SCN NEWS
Item
- Title
- SCN NEWS
- extracted text
-
Ch 1.3
UNITED NATIONS
NATIONS UNIES
ADMINISTRATIVE COMMITTEE ON COORDINATION - SUBCOMMITTEE O INNUTRITION
May 1991
Extracts from:
SCN NEWS
A periodic review of developments in international nutrition
compiled from information available to the ACC/SCN
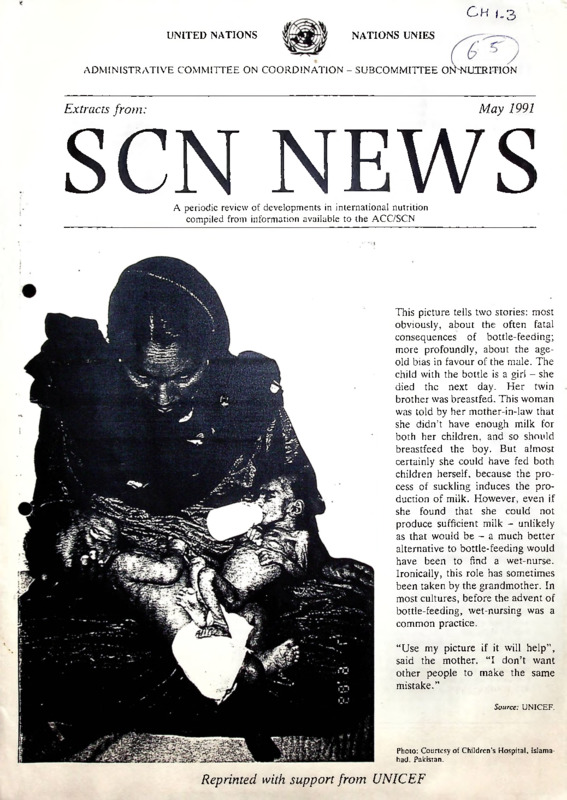
This picture tells two stories: most
obviously, about the often fatal
consequences of bottle-feeding;
more profoundly, about the ageold bias in favour of the male. The
child with the bottle is a girl - she
died the next day. Her twin
brother was breastfed. This woman
was told by her mother-in-law that
she didn’t have enough milk for
both her children, and so should
breastfeed the boy. But almost
certainly she could have fed both
children herself, because the pro
cess of suckling induces the pro
duction of milk. However, even if
she found that she could not
produce sufficient milk - unlikely
as that would be - a much better
alternative to bottle-feeding would
have been to find a wet-nurse.
Ironically, this role has sometimes
been taken by the grandmother. In
most cultures, before the advent of
bottle-feeding, wet-nursing was a
common practice.
“Use my picture if it will help”,
said the mother. “I don’t want
other people to make the same
mistake.”
Source: UNICEF.
Photo: Courtesy of Children’s Hospital. Islama
bad. Pakistan.
Reprinted with support from UNICEF
Extracts from SCN News - Mav 1991
The Lesser Child
“In a culture that idolizes sons and dreads the birth of a
daughter, to be born female comes perilously close of being
born less than human. Today the rejection of the unwanted
girl can begin even before her birth: prenatal sex determi
nation tests followed by quick abortions eliminate thou
sands of female foetuses before they can become daughters.
Those girls who manage to survive till birth and beyond find
that the dice is heavily loaded against them in a world that
denies them equal access to food, health, care, education.
employment and simple human dignity.
figures became 86% compared with 63%: and preschoolers
72% aeainst 65%: This also illustrates that the effects are
particularly severe in the first year of life, and suggests that
girls become relatively' better able to look after themselves
as they grow older. The morbidity patterns quoted, from
rural Tamil Nadu, show much higher incidence of diseases
such as respiratory infections among young girls; poig
nantly. the only condition in which boys are more affected
than girls is dental caries, perhaps resulting from the
observation made in “The Lesser Child that although
there are great variations in feeding practices across the
country, it is generally true that boys eat better than girls
even in privileged families. Sons are more likely to be given
milk, eggs, meat and fruit in their diet. As they grow older,
boys spend part of their earnings on food and snacks while
girls continue to eat the same unvaried diet at home.”
