SUMMARY CONCLUSION AND RECOMMENDATIONS
Item
- Title
- SUMMARY CONCLUSION AND RECOMMENDATIONS
- extracted text
-
CH -
7?
We have tried to collect and collate the available
information regarding the status of health of the
people of Karnataka. There are many gaps in the
information. It follows Finagle's law:
"The information you have is not what you want.
The information you want is not what you need.
The information you need is not whatyou can get.
The information you can get costs more than what
you want to pay."
While many were willing to help, others were
indifferent or even antagonistic. The data and
information about the health of the people belong
to the people. It is the duty of all to share the
information.
Some of the data are notreliable. Cross-checking
with other sources show disparities. We have tried
to use the most reliable sources and data.
>
As regards, the health of the people, Karnataka is
an 'average' state. It is neither at the forefront, nor
in the rear, compared to all the states in India.
If we compare Karnataka's health with the
neighbouring states and particularly with the
Southern neighbours. Karnataka has a long way to
goHealth is a right that can be obtained only
through meeting other basic rights. This comes up
forcibly when we look at the health status of the
disadvantaged groups-children, women and
tribals. Unjust structures and relationships lead to
ill-health.
1. EMERGING TRENDS
The emerging scenario-economic, social and
political-is not conducive to better health of all the
people. They tend to widen the gap between the
haves and have-rots. The new economic policy
favours the rich. The poor become relatively and
absolutely more poor and destitute.
The poor are more likely to be sick; sickness
leads to poverty.
2. COMPREHENSIVE HEALTH CARE
There is need for commitmentto comprehensive
primary health care and community health. But the
pressures on the State Govern ment seem to be to go
after sophisticated, costly secondary and tertiary
care.
The costly care makes it unaffordable to the
majority of the people. Even when the diagnostic
and therapeutic procedures are free, there are hidden
costs. Less costly but committed care with concern
and compassion is necessary if we are to reach the
poor, the lowly and the disadvantaged.
3. HEALTH IN THE PEOPLE S HANDS
We have to restore health care into the people's
hands. Health professionals and workers should help
this process, enabling the people to attain and
maintain their health. Government, Voluntary
Organisations and the private sector should work
towards it. There is need for a collective will to
create a community movement towards people's
health.
Decentralisation as envisaged by Panchayati
Raj, is expected to bring greater dividends in health
care. The community (and the people's
representatives) has to be strengthened and
organised. They must become knowledgeable and
skilled. There is need for changes in behaviour and
health practices. There is need for training.
4. FACTORS WHICH AFFECT HEALTH
OF THE PEOPLE
Many factors play a role in determining the
health of the people, apart from the quality and
extent of coverage of health care services:
• Food and nutrition, adequate in quantity and
quality
• Safe water supply and sanitary disposal of waste
• Education, particularly female education
• Employment and improved purchasing power
with equity
• Housing and shelter
• Prevention of pollution of air, water and soil
• Other relevant factors.
5. FOOD AND NUTRITION
Food and nutrition must be adequate in energy
and quality. The average person in Karnataka is
better off than many people in average parts of the
country but there are many areas which require
urgent and sustained attention.
In children (1-5 years), if we use the well-to-do
Indian children as standard, only 11.2% of male
children and 20.6% female children had normal
nutritional status (1988-89). If we use the National
Councilof Health Sciences, U.S. A. standard, it becomes
only 3.8% and 6.0% respectively. The situation is
highly unsatisfactory. Even mild malnutrition can have
deleterious effects on the development of the child in
the early years. This adverse effect (physical, mental
and behavioural) is likely to have continued ill effects
throughout life.
Most women are undernourished and anaemic.
This becomes worse during pregnancy. Only 14.5%
of pregnant Indian women have haemoglobin levels
considered adequate (11 .Og/dl or more). The situation
is considered similar for women in Karnataka also. It
affects maternal health and the outcome of pregnancy.
236
Added to the inadequacy of food is tood
adulteration and substandard food. Worse still is
contamination with pesticides.
With the new economic policy, with thrust
towards more export, there is danger of diversion of
land use from cultivation of food crops to cash crops.
