RF_DEV_3_C_SUDHA.pdf
Media
- extracted text
-
RF_DEV_3_C_SUDHA
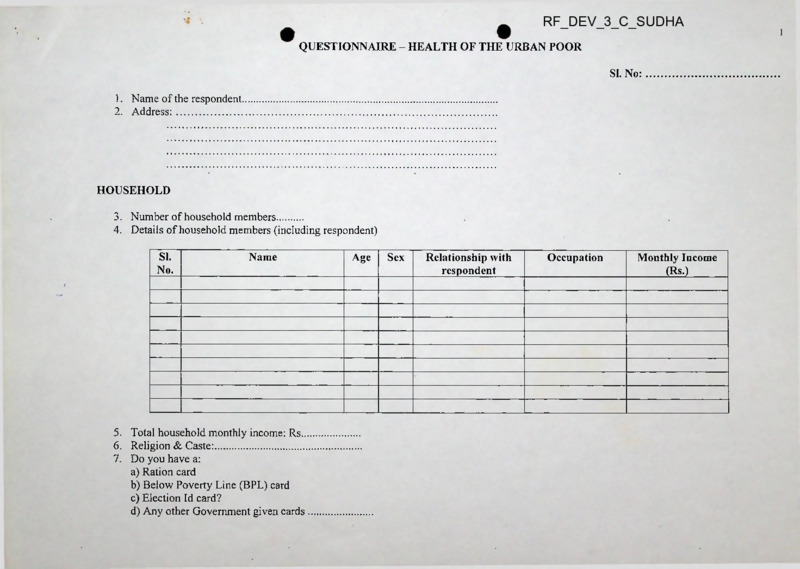
QUESTIONNAIRE - HEALTH OF THE URBAN POOR
SI. No:
1. Name of the respondent
2. Address:
HOUSEHOLD
3. Number of household members
4. Details of household members (including respondent)
SI.
No.
Name
5. Total household monthly income: Rs
6. Religion & Caste:
7. Do you have a:
a) Ration card
b) Below Poverty Line (BPL) card
c) Election Id card?
d) Any other Government given cards
Age
Sex
Relationship with
respondent
Occupation
Monthly Income
(Rs-)
2
FOOD & NUTRITION
8. Where do you buy rations from?
a) Ration shop
b) Other shops
WATER SUPPLY
9. Source of water supply:
a) Household water supply
b) Common tap
c) Other
10. How many times a week do you get water?
a) Everyday
b) Two-three times a week
c) Four-six times a week
d) Other
11. How do you store water?
a) Drums
b) Buckets
c) other
12. Do you cover your stored water?
a) Yes
No
b)
13. Do you face water shortages:
a) Yes
b) No
14. If so, when:
a) Always
b) Very often
c) Sometimes
d) During certain months (specify months)
15. Do you have to pay for the water you receive?
a) Yes
b) No
16. If yes, how much do you pay in a month?
3
17. Do you think the water you get is clean?
a) Yes
b) No
18. Do you boil your drinking water?
a) Yes
No
b)
SANITATION
19. Location of toilet
a) Household toilet
b) Paid toilet
c) Common toilet (unpaid)
d) Other
HOUSING
20. Type of housing ownership:
a) Own
b) Rented
c) Other
21. Type of roof:
a) Thatched
b) Asbestos sheet
c) Concrete
d) Other
22. Number of rooms:
a)l
b)2
c) 3 or more
CREDIT
23. If you need to borrow money, whom all do you approach?
a) Bank (name)
b) SHG group
c) Money lender
d) Other
4
24.
25.
26.
27.
How much money does your household borrow in a year?
For what purposes do you borrow money?
What is the rate of interest?
What do you have to pledge to get loans?
HEALTH CARE INFORMATION
28. Health centres accessed
a) Govt
b) Private
.’....................................................................... ’
c) Pharmacy
d) Other
29. How much do you normally spend on each illness episode? (Give some instances)
SI.
Name of Illness
Name of health centre/ Amount spent
Amount
No.
doctor/ consultant
on doctor/
consultant
spent on
medicines
30. Does any health worker visit your home?
a) Yes
b) No
31. If yes,
i) Who?
ii) How frequently do they visit you?
a) More than once a month
b) Once in 2-3 months
c) Other
iii) What do they come for?
32. Does anybody provide you education concerning prevailing health problems?
a) Yes
b) No
Other
expenditure
(travel, food, etc.)
Total expenditure
(Rs.)
5
IMMUNIZATION
(NOTE: PLEASE ASK THESE QUESTIONS ONLY IF THERE ARE CHILDREN IN THE HOUSEHOLD)
33. Have the children in the household been immunized?
a) Yes
b) No
34. Where were the children immunized?
1)
2) ...........................:...............................
35. What immunizations have they received? (Please check immunization card, if any)
ANTE-NATAL CARE
(NOTE: PLEASE ASK THESE QUESTIONS ONLY IF THERE ARE/ WERE EXPECTANT MOTHERS IN THE HOUSEHOLD)
36. Did you receive ante-natal care? (this question needs to be broken down into iron& folic, tetanus, nutrition, access to maternity care, etc.)
MEDICINES
37. Please list out any medicines used by people in the household in the last six months? (as far as possible get copies of prescriptions)
SI.
No.
Signature
Name of interviewer
Name of medicines
Which illness was it
used for?
Date
Organisation
Who
prescribed it?
How many
tablets/ or
how much
was taken per
day?
How long was
the medication
used for?
on
No'x/e.ro b<n?
6).
No
, zoo <g
Name
Phor> e.
£&. cctia
/^TH 7A \) n' \
CM 1
H
an. ass
2. S'5-5 o 3
C IUI c -^> frbJG-fl ^o
?8S^3~?7W
ixCo'in
)<oo^aye^(5 \ft\koo- Co.
<? 7
£>MA £
£
(sifL
C^’DS
Nav@ D.
lo.
o/
PROGRAMME SCHEDULE FOR ORIENTATION ON
RIGHT TO HEALTH CARE IN AN URBAN CONTEXT
rfrtd sorfesWi)
urfuaertd
soA.d
urfA E&ariE’dsJs’rf trao^rrrod
sj
CO
6
u
Time: 9.30 - 5.00
Date: June 23, 2006
Venue Fedina-Navachetana, No. 154, Anjaneya Temple Street, Domltir Village,
Bangalore - 560 071, Phone No. 080-25353190, 2535363, 9886648508
Objective (enorf^edrtVo):
1.
To provide information regarding the structure and functioning of the urban
health care system, drtd d,dedd ejdoBertj dedtdo djddofcd^ SSdoiratfo^r^o-
2.
To orient the participants to ‘right to health’ and the ‘right to health care’
3.
To explore how the participants could integrate ‘right to health’ as part of their
work, ejdjaert.d
dido,
gzbt oodd ararisraPi uVdQijira^oddd zedr» dzir
6
d <
campaign, ‘adosertjd dio,’ dodo, ‘edooerij dedcdo d^d’ tsz^oiradd wrt drariE'ddrd
Schedule (sacdoridod arid):
09.30-10.15: Introduction of participants and listing of expectations [NT/ EP]
zaarfdddoddd dodcdo dodo,
11.15:
10.15-
eaaSoETtadOod edd SOeS^rtVo
Understanding health (including various dimensions of health) [SJC]
advert dodd ado?
11.15-11.30: Tea Break
dara acrado
11.30-12.15: Understanding determinants of health [EP]
wtkraertjdd^ aqirodod yodrfVo
01.15:
12.15-
Understanding ‘right to health’ & ‘right to healthcare’ campaign [NT/ PS]
‘esdjafrt.d
ddo.d ’ dodo-o ‘ejdoafrtt> dfdoio dzfo.d ’ - esodi
6
01.15—02.00: Lunch Break zjjaead doado
02.00-02.45: Structure and functioning of the urban health care delivery system [SJC]
drtd ddedd zjdjacrt dccra d,ddo8o dratod
02.45-03.00: Tea Break
dasa acrado
03.00-03.40: Group Exercise [PS] rtoosj duoddi / ddr
03.40-04.00: Consolidation of responses and linking it to the day’s theme [EP]
d,34oJorttf ojaeaddra dodo di add adoJoi z&aedrf
04.00-04.45: Brainstorming about how the participants could integrate ‘right to health’
as part of their work; Specific follow-up action points. [FEDINA]
esdoaedd
dido,
oirad oed ddo„6 ddo„& 8wdd<0r-» MiJdQJjiraVzjdodo
aoioodd zedn
6
U 4
V
MdeJoaedd dodo, aordj zsacdoroJjafzsdoJo d/adi^drWo
04.45-05.00: Feedback and Evaluation [CFIC team]
drartrdde-d oaafomadd art dsaoJo dodo d?>eo,dradd
[PS: Prasanna Saligram, SJC: S. J. Chander, EP: E. Premdas, NT: Naveen Thomas]
Bangalore Statistics
1
Population 6,532,577 (2005)
Colleges 51
Area 2,190 km2
Universities 4
Density 2,978.6 per km2
Motor Vehicles 595,000
Birth Rate 19.1 per 1000
Autorickshaws 82,699
Death Rate 5.7 per 1000
Cars 281,093
Net Income USS 51.9 billion
Public Busses 4,035
Per capita income US$ 1,110.03
Telephone connections 916,065
...
Primary Schools 5,466
Internet connections over 60,000
High Schools 1,766
Religions 79.3% Hindu, 13.3% Muslim, 5.7% Christian
Pre-university schools 209
Languages 38% Kannada; Tamil, Telugu, English, Hindi
Literacy rate 83% (Male 88%, Female 77%)
Slum Population 8%
http://en.wikipedia.org/wiki/Banoalore Statistics
Statement 1.2
TOTAL POPULATION, SLUM "POPULATION ANDTHEIRPERCENTAGeIn MUNICIPAL
CORPORATIONS WITH POPULATION ABOVE ONE MILLION-2001
SI.No.
Name of Million Plus
Municipal Corporations
State/Union
territory*
2
3
1
TOTAL
Total
population
4
Total slum
population
Percentage of slum
population to total
population
5
6
73,345,775
17,696,950
24.1
1
Greater Mumbai
Maharashtra
11,978,450
6,475,440
54.1
2
Delhi
Delhi
9,879,172
1,851,231
18.7
3
Kolkata
West Bengal
4,572,876
1,485,309
32.5
4
Chennai
Tamil Nadu
4,343,645
819,873
18.9
5
Bangalore
Karnataka
4,301,326
430,501
10.0
6
Hyderabad
Andhra
Pradesh
3,637,483
626,849
17.2
7
Ahmadabad
Gujarat
3,520,085
473,662
13.5
8
Surat
Gujarat
2,433,835
508,485
20 9
9
Kanpur
Uttar Pradesh
2,551,337
367,980
14.4
1Q
Pune
Maharashtra
2,538,473
492,179
19.4
11
Jaipur
Rajasthan
2,322,575
368,570
15.9
12
Lucknow
Uttar Pradesh
2,185,927
179,176
8.2
13
Nagpur
Maharashtra
2,052,066
737,219
35.9
14
Indore
Madhya
Pradesh
1,474,968
260,975
17.7
15
Bhopal
Madhya
Pradesh
1,437,354
125,720
8.7
16
Ludhiana
Punjab
1,398,467
314,904
22.5
17
Patna
Bihar
1,366,444
3,592
0.3
18
Vadodara
Gujarat
1,306,227
186,020
14.2
19
Agra
Uttar Pradesh
1,275,134
121,761
9.5
20
Thane
Maharashtra
1,262,551
351,065
27.8
21
Kalyan-Dombivli
Maharashtra
1,193,512
34,860
2.9
22
Varanasi
Uttar Pradesh
1,091,918
137,977
12.6
23
Nashik
Maharashtra
1,077,236
138,797
12.9
24
Meerut
Uttar Pradesh
1,068,772
471,581
44.1
25
Faridabad
Haryana
1,055,938
490,981
46.5
26
Pimpri Chinchwad
Maharashtra
1,012,472
123,957
12.2
27
Haora
West Bengal
1,007,532
118,286
11.7
http://www.censusindia.net/results/slum/slum2.html
Bangalore's population up 61 p.c. in 10 yrs
BANGALORE, OCT. 11. The Director of Census Operations, Mr. H. Shashidhar, today released figures pertaining to
the ward-wise population, the number of children up to 6 years of age, and the number of literates in the 100 wards of
the Bangalore Mahanagara Palike.
The BMP, within its municipal limits, has a population of 42,92,223, accounting for 75.48 per cent of the total
population of the Bangalore urban agglomeration, with 22.40,956 males and 20,51,267 females.
The decadal growth rate of the population of Bangalore was as high as 61.36 per cent. This high growth rate can be
attributed not only to the extension of the municipal limits of Bangalore city, but also to the ever-increasing
population.
Bangalore has 4,56,325 children up to the age of six, which constitutes 10.63 per cent of the total population, as
against 13.15percent in 1991.The sex ratio registered a slight increase from 913 in 1991 to 915 females for every
1,000 males in 2001. However, the sex ratio for the child population decreased from 961 to 937.
In consonance with the overall trend noticed in the State, the literacy rate of Bangalore's population increased by 4.20
percentage points in comparison to the 1991 census. In other words, 32,93,853 persons or 85.87 per cent of the
population aged over seven years have registered themselves as literates, as against 18,86,654 persons (81.67 per cent)
in 1991.
With the new Census figures, the number of urban agglomerations (UAs) in the country with a population of five
million or more has gone up to six, with Bangalore and Hyderabad being the fifth and sixth cities in that order. The
first four urban agglomerations of Mumbai, New Delhi, Kolkata and Chennai have retained their positions, and the
Bangalore UA, which occupied the sixth position in 1991, has now moved up to fifth, pushing Hyderabad to sixth.
hltp://www.hinduonnct. com/2001/10/12/stories/0412402e.htm
Bangalore - Demographics
As of2005 Bangalore had a population of over six million, making it the 3rd most populous city in India and the 27th
largest city in the world by population. With a decadal growth rate of 38%, Bangalore was the fastest-growing Indian
metropolis after New Delhi for the decade 1991-2001.1221 Residents of Bangalore are referred to as Bangaloreans.
While Kannadigas accounted for 38% of the population, sizable minorities from Tamil Nadu, Kerala, Andhra Pradesh
and Maharashtra exist.1221 Scheduled Castes and Tribes account for 14.3% of the city's population. Kannada, the
official language of the state of Karnataka, is widely spoken in Bangalore, as are Tamil. Telugu, Urdu and Hindi.
English is the lingua franca of the city's white-collar workforce.
According to the 2001 census of India, 79.37% of Bangalore's population is Hindu — roughly the same as the national
average.1212 Muslims comprise 13.37% of the population, which again is roughly the same as the national average,
while Christians and Jains account for 5.79% and 1.05% of the population, respectively, double that of their national
averages. Women make up 47.5% of Bangalore's population. Bangalore has the second highest literacy rate (83%) for
an Indian metropolis, after Mumbai. The city's workforce structure is predominantly non-agrarian, with only 6% of
Bangalore's workforce being engaged in agriculture-related activities. Roughly 10% of Bangalore's population lives in
slums1341 — a relatively low proportion when compared to other cities such as Mumbai (54%) and Nairobi (60%).1221
Bangalore's per capita income, at 2001 levels is USS 1,110.03 (Rs. 53,62s).1221
The 2004 National Crime Records Bureau statistics indicate that Bangalore accounts for 9.2% of the total crimes
reported from 35 major cities in India. Delhi and Mumbai accounted for 15.7% and 9.5% respectively.1221.
http://en.wikipedia.orR/wiki/Bangalore
PROGRAMME SCHEDULE FOR ORIENTATION ON
RIGHT TO HEALTH CARE IN AN URBAN CONTEXT
ddd
escLraerW SoA.rf torf zdysriE'ddE'd anodTOErroci
u
0
n
n
Time: 9.30 - 5.00
Date: June 23, 2006
Venue Fedina-Navachetana, No. 154, Anjaneya Temple Street, Dotnlur Village,
Bangalore - 560 071, Phone No. 080-25353190, 2535363, 9886648508
Objective
1.
2.
3.
To provide information regarding the structure and functioning of the urban
health care system,
eTsd. riedafo djd^abd^
To orient the participants to ‘right to health’ and the ‘right to health care’
campaign. ‘esdjafrtjd
d>^ ‘esd/aert rferfoi)
wzpoirarfd
drorirdilrd
To explore how the participants could integrate ‘right to health’ as part of their
work. odraertd
esVdtSSiS.'aVj.djdd torin ddr
A d8,?h
o 4 ddi& owitd lasrijjah
•
Schedule (zraoJae’^dod add):
__ —
09.30-10.15: Introduction of paiTi'cipants_and'HSling of expectations [NT/ EP]
j^artdtuTbddd do doh do^ dr MoOrrraddod tsdd DOeS rfVa
11.15:
10.15-
Understanding health (including various dimensions of health) [SJC]
tsd/aert aodd a>Fi>?
11.15-11.30: Tea Break
daoa boo do
11.30-12.15: Understanding determinants of health [EP]
ejduaeddefc, Sdroxbd eodrttf)
12.15—01.15: Understanding ‘right to health’ & ‘right to healthcare’ campaign [NT/ PS]
‘esdjafrt.d
a dth,d ’ dodo-o ‘esd^d6 ricwoJj d8>d ’ — «0d,
01.15-02.00: Lunch Break zp/aead dorado
02.00-02.45: Structure and functioning of the urban health care delivery system [SJC]
rfrtd d^d^rid esdja^rt :4?S3a dd^od drad^
m ac n-> nn
02.45-03.00:
-r
n
i
lea Break
_ <7.yOrr)
.
.
"
* hoev
Is
hec-x-LT/i c
,
doeo Mq'fct. i35Sk System
• no co.
c)r>
woA.
- rnkj- fe
daora buodo
03.00-03.40: Group Exercise [PS] rfooa^ d.dod>J8 / ddr
you.
b'r'r$ a cP
03.40-04.00: Consolidation of responses and linking it to the day’s theme [EP]
&g,e£ucto dj^
orfd ddo±>Se d/aedd
04.00-04.45: Brainstorming about how the participants could integrate ‘right to health’
as part of their work; Specific follow-up action points. [FEDINA]
esdjaertjd
oirad
Mdel/aetfd dodj,
dddt s!d5t
BaoJjE’oJjaearfab
/3r>
experije.oce/coo-.-io'
eVdQij^jjVuddd^ dotaodd wij
04.45-05.00: Feedback and Evaluation [CHC team]
drortg-ddE-d snabrrrodd urtn dSSofo
-J '-J dDib-o dS>e>drodd
6
[PS: Prasanna Saligram, SJC: S. J. Chander, EP: E. Premdas, NT: Naveen Thomas]
co
ro-^,
.
/
r 0 r / /€. ;
£'C''
<D '^up3
/■
hx do
c/o
Ap^cdp'c ac/'on
c'-i
$pP/></s\
cP'mmypSp bdW
/ /<£
it- -A^y
8
d'k^D (l/Ju. //d /(/ 3 ~p/i P^'-C ‘
P-d>
X A/m/aX
CO-u
-X Xz> a lc/1
§ s(j>ty\.t^
co
z>o/-
kocdtt
p^'ncu^
' acu^eLtp
dc^'c'^‘
h e /-ojat r\ cn
pK
dp
-/'pt^Jp '-'-Un
c^-u-dic/
^-o/-
^y^/c-ra
t.o>
cd
prcPoa/ .
(Xdd^coA cf- .
3-
^7~o
otyU- ^o<cyz>
8'
d~v
db
c^&Ucc^j
A/bo-v £>y
df-c m&cda cLi, m
-/\ame a.
3ciV'-ol(^
de
p<^lol'3
pry^/e^h
(d-p/etwtJ-
3/<h)Os
/"kt
dovc^Lc
hdcb i\
Mil
ocrh"^,
cp fe\
cL/'z
fke
c cr>xJtP~ ctccfaff^
pp c -c
r^r/^o-Qe .
C^ kc/ Aiy d)
itk. -d-coo.t^i
pilr>'t~^
th
/P
C<s>tor>-}C(i^^'(A .
p cph> C^ci' p
p- --/del
Jb^)-P(j\
c^le
e-Si
//sett' (oil <y
—5
<2©/h/nuw /y
h-lo\.c> F’drrypU/^-<T.oX'X'covn./
cd
hit
^C/^/'ers,
Ott^d
pO-Dj(-'C^ CCtxe
£y^./>hr>
P/rcif'Ce' t^-e
Cc /& CAt'C,/1^'
p-
WORLD BANK (WB) LOAN
to
KARNATAKA HEALTH SYSTEM
DEVELOPMENT AND REFORM
PROJECT (KHSDRP)
for
IMPROVING HEALTH OUTCOMES
Presentation
based on
review of following WB documents:
• Project Appraisal Docu:cent
• Integrated safeguards datasheet
• Indigenous People’s Plan
By:
Naveen Thomas, CHC
October 6, 2006
1
Context
c ___
. . :,
.
'.
• State Govt, expenditure on health and family
welfare (SGEHFW) as % of total Govt.
expenditure, fell from 5.62% in 1997 - 98 to
3.62% in 2003 - 04.
• GEHFW on an average, falls 10.8% short of
the allocated budget; It was 13.7% in 2001-02
• 70% of SGEHFW is on salaries.
® 43% staff absent on a day of announced visit.
• WB support will account for 7% of SGEHFW
Context (cont’d)
czzzzzzzz
• For every 1 Re. spent which benefits the
poorest 20% of population, 2.08 benefit the
wealthiest 20% of the population (Average in
Karnataka for expenditure by the Govt, on
HFW); India: 2.14%
• 36.6% people - live BPL in Karnataka
• 45% of outpatient visits at primary care were by
people living BPL
• Over 10 years - govt, expenditure of primary
care decreased; tertiary care increased greatly
2
Context (cont’d)
, ..
)
• Out-of-pocket (OOP) payments account for 80%
of health care expeniture
• 23% of ill people DO NOT SEEK formal care due
to financial reasons
• 24% of hospitalised people fall BPL b’cos of
medical costs
• 2004: Average cost per episode of hospitalisation
was Rs. 2,614 in public facilities (including bribes)
Rs. 12,724 in private facilities.
