Report of Cyclone Relief Work done in Andhra Pradesh, handwritten account by Dr. Thelma Narayan
Item
- Title
- Report of Cyclone Relief Work done in Andhra Pradesh, handwritten account by Dr. Thelma Narayan
- extracted text
-
RF /O M
1 RNj- 2a/Su
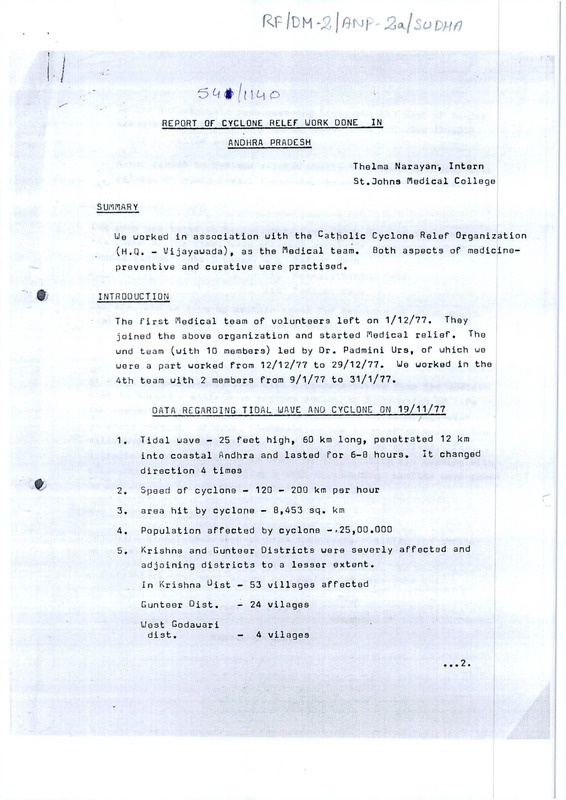
REPORT OF CYCLONE RELEF UORK DONE
IN
ANDHRA PRADESH
Thelma Narayan, Intern
St.Johns Medical College
SUMARY
We worked in association with the Catholic Cyclone Relef Organization
(H,Q. - Vijayawada), as the Medical team, Both aspects of medicinepreventive and curative were practised.
INTRODUCTION
The first Medical team of volunteers left on 1/12/77. They
joined the above organization and started Medical relief• The
und team (with 10 members) led by Dr. Padmini Urs, of which we
were a part worked from 12/12/77 to 29/12/77. We worked in the
4th team with 2 members from 9/1/77 to 31/1/77.
DATA REGARDING TIDAL UAVE AND CYCLONE 0N.19/11/77
1.
Tidal wave - 25 feet high, 60 km long, penetrated 12 km
into coastal Andhra and lasted for 6-8 hours. It changed
direction 4 times
2.
Speed of cyclone - 120 - 200 km per hour
3.
area hit by cyclone - 8,453 sq. km
4.
Population affected by cyclone -.25,00.000
5.
Krishna and Gunteer Districts were severly affected and
adjoining districts to a lesser extent.
In Krishna ^ist - 53 villages affected
Gunteer Gist.
- 24 vilages
Uest Godawari
diet.
4 vilages
...2.
6.
In the catastrophic zone covering Diviseema and part of Bandar
taluq’s over
50,000 people are feared dead and also 100,000
heads of cattle lost.
7.
Havoc caused by cyclone related mostly to property,
Tidal wave
related to human lives, livestock, houses, property crops.
Camp and organization
Our camp was based at Nagayalanka, Oivi Taluk Krishna dist, on
the funge of the tidal wave affected area.
It consisted of 60-70
people divided into 3 teams
ii
Relief team
Rehabilitation Team
iii
Medical team
- i
The aims was to take up certain areas for development which would
consist of 3 phases -
i
Immediate relief
ii
Intermediate phase
iii
Long term development phase
at first an exploratory team with a representative from the medical
want to survey a village as regards amount of destruction of life
and property, and relief measures already taken by other agencies
to avoid overlop
of work.
Information was obtained by meeting the
village president/Sarpanch and by going around the village.
The
villages chosen were those in which no organization was working with
a long term project.
6 villages with surrounding
hamlets were taken
up and alloted by the Govt, to this organization.
Hethod of uork in a village
Immediate relief consisted of providing food, clothing and shelter
ie building long community hute
a statistical team went around collecting baselive data viz
Male
Nuber of living
I
F emale
Census
Number of dead
3
Socioeconomic survey regarding
II
Housing
Occupation
Property
Education
( see charts)
on the basis of this, requirements were calculated and
plant drawn
up.
Medical work
(during first stay)
When wer arived. there were 3 clinics established
i)
At Nagayalanka population - 9000
It also covered surrounding villages
ii)
At Mandapakala
iii )
population - 1,311
Mobile clinic - going from village to village covering
a population of - 2,458
clinical work was done during the day. Daily statistics of cases
were kept with a graph shows of the distribution pattern of diseases
This uas classifed as follows:
t
1)
2)
3)
4)
5)
6)
Total number of cases
^iarrhoea and ^ysentry
Gastroenteritis'^
Respiratory Tract Infections
□ther Infections
Miscellaneous
Our team leader kept in contact with the D.M.O. at the nearest P.H.C.
at Avanigadda 18 km away. They were very helpful and supplied us
with DDT, bleaching powder, lime and drugs to supplement out own
stocks of medicine.
. . .4
4
Most of the population were already innoculated against typhoid and
Cholera and there were no epidemics.
