called acute onset and is part
of Type I diabetes. In some instances,
the genetic factors may not be adequate
to push the events to happen so rapid
ly. It may take several years for all the
beta cells to die and the disease to man
ifest. Unfortunately, until 90 per cent
of the beta cells die, there may be no
symptoms. Even then, it would be
apparent only under stress, such as
after a surgery, an infection and so on.
There is another form of Type I dia
betes, where the progress of the disease
is slow because of several factors in the
environment that arc not yet clearly
known.
Type II diabetes occurs when the
beta cells do not secrete adequate
insulin or when the insulin docs not
for some reason convert all glucose into
energy. Medicines are generally pre
scribed to induce the beta cells to pro
duce more insulin. And where the
insulin is not active, diet is controlled
or altered. Some patients may also
require insulin.
t> What are the types ofdiabetes and the
treatment methods!
Diabetes was classified as insulin
dependent diabetes mellitus (IDDM)
and non-insulin dependent diabetes
mellitus (NIDDM), based on its treat
ment, until 1997. In 1998, the World
Health Organisation recommended
the classification of diabetes as Type I
(a and b) and Type II, based on etiol
ogy (the origin and cause) of the dis
ease. .
In countries such as India, where
the estimation of auto-antibody mark
ers is not done routinely, the diagno
sis is made on the basis of clinical
criteria.
E> Why is the auto-antibody marker test
not routinely done in India!
Solely because of the absence of the
facility to diagnose the auto-immune
form of diabetes. Insulin assay that is
done in India only helps find out how
much insulin the beta cells secrete. It
does not reveal the health of the beta
cells.
► Diabetes is notfatal, but what are the
complications it can lead to!
Diabetes by itself is not fatal, but if
the blood sugar level is allowed to
remain high, it glycosolates certain tis
sues. That is, over a period of time glu
cose gets deposited on tissue walls,
thickening them with plaque and mak
ing it difficult for blood to flow. This
results in complications as it may pre
vent blood from flowing freely into the
brain and lead to a stroke, or to the heart
and cause a heart attack, or to the small
arteries and lead to a loss of sensation,
and so on. Thus, the implications ofdiabetes are severe.
By keeping the blood sugar level
under control, the complications can
be delayed. But, now, with consider
able research going on in various areas
of Type I diabetes, a cure, or preven
tion, appears possible. ■
FRONTLINE. MARCH 30. 2001
c
Type 11 diabetes is a metabolic disor
der that results from rhe body’s inability
to produce enough insulin or properly use
the insulin produced. It occurs in two
forms. First, owing to obesity, unhealthy
lifestyle or rhe consumption of the wrong
kinds of food. The second type is caused
by the inability of the beta cells in the pan
creas to secrete enough insulin. Often,
Type II diabetes can be controlled
through diet restrictions and changes.
But many patients may also need oral
medication and/or insulin.
Type II diabetes is common among
the elderly and may not show up until
very late. Thus many people arc not aware
of their being diabetics until th;- condi
tion becomes severe and leads'/? impli
cations. The incidence ofTy-.c I p. ibctcs
is under-reported as usually .!y the com
plications, such as heart or ie;:J failure
get reported.
Then there is the rare type called ges
tational diabetes - a tempon;ry form ol
insulin resistance that usually occurs dur
ing pregnancy as a result of excessive harmone production, or the oancreas’
inability to make rhe • iduiouai in. uiin
that some women need. Gc'.taci-mal dia
betes is found in 2 to 5 per cent of preg
nant women and usually disappears after
child-birth. However, women with this
problem are at a higher risk of develop
ing Type II diabetes later.
There are “other specific types” of
diabetes - those caused by genetic trans
mission, surgery, drugs, malnutrition,
infection and illnesses.
According to Prof. Rolf Zinkernagel,
the 1996 Nobel laureate for Medicine and
Physiology, the incidence of immunemediated diseases such as diabetes, as also
their types, varies with age, ethnicity, sex,
genetics and the environment. Thus, for
example, in the United StatesType II dia
betes is more common among AfricanAmericans (1.7 times) than the
population in general, and native
Americans and Latin Americans are twice
as prone to diabetes as the general popu
lation. Type I diabetes affects children and
adolescents, especially girls. In India, dia
betes is reported more among the urban
population (10 per cent) than the rural
population (between 2 and 4 per cent).
HE Chennai conference, which
brought together some 200 interna
tional experts on diabetes and immunolo
gy, discussed the progress in research and
devised methods to interpret the results.
It was revealed at the conference that
research on the disease is at an advanced
T
FRONTLINE. MARCH 30. 2001
stage and various groups are trying dif
ferent vaccine approaches for its preven
tion. Some researchers have reached the
second phase of clinical trials while oth
ers are trying the DNA (deoxyribonucle
ic acid) route to find a vaccine.
Simultaneously, population screening is
going on in several parts of the world to
predict the occurrence of the disease and
to identify people who would benefit
from vaccines. According to Prof. Hans
Wigzcll, Chairman, Committee for the
Nobel Prize for Medicine and Physiology'
and President, Karolinska Institute, a
vaccine for diabetes (for Type I) can be
expected in less than five years.
A vaccine for d'abetes will especially
benefi'. i.ic high-iisk groups - the firstdeg ee rciitives of dh.'beties, women who
hr- diabetes during pregnancy, and
cltiicLcn born to oidcc w mien. The cost
of the vaccine, according to Dr. Sanjecvi,
would depend on who develops it. If a
government institution docs it, the price
would be low, but if a private biotech
nology company does it, then it would be
different. Several companies, such as
Peptor in Israel and DiamcdTherapeutics
in Sweden, have reached the second phase
of clinical trials of their vaccines.
The U.S. is close to completing the
Diabetes Prevention Trial I (DPT I). The
largest such programme in the world, the
DPT, which covers 90,000 people (firstdegree relatives ofType I diabetics), is run
by the National Institutes of Health and
involves several institutions across rhe
country. Insulin was administered in
small doses to those with auto-antibody
markers but who had not developed dia
betes. According to Prof. Desmond A.
Schatz, Medical Director, Diabetes
Centre, College of Medicine, University
of Florida, the trials are being carried out
on two categories of people - high- and
medium-risk groups. While the trials on
the former were over and the results
would be known in May, the results of
the trials on medium-risk group trials are
expected by mid-2003.
Another major trial, ENDIT
(European
Nicotinamite
Diabetes
Intervention Trial), is under way across
the Continent. Under this, a particular
component identified in the vitamin
groups that is found to prevent beta cell
deaths is administered to the test group.
This pre-diabetes intervention prevents
the onset of full-blown diabetes. This trial
is to conclude in 2003.
Apart from the work on treatment
and prevention, several groups are work
ing on a cure such as islet transplantation
(that is, replacing dead islets with live
ones). The University of Alberta,
Edmonton, Canada, has developed an
efficient technique - called the
Edmonton Protocol - of islet isolation
from cadavers. As the pancreas is at the
bottom of the abdomen, during organ
harvest from brain-dead persons, doctors
go to it last. As a result, rhe percentage of
live beta cells decreases drastically. The
researchers ar Edmonton have come up
with a technique to go to the pancreas
first thereby recovering more number of
live beta cells. Millions of live islets are
necessary for one diabetic. Islet isolation
from one cadaver can benefit up to two
diabetics, depending on the live beta cells
harvested. While many centres in the
world specialise in human islet trans
plantation, some scientists are also work
ing on xeno-transplantation - from pigs,
whose islets are of the type closest to that
of humans. (The commonly used insulin
is also the porcine variety.)
At the Chennai conference, the major
presentations included those by Dr. Rolf
Zinkernagel (on immunity and auto
immunity), Dr. Jay Sltylcr (on DPT I, the
largest interventional trial in the U.S.),
Dr. Franco Bottazo (on islet cell antibod
ies), Drs. Ake Lernmark, George
Eiscnbarth and Jetty Palmer (GAD65>
IA2and insulin antibodies), Dr. Jonathan
Lakey (on the Edmonton Protocol), Drs.
H. Edlund, N. Kenyon, A. Peck and D.
Pipeleers (on stem cell approach for Type
I cure), and Dr. V. Seshiah (on malnutri
tion-modulated diabetes).
Apart from governments, research on
diabetes is Rinded by many organisations
such as the Juvenile Diabetes Foundation
International, which has pumped in a lot
of money and resources. The U.S. gov
ernment has allotted $100 million to
enable 10 U.S. universities to adopt the
Edmonton Protocol of islet isolation.
Says Rolf Zinkernagel: “While a lot
is understood about the immune system’s
relation with the diseases with quick
onset, the slow-progressing ones, such as
diabetes and tuberculosis, are the ones we
need to concentrate our efforts on.”
According to Hans Wigzell, governments
should realise the urgency for research in
these areas and allocate more funds in
money and resources. Although all
research is for public good, it matters who
produces the vaccines, as that would
determine the price. And this is why gov
ernments need to be educated on invest
ing in vaccine research, which would
finally lead to a fall in private as well as
public health costs. ■
89
■ COMMENT
The power crisis and
a paradigm crisis
After having been taken for a ride by the ideology of centralised electrification, people are
now being taken on another, equally dangerous spin by the ideology of privatisation.
WALDEN BELLO
N many developing nations today,
state-owned centralised power >• Meirs
are mired in mismanagement. ccr.;
and debt. And in country’ after co'.D’ .
influential multilateral agencies -J.
the Asian Development Bank (ADBj
the World Bank have come up w: th acuieall: privatisation and deregulation. This is
the case in India, Thailand, and the
Philippines.
Yet the state ownership versus privati
sation debate obscures the complexities of
the crisis of power generation and deliv
ery'in the Third World. For what is behind
the troubles of giant agencies such as the
Electricity' Generating Authority of
Thailand (Egat) and the National Power
Corporation (Napocor) in the Philippines
is not the natural inefficiency of state
managed enterprises but the crisis of the
paradigm that underpins them: cen
tralised electrification.
Centralised technologies are inextri
cably linked with the politics of domina
tion of countries by central elites - by
technocrats, urban elites and local and for
eign big business. Behind the crisis of these
technologies is the unravelling of a long
time developmentalist alliance among
technocrats, multilateral agencies and pri
vate corporations dedicated to foisting
devastating technologies on developing
nations in the name of a vision of moder
nity and the search for profitability. The
power industry, in particular, illustrates
this destructive symbiosis of modernity
and profitability.
One of the earliest expressions of rhe
sense that generation and distribution of
power was a central test of modernity was
made by Lenin in 1921, when he defined
socialism as Soviet Power plus Electricity.
But it was not only Leninists who equat
ed electric power with rhe desirable soci
ety'. Jawaharlal Nehru, the dominant
figure in post-Second World War India,
I
90
called dams rhe temples of modern India,
a statement that, as author Arundhati Roy
points out, has made its way into prima
ry scncoi textbooks in every Indian lange. Big dams have become an article of
'.mbine<tricI; linked withnationalism.
! question then* utility .
ks almost
sedition.
HElechiKiing''.a: Flu.j. ,-wer
JL development (or -h- pcj-oecotkl
World War period was hat of creating a
limited number of power generators giant dams, coal or oil-powered plants, or
nuclear plants - at strategic points which
would generate electricity that would be
distributed to every nook and cranny of
the country. Traditional or local sources
of power that allowed some degree of selfsufficiency were considered backward. If
you were not hooked up to a central grid,
you were backward. Centralised electrifi
cation with its big dams, big plants and
big nukes became the rage. Indeed, there
was an almost religious fervour about this
vision among technocrats who defined
their life’s work as missionary electrifica
tion or the connection of the most distant
village to the central grid.
It was, it must be noted, a grand mis
sion that was supported in India,
Thailand, South Vietnam and the
Philippines by millions of dollars worth of
grants from rhe U.S. Agency for
International Development (USAID).
Not surprisingly, this generosity was not
unconnected to the less than salutary mis
sion of pacifying rural areas permeable to
communist agitation.
In any event, in the name of mission
ary electrification, India’s technocrats,
Arundati Roy observes in her brilliant
essay, ‘The Cost of Living’ {Frontline,
February 18, 2000), not only built new
dams and irrigation schemes but also took
control of small, traditional water-har
vesting systems that had been managed for
thousands of years and allowed them to
atrophy. Here Roy expresses an essential
truth: that centralised electrification pre
empted the development of alternative
power systems that could have been more
decentralised, more people-oriented,
more environmentally benign, and less
capital intensive.
Centralised electrification, like every
ideology, served certain interests, and
these were definitely not those of the ordi
nary masses. The key interest groups were:
* key bilateral and multilateral develop
ment agencies. In Asia, the World Bank
and the ADB became the biggest funders
of centralised power technologies for
export to Third World countries while
USAID supported rural electrification.
Centralised power development provided
a grand rationale for the existence and
expansion of these institutions into giant
bureaucracies;
* big multinational contractors like
Bechtel or Enron, which made tremen
dous profits building dams or providing
power consulting services;
★ exporters of power plants, including
nuclear plants, like General Electric and
Westinghouse, whose costs were sub
sidised by government export agencies like
the U.S. Eximbank, with the taxes of cit
izens in the developed countries;
★ powerful local coalitions of power tech
nocrats, big business and urban-industri
al elites. Despite the rhetoric about rural
electrification, centralised electrification
was essentially biased toward the city and
industry. Essentially, especially in the case
of dams, it involved expending the natur
al capital of the countryside and the forests
to subsidise the growth urban-based
industry. Industry was the future.
Industry was what really added value.
Industry was synonymous with national
power. Agriculture was the past.
Aside from being an element in coun
terinsurgency programmes, rural electri
fication was simply a small concession to
the countryside to pacify opposition to
FRONTLINE, MARCH 30. 2001
CoverStory
Diabetes, the Ihv,
Killer, has bscKw v
pandemic
;±3
country,
at h
stalking our children
with
D1NESH PARAB.
32 EE3Z53 Nov 17,2002
j
By SANDEEP PHUKAN
In and out of jams
here there is traffic, there are
bound to be traffic jams. On
Diwali, to their great disgust, mobile
phone users discovered cellular traffic
jams. No one could send SMS
greetings as all routes were busy and
frustration peaked northward when
mobile phone screens flashed the stock
reply: Message not sent. But what you
see is not what you get, as a Hutch
subscriber discovered. Determined to
send her greeting to her friend, she
kept resending the message. Afim
seven such failed attempts, she gut n
SMS from the friend. “Is everything
OK? Uv msgd diwali greetings 7
times." Well, the more the merrier.
W
Illustrations/BH/\SKARAN
Carrot on a stick
he city is getting yet another cellular operator, Idea—a consortium by Birla,
Tata and AT&T. But what's good news for users is bad news for the
competition. Faced with the possibility of an exodus of existing subscribers,
mobile phone companies are at their enticing best. While Hutch has promised a
free holiday in Thailand for lucky subscribers who prefer to remain with it, Airtel
has a host of lucky gifts on offer—from a C-class Mercedes to a holiday in
Australia. And the longer a subscriber stays with Airtel, the greater are the
chances of winning. Little wonder people say an ‘idea’ can change your life!
T
In high spirits
ith student elections at
Jawaharlal
Nehru
University round the corner,
campus security has been
tightened. No visitor or vehicle is
allowed in without being personally
screened by senior security officer
Dipanjan Chakraborty and Group
4 Securitas, a private security
agency. But Diwali brought with it
a lessening in the efficiency. A
visitor found a guard inebriated
and when Chakraborty went to
check it out, the guard asked him
to put it down to Diwali spirit.
Hardly amused, Chakraborty
suspended him, ensuring that his
evening of lights was suitably
dimmed.
W
General’s drill
unctuality is not the forte of
politicians. But B.C. Khanduri,
Union minister for road transport and
highways, is an exception to the rule.
The former Army major-general
invariably arrives at official meetings
ahead of schedule. His reputation
nearly suffered a crack on November
2, when his car was caught in the
throng of pre-Diwali shoppers on the
roads. But despite being nearly half an
hour late for the meeting, he was still
the first person at the venue—even
before the hosts!
P
Nov 17,2002 unarfiAil 31
By STANLEY THOMAS
t’s Saturday evening and
Mumbai pulsates with a
restless energy. Shashank
Joshi is restive too as he
takes an emergency call at
his clinic in Opera House, a business
hub in the city’. Then, as neon signs
flicker to life and shoppers vie for space
with sedans on the streets, he grabs his
satchel and cell phone :nd dives into
his California Gold Maruti. As it races
toward suburban Bandra, the siighthui.lt endocrinologist sit-, back spotting
a lilac shirt and lots of worry lines.
Just past seven, he jumps off the
car and rushes into the lobby of
Lilavati Hospital, one of Mumbai's
snazziest. He swerves past groups of
relatives, a giant Ganesha statue and
turns into a corridor. For a moment he
locks eyes with the priest at the
T
entrance of the prayer room on the
way, but doesn’t stop. In seconds he is
in the casualty' and heads towards a
curtained enclosure. A white-coated
assistant steps aside, another woman
with red-rimmed eyes makes way, and
Dr Joshi comes face to face with Varun
Chandok.
The six-year-old boy sitting at the
edge of the bed with a blank look has
been brought in by his panicky' parents
from Chembur, another suburb.
Suspicious of his listlessness, frequent
thirst and urge to ease the bladder
umpteen times, they had got a blood
test done. The result left them in a
daze. Varun’s blood glucose level
measured 475 milligram/decilitre, far
higher than the normal reading that
ranges between 80 and 120 mg/dl.
Joshi knows the boy is in a
precarious condition and that, if his
blood sugar level is not controlled, he
can slip into diabetic ketoacidosis, a
condition akin to coma. For now he
keeps the information to himself, as
the woman with red-rimmed eyes,
Bharat
Gandhi
The Type 1 diabetic was rushed to hospital
in coma six months ago and had to be
hooked on to the respirator. The cricket
crazy lad again slipped into a mini coma
three months ago when he went on a
picnic and skipped an insulin dose.
,A
Pushpalatha
“I don’t v/ant to go to school,” she
says. Her teacher thrashes her
almost daily because she grabs
her lunch box soon after reaching
class. Excessive hunger and
thirst characterise many of the
Type 1 diabetics.
Varun’s mother, turns to him
pleadingly: “He has never had a health
problem before.”
As her eyes turn misty again and
Varun’s father chews his nail endlessly,
Joshi’s mind races to the case of Bharat
Gandhi, a teenager who was brought
to him with diabetic ketoacidosis and
needed to be put on the respirator. If
only he could tell Varun’s parents that
their child too was showing symiptoms
of ketoacidosis.
Such children are normally rushed
to doctors with complaints of
weakness and polyuria—excessive
urination as in the case of Varun—
besides nausea, low blood pressure
caused by dehydration, weight loss and
sometimes abdominal pain. These are
children caught in a bind: their blood
glucose level shoots up while insulin—
the hormone that deposits glucose
(sugar) from the blood into cells in the
body to use as energy—plays hide and
seek. Fast depleting insulin had caused
Varun’s body to break down fat instead
for energy, in the process creating
chemicals called ketones. And
excessive ketones in the blood stream
had led to ketoacidosis, a life
threatening condition.
