8861.pdf
Media
- extracted text
-
(Reference iMalerutfs -1
SEX SELECTION IN INDIA: ISSUES AND APPROACHES
^^Smiuftabk
5fwos India ^gionaCOffice, (Bangalore
IT1*
February, 2005
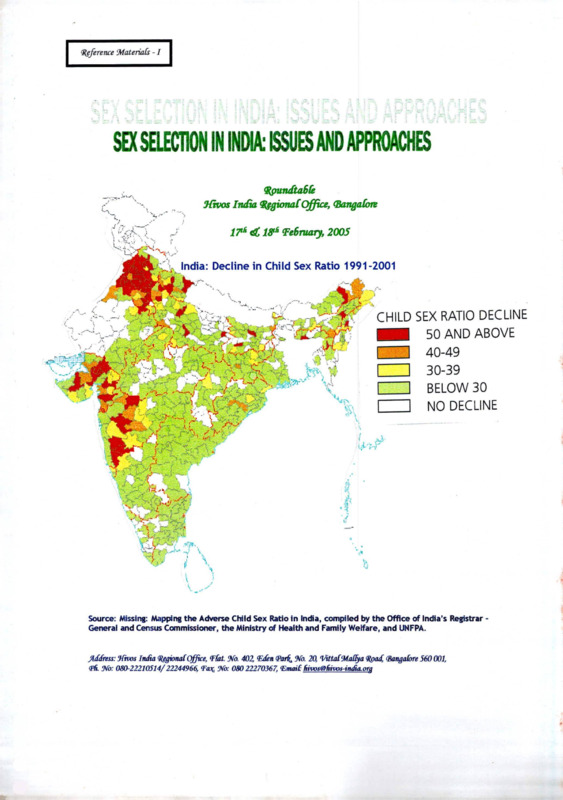
India: Decline in Child Sex Ratio 1991-2001
"“vj
*
ws\
CHILD SEX RATIO DECLINE
|
| 50 AND ABOVE
I ~~| 40-49
I
I 30-39
I
I BELOW 30
I
I NO DECLINE
4
I
Source: Missing: Mapping the Adverse Child Sex Ratio in India, compiled by the Office of India’s Registrar General and Census Commissioner, the Ministry of Health and Family Welfare, and UNFPA.
Jkfdress: Jfivos India RegionalOffice, (Flat. No. 402, (Eden (par^ No. 20, VittaliMalfya Road (Bangalore 560 001,
(Pfi No: 080-22210514/22244966, <Fa^ No: 080 22270367, Email lnvos@Iwws-iiuRa.org
u
(Rgference Materials -1
u
c
SEX SELECTION IN INDIA: ISSUES AND APPROACHES
Utivos India ^gionalOffice, (Bangafoit
L
18^ ‘February, 2005
India: Decline in Child Sex Ratio 1991-2001
<_
<-
I
I
Source: Missing: Mapping the Adverse Child Sex Ratio in India, compiled by the Office of India's Registrar General and Census Commissioner, the Ministry of Health and Family Welfare, and UNFPA.
address: JCtvos India Q^^ionalOffice, (Flat. No. 402, (Edm <Par^ Na 20, VittafMal^a ^pad^ (Bangalore 560 001,
<Pfi No: 080-22210514/22244966 Ta^ No: 080 22270567, (Email: fdvosSkivos-in£a.org
(
Background Note for
the Roundtable
Roundtable on Sex Selection in India: Issues and Approaches
Hivos India Regional Office
17th- 18th February, 2005
Bangalore
Introduction
Hivos (Humanist Institute for Cooperation with Developing Countries) supports many
institutions in the voluntary sector in India which have been addressing issues of
women’s equality in their communities. Hivos’ work in the country is determined by its
partners’ priorities and shared commitments. The Hivos India Regional Office in
collaboration with its partners, its activist friends and fellow development specialists felt it
would be useful to invite representatives of its partner and non-partner organizations,
members of the medical and legal fraternities, media representatives, and members of
the Government to deliberate on the deteriorating situation of women in the country with
special focus on the cluster of issues centered around sex selection in India. Various
factors that have a bearing on the issue have been discussed - patriarchy, son
preference, attitudes and beliefs that discriminate against girl children, population
policies, medical ethics, violence against women and legal reforms. The practice of
elimination of girl children must be stopped and this is possible only through a
convergence of social action and social commitment that brings together different actors
and institutions with their own responsibilities and expertise. How can we carry forward
in social and political practice a history of serious actions that will lead to fundamental
changes in the present social systems of increasing gender inequality and the practice of
sex selection?
In this meeting we hope to draw on the wisdom of earlier meetings to map the contours
of the challenges as they stand now, to pinpoint the similarities and the differences in
approaches and to sharpen the dialogue on future strategies which will put an end to this
state of affairs.
The Process
In 1992 this office of Hivos held a national meeting on the position of women in India in
association with the Centre for Women’s Development Studies. That was the beginning
of focused efforts to work with partner organisations that were committed to the
establishment and realization of women’s rights. We have learnt a great deal from
CWDS and from our partners’ stands on issues pertaining to women’s equality and
position in social life. This meeting is a result of the several dialogues we have held with
different organizations and individuals. In many ways this meeting is being convened by
all the members present! As a preparation for this meeting, Dr. Sabu George from
CWDS was kind enough to agree to draft a report which can be widely disseminated to
partner and other community organizations after this meeting.
1
Many participants have forwarded useful material; a selection of these documents will be
put together in a reference materials folder for all participants. Key articles and press
write-ups will be circulated to our partner organisations. Based on discussions at the
roundtable, Hivos intends to bring out a final report.
Issues
It is clear from anecdotal evidence, testimonies of women and press reports that there is
concern about the growing climate of discrimination against women in India and about
the specific collusion between parties which culminates in the commission of atrocities
against women and girl children. Both these aspects have to be addressed - the
environment that condones collusion and the act of collusion itself. Regarding the first,
one is compelled to question whether the women’s movement has been proactive
enough about safeguarding the interests of the girl child. The issue of the girl child came
into prominence in the eighties, not before that. In the years since then, though there
have been ongoing attempts to raise awareness in different spheres of society, the
situation prevailing today demonstrates that the issue has not been internalized
adequately by all concerned - perhaps even in the women’s movement. Similarly, the
child rights lobby has not seriously looked at gender in childhood. Women’s
organizations have expressed a need for stronger advocacy for the girl child by all
actors.
The present sex ratio imbalance could not have happened without the highly unfortunate
relationships of convenience and connivance that have developed between medical
professionals and those seeking their services. Despite existing safeguards in the
legislation against misuse of medical technology, the problem of sex selection persists in
an environment of traditional-patriarchal values, just as do child marriage and dowry.
This environment makes the issue of redressal and social change a highly complex and
several leveled issue. The weakness in the implementation of social legislation is well
known not only in the area of gender but also in areas such as child labor, untouchability
and dalit rights. Again, in order to really make an impact, we must look at both levels the environment that creates the strong demand for sex selection, and the inability of
legal mechanisms to regulate the actors who cater to that demand with a ready supply of
technology and services. Intervention strategies should address both demand and
supply, but how to sequence or synchronize? Both are essential; perhaps different
groups with different approaches are needed, but focusing on the basic fault line.
While attempting to analyze the efforts made during the past two decades to address the
problem of sex selection, we realize that
■
■
Single issue campaigns leading to highly critical changes in law and society need
to be understood and replicated.
Wider environments of neglect and derogatory attitudes towards women resulting
in the lowering of full citizenship rights need to be explored and understood so
that community-level activists can design campaigns to effect sweeping changes
in health services, health care accessibility, availability of reproductive health
rights information to women and men everywhere, and the premises on which
inequality is built - prejudices that assume the stature of facts and norms in social
life.
2
Poverty, structural processes that result in the disempowerment of people and loss of
their access to and control of resources have been central to Hivos’ financial support.
However, it is clear that the issues being discussed at this roundtable concern
communities who may or may not belong to immiserised populations. Indeed this calls
for differing forms of interventions and efforts at the field level and different kinds of
efforts by social development organizations. The problem is so deep-rooted, spanning
the household and community levels, that it offers multiple long-term challenges to social
development organisations. While the law under Section 23 (2) of the PNDT Act makes
the offence of sex determination a non-cognizable, non-bailable offence, the lax
enforcement machinery robs the law of effectiveness. Purveyors of ultrasound
equipment contribute to the ultimate dispensability of women by making the machines
very easily available. The ‘portability’ of equipment also implies the ‘invisibilisation’ of the
problem itself as far as localities, public policy, and regulatory mechanisms stand. The
problem does not lie with technologies but in the indiscriminate use of them. The culture
of social acceptance of sex selection and the willful practice of eliminating girl children
speak of the wider, growing climate that perpetuates gender inequality. This is of
particular concern given the rapid changes in technology that make regulation and
control difficult. Thousands of institutions and individuals across the country are
complicit in a crime that is tantamount to human rights violations of a kind that is likely to
result in genocide as pointed out by many activists and scholars.
With the view of building a commonality of purpose and a shared sense of reality, the
roundtable will try to foster a dialogue across the diversity of approaches, situations and
interpretation. It is our hope that the specialists gathered at the roundtable will
underscore the immediate and long term consequences of sex selection, and highlight of
the magnitude of the problem as reflected in the 1991 and 2001 censuses. Other
sessions will touch upon the central role of population policies and a “target-driven
population control” agenda particularly when implemented in a patriarchal society. The
two-child norm, and the focus on controlling ‘numbers’ is a feature of all state policies,
accelerating the decline in girl children. Decline in quality and accessibility of
reproductive health care services have also contributed to the state of affairs and the
roundtable will focus on these aspects of social reconstruction of a more equal society.
The responses that have emerged to this range of violatory practices- social
mobilisation, appeals to the judiciary for clear regulatory mechanisms, media campaigns,
debates on ethical choice and the culpability of the medical profession (including
incorporation of ethics in the medical education curriculum) and public policy advocacy
will be of special interest at the roundtable. We hope that this discussion on responses
will yield new insights on a question that is crucial for Hivos as a development institution
and for all civil society actors:
How can broad-based community organizations working on classical issues of class,
caste and gender divides join with the large number of social organizations already
active on several aspects of this growing crisis?
This question needs to be addressed in the context of communities that are in flux, as a
consequence of pervasive social change at multiple levels flowing from the processes of
modernisation, golobalisation and sanskritisation.
3
1
We hope that this dialogue between single-agenda campaign leaders and
representatives of community development organisations that draw on wider social
bases will strengthen future strategies for political and social action.
In Conclusion
With these objectives in mind, we have drawn up a schedule for the roundtable that will
provide time and space for exchange and intervention by all the participants. Differences
of opinions must be understood and overcome so that a few non-negotiables can be
drawn up by everyone. When talking to many of the participants we sensed that
everyone wishes to come to some convergence of perceptions and actions. In this sense
this meeting may be jointly owned, convened and carried forward by all present. We
hope that based on the analysis developed at the roundtable, recommendations for
social action will emerge for everyone to take home.
We look forward to meeting with all of you and we hope that this roundtable will be
useful for activists across the country who are trying to change the world of growing
divides, with special reference to the practice of sex selection. Free market logic, the
logic of technical totalitarianism which ruthlessly promotes the technical fix to deep social
issues, the exploitation of women’s bodies for social ends not necessarily theirs, the
minimalisation of women’s identity in the social mapping of ‘development and progress’,
the loss of historical memory when building the future by collective action, the threat of
several fundamentalisms ...these are issues the women’s movement has been
struggling with. We respect that struggle and we would like to see how the issue of sex
selection can be addressed further from the strength of the history of the women’s
movement. National attention needs to return more seriously (with sustained advocacy)
to the rights of the girl child.
Hivos India Regional Office
7th February, 2005
4
Draft
Programme Schedule
Roundtable on Sex Selection in India: Issues and Approaches
Hivos India Regional Office
17th-18th February 2005
Bangalore
THURSDAY 17 FEBRUARY 2005
09.30 - 09.40
Welcome and Introduction
Jamuna Ramakrishna, Ireen Dubel and Shobha Raghuram
09.40-10.30
Introductions
Participants will speak briefly about their work, gaps between theory and
practice and what they look forward to in the workshop (2 mins each)
Session I:
Historical Overviews
(15 mins presentation followed by 30 mins discussion to be initiated by Respondent)
10.30-11.15
Contextualising Sex Selection: Patriarchy, Position and Situation of
Women
C.P. Sujaya
11.15-12.00
What the Census Data Show
Satish Agnihotri
12.00-12.45
Campaign Efforts and Public Interest Litigation
Sabu George
12.45-01:00
Concluding Remarks by Chair
Chair: Vina Mazumdar
Respondent: Malati Das
01.00-02.00
Lunch
Session II:
Diverse Responses: Campaigns, Social Mobilisation, Legal Reforms
(15 mins presentation followed by 15 mins discussion to be initiated by Respondent)
02.00 - 03.30
Campaigns and Social Mobilisation
CASSA (Representative), Deepa Sinha, Lenin Raghuvanshi
03:30 - 03:45
Concluding Remarks by Chair
Chair: Akhila Sivadas
Respondent: Abha Bhaiya
03.45-04.00
Tea Break
1
04.00-05.00
Legal Reforms
Ossie Fernandes, Kamayani Mahabal
05:00-05:15
Concluding Remarks by Chair
Chair: Sabu George
Respondent: Elizabeth Vallikad
06.45-07.30
Steering Group Meeting
08.00
Dinner buffet at St. Mark’s Hotel
FRIDAY 18 FEBRUARY 2005
9.30 - 09.35
Steering Group Spokesperson- Recap of Highlights (5 mins)
Session III:
A Meeting Place of Diverse Worldviews and Perspectives
(15 mins presentation followed by 15 mins discussion to be initiated by Respondent)
09:35-11:30
Women’s Health
N.B. Sarojini
Campaign on PNDT Act in Gujarat
Trupti Shah
Effects of Two-Child Norm in Maharashtra
Audrey Fernandes
Maternal Health in Karnataka
Poornima Vyasulu
Chair: Shoba Nambissan
Respondent: Donna Fernandes
11:30-11:45
Concluding Remarks by Chair
Public Policy Advocacy
(10 mins presentation followed by 10 mins discussion to be initiated by Respondent)
11.45-12.45
Sex Selection & Pre Birth Elimination of Girl Child
Vibhuti Patel
Civil Society Perspectives
Sanjeev Kulkarni
Role of Media in Shaping Public Policy
Akhila Sivadas
People’s Health Assembly
Thelma Narayan
2
Chair: H. Sudarshan
Respondent: Basavaraj
12.45-01.00
Concluding Remarks by Chair
01.00-02.00
Lunch
Small Group Discussions on Priorities, Strategies, Alliance Building
02.00 - 03.30
Working Groups (11/2 Hrs)
03.30 - 03.45
Coffee/ tea break
03.45-04.15
Presentation of Reports
Chair: keen Dubel
04.15-04.45
Discussion
04.45- 05.00
Concluding remarks by Chair
Concluding Session
05.00-05.30
Open House Feedback Session
Final Comments
Jamuna Ramakrishna, Vina Mazumdar, Shobha Raghuram
Vote of Thanks
Reena Fernandes
3
List of Participants
Roundtable on Sex Selection in India: Issues and Approaches
Hivos India Regional Office
17th-18th February 2005
Bangalore
New Delhi
Ms. Abha Bhaiya
Jagori
C 54, South Extension Part II
Top Floor
New Delhi 110 049
Ph. No. 011 26257140/26264959
Fax. NO. 011 26253629
Email, jagori iaqori@Yahoo.com; bhaiyaabha@Yahoo.com
Dr. Sabu George
CWDS
25, Bhai Vir Singh Marg, (Near Gole Market)
New Delhi-110001
Telephone: 011-23345530/ 23365541/ 23366930
Fax: 011-23346044
Email: cwds@cwds.org; cwds@ndb.vsnl.net.in
Dr. R. Gopalakrishnan
Joint Secretary to PM
Prime Minister’s Office
New Delhi 110 011
Ph. No. 011 23015944
Email. rqopalakrishnan@pmo.nic.in
Dr. Vina Mazumdar
Centre for Women’s Development Studies (CWDS)
25, Bhai Vir Singh Marg, (Near Gole Market)
New Delhi-110001
Telephone: 011-23345530/ 23365541/ 23366930
Fax: 011-23346044
Email: cwds@cwds.org; cwds@ndb.vsnl.net.in
Dr. N.B. Sarojini
Sama Resource Group for Women and Health
C/o N.B. Sarojini
G-19, 2nd Floor
Marg No. 24, Saket
New Delhi 110 017
Phone: +9111-26562401/55637632
E-mail: samasaro@vsnl.com
1
Dr. Akhila Sivadas
Centre for Advocacy and Research (CFAR)
C-100/B, 1st Floor
Kalkaji
New Delhi 110 019
Phone: 91-11-2629 2787, 2643 0133, 2622 9631
Email: cfarasam@ndf.vsnl.net.in
Dr. C.P. Sujaya
A2, Diwanshree Apartments
30, Ferozeshah Road
New Delhi 110 001
Ph. No. 011 23320353
Email. aniali@del3.vsnl.net.in
Karnataka
Ms. Christy Abraham
ActionAid
139, Richmond Road
Next to Century Park
Bangalore - 560 025
Tel.No.25586682
Fax. No. 25586284
Email: christYa@actionaidindia.orq
Mr. Basavaraju
MGRDSCT
D.No.B/6/18, ’Sharada’
1st Main, KHB Office Road
Rajendra Nagar
Shimoga 577201, Karnataka
Tel: 08182-220867/227441
Email: kcbmqrdsct@yahoo.co.in
Dr. Malati Das
Additional Chief Secretary and
Principal Secretary to Govt
Planning and Statistics Department
Govt, of Karnataka, KGS-2
IV Stage, III Floor, M.S.Building
Dr B R Ambedkar Veedhi
Bangalore 560 001
Ph: 22252352, Internal Ph: 22092726
Fax: 22253694
Email: psrsplq@Yahoo.com; prs-plq@karnataka.qov.in
Ms. Donna Fernandes
Vimochana
No.33, Thyagaraja Layout
Jaibharath Nagar
Maruthi Sevanagar Post
Bangalore 560 033
Ph. No. 25492781
Email: awhrci@vsnl.com;streelekha@vsnl.net;
2
Dr. Sanjeev Kulkami
C/o. Tavargeri Nursing Home Pvt. Ltd
Near Kittur Chenamma Park
Dharwad 580 008
Karnataka
Ph. No. 0836 2448359
Resi. No. 0836 2743100
Email: sankulajeev@Yahoo.com
Dr. Sobha Nambisan
Principal Secretary to Govt. [Higher Education]
M. S. Building, Bangalore
Ph; No. 22252437
Resi. Ph. No. 26689583
Internal Ph: 22092494/22252437
Fax.No. 22253756
E-mail: prshiqh-edu@kamataka.qov.in
Dr. Thelma Narayan
Community Health Cell (CHC)
No. 369, Srinivasa Nilaya
Jakkasandra
1st Block, Koramangala
Bangalore 560 034
Ph. No. 5531518
Email: chc@sochara.org
Mr. Prasanna
People’s Health Movement (PHM)
Communication Officer Community Health Cell (CHC)
No. 369, Srinivasa Nilaya
Jakkasandra
1st Block, Koramangala
Bangalore 560 034
Ph. No. 5531518/51280009
Email: chc@sochara.orq;secretariat@phmovement.orq
Dr. H. Sudarshan
Vigilance Director
Lokayukta - Karnataka
Multistoried Building
Dr. Ambedkar Veedhi
Bangalore 560 001
Ph.No. 22257487
Mobile: 9448277487
Email: hsudarshan@vsnl.net: vgkk@vsnl.com
Karuna Trust
377, 8th Cross
1st Block
Jayanagar
Bangalore 560 011
Ph. No. 26564460
3
Dr. Elizabeth Vallikad
SJNAHS
Dept, of Obstetrics & Gynaecology
St. John's Medical College Hospital
Bangalore
560034, Karnataka
Tel: 080-25530724/ proj.off.22065271
Fax: 25530070
Email: emv2@vsnl.net
Dr. Suchitra Vedanth
State Programme Director
Mahila Samakhya Karnataka
631, 22nd Main, Near Sanjay
Gandhi Hospital, 4th T Block
Jayanagar
Bangalore 560 041
Ph. No. 26634845
Email: samakhya@vsnl.net
Dr Poomima Vyasulu
Centre for Budget Policy Studies (CBPS)
1st Floor, S.V. Complex
(Opp. Basavanagudi Policy Station)
55, K.R. Road
Basavanagudi
Bangalore 560 004
Ph. No. 56907402
Fax. No. 26671230
Ph. No. 9845231797
Email: poomima@cbpsindia.com
Bangalore based Guests
Dr. Saraswathi Ganapathy
Belaku Trust
No. 697, 15th Cross Road
J.P. Nagar llnd Phase
Bangalore 560 078
Ph. No. 26596933/26595594
Email: belaku@vsnl.com
Prof. Gita Sen (Health Watch)
Indian Institute of Management (IIM)
Bannerghatta Raod
Bangalore 560 076
Ph. No. 26582450
Email: qita@IIMB.ERNET.IN
Tamil Nadu
Ossie Fernandes
Human Rights Foundation (HRF)
10, Thomas Nagar, Little Mount, Saidapet
Chennai 600 015
Ph. No. 22353503
Fax. No. 22355905
Email: hrf@md3.vsnl.net.in
4
Mr. Jeeva/P. Pavalam
Campaign Against Sex Selective Abortion (CASSA)
11, Kamala 2nd Street, Chokkikulam
Madurai 625 002
Telefax: 0452 2530486, 0452 2524762
Email: sirdmdu@hotmail.com
Ms. D Sharifa
STEPS Women’s Organisation
Near Union Office
Pudukkottai 622 001
Telephone: 04322-220583
Email: sherifasteps@Yahoo.com
Mobile: 98424-20583
Orissa
Dr. Satish Balaram Agnihotri
Secretary, Department of Women and Child Development
Government of Orissa
Bhubaneswar
Orissa
Ph. No. 0674 2536775 (2928)
Fax. No. 0674 2406756
Email. sbaqnihotri@Yahoo.com; wcdsec@ori.nic.in
Ms. Bishaka Bhanja
C/o. P.C. Bhanja
Ramgarh, Tulsipur
Cuttack 753 008
Orissa
Ph. No. 0671 2361424
Mobile: 9437046508
Email: bhania@sathyam.netin
Andhra Pradesh
Ms. Dipa Sinha
MVF, No.201/202. Narayan Apartments
Sri Hanumanji Co-op. Housing Society
West Marredpally
Secunderabad -500026, A.P.
Tel: 040-27801320/ 27700290
Fax: 040 - 27808808
Email: mvfindia@hotmail.com
Maharashtra
Ms. Flavia Agnes
Majlis Manch
Bldg. No. 4, Block A/2
Golden Valley
Kalina-Kurla Road
Kalina, Mumbai 400 098
Telephone: 022-26661252/ 2666 2394
Fax: 022-26668539
Email: flaviaaqnes@vsnl.net;flaviaaqnes@hotmail.com
5
Dr. Audrey Fernandes
Tathapi Trust
425, Development Plant 77
Tilak Maharashtra Vidyapeeth Colony
Mukund Nagar
Pune 411 037
Ph. No. 020 24275906
Email: tathapi@vsnl.com
Dr. Kamayani Mahabal
CEHAT
Survey No. 2804 & 2805
Aaram Society Road
Vakola, Mumbai 400 055
Tel: (91) (022) 26673571/26673154
Fax: (91) (022) 26673156
Email: cehat@vsnl.com
Prof. Vibhuti Patel (Dr)
Head, P.G. Department of Economics
S.N.D.T. Women's University
New Marine Lines
Mumbai-400020
Email: vibhuti@vsnl.net
Uttar Pradesh
Dr. Lenin Raghuvanshi
Janmitra Nyas
SA 4/2A, Daulatpur
Varanasi 221002
Uttar Pradesh
Ph. No. 0542 586688/586676
Email: pvchr@yahoo.com
Rajasthan
Ms. Jaya Bharti
Astha Sansthan
attn. Dr. Ginny Shrivatsav
39 Kharol Colony
Udaipur, Rajasthan 313 001
Telephone : 0294-2451348 / 2451705
: 0294-2451391
Telefax
: fish trans@rediffmail.com; astha39@sancharnet.in
Email
Gujarat
Dr. Trupti Shah
Sahiyar (Stree Sangathan)
37, Patrakar Colony
Tandalja Road, Post-Akota
Vadodara-390 020
Gujarat, India
Telephone: 0091-265 513482 or 0091-265 334461
Email: sahiyar1@yahoo.co.in;rohit trupti@Yahoo.com
6
Rapporteur
Dr. Vijayalakshmi
Consultant Sociologist
416, Teacher’s Layout
Nagarbhavi First Stage
Nagarbhavi PO
Bangalore 560 072
Ph.No. 23213353
Mobile: 9448373353
Email: viiaYalakshmi@vsnl.com
Hivos Head Office, The Netherlands
Ms. Ireen Dubel
Senior Sector Officer
Gender, Women and Development
Raamweg 16
2596 HL Den Haag
The Netherlands
Ph. No: 00 31 70 3765500
Fax. No: 00 31 70 3624600
Email: i.dubel@hivos.nl
Netherlands
Dr. Sharada Srinivasan
Institute of Social Studies (ISS)
P.O. Box 29776
2502 LT The Hague
The Netherlands
Telephone: +31 70 426 0460/4260504
Fax: +31 70 426 0799
Email: srinivas@iss.nl
Staff of Hivos India Regional Office, Bangalore
For clarifications on logistics contact: Julietta Venkatesh/Hemalatha
For clarifications on financial and administration contact: Salim Vali
7
2.
National Population Policy 2000: A Critique
Jashodhara Dasgupta, KRITI
3.
Re-Examining Critical Issues on National Population Policy 2000
Devaki Jain and Mohan Rao
4.
Female Sex Selective Abortions: Some Issues
Mohan Rao, IDPAD Newsletter Vol. II, No. 1, January-June 2004
5.
The Two-Child Norm only leads to Female Foeticide
Madhu Gurung, www.infochanqeindia.orq/analYsis47print.isp
Role of Medical Establishment - Role of New Reproductive Technologies
1.
Social Justice and the New Human Genetic Technologies
Centre for Genetics and Society
2.
The Basic Science
Centre for Genetics and Society
3.
NGO moves Court over MCl’s failure to check Foeticide
Stop Selective Sex Abortions Stop Female Foeticide
www.datamationfoundation.orq/female/acourt.htm
4.
Sex Test law kills off Ultrasound
Kalpana Jain
Stop Selective Sex Abortions Stop Female Foeticide
www.datamationfoundation.orq/female/acourt.htm
5.
Sex Selection: New Technologies, New Forms of Gender Discrimination
Rajani Bhatia, Rupsa Mallik, Dhamita Das Dasgupta with contributions from
Soniya Munshi and Marcy Damovsky
6.
Sons are Rising, Daughters Setting
Dr. Vibuti Patel, HumanScape, Vol.X, Issue IX September 2003
7.
A Study of Ultrasound Sonography Centres in Maharashtra
Sanjeevanee Mulay and R. Nagarajan
Population Research Centre, Gokhale Institute of Politics and Economics
8.
Female Foeticide: The Collusion of the Medical Establishment
Lalitha Sridhar, www.infochanqeindia.org/features210print.isp
9.
Preimplantation Genetic Diagnosis for Gender Pre-Selection in India: A Counter
Argument to the Article by Malpani and Malpani
Rajiv H Mehta, Source: Reproductive Bio-Medicine Outline, Jan/Feb 2002, Vol.
4, Issue 1
10.
Court orders seizure of Illegal Sex Test Machines
Source: National Catholic Report, 3/8/2002, Vol. 38, lssue.18
ii
S
11.
Reproductive Technologies in India; Confronting Differences
Rupsa Mallik, Sarai Reader 2003: Shaping Technologies
Ethics
1.
Urgent Concerns on Abortion Services - EPW Commentary
Ravi Duggal, Vimala Ramachandran
2.
Negative Choice
Rupsa Mallik
Law - Human Rights
1
Female Feoticide or Crime against Humanity?
Kalpana Kannabiran
2.
Protecting the Rights of Giris
Dr. Erma Manoncourt, Deputy Director, UNICEF-lndia Country Office
3.
Rights of the Giri Child: Covered under Important National and International
Instruments
CASSA
4
Proposed Changes to the Medical Termination of Pregnancy Act, Rules and
Regulation in the Light of Concern about Sex Selection: A Response from the
Coalition for Maternal-Neonatal Health and Safe Abortion
5.
Treating Infanticide as Homicide is Inhuman
Lalitha Sridhar, www.infochanqeindia.orq/features211 print.js£>
6.
Memorandum to SCW to Relieve the Victims of Female Infanticide who are
Accused Guilty under Sec 302
Implementation of Existing Regulations - Obstacles and Bottlenecks
1.
Memorandum - Child Sex Ratio Vs Implementation of PCPNDT Law in Delhi
2.
Amendments to PNDT Act - Critical Appraisal of PNDT Act and Suggested
Amendments
CASSA
3.
The Role of the State Health Services - Emerging Issues
Dr. Reema Bhatia, University of Delhi
4.
A Merely Legal Approach cannot Root out Female Infanticide
Interview with Salem Collector J. Radhakrishnan
Stop Selective Sex Abortions Stop Female Foeticide
www.datamationfoundation.orq/female/acourt.htm
5.
The Role of Appropriate Authorities in Implementing the Pre-natal Diagnostic
Techniques Act 1994 and Roles (as amended upto 2002/2003) - Position Note
iii
for Discussion from State Level Consultation on the Role of the Appropriate
Authorities in Implementing the PNDT Act 1994 and Rules - 24 September,
2003
6.
Steps to be taken to implement the PNDT Act and Rules in Tamil Nadu from
State Level Consultation on the Role of the Appropriate Authorities in
Implementing the PNDT Act 1994 and Rules - 24th September. 2003
7.
A Critical Analysis of Tamil Nadu Government Cradle Baby Scheme
P. Phavalam, Convenor, CASSA
Campaigns and Interventions
1.
Tackling Female Infanticide: Social Mobilisation in Dharmapuri, 1997-99
Venkatesh Athreya, Sheela Rani Chunkath, Economic and Political Weekly,
December 2, 2000
2.
Indicators
CASSA
3.
Public Interest Litigation Filed in Supreme Court
CASSA
4.
Resolutions of Campaign against Sex Selective Abortion - Resolutions
CASSA
5.
Monitoring the Declining Child Sex Ratio - a Suggested Method
CASSA
6.
Minutes of the Two Days National Consultation on Enforcement of PCPNDT Act
iv
Gender Inequality; Patriarchy - Broad Overviews,
Analysis and History
[
s.rvi.o.U
■AZ'^r's
Sex Selection & Pre Birth Elimination of Girl Child
Dr. Vibhuti Patel, Professor & Head, Department of Economics,
SNDT Women’s University, Churchgate, Mumbai-400020.
E-mail- vibhuti@vsnl.net Phone-91-022-26770227, mobile-9321040048
Presented at A Round Table on Sex Selection
organised by HIVOS, Banglore on 17-18, February, 2005
Abstract
Consumerist Culture oriented economic development, commercialisation of medical
profession and sexist biases in our society, combined together have created a sad scenario of
‘missing girls’. Global comparisons of sex ratios shows that Sex ratios in Europe, North
America, Caribbean, Central Asia, the poorest regions of sub Saharan Africa are favourable
to women as these countries neither kill/ neglect girls nor do they use NRTs for production of
sons. The lowest sex ratio is found in some parts of India.
Deficit of women in India since 1901 -Violence against Women over the Life Cycle, from
womb to tomb- female infanticide, neglect of girl child in terms of health and nutrition, child
marriage and repeated pregnancy taking heavy toll of girls’ lives- Selective Elimination of
Female Foetuses and selection of male at a preconception Stage-Legacy of continuing
declining sex ratio in India in the history of Census of India has taken new turn with
widespread use of new reproductive technologies (NRTs) in India. NRTs are based on
principle of selection of the desirable and rejection of the unwanted. In India, the desirable
is the baby boy and the unwanted is the baby girl. The result is obvious. The Census results of
2001 have revealed that with sex ratio of 927 girls for 1000 boys, India had deficit of 60 lakh
girls in age-group of 0-6 years, when it entered the new millennium- Female infanticide was
practiced among selected communities, while the abuse of NRTs has become a
generalised phenomenon encompassing all communities irrespective of caste, class,
religious, educational and ethnic backgrounds. Demographers, population control lobby,
anthropologists, economists, legal experts, medical fraternity and feminists are divided in
their opinions about gender implications of NRTs. NRTs in the context of patriarchal control
over women’s fertility and commercial interests are posing major threat to women’s dignity
and bodily integrity. The supporters of sex selective abortions put forward the argument of
“Women’s Choice” as if women’s choices are made in social vacuum. In this context, the
crucial question is-
Can we allow Asian girls to become an endangered species?
Prenatal Diagnostic Techniques Act was enacted in 1994 as a result of pressure created by
Forum Against Sex-determination and Sex —preselection. But it was not implemented. After
another decade of campaigning by women’s rights organisations and public interest litigation
filed by CEHAT, MASUM and Dr. Sabu George, The Pre-natal Diagnostics Techniques
(Regulation and Prevention of Misuse) Amendment Act, 2002 received the assent of the
President of India on 17-1-2003. The Act provides “for the prohibition of sex selection,
before or after conception, and for regulation of pre-natal diagnostic techniques for the
purposes of detecting genetic abnormalities or metabolic disorders or sex-linked disorders
and for the prevention of their misuse for sex determination leading to female foeticide and
for matters connected therewith or incidental thereto”. The Pre-Natal Diagnostic Techniques
(Regulation and Prevention of Misuse) Amendment Rules, 2003 have activated the
implementation machinery to curb nefarious practices contributing for MISSING GIRLS. We
have a great task in front of us i.e. to change the mindset of doctors and clients, to create a
1
socio-cultural milieu that is conducive for girl child’s survival and monitor the activities of
commercial minded techno-docs thriving on sexist prejudices. Then only we will be able to
halt the process of declining sex ratio resulting into deficit of girls/women.
Introduction
Asian countries are undergoing a demographic transition of low death and birth rates in their
populations. The nation-states in S. Asia are vigorously promoting small family norms. India
has adopted two-child norm and China has ruthlessly imposed ‘one child per family rule.
Historically, most Asian countries have had strong son-preference. The South Asian countries
have declining sex ratios. This presentation tries to examine gendered socio-cultural and
demographic implications of new reproductive technologies, with special focus on sex
determination and sex-pre-selection technologies.
Sex Ratios - A Global Scenario
Sex ratios in Europe, North America, Caribbean, Central Asia, the poorest region- sub
Saharan Africa are favourable to women as these countries neither kill/ neglect girls nor do
they use (New Reproductive Technologies) NRTs for production of sons. Only in the South
Asia the sex ratios are adverse for women as the following table reveals. The lowest sex ratio
is found in India.
Table 1- Women per 100 men
Europe & North America
105
Latin America
100
Caribbean
103
Sub Saharan Africa
102
South East Asia
100
Central Asia
104
South Asia
95
China
944
India
L93
Source: The World’s Women- Trends and Statistics, United Nations, NY, 1995
There is an official admission to the fact that “it is increasingly becoming a common practice
across the country to determine the sex of the unborn child or foetus and eliminate it if the
foetus is found to be a female. This practice is referred to as pre-birth elimination of females
(PBEF). PBEF involves two stages: determination of the sex of the foetus and induced
2
termination if the foetus is not of the desired sex. It is believed that one of the significant
contributors to the adverse child sex ratio in India is the practice of female foetuses.”
Historical Legacy of Declining Sex Ratio in India:
In the beginning of the 20th century, the sex ratio in the colonial India was 972 women per
1000 men, it declined by-8, -11, -5 and-5 points in 1911, 1921, 1931 and 1941 respectively.
During 1951 census it improved by +1 point. During 1961, 1971, 1981 and 1991 it declined
by -5, -11, -4, -7 points respectively. Eventhough the overall sex ratio improved by +6
points, decline in the juvenile sex ratio (0-6 age group) is of —18 points which is alarmingly
high.
Table-2
Sex Ratio in India, 1901 to 2001
Decadal Variation
Year
Number of Women per 1000 Men
1901
972
1911
964
-8
1921
955
-11
1931
950
-5
1941
945
-5
1951
946
+1
1961
941
-5
1971
930
-11
1981
934
-4
1991
927
-7
2001
933
_____
+6
Source: Census of India, 2001
Prof. Amartya Kumar Sen, in his world famous article “MISSING WOMEN”, has
statistically proved that during the last century, 100 million women have been missing in
South Asia due to ‘discrimination leading to death’ experienced by them from womb to tomb
in their life cycles.
Dynamics of Missing Women in the contemporary India
Legacy of continuing declining sex ratio in India in the history of Census of India has taken
new turn with widespread use of new reproductive technologies (NRTs) in urban India. NRTs
are based on principle of selection of the desirable and rejection of the unwanted. In India,
the desirable is the baby boy and the unwanted is the baby girl. The result is obvious. The
1 “Missing...Mapping the Adverse Child Sex Ratio in India”, Office of the Registrar General and Census
Commissioner, India, Ministry of Health and Family Welfare and United Nations Population Fund, 2003
3
Census results of 2001 have revealed that with sex ratio of 933 women for 1000 men, India
had deficit of 3.5 crore women when it entered the new millennium.
Table-3
Demographic Profile
Population of India_________________
Males____________________________
Females
Deficit of women in 2001____________
Sex ratio (no. of women per 1000 men)
Source: Census of India, 2001.
102.7 crores
53.1 crores
49.6 crores
3.5 crores
933
Political Economy of Missing Girls
The declining juvenile sex ratio is the most distressing factor reflecting low premium
accorded to a girl child in India.2 As per the Census of India, juvenile sex ratios were 971,
945 and 927 for 1981, 1991 and 2001 respectively. In 2001, India had 158 million infants and
children, of which 82 million were males and 76 million were females. There was a deficit of
6 million female infants and girls. This is a result of the widespread use of sex determination
and sex pre-selection tests throughout the country (including in Kerala), along with high rates
of female infanticide in the BIMARU states, rural Tamilnadu and Gujarat. Millions of girls
have been missing in the post independence period. According to UNFPA (2003) 3, 70
districts in 16 states and Union Territories recorded more than a 50point decline in the child
sex ratio in the last decade.
1 To stop the abuse of advanced scientific techniques for selective elimination of female
foetuses through sex -determination, the government of India passed the PNDT Act in 1994.
But the techno-docs based in the metropolis, urban and semi-urban centres and the parents
desirous of begetting only sons have subverted the act.
Sex determination and sex pre-selection, scientific techniques to be utilized only when certain
genetic conditions are anticipated, are used in India and among Indians settled abroad to
eliminate female babies. People of all class, religious, and caste backgrounds use sex
determination and sex pre selection facilities. The media, scientists, medical profession,
government officials, women’s groups and academics have campaigned either for or against
their use for selective elimination of female foetuses/ embryo. Male supremacy, population
control and moneymaking are the concerns of those who support the tests and the survival of
women is the concern of those who oppose the tests. The Forum Against Sex Determination
and Sex Pre Selection had made concerned efforts to fight against the abuse of these
scientific techniques during the 1980s.
Science in Service of Femicide :
Advances in medical science have resulted in sex-determination and sex pre-selection
techniques such as Sonography, fetoscopy, needling, chorion villi biopsy (CVB) and the most
popular, amniocentesis and ultrasound have become household names not only in the urban
India but also in the rural India. Indian metropolis are the major centres for sex determination
(SD) and sex pre-selection (SP) tests with sophisticated laboratories; the techniques of
2 Patel, Vibhuti (2003) “The Girl Child: Health Status in the Post Independence Period”, The National Medical
Journal of India, AIIMS- Delhi, Vol. 16, Supplement 2, pp. 42-45.
3 UNFPA (2003) Missing, New Delhi.
4
amniocentesis and ultrasound are used even in the clinics of small towns and cities of
Gujarat, Maharashtra, Karnataka, Uttar Pradesh, Bihar, Madhya Pradesh, Punjab, West
Bengal, Tamil Nadu and Rajasthan. A justification for this has been aptly put by a team of
doctors of Harkisandas Narottamdas Hospital (a pioneer in this trade) in these words, “...in
developing countries like India, as the parents are encouraged to limit their family to two
offspring, they will have a right to quality in these two as far as can be assured.
Amniocentesis provides help in this direction”4. Here the word ‘quality’ raises a number of
issues that we shall examine in this paper.
At present, ultrasound machines are most widely used for sex determination purposes.
“Doctors motivated in part by multinational marketing muscle and considerable financial
gains are increasingly investing in ultrasound scanners.”5 But for past quarter century,
Amniocentesis, a scientific technique that was supposed to be used mainly to detect certain
genetic conditions, has been very popular in India for detection of sex of a foetus. For that
purpose, 15-20 ml of amniotic fluid is taken from the womb by pricking the foetal membrane
with the help of a special kind of needle. After separating a foetus cell from the amniotic
fluid, a chromosomal analysis is conducted on it. This test helps in detecting several genetic
disorders, such as Down’s Syndrome, neurotube conditions in the foetus, retarded muscular
growth, ‘Rh’ incompatibility, haemophilia, and other physical and mental conditions. The test
is appropriate for women over 40 years because there are higher chances of children with
these conditions being produced by them. A sex determination test is required to identify sex
specific conditions such as haemophilia and retarded muscular growth, which mainly affect
male babies.
?.
Other tests, in particular CVB, and preplanning of the unborn baby’s sex have also been used
for SD and SP tests. Diet control method, centrifugation of sperm, drugs (tablets known as
SELECT), vaginal jelly, ‘Sacred’ beads called RUDRAKSH and recently advertised Gender
Select kit are also used for begetting boys.6
Compared to CVB and pre-selection through centrifugation of sperm, amniocentesis is more
hazardous to women’s health. In addition, while this test can give 95-97% accurate results, in
1% of the cases the test may lead to spontaneous abortions or premature delivery, dislocation
of hips, respiratory complications or needle puncture marks on the baby. 7
Popularity of the test
Amniocentesis became popular in the last twenty-five years though earlier they were
conducted in government hospitals on an experimental basis. Now, this test is conducted
mainly for SD and thereafter for extermination of female foetus through induced abortion
carried out in private clinics, private hospitals, or government hospitals. This perverse use of
4 Patanki, M. H., Banker, D. D. Kulkami, K. V. & Patil, K. P. (1979, March). “Prenatal Sex-prediction by
Amniocentesis- Our Experience of 600 Cases”, Paper presented at the First Asian Congress of Induced Abortion
and Voluntary Sterilization, Bombay.
5 George, Sabu and Ranbir S. Dahiya (1998) “ Female Foeticide in Rural Haryana”, Economic and Political
Weekly, Vol. XXXIII, No.32, August 8-14, pp. 2191- 2198.
6 Kulkami, Sanjeev (1986) “Prenatal SD Tests and Female Foeticide in Bombay City- a Study”, Foundation for
Research in Community Health, 64-A, R.G. Thadani Marg, Worli, Bombay - 400018.
7 Ravindra, R.P. (1986, January) “The Scarcer Half - A Report on Amniocentesis and Other SD Techniques, SP
Techniques and New Reproductive Technologies” Centre for Education and Documentation, Health Feature,
Counter Fact No. 9, Bombay.
5
modem technology is encouraged and boosted by money minded private practitioners who
are out to make Indian women “male-child- producing machines.” As per the most
conservative estimate made by a research team in Bombay, sponsored by the Women s
Centre, based on their survey of six hospitals and clinics; in Bombay alone, 10 women per
day underwent the test in 1982.8 This survey also revealed the hypocrisy of the ‘non-violent,’
‘vegetarian,’ ‘anti-abortion’ management of the city’s reputable Harkisandas Hospital, which
conducted antenatal sex determination tests till the official ban on the test was clamped in
1988 by the Government of Maharashtra. The hospital’s handout declared the test to be
‘humane and beneficial’. The hospital had outpatient facilities, which were so overcrowded
during 1978-1994 that couples desirous of the SD test had to book for the test one month in
advance. As its Jain management did not support abortion, the hospital recommended women
to various other hospitals and clinics for abortion and asked them to bring back the aborted
female foetuses for further ‘research’.
Scenario During the 1980s:
During 1980s, in other countries, the SD tests were very expensive and under strict
government control, while in India the SD test could be done for Rs. 70 to Rs. 500 (about US
S6 to $40). Hence, not only upper class but even working class people could avail themselves
of this facility. A survey of several slums in Bombay showed that many women had
undergone the test and after learning that the foetus was female, had an abortion in the 18th
or 19^ week of pregnancy. Their argument was that it was better to spend Rs. 200 or even
Rs. 800 now than to give birth to a female baby and spend thousands of rupees for her
marriage when she grew up.
The popularity of this test attracted young employees of Larsen and Tubero, a
multinational engineering industry. As a result, medical bills showing the amount spent on
the test were submitted by the employees for their reimbursement by the company. The
welfare department was astonished to find that these employees were treating sex
determination tests so casually. They organized a two-day seminar in which doctors, social
workers, and representatives of women’s organisations as well as the family planning
Association were invited. One doctor who carried on a flourishing business in SD stated in a
seminar that from Cape-Comorin to Kashmir people phoned him at all hours of the day to
find out about the test. Even his six-year-old son had learnt how to ask relevant questions on
the phone such as, “Is the pregnancy 16 weeks old, etc.9
Three sociologists conducted micro-research in Bijnor district of Uttar Pradesh. Intensive
field work in two villages over a period of a year, and an interview survey of 301 recently
delivered women drawn from randomly selected villages in two community developed blocks
adjacent to Bijnor town convinced them of the fact that “Clinical services offering
amniocentesis to inform women of the sex of their foetuses have appeared in North India in
the past 10 years. They fit into cultural patterns in which girls are devalued”.10 According to
s Abraham, Ammu and Shukla, Sonal (1983) "Sex Determination Tests”, Women’s Centre, 104 B, Sunrise
Apartment, Nehru Road, Vakola Santacruz (E), Bombay.
9 Abraham, Ammu (1985, October). “Larsen and Turbo Seminar on Amniocentesis”, Women’s Centre
Newsletter, Bombay, 1 (4), 5-8.
10 Jeffery,Roger and Jeffery,Patricia & Lyon,,Andrew (1984) “Female Infanticide and Amniocentesis’” Social
Science and Medicine, (U.K) 19(11), 1207-1212.
6
the 1981 Census, the sex ratio of Uttar Pradesh and Bijnor district respectively, were 886 and
863 girls per 1000 boys. The researchers also discovered that female infanticide practiced in
Bijnor district until 1900, had been limited to Rajputs and Jats who considered the birth of a
daughter as a loss of prestige. By contrast, the abuse of amniocentesis for the purpose of
female foeticide is now prevalent in all communities.
In Delhi, the All India Institute of Medical Science began conducting a sample survey of
amniocentesis in 1974 to find out about foetal genetic conditions and easily managed to
enroll 11000 pregnant women as volunteers for its research. 11 Main interest of these
volunteers was to know sex of the foetus. Once the results were out, those women who were
told that they were carrying female fetuses, demanded abortion.12 This experience motivated
the health minister to ban SD tests for sex selection in all government run hospitals in 1978.
Since then. Private sector started expanding its tentacles in this field so rapidly that by early
eighties Amniocentesis and other sex selection tests became bread and butter for many
gynaecologists.
A sociological research project in Punjab in 1982 selected, in its sample, 50% men and
50% women as respondents for their questionnaire on the opinions of men and women
regarding SD tests. Among male respondents were businessmen and white-collar employees
of the income group of Rs. 1000/- to Rs. 3500/- per month, while female respondents were
mainly housewives. All of them knew about the test and found it useful.13 Why not? Punjab
was the first to start the commercial use of this test as early as in 1979. It was the
advertisement in the newspaper regarding the New Bhandari Ante-Natal SD Clinics in
Amritsar that first activised the press and women’s groups do denounce the practice.
A committee io examine the issues of sex determination tests and female foeticide, formed
at the initiative of the government of Maharashtra in 1986, appointed Dr. Sanjeev Kulkami of
the Foundation of Research in Community Health to investigate the prevalence of this test in
Bombay. Forty-two gynecologists were interviewed by Dr. Sanjeev Kulkami, who is himself
a gynaecologist. His findings disclosed that about 84% of the gynaecologists interviewed
were performing amniocentesis for SD tests. These 42 doctors were found to perform on-anaverage 270-amniocentesis tests per month. Some of them had been performing the tests for
10-12 years. But the majority of them started doing so only in the last five years. Women
from all classes, but predominantly middle class and lower class of women, opted for the test.
About 29% of the doctors said that up to 10% of the women who came for the test already
had one or more sons. A majority of doctors feel that by providing this service they were
doing humanitarian work. Some doctors feet that the test was an effective measure of
population control. With the draft of the 8th Five-Year Plan, the Government of India aimed
to achieve a Net Reproduction Rate of ond (i.e. the replacement of the mother by only one
daughter). For this objective SD and SP were seen as handy; the logic being a lesser number
of women means less reproduction. 14
11 Mazumdar, Veena (1994), “Amniocentesis and Sex Selection”, Centre for Women’s Development Studies,
Delhi, Occassional Paper Series No. 21.
12Chhachhi, Amrita & Stayamala, C. (1983, November) “Sex-determination Tests: A Technology, Which Will
Eliminate Women”, Medico Friend Circle Bulletin, India; No. 95, 3-5.
13 Singh, Gurmeet and Sunita Jain (1983). “Opinion of Men and Women Regarding Amniocentesis”, College of
Home Science”, Punjab Agricultural University, Ludhiana, India.
14 Kulkami, 1986, opcit.
7
Controversy Around Amniocentesis and other SD & SP Tests
Twenty years ago a controversy around SD and SP started as a result of several investigative
reports published in popular newspapers and magazines such as India Today, Eve’s Weekly,
Sunday and other national and regional English language journals. One estimate that shocked
many, from academicians to activists, was that between 1987 and 1983, about 78000 female
foetuses were aborted after SD tests as per Times of India editorial in June, 1982. The article
by Achin Vanayak15 in the same paper revealed that almost 100% of 15914 abortions during
1984-85 by a well-known abortion centre in Bombay were undertaken after SD tests.
All private practitioners in the SD tests who used to boast that they were ‘‘doing social work”
by helping miserable women, exposed their hypocrisy when they failed to provide facilities
of amniocentesis to pregnant women during the Bhopal gas tragedy, in spite of repeated
requests by women’s groups and in spite of many reported cases of the birth of the deformed
babies as a result of the gas carnage. Thus it is clear that this scientific technique is in fact not
used for humanitarian purposes, not because of “empathy towards poor Indian women ’ as
has been claimed. Forced sterilization of males during the emergency rule brought politically
disastrous consequences for the Congress Party. As a result in the post emergency period,
there has been a shift in the policy and women became the main target of population control.
SD and SP’s after effects, harmful effects of hormone based contraceptive pills and anti
pregnancy injections and camps for mass IUD insertion and mass sterilization of women with
their unhygienic provisions, are always overlooked by enthusiasts of the Family Planning
Policy. Most population control research is conducted on women without consideration for
the harm caused by such research to the women concerned.16
India has had a tradition of killing female babies (custom of DUDHAPITI) by putting opium
on the mother’s nipple and feeding the baby, by suffocating her in a rug, by placing the
afterbirth over the infant’s face, or simply by ill-treating daughters.17 A survey by India
Today, 15.6.1986, revealed that among the Kallar community in Tamilnadu, mother who
gave birth to baby girls may be forced to kill their infant by feeding them milk from
poisonous oleander berries. This author is convinced that researcher could also find
contemporary cases of female infanticide in parts of western Gujarat, Rajasthan. Uttar
Pradesh, Bihar, Punjab and Madhya Pradesh. In addition, female members of the family
usually receive inferior treatment regarding food, medication and education. When they
grow up, they are further harassed with respect to dowry. Earlier, only among the higher
castes, the bride’s parents had to give dowry to the groom’s family at the time of engagement
and marriage. As higher caste women were not allowed to work outside the family, their
work had no social recognition. The women of the higher castes were seen as a burden. To
compensate the husband for shouldering the burden of his wife, dowry was given by the girl’s
side to the boy’s side. Lower class women always worked in the fields, mines, plantations,
and factories and as artisans. Basic survival needs of the family such as collection of
firewood and water, horticulture and assistance in agricultural & associated activities; were
15 Vanaik, Achin (1986, June 20) “Female Foeticide in India”, Times of India.
16 Mies, Maria (1986 August) “Sexiest and Racist Implications of New Reproductive Technologies *. Paper
presented at XI World Congress of Sociology, 18-22, New Delhi.
17 Clark, Alice (1983) “Limitation of Female Life Chances in Rural Central Gujarat”, The Indian Economic
and Social History7 Review, Delhi 20 (1), 1-25.
18 Kynch, Jocelyn & Sen, Amartya (1983) “Indian Women: Well-being and Survival”, Cambridge Journal of
Economics, 7, 363-380.
8
provided by the women of lower castes and lower classes. Hence women were treated as
productive members among them and there was no custom of dowry among the toiling
masses.
Historically, practice of female infanticide in India was limited among the upper caste groups
due to system of hypergamy (marrige of woman with a man from a social group above hers)
because of the worry as to how to get a suitable match for the upper caste woman?19
Males in the upper class also thought that a daughter would take away the natal family’s
property to her in-laws after her marriage. In a patri-local society with patri-lineage, son
preference is highly pronounced. In the power relations between the brides and grooms
family, the brides side always has to give in and put up with all taunts, humiliations,
indignities, insults and injuries perpetrated by the grooms family. This factor also results into
further devaluation of daughters. The uncontrollable lust of consumerism and
commercialisation of human relations combined with patriarchal power over women have
reduced Indian women to easily dispensable commodities. Dowry is an easy money, ‘get rich
quick’ formula spreading in the society as fast as cancer. By the late eighties, dowry had not
been limited to certain upper castes only but had spread among all communities in India
irrespective of their class, caste and religious backgrounds. Its extreme manifestation was
seen in the increasing state of dowry related murders. The number of dowry deaths was 358
in 1979, 369 in 1980, 466 in 1981, 357 in 1982, 1319 in 1986 and 1418 in 1987 as per the
police records. These were only the registered cases; the unregistered cases were estimated to
be ten times more.
Academicians Plunged in the Debate:
In such circumstances, “Is it not desirable that a woman dies rather than be ill-treated?” asked
many social scientists. In Dharam Kumar’s20 words: “Is it really better to be bom and to be
left to die than be killed as a foetus? Does the birth of lakhs or even millions of unwanted
girls improve the status of women?”
Before answering this question let us first see the demographic profile of Indian women.
There was a continuous decline in the ratio of females to males between 1901 and 1971.
Between 1971 and 1981 there was a slight increase, but the ratio continued to be adverse for
women in 1991 and 2001 Census. The situation is even worse because SD is practiced by all
rich and poor, upper and the lower castes, the highly educated and illiterate - whereas female
infanticide was and is limited to certain warrior castes.21
Many economists and doctors have supported SD and SP by citing the law of supply and
demand. If the supply of women is reduced, it is argued, their demand as well as status will
be enhanced.22 Scarcity of women will increase their value.20 According to this logic, women
will cease to be an easily replaceable commodity. But here the economists forget the socio
cultural milieu in which women have to live. The society that treats women as mere sex and
19 Sudha, S. and S. Irudaya Raja (1998) “Intensifying Masculinity of Sex Ratios in India: New Evidence 19811991 ”, Centre for Development Studies, Thiruvananthpuram.
“° Kumar Dharma (1983, June 11) “Amniocentesis Again”, Economic and Political Weekly, (Bombay).
21 Jeffery Roger and Jeffery Patricia (1983, April) “Female Infanticide and Amniocentesis”, Economical and
Political Weekly, (Bombay).
Sheth, Shirish (1984, September) “Place of Prenatal Sex determination” , Larson and Turbo Seminar, Bombay
23 Bardhan Pranab (1982, Sept 5) “Little girls and Death in India”, Economic and Political Weekly (Bombay).
9
reproduction object will not treat women in more humane way if they are merely scarce in
supply. On the contrary, there will be increased incidences of rapes, abduction and forced
polyandry.
Agents Hired to buy the Brides and Forced Polyandry:
In Madya Pradesh, Haryana, Rajasthan and Punjab, among certain communities, the sex ratio
is extremely adverse for women. There, a wife is shared by a group of brothers or sometimes
even by patrilateral parallel cousins.24 Recently, in Gujarat, many disturbing reports of
reintroduction of polyandry (Panchali system- woman being married to five men) have come
to the light. In villages in Mehsana District, the problem of decling number of girls has
created major social crisis as almost all villages have hundreds of boys who are left with no
choice but to buy brides from outside.25
To believe that it is better to kill a female foetus than to give birth to an unwanted female
child is not only short- sighted but also fatalistic. By this logic it is better to kill poor people
or Third World masses rather than to let them suffer in poverty and deprivation. This logic
also presumes that social evils like dowry are God- given and we cannot do anything about it.
Hence, victimise the victims.
Another argument is that in cases where women have one or more daughters they should
be allowed to undergo amniocentesis so that they can plan a ‘balanced family’ by having
sons. Instead of continuing to produce female children in the hope of giving birth to.a male
child, it is better for the family’s and the country’s welfare that they abort the female foetus
and produce a small and balanced family with daughters and sons. This concept of the
‘balanced family’ however, also has a sexiest bias. Would the couples with one or more sons
request amniocentesis to get rid of male foetuses and have a daughter in order to balance their
family? Never! The author would like to clarify the position of feminist groups in India. They
are against SD and SP leading to male or female foeticide.
What price should women pay for a ‘balanced family?’ How many abortions can a woman
bear without jeopardising her health?
Do Women Have A Choice?
Repeatedly it has been stated that women themselves enthusiastically welcome the test of
their free will. “It is a question of women’s own choice.” But are these choices made in a
social vacuum? These women are socially conditioned to accept that unless they produce one
or more male children they have no social worth.26 They can be harassed, taunted, even
deserted by their husbands if they fail to do so. Thus, their ‘choices’ depend on fear of
society. It is true that feminists throughout the world have always demanded the right of
women to control their own fertility, to choose whether or not to have children and to enjoy
facilities for free, legal and safe abortions. But to understand this issue in the Third World
context, we must see it against the background of imperialism and racism, which aims at
control of the ‘coloured population.’ Thus/' It is all too easy for a population control
advocate to heartily endorse women’s rights, at the same time diverting the attention from the
24 Dubey, Leela (1983, Feburary)
(Bombay).
“Misadventure in Amniocentesis”, Economic and Political Weekly,
25 The Times of India, 8-7-2004.
26 Rapp, Rayna (1984 April) “The Ethics of Choice”, Ms. Magazine, USA.
10
real causes of the population problem. Lack of food, economic security, clean drinking water
and safe clinical facilities have led to a situation where a woman has to have 6.2 children to
have at least one surviving male child. These are the roots of the population problem, not
merely desire to have a male child”27.
Economics and Politics of Femicide
There are some who ask, “If family planning is desirable, why not sex-planning?”. The
issue is not so simple. We must situate this problem in the context of commercialism in
medicine and health care systems, racist bias of the population control policy and the
manifestation of patriarchal power.28 Sex choice can be another way of oppressing women.
Under the guise of choice we may indeed exacerbate women’s oppression. The feminists
assert; survival of women is at stake.
Outreach,and popularity of sex pre-selection tests may be even greater than those of sex
determination tests, since the former does not involve ethical issues related to abortion. Even
anti - abortionists would use this method. Dr. Ronald Ericsson, who has a chain of clinics
conducting sex preselection tests in 46 countries in Europe, America, Asia and Latin
America, announced in his hand out that out of 263 couples who approached him for
begetting off-springs, 248 selected boys and 15 selected girls.29 This shows that the
preference for males is not limited to the Third World Countries like India but is virtually
universal. In Erricsson’s method, no abortion or apparent violence is involved. Even so, it
could lead to violent social disaster over the long term. Although scientists and medical
professionals deny all responsibilities for the social consequences of sex selection as well as
the SD tests, the reality shatters the myth of the value neutrality of science and technology.
Hence we need to link science and technology with socio-economic and cultural reality.30
The class, racist and sexiest biases of the ruling elites have crossed all boundaries of human
dignity and decency by making savage use of science. Even in China, after 55 years of
“revolution”, “socialist reconstruction” and the latest, rapid capitalist development SD and SP
tests for femicide have gained ground after the Chinese government’s adoption of the “onechild family” policy.31 Many Chinese couples in rural areas do not agree to the one child
policy but due to state repression they, while sulking, accept it provided the child is male.
This shows how adaptive the system of patriarchy and male supremacy is. It can establish and
strengthen its roots in all kinds of social structures- pre-capitalist, capitalist and even post
capitalist - if not challenged consistently.32
27 Chhachhi & Sathyamla, 1983, opcit.
28 Wichterrich, Christa (1988) “From the Struggle Against ‘Overpopulation’ to the Industrialisation of Human
Production”, Reproductive and Genetic Engineering - journal of International Feminist Analysis, RAGE ,
Vol.l, No. l,pp. 21-30.
29 Patel, Vibhuti (2003) “ Locating the Context of Declining Sex Ratio and New Reproductive Technologies”,
VIKALP- Alternatives. Vikas Adhyayan Kendra, Mumbai.
30 Holmes, Helen Bequart & Hoskins, Betty B. (1984, April) “Pre natal and pre conception sex choice
technologies - a path to Femicide”, Paper presented at the International Interdisciplinary Congress on Women,
the Netherlands.
31 Junhong, Chu (2001) “Prenatal Sex Determination and Sex Selection Abortion in Rural Central China”,
Population and Development Review, Vol. XXVII, No. 2, PP. 259-281.
32 Patel, Vibhuti (1984, September). “Amniocentesis - Misuse of Modem Technology”, Socialist Health
Review, 1(2), 69-71.
