RF_DIS_5_A_SUDHA_PART_1.pdf
Media
- extracted text
-
RF_DIS_5_A_SUDHA_PART_1
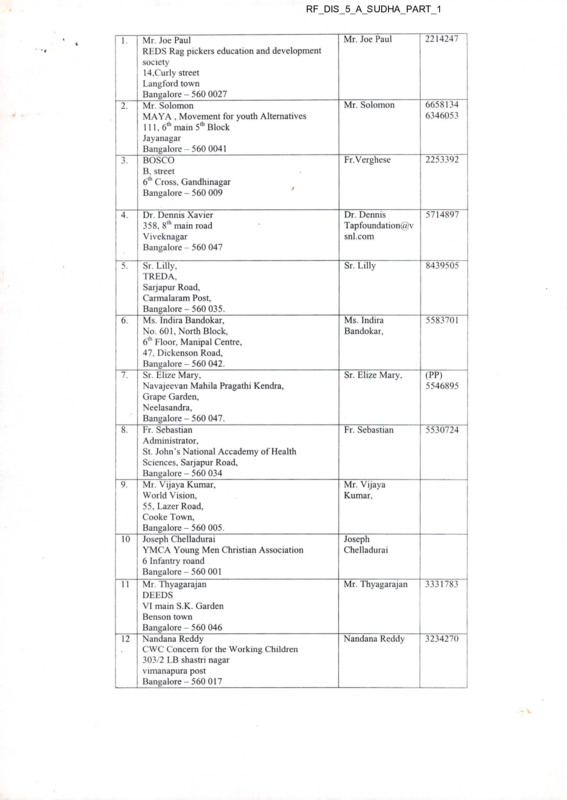
Mr. Joe Paul
REDS Rag pickers education and development
society
14.Curly street
Langford town
Bangalore - 560 0027____________________
Mr. Solomon
MAYA , Movement for youth Alternatives
111,6th main 5th Block
Jayanagar
Bangalore -- 560 0041
BOSCO
B, street
6l11 Cross, Gandhinagar
Bangalore - 560 009
Mr. Joe Paul
2214247
Mr. Solomon
6658134
6346053
Fr.Verghese
2253392
4.
Dr. Dennis Xavier
358, 8,h main road
Viveknagar
Bangalore - 560 047
Dr. Dennis
Tapfoundation@v
snl.com
5714897
5.
Sr. Lilly,
TREDA,
Sarjapur Road,
Carmalaram Post,
Bangalore - 560 035.
Ms. Indira Bandokar,
No. 601, North Block,
6'11 Floor, Manipal Centre,
47, Dickenson Road,
Bangalore - 560 042.
Sr. Elize Mary,
Navajeevan Mahila Pragathi Kendra,
Grape Garden,
Neelasandra,
Bangalore - 560 047.
Fr. Sebastian
Administrator,
St. John’s National Accademy of Health
Sciences, Sarjapur Road,
Bangalore - 560 034
Mr. Vijaya Kumar,
World Vision,
55, Lazer Road,
Cooke Town,
Bangalore - 560 005.
Joseph Chelladurai
YMCA Young Men Christian Association
6 Infantry roand
Bangalore - 560 001
Mr. Thyagarajan
DEEDS "
VI main S.K. Garden
Benson town
Bangalore - 560 046
Nandana Reddy
CWC Concern for the Working Children
303/2 LB shastri nagar
vimanapura post
Bangalore - 560 017
Sr. Lilly
8439505
Ms. Indira
Bandokar,
5583701
Sr. Elize Mary,
(PP)
5546895
Fr. Sebastian
5530724
1.
2.
3.
6.
7.
8.
9.
10
11
12
Mr. Vijaya
Kumar,
Joseph
Chelladurai
Mr. Thyagarajan
3331783
Nandana Reddy
3234270
13
14
15
16
17
18
Sr. Lauret Marie
Asha Deep
Montfortian Society
7/1 Venkatappa road
Tasker town
Bangalore - 560 051
Ms. Dona,
VIMOCHANA,
No.26, 17th Main,
HAL II Stage,
Bangalore - 560 008_____________________
Dr. Saraswathi Ganapathy,
Belaku Trust,
697, 15th Cross,
J.P.Nagar II Phase,
Bangalore - 560 078._____________________
Parsapara
71/2 First Floor
7th Cross, Bandappa road
Yeswanthpura
Bangalore APSA Association for Promoting Social Action
Nammane
Annasandrapalya
Vimanapura post
Bangalore - 560 017_____________________
Association of people with disabilities (APD)
6th Cross Hutchins road
Hennur Main road
Bangalore - 560 084
Sr. Lauret Marie
2864113
Ms. Dona,
5269307
/5360311
Dr. Saraswathi
Ganapathy,
6630463
Vnekatesh
3472701
Dr.Kshitij or
Mr.Laksha
5232749
5272111
Mr.
V.S.Basvaraju
5475165
5470390
604065
Welfare
19
St.
Lukes
Ragpickers
Programme
Pampa mahakavi road
Chamrajpet
Bangalroe - 560 018
20
Griha Karmika Okkoota
2, Mi Ilers road
Bangalore - 560 046
3330433
8/333083
8
21
Churches’ council for child and youth Mr.
Chakaraborty
care in south India
Lavelle road
Bangalore -560 001
Promod John
Prakruti
79,kariyanapalya
Lingrajapuram
Bangalore - 560 084
2210098/
2211412
Ms. Dorothy
5454653
22
23
New Horizon trust for disabled
354, 10lh main 100 feet road
Dodda Banaswadi
Bangalore - 560 033
5469550
1 o'
rl
s
PJ
a
pl
C3
CL
lQ
Q
CL
o
o
>
8
f—
X)
T
LL^
|CU
<2 .g
S
(X
0)
u)
ro
Q
O
0
O
££
a.
yr
X E Eg?
ZJ It!
.a_
3
15
c
■
O
Q
.2
*5)
CD
Z)
U)
JZ
UJ
’3
o
-I-
m
<
z
CO
O)
O
XJ
XD
aj
(
.-.'• ' I
ds
-JO
SI i ~|^. O
V4
(D
CO
0'
X L*O '*'
CO
r
3 £9
Is
4c$
J cO
ul cfl
a Io-
:6 r, jL- I'M
vT'3
6, I €
Zc?
\
i
I
i
l-'J1
di J4^
o
>7
!
-M
fT| '7 fl1,1
„«
< ’ FI
L
2|
-id
0=1
3!
k
7
n ■
crto(TO Pl q ~ij
5-j c
41 ^| -4| ±10 4^ & frq ?y
Cl
U
<
\D
L
Z
“7
fl
1no
?b o
ro o CT
Q) _g
Q
Q
; v?
. d
05
.,' I
Th <>
co
S’\° 5?
pg
L~
n
^0
?
1 "-i
K)
-I ’
zl
£ '< ' .'■
JJ
'4p
tn
L I
n
-y
8
I
a
IL
<4
T ~T T"
"iin I
I?
I3
r*
I
0
.
?
!
1
4
1
SI
§
^1ul Hl
>1 ^1 <
^1
d1
7|
^1
51 '
c
g 3
..........................................
j.
c
■^1
'
\q
rJ\^
^■)
j
r
L
IrSd
O-
CD
i /<
71^13
F
p
-1 j
H J■I ’4S-'S'- -4°R
■Us ^4
1
' ' I o
'C-5!;
Q_
<__
4
t
CL)
l|dj 0
U I1 2S 5lrf
i
a
o
-•$
1
tr. ..
S o
A
q
o Cl
a; |ci
i#| '■■> 4t-j
41i C £70- ?■• |4
UJ
co
>
UJ
tz
I 4
r.4
Z5
1
r
o
<
_L_
cd
a a ^1! tI rft s• bI-
E
o
H
r=
|f5
VJ|
o
o
H
H
tSq
d?
A
o
r-i
I r~;
TJ
c
I?
J Ji •>.n In
Hia
■7 HI? ish
IM
11 D a1*? S¥4?
5
'r
□
_j
a>
</
£o
f/x)
r>
|-
sT
”
•ij
u.
Q
=>
v>
ar
i
<O
!
O
-5 o O
H
o. .2
i—
2
cl
«jo
I
'r»
'4.
g E -£
m
H
,4$
i
w— "c
0(1)0)
ar
a| .S5
2
dA
Q.
O1
£H
H
®\a
£ t S
ro
~ ro ro
Q w E
z: s
Z
Q-
<>-
fe?<
S' '
\
£
£
• T____
0 ra
01 O
a:
H
z
-z
'Z
'*'7
CD —
CT^
c
\
<Z) ■
-O
"o 2?
O o
E CT
<
\
| ! S
iZ
ilz
z: o
o
!,2J
ro
>
Q
23
nJ
CD
CD
C
3
rro
c
o
E
El
UJ
O
■'
”^
h'
<D
B
s
rn
|Iii§
c
0
Is
/
I
■"■
z
-' ’
\-rA
#
G
‘.H
M
ri
^1
0
ri
0
1
I
xD
cr
?r
oQ
c<J
/ill
£ $
(>l
H
I
I;
cA
j
C\£
h"
QO
p
. ("J
oJ
<
'^r7
?
■ • ■ :^.^-^c. ;¥d
1I 1
1,1!
21 j id o
^gSKfegf jSKWgC«8g[
os
i gi~^a
I £ L ro _cd
/ 0
I .0)
IK
u?
I ™ I LU
C
<X
1 ’U0
li :
£ 2
a:
o
^J£
HCL
|a>
' CD
CL
J9
TO
3
r
TO
.
'^..:
o
LU
' ■■'•.■AU
— 'AA'p
s “ I1!
co
a5
a:
ID
c
V o
t
CD
0
TO
o).2?
<
S 8.
or o
CL
U
o ® S
2 '€ §
O
or
E’,
z
TO
TO
Q
CD
w I
TO
0
rr>
GO
o
o|
001
01
l_n
ri
°
0
TO
0
TO
0
g E£
X
o| (/)
£ OO
A
3 Q
C2
to
O
U4
OQ
O
I—
T
<
.Z'
□
o
</)
dVx?
CD
□
‘O. So
SCL
dl
• l-r
tff
od
c.
I
'U
i- :
8
^r“
'i
I kJlt> I
if;
idd
p'?) -..
MdddLkH
I ^Tii
o
CD
>
LU
p
-X
1 ft4;
1
I
P-Mi (5 '' r
P5?
r
LL!
O
-M
? K
.'
o
O
f
T
>
c2
c£
!^ P
■■
V|
E
ft®
d
Oi
2^1 S' ■ HIP
U;i I j
0
f-
.3
^'77 ,p
{■ I' I 1
CPU.
•o
■O
ro
x»
di
]?ni h
w
0
is ■
I
~~T’
Q}
Q)
CD
V)
S'
CL 9-^
Q
Si
<
ad
o
i
X
z
o
(D
o
■
!r
<;£
I
-U—ip I s I $
X LC
O
r
■^£>
'X
J
£ I
pr"
|
Zl
/ |
i >
I ob
Q d
d 9
^■'
a? ~
<a ^1 i Up I
ti- dp
I
o
£
(U
Z .£
’O J
3
o . J> 0
-S
c ‘b
-S
Q
tj
CD CU
$
J
v?
'\£
>
oo
<■
^r
H
I Vr|
w|
I
■?
CO
Bk.'
i—
r-01
;
Zi
to
C"
‘ f'
0"
vn
U
V
..........
■
j Mfw'’ ■ -
yfr •. ■
o'
Ig
J
F~
Oi
8 G>^ ro Q
£ t cu_a) •—-
o
nJ
I •§
I '£-CL 112••S 67
I w .5= _ |
I OJ
I1
CD
O
>
0)
Q.
£
hH >g
I <i)
' 8■®
a:_
H
i
r
OJ
ZJ
l
a.
CD
n5
ur
t CD
H
•6)^
CD
CD
a: o
CT §
■€ E
<u
ra
Q JS
V 2?
O|
ar
o
.2
o O)
co a;
00 I or
o
>
b U)
o O
Lil I
O s
H
-J
<
9
i— I
<
?
• a
.Lb
I
fc?
£
<?
■3
H ■
2? o
rj
r‘c
CD
2T
&
?
AC
Ef- OJ
AS
I
J
I
h' ■
j
tfc
A/
P
o
I
|
Jd
a
|T~ ~^7
«>'
cC
£.
uf^
rJ
Ji1
I c/y 1
ll
a2 II
u
JI ^1
sr!^i
li
c/'
r'J1
Q.
X
dz
r? i ?
£
t-
ro
_o
o
cu
1 C ,Oi
c
o
U ' r31 <
o
si hr5i/i
Jo'
!,
1/1
o
0)
CD
f
<__
1
i.
p
ru
I
<r|
J
' ■
c
i
I
'tl
? !
^ri r Pi
j_
±Xi
*?
K)
w
<) I
(J-
iL
L
V
p-L
s
B
B-'
11^'
IrEcKfrai :m§k £.1
X
"ki
'zl
fl
f
g
!■
V
nJ.
CJ-
ru
-<
D
ra
r^f' c
iG
IF
I
•r4
?
r ,
1- if I cir^rl |
rd
~T
<tl
I
® 0 ;
idJ
■^1
V 1
r
iX-
I -"S7
I
It11?
a1 1*
a I2 £
Sr
-X
I
kJ I
n
ni
X
CD —
CAJ
o v. .w o
c
ro t) O)
O
CL) CU
Q
s
•C'
'■^
c
lit
E-
ro
a>
E
7!o
X
•O
TD
XI
3
?
cJ
o
fi.L'
<
a
>l
ui
^l
'1 ?
'S 7
£
co
co
o
o| 0
b” I
il
0)
fe?
fc1’
>
H
u—
-J
QC
UJ
&•: .
'c
g? o
CL
STi
CD
MJ
° <? g-^.
_ Q
E
<
s
=>
CQ
ro s E Ecu
<D
co JS 3 3®
■'
m
a?
or
CD
(O
O
S
Si
<
£Z|
01
O
I!
>
’75
m
* 8
8
o
U
LU
ry
£'
f
J.
I..
pf -.
1 ..
2JU;
•-!
o
^S-3
co
>
a
.i'J
■c.:
1
i ■
S a
t
I
|ie
I
03
H—
w
o
1
§•
o
!
or
or
zo'SZ
S—
0)
D
<D
COW
o
Q ° 0-
or o
O
O ? S
-S t «♦E—•
m o
O
£ 5?
O)-£
£Z
.Q
Q
LU
55
>
IU
DI I
s
□
TO
TO
■
i
r-A
co
I-
:
LU
O'.
G
T
H |J
.i
\> w
!
H
• iP
r
0
0
m
{
A>
V
X]
oO
Cx-
<Q
6°
oi
Q
I
i
On
Ox
ry
n
i
( I
Tt
:i?
cJ
)
tz
n
I
I
1
a
r>
c E
3
H-
&
o s <D
f Sos
ffo
3 rg
a iX c>?
T
;i
n
i
Ci
><
o
rs\
r>
co
h ■
A pJ .....
1
y"
co
’co
c>
p
<
z
Q
or
LU
00
ZD
TO
TO
or,
2
z co
o ’cd
Q
o
CD
J
3
O
(si i
a? ro
CL
O
S-^
<
s
s
Z
7
a
UJ
Cl
‘.d
8 •§ -5 3 ly
z
•7
-
s
<
ar
o
o
or
CD
7:
ro co E
S
Bg| :
c
ro
0_
r
ro
LU
P
f
m
a
Pj
4
va__ I
I
o
I"!
I
J
ij_
s
CL
•J
3
Spin
H£cq-g^
o
P*
JlCi-I
■O
■O
co
o
XI r
o
c<)
co
<_
Li
t?
X LI-
u
<D
CO S
a
rrl
-j
2
31 3
31
si ,|
al| J5
1
i
JD
ro 'tS 4-2
CJ) "tzi
Q
p o
S? 2
Q<
co
vxT
H “T~ L
L Sy' -•C| ^*>
a «
fl
2v
c-<
AnrJ cp
—-
rd
I
El
Z
T ■J
I
ii1
El LL
I
I
&l
<5r ^1
'P
>1
‘ul
rd
Cl
<3
V'
r^
s^-
r1
rd
cd
I
cr
rp
Ot
rd.
\jD
(X)
O
•r>
o5
0~~
'.0
TC
ci- -5
v?l
I
C
I
44-1
4r -i?-
pi
"~~T
'X
■
I
rJ
o5V3
r-S
L>
—
rb
rh
I
1d
A
<X)
ill
E
>-
&
c|
Q
jo
Cf
>
uS
io.
Mr ~T
i
I
i
I
s
I
i
E
'T?
J
3H H E
15
i
I-
ci
I' ljL.
!LJ
IZ
■
' V- 4iai u I OC
■
c0
dH SlLh]
c-c
■/-'
$1
|
zS1
'J|‘
;p
I
L|c
s-
c
3
c!l
rb ■i.i
V®
I C"’
<51
§
lb
4 ~T
~r
q)
“Z
$A
kw
(£
cG
U
•z £
r
r
si J -I 4< E
if ?!
(11 1!
'A
-I
I
I
<ti
o =
c'
H
•'-d ■C
I
i
l'E
LL 4ii Ei
0)
? 5
o
2,1 d ,.L
V
E
o
lil
1
4i
co
co
o
zr
L
C'i
II
<r/
r>
. . ... .r_,:...
^1
s
j
"cd
CD
0)
'o
g? .£
CD
CL
1
»
O
CO
CO
o
’€
c
•H
E
(2i
■*-»
o s o
c
££
c E
llos
H
LU
CD
0
H
■
-J
<
■Z.
.2
o
0)
JD
Z3
■O
Q
LU
CO
>
LU
nil
CD
CD
a.
E
o
o
o
Q)
rs
17
0
k9
.<n
rn
t^)
Q
l=i
Tx
Q
Jo
^3-
9
Q
?5Q
A
3 ^3
$
CL
J-
5 o
CX
2 TO
<D
cQ
4$.
d?
3
2?^
“T- ~T
I ■
t
i
I
s
to
lii
—L
«’2
2
4
fe
9’
i
H
----------- F
is^
3
IgUif
-J k
|5 ■> Sp j
0 3 «a. < ■sli
,
£1 cc'■- 2l
o' X
k
jr'-lji
,
Cy
x '-1-
'L
O '■'-
co 2
LT "T
Hi ,
rl
7- ? -
'-•7
2
Q
3
I
I s;-ti
|7
£ -2
0
.2CD ‘-S5
2? 2
go
•E v'v . E •>" ■ v^Y\\VVy^vV-V. ;x'y X
J<d
I
EL
eJ
£P
r-t
rA
f/)
r
(x
J
61
^1
J3l
JI
<1
I
r-J
27
r
.e| 5 (rl
<c| f' 1
z\ ' tA I
o =
Q
O'
F^-
<
ro
I
0|
l£
30 J
ta
IL
1
gi--:
I-
cal
Z |3 L I
•i
.a
8
'Z? < Cl
<1 L ^j E I <H<$I
r Lr §sir
■ 4
4; Lz
? c"7 M I u
Itz
E Mlr
^7
li "J Sf
*ri- fep
Vri ’i
^/LL ^3
21
7 g oj j ?!/ -3ie| o
rg A OU 4 ^1' i
-4
r-\|
■‘{2
4
-LL
i
c$
?r
0 Ll 4^| cB
.A^0
r
ci
A
0
o
$
cu
CD
lx.
2i
CU
4-1
I
-’I
•U
H
a.
§
x5
A
Cjr>
p
co
co
CD
O
<
2T
Q.
El
~r
(0
2
2
o
co
or
Or
H
’S?
Z5
w
oJ
cu cu cu
U)
7
f
-_J
o
ni
z
z
Cl
Q w o
9
f-i:
ITJ
CD
O
o
O
7
Qi O
Qi
Li_
Qi
H
<
"c
£ o
E CD
O)-g
o cu
o
i
o:
11II
<
(Z
0
ctt\
S’
Q)
cn
CU
0)
•E? Q
Q____
s
)
I
J Is
LU
S’5
e
£ -S
Ia cr
g
<D
tr
ra
Z)
0
I1
LL
eg
CL
>-
I
A A1
Jl a
V
V
U-
.1
Cx
~T
~T
-Sr
ri
2
Q-
I
I
T-i
71
=t|
El
c/i
<tl
n
CO
T1
71
!7|
r\
r'-
(■>
.is
rr
ca
iteg
r
si
T
a
i
?!
?l
CO I
1 EL 2 A
' ts
s
•3!
|
J
cel
?l
4I
$1
Ek
on
OJ
<T
o
Q<
rK
0O
Oo
I
i
!■
!
MBR&
B^ViSEOj^ATION/U-JT UBERCUI ^SIS
■
CONTROL programme
.
T ubercuiosis Register
■
TB
No.
®-'^4
™
^lili
5:5
3.G
z\z
^'•3
2\ 3
53'3
91 ■
i I
.!
!
Bi
SMI;
p:
c i t~
03 n
2' <.C
_________
pt <) ^T3x<f-T~
PxiAO
■•3^ i\i
________ ^V*vuA
Kjc.
v£vtW
Q V-
IB
«
^3
I
14-3
3
V^VkA
-S2.
S/i-^
—
—'Xzca
pzy
2
“y-its^c_-r^x$ y - b{
2&
(j 0:
2,7^
L<?'3
J)
P
^<-3
£
£
c mi4
i
■a7^7
CT^C4
-F
-H,{.<,€■’<=;£. . v
av; V>cu5p2.
PrSA-
K j
i~
N
/\1
2^. C^SL Tjf /_£.'
--------------- 'f&C^ <-'■)- Q-OXLCSCii
.j
--------- ----------------------- -
n
P
l ~ r'>-' C,v
* 0 r* 'J
---- (T
J g^-u^)( p
ii-L
4
r
?
asjA x A_c>
r
__ p
A>
~ TsFij------
T-sl
■
Type of Patient
New Relapse llransFailure I Treat- Fot
case
ment
fer in
after
(N)
(R)
(F) default (c
H’3
crj
f
'
2X1^- £3 WA-ryyryj
5} 06 1
_£ q/
______
^y-AsftgJcii.A_
?
Year:
(D)
—
___ FF
—
m
(
3 2 -1
2Q-3
Date of Regimen/ Disease
starting Category class
treatment
Pulm./
(P/EP)
to A
%ci | 23-3
A/
Name of
Treatment
Centre
xpulm.
-
:r^
Complete address
—t
— Svfx vm\ ^3,._ __
ti g
i
Sex Age
M/F
S
w
Bl
Quarter:
Name
(in full)
2\ S
. BO
1
^fes
Date
of
regis
tration
\t-3
M
£
SUMMARY
• “Ax eciXv-J
ixtZEX_
VvA
New
I smear-positive
M
F
Relapse
—I
r
rh ;y
Smear-negative i^ra-pulmonarv
'nonary!
m
REVISED NATIONAL TUBERCUHTSig
.
■
TB
No.
.
■
ill
Date
of
regis
tration
"13
Name
(in full)
Quarter:
Sex Age
M/F
— VXWXL
_____
_
_b BlSsiC' Pr_ ffjA.tft -J
__
2^3
■
Complete address
(^0
.
CR
if
3a -2
__WA_
--------- <'n5vryj.. ?
fflf
Bl
S4<2€v< (2^
------ -21q
|oo
3o-3
I
^>.v) j4
___ ,J~
p——
ZA
J.
??■ i
■/
N
p
N
SkT
a s
ik
P
3X
?fc-3
e
X
^-0
-XT
?
ZS-3
W3
iffxXXSsi
<- T v*l I f
^-ce 3\-3
I - VO<^ t4
J
cr^
P
X-S A
B
r
m
A
31-3
iA s P1
■—r—-—-Y^~ ft-~ V.qxV'x
Type of Patient
____£L
z<i-3
2.^^
3t-3
II
\J Pc
■^dg
New Relapse iTransFailure Treat
case
ment
fer in
after
(N)
(R)
(F) default
xpulm.
I (P/EP)
jOow^.
if1____________ ft
3-3
I
/bs b-
5^0Voss
_______
--------
-F
Year:
\S<3
-4t> -t
-X1__X_'
—-^LL^-r
------
Date of Regimen/
[
Disease
starting Category
_ / class
treatment
Pulm./
_____
, iXXXDT
— ---
------ —ivC{- i
i
Name of
Treatment
Centre
sV^TT^—-
Ao-,,
^Q-3
r 'A
£ONTROLPROGRAMME
----- ----- —--
Tubercuk ‘S Register
v
?