Nov 17,2002 EEEEZS3 33
CoverStory
hinting at the lifestyle
changes among the affluent
that have caused a spurt in
Type 2 cases among the
She was diagnosed with
young. “But it is only half a
decade before it happens in
Type 1 diabetes four
the middle and lower level
years ago, when in class
schools of the country.”
three. Poor control over
Other predictions are more
sugar levels meant
alarming: the next decade,
frequent hospitalisation.
says one, could see diabetes
in one Indian child in five.
"I used to take a lot of
“There is a 100 per cent
sweets on the sly," grins
increase in the rate of
the girl whose dream is
diagnosis of Type 1
to become a (lector.
diabetes,” says Joshi. “It is
an epidemic among adults,
and it is an epidemic among children.”
Whatever the figures, India’s
children are being stalked by the Silent
Killer which has already become a
pandemic in the country. Ironically,
Children's Day on November 14 is also
World Diabetes Day. India already has
32.7 million diabetics, more than any
other country. And the disease is
showing no signs of let-up. In 1995, the
World Health Organisation reported
19 million cases in India. It was to be
25 million this year, but the revised
figures added seven million more. By
2025, WHO estimates some 57 million
patients in the country. Which means,
over three decades, there will be a 300
per cent increase in the number of
diabetics. “Indians with close family
members who are diabetics face the
risk of getting diabetes at a much
younger age, and the complications
they face are far more critical,” says Dr
Shishir Kumar, senior diabetologist at
Bombay Hospital.
worrying themselves sick as the dread
No one seems to be safe any more.
D-word is mentioned by the doctors.
A recent survey done in six Indian
“I have got children two weeks old with
cities indicated that 12 per cent of the
diabetes," says Dr V. Mohan, director
population could be diabetic. More
of the MV Diabetes Specialities Centre
worrying, says Dr Anil Kapur, vicein Chennai. “Type 1 diabetes can
chairman of the World Diabetes
happen anytime from birth to age 15.
Foundation, is the finding that 14 per
Type 2 diabetes traditionally used to
cent of the people in Indian cities have
start at around 55-60. Now we are
pre-diabetes, or impaired glucose
getting that too at the age of 10,
tolerance. In fact, 66 per cent of
12...151”
Indians are not diagnosed yet.
Studies in Chennai and elsewhere
Put the two figures together—the
have indicated that Type 1 cases are
diabetics and the pre-diabetics—and
increasing by the year. It may not have
the pandemic becomes apparent. “It
reached the staggering numbers seen
means that one out of eight Indians
in Japan and the US “but if you go to
living in a large city has diabetes, and
elite schools in the country, diabetes
that one out of four either has diabetes
is already happening,” says Mohan,
Shantala
Shamarao
As Joshi asks the duty doctor to put
him on human insulin injections the
boy, steadfast till now, breaks into sobs
at the sight of the syringe. He had
already been jabbed several times
during the day for various tests. Joshi’s
eyes soften at the boy’s agony but he
knows that Varun stands little chance
without the insulin.
Four hours later, as he hungrily
tears into a roti, the worry' lines are
intact on Joshi’s face. “Varun’s glucose
level is fluctuating, plunging to 45 then
shooting up to 376. Tests have
indicated serious problems."
Worry lines are appearing on the
faces of doctors across the country
these days. And parents can’t stop
34 mniarrasm Nov 17,2002
Cellular confusion
COMPLICATIONS
Diabetics face blood
vessel defects in the eye
Type 1 diabetics are insulin dependent for life because their
called microaneuryms,
body stops producing the hormone that helps convert food
besides retinal
into energy. The beta cells in the islet tissues of their
detachment.
pancreas, which secrete the hormone, are damaged. Insulin
antibodies—components of the immune system that would
They are more likely to
normally help fight infection—turn rogue and attack the
get cardiovascular
child’s own beta cells.
diseases. Ulcers and
wounds which don't heal
Beta cells —,
could lead to
amputations.
SYMPTOMS: Excessive thirst and
frequent urination are the most
Pancreas
common. Others include slow healing
Impaired blood vesselsto
the kidneys cause high
of cuts, unexplained weight loss,
blood pressure and
fatigue and blurred vision.
kidney failure.
They are also vulnerable
SECRET OF
to other diseases caused
by autoimmune
MY ENERGY:
response—when the body
Carbohydrates in the
does not recognise its
food are digested and
own cells and destroys
converted into glucose,
them—such as
which is stored in the
underactive thyroid.
liver or carried into the
I—Cell
Insulin -1
bloodstream. Insulin
RISK FACTORS
guides glucose (sugar)
The risk of getting T1
to the cells which
diabetes is 10-20 times
convert it into energy.
higher if an immediate
relative has the disease.
Glucose
And if one child has Type 1
diabetes, its siblings have
a 10 per cent risk of
developing it.
BLOCKADE:
When insulin is absent,
or deficient, glucose
cannot enter the cells
and remains in the
Bbod vessel
blood in high amounts,
causing confusion and
even coma.
CONSEQUENCES:
Excessive glucose in the
blood vessels is toxic and
ends up damaging their
walls, affecting circulation
and creating a host of
complications.
WHAT TO EAT: Include more fibre and less fat
to control blood sugar levels; take more of
cereals, dais, whole wheat atta, leafy vegetables;
avoid vegetables wth higher content of starch
such as beetroot and potatoes and fruits such as
bananas, grapes and mangoes.
Graphio/N.V. 1OSE
CoverStory
or is at a great risk of getting it,” says
Kapur.
The figures are alarming for
reasons other than the huge numbers
involved. Experts say that Type 2
diabetes, the kind that normally used
to hit people closer to retirement, is
occurring in Indians at least a decade
earlier than people in the west. In
India the mean age of onset of diabetes
is 42 years. With studies indicating a
six-year gap between the onset of
diabetes and its detection, most
Indians seem to be a candidate by the
mid-30s.
Try telling that to Timothy. With
two young children diagnosed with
Type 1 diabetes, or Insulin Dependent
Diabetes Mellitus (IDDM), the young
Bangalorean walks with a heavy' heart.
Daughter Aksa, 6, was diagnosed four
years ago and son Samuel, 4, showed
symptoms 18 months ago. Today, the
world of Timothy and his wife revolves
round the two young diabetics in the
family. “Aksa was taken to hospital
with fever and when the tests were
done, the doctor said she had diabetes.
I had no clue what diabetes was,” says
Timothy, who makes a living driving
an autorickshaw in the Garden City. It
was double trouble when Samuel too
was diagnosed. “We were devastated,”
Timothy says.
While the majority’ of patients in
India, as elsewhere, have adult onset
Type 2 diabetes, or Non Insulin
Dependent Diabetes Mellitus
(NIDDM), even a minuscule
percentage of child diabetics translates
into huge numbers in a country’ with
32." million diabetics. “On a global
scale, the rapid spread of Type 2
diabetes is worrying,” says Mads
Krogsgaard Thomsen, chief science
officer at Copenhagen-based insulin
producer Novo Nordisk. “But on an
individual, personal level, Type I
diabetes is far more serious. It is a
crippling disease because it attacks you
very young."
Often it cripples the family too.
"Many parents cannot accept the fact
that their child is a diabetic,” says
Kapur. “They go from one doctor to
another in search of the ‘right’
diagnosis. They waste valuable time.”
Emotional problems are followed by
economic ones. Timothy took a loan
36 v.n .^1 Nov 17, 2002
of Rs 50,000 to buy his autorickshaw
and the bulk of the money is still to be
repaid. He spent Rs 25,000 on getting
the various tests done on his children
before the Novo Nordisk Education
Foundation (NNEF) stepped in to
provide free insulin to the children,
among 800 children it is helping
countrywide.
Many others just cannot afford the
treatment. It costs more than Rs 1,500
a month to supply' a young diabetics
requirement of insulin, syringes, and
pay for the frequent pathological tests.
Sudha was eight when Dr Sharad
Pendsey met the newly diagnosed Type
1 diabetic. He recalls explaining to her
parents the importance of insulin. “I
found Sudha’s poor and illiterate
parents very attentive. Finally’ her
father asked me, ‘Doctor, does Sudha
have to take insulin every day for the
rest of life?’ I said yes. ‘What would
happen if she stopped taking insulin?'
'She would go into a coma,’ I explained,
‘and if left unattended she would die.’
He nodded calmly and I was happy
that my counselling had had the
desired effect.”
One month later, Pendsey learnt
that Sudha had died. Her father had
Narasimha Murthy
The 14-year-old has been living
with diabetes for the last six
years but dealing with the social
stigma is proving more difficult.
“Classmates taunt me saying
‘sugar, sugar’ when I am
around and they avoid me.”
stopped giving her insulin, knowing
full well what the result would be.
Stunned by such cases, Dr Pendsey and
his wife Swati formed the Diabetes
Research Education and Management
Trust (DREAM), whose aim is to help
poor children, especially' girls, with
diabetes. DREAM has so far
sponsored scores of children, who are
provided with free instdin, syringes
and blood sugar monitoring strips.
There are social problems to be
faced by' the young battling a
debilitating disease. “Can she get
married?” is a question that
Pushpalatha’s mother, Yamuna,
frequently poses to Shashikala
Thirunathan of NNEF. Pushpalatha,
6, often comes home complaining of
ill-treatment in school because of her
A DIETARY FOOD SUPPLEMENT
FOR DIABETIC PATIENTS
CERTIFIED
COMPANY,
fftSOWj
Mate IMi WCW a part off pwr My fet
CAAP
A DIETARY FOOD SUPPLEMENT
FOR DIABETIC PATIENTS
Introduced in capsule
form to avoid bitter and
sour taste of ingredients.
Melam R&D division has
found out that the use of
unique combination of
Turmeric, Fenugreek, Cloves,
Bitter gourd, Gooseberry and
Neem leaves can improve the
health of human beings.
A unique blend of Indian Spices, vegetables,
fruits and leaves in their natural flavour and form.
I DIETARY FOOD SUPPLEMENT
Ingredients:
Available in
powder form
Turmeric, Fenugreek, Cloves, Bitter gourd,
Gooseberry, Curry leaves, Neem leaves.
FOR DIABETIC PATIENTS
MELAM B35ACAAP - Energy every day
M.V.J. Foods (India) Pvt. Ltd., Cochin - 682 036.
Fax: 91-484-312370. E-mail: melam@giasmd01.vsnl.net.in Website: www.melam.com
Guiile-rComct
CoverStory
Come, play with DiaBetNet
By UTTA JACOB
t need not be the dread ‘D’ word
for the juvenile diabetic any
longer. Instead, a child can now
‘play’ diabetes down. Vikram Sheel
Kumar, a master's student at
Harvard Medical School and MIT’s
joint division of health sciences and
technology has figured that out.
Kumar worked on
the
assumption that motivating
children to test their blood glucose
levels frequently is not exactly a
cakewalk. So he roped in faculty
adviser Prof. Alex Pentland and
together they designed and
conceived a computer game—
DiaBetNet—in which children
punch in their glucose, insulin and
carbohydrate levels at least three
times a day and predict their glucose
level at the end of the day.
Just as kids play Super Mario or
Tetris on their Game Boys to get the
highest score, Kumar felt that
I
participants would be eager to increase
their DiaBetNet scores. “They will play
the game and say, 'Hey, I got that
right!’ said Kumar. “This way, there
will be something to look forward to.”
It takes a mix of meal planning,
exercise and insulin injections to keep
Type 1 diabetics properly regulated.
That’s where DiaBetNet comes in. The
Handspring (a hand-held wireless
device) helps check glucose levels and
teaches children how food and exercise
affect glucose, and to use that
knowledge to win.
The children must wear a wireless
accelerometer that determines how
much they exercise by measuring their
vertical motion. Each child will also
carry a blood glucose meter that will
plug into the serial port of a
Handspring. When a drop of blood is
fed into the meter, the reading will be
sent wirelessly through the
Handspring to a computer at the lab.
For the first three blood tests of
each day, the glucose level appears on
Kumar designed DiaBetNet (in
pic) for kids to punch in their
glucose, insulin and carbohy
drate levels and to predict
their 'scores'.
diabetes-induced behaviour. “I don’t
want to go to school,” she says. Her
teacher thrashes her almost daily
because she grabs her lunch box soon
after reaching class. Excessive hunger
and thirst characterise many of the
Type 1 diabetics but her teacher,
though not unaware of the condition,
refuses to understand her agony.
Yamuna’s complaints to the principal
have yielded little results.
H.M. Narasimha Murthy, 14, has
been living with diabetes for the last
six years—he points to the spots on
either side of his stomach where he
jabs himself six times a day with
insulin—but dealing with the social
stigma is proving more difficult.
“Classmates taunt me saying ‘sugar,
sugar’ when I am around and they
avoid me,” he says.
or a disease that causes so much
physical and mental distress,
experts have very simple explanations,
and sometimes none. They know a lot
about how Type 1 grips a child, but are
F
38 ESEE53 Nov 17, 2002
There is a 100 per cent increase in the rate of diagnosis of
Type 1 diabetes, says Dr Joshi (left, in pic). “It is an epidemic
among adults, and an epidemic among children.”
the hand-held device as a
number. The guessing
game begins later when,
rather than showing the
number reported by the
glucose
meter,
the
Handspring displays a
graph summarising the
child’s physical activity,
carbohydrate level and
prior glucose data for the
day. The more accurately
the child then predicts his
glucose level, the higher
the score. The most
correctly predicted result
is rewarded. It is even
possible to challenge other
members of the project on
the Internet through the
Handspring.
The clinical trials for
DiaBetNet was completed
with the Joslin Diabetes Center at
Harvard Medical School and the MIT
Media Lab and the results were
presented at the Diabetes technology
conference in Atlanta in October. Forty
children between the ages of 7 and 18
with Type I diabetes participated in the
four-w'eek trial. They were split into a
‘game’ group and a ‘no game’ group.
Kumar and his associates were thrilled
with the results—it showed how
DiaBetNet was feasible and
successfully used by the majority of the
patients.
“Beyond establishing feasibility for
a wireless system for diabetes
management, we wanted to determine
w'hether an interactive game could
motivate children to test their glucose
levels more often each day,” said
Kumar. “Though the size of our study
was small we did note that patients in
the ‘game’ group checked more often
each day than patients in the ‘no game’
group and that the mean glucose levels
of those in the ‘game’ group were less
than those in the other group. It gives
us reason to run a longer-larger clinical
trial to establish how long-lasting
these
effects
could
be.”
Kumar and a few colleagues have
founded a company called Dimagi, in
Massachusetts, for producing the
commercial version of DiaBetNet in
the US. “But before it reaches markets
like India, we need to do testing to
establish its relevance given the
basic availability of diabetes
management products (insulin,
glucose test kits, disposable glucose
strips) in the country,” said Kumar.
“One of the motivations for
founding Dimagi was to build a
health technology think-tank and
we are eager to work with diabetes
care providers in India to solve
some of these basic problems.”
DiaBetNet aims to create a diabetic
community for children. Children
get points not only for predicting
their own and others’ glucose levels
but also for offering useful advice
on strategy. Data for every player
will be available on a DiaBetNet
Web site, as well as rankings of the
top players and teams. Kumar said
that a stream of advice and
sympathy would rally children
when they find their scores
dropping. “Kids like the ability to
predict others’ levels, to be a part
of this larger community, and to
be able to learn about their illness,”
he said.
■
not sure why. So much is clear that
Type 1 diabetes is an autoimmune
disease where the immune system
attacks and destroys the insulin
producing beta cells in the pancreas.
“It is a disease that is irreversible,” says
Krogsgaard. “Once the cells are
destroyed they will never come back.”
Experts say there is a genetic
disposition
and
probably
environmental factors that trigger the
disease. Scientists have recently found
evidence that suggests a viral link to
diabetes. Their studies revealed a
marked difference between the way
the bodies of healthy individuals and
those newly diagnosed with diabetes
respond to a virus known as Coxsackie
B4. “The belief is that when the virus
hits you, it somehow triggers the
immune system into attacking the beta
cells,” says Krogsgaard. “But we don’t
know for sure.” The finding, however,
raises the possibility of developing a
vaccine for the disease.
Some experts also suggest that
those who are too early offbreast milk,
and too early on to cow’s milk, face a
heightened risk of getting T1 diabetes.
The fact remains that Indians are
genetically vulnerable to getting
diabetes. During his research in
Britain, Mohan found Indians in that
country with higher insulin levels in
their blood. “Ifthey had higher insulin
level and the same glucose levels as the
Europeans, it means the insulin is not
working. They have insulin resistance.”
Says Krogsgaard: “In India, once
we go out of the cities like Chennai and
Mumbai we find only 3 per cent ofthe
rural population suffering from Type
2 diabetes. But when the same people
move to urban areas, the number goes
up to 12 per cent.” This is because we
are genetically predisposed toward
turning everything we eat into fat. In
the old days we had what researchers
call the ‘thrifty’ or ‘distress’ genes
which deposited fat we ate in the body
for times of famine. “The body was
genetically tuned to store fat,” explains
Joshi. “And in times of famine it used
to utilise that fat to get energy. Now
we don’t need the fat-storing genes,
not at a time when food is in
abundance.”
However, the ‘thrifty’ genes
continue to store fat, leading to obesity
in some. “And when you become
increasingly obese the body becomes
insulin resistant,” explains Krogsgaard.
“In the beginning the pancreas will
compensate by making more insulin
needed for a healthy body. But beta
cells become stressed and exhausted
and they stop producing enough
insulin. Then you have T2 diabetes.”
Another important risk factor is
the waist-hip ratio. A lot of Indians
tend to collect fat in the abdominal
region. “That is a high risk for
diabetes,” says Kapur. “In the west if
you have a body mass index of more
than 27 then you are considered obese.
In India, when one moves from a BMI
of 23 to 24, which is still in the normal
range, people are becoming diabetic."
The results were startling when
Mohan did a comparative study of two
sets of diabetic parents from India and
Nov 17, 2002 UTl-.'gM 39
Are
You
Looking
Forward
Your
Future?
To
Presenting SmartScan™. a compact blood glucose monitoring
system. So sophisticated, you'll love to use it and so discreet, you
can use it anytime, anywhere.
With SmartScan™, it's possible to monitor your blood glucose
levels on a regular basis and maintain it within target* levels.
This way, it not only helps you prevent diabetic complications but
also ensures a better quality of life, today and tomorrow. So, you
can always look forward to a healthy future.
Simple, 3 step testing procedure.
Read result
Apply sample
Insert test strip
(Meter turns on automatically)
Feature rich.
