RF-TB-2.2.pdf
Media
- extracted text
-
70
different from that of an uninfected individual - Koch’s phenomenon. Years
later, the tuberculin test became the indispensable tool of the epidemiologists.
TUBERCULOSIS IN INDIA — THE PROSPECT*
I
S. SlVARAMAN**
So intense must have been his disenchantment with the failure of tuberculin
that he gave up research in the field of tuberculosis altogether and went on a
I am grateful to the Executive Committee
microbe hunting spree all over the globe. He visited several countries, inclu
of the T.B. Association of India for their kind
ding India and discovered the causative micro-organisms of several diseases ’.gesture
in inviting me to deliver the Wander
like cholera, sleeping sickness, relapsing fever, Rinderpest, Anthrax etc.
'•TAI Oration. Realising the honour that has
Robert Koch may well be described as the father of the discipline of
Microbiology. His techniques of making and staining of smears, culture techni
ques etc. are still in vogue today. He was responsible for making microbiology
as the basis of public health measures. Harley Williams has very rightly called
Robert Koch ‘the greatest technician in Medical Research’.
Honours came to him galore. He was elected a member of the German
Academy of Sciences and was awarded the Noble Prize in Medicine in 1905
for his outstanding work on tuberculosis. In his memorable address at the Noble
Prize Award function, he said with uncanny foresight “1 have performed my
investigations in the interest of public health, to which 1 hope they will bring
greatest benefit. To combat tuberculosis, I recommend prevention of infection
by isolation of the patient in hospitals or screening at home, disinfection of the
patient’s excretion, care of the patient in organised dispensaries, information
and health education of the population and, above all, of the patients and their
families and compulsory registration of all cases”. It is a great tribute to him
that the control of tuberculosis even today, 77 years later, is based, almost
entriely on these principles, except for the addition of chemotherapy which
became available in 1947 and has so revolutionised the management that
tuberculosis has ceased to be a puplic health problem in many developed
countries and isolation is no longer necessary.
The Centenary of the discovery of the bacillus is being celebrated this year
all over the world. Befitting tributes are rightly being paid to Robert Koch, a
colossus amongst medical scientists of all times. The Centenary should, however,
also be an occasion for taking stock of the state of tuberculosis control in our
country, consolidating our achievements and devising ways and means to
improve our strategy in respect of those procedures where our achievement
has so far been unsatisfactory. It is an irony that inspite of the technology and
know-how’ of control being available, tuberculosis still continues to be our
Public Health Enemy No. 1. With the revised strategy in respect of case-finding
and treatment in the rural areas under the National Programme, the added
impetus of tuberculosis being given a priority in the 20-Point Programme of the
Prime Minister, it should not be difficult to tame tuberculosis before the 20th
Century ends. This will be possible only if all medical and para-medical
personnel, voluntary organisations and the community as a whole put their
shoulders together with a sense of commitment in the fight against this scourge.
been bestowed on me by this award, I must
Confess that my contribution in the field of
^Tuberculosis research, compared to that of my
‘illustrious predecessors, is insignificant. Only
’.Stalwarts in our speciality have been selected
[’■'so far to deliver the prestigious Wander Oration,
'.•and this time the Tuberculosis Association has
achosen a humble Tuberculosis worker to dis
charge the responsibility. My distinguished
■fellow delegates must, therefore, hear with me
«if I make a deviation from the earlier Orations.
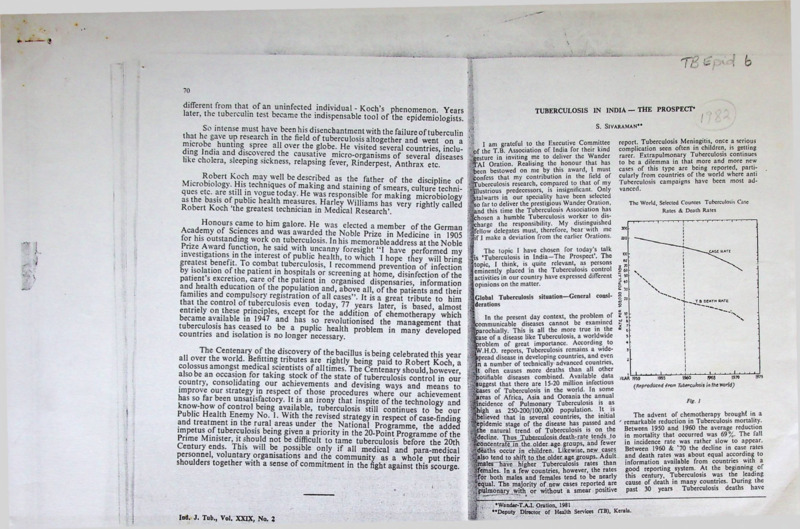
The World, Selected Countcs Tuberculosis Case
Rates & Death Rates
The topic I have chosen for today’s talk
is ‘Tuberculosis in India—The Prospect’. The
topic, I think, is quite relevant, as persons
eminently placed in the Tuberculosis control
activities in our country have expressed different
opinions on the matter.
Global Tuberculosis situation—General consi
derations
In the present day context, the problem of
communicable diseases cannot be examined
parochially. This is all the more true in the
case of a disease like Tuberculosis, a worldwide
Mproblem of great importance. According to
®V.H.O. reports, Tuberculosis remains a wide
spread disease in developing countries, and even
„ ;in a number of technically advanced countries,
‘4t often causes more deaths than all other
■‘notifiable diseases combined. Available data 7teAR two
1,75
^Suggest that there are 15-20 million infectious
(Reproduced from Tubercuhsis in the World)
,‘Stases of Tuberculosis in the world. In some
Jaretts of Africa, Asia and Oceania the annual
Fig. 1
>‘gincidcnce of Pulmonary Tuberculosis is as
Shigh as 250-200/100,000 population. It is
The advent of chemotherapy brought in a
-^believed that in several countries, the initial
idemic stage of the disease has passed and remarkable reduction in Tuberculosis mortality.
Between
1950 and 1960 the average reduction
e natural trend of Tuberculosis is on the
•^decline. Thuj^Tubcrculosis death-rate tends to in mortality that occurred was 69%. The fall
in
incidence
rate was rather slow to appear.
