SDA-RF-CH-2.3.pdf
Media
- extracted text
-
Page 1 of 1
SDA-RF-CH-2.3
Enter the Sunshine
department
Be our Partners in
Public Health
*
How will your work help the common man on the street?
Su khatme
«
Prof P V
Interdisciplinary School of Health Sciences,
University of Pune, Pune 411007, India.
Phone: 91-20-25691758
Telefax:
91-20-25690174
E-mail questions and comments to shs@unipune.ernet.in
#
http ://www. unipune. ernet. in/dept/shs/home.html
3/26/2002
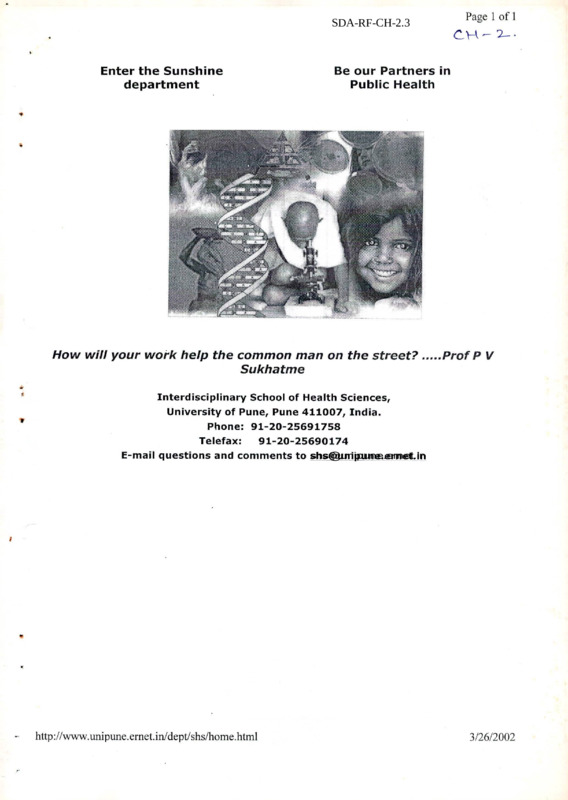
Figure 1
Maternal Mortality Rates (MMR) in
major states
INDIA
453
West Bengal
389
Uttar FYadesh
■'
1624
-
Tamil Nadu [
| 376
i
Rajasthan [
J 550
Punjab [
Orissa
1369
t
J 738
J 336
Maharashtra
1711
Madhya Pradesh
i
Kerala [
Karnataka [
187
I
1450
Haryana [
1436
I
Gujarat [
1389
i
Bihar [
1470
I
Assam [
.Andhra Pradesh [
J 544
1436
MMR 1992
Source : The Progress ofIndian States, UNICEF, New Delhi, 1995.
*
Finally, we may place Karnataka on the all India scale in respect of the life expectancy at
birth of its citizens (See Table 3). The International Conference on Population Development
(ICPD) had resolved in 1994 to target a life expectancy of 70 by 2005 and of 75 by 2015.
Against this. Karnataka has achieved a life expectancy at birth of 62 which is slightly higher
than the national level of 60. Kerala, Maharashtra, Haryana, Tamilnadu and Punjab alone
among the Indian states are ahead of Karnataka in this area.
5
The Interdisciplinary School of Health Sciences is one of the 44 departments of the Unive... Page 1 of 1
The Interdisciplinary School of Health Sciences is one of the 44 departments of the University of
Pune. The vision of late Prof P V Sukhatme (Padmabhushan), the School was established in 1989
through funding support from the University Grants Commission (UGC). The UGC was Chaired
during that period by Dr Manmohan. Singh, current Prime Minister of India.
The School has now evolved into a premier teaching institution in the field of Health Sciences. The
goal of the teaching programme is to train manpower, primarily students with an undergraduate
degree in the biological, social or clinical sciences to work in the field of public health.
The curriculum has a unique interdisciplinary approach, with an emphasis on learning through
extensive field work.
The School offers two Masters degrees :
- Master of Public Health(MPH) leading to a public health and epidemiology
specialization and
— Master of Health Sciences leading to specialization in biological sciences related
to health and disease, with primary teaching focus on human molecular genetics,
recombinant DNA technologies and their applications to human disease
diagnostics, vaccines, genomics of infectious agents etc.
