8862.pdf
Media
- extracted text
-
(Rgference Materials - II
SEXSELECHON IN INDIA: ISSUESAND APPROACHES
^mndiaSle
JGvos ImGa OfegionaCOffice, (Bangalore
17th
!1
s' >
gM
<
18^ <Fe6ruaTy, 2005
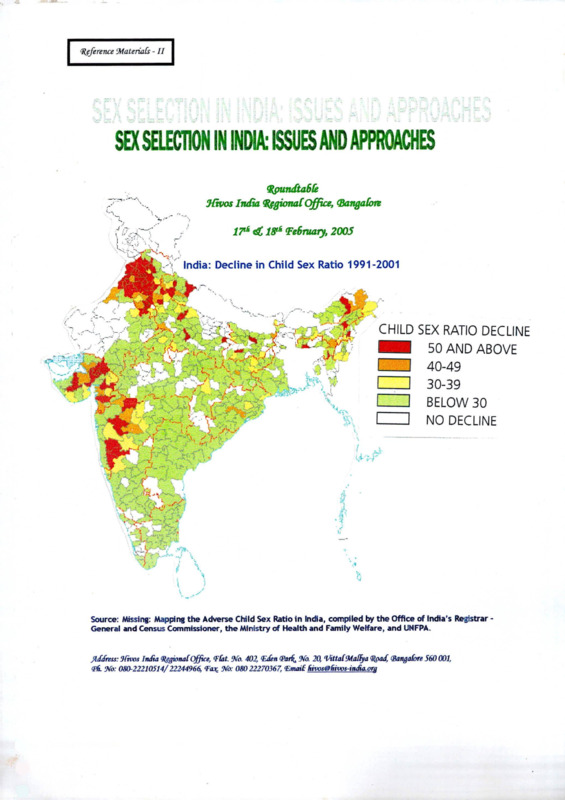
India: Decline in Child Sex Ratio 1991-2001
-
CHILD SEX RATIO DECLINE
50 AND ABOVE
I
I 40-49
f
H 30-39
7
I BELOW 30
___ I NO DECLINE
V
Si
'tW>
*
:
$
Vi
aJ-'
J-?
■f'
if
WTr
w
%
i
Source: Missing: Mapping the Adverse Child Sex Ratio in India, compiled by the Office of India's Registrar General and Census Commissioner, the Ministry of Health and Family Welfare, and UNFPA.
Jid/ress: Ilivos InJia RegionalOffice, I’(at. No. 402, {EJen (Parf^ No. 20, ‘VittalMalfya Q&aJ, (Bangalore 560 001,
<P6 No: 080-22210514/22244966, ¥0* No: 08022270367, ‘Email: 6ivos@liivos-iiuAa.org
^gference Materials - II
SEX SELECTION IN INDIA: ISSUES AND APPROACHES
Q&undtable
Mivos India (RegionalOffice, (Bangalore
IT* <£ 18* February, 2005
India: Decline in Child Sex Ratio 1991-2001
Source: Missing: Mapping the Adverse Child Sex Ratio in India, compiled by the Office of India’s Registrar General and Census Commissioner, the Ministry of Health and Family Welfare, and UNFPA.
^difiTss: Tdvos India (S^jional Office, Tlat. ‘\a 402, <Eden (Par^ Wo. 20, VittalMalfya
<Pii Wo: 080-22210514/22244966,
Wx 08022270367, ‘Email4mw^6ivos-in£a.org
(Bangalore 560 001,
2.
National Population Policy 2000: A Critique
Jashodhara Dasgupta, KRITI
3.
Re-Examining Critical Issues on National Population Policy 2000
Devaki Jain and Mohan Rao
4.
Female Sex Selective Abortions: Some Issues
Mohan Rao, IDPAD Newsletter Vol. II, No. 1, January - June 2004
5.
The Two-Child Norm only leads to Female Foeticide
Madhu Gurung, www.infochanqeindia.orq/analysis47print.isp
Role of Medical Establishment - Role of New Reproductive Technologies
1.
Social Justice and the New Human Genetic Technologies
Centre for Genetics and Society
2.
The Basic Science
Centre for Genetics and Society
3.
NGO moves Court over MCl’s failure to check Foeticide
Stop Selective Sex Abortions Stop Female Foeticide
www.datamationfoundation.orq/female/acourt.htm
4.
Sex Test law kills off Ultrasound
Kalpana Jain
Stop Selective Sex Abortions Stop Female Foeticide
www.datamationfoundation.orq/female/acourt.htm
5.
Sex Selection: New Technologies, New Forms of Gender Discrimination
Rajani Bhatia, Rupsa Mallik, Dhamita Das Dasgupta with contributions from
Soniya Munshi and Marcy Damovsky
6.
Sons are Rising, Daughters Setting
Dr. Vibuti Patel, HumanScape, Vol.X, Issue IX September 2003
7.
A Study of Ultrasound Sonography Centres in Maharashtra
Sanjeevanee Mulay and R. Nagarajan
Population Research Centre, Gokhale Institute of Politics and Economics
8.
Female Foeticide: The Collusion of the Medical Establishment
Lalitha Sridhar, www.infochanqeindia.orq/features210print.isp
9.
Preimplantation Genetic Diagnosis for Gender Pre-Selection in India: A Counter
Argument to the Article by Malpani and Malpani
Rajiv H Mehta, Source: Reproductive Bio-Medicine Outline, Jan/Feb 2002, Vol.
4, Issue 1
10.
Court orders seizure of Illegal Sex Test Machines
Source: National Catholic Report, 3/8/2002, Vol. 38, Issue. 18
ii
11.
Reproductive Technologies in India: Confronting Differences
Rupsa Mallik, Sarai Reader 2003: Shaping Technologies
Ethics
1.
Urgent Concerns on Abortion Services - EPW Commentary
Ravi Duggal, Vimala Ramachandran
2.
Negative Choice
Rupsa Mallik
Law - Human Rights
1
Female Feoticide or Crime against Humanity?
Kalpana Kannabiran
2.
Protecting the Rights of Girls
Dr. Erma Manoncourt, Deputy Director, UNICEF-lndia Country Office
3.
Rights of the Giri Child: Covered under Important National and International
Instruments
CASSA
4
Proposed Changes to the Medical Termination of Pregnancy Act, Rules and
Regulation in the Light of Concern about Sex Selection: A Response from the
Coalition for Maternal-Neonatal Health and Safe Abortion
5.
Treating Infanticide as Homicide is Inhuman
Lalitha Sridhar, www.infochangeindia.org/features211 print.jsp
6.
Memorandum to SCW to Relieve the Victims of Female Infanticide who are
Accused Guilty under Sec 302
Implementation of Existing Regulations - Obstacles and Bottlenecks
1.
Memorandum - Child Sex Ratio Vs Implementation of PCPNDT Law in Delhi
2.
Amendments to PNDT Act - Critical Appraisal of PNDT Act and Suggested
Amendments
CASSA
3.
The Role of the State Health Services - Emerging Issues
Dr. Reema Bhatia, University of Delhi
4.
A Merely Legal Approach cannot Root out Female Infanticide
Interview with Salem Collector J. Radhakrishnan
Stop Selective Sex Abortions Stop Female Foeticide
www.datamationfoundation.org/female/acourt.htm
5.
The Role of Appropriate Authorities in Implementing the Pre-natal Diagnostic
Technigues Act 1994 and Roles (as amended upto 2002/2003) - Position Note
in
for Discussion from State Level Consultation on the Role of the Appropriate
Authorities in Implementing the PNDT Act 1994 and Rules - 24th September
2003
6.
Steps to be taken to implement the PNDT Act and Rules in Tamil Nadu from
State Level Consultation on the Role of the Appropriate Authorities in
Implementing the PNDT Act 1994 and Rules - 24th September, 2003
7.
A Critical Analysis of Tamil Nadu Government Cradle Baby Scheme
P. Phavalam, Convenor, CASSA
Campaigns and Interventions
1.
Tackling Female Infanticide: Social Mobilisation in Dharmapuri, 1997-99
Venkatesh Athreya, Sheela Rani Chunkath, Economic and Political Weekly,
December 2, 2000
2.
Indicators
CASSA
3.
Public Interest Litigation Filed in Supreme Court
CASSA
4.
Resolutions of Campaign against Sex Selective Abortion - Resolutions
CASSA
5.
Monitoring the Declining Child Sex Ratio - a Suggested Method
CASSA
6.
Minutes of the Two Days National Consultation on Enforcement of PCPNDT Act
iv
1
Role of Medical Establishment - Role of New
Reproductive Technologies
CENTER FOR
GENETICS and SOCIETY
www.genetics-a nil-society.org
Social Justice & the New Human Genetic Technologies
Imagine a world in which well-off people planning to have a baby can buy all sorts of genetic
“enhancements” for their future child-better memory, perfect pitch, straighter nose, longer legs. Ferbhty
clinics craft upscale marketing and advertising campaigns with the message that responsible parents must
do whatever they can to give their child an advantage in a competitive world. Of course, only the wealt y
can access these technologies, and the poor fall further behind. Meanwhile, biotechnology corporations
are busy discovering the genes linked to “desirable” traits and hurry to develop artificial human
chromosomes and “gene cassettes” as well as to patent lucrative pieces of the human genetic code.
Cloning and Beyond: An Active Agenda
Such a world is not only being imagined, but actively promoted by a group of influential scientists
biotech entrepreneurs, bioethicists, and others. Their vision of “consumer eugenics (producing allegedly
superior human beings by means of commercially available reproductive and genetic procedures) is
finding its way into mainstream culture, sometimes accepted and even endorsed by major newspapers,
news magazines, and journals of opinion.
Many people have followed the recent headlines about
human cloning: a bizarre sect claiming to have produced
human clones; the difficulties of passing cloning policy at
the United Nations as well as in the U.S. and other
countries. But few people, including social and political
leaders, are aware of the technical and ideological ties
between cloning and the procedures that, if developed,
would enable a high-tech, free-market eugenics. Some of
these technologies may appear far-off and futuristic, but
they are already being widely used in animals.
uThe final ijoal of reproductive engineering j
appears to be the manu facture of a human
being to suit exact specifications of physical 1
attributes, class, caste, colour and sex.... I he |
powerless in any society will get more
disempowered with the growth of such
reproductive technologies. ”
-Saheli Women’s Resource Centre. India
The prospect of consumer eugenics is particularly threatening for groups that have been historically
targeted or disempowered. The underlying technologies—especially cloning and inheritable genetic
modification” (manipulating the genes of very early embryos, so that the child that develops from it will
have certain characteristics)-are of special concern to women because they are so closely tied to
reproduction and women’s health. Their use would dangerously transform the lives of women and
children, and exacerbate existing trends toward corporate-dominated “reproduction for pro it.
People of color and people with disabilities were targeted by eugenic practices of the twentieth centuty, in
which discoveries in genetics were used to justify scientifically dubious and morally indefensible efforts
The Center for Genetics and Society (www.qenetics-and-society.ora) is a nonprofit information and
public affairs organization working to encourage responsible uses and effective societa 9°^^® of
Where do we draw the line?
Pharmaceuticals
Diagnostics
Somatic
therapies
Creating
clonal
embryos
Creating
human
clones
Preimplantation
selection
Inheritable
genetic
modification
Genetic
castes
Posthuman/subhuman
species
to “improve” the human gene pool. Then, proponents relied on state-sponsored coercive methods such as
involuntary sterilization.
A resurgence of state-sponsored programs of eugenic sterilization (or worse) is, thankfully, unlikely in
most countries. Unfortunately, we do have to take seriously the prospect of a new commercial eugenics,
ideologically motivated by notions of “genes as destiny” and consumer choice, and economically driven
by life sciences corporations that could decide to develop and market species-altering technologies to
those who can afford them. The effects would be similar: the poor and disempowered would be deemed
inferior because of their “less fit” or merely “natural” genes, with all too predictable consequences for
their social, political, and economic well-being.
Responsible Policies for Powerful Technologies
A few applications of human genetic and reproductive
science thus open the door to forms of eugenic
engineering more powerful than any envisioned by the
state-sponsored eugenics movements of the twentieth
century. Many other applications are worthy of
support. There is no reason that we cannot distinguish
between the two, and put in place policies that would
foreclose the profoundly dangerous outcomes while
ensuring universal access to beneficial ones.
“The lessons of history have shown as what
happens when people are ordered as better and
worse, superior and inferior, worthy of life and
not so worthy of life.... H hat can happen when
the technology used in support ofgenetic
thinking is not the crude technology oj shackles
and slave ships, of showers that pour lethal gas ,
and of mass ovens, or even the technology of
surgical sterilization, but the fabulous, fantastic,
extraordinary technology of the new genetics
itself?...My children will not be led to genetic
technology in chains and shackles, or crowded
into cattle cars. It will be offered to them."
The United Nations has taken steps to draft a global
treaty banning reproductive cloning, and many
countries have already passed legislation that prohibits
the production of cloned or genetically modified
-Barbara Katz Rothman, City University of
children. Other countries, including the United States,
New York
have no such lugisiauwu.
legislation. rxnu
And aiuivugn
although uicuy
many people
nave
(_--------------------------------------- — ---- -——— ----are now aware that powerful new reproductive and genetic technologies are looming, there is still little
critical understanding of their political and social implications.
"Humans have long since possessed
the tools for crafting a better world.
Il here love, compassion, altruism
and justice have failed, genetic
manipulation will not succeed.
j
I -Gina Maranto, science writer
I Fortunately, that situation is beginning to change through the
efforts of advocates of women’s and human rights, social justice,
environmental protection and environmental justice, disability
rights, and responsible science. It will be far easier to prevent a
new eugenic future if we act before inheritable genetic
modification and cloning develop further, either as technologies,
as ideologies, or as business interests.
C E\ T ER FOR
GENETICS and SOCIETY
u w w. g e ii c t i c s - a ii d - s o c i e t y . o r g
The Basic Science
Reproductive Cloning
Reproductive cloning means creating a genetic duplicate of an existing organism. A human clone
would be a genetic duplicate of an existing person. Genes are strings of chemicals that help
create the proteins that make up your body. Genes are found in long coiled chains called
chromosomes. They are located in the nuclei of the cells in your body.
CELL NUCtfcUS
W!TH CHKOMOSOMLS
4?- ------- genc
PFOTE-M
SfJC
In sexual reproduction, a child gets half its genes from its mother (in her egg) and half from its
father (in his sperm):
SEXUAL REPRODUCTION
FEMALE
ZYGOTE
Q egg
To
BAPY
EF.13HYO
/'
K.
7
O
Q /
o
o
SPERM
This combination of genes is a fundamental basis for human variation and diversity.
In the case of clonal reproduction, all of the cloned child's genes would come from a body cell of
a single individual:
OR ASEXUAL nLr
-EMAlE
BAH-
: ON
Z’/BRYO
r\_y M’ClEL'S INSEHTED
■> \ »?4.a wsri ‘ rr."
The best known cloning technique, somatic cell nuclear transfer (SCNT), is shown abo\ e. The
nucleus from a body cell is put into an egg from which the nucleus has been removed. The
resulting entity is triggered by chemicals or electricity to begin developing into an embryo. If
that embryo were placed into a woman's uterus and brought to term, it would develop into a child
that would be the genetic duplicate of the person from whom the original body cell nucleus was
taken—a clone.
Research Cloning
Research cloning uses somatic cell nuclear transfer to produce a clonal embryo. Sometimes
called "'embryo cloning” or "therapeutic cloning,” it would begin with the same procedure that
would be used for reproductive cloning: the nucleus from a body cell is put into an egg from
which the nucleus has been removed. The resulting entity is triggered by chemicals or electricity
to begin developing into an embryo.
FEMALE
9
NUCLEUS
REMOVED
CLONAL
ZYGOTE
CLONAL
EMBRYO
o
o
■•
NUCLEUS INSERTED
BODY CELL
;SKIN. HA>Fi MUSCLE. ETC. ',
Instead of being implanted in a womb and brought to term as a cloned child, the embryo would
be used for research purposes—for example, to generate embryonic stem cells.
BLASTOCYST
O
0
o
O
HARVESTED
STEM CELLS
EMBRYONIC
STEM CELLS
"Z.OWAL
EMBRYO
NEAVE TISSUES
BONE TISSUES
MUSCLE TISSUES
FOR THERAPEUTIC USES
Most scientists agree that research cloning is not needed as a source of embryonic stem cells for
medical research —these can be obtained from embryos generated by in vitro fertilization.
Rather, researchers have proposed that research cloning may turn out to be useful for producing
‘‘customized” embryonic stem cells that could generate compatible replacement tissues for
individual patients. Replacement tissues generated in this way would presumably not be rejected
by a patient’s immune system, since their genetic make-up would be the same as that of the
patient.
Preimplantation Genetic Diagnosis (PGD)
Preimplantation genetic diagnosis (PGD) tests early-stage embryos produced through in vitro
fertilization (IVF) for the presence of a variety of conditions. One cell is extracted from the
embryo in its eight-cell stage and analyzed. Embryos free of the targeted condition can be
implanted in a woman's uterus and allowed to develop into a child.
o
X
o -o
o
o
o
FERTILIZED
EGGS
(ZYGOTES)
O —-s
►
x
o
o
o
TESTED FOR
PRESENCE OF
TARGETED GENES
SELECTED ZYGOTES
IMPLANTED AND
BROUGHT TO TERM
PGD allows couples at risk of passing on a serious genetic condition, such as Tay-Sachs disease,
to have a child that is fully genetically related to them and that does not carry genes for the
disease. It does not involve manipulation of genes in embryos; rather, it selects among embry os.
Because it allows the selection of particular traits in future children, PGD can be considered a
eugenic technology. Disability rights advocates in particular have been critical of its uncontrolled
use. They point out that the definition of “disease” is to some extent subjective, and that people
with disabilities can live full and happy lives. PGD is increasingly being used for less and less
serious conditions, and some US fertility clinics advertise PGD for the selection of a preferred
sex. PGD could also be used in attempts to select a future child’s cosmetic, behavioral, and other
traits.
Inheritable Genetic Modifications
The terms “human genetic modification” or “human genetic engineering” mean changing genes
in a living human cell.
There are two types of genetic modification. Somatic modifications involve adding genes to cells
other than egg or sperm cells. If you had a lung disease caused by a defective gene, scientists
might be able to add a healthy gene to your lung cells and alleviate the disease. The new gene
would not be passed to any children you may have.
Germline modifications (also called “inheritable genetic modifications”) would change genes in
eggs, sperm, or very early embryos. The modified genes would appear not only in any children
that resulted from such procedures, but in all succeeding generations. This application is by far
the more consequential, because it would open the door to the alteration of the human species.
Genes are strings of chemicals that help create the proteins that make up the body. They are
found in long coiled chains called chromosomes located in the nuclei of the cells of the body.
(See image on the first page.)
Genetic modification occurs by inserting genes into living cells. The desired gene is attached to a
viral vector, which has the ability to carry the gene across the cell membrane.
Ox VIRAL VECTOR
\
) CARRYING
' NEW GENE
CELL WITH
ORIGINAL
GENES
VECTOR
INSERTS NEW
GENE INTO CELL
NEW GENE IN THE
CELL ALONG WITH
ORIGINAL GENES
Proposals for inheritable genetic modification in humans combine techniques invoking in vitro
fertilization (IVF), gene transfer, stem cells and cloning:
Proposals for germline
engineering combine
the use of stem cells
and embryo cloning
cf
SPERM
EGG
©
STEM CELLS
© f Q
VIRAL VECTORS
CARRYING
NEW GENES
'
I
STEM CELLS ~
HARVESTED
& CULTURED
•«
COLONIES GROWN
PROM EACH STEM CELL
STEM CELL
WITH new gene
TEST COLONIES
FOR SUCCESSFUL
INCORPORATION
OF NEW GENES
I
NEW
GENETICALLY
ENGINEERED
DESIGNER
BABY
CLONING PROCESS
@
w /I
DS
....
As shown above, germline modification would begin by using IVF to create a single-cell
embryo, or zygote. This embryo would develop for a few days to the blastocyst stage, at which
point embryonic stem cells would be removed. These stem cells would be altered by adding
genes using viral vectors. Colonies of altered stem cells would be grown and tested for
successful incorporation of the new genes. Cloning techniques would be used to transfer a
successfully modified stem cell nucleus into an enucleated egg cell. This “constructed embryo’'
would then be implanted into a woman's uterus and brought to term. The child bom would be a
genetically modified human.
(Images courtesy of the Association of Reproductive Health Professionals)
rage i or
STOP SELECTIVE SEX ABORTIONS
STOP FEMALE FOETICIDE
Home
Appreciation
►
NEW DELHI: Aggrieved by a doctor's alleged admission on a television channel
that foeticide was his - and other doctors' - chief source of income, a women’s organization
has moved the high court against the failure of the Medical Council of India (MCI) to take
deterrent steps in this regard.
Femicide
Lodge Complaint
Laws & Acts
Programs/Projects ►
Articles
What's New
►
Links/Resources
►
Pledge Support
Our Inspiration
Admin
Forum
Search
Medical Ethics
NGO moves court over MCl’S failure to check foeticide
Seeking directions to the MCI to take action against the Mumbaibased doctor,
Mahila Jagran Samiti also wants the apex medical body to amend its code of ethics in view of
the Pre-Natal Diagnostic Techniques (Regulation and Prevention of Misuse) Act of 1994.
The PNDT Act makes the offence of pre-natal sex determination punishable by
removal of the guilty doctor from the register of the council and, consequently, cancel his/her
licence to practice.
The petitioners' grievance is that despite the fact that the Act was enacted eight
years ago, the MCI is yet to incorporate a provision for canceling the licence to practice.
In 1996, when the National Human Rights Commission (NHRC) tabled its annual
report focusing on sex-selective abortions, the MCI had given an undertaking that it would
amend its code of ethics in order to take action against erring doctors. But till date, it has not
done so. Provisions of the Act notwithstanding, Mumbai-based gynaecologist on August 16
last year had openly admitted during a talk show - US Newshour - on PBS Television that he
was a participant in "a widely corrupt system" and that such terminations are his chief source
of income. The programme was on the rampant practice of sex etermination in India.
The petitioner quoted him saying. Unless the government really puls its foot down
and decides to act really tough with the people who are doing this, I don't think there is any
way to curb this procedure."
"It is abundantly clear that although there is a law prohibiting sex determination, the
enforcement machinery works so slowly, or does not work at all, that doctors are confident
that they will not be penalized," the petition said.
Section 23(2) of the Act makes the offence a non-cognizable, nonbailable and noncompoundable punishable with imprisonment for five years and a fine of upto Rs 20,000.
Subsequent offences would attract an imprisonment of five years with a fine of upto Rs
50,000.
Once the doctor is convicted under the Act, the MCI is supposed to remove him/her
from its register, thus canceling his/her licence to practice. But MCI has not amended its code
even eight years after the Act was passed.
Back
Article in Hindi
Developed in National Interest by Datamation Consultants Pvt. Ltd. www.datamationindia.com
http://www.datamationfoundation.org/female/acourt.htm
2/19/200-
Page 1 of 2-
Female Foeticide
STOP SELECTIVE SEX ABORTIONS
STOP FEMALE FOETICIDE
Home
Appreciation
Sex test law kills off ultrasound by Kalpana Jain
►
Femicide
Lodge Complaint
Laws & Acts
Programs/Projects ►
Articles
What's New
►
Links/Resources ►
Pledge Support
Our Inspiration
Admin
Forum
Search
Medical Ethics
New Delhi: As the government, under pressure from the Supreme Court, cracks the whip to
implement a law banning sex selection, medical professionals are trying to devise
mechanisms for continuing with the legitimate use of ultrasound.
Ultrasound is used for determining the sex of the foetus, but it is an important diagnostic tool
as well.
The aim of the law, framed in 1994, was to penalize those who assist in the process of female
foeticide by determining, medically, the sex of the foetus. However, eagemess to implement
the law has resulted in checking the use of ultrasound even by those clinics which do not offer
any maternity services.
Recent interpretations of the law have made routine ultrasound scans for a pregnancy almost
impossible. Doctors are having to give reasons such as "history of aspirin" for an ultrasound
scan of a pregnant woman. And patients requiring diagnostic services for a heart, kidney or
another condition requiring an ultrasound, find doctors unwilling to provide the services.
"Until we get a clarification, even cardiologists are prohibited from taking their portable
ultrasound machines out. All free heart checkup camps too have been stopped for the same
reason," says the head of a branch of the Indian Medical Association, K K Aggarwal.
Chairperson of the Pre-natal Diagnostic Techniques Act advisory committee of the Delhi
government, Dr Sharda Jain, says that not only are doctors being harassed but foeticide
continues just the way it did earlier.
"If a woman comes to me in her third month of pregnancy and I refuse to abort, then she must
be finding a place to get it done, if she does not come back to me again," says Jain. "We have
been telling the government of places where people are sitting with these ultrasound
machines and termination of pregnancy too is taking place, but nothing happens."
Undoubtedly, the issues are complex and the problem of foeticide needs to be addressed at
several levels.
Member of the national monitoring board for the PNDT Act, Mira Shiva, agrees that the
sensitization of people responsible for its implementation in various states has not been
adequate.
However, national convener of the IMA's female foeticide campaign committee Vinay
Aggarwal, who tried to get doctors to be sensitive to the issue, is no longer so enthusiastic. "In
the name of implementation 'inspector raj' has taken over, which has done little else, except
getting ultrasound centers sealed."
Back
Article in Hindi
Developed in National Interest by Datamation Consultants Pvt. Ltd. www.datamationindia.com
httn7/www dAtAmationfniindAtinn nra/fpmnlp/atpQt htm
o/i o/onoz
Sex Selection: New Technologies, New Forms of Gender Discrimination
By Rajani Bhatia, Rupsa Mallik, and Shamita Das Dasgupta, with contributions from Soniya Munshi
and Marcy Darnovsky
October 2003
Introduction
With the advent of reproductive technologies that made it possible to detect the sex of a fetus
developing in a woman's womb came a new method of discrimination against girls and women.
Developed in the 1970s, prenatal_djagno§JicT.technQlQgies_h
mnniocentesis
proved profitable when maWed as a. method of sex selection. Using prenatal diagnosis to detect sex, a
person^ could choose not to have a child based on the sex of the fetus and opt for an abortion.(l)
Availability of these technologies and their promotion as tools for sex selection spread fast, primarily in
South and East Asia. Currently, they are the most commonly practiced method of sex selection around
the world.
Where its use is most .widespread, prenatal diagnosis for sex ^election reveals clear discrimination
against the'gfrl child, leading to severe gender imbalances in the population. In India, tor example, the
2001 census recorded a substantial decline in the child sex ratio from 945 to 927 females per^ 1000
males in just ten years. In urban areas the ratio declined even more dramatically from 9^5 to 903^girls
per 1000 males.(2) In China, the sex ratio at birth since the mid-1980s is only 100 girls per 107-120
boys.(3)
For decades, women's rights groups in these regions and disability rights groups internationally led the
struggle to expose the discriminatory use of these technologies. They sought, and tn many cases
succeeded in
in getting
Getting laws
laws passed
to regulate
regulate their
their use. But, due to poor oversight and implementation,
succeeded,
passed to
rampant misuse continues.
The U.S. Context
Adding to this climate, the powerful fertility industry (4) in the U.S. has recently developed and begun
promoting even newer technologies fonsex .selection. These include sperm sorting and pre-implantation
aenetic diagnosis (PGD), both of which carry the "added^eLofjLQlJ^mri^ abgrtion, a politically
contentious issue in the U.S. Both sperm sorting and PGD increase the likelihood oi_estabhshing a
pregnancy with a developing child of the desired sex. Because they are applied either prior to
conception of an egg by sperm (sperm sorting) or prior to implantation of a fertilized egg into a
women's uterus (PGD), neither process necessarily involves abortion. However, because neither is 10 J
percent accurate, some couples using these methods may still resort to use of PND followed by sex
selective abortion.
' : use of expensive assisted reproductive technologies commonly
Both PGD and sperm sorting require the
used in the fertility industr^ (like in-vitro fertilization or artificial insemination). The overall cost of
■ - For example, in 2001 the average couple using MicroSort, one
sperm sorting and PGD is very -high.
method of sperm sorting promoted in the
f U.S.
T T spent -nearly $10,000. MicroSort costs S3,200 a try and
most attempted it three times.(5)
Sex selection advocates in the U.S. promote the use of these techniques for what they call family
balancing" or "gender variety," a notion that presupposes.families.o.uglitto_haye children of both sexes.
In
In the
the U
U.’’S?
S’" arguments
arguments for
for sex selection seem to rest on the assumption that the only thing problematic
about its use is the elimination of females through sex selective abortions in societies where there is a
strong preference for sons, e.g., India and China. This, they say, is unlikely to happen in the U.S.
In recent months, sex selection ads have appeared in leading newspapers like The New York Times. Ads
in the North American editions of Indian Express and in India Abroad have specifically targeted South
Asians living in this country.(6)
The increased use and acceptance of sex selection in the U.S. would likely legitimize its practice
elsewhere and complicate the effort by rights-focused constituencies to develop societal and legal
mechanisms that can prevent current and future abuses, both here and abroad.
It is urgent that the unethical promotion and growth of an industry for sex selection is discouraged in
the U.S. In particular the high social cost, abuse potential, experimental nature as well as limited
efficacy of these methods need to be exposed. The practices of the profit-seeking fertility industry as a
whole require oversight and regulation (currently seriously lacking in the U.S.), in order to ensure
ethical use of all new reproductive technologies.
Sex Selection and Discrimination
Economic and social pressures to raise.male childrenJmthe U.S^ may be less than in other societies, but
they are not completely'absent. Furthermore, sex selection is by definition not gender neutral. While we
would like to believe that our preference for one sex over another is not influenced by bias, almost all
societiesJiaYe_inlernalized strong prejudices based on sex from which none of us are completely
immune. A decision to have a girl over a boy, or the ‘offer way around, will be based on gender
stereotypes. What if the child does not live up to our "boy" or "girl" expectations? Would the
disappointed parents feel they had not gotten their "money's worth?" What does it mean to think of a
child as a product with a price tag?
Sex Selection and Gender Violence
Son-preference is a^j^rpduct.pfJhe.ubiqujtQU^^i^chaL^giaL^stem. Unfortunately, this favoring
is hardly a harmless idiosyncrasy, as the valuing of male children is generally accompanied by the
contrasting neglect and mistreatment of daughtere’.TIistoricaliy, this degfaHation of girls has been
expressed in various ways," from female infanticide, to denial of nutrition and health care after birth, to
withholding education and empowerment opportunities to girls and women while they are growing up.
With the advancement in reproductive technology, pre-natal diagnostics followed by sex selective
abortion was added to this list of abuses.
Violence against girls and women often takes the form of deprivation and neglect. But, the dynamic ot
domestic violence can also involve control of women’s reproductive capacity. This aspect ot domination
can become part of a batterer's pattern of abuse.
In the South Asian context, giving birth to a son enhances a woman's status within the family, whereas
her inability to produce a male heir may result in humiliation^. contempt, abuse, and abandonment. Men
frequently blame their wives jor not,giving birth to.a male..child,Ja-laws may also openly threaten their
daughters-in-law with dire consequences if they are unable to produce a son.
abusive situations, a
woman may be forced to undergo testsJo identifyThe sex of her unbom^child, and then coerced to abort
if the fetus js female. Women may be beaten and/or divorced for not giving birth to sons. An abusive
spouselnay use the birth of a daughter as a pretext for violence towards his wife, and then be violent
towards the unwanted daughter. Such abuses occur in the U.S. context as well.
Sex Selection is Big Business
Since new techniques of sex selection require the use of assisted reproductive technologies (7) (like in
vitro fertilization and artificial insemination), the fertility industry can use sex selection to expand their
market to fertile couples. Fortune magazine estimates a U.S. market between $200 and $400 million per
year for the sperm sorting method, MicroSort.(8) In spite of their high price tags, invasiveness, and
risks, demand for these methods appears likely to be high. Surveys reveal that 25-35 percent of all
parents or prospective parents in the U.S. would use sex selection if it were available.(9) One fertility
specialist interviewed by the New York Times said he could fund all of his research until the day he died
if he honored the requests he got for sex selection.(10)
American companies are already turning profits on sex selection in South Asia. General Electric (GE),
for example, captured the largest market share for ultrasound scanners in India. GE sold a
disproportionate number of these machines in Northwest India where the female to male child sex ratio
is the lowest.(l 1) Another American company, Gen-Select, recently marketed dubious sex selection kits
in the Times ofIndia^M)
New Reproductive Technologies Used for Sex Selection
Prenatal diagnosis (PND)\ Developed in the 1970s, PND through techniques such as ultrasound
scanning and amniocentesis followed by sex selective abortion remains the most common method of
sex selection practiced around the world for the last three decades.
Pre-implantation genetic diagnosis (PGD)\ First tested on humans in 1990, PGD has found increasing
use during the last 5 years mainly by infertile couples undergoing in vitro fertilization (FVF) who are at
risk of having babies with certain genetic conditions. After fertilization of a woman's eggs by a man's
sperm takes place in the laboratory, genetic testing is performed on the resulting embryos (fertilized
eggs) to determine sex. Only embryos of the "desired" sex are implanted in the woman.
Disability rights advocates have raised concern about whether and where to draw the line on acceptable
uses of PGD. Screening out embryos of "the wrong sex" underlines how the method is already used
without reflection about its impact.on ho•w.peopje are valued (or devalued) in society. PGD has been
used to screen out embryos carrying a gene indicating an increased likelihood of deafness in future
generations of offspring.(13) Will PGD be used next to screen out undesirable hair and eye color? The
issues of sex selection are strongly related to forms of oppression based not only on gender, but also on
race, ability and class.
Since this method is experimental, it is not known whether the process of removing a cell from the
embryo for genetic testing may resulfin long-term health consequences for the resulting child.(14) For
women, IVF is an intrusive procedure that may have to be repeated a number of limes before a
successful pregnancy is achieved, if at all.(15) Risks include ovarian Hyper-stimulation syndrome, a
potentially life threatening condition, and multiple births.(16) Recent studies also suggest that infants
conceived by IVF have a higher risk of low birth weight and birth defects than those conceived
naturally.(17)
Sperm Sorting'. Since it is the sex chromosomes of a man's sperm that determine the sex of offspring,
sorting female from male bearing sperm is one method of sex selection. This is a pre-conception
method because it is used prior to fertilization of a woman’s egg, which is accomplished either by
artificial insemination or IVF. There are currently two methods to sort sperm, which were originally
developed to breed livestock of a particular sex. Since both are currently under experimentation for
humans, health risks are not fully known. When sperm sorting is used in conjunction with IVF, the
associated risks must again be taken into account.
Sperm sorting techniques remain unreliable. MicroSort, for example, had an average purity’ of 88
percent for female bearing sperm and 66 percent for male bearing sperm in 916 sorts conducted
between June 1994 and April 2000.(18)
Legal Status Regulating Sex Selection in Selected Countries
In the UK, stringent guidelines by the Human Fertilization and Embryology Authority (HFEA) regulate
the use of PGD. The HFEA recently held a public consultation to decide whether or not to regulate
sperm sorting.
The Council of Europe's Convention on Human Rights and Biomedicine states in Article 14, "The use
of techniques of medically assisted procreation shall not be allowed for the purpose of choosing a future
child's sex except where serious hereditary sex-related disease is to be avoided. (19)
In Canada legislation was introduced in May 2002 to make sex selection a crime if used for purposes
other than to prevent, diagnose or treat a sex linked disorder or defect.(20)
In India, the use of PND, PGD and preconception techniques such as sperm sorting for sex selection
have all been banned by the Pre-Conception and Pre-Natal Sex Selection/Determination (Prohibition
and Regulation) Act, 2001.
In China, a law was passed in March 2003 to ban PND for sex selection.
In the US, there is currently very little regulation of the fertility industry. The American Society of
Reproductive Medicine (ASRM), a trade association, issues policy recommendations on ethical use of
technologies, but clinics are not required to follow them. The ASRM issued guidelines in 2001 that
considered sperm sorting under certain conditions ethically allowable. Last year the ASRM confirmed
its policy recommendation against the use of PGD for sex selection. In spite of this, some U.S. fertility
clinics, such as the Tyler Medical Clinic in Los Angeles and the Sher Institute for Reproductive
Medicine in Las Vegas, perform and advertise PGD for sex selection.(20)
Rajani Bhatia is Coordinator of the Committee on Women, Population and the Environment
(http://www.cwpe.org). Rupsa Mallik is Program Director - South Asia at Center for Health and Gender
Equity (http://www.genderhealth.org). Other contributors represent Manavi, Inc.
(http://www.manavi.org) and the Center for Genetics and Society (http.//www.genetics-and-
society.org).
Footnotes
1. The authors believe that all women should have the right and access to safe abortion services.
2. Government of India; Census of India, 2001.
3. Banister, J. 'Shortage of Girls in China Today: Causes, Consequences, International Comparisons
and Solutions.’ 2003; presentation at PRB, Washington DC.
4. Dickens, B.M. "Can Sex Selection be Ethically Tolerated?" J Med Ethics’, 2002; 28.335-?6.
Robertson, J.A. "Pre-conception Gender Selection." American Journal of Bioethics, 2001; Vol. 1(1).
5. Wadman, Meredith, "Sex Selection: So You Want a Girl?" Fortune, February 8, 2001.
6. Sachs, Susan, "Clinics' Pitch to Indian Emigres," New York Times, August 15, 2001.
7. IVF - in vitro fertilization and artificial insemination
8. Wadman, Meredith, "Sex Selection: So You Want a Girl?" Fortune, February 8, 2001.
10.Ibl
Kolata, Gina, "Fertility Ethics Authority Approves Sex Selection." New York Times.
September 28,2001.
.
onno
11.
George, S.M. "Sex Selection/Determination in India," Reproductive Health Matters, -00^.
10(19): 190-92
12.
Weiss, Rick, "Screening Embryos for Deafness," The Washington Post, July 14 2003, p^A06
13.
Goldberg, Carey, "Screening of embryos helps avert miscarriages," Boston Globe, 6/1? J?.
14.
IVF success rate is around 25%. (Simoncelli, Tania, "Pre-Implantation Genetic Diagnosis
15.
and Selection," Political Environments #10, forthcoming)
I
16.
"Sex Selection: Choice and Responsibility in Human Reproduction, Human Fertilisation. &
Embryology Authority, http://www.hfea.gov.uk.
17.
Simoncelli, Tania, "Pre-Implantation Genetic Diagnosis and Selection," Political
Environments #10, forthcoming.
Wadman, Meredith, "Sex Selection: So You Want a Girl?” Fortune, February 8, 2001.
18.
Dickens,
B.M. ' Can Sex Selection be Ethically Tolerated?’ J Med Ethics', 2002; 28:335-36.
19.
Ibid.
20.
Zitner, Aaron, "Testing Embryos," Los Angeles Times, July 23, 2002; Marcus, Amy Dockser,
21.
"Embryo Screening Test Gains In Popularity and Controversy," The Wall Street Journal, July 25, 2002.
Date modified: May 18, 2004
i
1
<
f
Article by Dr. Vibhuti Patel,
Humanscape
VOL. X ISSUE IX SEPTEMBER 2003
‘Sons are rising, daughters setting’
Sex selection is a violation of law and unethical. But our patriarchal society continues to turn a blind
eye towards it or offer perverted excuses to justify its existence. Even the medical community has not
protested against the malpractices of its guilty peers
The recent controversy over Brihunmumbai Municipal Corporation filing a case against the Malpani
Infertility Clinic, Colaba, Mumbai, for violating the recently amended Pre-conception and Prenatal
Diagnostic Techniques (Prohibition of Sex"D¥termination)\Act (PNDT Act), 1994 has once again
brought the issue of the doctor’s participation in endangering lives of girl children into the lime-light.
Rated as India’s top five infertility clinics, if^_^^it^adyjsedJtie42ublia-.om how-to^elect the sex of
their child. Despite the highly reported concerns pi the ..Supreme Court, expressed in a PIL on the
subject for a very long time, the clinic continued to advertise, in defiance of the orders. So far 48 clinics
have been prosecuted for violation of the Act.
The legacy of continuing declining sex ratio in India__has_taken a new turn with the widespread use of
new reproductiveJ^F^Iogies (NRTs)74aljhe/ciiie& and__towns of India’. NRTs are based oh the
principle of selection of the desirable and rejection.of the unwanted (Patelu2002).
In South Asia, we have inherited the cultural legacy of strong son-preference among all communities,
religious groups, and citizens of varied socio-economic backgrounds. This preference is embedded in
patri-locality, patri-lineage, and patriarchy, and its result is discrimination in property rights and lowpaid or unpaid jobs for women. The Census of India for 2001 revealed that with the sex ratio of 933
women for 1,000 men, India had a shortfall of 3.5 crore women when it entered the new millennium.
According to the Chandigarh-based Institute for Development and Communication, during 2002-2003
every ninth household in the state acknowledged sex selective abortion with the help of ante-natal sex
determination tests. Commercial minded techno-docs and laboratory-owners have been usjng new
reproductive technologies for femicide for oyer two and a half decades. Among the educated families,
adoption of the smaTTfarriny“norm means a minimum of one or two sons in the family. The propertied
class do not desire daughters because the son-in-law may demand a share in property. The property
less classes dispose off daughters to avoid dowry harassment (although they do not mind accepting
dowry for their sons). The birth of a son is perceived as an opportunity for upward mobility while the
birth of a daughter is believed to result in downward economic mobility. Though the stronghold of this
ideology was north India, it is increasingly gaining ground all over India.
To stop the abuse of advanced scientific techniques for selective elimination of female foetuses
through sex-determination, the government of India passed the PNDT Act in 1994. But the techno
docs based in the metropolis and urban centres, and parents desirous of begetting only sons have
subverted the act. Avers Prof Ashish Bose (2001) “The unholy alliance between tradition (soncomplex) and technology (ultrasound) is playing havoc with Indian society”. In several states of India,
sex-selective abortions of female foetuses have increased among those who want small families of
one, two, or maximum three children. Communities, which were practising female infanticide, started
using sex-selective abortions. Many doctors have justified female foeticide as a tool to attain net
reproduction rate (NRR) of one i.e. to attain population stabilisation or, that a mother should be
replaced by only one daughter. There is an evident gender bias here too. To attain population
stabilisation, a fertility rate of 2.1 is envisaged. There is evidence to indicate a sex ratio in favour of
males and a prolonged duration of gender differentials in survivorship in the younger ages results in
the masculining of the population sex ratio.
Sex selection is a covert form of violence while female foeticide is an overt form against women, with
the use of tools like amniocentesis, chorion villai biopsy, sonography, ultrasound and imaging
techniques and assisted reproductive technologies (in which infertile couples are helped to produce
sons).
Socio-legal and ethical issues
Supporters of sex-selection tests for selective elimination of girls/female foetuses apply the law of
demand to validate their stand i.e. “reduction in the supply of girls will enhance their status”. Even
some Western scholars like Prof Dickens (2002), writing in the prestigious Journal of Medical Ethics
aver, "Son preference has produced, but might also mitigate, the sex ratio imbalance...If sons wish, as
adults, to have their own sons, they need wives. The dearth of prospective wives will, in perhaps a
sMr, «™. enhance <he soda. .a,ue o<
dominance”. This neo-classical logic of the law off de™nd “
J women without any respect to
social forces where patriarchy controls sexuality, fert~ y,
trary |n fact, shortage of women
her bodily integrity. Hence, the real e experiences speck to the^ontrar^
Qf
in Haryana, Punjab and the B1MARUrifX%hr^
evidence does not support
girls, forced polyandry, gang rape, and oh'^"Prostitu
.
was g72 and nQW as
such arguments. The sex ratio has steadily de
century the amount of dowry demanded
Ser — S^Sincreased^e =
t^.pu.at^ha^ and
Zile XVofXring5S— it has only universalised the s.ogan, so vociferous in
Haryana: “Sons are rising and daughters are setting !
th£y desjre. an argument
Is it then a question of giving women a choice to choose the sex o tn
y
even
given by many doctors to justify; their sex "Xc "
2001 (SeVen P
to accept that ethics have anything to with it Fo mst
Ma|pPnj when asked whether it was (j
years after the government passed the PNDT A ),
providing assisted reproductive services, I ;
ethical to selectively discard female e^ry are w£ hurtjng? unborn girls?”
-^i
asserted, “Where does the question of ethicsi comenn
'
d b the patriarchal system, and its
But what choice are we talking about f°r womei" *h
Alongside are threats of desertion, divorce,
supporters in the family and the society to produce sons? A ong&ae
are not mere threats,
ill-treatment, and even wife murder for sucha^,°mXomen are not taking decisions autonomously. How
but are often carried out. Under such a Ration,
the9question: Can we allow Indian
can there be choice without autonomy The ctwo
those wqho be|jeve that it is better to kill
women to become an endangered sp
fpmale child Their logic is not only short-sighted but
a female foetus than to give birth to. an unwante, aiven and therefore, not rectifiable. It is such
fatalistic. Their logic regards evils hke dowry to be^Go dgive,j and,^
By
)ogjc
thinking that creates advertisement copy I ke
2
xs-o
Needless tQ sayi investing in girls
xxt
Xconfon,
aX;for Oemand and darassmenf
;ex
of .fie
for dowry is indeed encouraging.
Integrity and accountability of the medical profession
The struggle by the socially conscious ^Xen is nw^rdecadls^W.'Vhe first strong movement
technologies which trigger violence agams
. ,
was started in 1984 in Mumbai, and resulted in
against doctors' unethical P^'^GoVin 1989 and then the national legislation through the PNDT
a law against it in Maharashtra and Goa n 1989. and t
dominated by vested interests in
Act in 1994. However, till the government move^d, medical^ouncils dom^ ^y^
the profession did not come forwar
viniatina the integrity of the profession. Even after the
XXSrtTpLS\W=t°.Ze«?“a,rt.d
moves .0 enforce fl. In connivance «llh ph.bfe
D, Sa” George. The Lawyers Cofleclive (Defhf) foogdl “ ^rt of the’e--
court d,reefed all
on 4 May 2001, to activate the state machinery for
imDlementation, and directed all bodies
state governments to take action for e ec tve> a
genetic laboratories, and genetic clinics to
under the PNDT Act, namely, genetic counse hng ce
qervices Thjs directive also triggered off
have registration and superv.sion to contmu^with t
jament amended the law by bringmg
attempts to plug loop-hopes m the 1994
X
ofPthe |aw. They put in place a stnng of
sex selection at a pre-conception stage unde
P
Brihunmumbai Municipal Corporation
checks and balances to ensure that the Act was effective.
Qf gender of foetus as per the
(BMC) has initiated a drive against the unau ^raphy centres are required to register themselves
directive of the ministry of law and jushce_ All sonegrap V
tratjon certjficate and the message that
with the medical officer of their wards. The disp y ^9$^ js mandatory at the centres.
ssx®
— ——
*
Balaji Telefilms because its top-rated television serial showed a young couple checking the sex of their
unborn child. The Commission approached the BMC and a first investigation report (FIR) was lodged
at the police station. After an uproar created by the commission, Balaji Telefilms prepared an
advertisement based on the Commission’s script that conveyed that sex determination tests for
selective abortion of female foetus is a criminal offence.
A study by Dr Sanjeev Kulkarni for the Foundation for Research in Community Health in 1984
indicated that 84 per cent of the gynaecologists in Mumbai admitted that they were performing
amniocentesis. In comparison, a study by Dr Sunita Bandewar for CEHAT found that 64 per cent of the
abortion service-providers were against sex selective abortions and another ten per cent said that they
were also against it but were compelled to do it. Those who were against it were vociferous in their
opinion: “It should be banned.” “It is inhumane and criminal.” “It is against medical ethics and human
rights.” “It amounts to discrimination against women.”
Interestingly, it took two decades of consistent campaigning by the socially conscious and health
activists using awareness and legislations to make some doctors realise that their act was unethical,
discriminatory, and inhuman. One is still not sure whether such doctors are convinced or are just
momentarily abstaining for fear of the law. Whatever it may be, by being party to the violence, the
profession has compromised its integrity. It is disconcerting, however, that not only does a sizeable
section of its members continue indulging in such malpractices, but the medical councils have not
shown any initiative to take to task doctors whose names have been publicised. The medical
profession cannot be let off as it waits for the police and appropriate authorities to chase violators of
the law, while its own legally constituted and empowered councils remain a mute spectator to such
gross violation of medical ethics. Till they put their act together, society will condemn the entire
profession for the misdeeds of some errant members.
References:
Bandewar, Sunita. Abortion services and providers’ perceptions: gender dimensions, Economic and
Political Weekly, Vol. XXXVIII, No. 21, 24 May 2003, pp. 2075-2081.
Banerjee, Piali. The battle against chromosome X, The Times of India, 25 November 2001
Bose, Ashish. Without my daughter-killing fields of the mind, The Times of India, 25 April 2001
Chattopadhyay, Dhinman. Child sex ratio on the decline in Bengal: report, The Times of India. 10
March 2003
Dickens BM, Can sex selection be ethically tolerated? Journal of Medical Ethics, No. 28, 2002. pp.
335-336.
Eapen, Mridul & Kodoth, Praveena. Demystifying the ‘high status’ of women in Kerala: an attempt to
understand the contradictions in social development, Centre for Development Studies, Kerala, 2001
Ganatra BR, Hirve SS, Walealkar S et al, Induced Aborin A Rural Community in Western Maharashtra:
prevalence and patterns, Mimeograph, Pune, 1997
Kannan, Ramya. More babies being abandoned now, The Hindu, 1 April 2002
Patel, Vibhuti. Women’s challenges of the new millennium, Cyan Publications, New Delhi, 2002
Sen, Vikram. 2001 Census of India - report for Kolkata, Director of Census Operations, West Bengal,
2002
Sridhar, Lalitha. (Women’s Feature Service), India: Killing in Cradle, POPULI - The UNFPA magazine,
Vol.28, No.2, September 2001, pp.10-12
Dr Vibhuti Patel is an economist and women’s movement activist. She works as Reader at the
Centre for Women’s Studies, Department of Economics of the University of Mumbai. She is also
Member Secretary of Women’s Development Cell of the University of Mumbai.
Send this page to your friends
Copyright ©Foundation for Humanisation. All Rights Reserved
by Dr Vibhuti Patel
Poster by Tushar V Mantri: ‘She has the right to live: Stop sex selective abortion'
Supporters of sex-selection tests for selective elimination of girls/female foetuses apply the law
of demand to validate their stand i.e. “reduction in the supply of girls will enhance their status”.
Even some Western scholars like Prof Dickens (2002), writing in the prestigious Journal of
Medical Ethics aver, “Son preference has produced, but might also mitigate, the sex ratio
imbalance...If sons wish, as adults, to have their own sons, they need wives. The dearth of
prospective wives will, in perhaps a short time, enhance the social value of daughters.”
84 per cent of the gynaecologists in Mumbai admitted that they were performing amniocentesis
Medical councils dominated by vested interests in the profession did not come forward to
declare doctors indulging in these practices unethical and making accountable those who were
guilty of violating the integrity of the profession. Even after the enactment of the PNDT Act,
they thwarted all moves to enforce it, in connivance with pliable government medical and civil
bureaucrats.
A Study of Ultrasound Sonography Centres in Maharashtra
Sponsored by the
Ministry of Health and Family Welfare
Government ofIndia
Sanjeevanee Mulay & R. Nagarajan
Population Research Centre
Gokhale Institute of Politics and Economics
Pune-411 004
January 2005
Gokhale Institute of Politics and Economics
Telephone: 020-25650287, 25654288, 25654289
Fax: 020-25652579
Email: gipe@vsnl.com
Website: http://www.gipe.ac.in
Contents
Chapter
Page
No.
Description
Contents
Acknowledgements
List of Tables
List ofFigures
List ofAppendices
i
a
m
vi
vi
Chapter 1
Introduction
1
Chapter 2
Ultra Sound Sonography Centres in Maharashtra: Distribution,
Type and Qualification of the Owners and Operators
6
Chapter 3
Child Sex Ratio and Ultra Sound Sonography Centres in
Maharashtra
18
Chapter 4
Findings of the Survey of Ultra Sound Sonography Centres in
Maharashtra
34
Chapter 5
Summary and Recommendations
59
References
Appendix 1
Appendix 2
Appendix 3
72
73
74
75
i
Acknowledgements
We take this opportunity to thank all those, who have been helpful in carrying out this
study. Since this study has involved private medical practitioners, who are not obliged to give
information to anyone, we needed great help from the state government officials. We are
grateful to Dr. P. P. Doke, Director of Health Services, Maharashtra, whose appeal to the
doctors made our job easy. We are also thankful to Dr. Ashok Belambe, Deputy Director,
State Family Welfare Bureau, Pune who helped us in getting the information from District
Appropriate Authorities.
The work m Mumbai was a challenge for us. Dr. Surekha Mehta, Special
Officer in the Department of Family Welfare and Maternal and Child Health, Municipal
Corporation of Greater Mumbai greatly helped our staff in getting the information from the 24
ward offices in Mumbai.
We owe a lot to her. Similarly, we are thankful to concerned
officials of all the Municipal Corporations and Appropriate Authorities at district/tehsil level
m the study area for helping us in carrying out the study. We express our gratitude towards Dr.
Gawhane and Dr. Ghanwat (officials of National Integrated Medical Association), who went
out of the way for helping us in identifying the doctors desirous of using the machine.
We are grateful to Ms. Madhu Bala, Director (PNDT), MOHFW for her guidance and
support in carrying out this study. We also thank Shri S. K. Das, Chief Director (PRC),
MOHFW, for his continuous support to carry out this study by us. We also acknowledge the
support extended by Ms. Sushama Rath, MOFHW.
We are grateful to Mrs. Vandana Shivanekar, Mrs. Deepali Yakkundi, and Shri.
Abhijeet Mahabaleshwarkar, for the help they provided in tabulation, computer processing and
typing of the report. We are thankful to Shri A.M. Pisal, Shri R. S. Pol, Shri Chintamani Jog,
Mrs. Priti Bhat, Shri Akram Khan, Shri A.P. Prashik, Shri Shirish Naikare, Miss Rima
Amrapurkar, and Miss Deepali Dixit for their valuable assistance in carrying out the field
visits. Lastly, we thank all the trained and untrained doctors who own the sonography centres
and the doctors who are desirous of using the sonography machine for providing the necessary
data and co-operation in spite of their busy schedule.
January 6, 2005
Pune
Sanjeevanee Mulay
R. Nagarajan
Population Research Centre
ii
List of Tables
fable
No.
Page
No.
Title of die Table
2.1
Number and percent of registered ultra sound sonography centres in
Maharashtra by I lealth Circles as on September 30, 2004.
7
9 9
Number of registered ultra sound clinics/centres in the districts of
Miiliarashtra as on September 30, 2004.
8
2.3
Number and percent of registered ultra sound clinics/centres in the
districts of Maharashtra, under PNDT Act, as on September 30, 2004.
9
2.4
Type of centre, qualification of owner of sonography centre and
qualification of operator of sonography centre in Maharashtra
10
2.5
Type of ultra sound sonography centres in Maharashtra
11
2.6
Qualifications of the owners of the ultra sound sonography centres.