Concentrate .fiT the older age groups, and fewer
>‘deaths occur in children. Likewise, new cases Between 1960 & ’70 the decline in case rates
/-'•also tend to shift to the older age groups. Adult and death rates was about equal according to
/.males have higher Tuberculosis rates than information available from countries with a
jiferriales. In a few countries, however, the rates good reporting system. At the beginning of
'7(or both males and females tend to be nearly this century, Tuberculosis was the leading
^cqual. The majority of new cases reported are cause of death in many countries. During the
. 'pulmonary .with or without a smear positive past 30 years Tuberculosis deaths have
S
■ .
Ind, J. Tub,, Vol. XXIX, No. 2
report. Tuberculosis Meningitis, once a serious
complication seen often in children, is getting
rarer, Extrapulmonary Tuberculosis continues
to be a dilemma in that more and more new
cases of this type arc being reported, parti
cularly from countries of the world where anti
Tuberculosis campaigns have been most ad
vanced.
•Wandar-T.A.I. Oration, 1981
*’Deputy Director of Health Services (TB), Kerala.
I
.«
72
TUBERCULOSIS IN INDIa-THB PROSPECT
S. SVAltAMAK
decreased to the point that in countries having
reliable statistics, Tuberculosis is responsible
for a very small proportion of deaths irom all
causes. However, in some countries including
ours, Tuberculosis continues to be the leading
cause of death among communicable diseases.
Even today, with all the modern facilities avail
able. millions continue to develop the disease
and many die of it.
Data on the risk of Tuberculous infection
has certain advantages over other epidemio
logical indices. But, unfortunately, this informa
tion is not available for many countries.
However, information available from a few
countries suggests that in the technically
advanced countries, the risk of infection is
low. According to Blciker of Netherlands
(1973) it is probable that in the majority of the
developed nations, the risk of Tuberculous
infection is below 5,'1000; may be 1-3/1000
and in a few countries this may even be below
1/1000. He concluded that the risk of tuber
culous infection was declining in the developed
countries by about 10% or more each year.
Some studies done or assisted by the TSRU
and 1TSC (International Tuberculosis Surveil
lance Centre) have helped to determine the
risk of infection and its trend in many countries,
both developed and developing. The risk
of infection in developing countries was thus
found to be between 1-4% (10-40/1000). Again,
in the developing countries the risk of Tuber
culous infection was seen decreasing only
slowly or it remained static.
Tuberculosis situation in the different regions
and countries of the world
Encouraged by the global eradication of
Smallpox, the question is being asked by many
as to whether Tuberculosis could be eradicated
next. To gain perspective on this question, the
U.S. Department of Public Health. Education
and Welfare division collected world statistics
from various sources and a world-wide status
of Tuberculosis has been critically assessed in
a book entitled ‘Tuberculosis in the World’
(1976). Antony M, Lowell, chief of the Statistics
and Analysis Section of the U.S.D.P. utilised
W.H.O reports, statistical publications from
various countries for compiling the data on the
world Tuberculosis situation and, wherever
necessary, available information was obtained
through
personal
correspondence
with
numerous National Health Service officials.
The data 1 furnish on the Tuberculosis situation
today regarding all countries except India are
only cxtracts/reproductions from this useful
book.
Ind. J. Tob., Vol. XXIX, No. 2
Western Hemisphere
From the statistics available for 1973, the
North-West territories of Canada, Mexico,
Guatemala, El Salvador, Honduras, Panama
Bahama Islands, Haiti, Puerto Rico, Guadc
loupe. Peru, Bolivia, Paraguay, Ecuador, Co
lumbia, French Guyana, Brazil and Argentina!
had a case rate above 50/100,000 population.
Of the above, the North-West territories oi
Canada, Peru, Bolivia and Paraguay registered!
case rates above 100/100,000 population. Bolivia
had a case rate of 413/100,000, one of the
world’s highest. This country' with a population*
around 5'million in 1972 registered 9,029 new
cases. About 53% of the population of Bolivia
consisted of Native Indians. In certain areas ofg
this Republic even 62% of the population was|
found infected with a 10% infection rate in the;
0-4 year age-group.
The lowest case rates in the region were;observed in Canada. U.S.A., Belize, the Canals
Zone of Panama, Cuba, Jamaica, Dominican’/
Republic, Virgin Islands, Bermuda, Martinique,!}
Barbados, Trinidad, Guyana and Surinam,
t'i
In Canada, the notification rate in 1973$
was 16.1/100,000 with a very low rate of 7/j
100,000 in certain areas and a high rate of:;
279/100,000 among the Eskimos. Case rate!
among the native Indians was 158/100,000. a
16.9% of all cases of Tuberculosis consisted J
of non-respiratory Tuberculosis. Tuberculosis’^
death rate in Canada in 1972 was only 2.1/
100,000. The Province of Ontario with 8 million's
residents forming 36% of Canada’s population:;
in 1973 accounted for 28% of their new’ cases.;
Of the 1176 new cases notified in Ontario
Province in 1973 only 39.5% were born in
Canada. 9.4% were native Indians and the rest S
51.1% were emigrants (Chinese, Indians,
Pakistanis and other Asians). A network of*a
units. Tuberculosis Clinics and Sanatoria make /j
up the system of Tuberculosis control in
Canada. About 83% of Patients arc treated as
out-patients and only 17% arc admitted for
treatment to hospitals. Prophylactic drug treat
ment is being given.
In the United States of America notification
rate of Tuberculosis was reported as 14.2/
100,000 in 1974. Death-rate had fallen by then
to 1.7/100,000. Maior reduction in case rate
was noticed in Pulmonary Tuberculosis. Extrapulmonary Tuberculosis manifestations appear
ed to be slowly increasing. All States, large
cities and county health departments have some
type of TB control programme as part of their
public health activities. Since 1960, Tuber
culosis control division of their Public Health 71
-f
Ind. J. Tub., Vol. XXIX, No. 2
u
TUBERCULOSIS IN INDIA-THE PROSPECT
S. JlVAWUls*
vice coordinates governmental, voluntary
I professional activities in Tuberculosis conI Even though the local or State Health
I
75
people of that continent in general arc very
high. Health resources arc scarce and its dis
tribution is unequal. The reforc Tuberculosis,
Malaria, Leprosy, Yellow fever, Trachoma etc.
flourish there. Tuberculosis is regarded as a
major problem in most of the countries of
Africa.
