BREASTFEEDING PROMOTION NETWORK OF INDIA
Item
- Title
-
BREASTFEEDING PROMOTION
NETWORK OF INDIA - extracted text
-
SDA-RF-CH-1.11
Mi
„MES LIVES
BREASTFEEDING PROMOTION
NETWORK OF INDIA
Editor Dr S Snnnasan
.ICHEBPV-6.:
OFFICIAL NEWSLETTER
VOL. 3.
MAY - AUG.
for •R : v -\1 !: ( 1R<'« I.ATIOS
Ph<.
36380/89 Ex'-80
All women must receive the support necessary for her to
be able to make tnat choice. This means that her fears
about not being able to breastfeed must be dispelled, for
example with advice on breastfeeding techniques, on
how to position the child or how to express milk by hand.
Breastfeeding contributes to all aspects of child sur
vival: it is the single most important measure to prevent But this also means that society should assist her, and
diarrhoea. Breastmilk contains antibodies and live cells even encourage her. to make that choice, while, of
which provide infants with their first immunization: and course not exhorting them to breastfeed and creating
breastmilk is the perfect food for infants which ensures guilt in those who are not able to breastfeed.
appropriate growth. Exclusive breastfeeding is the only The realities of today s workforce certainty contribute to
single human activity that fulfills conditions for good
many individual women’s decision not to breastfeed. It is
nutrition, health and care.
not only the job which forces a woman to choose be
BREASTFEEDING - A WOMEN’S
ISSUE
Children breastfed for at least four months tend to
have over all reduced rates of childhood cancers, and
they are less likely to show symptoms of asthma and
skin allergies. Some studies show that the develop
ment of the brain and consequently the IQ might be
higher in breastfed children compared to bottle-fed
infants of the same socio-economic status. Last, but
not the least, breastfeeding leads to unparalleled
psycho-social bonding between a mother and her
baby.
Now why it is a women’s issue ?
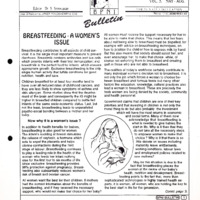
In addition to health benefits for babies,
breastfeeding is also good for women.
The infant's suckling at breast stimulates
the release of oxytocin, a hormone which
acts to expel the placenta and helps
uterine contractions during the third
stage of labour. Breastfeeding continues
to play a leading role in the health of the
woman who feeds her infant nothing
else for the first four to six months of life
since exclusive breastfeeding provides
98% protection against pregnancy. Breast
feeding also substantially reduces women's
risk of breast and ovarian cancer.
All women want the best for their children. If mothers
had the correct information about the benefits of
breastfeeding, and if they received the necessary
support, who would not make that choice for her baby?
tween breastfeed and formula feeds but many other
factors like education knowledge, cultural practices also
lead a woman to breastfeed. These are precisely the
tools women are being denied by the society, community
and health personnel.
Government claims that children are one of their key
priorities and that investing in children is not only the
moral thing to do but also probably the investment
which will have the most returns in economic
and social terms. Many of them now
acknowledge that breastfeeding is
what is needed to give babies the
start in life. Why is it then that they
do not take all the necessary steps
to empower women to make that
choice ? Why is it that there is so
little debate on issues including
maternity leave entitlements,
working conditions, labour laws
and employment policies related to
new mothers?
May be this situation is due to the
fact that breastfeeding places the
woman at the centre of her baby’s
health, nutrition and development. Breast
feeding points to the fact that, more than
sophisticated technologies or highly trained health ex
perts. it is women, all women, who are holding the key to
the best start in life for the generation.
Contd. page 3.
—| Editorial |-----------------------------------------------------------------
Training in breastfeeding and Lactation Management
Many mothers start artificial formula feeding to their
babies from early life, oven bolero Iho end of the first
month Hus practice seems to happen more ollon in
mothers who had institutional or hospital deliveries. A
single most important reason identified for this un
healthy practice is the lack of confidence among these
mothers who loll (hero was not enough breastmilk in
them loi Iho pmpoi and adequate growth of their ba
bies I ven when a mother feels confident about Iho
adequacy ol the breastmilk in her, relatives, neighbours
and visitors often pressurize and undermine this confi
dence Io make things woise, ovon Iho health care
piovidets including Iho family physicians, obstetricians
and child health specialists, either knowingly or un
knowingly give advices that lend to favour and support
aitilicial milk formula feeding from early months of life.