12
2.7
Qualifications of the doctors using the ultra sound sonography
machines in the centres owned by trained (Self Operated) and
untrained (Centres Employing Other Doctors) persons/doctors
14
2.8
Ultra sound sonography centres owned by trained and untrained
persons
16
2.9
Information regarding doctors attached to multiple (>=4) ultra sound
sonography centres
17
3.1
Sex ratio of child population in the age group 0-6, Maharashtra, 2001
19
3.2
The range in child sex ratio in the districts of Maharashtra, 2001
20
3.3
Change in child sex ratio between 1991 and 2001, by districts.
21
3.4
Sex ratio of child population in the Municipal Corporations of
Maharashtra, 2001
23
3.5
The range in sex ratio of child population in the tehsils of
Maharashtra. 2001
23
3.6
Top and bottom 10 tehsils by child sex ratio in Maharashtra (total,
rural and urban), 2001.
25
3.7
The correlation between number of ultra sound sonography (USG)
centres and child sex ratio and decline child sex ratio.
26
Contd...
iii
Table
No.
Title of the Table
Page
No.
3.8
Number of sonography centres for the top & bottom 10 tehsils in child
sex ratio.
28
3.9
Regression analysis of child sex ratio and availability of sonography
centres in Maharashtra.
29
4.1
Classification of centres by district and training status of the owner of
the centre
38
4.2
Classification of ultra sound sonography centres by its functional
status, kind of machine, year of installation of machine and cost of
machine.
39
4.3
Distribution of ultra sound machines by their make.
41
4.4
Approximate cost and year of installation and average cost of the
machine
42
4.5
Classification of centres by system of medicine studied by the owner
43
4.6
Classification of centres by purposes on which data are available
43
4.7
Classification of centres by reason for incomplete data
44
4.8
Classification of centres by number of obstetric sonography tests
earned out during July 2003-2004 by training status of the owner and
trimester (Tl, T2, T3).
46
4.9
Classification of non-obstetric sonography tests earned out during
July 2003-2004 by training status of the owner
46
4.10
Frequency of the operator's visit for centres with untrained owner
47
4.11
Classification of obstetric sonography tests by size and type of
untrained doctors.
49
4.12
Classification of non-obstetric sonography tests done by untrained
doctors by Kpe
50
4.13
Classification of sonography tests by functional status and training
status of the owner
50
4.14
Percent sonograph} testes done by training status of the owner and
trimester
52
Contd...
iv
Table
Title of the Table
No.
Page
No.
4.15
Percent sonographies done in first trimester cross-classified by percent
sonographies done in second trimester
53
4.16
Percent referred by allopathic doctors
55
4.17
Number of own clients by training status of owner
55
4.18
Frequency of supervisory visit by appropriate authority
57
4.19
AYUSH doctors desirous of having the sonography machine
58
List of Figures
Figure
No.
Title of the Figure
Page
No.
3.1
The relationship between child sex ratio (total) and number of
sonography centres in the districts of Maharashtra.
31
3.2
The relationship between child sex ratio (total) and number of
sonography centres per 1000 population in the districts of Maharashtra.
31
3.3
The relationship between decline child sex ratio between 1991 and 2001
and number of sonography centres in the districts of Maharashtra.
32
3.4
The relationship between decline child sex ratio between 1991 and 2001
and number of sonography centres per 1000 population in the districts of
Maharashtra.
32
3.5
The relationship between child sex ratio (2001) in Municipal
Corporations of Maharashtra number sonography centres per 1000
population.
33
List of Appendices
Appendix
No.
Title of the Appendix
Page
No.
3.1
Map showing the distribution of sonography centres (in dots) in
Maharashtra
73
3.2
Data used for analysis in Chapter III
74
3.3
Questionnaire used for the study
75
\i
Chapter I
Introduction
India is predominantly a patriarchal society. The perception that the family line
runs through a male makes men a precious commodity that needs to be protected and
given a special status. The dominance of men is reflected also in our marriage practices.
Dowry is a clear illustration of the same. In many parts of India, the dowries are so
staggeringly high that the parents have to incur their entire savings in getting their
daughters married off. Naturally, the daughters are cursed to an extent that even the birth
of a girl child in a family is sought to be avoided.
The women always have fallen prey to violence like rape, sexual abuse, dowry
harassment, etc. with no mechanism of fighting through effective laws. We are ashamed to
find instances of female infanticide occurring regularly. Female infanticide now in most
places has been replaced by female foeticide and more sadly, female foeticide has made
inroads into areas, where earlier there were no instances of female infanticide. Further, we
find that it has crossed the class-boundaries.
Female foeticide or sex-selective abortion is the elimination of the female foetus in
the womb itself. However, prior to the elimination, the sex of the foetus has to be
determined and it is done by methods like amniocentesis, chorionic villus sampling and
now by the most popular technique ultra sound sonography. Ultra sound sonography is the
least expensive test and can be performed around 12th week of pregnancy. After the
determination of the sex of the baby, if it is not desired, couples go for Medical
Termination of Pregnancy.
Pre-natal Diagnostic Techniques (PNDT) Act
In 1978, the government of India issued a directive banning the misuse of
amniocentesis in government hospitals. Thereafter due to the efforts of activists, a law to
prevent sex determination was passed in Maharashtra, known as Maharashtra regulation of
Pre-natal Diagnostic Techniques Act, 1988. Finally after a public debate all over India,
the parliament enacted the Pre-natal Diagnostic Techniques (PNDT) Act on September 20,
1994. It provides for the regulation of: (i) Use of pre-natal diagnostic techniques for the
purpose of detecting genetic or metabolic disorders or chromosomal abnormalities or
1
certain congenital malformation or sex-linked disorders; (ii) For the prevention of the
misuse of such techniques for the purpose of pre-natal sex-determination leading to female
foeticide; and (lii) For matters connected there with or incidental thereto. This act came
into force in 1996. Some amendments in the act were suggested later on. The amended
rules have come into effect from February 14, 2003.
Some important provisions of the PNDT Act:
♦ No genetic counselling centre, genetic laboratory, or genetic clinic (including
clinics or laboratories or centres having ultrasound or imaging equipment), unless
registered under the Act, shall conduct, associate with, or help in conducting
activities relating to diagnostic techniques that can be used to assess the sex of a
fetus.
♦ No person, including specialist in the field of infertility, shall conduct or cause to
be conducted or aid in conducting a pre-conception sex-selection technique on a
woman or man or both or on any tissue, conceptus, fluid, or gametes derived from
either or both of them.
♦ No prenatal diagnostic technique shall be used or conducted unless the person
qualified to do so is satisfied that at least one of the following conditions is
fulfilled: (i) the age of the pregnant woman is above 35 years; (ii) the pregnant
woman has undrgone two or more spontaneous abortions; (iii) the pregnant woman
has been exposed to potentially teratogenic agents such as drugs, radiation,
infection, or chemicals; (iv) the pregnant woman has a history of mental
retardation or physical deformities such as spasticity or other genetic desease; and
(v) any other condition as may be specified by the Central Supervisory Board
designated by the Act.
♦ No person conducting prenatal diagnostic procedures shall communicate to the
pregnant woman concerned or her relatives the sex of the fetus by words, signs,or
in any other manner.
Following bodies are appointed for the supervision of enactment of PNDT act
i)
Central Supervisory Board
2
ii)
State Supervisory Board and Union Territory Supervisory Board
hi)
Appropriate Authority and Advisory Committee
The Appropriate Authorities at district/tehsil level are the immediate supervisory
authorities. They have powers in respect of the following matters, namely:
a) summoning of any person who is in possession of any information relating to
violation of the provisions of this Act or the rules made there under;
b) production of any document or material object relating to clause (a);
c) issuing search warrant for any place suspected to be indulging in sex selection
techniques or pre-natal sex determination; and
d) any other matter which may be prescribed.
Every Genetic Clinic/Ultrasonography Centre/ Genetic Counselling Centre/Genetic
Laboratory has to have a registration with the Appropriate Authorities and shall be
required to pay prescribed fees. Every such centre has to apply within 60 days of
commencement of the Act. The Appropriate Authorities, after holding an enquiry and after
satisfying itself that the applicant has compiled with all the requirements of the Act, shall
grant a certificate. The certificate shall be displaced in a conspicuous place at the Centre.
Every certificate shall be valid for five years.
There is a prohibition of advertisement relating to pre-natal determination of sex
and punishment for contravention on any person or organisation involved in such
advertisement shall be punishable with imprisonment for a term extending to 3 years and a
fine which may extend to 10,000 rupees. Any subsequent conviction will lead to
imprisonment of 5 years and the fine of Rs. 50,000.
The centre needs to maintain records in terms of different forms to be submitted to
Appropriate Authorities. Form F containing the information on the men/women subjected
to any pre-natal diagnostic procedure, and form G containing the consents of the
men/women need to be maintained by the centre. Appropriate Authorities should maintain
the record of Form H containing the details about the application by centres. The centres
should send monthly report to the concerned Appropriate Authority. Every centre need to
3
display prominently a notice in English to effect that disclosure of sex of the foetus is
prohibited under law.
There is a code of conduct to be observed by persons working at the centre. It
includes mainly: (i) not engaging oneself or helping in sex determination; (ii) not
employing unqualified people; (iii) not conducting the tests in place other than that
registered to conduct or cause to conduct female foeticide.
The Appropriate Authorities have a power to inspect the centre and seal and seize
any ultrasound machine capable of detecting sex of foetus used by any organisation, if it
has not registered with them. The machines could be released if the organisation pays five
times the registration fees to Appropriate Authorities. However, Retherford and Roy
(2003) observe that, “The law contains loopholes. Government laboratories and clinics
are monitored much more closely, than private laboratories and clinics, which are only
required to register under the Act. Also genetic tests are monitored much more closely
than ultrasound tests”
The law is easy to circumvent for both physicians and clients. The PNDT Act
seems to have little impact on sex-selective abortions. Arnold, Kishor and Roy (2002)
estimate indirectly that more than 100,000 sex-selective abortions, following ultrasound or
amniocentesis, have been performed annually in India in recent years. Even if there are no
data available directly on sex-selective abortions, there are number of indirect indicators
on the basis of which one could estimate the extent of sex-selective abortions. The NFHS-
II data on use of ultrasound facility and on sex ratio at birth provide useful clues pointing
to existence of substantial number of sex-selective abortions (UPS and ORC Macro,
2000).
The Census of India (2001) came up with shocking results of decline in sex-ratio,
particularly of children aged 0-6 years and provided more direct evidence of sex-selective
abortions. At the same time, the sonography centres grew like mushrooms all over the
country.
In 2002, registration of ultra sound sonography centres became compulsory
under the PNDT Act.
determination tests.
However, it might not have affected the conduct of sex
It almost has become a money-making business.
The genuine
benefits in treatment and the money coming along with probably tempted the AYUSH
4
4
(Ayurvedic, Unnani, Siddha and Homeopathy) doctors to demand permission to allow
them to use the sonography machines.
Number of organisations negotiated with the
MOHFW. Before allowing them to use the sonography machines, it was decided to get
surveys done in selected states, mainly to know the extent of ‘untrained’ ownership and
tire purposes for which the sonographies have been carried out. Thus, the present study
was assigned to us with the following objectives:
>)
To know how many untrained doctors (allopathic and non-allopathic) are using
ultrasound machines and for what purpose; and
ii)
To analyse the secondary data on ultra sound sonography centres available with
the Appropriate Authorities designated under the ACT.
Chapter scheme
The present report is organised in five chapters. The first chapter of the report
briefly introduces the background for the PNDT Act, its salient features and the objectives
of the study. Chapter 2 presents the distribution, type and qualification of the owners and
operators of sonography centres in Maharashtra. The impact of ultra sound sonography
centres on child sex ratio in Maharashtra is analysed in Chapter 3. Chapter 4 presents the
findings of the survey of sonography centres in Maharashtra. Summary of the study and
the recommendations arising out of the study findings are given in Chapter 5.
5
Chapter II
Ultrasound Sonography Centres in Maharashtra: Distribution, Type and
Qualification of the Owners and Operators
As on September 30, 2004, Maharashtra had 4345 registered ultrasound
sonography clinics/centres in the entire state and this number is increasing continuously as
the new centres are being registered regularly throughout the state. Getting the total
number of sonography centres registered in the state in one place was a difficult job. The
information was not readily available with the State Family Welfare Bureau (SFWB), the
state Appropriate Authority for implementing the PNDT Act, when we approached them.
This indicates the lack of importance given for maintaining the data related to the
registered sonography centres at one place. Upon our request, the letters were sent by the
State Appropriate Authority to all the district Appropriate Authorities to supply the data on
number of sonography centres with the qualifications of the owner of the centre and the
operator of the sonography machine, and the type of centre. For this purpose the format
supplied by the Ministry of Health and Family Welfare was sent along with the letter to
collect the above data. We have received the necessary data from the district Appropriate
Authorities in September 2004. Five districts (Chandrapur, Bhandara, Washim, Buldana
and Nandurbar) did not send the details till we completed this report in spite of the
reminders by the SFWB. These five districts together have 124 sonography centres (2.9
percent) and also come from the region where the number of sonography centres is very
less in the state. The following section analyses the distribution, type and qualifications of
the owners and operators of the sonography centres in Maharashtra supplied by the district
Appropriate Authorities.
The sonography centres are unevenly distributed in the 35 districts of the state.
Maharashtra’s districts are further grouped into 8 health circles by the Directorate of
Health Services for administrative purposes. Table 2.1 shows the uneven distribution of
the ultrasound centres in the state by health circle. More than three fourth of the centres
(78 percent) are registered in just four health circles (Mumbai, Pune, Nashik and Kolhapur
circles). These four circles form as a contiguous region of Western Maharashtra. These
four health circles together have 16 out of 35 districts of the state. It means that 78 percent
of the sonography centres are located in just 46 percent of the districts of the state, a
highly concentrated distribution. The distribution of the sonography centres shown as dots
in the map clearly shows the concentration of centres in western Maharashtra (see
6
Appendix 1). It would be worthwhile to mention here that many of the low child sex ratio
districts of the state come from this region of Maharashtra. Also the decline in child sex
ratio between 1991 and 2001 is higher in this region compared to the rest of the regions of
the state. Mumbai health circle alone has one third of the centres. Mumbai and Pune circle
together have nearly half of the (48 percent) centres. Twenty-two percentage of the
sonography centres are evenly distributed (5 to 6 percent) in rest of the four health circles
(Nagpur, Akola, Aurangabad and Latur circles) located in central and eastern parts of
Maharashtra. These four health circles together contain 19 districts of the state. It means
that 22 percent of the sonography centres are located in 54 percent of the districts of the
state.
Table 2.1. Number and percent of registered ultrasound sonography centres in
Maharashtra by Health Circles as on September 30, 2004.
Sl.No. Name of the Health
Circle
1
2
3
4
5
6
7
__ 8
Total
Mumbai Circle
Pune Circle
Nashik Circle
Kolhapur Circle
Narpur Circle
Akola Circle
Aurangabad Circle
Latur Circle
No. of districts
in the Health
Circle
5
3
5
3
6
5
4
4
35
No. of registered
ultrasound
centres/clinics
1421
656
864
441
229
220
238
_________ 276
4345
Percent
Cumulative
percent
32.70
15.10
19.88
10.15
5.27
5.06
5.48
6.35
100.00
32.70
47.80
67.69
77.84
83.11
88.17
93.65
100.00
100.00
Source: State Family Welfare Bureau, Pune
Table 2.2 gives the distribution of the ultrasound centres in the Districts and
Corporations of Maharashtra. It shows that in Central and Eastern Maharashtra (Nagpur,
Akola, Aurangabad and Latur Circles) the number of centres is far less than the districts in
Western Maharashtra. Also the sonography centres are concentrated in the bigger cities of
the state. In the state as a whole, half of the sonography centres are located within the
Municipal Corporation limits.
The districts are also listed in the descending order according to the number of
registered centres in Table 2.3. It shows that just six districts (out of 35) of the state have
half (49.8 percent) of the sonography centres and all these districts come from western
Maharashtra. The population share of these six districts in the state is 38 percent. In 14
districts of the state the number of centres is more than 100 and 82 percent of the centres
7
Table 2.2. Number of registered ultrasound clinics/centres in the districts of Maharashtra as on
September 30, 2004.
Health
Circle
Mumbai
Name of the district/
Corporation_________________________
1
Raigad
2
Ratnagiri
3
Thane
4
Mumbai & Mumbai Suburb M. Corpn.
5
Navi Mumbai Municipal Corporation
6
Thane Municipal Corporation
7
Kalyan Municipal Corporation
Ulhashnagar Municipal Corporation_____
8
Nashik
Ahmednagar
9
10
Dhule
Jalgaon
11
12
Nashik
13
Nandurbar
14
Nashik Municipal Corporation_________
Pune
15
Pune
Solapur
16
17
Satara
18
Pune Municipal Corporation
Pimpri-Chinchwad Municipal Corporation
19
20
Solapur Municipal Corporation_________
Kolhapur
21
Kolhapur
22
Sangh
23
Sindhudurg
24
Kolhapur Municipal Corporation
25
Sangh Municipal Corporation__________
Aurangabad
Aurangabad
26
Jalna
27
28
Parbhani
Hingoh
29
30
Aurangabad Municipal Corporation_____
Latur
31
Seed
32
Nanded
33
Latur
34
Osmanabad
35
Nanded Municipal Corporation_________
Akola
36
Akola
37
Amrawati
38
Buldhana
39
Yawatmal
Washim
40
41
Amrawati Municipal Corporation_______
Nagpur
42
Bhandara
43
Chandrapur
44
Gadchiroli
45
Nagpur
Wardlia
46
47
Gondia
48
Nagpur Municipal Corporation
Total______ ____________________
Source: State Family Welfare Bureau, Pune
SI. No.
8
No. of registered
______ centres
106
56
170
833
71
86
77
________ 22
211
54
163
84
15
________ 129
160
99
209
276
45
________ 75
107
106
47
104
________ 77
27
34
36
12
________ 120
61
17
67
27
________ 48
64
20
47
37
14
________ 56
19
29
5
24
23
10
________ 166
4345
Total in
health circle
1421
656
864
441
229
220
238
276
4345
Table 2.3. Number and percent of registered ultrasound clinics/centres in the districts of
Maharashtra, under PNDT Act, as on September 30, 2004.
SI.
No.
Name of the
District
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
Total
Mumbai (Suburb)
Pune
Thane
Mumbai
Nashik
Ahmadnagar
Kolhapur
Satara
Nagpur
Sangli
Solapur
Jalgaon
Aurangabad
Raigarh
Amarawati
Latur
Nanded
Akola
Beed
Ratnagiri
Dhule
Sindhudurg
Buldana
Yavatmal
Parbhani
Jalna
Chandrapur
Osmanabad
Wardha
Bhandara
Nandurbar
Washim
Hingoli
Gondia
Gadchiroli
No. & % of registered sonography
centres
Number
Percent
Cmltive %
546
12.57
12.57
481
11.07
23.64
426
9.80
. 33.44
287
6.61
40.05
213
4.90
44.95
211
4.86
49.81
211
4.86
54.66
209
4.81
59.47
190
4.37
63.85
183
4.21
68.06
174
4.00
72.06
163
3.75
75.82
147
3.38
79.20
106
2.44
81.64
76
1.75
83.39
67
1.54
84.93
65
1.50
86.43
. 64
1.47
87.90
61
1.40
89.30
56
1.29
90.59
54
1.24
91.83
47
1.08
92.92
47
1.08
94.00
37
0.85
94.85
36
0.83
95.68
34
0.78
96.46
29
0.67
97.13
27
0.62
97.75
23
0.53
98.28
19
0.44
98.71
15
0.35
99.06
14
0.32
99.38
12
0.28
99.66
10
0.23
99.89
_____ 5_
0.12
100.00
4345
100.00
100.00
Percent of
population
2001
8.88
7.47
8.40
3.34
5.16
4.23
3.63
2.89
4.19
2.67
3.98
3.80
3.02
2.28
2.69
2.15
2.96
1.68
2.23
1.75
1.77
0.89
2.30
2.54
1.54
1.67
2.15
1.52
1.27
1.17
1.35
1.05
1.02
1.24
1.00
100.00
Chile sex
ratio (0-6),
2001
919
906
933
898
936
890
859
884
949
850
897
867
884
943
947
923
944
936
898
954
907
946
915
942
926
914
944
927
934
958
966
921
935
964
974
917
Sources: State Family Welfare Bureau, Pune. Directorate of Census Operations. Maharashtra. 2001.
in the state is located in these 14 districts itself. The population share of these 14 districts
is 64 percent in the state. In all these districts the percent of sonography centres is higher
than the percentage share of population in the state. All the districts in the central and
eastern region of the state have less percentage of sonography centres than their population
percentage. The table also reveals that, broadly, the districts with more than 100
sonography centres are distinctly having lower child sex ratio than the districts with less
9
(table 2.4 is given as a separate document)
I
10
than 100 sonography centres. The mean sex ratio for the districts with more than 100
sonography centres is 901 and for the districts with less than 100 sonography centres it is
937. This is a rough indication of higher availability of sonography centres and the decline
in child sex ratio. Gadchiroli district with the smallest number of sonography centres (five)
has the highest child sex ratio (974) in the state. Further, four districts, Gadchiroli,
Gondiya, Nandurbar and Bhandara, with less number of sonography centres (less than 20)
are having balanced child sex ratio (958 and above). Incidentally, these four districts also
have a higher share of tribal population.
Type of sonography centres
The following section analyses the characteristics of the registered sonography
centres. Type of centre, qualification of the owner and qualification of the operator of
sonography machines are the characteristics analysed. Out of the 4345 sonography centres
in the state, we have got the above information only for 4090 centres (94 percent) from the
district Appropriate Authorities as few districts did not provide this information in spite of
the reminders from the SFWB. Table 2.4 presents the details of type of centres and
qualification of the owners and qualifications of the persons operating the sonography
machines. Tables 2.5, 2.6 and 2.7 are extracted from Table 2.4 for easy readability.
Table 2.5. Type of ultrasound sonography centres in Maharashtra.
No.
1
2
3
4
5
6
7
Type of sonography centres
Genetic Clinic
Genetic Laboratory
Genetic Counselling Centre
Ultrasound Clinic / Imaging Centre
Private Hospital
Pathology Lab
Not Given____________________
Total
Number
Percent
739
32
41
18.1
0.8
1.0
2563
62.7
528
12.9
0.1
4.5
100.0
3
184
4090
Sonography centres are registered under different categories in the state (Table
2.5). However, most of these centres (63 percent) are registered as Ultrasound Clinic.
Eighteen percent of centres are registered as Genetic Clinic. Ultrasound Clinic and Genetic
Clinic together account for 81 percent of the centres in the state. Only very small
percentage of the centres is registered as Genetic Laboratory (0.8 percent) and Genetic
Counselling Centre (1 percent). Thirteen percent of the centres are registered as Private
11
Hospital. For nearly five percent of the centres the information was not provided by the
district Appropriate Authorities. These categories are given by the district Appropriate
Authorities at the time of registration. It appears that the Appropriate Authorities did not
pay much attention at the time of registration to classify the centres in the proper way.
Hence these classifications are not revealing the exact nature of the centres. However, we
feel that Ultrasound Clinic and Genetic Clinic are basically same and known as Ultra
Sonography Centres or USGs.
*
Qualifications of the doctors/persons owning the ultrasound sonography centres
As per the PNDT Act anyone can own a sonography centre provided that the
persons who operate the machine must have the necessary training in conducting the test.
Qualifications of the doctors/persons who own the ultrasound sonography centres are
provided in Table 2.6. One third of the doctors/persons who own the sonography centres
are Gynaecologists. Radiologists/Ultrasonologists own 21 percent of the centres. Nearly
four percent of the centres are owned by MBBS doctors with training or experience in
-.p
conducting sonography. These four categories together (Gynaecologists; Radiologissts /
Ultrasonologists; MBBS doctor with training or experience) account for the 58 percent of
the centres and can be considered as trained doctors/persons in ultrasound sonography.
One third of the Gynaecologists who own the centres may be mainly using the sonography
machines for obstetric purposes.
Table 2.6. Qualifications of the owners of the ultrasound sonography centres.
“sT
No.
1
2
3
4
5
6
7
8
9
Qualifications of the owners of the ultrasound
Number
sonography centres__________________________
Radiologist/Ultrasonologist (MBBS+DMRD)
863
Gynaecologist (MBBS+DGO)
1341
MBBS doctor with training
39
MBBS doctor with experience
111
AYUSH/BAMS doctor employing qualified doctors
231
Others*
428
MBBS
146
Not given
536
Trust/Govt. Hospital _____________________ _
395
Total___________________________________________ __________
4090 '
Percent
21.1
32.8
0.9
2.7
5.6
10.5
3.6
13.1
9.7
100.0
♦Gastroenterologist, Cardiologist, ENT specialist. Orthopaedics, M.D. Medicine etc. and Non-Medical Personnel
Doctors specialised in various other fields (Gastroenterologist, Cardiologist, ENT
specialist, Orthopaedics, M.D. Medicine etc. and Non-Medical Personnel) own nearly 11
12
percent of the centres. Six percent of the centres are owned by the persons/doctors
qualified in Indian system of medicine (AYUSH). Ten percent of the sonography centres
are registered in Trust/Govemment Hospitals. The district Appropriate Authorities did not
provide the qualification of the registered persons for 13 percent of the centres. We found
that qualification of the owner of the centre was not at all provided in the registration form
itself. Reported qualifications of the owners, as per the categories 1-4 in the table, broadly
reveal that trained and qualified people own most of the centres (58 percent) in the state.
Among the categories 5-8 in the table also some of them may be trained doctors in
sonography. Hence, the true extent of centres owned by the trained doctors/persons will be
slightly more than 58 percent. Similarly, the centres owned by the unqualified doctors
(AYUSH) will also be more than the figures given in the table because, the qualification
of the doctors/persons was not given 13 percent of the centres and 10 percent of the
centres are registered with trusts/hospitals. Private Hospitals may be owned by the trained
as well untrained persons/doctors. Leaving apart the cases with owners’ qualification not
given, it is observed that about 20 percent of the centres are with untrained owners.
Qualifications of the operators of the ultrasound sonography machines
As per the PNDT Act the doctors without any training or experience in the
operation of the ultra sonography machines can register a sonography centre on their
name. But, the person who operates the machine must have the necessary qualification/
training/experience to conduct the sonography tests. We have got the qualifications of the
persons who operate the sonography machine from the Appropriate Authorities. The
necessary data are given in Table 2.7 for the centres owned by the trained (self operated)
as well as untrained (sonography machine operated by a qualified person employed by the
owner) persons.
In the state as whole, 63 percent of the centres are ‘self operated’ i.e., owner
himself operates the machine. The remaining 37 percent of the centres are owned by the
persons who have employed the qualified persons to operate the machine. Out of these 37
centres, a few centres might have a qualified owner but they also employed sonologists.
Leaving these cases, the remaining could be taken as with untrained ownership. Roughly,
it could be estimated that about 30 percent of the centres are with untrained ownership. It
means that the majority of the sonography centres in the state are registered/owned by the
doctors/persons trained in conducting ultrasound sonography.
13
Table 2.7. Qualifications of the doctors using the ultrasound sonography machines in the
centres owned by trained (Self Operated) and untrained (Centres Employing Other
Doctors) persons/doctors.
Sonography centre owned by
Untrained Doctors
Qualifications of the doctors/persons using
SI.
Trained Doctors
(Employing other
(Self Operated)
No. the ultrasound sonography machines
____ doctors)
No.
No.
%
%
813
Radiologist/Ultrasonologist (MBBS+DMRD)
31.8
1146
74.7
1
1135
44.4
237
15.6
2
Gynaecologist (MBBS+DGO)
23
0.9
5
0.3
3
MBBS doctor with training
103
1.1
4.0
4
MBBS doctor with experience
17
5
0.2
AYUSH/BAMS
5
235
9.2
66
4.3
6
Others*
0.4
11
7
MBBS
232
4.0
Not given___________________________
9.1
62
8
Total______________________________
2557
100.0
1533
100.0
62.5
100.0
_____ % of trained and untrained doctors/persons
37.5
♦Gastroenterologist, Cardiologist, ENT specialist. Orthopedics, M.D. Medicine etc. and Non-Medical Personnel
Qualifications ofr the doctors using ultrasound machine in the centres owned by
trained doctors (self operated)
As we have seen earlier the trained doctors own 63 percent (2557 out of 4090) of
the sonography centres in the state. Among the centres owned by the trained doctors fortyfour percent of the doctors are gynaecologists. Gynaecologist mainly use the machine for
obstetric and ante natal purposes. Another one-third of the trained doctors are
radiologists/ultrasonologists. Gynaecologists and radiologists/ultrasonologists together
dominate (76 percent) the ownership of trained “self operated” centres. Five percent of the
trained owners are MBBS doctors with some training/experience in conducting
sonography. Nearly 10 percent of the machines are owned by “other” doctors (other than
gynaecologist and radiologists). Surprisingly 0.6 percent of the centres are owned by the
unqualified doctors (MBBS and AYUSH/BAMS) as per the data given by the district
Appropriate Authorities. This must have happened because of the wrong reporting in the
registration forms. A will be reported in the later chapter, a few AYUSH doctors operating
the machine were already found. Here also we did not get the qualification of the persons
using the machine for nine percent of the centres. The qualifications of the doctors in the
centres owned by the trained doctors broadly reveals that 81 percent of the sonography
machines are operated by gynaecologists, radiologists/ultrasonologists and MBBS doctors
with some training/experience in conducting sonography
14
Qualifications of the doctors using ultrasound machine iin the centres owned by
untrained doctors/persons (employing other doctors)
The qualifications of the doctors using the sonography machines in the centres
owned by the untrained doctors/persons (employing other doctors) reveal that, in threefourth of these centres radiologists/ultrasonologists operate the machines. Another sixteen
percent of the centres have employed the Gynaecologist for operating the machine.
Radiologists and Gynaecologists together operate the machine in 90 percent of the centres
owned by the untrained doctors/persons. Four percent of the operators are “other” doctors
and two percent are MDBS doctors with qualification/experience in operating sonography
machines. For the remaining four percent of the centres we did not get the qualification of
the doctors.
Qualifications of the persons using the sonography machines in the centres owned
by trained and untrained persons reveals the following: (i) in the centres owned by the
trained persons gynaecologist own large number of centres (44 percent) compared to the
doctors with other qualifications; and (ii) in the centres owned by the untrained persons
the radiologists/ultrasonologist are mainly (75 percent) employed to operate the sonography
machine.
District-wise sonography centres owned by trained and untrained doctors/persons
Table 2.8 further classifies the sonography centres according to the qualifications of
the owners for the districts of Maharashtra. The table reveals the following: (1) the
sonography centres owned by the untrained persons are much higher in western Maharashtra
compared to the other parts of the state; (2) the centres owned by the persons specialised in
Indian System of Medicine (AYUSH) is also higher in western Maharashtra compared to the
other regions of the state; (3) almost all the centres owned by the AYUSH doctors are located
exclusively in western Maharashtra; (4) in the areas falling under the municipal corporation
limits, majority of the sonography centres are mainly owned by the trained doctors; (5)
AYUSH doctors mainly own their sonography centres outside of the municipal corporation
areas i.e., AYUSH doctors exclusively operate in the smaller towns and interior areas of the
districts; (6) sonography centres located in central and eastern parts of Maharashtra are mainly
owned by the trained doctors and even among the centres owned by the untrained persons
allopath doctors own most of the centres compared to the AYUSH doctors; and (7) very few
AYUSH doctors own a sonography centres in central and eastern parts of Maharashtra.
15
Table 2.8. Ultrasound sonography centres owned by trained and untrained persons
SI.
No.
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
District
Trained
Pune
Pune M. Corp.
PCMC
Ahmednagar
Satara
Raigad
Kolhapur
Kolhapur M. Corp.
Sangli
Sangli M. Corp.
Aurangabad
Aurangabad M. Corp.
Solapur
Solapur M. Corp.
Nasik
Nasik M. Corp.
Mumbai & Mumbai SU
Ratnagiri
Ulhasnagar
Navi Mumbai M. Corp.
Thane
Thane M. C orp.
Kalyan-Dombivali M.Corp
Sindhudurg
Hingoli
Jalgaon
Dhule
Nagpur M. Corp.
Nanded
Parbhani
Beed
Gondiya
Yavatmal
Wardha
Osmanabad
Akola
Latur
Amravati M. Corp.
Total______________
Total percent
V-f-’
56
125
25
101
105
65
24
75
67
57
16
95
59
32
41
75
468
41
15
38
112
51
54
14
11
101
37
121
14
30
32
7
29
13
15
49
41
43
2354
63.7
___ Untrained
NG
Allopath
AYUSH
22
25
53
32
54
6
1
2
44
41
2
26
26
44
17
4
13
7
9
62
13
3
2
16
21
14
2
2
8
13
1
16
22
1
5
1
29
18
21
2
29
5
13
115
119
. 12
7
5
2
1
9
1 4
9
14
3
25
7
15.
11
2
15
15
1
16
42
6
9
5
30
3
5
16
4
4
1
1
7
6
9
1
7
1
1
20
3
__8
__ !_
574
231
536
15.5
6.3
14.5
Total
156
211
34
188
201
99
102
93
104
73
26
109
98
67
82
122
714
55
16
57
154
73
67
44
12
159
52
156
17
35
56
9
36
19
25
58
64
__52
3695
100.0
Multiple attachments of sonologists
Some sonologists are attached to more than one ultrasound centres. Either they
carry their own mobile ultrasound machine or they use the fixed machine owned by the
owner of the centre. This system effectively increases the number and spread of the
registered centres in an area/region. Although this issue is not important at the state-level
and may not have a significant role in influencing the functioning of the centres, it puts
16
forth interesting aspect of the functioning of sonography centres and hence we provide
some information on the same in Table 2.9. It is observed that 46 doctors, in the state as a
whole, are attached to 303 centres with an average of 6.6 attachments per doctor. The
average varies between the districts/corporations. It is also observed that such multiple
attachments are more common in the corporation areas. Truly speaking, the corporations
are expected to have ample number of sonologists, while in the non-corporation areas,
shortage could be experienced. Thus, the multiple attachments may not be out of shortage
of sonologists.
functioning?
Then the question arises, are these multiple attachments really
Or is it reported just to fulfil the requirement for registration?
This
alternative appears plausible at least in cases where the attachments are in the range of 8,
9, 10, 11 and what not? How is it possible to have attachments at these many places?
During the field work we came across a few cases, where some person was shown as an
appointed doctor for operating the sonography machine, but occasionally, the owner, not
trained in sonography, operates the machine. Another important aspect related to such
multiplicity of attachment is the quality of work. One sonologist in Pune has his own
centre reporting about 200-300 cases per month and is attached to 6 more places. Can
anyone imagine that the doctor could give justice to his patients? We have a strong doubt
about the genuine ity of functioning of such multiple attachments. We suggest that the
appropriate authorities should investigate into such cases.
Table 2.9.
Information regarding doctors attached to multiple (>=4) ultrasound
sonography centres
Place________________
Greater Mumbai MC
Navi Mumbai MC
Thane MC
Raigarh
Kalyan-Dombivali MC
Ulhas Nagar MC
Nashik MC
Nashik (Non-corporation)
Ahmednagar
Pune (Non-corporation)
Pune MC
Satara
Sangli
Latur
Nagpur MC___________
Total
No. of doctors
16
4
4
1
3
1
5
2
3
2
1
1
1
1
1
No. of attachments
96
30
34
8
15
4
38
16
24
11
6
46
17
5
4
8
_______ 4
303
Average
6.0
7.5
8.5
8.0
5.0
4.0
7.6
8.0
8.0
5.5
6.0
5.0
4.0
8.0
4.0
6.6
Chapter III
Child Sex Ratio and Ultrasound Sonography Centres in Maharashtra
Sex ratio is an important social indicator to measure the extent of prevailing
equality between men and women in a society and mainly reflect the sex differentials in
mortality. Contrary to the universal pattern, sex ratio is unfavourable to women in India.
Several reasons are cited for the consistently low levels of sex ratio and their further
decline over the decades in India. Some of the important reasons discussed in the literature
for the decline of sex ratio in India are: (1) neglect of girl child resulting in their higher
mortality at younger ages, (2) high maternal mortality, (3) sex selective female abortions,
(4) female infanticide, and (5) change in sex ratio at birth. The first part of the present
chapter briefly looks at the sex ratio of child population in Maharashtra and the second
part analyses the association/relationship between availability of sonography centres and
child sex ratios at the district level in Maharashtra.
Sex ratio of children in the age group 0-6 in the districts of Maharashtra
During the last decade (1991-2001), India and all the neighbouring states of
Maharashtra have shown rise in sex ratio of the total population but Maharashtra has
shown a decline indicating worsening position of women in the state. As per 2001 Census,
the sex ratio of the total population of Maharashtra (922 females per 1000 males) is not
only lower than all India sex ratio (933) but it has been declining from 936 in 1961 to 922
in 2001. It is, however, the sex ratio of the child population which causes more concern in
Maharashtra, as this group is not affected by migration. A decline in the sex ratio in the
age group 0-6 points towards the attitude and outlook towards the girl child. Universally,
the sex ratio at birth is favourable towards males and usually falls between 943-952 girls
per 1000 boys (or 105-106 male babies per 100 female babies). As per the 2001 census sex
ratio of the child population of India (927 girls per 1000 boys) is much lower than the
universal sex ratio at birth. In Maharashtra, the child sex ratio has declined by 29 points
from 946 in 1991 to 917 in 2001. It is not only much lower than the universal sex ratio at
birth, it is also much lower than those for the all four south Indian states (Kerala 963,
Andhra Pradesh 964, Karnataka 949 and Tamil Nadu 939) and Madhya Pradesh (931). Of
course, it is much better than the states like Punjab (793), Himachal Pradesh (897),
Haryana (820) and Gujarat (878). The drastic decline in sex ratio of child population
suggests the possibilities of neglect of girl child leading to higher mortality among girls
18
than boys and practice of female foeticide (Parasuraman, 2001; Kulkami, 2001; Premi,
2001; Bhat, 2002).
District-wise sex ratio of the child population shows that the sex ratio varies
between 974 in Gadchiroli and 850 in Sangli (Table 3.1). The districts with higher sex
ratio mainly come from eastern and central regions of Maharashta and most of the low sex
ratio districts come from western Maharashtra. Mainly the prosperous districts/areas of
Table 3.1. Sex ratio of child population in the age group 0-6, Maharashtra, 2001
Sr.
No.
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
Sex ratio of child population
in the age group 0-6
District
TotalI______ Rural
966
976
907
914
867
' 865
915
921
936
941
921
917
947
953
934
946
949
964
958
961
964
966
974
976
944
965
942
948
944
948
935
938
926
931
914
913
884
886
936
948
933
971
919
898
943
952
906
912
890
892
898
897
923
926
927
933
897
890
884
888
954
959
946
948
859
870
850
850
917
923
Nandurbar
Dhule
Jalgaon
Buldana
Akola
Washim
Amrawati
Wardha
Nagpur
Bhandara
Gondiya
Gadchiroli
Chandrapur
Yavatmal
Nanded
Hingoli
Parbhani
Jalna
Aurangabad
Nashik
Thane
Mumbai (Suburb)
Mumbai
Raigarh
Pune
Ahmadnagar
Beed
Latur
Osmanabad
Solapur
Satara
Ratnagiri
Sindhudurg
Kolhapur
Sangli__________________________
Maharashtra State_______________
Source: Director of Census Operations, Maharashtra. 2001.
19
Urban
895
888
871
890
927
945
935
898
939
939
946
941
897
910
929
919
915
917
882
916
915
919
898
914
900
878
898
912
895
914
857
911
925
832
851
908
Maharashtra have worst sex ratios e.g., Sangli (850), Kolhapur (859), Jalgaon (867),
Aurangabad (884), Satara (884), Ahmadnagar (890), Solapur (897), Beed (898), Mumbai
(898), Pune (906) and Dhule (907). The sex ratio of children in the entire Pune region is
very much unfavourable to females (below 900). On the contrary, the backward/tribal
districts like Gadchiroli (974), Nandurbar (966), Gondiya (964) and Bhandara (958) have
higher sex ratios in the state.
District-wise sex ratios of child population in rural and urban areas are also given
in Table 1. It shows that the sex ratio in urban areas of Maharashtra (908) is 15 points
lower than in rural areas (923). Except five districts, in all districts of Maharashtra, the
urban sex ratios are lower than the rural sex ratios. In 15 districts of the state the urban sex
ratio is 25 points lower than the rural sex ratio.
Table 3.2 gives the range of sex ratio for the districts of Maharashtra. As
mentioned above, the child sex ratio in the range of 943 to 952 is considered as ideal
because sex ratio at birth is 105-106 male babies per 100 female babies (100/106 = .943;
100/105 = .952). Anything below this range is considered to be a below normal sex ratio.
The table shows that sex ratio is above 943 only in 11 districts of the state. It means that
only in 11 districts of the state the sex ratio of child population is favourable towards
females and in the remaining districts it is unfavourable. In nine districts, it is below 900
indicating the severe imbalance of girls in these districts. In all, in 69 percent of the
districts the sex ratio is unfavourable to female children.
Table 3.2. The range in child sex ratio in the districts of Maharashtra, 2001
Maharashtra/
Region_____
Total
Rural
Urban_____
Distribution of districts according to child sex ratio
Below 900
900-942
943 and above
9 (25.7)
15(42.9)
11 (31.4)
8 (24.2)
10(30.3)
15(45.5)
14 (40.0)
19(54.3)
2 (5.7)
Total no. of
districts
35 (100)
33* (100)
35 (100)
* Mumbai and Mumbai Suburb districts are completely urban.
The range in sex ratio is also given for rural and urban areas of the district in Table
3.2. Rural sex ratio is above 943 in 15 districts (46 percent) whereas only in two districts
(6 percent) the urban sex ratio is above 943. It means that the imbalance of female children
in urban areas is prevailing throughout the state. The child sex ratio is below 900 in onefourth of the districts in rural areas and 40 percent of the districts in urban areas. The
20
classification reveals that in two thirds of the districts the child sex ratio is unfavourable to
female children and it is further worst in urban areas of the districts compared to the rural
areas. The abnormally very low sex ratios in urban areas of Maharashtra goes beyond the
limit as one would normally expect given the higher literacy and awareness in urban areas
compared to the rural areas.
Table 3.3. Change in child sex ratio between 1991 and 2001, by districts.
SI. No.
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
Sex ratio of child population in the
______
age group 0-6______
District
2001
1991
924
850
Sangli
Kolhapur
931
859
890
Ahmadnagar
949
867
Jalgaon
925
941
884
Satara
884
Aurangabad
933
898
Mumbai
942
898
Beed
939
907
Dhule
947
897
Solapur
935
914
Jalna
951
906
943
Pune
926
Parbhani
956
915
Buldana
945
923
Latur
947
944
Chandrapur
965
947
927
Osmanabad
941
921
Washim
942
961
Yavatmal
Thane
952
933
943
Raigarh
961
936
954
Nashik
935
Hingoli
953
934
952
Wardha
Sindhudurg
946
963
944
Nanded
960
964
Gondiya
978
966
977
Nandurbar
919
Mumbai (Suburb)
930
954
961
Ratnagiri
974
980
Gadchiroli
958
964
Bhandara
947
950
Amrawati
949
Nagpur
951
936
Akola_________________________ 929
917
Maharashtra____________________ 946
Source: Director of Census Operations, Maharashtra. 2001.
21
Change
between 1991
to 2001
-74
-72
-59
-58
-57
-49
-44
-41
-40
-38
-37
-37
-30
-30
-24
-21
-20
-20
-19
-19
-18
-18
-18
-18
-17
-16
-14
-11
-11
-6
-6
-3
-2
+7
-29
Decline in child sex ratio between 1991 and 2001
Comparison of sex ratios of total population of 1991 and 2001 in the state shows
that 23 districts have registered a decline in sex ratio and 10 districts have registered an
increase (Directorate of Census Operations, Maharashtra, 2001). But the comparison of
sex ratios of child population shows that every single district had experienced a decline
except Akola where it increased by 7 points (Table 3.3). The extent of decline is more than
40 points in 8 districts and in all these districts sex ratio is below 900. The districts which
have experienced higher magnitude of decline already had a lower sex ratio in 1991. The
range between highest and lowest child sex ratio has increased significantly between 1991
and 2001 in the state. The range between highest (Gadchiroli, 980) and lowest (Sangli,
924) child sex ratio in 1991 is 56 points whereas this range has increased to 124 points in
2001 (Gadchiroli, 974 and Sangli 850). Gadchiroli experienced a decline of 6 points and
Sangli experienced a decline of 74 points from 1991 to 2001. The decline in sex ratio from
1991 to 2001 generally goes down if one travels from west to east of the state with few
exceptions (Sindhudurg and Raigad). The developed districts of the state had experienced
higher magnitude of decline compared to the less developed districts. The magnitude of
the decline in the entire Time region is alarming.
Sex ratio of child population in the Municipal Corporations of Maharashtra
Maharashtra has 15 Municipal Corporations (MC) in the state. Sex ratios of child
population in the MCs are given in descending order in Table 3.4. Out of the 15 MCs only
three (Amravati, Nagpur and Nanded) are from the central and eastern regions of the state
and the remaining 12 are from the western regions. It shows that the child sex ratio for the
MCs is 910, which is lower than the child sex ratio for the entire state (917) and much
lower than the child sex ratio for rural areas of the state (923). Child sex ratio of MCs is
comparable with the urban child sex ratio of the state (908). Except Amravati MC, the
child sex ratio in all the remaining 14 MCs is below 943. In six MCs the child sex ratio is
below 900. Child sex ratio is below 930 in all the MCs from western regions. Child sex
ratios in MCs indicate the severity of the discrimination against female children in the
bigger cities of the state which goes contrary to the expectations.
22
explains nearly half (R2: 48 percent) of the variance in child sex ratio. The regression
analysis shows that the two variables representing the availability of the sonography
centres significantly reduce the child sex ratio at the district level in Maharashtra. It means
that the further spread of the sonography centres in the state will reduce the sex ratio
further. The graphs 1 and 2 with the regression line show these results.
Table 3.9. Regression analysis of child sex ratio and availability of sonography centres in
Maharashtra.
Regre
ssion^ Dependent variable
1
2
3
4
5
Child sex ratio_________
Child sex ratio_________
Decline in child sex ratio
Decline in child sex ratio
Child sex ratio in M.Corp
Independent variable
No. of USGs
No. of USGs/1000 popn
No. of USGs_________
No. of USGs/1000 popn
No. of USGs/1000 popn
Regression
Coeffcient
-0.289***
-927.742***
0.174***
523.857***
-443.276**
t
R2
N
4.663
5.465
4.095
4.222
2.751
43
.48
.37
.35
.37
3?
35
31
35
15
Number of sonography centres and decline in child sex ratio between 1991 and 2001
We have seen that the number of sonography centres have significant negative
effect on child sex ratio. This makes us to think that the decline in sex ratio is due the
availability of sonography centres. Hence, in place of child sex ratio we have used the
decline in child sex ratio from 1991 to 2001 as the dependent variable. The relationship
between the number of sonography centres and the decline in sex ratio is positive at one
percent level of significance i.e., the increase in sonography centres has significantly
increased the decline in child sex ratio in Maharashtra. Thirty-seven percent of variance in
the decline in child sex ratio is explained by the number of sonography centres. The
regression result for the effect of number of centres per 1000 population on the decline in
sex ratio is also positive and significant at one percent level. This regression explains the
35 percent variance in decline in sex ratio in the state. The graphs 3 and 4 with regression
line show these effects.
Number of sonography centres and child sex ratio in Municipal Corporations (MCs)
The regression of child sex ratio in 15 MCs of Maharashtra and number of centres
per 1000 population in MCs is also given in Table 12. It confirms the results obtained for
the districts, i.e., the relationship between the number of centres per 1000 population in
MCs and sex ratio in MCs is significantly negative. Hence, the increase in the further
availability of sonography centres in the MCs will contribute for the further decline in sex
29
ratio. The sex ratios in MCs are already very low at the level of 910 female children per
1000 male children. The graph 5 shows the regression line. The correlation and regression
analyses at the different levels of aggregation (districts, corporations and tehsils) confirm
the negative relationship between the availability of sonography centres and child sex ratio
in iMaharashtra.
Limitations of the analysis of association/relationship between child
sex ratio and
number of sonography centres
The above associations/relationships should be treated with caution as the
reference period for the data on child sex ratio and sonography centres are some what
different. Figures for child sex ratio come from the 2001 census. The number of
sonography centres is pertaining to the updated figures for September 2004. We do not
have the data on number of sonography centres in 2001. Obviously some of the
sonography centres were registered after the completion of the 2001 census. Only after the
implementation of the compulsory registration of sonography centres under the PNDT act
m 2002 the data is available with the Appropriate Authorities. In spite of this limitation,
the correlation between the number of sonography centres and child sex ratio in the
districts reveals the negative association between these two variables. Similarly,
availability of sonography centres and the extent of decline in child sex ratio are positively
associated.
30
Graph 3.1. The relationship between child sex ratio (total) and number of sonography
centres in the districts of Maharashtra (n = 31).
980;^;lc ilroli
3hJ!>dara
■
960
Ratnagiri
Nagpur
Raigarh
940
Nasrt*
' linWkrdha\^^
OsnlaP^aru^\^
' Cashim
920
"
Lan7l\^
" ■
JafeWan*
Dhule
5
o
Bid
900
lapur
Ol
o
To
cr
X
CD
co
Aurangabad
880
Jalgaon
Kofriapur
860
Sangli
o
840
Rsq = 0.4285
0
100
200
300
Number of Ultra Sound Sonography Centres
Graph 3.2. The relationship between child sex ratio (total) and number of sonography
centres per 1000 population in the districts of Maharashtra (n = 35).
980
’ adcbiroit
Bhandara
■
960
Ratnagiri
Amarawati
940
SinJhu^firg
RqJ&rti
"
AHeWiik
Hingoli Waittfaa
Thane
Osm“nafet>h:ani
1
Washim
"
■
Mumbai (S-buro'
920
Dhule
S
o
Bid
900
o‘
ro
Ahmadnagar
Aurangabad
880
cr
X
(D
CO
Mumbai
Solapur
CXI
Jalgaon
Kolhapir
860
p
O
Sardii
840
Rsq = 0.4751
0.00
.02
.04
.06
No. of Sonography Centres per 1000 Population
31
.08
.10
Graph 3.3. The relationship between decline child sex ratio between 1991 and 2001 and
number of sonography centres in the districts of Maharashtra (n = 31).
80
Sangli
5
o
60
■
Aurangabad
o
CD
Ia
DhulS*
40
Latur
20
Raigarh
led
Nashik
> ^aaCrSar
Ratnagiri
“Amarawati
Gaoc "defendara
O
Nagpur
0
C
I
Jalna
Partaudana
co
2
s
AhcQginacjar
Jalgaon
CM
s
Kolhapur
Akola
-20
Rsq = 0.3664
0
100
200
300
Number of Ultra Sound Sonography Centres
Graph 3.4. The relationship between decline child sex ratio between 1991 and 2001 and
number of sonography centres per 1000 population in the districts of Maharashtra (n = 35).
80
Sangli
Kolhapur
Jalgad^mad'^9af
60
o
o
CXJ
CD
CD
Satara
Aurangabad
Mumbai
B^Dhule
40
Solapur
Jalna
*une
BuBarttfiani
£
Latur
Cl
20
(Aded”
co
Gondia ■
Nandurcs
!
uroW
Mumbai (Suburb)
Bhandara
Ratnag id
Amffawati
Nagpur
0 Akola
I
Q
-20
Rsq = 0.3507
0.00
.02
.04
.06
No. of Sonography Centres per 1000 Population
32
.08
.10
Graph 3.5. The relationship between child sex ratio (2001) in Municipal Corporations of
Maharashtra number sonography centres per 1000 population (n = 15).
3
o
CM
cn"
c
,o
ro
o
e-o
Q
Tu
Q.
O
960
Amarawati
Nagpur
M
940
Solfed’d-Wa0hala
N^i MumbaJ"
920
Muml
»ub
pun«asik
900
PimP5ijfc^d
Kalyan-Oimbivali
880
5
s
.£
o
or
860
Sangli-Miraj-Kupwad
840
X
<D
CO
32
1c
O
820
Kolhapur
800
0.0
Rsq = 0.3680
.1
.2
No. of Sonography Centres per 1000 Population
33
.3
Chapter IV
Findings of the Survey of Ultrasound Sonography Centres in Maharashtra
As mentioned in the introductory chapter, this survey has been assigned to
Population Research Centres with the objectives of knowing the extent of ownership of
sonography centres by untrained persons and of knowing the purposes for which the
machines have been used. As per the minutes of the meeting held on April 7, 2004 at the
Ministry of health and Family Welfare (MOHFW), it was decided that:
i)
The data already available with the Appropriate Authorities (Civil Surgeons/ Chief
Medical Officers) about the sonography centres should be analysed;
ii)
About 200 centres (run by untrained persons) in a state should be visited and a
small questionnaire be canvassed;
iii)
For selecting a sample of centres, it was decided that the survey should be
conducted in those districts of the state which account for 75-80 percent of the
registered centres; and
iv)
Few AYUSH (Ayurvedic, Unnani, Siddha and Homeopathic) doctors of integrated
medicine may also be surveyed to know whether they are desirous of having an
ultrasound sonography machine for their line of treatment. About 50-100 centres in
a state may be surveyed.
Thus, in brief, about 200 centres run by untrained persons, and about 50-100 nonallopathic doctors were supposed to be the sample-size for our study. At the outset, getting
the sampling frame for centres run by untrained persons and selecting a proper sample
seemed easier, while there was no sampling frame for selecting AYUSH doctors.
However, even for centres with untrained owners we came across a number of
difficulties in getting the sampling frame for centres run by untrained doctors and selecting
a proper sample. They are as follows:
i)
The lists of sonography centres were not available with the state Appropriate
Authority (i.e. SFWB, Pune). Sometimes they were not available even with the
Civil Surgeons, who are the appropriate authority for the district. Occasionally, our
34
field team had to visit the rural hospitals at tehsil level to get the basic data, which
formed the sampling frame for the survey.
ii)
For Mumbai Corporation, which has more than 800 sonography centres, detailed
data were not available with the corporation office. Our field team had to visit 24
ward offices. One who has visited Mumbai, could imagine the amount of efforts
put in by us just to get the sampling frame. Apparently this was not the problem
with other states. The concerned officials stated that since Maharashtra
Government has appointed the tehsil officials as appropriate authorities they are
able to identify sonography centres even in interior areas, but as an effect
sometimes the records are not sent to the district authorities. On the other hand in
other states the appropriate authority is up to district level and hence the data have
to be with the Civil Surgeons.
Hi)
For selecting a sample of centres run by untrained persons, we needed information
on qualification of the owner. Surprisingly, the application form to be filled by the
owner does not ask for the qualification of the owner and hence the summarised
information also does not give details needed for sampling. We had to look into
each and every file to see whether any degree certificate of the owner is attached to
the application form or whether his signature carries the stamp revealing his
qualification. Even after doing all this investigation, we have not been able to get
complete sampling frame.
iv)
In order to save time and money (which was quite meagre, looking to the number
of centres for Maharashtra (4350 approximately)), we had decided to collect the
basic data regarding centres, select the sample and do the survey in one visit to the
district. However, this could not be done firstly, because of the problems stated
above, and secondly, the MOHFW requested us to collect the basic data in the first
round and to conduct the survey in another round. We had communicated to
MOHFW about the difficulties in getting the basic data. We also had appraised the
MOHFW officials about the problems in a meeting held at SFWB, Pune. As a
consequence, the officials at SFWB, Pune were requested to help us in this matter.