With many shared courses, the objective of the Health Sciences curriculum is to ensure that
students from a biological sciences background and with laboratory skills in microbiology,
biochemistry, genetics and molecular biology have sufficient community exposure and are aware of
the diseases of public health importance and of the public health priorities of the country, whilst
public health students from non-biological disciplines are made aware of the recent technological
advances in bio-medical sciences
http://www.unipune.ernet.in/dept/shs/courses.html
3/26/2002
Regional disparities in human development
There were serious regional disparities in the levels of human development of the Kannada
speaking people due to their dispersion in different political units, each of which had its own
priorities and policies. Developmental imbalances within the new state of Karnataka are a part
of its historical legacy. The new areas added to the princely state of Mysore in 1956 were at
different levels in most areas of economic and social development. Before independence, old
Mysore enjoyed the reputation of being one of the most progressive regions of the country. A
modern system of education was established in Mysore as early as in 1833. As a, result,
before independence, when only 16.6% of the country's population was literate, 20.3% of the
people of old Mysore came within this category.
In Bombay Karnataka, a modem system of education was established in Belgaum as early as
1826 and Kannada schools set up after 1836. By contrast, Hyderabad Karnataka did not have
a degree college in the district capital before the merger with old Mysore.
Basic health services were also a priority of the princely state of Mysore. In 1806, it was
perhaps the first state in the country to take up vaccination against small pox. A government
hospital was set up in Bangalore in 1846 and the first public health unit opened in Mandya in
1929. The state had established Public health centres as the principal units for basic health
care and undertaken extensive measures to control communicable diseases like malaria well
before independence. The government of Mysore in 1930 set up the first two birth control
clinics in the world. In the other two regions, however, progress in social services-health,
drinking water and roads-before reorganisation was not encouraging. Connectivity between
headquarters towns of districts and taluks was very poor in Hyderabad Karnataka region
before the merger.
*
Significant divergence in the availability of social infrastructure in different regions was not
the only major problem facing the new state of Mysore. The overall levels of literacy and
health had also to be substantially raised for the entire population. In 1956-57, the state had
an enrolment ratio in primary schools of only 36.5%. Per capita expenditure on education
was around Rs. 5 and that on medical services around 76 paise!
Th e condition of women in terms of marriage practices, inheritance rights and social status
continue to be a matter of concern in all regions of the state. Low age at marriage for
women, high female mortality rates, poor levels offemale literacy and high dropout rates
among girls still characterise Karnataka.
Karnataka and India
A bird’s eye view of where Karnataka stands today as far as human development is
concerned within the country as a whole is given below. A look at four indicators should
give us an idea of how far Karnataka has gone in providing basic health facilities to its
people. These are the gender ratio, the infant mortality rate, the maternal mortality rate and
life expectancy at birth.
As far as the gender ratio is concerned only Kerala has come close to the levels attained in
developed countries (See Table 2). In other states, the gender ratio (that is the number of
women per thousand men) is still adverse due to prevalent social and cultural factors. In
Karnataka, there are only 960 women for every 1000 men according to the 1991 census. This
is worse than the position in Kerala, Andhra Pradesh, Orissa and Tamilnadu. It is also
disturbing to note that the gender ratio has worsened between 1981 and 1991 in Karnataka
3
Centre of Social Medicine and Community Health (CSMCH)
Page 1 of 4
Centre of Social Medicine and Community Health
Faculty Profile | Program of Study
4
The Centre of Social Medicine and Community Health (CSMCH) is one of the eight Centres of
the School of Social Sciences. These Centres were conceptualised by eight Special Committees that
outlined the academic challenges that needed to be addressed by the Centres of JNU.The Special
Committee of the Centre of Social Medicine and Community Health, which visualised the objective
and the scope of the Centre, recognised the critical need of both delineating a field of enquiry in the
discipline and generating a data base for public health in India. It emphasised these needs and
placed them high on the Centre?s agenda along with the task of training both social scientists and
physicians of academically applying them selves to the huge tasks of public health in the country.
/
The recognition'tkiat the discipline of Preventive and Social Medicine needed to be strengthened was
the major impetusXQr establishing the Centre of Social Medkine and Community Health in the
Jawaharlal Nehru Univ&F^ity. The Centre was set up outside the confines of a medical college so that
it could enrich itself throbgh wider interaction with the various\disciplines of natural and social
sciences.