Such professional advices come in conflict with estab
lished practices and naturally confuse tho mother
further more.
Replacement of breastmilk with artificial milk formula
ovon in tho presence of breastmilk occurs so regularly
much before the appropriate time (4-6 months after
birth), tliat a strategy has to be dovised and imple
mented to curtail and dissuade this harmful practice.
The dangers of early introduction of artificial formula to
infants in the developing countries, where a majority of
population does not have access to safe drinking water,
aro well known. Many of these newborns and infants
develop repeated attacks of diarrhoea and chest infec
tions and suffer from ensuing malnutrition. Some qf
them even die of these infections and malnutrition. The
crux of the strategy to prevent this practice of early
introduction of artificial milk formula, is to educate and
convince all health professionals, health care delivery
workers and mothers logaiding tho advantages ol
exclusive broastlooding practices till Iho childion be
come 4-6 months old. Evon the other members of tho
family mainly tho husbands and the molhor-in laws
must also bo adequately motivated. Iho need ol tho
hour is development of training programs al all levels Io
disseminate the scientifically proven lacts regarding tlio
advantages and essentiality of exclusive breastfeeding
of infants, an important strategy in child survival pro
grams. Communication and other practical skills like
counseling must bo imparted besides theoretical knowl
edge in these training sessions.
bottle feeding. Invariably, the students were asked to fix
or attach the rubber teat properly on Io the mouth of Iho
loading bottles, an important skill to bo achieved by a
passing student. 'Hie students wore often seen memoriz
ing the compositions of artificial milk formula and the
subtle differences between them, before they went in for
their viva. Have things changed in tho past twenty years
or so ? It is difficult to answer this question. II at all,
changes have occurred in a tow colleges because of tlie
personal initiative of a few well meaning and motivated
teachers. Still there are institutions where the negative
aspects of the breastfeeding and positive aspects of
aitilicial formula feeding are highlighted, oilhor wittingly
or unwillingly.
As a post graduate examiner, it has been a common
experience to observe the inadequate training in this
important area. Students of child health are not in a
position Io answer the numtier ol lactiferous ducts and
the facilitating and inhibitory influences on breast milk
secretions, the anatomico-physiological dynamics of
breastfeeding, sucking and swallowing by the infants.
I
They are also not adequately prepared in communica
tion and counseling skills, very essential to convince the
mothers who are not confident about the adequacy of
breastmilk in them.
Many obstetricians and pediatricians who are sufficiently
informed about the advantages and necessity of breast
feeding have repeatedly expressed their practical diffi
culties in convincing tlie mothers to continue breastfeed
ing for a period of 4-6 months. Even in major leaching
institutions, mothers with twin deliveries - are not ad
equately motivated and their genuine doubts regarding
tho adequacy ol breastmilk for their twins' needs are not
dispelled from their minds I hose twins, though they aro
of adequate birth weights for survival, come back in the
neonatal period with diarrhoea and dehydration. Quite a
low of them even succumb in spite of best efforts. Tlie
only reasons for those episodes is withdrawal of breast
milk and substitution with artificial formula, often given in
bottles. All these deaths are avoidable If the mothers ate
given sufficient information regarding the advantages
and superiority of breast milk in the prevention of diar- (
rhoea and chest infections in their infants and about tlie
secretory dynamics and adequacy of breast milk oven to
feed twins and triplots. Health professionals who have
twins themselves can be trained to meet these mothers
and counsel them appropriately. Steps have been initi
As a pediatrician, my days as a post-graduate student
am remembered with regard to tho importance given to ated in this direction and training in breastfeeding and
breastfeeding and lactation management in Iho curricu lactation management aro being undertaken by various
lum. Retrospectively. I can definitely say this was woe bodies. Information regarding such similar training activi
ties in other areas are invited to be presented in ensuing
fully inadequate. Rattier, more stress was given to
issues of this bulletin.
artificial milk formula feeding. Even in the final Univer
Sincerely,
sity examination (both in diploma and degree courses)
Srinivasan.
questions were more focused on artificial feeding and
2 JfBPNI BULLETIN)
Contd. page 1.