Morocco, Spanish Sahara, Mauritania, Mali,
Togo, Swaziland and South Africa have a noti
fication rate exceeding 100/100,000. Many
countries such as Libya, Egypt, Senegal, Ghana,
Nigeria, Gabon, Congo, Zaire, Kenya, Angola,
Tanzania & Zimbabwe have notification rates
above 50/100,000. For countries like Sudan,
Algeria, Ethiopia, Somalia, Botswana, Zambia,
Ivory Coast etc. notification rates are not
available. Niger & Cameroon, however, have
notification rates below 24/100,000.
Though this continent on the whole has a
serious Tuberculosis problem, the sum total of
the problem is confined to a population of
about 30 crores (less than half the population
of India). Already control activities have begun
in some countries and the trend of Tuberculosis
can be expected to decline.
Asian conn tries (Fig. V) <£• countries of the Wes
tern Pacific region of W.H.O. excluding India
Among the countries of Asia high noti
fication rates have been recorded in countries
such as Saudi Arabia, Japan, Korea, Hongkong,
Vietnam, Malaysia, Singapore, Philippines,
Indonesia and most of the Islands in the Pacific.
Regarding Pakistan, Afghanistan and Bangla
desh, though reliable data arc not available,
there is every reason to believe that the problem
is probably at its worst in these countries.
Macao, an island in the western Pacific region,
with a high density of population of 16,250
persons/sq. k.m., has one of the world’s highest
morbidity and mortality rates recorded in 1973.
The morbidity rate was 469/100,000 population
and the mortality was reported as 76.1/100,000.
Afghanistan, Pakistan & Bangladesh
In Afghanistan, overall infection rate is
reported as around 50% of the population.
In Pakistan, available information shows that
prevalence of Tuberculosis in the 1970s was
as high as 4.7%, may be the highest now re
ported in the world. Bangladesh with a popu
lation of 70 million people reported 84%
infection and an infection rate of 46% in the
0-10 year age group. It would therefore appear
that Pakistan and Bangladesh probably nave
the most serious Tuberculosis problem in the
whole world.
Ind. J. Tub., Vol. XXIX, No. 1
Ind. J. Tub., Vol. XXIX, No. 2
TUBERCULOSIS IN INDIA-THE PROSPLCT
77
S. KVAXAMAN
Ytah 3
T16rT
U.S.S.R. consisting of l/6th of the Earth’s
Surface had an estimated population of 25
/.crores (1974). In early 1960s large scale anti
TB measures started in this country. In 1968
>it was further strengthened by enacting suitable
legislation for the improvement of Public
Wealth in general. The general Public Health
Jand special anti TB measures have resulted in
She improvement of epidemiological indices
i'.^n the U.S.S.R. During the period 1964-73
'^Tuberculosis morbidity dropped by 47.5% in
what country. This was especially impressive
»n children. Morbidity of extrapul monary Tuberijculosis also declined to the point that almost
Jgno eases of some forms of disease were notified
;yn the U.S.S.R. Genito-urinary Tuberculosis
Jwas the most common disease among the
’gextrapulmonary diseases.
■j
BCG vaccination is considered in the
• 'jU.S S.R. as the most effective preventive
■.^measure. Mass vaccination to the new born
Tand revaccination upto the age of 18 years and
Jin some cases upto 30 years are given. Chemo' iprophylaxis is considered second in importance
<i|as a preventive measure. With all the great
Ind. J. Tub., Vol. XXIX, No. 2
achievements in Tuberculosis control in that
country, they still consider Tuberculosis as an
important health problem that affects consi
derably the well-being of the people and the
economy of the country. Eradication of Tuber
culosis in the U.S.S.R., they believe, is one of
their important State tasks. Exact morbidity
and mortality positions arc not known.
In China, with the largest population among
the countries of the world, statistics of Tuber
culosis morbidity, mortality etc. were not
available to the W.H.O. in 1973. However,
those who have visited that country observed
that there has been a remarkable improvement
of Public Health due to elimination of most
serious infectious diseases including a reduction
in their Tuberculosis problem. All the same,
the extent and variety of literature that have
appeared on Tuberculosis control and treat
ment in Chinese Journals suggest that Tuber
culosis is still a disease of major concern in
that country.
Tn 1949, China probably had a Tuberculosis
prevalence of 3-9% and the estimated TubcrInd. J. Tub,, VIo. XXIX No. 2
S. SIVA RAM. AN
culosis mortality during that period was 230.
100,000 population. A decade of anti-Tuberculosis campaigning in China brought in a
decline ol Tuberculosis prevalence in their
cities to 1%. In 1958, Tuberculosis mortality
in Peking was 46/100,000 population with a
further reduction later.
Tuberculosis in children used to be very
common, especially Tuberculosis Meningitis
(I/3rd of Tuberculosis in children). Even during
1950s China was up-to-date in the treatment
of Tuberculosis and started using S.M., I.N.H.,
PAS, Viomycin etc. A nation-wide BCG vacci
nation began in China in the mid-fifties. Imme
diate goal was to vaccinate all new borns and
all healthy children below 15 years. By 1964
more than 90% of newborns were vaccinated.
Manpower to meet this programme was or
ganized by selecting teachers of Nurseries or
Elementary Schools and by training them in
Tuberculin testing and BCG vaccination.
Japan—Immediately after the second World
War. Tuberculosis was so widespread in Japan
that the morbidity rate for Pulmonary Tuber
culosis was 10%. The mortality also was as
high as 187.2/100,000 population. Anti-TB
measures started very early in Japan In 1951
a TB control Law was enacted. It laid down
methods for diagnosing and treating patients
and for protecting the population. ITie law
also allocated various tasks at Governmental
level and at each of the Prefectures. The law
thus provided for BCG vaccination and registra
tion of all new cases. Even compulsory hospitali
sation of patients was enforced. With such a
vigorous campaign, ably supportcd'by the Japan
Anti-TB Association, the achievement of Tuber
culosis problem reduction was unique. By
1973, the case rate had fallen to 118/100.000
population. In 1969, the case rate was 196.
Death rate (1973) was only 11/100,000 There
was a remarkable reduction in the notification
of cxtrapulmonary tuberculous disease
Philippines with40 million population scat
tered over7000 islands stretching over 1000 miles
had a very high notification rate of 328/100.000
(1972). Death rate during this period was
64/100,000. The trend of Tuberculosis in this
country however appeared to show a decline
since the year 1969.