“Born into indifference and reared on neglect, the girl child
is caught in a web of cultural practices and prejudices that
The book, though short, makes the compelling point very
clearly and repeatedly. But it continues to suggest that not
only long term changes must be brought about, particularly
The photograph on our cover is horrifying. Another baby
girl dies unnecessarily. The Department of Child Develop
ment. Government of India, with assistance from UNICEF,
has produced a compelling account of the plight of “The
Lesser Child".
“Through a haze of heat and pain, Sushma hears the dai mutter ‘Another daughter’ and bursts into
uncontrollable sobs. Throughout her third pregnancy she has fasted and prayed for a son. Burdened
by the guilt of having two daughters, she has supplicated every deity she knows, praying to Shiva, to
Santoshi Mata, even walking to the outskirts of the village to prostrate herself at the grave of the Pir
Baba. Now the sound of her mother-in-law's wailing fills the air ...”
Source: "The Lesser Child”, p. 4.
through education, but that there are also programmes that
can be effective now. “The glaring disparity between male
and female infant mortality rates, if plotted on a map. shows
a clear belt running across the north-western part of the
country, with a few pockets elsewhere, and this is where
immediate health and nutrition interventions must now
focussed.”
divest her of her individuality and mould her into a
submissive self-sacrificing daughter and wife. Her labour
ensures the survival and w'ell-being of her family but robs
her not only of her childhood but also of her right to be free
of hunger, ignorance, disease and poverty.
“We expect tommorrow's woman to become the pivot of
social change and development. Yet today we deprive her of
her rightful share of food, schooling, health care and
employment, then marvel that she does not come running to
get her children immunized, or when she refuses to send
them to school or practice good nutrition, hygiene and birth
control ... Unless the girl becomes a priority in health,
nutrition and education policies, can there be Health for All
by 2000. or universal elementary education, or social justice
and equality? It is already late. But perhaps not too late.”
“The ICDS (Integrated Child Development Services)
network is clearly one effective response to the problem of
early neglect of young children. Through its immunization.
nutritional supplementation and pre-school education com
ponents (which now reach ten million children) it can offset
the discrimination a girl faces at home and can lay the
foundation for healthy physical and mental development.
But an urgent answer has to be found for meeting the needs
of girls in the 6-14 year age-group, for this is when they have
either dropped out of school or arc too old for ICDS and are
nobody's concern. They have to wait until they are 15,
which is when they become another target group that the
health system recognizes - “women in the reproductive agegroup”. Perhaps it is time to enlarge the scope of ICDS
projects so that they can include girls between the ages of 6
and 14 years. This is an important period in a girl’s life,
when major biological, psychological and social changes
take place. . . . repeated adolescent pregnancies, common
in many parts of rural India, arrest this growth spurt and
prevent hill physical maturation of the girl, affecting not
only her own health, but also the survival and development
of her offspring.”
A number of key statistics are used to illustrate the
problem. The sex ratio (females per thousand males) is
shown to have declined during this century, for example
from 972 in 1901. 950 in 1931, and down to 933 in 1981;
variation in the sex ratio between states is also illustrated,
with a high value of 1032 in Kerala, dropping to below 800
even in some states (although migration may account for
some of this, it clearly does not account for all). Anthropo
metric data also tell a sad tale: data quoted from one area
show, for example, these differentials for growth retarda
tion (adding mild, moderate, and severe). In infants, the
prevalence among females was estimated at 79%, versus
43% in males - almost double; in one to two year olds, these
2
Extracts from SCN News - May 1991
OPERATIONAL TARGETS (Proposed in the Innocenti Declaration).