Donor supported health initiates
• Integrated disease surveillance
• Women and Child development
• TB and HIV/AIDS
- All the above are vertical programmes through
Gol Central Schemes (CS) or Centrally
Sponsored Schemes (CSS)
• Upgrading secondary level health care
facilities
- German government
3
Externally funded projects in health in
Karnataka during the decade of 90s.
Project
Period
Focus
IPP VIII (WB)
94-02, 00-02
Urban slums
Rs.(crores)
38.8 (26.2
state budget)
IPP IX (WB)
94-01
Rural PHcare
123.8
Raichur_Hos
96-01
350 bed multi
specialty
29.25
KHSDP-II
96-04
Infrastructure
, training
546
KfW
97-03
47 hospitals
44.1
RCH (WB)
99-03
FW services
91
pital (OPEC)
Recent externally funded projects in
health
SOCIETIES (Gol direct)
UNICEF
• State AIDS Control
• Child Development and
Nutrition
Project
• National TB Control
Program
• Water and Environment
Sanitation
• National Program for
• Education and adult
Blindness Control
literacy
OTHERS
• KfW second phase
4
Key highlights - KHSDRP
C
„..... : • 70% loan (about Rs. 663 crores)
I
• 30% own funding (about Rs. 302 c'orcs)
• Total: Rs. 966.63 crores (or USD 206.48)
• Maturity of 25 years; 10 years grace period
• Disbursements over five years
• Project effective period: Oct 2006 - March 2012
• Mid-term review after 2 % years
Key components
• Organisational development
- to expand coverage of existing programs
- through increased spending and better performance
• Innovations in service delivery and health financing
- Infrastructure
- Delivery of priority curative services
- Planning and delivery of public health services
- Accessibility to safe delivery and hospital inpatient services
• Project management, support, monitoring and
evaluation
5
Strategic documents
• Public Private Partnership - Dr. V. S. Patil
Kulkarni
• Reorientation of public health sector - Dr. M.
V. Murugendrappa
• Health financing alternatives in Karnataka Dr. Maathai Mathiyazhagam
6
Tel : 23443661
23328759
Fax : 23443661
niCIJNA SI VA SAINGHA
Community water and Sanitation Project
Sponsored by Water Partners International. USA
No. 22, Risaldar Street, Seshadripuram, Bangalore - 560 020.
E-mail: dssl 718@yahoo.com
Ref. No. :
Date :.
November 14, '06
Dear Shri Chander:
I have your communication dated 6th Nov.*06
on Consultation on Urban Primary Health Care
Training modules & National Health Assembly-II,
based on the health needs of the urban poor.
I will not be able to attend the programme which
you are having on 24th November ’06.
I would like to have a discussion with you
if you can spare sometime at my office on any
working day between 10 am and 12.30 noon. You
could just give me a ring and come. ' We have been
working with the urban slums for the last 1 3 to
14 years and it is quite possible that you might
be able to get an ideas from our experience.
Thanking you and with regards,
Yours sincerely,
(S. V.
Ijlr. 3. J. Ch and er,
society for Community Health
Awareness, Research & Action,
No.326, 5th Hahn, I Block,
Koramangala, Bangalore-560 034
Rama Rao.)
Consultation
&
on Urban Primary Health Care Training
National Health Assembly-II (NHA-2)
Date: 24 November 2006
Time: 10.00 a m. - 04.00 p.m.
Modules
Venue: Community Health Cell
AGENDA
Morning
10.00 - 10.30: Recap of urban health action.
10.30
- 11.30: Case study of a health module - “Hygiene promotion in urban areas".
11.00 - 11.30: Discussion on module preparation.
11.30
- 12.00: Presentation on Government initiatives to address urban health care needs:
>
Jawarharlal
Nehru
National
Urban
Renewal
Mission
(JNNURM)
-
Recommendations of task force on urban health care.
>
Healthy Urbanisation Project - World Health Organisation (WHO) in collaboration
with Bangalore Mahanagara Palike (BMP).
12.00 - 01.00: Discussion on responses of JABU to the above; action plan for module preparation.
Afternoon
2.00 - 2.30: Presentation on FORCES Study of Urban Anganwadis
2.30
- 3.00: Background and Introduction - National Health Assembly (NHA-2)
3.00 -4.00: Evolving an action plan for Urban Anganwadis in light of NHA-2
Addressfor Correspondence: Community Health Cell (Cl IC I. No. 359 (Old No. 367). Srinivasa Nilaya, Jakkasandra, I st
Main. 1st Block. Koramangala. Bangalore - 560 (134. Tel: 25531518. 25525372 (Contact Persons: S. .1. Chander:
9448034152: chander@sochara.orq-. Navccn Thomas: 9342858056. naveen@sochara.orq)
The Bangalore Healthy Urbanization project is a partnership with the WHO Kobe
Centre, (WKC) Japan, the World Health Organization (SEARO and India) and BMP.
In order to implement its 'Healthy Urbanization Project: (Optimizing the impact of social
determinants of health on exposed populations in urban settings for 2006 - 2007')
WHO Kobe Centre is in the process of establishing six Healthy Urbanization Field
Research Sites. They are San Joaquin (Chile), Bangalore (India), Kobe / Hyogo (Japan),
Suzhou (China), Ariana (Tunisia), and Nakuru (Kenya). In each of the sites, action
research projects will be developed through a capacity building process called the
"Healthy Urbanization Learning Circle" (HULC).
Some facts about Bangalore
Being the 6th Largest metropolis in India, Bangalore is a living witness to the changing
face of Indian cities. The city is an ever-increasing hub of industrial and technological
growth, changing rapidly, especially during the last two decades.
Bangalore's population is expected to cross 8 million by 2010. Those residing in low
resource settings account for nearly 40% of the current total population.
Reasons of rapid Urbanization
Search for employment.
Need for better educational opportunities (especially in low resource settings).
Infrastructure development - cheap labour attracts migrants from neighboring
states.
Search for better quality of Life.
Changes in production and marketing prices.
Poverty (lack of income).
Inadequate food and shelter.
Inappropriate and unplanned housing, physical overcrowding.
Improper sanitation, waste disposal and civic amentities.
Insecure employment and other stresses that result in communicable
and non - communicable diseases.
Use of harmful substances like tobacco and alcohol.
Environment pollution.
Poor education status.
Unsafe workplaces and lack of access to health systems leading to social inequites.
Bangalore Healthy Urbanization Project
Healthy urbanization is a coordinated series of health promoting, policy-related
activities, informed by evidence and research.
Health in this context is not a prescriptive concept (i.e. treatment of illness) but is
operationalized to address risk behaviours in the environment in which people live.
The National Institute of Mental health and Neuro Sciences, Bangalore, conducted a
situation analysis of various issues based on secondary sources of information that
needed to be addressed under the healthy urbanization project. The recommendations
included.
o
Need for evidence based policies and programmes.
o
Capacity enhancement of existing organizations and individuals.
o
Strengthen intersectoral collaborative mechanisms between health and related
sectors.
o
Information systems and research should be given priority.
o
Capacity of health systems to deal with non-communicable diseases need to be
enhanced.
o
Strengthening of health promotion practice (based on policy) recommended.
•
Targeted interventions based on evidence and good governance principles to be
initiated.
Bangalore Mahanagara Palike
BMP is the principal nodal agency to deliver services for the entire city especially
resource-constrained areas. Therefore, BHUP works very closely with BMP to bring
about healthy urbanization through action research.
The Bangalore Healthy Urbanization Project will address issues related to urbanization
such as.
o
Overcrowding, access to potable water and sanitation.
o
Education.
o
Transportation
o
Low and uncertain incomes.
o
Rights of women in terms of their access to healthcare, education and employemt.
o
Habits (including diet).
o
Violence (including domestic violence)
o
Demographic transition, which has resulted in the growth of elderly population.
o
Communicable diseases and high risk behaviour.
o
Risk factors like tobacco and alcoholism.
BHUP will have 7 research sites. Each site will have a Healthy Urbanization Learning
Circle (HULC). This will comprise of Health Centre Doctor, Social Organization, Board
of visitor from Health Centre and Local representative from the selected slum as
members.
1^
,,.._____ —
PROJECT OFFICE
Pobbathy Health Centre,
Sajan Rao Circle, V.V Puram, Bangalore - 560 004
Dr. M. Vijayalakshmi,
Chief Health Officer
98440 51125
BHUP Core Team
Dr. P.S. Thandava Murthy
Ms. Kameshwari
98867 40954
94491 57950
World Health Organization
Centre for Health Development
Kobe
World Health Organization
South East Asia Regional Office,
New Delhi, India
Dr. Susan Mercado
Davison Munodawafa (Prof.)
Regional Adviser Health Promotion
and Education
91-11-23370804 Extn. 26522
Teem Leader Urbanisation and
Health Equity
WHO Centre for Health Development
81-782303178
World Health Organization,
Office of the WHO
Representative to India
Dr. Cherian Varghese
National Professional Officer
Non Communicable Diseases
and Mental Health
011-23061955 Extn. 23133
Dr. Jostacio Lapitan
Ms. Vijayluxmi Bose
Technical Officer Urbanisation and
Emergency Prepardness (UEP)
81-782303178
Consultant
9811415443
Susan Loo
Technical Officer Policy Advocacy UHE
81-782303131
Page 1 ofi
Main Identity
From:
To:
Cc:
Sent:
Subject:
"fedina" <fedina@iqara.net>
<chc@sochara.org>
<navthom@yahoo.co.uk>
Thursday, June 15, 2006 6 04 PM
One day Training programme on 'A Rights based / political approach to health'
Dear Naveen,
In continuation to our discussion earlier this month, I would like to formally invite you and your collegues to
conduct a one day training programme on 'A Rights based/ political approach to health'. We would like to organise
this programme on the 23rd of June, (Friday) and the participants would mainly be the staff of FEDINA and a few
other people totalling to about 25 - 30 people.
As per our discussion, the training would have to focus on
1.
2.
3.
4.
The concept of 'Health' as a basic governmnet provided service
The present political scenario of health systems
Grassroot mobilisation to access the available health facilities
Mobilisation to approach the health system better.
That would be in a few points what the team is expected to learn from the training and I hope I have been able to
draw up a better picture for you. Do let me know if you need more information.
Looking forward to your response.
Regards,
Preethi Herman
6/16/2006
Consultation
&
on Urban
National
Date: 24 November 2006
Primary Health Care Training
Health Assembly - II (NHA-2)
Time: 10.00 a.m -04.00 p.m.
Modules
Venue: Community Health Cell
AGENDA
Morning
10.00 - 10.30: Recap of urban health action.
10.30
-11.30: Case study of a health module - “Hygiene promotion in urban areas”.
11.00-11.30: Discussion on module preparation.
11.30
- 12.00: Presentation on Government initiatives to address urban health care needs:
> Jawarharlal
Nehru
National
Urban
Renewal
Mission
(JNNURM)
-
Recommendations of task force on urban health care.
>
Healthy Urbanisation Project - World Health Organisation (WHO) in collaboration
with Bangalore Mahanagara Palike (BMP).
12.00 - 01.00: Discussion on responses of JABU to the above; action plan for module preparation.
Afternoon
2.00 - 2.30: Presentation on FORCES Study of Urban Anganwadis
2.30
- 3.00: Background and Introduction - National Health Assembly (NHA-2)
3.00 - 4.00: Evolving an action plan for Urban Anganwadis in light of NHA-2
Address for Correspondence: Community Health Cell (Cl IC)t No. 359 (Old No. 367). Srinivasa Nilina. Jakkasandra. 1st
Main. 1st Block. Koramangala. Bangalore - 560 03-1. I'ek 25531518, 25525372 (Contact Persons: S. J. Chander:
9448034152: chander(5>soctiara.ora: Naveen Thomas: 9342858056. naveeniSsochara orq)
Consultation
&
on Urban Primary Health Care Training
National Health Assembly-II (NHA-2)
Date: 24 November 2006
Modules
Venue: Community Health Cell
Time: 10.00 a.m. - 04.00 p.m.
AGENDA
Morning
10.00 -10.30: Recap of urban health action.
10.30
- 11.30: Case study of a health module - "Hygiene promotion in urban areas".
11.00 - 11.30: Discussion on module preparation.
11.30
- 12.00: Presentation on Government initiatives to address urban health care needs:
> Jawarharlal
Nehru
National
Urban
Renewal
Mission
(JNNURM)
-
Recommendations of task force on urban health care.
>
Healthy Urbanisation Project - World Health Organisation (WHO) in collaboration
with Bangalore Mahanagara Palike (BMP).
12.00 - 01.00: Discussion on responses of JABU to the above; action plan for module preparation.
Afternoon
2.00 - 2.30: Presentation on FORCES Study of Urban Anganwadis
2.30
- 3.00: Background and Introduction - National Health Assembly (NHA-2)
3.00 - 4.00: Evolving an action plan for Urban Anganwadis in light of NHA-2
Addressfor Correspondence: Community Health Cell (Cl IC), No. 359 (Old No. 367). Srinivasa Nilaya. Jakkasandra, I st
Main. 1st Block. Koramangala. Bangalore - 560 034. Tel: 25531518, 25525372 (Contact Persons: S. J. Chander:
9448034152: chander(5)sochara.orq: Naveen Thomas: 9342858056. naveen@sochara.orq)
PRE-GRANT REPRESENTATION BY WAY OF OPPOSITION
UNDER SECTION 25(1) OF THE PATENTS ACT
1970(39 OF 1970) AND RULE 55 (1) OF THE RULES
AS AMENDED BY THE PATENTS (AMENDMENT) ACT, 2005
The Patent Controller.
Delhi
Re: Patent Application No. 315/Del/2000 filed on 27 March 2000 titled “New Crystal
Modification of CDCH, And Pharmaceutical Formulations Comprising This
Modification”
S TATEMENT OF FACTS/ EVIDENCE
1. AIDAN (All-India Drug Action Network) was founded in the early 1980s as a
network of like-minded individuals and groups in India to fight for a people oriented,
rational, drug policy. AIDAN the opponents hereby make a representation by way of
opposition under § 25(1) of the Patent Act 1970, as amended by the Patents
(Amendment) Act, 2005 (the “Act”) against the grant of patent application, titled: “New
Crystal Modification of CDCH, And Pharmaceutical Formulations Comprising This
Modification" macle by Applicant Bayer Aktiengcsellschaft (the “Applicant”), bearing
Indian palcni application No.11 5/1 )cl/2()()0 filed oh 27 March 200(1 (the 'Application").
This representation ’-is proper under § 25(1) of the Act as the application has been
published but a patent has not been granted. Specifically, this representation is brought
under the grounds.as stated in § 25(1) (f), (h) of the act.
2. The Opponents are opposing the above-mentioned application for a patent under
section 25(1) of the Patents Act. All India Drug Action Network (AIDAN) is an
independent network of several non governmental organizations working tp increase
access and improve the rational use of essential medicines. They are also involved in care
and treatment of Tuberculosis patients as it is a major public health problem and a health
emergency. The existence of Multidrug and Extreme drug resistant strains has added to
the woe and is the single largest killer. The most effected are in productive stage and the
largest population of multidrug resistant strains are present in India.
The nonexistence of the effective drugs to treat multidrug resistant strains and alsc the
accessibility of the first line regimen of drugs are declining due to unaffordability. Of
particular concern to opponents is the impact of product patent regime on access to safe,
effective and affordable tuberculosis treatment.
3. The patent application was filed at the Patent Office in Delhi, therefore, the Patent
Controller has the jurisdiction to hear this pre-grant opposition in Delhi. Opponents
hereby request a hearing as per provisions under Rule 55(1) of the Patent Rules. 2005.
4. The present Application relates to a treatment of infections caused by bacteria like
acute bacterial sinusitis, acute bacterial exacerbation of chronic bronchitis, community
acquired pneumonia, bacterial conjunctivitis and uncomplicated skin/skin structure
infections. It is a broad spectrum antibiotic which is now being used to treat tuberculosis
caused by mycobacterium tuberculosis complex. Nine million new cases of tuberculosis
and nearly two million deaths ate estimated to occur around the world every year, making
it the leading cause of death among curable infectious diseases. The World Health
Organization declared tuberculosis a global emergency in 1993. This application is of
particular interest for the treatment of tuberculosis in HIV-positive people because it has
no interactions with antiretrovirals and may be potent enough to shorten the duration of
TB treatment, which currently stands at a minimum of six months which can be reduced
to three months. The DOTS programme initiated by Government is still in its initial
stages and has not reached the rural places of India. The accessibility of the first Ime
treatment comprising of Isoniazid, Rifampicin, Ethambutol, Pyrazinamide are prized at
Rs.4.90/10 tablets. Rs.57/10 tablets. Rs.24/10 tablets and Rs.65/10 tablets in total costs
Rs. 150. T his cost factor itself is a barrier and the current application which can be used in
Multidrug regime treatment is costing Rs.4, 735/10 tablets. If granted patent on this
application patent owner will have a 20-year monopoly, during which the owner is free to
set prices at levels impossibly beyond reach for the vast majority of those who are in
desperate need of treatment.
5. The most effective way to lower the cost of these essential medicines is to promote
competition, particularly within India’s vibrant pharmaceutical industry. However, in
order for there to be any effective generic competi’ion, it is imperative that patents not be
granted in India for uninventive, incremental improvements to already-known drugs.
Although India was compelled by its WTO obligations to introduce product patent
protection for pharmaceutical products through the Patents (Amendment) Act of 2005.
India retains full sovereignty in determining the standards that must be met with respect
to patentability. As such, India is under no obligation to follow the perilous path that
many developed nations have taken in setting loose standards for novelty and inventive
step that result in patent protection for incremental innovations, all .too often at the cost of
public health.
6. India's Patents (Amendment) Act, 2005 was passed in order to bring India into
compliance with its TRIPS obligations under the WTO, and introduced for the first time a
20-ycar product patent regime in this country. India, however, is also a signatory to the
Doha Declaration on the TRIPS Agreement and Public Health (the “Doha Declaration”).
which states, in part, “we affirm that the [TRIPS] Agreement can and should be
interpreted and implemented in a manner supportive of WTO members' right to protect
public health and, in particular, to promote access to medicines for all.” (emphasis
added).
7.
In part due to the recognition of its obligations under the Doha Declaration.
Parliament passed the Act with a few important provisions aimed at ensuring that a
product patent regime would not harm public health. One of the most important is § 3(d)
of the Act, a provision designed to discourage the pernicious but all-too-common practice
of “ever greening,” whereby pharmaceutical Companies artificially extend the life of their
monopolies by patenting trivial improvements to already existing drugs. Declaring that
“a new form of a known substance which does not result in the enhancement of the
known efficacy of that substance,” and the discovery of a “new use for a known
substance” are not inventions under the meaning of the Act, Parliament expressed
through § 3(d) its unequivocal rejection of ever greening.
8. The present Application falls squarely in the category of “inventions” that Parliament
intended in rejecting when it enacted § 3(d). The original patents for the active
ingredients of this drug were granted prior to 1995, when India first incurred its
obligations under the WTO. The sole “improvement” at issue is the conversion of the
active ingredient into a particular crystalline form that does nothing to improve the drug’s
efficacy. Granting the current Application a patent will do nothing but further enrich the
Applicant at the expense of human lives.
9. The Opponent humbly submits that the obligation to “promote access to medicines
for all" has been incorporated into the Act by Parliament, and that the Act. whenever
possible, can and must be interpreted in a manner that is consistent with the Doha
Declaration’s binding promise, as it is this Office that ultimately makes the decision that
will determine whether millions of people will have access to essential medicines. The
Opponents respectfully request that the Patent Office keep the Doha Declaration in mind
as it examines the present Application and interprets the applicable law.
GROUNDS
10.
The Opponent has closely studied the specification and claims made by the
Applicant in the Application and strongly believe that the invention is not patentab'e
inidci the following grounds of § 25( I) of the Act:
i.
s25(l)(f) - that the subject of any claim of the complete
specification is not an invention within the meaning of this Act.
or is not patentable under this Act, in particular under sec ion
3(d).
ii.
s25(l)(e)- that the invention so far claimed in any claim of the
; complete specification is obvious and clearly does not involve
any inventive step under this Act, in particular under section
2G)(a).
iii.
s25(l)(h) - that the applicant has failed to disclose to the
controller the information required under section 8 especially
form 3.
,
Accordingly, as permitted under s25(l) of the Act, which allows eln opposition to
be filed by any person after publication but before the grant of a patent, and Rule
55(1) of the Rules, the Opponent submits its opposition to the Application on the
grounds set out below.
11.
'
..
..
The Applicant has failed to meet its burden of showing that the alleged invention
described in the Application is entitled to a patent under the Act. The present ap[ .ication
merely relates converting a known pharmaceutical substance, CDCH into a monohydrate
form and making the monohydrate form in to prismatic crystals. - a process well known
in the art - in order to make the bulk manufacture of the drug substance more convenient
The applicant admits the active molecule CDCH is a well known substance used as a
broad spectrum antibacterial medicine disclosed in EP -A- 550903 and EP -A- 591808
attached herein as Exhibit A and B respectively. However, as will be explained below,
the conversion of a drug substance to its monohydrate crystalline form in order to obtain
certain benefits has been known in the pharmaceutical industry' for years, and is obvious
to one skilled in the art. Further, because whatever benefits may be derived from this
conversion does nothing to make the final drug substance more effective, it is not eligible
for a patent under s3(d) of the Act.
12 Despite the Applicant's admissions that the use of active molecule CDCH is
known the Applicant nonetheless claims that the alleged invention is patentable.
Specifically, the Applicant’s claims can be summarized as follows:
a.
Claim 1 relates to monohydrate form of active molecule CDCH.
b. Claim 2 relates to the prismatic crystal form of the compound described in
Claim 1.
l
< Imiii I • '< being dependent on Claim 1 and 2 .mil relate t<> the use of the
alleged invention as antibacterial compositions.