11
Action against SD and SP
How can we stop deficit of Indian Women? This question was asked by feminists, sensitive
lawyers, scientists, researchers, doctors and women’s organisations such as Women’s Centre
(Bombay), Saheli (Delhi), Samata (Mysore), Sahiar (Baroda) and Forum Against SD and SP
(FASDSP) - an umbrella organisation of women’s groups, doctors, democratic rights groups,
and the People’s Science Movement. Protest actions by women’s groups in the late 70s got
converted into a consistent campaign at the initiative of FASDSP in the 1980s. Even research
organisations such as Research Centre on Women’s Studies (Mumbai)), Centre for Women’s
Development Studies (Delhi) and Voluntary Health Organisation, Foundation for Research in
Community Health also took a stand against the tests. They questioned the “highly educated”,
“enlightened” scientists, technocrats, doctors and of course, the state who help in propagating
the tests.33 Concerned group in Bangalore, Chandigarh, Delhi, Madras, Calcutta, Baroda and
Bombay have demanded that these tests should be used for limited purpose of identification
of serious genetic conditions in selected government hospitals under strict supervision. After
a lot of pressure, media coverage and negotiation, poster campaigns, exhibitions, picketing in
front of the Harkisandas Hospital in 1986, signature campaigns and public meetings and
panel discussions, television programmes and petitioning; at last the Government of
Maharashtra and the Central Government became activised. In March 1987, the government
of Maharashtra appointed an expert committee to propose comprehensive legal provisions to
restrict sex determination tests for identifying genetic conditions. The committee was
appointed in response to a private bill introduced in the Assembly by a - Member of
Legislative Assembly (MLA) who was persuaded by the Forum. In fact the Forum
approached several MLA’s and Members of the Parliament to put forward such a bill. In
April 1988, the government of Maharashtra introduced, a bill to provide for the regulation of
the use of Medical or Scientific techniques of pre natal diagnosis solely for the purpose of
detecting genetic or metabolic disorders or chromosomal abnormalities or certain congenital
anomalies or sex linked conditions and for the prevention of the misuse of prenatal sex
determination leading to female foeticide and for matters connected therewith or incidental
thereto (L. C. Bill No. VIII of 1988). In June 1988, the Bill was unanimously passed in the
Maharashtra Legislative Assembly and became an Act. The Acts preview was limited only to
SD tests, it did not say anything about the SP techniques. It admitted that medical technology
could be misused by doctors and banning of SD tests had taken away the respectability of the
Act of SD tests. Not only this, but now in the eyes of law both the clients and the
practitioners of the SD tests are culprits. Any advertisement regarding the facilities of the SD
tests is declared illegal by this Act. But the Act had many loopholes.
Two major demands of the Forum that no private practice in SD tests be allowed and in no
case, a woman undergoing the SD test be punished, were not included in the Act. On the
contrary the Act intended to regulate them with the help of an ‘Appropriate Authority’
constituted by two government bureaucrats, one bureaucrat from the medical education
department, one bureaucrat from the Indian Council of Medical Research, one Gynaecologist
and one geneticist and two representatives of Voluntary Organisations, which made a
mockery of ‘peoples participation’. Experiences of all such bodies set by the government
have shown that they merely remain paper bodies and even if they function they are highly
inefficient, corrupt and elitist.
The Medical mafia seemed to be the most favoured group in the act. It, “ has scored the
most in the chapter on Offences and Penalties...last clause of this chapter empowers the
33 Patel, Vibhuti (1987) “Sex Determination and Sex Pre-selection Tests in India- Recent Techniques in
Femicide”, Reproductive and Genetic Engineering RAGE, Vol. II, No. 2, 1989, pp. 111-119.
12
court, if it so desires and after giving reasons, to award less punishment than the minimum
stipulated under the Act. That is, a rich doctor who has misused the techniques for female
foeticide, can with the help of powerful lawyers, persuade the court to award minor
punishment,” said Dr. Amar Jesani in his article in Radical Journal of Health, 1988. The court
shall always assume, unless proved otherwise, that a woman who seeks such aid of prenatal
diagnosis procedures on herself has been compelled to do so by her husband or members of
her family.” 34 In our kind of social milieu, it is not at all difficult to prove that a woman who
has a SD test went for it of her “free will”. The Act made the victim a culprit who could be
imprisoned up to three years. For the woman, her husband and her in-laws, using SD tests
became a “cognisable, non-bailable and non-compoundable” offence! But the doctors, centres
and laboratories were excluded from the above provision. The Act also believed in
victimising the victim. With this act, the medical lobby’s fear that the law would drive SD
tests underground, vanished. They could continue their business above ground. A high
powered committee of experts had been appointed by the Central Government to introduce a
bill applicable through out India to ban SD tests leading to female foeticide.
The Forum accepted that with the help of the law alone, we can’t get rid of female foeticide.
Public education and the women’s right movement are playing a much more effective role in
this regard. Some of the most imaginative programs of the Forum and women’s groups have
been a rally led by daughters on 22.11.86, a children’s fair challenging a sex stereotyping and
degradation of daughters, picketing in front of the clinics conducting the SD tests, promoting
a positive image of daughters through stickers, posters and buttons, for example, ‘daughters
can also be a source of support to parents in their old age,’ ‘eliminate inequality, not women’,
‘Dimolish dowry, not daughters’, ‘make your daughter self sufficient, educate her, let her
take a job, she will no longer be a burden on her parents.’ The Forum also prepared
“Women’s struggle to survive,” a mobile fair that was organised in different suburbs of
Bombay, conveyed this message through its songs, skits, slideshows, video films, exhibitions,
booklets, debates and discussions.
Recent Studies on Socio-Cultural Background of Son Preference and Neglect of
Daughters:
Recent studies have revealed that, in South Asia, we have inherited the cultural legacy of
strong son-preference among all communities, religious groups and citizens of varied socio
economic backgrounds. Patri-locality, patri-lineage and patriarchal attitudes manifest in,
women and girls having subordinate position in the family, discrimination in property rights
and low-paid or unpaid jobs. Women’s work of cooking, cleaning and caring is treated as
non-work. Hence, women are perceived as burden.35 At the time of marriage, dowry is given
by the bride’s side to the groom’s side for shouldering ‘the burden of bride’. In many
commumties female babies are killed immediately after birth either by her mother or by
elderly women of the households to relieve themselves from the life of humiliation, rejection
and suffering. In the most prosperous state of Punjab, the conventional patriarchal preference
of male children leads to thousands of cases of sex selective abortions.36 Recently a man
drowned and killed his 8-year old daughter and also tried to kill his wife for having borne
him the girl child. According to the Chandigarh (Punjab) based Institute for Development and
Jesani, Amar (1988) “ Banning Pre-natal Sex Determination — Scope and Limits of Maharashtra Legislation ”,
Radical Journal of Health, Vol. II, No. 4, March.
35 Patel, Vibhuti (2003, July-August) “Declining Sex Ratio and New Reproductive Technologies”. Health
Action, Vol. 16, No. 7-8, pp.30-33
36 Patel, Vibhuti (2003, June) “So Much for Son”, One India, One People, Vol 6, No.l 1, pp.45-46.
13
Communication, during 2002-2003 every ninth household in the state acknowledged sex
selective abortion with the help of ante-natal sex determination tests.37
Recently, Voluntary Health Association of India has published its research report based on
fieldwork in Kurukshetra in Haryana, Fatehgarh Sahib in Punjab and Kangra in Himachal
Pradesh that have worst child sex ratio as per 2001 Census. The study surveyed 1401
households in villages, interviewed 999 married women, 72 doctors and 64 Panchayat
members. It revealed that “The immediate cause for the practice of female foeticide is that
daughters are perceived as economic and social burden to the family due to several factors
such as dowry, the danger to her chastity and worry about getting her married.” 38
In this context, commercial minded techno-docs and laboratory owners have been using new _ _
reproductive technologies for femicide for over two and half decades. Among the educated
families, adoption of small family norm means minimum one or two sons in the family. They
can do without daughter. The propertied class do not desire daughter/daughters because after
marriage of the daughter, the son-in-law may demand share in property. The property-less
classes dispose off daughters to avoid dowry harassment. But they don’t mind accepting
dowry for their sons. Birth of a son is perceived as an opportunity for upward mobility while
birth of a daughter is believed to result in downward economic mobility. Though stronghold
of this ideology was the North India, it is increasingly gaining ground all over India.
Table 4: Index of Son Preference for Major States in India^ 1990
States________
Index of Son Preference*
Rank
Andhra Pradesh
13.8__________________
11___
Bihar_________
24.5 __________________
4 ____
Gujarat_______
23___________________
6 ____
Haryana_______
14.3 __________________
10___
Karnataka_____
20___________________
8 ____
Kerela________
11.7__________________
12 ___
Madhya Pradesh
27.1__________________
2 ____
Maharashtra
18___________________
9 ____
Orissa________
23.4 _________________
5 ____
Punjab________
20.3 __________________
7 ____
Rajasthan_____
25___________________
3 ____
Tamilnadu_____
9.2__________________
13 ___
Uttar Pradesh
21.6 _________________
_1____
West Bengal
14.3 _________________
10
All India
20
Index of Son preference =100 (E/C)
Where, E =the excess number of sons over daughters considered ideal
C= the ideal family size.
Sources: Rajan S.I., U.S. Mishra and T.K. Vimla (1996) “Choosing a Permanent
Contraceptives: Does Son Preference Matter?” Economic and Political Weekly, July p.20,
p.l980.The Third All India Survey of Family Planning Practices in India, ORG,
Vadodara, 1990. Calculated by Eapen and Kodoth (2001).
37 The Asian Age, Mumbai, 25-4-2003.
38 Voluntary Health Association of India (2003) “ Darkness at Noon- Female Foeticide in India”, Delhi.
14
BIMARU states (Bihar, Madhya Pradesh, Rajastan, Uttar Pradesh) were at the top of the rank
for son preference in 1990. Orissa was 5th in the rank. Avers Prof. Ashish Bose (2001), “The
unholy alliance between tradition (son-complex) and technology (ultrasound) is playing
havoc with Indian Society.” 39 Kerala ranked 12th in the index of son-preference. However the
sharp decline in fertility and strong preference for small family norm does raise the
possibility of enhanced gender bias. In several states of India- Maharashtra, Gujarat, Bihar,
Uttar Pradesh, Rajasthan, Madhya Pradesh, Punjab, Haryana and Tamilnadu sex-selective
abortions of female foetuses have increased among those who want small families of 1 or 2 or
maximum 3 children. 40 Communities, which were practicing female infanticide, started
using sex-selective abortions. 41 Many doctors have justified female foeticide as a tool to
attain Net Reproduction Rate (NRR) of 1 i.e. to attain population stabilisation; mother should
be replaced by only one daughter. 42 But here also there is a gender bias. To attain population
stabilisation, a fertility rate of 2.1 is envisaged. There is an evidence to indicate a sex ratio in
favour of males and a prolonged duration of gender differentials in survivorship in the
younger ages, results in a tendency to masculining of the population sex ratio.
Even this does not worry the western scholars who have no inkling of the ground reality in
the subcontinent. For example. Prof. Dickens avers, “Son preference has produced, but might
also mitigate, the sex ratio imbalance...If sons wish, as adults, to have their own sons, they
need wives. The dearth of prospective wives will, in perhaps short time, enhance the social
value of daughters, reversing their vulnerability and the force of male dominance.”43
Table-5
Sex Ratio and Literacy Rate of different States & UTs of India
State
India________
Andaman & Nicobar Islands
Andhra Pradesh
Arunachal Pradesh
Assam__________
Bihar___________
Chandigarh______
Chhatisgarh_____
Dadra & Nagar Haveli
Daman & Diu
Delhi___________
Goa____________
Gujarat_________
Haryana________
Himachal Pradesh
Overall
Sex
Ratio
933
846
978
901
932
921
773
990
811
709
821
960
921
861
970
Child
Total
Sex Ratio Literacy
(0-6 yrs)
Rate
927
65_____
965
81 _____
964
61_____
961
55_____
964
64 _____
938
48_____
845
82 _____
975
65 _____
973
60_____
925
81 _____
865
82 _____
933
82_____
878
70_____
820
69_____
897
77
Male
Literacy
Rate
76_____
86____
71 ____
64____
72 ____
60____
86 ____
78 ____
73 ____
88 ____
87 ____
89 ____
81____
79 ____
86
Female
Literacy
Rate
54_____
75_____
51 ____
44____
56____
34____
77____
52 ____
43____
70____
75 ____
76 ____
59____
56____
68
39 Bose, Ashish (2001) “Without My Daughter- Killing Fields of the Mind”, The Times of India, 25th April.
40 Patel, Vibhuti (2002) “Adverse Juvenile Sex Ratio in Kerala”, Economic and Political Weekly,
VoLXXXVII, No. 22 June 1, pp.2124-5.
41 Jeffrey, Roger, Patricia Jeffrey and Andrew Lyon (1984) “Female Infanticide and Amniocentesis”, Social
Science and Medicine, Vol. 19, No. 11, pp.1207-12.
42 Patel, Vibhuti (2002) Women fs Challenges of the New Millennium, Cyan Publications, New Delhi.
43 Dickens, B .M (2002) “Can Sex Selection be Ethically Tolerated?” Journal of Medical Ethics, No. 28, pp.
335-336.
15
927
Jammu & Kashmir 900
966
Jharkhand_______ 941
949
Karnataka_______ 964
Kerala__________ 1058
963
974
Lakshadweep____ 947
920
929
Madya Pradesh
917
Maharashtra_____ 922
961
Manipur________ 978
975
Meghalaya______ 975
971
Mizoram________ 938
975
Nagaland________ 909
950
Orissa__________ 972
958
Pondicherry_____ 1001
793
Punjab__________ 857
909
Rajasthan_______ 922
986
Sikkim_________ 875
939
Tamil Nadu_____ 986
Tripura_________ 950
975
Uttarpradesh_____ 898
916
Uttaranchal______ 964
906
934
West Bengal
963
Source: Census of India, 2001.
54
54
67
91
88
64
77
69
63
89
67
64
81
70
61
70
73
74
57
72
69
66
68
76
94
93
76
86
78
66
91
72
76
89
76
76
77
82
81
70
84
78
42
39
57
88
82
51
68
60
60
86
62
51
74
64
44
61
65
65
43
60
60
Overall literacy rates in all states and Union territories have gone up as compared with the
1991 census. Even states and Union Territories with high female literacy-Goa, Delhi,
Mizoram, Pondicherry, Lakshadweep, Kerala, Andaman & Nicobar, Daman & Deo,
Chandigarh have experienced decline in Child Sex Ratio. In a micro-study of Kolkata, the
Census Report observes, “ Out of 141 municipal wards, the percentage of child population
has declined in 134 wards since 1991. More importantly, the child sex ratio has declined
sharply, from a high of 1011 females per 1000 male children in 1951 to abysmal 923 in 2001.
This is the lowest child sex ratio for Kolkata in the last 50 years. A major cause for the
decline is 4sex selective foeticide'”.44 Rates of female foeticide have increased along with the
increase in female literacy rates. 45
This neo-classical logic of Law of Demand and Supply does not apply to the complex social
forces where patriarchy controls sexuality, fertility and labour of women without any respect
to her bodily integrity. Hence, the real life experiences speak to the contrary. In fact, shortage
of women in Haryana, Punjab and the BIMARU states have escalated forced abduction and
kidnap of girls, forced polyandry, gang rape and child-prostitution.46
It has been noted that the fertility rates in Kerala have declined over the past few decades and
currently the Crude Birth Rates (CBR) for the State is as low as 17.9 per thousand population
in 1997 (RGI, 1998). The Infant Mortality Rates (IMR) is also one of the lowest experienced
44 Sen, Vikram (2002) “2001 Census of India- Report for Kolkata”, Director of Census Operations, West
Bengal.
45 Chattopadhyay, Dhinman (2003) “Child sex Ratio on the Decline in Rengal: Report”, The Times of India,
10* March.
46 Patel, Vibhuti (1992) “Girl Child- An Endangered Species” in Viney Kripal(ed) The Girl Child in the 20th
Century English Literature, Sterling Publishers Private Limited, New Delhi.
16
among Indian States, about 12 per thousand live births again in 1997 (RGI, 1998). The
indicators of human well being in Kerala are among the best in relation to the different states
of India. With modernisation and changing life styles wrought by both external migration
and incomes from remittances there has been a qualitative change in the lives of the people.
There has been a proliferation of private health care in the state and this in addition to the
demand driven factors has contributed to the better access to health care in the state. One of
the factors associated with the proliferation of health care facilities, especially in the private
sector, has been the improvement in the availability of medical diagnostics. Medical
personnel have also sought the use of such facilities not only to improve diagnostics, but also
to avoid the complications of expensive litigation in the light of the inclusion of private
medical practice within the preview of Consumer Protection Act, 1986. All this has resulted
in the increasing trend of use of medical diagnostic facilities and increasing the cost of health
care for the consumer. A micro study in Trivandrum city found that the known number of
ultra- sonographs in the city alone was about 37, of which only 6 were in the public sector.47
Attitude Towards Women’s Health
Social discrimination against women results into systematic neglect of women’s health, from
womb to tomb. Female infanticide and female foeticide are widely practiced in BIMARU
(Bihar, Madhya Pradesh, Rajasthan and Uttar Pradesh) and DEMARU (Punjab, Haryana,
Himachal Pradesh and Gujarat) states.48 The overall sex ratio is favourable to women is
Kerala. But, in Kerala also, in the 0-6 age group, the sex ratio was 963, as per 2001 census.
Total 0-6 age-group population of Kerala was 36.5 lakhs. Out of this 18.6 lakhs were male
babies and infants and 17.9 lakhs were female babies and infants. Thus, 79760 female babies
and infants were missing in 2001 in Kerala. This masculanisation of sex ratio is as a result of
selective
abortion
of female foetuses after the use of ultra-sound techniques to determine sex
r
~
, 40
of the foetus.
In Andhra Pradesh, Chattisgarh, Goa, Gujarat, Haryana, Himachal Pradesh, Karnataka,
Kerala, Maharshtra, Manipur, Orissa, Pondicherry, Punjab, Rajasthan, Tamilnadu,
Uttaranchal and West Bengal; the juvenile sex ratio is lower than the overall sex ratio of the
respective states. A community- based study conducted by a doctor couple revealed that 16.8
% of abortions were after detection that foetus female.50
As a result of sex-determination and sex-preselection tests leading to selective abortions of
female foetuses, sex ratio of the child population has declined to 927 girls for 1000 boys.
Sixty lakh female infants and girls are ‘‘missing” due to abuse of amniocentesis, chorion villi
Biopsy, sonography, ultrasound and imaging techniques. Sex pre-selection techniques
prevent arrival of female baby at a pre-conception state. Even anti- abortionists use this
method to get baby boys, as it does not involve “Blood-bath”.
CEHAT study5 Showed that 64% of providers of NRTs revealed that they were against sex
selective abortions, 10 % of them stated that they too were against it but they had to do it.
47 Sumta and Joy Elamon (2000) “Medical Technology: Its Uses and Abuses in Trivandrum City”, Achyutha
Menon Centre for Health Sciences Studies, Thiruvanantliapuram.
48 Bose, Ashish (2001) “Without My Daughter- Killing Fields of the Mind”, The Times of India, 25th April.
49 Eapen, Mridul and Praveena Kodoth (2001) Demystifying the “High Status” of Women in Kerala, An
Attempt to Understand the Contradictions in Social Development, Centre for Development Studies, Kerala.
Ganatra, B. R, S.S. Hirve, S.Walealkar et al (1997)‘Tnduced Abortion in a Rural Community in Western
Maharashtra”: Prevalence and Patterns”, Mimeograph, Pune.
51 Bandewar, Sunita (2003) “Abortion Services and Providers’ Perceptions: Gender Dimensions”, Economic
and Political Weekly, Vol. XXXVIII, No. 21, May 24, pp. 2075-2081.
17
while 24% of them approved of sex selective abortions of female foetuses. Among them,
gender -based responses were quite interesting. 28% of total male and 17% of total female
providers supported sex selective abortions, 68% of total female and 61 % of total male
providers were against it. Those who opposed it, also said that “It should be banned”, “It is
inhumane & Criminal”, “It is against medical ethics and human rights” and “It amounts to
discrimination against women”.
Table-6: Population in the age group 0 to 6 years in 2001, India
infants and children - all
15.8 crores
male infants and children
8.2 crores
female infants and children__________________
7.6 crores
deficit of female infants and girls
60 lakhs
sex ratio of child population______ _________________________ ~ 927
Source: Census of India, 2001.
Sex ratio (number of women per 1000 men) of Greater Bombay has reduced from 791 in
1991 to 774 in 2001 in spite of rise in its literacy rate. Doctors are using code language so
that they can not be booked by police. They don’t give anything in writing and nor do they
maintain any records to avid medico-legal complications later. Economic globalisation has
made import of portable ultrasound machines and sonographic machines very easy. Bombay
branch of Indian Medical Association has circulated posters for awareness generation to stop
sex selective abortions of female foetuses.
Table-7
POPULATION OF GREATER BOMBAY
year______
Population
sex - ratio
literacy rate
1991
99 lakhs
791
84
2001_________
1 crore 19 lakhs
774__________
87
d
Source: Census of India, 2001
To stop female infanticide, the Tamilnadu government introduced 'Cradle Baby Scheme’
urging parents to leave their unwanted baby girls at cradles provided in hospitals, primary
health centres and orphanages and encouraging them to take them back if they changed their
minds?2 The cradle baby scheme was introduced in Tamilnadu in 2000.53 Between July 2000
and March 2002, Eighty two (82) babies were dumped in the cradles. The number rose to 140
between 1992-1996. In addition to these babies received at Salem Reception Centre, 19
babies abandoned at railway stations and dustbins in other districts were rescued by the state.
The babies are raised by shelter homes and orphanages run by NGOs. The government has
also resolved to set up 188 extra reception cradles in 6 other districts.54 Negative attitude
towards women’s health is the major reason for high levels of perinatal mortality and
morbidity including low birth weight babies.55 Girl child is discriminated against, even when
it comes to breast feeding, supplementary nutrition and care giving.56
52 Sridhar, Lalitha ( Women’s Feature Service) (2001): India: Killing in Cradle, POPULI- The UNFPA
magazine, Vol.28, No.2, September, pp. 10-12.
53 Philipose, Pamela (2000) “A Peddy Grain in the Mouth of An Infant”, The Indian Express, October,4.
54 Kannan, Ramya (2002) “More Babies Being Abandoned Now”, The Hindu, 1st April.
Wai, S. and Ruchi Mishra (2000) Encyclopaedia ofHealth, Nutrition and Family Welfare, Volume 1, Health
and Family Welfare in Developing Countries, Sarup and Sons, New Delhi, 2000. Pp.254-255.
International Institute of Population Science (2002) National Family Health Survey, NFHS-2, 1998-99.
18
Violence and Health Issues of Women Over the Life Cycle
As unborn children, they face covert violence in terms of sex-selection and overt violence in
terms of female foeticide after the use of amniocentesis, chorion villai biopsy, sonography,
ultrasound and imaging techniques.57 IVF (In Vitro Fertilization) clinics for assisted
reproduction are approached by infertile couples to produce sons. Doctors are advertising
aggressively, “Invest Rs. 500 now, save Rs.50000 later” i.e. “If you get rid of your daughter
now, you will not have to spend money on dowry”.
As girls under 5 years of age, women in India face neglect in terms of medical care and
education, sexual abuse and physical violence. As adolescent and adult women in the
reproductive age group, they face early marriage, early pregnancy, sexual violence, domestic
violence, dowry harassment, torture in case of infertility; if they fail to produce son, then face
desertion/ witch hunt. The end result is a high maternal mortality. Causes of maternal deaths
in our country are haemorrhage, abortion, infection, obstructed labour, eclampsia (blood
pressure during pregnancy), sepsis, and anaemia. Proliferation of NRTs should be analysed in
this context.
Important Research Studies on Missing girls
Human Development Report in South Asia 2000: The Gender Question recorded 3178 cases
of female infanticide in six districts of Tamilnadu in 1995. In Mumbai only, in 1984, 84% of
gynaecologists admitted that they were performing amniocentesis and there were 40000
known cases of female foeticide. Supporters of sex-selection tests for selective elimination of
girls/female foetuses, apply law of demand i.e., “ reduction in the supply of girls will enhance
their status.” but historical evidences don't support this argument. There had been a
continuous decline in the sex ratio since 1901 to 1971, from 972 women per 1000 men to 930
women per 1000 men respectively. In 1981 the sex ratio was 933 women per 1000 men,
slight increase but in 1991 it became the lowest in the history of the Census, 929 women per
1000 men. In 2001, the sex ratio for the total population is again 933 women per 1000 men.
Haryana had the most depressive scenario as a result of misuse of these tests. The current sex
ratio in Haryana is 861 men for thousand women, the lowest among the major states in India.
The current slogan is “ Sons are rising and daughters are setting.” The techno-docs owning
cars pay home visit to pregnant women’s home for extraction of amniotic fluid and deliver
the results in the next visit. As per the UNFPA study female foeticide has been the main
cause of widening sex ratio in Haryana. According to The Hindu, 19-10-2001."In the last six
years, number of sex-selective abortions has increased from 62000 to 69000 in Haryana and
from 51000 to 57000 in Punjab. This reckless scale has pushed the fertility rate down from
3.2 to 2.9 in Haryana and from 2.9 to 2.2 in Punjab. "Reduction of birth rate, at what cost?
A study was conducted in 9 provinces viz. Andhra Pradesh, Bihar, Gujarat, Haryana, Madhya
Pradesh, Punjab, Rajasthan, Tamilnadu and Uttar Pradesh, which were known for high rates
of abortion. This study revealed that the impact of sex-selective abortion is seen in terms of
widening gender gap among (O-6) age group, in Punjab and Haryana, two of the most
economically prosperous states.
37 Patel, Vibhuti (1992) ’’Girl Child: An Endangered Species?” in Viney Kripal (ed^ The Girl Child in 2(fh
Century Indian Literature^ Sterling Publications Pvt. Ltd., New Delhi, P.9.
19
Table 8
States_____
Punjab____
Haryana
Gujarat
Maharashtra
Sex Ratio among the States with Widespread Use of Sex Determination
Tests (0-6 year age group)
1991
875
879
928
946
2001
793
820
878
917
Source: Census of India, 2001.
Another argument that prenatal diagnostic tests give women a choice to select a child of
desired sex is also unacceptable as women's "Choices" are made within the patriarchal
compulsions to produce sons. Women are not taking decision autonomously. Threat of
desertion, divorce and ill treatment force them to opt for sex-determination and sex
preselection tests.
Between 1975 and 2003, there has been gross violation of The Medical Termination of
Pregnancy Act (1972) and Prenatal Diagnostic Techniques Regulation and Prevention of
Misuse Act (1994). Amniocentesis, chorion villai biopsy and pre-conception sex-selection
tests were provided by the technodocs on the door-to-door service basis in some states.
Private nursing homes and laboratories in several towns and cities in Maharashtra, Punjab,
Gujarat, Uttar Pradesh, Tamilnadu have provided these tests by charging extremely high fees
and without maintaining records so that they can’t be caught. Those who perform the SD and
SP tests are different from those who perform abortion so that the link cannot be established.
New Reproductive Technologies (NRTs) and Women
NRTs perform 4 types of functions. In Vitro Fertilisation (IVF) and subsequent embryo
transfer, GIFT (Gamete Intra Fallopian Transfer), ZIFT and cloning assist reproduction.58 In
Mumbai girls are selling their eggs for Rs. 20000. Infertility climes in Mumbai receive 4-5
calls per day from young women who want to donate their eggs.59
Contraceptive Technologies prevent conception and birth. Amniocentesis, chorion villai
Biopsy, niddling, ultrasound and imaging are used for prenatal diagnosis.60Foetal cells are
collected by the technique of amniocentesis and CVB. Gene technologies play crucial role
through genetic manipulation of animal and plant kingdoms.61 Genomics is “ the science of
improving the human population through controlled breeding, encompasses the elimination
of disease, disorder, or undesirable traits, on the one hand, and genetic enhancement on the
other. It is pursued by nations through state policies and programmes”.62
It is important to examine scientific, social, juridical, ethical, economic and health
consequences of the NRTs. NRTs have made women’s bodies site for scientific
experimentations.
58 Nandedkar, Tarala D. and Medha S. Rajadhyaksha (1995): Brave New Generation, Vistas in Biotechnology,
CSIR, Department of Biotechnology, Government of India, Delhi.
59 The Asian Age, 11-6-2004.
60 Patel, Vibhuti (2000): Sex Selection, in Routledge International Encyclopedia of Women- Global Women's
Issues and Knowledge, Vol.4, pp. 1818-1819.
61 Agnihotri Gupta, Jyotsana (2000) New Reproductive Technologies- Women's Health and Autonomy,
Freedom or Dependency? Indo Dutch Studies in Development Altematives-25, Sage Publications, New Delhi..
62 Heng Leng, Chee (2002)“Genomics and Health: Ethical, Legal and Social Implications for Developing
Countries”, Issues in Medical Ethics, Bombay, Vol.X, No. 1, Jan.- March, pp. 146-149.
20
New Reproductive Technologies in the neo-colonial context of the third world economies and
the unequal division of labour between the first and the third world economies have created a
bizarre scenario and cut throat competition among body chasers, clone chasers, intellect
chasers and supporters of femicide. There are mainly three aspects to NRT -assisted
reproduction, genetic or pre-natal diagnosis and prevention of conception and birth. It is
important to understand the interaction among NRT developers, providers, users, non-users,
potential users, policy makers, and representatives of international organisations. 63
Assisted Reproduction
The focus of assisted reproduction experts is on the healthy women who are forced to
menstruate at any age backed by hazardous hormones and steroids. The processual
dimensions involve- Use of counsellors, technodocs and researchers to know the details of
personal life of women to delegitimise victim's experience. Utter disregard for woman's pain,
carcinogenic and mutogenic implications, vaginal warts, extreme back pain, arthritis,
sclerosis, heavy bleeding, growth of hair on face, nose, chin, cheeks, joint pain associated
with uterine contractions for production of egg-cells are dismissed as Mood-Swings. Network
between stake groups has only one goal- impregnating women for embryo production which
in the technodocs’ language is assisted reproduction. Embryos and foetuses are used for cure
of Parkinson’s disease among influential and wealthy aging patriarchs. Side- effects on
women's health are totally ignored. Growth of moustache, deformation of teeth and dietary
requirements are totally ignored.
Political Economy of Assisted Reproduction
r
By using phallocentric and misogynist psychologists, psychiatrists, state and the politicians
(ever ready for plastic smile and neat presentation) have found a ruthless weapon to cretinise,
dehumanise, degrade, humiliate, terrorise, intimidate, and cabbagify women. Through
advertisement in newspapers, poor/needy women are asked to lend their womb for IVF on
payment of money. Through websites rich clients are sought.
Selective Elimination of Female Foetuses and Selection of Male at a Preconception Stage
Rapid advances in the field of new reproductive technologies has “created a situation where
there has been a breakdown of the moral consensus”64 with respect to medical ethics and
gender justice. Techno-docs refuse the see larger contexts, future implications and gender
implications.
Sharp remark of the Member Secretary of Maharashtra State Commission for Women
represents the concerns of women’s rights organisations in these words, “The attempt at
legitimising the vetoing of female life even before it appears, is worse than the earlier
abortion related violence in the womb, precisely because it is so sanitised and relies on
seemingly sane arguments against the policing of ‘human rights’ in a democracy in the
intensely personal matter of procreation. This needs to be resisted at all cost.”65
Diametrically opposite views come from Dr. Anniruddha Malpani, the most articulate
proponent of sex-preselection tests. When asked, “ Is it ethical to selectively discard female
63 Finnarage-Feminist International Network of Resistance to Reproductive and Genetic Engineering, Germany,
2000 and UBINIG: Women’s Declarations on Reproductive Technologies and Genetic Engineering”, Dhaka,
2004.
64 Rupsa, Malik (2003) “ ‘Negative Choice’ Sex Determination and Sex Selective Abortion in India”, Urdhva
Mula, Sophia Centre for Women’s Studies Development, Mumbai, Vol 2, No. 1, May.
65 Thekkekara, T. F. ( 2001) “On the Road to Extinction”, The Indian Express, December 5.
21
embryos?” he said, “Where does the question of ethics come in here? Who are we hurting?
Unborn girls?”66
My questions are: Can we allow Indian women to become an endangered species? Shall we
be bothered only about endangered wild life- tigers, Lions, so on & so forth? Massive
resources are invested in OPERATION TIGER. When shall we start OPERATION GIRL
CHILD?
Population Control Policies
There is a serious need to examine Population policies and Global funding from the
perspective of statisation of Medical Market and marketisation of the nation states in the
context of newly emerging culture of daily changes of sponsors. Financial economists have
reigned supreme to generate moment-to-moment existence among population so that they can
get an unending supply of cannon fodder for the NRT experimentation. Budgetary provision
on health has a hidden agenda of NRT. The victims are not given scientific details and by
labelling them as parasites and beneficiaries, their consent is not sought. It has burdened
women with backbreaking miseries. The nation states have been coached to implement the
use of NRT in Secrecy -in line with the programmes executed by G8 in Thailand, Indonesia,
Philippines and Bangladesh. To achieve population stabilisation, 2.1% growth rate of
population and NRR -net reproduction rate of l(i.e. mother should be replaced by 1 daughter
only) are envisaged. These have inherent sexist bias because it desires birth of 1 daughter and
1.1 sons. Those who support sex-determination (SD) and sex-preselection (SP) view these
tests as helpful to achieve NRR1. Recent study of Haryana revealed that out of 160 mothers
and grand mothers interviewed by AIIMS study team, 40 % supported SD on the ground that
it contributed to population control and prevented families from having series of females in
an attempt that a male was bom.67
This will further widen the gap between number of girls and number of boys in the country
.As it is 100 million women have been missing due to femicide (female infanticide, ill
treatment and discrimination leading to higher mortality rate among women/girls in the first
three quarters of 19th century and in the last quarter of 19th century due to misuse of SD and
SP) over a period of 1901 to 2001.
Gendered Power-relations and NRT
Search for ’’perfect' baby through genetic screening, ante natal sex determination tests, pre
implantation diagnosis, commercialisation of sperm and /or egg donation, commercialisation
of motherhood and hormonal contraceptives raise many socio-legal and ethical questions.
Division of labour among women to control women's sexuality, fertility and labour by
utilising homophobia and pitting women of different race, religions, age and looks to suit the
interest of NRT will serve the interest of patriarchy, medical mafia, pharmaceutical
industries, scientists, technodocs at the cost of vulnerable human beings as raw material. If
the NGOs don't want to get criminalised, they must dissociate from NRTs and divert the
funding for public health, library, education, skill building, employment generation as a long
term investment and channelise their energies towards formation of self-help groups.
It is important to understand that reproduction has an individual and a social dimension.
While examining birth control practices, an individual is a unit of analysis. While examining
66 Banerjee, Piali (2001) “The Battle Against Chromosome X”, The Times of India, November.25.
67 Bardia, A., Paul. E, Kapoor S.K. and Anand K (2004) “Declining Sex Ratio: Role of Society, Technology
and Government Regulation in Haryana- A Cpmprehensive Study”, Comprehensive Rural Health Services
Project, All India institute of Medical Sciences, New Delhi.
22
3
the population control policies we have to analyse pros & cons of NRTs, national
governments, population control organisations, multinational pharmaceutical industries,
public and private funded bodies, medical researchers and health workers who shape
women’s ’’choices’’- women’s autonomy or control at micro and macro levels. Thus choices
are not made in vacuum. NRT as a choice for some women (educated career women) can
become coercion for others (powerless and less articulate women). Hence it is important to be
vigilant about power relations determined by race, age, class and gender while examining
implications of NRT on different stake groups.
Informed consent and medical malpractice- Power relations in the medical market favour
the technodocs and the clients are not given full details of the line of treatment and its
consequences. . Respect for diversity, adoption of child/children is a far simpler and more
humane solution than subjecting women to undergo infertility treatment. Obsession about
creation of designer baby boys has made development agenda subsidiary.
Initiatives by the State and NGOs:
Prenatal Diagnostic Techniques (Regulation and Prevention of Misuse) Act was enacted in
1994 by the Centre followed by similar Acts by several state governments and union
territories of India during 1988 (after Maharahstra legislation to regulate prenatal sex
determination tests), as a result of pressure created by Forum Against Sex-determination and
Sex —preselection. But there was a gross violation of this central legislation.
In response to the public interest petition filed by Dr. Sabu George, Centre for Inquiry into
Health and Allied Themes Mumbai) and MASUM fought on their behalf by the Lawyers
Collective (Delhi)68; the Supreme Court of India gave a directive on 4-5-2001 to all state
governments to make an effective and prompt implementation of the Pre-natal Diagnostics
Techniques (Regulation and Prevention of Misuse) Act (enacted in 1994 and brought into
operation from 1-1-1996). Now, it stands renamed as “ The Pre-conception and Pre-natal
Diagnostic Techniques (Prohibition of Sex Selection) Act”.
Recently enacted Prenatal Daignostic Techniques (Prohibition of Sex Selection) Act, 2003
tightens the screws on sex selection at pre-conception stage and puts in place a string of
checks and balance to ensure that the act is effective.69 The Pre-natal Diagnostics Techniques
(Regulation and Prevention of Misuse) Amendment Act, 2002 received the assent of the
President of India on 17-1-2003. The Act provides “for the prohibition of sex selection,
before or after conception, and for regulation of pre-natal diagnostic techniques for the
purposes of detecting genetic abnormalities or metabolic disorders or sex-linked disorders
and for the prevention of their misuse for sex determination leading to female foeticide and
for matters connected therewith or incidental thereto”.
Uner the Act, the person who seeks help for sex selection can face, at first conviction,
imprisonment for a 3-year period and be required to pay a fine of Rs. 50000. The state
Medical Council can suspend the registration of the doctor involved in such malpractice and,
at the stage of conviction, can remove his/her name from the register of the council.
The Pre-Natal Diagnostic Techniques (Regulation and Prevention of Misuse) Amendment
Rules, 2003 have activated the implementation machinery to curb nefarious practices
contributing for MISSING GIRLS. According to the rules this all bodies under PNDT Act
namely Genetic Counselling Centre, Genetic Laboratories or Genetic Clinic cannot function
Basu, Asmita: “Sex Selective Abortions”, Lawyers Collective, Vol. 18, No. 11, Nov. 2003, pp.20-23.
Kamdar, Seema “ Sex Selection Law Tightened”, Times of India, 6-6-2003.
23
unless registered.70 The Bombay Municipal Corporation has initiated a drive against the
unauthorised determination of gender of the foetus as per the directive of the Ministry of Law
and Justice. All sonography centres are required to register themselves with the appropriate
authority- the medical officer of the particular ward. The registration certificate and the
message that under no circumstances, sex of foetus will be disclosed, are mandatory to be
displayed.71
The shortcomings of the PNDT Act (2003) lie in criteria set for establishing a genetic
counselling centre, genetic laboratory and genetic clinic/ultrasound clinic/imaging centre and
person qualified to perform the tests.
• The terms genetic clinic/ultrasound clinic/imaging centre can’t be used
interchangeably. But the Act does.
• Moreover, The amended Act should have categorically defined persons, laboratories,
hospitals, institutions involved in pre-conception sex-selective techniques such as
artificial reproductive techniques and pre-implantation genetic diagnosis.
• Who is a qualified medical geneticist? As per the Act, “ a person who possesses a
degree or diploma or certificate in medical genetics in the field of PNDT or has
minimum 2 years experience after obtaining any medical qualification under the MCI
Act 1956 or a P.G. in biological sciences”. Many medical experts feel that a degree
or diploma or 2 years experience in medical genetics can’t be made synonymous. 2
• As per the Act, an ultrasound machine falls under the requirement of genetic clinic,
while it is widely used also by the hospitals and nursing homes not conducting Pre
implantation Genetic Diagnosis (PGD) and PNDT.
Ban on the Advertisements of SD & SP Techniques
Another important initiative that has been taken is against any institution or agency whose
advertisement or displayed promotional poster or television serial is suggestive of any
inviting gestures involving/supporting sex determination. MASUM, Pune made a complain to
the Maharashtra State Women’s Commission against Balaji Telefilms because its top rated
television serial's episode telecast during February 2002 showed a young couple checking the
sex of their unborn baby. The Commission approached Bombay Municipal Corporation
(BMC) and a First Investigation Report (FIR) was lodged at the police station. After an
uproar created by the Commission, the Balaji tele-film came forward to salvage the damage
by preparing an ad based on the Commission’s script that conveyed that sex determination
tests for selective abortion of female foetus is a criminal offence. Now there is another battle
brewing. The women’s groups insist that the ad should be telecast for 3 months before each
episode, while the Balaji Tele-films found it too much.73
Conclusion:
We need to counter those who believe that it is better to kill a female foetus than to give birth
to an unwanted female child. Their logic eliminates the victim of male chauvinism, does not
empower her. The techno-docs don’t challenge anti-women practices such as dowry, instead
70 Handbook on PNDT Act, 1994, Department of Family Welfare, Government of India, for use by Appropriate
Authorities in States/ Union Territories, New Delhi, 2002.
71 Patel, Vibhuti (2003) “Sons Are Rising- Daughters Are Setting”, Humanscape, September.
72 Pradhan, Mandakini, Renu Singh, Manisha, Sarita Agrawal (2004) “The Shortcoming of Prenatal Diagnostic
Techniques Act”, Department of Medical Genetics, Sanjay Gandhi Post Graduate Institute of Medical Science,
Lucknow, India.
73 The Indian Express, Mumbai, 19-5-2003.
24
display an advertisement, “Better Rs.5000 now than Rs.5 lakhs later” i.e. Better spend
Rs.5ooo for female foeticide than Rs. 5 lakhs as dowry for a grown up daughter. By this
logic, it is better to kill poor people or third world masses rather than let them suffer in
poverty and deprivation. This logic also presumes that social evils like dowry are God-given
and that we cannot do anything about them. Hence victimise the victim. Investing in
daughter’s education, health and dignified life to make her self dependent are far more
humane and realistic ways than brutalising pregnant mother and her would be daughter.
Recently series of incidents in which educated women have got their grooms arrested at the
time of wedding ceremony for demand and harassment for dowry, is a very encouraging step
in the direction of empowerment of girls. Massive and supportive media publicity has
empowered young women from different parts of the country to cancel marriages involving
dowry harassment. They have provided new role models.
Hence, our slogans are
“Eliminate Inequality, not Women”, “Destroy Dowry, not Daughters”,
Say “No” to Sex-determination, Say “Yes” to Empowerment of Women,
Say “No” to Sex Discrimination, Say “Yes” to Gender Justice.
Philosophical and medical details of NRT need public debate without iron wall of secrecy, in
all Indian languages as NRT is penetrating even in those areas where you don’t get even safe
drinking water or food. Technologies for population control are primarily concerned about
efficiency of techniques to avert births rather than safety of women. Women have to put up
with the side effects of NRTs. New reproductive technologies are provider/doctor controlled,
not women controlled. Hence the women’s groups repeatedly state that NRTs have inherently
anti women bias. In the petition filed by CEHAT-MASUM in the Supreme Court of India and
supported by the women’s rights groups, Dr. Sabu George, the petitioner’s demand of
expansion of the scope of the Pre Natal Diagnostic Techniques Act to include sex pre
selection techniques and effective implementation of the PNDT ACT74 has not only been
accepted but also rules have been formulated for its implementation. The state governments
are also organising state level seminars for doctors from the government and private sectors
to focus on raising awareness to the fact of sex selective foeticide as a discriminatory
practice. They are also trying to deal with the issue from the point of view of responsibility of
science towards gender justice, medical ethics and human rights. Recent publication of
CEHAT “Sex Selection- Issues and Concerns” selected important writings of spokespersons,
who have examined the problem of “missing girls” from these angles.
There is a need to clarify the gender-just position from the anti- abortionist position. “Women
should have a right to their bodies and unconditional access to abortion is not in conflict with
the claim that sex selection and sex selective abortions are unethical. It is not the abortion
which makes the act unethical, but the idea of sex selection.” 75
We have a great task in front of us i.e. to change the mindset of doctors and clients, to create
a socio-cultural milieu that is conducive for girl child’s survival and monitor the activities of
commercial minded techno-docs thriving on sexist prejudices. Then only we will be able to
halt the process of declining sex ratio resulting into the phenomenon of missing girls. To stop
a gender imbalanced society we will have to convince doctors and clients, state and civil
society that “Daughters are not for slaughter”.
” Contractor, Qudsiya (2002) “Sex Selection and the Law”, Combat Law, Vol.l, No. 1,, April-May.
Madhiwalla, Neha (2001) “Sex Selection: Ethics in the Context of Development”, Issues in Medical Ethics,
October- December.
25
The Social Context of Sex Selection and the Politics of Abortion in India
Page 1 of 15
The Social Context of Sex Selection and
the Politics of Abortion in India
Radhika Balakrishnan *
Reviewing third world development strategies with an eye to the status of women adds a new and
important perspective. Women's position, relative to men, can be viewed from many vantage points; in
this chapter ! look at gender relations through the examination of the ratio of women to men in the —
population. I will argue as others have before me, that the sex ratio is the manifestation of an interplay
between biological and social factors. Identification of some of the key social, particularly
socioeconomic, reasons that explain the circumstances of women's excess mortality is crucial to the
formulation of development policy. Such an approach can indicate how certain development policies
may not only enhance the lives of women but, more important, save their very lives.
In this paper I will focus on the practice of sex-selective abortion within the cultural and material
context of India. In India, this practice is only the latest manifestation of a long history of gender bias,
evident in the historically low, and declining population ratio of women to men. In order to combat the
practice of using technology to abort female fetuses, one needs to look at the wider social and historical
context of gender bias on the population. I examine legal activism against amniocentesis by placing the
issue of sex-selective abortion against the larger backdrop of socioeconomic, cultural and ideological
factors that contribute to the neglect and murder of females beyond the fetal stage. I call for a radical
rethinking of our focus on technology, and question the underlying concepts of 'normality' that lie
uninterrogated.
Comparative Data
The relationship between economic well-being and population size has long been examined, since the
early theoretical work by Thomas Malthus (An Essay on Population was published in 1798). Catherine
Gallagher's interpretive research (1986) establishes the longevity of Malthusian ideology, which exhibits
a "zest" for checks in the population (death by starvation, infanticide) within the context of an
inexorable competition between population growth and economic well-being. Building on this, I use the
connection between the ideology behind the analysis of population growth and gender as the basis for
exploring the question of sex differentials. This Malthusian ideology, in conjunction with an
examination of existing power hierarchies based on gender relations, may shed new light on the
discussion of sex differentials in the population.
Comparative data on sex ratios worldwide indicate many differences between countries, as well as
between regions within national borders. A cross-national and intra-regional examination of
demographic variations in India highlights the impact of economic and cultural differences on the
relative number of women in any population.
In 1901, the sex ratio for all of India (female/1000 males) was 972; in 1971 the ratio had declined to 930
and after a small climb in 1981 to 936 the ratio in 1991 was 929. Table 13-1 compares the female death
rates of 10 Third World countries, selected because they represent a broad cross-section of the Third
http://www.hsph.harvard.edu/rt21/medicalization/BALAKRISHNANSocial Context.html
1/13/2005
The Social Context of Sex Selection and the Politics of Abortion in India
Page 2 of 15
World. This data does not control for emigration or under-counting of females by the census While
there are various problems with using Indian census data, especially when studying questions regarding
women, I agree with Sen that the sharp decline in the population cannot be answered by the under
counting of females alone (Sen and Sengupta 1983). The percentage of females to males over the last
few decades has shown a marked decline, barring the very small increase in 1981.
The biological sex ratio (rather than a cultural one) is commonly accepted as 105 males per 100 females
at birth (Kelly 1975). For example, the sex ratio in the United States is 105.5 males to 100 females
(below the age of one) (Miller 1981) Following birth, male infants have a lower chance of survival than
females primarily due to respiratory distress syndrome among males. Using a teleological argument, it is
hypothesized that the biological sex ratio compensates for the greater vulnerability of male infants
allowing the sex ratio to even out as children grow older (Miller 1981). Therefore, in a perfect world
where both sexes are treated equally, and the only reason for differential survival is the sex-linked
biological ability to survive in the same environment, the sex ratio will approach unity with the
possibility of a slightly higher female survival rate.
Table 13-1 Number of girls who die for every 100 boys who die
(Most recent year since 1986)
Country
< I Yr Old
Bangladesh
Egypt
Ne pal
Peru
India
Pakistan
S. Korea
Ecuador
Malta
Source:
93
100
97
89
109
89
86
89
52
1-4 Yr Old
112
122
110
102
300
126
105
105
133
Seager and Olson 1986.
Intra regional variations
There have been many studies that have analyzed the connection between social variables and sex ratios.
While a thorough analysis of the socio-cultural and gender dynamics as they relate to sex ratios is
beyond the scope of this chapter, I will briefly summarize key arguments pertinent to South Asia in
order to illuminate the complex nature of the association (see Balakrishnan 1990).
Since India is a country made up of many different cultural groups, the study of sex ratios permits an
analysis of the impact of cultural differences and socioeconomic practices on sex differential in the
population. Variances among regions are evident in language, food habits, clothing, inheritance patterns,
purdah (female seclusion), and female work force participation. Isolating the co-variates of intraregional variations in the sex ratio may illuminate which cultural practices enhance the ability of women
to survive (see Table 13-2).
I will summarize several studies from South Asia, predominantly from different parts of India which.
http://www.hsph.harvard.edu/rt21/medicalization/BALAICRISHNANSocial Context.html
1/13/2005
The Social Context of Sex Selection and the Politics of Abortion in India
Page 3 of 15
taken together, illustrate the complicated linkage of cultural, economic and social conditions which
increase female mortality. This review attempts to tease out the factors that have led a society as
complex as India’s to practice male preference to such an extent that the relative population of females is
significantly decreasing, even today (see Table 13-3). Karkal (1987) emphasizes the need for examining
connections between social practices and demographic variables; Caldwell (1982) hypothesizes that
increased payment of dowry costs may lead to deterioration in the status of women; Das Gupta (1987)
reminds us of the importance of kinship patterns and the economics of the family, and Kumar (1989)
calls for more investigation into women’s political mobilization. In my own work I suggest the need to
explore the relationship between access to property and sex ratios (Balakrishnan 1990). Finally, I review
key papers which illustrate the mechanisms through which male and female children are provided
differential care.
Table 13-2: Sex ratio in Indian states that show the greatest variation in sex ratios. (Number of
females per 1000 males)
Census years
Source
1901
’ll
’21
’31
’41
’51
’61
’71
’81
INDIA
972
964
955
950
945
946
941
930
936
Bengal
945
925
905
890
852
865
878
891
911
Bihar
1054
1044
1016
994
996
990
994
954
947
Kerala
1004
1008
1011
1022
1027
1028
1022
1016
1034
Mysore
983
981
969
965
960
966
959
957
963
Punjab I 832
780
799
815
836
844
854
865
886
I
Source: Mitra 1979.
Karkal (1987) argues that differences in female mortality rates for South Asia, in general, and India in
particular, are related to the relative status of women. Karkal disagrees with the widely accepted
argument that high female mortality rates are symptomatic of the poor health conditions prevalent in
Third World countries, or merely signs of innate biological differences between the sexes. Instead, she
attributes these differentials to the subordinate status of women:
It has been suggested that differentials in mortality of the two sexes reflect the differences in
their biological makeup. In societies such as India, high mortality forfemales is a reflection
of the role and status offemales, both within the family and in society at large, as much as
they represent the health consequences ofsocial, economic and cultural discrimination
against them. (Karkal 1987)
Table 13-3: Age-wise grouping of the percentage of females to males for the census years 1951,
1961, and 1971
Age
1951
1961 1971
http://www.hsph.harvard.edU/rt21/medicalization/B ALAKRISHNANSocial_Context.html
1/13/2005
The Social Context of Sex Selection and the Politics of Abortion in India
0-1
97.4
99.5
92.5
1-4
99.8
97.1
94.3
5-9
96.7
96.6
95.1
10-14 93.8
94.8
90.6
15-19 94.6
94.2
94.4
20-24 97.1
94.8
97.6
25-29 96.0
94.9
97.4
30-34 92.9
92.8
95.0
35-39 89.9
89.0
90.6
40-44 88.4
87.2
87.1
45-49 88.6
86.7
85.2
50-54 90.4
87.0
85.7
55-59 93.8
89.0
88.3
60-64 98.1
93.4
90.2
65+
Page 4 of 15
101.8 106.1 93.5
Source: Mitra 1979.
Caldwell, Caldwell and Reddy (1982), charting demographic changes in Karnataka state, describe
changes in marriage customs that may indicate why sex ratios have been declining in Karnataka.
The major change was the coming ofdowry. In the early 1950s the first dowries in
Bangalore were paid by some Brahmin families. Not until the beginning of the 1960s did
the first Brahmin landlordfamily in the study area provide a dowry, and not until 1965 was
this done by the first Vokkaliga (the major peasant caste) family. It is still not paid by
Harijans, although in the largest village they ceased paying the Tera five years ago, and the
payment is still small among some of the backward castes. Ne\'ertheless, they all anticipate
its arrival. In all castes, the bride's family now bears the major portion of the wedding
costs, and it is they who seek loans and sell land. (Caldwell, Caldwell and Reddy 1982)
Looking at family life in Punjab, Das Gupta (1987) reports that discrimination against girls is not
general, but closely related to individual family building strategies. Using data from 11 villages in
Ludhiana district, Das Gupta points out that excess female mortality is seen in girls who are bom to a
woman who already has one or more surviving daughters. The educational attainment of mothers is an
important effect modifier, such that mortality of daughters is 50 percent higher if mothers have no
education (relative to mothers with some education). Among women who already have one or more
surviving daughters, land holding size makes no difference to female child mortality.
Das Gupta also reports a gender differential in the allocation of food, clothing and medical care to
children, especially during the first two years of life; I people who owned land seemed to discriminate
less in terms of food allocation and health care expenditure than the landless.
http.7Avww.hsph.harvard.edu/rt21/medicalization/BALAKRISHNANSocial_Context.html
1/13/2005
The Social Context of Sex Selection and the Politics of Abortion in India
Page 5 of 15
Offering an hypothesis of how cultural practices in Punjab contribute to Punjab having one of the lowest
sex ratios in the country,' Das Gupta emphasizes that patrilineal descent is a key organizing principle of
the Jat kinship system.1 "There is no question of women owning land. If she should insist on her right to
inherit land equally under the civil law, she would stand a good chance of being murdered" (Das Gupta
1987). The resource flow is always from the woman's father to the man's family. This occurs even after
the initial payment of dowry.
Son preference is the interest of the lineage, whose continuity depends on sons alone. It is
also in the interest of the household, for whom daughters are transitory members .... Indeed
a woman's position in her husband's home is not consolidated unless she produces at least
one son. [Das Gupta 1987:94]
Das Gupta suggests that state policies or propaganda campaigns providing women the right to hold
property may be a primary way to, redress the high female mortality. The flow of resources is
unidirectional from the woman’s father to the man; a man inherits property and the wealth acquired from
his wife’s parents. These practices strongly reinforce son preference.
Das Gupta's study is important because it draws connections between inheritance patterns and sex ratios.
Gopalakrislina Kumar (1989) also emphasizes the importance of exploring the influence of women's
political and economic power to regional variation in sex ratios. Reporting that excess female mortality
in Kerala does not decrease with increases in life expectancy, Kumar emphasizes that sex differentials
stem from factors other than overall level of well-being. In particular, Kumar argues that Kerala disturbs
some of the convenient North-South topology described by others; existing theories are not easily
applicable to the case of Kerala.
Kerala is the only state in India that has historically shown an absence of sex bias. Kumar dismisses
arguments that attribute this positive sex ratio to male emigration; Kerala has shown this positive sex
ratio consistently over the past century. Relative to other regions of India, Kerala also has other
characteristics that suggest better gender equity: it has generally had the lowest fertility rates, the highest
level of female literacy, a high age at marriage and fairly good receptivity to contraception. Kumar
points to the preponderance of matrilineal inheritance as a possible explanatory reason for both the
positive sex ratio and the greater gender equity that set Kerala apart.
Land reform measures in Kerala required the partitioning of large landholding into smaller cultivating
units. Kumar suggests that this agrarian transformation pushed women in increasing numbers into the
labor market. Because these new wage labor opportunities are increasingly outside the agricultural
sector (in rural household industry or urban trade services), over 78 percent of women in Kerala perform
non-agricultural work. Kumar argues that, at a general level, there exists a relationship between female
participation and reduced discrimination. He suggests that further work that links women's labor force
participation and the gender dynamics within the household is vital.
Kumar also points to the manner in which increased social status of women translates into political
action. He asserts that the increased level of literacy throughout Kerala has led to many protest
movements.
Protest movements focusing on the advancement of low caste women seem to have been
particularly successful and the results were manifest from the 1920s onwards, particularly
in the expanding wage-earning opportunities and occupational diversification of the
Ezhava caste. Indeed, the occupational diversification may reflect the influence of these
factors. Grassroots pressures resulted ultimately in demonstrations demanding equal pay
http://www.hsph.harvard.edu/rt21/medicalization/BALAKRISHNANSocial_Context.html
1/13/2005
The Social Context of Sex Selection and the Politics of Abortion in India
Page 6 of 15
for equal work, and educational facilities for girls from destitute families. The impact of the
incipient radicalization of this period is difficult to underestimate [sic], andforms an
important element in an explanation of the relatively less disadvantaged position ofwomen
in more recent times (Kumar 1989).
This approach to understanding women's relative position is indeed new and much needed. The creation
of a grass roots movement that empowers women to claim an equal position in society is recommended
by many authors as a policy prescription. Though it is difficult to point precisely to such mobilization as
the crucial remedy, a more in-depth study of political movements in Kerala that dealt with women's
issues is warranted.
A close examination of the history of matrilineal inheritance as affects women's relative position and
status is also important to understand the dialectic between cultural practice and material condition
(Balakrishnanl990). 1 have examined the history of matrilineal inheritance in Kerala to better
understand the cultural and material impact of inheritance on sex ratios in Kerala. In my work, by
closely examining the history of Kerala, I show that access to property as well as women's labor force
participation has a definite impact on the population ratio. Focusing in particular on inheritance, we see
that if women inherit property, the burden that parents have toward their daughter is minimized.
Daughters have access to whatever the parents can accumulate. The birth of a daughter among the
Nayars is awaited, since only through her can the property be passed down. Daughter preference as a
cultural phenomenon is guided by real economic factors. Gender relations, examined through
inheritance patterns within a community, are therefore a determining factor in sex composition of the
population.
Nutritional Allocation
A gender difference in food allocation has been cited by many scholars as a key contributing factor to
the higher mortality of girls in South Asia. Chen (1982), D'Souza and Chen (1980) and Chen, Huq and
D’Souza(1981) use data from rural Bangladesh to investigate whether a decline in the sex ratio is due to
differential mortality rates by sex, and they examine household dynamics for important insights about
the value of females and sex ratios.
Chen (1982) shows that the predominance of males over females in Matlab is attributable to both
differential migration and mortality between males and females. Migration has accounted for an
increased number of women in the rural areas of Matlab, for male out-migration has been much more
common than female migration. The mortality patterns indicate that differential survival occurs, and
predominantly during childhood.
D’Souza and Chen (1980) indicate that there are higher female mortality rates than males shortly after
birth and through childbearing ages. They Point out that son preference in parental care, feeding
patterns, intra-family food distribution, and treatment of illness favoring males, are possible causes of
the differences in child mortality rates.
Chen, Huq and D'Souza (1981) examine the validity of the assumption that sex differentials in mortality
are due to son preference in the are as mentioned above. Utilizing extensive field data on dietary patterns
demonstrate that some of the disparities in nutritional status between the sexes can be attributed to sex
discrimination against females in intra-family allocation of food. They also indicate that male children
are brought to the hospital much more frequently than female children. These data provide important
evidence of the social mechanisms by which sex preference is manifest in access to health and nutrition.
http://www.hsph.harvard.edu/rt21/medicalization/BALAKRISHNANSocial_Context.htinl
1/13/2005
The Social Context of Sex Selection and the Politics of Abortion in India
Page 7 of 15
Chen’s research is important in that it highlights several methodological problems with Bangladeshi (and
Indian) data. Contradicting the National Bangladesh Nutrition survey, his data indicate that caloric
intake for females is less than that of males; for the population cohort ages 0 to4 years, females received
14 percent fewer calories than males. Chen calls for in-depth regional studies as a basis for improving
data collection and quality, and for providing comparable data for India. Indeed, his research provides a
solid understanding of the Madlab District. Its micro-perspective strength, however, renders it less
useful in under-standing the overall dynamics of sex differentials in a country like India.
Overall, this body of research demonstrates quite conclusively that the low sex ratio can be attributed to
the son preferential behavior on the part of the parents. Chen, Huq, and D Souza can only speculate as to
the reasons why females are undervalued in this area. A reversal of this trend, they argue, would require
an overall structural change in the role, status and economic value of women. Chen (1982) recommends
a closer examination of Kerala to be able to find the specific nature of Kerala’s society that would
explain its consistently high sex ratio. Chen sees that this problem cannot be easily addressed by minor
policy revisions (i.e., increased education of females). Long-term solutions rest in fostering an overall
change in the position of women.
Rather, it seems likely thatfundamental structural changes in the role, status and economic
value ofwomen in society will be required, in addition to the alleviation ofeconomic
poverty. (Chen 1982)
The authors conclude with the suggestion that an important social indicator for evaluating the
performance of development programs should be the reduction in sex differentials.
The range of factors emphasized by these studies makes it clear that gender preference is articulated at
numerous stages in a female life, and that it does not start or stop before birth. The entrenchment of
gender preference in social custom, and the number of female deaths is an urgent reminder that, while
sex-selective abortion is an important mamfestation of son preference, the significant decrease in the
female population occurs after birth and before the age of four. From 1978 to 1983, 78,000female
fetuses were reported to have been aborted following using amniocentesis (Kelkar 1992). During the
same time period, of the twelve million girls bom each year, only 9 million will live to be fifteen
(Patel 1991).
Abortion
It is within the context described above that we need to analyze the issue of sex-selective abortion. India
has allowed abortion on broad medical and social grounds since the Medical Termination of Pregnancy
Act was passed in 1971. Abortion can only be performed in institutions that are government-approved,
and by authorized physicians. By themid-1980s, with over 106 million women of reproductive age, only
4,600medical facilities and fewer than 15,000 physicians had received official approval. It has been
estimated that four to six million illegal abortions are conducted in India every year (Dixon-Muller
1993).
Therefore, access to safe abortion, although legal, is still denied to a majority of women. Technology
that allows genetic selection has posed a very complicated challenge to feminists. Son preference, and
the introduction of technology that helps in determining the sex of a fetus, leads to a great number of
female fetuses being aborted.
The problem of the abortions of female fetuses is one that is being addressed by feminists throughout
http://www.hsph.harvard.edu/rt21/medicalization/BALAKRISHNANSocial_Context.html
1/13/2005
The Social Context of Sex Selection and the Politics of Abortion in India
Page 8 of 15
India. In the face of increasing abuse of amniocentesis, Maharashtra state decided to ban this medical
procedure in 1987.
In one hospital, from June 1976 to June 1977, 700 individuals sought prenatal sex determination. Of
these fetuses, 250 were determined to be male and 450 were female. While all of the male fetuses were
kept to term, 430 of the 450 female fetuses were aborted. (Miller 1985)
Until recently, the technology was prohibitively expensive. Presently, however, as a result of increased
demand, amniocentesis is available on the market for as little as Rs.500 (and some claim that it is as
little as Rs. 50). Regardless of the cost, there is still serious concern over the consequences of this
technology in a culture saturated with son preference.