Preventive work done included — Remaining TABC innoculations, Tetrac
innoculations. Chlorination of walls, spraying of bleaching powder/
lime constructions of trench latrines for the camps, health education
to the villagers regarding environmental sanitations, nutrition,
boiling of wate
for children etc.
ObSBruations/Digcusaion
The population covered was not a normal population having first
1.
suffered an enourmous loss of life and property.
Most people had returned or had to be cqaxed back to their own villages
as all they had left was their land without which they wouldteesom
become beggains or slum dwellors in same town.
2.
3.
These people were building life afresh and were ideal ground for
community development.
4.
Every family had been disrupted due to loss of same or other or
many members causing a large social problem.
5.
The mental health problem was large and acute, the people still
dazed or depressed.
6.
These people were fairly well-off prior to the cyclone/and
poverty is new to them (see charts regarding property). To
avoid them getting used to obtaining
btaining things easily first for
the begging, some sail of cooperative ventive where they
provide at least the labour is desirable.
A team of village leaders could be the decision making and
negotiating body a system was noted in one village (Etimaga)
which was divided into 10 divisions, each of which had a
leader who would put up the requirements of that area and get
the work done. They themselves a had completed the hawesting
and started rebuilding.
7. Illiteracy and ignorance were found to be very widespread
(See charts) only 2-*3 persons are educated above the 10th
std. These could be involved in the development programme.
.5
I
// 9o
5
8.
The social problem of the Harijans was noted, They worked as
coolies as they did not own any land. In one area they had land
but without any irrigation facilities.
9.
Health
as this was a food grouing area the gneral health of the people
was good without much protein-calorie malnutritions. Anaemia
were found to a accute mainly in women and children.
- There were no epidemics of cholera, typhoid or gastroenteritis
due to early and complete 1nnoculations. The reamining few
were caused by us.
- There were no epidemics of cholera,
- Initially the graph showed a high incidence of respiratory
disease especially U.R.T.I This was due to i) exposure during tidal Weave and cyclone
ii) tack of adequate shelter and clothing
ill) Cold weather expecially at night
u
iv) Dust and fumes
This fact was brought to the notice of the organizers and priority
was given to providing ciotning
clothing ano
and snexter.
shelter. Large community
huts were built immediately. Individual families also started
building huts from palmyra leaves and bamboo provided by Govt.
uater was obtained mainly from tube wells. The feu open wells
were cleaned out by the army and attainated by the PHC staff,
subsequent chlornation was done by us. Tube well water was used
without purification generally. Some of the tubewells were
located close to drains/canals and were probably sucking in
water from them.. In one area an outbreak of Gastroenbntis was
found among usess of water of one such well. Cqses presenting
with diarrhoea and dysentry were advised to boil uaterf expecially
for children -nor very proclied suggestion for whole families.
Two cases of infective helpatits were seen.
- Cnviornmentai Sanitation was very poor following the hawoc
were additional factors viz occasional capaes and carcasses
uprooted trees, debris, staghout saline water. ^his combined
with the ignorance of villages concerning the subject. Towards
the latter half of out stay, there was a marked increase in the
number of flies with a corresponding gradual increase in the
incidence of diarrhoea and dysentry.
.. .6
I
I
Only spoiadic cases of gastroenteritis were seen who responded to
treatment on follow up no furthur cases were found in the surrounding
areas.
The D.PI^O. at Avanigadda was informed of the fly menace,
Bleaching
powder and lime were obtained and sprayed around the villages by
teams from the PHC and our camp.
A fairly significant number of evening fewers with chills presented
to us.
a few clinical cases of filaria with swelling were seen.
rest were ?
Halaria ?
Filaria
The
Mosquitoes were more around
nagagalanka and the canals of the Krishna river nearer the coast
there were pools of salt water brought in the tidal wave.
- Ngntal Health
The majority of cases needed only a sympathetic ear^ as everyone
in the area has a story to tell.
4-5 cases of hystenia were seen,
impossible
to
rub
out
the
experience
these people have had
it is
and many of them have told us that they wish that they too were dead.
But the most important thing is to give them same hope to start life
again and so the programme was called ’’Operation Hope”. Two priests
stayed at Geogepetta to encourage people to roturn to their land.
In that village not a single house remained, 100 people had died
and 146 were living comprising 40 families, in one large hut a kitchen
garden was planted to prove that the sail could still be productive.
Touls wore kept to bring back same
provide eggs villagers
semblance of nounalcy and to
4
7.
Bel/efs regarding auspicious times of entering and leaving
the dispensary, quite common in most parts of India, did not
interfere with our work, Except in one case when a women was
brought in with prolonged labour due to hand prolapse and
when we advised transfer to the nearest district hospital,
her relatives insisted her on taking her back to the hut and
then starting the journey to hospital again since the belief
is that if a patient is asked to leave a hospital and go to
another
with being given any treatment then the doctor has given
up hope and i»e., a bad omen.
©
The above observations helped us to understand the people
we were working with and in any such situation this is becoming
a very important factor. Dr. 3ohn Seaman in his paper in the
Lancet (ii) (1972) P866 echoes this need when he lists the
follow^ as the first lesson learnt from the Bangladesh experience
de says much more detailed information should be available about
C> Gtv
the nature of the society involved and that^ignorance of the
society and attitudes of the poor people was a problem felt
by all doctors in the camps.
- Media
 RF_DM-2_ANP-2a_SUDHA.pdf
RF_DM-2_ANP-2a_SUDHA.pdf
Position: 3106 (4 views)