All governments by the year 1995 should have:
*
*
appointed a national breastfeeding coordinator of appropriate authority, and established a multisectoral
national breastfeeding committee composed of representatives from relevant government departments, nongovernmental organizations, and health professional associations;
ensured that every facility providing maternity services fully practises all ten of the Ten Steps to Successful
Breastfeeding set out in the joint WHO/UNICEF statement “Protecting, promoting and supporting breastfeeding; the special role of maternity services”;
taken action to give effect to the principles and aim of all Articles of the International Code of Marketing
of Breast-milk Substitutes and subsequent relevant World Health Assembly resolutions in their entirety; and
enacted imaginative legislation protecting the breastfeeding rights of working women and established means
for its enforcement.
We also call upon international organizations to:
*
_
draw up action strategies for protecting, promoting and supporting breastfeeding, including global
monitoring and evaluation of their strategies;
support national situation analyses and surveys and the development of national goals and targets for
action; and
encourage and support national authorities in planning, implementing, monitoring and evaluating their
breastfeeding policies.
>-------------------------------------------------The Special Role of Maternity Services
A Joint WHO/UNICEF Statement entitled “Protecting, Promoting and
Supporting Breast-feeding, The special role of maternity services”, lays out
ten steps for maternity services; the Foreword by the Heads of the two
agencies stresses their universal relevance.
Foreword
In our world of diversity and contrast, we believe that
this statement on the role of maternity services in
promoting breastfeeding is striking for its universal
relevance. The principles affirmed here apply anywhere
maternity services are offered, irrespective of such labels
as "developed" and "developing". "North" and “South”,
"modern" and "traditional". And the health professionals
and other workers responsible for these services are well
placed to apply them by providing the leadership needed
to sustain, or if necessary re-establish, a "breast-feeding
culture”.
Ten steps to successful breast-feeding
Every facility providing maternity services and care for
newborn infants should:
1. Have a written breast-feeding policy that is routinely
communicated to all health care staff.
2. Train all health care staff in skills necessary to
implement this policy.
r 3. Inform all pregnant women about the benefits and
management of breast-feeding.
4. Help mothers initiate breast-feeding within a halfhour of birth.
5. Show mothers how to breast-feed, and how to
maintain lactation even if they should be separated
from their infants.
6. Give newborn infants no food or drink other than
breast milk, unless medically indicated.
7. Practise rooming-in — allow mothers and infants to
remain together — 24 hours a day.
8. Encourage breast-feeding on demand.
9. Give no artificial teats or pacifiers (also called
dummies or soothers) to breast-feeding infants.
10. Foster the establishment of breast-feeding support
groups and refer mothers to them on discharge from
the hospital or clinic.
While discoveries are still being made about the many
benefits of breast milk and breast-feeding, few today
would openly contest the maxim "breast is best". Yet
slogans, however accurate, are no substitute for action.
That is why we invite all those concerned with providing
maternity services to study this statement to see how they
are helping or hindering breast-feeding. Are they
encouraging and supporting mothers in every possible
way? We urge them, wherever they might be. to ensure
that their services are fully mobilized to this end and
thereby to bear witness to the unequalled excellence of
breast-feeding for infants and mothers alike.
Hiroshi Nakajima. M.D.. Ph.D.
Director-General
World Health Organization
Source: “Protecting. Promoting and Supporting Breast-Feeding The special role of maternity services." A Joint WHO/UNICEF
Statement. WHO. Geneva. 1989.
5
James P. Grant
Executive Director
United Nations
Children's Fund
Extracts from SC\ News - May 1991
Facts for Life
Of the many publications available emphasizing the importance of breastfeeding, one of the most accessible is Facts for
Life" sponsored by UNICEF, WHO and UNESCO in partnership with many of the world’s leading medical and children’s
organizations. Here are some specific messages on this topic.
What every family and community has a right to know about breastfeeding
Babies fed on breastmilk have fewer illnesses and less malnutrition thun babies that are fed on other foods.
Bottlefeeding, especially in poor communities, is therefore a serious threat to the lives and health of millions of children.
Source: "Facts for Life: A Communication Challenge." UNICEF. WFIO and UNESCO. 1989.
Bottlefeeding can lead to serious illness and death.