T
e?
N
■
:
SUMMARY
New
smear-positive
F
Hi
F-'SL
Smeanr^gative ^Extra-pulmonary
Relapse
i~ l f
M
M
’
r~
F
'
’
M
F
2_
-J..2_O
'•>-
rrcc4-¥.«sfc -.
-.■--•■*'<22;
2 • -.<?
...
ai
£
O
■O
0
o
o
r
-L
I
GY
I
Olso
E
e-
CD o —
‘W
c
o
E
.s .5
CD
03
D_
cu
0)
ro
u—
>
PS
a
LL.
ir
V)
c
—
Q
0
Z2
Q_
I—
UJ
E
—
CD
W
&
>
H
19
i L>
CD
I
a % E E cl
f?S’
<
01
0
I
I
■I
o
I
03
o
m
u
a>
H
2:
S'
C
QJ
°2 E
0
I ®o Q
-
L<
0
Y'
<a
6 2
01
CD
■' 9
21
V)
<0
03
~O
T3
r4
0
^3
<jl
ol
JI J
■R-l J
E
o
O
<
(t/I $
2:
^1
4 12
Q
LU
0
O)
W
>
<__
(y
X “-
LU
0
2
~r
0 ==
§2 £
Q
f2 d
->•
*$;
.
k!
<?S
■V-X3
i tt
b-7
r
U
c
£
dl
JJ-W
■
T1 Is
?i <L11< Si P
|3^l-gf
JJ o!<r 1? -si
1d
<3
oo|
ti
~1 '
I ‘ s ' i at?
[
J
.
(p ■
I
.« §
03 g
, I
I
3.1
^1
•S
Ji
di
(<l
I
JI
it
^1
I
<v1
S'
S'
T~
o
0'
C
i|?6|
o
£Z
U
I 7F
I
a
it
»r
1
I Ji Si
yl
B'di ,<J
■<?
li Isijl a .f-k 11
I
<1 <ll
J
JI •Si I
Zi
£ Jl I
^?l
fib '’: ?
.£!
Ji
L.
j
T
G
w I 5 c5| -
M
0Q|
>c
Ife
i
I■
I
............
cs
-
s
II f
c1
s
Q-
^•h
r:h
J !. y q)2 4i
'5 ■
.^>1^1
js:__ id
z
Ffd
I
lv> d H 'll N
J
-
J
rC
1
V J
t^l^
■' -i
Pi i
jiMhiisi
I cy
ST *
O
T
I
)
J
k'
o
. I-1 .■
o
"5
ex?
eV
P
s
__
'" "■ ’i'i^-^C1 ■? *• <>•■ •>•
<f
I
QO
o'
-'r-.'*k<.'>'‘,^>''*-:..«', -5^'K.<;:J
.
¥
;|
T I ‘
J
cu
fe-'
Jy.
<!
j. VT
' r-lJ
Jl
0
CD
i
^3
??
± G
I '
J >
•
0 2
I
rC
c2
CL
2
4
I
Q
7'- 'A
-J
■J! "S”
co
ro
<
<r
x
I
G
<0
J
-Q
CD
z
s
Q
<r Q
#;
jpc
□
o
CD
W
^■
IX
N
Cr
I—
O
is
V
or
erf
■^..---------------
o
H
k’ • ‘i
CZ)
a.
U)
1 feR'S
2
=□
V)
« 2?
o .2
*S)
Q
b—
1^
i—i
0
° S’ g
■s E £
0
□
<N
01 o
01
£L
LU
KJ
g-
“
Q
a.
3 14!
£ ro
s
z
.
0
a
-
z
Z
Q
22
rs
LU!
03 I
’ I
r03
u_
CD
CD
03_____
OJ
y
■ fe ■■■• '■'
kT'
Q
1 m ik
. <
!'j
t
J. ©
s
i
>
I
1
H
>,
I ’?
II
5
>
$
.r
I
)
,2b T
I
I
I
I
\
tr
i
-
/ £ 0<y^('T
6
■
ft
DEFINITIONS: THE REVISED NATIONAL TUBERCULQSiS CONTROL PROGRAMME
r
&
I
CASE DEFINITIONS
TYPES OF CASES
Pulmonary tuberculosis, Smear-positive
TB in a patient with at least 2 initial sputum smear
examinations (direct smear microscopy) positive for
New
A patient who has never had treatment for
AFB,
Or: TB in a patient with one sputum examination
positive for AFB and radiographic abnormalities
consistent with active pulmonary TB as determined by
the treating MO,
Or. TB in a patient with one sputum specimen
positive for AFB and culture positive for M. tb.
Pulmonary tuberculosis, Smear-negative
TB in a patient with symptoms suggestive of TB
with at least 3 sputum examinations negative for AFB,
and radiographic abnormalities consistent with active
I
r
k
r
pulmonary TB as determined by a MO, followed by a
decision to treat the patient with a full course of anti
tuberculosis therapy,
Or Diagnosis based on positive culture but
negative AFB sputum examinations.
Extra-pulmonary tuberculosis
TB of organs other than the lungs, such as the
pleura (TB pleurisy), lymph nodes, abdomen, genito
urinary tract, skin, joints and bones, tubercular
meningitis, tuberculoma of the brain, etc.
Diagnosis should be based on one culture-positive
specimen from the extra-pulmonary site, or
histological evidence, or strong clinical evidence
consistent with active extra-pulmonary TB followed by
tuberculosis or has taken anti-tuberculosis
drugs for less than one month.
TREATMENT OUTCOMES
Cured
Initially smear-positive patient who has
completed treatment and had negative sputum
smears, on at least two occasions, orre of which
Relapse
A patient declared cured of TB by a
physician, but who reports back to the health
service and is found to be bacteriologically
was at completion of treatment.________________
Treatment completed
Sputum smear-positive case who has completed
positive.___________________________ _____
Transferred in
A patient who has been received into a
initial phase but none at the end of treatment.
Or: Sputum smear-negative TB patient who has
Tuberculosis Unit/District, after starting
treatment in another unit where he has been
recorded._________________________ _
Treatment After Default
A patient who received anti-tuberculosis
treatment for one month or more from any
source and who returns to treatment after
having defaulted, i.e. not taken anti-TB drugs
consecutively for two months or more.
Failure
A smear-positive patient who is smear
positive at 5 months or more after starting
treatment. Failure also includes a patient
who was initially smear-negative but who
becomes smear-positive during treatment.
Chronic
A patient who remains smear-positive after
a MO’s decision to treat with a full course of anti-TB
therapy.
Pleurisy is classified as extra-pulmonary TB.
completing a retreatment regimen.
A patient diagnosed with both pulmonary and extrapulmonary TB should be classified as pulmonary TB.
mentioned categories. Reasons for putting a
patient in this category must be specified.
“Other”
Patients who do not fit into the above-
treatment, with negative smears at the end of the
received a full course of treatment and has not
become smear-positive during or at the end of
treatment.
Or: Extra-pulmonary TB patient who has
received a full course of treatment and has not
become smear-positive during or at the end of
treatment.___________________________________ _
Died
Patient who died during treatment, regardless of
cause.____________________ _ _____________ Failure
Smear-positive case who is smear-positive at 5
months or more after starting treatment. Also, a
patient who was initially smear-negative but who
became smear-positive during treatment.
Defaulted
A patient who, at any time after registration, has
not taken anti-TB drugs for 2 months or more
consecutively.
_____________________
Transferred out
A patient who has been transferred to another
Tuberculosis Unit/Districtand his/her treatment
results are not known.
1
tr'-
I
revised national tuberculosis_contrQl_pI1Q^B^MM^
Tuberculosis Register
Year:
Quarter
Sputu
Type of Patient
TB
No.
|.i itc\
|Y)
Tuna
3.1 01
3
3 VQ1
4-
3,vol
__ I fili al
4
1
3bol
65
164,01
______ ft Ml J
bO K>-4
_M_5 _y^_E__C21
ji^ndu Jc^_\bJtnA _
z.
~___________
/7. i\Q u
io p
^lo bQuni jUpriKftxgpftK
y
4h.?2£QL^- —______ i
j)n
_qS_kOh
-
_^-Ll52smTzr~_
filo hnvociy
lot- Cl
15.vol
10
Sex Age
M/F
Name
(in full)
Date
of
regis
tration
Name of
Treatment
Centre
Complete address
_______
Up kv)6hna?PCi
JCO-WACL_____ I
4
______
pYb-bkok^’C _
* (o~Xo pal
r
P
.1
p
M
iluoi flTo foabn — F
mu
~j<~p&iyofn Qi'lpyg-^
AJC_Aaama£ _£^_
2)S> ~i7c7QM (77c/ pt.nhUa nlc’^l^ _ A^iH c
_N0_il£
______
IS, k fbiayao? - ft - ________
L^: foTLaY_-oarjv^7n_Rdj
(Qmh
30 'BoTusTk^a 6blpny
UJIlCtoM.
___
Iq'l
di
______
1_J, lalWKxn bkat-b:__
IT Jqj)on ^C^cie fb
lQ-f __Yi'
b^l-lC
K/apY 7.C-^
_
3t-Y M.UI y_01c2d_
kT-ivl CkupeF
nMh
P
Cat /J
2>.i 61
cm Hi
3 i-01
J'
P
N
3,1.01
Cm d SP
N
CP
N
N
Oi
Niit
ib
N
irni bl
?
N
l~|lH
Cm 't ?
N
3?
A
SUMMARY
M
M
3il
?_
New
smear-positive
Relapse
Smear-negative Extra-pulmonary
* l.p. httensire Phsse
C P. Contiroation Phase
D
I
M
3
I
J____
IWllfr
t
0^
O
P
Id,io' (/ft-rT ?
Cm
t
3+
S'i Q| Cm
La
Cl
KS6
Cl.ol Cm
10.101
Lab No. Smear
Smear
N
ll.ol
ErdoUP
Pretreatment
Date of Regimen/ Disease
Treat Other
New Relapse Trans- Failure ment
starting Category class
fee in
after
case
Pulm./
treatment
default (O)
xpulm. . (N)
(R) (T) (F)
(D)
(P/EP)/
' i
-Q^l
■
■ ?- W;
■
?
I
REVISED NATIONAL TUBERCULOSIS CONTROL PROGRAMME
Tuberculosis Register
’
TB
No.
Date
of
regis
tration
Sex Age ?
M/F
Name
(in full)
Name of
Treatment
Centre
Date of Regimen/ Disease
starting Category crass
Pulm./
treatment
xpulm.
L.
Year:
OundtH
pp<>J r
PCb- fol lore
M
11 b0/
IL
H-vo 1
F
IS
llhtil
ryi
Vo SuKcm Ni^orf
j^ee cAe_WAbL
rtbOl
k?25!iT^
^0 (Z^.'yuPf
/6
/lb al
t-Jc 'pre.-n R)l<adCL-r
n
Nc GpariTifAk
Z^x^-Yo/y/z^/t
New
Relaf se Trans Failure
fer in
case
(N)
(R)
(T)
(F)
/b11 0 V €
Sub
■/r—
(D)
Smear
Lab No. Smear
Nft7
1^6
( + tuo
?
IM -ol
EY
N
n^i CrtT J.
?
N
&19
ir
<-
Car 1
?
N
I+- 3tfc Nfq
UC_YU yc
-A^l*______
—- o-----^afidlu tCa^Ciy ■
H.bol
Cm iti-
?
N
TU<j
Mi
Crf ijl 6?
N
/Wq
ib
ill 01
rt
lb
IS
/? iOl
___ 1 1
/9
l?.l..(>i
r
ZC - naf pA /2>jd
^0
/?.i.ol
1
rt
©Hi Fui'b
fanti/ld
32. 'i-C'iU CttUnpl'c
Ck£^t_
/3-^
5T ^a>M &,lol
Id’
dakgl^
/V^
?
New
smear-positive
M
3
F
Relapse
M
F
Smear-negative Extra-pulmonary
M
Z
F
M
F
i
3
6
I
1 i
‘
■"l ”
S3S~S«gJl.
•S
-A B
'
1'
Lj^
bicj
* l.P. Intensive Phase
** C.P. ContinuEbon Phase
SUMMARY
'2-■'B
Nf?
4^/
Io.I Ol
15.1.0)
I
L
Ti
(2,bo)
Jo
Part J CZ
o
End of
z< —
Qiicl^________
mart
N
ftnunda
Pre treatment
Treat Other
ment
after
default (0)
?
1DVoi (?fi7 1
■n
________
■YdUQ]_(X_
7o
Cr7 &
3 -bo I 6r Jzl
pl-Lari
£8-
I rA
____
Za;S^ 2bo|
Spu
Type'of Patient z''
(P/EP)
II
171.61
•
-' Complete address
Quarter
REVISED NATIONAL TUBERCULOSIS CONTROL PROGRAMME
Tuberculosis Register
TB
No.
21
H.LOi
Xi
i.o;
Sex Age
M/F
Name
(in full)
Date
of
regis
tration
__________________
r -
/S
y»AuX~> Al U.7 ?AZvA>.
P
Nd.-LoKfrunux
0>TUgj_C
VTfc-fl vi-o________
_LjJ __________
50
n•1 ‘<?1C' 6^cCC\-(
Hi.01
_Na
3(o
nQd.
i\J0
fV’D 6^
P^nA<on Mot>.ci|ld\
v\ no y6lez,-
M/Ol
P
tb I e
fl cJ-jeCi
^lo
_k^>Cn?
/OMCV
30
k^Ur/lOT_______
3/o Po; j up CuV/
f^o 6
30
_____
A~> -S %
CO
N
A,' . M
itn-ot
CftT 1
p
N
Via
Xi 1200
I
P
N
V. 14
4.1.ci
CP
/V
(A-io)
(k TH CP
N
?
N
?
N
07
di i CP N
KM
Aa) s V
iTi-ol ^1 3-
?
If
,O
.moi
HP N
M.M.H
ill 01 Pat AS
Ji-oWH1! U-l-01
/
lol
M
<5
-
Smear
C?
New
smear-positive
,
Pretreatment
New Relapse Trans Failure Treat Other
ment
fer in
case
after
(N)
(F) default (O)
(R)
(D)
F
M
F
End of I.P.
Smear
Lat
AffC.'
1
3y
Nt(^ 9/
3B>1
A'
Relapse
Lab No.
1+
14-
&
c
5^
I
SUMMARY
■
Sputu
Car 1
11. t?— _
P (_&•<£
per
rf'',v7
I
1
Type of Patient
'Yi .01
Aryia<pfa ccinC
30 Cotton fC I'^tOr Lf.»-g>;i
fbViCYOt^
36%
Date of Regimen/ Disease
starting Category class
Pulm./
treatment
xpulm.
(P/EP)
Zco'
67 ■
2jy_ _
J^^t'ori_£d_
_____
jf5u 4_/i______
He 0- ApFcuctf-
2C
Name of
Treatment
Centre
Clc hJvc-JxCindcy (,C1^^C u?o^<J
So
Hf-Oi
Complete address
Year:
Quarter:
Smear-negative Extra-pulmonary
M
F
M
F
2
3
* I.P. Intensive Phase
** C.P. Continuation Phase
s
4
■57'T'
•- 7.’
|
s »
IBS
l
REVISED NATIONAL TUBERCULOSIS CONTROL PROGRAMME
TB
No.
.W
Wi
55
Date
of
regis
tration
Sex
M/F
r'QowPPa.
44 Jokr,
w
Wr
3b
Name
(in full)
(£)/b ^UXWLt</
-
3
‘Tc: M-°L- Ch
M.C LJ
e>
iI
b'b; ^jfcO'rt?
C^1' e__
?0ful67
W pnw
IO| 5(^4 Cane
(
Mu-cM
(4? r'l 1-1
_L? .Ufw4^—. Bld .
I
tSs J_un cj A_cx_
F
P 50
*3
t'/.LOl
_414 _
4 0 7j_ _§>
KM
'VUoCa
apn_n
kd - Q? Iev'
Nt? £, ^'0 6*^4 _
iD ITu-Wol-gJQi'p.
■Year:
Sputun
Type of Patient
?
firX ?
N
Gw £-2.-0(
0 r^ l H
3.1.61
)
©MH
Z/.d
fv, p
2-2.of
N
M ^7
Mft?
60
/M^| 67
?
68
0
.F
Relapse
M
V5
f3t
__ *
Smear-negative Extra-pulmonary
M
F
I
1
'3
.3+
a
o-f-
^1.
* |.P. Intensive Phase
** C.P. Continuation Phase
SUMMARY
M
A AF5
T
p
?
New
smear-positive
Lab»
2+ ^7
EP N
C -I
Smear
ATTl^
3^1 ol
W
Lab No.
33 33&
5411
£-Zol 0
Smear
(D)
f.'
J ?
M-i-oi pCn -> *7
-11- EP
End of LP.’
Pretreatment
New Relapse Trans Failure Treat Othement
fer in
case
after
default
(O)
(F)
(T)
(N)
(R)
?
.l.cl 67 7
I
kco lo A' poiybM
6o ‘"'pkAgoncAVo
r'OaiV.'r.aM.OTOt
1^
Date of Regimen/ Disease
starting Category class
Pulm./
treatment
xpulm.
(P/EP)
► O.-V5
> _?_4_ 51° 0
-z' _ A Z? . 1 -r
iGunO-'Ti'
U|6 J
5^31 _2L
-qT
53 Oci33 01
4b sir
/>« $>5^
/S-/
IA bkl ''i^Mupct'
F
______
^/c CUKKannO
f I'. W U-r< S Ck Q> fl-Q
- 01 tyo XddTiyu-t?
Qjy c^-
©'vi>' tv
_£
Name of
Treatment
Centre
Complete address
Age
I
Quarter:
Tuberculosis Register
F
M
F
I
REVISED NATIONAL TUBERCULOSIS CONTROL PROGRAMME
Year: u*0l
Quarter:
TB
No.
41
4243
/joKAAm i'
uni -y^ 3 (J_______
II
Vo kunck.n /al Pun
46
44
L&n
O|
fp^lOn^ ___________ _
_
£) T k j y tt;1 £d, (S -
7U , i^&v^ Ptclu ct a__ _
33 ^7 Ct^yO ju. Pfet
(b
______
^kQ.TktXY
iC
MotUfeT;
_N_0 2_,^nian40.
Relapse Trans Failure
fer in
case
(N)
N
/y^'7u
Xi.ol 147 1"
2j M 10
?
?
Il L (?) c HL
A)
• b-£*
■So JI
_______
Qlo RzUo-______
‘2_
j/t Lcd-f lidring KicCU
P
n
H
6'8
(MO
Zoi'iC
lUSffi
lofc.
_NO_I
0k?« F
di
i
(R)
(T)
(F)
C
in
6‘P
N
V,H
16-1.0]
c’ B
CP
N
Li.iL. <?o
L’ 1
?
M
P
N
ACi->c a.i-s-i 6
/
n
I
irz
F
6
1
Relapse
M
F
hD
ri<5
NJCi
K<,
5f 75
Nl^
N
* I.P. Intensive Phase
'* C.P. Continuation Pnase
SUMMARY
M
Smear
NCCf
D
New
smear-positive
Lab No.
1^ o3
I
lU-L'i
Smear
J2L
End c
N
6>
12-Z.ol
Pretreatroent
Treat Otner
ment
after
default (O)
(4-
lb-Vo|
d-____
btorcul
C^-ol
A'.U
_
6o n^ MiAS^cn
■jjitEpk
0
zo /
•Jyp/noz_, CjUuyr
'i
1
61
Motj-i' Ho4r b"io*\
23 pl|
gpc>_ _
'si
2 S'
P
io&lu Au bntiM&iiyccM
^L
New
SF
r
Type of Patient
?
?
H
t^'1 io'"' e________
Ayr Sig ttufVYJnflgpPLt
Pu
l^
i
Date of Regimen/pisease
starting Category class
Pulm./
treatment
xpulm.
(P/EP)
IZ ol
12 -^L
2
Sex Age
M/F
Name
(in full)
Date
of
regis
tration
Name of
Treatment
Centre
Complete address
Smear-negative Extra-pulmonary
M
F
M
F
ci
ssa
i
OSS2A.22 I- ; 2
■
'
■
424422
-
■
REVISED NATIONAL TUBERCULOSIS CONTROL PROGRAMME
Tuberculosis Register
2ool
Year:
Quarter:
Sputo
Type of Patient
TB
No.
■3A ,
N1,
TsT
MMiLh------ _ n
Kum CiV' _
^■5T
5i A21^' Ol
_o!ftic.kL.
_ej 0_HBV6j_9nd vaj^a
___
17
^010-31^^1
ol
©IoTom^.
i—
r"
(>
I
e?
21- i oi <3 Th2-1.6]
Cl
(R)
(T)
(F)
Smear
(D)
LabNc.
N
'7^
N
39
N
i
N
I
G?
/.al
Pl-Sl
?
LI-o' L’
?
9-l-<j/
o
ft
AM T’
±lL._fe kta-_____ ________
MM M-o>
p
ft
(P
&c\Tde^
fl
—>_u. /fll _cl5"— —
k
p 27 oSfejji
it
_____
■—>1
H
lt
&
M
F
1 I
Relapse
M
F
J li
* I.P. Intensive Phase
r* C.P. ConSnuaton Phase
Smear-negative Extra-pulmonary
M
*£
ft t'C
0
F
M
F
I
7>
3 ft
rM a 7 ■.<
'
La
N^-t
0
SUMMARY
New
smear-positive
Smear
Lfo
3^-ol
—
P
(N)
End! of lUf-
Pretreatmerfl
Treat Other
ment
after
default (O)
—_
6 £1°
Z-4 c A P I
L (b^OT e
c- w
P9
to
case
fer in
e & cI M
JrrACnH-'j -I’M1
Icurtbavpab .
Relapse Trans Failure
d-'L-Ol
i
____
New
ft
‘
27 fitenUi' Avtude. , |7Jlb______
P
'I
5£ 210T
[\y ^pin £,8 •
Date of Regimen/ Disease
starting Category class
Pulm./
treatment
xpulm.
(P/EP)
L k> $.'7^ Mol
IltioM
u5)oJ)eTjlica^
cPu
■ftp
0 pf■ Yenti^bg/vA
______ _
51
Si
Complete address
Sex Age
M/F
Name
(in full)
Date
of
regis
tration
Name of
Treatment
Centre
'i
revised national tuberculosis
cONTROL PROGRAMME
Quarter:
Tuberculosis Register
SpHU-
Type of Patient
TB
No.
Name
(in full)
Date
of
regis
tration
bi
t,
^-—_____
i
------ £
3
1
go .1. ol
TSytyWiA Tuft- k-^tV1 HC^ .
- 9
N
6P
M
P
A)
-0 kclL^T—
IS
0\
NlU^oVnAkG Muttky_
______
1 C>l
_---------a5UT Q F71>--
j
IqtO _ _________
I
_jvcf0
Ktrx A.X A VO cxAA^d
6G
il
o^'U'P
f[p MCV/t t^lUbUK- f
____
lit
Nvi—
/6
2
Tp lfc b
/o\
_
<j lo Ail-KsO'
i_________
9
ip \jo-vU e€ V AJteb- L * >£
F
b®
c a
2£h
4^0
A
fi-.-----
ptOfo____ ____
Ct kr—L_kY----
li'
0
_
-
Smear
i
I
/'f 151M
s
‘j AP:
N
N
11- I d t li
L:3>cl
.A
Lab No.
(D)
e7
___
__ ' f MH
Smear
End of «■
iciti
t !
i
Pretreatrnent
Treat 1 Other
ment
after
default (O)
P
2i> •2-'0’
/ O'
<
(F)
(T)
(R)
(N)
N
J
1 01
bS”
fer in
case
<9
i,
h I n^jobU t/gMpU/
K)iU‘
4.
vA
26
bl,
I
Relapse Trans Failure
New
(P/EP)
'JLnjl'— ^1
d)
Date of Regimen/ Disease
starting Category class
PulmJ
treatment
xpulm.