The Changing Nature of Gender Relations
In order to convey- the complex nature of the crises of sex selection I will describe an incident from a
recent visit to India. While visiting a women’s reproductive health program m Gujarat, I was m a village
with an NGO (nongovernmental organization) representative, who had worked in the region for several
years. I asked my colleague the extent of abortions that occurred in this village, and whether, and how,
the NGO hospital handled abortions. She explained that the hospital had decided against providing
abortion services because of the increasing number of women who came for sex-selecnve abortions
(Though the hospital itself did not provide the technology for sex determination, there was a shop not
far away that claimed to provide the test.) Consequently, in the last few yearn there had been an mcrease
in the number of women and girls going to a traditional birth attendant for abortions. This factor
contributed to an increase in female mortality in the village.
Until recently, the community in this village had traditionally accepted sex outside of marriage and
premarital sex. Children bom to unmarried women were incorporated into the family. A recent censure
of unmarried pregnant women, my colleague suggested, had resulted from the introduction of television
and through its programs, a new perception that sex outside of marriage was immoral. Consequefrtly,
more unmarried women and girls were seeking abortions. Dowry and son preference were alsc> a
y
new phenomena; sex-selective abortion was only the most recent addition As we walked and talked to
people who were busy making clay pots I noticed a satellite dish in one of the mud huts, and many
villagers conversing while watching television.
This visit posed a very complicated set of issues for me, as I reconsidered jwlicy solutions to improve
reproductive health. There was an increase in the number of women dying from unsafe abortions
because the hospital would not provide abortions, but the hospital's policy was a response to the large
number of women requesting sex-selective abortions, based on information from an unauthonzed clinic.
This case illustrates the many technologies that are operative in changing the character of gender and
health relations. Technology was complicit here in enabling sex-selective abortion, and through
television having an impact on the sexual mores of the community to the extent that a premantai
pregnancy was ntw to be terminated. For feminists to be able to respond to the issue of sex-selective
abortion in a context where poor women do not have access to basic health care, we need to take accoun
of the multiple dimensions by which technology is affecting women's lives.
Legislative Strategy
http://www.hsph.harvard.edu/rt21/medicalization/BALAKRISHNANSocial_Context.html
1/13/2005
The Social Context of Sex Selection and the Politics of Abortion in India
Page 9 of 15
Amniocentesis was introduced to India by the All India Institute of Medical Sciences in 1975. It was
designed and promoted for detecting abnormalities in the fetus. Yet, couples who used this tec o ogy
increasingly aborted fetuses that were known to be female.
Subsequently, through an order of the Indian Council ofMedical Research theu^°f
amniocenteses was restricted to suspected cases ofgenetic diseases. Between 197
1985 three Circulars to government departments at the centre and in the states made use of
pre-natal sex determination for the purpose of abortion a penal offence (Menon 1993).
This ban on government institutions led to the commercialization of the technology;Jv'S® e teX were
providing sex determination tests through amniocentesis multiplied rapidly mid widely These tests w ere
made available in areas that did not even have potable water, with marginal farmers willingTo take loans
at 25 percent interest to have the test (Menonl993). Advertisements began appearing that blatandy
encouraged people to abort their female fetuses in order to save the future cost of dowry.
It was in this climate that feminists began to organize against this use -of amniocentesis^ In 1984 a
coalition was formed, the Forum Against Sex Determination and Sex Preselection. With the need to do
something fast and bring attention to this problem, one strategy they used was to campaign for
legislative action. They were successful in bringing about the Maharastra policy and have publicized the
incidence of sex-selective abortion (Menon 1993).
Drawbacks
focus on legal remedies, and the complexity of attempting to regulate technology.
The value of female "normality" is protected by the legislative restriction against using amniocentesis
for sex selection; but other social concepts of "normality" may be mdirectly endorsed by such a policy.
Amniocentesis is a technology providing genetic information. Societal norms establish which genetic
characteristics are abnormalities and which are normal. As feminists, we need to be very carefu
agreeing to the use of technology for one kind of genetic selection and not another After all, the
iiStifications used to abort female fetuses are often the same as those used by p^ple who want to abort
fetuses that have been diagnosed with "medical abnormalities." An "abnormal fetus and a female fems
are accorded similar drawbacks: expensive to maintain, less productive than normal (or mate) perso ,
detrimental to the parents' emotional and financial well-being, and is better off not being bom. Argu g
for restrictions against one specific application of genetic selection may suggest we are endorsing ofiier
applications of the technology, which themselves promote eugemcally-prescnbed notions of normality
and value.
How effective was the legal remedy that was sought? When there was pressure to restrict information
regarding the sex of the fems, the information did not disappear but went underground. The
consequences included reduced access to safe, legal and affordable abortion There is no guarantee tha
the clinics claiming to provide the illegal information are even conducting the test. Legalizing
criminalizing access to technology impacts primarily on government hospitals in the case of abortion,
although the procedure was legalized in 1971, access to safe abortion is limited to a few women because
of logistical constraints (see above). Criminalizing access to information on fetal sex has made the
information more expensive and abolished any possibilities for regulation or quality control.
http://www.hsph.harvard.edu/rt21/medicalization/BALAKRISHNANSocial_Context.html
1/13/2005
The Social Context of Sex Selection and the Politics of Abortion in India
Page 10 of 15
Rapid and frequent developments in medical technology further complicate our reliance on legislative
strategy to control the use of amniocentesis. Ultrasound is already used for sex determination; it is only
a matter of time before new blood testing techniques will make it possible to determine fetal sex from a
simple maternal blood test. These new kinds of information will be harder to police and regulate. The
expansion of medical technological in the service of sex selection threatens to concentrate our efforts in
the area of advocating for restrictions, diverting political capital from changing the existing social
structures and norms that encourage son preference and daughter neglect.
Possible Remedies
We need to approach this very difficult issue by going back to the broader question of the material and
ideological conditions that create a world in which women are dying. Bina Agarwal (1988) has
emphasized the connection between ideology and its material manifestations. In her critical evaluation
of India’s post-independence policies and their impact on women, she highlights the economic factors
which affect the relative valuation of males and females in the family. While stressing the importance of
cultural factors that lead to the high payment of dowry, thereby reinforcing daughter neglect, Agarwal
suggests wider interplay between economic position and cultural practice, thereby making the important
dialectical connection between ideology and material conditions.
A closer look at dowry and inheritance practices is wan-anted. just as position within a class system can
determine the number of children bom to different groups, so too the relative position within a gender
hierarchy can determine the sex of the children who survive. Further, within an economic system, sex
differences in the demand for labor and the reward for labor create incentives for the survival of one sex
over the other, thereby contributing to the sex ratio in the population. However, demands and rewards
for labor are not the only conditions that give incentives to sex-selective behavior. People who are not
dependent on the wage labor market may still exhibit sex-selective parenting if there is sufficient
economic reward guaranteed when one sex survives over another.
As Krishnaji (1987) points out, land-holding communities are less influenced by labor market
conditions. Nevertheless, inheritance pat-tems, including the connection to the payment of dowry,
provide incentives for sex selection.
In India, the character of wage and inheritance practices remains sex-specific. Wages that men and
women receive depend on a specific sexual division of labor, as well as the broader ideological
constructs that place women’s work in a lower position than men’s. The origins of particular systems of
sexual division of labor are beyond the scope of this study. But accepting the existing set of gender
relations that form, and are formed by, the dialectic between ideology and material conditions, I assume
that the patterns of inheritance as well are derived from existing sex-specified rules.
In most of India, both the sexual division of labor and the inheritance pattern that predominate establish
the male as more valuable, because he can earn higher wages and he inherits property. In general
practice, despite some carefully circumscribed legal rights, a woman has no right to her familial property
except for the right to be maintained until marriage. Most families that do not allow female inheritance
give property to a woman's husband and his family in the form of dowry (Liddle and Joshi 1986). The
amount given in dowry is determined by the groom's caste, his earning potential, and the specific
demands of his family. Wealth of the bride's family is not a significant determinant of dowry.
Payment of dowry is closely linked to the inheritance system. Das Gupta (1987) shows evidence of the
association between patrilineal inheritance patterns and payments of dowry’. When women do not inherit
http://www.hsph.harvard.edu/rt21/medicalization/BALAKRISHNANSocial_Context.html
1/13/2005
The Social Context of Sex Selection and the Politics of Abortion in India
Page 11 of 15
. property from their parents, a payment of dowry becomes a substitute.
The female child represents a heavy economic drain on her family. As a woman, she will either be
excluded entirely from the wage labor market or relegated to its least remunerative position. Her
exclusion from family property creates the impetus for large dowry payments at the time of mamage.
The male, on the other hand, receives better wages, inherits the wealth that is accumulated by his family,
and also gains a dowry.
Policy Implications
;
In India, dowry has been treated as a paramount social evil and many government programs have been
dedicated to education about the social evils of dowry. Women's organizations have actively
campaigned over the years to end that practice. Many stories of bride burnings and female infanticide
due to dowry have been publicized by the media. Brides have been murdered by their in-laws, so that the
groom can marry again and receive more dowry. These incidents cross class boundaries. The payment of
dowry is linked to, inheritance patterns. When women receive inheritance from their parents, dowry
payments are less frequently necessary.
However, while the elimination of dowry as a practice is most certainly an important goal, I feel that
looking at dowry alone without examining any other form of access to property is problematic. For
example, dowry is often viewed as a form of inheritance.
Most women see their dowry as the only share they will get of their parental property. In a
situation where women do not have effective inheritance rights, dowry is the only wealth to
which they can lay claim on. (Kishwar 1988)
If we view the decline in the female population as partially due to lack of access to property, several
policy options may be considered. Equal inheritance to family property can be campaigned for, while
continuing to work toward a corresponding decline in the practice of dowry. An increase in female work
participation and increasing wages for women will decrease the obvious material disadvantages that
females are seen to pose to the family.
A grass roots movement that works toward changing the ideology of sexism can be enhanced with
evidence that shows that access to property through inheritance and increased wages can impact on the
lives of women. Examples from regions in India where there have been, for example, matrilineal groups
can illustrate that the relationship between property and gender is not a concept imported from outside of
India.
I would argue that the strategy of seeking legislative restriction of sex-selective abortions has not been
effective in combating sex preference, and has decreased women's access to safe medical care. We need,
rather, to attempt more broad-reaching strategies that will address the economic and cultural roots of the
problem. One such strategy would be to advocate for female inheritance of parental property as an
alternative to dowry, as well as sustained efforts to reduce the level of dowry. Such reforms will require
more than legislative advocacy, but require changing cultural norms that effect women’s position in
society.
Although sex-selective abortion is appalling, we must not minimize the tragedy of the millions of girls
who are bom every day, but were never meant to survive.
http://www.hsph.harvard.edu/rt21/medicalization/BALAK.RJSIINANSocial_Contcxt.html
1/13/2005
The Social Context of Sex Selection and the Politics of Abortion in India
Page 12 of 15
A ckn o wledgements
Parts of this paper is taken from the research I conducted for my dissertation (Balakrishnan 1990), and
for this portion I would like to thank Temisan Agbeyegbe, Lourdes Beneria, William Milberg, Michele
Naples, Nina Shapiro and Robert Stuart. I would like to thank Arati Rao whose advice, editing and
support made finishing this paper possible. I would also like to thank Emanuela Toma and Pearl
Harrison for their technical and moral support. I would like to thank Gita Sen and Rachel Snow for
inviting me to be a part of this exciting collection, and for their and Jennifer Poulous' editing help.
Lastly, I would like to thank David Gillcrist for his support, in this paper and in all that I do.
Notes
1. Clothing expenditure is significantly bigger for boys than for girls, an important factor in a region
that can experience freezing temperatures.
2. Despite high rates of female literacy and a high age of marriage, the sex ratio in Punjab is one of
the lowest in the country.
3. The dominant group in this area are the Jats, a land owning caste.
References
Afshar, H. (ed.) 1985. Women, work and ideology in the Third World New York: Tavistock
Publications.
Agarwal, B. 1988. Who sows? Who reaps? women and land rights in India. Paper presented at the
Workshop on Women in Agriculture. Centre for Development Studies, in Trivandrum, India.
Balakrishnan, R. 1990. Access to property and its relationship to sex ratios in India. Ph.D. diss. Rutgers
University.
Bardhan, P. 1982. Little girls and death in India. Economic and Political Weekly, September 4.
. 1974. On life and death questions. Economic and Political Weekly (August): 1293-1304.
Caldwell, J., P. Caldwell, and P.H. Reddy. 1982. The causes of demographic change in rural South
India: A micro approach. Population and Development Review 8(4):689-728.
Chen, L. 1982. Where have the women gone? Insights from Bangladesh on the low sex ratio of India’s
population. Economic and Political Weekly, March 6:364-372.
Chen, L., E. Huq, and S. D'Souza. 1981. Sex bias in the family: Allocation of food and health care in
rural Bangladesh. Population and Development Review 7(l):54-70.
Clark, A. 1987. Social demography of excess female mortality in India: New directions. Economic and
Political Weekly, April 25:12-14.
Dandekar, K. 1975. Why has the proportion of women in India's population been declining? Economic
and Political Weekly, October 18:1663-1667.
http://www.hsph.harvard.edu/rt21/medicalization/BALAKRISHNANSociaI_Context.html
1/13/2005
The Social Context of Sex Selection and the Politics of Abortion in India
Page 13 of 15
Das Gupta, M. 1987. Selective discrimination against female children in rural Punjab, India. Population
and Development Review 13(l):90-95.
Dixon-Mueller, R. 1990. Abortion policy and women’s health in developing countries. International
Journal of Health Services 20(2):297-314.
D’Souza, S., and L. Chen. 1980. Sex differentials in mortality in rural Bangladesh. Population and
Development Review 6(2):257-270.
Forum Against Sex Determination and Sex Pre-Selection. 1983. Campaign against sex determination
and sex pre-selection in India: Our experience. Bombay.
Gallagher, C. 1986. The body versus the social body in the works of Thomas Malthus and Henry
Mayhew. Representations 14 (Spring).
Govind, K. 1993. Stopping the violence against women: Fifteen years of activism in India. In Freedom
from violence: Women’s strategies from around the world, ed. M. Schuler. New York: UIFEM;
WIDBOOKS.
Heyer, J. 1992. The role of dowries and daughters’ marriages in the accumulation and distribution of
capital in a South Indian community. Journal of International Development 4(4):419-436.
ICSSR. 1974. Toward equality. Government of India.
India. Office of the Registrar General. Census of India 1981. New Delhi.
Jain, D., and N. Banerjee, eds. 1985. Tyranny of the household: Investigative essays on women’s work.
New Delhi: Shakti Books.
Karkal, M. 1987. Differentials in mortality by sex. Economic and Political Weekly, August 8:13441443.
Kelkar, G. 1992. India stopping the violence against women: Fifteen years of activism. In Freedom from
violence- Women's strategies from around the world, ed. M. Schuler. New York. UIFEM; WIDBOOKS.
Kelly, N.U. 1975. Some socio-cultural correlates of Indian sex ratios: Case studies of Punjab and Kerala.
Ph.D. diss. University of Pennsylvania.
Kerala Bureau of Economics and Statistics (KBES). 1978. Women in Kerala. Trivandrum.
Kishwar, M. 1988. Rethinking dowry boycott. Manusbi: A Journal About Women in Society 48.
_. 1989. Toward more just norms for marriage. Manusbi: A journal About. Women in Society 53.
Koblinsky, M., J. Timyan, and J. Gay. 1993. The health of women: A global perspective. Boulder,
Colo.: Westview Press.
Krishnaji, N. 1987. Poverty and sex ratio: Some data and speculation. Economic and Political Weekly
22(23):892-895.
httn7/www hsnh.harvard.edu/rtZ I/medicaiization/tsALAKKlSHNANSociai ^oniexi.hiiiii
«
/1
1/
i^> r\ r\ r-
The Social Context of Sex Selection and the Politics of Abortion in India
Page 14 of 15
Kumar, G. 1989. Gender, differential mortality and development: The experience of Kerala. Cambridge
Journal of Economics 13(4):517-54.
Kynch, J., and A. Sen. 1983. Indian women: well-being and survival. Cambridge Journal of Economics
3/4(7):363-380.
Liddle, J., and R. Joshi. 1986. Daughters of Independence.. Gender, caste, and class in India. New
Brunswick, NJ.: Rutgers University Press.
Loudon, 1. 1986. Obstetric care, social class, and maternal mortality. British Medical Journal 239:606608.
Malthus, T. 1933. An essay on population, vol. 1. London: J.M. Dent.
Mamdani, M. 1972. The myth of population control: Family caste and class in an Indian village. New
York: Monthly Review Press.
Menon, N. 1993. Abortion and the law: Questions for feminism. Canadian Journal Of Women and Law
6:103-118.
Miara, M. 1991. The dilemma of sex selection ... the issue in India. Perspectives in Genetic Counseling
13(2): 1-2.
Miller, B. 198 1. The Endangered Sex.. The neglect of female children in rural India. Ithaca, N.Y.:
Cornell University Press.
. 1983. Son preference, daughter neglect, and juvenile sex ratios: Pakistan and Bangladesh compared.
Working paper no. 30, Michigan State University, Lansing, Mich.
_. 1985. Prenatal and postnatal sex-selection in India: The patriarchal context, ethical questions and
public policy. Working Paper no. 107, Michigan State University, Lansing, Mich.
Mitra, A. 1979. Implications of declining sex ratio in India’s population. Indian Council for Social
Science Research, Programme of Women's Studies I. Bombay: Allied.
Overall, C. 1987. Ethics and human reproduction: A feminist analysis. New York: Allen & Unwin.
Patel, S. 1991. The dilemma of sex selection-the issue in the U,S. Perspectives in Genetic Counseling 13
(2): 1-2.
Seager, J., and A. Olson, 1986. Women in the world: An international atlas. New York: Simon and
Schuster.
Sen, A. 1993. The economics of life and death. Scientific American (May):40-47._. 1984. Resources,
values and development. Cambridge: Harvard University Press.
Sen, A.K., and S. Sengupta. 1983. Malnutrition of rural children and the sex bias. Economic and
Political Weekly 13 (Annual Number).
Sen, 1. 1986. Geography of secular change in sex ratio in 1981: How much room for optimism.
Page 15 of 15
The Social Context of Sex Selection and the Politics of Abortion in India
Economic and Political Weekly, March 22.
Smyke, P. 1991. Women and health. London: Zed Books.
Radhika Balakrishnan, "The Social Context of Sex Selection and the Politics of Abortion in India" in
Power and Decision: the Social Control of Reproduction (Cambridge: Harvard School of Public Health,
1994), pp. 267-286.
Copyright © 1994 by Harvard School of Public Health, all rights reserved. Reprinted with kind
permission from the copyright holder. No part of this text may be reprinted or disseminated beyond
personal use without permission from the copyright holder.
[
/DAI A 1ZD TQUM AMQnnial
to the previous page
C’rtnfAYt htmi
]
Article
1 agt- i vi o
May 29, 2004
EPW Special Articles
Female Infanticide
The Colonial Experience
Archival records on female infanticide show the different perceptions, colonisers and their 'subjects' had on the issue. Colonial
officials characterised it as 'inhumane' and a 'crime'; on the other hand, castes which practised it, usually those higher in the
hierarchy, justified it on the grounds that they could not afford the huge dowries or the incalculable marriage expenses having a
daughter entailed. British efforts to stop female infanticide or change the social norms that contributed to the practice proved a
failure. The failure of the colonial state shows the resilience of institutionalised norms to which female infanticide was related
and about which little still remains known.
L S Vishwanath
Archival records on female infanticide during colonial rule tell us about castes which practised female
infanticide, societal and more specifically the institutional ramifications of the practice, how female
infanticide was related to caste dominance, status maintenance and dowry avoidance, the complications of
British revenue policies for the castes which practised female infanticide and finally, the strategies adopted
by the colonial rulers to get rid of the practice.
In December 1789, Jonathan Duncan, the British resident at Benares first found female infanticide among
rajkumar rajputs in Jaunpur district of Benaras division. The discovery was made when he was touring the
district to settle its revenues. Right from the time of Duncan’s discovery, the rajputs in north, west and
central India which means undivided Punjab, Rajasthan, UP Malwa and Saurashtra figure very prominently
in the records as a caste which resorted to extensive female infanticide. British officials reported in the 1817
that female infanticide was so extensive among the jadejas, a rajput clan in peninsular Gujarat, that whole
taluks inhabited by the clan were without any jadeja female children. In 1856, an official appointed to
investigate female infanticide in Benares division found after taking a census in 418 villages that rajput
female children were deficient in 308 villages; of these, 62 villages, nearly one-fifth had no rajput female
children below six years. The other castes, which the records say killed their female children, were: the lewa
kanbis and patidars of central Gujarat and jats, ahirs, gujars, khutris and moyal brahmins in north India
When the census enumerations were launched in the last quarter of the 19th century, we find that the same
castes, which the archival records say practised female infanticide also, figure in the census reports as
having low female sex ratios. Perhaps taking the cue from the records, the author of more than one census
report refer to the rajputs and lewa patidars as having a ‘stigma’ or ‘a tradition’ of female infanticide since
‘olden times’. The 1921 census reports classifies castes into two categories, namely, castes having 'a
tradition’ of female infanticide and castes without such a tradition (see table). This census provides figures
from 1901 to 1921 to show that in Punjab, United Provinces and Rajputana castes such as Hindu rajputs,
Hindu jats and gujars with ‘a tradition’ of female infanticide had a much lower number of females per
thousand males compared to castes without such a tradition which included: Muslim rajputs, Muslim jats,
chamar, kanet, arain, kumhar, kurmi, brahmin, dhobi, teli and lodha. What is interesting about this census
classification is that in Punjab, the Hindu rajputs are shown as having 822 (1901), 756 (1911) and 796
(1921) females per thousand males, while Muslim rajputs had 883 (1901), 841(1911) and 864 (1921)
females per thousand males. The Hindu jats had fewer females: 795 (1901), 774(1911), and 789(1921)
compared to 859(1901), 807(1911) and 820(1921) females per thousand males among the Muslim jats.1
Table: Sex Ratios of Castes in North India
Number of Females per 1,000 Males
Caste
Category
1901
1911
1921
A
A
A
A
B
B
B
B
795
808
822
799
859
883
871
924
774
802
756
763
807
841
836
947
789
811
796
778
820
864
845
936
Punjab
Jat (Hindu)
Khutri
Rajput (Hindu)
Gujar
Jat (Muslim)
Rajput (Muslim)
Chamar
Kanet
httn://www.enw.org.in/show Articles. php?root=2004&leaf=05&filename=7255&filety... 14/02/2005
Article
Ara in
Page 2 of 8
B
877
807
830
Jat (Hindu)
A
Rajput (Hindu)
A
Gujar
A
Brahmin
B
852
887
802
923
986
769
873
755
899
958
941
929
763
877
785
895
960
931
909
778
851
846
722
840
837
920
922
941
895
United Provinces
Chamar
B
Kumhar
B
931
Kurmi
B
970
794
830
834
925
916
908
911
Rajputana
Rajput (Hindu)
A
Jat (Hindu)
A
Gujar
A
Brahmin
B
Dhobi
B
Teli
B
Lodha
B
937
962
930
916
A= Castes with ‘a tradition’ of female infanticide.
B= Castes without a tradition of female infanticide.
Source: Census of India (Report), 1921, Vol 1, Appendix VI.
i?ndedaoron?r^,lZ1'1rhhe
Xta
SeemS t0 SU"eSt that the lower castes which did not
“s,r
much
taTZS'S
sansKritisation, acquisition of assets, modern education and dowry adoption can push the lower caster
uoS hat3 he^^T infantiCide'- 'ndeed reCSnt data for
chamars anTscSufed Stes in UP
Hfantlr H h * Jh rda *
65 are m0Vln9 ,n the direction of deficiency of females and possibly female
female tn mile etFlde’ ThUS '2 19°1’the chamars in UP had a female to male ratio of 986; but by 1981 the
tn ml? °
atl° cT-009 chamars ln the same state had dropped to only 880. Again in 1901 the female
Dreze and
nofe^
V 1981’
d°Wn t0 892' D'awin9 Motion to these Sgure!
Uttar Pradesh 2rnnnu'
‘ h? J u° far aS 9ender relations are concerned, the scheduled castes in
unar Pradesh are now more like the higher castes than they used to be”.
^f=ntreCa°rdS provide information on the lower castes being influenced by the higher so far as female
on inveX'a^^Tmid iSos6^^' E G Jenk|inson; the officiating magistrate of Saharanpur district found
ateo foun Sa C o tSkl th r PUre6r aT
rajpUtS in the district practised female infanticide. He
r'ro
.-J* *hat
Ot^er castes, the tuggas and kolis who had a ‘fair proportion’ of qirls all over the district
pactised female infanticide only in one tehsil. “They have probably” says Jenkinson "adopted the practice of
emale infanticide from the rajputs in the midst of whom they have been living for so many years"
Sex Ratios and Institutional Ramifications
When one examines the female infanticide records, what strikes one is the overwhelming evidence of the
038 68 lke h.e patldars’ rajPuts’ J'ats and ahirs - all of them were hypergamous-frying to maintain
their socio-economic status through dowry avoidance and female infanticide. British officials often speak in
female^5tOfdaJPtlJt8 °f hi9h StatuS seekin9 W marria9a a"iances' for their daughters ancI resortng to
aqhcu1tu?aan|Tnds Thomason0^'11'31 dov*ry pay.ment' which
lead
alienation of their hereditary
P?ovinS found in iX
mas'Slra‘e ° Azamgarh district (then part of the North-Western
fnrthrnmrnJ Thd
1836 th
'T0'19 a body of rajputs numbering 10,000 not a single daughter was
obtained an'JaXTri 9°rhS On ?
that the ba'S rajpUtS prefer 'h'9h alliances' which are “difficult to be
ahenation of L whnta
uhiCh they Can
bear and are almost certai" to cause ‘he
^nation of the whole or a great part of their hereditary lands. Hence the birth of a daughter is considered a
most serious calamity, and the unfortunate infant is very seldom spared.”
consioereo a
Steed lh95S9Lvan'ln^i[’UtdS?ad(at ?art a' eth°S 38 nOted by anthroPological studies [Hitchcock 1959,
Steed 1955] they generally did not take advantage of the avenues for social mobility, which opened up
httn://wvAv.epw.org.in/showArtieles.php?root=2004&leaf=05&filcname=7255&filety... 14/02/2005
*
Article
Page 3 of 8
is:
BEBS— “a
ble to pay revenue and doing away with the lucrative revenue contract system of precolonial times.
fter
8l“d>'of “» arcl'"al
«»
W>". found that In the 19th
«.X"±ZSI,dK in a running twte with the auction p^h.ser to aenrehow
horoH;/
I ?
hered,tary lands. Cohn further notes that faced with the orosoect of sale of thPir
raim itQi?e reY®9ue demands of the British and heavy dowry demands from the grooms’ side the
economy statu^TheVchos?
exPe"s7 ™arriages(s) of daughters and maintenance of their sociostatus. They chose the latter, avoided heavy dowries and practised female infanticide.
region^rsUhhe2Xfandnth/Way ^t\the
pafidars of Nadiad^Rn^JF n
h
1849 that
’
’
P
reVenUe COntract system of Pracolonial times in certain
P°llcy for the rnarria9e of daughters, we find the lewa
da Par9anas ‘oiling the collector of Kaira district, J Webb in
daughters in marriage incurring the expenses according to
former Jdm.w bu arn°n9st our people the expenses are daily increasing; whilst during the
the ® administratl0n (maratha rule), we used to obtain the management of the villages9from
lonsea tnfi
°Wn respons'blllty and therefore made the collections on our own authority
consequently our means were kept up; at present we have no such means.
Th® interviews of patidars and rajputs with British officials point to the new difficulties thev faced The
1847?
SinabiEto'nav ® mriemberS of thi® “ste told the same thing to the Ahmedabad collector te
ravoniio J ♦ nab,l,ty
pay ,and revenuP and large dowries demanded by the groom’s side since the
this problem had5^3female
do.es Provide a clue- However, it is not possible to say what impact
'
P °b'em had 0" female sex ratios and if female infanticide was accentuated due to British revenue
sexSfS;
aTno'Sfefe P,TO>l0n"“ Pert“’'
”ul<1 “ab">a
rflnndcqual?l‘ive and quantitative data in the historical records, which relate sex ratio to the social status
rajputs ’theHclan^h
dUrin9 the 19th Century' The
h ’ hL h controlled ‘he lar9est territory and occupied the topmost position in the raiout
ra^o!ts o?Renahrp radChy’ re®°rt?d to very extensive female infanticide. Thus in mid-19th century among
f B®nar®s dlvis'°n, the top position in the rajput hierarchy was held by the suryavamshis of Amroha
therajputs intee^eoten'A™1 Tt?ey ^RRRlled ?8 v'llages and were acknowledged to be the highest by all
to o^ 12Q nirk
? °f
that the su|7ava™shis had in the 78 villages 721 boys
that 10 of the survavam^hi^/u^ °f h9a' Tbat.is’ only 15 per cent were girls. The same census also revealed
mat 10 of the suryavamshi villages had no rajput girls and marriage of rajput girls was a “rare occurrence” in
position below he
reported to SncSn in lfimthJh c
less textens'vtamon9 the jethwa rajputs who held the number two
J
rTUt hJerarchy' Alexander Walker, the resident at Baroda
«4.a.Dzn™s
,h’tead
melpTfnr
enLalef sex rati0S than ofher lewa kanbis- The kanbis had 73 to 75 femates per hundred
Inuz
f L mal°/ part of .the 19th century lclark 1963]; from 1847 onwards, British local officiate talk of vprv
showpd'th6?^ fema'es ln what they called the 'aristocratic' patidar villages in Charotar A census of 1872
showed that the number of females in the 12 top ranking patidar villages^ ChaX ranged frem 39 to b!
http://www.epw.org.in/showArticles.php?root=2004&leaf=05&filename
7255&filety... 14/02/2005
Article
Page 4 of 8
girls to 100 boys below 12 years of age. The census of 1891, 1901 and 1911 also showed that the patidar
villages in Charotar had very low proportion of females. For example, the census of 1911 showed that five
of the 12 patidar villages under Baroda had less than 700 females per 1,000 males.
For Sikh khutris of Punjab, the records again suggest that the top rung in the hypergamous ladder
consisting of bedi khutris who claimed descent from Guru Nanak, the founder of the Sikh faith practiced
female infanticide more extensively than other khutris. The information on female infanticide for bedi khutris
range from Lake’s report of 1851 to the Punjab Board of Administration that “the bedees are an influential
caste of Sikh khutris ... who have destroyed all their female offspring for the last four hundred years" to
figures from the Punjab correspondence for the years 1848-49 to 1850-51 showing that the bedi khutris had
28 boys to only 10 girls in 1848-49, 24 boys to only 6 girls in 1849-50 and 20 boys to 12 girls in 1850-51.
Though the female infanticide records and later the census refer to low female sex ratios among jats, ahirs
and gujars in north India, detailed information on whether the top rung in these castes resorted to more
extensive female infanticide than those of lower status is not available. There is information that the princely
jat houses of Bharatpur, Nabha, Jind, Kythal, Patiala and Faridkot practised female infanticide ‘extensively’.
Since the lewa patidars, the jadejas and suryavamshi rajputs were acknowledged to be highest in the
hypergamous hierarchy in the respective region, they wished to maintain that position. Moreover, the top
stratum had restricted options in selecting eligible grooms. Consequently, they practised more extensive
female infanticide than others in their caste. The point is that for those at the top of the hypergamous
hierarchy, the complications of bringing up girls went beyond dowry avoidance. Going by the reports of
British officials in the records, this is how the establishment perceived the extensive female infanticide
among the high status patidars and rajputs. It seems to me to have substance and it may be erroneous to
regard it as the colonisers perception. As noted before, the British certainly complicated matters for the
castes, which resorted to female infanticide; however, it would be simplistic to suggest as some scholars
have done that the complications contributing to female infanticide were mainly due.to British revenue
policies or the support to the dominant castes by the political rulers.2 A close reading of the socio-political
history of Gujarat region shows that even during precolonial maratha rule and Muslim rule, there were
influential patidars in the Charotar villages who were tax collectors and rulers of villages. The maratha and
Muslim rulers tried to be friendly to the charotar patidars. Even during pre-colonial rule, the patidari or
narwadari villages which paid fixed revenues enjoyed a higher status than senja villages inhabited mostly by
kanbis who paid variable revenue [Shah: 2002]. Hence the complications of status hierarchy, hypergamy
and the friendship between the political authority and the local dominant caste existed before colonial rule.
Among Gujarati rajputs, the freezing of the political boundaries giving clans like the jadejas the highest
position among Gujarati rajputs happened before colonial rule. It is not possible to date it precisely but it is
safe to assume that the rajput territorial boundaries got frozen after the conquest of Gujarat by the Mughal
emperor, Akbar which gave the rajputs of peninsular Gujarat the top position in the regional rajput hierarchy.
Continuity and Change
Since caste census was discontinued after independence, it is difficult now to relate sex ratios to caste and
status within caste which one could do earlier on the basis of the female infanticide records and the census.
Nevertheless, it is possible to point to continuity and change which arguably has been a core feature of
Indian society for millennia. When one compares the information in the records on female infanticide to the
region specific census data on sex ratios since independence, one is struck by the fact that though caste no
longer figures now in the census, the regions which the records speak as having female infanticide are the
same. Thus while the records speak of undivided Punjab as having female infanticide among certain castes,
now it is Punjab and, Haryana which have shown very consistently as having not only low but also declining
female to male sex ratios since independence. The child sex ratio (girls per 1,000 boys aged 0-6) in Punjab
declined from 894 in 1961 to 793 in 2001. In Haryana, the child sex ratio plummeted from 910 in 1961 to
820 in 2001. Gujarat, Rajasthan and Uttar Pradesh, which figured in the records as areas where a number
of castes practiced female infanticide, continue to figure as areas with low female to male sex ratios. Given
the low female to male sex ratios in the jat dominated districts in UP and also in Punjab and Haryana, it is
not difficult to surmise that this caste which resorted to female infanticide in colonial times is now practising
female foeticide. A look at the districtwise sex ratios for Gujarat from 1901 to 1971 shows that compared to
other districts, Kheda district (Kaira during colonial days) which was the site of the patidar dominance since
precolonial and colonial times, has not only lower but also declining female to male sex ratio. The sex ratio
in Kheda district dropped from 897 in 1901 to 894 in 1971. It was only 865 in 1911 and 875 in 1931.
A suggestive pattern which emerges from the female infanticide records is that (a) the hypergamous castes
which practised female infanticide were dominant at the local level in parts of north and west India and (b)
they claimed kshatriya status and tried to cultivate a martial ideology. It is interesting to note here that the
http://www.epw.org.in/showArticles.php?root=2004&leaf=05&filename=7255&filety ... 14/02/2005
Article
Page 5 of 8
records never refer to trading or merchant castes such as the banias who were mostly urban based as
practising female infanticide. Nor do the kayasths who were scribes or took to service since medieval times
find a mention. Except in Punjab, the brahmins do not figure in the records in connection with female
infanticide in any other part of north, west or south India though they were dominant in some rural areas.
The records speak of the lower level rajputs and kanbis seeking wives from the kolis or tribals due to
shortage of marriageable women at the lower levels of the hypergamous hierarchy. Established brokers
were approached who procured women for a fee. Invariably the lower level rajputs and kanbis paid bride
price and brokerage. The deal was, however, kept a secret and generally came to light when the women
was ill-treated in her husband’s household. At the middle and lower levels of the status hierarchy among
kanbis and rajputs, families faced a double financial burden of dowry payment for marrying their daughter’s
hypergamously and bride price for marrying sons.
The caste specific information on female infanticide available in the records and the data on sex ratios for
regions are clearly indicative of how long the practice has been around in certain communities. The first
reference to female infanticide among jats in Punjab is in an 1857 publication by John Cave Brown on Indian
Infanticide. The census data for the colonial period and the recent 2001 census suggests that the jats in
Punjab have been practising female infanticide, now foeticide for over 150 years. For lewa patidars and
kanbis of central Gujarat, the first mention of low female sex ratios goes back to 1847. The long history of
female infanticide in these castes shows how well entrenched the practice is. There is no getting away from
the fact that the practice is embedded in the social structure of certain dominant castes. Unfortunately, for
reasons of status mobility and possibly other reasons we can guess, the other non-dominant castes are
following their bad example. Once we accept the fact that female infanticide is rooted in the social structure
of certain castes for a century and a half, the reality that it is not easy to eradicate it also needs to be faced.
The colonial ruler’s efforts to stop female infanticide may be instructive but perhaps inoperative in
democratic India.
Efforts at Suppression
The official records on female infanticide do not tell us everything we want to know, particularly how .the
castes, which practised female infanticide, viewed it. In addition, there is always the problem of an official
bias. Despite these limitations, the records show the very different perceptions of the coloniser and the
other. While the colonial officials who were called upon to deal with female infanticide in the course of their
official career, called it ‘inhuman’, ‘obnoxious’ ‘barbaric’ and ‘a crime’, the castes which practised female
infanticide in their interviews with the officials justified it by saying that they killed their female infants
because they could not afford huge dowries. This prompted officials like Walker to call the Jadejas an
‘avaricious’ lot who wished to keep their wealth intact by destroying their female children. The differing
yiewpomts3 bring out the fact that on one side there was a modern, reformist colonial state which viewed
female infanticide as an ‘obnoxious custom’ or a crime, which should be eradicated. On the other side, the
castes which practised female infanticide had well entrenched social norms such as dowry, hypergamy,
caste endogamy, clan exogamy and so on which made the marriage of daughters a very complicated affair
These castes did not regard female infanticide as a crime. That there was no meeting ground between these
perceptions is evident from the fact that British efforts to stop female infanticide or change social norms,
which contributed, to the practice were a failure. Coercion yielded temporary results. Starting from Duncan’s
efforts among the rajkumar rajputs of Jaunpur district in 1789 to the passing of the Female Infanticide Act in
March, 1870, British efforts to stop female infanticide covered a period of nearly hundred years. The
continuing low female to male sex ratios among castes known to practise female infanticide as revealed by
the census from 1891 onwards is proof enough that the British efforts at eradicating female infanticide did
not make a dent in the problem.
Jonathan Duncan was an orientalist by conviction. As the resident at Benares and as governor of Bombay
(1795-1812) he obtained written agreements signed by rajkumar rajputs in 1789 and jadeja rajputs in 1808.
The agreements stated that the signatories would thenceforth desist from killing their female children since
such an act was a sin according to the Hindu shastras. How successful Duncan was is clear from major
Ballantine s report of June 20, 1817 which showed that many talukas in Kathiawad inhabited by jadeja
rajputs had only one female child and some not even one. Ballantine cited the case of Drappa taluka, which
contained more than 400 jadeja families but “not a single female child in any of them”. As for the rajk’umars,
this paper had earlier mentioned the low female to male sex ratios in this rajput clan as revealed bv a
census.of 1856.
y
To stop female infanticide, the British tried persuading the castes, which practised it to reduce dowry and
wedding expenses. In the 1840s and 1850s meetings were organised in the North Western Provinces and
Punjab to obtain agreements from the castes that they will resort to ‘self-regulation’ by cutting down on
http://www.epw.org.in/showArticles.php?root=2004&leaf^05&filename=7255&filety... 14/02/2005
Article
Page 6 of 8
wedding expenditure. The agreements did not lead to any concrete result. Later, British officials admitted
that the agreements were a non-starter because the ‘problem’ of hypergamy, which mainly contributed to
expensive weddings of girls, had not been addressed. Perhaps taking a cue from this experience, the
British tried to curb hypergamy and encouraged reciprocal marriages to stop female infanticide.
Since the lewa kanbis who sought marriage alliances for their daughters in aristocratic lewa patidar families
of Charotar were excluded by the latter unless they offered a huge dowry, the kanbis formed endogamous
circles known as ‘ekadas’ or ‘gols’. These endogamous circles had rules, which were sometimes written on
stamp paper; the rules prohibited the members of the gol from marrying their daughter in a higher status
family or circle. To counter hypergamy and female infanticide, the British encouraged the formation of gols
and tried to strengthen the existing ones. British efforts bore fruit in terms of the number of gols formed; by
1872 there were 49 gols in Kaira district alone. However, the gols failed to check hypergamy. Ambitious
members of the gols flouted its rules and married their daughters hypergamously with large dowries. British
efforts to promote the gols started in 1847. A census of 1849 showed that there were in British Kaira, 72.84
kanbi females per hundred males. This moved by 1872 to a sex ratio of 73 kanbi females per hundred
males. In 23 years, the sex ratio ‘improved’ by less than one percentage point. It shows the degree of
success attained by the British in checking hypergamy and female infanticide by promoting endogamous
marriage circles. The efforts of Wilkinson in 1836 to curb hypergamy to stop female infanticide among the
rajput chiefs in central India and similar efforts of Mcloyd in 1853 among the bedi khutris of Punjab also did
not yield the desired results.
That the Female Infanticide Act of 1870 also did not produce any significant result so far as suppression of
the practice is concerned is evident from the census figures and comments of census officials. The author
of the 1911 (India) report says: “the figures for certain communities show that there is still in their case a
great dearth of females but there is very little direct evidence that it is due to actual infanticide and it may
equally well be the result of more or less deliberate neglect of girls”.There is evidence that deliberate
,gir,s was-there even before the Female Infanticide Act was passed. One is reminded of
W R Moores observation in his report of 1856. Designated as the infanticide commissioner, Moore was
asked to investigate female infanticide in the Benares division of the North Western Provinces and submit a
detailed report. When he asked the rajputs why they had no female children, they toldlhim: ‘Sookh jatain
ham (they dry up).
Post Independence Scenario
When one looks at the knowledge gained about female infanticide and the socio-economic institutions
related to it from the colonial period to the present, it is clearly diminishing knowledge which confronts the
researcher and all those deeply concerned with the problem. Based on the interviews of British officials with
castes which practised female infanticide, the records throw considerable light. The census till 1931,
continues to relate caste to female infanticide as the records do, but they are bereft of the kinds of
information which the records provide. What we find after 1931 and in the post-independence period is a
whole lot of regionwise statistics, which shows that female infanticide, has changed to female foeticide
wherever sex determination facilities are available. It is certainly alarming to find that the practice is
spreading like wild fire. However, none of the detailed information, which the records throw up on the socio
economic matrix in which female infanticide was located, is now available. This is an important point, which
needs stressing in the present day context. It is sometimes assumed that since female infanticide and
female foeticide is related to dowry, the problem will be solved once dowry is eradicated through efficient
law enforcement or some other method like generating public opinion against it. However, what leads to
dowry in the first place is often not asked. The colonial experience is instructive. From the use of the shastra
to coercion to social engineering, the colonial state tried almost everything to stop the practice. Its failure
shows the resilience of institutionalised norms to which female infanticide was related and about which we
still know so little. It is not surprising therefore, that facile suggestions are being made that this most blatant
form of discrimination against females can be tackled by somehow removing son preference and dowry.
Matters don t seem that simple. How does one tackle firmly entrenched institutionalised norms of which
owry and son preference are a part? Faced with a daunting task such as removing gender discrimination,
the governmental and non-governmental agencies who are doing their bit to solve the problem certainly
deserve praise and admiration. But we must know what we are up against and here the colonial records
and experience are a pointer.
Putting together the information in the records, anthropological studies and other sources, the perception of
the analyst of female infanticide during colonial rule is in terms of its caste specificity, hypergamy, hierarchy,
status maintenance, dowry avoidance and so on. However, is that all there is to analysing the records? Is
female infanticide just a matter of a sex ratios and statistics? Were the perpetrators of female infanticide all
heartless souls who steeled themselves from human emotions and sacrificed their female infants at the altar
http://www.epw.org.in/showArticles.php?root=2004&leaf=05&filename=7255&filety ... 14/02/2005
Article
Page 7 of 8
of pride and social status to protect their ancestral lands through dowry avoidance? Does not the element of
compulsion leading to female infanticide reported by more than one British official give some indication that
those who practised female infanticide felt caught up in the social structure of which they were a part?
Raising such questions is not to say that the practice is any way justified because of social compulsions.
Following Durkheim one may say that there is no wishing away the social compulsions and these need to
be addressed to get rid of female infanticide and female foeticide.
Finally, it is necessary to ask if female infanticide, now foeticide in urban centres, is the only one to persist
since colonial times. A number of pernicious social practices concerning women, which the social reformers
of the colonial era tried to eradicate, are still with us. Sati in UP and Rajasthan has been reported; child
marriage persists in rural India. The prohibition on widow re-marriage among upper caste Hindus and the
sanskritising lower castes is still to be reckoned with. Given the persistence of these customs, it can be
argued that modernity with its ideology of equality of the sexes intruded into Indian society without
significant changes in the position of women.
Address for correspondence:
Vishwanath@satyam. net. in
Notes
[This is a revised version of the paper presented at a workshop on ‘Missing Giris in India: Science, Gender Relations and the Political Economy
woriShop1]3 °r9an,Sed by the DePartment of Sociology, Delhi University on 30th-31st
thank Tulsi
30th-31st October,
October, 2003.
2003. II thank
Tulsi Patel
Patel for
for inviting
inviting me
me to
to the
the
1 I?6 fil9.ures
192J Census d0 not imply that castes, which convert to Islam, will not practise female infanticide. The records refer to the
path an khan^das of Jaunpur district in NWP who practised female infanticide in mid-19th century. The records also mention that the pathan
khanzadas were rajkumar rajputs before conversion and converted to Islam during the medieval period to ‘secure to themselves the
proprietary possession of a village’.
2 Alice Clark in her paper ‘Limitations on Female Life Chances in Rural Central Gujarat’, argues that “partly unwittingly and partly by feigning
blindness, British administrators ultimately supported the continuation of female infanticide and female child neglect’. Clark’s argument has
StkV'eW °nly °f the colonial Period- However, if we go back to pre-colonial rule, it is clear from the studies of scholars
Lbhah 1964, 2002] that in central Gujarat, the Maratha rulers allowed the patidars to maintain their high status by permitting them .to pay fixed
revenues. The British continued the same policy. As I have argued, the complications of status hierarchy and hypergamy existed before
colonial rule. Moreover, regardless of the practice of female infanticide by a dominant caste, the ruling political authority generally took into
account the local power of the dominant caste to collect taxes and maintain law and order.
3uPeICeuPt'OIl2SuOfrfemale lnf?nticide and ways of eradicating it varied within the British establishment. Some perceived it as an ‘abomination’,
which should be firmly eradicated since it was their duty as rulers to stop such customs. This view gained ground around the 1830s The earlier
generation of administrators like Jonathan Duncan and Monstuart Elphinstone were more cautious. They too regarded it as an ‘abomination’
out favoured a persuasive approach to suppress it. The missionaries, of course, viewed female infanticide, sati, child marriage and also
superstition as a sure sign of the ‘decadence’ of Hindu society.
References
Manuscript Sources
At the Bombay Secretariat Record Office
(i) Political Department, Vol 4, 2014 and 2181, 1848
(ii) Judicial Department, Vol 15, (No 237 of 1849), Vol 21 of 1849
(iii) Political Department, Vol 61, 1855; Vol 86, 1856, Vol 119, 1857, Vol 110, 1859, Vol 35, 1863' Vol 19 1867
(iv) Judicial Department, Vol 29, 1868
(v) Home Department (Judicial), No 1604, 1872
Printed Sources
(A) Selections from Records of Government.
(i) Government Records (1856): ‘North Western Provinces, Mr Thomason’s Despatches’, 2 Vols, Baptist Mission Press, Calcutta
Society’s^resT" Bombay ReC°rdS (1856): 'MeaSUreS Adopted for the Suppression of Female Infanticide in the Province of Kattywar’, Education
Government CenU-al^ress^0^5 ^1869^: ,|ntroduction of the Revenue Survey Assessment in the Kaira Collectorate’, No XIV (New Series),
Goven^ent Centra|rpent Reg°rd^ 0875): ‘Repression of Female Infanticide in the Bombay Presidency’ by H R Cooke, No XLVII (New Series),
(B) Reports
A Dozey ’Home^ecretan^ Press Calcutta6^ °f W R Moore’s ,nvestigation and Report Regarding Female Infanticide in the Benares Division,
(ii) Census of India, Reports, (1901, 1911, 1921) (Appendix VI), 1931. Punjab and United Provinces Census Reports, 1911. 1921
http://www.epw.org.in/showArticles.php?root=2004&leaf^05&filename=7255&filety ... 14/02/2005
/
Article
Page 8 of 8
(C) Other Sources
Brown, John Cave (1857): ‘Indian Infanticide, its Origin, Progress and Suppression’, W H, London.
Clark, Alice (1983): ‘Limitations on Female Life Chances in Rural Central Gujarat’, The Indian Economic and Social History Review, 20 (1).
Cohn, B S (1987): 'Structural Change in Indian Rural Society 1596-1885’ in An Anthropologist among the Historians and Other Essays, Oxford
University Press, Delhi.
Durkheim, Emile (1970): Suicide, Routledge and Kegan Paul, London, (Reprint).
Dreze, Jean and Amartya Sen (1995): ‘India: Economic Development and Social Opportunity', Oxford University Press, Delhi.
Hitchcock, John T (1959): The Idea of the Martial Rajput’ in Milton Singer (ed), Traditional India: Structure and Change, The American Folklore
Society, Philadelphia.
Pocock, D F (1971): ‘Kanbi and Patidar: A Study of the Patidar Community of Gujarat’, Oxford University Press, London.
Shah, A M (2002): Exploring India’s Rural Past, Oxford University Press, Delhi.
Steed, Gitel P (1955): ‘Notes on an Approach to a Study of Personality in a Hindu Village in Gujarat’ in Mckim Marriott (ed), Village India,
University of Chicago Press, Chicago.
Vishwanath, L S (2000): ‘Female Infanticide and Social Structure’, Hindustan Publishing Corporation, Delhi.
http://www.epw.org jn/showArticles.php?root=2004&leaf=05&filenanie=7255&filety... 14/02/2005
MAM Y bACBij Ob UJbMDEK IMB^UALll Y
Frontline
Page 1 ot1
Volume 18 - Issue 22, Oct. 27 - Nov. 09, 2001
India's National Magazine
from the publishers of THE HINDU
COVER STORY
MANY FACES OF GENDER INEQUALITY
An essay by Amartya Sen.
Table of
Contents
Mobel Laureate Amartya Sen's work on gender inequality is of seminal importance. His work
on the theory of the household represents the household not as an undifferentiated unit but
as a unit of cooperation as well as of inequality and internal discrimination. He has worked
ems of discrimination against women------------in the development
process, on
survivorship
---- - —J71VVVOJ,
Mil dUl
vivviomp
ditterentials between men and women under conditions of social discrimination against
women, and on women’s agency in the process of social development. Along with his
academic
collaborator .Jean Drze,' Professor Sen Xproposed
and popularised the concept of
I
------ X---- MMX* ^Vj/Uiiuiovu UXV VUULCUl Oi
missing women” - estimated to exceed 100
the world - which has given ns
us a
1,°0 million
mil.lion round 1116
new way of understanding and mapping the problem.
In this Cover Story essay, which is based on the text of his
SHANKER CHAKRAVARTY
inauguration lecture for the Radcliffe Institute at Harvard
University, Professor Sen takes a comprehensive and deeply
concerned look at the "many faces of gender inequality."
Focussing on South Asia, he discovers in the data thrown up by
the Census of 2001 an interesting phenomenon - a split India,
"something of a social and cultural divide across India, splitting
the country into two nearly contiguous halves, in the extent of
anti-female bias in natality and post-natality mortality." He
concludes by identifying the principal issues, emphasising the
need to "take a plural view of gender inequality," and calling for
a new agenda of action to combat and put an end to gender
inequality.
Frontline features this important essay by Amartya Sen as its Cover Story.
I. Seven Types of Inequality
IT was more than a century ago, in 1870, that Queen Victoria wrote to Sir Theodore Martin
compJammg about this mad, wicked folly of 'Woman's Rights'." The formidable empress
certainly d!d not herself need any protection that the acknowledgment of women's rights
might offer. Even at the age of eighty, in 1899, she could write to AT. Balfour, "We are not
interested in the possibilities of defeat; they do not exist." That, however, is not the way most
people s lives go - reduced and defeated as they frequently are by adversities. And within each
community, nationality and class, the burden of hardship often falls disproportionately on
^vomen.
,-n!nUabetW®en 'yomen and men can take very many different forms. Indeed, gender
inequality is not one homogeneous phenomenon, but a collection of disparate and interlinked
hv.f>://www.flonnet.com/fl 1822/18220040.htm
3/4/200
MANY FACES OF GENDER INEQUALITY
Page 2 of 15
problems. Let me illustrate with examples of different kinds of disparity.
(1) Mortality inequality: In some regions in the world, inequality between women and men
directly involves matters of life and death, and takes the brutal form of unusually high
mortality rates of women and a consequent preponderance of men in the total population, as
opposed to the preponderance of women found in societies with little or no gender bias in
health care and nutrition. Mortality inequality has been observed extensively in North Africa
and in Asia, including China and South Asia.
(2) Natality inequality: Given a preference for boys over girls that many male-dominated
societies have, gender inequality can manifest itself in the form of the parents wanting the
newborn to be a boy rather than a girl. There was a time when this could be no more than a
wish (a daydream or a nightmare, depending on one's perspective), but with the availability of
modem techniques to determine the gender of the foetus, sex-selective abortion has become
common in many countries. It is particularly prevalent in East Asia, in China and South
Korea in particular, but also in Singapore and Taiwan, and it is beginning to emerge as a
statistically significant phenomenon in India and South Asia as well. This is high-tech sexism.
KAMAL KISHOiy/REUTERS
A woman worker in New Delhi.
jf
. i
*
_ (3) Basic facility inequality: Even when demographic
M characteristics do not show much or any anti-female bias, there
are other ways in which women can have less than a square
deal. Afghanistan may be the only country in the world the
government of which is keen on actively excluding girls from
schooling (it combines this with other features of massive
gender inequality), but there are many countries in Asia and
Africa, and also in Latin America, where girls have far less
opportunity of schooling than boys do. There are other
deficiencies in basic facilities available to women, varying
■; from encouragement to cultivate one's natural talents to fair
MS - I participation in rewarding social functions of the community.
(4) Special opportunity inequality: Even when there is relatively little difference in basic
facilities including schooling, the opportunities of higher education may be far fewer for
young women than for young men. Indeed, gender bias in higher education and professio.
training can be observed even in some of the richest countries in the world, in Europe and
North America.
Sometimes this type of division has been based on the superficially innocuous idea that the
respective "provinces" of men and women are just different. This thesis has been championed
in different forms over the centuries, and has had much implicit as well as explicit following.
It was presented with particular directness more than a hundred years before Queen Victoria's
complaint about "woman's rights" by the Revd James Fordyce in his Sermons to Young
Women (1766), a book which, as Mary Wollstonecraft noted in her A Vindication of the
Rights of Women (1792), had been "long made a part of woman's library." Fordyce warned
the young women, to whom his sermons were addressed, against "those masculine women
that would plead for your sharing any part of their province with us," identifying the province
of men as including not only "war," but also "commerce, politics, exercises of strength and
dexterity, abstract philosophy and all the abstruser sciences."1 Even though such clear-cut
beliefs about the provinces of men and women are now rather rare, nevertheless the presence
of extensive gender asymmetry can be seen in many areas of education, training and
professional work even in Europe and North America.
i o://www. flonnet.com/fl 1822/18220040.htm
3/4/2004 ‘
■O'
(5) Professional inequality: In terms-of employment as well as promotion in work and
occupation, women often face greater handicap than men. A country like Japan may be quite
egalitarian in matters of demography or basic facilities, and even, to a great extent, in higher
education, and yet progress to elevated levels of employment and occupation seems to be
much more problematic for women than for men.
in the English television series called ”Yes, Minister,” there is an episode where the Minister,
full of reforming zeal, is trying to find out from the immovable permanent secretary, Sir
Humphrey, how many women are in really senior positions in the British civil service. Sir
Humphrey says that it is very difficult to give an exact number; it would require a lot of
investigation. The Minister is still insistent, and wants to know approximately how many
women are there in these senior positions. To which Sir Humphrey finally replies,
"Approximately, none."
(6) Ownership inequality: In many societies the ownership of property can also be very
unequal. Even basic assets such as homes and land may be very asymmetrically shared. The
absence of claims to property can not only reduce the voice of women, but also make it harder
for women to enter and flourish in commercial, economic and even some social activities.
This type of inequality has existed in most parts of the world, though there are also local
variations. For example, even though traditional property rights have favoured men in the
bulk of India, in what is now the State of Kerala, there has been, for a long time, matrilineal
inheritance for an influential part of the community, namely the Nairs.
K. GAJENDRAN
At a family welfare centre in Tamil Nadu.
(7) Household
uuuavuviu inequality:
illilly. There
1 llviv dIC,
are, UJLldl
often cHOUgn,
enough,
basic inequalities in gender relations within the ' - ’
family or the household, which can take many
different forms. Even in cases in which there are no Ep
-M'
overt signs of anti-female bias in, say, survival orEfia
son-preference or education, or even in promotion to
higher executive positions, the family arrangements
can be quite unequal in terms of sharing the burden
housework and child care. It is, for example, quite common in many societies to take it for
granted that while men will naturally work outside the home, women could do it if and only if
they could combine it with various inescapable and unequally shared household duties. This
is sometimes called "division of labour," though women could be forgiven for seeing it as
accumulation of labour." The reach of this inequality includes not only unequal relations
within the family, but also derivative inequalities in employment and recognition in the
outside world. Also, the established fixity of this type of "division" or "accumulation" of
labour can also have far-reaching effects on the knowledge and understanding of different
types of work in professional circles. When I first started working on gender inequality, in the
1970s, I remember being struck by the fact that the Handbook of Human Nutrition
Requirement of the World Health Orgamsation (WHO), in presenting "calorie requirements"
for different categories of people, chose to classify household work as "sedentary activity,"
requiring very little deployment of energy.^ I was, however, not able to determine precisely
how this remarkable bit of information had been collected by the patrician leaders of society.
I
II. Focussing on South Asia
It is important to take note of the variety of forms that gender inequality can take. First,
inequality between women and men cannot be confronted and overcome by any one set of all-
h. .,://www.flonnet.com/fll 822/18220040.htm
3/4/200
MANY FACES OF GENDER INEQUALITY
Page 4 of 15
purpose remedy. Second, over time the same country can move from one type of gender
inequality to harbouring other forms of that inequity. I shall presently argue that there is new
evidence that India is undergoing just such a transformation right at this time. Third, the
ditterent forms of gender inequality can impose diverse adversities on the lives of men and
boys in addition to those of women and girls. In understanding the different aspects of the
evl, i gender inequality, we have to look beyond the predicament of women and examine the
problems created for men as well by the asymmetric treatment of women. These causal
connections, which (as I shall presently illustrate) can be very significant, can vary with the
form of gender inequality. Finally, inequalities of different kinds can also, frequently enough,
feed each other, and we have to be aware of their interlinkages.
Even though part of the object of this paper is to discuss the variety of different types of
gender inequality, a substantial part of my empirical focus will, in fact, be on two of the most
kinds °f gender inecluality> namely, mortality inequality and natality inequality. I
shall be concerned, in particular, with gender inequality in South Asia, or the Indian
subcontinent. While I shall separate out the subcontinent for special attention, I must also
warn against the smugness of thinking that the United States or Western Europe is free from
gender bias simply because some of the empirical generalisations that can be made about the
subcontinent would not hold in the West. Given the many faces of gender inequality, much
would depend on which face we look at.
For example, India, along with Bangladesh, Pakistan and Sri Lanka, has had female heads of
governments, which the United States or Japan has not yet had (and does not seem very likely
to have m the immediate future, if I am any judge). Indeed, in the case of Bangladesh, where
both the Prime Minister and the Leader of the Opposition are women, one might begin to
wonder whether any man could possibly rise to a leadership position there in the near friture.
To take another example, I had a vastly larger proportion of tenured women colleagues when
I was a Professor at Delhi University - as early as the 1960s - than I had at Harvard University
in the 1990s, or presently have at Trinity College, Cambridge. To take another type of
example (of a rather personal kind), in preparing my last book, Development as Freedom,4
when I was looking for a suitably early formulation of the contrast between the instrumental
importance of income and wealth, on the one hand, and the intrinsic value of human life, on
the other (a point of departure for my book), I found it in the words of Maitreyee, a woman
intellectual depicted in the Upanishads (from the eighth century B.C.). The classic
formulation of this distinction would, of course, come about four centuries later, from
Aristotle, in Nicomachean Ethics, but it is interesting that the first sharp formulation of the
value of living for men and women should have come from a woman thinker in a society ti
has not yet - three thousand years later - been able to overcome the mortality differential
between women and men.
Indeed, in the scale of mortality inequality, India - as well as Pakistan and Bangladesh - is
close to the bottom of the league in gender disparity. And, as I shall presently argue, natality
inequality is also beginning to rear its ugly head very firmly and very fast right at this time in
the subcontinent.
III. Exceptions and Trends
In the bulk of the subcontinent, with only a few exceptions (such as Sri Lanka and the State of
Kerala in India), female mortality rates are very significantly higher than what could be
expected given the mortality patterns of men (in the respective age groups). This type of
gender inequality need not entail any conscious homicide, and it would be a mistake to try to
explain this large phenomenon by invoking the occasional cases of female infanticide that are
reported from China or India; these are truly dreadful events when they occur, but they are
'www.flonnet.com/fl 1822/18220040.htm
3/4/2004 g
■VIZVIN I
ur
± i
relatively rare. Rather, the mortality disadvantage of women works mainly through a
widespread neglect of health, nutrition and other interests of women that influence survival.
It is sometimes presumed that there are more women than men in the world, since that is wellknown to be the case in Europe and North America, which have a female to male ratio of 1.05
or so, on the average (that is, about 105 women per 100 men). But women do not outnumber
men in the world as a whole; indeed there are only about 98 women per 100 men on the
globe. This "shortfall" of women is most acute in Asia and North Africa. For example, the
number of females per 100 males in the total population is 97 in Egypt and Iran, 95 in
Bangladesh and Turkey, 94 in China, 93 in India and Pakistan, and 84 in Saudi Arabia
(though the last ratio is considerably reduced by the presence of male migrant workers from
elsewhere who come to Saudi Arabia).
It has been widely observed that given similar health care and nutrition, women tend typically
to have lower age-specific mortality rates than men do. Indeed, even female foetuses tend to
have a lower probability of miscarriage than male foetuses have. Everywhere in the world,
more male babies are bom than female babies (and an even higher proportion of male
foetuses are conceived compared with female foetuses), but throughout their respective lives
the proportion of males goes on falling as we move to higher and higher age groups, due to
typically greater male mortality rates. The excess of females over males in the population of
Europe and North America comes about as a result of this greater survival chance of females
in different age groups.