The SFWB officials invited the civil surgeons of all the districts; along with the
35
basic data on sonography centres. This helped us in getting data for most (not all)
of the districts. However, by then we had started our field work.
V)
As a proper sampling procedure, the sample size, which was fixed at 200 in the
first place, should have been allocated in proportion to the number of centres run
by untrained persons at the district level. However, the data were not available to
us for all the districts to start with and even if they were available, information on
owners’ qualification was missing in many cases. Thus, a proper sampling
procedure could not be followed. There was one more factor, which disturbed our
sampling plan. As per the e-mail dated July 14, 2004 the MOHFW asked us to do
the survey of 400 centres. Further, as we were proceeding towards the concluding
part of our field-work, we received a communication from MOHFW, saying that
we also should carry out a survey of ‘some’ centres run by ‘trained doctors’. All
these problems have disturbed our sampling plan.
•i-
vi)
The field-work in Mumbai was the most difficult part. Firstly, for getting the
information on owners qualification and for getting correct addresses, telephone
numbers etc, a visit to concerned ward-office was necessary. Secondly, the
distances, as is known, are quite large. Thirdly, the doctors, most of them, being
very busy it was difficult to get their appointments and fourthly, some of them did
not give the information readily.
vii)
Since the area for field-work was restricted to western Maharashtra (covering 80
percent of the total sonography centres in Maharashtra) and since, as mentioned
above the sample size and composition changed frequently, and further since field
work in Mumbai posed several problems, we were finding it difficult to complete
the target of 400 centres run by untrained persons. We could, at the end, complete
the field work of about 380 centres (including some run by trained doctors). To
repeat, the district-wise number of surveyed centres is not in proportion to the total
number of cenfres in the district.
viii)
Some of the surveyed centres were run by cardiologists and ideally should not have
been brought under the PNDT Act. However, since they are registered under the
36
Act and since according to the definition the ‘cardiologist’ is not trained, the
centres came under our survey. We have excluded them from the analysis.
ix)
Some of the surveyed centres are run by doctors with MBBS degree and some
training (not necessarily recognised) or little experience. We have clubbed them
under a separate category called '‘not properly qualified or trained’.
As mentioned previously, there was no sampling frame available for a survey of
‘AYUSH’ and other untrained doctors, desirous of using a machine. The MOHFW had
suggested that the field team should, on their own, enquire about such people and visit
them. However, we found that this may not be a proper procedure. Alternatively, we tried
a different approach.
In Pune, we have the office of the National Integrated Medical
Association (NIMA), Pune Branch.
We came to know that this association of Non-
allopathic doctors had played an active role in the negotiations with the MOHFW
regarding the demand for permission to operate sonography machines. We contacted the
chairman and vice-chairman of this association (NIMA) and obtained a list of AYUSH
doctors registered with NIMA. The Pune branch of NIMA has 400 AYUSH doctors
registered with it. From this list we prepared a list of about 100 hospitals of ISM &
Homeopathy. This became the sampling frame for the survey of desirous doctors. We
tried to contact them through personal visit, telephonic contact or by post. The response
was not bad. Out of about 100 doctors, about 80 doctors could be contacted and out of
them 52 are desirous of using the machine. A small schedule was filled for these people.
Findings of the Survey of Ultrasound Sonography Centres run by Untrained Doctors
As per the guidelines of MOHFW, a schedule was supposed to be administered to
the doctors.
The questionnaire contained questions on type of machine, registration
number, qualification of the operator, number of referrals by both allopathic and nonallopathic doctors, the purpose (obstetric/non-obstetric) of sonography, the classification
of obstetric sonographies by trimesters, etc. With a purpose of assessment of observance
of PNDT act, we had prepared a check-list about maintenance of records, sending timely
reports, supervisory visits, etc. The field work for the study was carried out during the
months of August-November 2004.
37
We start with the sample composition. Table 4.1 gives the same. As mentioned
previously, the sampling frames could not be prepared accurately and hence no statements
about the sampling fraction can also be made. However, roughly it could be estimated that
there were about 1100 centres run by untrained doctors in Western Maharashtra (including
Mumbai, Konkan, Khandesh, Pune division and Aurangabad) and we have tried to cover
about 300 in our sample survey. It is broadly observed that in the corporation areas, the
proportion of centres with untrained owners is lower, while in the non-corporation areas,
the same is higher. For instance, in the district of Pune, it is about 20 percent, while in the
Ahmednagar district, it is about 46 to 50 percent. This trend is in the expected direction,
since generally, the proportion of untrained doctors (untrained in sonography) is expected
to be higher in rural areas/small towns.
Table 4.1 Classification of centres by district and training status of the owner of the centre
Sr.
No.
1
2
3
4
5
6
7
8
9
10
11
12
13
14
Total
Training Status of the owner
District
Mumbai
Thane
Raigad
Sindhudurg
Nashik
Jalgaon
Ahmednagar
Pune
Satara
Miraj
Sangli
Solapur
Kolhapur
Aurangabad
Trained
Untrained
Not properly
qualified/trained
Total
4
2
1
37
27
5
5
2
6
26
5
4
15
11
13
27
48
14
7
22
19
17
15
275
43
29
7
5
33
22
32
63
29
1
34
30
6
5
3
69
1
•
1
4
1
4
1
5
5
4
28
26
18
372
Table 4.2 gives the information on the status of the centre, type of machine and
year of installation and cost of the machine. Out of 372 centres, 297 i.e. about 80 percent
of the centres are attached to hospitals. This information is important in the context of
access to the facilities. If ‘sonography’ has an important role in current pattern of
treatment, the attachment of the centre to the hospital is beneficial both to doctors and
patients. On the other hand, for the general practitioners, particularly from ISM and
Homeopathy, individual centres are essential, since centres attached to hospitals do not
generally accept referrals and provide the services only to their own clients. In this
38
context, it is observed that for the cities like Mumbai and Pune the proportion of
independent centres is higher. For instance, in Mumbai, the proportion of independent
centres is 65 percent, while the same for districts with no big city, say Satara, is 3 percent.
Table 4.2. Classification of ultrasound sonography centres by its functional status, kind of
machine, year of installation of machine and cost of machine.
Classification of
ultrasound centre
Functional status
Attached to hospital
Separate Unit/centre
Not Given
Total____________
Kind of machine
Fixed
Mobile
On-call
Not Given
Total____________
Year of installation
1980
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
Not Given
Total
Training Status of the owner
Trained
Untrained
Not properly
qualified/trained
Total
50
17
2
69
219
54
2
275
28
297
71
4
372
63
3
2
1
69
207
40
25
3
275
28
28
28
1
1
1
2
1
1
5
4
2
6
6
6
15
23
29
43
61
36
17
19
275
1
4
3
2
10
6
21
13
3
3
69
1
2
2
4
4
3
5
3
1
2
28
298
43
27
4
372
1
1
1
2
1
1
5
6
2
8
10
11
21
33
39
67
79
42
21
21
372
In the second panel of the table, we find the classification of centres by type of
machine (fixed, mobile or on call). It is observed that about 80 percent of the centres are
having fixed machines, while about 12 percent of the centres function with ‘mobile’
39
machines. It is further observed that when the owner is trained, the mobile/ on call
machines are least used (7 percent) while, with ‘untrained’ owner, the use increases to 25
percent. Is it an indication of the situation that ‘untrained’ owners (some of them being
ISM & H doctors in small towns) are not in a position of investing in the machine and
hence have accepted the alternative of an operator with a ‘mobile’ machine on fixed days.
If this practice increases, we might face a situation described as ‘Doctors are carrying the
machines to interior areas and the villagers are having the benefits’. One would have liked
to see this dream come true, if it was for provision of general health services. But it has
happened only for sonography. What could be the reason? The obvious answer is ‘money’.
The money involved in the practice of ‘sonography’ is definitely much much higher. For
instance, the simplest sonography is done at the cost of Rs. 300. Further, the practice is
IS
very clean and safe; no infections, no risk, no emergencies, and no tensions. It is just a
little space and an appointed qualified doctor that would fetch a fair amount of monetary
benefits.
The information on year of installation could be helpful in assessing the trend of
‘untrained ownership*,
The third panel in Table 4.2 gives this information.
Few
interesting observations emerge from this table.
i)
Before the Act in 1994, 12 centres (out of 275) were functioning with an untrained
owner, while among the 69 centres with trained owners, there were 4 centres
functioning even before 1994. This indicates the untrained ownership is not a new
phenomenon.
ii)
After the compulsory registration initiated in 2002, the number of centres with
untrained owner is 114 (i. e. 40 percent), while the same proportion for centres
with trained owner is 19 out of 69 (i.e. 30 percent). Although, the proportions are
based on not necessarily random samples, the findings are indicative of
strengthening of the untrained ownership. What will be the consequences of such
a trend? Firstly, in case of untrained ownership, the sonography services are made
available through appointed operators and hence will be limited.
Secondly, in
absence of the operators, the owners may use the machine. During our field-work
we have got some evidence in support of the above statement. As far as the
untrained Allopathic (doctors) owners are concerned, we expect that their training
40
as medical graduates or postgraduates gives them adequate grounding so as to be
able to carry out the sonography tests.
But there could be reservations about
AYUSH doctors owning the centres. In fact, our field team had come across a
couple of AYUSH doctors owning and also operating the machine. By law,
AYUSH doctors are not allowed to use the machine. But thanks to the Appropriate
Authorities, the concerned doctors are using the machine openly.
Type of ultrasound sonography machine and cost of machine
Being non-technical persons, we do not intend to say anything about the type of the
machine in specific terms. However, just to have an idea, we give hereby the different
types of machines used by the respondent. Table 4.3 gives the information.
Table 4.3. Distribution of ultrasound machines by their make.
Machine Make
GE & Wipro
L&T
Toshiba
Aloka
Medison
ATL & Ultra Mark
PMS India
Siemens
Fukuda
Machine Make
Acuson
Esaote
Schimatzu
BPL
Toshbro
NA
NG
Other_______
Total
Frequency
94
67
47
35
19
17
15
11
8
Frequency
5
5
5
4
3
4
11
22
372
The figures clearly show that the machines manufactured by GE or Wipro and
L&T seem to be the more commonly used machines. Table 4.4 gives the classification of
the machines by the approximate cost reported by the owners. It is observed that the
median cost is around 4-5 lakhs. Thirty two respondents (9 percent) own machines costing
more than 10 lakhs. In short, having a sonography machine is definitely a costly affair.
As the next panel of Table 4.4 shows, the cost of the machine has increased over
time, as expected. How do we interpret these facts? One obvious implication is that unless
the owner is able to use it frequently, it might not be possible to recover the cost. But
surprisingly, the performance at least of the untrained owners is very poor like one
sonography a day on an average. It implies very weak chances of recovering the cost. In
our opinion doctors cannot take chances like this. Thus, either the performance is under
reported or the buyers of the machine do not find the cost heavy. The third alternative is
the recovery through the exorbitant charges, which could be demanded in case of sex41
determination. Although PNDT act is being implemented and we can not have direct
evidence of sex-determination there is enough indirect evidence to show that sex-
determination is being done. The proof of decline in child sex-ratio is a very convincing
reflection of the sex-determination tests.
Table 4.4. Approximate cost and year of installation and average cost of the machine
Approximate cost of the machine
< 1 Lakh
1- 2 Lakh
2- 3 Lakh
3- 4 Lakh
4- 5 Lakh
5- 6 Lakh
6- 7 Lakh
7- 8 Lakh
8- 9 Lakh
9- 10 Lakh
10- 15 Lakh
15-20 Lakh
20 - 25 Lakh
25-30 Lakh
Not Given
Total______________________
Year of Installation___________
1980-90
1991-95
1996-00
2001
2002
2003
2004
Frequency
10
21
22
67
63
47
21
16
2
1
11
11
6
4
71
373
Percent
2.7
5.6
5.9
18.0
16.9
12.6
5.6
4.3
0.5
0.3
2.9
2.9
1.6
1.1
19.0
100.0
Average cost of machine (in Rs. Lakhs)
4.71
4.41
5.60
5.72
4.25
7.51
6.64
In this context, it could be worthwhile to look into the classification of the owners
by system of medicine. It is observed that 113 out of 275 (i.e. 40 percent) are AYUSH
doctors (Table 4.5). Further, it is also observed that out of the 152 untrained allopath
owners nearly 100 are postgraduates in allopathic medicine. Just because they are not
qualified by definition, they are designated as ‘untrained’ owners.
In brief, about 40
percent of the ‘untrained’ ownership comes from AYUSH doctors and the proportion may
increase in future. Looking into its consequences, the authorities have to decide firstly,
whether to allow the AYUSH doctors to operate the machine and secondly, whether to
give them the training before allowing them to use the machine,
Among a few
gynaecologists, whom we tried to contact, there is a difference of opinion. One group
42
opines that there will be chaos if the AYUSH doctors are permitted to use the machine,
while the other group opines that, there is no harm in allowing them to use; unofficially, a
few of them are using it.
Table 4.5. Classification of centres by system of medicine studied by the owner
Training status of the owner
System of medicine studied by
the owner
Allopath
Non-Allopath
Both Allopath & Non-Allopath
Trained
Untrained
68
150
113
Not properly
qualified, trained
Total
28
246
113
1
1
(A Group of 12 doctors own)
Trust Hospital
Non-Medical
Not Given_________________
Total
1
8
3
275
69
1
8
3
372
28
Purposes for sonography — Availability of data
One of the objectives of this study is to know the main purposes for which
sonographies are being carried out. This would be revealed by the survey. As far as the
availability of data is concerned, it is observed (Table 4.6) that in case of 21 centres, no
data were available, in 190 cases, data were available for both i.e. ANC and Non-ANC
purposes, in 100 cases only ANC data were available, while in 61 cases only non-ANC
data were available. The proportion of not getting any data was higher (6 percent) in case
of untrained owners compared to 3 percent for the trained owners. Similarly, the
proportion of the centres with non-ANC data available is much higher (16 percent) for
untrained owners compared to the trained owners (1-2 percent). This might be due to large
number of MSs/MDs among the 'untrained’ owners, needing sonographies only for other
non-ANC purposes, while the sample of trained owners is overweighed by gynaecologists,
needing sonographies for ANC purposes.
Table 4.6. Classification of centres by purposes on which data are available
Training status of the owner
Availability of data on
purposes of sonography
Trained
Untrained
Not properly
qualified/trained
Total
Percent
ANC
Non-ANC
Both ANC & Non-ANC
None_______________
Total
27
1
39
____ 2
69
5
68
15
45
5
146
______ 16 __________ 3
28
275
100
61
190
21
372
26.9
43
16.4
51.9
5.7
100.0
Another interesting information is provided in Table 4.7 which gives the data on
different kinds of problems for getting partial data. Out of a total of 100 cases, 53 cases
relate to sonography centres dealing with non-ANC cases only. Incidentally in this case, a
question arises as to why are these centres made to register under PNDT act? A serious
thought needs to be given.
Table 4.7. Classification of centres by reason for incomplete data
Reasons for incomplete data
No ANC cases and other data not available
Non-obstetric data not available/ maintained
Both ANC and non ANC data not available
Only pre surgery diagnosis/cardiac cases
Only last three months data available
Don’t keep records/ copies
Recently Started
Trimester-wise data not available
Only non-ANC cases are done
Under renovation
Total
Training Status o: ? the owner
Not properly
Trained Untrained
qualified/trained
5
2
1
7
2
9
8
1
2
4
1
3
6
1
1
8
1
30
7
1
7
74
19
Total
7
8
2
17
3
5
10
9
38
1
100
Annual Performance: Obstetric ultrasound sonography tests
The performance is reported for both last three months and last one year. Here we
analyse the annual performance for the year, July 2003 to June 2004. The performance can
be classified into obstetric sonographies and non-obstetric sonographies. It is observed that
63 centres owned by trained doctors have conducted about 20000 obstetric sonographies,
I
while the number of sonographies for centres with ‘untrained’ owner is 31000. The
average number of sonographies for the three categories of sonography centres is as
follows:
Obstetric sonography tests
Trained
Untrained
Average obstetric sonography tests
325.3
153.5
Not properly
qualified/trained
73.5
It is observed that the performance of centres with trained owner is more than
I
twice that of the centres with ‘untrained’ owner. The difference could be due to the
difference in the extent availability of the operator doctor, difference in the regional
composition etc... Before we look into the reasons, let us examine the situation regarding
non-obstetric cases. It is observed that the centres with trained owner have carried out
44
about 19000 sonographies, while the centres with untrained owners have carried out about
45000 sonographies. The averages are as given below.
Annual performance: non-obstetric ultrasound sonography tests
Non-obstetric sonography tests
Trained
Untrained
Average non-obstetric sonography tests
534.5
248.8
Not properly
qualified/trained
290.4
Here again we find that the centres with untrained owners lag behind the centres
with trained owners and the lag is of the order similar to that found for obstetric
sonographies. One would like to know about the proportion of obstetric cases carried out
by a centre. The above figures tell about the overall performance. It would be interesting
to know about the proportion of obstetric cases at centres which conduct both types of
sonographies. It is observed that it is about 50 percent for the ‘trained’ category of centres,
and 46 percent for the ‘untrained’ category of centres. If we consider the overall
performance it is observed that the centres with ‘trained’ owners are carrying out 2-3
sonographies per day, while the centres with ‘untrained’ owners are conducting only one
(or slightly more) sonography per day. Is it not an indication of the machine lying idle,
particularly for the centres with untrained owners? One could identify the reasons for the
lower performance. However, it should be remembered that reporting biases also exist.
Before coming to this conclusion, one could have a look at the distribution of the centres
by performance. Table 4.8 gives the data on obstetric cases and Table 4.9 gives the data on
non-obstetric cases. It is observed that out of 62 centres owned by trained persons, about
60 percent have reported annual obstetric performance less than 100, while the same
proportion for the centres with untrained persons is 80 percent. Similarly, for non-obstetric
sonographies, 48 percent of the centres of ‘trained’ category report annual non-obstetric
performance less than 100, while the same for ‘untrained’ category of centres is 33
percent. Thus, it is clear that for obstetric sonographies the lag between the averages is
reflected also in the distribution, while for non-obstetric cases the lag appears not due to
the overall distribution but mainly due to 4 centres showing abnormal performance (more
than 2000). This implies that the performance in obstetric sonographies depends upon the
ownership of the centre, while performance in non-obstetric sonographies is not sensitive
to the ownership.
45
Table 4.8 Classification of centres by number of obstetric sonography tests carried out
during July 2003-2004 by training status of the owner and trimester (Tl, T2, T3).
Number of
sonography
tests
0-24
25-49
50-74
75-99
100-199
200-399
400-599
600-799
800-1000
1000+
N.G._______
No. of centres
Average____
Median
Number of Centres
Trained
T1
23
19
6
3
8
2
1
1
T2
12
9
12
5
12
8
2
1
1
Untrained
T3
16
9
9
4
13
8
2
T1
131
32
12
7
9
3
T2
76
50
20
14
27
11
2
3
197
29.4
18.8
3
203
63.3
37.8
T3
88
44
19
12
27
9
3
1
63
73.1
36.2
62
142.7
70.8
62
123,0
66.7
Not properly
qualified/trained
T1
T2
T3
7
3
5
3
5
2
2
1
1
203
61.5
32.7
10
9
9
19.9
34.7
25.1
Not Calculated
Table 4.9 Classification of non-obstetric sonography tests carried out during July 20032004 by training status of the owner
r
Number of sonography
tests
0-24
25-49
50-99
100-299
300-499
500-1000
1000-2000
2000+
No. of centres
Average____
Median
Number of Centres
Trained
Untrained
Not properly
qualified/trained
4
3
12
7
4
5
2
4
41
534.5
121.4
33
12
20
61
30
1
3
6
5
21
5
182
248.8
142.6
18
290.4
Not Calculated
Coming back to the reasons for lower performance of centres with untrained
owner, we present here some information about the availability of doctors/operators at the
‘untrained’ category of centres.
Limited availability of the doctors at ‘untrained’ category of centres could be
directly examined by examining the frequency of visits of appointed doctors. However,
the question regarding this was not incorporated in the original questionnaire. During the
46
field work it was thought that this is an important information and hence a question was
added. For centres with trained owner, this question was not asked, assuming that the
services are available on daily basis. Because of the reason given above the information is
not available for the entire sample. However, the sample for which the information is
available is adequate (164 out of 277) enough. Table 4.10 gives the relevant data. It is
observed that only about 29 percent of centres have a daily visit, while about 11 percent of
the centres have one/two visits in a month. If we call less than thrice a week as rare visit,
it is about 45 percent of the centres have a rare visit of the operator.
Thus, lower
performance of the ‘untrained’ category of centres could be partly explained by the limited
availability of the facilities. Apart from the explanatory nature, one has to think about the
utility of such centres.
Table 4.10. Frequency of the operator’s visit for centres with untrained owner
Sr. No.
T”
2
3
4
5
6
7
8
Frequency of the operator’s visit
Daily
Five days in a week
Thrice in a week
Twice in a week
Once in a week
On call
Twice in a month
Once in a month_____________
Total
No. of centres
47
1
9
9
46
33
13
___________6
164
Percentage
28.66
0.61
5.49
5.49
28.05
20.12
7.93
3.66
100.00
Role of AYUSH doctors.
Earlier it was observed that the performance of the centres with untrained owner is
much lower in comparison to the centres with trained owner. Limited availability of
operator doctor and limited need of the hospitals are some of the reasons for lower
performance. In this context, it is worthwhile examining the performance of centres owned
by AYUSH doctors as against other allopathic doctors untrained in sonography. Table
4.11 gives the relevant information, for obstetric cases for the three trimesters. The median
performances of the two types of centres are given below.
Trimester
First
Second
Third
________________ Median Performance
Centres owned by AYUSH
Centres owned by allopathic
________ doctors________
____ untrained doctors
16.1
19.6
28.4
49.5
44.0
23.3
47
The figures clearly imply that among the centres run by untrained doctors, those
owned by AYUSH doctors have lower performance pointing towards the limited use of
centres owned by AYUSH doctors. Table 4.12 gives the distribution of non-obstetric
sonographies carried out in the centres owned by AYUSH and other non-allopathic
untrained doctors. There is significant difference between the median performances the
two categories of centres. Thus, if in future, the AYUSH doctors are permitted to operate
sonography machines, the performance of such centres is not going to contribute
significantly to the total sonography performance.
Another factor which could explain the differentials is the functional status of the
centre such as ‘attached to hospital’ or ‘independent centre’. Table 4.13 gives the
performance classified by training status of the owner and functional status of the centre.
Median performance of these centres classified by above-mentioned characteristics is
given below.
Functional and training status of the owner__________
Centre owned by trained person, attached to hospital
Centre owned by trained person, separate centres
Centre owned by untrained person, attached to hospital
Centre owned by untrained person, separate centres
Median Performance
156.5
750.0
156.0
300.0
The above figures clearly indicate that a separate centre owned by a trained person
has the highest performance, as explained. At the same time it is also revealed that the
lower performance of ‘untrained category’ is partly due to the fact they have higher
proportion of centres attached to hospitals and these centres have a lower performance.
Trimester-wise sonography tests at the level of the centre.
In the last section, the data on the performance regarding obstetric and nonobstetric sonographies were analysed on overall basis.
For instance, among obstetric
sonographies, the number of them earned out during the three trimesters were examined
for the entire sample of centres with trained and untrained owners.
It showed that,
compared to the second and third trimester, number of sonographies carried out during the
first trimester are smaller in proportion. According to the doctors, the sonography during
the second trimester enables them to identify for the first time, deformities if existing, in
the baby and hence is very essential. However, it should be remembered that it is this
sonography which also could detect the sex of the baby. The sonography during the third
48
Table 4.11.
doctors.
Classification of obstetric sonography tests by size and type of untrained
First Trimester
Number of obstetric
sonography tests
0-24
25-49
50-74
75-99
100-199
200-399
1000 +
Total
Median
__________________ Type of Doctor
Ayush/BAMS/BUMS/BHMS
Other Untrained
Number
Percent
Number
Percent
69
77.53
65
58.04
19.64
12.36
22
11
6.74
6
6
5.36
1.12
1
6
5.36
1.12
7.14
1
8
1.12
1.79
1
2
2.68
0
0.00
3
89
100.00
112
100.00
16.1
19.6
Total
134
33
12
7
9
3
3
201
Second Trimester
Number of obstetric
sonography tests
0-24
25-49
50-74
75-99
100-199
200-399
400-599
1000 +
Total
Median
__________________ Type of Doctor
Ayush/BAMS/BUMS/BHMS
Other Untrained
Number
Percent
Number
Percent
43
45.74
34
30.09
29
20.35
30.85
23
6
6.38
14
12.39
4
8.85
4.26
10
10
10.64
15.93
18
2
7.96
2.13
9
0
0.00
2
1.77
2.65
_____ 0
3
0.00
94
100
100
113
28.4
49.5
Total
77
52
20
14
28
11
2
3
207
Third Trimester
Number of obstetric
sonography tests
0-24
25-49
50-74
75-99
100-199
200-399
400-599
1000 +
Total
Median
__________________ Type of Doctor
Other Untrained
Ayush/BAMS/BUMS/BHMS
Percent
Number
Number
Percent
33.04
52
37
53.61
22.32
25
19
19.59
10.71
12
9
9.28
5.36
6
6
6.19
17.86
20
7
7.22
7.14
2.06
8
2
0.89
2
1
2.06
2.68
3
0.00
0
100.00
112
97
100.00
44.0
23.3
49
Total
89
44
21
12
27
10
209
Table 4.12. Classification of non-obstetric sonography tests done by untrained doctors by type
Number of
non-obstetric
sonography tests
0-24
25-49
50-74
75-99
100-199
200-399
400-599
600-799
800-999
1000+______
Total_________
Median
__________________ Type of Doctor
Ayush/BAMS/BUMS/BHMS ___
Others______
Number
Percent
Number_____ Percent
19
29.23
13
11.30
7
10.77
5
4.35
5
7.69
7
6.09
1
1.54
7
6.09
18
27.69
26
22.61
7
10.77
33
28.70
6
9.23
8
6.96
1
1.54
8
6.96
1
1.54
3
2.61
0
0.00
5
4,35
65
100.00
115
100.00
102.5
162.2
Total
32
12
12
8
44
40
14
9
4
5
180
Table 4.13 Classification of sonography tests by functional status and training status of the
owner
Number of sonography tests
Functional status of the centre
Attached to
Separate
Not Given
Hospital
UniVCentre
Total
Trained
0-24
25-49
50-99
100-299
300 - 499
500- 1000
1000-2000
2000 +
Total
3
2
7
23
6
5
3
1
50
1
4
1
5
2
4
17
0-24
25-49
50-99
100-299
300 - 499
500- 1000
1000-2000
_______________ Total_____
Not qualified and not properly
trained
32
22
35
72
30
19
9
219
8
5
6
8
7
15
5
54
0-24
25-49
50-99
100-299
300 - 499
500- 1000
Total
5
3
5
5
7
3
28
1
1
2
3
2
9
27
8
10
5
5
69
Untrained
2
2
42
27
41
80
37
34
14
275
5
3
5
5
7
3
28
50
trimester is to assess the growth of the baby.
If one wishes to examine whether the
sonographies are done timely, it could be better to examine the trimester-wise proportions
at the level of centre rather than on overall basis. Table 4.14 gives these the data for both
trained and untrained owners.
The medians for the percentage shares of the three
trimesters are as follows:
Training status of the
owner____________
Owner Trained
Owner Untrained
Trimester
II
42.1
41.2
I
20.1
16.0
III
35.0
39.4
There is no significant difference between the distributions of sonographies carried
by trained and untrained categories of centres. However, it should be remembered that the
medians are based on independently tabulated distribution of centres. The sonographies of
a centre during first/second/third are not analysed as a package. It may be interesting to
observe the patterns examined at the level of individual centres.
Since a three way
tabulation is a complicated exercise and since the performance during 2nd and 3rd trimester
are close to each other, we have presented the cross-classification of sonographies carried
out during 1st and 2nd trimester in table 4.15. If sonographies are done observing the proper
time-schedule, one would observe the diagonal cells in table 4.15 filled. However, in
absence of the proper time-schedule, one would observe figures not necessarily only in the
diagonal cells. The panel for trained owners shows mainly the diagonal cells filled with a
few exceptions. However, the panel for untrained owners shows the left triangle, and not
necessarily the diagonal, filled. These observations indicate that some of the untrained
owners have not followed the time-schedule properly. For instance, there are 13 centres
which have conducted less than 20 percent sonographies in the second trimester. As
mentioned previously, sonography in the second trimester is an important component in
antenatal case. This irregularity can also be assessed by looking at the trend of proportion
of sonographies carried out in the second semester against the rising proportion of
sonographies in the first trimester. If we locate the intervals with a median, they could
serve as the trend values. The last column of the table gives the medians in terms of
intervals.
Ideally, if proper time-schedule is observed, the medians should go down
against rising proportions of sonographies in the first trimester. First panel of the table for
trained owners shows that the trend is smooth. However, the trend for the centres with
untrained owners does not show a smooth trend. For instance, the median does not go
51
Table 4.14. Percent sonography testes done by training status of the owner and trimester
Training status of the owner______________
Not qualified and
Untrained
Trained
not properly trained
Percent sonographies done in first trimester
0-10
11-20
21-30
31-40
41-50
51-60
61-70
71-80
81-90
91-100
14
15
18
6
3
(24.1)
(25.9)
(31.0)
(10.3)
(5.2)
1
1
(1.7)
(1.7)
Total
58
(100.0)
58
50
31
21
7
3
3
1
(33.0)
(28.4)
(17.6)
(11.9)
(4.0)
(1.7)
(1.7)
(0.6)
2
(1-1)
176
Total
75
65
49
28
11
3
4
2
1
2
(31.3)
(27.1)
(20.4)
(H.7)
(4.6)
(1-3)
(1.7)
(0.8)
(0.4)
(0.8)
(100.0)
240
(100.0)
1
(12.5)
2
2
(25.0)
(25.0)
2
1
(25.0)
(12.5)
9
9
28
66
79
30
16
1
1
(3.7)
(3.7)
(11.5)
(27.0)
(32.4)
(12.3)
(6.6)
(2-0)
(0-4)
(0.4)
3
(50.0)
1
1
(16-7)
(16.7)
1
(16.7)
(100.0)
6
(3.9)
(3.9)
(10.7)
(27.5)
(33.7)
(12.4)
(6.2)
(1.7)
Percent sonographies done in Second trimester
0-10
11-20
21-30
31 -40
41-50
51-60
61-70
71-80
81-90
91 - 100
1
2
7
15
19
6
4
2
1
1
(1.7)
(3.4)
(12.1)
(25.9)
(32.8)
(10.3)
(6.9)
(3-4)
(1.7)
(1.7)
7
7
19
49
60
22
11
3
Total
58
(100.0)
178
(100.0)
8
(100.0)
244
(100.0)
(5.0)
(8.3)
(12.2)
(26.1)
(27.2)
(11-1)
(6.7)
(1-7)
(0.6)
(1.1)
1
1
3
(12.5)
(12.5)
(37.5)
1
2
(12.5)
(25.0)
12
22
36
64
61
27
14
3
1
3
(4.9)
(9.1)
(14.8
(26.3)
(25.1)
(H.l)
(5.8)
(1.2)
(0.4)
(1.2)
(100.0)
8
(100.0)
243
(100.0)
Percent sonographies done in Third trimester
2
(3.6)
(10.9)
(20.0)
(30.9)
(20.0)
(9.1)
(3.6)
1
(1-8)
9
15
22
47
49
20
12
3
1
2
55
(100.0)
180
0-10
11-20
21-30
31-40
41-50
51-60
61-70
71-80
81-90
91-100
2
6
11
17
11
Total
52
(table 4.15 is given as a separate document)
53
Table 4.15 Percent sonographies done in first trimester cross-classified by percent sonographies done in second trimester
Training Status of Owner
0-10
11-20
Percent Sonographies done in Second Trimester
21-30 31-40 41-50 51-60 61-70 71-80
81-90
91-100
Total
14
15
17
5
2
1
1
55
Median
Interval
Trained Owner
Percent Sonographies done in First
Trimester
0-10
11-20
21-30
31-40
41-50
61-70
71-80
Total
Untrained Owner
Percent Sonographies done in First
Trimester
0-10
11-20
21-30
31-40
41-50
51-60
61-70
71-80
91-100
Total
Not properly qualified/trained
Percent Sonographies done in First
Trimester
0-10
31-40
41-50
81-90
Total
NC: Not Calculated
2
2
2
4
2
1
1
2
10
3
3
7
5
2
15
17
6
4
2
1
1
10
8
13
9
3
17
22
10
5
3
12
5
2
1
4
4
3
1
1
1
57
20
11
3
1
1
3
2
1
1
2
3
1
1
2
1
1
1
1
2
7
6
1
6
5
4
3
1
1
1
1
16
1
44
2
1
1
1
1
I
1
2
1
1
60
40-50
30-40
30-40
20-30
NC
NC
53
46
30
20
7
3
2
1
2
164
40-50
40-50
40-50
30-40
30-40
10-20
20-30
NC
0-10
3
1
1
1
6
NC
NC
NC
NC
NC
down for the first three intervals (0-10, 10-20, 20-30), indicating the lack of observance of
proper time- schedule. One should bear in mind that whenever own clients are there, one
could expect observance of time-schedule, but in case of referrals, the observance would
depend upon the doctors referring the patient and not on the centre. However, in our
sample, majority of the centres (80 percent) are attached to hospitals and hence we can
very well expect that the distribution of obstetric sonographies should have somewhat
fixed pattern. Contrarily, we find that there is some kind of deviation from regularity as
far as the untrained owners are considered.
What could be the reasons for this
phenomenon? One reason could be in the lack of expertise on the part of the owner
reflected in lack of timeless in the schedule of antenatal sonographies for the patients.
Another reason could be traced in the emphasis of the ‘untrained’ owners mainly on nonobstetric cases. Whatever be the reasons, it is to be noted that the utilisation of the
sonography facility by the untrained owners lacks both in quantity and quality as far as the
obstetric cases are concerned.
Referrals by Allopathic and Non-allopathic (ISM & H) Doctors
In order to know the extent of referrals by allopathic and non-allopathic doctors, a
question was included in the questionnaire asking for whether the patients are referred or
are own clients and if they are referred, their classification by type of doctor referring the
patients. It is observed that during the last year 76513 sonographies were of own clients
while 63984 were referred cases. Fifty centres have reported the data on referrals while
285 centres have reported the data on own clients. It is observed that the overall
percentage of referrals by allopathic doctors is 77.85. For ‘trained’ category of centre, the
percentage is 84.50 while for ‘untrained’ category it is 70.14. The figures indicate that the
referrals by allopathic doctors are relatively lesser for the ‘untrained’ category centres.
However, as observed in Table 4.16 there are 15 out of 38 centres (untrained category),
where the percentage of allopathic doctors are about 70 percent. Since majority of
‘untrained’ category of centres are from non-corporation non-city areas and since the non
allopathic doctors mainly practice there, we find a higher amount of referrals from ISM &
H doctors for ‘untrained’ category of centres.
As far as ‘own clients’ are concerned, once again it is found that the numbers are
smaller for the untrained category of centres (Table 4.17). The reason mainly lies in the
54
small size of hospitals in non-corporation areas, where the ‘untrained’ category of centres
are mainly found.
Table 4.16. Percent referred by allopathic doctors
Percent referred by
allopathic doctors
0-10
21-30
31-40
41-50
51-60
61-70
71-80
81-90
91-100
Total
Training status of the owner
Trained
Untrained
2
2
6
4
7
1
4
2
7
2
5
5
3
12
38
Total
2
2
6
11
5
2
7
7
8
50
Table 4.17. Number of own clients by training status of owner
Number of own clients
0-100
101-200
201-300
301-400
401-500
501-600
601-700
701-800
801-900
Total
Training status of the owner
Not properly
Trained
Untrained
qualified/trained
11
86
8
11
53
4
12
23
2
4
23
4
5
9
2
2
1
3
7
6
5
1
213
49
1
2
23
Total
105
68
37
31
16
9
8
10
1
285
Some observations about the maintenance of records, sending reports, supervisory
visits etc.
Along with the questionnaire administered to the centres, we also had prepared one
check-list in order to assess the observance of provisions of PNDT act in administrative
matters. The following extract gives some observations to start with.
The violation of the Act seems to be maximum in case of maintaining the records.
It is to be noted that majority of the doctors had not kept the copies of the form ‘F’ which
55
reveals the performance and form ‘G’ which is a consent form. In fact according to section
29 of the act, ‘All records, charts, forms, reports, consent under this Act and they shall be
preserved for a period of two years or for such period as may be prescribed?
Sometimes our field team had to scan through the original papers and in some
cases information was not at all available. In some cases data on obstetric cases only were
maintained. In short, the system of data maintenance needs some improvement.
Observance of provisions of PNDT act by the centres
No
Yes
Sonography centre functions in the same registered place
Change of place intimated to authorities
11
2
361
9
Operator is same as reported at the time registration
Change of operator intimated to authorities
43
15
329
28
Centres maintains form ‘F’
Centres maintains form ‘G’
62
62
303
303
43
318
.■5
Centres sends monthly report regularly
Supervisory visit by the Appropriate Authorities
Lastly, the information on supervisory visit of the appropriate authorities needs an
examination in order to evaluate the role of the authorities. Table 4.18 gives the data. It is
surprising to observe that in 66 cases, i.e. in about 18 percent of the cases, the visit was
rare, in 36 i.e. about 10 percent cases, no visit was paid, in 50 cases (i.e. about 13 percent),
the visit was paid once in six months and in six cases, it was once a year. In short in case
of 45 percent of the centres only, supervisory visits were somewhat regular. The regularity
of frequency of visits does not change according to the status of ownership. However, as
per the observations of our field team, the supervision in the corporation areas was better
than that in the non-corporation areas. It was told that conveyance charges for supervisory
visits are not reimbursed. But, this could be a stray observation. Whatever the reasons, the
fact remains that, supervision is not regular and strict and hence the authorities need to
give a serious thought to the same.
56
Table 4.18
Frequency of Supervisory Visit by Appropriate Authority
Frequency of supervisory visit
by Appropriate Authority
Never visited
Rare visit
Not a single visit since one
year/date of registration
Once in a year
Once in a six months
Once in three/four months
Once in two months
Once in a month
Frequent visit
Not Applicable
Not Given
Training Status of the Owner
Trained
Untrained
16
2
46
27
3
1
Not qualified and
not Properly Trained
4
6
4
37
6
8
16
12
2
33
5
33
1
7
1
7
1
1
66
24
3
1
Total
2
66
36
6
50
42
89
37
6
1
38
Findings on the opinions of the AYUSH doctors desirous of having the sonography
machine
As mentioned in the introductory chapter, it was proposed to contact 50-100
doctors, unqualified at the moment, but desirous of having the sonography machine.
Again as mentioned earlier in this chapter, it was impossible to get a proper sampling
frame for this category of respondents. Further, although the study was proposed for both
non-allopathic and allopathic doctors, we thought that for allopathic doctors, the training
facilities are available and hence they have no difficulty in translating their desires into
action.
The real problem is with the non-allopaths.
Therefore, we tried to use the
sampling frame for non-allopaths, which was available with Pune branch of NIMA. In all
100 doctors were contacted, either through a letter, actual visit or a telephonic call.
Out
of these, in 32 cases, there was no response, 53 doctors showed interest, while 15 of them
were not interested in having the machine, thus, leading to an extent of 72 percent
willingness to use the sonography machine. A few details about these doctors are given
below in Table 4.19.
It appears from the table that although the proportion of desirous doctors is good
enough, the other aspects are not that encouraging. For instance, only one-third of the
respondents intend to operate the machine by themselves.
Further, their use also is
limited. Nearly half of the respondents have referred only 17-18 cases per month. It is
57
generally observed that doctors of hospitals with larger bed-strength seem to refer cases in
large numbers. Although, these findings are based on a small sample, they do indicate that
hospitals with adequate bed strength only could utilise the machine properly.
Table 4.19. AYUSH doctors desirous of having the sonography machine
AYUSH doctors desirous of having the
sonography machine
Number
Percent
Willing to have sonography machine
Yes
No
38
15
71.7
28.3
Type of attachment
Hospital
Dispensary
N.G.
44
7
2
83.0
13.2
3.8
Mode of operation
Self
Operator
Both
17
21
15
32.1
39.6
28.3
Cases referred during last three months
0-49
50-99
100-149
150-199
200+
N.G.
24
8
6
3
1
11
45.3
15.1
11.3
5.7
1.9
20.8
Purpose of use
Obstetric
Non-obstetric
Both
Not Given
10
5
36
2
18.9
9.4
67.9
3.8
I Total
53
100.0
58
Chapter V
Summary and Recommendations
The Ministry of Health and Family Welfare (MOHFW) has assigned us the present
study and we got a good opportunity to examine the situation, although in a small way,
regarding a currently most important issue of tremendous expansion of sonography centres
and its consequences. There is an additional dimension to this study. The organisations of
doctors of non-allopathic medicine were constantly demanding permission, from
MOHFW, to use the sonography facilities. At present they are not allowed to use the
machine under the PNDT Act. They have to appoint a sonologist for their clinics. The
organisations of non-allpathic doctors have been negotiating with MOHFW on the
grounds of a Government Resolution which allows them to use modem testing procedures.
They also argue that since in interior areas, more than the allopathic doctors, these doctors
are practicing in large numbers and hence if the rural populace is to benefit from modem
medical procedures, the non-allopathic doctors should be permitted to use the sonography
machine, may be after undergoing training in sonography.
As a consequence of these persistent demands, the MOHFW decided to obtain the
information about the current use of sonography machines by untrained doctors, mainly
consisting of non-allopaths and the main purpose for which sonography is being carried
out. Subsequently, a meeting of the representatives of the Population Research Centre was
held at the MOHFW and the present study was assigned to PRCs of selected states, where
the number of sonography machines was adequate. This chapter presents the summary and
the recommendations of the study.
Distribution of ultrasound sonography centres in Maharashtra
As on September 30, 2004, Maharashtra had 4345 ultrasound sonography clinics/centres
in the entire state. These centres are unevenly distributed in the 35 districts of the state.
Maharashtra has eight health circles. More than three fourth of the centres (78 percent) are
registered in just four health circles (Mumbai, Pune, Nashik and Kolhapur circles) or in 16
districts located in the contiguous region of western Maharashtra. It means that 78 percent
of the sonography centres are located in just 46 percent of the districts of the state, a
highly concentrated distribution. The remaining 22 percent of the sonography centres are
59
08862
p
evenly distributed (5 to 6 percent) in rest of the four health circles (Nagpur, Akola,
Aurangabad and Latur circles) located in central and eastern parts of Maharashtra.
The concentration of sonography centres in the bigger cities of Maharashtra is very high.
In the state as a whole, half of the sonography centres are located within the Municipal
Corporation limits. Further, just six districts of the state have half (49.8 percent) of the
sonography centres and all these districts come from western Maharashtra. It is a clear
indication of a combination of higher aspirations of sonologists and higher capacity to pay
on the part of the people. The population share of these six districts in the state is 38
percent. In 14 districts of the state the number of centres is more than 100 and 82 percent
of the centres in the state is located in these 14 districts itself. The population share of
these 14 districts is 64 percent in the state. In all these districts the percent of sonography
centres is higher than the percentage share of population in the state.
All the districts in the central and eastern region of the state have less percentage of
sonography centres than their population share. The districts with more than 100
sonography centres are distinctly having lower child sex ratio than the districts with less
than 100 sonography centres. The mean sex ratio for the districts with more than 100
sonography centres is 901 and for the districts with less than 100 sonography centres it is
937. This is a rough indication of higher availability of sonography centres and the decline
in child sex ratio. Gadchiroli district with the smallest number of sonography centres (five)
has the highest child sex ratio (974) in the state. Further, four districts, Gadchiroli,
Gondiya, Nandurbar and Bhandara, with less number of sonography centres (less than 20)
are having better child sex ratio (958 and above).
Type of sonography centres
Sonography centres are registered under different categories in the state. However,
most of these centres (63 percent) are registered as Ultrasound Clinic. Eighteen percent of
centres are registered as Genetic Clinic. Ultrasound Clinic and Genetic Clinic together
account for 81 percent of the centres in the state. Only very small percentage of the centres
is registered as Genetic Laboratory/Genetic Counselling Centre (1.8 percent). Thirteen
percent of the centres are registered as Private Hospital. For nearly five percent of the
centres the information was not provided by the District Appropriate Authorities. It
appears that the Appropriate Authorities did not pay much attention at the time of
60
registration to classify the centres in the proper way. Hence these classifications are not
revealing the exact nature of the centres. With our field-work experience for the study, we
feel that Ultrasound Clinic and Genetic Clinic are basically same and are popularly known
as Ultrasound Sonography Centres or USGs.
Qualifications of the doctors/persons registered the ultrasound sonography centres
As per the PNDT Act any untrained persons in sonography can register an
ultrasound clinic provided that the person who operates the machine must have the
necessary training in conducting the test. One third of the doctors/persons registered the
centres are Gynaecologists. Radiologists/Ultrasonologists have registered 21 percent of the
centres. Four percent of the centres are registered by MBBS doctors with training or
experience in conducting sonography. These four categories together (Gynaecologists;
Radiologissts / Ultrasonologists; MBBS doctor with training or experience) account for
the 58 percent of the centres and can be considered as trained doctors/persons in
ultrasound sonography.
Doctors specialised in various other fields (Gastroenterologist, Cardiologist, ENT
specialist, Orthopaedics, M.D. Medicine etc. and Non-Medical Personnel) registered
nearly 11 percent of the centres. Six percent of the centres are registered by the
persons/doctors qualified in Indian system of medicine (AYUSH). Ten percent of the
sonography centres are registered in Trust/Govemment Hospitals. The District
Appropriate Authorities did not provide the qualification of the registered persons for 13
percent of the centres.
Qualifications of the operators of the ultrasound sonography machines
As per the PNDT Act the person who operates the sonography machine must have
the necessary qualification/training/experience to conduct the sonography tests. In the state
as whole, 63 percent of the centres are ‘self operated’ i.e., owner himself operates the
machine. The remaining 37 percent of the centres are owned by the persons who have
employed the qualified persons to operate the machine. It means that the majority of the
sonography centres in the state are registered/owned by the doctors/persons trained in
conducting ultrasound sonography.
61
Among the centres owned by the trained doctors forty-four percent of the doctors
are gynaecologists and one-third of them are radiologists/ultrasonologists. Gynaecologists
and radiologists/ultrasonologists together dominate (76 percent) the ownership of trained
“self operated” centres. Five percent of the trained owners are MBBS doctors with some
training/experience in conducting sonography. Nearly 10 percent of the machines are
owned by “other” doctors (other than gynaecologist and radiologists). The qualifications
of the doctors in the centres owned by the trained doctors reveal that 81 percent of the
sonography machines are operated by gynaecologists, radiologists/ultrasonologists and
MBBS doctors with some training/experience in conducting sonography
The qualifications of the doctors using the sonography machines in the centres
owned by the untrained doctors/persons (employing other doctors) reveal that, in three-
fourth of these centres radiologists/ultrasonologists operate the machines. Another sixteen
percent of the centres have employed the Gynaecologist for operating the machine
Radiologists and Gynaecologists together operate the machine in 90 percent of the centres
owned by the untrained doctors/persons. Four percent of the operators are “other” doctors
and two percent are MBBS doctors with qualification/experience in operating sonography
machines. For the remaining four percent of the centres we did not get the qualification of
the doctors.
Qualifications of the persons using the sonography machines in the centres owned
by trained and untrained persons reveals the following: (i) in the centres owned by the
trained persons gynaecologist own large number of centres (44 percent) compared to the
doctors with other qualifications; and (ii) in the centres owned by the untrained persons
the radiologists/ultrasonologist are mainly (75 percent) employed to operate the sonography
machine.
District-wise sonography centres owned by trained and untrained doctors/persons
Analysis of district-wise qualifications of the owners of the sonography centres reveals
the following: (1) the sonography centres owned by the untrained persons are much higher in
western Maharashtra compared to the other parts of the state; (2) the centres owned by the
persons specialised in Indian System of Medicine (AYUSH) is also higher in western
Maharashtra compared to the other regions of the state; (3) almost all the centres owned by the
AYUSH doctors are located exclusively in western Maharashtra; (4) in the areas falling under
62
the municipal corporation limits, majority of the sonography centres are mainly owned by the
framed doctors; (5) AYUSH doctors mainly own their sonography centres outside of the
municipal corporation areas i.e., AYUSH doctors exclusively operate in the smaller towns and
interior areas of the districts; (6) sonography centres located in central and eastern parts of
Maharashtra are mainly owned by the trained doctors and even among the centres owned by
the unframed persons, allopath doctors own most of the centres compared to the AYUSH
doctors; and (7) very few AYUSH doctors own a sonography centres in central and eastern
parts of Maharashtra.
Multiple attachments of sonologists
Some sonologists are attached to more than one ultrasound centres. Either they
carry their own mobile ultrasound machine or they use the fixed machine owned by the
owner of the centre. This system effectively increases the number and spread of the
registered centres m an area/region. It is observed that 46 doctors, in the state as a whole,
are attached to 303 centres with an average of 6.6 attachments per doctor. The average
vanes between the districts/corporations. It is also observed that such multiple attachments
are more common in the corporation areas.
The sex ratio of child population in Maharashtra
In Maharashtra, the child sex ratio has declined by 29 points from 946 in 1991 to
917 in 2001. It is not only much lower than the universal sex ratio at birth (943-952), it is
also much lower than those for the all four south Indian states (Kerala 963, Andhra
Pradesh 964, Karnataka 949 and Tamil Nadu 939) and Madhya Pradesh (931). Child sex
ratio in the districts of Maharashtra varies between 974 in Gadchiroli and 850 in Sangli.
The districts with higher sex ratio mainly come from central and eastern regions of
Maharashtra and most of the low sex ratio districts come from Western regions of the
state. Mainly the prosperous districts/areas of Maharashtra have worst sex ratios e.g.,
Sangli (850), Kolhapur (859), Jalgaon (867), Aurangabad (884), Satara (884),
Ahmadnagar (890), Solapur (897), Seed (898), Mumbai (898), Pune (906) and Dhule
(907). The sex ratio of children in the entire Pune region is very much unfavourable to
females (below 900). On the contrary, the backward/tnbal districts like Gadchiroli (974),
Nandurbar (966), Gondiya (964) and Bhandara (958) have higher sex ratios in the state.
63
The child sex ratio in urban areas of Maharashtra (908) is 15 points lower than in
rural areas (923). In 15 districts of the state the urban sex ratio is 25 points lower than the
rural sex ratio. Rural sex ratio is above 943 in 15 districts (46 percent) whereas only in two
districts (6 percent) the urban sex ratio is above 943. It means that the imbalance of female
children in urban areas is prevailing throughout the state. The child sex ratio in rural areas
is below 900 in one-fourth of the districts whereas in 40 percent of the districts the urban
sex ratio is below 900. The child sex ratio for the 15 Municipal Corporations of the state is
910, which is lower than the child sex ratio for the entire state (917) and much lower than
the child sex ratio for rural areas of the state (923).
Decline in child sex ratio between 1991 and 2001
Decline in child sex ratio from 1991 to 2001 shows that every single district had
experienced a decline except one (Akola) where it increased by 7 points. The extent of
decline is more than 40 points in 8 districts and in all these districts sex ratio is below 900.
The developed districts of the state had experienced higher magnitude of decline
compared to the less developed districts.
Sex ratio of child population in the tehsils of Maharashtra
Out of 353 tehsils in the state only in 37 percent of the tehsils, the child sex ratio is
IS
in the normal range of 943 and above. In the remaining tehsils it is below 943 and in one-
fourth of the tehsils it is below 900. The sex ratios of the rural and urban areas of the
tehsils reveal a shocking picture for urban areas. In 41 percent of the tehsils the rural sex
ratio is 943 and above whereas only in 17 percent of the thesils the urban sex ratio is
above this level. In half of the tehsils the urban sex ratio is below 900. The sex ratio of
child population in the urban areas of the tehsils reveals that not only the sex ratio is lower
in urban areas of the state it is lower even in smaller towns in most parts of the state.
The association between the number of sonography centres and the child sex ratio at
the district, corporation and tehsil levels.
It is generally believed that the recent sharp decline in child sex ratio is a result of
the rapid spread in the availability and use of the ultrasound sonography for sex
determination. This association is tested with the data we have collected for the study on
number of sonography centres at the district level. The correlation coefficients between the
number of sonography centres in the district and child sex ratios in the district (total, rural
64
and urban) are negative and significant at one percent level - a very clear negative
association between the availability of sonography centres and child sex ratios in
Maharashtra. The sex ratio of the child population in Maharashtra has declined by 29
points from 946 in 1991 to 917 in 2001. During this decade the sonography centres have
mushroomed m many parts of the country including Maharashtra. The correlation between
the number of sonography centres and decline in child sex ratio is positive and statistically
significant at one percent level i.e., higher the number of sonography centres in the
districts higher the decline in child sex ratio in the districts.
The alternate variable, the number of sonography centres per 1000 population (as
per the population in 2001) in a district helps us to capture number of centres in proportion
to its population size. The correlation between number of centres per 1000 population in
the districts and child sex ratio is negative and significant at one percent level for total,
rural and urban areas. Similarly, the same variable has a significant positive correlation
with decline in child sex ratio from 1991-2001. The number of centres per 1000
population is also negatively associated with the child sex ratios in the municipal
corporations at one percent level of significance. Tehsil level data also broadly indicate
that the higher availability of sonography centres at the tehsil level has a negative impact
on the child sex ratio of the tehsils. The tehsils with very high sex ratios in the state are
having a less number of sonography centres whereas the tehsils with the lowest sex ratios
in the state are having higher number of sonography centres.
We have done the bivariate regression analysis by taking the child sex ratio
variables (child sex ratio and decline in child sex ratio between 1991 and 2001) as the
dependent variables and availability of sonography centres (number of sonography centres
and number of sonography centres per 1000 population) as the independent variables.
Number of sonography centres and child sex ratio
The regression analysis shows that the effect of number of sonography centres on
child sex ratio is negative and statistically significant at one percent level. This single
independent variable alone explains 43 percent of variance in child sex ratio. Similarly, the
number of sonography centres per 1000 population exerts a significant negative influence
on the child sex ratio at the district level. The explanatory power of this variable on child
sex ratio is greater than the earlier variable. Centres per 1000 population explains nearly
65
half (R2: 48 percent) of the variance in child sex ratio. The relationship between the
number of centres per 1000 population in MCs and child sex ratio in MCs is significantly
negative. The regression analysis shows that the two variables representing the availability
of the sonography centres significantly reduce the child sex ratio at the district level in
Maharashtra.
Number of sonography centres and decline in child sex ratio between 1991 and 2001
The relationship between the number of sonography centres and the decline in sex
ratio is positive at one percent level of significance i.e., the increase in sonography centres
has significantly increased the extent of decline in child sex ratio in Maharashtra. Thirty
seven percent of variance in the decline in child sex ratio is explained by the number of
sonography centres. The regression result for the effect of number of centres per 1000
population on the decline in sex ratio is also positive and significant at one percent level.