• Slender, lightweight and contoured • Fits perfectly in the palm
of your hand • Accurate results just in
IS secs • Small sample
size - 2.5 pl • Touchable test strips • Confirms sufficient sample
size • Large, easy-to-read display • No cleaning necessary •
150
test memory with date and time • Automatic 14-day average
Why is frequent monitoring important for you?
Studies show that frequent blood glucose testing, as part of an
overall
diabetes
plan, can
help
you
lead
a
healthier
life
and
reduce long-term complications such as - heart disease, kidney
disease and retinopathy (progressive loss of vision) - by up to 60%'.
Ask your doctor about how easily the SmartScan™ meter fits
into your busy life. Because staying in control is
the smartest
choice you can make.
SmartScan'
COMPACT BLOOD GLUCOSE MONITORING SYSTEM
The future is waiting
• Your target levels may differ. Ask your doctor
f Diabetes Control and Complications Trial
To know more about SmartScan™. write to:
OFssmn
x
fl mew -/Jcfi»««©»> cen-puny
To find out how to keep better control over Diabetes, consult your doctor.
For diabetes and life.
Johnson House. 64-66. Senapati Bapat Marg. Mahim. Mumbai-400016. E-mail: Scrvicc@LifcScanlndia.com.
Tel: 91 22 4466801. Fax; 91 22 4469062. Visit us at www.LifcScan.com/lndia
CoverStorv
Testing time
AS HIGH BLOOD glucose levels
are the root of most of the
complications
of
diabetes,
maintaining glycaemic control is
central to treatment. A host of
devices are currently available—
both to monitor blood sugar levels
and to administer insulin. Regular
testing will help diabetics find out
what happens to glucose levels
when they eat certain kinds of food,
or exert on the playground.
Companies are introducing
newer and high-tech monitoring
systems that are smart, discreet and
accurate. These systems, such as
Lifescan's SmartScan, consist a
blood glucose meter and test strips
which measure the glucose level
withjustadropofblood. In just 15
seconds'.
Novo Nordisk revolutionised
the treatment of diabetes when it
introduced its state-of-the-art
insulin delivery
system NovoPen,
about the size of a
fountain
pen.
Today it is used by
some 2 million
people round the
world.
The
company recently
introduced Innovo,
another prefilled
insulin pen with
features such as built-in memory and
display to show when the last dose
was taken.
To help reduce the pain and
fear associated with injections, the
company has even launched a
unique product: PenMate, which
hides the needle tip thus reducing
needle phobia.
42 EEH333 Nov 17, 2002
Europe. Over a period of time, one
child out of four of the European
parents developed diabetes, and a
second child faced a risk of getting it
later. In the case of the Indian parents,
two of the children already had
diabetes at the time of initiating the
study, and the chances of the other two
getting it was about 95 per cent.
But genes alone do not explain the
surge in the number of diabetics in
India. “The explosion of cases now is
coming from environmental factors,”
says Mohan. The most important
factor is physical inactivity, he adds.
The Chennai Urban Population Study
(CUPS) looked at a middle income
group and a low income one in the city.
“We found that the low income group
(monthly income: Rs 1,500) who ate
less and exercised more had half the
levels of diabetes of the middle income
group (Rs 8,500 pm). By the time
income increased five times, the risk
of getting diabetes doubled.
Obviously, affluent Indians and
their kids are paying a price for those
frequent visits to fast food joints and
the crates of cola that they have been
downing, often plonking themselves in
front of their television sets to become
perpetual SOBs: Seated On Butts. Add
high calories to the competition at
work and school and the cocktail is
explosive. “The stress of preparing for
exams is enough to trigger diabetes in
some kids,” says Mohan. “Once you
have stress, counter regulatory
hormones such as cortisol and
glucagons increase in the blood. All
these are anti-insulin hormones.”
ot only will an Indian live with
diabetes for a longer time, he is
more
vulnerable
to
getting
complications at an early age. Any
diabetic, after 10 to 15 years of getting
the disease, has a much higher risk of
developing diabetic eye complications
leading to blindness, kidney failure,
neuropathy, and cardiovascular disease
leading to heart attacks. "By the time
he’s 25 he could get a heart attack, eye
trouble and kidney complications
needing dialysis,” says Mohan. The
Indian genetic profile is such that
many of the diabetics will be at greater
risk of getting heart disease than aT2
diabetic elsewhere.
N
Progress
in patches
ByTHOMMEN JOSE
dvances in medicine and
technology have made it
possible for diabetics to lead long,
productive lives. Though a cure is yet
to be found, researchers are devising
methods of administrating insulin
other than through injections.
PIUS: A new polymer that can allow
the development of insulin pill has
been discovered. When the polymer
is used as a pill coating, it allows
insulin to get into the bloodstream
without being destroyed by the
digestive system. But there are
apprehensions on the efficacy of an
insulin pill as dosing is often
variable. Two different drug
companies have pills that are in the
early stages of development and it
could be two years or more before
they hit the market.
SKIN PATCHES: There are two steps in
A
The Silent Killer also bleeds
society. Imagine the economic burden
on the family if a 35-year-old man with
two kids has to undergo dialysis
because of diabetes complications.
Imagine the burden on society, with a
million people like that who will not
be able to work because of their
condition.
The direct cost of treatment with
tablets and insulin in 1995 was
estimated at Rs 19,000 crore. By 2025,
it will cost Rs 57,000 crore. “Ifyou add
complications, at a very conservative
estimate that only 10 per cent of these
diabetics are going to need further
treatment for complications, then the
cost will be a staggering Rs 126,000
crore, estimates Mohan. “Who’s going
to pay? Will the government pay? Will
private industry pay? Will the
individual pay? No one can pay this
kind of money. It means people will die
simply because they cannot afford the
treatment.” Like Sudha.
People like Krogsgaard and Mohan
using patches. The patients first stick
an electronic adhesive patch, powered
by a small battery, on their skin. The
cells on the skin surface are painlessly
vapourised creating microscopic
openings through which the
medication can be delivered. Then, a
small patch which contains insulin is
stuck on to the skin.
INHALERS: Inhaled insulin is currently
on clinical trials and could soon hit the
market. These insulin pumps are the
size of a small flashlight. Rapid action
insulin, which is inhaled, coats the
mouth, throat and tongue and passes
quickly into the bloodstream.
Sugar monitors
NO MORE PAIN: The AtLast Blood
Glucose System, with a lancing device
and a blood glucose meter, allows
patients to monitor their blood sugar
minus the pain of sticking their fingers
for blood samples. It uses a disposable
test strip to obtain blood samples from
areas that have fewer nerve endings
like the forearm, thigh or upper arm,
so that it does not hurt as much as a
fingerstick.
WATCH THAT LEVEL: The GlucoWatch
are, of course, working overtime to
come up with ways so that people don’t
die of diabetes. “Research in the field
of T2 diabetes at the moment is the
most promising in the sense that the
understanding of the mechanism of
the action of insulin has become much
clearer today than it was a few years
ago,” says leading international
diabetologist Christian Binder. “New
drugs will come in the next 5-10 years.”
There is much excitement about
research in islet-cell transplantation to
help diabetics make up for the loss of
insulin-producing islet cells in the
pancreas. Shortage of donors is one
reason more such transplantations
have not taken place. “So we can cover
only up to 2 per cent of the need this
way,” says Krogsgaard.
His team has developed a
molecule, NN 414, which, when it goes
into the body, circulates to the
pancreas. In the beta cell when insulin
is secreted out into the blood stream,
a lot of other molecules also travel
technique has shown some promise in
treating people with Type 1 diabetes.
Also known as the ‘Edmonton’
technique, it uses cells from two or
more donor pancreases. The cells are
transplanted into the patient and
special medications are given to
prevent their rejection. One
drawback is that though the patient
need not take insulin again, the
medications to prevent rejection
has side-effects and must be taken
for a lifetime.
VACCINE: The world’s first drag that
stops the destruction of pancreatic
beta cells in humans has been
developed. It could prevent the
incidence of Type 1 diabetes in
people at high risk and could also
halt the progress in newly
diagnosed patients. Tests showed
that three injections of the
compound administered within six
months of diagnosis successfully
arrested the progression. After
treatment, the patients produced
insulin and required fewer
injections. There were no major
side-effects, either. To be marketed
post-2004.
GENE THERAPY: Researchers have
identified a gene called SHIP2
which apparently regulates insulin.
This discovery makes it a potential
target for gene therapy for the
treatment of Type 2 diabetes.
Many parents cannot accept
the fact that their child is a
diabetic, says Dr Anil Kapur
of the World Diabetes
Foundation.
along with it. These molecules are
believed to be the ones that trigger the
immune system to kill the cells. “By
resting the beta cells, when we give the
person insulin, we hope the immune
system will shy away from killing the
cells. Patients will then be able to treat
themselves with insulin and they will
also have some beta cell reserve,”
explains Krogsgaard.
Any breakthrough in research
(box, above) will come as a welcome
shot to the likes of Varun. Since being
diagnosed with Type 1 diabetes, he
had plunged into coma. “Fortunately,
he is now out of coma but will need
insulin three times daily with close
diet and blood sugar monitoring,” says
Joshi.
Varun is back home. In two weeks
his world has turned upside down but
the lad is determined to pull through.
Even endure the daily jabs till the
time researchers come up with
something that will restore the joys of
childhood.
Q
Biographer is a wristwatch-like device
that is intended to be used along with
fingerstick blood tests. The watch
extracts fluid through the skin by
sending out tiny electric currents. It
can be worn for 12 consecutive hours
and it produces three measurements
every hour, even while diabetics are
asleep. If glucose levels are perilously
low, it will sound an alarm.
New promises
ISLET CELL TRANSPLANT: This new
Nov 17, 2002 ESEEE3 43
OOO/ or 33 million of the world’s
/O diabetics are Indians.
4 OO/ of the people living in Indian
1.^/0 metros suffer from diabetes.
WHY INDIANS ARE
MORE PRONE
IN THE GENES: Indians are prone to the
Insulin Resistance Syndrome, which is
caused by abdominal fat, thin arteries
and high blood pressure.
STOREHOUSES OF FAT: One theory says
Indians have ‘thrifty’ genes, which
O/ more are in a pre-diabetic
/O stage and may get it later.
M
QfYV of diabetics in urban India
JU /O are below the age of 40.
enabled survival during famine by
storing fat in the abdomen. Now, this
tendency to store can lead to diabetes.
CHANGING LIFESTYLES: Rapid, lifestyle . .
changes and lack.of physical exercise'
has led to a spurt in the incidence oT
diabetes in.urban Indra..
“Diabetic complications
grow with age so I want to
do as much as I can now.”
Tamanna Varma, 25
The investment manager has been
fighting diabetes since she was 14.
Diagnosed with Type-ll diabetes, she
has got used to a controlled diet and
takes insulin regularly. Diabetes has
not diminished her ambition.
16
INDIA TODAY ♦ OCTOBER 6. 2003
□ By Supriya Bezbaruah
mart, articulate, energetic, determined, successful. Adroitly managing
crores of rupees at the age of 25, investment manager Tamanna Varma
enjoys living on the edge. Her bright smile and efficient manner, however,
shots
a drug called
insulin,
religiously
before
meals
day.
soothing
cup of
tea,
impulsive
ice cream
forhas
her.
Noevery
chocolates,
hide No
aof
poignant
secret
—
for no
thetaken
past 10
years,
her
life
hinged
on single
three
no mangoes, no unplanned meals as a teenager. When she started losing weight
inexplicably at the age of 14, little did she realise that those little joys of youth would
be forever forbidden. No one else did either. After an extensive range of tests for
almost every possible ailment, her doctors diagnosed her with Type-11 diabetes, a
disease earlier seen only in pot-bellied and middle-aged men and women.
Varma typifies the unique Indian twist in a global epidemic. Diabetes, a meta
bolic disorder involving high blood sugar levels due to the non-functioning of a key
hormone called insulin, has been on the rise across the world, affecting 150 mil
lion people. More than one-fifth, or 33 million, of them are Indian, according to the
I International Diabetes Federation (idf), resulting in India being dubbed the
j Diabetes Capital of the World at the recent 2003 idf conference in Paris. Indians
diabetics tend to be younger and are more likely to fall prey to complications ranging
from heart attacks and strokes to blindness and sexual dysfunction. Worse, almost
80 per cent of them don't even know they suffer from diabetes. The cost: an
estimated $2 billion (Rs 9.200 crore) annually, according to a British Medical
Journal report. “For developing countries like India, where most patients don’t have
f optimal control, the cost of this epidemic can be crippling." says Wim Wientjens,
I president-elect of idf Europe.
What makes Indians so vulnerable? From Chennai to Chandigarh, a plethora
i of recent studies by leading Indian doctors throws some light on the mystery. The
potent combination of genetics, a rapid rise in riches, and even one’s weight at birth
are possible culprits. But a range of new drugs and treatment methods have made
i a diabetic’s life easier than ever before.
“Everyone knows someone who has diabetes. It is that common in India," says
Ambrish Mittal, senior consultant endocrinologist at the Indraprastha Apollo
Hospital. Delhi. Recent surveys across the country buttress the fact. Diabetes is in
creasingly afflicting young and affluent urban people in India, reveals a survey of
the disease in six metros. The survey conducted by A. Ramachandran of the
Chennai-based M.V. Diabetes Research Centre (mvdrc) found that almost every
I eighth person living in a metro was diabetic. Worse, half of them were less than 50
S
cover story dubetes
years old and at the peak of their
working life. In comparison. Chinese,
Japanese, Americans and Britons tend
to be a decade older when the disease
strikes. "Diabetes is increasing as the
age profile of tire patients drops," says
K.P. Singh, senior consultant endocri
nologist at Fortis Hospital, Mohali.
aurav Kapur. 25. doesn't need sta
tistics to tell him that. Three years
ago. the fun-loving successful vee
jay went to the doctor when he
lost 15 kg. They conducted a battery of
tests, but not for blood sugar. “Who
would have thought 1 had diabetes?" he
asks. Finally, at the Escorts Heart
Institute in Delhi, a blood test revealed
the bitter truth—he was suffering from
diabetes. The doctor said, “We're sur
prised you are not in coma.” He adds.
“Looking back, I am amused by my lack
of awareness of the disease. 1 didn’t rea
lise the repercussions till much later.” To
Kapur, diabetes has meant giving up on
beer, sugar, oily food and red meat.
Worryingly, according to the survey,
another 14 per cent of metro resi
dents—most of them below the age of
40—showed a pre-diabetic condition
G
fests itself in early childhood. In Type II, sugar layer, rendering them ineffective.
or adult onset diabetes, insulin is pro The eyes, brain, kidneys, heart, even the
duced but cannot function as effi healing properties of the body are
ciently—a condition known as insulin ! adversely affected.
resistance. Starving and desperate, the ,
Where one lives and how much one
brain then directs the pancreas to churn j earns clearly make a difference to the
out higher amounts of insulin, not real risk of diabetes. That is what Diabetes
ising that the cells are blind to the hor- I India, a Mumbai-based organisation,
mone. Worse, high insulin levels discovered after conducting a compre
increase the transportoffatty acids, also . hensive study of the disease in villages,
obtained from the diet, into fat cells. It small towns and cities across India.
leads to fatty acids floating about in I Urban India was 4.57 per cent diabetic,
blood vessels too, causing cardiovascu- ■ while only 1.91 per cent of villagers
lar horrors. The glucose, meanwhile, ; were affected. Another study conducted
chokes other crucial proteins with a I in South India found an increase in
called impaired glucose tolerance (igt). Syndrome (irs) in Indians, which
This implies that in the next two includes hypertension, thinner arteries,
decades there may be a veritable explo and high cholesterol levels.
Simply put, glucose, obtained from
sion of the disease in India. It may have
already begun. In the 1970s, urban our diet, is our body's fuel. It is crucial.
diabetes prevalence was 2.1 per cent. Cells grab it from the blood and burn it
Now it is 12 per cent. In Ahmedabad. for energy. The gate through which glu
the incidence has risen from 3.8 per cose enters cells is controlled by insulin,
cent of the population to 7.8 per cent in a pancreatic hormone, which acts as the
17 years. In cash-rich Ludhiana, the ; key. Diabetes mellitus happens when
number of diabetics has almost doubled the body's insulin does not work. So glu
in the past decade to 20 per cent. The cose cannot enter the cells and its level
World Health Organisation (who) esti- | in the blood increases. The disease is of
mates a 170 per cent increase from 84 : two types. In Type 1, insulin cannot be
to 228 million diabetics in developing produced by the pancreas, and mani
countries by 2025. India will lead the
pack, followed by China and the US.
“It is the possible complications that ■
make diabetes a dreaded disease.” says
R.K. Gupta, senior endocrinologist at .
the Sir Ganga Ram Hospital, Delhi, j
People with diabetes are 25 times more
A combination of genes
likely to develop blindness, 17 times
and lifestyle changes
more likely to develop kidney diseases.
place urban Indians
30-40 times more likely to undergo a
at a risk of diabetes
major amputation. 2-4 times more
likely to suffer a heart attack and twice
as likely to get a stroke than a normal
individual. It is because diabetes forms
part of the larger Insulin Resistance
Cells need
SPREADING LIGHT: An awareness camp on diabetes. Many diabetics in
India don’t even know that they are suffering from the insidious disease
Diabetes Dossier THE WHOLE BODY IS AFFECTED
■ DIABETIC FOOT: Foot ulcer
ation, caused by nerve damage
and lack of blood supply, makes
diabetics 30 times more likely
THE CAUSE
Glucose
Type-11 diabetes with the rise in the
urbanisation level from villages (2.4 per
cent) to semi-urban areas (5.4 per cent)
and metros like Chennai (11.6 per cent).
Intra-city income groups also showed
considerable differences for both
diabetes and igt—the incidence of
diabetes was 12.4 per cent in the mid
dle-income class and 6.5 per cent in the
low-income class while that of igt was
7.5 per cent and 2.9 per cent. “Our
Chennai
studies
have
clearly
established the role of lifestyle in the
probability of diabetes,” says mvdrc
Chairman V. Mohan
BRAIN: Diabetics are 2-5 times more
likely to suffer strokes than non
diabetics, especially if they have
high blood pressure as well. Strokes
to undergo limb amputation.
are also more severe in diabetics.
This is because prolonged high
■ PROLONGED HEALING:
blood glucose levels weaken the
High blood glucose affects
blood vessels in the brain.
crucial proteins, so
wounds take long to heal.
EYES: Diabetics are 25 times
glucose. Insulin,
■ OC.AUHL
secreted by the
DYSFUNCTION: A
Insulin—*
pancreas, is the
common problem among
Glucose gate
■
key that opens
diabetics because blood
the cell gates
supply to organs is
for glucose.
affected.
more likely to go blind than non
diabetics. Retinopathy, caused
by damage to the eye capillar
ies. is most common. So are
cataracts and glaucoma.