Name of
Treatment
Centre
Complete address
Sex Age
M/F
|-A
2^
/V’A
,c
£1
ex
ci
2
N
* |.p. tatensive Phase
** C.P. Continuation Pnass
SUMMARY
New
smear-positive
M
F
Smear-negative Extra-pulmonary
Relapse
M
F
F
M
M
F
--------- '-^
'><‘9 %
J
’■
'
•A~ •
REVISED NATIONAL TUBERCULOSIS CONTROL PROGRAMME
Tuberculosis Register
TB
No.
Sex Age
M/F
Name
(in full)
Date
of
regis
tration
Name of
Treatment
Centre
Complete address
Date of Regimen/ Disease
starting Category class
Pulm./
treatment
xpulm.
it C|
fc. IM
fe! 10
_7/cbr)c^_______
io
tc/o ~^Qr40
J-Z?
-T3
J.L-^±
if
ofoMCinnct.
_____
3[O
------ hA.
_no_3_L1j2_____
c^w11< *v'-^y.
Cf/* Kg .r-xU-°T
it
2i_
New
Relapse Trans
case
fer in
(N)
(R)
(T)
Failure
(F)
V
7^
7^
o/
Sfri-jfy\,
_ku^-p cj_zv^-'w\4—
6 Jii
Lu? s’vc.
C
er
4
(^ui
P
N)
tfe^
7^
flu
77
ib
90
lb 3
f3>'(t/
no
—
JU?
F
JalMO.
~6lG
A
b^
5 I--el
J.C'W M rvyr-L
Lab No.
N
^5 s'
2^
XUxO'cd Jbpc<ckzru_5L_
Sk
______
/v- 2.^8, fc.^ Na^ai
/VUJU,_____________
HAKQ'f af) ci
c. ZocicJ
^ardSf)
r<>1 )o>b. 2
CL-
Cr^f
“7
IX^\
r
K(
Z ^01 C7
?
/V
Ib.Z-Ol
P
N
I
New
smear-positive
M
2.
■;73-3
Smear
End of I
3-f- /7
SUMMARY
i
(O)
(D)
9z3--vf
B -s' L
^7^r-±--
a„
Jl^j’0+
Lfnit-9^ _
R<A L^-vy' bA,G^-s< fvl
_____
PH
C !
x-\<3cu.j
j=^^Vi^C£Afilp_t^£L
______
>■■. .-A.\ ~
Pretreatment
x/
3A?
C~vpc-4_______
JThr^j
Other
c
C-K3.
tpfc b4-)Cr7
3
1^
77
AQ-><y>rt
Treat
ment
after
default
N
J
_ P F- ri
tt^
?
£L
- Spu
Type of Patient
(P/EP)
T1
I
Year:
Quarter:
F
Relapse
M
F
Smear-negative Extra-pulmonary
M
F
M
F
I
1
I
I
* I.P. Intensive Phase
r* C.P. Continuation Phase
L
iw:
<-> ,.£■
I
•
REVISED NATIONAL TUBERCULOSIS CONTROL PROGRAMME
I
Tuberculosis Register
TB
No.
Date
of
regis
tration
Name
(in full)
Sex Age
M/F
'y/id
2/ ’Pl ^!o Anl-g>Af
b?
lb X
3/o
kan Ppg. Ji
(91
v
Of
/S’^eemai'cih
S>lo A bda\ -Sab
Mayjd)Pi_ k-Uf^ATL
___2L_
26 A‘b A
Ot
2d
Jana ppg
01
01
01
%
^/d
0!
kkal.'J
^lo
A 11
Z»k iinalih
Complete address
N•
Ole N.
Name of
Treatment
Centre
Date of Regimen/pisease
starting Category class
treatment
Pulm./
xpulm.
(P/EP)
vMi*
H
lamnu'6)'on Ajeni-. k-Patyg .
00
P
p
Skaybu Valya.
'~cio Pet- Pau
35'
3S
t-
o f 2/
klk^L
G-2
cl
CoM^Peh
CttHonPCl- I'C'M Zoyot) &id, Gwcth'
__
Sp
New Relapse Trans Failure Treat Other
ment
case
fer in
after
default (O)
(N)
(R)
(T)
(F)
(D)
0 Ju 7
Lab No.
End of
Smear
7!^^
71/^
6?
![>5
C#
G?
Nec, UQ
t> x\
KP9Q ,u!j
7^
Cl
A
P
16^
l-P U£i
e1
'
■
/'la.
!ib
1+
129
2 3 s'
0
SUMMARY
7 <
Smear
C I1L
New
smear-positive
- ■?: v-; tf; smB
Pretreatment
p
Ik el p A/
Ik e & 6 P Al
& lot &
A /a
--------P
^eu) njMA7o» £J.
Type of Patient
ntj cl 6? /J
$772#
(jUbbcnPet
C £U
Year:
hk £1 ?
L_
31 k" Pcciya
-5l1£1£l£
W
9
t,te' k77
i~kaA?a?a /^TfaT^TgVg*
Ft qn £0^^
5o ^»mpoun
, ^ . .. d
J
0>x ] 0 'iiL
t
Quarter:
M
F
i
2_
I- 1
Relapse
M
F
I.P. Intensive Phase
** C.P. Continuation Phase
Smear-negative Extra-pulmonary
M
I
F
M
F
I
K
REVISED NATIONAL TUBERCULOSIS CONTROL PROGRAMME
Tuberculosis Register
TB
No.
9/
i <? A
-1
nJ.
_ -L&2?A_
____ QL
Sex Age
M/F
Name
(in full)
Date
of
regis
tration
Uryi
A'bjL Aoi76^_
2^ £d. AAdrtfln ^^3
r
AXVf4(ll<2_ _
’■'Z
lb
Nj
b&kind kiftalyg
.
£i/tuka Q)>t^, 2 ft , jj
fit**
C-
fcqkptr ft'-S3
±l^l^^_Cob};Qn^tr_^b>ii P
X?
Zb ,
Gi^1-t
Tio M
99
J A >' -vci
%
J/p A’Q'JQfaJtZ
I_____________ _______________
A3l*f tto(uv
1 IS
xjkaSAj kuMCv/
99
21
lt)D
p
AJ’/Xr, kert^Ao n^aifaHA t'
IS
n o io_,
I
7
Type of Patient
Sputi
New Relapse Trans Failure Treat Other
ment
fer in
case
after
default
(N)
(O)
(F)
(T)
(R)
Pretrealment
Smear
(D)
Lab No.
?
N
54-
's«r 6 5
?
N
Z-f- 277
N
?
d-F M
/l 2^1
7
1+
01
01
»Zl
M2; 01
?
>^i
14-
N
2+
p
01
N
3-7 23 It)
N
39
M
F
Smear
La-.
* I.P. Intensive Phase
* C.P. Continuation Ptaase
SUMMARY
New
smear-positive
End of I.F
l-l 133
Oil
0£i,
N
?
«A
uJ ato r PaJii] i£_ _
fad
Year:
10^
s
/? AL
aLl^Ata & l2 *1^
%
II.
UlApfly
- If ll fanu
V~
Date of Regimen/ Disease
starting Category class
treatment
Pulm./
xpulm.
(P/EP)
_____
__ 01
J/c jj
93 4??AJ 0)1
%
Name of
Treatment
Centre
IMv-
/
Of
%
Complete address
r
Quarter:
Relapse
M
Smear-negative Extra-pulmonary
F
M
F
(
M
F
I
:‘r3
I
7’1
■
,
r-V-T’
■
■:'.
‘
.
'WSB
'
-
iiS
,A; "A"
■'
'$>♦
^^9
Bf*
asefll
Ii 3
$
aj
<u
E
o
£
c\
ri
ra
-h
<3'
Z
cn
:
O
n;&
z
* :
J
a>
£
I
iHls
l
O
o
c
cS
ro
<D
o
V)
0)
Q.
(r)
LU
O
i
S
’
c
-J
O
01
H
Z
O
u
(/)
(f)
O
_j
D
U
01
LU
co
ZJ
H
<
CE
* %
z. 3
0)
w
co
o ro o=
S E zj
CD
o ? sE
O
y
CD
ID
£ E -bc
<D
-Q
ZJ
Z
o
H
<
5
V)
<n
•n
H
r
r4
CO
r~
4
w
Q
s
t
4
<T
^1
<D
Z|r-Q
a I
•u
■O
ro
0)
5a.
4
ii
Z
Q
••J
7/
b
I
I
I
I
I
I
Cl\
Q
7\r
T
I
I
I
I
2
-I
> L
<1
S-p
i ’Z
T
I
I
|:
I
I
I
^1^
iL 1II
i!
-------- U
oiy
^\ <c
i
a
Z
I
Yj
ft)
H
C.
<S) >
'll
^1
Zl8
J> O
ro ts cn
Q
E E
0)
t
f9 o
u
'T
"T
I
I
.1
P
aco
I
I
I
I
1
£1
4 <<
c
'A
C>
SI
.J!
o
e
r*
o*
r<
<q
s
2§ s
cx.
Q
T
I
E
o
O
H
d
2
g So0)
ro
Z
2
ai
Q.
a> <D
in
in
O
□
o
<
zf
<n
or
a.
<£
ro
a>
.to
Z
X
z>
u>
o
Ct
(iP ro
01 O
z
Zl
z
z
VA
0) o
« €
ro co
Q
co
<D
g
CO
■&
Q_
I
ro
i=
LU
e
b.
<
01
0
O
01
I
l
3or
in
s
i
.9
2
(D
I
O
H
t
ro
I
c
11?
Q.
>
I.
-w
■wi
O
o
3
I
I
I
I
I
I
T
I
I
'1n
-2
I
I
I
REVISED NATIG. AL TUBERCULOSIS CONTROL PROGRA ivnvIE
Tuberculosis Register
TB
No.
Date
of
regis
tration
Name
(in full)
Sex Age
M/F
Complete address
Name of
Treatment
Centre
I
1
Quarter:
Year:
Type of Patient
Date of Regimen/ Disease
starting Category class
treatment
Pulm./
xpulm.
New Relapse Trans Failure
case
fer in
(N)
CD
(R)
(P/EP)
J4
I
(F)
Treat
ment
after
default
Other
Pre
0
(O)
Smear
(D)
rrcKc _
IX iJctv
/piMflril, Xf Ks^'ac
-^LcfZr^^o.__________
2) 12 -414.3V
12
LC:
£
CS vA i
<^\k.<xs
___ jjki
7//
V\-
V2rft
CAT I
Voq<\ •
13
in -
___ _p
________ 3S
re
t
—
iA*
x\
K
2 q- K
i
va -c \^
A<r<v<c<<
IS"
ITlicco
-
11
I-
“
}lo_No oo,
A
__ ?\p< ^''Xf
iV\
Cpx^fs v
\% \-7<tc
Cwt
/
V
I
,
r ■
fl
r\«
bA
\ Tece
____
*;
SUMMARY
New
smear-positive
M
F
)
WWWPWS#
Relapse
M
F
Smear-negative Extra-pulmonary
M
F
M
F
i
ii >
\
I
»-j7^4*-—-
* IP. In
** CP. Cc
I g. 3
■ cu
S'
i'
ro
9j o
« *
to
<D
E
<n
■
1
C
c
(j,
O
£
jill'a
1 ■
«
•5
c
*C I[2
<D
*
Q-
*o
| 0>
H
UJ
1
<D
i
I i^
I
Rle
rr^ e
°->• I r
a:
I -2
I fV
3E
Z
O
V)
H
ro
U3
Q
t
(0
□
<D
0 <n
>
I
01 O
D.
O gS
_
Z
b
a
t
A
A
u € S
ra eg <JJ
O <n E
o
01
H
z
°o
°
tn
’S)
0)
<n
U>
0?
i
H
I
I
01
ID
(D
-j
01
in
3
co o
H
-J
<
Z
1
o
'm
O
A
o
I
I ir-J
I
I
p1 -q
I
I
i
Z)l4
I
2l
«T
I £1J <1
I
•*1
j • I pi 3 >1
5
’/ II
p.| ■
<1
^1
O
o
■■■«
J
■£ 2?
<D O
01
4
(/>
0)
■o
■o
l-'l ^1
ro
o
f’
Z1
>1J
>1
CL
E
o
O
I <1
z
in
—
>
in
oil
I
o
'v0
0
<__
x “CD S
r
if
ro
Z
.£
%
i
Cl
i
i
i
i
i
i
j.
T
I
I
I
ri
r
I
i
I
I
I
I
</l
<v
jo
el
o
CD
Is
s
E
cn
uil
S
5
<
1
1
I 5
OJ
E
cn
r
I
I
i
i
i
i 3
i
i ijl
5|
fl
i’\
Ti
cl
±1
j.
I
A
rl
rl
I
I
I
I
I
I
J.
0
o
d:
1
I
• <n£
'il
5
T
I
I
* t
I
!
Eh
1
i
1
0)
*
co
CL
j
(D
3
ro
U?
x—'
<0
C
c
— O
C
4)
Q.
>»
I
I
I
I
LL1
*5)
D
* h
<
z
o
I—
<
z
o
ir
i
LU
CD
>
LU
Ct
o
2
2.
Z 3 “
.
Z3
CO
0>
(X
S3<u H
E Efo
ra
zj UJ
Or
5
2
U)
0)
^c.
E
CO (0 16
O to E
T7
fs
01
’Ll
CD
*o
E
Is
ra O O
Z
H
’(/)
o
□
o
kQ
□
CO
0)
■O
■O
co
0)
Q
Q.
§
o
z Ju
i
o
v”
5
Q
u
3
H
H
d
c
"5r
TT"
•pi
Si
^c^
Ic
w
J 8. -
I
A
ci
f
T
<1
J
rb
I
I
jl y *!
J
z cx|
4
Is
| s I 5if
4' I
5”
li11
3
Bi
ik
_3_i
3q
si
51 </
"I-
<| CJ>~
<z"
<D
Q)
$
1-
<__
T
I
I
I
b'
5-1
I Ti(I
I
I
I
1
SI'i
o
$
(J
z.
X U-
(>
CD S
T“
I
11
I
I
I
I
I
I
1^ I
o
'n
11
i
I
i ■■
I
g
<
cz>
2
2
CL__________
CD
XI
-j
CD
O'
o go
o
m
g*
c
8S’,'§
3
Ct o
CD
-J
D
O
Ct
Lil
ra
E 8)
Ct
H
Z
o
0>
.= o
o
(/)
><
■
s
UJ
"c
-i
(fl
<0
>
5
<
or
o
O
ct
o.
o
il
8
1
it &
H
r
l
I
2?
co
lliia
<D
i I
o
o
16 75
o
I
I
I
I
I
I
I
1
“T
i
I
i
I
I
I
I
1
1;
A
I
I
•J
•1
i
6
O
I
I
I
I
I
I
1
T
J
J
■3l
21
u
v>
<J
.A
<4
-J
tJ
v>
r4
i
i
i
I
I
I
I
s
II <i
■ IS
1.
♦
X
O
§
0
OL.
V-'A
%-
o
8
a.
C
£
£
ipi
Q
§
aj£.S§
Etq-§
CD
>
1
ro
CL
</>
CL
>»
0
<D
t
CU
D
i
LU
o
S'
3
O
01
LU
CO
D
H
o
it-
CD
C£
<
CO co E
o co ■=
<0 7S J?
/>
<
z
Q
LU
0
>
LU
01
cn
s
Q
-EH
r
£ E £
‘c
I •r®Q QQ?
£
z R
r
o
o
u.
O
JD
□
H
I
A
r1
0)
cn
co
0)
•O
J
•g
ro
a>
o
/
Q-
E
o
O
c£
i
i
i
i
i
i
i
i
i
_i
S£
I
z ro
a>
D
rx
5i
□
a>
>
c$l
J
3
E
£ '€ "co
ro cu
D w a
3-|
<x
T
T
I
I
*
I
I
I
J I
tH
. ,1'I ?
►*-
d
Z4 g-.^1
< ■,
12h1
"0
J-l
<1 ‘■
^17
I
i
^1J
M| V-
J
I
J|
I
I
I
I
c
I
1
vl
I
L
T
o
co
<D
<__
s r
X LiQ
GO
I
d -'
<u =
'c
cn
£
T“
I
3
7.
o
w co _:
o ?
(D
a>
E
co
ZE
2
(?3_
<
Z
:
t- a
VI
z 3
£
o
I*
S
’
C
’K, ®
5)
a>
ar
cn
:
e
u
a:
z
o
o
I
o
<
o
.
S
>
§
"c cl'
E o)
CL
I
—
Q ° Q-
a:
*
c
C
LU
S
a
c
o
l
cn
ia
U-
£
0)
H
g.
<D
Q
ra
E
1
£ -c
§
i
i
i
i
i
i
1
'■i
i.?
“T
4!
1
I
i
i
i
i
i
i
i
i
r-
1.^
I r>
12
IS
Is;
i
I
I
I
I
I
I
I
I
I
I
i
i
i
i
J
i ■
i
i
5
?
1
~/?l
—I
,4
T
I
I
I
I
I
1
ZE
I£
1 e
!
u
4-
la .
&
c
2=6
* t
oj
o
i
(L
<•
ID
4
1
1o
"
o
ro
O
c
|
ra
c03
03
CL
03
0)
l?
«
>>
t or
oe
<
x
Ig
X
H
z 8 s-
o
03
o
HI
4
z 4-«
0)
o
o U)
Q
(/) 01
0)
o
-J
‘(J)
o o
Qi
u □
m o
kD 0)
i
H
-J
□
O w E
?■
Z ro
z
i
<D
B
A
f
0
\7
c/
O7
f
T
3 ?J
</V)>
31
^1'
03
"U
■o
03
03
C*1 C.
E
si
2I ‘
<
z
LU
oi
c*
<jl
H
cn
>
o
c4
ty
<u O
H
o
O
Q
LU
p
n
ra S
03
Z
5CL
o
?
c*
6
A
*o o 03
E c
Z
<
03
<__
X t
cn S
tr
to
J
!:'f
■'
(
n
>1I«» <1
I
I
I
I
I
J.
■j 4
-2| 4 $1
■M
M
P
1
zfl '
r
o0
rO
(A
£
I
I
'■'
e\
vr
$
o gg
303 ra |03
, 0)
2
>
Qi O
QI
H
i
Q
tn
gw
o
C/3
m
1.1 £S’
-I
I
E
22
(Z
S-§3 g.^
Q.
r
ro
CD
«^.-
ro $ E
S
<
cz
o
o
or
iiI’
z
<u y—.
5
I
I
| s£
03
Q.
■E
03
D
j
>
ro
>
i
2
UJ
I ■
I
I
I
I
j
rj
i
4|
I
I
I
I
I
n r
I
1
I
I
I
r 1
i
1
1n T 1
41
9? _
national tuberculosis
REVISED
I
CONTROL PROGRAMME
Year.
Quarter:
Tuberculosis Register
1
Type of Patient
Sex Age
Name
(in full)
Date of Regimen/ Disease
starting Category class
Pulm./
treatment
xpulm.
Name of
Treatment
Centre
Complete address
M/F
Treat Other
New Relapse Trans Failure ment
fer
in
after
case
(F) default (O)
(R)
(N)
co
____________
_£s£_ AO.
J ;
c^/
A! Watt
v
tA-
2o.
Lab No.
Sme
\ -V
I*-
?
-T-
Ei
0 months
Smear
(D)
(P/EP)
Pretreatment
C Y>rc V
•C^_____
\A:\2xM
va
(kcrvA
gas*
'A
N':
Q> Ws-____________
S\j2j2
l-'Lco
jku. _■— r
a
Ace
N
:
n
N
Cp<\ 'vx
* ? \ Intensive Phas
**
SUMMARY
New
smear-positive
M
F
Relapse
M
iF
Smear-negative Extra-pulmonary
M
\
F
M
F
3
i1
Continuation P
g'X^
d
z
I
to
(0
I
CO
o
OJ
£
CO
_________
i
<5
S
O
o_
?r
ro
i
illh
8
ci
I
ro
ro
<D
•ico
e
I H 11
OT
C
S
’
c
o
Q.
i
at
-
Ilf z
0)
-c
ra
□
O
<D
<O
CO
0)
Uli
p.
s
r
-4—*
CD
w
V)
o •-
ii
o
(D
</)
<75
o
_j
I’
01
co (0 co
CD
Q w ±5
A
in
Cfl
i
H
-J
E co
SJ
CTJ
z E
<
O
21
-J .21
T?
0)
I
□
<n
Q
o
XJ
ro
□
•dA
ck
£
in
o
§
X—
O
!j) I■
0)
l
I
o
cS
c
<v O
*0
Z ™
I
g> g
•S E
■^4 f
8
</l
E
H
<
Z
1W
Q
Ujl
>1
Si-
<1
L
iJ ■
0)
Q
?'y
ul ?■
lh'
U t
1\'-
I
rt
I.
o|"
tn
>
LU
01
X
<d z:
co S
TT
I
<D =
e a
c
z ■—
!
<D
in
4
(.^
o: o
*0
<0
<D
E
co
>
g’-a
CL
-JI
O
01
H
Z
; -i
1
I1 S'g>
<
O
O
3E
Z
Z>
co
il<E
w
2
s
UJ
W
Q_
<D
ro
<D
0)
1
il
I
a
I
I
I
I
I
I
I
_1
n
I
i
i
u
T1
IC
D
I
I
I
I
J
i
I
I
I
I
I
5
| I ■
05
o
I ‘ <DE
Ip
E
n
§
cn
'V.
ila
■O
* :
L
i
'
i
i'
<5
£
o
0
o
*
u
I
■>
?Hi6
6
■
co
i
>
o
o
s?
(0
u?
Q.
2
CL
>»
t
H
sE
g.
ro
a.
£
e
•5ro
</> s
o
&
a
5
LU
0)
12
a:
&
Z
<
<D
I
* 8
z S
0)
■e
co
O
LU
C\
I
CD
V)
CD
CD
u»
o
0
0
CD
0)
u
Di
LU
m
ZD
i i
-J
<
Z
O
<
!i !
? r;
Hl
•
o
CO
ro
□)
0)
E
Q w
E
s
CD
0)
Ct
o w
_J
D
O)
C
n
3
>
LU
Qi
I
z
I
</>
I
•I
2
C I
=J
£i
3
Sd
■O
•O
(0
a>
fl
CL
E
o
O
7
SLM <D
>■
<
sf
(D ^2
s
r
T
rl
I
I 3 i
10 I
I21 I
i
b
)
1
<D
ra -8
Q
.<2 §
Eg
V
i
1
$
r<
fA
2
£1
I l^b!
■/i 2
M
II'p I
I I2
=1
li
I
•
r
I
idc I
i
Ii
!f
I
I
I
I
§ 3
¥3
cjl
31Al
= sa>
£
Ci
£
X U-
0 2
i
is
o
z
o
LU
0
r^
5
<D
E ra <d
ro o Q
H
o
2
O
u.
<D
£5
£
3
£■
§
3
A
(A
a>
oo
I
f
>
* §.
c
3
or o
-I
co
\
tz
I
S’ co
QI
Q.
o
u
\
o
o
Di
H
Z
a
-5£
£2.a. S-fe
S
S
<
X.
0
3
(X
Eq?
-
co
C
GO
z
7
Z
C
%
c
C.
CD —
f
!
4
i
i
i
i
I
i
Ic
I-
I
i
I
r
1
i
i
i
i
is?
Hl| <
9l-<
is
-A-2 iJ
_^J
ZI
I
J
J
-71
Ll
''
H
T
I
I
I
I
I
I
I
I
■
H)
CO
6
z
>
c:
5 Tr°
Q
I
3
_J
I
co
co
o
!
Q-
Ir.
2
5
IL
A’
V'1
i'
V
2
2
o;&
j:
* :
U---- .4
■r1
fj
®
o
£
O_
c
I
c
o
2^| G,
i
i
ro
o
r
ro
UJ
re
Q_
>
c
- C?
w
c
<D
E £ t
CL
J
i
2
o
ra
>
§
t
S
’
c
H
ro
ct
»
cc
* h
t
ro
□
O
UJ
(
<D
or
o
o
il
Q.
II
!
!
