A STUDY FOR DRUG ACTION FORUM KARNATAKA
Item
- Title
- A STUDY FOR DRUG ACTION FORUM KARNATAKA
- extracted text
-
RF_DR_13_SUDHA
"H,(First <•
1
ALTti CELL
i ,j .. )Vlark3 noat-
p.ANGALO i£-56O001
LANCET, OCTOBER 11, 1986
jients how they felt that diarrhoea had affected their
sfcstvle- The frequency of attacks is obviously important
is by no means the only factor to be considered. Most
Orients with diarrhoea emphasised that it was the sudden,
.^predictable onset of the attacks that they minded most.
pn dose questioning it became apparent that the urgency
^•ceding an attack of diarrhoea could be so intense that
■
panents had actually been incontinent. The fear of
(^rrc embarrassed in a public place was common, and it was
jbvious that this fear often dominated the patient’s
Efestyle." A patient who experienced only one attack a week
ZJrjld be as incapacitated as a patient with daily attacks,
jj-pending on their circumstances. Many patients with
persistent postvagotomy diarrhoea are labelled neurotic, but
anxiety they show may be a secondary phenomenon,
rather than due to an underlying psychological
abnormality.*91112
We were disturbed to find patients who had
jost their jobs or had to change them because of diarrhoea.
also found that patients with physical disabilities were
particularly badly affected, even infrequent attacks resulting
in incontinence.
Most surgeons believe that postvagotomy diarrhoea
disappears with time. Many gastric surgery patients
experience a short period of diarrhoea after the operation,
shich settles spontaneously; this may have led to a false
complacency. Our study confirms that postvagotomy
diarrhoea does not disappear with time, and we believe there
is little improvement with time. The prognosis for the
patient in whom this side-effect develops is, therefore, not
good.
Ulcer recurrence is widely regarded as being the ultimate
failure of ulcer surgery, but since the introduction of the
Hj-receptor antagonists this may no longer be true.
Postvagotomy diarrhoea may be more difficult to treat than
ulcer recurrence; many of our panents found standard
treatments ineffective. We are now carrying out a study of
treatments for postvagotomy diarrhoea; nearly all patients
have had relief of diarrhoea with once-daily loperamide (to
be published elsewhere). However, any treatment for this
disorder would be required for the rest of the patient’s life.
40 years ago diarrhoea may have seemed a worthwhile
price to pay for safe and effective ulcer-healing. However,
there are now operations virtually free of functional
sde-effects.1314
" We believe it is difficult to justify' the
continued use of truncal vagotomy and drainage and
conclude that the risk of diarrhoea is sufficient reason to
avoid this type of operation whenever possible.
Correspondence should be addressed to S. A R., Department of Surgery,
University of Newcastle upon Tyne, Framlington Place, Newcastle upon
TyneNE2 4HH.
1. Dragstedt LR, Harper PV, Tovre EB, Woodward ER. Section of the vagus nerves to
ten years or more after vagotomy-pyloroplasty. Am J Gastroenterol 1971; 56:
99-108.
5.
6.
duodenal ulcer in 500 patients. Acta Chir Scand 1975; 141:657-63.
Cox AG, Bond MR. Bowel habit after vagotomy and gastrojejunostomy. Br Med J
1964; i:460-65.
Feggener GY, Pringle R. The long-term results of bilateral vagotomy and
gastrojejunostomy for chronic duodenal ulcer. Surg Gynecol Obstet 1963; 116:
gastrojejunostomy or pyloroplasty. Am R Coll Surg Engl 1969; 45: 193-211.
8. Barnes AD, Williams JA The change in bowel habit following vagotomy and
pyloroplasty - Br J Surg 1967; 54:218-20.
References continued at foot of next column
853
Drug Evaluation
USELESS DRUGS ARE NOT PLACEBOS:
LESSONS FROM FLUNARIZINE AND
CINNARIZINE
Joan-Ramon Laporte
Dolors Capella
Division of Clinical Pharmacology, Univcrsitat Autonoma de
Barcelona, Barcelona, Spain
A PAPER by Chouza er al1 on extrapyramidal signs and
depression induced by flunarizine raises doubts about the
safety of cinnarizine. Flunarizine, a difluorinated derivative
of cinnarizine, was marketed at the beginning of the 1980s,
12-14 years after cinnarizine.
In certain European countries cinnarizine is widely
prescribed for “chronic cerebrovascular disease”. Within
Europe the prescription of “cerebral vasodilators” is
perhaps greatest in Spain, even though other countries have
a higher proportion of old people in their populations. In
1985 8 million units of preparations containing cinnarizine
were prescribed, and in Spain 5-7% of the population over
the age of 60 may be on long-term cinnarizine. In 1984 the
total value of prescriptions of pharmaceutical products
containing cinnarizine and issued by the Spanish social
security system was 6200 million pesetas (about S43-5
million). By contrast, cinnarizine is not even on the market
in the USA, and in Europe its use varies widely.
It is not surprising, then, that extrapyramidal signs
attributed to cinnarizine were first reported from Spain. In
1985 Marti Masso et al2 described eleven patients aged
65 — 83 in whom parkinsonism developed after treatment
with cinnarizine for from 6 to more than 36 months at daily
doses of 150 mg. Subsequently Marti Masso reported a
double-blind, placebo controlled randomised trial of
cinnarizine 150 mg daily in 20 patients with mildly
incapacitating Parkinson’s disease.3 After 1 month, 4 of the
10 patients in the cinnarizine group had to be withdrawn
from the study because of worsening of their condition;
Webster’s score and other objective scores and indicators
significantly deteriorated in the cinnarizine-treated group.
Data on the pharmacokinetics of cinnarizine are scarce.
Although no information is available for elderly people, it
seems that the drug’s plasma half-life in young volunteers is
about 3 h.4 By contrast, flunarizine has an elimination half
life of 4-19 days and is much more lipophilic,5 suggesting
that it is more likely to accumulate and cause CNS effects.
The main indication for cinnarizine is “cerebral
arteriosclerosis” but randomised trials of cinnarizine have
been inconclusive, mainly because inclusion criteria and
outcome variables have not been well specified.6 Nor is the
evidence for the efficacy' of other drugs used as cerebral
vasodilators convincing.7
s. A. RAJMES AND OTHERS: REFERENCES—continued
9. Burge H, Hutchinson JSF, Longland CJ, ei al. Selective nerve section in the
prevention of post-vagotomy diarrhoea. Lancet 1964; i: 577-79
10 Connell AM, Hilton C, Irvine G, Leonard-Jones JE, Misiewjcz J J. Variation ofbowel
habit in two population samples. Br Med J 1965; ii: 1095-99.
11 Kennedy T, Connell AM, Love AHG, McRae KD, Spencer EFA. Selective or
truncal vagotomy? BrJ Surg 1973; 60: 944—48.
12. Johnstone EC, Allan JG, Geraghty BP, Russell Rl. Psychiatric disturbance and
post-vagotomy diarrhoea J Psychosom Res 1974; 18:205-08.
13. Gohgher JC, Hill GL, Kenny TE, Nuncr E. Proximal gastric vagotomy without
drainage for duodenal ulcer, results after 5-8 years. BrJ Surg 1978; 65: 145-51.
14. Johnston D, Humphrey CS, Walker BE, Pulvenaft CN, Goligher JC. Vagotomy
without diarrhoea. Br Med J 1972, iii: 788-90.
854
THE LANCET, OCTOBER 11, 1986
SUSPECTED EXTRAPYRAMIDAL ADVERSE EFFECTS OF CINNARIZINE
AND FLUNARIZINE (WHO COLLABORATING DRUG MONITORING
PROGRAMME)*
Suspected
78M
46 F
48F
68 M
. 73 M
69/F
64/F
68/M
64/F
42/M
48 F
60 F
68 M
69, F
Daily
C
c
45
c
c
(2
c
c
c
F
F
F
F
F
F
150
150
150
60-180
150
10
10
20
10
10
10
Duration
of
treatment
4 5 vr
5 days
14 mo
2 days
..§
1 yr
2 days
28 days
•t mo
11 days
6 wk
lyr
8 mo
Suspected
Improved
adverse
with
drug
reaction t dechallengc
ED+T
ED
T
T
AP
T
T
AP
T
T
T
ED
ED
No
Yes
Yes
No
No
Yes
Yes
Yes
No
Yes
Yes
No
•There is some delay in reporting from national centres to the WHO
Collaborating Centre, Uppsala, so numbers arc not up to date.
tC = cinnarizine; F = flunarizine.
TED = excrapyramidal disorder, T = tremor, AP = aggravated parkinsonism.
§It is certain that cinnanzine intake began before the tremor.
. =unknown
remedies for the elderly, constitutes an invitation to
prescribe them for every such patient in an irrational way by
spinal reflex prescription rather than by rational drug
prescription.
Why are drugs of this kind available in. important
pharmaceutical markets in Western Europe? Drug
registration authorities evaluating a new product will look at
efficacy and safety. If there is no benefit demonstrated and
the drug carries risks, the benefit/risk ratio is zero, and the
drug should not be on the market, especially if it is to be paid
for with public money through a national health or social
security scheme. The registration-of drugs of no proven
efficacy is potentially dangerous.. Such drugs should be
banned, and national health authorities should adopt clear
criteria for the evaluation of drug efficacy.
We thank the national drug monitoring centres of Belgium (Dr Ph.
Janssens), West Germany ‘.Dr G. Kreutz), Ireland (Dr A. I. Scon), Italy
(Prof L. Rossini and Prof L. Leone), and the Netherlands (Dr R. H. B.
Mcyboom) for permission to use their data.
Correspondence should be addressed to: J.-R. L., Divisid de Farmacologu
Clinica, Universitat Autonoma de Barcelona, Ciutat Sanitaria de la Vail d’
Hebron, P Vail d’Hebron sn, 08035 Barcelona, Spain
REFERENCES
Parkinsonism, tardive dyskinesia, akathisia, and depression induced by flunarizine.
Cinnanzine is mainly prescribed to old people with
intellectual impairment and/or focal neurological signs, in
whom extrapyramidal signs may easily be attributed to
spontaneous deterioration rather than drug-induced
parkinsonism. This may be why so few cases were notified
through the spontaneous reporting system that has been
operating in Catalonia since 1983: of 7 adverse drug
reactions attributed to cinnarizine, 5 were extrapyramidal
symptoms. The WHO International Drug Monitoring
Programme’s file in Uppsala contains 3 further repons of
extrapyramidal disorders and tremor associated with
cinnarizine (table) and 6 repons of extrapyramidal disorders
associated with flunarizine. The accompanying table shows
that extrapyramidal symptoms do occur at the
recommended daily flunarizine dose of 10 mg, even in
young patients, contradicting Amery’s points8 about
Chouza’s paper.1
Cinnarizine, flunarizine, and drugs with a similar
spectrum of indications (eg, co-dergdcrine and citicoline)
are used as “mass placebos” in some countries. The
successful marketing of these useless drugs—which are not
even mentioned in most pharmacology textbooks—suggests
that prescribers either accept the claims made by
manufacturers, being unable to conceive that a registered
drug can lack efficacy, or, while sceptical about those claims,
mistakenly believe that a drug without any proven benefit
will at least be safe.
Suloctidil, another “cerebral vasodilator” recommended
for cerebral and peripheral ischaemia, was withdrawn in
1985 because it was found to induce hepatitis, in some cases
fatally. Another dangerous “placebo” withdrawn in 1985
was cyanidanol, promoted as a hepatoprotective agent for
the treatment of hepatitis B and other liver diseases. Cases of
haemolytic anaemia, some fatal, were ascribed to it.
The main side-effect of placebos, however, is not likely to
be uncovered by any drug surveillance system. Misused
placebos may produce the false sensation, among doctors
and patients, that some treatment is being provided when in
fact nothing is being done except delay the diagnosis and
treatment of the disease underlying the patient’s symptoms.
The very existence of these drugs, promoted as all-purpose
3.
4.
5.
6.
7.
Med Clin 'Barcelona) 1985;85:614-16.
Marti Masso JF Cinaricina y enfermedad de Parkinson: Estudio doblc ciego frencei
placebo. Neurologia • Barcelona; 1986; 1: 55-57.
Morrison PJ, Bradbrook ID, Rogers HJ. Plasma cinnarizine levels resulting from oral
administration as capsule or tablet formulation investigated by gas-liquid
chromatography. BrJ Clin Pharmacol 1979; 7; 349-52.
Holmes B, Brodgen RN, Heel RC, Speight TM, Avery GS. Flunarizine: a review of
its pharmacodynamic and pharmacokinetic properties and therapeutic use. Dn&
1986; 27:6-44.
Laporte JR. Report on cinnarizine. In. Tognoni G, Garanini S, eds. Drug treatment
and prevention in cerebrovascular disorders. .Amsterdam: Elsevier North-Holland
Biomedical Press, 1979: 181-91.
Spagnoli S, Tognoni G. ‘Ccrebroactive" drugs: Clinical pharmacology
therapeutic role in cerebrovascular disorders. Dru?r 1983; 26: -14 - 69.
Point of View
STROKES IN MILD HYPERTENSION:
DIASTOLIC RULES
Lawrence E. Ramsay
Patrick C. Waller
University Department of Therapeutics, Royal Hallamshire
Hospital, Sheffield S10 2JF
Fisher* has reviewed evidence suggesting that the risk of
cardiovascular disease is related more closely to systolic than
to diastolic blood pressure, and suggested that routine
measurement of diastolic blood pressure could I*
abandoned. The report of the Medical Research Council
trial of treatment of mild hypertension2 appears to give some
support to this view. It stated that systolic blood pressure a1
entry to the trial was significantly associated with d*
subsequent development of strokes and all cardiovascular
complications, whereas diastolic pressure at entry was less
clearly related to the risk of complications. This conclusion
was certainly incorrect for strokes, as will be shown below»
and may also be incorrect for other cardiovascular
complications.
The MRC report also stated that there was no relation
between systolic or diastolic blood pressure at entry to _
study and the percentage reduction in stroke incidence wi
active antihypertensive treatment, and it concluded that
benefits of treatment were uniform over the range of bk*pressure studied. This conclusion is also incorrect. 1
benefits of preventive treatment have to be assessed
/ ^d^X^lC-Kt
^7S
291
Chapter 27. Antipyretic Analgesics
Table 27-2. Pyrazolone analgesics.
R,
Rj
-ch3
-ch3
Aminopyrine (amidopyrine)
-ch3
-ch3
Dipyrone (aminopyrinesulfonate,
methampyrone)
-ch3
-ch3
Rs
-H
X
Antipyrine
z
X
Phenylbutazone (Butazolidin)
Oxyphenbutazone (Tandearil)
Sulfinpyrazone (Anturane)*
ch3
-phenyl
-p-hydroxyphenyl
-phenyl
-OH
-OH
-OH
XH2-SO3Na
-C4 H,
-c4h,
—C2 H4 -SO-phenyl
•Uricosuric agent discussed in Chapter 40.
ated in the body to oxyphenbutazone, and this metab
olite is also available as a drug.
Antipyrine is slowly metabolized by hydroxyla
tion at liver microsomes, with a half-life of about 8
hours. Phenylbutazone and oxyphenbutazone are even
more slowly metabolized and are well reabsorbed by
the renal tubules, resulting in a half-life in excess of 2
days.
Sulfinpyrazone (Anturane), the metabolite of a
compound closely related to phenylbutazone, is a very
useful uricosuric agent.
Pharmacologic Effects
The therapeutic effects are similar to those of
aspirin-ie. these drugs are analgesic, antipyretic, and
anti-inflammatory.
Clinical Uses & Dosages
The pyrazolone drugs exert an antipyretic effect
in some situations in which aspirin is not completely
effective—eg, Hodgkin’s disease with fever unresponsive
to salicylates or chemotherapy. They are probably also
more potent as analgesics and anti-inflammatory agents
in arthritis, bursitis, and thrombophlebitis. There is no
justification for the use of aminopyrine or dipyrone.
A. Antipyrine: Antipyrine can be used orally,
0.3-0.6 gm every 4-6 hours, as an alternative to
aspirin. The volume of distribution of antipyrine or its
metabolite, N-acetyl-4-aminoantipyrine, may also be
used to measure total body water.
B. Phenylbutazone (Butazolidin) and Oxyphen
butazone (Tandearil): Butazolidin, Tandearil, and
Butazolidin Alka are among the 200 drugs most com
monly prescribed by physicians in the USA, suggesting
that they are often used as first treatment drugs rather
than as alternatives to aspirin. Yet the restrictions on
their use and the contraindications and cautions made
a part of the labeling by the manufacturer are so strin-
Tabfe 27—3. Pyrazolone derivatives: Dosages and preparations available.
Usual Adult Dose
Preparations Available
Aminopyrine*
Antipyrine
Dipyrone (Pyrilgin, Narone)*
300-600 mg/day
300-600 mg every 4 hours
325—650 mg every 4-6 hours
Phenylbutazone (Butazolidin)
100 mg 3-4 times daily
Oxyphenbutazone (Tandearil)
100 mg 3-4 times daily
Bulk powder
Bulk powder
Tablets, 325, 500, and 650 mg
Oral liquid, 500 mg/5 ml
Pediatric liquid, 250 mg/ml
Injection (IM), 500 mg, 2, 10, and 30 ml
Tablets, 100 mg
Capsules (Butazolidin Alka), 100 mg, with
antacids
Tablets, 100 mg
•Not recommended for any use. See text.
Chapter 27. Antipyretic Analgesics
292
gent and comprehensive that responsibility for any
adverse result of therapy would probably devolve on
the physician. The drugs should not be used without
reference to the package insert.
The use of these drugs is suggested or permitted
in acute rheumatoid arthritis or spondylitis, osteo
arthritis, psoriatic arthritis, “painful shoulder,’’ acute
superficial thrombophlebitis, and acute gouty arthritis.
The daily dose is stated to be 300-600 mg/day
by the labeling. A more conservative position limits the
daily dose to 200 mg. These drugs should be discon
tinued if no improvement is observed in 4—5 days.
Adverse Reactions
The toxicity of the pyrazolone analgesics restricts
their use.
A. Antipyrine: Antipyrine causes fewer side
effects than aspirin. Unlike aminopyrine, it has rarely
been associated with agranulocytosis. It has caused an
allergic erythematous rash, often about the mouth,
that leaves pigmented areas when it resolves.
B. Agranulocytosis From Aminopyrine and
Dipyrone: The unusually high risk of agranulocytosis
following the use of these 2 analgesics is generally
acknowledged. As is true for many therapeutic agents,
the quantification of the risk is difficult, and the drugs
continue to be used in some countries. Neither of the
drugs was used recently in the USA until dipyrone
reappeared during the period 1960-1964. Imports of
dipyrone rose from none in 1958 to 19,000 lb in 1962.
During the period 1960-1964, 18 cases of agranulo
cytosis associated with the use of dipyrone, one-third
of them fatal, were reported to the AMA registry. How
complete this reporting was cannot be established. The
dipyrone was probably not recognized by the physi
cian as a derivative of aminopyrine, emphasizing the
need to think of drugs in terms of general classes rather
than individual compounds. The use of drugs under
their trade names and the prescribing of proprietary
mixtures without first identifying the ingredients
undoubtedly also led to the misuse.
In the USA. any preparation or mixture contain
ing aminopyrine or dipyrone must now bear a label
warning that the drug may cause agranulocytosis and
that it should be used only when specifically indicated
and when less toxic drugs-eg, salicylates-have proved
ineffective or are not tolerated.
The characteristics of agranulocytosis are dis
cussed in Chapter 6. The reaction is allergic in origin
rather than dose-related and is due to the sudden
peripheral destruction of granulocytes.
C. Phenylbutazone: Phenylbutazone and its
metabolite, oxyphenbutazone, frequently cause side
effects, and serious toxic reactions are frequent enough
that their use should be greatly restricted. Dose-related
toxic effects include sodium retention and edema, dry
mouth, nausea and vomiting, peptic ulceration and
hemorrhage, and rare cases of renal tubular necrosis
and liver necrosis. Allergic reactions include dermatitis,
which may rarely progress to exfoliative dermatitis,
and agranulocytosis.
Phenylbutazone may cause a reversible leukemoid
reaction: of greater concern, however, is the possibility
(not yet well established) that its chronic use may be
associated with a high incidence of acute leukemia.
Administration of phenylbutazone increases the
effects of tolbutamide and warfarin.
References
Mills JA: Drug therapy: Nonsteroidal anti-inflammatory
drugs. N Engl J Med 290:781, 1002, 1974.
Roe RL: Drug therapy in rheumatic diseases. Med Clin
North Am 61:405, 1977.
Hunter J: Study of antipyretic therapy in current use.
Arch Dis Child 48:313, 1973.
Kimberly RP, Plotz PH: Aspirin-induced depression of
renal function. N Engl J Med 296:418, 1977.
Leist ER, Banwell JG: Products containing aspirin. N Engl
J Med 291:710, 1974.
Salicylates
Croft DN, Wood PHN: Gastric mucosa and susceptibility
to occult gastrointestinal bleeding caused by aspirin.
BrMed J 1:137, 1967.
Davenport HW: Salicylate damage to the gastric mucosal
barrier. N Engl J Med 276’1307, 1967. [See also
editorial, N Engl J Med 288:316, 1973.]
Genton E & others: Platelet-inhibiting drugs in the preven
tion of clinical thrombotic disease. (3 parts.) N Engl
J Med 293:1173, 1236, 1296, 1975.
Hill JB: Salicylate intoxication. N Engl J Med 288:1110,
1973.
Hollister LE, Ranter SL: Studies of delayed-action medi
cation, 4. Salicylates. Clin Pharmacol Ther 6:5,
1965.
Moser RB: Bibliographies on diseases of medical progress:
Salicylates. Gin Pharmacol Ther 8:333, 1967.
Smith AP: Response of aspirin-allergic patients to chal
lenge by some analgesics in common use. Br Med J
2.494, 1971.
Smith MJH, Smith PK: The Salicylates: A Critical Biblio
graphic Review. Wiley, 1966.
Vane JR: The mode of action of aspirin and similar com
pounds. Hosp Formulary 10:618, 1976.
Zimmerman HJ:
Aspirin-induced hepatic injury. Ann
Intern Med 80:103, 1974.
Phenacetin & Acetaminophen
Burry AF, De Jersey P, Weedon D: Phenacetin and renal
papillary necrosis: Results of a prospective autopsy
(sfCnS^^^^
$k (^^krY^/^
§-^ ^~c't.
347
Salicylate-like Analgesic-Antipyretics
nol). Official preparations include tablets (120 and
325 mg) and an elixir and syrup (120 mg/5 ml); a
solution (60 mg/0.6 ml) is also available.
The conventional oral dosage is 325 to 650 mg
every 4 hours for adults and older children. The total
daily dose should not exceed 2.6 g. For young chil
dren. the single dose is 60 to 120 mg. depending
upon age and weight; total daily dosage should not
exceed 1.2 g Acetaminophen should not be admin
istered for more than 10 days or to young children
except upon advice of a physician.
Phenacetin {acetopheneiidiri) is no longer an offi
cial drug. It is too insoluble to be prescribed in
aqueous solution, and is usually administered orally
in powder, capsule, or tablet form. In recent years
it has been employed primarily in analgesic mix
tures. The average single dose for adults is 300 mg:
the total daily dose should not exceed 2.4 g.
Therapeutic Uses. Acetaminophen or
phenacetin is a suitable substitute for aspirin
for its analgesic or antipyretic uses in patients
who are allergic to aspirin or when aspirin
is contraindicated, as in patients with gout
or peptic ulcer. Acetaminophen has some
what less overall toxicity and is preferred
over phenacetin. Neither drug is an effective
antirheumatic agent. An additional minor
convenience of acetaminophen is its avail
ability in a liquid dosage form for oral inges
tion.
Analgesia. For headache, dysmenorrhea, arthral
gia. myalgia, and similar disorders, a therapeutic
dose of acetaminophen or phenacetin may be given
every 3 or 4 hours. Self-medication over a period
of days is not advised. If ordinary' doses are ineffec
tive. larger amounts as a rule do not give relief.
Acetaminophen is definitely less effective than aspi
rin in patients with active rheumatoid arthritis, and
any relief obtained is due to the analgesic effect.
Analgesic combinations containing acetaminophen
and phenacetin are discussed below.
Aniipyresis. The use of acetaminophen or phen
acetin to reduce fever is similar to that of aspirin.
The indications and the rationale for reducing body
temperature are discussed in connection with the
salicylates.
Pyrazolon Derivatives:
Antipyrine and Aminopyrine
Antipyrine {phenacone) and aminopyrine {amido
pyrine) were introduced into medicine in the late
nineteenth century' as antipyretics and subsequently
were also widely used as analgesics and anti-inflam
matory agents. However, clinical use of aminopyrine
was sharply curtailed after its potentially fatal
bone-marrow toxicity was recognized, and anti
pyrine has also lost favor. Both drugs have virtually
disappeared from the therapeutic scene in the
United States, but antipyrine is still employed in
some countries, usually in analgesic mixtures. A
#76 ,
variety of related pyrazolon derivatives have enjoyed
sporadic popularity. The congeneric phenylbutazone
has limited usefulness as an anti-inflammatory agent
{see above).
Chemistry and Pharmacological Properties. Anti
pyrine and aminopyrine are closely related phenylpyrazolon derivatives. Their structural formulas are
as follows:
CH,
I
Antipyrine
Aminopyrine
The pharmacology and toxicology of antipyrine
and aminopyrine have been reviewed by Greenberg
(1950). Randall (1963). and Beaver (1965, 1966). In
both animals and man, the pyrazolon derivatives
exhibit analgesic, antipyretic, and anti-inflammatory
properties similar to those of the salicylates: Neither
antipyrine nor aminopyrine has been subjected to
adequately controlled clinical trial by current stand
ards. However, aminopyrine was considered the su
perior anti-inflammatory agent and equivalent to
aspirin for therapy of acute rheumatic fever. Unlike
salicylate, the pyrazolon derivatives are not organic
acids, are only slightly bound to plasma protein, and
do not have uricosuric properties. They do not cause
gastric irritation or produce the acid-base or meta
bolic effects of salicylate.
Aminopyrine Agranulocytosis. Aminopyrine and
its close congener dipyrone cause a high incidence
of agranulocytosis. This allergic reaction is charac
terized by the presence in the plasma of antibodies
to granulocytes (see Wintrobe, 1969). In rare indi
viduals. instead of frank agranulocytosis, each ad
ministration of aminopyrine produces a sharp fall
in total leukocyte count associated with a severe
chill, spiking fever, headache, and pain in muscles
and joints; the attack is over within a few hours. The
incidence of aminopyrine-induced agranulocytosis
has been variously estimated between 0.01 and
0.86%. The mortality rate has been 20 to 50% (see
Huguley, 1964).
Antipyrine. Reports of agranulocytosis attributed
to antipyrine have been rare. Nevertheless, because
it is closely related to aminopyrine and because it
is not superior to safer drugs, the use of antipyrine
as an analgesic and antipyretic is not recommended.
Whether antipyrine has clinically useful antirheu-
348
Analgesic-Antipyretics, Anti-inflammatory Agents
malic properties has never been adequately deter
mined. It is no longer an official drug.
Antipyrine is employed as a pharmacological tool
for measurement of total body water and for assess
ment of hepatic microsomal mixed-function oxidase
activity. Il is rapidly and essentially completely ab
sorbed from the gastrointestinal tract. Peak plasma
concentration is usually attained in 1 to 2 hours. It
is less than 10% bound to plasma proteins and is
distributed in various tissues in proportion to their
water content. About 30 to 40% of the drug is con
verted to 4-hydroxyantipyrine. This metabolite is
rapidly and almost completely conjugated with glu
curonic, and perhaps sulfuric, acid and excreted in
the urine. Only about 5% of unaltered antipyrine is
eliminated in the urine. Hydroxylation of the side
chain also occurs, but the fate of a significant frac
tion of the drug remains uncertain. The plasma
half-time for the unchanged drug is 7 to 20 hours
(see Brodie and Axelrod. 1950).
Antipyrine causes induction of the hepatic micro
somal enzyme system and modifies the biotransfor
mation of other drugs, including the oral anticoagu
lant agents.
Aminopyrine and Dipyrone. “Over-the-counter’
sale of aminopyrine in the United States has been
prohibited since 1938. and federal regulations re
quire that preparations of aminopyrine and dipy
rone bear a warning on the labels stating that the
drug may cause fatal agranulocytosis.
Although it is an excellent antipyretic, analgesic,
and anti-inflammatory agent, and despite its advan
tages over salicylate, aminopyrine ordinarily should
not be employed because of the danger of agranulo
cytosis. In some cases of prolonged intractable fever.
as in Hodgkin’s disease and periarteritis nodosa,
aminopyrine is capable of controlling the disability
and may be justified. Dipyrone, the methanesul
fonate derivative of aminopyrine, has similar phar
macological and toxicological properties, including
the potential to cause fatal agranulocytosis. It differs
only in being more soluble and available for paren
teral administration.
If used at all in the treatment of intractable fever,
aminopyrine or dipyrone should be employed only
after safer drugs and other measures have proven
ineffective, and only with proper supervision and
monitoring. Administration of dipyrone with chlor
promazine can result in serious hypothermia, and
such use is contraindicated. Dipyrone can aggravate
a bleeding tendency or prothrombin deficiency.
Salicylamide
Salicylamide, the amide of salicylic acid, is no
longer an official drug. Its effects in man are not
reliable, and its use is not recommended. The small
doses included in “over-the-counter” analgesic and
sedative mixtures are probably ineffective.
Although not metabolized to salicylate in the
body, salicylamide has antipyretic, analgesic, and
anti-inflammatory effects similar to those of salicy
late. It also has sedative and hypotensive effects.
However, the drug is very rapidly inactivated during
[Chap. 17]
absorption and the initial circulation through the
liver. Concentrations of active drug in the systemic
circulation are markedly influenced by the dosage
form, and they are disproportionately low after low
doses. Salicylamide may inhibit ths metabolism of
other drugs by the liver.
Analgesic Combinations and
Mixtures
Aspirin, acetaminophen, and phenacetin
are frequently administered with each other
and a variety of other drugs, including
caffeine, sedatives, and the opioid analgesics.
Concurrent administration of an opioid and
an analgesic-antipyretic, such as codeine and
aspirin, has a valid role in analgesic medica
tion. However, none of the mixtures of
analgesic-antipyretics, including the tradi
tional aspirin-phenacetin-caffeine combina
tion, has been shown to provide significant
advantage over medication with aspirin
alone.
Irrational analgesic mixtures, such as those
with a hazardous component or presumed
active ingredients that are in fact inert, can
be expected to disappear from the thera
peutic scene when the assessment of “overthe-counter” medications currently being
conducted by the FDA is completed and the
recommendations of its panel are imple
mented.
Combined Opioid and Analgesic-Antipyretic Medi
cation. In most controlled clinical trials, codeine,
65 mg. has been found to add significantly to the
analgesic effect of aspirin, 650 mg. The combined
codeine-aspirin effect can be duplicated by larger
doses of codeine alone, but considerations of toxicity
and abuse favor restricting the dosage of the opioid.
Thus, combined codeine-aspirin analgesia is justified
if aspirin alone in full dosage is ineffective. Gastro
intestinal and central side effects typical of the opi
oids are the price for the increased analgesia pro
vided by this multiple-drug therapy. Parenteral
opioids are still required for relief of severe pain.
In adequate dosage, other orally effective opioids
add similarly to the analgesic effect of aspirin. In
general, a dose of an opioid that given alone pro
vides uncertain analgesia adds only equivocally to
the analgesic effect of aspirin. Although it is likely
that an effective dose of an opioid adds to the anal
gesic effect of acetaminophen as it does to that of
aspirin, clinical documentation is required. The
usual arguments for and against the use of fixeddose mixtures versus concurrent but separate ad
ministration of the components apply to combined
opioid and analgesic-antipyretic medication (see
Chapter 1).
COIVIMUfilj
'-Til CLLL
B4fJGAt O ■/q ^Srl<3 *Oad
UMI-u.-iE. 5bu q0^
Coate, „
-jate of the Art/Review
nd p]
fork
rberese Southgate. MD, Section Editor
'o and goj^
Rational Therapeutic Drug Monitoring
^anTp^
Redman. MD. D J. Greenblatt, MD
1cy s.vntiro^'
Zang ea
rus type flj'
men in Xe,“
MANY drugs, the measurement
Concentrations in serum or plasma
’. become widely available and
nodeficienCj
\^pted as an important component of
abort study,’
*Lical decision making. While these
Lang W, e Jj, levels often do allow more
Lertive monitoring and titration of
^mission:
1985. Pres^? Ljapy, the information also has the
A>DS. Pan^
"t^ntial to be valueless or even mis
TC. et at s__ sing- Laboratories sometimes report
a serum concentration is in the
-.tic’1 range, when the patient is
ablem
=2 well and has no evidence of toxic
'<ts. Or, conversely, the drug is not
Epidemic^
Etpideinioi i ..-ectable in serum. Such discrepancies
r-xeen measured serum drug concenaiming PD,. -^ions and observed clinical drug
,•313^^' #cts may occur for numerous reaE Hadle
H2S. Tkic
This arfiplo
article will
will rovipw
review enmp
some
en: Preral.» yindples and problems associated
transmisstt cth therapeutic drug monitoring.
vaccine. Min wn0NALE FOR MONITORING
■rman HJ, e. 5ERUM DRUG LEVELS
k exposure ?■ For a serum drug concentration to be
e globulin, a
xcentially useful for purposes of ther-
x'cedlestidi .-eutic monitoring, at least two requi: of the aop; ses must be fulfilled.' First, the
>ng health 0 enjm drug concentration must reflect
127-1132.
>rr-
* concentration at the receptor site;
the intensity and duration of
je
pharmacodynamic effect must be
37’753-756.
anporally correlated with the recep.<■ site drug concentration. When
fciese two conditions are not met, as in
je case of anticancer drugs showing
sTects long after they' are gone from
■he serum, the likelihood of correlating
gram levels with therapeutic effect is
sisiderably reduced.
During long-term dosage with any
irag, the two major determinants of
is mean steady-state serum concentra
te are the rate at which the drug is
idministered (dosing rate) and the
mig’s total clearance in that particular
atient.2'1 The mathematical relation
slip is
enthal BG: I
mily contaa; «cond,
bom be Division ol Clruca! Pharmacology. Oepart■et ol Psycbatry and Medcne. Tulls University
neo ol MerSone and New England Metical Center.
Tram
naml requests to Drasxxi ol CUtrcal Pharmacology.
x< 1007 Tults-New England Metical Center. 171
■arson Ave. Boston, MA 02111 (Dr Greenblatt)
ian & CV
Oct 24/31. 1986-Vol 256. No 16
Mean Steady-State Concentration =
Dosing Rate
Clearance
Clearance is measured in units of vol
ume per unit of time, and describes in
quantitative terms the capacity of a
given individual to biotransform or
eliminate a given drug. Drug clearance
is usually accomplished by hepatic bio
transformation, renal excretion, or a
combination of the two. Thus, under
usual circumstances, the steady-state
concentration of a particular drug in a
given individual is directly propor
tional to the dosing rate (with the
exception of a few drugs with saturable
or nonlinear kinetics, such as salicy
late, phenytoin, and alcohol). Among
different individuals, however, any giv
en dosing rate is likely to produce wide
variations in steady-state concentra
tion, attributable to large interindividual differences in clearance (Fig 1). A
number of identifiable factors can alter
the clearance of drugs, such as age,
gender, body habitus, disease states,
cigarette smoking, and drug interac
tions.2" However, substantial unex
plained individual variation in drug
clearance is commonly observed even
among healthy, drug-free persons of
the same sex and within a narrow age
range.1" Therefore, dosage may not be a
good predictor of steady-state concen
tration.
“Therapeutic range” and “therapeu
tic index” are two concepts used to
quantitate the relationships of serum
concentration to efficacy and safety,
respectively. Some drugs have a welldefined therapeutic range. When the
steady-state concentration falls within
this range, the likelihood of clinically
effective and nontoxic therapy is maxi
mized. Direct measurement of the
serum concentration allows appro
priate upward or downward titration
of dosage in the individual patient, to
attain the desired level. Therapeutic
ranges, however, are not absolute (Fig
2). Levels at the “low” therapeutic end
have a significant likelihood of being
clinically ineffective, whereas levels at
the high therapeutic end have a signifi
cant likelihood of causing toxic effects.
In experimental pharmacology, “thera
peutic index” is defined as the ratio of
the median lethal dose to the median
effective dose. In clinical medicine,
however, therapeutic index is usually
estimated as the ratio of the highest
potentially therapeutic concentration
divided by the lowest potentially thera
peutic concentration (Fig 2). Some
drugs (such as gentamicin, digoxin, and
lithium) have a narrow therapeutic
range and therefore a low therapeutic
index. For such drugs, one can antici
pate considerable overlap among inef
fective, effective, and possibly toxic
concentrations, thereby increasing the
importance of serum level monitoring.
Serum drug concentrations may still
be of considerable value even when a
therapeutic range has not been defi
nitely established. Consider a patient
with no apparent clinical response to
drug therapy despite seemingly ade
quate dosage. A measured steady-state
concentration that appropriately re
flects the dosage rate suggests that the
patient may actually be a “nonrespond
er." If, however, the measured level is
very low or undetectable, this suggests
that the patient either is not taking the
medication (noncompliance) or has un
usually high metabolic clearance. An
other example is the patient with a
sign or symptom (such as loss of
appetite during digitalis therapy) that
could be attributable either to an
adverse drug reaction or to the
underlying disease itself." In this case,
a high serum drug level suggests that
the medication might be responsible
for the adverse effect; a low serum
level, on the other hand, could indicate
that the underlying disease, or some
other factor, explains the reaction.
Drug concentrations frequently are
measured for medicolegal reasons. In
cases of deliberate or accidental drug
overdosage, verification of the particu
lar substances ingested, and their con
centrations in serum, may have impor
tant therapeutic and forensic value.
“Screening” of current and prospective
employees for the presence of “illicit
drugs” is becoming increasingly com
mon, although these tests are usually
done on samples of urine.12
Drug Monitoring—Friedman & Greenblatt
2227
1 2 3 4 5 6 7 8 9101112131415
Digoxin, jzg/kg/d
Fig 1. —Relation of steady-state serum digoxin
concentration to daily dose per kilogram for 100
patients receiving long-term digoxin therapy
Correlation is poor (r=.O69), indicating sub
stantial variability in steady-state concentration
that is not explained by dosage (Hermann R.
Ochs. MD. unpublished data. 1979).
Toxic
Possbty
s
II
Therapeutic
<3 1
§
J?
Toxic
Possibty
Toxic
Therapeutic
Effective
Not
Effective
Wide
Therapeutic
Range
Parity
Effective
’noT~
Effective
Narrow
Therapeutic
Range
Fig 2.—Schematic relation of serum or plasma
drug concentration to clinical efficacy or toxicity
for hypothetical drugs having wide or narrow
therapeutic ranges (from Greenblatt and Shad
er2).
Finally, the availability of methods
for measurement of drug concentra
tions provides the impetus for clini
cians to increase their expertise and
understanding of pharmacologic and
pharmacokinetic principles of drug
therapy. Enhanced awareness of dose
concentration relationships, and fac
tors influencing these relationships,
may lead to an overall improvement in
the quality of drug treatment.13
drug distribution and
ACCESS TO ITS RECEPTOR
When a drug is given by an extravascular route of administration (orally,
intramuscularly, rectally, subcuta
neously, sublingually, transdermally,
2228
JAMA. Oct 24 31
1986-Vol 256. No 16
etc), or even by intravenous injection,
the entire administered dose does not
have immediate and complete access to
its receptor site mediating pharmaco
logic activity (Fig 3). After intravenous
injection, the entire dose reaches the
systemic circulation and by definition
has 100% bioavailability. However, the
drug is distributed not only to the
tissue where it is active, but also to a
number of other sites (Fig 4). Further
more, once the drug has reached the
systemic circulation, it also encounters
serum or plasma proteins. Drugs are
bound to proteins to varying de
grees.1415 The principal binding pro
teins are albumin and cq-acid glycopro
tein. The affinity of a drug for serum
protein limits its freedom to diffuse
across cell membranes, hence further
limiting its accessibility to the receptor
site.
When a drug is administered by an
extravascular route, it reaches the sys
temic circulation indirectly, often
yielding less than 100% bioavailabili
ty."' Oral bioavailability of drugs in
tablet and capsule form can be influ
enced by incomplete absorption due to
incomplete dissolution, which in turn
depends on packaging and drug parti
cle size. Oral solutions overcome the
dissolution problem. Other factors that
can influence oral bioavailability in
clude changes in gastrointestinal mo
tility, gastric and intestinal pH, mal
absorption
syndromes,
and
the
coadministration of foods and drugs
(especially
antacids,
antidiarrheal
agents, and chelating agents).
After absorption of the drug from
the gastrointestinal tract, systemic bio
availability may be reduced because of
metabolic transformation in the gut
wall, or by extraction from the portal
circulation during the “first pass”
through the liver. This is the case for
certain drugs characterized by high
hepatic clearance, including proprano
lol, lidocaine, tricyclic antidepressants,
opiate analgesics, neuroleptics, hydral
azine, nitroglycerin, verapamil, and
prednisone.1.
Incomplete bioavailability after in
tramuscular injection is also possible.
This has been attributed to poor drug
solubility at physiologic pH and precip
itation at the injection site after
administration of chlordiazepoxide, di
goxin, phenylbutazone, phenytoin, and
quinidine.1"
A number of recent studies have
evaluated drug absorption after sublin
gual or buccal administration.111'21 In
principle, this route of administration
delivers the drug directly into the
systemic circulation, bypassing both
the gastrointestinal tract, where some
drugs are degraded or metabolized, and
the portal circulation and consequent
first-pass hepatic extraction. For most
drugs evaluated to date, bioavailability
after sublingual dosage is equivalent to
or greater than that after oral admin
istration. A similar principle holds for
rectal drug administration, since ap
proximately 50% of the hemorrhoidal
circulation empties into the systemic
rather than the portal venous system.21
Finally, the transdermal23 or pulmo
nary route can be used to administer
some drugs.
For all these reasons, drug concen
trations in blood, serum, or plasma
often reflect pharmacologic action
more closely than administered dosage
alone.
"
FACTORS INFLUENCING
INTERPRETATION OF
SERUM DRUG CONCENTRATIONS
Total vs Free Serum
Concentrations
Although only the unbound or free
drug can passively cross cell mem
branes and interact with receptors,
free drug levels nonetheless are still
not routinely monitored. This is partly
because their measurement is techni
cally more difficult to perform than
that of total levels. Fortunately, for
most drugs, the ratio of free to total
serum concentration (free fraction!
usually remains relatively constant
during a given patient’s course of then
apy, with salicylate and ibuprofen24'
being among notable exceptions
Therefore, a doubling of the total con- al situa
centration will also lead to a doubling fading
of the free serum drug concentration at owered
steady state. In most clinical circutn- or total
stances, variability between patients in fa, phen
free fraction may also be relatively ally falls
small.26 When within- and between- *come a
individual differences in serum proteit Uternati
binding are small, monitoring of toti cute ph.
serum concentration should prove to bt ’ently el
as useful therapeutically as monitorta' ’farction
of free or unbound concentration.1"’' ,es. or it
In some conditions, however, drUf Creased.
binding to serum protein may be sub nd resul
stantially altered. For example, proteit rug level.binding of a given drug may be reduc* •■nical eff
(increased free fraction) when anotM iclude lid
drug displaces it from its bindini one. phen
sites.15"' Such interactions in then? »mide. F
selves are unlikely to be of dire*1 tund to se
clinical importance,15"’T"'J“ since tl» tine, dig,,,
increased “free” concentrations will b ’faainamii
only transient due to rapid equilibr* ety|proca
tion with tissues. However, the tot* ’tn hindin
drug concentration will consequent «ence.
fall, and may lead to a lowering of
therapeutic and toxic ranges for b
“trial S
total serum drug level (Fig 5).31 Uren"1 Proper cl
and hypoalbuminemia are other cH’u ’Cial for t
Orin) Monitoring—Friedman & Greer*’*
. ,j
Intramuscular,
Subcutaneous,
or Transdermal
IOK<
r fits
met
iptor.
e stj
part
echtthy
y, fa
i tou
ictioz.
nstaz
fthe
Fig 3.—Schematic diagram of pathways of drug absorption, distribution, elimination, and clearance
fen"atioK
Fig 4.—Estimated distribution pattern of benzodiazepine derivative nordazepam (desmethyldiaze•d cor tai situations in which serum protein
pam) in normal healthy woman (30% body fat), based on human autopsy studies.47 Nordazepam
ublfa; binding of drugs is reduced, causing
(desmethyldiazepam) is major metabolite of diazepam (Valium) and halazepam (Paxipam), and is
Lions lowered therapeutic and toxic ranges
principal active substance present in blood during treatment with clorazepate dipotassium
ircutt- for total drug concentration. For exam(Tranxene) and prazepam (Centrax).
tntsi: ole. phenytoin free fraction, which usuitiveb illy falls between 10/" and 2O'/'<, may
tweet oecome as high as 30'f in uremics.31
’Jfcnatively, <>i-acid glycoprotein, an
iroteif^BC'
phase reactant, may be tran
f tots
e to b siently elevated in acute myocardial
Itorin infarction, shock, severe burns, inju
ries, or infectious processes,"J causing
dni mcreused binding of some basic drugs,
sul tnd result in increased total serum
irotei irug levels without an enhancement of
educe dinical effect. Examples of such drugs
notht include lidocaine, propranolol, imipraindin nine, phenytoin, quinidine, and disopythen ’amide. For drugs not extensively
dire »und to serum proteins, such as cime:e tl Mine, digoxin, and gentamicin, lithium,
will 1 irocainamide and acecainamide (N•lilibn cetylprocainamide), changes in proe tot ein binding are of far less conseuentl lienee.
0°f y Iptimal Sample Timing
Jremi Proper choice of sampling time is
- din rucial for the interpretation of serum
■reenbi WA. Oct 24 31. 1986-Vol 256, No 16
Drug Monitoring—Fnedman & Greenblatt
2229
25.0'
Fig 5.—Influence of change in protein binding on total and unbound serum or plasma
concentrations of hypothetical drug at steady state. It is assumed that drug is being administered at
constant dosing rate (8 mg/kg/d), and that drug's total clearance is also constant. When free
fraction (FF) is 0.05 (left), total plasma drug concentration is 20 mg/L, and free concentration is
1.0 mg/L (dotted lines). If for some reason extent of protein binding is reduced, and FF is increased
to 0 to (right), steady state free drug concentration remains at 1.0 mg/L because there has been
no change in either dosing rate or clearance. However, total concentration falls to 10 mg/L Thus,
change in protein binding (free fraction) by itself causes no alteration in free drug concentration, but
win cause reciprocal change in total drug concentration (from Greenblatt and Shader7).
drug concentrations. In general, it
takes four times the drug’s half-life at
a constant dosing rate for the steady
state condition to be more than 90%
attained. Similarly, an increase or
decrease in dosage will require the
same time interval to reach the new
steady-state level (Fig 6). After initiat
ing therapy with long half-life drugs, a
considerable length of time may be
required for steady state to be attained
(Fig 7). Therefore, sampling before the
attainment of the actual steady-state
condition may lead to premature dos
age adjustments. This is of particular
importance for drugs such as theophyl
line that are administered to infants
§
and children.