Oceania Fig. VI.
Indonesia. Population of 125 million (1973)
scattered over 5 large and/3000 small islands
forms an arc between Asia and Australia.
This country launched TB control . activities
in 1952 when BCG vaccination received high
TUBERCULOSIS IN 1NDIA-THB PROSPECT
79
priority. Case detection by sputum examination
and treatment with supervised intermittent
treatment are now practised. Tuberculosis
problem is considered very high with a pre
valence rate of 0.6% sputum positive patients.
No doubt the problem of Tuberculosis in
the Western Pacific region is a major one with
some adverse factors. However, the population
involved in this region is below 30 crores (ex
cluding mainland—China).
Australia has a very low notification rate
of- 10.5/100,000 (1973). Tuberculosis mortality
during this period was also very low 1/100,000.
This is one of the lowest death rates prevailing.
In Western Australia, non-Australian bom
persons contribute 50% of the cases. Case
rate for non-Australians ranges from 18-31/
100,000 compared to 8-12/100,000 for Australian
born persons. Non-Australian born comprise
27% of the population.
New Zealand Population is 89% Europeans,
natives 8%, Emigrants from Pacific Islands 2%
and others I %. Overall notification rale in
NewZcaland was steadily declining until recent
years when due to large scale miiyaf;on, the
trend of decline has slo - down.
The Tuberculosis situation in our country
Tuberculosis is known to have existed in
India from time immemorial. It continues to
be a major problem of public health interest.
Until recently our knowledge regarding its
distribution in India in different age groups,
sexes, and also in different places was meagre.
Even today there arc widespread misconcep
tions regarding the diagnosis of the disease and
its treatment. If in the past, there were no health
statistics and no notification on the morbidity
and mortality, even today the system that pre
vails in India is far too incomplete and un
satisfactory. Though it is a disease of antiquity,
actual statistics on the incidence, prevalence,
mortality etc. of Tuberculosis became available
in any part of the world within the last hundred
years only (we know that the disease was proved
with certainty as a communicable disease, and
the causative agent was isolated only about
100 years ago).
For the first time in the history of Tuber
culosis in our country it was only in 1920 that
any epidemiological data on this disease was
collected. Sir Leonard Rogers, on the basis of
2? long years of postmortem studies conducted
in Calcutta, found that 17% of the total deaths.
were due to Tuberculosis. On the basis of the’
decennial estimate of crude mortality for
about 9%,of mortality due.to. all causes in that
.911-21, the Tuberculosis mortality for India population. The death rates were the highest
was computed for the first time as .800 per in 55 years and over—age group and the lowest
100,000. This was probably not a true estimate mortality was in the 5-14 years group. An
as the postmortem studies were on hospital increasing trend in mortality with increasing
deaths and it is unlikely that hospital deaths age was also noticed. According to Official
could truly represent the actual death rale. reports, Tuberculosis mortality for our country
It was Lancaster, who from Rogers’s estimates as a whole is 80-100/100.000. One thing is very
and from other available information computed clear, and that is, as in all countries of the
mortality for some of the Cities in India and world the mortality trend in India is certainly
reported that in most of the Indian Cities the one of decline. However, we shall not lose
mortality rate would be higher than 400 per sight of the fact that a mortality rate over
100,000. Later in 1949 Me Dougal estimated
population is the highest death rate
(Tuberculosis mortality m'h'ndia as 200 per 80/100,000
now in existence anywhere in the world. This,
i 100,000. FrimodL-Mollcr’s estimate during this
[period for" Madanappallc and surrounding no doubt, is highly disturbing.
J rural areas was 253 per 100,000. He also found
Tuberculosis infection as an index of the
I a rapid decline in the Tuberculosis mortality Tuberculosis situation in a country has growing
j in that area to a low level of 21.1 per 100,000 importance. For the first time in India, Dr.
I by 1954-55 (explained as a result of intensive Ukil in .Bengal, one of the pioneers in T.B.
i anti-tuberculosis measures introduced in that ’work introduced Tuberculin testing and BCG
area). A longitudinal study to estimate the vaccination in our country. Though countrywide
! Tuberculosis mortality was undertaken by Tuberculin surveys have not so far been carried
' Chakra borty et al from National Tuberculosis'
out in India, extensive testing was done as part
rhstitutc during the period 1961-68. They of our BCG Campaign from the year 1948.
found the annual cause specific death rate due With all' the“labunac and limitations inherent *
to Tubcrc_ulosis_as...84_perJ 00.000population \ in this effort, for the first time, it became
| aged 5 years and above and this represented
Ind. J. Tub., Vol. XXIX, No. 2
Ind. J. Tub.. Vol. XXIX. No. 2
k.
s. SiVA&AM.\N
possible for us to estimate the overall prevalence
of Tuberculous infection in the different age
groups. Without going into the details of those
findings—-well known to all of us. I wish to
mention that it became evident that infection was
widespread in our country both in the rural and
urban areas. The risk or chance of contracting
infection by a person in India was so high that
one had every' possibility of acquiring it before
one reached 20 years of age. Considerable work
in this line was done by Ukil, Benjamin, Sikaad
Pamra, Raj Narain, I.C.M.R. and the National
Tuberculosis institute. 1 wish to refer only to
one study done in South India by the National
Tuberculosis Institute from 1961-68. Prevalence
of infection in that population group was 30%
(25% for female and 35% for males). The
rate increased with age upto 45 years. In the
case of females there was a slowing down after
the age of 15 years in contrast to that for males.
The incidence of infection, a very useful epide
miological index, was also obtained from this
study which showed a rate ranging from 0.84%
to 1.5%. This broadly corresponds to the 1-2%
reported by Frimodt-Moller. The BCG pre
vention study done in Madras showed the
infection rate in the study area to be considerably
higher. For all purposes we can believe that
the annual infection rate in India today may be
anything between 1-2% or 10 to 20/1,000. Com
pared to the infection rate of 5/1,000 for many
of the developing nations and 1-3/1,000 for
the developed nations, our infection rate is at
least double the average of developing nations
and 10 times that of developed nations. In a
few of the developed countries, the infection rate
has fallen to very low levels of below 1/1,000.