This regression explains the 35 percent variance in decline in sex ratio in the state. The
correlation and regression analyses at the different levels of aggregation (districts,
corporations and tehsils) confirm the negative relationship between the availability of
sonography centres and child sex ratio in Maharashtra. The analyses also indicate that the
further increase and spread in the availability • of sonography centres in the
districts/corporations will contribute for the further decline in sex ratio. The sex ratios in
Maharashtra and MCs are already very low at the level of 917 and 910 female children per
1000 male children respectively.
Findings of the survey of ultrasound sonography centres
The survey was carried out in 372 sonography centres during August - November
2004. The questionnaire supplied by the MOHFW was canvassed for the survey and it
contained questions on type of machine, registration number, qualification of the operator,
number of referrals by both allopathic and non-allopathic doctors, the purpose
(obstetric/non-obstetric) of sonography, the classification of obstetric sonographies by
trimesters, etc.
With a purpose of assessment of observance of PNDT act, we had
prepared a check-list about maintenance of records, sending timely reports, supervisory
visits, etc. In all, the survey was conducted in 69 sonography centres owned by the trained
doctors/persons, 275 centres owned by untrained persons and another 28 centres owned by
‘not properly trained/qualified persons’.
66
Although, the prescribed objectives of the survey and the questionnaire did not
contain anything related to sex-determination, we have analysed the available data to look
for the relationship of sonography centres and the significant declines in child sex-ratios in
selected districts of Maharashtra. During the survey, one could not ask openly about the
sex-determination tests, since there is a ban on the same. However, we used to address a
simple question, ‘Do couples come to you asking for the sex-determination?’ and the reply
always would be, “Yes, they come, but I do not do the test. There are many, who do the
tests . This indirectly hints at the possibility of sex-determination tests being carried out in
non-negligible proportion.
The information regarding type of machine, cost of machine, performance, referral
etc. enabled us to have an assessment about the functioning of the sonography centres.
Type of machine and cost of machine tell us about the investment incurred by the owners.
It is observed that 80 percent of the owners have a fixed machine. Only 12 percent are
using the mobile machine. Although, a small proportion, its variation between ‘trained’
and ‘untrained’ category of centres provides an interesting observation. For ‘trained’
centres, it is just 7 percent, which increases to 25 percent for ‘untrained’ centres,
indicating the untrained owners’ tendency to make use of the ‘mobile’ facility in absence
of capacity to invest. In this context, it is further more interesting to observe the trend in
‘ untrained ownership ’.
The data on year of installation’ show that the untrained ownership has increased
remarkably after 2002. It means that these people must be operating even before
registration and new people must have taken the benefit of the ‘mobile’ facility and
registration with the help of an appointed person. For untrained owners, many of them
being AYUSH doctors with limited earnings, the cost of machine could be unaffordable
and hence the ‘mobile’ facility becomes helpful. At the same time, those ‘untrained’
owners, who have bought the machines at the rate of 5-6 lakhs must have done so, looking
to the treatment benefits and monetary benefits emerging from this investment. It should
be noted down that 40 percent of the sample of ‘untrained owners’ came from AYUSH
systems of medicine. The returns to this investment would be substantial if the utilisation
of the machine is adequate enough. In this context it is necessary to examine the data on
performance of these centres.
67
Performance of the Centre is collected in terms of both obstetric (three trimesters)
and non-obstetric cases. It is observed that 63 ‘trained’ centres have carried out on an
average 620 sonographies in an year, while the performance of untrained centres is 380 in
an year. Assuming 300 working days in an year, the average turns out to be around 2 for
trained’ centre and around ‘one’ for untrained centres. Is it not an indication of ‘under
utilised capacity’? Yes, if the figures are to be believed. In fact the experience of our field
team does not suggest such low averages. For ‘untrained’ centres, there are reasons to
believe in the reported figures for example limited availability of operators, majority of the
centres being attached to hospitals and hospitals having limited needs and dominance of
AYUSH doctors with still lower needs of sonography facility. However, what about the
trained’ centres? Attachment to a hospital has affected this category of centres also. Our
actual field experience and our expectation lead us to conclude that the performance is
underreported. Then the question arises, ‘what could be the reason for underreporting?
Does it smell of ‘sex-determination cases’? It seems plausible, because by not reporting,
chance of getting caught is nil and with exorbitant fees for the same, the centre runs in
spite of inadequate performance. One remark by a busy sonologist is worth noting down.
While discussing about sex-determination he said, “Sometimes, when a women with 3-4
daughters comes to me asking for sex-determination, Lam tempted to satisfy her demand.
However, I know that, if I do it, I shall not be able to have a sound sleep and as far as
money is concerned, why should I do it for money? For a simple case of ‘Thrombosis’. I
get Rs. 1000. Why should I bother? But I know, there are many doctors, who are doing
sex-determination”. The money mindedness has overpowered the moral values. Less said
the better.
Improvement in obstetric care is one of the significant advantages of sonography.
A number of gynaecologists reported that sonography has brought revolution in the
treatment of the pregnant women. They themselves wonder as to ‘how they could treat
pregnancy-related problems when sonography did not exist’. If the doctors do this
religiously, one is willing to accept the possible impact of the sonography facility. How to
test this? One way is to examine observance of some broad norms regarding the
sonographies in the three trimesters. It is understood that there is no norm regarding the
number of sonographies needed during pregnancy. It depends upon the need of the case.
However, we came to know that sonography in the second trimester is essential, since it,
for the first time, reveals deformities, if any, with the foetus. Similarly, sonography during
'
68
the third trimester reveals the growth of the baby and retardation, if any. Generally, the
first trimester sonographies are relatively less in proportion. Assuming that there should be
some time-schedule in carrying out obstetric sonographies, we tried to examine the
schedule followed by the centres and we observed that the sonographies carried out by the
‘untrained’ category of centres do not follow the time-schedule. Thus, the centre with
‘untrained’ owner fails both in quantity and quality.
In order to assess the need of the centres of different type, a question was
addressed about the referrals by allopathic/ non-allopathic doctors. As expected, more than
three-fourths of the referrals are by allopaths. Further, It is observed that for centres with
untrained owner, the proportion of referrals from allopathic doctors is slightly lower (70
percent). This indicates that particularly, the AYUSH doctors still not that conversant with
the utility of sonography and hence do not refer patients for sonography. This
phenomenon is also reflected in the responses of 53 AYUSH doctors desirous of using the
machine. Only one-third of them want to use the machine by themselves. They have on an
average referred only 17-18 cases per month. In short, it appears that those who were
negotiating with MOHFW were the selective ones. Community of AYUSH doctors as a
whole does not seem to be that keen on having the facility.
As mentioned in the main text, we had attached a check-list along with the
questionnaire in order to assess the observance of the PNDT act. There are few lapses in
some matters. But the worst situation is about the maintenance of records. Nearly 15
percent of the centres have failed in this. Similarly, at the level of Appropriate Authorities,
the lapses are observed and they are more serious. In only 45 percent of the cases, the
supervisory visits are regular.
Private doctors have literally no check. PNDT act is one such tool to have a check.
If it is implemented properly, misuse of sonography could be avoided and the doctors will
not be able to use it only as a money-making machine.
Recommendations
1. An important finding has emerged from this study.
There is a strong correlation
between availability of sonography centres and decline in child sex-ratio during 1991-
2001. This is a clear revelation of the sex-determination tests being carried out in spite
69
of the PNDT Act, 1994. It is further observed that the districts with sharp declines in
the child sex-ratio and higher availability of sonography are mainly from Western
Maharashtra, particularly, the sugar-belt of Pune division. Clearly, the declining sex
ratio is the consequence of availability of sonography centres, persistent sonpreference and capacity to pay. As the well-known demographer- Dr. Ashish Bose-
has said, ‘The unholy alliance between tradition (son-complex) and technology
(ultrasound sonography) has played havoc in Indian society. One recommendation,
naturally emerging from this type of scenario is “stop the expansion of sonography
centres”. However, this may not be a practical suggestion. One way-out could be a
recommendation in terms of disallowing registration to an untrained owner (AYUSH
doctors or MBBS doctors with no experience or training). Further, it is also suggested
that expansion in Western Maharashtra should be discouraged. Our study has observed
that the performance of centres with untrained owners is quite low - one sonography a
day - implying that there is ample idle capacity. In this connection, one thinks that
there is no need of increasing this idle capacity.
2. The ‘F’ Form supposed to be submitted by the centres has a column on sex
composition of the children. The data should be analysed along with the information
on MTPs. It would definitely help identifying centres where sex-determination tests
are being carried out.
3. Column on owner’s qualification should be added to the application form. In absence
of this it becomes difficult to assess the extent of untrained ownership.
4. Our study has pointed out to the lapses in supervision.
The condition in non-
corporation areas is worse. Appropriate Authorities should look into it seriously.
5. In spite of the provisions in the act, records are not maintained by the doctors. The
Authorities should appraise the doctor about the legal provisions.
6. We have doubt about the reporting of performance. Appropriate Authorities have to
have some machinery to avoid underreporting. From the point of view of utilisation of
the machine, new machines should not be allowed, if the performance is poor.
70
7. There should be standardisation in training. Sometimes registration is given on the
basis of a certificate given by some doctor.
8.
The functioning of doctors with multiple attachments should be carefully examined.
Sometimes this attachment could only be for completing the formality for registration.
9. The centres owned by cardiologists, logically, should not come under PNDT act. A
serious thought needs to be given.
10. In spite of the PNDT Act, there is evidence of sex-determination test being carried out.
This makes us think about the supervision, not only in quantitative terms, but also
about ‘who should supervise?’ A slight doubt arises regarding the supervision of a
doctor by doctor only.
11. Our study does not come out with any finding, which is favourable for AYUSH
doctors. Therefore, the authorities should think twice before allowing them to use the
facility.
************
71
References
Arnold, A., S. Kishor and T.K. Roy. 2002. Sex selective abortions in India. Population
and Development Review. 28(4): 759-785.
Bhat, M. 2002. On the trail of ‘missing’ Indian females: I Search for clues. Economic
Political Weekly, December 21, pp. 5106-5118
Bhat, M. 2002. On the trail of‘missing’ Indian females: II. Illusion and Reality. Economic
Political Weekly, December 28, pp. 5244-5263.
Director of Census Operations. 2001. Census of India 2001, Provisional Population
Totals, Maharashtra. Series 28, Paper 1 of 2001. Mumbai: Director of Census
Operations.
Director of Census Operations. 2001. Census of India 2001, Provisional Population
Totals: Rural Urban Distribution of Population, Maharashtra. Series 28, Paper 2
of 2001. Mumbai: Director of Census Operations.
International Institute for Population Sciences (UPS). 1995. National Family Health
Survey (MCH and Family Planning), India 1992-93. Mumbai: UPS.
International Institute for Population Sciences (UPS) and ORC Macro. 2002. National
Family Health Survey (NFHS-2). India 1998-99. Mumbai: UPS
Kulkami, S. 2001. Situational analysis of Maharashtra on population stabilisation and
related development issues: some areas of concern. Paper presented at the "State
level conference on health, development and population stabilisation issues in
Maharashtra”, organised by the Population Foundation of India during October 45, 2001 at Yashwantrao Chavan Academy of Development Administration, Pune.
Parasuraman, S. 2001. Declining sex ratio of the child population in India. News Letter of
the International Institute for Population Sciences, 42(3&4):29-39.
Premi, M.K 2001. The missing girl child. Economic and Political Weekly, 36(20): 18751880.
Retherford, R D. and T.K. Roy. 2003. Factors affecting sex-selective abortion in India and
17 major states. National Family Health Survey Subject Reports. Number 21.
Mumbai: International Institute for Population Sciences and Hawaii: East-West
Centre.
Appendix I : Map showing the distribution of sonography centres in Maharashtra
Appendix II
Data used for the analysis in Chapter 3
Districts
Gadchiroli
Nandurbar
Gondia
Bhandara
Ratnagiri
Nagpur
Amarawati
Sindhudurg
Chandrapur
Nanded
Raigarh
Yavatmal
Akola
Nashik
Hingoli
Wardha
Thane
Osmanabad
Parbhani
Latur
Washim
Mumbai (Suburb)
Buldana
Jalna
Dhule
Pune
Bid
Mumbai
Solapur
Ahmadnagar
Aurangabad
Satara
Jalgaon
Kolhapur
I Sangli
Child sex
ratio, 1991
Child sex
ratio, 2001
980
977
978
964
961
951
950
963
965
960
961
961
929
954
953
952
952
947
956
947
941
930
945
951
947
943
939
942
935
949
933
941
925
931
924
974
966
964
958
954
949
947
946
944
944
943
942
936
936
935
934
933
927
926
923
921
919
915
914
907
906
898
898
897
890
884
884
867
859
850
Decline in
sex ratio.
1991-2001
Number of
sonography
centres
-6
-11
-14
-6
5
15
10
19
56
190
76
47
29
65
106
37
64
213
12
23
426
27
36
67
14
546
47
34
54
481
61
287
174
211
147
209
163
211
183
-3
-17
-21
-16
-18
-19
+7
-18
-18
-18
-19
-20
-30
-24
-20
-11
-30
-37
-40
-37
-41
-44
-38
-59
-49
-57
-58
-72
-74
No. of
sonography
centres per 1000
_____ population
0.005
0.011
0.008
0.016
0.027
0.046
0.029
0.045
0.013
0.023
0.047
0.016
0.039
0.041
0.012
0.019
0.052
0.018
0.024
0.032
0.013
0.063
0.021
0.022
0.032
0.067
0.028
0.086
0.044
0.052
0.050
0.075
0.044
0.060
0.097
I
rage i 01
Print
[
Click here to close this window
.J
Features
Female foeticide: The collusion of the medical establishment
By Lalitha Sridhar
The PCPNDT Act prohibits sex selection by any means, before or after conception. But, as one
survey in Chennai of 29 ultrasound clinics found, for the medical fraternity it’s business as usual
“Women patronise scan centres; they want to know the sex of the child. So many of them come
without any pressure from their husbands or mothers-in-law. Doctors who promote scanning to
determine the sex of the foetus are only fulfilling a demand in society.” So says Dr K R
Balasubramaniam, president of the Tamil Nadu Medical Council. His blatant defence is only one
aspect of the collusion between the medical lobby and Indian legislators in not preventing the
death of that most vulnerable being in India - the female foetus.
The Pre-Conception and Pre-Natal Diagnostic Techniques (Prohibition of Sex Selection) Act and
Rules 1994 (as amended up to 2002) (the PCPNDT Act) mandates that sex selection by any
person, by any means, before or after conception, is prohibited. Then there is the legally binding
Code of Medical Ethics, constituted by the Indian Parliament in the Medical Council Act, 1956,
that many doctors conveniently ignore.
Doctors are legally bound to report medical malpractice. Says Dr Puneet Bedi, a Delhi-based
foetal medicine specialist and anti-foeticide activist: “In medical practice, by the very nature of the
profession, everything which is unethical is also illegal."
To the contention that the medical fraternity is colluding in the practice of female foeticide, Dr
Balasubramaniam says: “Doctors are not a special tribe removed from society. Therefore, the
faults of society will also be found among them.”
“Clearly," says a visibly angry Mina Swaminathan, gender activist, “Dr Balasubramaniam neither
knows law nor medicine. Given that he represents doctors in Tamil Nadu and speaks for them,
we can have a fair idea of the degree of medical malpractice that exists.”
“Female foeticide is a crime against humanity,” says Bedi. “Doctors as a community are involved.
The only surprise for people like us who have been talking about the problem for some time is
that people are surprised. Statistics, with all their limitations, ultimately reflect social realities. The
zeal with which female foeticide has been pursued in the last few decades had to get reflected in
the national census.”
The 2001 census registered a decline in the child sex ratio in 80% of the districts in India. The
juvenile sex ratio, which stood at 976 in 1961, fell to 927 in 2001, for the country as a whole.
Twenty of the 30 districts in Tamil Nadu have a sex ratio at birth lower than the biological sex
ratio.
According to government statistics, there are 2,379 registered scan centres in Tamil Nadu alone.
This, in a country that critically lacks medical health infrastructure. In Chennai itself, 147 private
nursing homes are allowed to carry out medical termination of pregnancy and sterilisation.
Seizure of equipment/machines for non-registration usually results in the release of machines
after payment of a fine. After that, it’s business as usual. There is virtually no monitoring of the
other requirements of the Act. Ninety per cent of deliveries in Tamil Nadu are institutional. Yet,
the sex ratio of children at birth is not registered or made available in the public domain.
In a surprise survey of 29 ultrasound clinics in Chennai, by activists from the Campaign Against
Sex Selective Abortion (CASSA), staff at one prominent hospital said they were unaware that any
httn: //www. i nfochan eei ndi a.ore/features21 Onri nt. i sn
16/09/2004
forms had to be filled out by patients. Of the 29, only one maintained the required records.
The PCPNDT Act mandates that any person conducting ultrasonography or any other pre-natal
diagnostic technique must maintain proper records. The Act requires the filling up of a written
form, duly signed by the expectant mother, as to why she has sought diagnosis. Violations are
punishable by imprisonment and a fine.
But one doctor said that during her three-year career she had never mentioned the MTP (Medical
Termination of Pregnancy) Act to any of her patients, as she is legally required to when an
abortion is performed. A register giving reasons for termination of pregnancy and the period
thereof also has to be maintained. But it rarely is.
At another facility, the reception desk claimed abortions were being performed. But the
gynaecologist said they were not.
One practitioner is on a National Monitoring and Reporting Committee for violations in the Code
of Medical Ethics, but receives numerous ‘standard’ referrals for ultrasonography every day.
Another facility had the 4D TV screen facing the patient for a full view of the examination.
One reputed hospital said 99% of its patients wanted to know the sex of the child. All deni®d
revealing it. Only one ultrasonologist boasted that he could determine the sex of the foetus at 45
days!
Near the one-room clinic of a medical graduate, in a residential suburb of Chennai, a banana
seller told visitors from a non-governmental organisation (NGO): “Abortion? Go there (pointing to
clinic).”
The National Health Policy makes no mention of gender, women’s health or monitory systems.
The Tamil Nadu government has not constituted a supervisory board, as mandated by the
PCPNDT Act, to monitor the implementation of the Act and Rules. Legislation has, for years,
lagged behind technology.
Already, the abortion pill (part of the state-initiated family welfare programme) makes surgical
termination of pregnancy redundant. New non-invasive drugs like antiprogestogen-mifepristone
derivatives, which, studies have shown, are 85-97% effective, are available over the counter.
The pressure to enforce the PCPNDT Act seems to have resulted in the opening out of abortion
options. The MTP Act offers protection to registered medical practitioners against any legal or
criminal proceedings arising out of harm or injury to women seeking abortions, unless the
contrary is proved.
Studies indicate that the risk of death is seven to ten times higher for women who wait until the
second trimester to terminate their pregnancies. Sex selective abortions are all second trimester
abortions.
Dr Saradha Jain, secretary of the Indian Medical Association, warns that the risk of maternal
morbidity/mortality needs to be given as much attention as the negation of women’s rights to
better health. Says P Phavalam, state-level convenor of CASSA: “The female foetus is
considered a disease and elimination is done as a service to mankind.”
The three chief pre-natal diagnostic tests that are being used to determine the sex of a foetus
(sexing) are amniocentesis, chronic villi biopsy (CVB) and ultrasonography. Amniocentesis is
meant to be used in high-risk pregnancies, in women over 35 years. This embryonic pre-natal test
requires the removal of 15-20 ml of amniotic fluid. The cells have to be cultured for three weeks,
or else there is an inaccuracy rate of 10-20%. CVB is meant to diagnose inherited diseases like
thalassaemia, cystic fibrosis and muscular dystrophy.
Ultrasonography is the most commonly used technique. It is non-invasive and can identify upto
50% of abnormalities related to the central nervous system of the foetus. But sexing has become
its preferred application. Depending on the ultrasonologist’s expertise, chances of a correct
prediction are 95-96%, with greater accuracy as the pregnancy advances. If the foetus is female,
a second trimester, even a third trimester abortion is carried out either by a doctor or a quack.
http://www.infochangcindia.org/features21 Oprint.jsp
16/09/2004
Print
Page 3 of3
of Salem, Dharmapuri, Madurai, Namakkal and Theni. But we have strong evidence to prove that
the practice is not restricted to these districts alone. Keeping IMR gender differential as the
indicator, female infanticide is observed in districts like Trichy, Perambalur, Thiruvannamalai,
Karur, Villupuram, Vellore, Erode and Dindigul. So, from the core area it is now spreading to the
peripherals. But the state is not keeping pace.
We are against schemes like the Cradle Baby Scheme. It implies that the government is
encouraging parents to dump unwanted girl-babies. Is that a correct message? Cradle Baby
centres exist in all 30 districts of Tamil Nadu - even in areas where there is no infanticide! Think
of the implications.
Also, the abortion law is liberal and there are no mechanisms to monitor the enforcement of the
MTP Act (Medical Termination of Pregnancy Act, 1971). The state’s indirect sanction to use the
MTP Act as a tool to reduce population size implies that sex selective abortion indirectly enjoys
legitimate sanction from the state. The official machinery and the law concern themselves solely
with female infanticide, which is actually not as alarming as foeticide now is. Foeticide committed
with the assistance of ‘ultrasound’ clinics is spiralling even in hitherto unaffected areas like
Perambalur. Scan centres are supposed to be registered but this is not done comprehensively.
Laws exist on paper only. We have agitated and provided authorities with lists of unauthorised
scan centres. They are pulled up, they pay a fine, get their machines released and go back to
business!
The PNDT Act (Pre-Natal Diagnostic Techniques [Regulation and Prevention of Misuse] Act
1994) was inadequate. It never once mentioned ‘sex selection’. The law was concerned only with
the foetus from conception to delivery. But sex selection is possible prior to conception, in a
laboratory, using genetic means. We filed a case against a doctor in Madurai who openly
advertised that he could make male embryos by selecting the required chromosomes. It is two
years now, but the case has not yet even come to trial. The judicial process reacts too slowly.
Indeed, sex selection is done even in western countries. We are hopeful that the new law, the
Pre-Sex Selection and Pre-Natal Diagnostic Techniques (Prohibition of Sex Selection) Act 2002
will overcome some of these drawbacks. As its name suggests, it is more comprehensive in its
coverage. Its impact is still to be analysed.
We found in our discussions with doctors and sonologists that prenatal diagnostic techniques are
widely used to confirm, monitor and manage pregnancies - almost all pregnant women resorting
to institutional deliveries are subjected to ultrasonograms at least four times during their
pregnancy, as directed by doctors. Even registered genetics labs, counselling centres and clinics
do not maintain records, as specified in Form G of the rules. Registration of abortions beyond 12
weeks should be universalised, including in private hospitals. The specific cause of termination
should be mentioned clearly - be it congenital malformation, genetic abnormalities or metabolic
disorders. The definition of ultrasonography should be made more explanatory to include all
imagery techniques such as ultrasonograms, Doppler scans, CT scans and MRIs, etc. If the
purpose of these prenatal diagnostic techniques is to detect abnormalities, then considering the
negligible prevalence of such disorders, this kind of rampant application amounts to abuse of
medical practice.
It is not only legislation and judicial pronouncements that play a significant role. As I explained
earlier, there are overwhelming social ground realities to be reckoned with. The practice of female
infanticide has been around for generations. It is a matter of grave concern that modern society,
which has emancipated women in so many ways, is yet to come to grips with the issue of female
infanticide and foeticide.
(Lalitha Sridhar is a Chennai-based freelance journalist)
InfoChange News & Features, August 2004
Shobha Raghuram
From:
Sent:
To:
Subject:
ephost@epnet.com
Wednesday, February 09, 2005 11:36 AM
s.raghuram@hivos-india.org
Vijayalakshmi, Sex selection articles
6990975.pdf (397
KB)
Record:
10
Preimplantation genetic diagnosis for gender pre-selection in
Title:
India: a counter argument to the article by Malpani and Malpani.
Authors:
Mehta, Rajvi H.
Reproductive BieMedicine Online; Jan/Feb200 2, Vol. 4 Issue 1,
Source:
pH, 2p
Document Type:
Article
Subject Terms:
*PREIMPLANTATION genetic diagnosis
*SEX preselection
Geographic Terms: INDIA
Abstract:
Responds to a commentary regarding the use of
preimplantation genetic diagnosis (PGD) for gender pre-selection in India. Opinion on the
debate over the intention of using PGD; Claim against conception of using reproduction
technology for sex
determination; Recommendation.
Full Text Word Count:
1078
ISSN: 1472-6491
Accession Number: 6990975
Persistent link to this record:
http: //search, epnet. com/login. aspx?direct=true&db=aph&an=6990975
Cut and Paste:
<A
href="http: //search, epnet. com/login. aspx?direct=true&db=aph&an=6990975’’
Preimplantation genetic diagnosis for gender pre-selection in India: a
counter argument to the article by Malpani and Malpani. </A>
Database:
Academic Search Premier
PREIMPLANTATION GENETIC DIAGNOSIS FOR GENDER PRE-SELECTION IN INDIA:
COUNTER ARGUMENT TO THE ARTICLE BY MALPANI AND MALPANI
A
The anchors emphasize that PGD, which is ”technology used for pre-conceptional sex
selection", should not be considered on par with ”post-conceptional sex determination
techniques ( which are actually sex deselection techniques, since they involve termination
of fetuses of the undesired sex)
The authors are of the opinion that since PGD does not
involve embryo destruction, there should be no "emotions” involved. This may not be true
for Indians where the Law of the land permits medical termination of pregnancy ( MTP) ,
irrespective of the sex of the unborn. The issue is not about destruction of fetuses or
embryos but rather about gender selection! MTP following sex-determination, either by
amniocentesis or ultrasound scanning, is illegal in India.
Indeed, Indian population censuses during the past few decades clearly indicated that in
contrast to other countries of the Western world, the number of females is far lower than
that of males ( http: //gende-rstats, worldbank, org) . UNICEF has widely publicized this
anomalous situation as ’the case of missing females’ ( http://gendericide.org). PGD for
gender selection cannot be considered mere destruction of embryos but selective gender
1
fetuses,
discrimination. Gender discrimination already occurs at various levels
infants, young girls and women. Law in India prohibits ail such discrimina 10 ..Do we now
need to enlarge the list of sex discrimination to XX embryos containing a bunch
L-..-. of
pluripotent cells and cells surrounding them? . There cannot be anyr <difference
--- ------ in laws
ultrasonography
governing sex-selection, whether it be by amniocentesis, i._
.
- - - or PGD.
for the misdse of PGD for
E SEE EE:
sKoEhi srEss
J“k
does. Society therefore has a right to express deep concern against procedures that woul
discriminate against one half of its social structure.
The authors state: "The hidden message is that Indians nd Indian doctors cannot be
trusted to use this technology responsibly, and while it can be safe!y used in the We st,
its use in India should be policed". One wonders what privileged insight the authors
to read this 'hidden message' which has escaped the attention of most of us.
To quote the authors once again: "The basic purpose of technology is to give Man more
control over his destiny than he has had in the past. Ct course, how he will use this
technology is difficult to predict". It is surprising that the authors find it difficult
to predilt how Man may utilize the technology of PGD for gender pre-selection. It is quite
obvious that considering the preference for a male chile in several sections of Ind
Society, individuals would be misusing it for selecting male embryos and promoting gender
discrimination against the female, albeit at a much earlier stage in human existence.
The authors have treated 42 cycles for 36 patients with PGD for family balancing in their
clinic but they do not state how many of these came m tor a male embryo selection,
would itself explain whether couples would-be oPtj-ng^ for this technology for gender
balancing or for rejecting the birth of a female child!
and’ figures? for their hypothetical example stating
The authors have misused statistics
-j
female
that couples who already have one Lt.--- child
-- -- and undergo a sex determination procedure,
the sex ratio will be more balanced in the selected group
abort the female fetuses so that
t
of families. This is the most distorted argument stating that abortion of female fetuses
would in fact ' balance' the gender ratio in the select group of families. The data from
.1.-- the
E-u sex ra lo, which is already skewed against
the Census of inoia,
India, 2001 clearly .u
show that
northern Indian states of Punjab and Haryana, have been further skewed in
women in the i
children under 6 years of age ( http://www.censusindia.net). In Punjab, there arefp
females per 1000 males in the whole population but onlv 793 girls per 1000 boys below th
al^of six. In Haryana, there are 861 females per 1000 males in the . whole population but
only 820 girls per 1000 boys below the age of six. Th
clearly indicates a P°ssi e
misuse of technology such as ultrasonography or amniocentesis and that it could be
Ss^ns^ble for this distorted sex ratio. With such data staring at us, how can one argue
that ' aborting'
female fetuses will bring gender balance?
It is absurd to presume that the affluent couples who go in for PGD "make^excellent
parents because they have taken the time and trouble to plan their family .Parent_ng
involves much more than planning the family and providing to the materialistic
reouirements of a child. Affluent parents need not necessarily make good parents, The
children of the patients treated by Malpani and Malpani (2002) would not be more than
.
year old and it is premature to conclude that these couples make "excellent parents
ano
thereby promote this technology.
The authors’ concluding statement "Haven' t the politicians interfered in our lives enough
already? Do we want to invite them into our bedrooms as well?" is m very poor taste
India is a democracy and legislation passed by our parliament meets the approval of the
elected representatives of the country after intense donate ana following guidance o
:Srt proSstonals from a given field. If personal views do not subscribe to those of
the majority, this is no reason why legislation, which a majority of our elected
representatives feel is for the good of Society, should not be passed.
gender
selection through PGD but it may not
Today, there may not be many clinics offering
<------ 3 3
---- ' which in
be long before this technology is marketed for so-can id gender ’balancing
action now and
reality would be gender pre-selection for a male child, should we not take
t
prevent furtherance of gender discrimination by PGD rather than wait for 10” yea s until
skewed even further?
Census 2011 and then panic on seeing an already distorted sex ratio
-- ---2
References
??? Malpani A, Malpani A 2002 Preimplantation genetic diagnosis for gender selection for
family balancing — a view from India. Reproductive BioMedicine Online 4, 7—9.
; www. rbmonline. com/ Article/4 40
??? Vol 4. No 1, 11-12 Reproductive BioMedicine Online;
10 ---December 2001
<http: //www. rbmonline. com/Article/440> on web II
By Rajvi H. Mehta, Hope Infertility Clinic, 12 Aga Abbas Ali Road, Bangalore 560 042,
India e-mail: mehtat@vsnl. com
Copyright of Reproductive BioMedicine Online is the property of Reproductive BioMedicine
Online and its content may not be copied or e-mailed to multiple sites or posted to a
listserv without the copyright holder's express written permission. However, users may
print, download, or e-mail articles for individual use.
Source: Reproductive BioMedicine Online, Jan/Feb2002, Vol. 4 Issue 1, pll, 2p
Item: 6990975
3
Shobha Raghuram
From:
Sent:
To:
Subject:
ephost@epnet.com
Wednesday, February 09, 2005 11:36 AM
s.raghuram@hivos-india.org
Vijayalakshmi, Sex selection articles
9685233.pdf (655
KB)
Record:
7
Court orders seizure of illegal sex test machines.
Title:
Source:
National Catholic Reporter; 3/8/2002, Vol. 38 Issue 18, plO,
l/9p
Document Type:
Article
*ABORTION
Subject Terms:
CHURCH
JUDGMENTS
*SEX determination. Diagnostic
Geographic Terms: INDIA
Abstract:
Reports that church groups in India have welcomed the
Supreme Court order to confiscate ultrasound machines from illegal clinics to fight femal
feticide in the country. Need for a change in people’s attitude towards women; Factors
which lead to female feticide
in India.
ISSN: 0027-8939
Accession Number:
9685233
Persistent link to this record:
http: //search, epnet. com/login. aspx?direct=true&db=aph&an=9685233
Cut and Paste:
<A
href="http: //search, epnet. com/login. aspx?direct=true&db=aph&an=9685233" >
Court orders seizure of illegal sex test machines. </A>
Database:
Academic Search Premier
1
Commentaries ■ PCD for gender selection
the Government of India to take legislative measures to prevent
selective abortions o' female fetuses. This seems to be a losing
battle. Many organizations concerned with this problem are of
the view that the only solution is social education, rather than
legislation. Changes in societal perceptions occur very slowly
in a democratic society. Female feticide must therefore be
considered to be a reality until this change takes place.
I had written on the subject of gender pre-selection earlier
(Anand Kumar. 1995) and suggested that the development of a
reliable, simple method for gender selection of offspring would
be an interim solution for the masses who have not as yet
reconciled to having a female child, so they could avoid female
feticide. Now 1 would like to consider the ethical issues of
gender pre-selection in the Indian context. Discrimination
against females from die fetal to the adult stage is a concept that
is not in consonance with modem social trends. Women
compete very effectively for jobs that were earlier considered to
be in the male domain and. strikingly, women most often do
much better in certain jobs than men. Despite this, there is still
a gender prejudice against women, and this is not exclusive to
Indian women in Western societies also continue to experience
such discrimination in public life, as well as in offices and
universities. A reduction in the number of females is therefore
an unacceptable proposition, not only to India but all over the
world. There is reason to believe that India, while still
upholding traditional beliefs in their ethos and culture, would
also like to be modem in their outlook. Reduction in the
.i (cspcrse - RH Me-',la
number of females is not a concept of modem societies and
therefore would not be acceptable by a very large section of
Indian society.
The article by Malpani and Malpani (2(X)l) suggests that
prenatal genetic diagnosis for selecting the sex of the embryo
before implantation is a solution to the problem.
Preimplantation genetic diagnosis (PGD) requires sophisticated
laboratory facilities that are not available in rural India. The
technique is expensive and affordable only by the rich, who are
few and far between compared with other, economically
weaker, sections of Indian Society. Malpani and colleagues’
suggestion of PGD offering a solution for the masses is
therefore impractical. Their contention that PGD offers a
medical technological solution to a societal malaise is
presumptuous. Reproductive biomedicine, like all other
medical technologies, aims to alleviate personal illness and not
attempt to offer solutions to societal problems.
If these are technical and ethical weaknesses of rhe article, one
wonders what purpose the article serves?
Reference
Anand Kumar TC 1995 Gender pre-selcetion: prevenuon or
perp -tuation of female deaths. Human Repmlucrwn 10. 13 Ft
Malpani A. Malpani A 2002 Preimplantatiun genetic diagnosis fw
gender selection for family balancihg: a view fn»m India.
Rcprnditt rive BithMi’iUcinc Online 4. 7 -9.
Vai 4. .\!o I. U - >1 Repmducfive BiM'dirine Online: w^j-brntmline^anU
^eh 10 Da cmber 2001
Preimplantation genetic diagnosis for gender
pre-selection in India: a counter argument to
the article by Malpani and Malpani
Rajvi H Mehta
Hope Infertility Clinic, 12 Aga Abbas Ali Road, Bangalore 560 042, India
e-mail: mehtat@vsnl.com
I he authors emphasize that PGP. which is •‘technology used
for pre-conceptional sex selection", should not be considered
on par with "posl-conceptional sex determination techniques
(which are actually sex deselection techniques, since they
involve termination of fetuses of the undesired sex)". The
authors are of the opinion that since PGD does not involve
embryo destruction, there should be no "emotions” involved.
This may not lie (rue for Indians where the Law of the land
permits medical termination of pregnancy (MTP), irrespective
of the sex of the un Torn. The issue is not about destruction of
fetuses or embryos but rather about gender selection! MTP
following sex-determination, either by amniocentesis or
ultrasound scanning, is illegal in India.
Indeed. Indian popu alien censuses during the past few decades
clearly indicated that in contrast to other countries of the
Western world, the number of females is far lower than that of
males (http://genderstats.worldbank.org). UNICEF has widely
publicized this anomalous situation as the case of missing
females’ (http://gendcricide.org). PGD for gender selection
cannot be considered mere destruction of embryos but
selective gender discrimination. Gender discrimination already
occurs at various levels - fetuses, infants, young girls and
women. Law in India prohibits all such discrimination. Do we
now need to enlarge the list of sex discrimination to XX
embryos containing a bunch of pluripotent cells and cells
surrounding them? There cannot be any difference in laws
governing sex-selection, whether it be by amniocentesis,
ultrasonography or PGD.
Arguing against the concerns for the misuse of PGP for non
medical reasons by ESHRE Task Force on Ethics and Law. the
authors give an analogy to cosmetic or re-constructive surgery
for non-medieal reasons. This analogy is misplaced and
a
Commentaries
PGD for gender selection - a response - 67/ Mehia
irrelevant because these surgical procedures do not in any way
affect the social matrix as gender pre-selection does. Society
therefore has a right to express deep concern against procedures
that would discriminate against one half of its social structure.
The authors state: *‘The hidden message is that Indians and
Indian doctors cannot be trusted to use this technology
responsibly, and while it can be safely used in the West, its use
in India should be policed*’. One wonders what privileged
insight the authors* had to read this ‘hidden message’ which has
escaped the attention of most of us?
To quote the authors once again: “The basic purpose of
technology is to give Man more control over his destiny than he
has had in the past. Of course, how he will use this technology
is difficult to predict”. It is surprising that the authors find it
difficult to predict how Man may utilize the technology of PGD
for gender pre-selection. It is quite obvious that considering the
preference for a male child in several sections of Indian Society,
individuals would be misusing it for selecting male embryos
and promoting gender discrimination against the female, albeit
at a much earlier stage in human existence.
The authors have treated 42 cycles for 36 patients with PGD for
family balancing in their clinic but they do not stale how many
of these came in fora male embryo selection? This would itself
explain whether couples would be opting for this technology
for gender balancing or for rejecting the birth of a female child!
The authors have misused statistics and figures for their
hypothetical example stating that couples who already have one
female child and undergo a sex determination procedure, abort
the female fetuses so that the sex ratio will be more balanced in
the selected group of families. This is the most distorted
argument staling that abortion of female fetuses would in fact
'balance* the gender ratio in the select group of families. The
data from the Census of India. 2001 clearly show that the sex
ratio, which is already skewed against women in the northern
Indian slates of Punjab and Haryana, have been further skewed
in children under 6 years of age (http:/Avww.ccnsusindia.net).
In Punjab, there are 874 females per 1000 males in the whole
population but only 793 girls per 1000 boys below the age of
six. In Haryana, there arc 861 females per 1000 males in the
whole population but only 820 girls per 1000 boys below the
age of six. This clearly indicates a possible misuse of
technology such as ultrasonography or amniocentesis and that
it could be responsible for this distorted sex ratio. With such
data staring at us, how can one argue that ‘aborting’ female
fetuses will bring gender balance?
It is absurd to presume that the affluent couples who go in for
PGD “make excellent parents because they have taken the time
and trouble to plan their family”. Parenting involves much
more than planning the family and providing to the
materialistic requirements of a child. Affluent parents need not
necessarily make good parents! The children of the patients
treated by Malpani and Malpani (2002) would not be more than
a year old and it is premature to conclude that these couples
make “excellent parents’* and thereby promote this technology.
The authors’ concluding statement "Haven’t the politicians
interfered in our lives enough already? Do we want to invite
them into our bedrooms as weli r is in very poor taste. India is
a democracy and legislation passed by our parliament meets the
approval of the elected representatives of the country' after
intense debate and following guidance of expert professionals
from a given field. If personal views do not subscribe to those
of the majority, this is no reason why legislation, which a
majority of our elected representatives feel is for the good of
Society, should not be passed.
Today, there may not be many clinics offering gender selection
through PGD but it may not be long before this technology is
marketed for so-called ’gender balancing’ which in reality
would be gender pre-selection for a male child. Should we not
lake action now and prevent furtherance of gender
discrimination by PGD rather than wait for 10 years until
Census 2011 and then panic on seeing an already distorted sex
ratio skewed even further?
References
Malpani A. Malpani A 2(X)2 Prcimplantation genetic diagnosis for
gender selection for family balancing - a view from India.
Reproductive BioMedicirtc Onlb'ii14. 7—9.
Copyright©2002 EBSCO Publishing
120 / Sarai Reader 2003: Shaping Technologies
Reproductive Technologies in India
Confronting Differences
■ n the last two decades the use of reproductive technologies (RTs) has become an
I inevitable and often indispensable part of women's lives.1 On the one hand, the increased
I knowledge and availability of a wide range of RT options has redefined ‘traditional' notions
of conception and procreation. On the other, the introduction of each new device or tech
nique has served to renew a growing flux in the way reproductive choice is understood. The
right to bodily integrity - defined as the inalienable right of women to have control and
autonomy over their bodies - has been central in the feminist understanding of choice.
Women's expanded access to reproductive technologies (RTs), including abortion, is an
essential corollary to this argument. Access to certain types of RTs have indeed saved
women's lives and often provided them with expanded choice with regard to reproductive
decision-making. However, there is a continued need to evaluate the role of RTs in gendered
terms and examine their role in providing women with real choice. This need becomes parti
cularly acute in the face of the growth of the non-medical use of RTs to satisfy individual and
sociocultural needs.
Women's bodies, in particular her reproductive functions, are increasingly being sub
jected to technomedical interventions to satisfy non-medical aspirations with regard to con
ception and procreation. The case of sex selection and sex selective abortion in India is a
classic example of both the non-medical use of RTs and of the misappropriation of the defi
nitions of reproductive choice. In light of this, and numerous other RT-related ‘events' in
India, there is need for an urgent reassessment of the way bodily integrity is defined in the
Indian context. This is imperative in order to be able to frame adequate norms and stan
dards for RT use in ways that do not limit women's access to RTs and at the same time find
ways to limit the gendered context within which they often find use. In this article some of
these issues will be examined in an India specific context in an attempt to illustrate a con
ceptual path that might serve to build bridges between different constituencies that are
increasingly positioned on opposite sides of a growing chasm.
Contextualising the Reproductive Rights Discourse
The feminist discourse on reproductive rights rests on the notion of procreative liberty
defined as the right to reproduce (positive right) and the right to avoid reproduction (nega
tive right). Both these rights carry with them an implicit assumption of first, bodily integrity
Scans / 121
- the right to control and autonomy over one's body - and second, an implicit assumption
of the use of varied RTs. For example, the negative right to avoid procreation can be
attained through access to abortion. However, this right based claim cannot be universalised and needs to be examined in a relational context (Menon 1995; Steinbock 1998).
In India, women's health and rights activists have often emphasized the need to define
reproductive rights and choice in gendered terms so that its fulfilment is not only dependent
on the availability of technical choice and information. It is indeed important to argue that
RTs cannot be viewed as a magic bullet that will help alleviate women s reproductive bur
dens’. When this is done with little or no effort to change the often oppressive arrangements
for reproduction, the result can be a reinforcement of gender based inequality. The misap
propriation of prenatal obstetric diagnosis and abortion, by families and medical community
alike, to systematically eliminate female foetuses is one example. The introduction of hor
monal and other provider-controlled contraceptives has also been the site of controversy.
Besides questions concerning the safety of these methods, the governments efforts to
achieve its demographic goals by using women as the vehicles for population control, while
disregarding*their safety and well-being, has been harshly criticised, n
Unfortunately, controversies surrouding the use of RTs have resulted in the consolida
tion of opinion, in line with moral and legal absolutes, rather than producing a constructive
dialogue between the different constituencies. As Birke pointed out, the problem with
moral absolutes is that they do not take [us] far, they tend to result in an insensitive poli
tics, which says little about the needs that gave rise to the discussion in the first place
(Birke et al 1990, p. 282). Hidden within these absolutes is the female person whose spe
cific context and needs often find no place in current discussions. Little or no account of
the social position of women, and the socially determined needs that position generates, is
taken into account when pronouncing judgments (Petchesky 1980). Just as pushing tech
nologies without addressing arrangements for reproduction often proves to be detrimental,
’banning' a technology without advancing non-exploitative definitions and methodologies for
use of RTs serves little purpose. There is an urgent need to undertake this task as increas
ingly "these technologies and the ’choice’ they offer are gaining considerable validity for
women who are its direct users" (Mallik 2002, p. 189). In the absence of choice in real
terms, these RTs often represent the only power base for women from which to negotiate
the terms of their existence (Rowland 1985). The legitimacy of the non-medical use of RTs
is a powerful example where women are as much the agents seeking sex selection as they
are victims of the social pressure to have sons.
There is a need to examine the introduction of certain types of RTs in India within a
framework that responds to the process of technological advance as a whole rather than
as isolated procedures. It is, for example, important to be able to illustrate the way the RT
industry has built its profits on the basis of reconstituting reproduction into varied ’patholo
gies’, more often than not through reinforcing gender based stereotypes and inequalities.
Previously, reproduction was regulated largely through sociocultural principles. Today this
reality remains unchanged and further overlaps with technomedical control. Together these
serve to create a complex terrain on which decisions about reproduction (by women) are
made. At the same time it is important to deconstruct, for example, how non-medical use
122 / Sarai Reader 2003: Shaping Technologies
of RTs for sex selection has gained legitimacy as a result of their potential to alter e
balance of power between individual men and women, as well as between women and insti
tutional control - something that is not fully understood (Gimenez 1991). It is evident that
the advent of RTs and their use, particularly non-medical use, has precipitated the need to
redefine our understanding of procreative liberty and, more specifically, issues of repro
ductive choice and autonomy.
Needs Interpretation - Who Defines the Female Lifeworld?
In India the varied interpretation of what women need has resulted in polarised debates on
the need and importance of talking about reproductive rights and choice; and within that
the need to expand women's access to RTs. Interpreting needs has been reduced solely to
a political idiom in which conflict is played out through inequalities, which are differentially
positioned and then symbolically challenged (Fraser 1989). The interpretation of needs with
reference to reproductive rights, choice and the role of RTs, for example, is often talked
about within a dichotomous and hierarchical framework that characterises socio-economic
and cultural-symbolic injustice as two separate injustices. Socio economic injustice and the
need for a politics of redistribution is often favoured over a politics of recognition tlrat talks
about cultural-symbolic injustice. The first step towards being able to frame a meaningful
discourse around reproductive rights and choice means bridging the gap between these
two struggles and illustrating the interconnectedness that exists between the two.
This understanding can be a first step towards building bridges between the two con
stituencies that are currently aligned as being those that fight inequality, and those that
stress difference and fight for recognition. In pooling resources it is possible to participate
more equally in what is currently an unequal discursive struggle to influence the agenda for
the development and use of RTs. Making a dent on the existing scenario, currently domi
nated by big pharmaceuticals, the medical community and the Indian state through its
undue emphasis on anti-natalist population policies, is a complex and difficult goal in both
theory and practice. The fragmented and varied nature of claims made by and on behalf of
women often acts as an impediment in countering the more homogenised discourse of
these powerful actors.
The deterministic role that RTs play in women's lives, and the fact that a woman s body
is often the site for this technological advance, is an irreversible fact today. Furthermore, it
is important to note that the wide range of RTs have the power to directiy impact social relations that govern procreation and conception. For example, sex selection and sex selective
abortion in India has dramatically redefined both conventional notions of biological repro
duction and kinship building, as well as altered the way women experience pregnancy and
motherhood. It is also an undeniable fact that in a culture which can only be described as
being extremely antagonistic to women there is a misuse of RTs. However, none of the
above should deter or undermine efforts to evaluate the potential of technologies in mak
ing real improvements in women's lives. Feminist activism should come together to under
take the collective task of developing a holistic vision of RTs that combines transformatory
goals to advance women's reproductive well-being within the need based context of
women's lives.
Scans / 123
NOTES
1.
For the purpose of this article the term 'RT' is used in its broadest sense to indicate the wide spectrum of
devices and techniques that facilitate fertility control, infertility treatment and prevent sexually transmitted infec
tions and disease.
REFERENCES
1.
Birke, L, S. Himmelweit and G. Vines Tomorrow's Child:Reproductive Technologies in the 90s (Virago
Press, 1990, London).
2.
Fraser, N. ’Struggle Over Needs: Outline of a Socialist-Feminist Critical Theory of Late Capitalist Political
Culture" (in Unruly Practices: Power, Discourse and Gender in Contemporary Social Theory Polity Press, 1989,
Cambridge) p. 161-87.
3.
Gimenez, M.E. "The Mode of Reproduction in Transition - A Marxist-Feminist Analysis of the Effects of
Reproductive Technologies' (in Gender and Society Vol. 5, No. 3, 1990) p. 334-50.
4.
MalliMR. "Sex Selection: A Gender-Based Preference for a Pregnancy" (in Reproductive HealthzMatters
Elsevier Science, Vol. 10. No. 19, 2002) p. 189-90.
5.
Menon, N. "The Impossibility of ’Justice': Female Foeticide and Feminist Discourse on Abortion" (in Con
tributions to Indian Sociology Vol. 29, No. 1 and 2, Sage Publications. 19S5, New Delhi) p. 369-92.
6.
Petchesky, R.P. ‘Reproductive Freedom: Beyond ’A Woman's Right to Choose" (in Signs: Journal of Women
in Culture and Society Summer, Vol. 5, No. 66, 1980) p. 1-85.
7.
Rowland, R. ‘A Child at Any Price? An Overview of Issues in the Use of the New Reproductive Technologies,
and the Threat to Women" fin Women's Studies International Forum Vol. 8, No. 6, 1985) p. 539-46.
8.
Steinbock, B. Rethinking the Right to Reproduce (Harvard Working Paper Series, Harvard School of Public
Health, http://www.hsph.harvard/HW papers/reproright.html, 1998. Cambridge).
9.
Young, I.M. "Unruly Categories: A Critique of Nancy Fraser's Dual Systems Theory" fin New Left Review
May-April, Vol. 222,1997, London) p. 147-160.
Ethics
i
!
I
l
i
EPW Commentary
March 6, 2004
Urgent Concerns on Abortion Services
While the Medical Termination of Pregnancy Act (MTP Act) has existed for 33 years, certified and legal abortion facilities
account for only a quarter of all such private facilities in the country. Neither the public nor private abortion services have fully
measured up to the needs of the abortion seekers.
Ravi Duggal, Vimala Ramachandran
For many decades now maternal health has been recognised as a crucial area of concern. Access, safety
and legality issues regarding abortion and abortion services in India have assumed serious dimension in
the context of women’s reproductive health needs. The Abortion Assessment Project-lndia (AAP-I). an allIndia research study that commenced in August 2000, was initiated with the objective of assessing
ground realities through rigorous research.
Facility surveys in six states, household based surveys in two states, nine qualitative studies in seven
states, a policy review and nine working papers undertaken in this project highlight the inadequate
attention given to abortion within the health and population policy of the country and reiterates the often
voiced concern that even the recent reproductive and child health programmes have failed to address.
Abortion facilities mapped in six states (Kerala, Madhya Pradesh, Orissa, Rajasthan, Haryana and
Mizoram) reveal that there are four formal (medically qualified though not necessarily certified/ registered
to provide abortions) abortion facilities per 1,00,000 population in India. This adds up to 40,000 facilities
or 48,000 providers (each facility averages 1.2 providers). Of the formal abortion providers 55 per cent
are gynaecologists and 64 per cent have at least one female provider, with each facility performing 120
abortions per year on the average. This adds up to 4.8 million, with one-third being conducted in public
facilities. There are more or less similar numbers of informal (traditional and medically non-quafified)
abortion providers handling about one-third of cases handled by formal providers. Based on these studies
our estimate is that about 6.4 million abortions are performed annually in India.
While the Medical Termination of Pregnancy Act (MTP Act) has been around for 33 years, certified and
legal abortion facilities account for only 24 per cent of all private abortion facilities in the country. The 380
facilities (285 private) across the six states covered in the study provide evidence that those who were
certified had obtained certification on an average within a month and of those who were not certified, 68
per cent had not even attempted to obtain certification. Thus the problem lies largely in the domain of the
medical professionals who have not shown interest in registration, probably because they do not want to
be accountable to the authorities. This is when two-thirds of the providers in the non-certified facilities had
the requisite training or qualification as per MTP Act to conduct abortions; thus a majority of uncertified
facilities are perhaps providing safe abortions. The latter was confirmed by the fact that with regard to
technical aspects and infrastructure facilities the difference between the certified and non-certified
facilities was small. Lack of ethics in medical practice and absence of self-regulation amongst the
profession is largely responsible for the present state of affairs - including the proliferation of sex
selective abortion.
Our studies also found that 73 per cent of abortions were conducted for less than 12 weeks gestation.
Dilatation and curettage (D and C) seems to be the preferred method for nearly 89 per cent of induced
abortions. Even amongst those who use vacuum aspiration the practice of check curettage is very
common. This obsession with curettage both adds to the cost of the procedure and contributes
substantially to post-abortion complications and infections.
While physical access seems to be reasonably good, social access remains restricted since providers,
especially in the formal and certified facilities, do not provide services to women if they come alone and/or
if the spouse or some close relative does not give consent In the household and qualitative studies
women said that the decision for undergoing an abortion is rarely their own; more often than not their
spouse or some relative decides for them. This affects the woman’s freedom to access such services. So,
to protect her confidentiality and privacy she may often resort to providers who may not be very safe. As
1
regards reasons for seeking induced abortions, only 15 per cent of them fall into what is permitted under
the MTP Act (failure of contraceptives, threat to the woman’s life, biological reasons), the rest were
unwanted pregnancy, economic reasons and even unwanted sex of the foetus. The household based
household surveys in Maharashtra and Tamil Nadu, qualitative studies and working papers all indicate the
prevalence of the practice of sex-determination and female-selective abortions.
Public investment in abortion services is grossly inadequate. Only 25 cent of abortion facilities in the
formal sector are public facilities, and 87 per cent of the abortion market is controlled by the private
sector; the average (median) cost of seeking abortion in the private sector is Rs 1,294, which is 7.5 times
more than the cost in public facilities. This constitutes a major barrier for women from poorer or other
disadvantaged social groups. The household studies under this project reveal that women from poorer
classes and from dalit and adivasis communities have significantly lower rates of induced abortion
because they often do not have the purchasing power to access abortion services from the private sector
or travel long distances to access public services. This makes a strong case for both strengthening as
well as expanding public abortion facilities across the country.
The eight qualitative studies revealed that the overwhelming reason for seeking abortion among married
women was to limit the family size. When women were asked to indicate the situations in whicn they
would seek abortion or had actually sought abortion, the majority of the women in studies conducted in
Maharashtra, Gujarat, Andhra Pradesh and Tamil Nadu reported limiting the family size as the main
reason for abortion. Equally disturbing was the finding that non-use of contraception rather than
contraceptive failure was reported to be the chief reason why the unwanted pregnancy situations
described above tended to occur. Actual contraceptive failure was reported in very few cases. Though all
respondents across studies reported knowledge of sterilisation as a method of limiting family size and a
majority of the women knew about the reversible methods of contraception such as condoms, oral pills
and IUD for spacing births, yet this knowledge did not translate into practice for a range of reasons - fear
about its effect on health, pain and discomfort, irregular supply and problems with obtaining
permission from husband. Use of condoms for contraception was rare. Paradoxically, there was a
perception that abortion was safe and did not have any long-term adverse health consequences. For
some respondents it was seen as a ‘safer* option than the use of IUDs and other spacing methods!
