RF-TB-2.10.pdf
Media
- extracted text
-
T
fj.i)
Ind. J. Tub., 1990, 37, 175
TUBERCULOSIS IN INDIA, PAST, PRESENT AND FUTURE*
Wallace Fox
Introduction
r *■
It was a great honour to be invited to deliver
this important oration for 1989 and 1 deeply
regret that the change in date of the annual
meeting made it impossible for me to deliver it in
person, as planned. Instead, I have produced a
more detailed text.
At the outset I must express my special
gratitude to Dr. S.P. Pamra, Dr. D.R. Nagpaul,
and to Dr. K. Chaudhuri and his colleagues in the
NTI and Dr. R. Prabhakar and his colleagues in
the TRC Madras who answered many questions
that I put to them and made available much
unpublished up to date data, and even undertook
special analyses. However, the views I express are
entirely my own. 1 hope you will consider them as
constructive contributions to what I regard as a
most challenging problem of a size and
complexity compounded by the large and growing
population, and the geographical area of India,
the limited resources which can be devoted to any
single problem, including health, and within its
budget, to a single disease.
I intend to highlight a number of what I regard
to be major aspects of tuberculosis control in
India. My emphasis is on the need to improve
research and evaluation, based on my background
of research into the principles of chemotherapy,
the role of new drugs and new approaches to
their service programme application, their
surveillance and evaluation and the problems of
patient and physician compliance. I have had
long-term collaborative programmes in both
technically advanced and many developing
countries of Africa, Asia and the far East,
stretching back to 1952 when I joined the British
Medical Research Council (BMRC). Above all,
my close participation for 35 yearsjn studies of
tuberculosis in India^ and its problems, my
contacts with many of the leading research
workers, clinicians and administrators, has
encouraged me to face the challenge of the above
title.
I first came to India in 1955 as a member of a
3-man BMRC group asked by the WHO to advise
the Indian authorities on studies relevant to the . \
chemotherapy of tuberculosis, espccialljl
ambulatory regimens, their potential, and
possible risks to the patients’ close contacts. The
visit led to the formation of the Tuberculosis
Chemotherapy Centre, Madras. The broad;,
background of its formation was recorded many
years ago in the first report of the home and
sanatorium study.1 In amplification, after 3 weeks
in India my 2 colleagues returned to the UKwhilst I visited a number of cities with
populations of at least 500,000 and with a sizeable
sanatorium service,, both basic requirements.
After assessing the tuberculosis services of
Bombay, Delhi, Calcutta, Madras, Bangalore,
Hyderabad, Ahmedabad, Indore and Nagpur, I
opted for Madras, which was soon to open with
support of WHO what was then called a training
and demonstration centre”. The Director of
Medical Services, Madras, Dr. Sangham Lal, and
his Scientific Adviser Dr. K.S. Sanjivi reacted
favourably when I suggested that a chemotherapy
research centre would be of much greater value,
and Dr. P.V. Benjamin, the then Tuberculosis
Adviser to the Indian Government said that he
would approve the change if the WHO and the
Indian Council of Medical Research (ICMR)
agreed. Both Dr. C.S. Mani and C.G. Pandit (the
2 relevant Directors) were enthusiastic loo. In
this way empty premises, with X-ray equipment in
the process of installation and a partially
equipped bacteriological laboratory and rooms
that could be adapted to patient interview and
examination became available in the compound
of the Madras Government’s main tuberculosis
clinic. I became the Unit’s first Director, under
secondment to the WHO, and had the task of
implementing the scientific direction of the
project which was the responsibility of the
BMRC. This entailed establishing and training a.
research group and setting up an outpatient clinic
and a domiciliary_servic£ from scratch as well as
supervising the Tuberculosis Chemotherapy
* Ranbaxy Robert Koch Oration - 1989.
Abbreviations arc listed on pages 209-210.
TU/mrPr UK
Convspondence: Prof. Wallace Fox, 28, Mount Ararat Road, Richmond, Surrey TW10 61 G, UK.
r-Cx
\ • /Qv, G?.'X Z
176
f.U-
1
* ' rvA‘'1 o: iao s
WALIACF, FOX
Centre’s (subsequently named the Tuberculosis
Research Centre) (TRC) patients in Tambaram
Sanatorium just outside^fadras where 100 beds
had been put at our disposal. Professor D.A.
Mitchispn came out to Madras in 1956 for a year
and built up the bacteriological and biochcniical
laboratory, essential for the controlled clinical
trials, set up other important research studies and
became a long-term consultant and collaborator.
I. remained in__M_adras for 5 years and
subsequently visited annually until my retirement,
but less frequently since.
. 1-0-1265, the Centre, which was originally set
up as a temporary project, became a permanent
uniLoflbcJCMR^with the generous help of the
Madras Government, which included making a
large and valuable compound available. This
enabled the ICMR to expand, and build a major
laboratory unit able to undertake research in a
wide variety of basic problems, with continued
financial support, of WHO.
In 1958, the National Tuberculosis Institute
(NTI) wasstartc_d in Bangalore, and was officially
opened in 1960 by Pandit Nehru, the then Prime
Minister. Its main objectives were 1) to formulate
an applicable, acceptable and economically
feasible national programme for tuberculosis, 2)
to train the necessary manpower to organise and
manage the programme, 3) to continue research
with emphasis on operational activities to evolve
the programme, 4) from the late 1970s, to
monitor the National Tuberculosis Programme
(NTP).
Thus, there were 2 institutes in South India
220 miles apart, Madras with the remit of the
intensive study of chemotherapy and it^scientific
basis as well as epidemiology, for example the
risk of contact infection from domiciliary therapy
of index cases and the level of drug resistance in
new cases of tuberculosis, and the NTI
concentrating essentially on training district
teams, thc_opcrational problems of programme
application and on epidemiology. In between,
both geographically and operationally, at
Madanapallc in Andhra Pradesh was a
missionary group directed by the late Dr. J.
Frimodt-Mollcr, whose main activities were what
can best be termed semi-service, supported by the
ICMR. He became a close friend and a staunch
supporter and admirer of the TRC, a provocative
and stimulating member of its project committee,
and for a number of years the independent
assessor of the Centre’s study radiographs, a time
consuming commitment.
Soon after the WHO team leader, Dr. Halfdan
Mahler, arrived in India in January 1959 toJoin
the NTI. He, Dr. Frimodt-Mollcr and I agreed we
three should aim to meet formally at least 3monthly and preferably more frequently. In
practice however because of the problems and
pressures of establishing and running the 2 major
institutions and the number of weeks in the year
-when one or more of us were out of the country
or on leave,,we only had one such fnrrnj\l meeting
by February 1961, when Dr. Mahler returned to
Geneva. Looking back over the years, I feel it is a
great pity that there have not been more frequent
detailed operational and tactical meetings
between the staff of the 2 major institutes in
addition to the eventual administrative
relationships established through the 2 scientific
advisory committees. A breakthrough was made
when Dr. N.K. Menon who had been the first
Indian Director of the Madras Centre became
the Director of the NTI and Dr. S.P. Tripathy,
then the TRC Director, and I went to Bangalore
in 1977 specifically to discuss direct collaboration
in a controlled clinical trial of short-course
chemotherapy. This was readily agreed ”byT)r.
Menon" and the Bangalore participation was in
the Lady Willingdon Clinic and the staff members
of the 2 units worked side by side and in harmony
with the clinic’s staff and the research
bacteriology was centred in the TRC, ensuring
standardised
bacteriological
tests.
The
collaboration was a great success (Dr. P. Jagota
of the NTI proved a gifted team leader with a
special talent for clinical research) but
unfortunately it was unexpectedly terminated, for
unforeseen administrative reasons which arose in
Bangalore, so that the NTI could only contribute
a 2-year period of observation of its patients
whereas Madras, as usual, completed a 5-ye?.r
follow-up2 which in this study was of particular
importance. One of the 3 regimens studied was of]
only 3 months’ duration, which I regard as one of /
the most important regimens ever studied,/
because of the light it shed on the striking]
potency of short-course chemotherapy.
J
(There have, of course, over the years, been
other groups who, in the course of their service
programme commitments, also conducted
valuable investigations, clinical, operational,
epidemiological and controlled trials. Those
WBF.RCULOSIS IN INDIA, PAST. PRESENT AND FUTURE
currently active may well be in a position to make
important contributions to the national
programme if they evolve along the lines referred
to on pages 204-205 and 208-209, that is, their
research activities being integrated into an overall
national plan.)
My first major conclusion is that I have no
doubt that every effort must be made hereinafter
to ensure that the 2 institutes (NTI & TRC) work
closely together, including resuming collaborative
controlled trials and other investigations. This has
become even more important for a number of
reasons, for example, because of the TRC’s direct
participation in monitoring and implement!ng
short-course chemotherapy in 18 District
Programmes (pages 182-185) and the need to
improve training facilities nationally (page 208)
and to monitor in special surveys important
factors such as drug resistance levels nationally
(pages 204-205).
Monitoring District Programmes
The roles of the National Tuberculosis Institute
(NTl) and the Madras Tuberculosis Research
Centre (TRC) and their interrelationship
1. 'The role of the National Tuberculosis Institute
(NTI)
(a) The NTI formulated the National
Tuberculosis Programme (NTP) and its
documentation. (/?) It produced a scries of
manualj^for members of the District Programme
Team (DPT), namely the District Tuberculosis
Officer (DTO), the Treatment Organiser, the
X-ray technician, the laboratory technician, and
the statistical assistant, and also a manual for
Peripheral Health Institutions (PHIs) as well as
an introduction to District Tuberculosis
Programme. Although these valuable manuals
arc essential for the District Programme Team,
they do not cater, in a simple form, for the
individual worker in the PHIs, an aspect that has
in recent years been a major concern of the
Tuberculosis Research Centre, Madras (see
below), (c) The NTI Newsletter,, a duplicated
magazine, was introduced in May 1964 and
appears quarterly. Il is distributed free with a
nalional distribution of about 700_ copies
including 371 district centres, 30 assistant
directors pfhealth services (tuberculosis), and a
number of State TB Demonstration Centres, TB
177
hospitals and sanatoria, State TB associations and
to over 100 undergraduate and postgraduate
medical institutions, and other research groups. It
also has an international circulation of over 100.
It publishes new and current state of knowledge
articles, especially those concerned with control
programmes, new concepts and research work,
and answers readers’ questions and summarises
the performance of the NTP. Over many years, I
have found it a useful forum and consider that
careful thought should be given to its role and
widening its scope and circulation. It covers
rather different ground from other relevant
publications in India such as the Indian Journal of
Tuberculosis and Lung India and almost certainly
has a different circulation, particularly being
aimed at workers concerned with TB control and
district programmes. Being free, it reaches a wide
audience automatically, so the target groups
should be carefully considered and the cost of
improving its production and enlarging its
circulation would be a valuable ihvcslment of
Central Government Junds. (J) The NTI has
monitored the National Tuberculosis Programme
since 1978^ Of the 437 districts of India, 371
(85%) have implemented a District Tuberculosis
Programme, each with a District Tuberculosis
Centre (DTC). Currently, about 14,000
Peripheral Health Institutions (PHIs) in rural
and semi-suburban areas function as microscopy
centres, X-ray centres or referral centres.
Nagpaul (1989) points out’ that the 14,000 PHIs
then participating represented only 63% of the
estimated total of about 22,000 PHIs (on average
60 per district). He stresses the seriousness of the
incomplete coverage and utilisation of the PHIs,
which he attributes to the distance of access for
the surrounding population. The PHIs report
monthly to the DTC on case-finding and
treatment and each DTC reports to the NTI and
the latter in its turn reports to the State and
Central Government. The NTI also reports back
to the DTC deficiencies observed and the
necessary corrective actions. Currently, 15% of
the DTCs and 30% of the PHIs do not report on
time, if at all, and although the DTC has the
responsibility of monitoring the PHIs, by 3monthly visits, surprisingly, only 50% are being iJ
supervised by any visits at all, a major and
important deficiency in the National Programme, [
in addition to the 66 districts whi(±_hav£ nol |
implemented a District Programme at alMThese
are”alarming observations, to say the least.
WALLACE FOX
178
Table 1. Case-finding calculated in thousands according to type of case in the National Tuberculosis Programme,
1978-1987 (Nagpaul, 1989)3
Years
1978
1979
1980
1981
1982
1983
1984
1985
1986
1987
Sputum positives 188
185
174
189
219
256
262
259
281
286
Suspect cases*
473
508
474
521
638
747
764
798
904
1000
Extra-pulmonary'
61
58
56
58
66
69
'll
76
95
114
Total
722
751
704
768
923
1072
1103
1133
1380
1400
*A11 active cases of pulmonary disease, not confirmed bacteriologically
■> <
Nagpaul3 presents overall figures on case
finding, calculated from the number of cases
reported annually from the districts with a DTP,
and estimates based on averages for the districts
not reporting (Table 1). There arc increased
numbers from 1982, the first full year of the 20
point national programme, which included
tuberculosis as a priority disease, but the trend is
least marked for the sputum-positive patients, the
most important target group. Nagpaul (1989)
calculated3 the total sputum-positive cases per
100,000 was 29 in 1978, 31 in 1982, 36 in 1983,
1984 and 1985, 37 in 1986 and 1987, and 38 in
I 1988.
There is evidence that over the recent decade
the PHIs are making a larger contribution to
case-finding (Table 2), and if this is really the
ease it is of considerable importance. A puzzling
finding, however, is the decline in the proportion
Table
of new specimens examined that arc positive for
tubercle bacilli to the figure of 4.7%, which has
halved since 1982. It might be that more
specimens arc being collected from symptomatic
patients including a high proportion who are
smear-negative but culture-positive (as occurred
in a survey in Kenya4,5 or of non-tuberculous
conditions (possibly under the pressure of
meeting set targets, a fashionable but, in my view,
questionable approach in operational conditions
without careful monitoring), or it may be related
to less satisfactory specimens being obtained, or
inefficient smear preparation or examination, or
even all three. It demonstrates the importance of
monitoring at a field level, and although this is a
District and State responsibility, in view of the
evidence that they often neglect basic tasks, the
need for a representative national sample of PHIs
whose case-finding is efficiently investigated is
self-evident. The decline to 11.5% in the average
bacteriological workload and new positive patients found in the District Tuberculosis Centiv (DTC)
and the Peripheral Health Institutions (Pills)
(modified and contracted from Nagpaul, 1989)3
1978*
Average
District
tuberculosis
centre
1988*
1982*
Peripheral
health
institutions
No.
% of
total**
District
tuberculosis
centre
Peripheral
health
institutions
No.
% of
total
District
tuberculosis
centre
Peripheral
health
institutions
No.
% of
total
New outpatients sputum
examined
2,859
1,575
35.5
2,895
2,690
48.2
3,359
8,489
71.6
New sputum positive cases
415
188
31.2
375
245
29.5
385
395
50.8
% of new patients positive
14.5
11.9
13.0
9.1
11.5
4.7
*Based on 313 districts in 1978, 353 in 1982 and 371 in 1988
**Total = amalgamated numbers for the DTC and the PHIs
TUBERCULOSIS IN INDIA, PAST, PRESENT AND FU TURE
proportion of positive cases in the DTCs equally
requires detailed investigation.
It may be mentioned cn passant that India has
a national rule for sputum examinati(»|^hich is
exee p U on a 1. I its tfiat any patient with a
spontaneous complaint of cough for~2 or more
weeks should have sputum examined by smear
for tubercle bacilli, in contrast to the widely used
durations of 4 or more weeks, or a month_.or
more. This decision was based on a careful study,
but in a single district of south India in 1966.6,7
The implications on the work load of smear
examination arc considerable and it would be
well worth while to repeat such a survey on a
wider scale across the country. If confirmed, it
raises the question of whether the widely used
“month” rule should not be reviewed in other
countries. If, however, the “month” rule proves to
be more appropriate to India the number of
specimens to be examined would be reduced by
at least a third. The balance between workload
and case yield is an important issue to investigate
and cost operationally.4,5 It would also be a
valuable opportunity to investigate the gain by
doing cultures as well and also relate them to the
duration of cough.
179
3) have been used under the NTP for all
categories of patients (Table 1). The
recommendation is an 18 months’ duration, with
the aim that all patients should receive or collect
at least a 12-month supply in this period.
Currently, the great majority of patients,
including all those not bactcriologically
confirmed, are still recommended treatment with
conventional regimens. Also, of those patients
bactcriologically confirmed in districts where
short-course chemotherapy has been introduced,
the evidence from the TRC’s 18 pilot districts is
that a high proportion still do not receive short
course chemotherapy, and that they too arc still
on the conventional regimens (Table 5).
The NTI is also monitoring the introduction of
the short-course chemotherapy programme
(Table 4). In addition to the 18 districts in which
the TRC is involved (see below),. short-courst
chemotherapy has been introduced into the
I National Programme for the treatment of smea^
positive patients aged 15 or more (Table 4),
irrespective of a history of previous chemotherapy
that is, it includes chronic failure patients^his is,
however, a policy wnich could lead to the creation
of strains resistant to rifampicin, to rifampicin
plus isoniazid, and to pyrazinamidc-resistant
Until 1986 only conventional regimens (Table
strains also, a very dangerous situation, and it is
important to know if this proves to be the case,
Table 3. Cunvnt conventional regimens for District
Programmes (1989) and the cost of a 12-month supply
and the speed with which it occurs in the patient
population. This decision was perhaps taken (1)
Number
i
Cost
iin recognition of the difficulty of obtaining an
of doses
(rupees)
Regimen
accurate history of previous chemotherapy,
12-months
12-months
especially in small peripheral health units, (2)
because some patients with a history of previous
365
73
TH
chemotherapy may have been given (or taken)
365
774
PH
too little medicament for their strain of organism
365
285
EH
104
331
s2h2
Table 4. Current (1989) short-course regimens in
2STH/TH
273
365
2SPH/PH
857
365
2SEH/EH
450
365
2SH/S2H2
488
148
r
T = thiacetazone, H = isoniazid, P = PAS,
E = ethambutol, S = streptomycin
The number preceding the drugs is the number of
months of their duration
For intermittent regimens, the number of doses of
drugs a week is shown by the suffix number
The aim remains an 18-month duration and supply.
The increase in the number of doses and the extra cost
can be calculated from Table 8.
District Programme conditions in India
Monitoring
centre
Regimen
Cost
Number
(rupees) of doses
2S2H2R2Z2/4H2R2
240
52
NTI
2EHRZ/6EH
485
240
Bangalore
2EHRZ/6TH
345
240
1)
2H2R2Z2/4H2R2
190
TRC
2)
2HRZ/6TH
295
52
240
Madras
3)
2HRZ/4H2R2
340
94
R = rifampicin, Z = pyrazinamide
Also see footnotes to Table 3.
WALLACE FOX
180
Table 5. Year by year comparison of the percentage of smear-positive patients put onto short-course chemotherapy in
each of the 18 districts monitored by the IRC (Prabhakar, personal communication)
District
North Arcot
Puri
Baroda
Thane
Ujjain
Dchra Dun
Karnal
Kanpur
Nagpur
Rajkot
Raichur
Sagar
Pondicherry
Vidisha
Aurangabad
Varanasi
Sabarkantha
West Godavari
Policy*
A
B
C
Percentage of patients put on short-course chemotherapy**
1985
1986
1987
1988
1989
66
88
64
72
46
43
61
64
49
64
43
49
68
79
44
64
47
86
55
67
32
72
44
85
51
68
59
82
48
89
36
26
16
75
27
44
38
12
32
59
30
37
31
18
33
51
39
79
50
36
64
53
54
87
73
30
53
68
76
91
45
82
39
58
60
24
52
80
46
64
60
30
48
76
48
62
59
40
50
81
33
61
70
44
36
70
76
81
83
80
* Defined on page 182
** 2 Districts had started the programme in 1983 and 8 in 1984
to have acquired drug resistance, or (3) in the
hope that at least some patients, whether with
primary or acquired drug resistance, would still
be cured. This may still be the case, dependent on
the pattern of drug resistance, the regimen of
short-course chemotherapy and the patient’s
compliance in taking it. In my view, as a
minimum, each District Tuberculosis Centre
should make strenuous efforts to obtain from
every patient brought under treatment an
accurate history of previous chemotherapy and its
details so that some information on the
proportion of patients in the district who give a
history of previous chemotherapy, its duration
and the regimen previously received is obtained
across the country. The NTI has experience of
districts whose reports it regards as accurate and
this group could be of special value.
personal communication). The three regimens of
the National Programme (Table 4) can be
modified to some extent. One is a fully
intermittent twice-weekly regimen for 6 months.
If streptomycin is not available or adverse
reactions to it occur, ethambutol can be used
instead. The other 2 have a 4-drug daily phase of
2 months, followed either by 6 months of
thiacetazone plus isoniazid daily or, if the patient
cannot tolerate the latter, ethambutol plus
isoniazid. Streptomycin can be given instead of
ethambutol in the first 2 months if the patient is
prepared to attend daily, otherwise the patient is
given a supply of oral medicament every 15 days
in the first 2 months and then a monthly supply
thereafter, to self-administer at home.
The developing countries face a dilemma.
Because of the problem of initial drug resistance
The rate of admission of districts to the short " in many, the total absence of sensitivity tests for
course programme has been very rapid : 1986-26,
epidemiological surveys or patient assessment,
1987-75, 1988-75, 1989-18. By October 1989, 194
limited culture facilities at best, and the difficulty
districts were using short-course chemotherapy
of obtaining an accurate history of previous
and the target set for April 1990,1 the end of the
chemotherapy it could be argued that ideally
seventh 5-year plan, was 275 f (Chaudhuri,
multiple drugs, up to 5, including, wherever
■-••.s.dh.v, .
"
J .• r
■
(
i
1
. 14.M.
<
TUBERCULOSIS IN INDIA. PAST, PRESENT AND FUTURE
possible, streptomycin and either thiacetazone or
cthambutol., should be given in the initial
intensive phase for all smear-positive patients.
This is a paradoxical situation for countries with
limited funds and so many other basic resources
that need strengthening, e.g. bacteriolog}'. It
highlights the problem of the chemotherapy of
tuberculosis in developing countries, the
apportionment of funds to the different
components of the programme and also the
difficulty of deciding what are the most
appropriate short-course regimens to introduce,
especially because of a need to avoid producing
rifampicin resistance in chronic failure patients,
_with drug-resistant strains already/
At a visit to the NTI which I paid with Dr.
Prabhakar injNovetnbcr 1989 we were shown a
summary-assessment made by the NTI, orte oflts
standard responsibilities. It covered 2 quarterly
reports of the performance of the District
Tuberculosis Programmes of & major State Avith
about 30 Districts. The NTI assessment clearly
set out deficiencies in the implementation of the
programme and in its reporting, commented on
case-finding and treatment, and named 6 districts
where the majority of the PHIs had not been
visited at all. It is also noteworthy that in the 15
districts which had reported on the staffing
position, only 2 had trained DTOs in situ and in 5
districts the statistical assistants were not trained
and in 4 more the post was vacant, these despite
the training programmes of the NTI (see below).
These are serious problems that can obviously
greatly undermine the efficiency of the State’s
programme, whatever regimens are used. The
value of the NTI reports is unquestionable in
highlighting major deficiencies for a State
prepared to take remedial action. A copy of the
State report also goes to New Delhi as does a
quarterly detailed summary report for all the
districts of India that returned a report for the
quarter in question, so that the Central
Government is informed too.
The NTL has had a long-standing problem of
recruitment of senior key scientific staff
members. In March 1989 of 17 such posts, there
were vacancies for a sociologist, a bacteriologist,
2 TB specialists, a senior statistical officer and an
epidemiologist. (The sociologist’s post had been
vacant for 3 years). Further, over quite a period
of time, some of the key posts have, of necessity,
been filled by encumbents approaching
181
retirement whose background was from other
disciplines, or administration. (These posts are
advertised by the Central Government and the
NTI is not represented on the Central
Government selection committee.) The staff
shortages obviously limit the amount of field
work and visiting that the NTI can undertake as
well as its operational research activities and it
has had to concentrate primarily on its large and
important commitment to training, which is very
relevant. The total number of personnel (which
constitute a District Programme Team) trained
up to 1989 is (a) medical officers 1104, (b) health
visitors/treatment organisers 1107, (c) laboratory
technicians 866, (tf) radiographic technicians 771,
(e) statistical assistants 793, (f) BCG technicians/
team leader 361 (this category was deleted from
team training for the last 10 years). The NTI docs
its field training not only in the Tumkur district
but nearby districts of other States. The NTI
currently runs regular training courses of 10-week
duration twice a year including, in one of them,
international candidates sponsored through
WHO. It also conducts educational activities as
seminar/workshops for District level and State
level administrators, and professors of medicine,
chest diseases, tuberculosis and community
medicine, many coming from medical colleges.