Breastmilk alone is the best possible food and drink for a
baby in the first four-to-six months of life.
*
*
*
*
•
*
From the moment of birth up to the age of four-to-six
months, breastmilk is all the food and drink a baby
needs. It is the best food a child will ever have. All
substitutes, including cow’s milk, milk-powder solu
tions. and cereal gruels, are inferior.
Even in hot. dry climates, breastmilk contains sufficient
water for a young baby's needs. Additional water or
sugary drinks are not needed to quench the baby's
thirst.
Breastmilk helps to protect the baby against diarrhoea.
coughs and colds, and other common illnesses. The
protection is greatest when breastmilk alone is given to
the baby during the first four-to-six months.
Other foods and drinks are necessary when a baby
reaches the age of four-to-six months. Until the age of
nine or ten months, the baby should be breastfed before
other foods are given. Breastfeeding should continue
well into the second year of life - and for longer if
possible.
Frequent breastfeeding, both day and night, helps to
delay the return of menstruation and so helps to
postpone the next pregnancy. But breastfeeding, on its
own. is not a reliable method of family planning.
*
*
*
*
*
*
*
Cow's milk, milk-powder solutions, maize gruel and
other infant foods given by bottle do not give babies any
special protection against diarrhoea, coughs and colds
and other diseases.
Bottlefeeding can cause illesses such as diarrhoea unless
the water is boiled and the bottle and teat are sterilize^
in boiling water before each feed. The more often "
child is ill. the more likely it is that he or she will
become malnourished. That is why. in a community
without clean drinking water, a bottlefed baby is 25
times more likely to die of diarrhoea than a baby fed
exclusively on breastmilk for the first four-to-six
months.
The best food for a baby who, for whatever reason,
cannot be breastfed, is milk squeezed from the mother's
breast. It should be given in a cup that has been
sterilized in boiling water. Cups are safer than bottles
and teats because they are easier to keep clean.
The best food for any baby whose own mother’s milk is
not available is the breastmilk of another mother.
If non-human milk has to be used, it should be given
from a clean cup rather than a bottle. Milk-powder
solutions should be prepared using water that has been
brought to the boil and then cooled.
Cow’s milk or milk-powder solution can cause poor
growth if too much water is added in order to make it go
further.
Cow’s milk or milk-powder solutions go bad if left to
stand at room temperature for a few hours. Breastmilk |
can be stored for at least 8 hours at room temperature
without going bad.
In low-income communities, the cost of cow's milk or
powdered milk, plus bottles, teats and the fuel for
boiling water, can be 25-50% of a family’s income.
Source: Facts for Life - A Communication Challenge." UNICEF,
WHO and UNESCO. 1989.
Source: Reproduced from "My Name is Today" (1986), TALC. P.O. Box 49,
St Albans. Herts AL1 4AX. U.K.
Recent Results - “Water supplementation in exclusively breastfed infants in the tropics”
This study from India, published in the Lancet on 20 April, showed that even in the heat, the breastfed infants studied
were better off without any additional water (or anything else). “Our findings show that exclusively breastfed infants can
adequately maintain water homoeostasis during summer months under the environmental conditions studied. Water
supplementation is unnecessary and offers no additional advantage for maintaining hydration status”, the authors state.
“Among the potential hazards of water supplementation in the developing world, diarrhoea secondary to enteropathogen
contamination and premature termination of breastfeeding are well documented. Our study also provides evidence of
diminished breastmilk intake in infants receiving supplemental water.”
6
Extracts from SCN News - May 1991
Everyone's Concern
Although the book is specific to India, the issue extends far
wider. Indeed, the same thoughts are exactly right for many
other places, whatever the child's gender. The book finishes
like this.