Occasionally, the need may arise to
hasten the attainment of therapeutic
concentrations. This can be achieved by
giving an initial loading dose, the sue
of which has been appropriately chosen
based on the desired therapeutic con
centration and the pharmacokinetic
characteristics of the drug.”'” How
ever, even the ideally selected
dose has potential disadvantages. T**
rapid attainment of therapeutic con
centrations precludes gradual adapta ■issi
'ffe,
tion to therapeutic or adverse dru?
effects, such as sedative, hypotensi'*
'eda
bradycardic, or anticholinergic proper
>yc.
ties.
’and
Once the steady-state condition h®
'ery
been achieved, the mean steady-st3“
ntd
serum drug level should remain
stant as long as the dosing ratea* Htie
,.Cer
clearance are constant (as indicated
the equation in the first section oft"® ■*>113
*t>l0(
article). However, the interdose 0
tuation depends on the dosage inter*
! the
A proportional increase or decrease
J
Multiples of HatfTrte
Fig 6.—'Time course (in multiples of half life) of mean serum concentration during attainment of
steady-state condition after starting therapy and after reducing dosage. Css indicates mean serum
concentration at steady state (from Greenblatt and Shader7).
Fig 7. — Time course of attainment of steady-state condition, assuming drug is given once daily.
Case A indicates drug with short half-life; case B, drug with long half-life (from Greenblatt and
Shader2).
Days
both the size of each dose and
interval between doses, such that
;
overall dosing rate remains consW®J i
does not change the mean steady;5
concentration, but will alter the >n . |
dose fluctuation (Fig 8). More frefl
|
Drug Monitoring—Inudnian S
2230
JAMA. Oct 24/31. 1986—Vol 256. No 16
1
&
drugs with narrow therapeutic indexes,
such as aminoglycosides or lithium.
Unfortunately, however, the time of
peak concentration can seldom be pre
dicted with certainty.
If the dosage interval is not regular,
or if the drug is taken intermittently,
then the best time to sample is not
necessarily so obvious, since there is no
single “trough” concentration (Fig 10).
Hours
pg g.—Interdose fluctuation ol serum drug concentration as function of dosage schedule,
ming that drug is given in overall total dosage of 500 mg/24 h. but with different dosing
doles. Note that mean serum concentration at steady state (Css) is same for each regimen,
and that interdose fluctuation is largest for once-daily therapy (from Greenblatt and Shader5)
•
Fig 9—Time course of serum drug concentra
tion at steady state during oral dosage every 12
hours, with illustration of optimal sampling time
Greenblatt and Shader2).
dosing is useful to minimize transient
effects due to high peak levels that
some people find objectionable, such as
sedation and drowsiness from certain
psychotropic drugs.35 On the other
hand, dosing schedules that require
very frequent dosing are inconvenient,
and may be associated with reduced
patient compliance.
Certain sustained-release formula
tions of drugs have been designed to
prolong drug action after each dose,
thereby allowing less frequent dosing.
If the rate of drug entry into the
systemic circulation precisely mimics a
fixed-rate infusion, then the serum
drug level will not fluctuate. Although
this is not an attainable ideal, some
sustained-release preparations do in
fact allow infrequent dosing, with only
JAMA. Oct 24/31. 1986—Vol 256. No 16
small fluctuations in serum drug con
centrations?'
At steady state, each discrete drug
dose is followed by an “absorptive”
phase, during which serum concentra
tions exceed the mean. Transient side
effects may be associated with the
absorptive peak. After peak concentra
tions are reached, the serum level then
falls as distribution and clearance pre
dominate. Just before the next dose,
levels are at a minimum during the
“trough” phase. Sampling shortly after
a dose, during the absorptive phase, is
not recommended for evaluation of
therapeutic efficacy since the measured
level does not necessarily correspond to
the peak. Furthermore, even if the
peak level was found to be in the
therapeutic dosing range, this would
not ensure therapeutic levels through
out the entire dosage interval. The
optimal time to sample for evaluation
of efficacy is just before the time of
dosing (Fig 9), to ensure that the
minimum drug level falls with the
therapeutic range. If the trough level is
found to be subtherapeutic, the clini
cian may elect to give smaller doses
more frequently while maintaining the
same total dose per 24 hours (Fig 8).
This change would reduce the interdose
fluctuation and possibly bring the
trough level to within the therapeutic
range. Measurement of peak serum
concentrations after an individual dose
may be of value when clinicians wish to
evaluate potential drug side effects
coinciding with peak concentrations.
Knowledge of both peak and trough
concentrations may be desirable for
Artefacts due to Collection Tubes
The Vacutainer brand of blood col
lection tubes is reported to contain
TRIS (2-butoxyethyl) phosphate, a
plasticizing agent. Blood samples
drawn into these tubes can give spu
riously low serum drug levels when the
serum is analyzed for imipramine,
alprenolol, propranolol, lidocaine, and
quinidine.33 The mechanism for the
lowering of serum levels appears to
involve displacement of drugs from
0,-acid glycoprotein (but not from
albumin) by TRIS (2-butoxyethyl)
phosphate. This in vitro phenomenon
results in an increase in unbound drug,
which quickly diffuses into and equili
brates with the red blood cells present
in the tube. Thus, when the serum is
aspirated after centrifugation, the re
sultant serum drug level is spuriously
low. However, the whole blood level is
unchanged. Any drug that is extensive
ly bound to aracid glycoprotein is
likely to be influenced by this collection
artefact.
Analytic Methodology
Knowledge of the methodology used
by a laboratory in analyzing serum for
drug levels may be of critical impor
tance for the clinician in interpreting
the results. Ideally, an assay procedure
for a particular drug should (1) resolve
compounds of similar structure, such
as the parent drug and its metabolic
products or other substances present in
the serum (specificity); (2) consistently
conform to accepted standards for
accuracy and replicability for the range
of concentrations encountered clini
cally; and (3) be sensitive enough to
quantitate levels well below the thera
peutic range. In addition, the need for
cost containment must always be con
sidered. Procedurally straightforward
analytic methods that can be auto
mated are generally less expensive and
therefore preferred. However, such
procedures, although less costly, may
not provide adequate specificity, accu
racy, replicability, and sensitivity'.
More complex and often more expen
sive analytic methods may be needed
,to provide meaningful serum concen
tration data.
Historically, spectrophotometry and
Drug Monitoring—Friedman & Greenblatt
2231
$
1O'r
0
4
8
12
24
Hours
Fig 10.—Plasma concentrations of drug at
steady state with four-times-daity dosing sched
ule. with individual doses given at times shown
by arrows. This complex dosing schedule
makes monitoring of plasma drug levels more
difficult (from Greenbtatt and Shader2).
colorimetry were the first methods
widely used in laboratories for mea
surement of drug levels.37 These proce
dures may require one or more solvent
extractions, often coupled with chemi
cal reactions, to yield a solution con
taining primarily the drug of interest
The absorption of visible, infrared, or
ultraviolet light at a specific wave
length by the drug in solution is used to
quantitate its presence. The level of
sensitivity is usually on the order of
parts per million to parts per thousand.
These methods are limited by poor
sensitivity and variable specificity,17
and high cost.
Immunoassays for drugs have be
come popular within the last 20 years.38
In principle, they rely on the interac
tion between a drug acting as an
antigen and an antibody to it. Since
most drugs are nonimmunogenic, they
first must be conjugated by a bridge or
linkage group to a substance of high
molecular weight, such as a protein. In
this conjugated mode, the drug behaves
like a hapten and is used to immunize
an animal. Antibodies may be gener
ated against the drug if the conjuga
tion bridge or linkage keeps the drug
sufficiently far from the larger protein
molecule. The necessity for an antibody
to seek out a hapten creates the inher
ent variability in specificity provided
by immunoassays. Some antibodies
may show cross-reactivity with metab
olites and congeners of the drug of
interest, thereby rendering the anti
bodies relatively nonspecific.”
In the radioimmunoassay (RIA),
drug present in a serum sample com
petes with a radioisotope-labeled
ligand for antibody binding sites. The
RIA procedures are stated to be very
sensitive, but require the use of
radioactive material and are costly.
Enzyme immunoassays substitute an
2232
.JAMA. Oct 24/31. 1986—Vol 256, No
enzymatic label for a radioactive one.
The inhibition of labeled enzyme activi
ty by antibody is the basis for the very
popular enzyme-multiplied immunoas
say technique. This technique is
claimed to be procedurally straightfor
ward and inexpensive, but is considera
bly less sensitive than RIA and can
have variable specificity, particularly
when applied to screening for drugs of
abuse in urine.12,10,11 Most nonisotopic
immunoassay labels are inactivated by
antibody; hence, they do not require
the separation of bound from free
labeled ligand as in RIA.
Chromatography is a method of sep
arating mixtures of substances based
on their physicochemical characteris
tics, so that one or more of those
substances may be specifically de
tected. The principal methods used in
drug measurement are gas-liquid chro
matography (GLC)12 and high-pressure
liquid chromatography (HPLC).13 Se
rum, or a concentrated extract thereof,
is injected onto a column through
which flows a mobile phase. For GLC,
the mobile phase is a purified gas such
as helium, nitrogen, or argon. For
HPLC, the mobile phase contains mix
tures of an aqueous buffer and an
organic solvent such as acetonitrile or
methanol. Separation of the serum
components by the mobile phase is
influenced by interactions with the
column’s stationary phase. Actual sep
arations are based on lipophilicity,
polarity, molecular size, temperature,
and boiling point (for GLC). The HPLC
separations may be further refined by
varying the pH and polarity of the
mobile phase. Often it is possible to
detect and quantitate the parent drug
and some or all of its important metab
olites simultaneously.
For some applications, a mass spec
trometer is coupled to a chromato
graph’s effluent and thereby acts as
the detector. This combination pro
vides the “gold standard" in specificity
and sensitivity in drug analysis. How
ever, mass spectroscopy is expensive
and requires complex instrumentation
as well as highly trained personnel.
When the drug mixture is well sepa
rated chromatographically, other less
complex detection systems usually suf
fice. In GLC, the most commonly used
detectors are flame ionization, nitrogen-phosphorus, and electron capture.
Flame ionization will respond to all
organic compounds. Nitrogen-phosphorus has enhanced response to nitro
gen- and phosphorus-containing com
pounds, and electron capture responds
to drug-containing electronegative sub
stituents such as halogens, nitrates, and
conjugated carbonyls. The sensitivity
of nitrogen-phosphorus and electron
capture is in the subparts-per-billion
range; that of flame ionization is on
the order of parts per million. Highpressure liquid chromatography most
commonly utilizes spectrophotometry ’,
fluorescence, or electrochemistry for
the detection and quantitation of drugs
after chromatographic separation. Flu
orescence detection is applicable to
molecules with rigid polyaromatic
structures or extensive conjugation
having the property of absorbing light
and then emitting.it at a lower wave
length. Electrochemical detection is
employed for the recognition of easily
oxidized or reduced groups such as
phenols, indoles, and secondary and
tertiary nitrogens. In favorable cases,
fluorescence and electrochemical detec
tion can extend sensitivity two orders
of magnitude beyond the spectrophoto
metric range.
The above information can be
extremely useful to clinicians in inter
preting serum drug concentration re
ports. Consider, for example, a “nondetectable” serum concentration report
This must be interpreted in light of the
lower limits of sensitivity of the partic
ular assay technique. If the assay
technique has a high degree of sensitiv
ity, a reported zero level may actually
mean that there is no drug present in
serum. Conversely, it may imply that
clinically important amounts of drug
may be present in serum, but the assay
is not sufficiently sensitive to quanti
tate levels in this range. At the other
extreme, laboratories may report very
high serum drug concentrations in 1
patient taking “usual doses” and hay
ing no manifestations of toxicity. This
might be attributable to the use of»
very nonspecific assay technique that
quantitates not only the drug in que*tion but also its metabolic products, *
possibly other endogenous unrelated
substances present in serum. FinaW'
laboratories may report widely
ant serum drug concentrations fro®
day to day in samples drawn under
identical conditions in a given pati
receiving a constant dose of a dr*
These variations could be due to van*
bility over time in the patient's
bolic clearance or extent of
’
absorption. They could also be attn
able to insufficient accuracy
j
laboratory determination, regardless
i
the method.
’
Laboratories should readily P7?'
'
to any inquiring physician all
j
analytic quality control Pr0C<<L^
Nonetheless, clinicians have niea &
their disposal to test and comp31* .«■
performance of laboratories. H 3
reference standard of the drugin
Druq Monitoring — Friedman
>ion is available, physicians may
-spike” drug-free control serum with
carious known concentrations of drug,
3nd send them “blindly" to the labora•' rnt|t mrv. This procedure should provide
ometr ■nformation
■’
- - on
the sensitivity and
try t; jcciiracy of the laboratory’s methodo•fdruj iQjry. Another procedure that can be
in. p|: ;?ed to test the replicability of deterk ruinations either within the same labo■omati fjtory or 'between ’laboratories
'
'
' to
is
ugatio- jplit a given serum sample into two
ig ligb jiquots. The aliquots can be then sent
■5 different laboratories and the
lion
•fsults compared. Alternatively, the
f east ame divided sample under different
uch ; resignations can be sent to the same
jboratory on different days. The labo•atory should quantitate the identical
1 det*. nearly identical results in these split
order jampies. When results on identical
iphou, samples differ by less than 10%, the
jboratory performance under these
an b ^himstances is acceptable.
1 int*
" we ....
Parent Drugs and
Active Metabolites
Many drugs used in clinical practice
are biotransfornied into other com
pounds that themselves are pharmaco
logically active.4145 When evaluating
the therapeutic effects of such drugs,
clinicians must integrate the relative
contributions of all active substances
present in serum. Physicians should be
knowledgeable of the metabolism of
the drugs they prescribe, and analytic
laboratories should automatically mea
sure concentrations of parent drug and
active metabolites. Consider, for exam
ple, a patient taking imipramine, which
is biotransformed to the active metabo
lite desipramine. Clinicians requesting
a serum imipramine concentration
should expect, and laboratories should
provide, simultaneous concentrations
of both imipramine and desipramine
present in the sample. In a few years,
this problem may become further com-
plicated by the appreciation of other
active metabolites of imipramine, such
as hydroxyimipramine and hydroxydesipramine."’
SUMMARY
The simple act of ordering a serum
drug level does not guarantee that the
information will be meaningful or use
ful. The interpretation of serum con
centrations can be profoundly influ
enced by such factors as the timing of
the sample, the patient’s clinical state,
the drug’s pharmacokinetics and me
tabolism, and the tube type and analyt
ic methodology used. The likelihood of
obtaining clinically meaningful and
useful results can be maximized when
these factors are taken into account.
This investigation was supported in part by
grants MH-34223 and AG-00106 from the Public
Health Service
We are grateful for the assistance and collabo
ration of Richard I Shader and Hermann R.
Ochs.
seferences
nonds
Koch-Weser J Serum drug concentrations as
1979;4:423-132
net 1980;5:246-262
18.
Greenblatt DJ, Koch-Weser J: Intramuscular 33.
Wilder BJ, Serrano EE, Ramsay RE: Plasma
injection of drugs. N Engl J Med 1976;295:542diphenylhydantoin levels after loading and main
546.
tenance doses. Clin Pharmacol Ther 1973;14:79719.
DeBoer AG, deLeede LGJ, Breimer DD: Drug 801
assay
absorption by sublingual and rectal routes. Br J
3-1. Greenblatt DJ, Bolognini V, Koch-Weser J, et
nsitiv. 1 Greenblatt DJ, Koch-Weser J: Clinical pharmaAnaesth 1984;56:69-82.
al Pharmacokinetic approach to the clinical use of
.-okinetics.
A
r
Engl
J
Med
1975,293:702-705,
96-120.
Greenblatt
DJ, Divoll M, Harmatz JS, et ah lidocaine intravenously. JAMA 1976;236:273-277.
ctualr
35.
Tomson T Interdosage fluctuations in plasma
Pharmacokinetic comparison of sublingual loraze
sent ii t Williams RL: Drug administration in hepatic
pam with intravenous, intramuscular, and oral
carbamazepine concentration determine intermit
y ths isease. N Engl J Med 1983,309:1616-1622.
lorazepam. J Pharm Sci 1982;71:248-252
tent side effects. Arch Neurol 1984;41:830-834.
f drug i Hoyumpa AM, Branch RA, Schenker S: The
21.
Scavone JM, Greenblatt DJ, Friedman H, et 36.
Kelly HW, Murphy S: Efficacy of a 12-hour
al: Enhanced bioavailability of triazolam following
sustained release preparation in maintaining ther
* assay fsposition and effects of sedatives and analgesics
- liver disease. Annu Rev Med 1978;29:205-218.
sublingual versus oral administration. J Clin
apeutic serum theophylline levels in asthmatic
|uant £ Dawson GW, Vestal RE: Smoking and drug
Pharmacol 1986^6208-210
children. Pediatrics 1980;66:97-102.
• othe metabolism. Pharmacol Ther 1982;15:207-221.
22.
DeBoer AG, Moolenaar F, deLeede LGJ, et al: 37.
Thienes CH, Haley TJ: Clinical Toxicology, ed
Powell JR, Donn KH: Histamine H;-antagonist
Rectal drug administration: Clinical pharmacoki
4 Philadelphia, Lea & Febiger, 196-1.
38.
Marks V: Immunoassays for drugs, in Richens
netic considerations. Chn Pharmacokinet 1982;
s in i inig interactions in perspective: Mechanistic con
cepts and clinical implications. Am J Med 198-1;
7.285-311.
A, Marks V (eds): Therapeutic Drug Monitoring.
d hav- "isuppl
23.
Breimer DD: Rationale for rate-controlled New York, Churchill Livingstone Inc, 1981
5Br.57-84.
-. Thh «. Greenblatt DJ, Sellers EM, Shader RI. Drug
drug delivery of cardiovascular drugs by the
39.
Blyden GT, Franklin C, Cho SI, et al: Cyclos
e of 2 nsposition in old age A’ Engl J Med 1982;
transdermal route. Am Heart J 1984;108:195-200.
porine blood concentrations determined by specific
24.
Levy G: Clinical pharmacokinetics of salicy versus nonspecific assay methods. J Clin Pharma
e tha- •W:10Sl-108S.
i Abernethy DR, Greenblatt DJ, Divoll M, et al:
lates: A re-assessment. Br J Clin Pharmacol
col 1986;26:367-371
que? : ations in drug distribution and clearance due
1980;10:285s-290s.
40.
Divoll M, Greenblatt DJ: The admissibility of
cts, or | bsity. J Pharmacol Exp Ther 1981^17:68125.
Lockwood GF, Albert KS, Gillespie WR, et al: positive EMIT results as scientific evidence:
elatk :
Pharmacokinetics of ibuprofen in man: I. Free and
Counting facts, not heads. J Clin Psychopharmacol
total area/dose relationships. Chn Pharmacol
1985;5:114-116.
inalh.110. Friedman H, Greenblatt DJ, Burstein E, et al:
A population study of triazolam kinetics,
Ther 1983;34:97-103.
41.
McBay A J: Cannabinoid testing. Forensic and
ibstracted. Clin Pharmacol Ther 1986;39:193.
26.
Levy RH, Moreland TA- Rationale for moni analytical aspects. Lab Management 1985;
free 11.
| Ochs HR, Greenblatt DJ, Harmatz JS, et al:
toring free drug levels. Clin Pharmacokinet 1984;
23(Jan):36-41.
9(supp) l):l-9.
42.
Sherma J; Gas chromatography, in Zweig G,
unde jyrum digoxin concentrations and subjective manof toxicity. Pharmacology 1980-^0:14927.
Greenblatt DJ, Sellers EM, Koch-Weser J: Sherman J (eds)- Handbook of Chromatography.
atien: Jestations
Importance of protein binding for the interpreta
Boca Raton, Fla, CRC Press Inc, 1972, vol 2.
drug ll
[ Morgan JR Problems of mass.urine screening
43.
Kabra PM, Morton LJ (eds): Liquid Chroma
tion of serum or plasma drug concentration. J Clin
varia &lor misused drugs. J Psychoactive Drugs 1984;
Pharmacol 1982;22:259-263.
tography in Clinical Analysis. Clifton, NJ,
28.
Froscher W, Burr W, Penin H, et al: Free level Humana Press, 1981
mete iiI&30S-317.
_____
(jlTX 11 Duhme DW, Greenblatt DJ, Koch-Weser J:
monitoring of carbamazepine and valproic acid:
44.
Drayer DE: Pharmacologically active metabo
seduction of digoxin toxicity associated with
Clinical significance. Clin Neuropharmacol 1985;
lites of drugs and other foreign compounds. Drugs
ribui measurement of serum levels. Ann Intern Med
8362-371.
1982^4:519-512.
29.
Sellers EM: Plasma protein displacement 45.
1374;80:516-519.
Atkinson AJ, Strong JM: Effect of active drug
esso ILJusko WJ, Gretoh M. Plasma and tissue
interactions are rarely of clinical significance.
metabolites on plasma level-response correlations.
protein binding of drugs in pharmacokinetics.
Pharmacology 1979;18:225-227.
J Pharmacokinet Biopharm 1977;5:95-109.
•j '-Jrug Metab Rev 1976;5:43-140.
30.
McElnay JC, D’Arcy PR Protein binding 46.
Potter WZ, Calil HM, Manian AA, et al
0V10 li
J Sellers
EM.EM: Binding of drugs to displacement interactions and their clinical impor
15.
Koch-Weser
J, Sellers
Hydroxylated metabolites of tricyclic antidepres
ills fl >eum albumin. Ar Engl J Med 1976;294:311-316,
tance. Drugs 1983;25:495-513.
sants: Preclinical assessment of activity. Biol
31.
Gugler R, Shoeman DW, Huffman DH, et al: Psychiatry 1979;14:601-613.
lures 526-531.
16.
Greenblatt DJ, Smith TW, Koch-Weser J: Pharmacokinetics of drugs in patients with the
47.
Friedman H, Ochs HR, Greenblatt DJ, et ah
^availability of drugs: The digoxin dilemma.
nephrotic syndrome. J Clin Invest 1975^5:1182Tissue distribution of diazepam and its metabolite
Qin Pharmacokinet 1976;1:36-51.
1189
desmethyldiazepam: A human autopsy study. J
pun 17. Blaschke TF, Rubin PC: Hepatic first-pass 32. Piafsky KM: Disease-induced changes in the Clin Pharmacol 1985,25:613-615.
plasma binding of basic drugs. Clin Pharmacokique metabolism in liver disease. Clin Pharmacokinet
report •jerapeutic guides. A’ Engl J Med \Ti2-2$T.22~of th. 51
• Greenblatt DJ, Shader RI: Pharmacokinetics in
panic- Chnical Practice. Philadelphia, WB Saunders Co,
B
•^4A, Oct 24/31. 1986—Vol 256, No 16
Drug Monitoring—Friedman & Greenblatt
2233
1488
THE LANCET, JUNE 28, 1986
Fallacy
Therapeutics
DOES PERITONITIS IN THE UPPER ABDOMEN
CAUSE PAIN IN THE TIP OF THE SHOULDER?
DANGEROUS AND INAPPROPRIATE DRUGS
Competition between manufacturers in flourishing
economic systems is said to benefit the consumer by way of
cheaper and better products. This may be true when, say,
television sets are being sold in sophisticated markets where
the consumer has a good idea of what- he wants and needs.
The argument crumbles when the.bpyer has an imperfect
understanding of the virtues and vices of what is on offer. In
Western industrialised countries the ordinary citizen
perceives, if somewhat dimly, what medicines can offer, but
is nevertheless prey to plausible suggestions. He is therefore
likely to take on trust that, because some aspects of health
screening are useful in some people, there may be wider
benefits to all—thus fostering a growing and often virtueless
industry in wellperson screening. He will accept advice to
buy branded products when the non-proprietary versions
differ not at all, except in price, and he will assume that,
because substances are labelled as health foods, herbal
remedies, and homoeopathic remedies that they are indeed
valuable. Some protection is available through the activities
of drug regulatory and consumer advisory bodies, but there
remains a wide and perhaps growing trend towards the
promotion of costly practices which vary from the mildly
deceptive to the frankly fraudulent.
Underdeveloped countries are beset by greater
difficulties. They are ill placed to afford expensive but
useless health care products, let alone the frankly dangerous.
They have unsophisticated consumers and tend to have
poorly developed regulatory and advisory systems. Against
this background it is hardly surprising that pharmaceutical
manufacturers, both international and indigenous, have
indulged in practices which would be obviously
unacceptable in Western countries. The World Health
Organisation essential drugs list is a straightforward attempt
to draw attention to the virtues of a limited range of generally
cheap drugs, but it has so far failed to secure the widespread
acceptance it deserves.
Health Action International has lately issued a
compendium1 of leaflets which detail the depressingly
widespread tendency to peddle dangerous and
inappropriate drugs in poor countries. It draws attention,
The General Hospital,
Birmingham
GEORGE T. WATTS
for example, to the widespread continued availability of
phenylbutazone and oxyphenbutazone as treatments for
mild self-limiting painful conditions, of chloramphenicol in
M. A. EASTWOOD- REFERENCES— continued
15. Heaton KW Gallstones. In: Vahouny GV, Kritchcrsky D, cds. Dietary fiber, basic
the management of minor infective disease, often of a nature
and clinical aspects. New York: Plenum Press, 1986.
unlikely to be responsive, and ofantidiarrhoeals, when water
16.
Eastwood MA, Kirkpatrick JR, Mitchell WD, Bone A, Hamilton T. Effects of
and electrolyte replenishment represent prime needs.
dietary supplements of wheat bran and cellulose on faeces and bowel function.
Br Med J 1973; iv: 392
The Health Action International pack on problem drugs
17.
Kntchevsky D. Lipid metabolism and coronary heart disease. In: Trowell H,
covers nine areas: antidiarrhoeals, cough and cold remedies,
Burkitt D, Heaton K, cds. Dietary fibre, fibre-depleted foods and disease.
London: Academic Press, 1985.
growth stimulants, antibiotics, contraceptives, potency
18.
Kay RM, Truswell AS: Effect of citrus pectin on blood lipids and faecal steroid
drugs, analgesics, drugs in pregnancy, and combination ■
excretion in man. Am J Clin Nutr 1977; 30: 171 -75.
19.
Jenkins DJ, Wolever TM, Taylor RH, et al. Glycemic index of foods: a drugs. Each section contains dismal records of inappropriate
physiological basis for carbohydrate exchange. Am J Clin Nutr 1981; 34(3):
and dangerous merchandising. The papers are individually
362-66.
referenced, but often to obscure sources which readers, even
20. Eastwood MA. Measurement of water-holding properties of fibre and their
faecal bulking ability in man. BrJ Nutr 1983; 50: 539-47.
in developed countries, will find it impossible to examine
21. Stephen AM, Cummings JH. Water-holding by dietary fibre in vitro and its
(such as newspaper articles). The pattern of writing is direct,
emphatic, and even strident, but given the list of
A wise student soon learns that he can save himself effort
by coupling understanding with fact. This is a great help
where embryology, anatomy, and clinical signs can be linked.
Pain—in particular referred pain—lends itself to this
approach. We soon learn, for example, that colic from the
ureter radiates to the groin and does not cross the midline
because each side of the urinary tract has a multisegmental
unilateral origin. We are therefore tempted, having found
such relations, to apply the process in reverse. Since the heart
and diaphragm originate from the cervical septum
intermedium, which descends to the centre and lower part of
the chest, we would expect referred pain in the area supplied
by the cervical nerves. Coronary occlusion frequently causes
arm pain, so we expect irritation of the diaphragm to do the
same. Nowadays we see basal pleurisy infrequently, but in
the past it was common, caused by pneumococcal and
tuberculous infection. As we expect, there is shoulder tip pain
with such disease.
We could assume that if irritation of one side of the
diaphragm gives shoulder tip pain, the same symptom would
arise from inflammation (peritonitis) on the abdominal side.
This is what is commonly taught. However, only part of the
diaphragm has a cervical origin. The rest is costal in
derivation. The central or cervical area is not greatly exposed
to the main peritoneal cavity. Most of all the right side is
protected by the liver, which also has a large bare area. The
greater part of the left side is isolated from the main cavity by
the spleen, stomach, liver, and the reflections of the lesser sac.
The most exposed part is that which is costal in origin, even
when the peritoneal cavity contains gas and acid. Therefore,
the pain is seldom referred to the shoulder tip: instead it is
referred to the lower chest area. When the patient with a
perforated ulcer is asked to sit up, pain between the scapulae
is almost invariably present, whereas pain in the shoulder is
very rare.
Thus if a patient has pain suggestive of a diaphragmatic
lesion and the pain is referred to the tip of the shoulder, we
should direct our attention more to the chest and its contents
than to the abdomen.
23. McBurncy Ml, Horvarth PJ, Jcraci JL, Van Soest PJ. Effect of in vitro
dietary fibre. Br J Nutr 1985; 53: 17 - 24
1 Prepared by Andrew Chetley and David Gilbert and published by the Intemanixud
Organisation of Cnnst’jnen Unions, Emmastraat 9, 2595 EG The Hague.
Netherlands.
1489
THE LANCET, JUNE 28, 1986
unsupportable actions it catalogues this tone is
understandable. The recommendations are generally clear,
entirely acceptable, and obviously necessary (rchydration
therapy before the use of antidiarrhoeals, ban oxyquinolines,
cold cures do not work), but they could sometimes be better
framed. Thus the recommendations for action on butazones
are really part of an extended (and appropriate) diatribe, but
lose force by being buried in the text; and the
recommendations about contraceptives stem not from drug
problems but problems of society (the second of HAI’s
recommendations here is to improve the status of women).
Virtuous as the Health Action International pack may be,
a more important approach might be directed at the vested
interests, not necessarily within the pharmaceutical
industry, which perpetuate such a sorry state of affairs.
Department of Therapeutics,
University Hospital,
Nottingham NG7 2UH
M. J. S. LANGMAN
In England Now
The great debate of the moment is, of course, whether or not the
Health Service is sufficiently funded. The Government—that is to
say, the Prime Minister—speaking ex cathedra, assures us, in tones
that brook no argument, that it is better funded than ever before in
its history.
But those of us at the business end, both as providers and
consumers, are not convinced. If money is adequate, why are wards
being closed? Why are nurses’ homes being sold off, on the wholly
fallacious theory that, in future, any girl wishing to take up nursing
can jolly wrell do it in her home town^ Why, as in our hospital, does a
secretary, when requiring a new pen, have to go to the Unit Admin
Office, between 9.30 and 10 on a Tuesday, carrying the old one with
her to effect an exchange? Why ... oh, why go on? We are told,
firmly, that things are fine and all of these problems must be but
figments of our imagination. Can we not see that the Emperor is
wearing the most beautiful suit of clothes?
No, we cannot However, let us, in all charity, assume that the
figures do show that, in real terms, more money is going into the
NHS, and ask where it is going, as patient care plummets. An awful
lot must go into administration. Now, fair enough, administrators
are necessary, but is not the very' substantial tail now’ wagging the
weak and emaciated dog? Look at the money that is spent (w’asted?)
every few years in “reorganisation”. Salmon. Area and District
Management Teams. Scrap the Area tier. Now Griffiths—down
with consensus, bring back despotism. Yet all of these schemes have
cost vast sums of money and certainly all have led to a proliferation
of the numbers of people not actually involved in patient care. The
latest changes are no exception. Every general manager must have
deputies; every chief must have his persona] Admiral Byng who can
be shot on his own quarterdeck if things go wrong “pour encourager
les autres”. Of course, we are told, this reorganisation is the answer,
which will streamline the National Health Service and maximise
resources into patient care. I have heard this before—several times.
This time it is the importation of fresh managerial blood which will
do the trick. This, perhaps, is the last of the old quaint English
eccentricities—that if you want something done, you appoint
someone with no knowledge of the subject. Provided a man was a
gentleman—and preferably an officer as well—he could be a
magistrate and know no law, rule an empire, and know nothing of
the culture he ruled. Many of the new managers are ex-servicemen.
Is running a Health district really no different from running a small
RAF station or a minor ordnance depot? Are the accounts really the
same as keeping an eye on the junior officers’ mess bills?
We all heaved a sigh of relief when, at long last, Donald
passed his finals. In those far-off days, every medical year had
one—a student who always struggled on the brink of
dissolution. No examination was ever passed at the first attempt
and it was usually only at the third or fourth try that success
finally rewarded effort. Indeed, with Donald, success was
achieved mostly because we all rallied round to tutor him. After
graduation he disappeared into an overworked practice in one
of our underdeveloped areas.
Our paths failed to cross until I met him again at our 30th year
reunion. He was impeccably dressed in a Savile Row suit and
his Rolls Royce was parked rather ostentatiously outside the
hotel entrance. He gave three cases of champagne to the
chairman to help with the jollification.
During the cocktails, conversation, and canapes phase we fell
to talking. His Harley Street practice was doing nicely, thank
you very much. He attributed his success to the fact that he had
discovered a new disease, and this had made him popular. I
lifted my eyebrows, inquiringly. Yes, he said, it consisted of
headache, backache, mild depression, and an urge to talk to
someone for about 15 minutes or so. It particularly affected
middle-aged women. But what had really made his name was a
feature never before described. Indeed, when he told his
patients of his finding, they were horrified that all the other
doctors had missed it. “You know those funny sounds you hear
through the stethoscope when you take a blood pressure?” he
said. I agreed cautiously. “Well,” continued Donald. “I found
in every’ case, without exception, that the diastolic blood
pressure was always higher than the systolic.”
Am I alone in thinking that this Christian name business is getting
out of hand? I know that we arc, in the NHS, supposed to be one
happy family, but do we have to go around using first names all of
the time as pan of the pretence?
I have always written my clinical letters to “Dear Dr Bloggs”,
never “Dear Jim”. At first, all the Bloggses used to be older than me,
and I would have felt it rude and presumptuous to be familiar. Now
the tables are turned; most of the Bloggses are but veritable children,
and I do not wish them to be familiar, so I retain the formality.
Now everyone expects instant intimacy. Junior administrators,
still with marked post-auricular dampness, take it for granted they
can use my Christian name, and are offended by the careful “Mr” I
employ for them. Even nursing officers seem to consider it their
right to call consultants by their first names, and to be so addressed
in return. It is, I suppose, all part of the quaint fallacy that, to work
together, we must all be chums (“and you shall call me Eric”),
whereas it is easier to work with people about whom you are neutral
and with whom you maintain a polite formality.
It all reaches its heights (or depths) with patients. I have for years
been fighting a losing battle against the practice of automatically
calling patients by their first names. The retired professional lady,
called “Miss Jones” all her life, does not want, I am sure, to have
chits of girls calling her “Molly”. Then there is the old man, always
called “Mr Smith” by his wife in public, or “Dad” in the family
circle, who suddenly finds complete strangers calling him “Jack”.
Mind, I have to concede that the use of first names is, marginally,
better than “Gran” or “Pops” or whatever other totally demeaning
soubriquet the young happen to favour for the elderly at the time.
But how much nicer would “Miss Jones” or “Mr Smith” be—more
dignified, more respecting of individuality, all those things to which
modern-day nurses pay lip service but ignore in practice.
938
JAMA, Sept 21, 1964
Council on Drugs
Agranulocytosis Induced by Dipyrone,
a Hazardous Antipyretic and Analgesic
Charles M. Huguley, Jr., MD, Atlanta
N INCREASING NUMBER of reports of agran.ulocytosis associated with dipyrone are being
received by the American Medical Association’s
Registry on Adverse Reactions. Between 1955 and
1959 only ten cases of leukopenia associated with
this drug had been reported to the Registry from
the United States, and none of these were in chil
dren. Since 1960, reports of 18 cases have been re
ceived, seven of them in children. Thirty-six percent
of these patients have died. Since it is probable that
many more cases of agranulocytosis occur than are
reported to the Registry, these data are a cause for
concern.
During the same period there has been a striking
increase in the use of dipyrone. Much of the dipy
rone used in this country is imported; domestic
production and sales figures are not available, but
US Tariff Commission figures show that imports in
creased from none in 1958, to 220 lb in 1959; 7,164
lb in 1960; 39,790 lb in 1961; and 18,879 lb in 1962.
This increase in the use of dipyrone is puzzling,
since the drug has the same pharmacological effects
and therapeutic indications as aminopyrine, of
which it is a derivative. Aminopyrine, on the other
hand, does not seem to be in frequent use in this
country, and only seven cases of leukopenia associ
ated with aminopyrine have been reported to the
Registry from the US since 1954. It may be sus
pected that many physicians who prescribe dipy
rone are unaware of its relationship to amino
pyrine.13
Some of the brands of aminopyrine and dipyrone
available in the US today are listed in the Table.
It has been suggested in England that no prescrip
tion for a drug or compound containing aminopy
rine or its salts be valid unless the prescriber has
indicated that it contains aminopyrine,3 and aston
ishment has been expressed that these drugs are still
A
From Emory University School of Medicine.
This article was written at the request of the Council’s Section on
Adverse Reactions.
being produced/ At this time, therefore, it seems in
order to review briefly the history of these drugs
and their relationship to agranulocytosis.
History
Aminopyrine was introduced as an analgesic and
antipyretic agent in 1897. Its general pharmacologi
cal properties are very similar to those of the salicy
lates, and it is an effective analgesic and antipyretic
compound. Cardon et al ’ have cited the older liter
ature concerning its effectiveness in a variety of
conditions. During the 1920’s it became very popu
lar, and by 1930 it was widely used throughout the
world. In the US it was reported that 30 million
prescriptions per year were written.’
Some Commonly Prescribed Brands of
Aminopyrine and Dipyrone
Aminopyrine
Aminopyrine (Lilly)
Amytal with aminopyrine (Lilly),
Cibalgine (amlnopyrineallobarbital) (Ciba)
Pyramidon (Winthrop)
Dlpyrone
Dipralon Forte (Arnar-Stone)
Fevanil (Carrtone)
Key-Pyrone (Key)
Migesic (Misemer)
Narone (Ulmer)
Novaldin (Winthrop)
Pydirone (Breon)
Pyralgin (Savage)
Agranulocytosis, an often fatal disease character
ized by an explosive onset of infection (usually a
sore throat) and a virtual absence of granulocytes
in the blood, was first described in 1922.7 In the late
1920’s, cases appeared in the US frequently, and in
1931 it was suggested that these were often related
to the ingestion of drugs that were coal tar deriva
tives.8 In 1933 Madison and Squier' established a
causal relationship between aminopyrine and agran
ulocytosis by reproducing the syndrome with a
test dose of the drug in patients who had previously
developed the disease while receiving aminopyrineKracke and Parker established tins relationship be
yond all doubt in 1935.10 Of the 172 cases of agranu
locytosis reported in the literature from September,
162
938
JAMA, Sept 21, 1964
0 001
Council on Drugs
Agranulocytosis Induced by Dipyrone,
a Hazardous Antipyretic and Analgesic
Charles M. Huguley, Jr., MD, Atlanta
N INCREASING NUMBER of reports of agran.ulocytosis associated with dipyrone are being
received by the American Medical Association’s
Registry on Adverse Reactions. Between 1955 and
1959 only ten cases of leukopenia associated with
this drug had been reported to the Registry from
the United States, and none of these were in chil
dren. Since 1960, reports of 18 cases have been re
ceived, seven of them in children. Thirty-six percent
of these patients have died. Since it is probable that
many more cases of agranulocytosis occur than are
reported to the Registry, these data are a cause for
concern.
During the same period there has been a striking
increase in the use of dipyrone. Much of the dipy
rone used in this country is imported; domestic
production and sales figures are not available, but
US Tariff Commission figures show that imports in
creased from none in 1958, to 220 lb in 1959; 7,164
lb in 1960; 39,790 lb in 1961; and 18,879 lb in 1962.
This increase in the use of dipyrone is puzzling,
since the drug has the same pharmacological effects
and therapeutic indications as aminopyrine, of
which it is a derivative. Aminopyrine, on the other
hand, does not seem to be in frequent use in this
country, and only seven cases of leukopenia associ
ated with aminopyrine have been reported to the
Registry from the US since 1954. It may be sus
pected that many physicians who prescribe dipy
rone are unaware of its relationship to amino
pyrine.1'1
Some of the brands of aminopyrine and dipyrone
available in the US today are listed in the Table.
It has been suggested in England that no prescrip
tion for a drug or compound containing aminopy
rine or its salts be valid unless the prescriber has
indicated that it contains aminopyrine,3 and aston
ishment has been expressed that these drugs are still
A
From Emory University Schoo! of Medicine.
This article was written at the request of the Council’s Section on
Adverse Reactions.
Q £
being produced? At this time, therefore, it seems in
order to review briefly the history of these drugs
and their relationship to agranulocytosis.
History
Aminopyrine was introduced as an analgesic and
antipyretic agent in 1897. Its general pharmacologi
cal properties are very similar to those of the salicy
lates, and it is an effective analgesic and antipyretic
compound. Cardon et al5 have cited the older liter
ature concerning its effectiveness in a variety of
conditions. During the 1920’s it became very popu
lar, and by 1930 it was widely used throughout the
world. In the US it was reported that 30 million
prescriptions per year were written.”
Some Commonly Prescribed Brands of
Aminopyrine and Dipyrone
Aminopyrine
Aminopyrine (Lilly)
Amytal with aminopyrine (Lilly) t
Cibalgine (aminopyrine*
allobarbital) (Ciba)
Pyramidon (Winthrop)
Dlpyrone
Dipralon Forte (Arnar-Stone)
Fevanil (Carrtone)
Key-Pyrone (Key)
Migesic (Misemer)
Narone (Ulmer)
Novaldin (Winthrop)
Pydirone (Breon)
Pyralgin (Savage)
Agranulocytosis, an often fatal disease character
ized by an explosive onset of infection (usually a
sore throat) and a virtual absence of granulocytes
in the blood, was first described in 1922.7 In the late
1920’s, cases appeared in the US frequently, and in
1931 it was suggested that these were often related
to the ingestion of drugs that were coal tar deriva
tives.” In 1933 Madison and Squier established a
causal relationship between aminopyrine and agran
ulocytosis by reproducing the syndrome with a
test dose of the drug in patients who had previously
developed the disease while receiving aminopyr*n®"
Kracke and Parker established this relationship be
yond all doubt in 1935.10 Of the 172 cases of agranu
locytosis reported in the literature from September,
940
AGRANULOCYTOSIS—HUGULEY
In 1934, the Council on Drugs condemned the in
discriminate use of aminopyrine and criticized the
confusing and uninformative names used for prepa
rations containing the drug. As shown by the partial
list in the Table, a comparable situation exists today
with the derivative, dipyrone.
Pharmacology.—These two drugs are almost iden
tical pharmacologically; sulfonation of aminopyrine
to dipyrone renders it more soluble without affect
ing other properties. Both compounds are demethyl
ated to 4-aminoantipyrine, a portion of which is
then acetylated to 4-acetylaminoantipyrine. Neither
of the parent compounds, antipyrine and 4-amino
antipyrine, has been used to any great extent sys
temically in this country and, although antipyrine is
used topically, there have been no reports of agran
ulocytosis attributable to it. The structural for
mulae of these parent compounds are shown in
Fig 3 and 4.
Efficacy.—Although it has been shown in animal
studies that aminopyrine is an effective analgesic
and antipyretic,1411 there are no reports of double
blind, randomized studies comparing either amino
pyrine or dipyrone with any other drugs to deter
mine their relative effectiveness. Nevertheless, there
is little question of the efficacy of these two drugs as
analgesics and antipyretics.’ Wolff and associates
studied the effect of a variety of analgesic drugs on
the pain threshold in man. The effect of equal doses
of aminopyrine and aspirin was identical.'’ For
many years, however, the lack of use of either
aminopyrine or dipyrone in this country has indi
cated that American physicians have obviously felt
that they had no advantages over salicylates and
similar drugs that would justify the danger atten
dant upon their use.
There have been only four articles in recent years
in the American literature advocating the use of
aminopyrine.’ '7"1 Of these, the report by Cardon
et al presents the most persuasive argument for the
occasional use of aminopyrine.’ Aminopyrine af
forded complete relief in six patients who had
severe febrile illnesses in which the major sympto
matology was referable to fever. Spear reported
that of 74 patients with Hodgkin’s disease whose
charts he reviewed, 62 had fever.17 He states that
aspirin "given in a haphazard fashion’’ failed to
relieve the fever in 31 of 35 patients but that in 18
of these patients aminopyrine, given every six hours,
afforded effective relief. One can, of course, specu
late on what might have been accomplished by the
regular administration of aspirin or another rela
tively safe antipyretic. Another article recommends
the use of aminopyrine for the treatment of diabetes
insipidus, although it is not clear why the authors
felt that the antidiuretic hormone was not accept
able therapy, since they had demonstrated its effec
tiveness in their patient as proof of the diagnosis.'8
The only other article advocating the use of amino
pyrine presents no data.1’
JAMA, Sept 21, 1964
The unfortunate aspect of these articles is that
the authors all minimize the incidence of agranulo
cytosis and state that the hazards of aminopyrine
have been overemphasized. These statements have
been refuted by Wintrobe and by Trimble,7' and
it is appropriate to consider just how dangerous
these drugs are.
Incidence of Agranulocytosis
Aminopyrine.—In a review article, Discombe cites
the use of aminopyrine in four series of over 200
patients each, in which nearly all patients received
the drug for at least 14 days and most for a much
longer period.3 The incidence of agranulocytosis
ranged from 0% to 0.91%. The total number of pa
tients in the four series was 1,272 and the total
number of cases of agranulocytosis was 11, or 0.86%.
Of the II patients who developed agranulocytosis,
eight died (0.63%). Even if we add to these the 103
patients of Simon and Metz,77 the 18 of Spear,17
and the 6 of Cardon et al,’ none of whom developed
a blood dyscrasia, we will have a total of 11 cases
and eight deaths in 1,399 patients, an incidence of
0.79% and a mortality rate of 0.57%. These are the
only figures that a diligent search of the literature
has revealed among patients who have received the
drug regularly over a period of at least two weeks
and who were observed during the period of ad
ministration.
Discombe3 estimates that, in countries in which
aminopyrine was freely available, there probably
were two to five cases of agranulocytosis per 1
million inhabitants per year. It is very likely that in
that era a large number of cases of acute sore throat
secondary to agranulocytosis were not diagnosed as
such and, even among those in whom the diagnosis
was established, many cases may not have been
reported. Dameshek and Colmes6 estimated that
there was one case of agranulocytosis for every
10,000 prescriptions of aminopyrine. This does not
take into consideration the fact that the disease ap
parently requires a period of time for sensitization
to occur, so that patients who received only a few
doses would not be expected to have a reactionMoreover, those who used the drug for a long pc*
riod very likely had prescriptions refilled, so that
10,000 prescriptions may represent less than 10,000
patients.
Dipyrone.—Aminopyrine and dipyrone are, 50
similar that there is no reason to suspect that they
are not equally likely to produce agranulocytoseThe first case of agranulocytosis associated 'V1
dipyrone was reported in 1935.' Later, a human
volunteer known to be sensitive to aminopyrine ***
given 0.65 gm of dipyrone, and he developed gram*'
locytopenia eight hours, later.73
The recent reports to the Registry on Adver*
Reactions certainly indicate the potential °f,~*^||
rone for producing agranulocytosis; since 195o>#
cases from the US and 9 from foreign countrw*
AGRANULOCYTOSIS—HUGULEY
Vol 189, No 12
have been reported to the Registry. An additional
14 cases have appeared in the foreign literature. Of
this total of 51 patients, 19 (37%) died.