I
The claims of the application relates to the inpnohydrate form of CDCH in a prismatic
crystal form. The conversion of an active molecule CDCH into monohydrate, admitted by
the applicant that CDCH as already known is insufficient to render the application
patentable under the Act. The applicant does not prove the fact that conversion of active
molecule CDCH to monohydrate form is an improvement in therapeutic efficacy,
therefore it is just a mere discovery of a new form of known substance and thus not an
invention under § 3(d) of the Act. The conversion of active molecules to monohydrate
forms to overcome the pharmaceutical manufacturing barriers is obvious and is a practice
well known to a people skilled in the art and not an invention under § 2(j)(a) of the Act.
Furthermore the applicant fails to disclose information to the patent controller required
under § 8 of the Act. Each of these separate and independent grounds for denying the
present application is discussed in further detail below
The Alleged Invention Is Not An Invention Under § 25(l)(f) and § 3(d) Of The Act
Because It Is The Mere “Discovery” Of A New Form Of A Known Substance.
13. The alleged invention is not patentable under the Act because it is. at most, the mere
"discovery” of a new form of a known substance. Under § 3(d) of the Act. the “mere
discovery of a new form of a known substance which docs not result in the enhancement
of the known efficacy of that substance” is not an invention within the meaning of the
Act. The accompanying Explanation to § 3(d.) states. "For the purposes of this clause,
salts, esters...combinations and other derivativeSjof known substance shall he considered
to be the same substance, unless they differ significantly in properties with regard to
efficacy.” (emphasis added).Because the alleged invention claims to be and is in fact
nothing more but only conversion of the active molecule in to monohydrate crystalline
form with no improvement on efficacy of the dpug.
14. The present invention is about conversion of CDCH to nonhygroscopic form
achieved by converting it into monohydrate form. The invention claims to overcome the
hygroscopicity problem thereby, enhancing the effect of flow characteristics and dosage
accuracy. The hygroscopic problem of active molecules is tackled by technologies which
are already known and practiced for many years in the pharmaceutical industries. The use
of desiccants is one of the widely used method employed in pharmaceuticals for
hygroscopic compounds, the most widely used is silica gel. (Still searching for
documents)
Attached herein as Exhibit C US 4568547 explaining the process of obtaining anhydrous
compound in presence of methylsulphonylmethane a carrier used to tackle storage
problems of hygroscopic compounds.
15. The presence of different pharmaceutical technologies proves that hygroscopicity
problem can be overcome by use ol already known method? and there is no heed to
convert the active molecule to monohydrate form.
16. As the foregoing shows, all of the substances contained in the present Application
are known. Nevertheless, the Applicant Claims and purports to stake ownership over the
following: Monohydrate of CDCH in the prismatic crystal form used ten treat bacterial
infections. It is very clear that the applicant fails to show any invention and it is only a
new form of a known substance with no enhancement on known efficacy under section
3(d) and therefore does not fulfill the criteria of patentability.
17. In light of the above arguments Claim 1 fails as it is a monohydrate form of already
known substance, (need to work more on this).
18. In order to meet its burden under § 3(d), the Applicant is required to present
evidence that the claimed invention (i.e., the monohydrate form of CDCH) represents an
enhancement in the known efficacy over the previously known substance, (i.e..
anhydrous form of CDCH). The Applicant does not and cannot satisfy this requirement.
The Applicant admits that the only active ingredient in the claimed invention is CDCH
See, e.g., Specification, p. 1, lines 5-10 2"‘ para. Accepting the fact that the active
molecule is converted to monohydrate form to make it non-hygroscopic and free Bowing
and in no way it has effected or enhanced the therapeutic activity of the active molecule.
19. This alleged “improvement” bears no relation to the ultimate therapeutic efficacy of
the active ingredients. It is, at most, a tool that may facilitate: (i) the mass production (ii)
of a particular dosage form of the active ingredients (i.e.. the tablet form). However.
there is no sound reason why the relevant comparison should be between the therapeutic
efficacies of an active molecule converted to monohydrate form versus that of a active
molecule without conversion to monohydrate form. The Applicant has put forth no
evidence to show that the therapeutic efficacy of an active molecule converted to
monohydrate form is greater than that of, say, anhydrous CDCH which can be
manufactured through different means.
The Alleged Invention Is Not An Invention Under § 25(I)(e) and § 2(j)(a) Of The Act
Hecaiise It Is Obvious To A Person Skilled In The Art and does not Involve any
Inventive step.
20. The applicant claims that to get non-hygroscopic, free flowing active compound the
active molecule is converted to monohydrate form which they claim is new. Conversion
ol an active molecule to monohydrate form is not a technical advance and is obvious to a
person skilled in the art. Attached here in is Exhibit D, E and F US Patent No.
5.068.440. US Patent No. 3.655,656 and US Paten; No. 4.504,657 which clearly explains
that hygroscopic materials arc difficult to handle and to get a non-hygroscopic form we
need to convert the active molecule to monohydrate form which is vers much obvious
and any person skilled in the art can obtain the same.
21. For the reasons already stated it would have been obvious to a person skilled in the
art, given the disclosures contained in the US Patent No. 5.068.440, US Patent No.
3,655,656 and US Patent No. 4,504,657 which clearly explains that hygroscopic materials
are difficult to handle and to get a non-hygroscopic form we need to convert the active
molecule to monohydrate form which is very much obvious and any person skilled in the
art can obtain the same.
22. Need to discuss on the claims.
23. For all of the reasons stated above, Claim 1 and its dependent Claims 2-5 of the
present Application also fail because they lack the inventive step required for
patentability. The claimed invention is obvious, to a person skilled in the art i.e. obtaining
monohydrate forms to over come the hygroscopicity of active molecule and it is very
well known in the pharmaceutical industrial practices. Under § 2(j)(a) of the Act.
“inventive step” is defined as “a feature of an invention that involves technical advance
as compared to the existing knowledge that makes the invention not obvious to a person
skilled in the art.”
24. The sole “innovation” that the Applicant claims with respect to the conversion of
active molecule to monohydrate form which is already known and practiced from many
years does not involve any inventive step and it is very much a common practice i.e.
obvious (to a person skilled in art) is carried through out the Pharmaceutical industries to
obtain a non hygroscopic and free flowing active molecule.
The applicant has failed to disclose to the controller the information required Under
§25(l)(h) by section 8 especially form 3.
25.
Section 8 of the Patents Act requires an applicant for patent to furnish the
Patent Office with detailed particulars of any patent applications for the same or
similar inventions made in any other country, and to undertake to update the
Patent Controller of detailed particulars of ever, other application made
subsequent to filing within the prescribed time. Under Rule 12(1 A), the
statement and undertaking under section 8 must be made within 3 months of
filing. Rule 12(2) requires the Applicant to inform the Patent Controller of
additional particulars within 3 months of the additional filing. The details
required by section 8 are clear from Form 3. and include status of the
application. Under section 25(1 )(h), a failure to comply with section 8 is a
ground for opposition and is therefore sufficient to reject an application in its
entirety.
26,
Thus the claims of the Application do not prove any efficacy of the drug and it is only
about the monohydrate form of the active molecule which is insufficient to render the
alleged invention patentable under the Act. 'Uli's is because the mere conversion of the
active molecule to monohydrate form to improve its flow characteristics is not an
invention and also obvious under section 2(j)(a), the alleged invention is not patentable
under section 3(d) as it is a new form of a known substance which does not result in the
enhancement of the known efficacy, it is anticipated in the prior art and is not Novel
Furthermore, the applicant has failed to disclose the controller the information required
under section 8 especially Form 3.
CONCLUSION
26. Given all of the foregoing, Opponents hereby humbly request that the Patent Office
reject the Application on the following grounds:
»
The alleged invention is a “mere discovery of a new form of a known
substance” and thus not an invention under § 3(d) of the Act;
•
Claim 1' and its dependent Claims 2-5 of the present Application fail for
lack of novelty;
•
All of the Claims in the present Application fail lor lack of inventive step.
•
The Application fails to meet the formal disclosure requirements under
section 8.
27. Opponents further request that the Office grant a hearing as per Rule 55(1) of the
Patent Rules.
Respectfully submitted,
On Behalf of the All India Drug Action Network,
Page 1 of 2
Community Health Ceil
From:
cehalpun@vsnl.com on behalf of SATHI [cehatpun@vsnl.com]
Sent:
Wednesday, Februaty 28,2007 12:57 Plvl
To:
Sama: Sunil Kaul; Thelma Narayan: Ab hijit Das; Abhijit dasjAmoerkharr.Asha Mishra-MP-BGVS;
ashagramirust Batwanl; cehat indore: chablj; D Barkatakl; indira chakravartN; Joe Varghese; rakhal
gaiiondo; gouranga_2k@yahoo.com: renu khanna; Sojal Band; Ajaykhare: Arnuiya Nidhi;
narendra@prayaschittor.org; Sulakshana Nandi
Cc:
Vandana Prasad; Sundar gmail; ekbal@gmait.com;Amit Sen Gupta
Subject: CommunityMonitoring in the NRIIM
Dear Friends,
Greetings,
We are writing this mail to you in the context of the process of Community Based Monitoring being
planned in the National Rural Health Mission. JSA members have been consistently raising the need for
such monitoring of the Mission at various levels. In the recently held AGCA (Advisory Group on
Community Action) meeting in New Delhi on 24'h Feb., a draft proposal which was mainly drafted by a
sub-group (Abhay Shukla, Abhijit Das and Narendra Gupta) and approved by the larger AGCA was
sanctioned in principle by representatives of the Union Health Ministry, Now a large pilot activity of
Community monitoring will be initiated in eight states, which would start in the states from April 07. .hi
tills scenario JSA State units in the pilot states should contact NRHM officials in the state, and argue for
the desirability of involving JSA constituents - as members in the bodies at various levels for
community based monitoring, and to help the process of forming and training committee members.
Following are some important highlights hi this proposal1. For the National Pilot of the community based m onitoring, the following eight States were
approved: Assam, Chhattisgarh, Jharkhand, Madhya-Pradesh, Maharashtra, Orissa, Rajasthan,
Tamil Nadu. (U.P. and Karnataka had also been suggested, but were presently not accepted by the
Health Ministry)
2, Three to five districts in each state would be identified, with a minimum of 3 districts per state,
Thia amounts to a total of 30 pilot districts spread across these eight states.
3, In each district, three blocks would be taken up (total 90 pilot blocks).
4. Three PHCs in each of these blocks would be taken up (total 270 pilot PHCs)
5. Five revenue villages in each PHC area would be identified (total 1350 pilot villages)
Committees at all levels would have about one-third representatives from Panchayati Raj institutions,
about one-third representatives of NGOs i CBOs or People’s organisations, and one-third representatives
of the Health department or other officials.
The following major activities are planned at various levels during the pilot which would be
implemented over the next one year:
a Preparation ofmodel Community monitoring tools and training material etc. at national level
b. State Preparatory meetings and Workshops
c. State mentoring team formation, finalization of state appropriate frameworks for monitoring
d. State Training of trainers - one state level workshop for Facilitators.
e. Training of Community Monitoring teans at different levels will be conducted by NGO
facilitators in the pilot phase.
f District workshop - one in each district Formation of District mentoring teams.
g. Block level training for members of a Block Community Monitoring team, including at least
two civil society membets.
h. Community mobilisation and formation of Community Monitoring committees at different
levels starting mom village level.
i. Orientation of members of Community Monitoring committees at all levels. Initiation of
work of these committees, witit discussion and action on various issues that emerge during
Page 2 of2
the p eri odic tn eeti.ngs,
j. Block and district level community monitoring exercises would include u public dialogue
(‘Jan Samvad’) or public hearing (‘Jan Sunwai’) process, once in each PHC and Block
during the pilot year, to later continue on annual basis.
k. Process documentation, state evaluations and end phase state workshops in all pilot states.
We have attached the suggested outline and framework of the community based monitoring with this
mail to give you some idea about the nature of activities involved in this process.
We would like to suggest that ISA organisers / affiliated organisations in the pilot states along with
other interested organisations may get involved in this activity, which would include selection of pilot
districts (3-4 districts per state) for the community based monitoring process, This is especially
important since designated AGCA members for each pilot state would be shortly visiting these states for
conducting preparatory meetings (probably in March -April 07), and to plan the state level workshop. In
these preparatory7 meetings, some civil society representatives would be involved and a brief mapping of
coalitions and organisations with experience of Community' monitoring activities would be done.
Since many of the visiting AGCA members would be quite aware of JSA, you may contact them and
share with them a list of organisations / coalitions which could be involved in the community
monitoring process, prior to their scheduled visit to the States for the preparatory meeting. While
suggesting organisations, priority should be given to organisations with a demonstrated experience of
monitoring Public health services, organising public dialogues or public hearings. Along with JSA
constituents, like-minded organisations involved in monitoring of health services, independent social
audit, or citizen ’s reports could also be actively involved.
Such lists may help AGCA members to specifically suggest to State Mission officials, to invite for the
State level preparatory meeting, JSA organisations and other organisations involved in monitoring. Hi is
would also help JSA. related organisations to get involved in entire process, including the monitoring
committees from State to PHC level.
You may also note that the time frame for State preparatory phase for all the eight pilot States is from
April 07 io June 07. In this timeframe, tire state preparatory meeting, final selection of pilot districts,
formation of State mentoring team, State level workshop and Training of trainers is expected to be
completed. Actual formation and orientation of monitoring committees in the districts would start from
July 07. Considering the relatively short timeframe, it would be good to initiate state level discussions
within JSA about this at the earliest.
It may also be mentioned that SATHI-CEHAT and Prayas would be organising a workshop on behalf of
JSA on ‘Community Monitoring of Health Services’ during NHA-2 to discuss and work out various
finfrier aspects of tills activity. We hope that this workshop would be an opportunity to nationally
discuss and plan participation of JSA constituents in this major emerging activity - which would give us
a platform to empower communities on Health, rights, would enable organisations to forcefully and
persistently raise various Health issues on behalf of communities, and to present suggestions for
improvement of Public health services at various levels.
Do let us know'your suggestions in this regard at the earliest, we can send further information which
may be required.
Regards,
Abhay and Dhananjay
SATHI-CEHAT
3 & 4, Aman E Terrace,
Dahatiukar Colony, Kothrud,
Pune -411029
Phone: 020-25451413,25452325
Section—II: Suggested outline of the Community based monitoring
activity
We are envisaging an interactive system of monitoring, where more than one level of
committee looks into the functioning of each level. The underlying concept is:
a. The Monitoring committee at each respective level reviews and collates the
records coming from all the committees dealing with units immediately below it.
This enables it to make an assessment of the situation prevailing in all the units
under its purview, and to make a report at its level.
b. This Monitoring committee also appoints a small sub-team drawn from its NGO
and PRI representatives who visit a small sample of units (say one facility or two
villages every trimester) under their purview and review the conditions there. This
enables the committee to not just rely on reports but to have a first-hand
assessment of conditions in their area. For example, the PHC committee
representatives would visit 2 villages and conduct FGDs there, in each trimester
by rotation. Similarly the Block committee representatives would visit one PHC
by rotation in each trimester.
c. The monitoring committees at PHC / Block / District levels would make an
assessment of the functioning of the major Health care facility at their respective
level (PHC / CHC / District Hospital). This obviates the need for a separate
committee to look into Health care facilities.
d. The Monitoring committee sends a periodic report (Quarterly for Village, PHC,
Block and District levels; Six monthly for State level) to the next higher level
committee enabling it to collate the report at that level.
Keeping this in mind, outlined below are a broad suggested framework for activities
at various levels, and a complementary suggested framework of organisation of
information for the Community based monitoring activity.
Suggested framework of activities according to levels
Level
Agency
Activity
Village
Village
Health
Sanitation Committee
(Quarterly for
Village,
PHC, Block and District
levels; Six monthly for State
level)
and a. Reviews Village Health
register,
Village health
calendar
b. Reviews performance of
ANM, MPW, ASHA
c. Sends brief three monthly
report to PHC committee
PHC
PHC
Monitoring
Planning Committee
Block (including CHC)
Block
Monitoring
Planning Committee
District (including District
hospital)
District Monitoring
Planning Committee
and a. Reviews and collates
reports from all VHSCs
b. An NGO / PRI sub team
conducts FGDs in three
sample villages under PHC
c. Visit PHC, review
records, discuss with RKS
members
d. Send brief three monthly
report to Block committee
and a. Reviews and collates
reports from all PHCs
b. NGO / PRI sub team
visits at least one PHC of
the
block,
conduct
interviews with MO and
make observations
c. Visit CHC and review
records, discuss with RKS
members
d. Send brief three monthly
report to District committee
and a. Reviews and collates
reports from all Blocks
b. An NGO / PRI sub team
visits at least one CHC of
the
District,
conducts
interviews with Incharge,
meets Block committee
members
and
RKS
members,
makes
observations
c.
Visits
District hospital and reviews
records, discuss with RKS
members
c. Send brief three monthly
report to State committee
State
State
Monitoring
Planning Committee
and a. Reviews and collates
reports from all Districts
b. An NGO / PRI sub team
visits 3 to 5 Districts,
conducts interviews with
DHO
and
District
Committee members, makes
observations on DH
c. Sends six monthly report
to NRHM / Union Health
Ministry
Mr. Ramkumar
APSA Association for Promoting Social
Action
Nainmane
Annasandrapalya
Virnanapura post
Bangalore-560 017
Ph. 25232749
Ms. Kalaivani/ Ruth Manorama
Womon’sVoioe
47/1 St. Marks road
Bangalore - 560 001
Ph no. 26642053, 22129568
Mr. Rajendra & Mr. Selva
Jana Sahyog
Urban Resource Centre
40, 8th cross
Sampangi Ramnagar
Bangalore - 560 027
Ms. Roopa
Foundation for Revitalisation of Local Health
Traditions (FRLHT)
No.74/2, Jarakbande Kaval,
Post: Attur, Via Yelahanka,
Bangalore - 560 064.
Ph no.28568000
Ms. Renuka
MILANA
95,1st Floor, Old race course raod
Opp Vannarpet officers colony
Austin town
Bangalore- 560 047
Ph no. 25545691/ 9845036638
FEDINA Navachena
7101,154, Anjaneya Temple Street,
Domlur village,
Bangalore 5600 071
Ph: 25353190, 25353190,25353563
I'li no. 22128565
Mr. Robert
Ms. Gopa and Ms.Jayamary
CISRS
/J, Millers road
Post Dox 4600
Bangalore 560 001
Ms. Ms Glory .Ms Anjalai and Ms Josphine
AVAS
131-A 80 feet road
Ashwath Nagar, RMV Extension
Bangalore- 560 094
Phone: 23516227
Ms. Regina and Usha
APD Association of people with
Disabilities
6th Cross Hutchins road
I lennur Main road
Bangalore - 560 084
I’li no. 547565, 5489594
Ms.Kathiyayini Chainraj
CIVIC
Bl. II floorl2th Cross Road. 4th Main Road
Vasanth Nagar,
Bangalore- 560 052
I'll no. 22110584
Ms. Tabbasum
VIMOCHANA
CIEDS Collective
33/1, Thygaraja Layout,
Jaibharath Nagar,Bangalore- 560 033
Ms.Sujaya Sumath
World Vision of India
422, 5th A Cross
11 block, Kalyannagar
Bangalore- 560 055
Ph no.25426072,25426098
Mr. Guru Raghavendra
Basic Needs India
114,4th cross, OMBR Layout
Banas wadi
Bangalore - 43
Ph no. 25459235, 25450562
Mr. Joe paul
Uthsaha
Krsihnappa building
Ejipura Main Road, Near Ejipura bus stand
18th cross, No. 93, Bangalore - 47
ph no.25702597/ 9845951677
S. Natarahan
Bangalore Maitry Sangha
(Vo CISRS, 73, Millers road
Post Box 4600
Bangalore 560 001
Mr. Hemanth
The Concern for the Working Children
303/2 LB shastri nagar
vimanapura post
Bangalore - 560 017
Mr. Veerabadhriah
CURDS
4 7, III cross, 10th main,
Hosahalli
Vijayanagara, Bangalore- 40
Curds mntajyhoo.co.in
9980172420
Ms Meena
BGKS
No.47,3rd cross, 10th main, Behind Sharada
school, Hosahalli, Vijayanagar, Bangalore-40
22129568
The Director / Ms. Prema
REDS
14,Curly street
Langford town
Bangalore -- 560 0027
Ph no. 22214217
Mr. Venkatesh
Pinaspaia
71/2 First Floor
7 III Cross, Bandappa road
Yeswanthpura
Bangalore -
Mr. Madhsudhan
KKNSS
No. 17,6th cross
Rangadasappa Layout (Pukkaraj Layout)
Bannerghata Road
Audogodi Post
Bangalore
The Director
Maithiri Sarvaseva Samithi
1300D I cross, I Main
New Thippasandar
HAL III stage
Bangalore - 560 075
Mr. Anthony
Center for Social Action
Christ College
Hosur road
Bangalore- 560 029
Dr. Maduban Desai & Dr.Neha
OASIS
66. diamond district
Kodihalli Airport road
Bangalore 560 08
Dr. Veda Zachariah
Sanjivini Trust
57, Langford Road,
Richmond Town,
Bangalore - 560 025.
Ph no 22212530
The Director
Deena Seva Sangha
Risaldar street
Sheshadri puram
Bangalore -560020
Ph no.23443661
FEDINA-NA VACHETHANA
Project Area - Bangalore, Karnataka
Funded by - CORDAID, Netherlands
Project Period - 1993 - till date
Emphasis: “Empowerment of senior citizens living in slums - to live in dignity”. Empowerment being
Confidence building, Building ability to negotiate and collaborate for collective action and critical
awareness of situation.
30% of the elderly in India are below the poverty line and their situation is affected among other
things by:
- Lack of economic resources (given previous occupations- domestic servants, carpenters and daily wage
workers)
- Desertion by families
- Social Exclusion- serious invisibility as a group
- Inadequate Governmental provision (meagre pensions)
- Inadequate to non-existent housing
- Irregular health screening and care
- No screening for mental health conditions
It was with the awareness of all such problems relating to the aged persons, that Fedina set up a subsidiary
Organisation, Fedina Navachetena in the year 1994. Fedina Navachetana aims to improve the conditions of
the elders and provide them the rightful place and dignity in the family in particular, and the society in
general. Fedina Navachetana works in 22 slums of the city. Regular medical camps on Diabetes,
Osteoporosis and Cataract are organised for the elderly. We also distribute free medicines to the needy
persons. It is a matter of immense pleasure to report that in the eye-camps organised by us, sight was
restored to several persons. These persons had lost their vision for almost a decade. Health volunteers in
each area are trained on vital preventive health matters such as hygiene, cleanliness and diet related
diseases and curative health issues such as access utilization of government facilities, epidemics and
control and administering first aid. The residents are taught the methods of preparing medicines from
locally available plants for curing several general aliments and high protein food with locally available
inexpensive food grains. Habitation has been provided for several senior citizens and efforts are towards
accessing government programs.