An integrated and holistic approach to the girl-child’s
development is essential for the creation of a new environ
ment in which she can be valued and nurtured. Our search
for brave new efforts to give the girl-child her due, to allow
her to evolve to her full potential, involves a process of
social mobilization that will make her everyone’s concern:
the media, the family and the community, as well as
government and voluntary agencies. By supplementing
formal schooling with non-formal education that conforms
to local needs and constraints; by enlarging the ambit of
child development programmes with the creation of new
channels to reach adolescent and pre-adolescent girls; by
reinforcing constitutional mandates through widespread
awareness of the rights of girls: these are only some of the
ways in which we can empower the girl child to enter the
mainstream of economic and social activity. And help her to
walk out of the maze of neglect in which she has been lost
for centuries.”
Source: "The Lesser Child" Dept, of Women and Child Develepment. Ministry of Human Resource Development. Govt, of India.
with assistance from UNICEF.
Breastfeeding — More Important than Ever
The benefits of breastfeeding and dangers of bottle-feeding as two sides of a complex set of issues are constantly becoming
better understood. Breastfeeding is well known to reduce exposure to pathogens in the environment, to give protection by
immunization, to provide anti-bacterial and anti-viral substances, and to supply the correct mix and density of nutrients; it
also has very little direct cost. Bottle feeding, in contrast, tends to be contaminated, non-ideal in terms of nutrients, and
not affordable to many families in poor societies.
New knowledge expands our realization of the sophisticated meshing of the newborn infant’s needs and the mother’s ability
to provide for them — not only to nourish but to protect1. A continuity has evolved to bridge the gap between the safety
of the womb and the shock of post-natal life, when the gut suddenly replaces the placenta as an interface with the world.
The immature infant gut is adapted to the nutrition and protection of breast milk. Antibodies from colostrum and then
breastmilk protect the gut and provide some immunity against other infections. Antibiotic activity in breast milk proteins is
being shown to be selective against precisely certain of the harmful bacteria that cause infantile diarrhoea. The protein of
breast milk is tailor-made to the infant’s needs, and is quite innocuous unlike many non-human proteins. The hazards of
sudden exposure of the fragile gut to foreign materials is now being realized. The gut matures in the first few months —
the recommendation for 4-6 months' exclusive breastfeeding is no accident.
But before this time, researchers are beginning to realize just how vulnerable the infant gut is. and protection by excluding
everything but breast milk is of crucial importance — for preventing contamination with pathogens and exclusion of foreign
materials.
The story goes on. The natural effect of suckling itself in delaying the resumption of fertility is better understood —
protecting’the infant from displacement by a new pregnancy, and the mother's health from excessive reproductive stress.
This process needs to be fostered throughout the world. “It is still true to say that the artificial feeding of our infants has
been the largest uncontrolled clinical experiment in human history2." Here we highlight a number of recent summaries
from the UN system on these issues, mainly compiled from material in SCN News. The first is known as the “Innocenti
Declaration". This is followed by the recommended steps for maternity services, from WHO and UNICEF. Messages from
“Facts for Life" (information was distributed with SCN News No. 4) are then extracted, giving succinct guidance on
breastfeeding, and clear warnings on bottle feeding. The next item emphasizes relations between population and nutrition
issues (from=t'he SCN’s recent symposium, article forthcoming in next SCN News), in particular the congruence of interests
centred on breastfeeding. This extract, printed with support from UNICEF, aims to bring together some pertinent material
to help promote and protect breastfeeding practices.
1.
2.
For a recent review see: "Infant Feeding: the Physiological Basis" Suppl. to Bull. WHO 67, 1989, edited by J. Akre;
reviewed in SCN News No. 6 p.56-7.
Minchin. M. Birth 14, 25-34 (1987).
3
Extracts from SCN News - May 1991
The Innocenti Declaration on the Protection, Promotion and Support
of Breastfeeding
The Innocenti Declaration on the protection, promotion and support of breastfeeding (cited below) was produced and
adopted by participants at the WHO/UNICEF policymakers' meeting on “Breastfeeding in the 1990s: A Global Initiative”
co-sponsored by the United States Agency for International Development (USAID) and the Swedish International
Development Authority (SIDA). held at the Spedale degli Innocenti, Florence, Italy, on 30 July - 1 August 1990. The
Declaration follows. Proposed operational targets are in the box opposite.