Some of these case reports illustrate the cross
reactions between dipyrone and aminopyrine. One
patient previously had agranulocytosis after receiv
ing aminopyrine.” Of several patients who had re
covered from dipyrone-related agranulocytosis, one
developed full-blown agranulocytosis within 24
hours after being given 0.6 gm of aminopyrine; one
reacted to a test dose of dipyrone itself”; and one
was shown to have a positive skin test, serum leuko
cyte agglutinins, and positive response to a test dose
with both dipyrone and aminopyrine. Three other
patients were tested with dipyrone for the presence
of leukocyte agglutinins, and the results in two were
positive.25 27
Comment
This recent increase in the use of dipyrone and in
cases of agranulocytosis and death resulting from it
must give us pause, particularly since so many chil
dren are among the victims. We must consider
whether there are any special advantages offered by
941
these drugs that warrant the risk of a serious and
possibly fatal reaction. From the articles urging the
use of dipyrone, it is obvious that those who pre
scribe it are chiefly taking advantage of its anti
pyretic effect. However, there are several effective
antipyretics on the market in addition to aspirin,
and there are also physical measures that may be
used to reduce acute pyrexia, particularly in chil
dren. The rather limited use of dipyrone and amino
pyrine in this country in the past suggests that most
physicians find these other drugs satisfactory, and
there is a widespread belief that there are practi
cally no circumstances in which aminopyrine or
dipyrone is indicated.4,2“ Admittedly, reports indi
cate that some patients with fever respond well to
aminopyrine after they fail to respond to aspirin,5 '7
but these would seem to be too rare to justify use
before a thorough trial of other drugs.
The question facing the medical profession is
whether the continued use of these drugs is justi
fied. Seven deaths, three of them in children, have
been attributed to dipyrone in the US in the past
four years. Have this many lives been saved through
use of the drug?
References
1. Blake, F.C., et al: Agranulocytic Angina,
Yale J Biol
Med 7:465, 1935.
2.
Hart, F.D.; Wraith, D.G.; and Mansell,
ulocytosis Successfully Treated With ACTH,
1:1273-1275 (June 14) 1952.
3.
Brit Med J
Discombe, G.: Agranulocytosis Caused by Aminopy
rine: Avoidable Cause of Death,
(June 14) 1952.
4.
Agran
Simpson,
R.G.:
Brit Med ] 1:1270-1273
Aminopyrine
Agranulocytosis,
Cardon, L., et al: Value of Aminopyrine, Ann
Intern
6.
Dameshek, W., and Colmes, A.: Aminopyrine Hyper
sensitivity, With Particular Reference to Effect of Drugs in
Production of Agranulocytosis, J Clin Invest 15:85-97 (Jan)
1936.
Schultz,
W.:
Uber
eigartige
Halserkrankungen,
Kracke,
Unusual Case,
9.
R.R.:
Recurrent Agranulocytosis.
Amer J Clin Path 1:385-390 (Sept)
102:755-
JAMA 105:960-966 (Sept 21)
Moeschlin, S., and Wagner, K.: Agranulocytosis Due
to Occurrence of Leukocyte
(Basel) 8:29, 1952.
12.
JAMA
Kracke, R.R., and Parker, F.P.: Relationship of Drug
Therapy to Agranulocytosis,
1935.
11.
1931.
Madison, F.W., and Squier, T.L.: Etiology of Primary
Granulocytopenia (Agranulocytic Angina),
759 (March 10) 1934.
10.
Report of
Agglutinins,
Acta Haemat
Moeschlin,-S.: Immunological Granulocytopenia and
Agranulocytosis; Clinical Aspects, Sang Par 26:32-51, 1955.
13. Merck Index of Chemicals and Drugs, 7th ed,
P. G. Stecher, ed, Rahway, NJ: Merck and Co, Inc., 1960.
14.
Benitz, K.F., and Hall, L.M.: Carrageenin-Induced
(March)
J Clin Invest 20:63-80 (Jan)
18.
1941.
Spear, W.: Use of Aminopyrine to Control Fever in
JAMA 180:970-972 (June 16)
1962.
Balsam, T., and Katz, H.M.: Diabetes Insipidus Suc
cessfully Treated With Oral Aminopyrine, JAMA 176:11121114 (July 1) 1961.
19.
Bauer, J.: Some Remarks on Properties and Thera
peutical Use of Aminopyrine (Pyramidon),
18:27, 1960.
20.
21.
Exp Med Surg
Wintrobe, M.M.: Toxicity of Aminopyrine, Letter to
the Editor,
Deutsch Med Wschr 48:1495, 1922.
8.
17.
Hodgkin’s Disease,
Med 48:616-634 (March) 1958.
7.
Toxic Appl Pharmacol 5:247-256
Wolff, H.G.; Hardy, J.D.; and Goodell, H.: Measure
16.
ment of Effect on Pain Threshold of Acetylsalicylic Acid,
Acetanilid, Acetophenetidin, Aminopyrine, Ethyl Alcohol,
Trichlorethylene, Barbiturate, Quinine, Ergotamine Tar
trate and Caffeine: Analysis of Their Relation to Pain Ex
perience,
and
Brit Med J 5334:887 (March 30) 1963.
5.
Drugs in Rats,
1963.
JAMA 178:1051
Trimble, G.X.:
(Dec 9)
1961.
Aminopyrine in
Hodgkin’s Disease,
Letter to the Editor, JAMA 183:153 (Jan 12) 1963.
22.
Simon, S.D., and Metz, M.H.: Amidopyrine and Cir
culating Leukocytes; Effect of Prolonged Administration on
Number and Type of White Blood Cells, J
21:1154-1157 (Aug) 1936.
Lab Clin Med
23.
Benjamin, J.E., and Biederman, J.B.: Agranulocytic
Leukopenia Induced by Drug Related to Aminopyrine,
JAMA 107:493-494 (Aug 15) 1936.
24.
Thygesen, J.: Medikamentel Agranulocytose,
LJgeskr
Laeg 124:146-147 (Feb 2) 1962.
25.
Dyrbye,
M.O.,
and
Hvidberg,
E.:
Medikamentel
Agranulocytose, Ugeskr Laeg 123:1307-1310 (Sept 22) 1961.
26.
Kalicinski, A., and Paszko, W.: Przypadek immuno-
leuko-trombocytopenii popiralginowej,
1971-1973 (Dec 23) 1957.
Pol Tyg Lek
aglutynin, Pol Arch Med Wewnet 27:1137-1146, 1957.
15.
Winter, C.A., and Nuss, G.W.: Pyretogenic Effects
of Bacterial Lipopolysaccharide and Assay of Antipyretic
Abroad, Med Letter on Drugs Therapeutics 3:44, 1961.
16-5
12:
27.
Kowalczyk, M., and Urasinski, I.: Przypadek Polekowej Agranulocytozy Wywolanej Obecnoscia Granulocyto-
Abscess as New Test for Anti-Inflammatory Activity of
Steroids and Nonsteroids, Arch Int Pharmacodyn 144:185195 (July 1) 1963.
28.
Aaron, H., et al: Aminopyrine Nonprescription Drugs
Issue No. 8
Editorial
useful are being investigated
scientifically. These include
acupuncture and hypnosis which are
being currently featured. In some
cases, alternate therapy can be
dangerous as was demonstrated by
the use of Laetrile.
Pain and Fever, one or both these
symptoms, account for the majority
of presenting complaints to a
physician. Viewed with a casual air,
they are often vital clues to reach a
diagnosis. Therefore, an update of
the pathology and management of
pain and fever is much called for.
can cure may also harm.
Unfortunately emotional overtones
cloud rational judgement. 'Weighing
Risks’, an article in this issue,
suggests a rational approach to this
problem. It examines the balance
between risk and benefit with relation
to not only drugs but also everyday
events.
Symptomatic treatment always vies
with specific therapy. Yet its value in
terms of relief obtained and
improvement in well-being is the
cornerstone of successful medicine.
Patients expect to be rid of
uncomfortable symptoms, even
before the disease runs its natural
course,- thus promoting the physician
to reach for the first analgesic and/or
antipyretic agent. In satiating the
demand for relief, there is sometimes
a subtle suspicion of an
accompanying risk.
One result of the fear that has been
induced by emotionally charged
allegations of drug risks is the revival
of fringe medicine — homeopathy,
herbalism, hypnosis, acupuncture
and iridiology. But alternate therapy
or fringe medicine has yet to prove
its worth under scientifically
controlled clinical trials.' The-recent
report of the Board of the Science
Working Party of the British Medical
Association on Alternate therapy
found no reason why it should not be
assessed by the same scientific
principles that are applied to
conventional practice.2
However, running parallel to this
demand for relief of unpleasant
sensations is the concern that what
2
The methods that were found to be
On the other hand, the close control
of pharmological and toxicological
testing has reduced the chances of a
drug being released for general use.3
Great strides have been made in the
field of adverse drug reporting and in
statistical methods of evaluating
risks. These have permitted a
scientific approach to determine the
true incidence rates of rare side
_
effects. As an example, two studies
O
designed to determine the incidence
of rare adverse drug reactions,
presented at the III World Conference
of Clinical Pharmacology and
Therapeutics held in Stockholm last
year have been reported. These
studies along with Weighing Risks
have resulted in Weighing Risks — A
Case in Point an article which
demonstrates the need to cultivate a
cautious and balanced attitude not
only towards the ‘victim oriented'
press reporting but also to apparent
‘scientific studies' which could be
pivotal in decision making. A
pertinent example relevant to this
issue of the Medical Bulletin is the
repeatedly quoted and outdated
estimate of the risk of aminopyrine
induced agranulocytosis by
Discombe and Huguely — despite
the fact that it was based on
evaluation of data from different
sources which are not comparable
and which were arbitarily collected.4
The results of these studies are in
conflict with all practical experience4
and have been disproved by the
recent International Study on
Agranulocytosis and Aplastic
Anaemia reported in the October
issue of the Journal of the American
Medical Association.5
References
1.
Editorial, BMJ. 1985. 291, 1744-5
2.
Woodward J. The Practitioner. 1986,
230. 687
3.
Editorial, BMJ. 1986. 293. 219
4.
Miescher PA and Pola W, Drugs.
1986, 32, Supplement. 4, 99
5.
ISAAA. JAMA. 1986. 256,
1749-1757
Pain — A Review
As different as one person is to
another,so is the experience of pain
felt by each individual'; so, too, the
resulting pattern of behaviour and
reaction. Pain is a personal, private
and subjective experience it is a hurt
we feel; this underlies the affective
element which is an integral part of
the pain experience.
But different though each person
may be to another, at another level
they are alike; likewise pain has its
commonly shared characteristics. It
is these characteristics, — the
emotionally neutral ones — that will
be discussed here. The affective
element is no less important but will
be dealt with briefly. In many cases
of chronic pain and, rarely, acute
pain the affective element can
drastically change the pain
experience as in the famous and
often cited example of soldiers on
the battlefield who do not feel injuries
when they occur2; or the less known
one of walking barefoot over hot
coals during neurolinguistic
programming3. In these cases a
strong emotion suppresses pain. On
the other hand,a once brave and
courageous person can be so
affected by chronic pain to become
a cranky, complaining, miserable
and irrational creature.
Pain is considered a protective
mechanism of the body which allows
recognition at a conscious level that
a harmful or potentially harmful
stimulus or situation threatens the
structural and functional integrity of
the body — and if uncontrolled,
subsequently of the mind too. It
allows the person to respond to
these threats with a battery of
responses that will result in
protection from,or avoidance of
these stimuli. These responses
range from a verbal 'ouch' to a
conscious decision to visit a doctor
and include postural adjustments,
avoidance of movements, affective.
autonomic and other physiological
and neurological responses. A
description of pain based on any
one of these responses does not
give a comprehensive view of the
pain phenomenon, and stresses the
need to take all the aspects of pain
into consideration while determining
treatment. To not do so can be
detrimental to the patient: for
example, a patient who has been
diagnosed as having 'psychogenic
pain' (on the erroneous belief that he
has a painless pain) is treated
exclusively by psychiatry.'
On the other hand,if it is decided that
the pain is ‘physical’, one somatic
treatment after another, each more
desperate than the earlier, is
prescribed.
Pain should be approached,
considered and treated at all levels.
This is all the more so in the cases of
chronic pain as pain is a sensation
which does not exhibit the
phenomenon of adaptation and can
therefore have many adverse effects
on a patients life.
Pain can be conveniently viewed as
acute or chronic; the difference being
that in acute pain the sufferer can
usually give a clear description of the
location, severity, fluctuation, mode
of onset and factors that aggravate
or relieve it. This sort of pain usually
responds well to analgesics. On the
other hand, descriptions of chronic
pain are comparatively vague and
are influenced by cultural, religious
and psychological factors; this pain
does not respond as well to
analgesics.
Furthermore,objective signs such as
pallor, tachycardia, mydriasis.
hypertension, sweating — (signs of
autonomic nervous system
hyperactivity) — are seen in acute
pain-and present a clinical picture of
anxiety? Chronic pain tends to cause
disturbances in work, sleep, social,
sexual and other functions and thus
comes close to a clinical picture of
depression? The point at which acute.
pain — which serves the purpose of
warning that something is wrong —
becomes chronic varies,but is
arbitrarily taken as six months.5
Pain is often experienced before
other signs and symptoms of the
disease occur. It is thus essential for
the physician to understand well the
sensory supply of the body surface
and also the viscera as well as the
differences in the quality and types of
pain to reach a diagnosis. The
sensory supply of the body surface is
illustrated in Figure 1. A given spinal
segment also supplies a visceral
Fig. 1; Sensory supply of body
surface.
area with autonomic nerve fibres.
The important nerves for
intrathoracic viscera are the first to
the fourth thoracic,while for the upper
abdominal,the sixth to the eighth.
Superficial pain has two components
— a quick pricking sensation,
followed by a burning pain a few
seconds later — this constitutes the
double response of Lewis. Visceral
and deep musculoskeletal pain have
the quality of cramping or aching but
can occasionally be sharp or
burning. While superficial pain can
be localized to a single sensory
segment both deep musculoskeletal
and visceral' pain cannot be localized
to closer than 2 to 3 segments and
are often indistinguishable from each
other; for example,the pain of renal
colic may resemble that of a tear in
the lumbar muscle in location and
quality. Likewise,a tear in a muscle in
the chest may resemble that of
angina.
Due to a greater cerebral
representation in the sensory supply
of the integumen as opposed to that
of the viscera, pain in the latter is
often referred superficially. The
location of the referred pain on the
3
points to arterial pulsation as a
cause. Sharp, stabbing and
recurrent pains usually result
from disease of nerve roots or
sensory ganglion. What is
important is to determine whether
the pain is steady or fluctuating.
A steady pain is found in peptic
ulcer, angina pectoris, gall
bladder colic and renal colic. With
the latter two. the word colic is
misleading as the pain is actually
steady6. True colicky pain
suggests the obstruction of a
hollow viscus6.
Table: Dermatomes to which visceral pain is referred
Spinal segments
Viscus
C 3-5, T 1-8, usually on
left occasionally bilateral
T2-5
T 5, occasionally T 6, 7, 8
T 7,8,9 usually bilateral
T 9-12, bilateral or on left
C 3-5
T 8-10 Right
T 8-9, occasionally 5-7
T 10, also T 11, 12, LI
T 11, 12, L1
T 10
T11.12
T 11, 12 L1, S3-4
T 10-12, LI, SI-4
Heart
Lung
Oesophagus
Stomach
Intestine
Diaphram
Liver
Gall bladder
Kidney
Ureter
Testes
Epididymis
Bladder
Uterus & Ovary
surface of the body lies in the
dermatome of the spinal segment
which supplies the affected viscera.
Table shows the sensory segments
to which pain in certain viscera are
reffered to. The paucity of pain
representation in the viscera is
eloquently described in the
accompanying extract.
Harvey (1628, see 1962 ed.)
remarked upon the absence of
sensation in the exposed heart of
Viscount Montgomery. Harvey
records, “I carried the young man to
the King (Charles I) that His Majesty
might with his own eyes behold this
wonderful case; that, in a man alive
and well, he might, without detriment
to the individual, observe the
movement of the heart, and with his
proper hand even touch the
ventricles as they contracted. And
His Most Excellent Majesty, as well
as myself, acknowledged that the
heart was without the sense of touch;
for the youth never knew when we
touched his heart ...”7
Occasionally an aberrant referral of
pain occurs. Pain spreads to areas .
next to those that are affected. This
happens due to pre-existing disease
in adjacent areas which have already
caused a partial depolarization in the
neurones supplying these areas;
which then easily become
depolarized by the new disease6. A
person with cervical arthritis might
thus have the pain of myocardial
infarction referred to the neck region.
Clinical Approach:
In dealing with a problem of pain a
detailed history, general physical
examination, neurological
4
examination and perhaps a
psychiatric evaluation are required.
The importance of a detailed account
from the patient on the history of the
pain cannot be stressed adequately
because it is on this information that
the physician can arrive at a
reasonable conclusion regarding the
cause of the pain.
History:
The following inquiries should be
made:
a)
The location of the pain: This
helps to identify the cord
segment involved'and will limit
the diagnostic possibilities to be
considered.
b)
Exacerbating and Relieving
factors: These pointers are
valuable clues to the possible
mechanisms producing pain.
Pain on swallowing focuses
attention to the oesophagus;
back pain which worsens on
sitting or walking suggests disc
disease, while similar pain
aggravated on lying down.
suggests intraspinal disease.
c)
Mode of onset: Pain reaching its
'full' intensity almost immediately
indicates rupture o.f a tissue as in
dissection of the aorta or in
perforation of a peptic ulcer
Time of occurrence: Pain that
occurs several hours after a meal
and which is relieved by food
suggests the action of acid on the
stomach or duodenal mucosa.
Joint pains'that are more severe
with the first movements after
prolonged rest point to arthritis.
e)
Quality of pain: A throbbing pain
d)
f)
Duration: Anginal pain rarely lasts
more than 15 minutes; in contrast
the pain of myocardial infarction
persists longer.
g)
Severity: Determining the severity
of pain based on the persons
judgement is difficult as people
differ in their tolerance to pain.
Pain should be taken to be
severe if it interferes with the
person's work, sleep or social
activities, is accompanied by
physiological signs or requires
therapeutic intervention.
After a systematic interrogation,
measures which reproduce and
relieve pain should be attempted,as
these, apart from confirming the pain
mechanism, convince the patient
that the doctor understands his
problem.
A psychiatric evaluation along with
the inquiry regarding pain should be
done and signs and symptoms of
depression,such as loss of sleep and
appetite, loss of weight, reduction in
social pain and sexual functions
should be noted especially in chronic
pain.
General Physical Examination:
Begin with the site of pain. Examine
the area for any swelling, deformity
and redness. Palpate for tenderness.
check if temperature of area is
raised.
Joints should be taken through the
full range of movement,noting if the
character of the pain changes.
Nerve trunks should be palpated and
stretched. A neurological
examination should be serfoi ■
I
there are any neurologic.'.:
abnormalities, one can assume that
the pain is due tc it.but one cannot
rule out the involvement of the
nervous system in the absence of
such abnormalities.
Laboratory tests and other
investigations are determined and
depend entirely on the possible
cause of the pain.
Management:
An important consideration in pain
management is the possibility that
the cause of pain can be eliminated.
Even if one cannot eliminate the
cause,it is possible to reduce pain
more easily if one is aware of the
origins of the discomfort.
Before considering the management
of pain, the pathway of the pain
sensation and the sites of drug
action should be clearly understood.
Figure 2 illustrates this in brief.
Though the main site of action of the
non-narcotic drugs is by the
inhibition of prostaglandins at the
periphery, somejike analgin,also
have a potent central nervous
system effect.
Paracetamol also possesses a CNS
effect,but its mode of action is
undead1 as it has a weak effect on
prostaglandin synthesis.
The side-effects of the non-narcotic
analgesics are also related to their
inhibition of prostaglandin synthesis;
the most common being the ability to
induce gastric or intestinal bleeding
and ulceration'-1. Other side-effects
include renal toxicity, hepatotoxicity
and allergic reactions. In cases of
hepatic disease or overdose of the
drug, paracetamol is potentially fatal.
Though rare, aspirin usage has been
significantly linked with the fatal
Reye’s Syndrome in children with
concurrent viral infections and
should therefore be avoided in
children. The use of this drug is now
banned in India for children under 12
years of age.
Though these drugs are classified as
effective in pain of low to moderate
intensity,this is not altogether true. In
cases of post-operative pain.nonnarcotic drugs are preferred to
narcotic analgesics.
What is, however., notable about the
long list of non-narcotic drugs is not
so much the difference between
them but the striking similarities in
drug action. Some of these drugs
such as aspirin and analgin also
possess anti-inflammatory and
antipyretic actions. Rather than
attempt to memorize the long list of
drugs and their minor differences,
the physician should familiarise
himself with a few preparations.
The weak narcotic analgesics may
be used for mild to moderate pain,but
as there is a slight euphorant effect,
they should not be used for long
periods of time as they carry the
potential for addiction. In these
cases the patient’s mental status
should be well assessed.
The potent narcotics have their use
in severe visceral pain, severe pain
due to trauma including post
operative care and the pain of
advanced malignant disease.
Fig.2 : Pain pathway and sites of action of drugs
Mention must be made here of the
recently recognised
neurotransmitters,encephalins and
endorphinsjn pain relief. These
endogenous peptides have a
profound and long-lasting analgesic
effect and have been found in
various parts of the nervous system,
namely,the periaqueductal gray
matter, medullary raphe, the neurons
in the dorsal horn of the spinal cord,
in the thalamus and the
frontotemporal cortex. Their action
is blocked by the opiate antagonist
naloxone and they are therefore part
of a natural endogenous analgesic
system. They also probably play a
role in the analgesic response to
opiates.
5
Another major inhibitory pathway in
the pons appears to inhibit the
nociceptive responses of the dorsal
horn neurons.
Guidelines:
The management of pain should
observe the following guidelines.
a)
b)
Identification of the cause —
Certain conditions can be treated
by particular agents, for example.
the pain of angina pectoris
responds to glyceral trinitrate;
trigeminal neuralgia and the
lightning pains of tabes dorsalis
to carbamezepine. Bone pain
from metastatic prostate cancer
responds to stilbestrol and post
herpetic neuralgia to
carbamazepine along with a
tricyclic antidepresant.
Begin with the simplest method
(or drug) but with early treatment
and adequate dosing. There is
strong evidence that if pain is not
treated for an extended period of
time, abnormal excitatory states
arise in the CNS so that treatment
which would have earlier relieved
the pain does so no longer.
Oral drugs are preferable to
parenteral drugs as they are
drugs with few side-effects and
low addictive liability.
c)
For the same reason, adequate
timing between doses and
adequate dosing is essential:
especially in chronic pain which
should be considered a serious
problem and treated so that the
patient is made as comfortable as
possible. Drugs and doses should
therefore be tailored to the needs
of the individual.
d)
More than one kind of treatment
should be utilized. This could be
drug combinations, adjuvant
analgesics, other drugs or
physical methods. Non
pharmaceutical methods of pain
control such as acupuncture.
hypnosis, biofeedback, relaxation
techniques and coping skills
should also be tried. Adjuvant
drug therapy mentioned above
includes psychotropic drugs
which are sometimes useful in
chronic pain since they alleviate
the associated depression and
improve the quality of life.
Benzodiazepines are useful if
anxiety plays a part; chloral
hydrate, if insomnia is present;
antiemetics counter the nausea
and vomiting associated with
short-term treatment with
morphine, and laxatives reverse
the constipation associated with
the long-term use of narcotic
analgesics.
Each case must receive a full trial of
analgesic drugs and other
concommitant physical methods to
relieve the pain. Destructive
methods such as rhizotomy or
cardotomy should be tried as a last
resort especially since these
procedures yield only temporary
relief: in some cases the pain that
recurs is worse than it was prior to
the operation.
References
1.
Stembach R A. Pain. A
Psychophysiological Analysis.
Academic Press, London, 1968. 2.
2.
Guyton A. C. Textbook of Medical
Physiology. Igaku Shoin/Saunders.
Tokyo, 1981, 613.
3.
BandlerR. Using your brain — fora
change. NLP, Real Peoples'Press
1985.
4.
Wyant GM, Chronic Pain, Drugs,
1983, 26. 262-267.
Pain. Cecil Textbook of Medicine,
Eds: Wyngaarden J.B. and Smith
L.H., W.B. Saunders, 1985. 17th
Ed. 2049.
5.
6.
Adams R.D. and Joseph JB. Pain.
Harrisons Principles of Internal
Medicine: Ed: Petersdorf R.G.. et
al, McGraw Hill, 1983, 10th Ed.
7-15.
Best and Taylors Physiological
Basis of Medical Practice. Ed:
Brobeck JR. Williams and Williams.
1979, 10th ed. 2. 16-2. 19.
8. Oxford Textbook of Clinical
Pharmacology & Drug Therapy, Ed:
Grahame Smith DG and Aronson
J.K: Oxford University Press. 1984,
533-548.
7.
9.
C.S.M. Update, BMJ, 1986,
292-1190
Novaloiii
Active ingredient: Analgin
■■■■MM
■■
■■
■■
■■
3)
'^■■■■■■■■■■■■■■■■■■ b
THE ESTABLISHED
ANALGESIC-ANTIPYRETIC
FOR
^■■■■■■■■■■■■■■■■■■■■■■■■M
PAIN
____________________________________ JIM
M«MMMMMM«M»1.
Further information available on request from
HOECHST INDIA LIMITED. Hoechst House. Nariman Point. Bombay-400 021.
jschst SB
Psychological Aspects of Pain
Psychological factors can influence
pain behaviour — to varying extents
— in a considerable number of
patients. The importance of this lies
in its effect on the management of
persons suffering from pain; patients
then need not undergo expensive
and lengthy investigations and, also
the development of many
psychological techniques based on
this, offers help even to those
suffering from pain due to somatic
reasons.
Both physiological and psychological
factors are responsible for the
existence, perception and
persistence of pain. At one pole are
patients with pain that is completely
psychologically determined; at the
the other end are patients where
pain is physically determined;
inbetween lie patients where an
interplay between somatic and
psychogenic factors exists — here
the character and experience of pain
is not fully accounted for by the
lesion.
In the psychological disorders that
are associated with pain, such as
conversion hysteria, depression,
anxiety and schizophrenia, it is only
when the underlying disorder is
corrected that the patient
experiences relief.
Symptoms of an underlying
psychiatric disorder may be
discovered by careful questioning.
The commonest psychiatric disorder
associated with pain is conversion
hysteria; the patient presents with
dramatic complaints, yet may show
indifference to the symptoms, for
example, the patient may smile while
talking about his pain. Patients with
this disorder often have a history of
previous episodes with remissions
and relapses.
Depression is another frequent
cause of pain; the patient gives a
history of feeling depressed before
the onset of pain. Questioning may
reveal that things which had
previously given him pleasure were
no longer so. In addition,
physiological parameters of
depression, such as loss of appetite.
decrease in sleep and loss of sexual
desire may be noted. On the other
hand, patients with organic illness
often become depressed as a result
of the pain, moreso in cases of
chronic pain. The schizophrenic
patient is likely to have bizarre
complaints with disturbances of
thought and behaviour.
attention from others is made
contingent on increasing activity
levels and decreasing complaints of
pain. Analgesics are given by the
clock and not when the patient
complains of pain.
Once a diagnosis is made, the
physician has a large therapeutic
armamentarium to draw upon;
placebo, biofeedback, hypnosis,
behaviour modification,
psychopharmaceutical agents and
psychotherapy,to name a few. A
psychiatric disorder like
schizophrenia responds to
antipsychotic drugs and
psychotherapy, as does depression
to antidepressants. It is important to
remember that a depressed person
is likely to improve with
antidepressants even if the
depression is secondary to pain due
to an organic lesion.
Biofeedback is yet another powerful
modality and has been found useful
for muscle tension headaches
(electromyography feedback) and
migrane (skin temperature
biofeedback) with as many as 70 per
cent of patients remaining free of
migrane one year after treatment. In
addition to these methods are many
other psychological ones;
psychotherapy, where the patient is
challenged to get well and to specify
realistic relationship, work and
recreational goals and the patient is
reinforced for objective evidence of
attempts to achieve the goals set.
Many patients respond to placebo,
but this does not necessarily mean
that the pain is psychogenic. What it
does mean is that the patient is a
placebo responder and that he/she
may yet have an organic lesion.
Probably the most powerful tool in
acute or chronic pain, organic or
psychologically caused, is hypnosis
in this state the person can distort
his/her perception of the pain to
warmth or pressure, thereby
preserving the signal functions of the
pain. Hypnosis can also be used to
induce analgesia or anaesthesia.
The advantage of hypnosis lies in the
absence of demonstrable
physiological risks. An example of its
usefulness was demonstrated by Dr.
James Esdale, a Scotish surgeon in
Calcutta who. in the pre-anaesthetic
days of the 1850s performed 500
major and 1500 minor surgical
operations under hypnosis. He often
undertook operations that in his day
were considered too dangerous to
contemplate.
Behaviour modification has also
been found very useful in pain
management. Pain is often
reinforced by rest, medication and
attention focused on the patient by
medical personnel and family
members. In this approach, patients
are reinforced for behaviour not
compatible with pain: rest and
Dr. J.D. Mirchandani. MD. DPM, FIPS.
Bombay
“It is important not to forget that
non-drug approaches often have a
great deal to offer to the patient
with pain and that a
multidisciplinary approach is often
preferable to a solely
pharmacological one."
"Consider the common experience,
for instance, of being able to
relieve quickly, by means of a hug
and reassurance, the distress and
suffering of a child who had tripped
and fallen. “
“In moments of excitement, stress
or competition, such as on the
athletic field significant injury can
be unattended by pain."
“Reassuring patients prior to
surgery can have a beneficial
effect on the course of
post-operative pain and
requirements of analgesics."
Louis Lasaqna — DRUGS. 32 (4),
1-7, 1986.
7
Facts on Fever
Fever is one of the commonest
presenting symptoms a general
practitioner encounters, but it serves
merely as an indicator — a sensitive,
objective and reliable one — of a
disturbance within the body except in
a few instances; It should not be
unnecessarily viewed with alarm and
panic.
These few exceptions are pyrexia of
moderate elevation in patients with
central nervous system disease,
decreased cardiovascular function
(the increased oxygen demand,
cardiac output and pulse rate
associated with fever can be
dangerous on the already
compromised myocardium in these
cases); a history of previous febrile
seizures (particular in children) and
in pregnant women (fever may be
teratogenic for the developing
foetus).' A potentially fatal example
is heat stroke, where temperatures
greater than 106°F (41.1 °C) are
common. Heat stroke is classified as
a hyperthermia syndrome; these are
cases where the hypothalamic
thermostat remains at the
normothermic level, unlike cases of
'fever' where the setting is at a
higher level. In hyperthermia the heat
loss mechanisms fail, causing
temperatures that in some cases
have been recorded as high as
112-113°F (44.4°C)2. Temperatures
higher than this are probably
incompatible with life; in fact,
irreversible brain damage is common
at temperatures of 108°F (42.2°C)
and convulsions are common at
106°F (41.1°C)’ Usually
hyperthermia is seen with cerebral
lesions that involve the
hypothalamus2. Another condition
that causes dangerously high
temperatures is malignant
hyperthermia; this is a group of
inherited disorders which results in
temperatures of 102.2°F to 107.6°F in
response to certain inhalational
anaesthetic agents, such as
haloperidol, cyclopropane, ethyl,
ether or muscle relaxants, especially
succinylcholinefAs with other causes
of hyperthermia, this should be
considered an emergency and
treated immediately. The most
effective measures in hyperthermia
are ice-water baths and, depending
on the cause, other measures, such
as dantrolene sodium, which is
8
specific for malignant hyperthermia,
paying special attention to hydration,
electrolyte and acid balance.
indicator of disease. (Rectal
temperature is usually 0.5 to 1°F
higher than oral temperature).
What is generally termed as 'fever' is
an elevation of the normal body
temperature which, depending on the
individual, varies between 97-99 F
(36.1-37.2’C). This includes the
diurnal variation of 1°F (0.6’C). It is
safe to consider an oral temperature
of above 99'F (37.2’C) as an
The following disease states are
accompanied by fever:
1.
All infections, whatever be the
offending micro-organism. The
majority of febrile illnesses of less
than 2 weeks duration can be
attributed to this.
Tissue damage due to any cause Fever is caused by many stimuli
Vascular accidents such as
which include bacteria, their
myocardial or cerebral infarction
endotoxins, viruses and other micro
or mechanical injury frequently
organisms, hormonal substances,
cause fever.
immune reactions and drugs; these
3.
Neoplastic diseases. Hodgkin's are termed exogenous pyrogens and
cause the release of endogenous
and other tumours of the
reticuloendothelial system can
present with fever. The
Genesis of fever
production of EP/IL-I is thought to
be responsible. Solid tumours
can cause fever which is probably
due to obstruction or infection
consequent to the tumours.
2.
4.
Drug fever and other conditions
that involve the immune
mechanism, such as connective
tissue diseases.
5.
Metabolic disorders, such as
gout, porphyria, Addisonian or
thyroid cases, are occasionally
responsible.
Pathogenesis Of Fever
The temperature of the body is
regulated almost entirely by nervous
feedback mechanisms and most of
these operate through temperature
regulating centres in the
hypothalamus. The principal area of
temperature regulation lies in the
preoptic area and, also, to some of
the adjacent parts of the anterior
hypothalamus. These areas contain
heat-sensitive neurons which
increase their firing rate in the
presence of endogenous pyrogen.
Fever is best understood using the
analogy of a thermostat. The
regulatory system at the
hypothalamus balances heat
production and heat loss. Heat
production is principally promoted by
increased shivering and by
peripheral vasoconstriction which
reduces heat loss. Heat loss occurs
by vasodilation (full vasodilation can
increase the rate of heat transfer to
the skin eight-fold and by sweating
(1°C) increase in body temperature
can cause enough sweating to
remove ten times the basal rate of
heat production).4
In fever, the thermostat is at a setting
higher than normal which causes
signals to increase heat production.
The tone in the muscles
consequently increases which
results in shivering, which commonly
occurs during a fever. Conversely,
when fever comes down, the
uncomfortable flushing and sweating
is due to the loss of body heat in
accordance with the temperature
'reset' at the hypothalamus.
pyrogen which is a product of
macrophages and monocytes.
Endogenous pyrogen has now been
identified as interleukin 1 (IL-l) and it
is believed to be the basis for many
of the reactions under the umbrella
of the ‘acute phase response'.2
peritoneum.
that occur during fever, controversy
IL-I is responsible for setting the
(Other granulomatous infections
hypothalamic thermo-regulatory
often surrounds its treatment.
that should be kept in mind
system at a higher level. The
Specific therapy should, of course,
include actinomycosis.
mediators responsible are
be initiated. Antipyretic drugs, such
candidiasis, histoplasmosis).
prostaglandins of the E series whose as aspirin,analgin or paracetamol.
synthesis is induced by (IL-I). PGE
should be employed, particularly
ii)
Bacterial endocarditis.
activates the heat - generating and
when fever poses a high risk, such
iii)
Bacteraemia due to Salmonella.
conserving mechanisms by inducing as in patients with a history of
Neisseria
and Brucella.
the synthesis of cyclic adenyl
seizures (especially children), with
monophosphate.2
heart failure, head injury, mental
iv)
Abscesses are a common cause
disorders or pregnancy.
and often arise in the abdomen
EP/IL-I is probably responsible for
and pelvis. Amoebic abscess or
other symptoms that occur during
Antipyretics are sometimes
hepatitis should be ruled out.
fever. It mobilises amino acids
associated with unpleasant
v)
Urinary and biliary tract
from muscles through a mechanism
sensations due to the sudden
infections.
mediated by PGE; these amino acids lowering of body temperature. This is
act as nutrients for other cells. The
mitigated by a liberal fluid intake and vi)
Viral infections caused by
myalgias experienced during fever
administering the prescribed
Epstein Barr or cytomegalo virus
and the muscle wasting that occurs
antipyretic drugs frequently and
are becoming more common in
in febrile states is therefore a result
regularly.
immunocompromised hosts.
of EP/IL-I production.2
b)
Neoplasms —A number of
If rigors are severe, an intravenous
neuplasias are associated with
EP/IL-I also activates slow-wave
injection of calcium or morphine
fever; at least 20 per cent of
sleep-inducing neurons which
sulphate or chlorpromazine is
FUO will have an underlying
explains the drowsiness and
helpful.
tumour as acause and the
prolonged sleep characteristic of
febrile illnesses.2
percentage of such patients is
Physical methods, such as tepid
water sponging, can also be initiated.
increasing.' These neoplasms
On the positive side, EP/IL-I plays a
include Hodgkin’s (in this case
key role in activating immune
Of the common antipyretics, aspirin
fever may be a principal
responses, in mobilising T. helper
should not be used in patients with a
symptom) and other lymphomas,
cells from marrow storage pools, in
history of salicylate sensitivity, or
leukaemias, solid tumours and a
inducing lysosomal discharge in
with a history of erosive pathologies,
trial myxoma.
neutrophils, and in generating
gastric ulcer patients with
c)
Granulomatous diseases —
chemotactic activity in neutrophils.2 It haemophilia and other diseases of
Sarcoidosis, if in an extraalso activates fibroblasts to
blood coagulation and even asthma.
pulmonary site, often presents
synthesize collagen and presumably It should also not be used in children
with fever. Fever is also a
contributes to tissue reparative
due to the potentially fatal Reye's
prominent feature in regional
responses.2
Syndrome. It is on this account that
enteritis. Granulomatous hepatitis
aspirin has, in U.K. and recently in
of unknown aetiology is also a
Manifestations of Fever
India, been banned for children
cause of FUO.
below the age of 12 years.
Subjective Symptoms
d)
Inherited disease — The
Fever of Unknown Origin (FUO)
commonest of the inherited
a)
Sensations of feeling cold or
diseases
presenting as FUO is
warm chills
Perhaps one of the most challenging
Familial Mediterranean Fever
b)
Headache
problems in general practice is FUO.
(FMF),
which
is common in
c)
Myalgia, arthralgia
Though the problem may ultimately
Armenians, Sephardic Jews and
d)
General malaise
become obvious, its elucidation
Arabs.
Inherited
hyperlipidaemia
requires a detailed and careful
e)
Drowsiness
(Type 1) can also present as
history, thorough physical
FUO, whereas it is a prominent
Objective Signs
examination, appropriate laboratory
sign in Fabry's disease.
examinations and occasionally even
a)
Elevated temperature
imaging techniques.
e)
Drug Fever — Allergy to
b)
Increased respiratory rate
antibiotics especially penicillin
c)
Wide pulse pressure
The term FUO should only be
and sulphonamide may be a cause
d)
Rapid pulse rate (except in
applied to those cases where the
for prolonged fever and can
typhoid fever and certain
duration of fever exceeds 3 weeks
compound diagnosis. Other
■ hypothalamic tumours)
and
where
intensive
study
of
the
drugs causing fever include
e)
Delirium
case for at least a week fails to
bromides, iodides, arsenicals,
reveal
the
cause.
6
Some
conditions
procanimide, thiouracil.
Laboratory Findings
that present in such a manner are
hydrallazine, phenytoin,
given below:
a)
Elevated ESR
barbiturates, quinidine and
b)
Increased neutrophil count
laxatives.6
c)
Decreased serum iron and zinc
a) Infections —
f)
Factitious Fever — There is a
levels
i) Tuberculosis and atypical
d)
Concentrated urine with high
small group of patients —
mycobacterial infections,
generally young women with FUO
specific gravity.
especially if extra-pulmonary and
— who complain of fever or
Management
involving the bone, lymph nodes,
contrive to cause the thermometer
genital or urinary organs or
Given the complexity of responses
to register high temperatures.
10
These patients are found to have
psychiatric problems.
Management
As it is assumed that patients are
categorized as having FUO after all
routine tests (Table) have been
carried out, the next question relates
to determining the cause of the
elevated temperature.
Table: Routine Tests
1.
2.
3.
4.
5.
6.
Total blood count
Blood culture
Urinalysis/urine culture
Blood chemistry
Chest x-ray
Stool examination
The causes are many, so it is
essential that the physicians re
evaluate the patient thoroughly.
Questions covering contact with
animals, place of residence and
recent travel, illnesses, drug intake
and localizing signs may provide a
lead to the affected organ system or
possible infectious agent.
Physical examination should be
repeated. Skin and mucosal lesions
must be searched for; lymph nodes
must be palpated with special
attention to supraclavicular and
axillary areas; careful palpation of
the abdomen, rectal and vaginal
examination should be done;
valvular anomalies should also be
searched for. Drug intake should be
curtailed for 48 to 72 hours.
Laboratory tests
There are no specific guidelines to
follow: tests should be aimed at the
most likely system that could be
affected, for example, if there is a
suspicion of a connective tissue
disorder, tests as to detect
rheumatoid factor, antinuclear
antibody and antistreptolysin titre
may provide a clue.
Special attention should be paid to
the abdomen, as many of the causes
of unexplained pyrexia lie within.
Treatment
This depends entirely on the
diagnosis which should be possible
in 90% of patients with FUO.5
Fortunately, of the remaining, the
majority recover sponatneously or
respond to medical or surgical
treatment.
References
1. Cecil Textbook of Medicine. Eds:
Wyngaarden JB and Smith LH, WB
Saunders. 17th Ed. 1985, 1430-7
2. Harrison's Principles of Internal
Medicine. Eds: Braunwald E et al,
McGraw Hill, 11th Ed. 1997,43-9
3. Harrisons Principles of Internal
Medicine, Eds: Petersdorf RG et al,
McGraw Hill, 10th Ed, 1983.50-8
4. Textbook of Medical Physiology, Ed:
Guyton AC. Igaku Shoin/Saunders,
7th Ed. 1986. 849-60
5. Harrison's Textbook of Internal
Medicine. Eds: Braunwald efal,
McGraw Hill. 11th Ed. 1987,50-6 .
6. Oxford Textbook of Medicine. Eds:
Weatherall BJ et al, Oxford University
Press, 1983. 5.469-72
11
The International Study on Agranulocytosis and Aplastic Anaemia (ISAAA)
Agranulocytosis and aplastic anaemia are
exceedingly rare blood dyscrasias which
have been loosely associated with several
drugs. Both disorders can be caused by
many environmental, biological and
chemical factors, including over 100
pharmaceutical drugs. Many of these drugs
have been implicated solely on the basis of
case reports, or without controls, or on
incomplete data reports.
Intentional rechallenge is ethically
unacceptable and specific laboratory tests
do not exist either to label the cause-effect
relation. Therefore, to obtain a reliable
estimate of the incidence of the risk of
agranulocytosis and aplastic anaemia, the
only reasonable approach medically
acceptable was to undertake a rigid
case-control epidemiological study.
This was the genesis of the International
Study for Agranulocytosis and Aplastic
Anaemia.
The study had a supervisory International
Honorary Advisory Board to guarantee full
independence between the organisers and
the sponsors. This Board comprised
eminent experts in medicine and
haematology whose members were Sir
Richard Doll (Oxford), Chairman, P.K.
Lunde (Oslo) and Soen Moeschlin
(Sweden).
Al! co-ordination and data analysis was
done at the Drug Epidemiology Unit at
Boston.
Carefully defined cases, diagnosed and
reconfirmed by an independent
haematological review committee, were
searched for in a time-span of four years.
For each diagnosed case, at least 4
controls were selected who could match
totally with the cases based on age, sex,
occupation, education, social status and
such features.
Specially trained staff questioned all cases
and controls. All haematological data
diagnosis was in line with international
diagnostic criteria.
The study covered 300 hospitals in 6
countries, i.e., Israel, IV. Germany,
Hungary, Italy, Spain and Budapest, with
more than 40 investigators specially trained
to determine drug exposure and other
related risk and disease factors.
12
Acupuncture in the Treatment of Pain
The late Dr Albert Schweitzer once
said, “Pain is a more terrible Lord of
Mankind than even Death Himself."
The truth of this saying is apparent to
all, yet forgotten when we are not
affected with the symptom. Most
physicians pay inadequate attention
to the treatment of this symptom as it
is a purely subjective phenomenon
which is difficult to assess objectively
in clinical practice. Different patients
have different pain thresholds and
hence respond differently to similar
ailments.
Western medicine is able to deal
adequately with acute severe pain
using narcotics which are however
unsuitable for prolonged use in
chronic pain due to their potential for
habituation and addiction. And the
range of analgesics available —
including the new range of non
steroidal anti-inflammatory drugs —
are occasionally inadequate to treat
chronic pain.
Acupuncture offers an effective
alternative to the problem of pain,
both in its acute and chronic form. At
present enough evidence exists of its
ability to relieve pain and to create
analgesia profound enough to carry
out surgery ranging from
Caesareans to Craniotomies and
open heart surgery. We are as yet
unable to define exactly how
acupuncture produces analgesia,
and several theories have been
propounded to explain the
mechanism of its action. As none of
these is able to completely explain its
action, it is probable that
acupuncture produces analgesia at
multiple levels and the true
mechanism is a synthesis of the
theories described below.
The ‘gate control' theory of Melzack
and Wall propounded in 1965 is the
most popular neurological theory for
the mechanism of action of
acupuncture in the treatment of pain.
According to this theory, perception
of pain is modulated by functional
gates within the central nervous
system. Under normal
circumstances, this gate is wide
open and pain impulses which are
carried by the small diameter fibres
get through quite easily. When
acupuncture needling is carried out,
a second stream of non-painful
impulses is set up via the large
diameter fibres which cause
overcrowding or jamming at the gate,
causing it to close. There is,
therefore, a competitive inhibition of
the pain impulse at the gate. This
gate is postulated to exist at the
thalamic level.
The action of acupuncture should
then be mediated through the large
diameter fibres. However, it was
seen that trans-section of the large
diameter fibres diminished but did
not abolish the analgesic effect. This
led to the finding that the autonomic
nerve fibres accompanying the blood
vessels were also stimulated by
acupuncture. The development of
the humoral theory of the action of
acupuncture was the result of this, as
it was seen that acupuncture
released morphine-like analgesic
substances both in the brain and
peripheral tissues. Over a hundred
neurotransmitters have been
isolated which play a role in
acupuncture analgesia. The two
major groups of these are the
endorphins and encephaiins which
are produced by the Ivsis of betalipotropm.
14
©
Pomeranz suggested that the
endorphins and encephalins
produced by a neuron,binds to an
opiate receptor on the terminal of an
excitatory neuron,partially
depolarizing the terminal membrane,
thus reducing the net depolarization
produced by arrival of a nerve
impulse.
Stimulation of different acupuncture
points augments the secretion of
different analgesic substance and
produces analgesia in different
areas. Stimulation of the
acupuncture point HEGU situated on
the dorsum of the hand between the
1 st and 2nd metacarpal bones leads
to production of alpha-and beta
endorphins in the ratio of 2:1.
Alpha-endorphins induce analgesia
in the region of the head and cause
a slight tranquilhsation. Hence.this
point is used to treat toothaches,
headaches, and;trigeminal neuralgia,
as well as to create analgesia for
tooth extraction and tonsillectomy.
Beta-endorphin creates analgesia all
over the body and is released by
stimulation of most acupuncture
points. These substances also cause
slight sedation which potentiates the
analgesic effect.
Acupuncture, contrary to popular
belief, is not very painful.
Acupuncture needles are normally
30 to 36 gauge (0.32 mm to 0.18 mm
in diameter), which is little thicker
than a human hair. The photograph
shows a little girl undergoing
acupuncture therapy.
In osteoarthritis, damage to the
articular surface causes pain. This
leads to a protective spasm of the
surrounding muscles to restrict
movement and pain.