Food security and nutrition can be affected by such
change as also the move to give large tracts of land to
industries.
6* HEALTH SERVICES
Karnataka, as successor State of Mysore, had
many advantages in health care services. Also the
location of certain bodies like the All-lndia Institute
of Mental Health, which was transformed in 1974
into the prestigious National Institute of Mental
Health and Neurosciences, helped. How did we
lose that advantage?
The characteristics of effective and efficient health
care are availability, accessibility and affordability.
With high cost of medical care, the poorer people
cannot avail of the services. It is necessary to make
available competent and compassionate care in all
circumstances.
The availability of essential drugs at all times
must be ensured. The state must have a drug policy
and also a State Formulary appropriate for various
levels of functions and expertise.
Karnataka has certain diseases peculiar to it such
as Kyasanur Forest Disease and Handigodu
Syndrome. It is necessary to conduct intensive search
into their causes and find means for prevention and
treatment.
7* HUMAN RESOURCES DEVELOPMENT
There is lopsided development of health human
power. There has been very large increase in the
number of doctors, whereas other categories of
health personnel lagged behind.
The capitation fee culture in Karnataka is playing
havoc in thequality of education. Started with medical
education, it has spread to nursing, dentistry and
education of other health personnel.
I
0
8. INDIGENOUS SYSTEMS
The people of Karnataka utilise the indigenous
systems and homeopathy to a large extent. There has
not been very much encouragement in the
development of these and other alternative systems.
CHILD HEALTH
Infant mortality rate is still unacceptably high. The
plan is to reduce IMR to 40 by 2000 AD from 71 in
1990. This is an achievable target. There will be no
excuse for not achieving this target and even better.
10* WOMEN'S HEALTH
Women suffer from all the common diseases
d additionally from some diseases peculiar to the
reproductive phase. Even among the diseases
common to all, women's health suffers because of
their disadvantaged position in thefamily and society.
Cervical cancer is very common and takes a big toll
by way of suffering and death. It is heartening to
note that Kidwai Memorial Institute of Oncology is
taking steps to prevent, detect and manage Cervical
Cancer through a community- based approach.
11* TRIBAL HEALTH
Tribal persons who live in non-forest areas and
alienated from their traditional environment have low
health and nutrition status. They are prone to a number
of diseases such as sickle cell anaemia. Government
health care services do not reach them effectively.
!♦ ENVIRONMENT
The environmental situation is totally
unsatisfactory. With the emphasis on starting new
industries without sufficient attention to the effect on
environment, the situation is getting worse. There is
contamination and pollution of rivers and other
water sources. Air pollution in cities and towns has
reached very high levels.
Garbage collection and disposal are very
unsatisfactory. The pollution control measures must
be applied more strictly.
13< INJURIES
The main cause of injuries, especially in the
cities and towns, is road traffic accidents. The
accidents may be caused by deficiencies in
• driving
• vehicles
• roads
The drivers must be wel l-trained. Driving I icences
must be issued only after rigorous testing and
determining competence. The road usage behaviour
has to improve.
Many of the vehicles are not roadworthy. Checks
must be applied on a regular basis.
The roads are in poor condition.
14* DISABILITIES
Karnataka has carried out a survey of persons
with disabilities. This is a remarkable achievement.
Because of various limitation s, we have detected,
probably, only the persons with severe or profound
disabilities. More refined methods will detect more
persons with mild and moderate disabilities.
Once detected, it is necessary to provide
rehabilitation and integration into the society.
Community based rehabilitation can reach those
needing care more effectively and with greater
coverage.
15* LAW AND ETHICS
There are many pieces of legislation affecting
health care. Unfortunately, they are not applied
effectively. The Consumer Protection Act was
expected to give quicker relief to those affected by
deficiencies inservice. But this has not been possible
with large numbers of complaints pending disposal.
There is need for the health professionals and
health care institutions to follow the codes of ethical
conduct. There is a change coming on from ethics of
trust to ethics of rights.
16< VOLUNTARY ORGANISATIONS
There are a large number of voluntary organisations
in health in Karnataka, but they are unevenly
distributed. Where they are active, there is marked
effect on all the health indices. There is a need for
better networking and playing advocacy roles.