Realising the distress situation, we at Fedina have committed ourselves to the betterment of the elderly,
especially residing in slums and have initiated the senior citizens of the slums to form self help groups,
collectively called as A1KYATA (Akila Karnataka Vayo Vriddara Okutta), a registered federation.
AIKYATA campaigns for public awareness of the problems, needs and rights of senior citizens. The main
objective of the campaign is to bring about change in policies. Fedina gives its constant support to
AIKYATA to achieve its goals.
DEMANDS OF THE CAMPAIGN
- A simple pension scheme without cumbersome procedures for senior citizens in slums, abolishing all
discriminatory clauses.
- Implementation of concession upto 50% in public transport buses for senior citizens of slums.
- Community centres for senior citizens in slums and also shelter for the homeless and abandoned senior
citizens
- Special provisions for treatment of senior citizens in primary health centres
Address:
Preethi Herman, Programme Coordinator, Fedina-Navachetana, No. 154, Anjaneya Temple Street, Domlur
Village, Bangalore - 560 071, Phone No. 080-25353190,2535363, 9886648508
http://www.borda.de/homepaees/india/fedina/modules/ciavconlent/index.php?id=6 (accessed on June 14, 2006)
Draft as 19/06/2006
Page 3 of 10
Dear Friends.
1. Suggestions about the Session 3. of 25lh March NHA-2 parallel session'
Presentation of the theme:
Realising Right to essential medicine
Ensuring Rational Drug Use
(20 mtsi
Dr Mira Shiva
(20 mts)
Dr. Anant Phadke/ Dr. Gopal Dabade
Developing Alternatives:
Locost
CDMU
Presenting proposal for future
Campaign/action
I shall circulate draft soon (5 mts)
Finalisation of Tasks
: Discussion by the participants (6X
5mts)
Conclusion
: (5mts.)
2. Parallel Session: Two on 23"': On Ensuring Access to Essential Medicines: If
required I can also make presentation
Please respond
Best Wishes.
Ainitava
Amifava Gaha <guhaamitava_(a hotmail.com> wrote:
Dear Friends.
Giving below the suggestion on the issues io be discussed in the Parallel Sessions on Key
Campaigns and Alternatives in Key areas: past experience, future plans* Session No III. on
Rational Drug Use. etc. scheduled on 25‘h.
Since issues related io rational use of medicines is a vvtdclv discussed area we do not need to
repeal or make large speech on this. In the workshop we need to take new emerging areas and
should try to grossly understand them
Major part of the discussion can be devoted to prepare future tasks. It is also welcome if such
tasks are div ided among the groups.
I suggest that the issues may be placed by one of the speakers for about 20 minutes which can be
followed by discussion by the others for about -10 minutes.
Similarly the updating of charter and tasks may be presented by one of the speakers which can
follow discussion for 30 minutes Conclusion and recommendations can be made at the end 15
minutes.
We may also be circulated (he Kolkata Declaration among the participants of the workshop
New Emerging Issues:
Pharmaceutical Policy:
1 he Govt, in order to formulate new policy had constituted two committee- Pronab Sen
Committee and a Joint committee on Draft National Pharmaceutical Policy. Based on the reports
of these Committees, the Ministry of Chemicals and Fertilisers had forwarded a note to the
Cabinet of the Ministers on 27th December. 2007 and enclosed a 'National Pharmaceutical Policy
draii.
I. The draft policy contains certain new and valid decisions but left many area uncovered which
needs to be discussed. Certain such areas arew
Weeding out of irrational and hazardous medicines.
w
Compulsion for production of medicines by the large and medium sector companies
w
Importation of expensive medicines
w
Consumer awareness
2. Apart from the concept ol counting all medicines in the National List of Essential Medicines
under price control all other recommendations in the policy on pricing arc not acceptable. I hcre
is no reason to enhance mark-up up to 200 percent replacing present limit of 100 percent
3. No measures had been proposed for controlling the unethical marketing practices.
-I. No concrete proposal for strengthening (he public sector medicine companies.
5 Promoting rational medicine use is absent.
Action: Alternative pharmaceutical policy in the line of Kolkata declaration should be prepared.
Issues Regarding EMR application:
Recent court case by Noverlis on Glccvcc has challenged the sovereign right of the Govt, to
change its domestic law and the right of the Patent Office to reject patent application, l ied up
with the interest of the multinational medicine company. Govt, appointed committee chaired my
Dr. R.A. Mashclkar had reported against the Patentability under frivolous claim.
The scope of availability of medicines at cheaper price manufactured by the national companies
are also endangered. Die Govt, has not yet shown required prompt action in defending its
sovereign law in the court
Data Exclusivity:
Post patent amendment issue which yet remains unresolved is data exclusivity permitting the
generic medicine makers to produce off patented medicines relying on the test data from the
patentees. The Govt. Committee appointed for the purpose has not yet reached to conclusion
Multinational lobby is highly active in this urea li is apprehended that most stealthily the Govt.
determine data exclusivity period which would help prolonging the patent period beyond 20
years.
Production ()iiisourcin^:
In absence of any compulsion on the companies to manufacture medicines within the country.
the multinationals are taking advantage to manufacture bulk medicines by the Indian companies
and re-exporting them at a ven high cost beyond the limit of price control I urge Indian
companies arc shifting towards this direction since they apprehending that being unable to market
patented medicines this contract manufacturing would provide their industrial activity. The
production profile of Indian company would surrogate from domestic consumption to export may
lead to shortage of essential medicines
New drugs for reproductive therapy
Future Actions:
At the Ministry Level: People's Pharmaceutical Policy should be prepared and presented to the
Govt as a demand from the people.
Meeting with selective Parliamentarians, political parlies can be held lor pursuing the demands.
Campaign booklet should be published in several regional languages.
State Campaign Committees should be formed Io popularise the demands and local actions.
To pursue code of ethics to be formed by the (iovt. to regulate promotion of medicines.
Public interest litigations should be Hied against violation of code, inaction by the state drug
control on fake medicines.
Meeting with the medical students to popularise demands and for rational use of medicines and to
develop appropriate medical curricula, guideline for local ethical committees preparation of
hospital formulary. etc
National Convention al Delhi bv end of 2007 on the demands.
Coordinate activity for production and procurement of medicines by the civic society initiatives.
Dear Amitava.
since it is campaign & strategy session & since Ainit & Chinu would have already dealt
with the kev concerns in the plenary . & Ainit would have dealt with IPR issues in the
teach in .we should focus on areas of Action., keeping tn mind what INDIVIDUALS can
do whereever they are located . what DIFFERENT ORGANIZATIONS can do & what as
JSA needs to be done .
Pharmaceutical Police Response .For the uninitiated it may be too complex therefore it
is better to locus on Few aspects while encoraging reading up of material which should be
made available eg Pricing . formation ol the Drug Regulatory authorilv
Koikola Declaration quick Revisit I hope you will bring lots of copiesfor workshop
participants as well as those who would like to buy copies .
Novartis Case
Addressing the Mashelkar Committee Report issue.
24th Mav is Dr Olle I lansson's Dav Anti Hazardous Drugs Dav As one of the Actions a
call to deal with Novartis’s Hazardous Action around Glivic could be given It is
possible that the judgement w ill be given before that.
Essential Drug shortages if they have been experienced mav need to be highlighted
Irrational & Hazardous drugs focus on few
Rational Drug use with focus on Antibiotics .or National Health Programmes
Amitava 20 minutes may be loo long since the lime is short !0 to 15 minutes introduction
of the issue .highlighting points which need discussion .
For the drugs issues the Rapporleures must be familiar w ith (he drugs issue & the
nuances to record the discussion in detail .
we can div ide the responsibilities amongst ourselves .
regards
Mira Shiva
dear Vandana .
Please check about the TRIPS TEACH IN which Ainit is facilitating . Is it being done in
collaboration with other organizations . Is there anything that needs to be done as
preperatory work . we hope Amifs father is well by then .
For the Drug panel Amit & Antirag were to be speakers .i beleive Anurag is unable to
come & it w ill be Chinu instead with Amitava also contributing .
For the Drug Campaign session which Amitava is coordinating I think the contemprarv
issues requiring wider & higher energy response will be dealt
Drug Policy Response
Novartis case
mashelkar Committee Response
Safety of medicines Irrational & Hazardous Drugs
Rational Use of Drugs
Essential Drugs ensuring access .
Dear Naveen.
It was nice to receive mail from yon. My home no. by phone is 033-26747094 where yon
may contact at any lime from 10 pm. to 8 a.m.
During day tiem after 3 p.m. yon may contact me at FMRAI office no. 033-24242862
Greetings.
Amitava
Dear Mira,
Your suggeations are partinent We should consider the following.
Drug Policy Response: Should be discussed since the ploicy is almost finalised
Novartis ease : can be taken tip in the action plan
Mashelkar Committee Response: Since the Committe’sreporl is withdrawn, we may
take it up lor future action
Safety of medicines Irrational & Hazardous Drugs: This can be taken in the policy
issue
Rational Use of Drugs : Already included
Essential Drugs ensuring access : Already included
Please try to include the issue ofCIPII I of WHO regarding TRIPS and R&D by the
developing countries. This may be taken up in the session you are chairing.
Greetings.
Amitava
XIII. Access to Essential Drugs in the Peoples health plan.
Ihc Peoples Health Charter had called lor " A rational drug policy be formulated that ensures
development and growth of a self reliant industry for production of all essential drugs, at
affordable prices and ol proper quality. I he policv should, on a priority basis:
• ban all irrational and hazardous drugs:
• introduce production quotas and price ceiling for essential drugs:
• promote compulsory use of generic names.
• regulate advertisements, promotion and marketing of all medications based on ethical
criteria:
• formulate guidelines for use ol old and new vaccines:
• control the activities ol the multinational sector and restrict their presence only to areas
where they arc willing to bring in new technology:
• recommend repeal of the new patent act and bring back mechanisms that prevent creation
of monopolies and promote introduction of new drugs at affordable prices:
• promotion of the public sector in production of drugs and medical supplies, moving
towards complete self-reliance in these areas."
The National Rural Health Mission and (he national health policy documents arc completely
silent on these crucial issues. This is surprising considering (hat two thirds of all health costs
goes to drugs and the health ministry itself as care provider has a lot to gain from price
regulation. The number of drugs under price regulation declined from 3-17 in 1977 to 7-1 in
199? and this trend continued till 2002 when the last government proposed a further reduction
to 30 drugs. Subsequent to the government change after a lot ol hesitation and delay a draft
proposal for bringing all the 35-1 essential drugs was circulated to the Cabinet by the Ministry
of Chemicals But here al the highest level this was turned down and sent back for
reexamination by a committee w here 11 of the I-I members arc representatives of the industry
What we have now is onlv some sort of vacuous promise by the companies themselves for a
voluntan reduction of drug prices with no mechanism in place to even sec whether they have
done so. While the government has introduced well institutionalized regulatory controls for
electricity rates, telecom rates, insurance premiums and even for trading ol' shares, its
reluctance to countenance any regulation for essential drugs points to a deeper malady in the
area of drugs- what we could call " corporate capture." W hat we have been seeing in this
period is an unchecked rise in drug prices and an almost complete surrender to corporate and
pharmaceutical interests- going far beyond what is needed to be compliant to the international
TRIPS agreement, which itself is discriminatory and against third world interests, hi this
period the government signed off its rights on drug patenting by agreeing first to the product
patenting and then to data exclusivity clauses( Corporate Capture’. Usually policy is made by
negotiation between different stakeholders with different stakes and different strengths.
Eventual policy outcome is a compromise based upon relative strengths. The term capture is
used to denote one stakeholder coming to command such influence that all the other positions
arc reduced to nothing- there is no negotiation . it is outright capture In pharmaceutical policy
we sec a good example of capture here the larger multinational pharmaceutical corporates
seem to have captured through their influence on linance and industries ministries all policy
making on pharmaceuticals reducing even other ministries, let alone peoples organizations or
civil society, to impotence.)
This has thus been a period of defeat and set back on the pharmaceutical front at the level of
policy. Even on such a dimension as procurement of drugs for its own health programmes, the
government has bowing to pressure from the World Bank the government agreed to a regime
of international procurement of drugs for aid-funded projects
.1 Peoples Health Plan t here fore:
At the level ofpolicy
I. Reiterates the demands of the charter as regards pharmaceuticals.
2.
Notes that the entire area ol pharmaceutical policy lies in a slate of "corporate capture"
and considerable mass mobilization and protest would be needed to expose the
tremendous profiteering that is going on and the price people arc paying in terms of
financial and health ruin due to this
. If the level o] strategy and implementation
1. Calls for a large investment in promoting the concept of rational drug use funded by the
stale and organized by health advocacy NGOs. I his campaign should be able to build
public awareness on this issue and facilitate the eventual stale action for stricter
controls on irrational drugs in the market As financial costs of such irrational drugs
arc crippling to households, such a campaign for behaviour change in drug promoters.
drug prescribers and in drug consumers must be seen as an essential component of
financial protection from high health care costs. Such a campaign would also build up
support for belter price and quality regulation of drugs. It would also campaign
against quacks, qualified and unqualified who prescribe large quantitative of
unwanted drugs and injections with no regards to ethics or health. Above all such a
campaign would expose the situation of "corporate capture” that exists in the
pharmaceutical sector.
2. Calls for ensuring provision of essential drugs at all times in all public health facilities
with adequate transparent arrangements lor procurement and distribution to enable
this.
3. Calls for ensuring that by provisioning ASHAs. anganwadi kendras and sub-centers
with a basic set of 12 to 3() drugs, there is universal access to al least the most basic
drues within the next three vears.
Suggested Guidelines for Parallel Sessions in NHA II at Bhopal, 24"'
March
Objectives of (lie Parallel Sessions:
11 To lake forward the process ol revisiting, updating die People’s Health Charter 2000 in
order to move towards an outline of Alternative People's I leallh Plan.
2) To get inputs from different parts ol India lor the Alternative People's I leallh Plan.
I he theme of the NHA-II in Bhopal is Defending the Health Kights of People in the l.ra
of Globalization". I he strategy, we are adopting is - reform and strengthen the Public Health
System and regulation of the private health sector, so that both together arc pan of a publicly
funded National Health Care System. which ensures universal access to health care, irrespective
ol ability to pay.
I he overall direction of the proceedings ol this NHA II including that of the parallel
sessions would have to be in consonance with this overall objective.
Hie People's Health Charter 2000 has twenty major points In each of the parallel
sessions in NHA II one or two relevant sections from the People's Health Charter would be a
point of departure. Il is expected that the outcome of each of the parallel session would be
updating, modifying. the concerned demands in the People’s Health Charter and move towards
Alternative People's Health Plan by taking into account the formulations in the draft prepared by
Sundaroflhc Alternative People’s Health Plan.
In each of the sessions, there would be two initial presentations of 15 minutes each - One presentation would be on the overall situation, as regards say child health or
availability of primary health care, or urban health policy etc. etc .
Building on this presentation, there will be a second presentation, which will revisit the
relevant paragraph in the Charter 2(100 and suggest modifications, updating, of the specific
demands. There will be suggestions about how these demands can he met by making specific
reforms in the health care system.(Some of the reforms do not need additional financial
resources). We thus move forward from merely making demands to pulling forth specific ideas
about how to meet these demands, i.e moving forward from People’s Health Charter to an outline
of Alternative People’s Health Plan
Huis in the session the relevant para from the Charter 2000 can be projected on the
screen to begin with and later other slides would suggest specific changes in additions to this and
also specific suggestions about the reforms that we suggest to fulfill these demands.
I'hcsc two presentations should be over in 30 - -10 minutes. This would be followed by a
discussion for an hour or so. We should consciously plan this session in such a way that there will
be adequate scope for discussion. We can begin with intervention by grass-root level activists
from different areas tn India Three-four discussants would be identified by the session
coordinators through prior consultation. I 'ach of these discussants would speak for about 5-10
minutes, commenting on the first presentations. I’hey may. based on their local experience.
express their support to the presentation and / or share the peculiarities in their own area and I or
suggest changes in the demands made in the initial presentation.
After the intervention of these discussants, the discussion would be thrown open for all
other participants oflhc session.
At the end of the discussion, in last 15 minutes or so an attempt would be made to
prepare a list of demands/reform measures about which there would be a consensus. I hesc
consensus demands/reform measures would be later shared with others in the plenary on day III
to present an outline of Alternative People’s Health Plan.
P1IM ll’IIl Leadership Workshop, Bhopal, 23-24 March 2007
Pl IM Global, in association w ith PI IM India and IPIIU is pleased io present a two day
leadership workshop lor selected Pl IM act iv isls from India and around the world.
Objectives
We hope that after the workshop participants will be.
•
more familiar with the history, development. structures, cultures, campaigns.
strategies and processes of Pl IM in .ill ns various manifestations:
•
inspired to redoubled efforts to build the people’s health movement in their own
localities, stales, countries, regions and globally.
•
enriched by new ideas, new strategies, new skills which can be applied in organising
Pl IM and in dev eloping and implementing campaigns and strategies Io achieve the
goals of PI IM: and
•
more familiar with the knowledge base, experience and analyses which undcrly the
People's Charier for Health
•
[other objectives / amended wording?!
Workshop v enuc
www.lakevicw<ishok com
Room to be adv ised
Preparation
On arrival participants will be provided with copies of:
•
Alma- VdJls'claialion (plus covering note with 'homework questions": What is the
significance of Alma-Ata? Is it dead? Why has it not been achieved? W'hal is
needed to realise the vision off PIIC more widely?)
(vv w w.euro.w ho.int AboulW 11( ^'Policy720010827 I)
•
People's ( harlcr for I lealtli (plus covering note with homework questions' W'hal
are the important bits? W'hal is missing? W hat are the more difficult bits (to
understand, lo achieve)? How to implement the vision0)
(w w w.ph movement-orgiesoii ices/pheharter)
•
Mumbai Declaration (wvvvv.phmovement.org/llles/md-english.pdf)
•
Cuenca Declaration (phmovcmcnt.org/pha2/papers/cucnca dcc.php)
•
GIIW GHA CD
•
GHA hard copy
•
GIIW based advocacy documents (health systems and W I IO)
•
PI IM bibliography
•
PHM T shirt
Further documentation on the Nl IA available from vyw vv.phm-india.org.
Participants w ill be asked lo bring for show-and-tell materials from their local PI IMs.
Participants will be provided with the Program for the \ll.\. including the parallel sessions on
Salurdav
Other resources to be developed:
•
Building PHM (one page check list of issues and ideas in organising the movement).
I page. Deien to coordinate writing?
•
I he Struggle for I Icallh (principles and strategies lor campaigns and actions to
realise the vision of the Charter). I page. I hclma to coordinate writing?
•
PPT presentations (globalisation (1)1). PI It and health systems (DS)
•
Communication technologies. I ses. traps, hints Lmail W eb sites, list serves. VOIP
teleconferencing (I page (ihassan to prepare?)
•
Guidelinese for '.\ better world is possible' 2020 Scenario l.xcrcise (DI. to
coordinate the writing of)
Draft program
Day 1 line
Thursday 22
S 30 pm
Friday 23
S.30 10 15
10 30 1 00
1 00 2.0(1
2.00 3.00
3 0o
4 oo
Activity
Informal mixing, badge wearing
checking package, chatting
Personal introductions, introduction to
1'1 IM. .ISA. plans tor the (wo days.
discussion of program
Short presentations: my background.
issues in my country. PI IM in my
country stale, challenges fur
development of PI IM and strategies.
aspirations lor this workshop
< Ipening of Indian Nl l.\
1 unch (and further socialising)
< h’ganisational history of PHM (Sawn
to Cuenca but with more detail about
organisational structures and processes.
including IPI III)
Overview of a limited number of
campaigning actions undertaken at (he
national and global levels with focus on
political analy sis and strategic action
Organising PI IM at national level
and organisational capacity
building a checklist of issues to
consider (also as handout)
faculty
Participants and faculty
Chairperson Deien
Supported by Ravi. Claudio. Jell
Lessons from JSA
Deien supported by Naveeu. Maria,
Dav id. etc
Brief plenary presentations followed In
sin.ill group discussions
Brief final plenary
PHM having an effect about
strategics and campaigning
(principles as one page handout)
4(Kt - I 30
4.30 -5 00
General discussion with individual
members talking about how these
checklists might work or need to be
changed m my country or stale
Break
Showing of the Cuenca DVD
Communication technologies (email.