HEART: High blood
sugar levels and
If the insulin is
Faulty insulin
z
Energy
deprived cell
defective, the
increased amounts
glucose gates
of fatty acids due
remain shut
to insulin, thicken
and cells don't
the arteries. Dia
get energy. The
betics are at four
patient feels
times greater risk
very tired.
of heart attacks.
■ Frequent hunger and thirst are
common signs of diabetes.
■ Weight loss, irritability and lack of
energy are other symptoms.
■ Frequent urination is also a sign.
■ A common sign is when wounds don't
heal, cramps and pain in legs.
INDIA TODAY ♦ OCTOBIHI 6. 2003
j
Diabetes occurs
if fasting sugar
level crosses
110 mg per 100
ml blood. Two
hours after meal,
it should be less
than 140 mg.
KIDNEY FAILURE: High blood glucose.
and blood pressure damage kidney
vessels. So diabetics are 17 times
more likely to suffer kidney failure.
cover story diabetes.
“I am amused
by my lack of
awareness of
the disease.”
Gaurav Kapur, 25
Three years ago, Kapur
started losing weight.
Puzzled doctors found
nothing amiss before a
blood sugar level test
pronounced severe
diabetes. Initially on a
strict diet, he later
decided to go in for
insulin therapy. He
now takes it regularly.
MYTHS AND REALITIES ABOUT DIABETES
MYTH: I AM NOT FOND OF SWEETS, SO I WILL NOT GET DIABETES.
REALITY: The onset of diabetes is not linked to intake of sweets. Diabetes is
more likely to hit people who don't exercise regularly or are overweight. Once a
person develops diabetes, however, sweets are best avoided.
MYTH: ONLY OVERWEIGHT PEOPLE SUFFER FROM DIABETES.
REALITY: Slim people are as much at risk of diabetes in India as are overweight
people because Indians suffer from a syndrome called the Insulin Resistance
Syndrome which is caused by abdominal fat and high blood pressure.
MYTH: I HAVE HIGH BLOOD SUGAR BUT I FEEL FINE. NO SYMPTOMS.
REALITY: Often, symptoms do not correlate with the blood sugar level.Going by
just symptoms can be very misleading because the high level of blood sugar
can seriously damage other organs like eyes, kidneys and heart.
MYTH: I WAS TOLD I CAN
HAVE ALCOHOL.
REALITY: Alcohol can worsen
blood sugar control, provoke
severe hypoglycaemia and even
react with antidiabetic drugs.
/lYTH-.ONCE ON INSULIN,
ALWAYS ON INSULIN.
TY: Medical evidence says
t early use of insulin can
diabetes from worsening.
20
INDIA TODAY
OCTOBER 6. 2003
The Diabetes India study also
showed significant regional differ
ences—western and southern India
showed highest prevalence while east
and central India showed the lowest,
with the north in between. “Western
and southern India are more industri
alised compared with the rest of the
country. So it is likely that they get the
least amount of physical exercise,”
explains Mumbai-based S.M. Sadikot,
president, Diabetes India.
While lifestyle changes puli the bag
ger, one theory says it is the “thrifty
genes” in Indians that put them in the
cross-hairs. These are genes that over
the centuries helped ensure survival
during famines by storing excessive fat
in the abdomen when there was plenty
of food. In modern times, bombarded
with rich food, the body' cannot cope,
leading to diabetes. This is precisely
what happened to Indians migrating to
western countries. Indians settled in
the UK and US have far higher rates of
the disease than any other ethnic
groups. Mexican Pima Indians living in
the US, and other US native Americans
who have since moved to an urban life,
also show epidemic rates of the disease.
Research by Pune-based doctor
Chittaranjan Yajnik showed that Indian
babies are born smaller than
Caucasian babies, but, surprisingly,
have just as much fat, all concentrated
cover story diabetes
“That I have to
inject myself
daily comes as
a huge shock.”
Sonic Purwal, 34
A busy IT professional,
Purwal went for a
routine preventive
health check up only
to find that he had
diabetes. Put on
insulin immediately,
Purwal has been
able to manage the
disease by regular
exercise and a more
disciplined lifestyle.
around the abdomen. Indian babies are
also born with much higher blood
insulin levels. All are markers for
diabetes in later life.
Genes may show the way, but diet
spells dooms. Low birth weight fol
lowed by obesity in later life has been
linked to insulin resistance syndrome.
Yajnik’s group had recendy shown that
it is not lack of food but specific lack of
micronutrients—like iron and zinc—in
mothers that lead to smaller babies
among Indians. “Most girls in India are
deficient in micronutrients from child
hood. Anaemia is rampant,'' says Geetu
Amarnani, chief nutritionist, Delhi
Diabetic Forum. One study by Raheja
Hospital. Mumbai, blames the refined,
processed and preserved foods which
are very popular but deficient in an im
portant fatty' acid called n:3 fat.
Sadikot blames a sedentary lifestyle
instead. “In India, it is more to do with
lack of activity rather than being over
weight because 40-50 per cent of the
diabetics are either underweight,
normal or just mildly overweight." he
explains. Interestingly, it is not confined
to human beings. Evolutionary bio
logist Jared Diamond noted that there
is a diabetes epidemic in the Los
Angeles zoo too, among primates like
chimpanzees, whose zoo lifestyle ap
proximates the high-calorie, low-exer
22
INDIA TODAY ♦ OCTOBER 6. 2003
cise lifestyle of many human diabetics.
Genes, pre-birth and post-birth
diet, lifestyles, whatever the reason,
Indians seemed to have pulled the
worst cards for this disease. With a di
abetic father, an American has a 20 per
cent chance of getting the disease. But
an Indian has a 30 per cent chance. If
both parents are diabetic, Indians are
at a 60 per cent risk, while Americans
are safer at 25 per cent.
irst generation Indian diabetics
are common, the disease often
creeping up without warning. It
took it professional Sonic Purwal,
34, completely by surprise. No one in
his family suffered from diabetes. But
two months ago, he was stunned when
a routine preventive healthcare check
up showed his sugar levels were so high
that he had to be put on insulin imme
diately. “Learning to inject myself and
realising that I would have to do this
every day for the rest of my life has
come as a big shock,” he admits. In two
months, his life has changed drastically,
but he looks at the brighter side. Now
he is more disciplined, his meal timings
regulated and regular exercise makes
him more energetic. “We have realised
how precious life is. Now all of us have
a healthier lifestyle,” his wife adds.
Several new products in the market
F
have made managing the disease eas
ier now. Thirty years ago, when a young
Delhi-based businessman Jitender
Mohan, then 35, was diagnosed with
diabetes, there were no disposable
needles. "I even had to learn to carefully
sterilise those large needles,” he says.
“Now it’s so much easier,” he says feel
ingly, bringing out what looks like a pen
case. Inside, what looks like an ordi
nary pen is a compact, injectible insulin
pen, costing Rs 1.200 which he can
carry anywhere, even in his shirt
pocket. “And since it is insulated, I don't
have to worry about finding a fridge to
keep the temperature-sensitive insulin
whenever I travel," he adds.
Timing and balance were once
crucial features of a diabetic's life. Their
vocabulary was entirely different—they
talked in terms of “million dollar
peaks". Those are the blood sugar
peaks after a meal. “Even in the middle
of an important business meeting, I had
to excuse myself and take my insulin
shot on time,” says Mohan. Timing the
insulin dose is vital. Too much, or too
early, ..and glucose levels dip precari
ously. Headaches, restlessness, dizzi
ness, blurred vision, and eventually
coma could follow. Now, a new slowreleasing insulin analogue, called
insulin glargine, has been launched in
India. One shot is enough for 24 hours,
cover story diabetes
"I miss sweets
and chocolates
but I am used
to it now.”
Kalpana Sharma, 10
Two years ago, Kalpana
started urinating fre
quently. No one had
imagined she would get
the adult version of
diabetes at such a
young age. Put on a
strict diet and exercise :
regimen, she has shed i
over 10 kg. With pills,
her sugar level is down.
WHAT’S NEW
Managing diabetes has become
easier with modern technology
HOME ALONE:
Easy to use
glucometers
monitor blood
sugar levels at
home. New
software sets
alert if sugar
levels rise.
NEW DRUGS: One shot
of Lantis, a slow-act
ing insulin, is enough
for a day. An Indianmade recombinant
human insulin from
Wockhardt is cheaper.
EASY INSULIN:
No more
syringes. Instead
patients use sleek
insulin pens that
can be carried in the
pocket. Also, insulin
pumps which are
inserted under the skin.
FOODS: Specially made for
diabetics, from chocolates
and jams to atta.
allowing for more flexible schedule.
There is another minor revolu
tion—no more daily pokes. Diabetic pa
tients today can also replace injections
altogether with an insulin pump—a
battery powered, computerised device
about the size of a deck of cards. It has
a needle or catheter implanted in the
body and a preset dose of insulin is
automatically administered. But at
$3,000 (Rs 1.4 lakh), it is too costly.
Insulin itself is seen as the last op
tion for diabetics. In India, patients are
first put on a diet-and-pills course.
From only a couple of types of anti
diabetes drugs a decade ago, now there
are a huge range of treatment options.
Prominent among them are sulphonylureas (which interferes with the
liver’s output of glucose), buguanides
(helps more efficient utilisation of
glucose in insulin resistance), sulphonylureas-i- biguanides and alpha
glucosidase inhibitors (which help in
the absorption of glucose).
It is also far easier to monitor blood
glucose levels today, with the new onetouch monitoring systems now avail
able in India precluding the chances of
falling into diabetic coma. Another de
vice—the HbAlc—monitors glucose
levels in the past three months by de
tecting the percentage of sugar coating
i blood haemoglobin. It is considered exi tremely accurate and takes only eight
minutes. A reading of more than 7 per
cent by this instrument spells danger.
And new software helps iT-sawy
people like Purwal to keep track of how
well they are fighting their disorder.
ven the availability of insulin is
easier now. Earlier, animal-based
insulin had caused ethical prob
lems. Now, modern biotechno
logy ensures that yeast or bacteria
churn out human insulin. Eli Lilly, the
world’s first manufacturer of insulin,
has a range of such insulin and insulin
analogs in the market. Recently,
Wockhardt, using a unique system,
launched India’s first “desi” recombi
nant insulin. This has brought prices
down to a more affordable Rs 120 per
vial. “The launch of Wosulin is part of
Wockhardt’s larger commitment to
diabetes management in the country,"
says Habib Khorakiwala, chairman,
Wockhardt. Following Lantis. a 24hour insulin developed by Aventis, an
inhaled form of insulin, Exubera. will
soon be available, making diabetes
management easier.
Indeed, to both multinational and
Indian pharmaceutical companies, the
Indian diabetes explosion spells an
opportunity. “Not just in the near
future, but in the long term too, the
single largest and most important busi
ness for Eli Lilly will be diabetes," says
E
OCTOBER 6. 2003 ♦ INDIA TODA\
cover story diabetes
Rajeev Gulati, managing director, Eli
Lilly India. For the company, India is
No. 1 in Asia, and among the most im
portant markets globally. Ranbaxy has
set up a separate dedicated division for
innovative cardiac and anti-diabetic
products. The total Indian diabetes
market is Rs 750 crore and is growing
at a rate of 15 per cent. The average
pharmaceutical industry growth, in
comparison, is 8 per cent. The potential
can be gauged by the fact that 30 new
players entered this market in the past
four years. Nearly 144 new diabetic
products were launched in the Indian
market in 2002 alone.
Controlling the Problem
Although Indians are genetically prone to diabetes, an
affluent, high-stress, sedentary lifestyle increases the
risks dramatically. But minor changes can help one cope.
YOU MUST...
EXERCISE REGULARLY: Even if this means walking to work or taking the
stairs instead of the elevator. A sedentary lifestyle is considered a
major cause of the diabetes epidemic in urban India.
EAT HIGH-FIBRE DIET: Though this varies from individual to individual,
food with high fibre content, like leafy vegetables, is good.
MONITOR BLOOD SUGAR LEVEL* Check blood sugar levels every three
months, especially if there is a history of diabetes in the family.
AVOID STRESS: Try and control stress and lead a regular daily routine.
According to some patients, yoga and even a regular massage have
helped them in reducing stress.
YOU MUST NOT...
IGNORE ANY SYMPTOM: Symptoms such as tiredness, cuts that do not
heal, frequent urination, frequent hunger and thirst, should not be
taken casually. Consult your doctor and get a check up done.
MISS A MEAL* Missing a meal will result in fluctuations in blood sugar
level, and can even result in dangerous hypoglycaemia (low blood
sugar level). Small frequent meals are advisable.
EAT FOOD RICH IN FAT: Fast, fatty, fried, refined, processed and pre
served foods should be avoided at all cost.
ut awareness remains low. “For
every diagnosed Indian diabetic,
at least two have the disease and
do not know it,” says Ashok
Jhingan, chairman, Delhi Diabetic
Research Centre. Even doctors are not
always up to date with the latest
technologies. “Here patients are less
compliant on medicine and doctors are
not aggressive enough, so the disease
is not controlled,” says Sandeep
Bhattacharya, director, Commercial
Operations, Aventis. As a result, it takes
15 years before a diabetic patient is put
on insulin by doctors, usually as a last
resort, although some studies show
that early use of insulin can help con
trol sugar levels better. Fear of injec
tions, and the risk of hypoglycaemic
coma, are some of the reasons why
Indians avoid using insulin. Eli Lilly has
launched many pioneering initiatives,
including diabetes education camps,
and a special diabetes kit for children
called HumaCare. Aventis, in co-opera
tion with doctors nationwide, is launch
ing a major database of its Lantis users.
Even as scientists grope for a cure
for diabetes, it may take several years
before a breakthrough. Only a few
genes which can cause diabetes have
been identified so far. “Till then, only a
broadbased preventive programme
involving all sections of society can
tackle this challenge,” says the
Ahmedabad-based diabetes expert
O.P. Gupta. Regular physical exercise, a
controlled diet and careful monitoring
of sugar levels would be a good begin
ning for most urban Indians.
B
with Kanika Gahlaui, Sheets Raval,
Arun Ram, Ramesh Vinayak,
Stephen David and Uday IVIahurkar
24
IVD1A TODAY ♦ OCTOBtH 6. 2003
Food related maladies - in relation to Lifestyle With special reference to
Diabetes.
Dr. Rangesh Paramesh M.D. (Ay),
Senior Medical Advisor, Research & Development Center, The Himalaya Drug Company, Bangalore 562123.
E-mail: dr.rangesh@himalayahealthcare.com
Food is one of the three pillars of life according to Ayurveda, the ancient Indian science of life. Sleep and
regimented lifestyle are the other two which contribute to a great extent the state of healthy living. The
optimum state of health is a goal toward which many strive. After all, every one knows that, in great
measure, primarily the physical well-being determines the quality of life. But deciding which approach to
a healthy life-style will best improve or maintain personal health is no easy task. It is virtually impossible
to read a newspaper, watch television, listen to the radio, or browse in a book-store without being
bombarded by information from experts and so-called experts on the art of staying healthy. It is no
wonder that confusion abounds.
Ahara, the food as it is known in Ayurveda, is defined as that which brings near or procure or being about
to fetch all the living beings the nutrition that results in strength (physical & immunological), complexion
(social) and enthusiasm (psychological) and subsequently survival. Ironically it is the same food which is
also the cause for the diseases and death. Hence the food bome diseases are in the focus.
Diet as a Tool for Health
( "Whenever
youfind
yourselfon
the side of
the
majority,
it's time to
pause and
reflect." Mark Twain
Modem day lifestyles are busy, stressful, and seem to produce time conflicts more than ever. With time
being so precious, it is no wonder that quick and easy foods are eaten over foods one needs to prepare.
Not until one gets ill, does one look at food as a possible problem in one’s life. This common notion
should change.
The food one consumes on a daily basis affects the health more than anything else. The skin protects the
body from the outside world, but what protects it when the outside world is internalized? All of the
materials one requires for survival (besides oxygen and sunlight) need to be ingested and then digested.
The easiest way to take control of the health is to take control of what one eats. If the physician inform
that most of the health problems are not diet related, they could be wrong.
The foods of today are nothing like the foods of the past. Modem foods are laced with nitrates,
preservatives, soy additives, plant byproducts, etc, and are heavily processed. Most livestock are
pampered with high caloric feed, injected with hormones and antibiotics, and not allowed to graze,
resulting in meat with different nutrients than those of wild game. Many of the modem foods touted as
"healthy" didn't even exist in our ancestor's diet. It is important to realize that what the majority of people
eat today is not optimized for the body, but optimized for convenience, taste, and preservation.
“It has
become
appallingly
obvious
that our
technology
has
exceeded
our
humanity ”Albert
Einstein
The knowledge and technologies have advanced at a tremendous pace, but the human body is still in the
Stone Age. One still have the genetic makeup of our Paleolithic ancestors. On an evolutionary scale, our
bodies have not been given the necessary time to efficiently utilize these new foods. It takes thousands
upon thousands of years to adapt to the dietary changes we have incorporated in our modem day diet in a
relatively short period of time. This sudden change in diet can account for many of the diseases that
plague modem society.
If one has been caught up in the mainstream by following a diet low in fat or high in processed foods, or
if they have developed a modem illness such as obesity, diabetes, Irritable Bowel Disease, Ulcerative
Colitis, Crohn's disease, rheumatoid arthritis, and other autoimmune diseases, one need not despair. A
Paleolithic diet can still be followed today. In fact, a number of diets that closely resemble that of our
ancestors have been used to alleviate modem day illnesses. The following is a list of these diets, and the
illness they have treated.
The Generic Low Carbohydrate Diet: Also called a high protein diet was made popular by the
cardiologist, Dr. Atkins. The program restricts the amount of carbohydrates one can eat in a day. As a
result, one can lose a fair amount of weight. Our ancestors did not have access to the refined sugar found
1
found in today's food. By restricting sugar-laden foods, we get one step closer to our optimum (our
ancestors) diet. A generic low carbohydrate has been used to treat obesity, diabetes, and heart disease.
The Specific Carbohydrate Diet: This diet was developed to treat illnesses of the bowel, such as
Crohn's and Ulcerative Colitis. It has also been used effectively to combat yeast infections and other
illnesses, including autoimmune diseases. The diet does not limit the amount of carbohydrates eaten,
just the kind of carbohydrates. The diet also stresses eating whole foods and limiting the amount of
processed foods one eats.
The Paleolithic Diet: Is the strictest of the three diets shown, but also offers the greatest health
benefits. It stresses whole foods with an emphasis on meats. The diet excludes all modem foods, such
as dairy, alcohol, legumes, and grains.
Diet & Diseases
Diet as a means of disease prevention has-with good reason-received a lot of attention from the
medical community and the popular media. An unhealthy diet has been linked in varying degrees to
six of the ten leading causes of death in America today: cancer, adult diabetes, atherosclerosis, stroke,
cardiac diseases, and liver cirrhosis. Of these, heart disease and cancer are responsible for the vast
majority of chronic illnesses and premature deaths. Whereas enormous strides have been made in the
treatment and cure of these diseases, medical science is now also investigating their prevention, with
special emphasis on how dietary modifications affect probability of disease. Obesity, the most
common nutrition-related health problem, is a contributing factor in a number of health problems,
including hypertension, arthritis, and certain types of cancer, adult diabetes, and heart attacks.