-j
o
or
H
Z
O
o
CO
tn
O
-j
l\ f
u
II
o
CH
LU
CD
O
H
-J
<
Z
o
H
• '~l
I n ■
<
f It
Q
LU
i
U
0
S’ co
CH o______
5
o g SE
r*
a ■■£
CO co To
Q w 2
H
*
I-
0)
E
</>
2
/»
>
F"
r>
A
X
jj
-♦-»
tn
*U)
0)
QI
‘ri
O
<D
£ E £c
o
CD
X2
□
>z
Q>
tn
’a5
o
□
5
C/
o O
H
■ jj
—>
1”
</>
2
TJ
TJ
ro
©
1
f.
■S.rJ
Ll
-\
aS
?l
<3
CL
E
o
o
1
✓4
■
A-
1
3
| il
I
I
I
I
I
I
I
0
S2
3!_
LU
X t
A
x
“T
ss
iS.
t
-^1
$1
CM
_L
r
I
i
i
i
i
i
c'TA
A
j
-1
I
I
I
I
I
I
I
I
I
I
A
I
I
1
I
J
1
d
-I I
•<,
J
ai
' I'd
M-o
1 eh A-'
T
J
!
d.i
>1 -d
<J d
d2
J
I
•■.<■■•
■td
-'Sk ALT
r-
i
>
i
(
s
Z
or I
K2
'a)
r»
Q
I S’
a:
0^
ID
2
0>
v>
a
.
v) • c st'
co E — ih
CO ■= 3> £
<D
<n
co
<D
•g o (X
<
!['
2
z 3 6-
0)
2
2
L3
CO
<D
E
co
¥7
O
3
iro Z
c
£ o?
J
cS
CL
f
-t
co
eiS
-v
§
z
* :
I
o
s
o
2r
c
o
sllia
i
£ E “>■§
ro
(D
>
2
76
Q.
i2
o
</> .E
2
>»
H
Ji
i
e
t
S
’
c
a.
&
CH
d ;
■4 ■
1 sg
J
t
ra
s
O
LU
z
7
Qi
o
O
a:
o.
0^1
o ro
o
Ql
H
Z
0
<n
’
o 5)
a
(/) al
w
O
o
-J
h.
)
E
aOJ €«J 76
-j
(/)
Q Zn >*o—•
O s
0)
■b
i- 'J
m o Q
Z
H
sZ I
a E c
£
~
cu 76 <D
□
I
r
D
H
_J
0)
JD
<
z
O
H
o
□
z
<1
6
</)v>
<D
•u
■o
ro
a)
Z
S2
>
LU
O'
Jl £i j>
^1
U<!
] ~>l
d cl
<
Q
UJ
TO
£
i
i
i
i
i
z
o
O
LJ
Q
<
X
Zz
d
r-i z1
-'I 5,
JI
I
I
I
I
I
I
I
I
I
I
■<
Q =
-a
a
e a
Ji
s
O g
5
1
£
ro
4
x- ro
CD
E
v>
2
1
2
i
f
T
I
T
"j
i
i
i
1
I
I
I
I
I
I
I
J.
3
i
J
I
I
I
I
rc'i
-V b I
I
^4
?,'L
cT
i
I
s
3
i
Wl
;T
J\ cd O\
-Id 11
rJ
r a
gi
I
I
I
1
~T
?b
£
1i iJ
<1
*1
CD
J
Q.
I
W -w
q-3
c-
I
tn S
‘7
i
IL Ji-1H
E
4f
£
«J
So
Q-
p
2
ci
CP
zi
cn
D
o o
or
UJ
co
1J
I
i,
g) §
Vvi
(<>
b'
f3
3
V)
ro
a>
E
cn
a5
Ct
s
. ■
CD C.
1 £•
i?
2
2
1
.•£> Q
Q____
<
3E
X
LU
Q.
S I
ro
§
I
bb ■
S'
I
1
I
I
I
I
I
J
r
I
I .
I
I
tl
5b
s
.i
r-^
i
i
i
i
i
i
i
f
■------ c
o
-■_.£
z
I£ e 3
3
c
CO
a. «
■°.
9j &
co
o
I
CZ)
• :
■4
—-4
4
£
IE
I '!
I
ro
CD
>
SL
ra
H
E
<D
•X3
OJ
1
*o
11 e
CL
<D
Q.
>*
H
i2
in c.
i>
&
E
cn
5
CD
CD
CD
a
ro
o5
Ct
CD
CO
12
2
<
cd
o1
o
>
w
5 o
<v
J
z &
,e g1
<D
S’ <5
cz o
0-
01
H
a>
0)
o •o CD
0)
(fll
(/)
o
01
CD
-J
Z)
3i
01
LU
CO
3
H
□
o
u.
<
Z
o
H
X'
,*5
o> §
->
a £
t <E
ro ro co
Q
£
Q
CD
Is
<D
E
CD 0 o
Z H
□
4
P
cz R
— kz.
f
cT
o
CD
X2
^4
r;
K-
m
co
CD
■o
■g
Q
Q
CL
E
o
O
tn 7,9° cl|
$1
<A
a
^1 ■
rl £ d
Z
1
7
1
<
Q
LU1
(D
>
LU
01
2
m m
co m
s
o
2
<v
.
CD
o
LUI
i
1 8^
t
L
S’
JS
<D
CL
Q:
! :
2
UJ
-21 S
5^ ^1
T
T
$]
q
tOl-
<D
CD
<___
xt
(D
CO S
I
I
d
fl
<D =
e a
4
2
u
^3 rx
ra T5 ct =
-Q)
I
l
I
I
I
I
I
I
1
.71
n
I
l
l
i1
■4
41
ZLL
s
M
r<
2
I
CT
•I
o
f
co
tf
•SO
Uj
r\
■g =
iS
• :
Fj
1
/
_o
g
s
2?
ca
Q.
i?
a>
v> c
c —
f
oj
<D
>
Q.
e as
t”
c=j
S’ CO
o
S’
<
7
o
o
0
<
ct
S’<6
ct o
ct
Q.
og
’SE
o
_J
0
z CO
u ’S)
-J
ZD
o
Ct
LU
CO
ZD
H
<
I
^3
r?\
7,
I 7
>?
or
co
’55
rS
R7
'zjjz
^0/
■zi
w
M
O
"U
v-
E
zl d Tvl
•dH1 C1J i‘\
qM
21 4
jl
CD
9
<__
5’.
cl
il
I
ft
>
.52 S
T~
I
I
I
I
I
I (
I >1
j
‘-t
A
^2
I
I
I
I
I
I
I
7
did
O’rz
I
I
I
L
J7
3 ■<
1^
^'
Ir
r
fl
i
II ?l
I
l
l
I
<i
rsL ±L
I
yi
i
»*
if
I <p J
I
I
I c.-
tn
£
I
l
l
l
<4
I
I
ci
iSi1
r
| £
hl
ifi
~XT T
2i
£
r
^■
CO 2
0)
I£
<r
7Z|
o
X
i
I
I
I
I
I
i
I
I
I
■>
o
O
Q
I
tl§
'1
r
5CL
fX
f
-I*i
Ij SiL
Si
.
■O
ra
a
r-»
i
??
C'A
Q-
§
r:
V
r^
7
o
□
ok-
0)
2 £0)
5
I
s
>
1?
\-\
<-
§
r(
S a
0
ro aj
o O
Z
h-
z
a
LU
<u
(X
iIs
<D
o
JCD
□
<
Z
o
Z3
<n
(<
(')
|
s
«
cu cu aj
Q w 2
o
o
<
P —
s
GO
1
3E
2
s gi-h
S
O
Ct
h-
c
ro
a>
E
co
CE
J37_s7 o
LU
3
i>
l-
1
O
>
e
(X____
cu
LU
Ct
g
J-
<u
■E
Ai
iE£
J9
1
$2
o
silJg
i
I
'
o
i_L
I
I
l
I
I
I
I
I
T
i
4~
L^J
I
si
3
f
w
--
6
z
■
£
!
0J
W'r'-'Te?-’-!
J
o
A
cn
cO
I
CL
ri
ca
<n
d1
z
z
\ £S
J
P
_ 0.
0
j
E
o
2
c.
a> ro
IS
LH
- Q
£ O
y
A
z
Z
* : •
- 4. -
■
Io
i
.7
<L
W.III.IIW! ^"—1,1
o
7Tg
2i^|
s
II
ra
a>
Q_
>-
f!
e
£u. 5
t
LI
o
in
i
11
ra in t 3m
0ro-=
O
01
H
Z
Q)
'□So
Q
(n QI
0 o
Q
3
O
■
y
I
or -=
in o
cn
D
H
-J
<
z
o
i
H
I u:,
In
<
z
T
Q
0:
in
01
fn
in
cn
>
O
JD
3
H
<i
r nv nr ~T~^
i
i
cj
0
CL
E
o
O
4l X
ri
0
CD
^IC? 7l
Zr
l>;
0
2i
t?
-771 '>
h
Ct 7
'7 <
d 6o
-I >
V
c| r
rJ
Cl V
Z -
I
i
x u0 2:
f
r
I
i
i
i
i
i
11
I
A
1':
r
I
I
l
JI
J1
p
.55 O
76 15 S’ 2
O
Z
“T
i
i
i
i
i
i
1
0
i
Lil
i
i
I
3Z-
{Is ..
6l
I A^l
I
I
i
1E'
V
I
I
i
■ lv
e
c7>
f
T
nr
i
'z>
H
<
0
"SCv1
ji
Ar
JI
Y'\i I'5
ni \ 11
:
'4 i
J
[l
i
0
"O
X)
ra
11
A
T
7-.■
3
11
>z
o
17 Vi
(/)
w
A
J
' y,
(A
*a
r'A
i
rS
j
't
T
Z
(D
J
s
Co
6<
11 s
</)
o
'P
J
0)
Z
<z.
Lu2
H
cf>
-0
(/)
U)
o
c*
E
2
</> o
1 < I
§
J
£
0
Q
t
0
£
r.)
O
r
.E S’
S’76
cr o
*0
0>
(fl
o
c?
0 o
CL
5
cc
0
W </) —
Q °
01
0
O
01
co
2
2
-z
1
<
7i E
5
5
<
i
z
'.v
I
i s
oc
13?
I
I
e
o
o
■C
ro
r
LU
<n
0
CL
H
i
I
76
r
'
.
■;i
i
4
1
r ~r
i
i
i
i
i
i
i
i
i
i
r
r-’k
»<-
i
^1
?
■
A
/. -
• fi
mA
ro
o
£ <No
.1
33
—i
C
g oe
I
•4
2;||
■ '-
•
J oB
r
-z
co
0)
£
ro "E
x 0
o
2
in
co
4-
<5
--------- -
6
z
s
1
,'i
2
2'
E
(f)
2^
<
.■ ’'; - f ''
■:r" -Ej?
■
iS.
• :
r
i
H
o
-•?W!
it
fW
.w|
a>
xz
O
J
XI
.92
To
O,
o
>
0)
■£
b I
&
I
' ‘'-iwl
1X1 I
<D
!
' • 3
11
co I
E <0 ®
(U
fl
2?
ro
o
tpl@
y
•«
O
I
I
J
I
f
1
IF
'xl
15 e
rl
CO
CD
a:
cn
<D
</>
:'2
O
CH
ro
D
Hili
s
5 o
.e %
a:
o
o
Di
S’
(to
O g>S
o ,
* 0)
z V)
o •*U)
o
CD
52
l01
(D
<D
H
I
<
o
H
<
Z
<n
</>
O
u.
O
J2
■o
■o
GJ
H
CL
□
UJ
52
>
LU
Di
a>
E
o
5
L
•4
J
A_
I <
CD
CD
<__
tSl
H sJ £1
zl ■M
3
<1 T
<' 1
|1
§ A
v>i nr
11
5 c
I
I
1J
t\
i <
'^1
1
tn o
Q
~c
ir
in
21 ?
~
s2
in 2
ISi
I
'1
2-
X L1-
z_
£
i
'- •]____
O
□
0)
C
Q
£
02
1
I
12
1
212
..
I
2
I
5i
c^l
-1 .>1 1 yl,J
I
2 i
d ; I
£
2' 3 I 11
c •
<o|
A
I
I ^|tL
O
o
^5
>
c
-
Z
o|
4'I
«/>
X
£ OQ
CJ
i/’
r-n
U
Q
VW
\
<
►—
fn
<D
a) E h>
O
CD
□
Ie
<2 € S
a 55 <P
Q
E
° (/)
LU
CD
A
ro w E -|^
o
Q
■r
E
cn
X
X
<D
Z
’J
Sc’
■C
H
'■‘•'’H ..Xra
a>
•2co
LL
21
D_l|
.1
!
5
I
I
I
I
I
I
I
’I 2 ’ J.I
I
I
I
I
I
I
I
5.
14 J!
^1^1 I
r6
I A
I
i
A
I
I
I
I
I
I
I
r
j
'I
t?
2.|
--K,
.
n 1
u 3
I.
p
I
I
1
I
i
I
j.
Wliil
r
''
i
REVISED nationalwbercj^^
re
Tuberculosis Register
Quarter .
Year.
_____ y
Tyt>e of Patient
3
•ft
Name
(in full)
Date
of
regis
tration
Sex Age
M/F
Complete address
Name of
Treatment
Centre
Date of Regimen/ Disease
starting Category class
Pulm./
treatment
xpulm.
(D
(R)
(N)
(F)
A
3
0 months
Smear
Lab No.
(0)
(P/EP)
V'V-\ G n
Pretreatment
Treat Other
New Relapse Trans Failure ment
fer in
after
case
default (O)
2-7
V
■Jc-2, rt
45 ci
5 ■
Lr> tS
-cc l m7-I
N
2I
r; o <-<
P I
/ q LtsR,^ .
1
14
.°5l
,r.
PM v :
" 1
AHPE—I q ■ C H ■
j-l ■S'Qi-
CAl't
__
tlA’A. 2£"l/’d
5^
I
11 3
■'X \
2
New
smear-positive
M
■ 1
Smear-negative Extra-pulmonary
Relapse
M
1
* ip. Intensive
** CP. Continual
SUMMARY
W\\\
x\ \ N
~~
F
M
'1
M
___
•
■W’
:-w
J
S0jf.
II
ro
a>
I
ro
o
£
tv
cn
I
H
m
s Jj
£
o
0> 1
r
co
o
a r------
«5 I
I
>
I
Isw
__
03 1
To
. CL
e 2
| 0)
CO I
I °-
I
a> I
8.
__
ro
-S I
Is
J2
OJ
Ct
I
Q
■c
CO
73
o
f
1i
i Ms
IDI
5
5
<
03
O
E S’
S’™
o
o
sS
</> I
c 2?
Ct O
Di
D-
o g|
2€s
£2 S
, O co £
o
£ <D
H
z' tn
o O)
o 0
r-0
*^5
0)
Eco
(/>1 01
Z
o
</>
D
0)
<’
z
o
m
L
I
I
I
1M II
I
I
5 I
hai
I
<n
UJI
CD
0)
>’
U1
Di
□
-4
i
i
i
i
i
i
i
=?
i
R II
in
(/>
O| O
0)
■o
-o(0
0)
UJ
sex
E
o
O
<D
CD
<
r
~t\
i
i
i
i
i
i
I
1
I
1
I
I
>1
1
e
rA
eA
<<
hi
i
i
i
i
i
i
\r
rd
ir
ij
i
i
i
i
i
I
I
I
I
I
I
►
ft
I®
'3
Bs
REVISED NATIONAL TUBERCULOSIS CONTROL PROGRAMME
I
r\•I
I
Tuberculosis Register
TB
No.
Date
of
regis
tration
Name
(in full)
Sex Age
M/F
Complete address
Name of
Treatment
Centre
Quarter:
Date of Regimen/ Disease
starting Category class
treatment
Pulm./
xpulm.
Type of Patient
New
fer in
case
(N)
(R)
F
W1
jjOd_._
3
01
jJamhVdii—
Md_^ U_brf)Gn.
103
‘r'l
/Of
^4;
107
aiAi
IO?>
-i/gj
1
eja
TEU
P>v<.£ypaJ
QbAcJLj KMtrt
& ru.
N
b'li’lt''
L,
yuyplc.enrf'n- 0-2,3
Z>A) a7<.
)^k(?vjA5
■7
55
P. d
b-U
End of I.P.-
2 months in CP.”
Enc of treat-n
Smear
Smesr
(O)
Smear
n
Lab No.
Smear
Lab No.
Lab No.
Cl
' Yu
AV
N
/r.’
f
N
Nf«
V
N
l~r
? N
I-t
?
f
-<0!.
N
»
Type of patient
SUMMARY
New
smear-positive
M
F
La?2
o
p
—N^/
TontMiuDc '
_FanCXfl_ A<«Ja
'I
Sputum examination
Pre treatment
(D)
P
0 15
Ay Tc^Md.
Ia
(F)
Other
N
A_M 321
1
JjpLkCld.sV
_Z^L
75--L
T9ilQ_!
6?
CD
o"
Treat
ment
after
default
Relapse Trans Failure
(P/EP)
Nd_S I fcurnbft*
/___
3> I. Pt ad. Nltf iLi'/Ob'
kri,
REVISED NA
Year:
Relapse
’ M
F
I.P. Intensive Phase
** C.P. Continuation Phase
Smear-negative Extra-pulmonary
M
F
M
New smear-positive
New smear-negative
New extra-puimonarv.
Relapse (smear-postage)
F
Failure (smear-posnswe;
Treatment After Default, .smear Others treated with CAT 11
•
■
I
I
iOS
- '
'■■■
rr ■
r
- •■' - g. "-
---''.
-r- >.’
- <V
-'..........................................................................................................................................................’
■
■?
....... ®r.... '
AA''7-'
83^
-
-------- -
1
y.acj^0
^CULOSlSCONTKOtPEOSE"^
NATIONAL TUBERCUL05 ----- Quarter.
R-^D-
ate
of
;gisation
Name
(in full)
Sex Age
m/f
Name of
Treatment
Centre
■
iff
Type of Patient
Regimen/ Disease
Date of
I class
I
starting I Category
I pulm./
treatment
I xpulm.
Pretreatment
0 months
Treat-Tother
Trans- Failure ment I
.Relapse
New
after
I ter in
1 default I (O)
Smear
Lab No.
case
(N)
(P/EP)
M
crw
ft
74
L — ’•
IM-t
I? 1
f
‘ LP. IntensJ
'* CP. Confin
’>■
/t
SUMMArY
New
smear-poSit've
M
Relapse
Smear-negative_
Extra-pulmonary
F
11
11
I
!
M
-
I
■ -'r f
1
I
o
tf)
4
z
/
• t
■■'a
<B
£
_O
C
$s|1q
c
,S 5<D
ro
!y
in
S
S
c
c
•“
S
O
T“ *
icr___
*
z 3 —
Z3
<D
°j
<n tn
r1
p,
i
o
c
(fl
0
u.
O
’□7
<D
D
cn
o
Qi
□
LU
cn o
u.
H
-J
1.
ji
J
u
f
I'
1
hl
<
Z
Q
£2
□
H
<
2
lJ)
»*r C
O <D
<D
0)
§
o'
cj
£ a
Ju a ,
w
i
Si <Si J 31 -c
^1 <71 -I 7^
ro
1s91.1 3 I'
41 "15
-.
£1
zl
TO
"O
I •
I
I
'T
41
-'^E l I{
-7
J|5
o! e
I Q
T
I
I
I
I
I
1
I
T
t
tlf
r Ji
1
I
4 ll
“T
u
£
<$-
ll
/.
i h
J
<D
O)
s
Q 2
o
I
I
I
I
I
I
I
I
1
£l
9'1
'I
41
"I
4?
o
i *.
<>4
i
i
I
r
I
I
si
C-J
i
1
O
r
I
I
I
o
I
i
I
-'1l I
xol -a
r
</J 5
T
I
I
I
I
I
c
<<
X “<D
p 6
T-
'i iv
u | J
<?
: I
($
I
JI. o
Q_
75 ‘b
8
t
ri
I %i
z|°
Q
2
z
I
•i
Ja
o
«shl
II
<D
V)
z ro
r)
£ E ±3c
o>
LU
Qi
tn
$
w
ol6
>
i
s
n
Z
Q
LU
CO
P
=3
((7?y
£
c
O Tn
§
2
tn
>
5
Q
i
AAI
d)
S
H
2
e_
O c
o
I
x~
5?(U :eCD 75E
I
ZE
X
~z
2
4
OL O
co
o
I
0) O
o
o
■
or
I
c ^r-
£
S’
a? cd
o
I
I
I
E — HI
i5 u
CL
'
1
~c
or
O
Qi
H
Z
£
H
O
QI
0
O
fi
<n
CL
0)
■E
cu
I
t2
Q.
>»
i
I
I
E
cu
<D
>
i
■'
(
o
L/>|
J
E
i
i
1
I
I
I
I
I
I
I
I
c
th
rC
i
i
f
i.
t
-
f
c
.zcx; 4«■
r-
J
iI
------- —
IB
No.
Hi
I
REVISED NATION AL TUBERCUL°S|S control programme
TubGrCylOSIS Register
Quarter: ------ -±
I Sex | Age
Name
(in full)
Date
of
regis
tration
Complete addresr
M/F
J
Name of
! Date of
Treatment
starting Category
treatment
Centre
xpulm.
New ipelaijse Trans Failure
fer in
case
(N)
CD
(R)
(f;
(WEP)
X
C\ . ic t z-u
2^
r
_l------>s_
_^c_ —
-^•^.■Ae.
-W\
____ _
A-A.
--------------------------------------------- *
Other
d€ tac-n
’•
0 'TCJTiihS
-
■
Smear
Lab No-
14"
C€
2 Of 3
Smea
i
1X2X1 __ k „
'
’*
TV \L CC
________ __ _____ ______ —------
S
?
—
i
C^ki
I
V-
'iill
—
f
(CT
O)
_t2Z—X
•. -‘T\o.VVA'>-'-•
Pretreatment
man-
i
A ZV- •^^,—
(c• • I
.___
Si
Cx?l- T
' t
St
Type of Patient
Regimen/ Disease
class
pjImJ
Year.
C
------ ---------------- i
-------
■
I fisUiT "
I
Vs .
~
- A'h 4\v»--x \yv-cX-. _
___ LZ
f >
IV) ’VT-su---- — -
?
^r4 V €-’A'
n'
I
<Ao]
Y<4
I
I
?
Gxk\o
•'A« o yc.
I
!
i-
—■t--
* ip. imensive Pnas?
” CP. Conrr.uaton Pr-4
SUMMARY
New
smear-positive
M
F
Reiaose
M
F
Smear-negative Extra-pulmonary
M
M
F
I
I
S
pj:
fe:
E-
! U! 3
■-■
•?r »-
pg!
ri;
o
o
te r r
♦J
fl i
I
T'
r
A'
I!
1
H
o
.9
"ST'
VO
o
J
is
f-
\ sf
?3
i
3
s>
■\l>
0
“
t
Q.HWflSM
I
I
J
lA
0- Li
o
,
0
LU
1 s
1
5
d
Q.
o
41
i’l
z
0
o
tn
0)
<f)
OH
CD
C)
o
<J)
Z)
o
co
o
CO
o
K
LU
□
D
o
XI
□
<
o
if
0
H
1 00
(i
si
a>
ra
0
1f
(V|
c-
0-
§i
L:
fl
l'»
r1
J
a,
E
</>
o.
o
' r//
U)
6\
0)
■h
s
.)
1
r-
ci
4
0
o4
_r-
y>
?1'’' ,’ I
,p ■
I
K
H
"I '
•e1 ?
3
f c
Ji
f I i
‘^11
a>
o
o
O
'7 I a
J?
Ji j J
E
•I
LL-
"T”
T
I
I
i
I
I
I
I
il
d!
-n
d?
fji
Ji-.
;L_
T
I
!
.
I i
•If
'A ' . .;;g
i!
a
ro
Z ~
I
I
I
I
53
<vj T5
Q
P -i
1
I
I
I
I
I
I
1
't- i
1
r.
I
La
I
$
rr
c
O
I
■/' I
a
'■
■;!• I1'’I
l
iLi i
(*1^
i
J___ 1
I
I
1
-I
H
I
I
•It
I
ii
J
•h §
O
ll
z-
3'i:
r
.J,
v«.s
vO
£
c/) S
-th i
■?'
AJ.