This spasm also pulls the joint
surfaces closerand increases
damage to the articular surface. This
again creates pain, setting up a
vicious cycle (see Fig below).
This cycle is difficult to break with
conventional medical treatment.
Acupuncture relieves the pain in
sittings,thus breaking the cycle
and affording the patient a pain-free
existence for 2 to 5 years before the
pain recurs.
In sciatica, we needle points which
lie along the course of the sciatic
nerve. This serves to relieve the pain
and relax the muscular spasm of the
paraspinal muscles, making
movement easier. This is effective in
giving relief from pain within 8 to 10
sittings in most patients.
Acupuncture is also effective in
relieving pain by needling areas
which are distant from the affected
area. In frozen shoulder, a needle
placed a few inches below the knee
next to the tibia and rotated
vigorously for a minute permits
immediate pain-free mobilisation of
the shoulder. This is one of the most
dramatic demonstrations of the
efficacy of acupuncture.
Acupuncture points are situated on a
series of pathways called meridians
which criss-cross the body. These
pathways are traditionally said to
allow the flow of certain life forces.
Needling is said to restore the
balance of these forces,the
disruption of which was thought to
cause disease.
Similarly, there exist acupuncture
points in the ear (over a hundred of
them) by the use of which it is
possible to treat most ailments. The
entire human body is represented in
the ear in the form of an inverted
human foetus. The facial area is
A young patient undergoing
acupuncture therapy.
represented in the lobule of the ear
and the feet near the apex of the ear.
This can be used to treat a wide
variety of ailments like headache.
hypertension, insomnia, gastritis.
sprains, sciatica, dysmenorrhoea
and pain anywhere in the body.
Acupuncture is a complete system of
medicine and. like all systems of
medicine, has a treatment for most
conditions.
The use of acupuncture needles
can be substituted in many cases
by stimulation with lasers. This is as
effective as acupuncture and is
extensively used for treatment in
children and thin individuals.
Electro-acupuncture.
cryoacupuncture, and acupuncture
using ultrasound, are other methods
which are used to stimulate
acupuncture points.
Acupuncture, the 5000-year old
Chinese system of medicine,is an
effective method for treatment of
pain both in its acute and chronic
forms. In skilled hands, it yields
results which border on the
miraculous. To quote Dryden, in
conclusion, is apt:
'For all the happiness mankind can
gain
Is not in pleasure, but in rest from
pain.”
Dr. Manik Hiranandani. M.B.. B.S..
D Ac. M.D F.F. Hom
15
Weighing Risks
Taking risks or avoiding them is
intrinsic to life. As we grow older we
veer away from the former towards
the latter with the quest for vanished
youth during the middle years
expressed by a shiftback, for a short
time, towards risk-taking again.
To grasp opportunity, one must act,
and inherent in this,is the element of
risk; opportunity and risk cannot be
separated. When fear paralyses
action, opportunity fades.
Understanding risk means learning
to balance fear and opportunity. In
this attempt strange paradoxes
occur which highlight the magnitude
in which risk is misunderstood, and
this is the basis for some of the
strikingly distorted perceptions of
risk!
Cigarette-smoking is deemed
responsible for half-a-million
premature deaths per year from lung
cancer and heart disease in the U.S.
alone — but this fact only gets a
small amount of coverage in the
news media even though the number
of smoking-related deaths is
equivalent to three fully loaded 747
jets crashing every day. Yet, when
an actual jet crash occurs, it is given
“Big Attention".
That 'bad news' sells is nothing new.
What is new is the instantaneous
dissemination of news — one of the
gifts of modern electronic
technology.
Many widely accepted human
activities are the very essence of
risking life or limb. (Table)
Quantifying or measuring risk
permits a rational approach which
can allow people to make their
choices based on information rather
than on imagination. Imormation is
crucial to this concept, but the
methods of generating the
information that one needs to assess
risk are often uncertain and.
moreover, the methods of
communicating this information, viz.,
expressing risk are usually
confusing, misleading and
emotionally charged.
To understanding risk, one has to
take a big step beyond the
Table: Risks estimated to increase chance of death in any year
by 0.000001 (1 part in a million)
Cause of death
Activity
Smoking 1.4 cigarettes
Cancer, heart disease
Drinking 0.5 litres of wine
Cirrhosis of the liver
Living in New York for 2 days
Air Pollution
Travelling 150 miles by car
Accident
Flying 1000 miles by jet
Accident
Living in average stone or
brick building for 2 months
Cancer due to natural
radioactivity
1 chest x-ray taken in a
good hospital
Cancer caused by radiation
Living with a cigarette
smoker for 2 months
Cancer, heart disease
Medical News, BMJ, 293, 1445,1986
journalistic view. It is necessary to
perceive the number of victims in
relation to the number of people who
did just what those victims were
doing,but yet managed to emerge
unharmed. This would be the
genesis of avoiding what is known as
Victim-Oriented Reporting.
Thursday, the average number of
traffic deaths is 75 per day. From
Friday through Sunday the average
number is 240 per day. In other
words, a 3-day holiday weekend
might be expected to produce 3 x 240
= 720 victims.
To illustrate the kind of
misinformation which victim-oriented
reporting can generate, have a look
at the following headline in the USA;
“411 DIE ON HIGHWAYS DURING
LABOUR DAY WEEKEND".
The alternate headline to the one
above should have been "CAREFUL
DRIVING ON LABOUR DAY
WEEKEND — 309 LIVES SAVED."
But human nature yearns for tragedy
or bad news. Good news in our
emotional makeup must take a
second place.
First spontaneous reaction — How
awful!!
An analytical look behind the
headline:
50,000 traffic accidents occur in the
U.S.A, every year, i.e., 137 per cent
per day of 411 in 3 days. Since
Labour Day weekend is 3 days, the
411 turns out to be the right average.
A closer analysis of that headline:
An average of 137 per day is
misleading as there is a strong
difference between weekday and
weekend incidents. Monday through
Victim-oriented reporting is designed
to leave us with anxiety and fear of
such things in no particular order —
the bomb, the next earthquake, a jet
crash, a chemical plant fallout.
passive smoking, AIDS. The list can
continue endlessly, as long as it sells
unpleasant events.
To give some order to these high
nsks we must have a “Scale for risk'
which integrates information so that
rational people can make rational
decisions about which hazards
present high risks and which are
accompanied by small risks.
The lack of acceptance of a uniform
standard for expressing risk is one of
the reasons that we haggle a great
deal about certain risk-related
issues.
Just as the Richter Scale in an
earthquake report tells us about the
severity of the quake, we need to
have an analogous risk scale so that
everybody can understand to what
extent, for example, a newly
discovered hazard affects our
already known health risks.
In making such a scale, it is
important to keep it very simple.
Instead of saying “the death rate
from homicide in the USA is 10.4 per
100,000 per year”, a simple way of
representing this figure is by saying
“the risk of one’s dying due to
homicide in a year's time in USA is 1
in 9615".
The number ‘1' means that the event
in question happens to you or to
someone else. The chances of ‘1'
becoming a victim to a hazard is his
or her risk.
The Risk Ratio is a ratio in which the
numerator represents the individual
who is actually harmed while the
denominator represents the number
of all persons who are exposed to
the same activity but have emerged
unhurt. For example, all airline
passengers, all persons with high
B.P., all cigarette smokers, etc. The
risk ratio varies from 1 : 1 to 1 : 100
million representing a scale of 0 to 8
(Fig.1), where each number
represents the number of zeros after
1.
A 1 :1 risk occurs when a person
contracts a disease such as rabies
which has the virtual certainty of
death.
There is no theoretical upper
boundary to the scale, but 8
represents this limit which has been
set by the present methods of data
collection. And so, now we see the
basis for making easily understood
statements such as "my risk erf being
killed as a passenger in an air crash
is 1 in 800,000 per trip or, if using the
above scale,the risk is between 5
and 6. Fig.2 compares the risk of
various activities.
For greater accuracy any risk
statement necessitates a time
interval to be expressed. In general,
either of two time intervals are used
per year or per event, i.e.. per trip or
a surgical operation or giving birth or
any such parameter.
17
numerically strong base against
which incidence of the event can
be compared. This kind of
methodology is the basis of the
Fig 3. Risk Scale (K. Heilmann and T. Urquhart)
International Study on
Agranulocytosis and Aplastic
__________________________________________
Anaemia which has been
presented in this issue.
1 :100 000 000 8-
1 :
10 000 000 7- . Rheumatic fever, tetanus, diphteria
1:
1 000 000 6- - Malaria, venereal diseases - 6
7
One could use the Risk Scale to
place some of the known side-effects
of drugs in relation to other risks of
life (Fig.3). As an example, the
occurrence of agranulocytosis
consequent to drugs occurs on this
scale with a frequency so low that
the chances of being struck by
lightening or even encountering a car
accident are very much higher.
-Digitalis (West-Germany 1982) 5.5
: UT AdJ? ST;
Drugs (West-Germany 1975) 5.4
-Contraceptive (Age 25-34; non-smokers)4.4
^Contraceptive (Age 25-34; smokers) 3.8
Lung cancer 3.4
1 :
1 000 3" ' Contraceptive (Age 35-44;. smokers) 3.2
,/.L -. - K Cigarette smokers (20/day) 2.3
1 :
100 2' Myocardial Infarction ()35 years) 1.9
1:
1 :
Medicine and surgery are both
naturally linked with risks.
Contemporary medicine could never
have brought solace to patients
without the accompanying risks of
therapy. Where would open-heart
surgery, valve replacement and the
like be today if the initial patients had
not taken the risk of undergoing the
surgeon's knife?
10 1-
10
—————-Like all activities, drug treatment is
also a calculated risk. HOW SAFE IS
A DRUG? — this question is often
asked. The safety of a drug is always
assessed first by studies on animals
and later in extensive clinical trials in
human volunteers under regulated,
approved ethically designed and
closely monitored clinical trials.
The sample size required for
detecting the occurrence of adverse
drug reactions (ADR) varies and
depends on the frequency of the
reaction. If the frequency of the ADR
is 1 : 10, then the number of patients
needed to have noted this would be
39 - 40. Similarly,for a 1 : 100 ADR,
390 - 400 patients would have been
required; for 1 : 1000, 3900 - 4000
patients and for a 1 : 100,000, a
corresponding 390,000 - 400,000
patients. It is therefore almost
impossible to detect rare ADR.
18
Therefore the next time such a
''sensational" news report appears,it
would be very necessary to recall
that the information is next to nothing
if not presented along with the
comparative data or the hidden facts.
However, two kinds of studies to
detect rare ADR have been
epidemiologically identified:
a) The cohort type: Individuals likely
to develop the disease are
studied even before they suffer
the pathology. They are followed
up for prolonged time periods to
determine when the exact
occurrence takes place. This
method obviously has
tremendous constraints in terms
of finance and time.
b) The case-controlled type: Every
case identified is compared with a
large number of controls who are
necessarily matched for all
identifiable variables with the
suffering case. In so doing it
allows the exploration of all
possible causal factors related to
the event, and also provides a
The risk of treating versus not
treating is often the genesis to know
how small risks can become the
basis of big controversies.
The problem with drugs is not that
their risks are greater than their
benefits. It is simply that we cannot
make up our minds about the risks
— which risks are tolerable and
which are not acceptable.
The tendency of people to worry
about rare side-effects and forget
about the benefit of the drug is due
to our failure to calculate risks, to
assess them and to compare them!
Prof. William Inman of the Drug
Surveillance Unit of the University of
Southampton has very aptly spelt out
the benefits of a drug versus the risk
of a drug-free existence, when he
says "One way to consider drug risks
is to ban all drugs. Ending all druginduced harm would add 37 minutes
to your life expectancy. Ending all
drug-related benefits would subtract
15 years from your life expectancy,
and also end the improvement in life
quality drugs give".
■
Weighing Risks —- A Case in Point
Many of us provoked to seek the
aid of analgin for various aches and
pains have often been perturbed by
conflicting reports.
patient-history.
Besides Hoechst AG, this study,
the first of its kind in the world and
in medical epidemiology, saw
Analgin, which belongs to the family participation very actively from the
of pyrazolone analgesics, was
Governments of Sweden, Hungary
discovered in 1918. Its discovery
and Bulgaria, the National Institute
was an important breakthrough in
of Health, USA and the WHO.
the field of analgesics, since it
offered doctors a safer alternative
Four long years elapsed before the
to the narcotic opiate analgesics
data produced results. The
International Study for
like morphine and pethidine.
The worldwide response to the drug Agranulocytosis & Aplastic Anaemia
(ISAAA
as it was called) would
was astounding and it soon
provide data on the drug-related
became the leading analgesic.
causality of both these blood
Somehow, through scattered,
dyscrasias.
unchallenged reports, it began to
At the lllrd World Conference of
be linked with 'agranulocytosis'.
Pharmacology & Therapeutics,
The essential mistake at the time
Stockholm, the ISAA study results
was that these vaguely distributed
were
finally presented. The findings
reports were not investigated and
clearly revealed that the past
proved then and there. These
doubts
on analgin's safety had
reports began to be repeatedly
been needlessly raised and the
quoted as retrospective data and
previous
incidence of
soon became the basis on which
agranulocytosis was grossly
adverse effects of the drug were
calculated and talked about. These exaggerated. The originally quoted
few reporting incidents generated a incidence for this disorder was the
astounding figure of 0.8%. i.e.,
snowball effect and analgin came
8000 cases per million.population!.
under the strict control of the
regulatory authorities in some
countries. Incidence rates for
agranulocytosis which were quoted
as long back as 2 decades ago
also became the basis to ban the
sale.of analgin in some countries.
Hoechst AG, at West Germany,
being a manufacturer of the drug
and concerned about the safety of
its products immediately took steps
to determine the true incidence of
this disorder and assess the safety
of analgin.
In 1979, a massive study was
initiated in collaboration with the
University School of Medicine at
Boston, USA, to determine the true
incidence rates associated with
analgesics, not only for
agranulocytosis, but also for the
dreaded disease, aplastic anaemia,
which has a fatality rate of about
50%. 300 hospitals from 6 countries
(West Germany, Israel, Bulgaria,
Hungary, Spain and Italy) covering
a total population of 22 million
people became the study base. A
team of experts examined all
laboratory material, i.e., slides of
blood and bone marrow to reach a
diagnosis independent of
This error in previous calculations is
totally mind-boggling — consider
therefore with such an enormous
figure, the incidence of
analgin-related agranulocytosis in
Bombay city alone should be of the
order of 56,000 cases.
Dr. Samuel Shapiro, member of the
ISAAA Study Group, accurately
summed up this high-blown error
when he stated at Stockholm last
year that “the original estimates of
agranulocytosis was an error of
many orders of magnitude.”
In fact, the study data presented
showed that the risk of getting
agranulocytosis following analgin
was as low as zero to a maximum
of one in one million users.
Along with analgin, the study also
showed that a few other drugs like
sulphas and commonly used
analgesics have the potential to
cause agranulocytosis, the
commonest being indomethacin.
which is surprising because this
substance was never suspected to
be a high-risk factor to get
agranulocytosis. Moreover,
indomethacin also was associated
with aplastic anaemia. This disorder
is unrelated to the use of analgin.
At this conference, it also became
evident that other major pain-killers,
like aspirin bear the risk of rare but
severe adverse drug reactions. The
risk of gastrointestinal bleeding is
substantially increased often to a
fatal end. Aspirin was also
associated to an appreciable
extent with aplastic anaemia. With
paracetamol, the other common
pain-killer, no association with
either disease could be found, but
the experts stated, there were not
enough cases of individuals
exposed to the drug.
Analgin is almost 65 years old. Yet
it continues to successfully vie with
its younger competitors for the
pride of place among not only
pain-relieving drugs, but also
among fever-reducing agents
because it has the twin combination
of proven safety and efficacy.
According to Dr. T. Floeter, Doctor
of Anaesthesiology who runs a Pain
Clinic in Frankfurt, “Analgin is
irreplaceable among peripheral
analgesics. Its therapeutic uses are
so broad and yet no case of
poisoning has been observed".
Current research indicates that the
drug is superior to aspirin and
paracetamol for the relief of pain
and fever.
All analgesics, like any drug, have
some element of risk involved with
their use because they, like any
other drug again, can cause a
hypersensitivity reaction in an
isolated patient, but this is an
extremely rare phenomenon and
the side-effects which are usually
talked about so loudly are so
extremely rare that most doctors
have an occasion to learn about
them only from textbooks.
Any drug at any time is always a
risk to the user, and drug-related
risk is always a concern. A risk-free
drug has yet to be found and
therefore every drug needs to be
evaluated not on the isolated case
of adverse effects, but on the vast
population who will benefit from its
use. Therein lies the answer to
what is colloquially known as the
risk-benefit ratio!
■
Emergencies in Clinical Practice
Acute Myocardial Infarction (AMI)
Approximately 40-50% of persons
who suffer an acute myocardial
infarction die within 20 days of the
onset. If one takes into consideration
that half these deaths occur within
the first and second hour after the
onset of the symptoms, the urgency
to provide prompt treatment is further
stressed by the fact that the majority
of these deaths are due to potentially
correctable ventricular fibrillation.
straightforward; with a careful
examination and history, the
following should be ruled out:
On auscultation, a fourth or atrial
sound is present and may be
palpated as a presystolic expansion
over the anterior aspect of the left
ventricle. With extensive myocardial
damage, a third heart sound is
present often accompanied by a
systolic thrust palpable over the 3rd
and 4th intercostals.
Differential Diagnosis
The clinical history of AMI is
20
2.
Examine cardiovascular system,
especially pulse, B.P. and heart
sounds. If possible take an ECG:
a) If pulse is less than 45/minute,
atropine 0.6 to 1.2 mg
intravenously or intramuscularly
may be given, especially if
hypotension is also present.
b) If pulse is irregular an
intravenous bolus of 50- .
100 mg xylocaine or lignocaine
can reduce the occurrence of
potentially fatal arrhythmias.
3.
If cardiac failure is present, 80 mg
frusemide should be given.
4.
If patient deteriorates and goes
into ventricular fibrillation,
defibrillate at once. Perform
external cardiac massage and
mouth-to-mouth resuscitation.
Aortic dissection
Pulmonary embolus
Pericarditis
Spontaneous pneumothorax
Acute pancreatitis
Spontaneous rupture of
oesophagus
7. Peptic ulcer
8. Cholecystitis
1.
2.
3.
4.
5.
6.
The most common presenting
feature in more than 80% of patients Management
is severe pain in the retrosternal area 1. Immediate slow intravenous
of the chest or epigastric pain.
injection of morphine 10-15 mg
Precipitating factors such as a heavy
results in rapid pain reduction and
meal, emotion and exercise may
reduces anxiety. Pentazocine is
have triggered off the attack but, in
not recommended as it may
many cases, AMI occurs at rest. The
induce hallucinosis and cause a
patient often describes the pain as
rise in pulmonary artery pressure.
having the same qualities as those
Morphine has an advantage in
during an anginal attack,but being of
that it causes peripheral
a more severe and persistent nature
vasodilation; postural
which does not respond to nitrates.
hypotension and bradycardia
Radiation to the neck, jaws, arms and
may result due to this, but is rare
fingers is commonly encountered.
and requires only postural
readjustment. Other alternate
Persons having no prior history of
analgesics are diamorphine,
cerebrovascular disease may
pethidine and methadone.
ascribe the pain to indigestion, as
belching and nausea frequently
If potent analgesics are not
accompany an attack. Sweating,
available, a 50% nitrous oxide/
weakness, giddiness, anxiety and
oxygen mixture can reduce pain
restlessness can also be present.
and distress; this can also be
The intensity and quality of the pain
varies with different individuals and,
in 10-20 per cent, pain may not occur
at all. This has been noted with
greater frequency in diabetics.
The patient is usually in obvious
distress, anxious, fearful and pale.
Physical examination may reveal
only a weak thready pulse and the
B.P. low ■— though a transient rise
due to anxiety and fear can
occasionally be found.
used during transport to a
hospital.
5.
Admit immediately.
References
1 Pentecost B. L. Myocardial Infarction,
in Oxford Textbook of Medicine: Eds:
Weatherall D J.. Ledingham JGG and
Warrell D.A.. Oxford University Press,
1983. 13. 174-179.
2. Acute Myocardial Infarction. Medical
Therapeutics Eds: Sainani GS. Joshi
VR. Mehta PJ, Bl Churchill Livingstone,
1987. 1st Ed.. 163.
Convulsions in Children
To be called to a child having a
convulsion is a disconcerting
experience. Often by the time you
reach him the fit is over. If it is not,
all you need do is to prevent him
hurting himself. When the jaws are
already in spasm you may cause
damage by forcing them open but a
gag may be used if the airway is
obstructed. The parents will be
alarmed and it is important to
behave in a reassuring way. Let
them see that you know what you
are about. Prevent them from doing
silly things. It is comforting to them
to see a cold compress being
prepared and even to help you or
Sister to put it on the head. In the
rare case where fits continue
without a return of consciousness
(status epilepticus) they must be
stopped, for prolonged convulsions
are incriminated as a cause of
temporal lobe epilepsy. Give
diazepam 5 to 10 mg by slow i.v.
injection or rectaliy. An alternative
is paraldehyde 0.1 mg/kg i.m. which
can be repeated after an hour,or,phenobarb 6 mg/kg i.m. Remember
that a plastic syringe cannot be
used for paraldehyde. After the fit is
over try to find the cause. This
varies with the age of the child. In
the newborn birth injury is likely.
Hypoglycaemia should be looked
for because it is easily missed and
otherwise disastrous. In the toddler
febrile convulsions are common
and in the older child epilepsy,
intracranial disease (meningitis) and
nephritis should be thought of.
About 1 child in 15 has a
convulsion and at least one-third of
these are simple febrile
convulsions. So be reassuring to
the parents. The outlook is good if
the child is mentally and structurally
normal and if the fits are brief,
albeit recurrent, complications of a
febrile illness (‘benign febrile
convulsions') as distinct from true
epilepsy precipitated by fever.
Reference
The House Physician’s Handbook C.
Allan Birch, S.J. Surtees, Richard
Wray, Fifth Edition, 1980, Churchill
Livingstone, p. 247.
in a Lighter Vein
THE PAIN SYNDROME
/T)
A pain sensation pulls a person
immediately into an isolated orbit in
which he remains alone with a
personalized experience, since pain
is a very private sensation. An
individual may try to express pain
verbally or through behavioural
changes which may not however
convey the actual sensation or
intensity of pain. This makes pain an
essentially abstract concept, though
it is a very tangible hurt — a hurt that
can be only insufficiently
communicated. Besides, pain perse
is seldom uniform in its effect on
people, because of the structural
differences among them, the
differences in their levels of
tolerance as also in their attitudes
which condition their total perception
of pain.
The Role of Pain Expressions in
Medical Diagnosis
Expressions of pain are of immense
value in medical diagnosis. The
physician is heavily dependent on
the patient's report of pain, itsnature, location, intensity, duration
and so on. By the virtue of the power
of articulation and expression,
human beings are better subjects
than animals for the study of pain.
The study of pain is difficult as not all
aspects of pain are available for
scientific enquiry. However,
externalised ‘behaviour’ due to pain
is observable and therefore can be
described in visible terms which
makes it less of an abstract concept.
Signs of writhing, gritting of teeth or
withdrawing from pain, for instance,
may find supportive verbal
expressions to describe the agony
one feels. Pain can be described in
neurological or in psycological terms.
By recording the verbal signals of
pain, medical science is greatly
assisted in discriminating varieties of
pain, both in their nature (muscular
ache, scalding, burning, stabbing,
smarting, throbbing) and degree
(severe, mild, bearable, etc).
Although these may be clothed in
culturally defined styles,one can
nevertheless zero in on certain
features to deduce the nature/source
of the pain.
Pain as a Defence System
Pain promptly set up an alarm to the
brain, putting it on the alert about
harmful, external influence on the
body. This new perception of pain as
a warning and a protective reflex
alters its role from a negative
concept to one of extreme
importance, since it attempts to
protect the body. This can even be
seen in the effective way in which a
reflex withdrawal prompted by a burn
or an electric shock, minimises
injury.
Pain Receptors
Pain signals are picked up by nerve
endings which are called pain
receptors. They mediate a response
signalling pain impulses to the brain
and setting off the first alarm that
something is wrong with some part of
the body. The central nervous
system helps locate the source of the
pain. Pain receptors are of various
types, each of which responds to a
different sort of tissue damage, such
as from a cut or that caused by heat
or chemicals. It is important to
remember the same kind of pain may
evoke varied intensities of responses
from different individuals, depending
upon the individual degree of pain
tolerance and the pain threshold.
Kinds of Pain
Pain sensations are of various types.
For instance, a sprain in the leg feels
different from the sharp pain due to
an abrasion; a pervasive toothache
feels different from a burnt finger or a
headache. Pain varies in duration
too. It can be intermittent, prolonged
or even chronic: in some cases, it
may persist for months or years,
disrupting the lives of the suffering
individuals. There is also the
“referred pain”, a situation in which
an area of the body may indeed hurt,
but the real origin of the pain may
reside elsewhere, in a region far
removed from the area. This
21
"referred pain" can lead to an error in
localization.
groups like the Jews and Italians
implicity encourage complaints of
pain, while others discourage it.
Kinds of Pain Responses
There are as many kinds of pain
responses as there are kinds of pain.
To cite some, neurological,
physiological, verbal, behavioural
and "affective" responses to pain
exist. From the medical point of view,
physiological responses are more
reliable than verbal expressions;
changes in blood pressure, heart
rate, dramatic changes in muscle
tension or sweating, help in arriving
upon objective data. And yet,
medical diagnosis does not
underestimate the “affective"
descriptions of pain as they come
closest to the essentially personal
experience of pain and its
uniqueness. All the classifications
talked about earlier— physiological,
neurological, behavioural, "affective"
— are confusedly abritrary, whereas
in reality they are mutually inter
related and integrated by the
individual who experiences pain.
Classifications that go against this
holistic view of pain are only resorted
to as clearing-aids for medical
diagnosis and treatment.
A Puzzling Phenomenon
When pain enters a less tangible
plane, it becomes more challenging
for the medical profession to
alleviate suffering. There are three
puzzling phenomena of pain which
are identified — insensitivity to pain,
phantom pain and the hypnotic relief
of pain. The first is by no means a
blissful condition,for often persons
who fall in this category have other
associated neurological defects. The
second, 'phantom pain; may occur in
a non-existent location as in the
imaginary pain in a leg which has
been amputated long ago. Hypnotic
analgesia is another area which
causes a patient to accept even the
worst, whatever iliogic it involves.
Conditioning
The familial, social and cultural
environment along wi’Ji
temperament and personality
‘condition’ a person. A neurologist,
physiologist or psychologist is each
dependent for his data on the
patient’s cultural conditioning,
upbringing, and discipline. For
example, the Irish are supposed to
be inhibited in their expressions of
pain,while the Americans tend to
"take pain in their stride” (which is
believed to result in less anxiety and
higher tolerance). Certain ethnic
22
Apart from cultural conditioning,
personality traits, such as an
extraverted nature, results in
relatively low anxiety states,
whereas a neurotic temperament
produces greater anxiety. Pain
tolerance also varies with the
presence or absence of sympathy
from the family or attendants.
Pain Threshold
Pain threshold (which is not quite the
same thing as pain tolerance) is
roughly the same in all people even
from diverse ethnic groups. In
patients with “low painful threshold’,’
pain occurs with negligibly painful
stimuli, while those with “high painful
threshold" may bear severely painful
stimuli uncomplainingly. Extreme
stress and shock are also known to
numb pain, for the brain
manufactures its own opiates,
resulting in what is medically termed
as "stress-induced analgesia.”
Coping with Pain
Coping with pain involves a thorough
understanding of the pain situation
which, in turn, requires education not
only in the endurance of pain, but in
understanding the limitations of
preferred relief as well. Two old
methods for minimising pain are
application of heat or. cold compress
to give a temporary respite from
pain. Massages and exercises have
also been tried. In electrical therapy,
electrical impulses of adjustable
intensity and frequency are applied
through small skin electrodes to
stimulate (cutaneous) nerve endings
and muscle fibres. This treatment,
however, is known to give relief only
as long as the stimulation is
continued. Surgical measures of
pain relief are undertaken in extreme
cases. Acupuncture is an ancient
treatment where needles inserted
into ‘acupuncture points' relieve
pain. Psychotherapy sets about to
change thoughts and ideas of the
patient simultaneously, and obliquely
appealing to the patient’s will in
coping with pain.
Pain Relief
Treatment in medicine has one
major aim — to relieve suffering.
Anaesthetics make surgery possible
without pain by preventing pain
signals from reaching the brain.
Local anaesthetics block the sensory
nerves which conduct pain. In
addition to anaesthesia are a variety
of substances that help in the safe
elimination of pain. Analgesics like
asprin, analgin and paracetamol are
given in effective doses and are
sometimes also given in anticipation
of pain, it is when it comes to chronic
diseases that the benefit-risk ratio of
drugs must be carefully weighed.
Modern therapy has now stretched
to para-medical areas. Ordinary,
everyday work is in fact looked upon
as an occupational therapy. Modern
medicine, therefore, drastically
curtails the duration of
convalescence. It encourages the
patient to get on to his feet as fast as
he can and on to his work
environment for that will surely help
in dispelling his pain symptoms.
Doctor-Patient Relationship
This relationship is so important that
it could be the cornerstone of
therapy. The doctor should
acknowledge the reality of the
patient’s experience, encourage the
patient to express himself and show
a willingness to understand what he
says. Medical ethics has developed
enough to understand the obligatory
need to give a patient all the
information he needs regarding his
condition.
Knowledge of his condition may help
the patient regain his confidence and
reduce his anxiety. For a good
doctor-patient relationship, it is
equally important for the patient not
to be passive but responsive and co
operative with the doctor who is,
after all, trying hard to contend with
the pain as much as the patient
does.
Pain is a reality. There is now a more
comprehensive, holistic view of pain
than before, which takes into
account the patient's mental agony
together with his physical suffering.
Medicine no longer dismisses
intractable pain as “psychological"
nor does it like the idea of making a
patient toss between "psycho" and
somatic’ evaluation. It realises that
it is our thinking here which is
dichotomised and not the pain
sensation in itself, which is inherently
physical, mental, psychic and
somatic, all in one.
Glimpses from Literature
users. Occasional use of aspirin
researchers, Dr. George Browning
caused major GIB in 25 persons per
and colleagues at the Medical
million users.
Research Council's hearing
The management of pain, especially research unit in Glasgow; they had
Even the common non-steroidal anti
chronic pain, presents a complicated thought that if blood was more
inflammatory drugs had an elevated
problem as it becomes an illness in
viscous, supply to the tiny vessels
risk of upper GIB, but evaluation of
itself. This is amply bourne out by the supplying the hair cells (stria
average number of years — over 10 vascularis) may be impaired, leading individual drugs was not possible
because of insufficient data.
— and by the number of doctors
to ischaemia and death of hair cells.
seen — 8 — by the patients who
The
unexpected
finding
led
to
the
Ill World Conference on Clinical
come to the Pain Clinic run by Dr
discovery that the variable most
Pharmacology and Therapeutics,
Floeterin Frankfurt.
closely linked to the degree of
Stockholm, Abstracts II, 1986, 326
deafness was red cell stiffness; stiff
Important in management is the
Clinical Evaluation of Drugs Used
red
cells
get
stuck
in
the
tiny
vessels
analysis of pain, namely, its origin,
in Fever
in the inner ear, leading to ischaemia,
i.e., whether central or peripheral,
death of hair cells and possibly even
Fever, especially when high, has
the intensity of the pain, its exact
location and the pattern of the pain. atrophy of the blood vessels
many metabolic and haemodynamic
Depending on this, the choice of an themselves. The lower viscosity of
effects; for example, the metabolic
plasma in people with stiffer red cells rate rises by 15 per cent for each
analgesic of central or peripheral
degree Celsius rise in temperature.
action, potent or mild, and the need is probably due to a homeostatic
mechanism to keep the overall
At the same time, the food intake
for additional local treatment is
viscosity of the blood near normal
reduces. This results in the
determined.
values.
catabolic processes becoming
Of the non-narcotic analgesics,
predominant and thus an essential
dipyrone or metamizole or analgin is The cause of the red cell stiffness,
need for antipyresis.
the single most important drug due to whether primary or secondary, is not
known. However, the finding makes
As aspirin has limited use in a febrile
its very wide therapeutic index or
a strong possibility for treating and
anorexic patient due to its
safety margin, its effectiveness and
preventing sensineural deafness in
gastrointestinal side-effects,
the combination of analgesic,
the future.
paracetamol and analgin were
antipyretic, anti-inflammatory and
compared for antipyretic efficacy at
antispasmodic properties. All these
General Practitioner, 24 January
the Kasturba Infectious Diseases
complement each other in pain
1986, 2
Hospital, as they both have clinically
management, for example, the relief
insignificant gastrointestinal side
of pain in biliary or renal colic is
Major Upper Gastro-Intestinal
effects.
assisted by its antispasmodic action. Bleeding in Relation to Aspirin
and Acetaminophen Use
Adult males, clinically considered to
It is, however, not only the total
have enteric fever, with a rectal
number of properties alone that is
Upper gastrointestinal bleeding
temperature of over 38.2°C were
decisive, but also the consideration (GIB) is a relatively common illness.
studied
in a random, double-blind
of side - effects and potential for
Three countries — the USA. Canada fashion. Fever and pulse rate were
abuse. Aspirin, which is important
and Israel conducted a hospital
continuously
monitored by a
in pain management and useful for based case - control study to examine
computerized machine for 8 hours
its antithrombotic effect with low
the relationship between aspirin or
and
thereafter
manually for 4 hours.
doses loses its usefulness at high
acetaminophen use and GIB.
Hepatic and renal function were
doses because of its serious G.l.
evaluated
prior
to the study and after it.
effects. Similarly with paracetamol, 57 persons were admitted with major
high doses and long-term use are
In a preliminary double-blind,
GIB. None of them had any earlier
frequently associated with liver
placebo-controlled study, the
known predisposing factors for GIB.
damage.
effectiveness of 1 gm analgin as an
They were matched with 2417
antipyretic was established, but the
patients
admitted
at
the
same
time
Dr T Fleeter, The Indian
occasional diaphoresis seen in some
for conditions judged to be
Practitioner, 1987, XL, 1
patients suggested the dose may be
independent of prior analgesic use.
too high in Indian subjects.
The latter served as controls. Drug
Red Blood Cell Defect Linked toTherefore, in a subsequent study,
use was specifically investigated for
Deafness
500 mg analgin was compared with
the week prior to the day on which
an equivalent dose of paracetamol.
Plasma viscosity, in a study of 140
symptoms of the disease first
The onset, degree of antipyresis and
people from a hearing clinic and the
occurred.
total duration of action were
general population, was found to
significant in favour of analgin.
correlate with hearing loss; lower
The results show that regular use of
plasma viscosity correlated with
aspirin — for at least 4 days —
higher degrees of hearing loss. This entails hospitalization for major GIB
U.S. Ajgaonkar, The Indian
finding was a surprise to the
in at least 82 patients per million
Practitioner, 1987, XL, 29
Analgesics in the Management
of Pain
23
1
ANALGIN - fl STUDY FDR DRUG ACTION FORUFl-KARNATAKA
1,
The Drug
A class of chemicals called PYRAZOLONES have been used
as medicines for over ninety years.
Pyrazolones include
Anti Pyrine„ fiminopyrine, Phenyl
Oxyphenbutazone» Sulfinpyrazone and a derivative of Affiin©pyrine called Dipyrone or Analgin* The pyrazolones share
drugs like
similar pain-killing,fever-reducing,
and also toxic properties.
inflammation reducing
Analgin being more water soluble
is amenable to use in injections and liquid oral prepara
tions (for children).
They are rapidly absorbed in the
stomach and intestine and spread in various tissues of the
body in proportion to their water content.
While 30 to 40%
of the drug is altered in the liver and eliminated in the
urine, 5% is eliminated unaltered.
The fate of a signi
ficant fraction is not known.
The range of actions of Pyrazolones is similar to that
of Salicylates (Aspirins)
except in reducing fever in
diseases like Hodgkins disease and Periarteritis nodosa,
mere aspirins are not completely effective.
The most important and potentially fatal adverse
e'fect of Pyrazolones (Analgin)
is Agranulocytosis.
This
is a condition where the Granulocytes which form the major
part of the White Blood Cell population and are the first
line of the body’s defence against infection are destroyed.
It is an allergic reaction and can occur suddenly even
a'tar a fraction of a dose in any person who has been
previously taking Analgin with no bad effects.
£ to 24 hours,
Within
the while blood cell count fall and
granulocytes disappear from the blodd.
They start re-
opearing 5 to 10 days after the drug is dtpscontinued and
rapid recovery occurs.
The incidence of agranulocytosis
las been variously estimated from 0.01% to 0.86%.
infection occurs now,
If
it starts as a sore throat of sudden
2
8
8.
Dipyrone,
Hoechst and the Boston Study, MFC Bulletin Dec 86
- Wilbert Bannenberg
9.
Drug marketing in the Third World :
Beneath the
cosmetic reforms, Lancet 07 January 1986
- Trisha Greemhalgh
10.
Dangerous and Inappropriate drugs
Lancet 28 Oune 19B6
- M.3.S. Langman
11.
A BUKO Campaign - A Drug Campaign Newsletter
12.
The Hoechst Medical Bulletin - issue No 8.
mfc Rational Drug Policy Cell,
1985
2
high f)ever and prostration, which even on proper treatment
onset,
carries a mortality of 20 to 50%.
The other adverse effects of Analgin documented in a
study are,
skin rashes, Dyspepsia, Fever,
and Bronchospasm.
Anaphylactic shock
Analgin can aggravate a bleeding tendency
and produces a serious fall in body temperature when given along
with Chlorpromazine.
Liver cancer in mice has also been reported
by ^Japanese.
Even now
a.
b.
the mode of action is not known;
which are the metabolites which cause agranulocytosis
and how is now known;
c.
Basic pharmacological data, like potential for
causing Cancer,
congenital malformations, kidney
and Liver damage and damage in elderly patients
are not known;
d.
Interactions with other drugs for diabetes,
hypertension etc.,
have not been investigated
--because Pyrazolones were introduced in the
pre-Thalidomide era when registration was easy.
2.
History and_Present Status
1897 - Aminopyrine was first introduced and became very popular
in 1920s for painkiiilimg and fever.
8y 1930s it's use
was world wide
1922 - Agranulocytosis was first described by U. Schulz.
1922 - Dipyrone or Analgin was introduced by Hoechst,
Not
being recognised as a derivative of Aminopyrine, it
gained popular use.
1933 - Madison and Squier established a causal relation
between Amidopyrine and agranulocytosis
1935 - Kracke and Parker established its relationship to
agranulocytosis beyond doubt
1938 - O.T.C.
sale in U.S.A was prohibited
3
3
Between 1955-59 - The American Medical Association Registry
on Adverse Reactions recorded only 10
reports of leucopenia (fall in W.8.C count)
and none in children
1960-64 - 18 cases reported (7 in children)
An increase in the import into U.S.A
of dipyrone from Nil in 1958 to 18,879 lbs
in 1962 was noticed.
1964
- Americal council of drugs - section one
adverse reactions studied the case of
Dipyrone (Analgin)
and questioned the
justification of continued use of this drug,
1960
- Great Britian and Canada revoked the licence
1965
- Australia and New Zealand issued an import
1974
- Sweden revoked Dipyrone licence
1976
- Norway revoked Dipyrone licence
1977
- U.S.A revoked Dipyrone licence
of Dipyrone
ban on dipyrone
1977
- Japan banned free O.T.C sale
1978
- Ireland and Singapore revoked licence of
1979
- Denmark revoked licence of Dipyrone
Dipyrone
5k986xxxx-HxMaiaysiaxbanpiEdxHip^K«Rts
1980-84 - An international study for Agranulocytosis and
Aplistic Anaemia was done in Europe - called
the Boston Study,
since coordination and
data analysis was done at the Drug epidemi
This was primarily
ology unit at Boston,
financed by Hoechst,
and the results
published in the JAMA of Oct 1986.
1983
- The G.O.I banned the manufacture and sale
1986
- Malaysia banned dipyrone
of Amitjopyrine.
19B6
- F.R.G banned O.T.C sale
In Netherlands, Dipyrone use is only allowed
for uncontrollable fever.
4
4
following reports of anaphylactic shock,
Italy, Egypt and
Saudi Arabia have prohibited manufacture of injectible
preparations
The F.D.A of U.S.A regards that "true risk associated with
this drug far outweigh any benefit derived from its use,
including use in Hodgkins and similar malignant diseases".
3.
The Issues
i.
According to Hoechst,
approximately 25 tonnes or
18.5 million doses of Novalgin are used world wide
everyday.
With most of the developed nations banning
or restricting its use,
it is obvious that it is sold
mainly in third world countries.
The countries which have banned Dipyrone have been
managing pain without Dipyrone by using equally
effective and sage analgesics.
ii.
The
'Boston Study' generated a lot of controversy,
since Hoechst used the results even before publication
for a misleading advertisment campaign showing the
occurence to be 1 per million.
The Hearing of the
German Federal Health Office finally confirmed the
assumption of 1 per 30,000 to 60,000 to be nearer the
mark, or one tablet per 70,000 consumed could cause
agranulocytosis based on this same study.
The limitations of this study are,
a.
that
it excludes all patients
i.
who die of agranulocytosis without receiving
ii.
who die without having a white cell count,
iii
who have undiagnosed agranulocytosis and
medical aid;
and
recover from it.
b.
The study does not look into other side effects
of Dipyrone,
like shock,
fall in B.P.,
Urticaria etc.
5
5
c.
The data presented in the intermediate and
final reports are inconsistent.
d.
Whereas 400 cases of agranulocytosis were
registered to assess risk properly, only
221 cases were analysed in the final report,
e.
and
There is extreme variability in data between
different countries and even within the same
country.
f.
Some data were seen to be clearly unreliable.
iii» The findings of the controversial
'Boston Study'
is
being utilised by Hoechst the largest manufacturer of
Analgin for sales promotion in Germany,
Gountries and the Third World.
Eastern Bloc
Unethical propoganda
practices with different types of promotional liter
ature in different countries is being practiced.Even
claims of anti-spasmedic action which is not
scientifically substantiated is being made.
Any
source of detailed scientific literature is virtually
non-existant beyond the literature supplied by the drug
companies.
iv.
Since 1985, Dipyrone (Analgin) has not found mention
in any standard medical text books,
except for naming
it as a drug which can cause agranulocytosis.
v. Even in our country,
Medical students do not learn
about Analgin while doing their Pharmacology.
4,
1.
In India
In 1983,
the G.O.I
banned the manufacture and sale of
Amidopyrine but not dipyrone.
The Drugs Consultative
Committee had recommended ban on FDCs of dipyrone also,
but this seems to have slipped from the banned list.
2.
The Government is the largest
manufacturer of Dipyrone in
this country.
6
6
3.
Analgin is among the largest selling analgesics in the
country with sales figures accounting for Rs. 70 million.
There are approaimately 200 formulations containing
Analgin,
including injectables,
and drops for newborns
and infants for colic.
4.
Analgin is available as O.T.C inspite of its being a
Schedule H drug in our country and the attitude of the
prescribing doctors as per a study (Lancet 86) was "if
I
prescribe it 30 times a day and it is available over the
counter it must be safe".
In a field study (Lancet 86)
it was seen that the pyrazolones made up the majority of
both G.P prescriptions and O.T.C sales of Analgesics.
One more of these drugs were given to over 50% of patients
requesting an analgesic.
5.
Drug action groups have initiated a campaign on Analgin
especially at ACASH,
Bombay,
D AF West Bengal ano AIDAN,
New Delhi.
6.
Analgin induced agranulocytosis does occur in India,
especially if one looks for it systematically as
Bombay haematologist B.C.Mehta has done.
a
He reports
12-15 cases of agranulocytosis a year, of which 10-12
are caused by Dipyrone or Dipyrone containing drugs.
by the risk estimation of the Boston Study,
Even
in India,
one person develops Analgin induced agranulocytosis
per day by other reasonable estimates,
it could be 15
times this figure.
5.
Wider issues
Developing countries like ours are ill placed to afford
expensive and useless health care products and definitely
not the frankly dangerous ones.
We have unsophisticated consumers and poorly developed
regulatory and advisory systems - this is fertile ground
7
7
for pharmaceutical companies to indulge in unacceptable
practices.
The vast majority of rural doctors working in nrofessional
isolation have no access to independent information on drugs
they prescribe.
Here,
the representative of the pharmaceutisel
company who is ill-informed himself and paid by commission
on drug sales becomes an ideal tool to promote the interests
of the Pharmaceutical company*
Thus,
it appears that the consumer is at the mercy of drug
manufacturers.
Other than an appeal to the Food and Drugs
Administration,
the Central government and the HRTP Commission
the consumer is virtually without recourse to any independent
body such as the judiciary.
The 3.3 Hospital Commission (Lentin
Commission)
enquiry reveals the ineffectiveness of these
agencies.
The consumer protection Act of 1996 is expected
to offer some hope.
In effect,
only a public outcry by the consumer can force
Voluntary withdrawal by or reform by drug companies.
— $ P i <1
REFERENCES
1,
The Pharmacological Basis of Therapeutics
2.
Review of Medical Pharmacology
3.
Agranulocytosis induced by Dipyrone,
- Goodman and Gillman 5th Edition,
- Meyers,
Dawet z,
Goldfien,
1975
6th Edition 1978
a Hazardous
antipuretic and Analgesic
- Charles M Huguley 3r. DAMA 21 September 1964
4.
Risks of Agranulocytosis and Aplastic Anaemia - A
first Report of the International Agranulocytosi§/and
Aplastic Anaemia study - DAMA 03 October 1986
5.
Analgin - Pain killers or man killers?
6.
Why Analgin should be banned - A bit of history
7.
Counterfact on Analgin (An untold story)
- Indian Express 24 October 1987
- Anant Phadke
Drug Disease Doctor Vol 3,
No 4 1988
- Arun Bal and Anil Pilgoankar
8
U !_AN-CET. OCTOBER 18, 1986
-vjuct—sphingolipidoscs (eg, Tay-Sachs disease),
%copolysaccharidosis
(eg,
Hurler
disease),
..^proteinoses (eg, fucosidosis), mucolipidoses (eg,
disease), and type II glycogenosis (Pompe
jjj^ase). Acid hydrolase deficiencies are due to a series
^single-gene mutations with the following results:
failure to produce immunologically detectable
• aizy1710 glycoprotein (CRM ); production of
cjtaJytically inactive or inefficient protein (CRM-);
reduced or absent post-translation processing of
rjre enzyme protein; excessive post-translation
processing; failure to glycosylate the enzyme protein;
failure to generate the mannose-6-phosphate
recognition marker which enables the enzyme
molecule to follow its correct path to the lysosome
after it has been glycosylated in the Golgi apparatus;
lack of an enzyme activator or protector protein; lack
of a substrate activator protein.
Each of the main types of gene-product
abnormality can be due to several different
abnormalities at the genomic level. Thus CRM
negativity may be due to a lesion of the gene directing
the synthesis of the enzyme protein (and this can itself
be due to premature insertion of a termination codon,
deletion of a major portion of the gene including the
coding region for the immunogenic site, mutation or
deletion of a start codon, or a splice-mutation);
transcription failure; translation failure. The CRMvariants of these diseases show a similar range of
genomic lesions which modify the activity of the
catalytic site on the enzyme molecule without altering
the immunogenic site. In addition to, or instead of,
modifying or abolishing the catalytic site, the genomic
lesion may lead to an abnormal gene product (the
enzyme) with reduced affinity between subunits,
reduced stability, increased susceptibility to
proteolysis, or reduced solubility with impaired
mobility in the reticular system and Golgi apparatus.