Also, almost all women were aware that sex selective abortion was illegal, and admitted that women
approach different facilities for ascertaining the sex of the foetus and for abortion. Awareness of the new
PNDT Act was far greater among women and service providers in comparison to the details of the MTP
Act Gtoup discussions invariably turned spirited when sex selection was discussed. While most
respondents admitted that sex selective abortion is indeed illegal, they expressed helplessness as their
status in the family and sometimes the very survival of their marriage depended on their ability to produce
sons. The studies also revealed that when couples have more than two female children, then female
selective abortion was approved by the family and condoned by the community. There was no social
stigma associated with sex selective abortion - especially for mothers with many daughters. Women from
Gujarat and Haryana also reported that while they were not comfortable with abortion per se, when it was
done for the sake of the family, then they accepted it
There was an overwhelming perception that private facilities were better. The reason for preferring private
providers was quite wide, suggesting that the women and their families do weigh the alternatives before
deciding where to go. Reasons cited by women were:
- Abortion in private facility takes much less time — everything is done in one visit, meaning that they do
not waste time waiting and going through formalities (as most government hospitals are not client-friendly)
and
that
everything
could
be
wrapped
up
in
one
visit
- Private doctors have better facilities and equipment and that they are not in a hurry to discharge women
soon after the procedure if they need rest for an hour or so before going home. In public hospitals, on the
other hand, given a shortage of beds women are asked to leave as soon as possible.
- Private doctors treat women with dignity and ensure confidentiafity.
It was accepted that while private providers are expensive, visits to the government hospitals were not
cost-free because women had to pay for medicines separately. They were sometimes required to make
2
repeat visits before the abortion was performed. The long waiting period implied that the time of the
service seeker and of the accompanying person (generally women do not go alone to impersonal lai^e
facilities) was wasted, leading particularly in poor families forgoing wages for that time. The cost, vaned
according to the type of provider and the gestation period. For example, the cost,n Pnvate
urban Gujarat varied between Rs 400-600, similar to what women in urban Andhra Pradesh had to pay.
In a two-day National Consultation with experts working on reproductive health issues across the country,
held in Delhi in November 2003, the following issues were flagged as needing urgent attention:
-
Changing the mindset of providers through their professional associations to accept
certification on a universal basis.
-
Integrating abortion services under primary health centres and community health centres
through a strengthened RCH programme which would automatically enhance women s
access to abortion care services.
-
Promoting safer technologies by changing the mindset of providers away from unnecessary
use of curettage.
-
Strengthening regulation of abortion facilities to evolve minimum standards for quality care
and accreditation.
-
Promoting safe spacing methods of contraception to reduce the need to resort to abortion as
a spacing method.
-
Broadening the base of providers by training paramedics for early trimester abortions as is
done in many countries like South Africa, Bangladesh, etc.
The need to widely display certification status of abortion facilities so that women can
recognize a safe abortion facility.
-
The need to educate providers on ethics of sex-determination tests and respecting the
provisions of the PNDT Act
-
The need for medical associations to get active in training abortion providers, especially
those in the private sector.
-
Promoting apprenticeship as a method of training.
-
Reskilling of traditional providers to play alternative roles like accompanying/supporting
abortion seekers to safe abortion facilities.
To conclude, the various studies undertaken under the aegis of AAP-lndia project clearly ind
neither the public nor private abortion services have fully measured up to the needs of the a
seekers. While private providers need to be regulated and made accountable to the law
educated about safer technologies for improvement of both safety and quality
„Jc:nn
public sector needs to extend its presence, especially in rural areas, as well as strengthen theprovi
and quality of existing services to measure up to the satisfaction of aborfaon seekers. The
phase being planned currently needs to factor the issues flagged above in their strategy if reproa
health and healthcare are to improve in India.
3
Negative choice
RUPSA MALLIK
■eproductive technologies
access to reproductive
(RTs) including abortion. Access to
* _*
reproductive and genetic technologies
has indeed provided women with
expanded choice as well as numerous
benefits with regard to reproductive
time,
decision-making. At the same time,
unregulated provision and use of RTs
has served to create new challenges and
NO engagement with abortion in India
~ g”der.based inequities,
can be undertaken without considering
this paper( a three-part
first the issue of sex determination analysis of
practice will be
Contemporary developments like
contemporary
ukc the
ujc
availability of diagnostic technologies
' ■ sex selection coupled with the
for
desire for smaller families (as a result
of population policies that enforce a
two-child norm) have served to> create
new dynamism in family building
new
strategies. The use of RTs creates the
potential to alter what was once
considered the ‘immutable processes’
of repeated child-birth (Edwards
sons to include
1999:2) to have
‘
discretionary
childbearing
’ (Goodkind
(SD) and sex selective abortion (SSA). undertaken. First, the context - son
to
prevent
the
birth of
profound preference, growth in the political 1996:115)
SSA
underscores
the
economy
of
diagnostic
technologies
and
daughters,
complexities that surround the abortion
debate in India. Today, more than ever, enforcement of a small family norm The emergence of this phenomenon,
there is wide-ranging consensus in through population policies - is however, should not be viewed as__a
sudden consequence
the availability
India that this practice is morally and discussed. Second, the key debates on
— ------5_______of_____________
ethically unacceptable and the urgency the issue - with regard to development of diagnostic technologic. It should bg
to address it has gained tremendous of RTs, the regulation of these seen as an additive strategy (Goodkind
momentum. However, the intersecting technologies as well as the discourse on 1996) withihlfie existing continuum of
~
o " t women and
‘spaces’ occupied by sex selective abortion — is examined. In conclusion, discrimination
against
female
children
that has resulted in
abortion and women’s right and access the emerging regional patterns with
excess
female
mortality
and the decline
to safe abortion create a number of regard to SD and SSA have been
in
the
sex
ratio.
the
thorny overlaps that make
illustrated,
consensus urging a ban on sex
determination appear laden with For women, family based relationships * This is an abridged version of a paper
with the same title written for the
ambivalence and contradictions.
are a source of support as well as Abortion Assessment Project.
The right to bodily integrity,
sanction. However, support often rests 1. While SD and SSA can mean the
defined as the inalienable right of
on conformity with predetermined selective abortion of foetuses of either sex,
women to have control and autonomy
norms, Traditionally, childbearing, in this paper discusses the widely prevalent
over their bodies, has been central to
particular the birth of a son, is one trend of aborting female foetuses in India.
arguments made by reproductive health
such norm that a large number of
advocates to demand for women’s
women in India have to abide with.
[CJhoices exist that did not before, people
make decisions about procreation in the
range of
context of an expanding
<
possibilities... the arenas of decision
making have proliferated, there are new
domains and social actors involved, new
alliances of medicine, ethics and law, not
to speak of commerce (Edwards, et al.
1999:2).
I
Discrimination
against
girl
It is within this adverse setting that the desire for fewer children is not
a
children is the direct outcome of son that the political economy of diagnostic necessarily
accompanied
by
;
technologies
needs
to
be
examined,
preference
for
a
fewer
number
of
sons,
preference. Mutharayappa, et al. have
described three major factors that result Currently, three types of technologies Till date, son preference continues to
in sons being favoured over daughters are available to screen and identify the be a significant determinant of family
in India. First, the continued belief in sex of the foetus - amniocentesis, planning strategies, although this is
the economic utility of sons as family chorionic villious sampling and strongest for birth orders two or mote
labour, wage earners as well as support obstetric ultrasound. Amongst these (UPS andORC Macro 2000).
As India undergoes its fertility
for parents during old age. Dowry also ultrasound is non-invasive and
serves as an economic incentive to have currentlythe most widely used method transition the conditions exist for an
I
•
'■ ’ i in SD and SSA.
sons just as it serves as a disincentive for sex determination. It is important to intensification
to have daughters. Second, socio- note that the use of ultrasound to <Retherford and Rd^(2003) use NFHS
ratio—
at------birth--as —
an
cultural factors like patrilineal descent monitor foetal and maternal health has data ohi~the
t— „sex
—----almost aa routine
routine iand
prevalence
and inheritance as well as other aspects become; almost
— indirect indicator to assess *.
of kinship building serve to create recommended component of prenatal and determinants of the practice. They
conditions
that
sustain
female care. Simultaneously, there is littlejhat argue that multiple factors influence
disadvantage and inequality. Third, distinguishes the provision of thejest the levels of SSA confounding the
within religion sons have been accorded for legitimate reasons and those for the effect of any single variable. Some of
the unique privilege of performing purpose of SD. Much rests on the the important—predictor—variables
various rituals, including the last rites ethical conduct of medical practitioners identified by them include a composite
variable of the child’s birth order and
for deceased parents. All these together and radiologists,
the mother’s number of living sons,
create a higher premium on having
education levels of women as well as
sons.
By the mid-eighties, ten years after the
rural-urban residence. The authors also
technologies were first introduced in
point out that the potenUaLfoJLSSA^o
Other related factors identified as the country, clinics had proliferated in
increase is greatest in states like UP^
intensifying discrimination against girls most parts of the country7, though Bihar and Rajasthan .where there is
during the past decades include mainly restricted to urban centres. For continual evidence of strong son
marginalization of female labour as a example, one study (1986) estimated preference. Currently, these states have
result of the shift to mechanized forms that there were 248 clinics and low sex" ratio at birth but with
of agriculture. The shift to cash crops laboratories, and approximately 16,000 increased availability of information y
too served~to create enormous wealth tests were performed in Mumbai and technology for SD this can change. £
within
certain
communities, metropolitan region annually (Lingam
particularly in North India, which led 1998). The growth in the number of
i
to higher demands for dowry and a clinics continued
continued throughout
throughout the
the For over two decades there has been a
female
” nineties. In a single district of Haryana, sustained campaign against SD and
heightened perception of _f,
,
liability_jvithih the:'household (George 65 ultrasound clinics have been SSA. A significant focus of activism
registered (Pushkama, The Week, has centred on the demand for laws that
1997, Miller 1981).
Modernization,
defined
as 2002). With growth in the number of banl sex determination and regulate the
use of diagnostic technologies,
i
increased access to education and clinics and easy availability of these medical
tests
there
has
been
a
corresponding
Recently,
the focus has simultaneously
communication technology, has also
contributed in the diffusion of SD and drop in the price of obtaining a test, been on the effective implementation of
SSA. This is notable in the role that which fluctuates between Rs 500 to the law. The history of the activism can
mass media plays in the spread of 1500, though some have pointed out be broadly divided into two phases.
that recent efforts to ensure effective The first decade of activism was
caste_valu^___ CS" - 4he
/yX' upper
— —
accompanying anti-female
bias, implementation
has dominated by the campaign by the
bias,
implementation of the ban on SD has
anti-female
- --------——
Adoption of
these norms
by served to double the cost of clandestine Forumj\gainst Sex Determination and
of these
norms
communities that have traditionally SD tests.
Sex Pre-Selection (FASDSP) and
been more egalitarian towards women
Recent efforts by the government resulted in the formulation of the Pre
" norm as well
** asj Natal
Diagnostic
Techniques
served to intensify to enforce a two-child
has
also
women voluntary desire for smaller families (Regulation and Prevention of Misuse)
against
discrimination
can potentially serve to exacerbate SD Act, 1994.
f
f P':
(Agnihotri 2000).
and SSA. Scholars have pointed out
.
o-'-y
SEMINAR 532 - December 2003
The second decade of activism be often seen as scientific progress that insisted on a boy, she wanted to get the
has been symbolized by renewed helps reduce women’s reproductive test done. Dr Verma was willing to do
activism on the issue of SD and SSA burden. This shortsighted view of it, assuring that the test was very
but most importantly
on the technologies as magic bullets makes simple. He added that if the sexof the
implementation of the PNDT Act, 1994 little or no effort to address the unequal baby was “not satisfactory”, they
and subsequent public interest litigation arrangement and disproportionate would carry out an abortion the next
(PIL) filed in the Supreme Court of burden that women bear with regard to day... he did not even conduct a
India
resulting
in
improved reproduction (Birke et al. 1990). The cursory medical examination and when
implementation as well as amendments case of SD and SSA is a stark example asked about the well-known dangers of
to make the existing law more effective, of how RTs can result in reinforcing the test dismissed it... “Today in the
A main feature of the amendment was women’s oppression.
morning I have done three tests.” He
bringing within its purview new
Feminist advocates
remain said that they had conducted 20 tests in
technologies used at the preconception divided with regard to defining a a week’ (Chaturvedi, The Statesman,
and preimplantation stage for sex position
on
new
reproductive 1994).
selection.
technologies. Some in the past (e.g.
Feminist IInternational Network of
doctors who admit to providing
Resistance
to
Reproductive
and
SD
c
i
a
i
m
do it as a result of client
Contention and controversy have
Genetic Engineering) have advocated a pressure. They cite instances when they
characterized key debates amongst the
blanket ban. Others emphasize the have refused tests and been labelled
various constituencies,,in particular the
ambivalent effects that RTs have on ‘bad’ doctors which in turn affects thenactivists who urged a ban and the
women’s lives. As a way out of this practice. Many others have argued that
medical community, some of whom
deadlock the debate on science and they are in fact doing a good deed by
opposed the ban. Three broad themes
technology can and should be framed preventing the birth of a female infant
underpin these debates and are
discussed in some detail. First, the role around two broad issues - that of who will subsequently be the victim of
political control and of morality and gender-based violence.
of RTs and the gendered context in
ethical standards (Nelkin 1992: x). For
‘Dr V.K. Vats in charge of the
which they find use; second, the
example the FASDSP’s demand to Hiralal Nursing Homes is completely
usefulness of regulatory frameworks to
regulate diagnostic technologies and unabashed about carrying out sex
guide their use; and finally, the dual
ban SD tests is an effective strategy determination tests. “It has been going
agenda of promoting the right and
that highlighted the disproportionate on for a long time and a handful of city
access to safe abortion while curbing
control of the medical community over people cannot decide what the rural
sex selective abortion.
the provision of these technologies and people want. In my opinion, it is better
‘FASDSP does not believe in
the absence of moral or ethical \ to abort a female foetus rather than
saying a categorical “no” to
standards in the use of that power. — give birth to her. In all probability, she
technology. But certain questions have
will be burnt for not bringing enough
to be asked: Is there a qualitative
difference between the various The medical community, till date, dowry’ (Dasgupta, The Telegraph.
technologies? If so, how does one remains slow to acknowledge its role in 1994).
‘It is one thing to legislate that an
identify it and if not, how does one fuelling SD. Doctors claim that the use
evolve criteria by which a distinction of amniocentesis and ultrasound is a individual should not be forced to
can be made to help determine those part of routine antenatal care to judge procreate against her will, and thereby
technologies that are desirable and the quality of the pregnancy. They protect legal access to contraception or
resist any attempts through law to curb abortion. It is quite another to derive
appropriate?’ (FASDSP 1992: 91).
The reproductive technologies the free provisions of these tests, and from this legal protection the belief that
need to be examined through a lens that over the years many have continued to individuals have the right to procreate
extends beyond the procedures to provide them freely in spite of the by any means possible. Hidden in this
include the socio-cultural and economic existing law.
discourse of means is the female person
context in which they find use. The
‘Dr M.L. Verma, the attending who is used’(Raymond 1993: 79).
most significant contribution of doctor on Saturday, met this reporter
To some, viz., members of
feminist analysis of RTs has been to when she visited the hospital posing as FASDSP, the need for regulation
demonstrate the gendered context a pregnant woman. The story trotted appears self-evident. But there are
within which these technologies are out was that she and her husband did many who oppose regulation. The
often used. However, RTs continue to not want the baby. But as her in-laws opposition comes from two quarters —
SEMINAR 532 - December 2003
*i requiring that they be prominently of strategies to address unsafe abortion
the medical community and certain
often conflated
conflated with
with the^usston
discussion
fantot Roups' The’iatter fear that displayed, among others, could help isis often
regulation of Stese technologies by law curb misuse.
t
”
on
curb misuse.
can potentially undermine the hardThe PNDT Act can be the first tighten
the MTP Act.
‘Yes, it is true that women seek
fought gains with regard to women’s step in a broader effort to regulate the
amniocentesis to have female foetuses
' "
*
pxlvwiw
reproductive rights, in particular
the
private health care sector. The law, as
currently implemented, fails in that it aborted, but should the state compel1 a
right to abortion. This does not mean <
\
/
she
does
not
tAV'W
V*
•
•
that these groups condone the practice
does AAVZV
not specify the-- ------------role that has beenI woman to rear a daughter
the played almost single-handedly by the want? A ban on sex determination tests
but rather that they differ on 1
private
private sector
sector in spreading SD and will impose unwanted pregnancies on
strategy to address it.
SSA across the country. It is worth women... [it] will restrict the jight of
In spite of efforts by the medical
’ ” i women for having abortions. It
* "D
community to water down the law, the noting that
SD was banned in all public Indian
will tell women that they can decide the
PNDT Act sets an important
L_r------ legal facilities in the mid-seventies.
1Having discussed
2 the
’ usefulness number of children, but not their sex
precedent to regulate RTs. One positive
of laws it is important to point out that (Kala, The Statesman, 1994).
effect of this law has been its ability to
rampant
growth
and they are at best a first step in
curb
rampant
growth
Type A
advertisement of SD clinics. Another addressing
deep-rooted
injustice,
Driven by Cultural Factors and
important outcome has . been to George (2002), one of the three
Family
Planning Goals (e^g.Tamil \adu)
highlight
Iti
the negative role of the petitioners of the PIL, points out that a
medical community in the widespread law and effective use of the judiciary
Women’s Parity
misuse of diagnostic technologies.
can bring pressure on the executive
(number
and sex of
branch of government to do a better job
living children)
of monitoring use of these technologies,
Framing a social problem in the
guide medical ethics that till date have
CulturalNorms
State Population
formal and specific language of law been seriously lacking with regard to
(e.g. son
Policies (eg. tw> SSA
has first clearly defined all the key SD and SSA and at the same time
preference)
childncim)
players and their roles in promoting the serve as a catalyst to address deeppractice and, second, put in place rooted patriarchal norms within Indian
High Rates
institutional mechanisms to enforce society. Other policy and programmatic
of Sterilization
norms that will regulate the practice. efforts,
however,
need
to
be
Type B
Legislation and regulation provide a simultaneously made to address the
Driven by Economic Factors
framework within which the role of factors
that
serve
to
sustain
(e,g. Punjab and Haryana)
multiple actors and institutions can be discrimination and violence again
concretely measured and evaluated. For
Prosperity
women.
instance, regulation has a critical
(High Per Capita Expenditure)
impact on the larger medical and
pharmaceutical industry that has The non-medical use of technology
uenaer |
High Gender
Low Female
sprung up around reproduction in and abortion for the sole purpose of sex
Gap in ■
SSA
Labour
Literacy |
Participation
general and SD in particular, of which selection must be distinguished from
women’s right and access to safe
doctors are only a part.
Upward mobility/Consumerism
t
The difficulties and gaps in abortion. Some within the medical
(increase in dowry payments)
v
of
technologies
like
community
have
argued
that
if
women
regulating the use <
obstetric ultrasound for SD should not have the right to abortion then by
Type C
_t extension they also have the right to
become the basis for an argument
Driven by Notions of Choice and
Autonomy (e,g. Delhi and
against regulation. A number of
c. choose the sex of the offspring and
Chandigarh)
therefore
SSA.
measures can be taken to ensure
effective implementation. For example
Sex
selective
abortion
is,
High Levels of
under both
both the
the MTP
MTP Act,
Act, 1971
1971 and
and the
the however,
however, not the result of an
under
Female Education
!
PNDT Act, 1994, specific sites have unintended or unwanted pregnancy. It
been classified for legal provision of is in fact the gendered preference for a
Prosperity (high
Access to
these services. Universal registration of certain type of pregnancy that guides
per capita
SSA
Information
these sites and listing of diagnostic the decision to undergo^sex; selective
s-----expenditure)
and Technology
abortion (MaUik 2002). The discussion
equipment, granting licenses <and
— —
SEMINAR 532 - December 2003
4
S.M. George (2002), Sex Selection/
Determination in India: Contemporary
Developments’. Reproductive Health
Matters 10(19): 190-92.
As India goes through a fertility s.M. George (1997), ‘Female Infanticide
transition,
regional patterns
are in Tamil Nadu: From Recognition Back to
emerging with regard to factors that PTenial?J R^ro^uAct^e Health Mattersappear to fuel sex determination and November, 10: 124-32.
D. Goodkind (1996), ‘On Substituting Sex
sex selective abortion within those
Preference Strategies in East Asia: Does
specific contexts (see diagram). The Pre-Natal Sex Selection Reduce Postinter-relatedness of these various Natal Discrimination?’ Population and
factors cannot be emphasized enough. Development Review 22(1): 111-25.
The intention, however, is not to Government of India (1996), The Pre
generalize or strictly allocate any one Natal Diagnostic Techniques (Regulation
type to a particular region/state but to anc^ Prevention of Misuse) Act, 1994. New
illustrate the complexity embedded in Delhi: Gazette of India.
International Institute for Population
the host of issues that constitute the
Sciences (UPS) and ORC Macro. 2000.
terrain within which SD and SSA takes National Family Health Survey (NFHS-2),
place in India. The objective is to 1998-99: India. Mumbai: UPS.
illustrate -v
the xawwxx
need xwx
for ~a multi-prong
ed h.B. Johnston (2002), Abortion Practice
__
utMouutw
ro—
Healthrisks posedby SD and SSA policy
mmatic approach
policy and
and progra
programmatic
approach in India: A Review of Literature. Mumbai:
that mightotherwise not occur
also withS which laws and their effective CEHAT and HealthWatch. May.
have an iroortant role L. Lingam (1998), ‘Sex Detection Tests
need to be highlighted. Tests like implementation
j
and Female Feticide: Discrimination
amniocentesis carry with them the risks to play.
Before Birth’, in L. Lingam (ed.)
of spontaneous abortion and infection.
Understanding Women’s Health Issues: A
Amniocentesis requires trained medical
Reader.' New Delhi: Kali for Women.
technicians to carry out the test, and References
R. Mallik (2002), ‘Sex Selection: A
even in those instances the possibility S.B. Agnihotri (2000), Sex Ratio Patterns Gender-Based
Preference
for
a
of injury to the placenta or to the foetus in the Indian Population: A Fresh Pregnancy’. Reproductive Health Matters
Sage 10(19): 189-90.
New
remains. There is evidence of tests Exploration.
Delhi:
Publications.
B.D. Miller (1981), The Endangered Sex:
being performed by untrained persons
F. Arnold, S. Kishor and T.K. Roy (2002),
with inadequate equipment and in poor ‘Sex Selective Abortions in India’. Neglect of Female Children in Rural
North India. Ithaca: Cornell University
conditions (Ravindra 1995).
Population and Development Review Press.
Separate laws - MTP Act to 28(4): 759-785.
R. Mutharayappa, M.K. Choe, et al.
reduce unsafe abortion and PNDT Act R Balakrishnan (1994), ‘The Social (1997), Son Preference and its Effect on
and the varied Context of Sex Selection and the Politics Fertility in India. National Family Health
that bans SD
implimentation strategies that stem of Abortion in India’, pp. 267-86, in G. Survey Subject Reports. Number 3,
from the diverse objectives of the two Sen and R.C. Snow (eds.) Power and March. Mumbai: International Institute
acts provide the possibility of Decision: The Social Control of for Population Sciences.
Reproduction.
Cambridge:
Harvard D. Nelkin (ed) (1992), Controversy’:
emphasizing the difference between the
School of Public Health.
two. Unsafe abortions can be reduced L. Birke, S. Himmelweit and G. Vines Politics of Technical Decisions. London:
Sage Publications.
through access to contraception, in (1990), Tomorrow’s Child: Reproductive
V. Pushkama (2002), ‘Where Have All
particular spacing methods as well as Technologies in the 90s. London: Virago the Girls Gone?’ Kerala: The Week, 7
emergency contraception, improving Press,
July.
the efficacy of those methods, better S. Chaturvedi (1994), ‘Boy or a Girl ? R.P. Ravindra (1987), ‘Struggle Against
antenatal care, among other things. They will Tell You for a Price’. Delhi: Sex
Determination
Techniques:
Unfinished Battle’.
Economic and
SSA, on the other hand, is part of a The Statesman, 22 May.
J. Edwards, S. Franklin, et al. (1999), Political Weekly 22(12f. 490-92.
family building strategy to ensure the
Technologies of Procreation: Kinship in
birth of only sons and can be addressed the Age of Assisted Conception. London: R.P. Ravindra (1995), ‘Myths About Sex
Determination Tests’. Facts Against
by
strategies
that
focus
on Routledge.
Myths. Mumbai: Vikas Adhyayan Kendra.
empowerment and education of women. Forum Against Sex Determination and
June. 2(3): 1-6.
Finally, there is critical need to build Sex Pre Selection (FASDSP) (1992), J.G. Raymond (1993), Women as Wombs:
on women’s own perspectives and ‘Using Technology, Choosing Sex’. Reproductive Technologies and the Battle
Development Dialogue. 1&2: 91-102.
Preference for
___________ Small Families__________
Sex selective abortion currently
accounts for roughly 11 per cent of
late-term, unsafe abortions^ in India
(Johnston 2002). It is important to
recognize that SD and SSA cannot be
addressed by placing limits on the
availability of abortions for women.
Rather, it will serve to heighten thenvulnerability. When SD and SSA are
viewed as a continuum it is evident that
effectively
curbing
SD
will
automatically lead to a reduction in
SSA and thus in unsafe abortions. On
the other hand it is easy to see that
arguments that favour curbing abortion
do little to address or reduce SD.
dilemmas with regard to seeking
abortion and, in particular, SSA
SEMINAR 532 - December 2003
Over Women's Freedom. San Francisco:
Harper Collins.
R.D. Retherford and T.K. Roy (2003),
‘Factors Affecting Sex Selective Abortion
in India*. National Family Health Survey
Bulletin^ 17, January. Mumbai and
Hawaii: UPS and East West Center.
SEMINAR 532 - December 2003
Law - Human Rights
FEMALE FETICIDE OR CRIME AGAINST HUMANITY?
For a hundred years in the late nineteenth century not a single female child was bom in the
royal house of the Raja of Porbandar.
Reviewing research on female infanticide in
contemporary India, Harriss-White, reiterating Amartya Sen, observes that the declining sex
ratio since the turn of the century points to the fact that the missing women are a social product.
Agnihotri’s painstaking documentation of district level data on sex ratio differences in the 5-9
age group, lead him to map a Bermuda Triangle of twenty four districts in North India where
the sex ratio of children averages 774 girls to a 1000 boys (Harriss-White 1999). Research
from the southern state of Tamil Nadu shows that two thirds of female infant deaths and forty
percent of female neo natal deaths are due to “social causes.
More recent work on sex
selective abortion, points to the abortion of one lakh female fetuses after sex determination tests
during pregnancy in the last three years, the more affluent sections of the Indian population
actively practicing ‘gender cleansing’.
While the Pre Natal Diagnostic Testing Act is seen as a solution to this problem, the magnitude
of the problem urges a re-orientation to the problem itself. Juxtaposed to this is the need to
make a clear distinction between the woman’s right to abortion and the right of the female fetus
against abortion. This question is further complicated by the fact that there is no clear gender
line between those that demand female feticide services and those that do not. It is women,
often older women in the family who make the most vociferous demands, and it is
t-
predominantly women in the medical profession who provide the services. The standpoint of
most doctors on this issue echoes the argument of procreative autonomy that has been
developed in US courts (see Dworkin 1996: 72-116). This right is one that developed with
respect to the right to contraception and was extended to argue that whether or not, or when to
have a child was part of the right to privacy, and that mothers especially had a right to
procreative autonomy. The relevance of the principle of procreative autonomy [and more
generally the right to privacy] to the Indian context is two-fold to begin with. First, with
respect to coercive family planning or population control programmes of the state, this right
includes the right to refuse family planning without detriment to the entitlement to state
welfare; it also includes the right to free, full and informed consent with respect to the use of
contraceptives. There is in this sense, an immediate link between the right to procreative
autonomy and the right to life and livelihood of the mother with respect to conditionalities for
receipt of welfare or participation in government [loans or the right to run for political office to
those with two children or less, for instancefand with respect to the dumping of hazardous
contraceptives on masses of poor women, a direct human rights injury.
On a second level the relevance is negative. While procreative autonomy must certainly
include the right to abortion, this right must be mediated by the state’s commitment to women’s
right against discrimination. The selective abortion of female fetuses, in this context, cannot be
interpreted as part of the right to procreative autonomy, since it is a practice of discrimination.
Yet, this is not an issue that is simple and subject to a linear interpretation. The very use of the
term feticide implies the acceptance of fetal rights and of the status of the fetus as a person,
veering dangerously close to the position of anti abortionists who raise the issue of fetal rights
as a limitation on the right to procreative autonomy. The problem in tackling the issue of
female feticide arises precisely on this score. Doctors and medical professionals tend to read
this demand as a matter related to procreative autonomy and encourage that autonomy in
i female feticide service seekers. Further if fetal rights are granted to female fetuses, they must
also be granted to other classes that are silently exterminated as well. The specific case of
disability may be raised here. It is accepted practice, medically, legally and socially to demand
and provide abortions if fetal abnormalities are detected. The effect is the same and pushes us
dangerously close to the eugenic standpoint. The rights of persons with disability must include
the right to be bom. The issue of abortion forces a synthesis ofjurisprudential reasoning with a
political reading of rights as they have been articulated in movements. Abortion, as a decision
of whether or not to have a child is a matter of procreative autonomy for the mother. Sex
selective abortion and the more recently discovered practice of sex selective conception
however invokes the right to life of women as a class which includes the right to be bom.
By this argument, female feticide must be seen as part of the practice of killing female
children. Female feticide alone already matches, even surpasses the worst episodes of
enmes against humanity in scale. There are clear correlations between the proliferation of
sex determination tests, increase in sex selective abortions [female feticide] and decline
<3
in sex ratio with urban areas showing sharper drop in the sex ratio than rural areas. And
not only do the numbers increase &ch year, but techniques for eliminating the birth of
girl children proliferate. The most recent method of exterminating girls that is on offer is
sex selective conception. Nussbaum provides a very useful and nuanced reading of the
intersection of privacy jurisprudence with questions of culture, difference, equality and
rights, arguing among other things that there must be ‘ a reliance on equality and equal
protection where the relevant issue involves systematic hierarchy and subordination
(Nussbaum 2004: 273).
The Universal Declaration of Human Rights opens with an assertion of the equal
inalienable rights of all members of the human family to inherent dignity and the
recognition that the aspiration of the common people for a world that is free is based on
their experience of barbarous acts, which have outraged the conscience of humankind.
Articles 1, 2, 3, 7, 16 (3), 22, and 25 (2) specifically relevant to the present purpose
address questions of entitlement to dignity and freedom without distinction of race,
i
colour, sex etc., assert the right to life, liberty, security of person and equality before the
law; the entitlement of the family to protection by the state; the entitlement to the
realization of social security; motherhood and childhood are entitled to special car- and
assistance. All children, whether born in or out of wedlock, shall enjoy the same-social
protection-, and finally that everyone is entitled to a social and international order in
which the rights and freedoms set out in the Declaration can be fully realized. Add to this .
a view of the Genocide Convention. For a crime to be defined as genocide, any of the
following five acts should have been committed with intent to destroy a group in whole
or in part; a) killing members of the group (b) causing serious bodily or mental harm to
members of the group (c) deliberately inflicting on the group conditions of life calculated
to bring about its physical destruction (d) imposing measures intended to prevent births
within the group (e) forcibly transferring children of the group to another group.
Female Feticide and female infanticide satisfy four of the five catena set out in the
Genocide Convention. Female feticide alone already matches, even surpasses the worst
episodes of genocide in scale. Conservative estimates drawn from the 2001 census
indicate 15 lakh missing girls in the 0-6 age group in a period of six years marking
sharp decline in the sex ratio. In the 0-6 age group, the 2001 census shows a decline in
sex ratio ftSm 945 girls for every thousand boys in* 1991 to 927. Punjab is at an
unspeakable 793. There are clear correlations between the proliferation of sex
determination tests, increase in sex selective abortions [female feticide] and decline in
sex ratio. And not only do the numbers increase each year, but techniques for eliminating
the birth of girl children proliferate. The most recent method of exterminating girls that
is on offer is sex selective conception. While much of this is advertised as serving the
interests of sex balance in families, “one baba, one baby,” the selection itself speaks a
different tongue. Both the doctor and the customer conspire to eliminate the possibility
of the birth of a girl, while sex selective abortions of male fetuses are unheard of. In the
light of Article 21 of the Indian Constitution, female feticide, by bringing about the
physical destruction of an entire class of persons by actively preventing births of
members of that class, is a direct infringement on the right to life, dignity and security of
person for surviving members of the class as also their mental well being, through the
i
creation of an environment of terror and hate engendered by such mass destruction.
Further, the sheer magnitude and brutality of the practice coupled with the guarantee of
impunity are masked by the terms in which feticide has been described to date: “A social
evil” because “girls are viewed as a burden by society” and because “doctors are greedy,”
resulting in a “shortage of girls” making it difficult for young men to find brides, we are
told! Girls are a commodity that can be bought and sold in the market, so why bother to
give birth to them? And the solutions then typically lie in awareness raising, and
educating people about the better ability of girls to look after them in their old age. It is
in the naming that the problem lies, and it is because of the naming that the problem
persists. Female feticide is not a social evil. It is gender cleansing — the extermination of
an entire generation of women, and by extension all future generations as well.
Meeting the definition of genocide on four out of five counts, but not being an act against
a national, ethnic, racial or religious group, rather a class of persons, it falls within the
ambit of
Crimes against Humanity.” The Rome Statute of the International Criminal
Court, in Article 7 defines “Crimes against Humanity” as “any of the following acts when
committed as part of a widespread or systematic attack directed against any civilian
!
J
population,
<5
with
knowledge
of
the
attack:
(a) Murder,
(b) Extermination;
(c) Enslavement; (d) Deportation or forcible transfer of population; (e) Imprisonment or
other severe deprivation of physical liberty in violation of fundamental rules of
international law, (f) Torture; (g) Rape, sexual slavery, enforced prostitution, forced
pregnancy, enforced sterilization, or any other form of sexual violence of comparable
gravity, (h) Persecution against any identifiable group or collectivity on political, racial,
national, ethnic, cultural, religious, gender, or other grounds that are universally
recognized as impermissible under international law; (i) Enforced disappearance of
persons, (j)
The crime of apartheid; (k) Other inhumane acts of a similar character
tentionally causing great suffering, or serious injury to body or to mental or physical
health. “Extermination” according to the Rome Statute includes the intentional infliction
of conditions of life, mterjflia the deprivation of access to food and medicine, calculated
to bring about the destruction of part of a population.
“Persecution” means the
intentional and severe deprivation of fundamental rights contrary to international law by
reason of the identity of the group or collectivity. Extermination through systematic
1
murder of newborn female infants and through abortion of female fetuses [under clause
(g) above] is part of the persecution of women as a class [clause (h) above].
In
accordance with the Statute then, female feticide meets the definition of a Crime against
Humanity strictly construed and not by analogy.
Article 25 of the Rome Statute addresses the crucial question of individual criminal •
responsibility. Clause (3) states that “a person shall be criminally responsible and liable
for punishment for a crime within the jurisdiction of the Court if that person: (a) Commits
such a crime, whether as an individual, jointly with another or through another person,
regardless of whether that other person is criminally responsible; (b) Orders, solicits or
induces the commission of such a crime which in fact occurs or is attempted; (c) For the
purpose of facilitating the commission of such a crime, aids, abets or otherwise assists in
its commission or its attempted commission including prowding the means for its
commission; (d) In any other way contributes to the commission or
commission of such a crime by a group of persons acting with
attempted
a common
purpose...(f) Attempts to commit such a crime by taking action that commences its
•i
O'
'<5
execution by means of a substantial step, but the crime does not occur because of
circumstances independent of^the person’s intentions.” Families that seek “female
feticide services,” but more importantly doctors and medical practitioners [and all
categories of employees in establishments with ultrasound or other diagnostic or fertility
treatment facilities] who use the facilities to either commit or aid in the commission of
female feticide, or, to use Satish Agnihotri’s phrase “Female Feticide Service Providers”
will be liable for punishment for perpetrating crimes against humanity under the
provisions of the Rome Statute in far more serious ways than contemplated by the current
legislation, which imposes extremely mild punishment for the first offence and then steps
it up gradually, the penalty structure itself defeating the purpose.
The conspiracy of
silence and non-reporting, especially by the medical fraternity, even when definite
information of the commission of this offence is available is yet another dimension that
must be addressed as also the collective responsibility of professional bodies like the
IMA for derogatory practices by members on a mass scale targeting an entire class of
persons, practices that use the professional training and qualifications that qualify them
for membership in these bodies. Clearly therefore the question of criminal responsibility
and liability must be structured on the basis of an understanding of the gravity of the
offence - not as a response to a “social evil”.
Any enactment of national legislation on female feticide must take cognizance of its
occurrence in radically new terms in order to effectively combat it, but more importantly,
to put an end to impunity, which is the hallmark of this practice today. While it may be
argued that the state has in fact taken steps to stop this practice through the enactment of
the PNDT Act, the ineffectiveness of the Act in real terms translates into state liability,
not
apathy
since we are not here speaking of individual crime but of mass
extermination, for which the mechanisms and the urgency of redressal cannot be a mild
legislation like the PNDT Act alone. This is one more reason why India must ratify the
Rome Statute.
b>’Kja~D ■
S | O
Workshop on Sensitising Media on Sex Determination
Goa, 2-4 May 2003
Presentation:
Protecting the Rights of Girls
by
Dr Erma Manoncourt, Deputy Director
UNICEF - India Country Office
Dear Colleagues, Ladies and Gentlemen:
It is indeed a pleasure, and an honour, to participate in this inaugural session and greet you on
behalf of my colleagues at Unicef and the United Nations Interagency Working Group on Gender &
Development. At the onset, I would like to express our appreciation to the organisers for this
reflection on the practice of sex determination and its contribution to the pre-birth elimination of
females.
This meeting comes at a very opportune time since you may recall that in 1990 the heads of the state of the
SAARC countries recognised the needs of girls and adolescents. At that time, they agreed that there are
vulnerable groups needing special attention and then prepared country-specific action plans to ensure their
survival, protection and development. Now, more than a decade later, it is timely and appropriate that to
take stock of what has happened and the situation of girt rights in 2003. It is important to judge ourselves not
by the long list of things we have done nor the amount of money spent on special campaigns or awareness
programmes; we must measure against the increased opportunities, better care and protection as well as
reduction in discrimination and/or outright violence that exist against young and adolescent girts.
I ve been asked to discuss the topic Protecting Girl Child Rights, as a prelude to examination of the issues,
and implications for the media. Last year during the UN Special Session on Children, India along with many
other countries, re-affirmed its commitments to child rights. As a result of the concluding deliberations, the
Assembly agreed on an far-reaching agenda entitled ‘A World Fit for Children,’ which sets a framework for
operationalising child rights into concrete actions, with particular emphasis on the girt child.
As such my brief remarks aim to provide a lens through which one may wish to examine the data,
discuss strategic communication interventions and make proactive advocacy decisions.
What do we know about the situation of girl children in India?"
A glance at the Indian Census 2001 figures shows that the demographic situation of women and girls
continues to deteriorate. The net deficit of females in India, which was 3.2 million in 1901, has now widened
to over 35 mi.'ion at the Census of India, 2001. Though the sex ratio of 933 females per 1000 males
recorded by the Census 2001 is an improvement over that of 1991, it continues to be indicative of a
population with gender discrimination. As a population should have, as a norm, at least 1050 women for
every 1000 men, because of the inherent biological superiority of women.
In respect to the child population in the age group 0-6 years (927 girls per thousand boys), the situation is
even worse, with the greatest decline has been in urban India as opposed to rural. The low child sex ratio is
cause of greater concern, as it appears to be a result out of wilful elimination of the female child in eariy
l
oSkend whir?’'0'? fam"'eS’The conse(’uence:: °f th's disturbing trend of falling sex ratios is indicative
of a trend, which w-,1 only .ncrease the vulnerability of women/giris due to their reduced number
What are the attitudes that appear give rise to this phenomenon?
UNICEV'sSto1 Stow m?theS and PeejUdi7 "a"5*9ir,S COntinUeS t0 raise considerable concern for
They are often rpnnirpd J™ 0 7 T! Often neg,ected ,n the,r access to nutrition, health care and education,
tha/beinq sent to school AndLT 9 n?™t0
fOr youn9er s,b,ings or to work in the household rather
de^rtS? °ther T’0 eCOn0miC factors’son Preference and practice of dowry have contributed to
SSTont r* in,?e
Ch",s heal'b' "u“on “Kl educa6on. 'r“ “woy “rougo adolescence are
to re ate X„ ° s
“J" 'nTOl,em“l 01
are at the tool el the life cycle WdlM beSsSle
,Pa^ddbhe dghls ol^lrtes^^wiil^the^^ger ^n^radon,C^uP|de!t be possM^o^build'aish'arad'and
the core
Pr0“i0" 0'taraan * °'8irtS “
oHhe^etoh1Pbm.n^ playf f" taclklin9 ne9ative consePuences of sex determination, such as the problem
d S Z S/T 3 V6ry Cntical P,ace in 311 discus^ns relating to hSman
A rights based aonXh inf^ ’ I f n'the r00t °f Child rightS ’the nght to be bom and sun/ive.
grits based approach introduces the following additional considerations in the sex determination debate: I
P'“ an'11,5
■ ™X°Sto „‘s"edX°Se " and
",h
'»
not iust obieZ n? fhildrea and kwomen are
Of rights - this means that they are rights holders
conE nf f
, 3 y- Th'S Chan9e in attitude initiates a Process thereby children within the
’
affect their hveseV Vin9
partic,pate in 1116 Pf0Cesses and ecisions that concern them and
peroplctivT SX™ alaCtiOnS’While 9°0d' are insufficient fram a Arrian rights
hXr/xs sss sr,s a need sha,ed in,eress
Clearly there is value-added from a righfc perspective that promotes the following via:
-
global legitimacy
indivisibility, interdependence and inter-relatedness
non-discrimination
participation
accountability - rights holders and duty bearers
empowerment
sustainability
—
y-
a
As you reflect and discuss over the next two days, I would ask you to keep in four guiding principles, which
are tne foundation for promoting gender justice, and therefore have a particular meaning for this discussion
on sex determination:.
Priniciple 1 - Gender equality starts early
Gender roles, attitudes and behaviours are established within the family and community setting. Creating an
environment where girls and boys are respected and cared for equally in early childhood is the first step
forbids5 break'n9 the inte^9ene^ationa, cyc,es of discrimination and disadvantage and ensuring equal rights
Principle 2 - Women's rights and girl's rights are interdependent
Only in societies where women have equal rights can the rights of girl children be fulfilled. Thus laws and
structures that guarantee equal rights for women are essential both for women themselves and for girls.
Principle 3 - Children's rights cannot be achieved without girl's rights
S nn^ld/u0Uld ^Uffer oiscrimination is one of the foundation principles of the Convention on the Rights
will remain oS of o^rreacb°f
POpU'at'On 3nd * the'r equality is not assured'the Convention goals
Principle 4 - Civil society pa tnerships are needed to end the margnalisation of women and girls
In order to support change and overcome resistance, new collaborative relationships are needed within
communities and civil society, reinforced and nutured by the media. For UNICEF, the participation of non
governmental organisations and media professionals is an indispensable complement to legislative and
policy efforts of the Government to mobilise for the rights of girt children.
The role of Media in promoting the rights of girls
Journalists and media professionals have long been champions of human rights - drawing attention to
violations and being instrumental bringing about change. They are the eyes and voice of all citizens
demanding the right to expose facts, tell the truth and express opinions.
The work of the media affects children's lives. It influences decisions made about them and the way in which
ey are regarded by the rest of the society. The journalists and media professionals who write the
ea ines, tel. the stories, select the images and set the tone of print and broadcast coverage play a vital
XcogniseT9 PUbhC
'nfluencin9 those who
children's ’'ves. It is a role that often goes
Media professionals can do much to expose shortcomings in the system, but they must also ensure that
eir s ones do not compound the problem. As you engage in addressing the issue of sex determination and
its negative consequences, I believe that you are faced with 3 key challenges:
Challenges :
thp'pRcro3’6 3 SenSe °f PUbl'C outra9e a9ainst violence against women and girl children, especially
U It* I
•
Dli
.
How best to sensitise political leaders on the "shame'' of gender violence, such as prebirth elimination
ot females, against women and girls?
How to empower individuals, families and local communities who are seized with the issue but hesitate
io act f
These questrons have no simple answers and will not be solved in this meeting; but they require continued
reflection and self-evaluation, plus a commitment to a human rights approach to development. So
what can you do, as media professionals, committed to children’s rights and gender equity? I don’t presume
to have a definite answer and there are many possible actions, but let me list a few actions for your
consideration. There is a need to:
•
•
Raise public awareness
Provide visibility to gender violence when and where it occurs
Break the gender stereotype and highlight biases when they occur
Give voice to girls and wc men
Give a balanced portrayal of implementation of the law and the social dimensions of the problem
Increase public dialogue on partnerships that aim to improve care for girls/women in their families and
communities and promote increased male responsibility in family life.
The emphasis given by UNICEF on promoting the rights of girls and women is captured in its Mission
statement: “UNICEF aims, through its country programmes, to promote the equal rights of women and girts
and^to support their full participation in the political, social and economic development of their communities’
Guided by the Convention on the Rights of the Child (CRC) and the Convention on the Elimination of All
norms of Discrimination against Women (CEDAW), UNICEF is fully committed to the goals of gender
equality and the empowerment of women and girls.
We, therefore, look forward to learning from this workshop - your reflections on the specific communication
interventions and innovations to fight against sex selection as a means of advancing children rights,
especially those of young and adolescent girls will be of interest to many. As an outcome of your
deliberations, I urge you to develop practical, do-able recommendations that can guide all partners working
to respect, protect and fulfil rights of the girt child as well as improve her quality of life. In conclusion, I wish
you success and hope that the time you will spend at this consultation during the next two days will go a
long way in promoting the achievement of the rights of the girl child in India.
Thank you
4
I
Kg$j£f:£ •
Child Sex Ratio
An Analysis of Census 2001 Results
Office of the Registrar General, India
2A Mansingh Road, New Delhi 110011
0R.T5.-rrr)
• ..c/’y .‘-V••
Sex ratio is an index of male-female
balance in population
ratio across different groups,
communities, areas bring out gender
imbalances in the society. For examples,
sex ratio in different age-groups, religions 5
scheduled castes, scheduled tribes
■■
At the Census 2001, sex ratio of
population stood at 933 females per
1000 males which is a marginal
increase from 927 recorded at the 1991
Census.
In contrast, child sex ratio in the age
group 0-6 showed considerable decline
from 945 girls per 1000 boys in 1991 to
only 927 girls per 1000 boys in 2001
Census
The sex ratio in the age-group 0-6 years
Is influenced by
• Sex ratio at birth
• Sex selective mortality at younger ages
The sex ratio at birth is usually a biological
constant with a value that lies between 943
to 954. Therefore, the sex ratio of in the
age-group 0-6 years is much lower than
the globally accepted constant.
Along with the data on population and
literates, the data on number of children in
the age group 0-6 years by sex was
obtained through manual aggregations in
the field at various levels immediately after
the enumeration was complete mainly with
a view to working out the effective literacy
rates by sex.
These numbers were utilised to work out
the sex ratio in the age group 0-6 years.
When it was found that the child sex ratios
in certain parts of the country have recorded
alarmingly low values it was decided to
highlight this fact in the first report on
Census 2001 known as
Provisional Population Totals
Paper 1 of2001
India
“It is dear that the sex ratio in the age group o-6 has
decreased at a much faster pace than the overall sex ratio of
the country after 1981. The decreasing sex ratio in this child
population perhaps has a cascading effect on the population
over a period of time leading to diminishing sex ratio in the
country. One thing is clear- the imbalance that has set at the
early age-group is difficult to be removed and would remain
to haunt the population for a long time to come. To say the
least, demographically the sex ratio of 927 of the population
in the age-group 0-6 does not augur well for the future of the
country. “
- Provisional Population Totals : Paper 1 of 2001 India
The rest is all history
Sex ratio of total population and child population in
the age group 0-6: 1961-2001
7'7'
1961
976
941
1971
964
930
1981
962
934
1991
945
927
2001
927
933
. 7:.
:h-! s :
Distribution of States by Child sex ratio -1991 & 2001
States/Uts
Child Sex ratio
2001
1991
HP, Punjab, Haryana Delhi,
Gujarat (5)^
900 & below
Punjab, Haryana (2)
901-950
Uttaranchal, DefiiLjtaja;
UP, MP, Gujantfr^^
Maharashtr^TN, (8)
951& above
Jlpf Biharf^ikkim, Arunachal ✓Sikkim, Arunachal Pradesh,
Pradesh, Nagaland, Mani^prf Nagaland, Manipur,
Mizoram, Tripura,
Mizoram, Tripura,
Meghalaya, Assam, WB,
Meghalaya, Assam,
9
Jharkhand, Chhatisgarh,
Jharkhand, Grim,
Chhatisgarh, AP, Karnataka, AP, Karnataka, Goa,
Kerala (15)
Goa, Kerala (18)
n, Uttaranchal, Rajasthan,
UPjJBihar, Orissa, MP,
Maharashtr^/TN. (8)
Distribution of districts by ranges of child sex ratio in the age
group 0-6 - India and major States 2001
■ ^^riuldisexjrati&aiid lumbenp:
^^^distnctsjSsh
i
I^sl
as 58001
0W
India
16
B5O
33
1
72
J
2» »50?
fiO(
213
245
12
591
5
3
4
14
f999J
liil
1.
Jammu and
Kashmir
2.
Punjab
10
7
3.
Haryana
5
12
2
4
Delhi
1
7
1
5.
Rajasthan
10
19
3
32
6.
Uttar Pradesh
22
35
11
70
7-
Bihar
2
25
10
37
2
IaJ H-' la 7—
08882
17
19
(
9
k 0<>C
G
ft A
£N
MG
'
Distribution of districts by ranges of child sex ratio in the age group
0-6 - India and major States 2001 (contd.)
A’-r’> ■ J32
888
SI
aS
SEesS
No.-
ip.anq^uinber^of
t
pi
1049]
8.
Assam
3
20
23
9.
West Bengal
1
17
18
10.
Jharkhand
3
15
18
11.
Orissa
12
17
1
30
12.
Chhatisgarh
1
13
2
16
13.
Madhya
Pradesh
14
Gujarat
15
Maharashtra
1
3
1
27
14
45
3
12
5
3
24
9
21
5
35
Distribution of districts by ranges of child sex ratio in the age group
0-6 - India and major States 2001 (contd.)
^^^hildgyr^^jiimbgdj^
RO
^7Uriiont-^<
No-: tci
thariS
|lQ00|
'
: i
16
Andhra
Pradesh
1
22
23
17.
Karnataka
12
15
27
18.
Kerala
1
13
14
19.
Tamil
Nadu
9
17
30
1
3
Top ten districts according to child sex ratio in the age group 0-6
India: 2001
SSENoJ
ion^urito^
>isi
LQ.
1
South
Sikkim
1036
2
Upper Siang
Arunachal Pradesh
1018
3
Pulwama
Jammu and Kashmir
1017
4
Bastar
Chhatisgarh
1014
5
Dantewada
Chhatisgarh
1014
6
East Kameng
Arunachal Pradesh
1011
7
Kupwara
Jammu and Kashmir
1010
8
Senapati
Manipur
1007
9
Mokokchung
Nagaland
1004
10
Badgam
Jammu and Kashmir
1003
Bottom ten districts according to child sex ratio in the age group 0-6
India: 2001
>■
i
Fatehgarh Sahib
Punjab
754
2
Patiala
Punjab
770
3
Kurukshetra
Haryana
770
4
Gurudaspur
Punjab
775
5
Kapurthala
Punjab
775
6
Bathinda
Punjab
779
7
Mansa
Punjab
779
8
Amritsar
Punjab
783
9
Sonipat
Haryana
783
10
Ambala
Haryana
784
Child sex ratio in selected states by residence 1991 & 2001
11 h In •-
™ -J»
India
948
Himachal Pradesh
-14
935
903
-32
966
934
900
-66
904
858
-46
Uttaranchal
952
914
-38
936
874
-62
Haryana
877
878
919
927
953
824
884
866
909
928
940
-13
949
809
789
886
880
924
-75
795
914
922
-53
-83
-5
-5
967
-10
967
973
-2
-13
955
955
950
Punjab
Rajasthan
Uttar Pradesh
Bihar
Assam
West Bengal
Jharkhand
977
969
986
-77
-23
-48
931
-25
-24
948
931
-5
-19
Child sex ratio in selected states by residence 1991 & 2001 (contd)
Orissa
969
954
-15
Chhatisgarh
988
982
-6
Madhya Pradesh
941
Kerala
958
905
923
965
954
964
-3
-20
-30
-14
Karnataka
944
925
953
979
963
I Tamil Nadu
945
931
Gujarat
Maharashtra
Andhra Pradesh
949
960
927
941
-22
-9
931
908
934
962
951
906
827
908
958
939
-25
-81
-26
-4
-12
+6
958
958
0
-14
955
951
-4
-19
Distribution of districts by child sex ratio in the age group 0-6 for
rural areas - India : 1991 and 2001
tncE|
Total
<
ter.ceni
kbsolui
’eireni
568 621,866,456
100
568
732,954,380
100
Less than 800
1
1,739,455
0.3
15
13,856,388
1.9
800-849
1
967,857
0.2
29
24,833,597
3.4
850-899
69
60,563,192
9.7
63
88,560,481
12.1
900-949
30.0
201
58.2
247
272,823,800
328,850,587
37.2
950-999
186,625,451
313 361,899,067
1,000 and above
28
10,071,434
1.6
13
4,029,527
0.5
156
44.9
Note: Excludes fourteen districts of Jammu & Kashmir where Census was not held in 1991, nine totally urban
districts and Kachchh and Kinnaur districts of Gujarat and Himachal Pradesh where 2001 Census was not
held in Feb-Mar 2001.
Distribution of districts by child sex ratio in the age
group 0-6 for urban areas - India : 1991 and 2001
ibpnlatia
rauo^
yen®
Total
565 215,383,755
100.0
568
282,380,679 100.0
Less than 800
0
0
0.0
24
13,405,562
4.7
800-849
5
1,126,912
0.5
53
27,780,152
9.8
850-899
68
23,129,902
10.7
107
52,524,605
18.6
900-949
261
110,785,366
51.4
247
124,129,800
44.0
950-999
216
78,588,567
129
64,082,576
22.7
1,000-1,049
1050
12
3
1,733,359
19,649
36.5
0.8
0.0
7
1
456,160
1,824
0.2
0.0
Note: Excludes fourteen districts of Jammu & Kashmir where Census was not held in 1991, Kachchh
district of Gujarat, Kinnaur district of Himachal Pradesh where 2001 Census was not held during
Feb-Mar 2001. Thirteen districts in 1991 and ten districts in 2001 are totally rural.