Thus the available annual rate of infection in
our country also depicts the serious nature of
our Tuberculosis situation.
Prevalence and Incidence of Tuberculosis in India.
For the first time in 1945 Dr. P.V. Benjamin
estimated from certain observations that about
2.5 million persons suffered from Tuberculosis
in our country. During 1955-58, when the
National Tuberculosis Sample Survey was
conducted in India under Dr. Benjamin’s initia
tive' (ICMR Survey), we got for the 6rst time
many useful baseline data which helped us to
appreciate the extent and nature of the problem
of Pulmonary Tuberculosis in our country
Since then we know that the disease was widely
prevalent throughout the length and breadth
of India and that even in rural India the preva
lence of the disease was almost the same as
in the urban areas. We also found that males
suffered more from pulmonary tuberculosis
compared to the females and that in the males
particularly the disease prevalence increased with
tuberculosis in india-tkh prospect
81
the increase in age. Two and half decades after present level of efficiency, has a potential of information that the bulk of the TB patients in
the National Sample Survey today, for rnakifig -Accelerating the natural decline.’’ The study the country stayed in the rural areas and Tuber
estimates of the Tuberculosis problem m our Undertaken by National Tuberculosis Institute culosis was widely scattered made it imparative
country we largely depend on The results of the K a rural South Indian population where virtua- that the programme in the country should be
NationaESurvey. This preSTcamenfw cettainly
no Tuberculosis control .facilities existed one that reached every nook and corner. There
fore, in the year 1959, Govt, of India established
unfortunate. However, after the National Sample Showed the following:
the National Tuberculosis Institute at Bangalore
Survey, seme other surveys have been carefully
to formulate a comprehensive, realistic and
conducted at Delhi, Madanapallc and Banga
["
V
“
The
annual
rate
of
Tuberculosis
infection
economically feasible Tuberculosis Programme
lore all of which show that the prevalence of
previously
uninfactcd
children
and
in
adults
for
the entire country. By 1962 National Tuber
bacillary cases of Tuberculosis was about_400/
100,000 population, a finding in agreement »."-was found to be about 1% (10/1000). The culosis Institute could evolve a programme for
I
’
T
ncidcnce
of
Tuberculosis
(confirmed
by
culture)
the country based on very solid scientific data
with the National Sample Survey. It was also
found that this rate did not appreciably change i ' v/as about J/1000 (excluding children below 5 obtained from the studies undertaken at the
until 1968. At least in the Delhi area a reduction •Wears), About 30% of newly detected cases National Tuberculosis Institute. Chemothera
of bacillary cases was noticed, bringing down its l.fiiamc from the population uninfected at an peutic Research Centre, Madras and other
prevalence to.2£M)-300/l 00,000 population. There Hlbariier survey. ** Prevalence of disease was a valuable studies and the experience gained from
is not much evidence for us to believe that this ugh times the incidence. Among cases found in the within the country and all over the world.
|initial survey 50% died within 5 years, about According to Dr. Banerjee "The findings of the
is happening in the rest of our country.
1:^20% continued to excrete bacilli after 5 years, sociological studies done at National Tuber
Without permanent and extensively spread rKnd the remaining 30% got cured spontane culosis Institute provided an entirely new
out diagnostic facilities, and notification of ously. There was no evidence of an increase in direction to the strategy for dealing with the
drug-resistance among the newly diagnosed problem of Tuberculosis in India. In the first
detected cases it is very difficult to give convincing
cases. The prevalence and incidence of infection place, as already a large number of patients
information on the incidence of Tuberculosis
showed a significant decrease during the 5 years were actively seeking treatment at various health
in our country. But some longitudinal studies
in the age groups 0-24 and 0-34, respectively. institutions, top priority was to be given in a
have been carried out in Defi^ B'Shga1 ore and
Madanapalle. The overall incidence' rate of At each survey, infection rate among the new national programme for providing services to
born, tested for the first time at the survey, also those who had a felt need (Programme ought
Tuberculosis from the studies done at Delhi
and Madanapalle, though not strictly compar showed a decline. The overall prevalence of to be a felt need oriented one). As those who
disease also decreased from the first to the 3rd had felt need sought treatment at institutions
able, was 340 and 410/100,000 . respectively.
survey, but showed a slight increase in the 4th. of general health services, Tuberculosis services
However, a"longitudinal study undertaken by
•However
this was below that found at the 1st ought to be provided as an integral component
the National Tuberculosis Institute in a rural
survey." Pamra in Delhi also found a slight of the general health services. Diagnosis and
population of South India found annual inci
dence rate for Tuberculosis as around .100/ •• decline in the prevalence of Tuberculosis in treatment of about 52% of infectious Tuber
100,000. population
It must however, be ,'jthc city area. This area however had a good culosis who were worried enough to seek
pointed out that whereas Bangalore rate was Ajpnd comprehensive anti-TB service. Frimodt- treatment on their own initiative would require
reported the decline in disease in six"?
based on fresh bacillary cascs_.only, the fwMoller
I^turns with a good tuberculosis service to~~be very great effort. Logistically it implied an administrativc effort to cxaminc_the_ sputa of as
Delhi, Madanapalle rates were in respect of
all cases judged as active, including abacillary i^jnot different significantly from the decline in as many as 30 mifiion cases of _chronLc_cough
cases. In any case one has to admit that an hS’the'ot hefsix control Towns without anyjpecia| who were reporting at over l_2jjOO.Jnpw_it is
service (Fimodt:Mollers 1981^
important information such as attack rate of /^tuberculosis
WjThcse'findihgs of Bangalore, Delhi aniTMadana^ about -20;000)7heaith institutions scattered all
Tuberculosis applicable to our country as a
over the country to identify about a million of
pallc
together
with the characteristic of Chronic infectious patients. Bangalore study revealed
whole is woefullyJacking.
• :Pulmonary Tuberculosis now increasingly seen that as many as 90%' of the patients _who visited
Regarding the trend of Tuberculosis in India, A in the country, the shift in the age group in which the different health institutions did not get any
Imore and more cases of tuberculosis arc seen facility-even to* get diagnosed as cases of Tuber
we have no statistical data applicable to the
country. That means we really do not know S — all indicate the declining trend of tuberculosis culosis and were sent back mostly with a bottle
how the Tuberculosis situation in our country !j in our country, however small it is. This, no of cough mixture."
has responded to three decades of BCG vaccina i| -doubt, is an encouraging feature of the Tubcrtion programme and the National TB Control •^culosis situation in India. Concerted action
In view of the sociological studies made by
Programme in operation for
o... and half & taken now will help us to bring down our Tubcr- the National Tuberculosis Institute, our National
A
culosis
situation.