Lack of an enzyme activator or protector protein, or of
a substrate activator protein, can be the result of a
^similar range of genomic lesions. Lysosomal storage
diseases that are due to lysosomal acid hydrolase
deficiencies have now been reviewed in a monograph1314
15
and the biosynthesis and intracellular migration
(“trafficking”) of these enzymes have been intensively
studied by several groups of workers.1415
In Salla disease16 there is abnormal lysosomal
storage and urinary excretion of N-acetylneuraminic
(sialic) acid,17 and -the disorder was provisionally
grouped with the glycoproteinoses.18 It is now clear
that the disease is attributable to a transport defect
whereby sialic acid cannot be transported out of the
lysosome.1’-20 Salla disease is an autosomal recessive
13. Wans RWE, Gibbs DA. Lysosomal storage diseases: biochemical and clinical aspects.
London: Taylor and Francis, 1986.
14. Komfeld S. Trafficking of lysosomal enzymes in normal and disease states. J Clin
Invest 1986; 77: 1-6.
15. von FiguraK, Hasilik A. Lysosomal enzymes and their receptors. Am Rev Btockem
1986; 55:167-93.
16. Aula P, Autio S, Raivio KO, et al. ‘Salla disease*. A new lysosomal storage disease.
Ard, Neurol 1979; 36: 88-94.
17. Renlund M. Clinical and laboratory diagnosis of Salla disease in infancy and
childhood. J Pediatr 1984; 104:232-36.
899
disorder which appears to be confined to individuals
of Finnish descent, and which derives its name from
the region of Finland whence most of the patients have
originated. Patients show muscle hypotonia and
psychomotor delay by 4—12 months of age; motor
incoordination, dysarthria, dyspraxia, and mental
handicap then become apparent. Some patients have
epileptic fits and muscle rigidity, torsion dystonia, and
signs of an upper motor neuron lesion may be
apparent later. Salla disease is the first disorder shown
to be due to defective transport of a monosaccharide
across the lysosomal membrane. The findings arc
consistent with sialic acid egress from the lysosome
being mediated by either a diffusional or facilitated
transport system, but it has not yet been possible to
demonstate the saturability of the system which is
required to establish the existence of a specific carrier
mechanism or carrier protein. Nevertheless, there is
some circumstantial evidence for the view expressed’
by Renlund et al that “a single gene product, a specific
carrier, mediates the transfer of NANA (sialic acid)
across the lysosomal membrane”.20
Cystinosis is no longer the exception among the
lysosomal storage diseases but the archetype of a new
subset of these disorders, and a disease due to defective
transport of vitamin B12 across the lysosomal
membrane is already known.21 One family has been
identified in which a lysosomal hydrolase deficiency
(Fabry disease) and a lysosomal transport defect
(cystinosis) occurred in different members of the same
sibship.22 The lysosomal transport defects may well
prove to be as important and varied as the diseases
caused by deficiencies of lysosomal hydrolases.
ANALGESICS, AGRANULOCYTOSIS. AND
APLASTIC ANAEMIA: A MAJOR
CASE-CONTROL STUDY
AGRANULOCYTOSIS and aplastic anaemia are rare but
commonly fatal complications of drug treatment. Their
rarity has made it difficult to assess the risk associated with
individual drugs; estimates have often been alarmingly high
or complacently low. Now the first findings from a large
case-control study offer some answers about analgesics.1
The impetus for the work was a stark difference of opinion
about the safety of the pyrazolone analgesic dipyrone. As we
noted last month,2 Hoechst, the major manufacturer of the
drug, needed clear evidence that it was acceptably safe, and
so sponsored the independent International Agranulo
cytosis and Aplastic Anaemia Study. Funds were also
contributed from Hungary, Bulgaria, and Sweden. The
18. Durand P, O'Brien JS. Genetic errors of glycoprotein metabolism. Berlin: Springer,
1982.
19. Jonas A. Studies of lysosomal sialic acid metabolism. retention of sialic add by Salla
disease lysosomes. Buxkcm Biophys R(} Cormnun 1986; 137: 175-81.
lysosomes in patients with Salla disease. Science 1986; 232:759-62.
21. Rosenblan DS, Hosack A, Matiaszuk NV, Cooper BA, Laframboisc R. Defect in
vitamin Bu release from lysosomes: newly described inborn error of vitamin Bu
metabolism Science 1985; 228: 1319-21
22. Gahl WA, Adamson M, Kaiser-Kupfer 1, et al. Biochemical phenotyping of a single
sibship with both cystinosis and Fabry disease. J Inker Meiab Dis 1985; 8:127-31.
1. International Agranulocytosis and Aplastic Anemia Study. Risks of agranulocytosis
and aplastic anemia: a first report of their relation to drug use with special reference
to analgesics. JAMA 1986; 256: 1749-57.
2. Anon. Dipyrone: hearing by the German drug authority. Lancet 1986; ii: 737.
900
study was coordinated and the data analysed by the Drug
Epidemiology Unit in Boston and supervised by a
distinguished honorary advisory board.
The study aimed to collect all cases of agranulocytosis and
aplastic anaemia that were admitted to hospital (community
cases) or that occurred during a stay in hospital (hospital
cases) in each of seven regions—Israel, Barcelona, Ulm,
West Berlin, Milan, Budapest, Sofia, and Stockholm/
Uppsala—with a total population of 22 3 million people.
The attempt to include the region of Sao Paulo failed. Great
care was taken to prove the diagnosis. Detailed drug
histories were obtained from the patients, focusing
especially on the seven days before admission
(agranulocytosis) or on the preceding six months (aplastic
anaemia). The interview included presentation of a long list
of generic and brand names. Controls for ±e community
cases were selected from patients admitted to the same
hospitals, but the prospective controls for the hospital cases
were too ill to be interviewed. Conclusions about individual
drugs had to be based on the community cases alone.
The annual incidence of verified cases of agranulocytosis
ranged from 1-7 to 9 0 per million in the different regions.
This of course excludes mild cases that were not recognised
and those that died before the diagnosis could be made.
Some cases might also have attended hospitals outside the
catchment area. The fatality rate was 10% among
community cases and 6% among hospital cases. Regional
fatality rates are not reported, perhaps because they might
be taken to reflect differences in the effectiveness of medical
care. The real meat of the report lies in the estimates of risk
associated with different drugs. A rate ratio (rr) for each drug
was obtained from the number of community cases and of
controls who had taken it in the seven days before admission
to hospital. One-third of the 300 community cases were
excluded because they were not interviewed (21 had died),
or because the day of onset could not be determined. For
dipyrone, but not for any other drug or group of drugs, the rr
varied greatly between regions, ranging from 1 and 2
(Budapest, Israel) to 21 and 31 (Berlin, Barcelona). These
huge disparities raise some doubts about the results, for they
were not due to differing incidences of agranulocytosis, but
to very high and perhaps untrustworthy figures for dipyrone1
use by the controls in Israel and Budapest. Despite the low
rrs for these two regions, 18% of their cases were apparently
due to dipyrone, hardly less than the 23% in the study as a
whole. Some of the doubts might have been resolved by
examining sales data, but none were used—although
Laporte, one of the investigators in the study, has presented
such figures.3 The estimate of the excess risk from dipyrone
is expressed rather oddly, as 1 1 per million takers during a
seven-day interval. The calculation underlying this estimate
is not explained. The peculiar denominator is difficult to
apply to real life. The risk for exposure during one year
could be up to 50 times higher. It would be expressed more
clearly as the number of cases per million defined daily doses
(DDD), or per 100 000 packs sold.
Other analgesics
significantly associated
with
agranulocytosis across regions were indomethacin (rr
estimate 9) and the butazones (rr 4). Numbers were too
small to allow estimation of rrs for other pyrazolones such as
amidopyrine which is an acknowledged cause of agranulo
cytosis, or for other anti-inflammatory analgesics (NS AI Ds)
J. Laporte JR, Came X, Ibariez L, Juan J, Vidal X. An epidemiological approach for the
etiological study of blood dyscrasias. Proceedings of the Bergamo meeting on phase
IV studies, October I9H5. Milan: Wichttng (in press).
THE LANCET, OCTOBER 18, 1986
which are not. Use of salicylates or paracetamol was not
associated with agranulocytosis or aplastic anaemia. These
findings reinforce the arguments for banishing dipyrone2
and where possible using paracetamol or aspirin instead.
The data on aplasdc anaemia also bring some surprises.
The overall annual incidence was 2-2 million, with a
two-year fatality rate of 49%. Analgesic use by cases and
controls in the period between six months and one month
before hospital admission yielded rrs for individual drugs or
groups of drugs. Histories of any exposure to indomethacin
(rr 13), diclofenac (rr 9), and butazones (rr 9) were
significandy associated with—aplastic anaemia. For
prolonged exposure to indomethacin or butazones the rate
ratios were around four times higher; but these were based
on small numbers. For the same reason, no rrs could be
calculated for pyrazolones other than dipyrone, or for
individual NSAIDs. The data thus do not incriminate other
NSAIDs, but they raise ±e worrying suspicion that
indomethacin, the butazones, and diclofenac may not be the
only ones to carry a risk ofaplastic anaemia. It certainly looks
as if indomethacin ought to join phenylbutazone as a drug of
last resort, but while data on the other NSAIDs are lacking it
seems premature to regard diclofenac as a second-line drug.
This study is the first of its kind, and the courage and
tenacity of the investigators in carrying it through despite
some serious setbacks must be applauded. It confirms that
dipyrone is a major cause of agranulocytosis and/that
phenylbutazone, indomethacin, and diclofenac can cause.,-.
aplastic anaemia. It is now up to all of us—prescribers, drug
regulators, and pharmaceutical companies—to use the
results in the best interests of patients.
RESEARCH ON HEALTHY VOLUNTEERS
CONCERN about drug safety has led progressively to more
stringent licensing requirements and more comprehensive
investigation of drugs before they are marketed. As a result,
more early phase trials are being conducted on healthy
volunteers; the wheel has now turned full circle with two
well-publicised reports of fatalities. The Medicines Com
mission responded by asking the Royal College of Physi
cians to set up a working party on research in healthy
volunteers. In its report* the working party attempts to
establish safeguards for such volunteers and recommends
procedures for compensation in the event of harm.
Volunteer experiments are in danger of becoming big
business. Several contract companies have been established
to sell volunteer studies to phannaceutical firms which lack
the necessary in-house capacity. Such developments pose
two important questions about those who carry out the work
and those who volunteer to participate. Firstly, the facilities
for early-phase studies have in some instances fallen weU
short of the ideal; in other cases, university or hospital staff
have used the resources of their department as a sort or
academic moonlighting. The report recommends that all
premises should be open to scrutiny. A distinction is drawn
between, on the one hand, NHS hospitals and university
departments, which should be inspected “where necessary
by or on behalf of the local ethics committee, and, on die
other hand, commercial institutions (including pharmaceu
tical companies) which “should” be subject to independtfit
scrutiny. Further, a register of approved commercial
institutions carrying out research on healthy volunteers £
_____________________ __________ _ _________ _—■—’
I. Research on healthy volunteers. A report of the Royal College of I’hysicuns- J
Phyuciiuu Lund 1986, 2(h 1-17.
Table 4.—Agranulocytosis: Use of Dipyrone in the Week Before the Index Day According to
Region
Region
No.* (%) of
Cases
No.* (%) of
Controls
Crude
Rate Ratio
Estimatef
Ulm, West Germany
6/28 (21)
5/237 (2)
12.7
12.2
West Berlin
6/17 (35)
2/72 (3)
19.1
20.9
305
Stratified
Rate Ratio
Estimate!
Barcelona, Spain
15/50 (30)
5/394 (1)
33.3
Israel
13/65 (20)
28/253 (11)
2.0
1.8
Budapest, Hungary
4/30 (13)
22/147 (15)
0.9
0.9
Stockholm / Uppsala.
Sweden
0/12 (0)
0/126 (0)
1/9 (11)
3/ 133 (2)
5.4
3.6
6/10 (60)
13/63 (21)
5.8
5.3
51/221 (23)
78/1425 (6)
5.2
Milan, Italy
Sofia. Bulgaria
Total
•Number of cases of controls who used dipyrone/total number in center
[Relative to no use in the week before the index day.
[Age and sex taken into account by the Mantef-Haenszef procedure, xi for,heterogeneity. 45.4; PC.001.
Table 5 —Agranulocytosis: Analgesic Use in the Week Before the Index Day
Drug
Cases
(221)
Controls
(1425)
Stratified
Rate Ratio Estimate*
(95% Confidence
Interval)
Multivariate
Rate Ratio Estimate*
(95% Confidence
Interval)
Dipyrone
Ulm, West Germany/West
Berlin/Barcelona, Spam
Any
27
12
21.3 (11.7-38.9)
23.7 (8.7-64.4)
12
7
16.5 (7.2-38.0)
20.4 (5.6-74.1)
17
50
1.5 (0.8-2.7)
0.8 (0.4-1 8)
10
23
2.0 (0 9-4.4)
1.2 (0.4-3 7)
>3 d
Israel/Budapest, Hungary
Any
>3 d
Other pyrazolones!
Any
18
58
2.1 (1.2-3.7)
1.2 (0.6-2 5)
>3 d
6
16
2.1 (0 8-5.4)
0.9 (0.2-3.1)
Salicylates
Any
43
129
2.4 (1.6-3.6)
1.6 (1.0-2.7)
>3 d
24
56
2.7 (1.6-4.6)
1.9 (1.0-3.8)
Acetaminophen
Any
25
78
1.6 (1.0-2.6)
1.0 (0.5-1.9)
>3 d
12
42
1 4 (0.7-2.9)
0.8 (0.3-2.0)
Butazones
Any
11
11
5.2 (2.2-12.0)
3.8 (1.3-10.7)
>3 d
8
6
6.7 (2 6-17.5)
6 3 (1.8-22.3)
10
7
6.7 (2 8-16.1)
8.9 (2.9-27.8)
9.0 (3.2-25.4)
14 2 (3.7-54.4)
Indomethacin
Any
>3 d
8
4
Other nonnarcotic
analgesics!
Any
5
24
1.5 (0 5-4.0)
0.9 (0.3-3.1)
>3d
3
19
1.0 (0.3-3.7)
0.6 (0.1-2.6)
•Relative Io no use in the week before the index day.
[Includes aminopyrine (six cases. 18 controls); aminopyrine/propyphenazone (five. 21); propyphenazone
(three, seven); antipyrine (three, five); aminopyrine/propyphenazone plus propyphenazone (one. one);
aminopyrine/propyphenazone plus antipyrine (zero, four); and propyphenazone plus antipyrine (zero. two).
"Aminopyrine/propyphenazone" refers to compounds the components of which were changed from aminopyrine
Io propyphenazone during the course of this study
[Includes ibuprofen (two cases, four controls); diclofenac sodium (one. five); naproxen (one, three);
proquazone plus piroxicam (one. zero); piroxicam (zero, throe); benzydamme hydrochloride (zero, two); niflumic
acid (zero, one), glafenine (zero, one); flurbiprofen (zero, one); ketoprofen (zero, one); clonixin (zero. one).
naproxen plus diclofenac (zero, one); piroxicam plus diclofenac (zero, one).
1752
JAMA, Oct 3. I986-Vol 256. No 13
terms for the use of thyrostatic drugs
(propylthiouracil, carbimazole, and
methimazole) and sulfonamides were
included because these agents were
associated, as expected, with agranulo
cytosis (thyrostatic drug use, 15% of
cases and 0.4% of controls; sulfona
the
mide use, 8% and 1%).
Excess risks were calculated using de^
the multivariate rate ratio estimates
Since the estimates were based on drug the
histories covering seven days befon ity
the index day, excess risks were calcu for
Wb
lated for a seven-day period.
for
Specific Methods:
spa
Aplastic Anemia
Bud
The effects of drugs used up to 18 mer
days before admission were assessed the
It
because there can be a considerab
delay between exposure and diagnosi Terr
Any use that took place less than : fron
days previously was ignored, becau The:
such use could well have occurred aft iate
the onset of the dyscrasia. The refer
Berli
ence category was no use of the d
ratio
under consideration during days
these
through 180 before admission. The dit
rate!
tribution of analgesic use among
rize t
1724 controls is given in Table 2; u
forth
rates were reasonably similar.
The multiple logistic models includ Ito r
the following factors: age; sex; get Rep
graphic area; date of interview; ret ratio
other
ability of the patient; person in
viewed; transfer from another hospi regior
histories of bruising, blood disorder, cj’"’fl
tuberculosis; histories of exposure preset
■ -z:
benzene, petrochemicals, or insect|l)lPyrc
cides; and the use of drugs during da)|. ‘n 1
29 through 180 before admission ( *:c use
drug groups were defined as for agra: day—t
ulocytosis). Thyrostatic drugs we^®"sw
used" by 4% of the cases and 0.4%
co
the controls and sulfonamides by 101 ona.
and 4%; again, separate terms w ‘
I
included for these drugs.
JL* ° 0
As with agranulocytosis, excess r4-- ‘ ;
calculations were based on the mul'4.^ 1[
variate rate ratio estimates. Si ^^Iges
these were based on drug histori
covering days 29 through 180 bef •nultiv
admission, excess risks were calcula ’"d but
the
for a five-month period.
^nfider
fcfazok
RESULTS
tami
Agranulocytosis
Table 3 gives estimated incide
all
rates by region. The overall ann
the c
incidence was 6.2 cases per million:
othe
ranged from 1.7 per million in Milan
be
9.0 per million in Budapest. Among
422 cases, there were 36 deaths ! ’Jrnbers
which agranulocytosis was the main
t thr
contributory cause, giving a fatal1
rate of 9% and an annual mortal1 : "ate i
fuced.
rate of 0.5 per million.
,n earl
The annual community incide
Intt.-rnational Agranulocytosis and Aplastic Anenu.i $
Oct
1318
THE LANCET, JUNE 7, 1986
Examples of apparent deception or lack of frankness listed
under category 4 touch the very heart of the demand for full
disclosure. Yet I believe most doctors would take the view
that patients should not be burdened with a serious diagnosis
which is merely probable or possible, if it does not affect the
current management.
Those in favour of patients’ having access to their medical
records argue that seeing these documents is in most
instances reassuring. I estimate that this would have been so
in approximately a third of the cases in the present series.
There is some evidence that reading the specialist’s advice to
stop smoking is more effective than merely hearing it. These
beneficial effects would, however, be appreciably reduced
once patients knew that the doctor realised that they would be
likely to read what he had written.
It is widely, though not universally, held that some medical
records contain information which should, in the patient’s
own interests, not be accessible. What is not sufficiently
appreciated is the high proportion of records to which this
reservation applies—at least in some specialties. In the
present sample, 42 out of 100 sets of notes contained at least
one comment likely to give rise to alarm or anxiety—an effect
which might persist despite explanation and reassurance.
Open access to medical records would profoundly affect the
specialist’s system of note-keeping. Besides having to develop
a plan for avoiding ambiguous or potentially worrying
symbols, he would be compelled to alter his hitherto frank
style. Where alarming or objectionable statements could not
be avoided, he would undoubtedly find some way of keeping
a second set of notes. Sensitive material would be
communicated to the GP verbally instead ofbeing committed
to writing, with the danger that it would be forgotten or
attached to the wrong patient.
Correcting misunderstandings and allaying fears fostered
by reading raw data couched in technical language would also
take more of the consultant’s (and presumably the general
practitioner’s) time. There would undoubtedly be a major
increase in cost to the NHS, both in paying for the additional
medical time and in arranging for the notes to be made
available to the patients under supervision. There would also
be a danger of defacement or loss.
The fundamental question is: What is best for the patient?
Medical science exists primarily for patients, not for doctors.
The answer surely is that the patient needs to have all the
information which would enable him or her to preserve or
restore his health to the maximum degree possible, and to
discharge his duties to his family and to society. The patient
should not be presented with information which is likely to
have the opposite effect.
CONCLUSION
I can appreciate that patients and potential patients want to
take greater responsibility for their own health, and they want
to have all the information available to enable them to do this.
This is right. They know that doctors sometimes fail to
provide them with important information and may make
inaccurate entries in their medical records. This is true. They
think that by insisting on seeing their records they would
avoid these problems. This is a mistake. Patients would be
overloaded with information, which their doctor would need
to explain—if he had time. More seriously, the notes and
letters in the record available to the patient would cease to be
frank.
What is needed is better record keeping and more time
spent in consultation with the patient; improved
communication in the traditional manner, rather than open
access to medical records. The findings of this small study
support the view that access to personal health data should be
limited to the disclosure of bare administrative details, such
as whether the inquirer is on a waiting list, and the name of
the consultant. Any patient who wanted to pursue the matter
further could then approach the consultant for more detailed
information.
REFERENCESI
Editorial. What’s in my file? Lancet 1985;-u_S12. 2
Jenkins S. Talking point. GMSC Voice 1986; 3: 9-11.
3
Self-Health March, 1986, 54-35.
I. Bird AP, Walji MTI Our patients have access to their medical records. BeMedJ 1986;
292: 595-96.
5. BaIJry M. Cheal C, Fisher B. Gillett M, Hue! V. Giving patients their own records in
general practice: Experience of patients and staff Br Med J 1986, 292: 596-98.
6. Editorial. Whose data are they anyway? BrMedJ 1986, 292: 577-78
Drugs and the Third World
DRUG MARKETING IN THE THIRD WORLD:
BENEATH THE COSMETIC REFORMS
Trisha Greenhalgh
Battle Hospital, Reading, Berkshire RG3 1AG
Eleven years ago Silverman and Lee, in Pills, Profits
and Politics, drew attention to the unethical marketing
tactics of certain US-based drug companies in Latin
America.1 Four years ago Dianna Melrose, in the
controversial Bitter Pills, claimed that western
multinational companies continued to make fat profits
from the “dumping” of harmful and therapeutically
useless drugs throughout the Third World.2 These and
other books have had impact, and standards of drug
marketing, as many would measure them, have risen.
However, from what I found during the four months
that I spent in India recently conducting a field study
into the prescribing practices of rural medical
practitioners3 the reforms in the drug industry seem to
have been a pyrrhic victory.
In India I introduced myself as “a foreign doctor
interested in diseases in this area” and followed 2400
patients through medical consultations. I recorded for
each patient the presenting complaint, the stated clinical
findings, and the drugs prescribed. In addition, I
collected promotional literature from medical journals
and drug company representatives, and sat in on
interviews between the representatives and local
doctors.
Examples of inexcusable marketing behaviour by
western-based companies can still be found. Merck
(India), in an advertisement that names Merck,
Darmstadt, West Germany, as its parent company,
promotes ‘Encephabol’ (pyritinol, a vitamin 8,
derivative) as a brain tonic that “improves the uptake
and utilisation of glucose in the brain”, and recommends
its use for “strokes, organic brain syndrome of the
elderly, post concussion syndrome, perinatal distress ■ • ■
(and) learning disorders”? I saw only two qualine“
doctors prescribe this drug—in both instances for 3
complaint of “weakness”—but I noted its unrestricted
sale over the counter in street pharmacies and bought it
THE LANCET, JUNE 7, 1986
myself from a market stall. Parke-Davis were still
promoting
the
anabolic
steroid
‘Adroyd’
(oxymetholone) for “underweight or asthenic patients,
convalescence from acute infectious diseases,... chronic
debilitating illness, osteoporosis, fractures, . . . (and)
decubitus ulcers”.4 I saw’ this product prescribed by
doctors for complaints of weakness, sore throat, and
fever.
Such aggressive promotion of useless and dangerous
drugs is indefensible, but I believe it is diminishing.
Only a handful of w’estem companies are still prepared
to risk their reputations in this way. However, this
practice is being replaced by a subtler one, whose effects
are more insidious, more widespread, and at least as
dangerous—namely, the inappropriate prescription of
drugs which are useful (even essential) in certain
circumstances but contraindicated in others.
Take the prescription of analgesics, for example. The
analgesic amidopyrine, its sodium sulphonate dipyrone
(analgin),
and
the
anti-inflammatory
drugs
phenylbutazone and oxyphenbutazone made up the
majority of both general practitioner prescriptions and
^^r-the-counter sales of analgesics in my study.
TTespite warnings on package inserts of the risk of fatal
blood dyscrasias, one or more of these drugs were given
to over 50% of patients requesting an analgesic.
European-based multinationals, including Hoechst,
Evans, Concept, Merck, and Glaxo (India), all obtain
considerable revenue from wide sales of these “second
line drugs”, even though (a cynic would say because)
their use has been severely restricted in the West.5,6
Chloramphenicol, whose use in the West is similarly
restricted, accounted for 11% of all antimicrobial
prescriptions in my study and was the commonest
antimicrobial sold without a prescription. Although
package inserts warning of the danger of aplastic
anaemia were supplied with each bottle, the practical
reality was, at best, that of a general practitioner
counting out loose tablets into an envelope and, at worst,
that of a pharmacist selling them over the counter one or
two at a time from an opened bottle. One pharmacist,
commended me on my interest in the package insert he
wras about to discard and explained, “This is legislation.
Government now approve to this drug”.
High-dose oestrogen-progesterone combination
^Bsparations have repeatedly been shown to be
teratogenic;7,8 in India they are allowed to be sold
specifically for dysfunctional uterine bleeding. Package
inserts warn that they should not be used in pregnancy.
Yet they continued to be prescribed as the cheapest and
most widely available pregnancy test in the country (I
never saw it prescribed for anything else), and I was sold
the drug at each of ten pharmacies where I requested a
pregnancy test.
'
A final example is the use of nutritional substitutes.
40 000 children in India still go blind every year because
the government cannot afford to fund a systematic
programme of vitamin A supplementation; yet over a
quarter of the country’s total drugs bill is spent on the
erratic and indiscriminate sale of vitamin and mineral
supplements. 729 such products are listed in the Indian
Pharmaceutical Guide, and they form the most
commonly prescribed class of drug in all the areas I
visited, accounting for 23% of all drugs dispensed.
General practitioners prescribed them for over half of all
patients, and many declared their belief that prescribed
1319
nutritional supplements were essential for health.
No-one can make a case for the banning of vitamin
syrups in a country where 90% of the children are at least
mildly malnourished, but to see vitamins in an expensive
form prescribed for children with the marasmus of raw
poverty begs the question: who takes responsibility for
their sales?
Phenylbutazone, chloramphenicol, and vitamin
supplements are useful and appropriate drugs in the
right clinical context. I prescribe them myself. And
tighter indications and sterner warnings are now' being
provided (ostensibly) to restrict their use. But the reality
is that these drugs continue to be used for trivial and
bizarre indications by doctors who have no real grasp of
their dangers and limitations.
Of the 26 general practitioners I interviewed not one
took seriously the possibility of fatal side-effects with
amidopyrine derivatives or chloramphenicol. Doctors
held the attitude that “if I prescribe it 30 times a day, and
it is freely available over the counter, it must be safe”. >_.
This attitude cannot be condoned, but it occurs in a
context where it cannot easily be condemned. The vast
majority of rural doctors work in conditions of extreme
material hardship and professional isolation. There is no
peer review, no clinical feedback, no system for
reporting or investigating adverse drug reactions, and no
access to independent information on the drugs they
prescribe.
Postgraduate
education
in
clinical
pharmacology is, for the rural doctor, the unchallenged
province of representatives from the pharnfaceutical
industry. Many representatives are paid only by
commission on the drugs they sell. The free samples and
financial incentives they liberally offer seem to be highly
effective in areas where the doctors themselves are living
well below' the poverty line. The representatives are, in
general, poorly informed of the indications for their
products, and often uninformed of serious side-effects.
Their sales techniques are simple—they generally show’
colour charts bearing pictures of the drug and a list of
indications in bold print. A flash-card from Glaxo
(India) states that “In DEBILITY and GENERAL
WEAKNESS, associated with tuberculosis, diabetes,
liver disease, cardiac disease, BECADEXAMIN (a
multivitamin/mineral supplement) helps healing,
promotes
growth,
restores
taste,
replenishes
deficiencies”. The verbal claims made by the
representatives surpass even such wide-ranging printed
texts, and the combination of eastern enthusiasm with
personal financial incentive adds a disturbing sincerity
to their affirmations. Far from being disdained by the
doctors, company representatives are welcomed w'ith
great ceremony as friends and fellow professionals in an
otherwise lonely subculture. I got the impression that
companies gained more sales through this curious
camaraderie than through any form of “promotion” in
the narrower sense.
In conclusion, the success of local and international
pressure groups in persuading multinational drug
companies to produce responsible advertisements and
comprehensive package inserts has been a pyrrhic
victory indeed. For some companies, the responsibility
which began with the package insert ends there, and
their directors have used the indications for which a drug
is now recommended as an official excuse for ignoring
the situations in which it is actually used. Cleverly
worded small print (in a language which most of the
1320
THE LANCET, JUNE 7, 1986
patients do not speak) provides the multinational
company with legal immunity and transfers the moral
accountability for drug deaths onto the poorly- informed
and professionally isolated Third World doctor, while
the dubious backstage behaviour of the company
representative is quietly ignored.
I have watched, in the slums of Calcutta, a young
mother spend two days’ wages on ‘Orabolin’ drops
(ethyloestrenol, an anabolic steroid), and feed the whole
bottle to marasmic twins through a rusty teaspoon. She
could not read a word of the warnings on the package
insert which I bought off her for a rupee, but she
responded to the picture of the healthy baby on the box.
Official legislation rarely can and almost never does
change realities such as these. India already has so many
cumbersome laws on the prescription and dispensing of
drugs that the government’s hands are consistently tied
by its own red tape trfid the administrative infrastructure
is pitiably inadequate for carrying out the volumes of
official instructions. I hope that I have shown that the
focus of reform must shift from the nitpicking of legal
loopholes to the reality of what is actually being
prescribed and dispensed, to whom and for what.
In Britain, no case of drug damage has gone as far as
settlement in a court of law. Thalidomide was not
Hospital Practice
THE FIVE-YEAR BURP SYNDROME
J. T. Wright
The London Hospital, Whitechapel, London El IBB
THERE is no argument about the cyclical nature of many
biological phenomena, such as sleep, ovulation, and
hibernation; that the higher functions of human beings are
also subject to cycles is, however, less evident—though well
accredited, for instance, in the manic-depressive psychoses
and in schizophrenic episodes. The somewhat fanciful urge
for a periodic change of sexual partner is, of course, the basis
for The Seven Year Itch, the 1950s film featuring Marilyn
Monroe at her best. Many years’ experience of the same
hospital outpatient clientele suggests that psychoneurotic
symptoms may also run in cycles. It is ff commonplace that
neurotic patients may change the focus'of illness from one
organ system to another with bewildering frequency. For the
purposes of this paper, however, I have selected patients with
recurrent gastrointestinal upsets in which the most common
symptoms are burping and the distension and discomfort that
proceed from this habit. Just a few of the patients included
have had recurrent cardiopulmonary symptoms such as chest
pain and overbreathing; their inclusion emphasises that the
syndrome described here is not after all specific to any body
system and that specialists in other fields will be perfectly
well acquainted with it.
THE PATIENTS
The patients studied were attending the London Hospital
outpatients department for the second time, at least two years
after the initial investigation. All were still complaining of
their initial symptoms, for which no organic cause was
evident. Patients reporting initially to another hospital and
then coming to the London Hospital for a second opinion are
not included. 43 patients (25 women, 18 men) are considered,
banned—it was voluntarily withdrawn following a
public outcry. It is time for another public outcry. It is
time the World Health Organisation gave financial and
scientific support for the continued education and
updating of Third World doctors in the difficult and
ever-changing subject of clinical pharmacology. It is
time the multinational drug industry stopped trumping
its ethical responsibilities with its commercial
obligations. And it is time the British Medical
Association had the courage to use its professional power
to demand that British-based drug companies be
morally accountable for the deaths their drugs have
caused in the Third World, .
x
REFERENCES
1. Silverman M, Lee PR. Pills, profits and politics. Berkeley; University of
California Press, 1974.
2. Melrose D. Bitter pills: medicines and the third world poor. Oxford: Oxfam,
1982.
3.
Greenhalgh T. A field study of drug utilisation in India. Soc Sci Med (in press).
4.
MIMS India, September 1984 (personal communication from the Voluntary
Health Association of India in October, 1985, confirmed that these
advertisements were still appearing in the same form).
5.
Discombe G. Agranulocytosis caused by amidopyrine. Br Med J 1952; i:
1270-73.
6. Huguley CM Agranulocytosis induced by dipyrone. JAMA 1964:189:938-41.
7. Janerich DT, Piper JM, Glebatis DM. Oral contraceptives and congenital limb
reduction defects. N Engl J Med 1974; 291: 697-700.
8. Hcinonen OP, Slone D, Monson RR, et al. Cardiovascular birth defects and
antenatal exposure to female sex hormones. N Engl J Med 1977; 296:67 - 70.
DISTRIBUTION’ OF INTERVALS BETWEEN OUTPATIENT VISITS
Years between
eutpatient visits
No of repeat
visits
2
3
4
5
6
749 19 14
7
8
9 10 11
12 13 14 15
502310101
35 being in the fourth to sixth decades of life at the time of
their first visit. Between them the patients paid 109 visits to
the outpatient clinic, 4 of them contributing four visits each
for the same symptoms at approximately 5-year intervals.
The table shows that 5 years was in fact the mode and also, by
elementary calculation, the mean interval between visits.
That the frequency of outpatient attendances was not due
to the whim of a small number of general practitioners is
attested by the fact that 46 GPs were involved and only 4
referred a patient more than once; it could, therefore, be
argued that subsequent referrals were more often due to a
change in general practitioner, though in most cases this was
another member of the same practice partnership.
DISCUSSION
What appears to the hospital clinician as a cyclical
phenomenon may be less evident as such to the referring
general practitioner, who in most cases will be aware that his
patient is prone to neurotic complaints. The common story
seems to be that following the first hospital investigation
reassurance so gained lasts for 2-3 years before confidence
wanes and symptoms become less tolerable. xMany patients
have the experience of a relative or friend being assured that
his or her symptoms were due to “nerves”, only to die of
cancer soon afterwards. Or the patient may express th?
feeling that symptoms “have gone on so long that surely
something (meaning cancer) might develop”.
The conscientious general practitioner will try reassurance
and symptomatic remedies for a further year or so and then,
yielding to pressure from patient or relatives and perhaps
with the feeling that 5 years is a decent interval, refer the
patient again. On the hospital side it is important to recognise
that such patients need explanation of their symptoms and
support, not reinvestigation.
ii
ii
ii
u
n
. Cl
C(
ir
w
G
sa
h<
re
to
A
82
di
-
Original Contributions
Risks of Agranulocytosis
land Aplastic Anemia
i A First Report of Their Relation to Drug
Use With Special Reference to Analgesics
; in the thre
international Agranulocytosis and Aplastic Anemia Study
risks of agranulocytosis and aplastic anemia in relation to analgesic drug
9 use were evaluated in a population-based case-control study conducted in
Europe and Israel. Analgesic use in the week before the onset of illness was
compared between 221 cases of agranulocytosis and 1425 hospital controls.
'ar Analgesics significantly associated with agranulocytosis were dipyrone (metam-
col sodium), indomethacin, and butazones (phenylbutazone and oxyphenbutaul zone). For dipyrone, the rate ratio estimate was 23.7 in Ulm, West Germany,
i West Berlin, and Barcelona, Spain, and the estimated excess risk for any
exposure in a one-week period was 1.1 per million. In Israel and Budapest,
Hungary, where the rate ratio estimate was 0.8, there was no evidence of
zs| excess risk. In all of the regions combined, the rate ratio estimates were 8.9 for
i.!f; indomethacin and 3.8 for butazones, with excess risk estimates of 0.6 and 0.2
J- per million, respectively. Analgesic use 29 to 180 days before admission was
(compared between 113 cases of aplastic anemia and 1724 controls.
’•<! indomethacin (rate ratio estimate, 12.7), diclofenac sodium (8.8), and
t butazones (8.7) were significantly associated with aplastic anemia, with
4it estimated excess risks for any exposure in a five-month period of 10.1, 6.8,
aS and 6.6 per million, respectively.
(J.4,W.4 1986256:1749-1757)
Mention, ms,
AGRANULOCYTOSIS
and
aplastic
ig adrr^ f'anemia are rare diseases that can be
ously iW
contindeoi caused by many environmental factors,
?)'h?geS including a variety of drugs.''1 There
. Lessor are, however, no reasonably accurate
n. oradja estimates of the overall incidence of
enlricutar 6
•wnias. hype either disease or of the risk associated
s; haHucira
See also p 1788.
gaslroinse
with any particular exposure, and reg
etNAandfi
>granuiocyi1 ulations concerning the various suspect
agents
vary from one country to anoth
/changes
xxj! 3 tfi
■er. In view of this situation, the present
?al and p&
1000. SLE international case-control study was
cur amort undertaken to obtain quantitative esti
IECALTD0 mates of the incidence of the two
3 was feta
diseases and the magnitude of the risks
ng 150.2
ME-®
in relation to various agents, particu
larly drugs.
The study is continuing in several
countries, but enough data have
already been obtained to enable us to
report on the overall incidence of each
disease and on the risks associated
with the use of analgesics.
Repnnt requests to Drug Epidemiology Umt. Boston
'Jrwersity School of Medcme, 1371 Beacon St. Brook*ne. MA 02146 (Dr Shapiro)
JAMA, Oct 3, 1986—Vol 256.-No. 13
METHODS
This population-based case-control
study5 was originally organized in
Israel (population, 3.9 million), Barce
lona, Spain (4.1), Ulm, West Germany
(5.3), West Berlin (1.8), and Milan, Italy
(2.3). After a pilot phase, data collec
tion began on July 1, 1980. Three
additional regions joined subsequently:
Budapest, Hungary (2.0 million), in
December 1981, Sofia, Bulgaria (1.1), in
August 1982, and Stockholm/Uppsala,
Sweden (1.8), in January 1983.
Efforts were made to identify all
cases of agranulocytosis and aplastic
anemia that resulted in hospital admis
sion (community cases) or that oc
curred during a hospital stay (hospital
cases). To ascertain potential cases,
study centers maintained regular liai
son with all hospitals in the regions at
intervals of no more than two weeks.
The present report is based on cases
identified up to June 30, 1984.
Potential controls for community
cases of both agranulocytosis and
aplastic anemia were selected from
among other patients admitted to the
same hospitals at about the same time,
who were of the same sex and approxi
mately the same ages as the cases.
The controls for the hospital cases
were to have been a random sample of
all hospital patients5 who were not
receiving cancer chemotherapy, immu
notherapy. or radiotherapy. In practice,
such a sample could not be obtained,
principally because patients with seri
ous illnesses frequently were inaccessi
ble for interview. Therefore, hospital
cases were not included in the analysis
of the effects of drug use.
Specially trained nurses or physi
cians administered a standard ques
tionnaire to potential cases and con
trols. For young children, a parent or
guardian was interviewed. Detailed
information was obtained about drug
use, day by day for the first seven days
before admission, week by week for the
three weeks before that, anytime in the
five months before that, and anytime
in the more distant past.
To ensure that drug histories were as
complete as possible, patients were
first asked about indications. With
regard to analgesics, they were ques
tioned about use for pain, headache,
backache,
toothache,
menstrual
cramps, muscle relaxation, muscle
International Agranulocytosis and Aplastic Anemia Study
1749
Table 1.—Agranulocytosis: Use of Analgesics by 1425 Controls in the Week Before the Index Day'
According to Diagnosis
Diagnostic Category, No. (%)f
Trauma
(N=787)
Infection
(N=396)
Other
(N=242)
Dipyrone
35 (5)
27 (6)
16 (5)
Other pyrazolones!
29 (4)
21 (6)
8 (3)
Salicylates
67 (8)
42 (10)
20 (7)
Acetaminophen
34 (4)
25 (7)
19 (8)
Drug
Butazones
6 (1)
3 (1)
2 (D
Indomethacin
4 (0.4)
1 (0.2)
2 (0.4)
Other nonnarcotic analgesics
16 (2)
3 (1)
5 (2)
•Two hundred ninety-nine controls for whom the index day was unknown are excluded.
fStandardized to the overall age, sex, and geographic distribution of the control series.
tAminopyrine, antipyrine, and propyphenazone.
spasms, arthritis, gout, cough, colds,
influenza, and other infections. A list
of generic and trade names was then
read. The list was based on marketing
data for each region and included
names that together accounted for over
90% of the sales of the common non
narcotic analgesic drugs (there were
too many trade names to ask about the
remaining 10%) as well as other drugs
generally suspected of causing either
dyscrasia. To minimize memory loss
further, patients were not interviewed
if they had been in the hospital more
than 28 days.
Data collected on potential confound
ing factors included, in addition to
medication histories, demographic in
formation such as age and years of
education, medical information such as
major illnesses and history of allergy,
and limited information on exposure to
radiation, petrochemicals, laboratory
chemicals, insecticides, and benzene.
Information on the clinical course of
the illness was recorded for all subjects
(for agranulocytosis, this included sys
tematic questions on the time of onset
of sore throat, fever, and chills). In
addition, for all cases (including those
not interviewed), blood smears, bone
marrow aspirates, and biopsy sections
were obtained, whenever available. All
available blood cell counts were re
corded, together with other relevant
clinical and laboratory information.
Definition and Selection of
Cases of Agranulocytosis
Potential cases were patients with a
granulocyte count of 500/mm3 or less
(<O.5X1O9/L) or a total white blood
cell count of 3000/mm3 or less
(<3.0xl0a/L) who were not undergoing
cancer chemotherapy, radiation thera
py, or immunosuppressive therapy. A
lower age limit of 2 years was specified
1750
JAMA, Oct 3. 1986 —Vol 256. No 13
because transient neutropenia in
younger children is commonly associ
ated with viral infections.7 There was
no upper age limit. The diagnoses of
potential cases were confirmed by a
committee of hematologists, who ex
amined the clinical and laboratory
data, including peripheral blood
smears, bone marrow aspirates, and
biopsy specimens. The review was car
ried out without knowledge of drug
use.
Final cases were patients with severe
selective neutropenia, defined as a
granulocyte count of 500/mm3 or less
(<0.5X109/L) with a hemoglobin level
of 10 g/dL or greater (>100 g/L) and a
platelet count of 100 000/mm3 or
greater (>100X109/L). Patients with
systemic diseases that can be associ
ated with neutropenia (eg, infectious
mononucleosis, systemic lupus erythe
matosus, leukemia, and malignant lym
phoma) were excluded. If a bone mar
row aspirate or biopsy specimen was
not available, the diagnosis was ac
cepted if the neutrophil count returned
to normal within 30 days (105 cases).
There were 422 final cases, of which
300 were community cases and 122
were hospital cases.
Because the major symptoms of
agranulocytosis—sore throat, fever,
chills, and headache—could each have
prompted the use of analgesic drugs,
there was a particular need for careful
timing of the day of clinical onset
(index day) of the illness, without
knowledge of drug use. The index day
was deemed to be the day on which
sore throat, fever, or chills first
occurred, as reported by the patient.
Of the 300 community cases, 47
(16%) were not interviewed for the
following reasons: death (7%), a delay
of more than 28 days (5%), psychologi
cal or medical reasons (3%), and fail
ure to locate the patient (0.3%). Among
the remaining 253 cases, there were sir
refusals (2%) and 39 (15%) for whom
the index day could not be determined,
leaving 208. Finally, 13 pilot cases with
an identifiable index day were also
included in the analysis of drug use,
giving a total of 221.
Definition and Selection of
Cases of Aplastic Anemia
Potential cases of aplastic anemia
were patients who were not undergoing
cancer chemotherapy, radiation thera
py, or immunosuppressive therapy and
who met at least two of the following
criteria: a white blood cell count of
3500/mm3 or less (<3.5X1OVL), plate
let count of 50 000/mm3 or less
(tgSOXlOVL), or hemoglobin value of
10.0 g/dL or less (<100 g/L) with a
reticulocyte count of 30 000/mm3 or t)
less (<30X109/L). As with agranulocy n
tosis, the diagnoses of potential cases ct
were confirmed, without knowledge of ae
drug use, by the committee of hematol th
ogists.
ft
Final accepted cases were patients
who did not have neoplastic or granulo
matous disease involving the bos em
marrow, systemic lupus erythemato ber
sus, hypersplenism, or other conditions Th
masquerading as aplastic anemia. Th" 113
bone marrow biopsy specimen, if avail
able, had to be compatible with the Da
diagnosis. In the absence of a biopsy
specimen, the diagnosis was accepted c dru,
there were at least two typical marro* stra
aspirates and if the clinical presenta Hae
tion and progression were typical (nil* inte.
cases). There were 168 final cases, « the;
which 160 were community cases a* atic
eight were hospital cases.
59,6
Because the presenting symptoms * agio
aplastic anemia (eg, fatigue or exces hient
sive bruising) are too vague to be timec ’■ors,
with acceptable precision, it was no multi
possible to determine the date of on*’ some(index day).
•iscr.
Of the 160 community cases, ’
The
(33%) were not interviewed for th '-sed |
following reasons: a delay of more th* ■»o dr
28 days (22%), death (8%), psycholo? :ssue,'
cal or medical reasons (1%), failure' •'ollow:
locate the patient (0.6%), and langus?
ftrnpor
difficulties (0.6%). The remaining ll> to use,
were combined with five pilot cas* ■*ter(
giving a total of 113 cases included e ati0 e,
the analysis of drug use.
J*d t,
x*rs s
Definition and Selection
*»» th
of Controls
’’’‘mat,
There were 2408 potential control
Of these, 27 (1%) refused to be in*? $°«cifi
viewed. The selection of final eontn*
from the remaining 2381 was m* . The ei
without knowledge of drug use. < > b,
categories were considered eligible: s- 'Sessed
International Agranulocytosis and Aplastic Anemia
I R
JMAOct
.3%). Amotu
. was patients with acute conditions
here were sk- ' i known to be caused, prevented by,
M for whod n° otherwise associated with analgesic
■ determine?
(eg. trauma and acute infections);
ot cases wje uhe5<, conditions were judged to be
J' were au ‘^dependent of analgesic use prior to
of drug ujj!.' \eir onset. The second category con-ted of Palients admitted electively
n of
f for long-standing conditions thought
ot
to influence analgesic use (eg,
nia
■J
hernia): these conditions were judged
astic aneiJ
anenv •o be independent of analgesic use
J?
it undergo,."
iation thej nrior to the date of admission. There
>-ere 1T24 eligible controls.
■ therapy
" In analyzing agranulocytosis, the
the followir-'
grol series was further restricted to
:ell county rent
sc with a known index day (as with
107L), platf ;hose
s■t " ‘ 7T
. << the
»nx> case
CH series): for those with trauma,
m. or. H ,’his was the day on which the accident
>bm value ( (jffUrred; for those with other acute
renditions (such as infections), it was
vw/mm f
jay on which symptoms com1 agrtmulot; ' nced; and for those admitted with
'tentOcas’■'
-c conditions, it was the day of
knowledge ( >mission. The index day could be
e of hemati (if,lerTnined for 1425 patients. Thus, the
■ ■ final comparison involved 221 cases of
/ere patie^ ^eranu]oc.vtosis and 1425 controls.
ic or granuh jn anajyZing aplastic anemia, the
ig the ba■
tr0] series was not restricted
an index day was not specified.