Sex ratio in the age group 0-6 population in million plus UAs
and cities: 1991-2001
^^^gglomeratior
l20W
1
Greater Mumbai
Maharashtra
934
911
2
Kolkata
West Bengal
954
939
3
Delhi
Delhi
917
866
4
Chennai
Tamil Nadu
962
959
5
Bangalore
Karnataka
948
938
6
Hyderabad
Andhra Pradesh
948
7
8
9
Ahmadabad
Gujarat
963
894
Pune
Maharashtra
Surat
Gujarat
Kanpur
Uttar Pradesh
Jaipur
Rajasthan
Lucknow
Uttar Pradesh
10
11
12
941
921
941
909
945
792
903
830
828
880
901
Sex ratio in the age group 0-6 population in million plus UAs and
cities: 1991-2001(contd.)
fegfeerf® i
jUiban^O
««
O+population);^;
?:
13
Nagpur
Maharashtra
944
939
14
Patna
Bihar
919
905
15
16
Indore
Madhya Pradesh
Vadodara
Gujarat
930
914
901
832
Bhopal
Madhya Pradesh
941
937
Coimbatore
Tamil Nadu
Punjab
923
818
956
17
18
19
20
21
Ludhiana
Kochi
Kerala
971
867
951
Visakhapatnam
Andhra Pradesh
965
963
22
Agra
Uttar Pradesh
894
803
23
Varanasi
Uttar Pradesh
964
903
24
Madurai
Tamil Nadu
942
950
>
Sex ratio in the age group 0-6 population in million plus UAs and
cities: 1991-2001(contd.)
BOsiiifl
■
ig’W -:
jt
20011*
■■■'”" population)^^
25
Meerut
Uttar Pradesh
928
864
26
Nashik
Maharashtra
931
904
27
Jabalpur
Madhya
Pradesh
947
891
28
Jamshedpur
Bihar
948
919
29
Asansol
West Bengal
946
963
30
Dhanbad
Bihar
945
941
31
Faridabad
Haryana
902
848
32
Allahabad
Uttar Pradesh
931
895
33
Amritsar
Punjab
862
770
34
Vijayawada
Andhra
Pradesh
949
936
35
Rajkot
Gujarat
909
821
935
897
Total
Ranges of decrease in child sex ratio in million plus UAs/
cities in 1991-2001
- ^decrease
No decrease
1-9
10-19
* N arrieJifithe^C i
Asansol, Madurai, Kochi
Dhanbad,
Bhopal,
Chennai,
Visakhapatnam,
Nagpur
Bangalore, Vijayawada, Hyderabad, Patna, Kolkata
Nashik, Jamshedpur, Jaipur,
20-29
Greater Mumbai,
Indore_______
30-39
Allahabad, Pune
40-49
Lucknow, Coimbatore, Ludhiana
50-99
Delhi,
Delhi, Faridabad, Jabalpur, Varanasi, Meerut,
Vadodara, Rajkot, Surat, Agra, Amritsar
100 and
above
Ahmadabad, Kanpur
The situation of girls is of particular concern in rural and remote areas under the
•
strong influence of community and religious leaders
The educational programmes should be launched to eradicate all forms of
•
discrimination against the girl children and the participation of customary religious
and community leaders must be ensured to overcome the negative influences of
traditions and customs.
•
Effective to educational and vocational system will allow for the harmonious and
informed development of children and skills to make free choices in their life and to
act in a context of gender partnership both at work and family.
•
Eliminate stereotype in educational material and incorporate the CRC in the school
and training curriculum to enhance the promotion and protection of rights of girls
and to eradicate gender discrimination.
•
Eradicate degrading and exploitation images of girl and women in media and
advertising. The values and models of behaviour that were portrayed contribute to
the perpetuation of inequalities and inferiority.
•
Legislative measures to ban all the traditions and customs contrary to the rights of the
child would create a meaningful deterrent and clearly contribute to changing attitude.
•
The national legislation of the State Parties should clearly recognise the principle of
equality before the law and forbid gender discrimination while providing for effective
protection and remedies in case of non-respect.
•
Law reforms should be undertaken in both the civil and penal spheres against those
provisions which deprives the comprehensive protection of the Convention, eg.
Linking the age of criminal responsibility to the attainment of puberty.
•
The situation of specific vulnerable group of girl children should be separately
addressed as they are deprived of their childhood enjoyment and the traditional
inferiority is further aggravated by the prevailing external situation.
•
Girls below the age of 15 often did household works as adults which is not considered
as a “real work”. They should be freed from the vicious circle by providing equal
chances, equal treatment and education.
•
There is an urgent need for gathering information and gender dis-aggregated data in a
comprehensive and integrated manner at the international, regional, national and local
2
Need for the Declaration of the Rights of the Child:
‘The child’ by reasons of his or her physical and mental immaturity needs special
safeguards and care including appropriate legal protection, before as well as after birth.
The rights of the girl child is ensured in Convention on the Elimination of all Forms
of Discrimination Against Women (CEDAW), in the following articles:
•
Discrimination against women, denying or limiting as it does their equality of rights
with men, is fundamentally unjust and constitutes an offence against human dignity
•
All appropriate measures shall be taken to educate public opinion and to direct
national aspirations towards the eradication of prejudice and the abolition of
customary and all other practices, which are based on the idea of the inferiority of
womfcn.
CEDAW Convention insists that the state parties have the obligation to ensure the equal
rights of men and women to enjoy all economic, social, cultural, civil and political rights.
Beijing Convention:
The Beijing Flatform for Action, adopted at the Fourth World Conference on Women,
included “the Girl Child” in its 12 critical areas of concern. It recognises that in many
countries, the girl child faces discrimination in all stages of life from birth through
childhood and into adulthood. It urges the government to take action to provide access
for girls to training and information, to enable them to articulate their views and to
promote the equality and participation of girls.
The strategic objectives formulated under Girl Child are as follows:
1. Eliminate all forms of discrimination against the girl child
2. Eliminate negative cultural attitudes and practices against girls
3. Promote and protect the rights of the girl child and increase awareness of her
needs and potential
4. Eliminate discrimination against girls in education, skills and development and
training
5. Eliminate discrimination against girls in health and nutrition
3
6. Eliminate the economic exploitation of child labour and protect young girls at
work .
7. Eradicate violence against the girl child
8. Promote the girl child’s awareness and participation in social, economic and
political life
9. Strengthen the role of the family in improving the status of the girl child
The General Assembly Resolution on Girl Child, adopted on 9th December 1998,
regarding the rights of the Girl Child:
It urges all States to enact and enforce legislation protecting girls from all forms of
violence including female infanticide and pre-natal sex selection, female genital
mutilation, rape, domestic violence, incest, sexual abuse, sexual exploitation, child
prostitution and child pornography and to develop age appropriate safe and confidential
programmes and medical, social and psychological support services, to assist girls who
are subjected to violence.
4
A response from the Coalition for Maternal-Neonatal Health and Safe Abortion
The Coalition for Maternal-Neonatal Health and Safe Abortion is a eroup of individuals and
/
of Health and Family Welfare, Government of India, to amend the MTP Act as a measure to curb
the practice of sex selective abortion. In this connection it has been proposed that access to
second trimester abortion be limited only for certain indications, and that the service be restricted
to certain (government) facilities.
Our position on sex selective abortion
Prenatal sex selection is a gender discriminatory practice that represents misuse of medical
technology for irrational and unethical purposes. The PNDT Act with its recent amendments is a
key measure tor outlawing and eliminating this practice. The Coalition fully supports the need
If
measures t0 eiiminate the practice of sex selection, including strict implementation
O1 JrlxjL/ i
Cl.
On amending the MTP Act
The MTx Act (10 Aug 1971, as amended with effect from 18 June 2003) has served a vital
health-protecting purpose by helping to reduce mortality from unsafe abortion, while giving
women the choice of not having to remain pregnant under certain circumstances. Yet despite the
provisions of the MTP Act, the large majority of induced abortions have over the years been
earned out in an unsafe manner outside the scope of the Act. These unsafe abortions have been
occam*8 from the time before sex selection became prevalent, and are an important reason for
e high maternal mortahty rate in India. We therefore feel that any amendments to the MTP Act
(and the accompanying Rules and Regulations) should only be for enhancing access to safe
abortion, especially for women subsisting below the poverty line, women living in interior areas
and those belonging to vulnerable age or social groups. While it is true that sex-selective
abortions usually take place in the second trimester, it must be borne in mind that a large
proportion of second trimester abortions takes place for a range of valid indications that fall
“Heer the purview of the MTP Act. Restricting access to safe and legal second trimester abortion
would nave the following consequences:
1.
More second trimester abortions, including those for valid indications, would become
illegal and unsafe, and hence contribute further to maternal mortality. This is likelv to
disproportionately affect pour, rural and dalit women and adolescents.
2.
Any effect of measures to restrict second trimester abortion on reducing sex-selective
abortion would be short-lived, because advances in ultrasound and invasive technologies
such as amniocentesis and chorion villus biopsy allow sex determination within the first
trimester. Restrictions on second trimester abortion might even drive sex determination
into the first trimester.
Sex selective abortions are a major social concern. They result from a combination of preference
for sons and avoidance of daughters within an environment that promotes low fertility.
Addressing people's preference for sex selective abortions would require a multi pronged
approach that includes but goes well beyond effective implementation and monitoring of the
PNDT Act. Those include measures to improve women's status such as stronger implementation
of the Dowry Prevention Act, changes in property accession iaws in favour of women,
programmes for economic empowerment of women and social security schemes for elderly
people, especially those who have only daughters. Preventing sex selective abortion would
therefore require much more than imposing restrictions on the use of medical technology - it
would involve actions beyond the traditional purview of health and family welfare agencies.
Also, given the prevailing international political environment, we are concerned that measures to
curb sex selective abortions might be used by interests and organizations that oppose enhancing
access to safe abortion, to promote their agenda.
We therefore call upon all concerned persons and organizations committed to women's health
and reproductive choice, to lend their voice to opposing measures to restrict access to safe
abortion through amendments in the MTP Act.
Comments on proposed changes in the MTP Act, Rules and Regulations
The following comments refer to the draft version of the MTP Act circulated by Ravi Duggal by
email on 27 Feb 2004, in response to the request from the Ministry of Health & Family Welfare
to coordinate the process of suggesting amendments to the Act.
MTP Act
We do not recommend any amendments in MTP Act because amending the MTP Act will open
all its provisions to scrutiny by Parliament. In the current scenario, this carries the risk of risk of
additional undesirable changes being introduced that might result in reduced access to safe
abortion.
Page 1, Clause 2d and Page 7: Clause 4.c.i & ii
Inclusion of ISM practitioners will increase access to safe abortion and we welcome this
amendment, however we feel that in light of the above concerns, making changes in the "Act" to
:l„de ISM Practitioners be postponed till the environment becomes more favourable to
improve access to safe abortion. The latter would include large-scale mobilisation of public
opinion on the issue of unsafe abortion. We however feel that the MTP Rules and Regulations
may be amended at this stage, since this requires action at the level of the nodal ministry, which
in tum is following a consultative process.
Clause 3.2.b (Page 2)
We disagree with the iproposed change that for pregnancies exceeding 12 weeks, opinion of 2
doctors, "of which at least one
from1 a public facility" be necessary'. Our reasons for
— is ---1a
----- ~
- - — —.
disagreeing with this change are:
(i) Sufficient numbers of government doctors, leave alone MTP certified doctors, are not
available or accessible in rural areas
(ii) In several states, government doctors themselves cany' out private practice, hence they would
get into an unfair competitive relationship with MTP trained private doctors and gynecologists
(iii) This measure would give unnecessary power and control over access to safe abortion, to
public sector doctors, and by extension to government officials and politicians.
Page 2: Clause 3.2.iii
This change (addition of social and economic condition) would be subject to interpretation by the
provider. If the provider takes a restrictive view of whether or not a woman faces social or
economic compulsions, she would not be able to access an abortion. Hence we feel that this
amendment (and the corresponding changes in the rules and regulations) is not required.
The MTP Rules
Page 7 Clause 4,c.i
We feel that differential training requirements for first and second trimester abortions are not
required for the following reasons:
i. This measure would restrict providers other than gynecologists and those who have done
residency in gynecology and obstetrics, from providing second trimester abortions. A decline in
numbers of trained and certified providers will become evident some years after these rules take
effect.
ii. There is little evidence to show that differentials in negative outcomes following abortion are
related to differences in the training of formal MTP providers.
iii. The advent of medical abortion (misoprostol, used as per WHO guidelines) has made second
trimester procedures simpler and safer.
We therefore propose that even for termination up to 20 weeks, sub rule (c) should apply i.e.
assistance of 25 (or more as considered appropriate) cases of MTP by a registered medical
practitioner in a training hospital or institute should enable them to perform terminations up to 20
weeks. Our suggestion in effect is to make a change to the amendment of 2003.
Page 9 Clause 5.8
This clause needs to specify a redressal mechanism in case the process of inspection or
certification/ rejection after inspection is delayed for an inordinate length of time. The options
for redressal could be application followed by direct certification by a higher authority (along
with an administrative inquiry of the district mechanism by the higher authority) or the filing of a
court petition by the applicant in some form.
Ml P Regulations
Form II
The reporting formats should include information on medical abortion. We suggest that
following indicators be included in form 11:
■
Number of women for whom medical abortion was initiated
Number of women in whom medical abortion was completed
Number of women lost to follow up
We further agree with changes mentioned in 4.4 and 5.5. However we feel that under reasons for
termination point (g) relating to social economic compulsions need not be added as explained
earlier.
’
r
Other
We suggest that a new addition be made to the regulations in the interests of improving the
quality of services:
Service management guidelines for carrying out medical termination of pregnancy, covering the
technique(s) employed by that facility, should be physically available in the print form on the
premises of all government and private MTP facilities. In case the facility or provider is using
medical abortion, then guidelines for the same should
The service
should be
be available
available on
on the
the nremises.
premises. The
service
management guidelines should be based on government approved guidelines for the same."
Kirti and Sharad E>. Iyengar. ARTH
Indu Capoor, Pallavi Patel and Yd. Smita Bajpai, CHETNA
K Pappu and Anuradha R. CINI
TK Sundari Ravindran, Thiruvanathapuram
For
Coalition for Maternal-Neonatal Health & Safe Abortion
Secretariat: ARTH, 39 Fatehpura, Udaipur 313004
Email: arthsoc@sanchamet.in
Page 1 of3
Print
Ij..- ■, '•
Click here to close this window
]
Features
‘Treating infanticide as homicide is inhuman’
By Lalitha Sridhar
Prosecuting women such as Karuppayee, the first woman in Tamil Nadu to be convicted of
female infanticide, is hardly the answer to the problem of female infanticide and foeticide, says P
Pavalam, state-level convenor of the Madurai-based coalition NGO Campaign Against Sex
Selective Abortion (CASSA). The role of the state and society in perpetuating the secondary
status of women is the real issue to be addressed
How has the issue of female infanticide survived, even flourished, in spite of awareness
and laws that should serve as a deterrent?
The female infanticide issue is not a new one. Sexual violence is spread over various cultural set
ups. Only the methods differ. It is not peculiar to India, or, within the country, to south India. In
Tamil Nadu, it is considered chiefly prevalent in the Madurai, Salem and Dharmapuri districts. But
it is spreading - so are ultrasound clinics - to Namakkal, Theni, etc. Official mechanisms do not
pay any attention to the spread.
The socio-economic background to the issue has to be understood. In Madurai district, the
practice was mainly prevalent within the Kallar community. It is important, however, not to
stereotype people. The Kallar men migrated and the women were employed in agriculture, which
catered to all their needs. Marriages usually took place among relatives. The dowry system was
not in vogue. Upto the 1950s, the status of women was high.
But life in the villages is not the same any more. Agriculture is an inconsistent employer. In many
villages, the quality of life for labourers has steadily deteriorated. Anti-women customs, some of
them imported from outside, have steadily gained ground.
When we conducted a survey in the Usilai area (Usimlampatti taluk), of the 120 girls who
participated in our questionnaire, 57 were Kallars, 39 dalits and 24 members of other backward
communities. From their responses we were able to assess the impact of new economic policies,
marriage customs, dowry, physical and mental violence, migration, even alcoholism, on the status
of women in society. Where the women’s position in society is significantly undermined, there is
female infanticide. This link is undeniably present.
What are the tools available to address the issue, and how well do they work?
We believe that gynaecologists, VHNs (village health nurses), adolescent girls, general
physicians, the entire health infrastructure, panchayat presidents, village elders, spiritual and
religious leaders, even teachers should speak out against infanticide. As activists, we find their
opinions significant. We have tried to engage them in our campaign against infanticide/foeticide.
It is very important to understand that in the worst affected districts the killing of girl-children is
sanctioned by society. Neighbours and family members are likely to know about the occurrence;
they even support such incidents. Some mothers are co-opted willingly. Like I said, this is not a
new phenomenon. It has only become bolder, more technology-assisted.
Unless young girls are raised to feel confident about their gender, to have self-esteem, we can
only firefight, not eliminate the phenomenon. The media too has a role to play. Films and
television serials stereotype the role of women in society. Scripts include lines such as: “I am
helpless because I am born a woman.” “If only I had not had a daughter.” “Daughters are a
burden we must carry till our death.” These only serve to emphasise the fact that there is no
escape from the problems of being an Indian woman.
The media does not give consistent coverage to the issue. There is a sudden rash of reporting,
particularly if the case is sensational or tragic. Take the example of Karuppayee. A case was filed
Print
against her and her husband in 1994. Her first-born male child and third-born female child met
with natural deaths. She strangled her fifth girl-child the day the baby was born. The Indian
Council of Child Welfare lodged a complaint. The police moved with great alacrity. By 1996, she
was convicted but her husband was let off because he was not present at the scene of the
‘crime’. Karuppayee made big news because she was the first woman in Tamil Nadu to be
convicted of female infanticide. She was interviewed umpteen times and attained the status of a
‘notorious celebrity’. Her case is pending before the high court and she is out on bail. The impact
of all this on her life has been terrible. She no longer wishes to meet the media and has become
a recluse. She prefers not to interact at all. We have interviewed over 25 women who have been
convicted. Many have been badly scarred by their experiences. It is true that, as a strategy to
instil fear in the minds of potential perpetrators, the media coverage served a good purpose.
Inasmuch as the media is concerned, there is no follow-up, no regular review of the case and the
campaign. The issue is too complex to label people either ‘good’ or ‘bad’.
In another case, where the husband was convicted, the wife herself was the complainant.
Although the man is in jail, and there was marital strife from the start, the couple made up and the
woman has had another child by him. Women are often completely subservient to male
patriarchal values and hierarchies. A woman often has no identity without her husband.
When the whole issue is centred around awareness-building and bringing about social change at
the fundamental level, sustained and balanced media support can be invaluable. However, it is
not forthcoming. We at CASSA have in fact noted that media coverage of our activities has
steadily declined in the last two years. It seems female infanticide is not newsworthy anymore.
CASSA opposes the conviction of mothers culpable of female infanticide. Please explain.
We believe that treating infanticide as homicide and charging the mother and other members of
the family under the Indian Penal Code is inhuman and excessively harsh. The social structure
and value system is fiercely patriarchal. Intense family and social pressures drive women to kill
their own babies. The woman is helpless and has no power over her own decisions. A woman
who participates directly or indirectly in the killing of her own child is actually in the deepest denial
of her self-value. She should not be punished and must be treated with sympathy and concern.
She herself is a victim.
Also, the impact of judicial action has been devastating. Families have been displaced, broken
up, older children have dropped out of school, convicted women have shown suicidal tendencies,
the event has caused financial indebtedness, and, when both parents are jailed, older children
have become destitute. When families are placed in remand, the social ostracism itself becomes
a punishment more severe than anything the courts can give. Besides, women in custody do not
receive post-natal care.
According to government data, there were 2,568 reported cases of female infanticide in Tamil
Nadu in 2000. Amongst these, only 16 were brought to book. What can the state do about the
rest? The role of the state and society in perpetuating the secondary status of women is the real
issue to be addressed. Otherwise, women are simply punished twice over. “If the baby is a girl,
don’t come back,” they are told. It is not a threat to be taken lightly when the woman’s survival
and that of her other children, depends on her family.
What are the other concerns?
It is our contention that IMR (infant mortality rate) gender differential and sex ratio at birth are the
two key direct indicators to understanding female infanticide and foeticide. Our studies have
shown that even if there is a slight improvement in IMR differential, it is negated by a decline in
the sex ratio at birth. In other words, districts where the practice of infanticide seems to be on the
decline show an alarming drop in sex ratio at birth (an indicator of female foeticide). There has
been a consistent fall in infanticide between 1996 and 2001 in all the blacklisted districts. It is
foeticide that is the real threat now. But this is poorly understood and addressed.
We are campaigning for the United Nations and the World Health Organisation to recognise IMR
gender differential and sex ratio at birth as standard indicators. Not only India, many countries like
China for example have son-preference. No standard official data is available as of now. This is a
great drawback.
With regard to female infanticide, the government is chiefly concerned with the notorious districts
Page 2 of 3
Print
Says Bedi: “In societies like China and India, infanticide has been practised with all kinds of social
sanction. The act of abortion, even the term ‘foeticide’ is designed to de-sensitise, clinically, the
act of foetal murder. The MTP Act further trivialised the issue of foeticide. There has been an
inability to discuss the issue of foeticide without the larger debate on abortion, which is legally
allowed and has been seen as a triumph of the women’s rights movement in the country.”
Some doctors feel that the resultant de-sensitisation has meant, unfortunately, that foeticide can
no longer be separated from gender unspecified abortions. Bedi adds: “We may have to, for
some time at least, revive the guilt of foetal murder. It would be calling a spade a spade.”
An excerpt from the Hippocratic oath, written 2,300 years ago, reads like an accurate prophecy of
' doom: “Our mistakes are not discovered by the patient (or their kin in case of the deceased)...and
even if they are...they may whimper but rarely scream...and the worst penalty a doctor has to
pay for his sins is disgrace...and it is surprising how little it (disgrace) bothers those who are used
to it.”
(Lalitha Sridhar is a Chennai-based freelance journalist)
InfoChange News & Features, August 2004
Page 3 of 3
Memorandum to SCW to relieve the victims of female infanticide
who are accused guilty under Sec 302
Context:
The prevalence of female infanticide is now well established in Tamil Nadu. According
to the data revealed by DANIDA Foundation, female infanticide in Tamil Nadu is 15.8 per
thousand live births.
This practice is rampant in Salem District where 54.3 female
children are killed for every 1000 live birth. Dharmapuri accounted for 42.1; Theni 36.1,
Madurai 20.4 and Vellore 24.6 (November 28, 2001: The Hindu). It has been reported
that in Dharmapuri alone 105 female infants had been killed every month through out
1997 (Christian Medical Journal of India, April - June 1998, citing a report from the
Pioneer) and 3000 female infants were said to be killed during the period 1998 - 1999 in
Dharmapuri (Dinamani dated July 10, 2000).
The intensity of this inhumane
phenomenon is getting worse in Theni and Salem as per .the data for the year 2000
(PHC records).
In 1994, a criminal case was registered against one Ms Karuppayee from Usilampatti, an
agricultural coolie worker, who was said to be indulged in killing of her new bom girl.
She was proved guilty and convicted for life imprisonment by Madurai Sessions Court, in
1996. Inspite of judicial pronouncement, the incidence is not scaled down
Issues and Concerns:
Our contention is that the IMR Gender Differentials and Sex Ratio at Birth are the two
key direct indicators to understand the incidence of female infanticide and feticide. The
statistical data from 1996 to 2000 are taken for analysis to understand the impact of the
deterrent nature of the judicial intervention to tackle the issue of female infanticide. In
the year 1996, Karuppayee was convicted with life imprisonment for the act of female
infanticide. This first case was highlighted by the media to a larger extent, as a strategy
to instill fear in the minds of the potential actors.
It is in this context, the IMR gender differentials for the period 1996 to 2000 in the
districts of Dharmapuri, Madurai, Namakkal, Perambalur, Salem and Theni is discussed
here.
The sex ratio at birth for the same period in all the above districts is also
interpreted.
If we carefully watch the trend, the following inferences can be made:
1. There is no reversal of the trend which is clear from the IMR Gender Differentials
Table.
2. If there is a slight improvement in IMR gender differentials, it is negated by the
decline in the sex ratio at birth. In other words, the districts where the practice of
infanticide seems to be reduced are showing an alarming decline in sex ratio at birth
(practice of female feticide)
3. The spiral effect of both these violence (female feticide and female infanticide) are
spreading to new areas. To illustrate, Perambalur showing a drastic decline with
regard to sex ratio at birth. The IMR Gender Differentials shows a drastic increase in
districts like Salem and Them’.
The report of State Human Rights Commission for the year 1998 quoted the following
data, after study and verification of data by the Commission with J.D of health services.in
Dharmapuri District
Data for the year 1997:
Name of the Block
Death due to social causes
Pennagram block
261
Nallampaatti block
226
Karimangalam
130
Palcode block
125
Morappur
110
Dharmapuri block
106
The commission as a result of the enquiry has only insisted on the awareness and as
matter of procedure requested the police to do an inquest into every death of female
child. Altogether there were 1260 deaths in 18 blocks in Dharmapuri District. What is the
procedure the State can follow in dealing with these cases?
There are reported cases of 2568 in Tamil Nadu in the year 2000 according to the
government data. Amongst them, only 16 cases are brought to book. From five districts,
the practice/violation has spread to 13 districts. From a particular community, it has
percolated down to other communities. It is in this context, it is imperative to assess
whether legislation and judicial pronouncement play a significant role or are there any
ground level realities.
Fundamental issues for reflection:
In a society where girls live under a constant threat of being sexually exploited both
within the family and outside, where the evil of dowry is so rampant despite anti dowry
laws, where daughters are killed and tortured, where a daughter-in-law or wife is thrown
out of the house for giving birth to girls, where there are no social and economic security
provisions for old age and parents having daughters are left alone after their daughters
marry without any physical, economic, financial and emotional security, where religious
beliefs enjoin that the last rites can be performed only by sons, what else can be
expected of parents.
This insight on
structural violence on women
has
not been understood by the
Judiciary.
We quote that “ educating them that there is no gender difference, women have equal
rights to men, women are assured of thirty percent reservation in government
employment and panchayat raj institutions. In the midst of these programmes, it is very
pathetic that the rural folk still remain unaware". The learned Judge views the whole
situation as an issue of awareness raising and leaving the structural issues in air. We
do not negate the role of education , but mere functional literacy will not solve the issue.
The issue of gender division of labour and discriminating values
and other Institutions
and the role of state
in perpetuating the secondary status of women still an issue to
be addressed In the case of Neelavathy who was convicted for the commission of
infanticide, the court never took cognizance of the victims state of mind.
The victim was expecting a male baby and the news of the birth of a daughter affected
her. She had all clinical symptoms of postpartum psychosis. When she had the mindset
that she would be respected only by giving birth to a male child and by giving birth to a
girl child, she has burdened the family. With that mind set, without understanding the
consequences of her act, she killed the new bom. Like Neelavathy, there are several
others who are the victims of patriarchal
values
and
they are suffering from the
illness of depression and mental agony. The court never takes into account the mental
health of victims of female infanticide at the time of commission of the act..
Any civilised state is supposed to protect the human rights of all the members of the
State. But, in the context of women, she is experiencing nothing but violence right from
womb to tomb. The state policies and state laws never render or reflect gender justice.
Moreover, the State itself is giving priority to urban over rural, profit over nature, elite’s
interests over ordinary people and male over female. This gender hierarchy is further
perpetuated by the caste hierarchies and market based production process which is
globalised.
In a society where women are not valued and considered as an object and not
a
subject, the entire goal of the society is based on profit motive and the right to life and
livelihood has not recognized as value. So women do not have any self value and they
have deny their self value in a painful way. They are pitted against themselves on each
other in the most merciless way. Underlying is the deepest denial of self-value and the
desperate preparedness for self-victimization. This requires exodus from victimhood to
sovereignty. Thus, the elimination of the female infants after birth is an act of self
victimhood
The net result, it could be claimed, is that the woman get punished twice over - once by
depriving her the right to be bom and to be alive and again by punishing her for killing
her baby girl; as expected of her by community custom and also as an act of mercy to
spare her daughter the agony and tears of her own life.
Profile of the victims against criminal cases had been filed under 302:
Society for Integrated Rural Development (SIRD), a Madurai based Non-governmental
Organisation has documented the socio-economic profile of 24 victims of female
infanticide. The focussed group discussion, several fact finding visits, reflection with the
victimised persons, their community have raised several questions.
Status of the cases:
■
In 20 cases, mothers are both exclusively and jointly victimised.
In 17 cases, the
father is both exclusively and jointly victimised. One sixth of the cases are filed in the
name of members of the natal family of the mothers.
•
In 19 cases the victims were released under bail. In one case, the victim is under
judicial custody for nearly 8 months. In only one case, the victim was acquitted. In
one case, the victim was convicted and released under conditional bail after 8
months imprisonment. In one case, the victim is under imprisonment.
Impact of judicial action against the victimised families:
■
One family has been displaced
■
Domestic violence is acute in 14 families and 2 couples are separated.
■
Suicidal tendency is seen in all the 24 cases and 3 women had attempted suicide
and one succumbed to death.
■
All the 24 families are in chronic depression and anxiety.
■
In 10 families the children remained as orphans when their parents were in judicial
custody.
12 families are indebted.
Denial of human rights to the girl children of the victimised families:
■
The girls of the victimised families pay the heavy penalty and labelled for being a
member of penalised families. They are forced to face very difficult circumstances
especially when the parents are under judicial custody.
The universally
acknowledged repository of caring and security, the family has proved to be a
physically, psychologically and sexually threatening environment for the growing
giris.
■
Education has become an expendable option and they are forced to have lesser
entitlement to care and attention. Their childhood is crowded with domestic chores
and the self-image the society creates for her is one of the worthlessness, servitude
and dependence.
■
The young girls’ prospect for all round development is severely constrained.
■
Societal discrimination and neglect override on the vulnerability of the children can
initiate a life-long downward spiral of deprivation and exclusion from the social
mainstream.
■
The labelling has negative implications for her marriage, physical mobility.
The
psychological scars left in the minds of these girls adds to their self-negation. They
are victims of extortion and additionally they are tormented and terrorised by the anti
social elements and their own relatives. The odds staked against them are too many
to oppose single handedly.
They also experience some type of psychological
distress in the aftermath of crime. Immediate reactions are fear, anger, shame, self
blame, helplessness and depression. Long term reaction can include sleeplessness,
loss of concentration and fear of being alone. Though they resent their situation,
they are forced to sell their labour to meet the basic needs of the family. So even
after the release of the victims from the judicial custody, they continue to work as
labourers.
■
In this context, how are we going to rectify the situation. The real pathology lies with
the criminal justice systems which bent upon punishing the already victimised victim
(mother of infant girl). So, whole criminal justice system needs through review in
favour of mothers.
It should uphold the rights of victim to represent herself
throughout the case starting from FIR to trial. And also, Judges should be sensitised
about the victims’ perspective.
Are these 24 women and their families more sinned against than sinning? Are we
punishing the victims of patriarchy rather than its perpetrators? Didn’t they kill the female
babies they had been taught to devalue from childhood, mainly to ensure their own
survival in their marital homes? “If the baby is a girl, don’t come back” is the injunction
not to be taken lightly. There is no massive education campaign to publicise the basic
biological reality that it is the chromosomes of the father that determine the sex of the
baby. Given the reality that vast stretches of rural India still reel under patriarchy in its
crudest forms, is it realistic to penalise its victims for not standing up to it? Whose fault is
it that the woman, who labourers more than the man, and subsists on much less, has
come to be perceived as a liability? Furthermore, State is now targetting men and natal
family members which would likely lead to even more violence on women,
As the
criminal action is repressive against the poor families, there is more family
disorganisation. As these families are labelled as criminals for the action which is
legitimised by the community, some of the families are supposed to displace.
It is
counter productive in some cases where there is more demand for dowry while
arranging marriages for their daughters.
So without addressing the root issue behind this social crime, the State is punishing the
victimised families.
6
The earliest efforts to eradicate Female Infanticide:
■
In 1808, Alexander Walker, Chief President of Baroda, encouraged the chiefs of
different clans to enter into deeds to renounce this evil practice of killing female
infants. Penalty was imposed on the violators.
■
An infanticide fund was also set up to defray marriage expenses.
■
He also extended cash awards to parents of girls.
■
Regulation 8 of 1803, declared female infanticide as cognizable and punishable
criminal offence,
s
■
In Punjab, it was diagnosed that the intense factional rivalry was the cause of female
infanticide. So the State established marriage bureaus.
■
Johan Strachey enacted a Special Act of 1870, applicable to North, West Province,
which suggested an enlarged police force, increased surveillance, regular and
thorough census and restriction on marriage expenses. It was also declared in 1872
that those clans which had a proportion of girls less than 40 per cent of the total
population were declared very guilty of crime of female infanticide. Thus the entire
community was deemed to be responsible for every criminal act of exterminating
female infants.
Art 6 of the Convention on Rights of Children, cast the duty upon the State to ensure the
maximum extent possible the survival and development of the child.
Art 21 of the Indian Constitution guaranteed the right to life of every person.
The underlying perspective in all the above efforts is that the State / Community are
always held responsible for the social evil of female infanticide.
But now, the
responsibility is shifted from State / Community to individuals and families. This is a
clear indication of the abdication of State responsibility and shifting the role to the
families. So it is imperative to view those who are indulged in this crime as victims and
not as criminals.
A case of reparation:
The protection and promotion of human right to a large extent is based on the concept of
state responsibility. In addition, when a society is legitimising the killing of girl children
and when the feminine gender of this patriarchal society has been victimised by brutal
forces of tyranny and oppression, reparation is a means to foster a process of healing,
7
not only for the sake of morality, but also to build a lasting right to survival. Reparation
also implies the acknowledgement that serious wrongs were done to another party.. In
the case of female infanticide, the state is the major violator.
Reparation as ‘justice’
should be extended to the victimised mother and children of the victimised families. As
their nghts have been violated and therefore they are entitled to redress.
It is an
imperative norm of justice that the responsibility of the perpetrators be clearly
established and rights of the victims and potential victims be realised to the fullest
possible extent.
Prayer:
"
We humbly request the honourable authority to direct the
e
concerned department not
to file cases of female infanticide under Sec 302 IRC.
"
As all the alleged accused are the victims marginalised by their social, economic
and cultural condition, we request the State to appoint a Special Defence Counsel for
the victims.
■
We also request the State to provide
compensation to the victims of arbitrary
detention.
■
We also request the state to identify the blocks with
high IMR gender differential
and evolve local specific programmes
‘
Under Panchayat raj Institutions all the panchayats has to constitute health
committees, and this committee can be entrusted to take care of the birth and
survival rights of the girl children.
A corpus fund can be created in every panchayat to support the families to rear the
girl children and for awareness raising. Like 1870’s The panchayat must be held
responsible for the death of girl infants and Panchayat will be denied of economic
sanction if found with the prevalence of female infanticide
^andinlathh ^nlenihi,
QCadll
io gidy 2002.
Implementation of Existing Regulations Obstacles and Bottlenecks
Memorandum
Child Sex Ratio Ks Implementation of PCPNDT Law In Delhi
The PCPNDT Act to check the use of pre-conception and prenatal diagnostic tests for
the sex determination has been in place since 2002 but sex determination and selection
has continued unabated State governments including the Delhi government stepped up
efforts to enforce the law through formation of appropriate authorities for monitoring
implementation of the Act at district as well as state levels.
Despite efforts, something is definitely amiss. The birth registration data made available
by MCD recently shows that the sex ratio at birth in Delhi between January and
June 2004 indicates that only 819 girls were born for every 1000 boys. In prosperous
and educated South Delhi zone a mere 762 girls were born for every 1000 boys. In
the Rohini part of northwest Delhi the sex ratio at birth is 784 and in Najafgarh, a
part of southwest Delhi, it is 792.
These figures are horrifying and very much point towards the need for strengthening the
implementation of the Act. The. Act requires the registration of all ultrasound machines as
well as clinics that provide these services. However, it is evident that registration does not
in itself translate into prevention of misuse. As of now 210 genetic counseling centers,
221 genetic laboratories, 458 genetic clinics, 65 ultrasound clinics, 25 mobile clinics, and
44 government facilities have been registered by the state PNDT authority. A total of 73
complaints have been registered in court mainly for non-registration. {Report submitted
by state PNDT authority for the quarter ended on June 2004)
We appreciate this opportunity to meet with you and to raise a few of our concerns over
the continuous decline in the child sex ratio in Delhi, the phenomenon of missing girls in
our society, and the poor implementation of the PCPNDT Act in the state. We would like
to know the steps being taken by the government to address this issue on an urgent basis,
a
and hereby make a plea to the government to take action on the following concerns:
Concerns on the implementation of the act
•
Implementation of PCPNDT law in the priority list of state government and seems
and another appendage of health system. We would like to know the threshold
limit of the situation to recognize and prioritise action on the issue and not
consider it as an appendage to the implementation of other schemes and
programmes
•
Almost all the cases registered in the court are pending without any results. Even
the six cases against the advertisement published about the facility for pre
conception and pre natal sex selection test are pending in the court
•
Registration of the clinics providing the Prenatal and Postnatal diagnostic
services has not been efficient there are many clinics around especially in East
district which has not been registered under this act
•
Regulation is poor; last two quarterly reports to be submitted under the act by
state PNDT authority have not been submitted to the central health ministry. Only
a single case was filed in 2003-2004 which is also pending.
•
Monitoring of the clinical reports from the registered clinics is not done and also
these records have not been made available to civil society, though the
information should ideally be in the public domain. Needless to say, the practice
of sex selection cannot be changed through law alone. However, for civil society
to be vigilant and to contribute to the government’s efforts, it’s important that
they are equipped with information. Evidence based advocacy is the need of the
hour.
•
Policing by doctors on doctors is not working, many complaints are settled within
the fraternity and the civil society very often is left clueless.
Immediate Steps need to be taken
1. Every month a monthly report to be made available by the state
government on the trends in sex ratio at birth through hospital records and
birth registration data to the public
2. Registration of all the clinics providing the Prenatal and Postnatal
diagnostic services in the state
3. Speedy trial of the pending cases in the court to ensure efficient and timely
delivery of justice
4. List of all ultrasound machines both mobile and others along with the
4. List
names of the owners and the clinics available in the state should be made
public
5. An immediate meeting with all the elected representative of the Delhi to
be called under the chairpersonship of the H’ble Chief Minister so that the
problem is addressed by each one of them in their area of work
6. To ensure that clinic records and registers and information on court cases
is available for public scrutiny and building concrete mechanisms for
partnership with civil society organisations/individuals in monitoring and
social auditing of the clinics registered under this law
7. Non-medical person to be given the powers of PNDT authonty. To
ascertain that the Appropriate Authority is a multi-member body. Its work
is further strengthened and monitored by the state advisory council that
consists of legal as well as social experts
Signed and endorsed:
1) Ms Kumkum Sangari (NMML)
2) Ms. Uma Chakravorty (DU)
3) Dr. Puneet Bedi (APPOLO
Hosp.)
4) Dr Mohan Roa (JNU)
5) AIDWA
6) Jagori
7) Sama
8) Deepalaya
9) CWDS
10) Action India
11) CHANGE
12) Datamation
13) HRLN
14) Haq
15) Lawyer’s Collective
16) CFAR
17) CSR
18) Joint Women’s Programme
<
19) MRYDO
20) Mobile Creches
21) VHAI
22) Prema
23) Child Survival India
24) CASP
25) CAFE
26) UNFPA
27) Saheli
28) Zubaan
29) Nirantar
30) Marg
31) Women’s Coalition of peace and
Development
32) Indian Alliance for Child Rights
33) Ekatra
34) A B Baliga Trust
35) Delhi brotherhood society
36) Ankur
lw
Amendments
to
PNDT
Act
■ ■
■
•
•
•
Save the Girl Child
Critical Appraisal of PNDT Act and Suggested Amendments
Context:
Like several other regulative legislations section 16 and 17 of PNDT Act establishes the
usual bureaucratic mechanisms for prohibition and regulation. Citizen groups who have
been fighting this issue for several years find little or no place within the format of this
law. They have a toothless mechanism in this law and it is very easy to defeat the law.
Even in a recent case filed by the campaign against the violator in 1999 (Crime No.
927/99, Madurai), The Joint Director of Medical Services, the District-level Appropriate
Authority is waiting for procedural directions, till date, from the concerned ministry, is a
proof to show the ineffectiveness of the law.
Sec 4(2) : States that the pre-natal diagnostic techniques should be conducted only to
detect the abnormalities such as I) chromosomal abnormalities, ii) genetic metabolic
diseases; iii) haemoglobinopathies; iv) sex-linked genetic diseases v) congenital
abnormalities vi) any other abnormalities or diseases as may be specified by the Central
Supervisory Board.
Critique: It is however found from the discussion with the doctors and sonologists,
that the pre-natal diagnostic techniques are widely being used to confirm the
pregnancy, to monitor the pregnancy, to better medical management and to assess
the growth of the fetus.
Sec 4(3): Details the conditions under which the pre-natal diagnostic techniques could be
used or conducted on a woman namely i) age of the pregnant woman is above thirty five
years; ii) the pregnant woman has undergone two or more spontaneous abortions or fetal
loss; iii) the pregnant woman has been exposed to potentially teratogenic agents such as
drugs, radiation, infection or chemicals; iv) the pregnant woman has a family history of
mental retardation or physical abnormalities such as spasticity or any other genetic
disease; v) any other conditions as may be specified by the Central Supervisory Board.
CASSA ®
Critique: Normally, almost all pregnant women resorting to institutional deliveries
are subjected to ultrasonogram atleast 4 times during her pregnancy, as directed by
doctors.
Form D/E/F as mentioned in Rules are not being maintained by Genetic Counselling
Centres, Genetic Laboratories and Genetic Clinics
Sec 5(1): Details that informed consent should be obtained from the pregnant woman
before conducting pre-natal diagnostic techniques and a copy of which should be given to
the pregnant woman.
Critique: In practice, even in the registered Genetic Counselling Centres, Genetic
Laboratories, Genetic Clinics, this section is not being followed and many of the
Genetic Centres are not maintaining records as specified in Form G of the Rules,.
Sec 5(2) says that no person conducting pre-natal diagnostic procedures shall
communicate to the pregnant woman concerned or her relatives the sex of the fetus by
words, signs or in any other manner.
Critique: This section should also include the referral doctors.
Sec 18: Talks about the registration of all Genetic Counselling Centres, Genetic
Laboratories, Genetic Clinics.
Critique: Though Sec 23(1) penalises the owner of unregistered Genetic Counselling
Centres, Genetic Laboratories, Genetic Clinics with imprisonment for a term which
may extend to three years and with fine which may extend to ten thousand rupees,
the State Appropriate Authority has not filed any single case against the violators
for non-registration.
Sec 19(1): Says that the advice of the Advisory Committee should be obtained before
granting a certificate of registration to the Genetic Counselling Centres, Genetic
Laboratories and Genetic Clinics.
Critique: In practice, this provision is not being followed.
2
Administrative Amendments:
1. According to Sec 15 of the Rules, the intervening period between any two meetings of
Advisory Committees should not exceed sixty days.
But in Tamil Nadu, the State Advisory Committee met only 4 times ( 3.11.1998,
16.3.1999, 27.4.2000, 15.9.2000), since its constitution on 6.2.1996. It should be
made mandatory that the Advisory Committee should meet once in two months.
2. The Advisory Committee should be authorised to inspect the records supposed to be
maintained by the Genetic Counselling Centres, Genetic Laboratories, Genetic
Clinics, as it is democratic body.
Government Order can be issued to direct all the pre-natal diagnostic centres to
submit a status report, every six months, along with copy of the form D, E and F.
3. It is not realistic to regulate all the various private Genetic Counselling Centres,
Genetic Laboratories, Genetic Clinics, that offer pre-natal diagnostic facilities
particularly that of ultrasonography.
If the purpose of these pre-natal diagnostic
techniques are mainly to detect the abnormalities, metabolic disorders or certain
congenital malformations, then, considering the negligibility of prevalence of such
disorders, malformations, abnormalities, and eligible pregnant mothers, all pre-natal
diagnostic services could be restricted in government clinics, to cater to the needs of
the people and to make regulation more effective.
A new legislation to register all the private medical institutions should be
enacted.
Legislative Amendments:
1. The Act does not spell out the proper procedure, to take cognizance of offence.
As a result, there is an unduly delay in filing a case.
Case Study:
(A complaint was filed against a medical geneticist in Madurai for violating sec
18 & 22, in March 1999 and as per sec 28(1 )(b), a notice of not less than 30 days
in the manner prescribed was given to the Appropriate Authority.
Repeated
reminders were sent. The District Appropriate Authority was requested to consult
the Public Prosecutor for necessary action. The Deputy Director (Prosecution) of
3
Madurai Court read the fact in the case and asked the Appropriate Authority to get
the instruction from the District Collector, to file a private complaint against the
medical geneticist.
The office of District Collector replied that the PNDT Act
does not spell about anything about the issue of instruction from the District
Collector)
Clear procedure should be laid down to penalise the violators under Sec 23(3),
by the appropriate authority.
2. Pre-selection techniques are widely being misused and researches on invention of
new pre-selection techniques are being undertaken seriously.
The definition of pre-natal should be widened to include such pre-selection
techniques. Or all the pre-selection techniques should be banned outright (A
Public Interest Litigation was filed in the Supreme Court by Dr Sabu George,
CEHAT and MASUM, to draw the attention of the State to the gross misuse of
reproductive technologies leading to adverse sex ratio against girls and to widen the
definition of the term ‘pre-natal’ to include ‘pre-conceptual’ .)
3. Women seeking pre-natal diagnostic techniques should be regarded as innocent in the
absolute sense. Punishing a helpless woman would make her more vulnerable to
pressures and would leave her with fewer options. It would also discourage
courageous woman from coming out to expose guilty doctors and family members.
The clause of punishment to women undergoing sex determination test should be
removed.
4. Registration of abortion beyond 12 weeks should be universalised, including
private hospitals.
5. Sex of the fetus for all second trimester abortions to be documented clearly
6. Specific cause of termination to be mentioned (Congenital malformations,
genetic abnormalities, metabolic disorders)
7. To make the PNDT Act meaningful, all the provisions of the Act and Rules
should be strictly enforced.
8. The definition of ultrasonography should me made more explanatory under Sec
2(i), to include all imagery techniques such as ultrasonogram, Doppler Scan, CT
Scan, MRI etc., which are used as pre-natal diagnostic techniques.
4
THE ROLE OF THE STATE HEALTH SERVICES-EMERGING ISSUES
BY: Dr. REEMA BHATIA
MIRANDA HOUSE
UNIVERSITY OF DELHI
DELHI.
reemagbhatia@yahoo .com
This paper focuses on the role of the state health sendees in altering the sex ratio in
rural Punjab.
The first section briefly looks at the structure of the health services in order to identify
the various categories of health personnel involved in delivering the health sendees.
This will also help to exactly identify the proximity and frequency of the contact with
the people.
The second section of the paper focuses on the causes and factors that lead the health
personnel to propagate elimination of women before birth.
The paper is based on data collected through extensive fieldwork in rural Punjab. The
third and the final section of the paper draw conclusions.
I
Introduction
In most populations, the world over, sex ratio1 is favourable to females. In India.
South Asia, West Asia, and Africa the situation is different. In India the overall sex
ratio has been favourable to males, and since 1901 the sex ratio has fallen from 972 to
933 in 2001.
The reasons for a sex ratio that is unfavourable to females could be due to a greater
undercount of fri^ales relative to males, greater emigration of females, more adverse
mortality conditions for females than for males and sex ratio at birth becoming more
favourable to males than in the past (Premi 1997).
1 Sex Ratio indicates the ratio of women to men in a given population. The definition of sex ratio used
here is the number of females per thousand males. The sex ratio that is lower and unfavorable to
women is said to be indicative of a lower status for women
I
In the initial censuses a lower female count was attributed to an incomplete
enumeration particularly in Northern and Northwestern regions of the country. Premi
(Premi 1997) points out that differential male and female undercount has nanowed
down from 1951, 1971,1981, and 1991. He indicates that this reason is not substantial
enough to explain the imbalance in the sex ratio. In addition, statistics on international
migration for India are scarce and are not sufficient to explain the unfavourable sex
ratio (Premi 1997).
The paper seeks to pinpoint some of the reasons for the lower number of females as
opposed to males. The focus is on the manner in which the implementation of the
health services and the prioritisation of the certain health programs particularly the
Family Welfare Program have had an impact on the number of girls being bom.
Since a sex ratio unfavourable to women is attributed to poor health of women
(among other things), interventions in the sphere of health are one of the ways
through which the government seeks to improve the status of women. The
implementation of the health programs is examined at the lowest level of the health
hierarchy in the rural areas i.e. the Male and Female Multipurpose Health Workers.
The sex ratio in Punjab is 874 (as per the 2001 census) females per thousand males in
Punjab. This is lower than the sex ratio of 882 in 1981 and is lower than the sex ratio
of 933 (2001) for the country as a whole. It is one of the most prosperous states of
India. In 1996-97 Punjab had a per capita net state domestic product of Rs. 18,1213 at
current prices; second only to Goa. Only 12% of the total population of Punjab is
below the poverty line. The figure for India is 36%. Agriculture is the single largest
sector of the economy with 83.5 % of the total geographical area under cultivation.
(NFHS-2,2001). In addition Punjab is a patriarchal and patrilineal society. An
agricultural based economy is indicative of a society with son preference.
Given the predominantly agricultural based economy, the economic prospenty of
Punjab, and the patriarchal kinship relationships it is critical to examine the extent to
which the implementation of the health programs has imbibed the intent and objective
of the health policies particularly in the sphere of equality of both the sexes.
II
Thrust on Targets
An examination of the implementation of the health programs at the village level
show that the Family Welfare Program is the main program that gets implemented.
2
often at the cost of all other programs. The major focus of the health bureaucracy is
on the achievement of targets for Family Welfare. Here too the focus is primarily on
achievement of targets through sterilization. Sterilization is primarily female
sterilization. Male sterilization is very rare. In the pursuit of the targets, the Welfare
component of the Program is lost and only the ‘Planning’ component remains. Thus,
it would not be wrong to call the program the Family Planning Program.
In order to take health services beyond the pursuit of targets the Government of India
introduced the Target Free Approach (TFA) since 1 April 1996 all over India and
under the system of decentralized participatory planning. TFA has been renamed as
Community Needs Assessment Approach (CNAA) from 1997. However, adoption of
the target free approach has not done away with the importance of meeting targets.
Informally targets continue to be of prime importance.
Ill
The Cultural Frame
The targets have to be met within a cultural framework of patriarchy and economic
prosperity. The workers by virtue of being a part of the same patriarchal society have
modified and negotiated the rules to fit in with the fertility behaviour and desires of
the people. There is a shared understanding of the fact that spacing between children
and sterilization is not an option till a family is 'complete with sons.
It is within then context of this culturally determined fertility behaviour framework
that the workers try to meet their targets for family planning and sterilization. Thus
there is an attempt to hasten the process of family completion .
They try to hasten this process through many ways. One of the major ways is through
pre-birth elimination of the female foetus. The entire health hierarchy is propagating
this as a means of planning for sons. Once the family is complete then a case for
sterilization is ready and you are one step closer to target attainment.
There has to be a direct attack on son preference as a way out of this maze created by
science and technology. There have to be well -developed links between rights of
women as a part of culture and with female autonomy.
Initiatives and efforts taken to address women’s issues have been inadequate,
distorted, vertical, and top- down and have rarely emerged out of concern for
women’s health. The only solution being offered for women’s health is for maternal
health. This too is extremely limited and is restricted to distribution of iron and folic
acid tablets and to tetanus toxoid injections. Here too only those women who have
been targeted for sterilization by the health workers receive iron supplements to pump
up their haemoglobin levels. Poverty, illiteracy, and a rural background further
compound the mariginalisation of women. The household factors like its type, gender,
and generational control also contribute to her marginalisation.
There is a total lack of a supportive structure to empower women. That can only be
achieved through cooperation of different departments working in the rural areas and
through the involvement of people themselves. Female autonomy should be the prime
focus. Economic empowerment of women can lead to female autonomy. Structural
reforms like land ownership can also do the trick. It is only then that the shackles of
patriarchy can be broken or modified to suit women too.
It is a case of son preference versus daughter dis-preference. There is not just a son
preference butthere is also a daughter dis-preference that leads people to take extreme
measures like elimination of unwanted female foetuses. Thus what emerges is that
science and technology are not external to culture but are very much a part of culture.
Science and technology have become a part of the culture in the sense that they are
abetting a desire for sons and the lack of desire for daughters.
It is this kind of an understanding of family planning that the entire health hierarchy
in Punjab including the health workers identifies with. The doctors and the rest ot the
health services hierarchy is aware of the fact that in Punjab temporary methods ot
family planning are not adopted till the desired family composition is achieved. The
desire to have sons is something with which the health hierarchy at all levels identifies
with. The traditional social structure is manifested in the primary health care deli\ ery
system at the hands of the health functionaries.
REFERENCES
International Institute for Population Sciences. 2001 National Family Health Survey
(NFHS-2) Punjab. Mumbai: International Institute for Population Sciences
Premi, M. K. 1997 Changing Population Profiles of India and Policy Issues in Ahmad
Aijazuddin, Daniel Noin, and H.N. Sharma. Ed. Demographic Transition - The Third
World Scenario. Jaipur: Rawat Publications.
4
rcniaic ruuiiciuc
STOP SELECTIVE SEX ABORTIONS
STOP FEMALE FOETICIDE
Home
Appreciation
►
A
1 VI .
■ a
’V’-
'A merely legal approach cannot root out female infanticide
Femicide
Lodge Complaint
Interview with Salem Collector J. Radhakrishnan
Laws & Acts
Programs/Projects ►
Articles
What's New
►
Links/Resources
►
Pledge Support
Our Inspiration
Admin
Forum
ft Search
Medical Ethics
Having set a trend, even if unwittingly, Salem District Collector Dr. J. Radhakrishnan is
overwhelmed by the fact that seven baby girls have been handed over to him since December
10. At his camp office in Salem, Radhakrishnan, a veterinary doctor by training, spoke to
Asha Krishnakumar about the poor social indicators of the district, the implementation of the
cradle baby scheme and the measures undertaken by the district administration to root out
female infanticide. Excerpts from interview:
Salem district has the dubious distinction of being one of the worst districts in the country in
terms of juvenile sex ratio. It is also the only district in southern India to figure among the
worst 50 districts in the country. What are the underlying reasons?
It is really a paradox that Salem, the fifth most prosperous district in Tamil Nadu, with a high
infrastructure index (134 compared to the national average of 100), is poor in social
indicators. The low juvenile sex ratio is a manifestation of several cultural, social and
economic factors. It also reflect the poor status of women and the son preference leading to
the doing away with girl babies. This is not a recent happening but a well-entrenched practice
that has spread to almost ail communities in the area.
How can such a deeply entrenched practice be stopped? Can the cradle baby and girl child
protection schemes address the problem adequately?
The cradle baby scheme is effective. Since 1992, 200 girl babies (10 of them between 1996
and 2001) have been saved by the scheme. In the last few months, legal measures have also
been used. More than a dozen arrests have been made on charges of killing girl babies and
some bodies have also been exhumed. This has instilled some fear among the people. Thus,
in less than five months more than 53 babies have been received in the government cradles
placed in the PHCs (Public Health Centres).
Since 1992, 2,576 girls have been enrolled in the district under the girl child protection
scheme. From January 1, 2002, the eligible age for enrolment in the scheme has been
brought down to one year. This will help save more girl babies.
However, it is important to look at the underlying reasons for the scourge. A high infant
mortality rate, poor female literacy, extensive higher order births and the dowry system are
issues that have to be addressed.
How is your administration dealing with these issues?