BRENNAN LINSLEY/AP
There is relatively little bias against women in
terms of health care and social status in subZr Saharan Africa.
I However, in many parts of the world, women receive
■BgiJ less attention and health care than men do, and
■ particularly girls often receive very much less support
■ than boys. As a result of this gender bias, the
J mortality rates of females often exceed those of males
Lea
J in these countries. The concept of ’’missing women’’
was devised to give some idea of the enormity of the phenomenon of women's adversity iin
mortality by focussing on the women who are simply not there, due to unusually high
mortality compared with male mortality rates. The basic idea is to find some rough and ready
way to understand the quantitative difference between (1) the actual number of women in
these countries, and (2) the number we could expect to see if the gender pattern of mortality
were similar in these countries as in other regions of the world that do not have a significant
bias against women in terms of health care and other attentions relevant for survival.
For example, if we take the ratio of women to men in sub-Saharan Africa as the standard
(there is relatively little bias against women in terms of health care, social status and mortality
rates in sub-Saharan Africa, even though the absolute numbers are quite dreadful for both
men and women), then its female-male ratio of 1.022 can be used to calculate the number of
missing women in women-short countries.^ For example, with India's female-male ratio of
0.93, there is a total difference of 9 per cent (of the male population) between that ratio and
the standard used for comparison, namely, the sub-Saharan African ratio of 1.022. This
yielded a figure of 37 million missing women already in 1986 (when I first did the
estimation). Using the same sub-Saharan standard, China had 44 million missing women, and
it was evident that for the world as a whole the magnitude of shortfall easily exceeded 100
million. Other standards and different procedures can also be used, as has been done by
Ansley Coale and Stephan Klasen, getting somewhat different numbers, but invariably very
hl t ://www.flonnet.com/fl 1822/18220040.htm
3/4/200
MANY FACES OF GENDER INEQUALITY
Page 6 of 15
large ones (Klasen's total number is about 80 million missing women).7 Gender bias in
mortality does take an astonishingly heavy toll.
How can this be reversed? Some economic models have tended to relate the neglect of
women to the lack of economic empowerment of women. While Ester Boserup, an early
feminist economist, discussed how the status and standing of women are enhanced by
economic independence (such as gainful employment), others have tried to link the neglect of
girls to the higher economic returns for the family from boys compared with girls.8 I believe
the former line of reasoning, which takes fuller note of social considerations that take us
beyond any hard-headed calculation of relative returns from rearing girls vis-a-vis boys, is
both appropriately broader and more promising, but no matter which interpretation is taken,
women’s gainful employment, especially in more rewarding occupations, clearly does play a
role in improving the deal that women and girls get. And so does women’s literacy, and other
factors that can be seen as adding to the status, standing and voice of women in family
decisions.9
An example that has been discussed in this context is the experience of the State of Kerala in
India, which provides a sharp contrast with many other parts of the country in having little or
no gender bias in mortality. Indeed, not only is the life expectancy of Kerala women at bi
above 76 (compared with 70 for men), the female-male ratio of Kerala’s population is l.bo
according to the 2001 Census (possibly somewhat raised by greater migration for work by
men, but certainly no lower than the West European or North American ratios, which are
around 1.05 or so). With its 30 million population, Kerala’s example also involves a fair
number of people. The causal variables related to women's empowerment can be seen as
playing a role here, since Kerala has a very high level of women's literacy (nearly universal
for the younger age groups), and also much more access for women to well paid and well
respected jobs. One of the other influences of women’s empowerment, namely a fertility
decline, is also observed in Kerala, where the fertility rate has fallen very fast (much faster,
incidentally, than China, despite the rigours of Chinese coercive measures in birth control),
and Kerala's present fertility rate around 1.7 or 1.8 (roughly interpretable as an average of 1.7
or 1.8 children per couple) is one of the lowest in the developing world (about the same as in
Britain and France, and much lower than in the United States). All these observations link
with each other very well in a harmonious causal story.
However, there is further need for causal discrimination in interpreting Kerala's experience.
There are other special features of Kerala which may also be relevant, such as feme’
ownership of property for an influential part of the Hindu population (the Nairs), openness to
and interaction with the outside world (with the presence of Christians - about a fifth of the
population - who have been much longer in Kerala - since around the fourth century - than
they have been in, say, Britain, not to mention Jews who came to Kerala shortly after the fall
of Jerusalem), and activist left-wing politics with a particularly egalitarian commitment,
which has tended to focus strongly on issues of equity (not only between classes and castes,
but also between women and men).10
IV. Issues that Need Investigation
I now move away from the old - and by now much discussed - problems of gender bias in life
and death (illustrated by the enormity of the size of "missing women") to other issues which
are in need of greater investigation at this time. We begin by noting four substantial
phenomena that happen to be quite widely observed in South Asia.
(1) Undernourishment of girls over boys: At the time of birth, girls are obviously no more
;r»-//www flnnnet.com/fl 1822/18220040.htm
3/4/2004
MANY PACES OP UEIWEK. IN EQUALITY
rage / 01 i
nutritionally deprived than boys are, but this situation changes as society's unequal treatment
takes over from nature's non-discrimination. There has, in fact, been plenty of aggregative
evidence on this for quite some time now.11 But this has been accompanied by some
anthropological scepticism of the appropriateness of using aggregate statistics with pooled
data from different regions to interpret the behaviour of individual families. However, there
have also been some detailed and concretely local studies on this subject, which confirm the
picture that emerges on the basis of aggregate statistics.12 One case study from India, which I
myself undertook in 1983, along with Sunil Sengupta, involved the weighing of every child in
two large villages. The time pattern that emerged from this micro study, which concentrated
particularly on weight-for-age as the chosen indicator of nutritional level for children under
five, brings out clearly how an initial condition of broad nutritional symmetry turns gradually
into a situation of significant female disadvantage.12 The detailed local studies tend to
confirm rather than contradict the picture that emerges from aggregate statistics.
In interpreting the causal process, it is important to emphasise that the lower level of
nourishment of girls may not relate directly to their being underfed vis-a-vis boys. Often
enough, the differences may particularly arise from the neglect of health care of girls
compared with what boys get. There is, in fact, some direct information of comparative
medical neglect of girls vis-a-vis boys in South Asia. Indeed, when I studied, with Jocelyn
Kynch, admissions data from two large public hospitals in Bombay (Mumbai), it was very
striking to find clear evidence that the admitted girls were typically more ill than boys,
suggesting the inference that a girl has to be more stricken before she is taken to the
hospital.1 Undernourishment may well result from greater morbidity, which can adversely
affect both the absorption of nutrients and the performance of bodily functions.
JORGE SILVA/REUTERS
A malnourished mother and her daughter in Guatemala.
(2) High incidence of maternal undernourishment: In South
Asia maternal undemutrition is more common than in most other
regions of the world.15 Comparisons of Body Mass Index (BMI),
which is essentially a measure of weight for height, bring this out
clearly enough, as do statistics of such consequential
characteristics as the incidence of anaemia.16
c-
(3) Prevalence of low birthweight: In South Asia, as many as 21 ••
per cent of children are bom clinically underweight (in accepted
medical standards) - more than in any other substantial region in
the world.17. The predicament of being low in weight in childhood
F /A
seems often enough to begin at birth in the case of South Asian
children. In terms of weight for age, South Asia has around 40 to 60 per cent children
undernourished compared with 20 to 40 per cent undernourishment even in sub-Saharan
Africa. The children start deprived and stay deprived.
(4) High incidence of cardiovascular diseases: South Asia stands out as having more
cardiovascular diseases than any other part of the third world. Even when other countries,
such as China, have greater prevalence of the standard predisposing conditions, the Indian
population seems to have more heart problems than these other countries have.
It is not difficult to see that the first three observations are very likely causally connected. The
neglect of the care of girls and of women in general and the underlying gender bias that they
reflect would tend to yield more maternal undernourishment, and through that more foetal
deprivation and distress, underweight babies, and child undernourishment. But what about the
hnp.7/www. flonnet.com/fl 1822/18220040.htm
3/4/200
MANY FACES OF GENDER INEQUALITY
PageS of 15
last observation - the higher incidence of cardiovascular diseases among South Asian adults?
In interpreting it, we can, I would argue, draw on some pioneering work of a British medical
team, led by Professor D.J.P. Barker.18
Based on English data. Barker has shown that low birth weight is closely associated with
higher incidence, many decades later, of several adult diseases, including hypertension,
glucose intolerance, and other cardiovascular hazards. The robustness of the statistical
connections as well as the causal mechanisms- involved in intrauterine growth retardation can,
of course, be further investigated, but as matters stand these medical findings offer a
possibility of causally interconnecting the different empirical observations related to South
Asia, as I have tried to discuss in a joint paper with Siddiq Osmani.19 The application of this
medical understanding to the phenomenon of high incidence of cardiovascular diseases in
South Asia strongly suggests a causal pattern that goes from the nutritional neglect of women
to maternal undernourishment, from there to foetal growth retardation and underweight
babies, and thence to greater incidence of cardiovascular afflictions much later in adult life
(along with the phenomenon of undernourished children in the shorter run). What begins as a
neglect of the interests of women ends up causing adversities in the health and survival of all
- even at an advanced age.
Given the uniquely critical role of women in the reproductive process, it would be hard
imagine that the deprivation to which women are subjected would not have some adverse
impact on the lives of all - men as well as women and adults as well as children - who are
bom of a woman" (as the Book of Job describes every person, not particularly daringly).
Indeed, since men suffer disproportionately more from cardiovascular diseases, the suffering
of women hit men even harder, in this respect. The extensive penalties of neglecting women's
interests rebounds, it appears, on men with a vengeance.
V. What Women’s Agency Can Achieve
These biological connections illustrate a more general point, to wit, gender inequality can hurt
the interests of men as well as women. There are other - non-biological - connections that
operate through women's conscious agency. The expansion of women's capabilities not only
enhances women's own freedom and well-being, but also has many other effects on the lives
of all. An enhancement of women's active agency can, in many circumstances, contribute
substantially to the lives of all people - men as well as women, children as well as adults. A c
many studies have brought out, the greater empowerment of women tends to reduce clu.
neglect and mortality, cut down fertility and overcrowding, and more generally, broaden
social concern and care.
These illustrations can be supplemented by considering the functioning of women in other
areas, including in economic and political fields.^1 Substantial linkages between women's
agency and social achievements have been noted in many different countries.
AVENTURIER PATR1CK/GAMMA
An Afghan mother and children at a refugee camp
in Pakistan.
There is, for example, plenty of evidence that
whenever social and economic arrangements depart
from the standard practice of male ownership, women
can seize business and economic initiative with much
success. It is also clear that the result of women's
participation is not merely to generate income for
np.7/www.flonnet.com/fl 1822/18220040.htm
-w
it w
3/4/2004
ivtaiN i racEd ur ueinuck irw^u/U-,11 x
A CA6W ✓
women, but also to provide many other social benefits that come from women's enhanced
status and independence. The remarkable success of organisations like the Grameen Bank and
the Bangladesh Rural Advancement Committee (BRAC) in Bangladesh is a good example of
this, and there is some evidence that the high profile presence of women in social and
political life in that country has drawn substantial support from women's economic
involvement and from a changed image of the role of women. While the Revd James Fordyce
might disapprove of "those masculine women," as he called them, straying into men's
"province," the nature of modem Bangladesh reflects in many different ways the increasing
agency of women. The precipitate fall of the total fertility rate in Bangladesh from 6.1 to 3.0
in the course of two decades (perhaps the fastest such fall in the world) is clearly related to
the changed economic and social roles of women, along with increases in family planning
77
facilities. There have also been cultural influences and developments in that direction.
Similar changes can be observed also in parts of India where women's empowerment has
expanded, with more literacy and greater economic and social involvements outside the
home.23
VI. Behind a Split India
While there is something to cheer in the developments I have just been discussing, and there
is considerable evidence of a weakened hold of gender disparity in several fields in the
subcontinent, there is also, alas, some evidence of a movement in the contrary direction, at
least in one aspect of gender inequality, namely, natality inequality. This has been brought out
particularly sharply by the early results of the 2001 decennial national Census of India, which
are now available. Early results indicate that even though the overall female to male ratio has
improved slightly for the country as a whole (with a corresponding reduction of the
proportion of "missing women"), the female-male ratio for children has had a substantial
decline. For India as a whole, the female-male ratio of the population under age 6 has fallen
from 94.5 girls for hundred boys in 1991 to 92.7 girls per hundred boys in 2001. While there
has been no such decline in some parts of the country (most notably Kerala), it has fallen very
sharply in others, such as Punjab, Haryana, Gujarat and Maharashtra, which are among the
richer Indian States.
Taking together all the evidence that exists, it is clear that this change reflects not a rise in
female child mortality, but a fall in female births vis-a-vis male births, and is almost certainly
connected with increased availability and use of gender determination of foetuses. Fearing
that sex-selective abortion might occur in India, the Indian Parliament banned some years ago
the use of sex determination techniques for foetuses, except when it is a by-product of other
necessary medical investigation. But it appears that the enforcement of this law has been
comprehensively neglected, and when questioned by Celia Dugger, the energetic
correspondent of The New York Times, the police often cited difficulties in achieving
successful prosecution thanks to the reluctance of mothers to give evidence of use of such
techniques.
I do not believe that this need be an insurmountable difficulty (other types of evidence can in
fact be used for prosecution), but the reluctance of the mothers to give evidence brings out
perhaps the most disturbing aspect of this natality inequality, to wit, the "son preference" that
many Indian mothers themselves seem to have. This face of gender inequality cannot,
therefore, be removed, at least in the short run, by the enhancement of women's
empowerment and agency, since that agency is itself an integral part of the cause of natality
inequality. Policy initiatives have to take adequate note of the fact that the pattern of gender
inequality seems to be shifting in India, right at this time, from mortality inequality (the
female life expectancy at birth is by now two years higher than male life expectancy in India)
to natality inequality.
http://wAvw.flonnet.com/fl 1822/18220040.htm
3/4/20(
MANY FACES OF GENDER INEQUALITY
Page 10 of 15
Indeed, there is clear evidence that traditional routes of changing gender inequality, through
using public policy to influence female education and female economic participation, may not
serve as a path to the removal of natality inequality. A sharp pointer in that direction comes
from countries in East Asia, which all have high levels of female education and economic
participation. Despite these achievements, compared with the biologically common ratio
across the world of 95 girls being bom per hundred boys, Singapore and Taiwan have 92
girls, South Korea only 88, and China a mere 86. In fact, South Korea's overall female-male
ratio for children is also a meagre 88 girls for 100 boys and China's 85 girls for 100 boys. In
comparison, the Indian ratio of 92.7 girls for 100 boys (though lower than its previous figure
of 94.5) still looks far less unfavourable.24
However, there are more grounds for concern than may be suggested by the current all-India
average. First, there are substantial variations within India, and the all-India average hides the
fact that there are States in India where the female-male ratio for children is very much lower
than the Indian average. Second, it has to be asked whether with the spread of sex-selective
abortion, India may catch up with - and perhaps even go beyond - Korea and China. There is,
in fact, strong evidence that this is happening in a big way in parts of the country.
There is, however, something of a social and cultural divide across India, splitting the counfrv
into two nearly contiguous halves, in the extent of anti-female bias in natality and po\
natality mortality. Since more boys are bom than girls everywhere in the world, even without
sex-specific abortion, we can use as a classificatory benchmark the female-male ratio among
children in advanced industrial countries. The female-male ratio for the 0-5 age group is 94.8
in Germany, 95.0 in the U.K., and 95.7 in the U.S., and perhaps we can sensibly pick the
German ratio of 94.8 as the cut-off point below which we should suspect anti-female
intervention.
The use of this dividing line produces a remarkable geographical split of India. There are the
States in the north and the west where the female-male ratio of children is consistently below
the benchmark figure, led by Punjab, Haryana, Delhi and Gujarat (with ratios between 79.3
and 87.8), and also including, among others, Himachal Pradesh, Madhya Pradesh, Rajasthan,
Uttar Pradesh, Maharashtra, Jammu and Kashmir, and Bihar (a tiny exception is Dadra and
Nagar Haveli, with less than a quarter million people altogether). On the other side of the
divide, the States in the east and the south tend to have female-male ratios that are above the
benchmark line of 94.8 girls per 100 boys: with Kerala, Andhra Pradesh, West Bengal and
Assam (each between 96.3 and 96.6), and also, among others, Orissa, Karnataka and the
northeastern States to the east of Bangladesh (Meghalaya, Mizoram, Manipur, Nagalai.
Arunachal Pradesh).
S. GOPAKUMAR
t'
B I fFi
r.
At the start of a new school year in Kerala.
J One significant exception to this neat pattern of
adjoining division is, however, provided by Tamil
are
Nadu, where the female-male ratio is just below 94,
which is higher than the ratio of any State in the
deficit list, but still just below the cut-off line used
for the partitioning (94.8). The astonishing finding is
not that one particular State seems to provide a
marginal misfit, but how the vast majority of the
Indian States fall firmly into two contiguous halves, classified broadly into the north and the
west, on one side, and the south and the east, on the other. Indeed, every State in the north and
the west (with the slight exception of the tiny Union Territory of Dadra and Nagar Haveli) has
strictly lower female-male ratio of children than every State in the east and the south (even
■E
I
n7/www flnnnet cnm/fl 1 «??/! 8290040 him
3/4/2004
1VLA1N Y r ACtSd Uf OBlNJJtSK UNUSUAL,! 1 Y
~ rage 11 ui i
Tamil Nadu fits into this classification), and this indeed is quite remarkable.
The pattern of female-male ratio of children produces a much sharper regional classification
than does the female-male ratio of mortafity of children, even though the two are also fairly
strongly correlated. The female-male ratio in child mortality varies between 0.91 in West
Bengal and 0.93 in Kerala, on one side, in the southern and eastern group, to 1.30 in Punjab,
Haryana and Uttar Pradesh, with high ratios also in Gujarat, Bihar and Rajasthan, in the
northern and western group.
The north and the west have clear characteristics of anti-female bias in a way that is not
present - or at least not yet visible - in most of the east and the south. This contrast does not
have any immediate economic explanation. The States with anti-female bias include rich ones
(Punjab and Haryana) as well as poor States (Madhya Pradesh and Uttar Pradesh), and fast
growing States (Gujarat and Maharashtra) as well as growth failures (Bihar and Uttar
Pradesh). Also, the incidence of sex-specific abortions cannot be explained by the availability
of medical resources for determining the sex of the foetus: Kerala and West Bengal in the
non-deficit list, both with the ratio of 96.3 girls to 100 boys (comfortably higher than the
benchmark cut-off of 94.8), have at least as much medical facilities as in such deficit States as
Madhya Pradesh or Rajasthan. If commercial facilities for sex-selected abortion are
infrequent in Kerala or West Bengal, it is because of a low demand for those specific services,
rather than any great supply side barrier.
This suggests that we have to look beyond economic resources or material prosperity or GNP
growth into broadly cultural and social influences. There are a variety of potential
connections to be considered here, and the linking of these demographic features with the rich
subject matter of social anthropology and cultural studies would certainly be important to
pursue. There is perhaps a common link with politics as well. Indeed, it has been noted, in
other contexts, that the States in the north and the west have, by and large, given much more
room to religion-based sectarian politics than have the east or the south, where religioncentred parties have had very little success. For example, of the 197 members of Parliament
from the Bharatiya Janata Party (BJP) and the Shiv Sena elected in 1999, as many 169 won
from States in the north and the west. Even if we take out the BJP members who. though
elected from Bihar or Madhya Pradesh, come from the recently formed relatively "eastern”
States of Jharkhand and Chhatisgarh (which, incidentally, do have "eastern" female-male
ratios above the benchmark line), the predominance of the north and the west in the
representation of the Sangh Parivar remains strong. It is not easy to settle, without further
scrutiny, how significant these regional, cultural or political associations are, and how (and
even in which direction) the causal influences operate. But the remarkable geographical
division of India into two largely contiguous parts in terms of female-male ratio among
children (reflecting the combined influence of inequality in natality and post-natal mortality)
does call for acknowledgement and further analysis. It would also be important to keep a
close watch on whether the incidence of sex-specific abortions will significantly increase in
States in which they are at this time quite uncommon.
VII. Summing up
I may end by trying briefly to identify some of the principal issues I have tried to discuss.
First, I have argued for the need to take a plural view of gender inequality, which can have
many different faces. The prominent faces of gender injustice can vary from one region to
another, and also from one period to the next.
Second, the effects of gender inequality, which can impoverish the lives of men as well as
women, can be more fully understood by taking detailed empirical note of specific forms of
http://www.flonnet.com/fl 1822/18220040.htm
3/4/200
MANY FACES OF GENDER INEQUALITY
Page 12 of 15
inequality that can be found in particular regions. Gender inequality hurts the interests not
only of girls and grown-up women, but also of boys and men, through biological connections
(such as childhood undernourishment and cardiovascular diseases at later ages) and also
through societal connections (including in politics and in economic and social life).
Fetching water, a scene from rural Rajasthan.
To have an adequate appreciation of the far-reaching
effects of disparities between women and men, we
have to recognise the basic fact that gender inequality
is not one affliction, but many, with varying reach on
the lives of women and men, and of girls and boys.
There is also the need to reexamine and closely
scrutinise some lessons that we have tended to draw
from past empirical works. There are no good reasons
to abandon the understanding that the impact of
women's empowerment in enhancing the voice and influence of women does help to reduce
gender inequality of many different kinds, and can also reduce the indirect penalties that men
suffer from the subjugation of women. However, the growing phenomenon of nata
inequality raises questions that are basically much more complex. When women in some
regions themselves strongly prefer having boys to girls, the remedying of the consequent
natality inequality calls at least for broader demands on women’s agency, in addition to
examining other possible influences.
Indeed, in dealing with the new - "high tech" - face of gender disparity, in the form of natality
inequality, there is a need to go beyond just the agency of women, but to look also for more
critical assessment of received values. When anti-female bias in action (such as sex-specific
abortion) reflects the hold of traditional masculinist values from which mothers themselves
may not be immune, what is needed is not just freedom of action but also freedom of thought in women's ability and willingness to question received values. Informed and critical agency is
important in combating inequality of every kind. Gender inequality, including its many faces,
is no exception.
Based on the text of an inauguration lecture for the new Radcliffe Institute at Harvard
University, on April 24, 2001. A shortened version of this paper was published in The New
Republic on September 17, 2001; this is the full text.
ENDNOTES
1. See William St. Clair, The Godwins and the Shelleys (New York: Norton, 1989), pp. 5048.
2. Bina Agarwal, among others, has investigated the far-reaching effects of landlessness of
women in many agricultural economies; see particularly her A Field of One's Own
(Cambridge: Cambridge University Press, 1994).
3. World Health Organisation, Handbook of Human Nutrition Requirement (Geneva: WHO,
1974); this was based on the report of a high-level Expert Committee jointly appointed by
the WHO and FAO - the Food and Agriculture Organisation.
4. Development as Freedom (New York: Knopf, and Oxford: Oxford University Press,
1999), Chapter 1.
■ f vx- //xxrtTmr
™rn/fl 1 899/1 8990040 htm
3/4/2004 f
1VLAJN I rALCd UP UBINUBK IINB^UAjLII I
rage u oi i
5. Presented in my "More Than a Hundred Million Women Are Missing," The New York
mX’XSS''' Dec”1’er 20-1”0, “d in
Women’”M,ish
“
The fact
that I had used the sub-Saharan African ratio as the standard, rather than the
European or North American ratio, was missed by some of my critics, who assumed
(wrongly as it happens) that I was comparing the developing countries with advanced
Western ones; see for example Ansley Coale, "Excess Female Mortality and the Balances of
the Sexes in the Population: An Estimate of the Number of 'Missing Females'," Population
and DeveJopment Review, 17 (1991). In fact, the estimation of "missing women" was based
on the contrasts within the so-called third world, in particular between sub-Saharan Africa
°nJ116 °ne hand and Asia and North Africa, on the other. The exact methods used were
nthA ?^bOrav Y dlSuCU"Sed ln my "Africa and India: What Do We Have to Learn from Each
er., in Kenneth J. Arrow, ed.. The Balance between Industry and Agriculture in
Economic Development (London: Macmillan, 1988); and (with Jean Drze), Hunger and
Public Action (Oxford: Clarendon Press, 1989).
B
6.
7. Stephan Klasen, '"Missing Women' Reconsidered," World Development, 22 (1994).
?07m
®0SerUp’ Women's Role in Economic Development (London: Allen & Unwin,
LIr J!- ’-i nenZWelg
T P- Schultz’ "Market Opportunities, Genetic Endowments,
ana Intraiamily Resource Distribution," American Economic Review, 72 (1982).
T J0I?en and c°0Perative Conflict," in Irene Tinker, Persistent
Inequalities (New York: Oxford University Press, 1990). See also J.C. Caldwell, "Routes to
Low Mortality in Poor Countries," Population and Development Review, 12 (1986)- Jere
MediSJc11'^ nL' Wo1 J’ 'How Does Mother's Schooling Affect Family Health, Nutrition,
Medical Care Usage and Household Sanitation," Journal of Econometrics, 36 (1987)- Jean
Dreze and Amartya Sen, Hunger and Public Action (Oxford: Clarendon Press, 1989).
facjrs in Ty "More Than a Hundred
w°men
(1990}- See also Jean Dreze and Amartya Sen, India: Economic Development and
Social Opportunity (Delhi: Oxford University Press, 1995), and particularly VK
Ramachandran, Kerala's Development Achievements," in Jean Dreze and Amartya Sen
1996)ndlan DeVelopment: Selected Regional Perspectives (Delhi: Oxford University Press’
11. See the literature on this cited in Development as Freedom (1999).
12. One of the earliest and pioneering studies was bY Lincoln Chen, E. Huq and S. D’Souza,
"Sex Bias in the Family Allocation of Food and Health
— ----- --i Care in Rural Bangladesh,”
Population and Development Review, 7 (1981).
13. See my joint paper with Sunil Sengupta, "Malnutrition of Rural Indian Children and the
Sex Bias, Economic and Political Weekly, 19 (1983).
ctmhXtTJOmt iPa^ With J°Celyn Kynch’ "Indian Women: Well-being and Survival,"
tC^hnd
?T?miCS’ 7 (1983)’
als° Resources, Values and Development
(Cambridge, MA: Harvard University Press, 1984).
F
15. See Peter Svedberg, Poverty and Undemutrition: Theory and Measurement (Oxford£'somhM SSH h°q h°T an^minating “d thorough analysis of comparative nutrition
in South Asia and sub-Saharan Africa.
http://www.flonnet.com/fll822/18220040.htm
3/4/200
many faces of gender inequality
Page 14 of If
p6:.Sle (1997?^^
S.f;5>smaill- ”Povert
y andpTT
Nutrition1 im *0Uth Asia’" in ^CC/SCN, Nutrition and
Poverty
XXT
First AbrAharn ’ I-T
TUtntlon Pollcy Paper No. 16 (Geneva: WHO, 1997) This is the
First Abraham Horowitz Lecture of the
°f
'jn,te<‘
s“
17 On this see Osmani, "Poverty and Nutrition in
South Asia" (1997), and also the
references cited there.
»d Ad”"
Development Report 1995 (New York: United Nation” 1996)
and DevelopmXev^SS)8'
c-“.
BaCk8r<,“nd PaPers' H“”“
°P™eSS “ ,”"»’atto“."
nftwJTnt StUdy °f 10Cal g°vemmental decisions in India brings out the substantial nature
Randomised Expo™, (“nd’a,” 1X^5^^^^
whereas^the "Indian
“tT' "1?"'“ fi«"“ “™r 'Wldren between 0 and 4,
ZX“e ‘St **“””“>XeneemI o'o^nTt taa^le mtSZdTm m“ hta
Dr2uX''
SfiihrioDrin "OpO°r^^^^^
Gupta, Selective Discrimination against Female Children in Rural Punjab," Population
■ >://www.flonnetcom/fl 1822/18220040.htm
3/4/2004 *
AIN Y rACES UP UPlNDbK UNJL^UAEll Y
Page
ot
and Development Review, 13 (1987); Alaka M. Basu, Culture, the Status of Women and
Demographic Behaviour (Oxford: Clarendon Press, 1992); Satish Balram Agnihotri, Sex
Ratio Patterns in the Indian Population (New Delhi: Sage, 2000).
[ Subscribe | Contact Us | Archives | Table of Contents]
[ Home | The Hindu | Business Line | Sportstar ]
Copyrights © 2001, Frontline.
Republication or redissemination of the contents of this screen are expressly prohibited
without the written consent of Frontline
<
Maternal Deaths and Near Deaths
Facts and Figures
Maternal death is defined as “the death of a woman while pregnant or within 42
days of termination of the pregnancy, irrespective of the duration and the site of
pregnancy, from an cause related to or aggravated by the pregnancy or its
management but not from accidental or incidental causes.
International Statistical Classification ofDiseases
Maternal Mortality:
Uttar Pradesh has the highest maternal mortality ratio in the country according to the
Sample Registration System of the Government of India (1997). In Uttar Pradesh for 707
cases out of every 1 lakh live childbirths, the mother does not survive. This is about 80%
more than the maternal mortality ratio of the country as a whole and over 3 to 4 times
more than most other states in the country.
Nearly 40,000 women of Uttar Pradesh lose their lives due to maternal mortality every
year in Uttar Pradesh. Every third woman who loses her life due to pregnancy and related
causes is from Uttar Pradesh. Three out of every 100 women in Uttar Pradesh have the
risk of dying in pregnancy and childbirth. The risk is far more for poor rural women.
According to the National Family Health Survey conducted in 1998-99, about 7^J<>
women had their deliveries without any trained supervisors. Anameia or low levels of
haemoglobin in the blood is considered one of the most important contributory factors of
maternal death. 48% of women in the state have anaemia.
.?
According to the WHO, over 90% of maternal deaths result from either of five causes bleeding ( 25%), infection (15%), high blood pressure (13%), obstructed labour (7%)
and unsafe abortion ( 13%). All these are preventable causes, and can be managed with
regular antenatal care, trained supervision during labour, appropriate referral and follow
up after delivery.
( all datafrom National Family Health Survey 2-1998-99)
Abortion:
Provision of safe abortion services to women who need it is not part of the
provisions of the UP State Population Policy 2000
Unsafe abortion is one of the most important reasons for maternal deaths. UP has the
highest estimated rate of abortion in the country. Over 20 lakh abortions take place in the
state of Uttar Pradesh every year of which about 60% are induced. Complications from
abortion are responsible for 15 - 30% of all maternal deaths in the state. Serious
I
uu V a 1 M '7—
08861
i.S(
<
(
complications of unsafe abortion include infection, bleeding, and injuries to the
reproductive tract.
(from study report ofJohns Hopkins University - w'ww.jhpiego.org/pubs/TR/tr516sum.htm)
Complications during Pregnancy:
WHO estimates that 15% of all pregnant women develop complications
serious enough to require rapid and skilled intervention if the woman is to
survive without long term disability
The total percentage of women in Uttar Pradesh receiving any antenatal care was only 36
% and only 5% had a check up in the last three months. Anameia or low levels of
haemoglobin in the blood is considered one of the most important contributory factors of
maternal death. Only 32% women report having received any iron and folic acid
supplements during pregnancy.
A large number of women in Uttar Pradesh had serious complications during their
pregnancy
Night blindness -14%
Blurred vision - 28%
• „ Convulsions - 16.6%
Swelling of the body, legs or face - 24.8%
Excessive fatigue - 44.5%
Anaemia - 30.9%
Vaginal blgeding 4.3%
Complications after childbirth:
Nearly 17 % women had very high fever and 9.4% had massive vaginal bleeding after
childbirth. 93 percent of women in UP did not receive any check up within two months of
delivery and only about 2% receive a check up within two days. In only 33% of these
cases ( less than 3% overall) is the mother’s abdomen examined. Of the 50 lakh
childbirths taking place in UP every year, in 48.5 lakh mothers no abdominal
examination is done after childbirth and 40 lakh mothers are not even visited after 2
months of her delivery.
(all data from National Family Health Survey 2- 1998-99)
Maternal Deaths and Near-Deaths In UttarPradesh
Case Studies
Illegal Abortion:
Lack of Emergency Obstetric Care:
> Adolescent Abortion:
Complication in pregnancy:
> Lack of Post-delivery' Care:
Kanpur
Hardoi
Sitapur
Manikpur
Mirzapur
Illegal abortion services by government health worker causes death
1. 35-year old Munni of village Ghatukheda, Block Bidhnu, district Kanpur went for
a check-up suspecting a seventh pregnancy. The government nurse performed an
illegal abortion that led to uncontrollable bleeding, and refused to refer her to a
hospital. As the bills at tlie private hospital became unaffordable Munni finally died
at home after almost a month of bleeding, infection and pain.
Munni, a 35 year-old mother of six children, was an inhabitant of village Ghatukheda,
Block Bidhnu, district Kanpur. In the summer of 2000, she went to the PHC at Bidhnu
after missing her periods, and was checked up by the Auxiliary Nurse Midwife (ANM)a government health worker who is not qualified to perform abortions but should provide
prophylactic services to pregnant women and refer them to the hospital if necessary. The
ANM advised her to come to the ANM Sub-centre for an abortion. The next day Munni
went to the Sub-centre with her husband. They paid the nurse Rs.500, and he waj asked
to wait outside.
After a couple of hours, the ANM returned the money and said he should take his wife
away since her bleeding would not stop. She refused to accompany them. The husband
took the help of a son of the village Pradhan who happened to be working at a private
hospital called “Ramshiv”. The doctor there operated upon Munni, but she kept bleeding
and the stitches also got infected. Munni remained in the hospital for over three weeks,
but finally the doctor advised them to stop spending money since she would not get better
anyway. She was taken home where she died around 24 days after her abortion.
Unregulated private practitioners kill mother and child
2. 35-year old Ramdevi was delivering her seventh child on 5th June 2003 at Mohalla
Kheda Bibi Jai in Hardoi district when a quack doctor Asma and colleague Pervez
hacked off the baby’s body leaving the head inside. She bled to death within a short
while. The local police initially refused to register the case, then personally removed
crucial evidence before taking the body for post-mortem.
Ramdevi, a 35 year old mother of six children lived in New Delhi where her husband
earned a meagre living. Unable to afford costs of delivery in Delhi, she had returned to
her marital home at Mohalla Kheda Bibi Jai in Hardoi district, Uttar Pradesh for her
seventh childbirth. She had never received services from any provider for ante-natal care
for any of her six previous deliveries.
On 5th June, 2003, she went into labour and the village dai was called. The dai diagnosed
that the baby was in tlie wrong position and expressed inability to assist in the birth. In
the meantime a local quack doctor Asma Khatun arrived on the scene and urged the
family to let her handle the case. The family members report that she charged1 Rs. 3000
for her fees and the medicines she would be using.
From seven in the morning to midday, Asma and later her colleague Pervez tried to
deliver the baby and would not let any family members inside the ‘clinic’. Finally the
family were allowed to send in a neighbour Tahira Begum, who saw the mother writhing
in pain near a pail of blood, while the headless body of the baby lay in a basin. At one
pm, Asma told the family that she would write out a referral slip and they should take
Ramdevi elsewhere. Initially she refused to accompany them, but later she took them to a
private doctor whom she already knew. The doctor declared Ramdevi dead on arrival and
asked them to take away the body at once.
The family took the body back home, but some of the relatives and neighbours went to
lodge a report at the nearest police station at Shahbad. The police refused to record what
they were saying. Later that evening, Ramdevi’s husband and father-in-law went to the
' x police station and found the colleague of Asma, Pervez, sitting with the policemen. Later,
policemen came to the house and. verbally abused the grieving family. They forced one of
tlie women relatives to remove from Ramdevi’s vagina the scissors entangled in the
umbilical cord, for which they provided light using a torch.
After this the police took the body away for the post-mortem, but no report was provided
to the family. At present, Asma and Pervez are in prison and have been refused bail.
Taking advantage of need for secrecy, government nurse causes student’s death
3. Radha (name changed) of village Vijnapur, block Mishrik, district Sitapur was an
eighteen year-old student who was four months pregnant. Her mother compelled her to
go to the local PHC for an abortion where the government nurse illegally performed a
procedure causing Radha to bleed to death in two days.
Radha (name changed) of village Vijnapur, block Mishrik, district Sitapur was an
eighteen year-old student who had a relationship with a boy at college, Govind (name
changed) and was four months pregnant. Her mother compelled her to go in for an
abortion and on 9th August 2003, they went to the Mishrik PHC where a nurse inserted
some medicine into her through a tube.
1 Without any receipt
)
After an hour, Radha started bleeding heavily. She stayed on at the hospital, where the
nurse performed the procedure again saying ‘a piece is still left inside’. The nurse
summoned the mother the next day and asked her to take Radha away. Telling
acquaintances that Radha was suffering from cholera, her mother and Govind arranged
for transport to take Radha to Sitapur. Radha died on the way, and Govind fled from the
scene. The villagers are unwilling to speak openly about what happened.
No attention by ANM to complications during pregnancy leads to woman’s
death.
4. 25 year old Nirmala, an extremely poor Dalit woman of village Sukhrampur, PO
Manikpur had a spontaneous abortion four months into her fourth pregnancy. She
received no medical attention and a month later developed complications. A private
doctor treated her over six visits without referring her elsewhere. Her symptoms
worsened and she consulted a new doctor. He gave her a ‘strengthening’ injection,
immediatelv after which she died in the clinic.
25 year old Nirmala, an extremely poor Dalit woman of village Sukhrampur, PO
Manikpur, had three children aged between 2 and 6 years. The government ANM’s
Subcentre at Unchadih is 4 km from her village. Nirmala was four months into her fourth
pregnancy when she started getting pains. She did not get to see a doctor, and two days
later, Nirmala had a spontaneous abortion on 2nd August 2003. Her mother-in-law
managed it at home.
After a month of rest, the bleeding and discharge had stopped, when suddenly Ninnala
developed fever. Her husband put her in a bullock-cart and took her to a private doctor at
Manikpur. “Doctor Lallan” gave her medicines for a fortnight, and this was repeated over
two visits. After the third visit, Nirmala developed pain and swelling in her thighs, to the
extent that she was unable to walk. The doctor said it must be due to a boil.
When even the sixth visit to “Doctor Lallan” failed to cure her, Nirmala was taken to
another doctor, Doctor B.K. Tiwari. He examined her and gave her an injection.
Immediately after the injection, Nirmala died in his clinic itself. The husband did not
even have Rs. 500 to hire a jeep to take the body home, so the doctor donated Rs. 200.
The doctor said he had given her a ‘strengthening’ injection and she died because she was
extremely anemic.
Neglect of post-deliver)' complication by government doctor leads to woman’s
death.
5. Somari, a 26 year-old mother of two children of Nikrika, Post Rampur 38, Tehsil
Madihan, district Mirzapur developed post-delivery complication seven days after
her birth at home with pain in her legs and body. She reached the nearest
government PHC in a state of collapse in a jeep that was hardly working, but the
doctor turned her away without even finding out why she had been brought there. A
series of four private doctors tried to treat her through intravenous drip as her
Somari, a 26 year-old mother of two children aged 8 and 4, was the wife of a poor Dalit
labourer, of Nikrika, Post Rampur 38, Tehsil Madihan, district Mirzapur. During her
third pregnancy, the local ANM Kusum Singh Dhansiriya had^given her both T1
injections and an examination. Sumari went into labour on 26 July 2003 and was
attended by the community women during the normal birth.
Seven days later, on 2nd August, 2003, she developed pain in her legs which spread all
over her body. The private doctor from Nikrika, Doctor Jawahir was summoned who
made a cursory check-up and started an intravenous drip. The first bottle was finishe in
the short span of half an hour, by which time Somari stopped speaking and moving, ic
doctor fled from the scene. By evening the family was alarmed at her condition and
began preparations to get her to a hospital. The only vehicle in the village was a run
down jeep which needed to be pushed to start and had no lights.
They drove to the PHC at Rajgarh by eight at night. They called for the doctor for a long
time. Finally the doctor came out on his roof and flashed a torch at Sumari. He did not
ask what the matter was with her. He declared that she was in a very critical condition
and they should immediately go to Robertsganj. The villagers suspect it was because t e\
looked too poor to pay too much for services.
There were only two of them and they could not get the jeep to start. There were no lights
either. They pushed the jeep to the Shahganj road where they arrived at the clinic of a
private doctor. The doctor started a drip and started examining her abdomen at which she
screamed in pain. At 3 am the doctor declared he could do nothing else seeing that she
was getting worse with the drip.
At 4 am Sumari was taken to the private hospital of Dr. Ayron at Mirzapur He too
started a drip, and gave her some medicines, but soon he
he too
too asked
asked the
the family
xami y to
to take
ta 'e her
ler
away to Mirzapur.
They took her to Dr. Meena Jain at a private hospital in Mirzapur. She examined Sumari
and asked them to take her away. They took Sumari back to Dr. Ayron, feeling that
private providers would provide better care than a government hospital. He as 'e t em o
take her to Allahabad. By that time Sumari was barely breathing. Deciding against
moving her anywhere else, they took her to a relative s house at MirzapUi wnere on re
night of 3rd August, Sumari breathed her last.
Maternal Deaths and Near—deaths in Uttar Pradesh
State Obligations
Uttar Pradesh has the highest number of women dying every year due to maternal related causes in all of South Asia. This violation of women’s right to life is all the more
serious since the deaths are all due to preventable or manageable causes. The documented
case studies from all over Uttar Pradesh clearly indicate that the state itself is violating
the rights of women to enjoy complete health and life through
> Lack of services
> Lack of intervention to regulate high-risk services of private providers and
> Collusion with the family in preventing women’s access to emergency care during
complications
At the same time, it must be remembered that the state is obliged under the following
Constitutional and policy declarations as well as international conventions and
agreements to protect, promote and fulfill women’s right to health and life.
1. The Constitution of India
Article 14 Equality before law: The State shall not deny to any person equality before
the law or the equal protection of the laws within the territory of India.
Article 15 Prohibition of Discrimination on grounds of religion, race, caste, sex or
place of birth : (3) Nothing in this article shall prevent the State from making any special
provisions for women ...
Article 21 Protection of life and personal liberty: No person shall be deprived of his
life or personal liberty except according to procedure established by law.
Article 38 State to secure a social order for the promotion of welfare of the people
(1) The State shall strive to promote the welfare of the people by securing and protecting,
as effectively as it may, a social order in which justice, social, economic and political,
shall inform all the institutions of the national life.
Article 47 Duty of the State to raise the level of nutrition and the standard of living
and to improve public health: The State shall regard the raising of the level of nutrition
and the standard of living of its people and the improvement of public health as among its
primary duties ...
2. National Population Policy 2000
16. Impaired health and nutrition is compounded by early childbearing, and consequent
risk of serious pregnancy related complications. Women’s risk of premature death and
disability is highest during their reproductive years. Malnutrition, frequent pregnancies,
unsafe abortions, RTI and STI, all combine to keep the maternal mortality ratio in India
among the highest globally.
17. Maternal mortality is not merely a health disadvantage, it is a matter of social
injustice. Low social and economic status of girls and women limits their access to
education, good nutrition, as well as money to pay for health care and family planning
services. The extent of maternal mortality is an indicator of disparity and inequity in
access to appropriate health care and nutrition services throughout a lifetime, and
particularly during pregnancy and child-birth, and is a crucial factor contributing to high
maternal mortality.
2. Convention on the Elimination of all forms of Discrimination Against Women
India has been an active party in the formulation ofand a signatory to this UN Treaty in
1979. It has also ratified this treaty in the Parliament in 1993, thus taking upon itself the
voluntary responsibility to ensure the following:
CEDAW Article 12 (2):
State parties shall ensure to women appropriate services in connection with pregnancy,
confinement and the post-natal period, granting free services where necessary, as well as
adequate nutrition during pregnancy and lactation
General Recommendation 24 [Article 12 (2)]
26. Reports should also include what measures state parties have taken to ensure women
appropriate services in connection with pregnancy, confinement and the post-natal
period. Information on the rates at which these measures have reduced maternal mortality
and morbidity in their countries, in general, and in vulnerable groups, regions and
communities, in particular, should also be included.
27. Stat^parties should include in their reports how they supply free services where
necessary to ensure safe pregnancies, childbirth and post-partum periods for women.
Many women are at risk of death or disability from pregnancy related causes because
they lack funds to obtain or access the necessary services, which include antenatal,
maternity and postnatal services. The Committee notes that it is the duty if the State
parties to ensure women’s right to safe motherhood and emergency obstetric services and
they should allocate to these services the maximum extent of available resources.
General Recommendation 24
31. State parties should also in particular
(e) Require all health services to be consistent with the human rights of women, including
the rights to autonomy, privacy, confidentiality, informed consent and choice
3. Concluding Comments of CEDAW Committee to Government of India Baseline
Report of 2000
The Committee notes with concern that maternal mortality rates ... are among the highest
in the world. (Para 49.)
The Committee urges the Government to allocate resources from a “women’s right to
health” perspective ... (Para 50)
Understanding Female Feticide
Save the Girl Child
Understanding Female Feticide
Issues and Concerns
Backdrop:
In India, right from her birth, a girl child is treated by the society, including her parents as a burden
because of various traditional belief and misconceptions of the society. The reaction of the family
members is different towards the girl’s rights right from the birth. Often, the girl is bom and
brought up in an atmosphere where the family would have rather preferred a boy in her place. This
attitude ofacceptance to large extent affects her existence. Those who survive are also discriminated
against and neglected in numerous ways.
The bias is rooted in a complex set of religious, economical, social and cultural factors. The degree
of bias may vary but it definitely exists at various levels at different stages in girl’s life affecting the
fundamental rights of the girl child to survival, development, protection and participation. The
mortality rate ofyoung girls of different age groups is much higher than young boys because of the
preference for male children, resulting in the neglect of girl children. The hatredness towards a girl
child has grown up so much and brought into the system of eliminating the girl child - the vulnerable
and unwanted gender, in the womb, before she sees the world. The sex ratio is already precarious
owing to the discrimination against daughters. Abortion of unborn daughters is bound to accelerate
the downward slide of female along the demographic ladder.
Thus, in our society where systematic neglect and discrimination against daughters and ‘son
preference’ attitude are so deep-rooted, the very birth of the girl children and their survival are at
stake leading to declining sex ratio. The pathetic situation is that women are forced to endanger
their own species either in the womb by practicing female feticide or at birth by practicing female
infanticide or after birth by way of neglect. This also indicates the denial of women’s reproductive
rights as human rights, which recognises that personal freedom and social entitlements are essential
to the advancement of human welfare. It is a very denial of women’s right to control their own
fertility, their own lives, their reproductive freedom to have children when they want, to be confident
thstt they will survive and to avoid unwanted child being.
Though the practice of killing female child soon after birth has existed in certain pockets of our
country and more in particular communities, female feticide - the practice of silent killing of female
fetuses in womb is wide across regional boundaries and castes.
CASSA
Technologies and declining child sex ratio:
Amniocentesis, Sex Determination Techniques arrived in India in 1975 primarily for the determination
of genetic abnormalities. Soon it came to be used more commonly for sex determination, leading
to sex selective abortions. In Bombay alone, 258 private centres for amniocentesis have sprung up
in short period, and 16 government-supported clinics provide the service as well, where the abortion
of female fetuses is on high as 99 per cent. Portable ultrasound units are more available in some
areas. Out of 8000 abortions preceded by amniocentesis in six hospitals in Bombay, as many as
7999 were female fetuses. It is estimated that between 1978 and 1982, there were over 78000
cases ofamniocentesis followed by abortion of females in India as a whole. However, these techniques
came to be widely used to determine the sex of the fetus and subsequent abortions if the fetus was
female. In view of the widespread misuse of this technique, an official directive was issued to the
government hospitals to prevent such misuse for sex determination. This led to the commercialisation
ofthe medical technique as private clinics mushroomed across the country. Sex determination
became a booming business in north and west India. There were a wide publicity that read “Spend
Rs.500 now and save Rs. 50000 later”.
In Tamil Nadu, ultrasonogram became a booming business. This technology is blatantly misused as
sex determination test. Many medical practitioners, in breach of professional ethics are unduly
tempted by the prospect of a lucrative business, have indulged in indiscriminate termination of
pregnancies. The invention and invasion of medical technologies even at the rural level has lead to
adverse sex ratio against females. This is a serious threat as there is a deliberate neglect / negation
on the part of the State as it silently permits this genocide by some medical practitioners using pre
natal diagnostic techniques such as ultrasonogram for profit motives. For a long time, the State
thought that it had no role or responsibility to stop this practice.
People’s Campaign for regulating the misuse of the Medical Technologies that were used as
sex determination test:
In 1982, an error in sex determination diagnosis at the New Bhandari Hospital of Amritsar resulted
in the abortion of a much-wanted son of an influential family. A controversy erupted which
snowballed into a major national issue.
Genesis of the Campaign at the National-level:
In 1986, Forum Against Sex Determination and Sex Pre-selection (FASDSP), a social action group
based in Mumbai, made a systematic attempt to initiate a campaign on the issue, thus pressurising
the Maharashtra government to enact the first ever law on the issue in India. The government
responded to the public pressure by enacting the Maharashtra Regulation of Pre-natal Diagnostic
Techniques Act, 1988. Then the Haryana Government passed similar legislation for its state.
2
As these test were very popular in Gujarat, Madya Pradesh, Uttar Pradesh and other States, a
nationwide campaign was launched by FASDSP against the abuse of sex determination and sex
pre-selection test. The nationwide support had resulted in the appointment of an expert committee
by the union government. The committee had after detailed dialogue and debate drafted a central
bill (The Pre-natal Diagnostic Techniques ((Regulation and Prevention of Misuse)) Bill, 1991) and
submitted it to the union government along with the detailed report and it became an Act in 1994.
The Central legislation titled “The Pre-natal Diagnostic Techniques (Regulation and Prevention of
Misuse) Act 1994” came into force since 1st January 1996.
Sex Determination Test:
The three major pre-natal diagnostic test that are being used as sex determination test are as follows:
1. Amniocentesis
2. Chorionic villi biopsy
3. Ultrasonography
1. Amniocentesis:
Amniocentesis is an embryo pre-natal test by which certain genetic defects and the sex of the
unborn baby can be determined. It is a procedure in which 15-20 ml of amniotic fluid is taken out.
The genetic disease or defect can be ascertained or analysed by chromosomal studies. The process
can be performed between 14 to 16 weeks of pregnancy and has nearly 1-2 per cent risk of abortion.
For accurate determination ofthe sex, the cells have to be cultured for 3 weeks, else inaccuracy rate
is 10-20 per cent. It is a useful tool to detect fetal abnormalities such as mongolism, haemophillia,
retarded muscular growth, Rh incompatibility and other gender related disorders. This test is
normally used for women after 35 years of age when the incidence of Down’s Syndrome babies
and deformed children increases.
2. Chorionic villus biopsy:
This test can be performed in the first 7-11 weeks of pregnancy. A plastic canula is passed through
cervix upto amniotic sac and a few chorionic cells, which occur at the site of future placenta,
surrounding the sac, are aspirated under ultrasound vision. These cells are cultured in a specific
solution. This technique is used to diagnose some inherited diseases such as thalassaemia, cystic
fibrosis and muscular dystrophy etc. These diseases affect tissues and organs, which develop after
the first few weeks. It is also possible to diagnose the congenital defects in an unborn fetus.
3
3. Ultrasonography:
Ultrasonogram is the most commonly used test under ultrasonography It is an imaging technology.
It is a non-invasive technology. This technology uses the ‘echo’ of sound waves to ‘visualise’ the
form of the fetus in the womb as early as from 11 to 14 weeks after conception. Through
ultrasonography, it is possible to diagnose 50 per cent of the abnormalities related to the central
nervous system. This technology has gained immense popularity in Tamil Nadu, to determine the
sex ofthe fetus. If the fetus is female, a second trimester and even third trimester abortion is carried
out either by a doctor or by a quack. The chance of correct prediction is 95 to 96 per cent depending
upon the expertise of the ultrasonologist. As pregnancy advances, the chance of accuracy also
increases.
After effects of these test
Amniocentesis:
The test procedure may damage the fetus and placenta resulting in spontaneous abortion and
premature labour.
■
■
The test procedure may also lead to hip dislocation and respiratory complications.
Infection which may lead to acute or chronic pelvic inflammation
■ Bleeding during and after abortion, leading to anaemia
■ Pulmonary embolism which may lead to death
■ Needle puncture mark on baby
■ Hip dislocation
Chorion Villous Biopsy:
■ Spontaneous abortion (4 to 12 per cent)
■ Wrong diagnosis (4 to 6 per cent)
■ Infection
■
Limb defects
■
Growth retardation of the fetus due to bleeding at the site of biopsy
Ultrasonogram:
The margin of error in the case of sex determination though small leads to sex selective abortion
regardless of the accuracy of sex determination.
Sex Selection Techniques:
X-Y Separation:
The various methods currently in use for X-Y separation are:
1. Ericsson Method
2. Albumen Column
4
3. Percoll Gradient
4. Sephadex Column
5. Modified Swim Up
6. Flow Cytometric Separation
After separating X and Y chromosome carrying sperms, the Y chromosome sperms are injected
back into the uterus to ensure that a boy is conceived. The success rate of this method is 65-70 per
cent.
The Pre-implantation Genetic Diagnosis (PGD):
As early as three days after fertilisation, one or two cells are removed from an 8-10 celled embryo
and tested. The selected embryo is then re-implanted into the uterus. The success rate is about 90
per cent for couples wanting girls and 70 per cent for those wanting boys.
Risk Factors Associated with Abortion:
Sex Selective Abortions are generally second trimester abortions as the sex ofthe unborn is known
late. In India, inspite the fact that abortions are legal, it is said that 20,000 deaths per year take place
as result of abortions alone in India and 100 fold have long term morbidity. According to Indian
Council of Medical Research, risk of maternal mortality is more than 10 fold, even if they are done
by experts in government approved institutions i.e. 26/100000 first trimester abortions, 322/100000
second trimester abortions.
Psychological problem, perforation of uterus, cervical tears, septicaemia, haemorrhage due to
incomplete abortion or injury, chronic pelvic inflammation, shock due to haemorrhage, trauma or
septicaemia, infection, infertility and even death are some of the abortion risks.
Situation in other countries:
As a result of selective elimination of female fetuses, the demography is massively effected. As
opposed to the normal birth ratio. South Korea has a ratio where male births exceed female births
by 14 per cent because of the differentially meted out abortions. China has a sex ratio of 944.
Because of‘One Child Policy’ imposed by the Chinese Government, there is a skewed sex ratio at
birth. The sex ratio at birth was 885 females for every 1000 males. The practice of prenatal sex
identification, primarily through the use of ultrasound but also through amniocentesis and chorionic
biopsy, has resulted in the abortion of many female fetuses. 97.5 per cent of all aborted fetuses in
the country are female.
5
Legislative provisions that can be used to curtail Sex Selective Abortion:
The Medical Termination of Pregnancy Act, 1971:
Ifthe very purpose ofthe PNDT Act is to regulate all the pre-natal diagnostic techniques and for the
prevention of the misuse of such techniques for the purpose of pre-natal sex determination leading
to female feticide, then PNDT Act should be read with Medical Termination of Pregnancy Act
1971.
The MTP Act Specifies:
1 The conditions under which a pregnancy can be terminated
2. The person or persons who can perform such termination
3. The place where such termination can be performed
The conditions under which a pregnancy can be terminated:
■ Medical: Where continuation of the pregnancy might endanger the mother’s life and cause
grave injury to her physical or mental health
■
Eugenic: Where there is substantial risk of the child being bom with serious handicaps due to
physical or mental abnormalities
■
■
Humanitarian: Where pregnancy is. the result of rape
Failure of contraception
The person or persons who can perform such terminations:
The Act provides safeguards to the mother by authorising only MDBS doctors having experience
in gynaecology and obstetrics to perform abortion where the length of pregnancy does not
exceed 12 weeks.
■
Where the pregnancy exceeds 12 weeks but is less than 20 weeks, the opinion of two Registered
Medical Practitioners is necessary to terminate the pregnancy
■
Where the pregnancy exceeds 20 weeks, it cannot be terminated except in cases where it is
immediately necessary to save the life of the pregnant woman
All MBBS doctors have to obtain a certificate from the Chief Medical Officer of the district
before performing MTP, otherwise it is considered illegal.
The place where such termination can be performed:
The Act stipulates that pregnancy shall not be terminated at any place other than a hospital established
or maintained by the Government or a private place approved for this purpose (MTP) by the
Government.
6
$
&
Penalties:
Conducting an abortion is punishable with
7 years imprisonment unless done in good faith to save the life of the mother
10 years imprisonment if
1. done without consent of the woman
2. the woman dies while inducing abortion
Also, the Act provides for 10 years imprisonment for
1. doing an act intended to prevent a child being bom alive
2. causing the death of 4 -5 months unborn child
Pre-natal Diagnostic Techniques (Regulation and Prevention of Misuse) Act 1994:
The main purpose of this Act is to regulate the use ofpre-natal diagnostic techniques and to prevent
the misuse of such techniques for the purpose of pre-natal sex determination leading to female
feticide.
The salient features of the Act:
> The Act compels the regi stration of all pre-natal diagnostic centres.
> The Act bans the use of medical techniques for the determination of sex of the fetus.
> The test can be conducted only in the registered pre-natal diagnostic centres.
> The test can be administered only by the trained professionals having prescribed qualifications.
The Act bans the advertising of the availability of facilities for pre-natal sex determination.
> The Act lays down that the pre-natal diagnostic test can be used only for detecting specific
>
conditions, under any one of certain given circumstances, like:
■ The age of the pregnant women should be above 35 years.
■ She must have had a history of two or more abortions or fetal losses
■ She must have been exposed to potentially teratogenic drugs, radiation, ]infection or
■
chemicals.
There must be a family history of mental retardation or physical deformities such as
spasticity or any other genetic disease
> The pre-natal diagnostic test should be administered only to detect the following abnormalities:
• chromosomal abnormalities
•
•
•
•
genetic metabolic diseases
haemoglobinopathies
sex-linked genetic diseases
congenital abnormalities
7
>
The side and after-effect of such pre-natal diagnostic procedures should be explained to the
pregnant woman concerned.
>
The test cannot be performed without the written and informed consent of the mother.
> A copy of her written consent obtained should be given to her.
>
The sex of the fetus should not be disclosed to the pregnant woman concerned or her relatives
by words, signs or any other manner.
Penalties:
Medical professionals who conduct pre-natal diagnostic techniques are subjected to supervision
and defaulters of the provision of the Act are liable for imprisonment from 3 months to 3 years and
fine of Rs. 1000/-, Rs. 10,000/-, Rs. 50,000/- for various categories of offences mentioned below:
•
Disclosing the sex of the fetus
•
Compelling the pregnant woman to undergo these techniques to find out the sex ofthe
fetus.
•
Advertisement regarding facilities of pre-natal determination of sex of the fetus.
•
Misusing the pre-natal diagnostic techniques contravening sex
Different Monitoring Mechanisms of the Act:
Central Supervisory Board - It is a 23 members forum, the functions of which are to advise the
Government on policy matters relating to use of pre-natal diagnostic techniques; to review
implementation of the Act and the rules made thereunder and recommend changes in the said Act
and Rules to the Central Government; to create public awareness against the practice of pre-natal
determination of sex and female feticide; to lay down code of conduct to be observed by persons
working at Genetic Counselling Centres, Genetic Laboratories and Genetic Clinics.
Appropriate Authority at the State-level - Director of Medical and Rural Health Services. The
functions of the Appropriate Authority are: to grant, suspend or cancel registration of a Genetic
Counselling Centres, Genetic Laboratories and Genetic Clinics; to enforce standards prescribed for
the Genetic Counselling Centres, Genetic Laboratories and Genetic Clinics; to investigate complaints
of breach of the provisions of this Act or the rules made thereunder and take immediate action; and
to seek and consider the advice of the Advisors’ committee on application for registration and on
complaints for suspension or cancellation of registration.
Advisory Committee at the State-level - It is a eight member body
Appropriate Authority at the District Level - Joint Director of Health Services in each District.
8
Key issues for discussion
Implications of decliming sex ratio:
1.
If the population of women decreases, it will have for reaching consequences. The society that
treats women as mere sex objects will not treat women in a more humane way, ifthey are scarce in
supply. On the contrary there will be increased incidences of rape, abduction and forced polyandry.
I.
Lack of food economic security clean drinking water and safe clinical facilities have led to a situa
tion where a woman has to have 6.2 children to have atleast one surviving male child. Howmany
abortions during 16-18 weeks can a woman bear without jeopordizing her health.
3.
Under the guise of sex choice woman are exacerbating their own oppression. Moreover this sex
choice is envisaged within the matrix of patriarchal society & it can be another way of oppressing
woman.
4.
Through social consequences of sex selection as well as sex determination tests, ther reality shatters
the myth of neutrality of science and technology.
5.
Class, race sexbiases ofruling elites have crossed all boundaries. After 53 years of socialist recon
structions sex determination for female extermination have gained ground after governments adop
tion of one child policy. This shows how adaptive the system of patriarchy & male supremacy is.
6.
Women’s political participation & her participation in all decision making bodies will be further
marginalised in a patriarchally construct state.
7.
Women are the primary source of social and biological reproduction. When this very resource is
exploited and destroyed (femicide) her under valued / unrecognised contribution to be national
economy will be more.
8.
Advocates ofpopulation control will continue cashing as socio cultural values that treat the birth of
a daughter as a great calamity and perpectuate modem methods (including sex preselection tech
niques) of massacure of features as a massive scale.
9.
It only shows the failure as the party of state that would reorganize and nurture the fundamental
equality between men and women through its policy imbalances and programmes and which was
guaranteed under the constitution of India.
10. Media : Both Print & Electronic media uses the sexist language. Sexist language is a symbolic
device that limits the activities of one sex but not those same activities of the other. Sexism in
language allows an ideology to legitimize the prescriptions and appraisals of every human endeav
our solely on the basis of gender.
11.
The powerlessness women experience in the present era can be partially attributed to the stereo
typing of role, portraying women as sex objects as commodities by the media esepecially the global
media for the global consumer and the industiy the women become categories classifiable by their
face and colouring concepts of female passivity and male sexual activity continue to pervade much
social life and the tendency to categorize women in terms of tlieir sexual availability to men is not yet
altered.
In conventional parlance, the cunent era in history' is generally characterized as one of globalization
technologies revolution and democratization. In all these three areas, media and communication
play a central perhaps even a defining role. Economic and cultural globalization arguagally would be
impossible without a global commercial media system to promote global markets and to encourage
consumer values.