Undergraduate and postgraduates in medicine
from nearby visit the NTI to learn about it as well
as the national tuberculosis programme. Clearly,
the reason a State is short of DTOs and statistical
assistants lies within the State itself, not the lack
of NTI training courses.
This current limitation of the activities of the
NTI is a serious problem which must be
overcome. Operational research and field
supervision was a major activity for many years,
and is essential for the evolution of the National
Programme in the light of field experience.
Despite the difficulties, the staff still undertake
some valuable operational research projects and
controlled trials, a recent example being
rcfcrence(8) and related reports, and publish
review articles, as well as the NTI Newsletter.
Thus, through the NTI, a framework exists to
identify a number of problems and deficiencies
but the patent weakness is the lack of means and
an organisational structure with which to. take
remedial measures. There is an obvious need for
the most careful consideration being given to the
creation of an effective and adequately staffed
182
WALLACE FOX
agency, with the authority to guide and assist the
States in improving their District Programmes’
performances.
The question arises whether, in addition to the
training courses centred on the NTI, a mobile
training team attached to the NTI should be
established. It could visit a State which has
declared a serious long-term intent and
commitment to upgrading its tuberculosis control
programme and run a training course for a large
y i number of staff of all cadres, including
5
administrators, team leaders and medical
officers, treatment organisers, X-ray and
laboratory technicians. Key staff from every or
most districts in the State could be trained and
university teaching staff too. There would thus be
a concentrated effort to upgrade and improve
knowledge and organisational and evaluatory
skills and this might well be the most costeffective way of training substantial numbers of
the main cadres and introduce modern regimens
most effectively. This approach could be
supported by a well orchestrated statewide
publicity campaign including the widescale use of
the media and aimed at community leaders and
the general public, so that a large and concerted
effort could be mobilised. The health service and
community’s expectations and demands would
also receive a stimulus and strengthening the
infrastructure would be an inherent component.
The team could pay further visits of shorter
durations, as indicated. This would offer much
wider benefits than the NTI training or retraining
in Bangalore of a limited number of individuals
from a number of different States. In my view,
this may well be the way forward, and might be
tried, in the first instance, in a single State to
work out the logistics of such an approach, and
move into a second State as soon as a broad
modus operandi is established.
Since writing this section I have just received
the April 1990 issue of the Indian Journal of
Tuberculosis. An editorial9 reports an important
project, the “Expanded programme of Health
Education and community involvement in the
National Tuberculosis Programme”, assisted by
USAID which started in July 1987 and comes to a
formal end in September 1990. The TB
Association of India and the State Associations,
collaborated with the Central and State
Governments. The project aimed to cover 250
districts in 23 States and 2 Union Territories, a
highly ambitious target! The editorial summarises
errors and the lack of a proper evaluation of the
components, a conclusion reached by the
National Institute of Health and Family Welfare.
Such projects are, in my view, operating with too
small an input and for too short a time and run
the risk of gradually dying out unless built into a
much broader based, better supported and long
term scheme, such as I have proposed above, but
full advantage should be taken of the lessons
learned from this project.
2. The role of the Tuberculosis Research Centre
(TRC)
In 1983 the TRC was asked to monitor the
working of short-course chemotherapy in 18,
districts, 3 groups of 6, studying 3 different
policies (termed A, B and C) based on 3 regimens
in order to document the applicability and
acceptability of short-course regimens under field
conditions. The eligible patients are sputum
smear-positive patients, aged 15 years or more
with no history of previous chemotherapy for
tuberculosis or for no longer than 2 months. Three
short-course regimens are being studied (Table
4). All the doses of Regimen 1, 2H2R2Z2/4H2R2,
are administered at a health facility under direct
supervision of the staff. For the daily regimen
2HRZ/6TH, Regimen 2, the patient attends
every 15 days to collect a supply to self-administer
at home, and Regimen 3, 2HRZ/4H2R2,
intermittent in the continuation phase, entails, for
the first 2 months, collection by the patient every
15 days for self-administration and then twiceweekly attendance for
the supervised
administration. The 3policies being studied are :
Policy A in which the patient is offered Regimen
1 but has a choice of Regimen 2, as an alternative.
Policy B is Regimen 2 with no alternative short
course choice.
Policy C is Regimen 3 with Regimen 2 as an
alternative.
(It is currently not the policy to retreat with
short-course chemotherapy if the patient
relapses, a decision which will need to be
considered as part of a general review of national
policies and priorities.) In 1987, in the-light-of
preliminary findings, the TRC’s remit was
Extended to concentrate on improving the
functioning and efficiency of these 18 districts’
programmes and to undertake relevant field
TUBERCULOSIS IN INDIA, PAST, PRESENT AND FUTURE
studies. The original remit was demanding of
-time and this extended remit is even more so.
Table 5 shows the percentage of smear
positive patients
put
on
short-course
chemotherapy in the 18 districts monitored by the
TRC. Even in 1989 the proportions arc
surprisingly low. This means that conventional
regimens are still widely used. There arc many
reasons why sputum-positive patients may not be
put on short-course chemotherapy. The NTI in its
duplicated Guidelines for the introduction of
short-course chemotherapy in the DTP lists
“Living too far off, too old or sick, clinic hours
not convenient, no transport facilities, travel too
expensive, likely to migrate, as well as “any other
reasons (not specified above)”. In addition it is
clear that there is not the drive or the will to
make such a switch to short-course chemotherapy
in many PHIs (sec below). A detailed analysis of
every PHI breach o£thcJ8 districts could be very
informative about the characteristics and reasons
'that in" the same district some PHIs arc and
others arc not involved in short-course
chemotherapy after the passage of several years
and despite substantial educational efforts and
stimulus and interest of the TRC. The TRC has
detailed computer printouts for its districts and
the PHIs already, which may well be very
informative on detailed analysis.
A second worrying feature is a summary of a
July 1986 to June 1987 cohort analysis of short
course chemotherapy in the A, B and C Districts
(Prabhakar, personal communication). This
clearly demonstrates the high drop-out rate in the
early months of treatment with the pilot
regimens. Thus, of patients (average number in
the cohort 425) in 4 Policy A districts who had
elected to attend for twice-weekly supervised
chemotherapy (see Table 4), 24% did not
complete a total of even 1 month’s treatment
before terminating their chemotherapy,
increasing to a total of 37% who did not complete
2 months’ doses, and that in all 53% did not
# complete at least 80% of the due doses (a
percentage widely regarded in India as the
minimum therapeutically satisfactory quantity).
Of 4 Policy C districts, in which patients (average
number 263) who agreed to accept the regimen of
daily self-administered chemotherapy for 2
months (this entailed only once a fortnight
attendance to collect a drug supply) followed by
twice-weekly attendance at a health facility for 4
183
months (Tabic 4) the corresponding 3 propor
tions were 12%, 26% and 49%. Of 13 districts (A,
B and C) (average number of patients 425), the
patients on the 4 A and 4 C Policies who had
opted to have the daily 8 months self
administered chemotherapy (Table 4) instead of
an intermittent regimen and 5 B Policy districts
where it was the only regimen offered, the corres
ponding proportions were 18%, 28% and 48%.
Thus it is evident that a high proportion of
patients in the 18 pilot district programmes do
not like the current fully or partially intermittent
6-months regimens they are offered (regimen 1
and regimen 3) almost certainly because of the
number of attendances entailed, and that they
prefer to chose a daily 8-month regimen which
entails fewer attendances, because they collect
15-day supplies to self-administcr at home. Even
so, there is still a high drop-out rate both earlv
and later on with all three regimens. This is|
evidence that shorter duration and fewer dose /
regimens in themselves are not adequate, and
that it is essential to improve the organisational
framework and infrastructure of the programme
and with them patient compliance to ensure
major improvements in the therapeutic results. J
A third deficiency is that in 1989 not all of the
PHIs in the 18 districts had even implemented a
District Tuberculosis Programme. Thus, 12 of the
18 districts had done so in 100% of the PHIs, 4 in
90-99% and 2 in only 70-79%.
A fourth deficiency is, considering the PHIs in
the districts that had implemented the DTP, only
9 districts had introduced short-course chemo
therapy in all of the PHIs, 2 in 90-99%, 4 in 7089% and 3 in 50-69% of the PHIs.
Yet another deficiency is the average
“completion rates”, that is patients receiving or
collecting 80% or more of the prescribed
chemotherapy, for the 3 policies A, B and C,
which have been studied for 4 cohorts. The
cohorts are from the inception of short-course
chemotherapy to October 1985, November 1985
to June 1986, July 1986 to June 1987, and July
1987 to June 1988.
The averages for the 4 cohorts for each of the
3 policies were as follows :
Policy A 46%, 57%, 51% and 54%
Policy B 48%, 42%, 52% and 48%
Policy C 52%, 46%, 52% and 51%
184
WALLACE FOX
These figures arc disappointing and a more
detailed review of individual districts gives no
grounds for encouragement. Thus, comparing the
completion rates for cohorts 3 and 4 show for the
latter an increase of 5% or above in 5 districts, a
decrease of 5% or above, also in 5 districts, and a
change of less than 5% in either direction in 8.
Thus, it is clear that there are a series of levels
where deficiencies exist and despite the efforts
and encouragement of the TRC, they remain
formidable. I do not believe that these arc early
days and that in a few years time the situation will
have improved substantially. To me this is a cause
for anxiety about what will happen under the
National Tuberculosis Programme where
monitoring and the substantial technical,
scientific and educational input of the TRC will
not be forthcoming. There is no possibility of any
mechanism by which a vast input of effort and
expertise and enthusiasm can be mobilised for
the districts already using short-course
chemotherapy which by now must be over 200, or
for the districts that will come in within the next
few years unless a radical policy change takes
place. One such radical change would be the now
State approach I have suggested (pages 181-182).
Unfortunately, the National 20-point Plan of
1981, which specifically included tuberculosis, led
to some minor initiatives that rapidly faded, and
the opportunity presented by the public
endorsement of the Prime Minister, Indira
Gandhi, was never energetically exploited.10
In November 1989 at my visit to the TRC, I
interrogated in detail Dr. Prabhakar and his
senior colleagues to clarify exactly how they
monitored the 18 districts. Briefly, a TRC visiting
team consists of a medically qualified research
officer, a bacteriologist, a statistician and a social
worker and Dr. Prabhakar also pays visits. Thirty
five visits were made in 1988. A single field team
visiting at any one time is the aim and 2 teams
visiting, strains the TRC’s resources. Al each
district visit 2 groups of local medical officers and
v?- 2 of paramedicals, both laboratory and treatment
. organisers, are involved in carefully planned
lectures and educational seminars. This is in
addition to the TRC staff visiting the DTC,
discussing with its team a TRC computer print
out which, as well as giving an overall summary,
includes a detailed tabulation of the performance
of every PHI. A visit takes, on an average, 10 days
and travelling expenses arc considerable since the
study districts arc in all parts of the country.
The TRC has had to prepare a series of policy
and instruction documents for its own staff to use
so that its teams systematically cover the
necessary issues at visits and obtain standardised
information. Also of particular interest to me arc
3 publications prepared (and revised in the .light
of experience).Tor field workers-in the District
Programmes, one dealing with “Treatment r«»
Aspects in a District TB Programme”, a second
summarising “The District Tuberculosis
Programme Salient Features” and a third
“Instructions to Laboratory Technicians on
Sputum Migroscopy”. They are simple, and are
still being improved (professional expertise on
layout and presentation would now be
advantageous) and of value as an aide memoire
for individual field workers, and are especially
necessary in the smaller institutions where the
numbers of possible and actual cases of
tuberculosis seen are inevitably few. Their object
is very different from the detailed manuals
prepared for the members of the District
Tuberculosis Team by the NTI.
I
It is patently unnecessary for every district or
State to produce its own set of simple instruction
documents and the aim should, in my view, be to
produce a model set primarily by the
collaborative efforts of the TRC and the NTI,
since both have direct and overlapping national
responsibilities. They too should seek advice from
a limited number of knowledgeable critics from
other parts of the country to broaden the input of
experience. Where there are local conditions in
individual States or districts which require
modifications to the model set, these can, of
course, be introduced locally. Ideally, they would
be discussed with the NT1/TRC team to see if
they are really necessary, and, if of general
interest, can be reported in the NTI Newsletter. It
is important to consider the use on a substantial
scale of improved simple manuals and, in
particular, to evaluate under field conditions what
they achieve, before they are introduced
nationally.
I have urged the TRC to publish its approach
to supervisory visits to districts, explaining its
procedures and also to document the cost in time,
effort and finance of such visits, with the current
objectives, or if the objectives were limited to
monitoring activities or operational research.
Obviously, there are financial and staff
constraints on such visits and this is why it is
»
TUBERCULOSIS IN INDIA, PAST. PRESENT AND FUTURE
important that they be costed. With 437 districts
in India the primary aim must be to raise the
average standard as rapidly and economically as
possible, not just to concentrate on producing a
limited number of outstandingly efficient districts.
These will emerge in any case, when a district
team, especially its leader, is of high quality and
receives full support from the State Director of
Medical and Health Services.
It is clear that if every DTO and his trained
colleagues were paragons of efficiency, energy
and enthusiasm, the TRC’s role at a field level
could be limited to operational research and
epidemiological and sociological studies, but this
is not the case and, realistically, is unlikely ever to
be so. The NTI’s role would also be much easier
to perform if every district reported to it, and did
so punctually, providing all the stipulated
information, and the PHIs were visited regularly
by the DTOs, as is intended in the National
Programme.
The NTI regards the information on short
course chemotherapy it currently receives as
unsatisfactory. In part, this is because the district
statistical assistants have not been trained in the
preparation of the new reports and currently the
details required are complicated for the PHIs to
complete (Chaudhuri, personal communication).
The reporting instructions and forms adopted by
the TRC and the NTI also had differences which
have created problems for both groups and these
arc in the process of being ironed out. The TRC
has the great advantage of a well trained
statistical assistant from its own staff, working in
16 of its 18 pilot districts. A similar NTI
appointment (and so responsible to the NTI) for
each district should be considered, and tried out
on a pilot scale.
185
especially if oral, when monthly supplies are given
from the outset, is the fewer attendances they
need to make.
^1 predicted ip 198310 that the introduction of
short-course" chemotherapy in India would
inevitably mean that data would need to be
collected for both conventional and short-course
regimens for a number of years, and the
additional recording and its complexity would put
extra responsibility and strain on staff at every
level, and especially in the district programmes
and this is indeed the case. When short-course (6month) chemotherapy was declared the National
policy in Algeria it took 3 years to introduce
despite a population of approximately only 20
million, and adequate funds to purchase all the
necessary drugs for the new national short-course
regimen from the outset. In Tanzania, a country
with a slightly larger population, despite a
declaration of a National Commitment to
Tuberculosis Control in the mid-1970s (and other
advantages), and the implementation of the
programme by the International Union Against
Tuberculosis from 1978 and several years
building up a framework based on standard
duration chemotherapy, it still took (Styblo,
personal communication) 4 years to introduce
short-course chemotherapy to all 20 Regions of
the country.
It is now essential to review what information
is being collected about district programmes both
by the NTI and the TRC and whether it is in the
best form and whether indeed it is all necessary.
It may be possible to design reporting forms with
one section with information which must be
provided by every district and on a second section
information which, though not obligatory, would
be valuable. Further, the issue arises on the
It will also be appreciated that a sudden switch ' relative emphasis in data collection to be given to
from conventional chemotherapy, even in a ; bactcriologically confirmed and unconfirmed
cases, as well as to short-course and conventional
district programme, and much more so in a whole
chemotherapy,
and new and retreatment cases.
State, is not possible because, in addition to the
provision of the new drugs and adequate
There is now an urgent need for a detailed
instructions on their use and introduction, the
analysis of the data collected by the TRC with a
staff and patients, the administration and
full presentation of the findings and as full an
community leaders all have to understand and
explanation of them as possible and an
accept the new policy. Inevitably, conventional
assessment of their implications. Careful
chemotherapy regimens remain among the list of
consideration needs to be given to the question of
options for smear-positive pulmonary disease,
which of the regimens currently studied should be
and are to be used, according to current policy,
persevered with. My own view is that the evidence
for all smear-negative disease. The attraction of
a
of unacceptability
on a wide ___
scale__________
in District
conventional duration regimens to the patients,
Programmes is already clear for the fully
186
WALLACE FOX
supervised intermittent regimen. What is not
clear is for what section of the patients it is
suitable. Has it, for example, been acceptable in
the urban areas, suburban areas, and in areas
close to PHIs? Are there any other identifiable
factors that are associated with improved or
impaired cooperation? The TRC may well have
answers to the important issues from the data
already collected. The TRC’s annual reports and
the publication of conference presentations give
interesting yet tantalizing tabulations. Inevitably
the tables ancMext_ are inadequate to give a
balanced and interpretable picture of the
achievcmcnts_ and failures—of .District .
Programmes and how best to proceed with or
modify the approaches.
Tables 3 and 4 show the cost and the number
of doses in each regimen, whether conventional
or short-course. I think of these regimens in
terms of the number of “units of patient
compliance” each regimen requires if the patient
is to receive every dose. For example, the units of
compliance for a fully self-administered daily oral
regimen are a small number of attendances to
collect drug supplies, but a large number of doses
for the patient to swallow to complete the course.
In contrast, at the other extreme, for a fully
supervised intermittent regimen the number of
attendances is relatively high, but the number of
doses, all taken under full supervision is small.
This approach helps us to sec current and new
regimens in terms that are relevant both to the
patient’s convenience (and so compliance) and
the workload of the treatment services.
Among the 18 pilot districts under the TRC
are 2, namely, North Arcot and Pondicherry,
geographically convenient to Madras, in which
the TRC has been monitoring the programme
intensively, including (1) the efficiency of the
equipment, radiographic and microscopy, (2) the
bacteriology, pre-treatment, at the end of
chemotherapy, and at follow-up, and (3)
undertaking operational and sociological studies.
On the laboratory side it obtains pre
treatment smears, cultures and sensitivity tests,
which latter need to be related to the history of
previous chemotherapy and to failure during
chemotherapy and bacteriological relapse when
these events occur, and the drug sensitivity of the
strains at the lime, as well as to the regimen the
patient received. Thus, it is collecting invaluable
information on the levels of drug resistance in the
patients on presentation for treatment, and
changes in the levels over a period of time and on
the emergence of drug resistance in individual
patients. Again, a detailed analysis and a full
presentation and discussion of the findings is
urgently required.
Clearly, these 2 districts might be quite
unrepresentative of the situation around the
country, and there is a need for a network of
centres able to monitor drug resistance along
similar lines (pages 204, 205).
Operational studies by the NTI and TRC
The TRC, like the NTI, has also undertaken in
its recent remit operational studies relevant to
District Programmes. For example, it has studied
the use of the address cards system in North
Arcot District to see whether it is successful in
obtaining accurate patient addresses in small
towns and villages, as it was in large towns of
Tamil Nadu.11 Il has also studied policies of
motivation in 2 different treatment centres under
field conditions, an extension of an approach that
had previously been studied in the TRC
patients,12 as well as by the NTI in the Bangalore
area.13 Like the NTI it has also studied patient
awareness of symptoms and their utilisation of
the available resources of primary health care
under District Programme conditions, studies
that can produce surprising and unexpected
information. For example, in Hong Kong a
collaborative survey with the BMRCTonclusively
demonstrated the need for better education of
the general public14 about tuberculosis and the
existence of a free Government service. Two
subsequent surveys15 showed how difficult it is to .
run a successful case-finding campaign using the
mass media (television, the newspapers and
posters), as assessed by studying whether the
number of symptomatics attending and cases of
tuberculosis diagnosed before, during and after
the publicity campaigns were increased.
Fully Supervised Intermittent Chemotherapy
I have, for well over 20 years, advocated the
importance in urban areas of India of organising
fully supervised intermittent chemotherapy in a
way convenient to the patient so as to improve
compliance. I suggested that the administration
of each dose should be near the patient’s home or
place of work or en route between them,
whichever was most convenient for the individual
patient as in studies in Czechoslovakia16 and
TUBERCULOSIS IN INDIA. PAS T, PRESENT AND FUTURE
Britain.17 Fully supervised intermittency,
especially in short-course regimens is now
receiving emphasis both in the Indian National
Programme as well as in the TRC’s Pilot Districts
and so I intend to repeat yet again largely
verbatim but also with some expansion what I
wrote in 1984, using the same data I had obtained
for the year 1983 for Madras City.10
In 1983, the possible sources of supervised
chemotherapy in Madras City were (and still are)
numerous. Madras City had a population ofj.3
million and a geographical area of 169 sq km. The
Madras Corporation had ^9 dispensaries as well
as 40 maternal and child welfare clinics with
enough space and facilities to organise with safety
fully supervised intermittent chemotherapy for
tuberculosis, and, if need be, to give streptomycin
injections. There wore 14 J^ate.hospitals, .4
Centra] Government hospitals and 10
dispensaries, 2 Employees’ State Insurance
hospitals and 31 dispensaries, 20 voluntary
organisations (including missionary hospitals), 20
Service Clubs clinics, including Rotary and Lions,
15 Jain Medical Relief centres, and some 3,000
general practitioners.
If it were possible for the purpose of full
supervision of tuberculosis chemotherapy, to
break down in Madras City the artificial
administrative divisions between the units under
the Corporation, State, Central Government,
Employees’ State Insurance Scheme and the
various voluntary agencies, then it could be made
much more convenient for patients to attend
nearby facilities for supervised chemotherapy.
Recommendations have been made in editorials
in the Indian Journal of Tuberculosis in 1981r819
that general practitioners too could be involved in
the programme and, provided they keep suitable
records, should have free X-ray and
bacteriological facilities as well as free
antitubcrculosis drug supplies. It docs seem to me
that the medjeal profession should really make
strenuous efforts to set up in one or more cities,
both large and small (why not including Madras?)
an organisation that cuts across artificial
administrative barriers between different
agencies. If this were achieved it could lead to a
substantial proportion of patients in urban India
being conveniently and more effectively treated in
this way. (The overall management would remain
the responsibility of those with the necessary
skills and facilities.) There is no doubt that the
187
effectiveness of intermittent regimens, both of
conventional duration and short-course, depends
on their acceptance by the patients, which in its
turn depends on the efficiency and flexibility of
the organisation of such regimens. There is no
inherent reason why the same approach might
not be tried in small towns. In fact, an
appropriate and flexible exploration of what
proportion of patients could have convenient
access to intermittent chemotherapy in a District
Programme has yet to be undertaken. The
detailed analysis of the accumulated data
obtained by the TRC might, in fact, give pointers
for further exploration. Also, it must always be
remembered that if an efficient primary health
care network does come into existence this might
radically influence the situation.
Stead and his colleagues in the USA20
successfully used short-course chemotherapy
unsupervised twice-weekly intermittent for most
of its duration and in subsequent studies, but this
depends on patient self-administration, and lacks
the assurance provided by full supervision of
every dose of intermittent chemotherapy.
Finally, the importance of voluntary agencies
interfacing with official agencies cannot be
overstressed and this again is an area where
concerted efforts are necessary. The need to
educate and involve the general practitioners who
represent such a large sector of the tuberculosis
treatment services and are often the first point of
contact with the patient is another important
priority. The TB Association of India had done
this on an inevitably limited scale because of
financial
constraints
(Pamra,
personal
communication), but what is needed is a national
implementable plan. The involvement and good
will of practitioners of indigenous systems of
medicine could also make a valuable
contribution, and they must not be overlooked or
dismissed without searching consideration of
their role in the community and what
contribution they might make to the National
Tuberculosis Programme.