The health is influenced not only by how much one eats, but what one eats. While many experts have
been advocating a low-fat, low-cholesterol, high-complex-carbohydrate diet to combat heart disease,
evidence has been mounting that virtually the same diet may also reduce the risk of other diseases.
To control weight and minimize other food-related health problems, one needs to become
knowledgeable about nutrition. Although Americans are more concerned about eating healthfully
today than in the past, the abundance of conflicting, misleading, or outright false information about
diet can be bewildering. Indeed, sorting out reliable nutrition advice from the plethora of
misinformation (i.e., popular diet books such as Fit for Life or How to Be Your Own Nutritionist) can
be difficult.
Foodborne Diseases
Definition of foodborne illness: Foodborne illnesses are defined as diseases, usually either infectious
or toxic in nature, caused by agents that enter the body through the ingestion of food. Every person is
at risk of foodborne illness.
There are three main types of causative agents that bring about illnesses from food: - Pathogenic
Bacteria, Viruses, and Chemical toxins in food either naturally occurring or introduced to a food.
Magnitude of foodborne illness:
Foodborne diseases are a widespread and growing public health problem, both in developed and
developing countries.
•
The global incidence of foodborne disease is difficult to estimate, but it has been reported that
in 2000 alone 2.1 million people died from diarrhoeal diseases. A great proportion of these
cases can be attributed to contamination of food and drinking water. Additionally, diarrhoea is
a major cause of malnutrition in infants and young children.
•
In industrialized countries, the percentage of people suffering from foodborne diseases each
year has been reported to be up to 30%. In the United States of America (USA), for example,
around 76 million cases of foodborne diseases, resulting in 325,000 hospitalizations and 5,000
deaths, are estimated to occur each year.
•
While less well documented, developing countries bear the brunt of the problem due to the
presence of a wide range of foodborne diseases, including those caused by parasites. The high
prevalence of diarrhoeal diseases in many developing countries suggests major underlying
food safety problems.
2
•
While most foodbome diseases are sporadic and often not reported, foodbome disease
outbreaks may take on massive proportions. For example, in 1994, an outbreak of
salmonellosis due to contaminated ice cream occurred in the USA, affecting an estimated
224,000 persons. In 1988, an outbreak of hepatitis A, resulting from the consumption of
contaminated clams, affected some 300,000 individuals in China.
Major Foodborne diseases from microorganisms
•
Salmonellosis
•
Campylobacteriosis
•
Cholera
•
Infections due to enterohaemorrhagic (causing intestinal bleeding) E. coli, and listeriosis
Other food safety problems: some major examples are:
•
Naturally occurring toxins, such as mycotoxins, marine biotoxins, cyanogenic glycosides and
toxins occurring in poisonous mushrooms periodically cause severe intoxications.
•
Unconventional agents such as the agent causing bovine spongiform encephalopathy (BSE, or
"mad cow disease"), is associated with variant Creutzfeldt-Jakob (vCJD) Disease in humans.
•
Persistant Organic Pollutants (POPs) - Dioxins and PCBs (polychlorinated biphenyls).
•
Metals: such as lead and mercury, cause neurological damage in infants and children.
Exposure to cadmium can also cause kidney damage, usually seen in the elderly. These (and
POPs) may contaminate food through pollution of air, water and soil.
Costs of foodborne diseases
Food contamination creates an enormous social and economic burden on communities and their health
systems. In the USA, diseases caused by the major pathogens alone are estimated to cost up to US $35
billion annually (1997) in medical costs and lost productivity. The re-emergence of cholera in Peru in
1991 resulted in the loss of US $500 million in fish and fishery product exports that year.
Food safety is an increasingly important public health issue. Governments all over the world are
intensifying their efforts to improve food safety in response to an increasing number of food safety
problems and rising consumer concerns.
Why do foodborne diseases emerge?
New foodbome disease threats occur for a number of reasons. These include increase in international
travel and trade, microbial adaptation and changes in the food production system, as well as human
demographics and behavior:
•
The globalization of the food supply :
•
The inadvertent introduction of pathogens into new geographic areas :
•
Travelers, refugees, and immigrants exposed to unfamiliar foodbome hazards while abroad :
•
Changes in microorganisms :
•
Change in the human population
•
Changes in lifestyle: Greater numbers of people go out and eat meals prepared in restaurants,
canteens, fast food outlets, and by street food vendors.
Diabetes & Lifestyle Changes
The disease is described several centuries ago in Ayurvedic literatures, which have recorded the bad
lifestyle as the principal cause of this disease. It is said that sedentary lifestyle including excess sleep,
food very rich in carbohydrates like fresh rice, cane sugar products, milk products especially curds,
animal protein, dietary fats.
3
"The world is facing a growing diabetes epidemic ofpotentially devastating proportions. Its impact
will be felt most severely in developing countries. The World Health Organization and the
International Diabetes Federation are working together to support ongoing initiatives to prevent and
manage diabetes and its complications, and to ensure the best quality of life possible for people with
diabetes worldwide. Together we are helping to provide countries with the means to face the
challenges that lie ahead. It is time for diabetes action now ”. - WHO.
DIABETES is a life-threatening condition
•
Worldwide, 3.2 million deaths are attributable to diabetes every year.
•
One in 20 deaths is attributable to diabetes; 8,700 deaths every day; six deaths every minute.
•
At least one in ten deaths among adults between 35 and 64 years old is attributable to
diabetes.
•
Three-quarters of the deaths among people with diabetes aged under 35 years are due to their
condition.
A full and healthy life is possible with DIABETES
•
Studies have shown that, with good management, many of the complications of diabetes can
be prevented or delayed.
•
Effective management includes lifestyle measures such as a healthy diet, physical activity,
maintaining appropriate weight and not smoking.
•
Medication often has an important role to play, particularly for the control of blood glucose,
blood pressure and blood lipids.
•
Through the provision of optimal health care the risk of developing diabetic complications
can be reduced substantially.
•
Helping people with diabetes to acquire the knowledge and skills to manage their own
condition is central to their leading a full and healthy life.
In many cases, DIABETES can be prevented
•
The prevention of type 1 diabetes is not yet possible and remains an objective for the future.
The prevention of type 2 diabetes has been shown to be possible and requires action now.
•
Trials have shown that sustained lifestyle changes in diet and physical activity can reduce the
risk of developing type 2 diabetes. For example, the Finnish Diabetes Prevention Study
showed that a better diet, increased physical activity and modest weight loss could
substantially reduce the development of type 2 diabetes in middle-aged adults at high risk.
•
In all the studies conducted so far in people at high risk, lifestyle changes have been
substantially more effective than the use of drugs.
•
The scale of the problem requires population-wide measures to reduce levels of overweight
and obesity, and physical inactivity.
•
Informed policy decisions on transport, urban design, and on food pricing and advertising can
play an important part in reducing the population-wide risks of developing type 2 diabetes.
Ayurvedic literatures have advocated the treatment such as less fat in the food, and physical exercise,
besides dry massage and sauna which help to reduce the body weight or obesity.
4
Issue no. 37 April-June 2004
Health Dialogue
A forum for the exchange of news and views on primary healthcare in India
Diabetes
Is \\ iabetes is
■
«
no longer
the disease of
the rich or the aged.
Known as the “Silent
Killer", it is reaching
epidemic proportions
and according to the
World Health
Organization (WHO)
approximately 177
million people
worldwide have
diabetes. India has an
estimate of 32.7 million
diabetic people.
To compound this
problem, diabetes is no
longer behaving the way it did in the
Pjji. In recent years it has been
n^rced, class distinctions and age
have been blurred and it is now
increasingly common even among
migrant labourers in Indian cities.
Delhi Government has recently
introduced Diabetic Awareness Camps
in schools to help children fight
obesity and diabetes.
Dr Paul Zimmet, Director, Inter
national Diabetes Institute, Australia
or think that you could have diabetes,
get your blood tested and make sure
of your status without further delay.
But more importantly, the key is,
NOT to let your diabetes diagnosis
paralyse you. The sooner you start to
act, the sooner you will start feeling
better and will be able to get your life
back under control.
It is also important to realise that
your diabetes is not the same as the
next person’s, so
do not pop another
person's pills.
Sounds ominous? Sure, but should
that scare us? The answer is No.
While diabetes is a serious disease, it
is well within one’s power to control
both high blood sugar and the
complications it can cause.
And finally,
remember
diabetes is not the
end of the world.
Wasim Akram, the
legendary cricketer
has it but he did
Wasim Akram
not let this hamper
his game. This is what he has to say,
“The best way to control the sugar
levels is to exercise." Indeed, exercise
and proper diet are the two important
keys to control diabetes.
If you have diabetes, take your
doctor's advice seriously. If you are at
risk for diabetes, that is, if you have a
family history of diabetes or are obese,
This issue focuses on the manage
ment of diabetes and lists out tips for
care.
Editor
Get set, go...
predicts “Diabetes is going to be the
biggest epidemic in human history.”
page 2-3
Overview
page4&5
Diabetes Management page 6
page 7
Nature Cure
page 8
Foot Care
page 9
Care of Organs
page 10
Diabetes in Children
page 11
Teach Yourself
page 12
Resources
Diabetic Conditions
OVERVIEW
What is diabetes?
A recent survey indicated that Asians are more prone to
diabetes. Change in lifestyles, food habits and stress are
some of the causes for this
D
The term ‘diabetes’ come from the
Greek word ‘siphon’ based on the
observation that diabetic people lose
fluids in urine almost as quickly as they
quench their thirst.
There are three main types of
diabetes: Type 1, Type 2 and
Gestational diabetes
With Type 1 diabetes, the pancreas
loses its ability to monitor and control
blood sugar. This type used to
account for less than ten per cent of
diabetes and even though genetics
does not completely predict the
disease, having a family history of
Type 1 diabetes may be the single
most important risk factor.
of a limb or other appendage or
outgrowth from body.
Glucose tolerance test3 — Test
for diabetes mellitus where a
person is given a specific amount
of glucose and the urine and
blood are tested at regular
|
intervals.
Many people think that it
comes from eating too much
sugar. But that is not the case.
Researchers have also come to
realise that while it takes several
forms, it is fundamentally similar but
differ in many important ways.
Amputation3 — Surgical removal
Polycystic ovary3 — Congenital
disease where several cysts form
in the ovary at the same time.
iabetes Mellitus or
diabetes is an illness in
which the body cannot
automatically control the level of
sugar (glucose) in the blood.
In a healthy body, the
pancreas releases the hormone
insulin, which converts blood
sugar into energy. Diabetes
interrupts this process. A
diabetic fails to produce enough
insulin — a hormone made by
the pancreas needed to
transport glucose to muscles
and other tissues to provide energy —
effectively.
This box explains
some of the
technical terms
used in this issue.
Insomnia7— Inability to sleep.
Gangrene8 — Death and
putrefaction of tissue usually due
to loss of blood supply. .
Dribbling9 — To flow or fall in
drops or in an unsteady stream.
This type will need an outside
supply of insulin and therefore, will
have to be injected with insulin. That is
why Type 1 is sometimes referred to
as Insulin Dependent Diabetes Mellitus
(IDDM).
Although the reasons are not
known, the incidence of Type 1
diabetes appears to be rising steadily.
Type 2 diabetes, known as adult
onset diabetes, is the more common
form of diabetes and accounts for 90%
to 95% cases of all diabetes. With
Type 2 the pancreas does not
completely shut off insulin production,
but instead the body’s use of insulin
becomes impaired. Unlike Type 1,
Type 2 develops slowly over time and
the symptoms do not show right away.
It usually strikes people above 40,
but in recent times even children have
been known to have it. In Japan for
example, 80% of new cases in children
are Type 2, some as young as nine years.
The cause of Type 2 has much
more to do with lifestyle habits and
obesity could be the biggest culprit.
With doughnuts, burgers and colas
becoming the popular food for
teenagers across the country, the
caloric intake is far too unhealthy. But
other important factors are genetics,
physical inactivity, wrong diet and age.
Gestational diabetes — This is
detected during pregnancy and is
caused by the hormones produced by
the placenta which hinder insulin
function. Symptoms are similar to Type
2 diabetes. Women detected with
Gestational diabetes should be careful
with their lifestyle habits to avoid
problems in later years.
How to treat it?
There is no cure for diabetes. But it
can be controlled effectively with
medicines, correct diet and exercise.
Health Dialogue, Issue no. 37, April- June 2004
OVERVIEW
TAKE-CHARGE TIPS
Learn how to test your own
blood sugar (by using test strips
and blood glucose meter).
Use the result to determine
your average blood sugar
levels and how they tend to
fluctuate throughout the day.
Learn from your doctor or
diabetes educator about how to
stabilise your blood sugar with
diet and exercise.
Schedule an eye examination
for a month after your diagnosis.
High blood sugar can temporarily
cause blurry vision, a complete
visual examination to screen for
more permanent damage after
a few weeks of having brought
blood sugar under control.
Read everything you can about
diabetes.
your diet, cut fats and most importantly
exercise. Get regular check ups done
and monitor your blood sugar.
If you are diabetic or have a family
history of diabetes, a little bit care
could take you a long way. Diabetes is
not just physical disorder. Like any
chronic condition it is also an ongoing
emotional challenge. You are likely to
face anger, frustration and even
feelings of depression. Learning to
cope therefore, is important.
Symptoms
When to test for Diabetes?
Because risk increases with age, it is
advised that diabetes tests should be
taken routinely at three-year intervals
for everyone after the age of 35 years.
In addition, it is recommended that
for people with a higher risk, the tests
should be more frequent.
This includes:
The following are some pointers:
° Persons with a parent or sibling with
diabetes
8 Excessive thirst
® Increased appetite
• Frequent urination
• Blurred vision
» Frequent infections
• Tingling in your hands and feet
• Sexual dysfunction
Test for diabetes
Today testing for diabetes is simple
and fairly accurate. Apart from the
traditional finger prick to draw out a
drop of blood, today the market is
flooded with easy-to-use test strips,
0 Adults who are at least 20% above
ideal body weight
• Women who have given birth to
babies weighing more than nine
pounds (4 kg)
° Women who have had diabetes
during pregnancy
• Persons with high cholesterol
° Persons with high blood pressure
® Persons identified with abnormal
glucose tolerance
° Women with polycystic ovary
syndrome
For children:
Over weight children with two or more
additional risk factors, should test
every two years.
DOES STRESS CAUSE DIABETES?
Fact: Stress makes the body
release hormones like cortisol.
Prevention is better
than cure
We are a generation that is
vulnerable to this disease
because our lifestyles have
changed dramatically. Stress,
coupled with bad eating habits
and lack of exercise make us
easy targets. It is therefore,
important to adopt a healthy
lifestyle. Be positive, change
Sometimes you might be advised by
your doctor or health visitor to come
without eating or drinking anything
before the test (fasting). See a doctor
for a full evaluation.
While the signs of diabetes can be
subtle at first, they are not something
you can ignore for long. The longer the
diabetes progresses, the more likely
symptoms are to become obvious and
troublesome.
o Fatigue
Diabetic patients must also pay special
attention to their eyes and feet. Since
it is a multi-system disease, that is, it
can affect one's heart (increase the
risk of a heart attack), kidneys (long
term high blood glucose can damage
small blood vessels in the kidney which
could result in kidney failure), eyes
(damage small blood vessels in the
which can lead to vision blurring)
i^m/e endings and circulation
(this could lead to loss of
sensation, which could result in
foot ulceration and even
amputation).
blood glucose meters etc. to check
ones blood sugar level.
Fact: Stress hormones make
blood sugar go up.
Fact: High blood sugar and belly
fat contribute to insulin resistance
and eventually to diabetes.
Conclusion: Stress causes
diabetes.
(Source: Diabetes Care)
Avoid stress
Health Dialogue. Issue no. 37. April-June 2004
DIABETES MANAGEMENT
Taking charge of your
Diabetes
What is diabetes?
es occurs when a person's
doesn’t make enough
n or doesn't use insulin
the right way. Insulin helps your cells
use blood sugar for energy. Diabetes
causes the sugar to build up in your
blood.
Diabetes can generally be classified
as Type 1 or Type 2. If you have type
1, your body makes little or no insulin.
If you have Type 2, your body makes
some insulin but can't use it properly.
Most adults with diabetes have Type 2.
What health problems can
diabetes cause?
Over time, high blood sugar levels can
damage your eyes, blood vessels,
nerves and kidneys. Damage to your
nerves can lead to foot sores,
problems with digestion and
impotence. Damage to your blood
vessels increases your risk of heart
attack and stroke. Many of these
problems can be delayed or prevented
with treatment.
How is diabetes treated?
The goal in
treating
diabetes is
to keep the
level of
sugar in your
blood as
close to
normal as
possible—
not too high
(called hyper
glycaemia)
or too low (called hypoglycaemia). You
can do this by eating right, by
exercising and by taking insulin or
Tips on blood sugar testing
♦ Wash your hands and dry them
well before doing the test.
♦ Pay attention to expiration dates
for test strips.
♦ Let the drop of blood be big
enough.
medicine if your doctor prescribes it.
Regularly checking your blood sugar is
a key to helping you control it. Blood
sugar checks can help you see how
food, exercise and insulin or medicine
affects your level. Checking your blood
sugar also allows you and your doctor
to change your treatment plan if
needed.
How do 1 check my blood
sugar level?
To check your blood sugar level, you’ll
need to prick your finger to get a drop
of blood for the test. Spring-loaded
devices, which prick your finger when
you press them against your skin,
make this simple and less painful.
Call your doctor if:
» you start feeling very thirsty and
are urinating more.
• you feel sick to your stomach or
vomit more than once.
♦ you start breathing deeper and
faster.
♦ your breath smells sweet.
♦ you start to tremble, feel weak
and drowsy, and then feel
confused or dizzy, or start seeing
double.
» you feel uncoordinated.
After you prick your finger, you place
the drop of blood onto a test strip. The
test strip will change colour. You then
either insert the strip into a blood sugar
meter or compare the colour of the
strip to a colour chart to figure out your
blood sugar level.
How often should i check my
blood sugar level?
Check your blood sugar as often as
your doctor suggests. You'll also check
♦ Be sure your meter is set right.
o Keep your meter clean.
♦ Check the batteries of your
meter.
® Follow the instructions for the
test carefully.
♦ Show the results to your doctor.
it more often when you feel sick or
stressed, when you’re changing your
medicine, or if you’re pregnant. People
taking insulin may need to check their
levels more often.
Keep track of your blood sugar levels by
writing them.down. You can also keep
track of what you’ve eaten and how
active you’ve been during the day. This
will help you see how eating and
exercise affect your blood sugar level.