6 6 RECOGNISING that
communications strategy involving all media and addressed
to all levels of society. Furthermore, obstacles to breast
feeding within the health system, the workplace and the
community must be eliminated.
Breastfeeding is a unique process that:
provides ideal nutrition for infants and contributes to
their healthy growth and development;
* reduces incidence and severity of infectious diseases,
thereby lowering infant morbidity and mortality;
* contributes to women's health by reducing the risk of
breast and ovarian cancer, and by increasing the spacing
between pregnancies:
* provides social and economic benefits to the family and
the nation;
* provides most women with a sense of satisfaction when
successfully carried out: and that
*
Measures should be taken to ensure that women are
adequately nourished for their optimal health and that of
their families. Furthermore, ensuring that all women also
have access to family planning information and services
allows them to sustain breastfeeding and avoid shortened
birth intervals that may compromise their health and
nutritional status, and that of their children.
All governments should develop national breastfeeding
policies and set appropriate national targets for the 1990s.
They should establish a national system for monitoring the
attainment of their targets, and they should develop
indicators such as the prevalence of exclusively breastfed
infants at discharge from maternity services, and the
prevalence of exclusively breastfed infants at four months of
age.
Recent research has found that:
these benefits increase with increased exclusiveness1 of
breastfeeding during the first six months of life, and
thereafter with increased duration of breastfeeding with
complementary foods, and
* programme interventions can result in positive changes
in breastfeeding behaviour;
*
National authorities are further urged to integrate their
breastfeeding policies into their overall health and develop
ment policies. In so doing they should reinforce all actions
that protect, promote and support breastfeeding within
complementary programmes such as prenatal and perinatal
care, nutrition, family planning services, and prevention
and treatment of common maternal and childhood diseases.
All healthcare staff should be trained in the skills necessary
to implement these breastfeeding policies. ??
6 6 WE THEREFORE DECLARE that
As a global goal for optimal maternal and child health and
nutrition, all women should be enabled to practise exclusive
breastfeeding and all infants should be fed exclusively on
breast milk from birth to 4-6 months of age. Thereafter,
children should continue to be breastfed, while receiving
appropriate and adequate complementary foods, for up to
two years of age or beyojtd. This child-feeding ideal is to be
achieved by creating an appropriate environment of aware
ness and support so that women can breastfeed in this
manner.
Attainment of the goal requires, in many countries, the
reinforcement of a "breastfeeding culture" and its vigorous
defence against incursions of a “bottle-feeding culture.”
This requires commitment and advocacy for social mobiliza
tion. utilizing to the full the prestige and authority of
acknowledged leaders of society in all walks of life.
Efforts should be made to increase women's confidence in
their ability to breastfeed. Such empowerment involves the
removal of constraints and influences that manipulate
perceptions and behaviour towards breastfeeding, often by
subtle and indirect means. This requires sensitivity, con
tinued vigilance, and a responsive and comprehensive
1.
Exclusive breastfeeding means that no other drink or food is
given to the infant; the infant should feed frequently and for
unrestricted periods.
4
Extracts from SCN News - May 1991
“Nutrition and Population”
3 s'mPos'um on “Nutrition and Population" at its annual session, hosted this year by UNFPA in New
hil
dnnrT ebruar}' 1991. The SCN. with representatives of all concerned UN agencies and with participation of
bilateral donors, approved a statement on the issues including the following.
Breastfeeding provides one link between nutrition and
family planning with mutually beneficial effects at the level
of the individual mother and child. Exclusive breastfeeding
for 4-6 months is advised. Lactational amenorrhoea,
prolonged by breastfeeding, is of great benefit through
increasing birth intervals. There is an opportunity at this
time for counselling on modern family planning methods, in
particular those deemed most appropriate for lactating
women.
policy formulation, programme planning, training and the
support of community level initiatives present several
challenges.