It is women who are the holders of the possible re
source for everyone's future. As for many other’ com
modities’ produced by the less powerful, breastmilk is
undervalued and those who produce it. women, are
kept in the dark about its value and not supported to
exploit to their full potential.
It is time society supports these commitments and
ensures legislative and other measures to carry out its
responsibilities to protect and support breastfeeding in
the county, this is very much a women's issue.
We have a legislation to control marketing of breastmilk
substitutes which has come into force since December
1992 and prohibits free or subsidized supplies of infant
formula and bans all types of aovertisements. This
legislation is to control some of the bad practices
adopted by the industry and not to exhort women to
breastfeed.
We need a legislation to empower all women to have an
access to the right information and improving existing
maternity leave benefits. This is then all women should
choose by themselves between the two, Breastfeeding
and Artificial Feeding.
Arun Gupta.
I "We allowed
tke companies
I to touck the I ives
I of our babies?
I not because we
| did not care, but
| because we did
| not realise the
| consequences
| of granting suck
| a previlege."
Dr. N.CIavano
Phillipines
BREASTFEEDING PAPER OF THE MONTH -JUNE 1993.
BPNI team from Davangere. Drs. N. Kesaree, C.R.
Banapurmath, Shobha Banapurmath and
Kalllnath Shamanur.
"Treatment of inverted Nip
ples using a disposable
syringe"
Published in Journal of
Human Lactation 9(1),
1993 27-29 and declared
to be breastfeeding paper
of the month June 1993 by
UNICEF Headquaters,
New York.
The nozzle end of a 10 ml.
plastic disposable syringe
is cut off (Figure A: Step
one). The piston is intro
duced from the ragged cut
end side (Step two).
The mother then applies
the smooth end to her breast and pulls on the piston
gently and holds in that position for about ajninute
(Step three). Nipple protrudes out into the‘ syringe.
The mother reduces the traction whilerele’asing the
syringe. The nipple stays protruded for sometime and
immediately the baby is put to the breast. As the
nipple is easily taken into the mouth, the baby is able
to suckle in a proper position.The nipple retracts
again after a while but not
to the same extent. The
procedure is repeated sev
eral times a day for a cou
ple of days.
This corrects the retraction
permanently in almost all
cases due to the following
actions:
1) Suction by syringe fol
lowed by
2) Suckling by the baby.
It is a simple method to
follow. Physician ora nurse
has to demonstrate only
once and the mother learns
the procedure without any
difficulty.
fBFNI BULLETIN) f~T)
World Breastfeeding Week (WBW)
1-7 August, 1993
Thame for 1993.
BREASTFEEDING. WOMEN AND WORK
MOTHER-FRIENDLY WORKPLACE INITIATIUE
WHY WOULD BRI ASIFEEDING WEEK?
The world Alliance for Breasteeding Action (WABA)
organises World Breastfeeding Week (WBW) as part of
its global mobilization strategy to increase public aware
ness on the importance ol breastfeeding. From 1-7
August every year, communities around the world cart)
paign to revive and maintain a natural breastfeeding
culture worldwide. Although WABA works on the promo
tion of breastfeeding all year round, it uses WBW as a
particular time when attention of tho wider public can lie
locussod and activities can bo concentrated. WBW also
allows WABA to coordinate ellorts to meet the targets of
tlio Innocenti Declaration. This Declaration states that by
199f> all governments should have
" a National Breastfeeding Coordinator and a
multi sectoral National Breastfeeding Committee;
■ ensured that every facility providing maternity
services practice all ten of the Ten Steps to Successful
breastfeeding as outlined jointly by WHO and UNICEF;
‘ ensured that the International Code of Marketing
of Breastmilk Substitutes is implemented, and
‘ enacted imaginative legislation protecting the
breastfeeing rights of working women and established
moans lor its enforcement.