Tuberculosis Control Programme is sociologi
decades. Therefore, opii..uiis are varied. Accord
ing to Dr. Nagpaul (1978) “there arc reasons to
cally oriented and is an attempt to meet a felt
believe that India had more than one epidemic
need. It is also cpidemiologically aimed in order
Tuberculosis Control Activities in India
of Tuberculosis since the time of yore. The
to cut the transmission of infection. Another
present epidemic might have started in the 17th
The National Tuberculosis Sample Survey good thing about our National Tuberculosis
century. There is evidence that the present
revealed the urgent need for a nation-wide TB control programme is that it is operationally
epidemic has been declining since the turn of the
Control Programme in our country. The new flexible, or it has a flexibility that will allow for
20th century. The natural decline at present
nt situation. The number of new tuberculosis cases
•‘Prevention trial in Chinglcput showed a dil
is very slow, probably because of the prevailing
in that population. The disease in the infected group
developing from the initially uninfected was particularly
poverty, malnutrition and over crowding The
District Tuberculosis programme, even at the y was 17 time morc-a really peculiar and noteworthy phenomenon.
Ind. J. Tub., Vol. XXIX, No. 2
Ind. J. Tub., Vol. XXIX, No. 2
■j
83
TUBERCULOSIS IN 1ND1A-THB PROSPECT
8i
5. SVaXAMAN
local, sociological, administrative, operational
and other variations.
Our National Control Programme is defined
as “an organised effort wihich aims to bring
under control the problem of Tuberculosis in
the community through defined objectives,
activities and resources. It comprises of wellknown anti-TB measures knit into a compre
hensive, practical, acceptable and economically
feasible programme.'’
The objective is to reduce Tuberculosis in
our country sufficiently quickly to the level where
it ceases to be a public health problem.
The operational objectives laid down are:
Table. 1
Health Services, New Delhi shows that out of
400 districts in our country’, there are only 320
districts with TB control programmes which
means that l/5th of the districts in India arc
without a programme. In an average Indian
district there arc about 50 implementable peri
pheral health institutions. The report shows
that the programme has been implemented on
an average only in 33 peripheral institutions. It
would appear from the report that about 34 %
of the peripheral health institutions in the
country are without a programme in the already
established District TB control programmes^
Thus, on the whole about 47% of the country i
cven_LQda.y-is-nol-covcred by the-TB-control]
programmes. This geographical coverage 1T*
reported as fairly satisfactory. I beg to differ
and say that this is rather unsatisfactory.
“To vaccinate with BCG a majority
of the eligible (if possible more than
Average case detection performance of a
70%) in the community, in an efficient District Tuberculosis Control Programme in
manner.
our country can be judged from the quarterly
reports issued from the Directrate General of
(2) To detect maximum number of TB Health Services. According to the report for
patients with symptoms from among the the period ending December 1980, a total of
out patients attending Health institu 1,23,353 cases of Tuberculosis werc’diagnosed
tions and to treat them adequately; in through the reporting District TB Centres.
doing so, to give priority to sputum Of these 10,293 were cases of cxtrapulmonary
positive TB patients.
Tuberculosis.
N.T.P. (INDIA)-Case Detection in an Average Quarter
D.T.Cs.
CASES DEIKTCD
TOTAL
P.H.Is.
123,355
All types
91.645(66-2) 41.708(530)
Pulmonary '
Tuberculosis •
(bacillary)
19,203(641) 10)800(359) 30.083(243)
Pulmonary
Tuberculosis
:
54.034(651) 29,143(34-9) 83.177(675)
;
(abacillary)
;■
Extra Pulmonary
Tuberculosis
8,328(825)
1,765(175)
10,095(82)
Figures in brackets sho* percentage value
(I)
To undertake the above, activities from
all health institutions, as an integral Table I
part of the general health services”.
Table shows average case detection perfor
It is not only the Government medical insti mance in our N.T.P. in a quarter (quarter ending
tutions wherein the control activities are to be December 1980). Of the cases detected 8.2%
organised. Private medical institutions and were cxtrapulmonary tuberculosis and the re
practitioners should be involved in aUJhc_act£ maining were pulmonary tuberculosis. Bacillary j
vitics in the manner posiblc. A District T.B. cases of pulmonary tuberculosis constituted
Centre, OriS fUr eveiy districr, located at the 24.3% of the total :and abacillary pulmonary
district headquarters is to form the nucleus of tuberculosis cases formed the balance 67.5%.
the District TB Control Programme. According
When we look at the performance of D.T.Cs j
to Dr. Nagpaul, "applying the National
Sample Survey findings to the average Indian and P H.Is in our N.T.P., we sec that the P.H.Is ,
district, it was estimated that there would be contribute only 33.8% of all cases detected. The I
5000 infectious Tuberculosis p.irienfy
3-4 bulk of cases arc even today detected in the
times that number with X-ray shadow suggestive D.T.C.s Another interesting observation is that
of the diseaseTnit sputum "negative, to be dealt even in the P.H.Is cases of Pulmonary tubercu
with at any time. This pool of ‘cases’ and ‘X- losis detected are largely abacillary and not
n direct
ray suspects’ constitute the problem of Tubercu bacillary which means that
losis in a district Programme performance sputum microscopy, our literal medical institu
potential studies have shown that District TB tions arc relying on other methods including
Control Programme-is-capable of discovering X-ray examination for case detection. There
in on^^i_46%^onhc entire.pQoLQLinfectiQiis fore, we can conclude that the case detection in
P.H.Is on the whole is poor and the outlook is
cases in the district.’’
not one of detection of infectious cases of
pulmonary tuberculosis by sputum examination.