New Approaches to Patient Compliance
(A)
Background
Obtaining continued patient compliance in
long-term therapy for tuberculosis after the rapid
disappearance of their symptoms and early return
to their normal state of health is a universal
8
188
WALLACE FOX
Czechoslovakian study) and administrative
problem. In 1956 we developed in the then
problems such as whether peripheral health staff
Tuberculosis Chemotherapy Centre, Madras, a
could distribute or supervise antituberculosis
coordinated approach to patients under
chemotherapy were resolved. For this reason I
ambulatory domiciliary treatment for pulmonary
had regarded daily self-administered chemo
tuberculosis. This included (1) the involvement of
therapy as the only practicable policy for
the family as well as the patient during the pre
widescale rural use in India, supervised wherever
treatment diagnosis and assessment period, (2)
possible by the family or by local responsible
frequently repeating during therapy the need to
community members. The position has, however,
take the medicaments regularly and emphasizing
changed and I present in section C a further
the family’s or a neighbour’s role in supervision,
suggestion which I regard as being of substantial
(3) a policy of restricting the medication to
potential importance, not least because it opens
antitubcrculosis
chemotherapy
whenever
up new fields of laboratory research in vitro and
possible, (4) surprise visits to the home to (tf)
in vivo and in controlled trials in patients, but, in
check the patient’s stock of pills and (b) to collect
due course, hopefully, in operational studies
a urine specimen to test for antituberculosis
under service programme conditions also.
drugs, and (5) taking speedy absconder action if a
patient failed to attend when due.* It was, in fact,
I should add that it was the patient compliance
the continuing problems of patient compliance
problem which had led us in the BMRC to
despite their urban domicile, which led us to
explore both short-course chemotherapy and
explore
fully
supervised
intermittent
then intermittency combined with short-course
chemotherapy in Madras which I had already
chemotherapy studying regimens based on
come to realise by 1958 might be an alternative
isoniazid and rifampicin. Also, pyrazinamide was
approach in urban conditions and for which
reintroduced into primary chemotherapy in the
evidence of possible effectiveness subsequently
very first study which was conducted with our
arose from studies in the Centre of the serum
collaborators in East Africa.2324 This was a study
profiles in patients on isoniazid.21 The in vitro and
of 4 daily 6-month regimens, streptomycin plus
in vivo studies of Mitchison and his colleagues
isoniazid, streptomycin plus isoniazid plus
have explained the underlying mechanisms and
rifampicin, streptomycin plus isoniazid plus
the role and limitations of individual drugs.22 Two
pyrazinamide, streptomycin plus isoniazid plus
further advantages of intermittent chemotherapy
thiacctazone, compared with, as a control, a
were the reduction in drug costs (an important
standard 12-month regimen of streptomycin,
issue) and the reduced risk of drug toxicity,
thiacctazone and isoniazid for 2 months followed
provided appropriate dose sizes and rhythms
by thiacctazone plus isoniazid. The culture
f were used. I had always visualised full supervision
negativity rate at 2 months was significantly
as organisable in urban areas for patients with
higher for the rifampicin and pyrazinamide
reasonably convenient access to the treatment
regimens than for the thiacctazone and 2-drug 6services and it was in fact the preferred regimen
month regimens, and the relapse rates were also
by both patients and staff in a programme
strikingly lower, 3% and 8% respectively,
involving all new patients in a large area of
compared with 22% for the thiacctazone and
Czechoslovakia with substantial urban and rural
29% for the 2-drug combination (the latter
populations set up as a collaborative investigation
difference being statistically non-significant).
between the BMRC and Dr Polansky’s group.16
Nevertheless I had not regarded full supervision
(B) New formulations in the field of leprosy and
as suitable for rural areas in developing countries
tuberculosis
except for patients near to treatment facilities, or
Leprosy
until an effective primary health care
infrastructure had been set up or existed (as was
In recent years, stimulated by the
virtually the way supervision was organised in the
♦ For every patient admitted to treatment a full list of addresses was obtained, namely 1) the patient’s home
address, 2) the addresses of his relatives and friends in Madras city, and 3) how often he visited them, 4) ii
employed, the place of work, 5) if children were at school, its address, 6) the address of his native place. If a
patient failed to attend and the home was locked and the neighbours did not know where the patient or the
family was, a systematic approach to the above alternatives was made until the patient was traced. (Adequate
transport and devoted trained home visitors for this purpose were available.)
TUBERCULOSIS IN INDIA. PAST, PRESENT AND FUTURE
developments with the contraceptive pill, an
increasing number of medicaments arc packed
commercially in “bubble” or “calendar” packs
with a day’s, week’s, fortnight’s or month’s supply.
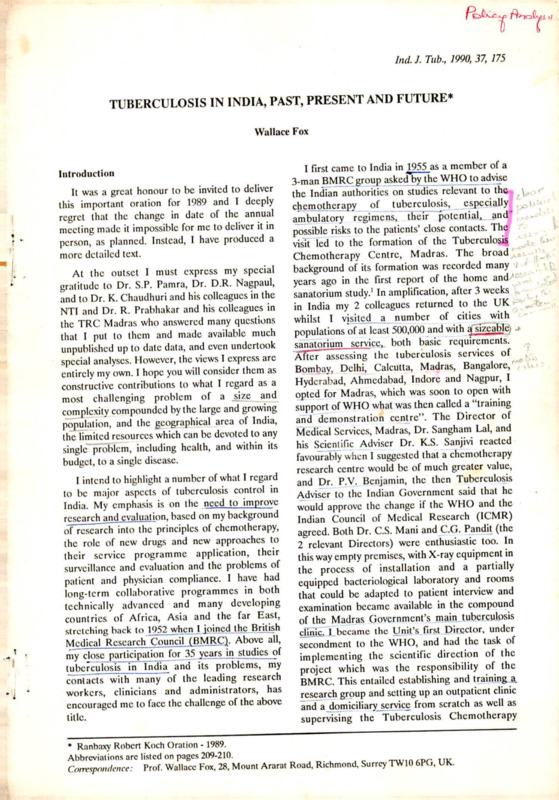
In the field of leprosy this approach has also been
adopted in large-scale pilot investigations. Fourweck calendar packs have been produced for
paucibacillary and for multibacillary (Fig. 1)
patients using WHO drug and dosage
recommendations, in Danish International
Development Agency-assisted projects in 4
hyperendemic districts in India, namely in Orissa,
in Tamil Nadu, and 2 in Madhya Pradesh. In the
Philippines a project supported by the Sasakawa
Memorial Health Foundation and WHO has
been implemented since 1985 and recently in
Thailand the government has introduced blister
packs in a few provinces with both specialised and
semi-integrated leprosy control programmes. The
leprosy mission of South Africa has in Transkei
produced low technology packs which have been
used successfully for several years.25 Such
preparations lend themselves to important
operational studies designed to assess whether,
and, if so, how much gi eater cooperation is
189
obtained by using the packs compared with . /i,
dispensing the same duration drug supply in the
standard way. Even though urine testing26 and
surprise checks of the calendar pack would be
very suitable measures of compliance, I am
unaware of any publication reporting attempts to
assess the benefit from the use of the packs. Such
an approach is important in its own right, but is
also necessary to measure other strategics aimed
to improve further, by whatever means, the
regularity achieved by the use of calendar packs.
Tuberculosis
Turning to tuberculosis, in the ..Philippines the
use of short-course chemotherapy in the National
Tuberculosis Programme was adopted nation
wide in August 1986 for sputum-positive patients,
or those 'with a lung cavity, after 2 negative
smears. Valcza and McDougall (1990) have
reported in a letter in the Lancet27 that in the
Philippines, between September 1986 and
September 1989, over a quarter of a million
patients had a 6-month regimen as two calendar
blister pack preparations.First, one of rifampicin,
isoniazid and pyrazinamidc daily, was given for 2
■>
illisfla
«.
.
■. c
•<-
J
iFig. 1. A 4 weeks calendar pack for multibacillary leprosy, as used in the Indian pilot project. The first dose
(supervised) is rifampicin 600 mg, clofazimine 300 mg and dapsonc 300 mg. The 27 self-administered daily doses
are clofazimine 50 mg and dapsonc KM) mg (Pharmanova, a division of Scanpharm A/S, Copenhagen, Denmark).
190
WALLACE FOX
months. A week’s supply was provided in a single
pack (Fig. 2), but the dimensions arc quite
considerable (15 cm by 10 cm). This was followed
by much smaller weekly calendar packs of
isoniazid and rifampicin daily in the continuation
phase of the next 4 months. There is no cohort
analysis and the data they present do not enable a
clear picture of what gain has resulted from the
use of the calendar packs, but it is reported to
have proved highly acceptable, both to patients
and staff, as an improved approach. They also
state "the__ pace of implementation has
outstripped objective assessments of (heir value,
notably in improving compliance”. (A committee
on the National Consensus on Tuberculosis in the
Philippines representing the Lung Centre of the
Philippines and the Quezon Institute, both
Governmental, has recommended the addition of
a fourth drug due to the high incidence of
resistant cases locally. The Department of Health
has not yet expressed its official view). More
recently a blister pack preparation containing
ethambutol in addition to the other 3
medicaments for the first 2 months is being
marketed in the Philippines (Lederle SCC Kit).
Because of the bulk, each blister pack contains a
day’s supply, a move away from the calendar
presentation. Ciba-Geigy are also marketing in a
number of countries individual daily blister strips
with 2 tablets of rifampicin plus isoniazid, each
containing 300 mg of rifampicin and 150 mg of
isoniazid, and cither 3 or 4 scored tablets of
pyrazinamidc, each of 500 mg, that is the 3 vital
drugs for the first 2 months of bactcriologically
confirmed pulmonary tuberculosis.
The indisputable advantages of the blister
packs arc that they are easier to dispense than
separate medicaments, make it easy for the
patient to know the dosage of each drug to take
daily, and provided the appropriate plastic is used
for the pack, the medicaments arc protected
against hot and humid tropical climates, and the
increase in cost of this type of formulation
(estimated at 5% in the Phillipine study)27 is
small, but might be more (up to 15% has been
quoted) for less expensive regimens. However, it
is clearly important to study, by both surprise
checks of the calendar pack and excretion of the
drugs in the urine, whether patient compliance in
ingesting the daily dose is improved. These arc in
addition to the patient remaining on treatment as
measured by the regularity and punctuality of
attendance to collect supplies, and what
proportion of patients do so for the full duration
of treatment and for those who drop out
[ >
r i fl
W-
'
£
kJ
o^f2’
calendar pack in 2 month intensive phase of short-course chemotherapy for tuberculosis in the
Philippines. A daily dose is rifampicin 450 mg, isoniazid 300 mg and pyrazinamidc 1000 mg and is sclfadministered by the patient at home.27
191
TUBERCULOSIS IN INDIA. PAST, PRESENT AND FUTURE
prematurely the reason why. Also, what are the
therapeutic results in the latter as compared with
the outcome in the patients who complete the
course? The real proof of therapeutic benefit is
fewer failures during treatment and a lower
relapse rate when compared with dispensing the
same medicaments in ordinary containers (in the
developing countries often an envelope or
wrapped in a piece of newspaper). It is relevant
that therapeutic benefits are much easier to
measure in patients with pulmonary tuberculosis
than in leprosy, because clear-cut bacteriological
culture assessments can be made during
treatment as well as bacteriological relapse after
stopping, which, if it occurs, usually docs so
within the first year or two of follow up.
(C) Converting an intermittent regimen into a
daily regimen-a research problem
In the light of these experiences with drug
packs, an important research approach which I
now wish to suggest is the possibility of
converting a fully supervised intermittent regimen
to what, from the patient’s point of view, would
be a daily regimen. This could be achieved by
using calendar packs for 1, 2 or 4-wcek periods,
but ensuring that every day the patient has at
least one pill to take. Table 6 illustrates research
daily calendar pack options, as alternatives to a
fully supervised intermittent regimen ol
ethambutol,
isoniazid,
rifampicin,
and
pyrazinamide given 3 times a week for 2 months
followed by rifampicin and isoniazid, also fully
supervised, twice a week for 4 months (a month is
usually a lunar month in clinical practice). The 3times weekly regimen could be spread over a 6day period in the way illustrated in the table
giving rifampicin plus ethambutol one day and
isoniazid plus pyrazinamide on the next in a
calendar pack for the patient to sclf-administcr at
home. There is good evidence that both 2-drug
combinations achieve a high level of effectiveness.
Isoniazid and pyrazinamide was compared with
isoniazid and PAS in the era when 2-drug
combinations were used and was at least as
effective as the latter.28-29-30 Rifampicin plus
ethambutol as retreatment for failure patients in
Hong Kong was surprisingly effective (ranging
from 79% to 87% success rates) when given,
1 daily, twice a week and even once a week, or once
° a week after a 1-monlh daily phase.3132 Sunday
could cither be a placebo (P) day or an extra dose
of isoniazid could be given.
Table 6. Convening a supervised intennittent regimen to
a daily regimen in calendar pack form*
A Research Approach
First 2 months
Next 4 months
Fully Unsupervised Fully Unsupervised
Day
supervised calendar supervised calendar
of
packs
dosage
packs
week dosage
Mon
EHRZ**
RE
RH
RHor RH
HZ
P
H
RE
P
H
RH
RH
RE
P
H
Sat
HZ
P
H
Sun
PorH
P
H
Tue
Wed
EHRZ
HZ
Thur
Fri
EHRZ
RH
♦The essential first step is to study every dose of both
types of regimen given under full supervision (ref 35
and pages 191-192)
**For definitions see footnotes to Tables 3 and 4
P = Placebo
In the continuation phase, instead of twiceweekly fully supervised rifampicin plus isoniazid
there arc daily blister pack options (Table 6).
Thus the twice-weekly regimen could remain
unchanged and on (he rest of the days the patient
could receive a placebo (P) tablet or alternatively
an extra dose ol isoniazid. There are a number of
other regimens given intermittently throughout,
or daily initially and then intermittent, but the
principle proposed would still apply. The
evidence from India is that currently patient
compliance with all the regimens so far tried
under District Programme conditions is
disappointing as in so many developing countries,
and for India fully intermittent regimens in rural
areas. Hence the need for a radical change of
approach, which the calendar format would offer
if impeccably conducted research shows it to be
justified. It is unlikely that sociological enquiries
and the study of non-cooperative or failure
patients are going to solve the problem in
tuberculosis since it applies to all long-term
therapy of any disease and very often short-term
therapy too, as well as to prophylaxis.33 Much has
been published since then, including books on the
subject,34 but the basic general problem remains.
(D) The role of the Tuberculosis Research
Centre (TRC) in exploring (C) above
Professor Mitchison and 1 had discussions
x
192
WALLACE FOX
several years ago with our Madras colleagues
about the need for a study of an intermittent
regimen compared with the same drugs
presented in pairs to make a daily regimen. The
Centre undertook a pilot study of the daily
regimen approach, which has provided evidence
to justify a carefully conducted controlled clinical
trial along the lines discussed in (C) above. The
claims for calendar pack preparations from
workers in the field of leprosy, including India
itself, provide further justification for converting
an intermittent to a daily regimen as I suggest in
section (C), as well as the recent report on
tuberculosis from the Philippines.27 The essential
first step is to obtain accurate information of
effectiveness and toxicity of the 2 approaches
under strictly controlled trial conditions when
every dose of both regimens is fully supervised.35
This will establish whether a substantial scale
field trial of a calendar pack preparation should
be launched, again with a proper evaluation of
patient compliance. The target is an effective, less
toxic, cheaper, more acceptable and more easily
dispensed regimen, protected from the
environmental temperature and humidity when in
the patient’s charge. Such a study under strict
supervision of every dose of both regimens, which
is an essential feature of the study design, will
start shortly in the TRC and its sub-centre in
Madurai. It is only such a study that can establish
whether the regimens in this form merit, in due
course, comparative field trials using calendar
pack preparations. Such field trials too, if and
when this stage proves justifiable, will need very
careful design, planning and execution, if the
findings arc to carry conviction. I do not advocate
this approach being used in routine clinical
practice for it is an hypothesis to be carefully
tested first.
(E)
The underlying mechanisms
This is a complicated issue and I have no
pretensions to being a laboratory scientist, so I
write from my own viewpoint. In the early days of
chemotherapy it was regarded as essential to
maintain continuous minimal inhibitory
concentrations of each medicament throughout
the 24 hours. For this reason the administration
of the drugs was in divided doses, 4 times a day
being a common rhythm in the early days for
PAS.36-’7 An important step forward was made
from two observations in the late 1950s and early
1960s in Madras. First, that patient non-
compliance was not solely a problem of bulky
PAS (a view strongly held in WHO circles at that
time) but that it applied equally to isoniazid and,
indeed, to placebo also.38 Secondly, 400 mg of
isoniazid a day was more effective when given
alone to patients with smear-positive cavitary
disease in one dose than when given in 2 doses of
200 mg.31' This was so even though all the patients
on the divided dose, whether rapid or slow
inactivators of isoniazid, had a continuous level of
serum isoniazid above the minimal inhibitory
concentration of the drug, which was not the case
with the single 400 mg dose a day.21 Obviously
one dose a day makes less demands on patient
compliance and family supervision than 2 doses a
day.
Another view which was held in the early days
of chemotherapy was that it was essential to give
the drugs in combined chemotherapy together, in
order that each drug protected the other or
others from the emergence of drug resistance.
Indeed, there was a period in the 1950s and early
1960s of strong advocacy of studying the serum
level 6 hours after a dose of drug and relate this
to the ability of dilutions of the scrum to kill the
individual patient’s tubercle bacilli (the specific
scrum antimycobactcrial activity test) not only to
isoniazid and streptomycin but other drugs,
including
PAS,
kanamycin,
viomycin,
thiacctazone, cycloserine and pyrazinamide.40 The
National Jewish Hospital, Denver, Volumes of
the period, e.g. Volume 21,41 make fascinating
reading, and the stimulating work of Gardner
Middlebrook (an outstanding figure), William
Russell Jr, William Dye, Irving Kass, Sidney
Dressier, Maurice Cohn and their colleagues and
its scale in a single group reminds us of an era
(and of the earlier pioneers) when there was
great worldwide interest in tuberculosis
chemotherapy and the underlying mechanisms,
new drugs and their optimum clinical use. This is
in sharp contrast to the current era when the
pharmaceutical industry is loath to bring
promising new antitubcrculosis drugs to the state
of clinical trial, although they are badly needed
for the third world countries. (The technically
advanced countries too would be beneficiaries of
their study in the third world countries, as has
happened for many years with ambulatory
chemotherapy
and
standard
duration,
intermittent and short-course regimens).42
Questions of additive or synergistic activity
IWERCUIjOSIS IN INDIA. PAST. PRESENT AND FUTURE
and antagonism between drugs arise. The
construction of isobolograms, standard practice
for nontubcrculous antibacterials have been
studied for non-tuberculous mycobacteria.4344
Appropriate animal experimentation is obviously
important.
A simple view, which may well be largely
correct, is that each bactericidal drug will
eliminate dividing bacilli drug-sensitive to it if it is
given separately and that it is only doubly
resistant strains that might multiply when a 2drug combination is given, but that even when
given together, doubly-resistant strains are less
likely to respond to a 2-drug combination than a
fully sensitive strain or a strain resistant to one
drug. This was the basis for the view that the
addition of extra drugs at the start of
chemotherapy was desirable when there was any
likelihood that initial drug resistance might be
present. We must also remember that the
patient’s host resistance is a “drug” and can be a
very powerful one as testified by extensive healed
and calcified pulmonary tuberculosis lesions that
had never been diagnosed, much less treated, in
the pre-chemothcrapy era. Mitchison45 has
emphasised that in the prevention of drug
resistance the early bactericidal activity of drugs
and the sterilising capacity of drugs must be
considered separately. The overall evidence is
that important features in the construction of
effective regimens include (1) the drugs given, (2)
the total quantity of each drug a week, and (3) the
interval between doses. The aim is, in fact, to use
each drug in its optimal way taking into
consideration its pharmacokinetic characteristics,
its type of antibacterial effect and its toxicity.
There is also much evidence of the lesser need
for potent combinations in the continuation
phase, and that intermittency, even at a frequency
of once a week, with rifampicin and isoniazid, is
an effective continuation regimen46 (in the rural
areas of Hong Kong, rifampicin, isoniazid,
streptomycin and ethambutol.47) Indeed there is
now a possibility that other rifamycins might well
be effective at longer intervals than weekly in the
continuation phase.48
Drug Combinations and the Bioavailability of
Rifampicin
Combined preparations of antitubcrculosis
193
drugs have been widely used since soon after the
introduction of isoniazid in 1952. Combinations
of isoniazid with PAS, thiacctazonc, ethambutol
and rifampicin have been marketed on the
grounds that (1) it is more convenient for the
patient to take isoniazid and a companion drug
together rather than separately, and (2)
monotherapy, especially with isoniazid alone with
its greater risk of the emergence of isoniazid
resistance, is avoided. Isoniazid monotherapy was
a tempting choice for patients because of its small
bulk, when compared with, for example, 10 grams
of bitter PAS sodium. However, a special
problem has arisen about the bioavailability of
rifampicin and the quality control of combined
preparations containing rifampicin.
Fixed combinations of isoniazid and rifampicin
have been widely used for many years. More
recently, a fixed combination of rifampicin,
isoniazid and pyrazinamide developed by Lepetit
is now marketed in the UK by Mcrrel Dow.
Similar preparations arc available in other
technically advanced countries too. Since the late
1970s, my BMRC colleagues, Professor
Mitchison, Dr Gordon Ellard, and I were closely
involved in the design of 2 such combined
formulations by Lepetit : one was for daily
regimens (Rifatcr 2* which contained 50 mg
isoniazid, 120 mg rifampicin and 300 mg
pyrazinamide per tablet). The other was for
intermittent chemotherapy which required
different proportions of the 3 drugs (Rifatcr 3,
which contained 125 mg isoniazid, 100 mg
rifampicin and 375 mg pyrazinamide per tablet).
Early unpublished studies conducted by Professor
Acocclla and his Lepetit colleagues showed that
scrum levels of isoniazid, rifampicin and
pyrazinamide after giving them in 3 combined
Lepetit preparations (Rifater 1, 2 and 3) were
closely similar to those achieved when the same
quantities of the 3 drugs were given to volunteers
as separate formulations in cross-over design
studies in Italy. In a further Lepetit preparation
(Rifatcr 4), unbeknown to the firm’s research
group the pharmaceutical section had altered the
order in which the 3 drugs were mixed. The
consequence was a striking and alarming
reduction in the absorption of rifampicin in the
bioavailability studies (Acocella, personal
communication).
* The first formulation (Rifatcr 1) was never taken to clinical trial because of the low dosage of pyrazinamide it
provided.
196
WALI^XCEFOX
In my view the only safe policy currently is,
therefore, to avoid the use of fixed triple
combinations of rifampicin, isoniazid and
pyrazinamide unless their origin is from sources
with impeccable reputation and quality control,
and with
unquestionably
“demonstrated
bioavailability" as emphasised by Pamra,58
Reichmann61 and the above (1988) editorial.59
This is especially important in the many
developing countries which, like India, already
have high levels of initial drug resistance to
isoniazid and to streptomycin. If such a policy is
not followed there will be a high risk of using
preparations with a poor bioavailability of
rifampicin which could have disastrous
consequences both for the individual patient and
the national programme for it could lead to a
high failure rate with short-course chemotherapy
and eventually much more resistance to isoniazid,
to rifampicin, and isoniazid plus rifampicin. In
this connection the responsibility that many
countries have accepted under the WHO
certification scheme for drugs to be exported arc
highly relevant.62 Now the onus must clearly be
for the manufacturers to provide adequate batch
data for all triple combinations before they arc
marketed even in the country of origin, an issue
that clearly falls within the WHO ambit and
which applies, on current evidence, to all
production in every country, and possibly the
double combination too.
I now, however, view the situation from a
different and important point of view which I
consider calls into question the alertness and
awareness of the pharmaceutical industry in
relation to quality control exercised over the
production of rifampicin-containing combina
tions, certainly the triple formulation, and
possibly even the combination of isoniazid and
rifampicin as marketed in the developing
countries, which is also a most worrying aspect.
In the investigations of Ellard et al.4- of the 2
Rifater formulations referred to above, not only
were plasma levels of rifampicin, isoniazid and
pyrazinamidc estimated, but also the urinary
excretion of the 3 drugs and their principal
metabolites. Both sets of measurements indicated
the excellent bioavailability of each of the 3 drugs
in the 2 combined formulations. These findings
clearly confirm the evidence previously obtained
over a decade ago by a group working in CibaGeigy in Basle. Brcchbuhler and his colleagues63
published in 1978, that the renal elimination of
rifampicin plus dcsacetyl rifampicin provides a
reliable and much more convenient method of
assessing rifampicin bioavailability than
estimating areas under plasma concentration
curves.