/<
Over the past 25 years, the Centre has acquired the rich experience of evolving problem-oriented
interdisciplinary academic programmes in addition to building an active research base. At the same
time, efforts have also been made at constructing ihstttuti on a I links with policy maklpg.
Under the overall objective of creating academic programmes for making health services meaningful
to the people of the country, the CSMCH set out its objective to understand the health problems and
health needs of the Indian people with a view to find workable solutions for them in the existing
social structure and to examine the social structure itself to delineate the structural constraints
which limit the scope of health interventions.
The task obviously requires an intfc^-disciplinary approach involving disciplines such as sociology,
anthropology, psychology, econornhs^, history, politics, demography, statistics and public
administration, apart from the discipline^that are traditionally included in public health. It was for
this reason that the Centre was located in the School of Social Sciences.
Thrust Areas and Perspective plans
The Centre is poised to take up new challenges in the late nineties as public health has emerged as
an important area of research at the national and international level. The following are the thrust
areas of the Centre:
- Health service systems research;
- Epidemiology of diseases with special reference to communicable diseases, their resurgence and
new epidemics;
- Quantitative epidemiology;
- Nutrition and health with a special focus on the vulnerable;
- Population policies;
- Environment and health including worker?s health;
- Medical sociology, medical anthropology and health economics;
- Political economy of health;
http://www.jnu.ac.in/Academics/Schools/SchoolOfSocialSciences/MedicineCenter.htm
3/26/2002
Nearly a quarter of all mothers did not receive a single dose of tetanus toxoid; threefourths of births were to mothers who had received iron and folic acid tablets.
While knowledge about contraception is nearly universal, this remains mostly limited to
female sterilization, with 41% of currently married women being sterilized.
Table 6
Table 7
HDI ranking oftop 5 and bottom 5
districts of Karnataka at the
global level
D istrict
Kodagu
Bangalore Urban
D akshina Kannad
Uttara Kannada
C hikm agalur
Mysore
B e Ila ry
B id a r
G ulbarga
R a ic h u r
A
STATE
TND IA
W ithin State
1
2
3
4
5
Te
17
18
19
To
(0.630)
(0.60J)
(0.5 92)
(0.533)
(0.52 4)
(0.440)
(0.4 2 9)
(0.419)
(0.412)
(0.399)
(0.47 0)
(0.439)
G lob al
level
104
£10
11 1
123
124
133
135
138
139
142
131
134
N.B. : Figures in parentheses relate to HDI
values
Gender-related
Health Index
District
Bangalore Urban
Bangalore Rural
Belgaum
Bellary
Bidar
Bijapur
Chikmagalur
Chitradurga
Dakshina Kannada
Dharwad
Gulbarga
Hassan
Kodagu
Kolar ___________
Mandya
Mysore
Raichur
Shimoga
Tumkur
Uttar Kannada
STATE
GHI
1991
0.696
0.619
0.610
0.484
0.523
0.523
0.626
0.613
0.807
0.546
0.530
0.596
0.718
0.588
0.545
0.569
0.536
0.553
0.567
0.677
0.546
■
The survey also showed that while vaccination of children is fairly good for BCG. DPT
and polio, measles coverage continues to be low. With measles immunization coverage
at 67.3%, a tremendous effort is required, to increase the overall coverage.
■
Childhood diarrhoea is another area of concern; nearly 60% of children with diarrhoea
are not given ORS, nor the recommended home solution, nor even increased fluids.
While the prevalence of leprosy has declined considerably in the last few years from 4.08 in
1985-86 to 0.36 in 1996-97, HIV is emerging as a public health problem, with several
dimensions which are not yet full understood. Official surveillance centres have detected
3265 HIV positive cases and 120 AIDS cases. There have been 163 deaths due to AIDS.
Apart from the fact that existing data does not really capture the full dimensions of the AIDS
and HIV issue, other aspects of surveillance, counseling, etc. also need attention.
10
Centre of Social Medicine and Community Health (CSMCH)
Page 2 of 4
- Demographic history
The
ew areas that we need to initiate work in are:
Democratisation and decentralisation as alternative strategies for the delivery of health care;
Non-healtl
;ervice inputs into health;
* ^X^Urban health;\.
Health legislation;'
Bio-ethics;
Indigenous systems and^primary health care;
International trade, legislation and health;
Top
Academic Programmes
MCH Programme of Study
Physicians and nurses are offered admission to the Master of Community Health which is a pre-Ph.