What should my blood sugar
level be?
Consult with your doctor about what
range of blood sugar levels is best for
you. A level of 80 to 120 before meals
is often a good goal, but not everyone
with diabetes can get their blood suctf<
levels this low.
Be sure to ask with your doctor
about what to do if your blood sugar
level isn't within the range that’s best
for you.
How does food affect my
blood sugar level?
Every time you eat, you put sugar in
your blood. Eating the right way can
help control your blood sugar level.
As a general rule, just following a
healthy diet is wise. Your doctor may
help you find a dietitian who can help
you learn how to make wise food
choices. See the box for some tips on
eating right.
Health Dialogue. Issue no 37, April- June 2004
DIABETES MANAGEMENT
Tips on eating right
Eat at about the same time every
day. This helps to keep your insulin
or medicine and sugar levels steady.
♦ Try to eat thrice a day. Have a
snack at bedtime if you're taking
medicine or insulin. Avoid other
snacking unless you’re exercising or
treating hypoglycaemia.
* If you’re overweight, lose weight.
Even losing just a little weight, such
as 5 to 15 pounds, can lower your
blood sugar levels.
♦ Eat plenty of green leafy vege
tables, grains and fruits. Fiber helps
^/ou feel full.
♦ Eat fewer “empty” calories, such
as foods high in sugar and fat, and
alcohol.
What about smoking and
alcohol?
You should stop smoking as soon as
possible. It's probably okay to drink
some alcohol. But it’s best not to have
more than about one serving a day
with a meal. A serving is 4 ounces of
wine, 12 ounces of beer or 1.5 ounces
of hard liquor. If you drink on an empty
stomach, you risk causing a drop in
your blood sugar.
Will exercising help my
blood sugar level?
Yes. Exercising is especially good for
people who have diabetes because it
can help the body better use insulin,
resulting in a lower blood sugar level.
Exercise is also good for your heart,
your cholesterol levels, your blood
pressure and your weight — all factors
that can affect your risk of heart attack
and stroke.
Exercise also seems to make
people feel better about themselves
and feel less anxious.
Talk with your doctor about starting
an exercise programme. He or she can
help you make a plan.
What is a glycosylated
haemoglobin test?
It’s a blood test your doctor may do.
One common type of glycosylated
haemoglobin is haemoglobin A1c. The
haemoglobin AIc level helps to show
how well your blood sugar has been
controlled during the previous 1 to 3
months. It helps your doctor to see
how effective your treatment is and
decide if any changes are needed.
Source: www.familydoctor.org
Your Guide to Start Right...
Good diabetes care always begins at home with daily blood sugar tests that are done often enough to achieve your blood sugar goals. This
monitoring is essential for providing a record from which changes in therapy can be made to reach a level of control that is best for your overall
health. It is also the cornerstone for feeling at your best each day and preventing unwanted complications. The best record is a complete one. a
i sample log of typical food choices and quantities and blood sugar readings.
Below is a chart which describes the types of laboratory tests one should have performed and the frequency at which to perform them.
Lab Test
Type
Frequency
Purpose and Goal
HbAlc
or
Fructosamine
Blood
4 times a year
Averages the blood glucose levels for the past 2-3 months.
Goal is 7% or under when normal is 4-6%
Averages the blood glucose levels for the past 2-3 weeks
Lipid Profile:
Tot Cholesterol.<200
LDL:<100
_ HDL:>35 men
■ >45 women
Triglycerides:<200
Blood
fast for
8 hours
Yearly
Measure of fats and lipids in the blood. Provides good
determination for risk of heart disease.
Microalbumin
Urine
Yearly
Determines kidney disease at an early stage.
Serum Creatinine
Blood
Yearly
Determines kidney disease at a late stage
24-year Protein or
24-hour Creatinine
Clearance
Urine
Urine and Blood
As needed
Determines function of the kidney at an early stage
Blood
When visiting a healthcare professional, the following should be checked and discussed:
Blood pressure
♦ weight
• foot exam
♦ Blood glucose readings record
< Review of diet, exercise and medications or insulin
Every year be sure to have the following:
A dilated eye exam
A detailed foot exam
♦
Your seasonal flue shot
Source: http//www.diabetesnet.com/diabetes_information/index.php
Health Dialogue, Issue no. 37, April-June 2004
DIABETIC CONDITIONS
Managing Hypoglycaemia
Hypoglycaemia & Hyperglycaemia are two conditions that threaten diabetes if they are not careful about their sugar
level. If monitoring reveals that your blood sugar has dropped below 70 mg/dl, your glucose levels are too low and you
are in danger of hypoglycaemia. Do not wait for such symptoms as mental confusion, rapid heartbeat, sweating and
double vision to occur before you act. They often show up when blood sugar drops dangerously low.
Follow these steps
AT: Start by consuming 10-15
E
gm of a fast acting carbohydrate
to get glucose into the blood as
quickly as possible. This could be
two spoonfuls of raisins, half cup of
juice, half cup of any soft drink (not a
diet cola) two teaspoonful of sugar, a
sweet or two, half a chocolate bar or
even a small portion of gur.
REST: Take it easy for at least 15
min. or while the carbohydrate goes
to work
TEST: Take another blood test to
check if your glucose levels have
improved. Once your glucose levels
have improved and if you have another
hour or so left for the next meal, then
eat another small snack (some salt
biscuits) to help tide you over.
Important Tips
♦ To protect against hypoglycaemia,
do not exercise if your blood sugar is
below 100mg/dl.
♦ Blood sugar can continue to fall
long after you have exercised. So be
alert and watch for signs of hypo
glycaemia until 24 hours after the
workout.
♦ Always carry a snack/biscuits/
toffee.
* Staggering your food intake
throughout the day helps to keep your
blood sugar on an even keel.
* Avoid three big meals in a day,
instead take five smaller meals.
«■ Always carry an identity card
with your diabetes status written
clearly along with your name, address
and emergency telephone nos.
Understanding hyperglycaemia
Hyperglycaemia is arbitrarily defined as a glucose level of less than 12 mmol/1. It can result from non-compliance with
treatment. Most patients forget to take their tablets/insulin from time to time. If one dose of tablets/insulin is forgotten
within 1 hour of the usual time, take as usual. If longer than this, omit the dose and take the usual dose when the next
one is due. DO NOT double the following dose. Accept that blood glucose levels will be temporarily raised.
Causes
♦ Untreated diabetes
♦ Too much food
* The wrong type of food
♦ Infections/illness
♦ Insufficient tablets or insulin
(incorrect dose)
♦ Overuse of particular injection sites
- leading to fatty lumps
♦ Poor injection technique
♦ Reduction of activity
♦ An increase in drugs affecting
glycaemic control (e.g. steroid
therapy)
♦ Stress—life changes (retirement,
bereavement)
* Weight increase.
MONITORING: THE PRIMARY CARE TEAM
0 Patients should monitor their
own general health and well-being,
diabetes control, eyesight, weight,
dental care, care of the feet and
footwear.
0 To promote health and reduce
risks of complications, you should
teach them how to monitor their
diabetes control (urine/blood glucose
levels). This monitoring allows them
to check their own control, take
responsibility for their condition and
as far as possible maintain
independence.
0 If you suspect that the person
with diabetes has hypoglycaemia
(from discussion of symptoms or
reports of (‘dizzy spells'), blood
glucose levels should be checked and
medication or insulin reduced.
0 Hyperglycaemic episodes will ...
need an increase in tablets or insuli^
0 You will have to decide with the
patient whether any change in
therapy is needed, e.g. diet alone to
tablet therapy combination tablet
therapy to combination tablet +
insulin therapy to insulin therapy— all
in association with dietary guidelines.
0 Decisions about adding tablets
or insulin should be taken in
consultation with the doctor and the
person with diabetes.
0 By monitoring dietary habits,
changes in weight, lifestyle and other
medical problems (particularly in
elderly people), you can decide when
possible review and changes in
treatment are necessary.
Health Dialogue. Issue no. 37. April- June 2004
NATURE CURE
Naturopathy & Diabetes
The market is full of alternative therapies and some of
them can indeed be tempting especially if you are faced
with injecting insulin every day
o use these remedies
(Ayurvedic, Homeopathy or
Chinese herbal medicines) is a
personal decision, but it is better to
approach them with caution. To begin
with do not assume that “herbal”
means “safe". Medicinal herbs do have
effects on the body. But more
importantly, even if they work for you,
$you should never substitute it for your
T
regular insulin or medication, but
instead use it to complement your
allopathic medicines. And finally it is
extremely important that you monitor
your blood sugar closely if you take
these remedies. First to find out how
effective the herb is and second to
monitor your blood sugar for your own
safety.
Among the herbs that show the most
promise for lowering blood sugar are:
Jamun (Gymnema Sylvestre) - is a
very popular black
blue fruit in the
north of India, and
have been used to
treat diabetes for
more than 2000
years. It is thought
that it works by
boosting the
activity of the enzymes that help cells
use glucose or by stimulating insulin
producing beta cells in the pancreas.
The herb is not known to cause side
effects.
i.':ethi (Fenugreek) - A spice that is
found in most Indian
kitchens. Small
studies conducted
have revealed that
methi seeds can
lower blood glucose.
Lab research shows
that methi seeds
contain an aminoHealth Dialogue. Issue no. 37. April-June 2004
acid shown to boost the release of
insulin.
Karela (Bitter Gourd) - This common
vegetable has
been a local
remedy for
diabetes for a
long time. A
number of
studies in small
groups of
people who
were diagnosed with Type 2 diabetes
suggest that it indeed might have
some benefits. It is consumed as
juice or in powder form and it is
thought to help cells use glucose
through such active ingredients as
plant insulin. Other substances in the
bitter gourd are thought to block sugar
absorption in the intestine.
A word of caution -Some side
effects like headaches and
gastrointestinal distress have been
reported. It should not be taken during
pregnancy.
Ginseng - An increasing popular
remedy in India. However, research
about its effect
to lower blood
glucose is far
from
1 ».
conclusive.
(.
Ginseng is
'*
_
known to cause
excitability,
which in turns
makes people more active, and this
might lead to burning up more
calories.
Ginseng is expensive to cultivate,
so what is marketed is often
adulterated with other substances like
caffeine.
Side effects could include
headaches, increased blood pressure
and Insomnia.
(Source: RD)
SOME MYTHS
Myth: If you have diabetes, you
can never eat sugar again.
Truth: People with diabetes can
eat sugar but these treats should
be a part of a careful meal plan.
Myth: I just have a touch of
diabetes.
Truth: Either you have diabetes or
you don’t. Even if your type 2
diabetes does not require insulin
injections, it still demands medical
attention and careful calorie
management.
Myth: I feel fine, so my blood
sugar is fine.
Truth: High or low blood sugar
does not always produce
symptoms. Regular monitoring is
the only way to know where you
stand.
Myth: I am, a pro at self-manage
ment, check-ups are just a waste
of time.
Truth: Your treatment programme
is never a done deal, Thanks to
ongoing research; the best way to
keep up is to keep up with regular
doctor visits.
Myth: If I don’t need insulin my
diabetes is not serious.
Truth: Diabetes is always serious.
Even if diet and exercise keep
your blood sugar in check, your
cells are still insulin resistant and
your condition could get worse if
you do not control it.
FOOT CARE
Care for your feet
If you are diabetic, then you have to be vigilant about
your eyes, kidneys and feet
homas, a diabetic, was
meticulous about his insulin
shots, diet and exercise. But he
slipped up when it came to his feet. It
was not deliberate though. His age
made bending
difficult and
his failing
eyesight did
not help
either. A new
shoe proved
to be his
undoing. A
small shoe
bite was the
beginning of
the end. The
wound
refused to
heal.
Medication
and dressing
did not help.
The infected
area turned blue (which his eyes failed
to see) and it was not till his wife
complained of a foul smell did the
alarm bells ring.
T
He immediately went to see his
doctor, who without wasting time
admitted him and got ready to
amputate his foot. Gangrene left him
with no choice.
Many diabetics end up losing their
toes or foot. Taking care of your feet is
important. Poor circulation from
damaged blood vessels slows healing
and makes feet more prone to
infection, while nerve damage can dull
sensation and leave you oblivious to
injuries that can quickly get out of
control.
And therefore, it is important to be
extremely careful of one's feet. Cuts
MUST DO’S
•
Find out all you can about
diabetes and check with your
medical care team.
•
Inform others about your diabetes:
your family, friends and your
colleagues.
while clipping of toe nails, in-grown
nails, chapped feet, broken skin, or
small shoe bites should not be ignored.
Give your feet a good check once a
day, both with
your eyes and
hands. Besides
blisters, cuts or
bruises check
for discolour
ation. A paler
or redder tint
could indicate
your footwear
is not the right
kind. Also
check for areas
of coldness
(indicates poor
circulation) or
warmth (could
indicate
presence of
infection) and
swelling. Use a
mirror to see the bottom of your foot
and if your vision is poor ask a relative
or friend to check for you.
Wash your feet everyday with luke
warm water. Avoid soaking the feet as
it will soften the skin and make you
more vulnerable to infection. Dry feet
by gently patting dry the water. Avoid
vigorous rubbing down. Take care to
dry between the toes to avoid fungal
infection. Use moisturising cream or oil
to prevent dryness and cracking.
Clip your toe nails with care and if
need be ask for someone to help.
Wear clean and good fitting cotton
socks and proper shoes.
Have your doctor check your feet
when you visit him.
• Go for regular checks.
® Be in control of your diabetes on
a daily basis.
•
Monitor your own sugar levels
and change treatment as advised.
Keep a record of your blood (or
urine) tests.
-.
’<>
• Know when to seek help and
where, particularly in an
emergency or if you are ill.
« Discuss your fears with your team.
® Ask questions and repeat if not
answered; prepare them before
your appointment.
• Follow a healthy lifestyle by
choosing healthy food,
controlling your weight, taking
physical exercise and not
smoking.
• Examine your feet regularly. If
you find this difficult, try to
arrange for someone to do this.
• Recognise signs of low/high blood
glucose levels and how to
prevent.
• Be aware of the long-term
complications of diabetes, the
importance of early detect and
the relevance of reducing blood
glucose (sugar) levels to reduce
the risk of complications.
o Carry personal identification card
with your diabetic status and
details of who can help.
®
If you are female and hoping to
have a baby, get advice on your
diabetes before trying to conceive.
Health Dialogue, Issue no. 37, April- June 2004
CARE OF ORGANS
Care for your kidneys
t takes years of blood sugar abuse
for your kidneys to pack up. But
between 20% to 40% of diabetic
patients develop kidney problems and
diabetes is among the leading causes
of kidney failure. Total loss of renal
function will ultimately require dialysis
where the patient is hooked up on a
machine for two to four hours for the
blood to be cleansed. The other option
is a kidney transplant.
can notice
puffiness of
the eyes and
swelling of
hands and
feet— classic
symptoms of
a diseased
kidney.
The kidneys produce and eliminate
urine through a complex system. Blood
flows through at high pressure and
♦y) urea, toxin and other wastes are
flushed out in the form of urine.
♦ Control
blood sugarClosely controlling blood sugar is the
single most effective way to keep
kidney at bay.
Over time, high blood sugar
destroys these small centres and the
kidney fails to flush out the toxins or
keep the nutrients from being expelled.
Small amounts of protein or albumin
can be detected in the urine and you
♦ Check blood pressure - Monitoring
of blood pressure can halt damage to
the arteries in the kidney.
I
What you
can do:
0 Visit the doctor - If you have
swelling, pain in the lower back.
0 Protect against UTI - Urinary Tract
Infections (UTIs) are common in
people with diabetes. If you feel a
burning sensation when you urinate,
constantly having to go, pain in the
lower abdomen, or notice your urine is
cloudy or has traces of blood, then
chances are you have urinary tract
infection and are in need of treatment.
Dribbling of urine is a common
symptom.
0 Watch the pills you pop - A wide
range of drugs can be hard on the
kidneys. Check with your doctor and
watch for warnings on the cover/strip
about taking it if you have kidney
disease.
♦ Cut back on protein - If you have a
kidney problem, be careful about the
protein intake.
Care for your eyes
iabetes is one of the leading
causes of blindness in adults.
Like the kidneys, the eyes are
nourished by small blood vessels and
diabetes can easily damage these blood
vessels.
If this damage is not attended to
promptly then it could lead to vision
loss.
Most diabetes related damage of
the eye takes place in the retina,
where the weakened blood vessels
can puff up or rupture (nonproliferative
retinopathy) and make your vision
blurry. If this damage is unchecked, it
could develop into more serious
haemorrhages and pressure build up
in the eye, leading to scarred tissues
or even the retina starts tearing away
from the eye.
Do not take even minor changes in
examination immediately after
diagnosis and then get their eyes
checked once every year.
D
Health Dialogue. Issue no. 37. April-June 2004
Apart from this, should you
experience any of the following, visit
your ophthalmologist immediately:
♦ Double vision
0 Vision is blurry
0 Vision is distorted. That is, straight
lines start looking wavy.
♦ Spots or lines seem to float in front
of your eyes
your vision lightly. You may not be
able to detect any serious changes in
your ability to see, but your doctor will
be able to do so. Most diabetic centres
recommend that persons with Type 1
diabetes get their eyes examined at
least once in three years. Persons
with Type 2 should have an eye
♦ Flashes of bright light
♦ Pain or pressure in your eyes
♦ Hazy vision and narrower field of
vision
♦ Difficulty in seeing in dim light
» Difficulty in colour identification.
especially blue and yellow.
Q
DIABETES IN CHILDREN
Juvenile Diabetes
According to a national survey, two in five Delhi students have diabetes and
high cholesterol (Type 2) is becoming increasingly common even among young
school children. About a decade ago, a ten-year-old diabetic patient would
have been startlingly rare. Not any longer. Doctors are now struggling to treat
even six-year old.
dietician and follow
instructions.
As the child grows up he/
she will be able to
understand why this
treatment is necessary and
will also cooperate.
Educate the child whenever
he/she shows a curiosity or
a willingness to learn.
Do not scare the child,
instead be positive and
encourage positivity in your
child too.
reating diabetes (both Type 1 &
Type 2) in children is more
challenging as children often fail
to take their problem seriously.
T
As a first step parents have to be
extra alert and learn to identify
hypoglycaemia and hyperglycaemia,
since the child is often at a loss to
express its feeling.
Expect some opposition to change
in food habits and may be even open
rebellion over insulin injections and
blood sugar tests. But do not give in.
Children need more blood sugar for
normal development. Consult a
RURAL MIGRANTS PRONE
TO DIABETES: STUDY
Rural people who migrate to urban
areas in search of better prospects
and reside in slums, are at high risk
of getting diabetes and hypertension
compared to those who choose to
remain in villages, a study has said.
“Rural population usually has a
low risk of development of diabetes
and hypertension but migration to
metropolitan cities exposes them to
several adverse lifestyle and
environmental influences,” Dr Anoop
Mishra, a professor in the depart
ment of medicine at All India Insti
tute of Medical Science (AllMS)
said.