Iistscrvs websites. V( >|p tele
conferencing) Practising on Skype and
Paltalk Working with the media
1 him. (.ihassan and 1 )a\ id 1
5.00 -0 !/0
6 00
7 00
Saturday 24th
8 00 8 30
8 30 10 00
10.00 lit 30
11.00- 1 00
I 00 2.00
2.00 4 00
4 00 4 30
4.30 5.00
5.00- 5 3o
5 30 •
IntrixJucing inorc folk from .ISA. 1’1 IM
SC. (ilobal Secretariat etc Brief
personal introductions in all Informal
conversation about organising PI IM (no
set pieces) and having an impact on the
struggle for health
informal, refreshments, dinner etc
Ml IA Cultural Program
gathering, chatting
Alma-Ata Declaration. People’s
Charier lot 1 leallh and Cuenca
Declaration What is the significance
of Alma-Ata" Is it dead" Why has it
not I'een achieved"
\boiit the PCI 1 What arc the important
bits, what is missing, what are the more
difficult bus. how to implement the
v tsion"
Pee and tea
N1IA2 Ten parallel workshops on a
variety of topics 1 he workshops are
around campaigns and w ork m progress
and on building linkages between
groups
lunch
Scenarios of change exercise A belief
world is possible
Sketch some key features of a better
w orld by 2020
Sketch a plausible historical scenario
by which this belter world ‘was’ (could
be) achieved
Implications for Pl IM strategics how
can we make n happen '
Pec and tea
About IPI III Learning from Cuenca.
possible uses of IPI II ‘ courses in
different regions, priorities for IPIIII
content in different regions
Feedback, evaluation and w rap up
Informal lefreshments. dinner etc
Sunday 25th
9 00- 12 00
12.00- 1 00
In continental dialogue (N1 IA >
.Alliances t Nil A >
Bringing in more of the people involved
loi a longer term in PI IM (preferably from
wide range ol places) into a general
conversation, getting to know you.
chewing informally over the issues of
organising and strategising
1 lomcwork questions to be thought about
before hand
Brief introduction (5 )
Small groups (with faculty ) to work
through A A and PCI 1 (3<>‘ >
Plenurv reports and plenurv discussion
(20*)
Faculty Deien. Maria. Maija. David
Perhaps participants could take 45
minutes to one hour (eg 12-1) and spread
out in pairs (Indian and other) among the
different workshops and then return lo
report back
Brief introduction i?’ >
Small groups (3) (with faculty) to work
through scenario (.30')
Plenurv reports and discussion (20’ >
1 acuity Deien Maria. Maija
DI Mana Deien
List of delegates and their Accommodation
1
State
01
02
03
04
05
l.ahi Shadi Hall. Sear
PI IQ,Shahhan
Choraha,
Jahangirabad,
Bhopal.
75
UP
Hihar
Jharkhand
1 limachal
Pradesh
70
50
100
Kerelti
26
06
Karnataka
100
07
Andhra Pradedh
120
08
Tainilnadn
100
09
Maharashtra
50
10
CMAI
50
II
l-MR \l
20
12
Chait isgarh
225
13
Sr. Mouli
20
II
Asani
01
15
, Accommodation
Haryana
05
Sainik Resthouse,
Banganga, Bhopal
AICUF Asharam,
near campion School
.Arora Colony,
Bhopal.
20
30
Youth Hostel, Near
Hotel Palash
Banganga
Bhopal.
Gli.lRAT Bhavan.
Tulsi Nagar, Near
Link Road No. 1
Bhopal.
[Narmada Mandir|
Bhavan. Near Bal;
[bhavan, Tulsi NagarJ
Bho^il;.
16
17
Punjab
Gujral
05
50
18
Rajasthan
100
19
M.P.
200
Gandhi Bhavan
20
Bangladesh
100
PWI) Rest 1 louse
No. -2. Banganga
Bhopal”
21
22
9.3
24
25
AIDW A
Delhi
Uttaranchal
Orisa
Other Delegates
•10
20
50
50
Kamla Agrarawal
Dharam Shala, Near
Apsara Talkies,
Raison Road Bhopal.
NHA II WORKSHOPS i OR 24.3.07
11 am - 1pm
2pm - 4pm
Urban Heaith
Tribal Health
PHRN
PHRN
devanshrchanchani@ext.icicibank.com
Suranjeen Prasad, suranieen@gmail.com
Children’s Right to Food; Action for
Children’s Right to Food; Action for
Children Under Six
Children Under Six
CIRCUS. BPNI, Action Aid MP
CIRCUS BPNI Action Aid MP
Dipa Sinha dipasinha@gmail.com
Dipa Sinha dipasinha@gmail.com
Radha Holla
Radha Holla .
radhahb@yahoo.com
radhahb@vahoo.com
malini@actionaidmdia.org .
malini@actionaidindia org .
robho@actionaidmdia.org
robhoffiactionaidindia.orq
Alternate Health Practices and Sustainable
Health Rights of Positive People
Development
Positive women's network
Medical Mission Sisters Organization
Sunil George mail2sunilgeorge@gmail com
Sr Molly Vadaken
Kousalya Periasamy
pkousalva@omail. com
mmsktvm@sancharnet in
Human Resources for Health Care
Bhopal Gas Tragedy
CMAI, CHAI, CHC
MP JSA
Joe Varghese. |varqhese@cmai.orq
aiavkharebpl@qmail.com
Sexuality Minorities and Sex workers
PRIs and Health
Sangama
Hunger Project. MP
Sandeep Nayak
sathyasree
advocacy@sanqama.orq_
_ ______ |
I sandeepnaik@rediffmail.com
Violence Against Women
Sex Selective Abortion
Cehat. Masum. AIDWA
AIDWA, CMAI. JSA-Raj. MP VHA
kamavni@qmail com
mpvna@sancharnet.m .
mpvha@rediffmail.com
Joe ivarqhese@cmai.org
Tejram iatieiram@yahoo.co in
Sudha aidwa@rediffmail com.
sudhaaidwa@vahoo co. in
Disability
Mental Health
CEHAT. Basic Needs and Bapu Trust
CHC Bangalore. CBR Forum. Action Aid MP
Kamaym
Mahesh Chandrashekhar
cehatinumbai@vahoo co.in
mahesh mobility@yahoo.com
kamayni@qmail.com
malini@actionaidindia org ,
robho@actionaidindia.org.
Environment and Mining
Community Based Monitoring
CHC,
SATHI-Cehat and Prayas for JSA
Rakhal Gailonde subharakhal@qmail com.
narendra531@rediffmail.com
narendra@prayaschillor org
Abhav cehatpun@vsnl.com
Public Health Act
Patents and IPRS
JSA teach in
Gujarat JSA
Renu Khanna.sahajbrc@yahoo.com
Amil Sen Gupta c.tddsf@bolnet.in.
ctddsf(a)vsnl com
Micronutrients
Pulse Polio
JSA teach in
JSA teach in
Vandana Prasad chaukhal@yahoo.com
Anant,cehatpun@vsnl com
Indira. indirachakravarthi@vahoo com
KOLKOTTA DECLARATION on PHARMACEUTICAL POLICY
Adopted in (lie
National Seminar on Pharmaceutical Policy and Access to Essential Medicines
Kolkata on 16-17 April. 2(105
The National Seminar on Pharmaceutical Policx and Access to I•’sscntial Medicines organised b\
Jan Swasthxa Abhiyan. Federation of Medical and Sales Representatives’ Associations of India.
National Campaign Committee for Drug Policy and All India Drug Action Network and
supported b\ the World Health Organisation. India countrx office discussed different aspects of
the country's pharmaceutical policy. I he seminar was attended bx one hundred and twenty eight
activists, academics and experts from all parts of the countrx that deliberated on diflcrcnl issues
related to the pharmaceutical sector in India.
I he Seminar noted that (he country's record in controlling diseases that affect large sections of
the people has been far less than satisfactory. The countrx faces new challenges in the form of
increased incidence of "lifestyle" diseases and infections such as IIIV-AIDS I his ominous
situation admitted in (he National Health Policy-2002 needs to be addressed seriously Disease
pattern and common ailments highlighted in NI HS-2 survey should also be taken in
consideration.
The seminar also noted the new situation created b_\ the policy of globalisation privatisation.
liberalization and the new product patent regime which together have threatened the national self
reliance as well as availability and affordability of essential medicines. The seminar also felt
concerned about the worsening situation on the drug price front with its disastrous impact on the
poor.
Given the above the Seminar resolves the following suggestions be considered while making the
National Pharmaceutical Policx.
Formulation of National Pharmaceutical Policy:
The seminar expressed the need to formulate a National Pharmaceutical Policx that addresses the
critical issue of universal access to essential medicines and of national self-reliance. I his policx
should be prepared by an intersectoral committee ol the Ministry of Health & Family Welfare and
Ministry of Chemicals & Fertilizers after discussions w ith all sections (hat have a stake in the
pharmaceutical sector, The two should jointly constitute a National Drugs and Therapeutic
Authority, which should be a statutory body with powers to regulate all aspects of the National
Pharmaceutical Policy Apart from experts, this body should also include representatives from
health movements.
National Essential Medicines List
I.
The Govt., based on epidemiological data, should update the National Essential
Medicines List (NEME) and also prepare a Graded Essential Medicines List that is
appropriate for each level of the health care system. The National List needs to be
adopted by different stales and adapted by them based on local conditions and disease
pro 11 le.
2.
The Govt. should monitor and ensure the availability of Medicines listed in (he EMI.
Production of these medicines from the basic stages should be ensured through
production control mechanisms.
3.
It should be made mandatory that the procurement and use of medicines in Govt.
hospitals and public sector undertakings be done based on the NEME .Such procurement
Deleted:
should be through transparent procedures. Regular training and incentives to promote use
of medicines in the NF. Ml should be provided.
Irrational and Hazardous Drugs
I.
Given the proliferation of irrational and hazardous medicines in the market, a special
committee of the DIBA should be set-up to weed out all such medicines including
irrational Fixed Dose Combinations (I-DC) within a stipulated period. Hence forth
medicines and Fixed dose combinations which arc not mentioned in standard text books
and other such authentic sources of pharmacological information should he banned and
should not be allowed to be marketed. All existing medicines should he re-evaluated at
regular intervals on the basis of expert opinion on their rationality efficacy and need.
2.
Injectable contraceptives, transdermal implants and anti fertility vaccines should not be
used in the National Family Planning Programme.
3.
/Adverse Drug Reaction (ADR) Monitoring Centres should be set up in all slates of the
country and be provided with sulTicienl resources.
4
W hen a substantial number ol ADRs are reported either in India or abroad for a drug, the
same should be referred to the D I AB for withdrawal
Generic Drug Use
In order to encourage use of medicines in generic names, all medicines sold under generic
names should be exempt of duties and taxes. All packages ol medicines should carry the
generic name more prominently than the brand name
Medical Education
The curriculum lor medical education should include the concepts of essential drugs and rational
prescription practices.
Indian Patents Act
1
I he Govt. should keep advocating for keeping TRIPS out of WTO prov isions and
advocate for reopening the issue of exempting the developing countries from Product
Patent.
2.
I he Govt, should ensure that ail the flexibilities in the Act arc used to promote health and
development of the indigenous drug industry.
3.
The Govt, should closely monitor the application of Patentability criteria for granting of
Patents to ensure that triv ial Patents are not allowed and ever greening of existing Patents
does not take place.
4.
The Govt, should liberal!} interpret the Doha Declaration of 2001 by declaring situations
of emergency/urgency in the case of diseases that are present in epidemic or endemic
forms or where their prevalence constitutes a health emergency. In such situations
Compulsory licenses should be issued without delay.
5.
Govt, should also facilitate the issue of compulsory licenses to remedy situations of non
availability or high price of a patented drug or where an export market exists and is not
being addressed.
Drug Production and Availability
I
Io ensure produetion from the basic stage, ratio parameters between manufacture ol
formulation and bulk drugs should be reintroduced.
2.
Production Control mechanisms should be introduced to ensure that all manufacturers
produce a certain proportion of drugs from NLMI. that arc I'sscnlial.
3.
I he new policy of allowing 100% equity participation of MNCs in the pharmaceutical
sector needs to be changed and majority equity participation by the multinational
companies should only be permitted if new technology is brought in by them for
manufacturing and research.
4.
Restrictions in the form of tariffs and other non-tariff measures should be imposed on the
import of bulk drugs or formulation for which adequate production capacities exist in (he
country.
5.
Prevailing systems of loan license or third party license should be abolished. Mention of
the name and address of die manufacturer should be clearly indicated on the label of each
medicine, and the license holder should be held responsible for all complaints.
compensation and replacement ol medicines
Drug Pricing
I.
All drugs should be brought under price control given the fact drug expenditure in India
is more than half the health care expense and also because more than 80% ol health care
expenditure is met by patients themselves. Mechanisms that arc transparent and easy to
administer should be pul in place to control prices and the system of price control should
benefit the efficient producer. In no case should the mark up allowed be more than 100%.
2.
I rade margin, those to including wholesalers and retailers should not go beyond 30%.
3.
National Medicines Pricing Authority should be established as a quasi judicial body
which should be given sufficient legal power to punish manufacturer for violation of
ceiling prices.
4.
lor imported medicines, provision of cost data and manufacturers price certificate should
be made mandatory.
5.
.All cancer and IIIV/AIDS medicines and orphan medicines should be exempt from all
taxes and duties, including import duties.
Public Sector
The production of drugs for the poor and the neglected diseases can only be ensured by
making public sector companies major producers in these areas. Public sector medicine
companies such as IDPL and HAL should be revived and they should be provided with the
support in the form of sectoral reservation, preferential treatment in the cases of Govt.
purchases, etc. These companies would need to he provided a leading role in drug
manufacture in the case of compulsory licenses issued in situations of national emergency
and extreme urgency. New public sector companies should be promoted for producing those
essential medicines that arc not being produced by private companies at an affordable cost.
Research and Development
1.
A major national effort should be made io increase original drug research based on lhe
strength of our national research institutes, laboratories and the Universities and also on
lhe biodiversity and lhe medicinal plant wealth of our country, lhe research institutions
should be provided with adequate funds lor drug research .Regional drug research centres
may be established in slates where infrastructural facilities arc already available.
Universities should be encouraged to offer courses so as Io produce adequate and high
quality human resource pool lor modern drug research related activities. The Public
Sector should be promoted to play the leading role in R&D activities
2.
Public funded Research Laboratories should co-ordinate their activities, lhe research
activities of publicly funded research organisations should not duplicate empirical drug
discovery projects in lhe pharma R&D model, but should concentrate on generating the
knowledge base for the identification and exploitation of new intervention points for
medicines.
3.
All medicines developed in lhe country should be exempt from taxes and duties for It)
years.
4.
A comprehensive legislation on lhe ethical conduct of clinical trials should be enacted in
line with lhe Helsinki Declaration and other international covenants. treaties and
declarations so as io provide for strict guidelines for obtaining informed consent, for
protection of the health of subjects of such trials
5.
Outsourcing of clinical trials for MNCs should be closely monitored by a specially
constituted Standing Ethics Committee set up in each stale.
6.
All information about protocols and the results of lhe clinical trials approved by lhe
DGC1 should be in the public domain.
7.
Phase IV of the clinical trials should be mandatory and should not be replaced by the
PMS studies by he pharmaceutical companies.
Quality Control and Drug Information
( onsumers should be allowed to get tested medicines of doubtful quality al any Goxt
approx ed lest laboratory
8.
New colleges of pharmacy should be opened io eventually ensure that all retail
pharmaceutical outlets haxe the services of a trained pharmacist
9.
I he outdated Magic Remedies \ct should be replaced by a new Act.
If) Io disseminate unbiased information of medicines. (ioxi. should develop an independent
process for information. I he National Formulary should he updated and published
regularly Standard treatment protocols and guidelines for common ailments anil for
ex cry tier of the health system should be prepared and disseminated Doctors.
pharmacists and staff nurses should be trained in treatment protocols and guideline. All
hospitals and medical centres should be encouraged to prepare and use their own
formularies.
Drug Promotion
I.
2
A National F.lhics Committee on Promotion of Medicines (Nl'CPM) in which there is
adequate representative of ctxil society organisations should be formed to monitor all
promotional efforts
A code of ethics for marketing of medicines should be adopted by Nl .CPM and made
obligatory for all the manufacturers.
Ml promotional materials for health professionals should be screened and approved by
Nl CPM and all advertisements in the regional press be scrutinized and approved by a
state lex cl llhical Promotion Committee.
4.
Gifts except minor items, inducements, sponsoring of meetings and entertainment of the
members of the medical profession and those who arc related to drug prescription.
purchase etc by drug companies should be banned so that these do not influence
prescribing practices.
5.
Drug companies should contribute funds to the drug control authority for the conduct of
Continuing Medical I ducat ion programme for doctors
6.
A cap on drug promotional expenditure drug companies should be fixed and enforced.
VII Sir Dorabji Tata Symposium
March 11, 2006
Panel Discussion
Towards the Social Vaccine - research challenges on
the social / determinants of HIV / AIDS
Panelists :
Dr. Ravi Narayan
Community Health Advisor,
Community Health Cell, Bangalore
(ravi@phmovement.org)
Dr. Jayashree Ramakrishna
Additional Professor & Head,
Department of Health Education, NIMHANS, Bangalore
Qayashree.Ramakrishna@gmail.com)
Ms. Sanghamitra Iyengar,
Director, Samraksha, Karnataka
(si@samraksha.org)
1
1.
INTRODUCTION
The HIV / AIDS pandemic is one of the greatest humanitarian crisis of our times and also
one of the most complex research and programme challenges in public health practice
today. While new drugs and vaccines and other 'magic bullets' need to be developed, as
researchers work on the bio-medical aspects of HIV-AIDS leading into the frontiers of
molecular biology, pharmacokinetics and other related areas, there is urgent need for
researchers to also study the social determinants of HIV I AIDS and explore the social,
economic, political, cultural and other factors that contribute to the evolving socio epidemiology of HIV / AIDS and affect the health systems response to it. This alternative
area of research is not just 'operations research' or 'evaluation and health systems
management of public health programmes', but an area of research that could lead to a
deeper understanding of the complexity of the pandemic and the complexity of the socio
medical response required to address this complexity. Without progress in this area of
research leading to perhaps a more comprehensive programme that could be entitled a
'social vaccine', there is a danger that we may loose the battle against this new health
challenge and the loss would represent a failure of research methodology rather than a
programme failure in public health. A panel discussion at the VII Sir Dorabji Tata
Symposium on March 11, 2006, tried to explore these social determinants - so that
discussion, debate, research and response towards a 'social vaccine' could be stimulated.
The Panelists on this session discussed this theme in three different ways:
a)
Dr. Ravi Narayan identified the larger social determinants of HIV-AIDS that are
emerging from health systems and health policy research.
b)
Ms. Sanghamitra covered some experiences from North Karnataka focusing on
determinants which include both positive and negative experiences of sexuality and
sexual behaviour. She also emphasised that responsible sexual behaviour, involves
both individuals and communities and that there is evidence that social norm change is
not only possible in these areas, but may be one of the most effective ways of halting
and reversing the HIV epidemic in India.
c)
Prof. Jayashree Ramakrishna, (who unfortunately could not attend the panel) sent a
presentation that focussed on stigma and discrimination and the association of this
with our notions of sexuality and morality. The presentation also focussed on the
relationship between structural factors such as gender and socio-economic class on the
ability to manage stigma, drawing upon studies in Bangalore and Pune. It highlighted
that the language of scientists and public health specialists often contribute to stigma
and changing attitudes of health care providers can go a long way towards mitigating
stigma.
d)
Dr. Narayan then integrated all the components of actions that emerged from the
above reflections on social determinants into the concept of a social vaccine. This
consisted of a series of potential programme components. He also made a plea for a
greater paradigm shift in medical and health research to take this line of research and
public health system development further.
2
2.
SOCIAL DETERMINANTS OF HIV-AIDS (RN)
A review of public health literature on the research and health challenges of HIV-AIDS is
increasingly focusing on a large number of social determinants that affect the evolution
and spread of the disease as well as affect the access, response and outcome to
programmes evolved to meet this health challenge. These include:
1.
Poverty and equity
2.
Class and caste differentials in society
3.
Gender relations and discrimination
4.
Access to primary health care
5.
Sexuality, sexual behaviour and norms
6.
Stigma and discrimination
7.
Levels of community awareness and mobilization
8.
War and social conflicts
9.
The state of development of medical ethics and the concept of patient rights in society.
In addition, the new economic paradigms are leading to changes in health system
responses that affect indirectly the spread of the HIV-AIDS epidemic or our ability to
respond to it in systemic ways. These include the following:
1.
Erosion of public health systems
2.
Privatization and commercialization of health care
3.
Inadequate occupation health and safety
4.
Enhanced migration and displacement due to unplanned or inadequately evaluated
development strategies
5.
Social aspects of natural and man made disasters
6.
Provisions of WTO and TRIPS and its effect on drug policies and availability of essential
drugs
7.
8.
The continuing debt crisis of national and state governments, and
The global macro economic policies and international financial trends affecting national
economic policies and health budget.
All these factors have been identified by a People's Charter on HIV and AIDS that was
developed through an active participatory process involving people from various walks of
life, including persons living with HIV/AIDS (1).
3.
COMPLEXITY OF RESEARCH CHALLENGE (RN)
While the current symposium has been primarily discussing bio-medical and molecular
biological challenges of HIV-AIDS treatment and prevention including HIV Virology; tissue
pathology; clinical and laboratory monitoring; opportunistic infections including fungal and
visceral leishmaniasis; ARV therapy; HIV drug resistance; therapeutic vaccines; preventive
HIV vaccines; microbicides and non human primate models - there is urgent need also to
study the larger social determinants mentioned above. The research challenges in
3
HIV/AIDS should ideally include work at both levels so that we understand better the
complexity of HIV/AIDS as shown in the diagram below.
RESEARCH CHALLENGES ON THE SOCIAL DETERMINANTS OF HIV/AIDS
4.
BEYOND THE VIRUS - NAGGING QUESTIONS ABOUT THE HOST (SI)
As antiretrovirals suddenly brought hope and new life to many, we are hopeful of the
advances in Science in new areas and the new research in Microbicides and the AIDS
vaccine. Every effort is being made to speed up these advances, and there is a feeling of
optimism.
At a time of such hope and expectation, we also need to listen to those nagging voices
from the community, which repeatedly ask the following questions:
1.
2.
3.
Is a Clinical Vaccine or Microbicides alone the answer to halting or reversing the HIV
pandemic? •
Do we need to go beyond the agency of the virus to look at agency of the host?
Is the interaction between the virus and the host merely clinical?
These questions are serious ones. They raise the forgotten issue of human agency and
how HIV is more than a medical issue. Its social and behavioural dimensions, which we
tend to forget in the excitement of scientific advances in microbicide and vaccine trials,
come back to haunt us.
Ethical issues surrounding access, availability, use and misuse of the vaccine still need to
be resolved. Women's groups are hopeful of the microbicide but concerned about the
impact of the vaccine. Whether its protection will extend to women? whether it will extend
only to consensual acts? or would it encourage co-ercive acts against women? Would
gender inequities and gender violence be addressed, or swept under the carpet with the
availability of the vaccine or microbicides?