The similarity in the results obtained in these 2
studies are noteworthy. Brcchbuhler et al.63
extracted rifampicin and dcsacetyl rifampicin into
toluene and measured the absorption of the
extract at 478 nm. In this way they showed that
after giving doses of 600 mg rifampicin in their
standard formulation, some 13% of the dose was
excreted in the urine within 24 hours. Ellard et
al.49 used the colorimetric method54 of Sunahara
and Nakawgawa (1972), in which rifampicin and
dcsacetyl rifampicin are extracted from urine into
an equal volume of isoamyl alcohol and the
absorption of the extract measured at 475 nm.
They recovered 15% of the dose of the standard
formulation and 14% of the 2 Rifater combined
formulations in the urine within the same time
period. Furthermore, the more detailed kinetic
studies of Brcchbuhler et al.63 suggest that
rifampicin bioavailability studies could probably
be conducted using urine collected just over the
first 8 hours following dosage, since 78% of the
total urinary excretion occurs during this time.
A further valuable precaution would, of
course, be to confirm the completeness of the
urine collections using the simple colorimetric
alkaline picrate method.
These urinary methods are clearly both much
easier and cheaper to organise and undertake
than the invasive and much more technically
demanding scrum assays. They fall well within the
scope of at least some laboratories in many
developing countries, and, of special importance,
the National Drug Supervisory laboratory as well
as the State level reference laboratory in a
country such as India. Thus, drug regulatory
bodies can, in fact, exercise effective quality
control. They can also insist that the
manufacturer checks each batch, a practice
already common in the field of vaccine
production.62
Cross-over studies can therefore readily be
designed to compare the bioavailability of
rifampicin in combined formulations with that in
standard formulations of the same rifampicin
alone. Aliquots of urine samples can now be used
TUBERCULOSIS IN INDIA, PAST, PRESENT AND FUTURE
to test the ability of selected laboratories in
developing countries to perform the urine assay
accurately with other aliquots being assayed in
reference laboratories in technically advanced
countries. Parallel scrum/plasma samples can
also be obtained in selected studies for testing
abroad to confirm the urinary bioavailability
conclusions.
It would be valuable to know what batch
quality control the pharmaceutical firms in the
technically advanced countries who arc marketing
the triple combination have been using in the past
as well as currently, and I hope that this
information will be forthcoming because it may
provide further guidance.
In my view, there should be a meeting of the
WHO and its expert advisers with representatives
of some major pharmaceutical firms marketing
the triple combination, so that what might be
regarded as “a case study” of the manufacture
and marketing of the triple combination can be
undertaken. This would review quality control,
past and current, and what procedures should be
followed in future, and how best to organise
further parallel studies of urinary excretion and
serum levels, which might well need to involve the
WHO. The WHO could inform Governments of
the recommendations reached. Such a review
should also include the manufacture of
preparations of isoniazid and rifampicin which
might well be a majoi problem too. I have been
informed from a reliable pharmaceutical source
that experience shows that there arc significantly
more batch problems with the manufacture of
rifampicin and isoniazid than with rifampicin
alone (Acocclla56 had found that 1 of 3 double
combinations was deficient in the bioavailability
of the rifampicin) and it is likely that the same
happens when a third drug is added, in this case,
pyrazinamide.
Antituberculosis Drugs in India
There are a number of important aspects of
antitubcrculosis drugs in India which have to be
considered. Their national availability, cost and
quality, and the regimens used and their
availability and acceptability to the patients, are
all of great importance.
1.
Bulk supplies of antituberculosis drugs
In 1983 the Adviser (Drugs) to the Govern
ment of India gave me information on the metric
197
tonnes of each antituberculosis drug available in
India for the year 1982-83 as well as the licensed
capacity (that is the maximum quantity which can
be made available either by manufacture in India
or importation) and the amount imported. These
figures, required for the Merck Oration10 were, as
I had been warned, not easy to come by, nor wqs j
permission to publish them. From these data I
calculated the number of patients who could be
treated daily for a year as a convenient measure
for comparisons from year to year related to the
number of new patients diagnosed.
The bulk supplies of antituberculosis drugs
available in India annually from 1982 to 1986 are
informative (Table 7). Unfortunately, the 1982-83
figures arc the only official Government figures.
The rest of the figures are from unofficial
sources, but I have been advised that there is no
reason to doubt their reliability. They show that
adequate quantities of isoniazid were available
with a drop in 1985-86, a year when isoniazid was
unavailable in many Government treatment
centres because the producers, who were mostly
the smaller firms with limited resources, could
not make a profit if they supplied it at the price
the Government had fixed.65 There were
adequate stocks in the local markets at a higher
cost, yet Government units had no option but to
give the patients prescriptions for them to
purchase this essential medicament themselves!
Unfortunately, such shortages still occur and
Prabhakar (personal communication) recently
(1989) encountered an isoniazid shortage in a
district in one of the major States. This re- i:
emphasises the importance of satisfactory drug
ril,A
manufacturing and importing policies, ordering,
stocking, and distribution system throughout
every State, including all the PHIs involved in the
programme.
It is clear from Table 7 that nationally PAS has
a very minor role, that the use of thiacetazone is
declining, whereas in contrast the use of
ethambutol has increased substantially. In this
respect a view has grown up over the years in
India that thiacetazone is frequently toxic and
unacceptable to the patients, although no
evidence that I am aware of has been produced to
confirm that the level and severity of adverse
reactions is particularly high or that divided
doses, as recommended, docs not usually resolve
indigestion. Ethambutol has been widely
advocated, advertised and accepted as a safe
WALLACE FOX
198
Table l.Antituberculosis drugs in India
(metric tonnes)
Drug
Licensed*
capacity (1.4.83)*
Number of patients who could
Total available
be treated daily for a year
1982-83*
1983-84
1984-85
1985-86
1982-83
1985-86
Isoniazid
433
199
152
205
113
1,817,000
1,031,000
PAS and salts
1,090
288
217
119
107
79,000
29,000
Thiacctazonc
153
49
38
47
18.25* +
895,000
333,000
Ethambutol
121
123
207
269
295* *
421,000
1,010,000
Pyrazinaniidc**
3
17
34
14.5
52**
31,000
94,000
Rifampicin**
0
25
75
67
71
152,000
429,000
Streptomycin
490
247
248
235
188
902,000
686,000
•Licensed capacity = maximum quantity of drug which can be manufactured or imported
*Thcsc figures were provided by the Adviser (Drugs) to the Government of India
**A11 imported
* * Figures for year calculated from supply in first 10 months.
substitute. However, it may cause irreversible
ocular damage which, although uncommon when
appropriate dosages are used, is still a risk. In
many developing countries, including India,
ocular lesions with impaired vision are
particularly common in the general population.
The widespread use of ethambutol under field
conditions with supervision by relatively
untrained paramedical staff with little access to
skilled medical staff might well prove hazardous.
Because of the increasing use in district
programmes in developing countries, this risk
must not be overlooked and special care in young
children, the elderly and in impaired renal
function, is necessary. Publications from India66-67
warn caution, and consideration should be given
to organising studies to establish what risk exists
in District Programme conditions.
date. The Tuberculosis Association of India65 was
also unable to obtain the official Government
figures on a regular basis (Pamra, personal
communication).
The use of pyrazinamide is increasing and this
is likely to continue as the switch to short-course
chemotherapy increases because it is one of the 3
major drugs in this type of regimen. The use of
streptomycin shows evidence of decline, and this
too is likely to continue because limitations of
cadres of staff permitted to give streptomycin
injections and the advent of AIDS (not the only
risk) raises further cause for concern about
injections under field conditions.
In my view the information on licensed
capacity and quantity of each drug should not
only be made freely available but should be
published annually in the appropriate respiratory
diseases journals, in addition to the Indian
Journal of Tuberculosis and the NTI Newsletter
so that the medical profession can discuss and
decide if they are appropriate. In considering the
quantities it is also important to know about
exportation. Indeed, steps should be taken to
obtain and publish the official figures from 198283 up to 1989, as soon as possible, so that we can
get up to date and also check whether the figures
from 1984-86 in Table 7 are accurate, and also
take into account the influence of exportation. If
there are good reasons why export figures need to
be kept confidential at a Governmental level,
then the publication of the annual supply of each
drug available in India should be reported. In
198768 it was reported that exports of bulk drugs
and formulations were worth over Rs. 217 crores
and that the Indian pharmaceutical industry is
one of the most diversified and integrated
industries in the entire third world.
How much more valuable the information in
Table 7 would be if it contained the official
Government annual figures and was fully up to
This is a period when (he regimens used in
India are changing year by year and from State to
State and are likely to do so for many years to
TUBERCULOSIS IN INDIA, PAST, PRESENT AND FUTURE
come, as short-course regimens are progressively
introduced and modified in the light of further
knowledge of their efficacy and of service
programme experience.
2.
The number of doses of drugs in a regimen
Rather than consider the number of patients
that could be treated daily for a year, as above, it
is more realistic, with the introduction of short
course regimens, to consider the quantity of each
drug likely to be given to a patient in an effective
regimen, and then calculate how many patients
:ould be treated with that regimen from the bulk
supplies available.
For example, there are a number of highly
effective 6-month daily regimens containing
rifampicin throughout that require 180 doses. We
know, however, that 60 doses of rifampicin is an
important quantity which might be given in
several very effective ways, for example daily for 2
months, 3 times weekly for over 4 months, and
twice-weekly (only 52 doses) for 6 months. The
bulk supply of rifampicin available for the year
1985-86, if none was exported and its use was
restricted to tuberculosis (it is also used in
leprosy and other infections), would be enough to
provide 60 doses for more than l/z million
patients receiving 450 mg doses and just under 2
million on 600 mg doses! On the basis of
information provided by Dr SK Noordeen of
WHO of the therapy policies in India, I have
calculated that in 1986 it is likely that the quantity
of rifampicin used for the treatment of 300,000
leprosy patients, of whom I have assumed one
third were multibacillary and two thirds
paucibacillary, was 4 metric tons. These
requirements for leprosy reduce the above
calculation in Table 7 by 100,000 patients on 600
mg. Thus, the leprosy programme was a minor
consumer of rifampicin. Although the quantity
now used has increased substantially with
intensification of the treatment programme with
regimens that include rifampicin, leprosy remains
a minor consumer compared with the rifampicin
production.
It is of particular interest to consider
pyrazinamide because its only use is as an
antituberculosis drug, important because of its
unique sterilising role.10 It is given as a maximum
of 60 doses when it is prescribed daily for 2
months, a widely used duration and rhythm, even
199
in the technically advanced countries. In the
service programme in Hong Kong it is currently
given 3 times a week for 4 months (an exceptional
duration but still less than 60 doses) in a fully
supervised 6-month intermittent regimen. In
District Programme conditions in India it is being
given either as 60 daily doses or twice a week for
the first 2 months (16-17 doses) for smear
positive patients, and is currently being studied in
Madras in a controlled clinical trial, given 3 times
a week for 3 months (39 doses). The 52 tonnes
bulk supply in 1985-86, if none had been
exported, would provide enough pyrazinamide to
give 60 doses to nearly 600,000 patients, or a
twice-weekly supervised dose for 2 months to
over 2 million patients. I might add, en passant,
that a small proportion of the metric tons arc of
morphazinamide, although in a detailed review of
the literature a few years ago I could find no
evidence whatsoever to justify its use instead of
pyrazinamide. The claim of lesser toxicity is
misleading since it is less active than
pyrazinamide. In my view its use should be
stopped.
Since the regimens that contain rifampicin
and/or pyrazinamide which are recommended
for the National Programme are those in Table 4
monitored by the NTI, it is clear that there were
apparently very large supplies of both of the
drugs in India. The impression these figures in
Table 7 give is of an excess of at least some drugs
rather than a shortage. This again underlines the
need to know what the Indian consumption
actually is.
3.
The cost of individual drugs currently used
in District Programmes
The latest cost of doses of individual drugs is a
basic figure, for from it the cost of any regimen
can be calculated. By far the cheapest drugs
(Table 8) are isoniazid and thiacetazone. The
substitution of ethambutol, which is 7 times as
expensive as thiacetazone, as a companion drug
to isoniazid results in a fourfold increase in price
of ethambutol plus isoniazid as compared with
thiacetazone plus isoniazid, and PAS produces a
tenfold increase in price. If rifampicin is the
companion drug, the average cost of a dose of
isoniazid plus rifampicin is no more than of
isoniazid plus PAS, and in practice rifampicin is
given for a much shorter period of time and many
fewer doses are given. Pyrazinamide, expensive in
WALI jXCE FOX
200
Table 8. Cost per dose of antitube/vulosis drugs in
Madras (April 1989)
Drug and dose
Isoniazid 300 mg
Thiacctazone 150 mg
Streptomycin 0.75 g
Sodium PAS 10 g
Ethambutol 800 mg
Pyrazinamide 1000 mg
Pyrazinamide 1500 mg
Pyrazinamide 2000 mg
Rifampicin 450 mg
Rifampicin 600 mg
Price per dose (rupees)
0.11
0.09
2.76
2.01
0.67
1.65
2.37
3.30
1.86
2.48
individual doses, is given as a maximum number
of 60 doses. Streptomycin is the most expensive
individual drug with the added cost of the
injection, the restriction to individuals authorised
to give them and the increasing concern about the
transmission of infections.
It must be added that drug costs in India do
fluctuate rapidly, some increasing and others
decreasing, so the cost of regimens must be
calculated annually.68 Hence also the desirability
of bulk purchase arrangements for as long a
period in advance as can be negotiated, especially
those purchased from abroad.10
(4)
Who pays for antituberculosis drugs?
The Planning Commission of the Central
Government (“Hindu” 6.7.83) turned down the
recommendation of a Health Ministry Task Force
that it should provide all the antituberculosis
drugs required for the National Tuberculosis
Programme free. Instead, it is adhering to the
policy of providing 50% of the drugs supplied to
the State Government clinics and to other
schemes shared equally by the Central and State
Governments. Again, I wish to repeat my view10
that the medical profession must make a
concerted and sustained effort to have this
decision reversed. In addition to the psychological
effect of the Central Government showing its
commitment to giving priority to Tuberculosis
Control as recommended in the National 20point Plan, the provision of 100% of the
necessary antituberculosis drugs would remove
the shortages because of States underbudgeting
for tuberculosis drugs on financial grounds, in
relation to their own health priorities.
(5) Quality control of antituberculosis drugs
There are a limited number of antituberculosis
drugs relevant to district programmes in India
(Table 8) and it is important that their quality is
monitored. This is no easy task in a country,
which, in addition to major manufacturers (or as
in the case of rifampicin and pyrazinamide, of
imported powder) has a very large number of
small firms preparing medicaments in what, in
pharmaceutical terms, can only be regarded as
unsatisfactory conditions, with, at best, suspect
quality control, if any at all.65,68 The method of
packaging for hot humid conditions, of storage by
the distributors and their outlets, and the sale or
use of drugs that have passed their expiry dates,
are also relevant, especially in rural areas. The
question arises whether the sources of reliable
antituberculosis drugs should not be reviewed
and monitored to the satisfaction of an expert
group, so that order is brought into what is, to say
the least, a difficult and confused situation.
General practitioners who represent a major
sector of the prescribers of antituberculosis
therapy must also be kept informed of the need to
adhere to high quality formulations, and be given
guidance as to which they are. They should advise
their patients about reliable stockists, and this is
particularly important in District Programmes
and in rural areas.
It is relevant that the TRC keeps a careful
check on the quality of drugs which it uses in
controlled clinical trials to be sure of their
potency and this is a wise precaution. It has also
conducted a study which showed that the
rifampicin, isoniazid and pyrazinamide used in
the North Arcot district programme conditions
remained potent when stored for up to 30 months
in circumstances far from favourable, although
not fully documented (GS Sarma, personal
communication), a study that could well be
repeated in areas of high temperature, high
humidity, or both. The aim, however, should be to
ensure refrigerated storage whenever possible, be
it bulk supplies in a Central or State Government
store or the stock of a peripheral dispensary or
pharmacies where general practitioners’ patients
may take their prescriptions.
Pre-treatment Drug Resistance
A knowledge of the level of primary drug
'' —1
1
• -
’
TUBERCULOSIS IN INDIA, PAST, PRESENT AND FUTURE
resistance (that is resistance of strains in newly
diagnosed patients who have had no previous
chemotherapy) or of initial drug resistance, which
includes in addition (1) not only such patients, but
(2) patients who have unknowingly received
antituberculosis chemotherapy, for a chronic
cough without adequate investigations, and were
not informed what their medicaments were, (3)
or had knowingly had previous chemotherapy and
concealed the fact for fear that they would not be
retreated. In developing countries representative
surveys to monitor the levels of drug resistance in
newly diagnosed patients arc of importance,
especially to isoniazid, and now, above all, to
rifampicin, especially if they have a large private
sector, as in India, and rifampicin is also being
used on an increasing scale in the public sector.
In technically advanced countries, it is usually no
problem to identify with certainty primary drug
resistance, but they also have a special need to
monitor the trends in immigrants and in
disadvantaged sections of the community.
In the early days of chemotherapy there was a
fear that the careless use of the then available
drugs, streptomycin and PAS, and from 1952
onwards isoniazid, could lead to a build up of
chronic excreters of drug-resistant strains who
would progressively spread primary drug
resistant infections leading to very high levels of
primary resistance in new cases, and rendering
the available drugs increasingly less effective in
therapy.
The BMRC monitored this possibility in 2
surveys, the first in 1955-56 on a weighted
random sample of 80 chest clinics drawn from the
450 of the whole United Kingdom69 and the
second survey in 196370 sampled 125 clinics since
the total of new cases per annum had declined.
All new patients attending the clinics with
pulmonary tuberculosis had bacteriological
specimens sent to Professor Mitchison’s
laboratory in the Royal Postgraduate Medical
School, London, for smeqj-, culture and sensitivity
testing, until each had achieved its quota. The
level of isoniazid resistance in new cases of
British and Irish patients (the vast majority of the
cases at that time) was 0.6% and 1.3%
respectively and for streptomycin it was 2.2% and
2.8% respectively, very reassuring findings. In
1978-7971, 198372 and 1988 (unpublished) the
BMRC conducted surveys of all newly-diagnosed
patients notified by statutory requirement in
201
England and Wales in a 6-month period (12
months’ periods in children and young adults in
the second and third surveys). Because the total
number of patients had declined substantially
since the 1960s, such comprehensive surveys were
feasible. There was, moreover, increasing interest
in following the trends in the white population
and the now larger immigrant groups. No
relevant information on ethnic origin,
bacteriological status or radiographic severity of
chest lesions was available from the notification
system, so special surveys were necessary. In
addition to a detailed review of pre-treatment
characteristics of the disease, whether pulmonary
or extrapulmonary, or both, we also had a special
interest in knowing the regimens of
chemotherapy then being prescribed and their
duration and, in the 1983 survey, the results
achieved as well. It will be seen (Table 9) how
little drug resistance there was in the white ethnic
population in each of the 3 surveys and that in the
1988 survey, where information on the patients of
Indian ethnic origin was available (separately
from those of the Pakistani/Bangladcshi ethnic
group) the findings arc very similar. It will also be
seen that considering all ethnic groups combined
the overall level of drug resistance in England
and Wales remains low. Rifampicin resistance is
not a problem, nor is resistance to ethambutol
and the most frequent resistance is to
streptomycin, a drug whose use is, in any case,
progressively declining.
In developing countries, it is less easy to
conduct representative surveys, but we have done
so in 3 surveys in a weighted random sample of 11
of 30 districts of Kenya over a 20-year period,
196473, 197474 and 1984.75 The same central
reference laboratory in Nairobi using standard
BMRC techniques did the cultures and sensitivity
tests, supervised by the same senior laboratory
technician seconded from Professor Mitchison’s
Unit. It was possible to do such surveys because
Dr Pierce Kent (subsequently Director of the
East African Tuberculosis Investigation Centre)
had established in the mid-1950s a treatment
register in each district and every patient brought
under treatment in the district had their
identification details recorded in the register. The
same district register system was specifically
introduced in Tanzania by Dr R Doyle so that it
would be possible to conduct the first
representative survey in 1969,76 and a second one
in 1978/8077 at a time when the National
WALLACE FOX
202
Table 9. Results of pre-treatment sensitivity tests to Isoniazid, Streptomycin, Ethambutol and Rifampicin for previously
untreated patients with respiratory disease notified in 1978/79, 1983 and 198tf in England and Wales
1978/79 survey69
Initial resistance
White
%
No.
%
12
%
No.
No.
%
No.
%
No.
2
3
4
8
2
Indian
White
All ethnic
groups
White
All ethnic
groups
No.
1988 survey*
1983 survey70
%
All ethnic
groups
%
No.
10
Isoniazid alone
Streptomycin alone
3
Ethambutol alone
Rifampicin alone
0
0
Isoniazid and
Streptomycin
3
0.4
8s
0.7
1
0.2
10
1.2
2
0.4
1
0.6
7*
0.8
Total with a
resistant strain
13
1.6 32
3.0
10
1.6 39
4.6
13
2.4
6
3.6 32
3.8
Total with a
sensitivity test result 801
100 1070
100
623
855
100
543
100
165
840
100
7
1 H
L- 1.2
J
°J
6
U 2.2
0
100
0
0
0 —1
o0 -J
1 n
1—3.0
2.0
1
0 -J
-f J
100
k-3.0
*J. Darbyshirc, personal communication
sOnc resistant to Rifampicin as well
*Onc resistant to Rifampicin as well, another to Ethambutol
Programme was in a state of reorganisational
upheaval and the registers were not properly
kept. As with Kenya, the central laboratory used
BMRC methods, and was supervised by a
seconded senior technician from Professor
Mitchison’s Unit. This district register approach
has been adopted in other countries, becoming,
for example, in the last decade a standard and
central feature of the International Union
Against Tuberculosis and Lung Disease mutual
assistance programmes.
The findings for Kenya on drug resistance arc
given in Table 10. They arc very similar over the
whole 20-ycar period. It is very encouraging that
they show no evidence of a build-up of initial drug
resistance in previously untreated eases. It must
be added, however, that the great majority of
Kenyan Africans arc treated in the government
health service and that there was very little
competition from private practitioners, especially
during the earlier surveys. Further, the evidence
is that the rate of new' registrations of pulmonary
tuberculosis per 100,(XX) of the population of
Kenya in 1964 was 65.9, in 1974 51.1, and in 1984
42.7, which probably represents a genuine decline
rather than a less efficient diagnostic service, the
change in rate between 19€>4 and 1974 being a
decrease of 22% and between 1974 and 1984 a
decrease of 16%. However, the estimated
population in millions in the survey districts was
3.39, 4.94 and 7.24 respectively over the 20-ycar
period, so that in absolute numbers there were
more cases in 1984 than there were in 1964 and
1974. (The findings of HIV infections and the
association with tuberculosis is a dramatic event,
which may not, however, necessarily influence
patterns of drug resistance, but speculation is no
substitute for hard facts.) The resistance figures
for Tanzania arc also shown in Table 10.
Turning now to India, the problem of
conducting surveys is totally different in such a
large country with a population of over 8(X)
million in 437 districts. Even so, I would remind
you of 2 important ICMR surveys™79 coordinated
from the TRC by Dr PRJ Gangadharam in the
1960s using MRC laboratory methods and ways
of defining drug-resistant strains which had been
introduced by Professor Mitchison in 1956. The
methods have been unchanged ever since. India
has the great advantage of having in Madras a
national reference laboratory, which is widely
recognised as an international reference
laboratory too.