237
DISIRIC1S ACCORDING IO INILGRAILD INDtX Of DEVLLOPMtNI
GO
CO
1.
Category
Rank
District
I.D.
Rank
District
I.D.
Rank
District
I.D.
Highly Developed
1.
Bangalore
266.48
1.
2.
Mandya
Dakshina
Kannada
Bangalore
Shimoga
124.78
1.
Mandya
114.64
120.57
113.84
107.75
2.
Dakshina
Kannada
107.09
3.
4.
II.
Developed
2.
3.
4.
5.
III.
1991-92
1981-82
1971-72
Developing
6.
8.
9.
10.
11.
Dakshina
Kannada
Shimoga
Mandya
Dharwad
148.69
126.60
123.12
114.02
5.
6.
Kodagu
Bellary
Mysore
87.91
87.54
85.52
3.
4.
Bangalore
Shimoga
98.26
94.55
Mysore
Kolar
109.69
105.72
8.
9.
81.93
81.70
5.
6.
Kodagu
Hassan
81.88
Belgaum
Kodagu
UttarKannada
Raichur
99.61
10.
11.
12.
13.
Kolar
Uttar
Kannada
Hassan
Bijapur
Belgaum
Chikmagalur
80.45
13.
Kolar
Belgaum
Uttar Kannada
Mysore
Dharwad
Chickmagalur
Chitradurga
14.
15.
16.
17.
18.
19.
Bellary
Bijapur
Tumkur
Bidar
Raichur
Culbarga
69.15
66.14
94.80
93.79
91.24
80.96
80.82
80.26
79.83
8.
9.
10.
11.
12.
IV.
Backward
12.
13.
14.
15.
16.
17.
18.
19.
Chitradurga
Chilkamagalur
Bellary
Hassan
Tumkur
Bijapur
Bidar
Culbarga
86.37
85.54
82.21
78.28
76.35
70.59
14.
15.
16.
17.
18.
19.
Chitradurga
Dharward
Tumkur
Bidar
Raichur
Culbarga
58.23
48.06
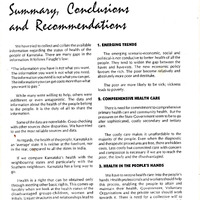
I.D. Index of Development
Source: Karnataka at a Glance, 1991-92: Directorate of Economic and Statistics, Bangalore.
72.39
71.66
60.80
60.35
50.94
40.48
80.45
79.52
78.59
77.82
76.12
74.11
73.23
64.94
59.25
57.75
50.76
17- REGIONAL DISPARITIES
There are many regional disparities, which affect
health. If we use selected economic indicators of
development, we can see wide disparity between
the districts.
Bangalore Rural and Urban are clubbed together.
18. RECOMMENDATIONS
Recommendations have been made in each
chapter. Below are some important ones:
1. DISPARITIES
Improve health care services in the backward
districts and areas, enabling them to catch up with
other more developed districts and areas.
Have a more equitable distribution of health
care services even within the district/area.
2. COMMUNITY PARTICIPATION
Organise the community to take action for health
Train the people and people's representatives
(under panchayati Raj and Municipalities Acts) to
plan and make decisions.
Ensure that the health functionaries accept the
rights of the people to plan, make decisions and
ensure their implementation. Health personnel
should help.
3. EQUITY WITH QUALITY
Service for the poor cannot be poor service
Have regulations to improve quality of care,
whether in the Government, Voluntary or Private
Sector and implement them. These regulations
must be promotive and enabling and not merely
punitive.
4. HEALTH PERSONNEL
Education of all health personnel must be value
based. They must be motivated to provide
continuously improving health care.
Abolish the capitation fees system
Have a proper balance in the development of
different categories of health personnel to meet the
needs of the state.
Improve the competence and managerial capacity
of all health personnel at all levels.
The practice of health care must be ethical.
Train all health personnel in medical ethics and
bioethics.
5. PUBLIC HEALTH
• Have a public health approach, taking
appropriate health sustaining measures.