4
These questions need deliberation. As a society, we are looking at quick fixes. At a recent
Psychotherapy Conference in New York, O'Donohue took the audience by storm. He totally
lifted them out of their existing paradigm of thinking and questioned the "ever briefer,
more technical, symptom-focused, evidence-based, standardized therapies" making ever
greater use of psychopharmacological agents. Analysing the phenomena of his astounding
appeal, Mary Sykes(2) found that contemporary professionals were struck by the critical
areas, that were neglected in the " highly logical" approach, that they had been taking.
Respecting the inner agency of the individual, "helping people retrieve what had been lost
to them; wakening and bringing home their fundamental wholesomeness." was the old
mantra which had been brought back with an exhilarating sense of personal possibility.
We, in HIV prevention, have fallen into the same rut. We feel that as clinicians, health
educators and scientists we can change the behaviour of individuals with drugs, vaccines
or didactic health education. Whatever tools for prevention we may use, we need to look at
other factors that affect the individual's ability to use them. For example, issues of gender
power inequities which make women vulnerable have to be addressed, not just provision of
means to protect them in a coercive interaction. We need to recognize that HIV
transmission is embedded in a context of denial, taboos and power inequalities. Most of the
sexual transmission of HIV takes place in privacy, intimacy and secrecy. In this context of
secrecy, there is no accountability. It is known that all behaviour change, whether it is the
practice of safe sex or taking a vaccine when it is available, is dependent on the
responsible behaviour of individuals. Therefore, the issue is about not just advocating
responsible behaviour, but ensuring it.
When sexual activity is hidden and there is no discourse around it, responsible behaviour
becomes difficult to enforce even through social pressure. What is required then, is to talk
about the factors influencing HIV spread such as the lack of open and free discourse on
sex and sexuality; and the social, legal, moral and cultural taboos on forms of consensual
sexual interactions outside marriage.
We have forgotten the forces that have shaped individuals' social and sexual behaviour;
the family, their peers and their community. If responsible sexual behaviour has to be
achieved, these forces have to be harnessed again. Larger social norms have to be
addressed, so that behaviour change is sustained and sexual behaviour like social
behaviour is held accountable.
Indian society is in transition and study after study quotes the high level of sexual partner
change in both rural and urban India.(3,4,5,6,7). Samraksha's own study of Sexual
Networks, Risk and Vulnerability across 5 districts of North Karnataka with Synovate's
Social Research Wing (8), revealed that of the 2500 men interviewed (selected through a
random sampling of households), 41% reported having had multiple sexual partners. They
were from all walks of life, all occupations and all ages between 18 - 60. People spoke
freely but asked for confidentiality, which signified a lack of social sanction. Most were
consensual, but coercive acts were also reported. These included both paid and unpaid
sexual acts. What was significant was the reason given for having many sexual partners.
Topping the list was ”1 have money" followed by "Anonymity and easy access"
These highlight clearly the gender-power dimension as well as the loss of accountability
structures in the anonymity offered by modern living.
In this dismal picture, Samraksha would like to share its experience of a new model of
building a social force towards positive and responsible sexuality in the era.
5
This prevention model works with small geographical units eg a village or a town ward.
With a highly intensive focus over a very short time, using the tool of perspective building
on HIV prevention and impact reduction , Samraksha was able to achieve some significant
results The methodology has been to initiate community conversations on sex and
sexuality, risk and vulnerability and protective mechanisms across every segment of that
geographical unit. The strategy and activities have included letting communities question
existing norms, explore newer ones, bringing in public discourse on taboo areas, creating
cultural and social channels for that discourse, building gender ,caste and economic
perspectives, letting women examine power relations, risk and vulnerabilities. These were
done through a range of interactive and reflective exercises and processes, using culturally
appropriate media.
In the last 2 years, 680 villages have undergone a first round of the process. Over 400
villages have undergone a second round of that process. Process indicators are highly
encouraging. Just to cite a few,
A greater acceptance of risk and community support for behaviour change to
safe sex practices: seen through increased condom stocking in the
community, at public places including Panchayats; increased condom
acceptability by sex workers and an overall increased condom uptake
2. Decreased denial of sexual practices/ networks and increased tolerance for
them. This is seen though the changing language of public discourse; a shift
from morality laden statements to condoms, education of school children
and youth. From sex workers as the cause to personal risk acceptance by
men has been a significant shift.
3. Decreased blaming/shaming and decreased episodes of discrimination
against people living with HIV and AIDS denotes an acceptance of the
community of the need to act on these beliefs
1.
Conclusion
To conclude, an equal emphasis on social determinants of the epidemic is needed to respond
to the epidemic on the social dimensions as well.
Studies in understanding these determinants is critical, as the paucity of research
done with scientific rigour, leads to a neglect of important issues in planning
interventions in the area of HIV and AIDS. If we acknowledge that HIV is a medical
problem embedded in a social context, the medical research needs to be
contextualised in a body of wider social science research.
Support of action research to initiate and measure interventions is also needed. There are
numerous indigenous and culturally diverse responses to HIV/AIDS in India now. In order to
measure their efficacy as well as draw out critical features that will lend themselves to be
replicated, efforts will have to be made to document and disseminate these diverse and
indigenous civil society led preventive responses. This is indeed important if HIV/AIDS research
is to be holistic and comprehensive.
6
5.
STIGMA AND DISCRIMINATION AND ITS ASSOCIATION WITH NOTIONS OF
SEXUALITY AND MORALITY (JR)
"When the history of AIDS and our time is written, the inextricable links between
health and social stigma, discrimination, human rights, and dignity may be
recognized as our most important contribution
Jonathan Mann
HIV/AIDS Stigma and Human Rights
At one level Stigma and discrimination seems embedded and entrenched in society. It
is built on the basic divisions of society that is used to categorise and make sense of
social life - eg. Who is good and bad, what is valued, etc.. It rests on the fundamental
divisions that we all draw between 'us' and 'them.' These societal categories are not
fixed but change with time, place and situation. All of us are a part of a society and
culture, all Of us internalise values and morals, and we seldom question these.
Stigma and discrimination have been closely linked to health conditions. In fact, before
HIV/AIDS, leprosy was seen as the sin qua non of stigma. However, it is with the
advent of HIV/AIDS that there has been a refocus on the study of stigma, after the
seminal study by Goffman (9) a social interactionist saw stigma as a product of social
interaction and a deviant behaviour, it affected the very core of personhood, a person's
identity. Stigma represented a devalued and discredited identity. The pernicious aspect
of stigma is that it is not only how others perceive the stigmatised but how the
stigmatised perceive themselves. This causes untold anguish and suffering.
Discrimination may be seen as 'enacted' stigma, where people are treated 'differently,'
Morality, Sexuality and Gender
In terms of HIV/AIDS we need to look at the stigma of HIV/AIDS in relation to our
notions of sexuality, our hesitancy to speak about sex, much less educate youngsters
about it, the intimate link between gender and sexuality and differential moral
standards. We only have to reflect honestly to recognise the discrepancy between
popular rhetoric about 'Indian" culture (as though there was a monolithic Indian
culture) and the reality on the ground as evidenced by STI rates.
The agenda is to impose 'moral' standards. Whose moral standards? In India at least it
is determined by the 'middle class' who draw upon 'traditional' Indian culture (which
precludes art, dance, literature to which sexuality is central) and a 'Victorian" legacy.
In the recent past in India and currently in the US and in the programmes funded by
the US government, the ABC policy is espoused. Abstinence and faithfulness is
propagated and the use of condoms neglected. Of course this might be a reaction to
the perception that HIV programmes unduly focused on condoms. However this has
adversely affected programmes for young people for whom the first two may not be
realistic choices
Morality and Power
I want to look at how the same stigma plays out in the international arena. It is not
only a country's policies that affect people in that country. The US administration in
June 2005 notified U.S. organizations providing HIV/AIDS-related services in other
countries that they must sign the pledge to be considered for federal funding opposing
prostitution' and sex trafficking. This notification conflated prostitution and sex
7
trafficking. Note the language the term 'prostitution' is used instead of sex work. The
idea is to name them and shame them.
Many groups doing pioneering groundbreaking work lost their funding. However, on
19 May 2006 U.S. District Judge Emmet Sullivan ruled that a U.S. policy requiring
recipients of federal HIV/AIDS service grants to pledge to oppose commercial sex work
violates the groups' First Amendment right to free speech and was thus
unconstitutional.
Public Health and Stigma
The language of public health can in itself be stigmatising. When twenty five years
ago AIDS was recognised and the modes of transmission ascertained the focus at once
turned to 'high risk groups.' A classic case of us and them. However, in time it was
appreciated that it was high risk behaviour and not membership to a group that put
one at risk. Still the notion persisted in form or another - 'targeted interventions' ,
focus on 'key groups' etc. Areas of high prevalence were seen as epicentres, hot spots,
these geological metaphors evoking images of disasters - earthquakes, volcanoes
exploding, waiting to happen. The people who were infected were referred to in a
dehumanising fashion as 'vectors.'
The consequences of this stigmatising language are many.
1. In India at least it detracts attention from the 'generalised' epidemic, HIV infection
in the general population - in people who do not belong to 'high risk groups' and
some who do not even have ’ multiple partners.'
2.
It serves to reinforce stereotypes, prejudices and biases that we all have. It
cocoons us from the HIV patient as being among the 'others.'
3.
This notion of static groups also detracts attention from the dynamic nature of
society. Eg., 'brothel' based sex work patterns may be changing, 'family based,'
occasional sex work may be increasing.
Gender, Social Class and Disclosure
A study conducted in NIMHANS, by Prabha Chandra revealed that poor patients had
little control over who learnt of their HIV status. This study was conducted before
antiretroviral drugs became available. In contrast, a study conducted in Pune among
middle class patients attending a NGO clinic, where antiretrovirals were available,
showed they had more control over who they revealed their status to. Stigma
management is thus related to access to resources and social class. The following
tables show that even among the middle class women there is less control on
managing information/stigma. (Table 1, 2, 3).
8
Table 1
Disclosure of HIV Positive Status to Men
,(48) and Women (29) by HCP (58) and Lab
Table 2
Pattern of Disclosure of HIV Status to
Men (42) and Women (16) by HCP
(58)
Percentage
Table 3
Disclosure of HIV Status by Laboratory Personnel to
Men (6) and Women (13)
The National AIDS control policy explicitly states that pre-test and post test counselling is
essential and the a competent person should reveal their status.
Can you tell why in the above table 45% women learn about their status from the lab as
compared to 13% men? Why do most men learn about their status from health care providers.
The difference between the gender in terms of the source of HIV disclosure is statistically
significant at p = 0.002
Similarly, in the case of men, their status is revealed to them in private, while this happens in
less than ten percent of the women as illustrated by the next table. A third of women learn of
their status along with their spouse, or through their natal family, A surprising 25% men learn
of their wife's status before she knows her status. This might also be reflection of the fact that
many married women contract infection from their husband, and HIV status may be checked in
an antenatal care setting.
Conclusion
From the above discussion and study results we have seen the intricate relationships between
social structural factors that affect stigma and discrimination. Thus the strategies that we adopt
to mitigate these need to take these factors into consideration and not merely focus on the
individual.
6.
COMPONENTS OF A PROGRAMME TOWARDS A SOCIAL VACCINE (RN)
Research on social determinants including issues such as poverty and equity, gender
relations, sexuality, morality, stigma and other factors will help us understand the
HIV/AIDS pandemic better. It will also help us identify programme responses that go
beyond just the concept of ARVs and condoms. Many civil society groups and NGOs who
are deeply involved in the HIV/AIDS pandemic are beginning to develop many programme
responses based on this new understanding. These include:
Life skill education for youth and vulnerable groups on health and responsible sexuality
- the focus being on building healthy and non exploitative relationships rather than
only condom use for safe sex.
b) Local level peer educators and health promoters especially among youth and women to
discuss the key messages of health and responsible sexuality and to help people make
responsible-and informed decisions.
c) Strengthening primary health care access to diagnosis, treatment, counseling and care
with focus on women and marginalized sections of the community - who are often
unable to access care even though they are most in need due to structural and other
blocks in this health care system.
d) Community organisation, self-help groups and village health committees to strengthen
local capacities to identify and tackle the problems.
e) Positive people's networks to demand, empower, enable and monitor programmes
responsive to their social, economic, cultural and political situations.
These programmatic shifts are taking place very slowly because of the dominant
biomedical projects in international public health collaboration that is focus on highly
selectivised, top-down vertical, distribution strategies of ARVs and condoms only. This has
to change and this change will come only when researchers begin to shift focus of their
research evidence and understanding of the problem.
a)
7.
THE NEW PARADIGM SHIFT IN RESEARCH (RN)
There is a Paradigm shift required to enhance research towards a 'social vaccine' which will
be a much more comprehensive response to the HIV/AIDS problem building actively
beyond the present pre-occupation with a bio-medically oriented vaccine / drug response
to the epidemic.
10
The Paradigm shift for Research in HIV / AIDS
Parameter
Social / Community
Approach
Biomedical Approach
Focus
Dimensions
Individual
Physical, Pathological
Technology
Drugs / Vaccines
Type of service
Providing / Dependence
Creating
Passive beneficiary
Community
Social, Economic, Political,
Cultural and Ecological
Education, Awareness &
Social Mobilization
Enabling / empowering /
Autonomy building
Active participant
Molecular biology
Socio epidemiology
Pharmaco therapeutics
Behavioural
sciences /
social determinants
Social policy and political
economy
Patient
Research
Clinical epidemiology
As shown in the above diagram, this paradigm shift in research focus includes shifts in our
attitude to the dimensions of research, to the type of processes to be organized; the type
of service and our attitudes to the patients. It involves a focus on the community; a focus
on education, awareness building and social mobilization; a focus on programmes that are
enabling, empowering and autonomy building and a focus on people as active participants
not just passive beneficiaries. Even within the Research agenda, the focus will move
towards socio epidemiology focusing on social determinants and behavioural factors and
additional research on social policy and political economy of health.
This paradigm shift will also require new partnerships between the medical / laboratory
researcher and the public health researcher / activist. The quest for the social vaccine
arising out of research activities in this new paradigm is an exciting prospect for the future.
IS THE RESEARCH COMMUNITY IN OUR COUNTRY
READY TO ACCEPT THIS CHALLENGE?
IF SO, A SOCIAL VACCINE MAY DEVELOP SOONER THAN WE
IMAGINE!!
References
1.
People's Health Movement (2004), People's Charter on HIV and AIDS by People's Health Movement
Secretariat, Bangalore (www.phmovement.orq).
2.
Mary Sykes Wylie, Rediscovering the Mystery, Psychotherapy Networker, April, 2006
3.
Madhivanan et al, Sexual Behaviour and STIs among men at high risk for HIV infection in Mumbai
India; http://ari.ucsf.edu/science/posters 2005/madhivanan.pdf
4.
ICMR Bulletin, Vol 30, No: 12, December 2000; A World AIDS Campaign where Men make a
Difference: A challenge for the men in the Third Millenium!
5.
Research Update 2005, No: 4, Population Council; Promoting Role model of Reponsib/e Men:
Gatekeepers' Views on Young Men's Sexual and Reproductive Health Needs in Uttaranchal
6.
Akhila,
Vasan;
Sex
books
http://www.infochanqeindia.org/index.isp
and
the
Mediation
of
Masculinities,
11
7.
Eknath Naik, Arun Karpur et al; Rural Indian Tribal Communities: An emerging high-risk group for
HIV/AIDS, BMC International Health and Human Rights 2005, 5:1
8.
Situational Needs Assessment of 5 districts of North Karnataka; Profiling Sexual Networks, Risk and
Vulnerabilities to HIV.; Samraksha an Synovate Social Research Wing, January 2005.
9.
Goffman, Erving. Stigma. Notes on the Management of Spoiled Identity. Englewood Cliffs, NJ:
Prentice-Hall, 1963.
10.
Narayan, Ravi, 2001, Beyond Biomedicine : The Challenge of socio-epidemiological research in
Trends in Malaria and Vaccine Research - The Current Indian Scenario, ed., Raghunath, D & Nayak
R, proceedings of the Second Sir Dorabji Tata Symposium, Tata McGraw Hill, New Delhi, 2001.
11.
Narayan, Ravi, 2002, The Community Health Paradigm in Diarrhoeal Disease Control in Diarrhoeal
Diseases : Current Status, Research Trends and Field Studies ed., Raghunath, D & Nayak R,
proceedings of the Third Sir Dorabji Tata Symposium, Tata McGraw Hill, New Delhi, 2002.
12.
Bhan, Anant, 2003, Public Health Aspects of Acute Respiratory Infections in Trends in Respiratory
Diseases - The Environment and the Infection, ed., Raghunath, D & Nayak R, proceedings of the
Fourth Sir Dorabji Tata Symposium, Tata McGraw Hill, New Delhi, 2003.
* 5jc *
12
Disability
Emerson says, “ A hei’O IS DO braver
than an ordinary man, but he is
braver five minutes longer”
The dictionary definition of a 'Hero' is an
exceptionally skillful individual, one who fights
against the odds. And wins. Going by this, at the
Association of People with Disability (APD),
everyone we work with would excel in the test
to be a Hero.
The vision that propelled our mission was the
resolve to not study disability, but instead to
highlight ability.And ensure people with disability
a place in mainstream society.An individual’s
disability can be limiting, but with help, we can
transform that person into a contributing
member of society. A magical process, which, for
the past four and a half decades, has inspired us
to create more programs, to reach more people
in need. Spearheaded by the determination to
provide'Equal Opportunities’, we now support
overlO.OOOpeople with disability, provide them
with training, therapy, education and help them
find a new purpose in life.And in doing so, find
a new meaning in ours.
Organising
self-help groups
The gofden opportunity we are
seeking is not in luck or chance, it
We agree with Orison Harden.
Proxy revolutions do not work.Any movement,
to be effective, has to be fought by the people who
will benefit by the change.The challenge also being
sensitising the larger community, by involving them
in the rehabilitation of people with disability.
Among the various activities we conduct under
this program, the first is to identify those who
need support. Once identified, we work at building
their capacity, provide them with training and
vocational skills and concentrate on their health
and educational needs.They are encouraged to
build on their collective strengths and form
self-help groups to create a common platform
to redress their concerns.There is no joy greater
than to watch those we've supported turn
self-reliant. Help though is still required at the
macro levels, thus we regularly network with
existing government and non-governmental
organisations to ensure the needs of a person
with disability are better understood.The road
of opportunities has been discovered, through
our work we hope to carry the trail forward.
<S>©
THE
ASSOCIATION
OF PEOPLE WITH
DISABILITY
Therapy
Zig Ziglar makes a pertinent statement in saying,
"You are the only person on
earth who can use your ability.”
The people we work with have varied forms
of disability, thus we lay equal emphasis on
training and education as well as mobility and
therapy.We provide therapeutic interventions
and suitable aids and appliances to enhance
functional ability and help achieve independent
mobility through various interventions.
Thanks to your support, some of us can walk with help,
kick football and fight for the best desk in class.
Others quickly wheel their way out of school when the
bell rings, to join their gang of friends.
Yet many others give colour to their dreams on pots,
Our Orthotic Appliance and Training Centre
manufactures customised aids, appliances and
artificial limbs and also co-ordinates with
schools and institutions in creating barrier-free
environments.The Physiotherapy Unit reaches
people at grass root levels and more importantly
transfers skills to families, communities and
voluntary organisations, so that, independent
of us, they can provide care to people with
disability. Dealing with disability also creates
concern for the minimisation of its incidence.
This is where our Community Health Work
steps in.Through immunization programs and
nourishment supplements.it seeks to improve
the health status of people and prevent the
incidence of disability in their families and in
the community.The beautiful thing about
healing is that it also heals the healer.
glass and sometimes, the walls!
Our smiles say ‘thank you’ in ways
that words just cannot.
For over 48 years. The Association of People with Disability (APD) has
empowered many children and adults with disability to believe in their
abilities. We need funds to carry forward our work in educating, training
and encouraging people with disability to become self-reliant. We need
funds for food and?clothes, crutches and wheelchairs, books and blackboards, training and development and many other valuable things. All
your generous donations go to provide these things to people who really
ne ”^|hem. Please contribute whatever you can as you have always done.
O*
*
J
Would you like to share a smile around?
Please tick...
Tick
Rupees
Toward
750/1000
Midday Meal / with Sweets
(foronechild)
1000
Books and Uniform / per child / per year
3500
Education in School with facility for special interventions
5000
Comprehensive Education / per child / per year
8000
Vocational Education / per child / per year
1500-4000
______________
Mobility aids and appliances
{calipers, special seats, braces etc.)
Any amount you wish to contribute
Name - ----------------------------------------------------------------Address ________________________________________
Email
______________________________________
Phone ----- -----------------------------------------------------------CrA ;e/DD No----------------------------- Dated------------------
THE
ASSOCIATION
OF PEOPLE Wi n I
DISABILITY
for Ks. - -----------------------------------------------------------------Please send your cheques / demand drafts in favour of
'The Association of People with Disability' to
The Association of People with Disability
6th Cross, Hutchins Road, Off Hennur Road,
St. Thomas Town Post,
Lingarapuram, Bangalore-560 084 Or call us for more details
Ph: 080-25475861 / 25489594 Fax : 25470390.
E-mail: ablehand@vsnl.com / apdblr@dataone.in www.apd-india.org
Your contribution is eligible for tax exemption under Section 80G of the Income Tax Art.
from ARD fcJr
her disability.
to support
with disab.il
Education
Education is the
movement from darkness to light."
Allan Bloom once said,
How appropriate, as the light at the end of the
tunnel for disability can only be seen by ridding
society of the dark‘exclusion’ factor.The need to
communicate, to learn is common to all children.
It is only the teaching skills that differ. Thus‘inclusion’
in mainstream schools is necessary and an important
aim of our Education program.
Teachers, as much as children, are an integral
part of this process and we provide special skills
required to understand specific needs to deal with
specific situations. Proof that it works is the fact
that our Education program is studied as a success
story both in urban and rural areas. Credit goes to
the model school - Shradhanjali. A pioneering
effort by APD, it is a school for holistic
development and education, where children with
severe and multiple disability learn and play with
children without disability. Pre-education is taken
care of through community based group activities,
anganwaadis and pre-schools. We've seen the light
And would like people like you to pass the torch on.
and employment
Archimedes once said, 'Give iTie a lever
long enough and a fulcrum on
which to place it, and I shall move
the WOldd. Training, education and
healthcare is not our end goal. Providing
economic independence is. A pioneering APD
training and work opportunity is horticulture.