Our National Tuberculosis Programme Today
This only means that the very philosophy of our
Quarterly progress report of the District N.T.P. has not been understood/appreciated by
TB Control Programmes for the period ending persons working in the general health institu
1980 issued from the Directorate General of tions. -•/
(3)
Ind. J. Tub., Vol. XXIX, No. 2
I] It is rather difficult to get figures of T.B,
Btients detected each year in our country. On
to average about 5-6 lakhs patients of all forms
fre detected through reporting D.T.Ps. (All
S.T.Ps do not send reports and some reports
re incomplete). If we guess that an equal
umber of patients are also detected in our
ounlry from institutions not covered by D.T.Ps.
ossibly 10-12 lakhs patients are detected each_
'ear. This means that only 10-15% of the total
f.B. patients (if the total tuberculosis prevapnee i¥~E2'%rarc~detcctcd ~cach-ycar-in-fndia.
• About case holding, particularly successful
rcatment completion by patients, information
? not available in the quarterly reports. However
iccording to Dr. Nagpaul’s estimate about
|5% of detected patients arc cither cured or
jccamc sputum negative in a period of one year
n an area covered by D T P.
As regards BCG vaccination coverage, we
fave no data. Moreover the ‘indirect protective
iction’ of BCG has been reported as zero by the
yfadras study.
Spidomiological Model
As the evolution of Tuberculosis starting
irom infection—disease—recovery or death is
iow better known, one can prepare an cpidcniological model for tuberculosis in a commulity or country. A simple model prepared by
Jr. Azuma (Japan) which is a modification of
Vaalcr's model is Shown-iirFiprVH:----------This model subdivides a given population
into six groups. Numerical values of these
{roups arc called ‘variables’. Variables vary
vith time and are therefore not constant.
SIMPLE EPIDEMETRIC MODEL
OF TUBERCULOSIS
(modified from Waaler’s model)
newborn
Infected
s 5 years
'1 ^°rn F H
z| infected
years
—Ji >5Infected
'
|
BCGt . t
protected j
Bacilli
Deaths
Cured
Fig- 7
Numerical values for the flow between variables
are called “parameters”. Birth-rate, Infectionratc, BCG vaccination coverage, protective
effect of BCG, case rates (annual incidence
of the disease) death-rate, (crude and cause
specific) and cure rate with or without a pro
gramme are some of the parameters for the
above model. If initial values of variables are
known, and values of parameters are available.
the dynamics of tuberculosis in a community
becomes clear. Such a model approach is
particularly useful in India for predicting the
trend of tuberculosis. As reliable values for
most of the parameters arc not available for
our country, determination of the future trend
Ind. J. Tub., Vol. XXIX, No. 2
«4
S. SIVARAMAN
of tuberculosis becomes difficult. However, Dr.
Nagpaul worked out the trend of tuberculosis
problems in our country using a very simple
model.
According to him, the District Tuberculosis
Programme, even at the present level of efficiency,
has a potential of accelerating the natural
decline of tuberculosis in India. He very roughly
calculated that without other epidemiological
‘flows’ there would be 4.8% annual decrease in
our problem over and above the natural decline.
Table 2
Estimated Sputum Positive Cates in Average Indian
District with & without District Tuberculosis programme
at the end of one year
| fate of prevalence cases during one year
i
1
Dead I Cured [Aiaihr'M ,Cases Nc.of
(sputum 1 (Sputum 1 (sputum 1 added Cares
necathe) negative), positive) (inci- at tt
(Preva
lence)
Without pMcrw *>5000
(natural time-freed
700
1000
5500
With programme 4.224
diagnosed
590
B15
2789'
Diagnosed
776
Total
5.000
1700
5.000
1.700
4.761
272 \
737 1 1.202
5.061
Reproduced from "Tuberculosis in India" by Dr.
Nagpaul Journal of the Indian Medical Association
In the estimate of Dr. Nagpaul, expected
reduction in the prevalence in an area without a
programme due to death occurring in the
patients was at the rate of 14% a year. This was
the crude death rate for the country. The same
rate was applied for patients not diagnosed in
an area with a programme. However, a rate of
19% was applied in calculating reduction by
death in the group of patients detected in the
programme area. This appears to be some
what unlikely. If the rate of 14% was also
applied to the group of detected patients in the
programme, the estimated problem reduction
would be 4% instead of 4.8%.
Earlier, 1 worked out that our N.T.P. has
achieved onlv about 50% geographical coverage.
Therefore with the type of programme that we
now have, the annual problem reduction, will
be around 2%. If the programme docs not
change in coverage and efficiency and the general
conditions of living standard remain static.
by 2000 AD our problem will be that of 5.3
million cases of Pulmonary Tuberculosis.
TUBERCULOSIS IN JNDIA'THE PROSPECT
Fig. vm
*3 3
If the rate of growlh of population noticed
during the last two decades is to continue for the
coming two more decades, our population would
touch 1000 million mark by 2000 A.D. With
all our efforts in family planning programme,
the decade growth rate of population in India
was 24.80 for 1961-71 and 24.75 for 71-81. If
this unfortunate thing continues, the prevalence
of Pulmonary Tuberculosis by 2000 AD would
be 0.5% and 0.12% for total problem and pre
valence of infectious cases respectively. To
arrive at the above figures, the problem of
Tuberculosis in India in 1980 was arbitrarily
considered as the one found by. Dr. Pamra for
Delhi area in his 5th survey (1972-7.3), i.e.2.8/
TUOO (Bariliary cases) and~12>T000 (Total'active
cases). This was accepted for calculation 'pTTrposes as the all India prevalence rate since no
other reliable figures were available. Prevalence
for 1973 in Delhi where active anti-TB measures
were in operation could justifiably be ..pplied
as the near true all India t -valence rate for the
year 1980. All these approximations have been
made to have an idea of the possible effect of the
programme in our country.
ESTIMATED TUBERCULOSIS PREVALENCE IN INDIA
FOR THE PERIOD FROM 1900 TO 2000A D.
It would thus appear that Tuberculosis will
have a slow downward trend in the next two
decades to come and tuberculosis may continue
as a major public health problem for many
years. I am not trying to say that the problem
cannot be tackled in a period oC20-30 years. athat a T.B. Control Law, if enacted, could help produce the desired impact on the growth of
If Japan could lower their problem considerably ■>sus in fixing standards for case detection, case our population, the same might get repeated
during the past three decades, wc could also ..^holding, classification or various forms of in the Primary Health Care Programme. Such
achieve it provided wc work together to create a ^disease,
an eventuality should not occur.