II10 goals of WBW 1993 are:
* To create public awareness of tho rights of working
women to breastfeed.
‘ To facilitate and protect cultural/traditional prac
tices which are supportive to tho breastfeeding mother
working at or away from homo;
‘ To involve community loaders and other
popular groups (ecological, women and development
groups) to develop tho social support neodod for women
in all sectors to combine breastfeeding and work.
Baby Friendly Hospitals
Following hospitals in India have
been certified to be Baby Friendly
Hospitals, which follow 10 steps to
successful breastfeeding.
DELHI
Jaipur Golden Hospital
MADRAS
Kaslurba Gandhi Hospital
CSI Kalyani Hospital
Institute of Obstetrics & Gynaecology
R.K. Maternity Hospital
Vijaya Hospital
Public Health Centre
HSRM Hospital
Nagamani N I lospilal
Perumal Pet Health Post
Shenoy Nagar Health Post
Ayanavaram Health Post
(*T) (BPNI BULLEIIN)
Sanlhomo Health Post Hospital
Poonnammal Women and Children
Hospital
Saidapet Health Post
Mondithope Health Post
Durgabai Doshrnukh Hospital
Vadapalani Zone P.P.P.
Voluntary Health Services Hospital
Sanjoovanaryan Pot Health Post
Rajah Muthiah Medical College and
Hospital
Jyothi Nursing Home
BOMBAY
L.T.M.G. Hospital
B.V.L. Nair Hospital
RN. Cooper Hospital
Nandini Hospital
Jaslok Hospital
K.E.M. Hospital
Municipal Maternity Home
WORLD BREASTFEEDING WEEK AUG 1-7
CONSENSUS DOCUMENT
ON
INFANT NUTRITION
Let’s All Say The Same Thing
Conflicting messages on infant nutrition over the years has caused a great deal of confusion among
mothers. It is the baby who loses out.
Protect the infants cf this Nation. Share the following messages with every mother you come in touch
with.
1. Start breastfeeding within one hour of birth in normal
deliveries and 4 hours in C-section deliveries
2. Only mother’s milk is required in the first 4 to 6
months. No need for any supplements of water, milk
or other fluids and foods
3. Avoid bottle-feeding at all ages
4. Solids, preferably home made, should be started after !
4 months and definitely not later than 6 months
BREASTFEEDING PROMOTION
NETWORK OF INDIA
1’0 Sox-10551 Delhi 11003',.
es : 7227:52. 7211435
7.1.x : 91-1 !-572661 2
B P n I
BREASTFEEDING,
WOMEN AND WORK
MOTHER-FRIENDLY WORKPLACE INITIATIVE
World Breastfeeding Week (WBW) 1 - 7 August, 1993
WHY WORLD BREASTFEEDING WEEK?
The World Alliance for Breastfeeding Action (WABA) organises World Breastfeeding Week (WBW) as
part of its global mobilization strategy to Increase public awareness on the importance of
breastfeeding. From 1-7 August every year, communities around the world campaign to revive and
maintHin a natural breastfeeding culture worldwide. Although WABA works on the promotion of
breastfeeding all year round, it uses WBW as a particular time when attention of the wider public can be
focussed and activities can be concentrated. WBW also allows WABA to coordinate efforts to meet the
targets of the Innocenti Declaration. This Declaration states that by 1995 all governments should have:
• a National Breastfeeding Coordinator and a multi-sectoral National Breastfeeding Committee;
•
ensured that every facility providing maternity services practice all ten of the Ten Steps to
Successful Breastfeeding as outlined jointly by WHO and UNICEF;
•
ensured that the International Code of Marketing of Breastmilk Substitutes is implemented; and
*
enacted imaginative legislation protecting the breastfeeding rights of working women
and established means for its enforcement
BABY-FRIENDLY HOSPITAL INITIATIVE (WBW 1992):
WABA launched the first WBW on the theme of the Baby-Friendly Hospital Initiative (BFHI), on 1
August 1992. The aim of the BFHI is to encourage all institutions and facilities providing maternity
services to practice the 10 Steps for Successful Breastfeeding as suggested in a WHO/UNICEF Joint
Statement This initiative has made almost 70 countries around the world recognize the importance of
breastfeeding and encouraged them to initiate activities and programmes in support of breastfeeding.