A unique way to provide a different kind of
therapy and livelihood, it is one of our most
successful case studies. Started in 1987,
the horticulture centre trains people with
disability in gardening.They then find gainful
employment with firms and individuals as
gardeners and achieve self-reliance.
To equip them for the future, we also train
them in new mediums like IT. Our Information
Technology Unit trains people with disability in
Computer Applications, Desktop Publishing,
Auto CAD and muitimedia.The Industrial Training
Centre (ITC) imparts training in electronics, fitter
and welder trades.The Career Guidance and
Placement Cell plays a key role here. It works to
identify appropriate vocational training and then
creates job opportunities and promotes group
and self-employment by proactive networking.
Working for a living comes naturally to most of
us. Some though have to work to achieve that.
Support
This was just a brief overview of what we do.
Working with people with disability over the
years has inspired us and made us believe that
anything is possible, if we believe it to be so.
And we do. APD is dedicated to reach as many
people with disability as it can, and make them
realise that they are, in fact, able. Write in or call
us if you’d like to help or know more about what
APD does.The generosity and support of our
sponsors, friends and well-wishers continues to
and always will inspire us. In conclusion, we'd like
to share a thought we live by. "We make a living
by what we get, we make a life by what we give."
s
iJi
1
a
j
The Association of People with Disability
association
of PEOPLE with
DISABILITY
6th Cross, Hutchins Road, Off Hennur Main Road, Lingarajapuram,
StThomasTown Post, Bangalore-560 084 India. Phone (91-80) 25475861 7 25475165
Fax (91 -80) 25470390 Email: apdblr@eth.net 7 ablehand@vsnl.com www.apd-india.org
I
You can i
port us by:
0 Sponsoring one mid-day meal at
Rs.1000/o Sponsoring education of a child at
Rs.5,000/- a year.
© Sponsoring a vocational trainee at
Rs.8000/- a year.
o Sponsoring or donating Utility Items like
Furniture, Computers, Stationery, Kitchen
Items.
© Sharing your knowledge and expertise.
o Mobilizing resources for our programmes.
o Being a Volunteer.
o Propagating the spirit of APD.
Donations to The Association of People with
Disability are exempt from Income Tax under
Section 80 G. For further clarifications please
contact us.
We run var;'s programmes which
fall under foiling categories:
Education: We offer schooling to
children with disability and reach out to
children in rural and urban
communities
Training, employment and
livelihood : We offer training and
placement to young people with
disability in Information Technology,
Industrial Training and Industrial
Sewing Skills and reach out to disabled
youths in Urban and Rural
Community.
Therapeutic serviceSFnrough our
physiotherapy, spinal cord and
orthotic units we help disabled people
adjust to their new situation and
provide them with mobility aids.
Networking and advocacy We
organize self-help groups to empower
people with disability to access
resource.
Horticulture Units We have two
horticulture units at Jeevan Bhima
Nagar and Kyalasanahalli and train
people with disability in gardening
and landscaping.
fled) dd &e
araelfa^aaddb:
ddbj sacdbE-^dbri^
es^1
Q)
SIS sratra dbdd a>odb
tnjaud ddari
dba.1000/-
ajodJ dbrbad
cftesjej6 <3^ &?€29e9C9
Strati dd dlra.sooo/-
AraetarraO^ dddeA
cD<5)^
Sooda Sdd enratad ddari
2500/—
aaodb esdjtbrah aiaard iSjaeurrofi^ aidde^cdb dd
<±0.8000/-
a>a> d^ dd ddde.3 esd^d^cda £ra*E7$ dd dja.sooo/rira^cdbog. ae<±raed£drarisb. eadridod ddorieb, dead
roadbQrieb da<±? ga^dd (rodccbo^ drtbrii±>.
adb,<s dOra£ db<±>
-* eradddb,
sp
<X aooas&radadodb.
V
a esdLraeAOlieda!''
esg’tiedc" as®
ddt^ saobbr^dbrides doddjajortedjj sigdedodbd)dj.
5jQi>o ded^oad ded) saaitradrSodaaaddj.
d) & a. o±>
adaesta
db^j e/uaadddbj ddOdadido.
aes^j aeciid <j!d dcraceb^ esGrecdj <30ri acdbdbd dS^ed
soa esaodbu
dasd
m esnaoixSOrl dbo^ suafidbsid.
gj
dbaa>v3ri dodcdbdb.
(P
ci dod*r<?>.
6de esddd, da<\5« dd, drajacb dbbaocdd, dou® tpadbFo®
tPa® esoeJ, uoricraajdjdo, doritOadb-560084,
dbadsrerf : (91-SO) 25475165 / 25489594
dS$S^ ; (91-80) 25470390.
q - dbeu® : ablehand@vsnl.com / apdblr@dataone.in
dsb® ^£3* : www.apd-india.org
?
r
(
;
da&a dodcdba ddd ado dsidri^Btf “esoriadocLra dd
aodo^ fsgdeaoaad Hedd drfdeo
adraddad dcosrad 5aoi>E-&dr&>da^d.
f
d> a cda erooiaE-ddarld Abb dOdcda
ddro:
d>.*.aoi> daaao erodes) dda^cda adra FsaOdodcroftcb.
dorhiraBd M$rdsrafa a>odavd 32 sradbErisb srarira daaeeaad
adcda ^e£>aaadd)d dada asdaavadd esddb aosadari saeagAd
200 darid sradrides esoriadea daddda, oaaaed. riaeadaud
ddcasaft sacdar adr&djtSd. sjnaoau ddagjcda sradoiadjj
(SIS)
ddrScaaod' adde ddriAcdaddri ddduaria^G^,
<2i5s.<as5.<jo'.1?l esdaiAetaroaddBri
dd^ocbod sradcdada.c<
-•
naaaera sroairaeaKja AdeBcda esddradu dddbad. gdodd
daaaa^ erodes), esoriadea daddda^daaaa^aa&Sri ddagjcaand.
aediaaoraBid ^dea^ ddeJeA dada erodasgeri:
oiud esoriadoddbj es®rdsran daoeddrarijawdbdda dodccb
gdaaaa riaBcdaaRd. de aejdes dododaa doridaada drid dodo
ngdraodd.
daaeeaad,
aJdaawagjd esod oaajjd deaaaacb
asdrides dedaaPi esoriadeaflri draA>^ dogsad. dyaaBsa
ddded, djoaBsa draori e^do^ ddde^
dodo doad
erodjajerradsasiritfdbj ddcdsos ddjddsTOjRdj^d, gddLroo&ri
dJa^ ddde^risad ^doiraeddd, esaLrarecsaJ. ddojcraoi)
E^ddrdA, ddjonaoi) escUaerij ddde^cdbdbj dodccbes sarira
uaajd sidd daard dsda daardedd ddded dodrid
ddoiraeridLraoari deQ esoriadoddbj djaa^sra&dri dduarbdd.
qdod dda dorte djaecarradaa dddedcdbdbj deg esoriado
oioddOri aeduarbdd.
sraSedii zra^oirodb
asai (4>ACdjaeq5d*):
?rag^ado±>oda
esoriaAodoi) g)ddsdda±> adrddocbj ddbaro ^rarinanGb,
siadeOd aajcdjado, d«d, aaa® aad crarLra d^dodd
duodts^rid dxrao^
aitsg aedodd. esde Bed dLrae? sadsra
doAddridd^ a>dfidjdcb, esdjrW doiroOaa aarira ddded
^eod. doaA rraodjar doiraBaa SeodrtedSj dorisLradb drid
dads rgdbaodd gdesirido dddbdd.
drid dado rradaere ddx>aao±> e»qn>ad dlddedd aao±>e-^si>:
esgsrdEjafi a>odbHadbd esoriadodd^ rbcbdd esdddjj
ddraLraedbarosraa gjddeddrirawd ddoaad djja^aia&doJjo
regdooarisarbdod daaci>d)db de aaocbfgdod gdaaro erodes).
de fed^dcdao doridaaBd 32 nadarrisb. daaeeaad dada
ajdaavaa^d aoarlra craa^d esded asdridea gjdsJedd
wacdae-^dariddbj ddduariadd.
■sjddaaoari ddaacaacda odLraer^ sacdarddarivad Ssb esspd^a,
esaPcJjdd saaadd, daad esdraer^ adrdd, gdlrad aaead slasi^d
dedridda,C( adraodadd.
i»
ead dogiud dada daaeaad:
esoriado d^Arisb ddaaaido esdaadad dsbridda^dddadjaoda
dAcdasroa es^d^acdao aaarid&doa esoriado dod-dodrid
aaeaddfdri gjaddsaarbdod eacdae'^darlddao) oasajd^od
dddoariaad. dodcdba esoriadod sj-dasaoia riaogjriddbj
dasa. esdd d^rid sari erarj^d daoaaa, dvecda doddLra^oriddbj
cearlra daead^riddOj ddodaodu ddddajBjft daatdad
eracdarddaridda,<x ddda^d.
-•
s&steri
atoerad aaddorid
dr
Fdodsd
tSSirae a?5 asaoSrttfSjUa&raoda asfc dod sacCortSA) £>da
gec&arron ad^rt), saeri Ssb&>;*3crod. aesSj dso±>£>
^odOTbdart Jladgsa aafccfcritfsfc
ad> daab adad£
siiO--COjO goZjdi............ ...............
dddd $.fofc rtJOrttfjS), jjaddadjda ad.dd.daAd
zfoal: z±e3:............................... sstf
a
oo3i£d ssSeXb:......................................d^d rtodj............................
sdrt^................................................... odZ^Jdrt......................................
“HoSs, dd.SnaA, dS ?i)d^rraft a, ts, g, d?...rtsb” coozj odb
aojadrtoi>S>4 axiaddoOcb "addSdarf aafcsbrftfKbj add:
ct<£>^ d3 stodj^cdosb* ajsoTtra^.
asS>s acs^jpa^cS e>, a, <g, d?...oiradw dS adgSoii a, a, <a,
93...oi>s», Sas azaa^j st®a.
d?5 sbdi^ato ZoOo&ort, u0oi>a<i, aziao d.dcaOateA
caoBrLra a^rt^ssaAd^, ctezsadejs 5? djsj
^eSSCLfSCFudcSSddi ^dd..........................................................
G-JOijji ^cod......... .
.............
........................................................................d/ad^ar^..............................
&&F
SjOJj^QiO
d/sdso^r*^
a
ZjOduFSWuoiCJad
coZ^di,
zj'S’oiiauasjaotS) 'gddfld ao*d>rW&>, szaa^ djadssa
adaad xayf zJozjo?>ioztra adsj Aeddorua d^ zt>dod
.Reidas,, &>rtda Mossad, ;*d3d zsaaS, ad^ad dJod dcS
dda rt>&. ada rtadoJxra 'adz aAdfl.
B
fc
sozpadoirt&iaoart.
£S73Zj,
san
ziortsbacb
doSd zOdO, so.d.ax1
agpOex4, ^caiedo4’
zSortebacb £rtd
ddnaeaad atod, aied draea
ai>da sieds aeS i-JAi
dbdfidda&dd dd crata^
u
-*
sadasae ddd abede ddoeoe ddccb abee^j
Look right, look left and
again right before
you cross
Walk on the footpath not on road
eseag dt^risf abed atradde naea
Cross at the Zebra Stripes only
aradsae dtpa^de add aicbcb acbscbaJ
dosadd atoa atraa zje> aradde ddoaoe
If there is no footpath walk on
the right facing oncoming traffic
d^oaSrisi) cSeetai grtari edajaoi^
da5 abcfejd gse srarieedd
sraaSsJriti) afoaSeabscbarari
tg&s* aej^oo'aod e?sfs|
adetsdcb.
aoscbd eraddritf
&oaaosood
dd dbed ^dsSea
Do not step off the
traffic island when
vehicle are passing by
Do not run out
from behind
parked cars.
afossad s^peserc6 dsb,
da^d odd daracdJdd^
aftSosoe.
The Policeman is
our friend
Take his help
deS esa^d abmoad aedd ©srad
ds> adsrad KiEbaase? ^oss^sgai)
drSoii <i>ee3
eusrad
dadcb Qp
Never play
on the road
aorfd
o ftaSddnix
cj
«
dcSoi; shed
esaradao
aoscbd
sraddrid ae
eusrad
asdcb
Never throw
fruit skins
the road
Never play
near stationary
vehicles
gse da? adgjadd) a-ocb
assgriseabdd
da?
ddcdbadd es®r^ es^a ast^a©
a&sfe 5a>S3®a3saet36E'
dbee? gjoirarf^ao
dud gcbsi d^o±>»
esse sarjdosood 30
Never stand on the
footboard of bus
aiesabsl fflAaod
geccbeo escjisra
ao3ex> gjccbs^ea
Never jump on
or off a moving bus
dtS
_o
<a
desid
q
e
strade
deScdbcd^j ^eoirafl ®o3d ®d> a^nb) sbd^srafl strf
aec±>d Klroaisra ^©ddda
ajraaccb Soared austere SjodririJ
Q
SDfrjSS seas sL'srfSn'B / d-jSssitd z^sassod ztoirtw
usSzrsuj a.SjzedzS,'® ?ioSrt<b
MANDATORY / REGULATORY SIGNS
CAUTIONARY / WARNING SIGNS
SIGNS GIVING ORDERS-MOSTLY CIRCULAR
MOSTLY TRIANGULAR
STRAIGHT
PROh.BiTED
OR NO ENTRY
bluock
ALLUDE
VEHCLES
PROK&TEC
CARTS
PRvHBtTED
ONEWAY SIGNS VEHICLES
PROHRTEDINOHE
DIRECTION
TONGAS
PROHIBITED
HANDCARTS
PROHIBITED
RiGHT HAND
CURVE
LEFTHAND
ClRE'E
STEEP
CYCLES
PROHIBITED
ASCENT
STEEP
DESCENT
IIAFRO.V
POADATIEAO
POAbWDtirAl 8.AD
BRIDGE
ROAD
PEDESTRIAN
CROSSTiG
5LKXX
Mf.fl AT
CATTLE
FALLING
ROCKS
® ® ® ® ® <8)
PEDESTRIANS
PBMBna
RGhTTURN
PROHBIEO
LEFT TURN
PROHIB-TED
UTURN
PROHIBITED
OVERTAKING
PROHIBITED
PROHBiTED
PARKING
OR STANDING
LIMIT
LIMIT
LIMIT
LIMIT
LOAD
LIMIT
AXLE LOAD
LIMIT
RESTRICTION
ENDS SIGN
COMPULSORY
TURN LEFT
COl.'PLl.SORr
AHEADOMY
COMPEL SC=Y
TURNRIGHT
fOSUSOR.
AHEADOR
“URN RIGHT
COMPltSCRr
AHEADOR
TURN LEFT
COMPOSE
KEEP LEFT
COMPULSORY
CYCLETRACK
COMPULSORr
SOUND HORN
CYCLE
CROSS-NG
ZL
HAIR PIN BE NR
MEDIAN
S’DEROAD
RIGHT
STAGGERED
INTERSECTIONS
GAP IN
ECAD
KjUGhROAD
slippery
FOUND ABOUT
M.AJORFOAD AHEAD
(50-KOMETRES1 i200MEIRESi
LN-GUARDED LEVEL CROSSNG
FERRY
DAI CERCUS
DIP
<50-100METRES) (200 METRES)
GUARDED LEVEL CROSSING
ds3 acdbsbridaik saadadjcb dsb,
ca
LOOSE
GRAva
Y • INTERSECTION
SDE ROM)
LEFT
HUUI'OR
dsccbab,
a>odeabgJEicdcdx
d^ccbcdid
_a
cl
u
ol
LEFT
RR/ERSE EE r ID
VEHICLES
PROH BRED IN
BOTH D’F.ECTlOf;S
fcoojidj sjadd dsssbsrari
esdodOiddessd dossad acxbdartdo
e±ro&3 Se!±)g5 KiSa^aTO
^XX3Z5 2 ^C5rt«?o
e)
aaaofja wdrsadd wde gjadrfddo, duaoddasadcfa.
INFORMATION SIGNS
MOSTLY RECTANGULAR
add aaadd daadcb ajcrooi^aaft ddd*
|
fBANGALOPE |
<4
HQSUR~||-| TUMKUR F»
BANGALORE
dbd.ajad
drea wadddda,4 duaeddaadda.
□
-* TUMKUR
•*- HOSUR
drtd d.dcddC do* asadcs6', dofteddaoi; ooadcsWd^
Sde^dusAd.
DIRECTION SIGN
ADVANCE DIRECTION SIGN
DIRECTION SIGN
|HYDERABAD)
VIJAYAWADA
MADRAS
PLACE
IDENTIFICATION
RE-ASSURANCE SIGN
SIGN
Ila
PETROL
PUBUC
TELEPHONE
HOSPITAL
PUMP
addx^O dozsad
deroodderodds.
d^od©
-» "
Sdd<?
QAeSd
<s
ro>d?j
acortd adedd d,dedd© sjaddrt^d^ SOdaiaddo.
EATING
PLACE
RRST-AIO
POST
LIGHT
REFRESHMENTS
RESTING
PLACE
HOTHROUGH
ROAD
NOTHROUGH
SDEROAD
dadddC djafcb
W^d233dd3.
ddoi>
doAed
ddd
gjawdri'v‘©mw
^wOAod
cd —’
do±rar3dJ5sdd5.
srodddrarttfdsj
ddow
doo©
. ••
’
:.je‘
A
PARK
THIS
S©£
PARKING
BOTH
SiOES
SCOOTER
& MOTOR
CYCLE
CYCLE
STAND
ailraeSBarttfig (ddedasan aaua osartsfo) dz& dood
sraeSrt Sjaodjaoi-Sjadcfc.
Q
TAXI
STAND
STAND
daocraorisb dedd driari
AUTO
RICKSHAW
STAND
CYCLE
RICKSHAW
ROOD
GUAGE
ajadd dcaoddaaaari de?
erodoireeAdsjadds.
STAND
asaddd)
Scddddj.
e q
dd>d) ddoiogsart ddde djao djadd
dosrad accbdo zraes&,
©dsradd^cbj d&&
eaaejpoeeopocprecjs 'cppppass ‘ esaes^faes? 'qsppcpcpo® p p
cpeesaesp© e3*2 cpo^a pcs pjapqs §ep
CJECPOGSp T^CpDSOCjfi© pO3CpOJ2 P2J29S2
sbd^d tffimdrid feosa tbda stooaa deaccbstj5 de^risi)
•
freest)
sborte
ax>c3
rbdb
sb^
eJcO
s3es?a edss£3
ddrQrija dcra Mossad dbddd
Safety Always for Every Road user
djddb doasad, dbdfid araed esdsrad d&d aid
doddsacb ddd doajad ^aesedd &oaod
t)
dd mrisnadcbdde adb, giadd adod?
ddbd riradj aet^ja ddsa,dd goes e>od!i
©sededd doirad eidspadd aadra
Over Speeding - Cause for Accident
doasad djaesed5 ada,S dad,
add dasaccbddD,oi ddosoe
S'-'
The Policeman is your friend take his help
sradd aaod djadosrad dsaaJje4 a^jaeaa6 addaredda
Don’t use mobile phone while driving / riding vehicles
aed) ©agd doi>doaadd aredd aaed dradbd ed$d acbdtso
Don’t drive if you are minor
addd ddda asanadd araddddb desdascbaaad addaRfa
Avoid over loaded vehicle
dje&darisa asadsa ad^ doaodddbried
q§4>a« accbdbddd^ 3H& / dee
Ask your Friends / Relatives to follow the same
dd dbt^d dda das
dea3, da naadd ®d®ad asd
asm
INDIAN INSTITUTE OF SCIENCE
BANGALORE - 5600'12
Centre for Sustainable Technologies, CST (formerly known as ASTRA,
Application of Science and Technology for Rural Areas) is an
interdisciplinary research and development centre at Indian Institute
Bath water heating
e
Stove for agro-processing / cottage / small scale industries
(areca boiling, silk reeling, ayurvedic medicine, jaggery, fabric
dyeing etc.)
of Science, promoting sustainable technologies, particularly focused
on advancing sustained rural development. Technologies developed
at CST are; environmentally sustainable, lower in cost, resource use
efficient and based preferably on local resources.
CST is over 30 years old and has developed and sustained high
quality R & D teams in several areas such as; bioenergy (biogas and
biomass gasifires), efficient wood burning devices (cook stovt^^d
Specifications
Open top down draft gasification system using woody
as well as non-woody biomass fuel
Large-Scale cooking (in hostels, school mid-day meals etc.)
e
1 to 1000 kW capacity for power generation
100 kWth to 5 MW th for heat application
Specific fuel consumption 1-1.2 kg/kWh
Atmospheric pressure steam generation for aromatic oil
manufacture, rubber vulcanization, stifling of cocoons,
lime-stabilized compressed block curing
e
3.5 kg of biomass to replace 1 litre of fossil fuel
Driers for vegetables and fruits, cardamom, areca, coconut,
tobacco.
Alternative BuildingTechnologies
Efficient brick and lime kilns.
agro-products driers), alternate building technologies, water
treatment, forestry sustainable biomass production and climate
change.
Biogas,
i
In addition, CST is aiming to pursue R&D in areas such as sustainable
water and sanitation, information and communication technology,
waste treatment and recycling and climate change mitigation.