Q
Issues of Concern :
The advertisements, the serials & coverage about any women s issue usually present women s
situation as static and inevetable. The women are shown as passive child like victims completely crushed
by the weight of the circumstances and unable to understand what is happening. They themselves seem
to be the problem, as though it is the women’s own inadequacy which makes her axious and depressed,
rather than the fault of existing gender division of labour and gender based values and the patriarchal
construction of family and state and community.
According to the present image portrayed by the media, it is something to do with her personal
and no political action to change things.
The publication of ad’s such as do you want a boy, spent Rs. 150, you can save Rs. 1,50,000
later are quite insulting demeaning and embarassing women.
The sex preselection tests has been advocated as media achievements of science. But the same
microsoft techniques is converted in India to eliminate feminive gender.
Media hardly tries to link science and technology and cultural meeting. They never give the other
view that now these technologies are used to appress women. More importantly how these technologies
are used to eliminate the weaker races. The racist & sexist ideology try every scientific innovation or
technology should be clearly articulated and put to public debate. Most important the last but the con
cern from the media is the absence of political position regarding women s issues. Especially her \ eiy
right to life and survival. No paper has issued any editorial for the decliming child sex ratio, disincenth e
policies of every welfare scheme for woman, National population policy etc.
When India is a party to CRC convention the very local question before us is to do we need
prenatal diagonostic techniques at all? Why don’t we advocate the state & society to accept children
with deformities. Are we not promoting the racist and sexist technologies by the imperialist nations?
What is the position of media in all these issues.
Mostly media has confined women’s problems to seperate programs or separate papers ot the
news paper. By doing so, it has isolated them from mainstream problems and their assigned them a low
social value. Portraying women as equals is a subject that has been given low priority.
Conclusion: While we have raised several areas of concern to before the media group we also
acknowledge the fact the media is the one which has brought the attention of state and public about the
incidence and intensity of these violences against women namely sex selective abortions. Our onl\ ap
peal before the media is to ethically take a political position to protect the right of a girl child, very right
to survival and life and promote women’s rights as human rights.
10
A Perspective Paper on
Understanding Female Infanticide and Feticide
Backdrop:
Gender violence is a phenomenon that exists in all cultures. The direct pattern of
violence on women within the family and work place are in the forms of physical
attack, brutality inflicted on women by marital partner and family members,
suspecting the wife's fidelity, squandering the meager earnings on alcohol, dowry
harassment, rape, molestation, eve-teasing kidnapping etc. According to the
figures released by the National Crime Records Bureau, a rape is committed
every 54 minute, a kidnapping every 43 minute, a dowry death every 102 minute,
eve-teasing every 51 minute, and an act of domestic violence every 7 minute.
The magnitude of the problem can be gauged from the fact that for every case
reported, hundreds go unreported.
*
There is yet another pattern of violence, the violence constituted by violation of
rights or denial of rights that often operates not only on personal but societal and
cultural levels. The present system is so oppressive to women. Men, women
and society as a whole act to perpetuate the system that results in various forms
of abuse. Thus women are victimized from different dimensions. All these
victimisation are manifested in different forms like subordination and extreme
forms like suicide, female infanticide and feticide.
Globalisation and the modernisation fo economy are not serving as an
emancipating force but as a further means of patriarchal control. The
globalisation injected materialistic and selfish values.
The unsustainable
development as a result of globalisation, policies of structural adjustment and
liberalisation victimised women leading to feminisation of labour and feminisation
of poverty.
If we analyse the complex aspect of the role of women in female infanticide, it is
quiet apparent that they actually inflict violence upon themselves as forced by the
patriarchal values. They internalise the gender bias in favour of male children as
imposed by societal, cultural and political forces. Eventually they resort to the
heinous practice of female infanticide and feticide in secret at the cost of
endangering their physical and psychological health. The following analysis on
the profile of the victims of female infanticide will enable us to draw insights in
understanding the issue and the possible strategies to address the same.
Analysis of the Profile of Victims of Female Infanticide and Feticide
Analysis of 28 cases who depose before the jury team:
1. Nature of the Violence vs No. of families
Nature of Violence
No. of families
Female Infanticide:
1. Case filed
14
2, Case not filed.
5
Female Feticide
4
Surrendering in cradle
baby scheme
5
In reality feticide is more practiced than infanticide. As there is no evidence in
the case of feticide, it appears that the cases of infanticide .is more.
2. Caste vs No. of families victimised
I
i
Caste
Families
BC / MBC
19
SC
9
Caste:
According to Athreya and Chunkath (1999) the female is treated as an
endangered sex in all agrarian, castes-landlord. peasant or labourer-practise.
The analysis of the 28 cases reveals that the incidence is more in the most
backward communities (19) than the dalit communities. Though the practice of
female infanticide may have been initiated in caste which have numerical and
social dominance, it now appears to cut across caste.
It is very likely that the practice of female infanticide by thedominant/landlord
caste of the local community serve to legitimise and provide social sanction to
the practice and contributes substantially to its spread amongst all castes.
(Athreya 1998)
2
3. Occupation vs No. families victimised
Occupation
Families
Agriculture Work
Agricultural Coolie
10
Petty business
Quarry Worker
Kiln Chamber
T
T
T
T
T
Domestic Work
Worker in unorganised
sectors
The practice is high in agrarian families (19). The incidence of female infanticide
has now probably spread to more other occupational groups from agrarian
families which are the core-area.
4. Birth order of the child killed vs No. of families victimised
Birth order of the child
Families
Second child
6
Third child
8
Fourth child
4
Fifth and higher
10
Studies show that the birth order of the girl child seems to have a considerable
bearing on female infanticide. The study conducted in K.V.Kuppam block in
Thiruvannamalai district of Tamil Nadu showed that out of the total cases of
female infanticide discovered, only one involved a first born daughter. The
pattern seems to correspond to 'the parity-specific female child neglect’ common
in North India. Thus most of the victims are daughters who have a birth order
greater than one and a surviving older sister. According to the Birth Order in
selected Health Unit Districts like Dharmapuri, Madurai and Dindigul in Tamil
Nadu (1995), out of the total cases of female infanticide discovered, the
elimination is more as the birth order increases. The third child in most cases is
eliminated. Of the 28 cases documented, the child is eliminated when the birth
order is more than one.
3
5. No. of children vs No. of families victimised
Children
Families
1 Girl
5
~1 Boy
7
7
7
7
T
2 Girls
3 Girls
1 Girl + 1 Boy
2 Girls + 1 Boy
3 Girls + 1 Boy
3 Girls + 2 Boys
4 Girls + 1 Boy
3
7
7
Our study revealed that one of the precipitating factors for female infanticide was
the number of girl children in the family. Since, the status of daughters is viewed
as a financial burden in the context of deteriorating economic condition the
women are forced not to have daughters so that their daughters don’t have to
share their fate, which is an act of self-negation.
6. No. of Women underwent permanent sterilisation vs No. of families victimised
No. of Women underwent
permanent sterilisation
Soon after killing of the
female infant________
After judicial intervention
Families
After giving birth to another
child
Women do not underwent
sterilisation
5
6
2
15
In the eventuality of giving birth to female babies and eliminating them 13 victims
had gone for sterilisation. There are 15 women still in the desire of getting a
male child. This data only attempts to prove the denial of rights to women’s bodv
and sexuality.
7
1. Complainants vs No. of families victimised
Complainants
Families
Public who witnessed the
killing_______________
VAO
9
Relatives
1
NGOs
2
Health workers
1
1
VAOs and NGOs seems to be the watch dog for the incidents.
8 Details of accused vs No. of families victimised
Accused
Mother_____________
Father______________
Mother and Father
Mother, Father and
Mother’s side members
Families
. 2
2
5
5
9.Details of charges vs No. of families
Sections
Families
302 IPC
9“
302, 201,202, 34IPC
3
315,201 IPC
2
10. Details of position of the case vs No. of families victimised.
Present position of the
case
Families
Bailed out
12
Conditional bail
2
Imprisoned and bailed
out on condition and
filed appeal petition
Case under trial
2
3
11. Effect of legal action vs No. of families victimised.
No. of families
Female Infanticide
Female
Surrend-
Cases
Cases not
Feticide
ering in
filed
filed
Disturbed at the psychological I
level_____________________ |
Suicidal thoughts
14
5
4
5
Suicide attempts
1
Conflict between spouses
10
4
2
2
Conflict between spouses and
in-laws_____________
Separation between spouses
11
Indebtedness
13
Criticism in the community
13
2
2
1
Physical ailment
11
7
2
2
Children left uncared
10
School dropouts
3
Disability in academic
activities
9
Effect
Cradle
10
1
1
Status of the cases:
■
In 12 cases, mothers are both exclusively and jointly victimised. In 12 cases,
the father is both exclusively and jointly victimised. Five of the cases are filed
in the name of members of the natal family of the mothers.
■
In 12 cases the victims were released under bailln two case, the victim was
convicted and released under conditional bail after 8 months imprisonment.
In one case, the victim is under imprisonment. In three cases the case is
pending before the Sessions Court.
Impact of judicial action against the victimised families:
°
One family has been displaced
Conflict between spouses is seen in18 cases, conflict between spouses and
in-laws are observed in 12 cases. Out of 12 families, in three families, the
children had become drop-outs. In 9 families there is a disability inacademic
activities of the children.
6'
■
Suicidal tendency is seen in all the 10 cases of female infanticide and 1
women has attempted suicide.
■
All the 28 families are in chronic depression and anxiety.
■
In 10 families the children remained as orphans when their parents were in
judicial custody.
■
13 families are indebted.
Denial of human rights to the girl children of the victimised families:
■ The girls of the victimised families pay the heavy penalty and labelled for
being a member of penalised families. They are forced to face very difficult
circumstances especially when the parents are under judicial custody. The
universally acknowledged repository of caring and security, the family has
proved to be a physically, psychologically and sexually threatening
environment for the growing girls.
■
Education has become an expendable option and they are forced to have
lesser entitlement to care and attention. Their childhood is crowded with
domestic chores and the self-image the society creates for her is one of the
worthlessness, servitude and dependence.
■
The young girls’ prospect for all round development is severely constrained.
■
Societal discrimination and neglect override on the vulnerability of the children
can initiate a life-long downward spiral of deprivation and exclusion from the
social mainstream.
■
The labelling has negative implications for her marriage, physical mobility.
The psychological scars left in the minds of these girls adds to their self
negation. They are victims of extortion and additionally they are tormented
and terrorised by the anti-social elements and their own relatives. The odds
staked against them are too many to oppose single handedly. They also
experience some type of psychological distress in the aftermath of crime.
Immediate reactions are fear, anger, shame, self-blame, helplessness and
depression.
Long term reaction can include sleeplessness, loss of
concentration and fear of being alone. Though they resent their situation,
they are forced to sell their labour to meet the basic needs of the family. So
even after the release of the victims from the judicial custody, they continue to
work as labourers.
■
In this context, how are going to rectify the situation. The real pathology lies
with the criminal justice systems which bent upon punishing the already
victimised victim (mother of infant girl). So, whole criminal justice system
needs through review in favour of mothers. It should uphold the rights of
victim to represent herself throughout the case starting from FIR to trial. And
also, Judges should be sensitised about the victims’ perspective.
^7
Statistical Highlights:
Dharmapuri, Salem, Namakkal, Theni and Madurai Districts are the black-listed
districts for the practice of female infanticide. Mushrooming of scan centres in all
these districts have replaced the intensity of practice of female infanticide to
female feticide. According to the Census for the year 2001, Dharmapuri, Salem,
Namakkal and Theni have juvenile sex ratio below 900. Thus, to understand the
trend of such practice in these districts, the data of Sex Ratio at Birth and IMR
Gender Differentials are analysed. The datum is presented in graphical forms.
Inferences:
In all the six districts, the sex ratio at birth continuously decreases each year from 1996 to
2001. Though the practice of female infanticide still continue in all these districts as the
IMR is still considerably high for girl children, There is neither a steady increase or
decline in IMR Gender Differentials.
Inferences - Theni District:
■ It is evident from the above table that the sex ratio at birth for the year 2001 2002 as compared to the period 2000 — 2001 shows an alarming decline.
■
There is a declining trend in sex ratio at birth in 16 PHCs.
■
The difference fall off by more than 100 in 9 PHCs.
■
The decrease is higher in Odaipatti PHC (343). ie. the ratio fall off from 1073
in 2000 to 729 in 2001.
The sex ratio at birth is lowest in Erassakkanaickanur, that is 679, for the year
2001.
Only in 5 PHCs the sex ratio at birth is higher than the biological sex ratio at
birth of 971 female infants for every 1000 male infants, during the period 2000
and 2001.
■
■
■
In Rajathani and Theni Primary Health Centres, the sex ratio at birth
increases and the data shows that the practice of female feticide is wiped out
in these areas.
■
7 PHCs such as Devaram, Chinthalaichery, Odaipatty, Mottur, Dombuchery,
Devathanapatti and Genguvarpatti could be noted as high risk prone areas as
both the practice of female infanticide and female feticide is getting intense.
Similar trend is observed in other black-listed districts such as Madurai,
Salem, Namakkal and Dharmapuri.( Refer the enclosed data)
Inferences for other districts:
Thiruvannamalai and Trichy:
In the case of both Trichy and Thiruvannamalai both Sex ratio at Birth and IMR
Gender Differential show a negative trend only in few selective blocks. The
reasons need field-level investigations. But depending upon the incidence and
intensity of these few blocks, the overall ratio of the districts varies. The
difference between these districts and black-listed districts is that the
phenomenon is more or less seen in most of the blocks with regard to black
listed districts where as it is restricted to few blocks in the former districts.
Issues:
1. With regard to female infanticide, the government is concerned with Salem,
Dharmapuri, Madurai, Namakkal and Theni. But we have strong evidence to
prove that the prevalence is not restricted to these districts alone. Keeping
IMR Gender Differential as indicator, the prevalence is observed in districts
like Trichy, Perambalur, Thiruvannamali, Karur, Viluppuram, Vellore, Erode
and Dindigul. In all these districts, IMR Gender Differentials show a negative
trend. So from the core-area, it is now spreading to the peripherals. How the
State is going to view the incidence in other districts.
2. It is a myth that the prevalence of infanticide is restricted to certain selective
communities like Vanniyar, Piramalai Kallar and Gounder. From the field
level data, it is proved that it cut across caste. To add to that the practice is
seen in dalit communities too.
3.
It has been argued that the prevalence is restricted to agrarian communities.
The field level data shows that the practice is now spread to other non
agrarian occupational groups.
4. With regard to female feticide, at birth sex ratio is the direct indicator. From
the enclosed data, it is very evident that there is a declining trend in at birth
sex ratio ratio, in districts where there is an easy accessibility to sex
determination. What is threatening us is that the sex at birth shows a
consistent declining trend for a period of 1996 to 2001 in all the black-listed
districts. The unwarranted invasion of medical technologies and unregulation
of private practice and non-enforcement of PNDT Act have ended up in good
number of scan centres. The medical community is a benefactor to all those
who wanted to eliminate their girl children, by doing the sex determination and
sex selective abortion.
5. As the abortion law is liberal and there is no mechanism to monitor the
enforcement of MTP Act, and State’s indirect sanction to use MTP as a tool to
reduce the population size, the sex selective abortion has a legitimate
sanction, indirectly from the State.
-a
6. The State is focussing its attention to the visible form of elimination — female
infanticide. In reality, the real culprit to natal inequality is sex selective
abortion. That does not mean that infanticide is also not a cause. State
allocates budget and advocates programmes only to address the issue of
female infanticide which is evident from the non-inclusion of at Birth Sex Ratio
as a health indicator.
7. With regard to victims, the early marriage, the prevailing economic condition,
increasing newer forms of violence and the consumer cult adds to their
vulnerability. Govind Kelkar argues that violence is an act of aggression
usually in interpersonal interaction or relation. It may also be aggression of
an individual woman against herself such as suicide, sex determination and
female infanticide. It implies that when the body — and indeed the self — is
vulnerable to violation, individual has a very different notion of what is one’s
body and what is done to one’s body.
Given that violence is not limited to
one group, it can be perpetuated by those in power against the powerless or
by the powerless in retaliation against coercion by other to deny their
powerlessness. This is a good analysis to understand the participation of
women in eliminating their own gender.
8. All the victims have experienced inhuman treatment in the sense many of
them have been arrested within few days of their deliveries No post-natal
care was extended to them.
9.
The Court has not taken the cognizance of the mental health of the victims.
To quote, Chinnapappa, Neelavathy and Chinnasamy were arbitrarily
arrested. From our field study, it is proved beyond doubt that all these
persons showed clinical symptoms of depression and with regard to
Neelavathy, she was suffering from postpartum psychosis.
10. Most of them have been charged with IPC 302 which we feel is a greater
punishment for a social offence. They should not be viewed as criminals and
by punishing them, the State is doubly victimising the already victimised
families. The deterrence has ended up in the emergence of new form of
violence namely feticide and it cut across class, caste and other hierarchies.
by JiLr^e^ rDi^cd^ o{ S^D. durbi^ the 7)u^
oryajiiMid bi/ Qiunil QCadu Stale QaniHibsioa far lOoaien in Ohennai on 10th Quhj,
2002.
Demography - Census Statistics and Analysis
n
Survival of the Girl Child
Tunnelling Out of the Chakravyuha
Results of the first population census of the millennium reveal a number of significant changes
in the sex ratio patterns in the country. Firstly, the sex ratio decline among children in the
0-6 age group turns out to be sharper in the urban areas (32 points) than in the rural. Second,
the traditional north-south divide stands significantly modified and the ‘northernisation ’ of sex
ratios is rapidly taking the urban route. The sharp decline in the urban female/male f/m)
ratios among children cannot be explained away by any of the three popular escape hatches of
yesteryears, i e, migration, undercount or biologically ordained high sex ratios at birth.
This decline clearly points to one factor, sex selective abortion or female foeticide that has
gained currency during the 1980s and more sharply in the 1990s.
Satish B Agnihotri
I
bhimanyu, the legendary prince of Mahabharata, died
during the epic war, trapped insidechakravyuha; the
JL jk.wheel shaped formation of the enemy columns. His death
was destined while he was in his mother’s womb. Many an Indian
girl children seem destined to die likewise today and in their case
the chakravyuha has invaded the womb itself resulting in their
death even before they are bom! Provisional results of 2001
Census give rise to both alarm and despair on this score.
How can we begin to rescue the girl children out of the
chakravyuha of sex selective abortions? Do we wait for a ‘revo
lution’, or for that illusive entity called ‘political will’ to be forged
or for the miracle of total enforcement of the PNDT act to happen
or expect a change of heart among the foeticide service providers
who worship profit at all costs?
We first need to.piap the contours of the problem by locating
the ‘epicentres’ of female child deficit. We need next to move
to a mix of possible, even if partial solutions, to mitigate the
situation rather than seeking a blue-print for a perfect solution.
That will be like ‘Waiting for Godot’.
In short term, we need to support and strive for universal
coverage in survival inputs like immunisation, supplementary
nutrition or even birth registration to minimise the gender gap.
As girl children usually face discrimination in accessing these
inputs, universalisation benefits them more. But in the longer
term, we need to create objective conditions so as to minimise
die ‘unwanledness’ of a girl child. This necessitates a modicum
of economic and physical security being guaranteed to women.
At the same time, the civil society must also debate the ethical
dimension of sex-based elimination of a segment of the popu
lation. This could well be the thin end of the wedge that provides
in its wake currency to eliminate other segments of population
based on other criterion. We must also question the current model
of development, where discrimination necessarily appears to
accompany development. Success stories of alternative ‘devel
opment’ must be provided visibility and highlighted as role
models for the society to follow.
Sex ratios in the Indian population are becoming rapidly mas
culine. A marginal increase of 6 points in the female to male
ratios ofthe overall population; 933 in 2001 from 927 in 1991, has
not given rise to much euphoria as it did in 1981 [Chhabra 1981,
A
Economic and Political Weekly
October 11, 2003
Padmanabha 1981] and rightly so. This is because there has been
a sharp decline of 18 points in the f/m ratios among children
(0-6 years) during the same period. This pattern; the RGI warns
us, will continue to haunt the society for decades to come (Paper 1
of 2001), unless of course, corrective measures are taken.
Results of the first population census of the millennium reveal
a number of significant changes in the sex ratio patterns in the
country. Firstly, the sex ratio decline among children in the 06 age group turns out to be sharper in the urban areas (32 points)
than in the rural. Table 1 provides state level data on the changes
in sex ratio between 1991 and 2001 in the rural and the urban
population. It can also be noticed that the decline in urban f/m
ratios among children in most of the states is significantly larger
compared to that in the rural areas.
Above pattern is seen more sharply in the distribution of the
decadal decrease in sex ratios in the rural and the urban areas
in different districts of the country. Figure 1 gives these distri
butions. While the mean decline in rural areas of the districts
is 16, it is as high as 28 in the urban segment. Further, the number
of districts where the f/m ratios have declined by 60 to 100 points,
is much higher in the urban areas.
The second important change is of the breach in the much
written about north-south divide in the sex ratio patterns1 across
the Narmada-Sone or the Bharuch-Chhotanagpur axis. This can
be seen from Figure 2 which maps the urban f/m ratios among
children in 0-6 years age group. Four broad categories of districts
can be identified by f/m ratio; below 865, between 856 and 910,
between 910 and 960 and above 960. Districts in the first two
categories are the ones where the female deficit is strong. These
are no longer confined to the north of Narmada but have moved
considerably southward, making ingress into nearly entire Gujarat,
a number of districts of Maharashtra, and surprisingly, certain
pockets of Orissa. The traditional north-south divide stands
significantly modified and the ‘northemisation’ of sex ratios [a
term used by the Caldwells 1990] is rapidly taking the urban
route. Even the north-east is not unaffected from this malaise,
urban Kamrup that is essentially Guawahati shows a f/m ratio
of 888 for children in the 0-6 years age group.
Sharp decline in the f/m ratios among children in urban areas
cannot be explained away by any of the three popular escape
hatches of yesteryears, i e, migration, undercount or biologically
ordained high sex ratios at birth. Unlike adults, children below
4351
Figura 11 Urban and Rural Daclina in the FMR06 between 1991
and 2001, Diatrictwiee
Rural
200 T"
150
100
50
StdDev>27.22
M*an - 14
ty-568.00
0
o
'<b
%
DIF06R
Urban
2M
—------ r-
150
IM
50
StdDev>40.M
Mean - 28
*
X>
O
%
%
%
%
%N-562 00
DIF06U
Figure 2: Female to Male Ratios (Urban) among Children
(0-6 Years), Census 2001
No X.
data
H Below 865
£ 866 to 910
_ 911 to 960
lj Above 960
|—i Missing
•
—Data
that has gained currency during the 1980s and more sharply in
the 1990s. The sex of the foetus is identified through techniques
ofamneoccntesis or use ofultrasonography. Abortions are carried
out either as an ‘attached’ service’ or independently. Compared
to female infanticide, this became a more acceptable mode of
disposing of the ‘unwanted’ girl child. Infanticide is an overtly
‘barbaric’ practice, carried by non-professional and less powerful
persons, e g, traditional ‘dai’s or an old lady in the household.
It does not allow parents to distance themselves from the event,
i e, killing of the child, and be free of any guilt [McKee 1984].
Sex selective abortion, on the other hand, is carried out by
‘professionals’, superior in the power hierarchy. They use sci
entific techniques, hardware and skills; sanitise the process of
eliminating the foetus and reduce the burden of guilt on parents.
Concentration of medical facilities and professionals in urban
areas, and, more important, their absence from the rural areas
is well known in our society. Naturally, the facilities for sex
selective abortions and other sex selection techniques will be
available in the urban areas first and that is precisely what we
are seeing in the results of 2001 Census.
It is important to highlight here the importance of state specific
analyses of the problem. Many a nuance of the state level decline
are not revealed in the national perspective. This can be elaborated
with the example of Orissa, a state where it was hard to imagine
such widespread decline in sex ratios even ifthe decline is confined
to urban areas. The spatial pattern ofthe decline is shown in Figures
3a and 3b. In 1991, only two districts, Kendrapada and Jagatsingpur
had low frm ratios, 942 and 941 respectively. But in 2001 as many
as 12 districts had frm ratios below this level, lowest being in
Nayagarh (901). The contiguity of these 12 districts is striking;
low f/m ratios show a remarkable cluster and not a scatter.
But the contiguity of districts with very low f/m ratios in urban
population is more disturbing (Figure 4). Three adjoining dis
tricts, Ganjam, Nayagarh and Boudh have f/m ratios (urban)
below 860; a figure comparable to some ofthe districts ofHaryana
and western UP. These are flanked by Kandhamal (896), Angul
(898) and Dhenkanal (902), Khordha (908) and Gajpati (920).
Two districts, Kendrapada (916) and Jagatsingpur (889) are not
contiguous but separated by a strip ofJajpur (926), Cuttack (948)
and Puri (930); even these ratios are not quite high. The belt of
low f/m ratio also stretches along the Bolangir (921), Bargarh
(938) and Jharsuguda (931).
It is plausible to argue that the low urban f/m ratios for the
0-6 age group could also be attributed to statistical fluctuations
due to the small population size. This is especially so for urban
child population of Nayagarh, Boudh and Kondhmal. It is in
triguing however, as to why the ‘fluctuations’ should point in
the same direction. Further, even if we add the urban population
of these contiguous districts, f/m ratios in the 0-6 age group will
remain low. The ‘fluctuation’ argument does not therefore help.
It is possible to take this kind of analysis to sub-district level
and quite fruitfully. This part of the research is currently under
way and is progressing as per the availability of the Census 2001
sub-district data.
I
Source: Census of India.
*
6 years do not migrate sex selectively; urban areas should suffer
much less from undercount than adjoining rural areas and bio
logically, sex ratios at birth cannot become masculine so rapidly.
The rapid decline in the urban f/m ratios among children clearly
points out to one factor; sex selective abortion or female foeticide
4352
How does the lowering of f7m ratios in urban areas affect the
rural segment of the population? It is necessary to study this
pattern and anticipate the changes that are likely to occur. We
have talked of the ‘foeticide service providers’ operating from
the urban centres in the previous section. As their practice and
the profit2 ‘roars’ in the urban area, the doctor-entrepreneur starts
Economic and Political Weekly
October 11, 2003
1 f
Figure 3ai FMR among Children 0-6 Yeare (Girls per 1000
Boys) i Orissa 1991
lUAMKIlANl)
MaywMaaJ
-
Bargark SaatMlpal
‘^Ck^nepar 'k,
Ml
»teaka<
Boadh
BoUnflr
)
>padi
Cattack
Kandhai
j / r.rf
Kalahaadl
N|
941 and below
I
1941 to 980
|
| Above 980
Matkangl
.ANDHRA
PRADESH
Figure 3b: FMR among Children 0-6 Years (Girls per 1000
Boys) : Orissa 2001
JltAKKHANO
;
\
Maywkbaa|
ffSjk z'/
0
Kr-Qte/)
B.Vck\S“U*’
Bate^lr
Kaadha.
Kateteedl
<bSM 941 and below
Rayageda1
Karapaf
^zOfakaacI*
•
/
ANDHRA
J
rttADESH
I
1 941 to 980
I
I Above 980
r- '
r
Figure 4: Urban FMR among Children 0-6 years (Girls per 1000
Boys) : Orissa 2001
Saadargark
niARKIUND
MayarkkaaJ
Keaajhar
Balaa<
Sambeli
■BbaMk'
^Cattack
J
-T-
Kalahandl
Ni
Raya gada'
■■■ 900 and below
■■■ 901 to 920
Karapat
l*5££l 921 to 940
I
I 941 to 980
I
I Above 980
attracting clients from the rural catchment. At the same time, the
number of such ‘service providers’ increases and in many in
stances, they start providing mobile service. Gradually a larger
segment of the rural population starts availing ofthese ‘services’.
As the use becomes widespread the sex ratios in the child
population become more and more masculine in the concerned
area and tell tale signs appear through the sex ratio figures.
High school physics text books describe a phenomenon called
‘sympathetic resonance’. Imagine two cloth-strings on which
clothes are kept for drying. If one string is shaken, up and down
vertically, the other string does not respond initially. If the
oscillations persist, the second string slowly begins to respond.
Gradually its oscillations become comparable to those of the first
string. In the extreme case of ‘coupled oscillations’, it is possible
for a bridge to collapse as soldiers march in unison and the rhythm
of their march coincides with the ‘natural’ frequency of the bridge.
The response of the rural sex ratios to growing masculinity
of the urban sex ratios follows a similar pattern [for details sec
Agnihotri 2002]. Initially these remain indifferent to the changes
taking place in the urban f/m ratios. If we draw a graph showing
the urban f/m ratios on x-axis and the rural sex ratios on the
y-axis, we can expect a horizontal line. This is indeed the case
in most of the eastern and the southern states (with exception
ofTamil Nadu and Orissa), Chhattisgarh and Jharkhand as shown
in Figures 5a to 5i. This pattern has remained the same in these
states for both 1991 and 2001.
In the states where the rural sex ratios have ‘begun responding
slowly’, the line starts sloping downwards. As the urban f/m ratios
decline, rural ratios decline but not very strongly. Bihar, Orissa
and Uttaranchal are examples of such states (Figures 5k To 5m).
In the list of‘strongly responding’ states, the line slopes further
downwards. Here the rural f/m ratios decline quite strongly, say
by 50 to 90 points for a decline by 100 points in urban f/m ratios.
These states are Punjab, Haryana, UP, Himachal Pradesh, Gujarat
and Maharashtra (Figures 5n to 5t). In Himachal and Maharashtra,
the deterioration between 1991 and 2001 is sharp, while in Gujarat
it has been bad in 1991 itself. Rajasthan presents an interesting
case where the situation appears to have improved. But this needs
further and a more detailed look.
Among southern states, Tamil Nadu presents alarming trends
for both 1991 and 2001. Unlike most other states, the rural f/m ratios
among children in a number of districts have been lower than the
urban ratios and have declined faster than the urban ones too.
This analysis will remain incomplete without mentioning the
‘terminal cases’ or districts where rural f/m ratios 06 are signi
ficantly more masculine compared to the urban f/m ratios among
children. Table 2 gives a list of districts where the rural f/m ratios
06 are a) below 920 and b) less than 10 points or more compared
to urban f/m ratios 06. First of the three discernible clusters
comprises of districts from Punjab, Haryana and Delhi along with
Kangra (836) in Himachal and Haridwar (850) in Uttaranchal.
The second cluster is in Bihar comprising of Daibhanga (884),
Sitamarhi (896), Saharsa (897) and Munger (905). The third cluster
is in Tamil Nadu with Salem (763), Theni (873), Namakkal (882),
Dharmapuri (869) and Madurai (903). These districts may have
an earlier history and prevailing pattern of infanticide co-existing
with or replaced by provision of foeticide.
MattuuigiK
y-v/J ANDHRA
PRADESH
>
Note: The boundaries and the names shown and the designations used on
these maps do not itrply official endorsement or acceptance by the
ChitedNations.
Economic and Political Weekly
October 11, 2003
I
The patterns above are linked to a question agitated for some
time now in the received literature. Bardhan (1974) had pointed
out how the relatively poorer regions in the country, e g, Kerala,
4353
Figure 5a
Figure 5e
Child Sex Rat ioo: Andiua: Urban-Rural
Child Sex Ratios: NE: Urban-Rural
1000
1
i
1000
900
6
900
I
I
800
• E
700 4—
700
800 I—
800
1000
900
Andhrat 2001
Andhra 1991
NE2001
A
NE1991
1000
900
800
Urban FMRs (0-6 Years)
Urban FMRs (0-6 Years)
Figure 5f
Figure 5b
Child Sex Ratios: Assam: Urban-Rural
Child Sex Ratios: Kerala: Urban-Rural
-jjj-1000
CD
©
1000
12
CD
0)
>
CD
O
tn
CH
S
CD
o
900
tn
01
y = 0.5838x + 398.31
R2 = 0.34 (1991)
g
800
E 700 4-
2
3
01
01
800 ------800
900
800
700
1000
900
♦ Kerala 2001
—A— Kerala 1991
♦
900
♦ Assam 2001 A Assam 1991
1000
Urban FMRs (0-6 Years)
UrbcnFMRs (0-6 Years)
Figure 5g
Figure 5c
Child Sex Ratios: WB: Urban-Rural
Child Sex Ratios: Karnataka: Urban-Rural
ro 1000
o
2 1000
CD
>
>
CD
O,
900
y = 0.3511x + 628
R2 = 0.22 (1991)
tn
01
S
CD
O
tn
CH
800
900
S 800 —
LL
2
or 700 4—
700
800
1000
900
Karnataka 2001
Karnataka 1991
2
£ 700 700
♦ WB 2001
UrbcnFMRs (0-6 Years)
900
800
1000
Urban FMRs (0-6 Years)
AWB1991
Figure 5h
Figure 5d
Child Sex Ratios: Jharkhand: Urban-Rural
Child Sex Ratios: Chhattisgarh: Urban-Rural
gco 1000
'
2 1100
<D
CD
©
>
> 1000
A 900
2,
CD
O,
900
tn
CH
800
u.
2D 700 4—
D
CH
U.
01
700
♦ Chhattis2001
4354
800 ------
2
800
900
Chhattis 1991
1000
1100
Urban FMRs (0-6 Years)
700 4—
700
♦ Jharkhand 2001
800
a Jharkhand 1991
900
1000
Urban FMRs (0-6 Years)
Economic and Political Weekly
October 11, 2003
I
1 1
S 1000
>
co
o^
co
01
900
Figure 5i
Figure 5m
Child Sex Ratios: Orissa: Urban-Rural
Child Sex Ratios: Haryana • Urban-Rural
21000
co
y = 0.3967x + 587
R2 = 0.31 (2001)
S 800 -
ti
ro
3
01
y = 0.4479x+483.16
R2 = 0.2555
900
y = 0.5581k + 443
o
R2 = 0.26 (1991)
tr 800
co
♦
y=0.6746x+27829
E
700 -I—
R2 = 0.3788
5 700
700
CT
800
900
800
Child Sex Ratios: Bihar: Urban-Rural
>
A
o
900
*2 1000
co
y = 0.2724k + 687
R2 = 0.07 (2001)
▲ i
y = 0.3174k + 649
R2 = 0.14 (1991)
cn
u_
800
y=0.6763k+310
R2=0.51 (2001)
>
o 900
y=0.6494k+320
R2=037(1991)
in
tr
s 800
UE
§ 700 4-
tr 700 4-
(t
700
800
♦ Bihar2001
900
Urban FMRs (0-6 Years)
▲ Bihar 1991
700
800
♦ UP2001
A UP 1991
1000
900
1000
Urban FKf^s (0-6 Years)
Figure 5k
Figure 5o
Child Sex Ratios: Uttaranchal: Urban-Rural
Child Sex Ratios: Himachal: Urban-Rural
~1000
giooo
(0
(D
cc
>
O,
Urban FMRs (0-6 Years)
Child Sex Ratios: UP: Urban-Rural
E 1000
0)
1000
Figure 5n
Figure 5 j
co
900
♦ 2001 Haryana ▲ Haryana 1991
Urban FMRs (0-6 Years)
♦ Orissa 2001 ▲ Orissa 1991
700
1000
900
y = 0.3571k + 572
R2 = 0.28 (1991)
CO
or
2 800
♦
>
Al
LL
co 900
o,
co
a: 800
y= 1.0901k- 28.8
R2 = 0.33 (£001)
# A
y=0.1131X + 852
R2 = 0.03 (1991)
ro
3
or 700 -I—
700
800
900
♦ Uttar. 2001 a Uttar 1991
1000
Urban FMRs (0-6 Years)
E
3
a: 700 4-
700
800
♦ Himachal 2001
A Himachal 1991
900
1000
Urban FM^s (0-6 Years)
Figure 5p
Child Sex Ratios: Rajasthan: Urban-Rural
Figure 51
Child Sex Ratios: Punjab: Urban-Rural
^1000
2
co
CD
900
£ 900
o
co
01
S
E
3
01
_1000
2
y = 0.9173k + 92.6
R2 = 0.70 (1991)
o
>
A
900
CO
gcr 800
800
700 4700
y = 0.9424k + 48.7
R2 = 0.58 (2K1)
800
♦ 2001 Punjab a Rjnjab 1991
Economic and Political Weekly
900
E
cr
1000
Urban FMRs (0-6 Years)
October 11, 2003
A
Ct
A
y = 0.5202k+454.1
R2 = 022(2kl)
700 4700
4 Rajasthan 2001
800
A Rajasthan 1991
y=0.9622k+40.3
R2 = 0.58 (1991)
900
1000
Urban FWs (0-6 Years)
4355
Figure 5q
Child Sex Ratios: MP: Urban-Rural
1000
E?
ro
<D
>
o
900
y = 0.8512x ♦ 165.77
R2 = 0.53 (2001)
= 0.0822k + 868.23
R2 = 0.1281
<n
or
800
O'
700 J—
700
800
♦ MP 2001
A MP 1991
900
1000
Urban FMRs (0-6 Years)
Figure 5r
Child Sex Ratios: Maharashtra: Urban-Rural
"E1000
co
®
y = 0.918x + 97.5
R2 = 0.54 (2001)
>CD
O
CO
Ct
A
900
g 800 -
y =0.3912x + 589
R2 = 0.19 (1991)
1D
(Y 700 -I—
700
900
800
♦ Maharashtra 2001 ▲ Maharashtra 1991
1000
appcar to treat their daughters better that the more prosperous
states in the north-western India. Within a given region too, Miller
(1981) has discussed the differences in sex ratios among the
‘propertied classes’ and others. Most recently, Premi (2001) has
stressed the need to examine as to why the largest decline in the
child sex ratio (0-6 years age group) has occurred in the welldeveloped districts.
At a different level, sociological and anthropological literature
provides many instances of increased female subordination among
the more prosperous groups [e g, Goody 1990; Papaneck 1990;
Berrcman 1993). This leads to unequal access to life sustaining
resources c g, food, nutrition, health care, for the female members
(Dasgupta 1987; Miller 1981 ]. In a harsher manifestation of this
inequality, direct denial of life chances through infanticide or
sex selective foeticide can take place among these groups.
Concerns over the masculinity of sex ratios in the wake of
prosperity at district level is one matter; corroborating this with
quantitative data is another. As the mainstream population census
data did not provide sex ratio data by prosperity level, this
important issue has remained unaddressed in the demographic
literature.
One exception to this trend was Krishnaji (1987) who analysed
the National Sample Survey Organisation (NSSO) data on family
composition and the prosperity level represented by the Monthly
Per Capita Expenditure (MPCE) class. The household consumer
expenditure surveys of NSSO provide data on the composition
of the household in terms of the adult and the child (0-14 years)
population by 12 different Average Monthly Per Capita Expen
diture (AMPCE) classes. As the AMPCE reflects per capita
UrbcnFMRs (0-6Years)
Figure 5a
Table 1« Decline in HGta (Fen&lee per 1,000 sales)
in the 0-6 Year Population, 1991-2001
State
FMR06U01
FMR06R01
FMR06U91
FMR06R91
Decline Dadine
U
R
India
903
Punjab
789
Dadra and Nagar Havel i* 885
827
Gujarat
809
Haryana
935
Daman and Diu*
866
Delhi*
880
Uttar Pradesh
858
Himachal Pradesh
874
Uttararehal
844
Chandigarh*
919
Goa
934
795
995
905
824
920
853
922
900
914
852
948
935
936
977
909
884
996
917
928
904
913
879
953
948
952
1015
937
877
933
900
927
955
898
891
972
32
147
92
81
76
62
51
48
46
39
35
35
14
157
20
32
53
13
48
4
55
-16
39
24
Andaman and Nicobar
Islanfe*
Maharashtra
Bihar
Madhya Pradesh
Nagaland
Assam
Orissa
Rajasthan
Qtstti^axh
Jharkhand
Sikkim
Karnataka
Lakshadweep*
FCndicterr^'*
Tripura
West Bengal
Tamil Nadu
Meghalaya
Mizoram
Andhra Pradesh
Kerala
Manipur
Arunachal Pradesh
976
923
940
941
983
967
954
914
962
973
991
954
1010
971
978
967
931
977
978
965
964
956
957
970
934
950
931
959
955
949
909
960
950
936
951
932
962
959
955
955
968
965
962
958
972
946
973
953
953
944
1001
977
969
919
988
985
967
963
951
963
968
969
945
989
973
979
958
975
986
31
27
26
25
24
24
23
22
19
19
12
12
11
11
11
7
4
4
4
3
-3
30
14
4
17
10
15
4
6
13
-24
9
-59
-7
-10
3
14
Child Sex Ratios: Gujarat: Urban-Rural
*2 1000 <n
<D
>
900.O
y= 0.7472x+275.4
R2 = 053(2kl) 0
y = 0.5412k+440.4
R2 = 022(1991)
V)
tz
S 800
ro
or
700 +700
800
♦ Gujarat 2001
A Gujarat 1991
900
1000
Urban FMRs (0-6 Years)
Figure 5t
Child Sex Ratios: IN: Urban-Rural
^1000
co
<D
o,
y = 1.172x- 180.77
R2 = 0.40 (2001)
i
900 - -
co
S 800 —
uy = 1.3416k -327.85
co
5 700 —
R2 = 0.36 (1991)
700
♦ TN 2001
4356
800
a TN 1991
900
1000
Urban FMRs (0-6 Years)
940
908
924
906
935
931
927
886
941
931
925
939
920
951
948
948
951
964
961
958
958
980
981
Economic and Political Weekly
-8
-35
12
-6
14
-6
19
29
October 11, 2003
I
expenditure, the family size does not affect the measure and it
can be taken as a good surrogate for prosperity.3
Very recently, while all eyes had been fixed on the results of
the 2001 population census for data on sex ratios, NSSO report
on the 55th round reported an important and disturbing
observation. The report (No 457: 17), blandly provides the fol
lowing information (Table A) based on a survey of over 1.20
lakh households in the country (rural 75 per cent and urban 25
per cent);
Table A: Demographic Differences between Lowest
and Highest MPCE Classes
Etpulatim
n-wnyt-pr-i
r
Sex ratio
Sexratio (acblts)
Sexratio (childrm)
____________Rural
Bottom 5
Top 5
Per Cent Per Cent
1005
1067
946
858
873
804
m
941
966
900
___________ Urban
Bottom 5
Top 5
Percent Percent
949
993
903
837
840
819
ffi
900
908
883
Source: Report of the National Sanple Survey Organisation, NSSO No 4 57
Level andPattern of ConsumerExpend! ture in India : 1999-2000.
This information is significant. It shows how masculine the sex
ratios are among the prosperous groups both in rural and in urban
areas. It also points towards a trend of more masculine sex ratios
in urban households compared to the rural households.
Before invoking the escape hatch of migration to explain away
these findings, it will be useful to remember that the sex ratio
among children does not suffer from sex selective migration.
Further, the difference of 142 points in rural and 84 points in
urban households between the bottom 5 per cent and the top
5 per cent of the households is too large to be explained away
by migration. The observed distortion in the sex ratios is clearly
man-made.
Before proceeding further, it is pertinent to look at the sex ratio
figures by the 12 different AMPCE classes. Table 3a gives the
details of the AMPCE classes, number of households surveyed,
mean AMPCE in each class and the sex ratios among these for
the total as well as the child (0-14 years) population in rural areas.
Table 3b gives corresponding information among the urban
households.
A consistent decline in the £7m ratioss (females per 1000 male
population) as one moves up the AMPCE range is clearly dis
cernible. This is so for both rural and the urban households and
for the 0-14 years as well as total population.
Figure 6a and 6b show the relationship between prosperity as
measured by the variable logAMPCE and the sex ratios for total
as well as the 0-14 year age-group population. The two have
strong negative correlation and the relationship between the two
can be expressed as;
f/m ratios(All-age) = 1405 - 175.3 x LogAMPCE (Rural)
Adj R Sq = 0.76
f/m ratios(0-14 yrs) = 1432 - 204.2 x LogAMPCE (Rural)
Adj R Sq = 0.92
The constant term and the slopes are significant at 1 per cent
level and so is the f - value in both the equations.
For urban areas the relationship can be linearly described as,
f/m ratios(All-age) = 1368 - 163.1 x LogAMPCE (Urban)
Adj R Sq = 0.76
f/m ratios(0-14 yrs) = 2188 - 728.5 x LogAMPCE (Urban)
Adj R Sq = 0.65
Once again, the constant term and the slopes are significant
at 1 per cent level and so is the f-valuc in both the equations.
However, as Figure 6b indicates, the relation can more correctly
Economic and Political Weekly
October 11, 2003
TtablaZ: S^xtij/State/OdmTmzltxxry/lJlBtxlct
F/MRatios in the 0-6 Etapulaticn
FMR06R
FMR06U
FMR06T
0-6Rural
0-6 Urban 0-6 (R+U)
2
^tiala
SangiTjr
Rupnagar
Aroala
Rewari
Southwest
Delhi*
South
Sikar
i
Meerut
Mau
Darbhanga
Sitararhi
Saharsa
Manger
Ri^rupur
Jczhat
Sdlakandi
Pxi
Shcpal
Tikangarh
Sclapur
Kashim
Salem
Theni
Kasakkal
ttHTraapuri
Jtadurai
927
929
836
754
770
784
791
784
814
845
865
886
882
876
854
902
897
885
896
900
915
925
901
903
921
931
919
897
921
826
893
896
878
927
903
966
84 9
774
786
798
800
812
830
852
866
888
891
894
861
917
956
906
913
939
948
966
932
959
930
936
939
914
945
910
911
919
928
950
934
911
836
747
764
779
787
772
811
798
853
870
880
873
849
898
883
884
896
897
905
903
895
900
920
916
915
890
917
763
873
882
869
903
Leh (Ladakh)
Kangra
Patehgarh Sahib
Urban06
DiffO6R-U
Percent
22
34
4
28
31
29
30
31
16
86
92
90
19
13
43
22
19
6
5
7
24
35
15
5
12
75
15
29
17
45
54
38
15
53
31
-55
-14
-27
-22
-20
-13
-41
-19
-54
-14
-18
-11
-20
-12
-19
-73
-22
-17
-42
-43
-62
-36
-60
-10
-20
-25
-24
-28
-147
-39
-37
-59
-47
Table 3a: Sex Ratio by MPCE Class, India (Rural) NSSO Survey
Round 55, July 1999-June 2000
PCE
CLASS
0-225
225-255
255-300
300-340
340-380
3S0-420
420-470
470-525
525-615
615-775
775-950
> 950
AMPCE
No of
Hhs
Log
AMPCE
f/mRatio
(0-14)
f/mRatios
PEI)
191
242
279
321
361
400
445
497
567
686
853
1345
2547
2451
5147
5588
5892
5895
6783
6635
8253
9383
5337
7474
2.28
2.38
2.45
2.51
2.56
2.60
2.65
2.70
2.75
2.84
2.93
3.13
946
951
950
925
914
948
895
832
853
820
854
804
1004
990
988
971
946
955
940
904
921
904
908
858
Table 3b: Sex Ratio by MPCE Class, India (Urban) NSSO Survey
Round 55 July 1999 - June 2000
PCE Class
AMPCE
No of
Hhs
Log
AMPCE
f/mRatio
(0-14)
f/mRatios
WD
CO - 300
300 - 350
350 - 425
256
326
389
464
537
619
719
841
1010
1286
1692
3074
1585
1586
3290
3886
3926
4374
4785
5150
5677
6651
3901
4113
2.41
2.51
2.59
2.67
2.73
2.79
2.86
2.92
3.00
3.11
3.23
3.49
903
977
948
894
915
885
875
840
795
798
810
819
949
988
961
941
958
913
896
871
848
815
847
836
425 - 500
SCO - 575
575 - 665
665 - 775
775 - 915
915 - 1120
1120 - 1500
1500 - 1925
> 1925
4357
Figure 6a: Sex Ratio* by Prosperity: Rural India 1999-2000:
NSSO 55th Round
1050
1000
.2 950
& 900
^eso
of rice may have disappeared, can co-exist with strong inequality
in access to protein or more crucially in the access to medical
care. The net result will still be that the survival of the girl child
may get more adversely affected. The NSSO data so far indicates
this to be the case. Finally, it can be shown from analytical
considerations that it is not the prosperity per se, but the female
contribution to prosperity that is relevant in deciding her lot; a
result intuitively obvious to sociologists and anthropologists, but
not necessarily so in economics.
800
750 ------2.00
17
2.20
2.40
2.60
2.80
3.00
3.20
Against this backdrop of despair, how do we rescue the girl
child out of the chakravyuha? Her situation is, to use an analogy
from physics, like that of a particle in a well. Imagine a ball in
Figure 6b: Bex Ratios by Prosperity: Urban India 1999-2000:
a bowl-shaped pit. The walls of the pit provide the barrier that
NSSO 55th Round
the ball must overcome in order to get out of the pit. The higher
1050
y - 2188-728.Sx+96.4X2
the barrier, the more difficult it is for the ball to overcome it.
R2- 0.81
1000
The extreme example of this is the black hole where the barrier
is so high that even light is unable to escape out of it.
o 950
Traditional solutions offered by classical physics essentially
require enough energy to be imparted to the ball so that it
s 900
$ 850
overcomes the barrier. Either the kick imparted to it has to be
sufficiently strong or one could just pick it up and place it outside
800
the pit or, radically, break the barrier to allow the ball to roll
y - 2367-877.Bx+122.68X2
p2«0.73
out. In short, single drastic solutions are on the offer. But in reality
750 --------2.00
4.00 particles do emerge out of these barriers even without such solu2.50
3.50
300
3.50
4.00
A
Logof anpge
tions. Alpha particles breaking from the stranglehold of the
nucleus and even black holes emitting matter. How does it hapbe described as a quadratic one (the adj R Sq values marginally pen? Quantum physics tells that they ‘tunnel’ through the barrier;
improve);
a non-radical solution indeed but does help them break free.
fZm ratios(All-age) = 1368 - 728.5 x LogAMPCE +
We can likewise wait for radical solutions to happen i e, for
96.4 x (LogAMPCE)2
a revolution,4 for the perfect enforcement of the PNDT act, for
the emergence of that elusive entity called the political will or
ffm ratios(0-14 yrs) = 2367 - 877.5 x LogAMPCE +
122.7 x (LogAMPCE)2
await a change of heart among foeticide service providers who
Above pattern is not ‘one off. A similar trend is seen in the worship profit at all costs. While each of these solutions must
43rd and the 50th round. It is observed not just at all-India level be explored, it is useful in the meantime, to look at some seem
but in different states as well (Agnihotri et al 2003: Forthcoming).
ingly non-radical solutions as well.
What is disturbing is that the lowering of the f7m ratios has
One such set of solutions is to consolidate the position of the
intensified in most regions across the three rounds.
girl child in areas where barriers to her survival have not yet
This analysis is important for another reason. As against the become formidable. Even in these areas, gender inequalities in
observed reality of increased female subordination in the wake respect of basic entitlements do operate, e g, in birth registration,
of prosperity, certain economic literature expresses a ‘prosperity in immunisation, in nutrition or in schooling. It stands to reason
optimism’. Briefly speaking, it is similar to the ‘trickle down’
that any effort towards complete coverage will reduce the gender
hypothesis based on an inverse U shaped relationship (Kuznets gap in the coverage. Attempt should therefore be made for
curve) between inequality and prosperity. It tells us that inequali complete coverage as an anti-dote to the gender gap. Three
ties initially increase as nations become prosperous. Beyond a specific examples from the field will amplify this.
Data on nutritional status of children in the 0-3 age group in
‘turning point’, however, these decline as fruits of prosperity
trickle down to the lower strata as well. Similar relationship holds, the ICDS do show a gender gap in the incidence of moderate
some economists argue [Haddad and Kanbur 1992], in the house and severe malnutrition.5 I have seen this in respect of at least
hold domain. Inequalities rise with prosperity initially reaching three different states; Orissa, West Bengal and Maharashtra. Data
a maximum at the ‘turning point’ of prosperity level. Beyond show that girls in this category often outnumber boys and the dif
it these reduce and everybody lives happily ever after.
ferences in the incidence of moderate and severe malnourished
I have elsewhere [Agnihotri 2002: Chapter 8] argued against between them are statistically significant. Further, the gender gap
this ‘prosperity optimism’ on three counts. First, the existence appears to aggravate during lean seasons when malnutrition
ofa U-shaped relationship begs three important questions; at what peaks;; an observation supported in literature [Behrman 1988].
level of prosperity does this turning point come, how attainable
The implications of these patterns were brought home dramati
is it and most important, how severe is the inequality at this turning cally before me during a zonal ICDS review meeting conducted
point. Second, at this turning point the inequality is at its peak, by me as the secretary to government of Orissa in the women
As such one has to prosper a lot more before it comes down to and child development department at Sambalpur, in 1999. I did
some ‘acceptable’ level. Third it is naive to assume that the on purpose ask a couple of ICDS project officers to read out
the gender break-up of moderately and severely malnourished
inequality in terms of different life sustaining inputs behaves
identically. A prosperity level at which inequality in consumption children in different sectors in their project. As they started
Log of AMPCE
♦ 0-14 year, Age-grcup • Total Population
4358
Economic and Political Weekly
October 11, 2003
»
reading out the statistics, it was clear that girls were invariably jsense. A substantial part of this perception is shaped by the
outnumbering boys. This explicit revelation created a sudden if prevailing status of women,
uncomfortable silence in the meeting hall with many project
Received literature is nearly unanimous that high workforce
officers murmuring that they too had seen a similar pattern. It participation by women, goes together with higher sex ratios
did dawn on most of them that a campaign to eliminate severe [Murthi et al 1995]. It is not, however, a necessary condition
and moderate malnutrition, benefited the girl child more. Inter for high sex ratios, if culture takes care of survival [Agnihotri
estingly all the anganwadi workers, sector supervisors and project 2000]. However, a distinction needs to be made between wageofficers in Orissa are women and yet, the point had to be explicitly work where women have control over their earnings and work
made with supporting data.
not explicitly linked to wages e g, dairy activity, where the
A similar and explicit recognition came iup
a recently during
‘
a blessing may be mixed depending on the control women have
review meeting of a UNICEF-supported intervention in certain over the earnings [Sharma and Vanjani 1993].
Among non-poor households, the dynamics of withdrawing
blocks of West Bengal. This project ‘positive deviance’ aims at
improving nutritional status of children on a sustainable basis women from workforce for purposes of ‘status production’
through mobilisation of mothers and the community. Initial results [Papanek 1989] in the wake of prosperity needs to be noted. But
indicate that the nutritional status of girl children improves more this creates a conflicting situation for the concerned woman; her
for the simple reason that they are the more deprived to begin with, status within the society goes up while her bargaining power
Gendergaps also mark child immunisation especially for dropout within the household declines. She therefore hopes for the best
between, say, the first and the third dose of the DPT. Once again, but is not ‘prepared for the worst’. Once withdrawn from the
an NGO, Shibpur Peoples’ Care Organisation (SPCO) that has labour market, her ability to re-engage with it is erodes steadily,
taken up a campaign for complete immunisation of all children often sharply, giving rise to an increasing sense of insecurity.
in seven gram panchayats ‘realised’ that girls benefit more on Basu (1992: 222) has summed this up very aptly when she
this account. The reason again is simple; they were the more observes “probably the best placed mother is one who does not
work herselfbut knows thatthere are no restrictions on her finding
deprived to begin with.
It is necessary therefore, to remove the ‘veil’ of aggregation work ... should the need arise”.
Creation ofemployment avenues for women from the non-poor
from the data, look at the critical gender gaps and press for a
universal coverage in order to give the girl child her due. The households has to take into account above observations. Our
reality, however, is that the genderwise break-up ofdata are often policy preoccupation today is mostly with workforce participanot provided, and when provided often not analysed by gender, tion of women from poorer households. That is useful in the
In one unusual case, the gender break-up has been dropped from poverty context. But if we wish to create a dent in the epicentre,
routine reporting in the name of efficiency in a department flexible employment avenues must be created for women from
non-poor households. Once women are able to access these ‘...
entrusted with responsibility of women’s development.6
Three unintended outcomes of this ‘universal’ coverage can should the need arise’, their status within the household will
be anticipated. In less regressive regions, it consolidates the perceptibly go up. This is important since the social dynamics
‘female friendly* milieu while in others it improves her ‘entitle- within this class creates role models for the upwardly mobile
ments perspectives’, even ifnon-radically. Second, a ripple effect groups.
However, a parallel campaign has to be mounted about the
across entitlements takes place. Complete coverage in
immunisation can, for example, pave the way for complete birth deteriorating crime situation in the public sphere as it affects
registration ofgirl children. Finally, as we move closer to complete women more adversely than men. The tendency to withdraw
coverage, the service delivery infrastructure and social attitude women from external employment is also influenced by the safety
perceptions about the workplace and the road leading to it! This
towards girls may both improve.
It is necessary therefore, to follow this strategy for basic is one area where activism, civil society groups, media and
entitlements like registration, nutrition, immunisation and more judiciary has to play a proactive role to merely expedite judicial
important literacy/schooling. As universalisation is the stated processes. I am quite convinced that it is the swiftness and
goal of the state for these entitlements, this strategy needs serious certainty of punishment and not the harshness of a punishment
consideration by both civil society and the state. But the next that acts as a deterrent. The proactive role should identify to begin
climb is steeper still. How to stem the alarming increase in sex with, the weak links in the criminal justice processes because
a chain snaps not at its strongest link but at its weakest one. The
selective elimination of the girl children?
devil truly lies here in these weak links.
Two specific interventions need to be mentioned here which
V
may contribute to reduce the ‘unwantedness' of daughters. The
One front on which the activist groups are fighting hard is first relates to mobility in the non-metro urban towns. Girls do
implementation of the PNDT Act 1994.1 have myself provided not enjoy the same mobility as boys do because their access to
modest methodological inputs in this regard. These helpr highlight two-wheelers, especially bicycles, is limited. I seriously think
the emerging ‘epicentres’ of female child deficit at the district this must go. It is anecdotal, but not uncommon, to find parents
and sub-district level and may perhaps help take more effective mentioning
mentioning that
that daughters
daughters cannot
cannotrun
runerrands
errands as
as the
thesons
sons do
do as
as
implementation. It is useful to remember, however, that f/m ratios they lack of mobility. Riding bicycles should become part of a
have been low well prior to the 1990s due to excess female child movement for girls.
The second issue is of married adolescent girls. Notwithstand
mortality in the 1-4 age group, and in many a states in the post
ing the legal age of marriage being 18 years, a large percentage
neo-natal period itself.
Roots of sex selective elimination need to be traced to the of number of girls get married below this age (RCH 1998-99),
perceptions about ‘unwantedness’ of the girl child and tackled the percentage in some districts going as high as 70 per cent,
at that level. These perceptions are shaped primarily through These girls find their social communication avenues sharply
viewing a daughter as a liability in economic and physical security curtailed after marriage (Judith Bruce: personal communication).
Economic and Political Weekly
October 11, 2003
4359
Further, they cannot become part of any SHG as they are below
18 years of age. They thus get initiated into an unequal position,
burdened with the task of social and biological reproduction at
low information base. It is necessary to bring this group into the
fold of SHG activity as trainees or affiliates so as to improve
their social communication avenues if not economic power.
There is a view that the role of SHGs is exaggerated and these
are mostly insensitive to social issues once they pursue economic
goals. The solution to this, in my opinion is not to write these
off, but to sensitise them to social issues. In any case the im
portance of gaining economic security for oneself through parti
cipation in SHG cannot get negated merely because the person
does not become sensitive to an activist’s level of satisfaction.
Finally, a specific intervention to highlight the supporting role
of daughters to parents in old age. There is a growing realisation
in metros and rural areas alike that sons do not necessarily look
after parents in old age these days. In both these areas, son-drain
due to long distance migration is significant and there is a
considerable, anecdotal again, evidence to show that it is the
daughter who comes to help in the time of need or crisis. There
is a strong need to highlight this role through visual media.
VE
Notes
[This is a revised version of the 2nd annual lecture on Girl Child delivered
under the auspices ofthe Indian Alliance for Child Rights (IACR). The views
presented here arc author’s own and not of UNICEF.]
j
1 More appropriately a north-west and south-east divide with more masculine
sex ratios in the former and less adverse f/m ratios in the latter (See c g,
Sopher 1980; Miller 1981 and 1989 and Agnihotri 2000. Miller (1989)
talks in particular of the growing masculinisation of the f/m ratios between
1971 and 1981.
2 None of these foeticide service providers, who often claim to be rendering
‘national service’ provide the service free; even for some of their poor
clients!
3 Question regarding different saving levels or disposable and non-disposablc
income for the same MPCE level can be raised here. But by and large,
higher per capita expenditure will indicate higher prosperity.
4 While one may agree or disagree with the governance in North Korea,
son preference there is next to nil in stark contrast to the strong son
preference in South Korea traced to religio- cultural context of a Confucian
society (Goodkind, 1999).
5 I am quite puzzled by the persistent divergence on this issue between the
ICDS data and the survey data from, say NNMB and NFHS which seem
to indicate a much lower or insignificant gender gap.
6 The ICDS reporting format had reportedly been ‘modified’ with an aim
to reduce drudgery at the field level and what gets dropped is the gender
wise break up ofnutritional status. I strongly hope my information is either
incorrect or outdated!
It is important to debate here the ethical dimension ofsex-based
Qt6nC6S
elimination Ofa segment ofthe population. Once this is sanctified, Agnihotri, S B (2000): Sex'Ratio Patterns in the Indian Population -A Fresh
Exploration, Sage, New Delhi.
it could well be the thin end of the wedge that provides in its
- (2002): ‘Setting Daughters’ of Urban India: Locating the Epi-Centres of
wake, currency to eliminate other segments of population based
Female Deficit’ Proceedings ofthe International symposium on Girl Child
on other criterion whether religion or caste or the colour of the
- January 2002, UPS, Mumbai.
Bardhan, P K (1974): ‘On Life and Death Questions’ Economic and Political
skin or the shape of the nose!
Weekly, Special Issue No 9: 1293-1304.
Development, frankly, cannot be viewed in isolation; it is
Basu, A M (1992): Culture, theStatus of Women, and Demographic Behaviour,
important to know how it combines with discrimination,
gender
Clarendon Press, Oxford.
___ , o____
based one in
i particular.
’ ’
If we remain underdeveloped and yet Behrman, J (1988): ‘Nutrition, Health, Birth Order and Seasonality: Intra....... that is the worst case scenario.Household
Allocation among Children in Rural India’ Journal of
aggravate discrimination,
If
Development Economics, 28.
underdevelopment co-exists with lack of discrimination, life gets
Berreman, G D (1993): ‘Sanskritisation as Female Oppression in India’ in
tolerated but not enjoyed. But highly developed society with high
Miller, B D (cd), Sex and Gender Hierarchies, Cambridge University
discrimination levels as
in our ‘epicentres
is not a_________
great goal
_______
______ ’ ______
Press, Cambridge, 366-392.
for women either. We must, therefore, strive to become a society
Sun'ival in
...i
---- jdevelopment
.