D. programme. The student is required to complete and acquire a cummulative grade A- (FGPA6.5)
in the MCH programme before he/ she is admitted to the Ph. D. programme.
Eligibility for the Programme
♦
For admission to the MCH programme, the minimum requirement is a good MBBS degree or M. Sc.
in Nursing and one year experience in community health. The procedure for receiving applications,
screening and selection of candidates are laid down by the University.
Duration of the Programme and Credit Distribution
The Master of Community Health Programme is spread over 18 months, spanning three academic
semesters, including summer and winter vacations. While the students work for their course during
the semester, the inter-semester vacations are utilised for field work. In this programme, a student
has to earn a total of 36 credits. Of these, 9 credits are allocated to field-work and 27 credits are
allocated to course work. There are two types of courses- core courses and optional courses.
The credit distribution is as follows:
Core Courses: 14 credits
Optional Courses: 13 credits
Assessment of Students and Grade System:
The Assessment of a student is based on the students term papers, and end-semester written
examination and a viva-voce examination.
Course Outlines
The objective of the course structure of the MCH programme of studies is to expose the students to
the core areas in the field of Community Health and then allow them to ventures out into specific
areas in greater depth by selecting optional courses.
http://www.jnu.ac.in/Academics/Schools/SchoolOfSocialSciences/MedicineCenter.htm
3/26/2002
Crude Death Rate
The SRS estimate of the Crude Death Rate (CDR) in Karnataka for 1996 was 7.6 per 1000
population; again, it was higher - 8.6 - in rural areas and lower - 5.4 - in urban areas.
Decline in the CDR has been rather slow - 12.5 in 1975, above 10 but below 11 between
1980 and 1984 and ranging between 9.8 and 8.8 between 1985 and 1994. the CDR by district
has been estimated only for 1991 when it was 8.5 in the state; varying, nevertheless, from 7 in
Dakshina Kannada and Shimoga districts to 105 in Gulbarga. It was 10.5 in Bidar, 10.4 1
Bijapur and 10.3 in Dharwad.
Crude Birth Rate
The SRS estimate of the Crude Birth Rate (CBR) in Karnataka in 1996. was 22.7 per 1000
people; it was 24.2 in rural areas and 20.3 in urban areas. The CBR in Karnataka has been
fluctuating rather widely. It was 29.5 in 1975, 30.9 in 1984 and 1985, 30.1 in 1988 and 26 in
1994. According to the 1991 estimate, the CBR in Karnataka was 26.4; it ranged from 25.2 in
Chikmagalur and Dakshina Kannada to 30 and above in Bijapur, Gulbarga, Bellary, Hassan
and Raichur districts.
Maternal mortality rate
The maternal mortality rate of 450 per 100,000 live births in 1992 was still high when the
national average was 453; Significantly, neighbouring Tamilnadu had a maternal mortality
rate of 376 at the same time.
*
Gulbarga division, comprising the districts of Raichur, Gulbarga, Bidar and Bellary', along
with Bijapur district of Belgaum division, tends to be the most backward in terms of
demographic, social and health indicators. When the decadal population growth rate declined
in all districts except Bidar, Bijapur, Gulbarga and Raichur in the eighties, the annual
compound growth rates of these four districts increased from 1.99% in 1971-1981 to 2.25% in
1981-91, suggesting that decline in mortality has been more than the decline in fertility.
Expectedly, the lowest mean age at marriage (17.7 in 1981) is in the districts of Gulbarga
division, while Mysore division has both the highest mean age at mamage (20.4) as also the
most favourable sex ratio (993); the sex ratio in Gulbarga division is 964. The HDI ranking of
lowest 5 districts shows clearly that Gulbarga division is lagging behind the rest of the state
(See Table 6) and the Gender Related Health Index also depicts the backwardness of this
division (See Table 7).
■
The National Family Health Survey (1992-93) showed that mothers received antenatal
care in the case of 84% of the births in the four years preceding the survey, though
mothers in rural areas were less likely to visit an allopathic doctor for antenatal care: but
only 45% of the children bom to non-literate mothers received antenatal care from
allopathic doctor compared to 88% in the case of those who had completed middle
school.
While only 38% of live births were delivered in health institutions, one half of the
deliveries were attended by doctors or nurses and midwives; 22% of births were
delivered with the assistance of traditional birth attendants.