CURRENT R&J) AREAS
CST has developed a range of biogas technologies that use cattle
dung, herbaceous biomass and municipal solid waste. CST has also
disseminated; i) dung based community biogas plants, ii) solid-phase
biomass based biogas plants, urban solid-waste biogas digesters,
and iii) coffee and agro processing effluent treatment plants. The
technologies developed and disseminated at CST are:
Efficient wood burning devices
Optimized biogas plant designs for cattle dung
Biomethanation technologies
©
Biomass gasification
©
Plug flow like reactor for solid feeds, leafy biomass and urban
solid waste
Water treatment
©
Solid-phase stratified bed fermenter
Sustainable biomass production, forestry, bioenergy^gnd
climate change
0
High rate multifeed reactor for coffee effuents, leaf biomass
and agro industry wastes
Alternative building technologies
Environment Quality Assurance and Impact Studies
Vermicompostfrom digested feed
Centre for Sustainable Technologies (ASTRA) and the Department
of Civil Engineering are involved in developing and disseminating
Alternative Building Technologies. There are more than 30,000
structures using alternative building technologies spreading
across the country. Some of the technologies are: Stabilised mud
blocks, fly ash blocks, composite mortars, filler slab roofs,
ferrocement and ferroconcrete roofing systems, composite beam
and panel roofs, masonry vaults, and domes, containment
reinforcement for earthquake resistant structures, etc. Some of
the major advantages of these technologies are: energy efficient,
eco-friendly, decentralised production systems, cost effective and
amenable for small scale production.
Water Purification & Defluridation ofWater
Providing safe potable water in rural areas is a major challera^
in India. In India nearly 70% of drinking water sources
contaminated.
Conversion of digested feed to edible mushrooms
Energy EfficientWood Burning Devices
Biomass Gasification
Biomass (fuelwood, agricultural residue, cattle dung) is the dominant
fuel used in rural areas. Biomass use as fuel is characterized by; low
efficiency of use, shortage of fuelwood, exposure to smoke,
drudgeryforwomen and loss of tree resources.
CST has developed a large number of energy efficient wood burning
devices for,
Biomass gasification technologies have been developed for meeting
requires low maintenance and costs paise 15 to 18/litre and
defluridation of water prevents dental and skeletal fluorosis.
the needs of electricity and heat. Biomass power for village
electrification and industrial applications has been implemented
using gas engines. Gasifier has been used to substitute fossil fuel in
kilns, furnaces and other end uses for heat applications.
Domestic cooking (many types - 2/3 pan efficient stoves)
Fluoride Treatment: A new method to treat fluoride-contaminated
water using magnesium oxide has been developed. This method
relies on precipitation, sedimentation and filtration techniques and
is efficient for a range of ground water chemistry conditions. It
Silver based Household Water Purifier: Ceramic beads or candles
coated with microbistatic agent namely, silver is used under
conditions and methods where only a small quantity of silver is
released into water passing through the filter where most bacteria
■
CrOO.
are either killed or rendered unable to multiply rapidly. The devices
are designed for use iru continuous and batch-operated mode,
taking < 15 minutes for rendering water safe at typical microbial
loads. The cost for treating 1 litre of water is paise 1 -2.
Sustainable biomass for Energy, Forestry,
Bioenergy &Climate Change
Wstainable biomass production is prerequisite to sustainable
bioenergy. Biomass production for energy, bioenergy technologies
and forestry activities are attractive opportunities for climate
change mitigation. CST has conducted the following studies:
Sustainable biomass production potential for energy
Carbon sequestration potential of forest-sector and different
forestry activities
o
Bioenergy for fossil fuel substitution and carbon abatement
o
Clean Development Mechanism (CDM) projects in forestry
and bioenergy
o
All rural electricity needs can be met (> 100 TWh/year)
from bioenergy
Afforestation/reforestation in degraded lands can sequester
170 million tonnes of carbon annually in India
Sustainability and Human Settlements (Habitats)
Sustainability is well recognised as a fundamental rider underlying all
aspects of Science and Technology concerning human settlements.
Habitats include human settlements and their (urban and rural) living
environments. Research into sustainable human settlements involves
understanding the living environment process, which includes
interaction between the built - and natural environment. Potential
research into sustainable human settlements includes:
o
e
Building comfort studies and Climate - responsive buildings in
tropical regions
o
Building Integrated Photovoltaics (BIPV)
o
Integrated Water and Sanitation in Habitats
®
Green Buildings (design and evaluation)
------------ 4-----------Chairman
Prof. N.H. Ravindranath,'rav@ces.Ssc.emet.in
[Sustainable forestry, bioenergy, climate change]
Faculty
Dr. Monto Mani, monto@astra.iisc.ernet.m
[Sustainable human settlements, green/eco architecture, domestic water &
sanitation]
Dr. H.N. Chanakya, chanakya@astra.iisc.ernet.m
[Biomethanation, water purification, sustainable agriculture]
Dr. 5. Dasappa, dasappa@cgpl.iisc.ernet.in
[Biomass combustion and gasification]
H.l. Somashekar, somu@astra.iisc.ernet.in
•
Bioenergy can reduce C02 emission by 40 Mt Carbon
A annually in India
[Dissemination of bioenergy technologies, wood-burning devices]
Associate Faculty
Prof. B.N. Raghunandan, raghubn@aero.iisc.emet.in
[Combustion & propulsion, natural resources]
Environment Quality Assurance and Impact Studies
Prof. M. Sudhakar Rao, msrao@civil.iisc.ernet.in
[Water quality and hazardous waste management]
Prof. B.V. Venkartarama Reddy, venkat@civil.iisc.ernet.in
[Alternative building technologies water management]
Dr. TV. Ramachandra, cestvr@ces.iisc,ernet.in
CST is not only developing environmentally sustainable
[Energy planning, GIS for resource use, lake and ponds]
technologies but also has laboratory and technical expertise for
Dr. R Balachandra, patilb@mgmt.iisc.ernet.in
environment quality assessment and impact studies:
e
Conducts studies on water, soil and air quality
o
Has Environment Quality Assurance Laboratory
a
Undertakes research and consultancy projects
'
[Renewable energy, energy economics, optimization]
-------------------- 4--------------- -—
Contact Address
Chairman - Centre for Sustainable Technologies
Indian Institute of Science, Bangalore - 560 012
Phone: 91-802334 8575; Fax: 91-80-2360 0683/2360 0085
E-mail: chairman@astra.iisc.ernet.in,-
Website: www.cst.iisc.ernet.in
HELP
Personal Data
IpeS'-i
1993 XjoiiS6 §°oe$&>o£> ath£>5
sJ 3o£5;&
Q
CX O 2oi&>ex> £SR>
(E>doSo3Bo ssSftoa. 8-006® c(Y (SoaspeoSS epoo Ep&yco rb6o3
Name
8€>c£baspy>3, esepA ^SxpYje5a;& j5sSpd&8o ?3ft>
sP^Ejl^ EuSfi 8-3) epoo spepco epoo& esocSep tSpcpoiSa “P^) o^cXbo.
Address
'Sp^i JSorO epoo Sp&ge 366Sira§sjj'to, cp6|gg<3a3& art>o5^ &;6y Skpeo,
sioagorp |3oM a^GS. es8g, (PEepSB £fe>&o& Kj3;6 SStpo epooAe
Phone (O)
S3£b§°3 ?6s5paoS5§ 36R sp63 S&§°^)oaL>& "S'eSj ByhSpOoB.
&rp2o ea^o86o (Ss°^o Sep £>8 (a>o8 (tpsSpSJ Terre des
homines (Germany ) SbSdxo Yolks XVagan XSs$oso8o§6 "Sp^ (tpBpoS6
bpo s',6(^£g3rogb 5g3ogorp;&, epo s°6(i&e>& &6P> a&S5 ^BjodtjoS6
3°to epB-5’oo& eacSfSZj) rtdbex So’grao, epoo Sp&goo 388§t6p spB
6£ra,
XjjJpasoeBo 32$ 3o°o (oiaS^DaS6 bpoo 388§ra
Date of Birth
?6o$poj (Child Protection committee) epoo 3cyg?)^)^ (rpaSo^ccoS6
3cpg&oo, &jfcqygd±oeo, eSgaotfboca6 Saa ■&8oi5) $£$&) ssR^obSiS
Class
(Parents Teachers Association), epoo®5 33^8, r'Pczb^e^ ogKPoe^Gbta
BANK ACCOUNT INFORMATION
rp8 aprtidpsSpgJY 36gS56Soc5j| epB-poo spccotS6 ge| &5j (Child Clubs;.
(rpjbrpcoeS6 afiodit)
epooo, c&e38, S'3®8 gpoo'g B^a, s>eygtpcpoo,
a°8syge^oo3 8ai>& ep3x s=3=Ca§bofc>p
“epoo ?5o$poo” StogjtoSSc&Bo aSftoB.
wJp^&o^e sds>&§°j3oC»&
■Jpe^ ^>oS E>ao3?5 SeeoIpoS6 8s ScpB 2009 ?5on g6 ^S)
ip^S dp^oBorpExo
£a g6 £S> sfoSS g> & esCi(|Pci5po^o, XSpiSBe»^> 3p&
3(6^
Mobile
(R)
School / Office Address
Phone
Name
Roll No
Branch
A/c No
SPECIAL EMERGENCY INSTRUCTIONS
Blood Type
Allergic to
Doctor..........................................................
Phone
Solicitor
Phone
Tax Consultant
Phone
Travel Agent
Phone
s»&oy 8o33o?E?5arp
u’&Ss0sS°S ?)Siguoa8’ & Sa.1DS.&o,’S
HELP had constructed 7 Additional Class Rooms in the 7 target Villages.
These additional class rooms are being used by 300 children in 4 Tsunami
effected mandate of Prakasam District with the support of Volks Wagan &
Terre des hommes (Germany)
S36&5-1 : 18 rio.o
aroei
d&LuocmS StyoS:
es6^cf-3 : TiCSo
Sb
3iG$gbo. So
January
iSgra
eShiSoeS (a7°c520i?p^e5
s.o&.&o
February
HELP conduct the Bc'^ata (Back to School) campaign every year in the target villages
jointly with Dept, of Education Created Awareness in the target communities, through
Relies & IEC material about the need of education to children and admitted 800 children
in schools from the inception of the programme with the support of VW & Tdh(G)
2009
1
Right to Education
(Article 28 - CRC)
1
2
3
4
5
6
7
14 !
"1
8
9
10
11
12
13
15
16
17
18
19
20
22
Q
‘
23
Olst
International Development Week
02nd
World Wetlands Day
02 nd
Cancer Survivors Day
11th
World Day of the Sick
bun
211
24
25
18th
Festival of Women as Cultiraiors
23rd
World Magicians Day
28ih
National Science Day
International Mother Language Day
26
27
28
Play equipments like See - saw, Horizontal Bar, Double Swing etc. was
given to all the 10 schools in the target villages, approximately 1100
children are enjoying during their holidays and otter school hours with
this facility we have provided with the support of VW & Tdh(G)
esggd-8 :
rt>aoSj).
saSSeJ-9 :
So
S'ex> S&oiitio.
oSS^-10: Sb& 3c3
ssSjkl &oO So
Sb iSSiSol&oS6 rSPesohPPfcio.
2009
2009
01-7th
02nd
07th
14th
18th
s&So-ll: ®3Sj’(5ra&
S’SieSo, Aio XboO &&&
®6g£-12:
&
ej
’iiSa
’BS SOcxbtSci&iio. G3°6 SCiGfeo
Q
CO
azgo&eo cSSaStoaxS
10 Child Protection Committees were formed in all the target villages. Awareness
was created Througb-^iinings & IEC Material.
A pre paid post card was made available at all the strategic locations in the target
areas, which will enable children to inform about their issues to CWC, Prakasam with
the support of VW & Tdh(G)
CS&joS
i
1
Prevention of Blindness Week
International Children's Book Day
World Health Day
Fire Sen ice Week
World Haritage Day
National Public Relations Day
Right to Protection
1
3
4 |
(Article 34 - CRC)
araeegaor?
c3soi6. ffefle ri>0ox3
O
5
6
7
8
9
10
12
13
14
15
16
17
19 ____ 20
21
22
23
24
27
28 ....___ 29
i30]
on
ed
26
22(h
29th
30th
World Earth D
International Dance Day
Anti-Child Labour Dav
111
(WJSTERLEVE!
Ml
2-20C
Right to Participation
Mon
(Article 12 - CRC )
Children participation is ensured in all the Activities in the target areas.
From Planning to Implementation & Monitoring of the activities through
Child Clubs & Child Groups with the support of VW & Tdh(G)
ue
01-7th
pi st
|03rd
05th
08th
^9th
Prevention of Blindness Week
International Labour Day / May Day
World Press Freedom Day
National Labour Day
World Red Cross Day
Universal Family Week
b
tiB£t5-14:
Thu
>ed
11 th
13^
I5th
2-1 th
Fri
Sat
National Technology Day
Mother's Day
International Family Day
Common Wealth Day
No Tobbacco Day
■ International Childrens Day
J'
cssSeSS
30cxb<5<£b4oo.
SB aSjS>°
rt>8oO
^^6ot3’e&&o47>56 & eSSiSoi&o SesSS6
Si
June
2009
15: Scrfa’ s°S
aagoO &rt?5oe5a56&" &>£> ssotSOS6
feSto. sSriPtSioSvig.
S&&5-16: Ss”OeSo I s5c§<S«5 ^as”3§ :5°&^
s?5s'e-17: SSjdS SjBsg^o "S:odb§5s5fc:o, J5&»a”6 3»ijspe °7(P°
'S5ioi5c6£J3^2£.Gi^o7b ©SmST'S a>oiS>§°^ S>&).
10
04th
I
05th
08th
17th
11
International Day Of Innocent /
Children Victims of Aggression
World Environment Day
World Oceans Day
Fathers Day
World Day to Combat
Desertification and Drought
y^Zed* f
I
"’'Jhu
A bi-monthly publico'^p Tuniga (in Telugujis being wholly managed by the
children themselves, wth a little support from the Organisation. Children in the
target area are capacitated with advocacy trainings so that they can express
their issues effectively with the support of VW & Tdh(G)
I Ith
23rd
19
HELP initiated establishment of 10 libraries in project villages to provide information
needed for children and adults. Wide varieties of IEC materials are published to
dessiminate the information about Child Rights, abuse, exploitation and Child
labour to Children & Community with the support of VW & Tdh(G)
World Population Day
National Flag Adopton Day
20
'3:o£>^o(56, srS S5s>s=6oS” "SSh
e36gc5-19: opcy’SfSarS,
e?o<3
agseS-20: £Wt5o(&o itoo© tSXJon”
s22oo ri&Sj&rWjctoB SxQoo
August
eS^-21: St&
S’ltfeS, $>jg>«3 Sj’oiSiao
eS^t5'-22: &J» £6cs’&Si3 6s=ra 3i$6JK?'s>oc5
eBg£-23: && SSs? -3°6SS a°6je§o 5joi5 && So^rtSuS ^asSo
hiSsSto’aS |<5ek^ 3«%,
(&$ 3”oS &&%
10 Village level CMU Clubs & 60 Child Groups were formed and Networked into
Mandal & District level. These Groups & Clubs are periodically assembling &
discussing on their Issues and raise their voices at different forums with the support
of VW & Tdh(G)
■
Right to Expression
(Article 12 - CRC )
Mon..
/ '''Xi
_JTue
Thu
?
r.fSl-
01-7th
05th
08th
14th
14th
Sat
Fri
Nation: 1 Nutrition Week
Teacher ’s Day
Internal onal Literacy Day
Sancha, 'ika Day
Internal onal Cross-Cultural Day
1
2
3
4
5
i
ft
16
7
8
9
10
11
12
113
14
15
16
17
18
19
I 20
21
22
23
24
25
26
I 27
28
Child Groups are Expressing & Advocating their issues through Media
like Recording Cd’s, Cultural Campaigns & Press Meets with the support
of VW & Tdh(G)
_29_ ___ 3(L
16th
17th
23th
24tlt
27th
28th
Ozone Day
International Day For Peace
World Deaf Day
Girl Child Day
World Tourism Day
World Heart Day ’
®63<5-24: && Sosj’ji aS'rfro,
S?o<3
636^0-25: &>{£> ao6§ t&tiorp
Sty6
Sb 26333 26£5p(5&>o.
es§g£-26:
336^oS£ s»3 s>s5&5o6ss’& Sjrgtxcd l&Sbejgo &oa
225c&o Szo3
September
2009
October
01st
O3rd
05th
9th
13th
ec^C-27: «5ooO foti&ccorS rfiSeSo oQojfe”
£o J)Ci;rta$u&
S>oB &>&|j
S6&5-28: SB; s>oB s5«&j
sg^e-29: St>
& ^&tg^'&os>oaoi3 aeS&o &>&(xl>:&,
3eoS5e& rvBgoB 2i53oB acScRSj S°oc5
World Elders Day /
Universal Children’s Week
Child Protection Day
World Habitat Day
World Mental Health Day
International Day for Disaster Reduction
16th
17th
29th
30th
Capacity building Apings to teachers and Government officials was given to update
them with the latesunformation related child rights and issues with the support of VW
& Tdh(G)
Trainings to Teachers and
Govt. Officers on CRC
World Food Day
Anti Poverty Day
UNO Day
World Thrift Day
1
Tue
15th
16th
19th
20lh
25th
CRC week celebrations are held during 14-21 November every year.
Various compitetions are held for the children during this week. Interfaces
are planned with policy makers & Planners, media and police with the
support of VW & Tdh(G)
^¥ed
National Cooperative Week
International Day lor Tolerance and Peace
National Integration Day /
Child Abuse Day
CRC Day
International Day on Violence against Women
.. Thu ...
Fn
&
.
1
2
3
6
7
8
9
10
13
14
15
16
17
20
21
22
23
24
27_
28
29
JO
31
®0&!>-30: So
n°<s S’&j, & '4>S5”rs
s’oo XiSijcXbo eatoeMM&tS “^P<303(5-32:
So O&&,
SP Sdi&oc” aoctuo
_
e> estsWiS
e)
ssose-33:
si>oei>e>& swiSoo. £sc&»fi> 3d&i>o, 5°?ot>o
JS[OV6ITllO0T
Telephone n^pbers of
Dist. Collectors
Telephone numbers of
Superin+endets of Police
SM3
District
Telephone
Office
District
Resi
1.
ADILABAD
08732 221533
08732-226538
2.
ANANTAPUR
08554-240105
08554-274602
3.
CHUT00R
08572-226528
08572-226760
4.
CUDDAPAH
08562-221901
08562-244303
5.
EAST GODAVARI
0884-253000
0884-251644
1.
ADILABAD
Telephone
Office
Rest
08732-226203
08732-226202
08534-2 KSl)l>
08554-240801
08572-227200
08572-227201
cclectci adb@3p.gav.!n
2.
elector atp@ap gov.in
3.
elector ctr@ap.gov.in
MOA’AH
08562-24431)1
08562-244437
5
Ca'sctDT cdp@ap.gov.in
tASI G00AVAHI
244070
0884-2361200
244168
0884-2361300
CoSector eg@ap.govin
GUNTUR
0853-2234000
0863-2252100
7.
KARIMNAGAR
0878-2262303
0878-2242303
8.
KHAMMAM
08742-220000
08742-225005
T“
9.
KRISHNA
08572-223600
08752-223565
10.
KURNOOL
0S518-225600
08518-225700
6.
GUMIUB
0803-2234200
0063-2234550
7.
CoSector gni@ap.govin
HYDERABAD
040-23207833
0878-2242303
Col-actor hvd@ap gov.in
kAA;MMZgA!i
08722-2242541
08722-2242028
IT
Co-lactur kmnr@ap.guv.in
KHA.MMAM
00742-224012
08742-224917
ID.
CoL'cctor Kmm@ap.gov.in
KiHSHNA
O0672-?528d2
08762-252000
252222
223770
MAHABUB NAGAR
08542-243300
08542-243399
....
4.
6.
11.
MTfuM
Cd cctor krsn@ap.gov.in
11.
kuhnOOl ’
’
08510-220396
08518-220131
Collector knl@ap.gov.in
12.
MaHAMNaGAH
08542-242210
08542-242323
12.
MEDAK
08455-256600
08455-256700
NALGONDA
08682-232306
08582-232304
13.
Collector mbhr@ap.gov in
MEUAk
00455-276555
244136
08456-276712 "
13
14
NEllORE
0851-2331700
0661-2331633
14.
el ector mak@ap.BOv.in
NALG0NUA
08682-23Z332
08682-232940
276556
232345
Collector nig@ap gov.in
15.
NIZAM ABAD
08462-232203
08462-232309
1b.
NELLORE
0061-2331999
0861-2325025
2331235
Coilectsr n!r@ep.gov.in
08462-231552
16.
PRAKASAM
08592-231300
08592-232701
IS.
17.
RAN3A REDDY
040-2551600
040-2551601
17
PRA&sAM
08532-231222
08592-231443
18
Wector org@ap.govjn
HANGA REDDY
040-23235642
040-23315154
19.
Cc-iectnr nlq@ap.gnv.in
SRIKAKULAM
08942-222555
08942-222505
20.
VISAKHAPATNAM
0891-2563257
0891-2526999
21.
CoCector vsk@ap go-v.in
^ZJANAGARAM
08922-226720
08922-276177
22
Collector vznm@apgov.in
WARANGAL
08712-25/8315
08/12-2578017 ’
00812-230051
08812-230151
UZAMABAU
08462-231002
231602
CoSector nzb@ap.gov.in
2551602
18.
19.
20.
21.
SRIKAKULAM
V1SAKIIAPATNAM
VIZ1ANAGARAM
WARANGAL
08942-222508
0891-2551550
08922-226163
0870-2578114
08942-222556
0891-2754431
08922-226937
0870-2578115
2577518
22
WEST GODAVARI
08112-232662
222648
Collector wgl@ap.gov.in
08812-230503
230760
23
G
VI:si uoavahi
Coilcctor wg@ap govm
231844
€36^-42: aDOCO, wgco.
3£c& spo©
a,£oe3££ rbQoO o6n°z3°J6
&oc°D. loo£b^° '^es^o^&s
foQoQ SDc&Sdip©.
gsS£(S-43 : (&&>«$ c^osc^cr ££££ sj^eSc&j g>£xx> ^c&Csofi5
S'cPo (aS^s^ex) ^°§>oOXS
(oSfiSS ?o£osoSo<&>^ rF&>
?6o£do
Sd^souy’O.
Child Rights Resource Centre
2nd Lane, Sujatha Nagar, Lawyerpet Extn.,
ONGOLE - 520 002. Tel: (08592) 221209 / 270664 / 281738
E-mail: helpap2002@yahoo.com website : www.helpap.inwww.traffickinginap.com
Position: 1371 (11 views)