South Asia, Health transition working paper No 7, NCEPH, Australian
where
goes hand in hand with absence of discrimi7
National University, Canberra.
nation against its women.
Chhabra, R (1981): ‘India's Sobering Census’ People, 8(3).
We must, therefore, question the current model of development Dasgupta, M (1987): ‘Selective Discrimination against Female Children in
Rural Punjab, India’ Population and Development Review, 13: 77-100.
where discrimination necessarily appears to accompany devel
Goody, J (1990): The Oriental, the Ancient and the Primitive, Cambridge
opment. It is not that success stories of alternative ‘development’
University Press, Cambridge.
do not exist; Kerala, Goa or Manipur provide examples where Haddad, L and Kanbur, R (1992): ‘IsThere an Intrahousehold Kuznets Curve?
Some Evidence from the Philippines’ Public Finances 47.
social indicators have developed, but not at the cost of gender
equity. This is the role model that the society has to follow and Krishnaji, N (1987): Toverty and Sex Ratio - Some Data and Some
Speculations?’ Economic and Political Weekly 22(23): 892-97.
not the model of the Punjab, Haryana and western UP where McKee, L(1984): ‘Sex Differentials in Survivorship and the Customary'
discrimination appears as ‘inevitable’.
Treatment of the Infants and Children’, Medical Anthropology, 8(2)
91-108.
But that necessitates that the fight against gender-based dis
B D (1981): The Endangered Sex, Cornell University Press, Ithaca,
crimination has to become part of the larger fight against all other Miller,
New York.
discriminations. In fact gender based discrimination gets aggra Murthi, M, A Guio and J Dreze (1995): Mortality, Fertility and Gender Bias
vated when combined with other inequalities. It becomes nec
in India: A District Level Analysis, DERC Discussion paper no 61, School
of Economics, London.
essary therefore to identify the most unreached and the most
Padmanabha P (1981): ‘The Decisive Decade: A Note on the Provisional
unserved, within the gender domain and advocate strongly for
Results of the 1981 Census of India’ Yojana: 25(9).
improving their lot. Just as different inequalities multiply the Papanek, H (1989): ‘Family Status Production Work- Women’s Contribution
to Social Mobility and Class Differentiation' in Krishnaraj, M and
misery ofthe affected, reducing these together also gives multiple
Chanana, K (eds) Gender and the Household Domain, Sage, New Delhi,
benefits. Willy-nilly we are talking here of eliminating the
96-116.
chakravyuha of discrimination altogether rather than its specific
Premi, M K (2001): ‘The Missing Girl Child” EPW, 36(21), May 26,
manifestation we began with, so that no child dies an avoidable
1875-80.
RGI (2001): Provisional Population Totals; Paper-1 of2001, Office of the
death, let alone a girl child. RTil
Registrar General and Census Commissioner, New Delhi, India.
Sharma, M and U Vanjani (1993): ‘When More Means Less - Assessing the
Address for correspondence:
Impact of Dairy Development in the Lives and Health of Women in Rural
sbagnihotri@yahoo.com.
Rajasthan (India)’ Social Science and Medicine, 37(11): 1377-89.
4360
Economic and Political Weekly
October 11, 2003
Perspactives
Trends in Sex Ratio
A Review in Tribute to Asok Mitra
The 1991 Census counted 927females to every 1,000 males in the
Indian population. That was an all-time low level in the recorded
female-to-male ratio. It laid to rest the sanguine prospect
generated by the previous census, which showed an improvement in
the ratio: to 934 in 1981 from 930 in 1971. Indeed, there has been
a secular decline in the sex ratio from the beginning of this century.
Some probing into what lies behind the long-term trend and its re
establishment in 1991 suggests - as the studies reviewed here do that a further decline in the ratio is quite probable when the first
count is made in the next millennium.
< * N Krishnaji
or Asok Mitra, the steadily deterio|—4 rating sex ratio was an obsessive
A concern over more than six decades.
Presiding over the 1961 Census, he
publicised the influential work of Pravin
Visaria, which was the first major effort
to understand the worsening deficit of
females in the Indian population [Visaria
1971]. That study put an end to earlier
speculations about undercounting of fe
males as a plausible explanation, and
clearly established higher female morta
lity in several age groups as the prime
reason for low female ratios.
Asok Mitra returned to the question of
worsening female deficits, after reading
the results of the 1971 Census. He wrote
what perhaps is the most comprehensive
review of the social malady [Mitra 1979],
covering all that is relevant. He discussed
at length the possibility of undercounting
of females in the different censuses and
went on to the nature and extent of higher
female mortality under normal conditions
and under famines. He analysed the un
derlying causes such as the neglect of girls
and the risks associated with frequent child
bearing. Finally, he paid attention to the
economic and cultural environment that
generates discrimination against females.
After carefully describing and analysing
data from diverse sources, he listed in
detail what we ought to investigate further
to understand the trends in sex ratio. This
tribute to Asok Mitra reviews some recent
studies on the trends in sex ratio.
The balance tilted against females during
Economic and Political Weekly
the 1980s and produced the lowest ever
sex ratio of927 in 1991. It came as some
thing of a surprise, not only because it was
a reversal of the trend during the 1970s,
but also because the data from all available
sources suggested a narrowing down in
gender-differentials in mortality during
the 1980s. Since on a countrywide basis
a possible sex-selective migration could not
have been a major factor, the decline in
the female ratio, during a period when the
gender gap in death rates was narrowing,
clearly pointed to the possibility that larger
female deficits were occurring at birth itself.
Initially, demographers did not see it that
way. Looking at the 1991 ratio as some
thing of an intellectual puzzle deserving
attention, they attempted to resolve it in
otherways. Srinivasan (1994), forexample,
raises once again the phantom of under
enumeration of females. Let us remember
that Mitra has examined this at length (in
the 1979 paper cited earlier) and concluded
that
that while
while the
the undercount
undercount of
offemales
females could
could
have been a factor in the earliest censuses,
beginning in 1871-72, all evidence pointed
'
'
t in the
to the progressive
improvement
‘
* comaccuracy
in counting. ’Indeed,
other
---.
petent demographers have come to similar
conclusions. How, then, does Srinivasan
square this with his suggestion of under
counts of females? He says (1994:3234):
The extremely volatile political and social
climate that prevailed in many parts of the
country because of the issue of reserva
tions (Mandal Commission recommenda
tions supporting reservations of jobs and
seats in colleges on the basis of caste) and
the ‘ratha yatras’ or massive processions
April 1, 2000
organised by the Hindu fundamentalist
groups over the Ayodhya temple issue
during the six-month period prior to the
census, might have contributed to the
under-reporting offemales by households.
That women had gone into hiding under
political turmoil is a curious suggestion.
Srinivasan, however, puts this to test by
examining sex ratios in districts through
which ‘ratha yatras’ passed, and contrast
ing them with districts with no ‘ratha yatra’.
He finds much evidence in support of his
hypothesis involving politically disturbed
conditions as a factor behind female
undercounts. He is, ofcourse, not unaware
of female foeticide as a possible contri
buting factor. Here is what he says in the
context (1994:3234):
Another factor that has been advanced by
women’s groups and others for the decline
in the sex ratio is the increasing incidence
of female foeticide in the country through
the use of the modem techniques of ultra
sonography and amniocentesis that help
to identify the sex ofthe baby at very early
stages of pregnancy. When these procedures
determine at an early stage of pregnancy
that the foetus is female, it is more likely
to be aborted. However, these procedures
have found favourable response in the late
80s and the early 90s only in the large
metropolitan cities of Bombay, Calcutta,
Madras and Delhi where the facilities for
such techniques were available. Even to
increase the sex ratio at birth in the Indian
society by one point, for example, from
106 to 107 [here the ratio is male to female,
by convention in demographic literature],
about 60,000 female foetuses have to
aborted [during a year or a decade?].
In the sequel, he cites with approval the
work of Rajan and his colleagues,
who
_
advance the novel hypothesis ofa possible
double count of males leading to a fall in
the female ratio [Rajan et al 1991 ]. These
authors begin by accepting that female
counts have been improving in accuracy
over the different censuses; they recognise,
therefore, that underenumeration of fe
males could not have been a major factor
behind the low 1991 ratio. They present
data to show that gender differences in
death rates have been narrowing down;
and further make references to the work
of other demographers, pointing in the
same direction. Logically, all this should
have led them to a serious consideration
ofthe trends in sex ratio at birth. However,
they express much impatience with the
1161
suggestion that female foeticide and infan
ticide, promoted by son-preference, could
have contributed significantly to the fall
in the sex ratio; they assert that sex selec
tion at birth through the emerging techno
logy of sex determination is largely an
urban phenomenon. Their own inference
about double counts of males turns out to
be a purely speculative one. The under
lying argument is that migrant males were
probably counted twice, at places of origin
and destination of migration. The analysis
they present in support is based on sex ratio
trends separately in the (0-10) and 10+ age
groups. They find the bigger female defi
cits in the 10+ group, supposed to contain
the migrant males. However, in the ab
sence ofage data, they use estimates, which
now, after the release of official age data,
can be seen to have gone haywire. Indeed,
similar exercises done later conclusively
show that drastic reductions in the sex ratio
have taken place in the (0-4) age group.
The two examples above suffice to show
the bias, and consequent haste, in the initial
responses to the 1991 fall in the sex ratio.
However, as reliable data accumulated,
and demographers took closer interest, it
became increasingly clear that high female
deficits in early childhood were primarily
responsible. Indeed, this has now been identi
fied as a manifestation of an increasing
gender bias, which, moreover, is taking an
altogether new shape, different from what
it used to be. It is difficult to fully review the
extensive literature on the subject. Instead,
we refer below to a few studies that bring out
this changing map of the sex ratio in India.
The point of departure of a recent study
[Das Gupta and Bhat 1997] is the obser
vation that in several east Asian countries,
notably South Korea and China, there have
been steep decreases in the female ratios
among children as a consequence of sig
nificant declines in fertility. Most of these
societies have a cultural tradition of strong
preference for sons. It is suggested that the
well-established preference for male prog
eny combined with an emerging prefer
ence for small families will result in a loss
of girls either before or after birth. Easily
accessible procedures for sex determina
tion during pregnancy promote female
foeticide. This has a particularly strong
influence at higher parities: if the first birth
is female, the next pregnancy has dimin
ished chances of going to full term if the
foetus is female. A female baby bom under
these conditions has reduced chances of
survival. Thus the unborn female baby
shares with the bom female infant high
risks of elimination, as technology re
inforces traditional biases.
1162
All this has been documented well in the
Chinese case. The following paragraph
from a study on sex ratios at birth in China
[Zheng Yi et al 1993] neatly sums up what
has happened in China:
Strong male domination and discrimina
tion against women have a long history and
have not yet been fully eradicated in spite
ofgreat progress made in China, especially
during the second half of this century. The
current family planning policy does not
allow couples to have as many children as
they desire, but social and cultural traditions
and daily living conditions make it very
important to have a son, especially in rural
areas. Meanwhile, economic reforms and the
open door policy have promoted economic
growth and improvement in the standard
of living. Progress in medical technology
has made prenatal sex identification and
sex-selective abortion feasible. Therefore,
people with a strong desire for a son usually
have the resources to bribe medical per
sonnel to perform an illegal examination
and to use sex-selective induced abortion
to achieve their desire. This practice is not
unique to China but is also found in some
of the other developing countries experi
encing rapid economic development, tech
nological progress and fertility decline.
Only a few changes in the above text are
needed to describe the Indian situation.
Das Gupta and Bhat examine all the rel
evant data and go on to estimate the number
of girls ‘additionally’ missing, between
1981 and 1991. As we know, the female
ratios were low even in 1981 because of
the ‘traditional’ higher female mortality,
at different ages. The worsening of the
female ratio meant that there has been an
‘additional’ deficit of 1.8 million girls and
women. The authors say:
Of the total of more than 1.8 million
‘additional missing females’ of all
ages...more than 61 percent were children.
There has been only a 0.22 per cent
increase...in the percentage ‘missing’ above
the age 7...In Kerala, Punjab and West
Bengal, the number of females aged 7+ in
1991 actually exceeded the number esti
mated on the basis ofthe sex ratios of 1981,
which shows an improvement relative to
males in survival at these ages. This is
consistent with other data which suggest
that declining fertility in India has led to
a reduction in excess mortality of adult
females, especially at peak reproductive
ages, whilst increasing discrimination
against female children...
The point being made is that fertility
decline has had beneficial effects on the
survival of women in the reproductive age
groups, through fewer births and a reduc
tion in the associated mortality risks. That
brings us to the question of death rates
among female children. Demographers
have generally found no significant wors
ening in the gender differentials in child
mortality during the 1980s. But these
differences persist, and male children have
still higher chances of survival. These
findings, along with the clear worsening
of female ratios among children, clearly
suggest an increase in sex-selective abor
tion and female infanticide, although the
latter may be of a relatively small magni
tude. Sex ratios at birth (SRBs) thus be
come crucial to our understanding of the
changing patterns of female deficits in the
overall. Unfortunately, reliable data on
SRBs are lacking, given the incomplete
registration of births. Das Gupta and Bhat,
however, put together the available, sug
gestive evidence in this respect. They
conclude with the portentous remark that
“pre-natal sex regulation may replace post
natal regulation as a method of controlling
the sex composition of families, because
the psychological burden of abortion is
lower than that ofneglecting a living child”
(1997:314). That is the new shape gender
bias is taking. It is changing the regional
spread ofthe bias as well, with the emergence
of a new type of gender bias in the south.
The lack of data on the sex ratios at birth
is made up to some extent by the effort of
S Sudha and S Irudaya Rajan (who, with
his colleagues, had earlier advanced the male
double-count hypothesis to explain the 1991
fall in the female ratio). They make use of
reverse survival methods based on avail
able information to estimate sex ratios at
birth and find an increase in the masculinity
at birth in several parts of the country.
Examining the sex ratios in the population
and among children, along with their own
estimates ofthe ratios at birth, they conclude
that pre-natal sex determination, neglect
of girls and female foeticide are among the
factors that have contributed to the female
demographic disadvantage obsen ed in the
1991 Census [Sudha and Rajan 1999].
This study documents the spread of
female foeticide and infanticide, using
diverse sources, including field studies
done by some non-governmental organi
sations (NGOs). For example, it refers to
the work of Adithi (an NGO) in several
districts of rural Bihar, reporting how
female infanticide is carried out routinely
— even now, as we near the end of the
century - by ‘dais’, traditional birth atten
dants, who still conduct many deliveries.
The killing is at the behest of senior males,
overriding the protests of the women in
the family [Adithi 1995]. The authors refer
also to the work of Chunkath and Athreya
(1997) and others on the spread of female
Economic and Political Weekly
April 1, 2000
infanticide in some districts ofTamil Nadu,
including Salem, Dharmapuri and Madurai,
following the rapid decline in fertility in
these areas. The estimates of the magni
tude of female infanticide presented by
these different sources are truly shocking;
the national total, when assessed, will be
even more so. With such accumulating
information on female infanticide, and the
manner in which clinics for sex determi
nation have been mushrooming all over
the country, including its rural parts, demographers are no longer sceptical about how
sex ratios atbirth have been skewing further
in favour of preferred male progeny.
A north-south economic and cultural
divide has been identified in the literature,
with associated differences in demographic
structures. The pattern in the north (and
the north-west) has been characterised by
traditionally higher rates of mortality and
fertility and larger gender differences in
death rates (in contrast to the south).
Coincidentally, these regions had lower
female ratios among workers and in the
population. All this meant that women in
the ‘north’ had a much lower status, de
fined in a very broad sense. This of course
is a rough generalisation because many
sub-regions do not fit into the neat pattern,
and the regions in the east display many
unique features although the female ratios
there tend to be far better than in the north.
These variations are attributed to both and
economic cultural factors.
The economic argument is that women
in the south had a greater economic role.
Paddy, the main crop cultivated in the
south, unlike wheat in the north, gave
women work in fields and an independent
income. Families were less patriarchal and
income-earning gave women a voice of
their own. However, other cultural factors,
nothing to do with work, are given more
importance in explanations of regional
patterns in the sex ratio. One such factor,
frequently cited, is endogamy in marriage,
which was widely practised in the south.
This system was associated with greater
reciprocity in marriage transactions, and
presumed to have fostered greater female
autonomy: it placed less importance on the
number of sons (than in the north) as a
measure of reproductive success of a
woman. On the other hand, in the north,
exogamy was common and was associated
with the dowry system among many castes.
This was a factor behind the strong pref
erence for sons. Likewise, the system of
hypergamy (the practice of giving away
daughters in marriage to grooms belong
ing to a higher caste, or what amounts to
the same, sons bringing in brides of an
Economic and Political Weekly
inferior caste along with dowries) also led
Similarly, fewer children per family may
parents to regard girls as a 1liability.
........
The mean better care for all children including
search for a suitable boy was difficult and girls. But, unless sex determination and
the dowry taxed many beyond their means. female foeticide are halted, there is a distinct
Female infanticide and neglect of girls possibility for a further Toss’ of girls.
were options chosen to eliminate unwanted
In this context, we may refer to another
females. (As recently as September 17, factor that has not received adequate atten1999, there was a report in The Times of tion in the Indian literature. Recent studies
India, Mumbai, on a village called Devra on gender differentials in mortality in western
in Rajasthan. There, a girl child not only countries show that these differentials,
survived - through a series of accidental traditionally in favour of females, are now
circumstances - but also brought a ‘barat’ narrowing down; that is, the female demo
-a groom’s marriage party-to the village graphic advantage is getting eroded. This
for the first time after 110 years. Girl chilis attributed to the fact that in many ofthese
drenwere
wereroutinely
routinelykilled
killedin
insuch
suchvillages.
villages, countries, work participation rates among
dren
The
Theearly
earlyIndian
Indiancensuses
censusesreported
reportedvillages
villages women are rising, they are increasingly
with
with no
no girls
girls in
in some
some parts
parts of
ofthe
the north
north entering stressful occupations, and finally
west. Presumably, such villages still exist.) their life styles are assuming forms associated
Alaka Maiwade Basu, reviewing the with risks of heart disease [Trovato and
relevant literature raises the question whether Lalu 1996]. All this has implications for
these economic and cultural explanations India, although only a few women, in urban
for regional variations in gender bias are areas, are taking up stressful careers. Rural
ofany validity to the changing demographic women no longer lead secluded and peacepatterns. The question is pertinent because ful lives. The stresses and strains of living
endogamy is disappearing in the south, are getting fairly similar in rural and urban
and the dowry system is becoming univer areas. Over a period oftwo or three decades,
sal. The north-south divide in this respect the forces integrating rural and urban living
is wearing thin. More importantly, even if patterns are likely to become stronger. This
one accepts that in the south women have is an additional factor that may worsen female
a higher status - and that it has been life disadvantage in India as a whole.023
improving, as measured by conventional [This is a revised version of the introduction to
indices such as literacy, life expectation a book being brought out in memory ofAsok Mirra
and work participation - it is not clear how by the Centre for Women’s Development Studies,
New Delhi.]
such a relatively high status can reduce the
preference for sons. Indeed, the emerging References
evidence shows, if anything, that the pref Basu, Alaka Malwade (1999): ‘Fertility Decline
erence is getting stronger and leading to
and Increasing Gender Imbalance in India,
Including a Possible South Indian Turnaround’,
female foeticide on a noticeable scale.
Development and Change, 30, pp 237-63.
These considerations make Basu to put
Chunkath, Sheela Rani and V B Athreya (1997):
forward the hypothesis that “a kind of
‘Female Infanticide in Tamil Nadu’, Economic
regional convergence is takingplace”, with
and Political Weekly, 32 (17), pp WS22-WS29.
new forms of bias emerging
in the south Das€T?Gupta, Monica
and
P N Mari Bhatrz’ (1997):
°
w
_ _i•
_ j _______ __ . .1 > «
‘Fertility r-v
Decline
and
Increased Manifestation
[Basu 1999:2433, italics in original]. The
of Sex Bias in India’, Population Studies, 51,
observation of deteriorating female ratios
pp 307-15.
among children in all the southern states Mitra, Asok (1979): Implications ofDeclining Sex
Ratio in India, Allied Publishers, New Delhi.
barring Kerala supports the hypothesis.
Basu says, as did others we have referred Rajan, Irudaya et al (1991): ‘Decline in Sex Ratio:
An Alternative Explanation?’, Economic and
to earlier, that the recent fertility decline,
Political Weekly, 26, pp 2963-64.
combined with a persistent son preference, Srinivasan, K (1994): ‘Sex Ratios: What They
Hide and What They Reveal’, Economic and
is producing this type of regional conver
Political Weekly, 29, pp 3233-34.
gence. It is in this context that she makes
a detailed review ofthe dramatic reduction Sudha, S and S Irudaya Rajan (1999): ‘Female
Demographic Disadvantage in India 1981-1991:
in fertility levels in Tamil Nadu. Along
Sex Selective Abortions and Female Infanti
with fewer children, female infanticide
cide’. Development cmd Change, 30, pp 585-618.
has appeared in several parts of the state, Trovato, Frank and N M Lalu (1996): ‘Narrowing
Sex Differentials in Life Expectancy in the
This perhaps signifies the shape of things
Industrialised World, Early 1970s to Early
to come in other southern states as well.
1990s’, Social Biology, 43, pp 20-36.
The preference for sons may turn out in Visaria, Pravin M (1971): The Sex Ratio of the
Population in India, Monograph No 10, Census
the next few decades to be a major determinant
of India 1961, New Delhi.
of sex ratios. It may outweigh the demo
Zheng Yi et al (1993): ‘Causes and Implications
graphic gains that may be expected. For
of the Increase in China’s Reported Sex Ratio
example, improvements in maternal mortal
and Birth’, Population and Development
Review, 19, No 2, pp 283-302.
ity may result from fewer births per woman.
April 1, 2000
--------_______________ J-.—______ 1
T> YT
___ :
TM___ A
ZinA'TX,
t
1163
DECLINING CHILD SEX RATIO - A CONCERN
The child sex ratio is declining at a very fast pace in India. The Juvenile sex ratio in 1961 was 976.
and it fell to 927 in 2001.
Table-1
Sex Ratio in the age group 0-6years
Census year
1961
1971
198?
1991
2001
Var. within a i
decade
i
Over all Sex
ratio
976
964
'■ -12
962
-2~
945
j
- -17
927
[
•-18
Source: Census of India, 2001
Table-2
Dist ribution of districts by ranges of child sex ratio, 1991-2002c(Provisionalj
| Range of sex
Census years
ratio (0-6)
1991
2002 (Provisional)
Total______
577
577
Less than 800
16
800-849
32
1_
850-899
68
_7_1_
900-949
208
181
242
950-999
306
1000-1049
21
8
Source: Census of India, 2002:provisional
The declining sex ratio is a clear indicator of the extent of inequity between male and female in the
society. The female has always been the unwanted sex among the children in the Indian society. The
cultural bias against the unwanted sex has been intense and the practice of female infanticide has been
prevalent for centuries in several parts of India. The cultural legacy of strong son preference and
neglect of daughters is inherited by all communities, religiows groups and socio-economic
backgrounds. The gender bias is rooted in a complex set of religious, economic, socio cultural factors
further exacerbated by globalization.
If boys are preferred for their economic socio-cultural utility, daughters are only of secondary'
importance in our society. This renders them vulnerable to all forms of violence. Girls under 5 years
of age in India face foeticide, infanticide, deliberate neglect in terms of child care, medical care,
education not only this they face sexual abuse, physical violence and also bear the burden of child
labour within their own homes. Females in the’reproductive age face early marriage, early pregnancy,
sexual violence, domestic violence, dowry harassment and torture in case of infertility. Not only that,
if they fail to produce a son they face desertion, humiliation and witch-hunt. The pathetic situation is
that the women are forced to endanger their own species either in the womb by practicing female
foeticide or after birth by the way of neglect. The devaluation of girls is blatantly stated in the findings
of the Census of 2001.
action India
1
Action India Campaign
Action India was part of the women’s movement in the 1980s when the campaign against female
oeticide was for the first taken up in India. Until then, no voice had been raised on the growino
imbalance in the sex ratio even though demographers were aware of the decline visible since 190 L
he findings of the census 2001 of the drop in birth of girls in the last decade shook the nation. Voices
from the grassroots were heard, our community based health workers decided to initiate a campaign
immediately in the capital city. A street play was prepared “nks”kh dkSu”, songs written, leaflets,
pamphlets and posters were printed with the message to value your daughters, love them and care for
them directly addressing the family.
In Nov. 2001, the KARVAN Network was formed of NGOs brought together by the Delhi
Commission for Women. On 21 Nov, the
to sifauH was inaugurated at Bhartiyam, New
e u, where 2000 women gathered to take forward the campaign to their working areas to reach out
to a eve s of the community. Surrounded by colourful banners the message of the PNDT Act was
spe t out in simple but cleared terms. Sex determination was illegal and ultrasound clinics were to be
registered. A puppet show was specially created to educate the public of the PNDT Act. and a
pamphlet was handed out to viewers with information on the law.
The K AR VAN Campaign was supported by 60 NGOs and CBOs and was successful in traveling to far
tlung areas of Delhi over a period of 6 weeks from Nov 2001 to Jan 2002.
partners colJectiveIy bad done some spadework in the form of survey of an Opinion Poll of
persons across Delhi, to seek the causes of the decline in the birth of girls, as well as assess the
perceptions of people on different aspects of the issue. Action India as an independent effort also did a
small survey in Nandnagri and Seemapuri to know the prevalence of the service providers of these
tests and also the perception of the doctors providing such services and their awareness of the law.
Second phase of the campaign
To go further in the cause a need assessment survey has been conducted bv Action India with the
suPPortof two network partners MYRADO, Najafgarh in the soi ih-west Delhi and Child Survival
India, Narela in the north-west Delhi with the following objectives:
1. To focus on the most affected areas where the sex ratio is lowest in the capital as per the
census, and work out a strategy for intervention.
2. To-----initiate
j a dialogue with the stakeholders in the community, particularly the opinion leaders
and the service providers.
3. To design the communication and awareness package for the grassroots advocacy specific to
the context to inform and educate the public about the PCPNDT Act 2003.
4. To make a case for violation of the fundamental right of a woman to be bom and live with
dignity as stated in Article 21 of our Constitution.
The study was designed and research by Ms Ifat Hamid.
SOME HIGHLIGHTS OF THE SURVEY
This Survey was conducted in two areas of Delhi: Najafgardh block in southwest and Alipur block in
northwest. 3500 women were surveyed in five villages of Najafgardh Block (Premnagar, Gopalnagar,
Dharampura, Maksudabad, Najafgard kasba) and three villages of Alipur Block (Kherakhurd,
iera a an, Nayabaans) with the help of questionnaire. The community workers of the network
partners MYRADO and Child Survival in the Najafgard and Alipur block respectively did the survey
after proper orientation.
J
action muia
2
Tablc-3
ZONES
Delhi_____
North West
North_____
North East
East______
New Delhi
Central
West______
South West
South
Sex ratio
(0-6 Years)
865
854_______
870
867________
868
882
902
858
845______
I 886
Table-4
0-6yrs [Bo
ys
26
Total
07
Najafgarh 14
56
Block
11
Alipur
Block___
Education of the Mother did not show any improvement
among the educated as well as uneducated mothers.
Giri
s
208
9__
110
0
989
1-5 class_______
6-9 class_______
10-12 class_____
Graduation
Ig^BM
801
755
859
in the sex ratio. The sex ratio is low both
Table-6
Table-5
Education of the
Sex ratio
_____ 0-6 yrs
Boys I Girls
I—IB
127
137
329
412
62
262
376
55
IT
Sex ratio
818
927
796 ___
912
887
611
Landed
Landless
Boys
597
2016
0-6 yrs
Girls
460
1629
Sex ratio
778
1
808
]
As we see, the sex ratio in the group of uneducated mothers is 818, while the mothers who are
postgraduate show a much lower ratio of 611.
Land as a factor: The child sex ratio is below 850 in both the groups though the landless show
slightly better ratio.
Economic profile shows some parity /leveling in the sex ratio at the highests~ levds in^tur
survey Rs 15000-20000+. Interestingly the poorest income group between
sex ratio than the middle income between Rs 2500-10000
Table-7_______________ ____
0-6yrs
Family monthly
Sex ratio
Girls
Income
Boys
action India
501-1500
198
”T75
1501-2500
462
380
883
822—
2501-3500
407
766
3501-5000
531
62?
479
766
5001-10000
662
726
794
10001-15000
15001-20000
75
24
20001+
8
”67’
89T
24
1000
8
1000
3
Family planning and the composition of children
While interviewing respondents were asked a question whether they have done family planning,6. /o
of the respondents responded with a YES. While asking this question we did not define family
planning. On the basis of their response we tried to see if there is any difference in the sex
composition of the children in the respondents who according to them have done family planning, and
the respondents whose responses were NO. Our findings reveal the following.
Table-8
i
2 children
2 Boys
2 Girls
1 Boy- 1 Girl
Planned
35%
5%
60%
Not planned
22%
22%
56%
3 children
3 Boys
3 Girls
2 Girls- 1 Boy
2 Boys-1 Girl
Planned
11%
2%
35%
52%
Not planned
6%
8%
54%
33%
4 children
4 boys
4 girls
Planned
6%
0
53%
19%
22%
Not planned
4%
3%
26%
47%
21%
2 boys- 2 girls 3 girls- I boy
3 boys- I girl
Social, demographic and legal awareness about the issue in the community
1. Most of the women are aware that father •is responsible for the! sex of the child but the social
pressure not only from their in-laws but also from their own parents compels them to want a
SOn-
•
Al
•
2. Most respondents did not admit that they know about any sex selective tests. 11 le same ime
they admitted that the girls are decreasing because of the availability of the ultrasound and other
sex detenuination tests.
.
3. The respondents were well aware of the social and biological consequences of this decline
4. With regard to PCPNDT Act as well as MTP Act, the level of legal awareness of the
respondents was very poor.
TESTIMONIES
Caste: Jal
Education: 12th pass
Sunita, 39, had been happily married for 20yrs.She had two young daughters (elder one in I Ind
college) and twin sons. But fate had something planned for her. About 2yrs back, she lost both her
sons in a road accident. In a Jat family with large landholdings, it became a major issue an t ley were
told that they would not get a share of family property as they now had just two daughters and no son.
Sunita consulted doctors for recanalisation (reversing the tubectomy), but the doctors
hope. She could not bear frequent bickering and tensions at home and thus decided to get er us an
remarried to beget a male heir for the family. Last year, she got her 42yr. old husban
£a
20yr. old deaf and dumb girl from a neighbouring village. The young second wi e u i e
er
assigned duty soon and recently gave birth to a baby boy. Sunita s in-laws and her hus an are verx
happy now.
Desperation for the male Child
action india
4
i *
Caste: jat
Education: B. A
Sarita, 29, was married in a joint family, wherein her husband is the second son. Her elder sister-inlaw had two daughters. Sarita also had a daughter as her first baby. Her in-laws were not very happx
and next time when she became pregnant, she was forced to undergo abortion as the ultrasound
revealed a female foetus. The same story was repeated thrice and Sarita repeatedly went in for three
abortions in the next 7 yrs. The fourth time, the ultrasound reported a male baby and the family
became very happy and made a lot of preparations for welcoming the male child. Unfortunately, the
ultrasound report proved wrong and Sarita gave birth to her second daughter. Sarita s own words are.
“Yeh to baar baar aayi aur gayi,lekin isne aana hi tha”. The pressure to have a male child is still there
on Sarita. But her health has deteriorated. The male child still haunts her.
The Unending wait...
CONCLUSION
Crimes against women are soaring /on the rise. According to National Crime Report Bureau there
has been 29.2% increase of crimes against women in 1998 as compared to 1994 and 92.25% increase
as compared to 1990.
There is a “choice” today to eliminate daughters in the womb. Sex selective testing technology is
widely available in urban and rural areas. The MTP Act is overlooked by the demand and supply
nexus between the family and medical profession. There is social legitimacy to the killing of the
female foetus, no one suffers any shame or guilt for this act. The value of a daughter s life is
diminishing even as the preference for sons is rising.
The whole issue of female foeticide has to be understood in the wider context of an increasing male
bias and continuing gender gap. Although discrimination against girls by their own families is not a
new phenomenon, the recent fall in child sex ratio is a cause of fresh concern, or should be because of
its increased intensity and wider spread than ever before. Eliminating females before birth is now a
wide spread phenomenon across class, caste, region and religion. The tendency of falling child ratio
has now affected all parts of the country since 1991. A strengthening of male biased norms and values
across all caste and classes has grown simultaneously with economic development. What we need to
understand is in what way the increasing male bias and economic groulh are connected. The complex
connection between development process and social change are often contradictory as we find the
lowest sex ratio in the most developed states of Punjab, Haryana. Gujrat. Himachal Pradesh, which
has a high female literacy, shows a sharp decline in sex ratio in the last decade.
Declining sex ratio is a political issue besides a social issue. It cannot only be the hostile social
attitude towards the girls that is leading to the female Foeticide but it is more the factors that
perpetuated it. To meet the challenges of the declining ratio, first and foremost the females right to life
with dignity has to be valued by the society and the state. This means combating male child
preference and its associated legitimacy. Not only that we have to intervene to make both the service
providers and the service seekers accountable.
Society has to be motivated to value the girl child and also articulate concern on the issues so that the
demand for PNDT services are no longer required. There is need to gear up the activities to make the
medical professional accountable for the unethical practices and demand for the strict implementation
ofPCPNDT Act 2003.
Action India
Campaign against Female Foeticide
Media workshop on “Sex Selection and Female Foeticide” 6,h -8lh April 2004 at IIC, Conference Hall
No.2
action India
5
Female Demographic Disadvantage in India 1981-1991:
Sex Selective Abortions and Female Infanticide
S. Sudha and S. Irudaya Rajan
ABSTRACT
Using evidence from a number of sources (including the 1981 and 1991
censuses of India, prior research, and NGO reports), this article examines
whether bias against girl children persists during periods of development and
fertility decline, whether prenatal sex selection has spread in India as elsewhere
in Asia, and whether female vs. male child mortality risks have changed. The
authors present estimated period sex ratios at birth (SRBs) calculated by
reverse survival methods along with reported sex ratios among infants aged 0
and 1, as well as sex ratios of child mortality probabilities (q5), from the two
censuses. The findings show an increase in ‘masculine’ SRBs and persistent (or
even worsening) female mortality disadvantage, despite overall mortality
decline, due to selective neglect and the spread of female infanticide practices
in some areas. Research and reports indicate the increasing use of prenatal sex
selection in some regions. In India, preference for sons appears to be
undiminished by socio-economic development, which interacts with cultural
sources of male bias. The increased masculinity of period SRBs in some areas,
together with persistent excess female child mortality and female infanticide,
creates a ‘double jeopardy’ for girl children. Legislation curbing prenatal sex
determination and policy measures addressing societal female devaluation
have had little impact, suggesting that female demographic disadvantage is
unlikely to improve in the near future.
INTRODUCTION
Highlighted by sensational titles such as ‘The Endangered Sex’ (Miller, 1981)
or ‘More than 100 million women are missing’ (Sen, 1992), studies have long
pointed to the unfavourable life chances of females versus males in parts of
East and South Asia. This female disadvantage is particularly concentrated
in infancy and childhood years, and is rooted in long-standing social patterns
of preference for male children. Practices regulating the numbers of female
This is a revised version of Working Paper No. 288 of the Centre for Development Studies,
Thiruvananthapuram. It has been presented at the CDS-UNRISD Workshop on Gender, Poverty
and Well-being, Centre for Development Studies, Thiruvananthapuram (24-7 November 1997),
and at the T. N. Krishnan Memorial Seminar, Centre for Development Studies, Thiruvanantha
puram (7-9 September 1997).
Development and Change Vol. 30 (1999), 585-618. © Institute of Social Studies 1999. Published
by Blackwell Publishers Ltd, 108 Cowley Rd, Oxford OX4 1JF, UK.
Copyright © 2000. All rights reserved.
586
S. Sudha and S. Irudaya Rajan
children in a family traditionally included the post-natal methods of female
infanticide, abandonment or out-adoption of girls, under-reporting of female
births, and selective neglect of daughters leading to higher death rates. Lately
in China and South Korea, prenatal sex determination and selective abortion
of female foetuses have been increasingly implicated (Asia-Pacific Population
and Policy Report, 1995; Johansen and Nygren, 1991; Park and Cho, 1995;
Yi et al., 1993). When fertility declines and preference for male children
remains strong, parents still take steps to ensure the birth and survival of
sons, and prenatal sex determination and selective abortion of females are
apparently preferable to female infanticide or abandonment of baby girls.
Prenatal sex selection techniques appear to substitute for post-natal methods
in these regions, as shown by increasing masculinity of sex ratios at birth,
coupled with more equitable sex ratios of infant and child mortality
(Goodkind, 1996). That is, fewer girls are allowed to be born, but those who
are born are more wanted and tend to survive.
These issues are also significant in South Asia, which shares with East Asia
a long-standing tradition of son-preference. In India, the issue has mostly
been examined in terms of the masculinity of the population sex ratios
observed since the first census taken in 1871 under the British Raj (Irudaya
Rajan et al., 1991; Kundu and Sahu, 1991; Raju and Premi, 1992; Srinivasan,
1997; Visana, 1969). The persistent preference for sons and disfavour toward
daughters, leading to the phenomenon of‘excess female child mortality’1 and
highly masculine juvenile sex ratios (counter to the global norm of female
mortality advantage and moderately masculine sex ratios among children)
have been discussed as key factors in this imbalance (Agnihotri, 1996;
Kishor, 1993; Miller, 1981; Saith and Harriss-White, this volume).
An important dimension of inquiry, that of changes in the relative pattern
of births and survival of male versus female children in India, has been
comparatively neglected, mainly due to lack of data. Indian authorities do
not routinely publish data on sex ratios among births reported in the Census
or Sample Registration System enumeration years. A few regional studies
suggest that cohort sex ratios at birth are anomalously masculine in some
parts of the country, particularly in the North (Clark and Shreeniwas, 1995
for Gujarat; Mason et al., 1992 for Karnataka; Irudaya Rajan, 1996 and
Visaria and Irudaya Rajan, 1996 for Kerala). Therefore, it is not clear
whether parents in India, as in East Asia, are substituting prenatal for post
natal discrimination against girl children, or whether bias against females is
lessening over time. One all-India study has examined changes in juvenile sex
ratios (ages 0-4) between 1981 and 1991, alongside trends in mortality sex
ratios and fertility rates, and concluded that during fertility decline in India,
1.
“Excess female child mortality’ refers to t'
the phenomenon of higher death rates of females
among infants and children than males, -i
in contrast to the ‘normal’ pattern of higher
mortality among males.
Copyright © 2000. All rights reserved.
Female Demographic Disadvantage in India 1981-91
587
parents are not substituting prenatal for post-natal discrimination against
girls, but are combining these two strategies. Male bias thus appears to be
intensifying (Das Gupta and Bhat, 1997).
Our study explores this issue further, with more region-disaggregated and
age-focused data. Using the 1981 and 1991 censuses of India, we present
ratios among numbers of boys and girls aged 0 and 1 (taken together to
minimize the effect of age misreporting). Next, using an unorthodox
application of the technique of ‘reverse survival’ we estimate sex ratios at
birth for these two census years. We also present sex ratios of child mortality
probabilities (q5) from the censuses for these two time points. We examine
variations by rural/urban residence and state/region, drawing attention to the
specific sub-regions of India where changes have taken place over the decade.
We summarize what has been reported about the incidence of prenatal sex
selection and female infanticide in India, and place the evidence within the
context of social and economic development in India, especially relating to
the situation of women.
The rest of this article presents critical syntheses of prior research and
reporting on gender-specific demographic trends in India. Arguments con
cerning the possible impact of social and economic development on gender
stratification, and the consequent differences in the valuation and wantedness
of male and female children, are summarized. Subsequently, the observed
and estimated birth and mortality ratios calculated from the censuses are
presented. The concluding section discusses the implication of the arguments
and findings.
GLOBAL PATTERNS IN SRBs
Sex ratios at birth (henceforward SRBs), refer to the ratio of male to female
children born in a specific period, such as a year, or among all the children
ever bom to cohorts of women. In most human populations, more boys than
girls are conceived, and despite greater male than female foetal wastage, more
boys than girls are born. This leads to a fairly stable SRB observed among
human populations in countries with good vital registration, of approx
imately 104 to 106 boys per 100 girls (Johansen and Nygren, 1991). Sub
sequently, mortality rates at every age are slightly greater for boys than for
girls due to a combination of biological and behavioural factors. Thus, with
increasing age, the population sex ratio balances out to a slight female
dominance overall. Most societies irrespective of level of income or develop
ment exhibit this pattern.
In societies that have a marked preference for male children, however, a
different pattern is seen. In South Asia, population sex ratios are persistently
male dominant. In East Asia, period SRBs appear highly masculine
especially in recent years. In South Korea and China respectively, both
of which have good coverage of vital registration, SRBs as high as 112 and
Copyright © 2000. All rights reserved.
588
S. Sudha and S. Irudaya Rajan
113 males per 100 females have been observed among all births. First order
births are within the normal range (approximately 104-6 in each society).
Second and higher order births, however, soar up to 120 and more for China,
and third and higher order births to 185 and more for South Korea (AsiaPacific Population and Policy Report, 1995). Clearly, therefore, biological
patterns of SRBs are in these regions being overwhelmed by behavioural
factors rooted in parents’ preference for at least one male child (Coale and
Banister, 1994; Hull, 1990; Johansen and Nygren, 1991). These skewed SRBs
combined with anomalously masculine sex specific survival rates have
generated the problem of millions of‘missing’ females in East and South Asia
(Coale, 1991; Sen, 1992).
Several mechanisms are advanced to explain the phenomenon of
excessively masculine SRBs. In China, mechanisms include non-reporting
of female births (leading to omission of girl children in all subsequent official
records, tantamount to denying their social existence), abandonment and/or
out-adoption of girls, and female infanticide (Hull, 1990; Johansen and
Nygren, 1991). All these mechanisms can be viewed as varying types of
discrimination against female children. Lately, in China and South Korea
where there is a combination of lowered fertility, continued strong son pre
ference, and widespread access to medical facilities, the increased use of
prenatal sex determination techniques leading to abortion of female foetuses
is implicated in the phenomenally higher masculine birth order sex ratios
observed there (Asia-Pacific Population and Policy Report, 1995; Park and
Cho, 1995; Yi et al., 1993).
REGIONAL TRENDS IN JUVENILE SEX RATIOS IN INDIA
In India, most analyses focus on juvenile sex ratios rather than sex ratios at
birth. This is firstly because of the concern that excess female child mortality,
which arises from the selective neglect of girl children compared to boys,
manifests itself in childhood years rather than around the time of birth (Das
Gupta, 1987; Dyson, 1988). Secondly, data on period sex ratios at birth are
difficult to obtain in India, as the Census of India does not publish this
statistic. Such data are only occasionally published by the Sample Registra
tion System (SRS) of certain states, and thus nation-wide or time-trend
analyses are ruled out. Vital statistics registration is of varying quality and
completeness in different parts of the country, as are hospital records. Thus
all-India or time-trend investigations of period SRBs are difficult, although
some intra-state analyses are emerging (Visaria and Irudaya Rajan, 1996, for
Kerala).
Regional analyses of juvenile sex ratios in India on the whole indicate that
more masculine juvenile sex ratios and higher female than male child
mortality go hand in hand (Agnihotri, 1996; Clark and Shreeniwas, 1995;
Das Gupta, 1987; Das Gupta and Bhat, 1997; Kishor 1993). That is, higher
Copyright © 2000. All rights reserved.
t
Female Demographic Disadvantage in India 1981-91
589
juvenile sex ratios at ages 0-4 are accompanied by higher female than male
child mortality at ages 5-9. A well-known regional pattern is observed: the
Northern and Northwestern parts of India, including the states of Punjab,
Haryana, Rajasthan and Western UP, are areas most unfavourable to the life
chances of female children. Other parts of the country, including the East,
Central area and the South, exhibit more balanced rates.
A broad generalization has been made: the North/Northwestern regions of
India fall within the so-called Northern cultural and demographic zone,
distinguished by higher fertility, higher mortality, more masculine sex ratios,
and lower status of women. This zone traditionally had a wheat-based
agrarian economy (where women are less involved), and social systems
marked by dowry, exogamous marriage2 and the seclusion of women. In
contrast, the South is broadly characterized by rice-based agrarian systems
(with a greater role for women), endogamous marriage systems, marriage
payments that are more egalitarian between brides’ and grooms’ families,
and less seclusion of women. Women’s literacy and education levels are also
much higher in the South than the North. The status of women is higher in
the South, which also has lower fertility and mortality rates, and more
‘normal’ sex ratios (Dyson and Moore, 1983).
Other scholars rightly stress that the simplistic dichotomization of India
into ‘Northern’ vs. ‘Southern’ zones is inadequate. The rice-cultivating
Eastern region could never be fitted into either pattern. Within-region vari
ations have been ignored in the dichotomization, such as the ‘belt of female
infanticide’ in the Salem/Dharmapuri/Madurai districts of Tamil Nadu
noted by Chunkath and Athreya (1997). Alternative spatial patterns ranging
from five to nineteen clusters of India’s districts have been proposed, taking
into account ecological and economic sub-regions, areas with greater pro
portions of Scheduled Caste/Scheduled Tribe populations (who are
characterized by more gender-egalitarian cultures), and other criteria. Even
in these alternative groupings, however, juvenile sex ratios appear most
masculine in the North/Northwestern region of India. A so-called ‘Bermuda
Triangle’ for the female child exists in a zone of twenty-four districts
including parts of Haryana, Western Uttar Pradesh, some of Rajasthan, and
the ravine areas of Madhya Pradesh (Agnihotri, 1996).
2.
Exogamy refers to the practice whereby the bride marries outside her natal kin, clan or
lineage circles or village. It is argued that exogamous marriage makes women more
vulnerable, by separating them far from their natal kin, and placing them in the position of
outsiders in their marital families, until they ‘prove themselves’ by giving birth to sons and
by bringing dowry and other gifts from their natal home. Conversely, endogamy refers to
the practice of marrying within specific kin, clan or lineage circles or inside one’s natal
village, and is less detrimental to women.
Copyright © 2000. All rights reserved
08861
590
S. Sudha and S. Irudaya Rajan
FEMALE DEMOGRAPHIC DISADVANTAGE IN THE CONTEXT
OF DEVELOPMENT
Globally, it should be pointed out that gender-imbalanced demographic
measures are by no means simply associated with poverty or ‘under
development’, such that poorer nations have more female disadvantage.
African, Latin American and Caribbean nations, all with varying develop
ment philosophies, levels of poverty and living standards, exhibit ‘normal’
sex ratios at birth and of mortality. Any gender inequalities these countries
may have is apparently manifested in other domains. On the other hand,
countries such as China, South Korea and India which have a socio-cultural
pattern of preference for male children, irrespective of level of development
and philosophy of economic organization, exhibit gender imbalances in
demographic measures that persist over time.
In India, too, the relationship between social and economic development
and female disadvantage is not clear-cut. On the broadest level of general
ization, the process of development in India has been mostly to women’s
detriment. The 1974 Report of the Committee of the Status of Women in
India (GOI, 1974) was the first to point out that despite the progressive
promises and provisions of the Indian constitution, development since
Independence had been accompanied by a deterioration in women’s situ
ation, indicated by worsening sex ratios, declining female work participation
rates, and persistent shortfalls in literacy and female mortality.
Neither has the trend since that time been positive. The majority of Indian
women are involved in the agricultural sector, and have been adversely
affected by agrarian development. First, while land reforms focused on
redistributing land to the landless, in practice ownership was invested in the
household head, always seen as the senior male. Women’s alienation from the
most critical productive resource was thus progressively institutionalized.
Women’s use rights in land, where they exist, are exercised during the
goodwill of the male kin who have effective control over the land (Agarwal,
1994).
Second, although the Green Revolution dramatically increased food
production and allayed fears of population growth outstripping food supply
in India, it adversely affected women’s work participation. Evidence from
Punjab, Haryana, UP, and Tamil Nadu shows that the Green Revolution
narrowed the range of agrarian tasks, displaced women from traditional
occupations, and placed them at the bottom of the new labour hierarchies.
Women’s occupations became increasingly impermanent and casualized due
to technological changes coupled with traditional norms about the gender
based division of labour (Kapadia, 1992; Nayyar, 1989; Nigam, 1988; Sen,
1982). Although the initial impact of Green Revolution technology was to
increase the demand for labour to fertilize, weed, and harvest the new High
Yielding Varieties (HYVs), this trend was short-lived, and tended not to
involve women. For example, farmers in Gujarat utilizing HYV technology
Copyright © 2000. All rights reserved.
Female Demographic Disadvantage in India 1981-91
591
preferred male to female labour since they felt that men were more
efficient, more suited to the ‘high-technology’ innovations, could work for
longer hours at a stretch, and could fulfil demands for group labour.
Although women received lower wages than men for the same work, they
had no training for even the simplest new tasks such as spraying, and were
thus excluded (Hirway, 1979). In Bihar as in Gujarat, female work
participation grew substantially less in irrigated districts, and the rise of
mechanized dehusking and flour-making industries deprived women of
significant work they had hitherto performed (Hirway, 1979; Sinha, 1988).
Varghese (1991) states that rural Indian women’s paid work participation is
declining, and that women are highly concentrated (approximately 80 per
cent of female workers) in the agricultural labour and unpaid family work
sectors. The increased casualization of female labour is accompanied by
consistently greater unemployment among women than men. He concludes
that the ‘female marginalization thesis’ is supported in the Indian agrarian
context.
Non-farm opportunities have not kept pace with the displacement of rural
women. Though Deshpande (1992) shows that many urban women workers
are absorbed into new occupations such as in export processing zones, and
argues that despite low wages and poor working conditions they contribute
up to one third of household income, pull their families above the poverty
line, and thus gain a measure of respect and autonomy, Ramaswamy (1993)
argues that the vast numbers of women (94 per cent of the total female work
force) in the unorganized occupational sector indicates the failure of the
Indian planning process with respect to women. The organized sector,
depending on newly emerging technologies, offers little to the many women
displaced from rural or sunset industries. There are opportunities only for
those with education and skills. Though female literacy is rising, parents in
much of India do not encourage their daughters to attend more than a few
years of school, since higher education is seen as an unprofitable investment
in girls who will marry and move to their husbands’ households. Much of the
impetus for girls’ education comes from the increasing demand for literate
brides on the part of young educated men. Women thus cannot compete for
the new opportunities in significant numbers. Moreover, the masculine bias
of the organized sector tends toward decreased security of even those women
involved, as Indian trade unions usually downplay the needs of women
workers, who have had to set up parallel organizations as a result. Ramas
wamy (1993: 323) concludes that in India, ‘developmental processes have
only pushed women to states of survival’.
However, development has marginalized women in other less affluent
nations too, which none the less continue to exhibit gender-balanced
demographic measures. The fact that economic development devalues
women is not sufficient on its own to make families discriminate against
daughters. It is pointed out that both economic and cultural factors are
jointly responsible for the variations in the status of women, and consequent
Copyright © 2000. All rights reserved.
592
S. Sudha and S. Irudaya Rajan
sex differentials in the wantedness, birth, care and survival of male and
female children (Kishor, 1993).
Socio-cultural trends in India also place women at an increased dis
advantage. The traditional patrilineal, patrilocal, and exogamous marriage
and kinship systems prevailing over much of the subcontinent have always
placed women in a low-status, precarious position, until they earn their place
in the patriline by bearing sons. Although the southern part of the sub
continent had more endogamous and egalitarian marriage systems, with
matrilineal family forms in many Southwestern coastal communities, social
change in these regions has tended to move towards normatively patrilineal
systems. Significantly, scholars also note the spread of dowry3 nationwide to
communities and castes where it had never been the custom. Insufficient
research attention has been paid to this phenomenon. The bulk of socio
logical or anthropological research in India on the topic of kinship is abstract
and descriptive in nature, viewing women as objects of study and exchange,
and not problematizing t^e underlying causal and consequential gender
relations (Agarwal, 1994; Ramaswamy, 1993). Some scholars have begun to
address this issue (for instance, Palriwala and Risseeuw, 1996), but there is
little scrutiny of the relationship between kinship organization, gender
relations, and women’s life and death chances.
Some attribute the spread of dowry to the process of ‘Sanskritization’,
whereby lower castes achieve upward caste and class mobility by emulating
the customs of the upper castes, including dowry and female seclusion.
Others attribute the changes to the young age structure of the country: the
greater ratio of young marriageable girls to potential mates in the higher age
group increases the ‘price’ of grooms (Rao, 1993). The rise of consumerism is
also implicated, drawing people into a growing web of expectations and
demands. The continued importance of kin networks for economic resource
mobilization, the spread of the dowry custom, the growing amounts of dowry
changing hands, and the increasing importance of resource acquisition
strategies for family status enhancement, have led to the concentration of
wealth in families where the ratio of male children is greater, and female
children are therefore increasingly seen as liabilities (Clark, 1987- Hever
1992).
The socio-economic bases of female mortality disadvantage have been
examined with all-India level, and smaller-scale, localized analyses. All-India
studies suggest that districts with higher indicators of conventional develop
ment, such as urbanization, industrial output, and agricultural productivity
had significantly lower female vs. male survivorship, while girls in areas with
a greater concentration of Scheduled Caste/Scheduled Tribe populations
3.
Dowry is the transfer of wealth, in the form of money, gold, consumer goods, or other
assets, from the bride’s parents to those of the groom. Although the custom is supposed to
provide the bride with pre-mortem inheritance of her share of her family’s property, in
practice, she has little control over the dowry, and her in-laws dispose of it as they wish.
Copyright © 2000. All rights reserved.
Female Demographic Disadvantage in India 1981-91
593
(with largely more gender-egalitarian norms than the Indian mainstream),
endogamous marriage patterns, and greater female empowerment measured
by women’s labour force participation and education, fared better
(Agmhotn, 1996; Kishor, 1993; Murthy et al., 1996). These studies identify
a constellation of economic and cultural factors jointly affecting female
mortality disadvantage, improving on earlier and simpler models of female
agrarian labour force participation alone (Bardhan, 1974).
The findings of smaller-scale studies do not, however, lend themselves to
such consistent generalizations. The role of women’s education in amelior
ating female child mortality disadvantage might seem self-evident, and the
district-level studies cited above support the notion. However, smaller-scale
studies in rural Punjab and Gujarat indicate that mothers with some educa
tion might actually be more efficient in discriminating against their daugh
ters, particularly in asset-poor households. Schooling may make women
more aware of health, hygiene and nutrition, but female education alone is
not enough to transcend the nexus of conditions that leads families to
consider daughters a liability. Education often domesticates women rather
than liberates them (Clark and Shreeniwas, 1995; Das Gupta, 1987).
Regarding the role of economic assets, studies in rural Tamil Nadu suggest
that female child mortality disadvantage is greater among the landed and
upper-caste groups, where women are also more secluded and have lower
rates of work participation (Harriss-White, 1998; Heyer, 1992). In one Green
Revolution community of UP, and in a dairy co-operative region of rural
Gujarat, however, lower caste and landless groups are the ones where
daughters appear in greater jeopardy (Clark and Shreeniwas, 1995; Wadley,
1993). While the specific castes involved depend on local conditions, the
common factor is the family’s effort to acquire land or other economic
advantages through mobilizing kinship networks and manipulating the
marriages of their sons and daughters. In a patrilineal kinship system where
marriages are arranged on principles of dowry and hypergamy, and where
women are objects of exchange along with other forms of wealth, excess
female mortality is argued to be an inevitable outcome (Clark, 1987).
Contradictions notwithstanding, a pattern is discernible where increasing
economic marginalization and social devaluation make daughters increas
ingly viewed as liabilities. Productive activities and resources are increasingly
concentrated in the hands of men. Conventional socio-economic develop
ment accentuates rather than ameliorates this trend. Families therefore
respond by discouraging the birth and survival of female children. Numerous
studies document widespread gender inequality within households in the
allocation of food and health care; women and girl children have last
priority. This directly heightens female child mortality (reviews in Agarwal
1994; Kishor, 1995; Miller, 1997). The role of selective neglect of daughters in
excess female child mortality has been more extensively researched in the
Indian context, and is not addressed in this paper. We instead scrutinize the
related practices of female infanticide and foeticide, which have been less
Copyright © 2000. All rights reserved.
594
S. Sudha and S. Irudaya Rajan
examined in India for reasons obviously connected with the sensitivity of the
issues. The main findings not surprisingly come from the documentation
efforts of women’s groups and NGOs active in these fields rather than from
academic research.
FEMALE INFANTICIDE IN INDIA
Infanticide is an age-old post-natal practice among human populations to
regulate the numbers of children and eliminate less wanted offspring. The
practice of ‘exposing’ girls or weak or deformed babies was noted in ancient
Roman and Greek society in the West (Scrimshaw, 1984). Little is known
about female infanticide in India prior to the advent of British observers
(Miller, 1987). However, since then, female infanticide has been widely
recorded among upper caste (especially Rajput) groups in Northern and
Northwestern India.,
Historically, the main reasons for this practice in India included the system
of hypergamy, whereby women must marry into a social sub-group above
their own. Among the uppermost castes this was impossible. Since it was
unthinkable that the rules of hypergamy could be transgressed, or that girls
could remain unmarried, girls in these groups were killed and boys married
females from sub-castes slightly lower than their own. Nineteenth century
records show large groups of villages in Rajasthan and Gujarat, comprising
several hundred upper-caste households, where no female child had been
allowed to survive for many generations (Vishwanath, 1996). In that era
female infanticide was also part of a set of household strategies among these
same land-owning upper-caste groups, to acquire further holdings and
improve and consolidate their socio-economic status. This was achieved
through manipulating the marriage of sons and acquiring dowry from
daughters-in-law; daughters, as dowry-takers, were clearly a liability in this
scheme of things (Clark, 1983). Thus, the twentieth century socio-economic
processes linked to female societal devaluation and demographic disadvant
age discussed in the previous section, are foreshadowed in the nineteenth
century.
Similar processes are suggested to explain the spread of female infanticide
in modern India. Female infanticide has been recently noted among some
castes in remote village clusters in South India, in Tamil Nadu state, a region
where this practice was historically little known. Increasing landlessness and
poverty, an escalating dowry custom, high gender differentials in wages, low
education among women and few economic opportunities for them are
suggested as reasons (Chunkath and Athreya, 1997; George et al., 1992).
Newspaper reports describe the conditions of poverty and misery of the
families who turn to female infanticide, and their suspicion of alternatives
such as adoption offered by the Government and grassroots organizations in
the region (Aravamudan, 1994). Government plans to tackle the problem
Copyright © 2000. All rights reserved.
Female Demographic Disadvantage in India 1981-91
595
range from a ‘cradle baby’ adoption system for unwanted girl children, to
economic incentive packages for women who only have daughters and who
agree to undergo sterilization. The coercive design of some of these schemes,
and corruption and inefficiency in their management, have led to their falling
short of their targets and having a very limited impact on the problem. In
1995, an estimated 3174 female infanticides occurred in Tamil Nadu state
(George, 1997).
In rural North India, the historic practice of female infanticide apparently
never died out. Jeffery et al. (1984) state that up to the 1900s female infanti
cide was practised among Rajput castes in Bijnor, UP state. Their study in
the 1980s in villages around Bijnor town noted that part of a traditional birth
attendant’s duties continued to be disposal of unwanted (i.e. girl) children at
birth. They also report that the practice is spreading across the social
spectrum to caste groups among whom it had never been practised.
The same observation is made in rural Bihar state. In 1995, Adithi, an
NGO working in rural Bihar and having an excellent rapport with its target
population, conducted an in-depth investigation. It revealed that female
infanticide, foeticide, and excess female child mortality due to selective
neglect were widespread in the eight districts studied. Infanticide was carried
out by dais (traditional birth attendants), who were coerced by the senior
male kin of the woman giving birth, overriding the protests of the women in
the family. Fear of reprisals, poverty, lack of alternative occupation, and
socialization to obey the commands of those in authority led the dais to
comply. Other medical practitioners such as compounders and doctors also
carried out infanticide when approached by the family members of a
newborn girl. There was no difficulty in committing infanticide, because the
birth and death followed quickly upon each other, with no certificate
recorded for either event. Unscrupulous medical practitioners also conducted
abortion of female foetuses, especially after techniques like sonography
became widespread. The traditional skill of dais in identifying the sex of a
foetus in the seventh or eighth month of pregnancy is also used to avert the
birth of a daughter. Estimating a count of 68,000 dais in seven contiguous
and culturally similar districts of Bihar, and that each dai killed about two
infants a month (according to the interviews), Adithi (1995) estimates that
the number of female infanticides each year in these districts could total as
many as 1,632,000.
The Adithi report noted that whereas previously only upper castes such as
Rajputs and Brahmins practised female infanticide, the custom has now
spread to all other groups in the rural spectrum, including Scheduled Tribes,
Christians and Muslims. The main reasons are the spread of dowry with
exorbitant demands, due to marginalization of women from traditional
occupations and the concentration of income in the hands of men, with the
consequence that women’s seclusion and dependence on men increased, and
men began to assert their right to emulate upper caste customs, including the
practice of female infanticide. Emulation of upper caste social customs would
Copyright © 2000. All rights reserved.
596
S. Sudha and S. Irudaya Rajan
enable the men to tap into upper caste economic networks to further upward
class mobility. This spread of female infanticide across the Indian rural
spectrum supports the arguments made above about the association of
women’s social devaluation and economic marginalization with female
demographic disadvantage.4 The underlying socio-economic processes, first
analysed for the nineteenth century and intensifying in the twentieth century,
can be seen as going hand-in-hand with the persistence of excess female child
mortality and the spreading infanticide custom. The question of whether
some families turn to female foeticide as an option thus arises.
PRENATAL SEX DETERMINATION AND SEX-SELECTIVE ABORTION
IN INDIA
Unlike countries in East Asia, statistics on period sex ratios at birth, which
would have enabled us to assess the birth patterns of boys versus girls and.
thereby make direct inferences regarding sex selective abortion, are not
available for India. Statistics on abortion are also incomplete and largely
unavailable. In order to examine the possibility of the spread of female
foeticide in India, we thus turn to other kinds of evidence. In this section, we
summarize reports from a variety of sources about the increasing availability
and use of prenatal sex selection techniques. In the next section, we estimate
sex ratios at birth from the available census data. We then discuss the picture
that emerges from these complementary pieces of evidence.
Abortion was legalized in India in 1971, after a 1965 UN mission to India
recommended this step to strengthen the population policy, and the report of
the 1966 Shantilal Shah Committee also advocated it to reduce the numbers
of illegal and unsafe abortions. Although the stated reasons for passing the
Medical Termination of Pregnancy (MTP) Act were humanitarian (to ‘help’
victims of sexual assault), health-related (to provide an alternative to those
whose contraceptive measures failed) and eugenic (to reduce the numbers of
‘abnormal’ children born), there was a strong population control motivation
underlying the passage of the Act (Menon, 1996).