“Change in lifestyle of the people
living in urban slums is having a fall
out on their health in terms of increased
risk of Type 2 diabetes, a disease
which was earlier thought to be
associated with affluence,” he said.
Make sure he/she has a
bedtime snack and that the
child does not skip its
meals.
A total of 532 people, including
362 women, in an urban slum in a
south Delhi area, were studied for
the disease. Pregnant women,
disabled, drug users and acutely ill
people were excluded, Mishra, who
led the study, said.
If the child is nine or
above, encourage him/her
to inject himself/herself.
Monitor and supervise the
child as it grows into
adulthood and you are sure
he/she is capable of
handling it himself/herself. Kindly make
sure the child carries the identification
tag at all times identifying him/her as
diabetic.
Contrary to the widespread
assumption even among the experts
that obesity and diabetes are not a
crucial problem in urban slums due
to high prevalence of malnutrition
and low socio-economic conditions,
the team found that about 10 per
cent of the people over 30 years had
Type 2 diabetes while about 27 per
cent were found to have
hypertension.
DO NOT LET
A DISABLED
“Over 11 per cent males and
about 10 per cent females over 30
years were found to have the
disease while the obesity was more
prevalent among women,” Mishra
said. The team found that the onset
of Type 2 diabetes was also linked
with high waist-hip ratio.
CH!LD
GET
FAT!
“Children who are obese are more
vulnerable to Type 2 diabetes," he
said.
Source: PTI
Health Dialogue, Issue no. 37. April- June 2004
TEACH YOURSELF
DIABETES AT A GLANCE
SHOTS MADE SIMPLE
f you are insulin dependent and need insulin injections regularly, do not get
alarmed. It can be scary at first, but most people quickly get used to them.
Learn to inject yourself by following some basic steps. First, wash your
hands with soap and water and check the bottle to make sure you are using the
right insulin. Get the syringe, alcohol wipes and your insulin. Relax. Tense
muscles can promote tightness that can make it harder for the needle to enter.
/
Type 1
Characteristics: Sudden onset;
pronounced thirst and hunger,
frequent urination; fatigue, nausea
and vomiting; weight loss.
Age at onset: Usually 20 or
younger.
Turn the bottle and
syringe upside
down so the tip of
the needle is
submerged in the
insulin. Now pull
the plunger back
once again drawing the insulin until
you reach your dose mark.
Gently roll the bottle between your
palms (shaking it can make the insulin
less potent) check its appearance,
except for regular insulin which should
look clear, the contents should look
uniformly cloudy. Do not use if its
clumped or settled at the bottom or if
the bottle has a frosty look.
After wiping
the stopper/
cover with an
alcohol wipe
take the
cover of the
syringe and
Ah, pull the
plunger back
until it
reaches the dose you need as marked
by the lines printed on the syringe
side.
Stick the
needle
through
the
stopper
and
press the
plunger
down so
all the air in the syringe goes through
the bottle.
Health Dialogue, Issue no 37. April-June 2004
Physical Condition: Usually lean
or normal weight.
Cause: The immune system
destroys the pancreas cells that
produce insulin.
Mainstay of treatment: Insulin
injections.
Type 2
If you see any
air bubbles
(which dilute the
insulin strength)
push the plunger
back in and draw
the insulin again.
Repeat this
process until you
have the right dose and no bubbles.
Characteristics: Slow, difficult-todetect onset; pronounced thirst:
frequent urination; fatigue; slow
wound healing; tingling hands or
feet; frequent infections; weight
loss.
Cleaning the injection site, (preferably
outer thigh, upper arm or stomach) with
an alcohol dipped cotton swab and wait
for the area to dry. Pinch a fold of the
skin and push the needle in at a 90
degree
angle.
(Insert
the
needle
quickly,
slowness
and
hesitation can make it hurt more) If you
are thin, consider using a short needle
or inserting it at a 45 degree angle to
avoid injecting into muscle.
overweight.
Push the plunger down; release the
skin and pull the needle out. Press the
cotton swipe on the needle mark as you
remove the needle. Keep pressing for a
few seconds but do not rub the area.
Source: Diabetes Care
Age at onset: Usually 40 or
older. However, in recent times
younger people are getting Type 2
diabetes.
Physical Condition: Usually
Cause: Lack of exercise, poor
diet and resulting obesity;
genetics.
Mainstay of treatment: Lifestyle
changes, possibly supported by
insulin and drugs.
Gestational
Characteristics: Pronounced
thirst, frequent urination, fatigue
and other symptoms similar to
Type 2.
Age at onset: Child-bearing years
Physical Condition: Pregnant
Cause: Hormones produced by
the placenta hinder the function of
insulin.
Mainstay of treatment: Lifestyle
changes, possibly supported by
insulin injections.
RESOURCES
Useful Addresses
..
.... Foi.
Gopalpuram, Chennai 600 086.
~ ’■.
. 6, Conran Smith Road,
Juvenile Diabetes Foundation, India is a international organisation
dedicated to the welfare of children and young adults with diabetes within
India.
Health Dialogue
Health Dialogue is published
quarterly by the Christian Medical
Association of India. It has a
circulation of over 20,300 in India.
Christian
Medical
Association of
India
Diabetes Research Centre, (WHO Collaborating Centre for Research,
Education and Training in Diabetes), 4, Main Road, Royapuram,
Chennai - 600 013.
Diabetic Association of india, 127, MG Road, Maneckya Wadia Bldg,
1st Floor, MG Road Fort, Bombay 400 001, Tel: 91-22/273813
Editor
Ms Reena Mathai Luke
Editorial Co-ordinator
Diabetic Association of india, Raheja Hospital Road, Mahim 400 016,
Mumbai, India, Tel +91-22-4467569/70, E-mail info@rahejahospital.com
Diabetes Education and Treatment Center, Kantiwikha Road,
Panjagutta, Hyderabad 500 082, Andhra Pradesh, India.
Nutrition Foundation of India, C-13, Qutab Institutional Area, New Delhi
110016, Ph:26962615.
Ms Sumathi Morgan
Editorial Advisory Group
Dr Vijay Aruldas
Ms Reena Mathai Luke
Dr Shanti Ghosh
Dr Sukant Singh
Dr Sunita Abraham
Design & Production
Ms Susamma Mathew
Mailing List
Useful Sites
Ms Shalini Dayal
Diabetes Clinic Online Consultation
Published by the General Secretary
CMAI, Plot No. 2, A-3
Local Shopping Centre. Janakpuri
New Delhi - 110 058
Telephones: 25521502,25599991,
25599992,25599993
Fax: 011- 25598150
E-mail : cmai@cmai.org,
cmaidel@vsnl.com
Website: http://www.cmai.org
www.diabetescliniconline.com — It is the online consultation for diabetic
patients and provides useful information for doctors.
www.diabetesindia.com
www.familydoctor.org
http//www.diabetesnet.com/diabetesjnformation/index.php
Dear Reader,
We appreciate your interest in our magazine and would like
to record our thanks for the same. However, with the
steep increase in production costs, bringing out each
edition of ‘Health Dialogue’ (HD) is an uphill task. The
printing and paper costs alone for a single copy of HD is
Rs. 14/-. We would therefore, appreciate your support to
supplement these costs, by donating Rs. 100/- for two
years' supply of HD. Please send a crossed cheque or
Demand Draft payable to Christian Medical Association of
India, New Delhi.
Bangalore Office:
HVS Court, 3rd Floor
21, Cunningham Road
Bangalore- 560052
Telephones: 080-22205464, 22257844
E-mail: cmaiblr@vsnl.com.
heaBithlink
WORLDWIDE
Healthlink Worldwide (formerly
AHRTAG)
Cityside, 40 Adler Street,
London, E1 1EE, UK
Telephone +44 20 7539 1570
Fax +44 20 7539 1580
E-mail info@healthlink.org.uk
http://www.healthlink.org.uk
The views expressed in Health
Dialogue are not necessarily those of
the editorial advisory group.
Printed at: New Life Printers Pvt. Ltd.
Health Dialogue, Issue no. 37, April- June 2004
S MEDICINE
Dealing with renal disease
Cross-blood renal transplantation can go a long way in the treatment of end-stage renal disease, but
even more important is the control of diabetes and hypertension.
ASHA KRISHNAKUMAR
HE number of people suffering from
end-stage renal disease (ESRD), that
is, a condition in which the kidneys func
tion at less than 10 per cent of their capac
ity, is rapidly rising the world over and
threatening to become a major public
health problem.
In India, several lakh people suffer
from ESRD, which requires long-term di
alysis or renal transplantation. In the
United Stares there are over 300,000
ESRD patients and in Europe more than
250,000.
The kidneys maintain the internal
body environment for the optimum func
tioning of various organs by getting rid of
various metabolic byproducts such as urea
and uric acid and by maintaining the pH
and electrolyte level of various
body fluids. They filter 180
litres of blood every day. The
kidneys also perform hor
monal functions such as the
activation of vitamin D and
the production of erythroprotein, which is responsible for
the functioning of bone-marrow.
There are two types of
kidney failures. One is acute
failure, when there is a reduc
tion in the blood supply to
the kidneys or when a nephrotoxin is administered. It is
potentially reversible. The
other failure is chronic, which
is caused by urinary infection,
allergic reactions, diabetes
and hypertension. It is irre
versible. When a chronic fail
ure patient cannot survive
without dialysis or transplant,
the padent is said to be suf
fering from ESRD.
Dialysis purifies blood.
There are two types of dialy
sis. One is haemodialysis. It is
done by a sophisticated ma
chine in hospitals. A patient is
usually required to undergo
haemodialysis two or three
times a week, which would
T
86
cost about Rs. 10,000 a month. The sec
ond is continuous ambulatory peritoneal
dialysis (CARD), which can be adminis
tered by a patient on himself/herself by
implanting a catheter in the peretonial
(abdominal) cavity. It costs Rs.20,000 to
Rs.25,000 a month and provides better
quality life.
Haemodialysis was first done over 50
years ago. Only in 1960, with the devel
opment of the indwelling arteriovenous
teflon shunt, called the Quinton-Scribner
shunt, was maintenance haemodialysis in
troduced for patients with ESRD. At
about the same time, advances in immu
no-suppression, such as the development
of 6-mercaptopurine (Purinethol) and its
derivative azathioprine sodium (Immuran), led to the procedure of kidney trans
plantation. Widespread use of peritoneal
dialysis began in the mid-1970s and is
used by over 100,000 patients the world
over.
Neither haemodialysis nor peretonial
dialysis offers a cure. Transplantation is a
more stable form of therapy and leads to
complete
rehabilitation,
particularly
among younger ESRD patients. Trans
plantation, done from a live donor or
from a cadaver, costs over Rs.2 lakhs and
the annual cost of maintaining the patient
with immuno-suppresants is about Rs.l
lakh.
According to the nephrologist Dr. R.
Ravichandran, Director, Madras Institute
of Nephrology, Chennai, most kidney
problems remain undetected until they
become ESRD. Even among those detect
ed, most patients cannot afford the cost of
dialysis or transplantation and treatment
with immuno-suppresants. Add
ed to this are the myths and half
truths associated with renal dis
eases. Says Ravichandran: “Most
times the patient and his family
are left fatigued, confused and
depressed.” Realising the com
plexity of the problem faced by
ESRD patients, Ravichandran
and Dr. P.B. Sivaraman, Profes
sor in the Department of Urol
ogy at the Government General
Hospital in Chennai and con
sultant urologist, Malar Hospi
tals, who have been treating
ESRD patients for over two dec
ades, set up the Balaji Medical
and Educational Trust five years
ago, ro subsidise treatment costs,
create awareness about the dis
ease, and screen the population
for diabetes and high blood pres
sure - the main causes of ESRD.
Some organisations such as the
Tanker Foundation subsidise di
alysis. But that is not enough,
they say.
The rising incidence of
ESRD the world over has led to
social problems primarily because
the number of patients wanting
kidneys for transplantation has
increased manifold while the
availability of donor and cadaver
FRONTLINE. MARCH 26, 2004
A viewer, particularly one who ac
cepts the theological import of the story,
is thus caught in a sadomasochistic para
dox, as are the disciples for whom Jesus,
in a flashback that occurs towards die
end, promises to lay down his life. The
ordinary huma\ response is to wish for
the carnage to stop^in impulse that seems
lacking in the dissolute Roman soldiers
and the self-righteous^- Pharisees. But
without their fathomless cruelty, the story
would nor reach its necessary end. To halt
the execution would thwart divine provi
dence and refuse the gift of redemption.
The paradox of wishing something
horrible to stop even as you want it\to
continue has as much to do with movie
going as with theology’. And Gibson, ei- \
ther guilelessly or ingeniously, has ex
ploited the popular appedte for terror and
gore for what he and his allies see as a
higher end. The means, however, are no
different from those used by virtuosos of
shock cinema like Quentin Tarantino At a theatre in New York, a group called “Jews for Jesus” hands out flyers for the
and Gaspar Noi, who subjected Monica first showing of the film, on February 25.
remove every trace of controversy and in
Bellucci to such grievous indignity in Irri- vie suspense to slasher-film dread.
versible. Gibson is temperamentally a
Throughout, Gibson lays on Deb tolerance from a story that rests squarely
more stolid, less formally adventurous ney’s canned sublimity with the heaviest on the theological boundary separating
film-maker, but he is no less a connoisseur possible hand, and he indulges in equally Christianity from Judaism. That Gibson
of violence, and it will be amusing to see unsubtle visual and aural effects. Judas’ 30 did not attempt to transcend these divi
some of the same scolds who condemned pieces of silver fly through the air in slow sions may be regrettable, but to condemn
Tarantino’s “Kill Bill: Vol. 1” sing the motion, and the first nail enters Jesus’
The Passion ofthe Christ for its supposed
praises of The Passion of the Christ.
palm with a thwack that must have taken bigotry is to miss its point and to misstate
Gibson, from the moment he began hours of digital tweaking to articulate.
its problems.
speaking publicly about this project, em The thuddingly emphatic storytelling
The troubling implications of the
phasised his desire to make his “Passion”
(along with the ancient languages) makes film do not arise primarily from its reli
as realistic as possible. To that end the the acting almost beside the point, gious agenda: an extreme, traditionalist
dialogue is in Aramaic and a dialect of though it is hard not to be impressed by Roman Catholicism that has not prevent
Latin, which takes some gening used to Caviezel’s endurance. The only psycho ed The Passion from resonating, oddly
but which dispenses with the stilted, awk logical complexity in this tableau of good enough, with many evangelical Protes
ward diction that afflicts so many biblical ness and villainy belongs to Pontiu^Pilate tants. What makes the movie so grim and
epics. The absence of identifiable movie and his wife Claudia, played by twd very ugly is Gibson’s inability to think beyond
stars (with the exception of Bellucci, who capable actors, Hristo Naumov Shopov the conventional logic of movie narrative.
comports herself with fitting modesty) al and Claudia Gerini, who I hope will be In most movies - certainly in most mo
so adds an element of verisimilitude. But come more familiar to American audi vies directed by or starring Gibson - vio
the style and tone of The Passion are for ences.
\
lence against the innocent demands
from what is ordinarily meant by realism.
righteous vengeance in the third act, an
The first pan, which takes place in the
S The Passion ofthe Christ anti-Semi expectation that Gibson in this case whips
murk and gloom of night (shot by the
tic? To my eyes it did not seem to up and leaves unsatisfied.
superb cinematographer Caleb Descha traffic explicitly or egregiously in the toxic
On its own, apart from whatever be
nel), has the feel of a horror movie. As iconography of historical Jew hatred, but\ liefs a viewer might bring to it, The Pas
Jesus prays in the garden of Gethsemane, more sensitive viewers may disagree. The sion of the Christ never provides a clear
the camera tiptoes around him like a Pharisees, in their tallit and beards, are sense ofwhat all of this bloodshed was for,
stalker, and John Debney’s score is a high- certainly shown as a sinister and inhu Van inconclusiveness that is Gibson’s most
toned creep show of menacing orchestral mane group, and rhe mob they command Serious artistic failure.
undertones and spine-jabbing choral ef is full of howling, ugly rage. But this on
\ The Gospels, at least in some inter
fects. A slithery, effeminate Satan (played, screen villainy does not seem to exceed pretations, suggest that the story ends in
the end credits reveal, by a woman named what can be found in the source material.
forgiveness. But such an ending seems be
Rosalinda Celentano) slinks around like
A few weeks ago Gibson reportedly yond Gibson’s imaginative capacities.
something in a Wes Craven nightmare, expunged an especially provocative line of Perhaps he suspects that his public prefers
and Judas, reeling from his betrayal, is dialogue that referred to the Jews: “His terrorAftiry and gore. Maybe Homer
menaced by demon children with pointy blood be on us, and on our children.” Simpsoh was right after all.
teeth and milky eyes. When daylight That line comes from the Book of Mat
dawns, the mood shifts from horror-mo thew, and it would take a revisionist to
New York Times Service
I
FRONTLINE. MARCH 26. 2004
85
S. THANTHONI
In a haemodialysis centre at the Tamil Nadu Kidney Research Foundation in Chennai.
organs has not. A cadaver organ is hard to
come by and live related donation is nor
happening at the desired level, leading to
a thriving trade in kidneys; the organs are
sold mostly by the poor and the vulner
able.
According to Ravichandran, it is im
portant to increase die live related donor
pool, apart from strengthening the infras
tructure to harvest cadaver organs. One
way of increasing the live related donor
pool is by accepting cross-blood dona
tion. A new technique that was explained
by Japanese nephrologists Dr. Kazunari
Tanabe and Dr. Hiroshi Toma (see in
terview) recently in Chennai. According
to Ravichandran, though relatives of
ESRD patients often want to donate a
kidney, they are unable to do so because
of blood group mismatch. The new tech
nique removes antibodies from the pa
tient’s blood before the transplant. It can
increase the donor pool by over 20 per
cent.
The technique was tried in India in
1984, in Mumbai. But because of prob
lems with filteration techniques to re
move the antibodies from the patient’s
blood, it was not successful. “But now,”
says Ravichandran, “with new develop
ments in filteration technology, we
should be able to do it without any prob
lem.”
With the introduction of cross-blood
group transplantation, there is a very
good case for scrapping Clause 9(3) of the
Transplantation of Human Organs Act
(1994), which allows for live unrelated
donations on emotional grounds leading
to trade in kidneys. Often, the reason cit
FRONTLINE. MARCH 26. 2004
ed for sourcing a kidney from an unrelat
ed donor on “emotional grounds” is:
“The blood group of the patient does nor
match with any eligible close relative.”
Now that excuse will not hold water with
the introduction of cross-blood trans
plantation.
On the flip side, the cross-blood
march will open up a number of social
issues. For instance, there is the possibility
of a rise in kidney sales once the con
straint of “same blood group” march too
is gone. But Ravichandran is confident
that this will lead to at least a 20 per cent
rise in live related donation.