.er conditi^.^,
fina| comparison involved
anemia. TJ 3 cases an(j 1724 controls.
men, if av*
ble with 6 Data Analysis
• of a bit#
ratjos for various categories of
as accepta<jrug exposure were estimated from
pical manVsiratified data using the Mantelcal Preseni }|aensze| method,s and 95% confidence
typical (K jnlen-als were calculated according to
inal cases,.;^ method of Miettinen.9 The stratifiity cases s.jatjon variables were age (<40, 40 to
60 to 69, and >70 years), sex, and
symptonii;rt.p0n t0 control simultaneously all
rue or e®joentjfied potential confounding fac
ie to^e ht^rs, rate ratios were also estimated by
1, it^33 Multiple logistic regression,10 using
date of (Wiomewhat different models for each
Byscrasia (see below).
ty cases, 5 The most recent census data were
■wed for
to estimate the incidence of the
of more th vo dyscrasias. Then, for each drug at
), psychok sue, the excess r sk was estimated as
%>), failun #||ows; the etiologic fraction (that
and Jangs roportion of the disease attributable
emaining > use of the drug) was calculated"; the
pilot czfaiier estimate, together with the rate
:S includagatio estimate and incidence rate, was
sed to calculate risk estimates for
jsers and nonusers9; the excess risk
•n
jras the difference between the two
it i mates.9
itial conti
I
to be inSpecific Methods:
final contiflranulocytosis
1 was n The effects of drug use in the seven
-ug use. sys before the index
day
____ ____
„ were
d eligible ssessed, because drug-induced agrantic Anerriafcw. Ocl 3, 1986—Vol 256, No 13
Table 2 —Aplastic Anemia Use of Analgesics by 1724 Controls in Days 29 to 180 Before
Admission According to Diagnosis
Diagnostic Category, No. (%)'
Trauma
(N = 796)
Infection
(N=579)
Other
(N = 349)
130 (20)
179 (24)
109 (26)
Drug
Dipyrone
Other pyrazolonesf
154 (19)
124 (22)
77 (26)
Salicylates
378 (45)
295 (52)
150 (40)
Acetaminophen
143 (23)
156 (22)
82 (20)
Butazones
19 (2)
9 (2)
12 (3)
Indomethacin
10 (1)
4 (1)
4 (1)
Diclofenac
7 (0.7)
4 (0.6)
6 (1.9)
Other nonnarcotic analgesics
29 (3)
8 (2)
8 (2)
'Standardized to the overall age, sex, and geographic distribution of the control series.
tAminopyrine. antipynne, and propyphenazone.
Table 3.—Agranulocytosis: Annual Incidence Rates According to Region, July 1980 to June
1984
Community
Total
No.
Rate/
Million/y'
No. of
Hospital
Cases
No.
Rate/
Million/y*
67
3.5
55
122
6.3
48
21
2.3
17
38
4.6
4.1
48
62
4.2
23
85
5.7
Israel
3.9
48
64
5.6
12
76
6.5
Budapest, Hungary
2.0
31*
42
7.2
10
52
9.0
Stockholm / Uppsala,
Sweden
1.8
18*
19
7.0
3
22
8.0
Milan, Italy
2.3
45§
13
1.5
2
15
1.7
Sofia, Bulgaria
1.1
23"
12
5.4
0
12
5.4
Population,
Millions
Interval,
mo
Ulm, West Germany
5.3
48
West Berlin
1.8
Barcelona, Spain
Region
Total
22.3
4.4U
6.25
'Standardized to the age and sex distribution of the study population.
t December 1981 to June 1984
^January 1983 to June 1984.
§ October 1980 to June 1984
•'August 1982 to June 1984
51 Calculated as a population weighted average of the age- and sex-standardized region-specific rates.
ulocytosis is frequently characterized
by a short induction period.3 Use that
took place on or after the index day or
more than a week previously was
ignored. The reference category con
sisted of those not exposed to the drug
under consideration in the week before
the index day. The control distribution
of analgesic use according to three
diagnostic categories is given in Table
1. The rates of use were relatively low
and there was some variation across
diagnosis, but in general the rates were
similar.
The following factors were included
in the multivariate models: age; sex;
geographic area; date of interview; reli
ability of the patient (as assessed by
the interviewer); person interviewed
(patient, parent, or guardian); transfer
from another hospital; histories of
allergy', blood disorder, blood transfu
sion, or infectious mononucleosis; expo
sure to insecticides; the use in the week
before the index day of dipyrone, other
pyrazolones, salicylates, acetamino
phen, indomethacin, butazones (phenyl
butazone and oxyphenbutazone), other
nonnarcotic analgesics, thyrostatic
drugs, sulfonamides, a combined cate
gory of other drugs generally suspected
as causes of agranulocytosis (eg, phe
nothiazines and gold); and, finally, the
use of any nonsuspect drugs. Separate
International Agranulocytosis and Aplastic Anemia Study
1751
Table 4.—Agranulocytosis. Use of Dipyrone in the Week Before the Index Day According to
Region
Region
No.* (%) of
Cases
No.* (%) of
Controls
Crude
Rate Ratio
Estimate!
Stratified
Rate Ratio
Estimate!
Ulm, West Germany
6/28 (21)
5/237 (2)
12.7
12.2
West Berlin
6/17 (35)
2/72 (3)
19.1
20 9
30 5
Barcelona, Spain
15/50 (30)
5/394 (1)
33.3
Israel
13/65 (20)
28/253 (11)
2.0
1.8
Budapest, Hungary
4/30 (13)
22/147 (15)
0.9
0.9
Stockholm / Uppsala,
Sweden
0/12 (0)
0/126 (0)
1/9 (11)
3/133 (2)
5.4
3.6
6/10 (60)
13/63 (21)
5.8
5.3
51/221 (23)
78/1425 (6)
5.2
Milan, Italy
Sofia, Bulgaria
Total
•Number of cases or controls who used dipyrone/total number in center.
tRelath/e to no use in the week before the index day
!Age and sex taken into account by the Mantef-Haenszel procedure, xi for heterogeneity, 45.4; P<OO1.
Table 5.—Agranulocytosis: Analgesic Use in the Week Before the Index Day
Multivariate
Rate Ratio Estimate’
(95% Confidence
Interval)
Drug
Cases
(221)
Controls
(1425)
Stratified
Rate Ratio Estimate’
(95% Confidence
Interval)
Dipyrone
Ulm, West Germany/West
Berlin/Barcelona, Spain
Any
27
12
21.3 (11.7-38.9)
23.7 (8.7-64.4)
12
7
16.5 (7.2-38.0)
20.4 (5.6-74.1)
17
50
1.5 (0.8-2 7)
0.8 (0.4-1.8)
10
23
2.0 (0.9-4.4)
1.2 (0.4-3.7)
>3 d
Israel/Budapest, Hungary
Any
>3 d
Other pyrazolones!
Any
18
58
2.1 (1 2-3.7)
1.2 (0.6-2.5)
>3 d
6
16
2.1 (0.8-5.4)
0.9 (0.2-3.1)
Salicylates
Any
43
129
2.4 (1 6-3.6)
1.6 (1.0-2.7)
>3 d
24
56
2 7 (1 6-4.6)
1.9 (1.0-3.8)
Acetaminophen
Any
25
78
>3 d
12
42
Butazones
Any
11
11
5.2 (2 2-12.0)
3.8 (1.3-10.7)
>3 d
8
6
6.7 (2.6-17.5)
6.3 (1.8-22.3)
10
7
6.7 (2.8-16 1)
8.9 (2.9-27.8)
8
4
9 0 (3.2-25.4)
14.2 (3.7-54.4)
Other nonnarcotic
analgesics!
Any
5
24
1.5 (0.5-4.0)
0.9 (0.3-3.1)
>3 d
3
19
1.0 (0.3-3.7)
0.6 (0.1-2.6)
Indomethacin
Any
>3d
'
1.6 (10-2 6)
1.0 (0 5-1.9)
1.4 (0 7-2.9)
0.8 (0.3-2 0)
•Relative to no use in the week before the index day.
flncludes aminopyrine (six cases. 18 controls); aminopyrine/propyphenazone (five, 21); propyphenazone
(three, seven); antipyrine (three, five); aminopyrine/propyphenazone plus propyphenazone (one. one);
aminopyrine/propyphenazone plus antipyrine (zero, four); and propyphenazone plus antipyrine (zero, two).
•'Aminopyrine/propyphenazone" refers to compounds the components of which were changed from aminopyrine
to propyphenazone during the course of this study.
^Includes ibuprofen (two cases, four controls); diclofenac sodium (one, five); naproxen (one. three);
proquazone plus piroxicam (one, zero); piroxicam (zero, three): benzydamme hydrochlonde (zero. two), niflumic
acid (zero, one); glafenine (zero, one), flurbiprofen (zero, one); ketoprofen (zero, one); clonixin (zero, one);
naproxen plus diclofenac (zero, one); piroxicam plus diclofenac (zero. one).
1752
JAMA. Oct 3. 1986-Vol 256, No 13
was
com
(fat
mill
not
natc
bed
the
deat
Pi
ther
ity (
for
Whc
for
Specific Methods:
spec
Aplastic Anemia
Bud:.The effects of drugs used up to ISO men
days before admission were assessed. the i
In
because there can be a considerable
delay between exposure and diagnosis were
Any use that took place less than 29 frorr
days previously was ignored, because Thei
such use could well have occurred after late
the onset of the dyscrasia. The refer tn a
ence category was no use of the drug Berl
under consideration during days 29 ratic
through 180 before admission. The dis thes>
tribution of analgesic use among the rate!
1724 controls is given in Table 2; usage rize
furtl
rates were reasonably similar.
The multiple logistic models included two
Re
the following factors: age; sex; geo
graphic area; date of interview; reli ratio
othe.
ability of the patient; person inter
viewed; transfer from another hospital regie
histories of bruising, blood disorder, or sma]
tuberculosis; histories of exposure to presi
benzene, petrochemicals, or insecti dipy:.
In
cides; and the use of drugs during day?
29 through 180 before admission (the ic u<
daydrug groups were defined as for agran
ulocytosis). Thyrostatic drugs wert cons<
used by 4% of the cases and 0.4% ot and ,
the controls and sulfonamides by 10* relon
and 4%; again, separate terms wen mate
'95%
included for these drugs.
Israe
As with agranulocytosis, excess ris
1-8).
calculations were based on the muloanalf
variate rate ratio estimates. Since
these were based on drug historic agra
'mul
covering days 29 through 180 beta*
and I
admission, excess risks were calculate
use i
for a five-month period.
ennfi
Pyra:
RESULTS
aceta
Agranulocytosis
narct
Table 3 gives estimated incident
»ere
rates by region. The overall anna*
'n th
incidence was 6.2 cases per million;‘‘ and ,
ranged from 1.7 per million in Milan f not
9.0 per million in Budapest Among
’um!
422 cases, there were 36 deaths &
restr
which agranulocytosis was the main/ '■east
contributory cause, giving a fatal/ ■he r
rate of 9% and an annual mortal11-'
rate of 0.5 per million.
In
The annual community incident
terms for the use of thyrostatic drugs
(propylthiouracil, carbimazole, and
methimazole) and sulfonamides were
included because these agents were
associated, as expected, with agranulo
cytosis (thyrostatic drug use, 15% of
cases and 0.4% of controls; sulfona
mide use, 8% and 1%).
Excess risks were calculated using
the multivariate rate ratio estimates.
Since the estimates were based on drug
histories covering seven days before
the index day, excess risks were calcu
lated for a seven-day period.
international Agranulocytosis and Aplastic. Anemia
•c dr^ .• s 4 4 per million. Among the 300
-mmunitv cases there werc 29 deaths
e,
.fatality rate, 10%; mortality, 0.4 per
es
*-s Weir. illion). The hospital incidence could
j*. estimated because the denomi
granuk,
15% .J: nator (the number of person-years of
sulfon,: ned occupancy) was not known; among
• he 122 hospital cases, there were seven
'd usiJ deaths (6%).
, .
, ,
.
Preliminary analysis revealed that
itimaw: Preliminary
on drJ there was significant regional variabils befor itv (P< 001) in the rate ratio estimate
re caQ for the use of dipyrone (Table 4).
' Whereas the crude rate ratio estimate
J for all regions was 5.2, the region•' specific estimates ranged from 0.9 in
{ [hjdapest to 33.3 in Barcelona. AdjustP to Uf ment for age and sex did not change
issessg the estimates materially.
iderab.
In the separate regions, numbers
agnoj’ were too small to control confounding
than S from factors other than age and sex.
becan^-Therefore. to provide stable multivar■ ed a®ate estimates, the data were grouped
,e refe in categories of high rate ratio (Ulm,
he dr; Berlin, and Barcelona) and low rate
days { ratio (Israel and Budapest). Results for
The dr these categories are presented sepaong 3 rately. It was not clear how to catego2' usi rize the data from Milan and Sofia, and
| further data on dipyrone from these
includl two regions are not presented.
ex' M Regional heterogeneity in the rate
■w’; irf ratio estimate was not evident for any
i intalother analgesic drug, although in each
lOspMregion numbers for most drugs were
>rder (small. Overall results are therefore
isure’tpresented for analgesics other than
insect dipyrone.
ng d? In Table 5 two categories of analgesion (tj'ic use in the week before the index
- agrjday—any use and use for at least three
s ^consecutive days—are given for cases
0 4% (and controls. In Ulm, Berlin, and Barbv Kf.n'lona' (he multivariate rate ratio esti1S ™mate for any dipyrone use was 23.7
■<5% confidence interval, 8.7 to 64.4); in
Jsrael and Budapest it was 0.8 (0.4 to
ess
In all regions combined, other
gyinalgesics significantly associated with
iistorfagranulocytosis were indomethacin
, ^Umultivariate rate ratio estimate, 8.9)
lcu]al uid butazones (3.8). For any salicylate
ise the estimate was .1.6-(lower 95%
nnfidence limit, 1.0). The estimates for
lyrazolones other than dipyrone (1.2),
icetaminophen (1.0), and other nonicidar
icig
- arcotlc analgesics as a group (0.9)
jjrere
all close to unity. Individual drugs
annt
Ilion;H-in the categories of other pyrazolones
could
4ilan,>nd other nonnarcotic analgesics
ongi?ot be evaluated because of small
ths I lumbers. When the analysis was
main estrieted to use that took place on at
east three consecutive days, none of
ort he rate ratio estimates was materially
educed.
icidei In earlier studies111'1 the risk associOct 3, 1986—Vol 256, No. 13
Table 6 —Aplastic Anemia: Annual Incidence Rales According to Region, July 1980 to June
1984
Region
Population,
Millions
Interval,
No.
Rate/
Million Zy*
Ulm, West Germany
5.3
48
56
2.9
West Berlin
1.8
48
18
2.2
Barcelona, Spain
4.1
48
36
2.2
Israel
3.9
48
21
1.6
Budapest, Hungary
2.0
3tt
3
O.6
Stockholm/Uppsala,
Sweden
1.8
184
2
.
Milan, Italy
2.3
45”
27
3.1
1.1
23,1
5
Sofia, Bulgaria
Total
20.5
.§
2.6
2.2#
’Standardized to the age and sex distribution of the study population.
fDecember 1981 to June 1984.
t January 1983 to June 1984
§The incidence was not calculated for Stockholm/Uppsala, Sweden, for methodological reasons (see text).
'’October 1980 to June 1984.
5I August 1982 to June 1984.
it Calculated as a population-weighted average of the age- and sex-standardized region-specific rates
ated with the use of pyrazolones for 14
or more days was reported. In this
study, in Ulm, Berlin, and Barcelona
only one case and five controls who had
used dipyrone within one week of the
index day had taken the drug for 14 or
more consecutive days; in Israel and
Budapest the corresponding numbers
were five and ten (multivariate rate
ratio estimate, 2.2; 95% confidence
interval, 0.5 to 10.4). With regard to
other drugs, there were sufficient data
to examine 14 or more consecutive days
of use only for salicylates: there were
12 exposed cases and 24 exposed con
trols (multivariate rate ratio estimate,
2.9; 95% confidence interval, 12 to
7.1).
Estimates of excess risk were calcu
lated for those analgesics (dipyrone,
butazones, and indomethacin) for
which the lower 95% confidence limit,
based on a history of any use in the
week before the index day, was greater
than 1.0. For dipyrone use in Ulm,
Berlin, and Barcelona, the estimated
etiologic fraction was 27%, which
translated into an excess risk of 1.1 per
million. For butazone use in all regions
combined, the etiologic fraction was
4%, giving an excess risk estimate of
0.2 per million. For indomethacin use,
the etiologic fraction and excess risk
were 4% and 0.6 per million, respec
tively.
Aplastic Anemia
Table 6 gives the estimated incidence
rates by region. Stockholm/Uppsala is
omitted because bone marrow biopsies
are not done routinely in Sweden, and
many potential cases were not con
firmed due to insufficient information.
The overall annual incidence of aplastic
anemia was 2.2 per million (range, 0.6
to 3.1). Of the 168 cases, 159 were
followed up for two years: 78 had died,
giving a two-year fatality rate of 49%.
In Table 7 the distribution of
analgesic use in days 29 through 180 is
given for 113 cases and 1724 controls
according to use at any time in that
interval, use for at least four days in
any seven-day period, and use for four
or more days a week for at least four
weeks. Histories of any exposure to
indomethacin (multivariate rate ratio
estimate, 12.7), diclofenac sodium (8.8),
and butazones (8.7) were significantly
associated with aplastic anemia. In
addition, with limited numbers, the
rate ratio point estimates for the use of
indomethacin (52.0) and butazones
(34.5) were higher when the drugs had
been taken on four or more days in one
week and when such use had lasted at
least four weeks (49.9 and 43.4). For the
use of dipyrone, other pyrazolones, and
acetaminophen, there were no statisti
cally significant positive associations.
For the use of salicylates on four or
more days in any week, and for the use
of any drugs in the category of other
nonnarcotic analgesics, the estimates
were 2.9 and 2.2, respectively, but these
results were not statistically signifi
cant.
Excess risk estimates were calcu
lated for those drugs significantly asso
ciated with aplastic anemia (indometh
acin, diclofenac, and butazones) when
used any time in days 29 through 180
International Agranulocytosis and Aplastic Anema Study
1753
before admission. For indomethacin
the etiologic fraction of 6% translated
into an estimated excess risk for any
use in a five-month period of 10.1 per
million. For diclofenac, the correspond
ing estimates were 5% and 6.8 per
million, and for butazones they were
7% and 6.6 per million.
COMMENT
Agranulocytosis
The use of dipyrone was associated
with agranulocytosis in some of the
regions under study, but not in others.
Overall, indomethacin and butazones
were also associated with an increased
risk. In addition, there was an associa
tion of borderline significance for salic
ylate use, which was somewhat more
pronounced for use that lasted 14 or
' more days. There was no statistically
significant evidence of association for
pyrazolones other than dipyrone, acet
aminophen, or the heterogeneous cate
gory of newer nonnarcotic analgesics,
although for none of these drugs could
increases in risk of twofold to fourfold
be ruled out
The associations for dipyrone and
butazones were expected on the basis
of previous evidence.1-1'11’22 With regard
to indomethacin, however, although
there are case reports,23 there are no
studies that suggest an appreciable
increase in the risk of agranulocytosis.
With regard to salicylates, there are
only a few case reports suggesting that
they cause agranulocytosis,116251 and
since the statistical significance of the
association in this study is borderline,
it must be interpreted with caution.
The lack of association with the use
Table 7.—Aplastic Anemia: Analgesic Use in Days 29 to 180 Before Admission
Drug
Dipyrone
Any
Controls
(N=1724)
Stratified
Rate Ratio Estimate*
(95% Confidence Interval)
Multivariate
Rate Ratio Estimate*
(95% Confidence Interval
0.5 (0.2-0.9)
19
418
0.7 (0.4-1.2)
6
34
2 4 (1.0-5.8)
1.6 (0.4-5.7)
>4 d/wk for >4 wk
1
16
1.1 (0.1-8 8)
0.9 (0.1-12.9).
Other pyrazolones*
Any
27
355
1.0 (0.7-1.7)
1.0 (0.5-1.7)
>4 d in any wk
6
26
4.9 (1.9-12.3)
0 7 (0.2-2.7)
>4 d/wk for >4 wk
2
11
4 5 (0.9-21.5)
1.2 (0.1-10.5)
59
823
1.1 (0.8-1.7)
1.0 (0.6-1.6)
>4 d in any wk
11
58
3.8 (1.8-8.2)
2.9 (1.0-8.6)
>4 d/wk for >4 wk
5
33
3.9 (1.3-12.1)
2.9 (0.7-10 9)
Acetaminophen
Any
25
381
1.3 (0.8-2.1)
1.5 (0.8-2.7)
>4 d in any wk
5
49
2.2 (0 8-6.2)
0.9 (0.2-3.5)
>4 d/wk for >4 wk
2
26
2.5 (0.5-13.4)
3.9 (0.7-21.5)
Butazones
Any
9
40
4.3 (2.1-8.8)
8.7 (3.4-22.3)
>4 d in any wk
7
13
12.2 (5.3-28.0)
34.5 (9.4-127)
>4 d/wk for >4 wk
5
4
34.4 (12.5-94.9)
43.4 (7 9-239)
7?
18
7.2 (3.0-17.3)
12.7 (4.2-38.3)
>4 d in any wk
4
4
13.6 (4 3-43.4)
52.0 (10.6-255)
>4 d/wk for >4 wk
4
3
16.2 (5.2-50.6)
49.9 (9.0-278)
Diclofenac sodium
Any
7
17
7.4 (3.1-17.6)
8.8 (2.8-27.3)
>4 d in any wk
2
4
10.5 (2.5-44 2)
7.2 (0.6-82.7)
>4 d/wk for >4 wk
0
1
0.0
0.0
Indomethacin
Any
Other nonnarcotic analgesics*
Any
wit
be
th:
wb
dif
wh
Cases
(N=113)
>4 d in any wk
Salicylates
Any
of
su
is
dij
ret
an
dn
sm
rin
rat
pal
ex]
ty
res
be
ma
not
wa
cas
to.
otb
ver
sis
dis.
spe
in
We
clir
tai;
trc
Pin
the
juc
ic
dis1
sin>
cat
<fe
aci
an:
•hf
tha
_
...
9
45
3.4 (1.6-7.3)
2.1 (0.8-5.9)
>4 d in any wk
6
18
9.8 (3.5-27.1)
2.2 (0.4-11.4)
njr
>4 d/wk for >4 wk
3
14
7.4 (1.8-31.5)
0.8 (0.1-6.1)
13
Uli
•Relative to no use in days 29 to 180.
flncludes aminopyrine/propyphenazone (12 cases. 124 controls): aminopyrine (six, 104); propyphenazone (six. 48): antipyrine (three. 42); aminopyrine plus antip><1* ■•o
(zero. 18); propyphenazone plus antipyrine (zero. 15); aminopyrine/propyphenazone plus antipyrine (zero, three); aminopyrine/propyphenazone plus propyphenazone (^
two); aminopyrine plus metiphenazone (zero. one). “Aminopyrine/propyphenazone" refers to compounds the components of which were changed from amtnopynf*3 :
propyphenazone during the course of this study,
^Includes piroxicam (three cases, eight controls); benzydamine hydrochloride (one, ten); naproxen (one. seven); niflumic acid (one. one); indoprofen (one. zero); nap*0**, i ^n<,
plus ketoprofen plus piroxicam (one. zero); naproxen plus oxametacin (one. zero); ibuprofen (zero, six); glafenine (zero, two); clonixin (zero, two); ketoprofen (zero. b* i fin
chlorthenoxazine (zero, two); etofenamate (zero, one); sulindac (zero, one); flurbiprofen (zero, one); Hufenamic add (zero, one); ibuprofen plus ketoprofen plus sulindac (^
one).
1754
JAMA. Oct 3. 1986-Vol 256. No 13
international Agranulocytosis and Aplastic Anemia
ne
of pyrazolones other than dipyrone was
‘e bas>v surprising- Aminopyrine, in particular,
regajjj -s not only chemically closely related to
Ithoiig^' Jnvrone, hut has been shown on
are tfc’: rvchallenge to cause agranulocytosis,2,
■eciabU 3nfj antibodies cross-react with both
cytosi^ drugs2' However, numbers were too
ere aij .mall to assess the effect of aminopyng thjji rjnc separately.
,,il W
Most difficult to interpret is the wide
‘
regional variability in the association
derlinJ
dipyrone use, which is unlikely to
tion. j jx, dUe to chance. It is worth noting
the use" that in Ulm, Berlin, and Barcelona,
s n-here the rate ratio estimate was 23.7,
■; dipyrone was not commonly used,
u-hile in Israel and Budapest, with a
s ~ ; rate ratio of 0.8, use was common. This
mate- ! pattern may provide a clue to the
|n|en< ^planation for the regional variabili9>
' 1 The possibility that the present
~----- 4 re5ults are biased or confounded must
——considered. Clinically mild cases
!9) < may in some instances have been diag\ nosed preferentially if a suspect drug
7)
If was taken, but the number of such
—----- 1 rases would have had to be substantial
_ __ 10 affect the results materially. At the
>.5) J other extreme, it is possible that some
t very severe cases died before a diagno5)
' sis could be made. If the severity- of the
—-----i disease was related to the use of any
_ ___ _f specific drug, this could have resulted
19) | m underestimation of the rate ratio.
| We judge it likely that virtually all
7)
i clinically severe cases were ascer~
I tained.
_ ___ J Almost 100% of the potential con.5) i trols were successfully interviewed.
f Final controls were only included in
.3)
the analysis if they had conditions
------- rjudged to be unrelated to prior analges
! ic use; it was reassuring that the
■9) ; distributions of use were generally
j similar across the major diagnostic
3) ^categories.
—The symptoms of agranulocytosis
S5^ j I fever, chills, sore throat, and head8) ’ ache) are also indications for the use of
j analgesics. Despite attempts to date
‘ the onset of the illness, it is possible
that incorrectly reported or unreported
symptoms could have .induced analges
ic use that was erroneously classified
as occurring within the etiologic peri,)
fod, resulting in overestimation of rate
------ jratios. If similar misclassification oc__ ,‘curred in controls with conditions such
I)
*as appendicitis, this would have re3^suited in underestimation. For these
treasons, particular attention was paid
3ntl^f10 the use of analgesics for three or
^V^’more days, since there was greater
(assurance that such use antedated the
nap«».onset of the illness. The results con’r°. ^firmed the overall findings. It is also
“reassuring to note that had the con-
ia_
g
x_
cJjAMA. Oct 3. 1986—Vol 256. No 13
trols been restricted to those for whom
the index day was known beyond doubt
(trauma), the findings would not have
been changed materially.
There may have been information
bias, since it is widely known that
agranulocytosis can be caused by
drugs. Before the interviews for this
study were conducted, many of the
cases had been questioned repeatedly
about drug use. Thus, the memories of
the cases were stimulated before they
were interviewed while those of the
controls were not. Three approaches
were used to reduce information bias.
First, the patients were interviewed
within 28 days of admission. Second, a
standard and detailed questionnaire
was used. Third, three or more consec
utive days of drug use, presumably less
subject to differential recall, was ana
lyzed. Despite these precautions, infor
mation bias probably was not com
pletely avoided. Such bias is of concern
mainly for drugs already under suspi
cion as causes, such as dipyrone, and
would have resulted in overestimation
of the risk.
Information bias may partially ex
plain the regional variability of the
association with dipyrone use if the
intensity of questioning of the cases
before interview differed according to
study center. Another possibility is
that the recall of dipyrone use by the
controls varied among the regions. The
drug was available under many more
brand names in Ulm, Berlin, and Barcelona27-2, than in Israel2* and Buda
pest.21 Controls in Ulm, Berlin, and
Barcelona could have used dipyronecontaining preparations with unfamil
iar names and not have recalled their
use, with resultant overestimation of
the risk in those regions.
The possibility of underascertain
ment of analgesic use among the con
trols should be checked, if feasible, by
comparing the rates with data such as
defined daily doses.31
Potential confounding by age, sex,
region, concomitant drug use, and vari
ous other factors was controlled simul
taneously by multivariate analysis. It
remains possible that confounding was
incompletely controlled.
On balance, we judge that the results
are not materially biased. In particu
lar, the regional variability in the
association with dipyrone use is so
great that it is more plausible to
assume that some unidentified factor,
present in some regions, but not in
others, acts together with dipyrone to
increase the risk.
The excess risk for dipyrone use, as
estimated in this study, is discordant
with the findings of others. Discombe12
and Huguley'’ estimated, respectively,
that 0.867; and 0.79% of patients who
use aminopyrine for 1-1 or more days
develop agranulocytosis. Huguley sug
gested that this risk also applied to
dipyrone. As has already been pointed
out,32 these estimates were biased. Cor
responding estimates for dipyrone de
rived from the present data suggest
that in Ulm, Berlin, and Barcelona,
where the association was strongest,
the excess risk attendant to at least 14
consecutive days of use is 3.3 per
million, or 0.0003% (derived by multi
plying the excess risk by three,
because, as defined in this study, a
14-day period of use could have com
menced up to three weeks previously;
the assumption is made that the risk
per unit time is independent of the
duration of use). In the other regions,
the excess risk appears to be even
lower.
Bbttiger and Westerholm21 suggested
that agranulocytosis occurs in about
one of every 3000 dipyrone users. This
estimate is also much higher than the
present one, but its validity is in doubt.
First, there were repeated government
warnings about the dangers of dipy
rone, and it is possible that dipyroneassociated agranulocytosis was prefer
entially reported to the Swedish
Adverse Reaction Registry. Second,
and more important, the consumption
of dipyrone declined dramatically dur
ing the period of observation, and it
remained low thereafter, probably be
cause of the warnings. The denomina
tor of dipyrone users was estimated
from prescription records at a time
when consumption was virtually at its
lowest, whereas the numerator was
not, resulting in a risk estimate that
was too high.
Other studies have ruled out risks
for dipyrone users of more than one in
1000'“ and one in 133 00034 although
they did not provide estimates of the
actual risk.
With regard to indomethacin and
butazone use, the excess risk of agranu
locytosis has not previously been esti
mated. The data were too sparse to
explore possible regional variability for
these drugs.
Aplastic Anemia
The analgesics significantly associ
ated with aplastic anemia when taken
29 to 180 days previously were indo
methacin, diclofenac, and butazones,
with estimated increases in risk of the
order of tenfold. In addition, for two of
the drugs (indomethacin and buta
zones), with limited numbers, there
was a suggestion that the risk was
higher if they were taken regularly and
International Agranulocytosis and Aplastic Anemia Study
1755
for a sustained period.
There was no evidence of an associa
tion with the use of dipyrone or other
pyrazolones. Within the latter catego
ry, however, numbers were too small to
evaluate individual drugs. For salicy
late use of four or more days’ duration,
the rate ratio estimate was somewhat
elevated, but this result could have
been due to chance. Similarly, the
association with the use of a mixed
group of the newer nonnarcotic analge
sics other than diclofenac could also
have been due to chance. However,
since individual drugs in this category
have been implicated in case reports as
possible causes of aplastic anemia,23
these agents require further study.
The butazones are a well-recognized
cause of aplastic anemia,20,35'36 and the
association identified in this study was
strong, although based on small num
bers. There have been case reports
linking indomethacin use with aplastic
anemia,23:n'B but the strength of the
association observed here is surprising.
Diclofenac has been implicated in case
reports,39 and the present study gives a
quantitative estimate of the risk. This
result needs to be confirmed in further
studies.
Potential methodological problems
must be considered. The diagnosis of
aplastic anemia is virtually inevitable
in all cases and selective enrollment
dependent on drug use was therefore
unlikely. The incidence reported here
was lower than in other studies,35,l°'11
but this could have been due to the use
of different diagnostic criteria. As for
the controls, their conditions, most of
recent onset, should have been inde
pendent of the use of analgesics 29 to
180 days earlier. Consonant with this,
the distributions of analgesic use
across diagnostic categories were simi
lar.
About 8% of the cases were not
interviewed because of death and 22%
because they could not be interviewed
within 28 days. If the use of any drug
was selectively associated with severe
or rapidly fatal aplastic anemia, this
could have resulted in underestimation
of the risk.
It was impossible to time the onset
of aplastic anemia because symptoms
such as fatigue or easy bruising are too
vague. In the days or weeks before
admission, episodes of infection or
fever due to as yet undiagnosed aplas
tic anemia could have provoked the use
of analgesic or antipyretic drugs. For
this reason, drug use that took place
within the 29 days before admission
was not analyzed. It must be acknowl
edged, however, that 29 days is an
arbitrary cutting point and that in
1756
JAMA.OcI3.1986-VoI256.no 13
some individuals the illness may have
remained undiagnosed for many
months. Thus, drug use that com
menced more than a month before
admission may sometimes have been
provoked by early symptoms and the
effects of some analgesics (eg, salicy
lates) could have been overestimated.
All of the results for aplastic anemia
must therefore be interpreted with
caution. However, for the use of indo
methacin, butazones, and diclofenac,
the rate ratio estimates were so high
that it is doubtful that they could be
entirely accounted for by occult aplas
tic anemia having provoked their use.
It is widely suspected that some
analgesics can cause aplastic anemia.
Butazones, for example, were given
considerable publicity while the study
was in progress. Had there been differ
ential recall, it should have been least
marked among those who used analge
sics the most. The associations with the
regular use of indomethacin and buta
zones for more than a month suggest
that information bias was not a major
problem.
As with agranulocytosis, confound
ing by concomitant drug.use and vari
ous other factors was controlled by
multivariate analysis. Again, it is pos
sible that confounding was incomplete
ly controlled.
This study is the first to provide
excess risk estimates of aplastic ane
mia in users of analgesic drugs. Their
interpretability is limited, however,
because of small numbers. In addition,
the present findings suggest that the
magnitude of the risk may be a func
tion of both the frequency and the
duration of use, at least for certain
drugs. How to select an appropriate
measure of risk is therefore unclear.
Given the uncertainties as to onset of
the disease and timing of relevant
exposure, we elected to estimate the
excess risks associated with use of a
given drug on one or more days in a
five-month period.
GENERAL CONCLUSIONS
In the regions in which this study
was conducted the incidence rates of
agranulocytosis and aplastic anemia
are low. Aplastic anemia is less com
mon than agranulocytosis, but the
fatality rate is higher. The fatalny
rates of the two diseases, as well as
their incidence, must be considered in
interpreting the results for analgesic
use. However, inferences about the
public health impact of analgesic use
cannot be more widely generalized to
other regions of the world if a fatal
outcome of agranulocytosis is more
common because of factors such as
malnutrition or inadequate medical
Set
care.
hoi
In considering public health implies
ME
tions, it is necessary to compare anal
gesics not only in terms of blow nez
dyscrasias, but also in terms of otha Ou
serious adverse effects. What matten
ultimately is the total risk of morbidity Rei
and mortality. Many of the conditions
that have been attributed to the use d
analgesics may occur more commonh Pub
than agranulocytosis or aplastic ane
mia. These include thrombocytopeni
purpura, hemolysis, shock, nephrotoi
icity, hepatotoxicity, and gastrointesti Med
nal disorders such as major uppe zneigastrointestinal tract bleeding. The lat
ter condition is the most importair.
since of those that are life threatenin
drag
it is by far the most common.12 Quanti
tative estimates of the risk of bleedin
have been published for some of th
drugs considered here (eg, aspirin110? >19.
whereas for others (eg, dipyrone) nos
are available.
There were some large relatis
increases in risk in this study: agrant
locytosis among users of dipyrone (i
some regions), butazones, and ini
methacin, and aplastic anemia amoa
10. .<
users of butazones, indomethacin, as
diclofenac. However, it is more imps
tant to note that the absolute risk
associated with all of these dra
appear to be very low: for exposin’
occurring in a seven-day interval, th
estimated excess risk of agranulocytt
sis ranges from 0.2 to 1.1 per millit* ;:P>T
for exposures occurring in a five-moi
interval, the estimated excess risk <
aplastic anemia ranges from 6.6 to 18per million. It is the latter estimate
that provide measures of the incident *
. th.
of blood dyscrasias attributable 4. ■
these drugs.
This study was sponsored by Hoechst -lj
Frankfurt, Federal Republic of Germany. PW>‘
support was also provided by the governments |
Hungary and Bulgaria and by the Corporation^
Swedish Pharmacies The study was supervisee?
an Honorary Internationa! Advisory Board "V.-.
members are Sir Richard Doll. FRCP.
Oxford. England. Chairman; Per Knut M.
MD, Oslo; and Sven Moeschlin, MD. Soloth-y
Switzerland.
This study would not have been possible witf*t
the cooperation of over 300 hospitals in
participating centers.
I
Participants in the International Agranulod*g
sis and Aplastic Anemia Study are as follows |
Chairman: Micha Levy, MD. Jerusalem
Coordination and Data Analysis (Drug
miology Unit): Dennis Slone. MD.t Samuel
ro, MB, FRCP(E), David W. Kaufman.
Theresa Anderson. RN. Lynda J. Blair. RN. P>--.
via T. Cook. MPH. John J. Farrell, Leoni"1.}
Gaetano. MS. Robert Matis, MS, Judith PMS. Carol L Wells. MEd, Boston
Investigators; Joan-Ramon Laporte, MD.
Iona, Spain; Helmut Kewitz, MD, Berlin; G)
Retsagi, MD, Susan Hollan, MD, Budapest; •
Uvy. MD. Zvi Stern, MD. Jerusalem.
international Agranulocytosis and Aplastic Anemia
medic^
yognoni, MD, Milan. Italy. Vitan Vlahov MD,
c^fia. Bulgaria; Bengt-Erik Wiholm, MD, Stock^Ini; Hermann Heimpel, MD, Wolfgang Heit.
mplica jjD. Him, West Germany
"e ana]. Data Collection. Xavier Carne, MD, Luisa IbaMD, Barcelona, Spain; Marlind Klein, RN,
f blooj
)f oth^ fhrista Scott, RN, Berlin; Edit Czink, MD, Andras
matter,
orbiditj references
nditior^ I Swanson R, Cook R: Drugs. Chemicals and
e use# flood Dyscrasias. Hamilton, Ill, Drug Intelligence
mmonlj publications, 1977,
9 Do Gruchy GC: Drug-Induced Blood Disorders.
Lie arif. Oxford, Blackwell Scientific Publications, 1975.
■•topenj.
Gird wood RH (ed): Blood Disorders due to
>h rotox [rrufi^ an(l Other Agents. Amsterdam, Excerpta
tintesti. ^pdica, 1974.
4. Heimpel H, Heit W Drug-induced aplastic
’ uppe j^eniia: Clinical aspects. Chn Hematol 1980:9:611The lat
portant 5/The International Agranulocytosis and AplasAnemia Study. The de&’gn of a study of the
Stenin;
drug etiology of agranulocytosis and aplastic
Quanti anemia. Eur J Chn Pharmacol 1983;24:833-836.
□leedin; k Miettinen OS: The ‘case-control’ study: Valid
■ of thj selection of subjects. J Chronic Dis 1985;38:5-13irin*3*1, 549Portnoy B, Hanes B, Salvatore MA, et al. The
le) tO tfripheral white blood count in respirovirous
infection. J Pediatr 1966;88:181.
relativi g. Mantel N, Haensze) W. Statistical aspects of
agranu •he analysis of data from retrospective studies.
JSCI1959:22719-748
rone (i; 9. Miettinen OS: Estimability and estimation in
d ini case referent studies. Am J Epidemiol 1976;
. anion; 103:226-235
cin, an 10. Armitage P: Statistical Methods in Medical
Research. New York, John Wiley & Sons Inc, 1971,
e impor pp 380-38-1
te risk jl. Miettinen OS: Proportion of disease caused or
e drug prevented by a given exposure, trait or interven
eposure tion. Am J Epidemiol 1974;99:325-332.
12.
Discombe G: Agranulocytosis caused by ami
-val, th dopyrine- An avoidable cause of death. Br Med J
ulocyte 1952:1 1270-1273.
13.
Huguley
CH: Agranulocytosis induced by
million
a hazardous antipyretic and analgesic.
e-montl Jdipyrone,
AhiA 1964;189:938-941.
risk it 14. Madison FW, Squier TL Etiology of primary
6 to io: granulocytopenia (agranulocytic angina). JAMA
jtimate 1934:102:755.
ncideno 15. Moeschlin S, Wagner K. Agranulocytosis due
to the occurrence of leukocyte-agglutinins. Acta
able ti Haematol 1952;8:29
16.
Moeschlin S: Leucocyte-autoantibodies. Acta
Haematol 195820:167.
Laszlo, MD, Budapest; Michal Beiski, RN, Frances
Simon, RN, Zina Toledano, RN, Jerusalem; Carlo
LaVecchia, MD, Paola Liati, MD, Maria G Zurlo,
MD. Milan, Italy; Nina Bacracheva, MD, Sofia,
Bulgaria; Kerstin Jacobsen, RN, Maria Sandberg,
RN. Stockholm; Imelda Bayer, RN, Rosemarie
Kreuzer, RN, Dim, West Germany
Hematology Review Committee
Hermann
Heimpel, MD, Wolfgang Heit, MD, Ulm, West
Germany; Giorgio Lambertenghi-Delihers, MD,
Milan, Italy; Aaron Polliack, MD, Jerusalem
t Deceased
17.
Palva IP, Mustala OO: Drug-induced agranu
locytosis with special reference to aminophena
zone: 1 Adults. Ada Med Scand 1970;187:109-115.
18.
Westerholm B, Reizenstein P: Drug-induced
agranulocytosis, in Baker SB (ed): Correlation of
Adverse' Effects in Man With Observations in
Animals. Amsterdam, Excerpta Medica, 1971, vol
220, pp 217-221
19.
Kantero I, Mustala OO, Palva IP: Druginduced agranulocytosis with special reference to
aminophenazone: IV. Children. Acta Med Scand
1972:192327-330.
20.
Bottiger LE, Westerholm B: Drug-induced
blood dvserasias in Sweden Br Med J 1973;
3:339-3-13
21.
Bottiger LE, Westerholm B: Drug-induced
blood dyscrasias. Ada Med Scand 1979:205.457461.
22.
Bottiger LE, Bottiger B: Incidence and cause
of aplastic anemia, hemolytic anemia, agranulocy
tosis and thrombocytopenia. Add Med Scand
1981;210:475-479.
23.
Arylalkonic acid nonsteroidal antiinflamma
tory drugs (ibuprofen, fenoprofen, naproxen, tolmetin, sulindac, indomethacin): Suspected new,
rare or serious adverse drug reactions reported to
the division of drug experience: Aplastic anemia,
agranulocytosis, thrombocytopenia, in ADR High
lights. Food and Drug Administration, 1980.
24.
Israels MCG: Drug agranulocytosis and mar
row aplasia. Proc R Soc Med 1962*^5:36.
30.
Utmutato a Gyogyszerkeszitmenyek Rendelesere. Budapest, Medicina Konyukiado, 1980
31.
Nordic Statistics on Medicines, 1975-1977, Part
II.
Uppsala. Sweden, Nordic Council on Medicines,
1978. pp 17-23.
32.
Shapiro S: Agranulocytosis and pyrazolone.
Lancet 1981;1:1471
33.
Gross R. Horstmann H, Vogel J. et al: Zur
Epidemiologic und Klinik der medikamentosallergischen Agranulozytose. Med Welt 1967;
31:1767-1779.
3-1. Varonos DD, Santamouris S, Karambali S:
The incidence of dipyrone-induced agranulocytosis
in Greece during 1975. J Int Med Res 1979;
7:561-568.
35.
Bottiger LE, Westerholm B: Aplastic anemia:
I.
Incidence and aetiology. Ada Med Scand 1972;
192:315-318.
36.
Inman WH: Study of fatal bone marrow
depression with special reference to phenylbuta
zone and oxyphenbutazone Br Med J 1977;l:15001505.
37.
Canada AT Jr. Aplastic anemia after indo
methacin. N Engl J Mod 1968278:743.
38.
Frederick GR, Tanaka KR. Indomethacin and
aplastic anemia. N Engl J Med 1968:279:1290.
39.
Porzsolt F. Asbeck F, Heit W, et al: Panmielopathie nach Einnahme von Diclofenac. Dtsch Med
Wochenschr 1979;! 04.986-987.
40.
Aoki K, Fujiki M, Shumiza H, et al: Geograph
ic and ethnic differences of aplastic anemia in
humans, in Najean Y (ed): Medullary Aplasia. New
York, Masson Publishers USA Inc, 1980, pp 79-89.
41.
Szklo M, Sensenbrenner L, Markowitz J, et al:
Incidence of aplastic anemia in metropolitan Bal
timore: /X population-based study. Blood 1985;
66:115-119.
42.
Allan R, Dykes P: A study of the factors
influencing mortality rates from gastrointestinal
hemorrhage. Q J Med 1976;45:533.
43.
Levy M: Aspirin use in patients with major
upper gastrointestinal bleeding and peptic ulcer
disease. N Engl J Med 1984;290:1158-1162.
41. Coggon D, Langman MJS, Spiegelhalter D:
Aspirin, paracetamol and haematemesis and melena. Gut 198223:340-344
25.
Ruvidic R, Jelic S: Haematological aspects of
drug-induced agranulocytosis. Scand J Haematol
26.
Magis CC, Thierfelder S, Saint-Paul M, et al:
Etude serologique d’une agranulocytose allergique
a 1’amidopvrine. Nouv Rev Fr Hematol 1962;
2:602
27.
Catalogo de Especialidades Farmaceuticas.
Madrid, Consejo General de Colegios Oficiales de
Fannaceuticos, 1981, p 1570.
28.
Catalogo de Especialidades Farmaceuticas.
Madrid, Consejo General de Colegios Oficiales de
Fannaceuticos, 1983, p l287.
29.
Yosselson-Superstine S: Handbook of Drug
Information and Consultation. Jerusalem, The
Magnes Press, 1980.
■c#
ly. Parti
•nments c
» ration c
lervised b'
>ard who*
:CP, FK
M. Lund
Solothun
)le with®
rils in th
anulocyv
follows:
m
rug EpitkJ
iuel Shap’
nan, ScT^
RN, Patti
>eonardj|
International Agranulocytosis and Aplastic Anemia Study
1757
Editorial
Analgesic Risks and Pharmacoepidemiology
Knowledge of uncommon adverse drug reactions ordinarily
derives from case reports based on clinical observations. Size
limitations of clinical trials preclude identification of rare
adverse reactions.1 Yet individual case reports have two
problems. First, an observed clinical event may be coinciden
tal to a particular drug exposure, be linked to the disease
being treated, or be due to other drugs. Only in the unusual
instance when rechallenge and reappearance of the event
are described can causality be clearly inferred from a case
report. Second, individual case reports cannot generally
provide a basis for incidence estimates.1 For prospective
clinical decisions, the issue is not whether a drug might
cause a reaction, but how often this happens.
See also p 1749.
Thus, the extraordinary study of the relationship between
analgesics and aplastic anemia and agranulocytosis in this
issue of The Journal is most welcome and important.2
Because these conditions are rare, a case-control study is the
only practical means to examine their epidemiologic charac
teristics and associations. To assemble 588 carefully defined
cases at 300 hospitals involved work in seven countries by
more than 40 investigators during a four-year period.
Patients and nearly 2000 controls were interviewed to
determine drug exposures and other risk and disease factors.
Effort was made to avoid bias in case and control selection
and data collection. This enormous study sought all cases in
a total defined population of 22.3 million so that reasonable
estimates of incidence could be derived.