In 1975, amniocentesis techniques for detecting foetal abnormalities were
developed in India, at the All India Institute of Medical Sciences, New Delhi.
It was'soon known that these tests could also detect the sex of the foetus, and
doctors at the Institute noted that most of the 11,000 couples who volun
teered for the test wanted to know the sex of the child and were less interested
in the possibility of genetic abnormalities. Most women who already had two
or more daughters and who learnt that their expected child was female, went
on to have an abortion (Chhachhi and Sathyamala, 1983).
4.
Violence against women is growing, within and outside the home. Bihar has extremely low
female literacy: 23.1 per cent (Adithi, 1995).
Copyright © 2000. All rights reserved.
$
Female Demographic Disadvantage in India 1981-91
597
Between 1977 and 1985, in an effort to curb this misuse of the technique,
three circulars were sent to Central and State government departments
making the use of prenatal sex determination for the purpose of abortion a
penal offense (Kulkarni, 1986). Women’s groups, civil liberties groups and
health movements also launched a campaign against prenatal sex deter
mination and female foeticide (termed ‘femicide’). In 1984, a broad-based
coalition, the ‘Forum Against Sex Determination and Sex Pre-selection’
(FASDSP) was formed, with headquarters in Bombay, to monitor all aspects
of the situation, and document the growing use of the technique, and the
legal and policy steps taken against it. As a result of these efforts, the state
government of Maharashtra passed the Maharashtra Regulation of the Use
of Prenatal Diagnostic Techniques Act in 1988. The states of Punjab,
Gujarat, and Haryana followed suit and the Central Government passed
the Prenatal Diagnostic Technique (Regulation and Prevention of Misuse)
Act in 1994. The Act states that determining and communicating the sex of a
foetus is illegal; that genetic tests can be carried out only in registered
facilities; and only offered to women who meet certain medical criteria, such
as being over the age of 35, having a family history of genetic disorders, and
so on.
However, these acts are full of loopholes. Most restrictions pertain to
government facilities. Private laboratories and clinics are not banned from
carrying out tests that can be used to reveal a.foetus’s sex: they must only be
registered. While they are forbidden to communicate the foetus’s sex, many
evolve covert methods by which to do so. Second, the government can over
rule the decisions of the body set up to monitor facilities, which is empowered
to suspend or cancel the licences of offending clinics or laboratories. The
government can also exempt any facility from the Act. While in Maharashtra
the monitoring committee included representatives of NGOs, the State
Directorate of Medical Education and Research, and the Indian Council of
Medical Research, the Central Government Act appointed only two State
employees as regulators. Given the dubious record of the State as a monitor
ing body, the Act is thus considerably weakened. Further, an ordinary citizen
cannot directly move the courts, but must approach the monitoring body,
which can refuse to release any records if it is deemed in the public interest to
keep them sealed. Moreover, these regulations cover ultrasonography facil
ities to a lesser extent, and this technique is also being widely used for sex
determination. The possibility that newer technologies will be developed to
determine a foetus’s sex has not been allowed for (Arora, 1996; Menon, 1996;
Sengupta, 1992). The result of such partial regulation is that sex determina
tion facilities have privatized, commercialized, and mushroomed. Doctors
indicated that despite bans, they would continue to communicate the sex of
the foetus to parents who wanted to know, verbally rather than in writing,
and would hike the test fees to compensate for the legal risk. The
Maharashtra bans did not have much impact as sex determination facilities
continue to operate in that state (Kishwar, 1995). One study asserts that sex
Copyright © 2000. All rights reserved.
•1
(»
598
S. Sudha and S. Irudaya Rajan
selection continues to be the major purpose of prenatal diagnosis in India
(Wertz and Fletcher, 1993).
Systematic studies clearly indicate the increasing spread and acceptability
of the techniques. A 1982 study in Ludhiana, an urban area in Punjab state,
randomly sampled 126 individuals, of whom approximately half each were
male and female and most of whom were educated and middle class. All the
respondents had heard of the amniocentesis test; 66 per cent of them thought
it was intended for sex determination; few knew that it was actually for
detecting foetal abnormalities. While 73 per cent of the women and 59 per
cent of the men believed that a girl should be aborted if the couple already
had two or more daughters, only 25 per cent of the respondents felt that a
boy should be aborted if the couple already had two or more sons. The
reasons given indicated the nature of male-dominated society, dowry prob
lems, greater responsibilities in bringing up daughters, and social pressure to
bear sons. Over 71 per cent of the respondents felt that amniocentesis as a sex
determination test should not be banned (Singh and Jain, 1985).
u
These results were uncannily echoed over a decade later, in rural
Maharashtra state, among six villages of Pune district, three with road and
access to a health facility, and three others more remote and without these
amenities. Results indicated that 49 out of the 67 women interviewed indepth were aware of ultrasound and/or amniocentesis techniques and 45 per
cent of those who knew approved of aborting female foetuses. Only four
women were aware that such tests were actually for the detection of foetal
abnormalities (Gupte et al., 1997). The spread of awareness of these
techniques to rural areas is thus clearly documented.
The increase in number and reach of facilities offering sex determination
and abortion is also clear. In the early 1980s, Jeffery et al. (1984) noted that in
villages adjacent to Bijnor town in UP state, clinical services offering sex
determination and abortion had already appeared. The first newspaper
reports of private clinics offering sex selection techniques appeared in
1982-3, in cities such as Amritsar, Bombay, and Delhi. Within two to three
years, the numbers of such clinics rose to several hundred in the larger cities,
and several dozen in smaller towns in Maharashtra, UP, Punjab, and Gujarat
states. A few clinics reportedly had begun to offer services from the late 1970s
onward, but were brought to widespread public attention and formed the
subject of a Parliamentary debate only in the early 1980s, after a senior and
well-connected official’s wife underwent an abortion of a foetus that was
mistakenly diagnosed as female but turned out to be male (Ahluwalia, 1986).
The ensuing media storm ironically only served to increase awareness of the
techniques.
The use of these techniques thus became widespread not only in towns, but
also among rural areas with access to a road or transport system to the nearest
town. Newspaper reports describe mobile sex selection clinics, offering ultra
sound detection and immediate abortion if the foetus is female, in smaller
towns of Haryana state in the mid-1980s. The clientele included farmers who
Copyright © 2000. All rights reserved.
Female Demographic Disadvantage in India 1981-91
599
had come from villages half-an-hour away by road (Vishwanathan, 1991).
Remote districts that lacked basic amenities such as drinking water or
electricity were reported to have sex determination clinics; where refrigeration
and cold chain facilities for vaccinations were not available but amniotic fluid
samples were sent in ice packs to towns for testing (FASDSP and Saheli
Women’s Resource Centre, nd, cited in Menon, 1996). Grassroots workers
and concerned medical practitioners have observed an increase in female
foeticide in all segments of society in rural Bihar state, especially after
sonography techniques became common. Unscrupulous doctors identify the
sex of the child, and provide abortion if it is female (Adithi, 1995).
Nor is the cost of the test (ranging over time from Rs 500 to over Rs 1000)
a barrier. While we may expect that the largest consumers of such tests will be
those with at least a modicum of disposable income, education, and aware
ness of medical technology, landless labourers and marginal farmers are also
apparently willing to take out loans at high rates of interest to avail
themselves of these tests (FASDSP and Saheli Women’s Resource Centre, nd,
cited in Menon, 1996). In 1981-2, the approximate average daily wage of a
skilled male agricultural worker in Punjab was Rs 25, that of female and male
field or other workers ranged from Rs 10 to Rs 13. In Haryana, the figures
are Rs 18 for skilled workers, and Rs 7-15 for female and male field and
other workers. By 1991-2, the figures were Rs 84 for skilled male workers in
Punjab, Rs 77 in Haryana, and around Rs 40 in Bihar and Tamil Nadu. Field
workers in these states earned Rs 30—40 in Punjab/Haryana, and Rs 20—5 in
Bihar and Tamil Nadu (Government of India, 1983; 1993). Thus, even taking
the seasonality of wages, other expenses, and rural indebtedness into
account, affording the price of a sex determination test would not be totally
out of the question even for the poorer sections of rural society, especially in
the relatively rich states of Punjab and Haryana. The logic underlying the
motivation is illustrated by the now infamous slogan*. Better Rs 500 today
than Rs 500,000 tomorrow’ that was widely used in the early 1980s to
advertise sex determination clinics until protests from women s groups put a
stop to it. The slogan may no longer be used, but the underlying logic — that
an expenditure now (on the test) will save many multiples of the sum later
(on dowry, if the foetus is a girl) — still holds.
Performing the tests has become an extremely profitable practice for
doctors. A rough calculation may be made, that if the fee for a test is
currently around Rs 1000, and a clinic performs ten to twelve such tests a
day, based on a six-day work-week, a clinic can gross up to Rs 2.8 lakh (one
lakh = one hundred thousand; currently approximately 42 rupees = 1 US $)
per month. Some newspaper reports describe the tremendous wealth
amassed by practitioners offering this facility, and how training doctors in
the techniques has itself become a lucrative business. Nor is this trend toward
exploitation confined to the ‘modem’ medical sector. In March 1991, health
and consumer groups in Gujarat successfully lobbied the State Government
to ban a best-selling herbal pharmaceutical product called ‘Select’ that,
Copyright © 2000. All rights reserved.
I
600
S. Sudha and S. Irudaya Rajan
according to the manufacturer’s claims, used an ancient Ayurvedic technique
called ‘Punsavana Prayog’ to change the sex of a pregnant woman s foetus to
male (VHAI, 1992).
Attitudes of medical practitioners reveal that they view sex determination
tests as a ‘humane’ service they provide to couples not wanting any more
daughters; as a regrettable but unavoidable result of the preference for sons
in Indian society which they feel powerless to change; and as a necessary
weapon in the ‘population control’ arsenal (Kulkarni, 1986). Many also
argue that aborting a female is preferable to condemning an unwanted
daughter to a lifetime of neglect and abuse. These attitudes are also echoed
among large sections of the general public (Ravindra, 1995). Further, some
.eminent economists also endorse the argument that abortion of females is
preferable to neglect, and assert that if the sex ratio of India further worsens
as a result of these technologies, then the law of supply and demand will
operate and raise the value of women; thus curbing these tests and techno
logies is unnecessary or even retrograde (Kumar, 1983a, 1983b). v'
Making even approximate computations of the numbers of such pro
cedures occurring in India is difficult. One retrospective estimate (Saheli
Women’s Resource Centre, cited in Arora, 1996) suggested that betv/een 1978
and 1982 nearly 78,000 female foetuses were aborted after sex determination
tests. Arora (1996) also cites a statistic purporting to come from the Registrar
General of India, that based on hospital records alone, 3.6 lakh female
foetuses were aborted in India between 1993 and 1994.
ESTIMATING SEX RATIOS AT BIRTH IN INDIA
To complement such reports, and to assess the geographical spread and the
magnitude of impact of the increasing use of prenatal sex selection in India,
we use data from the 1981 and 1991 censuses. We present sex ratios of
children aged 0 and 1, i.e. under age 2. We then estimate sex ratios at birth by
means of the ‘reverse survival technique’ (UN Manual X, 1983: Chapter
VIII), using the counts of boys and girls aged under 2 and observed male and
female q2 mortality probabilities in the 1981 and 1991 Census of India
records, fitting to a South Model Coale and Demeny Life Table (Coale and
Demeny, 1966). In essence, the technique is based on the notion that children
aged x are the survivors of births that occurred x years ago. Therefore, it is
possible to take the numbers of children observed at age x, and observed
mortality probabilities for children in that population and, using a model life
table suitable in shape and level of mortality for the population in question,
‘resurrect’ the numbers who have died. Here, we ‘resurrect’ the numbers of
boys and girls under age 2 who died prior to the census enumeration, add
them to the numbers of reported males and females aged under 2, and take
the ratio of male to female children in the resulting total, to estimate a sex
ratio at birth.
Copyright © 2000. All rights reserved.
Female Demographic Disadvantage in India 1981-91
601
The authors warn that the reverse survival technique is sensitive to age
misreporting, especially for children aged 0 or 1. Das Gupta and Li (in this
volume) state that Indian census data show marked age-heaping, especially at
young ages. Our estimates overcome this potential danger by basing calcula
tions on children aged 0 and 1 taken together, i.e. those under age 2.
(In calculations not presented here, we examine sex ratios among infants aged
0, and the results are very similar to those among infants aged <2; none
differed by more than 2 per cent.) Moreover, we use this technique to
generate sex ratios among children ever bom, not to present or evaluate
estimates of actual fertility. Even if there is a nation-wide tendency to under
report the numbers of females (a contention doubted by Visaria, 1969), the
comparison we present, that is the trend over time in sex ratios, should not be
affected. In the absence of reliable statistics on abortions or on period sex
ratios at birth, we argue that infancy sex ratios and estimated SRBs provide
information that can illustrate and evaluate the impact of continuing
son preference in India, under conditions of social change, economic
development, declining fertility and mortality, and spread of new medical
technologies.
It was pointed out some time ago that the distribution of prenatal sex
determination facilities in India was greater in areas where females were more
devalued, i.e. the North/North-west (Patel, 1988). During the decade covered
in this study (1981-91), reports suggest that such techniques were more
widely available in urban areas, although there is every indication that their
awareness and use spread into the rural hinterlands too. Urban areas are
characterized in developmental terms by higher female literacy, more non
agrarian employment opportunities, more paid employment opportunities
for women, and better infrastructure, including availability of health
services. Moreover, a more egalitarian ethos may accompany increasing
education, income, and exposure to diverse groups and thoughts.
Thus, while scrutinizing the estimated SRBs, one might contrast urban/
rural SRBs over the decade, to investigate whether urban SRBs grow
progressively more ‘normal’ with improved education and greater accuracy of
reporting/recording births, and decreasing scope for female infanticide or
abandonment of girls. On the other hand, if gender stratification in India is
intensifying, attested by the increase of phenomena such as dowry and
economic marginalization of women, many urban families would not
necessarily have greater incentive to welcome daughters. They would also
have more access to the means to avert their birth, i.e. prenatal sex deter
mination and selective abortion, which may be seen as more acceptable and
practicable alternatives to female infanticide, abandonment, or non
registration of girls’ births. In fact, families with some amount of education
and disposable income might have better access to these techniques and thus
be more efficient in discriminating against their daughters. Particularly with
fertility falling in many parts of the country, with urban areas in the
forefront, Indian families may take steps to ensure that at least one son is
Copyright © 2000. All rights reserved.
602
S. Sudha and S. Irudaya Rajan
bom to them, as do Chinese or Korean families. Thus, if urban SRBs grow
anomalously masculine over the decade, the most likely cause is the increas
ing use of prenatal sex selection techniques rather than under-reporting,
infanticide, or abandonment of baby girls.
Appendix Table 1 presents the observed sex ratios among infants aged
under 2, and the corresponding estimated SRBs for rural and urban areas of
each state, for 1981 and 1991. Ratios are presented here as males per 100
females. There is, by and large, little difference between sex ratios at ages 0
and 1, and estimated sex ratios at birth. As may be expected, once mortality
at infant ages is taken into account, most ratios lessen, but only very slightly.
However, in some states, predominantly in rural areas, the ratios heighten
slightly, such as in rural MP, North-eastern states (Mizoram, Nagaland,
Arunachal Pradesh, Tripura), and the South (rural Kerala, Tamil Nadu and
Karnataka, urban and rural Maharashtra and Orissa). In 1991, far fewer
regions show this pattern: Himachal Pradesh, and urban parts of Sikkim,
Goa, Dadra and Nagar Haveli, and Pondicherry. The ; census was not
conducted in Assam in 1981, and in Jammu and Kashmir in 1991, thus the
corresponding Table and Figure entries are blank.
Spatial and Temporal Trends in Estimated Sex Ratios
at Birth
The spatial distribution of trends in estimated SRBs from the two
censuses are presented in Figure 1, which identifies rural and urban areas
of those states with ‘abnormally’ masculine SRBs (i.e. >107). The actual
sex ratio values on which Figure 1 is based are presented in Appendix
Table 1.
Figure 1 shows that in 1981, most parts of the country exhibited SRBs that
were not ‘abnormally’ masculine. The few masculine regions were mostly
within the North/North-westem zone such as urban Punjab, Jammu and
Kashmir, and Chandigarh, also urban Gujarat in the West, and, surprisingly,
the Lakshadweep Islands off India’s South-west coast. Appendix Table 1
shows that the ‘masculine’ SRBs mostly have values at the lower end of the
range (107-110). Thus, in 1981, we can conclude that SRBs in India were in
general not very masculine. Appendix Table 1 bears this out by showing all
India values within the normal range.
In 1991, Figure 1 shows a greatly changed picture. We see masculine SRBs
not only in the urban areas of the North/North-western zone (Himachal
Pradesh, Punjab, Rajasthan, Haryana, Delhi, and Chandigarh), but in the
corresponding rural areas, and a spread of anomalous masculinity outward
from this zone to urban areas of Central and Western zone states, namely
Gujarat, UP, MP, Bihar, Maharashtra, and Goa. Arunachal Pradesh, Assam
and Sikkim in the North-east also have masculine SRBs. Appendix Table 1
shows a stark shift toward excess masculinity, with SRB values in the range
Copyright© 2000. All rights reserved.
I
Female Demographic Disadvantage in India 1981-91
603
Os
Os
I
0)
£<D
.
tn
o
o
o
o
7
Sis
□ a:
•2
.22
.E5
i 3" 31
<
o
o
o
C§
I • °
I
©
s
□J
£Co
D
a.
2
2
V)
g
CM
CL
O
o
£
a?3
£
Ch
5
604
S. Sudha and S. Irudaya Rajan
of 107-118. The lowest abnormal values are 107 for urban Bihar, UP, and
Goa, and the highest values reach 118 for urban Punjab and 116 for urban
Haryana. Appendix Table 1 shows that the all-India urban area SRBs now
reach 108, reflecting the increase in masculinity of urban SRBs of many
states. The Southern states’ SRBs appear normal in both decades. The
Lakshadweep Union Territory (off the Kerala coast) that had masculine
SRBs in 1981 is in the normal range in 1991.
For 1981, Appendix Table 1 shows some states (Andhra Pradesh and
urban Tamil Nadu in the South; Manipur, urban Nagaland, Meghalaya and
Arunachal Pradesh in the North-east; Madhya Pradesh, urban Orissa and
rural Bihar in the Centre; Rajasthan and urban UP in the North/North-west;
urban Dadra and Nagar Haveli) have SRBs that may be seen as feminine
(below 103). We speculate that this might be due to under-reporting of
infants that might have been born alive but died shortly thereafter. They
would not be enumerated, and would thus not show up in either the counts of
infants, or the mortality statistics. Since neonate and infant boys have higher
mortality than girls, boys may be over-represented in the uncounted children,
leading to unusually feminine SRBs. In 1991, the phenomenon of. excess
femininity of SRBs has greatly lessened, now noted only in Dadra and Nagar
Haveli, Nagaland, and rural Arunachal Pradesh, Manipur, Meghalaya,
Andamans and Lakshadweep, and MP. This could be due to improved
enumeration and tabulation, or lessening of male infant/child mortality due
to the improvement in health facility coverage, or to the general country-wide
trend toward the masculinization of SRBs.
We conclude that while SRB figures have grown anomalously masculine
across several states, the numerical magnitude of the impact of sex selective
abortion in India is not great as yet, at least according to these Census
records. In East Asia, the impact of such practices amounts to about 5 per
cent of female births (Asia Pacific Population and Policy Report, 1995). In
India, the impact is less than this. Since the 1991 all-India rural SRB was
within the normal range, if we examine the change in all-India urban SRB
from 104 in 1981 to 108 in 1991, and consider that an SRB of 106 is the upper
bound of ‘normal’, then only 2 per cent of female births are affected. This
translates to a shortfall of some 74,600 female births (all-India urban),
mostly in the North-west zone. Since official records of induced abortion in
India are notoriously flawed and incomplete, Mishra et al. (1998) have
estimated the likely number of abortions occurring in India using National
Family Health Survey data (1992-3). They show that the possible numbers of
induced abortions for all-India were over 207,000. However, the fact that the
numerical magnitude of sex-selective abortion as judged from Census records
is not very great, does not diminish the gravity of the issue, for two reasons.
First, since Census records are only picking up the ‘tip of the iceberg’ of this
phenomenon, the reality is probably greater than the figures show. Second,
even Census records indicate that the phenomenon is increasing over time,
which is itself a grave cause for concern.
Copyright © 2000. All rights reserved.
Female Demographic Disadvantage in India 1981-91
605
SPATIAL AND TEMPORAL TRENDS IN FEMALE DISADVANTAGE IN
CHILD MORTALITY PROBABILITY
We examined evidence that prenatal sex determination and selective abortion
of female foetuses occurred on an increasing scale in India during the decade
1981-91, in specific urban areas. We also reviewed studies and reports that
female infanticide is spreading across the rural Indian spectrum. We now
turn to the examination of sex-specific child mortality probabilities, to
examine whether girl children in India continue to face heightened mortality
risks vis-d-vis boys. In Appendix Table 2, we present sex ratios of under-5
mortality probabilities for children (q5) for 1981 and 1991, for each state,
for rural and urban areas. Mortality ratios that indicate female disadvantage
(i.e. male to female q5 ratio < 100) are considered anomalous. Ratios that
show male disadvantage are considered ‘normal’. Figure 2, based on this
table, maps the spatial and temporal distribution of female mortality
disadvantage.
Figure 2 shows the spatial distribution of trends in mortality sex ratios
across 1981-91, identifying rural and urban areas of those states with ratios
showing female disadvantage. In 1981, all the Northem/North-western states
(except Himachal Pradesh and urban Jammu and Kashmir) had excess
female child mortality, in urban and rural areas. In 1991, all these areas
continued to exhibit female mortality disadvantage, with the exception of
Chandigarh, which along with urban Dadra and Nagar Haveli and
Andaman Islands, were the only regions shifting to ‘normal’ female vs.
male child mortality risks. Furthermore, in 1991, female mortality dis
advantage appeared in areas that were ‘normal’ in 1981, namely rural and
urban Orissa, Goa, and Karnataka, and rural Tamil Nadu (in keeping with
reports of female infanticide in that state). Thus, the phenomenon of excess
female child mortality not only persisted over the decade, but also actually
spread across more of India.
Overall, levels of child mortality in India declined considerably from
approximately 152 per 1000 (both sexes, all India) in 1981 (Government of
India, 1988: 5), to 96 per 1000 in 1991 (both sexes, all India, in Irudaya Rajan
and Mohanachandran, 1998, based on 1991 Census records). Appendix
Table 2, however, shows that the sex ratio of mortality actually became more
male-biased during 1981-91, indicating that mortality fell more for males
than females, and that females still have higher mortality than males. Positive
changes (i.e. lessening female mortality disadvantage 1981-91) are seen in
only a few areas, such as Himachal Pradesh, the Union Territories of Delhi
and Chandigarh, rural Punjab, urban Rajasthan, West Bengal, Mizoram,
Dadra and Nagar Haveli and Andaman Islands. However, of these areas,
only the small regions of Chandigarh, Mizoram, Dadra and Nagar Haveli
and Andaman Islands show ‘normal’ male to female mortality risk ratios in
1991, the other regions still exhibit female disadvantage. Increasing female
disadvantage appears in many North/North-western and Central states:
Copyright © 2000. All rights reserved.
o
o
O\
Figure 2. Spread of Female Disadvantage in Mortality Probability, India 1981 1991
1991
1981
>o
<Mmnw and Katfnr■
ArurwcJM
Praoaah
•O
Ar*a*al
Prada*
Oanlgaor
•O
K-
•O
•O
OaW-
• O^
•o
R*aa**
•o
Madhya Prada*
MM
•o
.•V
M*OfM
Tnpura
Ma*ya Prada*
CMarar
Onwa
•o
Prada*.
Goa -
>•0
Goa
• FontMtwry
Tarn!
.Nadu
Tr<xn
[-------- Muon
Mah««ir*»
OnMl
Andhra
Prada*.
Lak*arMap •
lalanda .
'S'
•o
---------- Mnram
DMatMagvH**)-
olftatNagarHav*-
f-Mg^nd
AMWn
•o
Ww
X-NagMand
Z_Ma^>Maya
A1MM
S2
,•0
'ora**
UK* Prada*
SMwii-
UH* Prada*
• l
co
TamJ
iNadu
AndamantlCcat*
wand.
0
MdamantMcobar
IdanN
,
I
§
‘a
*
‘i
%
Female Disadvantage in Mortality Probability (q5) is
q5 Sex Ratio < 100m / lOOf
t
>5
SRM < 100 Urban
O
SRB< 100 Rural
Copyright © 2000. All rights reserved.
a
Female Demographic Disadvantage in India 1981-91
607
rural Rajasthan, urban Haryana, all of UP, Bihar, MP, and Gujarat, which
all had female mortality disadvantage in 1981. Orissa, which had ‘normal*
mortality sex ratios in 1981, shifts to female disadvantage in 1991. In South
India, Karnataka, Goa, and rural Tamil Nadu also shift from ‘normal’ ratios
to female disadvantage. Thus, substantial parts of India in 1991 exhibit
persistent excess female child mortality, in keeping with research document
ing persistent selective neglect of girls.
While the 1991 Census mortality figures for Kerala also indicate female
disadvantage, infant and child mortality is generally so low in this state,
that a small absolute difference between the sexes has translated into a
large difference in the ratio in this case. Thus, in the case of Kerala, we do
not suggest at this time that excess female child mortality has suddenly
emerged in this state, since, unlike Tamil Nadu, no study has identified this
phenomenon here. This logic also applies to some Union Territories and
states in the North-east, that indicate extreme values of the mortality sex
ratios. Values in 1981, such as 152 for urban Meghalaya or 128 for urban
Sikkim, are an artifact of small sex differences in low reported levels of
mortality.
To contextualize the scenario of birth and life chances of boys and girls in
India, Appendix Table 3 shows fertility trends in different regions of India
1982-94. This decade witnessed a moderate fertility decline in the country
as a whole (20 per cent), from a TFR of 4.5 in 1982 to 3.5 in 1994 (SRS
Reports). However, we observe dramatic declines in the South, such
that Kerala now has below replacement fertility and Tamil Nadu is at
replacement level, and Karnataka and Andhra Pradesh are below the
national average. The Eastern states register moderate declines, as do Gujarat
and Punjab. The other Central and North/North-westem states record more
modest gains.
The demographic picture that emerges for the period 1981-91 is one of
all-India declines in fertility and mortality, worsening sex ratios of child
mortality in many major states, and increasing masculinity of SRBs in the
North/North-west, and in urban areas of some Central states. Prior studies
showed that higher birth order females were at the greatest risk of mortality
in Northern and North-western India (Das Gupta, 1987; Kishor, 1995). It is
therefore argued that with declining fertility, the proportion of births of
higher order would decline, lowering excess female child mortality overall.
Since the mortality ratios have not shown lessening female disadvantage in
the face of declining fertility, this contention is clearly not upheld. Further
more, SRBs in the North/North-west regions indicate increasing sex selection
to ensure that the greater proportion of babies bom are of the wanted
(male) sex. Thus, excess female child mortality appears combined with
prenatal sex selection in a specific zone of the country — the North/Northwest — to create a ‘double jeopardy* for Indian daughters there, with
increasing female mortality disadvantage in other regions that have ‘normal’
SRB patterns.
Copyright © 2000. All rights reserved.
S. Sudha and S. Irudaya Rajan
608
CONCLUSION AND DISCUSSION
The first point we highlight is the great need for suitable data to be collected
and released in a timely manner by the Government of India. The decennial
census does collect information on the number and sex of births in the
enumeration year. Statistics on period SRBs for all parts of India could be
directly furnished, removing the need for indirect estimation to illuminate
this important question. In our findings, it should be kept in mind that the
SRBs have been estimated based on the reported numbers of infants aged
under 2 years, and thus may be affected by any under-registration of female
' births or female infanticide, though we argue otherwise.
However, even with indirectly estimated measures, there is a clearly
marked shift toward increasing masculinity of SRBs in North/North-west
India, and urban areas of Central India. This suggests the rising use of
prenatal sex determination and sex selective abortion there. The studies and
reports we summarize, and the spatial distribution of the SRB figures we
present, indicate plausibly that prenatal sex selection techniques are being
increasingly used in these (regions. The trend initially began (as might have
been expected for a medical technological innovation) in urban areas and
spread out over time to the rural surroundings, especially concentrated in
those regions of the country that have a socio-cultural history of disfavour
toward women. As we saw, in 1981, only urban areas of the North-western
region had somewhat abnormal SRBs. By 1991, urban and rural parts of the
North-west, and urban parts of Central regions, all had masculine SRBs,
some with very high values. Since the increased masculinity is seen in urban
areas, we cannot attribute the trend to increased under-reporting of girls, or
rise in female infanticide, both of which are less likely to be successfully
carried out in urban areas.
Some argue that increasing masculinity of SRBs could be caused by
development, especially in the health sector, because improved health condi
tions provide better life chances to male foetuses that are by nature more frail
and prone to die. The trend in many parts of India between 1981 and 1991 of
SRBs moving from excess femininity to normal masculinity may be due to
this factor. The intense masculinity in the North/North-west region is,
however, a little difficult to attribute entirely to improved health. If improve
ments in health were mainly at the bottom of increasing masculinity of SRBs,
then regions such as Kerala and urban areas elsewhere in the South would
also have witnessed much more masculinity of SRBs than they have. We
thus conclude that improved male survivorship is in itself an insufficient
explanation for the temporal and spatial trend in sex ratios in India. Since, as
discussed above, other alternative explanations such as female infanticide
and under-registration of births are less likely in urban areas, the spread of
prenatal sex selection is further implicated.
Evidence indicating women’s increasing economic marginalization and
greater socio-cultural devaluation underlines the contention that develop-
Copyright © 2000. All rights reserved.
Female Demographic Disadvantage in India 1981-91
609
ment in India has generally been to the detriment of women, and further
research investigating how these trends are causally linked to female demo
graphic disadvantage is needed. Families in India respond to developmental
stresses by increasing discrimination against daughters, since this strategy fits
with the matrix of choices deemed culturally acceptable, which are largely
patriarchal in nature. Alternative strategies such as investing in girls’ educa
tion, ensuring daughters’ inheritance, and including females in the produc
tion process, are less considered. Resisting dowry pressures generated by a
‘groom shortage’ by marrying women to men their own age or younger, or
leaving them unmarried, or finding a spouse of another caste or community,
appear unthinkable. Despite gains in education, longevity, and income for
some groups of women, large sections of Indian society apparently still
consider daughters a liability, and may prefer to avert their birth. While
infanticide in earlier eras had been confined to certain limited caste and
geographical groups, neglect of daughters, female infanticide and foeticide
now appear widespread in some parts of India, and have pervaded groups
and classes where they were hitherto unknown (Adithi, 1995; Harriss-White,
1998; Jeffery et al., 1984). Selective neglect of daughters persists. In fact, the
co-existence of female foeticide, infanticide, and selective neglect of girls
renders the distinction between pre- and post-natal sex selection techniques
invidious: the bias against girls is entrenched, and the choice of methods may
depend on convenience rather than conscience. Some scholars have gone so
far as to term the persistent and multi-layered bias against girls, as ‘gender
cleansing’ (Harriss-White, 1998).
However, while the aggregate statistics for 1981-91 indicate that pre- and
post-natal sex selection methods co-exist in many regions, conclusions
regarding additive rather than substitutive strategies should also consider
whether some local differences are being obscured in the aggregate. A study
of a rapidly urbanizing and changing rural area near New Delhi revealed that
local parents of the Jat community had an ideal family composition of two
sons and one daughter, and thus formed the clientele of the flourishing local
sex determination clinics. However, the subsequent infant/child mortality
rates among their children did not reveal female disadvantage any more
(Khanna, 1995, 1997). This suggests that a pattern of substitution is indeed
occurring. More such micro-level studies would better illuminate whether
within any region, some families use certain strategies and others follow
other methods, or whether the same groups are indeed following both
strategies. Future research should prioritize examination of demographic
behaviour, development trends and policies in India from a gender perspect
ive, and focus on the nexus between macro-level cultural and economic
structures and micro-level household organization and strategies.
The contention that selective neglect or infanticide affect mainly higher
birth order girls and that therefore the gender imbalance in demographic
rates and indicators should decline with decreasing fertility and mortality is
clearly not upheld in this study. Consider that if the Jat families in the study
Copyright © 2000. All rights reserved.
L-
610
S. Sudha and S. Irudaya Rajan
just referred to could actualize their desired family size and sex composition,
the community would show a TFR of 3.0 and an SRB of 200! In fact, the
ideational shift to controlled fertility that includes acceptance of modern
means of contraception has, in India, also meant a growing societal accept
ance of medical technologies surrounding conception, prenatal sex selection,
and abortion. Abortion selectively directed against female foetuses is
acceptable to large sections of society in the name of ‘population control’,
or couples’ greater reproductive choice. The secular societal trend that
increasingly devalues female lives remains largely unquestioned.
The argument that an adverse sex ratio will lead to a shortage in the supply
-of women, which will drive up their value since demand will remain high, is
also unconvincing. The sex ratio in India has been noted to be adverse to
females, and more or less steadily worsening, since the first recorded Census
of 1871. The population sex ratio of India declined from 972 females per
1000 males in 1901 to 929 per 1000 in 1991. In this same period, the status of
Indian women has been steadily eroded, despite gains made in some sectors”
by some groups of women. A ‘shortage’ of women does not lead to their
increasing valuation,; but to greater restrictions and control being placed over
them. The increasing intensity of violence against women in all domains of
life is testimony to this. Scholars predict increased social unrest in China once
the shortage of females to males of the appropriate ages in the marriage
market is felt, as a result of the skewed SRB patterns there (Tuljapurkar et al.,
1995). The same might be said for India.
The trend toward greater use of prenatal sex selection despite legislative
proscription, combined with persistent female disfavour in mortality ratios,
combines to produce a scenario that is not likely to improve in the near
future. These demographic phenomena are themselves only symptoms of the
worsening situation of women in the Indian socio-economic developmental
context. Policy measures addressing women’s societal devaluation have
either not been implemented, as in the Central Government scheme proposed
in early 1997 of cash subsidies to girl children in all families identified as
poor; or have had very limited impact, as illustrated in Tamil Nadu state’s
cash subsidy schemes or ‘cradle baby’ schemes (George, 1997). NGO
strategies to tackle infanticide or female devaluation range from the very
long-term (consciousness-raising), to the confrontational (reporting suspi
cious female infant deaths to the police), to the ineffective (attempting to
dissuade parents from infanticide). Examples of plans that have successfully
involved women and men in local development efforts are rare and recent,
and their impact on demographic behaviour is as yet small.
Furthering the legislative drive against discriminatory practices, on
9 January 1996, the Indian Government announced a ban on the abortions
of healthy female foetuses identified during permissible genetic tests. Under
the new law, mothers, fathers, and doctors can all be punished with fines
ranging from $300-51500 and prison terms from three to five years, escalat
ing for repeat offenses. Critics point out that women are rarely the primary
Copyright © 2000. All rights reserved.
Female Demographic Disadvantage in India 1981-91
611
decision-makers in the use of these technologies, and such legislation places a
dual punishment on them. It is feared that women will be driven to seek
terminations of unwanted pregnancies under illegal conditions, in a country
where the majority of abortions are already reported to take place illegally. It
remains to be seen how effective new legislative measures will be in reversing
the trend of female foeticide, when past actions have not shown marked
success. Our review of the literature suggests that any policy measures must
not focus primarily on restricting technology used to women’s detriment, but
must also address the root causes of devaluation of Indian women, or they
will not succeed in eradicating discriminatory practices but will drive them
underground where they will continue to flourish.
ACKNOWLEDGEMENTS
This research was supported by a grant from the UNFPA Population and Sustainable
Development Programme at the Centre for Development Studies, Thiruvananthapuram, as a
‘Research in Support of Training’ activity. We are grateful to the office of the Registrar General
of India for providing the data and to the Centre for Development Studies for institutional
support. We thank Dr P. Mohanachandran for technical advice, Dr R. Homan for
programming help, and Ms A. Mini for research assistance. We are grateful to Tom Swasey
and John Vogler of the Carolina Population Center for assistance in preparing maps. We thank
Sarthi Acharya, Cecile Jackson, Helen Lambert, Alec Mercer, Uday Shankar Mishra, Richard
Palmer-Jones, and Shahra Razavi for their helpful comments. The following NGOs generously
shared their information with us: ADITHI, Patna; JAGORI, New Delhi; MATRIKA, NewDelhi; M. S. Swaminathan Research Foundation. Chennai. S. Sudha thanks family and friends
for child care, inspiration and moral support without which this paper could not have been
written.
Copyright © 2000. All rights reserved.
S. Sudha and S. Irudaya Rajan
612
appendix
Table 1. Sex Ratios at Ages 0+1, and Estimated Sex Ratios at Birth:
1981-91
1981
1991
Sex ratio (M/F)
Sex ratio (M/F)
Observed ratio
Observed ratio
Estimated SRB
0+1
i
Estimated SRB
0+1
State/Region
Rural
Urban
Rural
Urban
Rural
Urban
Rural
Urban
INDIA
North!Northwest
Himachal Pradesh
Jammu & Kashmir
Punjab
Rajasthan
Haryana
Delhi (UT)
Chandigarh (UT)
Uttar Pradesh
103
104
103
104
106
108
106
108
105
105
107
103
109
105
112
104
105
110
108
103
’ 107
104
103
102
105
105
105
101
108
105
111
103
105
110
107
102
106
106
107
102
108
113
109
117
108
114
111
110
107
119
111
117
111
109
109
117
107
113
110
110
106
118
110
116
110
109
108
102
101
105
102
101
104
104
102
108
101
103
105
101
102
104
106
102
104
103
101
107
105
104
105
107
103
107
103
104
103
108
108
112
108
104
106
105
102
106
106
103
103
107
107
111
109
103
107
102
104
103
103
103
101
102
100
105
101
105
100
103
104
105
104
101
99
104
102
102
102
106
101
104
100
103
104
105
104
100
98
104
105
102
99
101
101
104
103
105
105
108
104
103
103
109
104
105
123
103
104
103
99
101
101
104
102
105
104
107
104
102
103
109
104
105
124
102
101
103
102
107
102
102
104
103
102
104
103
106
102
101
104
106
103
105
105
106
104
105
105
105
103
105
105
106
103
105
105
94
104
109
99
103
95
108
103
103
100
102
101
103
104
106
94
105
100
102
103
106
101
106
Central
Bihar
Madhya Pradesh
Gujarat
Maharashtra
Orissa
Goa
East!Northeast
West Bengal
Assam
Mizoram
Nagaland
Meghalaya
Arunachal Pradesh
Tripura
Manipur
Sikkim
South
Kerala
Andhra Pradesh
Tamil Nadu
Karnataka
Union territories
Andamans
Lakshadweep
Dadra Nagar Haveli
Pondicherry
102
109
98
102
110
100
102
114
ri
101
103
------
Notes'. Any value above 107 can be considered ‘excessively’ masculine. The census was not
conducted in Assam in 1981, or in Jammu and Kashmir in 1991.
Source. Censuses of India 1981 (Government of India, 1988); and 1991 (Government of India,
1991).
Copyright © 2000. All rights reserved.
Female Demographic Disadvantage in India 1981-91
613
Table 2. Sex Ratios of Child Mortality: 1981-91
1981
1991
Sex ratio of child mortality q5 m/f Sex ratio of child mortality q5 m/f
State/Region
Rural
Urban
Rural
Urban
INDIA
93
98
89
95
North)North west
Himachal Pradesh
Jammu & Kashmir
Punjab
Rajasthan
Haryana
Delhi (UT)
Chandigarh (UT)
Uttar Pradesh
104
97
87
89
81
85
88
83
107
102
92
89
89
95
99
86
108
110
92
85
81
89
107
79
92
90
82
96
110
82
87
96
101
103
92
106
90
98
106
101
94
103
72
92
100
93
80
96
79
92
104
86
82
91
152
108
116
107
105
91
104
94
106
Central
Bihar
Madhya Pradesh
Maharashtra
Orissa
Gujarat
Goa
EastjNortheast
West Bengal
Assam
Mizoram
Nagaland
Meghalaya
Arunachal Pradesh
Tripura
Manipur
Sikkim
99
99
107
106
105
106
105
104
120
111
132
126
152
108
103
128
92
103
113
100
104
104
102
90
110
South
Kerala*
Andhra Pradesh
Tamil Nadu
Karnataka
113
105
101
101
101
107
104
102
94
103
88
96
88
108
100
97
Union territories
Andamans
Lakshadweep
Dadra Nagar Haveli
Pondicherry
107
121
113
103
92
105
97
104
112
136
133
107
102
91
136
103
*See explanation in the text. For all other cells, any value < 100 can be considered to indicate
female disadvantage.
Sources: 1981: Government of India (1988); 1991: Irudaya Rajan and Mohanachandran (1998).
Copyright © 2000. All rights reserved.
5. Sudha and S. Irudaya Rajan
614
Table 3. Profile of Fertility Decline in Major States of India (1982-94)
Total fertility rate (TFR)
State/Region
1982
1994
% decline
INDIA
4.5
3.5
22.20
North/North-west
Rajasthan
Uttar Pradesh
Haryana
• Punjab
5.3
5.7
4.9
4.0
4.5
5.1
3.7
2.9
15.10
10.10
24.50
27.50
Central
Bihar
Madhya Pradesh
Gujarat
Maharashtra
Orissa
5.6
5.3
4.2
3.8
4.3
4.6
4.2
3.1
2.9
3.3
17.90
20.80
26.20
23.70
23.30
East
West Bengal
4.1
3.0
26.80
South
Andhra Pradesh
Karnataka
Kerala
Tamil Nadu
3.9
3.6
2.9
3.3
2.7
2.8
1.7
2.1
30.80
22.20
41.40
36.40
Source: Government of India (1982, 1994).
REFERENCES
ADITHI (1995) Female Infanticide in Bihar. Report prepared by Viji Srinivasan. Vijay Parinita,
Alice Shankar, Medha Mukul and Anita Kumari. Patna: ADITHI.
Agarwal, Bina (1994) A Field of One’s Own: Gender and Land Rights in South Asia. Cambridge:
Cambridge University Press.
Agnihotri, S. (1996) ‘Juvenile Sex Ratios in India: A Disaggregated Analysis’, Economic and
Political Weekly 28 December. S3369-S3382.
Ahluwalia, Kishwar (1986) ‘Amniocentesis, the Controversy Continues’, Times of India 8 March.
Aravamudan, Gita (1994) ‘Whose Baby is She Anyway?’, The Hindu 16 October.
Arora, Dolly (1996) ‘The Victimizing Discourse: Sex Determination Technologies and Policy’,
Economic and Political Weekly 'XXXlfJ'): 420-4.
Asia-Pacific Population and Policy Report (1995) ‘Evidence Mounts for Sex-Selective Abortions
in Asia’, Report No. 34 (May-June). Honolulu, HI: East-West Center, Program on
Population.
Bardhan, Pranab (1974) ‘On Life and Death Questions’, Economic and Political Weekly Special
Issue (9 August): 1293-1304.
Chhachhi, A. and C. Sathyamala (1983) ‘Sex Determination Tests: A Technology which will
Eliminate Women’, Medico Friends Circle Bulletin 95: 3-5.
Chunkath, Sheela Rani and V. B. Athreya (1997) ‘Female Infanticide in Tamil Nadu: Some
Evidence’, Economic and Political Weekly XXXI 1(17): WS22-WS29.
Copyright © 2000. All rights reserved.
Female Demographic Disadvantage in India 1981-91
615
Clark, Alice W. (1983) 'Limitations on Female Life Chances in Rural Central Gujarat’, The
Indian Economic and Social History Review 20: 1-25.
Clark, Alice W. (1987) ‘Social Demography of Excess Female Mortality in India: New
Directions’, Economic and Political Weekly XXII(17) Review of Women’s StudiesWS517-WS521.
Clark, Alice W. and Sudha Shreeniwas (1995) ‘Questioning the Links between Maternal
Education and Child Mortality: The Case of Gujarat’, paper presented at the Population
Association of America Annual Meeting, San Francisco (April).
Coale, Ansley (1991) ‘Excess Female Mortality and the Balance of the Sexes in the Population:
17(3^S517at23Of thC NUmbCr °f *<Missing Females” ’, Population and Development Review
Coale, Ansley and Paul Demeny (1966) Model Life Tables and Stable Populations. Princeton,
NJ: Princeton University Press.
Coale, A.J.^and^L Banister (1994) ‘Five Decades of Missing Females in China’, Demography
Das Gupta, Monica (1987) ‘Selective Discrimination against Female Children in Rural Punjab,
North India’, Population and Development Review 13: 77-100.
Das Gupta, Monica and P. N. Mari Bhat (1997) ‘Fertility Decline and Increased Manifestation
of Sex Bias m India’, Population Studies 51: 307-15.
Deshpande, Sudha (1992) ‘Structural Adjustment and Feminization’, Indian Journal of Labour
Economics 35(4).
Dyson, Tim (1988) ‘Excess Female Mortality in India: Uncertain Evidence on a Narrowing
Differential’, m K. Srinivasan and S. Mukherjee (eds) Dynamics of Population and Family
Welfare, pp. 350-81. Bombay: Himalaya Publishers.
Dyson, Tim and Mick Moore (1983) ‘On Kinship Structure, Female Autonomy and
Demographic Behaviour in India’, Population and Development Review 9(1): 35-60.
FASDSP and Saheli Women’s Resource Centre (nd) ‘Information Sheet on Sex Determination
and Sex Preselection Techniques’, on file with Jagori (NGO) New Delhi.
George, Sabu R. (1997) ‘Female Infanticide in Tamil Nadu, India: From Recognition back to
Denial?’, Reproductive Health Matters 10: 124-32.
George, Sabu, R. Abel and B. D. Miller (1992) ‘Female Infanticide in Rural South India’
Economic and Political Weekly XXVII(22): 1153-6.
Goodkind, Daniel (1996) ‘On Substituting Sex Preference Strategies in East Asia: Does Prenatal
Sex Selection Reduce Post-natal Determination’, Population and Development Review 22(1):
111—26.
Government of India (1974) ‘Towards Equality: Report of the Committee on the Status of
Women’. New Delhi: Department of Social Welfare.
Government of India (1982) Sample Registration System: Fertility and Mortality Indicaterors. New
Delhi. Office of the Registrar General of India, Ministry of Home Affairs.
Government of India (1983) Agricultural Wages in India, 1980-81. New Delhi: Ministry of
Agriculture, Directorate of Economics and Statistics. Department of Agriculture and Co
operatives.
Government of India (1988) ‘Census of India 1981. Child Mortality Estimates of India’.
Occasional Paper No. 5, Demography Division. New Delhi: Office of the Registrar General
of India, Ministry of Home Affairs.
Government of India (1991) ‘Census Data C Series, Social and Cultural Tables’. New Delhi:
Office of the Registrar General of India.
Government of India (1993) Aricultural Wages in India, 1991-2. New Delhi: Ministry
of Agriculture, Directorate of Economics and Statistics, Department of Agriculture and
Co-operatives.
Government of India (1994) Sample Registration System: Fertility and Mortality Indicators. New
Delhi: Office of the Registrar General of India, Ministry of Home Affairs.
Copyright © 2000. All rights reserved.
616
S. Sudha and S. Irudaya Rajan
Gupte, Manisha, Sunita Bandewar and Hemlata Pisa! (1997) ‘Abortion needs of Women in
India: A Case Study of Rural Maharashtra’, Reproductive Health Matters 9: 77-86.
Harriss-White, Barbara (1998) ‘Gender-cleansing: The Paradox of Development and
Deteriorating Female Life Chances in Tamil Nadu’, in R. Sundar Rajan and U. Butalia
(eds) Gender and Modernity in Post-Independence India. New Delhi: Kali for Women.
Heyer, J. (1992) The Role of Dowries and Daughters’ Marriages in the Accumulation and
Distribution of Capital in a South Indian Community’, Journal of International Development
4(4): 419-36.
Hirway, Indira (1979) ‘Female Employment in Rural Gujarat: Some Issues’, Indian Journal of
Labour Economics 22(1).
Hull, Terence H. (1990) ‘Recent Trends in Sex Ratios at Birth in China’, Population and
Development Review 16: 63-83.
Irudaya Rajan, S. (1996) ‘Sex Ratios in Kerala: New Evidences’, paper presented at the
workshop on Target Free Population Policy, Health Watch Kerala, Trivandrum
(27 September).
Irudaya Rajan, S. and P. Mohanachandran (1998) ‘Infant and Child Mortality Estimates based
on the 1991 Census of India: Part I’, Economic and Political Weekly XXXIII(19).
Irudaya Rajan, S., U. S. Mishra and K. Navaneetham (1991) ‘Decline in Sex Ratio: An
Alternative Explanation’, Economic and Political Weekly 21 December: 2963-4.
Jeffery, Roger, P. Jeffery and A. Lyon (1984) ‘Female Infanticide and Amniocentesis’, Social
Science and Medicine 19(11): 1207-12.
Johansen, Sten and Ola Nygren (1991) ‘The Missing Girls of China: A New Demographic
Account’, Population and Development Review 17: 35-51.
Kapadia, Karin (1992) ‘Every Blade of Green: Landless Female Labourers, Production and
Reproduction in South India’, Indian Journal of Labour Economics 35(3): 266-76.
Khanna, Sunil K. (1995) ‘Prenatal Sex Determination: A New Family-building Strategy’,
Manushi 86: 23-9.
Khanna, Sunil K. (1997) ‘Traditions and Reproductive Technology in an Urbanizing North
Indian Village’, Social Science and Medicine 44(2): 171-80.
Kishor, Sunita (1993) ‘May God give Sons to All: Gender and Child Mortality in India’,
American Sociological Review 58: 247-65.
Kishor, Sunita (1995) ‘Gender Differentials in Child Mortality: A Review of the Evidence’, in
Monica Das Gupta, Lincoln Chen and T. N. Krishnan (eds) Women's Health in India: Risk
and Vulnerability, pp. 19-54. Bombay: Oxford University Press.
Kishwar, Madhu (1995) ‘When Daughters are Unwanted: Sex Determination Tests in India’.
Manushi 86: 15-22.
Kulkami, Sanjeev (1986) ‘Sex Determination Tests and Female Foeticide in the City of
Bombay’. Report commissioned by the Secretary to the Government, Department of Health
and Family Welfare, Government of Maharashtra.
Kumar, Dharma (1983a) ‘Male Utopia or Nightmares?’, Economic and Political Weekly
15 January: 61-4.
Kumar, Pharma (1983b) ‘Amniocentesis Again’, Economic and Political Weekly 11 September:
1075-7.
1075
—7.
Kundu, Amitabh and Mahesh Sahu (1991) ‘Variation in Sex Ratio: Development Implications'.
Economic and Political Weekly 12 October: 2341-42.
Mason, William, Alan Bitties, Marco Spinar, Sudha Shreeniwas and D. Natasha Singarayer
(1992) Sex Ratios in India: Studies at National, State and District Levels’, in L. M. Schell,
M. T. Smith and A. Bilsborough (eds) Urbanization and Ecology in the Third World.
Menon, Nivedita (1996) ‘The Impossibility of “Justice”: Female Foeticide and Feminist
Discourse on Abortion’, in Patricia Uberoi (ed.) Social Reform, Sexuality and the State,
pp. 369-92. New Delhi: Sage Publications.
Miller, Barbara (1981) The Endangered Sex: Neglect of Female Children in Rural North India.
Ithaca, NY: Cornell University Press.
Copyright © 2000. All rights reserved.
Female Demographic Disadvantage in India 1981-91
617
Miller, Barbara (1987) ‘Female Infanticide’, Seminar 331: 18-21.
Miller, Barbara (1997) ‘Social Class, Gender, and Intrahousehold Food Allocations to Children
in South Asia’, Social Science and Medicine 44(11): 1685-95.
Mishra, U. S., Mala Ramanathan and S. Irudaya Rajan (1998) ‘Induced Abortion Potential
among Indian Women’, Social Biology 45(3/4): 278-88.
Murthy, Mamta, Anne-Catherine Guio and Jean Dreze (1996) ‘Mortality, Fertility and Gender
Bias in India: A District-level Analysis’, Population and Development Review 21(4): 745-82.
Nayyar, Rohini (1989) ‘Rural Labour Markets and the Employment of Females in PunjabHaryana’, in A. V. Jose (ed.) Limited Options: Women Workers in Rural India, pp. 234-53.
Geneva: ILO.
Nigam, Namita (1988) ‘Employment Pattern and Educational Status of Female Workers in
UP’, Indian Journal of Labour Economics 31(4): 340-53.
Palriwala, Rajni and Carla Risseeuw (eds) (1996) Shifting Circles of Support: Contextualizing
Gender and Kinship in South Asia and Sub-Saharan Africa. Walnut Creek, CA: AltaMira
Press.
Park, Chai Bin and Nam-Hoon Cho (1995) ‘Consequences of Son Preference in a Low-fertility
Society: Imbalance of the Sex Ratio at Birth in Korea*, Population and Development Review
21(1): 59-84.
Patel, V. (1988) ‘Sex Determination and Sex Pre-selection Tests: Abuse of Advanced
Technologies’, in Rehana Ghadially (ed.) Women in Indian Society, pp. 178-85. New
Delhi: Sage Publications.
Raju, Saraswati and Mahendra K. Premi (1992) ‘Decline in Sex Ratio: Alternative Explanation
Re-examined’, Economic and Political Weekly 25 April: 911-12.
Ramaswamy, Uma (1993) ‘Women and Development’, in A. N. Sharma and S. Singh (eds)
Women and Work: Changing Scenarios in India, pp. 323-37. New Delhi: B. K. Publishing
Corporation.
Rao, Vijayendra. 1993. ‘Dowry “Inflation” in Rural India: A Statistical Investigation’,
Population Studies 47(2): 283-93.
Ravindra, R. P. (1995) ‘Myths about Sex Determination Tests’, in Facts Against Myths: Vikas
Adhyayan Kendra Information Bulletin 11(3) June (Bombay).
Scrimshaw, Susan (1984) ‘Infanticide in Human Populations: Societal and Individual
Concerns , in Glenn Hausfater and Sarah B. Hrdy (eds) Infanticide: Comparative and
Evolutionary Approaches. New York: Aldine Publishing Company Hawthorne.
Sen, Amartya (1992) ‘More than 100 Million Women are Missing’, New York Review of
Books December: 61-6.
Sen, Gita (1982) ‘Women Workers and the Green Revolution’, in Lourdes Beneria (ed.) Women
and Development, pp. 29-60. New York: Praeger Publications.
Sengupta, Amit (1992) ‘Prenatal Diagnostic Techniques Bill: Loopholes Galore’, Women's
Equality (newsletter) April-June.
Singh, Gurmeet and Sunita Jain (1985) ‘Opinions of Men and Women regarding Amniocen
tesis’, Journal of Family Welfare XXXI(3): 13-19.
Sinha, R.P. (1988) ‘Technological Change in Agriculture and Women Workers in Rural Bihar:
A Case Study’, Indian Journal of Labour Economics 31(4): 306-16.
Srinivasan, K. (1997) ‘Sex Ratios in India: What they Hide and What they Reveal’, in S. Irudaya
Rajan (ed.) India's Demographic Transition: A Reassessment, pp. 89-94 New Delhi: MD
Publications.
Tuljapurkar, Shripad, Li Nan and Marcus W. Feldman (1995) ‘High Sex Ratios at Birth in
China’s Future’, Science 267(5199): 874-6.
UN (1983) ‘Manual X: Indirect Techniques for Demographic Estimation’. Population Studies,
No. 81. New York: United Nations, Department of International Economic and Social
Affairs.
Varghese, N. V. (1991) ‘Women and Work: An Examination of the “Female Marginalization
Thesis” in the Indian Context’, Indian Journal of Labour Economics 34(3): 203-9.
Copyright © 2000. All rights reserved.
618
•S'. Sudha and S. Irudaya Rajan
3S
“,"<l
■»» «»S= K.Boof
women in Indian Society, pp. 179-202 New Delhi
Publications.
° h
™L
P„p.,„ion
-ru
. ~ ,
*
oz Znd Thousand Oaks, CA: Sage
VishwanaIhan Pre™ (1991) 'Haryana’s Urban Convicts’, Times of India 14 April
1’" R“' N"‘
..B
Y1’Ratio’at'Birt^in9^^
Implicatl0ns °f the
Increase in the Reported Sex
in the Reported Sex
Ratto at Birth m China’, Population and Development Review 19(2): 283-302.
S Sudha was a post-doctoral fellow at the Carolina Population Centre
sY.rib
Y °ri N°rth Carolina’ ChaPel
NC 27516-3997, USA (e-mail
fellow Centre for D 1
' q "a' tten, she was an associate
Indh A
f Deve‘°Pment Studi«, Thiruvananthapuram, Kerala
investigiine0 wd?hSt
demo8raPh^; her research interests include
mnnet r 8 .T"’1561118 outc°mes over the life-course, focusing on the
unpact of social structures such as gender, ethnicity and the state. Her recent
facmrs on^chTd ’3
°f
°f ethnicity-state P^cy and family
heakh ™
r
' edacatl0n ln Malaysia, and the role of ethnicity in
i
health care preferences of elderly pe:rsons in the southern United States.
SmSsdaThu>ajan iStbn aSS°Ciate fell°W at the Centre for Development
v nl netil) He has
Kera‘a’
(e’mail: ^"©giasmdOl.
nonula inn ' d d C°"duCted research
hi^orical and social demography
Ea He si
Planmng’ age'ng’ and studies °n
S
2 rc h co-nuthor of a recent book, India’s Elderly: Burden or
Challenge^ (Sage, New Delhi) and is a member of the team which has just
completed the Kerala Migration Survey.
J
Copyright © 2000. All rights reserved.
Population and Health Policies
~ I"
t
(
National Population Policy :
Small Family Norm & Sex Selection
ARNanda
Executive Director, PFI
■•6
n
Paper Presented at the Seminar on
The New Paradigm of Development and Sex Selection
Organized by
Nehru Memorial Museum & Library (NMML)
& Action India
at
Teen Murti Bhawan, New Delhi
August 6- 7, 2004
National Population Policy: The Small Family Norm & Sex Selection
National Population Policy-An Overview
effective devekL^^'r" P°!lcy
•AR Nanda
of 2000 is a significant move towards a human? and
and is the ref 611 l°
3t
,ssucs
016 perspective of social development \
shift from p4renC^ P°int for
CUITent
based approach to the subject. It reflects a
soecial rnnr ler demoSraphically driven target oriented approach to one that addresses the
on Pon.°f "eProductive
child health. As a signatory to the International Conference
between n
eve^0Pment (ICPD) Plan of Action in 1994, India focused on inter-linkages
develonm,
tH?n’ deve!°Prnent and gender. NPP, 2000 asserts the centrality of human
icc.iAo f ;n ’ gender equality and equity, adolescent reproductive health and rights among other
issues to stabilising the country's population.
ancT'f^QOO *S In fact 311 affirmation and articulation of India’s commitment to the ICPD agenda,
orms the blueprint for population and development programmes in the country. The
^vern lng concern of the NPP 2000 is economic and social development and human well being.
see s to provide quality services and supplies, information and counselling, and a basket of
servic CCpllVC cb°*ccs- It will enable people make informed choice and access quality health care
t a so states that stabilizing population is not merely a question of making reproductive health
services accessible and affordable, but also of increasing the coverage and outreach of primary .
an secondary education, extending basic amenities like sanitation, safe drinking water and ■
lousing, empowering women with enhanced access of education and employment.
The NPP affirms the commitment of government towards:
*v-
oluntary and informed consent as the basis for availing of family planning services.
arget free approach in administering the family planning services.
^mproving the health and nutrition status of women.
a nJ mortal ity*
survival initiatives to bring about reduction in infantand child morbidity
driven abz^don
Plann{ng and implementation which will promote need-based, demandscrviccs
°CatIon sPcc,fic, integrated and high quality reproductive and child health care
The National Population
opulation Policy (NPP), 2000 is gender sensitive and incorporates a
comprehensive and holistic
: approach to health and education needs of women, adolescents and
(he girl child.
2000 is. to address the unmet needs
for contraception,
basic reproductive
L
Personneb and to provide integrated service delivery of
replacement levels bv ?n n
medium term objective is to bring the TFR to
strategies. The lonp t
k- °.U . V1g°rous implementation of inter-sectoral operational
consistent with theg
°bjeCtive is to achieve a stable population by 2045, at a level
environmental protection111^111^
SUSta^na^^e econ°niic growth, social development and
•;
- 3—
Emphasizing the goal of TFR 2.1 by 2010 without linking it with other sodo-demographic
goals (like reduction of IMR & MMR, 100 percent registration of births; deaths etc, delaying age
at marriage etc), is a matter of concern. The details of socio-demographic goals and strategic
themes are enclosed in annexure-1.
10,h Anniversary of ICPD
The International Conference on Population and Development (ICPD) held in Cairo in 1994, was
a milestone in the history of population and development as well as in the history of women’s
rights. It heralded a paradigm shift in the approach to population and development, placed
women's equity center stage and introduced the importance of rights based programming. This
year 2004 marks the 10th anniversary of the ICPD, the mid-point of it’s 20 year programme of
action. In India a number of events and activities are taking place to commemorate ICPD + 10. A
series of planning and preparatory meetings were held with civil society and experts in last few
months to identify population issues requiring priority attention. In these meetings a key theme
which was identified as an issue requiring urgent attention was the theme relating to “Missing
Girls”. This theme captures some of the foremost concerns in population issues viz. declining
child sex ratio, sex selective abortions and two-child norm.
Sex Selection and Child Sex Ratio (CSR) in India:
While the improvement in overall sex ratio is noticed in the census 2001 what is most alarming
is the decline in the Child Sex Ratio (CSR), i.e the sex ratio of children in the age group of 0-6
years.
Census 2001 showed a decline of 18 points from 945 in 1991 to 927. The decline of child sex
ratio is so wide spread that out of the 28 States and 7 Union Territories, only 4 States namely
Kerala (5 points increase), Tripura (8 points increase), Mizoram (2 points increase) and Sikkim
(?/ P°ints increase) and only one union territory, Lakshadweep (33 points increase) are free from
this socially harmful and degrading phenomenon. Details attached in Annxure - II.
The Stales and Union Territories that have shown large declines in child sex ratio are Punjab (82), Haryana (-59), Himachal Pradesh (-54), Gujarat (-50), Chandigarh (-54) and Delhi (-50)
though they are economically quite developed with high female literacy rates. There are 122
districts spread over 14 states having CSR less than 900.