______ J
6
u
•4
J
■‘■'a
7i(
(/)
>
H-T
II
i
1
M)
<14 t
'"T
LiI Vp
•jd
8
■u
lg
(D
8<c
ai
o
Lro
z. F§” o
I
cc
5
LU
LU
01
1
't
r
a) c
2
x
'.l-
■1
3
Q
:
s
<y
$
|i
&8
o
01
H
is
z
■§ g
0
M
g'
£
fe
t
ro
a>
r!lE
cn
1
1
11I £
>
4
§
2^|0-
d
ij
£
a> « r?
«
kA
£?
o
I
Cj
I
i
...
-u...
---- --------------------------------
I
REVISED NATIONAL TUBERCULOSIS CONTROL PROGRAMME
!
Tuberculosis Register
TB
Date
No.
erf
Sex Age t
M/F
Name
(in full)
Name of
Treatment
Centre
Compiste address
regis
tration
j
'_____________
r
!
Date of Regimen/ Disease^
New
starting Category dass
FhjImJ case
treatment
(N)
xpuim.
Pie3')
I
Sputum e:
Type erf Pasent
Relapse Trans Fassre
fer in
(R)
(D
(?)
Treat Other
ment
after
default
(O)
Pretreatment
Endofl.P.’
0 <wft
2 or 3 mon'Jhs
ar^ar
(D)
—I
Cx&2ys_
V
?-cr i
Year
Quarter:
■ j L
V
<vc <AL
n\A^\
tc.
itV \
I
K\
Lafc Na-
\\A*
IS \G)
VA
-I
------
Smear
. 3
L?
Gd
Lab No.
poo
I
I
o\\-,
<'=-V \A
------
I
t
T
1
I
u^c-.-yx.
3f
~?'-'
V-
i
r-'
-AAt"
■'
___ ^/v
\XA
r
v(--4
I
r'Gc,
Cf I Si
i
1
* IP. Intensive Phase
” CP. Continuation Phase
SUMMARY
New
smear-positive
M
-----------------------
• F
Relapse
M
TT
Smear-negat!v=
M
F
Ex^cpulmonary
V
F
3
i|
H-
m
I
cn
<5
..
I
J
-
I
:-
^JSW
I
iit
•
o
I
I?
&
CM
?
C>
z'
i
■x
II
I
1
ns
<*>
_5
’’x
- k
!
2
11
< i
’
)
• r
■
fe' ,
J
till
i
11.1
§
I
« fS S m
Ig
i
n
£
n.ro g
<D
>
I
‘B
.G
o
£r
■'S
f
ste
iitg
■
(D
oo
o
b
o
al
LU
ffi
Z)
rs I
a
Qi
W
II
o
□
o
w
2
"O
£
•§
$
g
E
u
CL
LU
Di
eX
<s
I
n
i;
i I »-■
< *
i
i
i
i
311
1^1 J±
t:
e
V
cu.
7
F
I
I
-P
0cl.!P 1^.
J
,
(J I
i Ij
t
li
bi Sflii
\ I
T
I
I
I
I
II
I
■'
ill i
p
_j...3e 7
i
i
}.\ i'
fl I i
Va
;£
Q
X uQ) ^^•
s
-T-.
51
cS
■•■1
11
r
L
(fi
>
i
3
*?
1
41
>
§
a
y
<
A
•Z
Q
LU
W
I3
3
o
4
Zij- 31 lit la
0)
P
9
3
I7 1?;^
O
2
R
V'1
J
I
I
I
I
U)
To
<
s
0)
8 CDCD
tn
u
U S
I
'L
0.
ft r
%-
V
or c.
■5 s
o
!
3
T
V?! '
§
£
i
!
ft-
53
2
co
gs
I
gr
■
I
e
h
I if
,
N®
2q
7“
«
£
Pi- 1
i I
.il jj
2m
s 'X .<h o
co o
O
i
i
i
I
51 <
nt
I
I
I
I
l'ft
o
I
I
I
I
I
I
I
I
7
l<^
i1
7
5>b
o
i
i
i
i
i
i
I
I ?
zf II
4,1 7
Til'
i\^
I') I
O
I i-^
l£
c
U
j
po
•— *
r
I
"T“
<Al|
I
I
I
I
1
p, :
' I:
ii;
r
mA
'B;
:• :v' i f
'"-17
,
III? II
IwiO'
$
o
1 i i ■?
B!
&
«
ul s
jlb' -K \
| fi
$
1
CT
r’
L':
S
£
si
I
0
___
aid
• r
..{:
Q
05
0
Q.
e
I
LU
2o
W
£
hilg
If]
I
1
1
Sr
iV
o
z2'
c^1
r
5
J
Ii
lV
ill
u.
I
xsH
I
V
;i K'
3.
!R
w
Q
I
Q
A
<
a
t
vT
rA
I
I
I
I
I
CO
0)
®
Io
fJL„.
■<
^l-3
0| J
i
jl >1 Ah
?p
_9
1
A
iH
p-
go
-" I ■
-J f
fl
I
I
yi^'
il <}
5
o
co
rO
A
ci»
^1
J------
p
ub’
T
I
I
I
I
I
I
I
II
jl
_.L
0
ll P
<Zl2
£ £ .Li... w
a
0
t\i
I’H
I
cJ! 5! l
-11 >ji
3-!
1
ir|
I
-M
•’4
Z £
L7 I
~T“
vi
“V
W-R®W
f
t/.
I
2
s
I
I
3
A5
5
<C
Z3
U
0>
R
V
-K
0)
=1
</)
<D
o
X2
■z
1
I
<
(Z
ft
w
I
n
i
8 0)
<■
?
£1.
Hz
!'
2
>
11 e
o
4-»
I
s
2 s
AsL.
‘g
a-
ro
sE
g
d)
•b
;■
s?
>
I
fl
I-
I
o
p>
!
A
1 §
ri
|O
jy®
T
2
.4
I
«
&
,r -
/
Ii
•?
p
IMO
A_
A.
i" I
7
■
A
'<A
■
I
ill
ill
s
:
1
IF
4
T
J
x-
I
.I
i1
£
o
a
5
o
<r
I
I
&)
91
?l
6I
<1
JL
ri
I
IB
J
i
V\
A
\
F
•a.O
■-
f j
■■
I
'
fiStts -
-
I
J
i Wftw'
iMt
J
\ T/pi
{•-£: t'■Ai ' 4]
,<’L ;'-- ’ ’ A *4
. s A- ■ •-•■■.•
I
IByiSEp NATIONAL TUBF.RCULGS1S CONTROL PROGRAMME
ft
Tuberculosis Register
•.
I
TB
No.
Date
of
regis
tration
Name
fin f JI)
Complete address
Ssx
MSF
Sputum exanrar
Name of
T Data of Regimen/ Disease
Treatment
Centre
staffing Categoiy
treaimEnt
class
PulmJ
xpulm.
_______ I
c-
•>
_3l33_’ \e <c^ecv%s.______
>A-C
<CK> W\
9
21--'
r\x
p
t -
rype of Patient
I SygemE
New RJar.se Trans Faikiri‘ | Treat Other
ment
fer in
case
after
defauft
(0)'
(N)
(F)
(R)
CO
(REP)
A’S
!
Ysar:
Quarter:
-.ffC-fc
JS^O-
j
3a \- o \
-
I
v\
Sl-ci c)
i
\s
--------------- ■“<“?---------- <>
4 ar
Srrear
Lab No.
£:±
A>
:
A
1------------------ T ' V' • c
2nx
<D)
3
n-
Eno of I P-*
2 or 3 months
I
’T^Cka. —__________.___________
1
vuV
<
3- ^ ci
a-
& &
p-a
*4
\ A,-,
YCV
_
• p V_a<.VV<
\T^ V/xc, -
.;P-U L
I
CsJk <S
i
i
t
6‘.
3-2.-CI
XXS
V
T
gr
f^oA" \X\
—------
*
sssve Phase
” c? OfauatioH Phase
II
SUMMARY
New
smear-positive
F
Relapse
M
F
Smear-negative Extra-pd nonary
M
F
M
F
Sn*
■ -y;
REVISED NATIONAL TUBERCULOSIS CONTROL PROGRAMME
W
■
Quarter:
TB
No.
Date
of
regis
tration
Name
(In full)
Sex Age
M'F
v>\
IL
Name of
Treatment
Centre
Complete address
S^CLJ £?i<
X-
Date of Regmvrrv ptsease
starting Category | class
Pul mJ
treatment
xpuim.
(PEP)
I
f
^ --vrv Vt
Sputum examt
______
FSfeu-«
New jRe^sse Trans Failure Treat Other
ment
fer in
case
after
default
(O)
(F)
(N)
(R)
(D)
W^-
CD
S«S^ -3»D.
___
Smear
r
9i
G_V
End of I P-*
2 Of 3 months
.
2 m<
I ab No.
\°A'!
F
c-4^-
VA
?, X. ei
^Lx-^u
-c «-'- v- ’
r—
r
4,
-t
74;
1'7-c I
?
P-T
2T
-V
V C m'
N<*
\
Vxiexa
VXb\„
<• c<
Tc ~s.
■
^fe.Vrvt-
V'\
A& v ci
V
'
5l?<
"V ■J.-'Ls^
p
V I
4
■
■Q-X~>
V-\Q- VY2-, >V*K
-------------
r
J
* l ».f»e Phase
** •-jBtTtaton Phase
SUMMARY
New
smear-positne
M
F
Relapse
M
Smear-negative tjctra-pulmonary
F
F
r'
M
F
Srr
m
S
1^ Se
ry
! £
.
1
•tf
0>
E
2
o
ih
cu I
g.
(D
o
s
I 3
M
7
«
b
CM
J
!13
A
iji
■■■
.srj*
< ■ M’ ”
'
I
' 4
5 1
ro
n.
I
a
S
2
■
O
QI
o ’tncn
u
co
o
£Z
V)
c
—»
roo
tfl
Q^£
*l yO
H
-J
<
‘S g <D
a> £ £
J2
Z5
OT
!«
0>
ex
0)
5
E
Z
Q
112
0
a
■ s
>
IX
(J
V0
!|! I
(j
i
4
J
I
w
0)
A
a-
3
_A.
I
5
/Tn
±
0
cl
J
X 4</! 2
i,2
5
'V
-I
S'
Fl
«u
.i
pF
t\
——J—
?l~ ]l
ii
,jn
I
B-i]
fl
5
-..
(PI
I
<i£
I
^1
1
{I
I
An
nrji
yl i'r^ 5| "
W
^4 I
^1 f 7^? ^,1
11
I
Ji
A
2^
Al:
i\^
R i iii
*1 5
to
Bn;'.-J
rv
>
ti
s
A
■h] £
H
PS
-D
'
CPI
51
rf
vZl
d
Ji
Z\
?i
i
I
I
/]
J
A
cA
T
I
I
“"T
cii
£
GO
c/>
__ I
*/!
5c^
er1 J
1
F
L
~T
I
w 1
-'I
r*
f
“V
i||
^1
Si I
I I Jjj
J.
'±
I
_2L
ut
T
I
I
I
Jl
_L
:4.
3
3E
"Z-
1
ip
-JL
<
z
I
II1
felyw?
J
O
U
1
</)
s
t
■■■
?'
u
K »
K g
2
I
I -o a 9-fe
f <►•
O|
1
I E
Z
S8s
co
2 S
co rq TO
o
el
§
I
•li
18
O
tri
O.
1
£
? 5?
<
cz
0
‘WiWf?
'■f
2 so
[A
id
J
A
G?
**
<u
US
i,
<u
^o
n)
IXJ
I
gills
Ij^
I'w
b®
|||
1_1_
<5
■ •-'’P ''i
i
I
L
-i
■. i,fe
u
I
I I
■■}
Ji
A
i
’ ’’^
»W
■?“
to
\r-
Il I
I
f
r
IK
i
i
i
JA
*b
I
Ji IIr
|
■<
■$
■
r
m
V I
I I
F ■ ;L
A
M
Hi
s.
___ J?/ „
REVISED NATIONAL TUBERCULOSIS CONTROL PROGRAMME
Tuberculosis Register
■
I
■
—■-?■■■ ■ ■
——
{ Date
J
cf
• reysj iafon
TB
No.
Quarter
Sputum examinatk
II
‘'4arre
in fi/Q
Age
Complete address
Name of
Treatment
M/F
Centre
t
Va-vum
Type of Patient
Dale of Regimen/ pissase
staling Categoey class
PiMtJ
treatment
CD
XpU^T<PS’i
\s>
_
VAo_
_S_2 ta /_bZ?27L2?2.----------
__ X3 AA o, o~> _
I--------
c
X
o
-.■J
(H
(0)
End of IP*
2 or 3 months
L"St
i®2®. -mear
i
Lab No.
\<vA<n
r
±
c-
C?Jt 3-
i -;-
Ssurts
G-v
^•7.-° I
\a -0 ’
Other
New Relapse Trans Faiiure Treat
ment
case
fer in
after
default
(N)
’ ;D).
V^QX-ek.'u /VWX2-
5
t-----------------------
A3
n'c<-
i
?
I
A A j’^.
17-
X
l-i
i
4<
________ ■
A>
4
k ‘.
'
r"—c-%-
5
LA • 7 • TATn
±d—
V
"i
I r-i
*
iKETiei^e
* CF CsrjaKSiPhsse
SUMMARY
New
smear-positive
M
\
F
Reisse
W
|
I
F
Smear-neg alive Exra-pulmonary
M
s
F
U
1
F
nt
2 months
4 orSor
Smear
:
£'5 SI
Is flr
.13
; •
p#
iD. ‘oilia
u —
(/)
MM
II
“
}n
5
I
»lw
ra
o
>
JJ tltJ
■f
r
• i
■
§
?x
I
'
'
■•
llJ
2
s
s
'tglw
■•■'sSsfesd
-J
o
g.
<u
G?
&:
Z)I w
o
o O)
CD
<fJI
0>
I
re
■»<
O
11
g X)s
□
< h-
g
<
z
Q
LU
.'
. .....
'.?.
.4--*vS
«n
!~
LU
s
I
I
? I
I
I
I
-I
0)
3O-
flj 11
g
<3
iP
L
X
d) '\-
<
cn S
I
i
„„
Is
vjL
cfl
—r- ’*< *yjfA W M.- <4
421
U)
a®
i
j>
<r
0)
]11
It
>| V
C
T
.4
I
I
I
l
1!
4
f
10»-
Zl
I
;<
4^
21
t1r4 J)ii "I? H
'j' A
t?i| u ;k
t JI
V>! 7
I (.'
4
I1i
2|
T
I
I
7
II■'’life
I im
SB
i
i
I
I
4Ji1
I
T
I
I
5
<3
I
I
i
cjj
4.1
I____ I
s
?
JI I
I
3
I
I
I
1
fl-
<
!rWW^<
■>
A i
V
■
.■
!
T
I
I
111
y j
1
i
11 I
hi
_£
A
<
:
J :
41
2l^_i
d
tfl
'
<I
I
I
I
±
i
I
I
< i
l.L
T
stlfe- '■
ri if
i
$.1^ l
b^i
l>|
'I
Sw
l$
2e
H
'A
ii/
I ‘
1'
r1
O'
z f6
1
i
si A
}
3
v
i
4/
..—
o
1
A
ll
3
'5 t a>
□
0)
§
:-e
L''
3
:
' if! |
£
0-
r?
a:
w
ra
CO
®b
IB;
I iH
I
r/)
15
<e
*lW
CD
i-->
•1
!i q
(I1
34
36
7
ip
s
X
LB
ts
11 e
III
Hs1
■Il
£
§E
fs
£L
'-t
iw(s:
li
o
0
<n
O
■a
V,
g
•• •-■
!
Lv4i© r*<
o
rx
CO
*<5
»
I
I
A
• -wr*- ••*•■**
■
___
®Pi5
£_E
o
(U
Q_
g
H “V J H
g.
~
i
B
.
s
Q
;-
I
s._ Li!_ iL
t
I II
I I
—
$
&
filli c
£ <2
-_— -
—•9
it
K
9i
r.
-. &
■s
_ . .
V'
■
I
Iw
i’sms
T"
illflu
*
t* I
\A
T7
'“
’ Cx'
10
s
■?
V I
sJ
2
£j
w—- , V'.
5i’
.■U «i
* »
'W
o
o
0
A
HL.
is
>•
'S;’
..141
o
I
£
’8
o
ex
i
/*J .'£'■•“’■'^;# •v'
'i
LU
S
.:
J
/S
s
w
SfflHi
'Ji’A
s'l
J
7
_3.
rJ
1
o
J? £ s
S i§ s
O
!Z
<p
a « 8
o
w
c6
o
'Si
o § 0
Di
||Sq
o
co
To
-2
:□
LU
o
Cfl
p u.a>
< rs
o
<
o.
go
f
d4
ii
J;
Q.
E
o
o
i
51 ■
I
I
I
.1
J5
31
i
OMsp
f?
1
L-.
(V
ro
Q
.2? O
o 2
(3
1LZ
u
~T
I
I
I
I
I
5^
'-'I
r
c
I
A
T
i
I
I
I
I
1
T
I
I
i!
1
J
r
i
u
J_____
I
J
•x
>•
H I
i i I1' 71
J
'■ S
§
17
I ’ Is
3
i
I
tZ)
17
kt29
I i
I
^1
7
i
I
I
I
I
I
I
I
i'p
ii
o
i
T
I
I
I
I
i
F
<•
Lo
It®-
I tr
! Ii
I fi
! Il
i
«i
hO
fl
I I
C
-II
(X
i I As )
c3
_.L
k0
n
s
IF
r e;3 51 ivjll
»'6
p d
L
QI
;i
r.0|I 7
'r 2
~T
JI
i?
Z S
lr
8$
t
I
ij'p c I
c*
■
5
“7
LU
.. 2
o-
5
3
i
~T
I 77
7T
I
i
d ; fl
^i
$2
>
el
tr
33
<»
j; ij
3
je
S'J
ra
o>
o
r4
3
3
T ?
I
w
uJ
(.X-
LU
,;;JW
l»
'/
$
fl
>
d
o
or
o
ar.
£
0-'
s0
o
c
u
CL
' f -..-.I
>
§
I &
IR
I«fi
s
I’-
III
ul
£ p
E jb
fir
'■ "II
■ j.
I£ a
£L~
-rW^.»
■
I
llifa
k
I
I
I
?
R-
I
it
ri
IS •;?
‘1
l
I ri
i'-
N
J0 I
b 5
III 111.
g.
I
co
E
2
V,
B
•^A
f
z
I5
j_
L
____
m■■"■
2
■
1|
H
ai ft
• t
*
~“-jy • jaKapa^- \
e»
t®
IB
£n
1HI§
I
<£
w c;
o§. i
' ■
((DY
A
J
I i tr
1
>
cn
1.
jiE
i
i g
ni 7
is n
Q
Li'
2
e
h
$8
. |
--
K
"'IS
W 1
Z
o
o
12
co
o
m
Z3
O
u.
O
JO
□
O
£
<
Jp
L?I
<v
i
I
"r-
I
<!•>
s
,
■
I
I I
fl
L' b-■■ ^{i
<D
•
/> —' <y.:?•e'-z-.'
s
4r-0
ii
III
ro >>
c'
i
i
i
i
!
-L
«* >
. <'
£
,u
L JB
Ij h i
s|<
£ £
I
rT! o
ol \
c“'
11
T
I
nni '~~Ti
I
ip
11
LIL
u-p_
i
I
i
I
i
I
i
i JI
L
f
’I
T
I
~n~r~
i
I
I
I
I
I
/J
-<1
J
t>
A
'V
o' •
? I, ^1
Lx/ tx/.'jl
o
(k
n
I
J
A
,
I
’■|
I
Y 1
’■I
I .‘*1
I£[
Q
iff
h!
11
u’
r
Vs
f
:f1
ci
bn
(i
L''
4
n
I
■ iv 1
J
ii
Mi1 ’
x■ ?!
4* Jl ■&1
□_ 3ili LiH
111
c>i y AI
■’
f . .. ./
E
io
I
’ I
i
4
X
ii h
n
t'pl ih
KI
i
Z (0
B
0
si«
Jg
3
-A
^4>i
L
01
vl1V i
i
L M
1
co
«>
t s'
j
1
I
I
L [L
CZ>
5
o
rt
J
c*
or
.52
o
in
5
cl
o 55 o
VD
O
Oe-
5
o
al f
t)
1.
( >'
1
Sfl
a>
1
=>«/2>
j.
a -
H
y
" L- ••’
5
o
ti:
a
-I
$
LU
£*
i
<D
■i
-X
hi
2
o
•<S>
;
I
r fl 1i
! S i
I
11
gg(
,’.i ■
»
!■ :B
w
I
I I1 F
IF 1I
hl BBp
"
i FLr’
i I ■
■
i b
||i1
;
z
H
If y
i
/
1
h
'
i
.
ggyisg^ national .tuberculosis control program
I
I
Tuberculosis Register
Quarter:
T
IB
No.
Date
t
of
regis
tration
i
N'an»
(in fa|)
CoTipleie address
Name of
Treatment
Centre
?
-yV^-
&\
I Sex | Age
m/f!
TAS^ 1—Xt), \o'j^- Gt ’=-5?^
----- ¥
.Yean
Date of RegmynJ
Type of Patient
soese
starting Category ’ -Jass
New Rek-pse Trans-[Failure I TreatOther
treatment
jPuimJ case
fer in
H*nt
XpdfTL
(N)
(R) CD
(F) default
after (O)
(N)
(R)
(0
P^P)
I
(D)
S-’i '€> 5
I
Sputum examt
| gjgggreat
| *rsx |£3bNo.
nr
0^5
liV
S-3-cm
>■
p
v<
I
1
f n
D J>
2S-
... _ _______
______ -g^S V
_Vz\,'v-x^.-__p
—
----- jV'VV’-tVG e-3
V
\
■s\
I
iz. ^2. IS-SfL
Vb
1-0'
f
I
—
’3
oi ■ y
vj i _
-3
!
Smear
> A:'V
----- --------
v^«-< v^o)
i '_
I
J_________
t-
v
______________ "’"''•S -V—-
Ki e<
I
_____
I
I
SUMMARY
New
smear-pos.tve
Relapse
M
F
AC
Lab No.
y.
|
H q
l_-l-
2m
End eft P.*
2 or 3 months
i- Ppi
i
Cx-
\.“5ZS
|
: 2 rrenstve Phase
"
'station Phase
Smear-negative Extra-pulmonary
M
SfT
■V’':
■<
■■.-/
■'■ ■
■■-.'Sr
Jv-
LfcWS
NATiON'AL tuberculosis control programme
i
I
i uberculosis Register
IB
Dsh
No.
a
Name
(in full)
Sex Age
M/F
Aeg’srsiio-
_>
£
Complete address
■ Nsneof
j Teatmenf
i Centre
Quarter.
Type of Patent
I Date of RecamerJ Disease
starting Category
class
treatment
PulmJ
New Relapse Trans
case
fer in
(N)
0) j
xpulm.
(F7EP)
vAjX.
\jkl. S^^S^CXc^Q
VA
AA-WtMi
c/v'---- v-S
V2_-1't!. - — 4-T^±-___ c
Ca: A
"S -D }
Treat Other
ment
afier
default (O)
(D)
I2mor
i
---4
4ts»«^
Sin*
fR)
M
^•1
V
v
~T—--------------
Vctrz. _
€ "r
Ag-e-)
,Year_
i
A
A\j>
v3£-<
------ V - S.-TV VA
! AT
■— I
i
I
jA'-^V c -k.
G'l
t
pc
1
t■
v <■*?<.»- <-T'
1 n?
V
1
GV^'
I
i'
w.
v'--k<^c\c=»sx-A*
LJ
ifes
L_
_ ___ _
\5^°
I
rA
-1_ _——-
f!
_____
hk Y-Oj
■t—
vA
I
I
“T~---------4*><
v\
X<—A .
I TAss IT ,
1
y •X*C|
~~
£5“ _^*£.