The study found that agranulocytosis and aplastic anemia
are indeed rare conditions with overall annual incidence
rates of 6.2 and 2.2 per million population. For agranulocyto
sis, strongly positive associations were found for phenylbu
tazones, indomethacin, and dipyrone, but their excess risks
were small, ranging from 0.2 to 1.1 per million; Considerable
variation by region in the risk ratios for dipyrone was found
and discussed, but it remains unexplained and disturbing.
While the variation may be due to differences in populations
or medical practice, one must be concerned about hidden
biases or methodological problems that could affect other
results of the study. For aplastic anemia, excess risks of 6.6
to 10.1 per million were found for phenylbutazones, diclofen
ac sodium, and indomethacin, and increasing risk for
phenylbutazones and indomethacin was found with increas
ing intensity and duration of use. While the indomethacin
results are somewhat surprising, they are consistent with
evidence from an earlier study of aplastic anemia and
agranulocytosis done by Inman'1 in the United Kingdom.
Phenylbutazone risks appear to be lower than previously
found and thus merit critical examination. The relatively
low use rates during the period of the study for many newer
nonsteroidal antiinflammatory drugs prevented the drawing
of meaningful conclusions about the relationship of these
drugs to hematologic toxicity.
Why is this study important to the clinician? First, it
examines multiple drug exposures: too often only a single
drug is studied. If defined risks are to he clinically useful,
1708
JAMA. Oct 3. 1986—Vol
'.
1
they must be available across a therapeutic drug class sc
J
that comparisons can be made. Next, though aplastic anemi flsSSsE
and agranulocytosis are rare effects of analgesics, benefit^JlAia
must always be weighed against quantified risks. Hematofc-J
logic toxicity is noted in labeling information for hundred®®?”
of drugs, yet because precise incidence data are seldo
available, clinical decisions about monitoring blood coundK£g£?
and use of drugs are based on intuitive perception of risk. K
Lest the study be misinterpreted, it must again br;
emphasized that what counts is total drug risk. Gastrointeif
tinal and other organs are far more frequently adverse 1^,:.^.
affected by analgesics than the hematologic system. Eve®ifc■
the highest rates found in the study do not greatly exceed
•.
mortality rate of five per million exposures for these drug£^®^,f
While no firm cutoff can be set for declaring any drtdSjtei';
absolutely safe, it should be recognized that when drudKgf. ■:
induced mortality is found to be below five or ten p«B&*
million, differential distinctions about the safety of one dnni^gar
compared with another will be difficult to ascertain arg/support scientifically. Thus, choices of analgesics, once
need for them is clear, should not be made solely on the basr??T;‘’of the hematologic toxicity described in this study.
The presentation of an impressive pharmacoepidemiology
study reminds us how few such studies are carried out. fl
examine risks of marketed drugs, appropriate cohorts fl
case series and comparison populations must be located ■
the community. Dealing with confounding by indication afl
other complexities of observational studies of ill patienfl
requires carefully designed approaches and sophisticate
analyses. Who will fund and conduct such studies? Usufl
sources of research support find that most pharmaceutiiij
safety issues are too mundane or are lacking in bas j
scientific significance. Regulatory bodies have few funds f W
research. The pharmaceutical industry, while not homog 1
neous, largely commits its postapproval research funds , "
clinical trials having potential for product enhancement. T, If
result is that there are few academic or industry-bas^
pharmacoepidemiologists in the United States or elsewhe®
There are no easy remedies for these funding and manpo»4|
deficiencies. Certainly the starting point is a recognitigl
that epidemiologic studies of postmarketing drug safety
in the interest of the medical community; the governntt h susceptibi
and the pharmaceutical industry. Drug development d
not stop when marketing begins. To improve drug thera
pharmacoepidemiology must be fostered and practiced.
The opinions expressed are those of the author and do not necess;
represent those of the Food and Drug .Administration.
Gerald A. Faich. MD. MPH
Office of Epidemiology and Biostatis t Indications
tgs: Serious
Center for Drugs and Biologies
lactic) reactir
Food and Drug Administration
sapy; these r
Rockville, Md
with a histoi
ais with a hit
1. Faich GA: Adverse drug reaction monitoring. .V Etytl J Mid '
cad severe i
311:1589-1592.
and vice vt
2.
The International Agranulocytosis and Aplastic Anemia Study: Ri^k
agranulocytosis and aplastic anemia: A first report of their relation to J tiquiry siioul
ty reactions
use with special reference to analgesics. JAMA 1986;256:1719-1757.
ergens.
3.
Inman WHW: Study of fatal hone marrow depression with sp
’
SANAPHYL
reference to phenylbutazone and oxvphenbutazone. Hr Mid J 1977;1 1;
EMERGENCY
1505.
N. INtRAVI
EMEN I INC
■ ts.Vf ■
BG. feAN N (
'T)/- fin&vvt'
be
^(tjt<oPvicr>J
\.: ..
'
.1
generic .-rsnr o'.’ An tiffin
. oJoii
]>?riv >.tivo.
Orc It .
Ofier
Dinyrone, ilnt r.itol,
Methapyrone, Sul,'urine m i I'• t nn.i. lopyrino io'.'tinosulfonate Solium.
A group of compose 1:: c-J'ol winonh'-:. ronq
is close congener of Aniloin. Aminophen iron • is
also known 'i:; Dipyrine, Aminopyrino, Ami Jon • >.:>e,
Amidonyranolinn, Amidofabrin. The two grov.; . of ■
drugs have similar pharmacologic al and toxica logical
properties,
including the gotonti il
agranulocytosis.
soluble and
to ctur. ?
fatal
Anilgin 1 iffern only in ' .r ; :>•; more
iv ill iblc Cor r irontere.1 admini s tr ition.
Aminophenazone/Amidopyrine v/as. use 1 for 70
years for its potent not i infl nnm-jCary m l ■ Igesic.
action. But early in the thirties, it was found
that Amidopyrine causes agreimilocytocis; and was
identified .as a major cause of Irug-induced .igranulocytosisrf It was therefore placed under prascription
control by the P.O. A. of the U.S.A. in 19 33. /I/.
With the advent of better, safer • antiinflamm it.ary,analgesic agents, this drug gradually fell i. to disuse.
But in India, it was widely sold by drug companies
till fixed lose combination of •■midopynine •.-ns banned
bv the Drug Controller of In ilia from 31st Or cober 1982
Tn 1979-8.0, .95.tonnes ( I ) of amidopyrine was
imported in India.
ANALGIN, which is the sodium sulfonate
derivative of this notorious Amiodopyrine, was
introduced by Hoechst in 1922. Since 1931, the
group of pyrozolones to which Analgin belongs, has
been suspected of causing agranulocrytosis, and in
1934 this connection ' w-as proved. Yet till the 1960’s
this drag was widely used. But evidence accumulated
in respect of.Analgin-induced agranulocytosis and
hence gradually this drug was also discarded in the
West in 1960-70*s ( Swedent Norway, Australia, NewZealand, U.S. Canada.. . etcJj^Thus in the 1.9"Z5 edn.
of the aMa Drug Ev.ilu-.rtlons, American Physicians
we re to Id s
rnf.ort
' Its only -jn.'L.i. Ci. ib.i > n.-c j ... ir
reduce fever •vbern sifer measures have failed.
Because cH?y.r->ne rnv.- . roduco f it J ngranulot ■Otheir bl >r> 1 lyscras.l.•:
, :| p-- ,!fu; ;1 rr.
1.1. ■ u ■ ; , > I
, r1 i | r. #
c ?.nnou be con lone.], "
I
19 7 /■-■? I i. !• > 0.1
, ,,
. ,
,
mi. |r. ,
( .. _ p;p—pc>7. ) "
O’
,
11-1 ;rj
V • !• I
lr
the U.S.A. (
in the J9yQ edition,
.341 ).
not even listed.
h.i become ob.ee le‘ n in
i'
From 196r, o:r->ir-ln it was •■
or banned in :.i my cotin trier.
.cold in India
-z
. =
-s- war. st ite-! tn-t the
in large
is
: Jr-awn
i.t contin
m > > i ii>,! vs<->’
trivial
reasons.
It is also avail ihj. j Ln Iroos ( ’• J t j ioi>- )
arid is include-; i.-.
of tv.-i oyxt? Sf«Sv'ic.^cs~
I.
Baralgan;-Trigdn, Maxigan, So l5(llLsol. . .etc.)
Analgin induced aqranuloc'-tonis :
Agranulocytosis is the most import nt
adverse reaction of An ilgin.y
• 3>The incidence of aminopyrinc : in-l:ccd agranulo
cytoslri has boon variously estimate.! between 0.01 %
and 0.86 %pthe mortality rate being 20% - 50%. /S’/.
p'
____
Exact mech inism of trits disease
is not knovni. It is likely that the antibodies
resulting •from the drug allergy destroy the rhite
cells in the peripheral blood and probably in the bone
marrow too. It could also be duo to development ,
of luous syndrome ( a systemic illness chara
cterised by skin lesions where antibodies produced,
damage the patient's ovm tissues. ) The third
theory being toxic depression of bone rnarrov;
■resulting from ..9F0longed administration of a drug.
The possibilities of occurance of agranu
locytosis are greater in adult s above age of 40
than in men.
/ 4/
■years-and more often in women
vi
10 <
Vo
sP
I
The clinical symptoms ofYfejafls-iifhHggrse are[ !r*'“
onset of abrupt high fever, rigors, occasional
evidence of acute localised infections like :
pharyngitis or an abcess.
Patient may even die
due to infection.- If patient survivor- tho i ■ fa
ction, ihen ho/she could ho c-ro.l within 2-3 •.,o?ks
of complete withdrawal of the drug.
Evon <•' tor
recovery tho sensitivity jaor.u.sts for lone; ueriods
long' is
vi
-ts com i-.ham i.o. if tho ■ 'tient
takes this drug rg lin ’ tho
. of the Bureau of
i Luo 1:0 will pro-
)rtigs in tho n.c.
tly
found th it
" agranulocytosis c innot he • •foe tivoly pr^v •
’ by
frequent ex uni notion of treat '.i patients sLrico this
condition can occur
t' i in ■ cow hours fol lo --’. zi admi—
-nistrition of this drug to i sr' i’.ti.vo ii liv’ 1-ial. /5/„
Boston Study ( Intern ition ?.l / \-;r inulocy to.-i.p > . 1
X.-S
Aplastic Anomi
Estimates of the ill. -nd ml: ri..-,k of
gr -nu-
locytosis very considerably an i a l.-irge multicnntric.
stO.dy was 'planned to provide i more precise o.-• himate.
./m
Thi;,oaso
control study of drug induced agr mulocytosis, with
particular emphasis.on nyrozolones ( including
Filipyrone ).
Tho c‘”. iy
coyered !a population of 22.4 million people from Israel,
/test Berlin, Milan, Barcolon •, Budapest, Sof.i ., Stockholm .
and an area around Ulm. The data jwas- collected for
a period of five years. ----- - --------—:------------------------------■
It is a little misleading to c .11 this study is
Boston study since only the data of this study were
apalysed.^at Boston. It was primarily fin incc-1 by
Hoechst, with some finding help from Hungary and
Bulgaria and Sweden. We, therefore, call it as
Hoechst Study. Hoechst and other manufacturers are
misusing the findings of this study to create on
impression that, this study has proved that Analgin
is not more hazardous than other analgestics. But it
should be point-.d out that though source of the earlie r
estimates can be faulted anl were overestimates, the
data, the analysis and conclusions of this ISAAAstudy and also- highly controversial; and this study
is in no way conclusive.
■
‘-'raar. ..-s-r.i-ry-nTnr-r-JTTTrr'iiiHHciaTtiyrrn'arnd-jj w
Limitations
of,■•—nthe
ISAAA-studv s
1
ull
Dr, A.Horxhedmer of Charing Cross Hospital
Medical School, UK and Dr. John YudJcin have pointed
oat that the study does not provide the trae incidence
of drug induced adranulocytosis, because w the study
excludes all patients Cap who die of agranulocytosis
without, receiving medical care, (b) who die of it
without having a white cell count and (a) who have
undiagnosed agranulocytosis and recover from it.,«S
Thus according to then the study would yield only a
•minimum estimate’ of both 8 incidence & morality*
while the ’actual incidence could be higher.
Dr. Willbert Bannenberg has pointed out many
other* limitations of this study-6.
(Contd....
1
S’"
* The study does not look into other side/e£f acts of
"
dipyrone such a .3 shock;, hypotension. Urti
caria, Lyell syndrome, Moscowitz syndrome-.etct “he data in the intermediate results published in the
Lancet (25th l?eb9B4) and those in tie final
report are inconsistent- There is a three
fold increase in the use of Analgin in the
control group in the final report as compared
to the intermediate report .
*' Whereas 400 cases of agranulocytosis were required to
assess the risk properly, in the final analysis,
due to a large percentage of exclusions, only
221 cases are analysed in the final report-
* There .is extreme variability in the incidence of
agranulocytosis not only amongst different
countries but even between community and
hospital cases in the same countries0 The
group is propebly not representative of the
general population. 27% of them mentioned the use of an
analgesic! the weak before their interview I A
higher consumption of analgesics in the control leads
to a lower figure of relative risk.
n
tiSome data are clearly unreliable, For example, the data
collected through interviews indicated that the consumption
of pyjizolone in Isrel was 5 times more than in other
countries, whereas the Index of Medical Specialities (IMS)
Sales data shows that Israel actually uses 3 to 4 times
less dipyrone ° - the difference in these two data is
tr®nty-f'“■’-d
I
'
It may bo mentioned that one of ths two chiefinvestigates and its study—director, Prof. M.Levy was
blasted in favour of Analgin. This is clearly seen in
‘his paper 8 “Adverse Drug Reactions to Analgesic Antipyretic Drugs.13 This pq?or, circulated Joy Hoechst.
starts by claiming (on page No-1) that w °ipyrone is
widely used in many countries, including numerous
countries where medical knowledge and practice are well
advanced.” But it does not mention that it is banned
or withdrawn or severely restricted in developed countries
like s Australia, USA, UK, Greeae, Denmark, Norway,
Sweden, West Germany, Japan, In this paper, prof.
Levy likewise, selectively gives facts and figures
which favour the continued use of Analgin,
£jisi® 3 d Ing, j > rpp a-ga nd a s
Thus this so called Boston-Study is by no
means conclusive. Secondly, even the results of this
controvdrsial study ar*? being propagated by Hoechst in
a misleading manner, Hoechst claims that this study has
shown that the .risk of agranulocytosis due to Analgin
is only 1 in 1 million. It must be noted that this
risk of 1 in 1 million exists if one or more tablets
are taken in one week only, If dipyrons is ussd for
longer' periods, the risks will be greater, This was
confirmed by Shapiro, the epidemiologist and Admini
strative Director of this study, during the pressconference Ln Stockholm. Wilbert Bannenbergt7/has
estimated the risk ©S a^of 1 case of agranulocytosis
per 70000 packages of dipyrone—an estimate based on
the data of this Hocchsto-Study; but one which takes
into account the usual pattern of consumption of
analgin and hence is a more appropriate way of quoting
risk figures. LancQt has also pointed out. that ” The
estimate of the excess risk from dipyrone is expressed
rather oddly, as 1,1 per million takers during a seven
day interval. The calculation underlying this estimate
is not explained, The peculiar denominator is difficult
to apply to real life. The risk of exposure during
on® year could ba upto 50 times higher, It would be
expressed mor® clearly as the number of cases per
million defined daily doses (DDD) or per 100,000 packs
aold,""^®^ On 19th Oct’86, the Gernam Padcx'al Health
Office (BGA) conducted its second hearing on the risks
an3 benefits of dipyrone. In this hearing also the
present! ng of risks in the odd may of so many million
takers per week was criticized toy many scientists.
After expressing the risk in usual terms, the risk was
estimated to bejiin 30,000 to 1 in 70,000 per usor and
year. The speaker of the FRG*s Pharmacists Association
concluded that it took him a long time to understand that
the risk of agranulocytosis is as high as it was
_a
already estimated in the .1901 hearing.
Even if we accppt the controversialminimum
risk of agranulocytosis as given by this Hoechst-study,
we get 7000 cases of analgin-induced agranulocytosis
per year because every year, according to Hoechst, about
10000 tonnes of Analgin is consumed in the world, more
than 25 tonnes a day J, The mortality in agranulocytosis
in Europe, Eastern-bloc]: countries and third-world is
around 10%, 25% and 50% respectively. This means 1500 to
2000 deaths per year due to Analgin induced agranulo
cytosis 8!J^
Aqramilogytoals-ln Xndjat
Many medical practitioners say that they have
used plenty of analgin for years, but have not came
across a single case of agranulocytosis. This is because
of the fact that by and large, cases of agranulocytosis
go undetected in India. The clinical picture of agranu
locytosis abrupt onset of high fever, throat-pain,
rigors, occasional evidence of acute localized infectionis difficult to distinguish from that of infective fever,
so commonly found in India. The patient may recover
•spontaneously or die of fulminating infection, without
being investigated haematologically. Since the onset
of agranulocytosis is not immediate, it is hardly ever
suspected.
induced agranulocytosis does occur in
India,, One has to only look for it systematically.
i'his is what is being done, by Prof. B.C. Mehta., the
leading haema to legist from eombay. ,Je has communicated
his experience “ Xn my haematological-practiae,
X encounter 12-15 cases of agranulocytosis in a year.
Of these, 10-12 cases are caused by Dipyrone er Dipyrone
containing drugs.Dr.. Mehta has estimated that
even assuming the risk estimation of the Hoechst-study
to be correct? in India, one person develops Analgin—
induced agranulocytosis per day.
coMHM®'* ”3. Ma,k. «<■»->
~g-
"'’•‘"'SoM-WOW’
Risk ch io to Aspirin, Paracetamol ; md Analgin s
Hoechst has tried to create an impression that all
^on~sUu>AX»xaa.i /-.rci-inf lammatory Drugs ( NSAID ) cause
agranulocytosis, and there! is nothing special about
dipyrone.'”"^
Even Prof .1-1. Levy has also tried to
argue in this fashions ( in his paper mentioned earlier).
He has even quoted, uncritically, one estimate v.iiich
says that paracetamal induced agranulocytosis may
account for as much as 10% of all cases of this dis
order. ®ut the fact is that none of the standard
sources seriously implicate Aspirin., paracetamol in
the causation oif agranulocytosis. Even in this HoechstStudy, the relative risk (relative to not taking the
drug ) of different analgesics for causing agranulo
cytosis shows a vast difference between Analgin and
other minor analgesias. The following table gives
the relative risk as found in this study s—
Relative Risk of Agranulocytosis’
Name of the Drug
After any exposure to the drug
DipyrCiiie (in Ulna,
Berlin,. Barcelona
Centres).
Dipyrone (in Israel,
Budapest Centre?) «
Solleyletss
...
Paracetamol
...
Butazones
...
Indomathacin
...
Other JISAIS
... .
for three or
mors lay’;
23 .7
20.-1
0.8
1.6
1.0
3.8
8.9
0.9
1.2
1.9
0.8
6.3
14.2
0.6
12
It has been argued by Prof. Levy (Adverse
drug reactions...op.Git.p.3 to 5) that Aspirin, also
causes death on a/c of its nephrotoxicity and by causing
acute gastrointestinal bleeding. But he conveniently
forgets that to a varying extent, all NSAIO# cause
nephropathy and gastric bleeding. (Gastric bleeding
is partly due :o the systemic effect of the anti
prostaglandin effect of NSAIDs and even injectable
Analgin can also cause gastiic bleeding?) Secondly,
the risk due aspirin induced gastric bleeding or
the risk, due to Peye’s Syndrome can be considerably
reduced by avoiding its use in susceptible patients,
whereas analgin induced agranulocytosis is unpredictable
and unpxeventable. Similarly accidental oc suicidal
poisoning due to paracetamol overdosage cancot be
compared to the risk associated with Analgin.
Qthfir side—Effects of
Analgin
a—
€• 0000 0 00 0 €>000
Injectable dipyrone can cause severe
hypotension, as x7e.ll as anaphylactic shock and for this
reason, injectable preparations for dosages higher
than 1 gm., and intravenous preparations have been
,.1,
withdrawn from Italy, Saudi-Arabia and Egypt.
In
many developed countries, analgin in any form is not
marketed at all (see later.) It may bo noted that
the German Federal Health Office recorded 9 4 lethal
cases after intake of dipyrone in FRG from July*81 to
-July* 86? Out of these 46 deaths were due to ha emo tological reactions whereas 39 deaths were due to
-14
.allergic reactions.
Dinvrone can also aggravate a bleeding
’tendency'or prothrombin deficiency. It is contrain
dicated for* use with chlorpromazine as it can cause
..
, —15
♦
severa hypothermia.,
There are seme other problems with Analgin
--'16
'
as enlisted by Uannenberg.
'•______________________ __ _______
>
—1—1 "
/Genuine ther^beuttc need ?
I
/Analgin is a very potent antiinflammatory
analgesic/ antipyretic.
But no^v safer, powerful agents
are ava^lbble v-ith the advent/f propionicyacid derivativ
( Xlauprofen, Ketoprofen.. ."etcTt
" even after ICO years of use, the mode of
action is still unknow.
-unknown is also which metabolite causes
agranulocytosis or other side-effects ( and how.) It is
known, for example, that the drug aminophenazone, banned
■jorldwJ.de because of severe side—effects, has some simil ar
metabolites as dipyroncs does this mean that dipyrone
metabolites cause the same side-effects .?
-basic pharmacology data ( e.g. use in renal,
liver, or elderly patients J carcinogenicity, terato
genicity are not yet known, as it was developed before
the 8thalidomide scandal8 and could therefore get easier
registration.
-there axo 2 Japanese reports that link
dipyrone to a significant increase in hepatoma toxicity
studies with mice. Hoechst has never challenged these
reports«>
-Interactions with other drugs such as anti
diabetics Have never been investigatedooo.
Analgin is a very potent antiinflammatory
analgesic, antipyratic. But now safer, powerful agents
are available with the advent of propionic acid deriva
tives ( Ibuprofen, 1'etoprofen.. .etc.)<i V9"* G"r^
Ijii
j | I
When parenteral analgesic is required
for acute, severe pain, Inj. pentazocine 5( Portwin)
a very potent, safer analgesic is now available.
Many surgeons in India novz use Pentazocine ( long
’.dth stemetil/slquil to prevent pentazocine induced
vomiting ) postoperatlvely. ( Most doctors do not
aPPly for registration to get morphine, pethidine.)6^^
■.
yobv.-t" <suAjr^zv-->Vs?
"f-—fez..
zz..o-^?\s v\?.
z-Vz.
v-.z-j
.— .d
(Oi- s.—<+° V<'v aaer<x~—
It nas been argued that --nJ« Baralgan, 4«
KSBenfcialxtoxtrsrctxrenoixGciliE which contains Analgin plu
a spasmolytic agent, is essential to treat renal colic.
But the canbination of Inj. Pentazocine with, Injection
Buscopan is used by many doctors with equally good
results B It may be noted that in mai?.y countrl.es
Analgin, Saralgan are not marketed, yet the doctors
there successfully treat such cases. Same is the
capa with post-operative and other such cases of acute,
severe pain. Thus there is no merit in the argument
that analgin is essential to treat such caseso
Hoechst has been claiming that Analgin
has an antispasmodic action and hence Analgin-containing
Baralgan is more effective. This claim has not been
scientifically substantiated. When Association for
,,
H
z
r----------------Consumer Action for Safety and *aealth ( ACASH J^asked
Hoechst to provide reference-papers to scientifically
back up this claim, Hoechst did so only after a lot of
prodding by £'.CASH. These reference-papers were given
bv ACASH to leading Pharmacologists in Bombay and Baroda.
All these experts afciticisod these papers. For examples
Satoskar, the author of the Textbook of Pharmacology
stated that only 8 B..«ona reference indicates that
dlwyrone has smooth muscle activity. This reference is
Of: 195(5 ...The references do not give any comparison
between various NSAIDS as regards this property.....
Dr, Shallgrajn, professor of Pharmacology, Grant Medical
College, Bombay commented s '’.....(this reference) is
published in current Therapeutic Research—a journal
knowfii to publish anything from rubbish to sublime....”
About a second set of references provided by Hoechst,
L:'.r.of» ^haligx'am had this to say-—This is the most
unscientific of reviews. The author’s claim regarding
spasmolytic effect ( of dipyrone )’ is empirical and
l?cks details required for verifying the authenticity.
It. is no wonder, therefore# that none of the standard
textbooks of Pharmacology mention about any spasmolytic
action of dipyrone.
Some doctors feel that injectable Analgin
is necessary to reduce high fever. This is not true.
Oral aspirin# paracetamol and cold sponging is quite
effective. In case of hyperpyrexia# ice-cold sponging,
ice-cold enema, rehydration is more important than drugs?
hyperpyrexia can not be countered with anti-prostaglandin
effect of these drugs.
I! ■
Conclusion 3
///o have to conclude that since the risks
associated, with use of analgin are of very serious nature
and since there are now better substitutes available.
Analgin should. no more be used. That is why standard
authorities have, over a period of time, cast their
opinion against the continued use of Analgin. According
to the 5th edition of Goodman-Gillman, antipyrine, dipyrone
can be used in certain cases. Xn some cases of prolonged
intractable fever, as in Hoogkin*s disease and Periarteritis
nodosa, they are capable of controlling the disability and
<.'17
may be justified. "
Even in such cases they should be
employed only after safer drugs and other measures have
proven ineffective. They should be used under proper
supervision and monitoring, ^^he F.D.A. of U.S,, regards
that 11 true risk associated, with this drug farjany benefit
derived from its nee, including use in Hodgkin s disease
end similar malignant diseases.” ~"S The 7th edition (1985)
cf Goodman-Gillman doos not mention this use of Analgin.
A,-it inn taken in other countries s
Analgin has baen
prohibited, withdrawn or not. available in Australia, U.S.A.
t,K., Denmark, Norway, Sweden, Venezuela, Singapur and is
under restricted use, strictly under prescription, in
I srael, West Germany, Saudi Arabia, Japan, Phi Llippines,
Peru, Greece, Mexico,
Following reports of anaphylactic shock,
Italy, Egypt, Saudi Arabia, have prohibited meinufacture of injectable preparations with dos-ges
higher than 1 m and intravenous preparation-.:.
Au cA-o'i-/
& dear, prescriher, would you keep y risking
your patients' life for such low medical benefit of
using Analgin ? Certainly not; Please STOP USING
ANALGIN in any form. Ask the Government’ to ban this
obsolete drag.
STOP USING.ANT GF THESE DRUGS s
Av if ortan,
■
Bax-algan.,
Codol3 ic.
Ana Igin,
Novalgin,
Novalgin-quinine,
Paraagina,
Promalgin,
Sedyn-A-Forte0
UItragin,
Zimalgin-A,
Esgipyrin,
Ki Inane,
Oxalgin,
Spasniaol,
Spasmolysin,
Spalcin,
Buscopan-compositum,
Orphalgin,
Symalgesic,
Algesin—0 . . « . e ccJo >... etc...
REFERENCES;
h'HO Drug information, Jan-Mar'77 s PDT/DI/77.1
Goodman-Gillman, The E’harmacological Basis of “herapeutics,
!5th Bdn. 1975, p.347, 343.
* Consolidated List of I’roducts whose consumption and/or
sale have been banned, withdrawn, severely restricted or
:aot approved by Govt." United Nations, Ilnd issue,'86, 62.
Huguley C.M.Jr.Agranulocytosis induced by Dipyrone, J.A.M.A
1964, 189 3 933-941.
■Jr. Sunil JhParekh, Agranulocytosis - Diagnosis, Management
and Pathogenesis.
1J»N. Consolidated list, op. cit» p-62.
■filbert Bannenberg, Dipyrone, Hoechst & the Boston Study,
miraeo, Health Action International, Oct*06, reprinted in
the Medico Friend Circle Bulletin, Deer.’86.
(Ctd.
7)
8)
9)
Bannenberg, op. cit.
Lancet, Octo. 18, 1986, p.899—900
PHARMA BRIEF, Health Action
International (Dj,
10$
Letter from Dr. B.C. Mehta to the. Editor,
Journal of Association of Physicians of
India (J.A.P.I.) s 19.5.84, Ngst
11)
How safe is a safe drug 1 HOQChst A.G.,
Frankfurt, p.6
SCRIP, No.1128, August 13, 1986, p.23.
(report of the ISAAA-study)
UN Consolidated List, op.ait. pp-52, 63
PHARMA BRIEF op. ait. p.3
Goodman-Giliman (ad.)! The Pharme.eelogical
basis of Therapeutics, Sth Edn.1975,
p. 347-340.
W. Bannenberg, op. ci t.
Goodrr.a n-Glllman, op .cit.
UN Consolidated list, op.cit. p-61
UN Consolidated list,, op.cit. p-62.,
Fortyfour problem drugs, International
Organization of Consumers’« Union (IOCU),
Penang, Malas-a, 1981, p.36.
12)
13)
14)
IS)
1.6)
17)
18)
19)
l \ 7 G( }->. 3 .
.
JM
tv\J.f^~ eceWIfDecl^ «, A«fen
ArtXfi^.
} HAT
ANALGIN—A STUDY
1
F«a'R
L>
P
. The, Drug
A class of chemicals called PYRAZOLONES have been used
as medicines for over ninety years. Pyrazolones include
drugs like Antipyrine, Aminopyrine, Phenylbut'zone,
oxyphenbutazone, sulfinpyrazone and a derivative of
aminopyrine called dipyrone or analgin. The pyrazolones
share similar pain killing, fever reducing, inflammation
reducing and also toxic properties. Analgin being more water
soluble is amenable to use in injections and liquid oral
preparations (for children). They are rapidly absorbed in the
stomach and intestine and spread in various tissues of the
body in proportion to their water content. While 30 to 40%
of the drug is altered in the liver and eliminated in the urine
5% is eliminated unaltered. The fate of a significant fraction
is not known.
The range of actions of Pyrazolones is similar to that of
Salicylates (Aspirins) except in reducing fever in diseases
like Hodgkins disease and Periarteritis nodosa, whore aspirins
are not completely effective.
The most important and potentially fatal adverse effect
of Pyrazolones (Analgin) is Agranulocytosis. This is a
condition where the Granulocytes which form the major part
of the white blood cell population and are the first line
of the body's defence against infection are destroyed.
It is an allergic reaction and can occur suddenly even after
a fraction of a dose in any person who has been previously
taking Analgin with no bad effects. Within 6 to 24 hours,
the white blood cell count fall and granulocytes disappear
from the blood. They start reappearing 5 to 10 days after
the drug is discontinued and rapid recovery occurs.
The incidence of agranulocytosis has been variously estimated
from 0.01% to O.BS/o. If infection occurs now, it starts
as a sore throat of sudden onset, high fever and prostration,
which even on proper treatment carries a mortality of
20 to 50%.
The other adverse effects of Analgin documented in a study
are: skin rashes, dyspepsia, fever, analphylactic shock
and bronchospasm. Analgin can aggravate a bleeding tendency
and produces a serious fall in body temperature when given
along with Chlorpromazine. Liver cancer in mice has also
been reported by Japanese.
2
Even nou—
a.
b.
which arc the metabolites which cause agranulocytosis
.and how is not known;
c.
basic pharmacological data, like potential for
causing cancer, congenital malformations, kidney
and liver damage and damage in elderly patients
are not known;
•
d.
2.
,
the mode of action is not' known;
interactions with other drugs for diabetes,
hypertension etc., hav
not been investigated
bacause pyrazolones were introduced in the
pre-Thalidomide era when registration was easy.
History and _present status
1897
Aminopyrine was first introduced and bec.ame very
popular in 1920s for pain killing and f-’ver. By 1930s
its use was world wide.
1922
Agranulocytosis was first described by U. Schulz
1922
Oipyrene or Analgin was introduced by Hoechst. Not
being recognised as a derivativa.of Aminopyrine,
it gained popular use.
1933
Madison and Squier established a causal relation
between Amidopyrine and agranulocytosis.
1935
Kracke and Parker established its relationship to
agranulocytosis beyond doubt
1938
O.T.C.
19551959
The American Medical Association Registry on
Adverse Reactions recorded only 10 reports of
leucopenia (fall in UBC count) and none in children.
19601964
18 cases reported (7 children).
An increase in the import into USA of dipyrone
from nil in 1958 to 18,879 lbs in 1962 was noticed.
1964
American Council of Drugs—Section One: adverse
reactions: studied the case of Dipyrone (Analgin)
and quastioned the justification of continued use
of this drug.
sale in U.S.A,
was prohibited.
. . . .3
3
1960
Great Bri tian and Canada revoked the licence of
Dipyrone
1965
Australia and Nou Zealand issued an import ban
on dipyrone
1974
Sueden revoked Dipyrone licence
1976
Noruay revoked Dipyrone licence
1977
USA revoked Dipyrona liceneo
Japan banned free D.T.C. sals
197B
Ireland and Singapore revoked licence of dipyrone
1979
Denmark revoked licence of Dipyrone
19801904
An international study for agranulocytosis and
aplastic anaemia was done in Europe—called the
Boston Study, since coordination and data analysis uas
done at the Drug Epidemiology Unit at Boston.
This uas primarily financed by Hoechst, and the results
published in the JAMA of Oct 1986.
1983
The Government of India banned tho manufacture and
sale of Amidopyrine
1986
Malaysia banned dipyrone.
FRG banned DTC sale
In Netherlands, Dipyrone use is only allowed
for uncontrollable fever.
Following reports of anaphylactic shock, Italy, Egypt and
Saudi Arabia have prohibited manufacture of injectible
preparations.
3.
i.
TJ1B.
sue s_
According to Hoechst, approximately 25 tonnes or
18.5 million doses of Novalgin. are used uorld wide
everyday. With most of the developed nations banning
or restricting its use, it is obvious that it is sold
mainly in third uorld countries.
The countries which have banned Dipyrone have been
managing pain without Dipyrone by using equally
effective and safe analgesics.
4
4
The 'Boston Study' generated a lot of controversy.
since Hoochs t used ths results even before publication
for a misleading advertisement campaign showing the
occurrence to ba 1 per million. The hearing of
the German Federal
Health Office finally confirmed
the assumption of 1 per 30,000 to 60,000 to be
nearer the mark, or one tablet per 70,000 consumed
could cause agranulocytosis based on this same study.
The limitations of this study are that—
a.
it excludes all patients
i.
who die of agranulocytosis without
receiving medical aid;
ii.
who die without having a white cell count; and
who
iii.
have undiagnosed agranulocytosis and
recover from it.
iii.
b.
it does not look into other side effects
of dipyrone, like shock, fall in BP, Urticaria
etc.
c.
the data presented in the intermediate and final
reports are inconsistant
d.
whereas 400 cases of agranulocytosis were
registered to a sess risk properly, only 221
cases were analysed in the final report; "
e.
thare is extreme variability in data between
different countries and aven within the same
country; and
f.
some data wore seen to be clearly unreliable.
references contd...from page 6
9.
(
The findings of the controversial 'Boston Study' is being
utilised by Hoechst the largest manufacturer of.
Analgin for sales promotion in Germany, Eastern Bloc
countries and the Third World.' Unethical propaganda
practices with diff rent types of promotional literature
in different countries is being practiced. Even claims
of anti-spasmodic action which is not scientifically
substantiated is being made. Any source of detailed
scientific literature is virtually non-existant beyond
the literature supplied by the drug companies.
Drug marketing in the Third World: Beneath
the Cosmetic Reforms, Lancet, 7 Jan 1986,
Trisha Greemhalgh.
,
...5
5
iv.
Since 1985, Dipyrone (Analgin) has not found mention
in any standard medical text books, except for naming
it as a drug which can causo agranulocytosis.
v.
Even in our country, medical student' do not learn
about analgin while doing their Pharmacology.
4 • JLD_JLCLE!A.€L
i.
In 1983, the Government of India banned the manufacture
and sale of amidopyrine- but not dipyrone. The Drugs
Consultative Committee had recommended ban on FDCs
of dipyrone also but this seems to have'slipped from
the banned list.
ii.
The government is the largest manufacturer of dipyrone
in this country.
iii.
Analgin is among the largest selling analgesics in the
country with sales figures accounting for Rs 70 million.
There are approximately 200 formulations containing
Analgin, including injoctibles and drops for newborns
and infants for colic.
iv.
Analgin is available as OTC in spite of its being a
Schedule H druo in our country and the attitude of
the proscribing doctors as per a study (Lancet 86)
was "if I prescribe it 30 times a day and it is
available over the counter, it mi st be safe,". In a
field study (Lancet 86) it was seen that the pyfzolones
made up the majority of both GP prescriptions and OTC
salas of analgesics. One more of these drugs were given
to over 50% of patients requesting an analgesic.
v-
Drug action groups have initiated a campaign on Analgin
especially at ACASH, Bombay, OAF-West Bengal and AIDAN,
Neu Delhi.
vi.
Analgin induced agranulocytosis does occur in India,
especially if one looks for it systematically as a
Bombay haematologist BC Mahta has done. He reports
12-15 cases of agranulocytosis a year, of which 10-12
are caused by Dipyrone or Dipyrone containing drugs.
Evan by the risk estimation of .the Boston Study, in
India, one person develops analgin induced agranulocytosis
per day by other reasonable estimates, it could be
15 times this figure.
references from page 5 contd..
• a . ■ « 6
Dangerous and Inappropriate Drugs, Lancet,
28 Oune 1986, MOS Langman.
11.
A BUKO Campaign—A Drug Campaign Newsletter, mfc
Rational Drug Policy Cell, 1985.
12. The Hoochst Medical Bulletin, Issue No.8.
10.
,
6
5. Mider Issues
Doveloping countries like ours arc ill placed to afford
expensive and useless health care products and definitely
not the frankly dangerous ones.
Me have unsophisticated consumers and poorly developed
regulatory and advisory systems—this is fertile ground
for pharmaceutical companies to indulge in unacceptable
practices .
The vast majority of rural doctors working in professional
isolation have no access to independent information on
drugs they prescribe. Here, the representative of the
,
pharmaceutical company who is ill-informed himself and
paid by commission on drug sales becomes an id -al tool to
promote the interests of the Pharmaceutical company.
Thus, it appears that the consumer is at the mercy of drug
manufacturers. Other than an appeal to the Food and Drugs
Administration
the Central Government and ths MRTP
Commission the consumer is virtually without recourse to
any independent body such as tho judiciary. The 03 Hospital
Commission (Lentin Commission) enquiry reveals the ineffective
ness of those agencies. The Consumer Protection Act of 1986 is
expected to offer some hope.
In effect only a public outcry by the consumer can force
voluntary withdrawal by or reform by drug companies.
--S P TEKUR, Community Health Cell
4 7/1 St Mark's Road, Bangalore 560001
References:
1.
The Pharmacological Basis of Therapeutics,
Goodman and Gillman, 5th Ed., 1975.
2.
Review of Medical Pharmacology, Meyers,
6th Ed., 1978.
3.
Agranulocytosis induced by Dipyrone, a Hazardous
antipuretic and analgesic, Charles M Huguley Or.,
3AMA 21 Sept 1964.
Oawetz, Goldfien,
Risks of agranulocytosis and aplastic anaemia—A first
report of the International Agranulocytosis and Aplastic
Anaemia study, 3AMA 3 Oct 1986.
5.
Analgin... Pain Killers or Man Killers? Indian Express
24 Oct 1987
6. Mhy analgin should be banned—a bit of history, Anant Phadke
7.
Counterfact on Analgin (an untold story), Drug Disease
Doctor Vol 3, No.4, 1988—Arun Bal and Anil Pilgaonkar
8.
Dipyrone, Hoochst and the Boston Study, mfc Bulletin
Dec 1986, Milbert Bannenberg.
4.
—references contd....page 5
46. 5
**A '4
Amavgi/j pg
-a- nopy
■
---5 <■$
_4_ 1 _ fc Amalfi w *„T
- |§_£VA
4A cl&^
|
ee^cdc
PyR.AzoL0^e^
k^v^- b-eg44/ nzve4 <?vC vv\&dd&C w<^5
ovc^ MAe^y v^€«rr .
PyA^vg^tpw^ AkvoLvcX<g/ dy'^-y Ulc& At^ri pyj^ifoe^ AMiNOPyRiMe,
PPL-Nyu fiuTAZOKie ; ^yypHe^/^uTAzohjp, £vl.P)tjP'ypaz&avet Md
a <4cawzM<c^
c^lzcd. b)pypc>K/p oyj ' - AaMA|^.
ItvC'
<,Pu7i/i,o r^vkv^wv pAw'kZllwiy,
•
ZVvlA,
.^VfW- /C^AvvOI/A^ . Avv^C^PVi7v-i/A;^y(yVi/ -zvt Awcwv^■d/pi'dty
avv tM'
<AmMv CVwzX. zMAcstvvve- cvkA- S.p/M(h.d Aw uzM/ims
bvCSviZS (?{
tV\.C' b~C>d/y /WI/
tv<Tw tv
l/JcCtv\.. Cvydevtt.
$0 to li'O^o 0^ 'ttvd (jCwcQ- 4s (Xylte^vc-vC -vuu tt\.c Pk/^'V1 ix^\ct
ctvwvvv^fZ^L aAi tG<z U'Wukvc-1
As GtvvwAu7vtect Wnzvic^e.^/.
focXVVvt jv«(A<W VS wt kvWWiTW.
-vt-r • Am/^VSX 'Vt
_.
f
/^V€-
'VCM/^
xc
C>^
GtvwitcVt to t L v,<xt (>i
> M\
/VX A-VtCAwi
■vffy .tcv-vv Aw Avseev axs
AeMMplPd&L£>
Akx ^<A^4cwvs <4Cs€zCzx- Pwurl
kuvJ^Sc'G iAIaXul
M^xwAaS OM kvot Cow^> letcty
>5
/Vi/vup^t^WiZ' Avv<{
0-1
]/\G^PJ\l\IVLOCy~TO^IS*
G^RJXNUl-OC'^'X^
/Ma aS Ct 0<7wd/utCc»v wMw<s tp^c-
wPvvoVv
jy-Vyv ~tbx& l*VV^i/U
C^-lC ptTI^'VxZ-Ct'tcC'Vv
Uzw-a
0</\c.' L'tzyz.-'
Aw^> cic-iWeny^^.
It As cvv
SA/uAcAe/wby
tC\^& kV/'v'vfz fitcc~i\-
\c.(^cd?ovZ at^(L caa^i &ca^
^U^W" Ct^
h/t vo Gv^VS z(3'€Z/v'V 4>a
AU/vtt'vvvb
pot^vctiAdtcj
Pviy^otovvX. (A^t^Cn) As
i*j-
/ct 'Cjdt Co^wtl ^-^LC cVhX
Q> iv P-Lj-lyv^
\z> t>lwd.
TZ-iza; S’tzvvZ*
/ tt-AZ^- cVt-WL <vs ciCSC^IAvwzd
'Vt/j OCCAA^<> t
AzvCAitWl^C
>■
<t S6<J?A/ts' (AA CA $CA€
••W\^CotvCn'V OC.QiWvl
'
■
2.0 b) *50^ '.
' tA^-A)tvw&'Vut C-tVi/vv^' iA, Vvi/O> t^UlZ^
TivC-
otTvUu aXv^uS^- €^<,<X2 o7
^k/uuu rutA^UX
d rov\cl'vv^p^>v\
■v&w M/ttw aXcmzS.
(X s^^vCevix
•VUCdr
wlvvciy CAVKIZ
iv>virT<VTV
|2>AJUc-' j9^u«?wvuvAV/p^c/^izC/X
Xzvt'Ay,. LbX& p&L'i/'/JZaX ^Oy
CzTVvvt/v^ ‘ CAia^&vuv /tvC
tx;
L-W'-Cy AxLW\,A&yZ'
X
,
<?'Uu''V X-vtzs^S
y^y- X
l>^f^pC,'vL'C'vV<1/Ui?>v
Y\XL\£/vXj
I
'
zvt/v tf'Z./^yuz
JL^Yi/yy,
M^gAJT ^J'TATUf.
^TATUf,
^'"YY\,v<,yC)pAp./x4/^\jc.y
^^tL^ikvCx
!
f~
/\ji.£p^'Cv-^J^\,t-rxi
°b
-~.
i/OCXS
&i/y£'b
-
/WA-CXoX-uvc€_/t
AM.X
l<230s.-
Zt b
twe
lv^
le?22 -
_ ,(7
/\^Y^yvvZoc^Cos^
192-2 -
D^pv^o-^. <?v/4wd.^ wwAfrflK.^^^v. SCl-iUt-l.
19
A1AJ>KOA/ wX
33 -
-
R&A,.J£&'Ay
(^
^U/£R
A'Ywl^Lo Ti-t.y'y-i/ZV?^
(X^<VAywvto(>L<|'fe&V5
PAgK£R
<RACIi6
b&t^v-vxA. <Xc>'Vu£>6’
Lb
lc)2>(& -
vJ
CxJ-pyLA UM-AC-.
0(X/v\,i>(x2. , /\^.L.(^tto~k\, b<-XX<!(y^
/93£>
eTl
L^'W^\t^p-vZzV5x- VW (XO-OQ'-f-oy
• c/v^'i
<AU\X
*
'kA-iLsm'y
/uvv &Lilc'Jlyx
0\/\Asd.
>
O
(>-6aA'Vi,iCz ■,’y'\Z’^)O'^cr>v<-£ ' '^e-xc^
UlSTOKy
5i
’L
£<K>'.
14
X'b^.'tpY'/i/i//vX<.’TiX /
/l/Y\^i~ /^Uucq/VA .
I'V-T' ftv
'
L-.. /
b.e.&vx/
Czvwc^/%ku kvsaZ^ liiti
hj l/l)LvvcZi/ &i/vC 'tViZ^y Wve'k&Z'O'b tcs
tfwxjL
Vizu^-x
L , y ni- „
C l vlc^ p7',cn'v^7<wu^ .
/US
^SlU „ A^^X^vh
£tvuX 'i^Ycx^/tcex.
C Aw (A/pAwA/vaXc - A. k) Li.
.0^
nZ-MC AyJ-'idiiv) (
PiaHiT
/Yyv^t^pzvq Xo^Vt-krt/^J
®^>z' ^V^A-l^Oy
Avv?V^kujta.otvfr SX-vDC^. X Pwxdl.
Za)
t
jc\j'^/l^h ^A^^ty^tZcrVv , bi?bvvC^ ^-&vv 0V\> ^O^C/1^
(TVAA’e-t f ■
(XvtX
1^.
6Sttkvu^"tfX ,jvc>vvu O'Ol^/o
("vA<. b^'vy,
O,TC, Sc^lc
'
<vv-v
(7,^,4, Wft* ^xuotw^^X .
’'Tbz, ^v^e.'vbcxy^. ^'I^Xvca-1 /^-^ec-u{toiy\
O-vv
£■/.
IO‘\&yoy&
■^c&cy'eti d-
At^ve/viZ/
tOvvCC’n^KM'v^V (4tXL{. wv l/V./^.C- C-Owwt} , CMaA uwi^ -va
/
I
^(?0
C if
' ‘
■ I
-
(2
.'Upo'i^.ci
w'MZ' 4/uvu^>€-'ZC*,(
qzW /l/v vC<\£
N'.1 (.. ,vv»
tp
1
a<iv<. ■/_<:
>
OCVvAzCv vviax'zC
19(^0 —
vtfAA- ,
Ctni.v.{4 a-/
^/z-vcZv^
L'U 1Z
C^. U\x
6^/
rfx
n?4-t<$
■^J'VCzL
ivoi-Ccz. d
- S^-cA^-n
<V ^'- C^c
-ui^r-^'ovvs
d-Lwt^L
^jVv'iXuy’i 0-a-vC ^p-P")-, i
IS/STt? f-'l'-j /i/va l^b ’2-
cPvw
Av>/4,
(JT £v\ Cst VtL
’
7
(^'
C^jti£HVv
ftVvS,
/,’Cvc
lA)'^
.Cl
CA) -CA
OS' [vyx Q
DCh^b ■
UJ<r<A
^rtyia
^fvvi^i^ceJ be/ /-foetus.