More and more hospitals are now converting their institutions into baby-friendly facilities. WABA's
Baby-Friendly Hospital Initiative Action Folder has been a key instrument in aiding groups promote tiie
BFHI.
MOTHER-FRIENDLY WORKPLACE INITIATIVE (WBW 1993):
The challenge now for WABA is to take baby-friendliness outside the hospitals into other parts of society,
For WBW 1993, WABA intends to highlight the situation of breastfeeding mothers in their workplace to
create environments supportive of breastfeeding everywhere. The Mother-Friendly Workplace Initiative
(MFWI) is WABA’s theme for next year. WABA hopes that through this initiative, the home, streets,
markets, farms, offices, factories and other workplaces - both formal and informal - will become more
mother-friendly work environments. We realize that although this is an enormous and difficult
challenge, nevertheless, it is one which is vital. The initiative therefore needs concrete adion to support
the rights of women and children to breastfeed. Our common task is to ensure that worsen are able to
successfully combine breastfeeding and work, be it work at home or jn_paid employment
The goals of WBW 1993 are:
'
•
'
*
■
'
To create public awareness of the rightsof working women to breastfeed;
To facilitate) and protect culturnl/traditional practices which are supportive to the
breastfeeding mother working nt or away from home;
To involve community lenders and other popular groups (ecological, women and
development groups) to develop the social support needed for women in the informal and agrarian,
sectors to combine breastfeeding and work;
To have more trade unions demand maternity rights and provide a supportive work
environment for all women workers who choose to breastfeed (eg. a creche, better transport, etc.);
To ensure that national legislation to protect the breastfeeding rights of working women is
implemented in as many countries as possible; and
To make ns many workpl.ices as possible become Motlior-Friondly.
Suggestions for Action: •
•
•
•
•
•
•
•
discuss with co-workers and friends the importance of breastfeeding;
set up a (mother) support group at your workplace to discuss how to make your work environ -nent
more suitable for breastfeeding; take these ideas to your employer,
contact your union, if you have one, or the closest worker support group or community
representative to discuss breastfeeding and the need for adequate maternity' entitlement? and a
supportive work environment for breastfeeding;
be more involved with union decision making and help get breastfeeding support mechanisms on
the list of priority demands;
find out about maternity legislation in your countiy and start to collaborate with your employer on
implementing such legislation at your workplace;
contact groups working on breastfeeding in your country/region and inform them about the MFWI
to coordinate efforts;
involve the media in publicising the Initiative;
if you’re an employer, adopt measures necessary for a supportive work environment and be an
example to other employers;
WABA plans to produce an Al'llt’llJ-L'llltr and a basic information kit for WBW 1993. WABA invites
volunteers to help translate these materials into local languages for popular mobilization in your country.
if you need more information or have any interesting ideas for WBW 1993 in terms of publications,
advocacy and display materials, uetivities/progrummes, networking, etc., please contact either one of the
following:
Surah Amin
WABA Secretariat
1’0 Box 1200
10850 Penang
Malaysia
Tel: 60-4-884 816
Fax: 60-4-872 655
WABA
Marta Trejos, Coordinator
Social Mobilization Task Force
CEFEMINA
Apartado 5355
1000 San Jose, Costa Rica
Tel: 506-244 620
Fox: 506-346 875
WABA is a global network,of organizations and individuals who believe
breastfeeding to be the right of all children and mothers, and who
dedicate themselves to protect, promote and support this right WABA
acts on the InnoconG DeclaraUon and works in close liaison with
UNICEF.
- Media
 SDA-RF-CH-1.11.pdf
SDA-RF-CH-1.11.pdf
Position: 3497 (3 views)