•'jjUliUdbL,, iiUUllllHIUll
notification Ul
of IIIVIVIViiv;
morbidity & n.«.
mortality
.......
favourable situation.
j-'|ctc
[etc. Such a T.B. Control Law will ensure better
Before 1 conclude, a word about the Father
.'•^participation by individuals and institutions and
If our national Tuberculosis Control Pro W.nlso create an awareness of the problem and of French Phthisiology and former Secretary
gramme docs not function properly, it is not ds,programme in the minds of the lay public. Any General of the International Union against
due to any inherent defect in the programme.
[developmental activity, and no doubt a pro- Tuberculosis. Professor Etinnic Bernard. In a
On the contrary it is the poor coverage, and
l.grammc like Tuberculosis control needs the tribute to this great man who passed away on
operational and managerial problems that arc .•;d knowledgeable cooperation of many for its the 6th June, 1980, the Bulletin of the Inter
responsible for the poor performance. As our • •1 success. T.B. Control Law if enacted would be a national Union in its December, 1980 number
learned President once said it is in short due to ,3’short cut in achieving such cooperation. It is published his short life sketch. I wish to quote a
human failure that the programme docs not is® also unlikely to interpret such an enactment as few lines from this memorial. "Some morning,
function properly, a human failure in which wc
when I left the Hospital, I wanted to shout at
undemocratic.
all have contributed. It is upto us to decide
those who passed by and seemed so indifferent.
what we should do to control our Tuberculosis
The much talked of "Health for all by 2000 It couldn’t go on like that, and one morning I
problem. It is again upto us to din into the cars
AD” and “Primary Health Care" which is had the conviction—not the evangelical convic
of our decision makers the seriousness of our
s,ralc?y f°r achieving the above concept tion of the Christian, but a conxiRlifln, nonTuberculosis situation and what is to be done
has been accepted in India. A well thought thelcss, that the struggle against the scourge
in the matter. There is very little justification
out and planned Primary Health Care, properly of Tuberculosis would hehceforth~Fc_my voca
in not having a countrywide programme. By a j® established, will go a long way in carrying out tion. This conviction has never left me in more
countrywide programme, I mean a programme
a our TB control programme most successfully. ’ than forty years.” This was what he used to feel
in which every medical practitioner and insti
T However, wc have to take lessons from our in the early days of his career as head of a
tution in our country discharge their duties in
® Family Planning and National TB Control hospital department treating Tuberculosis in
the matter of controlling this malady. If suitable -j Programme. If like the Family Planning Pro- women, and what he did thereafter. Wc in our
legislation is to be enacted, it is again upto us to 75 gramme into which a sizeable amount of our country will have to shout at our fellow men
advise our decision makers. I have often felt
3 scarce resources have been pumped did not in the medical profession and tell them that
i
Ind. J. Tub., Vol. XXIX, No. 2
Ind. J. Tub., Vol. XXIX, No. 2
•i
j
-
-86
5. SIVARAMAN
we can no longer be indifferent to our Tuber
culosis situation. Jointly we may .then. shput
to the decision makers and tell them what is
to~be--done.--------- —----
13.
International Union Against Tuberculosis, Tuber
culosis: Japan, At the Cross Roads No. 31, 1973,
P. 4.
14.
Krishnuswami, K.V.,; Supplement to Indian Journal
of Tuberculosis; 1975, 22.
15.
Lowcl, A.M., Tuberculosis in the World, U.S
Department of Health, Education And Welfare.
Atlanta, 1975.
16.
Nagpaul, D.R.; Journal of Indian Medical Asso
ciation, 1978, 71, 44-48.
I.
Azuma, Y. Tuberculosis control. Research Institute 17.
of Tuberculosis, 1979, P. 68.
Nambiar, M.V.U.; Census of India 1981 Series 10,
Paper 1 of 1981.
2.
Bancrji, D., Social aspects of Tuberculosis in India, 18.
Text Book of Tuberculosis, 1981, P 528.
Pamra, S.P.; Clinics in Chest Medicine, 1980, 1,
265.
Before 1 finish, let me thank all of you for
listening to me so patiently. 1 take this oppor
tunity to thank the House of Wanders for the
keen interest they show in the activities of TB
control in India and particularly for instituting
the Wander TAI Oration.
REFERENCES
3.
Bulla, A., WHO Chronicle; 1977, 31, 279.
4.
Chakraborty, A.K., Gothi, G.D. ct al, Indian
Journal of Tuberculosis, 1978, 25, 86,
5.
Coudrcau. H., Bulletin of the International Union
Against Tuberculosis; 1980, 55, 83.
6.
District Tuberculosis Programme, National Tuber
culosis Institute, 1977.
7.
Farga, V., Bulletin of the International Union
Against Tuberculosis, 1978, 53, 3.
8.
Frimodt-Mollcr, J., Bull. WHO, 1960, 22, 61.
jmirimodt-MoIlcr, J.; Ind. J. Med. Res; 1981, 73
(Suppl.) April 1981, P. 63.
10.
19.
1980.
20.
Rai Narain, ct al; Bull. World Health Organisation,
1974, 51.
I
21.
Styblo, K., Mcijcr, J.: Bulletin of the International iUnion Against Tuberculosis 1978, 53, 283-293. ’J
22.
Styblo, K., Bulletin of the Interna lion? 1 Union g
Against Tuberculosis, No. 3, 1978, 53, 141-152. |
23.
Tuberculosis Prevention Trial,
Res. 1979, 70, 361.
24.
Tuberculosis Survey in England and Wales 1971,
tubercle; 1973, 54. 249.
Gothi, G D., ct al, Indian Journal of Tuberculosis,
25.
1979, 26. 121-133.
11.
Gothi, G.D., ct al, Supplement to the Indian Journal
of Tuberculosis; 1978, 25, 8,
12.
Hitze, K , Bulletin of the International Union
Against Tuberculosis; 1980, 55, 13.
26.
Ind. J. Tub., Vol. XXIX, No, 2
Quarterly Progress Report, Directorate General
of Health Services, quarter ending December. $
Indian J.
Med.
Tuberculosis in a rural population of South India.
a five year epidemiological study, Bull. World
Health Organ.; 1974, 51. 473-488.
World Health Organisation, Expert Committee on
Tuberculosis- Ninth Report, W.H.O., Tech. Rep.
Scr. No. 552, 1974.
Position: 1960 (7 views)