The first ICMR survey78 was conducted in
patients with
no
history
of previous
chemotherapy. Nine centres were chosen (Table
11), 8 because they were on convenient air routes
to Madras and were eager to cooperate, the
TUBERCULOSIS IN INDIA. PAST, PRESENT AND FUTURfi
203
Table 10. Kenya/BMRC and Tanzania/BMRC tuberculosis surveys
Initial Bacteriological Status
(in untreated patients)
Kenya
Prc-trcatment sputum
196473
Tanzania
197474
198475
196976
1978-8077
Cultures
Total tested
864
984
Positive (%)
74.5
77.0
981
76.4
1204
55.5
68.3*
632
702
718
636
555
Isoniazid alone
8.9
7.3
Streptomycin alone
0.8
1.4
Both drugs
1.4
1.4
7.1
0.5
1.3
4.9
3.0
1.4
7.6
0.7
1.8
932
Dmg resistance
Total tested
Resistant (%) to
*This higher proportion was because in the evolving National Programme, only a doctor could authorise a smear
negative patient to be brought under treatment
sputum samples could be kept refrigerated and
sent al frequent intervals to a special survey
laboratory set up in the Madras centre by Dr
Gangadharam. The levels of drug resistance are
substantial (Table 11). However, there is
evidence that this is not primary drug resistance
but initial drug resistance and that the
interrogation of patients about their history of
previous chemotherapy was often inadequate.
Thus, in the Government Tuberculosis Institute,
Madras patients, the level of initial resistance was
similar to the overall average for ail the other
centres in the study. However, patients with no
history of previous chemotherapy were referred
to the Tuberculosis Chemotherapy Centre which
was sited in the same compound because they
were eligible for admission to controlled clinical
trials in the Centre. They were reinterrogated
very carefully by medical staff with much
experience in obtaining accurate histories who
also had the time to do so. In addition, all
prescriptions, all medicaments and empty
containers patients still had were inspected and,
when in doubt, private practitioners who had
prescribed pills and injections were also visited, if
need be with the patient, to see if these were
antituberculosis drugs or, as they often then were,
vitamins. As a consequence of excluding further
patients found to have had a definite history of
previous chemotherapy, a reanalysis of the rates
of pre-treatment drug resistance to isoniazid and
to streptomycin (shown in brackets in Table 11)
when these results became available several
weeks later, were strikingly lower than in the
patients regarded as new and previously
untreated, by the Government Institute medical
staff.
In a second 1CMR survey79, also coordinated
by Dr Gangadharam, involving the same 9
centres, not only patients with no history but also
those with a history of previous chemotherapy,
Table 11. ICMR dmg resistance survey in patients with
no history ofprevious chemotherapy (1964-65)7S
Centre
Number of Percentage with resistance to
cultures ---------------------------------------with results Isoniazid Strepto- One or
mycin both drugs
Patna
202
223
221
191
213
245
217
196
130
14
11
20
18
13
15
13 (3.7)*
11
18
13
8
19
20
9
10
12(4.3)
10
14
21
14
29
27
18
18
18
15
27
All centres
1,838
14.7
12.5
20.4
Amritsar
Bangalore
Bombay
Calcutta
Delhi
Hyderabad
Madras
Nagpur
*The figures in brackets are the levels of resistance
after excluding patients who on detailed interrogation
in the TRC gave a history of previous chemotherapy,
several weeks before the sensitivity test results were
available.
WALLACE I'OX
204
were interrogated and its duration recorded.
Specimens from all the patients were sent to
Madras for examination in the special laboratory.
The levels of drug resistance in patients with no
history of previous chemotherapy (Table 12) are
similar to those of the first survey, but increased
with the duration of previous chemotherapy.
These findings are similar to those of a 1962
survey in Hong Kong,80 also conducted in
outpatient clinics, the bacteriology and sensitivity
tests being undertaken in the London laboratory.
The somewhat higher rates in Hong Kong may
well be due to a larger scale use of
antitubcrculosis drugs, and for longer periods,
not only in the Government service but from the
large number of private practitioners who were
treating tuberculosis before the patients
registered themselves in the Government service
for the first time. A similar survey is currently
being repeated in Hong Kong where ambulatory
short-course chemotherapy has been used on a
wide scale for nearly a decade, so the findings will
be of special interest.
The TRC Madras also has figures of drug
resistance in patients diagnosed in Madras city
since 1956 in an area of intake within the city
(enlarged somewhat over the years) and admitted
to a series of controlled clinical trials (Table 13).
There has, in fact, been an increase in the level of
drug resistance to isoniazid, to streptomycin and
to both drugs over the years, which has levelled
off in recent years. The increase may, in part,
represent a genuine increase in primary
resistance, but it is almost certain that patients
over the years have become increasingly skillful in
concealing
their
history
of
previous
chemotherapy and there may have been
Table 12. ICMR ding resistance sun>ey in all patients
with or without a history of previous chemotherapy
(1965-1967) (comparison with Hong Kong)
ICMR survey70
Duration Number
of chemo
of
patients
therapy
(months)
None
016-
851
46
143
189
Hong Kong survey
(1962)80
Resistant Number
to H or S
of
or both
patients
(%)
22
26
46
74
302
37
96
73
Resistant
to H or S
or both
(%)
19
27
66
94
variations in the standards of interrogation, which
had been conducted with almost obsessional
fervour in the early years of the Centre so that, in
fact, the inclusion of patients with other reasons
for initial resistance has increased.
The Madras centre has, over the years,
accumulated much information on drug
resistance in children, including child contacts of
the patients in the chemotherapy studies and in
studies of tuberculous meningitis, tuberculosis of
the spine, abdominal tuberculosis and from the
BCG study families, which it look over in the
later years of the study. It is important that these
data should be assembled and analysed since a
child, especially if young and with a primary
lesion, is much less likely to have had previous
chemotherapy for tuberculosis than an adult
eager to conceal a previous history. Reliable
information on the pattern of drug resistance in
paediatric practice is in my view, especially
important, as it is likely to be a better reflection
of the current trend of drug resistance than is
provided by the older age groups, many of whom
may have been originally infected 40 or more year
ago, prior to the era of chemotherapy.
An important issue now is what will happen to
the level of prc-trcalmcnl drug resistance,
especially to rifampicin as its use in district
programmes
based
on
short-course
chemotherapy progressively spreads, when there
is already a substantial level of initial drug
resistance to isoniazid, and an even higher level in
patients who admit a history of previous
chemotherapy.
It is clear that with the introduction of new
regimens of short-course chemotherapy and in
district programme conditions there is now a
need to undertake as representative surveys as is
possible of pre-treatment drug resistance in
India. The emphasis will increasingly be on
isoniazid and rifampicin, the 2 key drugs in short
course chemotherapy (tests for pyrazinamide
resistance are technically more difficult and
unlikely to be so relevant). I see the need for a
number of laboratories, each with a bacteriologist
with an interest and knowledge of tuberculosis
bacteriology, and equipped to use the same
laboratory techniques for smear, culture and
sensitivity tests and defining drug resistance by
using the approach adopted in the Madras centre,
and closely associated with Madras for reference
TUBERCULOSIS IN INDIA, PAST, PRESENT AND FUTURE
205
Table 13. Prevalence of initially drug-resistant strains in newly-diagnosed previously untreated patients
(Tuberculosis Research Centre, Madras)
(Prabhakar, personal communication)
Study
Period
of intake
Number
of patients
H
resistant (%)
S
resistant (%)
SH
resistant (%)
I
III
K
Va
Vb
VII
VIII
IX
X
XI
XII
XIII
XIV
XV
XVI
1956- 1957
1957- 1958
1961
1961- 1962
1962- 1963
1963- 1966
1967- 1968
1968- 1969
1970-1972
1972-1974
1974-1977
1977-1980
1980-1985
1985- 1986
1986- 1988
173
325
99
159
235
538
389
239
465
651
652
507
1(X)4
71
317
3
6
6
4
6
6
8
9
9
3
0
3
2
1
0
10
12
purposes. Such laboratories need to be in or near
cities with ready access to airlines and might be in
a university department, a general hospital or a
tuberculosis hospital. What is particularly
important is that the laboratory should be closely
associated with a doctor active in the field of
tuberculosis, with epidemiological and clinical
interests and who is ready to be a local
coordinator of relevant studies, for example,
participating in controlled clinical trials or in
surveys of alternative strategics for tuberculosis
control under district programme conditions and
the involvement of a statistician would also be of
great value. Tuberculosis^ in India needs an
expanded research and "evaluation capacity,
capablc o^ covering different regions of. the
country. Such a network would obviously take
time to establish but as it evolves, increasingly
representative information on drug resistance
and other issues in addition would become
available and the surveillance of tuberculosis
would progressively improve. In any case, an
efficient smear and culture service would be
invaluable, both in identifying the most infectious
cases and in supervising and monitoring the
efficiency of peripheral diagnosis by smear
examination, and the results of therapy. Such a
network could play a major training role in
District Programmes and in educating medical
4
1
9
3
6
2
7
4
4
1
9
4
12
5
6
5
6
7
6
10
11
8
11
12
13
11
11
9
students, and recently qualified doctors.
Initial Drug Resistance and Response to
Chemotherapy
Over the years the BMRC has accumulated
from its collaborative studies, all using the same
BMRC methods of cultures and sensitivity
testing, an impressive amount of important,
informative and encouraging information on the
response to treatment with short-course
chemotherapy in the presence of initial drug
resistance. I have summarised the major findings
on several occasions in review articles10 and a
detailed analysis and report was published in 1986
by Mitchison and Nunn.81 The TRC also has a
large body of corresponding data on patients with
initial drug resistance using the same BMRC
laboratory methods and treated by short-course
chemotherapy, some already published but to
which we have never referred. A report of the
TRC’s accumulated data along the same lines
would be invaluable too. Such data arc virtually
unobtainable from the controlled trials of new
cases reported from the technically advanced
countries, because they have changed the
regimen when a drug-resistant strain was found
to have been present at the start of treatment and
still do so. This is impracticable in the developing
206
WALLACE FOX
countries and certainly not a high priority
problem. The NTI has recently reported on 100
patients with isoniazid-resistant strains pre
treatment, treated by 3 alternative regimens. The
data on the emergence of rifampicin resistance is
of special interest, even though the drug
sensitivity test techniques were unfortunately not
reported.82
Extra-Pulmonary Disease
Extra-pulmonary disease is a decreasing
problem in technically advanced countries. For
example, the one lesion at all frequent in the UK
is glandular tuberculosis but even then a high
proportion of the patients are of immigrant
ethnic origin. It is in the developing countries,
where there arc still, unfortunately, substantial
numbers of patients with a variety of extrapulmonary lesions, many often florid when they
present, that studies can be undertaken to define
the best methods of therapy. Again, there is no
question but that controlled clinical trials are the
most fruitful approach because there is a
comparison of alternative regimens or policies.
My own BMRC group coordinated a series of
studies of alternative treatments of tuberculosis
of the spine on behalf of a BMRC Working Party.
This programme was established in 1964 because
of an important controversy between Professor A
Hodgson in Hong Kong, who advocated radical
surgery with a bone graft in addition to
chemotherapy, and Mr PG Konstam, also a
surgeon, working in Nigeria who advocated
ambulatory chemotherapy as the best approach.
The Working Party organised studies in Korea,
Hong Kong, Rhodesia, South Africa and Madras,
studying a variety of different orthopaedic
approaches, including bed rest, plaster jackets,
surgical debridement, radical surgery and a bone
graft, as well as ambulatory chemotherapy alone
from the outset, and both standard duration, and
in recent years, short-course regimens. The
Madras study83 was a collaborative investigation
between the ICMR and the BMRC Working
Party and it was the TRC which played a pivotal
role in the local coordination. This was important
because six different institutions were involved in
the admission of patients. The collection,
checking and recording of data and its transfer to
London so that the two groups had parallel
information would not have been possible
without the TRC which also took the high quality
standardised radiographic series of the lesion and
ensured a high coverage in a long-term follow-up.
In summary, the outcome of the large series of
studies is that ambulatory short-course
chemotherapy is remarkably effective.
My own group, Professor Mitchison, and Dr
DG Gibson, Brompton Hospital cardiologist, and
others have also collaborated with a Transkei
team (Dr JIG Strang and his colleagues) in
undertaking unique controlled investigations of
the therapy of constrictive pericarditis and
tuberculous pericarditis with effusion, both
conditions being surprisingly frequent, 383 cases
being diagnosed during a 4-ycar period in
approximately a 3 million population.8485 A long
term follow-up of both studies is in progress and
will surely illuminate not only our knowledge of
the therapy of these conditions but of the long
term course of the lesions also. This will be
especially informative about the evolution of
constrictive pericarditis.
In my view one of the major contributions of
the TRC is its investigation of extra-pulmonary
disease which is a considerable national problem
(Table 1) and it is important to find for each type
of lesion the optimal treatment most convenient
for the patients and least demanding of resources
(including hospitalisation) and staff time. In
addition to the study of spinal disease it has
undertaken a scries of studies of the treatment of
tuberculous meningitis86 including a current
controlled trial. Il is investigating the therapy of
brain tuberculomas, and of abdominal
tuberculosis, also in randomized controlled trials.
In has also undertaken an important investigation
of the treatment of paediatric lymphadenitis.87
This latter study is of particular interest becausp
of the striking severity of the lesions that have
been treated and a controlled trial of two 6-^
month regimens is currently in progress. These
studies illuminate our knowledge of the role of
short-course chemotherapy in these important
extra-pulmonary lesions and the technically
advanced countries will also be obvious
beneficiaries on the infrequent occasions when
such lesions arc encountered.
Another important consequence of these
investigations is that they have all been conducted
in collaboration with the experts in the fields in
question in Madras, such as orthopaedic
surgeons, gastroenterologists, both medical and
surgical, and 2 neurological teams, so that there is
TUBERCULOSIS IN INDIA. PAST, PRESENT AND FUTURE
cross fertilization between the specialities
including university and teaching hospital groups,
so that teachers and hence medical education too
have benefited. The implications, therefore, are
not just restricted to developing countries or to
practitioners with a special interest in
tuberculosis. I have no doubt that the groups in
other specialities in Madras who have
collaborated with the TRC will use the
methodology of the controlled clinical trial more
widely and with greater skill and better follow-up
in consequence of their association with these
investigations. Had groups in other centres in
India been submitting patients to a multiccntre
study following the same protocol, the speed of
intake to the studies would have been faster, the
outcome more rapidly available, and there would
have been a wider spread of the specialised
methodologies to other parts of the country.
It must be added that the management of
extrapulmonary tuberculosis in individ u al
patients should always involve tuberculosis
experts because ,it is they who are up to date in
the choice of regimens, arc fully aware of the
problems of patient compliance, and have the
experienced staff who understand the important
need for careful supervision of chemotherapy,
and have the organisation to take early and
positive absconder action, if the need arises.
The Utilisation of Tuberculosis Beds
Currently the tuberculosis beds in India
number approximately 47,000, of which 8,643 are
maintained by voluntary organisations. Some
agencies, e.g. the railways and the Employees
S£atc Insurance scheme, reserve TB beds in the
States but they also have their own TB hospitals.
The indications for hospital admission are : 1)
emergencies, such as haemoptysis and
spontaneous pneumothorax, (2) critically ill
patients, (3) patients in need of surgery, and (4)
socio-economic considerations. There is also no
doubt that unsuitable patients arc not
infrequently admitted through influential
channels. The official recommendation is that
domiciliary treatment is the treatment of choice.
A high proportion of patients in India prefer
ambulatory chemotherapy and even the
recommended categories refuse admission for
socio-economic reasons, and early self-discharge
is common, with loss to follow-up (Nagpaul,
personal communication). A 1988 editorial in the
207
Indian Journal of Tuberculosis88 is critical of the
advocacy of hospitalisation and the construction
of cheap cottage hospital beds.
I have summarised elsewhere the advantages
of treating even very ill patients in ambulatory
domiciliary conditions within the family from the
very outset and have listed some of the
misapprehensions and fallacies of the advocacy of
hospitalisation for the first 2 months, as the ideal
norm,89 based on the fallacious views and beliefs
such as that this ensures the patient receives and
needs every dose of a daily regimen. These issues
are also considered in a recent WHO
Publicati°n»
India now urgently needs a review of the' ,56s ,
utilisation of the tuberculosis beds including bed
occupancy rates, the areas from which the
patients are admitted, not only urban, suburban
and rural, but the distance from each patient’s
abode. The actual reasons for each hospital
admission, the classification of the_lesions both
bacteriologically and radiographically, the
duration of hospital stay, the regimens
prescribed, and the frequency and timing of self
discharge and losses to follow-up. How many
beds should be devoted to retreatment of failure
patients, which directs both staff time and
financial resources away from case-finding and
the therapy of new cases? The staffing structure,
with particular reference to the nursing and
medical staff numbers and their training is
needed. The cost of a bed when occupied and 7
when unoccupied needs calculating for each •
institution, because these vary widely.
With adequate background information,
rational policies can be recommended about the
use of tuberculosis beds and whether expansion,
contraction or relocation is indicated, or whether
the funds might not be put to better use. For
example, how many diagnostic cultures could be
performed for the cost of a single patient day in
hospital on short-course chemotherapy? Might
the provision of more health visitors for the
ambulatory programme yield better dividends?
Tuberculosis hospitals in India, as in many
developing countries, range from the very good to
the almost unbelievably poor (as I have recently
seen in a major State institution) with minimal
patient records which did not even contain the
regimen, the date of its start, the bacteriological
status (which had often not been assessed, even
by smear examination), and medical staff with no
208
WALLACE FOX
knowledge of tuberculosis or interest in the
disease and whose main concern was to be
transferred back to an urban area. Finally, each
State must take an overview of the use of beds in
relation to competing health priorities.
Improving Research and Training Facilities in
India
Laboratory, clinical and epidemiological
research, and the design and conduct of
controlled clinical trials in tuberculosis require
special training. Studies must be well planned and
conducted if they arc to provide reliable data, and
the analysis and presentation of results must be
dependable. Methodologies have already been
well established. Thus, excellent controlled
clinical trials, the findings of which have been
accepted worldwide, have been conducted in the
TRC, Madras, since 1956. There is, therefore,
available an exceptional resource to train
clinicians and their teams (social workers, public
health nurses, health visitors), bacteriologists,
laboratory scientists and all their technical
support staff, in laboratory aspects, and, of
special importance, statisticians and their
assistants. An understanding of the underlying
issues involved in the conduct of research,
especially controlled trials and epidemiological
surveys in tuberculosis, is particularly necessary
because of its chronicity. A close liaison between
clinical, epidemiological, laboratory and
statistical staff is, therefore, a key feature of an
effective research group.
Studies involving controlled clinical trials
(whether of pulmonary or extrapulmonary
disease) arc particularly important and much
more informative than a study of patients treated
with a single regimen or a single policy of
management. There are, for example, at least six
groups in India currently studying the diagnosis
and treatment of brain tuberculomata stimulated
by the special interest in brain scans. The only
centre currently investigating alternative
regimens in a randomised controlled trial is the
Madras group. This is a pity because the aim is to
find the most effective and quickest cure with the
least toxicity and which makes the minimum
demands on patient compliance and so the least
disturbance to the lives of the patient and the
family. The comparative aspect is the great forte
of well conducted randomised controlled trials.
An important feature of well conducted
controlled clinical trials is to achieve an adequate
intake of patients and a long-term follow up
because of the need for an accurate assessment of
relapse rates and late sequelae. In the home and
sanatorium study1 all (100%) of the 193 patients
admitted were followed up to 5 years or until
death, even those excluded from the main
analysis.91 The close family contacts were
followed up too by tuberculin testing and chest Xray for 5 years to compare the infection and
disease rates in the 2 groups. A chest X-ray was
obtained in over 99% of the surviving contacts at
5 years, including some who had emigrated to
Pakistan.92 Very high coverage has always been a
feature of the Madras studies and a 5-year follow
up of patients the norm. This has been the result •
of a carefully planned organisation (pages 187
and 188) and the attitude of the staff to the
patients and their determination that every
patient would be followed up, whatever time and
effort this entailed. In multicentre trials such
exceptional coverage is less easily achieved.
Nevertheless, if the coordination, both local and
central, is skilled and close contact with the
centres is maintained a high level of long-term
coverage and very complete data collection on
each patient can still be achieved.
The NTI has also had a long research record,
inevitably more orientated to epidemiological,
operational and sociological investigations, but
there has also been an important controlled trial
component because of its value in comparing
alternative approaches and interventions.
A high proportion of all controlled clinical
trials in tuberculosis, both in technically advanced
and developing countries, are uninformative
because they are too small or because the drop
out rate is high and the period of observation too
short. The aim for India should be to evade these
major deficiencies because they are avoidable as
the TRC and the NTI have shown. The TB
Association of India’s 6 controlled trials were
hampered by inadequate budgets for the research
and the consequences that stemmed from this
basic fact (Pamra, personal communication).
In the same compound as the TRC is another
ICMR unit, The Institute for Research in
Medical Statistics (Madras Chapter). Its director,
Dr. S. Radhakrishna, was the Head of the
Statistics Department of the Madras Centre from
1956 to 1975 and so has had exceptional
experience of tuberculosis research and is a gifted
TUBERCULOSIS IN INDIA, FAST, PRESENT AND FUTURE
teacher. His unit’s programme is now wide
ranging, covering many medical fields and
includes operational, surveillance and sociological
research.
There are, therefore, in South India 3 major
institutions with an unusual experience and
capacity to train not just district programme
teams and various categories of leaders of the
profession including administrators, but to train
important categories of research workers,
clinical, epidemiological, laboratory (especially
bacteriological) and statistical as well. It is clear
that careful consideration should be given to how
best to use these resources, involving both the 2
Madras units and NTI. My own view is they
should at least train research workers in all the
necessary specialities, for this could lead to major
improvements both in the scale and the national
standard of tuberculosis research (pages 204 and
205) including the investigation of the vital
operational problems which seem so intractable
as currently viewed.
Conclusion
Although the National 20-point Plan has had
some modest impact on the tuberculosis
programme, a golden opportunity to launch a
national crusade against the disease, under the
stimulus of your late Prime Minister, Indira
Gandhi’s support, has to a large degree been so
far missed. The switch to short-course
chemotherapy was, to some extent, inevitable.
There were pressures of the demands of private
practitioners to have access to the modern potent
rifampicin for sbori-CQurse xhemotherapy and of
the patients who could afford to pay for it too, in
addition to Government staff, both Central and
State, eager to have it available, and the
pharmaceutical industry naturally pressing to
open the Indian market. Even so, the speed with
which it has been introduced without major
strengthening of the individual units of the
infrastructure, and in many States any
improvement of the broad framework or removal
of as many of the obvious deficiencies as possible
in organisation, training and supervision, could
prove disastrous. It might lead to so much drug
resistance to isoniazid, to rifampicin and to both
drugs in patients newly presenting for treatment
as
eventually
to
render
short-course
chemotherapy, based on the currently available
drugs, no longer effective at a community level,
unless the infrastructure, and with it, patient
209
compliance, is greatly improved, a subject I have
emphasised in this paper and repeatedly
elsewhere.
In my view, the time has unquestionably come
for India to set up a long-term adequately
funded National Tuberculosis Standing
Committee (a term I prefer to a Task Force)
with wide terms of reference and authority
appropriate to its important national role It
may well need its own small whole time
secretariat. The membership must be the real
experts in the field drawn from an appropriately
wide range of disciplines (selected on the basis of
ability and not seniority). They must review and
rethinkjhe nationaljpolicies and in particular
their priorities, the organisation and especially
whether regionalisation has a role or a mobile
team or teams able to undertake intensive and
large-scale training at a State level, the many
issues that ensue with drug supplies, the
regimens, the monitoring, the involvement of the_
community, the framework for establishing a
substantially larger scale of high quality
operational research and training. The major
centres in the South, the NTI and TRC, as
currently staffed and constituted, are clearly not
enough in a country's large as India. The ICMR
obviously has a key role, and the Technical
Committee of the Tuberculosis Association of
India could be a further valuable resource. Also,
the relationship of the Central Government and
the States in the implementation must be
carefully interfaced. The funds for research will
also need to be substantially larger to achieve
better policies of case-finding, diagnosis,
regimens and their successful implementation
under programme conditions. However, the
prize is great and the cost would be relatively
small, especially if related to the cost of
continuing rectifiable failures of the National
Programme which already absorbed large sums
of money even as estimated in 1986’3 by a
previous Adviser in Tuberculosis to the
Government of India.
Abbreviations used in this Report
= National Tuberculosis Institute,
Bangalore
= Tuberculosis Research Centre,
TRC
Madras
BMRC = British Medical Research Council
ICMR = Indian Council of Medical Research
WHO = World Health Organization
NTI
210
WALLACE FOX
NTP
DPT
DTO
DTC
PHI
=
=
=
=
=
National Tuberculosis Programme
District Programme Team
District Tuberculosis Officer
District Tuberculosis Centre
Peripheral Health Institution
References
1.