Several questions have been raised with regard to trends in child sex ratio in the last decade. The
indications are that this alarming trend is due to large scale practice of female foeticide. Female
foeticide or sex selective abortion is the elimination of the female foetus in the womb itself. The
decline in child sex ratio may be due to different factors.such as neglect of female children
resulting in their higher mortality at younger ages, female infanticide and female foeticide.
Female foeticide refers to a practice where the female foetuses are selectively eliminated after
prenatal sex determination thus avoiding the birth of girls.
The factors Responsible for Female Foeticide are:
•
•
The obsession to have a son
The discrimination against the girl child
The socio-economic and physical insecurity of women
The evil of dowry prevalent in our society
The worry about getting girls married as there is the stigma attached to being an unmarried
women.
r
•
- li•
Easily accessible and affordabL
'e procedure for sex determination during pregnancy
Failure of medical ethics
The two child norm policy of certain stare governments.
chilXom^ohcy ^ootedb °f the.,rnportant factor responsible for female foeticide is the "Two
>unn Policy adopted by certain state governments.
Small Family Norm vis-A-vis Two Child Norm
•
•
basket ofconhT6 °{t^c
2000 is provision of quality health services and supplies and a
make informpH
C^0IjeS* PeoPie raust be free and enabled to access quality health care,
spirit that thp
Hd?pt methods for fcrtility regulation best suited to them” - it is in this
"two child
sPea^s of the ”small family norm'\ No where the policy advocates for
taikin o
„ owcver» ’s unfortunate and some times even’disturbing to note that while
A/tc /,e/rOUt NPP smaUfamily no rm" is often misinteipreted as "two chUd norm" (Which .
childrr eJlnite c^ercive connotation). "Two child norm" implies that the state promotes two
A “tw °
a sys*CTO of incentives and disincentives/.punishments for achieving it.
vo c n norm has the potential to cause immense harm to women’s health in the existing
cia situation where son preference is high and women’s status is very low. One of the gravest
risks includes increase in sex selective abortion and consequent reduction ofgirl children.
foci that compulsion to have no more than two children would result in increased female
oetici c. This happened in China when government declared that no couple should have more
an one child. The "one child policy" in China appears to have created more societal and
ami y problems like skewed sex ratio, female infanticide and foeticide, rather than helping in
smooth stabilizion of population. There are thus lessons to be learnt from the Chinese’ experience
in governance. We tend to misrepresent the Chinese story, whenever wc compare the Indian
si uation or advocating coercive polices like "two child norm " and the concomitment regime of
incentive and disincentives to solve our population problem quickly.
The
child norm policy of certain state governments which are not in harmony with the
NPP can become an important factor responsible for exacerbating female foeticide in these states
in future.
-
"
Annexure -1
National Population Policy (NPP), 2000
Socio demographic goals for 2010
1.
.Address the unmet needs for basic reproductive and child health services, supplies and
infrastructure.
2.
3.
4.
5.
6.
7.
8.
9.
10.
I
11.
12.
13.
14.
••
Make school education up to age 14 free and compulsory, and reduce op outs at
primary and secondary school levels to below 20 percent for both boys and gir s
Reduce infant mortality rate to below 30 per 1000 live births.
Reduce maternal mortality ratio to below 100 per 100,000 live births.
Achieve universal immunization ofchildren against all vaccine preventable diseases.
Promote delayed marriage for girls, not earlier than age 18 and preferably er
years
of age.
.
. ,
Achieve 80 percent institutional deliveries and 100 percent deliveries by trained
persons.'
Achieve universal access to information/ counseling and services for ferti ty regu ation
and contraception with a wide basket of choices.
Achieve 100 percent registration of births, deaths, mamage and pregnancy.
Contain the spread of Acquired Immunodeficiency Syndrome (AIDS), an P5®m0
greater integration between' the .management of reproductive tract infechon (RT1) and
sexually transmitted infections (STI) and the National AIDS Control Organisation.
Prevent and control communicable diseases.
Integrate Indian Systems of Medicine ((ISM) in the provision of reproductive and child
health services, and in reaching out to households.
Promote vigorously the small family norm to achieve replacement levels o
Bring about convergence in implementation of related social sector programs so
family welfare becomes a people centered programme.
Strategic Themes
i.
ii.
iii.
iv.
v.
vi.
vii.
viii.
ix.
x.
xi.
xii.
Decentralized Planning and Programme Implementation
Convergence of Service Delivery at Village Levels
Empowering Women for Improved Health and Nutrition
Child Health and Survival
Meeting the Unmet Needs for Family Welfare Services
Under-Served Population Groups
Diverse Health Care Providers
Collaboration with and Commitments from Non-Govemment Organizations and the
Private Sector
Mainstreaming Indian Systems of Medicine and Homeopathy
Contraceptive Technology and Research on Reproductive and Child Health
Providing for the older population
Information, Education and Communication
6Annexure- II
Child Sex Ratio in the States
States
~
—
Punjab
Haryana ______
Chandigarh ____
Himachal Pradesh
Jammu & Kashmir
“Delhi
Rajasthan
IJttar Pradesh____
Bihar_____
Orissa__________
Madhya Pradesh
Uttaranchal______
Jharkhand_______
Chhatisgarh______
Sikkim ________
Arunachal Pradesh
Nagaland________
Manipur_________
Mizoram ______
Tripura__________
Meghalaya
Assam___________
West Bengal______
Gujarat__________
Daman & Diu
D&NHaveli
Maharashtra______
Andhara Pradesh
Karnataka________
Goa ___________
Lakshadweep_____
Kerala___________
Tamil Nadu_______
Pondicheny______
A & N Islands_____
India
Year
1991
£75
879
899
951
NA
. 915
916
927
953
967
941
948
979
9£4
965
982
993
974
969
967
986
975
967
928
958
1013
946
975
960
964
941
958
948
963
973
yno
Distribution of States/UTs by Districts having less than 900 Child Sex Ratio.
Sr. No.
States/UT______
1
Uttar Pradesh
2
Haryana________
3
Punjab
4
Gujarat
5
Rajasthan______
6
Maharashtra
7
Delhi__________
8
Madhya Pradesh
9
Himachal Pradesh
10
Tamil Nadu
ll
12
13
14
Total
Bihar_________
Jammu & Kashmir
Chandigarh (U.T)
Uttaranchal
■
2001
793
820
845
897
937
865
909
916
938
950
929
906
.966
975
986
961
975
961
971
975
975
964
963.
878 _
925
973
917
964
949
933
974
963
939
958
965
927
No. of Districts
24
18
18
16
.10
~
-
9
8
5
4
4
2
2
1
1
122
-7
Annexure- II
Child Sex Ratio in the States
States
Punjab________
’ Haryana q______
Chandigarh______
Himachal Pradesh
Jammu & Kashmir
Delhi '
.
Rajasthan _______
Uttar Pradesh
B ihar___________
Orissa___________
Madhya Pradesh
Uttaranchal_____
Jharkhand________
Chhatisgarh______
Sikkim___________
Arunachal Pradesh
Nagaland ________
Manipur
Mizoram
Tripura
Meghalaya
Assam_____
West Bengal_______
Gujarat
Daman & Diu
D & N Haveli______
Maharashtra____
Andhara Pradesh
Karnataka _____
Goa
Lakshadweep
Kerala
Tamil Nadu
Pondicherry
A & N Islands____
India
Year
1991
875
879
899
951
NA
915
916
927
953
967
941
948
979
984
965
982
993
974
969
967
986
975
967
928
958
1013
946
975
960
964
941
958
•948
963
973
945
Distribution of States/UTs by Districts having less than 900 Child Sex Ratio.
Sr. No.___ Statcs/UT__________________ _______
1 __ _ Uttar Pradesh
2 ____ Haryana__________________________ _____________ _____
3 ____ Punjab_____________________________ _________________
4
Gujarat
2001
793
820
845
897
937
865
909
916
938
950
929
906
966
975
986
961
975
961
971
975
975
964
963
878
925
973
917
964
949
933
974
963
939
958
965
927
No. of Districts
24
18
18
16
5 __ • Rajasthan______
, '__________ _____ _
6. __ Maharashtra_____________ - .
. • .___________ 1_
7 ___ Delhi___________________________
8 ____ Madhya Pradesh______________ ________________________
9 __ _ Himachal Pradesh__________
10
Tamil Nadu
10
9
11 ___ Bihar_______________________________________ ___ _____
12 ___ Jammu & Kashmir___________________ _____________ _
13
Chandigarh (U.T)_____________ __________________
14
Uttaranchal
Tdtal
2
2
1
1
122
8
5
44
National Population Policy 2000:
A Critique
Jashodhara Dasgupta
KRITI
A Resource Centre on Women’s Health and Rights
(A Unit of SAHA YOG, Lucknow)
Paper Presented at the Seminar on
The New Paradigm of Development and Sex Selection
Organized by
Nehru Memorial Museum & Library (NMML)
& Action India
at
Teen Murti Bhawan, New Delhi
August 6-7, 2004
v
The National Population Policy: A Critique
io healthcare which
SriataT?
de™l»P"'="l ™1 access
“m
-“Xis
.0 heely „d
wim7nWa^Xyra^
00 mee‘ing 1116 health needs of individual
NPP 2000 consistently avoids^
dem.ographic
In keeping with this, the
“population suZioX.
J ‘>P^on control” and talks instead of
“population explosion” in
and entrenched convictions about the
current understand'
r«i d’a‘ 71113 ’S 3 “^S60115'Stance in consonance with the
=lXra.the
'
Xs toeeh S
Similarly the decimaXf ind?8e„0 “
.TesXed no oX
X“',1” Sh“kint! deCli"C in ,he
“*
' cnstable' lsXofXX e
d'a,hS ‘ach
»«»■"« of <he qualitative
P
he population that remain largely unaddressed in the NPP 2000.
Xe„y XlXdXXJdX d' :ery 'n<l ,he NPP
given the steeply decSad^e
hM
°ld def’Cit of females?” In fact,
country, the NPP nSZt0 exn ^tl
m°St deVel°Ped
of *e
this trend. One way X,
^guards for halting and reversing
monitored and followed un anothp 0 ° enSU^^e blrthS °f glrl children would be closely
the small family norm and nrn
F
co\1*d have been to tone down the rhetor
nc- on
affluent, developed^d^d.J- t d afnrmat‘VC action for gid children. The fact that
the sex ratio show^ tta the sSS X
Sh°Wed the SteePest decIine in
500 for survival of the
Cash,JlnCentIve of the Malika SarnriddhiYojana ( Rs
ival of the girl child) would not be an effective in halting the trend.
1 ,
'
“sustainable Gnomic
---------------
SdcvetoSSd ”Stab'e P°PUlatiOn by 2045” which
be consistent with
cufrentiy in their reprLtuctfvfye^ ’" 3 hi8h P^^on of the population being
Appends Three, para 5, NPP 2000'
The NPP 2000 is a consolidation of the earlier post-ICPD policy directions away from the
long-standing ‘target-oriented’ approach in the family welfare programme. It represents a
bold deviation from the earlier “top-down control” thinking on population, and brings in
fresh concepts like women’s empowerment, social development and holistic strategies to
improve the quality of life of the people. At the level of service delivery, the NPP
represents a move towards a more decentralized model of management and advocates
partnering with the private sector. All these paradigm shifts needed to occur in contested
areas of power, and do not occur by default As such the new policy needed very strong
support not only from its patrons but also from the marginal groups whose interest it was
representing, from civil society and media. It also needed a strong implementation
system. However, the reality was quite different If we re-examine the problem analysis
for the new policy, there emerges a certain level of ambiguity, since the demographic
imperative still informed the understanding of most of the players in the policy process. It
was obviously difficult to forge an unequivocal consensus understanding of what the
policy was actually attempting to change. Even after formulation, the Population
Commission went so far as to say that the policy approach needed to be fundamentally
changed to a ‘control’ approach. The ownership of the policy was therefore somewhat
limited among those who were to steer its implementation.
At the level of policy implementation, the governance structure to manage the
implementation was the MoHFW but the states were permitted to formulate their own
policies despite Population being a Central subject. There was urgent need to review' and
amend existing national or state-level laws and policies to ensure system-wide coherence
with the new approach of the NPP 2000 and achieve its goals. Unfortunately, the
continuing dominant paradigm of population control led to many of the state policies
contradicting the NPP and thus aggravating the negative population trends in the country.
Some of the state policies formulated after the NPP 2000 openly announced a return to
target-onented approaches, long discarded in family planning policy and programming.
Targets were re-instated in the state of Uttar Pradesh (State Population Policy 2000).
Andhra Pradesh already had a Population Policy that contradicted the target-free
approach of the NPP 2000, and openly used incentives and disincentives to enforce the
two-child norm. Attempts were made in the state policies of Maharashtra and Gujarat to
bring in draconian provisions that would even violate constitutional rights.
Some states had already made laws that conflicted with the NPP such as the provision for
disqualifying persons having more than two children in holding and contesting Panchayat
positions (also known as the two-child norm). None of these laws were revoked as
conflicting with the NPP 2000. Rajasthan was the pioneer in introducing this norm for
Panchayats and municipalities in 1992, later incorporating it as a disqualification within
the Panchayati Raj Act of 1994. Later a number of other states Haryana (Panchayati Raj
Act, 1994), Andhra Pradesh (Panchayat Raj Act of 1994), Orissa (Amendment to Orissa
Gram Panchayat Act 1994) also opted for this norm forelections to Panchayat bodies.
Madhya Pradesh was the latest state to have included two-child norm in their panchayat
legislation through a special amendment in its panchayat law in May 2000. It has also
commitfd^XOn^tO. inc!udeeIections t0 municipalities, agricultural produce marketing
RhnnTh J°bK 10 th°Se Wh°
nOrm- A Study by Mahila Chetna Manch of
hopal shows that a number of disqualified representatives had resorted to induced
bortion to avoid the birth of their third child and many woman were compelled to
Pre^™ination tests. Uttar Pradesh had produced a similar Population
i v ?n 2002 that womcn und health organisations were able to stop after a
ruggle Yet even as I speak today, there is a similar Bill tabled in the U.P. Sure
Assembly, which has the tacit approval of almost all the political parties.
The application of a two-child norm is based on the fallacious assumptions that
compelling people to have smaller families leads to an improvement in the overall
development status, that choice of number of children is independent of the sex of the
children, and that contraceptive services are universally available. But given that son
preference has long emerged as a social reality in most parts of India, while planning for
fewer children, most families would prefer a certain number of sons as insurance for
future welfare. The NPP also encourages sterilisation after two children through a variety
of incentives . The technologies for sex pre-determination are more easily available than
appropriate contraceptives and providers are always ready to conduct sex-selective
abortions. Although the NPP mentions 'strict enforcement of the PNDT Act’, it is open
knowledge that convictions under this Act are rare and difficult.
As a result, the promotion of‘small family norm’ or ‘two-child norm’ has a dangerous
possibility of aggravating the already declining sex ratio rather than leading to
development. The ‘norms’ are leading towards a future instability in the population,
where men will largely outnumber women. In fact the substantial evidence of the NPP’s
commitment to improving the status of women and achieving gender equality is
outweighed by the fact that the ‘small family’ approach is slowly doing away with
womcn altogether. This is ironical in a country whose Constitution was among the first
globally to grant women equal status in all matters, and which ratified the international
Convention on Elimination of All Forms of Discrimination Against Women (CEDAW)
ten years ago.
To conclude, the NPP 2000 is a commendable statement of political will, but for the
reasons given above, it remained vulnerable to misinterpretation and dilution in
implementation. In its translation and implementation at the state level, the NPP 2000 has
in the last four years been substantially altered in both letter and spirit. The demographic
imperative unfortunately continues to shape the thinking of lawmakers, law-enforcers,
and providers aI1 over the country, despite evidence to the contrary. The need
ot the hour is to honestly question whether such ‘norms’ about family size are necessary
tor development and population stabilization, given that the growth rates and total
e i ity rates are already low and there is already a substantial unmet need for
contraceptive services. It may be more judicious to promote other norms that lead to a
more stable future population.
Promotional and Motivational Measures for Adoption of the Small Family Norm, para 46, NPP 2000.
National Population Policy
Save the Girl Child
Re-examining Critical Issues on National Population policy 2000
- by Devaki Jain and Mohan Rao *
National Population Policy:
The policy announced ’’affirms commitment of the government towards voluntary and
informed choice and consent of citizens while availing of reproductive health care
services, and continuation of the target free approach in administering family planning
services” (001:2000:2).
The immediate objective of the National Population Policy (NPP) is to meet the unmet
need for contraception and health infrastructure. The medium-term objective is to bring
the total fertility rate to replacement levels by 2010 through inter-sectoral action and the
long-term objective is to achieve a stable population, consistent with sustainable
development, by 2045. Towards this end the goals set out include:
•
Making school education free and compulsory up to age 14
•
Reducing IMR to below 30 per 1000 live births
•
Reducing maternal mortality ratio to below 100 per 1,00,000 live births
•
Promoting delayed age at marriage
•
Achieving 80 per cent institutional deliveries and 100 per cent deliveries by
trained persons
•
Creating universal access to information and counselling and services for
contraception with a wide basket of choices
•
Ensuring 100 per cent registration of vital events — births, deaths, marriages and
pregnancy; and prevention
•
Controlling communicable diseases, especially AIDS.
The strategies to achieve these goals include:
•
Decentralised planning and implementation through panchayat raj institutions
(PRls)
CASSA
•
Convergence of health services at the village level
•
Empowering women for improved health and nutrition
•
Ensuring child survival interventions
•
Involving diverse health care providers
•
Developing increased partnership with NGOs and the private corporate sector
•
Encouraging a range of clinical, laboratory and field research on maternal, child
and reproductive health care issues.
Areas of concern:
The NPP, following the ideas of the Swaminathan Committee Report had attempted to
move away from both the two-child norm and target-based approach.
There was
however a subtle disincentive approach in the sections dealing with the institutional
arrangements for delivering the policy. At the same time, the NPP also emphasised the
importance of high quality social development services at the ground level as being the
most crucial arrangement for enabling people who would like to have fewer children to
exercise that will.
At the conceptual level, the question to be asked is do we have a population policy or a
family planning policy? Imbricated in a population policy ought to be a vision for
development, with macro-issues of income, employment, food, health and rights as the
focus and not merely strategies for generating acceptance of contraceptives.
Second,
what are the instruments for such policy? How are macroeconomic forces shaping the
enabling conditions necessary for health and family planning?
What, then, are our
priorities with specific reference to the poor? How are issues of livelihood, poverty,
inequality, hunger and ill health reflected in the NPP? Finally, there was a need for
reconsidering some of the tools to attain the goals of the NPP, specifically the move to
induct long-acting, provider-controlled and women-centred hormonal contraceptives in
some states and policies of incentives and disincentives in all of them.
It is clearly necessary to distinguish between the philosophy and actions towards a
population policy, and those towards a family planning policy.
The former should
2
include, besides demographic concerns, larger issues of sustainable and equitable
development.
In this context it is necessary to spell out the links between macro
economic policy and population.
The government’s repeated stress on the need to
stabilise the size of the population as a precondition for economic development misjudges
the linkages, and sidesteps the lack of effective and equitable development policies. The
NPP is not linked to an effective and equitable health policy. The fact that health itself
receives low priority among planners is a matter of great concern. It is desirable, and
eminently possible, that at least 5 per cent of GDP be earmarked for health.
It is
unambiguously clear that the state, and state alone, can play the necessary role in the
universal provision of comprehensive primary health care, irrespective of people’s ability
to pay. It is deeply disturbing that the NPP appears to regard primary health care as
merely primary level care.
The increase in the incidence and prevalence of communicable diseases, in infant
mortality rates and in maternal mortality attests among other factors, to the erosion of
public health services in the country. There is an urgent need to arrest this alarming
trend. The dilution of the state’s commitment to public health, and the subsidies given to
the private and NGO sectors in the name of efficiency and increasing inaccessibility to
health care for the people of the country.
There is an urgent need to regulate the private
sector that is currently not accountable to any institution, while simultaneously improving
managerial and supervisory capacities in the public.
Disincentives, incentives and targets have no place in a family welfare programme. First,
they are unnecessary, as birth rates have commenced a decline in large parts of the
country. Second, as experience in the past indicates, they are ineffective and serve only
to generate false programme performance data.
Third, the financial allocations for
incentives are a drain of scarce resources that ought to be utilised for strengthening
Primary Health Care.
Fourth, they inflict damage on the credentials of a so-called
welfare programme by deeply alienated people the poor and the powerless in particular,
from the health care system. Finally, they profoundly violate democratic rights. Indeed,
3
considering the NPP is framed in the discourse on rights, it is fundamentally at variance
with policies of incentives, disincentives and targets.
There is an urgent need to strengthen MCH services that have suffered as a consequence
both of the collapse of the public health system and the focus on the family planning
programme. At the same time, there is a need to promote user-controlled, safe, effective
and temporary methods of contraception. Equally important is the need to monitor and
systematically study the health implications of contraception, including sterilisation.
Strengthening the PRIs is an important step in the right direction even though the
experience has not been the same all over the country. They have a crucial role in the
planning, monitoring and implementation of all health and family welfare programmes,
but cannot supplant the role of the state. The existing data collection system leaves much
to be desired. This has to be strengthened as part of the overall strengthening of the
health care system rather than by initiating parallel systems of data collection or
launching ad hoc studies.
Research should be an ongoing activity of all health and family welfare programmes
rather than end-term project appraisals that lead to neglect of process oriented research.
Research funding should not be centralised but should be available at different levels for
appropriate, epidemiologically and socially relevant inter-disciplinary health research.
There is no place for donor-driven agendas of research that are all too frequently
epidemiologically misplaced. In this context, there is an urgent need to strengthen public
institutions of research that at one time produced nationally and internationally acclaimed
epidemiologically relevant studies but are now suffering the consequences of systematic
neglect and fund cuts. PRIs should be involved in the ethical review of research since
ideas of informed consent have proved problematic in the Indian context. There should
be a renewed focus on the family, on groups such as landless labourers, dalits, and other
marginalised groups especially in the light of globalisation and SAP
‘Excerpts from the report - Economic and Political Weekly dated 9th April 2001
4
Issues
Female Sex Selective Abortions: Some Iss
^m^°rtant article’ Mohan Rao, professor at the Centre of
Social Medicine and Community Health, Jawaharlal Nehru Universitv
draws attention to the magnitude of the problem and argues ihat
ong with the spread of conservative ideologies, state policies are
dZloTs ^ tO
of traditional Li female
■ >
laeoiogies and m engendering masculinity.
?
Tie human race sometimes uses
the most modern means in the
or
the fatal promise of immortality
advJSd rXX
XX?
technology industry
to abort female
fetuses in the
country, in what is j
referred to as Sex L
Selective Abortions |
(SSA)1, or indeed I
select only male I
embryos
for |
implantation. There I
has been much B
concern, even in "
official circles, and a gj
huge amount of B
academic
and k
journalistic literature. K
I do not intend, in |
i
■
«
1“'
’r°eredby
-
sS‘s
I
I
Code: the most patriarchal Hindu and
steady dedine of the sex ratio
SXSS dedir^d^^a^m
feminists are not.
feminists are not.
The female male ratio (FMR) in
the world
is th<! number “I
the
f'^^oosandmafes.^o.
Onsosftrewupahappytigure
r
-
females per thousand male!
optimistic thouc
1 indicated a halt
decline in th
—? ratio. The 1991
however put p
this optimisr
revealed a fu
decline to 927
1981 figure, it i<
accepted
demographers,
caused by a signii
under-countin
females due i
. decline in the qi
of the 1971 cer
Demographers
agreed that the 1
and 2001 Censuses are free from
infirmity. This is to say that the 2
census figures, of 933 females
thousand males, are real and indica
of an improvement in the ove
survival of females. Have we tl ’
turned the comer?
this paper, to review this literature, but
instead, after a brief description of Western Europe has a figure of 1,064
females |
some selected studies, discuss some ---------- ; per thousand males and
Africa,
1,015. Asia as a whole has
..-s
of the arguments that enfold the issue,
FMRs
of
953,
but
India
shares
sometimes occluding it. It is admittedly
a profoundly complex issue - touching extremely negative sex ratios with a
at the heart of Indian society, of caste, number of her neighbours in Asia.
class, religion and region. Above all, Values of less than 950 females per
its is about patriarchy which finds thousand males are found in countries
The Sex Ratio could turn femin
support in the most unlikely quarters. of West Asia (940), Pakistan (929), simply
because more men than won
India
(933),
Bangladesh
(939)
and
It is also a concern with the
have
migrated.
But tire Juvenile or O
ch
'
na
(941),
an
arc
of
anti-female
strangeness of bedfellows that politics
Sex Ratio (CSR) is not subj'ect to t
around this issue throws up, as indeed countries' cutting across religions,
limitation. And it is this that is dee
around the debates on the Uniform Qvil
In India, there has been
a worrying. Despite the slight over
..JPAD New sletter Vol. II, No. 1 January - June 3X14
Issues
improvement in the SRr the CSR in
India as a whole has declined
significantly - from 945 in 1991 to 927
in 2001. It is estimated that there are
35 million missing females in India as
per the 2001 census (Patel 2004).2
a decline from 914 in 1991 to 844 in
2001; Mehesana had a figure of 899
in 1991 but 798 in 2001; only eight
districts continue to record a CSR of
more than 900 girls as compared to
20 districts in 1991. In Maharashtra,
This decline in the CSR has been eight districts of central and southern
particular notable in Himachal Pradesh Maharashtra have shown sharp dedine
(897), Punjab (793), Chandigarh (845), t0 less than 900 9iris per 1000 boys.
Haryana (820) and Delhi (865), the Except
r
■ ' for
' three, all districts of
classical region of the north and west Rajasthan recorded CSR of less than
referred to by Oldenberg as the 950 9iris- The majority of districts of
Bermuda triangle for missing females
record
of ,ess than 900 girls;
(Oldenberg 1992).3 In all these states ^e prosperous South Delhi dedining
the number of female children per from 912 in 1991 to 886 in 2001, South
thousand male children in the 0-6 years West Delhi from 904 in 1991 to 845 in
age group declined by more than 50 2001. In Haryana, the state average
between 1991 and 2001. Gujarat has declined from 879 in 1991 to 820
(929) and Maharashtra (946) have in 2001, with almost all districts
also unfortunately joined this group of revealing figures of fess than 850 girls
to a 1000 boys. In Punjab, the state
states.
average has dedined from 875 in 1991
A part of the declining CSR is due
to 793 in 2001, with none of the
to continuing anti-female rates of infont
districts recording more than 850 girts
and child mortality. But more
per 1000 boys In Himachal Pradesh,
significantly, there has also been a
the state average declined from 951
marked masculinisation of the Sex
in 1991 to 897 in 2001, with eight out
Ratio at Birth (SRB) In India a figure of
of 12 districts showing less than 950
105 male births for 100 female births
girts. In Tamil Nadu, the state average
is considered the norm.4 However,
has declined from 948 in 1991 to 939
estimates of the SRB for 1998 reveals
in 2001; in Salem the epicentre of
an all-India figure of 111 males per
female infantidde the CSR dedined to
100 females. This is indicative of sex826 girls per 1000 boys.
selective abortion (SSA) of females
(Premi 2001).5 Figures above this
The dedine in CSR has spread to
national average of the SRB are seen regions and populations hitherto
in Gujarat (113.9), Haryana (123.3), considered immune, namely the states
Punjab (122.8), Rajasthan (114.8) and of the south and west of India and
Uttar Pradesh (118).
populations of SCs and STs. Indeed the
A 2003 report simply tided Missing, masculinisation of CSR has been
prepared by the United Nations particularly precipitate among the
Population Fund (UNFPA), Ministry of Scheduled Castes population
Health and Family Welfare and the (Agnihotri 2000).7 What is also
Census Commissioner, which mapped interesting is that the decline is more
the adverse CSRs in India captures the marked in the more developed and
decline in the number of girls (UNFPA better-off regions and in more literate
2003).6 It reveals that 70 districts in and better-off social groups.
16 States and Union Territories have
A large number of explanations
recorded a more than 50-point dedine have been proffered for the
in the CSR between 1991 and 2001. devaluation of female lives in India.
For instance, in Gujarat, Rajkot shows These range from marriage and
"Asia as a whole has
FMRs of953, but India
shares extremely
negative sex ratios with
a number ofher
neighbours in Asia.
Values ofless than 950
females per thousand
males are found in
countries of West Asia
(940), Pakistan (929),
India (933), Bangladesh
(939) and China (941),
an arc ofanti-female
countries, cutting across
religions."
"This decline in the CSR
has been particular
notable in Himachal
Pradesh (897), Punjab
(793), Chandigarh
(845), Haryana (820)
and Delhi (865), the
classical region of the
north and west referred
to by O/denberg as the
Bermuda triangle for
missing females."
IDPzYD Newsletter Vol. Il, No. 1 January — June 2004
21
Issues-
I
I
"I would suggest that
along with the spread of
conservative ideologies,
state policies are also
actively contributing to
the reinforcement of
traditional anti-femaie
ideologies and. in
•
. .
engendering
masculinity."
I
I
I
I
7
"What is often not
recognised is the
withdrawal ofthe state
- from health,
education, employment
generation and actively
combating anti-women
traditional values —
engenders both the
feminisation ofpoverty
and the shrouding and
enfoldment of women,
sacrificing them to the
altar of the family."
IDP/\D Newsletter Vol. II, No. 1 January - June 2<XM
kinship patterns, to female work
participation rates in wheat and rice
cultivation, to laws governing
inheritance of property and so on.
Evidence of this was evident as early
as the 1961 Census, as revealed by
Krishnaji, which showed a significant
relationship between landholding and
negative sex ratios (Krishnaji 2000).8
Harris White (Barbara Harris White et
a/1996)9, Judith Heyer (Heyer 1997)10
and Alice dark (dark 1987)11 have all
drawn attention to the imbrications of
Brahminical marriage patterns among
other castes, the interlocking of class
and social mobility and the spread of
dowry. I would suggest that along with
the spread of conservative ideologies,
state policies are also actively
contributing to the reinforcement of
traditional anti-female ideologies and
in engendering masculinity.
One of the earliest studies on the
subject found 430 of 450 women in an
urban clinic who, when told that the
sex of the baby was female, wanted
to have an abortion. In contrast, all 250
cases where the baby was male
continued with the pregnancy, even
with risk of genetic disorders
(Ramanama and Babawale 1980).12 It
is often argued that women
themselves accept and endorse sex
selection but are they in feet making a
choice? Some researchers certainly
seem to think not. The decision is
often a response to intense pressure
to produce male heirs, often through
implicit threats of violence or husband's
remarriage. Most women make their
choices in the context of their families
and the patriarchal system that does
not favour the birth of a female child
(Oomman and Ganatra 2002).13
That we have a problem of large
magnitude is realized. Yet the early
steps to deal with this have been
extremely problematic indeed. The
Indian Medical Association has been
reluctant to take action against erring
members. But it joined UNICEF and
the National Commission of Womer
organising a meeting with so-call
religious heads, the very struts
patriarchy, and some among thei
defenders of widow immolatio
Although a large number of progressr
women's groups and health groui
boycotted this meeting, Madhu Ktshw
defended this as "cost -offectjve*(Rc
2001).14
Although all religious heac
present at this meeting condemne
SSA, the moot question of course i
why groups, who in the past ha
opposed widow remarriage amon<
Hindus and more recently, afte
Deorala, supported widow immolation
have now become progressives ir
opposing SSA. The answer of course
is the familiar anxiety about so callee
Muslim rates of population growth.
Earlier Mr. Giriraj Kishore of the Vtshwa
Hindu Parishad had condemned access
to abortion in India, arguing that Hindu
women disproportionately aborted
fetuses (Ibid).15 I need hardly add that
lack of access to safe abortion is one
of the leading causes of the high
maternal mortality rate in the country.
What is often not recognised is
the withdrawal of the state - from
health, education, employment
generation and actively combating anti
women traditional values - engenders
both the feminisation of poverty and
the shrouding and enfoldment of
women, sacrificing them to the altar
of the family. Thus the 1990s have seen
a sharp increase in violent crimes
against women, especially dalit
women (Human Rights Watch 1999).16
It has also witnessed a significant
increase in so-called honour killings,
especially in the same areas of north
and west India that have also seen an
increase of SSA (Chowdhry 2000).17
Particularly sharp increases in dowry
deaths have also been documented in
these regions. As Chowdhury has
revealed in her study, in all these
cases, it is almost impossible to obtain
Issues
state action (Z/?/d).18
selection actionable. They also sought
Punitive and coercive population to create structures for the registration
policies, especially those announced by and monitoring of all facilities offering
several states, are an invitation to these services, as well as tightening
female SSA. Not curiously, a large punitive measures for the violation of
number of respondents in a study of the
Act.
Not
surprisingly,
female infanticide in Salem district representatives of the medical industry
explicitly stated this. The women
that has contributed to the dismal
interviewed felt that they could not scenario of the adverse sex ratios in
accept sterilisation as it interfered with the country — objected to the
their ability to work on the fields. What proposals on the grounds that such
they were doing, they argued, was technologies were essential for
"traditional" and achieved precisely bringing down unconscionable levels
what the Government of India wanted. of maternal mortality and for reducing
A study in Mumbai revealed that a the incidence of congenital
majority of doctors performing sex- abnormalities.^
-----While it is indeed true that the
selective abortions stated that they did
so in order to control population
Maternal Mortality Rate in the country
growth (FRCH Study cited in Gupta
is high and needs to be reduced, it is
2000).19 The clients were largely
"Representatives of
nevertheless true that the contribution
educated and came mainly from the
such technologies can make towards health groups and
middle classes.20
this is extremely limited, if not non
women's groups
Some feminists referring to the existent. As epidemiological
.
data on pointed out that the
issue in terms of reproductive rights maternal deaths in the country indicate,
and choice ironically--justify. SSA. This even within the reproductive age group medical profession's
argument goes that people have no use of 15-45 years, causes related to commitment to bringing
for abstract concepts as sex ratios. The reproduction account for merely 12 per down congenital
lives of Indian women were so terrible cent of all causes of death. Even within
abnormalities is highly
that this technology offered them an the reproductive age group of women,
element of choice, indeed of anaemia and communicable diseases selective and thus
empowerment. Over time a decline in take a far higher toll. Excluding these deeply suspicious (Delhi
the supply of girls might improve the major causes of death, the most Science Forum 2002)21."
demand
for girls and thus their status. significant factor is lack of access to
...
-What this argument misses out is safe and effective natal care. In the
extremely important: women are not absence of these, to argue that prein ^JI!
f
rC?nL^en3.when they natal diagnostic technologies are
exercise this "right" to SSA.
necessary to bring down the MMR is
The appeal of the reified concept
of rights was also evident during the
hearing of the Parliamentary
Committee on the Empowerment of
Women on the issue of Pre-Natal
Dia9nosticT^hniqu^ (Regulation and
Prevention of Misuse) Amendment Bill
2002, that considered representations
from the public to proposed
modifications in the PNDT Act. The
modifications, in essence, sought to
include a range of pre-implantation
diagnostic techniques in the purview
of the Act, making their use for sex
c,ear|y spurious.
Representatives
Representatives of
of health
health groups
groups
and women's groups pointed out that
the medical profession's commitment
to bringing down congenital
abnormalities is highly selective and
thus deeply suspicious (Delhi Science
Forum 2002)21. Some years back,
when health groups and women's
groups were involved in a campaign
against high dose oestrogen
progesterone based contraceptives,
since banned, on the grounds that they
induced congenital abnormalities in
1DPAD Newsletter Vol. II, No. I januan - June 2004
2.
Issues
foetuses exposed in utero, the medical
profession completely disregarded the
existing scientific information and
campaigned against the ban (Rao
2004).22
technology industry to seek markc
There is no doubt that India constitu
a large and lucrative market estimat
at Rs.126,270 crore in 19
(Srinivasan 2004).23
It was also pointed out that
What this calls attention to,-abo
scientific evidence on the prevalence all, is the urgent need to monitor a
of congenital abnormalities in India is
regulate all public health technologi
woefully inadequate. There is also no and practices, especially given the fe
data to substantiate the claim that that India has the dubious distinctic
ultra-sound and such other of being one of the largest unregulati
technologies that have been so private health care markets in tt
cavalierly used have indeed brought world. This is the case with pre-nat
down the prevalence of congenital and
________
natalwh
diagnostic tests as wit
ina,mbent
A'suXe
those who wish to continue to use such
What this underscores is technologies on this ground to furnishi carried out by Women's Centre
i Mumbai, revealed that between 198
data in support of their daim. On the; and 1986, the number of dinics offerin.
not epidemiological
other hand, those who wish to curtail sex-determination tests in Mumba
priorities or indeed
the misuse of these technologies, have alone increased from 10 to 600 (citec
concerns about
data on increasing masculinisation of
women rs health but the both the CSR and the Sex Ratio at Birth, in Gupta 2000).24 In the year 1985
alone, 40,000 female fetuses were
power of the global
attesting to SSA on a large enough aborted in Mumbai.
reproductive technology scale not warranted by the prevalence
Representations
to
the
rates of congenital abnormalities.
industry to seek
Parliamentary Committee pointed out
From a public health perspective, that the limitations of legal action alone
markets. There is no
then,
there is very little role for such
doubt that India
to curb female sex selective abortions
technologies. Doctors can perhaps be
are
very real. Yet, they are nevertheless
constitutes a large and
forgiven for not reflecting on Say's Law
crucial
in a sodety to establish norms
lucrative market
that supply creates its own demand. of ethical medical practice.
estimated at Rs.l26f27O They have evaded the responsibility of
In a sense rising to the defense of
creating an injection culture in our
crore in 1998
the medical industry, Madhu Kishwar,
population just as they now evade the
(Srinivasan 2004).23
the leading feminist-revisionist,
responsibility of a "tests" culture. But
they cannot be forgiven for not knowing pleaded against widening of the ambit
that the prevalence of congenital of the law. Kishwar argued that
abnormalities in 1.5 per cent of all women in India exhibited choice,
indeed agency when they undertook
pregnancies; that of these, possibly
sex-selective
abortions. It is not for the
only fifty per cent can be identified by
state
to
intervene
in the family— the
non-invasive technologies. Yet there
deeply
personal,
she
said. On the other
has occurred an epidemic of the
hand, Kishwar also argued that a
spread of sonogram and ultra-sound
clinics in a completely unregulated corrupt state merely brought in laws
in order to increase levels of
manner. Indeed Pre-Implantation
corruption.
Indeed she argued that
Diagnostic Techniques (PDTs) are
already available in our metropolitan doctors were by and large helpless,
coerced into performing SSA by
cities.
influential people. What was forgotten
What this underscores is not of course is that far from showing their
epidemiological priorities or indeed <
agency, women who took recourse to
concerns about women's health but the :sex-selective abortions were doing so
power of the global reproductive iunder pressure from families, and
.4
IDPAD Newsletter VoL II, No. 1 January - June 2004
Issues
were thus victims of patriarchy (Bhalla
2004).25 What this also reveals is the
miraculous power of the concept of
reified rights to turn things on the
head, and indeed become part of the
arsenal to further oppress and
subordinate women.
particularly the rights of the child.
Similarly, the use of contraceptive
targets results in undue pressure being
put by service providers on clients"
(NHRC: 2003:l-2).27 Ironically
Ironically just
just aa
few days later, on the 31st of July 2003,
newspapers announced that a three-
The National Population Policy,
2000, emphatically rejected any
element of coercion or disincentives in
the implementation of the family
planning programme. Yet in
contravention of the NPP, and indeed
the commitments made by the
Government of India at the ICPD in
Cairo in 1994, several state
judge Bench of the Supreme Court
upheld a Haryana Government law
prohibiting a person from contesting
or holding the post of sarpanch or
panch if he or she had more than two
children.
Unfortunately the fears of the
health groups and women's groups
have come true. It has been reported
study also found an increase in the
number of pre-natal sex determination
tests, followed by SSA. It also found
an increasing incidence of desertion,
divorce and the "donation" of children
in adoption. Yet another study
concluded, "women, especially from
marginalized groups suffered the
consequences of the Act from causes
beyond their control (Sama 2003:2).29
It is now abundantly clear that
given the ideology of son-preference
in the country, particularly marked in
the high fertility areas, a vigorous
pursuit of the two- child norm is an
invitation to female SSA. Indeed, it was
the explicit recognition of this link that
compelled the Chinese government to
modify its one-child per family norm.
governments have announced f
that’ a studyz commissioned by the
P??Ul^tiO21.POliCieS.thit
a String Ministry of Health and Family Welfare
of disincentives and a Two Child Norm did indeed find expectedly dolorous
for Panchayats. Women's groups and outcomes with the imposition of the
health groups had protested to the Two-Child Norm for Panchayats. The
National Human Rights Commission study, covering A.P., Haryana, M.P.,
that such a norm was discriminatory Orissa and Rajasthan concluded
and would lead to a further increase diplomatically: "The way the norm is
in SSA (Rao 2003).26 Subsequently
S ‘
conceptualized and currently
the NHRC in a Declaration stated:" Note implemented is not without serious
further that the propagation of a two- unintended negative consequences"
child norm and coercion or (The Hindu 2003:5).28 Thus 75 per
manipulation of individual fertility cent of those disqualified from
decisions through the use of incentives contesting elections to the PRIs were
and disincentives violate the principle from the SC, ST and-OBCs.
____ In Orissa
of voluntary informed choice and the and A.P., 55 per cent and 48 per cent
human rights .of the people, of those disqualified were women. The
A recent study of abortion in
Maharashtra found that a large
number of doctors were performing
SSA even though they knew it had been
banned (Bandewar 2003).30 Their
reasons were many: that it was for
the woman's sake - to save her from
illegal abortions; that if they did not
do it, other doctors would; above all
that it for the good of the country since
it brought down population growth.
The fight against SSA is thus a fight
against anti-women population and
health policies; it is also a fight against
a medical system profoundly
dismissive of wider social concerns in
the rush for profits. Above all, it is a
battle for women's democratic rights
to equality in property and against anti
female religious world-views.
Centre ofSocial Medicine and
Community Health, Jawaharlal
Nehru University, New Delhi
IDPAD Newsletter Vol. II. No. 1 Janu.irv
lune 2'>04
25
Issues
References
1. Foeticide is the word used by right-wing, pro-life groups,
especially in the USA - who express their views often
through bombing dinics or killing doctors who perform
abortions - and the Vatican. Feminists, who recognize a
woman's right to abortion, and indeed still have to fight for
it, therefore use the phrase Sex Selective Abortion (SSA),
or Pre-Birth Elimination of Females (PBEF).
2. Patel, Tulsi (2004), "Missing Girls in India" Economic
and Political Weekly, Vol.39, No.39.
3. Oldenberg, P. (1992), "Sex Ratio, Son Preference and
Violence in India", EconomicandPolitical Weekly, Vol.XXVII,
No. 49.
4. Under normal conditions, i.e. conditions under which
both males and females are exposed to the same mortality
risks, more boys are bom than girls. This is considered
nature's means of maintaining the parity of the sex ratio,
since boys are biologically more vulnerable than females
in infancy.
5. Premi, M.K. (2001), "The Missing Girl Child", Economic
and Political Weekly, Vol.XXXVI, No.21.
6. UNFPA (2003), Missing: Mapping the Adverse Child Sex
Ratio in India, New Delhi.
15. Rao, Mohan (2001), "Female Foeticide: Where C
Go", Issues in Medical Ethics, Ibid.
16. Human Rights Watch (1999), Broken People:
Violence AgainstIndia's 'Untouchables', Books for Chi
Bangalore.
17. Chowdhry, Prem (2000), "Enforcing Cultural Cc
Gender and Violence in Northern India" in Mary.EJohr
Janaki Nair (Eds.), A Question of Silence? The St
Economies ofModern India, Kali for Women, New De
18. Ibid.
19. FRCH Study cited in Jyotsna Agnihotri Gupta (20
New Reproductive Technologies, Women's Health
Autonomy: Freedom or Dependency?Sa^e, New Delh
20. This of course calls into question the almost autom
relationship between female education, autonomy .
empowerment that has too many utilitarian takers to
enumerated.
7. Agnihotri, S.B. (2000), Sex Ratio Patterns in the Indian
Population: A Fresh Exploration, Sage, New Delhi.
21. Delhi Science Forum(2002), Memorandum to Marge
Alva, Chair, Parliamentary Committee on the Empowerm
of Women, 6th September 2002, New Delhi.
8. Krishnaji, N. (2000), "Trends in Sex Ratio: A Review",
Economic and Political Weekly, Vol. XXXV, No. 14.
22. Rao Mohan (2004),"Sex Selective Abortions: So
Concerns", IW/7?e/7's Equality, Nos. 1-2.
9. Harris-White, Barbara et a! (1996), "Development,
Property and Deteriorating Life Chance for Giris in India: A
Preliminary Discussion with Special Reference to Tamil
Nadu", paper presented at the Silver Jubilee Seminar, MIDS.
23. Srinivasan, Sandhya (2004), "Selling the Parenthc
Dream" in Mohan Rao (Ed.), The Unheard Screa
Reproductive Health and Women's Lives in India, Zu ba.
New Delhi.
10. Heyer, Judith (1992), "The Role of Dowries and
Daughters' Marriages in the Accumulation and Distribution
of Capital in a South Indian Community", Journal of
Internationa!Development, Vol.4, No.4.
24. Gupta, Jyotsna Agnihotri (2000), Op cit
11. Clark, Alice W., (1987), "Social Demography of Excess
female Mortality in India" Economic and Political Weekly,
Vol.XXII, No.17.
12. Ramanama A, Bambawale U, (1980), "The Mania for
Sons: An Analysis of Social Values in South Asia", Social
Science and Medicine, Vol. 14B, No.2.
13. Oomman, Nandini and Ganatra, Bela R. (2002), "Sex
Selection: The Systematic Elimination of Giris" Reproductive
Health Matters, Vol. 10, No. 19.
14. We live in a world of no certitudes except the illusion of
choice offered by the market. Is this the reason for the
unthinking popularity of such phrases? How else does one
explain the fact that Madhu Kishwar argued that it is
necessary to involve so-called religious leaders in a
campaign against SSA since it is cost-effective (The Times
26
of India, 17th July 2001)? Sadhvi Rithambra, best I
for her anti-miqprity positions, was part of this allie
have argued elsewhere against the unholy anti-f
alliance this issue has brought together (see Isst
Medical Ethics, Vol.IX, No.4, October 2001).
lDPz\D Newsletter Vol. II, No. 1 January - Ju nc 2(KM
25. Bhalla, Manisha (2004), "The Land of the Vanish
Girls: Sex Selective Abortion in Punjab" in Mohan Rao (E
Opdt
26. Rao, Mohan (2003), "Two Child Norm and Panchaye
Many Steps Back", Economic and Political Weet
Vol.XXXVII, No.33.
27. National Human Rights Commision (2003), Dedarab
National Colloquium on Population Policies, New Delhi.
28. "Two Child Norm Brings Little Relief for Women",
Hindu, July 2nd 2003.
29. Sama (2003), "A Draft Report of the Study on
Implementation of State Population Policy on PRIs and
Women" unpublished report, New Delhi.
30. Bandewar, Sunita (2003), "Abortion Services c
Providers7 Perceptions: Gender Dimensions" Economic.
Political Weekly, Vol.XXXVIII, No.21, May.
r inn
[
A
Click here to close this window
]
Analysis
“The two-child norm only leads to female foeticide”
By Madhu Gurung
Commenting on the serious decline in the 0-6 sex ratio in India, leading demographer Ashish
Bose states that the government’s policies are all wrong. The two-child policy has got mixed up
with female foeticide. Government slogans like ‘Beti ya beta, dono ek hairi make little sense. And
financial sops for couples having a girl-child can make no dent in the traditional preference for
sons in India
Census 2001 figures, released recently, showed that the child sex ratio has dropped even further - from 941
in 1991 to 927 in 2001. States such as Punjab, Haryana, Himachal Pradesh, Chandigarh and Delhi nov\
have fewer than 900 girls per 1,000 boys. What are the causes and implications of this shocking drop in se>
ratio?
Leading demographer Professor Ashish Bose recently conducted a study of female foeticide in Punjab
Haryana and Himachal Pradesh, which showed that “demographic fundamentalism” or preference for a boy
child is on the rise in the country, resulting in a declining sex ratio. In this interview, Prof Bose discusses the
sex ratio figures and also comments on the recent controversy over the growth-rates of population in India bj
religion.
What are the most significant findings of Census 2001?
The latest Census shows that the juvenile sex ratio, which had become a concern in the 1991 Census, has
gone down even further. In 1991, the national average for the child sex ratio, in the 0-6 age-group, was 945
Several states, including Punjab, Haryana, Himachal Pradesh and Uttar Pradesh, had fewer than 900 girls
per 1,000 boys. However in Census 2001, in Punjab, Haryana, Himachal Pradesh and Gujarat alone, the se>
ratio had plunged. In 1991, all districts of Punjab except Nawanshahr, recorded a child sex ratio lower thar
900. In the 2001 Census, while Nawanshahr recorded a child sex ratio of 810 girls per 1,000 boys, mors
alarmingly, 10 of the 17 districts of Punjab recorded fewer than 800 girls per 1,000 boys.
The past decade also saw a worsening sex ratio in Haryana. In 1991, not a single district recorded less thar
800. In 2001, Haryana’s well-known districts like Kurukshetra, Kaithal, Ambala, Sonepat, Rohtak, al
recorded figures less than 800.
Gujarat, in 1991, enjoyed a sex ratio of 900 girls for every 1,000 boys, but the 2001 Census throws up c
dismal picture. There is a sharp decline in a large number of its districts. Of the 20 districts in Gujarat, onl^
eight recorded a child sex ratio of 900, the rest of the districts were very low. In fact in Rajkot and Mahesana
the situation is alarming and showed a ratio of just 798 girls per 1,000 boys.
In Himachal Pradesh too there is a drastic drop in the child sex ratio, especially in districts adjoining Punjat
and Haryana. What was deemed a normal sex ratio of more than 950 in 1991, had dropped drastically ir
Himachal Pradesh, eight out of 12 districts being the worst. Most of the prosperous northern states have
recorded more than a 50-point decline in the child sex ratio in the past 10 years.
In Rajasthan, more districts have recorded child sex ratios lower than 950, and it’s slightly better amongs
predominantly tribal populations. But even there, there has been a drop in child sex ratio especially ir
Chittorgarh and Udaipur. The child sex ratio has declined in Aiwar, Sikar, Jaipur and Jhunjhunu districts. This
could be attributed to the two-child norm pushed actively by the state government.
In 1991, Delhi’s child sex ratio was lower than 950. Ten years later, the 2001 Census shows that almost al
districts recorded a child sex ratio less than 900, with its more prosperous southwestern part showing c
decline from 904 girls in 1991 to 845 girls in 2001.
In Maharashtra, in Jalgaon, Aurangabad, Beed, Solapur, Sangli and Kohlapur districts, the child sex ratio has
gone from bad to worse. Maharashtra’s eastern districts like Nagpur and Jalna also show a significant drop.
Of all the southern states that come up on the map of worsening child sex ratios, is Tamil Nadu. Little seems
to have changed since 1991. Dharmapuri, Namkkal, Theni and Madurai districts had recorded a low chile
sex ratio in 1991. But the recent 2001 Census shows that the problem has spread to Tiruchi, Cuddalore anc
i *7/i i nnnd
r rm i
Vellore districts. In 1991, Salem had recorded the lowest child sex ratio at 830 girls which, the latest 2001
Census shows, has further declined to 826 girls per 1,000 boys.
What are the reasons for the decline in sex ratio? Census 2001 shows that during the 1991-2001
decade the overall sex ratio increased from 927 per 1,000 to 933 per 1,000 (an increase of six points).
But during the same decade the child sex ratio (0-6 years) dropped from 945 to 927 (a decline of 18
points) while the sex ratio in the 7+ age-group increased from 923 to 935 (an increase of 12 points).
When you talk of the Indian Census, it is important to understand that our sex ratio is defined as the number
of females per 1,000 men, unlike the West where sex ratio is the complete opposite and defined as the
number of males per 1,000 females. Like China, in India too masculinity is increasing. But having said that, I
also want to say that in India we have a poor civil birth registration system and most of our data are from
hospitals where births have been registered. In India there are thousands of births that go unreported. So
what we have is really biased data, not very reliable, but these are data constraints that we have to work
with.
If you analyse in detail, India has 28 states and seven union territories that add up to 35 administrative units.
We have data of 593 districts that were there in 2001, now the districts have gone up to 600. We have to
demographically map them. Your figures are correct - those are the figures we have arrived at.
The phenomenon of declining sex ratio that showed up in Census 2001 is worst in Punjab, Haryana,
Chandigarh, Delhi, Western Uttar Pradesh, Gujarat and Maharastra. This defies all demographic theories as
these are prosperous states. You expect that when people live better, have better education and economic
security, there will be less of a traditional bias against the girl-child; but in India, like China, it has only
worsened the situation. Suppose like China, instead of just one, we had a two-child policy, then the Jats and
Punjabis would ensure that they had two sons.
In India, there is an unholy alliance between tradition and technology. Tradition is marked by sonpreference. Technology started in the '80s with amniocentesis, most readily available in Punjab, the state
made most prosperous by the Green Revolution, and having a long tradition of son- preference. Today
ultrasound is the sex-selective technology that is widespread in most prosperous states.
The reasons are easy to define - prosperity ensured better infrastructure, more machines and more doctors
to perform the tests. People had money-power to pay for the technology and of course, as infrastructure
improved, people could access the clinics easily. All this made foeticide rampant. If we look at the historical
perspective of Punjab, where the sex ratio is the worst, the state has a long martial tradition, and women
were seen as liabilities. Sons were preferred as they could carry on the martial tradition.
The new factor in Punjab is migration. Punjabis are the most eager to migrate to the West. The propensity to
migrate is higher for young boys than for young girls. In Chandigarh, most young people are looking towards
New Zealand for migration because that country is also agriculture-oriented.
In Haryana, the Jats have their own tradition of land ownership, so sons are preferred. It is a dismal
situation. In the future, Punjabis will have to marry non-Punjabis, probably girls from Bihar and UP, which
are demographically surplus-populated states.
Son-preference has spread even to south India. Social wokers are saying the reason is patriarchy, or
women having internalised the value systems of men. The whole phenomenon is supply-driven rather than
demand-driven and women feel they have a better self-image and status in society if they have sons.
A UNFPA report in 1997 pointed out that if Kerala’s sex ratio of 1,036 females per 1,000 males
prevailed in the entire country, there would be close to 32 to 48 million missing women. In the light
of the Census 2001, what is your estimate of missing females?
This was a romantic expression coined by Amartya Sen. You cannot arrive at figures like that because you
must look at the individual family unit. For me this is a non-issue because much more fine-tuning is required
to understand the social phenomenon of declining sex ratio. All this is hypothetical and good for newspaper
headlines.
Does the latest census show that the DEMARU trend (an acronym you coined standing for Daughter
Eliminating Male Aspiring Rage for Ultrasound) has proliferated in the states and reflects a skewed
sex ratio?
Yes, it is spreading, and the reason is better infrastructure, better education, which ensures more doctors,
and overall prosperity, which ensures people’s ability to pay. The next Census will also show the declining
sex ratio. I was in Rajasthan on fieldwork, collecting data along with a team, and we had a questionnaire we
had prepared, and I had some young people going around the villages asking the same question. The
question was: how many sons do you want? And almost everyone had put down two sons, so I decided they
had all sat together and put it down. So I went around and met a woman on the road and asked her the
same question and she said she would like at least two sons. When I asked why, she said, why do you have
two eyes?
l-'Wr-x'//’tirtxrxir irrfrxr'l^nn rroinrli
'ar/pn<>lv<;iQZ17r»rint icr>
17/1 1/2004
In your booklet Darkness at Noon, in a chapter on societal action, there is a doctor who is quoted as
saying that prenatal tests should be permitted if the first child is a daughter so that couples can
have a planned birth, that is, a son thereafter. After this they can go in for sterilisation. What do you
say?
I think the government’s two-child norm and female foeticide have got mixed up, through no fault of either
the government or the people. The famous family planning slogan, Hum do hamare do, mathematically adds
up to only three possibilities — that people have two sons, two daughters, or one son and one daughter. Two
daughters are usually not acceptable - culturally or economically, because they have to be married off.
While one son and one daughter are tolerable, the ideal situation people strive for is two sons. When a vast
majority of people are poor, with no health or social security, sons make the best survival strategy. Slogans
like Beti ya beta dono ek hain make little sense. How can they be equal for people, when girls have to be
married off and sons can be used as crutches?
It’s nonsense when people say Hindus need sons for cremation rights. Who is thinking of death, when
survival is questionable on a day-to-day basis.
As for the government’s sterilisation incentives, it has not really worked because they pay a pittance. Its
barely Rs 200, or Rs 500 at most. Money-power cannot be invoked over this social phenomenon. Schemes
like sterilisation are only good on paper, but do not have the desired impact.
An amendment to the Pre-natal Diagnostic Tests (PNDT) Act was instituted on January 14, 2003. Has
it helped? What should the ideal government policy be?
Without insulting the Supreme Court order, it has not helped. How can anything help against demographic
fundamentalism? How can anyone question why sons are required over girls? However, I am not opposed
to the law as it creates an enabling environment to create awareness against female foeticide.
Our doctors are cleverer than our policemen, our law demands evidence and not a single one has been
caught with anything incriminating. Sex determination tests are the chief money-spinners. The Supreme
Court has ordered that all ultrasound machines have to be registered, but who will supervise this - the chief
medical officer, who is also a doctor? How can he complain against other doctors? The truth is the PNDT
Act is not implementable.
As to what should be the ideal government policy, one suggestion that I have given the government is to hire
private detectives who should collect incriminating information against doctors who flout the PNDT Act,
something like Tehelka... create a stir to get people working and rethinking.
Do you feel the girl-child schemes and financial help offered by the government are enough? Is there
any one state where the girl-child policy has worked?
There may be marginal impact or no impact in most states, however well-meaning the government schemes
may be. Schemes have to be innovative, imaginative and implementable. Sure, in states like Goa, Tamil
Nadu, Andhra Pradesh and Kerala, the government family planning programme has worked, but not in
states like Bihar and Madhya Pradesh. But there is not one state where the girl-child policy has been
successful or the census data would not show up so negatively.
In Bangladesh, most of the schools I visited had more girls than boys, when culturally they have the same
biases as us in India, and I learnt it was because each girl who came to school could take home a bag of
rice for every month she stayed in school. Yes, such schemes may have their pluses and minuses. But we
have to examine schemes that give people incentives, education to the girl-child that would enable her to
earn in the future, and flexible school hours that ensure she stays in school and also contributes to the
family income.
What are your recommendations? Is government policy addressing the problem?
Female foeticide is the result of an unholy alliance between the traditional preference for sons and modem
medical technology, the increasing greed of doctors, the rising demand for dowry that makes daughters
financial burdens, the ineffectiveness of the PNDT Act and the liberal Medical Termination of Pregnancy
(MTP) Act, and the lack of any serious involvement of civil society in fighting this menace. The gender
balance cannot be restored unless we make a frontal attack on all the players and stakeholders.
One possible way could be job reservation for women, because without economic empowerment, political
empowerment will not be enough. However, this may not be acceptable to the government. I suggest a
three-tier model involving the government, NGOs and panchayati raj institutions, with technical back-up from
academic experts, social activists and management experts. Local initiatives by NGOs and individuals with
vision in such fields must be permitted. No more additions to the already existing government schemes are
recommended.
Funds must be made available to organisations, especially in the health sector, to initiate an awareness
campaign through the electronic and print media. A nation-wide campaign must be launched to recognise
and spell out all forms of gender violence and the disastrous consequences of the demographic imbalance.
The role of the father in determining the sex of the child must be highlighted. All suspected cases of female
http://www.infochangeindia.org/analysis47print.jsp
17/11/2004
mill
foeticide must be examined by state commissions and women’s organisations, and action to punish erring
doctors must be undertaken. The PNDT and Dowry Acts must be implemented in letter and spirit. The
government should consider empowering reputed NGOs to deal with cases of female foeticide on a trial
basis. There has to be vigilance at the local level and state supervisory boards and authorities at the district
level have to be activated.
While recommending continuation of the governments sterilisation programmes, the concept of a small
family norm should be left to the zilla parishads, panchayat samitis, panchayats and gram panchayats, to be
handled at the local level. Financial sops to couples that have two daughters and agree to sterilisation are
not effective because reproductive behaviour cannot be manipulated by such incentives. It would therefore
be better to invest in special incentives for girls in the employment market, empowering them in terms of
their earning capacity. This could ideally be handled by the Planning Commission instead of the Ministry of
Health and Family Welfare, as is being done now. Years of propaganda have made people accept the small
family norm of one son and a daughter or even two sons and a daughter. The Ministry of Health and Family
Welfare should continue to propagate its population policy without emphasising the two-child norm, as it only
leads to female foeticide.
High priority has to be given to field studies and research. There has to be collaboration between
universities and research institutes, with NGOs that are qualified in this field. Only then can meaningful
intervention strategies be evolved.
What are your comments on the recent ‘by religion’ growth rates?
When we talk about communities, it is important to point out that no two communities grow at the same rate.
The newspapers write things to sensationalise their papers. What is important to know is that there is no
decline in the population in any community in India barring the Parsis. In absolute terms, the proportion of
population of each community must add up to 100. These proportions will depend on the growth-rate of
population of different communities. So when I say that the Muslim population has gone up, that does not
mean that the Hindu population has gone down. The Hindu population has also gone up, but the proportion
has gone down.
Three things affect population growth: natural increase in population (that is birth minus death), net migration
and geographical territorial adjustments (if any). In 2001, the census was conducted all over India. But in
1991, the census could not be conducted in Jammu and Kashmir (J&K) because of disturbed conditions,
and likewise in Assam in 1981 census enumeration did not take place. So it is important to compare the
comparables. Now that J&K has been enumerated in 2001, adjustments have to be made comparable to the
1991 Census.
So all I can say is that all over the world, the Muslim growth-rate is higher than the non- Muslim growth-rate.
But in Muslim-dominated countries, where they do practice family planning, the growth-rate is less than in
countries where Muslims are in a minority - as in India and Nepal, where there is some resistance to family
planning.
Community-wise, in India, the Parsis have the lowest growth-rate, in fact it is running in minus. The Muslim
growth-rate is 29.3%, the Hindu growth-rate is 19.9% and the Sikh growth-rate is the lowest at 17%. The
Sikh growth-rate was 25% in the 1991 Census, so it has dipped drastically. The Christian growth-rate is
25%.
(Madhu Gurung is a Delhi-based journalist and consultant working on gender issues.)
infoChange News & Features, November 2004
i-nfXr'hancrAlndinrcr/AnV«s1 <?47'nnFit. 1SD
17/11/2004
Position: 2144 (6 views)