The revival of the cradle baby scheme under the 18-point programme of the present
government, has given us a major boost. We have, with the support of Danida (Danish
International Development Agency), set up a toll-free help line over which suspected
infanticide cases can be reported. We have made a few arrests, and also exhumed some
bodies, thanks to the help line.
These legal measures have made people turn to the government cradles to leave unwanted
girl babies; they no longer kill the babies. And, after December 10, many are handing over
their babies to me. Interestingly, all parents ask for a certificate that they have surrendered
their babies.
We are also trying to put in place monitoring systems. For instance, we have set up
monitoring committees at the district, block and village levels. All the 385 village panchayats
now have a monitoring committee comprising the panchayat president, the village
administrative officer, the health nurse, a noon-meal scheme worker and a representative
from a non-governmental organisation. The committee meets once a month to discuss the
problems that work against ending the practice of female infanticide. The committees send
the details of the meetings to the Collector.
http://www.datamationfoundation.org/female/ainterviexv.htm
2/19/200<
Page 2 of 2
male Foeticide
Various departments such as Health, Family Welfare and Education are being sensitised on
the issue. The Health Department, for instance, is geared to monitor all pregnant women and
improve the PHCs while the Family Welfare Department is to promote family planning; now
only 11.5 per cent of sterilisations and done in government hospitals and PHCs.
Our focus is also on increasing literacy among women. While there are over 1,200 primary
schools, there are only 155 middle and 67 secondary schools. Some primary schools are to
be upgraded soon.
Simultaneously, a massive awareness campaign against the scourge, with focus on
education, is being undertaken. More than 180 of the 385 villages have been covered. Also, it
has been decided to talk about the issue at every government function. A massive door-todoor campaign has been planned next month with help from the women's wing of the National
Cadet Corps. We are also getting the help of NGOs such as Poonthalir, World Vision,
Community Service Trust and VRDP (Village Reconstruction and Development Programme)
for the campaign. The Community Services Trust's theatre group has already started its
campaign in the villages. We are also in the process of starting a massive anti-dowry
campaign.
Foeticide is not rampant in this area, as it is in some other areas in Tamil Nadu. However, we
have registered all the 105 scan centres in the district.
The idea is to provide a humane approach; a merely legal approach will not help us get to the
root of the problem of female infanticide.
Have these programmes, started five month ago, had any impact?
It is too early to talk of results. But there have been some changes, For instance, the recorded
causes of child deaths 'due to social causes' has now come down to 10 per cent from 40 pr
cent. Similarly, the number of infant deaths, which was 260 a month until mid-2001, has come
down to 150 now. This is only an indication of the improvement. We hope to get better results
soon.
Back
Article in Hindi
Developed in National Interest by Datamation Consultants Pvt. Ltd. www.datamationindia.com
CAMPAIGN AGAINST SEX SELECTIVE ABORTION
Convenor: 11, Kamala 2nd Street, Chinna Chokkikulam, Madurai 625 002.
Telefax: 0452-2530486 Ph: 2534762, e-mail: sirdmdu@hotmail.com
Co-convenor : No. 10, Thomas Nagar, Little Mount, Saidapet, Chennai - 600 015,
Ph: 044-22353503/ Fax: 044-22355905, e-mail: hrf@md3.vsnl.net.in / hrf@xlweb.com
/
\
_ .
___
State-level Consultation
X
on
The Role of Appropriate Authorities in Implementing
the Pre-natal Diagnostic Techniques Act 1994 and Rules
(as amended upto 2002 / 2003)
24th September 2003
J
V
POSITION NOTE FOR DISCUSSION
I. Need for the Consultation:
Over the last 50 years, the sex ratio has fallen in our country from 946 women
per 1000 men in 1951 to 933 women in 2001. The Juvenile Sex Ratio was 976
in 1961 and fell to 927 in 2001. In Tamil Nadu, the practice of eliminating female
children soon after birth in several parts of the state unfortunately still continues
despite actions taken by the State and NGO’s. This is considered an important
factor for the declining child sex ratio. The Juvenile Sex Ratio (0-6 years) has
been dramatically dechning in Tamil Nadu over the last 60 years. The JSR for
Tamil Nadu was 995 in 1961 and declined to 948 in 1991 and fell to 939 in 2001.
(Census 2001 Data). ‘Sex selective abortion with the invent of sex determination
technologies and sex selection technologies are bound to accelerate the
downward slide of females along the demographic ladder. According to
UNICEF’s estimate, nearly 50 lakh female feticide is taking place in India each
year. IMA’s shocking data reveals that 5 million female fetuses are aborted
annually.
According to this data, four of Tamil Nadu’s-30 districts report JSRs (rural and
total) below 900.
Rural JSR are as low as 763 in Salem, 869 in Dharmapuri,
873 in Theni and 882 in Namakkal. Of 201 taluks in the State, 28 taluks from 11
districts report JSR (rural) below 900. Teh of these have JSR below 850-five
from Salem, three from Dharmapuri, and one each from Madurai and Vellore.
Six of these ten have JSR (rural) below 800.
Infant Mortality Rate (IMR) is the best indicator to understand the incidence and
intensity of the practice of female infanticide. The general fact is that infant
mortality rate of male is higher than female. On the contrary, if IMR of female is
higher than male, then we can conclude that the practice is prevailing. To be
i
more specific, the analysis of early neo-natal deaths and late neo-natal deaths
will reveal the incidence of female infanticide.
The US Department.of Commerce has proved that the natural female to male
sex ratio at birth is 100:103 - i.e. 971 female children for every 1000 male
children, which is a biological sex ratio at birth. Thus a deviation from this ratio
will indicate sex selective abortion or female feticide.
The at birth sex ratio obtained from PHCs for the years 2001, 2002 and 2003
reveals that there is a significant increase from 879 per thousand in 2001 to 922
per thousand in 2002 and there is a dramatic decline in 2003 (up to June) to 888.
What could be the factors contributing for this dramatic changes?
II. Some Important Provisions of the Prenatal Diagnostic
Techniques Act, 1994 (as amended upto 2002):
Recognizing the growing use of sex-selective technologies to identify and abort
female feotusis the government of India enacted the Pre-conception and Pre
natal Diagnostic Techniques (Prohibition of Sex Selection) Act 1994 Despite
limitations it is one measure to address the social injustice inflicted on women by
the abuse of medical technologies and unethical practices of doctors. The Tamil
Nadu Government is one of the few States attempting to strictly implement the
Act and is credited with a maximum registration of ‘scan’ centres, which is a
mandatory requirement under this law. There is a need however to strengthen
the enforcing mechanisms by incorporating the directions given by the Supreme
Court and the recent 2002 amendments to the Legislation and Rules.
Government of Tamil Nadu needs to take measures on an urgent footing to
recognise the important indicators as part of the vital statistics and to monitor the
incidence and intensity of female infanticide and female feticide. More stringent
actions by the Government will contribute to an increased deterrence against the
practice of infanticide and foeticide.
The purpose of the Act is to provide for the prohibition of sex selection, before or
after conception, and for regulation of pre-natal diagnostic techniques for the
purposes of detecting genetic abnormalities or metabolic disorders or
chromosomal abnormalities or certain congenital malformations or sex-linked
disorders and for the prevention of their misuse for sex determination leading to
female feticide.a
The Act which was originally titled as “The Pre-natal Diagnostic Techniques
(Regulation and Prevention of Misuse) Act 1994” was amended as “The Sex
Selection and Pre-Natal Diagnostic Techniques (Prohibition and Regulation)
Act 1994". '
7
Under the new Act, Sex Selection before or after conception is prohibited.
2
The newly amended act defines the following terms: embryo, conceptus,
fetus, sex selection, sonologist or imaging specialist,
Genetic Clinic . includes vehicle, where ultrasound machine/imaging
machine/portable equipment is used which has the potential for detection of
sex during pregnancy or selection of sex before conception.
Genetic Counselling Centre, Genetic Laboratory, Genetic Clinic should
employ or take services of any person, on honorary basis or on payment, only
those who possess qualifications as prescribed under the Act.
No person is permitted to render services to non-registered GCC, GL or GC;
Ultrasound machine or imaging machine or scanner or any other equipment
capable of detecting sex of the fetus should not be sold by any person to
GCC/GL or to any other person not registered under this Act.
The conduct of pre-natal diagnostic techniques is permissible if the person
qualified is satisfied for reasons to be recorded in writing that any of the
following conditions exist.
•
•
•
•
•
■
age of the pregnant woman is above 35 years
■
she has been exposed to drugs, radiation, infection or chemicals
■
she has undergone two or more spontaneous abortions or fetal lose
■
she has a family history of mental retardation and/or physical deformities
No one including a relative or husband can compel the pregnant woman to
undergo pre-natal sex determination techniques
No one including a relative or husband of a woman can seek or encourage
the conduct of sex selection technique on her or him or both.
Her written consent should be obtained in the prescribed form in the case of
invasive techniques like pre-implantation genetic diagnosis, amniocentesis,
chorionic villi biopsy, fetoscopy, fetal skin, organ biopsy, cordocentesis etc.
She should be explained the side and after effects before administering
invasive techniques.
A copy of the written consent should be given to her.
The person conducting ultrasonography on a pregnant woman should keep
complete record in the prescribed manner.
The person conducting pre-natal diagnostic procedure should not
communicate the sex of the fetus to any one including the pregnant woman or
her relatives.
Central Supervisory Board should meet atleast once in six months
Constitution of State Supervisory Board/Union Territory Supervisory Board in
each State/Union Territory.
Functions of State Supervisory Board:
To create public awareness against the practice of pre-conception sex
selection and pre-natal sex determination
To review the activities of the Appropriate Authorities in each State
To monitor and review implementation of the provisions of the Act and
Rules
To send report in respect of various activities under this Act to the CSB
and Central Government.
State Supervisory Board is a 21-member body. The Minister of Health and
Family Welfare is the Chairperson and Secretary incharge of Department of
Health and Family Welfare is the Vice-Chairperson.
It should meet atleast once in four months.
Appropriate Authority:
The Appropriate Authority will be a three-member body. (Director of Medical
and Rural Health Services, an eminent woman .representing women’s
organisation, an officer of Law Department)
Functions of Appropriate Authority:
To grant, suspend, or cancel registration of Genetic Counselling Centre
(GCC), Genetic Laboratory (GL) or Genetic Clinic (GC);
To enforce standards prescribed for GCC, GL or GC;
To investigate complaints of breach of the provisions of PNDT Act or the
rules and take immediate action
To seek and consider the advice of the Advisory Committee,
on
application for registration and on complaints for suspension or
cancellation of registration.
To take appropriate legal action against the use of sex selection
techniques by any person at any place, brought to its attention or suo
moto and also to initiate independent investigations in such matters.
To create public awareness against the practice of sex selection or prenatal determination of sex.
■
To supervise the implementation of the provision of the Act and Rules.
To recommend to the CSB and SSB modifications required in the Act or
Rules in accordance with changes in technology or social conditions.
To take action on the recommendations of the Advisory Committee on the
complaint received and investigated by the Advisory Committee.
4
Powers of the Appropriate Authority:
They have powers as are vested in a Civil Court under the Code of Civil
Procedure, while trying a suit in respect of the following matters:
■
The summoning and enforcing attendance of any person and examining
him on oath or on solemn affirmation
■
The discovery and production of any document or material object
producable as evidence;
■
The reception of evidence on affidavits;
■
Issuing of any commission for the examination of any witness;
■
Issuing search warrant for any place suspected to be indulging in sex
selection techniques or pre-natal sex determination
Advertisement in any form about the availability of facilities such as sex
selection and sex determination is banned under the Act. Internet is also
included as a medium of advertisement in addition to other forms of means of
communication such as electronic, print format, hoarding, wall painting,
signal, light, sound, smoke or gas.
Any person publishing and / or issuing advertisement relating to pre
conception and prenatal determination of sex is liable to punishment which
may extend to 3 years and with fine which may extend to Rs. 10000/-.
Any medical professional who contravene any of the provisions of the Act is
punishable with imprisonment for a term which may extend to three years and
with fine which may extend to Rs. 10000/- an on any subsequent conviction,
with imprisonment which may extend to five- years and with fine which may
extend to Rs.50000/-.
The Appropriate Authority should communicate to the Medical Council of
India, the name of the medical practitioner who contravened the provisions of
the PNDT Act, to suspend the registration till the disposal of the complaint, if
the charges are framed, and for removal of his name for a period of five years
for the first offence and permanently for the subsequent offence, if convicted.
Any person seeking the aid of GCC, GL or GC for sex selection or for
conducting pre-natal diagnostic techniques for purpose other than specified in
the Act is punishable with three years imprisonment and Rs.50000 as fine for
first offence and five years imprisonment and Rs. 100000 as fine for
subsequent offence.
Pregnant women are exempted from punishment unless proved otherwise.
5
III. Significant Changes in Prenatal Diagnostic Techniques
Rules:
The provider of ultrasound machines/imaging machines or any other
equipment capable of detecting sex of the fetus should send once in three
months a list of those to whom the machine/equipment has been provided, to
the State Appropriate Authority.
• The person / centre who is buying any such machine or equipment or any
other equipment capable of detecting sex of the fetus should file an affidavit
that the machines shall not be used to detect the sex of the fetus or selection
of sex before or after conception, to the provider of the machine and to the
Appropriate Authority.
• The person / centre who is buying any such machine or equipment or any
other equipment capable of detecting sex of the fetus should display
prominently a notice that they do not conduct any technique to detect sex or
selection of sex of the fetus before or after conception.
• The provider of such equipments should sell them to the person/centre
registered under PCPNDT Act.
• The registration fee has been revised.
• Form of Consent (Form G) is now made applicable only to invasive
techniques.
• Self-referral to ultrasound clinic/imaging centre/genetic clinic is permitted.
• Th® Central Supervisory Board has laid down a representative list of
indications for ultrasqund during pregnancies. ■
•
IV. Some steps taken by Government of Tamil Nadu to
enforce PNDT Act 1994, (as amended upto 2002).
•
Pre-Natal Diagnostic Techniques (Regulation & Prevention of Misuse) Act
1994 of Government of India was published by a Gazette Notification on
20th September 1994.
•
The Act came into force in Tamil Nadu with effect from 01.01.1996 by a
Gazette Notification published on 21.12.1995.
•
A press Notification was published calling for registration under the Act by
those practicing pre-natal diagnostic techniques (ultrasound) who are
engaged in Genetic Counselling / Genetic Clinics / Genetic Laboratories
and other related activities. However it did not evoke much response.
•
In order to enforce the Act more effectively the Government of Tamil Nadu
constituted a State Advisory Committee by a Government Order vide
G.O.MS No.66 Health dated 06.02.1996.
•
This was also notified in the Government Gazette. IIn G.O. Ms. No.431,
Health dated 31.07.1996 the State Government: also ordered the
constitution of District Advisory Committee.
6
•
At the State level the Director of Medical and Rural Health Services has
been nominated as the Appropriate Authority to implement the Act. At
District level the Joint Director of Health Services of the district concerned
has been nominated as Appropriate Authority with members.
In G.O.Ms.No.431, Health dt.31.7.98, the Government has issued orders
constituting District Appropriate Authority and District Advisory
Committees to advice on implementation of Pre-Natal Diagnostic
Techniques (Regulation & Prevention of Misuse) Act 1994.
The Joint Director of Health Services of the Districts who are the
Appropriate Authority and convenors of the Advisory Committees were
instructed to convene the meeting of the Advisory Committees and to take
suitable action for implementation of the Act.
•
In a recent press release, the Government have also warned Doctors who
are found indulging in malpractice’s regarding sex determination that they
remain liable to lose their registration for Medical practice.
•
The Government of Tamil Nadu has also issued warnings that offences
under the Act such as non-registration and misusing diagnostic techniques
and technology to disclose the sex of the foetus are punishable as
cognizable, non-bailable and non-compoundable offences punishable upto
3 years of imprisonment and fine upto Rs.50,000/-. These equipment’s
(Scan) are strictly to be used for diagnostic purpose only for the
exceptions under the Act.
•
In G.O.Ms.No.298 of Health and Family Welfare (R1) Department, dated
31.10.2001,
the Government have issued orders constituting Taluk
Appropriate Authority and Taluk Advisory Committees to advice on
implementation of the Act.
•
In G.O.Ms.No.4 of Health and Family Welfare Department, Chennai dated
13.1.2003, the Government have issued orders reconstituting State-level
Advisory Committee.
• The Appropriate Authority took active measures to register the scan
centres by issuing special advertisements periodically.
• The Appropriate Authorities organised awareness programmes through
electronic and print media and issued stickers regarding the prohibitory
clauses of the Act.
• The Appropriate Authority has reopened the file of Dr Chandrasekar,
violator under Sec 22 (1).
•
From information available the total number of ‘Scan’ Centres (genetic
clinics / laboratories / counselling centres) registered so far is 2034. Due
to constant vigil, 79 unregistered Scan Centres have been seized and
sealed. Cases have been filed against 21 Scan Centres and Judgments
delivered for 16 cases convicting the offenders with fine.
7
A few more significant changes in the Act and Rules
The Pre-conception and Pre-natal Diagnostic Techniques (Prohibition of Sex
Selection) Act 1994, despite all its limitation is one weapon to address the
social injustice inflicted on women by the abuse of medical technologies.
• The incorporation of a representative list of indication for ultrasound during
pregnancy in the Rules itself is a recent legal development which will only
legitimise the legal practice and technology that is engaged in this human
rights violation.
• Prohibition of pre-conception sex selection is a useful amendment in the
context of mushrooming of fertility clinics.
• The inclusion of accountability of manufacturing companies to the Appropriate
Authority regarding pre-natal diagnostic technologies and sex selection
techniques is an important strategy to address the issue of female feticide.
• Powers of a Civil Court given to the Appropriate Authorities and clear
procedures are important steps in strengthening the enforcement
mechanisms.
• The inclusion of referral doctors as part of GCC is an important amendment.
• The new amendment to reconstitute the Appropriate Authority as a threemember body, constitution of State Supervisory Board and decentralisation
of Appropriate Authority at taluk level are important provisions.
• The constitution and functions of Advisory Committees is a step forward so
that issuance of registration and cancellation of clinics can be monitored
strictly.
•
V. Non-action against the prohibitory
advertisement and technologies:
clauses
on
Bharat Scans issued an advertisement dated 7th April in ‘The Hindu’ and
‘Business Line’ with regard to 4D Real Time Ultrasound Scanner, advertising this
technology as .a ‘window to the womb’ and providing ‘informed choice’. These
advertisements are in violation of Sec 22(1), 22(2) and 6(a) of PNDT Act. Inspite
of repeated memorandums from CASSA, requesting the Appropriate Authority to
initiate legal proceedings against Bharat scans for such an advertisement and
also against The Hindu, Business Line for publishing such advertisement, no
action legal or otherwise was initiated. There is also an advertisement in website
and in “Outlook”-on the sale of ‘Genselect’, a bill and douch kit from US firm,
which claims to help couples choose the sex of the child before conception. As
this advertisement is violation of Sec 22(1), 22(2) of PCPNDT Act, CASSA
submitted memorandums to the Appropriate Authority to take legal action against
the violators. Again no action was taken. Why is that no action was not
instituted against the violators by the Appropriate Authority inspite of the
repeated memorandums submitted by CASSA and its members?
8
VI. Main Highlights of the Interim Orders passed by Supreme
Court in case 301/2000:
Summary of the
4th May 2001:
First Interim Order of Supreme Court passed
on
Directions to the Central Government:
•
•
•
The Central Government is directed to create public awareness against the
practice of pre-natal determination of sex and female feticide through
electronic media.
The Central Government is directed to implement with all vigor and zeal the
PNDT Act and the Rules framed in 1996.
It ordered that the intervening period between two meetings of the Advisory
Committees should not exceed 60 days.
Directions to State Government / Union Territory Administrations:
•
•
•
Constitution of Appropriate Authority at the district an<2 sub-district levels and
also appointment of Advisory Committees to aid and advise the Appropriate
Authority in discharge of its functions.
Create public awareness against the practice of pre-natal determination of
sex and female feticide through advertisement in the print and electronic
media.
Submit report on the implementation and working of the Act once in three
months to the Central Supervisory Board.
Directions to Central Supervisory Board:
•
•
•
The CSB shall issue directions to all State / UT Appropriate Authorities to
furnish quarterly return to CSB, giving a report on the implementation and
working of the Act.
The CSB shall examine the necessary to amend the Act, keeping in mind
emerging technologies and difficulties encountered in implementation of the
Act..
CSB should take efforts to create awareness about the practice of pre-natal
determination test and female feticide and ensure the implementation of the
Act.
Directions to Appropriate Authorities
•
•
Take action against non-registered bodies and against those who issued
any advertisement in violation of sec.22.
Take action against all bodies and persons without a valid certificate of
registration.
9
Summary of the Second Interim Order passed on 19.09.2001:
•
•
•
•
Supreme Court directed the Appropriate Authority to file complaints under
Section 28 of the Act for prosecuting offenders.
The Appropriate Authorities are directed to search, seize documents,
records, objects, ect., of unregistered bodies under Section 30 of the Act.
It directed all the State Governments / Union Territories to implement the Act
and submit the compliance report (Quarterly return) as directed by the order
dated 4th May, 2001 as well as this order within six weeks from today.
The Supreme Court directed the concerned authority in the State of
Tamil Nadu to provide an appropriate form for getting registration to the
clinics having ultrasound machines and the Honourable Supreme Court of
India has further directed that if they are complying with the necessary rules
and regulations, the authority shall grant registration immediately.
Summary of the Third Interim Order Passed on 7.11.2001:
Supreme Court will wait for a period of three weeks from 7.11.2001 for the
constitution of National Inspection and Monitoring Committee by the CSB for the
implementation of the Act.
Summary of the Fourth Interim Order Passed on 11.12.2001:
Supreme Court directed the manufacturing companies of ultrasonogram to
supply information as to how many machines they have sold to various clinics
within the last five years including their names and addresses and also service
contract to those clinics or individual as the case may be.
1. Uma Parameshwaran, CEO, Wipro Ge Medical Systems Ltd. 1,
Corporate A Towers, Golden Enclave, Airport Road, Bangalore - 560017.
2. Toshbro Shimandzu Ltd. Khetan Bhawan, 2nd floor, Mumbai - 400020.
3. Erbia Engineering Co.Ltd., 2E/12, 4th Jhandewalan Extn., New Delhi 110005.
4. V. Prabhakar, CEO, ATL India Ltd., 79 & 94, Developed Plota, Perungadi,
Chennat- 600090.
5. Lareen & Toubro Ltd. (Medical Equipment Divn.) L&T House, 10, Club
House Road, Anna Salai, Post Bag No. 55247, Chennai - 600002.
6. International Medical Services Pvt.Ltd., 17 Industrial Estate, Maruti
Comples, Gurgaon- 122015.
7. A.K. Khosla. Chairman, General Electric Co. of India Ltd., E-16, Greater
Kailash, Part-1, New Delhi - 110048.
8. Rajeev Dayal, President & CEO, HCL Picker Ltd., D-3, Community
Centre, Poorvi Marg, Vasant Vihar, New Delhi - 110057.
9. Siemens Ltd., Mahape Workshop Shilphata Road, Behind MIDC Area Off
Thane Balapur Road. vill. Mahape, Thane - 400601.
The Supreme Court also directed the Central Government to frames appropriate
rules with regard to sale of ultrasound machines to various clinics and issue
directions not to sell machines to unregistered clinics.
10
| Summary of the Fifth Interim Order passed on 29.01.2002: |
The Appropriate Authorities are directed to follow the mandatory procedure
prescribed under Sec 19 of the Act before granting certificate of registration to
any person or organisation using the said machines / scanners.
It has suggested that the Union of India / concerned authorities can obtain
information about the user of the ultrasound machines / scanners from the
following Associations:
1. Indian Medical Association
2. Indian Radiologists Association
3. Federation of Obstetrics And Gynaecologists Society Of India (Fogsi)
Summary of the Sixth Interim Order passed on 05.03.2002:
The Supreme Court directed all the Health Secretaries of Bihar, Delhi, Gujarat,
Kerala, Jarkand, Orissa, Uttar Pradesh, Pondicherry and West Bengal to appear
in person on 9th April 2002, to report on the status of registration against the data
given by the manufacturing companies.
Summary of the Seventh Interim Order passed on 09.0’4.2002:
The Supreme Court has directed the State / UTs to take necessary actions
against the person who had not registered their ultrasound machines under
PNDT Act.
Summary of the Eighth Interim Order passed on 30.04.2002:
Supreme Court directed the concerned officers to seize and seal the machines of
the unregistered clinics within four weeks from 30.4.2002 and file necessary
affidavits indicating status of further actions taken and the information gathered
so far on or before 5th August 2002.
Summary of the Nineth Interim Order passed on 07.05.2002:
The Supreme Court of India directed that concerned officers to take further steps
for finding out unregistered clinics. If such unregistered clinics are found to be
operating in any part of the State, the concerned offices are directed to seize and
seal the said machines, and they are also directed not to permit them to
operate. All the States are directed to file necessary affidavit on or before
5th August, 2002.
Summary of the Tenth Interim Order passed on 18.10.2002:
The Supreme Court has issued directions to the Centre, all States and UT to file
a status report regarding the implementation of various order passed by the Apex
Court since May 2001. It has granted 6 weeks to file the response.
11
VII. Experience in Other States:
As the former Appropriate Authority of Karnataka was also the Chairperson of
State Commission for Women, she had the civic powers to send summons to the
violators, to call for enquiry, ask for evidences and can inspect, raid, seize the
documents and hence monitoring the implementation of the Act was more
effective. Moreover, the Appropriate Authority independently, on a suo motu
basis took action against the violators. The Appropriate Authority tried test cases
and took action against the violators if the evidences are relevant to the
provisions.
In Punjab, Dr Dahia was transferred from Faridabad to Chandigarh because he
was taking appropriate action against defaulting clinics. The newspaper reports
place lot of evidences. In the view of Supreme Court, if efficient officer is
transferred only because he was taking action against the defaulting clinics, then
certainly the action of the State Government is an unjustified one. The Supreme
Court ordered the State of Haryana through its Health Secretary to file necessary
affidavit stating reasons for transfer of
Dr Dahia.
During the Southern States Consultation held in Bangalore, in the month of April
2002, hosted by the Appropriate Authority of Karnataka and organised by Central
Supervisory Board, the following observations were made:
•
•
•
•
•
The scan centres with the military hospitals and railway hospitals could not be
registered as there is an administrative jurisdiction between the State and the
Centre.
The Appropriate Authority had technical difficulties in maintaining the seized
machines.
There is no effective monitoring mechanism for MTP Act.
The referral doctors are not included within the ambit of the Act.
The linkage between the sonologist and the gynecologist is not legally
recognised by the PNDT Act.
VIII. Medical Termination of Pregnancy Act, 1971:
It is important to mention that the PNDT Act has an important link with the
Medical Termination of Pregnancy Act, 1971 and Rules 2003.
Highlights of the Amendments:
District Level Committee consisting not less than three and not more than five
members will be constituted to approve the place for termination of pregnancy.
The termination of pregnancy by a person who is not a registered medical
practitioner shall be an offence punishable with rigorous imprisonment for a
term, which shall not be less than two years, which may extend to seven
years.
12
Whoever terminates any pregnancy in a place other than the approved place
shall be punishable with rigorous punishment for a term, which shall be less
than two years but which may extend to 7 years.
The owner of a place, which is not approved, shall be . punishable with
rigorous imprisonment for a term, which shall not be less than 2 years but
which may extend to 7 years.
Steps to be taken under MTP to strengthen PNDT Act:
•
•
•
•
•
All the records under MTP Act should be duly maintained.
The recording of the gender of the fetus aborted during second and third
trimester should be made compulsory.
Action against persons other - than medical practitioners indulging in
termination of pregnancy must be punished.
The Government must review the legalisation of medical termination of pill, as
there is wider scope for misuse to eliminate female fetuses.
The Joint Director of Health Services should display prominently, the list of
medical practitioners and hospitals registered under MTP Act, in all PHCs.
IX. Ethical Issues:
In India, inspite the abortions are legal, it is said that 20000 deaths per year take
place as result of abortions alone in India and 100 fold have long term morbidity.
According to ICMR, risk of maternal mortality is more than 10 fold even if they
are done by experts in Government Institutes i.e. 26/100000 first trimester
abortions, 322/100000 second trimester abortions. In addition to that, repeated
abortions may result in sepsis, shock, haemorrhage, anuria or oliguria, infertility,
chronic pelvic inflammation etc. (Family Medicine)
Dr Saradha Jain, Secretary of National IMA, warns that the risk of maternal
morbidity and maternal mortality need to be given much attention as an issue of
negation of women’s right to better health. Studies indicate that risk of death is 7
-10 times higher for women who wait until the 2nd trimester to terminate the
pregnancy. Sex Selective Abortions are all second trimester abortions.
According to Dr Vinay Agarwal, (Former Joint Secretary, National IMA), the
frightening fact is that in places where advanced technology is not available for
determining the sex of the fetus in the early week after conception, people turn to
scanning where sex is identified by the 6th or 7th month of the pregnancy and
then if the fetus is a female, they undertake abortion even beyond 20 weeks
which at times may even require a cesarean sections
From the above paragraphs, it seems true that the sex determination and sex
selective abortions are continuing, as doctors continue to violate the PCPNDT
Act and MTP Act. In these circumstances what Joint Directors of Health
Services under PCPNDT Act and Appropriate Authority under MTP Act can
do to contain these unethical practices.
13
Technological Interventions in Pregnancies: The prevalent gynaecological
practice necessitates the use of ultrasound even to confirm the pregnancy and
there are three to five ultrasound scans indicated in all the three trimesters.
Clinical diagnosis-is rarely practiced and the continuing of the very-pregnancy is
monitored by technologies. This unwarranted access to the technologies for
normal pregnancies leads to the misuse of the technologies
Commission for referrers - The corrupt practices such as commission from the
GC and GL to the referral doctors is not only an ethical issue. It also corrupts the
doctors and other para medical persons who are dealing with the patients.
Accountability and Transparency to the patients and to the society - As the
same Joint Director of Health Services is responsible for the implementation of
MTP Act and PCPNDT Act, she/he can take rndepehdeht initiative to monitor
both public and private hospitals for the occurrence of second trimester
abortions. If more number of pregnant women are undergone second trimester
abortions, she/he can initiate an interrogation process on the respective hospitals
or institutions.
X. Reforms I Measures in Enforcing the PNDT Act:
Budget Allocation-As many of the GCC/GC/GL/lmaging Centre/Ultrasound
Clinic are not aware of the latest amendments and supreme court directions, the
State Government should take necessary steps to allocate more funds to
strengthen the monitoring mechanism and for wide propaganda to issue
periodical advertisements and various directions regarding the latest
amendments and Supreme Court Directions. The corporate sector must be made
to sponsor advertisements for this public cause on Television, Radio and in the
print media.
Notification and enforcement of the Private Nursing Homes (Hospitals) Act
which was passed by the Legislative Assembly. This is very necessary for
making Private Hospitals accountable to Public Monitoring and make mandatory
for private hospitals to furnish all records for government and public scrutiny.
Awareness programmes-Government of Tamil Nadu / Appropriate Authority
must organise / support more awareness programmes on the Act / Rules and
ethics of not practicing feoticide this must be done in all villages and towns
involving local-government representatives and ngo’s.
Registration of GCC/GC/GL/Ultrasound Clinic/lmaging Centre under each
category-ln order to enhance the monitoring functions of civil bodies like
CA8SA, it is suggested that the Appropriate Authority brings public documents
which explains the classification of registration of GCC/GC/GL/Ultrasound
Clinic/lmaging Centre, on a periodical basis.
Monitoring the sales of machines by companies-The Appropriate Authority
should strictly. monitor the sale of pre-natal diagnostic techniques, sale of
14
pre-conception sex selection techniques by the manufacturing companies to the
registered and unregistered clinics this information should be made public in two
important newspaper dailies.
Constitution of State Supervisory Board, Appropriate Authorities at
different levels and Advisory committees-ln order to
strengthen the
enforcement mechanisms, the newly amended Act suggested to constitute State
Supervisory Board, Appropriate Authorities and Advisory committees at State,
District and taluk levels. These enforcement mechanisms are not constituted at
the fullest extent, The Government of Tamil Nadu should expedite the process.
Meetings of Board / Appropriate Authority / Advisory Committee - As per
the provisions of the Act and Rules and as per the directions of the Supreme
Court, the enforcement authorities will be directed to convene periodical
meetings, to strengthen the monitoring process.
Suo motu investigation against violations such as advertisement on sex
determination and sex selection, non-maintenance and disclosure of records, sex
determination through oral communication, disclosure of sex, records of
abortions sex-wise, etc., will strengthen the implementation of the Act. . In the
newly amended Act, suo motu action against the violation is clearly warranted.
The Appropriate Authorities, following the model of Karnataka State should take
independent initiative to take action against violators. Steps should be taken to
ban advertisement regarding sex selection in other forms of medicine.
Need for deadline in registering the centre-The Appropriate Authority should
immediately finalise the deadline for registration of all ‘Scan’ centres (Genetic
clinics / laboratories / counselling centres) and take immediate action against the
defaulters (non-registration) for the non-compliance of the provisions of the Act.
Legal Action taken against the violators - The Appropriate Authority through
MCI should periodically publish the data on the status of various action taken by
the Appropriate Authority against the violators.
Role of Advisory Committee in registration - We suggest that the Advisory
Committee can be consulted while issuing registration and cancellation of the
GCC/GC/GL/Ultrasound Clinic/lmaging Centre.
Functioning of Advisory Committee: Immediate action should be taken for the
constitution and regular functioning of advisory committees.at district and taluk
levels. There is no representation for Social Workers though the Act clearly spells
about inclusion of social workers and representatives of women’s organisation in
Advisory Committee..
Maintenance of records - The Appropriate Authority will be directed to ensure
the maintenance of records by GCC/ GL IGCI ultrasound clinic and imaging
centre as per the rules of the PNDT Act.
15
Registration of all referral hospital / institute / nursing homes to GC, GL,
Ultrasound Clinic / Imaging Centre as GCC must be ensured by the
department, as per the definition of Genetic Counselling Centre.
Union and State Government, Census of India and other statutory bodies
responsible for periodical data collection and recording should be persuated to
include Sex Ratio at Birth as one of the health indicators.
Stricter enforcement of the Medical Termination of Pregnancy Act (MTP Act
& Rules).
XI. Need for reviewing the pre-natal diagnostic and
pre-conception sex selection technologies:
In a son-preference society, it is suggested that any newly introduced technique
or technology should be reviewed by the expert committee constituted by the
parliament and must be permitted only after assessing the pros and cons of the
applications of these technologies on the rights of the girl child. The Central
Supervisory Board constituted under PCPNDT Act should instruct all the
manufacturing companies to apply to the Central Supervisory Board before
selling the same to the consumer.
Recommended Amendments in PCPNDT Act:
•
•
•
•
•
•
There should be a direct penalty clause for disclosure of sex by the medical
practitioner and his/her agents.
There should be a direct penalty clause for non-maintenance of records
The referral medical geneticists who are referring the pregnant woman for
undergoing ultrasound scan/pre-natal diagnostic test/pre-natal diagnostic
procedure should maintain records comprising the details of the pregnant
women, reasons for such test/procedures and details of imaging specialists.
The Chairperson of State Women - Commission and the Director of
Prosecution of State should be included as members in the State Supervisory
Board
The sex of the fetus should not be revealed to the referral doctors too and this
should be explicitly stated in sec 5 (2).
The Appropriate Authority is allowed to tale legal action against the use of
any sex selection technique by any person at any place, suo motu or brought
to its notice and also to initiate independent investigations in such matter.
The Appropriate Authority should have similar function in case of sex
determination.
Recommended Amendment in Rules:
•
There is no common reporting format for the equipment providers and
GCC/GL/GC/ Ultrasound Clinic/ Imaging Centre
16
Steps to be taken to Implement
the PNDT Act and Rules in
Tamil Nadu
• Public awareness against the practice of pre
natal determination of sex and female feticide
through print and electronic media.
• Conducting Advisory
every two months
Committee
Meetings
• Constitution of Advisory Committees at the
District level to aid and advise the Appropriate
Authority in, discharge of its functions. Scan
owners not a member.
• Create public awareness against the practice of
pre-natal determination of sex and female
feticide through advertisement in the print and
electronic media.
• Submit report on the implementation and
working of the Act once in three months to the
Central Supervisory Board.
ptjvr av-
th
f
.
2.^-.
03
1
• Take action against non-registered bodies and
against those who issued any advertisement in
violation of sec.22.
• Registration at District Level S.C. 2001
• Take action against all bodies and persons
without a valid certificate of registration.
• Appropriate Authority to file complaints under
Section 28 of the Act for prosecuting offenders.
• The Appropriate Authorities are directed to
search, seize documents, records, objects, etc.,
of unregistered bodies under Section 30 of the
Act - team.
• Submit the compliance report (Quarterly return)
as directed by the Supreme Court order dated
4th May, 2001.
• Frame appropriate rules with regard to sale of
ultrasound machines to various clinics and
issue directions not to sell machines to
unregistered clinics. Appropriate Authorities
can obtain information about the user of the
ultrasound machines I scanners from the
following Associations:
2
(1) Indian Medical Association, (2) Indian
Radiologists Association, (3) Federation of
Obstetrics And Gynaecologists Society Of
India (Fogsi)
• The Appropriate Authorities are directed to
follow the mandatory procedure prescribed
under Sec 19 of the Act before granting
certificate of registration to any person or
organisation using the said machines /
scanners.
• Appropriate Authorities to seize and seal the
machines of the unregistered climes within four
weeks.
• Appropriate Authorities take further steps for
finding out unregistered clinics - seize and seal
the said machines and not to permit them to
operate.
• The Supreme Court has issued directions to the
Centre, all States and UT to file a status report
regarding the implementation of various order
passed by the Apex Court since May 2001. It
has granted 6 weeks to file the response.
Publish Report for 2002 — Minutes of Advisory
Board.
3
• Constitute the S. Supervisory Board and Multi
Member
Appropriate
Authority
at
State
Level - 3 months of February 4th 2003.
• Nominate a women / 3 eminent social worker
/activists/social worker
Measures in Enforcing the PNDT Act:
• Increased Budgetary Allocations - PNDT
• Notification and enforcement of the Private
Hospitals Act
• Clinical Establishment - Notified / Rules sent to
Government
• Registration
of
GCC/GC/GL/Ultrasound
Clinic/lmaging Centre under each category
• Monitoring the sales of machines by companies
• Constitution of State Supervisory Board,
Appropriate Authorities at different levels and
Advisory committees
• Suo motu investigation against violations such
as advertisement on sex determination and sex
4
selection, non-maintenance and disclosure of
records, sex determination through oral
communication, disclosure of sex, records of
abortions sex-wise, etc
• Need for deadline in registering Scan Centres finalise the deadline - take immediate action
against the defaulters
• Joint meeting of JD + Magistrates and format
for reporting : Public prosecutors / police take
action immediately on mobile SCANS not
registered.
• Legal Action taken against the violators - The
Appropriate - Authority through MCI should
periodically publish the data on the status of
various action taken by the Appropriate
Authority against the violators - How is the
prosecution proceeding in cases filed.
• Role of Advisory Committee in registration - We
suggest that the Advisory Committee can be
consulted while issuing
registration and
cancellation of the GCC/GC/GL/Ultrasdund
Clinic/lmaging Centre.
• List of Registered Centres / Family Welfare
Department
5
• Display of doctors at PHC
• Action against Campaigns for sale of machines
to unregistered.
• Functioning and Composition of Advisory
Committee’s - inclusion of social workers and
representatives of women’s organisation
• Medical students curriculum - introduction
• Maintenance of records - The Appropriate
Authority will be directed to ensure the
maintenance of records by GCC/ GL ZGCZ
ultrasound clinic and imaging centre as per the
rules of the PNDT Act.
• Awareness — Sonologists / Radiologists.
• Registration of all referral hospital / institute /
nursing homes to GC, GL, Ultrasound Clinic /
Imaging Centre as GCC must be ensured by the
department, as per the definition of Genetic
Counselling Centre.
• What is - Genetic Counselling - Chromosome
abnormation
• Sensitise the judicial system on the law - public
prosecutors also — judicial academy
• District Advisory Authority Composition G.O.
6
A Critical Analysis of
Tamil Nadu Government Cradle Baby Scheme
Backdrop:
The extreme form of gender violence, in the form of female infanticide is deeply
entrenched in the patriarchal structure of the society.
The practice has the social
acceptance and has therefore been legitimised. It is difficult to deal such socially
consensual behaviour. Though the practice of elimination of female children soon after
birth is prevalent in many States in India, Tamil Nadu was the first state, which
•acknowledged the existence of female infanticide.
In 1992, the ‘National Plan of Action’ for children was framed, which includes the
objective of removing gender bias in improving the status of child in society so as to
provide her with equal opportunities for her survival and development. Various schemes
have been formulated by different States to protect the girl child from gender
discrimination. These schemes include both long term and short term measures.
The Tamil Nadu Government has introduced
two schemes to tackle the problem of
female infanticide. The first was the ‘Cradle Baby Scheme’, which was started in the
year 1992. This scheme was formed as a short term measure, to address the heinous
practice of female infanticide. The scheme involves, placing cradles for the unwanted
girl child at all the primary health centres, Hospitals, Orphanages and Children's Homes
to offer shelter and upkeep for the baby girls who have been abandoned by their parents
due to various social circumstances.
The scheme was under the administration of
Social Welfare Department. A Reception Centre was started in Salem in 1992. The
primary objective of the Reception Centre is to rescue the girl child and look after her
with due care and affection till she is handed over to an adoption agency/orphanage. It
is necessary to critically review this ‘Cradle Baby Scheme’ in terms of both its content
and implementation, to understand the effectiveness and relevancy to address the issue.
Status of Cradle Children:
As many as 136 babies were abandoned in Government cradles between 1992 and
1996 during the AIADMK Government.
Of these, 47 have been given for in-country
adoption, 12 children were taken back by their parents, 40 children are brought up in 8
Voluntary Institutions, 39 children died in the early stages itself due to diseases.
The then DMK Government derailed the scheme subsequently. Yet, during this period,
the abandoned children were rescued and given for adoption by the adoption agencies.
The number of children received during this period 14,7,1997 to13.5.2001 were 10 of
wh.ch one parent had taken the baby back.
The present Tamil Nadu Government
revived the Cradle Baby Scheme at a total cost of Rs 12.96 lakhs, vide its GO Ms
No.158 dated 24.10.2001.
The Government accorded sanction for starting four
Reception Centres, one each at Madurai, Theni, Dindigul and Dharmapuri, and also for
starting of 188 Cradle Points in all the Primary Health Centres/Selected Additional
Pnmary Health Centres and in the office of the District Social Welfare Officers in the
following districts viz. Madurai, Theni, Dharmapuri, Namakkal and Erode. Cradle Baby
Scheme was started in Usilampatti on 28°' July 2001 and 6 Cradle Points were set up.
After the announcement of 2002 Budget, 30 more Cradle Points were set up. Cradle
baby scheme was launched April 14, 2002 in Dharmapuri, set up cradles in 40 places.
! Districts
No. Of
Abandoned |
Total
babies
surrendered
Ti
No. Of
Children
Adoption/
Children
taken
foster
died
back by
care
parents
| Madurai
22
31
53
( Theni
4
0
4
Not
available
1
Not
available
10
1
1
9
120
Not
available
9
Not
availabel
Not
available
0
Not
available
0
41(F)
7(M)
0
0
0
Not
available
Not
available
before
1.4.2002
14 female
babies.
After
1.4.2002
11 babies
(3M+8F)
5
2
24
Not
available
Salem
(1997-2001)
Salem
(since
13.5.2001)
Dharmapuri
Dindigul
Namakkal
Not
available
The reception centre in DSWO, Madurai has not been functioning, the children received
in the cradle points are sent to the two adoption agencies in Madurai.
These two
agencies submit report about the status of the cradle children every month. The DSWO
also visits these centres and monitor the implementation of the scheme.
The present procedure is that if the DSWOs have not equipped to receive female babies
and act as reception centres, the female babies are received/rescued at the Cradle
Points and then handed over to the adoption centres and the information
communicated to the DSWO.
was
The adoption agencies also do have powers to directly
receive/rescue female babies. If DSWO acts as reception centre, the female babies
received/rescued will be handed over to the reception centre and the reception centre in
tum will hand over the babies to the adoption agency. There are 19 licensed agencies
to take up in-country adoption. These agencies are functioning in Chennai, Coimbatore,
Trichy, Thoothukudi, Madurai, Hosur, Dindigul, Salem, Nagapattinam and Thirunelveli. 8
agencies out of 19 are recognised to do intercountry adoption .
Issues and Concerns:
The Executive of the State and the Districts are formally inviting the parents to abandon
their unwanted, newly bom girl infants.
Under this scheme, a father is permitted to
abandon the second girt child of his third wife; another family is permitted to abandon
their 7 year old girl child; any parent can leave the girl child of any age if they decide to
abandon their girl children.
Though the State claims itself as the ultimate custodian of any abandoned children, it
legitimises the abandonment of girl child alone, which itself proves the patriarchal
construction of the State.
Instead of addressing the long-term issues of eliminating
gender discriminatory values and gender division of labour, it is simply permitting the
parents to abandon their girl children. The wider issues never draw the attention of the
State.
The issue before us is to see whether this intervention really addresses the issue before
us - protecting the rights of the girl children.
3
Perspectives
drawn from
international
and
national
instruments to review the scheme:
Convention on the Rights of the Child is the major international instrument to protect the
rights of the children. The Convention reiterates and elaborates principles enshrined in
the Constitution of India. By ratifying the Convention, the Government and the people of
India have renewed their commitment to children.
It is an accepted fact that the
balanced development of a child - emotional, physical and intellectual, can be best
ensured within the family, or where this is not possible, then in familial surroundings.
The preamble,of ..th# -Convention clearly states that the family is the fundamental pillar of
society and the natural environment for the growth and well being of all its members,
particularly children.
It is the major source of development of children, by way of
providing nurturance, emotional bonding and socialisation.
CRC Provisions:
According to Article 7 of the Convention, the child has the right to be cared for by her
biological parents.
Art 9 enjoins upon the State to ensure that children shall not be separated from his or
her parents and in case of separation from one or both the parents, the State should
respect the rights of the child to maintain personal relationship with both parents.
Art 18 mentions that both parents have the primary responsibility for the upbringing and
development of the child. For the purpose of guaranteeing and promoting the rights set
forth in the present Convention. States should render appropriate assistance to parents
in the performance of their child-rearing responsibilities.
Violation of CRC Provisions:
India, being a signatory to this convention, should follow the principles and provisions of
CRC.
For many reasons, parents feel that they cannot bring up their own newborn
female babies and want to abandon them.
to upbring their children.
But parents have the primary responsibility
In such a condition, it is the duty of the State to provide the
necessary assistance to parents to keep the child with them rather than separating the
child from the parents.
But the ‘Cradle Baby Scheme’ encourages the parents to detest
their unwanted female babies.
Thus the right to be cared by the parents is denied only
to girl children just because they are born as a female.
Legal Provisions for Deprived Children:
For children deprived of a family environment, it is the duty of the State to create a new
family, a new home. Adoption is considered as the best support system to provide a
stable and long-term familial environment. In the wake of reports of malpractice in the
process of adoption, the Supreme Court issued a series of directions with regard to the
detailed procedures to be followed on adoption. Accordingly the Government of India
issued Revised Guidelines on Adoption of Children.
This is the major national
instrument to protect the rights of the abandoned and destitute children. Cradle Baby
Scheme is reviewed in the context of CRC and Revised Guidelines to Regulate Matter
. 4.,..-.:. ^ . ■ Relating to Adoption of Indian Children.
As per the ‘Revised Guidelines to Regulate Matter Relating to Adoption of Indian
Children', while parents are surrendering a female child, the parents should be
counselled and fully informed by the agency concerned of the effect of their consent for
adoption and the aftematives available for the care and maintenance of the child.
The
surrender document should be executed at the freewill of the biological parents/parent
with no compulsion, payment or compensation of any kind on the part of the agency.
The parents should be informed that they have the right to reclaim the child within 60
days from the date of surrender. Further, the parents should be made aware that after
the period of 60 days relinquishment deed will become irrevocable and the agency will
be free to place the child in adoption or guardianship within or outside India.
The
surrender document should be executed on stamped paper in the presence of two
responsible witnesses whom the recognised agency shall be able to produce, if
necessity arises. In case, if a child is found abandoned or is picked up as a destitute,
then a report should immediately be lodged with the local police station along with a
photograph of a child. The Collector of the District must be informed, who in turn must
immediately inform the nearest recognised adoption agency. Police should immediately
undertake an inquiry to trace the parents of the child.
Denial of Child Rights:
•
In reality the above guidelines are not followed. On enquiry, many parents told that
they had surrendered their female babies either at the cradle points or at adoption
agendes and the parents executed no relinquishment deed. Except the reception
centre in Salem, no other centre is executing surrender document
•
No biological parents were counselled to keep their own children. Fearing that the
parents would kill the female babies, they immediately receive the babies.
Usually the newborn female babies are surrendered at the early or late neo-natal
period. By receiving the babies at this stage without conselling the parents, is the
sheer denial of mother's milk to the baby. But, every child has a right to be breast
fed by the mother.
•
In the absence of execution of relinquishment deed, parents have no knowledge that
they have rights to claim back the child within 60 days.
•
It is also impossible for the biological parents to trace their child if they want to take
them back in the stipulated period of 60 days. (An infant handed over at a reception
centre set up in Dharmapuri, as part of the cradle baby scheme in the Dharmapuri
Government Hospital was missing).
As the parents details are not available with the adoption agency, the child would be
denied of the right to know her biological parents.
•
Thought many parents surrendered their female babies, records are created as
though they were left abandoned.
•
In the case of abandoned child or picked up as a destitute state, no serious effort is
being taken up by the police to trace the whereabouts of the biological parents.
In the absence of relinquishment deed, the waiting period extends longer, inspite of
identifying prospective adoptive parents as the adoption agency ought to obtain a
certificate of orphan from the Juvenile Welfare Board.
Thus the whole process is a blatant denial of survival rights, human rights and child
rights.
Implications of expansion of the present scheme:
In response to members’ plea to extend the scheme to the entire state to curb female
infanticide, the government had decided to set up reception centres in all primary health
centres-Social Welfare Minister B.Valarmathi said during her reply to the debate on
€
the demand for grants for the social welfare department.
Under the scheme, the
parents, who do not wish to keep their girl babies, could drop them in the government
cradles kept the reception centres.” (Hindu, April 27, 2002). Thus the State advocates
the parents to dumb the unwanted female babies in the cradles.
If the main purpose of this scheme is to address the issue of female infanticide, what is
the necessity to introduce such scheme in districts where such practice is not heard off.
We are afraid that the expansion of the scheme only legitimised the abandoning of
female children. It proves the patriarchal construction of the State.
The implications
need to be studied.
Vafit,
^riny
by
fJMtf>enor
durlny tht rpllblb;
by JanlJL
10“' 54z/,y 2002.
7
Campaigns and Interventions
Tackling Female Infanticide
Social Mobilisation in Dharmapuri, 1997-99
The heinous practice offemale infanticide (FI) is widespread in several Indian states - even
in states which boast of a better record in reducing gender inequality. These include the three
southern states, minus Kerala, but also Maharashtra. FI is not merely not dying away,
it is emerging as a disturbing new phenomenon. That eradication of this practice is not on the
agenda of the central or concerned state governments or even of the major political
parties reflects the gender insensitivity in our society and polity. However, in Tamil Nadu over
the last four-five years, a serious governmental effort is on to address the issue.
Evidence from a set of interventions in Dharmapuri district suggests that with political will,
widespread generation of awareness and social mobilisation, a dent
can be made in eradicating the evil of FI.
Venkatesh Athreya, Sheela Rani Chunkath
"V "V Then the practice of female inY/V/ fanticide in Tamil Nadu was first
▼ V highlighted by the print media
in 1986, the focus was on the taluk of
Usilampatti in Madurai district. It was
widely presumed that the practice was
confined to this particular region, and that
only a specific community practised it.
Studies that we have carried out since and reported in Frontline, July 11, 1997
and Economic and Political Weekly, April
26, 1997 - have established that the prac
tice is widespread in a contiguous belt of
districts running south to north along a
western corridor of the state. The belt runs
from Madurai to Theni in the south through
Dindigul, Karur, Namakkal and Salem to
Dharmapuri and Vellore in the north. Data
on female infant deaths due to ‘social
cause’, an euphemism for female infanti
cide from primary health centre (PHC)
records show that, on an average, around
3,000 cases of FI occur in a year in Tamil
Nadu (Table 1). This amounts to around
one-sixth to one-fifth of all female infant
deaths in the state. Of these Dharmapuri
and Salem account for 1,000 to 1,200 each.
Tackling a deep-rooted social phenom
enon like FI clearly requires concerted
efforts at several levels, and multiple
interventions and strategies. A purely law
and order approach, treating FI as a crime
(which it certainly is), and going about the
business of punishment under die laws of
the land, would drive the phenomenon
underground, rather than reduce or elimi
nate it. The occasional slapping of a
case would have an inhibiting effect, but
here, the guilty would most often remain
Economic and Political Weekly
unpunished leading to a miscarriage of
justice. The mother, grandmother or an
elderly female relative of the infant, who
are usually compelled (or otherwise pres
sured) by the patriarchal male leadership
of the family (or neighbourhood social
group) to carry out the actual act - would
be arrested and punished. Those who incited
the crime - often the father of the infant
threatening to throw out the mother if she
did not kill the female infant — would
escape the long arm ofthe law by concoct
ing suitable alibis.
The need to address a difficult issue like
FI, which flourishes precisely because it
has acquired social legitimacy in areas
where practised, has to be done sensitively
and not seen as a law and order issue. The
implication of this proposition, however,
is not the suggestion sometimes made that
the state should rely on non-governmental
organisations (NGOs) to tackle the prob
lem. Quite apart from the fact that some
times NGOs end up counselling the already
harassed mother, being unable to put
pressure on her husband or the community,
there is the critically important question
of scale. In a context where the practice
is prevalent over an entire block (panchayat
union) or district, NGO interventions are
bound to be of limited reach. It is evident
that upscaling operations to cover an entire
block or district definitely requires involve
ment of government machinery.
Besides, there is also the question of
political and social legitimacy. Ensuring
the involvement of the community is criti
cal for the success of any intervention on
FI; thus elected local bodies - legitimate
December 2, 2000
political entities of local governance should be centrally involved.
TNAHCP Initiative
The district of Dharmapuri is one of the
five project districts under the third phase
of the Danish International Development
Assistance (DANIDA) assistedTamil Nadu
Area Health Care Project (TNAHCP) being
implemented by the government of Tamil
Nadu with assistance from the government
of Denmark. While the TNAHCP’s broad
objective is improvement of public
primary health care, it was decided to focus
on the issue of female infanticide in
Dharmapuri, a decision that made sense
when viewed against the fact that FI deaths
accounted for around half of all female
infant deaths in the district.
A strategy to tackle FI in Dharmapuri
through a process of social mobilisation
was developed by the TNAHCP. The art
of street theatre, as part of a multi-media
approach, was identified as an important
tool in this strategy. The use ofthis art form
as a tool of social communication goes
back to the days ofthe freedom movement.