• Improve the environment
• Reduce pollution of all kinds. Apply swift and
effective pollution control measures.
• Create health awareness among all the people,
leading to action.
• Bring about improvement in life-styles. Take
measures to curtail smoking and drinking.
6. WATER SUPPLY AND SANITATION
• Improve quantity and quality of water supply
• Have proper disposal of liquid and solid waste
7. HEALTH INFORMATION
• Correct and complete data and information are
required for planning and action
8. NUTRITION
• Comprehensive studies must be conducted to
get enough accurate data as regards nutritional
status, disaggregated according to age, socio
economic group, etc.
• Take action to correct all degrees of malnutrition,
including deficiencies of micronutrients.
• Improve the nutrition of children in the early
formative years
9. FINANCING HEALTH
• Increase the budget allocation substantially for
health and health related activities.
• Improve the utilisation of the amounts allocated.
• The allocation must be equitable with
proportionately higher allocation for
comprehensive primary health care.
• Have a comprehensive insurance scheme,
ensuring equity and quality of care for all,
irrespective of capacity to pay.
10. ALTERNATIVE SYSTEMS OF MEDICINES
• All recognised systems of medicine must be
supported and made available, leaving the
choice and utilisation to the people.
11.INJURIES
• Enforce the rules of safe behaviour on the roads,
factories and elsewhere.
• Insist on fitness of drivers, roads and vehicles.
• Improve environmental safety
• Improve trauma and rehab ilitation services.
23»
•r
12. HEALTH CARE SERVICES
• Monitor continuously and evaluate periodically
Government health care services-inputs,
activities, outputs and impact, developing
qualitative, quantitative and process indicators,
• Weed out corruption at all levels and in all areas
of health care services.
• Health CareServices must be watchful of emerging
health problems such as AIDS and other more
• persistent problems such as tuberculosis and
take appropriate action.
13. SPECIAL NEEDS
• The special needs of the vulnerable groups such
as tribals, urban poor, women, children, elderly
and other disadvantaged persons must be met
urgently.
• There is need for better antenatal and delivery care.
• Take measures to achieve the target of Infant
Mortality Rate to be reduced to 40 or less, by
2000 AD.
• The special needs of women must be met. These
include the special needs during adolescence,
reproductive age and later.
• Allocate more funds and utilise them better for the
health of the tribal people.
• Special illnesses like sickle cell anaemia require
greater attention.
14. MENTAL HEALTH
• Have district level mental health units (psychiatrist,
clinical psychologist, psychiatric social worker
and psychiatric nurses) in every district.
• The district unit will work in close collaboration
with the district hospital.
• Integrate mental health care with primary health
care.
240
•I
15. DISABIL TIES
• Extend the survey conducted to detect mild and
moderate Usabilities and their causes,
• Take meas ures to prevent or reduce disabilities
• Rehabilitaieand integratepersonswithdisabilities
into the society.
• Adopt community-based rehabilitation as probably
the best method to ensure adequate coverage.
16. RATIONAL USE OF DRUGS
• Enunciate and implement a Rational Drug Policy
• Have an essential drug list and formulary
appropriate for each level of use and expertise
available.
• Make available all essential drugs at all times and
places.
• Weed out corruption in the matter of drug
purchase and supply.
17. VOLUNTARY ORGANISATIONS
• Governmentshould see Voluntary Organisations
as true and equal partners and be supportive of
their efforts.
• They must be seen not merely as implementors of
Government Programmes but also as innovators,
issue raisers and trainers.
• Voluntary Organisations must enable the people
to plan, decide and take action for better health.
REFERENCES:
1. NCOs in the Nineties, Desmod A.D. Alareo, May 1992.
2. The Third Force in Health Care—Voluntary Sector: Role of
Voluntary Organisation in Health & Family Welfare in India,
1992 - Dr. Ashok Sahani - ISHA.
3. Collaboration with Non-governmental Organisations in
Implementing the National Strategy for Health for All,
COI, Ministry of Health & Family Welfare, New Delhi,
April 1985.
- Media
 CH-18.pdf
CH-18.pdf
Position: 450 (53 views)