These include the following:
At an individual level, the health and nutritional status of
the mother (particularly the adolescent mother) is a
fundamental concern, in term of her nutritional resources,
reproductive and productive roles and family planning
needs. Increasing the length of birth intervals will reduce
the likelihood of cumulative reproductive stress in the
mother and improve her ability to adequately care for her
Skild. The individual child too will benefit from birth
™acing and maternal health through more adequate feeding
and care practices.
-
appropriate training of health and family planning
workers; the motivation to support and counsel women
should emerge from common goals;
-
reconciling programmatic priorities of agencies that
differ in their support for the concept and practice of
integrated breastfeeding and family planning strategies;
-
recognition of constraints on exclusive breastfeeding
due to competing demands on women's time, misinfor
mation and other factors, hence the need for appropri
ate programmatic support to enable women to practise
breastfeeding;
resource mobilisation to provide relevant information,
education and communications to promote the practice
of breastfeeding and the adoption of contraceptives,
including research on beliefs and obstacles to family
planning and infant feeding."
“These are major reasons why family planning and nutrition
services and information should be integrated. Programma
tic considerations as to how to bring this about, in terms of
From: "If Queen Victoria had known about LAM"
An editorial with this title in the Lancet (Vol 337, pp 703-4, March 23 1991) starts by explaining the important role of
breastfeeding in child spacing, and notes that what Queen Victoria, who had 9 children “. . . failed to grasp was that, by
putting every one of her babies to a wet-nurse the day it was born, she was destroying the role of breastfeeding in the
spacing of pregnancies". Recent research clarifies why: “. . . In examining the proximate determinants of natural fertility,
Bongaarts found that lactation-induced amenorrhoea was the single most important variable determining fertility". This
has led to recommendations on family planning. "A consensus meeting sponsored by the World Health Organization,
Rockefeller Foundation, and US Agency for International Development in Bellagio. Italy, on the contraceptive effect of
lactation [concluded] that if a woman feeds her child on demand for up to 6 months after delivery and has not
menstruated, then she has only a 2% chance of conceiving - a “failure” rate similar to that of most modem methods of
reversible contraception".
The International Code of Marketing of Breast-Milk
(^Substitutes: 10 years later
On 21 Mav 1981. bv resolution WHA34.22. the Thirty-fourth World Health Assembly adopted the International Code of
Marketing of Breast-Milk Substitutes in the form of a recommendation, in the sense of Article 23 of the WHO Constitution. A
synthesis of action taken in countries from 1981-90. from information available to WHO. is given in the WHO document “The
International Code of Marketing of Breast-Milk Substitutes: Synthesis of Reports on Action Taken (1981-1990)".
WHO/MCH/NUT/90.1. issued in English. French and Spanish, which may be obtained from the Nutrition Unit. WHO Geneva.
The intention in synthesizing all the information is to provide an overall picture of the steps that more than 150 countries and
territories have taken during the last decade - individually, and in some cases collectively, through regional and interregional
forums — to give effect to the principles and aims of the International Code.
Many non-governmental and other organizations have responded to the responsibility put forward in the Code (Article 11.4) for
implementation and monitoring. The International Baby Food Action Network (IBFAN) is a coalition of more than 140 citizen
groups in 70 developing and industrialized nations. The network promotes optimum child feeding practices world-wide and
monitors compliance with the International Code of Marketing of Breast-Milk Substitutes, which it helped to develop. IBFAN
regularly informs WHO of the activities of its affiliates in support of appropriate infant and young child feeding practices.
including research, social support for women, breast-feeding promotion, and implementation of the International Code. The
1991 State-of-the-Code bv Country - IBFAN’s survey of measures taken by governments to implement its provisions - shows
the position ten vears after the Code was adopted by the World Health Assembly in May 1981. A booklet "Protecting Infant
Health: A Health Workers’ Guide to the International Code of Marketing of Breast-Milk Substitutes" is now available, from the
International Organization of Consumers Unions (1OCU was a founding member of IBFAN). in 16 languages (Address: PO
Box 1045. 10830 Penang. Malaysia).