4
9
Centre of Social Medicine and Community Health (CSMCH)
Page 3 of 4
The course title, credit allocation and the broad content of the core courses and the optional courses
are as follows:
Core Courses
Course No.
Title
Credits
SM 620
Comparative Studies in Health
2
SM 602
Epidemiology
3
SM 603
Health Services and the Community
2
SM 604
Research Methodology
2
SM 605
Review of Current Issues In Community Health
4
Optional Courses
Course
No.
Title
Credits
SM 611
Population Problem and Family Planning Programme in India
3
SM 612
Communicable Diseases
3
SM 613
Nutrition and Maternal and Child Health
3
SM 614
Hospital Administration and Medical Care Services in India
2
SM 615
Vital Statistics and Health and Information System
2
SM 616
Health Manpower Planning in India
2
SM 617
Health Planning and Health Economics
2
SM 618
Community Health Nursing Education and Administration
3
SM 619
Rural Health Services Systems
2
SM 621
Operational Research and Systems Analysis in Community Health
Research
2
SM 640
Workers Health in India
2
Top
Education Programmes for Social Scientists
M. Phil. In Social Sciences in Community Health
The education and Training programmes for social scientists have been evolved with the idea of
making social scientists more effective members of a health team. The effort is to widen their social
science perspective through the prescribed courses. Apart from strengthening the understanding of
their basis disciplines, these courses underline the need for an integrated approach in the field of
applied social sciences and offer the student an opportunity to understand the problems of
community health. Students with a Master's degree in social sciences are eligible for admission to
programme of study.
Eligibility for Admission
The procedure for receiving applications, screening and selection of candidates are being laid down
by the University.
http://wwwjnu.acjn/Academics/Schools/SchoolOfSocialSciences/MedicineCenter.htm
3/26/2002
\
easily understood. Between 1951 and I960, life expectancy at birth in Karnataka was 41
years for men and 39 years for women- two years greater for men than for women. Between
1971 and 1980, however, life expectancy for women surpassed that for men., it was 56 years
for women and 55.5 years for men. In 1997, LEB was 66.3 years for women and 65.1 years
for men, still below the ICPD goal of a life expectancy at birth greater than 70-years by 2005.
At the national level, life expectancy at birth was 41 years for men and 40 years for women
between 1951 and 1960 and 51 years for men and 50 years for women between 1971 and
1980; it is expected to become 63 years for men and 64 years for women between 1996 and
2001. Comparing life expectancies for men and women in Karnataka with those for the
country, it is clear that between 1951 and 1960, the LEB for men in Karnataka was aligned to
the national rate; for women however it was greater by one year at the national level than in
Karnataka. Between 1971 and 1980, life expectancy was greater by 4.5 years and 6 years for
men and women respectively in Karnataka than for the country.
Comparing different districts in terms of life expectancy at birth, in 1981, it is seen that while
life expectancy at birth in Karnataka was 57.71 years, the highest life expectancy of 65.53
years was in Dakshina Kannada district and the lowest of 57.09 years in Chitradurga,
Dharwad and Gulbarga districts. Mandya and Shimoga districts had LEBs equivalent to the
state average of 57.71 years. In 1981, life expectancy was higher than the average in 9
districts, lower in 8 districts and average in 2 districts.
In 1991, life expectancy at birth in Karnataka was 62.07 years; it was 60.6 years for men and
63.61 years for women. Thus, in 1991, not only was life expectancy higher for women than
for men; the gap was also wider than before. Dakshina Kannada district registered the highest
life expectancy of 68.82 years and Bellary the lowest of 60.32 years - a difference of 8.5
years. The highest life expectancy for men, 65.34 years, was in Dakshina Kannada district
and the lowest, 57.12 years, in Bellary district. Life expectancy for men was lower than the
state average in 9 out of 20 districts.
The highest life expectancy for women, 72.49 years, was in Dakshina Kannada district and
the lowest, 63 years, in Tumkur district. The next highest is Kodagu district with a life
expectancy of 71.87 years. Close to the lowest life expectancy in Tumkur district was Bellary
with a life expectancy of 63.15 years. In all districts, without exception, life expectancies at
birth were higher for women than for men but differences between life expectancies for men
and women varied from one distnet to another. The difference in life expectancies for men
and women was about 9 years in Kolar and Hassan districts and only 0.62 years in Bangalore
(Urban) district.