Later, it was the Kerala Sastra Sahitya
Parishat (KSSP), a people’s science move
ment, which first demonstrated, in 1980,
the potential of itinerant street theatre or
‘kalaipayanam’, (‘kalajatha’, as KSSP
called it) as not only a tool of communi
cation, but also a powerful tool of social
mobilisation. More recently, the strategy
of ‘kalaipayanam’ had been effectively
utilised in the mass literacy campaigns of
the 1990s to motivate and mobilise the
community on the issue of literacy. It was
4345
based on these experiences that the
TNAHCP leadership decided to utilise the
kalaipayanam strategy in Dharmapuri, both
to mobilise the community against female
infanticide and to promote community
involvement in public health.
In the first instance, it was decided to
develop itinerant street theatre troupes
‘kalaipayana kuzhukkal’ to create aware
ness on the issue ofFI and generate a nuclei
of activists throughout the district who
would pursue the issue in a sustained
manner. This strategy involved several
steps:
- Production of appropriate street plays
and songs to motivate people to act col
lectively against the practice of female
infanticide.
- Identification and training of committed
social activists who would make up the
troupes travelling from place to place
spreading simple yet powerful messages
against female infanticide.
- Ensuring that each troupe consisted of
roughly equal numbers of young women
and men and that the members of a team
touring a particularpanchayat union (block)
were drawn as far as possible from that
panchayat union.
- Approaching the presidents and mem
bers of every village panchayat, and en
listing their cooperation in hosting the
troupe visiting the village; arranging its
performance and ensuring that a large
proportion of the panchayat population
witnessed the programme.
- Motivating the district and grass roots
health officials and functionaries to
play an active role in the entire exercise
from production of plays and songs to
actual conduct of the kalaipayanam
programmes.
- Procuring and supplying the necessary
equipment and taking care of the logistics
of accommodation, transport, etc.
mum essential steps involved in deploying
the kalaipayanam strategy reveals that it
is not a quickfix, easy-to-apply tool for
social mobilisation, but in fact, requires
considerable preparation as well as a high
degree of involvement and commitment.
It is also important to stress the role of
voluntarism and creativity in designing,
producing and performing the skits and
songs, as these are crucial for an effective
performance and a heightened awareness.
Uninvolved professional troupes hired for
the purpose could be disastrous. Critical
to the production of effective skits and
songs is a deep understanding of the social
4346
phenomena and processes underlying the break many feudal social barriers, institu
horrendous practice like FI, and a sensitions and prejudices, and proved espe
tivity to the feelings and dilemmas of the
cially empowering for the women, many
people that lead to FL All this constitutes of whom had received only a modest
a tall order. The TNAHCP leadership, being amount of schooling and had little expo
fully aware of this, made adequate prepa sure to the world outside their own vil
rations, paying careful attention to detail, lages. The actual kalaipayanam - during
and enlisting the assistance of street the which members of each troupe consisting
atre experts. The participation of literacy typically of around eight women and as
and social activists, many of whom came many men stayed together for over 40
fromTamil Nadu Science Forum, apeople’s days and presented around 130 to 150
science movement in training and actual programmes in as many villages - carried
kalaipayanam, as well as the active involve this process further. At the end of the
ment ofthe project officials, greatly helped kalaipayanam many ofthe 300-odd women
in ensuring quality. The programme and men had grown in self-confidence and
managers worked closely with the social emerged as articulate activists with con
activists and street theatre professionals to siderable leadership potential.
ensure that the scripts of songs and skits
The process of preparing for and
were consistently gender sensitive and also conducting the kalaipayanam also helped
hadajudiciousblendofhumourandpunch, forge closer ties between the project
without compromising on content.
officials and field functionaries of the
Dharmapuri had a population of24 lakhs government’s health department, especially
in 1991, and the figure would have been the village health nurses, on the one hand,
around 27 lakhs in April 1998 when the and the panchayat representatives and social
kalaipayanam hit the road. The district is activists in the community on the other.
administratively divided into 18 blocks While the project funded the production
and three municipalities. It was divided for of skits and songs, the training and the
purposes ofhealth administration into two travel of the troupes and other related
health unit districts, namely, Krishnagiri expenses; the local community in most
and Dharmapuri. It was decided to produce instances provided hospitality to the
the plays with the help of the district level troupes, made the necessary on-site arrange
street theatre troupe, which had emerged ments for the performance and mobilised
during the district’s literacy campaign the people to watch the programmes. This
between 1994 and 1997. In the process, process led to the emergence in many
this troupe emerged as the master-trainer villages of a local leadership consisting
troupe, which was then used to train 18 of panchayat representatives, social
block level troupes. The process of idetr activists, local health functionaries, etc,
tification and training of troupe members for which tackling FI would be a continu
was itself instrumental in spreading the ing agenda.
word around among the people about the
Over a period of40-odd days, from April
kalaipayanam. It was also very significant 26 to June 6,1998, the 18 troupes covered
in social terms as it involved bringing over their respective blocks and completed close
350 young rural women and men to stay to 3,000 performances. Close to seven or
together in a camp for 15 days. This helped eight lakh people - roughly a third of the
TabIe 1; Female Infanticide Deaths (fiD) in Tami] Nadu 1994-99
The above brief description of the mini- _________________
Health
1999
Health Unit
Unit District
District
1994
1995
1996
1997
1998
947
Dharmapuri
Krishnagiri
Dindigul
Erode
Madurai
Theni
Namakkal
Salem
Thiruvannamalai
Tirupathur
Kallakurichi
Vellore
109
43
288
352
32
938
0
143
1I
0
Total - Tamil Nadu (*)
3004
51
982
2
176
8
1
1081
138
75
83
158
402
25
781
11
142
15
32
1048
196
73
77
125
281
107
1118
16
139
44
1
73
260
147
1326
10
158
24
0
3226
3002
3317
3417
1048
151
116
69
251
320
985
255
60
93
657
320
60
70
79
231
136
1223
33
142
44
6
3006
Note-.
(,•) including FI reported from other HUDs, reporting one or more FI death in one or more of the
years 1994 to 1999.
Source: PHU records.
Economic and Political Weekly
December 2, 2000
district’s rural population - watched the
programmes directly, while practically
every one either knew of it beforehand or
came to know of it afterward. A subse
quent evaluation study has shown that
the programme’s direct plus indirect reach
was nearly universal, and the programme
messages had effectively reached more than
a third of the district’s rural population,
Involving Elected Local Bodies
The kalaipayanam had a significant
impact - through both its process and its
outputs, and indirectly as well as directly
- on the community in terms of enhancing
consciousness and generating core groups
in villages committed to working for elimi
nation of FI. However, it was also clear
that, without follow-up activity, the
momentum could not be sustained. This,
in turn would require sustained and sustainable efforts over a longer period of
time, much of which would have to be in
non-campaign mode. Taking these aspects
into account, the project leadership de
cided to build a long-term intervention
strategy around the elected local body
leaders. During 1999, panchayat union level
conferences of elected panchayat presi
dents, health functionaries and social
activists were held in all the eight panchayat
unions of Dharmapuri health unit district
(HUD). At each of these conferences, the
panchayat presidents committed them
selves to working for elimination of
female infanticide. Thus, a serious effort
to address the issue of a deep-rooted
phenomenon like FI, by promoting com
munity involvement, has been initiated.
Decline in FI Incidence?
It is too early to speak with certainty of
a declining trend of FI. It is also clear that
a phenomenon like FI, with its strong roots
in objective conditions - a patriarchal
society with strong son preference;
universalisation of the small family norm
with the emergence of aspirations to a
higher lifestyle not easily achievable among
wide sections of the population and an
increasingly consumerist ‘development’
process that commodifies women and
promotes dowry, violence against women,
etc, cannot be tackled and uprooted easily.
Yet more than three years of sustained
work under the TNAHCP involving the
local people. In the initial preparatory work
to create awareness and kalaipayanam in
1996-97, have not been without impact.
We have community-based data on female
infanticide deaths from primary health
Economic and Political Weekly
centre (PHC) records for Dharmapuri for
the period 1996 to 1999. The blockwise
data on female infanticide deaths is pre
sented in Table 2. The table also shows
the excess of female infant deaths over
male infant deaths. What emerges clearly
from the table is that there is a distinct,
if slow, trend of reduction in the number
of female infanticides in Dharmapuri district. The number declined from 1244 in
1997 to 997 in 1999. A closer examination
shows that the trend of decline is more
unambiguous with regard to the
Dharmapuri HUD, where panchayat union
level conferences against FI have been
held. In the case of Dharmapuri HUD, the
number of FI deaths have declined from
1081 in 1996 to 1048 in 1997,985 in 1998
and 657 in 1999. IfFI deaths are compared
blockwise in Dharmapuri HUD for 1998
and 1999, one finds that, with the solitary
exception of Harur block, all other blocks
report a significant reduction. A compari
son ofthe reported number ofFI deaths with
excess female infant mortality for these
blocks also suggests that there is not much
concealment of FI deaths, except possibly
in Dharmapuri and Pappireddipatty blocks.
In the case of Krishnagiri HUD, initial
reports of the extent of female infanticide
suggested that the situation was much less
acute than in Dharmapuri HUD. The focus
was therefore on Dharmapuri to begin with.
In subsequent years mainly due to the
increased process of sensitisation initiated
by the TNAHCP project reporting of FI
deaths from Krishnagiri improved. Never
theless, it still remains that the number of
FI deaths in Krishnagiri is much less than
in Dharmapuri. Moreover, the fact that
excess of female over male infant deaths
had peaked by 1998 and declined in 1999
also suggests that the kalaipayanam inter
vention has had a significant positive impact
in Krishnagiri.
To understand what may be happening
in Dharmapuri HUD, it is instructive to
compare the FI deaths in other districts,
which have reported significant numbers
of female infanticide deaths. The data is
Table 2: Excess Female Infant Mortality (F-M) and Number of Deaths (FID)
Blockwise, Dharmapuri HUD, 1996-99
1996
(F-M)
FID
1997
(F-M)
FID
1998
(F-M)
FID
1999
(F-M)
FID
Pennagaram
Nallampalli
Morappur
Palacode
Karimangalam
Dharmapuri
Harur
Pappireddipatty
Total Dharmapuri HUD
Uthangarai
Bargur
Shoolagiri
Thalli
Hosur
269
197
134
106
129
111
43
33
1022
86
33
20
6
32
79
7
13
42
311
1333
265
185
101
138
132
129
31
57
1038
66
68
66
9
21
29
98
-10
34
89
470
1508
195
160
83
75
80
58
75
55
781
54
73
22
26
Krishnagiri
248
207
96
149
133
132
20
29
1014
60
55
18
14
2
42
130
16
31
61
429
1443
Kaveripattinam
Kelamangalam
Veppanapalli
Mathur
Total Krishnagiri HUD
Total Dharmapuri district
262
232
134
127
123
122
43
38
1081
98
20
15
0
0
5
0
0
0
0
138
1219
262
226
109
125
130
106
48
42
1048
48
25
20
3
1
3
69
0
0
27
196
1244
279
68
86
138
106
109
47
52
985
47
49
23
3
0
4
70
7
4
48
255
1240
31
132
38
70
439
1220
189
132
72
49
76
36
71
32
657
66
28
18
18
6
12
102
5
65
na
320
977
Source: Same as Table 1.
Table 3: Excess Female Infant Mortality and FI Deaths, Select HUDs in Tamil Nadu
HUD
1996
(F-M)
FID
1997
(F-M)
FID
Dharmapuri
Krishnagiri
Salem
Namakkal
Theni
Madurai
Dindigul
Erode
Tirupathur
1022
311
871
137
402
185
64
77
83
1014
429
1137
154
257
237
112
20
100
1081
138
781
25
402
158
75
83
142
1048
196
1118
107
281
125
73
77
139
1998
(F-M)
FID
1999
FID
(F-M)
1038
470
1218
216
295
88
137
27
144
781
439
1187
160
305
184
82
16
217
985
255
1326
147
260
73
60
93
158
657
320
1223
136
231
79
60
70
142
Source: Same as Table 1.
December 2, 2000
4347
presented in Table 3. Salem and Namakkal blocks are outside the core FI region of
show an upward trend between 1996 and Madurai - Theni - Dindigul - Namakkal
2000, while Dindigul, Erode and Tirupathur — Salem - Dharmapuri, serve to remind us
show little change. Madurai and Theni, that we are literally sitting on a volcano.
taken together, show some decline in the
The horrendous situation in Salem number of FI deaths. It is plausible that Namakkal, where FI deaths have been
in Madurai, Theni and Dindigul, efforts of increasing, serves as a reminder that pro
non-governmental organisations over the active government intervention ofthe kind
last decade and a half (including a carried out in Dharmapuri is critical to
kalaipayanam initiative in 1995-96 in which preventing such increases and rolling back
the present authors were involved), as well the incidence of female infanticide.
as sensitisation initiatives since 1997 under
There is considerable anecdotal evidence
the Reproductive and Child Health (RCH) of the spread of the practice of female
project, have contributed to some extent foeticide to several medium and large towns
to the reduction in FI deaths. Dharmapuri in Tamil Nadu. Increasingly, female foe
HUD shows a consistent trend of decline ticide is coming to be perceived as a viable
in the number ofFI deaths and also reports option in semi-rural areas around the urban
a declining trend of excess female infant periphery, and in the urban areas proper.
mortality.
This should hardly be surprising. Wide
As Table 2 shows, the trend decline in spread acceptance ofthe small family norm
FI deaths is consistent across blocks, except in Tamil Nadu (partly a result of govern
for Harur and Pappireddipatty, which are mental efforts, and partly an outcome of
the ‘low’ FI blocks in the district, and rising but not easily realisable aspirations
whose reported increase may largely for a ‘good life’) in the context of the
reflect growing awareness and improve prevailing socio-cultural ethos of strong
ments in reporting in the period 1996-99. son preference is bound to imply an
The reported declines in FI deaths also incipient threat to higher order female
appear largely credible when one looks at foetuses and infants. The already existing
the corresponding excess female infant social legitimation of female infanticide
mortality figures, with the difference makes the transition to the practice of
between the two varying within a fairly sex-selective foeticide considerably
small range.
easier. In short, while a beginning has been
made in the fight against female infanti
Sustaining the Momentum
cide in Tamil Nadu through an innovative
The fact that a series of well-planned effort, that offers important lessons for
intervention involving community other states, the road ahead is far from
mobilisation, and carried out jointly by easy. The broadest possible coalition
health functionaries, panchayat leaders and against female foeticide and infanticide
social activists, has resulted in a distinct needs to be built and sustained. This implies
decline in female infanticide deaths in a commitment to developing a people’s
Dharmapuri HUD is welcome. However, movement involving both ‘civil society’
there is no room for complacency. Firstly, and the state.GQ2
the phenomenon of FI has strong social
roots and social sanction in the region
References
under discussion, and the dent made can
not be assumed to be sustainable. Sec Athreya, V (1998): ‘Social Mobilisation for
Change’, Frontline, October 8.
ondly, the one-shot mobilisation effort
Athreya, Venkatesh B and Sheela Rani Chunkath
needs to be followed up by creation and
(1996a): ‘Fighting Female Infanticide’, The
sustenance of grass roots structures that
Hindu, March 17.
would be constantly active in the struggle - (1996b): Literacy and Empowerment, Sage
Publications, New Delhi.
against female infanticide. Thirdly, a whole
host of economic and social structures and - (1997a): ‘Bom to Die’, The Hindu. March 30.
‘Gender Discrimination Strikes’,
processes that reinforce patriarchy, devalue - (1997b):
Frontline, July 11.
and commodify women, and promote such -(1997c): ‘Infant Mortality in Tamil Nadu: Some
phenomena as dowry will need to be
Disquieting Features’, Frontline, July 11.
addressed seriously if a sustained reduc - (1997d): ‘Trends in Infant Mortality: A
Comparison among Southern States’, paper
tion leading ultimately to elimination of
prepared for the T N Krishna Memorial
FI is to be achieved. The fact that the
Symposium, September 7-8, Thiruvananthapractice of FI has occurred in nearly 140
puram.
blocks (out of 387 in the state) during the - (1998a): ‘Caste and Female Infanticide in Tamil
last four years, and that at least halfofthese
Nadu - Some Reflections’, paper presented for
4348
the workshop on South Indian Fertility
Transition, April 6-8, 1998, Thiruvananthapuram.
- (1998b): ‘Gender and Infant Survival in Rural
Tamil Nadu’, Economic and Political Weekly,
October 3-9.
Clark, A (1983): ‘Limitations on Female Life
Chances in rural Central Gujarat’ in The Indian
Economic and Social History Review, Vol 20,
No 1, pp 1-25.
Chunkath, Sheela Rani and Venkatesh, Athreya
(1997): ‘Female Infanticide in Tamil Nadu Some Prima Facie Evidence’, Economic and
Political Weekly, April 26.
Drezc, J and A K Sen (1995): India: Economic
Development and Social Opportunity, Oxford
University Press.
Government of Tamil Nadu (1998): Policy Note
on Health.
Hausfater, Glen and Sarah Blaffer Hrdy (eds)
(1984): Infanticide: Comparative and
Evolutionary Approaches, Aldine Publishing
Company, New York.
Johansson, Sheila Ryah (1984): ‘Deferred
Infanticide: Excess Female Mortality during
Childhood’ in Glen Hausfater and Sarah Blaffer
Hrdy (eds), Infanticide: Comparative ana
, Evolutionary Approaches, Aldine Publishing
Company, New York.
Krishnakumar, Asha (1992): ‘Beyond Symptoms:
Will the Government’s Measures Help?’,
Frontline, December 4, pp 105-06.
Krishnaswamy, S (1988): ‘Female Infanticide in
Contemporary India’ in R Ghadially (ed),
Women in Indian Society: A Reader, Sage
Publications, New Delhi.
Miller, B D (1981): The Endangered Sex, Cornell
University Press, Ithaca, New York
Nagaraj, K (1998): ‘Demographic Transition in
Tamil Nadu: Social Capillarity in Action?’,
MIDS, Chennai (mimeo).
Nath, Viswa (1973): ‘Female Infanticide among
the Lewa Kanbis of Gujarat in the Nineteenth
Century’ in The Indian Economic and Social
History Review, Vol 10, No 4, pp 386-404.
Panigrahi, Lalita (1972): British Social Policy
and Female Infanticide, Munshiram,
Manoharlal, New Delhi.
Sabu, George, Abel Rajaratnam and B D Miller
(1992): ‘Female Infanticide in Rural South
India’, Economic and Political Weekly.
May 10, pp 1153-56.
Srinivasan, Viji (1992): ‘Death for the Female:
Foeticide and Infanticide in Salem District’,
Frontline, October 9, pp 82-85.
Venkatramani, S H (1983): ‘Bom to Die: Female
Infanticide’, India Today, June 15.
Economic and Political Weekly
available from:
Popular Book House
75 Deccan Gymkhana
Pune - 411 004
Maharashtra
Economic and Political Weekly
December 2, 2000
■■■■■■I■HHI■I■
Indicators
Save the Girl Child
Backdrop:
The child sex ratio (0-6 years) has been dramatically declining in Tamil Nadu over the
last 60 years. The girl child sex ratio for Tamil Nadu was 1010 in 1941 and declined to
948 in 1991 and fell to 939 in 2001.
The declining sex ratio, or increasing severe imbalance in the ratio of males to females in
the population, is a grave danger facing the country in general and Tamil Nadu in
particular.
Together with female infanticide in Tamil Nadu there is an increasing
prevalence of female feticide.
The rapidly increasing and widespread availability of
modem scientific devices and technologies such as amniocentesis, chorionic villi biopsy,
sex selection X-Y separation of Pre-implantation Genetic Diagnosis (PGD) practice and
now the even cheaper, simpler and less obvious technology of ultra-sound, have led to
widespread misuse.
Female feticide is not a practice confined to certain groups or
regions. This practice is now spreading across caste, class, geographical boundary and
rural-urban divide.
Indicators of Female Infanticide:
Infant Mortality Rate (IMR), the number of infant death in a year is the best
indicator to understand the incidence and intensity of the practice of female
infanticide. The general fact is that infant mortality rate of male is higher than female.
On the contrary, if IMR of female is higher than male, then we can conclude that the
practice is prevailing.
The period of infant death includes early neo-natal (0-7 days), late neo-natal (8 - 28
days) and post neo-natal (29 days - one year) periods. If the IMR gender differential
(IMR of female - IMR of male) is higher, it is an indicator to understand the
incidence of female infanticide. The analysis of early neo-natal deaths and late neo
natal deaths and the gender differential during this period will reveal the prevalence and
intensity of female infanticide
CASSA
From the data and field experience, female infants are normally killed before the
completion of thirty days (inclusive of early and late neo-natal period), after which they
normally escape from killing as the mother and generally the family develops an
attachment to the female child.
Still one can argue that the post neo-natal deaths of
female infants can be equated to female infanticide as it is a sheer neglect on the part of
the parents in terms of girl child’s nutrition and health care, ultimately resulting in
elimination.
Table 1: IMR for the year 2000 - Theni District (PHC Data)
Total Birth
Early
Neonatal
Mortality
(0-7 days)
Male
11810
147
Late
Neonatal
Mortality
(8-28
days)
48
Female
10608
335
89
Total Birth
Post
Neonatal
Mortality
(29-1
year)
112
IMR
101
525
Late
Neonatal
Mortality
Rate
4.1
Post
Neonatal
Mortality
Rate
9.5
IMR
8.4
9.5
49.5
307
Table 1 (a):
Male
11810
Early
Neonatal
Mortality
Rate
12.4
Female
10608
31.6
26
Dharmapuri Dist - for the year 2000 (PHC Data):
Table 2:
IMR
Total
Early Neo-natal
Late Neonatal
Post Neonatal
Births
Mortality
Mortality
Mortality
Male
14789
259
80
120
459
Female
13283
663
112
103
878
2
Table 2(a):
Total
Early Neo-natal
Late Neonatal
Post Neonatal
Births
Mortality Rate
Mortality Rate
Mortality Rate
Male
14789
17.5
5.4
8.1
31
Female
13283
49.9
8.5
7.7
66.1
IMR
Tables 1, 1(a), 2 and 2(a) clearly show that in both Theni and Dharmapuri districts,
the IMR of female exceeds the IMR of male. The IMR differential clearly indicates
the practice and intensity of female infanticide. It is very obvious if we correlate the
early and late neo-natal mortality rates for both the gender. From the above tables,
it is evident that the IMR gender differentials is higher and to be more specific,
more killings take place during early and late neo-natal periods.
Indicators of Female Feticide:
The sex ratio at birth is the direct indicator of female feticide. 10 million girls are
bom in India every year and almost 2 million female fetuses are aborted annually after
sex determination.
But IMA gives a shocking note that 5 million female fetuses are
aborted annually. In Tamil Nadu, the sex ratio at birth is below 900 in many of the blocks
and districts.
The US Department of Commerce has proved that the natural female to male sex ratio at
birth is 100:103 - i.e. 971 female children for every 1000 male children, which is a
biological sex ratio at birth. Thus a deviation from this ratio will indicate sex selective
abortion or female feticide.
Data collected from three Primary Health Centres of Usilampatty Taluk of Madurai
District for the year 1998 reveals that the sex ratio at birth are 718, 888 and 787
respectively. According to Department of Public Health Survey 1996, the sex ratio is
below the biological sex ratio at birth in the districts of Kancheepuram, Dharmapuri,
3
Viluppuram, Salem, Erode, Nilgiris, Coimbatore, Dindigul, Trichy, Perambalur,
Thanjavur,
Pudukottai,
Madurai,
Kanyakumari and Nagapattinam.
Virudhunagar,
Ramanathapuram,
Tirunelveli,
According to V.S.Survey for 1998 (Danida Tamil
Nadu Area Health Care Project), the sex ratio at birth is below the natural female to male
sex ratio in 21 districts.
Table 3:
Theni District for the year 2000
Sex Ratio at Birth
Rural
886
Urban
939
Combined
898
Sex Ratio in 1 year
857
945
877
Table 4: for the year 2000
Dharmapuri District
Sex Ratio at Birth
898
Sex Ratio in one year
866
From table 3 and 4, it is evident that the sex ratio at birth as compared to biological sex
ratio at birth shows an alarming decline. This reduction clearly proves the incidence and
intensity of female feticide in these two districts, thanks to the proliferation of medical
technologies such as scan centres, Pre-implantation Genetic Diagnosis and the inactive
nature of the State to enforce the PNDT Act.
Girl Child Death Rate:
The high death rate of female children through out their childhood life is also attributed
to declining sex ratio against females.
Poor nutritional and health status of the girl
children due to neglect of parents and negligence of the State and the subsequent higher
morbidity are the reasons for high death rate of female children. The sex ratio of children
in selected districts according to 2000, in the following table, will clearly reveal it.
4
Name of the district
0-5 years
5-10 years
10-15 years
Virudhunagar
905
645
733
Viluppuram
772
673
835
Salem
905
774
713
Erode
646
771
804
Source: Report of the Survey in Tamil Nadu April 2000, Dept, of Economics and Statistics
In the words of Dr V.B.Athreya, the decline in birth rate is brought out at the cost of
grave gender inequality, which has its own devastating long run consequences.
Universal i sat ion of small family norm without the concomitant attack of son preference
and in the context of the largely commercialised medical profession for whom ethical
concerns are not high on their agenda, and an overall permissive atmosphere where State
and community intervention is generally frowned upon can be disastrous for the gender
balance of the population.
Women’s powerlessness caused by both inequality and abuse and perpetuated by the
patriarchal family, state and community threatens the very survival of girl child both
before birth and soon after birth.
Their rights are violated by acts of elimination from
those they should be able to count upon to protect them. It is a tragic irony that the girl
child is in the greatest danger in the place where she should feel more secure, in the
womb of the mother
5
Definition of different terms:
Female Infanticide: Intentional killing of baby girls after birth on account of the fact that
she is “female”
Female Feticide: Intentional killing of fetuses in the mothers’ womb, after determining
that it is female
Number of infant deaths in a year x 1000
Infant Mortality Rate
Total number of live births in a year
Number of infant deaths within 7 days of birth
in a year x 1000
Early Neo-natal Mortality Rate
Total number of live births in a year
Number of infant deaths from 8 days to 28
days of birth in a year x 1000
Late Neo-natal Mortality Rate
Total number of live births in a year
Number of infant deaths from 29 days to one
year of birth, in a year x 1000
Post Neo-natal Mortality Rate
Total number of live births in a year
Number of live female births x 1000
Sex Ratio at Birth
Number of live male births
6
Public Interest Litigation
Save the Girl Child
Public Interest Litigation Filed in Supreme Court
Public Interest Litigation for the Enforcement of the PNDT Act:
The Centre for Enquiry into Health and Allied Themes (CEHAT) - Mumbai, the Mahila Sarvanggeen
Utkarsh Mandal (MASUM) - Pune and Sabu M.George filed a writ petition (Civil) in the Supreme
Court vide No.301 of 2000, with the complaint that the PNDT Act is not implemented by the
Central Government or by the State Government. They contended that techniques such as pre
implantation genetic diagnosis (PGD) violated the Act. They sought a ban on advertisements
relating to all sex selection techniques before or during pregnancy. They sought directions to the
Central and State governments to implement the PNDT Act in full by appointing appropriate
authorities and advisory committees at the State and district levels as the appropriate authorities did
not function in most States and periodical meeting of Central Supervisory Board.
The Court issued notices to the concerned parties on9.5.2000. It took nearly one year for the
various States to file their affidavits in reply / written submissions. After considering the respective
submissions made at the time of hearing of this matter, as suggested by the learned Attorney General
for India, Mr. Soli J.Sorabjee following directions were issued on the basis ofvarious provisions for
the proper implementation of the PNDT Act.
Summary of the Interim Order of Supreme Court passed on
Directions to the Central Government:
•
May 2001:
The Central Government is directed to create public awareness against the practice of pre-natal
determination of sex and female feticide through appropriate releases programmes in the electronic
media.
•
The Central Government is directed to implement with all vigor and zeal the PNDT Act and the
Rules framed in 1996. Ordered that the intervening period between two meetings of the Advisory
Committees should not exceed 60 days.
Directions to State Government / Union Territory Administrations:
•
•
•
Constitution of Appropriate Authority at the district and sub-district levels and also appointment
of Advisory Committees to aid and advise the Appropriate Authority in discharge of its functions.
Create public awareness against the practice of pre-natal determination of sex and female feticide
through advertisement in the print and electronic media
Submit report on the implementation and working of the Act once in three months to the
Central Supervisory Board. The report should include the registration details and action taken
against non-registered bodies, complaints received under this Act and details of awareness
campaigns
CASSA
Directions to Appropriate Authorities:
•
Take action against non-registered bodies and against those who issued any advertisement in
violation sec 22
The Central Supervisory Board and the State Government / Union Territories are directed to report
to this Court on or before 30,h July 2001 and listed the matter on 6.8.2001 for further directions.
Response submitted by Tamil Nadu Government:
The Tamil Nadu government in its counter affidavit stated that it has appointed the Appropriate
Authorities and the Advisory Committees both at State and District levels. Admitted that the Preimplantational Genetic Diagnosis (PGD) could be misused to identify and to discard the female
embryo before an embryo is implanted in the uterus of a woman and therefore it is necessary to
bring the above said exercise for Pre-implantational Genetic Diagnosis also within the purview and
meaning of the Act whether it is pre-natal or pre-implantational genetic procedure with suitable
amendment to the Act for strict Governance and enforcement of the Act in letter and spirit.
Submitted that on and from the commencement of this Act, as many as 940 Genetic Clinics/
Laboratories in the State of Tamil Nadu have obtained the proper application forms from the office
of the Director of Medical and Rural Health Services, Chennai - 6 for registration as per the Act of
which only 602 applications have been received in the office of the Director of Medical and Rural
Health Services for issue of registration certificates. As many as 561 registration certificates have
been issued against 602 applications received as on date and only 41 applications received in the
office ofthe Director of Medical and Rural Health Services are under process. It is further submitted
that keen efforts are being taken to get the Genetic Clinics/Genetic Laboratories functioning without
authorisation duly examined and registered for further regulation as per the Act. Stated that the
Tamil Nadu Government has filed two cases under PNDT Act.
2
MMHIM|
Resolutions
Save the Girl Child
Resolutions of Campaign Against Sex Selective Abortion
Legislative Reforms:
•
Strict implementation of the Pre-natal Diagnostic Techniques (Regulation and Prevention of
Misuse) Act 1994 and compulsory registration of all Genetic Counselling Centres, Genetic
Laboratories and Genetic Clinics.
•
Take stringent action against the violators of the of Pre-natal Diagnostic Techniques (Regulation
and Prevention of Misuse) Act 1994, by formulating suitable procedures which empower the
Appropriate Authority to take action.
•
Stop all medical technologies that imbalances the birth ratio of female children.
•
Strictly enforce all progressive legislation and enact legislation to protect the rights of the girls
and women.
■
Enacting a central legislation for ensuring the registration and monitoring the functioning of all
private clinics as there is a growing trend in commercialisation of medical profession.
■
To bring out necessary amendments in the PNDT Act and MTP Act which takes away the
punishment for women, empowering the Advisory Committee for monitoring the pre-natal
diagnostic centres, to broad base the definition of the word ‘pre-natal’, ‘ultrasonography’,
submission of status report on the usage of pre-natal diagnostic techniques and abortion once in
six months, strict enforcement of MTP Act etc. (For details refer back)
Administrative Reforms:
•
The Health Secretary should issue necessary GO for periodical reporting of births, deaths and
abortions by all the private hospitals and Government hospitals, to the State and this should be
made public on request.
•
Registration of all births and deaths should be made compulsorily at the village-level, through
the statutory health committee formed under Panchayat Raj Institutions..
•
Activate the Health Committee at the panchayat level to monitor the health services at the
village level.
•
Sex of the fetus for all second trimester abortions to be documented clearly
•
Publish a scientific report every year on the causes for the declining child sex ratio and the steps
taken by the government to stop the decline trend.
CASS A
•
borm Monitoring ( ell at the panchayat level to look into the incidence of atrocities on women
and girl child
•
Maintain the disaggregate data by sex and age related to children and make it open to public
Policy Initiatives to be taken by the State:
•
Registering and monitoring of all pregnancies from 6,h weeks onwards and not from 12th weeks,
to avoid selective elimination of female fetuses and to improve the health status of pregnant
mothers.
•
Increase the age of marriage age of girls from 18 years to 21 years.
•
Provide compulsory, free, quality education to all girl children up to secondary school level.
•
Extend 50 per cent representation to women in all decision-making bodies ofthe State to introduce
a feministic political culture conducive to women-friendly political action.
Eradicate child labour and guarantee employment for adult women
•
•
Bring policy and legal measures to ensure that women have rights and control over productive
resources, for the economic empowerment of women.
•
Provide life-sustaining resources such as health, nutrition, water, education etc., to all the children
without gender bias.
•
Entrust power to panchayats to maintain a register of demographic profile with the details on
vital statistics
•
Frame the child policy and girl child policy to protect the interest of the girl children
•
Extend gender sensitisation training to policy makers, planners, administrators and implementors
at all level.
•
Promote gender perspective into all policies and sectoral programmes
2
CAMPAIGN AGAINST SEX SELECTIVE ABORTION
11,3(amala.2ii(lS(fui, &iuma ^hokkiludaiii,JHadurai- 625 002.
QyiitMie. S
: 25304S6A 2524762 e-iitfiil.com
Qd.o-,10-(cJltOHi(u.Qla(jai', dLittleJHount, Saida pet, dbennai 600 015.
rf)lt()ue: 044 2353503 Q^ax: 2355905
MONITORING THE DECLINING CHILD SEX RATIO - A
SUGGESTED METHOD
Position Note to include Sex Ratio At Birth, Infant Mortality Rate Gender
Differential and Under Five Mortality Rate Gender Differential as indicators
to calculate the Demographic Index, Human Development Index and
Gender-related Development Index.
The United Nations’ Declaration of ‘World Fit for Children’ and Plan of Action’ directs
every member State to reaffirm their commitment to promote and protect the rights of
children.
Through national actions and international cooperation, government of
member States committed themselves to promoting healthy lives, providing quality
education, protecting children against abuse, exploitation and violence, and eliminate
malnutrition. They pledged to achieve these goals, ‘to change the world, not only for
children, but most importantly with children’.
United Nation has set ‘Millennium Development Goals’ and the eight goals are:
1.. Eradicate extreme poverty and Hunger, 2. Achieve universal primary education,
3. Promote gender equality and empower women 4. Reduce child mortality 5. Improve
maternal health 6. Combat HIV/AIDS, malaria and other diseases 7. Ensure
environmental sustainability 8. Develop a global partnership for development and the
Member States of United Nation have pledged to meet these goals by 2015, six of which
are directly related to children.
If we are to meet the goals of “ A World Fit for Children’ and attain the Millennium
Development Goals, if we are to make the world truly fit for all children, the survival
rights and participation of children of both the gender in the development process must
be ensured.
The UN Convention on the Rights of Children places an obligation on the Indian State to
protect and promote the rights of children.
/
Convention on the Rights of Children:
Art 2: The child should be protected from discrimination of any kind in terms of race,
colour, sex, language, religion, political, national, ethnic, property, disability and birth or
other status.
Art 6: State parties should ensure the children’s inherent right to life, survival and
development of the child.
Art 24: State Parties recognise the right of the child to enjoyment of the highest
attainable standard of health and to facilities for the treatment of illness and rehabilitation
of health. State Parties shall strive to ensure that no child is deprived of his or her right
to access to such health care services. State parties shall take appropriate measures to
diminish infant and child mortality.
The rights of the girl child is ensured in Convention on the Elimination of all
Forms of Discrimination Against Women (CEDAW), in the following articles:
•
Discrimination against women, denying or limiting as it does their equality of rights
with men, is fundamentally unjust and constitutes an offence against human dignity
•
All appropriate measures shall be taken to educate public opinion and to direct
national aspirations towards the eradication of prejudice and the abolition of
customary and all other practices, which are based on the idea of the inferiority of
women.
CEDAW Convention insists that the state parties have the obiigation to ensure the equal
rights of men and women to enjoy all economic, social, cultural, civil and political rights.
Beijing Convention:
The Beijing Flatform for Action, adopted at the Fourth World Conference on Women,
included “the Girl Child” in its 12 critical areas of concern. It recognises that in many
countries, the girl child faces discrimination in all stages of life from birth through
childhood and into adulthood. It urges the government to take action to provide access
for girls to training and information, to enable them to articulate their views and to
promote the equality and participation of girls.
Review on the existing health indicators of Millennium Development Goals:
The progress of the children world over is usually measured with the agreed indicators
like Under Five Mortality Rate (U5MR) and Infant Mortality Rate(IMR).
2-
Both these
measurements are principal indicators of children’s well being. Both U5MR and IMR are
known to be the result of a wide variety of inputs: the nutritional health and health
knowledge of mothers; the level of immunization and ORT use; the availability of
maternal and child health services (including prenatal care); income and food availability
in the family; the availability of clean water and safe sanitation and the overall safety of
the child's environment.
According to data quoted by UNICEF in ‘The State of the World’s Children 2000’, the
difference in U5MRs between developing and industrialized nations has increased, and
in some developing countries, the rates are now more than 50 times higher than in the
industrialised world.
In countries where the U5MR for girls exceeds that for boys,
gender discrimination is thought to be a factor. U5MR rate for girls is disproportionately
high in many countries of South Asia and Sub-Saharan region and in some of the
countries in East Asia and Pacific Region and East European Region. Elsewhere in the
world, women generally experience lower mortality than men at almost all ages (Visaria
2002).
Hence sexwise disaggregated for all countries needs to be made available
including for USA and other European countries.
Though the organisations like UNICEF, UNDP have recognised the prevalence of
gender discrimination in the above countries, they have not included IMR Gender
Differentials and U5MR Gender Differentials as part of the Demographic Index,
especially under Human Development Index and Gender-related Developrhent Index.
India scores 54th position amongst 178 countries in the U5M and U5MR is 93 and IMR is
67 for the year 2003 (Source: The State of World’s Children 2003). Though reduction in
IMR is kept as an indicator as well as goal by UN, the IMR Gender Differential to assess
the prevalence of female disadvantage at the post-natal period is not consider as an
important indicator of demographic index.
The need for inclusion of ‘Gender Differentials’ and ‘Sex Ratio At Birth’ is discussed in
the following paragraphs based on the experience of Campaign Against Sex Selective
Abortion (CASSA) at the National and Regional level.
Demographic Data of India to assess the female disadvantage - A Case
Study:
The Constitution of India places an obligation on the Indian State to protect and promote
the rights of the children.
3
Constitution:
Article 14 : Equality before law
The State shall not deny to any person equality before the law or the equal protection of
the laws within the territory of India.
Article 21 : Protection of life and personal liberty
No person shall be deprived of his life or personal liberty except according to procedure
established by law.
Results of the first population census of the millennium for India reveal a number of
significant changes in the sex ratio patterns in the country.
One finds for the country as
a whole a sharp decline in Juvenile Sex Ratio (JSR) from 945 in 1991 to 1927 in 2001.
The decline is even sharper in several states. The JSR has declined from 951 to 897 in
Himachal Pradesh, 875 to 820 in Haryana.
In Gujarat, it has declined from 928 to 878
and in Maharashtra from 946 to 917. The general decline in the’JSR practically across
the entire country is breaking the traditional pattern of north- south divide in sex ratios.
The sex ratio in the Indian Population are becoming rapidly masculine.
A marginal
increase of 6 points in the female to male ratios of the overall population; 933 in 2001
from 927 ini 991.
But there has been a sharp decline of 18 points in the female/male
ratios among children (0-6 years - JSR), during the same period (Source: Census
Data). The JSR includes 'Sex Ratio At Birth’, ‘Infant Mortality Rate’ and ‘U5 MR’. The
disaggregated data of all these indicators clearly reveal the prevailing female child deficit
in the country.
The negative score in Gender Differential in IMR (IMR Male - IMR
Female) is largely attributed to the existing practice of female infanticide.
Sex ratio at birth is nearly constant - within the range of 104 -107 male live births per
100 female live births (Agnihotri, B.S. 2000; McKee. 1984, Visaria 1971). This is called
the biological sex ratio*. Therefore the biological sex ratio ranges from 971 to 935 per
1000 girls or 952 average. Thus a deviation from this ratio will indicate sex selective
abortion or female feticide.
The higher death rate of female children (0-5 years) is also attributed to declining
juvenile sex ratio.
Poor nutrition and health status of girl children due to neglect of
parents, negligence of the State and the subsequent higher morbidity are the reasons for
the high death rate of female children.
From our investigation as a campaign, we remain unconvinced about the rationality of the argument
Because this implies serious political and gender implications. The campaign is investigating this matter
runner. For the present, we are proceeding with this argument.
The rapid decline in female/male ratio among children clearly points out that sex
selective abortion or female feticide is the major contributing factor.
Sex Selective
Abortion is carried out by professionals, superior in the power hierarchy.
They use
scientific techniques, hardware and skills; sanitise the process of eliminating the female
fetus and reduce burden of guilt on parents.
Rajan and et al., have used the reverse
survival technique ** (UN 1983, Chapter VIII) and worked out the estimated SRB at the
district level.
Patterns in Estimated Sex Ratio at Birth (m/f) and
U5 Sex Ratio (f/m) in India, 1981 - 1991
1981
N districts
398
Mean______ 101.5
SD_______
3.6
N Districts
225
in Range (%) (56.5)
147
(36.9)
26
(6.5)
Estimated SRB M/F
Range
1991
452
104,0
3.9
<102
136
(30.1)
102-107
231
(51.1)
>107
85
(18.8)
1981
398
105.1
13.2
167
(42)
231
58
U5 Sex Ratio F/M
1991
452
104.3
13.6
<100
192
(42)
100 +
260
58
(Source: Irudaya Rajan et al., Economic and Political Weekly Oct 11-17, 2003 Vol. XXXVIII No.41)
The above Table describes the underlying data on estimated M/F SRB and F/M U5 Sex
Ratio.
The average all India estimated M/F SRB grew a little more male-dominant
(within the normal range) over the decade, and the F/M U5 Sex Ratio barely changed.
The proportion of districts with masculine estimated SRB tripled from 1981 (about 6 per
cent) to 1991 (about 18 per cent). The proportion of districts with female disadvantage
U5 SR remained at around 58 per cent and grew more dispersed in location and range.
Thus, gender gap in child mortality did not diminish in this decade.
The period SRB is a strong indicator of prenatal sex selection and is thus emerging as a
significant data need for India.
Rajan et al.,
have treated
SRB
values
more
masculine than 107 M/F as an indicator of weeding out of girls, either through prenatal
sex selection, or underreporting
female births.
They have found out that Female
disadvantage remains strong in the northern belt and also deeply penetrates all four
major southern states and in north- east.
1>
This technique is based on the notion, that children aged x are the survivors of births that occurred x
years ago. Therefore, we can take the numbers of children recorded at age x and observed mortality risk for
children in that population, and. using a suitable model life table for the population in question, 'resurrect' the
numbers who had died. From the result we take the ratio of male to female children and estimate SRB
S'
Thus it is very important to infer that girls in India is experiencing a 'double jeopardy' of
increasing prenatal elimination concurrent with persistent post-natal risk. On the one
hand, the average estimated SRB in India grew 3 percentage points more masculine
between 1981 and 1991. At the same time, the average gender gap in child mortality
still shows female disadvantage. That is, in the aggregate, in India pre and post-natal
risk to daughters may run concurrently, a scenario that suggests intensifying gender
bias.
Interpreted as a restriction of girl children's right to live, female disadvantage in child
mortality is rightly taken as one of the most significant indicators of gender bias in India.
This phenomenon is not due to greater natural fraility of girl children, but results from
parents practices discouraging the life chances of unwanted daughters through selective
negation at the fetal level or infanticide. Despite socio economic development, fertility
decline and falling mortality for both the sexes, the male- female' child mortality gap did
not shrink during 1981-1991 (Das Gupta and Bhat 1997), but also hitherto egalitarian
parts of the economy (Basu 1999 and Rajan., etal).
In countries such as China and South Korea,
with diverse development trajectories and
standards of living compared to India, but nevertheless sharing
a strong cultural sonpreference, prenatal sex selection techniques
seem to be replacing post-natal method
(Yi et al 1999, Good kind 1996). That is, SRB are
growing abnormally masculine while
sex ratios of infant/child mortality are growing more egalitarian. Fewer girls
are being
born, but those born are more wanted and tend to survive.
Even then, SRB as an
indicator of female disadvantage before birth
is very relevant even in countries like China
and South Korea.
Before we conclude, we like to place the Tamil Nadu experiences from information
available with the campaign.
Demographic Data of Tamil Nadu
to assess the female disadvantage - A
Case Study:
In India, for states like Kerala, Tamil Nadu and Goa, registration of births is nearly total.
(Seminar - Dec 2003, The Missing Girls by Leela Visaria) Hence, it is possible to
calculate the sex ratio at birth from actual births.
The CASSA has been investigating government data with regard to Sex Ratio at Birth
and IMR Gender Differential. Data collected from PHCs of Tamil Nadu are analysed to
understand the extent to which female births are prevented from occurring.
6
a
In Tamil Nadu, which is known for the practice of killing female child soon after birth in
certain agrarian pockets of the State is now again being focused for the declining child
sex ratio. The Juvenile Sex Ratio (0-6 years) has been dramatically declining in Tamil
Nadu over the last 60 years. The JSR for Tamil Nadu was 995 in 1961 and declined to
948 in 1991 and fell to 939 in 2001. (Census Data).
In Tamil Nadu, the JSR was below
900 in Theni, Namakkal, Salem and Dharmapuri.
According to the census of2001, four of Tamil Nadu’s 30 districts report JSRs (rural and total) belcw900. Rural
JSR are as lew as 763 in Salem, 869 in Dharmapuri, 873 in Theni and 882 in Namakkal. Of 201 taluks in the
State, 28 taluks from 11 districts report JSR (rural) belcw 900. Ten of these have JSR belcw 850-five from
Salem, three from Dharmapuri, and one each from Madurai and Vellore. Six of these ten have JSR (rural)
belcw 800.
In Chennai the Sex Ratio at Birth for the period 2002 - 2003 was 906, which was much
below the biological sex ratio. The inference is that the incidence and intensity of female
feticide is Chennai (urban) is on the increase. In the same way, the sex ratio at birth for
the districts, Salem, Namakkal, Theni and Madurai were analysed.
In Salem, of the 20 blocks, in 19 blocks the sex ratio at birth was below the biological
sex ratio for the period (2002 - 2003). SRB for this period shows a negative trend in 16
blocks when compared to the previous year (2001 - 2002).
The SRB for the Salem
district in the period 2001 - 2002 was 928 and declined to 888 in 2002 - 2003.
In Theni the SRB for the period 2000 - 2001 was 886 and declined to 863 in 2001 2002. Theni has 24 Primary Health Centres. The SRB declined by less than 50 points
in 3 PHCs, between 50 - 100 in 2 PHCs; 100 - 200 in 3 PHCs; 200 - 300 in 3 PHCs
and more than 300 in one PHC. Similar trend is observed in Madurai and Namakkal
Districts. The data made it clear that the sex selective abortions contributes More for the
sex ratio imbalance than the practice of female infanticide.
According to the PHC data for the year 2000, the IMR Gender Differential is negative in
12 districts in Tamil Nadu and the difference is higher in Salem District (-65.4). The IMR
gender differential is two digits in Dharmapuri, Madurai, Namakkal, Salem, Vellore and
Theni Districts of Tamil Nadu.
Further 20 districts have sex ratio at birth lower than the biological sex ratio. This shows
that the practice of female feticide is prevalent in almost all the districts in Tamil Nadu.
In Tamil Nadu 95 per cent of the births are registered. Hence, the data on SRB is a valid
data.
'4
Double Discrimination against girls at pre and post natal period - Tamil Nadu:
Sex Ratio at Birth
1996
2000
902
894
921
916
861
891
977
915
880
869
912
900
Dharmapuri
Madurai
Namakkal
Perambalur
Salem_____
Theni
IMR(Gender Differential)
1996
2000
-42
-37
-8
-13
-12
-23
___ 0
-7
-32
-65
-21
-39
The above table only proves that girl children are discriminated before and after birth. In
the absence of accurate information on such vital events, we have to depend on the
census data on Juvenile Sex Ratio. Other things being equal, the juvenile sex ratio does
not undergo significant changes over time. In India, with a somewhat faster decline in
female child mortality compared to male child mortality, the juvenile sex ratio should over
time become more favourable to girls. However, contrary to this expectation, the defict
of girls increased.
However, it would have been much more public knowledge and transparent if this data
was part of the vital statistics and Human Development Index and Gender-related
Development Index.
For organisations and government, very concerned about the
Juvenile Sex Ratio, the institutionalisation of SRB, IMR Gender Differential, U5MR
Gender Differential are very important, as they are vital indicators of status of girl child
and women. CASSA has made attempts to influence State Planning Commission and
National Planning Commission to consider this seriously.
CASSA has already made
representation to the Ministry of Health and Family Welfare and Department of Health
and Family Welfare to immediately take steps to provide this information in all their data
and Atlas.
Keeping these perspectives in mind, CASSA is presenting this paper to draw the attention of the scholars to
support the rationale of inducting Sex Ratio at Birth, IMR Gender Differential and U5MR Gender Differential as
indicators at the national and international level. Unless, goals are set for reducing gender gap, the millennium
goals cannot be achieved.
QirenlateiL btj
of ffoeoftle £ 'Jfealth
(Itwhuj the
chilei'iiatieiial C^orttm for CDefenee
in JJhtmbiti ott 1^' and /5^' of (January. 200-4 and duriuy.
the Qoeuultatioti on ^JHiisiiiy. 4jiids: cd Qxue of the Jdisuie of JHedieeil (Jechnoloejtj”
on 1J
(January 2004, at '70S(J- JHeet in JHuiubai, jointly eo-o rdmated by.
*
(Vimocl-uma. and QcdSScd-
Minutes of the two days National Consultation on
Enforcement of PCPNDT Act
CEHAT, a Health Action Group has been advocating against Sex Determination and Sex
Selection for more than two decades. CEHAT along with MASUM and Sabu George
filed a PIL in the Supreme Court regarding the enforcement of the PNDT Act. Supreme
Court has passed various interim orders and while disposing off the petition, pulled up
the State Appropriate Authorities and pushed them for rigorous implementation of the
Act and strict vigilance on medical professionals conducting sex selective diagnostic
tests. In its final order it was also spelt that the parties could approach the Supreme
Court in case of any difficulty in implementing the directions mentioned by it.
In this context, CEHAT called for a National Consultation on Enforcement of
PCPNDT Act, in Mumbai on 27th and 28th November 2004, with the following
objectives:
Review of the status of implementation of PCPNDT Act in the country after the final
order of the Supreme Court
*
Form a network of NGOs working on the issue who would work collectively towards
monitoring the implementation of the Act
*
Review the existing advocacy material on the issue of sex selective discriminatory
practice
CASSA was invited to represent Tamil Nadu and on behalf of CASSA, Phavalam and
Gandimathi participated and presented the status of enforcement of PCPNDT Act in
Tamil Nadu by our State and CASSA’s efforts in enforcing the Act.
Representatives
from 17 States / UTs participated. Each participant presented a paper on the efforts
taken the respective organisation and the State on the enforcement of the Act.
Status of enforcement of the Act in different States, Economics and politics of
Technology, Over medicalisation of Pregnancy, Need for strict enforcement of Medical
Ethics were the primary focus of discussion, during the 2 days National Consultation on
Enforcement of PCPNDT Act.
Main Deliberations and the outcomes were as follows:
*
Amniocentesis and
CVB were the widely prevailed technologies for sex
determination and sex selection at the time to framing legislation to regulate the pre-
natal diagnostic technologies. The PNDT Act was framed and enacted regulating
these
technologies,
which
Is
inappropriate
ultrasonogram predominate other technologies.
revamped,
keeping
in
mind
in
the
present
context
where
The present PCPNDT should be
the widely prevalent technologies
and
newer
technologies of sex determination (pre conception sex selection and medical
termination pills)
There was also a concern voice about the time limit in which the court should give
judgments on the cases filed.
The powers of statutory bodies like the State and National Human Rights
•
Commission and Commission for Women needs to be used in the implementation of
the Acts.
Proper record keeping is the primary area/component to ensure the enforcement of
•
the Act. The Act also clearly spells about the importance of record maintenance.
But there is no punitive clause for non-maintenance of records.
Act should be
amended appropriately.
•
The referral doctor should be brought within the ambit of the law.
•
The need to interlink PCPNDT Act and MTP Act was felt to identify the culprits.
•
The provision of 15 days notice to the Appropriate Authority by a person making
complaints should be removed, as this provision would provide chances for the
violators to hide the material evidences before the appropriate authority initiate
investigation.
•
Violation of PCPNDT Act is a criminal offence. Act should be amended appropriately
to attract CrPC provisions and the role of police in the investigation.
•
Court Directions should be sought to define arrest and lay down arrest procedures.
•
Time limit for disposal of cases under PCPNDT Act should be spelt down.
•
The Appropriate Authorities should initiate Suo motu investigation against violations
such as advertisement on sex determination and sex selection, non-maintenance
and disclosure of records, sex determination through oral communication, disclosure
of sex, records of abortions sex-wise, etc., which will strengthen the implementation
of the Act.
*
CEHAT can act as a resource agency to pool and disseminate information.
•
Small committee to be constituted to review the Act and lobbying for amendment.
*
The issue of sex determination, sex selection and declining child sex ration should
be linked up with other instruments like CEDAW and Beijing +10.
*
Study should be conducted to study the degree of correlation between the number of
scan centres and poor sex ratio.
*
Demography lobby to include Sex Ratio at Birth, Infant Mortality Gender Difference
and Under Five Mortality Gender Difference in Human Development Index and
Gender Development Index.
•
Need to initiate joint action with different interest groups and medical forums like
FOGSI, IMA and Medical Council.
*
The focus of intervention needs to shift from awareness to mass mobilisation and
action.
♦
Lobby to enact central legislation to regulate all the Private Clinics, Private Medical
Colleges and Medical Market, for making them accountable to Public Monitoring and
make mandatory for private hospitals to furnish all records for government and public
scrutiny.
•
Needs to file many cases and use the existing law and document the shortcomings
in the law.
•
A need to lobby against the population policies propagating two-child norm.
•
Need to review the birth and death registrations systems in each state and make
recommendations to improve the same.
•
Need to place the issue of sex selective abortion in the umbrella of violence against
women and girls. It also needs to be reviewed in the context of globalisation and
privatisation.
•
Need to go back to the Supreme court with the experience and problems faced
during implementation of the Act and documentation of cases from various States on
failures of the Act.
*
Need for a strong network of organisations working on the issue and plan
standardized campaign against sex selection.
Outcomes:
*
NATIONAL CAMPAIGN
AGAINST SEX
SELECTION,
a
network of
organisation working on the issue was formed.
*
Observe 29th January 2005 to 2nd February 2005 as “National Week for
Campaign Against Sex Selection”. The network organisations can chalk
out the strategy in their respective State, in consultation with their
member organisations, to work on this issue. Common Action in all the
State and Union Territories be organised on 29th January under the
banner “National Campaign Against Sex Selection”.
Get the attention of the international community on the issue by
presenting it in the Beijing Ten Conference
*****
r
FOR PRIVATE CIRCULATION ONLY
Position: 770 (20 views)