I
C=>^
T
a r
AX
------------ } S'
-• £Z __
.:
■
i----
—H
__ rpct-ATx''^
~
i 2t?±
'"s-s:
—L-------- ---------I
yo'
VA
r~
I
si
. p W^e?h2^e
«u £E c^tinuation-
SUMMARY
New
smear-fxssve
V.
k
F
Relapse
F
Smear-negative Extra-pjnTCnary
M
F
\
M
J
-
i
’c
'• ■
■T'<
*V-,
*—•? -
REVISED NATIONAL TUBERCULOSIS CONTROL PROGRAMME
Tuberculosis Register
0
IB
i
Date
of
regis
tration
L
Sterne
(s&J)
Sex Age
M/F
Complete adcress
I
tA-
*X2)V)
^2
i
Date of Regimen/ Disease
starting Category class
PulmJ
treatment
xpulm.
(P/SP)
Year:
2)utum ex?r
Type of Patient
------ r
New Relapse Trans Failure Treat Other
ment
fer in
case
| after
(N)
(T)
(F) ; default (O)
(R)
VA.^--^4*
VxTo
3 tK*6
P)
\TV
------
k2_'Vo\
Name of
Treatment
Centre
kV
Quarter
o
« X'V
■V-*=^
4°
-
2
4
Smear -ah No.
f
IT
5r\\
lt'2 -t) \
CZ.
I V-C
EndTlP-*
2 cr SmofiSis
I
j_______i____
>
'A''
■“V
Qdt- \x\
I
■T^Vr^jt—
i
-----
2A
------
\S>0 > 3T
tS---------- </ T-A* SrX
*
■wk;
!
-
j A'T-A -
T
rA
\x\
V'e-l G\
Gt
4^x3^ -
i
I
■ p Mtasive Phase
S’. Cotmuation Phase
SUMMARY
New
smear-positive
M
■
F
Relapse
M
Smear-negative Extra-pulmonary
M
p
M
I
F
-’StM (>
j=f
R EVIS E D N AT 10 NAL TUBERCULOSIS CON! RO
_
Quarter
Tuberculosis Register
Spbtunt examinat1
■
Type of Pa^er.t
r
TS
No.
Date
of
regis
tration
Name
(in full)
4 ol xx
H-T-o| - ---------------
—
\y
Name of
Treatment
Centre
Complete address
Sex Age
M/;F
tsQC
lA> V-
_____
2_____
p
Dale of Regimen/ Disease
sorting Category class
Pulm./
treatment
xpulm.
(P/EP)
New jR-etecse Trans
fer in
case
(R)
(N)
(H
(D
Trea merl
afte'
Other
defa*- ’ i
(O)
Endoti-P-*___
2mcntf
2 or 3 tnoolbs
Smear
I ah No.
4 or 5
Sm=a
(D)
, S 4^4
s>
VGq,^---
\ir4^
ife-yo/’
ou)
—| gr\p
Hr, JbAC t_2^ C -C B-VA
2-kUlct
_
tx;^
?
____ —
SL
kt s*c#!
\'o S-0) U '1k■ £JHTQ2_______ \
U-J-c; ■
4G
_K1O U^o_
A_LV^- cL-JO-
?
------------ YA- U-XA-O
_________________ _
— f
ee
i
Yk |
C_sA-\"
___ G?
1
I
in'Z'O]
_ c
<
S’C r±x^ _<• w c
1
-
•<7<
Pnase
* -■ -^MtionPhsse
SUMMARY
New
smear-positive
c
m
fF
V
F
\
u
*7'>——s-
rc-pulpona.y
Smear-negative
Relapse
I
V
F
«r
Ig.
1
a.
3
rJL
O'*
“■-av
1 •>
A
l< -
4-
* «
™_JiL —
'*
—-Hk
W'
I•
n
fi
TO
<D
w
? ■= c
0)
J'l
I i
ii!
U 5
.:
Hi
a
UJ|
%
2
<u
?'
Ia>
<2_____
Hs
u
<D
IMM
r
o g> S
5
o .2
o *5)
$2 Qi
111 §
m
□
llf
H
^’i ■
sh ;
!
<
J
11 ^1
I
0
XJ
□
qI
<
z
tn
n
>
LU
!/ 1
7'1
1_
2b 1
u
ll
II
I
-'!ll
I
I . 11
I
I
I &
JS
O
r**«
o
r-'-i
Jo
.
T
I
0"
i.
I
I
I
I
I
I
I
/:
?l
•51
CO
■:'!li
i.'l''
||p3
I
•1
I
!
s
c
,7>
iOi
M
^"V
U"T
I
I
d
‘7
7
o
\/)
0>
IF
I
'F Wiki
I
I
I
I
j ’.; \
I
i ■
[ ’ ! rt'
'■
I
A
crV
£1
I
°,f I
113
I
~0'
__
f2 6
»!
I
J
r! ■■
1
6I
Joi
1 L^l 4
I
II
5
n-
-1/ /i
3L
"c*
ro
£
<z>
f’y
I1'
I
I
I
I
i
•j'l d
$
0
!’ I
H
/)
"Tf
6^
i
il i
(h
r
i—r T
I 7]7
I Ul I
»
I
cr
C)
i-
I’
cP
31
e\
4H
rt-
rn
a
i|
I
ll
^1 t0Ji ■Ik I 4 I
'I
uI
II
J
3
Jrii/ "I 71 iH i
d> J
•■V/Vj*;
I
£
j
'3ii hi^tf
H
(V-
Yk
i
W
s
u
u.
tv
<p
7'-
• Mrf
w
7
r
sis
Q
7
OT
3
9
I -
3
2
c? I
rjr-
z H
o
Q
LU
4
tx/
'J
Q w g>
tn
gjp
7
(
o
cn
o
H
Z
7
7
0_ _ ■J
11
£
g0.
2
ia
&
tA
i ■ i ' •■
■'■- I.
' i
£
CL
_s g
r
Iffl ’ ■ 11 illol
u.
.1ro I £
>
i il
I -
iyj
I g
illfa
I’ “
io
i
n
el $
F’' '
1
-J
Iti
M
□
-yx'
z
V
1
s
■”T'T
t
4’1
I
I
■I
Nil
w
(
.n
a)
1 111
co
■
in
fi
■'
s
<
7
V)
!s
IJ *■y]
iI
' \- :Xd47 ,-^ - -1
1; • ?’ ■
’■ . / \4\7X,. 4
J
'd
'T, .1
-I
I
:’
y-i
cz)
’■'
4”
L
crA
1-
*£
4
’
'
\
t
I
-------- J
■
to
§
8
H
1
«&
iyh
I
1L
»I
i l’
aU
H*
£
MJ
111
S
o
a>
£ jn
o
Z)
o
ac
ijj
co
:
**♦
H
"
ft 48
-u
IS i
<
3
Ji
fi
n
11
L-J
V)
£
*O)
0)
0^
a)
w
h'§
c?
a
<p
XI
□
ii
4 7j
j
CL
I
I-
<
hiiJ
fxO|
p o•
a
UJ
J____
UJ
4
<nSt
a:
i
r')
c7
i
i
I
I
.sb
£
n
I
i
i
7 I IF i 4
z&
P O
i
i
n
r i
!
i
i
i
■" i
i pjf
I
r*
th
-44
4
1°
do
do
I
iI
iI
I
I
I
I
I
I
I
' I
I
^‘i l' ir
I
I
a
■~T'”
I1 il
£U
'if
I
I
I
I
I
I
Sil
1
s
I
a 1
i
i
i
I
I
,_U
I
ft
!
If
!
\w
l!
\I
fff
.FJ '•
&
(fy)
C )
O ’
••
‘ft
n^.
I
?l
ft i
R
■'.
>-
r-
1
li
f
d' i
J 4;
.7
JI
3ft
—r"-—! TH'
lwr ,xel„
s.y
'V
<).- I r. $1
d
?
■,^..s~
■ ■
I
I
Q*
71
:r
bl /
I
4I z
r'l <
Pw
s
.
w/l5 F 4
i
71 I
a>
2:
T
I
I
■j’1
■b
'fl
■.' ■
t'
IiF
11 Wli' I
ill's lie 4l"I
cn
2!
■i
A
:7
2
co
■,7 7
O
■I
j
_...4
r
'
8.
IU
(<)
'J
O (F 0)
Q
>M
-
5
<A
a
ft.ftftaS
iZ\
Ct Q___
(C
DC
o
(.^
S’ K
a.
2
w
O
i •& &
o
O
a
■ i
ae
P o
,'
iZ)
a>
f£
1o
<
Ct
Q
7
A
a
ZJE
2
<1' z—>
S
-4^'
!?■
«j
£
17®
i
I
£ ■
<
ftfll
ills|l
i
a
« .E
al
LU
•3
:
>
■
-
i
. IfF fl„
' i rfrf
REVISED NATIONAL TUBERCULOSIS CONTROL PROGRAMME
fi
Tuberculosis Register
r.’.i
N
1II-
TB
No.
Date
of
regis
tration
Name
(<n trull}
? Sex
Age
Compete address
! M/F
Name of
Treatment
Centre
Quarter
Type of Patient
Date of Regimen/ Drseasal
starting Category class
New Relapse Trsr.s- rzSusti Treat- (.Other
men*
treatment
Pulmj case
fesr in
after
xocirr.
(N)
(R)
CO (H default (O)
Spa? jit
'I
(D)
t
Q\
Prefegmerl
annrts
Snear Lab No.
End or LP.*
2 or 3 <~KJi.ihs
Smear
uab b
CjxV l\\
If
3V10I r-C^-’i------------v’
A r
O=>^'
?
^--X 'O'; Cs^T
A* >•
i
!
2-r
(Ao \*£.% .
°lL
'->-S
-—
<2>- ^-3.
7
- -s-------- x-------- L.
C 5^>
___
>■
i
h1
i
t 7». vti-----------
i
I i:
!ii
-i
T
«:
Li
'
r222-^^
C-*XMC yA->XVk
p
■--
A p5!-/
14
>r_^=-<\ — j
j
Ai fxf'o
K- *A-
>■
>
r . \A
p IA
K
!
!
O
f
4
SUMMARY
New
smear-positive
M
F
Re'apse
V
F
* £P. fasn5.w Phass
* CP. Cortr usson Phase
Smear-"reg stive Extra-pulmonary
M
F
M
r
L
r
B=
8K
7 ^.' v‘
-T
3
<c - >
'
Msb
<u
co
9,$
• J
$
t?>
IlsS
sW}
.
•:'; 'v/ •
:
1———
I5
iii|3
I £
CD
co
<D
yj
CL
3L-------- --
4>
I
&
H
■
'hPg._
I
SE
2E
kj
3
0
I
6
•egg
?2 '€ £
s§ ?.
d
o , ’Sh
o
I
cr*
<n
cn
i3!
gl
co
■
<(
o
p
w
s
-
iiS
ji_
S
- •f
•;yj
I |Hg
&
o
o
QI
i
a:
H
0
xJ
O
G
I *S
1
Pr
- •I
.
t
1
d
Irz. f>LI 3
yI
Ijk;
(A
>1
Uli
n
nil
X
’±
<D ^2
(J) s
..j_
I
'll
■w
I
p.
.
■
Q
-T*iS^
II I II
I
I
1
1
I
I
I
I
i
i
I
I
I
I
WM:ii
I !
I
I
1
r
r
1
1
1
•S2 .2
I.
gg I
I
1
n
»I
1
1
I
i—n
r r~
I
i
1
___ 1
T
1
1
1
.
I
I
i
T
I
Vx)
"I
CD
H iTT
I
I
I
I
I
I
I
I
I
I
I
I
W!
'-I
.
jl
<1
> _
ffl
i
T |T
<
>
Hi'
I
a S a>
UJ
10)
:■■'v
p
I o
I “5
Uli
CD o
o1 o I -cu
H■ n I ro
<D
_1
□
< H I 5Q.
z
o
<3
H
□1
L.
I
:z
Q
111
(f)
2
.
r
______
’W
|P|
!
I
I
I
I
1
i
1
i
i
i
i
i
1
1
1
1
1
“T"
i
i
i
i
i
l
l
I
I
I
I
I
I
I
I
1
i'IR
®F
I
I
IB1
ii ®
; ’’’. 1
! !• ■ t
v<
■ I
cT
i
'
IfF 1
Qmcri 24-03.2001
focb&aed d^ddeSocb^ eg^Q^d
^ocfordidb. 7oc5afc<^ csa.ed.23. djaoddE^, e^djyr^ sbgb. d^Sdotd tfejya
cwaaJocb d^o^jri^) aoarto daar&d oafc^ dpi) djaert assadesa tmo^oA)
©d6dp spadsa.
Zodbr^ a^sacd csa. oaedfedrsas^ddcb
■
rap
dpi)
djaerfc^)
si^iaf
24.03.18823^
fedjazoo^ddj.djae^f?^
<£ozo Tiras^radaaoci audci^d aod)
o
19960od
^Qe add,
djaedAdefe3td).
©3 v
eja^eOcdbo
dodd
8oac±>
oOddode a^ gpixlraeri
aswddreocbsb. CUCZjVUWUU^.
asSsrecio^ esd&sba^ aoSd.
IdCUeJGOObiyCMJaK^
24.03.2001 dodd css. crazod^r ss^ddd
d^oddd^ed d^ddracddd^ ©dOTdSd^d.
S)?L edbaert tsjotS obb sj.sad co.coofc&b EiuadcS taocb zjarl e^^cb
dpi) cftea^d^ H±uacb cfeto^
^cxbrfbaeri ebf^^oahTO d. £3/3 cdo^a
dpi) dbaehri'db cdaaroslyB TjaShetsarb^cj^d.
3s cbaer^ sba^cdd 7oa£)3
7doaio±)<£)
siiadodobbTOhd.
D
co
©odd
§p±) djaerfc^) 30edd cd©^ ©onart^oiua zactoabcb,
sbja^,
djO^d*^,
deeo,
^^eo^ocb,
^ctebo^o,
ddsb
6
' jco .
^o^ao dbaehrfc?oG> z^edoebc^Od djaeri^) Sodcid^ao
d.
sa^dbaedcd dpcbe^j djafhoOoocd fcSedcbbcddd ^dcia^a, zach^/d.
«
©cdd
©daOocd
c&aci
n) cdb rOj-ooijafl
dEb.e» desfcte), cra^dsajd dadf^oi) s^aad 140
ad ipi)
dpi)^) Tfcbastfde^
co
g^&ae^Gr
aodc&^Ootf
^ocb
gjOraSDAcS.
1
t
(Sea^docb,
9,
^dde)
SojaoScde) d.
dj3 EisaF 5 og, ad ds diaedOod T^oioScra<5. «odd d,3
o
cdSDd^
z^zdj
gpi>
§p±)
35
od, ad
diaehocto
d^efloio
dfitehrisb efepdtD, dpi) doenaraoritfsbj
dbdra
djaodasad.
sidde^
gp±>
djaerroradri^b^ djaehocbo z^oct) d^rd^ 10 Bod 15 ad^ ds Tjjaeodd^
i
I
!
E I
doddbSe^d.
I
^Efoaori gp±> daehrWsbt sgjarar
sSed 5±>e<9wciE® oera.cia
rbrasjartOaiicb cdowrff 3s siEard dx>aJ6 j^acdraoi) aetob.
Aacd ddr
ajsTifi Too^ A>o?3rte A>3bGacid) gpJddoeridsi^ ^drtojd dx>aJ6 ddoissraPi^.
Q
^8
cdddd ^o^r7^£3rt<& 2O3i) d^so^h To^rdd §crb ^cxbo^^) ^abr^dd,
3oe)rLfe)
<Spi>
cI)OciJy^
ct^ed
^cddo^Ce)
^obr^dddQoixQco
^scbd dbaehrte©, ^p±> draeric^) ^23^ ^siraraci©,
aSzsbso.a. dob,
^frbE^dbod, e9obd gpb djaehrted^ 3ocb b^cb Sdc^ed^b d^ade),
o^eccb
e>obddb zSeddd) Tbddd^rbdo^ djsdzoddcb.
ddx cra&>.d€)_
crac^eob
o±>^Q±»h
gpbd^eb cdobobjK) ©aobr^bdd^ cra^d cdcj^ 27
b3
©b^drba^c^hd.
sacbr^Bbd)
a
»
80
gp±>
cSjaeri
geori^at^
tss
<£>?jerafV3.
&obo3/teo dob’dbbd^ ^ocb cra«6
a^rb b3 ^Qbr^ddddd4 ?^d^d6 «d^ed6 ToedrtecD, a©erfriraiS>^ rie>4i
dd^d^
gpb
dbedddb4
c^rb
d^dd^eo
dd^obd^
djaefW
e1)e5o±>
d3 bde erodd^h ^dhdejshd.
_D
5)0^^ crae^/odd dcdd d^fci^Qbo^.Ee) ^cbrbddddd, do3>do^^h
ad zjs.ob®
ddassod
arartra
Scod,
-sisardd
djarir
Tiradcdao^
^d£)cdOG)
»
c3
^dd^drU^o^rb^ d.
djadede ddrdS dortejacb dda^ drib s^cDS ddsb,
-°
eJ
dortebcb drib zSe^obd^ WOSb^ obd^otoh e9dd^d dj^a ^obretoco^
dboahd.
dbdde ddrd^ raobd£>bb
23^,cbdr
dbdb,
obb^oirah
zSe^rb^
^obr^dddd^
KxDbr^drbTh^d.
dSb^bs^crahd.
24.03.2001 bodd
CO
saobrbddddd, ££),bo$^ e9dd^drtQ^dcrarbd)Cb.
ct
v_J
x>
oaa.eoi)
dOst^
eJ;
w
Spi>
^^0
23^^b,
djaed&ocbo^ra
ddod6
^8
bs
&!d_r»eb
23dp±)<£)
^3
cra^d cdo^ zSe^H'db
<
saobr^dadd^
3oO^c3e)f^
do3•
(^dd^drtoS’dco c^obrobsrad d^dej^hd.
esdjaert
a
^cdor^drcb
d)dd
ddsb^
ddco^obcb
ToEioGraocb
sirorird&rri'S'rt 3-^ddjc5es!odd dp±> draedd d^iri'*>^) drachrW^ 6o^d
codd sJo^d saoiir^didiO^ &s?Acbdod ^djde Sddraedessddsi^ sirad3d)d>
ASdjsad©,
d^dco
ds
draeddsbj
^HW.CO
ddd^to
eJ
aoiioS/teo
odjaeria 3«bd«5o±>sb4 &^c£)E3x±).
&»ab3)dx
d^JSddiafdessddd^
djacholo Ad4d dd
^dab4
eroddejsddd, Afsbdad stab, Sdiv^ri gjaotoctbs^ Sdd?^ ©d£» d^Ood
daoeij&o^deS), Tb^, dtodja d073ddsb4 edj/terajfi ^toj&a^deeb.
zaad,
eJ
gddjacdzzrad djaa&aod<9, ®s>d adjaedeS
aaji
doframri*
mddj^odddh ddsedddd^ doddo^dco ^EdddddjS
asdrtid mda^ddod SEda
addsecdd dd, Edcfd ddsendradd^b dsddd^cd^ dedoddEdOd ^dcddEd)CdOo<d 2d^^
dedd^cOdd^doo ^draEJ^dd^dd.
o
enddd^23edd dodd ©cdS* Edddzd^ Edddzd^edd,
&pd
Tid^a^ddedd.
1962dod:
Od23d6
O323
ddd^d 23.n).23. zddZdd^cddG^dd^ cBdSddEdod d^dzdedd.
3p±)
dpdd
djaeri
dJded
cd OddO P©e)
^oddo^rad
7^07?
oio
roo^oxu
Q
saocbr
Sejoddrdjcdd^
^do^dEddh
Od23.
7o5e>rdcd
©dotjr^dd^
oddrbraEddh
ddodctoh
cra23d T^drdd
z^oQuS, cdej^
cdOT 23eJ3d^eudo
aodrbd
d$doddddd4 dcd^
dod ddddd^d,
asdrbd TtooddEddd*
Ed^cdd^ 2do£)rf,
d^dfeS&xbdd,
djdd 23ejdo gpdddjded ^oddo^ra TdoT^d^d.
ToOT^d^ e?djded6
Edd^,
Tostjd^d©, MdsteSodd^ EddJdaToco edesdcd T^dEddh^d^^ ^dhTtosd, zdoftrf.
abddjd od&.tdc) Ed.d.d EddSb, edited, Td^dodddd TosSd^e^dd^d^ Eddd^, a^d
°t
««„©„ esdiaeri^ !s&>rar
s3A^«od asarta TSstroa
straSoSo^sb,
'X’
O
D
EdddSoS &dpd^dd4 EdEdrteid^ zooftcl
-ds doT^oddd Edd^^EdprarEJdh dstrass
TSeESodddd^ EdJdcddEdjcde^rf zded e>od do7?d^d/d4 djdcd ©dEda^lidOEdd escdca^
cdd&Sj^ dpdd d&edEddd* ^oddo^ded daododddEddhrf.
s5.aLot>>
craKdeccb
o D
T^oldo
stoajo^cb
asartja
ssabraeS arfregtecb,
Too^ T^oT^d^d ^d^b, T^rKcd&i) efe Q^Qod
g^zddraodd e^oriEJsh edL^er^
dpldd^ed
cdd^d, ^^Ed^cdd^ T^cddd&jtd^ cddJsQ^)
^oddrcU^ed^ ^odb cra«d dpdd djseri cdoddo^ra ssoddr^ddd^ mddcon) ^3
djdeHddd. ddjdelide23d,wd ddsddde) cdo djs Tod.cdd EUd^. dooTd^dodd Edddd
^O23rfoe^.
21 ooOCd^
©
21
o
Cyct/
f
7
"V
"TK
•771
As^o
I
A/(A.
Au.
f
A
r.
f
J?-?
^7r
%
&>
■
f^C-
Dear
Subject: A study on the patient’s perspective regarding TB treatment
Greetings from Community Health Cell!
2V>
oJl-Si— O—5-P
.
5
•£'‘11
/Yeu-may-be aware that tuberculosis contmues to be causing a lot ot
~suffeHng to the-patient'mid her B his family in many waysYThe poor kt
affected more because of their pM-"socio economic status.flt is hoped that
the finding of the study would help in
poh^y chMftW^r^
vSfcyKj
In Ihis connection we would like to request you to give the names of TB
patients from the slums where you are working, who
from the govemment^Ae private health institutions^ We may select some
of them for die study and we would need your W
6
would appreciate if you could send the list before^^M^2001.
..< ry'--'--:.
With Best Wishes!
Yours sincerely,
For Community Health Cell
S.J.Chander
'V
'.1
?>
WTBD brief access
Paue 1 o^'5
World TB Day 200! Brief
English
French
Spanish
World TB Day — 24 March 2001
"DOTS: TB cure for all"
" IVe have heard Ministers agree that no one should be denied access to DO TS. This means that DOTS
should be available to all who need it, wherever they live, whether they are young or old, man or woman,
homeless or housed, jaded or free. "
Dr Gro Harlem Brundtland. Director-General. World Health Organization
Ministerial Conference on TB and Sustainable Development. Amsterdam. 24 March 200G
The theme for World TB Day 2001, ’’DOTS: TB cure for all”, calls for equitable access to TB services for
anyone who has TB, free from discrimination—rich or poor, man or woman, adult or child, imprisoned or
free, and including other vulnerable groups such as people with HIV or drug resistant TB TB cure for all
contributes to the fulfilment of everyone’s right to the enjoyment of the highest attainable standard of health
The tw o main objectives of this year's campaign are:t
1) To mobilize political leaders and decision-makers around the world about the situation of TB sufferers, the
implications of TB for human development, and the fact that there is no excuse for inaction in the face of an
available, cost-effective cure
2) To raise awareness that a cure for TB is available and that accessing and completing TB treatment, without
stigma and discrimination, is an important step in realizing one’s right to the highest attainable standard of
health and well-being.