But medically, this kind of transplan
tation is significant and may be useful
especially as the number of ESRD pa
tients is rising sharply. For instance, in die
last decade, the prevalence of ESRD has
almost doubled in most countries and on
an average the rate is more than one in
every 1,000 persons. The figure is much
higher in developing countries. The in
cidence of ESRD is similar to that of
AIDS (Acquired Immune Deficiency
Syndrome) and 10 times greater than that
of Hodgkin’s lymphoma. On an average,
the incidence of ESRD is increasing at 5
per cent a year.
The rising incidence of diabetes
(fuelling an increase in diabetic nephro
pathy) and hypertension is said to be the
major reason for the sharp rise in ESRD
cases. Diabetes is the cause for over 40 per
cent of ESRD cases. Among ESRD pa
tients, those with Type II diabetes out
number patients with Type I diabetes by
almost three to one. Over 25 per cent of
ESRD cases are related to hypertension.
Glomerulonephritis accounts for over 10
per cent of new ESRD cases, and cystic,
hereditary and congenital diseases togeth
er constitute another 4 per cent of cases.
With significant developments in
pharmacology, the mortality rate has de
clined in dialysis patients in recent years
and is much lower in patients who have
undergone kidney transplants, particular
ly those having received the organ from a
live related donor. Increased clearance of
nitrogenous solutes through improved di
alysis membrane technology has resulted
in enhanced nutrition and fewer infec
tion-related complications. Improve
ments in general medical care may also be
contributing to the decrease in mortality.
Patient survival rates after a renal trans
plantation has also improved dramatically
in the last two decades. The five-year sur
vival rare is more than 90 per cent. Recip
ients of cadaver kidneys have a one-year
survival rate slightly lower than recipients
of live donor kidneys.
According to Ravichandran, the best
method is live related donation and it is in
that context that cross-blood group trans
plantation would go a long way.
According to Dr. M.K. Mani of
Apollo Hospitals, Chennai, the primary
goal should be the prevention of ESRD.
Aggressive treatment for hypertension is
likely to reduce the incidence of ESRD.
Screening for diabetes and hypertension
may be important in reducing ESRD
rates. Mani’s project in Sunkuvarchathram, a suburb of Chennai, is a success
story. Regular screening for hypertension
and diabetes has more than halved the
risk of ESRD among its population. ■
87
I MEDICINE
in India, it seems to occur in 100 per
million people every year, while in Japan,
it may occur in 200 per million people.
In Japan, we do 700-800 transplants a
year. Our hospital does 20-25 per cent of
all transplantations done in our country.
Since 1971, we have done 2,000 trans
plantations in our hospital.
► How does the incidence vary with
industrialisation?
Toma. With industrialisation peo
ple’s lifestyles change, food habits
change. People become sedentary, they
do not exercise, and so on. Of course,
genetics has an important role in getting
diabetes, but lifestyle change is a very
important reason for increase in the in
cidence of die disease.
► Does the incidence of ESRD (end
stage renal disease) vary with sex, age,
ethnicity and geographic location?
Tanabe. Not with sex. But age
seems to be important, as Type II dia
betes, whose incidence increases with
age, is die major cause of the ESRD. In
Japan and the United States, the average
age of a person undergoing dialysis is 63.
1 have not seen any study on the in
cidence of the disease across ethnic
groups. But I do know that in the U.S.,
African-Americans are more prone to the
disease compared to Caucasians.
► What are the treatment options for
chronic renal failure?
Tanabe. There are only two options
— dialysis or transplantation. There are
two types of dialysis - haemodialysis and
CAPD (continuous ambulatory peretoneal dialysis). But neither is sufficient to
remove all the uric toxins. Normally,
haemodialysis is done thrice a week, each
session lasting four hours. That is 12
hours a week of haemodialysis, or less
than 10 per cent of the hours in a week.
In such a situation, only 7-8 per cent of
uric toxins can be removed, with close to
90 per cent remaining in the body. This
leads to chronic uremia, which may
cause athelosclerosis (heart disease) and
bone diseases that shortens the life span.
But renal transplantation completely
resolves these kinds of problems. Of
course, the recipient has to be on immuno-suppresant medicines, which can
cause side-effects. Earlier there used to be
tremendous side-effects such as steroidinduced osteoporosis, athelosclerosis and
so on. But now we sometimes take pa
tients off steroids, prescribe low dosages
of steroids and cyclosporin, or put pa
tients on Tactrotimus (IL-2 inhibitor)
and so on, and thereby minimise the
side-effects.
► So, are the protocols of treatment
changing?
Tanabe. Yes, treatment protocols or
drug combinations are changing to min
imise the side-effects. Pharmacology has
improved so much that transplant pa
tients have practically little or no side-
Dr. Hiroshi Toma.
Dr. Kazunari Tanabe.
Research on to
ensure graft survival’
Interview with Dr Hiroshi Toma and Dr. Kazunari Tanabe.
Dr. Hiroshi Toma, Director of the To
kyo Women’s Medical University, and
Dr. Kazunari Tanabe Assistant Profes
sor in the Department of Urology, Kid
ney Centre and Head of the section of
Kidney Transplantation and Renovascu
lar Surgery at the university, form one of
the leading kidney transplant teams in
Japan. Since 1971, they have performed
over 2,000 transplants, more than 200 of
them across blood groups. According to
Tanabe, in the past decade the donor
pool increased by over 20 per cent in
Japan because of cross-blood group
transplantation.
The two doctors were in Chennai on
an invitation from the Madras Institute
of Nephrology, which is celebrating its
15th anniversary, and the Balaji Medical
and Educational Trust, which is cele
brating five years of its existence. They
spoke to nephrologists about their expe
riences in cross-blood group transplanta
tion. Excerpts from an interview they
gave Asha Krishnakumar:
> What are the main causes of the in
crease in the number of patients with
chronic renal failure the world over?
Tanabe. About 20-30 years ago,
chronic glomerular nephritis (an inflam
matory disease of the glomerula, the fil
ter in the kidney that removes uric
toxins) was the main cause of chronic
renal failure. But today, diabetes and hy
pertension, which are increasing rapidly
throughout the world, seem to be the
major reasons. I think diabetes is the sin
gle most important factor for the in
creased incidence of chronic renal
failure.
In Japan, the number of patients
needing dialysis has increased three
times, from 10,000 ten years ago. Some
10 per cent of the Japanese people are
diabetic and 40 per cent of them end up
with chronic renal failure.
> What is the incidence ofchronic renal
failure?
Toma. Though we do not have the
exact figures, I believe the incidence va
ries with industrialisation. For instance,
S3
FRONTLINE, MARCH 26, 200-i
eheas. Twenty years ago, one could easidentify a transplant patient, with
bloated face, increased weight and so on
due to the intake of steroids. But, now, it
is very difficult to make them out from
normal people.
► What kind of research — pharmac
ological, treatment methods and diagnos
is — is going on?
Tanabe. A lot of work is going on to
ensure graft survival. Short-term graft
survival is not a major problem. A fiveyear graft survival with cyclosporin and
tacrotimus is over 90 per cent. But our
concern is primarily on increasing long
term graft survival rates - 10 to 20 years.
In Japan, rhe graft survival rate 16 years
after transplantation is 50 per cent. To
better that and to be able to prevent nonimmunological injury to the kidneys, we
need more effective immuno-suppresants.
Non-immunology injury that reduc
es the graft survival rate depends largely
on the age of the transplanted kidney
(the older the kidney, the lower the sur
vival rate). But conditions such as dia
betes and hypertension that damage the
kidneys, as also obesity, lower the graft
survival rate. These are things a trans
plant patient should be very careful
about. Thus, a lot of work is going on to
study the effects of immunological and
non-immunological kidney injury on the
graft survival rate.
Also, after transfusion or the first
transplantation, patients may have anti
HIV (human immunodeficiency virus)
antibodies. This is very harmful to the
kidneys. Over 20 per cent of the people
have these antibodies and they are highrisk sensitive recipients. They pose a big
problem during transplantation. A lot of
work is on to improve graft survival rates,
especially in the long term.
For non-immunological factors we
need to use effective hypertension drugs
that protect kidney functioning. Work is
on in this area as well. Apart from choosing
the appropriate drugs, it is important to
focus on the diet to prevent hypertension
and so on. A lot of work is on in the
management and treatment widi a view to
increasing long-term graft survival rates.
We have to accept high-risk patients,
we cannot refuse anybody. We accept
older patients, AB incompatible patients,
and those with high complications such
as vascular and heart diseases owing to
diabetes. A lot of clinical research work is
on to improve the management and in
crease the long-term graft survival of
such high-risk patients.
At the basic level, we are concerned
FRONTLINE. MARCH 26, 2004
lems as the Japanese are reluctant to
donate organs as they cannot accept
brain death. There are over 10,000
ESRD patients waiting for a kidney and,
we get only about 100 cadaver organs in
a year. Several patients die just waiting
for a kidney. So, we have no choice but
to expand our live kidney donation pro
gramme. Live unrelated donation is nor
allowed in Japan; it is illegal.
► How do you increase your donor pool?
Tanabe. We are focussing a lot of
work to increase our donor pool. For
instance, in 1989, we started the cross
blood transplantation programme. Fif
teen years ago, 15-20 per cent of the
recipients who had relatives to donate
were found to be AB incompatible and
hence could not get a transplant done.
“We hope cross-blood
But after we started this programme,
transplantation
those 20 per cent of patients who have
and laparoscopic
relatives willing to donate but do not
have matching blood group have bene
harvesting of
fited. This has led to a big increase - at
kidneys will
least by 20 per cent - in the number of
increase the donor
transplantations in Japan. In our hospi
tal, we have done over 200 transplanta
pool significantly.
tions across blood groups. In Japan over
It may not be
10 hospitals do across-blood group trans
dramatic or happen
plantations against only two or three
centres in the U.S.
overnight, but
In the U.S., the laparoscopic or key
it will certainly
hole surgery to remove the donor kidney
improve gradually.”
for transplantation has increased the
number of relatives coming forward to
donate as it means no blood, less pain,
there is no need to use immuno-suppre- and shorter hospital stay. This has en
sant drugs and there is no immunolog hanced the donor pool. Thus in the U.S.
ical injury to the kidney. There would be live donation increased from 10 per cent
no reason for the donor kidney to be to 60 per cent last year.
rejected in this case as the immuno-comSo, we hope cross-blood transplanta
petant cells of the recipient become com tion and laparoscopic harvesting of kid
patible with that of the donor’s. In this neys will increase the donor pool
process, the recipients may have some significantly. It may nor be dramatic or
infections. That is what we need to over happen overnight, but it will certainly
come.
improve gradually.
> This is very interesting How does one > What is the procedurefor doing across
do this?
blood group transplantation?
Tanabe. There is no established
Tanabe. The antibodies of blood
technique as yet. The Harvard Medical groups A and B are removed from rhe
School tried doing this, but there are still patients before surgery by a procedure
some problems. We are also trying to do called Double Filtration Plasma Pheresis
this at our centre. We are now working (DFPP). This is done several times till
on monkeys and mice. Monkeys are dif the antibodies against rhe blood group
ficult as they are very similar to humans, disappear from rhe patient. Then rhe
with a very complicated immuno-sys- transplantation is performed. The plas
tem. We hope to complete this research ma removed from the patient is again
work in the next five years.
separated into albumin and globulin and
► Throughout the world, there is a big the former is returned to the patients.
gap between donors and the number of This minimises risk as only the antibod
people waitingfor a kidney. What is the ies are removed.
situation in Japan?
> Does the graft survival rate vary with
the same blood group and across blood
Toma. It is very difficult to get do
nor organs. We also face a lot of prob group transplantations?
about strengthening the immune sys
tems or tolerance levels to accept the do
nor organs and, at the same time, keep
up the defence mechanisms against bac
teria, viruses and other such germs.
Achieving this has been the main strug
gle since the beginning of the organ
transplantation programme. But we have
not been very successful in this till now.
One of the most interesting research
works in this area is doing bone marrow
transplantation on the recipient from the
donor so that the immunology of the
donor also gets transferred to the recip
ient. Then the donor’s kidney is trans
planted onto the recipient. In such a case
89
Statement
about
ownership
&
other particulars about newspaper
“FRONTLINE
(FORTNIGHTLY),"
Chennai, as required to be published
under Section 19-D Sub-section (b) of
the Press and Registration of Books
Act read with Rule 8 of the Registration
of Newspapers (Central Rules) 1956.
FORM IV
FRONTLINE (FORTNIGHTLY)
Place of Publication — CHENNAI.
Periodicity of Publication —
FORTNIGHTLY
3.
Printer and Publisher.
Mr. N. Ram, Indian
43-B. Kasturi Rangan Road,
Chennai-600018.
4.
Editor In Chief'
Mr. N. Ram. Indian,
43-B, Kasturi Rangan Road.
Chennai-600018.
5.
Names and addresses of individuals
who own the newspaper and partners
or share holders holding more than one
per cent of the total capital — Proprietors:
Kasturi and Sons Limited.
1.
2.
EQUITY SHARES:
Mrs. G. Narasimhan,
260.T.T.K. Road.
Chennai-600018.
Mr. N. Ram,
Miss. Vidya Ram,
43-B, Kasturi Rangan Road,
Chennai-600018
Mr. N. Murali,
Miss Kanta Murali,
Mr M. Krishna.
260-A, T.T.K. Road.
Chennai-600018.
Mrs. Usha Narayanan,
275-C. T.T.K Road.
Chennai-600018.
Serendipity Investments (P) Ltd.,
43-A, Kasturi Rangan Road,
Chennai-600018.
Ms Aparna Ravi,
120, East 83rd Street,
Apt 3C, New York-10028.
Mr. G. Kasturi.
Mrs. G. Kasturi,
Mr. K. Balaji,
Miss Madhumitha Balaji.
Mr. K Venugopal,
Miss Divya Venugopal,
Miss Lavanya Venugopal,
43, Kasturi Rangan Road,
Chennai-600018
Mrs. Lakshmi Srinath,
60,1st Main Road, R.A. Puram,
Chennai-600028
Mrs. Menaka Parthasarathy,
32, Kasturi Rangan Road,
Chennai-600018.
Mrs. Nirmala Lakshman,
Mr. Narayan Lakshman,
Mr. Snram Lakshman,
30-A, Kasturi Rangan Road,
Chennai-600018.
Mrs. Nalim Krishnan,
7-A, Parthasarathy Gardens,
Chennai-600018.
Ms. Malini Parthasarathy,
280, T.T.K. Road, Chennai-600018
Mr. R. Ramesh,
Mrs. S. Rangarajan,
7, Parthasarathy Gardens,
Chennai-600018.
Mrs. Vijaya Arun,
122, St. Mary's Road,
Chennai-600018.
Mrs. Akila Vijay Iyengar,
8, Paterson Hill,
#12-12, Paterson Tower.
Singapore-238567.
I, N. Ram, hereby declare that the
particulars given above are true to the
best of my knowledge and belief.
N. RAM
Signature of Publisher
1-3-2004
90
functioning of kidney tissues,'fading l0*».
Tanabe. When we started the cross
blood group transplantation in 1989, a rapid progression of kidney failure.
there was a difference in rhe graft’ survival now many patients have diabetes, hyper_
rate within five years after transplanta tension, glomerular nephritis and so
tion and was the same after that. But, If we remove the whole kidney in case of
now, with the use of newer and better tumours in all these patients, then they
drugs, the graft survival rates are the will be left with only one kidney, thereby
same for both - over 95 per cent for increasing the risk of ESRD. Hence we
three years - and the rejection rates are prefer to spare the kidney tissues and
also similar. The rejection rates are high remove only the tumour, without dis
er and the graft survival rates are poorer turbing normal kidney functions. But we
for the anti-HIV antibody positive or have to pay attention to the recurrence of
hyper-sensitive patients. Thus, the im the tumour. So, we also remove the re
munological barrier for
gion around the tu
mour to reduce the
the highly sensitised
recipients is much
risk of recurrence.
“It is very difficult
higher than the AB in
This procedure was
to
get
donor
compatible transplan
started in the U.S. in
organs. We also
tations.
This
is
the 1980s.
because the anti-HIV
► As the kidney has a
face a lot of
antibody is much
lot of blood vessels,
problems as the
more difficult to re
does it require some
Japanese are
move and recurs eas
special technique to re
ily; it destroys the
reluctant to donate move the tumour?
kidney easily. So, we
Tanabe. Yes. It is
organs as they
desensitise the recip
a difficult surgery.
cannot accept
ients who are antiSmall tumours are all
HIV antibody positive
right. It just needs to
brain death.”
and then perform rhe
be cut and stitched up.
transplantation.
But the real problem is
► Do patients undergoing cross-blood with the bigger ones. We study the area
group transplantation need to use more carefully for the arteries and veins, cool
immuno-suppresants than in the case of the kidney, cut out the tumour and then
close the blood vessels. But if the tumour
same-blood group transplantation?
is too big, we remove the kidney from
Toma. There is no difference in the
use of immuno-suppresants. Only, the the body, cool it, take out the tumour,
antibodies need to be removed from the close the blood vessels, and then put it
donor blood before transplantation in back into the body. This takes a long
time. This is a new technique but we
the case of cross-blood group graft.
We also do laparoscopic springecto now do it routinely in our hospital.
my (removing the spring; a two-hour > What is your view on kidney
procedure) on rhe recipients before rhe commerce?
Toma. The International Society of
transplantation, as spring - the oasis in
rhe bonemarrow - is a ver}7 important Transplantation and the Japanese Socie
organ for immuno-response. The spring ty of Transplantation are strongly against
has a lot of B-cells that help in producing the buying and selling of organs. We are
every kind of antibodies. Thar is why we for totally doing away with trade in kid
remove the spring to remove rhe anti ney. The only long-term solution for any
bodies. In the early 1980s, without country is to focus on preventive mea
springectomy, cross-blood group trans sures, concentrating on diabetes, glomer
plantation was not successful. But now, ular nephritis, hypertension and so on,
with newer and more powerful immuno- the main causes of renal failure, and at
suppresants, die Mayo Clinic in rhe U.S. rhe same time step up research work to
does cross-blood group transplantations decrease rejection and increase graft sur
successfully, even without springectomy. vival rates, which include the develop
But nobody knows the long-term results. ment of better immuno-suppresant
Just to be on the safe side, we do sprin drugs.
gectomy before cross-blood group trans
As one gets older, regular check-up is a
must as early detection can make a lot of
plantations.
► What ways do you adopt to save the difference to managing the kidney without
kidney?
going in for dialysis or transplanrarion. To
Tanabe. When there was a tumour
detect problems in children, it is important
in the kidney, we used to remove the to educate paediatricians to detect kidney
whole organ. This resulted in the loss of problems early.
FRONTLINE. MARCH 26. 2004
Position: 847 (18 views)