Tuberculosis Chemotherapy Centre, Madras. A
concurrent comparison of home and sanatorium
treatment of pulmonary tuberculosis in South
India. Bull Wld Hlth Org 1959; 21 : 51.
2.
Rani Balasubramanian, Sivasubramanian, S,
Vijayan, VK et al. Five-year results of a 3-month
and two 5-month regimens for the treatment of
sputum-positive pulmonary tuberculosis in
South India. Tubercle, 71, December 1990.
3.
Nagpaul, DR. India’s National Tuberculosis
programmc-an overview. Ind J Tub 1989; 36 :
205.
4.
Aluoch, J. Swai, OB, Edwards EA et al. Study of
case finding for pulmonary tuberculosis in
outpatients complaining of a chronic cough at a
District hospital in Kenya. Am Rev Respir Dis
1984; 129 : 915.
5.
Aluoch, J., Swai, OB., Edwards, EA et al.
Studies of case-finding for pulmonary
tuberculosis in outpatients at 4 District hospitals
in Kenya. Tubercle 1985; 66 : 237.
Krishnaswami,
KV.,
Tripathy,
SP.,
Vaidyanathan, B., Fox, W. A study of the
accuracy, and factors influencing accuracy, of
home addresses of patients obtained by registry
clerks and address cards in four large towns in
South India. Tubercle 1980; 61 : 197.
12.
Krishnaswami, KV., Somasundaram, PR.,
Tripathy, SP., Vaidyanathan, B., Radhakrishna,
S., Fox, W. A randomized study of two policies
for managing default in out-patients collecting
supplies of drugs for pulmonary tuberculosis in
a large city in south India. Tubercle 1981; 61 :
103.
13.
Sectha, MA., Srikantaramu, N., Aneja, KS.,
Singh, H. Influence of motivation of patients
and their family members on the drug collection
by patients. Ind J Tub 1981; 28 : 182.
14.
Allan, WGL., Girling, DJ., Payers, PM., Fox, W.
The symptoms of newly diagnosed pulmonary
tuberculosis and patients attitudes to the disease
and to its treatment in Hong Kong. Tubercle
1979; 60: 211.
15.
Hong Kong Chest Service/British Medical
Research Council Survey of patients presenting
to the government chest service in Hong Kong
and the effects of active tuberculosis case
finding by publicity campaigns. Tubercle 1984;
65 : 173.
16.
WHO Collaborating Centre for Tuberculosis
chemotherapy, Prague. A comparative study of
daily and twice-weekly continuation regimens of
tuberculosis chemotherapy including a
comparison of two durations of sanatorium
treatment. Bull Wld Hlth Org 1971; 45 : 573.
17.
British Medical Research Council. Co-operative
controlled trial of a standard regimen of
streptomycin, PAS and isoniazid and three
alternative regimens of chemotherapy in Britain.
Tubercle 1973; 54 : 99.
6.
Baily, GVJ., Savic, D., Gothi, GD., Naidu, VB.,
Nair, SS. Potential yield of pulmonary
tuberculosis cases by direct microscopy of
sputum in a District of South India. Bull Wld
Hlth Org 1967; 37 : 875.
7.
Nagpaul, DR, Savic, DM, Rao, KP, Baily, GVJ.
Case-finding by microscopy. Bull Int Un Tuberc
1968;41 : 148.
8.
Jagota, P., Gupta, EVV., Rao, BSN, Parimala,
N, Baily, GVJ. The acceptability and efficacy of
two regimens of short-course chemotherapy
under conditions of an urban tuberculosis
programme. Ind J Tub 1983; 36 : 18.
(IS)
Editorial.
General
Practitioners
Tuberculosis. Ind J Tub 1981; 28 : 43.
19.
Editorial. Tuberculosis service at the periphery.
Ind J Tub 1981; 28: 161.
9.
Editorial. Expanded programme of health
education and community involvement. Ind J
Tub 1990; 37 : 55.
20.
10.
Fox, W. Short-course chemotherapy for
pulmonary tuberculosis and some problems of
its programme application with particular
reference to India. Lung India 1984; 2 : 161.
Also published in Bull Int Un Tubcrc 1985; 60 :
40.
Dutt, AK., Jones, L., Stead, WW. Short-course
chemotherapy for tuberculosis with largely
twice-weekly isoniazid-rifampicin. Chest 1979;
75 : 441.
21.
Gangadharam, PRJ., Devadatta, S., Fox, W.,
Narayan, C., Nair, N., Selkon, JB. Rate of
inactivation of isoniazid in South Indian patients
with pulmonary tuberculosis. 3. Serum
concentrations of isoniazid produced by three
regimens of isoniazid alone and one of isoniazid
plus PAS. Bull Wld Hlth Org 1961; 25 : 793.
li.
Radhakrishna,
S„
Satagopan,
MC.,
and
TUBERCULOSIS IN INDIA, PAST, PRESENT AND FUTURE
22.
Mitchison, DA., Dickinson, JM. Laboratory
aspects of intermittent drug therapy. Postgrad
Med J 1971; 47: 737.
23.
East African/British Medical Research Council.
Controlled clinical trial of four short-course (6month) regimens of chemotherapy for treatment
of pulmonary tuberculosis. 2nd report. Lancet
1973; 1 : 1331.
24.
East African/British Medical Research
Councils. Controlled clinical trial of four short
course (6-month) regimens of chemotherapy for
treatment of pulmonary tuberculosis. Third
report. Lancet 1974; 2 : 237.
25.
26.
International Tuberculosis Conference held
September 10th to 14th, 1961, at Toronto.
Excerpta Medica, International Congress Series,
No. 44, 1, 307, Amsterdam 1962.
34.
Haynes, RB., Taylor, DW., Sackett. DL (Eds).
Compliance in Health Care. The Johns Hopkins
University Press, Baltimore, Maryland, 1979.
35.
Fox, W. The current status of short-course
chemotherapy. Bull Int Un Tubcrc 1978; 53 :
268.
36.
Wiseman, LA. Calendar (blister) packs for
multidrug therapy in Leprosy : an inexpensive
locally produced version. (Letter) Lepr Rev
1987; 58 : 85.
Medical Research Council. Treatment of
pulmonary tuberculosis with streptomycin and
para-aminosalicylic acid. Br Med J 1950; 2 :
1073.
37.
Medical Research Council. The prevention of
streptomycin
resistance
by
combined
chemotherapy. BrMed J 1952; 1 : 1157.
Ellard, 6. Drug compliance in the treatment of
leprosy. Lepr Rev 1981; 52 : 201.
38.
Fox, W. The chemotherapy and epidemiology of
tuberculosis. Some findings of general
applicability
from
the
Tuberculosis
Chemotherapy Centre, Madras. Lancet 1962; 2 :
413.
39.
Tuberculosis Chemotherapy Centre, Madras. A
concurrent comparison of isoniazid plus PAS
with three regimens of isoniazid alone in the
domiciliary treatment of pulmonary tuberculosis
in South India. Bull Wld Hlth Org 1960; 23 :
535.
40.
Dye, WE., Kass, I., Gill, R. Laboratory
evaluation
of
the
specific
serum
antimycobacterial activity test. Antimicrobial
Agents and Chemotherapy 1961; 22 : 20.
41.
National Jewish Hospital at
Denver.
Contributions to the study of tuberculosis and
diseases of the chest, Vol. 21 1957-1960. Denver
1962.
42.
World Health Organization. Tuberculosis
control. Report of a joint IUAT/WHO Study
Group. WHO Technical Report Scries 671,
Geneva, 1982.
43.
Banks, L, Jenkins, PA. Combined versus single
antitubcrculosis drugs on the in vitro sensitivity
patterns of non-tuberculous mycobacteria.
Thorax 1987; 42 : 838.
44.
Banks, J. Treatment of pulmonary disease
caused by opportunist mycobacteria. Thorax
1989; 44 : 449.
45.
Mitchison, DA. The action of antituberculosis
drugs in short-course chemotherapy. Tubercle
1985; 66:219.
46.
Singapore Tuberculosis Scrvice/British Medical
Valcza, FS., McDougall, AC. Blister calendar
packs for treatment of tuberculosis. Lancet
1990; 1: 473.
28.
Phillips S., Horton, GE. Pyrazinamide-isoniazid.
Comparison with isoniazid-para-aminosalicylic
acid in active pulmonary tuberculosis with the
choice of regimens determined by chance. Am
Rev Tuberc 1956; 73 : 704.
29.
A United States Public Health Service
Tuberculosis Therapy Trail. Sequential use of
paired combinations of isoniazid, streptomycin,
para-aminosalicylic acid, and pyrazinamidc. Am
Rev Rcspir Dis 1959; 80 : 627.
30.
Matthews, JH. Pyrazinamidc and isoniazid used
in the treatment of pulmonary tuberculosis. Am
Rev Rcspir Dis 1960; 81 : 348.
31.
Hong Kong Tuberculosis Treatment Services/
Brompton Hospital/British Medical Research
Council. A controlled clinical trial of daily and
intermittent regimens of rifampicin plus
ethambutol in the retreatment of patients with
pulmonary tuberculosis in Hong Kong. Tubercle
1974; 55: 1.
32.
33.
211
Hong Kong Tuberculosis Treatment Services/
Brompton Hospital/British Medical Research
Council. A controlled clinical trial of daily and
intermittent rifampicin plus ethambutol in the
retreatment of patients with pulmonary
tuberculosis : results up to 30 months. Tubercle
1975; 56 : 179.
Fox, W. Self-administration of medicaments. A
review of published work and a study of the
problems. In : Proceedings of the XVIth
212
WALLACE FOX
Research Council. Controlled trial of
intermittent regimens of rifampicin plus
isoniazid for pulmonary tuberculosis in
Singapore. Am Rev Respir Dis 1977; 116 : 807.
47.
48.
49.
50.
51.
52.
53.
Hong Kong Chest Service/British Medical
Research Council. Study of a fully supervised
programme of chemotherapy for pulmonary
tuberculosis given once-wcckly in the
continuation phase in the rural areas of Hong
Kong. Tubercle 1984; 65 : 5.
Mitchison, DA., Ellard, GA., Grossct, J. New
antibacterial drugs for the treatment of
mycobacterial disease in man. Br Med Bull
1988; 44 : 757.
Ellard, GA., Ellard, DR., Allen, BW et al. The
bioavailability of isoniazid, rifampin, and
pyrazinamidc in two commercially available
combined formulations designed for use in the
short-course treatment of tuberculosis. Am Rev
Respir Dis 1986; 133 : 1076.
Hong Kong Chest Service/British Medical
Research Council. Acceptability, compliance,
and adverse reactions when isoniazid, rifampin,
and pyrazinamidc are given as a combined
formulation or separately during three-times
weekly antitubcrculosis chemo-therapy. Am Rev
Respir Dis 1989; 140 : 1618.
Goiter, LJ., O'Brien, RJ., Combs, DL., Snider,
DE. United States Public Health Service
tuberculosis therapy trial 21 : preliminary results
of an evaluation of a combination tablet of
isoniazid, rifampin and pyrazinamidc. Tubercle
Suppl 1987; 68 : 41.
Combs, DL., O’Brien, RJ., Geiter, LI. USPHS
tuberculosis short-course chemotherapy trial 21
: effectiveness, toxicity, and acceptability. An Int
Med 1990; 112 : 397.
Algeria Working Group/British Medical
Research Council Cooperative Study. Short
course
chemotherapy
for
pulmonary
tuberculosis under routine programme
conditions : a comparison of regimens of 28 and
36 weeks duration in Algeria. Tubercle Vol. 72,
March 1991.
54.
Cavenaghi R. Rifampicin raw material
characteristics and their effect on bioavailability.
Bull Int Un Tuberc Lung Dis 1989; 64 : 36.
55.
Aspesi, F. Dissolution testing. Bull Int Un
Tuberc Lung Dis 1989; 64 : 37.
56.
Acocella, G. Human bioavailability studies. Bull
Int Un Tuberc Lung Dis 1989; 64 : 38.
57.
Long, MW., Snider, DR., Farer, LS., US Public
Health Service cooperative trial of three
rifampin-isoniazid regimens in treatment of
pulmonary tuberculosis. Am Rev Respir Dis
1979; 119:879.
58.
Pamra, S. Discussion. Bull Int Un Tuberc Lung
Dis 1989; 64 : 40.
^59)
Editorial. Multi-drug formulations. Ind J Tub
1988; 35: 161.
60.
Satellite symposium on quality control of
antituberculosis drugs. Bull Int Un Tuberc Lung
Dis 1989; 64 : 36.
61.
Reichman, Discussion. Bull Int Un Tuberc Lung
Dis 1989; 64 : 42.
62.
WHO Certification Scheme on the quality of
pharmaceutical
products
moving
in
international commerce : Guidelines for use.
WHO Drug Information 1989; 3 : 109.
63.
Brechbuhler, S., Fluehler, H., Riess, W.,
Theobald, W; The renal elimination of
rifampicin as a function of the oral dose. A
convenient way to assess relative bioavailability.
Arzneim. Forsch./Drug Res. 1978; 28 : 480.
64.
Sunahara, S., Nakagawa, H. Metabolic study
and controlled clinical trials of rifampicin. Chest
1972; 61 : 526.
65.
Editorial. Availability of anti-tuberculous drugs.
70 . irn
Ind JTT..L
Tub inoc.
1985; 32
: 169.
66.
Dubey, GR„ Shah, RC., Kamat, ST et al. A
study of efficacy and toxicity of short-course
chemotherapy with ethambutol, rifampicin,
pyrazinamidc and isoniazid in pulmonary
tuberculosis. Lung India 1985; 3 : 115.
67.
Tiwari, US., Mishra, BP. Ocular toxicity of
ethambutol. A clinical study. Lung India 1987;
5:111.
68.
Editorial. The new drug policy. Ind J Tuberc
1987; 34 : 179.
69.
Fox, W„ Wiener, A., Mitchison, DA., Sclkon,
JB., Sutherland, I. The prevalence of drugresistant tubercle bacilli in untreated patients
with pulmonary tuberculosis : A national survey,
1955-56. Tubercle 1957; 38 : 71.
70.
Miller, AB., Tall, R., Fox, W., Lefford, MJ.,
Mitchison, DA. Primary drug resistance in
pulmonary tuberculosis in Great Britain :
Second national survey, 1963. Tubercle 1966;
47 : 92.
71.
Medical Research Council Tuberculosis and
Chest Diseases Unit. National survey of
tuberculosis notifications in England and Wales
1978-79. Br Med J 1980; 281 : 895
TUBERCULOSIS IN INDIA, PAST, PRESENT AND I-VFURE
72.
Medical Research Council Tuberculosis and
Chest Diseases Unit. National survey of
notifications of tuberculosis in England and
Wales 1983. Br Med J 1985; 291 : 658.
73.
East African/British Medical Research Council
Co-operative Investigation. Tuberculosis in
Kenya : a national sampling survey of drug
resistance and other factors. Tubercle 1968; 49 :
136.
74.
East African and British Medical Research
Council
Co-operative
Investigation.
Tuberculosis in Kenya : a second national
sampling survey of drug resistance and other
factors, and a comparison with the prevalence
data from the first national sampling survey.
Tubercle 1968; 59 : 155.
75.
A Kenyan/British Medical Research Council
Co-operative Investigation. Tuberculosis in
Kenya 1984 : a third national survey and a
comparison with earlier surveys in 1964 and
1974. Tubercle 1989; 70 : 5.
76.
An East African and British Medical Research
Council
Co-operative
Investigation.
Tuberculosis in Tanzania : A national sampling
survey of drug resistance and other factors.
Tubercle 1975; 56 : 269.
77.
Tanzanian/British Medical Research Council
Co-operative Investigation. Tuberculosis in
Tanzania : A national survey of newly notified
cases. Tubercle 1985; 66 : 161.
78.
Indian Council of Medical Research. Prevalence
of drug resistance in patients with pulmonary
tuberculosis presenting for the first time with
symptoms at chest clinics in India. Part I.
Findings in urban clinics among patients giving
no history of previous chemotherapy. Ind J Med
Res 1968; 56 : 1617.
79.
80.
81.
Indian Council of Medical Research. Prevalence
of drug resistance in patients with pulmonary
tuberculosis presenting for the first time with
symptoms at chest clinics in India. Part II.
Findings in urban clinics among all patients,
with or without history of previous
chemotherapy Ind J Med Res 1969; 57 : 823.
Hong Kong Government Tuberculosis Service/
British Medical Research Council Co-operative
Investigation. Drug-resistance in patients with
pulmonary tuberculosis presenting at chest
clinics in Hong Kong. Tubercle 1964; 45 : 77.
Mitchison, DA., Nunn, AJ. Influence of initial
drug resistance on the response to short-course
chemotherapy of pulmonary tuberculosis. Am
Rev Respir Dis 1986; 133 : 423.
213
82.
Jagota, P., Srinivas, TR., Parimala, N.,
Chaudhuri, K. The fate of resistant cases treated
with three different drug regimens of short
course chemotherapy under programme
conditions. Ind J Tub 1990; 37 : 83.
83.
Indian Council of Medical Research/British
Medical Research Council Working Party Study
in Madras, South India. A controlled trial of
short-codrse regimens of chemotherapy in
patients receiving ambulatory treatment or
undergoing radical surgery for tuberculosis of
the spine. Ind J Tub 1989; 36 : (Suppl) 1.
84.
Strang, JIG., Kakaza, HHS., Gibson, DG.,
Girling, D.J., Nunn, AJ., Fox, W. Controlled trial
of prednisolone as adjuvant in treatment of
tuberculous constrictive pericarditis in Transkei.
Lancet 1987; 2 : 1418.
85.
Strang, JIG., Gibson, DG., Mitchison, DA et al.
Controlled clinical trial of complete open
surgical drainage and of prednisolone in
treatment of tuberculous pericardial effusion in
Transkei. Lancet 1988; 2 : 759.
86.
Ramachandran,
P.,
Duraipandian, M.,
Nagarajan, M., Prabhakar, R., Rarnakrishnan,
CV., Tripathy, SP. Three chemotherapy studies
of tuberculous meningitis in children. Tubercle
1986; 67 : 17.
87.
Jawahar, M.S., Sivasubramanian, S., Vijayan, 5
U.K. et al. Short course chemotherapy for
tuberculous lymphadenitis in children. Br Med J
1990; 301 : 359.
88.
Editorial. Hospitalization for pulmonary
tuberculosis. Ind J Tub 1988; 35 : 1.
U9.
Fox, W. Tuberculosis case-finding and
treatment programmes in the developing
countries. Br Med Bull 1988; 44 : 717.
90.
World Health Organization. Tuberculosis
control as an integral part of primary health
care. WHO, Geneva, 1988.
91.
Dawson, JJY., Devadatta, S., Fox, W et al. A
5-year study of patients with pulmonary
tuberculosis in a concurrent comparison of
home and sanatorium treatment for one year
with isoniazid plus PAS. Bull Wld Hlth Org
1966; 34 : 533.
92.
Kamat, SR., Dawson, JJY., Devadatta, S et al. A
controlled study of the influence of segregation
of tuberculous patients for one year on the
attack rate of tuberculosis in a 5-year period in
close family contacts in South India. Bull Wld
Hlth Org 1966; 34:517.
93.
Gupta, SP. Financial implications of
tuberculosis control. Ind J Tub 1986; 33 : 101.
L
yj _> uSr'o • ' 1
-
..L-VOX'.^ ri)
t •
-• 4-c
L
!
0 l/^>y ^H-C?.e-y^.»<2
•
I
O'*-« ‘
p
■ •
’ • < ■ ■ '■' *'
,
■
■
Xu^j-loa*’. ? 4 -et^-a . x-c.. .,
lv- cur
h
l^C* <
_jui-
>xc
i
• -_ .-
■ /
k
h" 0
f '■' •■' *■■ ' c’
J-> t
’
I'
< • <u6
'
1
* C -Q—
^j’ ' f^LLi^p
-
C='-tJ -
A-
»^'
I
o) fM-GL
fl
/JAXX
;
■kC ”
-■ ■*-
6
-B"
j
i. 6t>cU
^xv-Me-r Q 7et &
,
G. M2.i
>.->-< ^. ^‘■
oX^-V^5^-
e^sM ■
,V pu
T€rx
^>'0
C'
/
J
‘
*)
i
I
!
♦
i
I
I
111
IMPACT OF TREATMENT PROGRAMME ON TOTALITY OF IB PATIENTS
FIG. I
OVERALL SU< CESS RATE
Ind. J. Tub., 1938, 35, 110
DIRECT IMPACT OF TREATMENT PROGRAMME ON TOTALITY OF
TDBErSlOCS PATIENTS IN THE COMMUNITY"
i
crculosis treat-
radiographic, bacteriological and other inve t
('r
Xffie^ScutiV efficiency
their prescribed
of^ombinS; of anti-tuberculosis drugs em-
Ml
as the ‘ relaiive efficacy-of chemotherapy m
patients n^t%omplcting the prescribed duration
I
same, whatever the basic level of component.
The increase in the overall success rates(S)
following a 10% increase in case-finding effici
ency is set out in Table 3. for various levelt of
case-holding efficiency and chemotherapy
efficiency but keeping the relative efficacy of
chemotherapy in patients not completing tne
prescribed course at 50%. Itjs dear that the
increase in overall success rate tends to increase
with case-holding and chemotherapy dDciency
levels. Indeed, when they take values of 95/□
and 95%. the increase in success rate becomes
as high as 9.3% (cf 5.4% above).
If the case-finding efficiency is increased
from 30% to 40%. but all the other efficiencies
remain unaltered, the overall success rate turns
out to be 21.6%. ie. there is an increase of
5 4% The increase is the same for a 10/0 m
crease from 40% to 50%, 50% to 60%. - or
90% to 100% (Table 2). i e-. it is independent
of the base level of the case-finding efficiency.
i
chemotherapy efficiency (case-finding and case
holding efficiencies being fixedVItmay there^
ease-hohlim
eHieiencics
efficiencies being
being fixed
fixed al
at 35". and .80' _______
Increase
Overall
Case-finding
success
efficiency
86”2%^
30%
5.4",.
21.6%
40".,
5.4".,
50%
60",,
32.4".,
70"„
37.8".,
80%
43.2%
90"..
48 6".,
100%
54.0"„
*
|
i-
SUCCESS (40"',)
L£1
78
1
iUCCI SS (80",.)
i
!
162
i-mtc 9.
that in Table 3. I lowcver. a close comparison
Fable
4. Ml
At cuuvur
current t.nv.vnvj
efficiency iv.J.to
levels of casefinding (30".,) and chemotherapy (80%). the of the two tables (Tables 3 and 4) shows that the
2";,(ci‘ 5.4%
in Table .3). The increases in overall success rate are consistently
ncrcase i»
is only
only 11 2"„(cf
5.4
pattern of the findings is very similar and appreciably greater for a specified increase
general f.............
I able 3
fncr. ase in overall vuceesv rate following IO"., increase in cns.-lmding elficiene,, al various levels of ease
holding and chcmotherapi el/iei< nev
Efficacy of
chemotherapy*
80".,
85".,
90",,
95"„
5.4%
5.4",,
5.4".,
5.4':,.
5.4"..
Tuberculosis and Chest Diseases, held at
Range
Case-holding efficiency (",,)
35
55
75
95
Tt
6.2
6.6
7.0
7.4
7.0
7.4
7.9
8.3
7.8
8.3
8.8
9.3
6.1
6.4
7.8
6.4
9.3
•In those completing the course
Table 4
Inciease in overall success rale following
n'C •" c.uve-hnlding efficiency, al various levels of case
finding and chemotherapy efficiency
Range
I ase-lindmg^efficwn£y_(",,)^______
Efficacy of
»
. :..
overall
The corresponding increascs^iiUhc
'rate ‘(S) following a 10% increase in
success rate (S) following
only the case-holding efficiency are set out in
•Special lecture delivered at 42nd National Conference on
J_
195 I
|
j 105
16.2" . IS OVERALL SUCCESS
50",.
40".,
27.0"..
NOT COMF1 ETED
COURSE (65"„)
COMI’LETl D
COURSE (35%)
80",.
Table 2
are all proportions.