The theme, ’’DOI'S: TB cure for all”, promotes the principles of the Amsterdam Declaration to Stop TB
Through the Declaration, countries committed themselves on World TB Day 2000 to expand DOTS coverage
with the goal of making DOTS accessible to all who need it. They noted "with grave concern that the
magnitude of the suffering and death caused by TB is both alarming and unacceptable". The Declaration
further states that:
• Access to life-saving tuberculosis control programmes providing safe, high-quality drugs opens doors
to life's opportunities by getting people back to work and school
• Effective treatment and cure of tuberculosis is one of the most tangible interventions available to extend
the life of persons with HIV/AIDS
’’DOTS: IB cure for all” reflects the important role of governments and the private sector in providing TB
drugs and services It points to the need for health services to be patient-centred and non-discriminatory. It
challenges DOTS providers to continue to reach out and adapt DOTS to the needs of their TB patients. It
highlights the crucial role of DOTS workers and the community in ensuring that the right to health for each
patient becomes a reality, even in remote communities and among minority populations. It is a call to civil
society to provide an environment that encourages everyone with TB to seek treatment and cure DOTS is
used here in its broadest sense as an umbrella term for all DOTS-based strategies, including DOTS plus for
multidrug-resistant TB and TB/HIV
Home.New Stop TB Movement
'
Paiie I of 1
Stop TB Hone
the Stop TB Snitiptive
vf.'z III-1 I tttr’r>e-'>n
'■ •
Jt.'r jui'.dmy,
Hi- M’lfi !'!l n
-4;for“artnership
lobal
Action
Latest updates
VJhat is Stop TB?
World TB Day - 24 March 2001
"Dots: TB cure for all"
A>)out TB
Working groups
Stop TB Pai'triers
vJ Vacancies
J
1 ■"-fife
Countries
World TB Day
GDF
My Story
Join Stop TB
Resources
Events
hosted b\ W
< II
|
5.4 j
I
ft' f
2
*
w
World TB Day 2001 "DOTS: TB cure for all"
Contact Us
calls for equitable access to TB services for
anyone who has TB, free from discrimination— Fl Site Map
rich or poor, man or woman, adult or child,
Search
imprisoned or free—and including other
vulnerable groups such as people with HIV or
MASSIV>
drug-resistant TB TB cure for all contributes
t0 the fulfilment of everyone’s right to the
enjoyment of the highest attainable standard of
health.
Click here to obtain the World TB Day Material
Pack online.
WTBD brief access
Pane 2 of 5
TB Treatment for All" was also the theme of a 2000 campaign (www.iuatld.org) launched by the
International Union Against TB and Lung Disease (IUATLD), inspired
inspired by
by Archbishop
Archbishop Desmond
Desmond Tutu
Tutu
Archbishop Tutu made a moving and passionate declaration to attract the world’s attention to the fact that
despite the existence of a powertul and inexpensive tool to combat the disease, fewer than 25% of TB
sutterers worldwide have access to affordable and effective treatment strategy.
Desmond Tutu spoke on behalf of tuberculosis patients everywhere urging that governments, the United
Nations and development agencies the world over, take this responsibility seriously and make TB treatment
and cure available to everybody who needs it to stop the TB epidemic. "Every person with TB has the right to
treiated:!Or h'S °r her diSeaSe- TB Can be cured this scourSe can be defeated. So let us stop denying them
this basic human right”.
'
J 6
Back to Home Page - Top of Page
/
To
S J Chancfer
367 Srinivasa Nilaya
Jakksacfra 1 main 1st dock
Koramangala Bangalore 560 034
Sub; invoking GPs inTB Control
Dear Chandai,
Th Jinks for the letter. As per your requirement I am sending the addess list of our iwmlxxs. .
You can select as per your specification I will be announcing the same in old CME pro^amme on 25th Feb
2001.
Thaniing you.
Yours truly
Dr Mohan
Hon Secretary- IAGP
613 2nd main first Stage
Indranagar Bangalore 560 038
dpanohaiig^vai^com
V
i
\
ngalore
MMT nOAO
B.E.L COLONA x
©
8AMJAVIMAGAR
i|6
HES8AL
/.iqUStrttyhgi/y
NX^'f
o
\\XjwathixereV " SACKIDANA «D
©
V4
VESHWAPJTPUR
GANSANAGAR
li GUTTAHALU jI
©
R.T. .'IAGAR
wan avt'iuti.!
"TWahalaksh?jhpura
sadashivaI
NAGAR
0
o
©
AS>!OXA
^JUMKURWOACJA*-
o
'W
NAGAR
Fk
j
o
I PALACE
GROUi JDS y
.1 if •
k***i»4
BASAVESW AHA NAGAR
SRIRAMPURi
8HIVA
NAGAR
.
///8HIVAJI
y .. i NAGAR
INDIRA
iiooon ?•'•>
“ ™ "XX
KEMPfjpunA AC
SOWIESHWARAPI RA
CHOW -URPALYA
©
VUAV
AUSTIN
TOWN
(D
'■’''wi xoac
©
o
ARANQAN GUDOA
8Ai\lAS HAl'JICAR
J »YA NAGAR
(D
gte
. -NASAR.
"0A0
L.
IJ
m*4G no ac
f!#
t
Ind. J. Tub., 1995, 42, 101
Original Article
PERFORMANCE OF NATIONAL TUBERCULOSIS
PROGRAMME IN 1993: AN APPRAISAL*
///
L. Suryanarayana1, K. Veinbu2, R. Rajalakshmi’ and C. Satyanarayana'
fSummary : National Tuberculosis Institute^
5
•V3N’H
!•
; ‘MHr.KS
H
i
31
(NTI), Bangalore has been monitoring the
National Tuberculosis Programme (NTP)
since 1978. District Tuberculosis
Programmes (DTPs) numbering 390
registered by Directorate General ot Health
Services (DGHS), are covered under such
monitoring. The percentage of DTPs
implemented accounts for 81% ot the total
districts and 64% of such DTPs have been
covered under Short Course Chemotherapy
(SCC). As far as Peripheral Health
Institutions (PHIs) are concerned, 56% of
the available health institutions (His) have
been implemented. Reporting efficiencies
of the DTPs and the PHIs are 78% and
70%-respectively. Only 41% of the PHIs
have been supervised by the respective
District Tuberculosis Centres (DTCs) (i.e.,
at least once in a quarter). The smear
positivity rates are 12.3% and 4.8% at
DTCs and PHIs respectively. As far as
case detection efficiency of smear positive
cases is concerned, DTCs have achieved an
efficiency of 71%,and PHIs 36%. Quality
of X-ray reading and smear microscopy,
as reflected by smear confirmation rates,
among the pulmonary cases diagnosed are
20% and 24% respectively. Treatment
completion rates derived from the annual
cohort analysis reports are 34% for standard
regimens, 44% for SCC Regimen A and
52% for Regimen B. Out of the 276 DICs
reporting on the availability of trained
man-power and equipment, trained District
Tuberculosis Officers (DTOs) are posted
in 56%, X-ray Technicians in 60%,
Laboratory Technicians in 73%, rI reatment
^Organisers in 73% and Statistical Assistants^/
/in 46% of the DTCs. Only in 15% of the^
DTCs is there a full complement of trained
staff. As far as equipment is concerned, Xray equipment Is available in 84%,
microscopes in 96% and vehicles in 76%
of the DTCs. Achievements in all aspects
fall short of the expectations in fulfilling
the objectives set for NTP; therefore,
concerned • authorities have to take
appropriate remedial measures to achieve
the goal of NTP.
Introduction
NTI has been monitoring (he NTP since
1978. Monitoring is a continuous assessment of
certain key indicators of the programme through
periodic reports. Repons contain information on
case-finding and treatment activities and oilier
related aspects. The reporting under NTP involves
two tiers: the first tier is the Pills which report
to DTC and the second tier is the DTCs which
reports to the state and national levels. Reports
received al the Nd I are analysed in respect of
some key indicators developed as a result of
operational studies carried out al die NTI. The
results of the analysis are communicated to die
concerned disiricts/statcs for taking necessary
corrective actions.
Objective
This paper appraises the performance of
NTP in terms of implementation, reporting,
supervision, performance of case-finding and
treatment activities and availability of trained
manpower and equipment, for the year 1993.
• Paper presented at 49th National Conference on Tuberculosis and Chest Diseases. Pondicherry. 6-9 October. 1994
I. Chief Medical Officer. 2. Statistician. 3. Statistical Assistant.
National Tuberculosis Institute. No. X. Bellars Road. Bangalore 560003
Correspondence : Dr. C. Suryanarayana. Chief Medical Ollicer
NTI. No. 8 Bcllary Road. Banvalore 560 003
■
•
...
id
SURYANARAYANAET AL
102
positive cases
community*
Material & Methods
Four quarterly DTP Reports on case-finding
and treatment activities and Annual DTP Reports
on cohort analysis of the treatment results for the
prescribed cohort periods emanating from the
different DTPS constitute the material for this
paper. Reports received at NTI have been
scrutinised and consolidated state wise and on All
India basis. Incomplete and/or grossly incorrect
reports have been excluded from the analysis. In
all 1194 Quarterly Reports out of 1223 received
(1560 expected) have been considered for assessing
die case-finding activity. For the determination
of die treatment outcome, only 152 out ot 5/«
Annual Reports expected for Standard Regimen
(SR) for the cohort period July 1990 to June
1991,and 94 out of 234 reports expected from
SCC-DTPs (cohort period Jan-Dec 91) have been
considered. Data arc presented for DTC and PHIs
(iv)
Smear positivity irates, out of total spurn
examined are expectedt to be as follows:
Al DTC : 18%3
Al PHI : 8%
The above figures3 of expectations (based
of reasonably good performing
on achievements c. -D I'Ps) arc lower than the potential arrived at in
die operational studies conducted at NTI4-5.
Smear Confirmation of Pulmonary Cases
C.
i)
Expectations for the above indicators are
arrived at on the basis of :
(i)
(ii)
Population aged1 5 and above as per
mid 1993
1 — estimated population,
implenufH
of snidtfr
r<
"vsA
D * v^s will
the noiuc
sanciinrvd
stipuLmuDTPs inn
regisierd
fulfill ’He
enables T
Centra* f
cquipmrnl
Radiognp
in the
adininHU*.
they arep
chest chin
that all de.
under thi:
tubcrculoi
NTI4.
Case - finding
Sputum examinations, and
Detection of smear positive cases.
•Arfi
distric's-^
1991
Only ift’o
80% mrcspcd
48% of t
terriv'.^'
district
implonWf
the basis of 8rX« smear positivity rate.
The expectation is that 35% of pulmon^
cases deiccteu
detected arc
are smvcu
smear positive3 which is less
dian 55% potential as per studies conducted at
terms of
1)
It is
is expected
expected that
dial in
It
in an average district
....................
:
j
o
f
1.8
million,
DTC detects
with a population c.
500 smear positive cases per year @ 18% of die
conducted
total number of sputum (examinations
---------and PHls detect 2,0()6 smear positive cases on
Supervision
Efficiency of case-finding is measured in
II
(i)
(ii)
(d)
DTC is K)0%.
<1
patiedf-1
of tr(<yai<
trcathffii
liewtyt'iT/
Sputum Smear Positivity Rate
(c)
^T.
'(‘da
Achievements of a reasonably good
performing DTP in the country.
(v)
The expectation in respect of implementation,
reporting by DTCs to higher levels, and by
PHIs to DTCs and supervision of PHIs by
r
ii)
Coverage of PHIs under DTP and
Implementation, Reporting efficiency &
(a)
(b)
above
com pF.
>75% of
the
patients2.
Efficiency of a DTI’ is assessed by comparing
its achievements with the expectations. Expectations
from various activities are as follows :
B.
in
52% action taking by the tuberculosis
(iii)
separately, representing the average pcrtormance
of each district in a State for 17 big States and
collectively for 8 small Slates and 5 Union
Territories (as si. no. 18) in each Table.
A.
of 0.4%
Treatment outcome
Treatment Completion Rate
Standard Regimen (SR): Expectation here
is determined by percentage of patients making/
completing 12 or more drug collections/
consumptions over the treatment period of 18
months and is 100%.
Short Course Chemotherapy (SCC) :
.....................
Expectation is determined by the percentage of
ptients completing 75% and above of
expected
druo collcctions/consumptions and is 100 /o Hus
is based on the fact dial cure rate of 85 /o and
Prevalence rate of bacteriologically
? €: •
1I
'il
Ii
c
To in
the
•^bjculosis
and
good
country-
PERFORMANCE OF NATIONAL TUBERCULOSIS PROGRAMME
above can be achieved only when all the patients
comply with the collcction/consumption of
>75% of the expected drug collections6.
I11
il
ii)
1
II
Cure rate
Cure rate is percentage of smear positive
patients converting to negative status at the end
of treatment period out of those initiated on
treatment. Expected cure rate is > 85% among
newly diagnosed patients according to the WHO
Guidelines7.
sputa
■I
103
Out of 390 implemented DTPs, (64.6%)
252 DTPs have been covered under SCO. Only
Gujarat has die distinction of covering 100% of
the districts under SCC. Only 5 States (including
Gujarat) have covered 80% or more of the DTPs
under SCC. Four States have implemented less
dian 50% and Bihar accounts for die lowest
percentage of 19. Small States/Uls have a
coverage of 77% of DTPs under SCC.
Here, it is suggested dial emphasis should
be on consolidating the gains of SCC in the
entirety of the implemented districts instead of
extending it piecemeal to new districts (DlPs).
OBSERVATIONS & DISCUSSION
Implementation of Bills
2)
I
TUt'rtgc district
jrre detects
1)
Il
Al national level, 390 DTPs out of 480
districts (81.2%) in different States/UTs (as per
1991 census) have been registered by DGHS.
Only 12 out of 17 big Stales have implemented
80% or more of the districts available in the
respective States. Assam has implemented only
48% of the districts. Small States & Union
territories pul together have only 45% ol the
districts implemented. No new I)IPs were
implemented during 1993.
of the
p.frv; conducted
cases on
u-inVi-.
- ^ipns (based
A^ipcrfonning
t miP^ri70^ al in
~ sdau NT I ■
^♦nary Cases
"
nulmonary
.ch is less
conduGtcd at
}:1 Expectation here
^■patients making/
collections/
w!|t period of 18
^I.rapy (SCC) ■
b,A).»e percentage ol
;?.,ye of the expected
wand is 1<X)%. This
,C; rate of 85% and
--------
Implementation ot I) IPs (I able 1)
IIII
I
1I
Some Slates have reorganised the originally
implemented districts (D TPs) into varying number
of smaller districts for administrative and other
reasons. Certain Stales have created additional
DTCs within the existing DTPS. It has come to
the notice of the Nil that certain States have
sanctioncd/crcaied splinter DlPs without the
stipulated infrastructure. 1 his needs to be avoided.
DTPs functioning in such districts may gel
registered by DGHS in course ol time, after they
fulfill the prerequisites. Registration by DGHs
enables the DIPS to gel assistance from the
Central Government such as vehicles. X-ray
equipment. 50%’ ot the drugs and Mass Miniature
Radiography (MMR) film rolls. Ninety districts
in the country remain unimplcmcntcd due to
administrative and financial constraints, though
they are providing tuberculosis services through
chest clinics or in some other form. It is essential
that all the districts in the country arc implemented
under the programme to have lull coverage ot
t ubereu losis scrv ices.
It is expected that there should be one
Primary Health. Centre (PHC) for a population
of 30,000 in plain areas and 20,000 in hilly areas.
The expected number of PHIs in the country
works out to 29,794 but there arc about 29,500
health institutions (His) of various categories
available for implementation. Out ol these, otdy
16,830 i.e. 56% of die His, have been implemented
under the programme. Only lour Slates have 80%
or more of the His implemented under D TP. Four
other States have achievement of less than 50%
in this respect. Small States & UTs have a
coverage of 56%. Among the DI Ps covered
under SCC, the coverage of PHIs under SCC is
47%- at all India level (not given in Table).
Since the His situated mostly in rural areas
cater to large proportion ol population in the
country, the stress should be on implementing all
of them under DIP, in general. In case ot Dlls
covered under SCC, all Pills should be brought
under SCC, before extending the SCC to other
DlPs.
a:
Reporting by I)IPs (lable 2)
At national level, 78% efhcicncy of reporting
overall.
Only 10 big States and all. Small
is
States and UTs pul together have a reporting
efficiency of > 80%. Bihar has less than 50%
efficiency.
Reporting is a prerequisite for cl fee live
monitoring ot the programme. Hence, il is
so?
■
SURYANARAYANA ETAL
104
Table 1 : Implementation of. DTPs
%
No.
%
3
4
5
6
7
23
23
100
19
83
59
48
8
73
41
23
11
19
15
51
63
6
Bihar
32
19
100
19
100
89
Gujarat
19
11
69
3
Haryana
16
12
11
92
6
Jammu & Kashmir
14
10
71
Karnataka
20
20
1
2
Andhra Pradesh
Assam
2.
3.
4.
5.
7.
8.
10.
11.
12.
13.
14.
15.
16.
17.
•i 1i
I
18.
Si:l
1.
Ai4-
2.
A^u
BU
58
5.
rice
55
224
6.
rm
70
44
7.
7
Jan
14
70
Ill
8.
Kn
100
55
14
7
■Kxr
86
58
9.
12
80
S3
45
100
36
Madhya Pradesh
45
100
26
87
Maharashtra
30
75
30
13
100
8
62
63
13
100
4
33
56
12
12
96
10
37
53
Orissa
Punjab
10.
■
■
11.
Mj
12.
Or
13.
Hi
-
Ra
Rajasthan
28
27
88
Tn
Tamil Nadu
73
14
15.
16
77
22
54
30
Ut
63
89
30
16.
56
94
11
69
36
17
16
26
45
20
77
56
Uttar Pradesh
West Bengal
Small States
and UTs
INDIA
58
17.
18.
A
IN
■
480
390
81
248 @
64
56
'
■ \-
@ Excludes 4 districts monitored by TRC. Madras
,7; 1 sl_.
'
1/
in
1
U1P
Go
Kerala
9.
SI
No
4.
Himachal Pradesh
6.
a-
Pills
imple
mented
No.
No
1.
% of
DTPS under
SCC
Functioning
DTPS
No. of
dis
tricts
States/
UTs
SI
1
PHIs and introduction of SCC according to Slates - 1993
......
* •
■
1
I
performance of national tuberculosis programme
lies - 1993
Table 2. Position oj Reporting <6 Supervision in DTPs
I
% Of
Pills
imple
mented
SI
No
8
1
i
States/
UTs
105
according to States-1993
Quarterly DTP Reports
Received
%
Pills
Reported
%
3
4
5
6
7
92
81
88
86
43
44
41
93
57
28
128
56
44
37
17
Expected
2
Pills
Supervised
%
1.
Andhra Pradesh
2.
Assam
'S
3.
Bihar
89
4.
Gujarat
76
73
96
5.
97
58
I laryana
47
44
37
84
84
Himachal Pradesh
36
44
27
61
50
23
40
24
60
68
29
68
85
77
59
48
36
75
46
18
180
129
72
57
16
120
92
77
87
69
52
49
94
81
34
31
59
41
224
> I
I
6.
7.
Jammu & Kashmir
8.
Karnataka
55
9.
Kerala
S3
10.
Madhya Pradesh
75
11.
Maharashtra
63
12.
Orissa
13.
Punjab
48
43
90
14.
62
Rajasthan
108
88
81
52
36
64
63
98
62
39
196
88
67
42
35
55
22
14
104
85
82
66
44
1560
1223
78
70
41
44
111
56
53
77
I
30
36
56
56
I
}
I
II
II
1
.i:
80
15.
Tamil Nadu
16.
Uttar Pradesh
224
17.
West Bengal
64
18.
Small Stales & UTs
INDIA
i
4
!'
I
4“
ti
SURYANA.RAYANA ET AL
106
expected drat all die implemented DTPs submit
dieir quarterly and odicr reports to die Central
and State audioritics in time. As such, States have
to achieve die desired expectation of 100%.
About 3% of die reports received from Dlls
could not be considered for analysis due to large
number of discrepancies and inconsistencies.
Shortcomings in reporting, in terms of quantity
and quality are attributable to lack of trained
Statistical Assistants in DTPs. Also, rcmtmlers/
feed-back reports sent by NTI to die DTPs do
not seem to have been token note of by State/
throughout the district. Reasons for the low
performance in this regard are: i) non-avarlabihty
of trained personnel in the DTC, ii) non-availability
of vehicle, iii) diversion of available vehicle to
other programmes, iv) inadequate provision of
budget for vehicle and travel expenses and v)
lackof motivation of concerned staff even thoug i
facilities are available. Suite authorities have to
take appropriate measures to overcome die above
deficiencies.
Reporting by PH Is (Table 2)
-At DTCs
Bihar and West Bengal.
1;
Shortfall in diis regard is mainly due to
inadequate supervision of PHIs by the personnel
of Hie DTCs and higher dstncl level oilicers.
Medical Officers of PHIs need to be sintably
motivated by district level officers in despatch
of mondily reports to DTCs regularly and m tune.
Takino into account the efficiency of
reporting by DTPs (78%) and PHIs within them
(70%), die overall picture is truncated, rcllectmg
only 55% of die: expected reports from all the
DTPs in die
llic country. Steps are to be
I-- taken
------ by
the administrative authorities at S.
State/UI
—- - level
l0 improve thp.
the nerformance
performance inin (his
this respect.
respect.
5)
At D I
spu .1 pos
Andhra IYr
15.0% spin
sputum pos
15.0%. Six
could attaii
5.8% to 91
Efficiency of Case-finding
At all India level, only 70% of the PHIs
have reported to their respective DTCs compared
With the expectation of 100%. Only five b.g
States have achieved an efficiency of >80 A m
this respect. Reporting by PHIs is particularly
poor (less dian 50%) in three States viz... Kerala,
H
Achievemtf
(Tables 3 .
PERFORMANCE OF NIP
District authorities.
4)
should be x
observed sh
of Laboraw
of the Pin*
2.5% of 51
symptom aM
most of lift
case deteci
Supervision (Table 2)
• i 41% of the Pills
At national level, only
..J
\
j
the
have been supervised by t.-~ DTC staff al least
Maharashtra (69%) and
once in a quarter. Only
I
achieved efficiency of
Karnataka (59%) have
States
could not achieve
more than 50%. Seven
even 30% efficiency oni this score. Supervision
Pills by the key personnel ol the ^1^’
programme to ensure mamtenanee of work
standards, replenishment oi supplies and equipment
At national level, diough die efficiency of
sputum examinations is more dian 100% (not
shown in Table), die efficiency of case detection
'(sputum positive cases) is of die order of 71%
only. Four States and all small States and IT s
put together have achieved more dian 100 A
efficiency. Eight other States have achieved more
dian 50% efficiency and five States could achieve
only less than 50% efficiency. The performance
of Bihar is die lowest (15%), closely followed
by West Bengal (21%). Since trained personnel
are expected to be available at DTCs, perfomiancc
of 71% case detection is inadequate. Suitab e
remedial measures need to be taken by concerned
At
4.8%. Only
more than
positivity n
have attaim
pcrformanc
ranges fror
Expcc
positivity T
all 'car x
she > achi
average of
is quite di:
State authorities.
At PH Is (Table 4)
Al all India level, the efficiency of sputum
examinations is 61%. While Maharashtra and
Small States and UTs could achieve more than
80% efficiency, the performance ot all odier
States is not satisfactory. Eleven out of 17 States
could achieve efficiency of less than 50%
[performance of West Bengal (10%), Assam
(15%) and Bihar (18%) being very poor]. As
regards detection of sputum positive cases, die
alf India average is only 36%. Only two big
States (Gujarat & Maharashtra) have achieved
more than 50% efficiency. The performance of
14 Slates is even below 30% efficiency.
The
achieving tl
for strengtl
DTC and
supervision
providing
Technician;
ensuring si
stains. Mic
in proper *
Smear Co
pulmonary
It is relevant io point out that all the
eligible chest sympiomalics attending the PI Us
Tabic
■'
•
•
PEKI-ORMANCE OF NATIONAL TUBERCULOSIS PROGRAMME
)r the low
-availability
ravailability
• vehicle to
jrovision of
ises and v)
even though
tics have to
ic the above
j
should be subjected to smear examination. The
observed shortcomings arc due to non-availability
of Laboratory Tcchnicians/Microscopists in most
of the PHIs. Generally, it is expected dial about
2.5% of die new outpatients would be chest
symptomatics. Vast improvement is needed in
most of die Stales to step up die efficiency of
case detection, both at DTC & PHI levels.
I
efficiency of
i 100% (not
asc detection
>rdcr of 71%
ties and UTs
dum 100%
chicvcd more
could achieve
performance
scly followed
icd personnel
;, perfonmmce
date. Suitable
by concerned
ncy of sputum
iharashtra and
eve more than
i of all oilier
ml of 17 States
jss titan 50%
(10%), Assam
very poor]. As
ilive cases, the
Only lwo big
have achieved
performance of
tfficicncy.