Infant Mortality Rate
The Sample Registration Scheme has estimated the Infant Mortality Rate (IMR) in
Karnataka as 53 per 1000 live births in 1997; but the estimates of 63 for rural areas and 24 for
urban areas reveal the still large rural-urban difference which is typical of the country as a
whole. The urban IMR in Karnataka (24) in 1997 was lower than that in all states except
Kerala where it was 15. The country level IMR was 71; it was 77 in rural areas and 45 in
urban areas.
4
In 1981, the IMR for the state was 81 but it varied widely from one district to another,
ranging from 55 in Dakshina Kannada to 100 in Bijapur. In 1991, the IMR for the state was
74, down by 7 points from the 1981 level. At the district level, it ranged from 29 in Dakshina
Kannada to 79 in Bellary.
8
Centre of Social Medicine and Community Health (CSMCH)
Page 4 of 4
Duration of the Course and Credit Distribution
The course work shall be completed within the first two consecutive semesters and the whole M. Phil
programme (including dissertation) within the first four consecutive semesters.
The course work and dissertation together carry total of 24 credits . Distribution of credits for
various courses is as follows:
1. Core Courses: 12 credits
2. Optional Course: 6 credits
3. Dissertation: 6 cridits
Tog
http://www.jnu.ac.in/Academics/Schools/SchoolOfSocialSciences/MedicineCenter.htm
3/26/2002
Table 4
Estimates of crude birth rate and crude death
rate by district, 1991
C BR
Bangalore___________
B e 1 g a u m_____________
B ellary_______________
B i d a r_________________
B i j a p u r_______________
C hikm agalur_______
C h itra d u rg a_________
Dakshina Kannada
D harwad_____________
G u 1 b a r g a____________
Hassan_______________
K o d a g u______________
Kolar_________________
M a n d y a______________
M y s o r e_______________
Raichur______________
Shim o g a_____________
T u m k u r______________
Uttar Kannada______
KARNATAKA
I
C D R
26 .2
27.3
3 0.0
29.9
30,1
2 5.2
27 .4
2 5 .2
29.3
30.1
3 0.0
25.8
2 8.0
27.9
26.6
3 0.0
2 5.9
27 .4
26.4
26.4
7 .6
8.0
9.7
1 0.5
1 0 .4
8 .4
8.6
7.0
1 0 .3
1 0 .7
8 .2
7 ,9
8.6
9.1
8.8
9.5
7.0
8.2
8.5
8.5
Source : Estimates of Vital Rates for Districts of
Karnataka 1951-91 by Dr. P .J. B hattacharjee.
Director, Population Centre, Government of
K a rn a ta k a .
*
Life Expectancy at Birth
Life expectancy at birth (See Table 5) is the measure which is most often used and the most
Table 5
L i Te
expectancy
at birth in
D i s tric t
4
K arnatak
Males
by
district, 1991
Fem ales
Total
Bangalore Urban
6 5.48
6 6.10
6 5.78
Bangalore Rural
6 4.40
6 9.09
6 6.69
B e Ig a u m
6 4.06
6 6.15
6 5.08
B ellary
5 7.12
6 3.15
6 0.32
B id a r
6 1.23
6 6.38
6 3.74
B ij a p u r
5 9.33
6 6.38
6 2.76
C hikm agalur
6 2.47
6 6.87
6 4.62
C hitradurga
5 9.49
6 4.47
6 1.92
Dakshina Kannada
6 5.34
7 2.49
6 8.82
D h a r w ad
6 0.13
6 5.56
6 2.78
G u 1b a rg a
6 1.23
6 6.87
6 3.98
H assan
6 1.02
7 0.00
6 5.40
K oda g u
6 4.41
7 1.87
6 8.04
Kolar
5 8.54
6 7.42
6 2.87
M a n dya
6 0.12
6 8.03
6 3.97
M y so re
5 9.02
6 7.71
6 3.25
R a ich u r
6 1.76
6 9.53
6 5.55
Shim o g a
5 9.33
6 5.00
6 2.09
Turn k u r
5 8.39
6 3.00
6 0.64
Uttar Kannada
6 4.06
7 0.00
6 6.96
Source : Estimated
E s tim
by K .R . Narayana. Deputy Director,
Census Operations, Bangalore
7
Position: 1757 (8 views)