I
I
~ sr
Case-finding
Case-holding
Chemotherapy
Patients who do not complete
prescribed Course of treatment
(Fig. 1).
the.
More generally, if X, Y
\ and
—- Z
- denote
---- tethe
efficiencies of case-finding, case-holding and
chemotherapy and K denotes the relative
efficacy, the overall success rate (S) is given by
S=XZ{Y+(1—Y)K}, where X, Y, Z, K and S
300
Efficiency
Relative efficacy
Actual efiicacy
".XI’’...Ob i.
r 'i
Table 1
Factors affecting overall success rale
Factor
4’
DETECTED (30?,',)
f ' ----------------
of treatment.
CSt'fisp-
1000
fore be concluded that the increase in the overforea s^fi^-se in the
z- Available information (Table J) indicates
that in the National Tuberculosis Programme.
the efficiencies are about Wi for
(Nagpaul. 1967), about
(National TB Programme. 1.979), about 80 „
for chemotherapy (Radhakrishna. '’W), an<l
c. - Mo
TOT,\L CASES
s. Radhakrishna*’
The direct impact of any
t cTklui Lz v
o-'FEXit.-kCv.La ex-.'
J
chemotherapy*
80'.'„
LJi____
t
°!L
11
*ln those completing the course
30
g
50
2.0
2.1
2.1
70
90
s
3.6
3.8
-I 0
4.3
1.1
3.8
1.3 4.0
1.4 -4.3
112
S. RADHAKRISHNA
IMPACT OF TREATMENT PROGRAMME ON TOTALITY OF TB PATIENTS
of low case-holding efficiency; such a situation
_______
_
continue to have a place, the focus has to
could
lead to a dangerous
increase in the level
of
community,
with
C. drug resistance
----------- in the------------:7. -■*
t all : faift in a big way to operational research ascts under programme conditions, UnTortuits consequent‘ epidemiological implications.
lely, very little attention has been devoted to
Next, the increases in the overall success
With standard regimens that are currently
esc aspects in the last three decades. A brief
rate(S) following al0% increase in the efficacy
of chemotherapy are set out'in Table 5 At in vogue in the treatment programme and have
view of the limited research undertaken in
ese areas by institutions such as the National
VU..VUL
—- an efficacy of approximately 80%, we need a
current L.vlo
levels ^7
of case-finding (%%)
(30%) -..d
and .caseholding
success rate
notutng (35%),
tJO/ol, the
me improvement in
insucccss
taic case-finding efficiency of 65% provided we can uberculosis Institute. Tuberculosis Research
. only
... ~2.0%.
r.r.r ..
-----efficien
ensure case-holding efficiency of 95%. If case_________________
•ntre and the New Delhi TB Centre was made
is
However, if both these
ir[ier (Radhakrishna, 1983).
cies begin to increase, the benefit from better holding efficiency cannot be raised to such a
high
level
but
can
be
made
80%.
the
level
of
chemotherapy per se will also increase; for in‘ J ’is "''
n/ If better
Short-course chgafttlicrapy has been destance, if both case-finding and case-holding case-finding
efficiency
required
70%.
efficiencies increase by 40%,‘’to 70% and 75%, chemotherapeutic regimens are introduced^and
onstrated toTe very highly cffcciive in clim11 trials; practically all patients have a favourespectively, the 1...
increase5 in overall success the efficiency of chemotherapy is raised from
rate for a 10%
1"% increase in chemotherapy 80",, to 90%, a case-finding efficiency of 60"., •; We response, i.e bacteriologically quiescent
[sease at the end of the course of treatment,
efficacy is 6.1%, as compared to the earlier and a case-holding efficiency of 85% are re
id relapses occur in no more than 5’., of the
quired; alternatively, these could be 65% and
2.0%.
atierits. In consequence, short course regi70% respectively. Even if very highly effective
lens
have already been introduced into the
A modest target in the national tuberculo (95",.) short-course chemotherapeutic regimens
Jistricl
Tuberculosis Programme in 18 districts
,
containing
Rifampicin
and
Pyrazinamide
are
sis programme could be to successfully treat at
D me
the couuuy,
country, auu
and pm,,
plans are afoot ----to bring
least 50% of the totality of tuberculous patients introduced in the programme, unless case~ ’ 6'' sets
—out. various h0]ding efficiency is 75%. and case-finding
jore districts into this activity. This developin the community, fable
ient presents both a tremendous opportunity
‘‘mixes” of case-finding, case-holding and efficiency is 60% (or 90"„ and 55%, rcspec
nd a stiff challenge. It is vital that this special
chemotherapy efficiencies that are the needed lively), the modest target of successfully
iput (short course chemotherapy) should be
for the attainment of this objective. When treating 50",', of the tuberculous patients in the
tilised as an occasion for injliating qualify
deriving these, it has been assumed that the community cannot be attained.
: esearch on operational aspects in particular,
efficiency of case-holding will always be higher
The major implication of this mathematical
nnovative strategies must, to begin with, be
than that of case-finding, or at least the same
a.. is ,i.«.
but never lower. Such a stipulation is necessary study
that there should be: a drastic reoricn- < xplored empirically under D I P conditions.
applied
if we are avoid a situation where large numbers tation
-----of
e priorities in ---i:~j research in tuberof patients are diagnosed and brought under culosis. While controlled clinical trials to eva.
luatc new drugs and combinations and to evolve
treatment because of better case-findingw efficiency, but very few complete the course because better regimens under experimental conditions g
(10%) in case-finding efficiency compared to
the same increase (10%) in casc-holdingefficiency.
Ii
-3
Table 5
/«/ ;•„ increase in cncimn
Increase in overall success rate following l(>"„
chemotherapy ef/icieney, at various levels of case. J'
t
I I•
- /V - . . _ ..
finding
andI case-holding
efficiency
Case-finding
efficiency
30
50
70
90
35
’2 0
3.4
4.7
6.1
Case-holding efficiency
55
75
~ 32.r
95
2.9
~
■Vo
4.9
6.8
88
V
5
I
Table 6
Combinations leading to overall success rate of 50",,’
Efficacy of chemotherapy"’
80";,
85°„
90",',
95%
Case-finding efficiency
65%
70%
60%
65";,
70"„
60".,
65%
55%
60%
Case-holding efficiency
95",.
80"„
95",.
80"„
70‘!„
85"..
70".,
90".,
75".,
•With the stipulation that the efficiency of ease-holding i« at least as high as that of case-finding.
••In patients completing the prescribed course of treatment. In the others, the efficacy .is taken to b1-'
half this efficiency.
3
I
113
and those that appear promising must then be
evaluated scientifically, with adequate replica
tion and controls. These investigations need to
be directed towards vital aspects such as im- I
proved case-holding and case-finding efficien
cies, smooth drug delivery systems and reliable
documentation.
I
REFERENCES
Daily. G.VJ.. Rupert Samuel. G.E. and Nagpaul,
D.R. A concurrent comparison of an unsuper
vised self-administered daily regimen and a fully
supervised twice-weekly regimen of chemo
therapy in a routine out-patient treatment pro
gramme. Indian J. Tuber., 1974, 21, 152.
Nagpaul, D. R District Tuberculosis
Control
Programme in concept and outline. Indian J.
Tuber.. 1967. 14, 186.
National
Tuberculosis Programme—Report for
IVth quarter (sputum positive cases), 1979.
Radhakrishna, S. National Tuberculosis Pro
gramme - Relative merits of enhancing the ope
rational efficiency of different components of
the treatment programme. Indian J. Tuber.,
1983. 30, 3.
Ind. J. Tub., 1988, 35, 117
116
P. VBNKATARAMAN, A.S.L. NARAYANA AND R. PRABHAKAR
ted from leprosy patients three hours after the
administration of clofazimine (and dapsone),
7 specimens (26%) gave a positive reaction by
the chloroform method. No specimen was
reported positive by the benzene method by
any of the three readers, a significant differe
nce (P=0.01).
Reader variation : Of 700 tests (by each
method) from pitients receiving rifampicin,
one reader disagreed with the other two on
five occasions by each of the two methods.
In the remaining 695 tests, identical results
were reported by all three readers.
In the case of the 27 urine specimens con
taining clofazimine, on 11 occasions one
reader disagreed with the other two by the
chloroform method, while there was no dis
agreement on any specimen by the benzene
method.
Discussion
Tests for the detection of rifampicin in
urine have been described using simple extrac
tion of the urine with either chloroform or
benzene. Both tests gave 98-100% positive
reactions between 3 and 11 hours after the
administration of approximately 15 mg/kg
body-weight of rifampicin in this study.
r
I
The tests described by Eidus and Harnanansingh (1969) yielded 100% positive reac
tions from two to eight hours after 300 mg
dose using urine and chloroform in the ratio
of 5:1. The microbiological method of
Mitchison et al (1970) yielded positive results
upto 12 hours after the conventional dose of
600 mg. This test, though simple, can be
performed only in laboratories equipped to
carry out microbiological work, and further,
it requires at least 24 hours before the results
are available.
The present method using chloroform is a
simplification of the Eidus and Harnananstngh (1969) procedure and can be performed
even under field conditions. The tests are
simple, specific and sensitive, and no positive
.
" '
reactions were obtained among the O-hour
specimens or among specimens from patients
receiving other anti-tuberculous drugs with
either test. Clofazimine, which also yields a
reddish coloration of the urine similar to
rifampicin, gave positive reactions only with
the chloroform method Further, chloroform
has a tendency to form an emulsion with the
alternative tuberculosis control strategies and their
aqueous layer, necessitating centrifugation on
POTENTIAL IMPACT
some occasions (Eidus and Harnanansingh, ■
1969). Also, chloroform being heavy, forms :
V. SiVARAMAN*, V. Balu,** and V. Fi.gka**
the lower layer, and hence, there is a refiec
tion of the upper aqueous layer, especially in
dark-coloured urines, which might interfere :
dicate a rising trend of case finding
The merits and demerits of various tuber
with the reading. Finally, chloroform is twice ; culosis control strategies have been engaging
coverage.
as expcrretvtT as benzene. Thus, the benzene
the attention of the programme planners
method appears to be superior to the chloro ' jince the very evolution of the national tubcrThe modifications now made in the model
form extraction procedure. The benzene • culosis programme. Among the parameters include the following.
extraction procedure in this study yielded
used for finding the suitability of the stratc98-100% positive results for rifampicin in
(1) Birth and Death rates were calculated
cies one can cite (i) Operational feasibility,
urine between 3 and 11 hours after oral admi (ii) Resources involved, (iii) Cost effectivf- by applying b 0.9817 and d=0.9674 to
nistration of the drug. In clinical practice. | mss. Another parameter which can be used 110=0.0439 & DO 0.0223 (This is to faci
this means that if the drug is self-administered j% the long term epidemiological impact, litate operation by computer and agrees very
in the morning, on rising, or a supervised . ■%hich can be assessed through epidemetnc closely with the initial parameter used).
dose is given on attendance at a clinic, then ( ^models. Such models in the Indian context1
positive results could be expected at any time i lhave been discussed before by Waaler et al
(2) It is assumed that BCG does not
between 3 hours after the administration of I1(1974)- Nair (1977), Sivaraman and Umasankar offer any protection, other assumptions made
drug to midday or late in the evening.
in
the
previous paper (Sivaraman and Uma1(1979).
sankar lor fit) remain valid but different
Acknowledgement
| The aim of this paper is to present the operational and technical input data arc used
fuse of a model to assess the impact of possi- depending upon the programme envisaged.
The authors thank the clinical and nuts- j|ble alternative strategics with a view to help
ing staff of this Centre for collection of speci ?in decision-making on choice of a suitable
These changeg and the longer time hori
mens, and Shri KJ. Ilamparnan and Shri I*. -strategy.
zon envisaged entail time consuming and
Peter for technical assistance and reading th:
cumbersome calculations. Hence a compu
tests. The valuable suggestions of Prol
ter programme has been written in Basic and
I. The Model
Wallace Fox in the preparation of this manus- |
run, and outputs analysed.
cript are gratefully acknowledged.
An cpidemetric model is a mathcmalical
II. Siinulalions Done
-representation
of
the
epidemiological
situa
REFERENCES
tion in a community. The construction of the
(I) ----A hypothetical
non-interference sittiaEidus, L. and Harnanansingh, A.M.T. : Simple pm ’model rests upon grouping of population in
different epidemiological classes determining tion when no control programme is operated,
ccdurcs for checking rifampicin in urine. Amer
their sizes and transfer rates and on a series
Rev. Resp. Dis., 1969, 100, 738.
(2) The past programme from 1961 to 1986
of established facts and assumptions. A simu
lation model of tuberculosis epidemiology has been simulated by feeding the model with
Hobby, G L. : Practical methods of detecting majw
Tub
evolved by Azuma (1976) has been shown to the data on operational parameters obtained
anti-tuberculosis drugs in the urine Adv.
/
be suitable to Indian conditions with slight from N.T.P. reports.
Res , 1964, 13, 98.
'modifications (Sivaraman and Umasankar loc
Mitchison. D.A., Allen. B.W. and Miller. A.O
(3) As for the future. 4 alternaiive strate
-,cit). Predictions have been made upto the
Detection of rifampicin in urine by simple micro
year 1986. The predictions were very close gies are envisaged :
biological assay. Tubercle. 1970, 51, 300.
not only to survey results from National
(a) The case finding coverage maintains
Tuberculosis Institute and New Delhi TubcrRao, K.V.N., Eidus. L , Jacob. C V. and Tripath) , culosis Centre but also to predictions from a the same trend noticed in the previous years
S.P. : A simple test for the detection of pyrazinabut short course chemotherapy is introduced
more sophisticated model.
mide and cycloserine in urine. Tubercle, 196!. ’
with clfcct from 1988.
46, 199.
Need for taking a fresh look at the projec
(b) Same as (a) above but short course
tions and conclusions drawn from the previ
Rao, K V.N., Eidus, L., Jacob. C.V., Radhakrishm
ous model has arisen, not only because the chemotherapy introduced with effect from
S. and Tripathy, S.P. : Sodium nitroprusside tes
1990.
previous predictions were made only upto
for the detection of isoniazid and acetylisonia/ithe year 19S6 but also because of the follow
in urine. Tubercle, 1967, 48, 45.
(c) Same as (a) above but short course
ing subsequent developments.
chemotherapy is introduced with effect from
Venkataraman. P., Eidus, L, Tripathy, S.P. an:
(1) Demonstration of a very low efficacy 1996.
Valu. S. : Fluorescence test for the detection (■'
for B.C.G.
ethionamide metabolites in urine. Tubercle, 196’
(d) Efforts arc made to realise the full
(2) Possibility of using short course
48, 291.
potential of
the district
tuberculosis
chemotherapy.
(3) Data from N.T.P. reports which in- programme
s
••Assistant Sin geon
’Medical Superintendent
T.B Sanatorium, Gorimedu, I’ondichcrry-fiOS 006
TUBERCULOSIS control strategies
V. SIVARAMAN, V . BALU AND V. FLORA
118
111. Computation of Input Parameters for
Different Simulations
(1) Non-interference situation serves as
a base line and is obtained by assigning the
value O to case finding coverage and treat
ment regularity.
(2) Past Programme : Annual reports on
the performance of DTPs are being published;
(N.T.l. 1985-1986) the reports
indicate
that the number of sputum positive cases
diagnosed per DTP has risen from 536 in
1981 to 735 in 1985! If it were assumed that
the number of sputum positive cases prevalent
in an average DTP is around 6,000, the case
finding coverage thus has varied from 9% to
12%. From this a “guesstimate” of case find
ing coverage in 1961 has been arrived at and
is assumed to be 6% From these annual re
ports it is also known that the percentage of
patients completing chemotherapy has been
more or less stationary at 27% from 1981 to
1985. The cure rate among patients com
pleting 80% or more of prescribed treatment
is set at 65%. The cure rate in those incompletelv treated and not treated is assumed to
be 10%.
(3) Future Programmes
(A) The case finding coverage and the
percentage of patients completing 80% and
more of treatment are the same as before.
Introduction of short course chemotherapy is
simulated by assigning a higher treatment
completion rate of 45% and a higher cure
rate among fully treated 75% as well as
among inadequately treated (21%). Death rate
among incompletely treated will be assigned
the value of 13% (Death rate among lost
cases).
These figures are derived from the findings
oftheTRC study on application of short
course chemotherapy under programme con
ditions in North Arcot.
The trend in case finding coverage (observ
ed in the past and predicted for the future) is
shown in Figure 1. The varying parameters
in different simulations are summarised in
Table I.
72I
I
/
Results
The reduction in the various indices
brought about by alternative strategies is
shown in Table II.
60-
The postponement of introduction of short
course chemotherapy by 8 years (1996 in
strategy C. 1988 in strategy A) has led to a
marginal drop of reduction potential, the
difference being 0.7% for problem reduction.
0.6%, 0.5% and 1.2% for prevalence, mortality and risk of infection respectively.
The likely epidemiological situation in
1995 is shown in Table 111. Here also it is
seen that differences between strategies A, B,
and C are only marginal while a full poten
tial programme is likely to lead to considerable improvements.
-> 48Cy>
p
1
2
£
The trend in prevalence of disease and
the risk of infection with alternative strate
gics is shown in figs. 2 and 3. As the trends
with A, B and C arc very close only B is
shown. It is seen that there is a rise in pre
valence rate with programmes A & B after
1999.*
The conclusion to be drawn is that no
effort should be spared to increase the case
finding coverage otherwise the tuberculosis
problem is likely to worsen. Radhakrishna
(1983) has observed that the overall success
of the programme rests much more heavily
on improving the efficiency of case finding and
case holding than on evolving more and more
effective drug regimens under study conditions.
119
24o
12-
a
■
1961
73
81 85
97
2009 " 13
Another interesting feature is that the
absolute number of cases goes on increasing
Years .*'■ "ia—--(B & C) In these simulations only the with all strategies although the prevalence rate
Pig. /. Trend in case TinJing coverage
decreases.*
In
this
connection
the
following
year of implementation of short course
Tabic I
chemotherapy 1990 in B. and 1996 in C, is observations by Waaler (1982) are relevant.
“The population of India increased by 2.2%
Parameters ssed in different simulations
different from the previous one.
per year between 1971 and 1977 and that
Non InterPast I’rogsee
(D) Operational studies carried out in aged 55 and more, increased by 11% per year
ferenee
A. B C
National Tuberculosis Institute have shown with 8% of the population above 55 years of rBRChNTAGJ. REG.
0
27%
45%
age
and
with,
say
a
3
times
higher
incidence
that if D.T.P. is implemented as per manuals.
85% cure rate among fully treated, 48% treat above this age, this demographic change AMONG reg : Cure rate
65%
75%
ment completion rate and 33% case finding alone will increase the tuberculosis problem
Death rate
4%
4?i
coverage can be achieved. In this simulation, by 3.4% Even an annual reduction in the
------ 1RREG : Cure rate
it is assumed that the case finding coverage overall rate of 2.2% per year (equal to the AMONG
—
10%
21%
increase
in
the
population)
cannot
prevent
increases steadily over the years from 12.7%
'______________ Death rate
an increase in the absolute number of cases" _____________
- _____________ >7%__________ 13%
in 1986 to 33% in 1995.
__ _____ ______________________________
REG : Patients completing Treatment
1RREG : Patients with incomplete treatment
•Detailed tables may be obtained directly from the author, if so desired.
Future
Prog-D
27%
85%
4%
10%
17%
V. SIVARAMAN, V. BALU & V. FLORA
120
121
TUBBRCULOSIS CONTROL STRATEGIES
/40
NIS
120
NIS
ki
100
IF)
£
Q
U.
o
I
B
lai
80
B
2:
o
CJ
60
2
s
Uj
D
o
40
D
ic
Q:
Q:
1971
1961
91
81
YEARS
0.
YEARS
2001
2001
20
Fig. 2. Trend prevalence of disease with different strategies
1971
'81
'91
2001
2011
Fig. 3. Trend of risk of infection with two different strategics
Table II
Table III
Polenlial impact of alternative strategies
TB Cases TB Pro
blem*
Prevalence (Per thousand) Risk of Infection (5
TB Mortality
Strategies
Num- Reduc- initial Final Reduc- Initial Final Reduc- Initial Final Redta-
No.TB Pro
gramme
253553
. Introduc
tion of SSC in
1988
ber
226126
tion % (1987)
0
10 82
(2012)
0.4612 0.5829
0.4234 0.3993
Prevalence of Disease
(Per 1,000)
tion % lion"
tion
+ 12.8”
5.7
2.85
2.51
B. Introduc
tion of SCC
in 1990
226551
10.65
Introduc
tion of SSC
in 1996
227900
10.12
0.4234 0.4018
5 1
2 51
D. Full po
tential of
DTP.
211702
16.51
0.4234 0.2905
31.4
2.51
0.4234 0.4001
Possible epidemiological situation in 1995
5.5
2.51
3.26
+ 12.6”
2
2.46
2.46
2
114
0.87
0.87
1.30
0.79
0.80
+ 12.V
9.2
S
Risk of Infection
(Per 100)
NON INTERFERENCE
2.77
1.10
Introduction of
SCC in A.
11988
2.40
0.82
B.
1990
2.41
0.82
C.
1996
2.49
0.84
2.28
0.64
Full Potential of Programme
C.
I
tuberculosis.
’Defined ai number of years
year* of active infectious
it
**ln this situation there is no reduction,, only a rise.
2.47
1.89
1.5
35
0.87
0.87
0.87
0.33
8
62
The implications for the programme planner
are clear, namely, the workload for the tuber
culosis programme personnel is likely to in
crease both at the periphery and at DTC. To
cope wilh it. more staff is likely to be required.
Of course with the concept of integrated
health care the burden has to be shared by
multipurpose workers and a global view of the
V. SIVARAMAN, V. BALU AND V. FLORA
122
workload from different Jiealth programmes
has to be taken and staffing pattern might
need a dynamic change.
Acknowledgement
We are grateful to the Director, Health
and Family’Weifare, Pondicherry for permission to present this paper; Thiru Kumararaja
for his kind help in writing the computer
programme and running it in the Computer;
to Thiru Venkataramani for placing the
Computer service at our disposal.
REFERENCES
Waaler, H.T.. Gothi. G.D., Bailey G.VJ. Tub
26.4 Nair S.S. (1974) Bull. Wld. Hlth. Org. 51, 473.
Nair SS (1977) Ind. J. Pub Hlth 111, 31
Sivaraman, V. and Umasankar, V. : A Simulatioi
Model of Tuberculosis Epidemiology Adaptabilit
to Indian Condition; 1979, 26, 4.
Azuma Y. (1975) Bull Wld. Hlth Org. 52, 313
Nn NowS|Ctler (i985) 21/2. 38.
NTl Newsletter (1986) 22/2. 38
Radhakrishna, S. : National Tuberculosis Programm
—Relative Merits of Enhancing the Operational:
Efficiency of Different Components of the Treat
ment Programme; 1983. 30. 3.
Waaler. H.T.; Tuberculosis and Socio-Economic
Development; Bull. I.U.A.T., 1982, 57, 202.
Medical
Medical Council
Council of
of India invites nominations for Silver Jubilee
Research Awards-1988 under the following categories :
(1) Original and outstanding work in the field of medical and
allied sciences in India(2) Aid or assistance to research projects.
(3)
(4)
Travel Fellowships.
Establishment of Endowment Chairs. Professorship and
exchange scholars in different institutions.
For details, contact the Secretary. Medical Council of India.
Aiwan-E-Ghalib Marg, Kotla Road, New Delhi-110 002.
3
i
Definite cavitation was observed in 4 to 33 per cent of the
•active’ and ‘probably active’ cases, this percentage being
generally lower in cities.
The survey showed that the differences, if any, in morbidity rate,
between cities, towns and accessible villages were much smaller than
expected. Though the incidence of tuberculosis in villages was generally
lower than that in the citiesand towns, the difference was not marked. The
villages covered by the Survey were either those that had roads or tracks
for the transport of X-ray machines or a few others that were very close
to such roads. The places therefore were those that had possibility of
dissemination of the disease through normal channels of communication.
The exact incidence of the disease in remote villages and mountainou.
areas is still not known, but attempts are now being made to survey
some of these ‘inaccessible’ villages with the help of portable X-ray units.
The Survey also showed that the incidence of tuberculosis was signi
ficantly higher in the population living in insanitary conditions than in
7.