(Sources: WHOIMCHINUTI90.lt UNICEF)
7
Extracts from SCN News - May 1991
Some quotes
"Promoting breastfeeding while countries undergo change
will allow women to retain valuable traditional practices
while adopting important western ones, such as modern
forms of contraception, institutionalized births and employ
ment outside the home. Promoting breastfeeding will also
contribute to the effectiveness of family planning programs
and allow those programs to work in concert with health and
nutrition efforts. Projects with fertility limitation goals
should therefore include breastfeeding promotion programs
as complements to other services."
"From the standpoint of nutritional needs, physiological
maturation, and immunological safety the provision of
foods other than breast milk before about four months of
age is unnecessary and may also be harmful. On the other
hand, many infants require some complementary feeding by
about six months of age. There are a number of well known
disadvantages and risks involved in too early complemen
tary' feeding, including interference with the infant’s feeding
behaviour, reduced breast-milk production, decreased iron
absorption from breast milk, increased risk of infections and
allergy in infants, and increased risk of a new pregnancy/’
Source: Alan Berg and Susan Brems. “The Case for Promoting
Breastfeeding in Projects to Limit Fertility". World Bank Technical
Paper No. 102. 1989.
"Even under conditions of extreme malnutrition, a lactating
mother will continue to produce adequate milk for the baby,
if necessary consuming her own body tissue; in some
developing countries women lose weight during lactation.
Sadly, those women who are least prepared for the
nutritional stresses of lactation are also those who have the
fewest choices. As a result of poverty, they are in no
position to purchase or use milk formula in any S2^
manner . . . and failure to breastfeed can be near a del9
sentence for the infant ... far more attention needs to be
paid to the possibility of giving supplementary food to
lactating mothers and to the adequate nutrition of young
women around the age of puberty. Extra food for the
mother can cost as little as one tenth the cost of artificial
food for the baby.”
Source: “Infant Feeding: The Physiological Basis" Supplement to
volume 67. 1989. of the Bulletin of the WHO. Edited bv James Akre
p.55.
"Yesterday, merely because mothers were not effectively
empowered with the knowledge, were not adequately
motivated and not adequately supported to breastfeed. 3 to
4.000 infants and young children died. Today 3 to 4,000
died: 30 days ago another 3 to 4.000 died."
Source: James P. Grant, Executive Director of UNICEF, in
Opening Statement to the WHOIUNICEF Policymakers Meeting on
"Breastfeeding in the 1990s: A Global Initiattve", Florence. 30 July
1990.
"As many as 4-5 million children die every year and many
more suffer nutritional consequences of diarrhoeal diseases
even with all the advances in knowledge and technology
during the last three decades . . . There can be no doubt in
any of our minds that breastfeeding directly reduces
diarrhoea mortality and morbidity in the young infant . . ."
Source: Lancet, 337, 703 (1991)
"Breastfeeding should be promoted in the context of health
and well being of the woman.”
Source: Dr Nafis Sadik. UNFPA Executive Director, in Opening
Statement to the WHOIUNICEF Policymakers Meeting on "Breast
feeding in the 1990s: A Global Initiative", Florence, 30 July 1990.
Source: Dr Hiroshi Nakajima, Director-General of WHO (Press
release WHO!49. Dec. 1988)
The ACC/SCN is the focal point for harmonizing the policies and activities in nutrition of the United Nations system. The UN
members of the SCN are FAO, IAEA, World Bank, IFAD, ILO, UN, UNDP, UNEP, UNESCO, UNFPA, UNHCR, UNICEF,
UNRISD. UNU, WFC, WFP and WHO.
SCN News aims to provide information useful for those concerned with international nutrition. Publication of items in
SCN News (and in this issue which is mainly extracts) does not imply endorsement of views given, nor necessarily the
official positions taken, by the ACC/SCN and its member agencies. The status of quotes and other material is generally
indicated in the text and/or sources.
8
- Media
 SDA-RF-CH-1.3.pdf
SDA-RF-CH-1.3.pdf
Position: 3497 (3 views)