Achievement of Sputum Positivity Rates
(Tables 3 & 4)
At DEC level, only Maliaraslitra has achieved
sputum positivity rate of about 20.7%. Gujarat,
Andhra Pradesh and Rajasthan have more than
15.0% sputum positivity. Seven other Stales have
sputum positivity rate in the range, of 10.0%15.0%. Six big States and small States and UTs
could attain smear positivity rale in the ram’e of
5.8% to 9.8%.
■
At PHI level, the national average is only
4.8%. Oidy West Bengal & Gujarat have achieved
more than die expectation of 8.0% sputum
positivity rate. Karnataka, Maharashtra and Punjab
have attained > 5.0% sputum positivity rale. The
performance of ad other Stales and UTs which
ranges from 1.9% to 4.6% is not satisfactory.
Expecting that DTCs should achieve 18%
positivity in detection of smear positives among
all smear examinations carried out, while Pills
should achieve al least 8% positivity, the all India
average of 12.3% for DTCs and 4.8% for Pills
is quite discouraging.
I
I
The poor performance by the States in
achieving the desired sputum positivity rales calls
lor strengthening of laboratory sendees, both at
DIC and PHIs. And proper and adequate
supervision by DTOs. This could be achieved by
providing adequately trained Laboratory
Technicians both al DTC and PHI levels and
ensuring supply of good quality chemicals and
stains. Microscopes also need to be maintained
in proper working condition.
Smear Confirmation among all
pulmonary cases
ul that all the
aiding the PHIs
I able 5 gives percentages of sputum positive
4'
■■■■■
V.
107
eases confirmed among pulmonary cases, (smear
positive and X-ray suspects), both at DTC and
Pills.
It may be observed dial die confirmation
rate is only 20% in die case of DTCs and 24%
in respect of PHIs, at national level. It is expected
dial diis rate should be about 30-35% (as in a
reasonably good performing DTP) at DTC level.
This confinnation rate is more relevant in
DTCs where ease-finding is based upon
MMR screening followed by smear examination.
In the ease of PHIs, the diagnosis is by
smear examination preceded by symptom
screening.
At D1C level, only the performance of
Andhra Pradesh, Karnataka, Maharashtra and
Orissa could he considered as satisfactory. Five
other big States have achieved confirmation rale
in the range ol 20-29%. The performance of
Assam and Bihar is very poor (i.c. below ten
percent).
At PHI level, three States - Andhra Pradesh,
Orissa and Maharashtra have achieved >35%
confirmation rate. Six other big and all small
States mid UTs have attained 20-29% confirmation
rale, while all oilier States are below dial level.
The performance of Bihar and Himachal Pradesh
is very poor.
Bacillary confirmation rate of pulmonary
cases rellects the quality of X-ray reading by
Medical Officers. Confirmation rate around
35% could lie considered as reasonably good,
while rates below 35% indicate over-reading
of X-rays, assuming that the quality of laboratory
services is of reasonably good standard. In
such cases, quality of X-ray reading by Medical
Officers needs to be reviewed. The NTP aims
at detection and treatment of smear positive
cases on priority basis in order to cut the chain
of transmission of the disease. But, in reality,
it is the X-ray cases (smear negative but Xray positive) which outnuml>er the smear
positive cases by about 3*/2 times. T his causes
wastage of scarce resources as all may not be
tuberculosis cases.
SURYANARAYANA ET AL
108
District) according to Stales-1993
Table 3. Case-finding in DTCs (Average per
SI
States/
No. UTs
2
1
k
L
5
4
ij
r.
ft
1.
Andhra Pradesh
2.
Assam
3.
Bihar
4.
Gujarat
5.
Haryana
6.
Himachal Pradesh
7.
Jammu & Kashmir
8.
Karnataka
9.
Kerala
10.
Madhya Pradesh
n.
Maharashtra
12.
Orissa
13.
Punjab
14.
Rajasthan
15.
Tamil Nadu
16.
Uttar Pradesh
17.
West Bengal
18.
Small States & UTs
INDIA
New sputa
examined
(No)
+ve
cases
found
Positivity
rale
(%)
Expected
sputum
+ve cases
Effi
ciency
%
4
5
6
7
3
581
16.3
812
72
3558
96
7.4
274
35
71
6.9
476
15
711
17.4
610
117
493
289
171
4743
10.4
5.8
121
107
2207
129
91
9.8
155
59
270
11.9
631
43
273
10.4
583
47
243
14.3
413
59
804
20.7
739
109
387
684
57
2931
13.2
13.0
474
65
2356
307
298
15.7
441
68
393
6.7
713
55
620
54
335
9.8
1124
21
231
13.9
89
194
173
8.0
12.3
495
71
1293
1036
4077
925
2278
2627
1703
3889
1897
5882
3435
1657
2151
2851
350
SI. StarisZ.
No Ull^!
1
2
1.
A'dh
2.
3.
Bfcu
4.
Gmi
5.
Hirr.
6.
Him
7.
Jam;
8.
Kan
9.
Kex7
10.
M$'
11.
Mdt
12.
Ori<
U.
Pun
14.
Raji
15.
Tmi
16.
17.
18.
Snr
& ’
INI
PERFORMANCE OF NATIONAL TUBERCULOSIS PROGRAMME
109
Table 4. Efficiency of sputum examinations & sputum positive cases diagnosed in PHIs
according to States-1993
Effi
ciency
%
New sputa examined
SI. States/
No UTs
7
Sputum + ve cases diagnosed
Sputum
positi
vity
rate
%
Expec
ted
Perfor
mance
Effi
ciency
Expec
ted
%
Perfor
mance
Effi
ciency
%
3
4
5
6
7
8
9
72
1
2
1.
Andhra Pradesh
23950
8705
36
1916
397
21
4.6
117
2.
Assam
6838
995
15
547
26
5
2.6
171
3.
Bihar
11888
2125
18
951
42
4
2.0
4.
Gujarat
27162
14229
52
2173
1193
55
8.4
5.
I laryana
8375
4881
58
670
181
27
3.7
6.
Himachal Pradesh
6050
1608
27
484
30
6
1.9
j
7.
Jammu &. Kashmir
3875
1133
29
310
35
11
3.1
'■'i
8.
Karnataka
31575
8372
27
2526
528
21
6.3
9.
Kerala
16050
4226
26
1284
112
9
2.7
10.
Madhya Pradesh
17125
4194
24
1370
124
9
3.0
11.
Maharashtra
27700
23226
84
2216
1346
61
5.8
12.
Orissa
21538
10265
48
1723
361
21
3.5
13.
Punjab
13288
9653
73
1063
484
46
5.0
14.
Rajasthan
11688
2705
23
935
111
12
4.1
15.
Tamil Nadu
27450
18641
68
2196
562
26
3.0
16.
Uttar Pradesh
15500
9966
64
1240
351
28
3.5
17.
West Bengal
28112
2744
10
2249
262
12
9.5
18.
Small States
& UTs
3342
• 3588
107
267
117
44
3.3
INDIA
13862
8416
61
1109
404
36
4.8
35
I
15
107
59
43
47
59
57
i
65
I
109
68
55
54
21
194
71
I
I
i
I
1
i
IL
SET?'
p;.'-
.4
SURYANARAYANA CT AL
110
Table 5.
and PH Is according to States-1993
Cob
PHIS
DTC
|?S
SI
No
States/
UTs
I
2
L
r
I
4
4'
I
4'- '
4
refe
a gi
of
Pulmonary
cases
Sputum
+vc
%
Pulmonary
cases
Sputum
+ve
%
3
4
5
6
7
8
30
1087
397
37
1.
Andhra Pradesh
1918
581
1088
96
260
26
10
2.
Assam
9
yea
bee
arc
71
6
42
8
a)
3.
1098
538
Bihar
711
28
5061
1193
24
Gujarat
2546
832
181
22
Haryana
493
28
5.
1786
783
129
436
30
7
Himachal Pradesh
16
6.
341
91
241
35
15
Jammu &. Kashmir
27
7.
270
33
528
25
8.
826
2148
Karnataka
1530
273
698
112
16
Kerala
18
9.
1306
243
589
124
21
Madhya Pradesh
19
10.
Maharashtra
804
30
3886
35
11.
2670
1346
387
34
361
37
12.
1136
986
Orissa
1687
484
29
Punjab
307
25
13.
1244
1177
298
25
111
22
Rajasthan
506
14.
393
19
562
15
15.
2057
3852
Tamil Nadu
335
12
351
19
16.
2802
1808
Uttar Pradesh
2375
262
11
West Bengal
231
15
17.
1504
173
106
22
919
484
Small Slates & UTs
19
18.
1711
350
20
1704
404 ■
24
INDIA
4.
XT
TRI
Confmnation of sputum positive cases among pulmonary cases in DTCs
b)
(a)
Re
coi
anof
ref
co
av
pa
sc';
tie
co
m
fa
cc
sa
P«
tn
4
4(
lc
tc
• t
1
!
PERFORMANCE OF NATIONAL TUBERCULOSIS PROGRAMME
!
I
nCs
TREATMENT OUTCOME
iI
%
Cohort Periods
Analysis of treatment outcome is done with
reference to smear positive patients diagnosed in
a given cohort period which is fixed on the basis
of optimum treatment period.
8
0
In diis paper, die Annual Reports for the
year 1992, received from DTPs during 1993 have
been considered. The prescribed cohort periods
arc as under:
8
a)
For standard regimens, for which the optimum
treatment period is 18 months, the cohort
period considered is 1.7.1990 to 30.6.1991,
as the patients diagnosed during this period
were expected to complete optimum
treatment period in the course of 1992.
b)
For SCC, die cohort period is from 1.1.1991
to 31.12.1991. Patients diagnosed and pul
on treatment during this period were expected
to complete die treatment latest by December
1992.
(a)
Standard Regimens (Table 6)
37
24
22
7
15
i
25
16
I
21
6
35
1
37
4
29
1
22
2
15
1
19
,2
11
•>6
22
)4
24
a
I
!
I
I
■;!
I
.
I
I
IL.
-..
.
For die . year 1992, out of 378 Annual
Reports expected, (from DTPs relevant for the
cohort period), 247 Reports (65.3%) were received
and 152 of diem (61.5% of received and 40.2%
of expected) were analysed. Based on die analysed
reports, out of 81,180 patients included in the
cohort, treatment cards* of 74,210 patients were
available for analysis at the DTPs and 72,075
patients were initiated on treatment. It could be
seen diat only 34% of patients initiated on
treatment could make 12 or more monthly
collections of drugs. As patients making 12 or
more collections/consumptions are likely to have
favourable outcome in terms of bacteriological
conversion and hence deemed to have completed
satisfactory level of treatment, only 34% of the
patients could be considered to have completed
treatment. Completion rate is above 50% only in
4 States, between 40-49% in 4 States and below
40% in other States. The completion rate is the
lowest in West Bengal. It has not been possible
to work out cure rates due to non-availability of
111
results of final follow-up smear examinations for
most of die eases.
Cure rate is the best mediod for analysing
treatment outcome. It is determined by percentage
of patients becoming smear negative at die end
of the -treatment period out of those initiated on
treatment. Availability of final follow-up results
of smear examinations of all the patients initiated
on treatment is a prerequisite to arrive at cure
rates. Most of the DTPs do not subject die
patients to final follow-up of smear examinations.
In the absence of such data the next allcmativebut less reliable indicator - i.c. treatment completion
rate, has been considered. As die treatment
completion rale is very low, it is necessary that
case-holding is improved considerably by all
Medical Officers and Treatment Organisers
■concerned.
Il should be ensured that all cases diagnosed
arc effectively treated for the full period so that
the chain of transmission of disease by die smear
positive patients can be checked to a great extent.
Il is mandatory to subject patients to final follow
up smear examination and results recorded on the
treatment card which will facilitate calculation of
cure rates.
(b)
SCC Regimen ('fable 6)
A total of 119 Annual Reports were received
against 234 reports expected for the year. Out
of diese, only 94 (79% of received and 40.2%
of expected) reports were analysed.
As per die analysis, 2055 patients put on
Regimen A (2 S2H2R2Z2/4 II2R2) and 35,097
patients put on Regimen* B (2 EIIRZ/6 TH or
6 EH) were considered for analysis. It is observed
dial only 44% of the patients put on Regimen
A and 51.8% of the patients put on Regimen B
had collected > 75% of the doscs/collections
expected.
The completion rate is above 50% only in
2 big and one small State for Regimen A.
Number of patients put on Regimen A is too
small in many of die States reported.
As regards Regimen B, the completion nite
rr
••
/
SURYANARAYANA ET AL
112
SCC Regimen
SR Regimen
States/
UTs
SI
No
2
1
Andhra Pradesh
1.
3
i-
1
»•
I
5
6
7
8
9
10
391
47
4380
46
0
378
44
8732
56
20
10296
33
13
42
6
cost el
impact
of 55?.
which’
getting
of one
lias hi
shoukl
smean'
of cafci*
made j
patieiti
and •ct
Assam
7
Bihar
3
308
36
0
3.
Gujarat
14
14729
25
12
56
4.
28
1
0
5.
1388
32
3
25
Haryana
52
2
0
6.
84
19
1
68
Himachal Pradesh
78
47
0
78
1
155
Jammu & Kashmir
1
7.
22
11
911
1291
8.
6223
40
14
53
Karnataka
40
5
33
1849
9.
789
28
4
6
Kerala
52
2
25
40
258
47
11869
56
36
10.
Madhya Pradesh
10
4283
Maharashtra
8
3723
63
9
0
11.
40
4
29
1201
12.
5084
40
10
140
Orissa
53
3
63
738
13.
3696
59
7
19
Punjab
25
2
40
60
14.
5558
308
13
0
Rajasthan
415
33
46
Tamil Nadu
28
7
15.
1541
1596
6
36
4
23
44
16.
11267
351
15
9
Uttar Pradesh
14
29
1361
61
57
18.
2
1363
14
3
9
67
537
14
39
15
Small States
& UTs
885
72075
34
94
2055
44
35097
INDIA
152
West Bengal
* Cohort jx'riod: SR:
1st July 90 to 30th June 91
SCC: Year 1991
the ii
re-ew
both
2.
17.
ft
4
3
780
’•r
(
Regimen B
Regimen A
Comple
Reports
ted
analysed Inilia- Comple- Initia- Comple
12+
ted
ted
ted
ted
collec%
%
tions
%
Initia
ted
Reports
analyed
is a lx;
States?
40 to-*
comfit
that v
5.5^)
Regiir
of tl*i*
SR and SCC regimes according to States-1993
Table 6. Treatment completion* on
n
examii
complt
"'an be
.c tree
all car
to moi
out tht
Greater
tasks a
prognu
1
■ ‘"P
? W- of trairT
52
DTC a
■?. ?•’ observe
reporte*
ftT DTCs
comple
■ft-:
. •
Availa
& equ
T
I
1
I
PERFORMANCE OF NATIONAL TUBERCULOSIS PROGRAMME
is above 50% in six big States besides all small
States and UTs. The percentage varies between
40 to 49 in 7 States. Three States have achieved
completion rate less dian 40%. It could be seen
that only 2,055 patients out of 37,152 (i.e.
5.5%) have been put on intermittent SCC
Regimen A. This indicates the poor acceptability
of this regimen. Retention of this regimen in
the chemotherapy policy needs to be
re-examined.
993
i
£n B
Comple
ted
%
I
10
I he completion rate of 51.3% in respect of
both Regimen A and Regimen B put together is
neither commensurate with the effort put in nor
cost effective. This is not likely to have an
impact, on die epidemiological situation by way
of 5% reduction in Annual Risk of Infection,
which is defined as the proportion of population
getting infected with M. tuberculosis over a period
of one year. To achieve this reduction rate, it
has been suggested dial countries like India
should first achieve 85% cure rale among all the
smear positive patients before enlarging the scope
of case-finding activity further. Efforts should be
made to improve the treatment compliance by
patients to achieve a higher rale of completion
and consequent higher cure rate.
44
56
1
32
*
19
S
78
1
40
9
28
;s
47
59
56
•)1
9
38
59
■08
60
>96
46
553
44
361
61
537
57
!
III
I
II
5I
i
V-
M197
52
I
1
if
I
........
It would also be useful if follow-up
examinations are conducted for all patients
completing treatment period so that the cure rate
can be worked out to assess die real impact of
die treatment activity. The Medical Officers and
all concerned para-medical staff have not only
to motivate die patients suitably but also carry
out die work as prescribed in DTP Manuals.
Greater awareness and better devotion to the
tasks assigned, by all personnel involved in the
prognunmc, would help in achieving belter results.
It is pertinent to note dial only 127 (46%)
out of 276 DTCs had trained Statistical Assistants
(SAs). This would reflect both on die quality and
die number of reports received. Only 73% of the
reported DTPs had trained Laboratory Technicians
(LTs) and Treatment Organisers (TOs) which
would affect adversely die quality of case-finding
and case-holding activities.
Non-availability of trained key personnel at
DICs is due to : i) posts not being sanctioned
by Slate Governments, ii) sanctioned posts
remaining vacant, iii) lack of budget to depute
key personnel for training, iv) diversion of
trained staff to odier schemes/programmes.
The Slate Governments concerned have to
ensure that all key personnel tire trained in the
DTP and those trained are deployed in the
programme, avoiding diversion outside the DTP.
Il may also be seen that some of the D'fPs
have not reported the information on the availability
of trained manpower and equipment. It is observed
dial out of those reported, vehicles and X-ray
equipment are not available in some D'fPs. It has
also come to notice that allotted vehicles are
diverted to other purposes not connected with TB
Programme. It is also observed that adequate
budget for petrol and oil expenses, repair and
maintenance is not allotted which affects the
supervision and maintenance of die programme.
It is essential that the equipment is maintained
in good condition so dial the overall efficiency
of die programme docs not suffer.
Conclusions
a)
Measures are to be taken to implement all
the districts in die country under District
Tuberculosis Programme (Dl'P) and all the
health institutions available under the existing
DTPs.
b)
Reporting by OTPs needs vast improvement,
both in number and quality.
c)
It has to be ensured dial trained key
personnel, as full team, arc available in all
DTCs.
Availability of trained key personnel
& equipment
Table 7 furnishes the position of availability
of trained key personnel and equipment in the
OTC as on 31st December, 1993. It could be
observed that only 276 out of 390 DTPs have
reported particulars on these aspects. Only 43
DTCs (i.c. 15% of reporting DTCs) have full
complement of trained team.
113
' - -■
-' 3
" "Sa
■
W'
i
SURYANARAYANA ETAL
114
■ 7 availability of equipment in DTCs as on 31.12.1993
Table 7. Posting of trained key personnel &
according to states
States/
UTs
SI
No.
DTO XT
LT
TO
Equipment in order
DTCs
(No. of DTPS)
with full
trained
V
M
X
teams
SA
Availability of trained
staff
FuncStaff
tioning position
DTPs reported
5
6
7
8
9
10
11
12
13
4
1
2
3
20
20
18
15
21
1.
18
17
21
10
23
10
Andhra Pradesh
6
8
8
7
3
10
Assam
7
8
10
10
11
3
5
0
0
3.
Bihar
0
4
0
5
6
4
32
19
18
3
11
1
Gujarat
14
4.
12
19
18
19
19
1
5
6
0
8
5.
2
8
9
8
11
4
Haryana
3
4
4
I
1
5
6
5
2.
Ef
by
to
c)
Cr
irr
qu
ah
Pr
P<
ire
nc
0
C
th
to
g)
i
Himachal Pradesh
11
7
4
I
3
3
0
3
Jammu & Kashmir
3
4
5
4
10
0
Ft
oi
tc
15
9
2
17
8.
Karnataka
15
ACKN
6
11
14
17
13
20
1
3
1
0
10
9.
5
10
11
8
12
9
Kerala
23
26
22
21
18
10.
25
29
30
22
45
7
Madhya Pradesh
19
20
18
3
0
23
Maharashtra
5
22
24
22
30
8
11
9
9
1
6
Orissa
1
11
11
10
13
3
3
5
3
0
2
Punjab
1
11
11
9
12
12
14
2
18
Rajasthan
2
12
8
0
27
18
15
T
Ukc, ID
his vvkw
membe
for the
Sri M.'
Com pi
nssistm
kune’
14
15
8
15
Tamil Nadu
12
15
REEE
11
16
16
15
16
30
9
32
1.
16.
Uttar Pradesh
26
27
30
20
32
35
6
56
6
4
4
I
6
17.
2
7
7
5
16
6
West Bengal
11
15
13
3
13
19
17
127
43
232
266 212
6.
7.
11.
12.
13.
14.
15.
18.
Small States
& UTs
INDIA
■
26
19
16
13
390
276
156
167 202 203
w.
:■
X
i
d)
X-ray equipment (Col.
ID; m = Microscope (Col. 12); V
Vehicle (Cot. 13)
. ;7:'is#
I
•
I
1
PERFORMANCE OF NATIONAL TUBERCULOSIS PROGRAMME
I
993
115
d)
!
ipnunt in order
No. of DTPs)
c)
h'l!
V
12
13
ft
21
17
10
8
II
I
4
19'
19
18
8
8
6
5
4
3
17
14
10
10
29
18
23
22
•n
11
6
'Ji
11
2
J
12
16
15
32
27
7
6
19
17
266
212
•r?
S
232
Effective and adequate supervision of Pills
by the DTC personnel is very much required
to maintain the programme.
Case-finding activity in DTPs has to be
improved both quantitatively and
qualitatively, after ensuring that (he cases
already detected are treated adequately.
Priority is to be given to detecting smear
positive cases and initiating patients on
treatment based on X-ray evidence alone
needs to be discouraged.
0
Case-holding activity needs improvement
through considerable comprehensive steps
to achieve higher cure rales.
g)
For achieving the above objectives, adequate
organisational, administrative. Financial and
technical supports are very essential.
Report series No. 34; Indian Council of Medical
Research, New Delhi, 1959, 49.
2.
Bancrji D & Stig Andersen : Sociological study
of awareness of symptoms among persons with
pulmonary tuberculosis; Bull. Wld/Hlth/Org ■
1963; 29, 665.
3.
National Tuberculosis Institute ; Report on
performance of National Tuberculosis Programme
for the year 1993. National Tuberculosis Institute,
Bangalore.
4.
Baily G.V.J.; Savic D. Golhi G.D., Naidu V.B.
and Nair S.S; Potential yield ol pulmonary
tuberculosis cases by smear microscopy of
sputum in a district of south India; Bull. Wld.
Hllh.Orgn. 1967, 37, 875.
5.
Nagpaul D.R.. Naganathan N
Prakash M:
Diagnostic photofluorography and sputum
microscopy in tuberculosis case finding,
IVocccdings of the combined 29lh National
Tuberculosis Workers’ Conference & 9th
Conference of Eastern Region of IUAT, New
Delhi, 1974. 330.
6.
Chaudhuri K. Jagota P and Parimala N: Results
of treatment with a Short Course Chemotherapy
regimen used under field conditions in District
Tuberculosis Programme; Ind. J. Tub. 1993 40
83.
7.
World Health Organisation : Tuberculosis research
and development - Re|x>rt of a WHO working
group meeting. Geneva 9-11 Sep. 1991, WHO,
Geneva.
8.
Baily G.V.J.. Rupert Samuel G.E., and Nagpaul
D.R. A concurrent comparison o! an unsujxn’viscd
self administered daily regimen and a fully
supervised twice weekly regimen of chemotherapy
in a routine out patient department; Ind. J Tub
1974. 21 152.
ACKNOWLEDGEMENT
I
I
{
The authors are very grateful to Dr B.T.
Ukc, Director, National Tuberculosis Institute for
his wholehearted support and encouragement and
members of the technical Coordination Committee
for their valuable suggestions. They also thank
Sri M.V. Jaigopal and Sri S.G. Radhakrishna,
Computors in the Monitoring Section for their
assistance in compiling the data and Miss T.J.
Alamelu, Stenographer for her secretarial assistance.
REFERENCES
1.
I
J
Indian Council ot Medical Research : I ulxnculosis
in India - A sample survey. 1955-58. Technical
Position: 2142 (6 views)