SALIENT FEATURES OF WORK IN SELECTED
MEDICAL AND PUBLIC HEALTH FIELDS
t.
2.1.
COMMUNICABLE DISEASES
2.1.1.
Tuberculosis
National Tuberculosis Survey
For the effective planning of any measures against tuberculosis, it
is essential to have precise information about its prevalence. Attempts
had previously been made, on the basis of random surveys, to estimate
the prevalence of the disease in different parts of the country. It was,
however, considered essential to undertake a wider survey in an organised
manner for determining the precise incidence of the disease both in
urban and rural areas. Accordingly, a National Tuberculosis Survey
was started by the I.C.M.R. in 1955 and completed in 1958. This survey
was limited to pulmonary tuberculosis. Six zones around Calcutta, Delhi,
Hyderabad, Madanapalle, Patna and Trivandrum, which had mobile
miniature X-ray units, were included in the survey. Within each zone
the population to be surveyed was selected on a sampling basis, due
consideration being given to both urban and rural populations. The
technical direction in regard to field work. X-ray readings and laboratory
examinations was given by the T.B. Sub-Committee of the I.C.M.R. In
all, the survey covered 6 cities, 30 towns, and 151 villages, the total
number of persons submitted to radiographic testing amounting to 290,758.
Preliminary findings of the survey were given in the report of the
Council for the years 1950 to 1957. The final report of the survey was
published recently. The salient findings may be summarised as below :—
1. Prevalence rate for ‘active’ and ‘probably active’ tuberculosis
varied from 13 to 25 per 1,000 population in cities, towns and
villages in the different zones.
2. The rate of bacteriologically positive cases for 1,000 population
in these areas varied from 2 to 8.
3. Prevalence rates were lower for females than males, specially
in age groups above 35 years.
4.
5.
In general, the prevalence rate showed a steady increase with age.
In cities, higher prevalence among persons living in ‘kutcha’
houses than among those living in ‘pucca’ houses indicated the
possible effect of economic conditions.
A large majority of ‘active’ and ‘probably active’ cases had
moderately advanced disease.
2
6.
c
, iZ
<7
■
b-GX' < c-5j
7
those living in healthier surroundings.
In addition the survey served to indicate the probable number of
infective cases in the country as well as the number of ’active’ or
■probably active’cases. The estimated number of mfective cases was
in the neighbourhood of L5 million, and that of ’active or probably
active’ cases amounts to about 5 million. These figures are h.gher than
those roughly arrived at previously. The facts thus showed the need for
devoting greater consideration to the problem and indicated the necessity
for giving high piiority to anti-tuberculosis measures on a national basis.
While such measures should, in the first instance, be concentrated in
urban areas, steps should also be taken to extend them to rural areas at
an early date.
Assessment of efficacy of BCG vaccine
In view of the importance of the tuberculosis problem in the
country, the Government of India have been paying special attention to
the development of techniques for the control of the disease. Asa
practical measure a mass BCG vaccination camPa>gn was imtiated m
1950 By the end of 1958 more than 120 million persons had been
tuberculin tested, out of whom 42 million were vaccinated with BCG-
The value of BCG vaccination in the control of tuberculosis has
been well brought out in recent studies carried out in England and other
parts of the world. In 1954 and 1955, a study of the results of BC.G
Vaccination in regard to the allergy produced by it was undertaken by a
WHO team. This team reported that : —
A low-grade tuberculin sensitivity, presumably caused by
1.
^2
8
4
i
i
micro-organisms other than mycobacterium tuberculosis, was
widespread in the country ; and
2. the level of BCG-induced allergy was reasonably high and
J
uniform from group to group examined, though somewhat
lower than what could be achieved under controlled conditions.
‘
The study is being continued by an Indian team under the aegis
of the I.C.M.R. The results so far obtained have confirmed the findings
of the WHO team. The maximum allergy produced by the BCG
vaccination as observed in other countries, fell short of the allergy
j
produced by natural infection by 1 to 3 mm. Even after taking this fact *
into consideration, it would appear that allergy produced by BCG
vaccination in India was about 4 mm lower than that observed elsewhere.
It is yet early to expect the results of BCG vaccination to manifest
themselves in relation to the total incidence of tuberculosis in the
country, but in view of the lower allergy already noted, it is worthwhile
considering whether the BCG vaccine produced in India can be im
proved. Attempts are therefore being made to produce freeze-dried
vaccine to counteract the influence of climatic and other factors which
might be responsible for the production of a low grade allergy in India.
The question of BCG vaccination in the prevention of tuberculosis
was considered by the Tuberculosis Sub-Committee and the Communi
cable Diseases Advisory Committee at their recent meetings in Poona.
Both the Committees expressed the view that it would be necessary to
initiate a full-fledged study to further assess the effects of BCG vacci
nation todate. These recommendations will be considered by the
Governing Body in due course. However, it must be noted that such
an extended study will deal only with the question of allergy produced
after BCG vaccination. The value of BCG vaccination in the control
of tuberculosis can only be assessed later.
Tuberculosis Chemotherapy Project. Madras
The Tuberculosis Chemotherapy Project in Madras was started in
1956 under the auspices of the Indian Council of Medical Research in
collaboration with the WHO/BMRC and the Government of Madras.
The object of the project was to find out how effectively the new anti
bacterial drugs can be used in treating tuberculous patients in their
homes as compared to the treatment in hospitals. The study was also
utilised to ascertain the prevalence of tuberculosis in family contacts at
the time a case was detected as well as in the subsequent years.
A detailed protocol was drawn up for conducting the investigations,
indicating, among other things, criteria for the selection of pateints for
the study. For the purpose of comparing the effectiveness of domiciliary
treatment with that given in hospitals, 100 beds were reserved in tht
Tuberculosis Sanatorium, TambaramSo far over 600 patients and over 2,000 contacts were covered by
the study. The contacts of every patient were X-rayed before the case
was put on treatment and, as far as possible, all the contacts were
— contacts of both the
• groups of<■ cases
------ treated
followed up regularly. The
at home or in the hospital were included in the study. This is expected
to give an indication of the risk, if any, to which contacts were exposed
when patients were treated at homeInformation is being collected about the family structure and
living conditions of the patients. This is an important factor, as the
economic and environmental conditions in which the patients have to be
treated in their homes have to be taken into consideration.
The study also included an investigation to compare the diets of
sanatorium and domiciliary group of patients with a view to find out the
role played by the diet, if any, in the attainment of quiescence when
treatment is given with modern anti-bacterial drugs.
t
The study as planned would also indicate whether it would be possi
ble to secure co-operation of patients for long periods of treatment at home.
!
The Centre has developed a well-equipped laboratory which is
undertaking approximately 1200 cultures and 300 sensitivity tests a
month. Tests to identify the causative organism and virulence studies
of different strains are also being carried out.
Some of the virulence studies which were completed a few years
ago, yielded very interesting results. These studies covered 83 Indian
and 29 British strains of Mycobacterium tuberculosis and were carried
out in two laboratories in Britain and one in Madras. A majority of
them which were tested were all found to be of human type and all were
sensitive to streptomycin and isoniazid. Three strains of guinea-pigs
one bred in London, one in Madras and the third in both places were
used in those studies. The results showed that although Madras strains
were no less infective than British strains, they were definitely less
virulent in the guinea-pigs. The Madras strains were found to have a
wider range of virulence and only 30 per cent of them were as virulent
as British strains. The least virulent of the Indian strains caused little
more than local lesions. It is rather paradoxical that there is apparently
more human tuberculosis in India than in Britain even though the
Indian bacilli are less virulent to animals. The investigators believe
that since the disease is spread mainly by patients with chronic
cavitating lesions, it is perhaps possible that attenuated strains often
produce such lesions and continue to exist among people who are ill
[
6
and survive and under the circumsL'es Lly h^h vTZ"
greatest survival rate. These studies however brought forth /
'
inVi— -inslSS
6.
out a large number of sensitivity tests and is expected ^o play an im
portant part in drug resistance surveys.
P y
lm’
8.
The duration of the follow-up period of oatienta
•
? .o be,, minimum
ye.„ fmmTe .Ur. of“ mlobT Zm.
The follow-up of the first batch
of patients admitted in 1956 will be
completed by 1961.
In all, 193 patients were admitted to
at home (96 patients) w.th t^t inTnTtX (97
2.
Patients in both series were given the same chemotherapy for
the 12 months namely, isoniazid 200
-J mg. plus PAS (sodium)
10 g. daily (given together in the
same cachet in two doses)
far patients weighing 100 lb. (45 kg.)
or more. The dosage
was reduced for lighter patients, the
range of dosage being
ions1
,
ana from 0-18
too.Mg. PAS (sodium)/kg. body-weight.
Although all the survivors were examined at 12 months the
main analysis in this report concerns the 82 home and 81
twoad°rriUn;MaKen7i W|h°
had or^nisms positive to the
foil
‘‘I C °rn0 Previous chemotherapy and (c)
followed the allocated treatment regimen.
The intake of patients began on
24th September, 1956 and
ended on 24th September, 1957.
3.
4.
5,
In spite of the random allocation
The diet of the home and the sanatorium series was similar
before the start of treatment, but there were important differ
ences during treatment, the sanatorium diet being clearly
superior in terms of animal protein.
Despite some of these differences at the start and in the course
of treatment the study still showed that “the results of domiciliary
chemotherapy as carried out in the study, approach sufficiently closely
the results of sanatorium treatment to suggest that it is appropriate to
treat the majority of patients at home.”
The
X ne results
results of
ot the
the study
study ,on sanatorium treatment versu
versus home
treatment have been published in the Bulletin of the World
Orffamsatmn
91 51-144).
ki
A f
..
_
vvona Health
Organisation HQKQ
(1959, 21,
obtained may be noted:-""’
°f the results
1-
Series had more severe disease even at the time of admission
than the sanatorium series in respect of the extent of cavi
tation, total extent of the disease, and bacterial content of the
sputum, although they were similar in other respects ; the
pre-treatment differences between the series were greater for
females than for males.
Infection with primary isoniazid-resistant organisms occurred
in 3-6 per cent primary resistance to PAS in 2-6 per cent and
primary resistance to streptomycin in 2-2 per cent of the patients.
There is evidence that different criteria of interpretation should
be used for PAS sensitivity tests on Indian strains of tubercle
bacilli from those that apply to British strains.
for treatment, the home
I
The investigations reported so far, while of considerable interest,
leave two important questions still unanswered. Does the treatment of
cases at home expose the contacts to greater risk of infection because of
the source of infection remaining at home than does treatment of cases
in the sanatorium when the focus of infection is removed from home ?
Again, while the results of one year treatment of patients both at home
and in the sanatorium, are encouraging enough, what exactly happens
to them after the cessation of treatment ? Does their condition deterio
rate in any way, thus necessitating continuance of treatment for another
year ? Unless answers to these questions are available, it will not ob
viously be possible to recommend domiciliary treatment as a basis of
the national campaign for the control of tuberculosis. The data colleced during the course of the work are under analysis from these two
points of view. Preliminary analysis has, however, revealed that
domiciliary treatment of tuberculous patients for an year, drawn from
an undernourished section of the community and living in comparatively
unfavourable environment, does not in any way expose the contacts to
any additional risk of infection, even though the main case, i.e. the
source of infection, remains in the family till the patient becomes
bacteriologically negative. Preliminary analysis of data has also revealed
that continuation of treatment in the second year does not confer any
1
I
8
fl
further benefit. If these preliminary results are confirmed by a detailed
analysis of data, they would certainly provide the basis for the initiation
of a national tuberculosis control programme based on sound scientific
lines.
(d) In the Chemotherapy Centre at Madras, patients were selected
on random basis for observation and treatment which had to be continu
ed for several years. An elaborate machinery had to be devised in order
to ensure that the patients did take treatment and that too in the manner
indicated. The results mentioned above, were, therefore, arrived at
after a thorough check-up and a thorough follow-up of all the cases under
investigation. Obviously, such an approach would not be feasible in a
mass campaign. A special set up was. therefore, created in Madanapalle
in order to ascertain the applicability of domiciliary treatment on a
mass campaign basis. It will be recalled that work at Madanapalle
was conducted for a number of years under the Ministry of Health
as a joint project of the Government of India and the WHO.
Towards the end of 1958, the work of this centre was reoriented, keeping
in view the standpoint described above, and the technical execution of
the programme was entrusted to the I. C. M. R. During the year 1959
domiciliary treatment was started on 189 patients—some receiving PAS +
1NH and others receiving INH alone. It was soon apparent that it was
difficult to ensure that the patients continued under treatment according
to schedule. Four cases ceased treatment during the first month and
this trend increased as months went by. 92 per cent were continuing
treatment at the end of three months, 87 per cent at the end of six months
and 57 per cent only at the end of 10 months. It is too early, however,
to draw any significant conclusions from this. Nevertheless, the trend is
worth noting. At the end of six months, the sputum conversion rate
from positive to negative, was in the neighbourhood of 78 per cent.
This finding is encouraging. At any rate, this investigation when
completed will provide information on factors which will have to be
taken into account in instituting a mass campaign against the disease.
treatment of obvious cases of infection but also prevention of spread
of infection to those in close contact with active leprosy cases. Timely
prevention of infection in children is doubly important because they tend
to develop lesions much earlier than others. Many attempts have been
made to prevent infection among children, primarily by their segregation
at the earliest possible moment from infected parents. Such an
approach, it will be realised, is not easy to adopt, because of the various
socio-economic factors involved in the segregation of children from their
parents. Any lead, therefore, which may provide the know-how for the
prevention of infection in children, will be most valuable in the organisa
tion of a national campaign against this disease.
2.1.2.
Leprosy
The Government of India have embarked on a national campaign
for the control of leprosy by the establishment of treatment and study
units in different regions of India. The attempt is to make leprosy
cases free from infection with suitable treatment in order to prevent
spread of the disease. Recent experience, however, appears to show that
such a measure alone is not likely to control the incidence of leprosy.
The reason for such a presumption is obvious. Before a patient comes
up for treatment, he, in all probability, has already infected others, both
children and adults. The problem in leprosy, therefore, is not only the
There are yet other problems in leprosy. Sulphones have no doubt
been found very suitable for the treatment of the disease. Nevertheless,
there are not enough grounds to say that with adequate sulphone
therapy, the disease can be completely got rid of. It is, therefore,
necessary to try out other remedies as and when they become available.
There are yet other handicaps. It has not yet been possible to cultivate
the causative organism of leprosy in artificial media as can be done in
respect of many other bacterial infections. No suitable laboratory
animal, susceptible to leprosy, is available for the study of the evolution
of the disease under controlled conditions. The Council, recognising these
limitations, has had a programme of research during the last few years to
obtain, if possible, some information on these various problems. How
ever, it is only during the last two years or so that some insight has been
gained in them. Results obtained from the work carried out hitherto
are summarised below and future lines of work are also indicated.
(a) Evolution of the disease in relation to lepromin reaction
In the Acworth Leprosy Home, an elaborate investigation on the
evolution of the disease together with its reactions to lepromin amongst
those in contact with leprosy patients has been in progress for a number
of years. A detailed report on these observations has been published in
a recent issue of the Indian Journal of Medical Research. Four thousand
contacts have been under observation for a period of ten years. Of these
contacts, 60 have developed characteristic neural lesions of leprosy, while
73 have developed what are called primary lesions, e.g. hypopigmented
patches more or less erythematous and without sensory changes. It has
been established that ab initio every individual is lepromin negative and
that leprous infection is the most potent factor responsible for lepromin
positivity. It has also been found that tuberculous infection can induce
lepromin-positivity, but it plays a limited role in bringing about such a
change in the reaction. Follow-up study in a limited number of contacts of
11
10
quite an appreciable number developed progressive lesions,
significance of these findings is obvious.
neural patients has shown a significant reduction in lepromin-positivity
in those showing bacteriological regression. It has, therefore, been
suggested that continued maintenance of lepromin-positivity requires a
continual immunological inducement in the form of lepra bacilli. It has
been concluded that, in the evolution of leprosy, three phases can be
recognised (t) an initial transient phase which does not react to lepromin
(it) the sensitized phase which shows bacilli in the skin and reacts to
lepromin and (tit) the de-sensitized phase which is really the lepromatous
phase when lepromin reaction is negative. It would, therefore, appear
that lepromin reaction indicates the sensitivity of the patient to infec
tion and not the resistance of the individual towards infection. However,
some workers do not ascribe specificity to this reaction, as, in their
experience, similar reactions can be elicited with use of other non
specific substances. This study will provide a background to the efforts
that will be made for the control of leprosy through the administration
of BCG vaccine to which reference will be made later.
(c) Experimental transmission of human leprosy to laboratory animals
(t) At the School of Tropical Medicine, Calcutta, organisms
obtained from leprosy nodules of untreated human cases have been used
to infect laboratory animals like hamsters, white mice and a special breed
of black mice. The latter have yielded encouraging results. Over a
period of many months, these animals developed generalised infection
and acid-fast organisms were noted in many of their tissues and organs.
The possibility of contamination by tubercle bacilli or some saprophytic
acid-fast organism was excluded. It was also ensured that Stenfanski’s
bacillus which usually produces fatal infection in rats did not enter the
picture. This is the first time that successful infection of a laboratory
animal is produced with human lepra bacilli, but these findings obviously
require to be confirmed by further investigation in other laboratories-
(ti) Following an early lead obtained in the laboratory that the leprosy
organism has a special affinity to nerve tissue, attempts were made to
cultivate this organism in tissue culture with spinal ganglia tissues at the
Indian Cancer Research Centre, Bombay. This work is not entirely
financed by the Council, but is reported here as the results are of special
interest. The material for inoculation was obtained from leprosy nodules
of untreated human cases. It was observed that multiplication of
organisms took place very readily in such tissue cultures. Material from
the tissue culture was further inoculated in the fluid part of the tissue
culture medium, i.e. ’he portion without live cells. Growth was obtained
even in this medium. Further, the passage of the material from the
latter into the usual laboratory media also showed growth of acid-fast
organisms simulating the leprosy bacillus. In the absence of specific
immunological criteria it is obviously difficult to conclude that the
organism so cultivated is the leprosy bacillus, but presumptive evidence
appears to be rather strong. It has been ascertained that this organism,
labelled at present as ICRC bacillus, is not identical with any of the
known acid-fast organisms. Immunological tests conducted with it have
shown some degree of specificity. It is interesting to record that extracts
from these organisms give a reaction more or less similar to that obtained
with standard lepromin. Inoculation of the organism into special strains
of mice available at the Cancer Research Centre has also resulted in
lesions simulating early lesions of leprosy. The disease apparently does not
progress further in these animals. These results are extremely interest
ing and further work on this important aspect is proceeding. However,
th? workers themselves are aware that there is a need for caution in
(b) Effect of prophylactic treatment with sulphone in the development
of disease amongst contacts of leprosy cases
An attempt has been made to study the response of contacts to
prophylactic treatment with DDS. The long incubation period in
leprosy necessitates a correspondingly long period of observation before
the value of prophylaxis in this disease can be correctly assessed.
However, this difficulty can be overcome by observing the progressive
and regressive changes that occur in contacts under prophylaxis who are
in one or the other of the three stages, viz, (a) uninfected, (b) infected,
i.e. harbouring bacilli but without lesions, and (c) the stage of primary
lesions which precede the appearance of manifest lesions of leprosy.
The dosage schedule has been varied according to the period of contact :
those in contact for five years or under have been given only 5 mg. of
DDS twice a week, those in contact for 15 years or over received 25 mg.
twice a week, and varying dosages have been given to cases of contact
periods in between. The results of this study have given encouraging
results. In the normal course, the period required for the infection to
manifest itself in contacts varies from three months to four years in
children and a little over two years in adults. In the present seriesj
children found to be negative to infection at the time of commencing
prophylactic treatment tended to remain free from infection as compar
ed to those not so treated. The response to prophylactic treatment was
also similar in those contacts, who had the bacilli in the skin even at the
time the treatment was commenced. Majority of those treated did not
develop any lesions and many of them became bacteriologically negative.
In the case of the untreated group, the majority remained infected and
The
I
■mi
12
13
interpreting these results in view of the repeated claims of successful
cultivation of the leprosy bacillus by several workers in the past.
of suitable aplints have been designed and are being manufactured for
the purpose.
The basic question, however, is how do these deformities develop ?
If the mechanism underlying the process of development is known, it
will pave the way for evolving further ameliorative techniques. Some
basic principles of tendon transfer, tendon free-grafting and joint
function have been studied in anaesthetic hands and feet and compared
with those of healthy subjects. The relative vulnerability of different
nerves and different muscles has also been studied. Variation in the
temperature over the surface of the body has been considered to be an
important factor in the production of deformities. Indeed, the work
conducted at the Centre has paved the way for achieving good results
not only in the treatment of leprosy deformities but also in the treatment
of deformities caused by other paralytic conditions.
r
I
(fit) In order to elucidate the pathways by which lepra bacilli
metabolise nutrients, certain enzyme studies are being carried out at the
Indian Cancer Research Centre, Bombay, with organisms isolated from
lepromatous nodules by differential centrifugation. These studies have
shown, for the first time, the presence of several respiratory enzymes in
these organisms. Enzymes oxidising both lactate and pyruvate are also
demonstrable, of which those oxidising pyruvate appear to be less
stable. An interesting aspect of this study is the metabolism of amino
acids particularly glutamic acid and tyrosine by the lepra bacilli. These
two amino-acids are chosen, because the former is intimately associated
with nerve metabolism and the latter with pigment formation (in skin)
both of which are usually affected in human leprosy. The results do
indicate the presence of enzymes in the mycobacterium lepra which are
capable of metabolising the above amino-acids. Pursuit on these lines
may help to throw light on the biochemical mechanisms responsible for
hypopigmentation and nerve degeneration closely associated with human
leprosy.
(
Therapeutic Studies
A number of newer drugs for treatment of leprosy have been
tested for their therapeutic value. Some of them are S.U. 1906, diphenyl
thiourea (DPT), acidomycin, pomegranate extract, etc. It has been found
that both S.U. 1906 and DPT produce clinical improvement similar to
that with DDS. but neither of them is as effective as DDS in producing
bacteriological improvement. Acidomycin has been found to be of only
limited therapeutic value in lepromatous cases. Other drugs tested
have had no special therapeutic effect It would appear, therefore, that
for the present there is no drug which will replace DDS in the treatment
of leprosy.
Treatment of Deformities
The pioneering work at the Christian Medical College, Vellore, on
the treatment of deformities by suitable operative procedures, has been
reported previously. Efforts to develop further operative procedures have
been continued and special techniques have been developed for the
surgical reconstruction of the foot, the thumb and the nose. As a result
of the adoption of these techniques, it can be said that a majority of
leprosy deformities, which are not preventable, can be suitably corrected.
It has been possible to develop a programme of physiotherapy on the
basis of the results thus obtained, which may be useful in limiting
secondary deformities and in the correction of existing ones. A number
BCG Vaccination in the Prevention of Leprosy
In recent years, many reports have appeared indicating the utility
of BCG vaccination in the control of leprosy, particularly childhood
leprosy. The subject is no doubt controversial. Opinion is yet divided
as to whether one single BCG vaccination is enough or whether a
number of injections with BCG vaccine would be necessary to obtain
the desired degree of lepromin-positivity which is one of the criteria to
be observed in the assessment of the utility of BCG vaccination. A
recent small scale observation in this connection, on the incidence of
leprosy amongst BCG-vaccinated children in an area in India may
be mentioned. In the study, the closeness and duration of contact with
infected cases of leprosy was kept in mind. The study revealed that
only five cases of leprosy developed in 678 BCG vaccinated children
during the period of observation of five years, while 283 cases occurred
in 1651 children of the same group who did not receive BCG vaccina
tion. Further work in this regard is necessary.
The Leprosy Advisory Committee of the Council has taken note of
these results and has recommended the institution of a comprehensive
programme of investigation of the role of BCG vaccine and chemopro
phylaxis in the prevention of leprosy. It is essential, however, to plan
such a programme on sound scientific lines with considerable care, so
that the results may yield information of value for the initiation of ade
quate control measures against the disease.
2.1.3. Smallpox
As an unusual rise in the incidence of smallpox and cholera was
reported from many States in India during the early months ot 1958,
an Expert Committee on Smallpox and Cholera was constituted under
Position: 2677 (4 views)