Z\,C Pz?Ctb>y\
IjacC'l'iS b
Lv-Atb tls\jz/ /\£uM
b cj
£ l/\-0'^O)'UVl.
:
t
ivt^LZcn'^.
j/a k>iM
C-p/V uC-Wt^,
lj0f5&r]S7
fe
(\^>I?'V'O/C ■ |
\/\J.'C Uy\ ■'Yvvo ch c^ tV^- d^’Y-hc'^ct^L
i^KX-z
j2.(^./i.4.iLU^y
hc\rm^hv^
to
zt>/- <o
i/Q p yLcL.
. XWzCl/L^
/ % ' <9 4'VkZ{XXh>
LAxi^_d,
K)OVtxLi^p^'y,
tL'fe
vy
C'f<MxHx^l-,v -c<7 .
•X-^^eX-ut/'O
XXuL.iL'
L’^yL'
^Y\.cvL^-f9
'P'^X.C^A.
fiyx&vvYvfa yyyaJL
h^Lco>c-JXhoe^
^Xw xLCAtxT^e^A’
d-4w/=-
'-/
(CtC Lt-'ty
Aft'VVV -iA
(A/VX-CC'&p&S, in^lii
ct^.
XLu^’
|/ix£--
r4
^>'pl
&6$,h~Y\ pfctc^-
4' //V /\Jb/4
Ab/,. A
^ut> hiAWzfa^ zri H
/jvvv€^4^ f
QrLc\y\}^y C'Y’'yv-t
'Vly^'C-C'ka'^^CS^
/L-U't<yt;i.-L<t
(%-ua£
-Av’
s
z>toi-!-0^\,l^..(4-e^UA4CldL
J^p
4
S^izv
"Z/
6?>1/LX^.^
__ I
O4f
'-■$ aT^ip^y' plP.P~(r>'Z ,p
)A-^ z»>> 2gi_ ,1/yy
p^btpp~l<>.
'S
/tz4/l/Lx^^A.^Z^;^z
/v^t/Lz^-G^-
<
D/Yp1 I'vZ,
■
AiP.
ccw^
-
T
^l.<s
<4/ d
'fvVvi.^Z^ z
4-4- ^51
Zd'Z-S.
4P-.
A
0
7
CV/2>^R
'/^’)
/.ssu^s ■
I) COCC'/’toyxdovCO
lolc£-. ^>AVvX
Q&^£M/vCv& (ZoccC
6\/\jO ~Asbt
p-loCs'^CA-Z-CtL
CzC/i^vvmAyiZ, a-v-v^L
,C ^Zz7~yv-7_ SloocL
dL&veAoipcdL
te
A-€AzttXq^ CA/v^ pW^UC/^ /
0°'
Qirxs]etn&_
.CCS .
&A /O\A,\,(?JU' C^oh/xs. . ^jv/c-kv
/l/VA .U^-Avv
(}Y\.
Co ■
A/,'
Ph*
fC^X/vCi^.
tTv/y
ft-0'({t
frlA/v <OJ>p>C(Xj^
VV\'C/\a/x^O'(AC^C\S •
i)/W^5 /|TU-H,kWL3/r?vC(>i~rx z
”^i\z-
(SxzvCL^yZ <^itW'7 iVkwC-
ttxo ^-wipt-vC/CmM-
[z'V~)
- '
R^F^fZe FJC&S :
<^o'^>
’^/v/v vm/l^ op lA.
~Tixc
^y'C\A-t'V\,M-'V Lo
C.sij7
2.\
-
Fl aAsj&x*.
,
C'lzVxdS!
z
■Jifvwel^
^^'T^VuuvvliJtv^ Maix -wvctwco^
Tjrv&v^yYZ^tTcCz
19'7<7
<Jn
— C)0r?Xm4vi
b-yj
fycrCctj-Ce-yi , (j1^ &;/ AS 7S ■
Z?-< y>^z>O'>'z<^./
47'^vLj £<rt-
/Vl , £/>
OA/WZs
7^
a'Z)v/i.A,
C-FF-ci-u
2-Lf Oc'Y' <$"?
h .■
!4y''Azv^-
7.
CC'Vi/it.
,'^?'AZv^<^/VVa
A'^V?3zIzCcZ'
y>
l-'h^Cy^)'
iPF\^x^\
C-vxshrryl^
C^cr^J)
ITuf^OaZ-^ £>6>oAz^-
£■
b-i^r M
A^-VV-vVvC^ —
V<>0^>. No.Lj- /9<Sr£'
-
.
rVvCck
/'l/ fV^
L/M/\C&7~
/
An?(S P-^lflXoK
MFC- ^vdLcFF^ h^F:F>
oCwdP^-.
^1 "U^Q
Arppn^^
^s-Oizvi^V^1
07PT'M'i
tdo
F> - 7'/?/_f7/z9
^|
io
L-ft/w ccP 2,^dOI/vm 8c
H-
12.
A
fii/KO
~Tp&-
C^vp^ui^w
-
A
■ L-fo'yj- M^Ua._
0/5hf£Le77-£:(^
S t aneva- St oy ■ '
Institute of PI >, '• ■ 1
, . "
'
, ■ ■ f Sc
In
earlier ■- i u <1 i s (Ivanov, Staneva-Stoycheva, 1984)
'
.
'
we have found an
, ’ j
i 1 eu■
d
2
Vlaskovska M
Surcheva S
Ovcharov R
a non-narcotic
methamizole and the calcium
T hi e
effects
of
verapamil
on
carrageenan
hyperalgesia, release of
channel
blocker
and synthesis of p r o s t a g 1 a n d i n E 2
were studied.
beta-endorphin
and verapamil
It
was
found that a combined administration of
anal gesic
effect.
Analgin
prolonged
Hie
s t i m u 1 a ted release of
th the peak of
with
the
ma x i mu ra c o i n c i d i ng in
beta-endorphin
the
analgesic effect. Against tlie background of the action of c a1c ium
A 23187 the combination of analgin with verapamil inhibited
ionophore
PGE2
synthesis
more
The
combination of these
pharmacological
agents
is
suggested
to
exert
the
effect both at
different
levels,
central
and
peripheral ,
mechanisms involved in pain m o d u1 a t ion.
Farmakol Toksikol 1989 May-Jun;52 (3):25-9
Document 3
[Study
of
the
effect
of analgeton on the release of beta-endorphin
and its effect on chronic hyperalgesia]
Vlaskovska M
K rushkov I
The
effect
of
the
combined
preparation
analgeton
and its
componen Ls--an’al g i n
(metamizol,
no ramidopyrindimethansulfonate) and
am in ton
(2-amino-4-methyl-pyridinphosphate)
was
studied
on the
release
of
be t a-endo r ph i n and its influence on chronic hyperalgesia.
Experiments
were
carried
out in vivo and in vitro on white rats and
it
was established that analgin, aminton and analgeton stimulated the
release
of
beta-endorphin,
affecting
various regulatory levels.
Analgeton
in
contrast
to
analgin showed longer analgetic effect in
animals
with chronic hyperalgesia (adjuvant arthritis of white rats)..
Possibilities
for
pharmacological
control
of
chronic pain by
influencing the levels of endogenous opioids are di scussed .
Eksp Med Norfol 1989;28 (3):14-21
TI
AU
AU
AB
SO
TI
AU
AU
AU
AB
SO
TI
AU
AU
AU
AB
SO
TI
AU
AU
AB
Document 4
[An
evaluation
of the efficacy of treating rheumatoid arthritis w
preparations for local use]
Abdullaeva G K
Shak i mova BSh
made
of
the efficacy of local therapy of rheumatoid
Assessment
was
with
d i mex i de
during
a
double b 1 1 n d m e t h o d '■>f
arthritis
pat i e n t s
The
articular
index,
duration
of constraint in the
investigation.
the
strength
of
the
hand
were
taken as the leading
mo rn i ng
a nd
objective assessment of the drug efficacy. Applications
criteria
for
solution
of
dimethylsulforoxide give a statistically
of
a
50%
favourable
effect
as
compared
to the conventional
sign! f i c a n t
physiotherapeutic
methods
of treatment: ultrasound and p h o 11 o p h o r e s > s
s o1u t ion of
with
analgin.
Addition
of
analgin
to
a
50%
dimethylsulforoxide
intensities.
its
a n t i p h1o g i s t i c and analgesic
properties.
Revmatdogiia (Mosk) 1989 Oct-Dec; (4) : 35-9
Document 5
[ Thresho1 d s
of
the
electrical
excitability
of the pulp in va r i ou s
teeth
and
their
changes under the influence of analgin,
groups
of
a ni i d o p y r i n e and diazepam]
Moroz BT
Ignatov Iu D
Kalinin VI
Pulp
electric
excitability
thresholds
n different teeth groups and
their
changes
under effects of analgin, amidopyrin and diasepam were
electro-odontometry in 58 patients and in experimental
studied
using
recordings
of neuronal activity in rostral part of trigeminal complex
under
electrostimulation of molar and fang teeth. Baseline thresholds
of
pulp
stimulation
proved
different
in
anterior teeth group and
premolar/ m o1 ar group. Analgetic drugs used had more pronounced effect
in cases of molar pulp stimulation.
Stomatologiia (M o s k) 1989 Sep-0ct;68 (5) : 3 0 -2
Document 6
of
specific
type-III
glucocorticoid
receptors by
[T he
activation
pyrazolone series preparations]
Golikov P P
Nikolaeva NIu
K1 a d i e v A A
Experiments
were conducted on intact and adrenalectomized male
180-200
g)
with labelled corticosterone
rats
(weighing
to
study the effect of analgin and a m i n o p y
on
the
level
of type-III glucocorticoid receptors in the liver.
and
aminopyrine
in
doses of 10(-2) and 10(
of
labelled'
corticost
b1n ding
by
type-III glucocorticoid
receptors
of
the
hepatic cytosol and by blood plasma transcortin in
experiments.
The
effect of the agents depends on the dose.
model 1e d
a d m i n i s t r a t i o 11
of 140 ra g /10 0 9 of analgin to
I n t r avenous
equal dose of anal g 1 tl
and
intraperitoneal
of
an
adrenalectomized
rats also increases
p e c i f i c binding
f label] ed
corticosterone
by
type-III
glucocorticoid
cytosol.
The
importance
of
the
revealed
ne
pyrazolone series in stress regulation is di
ussed .
Paid F i z i o 1 E k s p Ter 1989 Jul -Au 9; ( 4) : 19 - 2 2
D 0 c u in e n t
[The
effe
non narco tic anal 9 e s i c s]
Stets VR
SIivko SF
The
effect
of
c li 01 i nerd i c
and
(P y r a z 01 1 n e
d erivati've)
using
a
"hot
M-( hoii nom i me tit
agents
analgesic
c li e m i c a 1
techni que.
compounds
e n t s on w 11 1
b e e n f 0 u 11 d
pain sens
so
of
other'
ageri Is. LD50 of LAS was similar to that of analgin arid A
was
s i 9 ri i f i c a n t1 y
less
Lhan that of am i dop y •' 1
LAS
toxicity
of ASA at i n I r amuscular a d m i n i s t r a t i o n to r a b b i t ,;j
Bioavailability
at
intravenous injection and significantly high®1
close
to
that
compared with i ntragastric administration.
Farmakol Toksikol 1988 Sep-0ct;51 (51:78-82
TI
AU
AU
SO
Document 16
Analgin, the killer [letter]
Mathur SL
Bhargava CS
J Assoc Physicians India 1988 A u g ; 3 6
TI
AU
AU
AU
SO
TI
AU
AU
AU
AB
TI
AU
AU
AU
AU
AB
(81:523
Document 17
A
comparative
study
of
ibuprofen
with para c e t a m o 1
oxyphenbutazone will i analgin combination in ophthalmic p r a c t i c e
Roy IS
Das A
Roy M
Indian J Ophthalmol 1988 Jan-Mar;36 (11 ;37 - 40
Document 18
[Complex
treatment
of
dental
plexalgia using physiotherapeutic
methods]
Sharov MN
Grechko V E
Puzin MN
A
total
of
66 patients with dental plexalgia have been examined and
treated
at the neurological dentistry department. A multiple-modality
scheme
for
the treatment of this condition is suggested, whose basic
methods
are
physiotherapeutic
ones:
longitudinal physiotherapy,
diadynamic
currents
with
a
narcotic mixture, L r i m e c. a i n or 1 y d a s e +
analgin
electrophoresis.
The treatment was effective in the majority
of patients.
Z h Nevropatol Psikhiatr 1988;88 (21:57-60
Document 19
[Effect
of multiple peroral use of analgin on the 1 i v e r ra o n o o x y g e n a s e
system in the rat]
Koleva M
Kai o i a n o v a F
D ob reva V
Mi tova S
given
Iy per os in d
mg/k9 to white m
some
indices
the liver NADPHmono-oxygenase
system.
AL
the
end
the
quantity
of
the
ni i c r o s o m a 1
pr
increase
of the cytochrome's content P-450 and b5. The f requeue i
P-450-dependent
biotransformations
c y t o c h r o ra e
and
an i 1 i ne
am i nopyr i ne
the end
ixth
month,
of
the
because of multiple drug application all t heS e
indices
re
in
the
mi ts
of
the control values. A change i
cytochrome
P-450,
is
established, whi
expressed
ma i n1 y
first
type.
The
Michaelis's
constant
Km for substrate ami nopy r n e
depends
on
the
duration of analgin i n t r o d u ction and increases u p
300% towards the control at the end of the sixth month.
Probl Khig 1987;12 :87-92
SO
11
AU
AU
AB
SO
TI
AU
AU
AU
AU
AU
AB
amounts
was
done
by
a
colorimetric
di chloromethane.
Arch Geschwulstforsch 1989:59 (2):79-84
method
after extraction with
Document 14
[Analgesic activity of pymadine]
M i tsov V
Bantutova I
The
analgesic
effect
of
4 - aminopyridine
(pymadine) was studied in
experiments
on
rats
and
mice
at
thermal
and chemical pain
stimulation.
Pymadine (1, 3 and 5 mg/k g) exerted the analgesic effect
when
administered
alone
and concomitantly with analgin and morphine
at
chemical
pain
stimulation.
During
thermal pain stimulation
pymadine
had
the
analgesic
effect
only
at
dosage of 5 mg/kg and
potentiated
the
action
of morphine given in doses of 3 and 5 m g / k g .
The
same
doses
of
pymadine
failed
to
influence
changes in pain
reaction induced by analgin at thermic pain stimulation.
Farmakol Toksikol 1983 Jul-Aug;51 (4):32-4
Document 1.5
[Analgesic
action
and
pharmacokinetics
of
lysine acetylsalicyl ate
administered in t rauuscu1 a r1y]
L i b i na VV
C11 a i k a L A
Kosheleva L P
K hadzha i I a I
Pich ugin V V
The
analgesic
effect,
acute toxicity and pharmac okine I i c s of lysine
acetylsalicylate
(LAS) , a water-soluble salt of acetylsalicylic acid
(ASA)
were
studied
as compared with a 50°. solution of analgin and a
4%
solution
of
amidopyrine
at intramuscular administration and ASA
admi n i ste red
i n t r a g as t r i c ally.
During
i n f 1 a m m at ion- i n d u c e d
pair' in
so
TI
AU
AU
AB
SO
analgetics.
Relative sensitivity of 11 o hi o zygotes i n < 1 e
,
all
three
elevation
of
drugs
concentration. The data oo Laine
wi th
I he
demonstrate the mutagenic i t y o f the analgetic s tested for 0 r osop'" la.
G e n e I i k a 1990 M a y ; 2 6 (5):856-62
Document 21.
[The effect of analgin on glucocorticoid receptors]
Golikov P P
N i ko1 ae va N I u
Scatchard's
analysis
was
used
to
examine
the specific bind in9 of
3H-acetonide
of
triamcinolone
(3 U- A T)
by Type II glucocorticoid
receptors
of
cytosol
from the liver of W i s t a r rats weighing 1. 3 0 - < 0 u
g.
It
was
found
that
a n a 1 g i n in concentrations of 5.0 and 10.0 m rl
inhibited
the
density
of
glucocorticoid receptors and increase trie
dissociate
rate
constant
of
3H-AT
from the receptor and decreased
3
H-AT
elimination
half-life
from
the
receptor.
Analgin
in
concentrations
of
0.04,
0.08,
0.16,
0.31 , 0.62, 1.25, and 2.50 tn M
lowered
the
association
cons t an L
of
the 3H-AT-receptor complex in
proportion
to
the
increase
of
analgin concentrations. Analgin was
found
to
have
uncompetitive
effects
followed by inhibition of the
density of Type II glucocorticoid receptors.
Eksp Klin Farmakol 1993 J u1 - A ug;5 6 ( 4) : 41 - 4
29199 of 29199 bytes transferred.
Activity duration 00:04:11
(HH:MM:SS)
Press E nt e r to continue.............
HJ 7rn
m4m
Welcome to SysO
t e tn Wipro UNIX System V ver.
m5m
You have mail
CLR
0000
NICNET>
M [7 D L A
INDIAN
4
release 2.5NIC +
1.
2.
3.
Search Mate Interface
Native Mode Interface
Online Document ordering
4.
5.
6.
List files
Capture a file
Delete a file
CENTRE
so
TI
AU
AU
AB
SO
TI
AU
AU
AU
AU
SO
TI
AU
AB
SO
TI
AU
AU
AB
Analgin) is mainly met aboil zed by phenobarbital - i nduc > b1e
(metamizol ,
P-4 50
(P-450PB)
.
We investigated the elimination of
cytochrome
the
use
of
plasma concentration curves (H P L C) an cl the
caffeine
by
of
me tajn i zo 1
by spectrophotometric determination of the
el i m i n a t i o n
in
urine
in 10 healthy young males, in 10 healthy young
me tabo1 i tes
no
OL-steroids
and in 10 healthy young females using
fema1 es
us i ng
of
s e x on the m i c r o s omal dr-ug metabo 1 i sm
OC-steroids.
No
i nf 1 ue nce
has
been observed. There was a
these
two
d rugs
activity
of
drug metabolism of hot h d r u gs i n
sign! f i c a n 11y
decreased
m crosomal
females
under
hormonal
contraception.
We conclude that OC-steroids
decrease the demethylation activity of both P - 4 5 0 M C and P - 4 5 0 P B .
Pharmazie 1985 J a n;4 0 (1) : 5 0-2
Document 26
inhibitors
on
the
nitrosat ion of drugs under
[Effect
of
non toxic
conditions simulating t h e human s t o tit a c h ]
Z i ebarth D
Schramm T
The
influence of sulphamic acid, sulfanilamide, p-aminosalicylic acid
and
ascorbic
acid
on
the
nitrosat ion behaviour of Analgin (active
agent:
nor amidopyrinmethane
sulfonate)
was
investigated
in the pH
range
between
1.2
and
6.0
under simulated conditions of the human
stomach.
Using
a
colorimetric
measuring
meth o d,
the
three
suitable as nitrosat ion inhibitors;
1ast-mentioned
compounds
proved
to
ascorbic
acid
because
of
its
better
preference
should
be
given
very
weakly acidic pH range. Sulphamic
inhibitory
capacity
in
the
it
stimulates
nitrosation
in this pH
acid
is
inadequate
because
The
distinct
inhibitory action of ascorbic acid was verified
range .
of
the human stomach in further 9 drugs
under
simulated
conditions
different rates, which contain the active
undergoing
nitrosation
at
clomipramine,
imipramine, desipramine,
agents:
aminophenazone,
phenoxymethylpenicilline,
ethambutole or
ampicilline,
o x a c i11i n e,
use
of
high
doses
of
ascorbic acid, no
piperazine.' Despite
the
complete
inhibition
of n i t r o s a t i o n could be achieved in the majority
of drugs investigated.
Arch Geschwulstforsch 1985;
(2):81-91
D o c u m e n 127
—
[Acute . kidney failure and acute
a large amount of analgin]
Konov A
Chernev K
Penkova S
Boshnakova Ts
Vutr Boles 1985;24 (l):133-6
toxic cholestatic hepatitis caused by
Document 8
[The diagnosis of drug hypersensitivity]
B a d i n a AK
The
author
revealed an i n c r e a s e of dienic conjugates in 391 patients
under
the
effect
of
drugs
in patients with drug intolerance and a
study
is
also presented in 46 patients with good tolerance to drugs.
It
is
shown
that
the
dienic
test
has an information value as to
intolerance
of
penicillin,
streptomycin, tetraole an, analgin,
novocaine and vitamin Bl.
Vrach Delo 1990 Dec; (12):46-9
Docunient 9
[Sensitivity
of
larvae of Drosophila melanogaster mutant mus(2)201Gl
to various analgesics]
Mikheev VS
I m i an i t ov E N
of
larvae
from
mutagen-sensi t i ve mus(2)201G1 mutant of
Sensitivity
melanogaster
to analgin, amidopyrine and antlpyrine (4-64
Drosophila
of
medium)
was
studied. Relative f r equ enc y of file s
m k m o1 /
ml
homozygous
for this mutation after combined development of homozygous
and
heterozygous flies in the medium with the analgetic was used as a
c ri ter ion
for
1 arva1
sensitivity.
Il
i s sh o w n that s e ns i t iv iIy of
SO
TI
AU
AU
AU
AB
TI
AU
AU
AU
AU
AU
SO
TI
AU
AU
AU
SO
TI
AU
AU
AU
AU
AU
AU
AB
py r a z o1 one- induced
were
requiring
the
pyrazolone
der i va
The
a1 1 ergo1 og i c
ents
w i th
pyrazolone- i n d u c e d
urt i car
the
patients had pollenosis, 6 patients ha
protein
and one patient to penicillin
egg
allergy
use was made of the natural
according
to A . D . Ado. The test app
all
the
35 patients suffering from py
It
represents
a
simple and accessible me
y
both
inpati e nts
al 1ergological
rooms
the
poly
examination
made
w it
t he
of
the
histograms de
appreciable
reduction
ntent of D-phagocytosing
The
latter
fact
might explain the presence of multiple
pyrazolone*induced
ur
patients
manifested
a
decrease
that
might
b
immediate
activation
of
the
al
pathway
of
pyrazolone derivatives.
Ter Arkh 1986;58 (10) : 7 6 - 8
in
Document 22
[Indomethacin in the treatment of ureteral colic
Bick C
Suckow B
Heil G
Experiences
are reported in the therapy of recurrent colics caused by
In
41
patients an initial treatment with indomethacin
suppositories
was
performed
which led to a removal of the colics in
group of 46 patients was conventionally
37
patients.
A
comparative
treated
by
means
of
an
i
therapy of a n a 1 g i n/p a p a v e r i n. In
order
i n less ri ess, on a average 10 to 15 injections were
the
hospital
dur i n 9
treatment. The importance of the
indomethacin
therapy
described lies
by
the
patient
as
well
as
in
t
frequent consultations of emergency physicians and hospitalisations
Z Urol Nephrol 1986 D e c ; 7 9 (12):705-8
Document 23
[Transplacental
passage
of sodium s a 1i <:y1 ate and analgin
trimester of pregnancy and labor]
Todorov S
Todorov I
K i u tukch i ev B
Khadzhiev A
Ruseva S
Akush Ginekol (S o f i i a) 19 8 5 ; 2 4 ( 4):3 0- 4
Document 24
poisoning
[Combined
metastatic 1 es ions of
Naumov V N
Krasnova RR
Galkina VS
Sud Ned Ekspert 1985
phenobarbital
and analgin c
with
the adrenals from cancer of the lung]
i ri
the
i ng
: 54 - 5
Document 25
me t am i 'o1
caffei ne
and
[Determination
of
an in v
women
with
and
wi L h o u t h o r m o n a 1
"'ethod
cytochrome P- 4 5 0 subspecies]
for char act ^f'ization
S i m on HU
Ortweiler W
S i eger t C
Splinter FK
Balogh A
T r aege r AM
metabolized by 3-methy1chol an threne-1nrfu
Caffeine
is
main
so
TI
AU
AU
AB
SO
TI
AU
AU
AU
AB
protein was established as well as
the
quantity
of
the
microsomalincrease
of the cytochrome's content P-450 and b 5 . The frequencies of
cytochrome
P-450-dependent
biotransformations
of
substrates
am i nopy r i ne
and
aniline are also of different directions. At the end
of
the
sixth
month,
because of multiple drug application all these
indices
are
in
the
limits
of
the control values. A change in the
catalytic
features
of
cytochrome
P-450,
is
established, which is
expressed
mainly
by strongly decreased affinity to the substrates of
first
type.
The
Michaelis's
constant
Km for substrate aminopyrine
depends
on
the
duration of analgin introduction and increases up to
3 00% towards the control at the end of the sixth month.
Probl Khig 1987;12 :87-92
Document 20
mineral metabolism in dry cows, p u e r p e r a n t s and
[Dynamic
as peels
of
calv e s]
P1 a n s k i B
Ab r ashe v M
It
is investigated the calcium, phosphorous and magnesium homeostasis
in
cows
in
the
dry
period,
cows
in
child-bi r th
and
calves i n
in
the
newborn
during the neonatal
connection
with
the
diarrhea
syndrome
in the growing up, with the
period,
with
the
respiratory
the
stillborn,
with e s fc r o u s and
sterility
in
heifers,
with
post estrous
metrorrhagia.
It
was
a s c e r t a i n e d a close dependence in
the
value
of
Ca,
P and Mg i n the different physiologic groups o f ■ a
given
farm.
It
was
ascertained
that the newborn from mothers with
values
of
Ca
of 2.5 m m o 1 /1 , P of 1.8 mmo1/1 and Mg of
lower
serum
0.70
m m o1/1 suffer from diarrhea, endotoxic shock, tetany etc. during
the
neonatal
period. Hypocalcemia is registered in the calves with a
respiratory
syndrome (2.20 ro m o 1 /1 ) , sterile heifers (2.39 mmo 1 /1 ) . In
all
cases
is
ascertained
hypophosphorosis
and hypomagnesemia
especially
i ri t h e calves w i 111 a respiratory syndrome (P - 1.24 and Mg
0.92 and Mg = 0.54
0.46 m m o 1 /1 ) , cows with a still born calves
mmol/ 1)
w i th
metrorrhagia
(P
0.93
and
0.71 mmo1/1)• The
ic
value
of
the
product
Ca
X
P
1e
relationship
between them is asce
comparison with
wh i ch Ca X P
the
ideal
11.11 and the r a t i o - -1 . 09 , in the
above
ment i oned
t he
product
decreases and the ratio
s.
The
graded which shows their mutual
11
was
estab1 i shed
e x p e r imentally that the addition with a
medical
the rat i o 11 o f th
green pea-oats and green rye during
spring
and sumine r, such as oa
winter for the pregnant cows has a
decisive
well
that
in
extra
situations
a component containing, calcium
gluconate, magnesium sulphate, sodium salicylate, analgin, 81 vitamin,
vitamin
C,
sodium
phosphate,
glucose
and sodium chlorate (if
necessary
sulfathiazole)
injected
s.c. 5 times to the pregnant cows
15-5
days
before
childbirth
a positive effect on the new-born
calves.
Vet Med Nauki 1987;24 (10):48-57
Document 21
[Clinico-immunological
and
allergological
characteristics of
urticaria caused by pyrazolone derivatives)
Poroshina luA
I. u s s L V
Ge r vaz i e va VG
The
authors
describe
the
results
of
clinical, allergological and
immunological
examination
of
35
patients
w 11h urticaria caused by
,
AU
AU
AU
AU
AU
AB
i gesi c
action
a ri d
pharmacokinetics
of
lysine acetyl sal
administered intramuscularly]
L i b i na VV
Cha i ka LA
Kosheleva LP
Khadzha i I a I
Pichugin VV
.
The
analgesic
effect,
acute- toxicity and pha r mac ok i ri e11 cs of lysine
acetylsalicylate
(LAS) , a water-soluble salt of acety1 sal icy1 ic acid
(ASA)
were
studied
as compared with’, a 50% solution of analgin and^a
4%
solution
of
amidopyrine
at intramuscular administration and ASA
administered
intragastrical 1y.
During
i n f'1 aroma t i on-i nduced
pain in
rats
LAS
exerts a pronounced analgesic effect exceeding the activity
of
other
agents. LD50 of LAS was similar to that of analgin and ASA.
than
that
LAS
toxicity
was
significantly
. ..
__
____ of amidopyrine
.... ............
TI
AU
AU
AU
AB
AU
AU
AU
SO
TI
AU
AU
AD
AB
30
TI
AU
AU
AB
ED e t e r m i n a t i o n
detector]
Yao SZ
m i c r o- amoun t
cl i p y rone
for
the
quartz
the
sample
iodide
is
added
to
iodine-potassium
immersed in the
frequency
shift
respect
x 10 ( - 6) mol XIover
a
range
from
2
10 (- 7 ) t
d i pyron
3.5-6 .5
according
to
the equation C (m o1/L)
by
commonly
caused
interferences
were
(Hz) .
No
significant
number
inorganic
substances,
amino
acids
and
a
The method has been suggested for determining di pyrone
substances.
ppm level and in micro-samples of mg
Yao Hsueh Hsueh Pao 19 8 9 ; 2 4 (2 ) ; 12 2 - 6
A
new
method
a
Document 12
[Effect of analgin on glucocorticoid receptors of the liver]
Golikov P P
K1 ad i ev AA
Nikolaeva NIu
experiments
were performed on intact and phlogogenic ally exposed
The
rats (weighing 130-210 g) . Glucocorticoid receptors were
mal e
a high-rate cytosol of the liver by using 3H-acet on ide
determined
in
triamcinolone.
Inflammation
was induced by subpl an tar administration
of
formalin.
In
the model experiments, analgin (10(-2) M) decreased
the
level
of glucocorticoid receptors in the rat liver cytosol. Tn a
m9/kg intraperitoneally, analgin after 90 min decreased
dose
of
250
content
of
glucocorticoid receptors and blood plasma
the
of
c o n c e r 11 r a t i o n s
the
exposed
rats.
The
mechanism
of
the
i v e r and blood p1 asma concentrations
glucocortico i d
receptors in Ihe 1liver
of corticosterone in analgin-treated animals is discussed.
2-5
Farmakol Toksikol 1989 Jul-Aug;52 (4)
Document 13
forms
of
diet
[Effect
of
various
on
the
nitrosation
of sodium
tablets) under s mulated conditions of the human
metam i zole
(a n a1 gin
stomach]
Z 1 ebar th D
K u 1 d m ae LA
Krebsforschung d e r A k a d e m i e d e r W i s s e n s c h a f l e n
Z e n t r a 1 i n s t tut
f
ur
d e r DDR, Robert-R o s s 1 e -1 n s t i t u t, Be rl n-Buch.
The
influence of a simple and a more complex diet on the formation of
nitrosometamizole
from
sodium
metamizole (analgin tablets) under
simulated
human
gastric
conditions
was estimated with extremely
different
nitrite concentrations. Only with the complex diet and only
with
low
nitrite
concentrations, the formation of nitrosometami z o 1 e
was
distinctly
lowered.
The
quantitative 'estimation of the formed
amounts
was
done
by
a
colorimetric
method
after extraction with
dichloromethane.
Arch Geschwulstforsch 1989;59 (2):79-84
Document 14
[Analgesic activity of pymadine]
M i tsov V
B an t u t ov a I
The
analgesic
effect
of
4-aminopyr idine
(pymadine) was studied -]■
experiments
on
rats
and
mice
at
thermal
and chemical pd-.
stimulation.
Pymadine (1, 3 and 5 mg/kg) exerted the analgesic effec(
when
administered
alone
and concomitantly with analgin and morphine
at
chemical
pain
stimulation.
During
ther mal pain stimulation
pymadine
had
the
analgesic
effect
only
at
dosage of 5 mg/kg and
potentiated
the
action
of morphine given in doses of 3 and 5 mg/hi;.
The
same
doses
of
pymadine
failed
to
influence
changes in p^,’
reaction induced by analgin at thermic pain stimulation.
so
qu i riazol i ne
and
trlazole
derivatives. At high
especially
that
of
pilocarpine increases drastically the toxii ity of
tn g / kg)
dose s
(10
an M-cholinoblocker atropine does not affect
analgin.
Contrast ngly,
pain
sensitivity,
however
blocks
completely the
considerably
the
of
all
the drugs studied. The role of cholinergic
analgetic
effect
m e c h a n i s tn s
i n t h e maintenance of pain sensitivity level and the onset
effect
of
non-narco tic a n alg e si c s as well as the
of
the
analgetic
cl i n i c a 1 value of the data obtained are discussed.
Anesteziol Reanima Lol 1989 N o v - D e c ; (6) : 2 4 - 7
TI
AU
AU
AU
AU
AU
SO
Document 8
[Postoperative analgesia by endolymphatic administration of analgin]
Pyshki n SA
Tkachev SV
Reznik lul
Bashtan LP
Malala VV
KI in Khir 1989; (12) : 55-6
TI
AU
AU
AU
AU
AB
SO
TI
AU
AU
AU
AB
SO
Document 9
Prescription audit of under six children living in periurban areas.
Prakash 0
Mathur GP
S i n g ii Y D
Kush waha K P
One
hundred and seventy two children were prescribed, in 212 episodes
of
illness,
antimicrobial agents (28.4%), followed by antidiarcheats
products (9.4%), analgesics (7.5«) and steroids
(10.9%) , nutritional
Ampicillin
(22.7%)
and cotrimoxazole (12.7%) were the m 0§ t
(6.8%) .
Tetracyclines, which are not
prescribed
antimicrobials.
common1 y
were
used in 7.1% of total
in
children
below
8
years,
i nd i ca ted
Penicillin,
a comparatively
exposures
of
chemotherapeutic
agents.
safe
and
u sef u1
drug,
wa s usad o 111y 1 ri 4.5% exposures. Analgin and
used frequently. Corticosteroids were, used for
fi y d r o x y q u i n o 1 lues
simple
ailments
diarrhea,
fever and jaundice. ORS was used in
only
13.9% episodes of diarrhea. A d v e r se drug reactions were noted in
30
(17.4%)
cases
and
death in 6 (3,5%) cases
The average cost per
prescription
for
neonates was Rs 32.43 and for a child was Rs 30.65.
Weight
of
the
children
was
not
taken prior to prescribing drugs.
There
is
need
for
prescription
audit as the e is high consumption
rate of drugs, with overuse of antimicrobial and nutritional products,
and misuse of steroids.
Indian P e d i a t r 1989 S e p ; 2 6 (9) : 9 0 0 - 4
D o c u m e n t 10
[Changes
in
thymocyte
DMA
template
activity
under
the effect of
agents acting on the central nervous system]
Golikov P P
Nikolaeva N I u
Alekseeva E A
Tiie authors studied the effect of phrenolon, am i t r i ptyi i ne , piracelani,
caffeine
(concentrations
of
10(-7), 10(-6) , 10(-5) M) , analgin, and
a in idopyrine
(c o n c e n (.rations
of 2.5 10 (- 7) , 2.5 10 ( - 6) , 2.5 10 (- 5) M)
on
the matrix activity of thymocyte DMA. The thymocyte suspension was
derived
from
the
thymus
of
adrenalectornized male rats. The matrix
activity
of
the thymocyte DNA was evaluated according to the ability
of
these
cells
to
reduce
the incorporation of 3H-uridine into
thymocyte
mRNA.
Biosynthesis
of
thymocyte
mRNA
reduced under the
effect
of
phrenolon,
amitriptyline, and analgin. When phrenolon,
a in i t r i p t y 1 i n e ,
ana1 g 1 n ,
and
amidopyrine
were administer e d t o g e I. h e r
with
triamcinolone
acetonide,
the
inhibiting
effect of the latter
agent
on
the
matrix
activity of thymocyte DNA increased; piracetam
and
caffeine
failed
to
produce
such an effect. The practical
significance
of
the obtained results in the clinic or emergencies is
d i scussed .
Patol Fiziol Eksp Ter 1989 May-Jun; (3):18-21
1
TABLE
B-COMPLEX
Brand Name
TABLETS
Elemental Vit.Bl Vit B2 Vit B6 Vit B12 Vit FA
iron in
mg.
mg.
mg.
mcg.
mg.
mg
Complex B
Glaxo
-
3
1
0.5
5
Libex
-
3.3
3.3
1
2.66
Becozyme -C
-
3
3
2
2
Ccbadex Forte
-
5
2.5
1
1
. 5
Loplex
-
0.5
-
-
10
2.5
.33
Nicacid
mg.
Cap.
panto.
mg.
Vit.C
mg.
Price in paise
for equivalent
doee Ibased on
price in June 81.
30
1
-
-1 tablet cf 4 paise.
30
-
50
14.6 ( IT = 44 paise)
10
5
40
9.3 ( IT = 46.5 paise)
7
1
20
4.45 ( 1 T=44.5 paise)
3
-
1 T = 4.25
25
F-COMPLEX INJECTIONS
Complex B glaxo
-
5
.5
1.5
5-25
Bejectal
-
5
1
2.5
-
-
0.75
2.5
2.5
-
0.5 ml : 17
0.5 ml ; 34
TABLE
MULTIVITAMIN
'Brand name
Vit.Bl
mgt
; Vit.B2
!
1 mg.
2
TABLETS
j Vit A
Vit.BBJ Vit. Bl 2 ! Vit. iNic. ‘ Ca1
; FA
!acid ! Panto.' I.U.
mg. ! mcg
j mg. '
i mg.
!
i
i
1
Vimgran
3
3
1
2
Vitaminets
Forte
10
2
3
1
Multivitapl-.n:
Forte
2.5
2.5
.5
1.25
0.1
.25
Vit.
D IU
mg.
' Vit. ]Mine- ; Iron
]rals ' solt
: c
, mgo ;
; mg
;
J__
____ L .
_
Price in paise
for equivalent
prices in June
1981).
20
5
5000
500
50
-
13.5 = 1 Tablet
10
10
4000
400
50
-
18
=1 Tablet
25
-
5000
3.7
38
—
10
(39.5 = IT)
MULT I VITAMIN SYRUP
Multivitaplex
3.5
Becadex
Visyneral
2.7
1
-
20
-
5000
1000
50
1.5
1.2
-
2.5
10
-
3000
500
40
-
1.5
0.6
1
2
10
2
5 ml = 38.65
5 ml = 21.45
3000
1000
50
—
MULTI VITAMIN DROPS
5000
5
2
1000
50
-
0.6 ml. = 14.2
Mn K 17.27
Zn
-
0.6 ml = 17.08
ABCDEC
Vitamin M
drops
1
0.4
1
-
1.5
1.2
.5
-
10
-
5000
1000
50
Alvite
Vi-Syneral
10
5
2
0.5
1
1.5
-
20
10
-
5000
5000
500
400
30
25
—
-
—
5 ml = 32.75
55
48
TABLE NO. 3
IRON WITH MULTIVITAMIN TABLETS
Brand Name
Vit
Bl
mg.
Vit
B2
mg o
Vit
B6
mg.
Vit
B12
mcg.
Vit
Folic: C
acid
mg
mg-__
Iberol
1
1
0.5
4.6
.33
25
1
100
5
50
3
50
-
Exifol
2
2
1
Fesovit
Fersolate
+ Complex B
Glaxo
2
2
1
-
-
3
1
.5
5
-
- -
66
5
Cap
Nic
panto. acid
mg
mg
Elemental
Iron. in mg..
Price in paise for equivalent
cose(based on prices in Jane f
5
52.5
6.3(1 tablet costs 19 paise.)
10
45
1 T i 59
15
45
1 T = 60.3
1
30
60
IRON WITH "folic" acid" and’ VIT B 12
1 T = 7.5 paise.
1
150
66
1 tablet = 34.3
emit in ic
10
1
150
66
1 T = 41.8
Macrafclin
with iron
Autrin
10
9
1
1. 2
-
90
66
70
Rediplex
10
1
100
68.6
1 T = 6.5
20.761&1T = 34.6)
(34.6 x 3/5)
21.3 (IT = 32)
(32x 2/3)
3.5
Ferplus
Fersolate
66
Imforon Fl2
668
3. 2
66.4
154
Uniferon Fl2
66.4
3. 2
66.4
76
(Tables prepared by Nitin Sane, Pune)
The following materials are available with Community Health
Cell (47/1 St Park’s Rood, Bangalore 560001) for references
1.
Guidelines to Drug Usage
2.
Consolidated list of products whose consumption and/or sale
have been banned, withdrawn, severely restricted or net
approved by governrasnts (United Nations Secretariat)
Essential drugs and developing countries
Rational Drug Policy, August 88 issue of HEALTH ACTION
(a CHAI-H FA publication)
3,
4.
5,
6.
7.
8,
9.
13.
11.
12.
Banned and bannabls drugs (VH”I publication)
Health Action Series 2 (rovised edition)
Gushadha mathu fisvu (&« 2,3(3)— Copal Dabade (KRVP publication)
The Pharmaceutical industry, drug policy and production—
A study* K Jaysraman
Hyth ano Reality of drug utilisation
Drugs for Primary Health Caro (Postgraduate Institute,
Chandigarh)
The use of essential drugs (UHO T'-> 722)
Ths rational use of medicine (VHAl)
Multinationals in drug and nharmacautlcal industry in India,
?•! S Majumdsr
13.
Measures for rationalisation, quality control and growth
of drugs and pharmaceutical industry in India (GDI)
14.
Healing without Medicine (reprint fro® UHE £ THERE IS ND
VICTOR) WI
15.
formulary therapeutic guides (Kurji Holy family Hospital, Patna)
16.
Pills, Pesticides and Profits, Morris Ruth, Ner York
17, Rational Drug Policy Statement, .IOAN’
IB. Ths case against EP Drugs, ACHf-K
19. Catting Essential Drugs to ths poo le, C -T'CT, No 53/73
20. A pill for uvery ill—cashing in on World Health—The New
International, November *Efi
21. Towarcs ® Pragmatic Drug Policy, A 3 Dudani (Sulabh India, Jan 37)
22,
Rational Study of Analgesics and Antipyretics (mfc)
COVER STORY
doctors to over-prescribe glam
orous and costly drugs with
limited medical potential. It is also
unfortunate that the drug pro
ducers always try to push doc
tors into using their products by
all means - fair or foul. These
Dr Ravi ftJarayan, MBBS MO DIH basic facts are more responsible
Community Health Cell Bangalqge
for o.stbr^ioris in drug production
and consumption than anything
else.
•'3'
rugs are the hallmark of Modern
Eternal vigilance is required to
Medicine. The 'healing professions’
ensure that the health care sys
throughout the ages have always
tem does not get medicalised,
used 'natural' or 'synthetic' products^^ that the doctor-drug-producer
for their medicinal value, to treat var
axis does not exploit the people
ious common ailments of people.
and that the abundance of drugs
Drugs, however, have never in the 4*3 does not become arrested inter
past dominated the medical scene
est in ill-health.”
as they have done in the second half
2
’’’
irjwigs are a serious
of this century. Today, the ‘pill
Indictment
of
every ///’culture is well established. It
"*
’’’ the medical profession
has ensured that we are probably
the most ‘drugged generation' of all
times. Not a very healthy thought!
Throughout the centuries, philo
sophers, social activists and con
cerned doctors have warned against.,
the dangers and problefris qtqyeruse^
or misuse of drugs by doctors and
the people.
The IndiarfSpituatiDTi
"There are two types
of physicians - those
who promote life and
attack diseases; those
who promote diseases
and attack life.”
- Charaka Samhita
The Indian Council of Meclical
Research.,and the Indian Council of
Social Sciences Researcnset up a
joint study group to study the health
situation in India and evolve an alter
native strategy for our commitment and the drug industry in the country.
to ‘Health for All by 2000 AD." This It confirms the growing evidence
high powered expert committee had that drugs are being pushed on an
some very interesting things to say unsuspecting public by devious
about the present situation of drugs methods which masquerade as
of nrug
drug companies
and prescribing practices, in theip^ 'sales
sales promotion’ or
Report published in 1981. (1J
4Kand ‘professional prescribing prac* “There is now an over-production
by doctors and health workers.
of drugs (often very costly) meancornrr|itted tb
for the rich and well-to-do whiles? Health^^d to be concerned about
the drugs needed by the poor this situgifon. The promotion of a
people (and these must be cheap) 'Rationatitfyg Use'by the medical
profession'^d health workers and
are not adequately available. This
skewed pattern of drug produc ultimately by the consumers - the
tion is in keeping with our inequi- patient community and the public, is
tous social structure which an important item on the agenda of
stresses the production of luxury HEALTH ACTION.
goods for the rich at the cost of Irrational Drug Use-some
the basic needs of the poor.;...
dimensions
* One of the most distressing
To understand the principles of
aspects of the present health Rational Drug Use. one needs to first
situation in India is the habit of identify and appreciate the elements
RATIONAL DRUG THERAPY
of irrationality in the present situa
tion A spate of reports appearing in
our newspapers and periodicals high
light these elements. Of all of them.
however, the report of the recent
‘Lentm Commission' and its shocking
findings are the most telling.
Irrationality in drug use arises out of
three sets of factors.
A Irrationality in drug production,
marketing a -d availability
8 Irrationality in prescribing practi
ces of doctors and health
workers
C Irrationality in drug use by the
consumer public.
All these taken together result in
the situation we find ourselves today.
A Irrationality in drug produc
tion, marketing and availa
bility
Industrial Policy
Drug policy continues to be part
of the industrial policy and not
/part of the health policy. Indus
trial growth and profit margins
determine the policy and not
hesjfh needs of the people.
□ ver abundance
There is a plethora of drugs pro4i?0ced in the country. The Hathi
Committee recommended 116
as essential and the WHO says
2O0ffire necessary. At present
there are over 60,000 formula
tions in the country.
Quality of drugs
Twenty percent of the drugs
available in the country are sub
standard and spurious. Many are
adulterated. Many apioid and
being sold after the|g$iry dates
are over.
Turmeric powder ^Tetracy
cline capsules and poor quality
intravenous fluids^Ig^e been
reported. The substandard ‘gly
cerol’ in J J Hospital highlighted
by the Lentin’report is another
example.
Unwanted Drugs
The formulations available include
the following;
i Banned drugs: Drugs which
have been banned in many
countries such as Lomotil and
Clioqujnol.
HEALTH ACTION AUGUST 1BBB • 5
COVER STORY
ii
RATIONAL DRUG THERAPY
Irrational
combinations: ★ Over-the-counter sales
Formulations which have
combinations that are anta
gonistic or irrational. The
Hath! Committee had sug
gested weeding out of atleast
23 such groups of prepara
tions. These were finally
banned by a gazette notifica
tion in July 1983 but continue
to be available.
iii
Hazardous or Bannable
drugs: Hazardous drugs
Sale of drugs over-the-counter
without doctor's prescriptions or
the necessary statutory checks
are not at all uncommon. This
results from inadequate drug leg
islation and even more inade
quate drug controls. Over-thecounter unauthorised sales of
prescription drugs, which now-adays do not even have the pre
cautionary product information
make the situation even more
hazardous.
which should not be available
without prescription or ade
quate medical supervision.
Preparations containing anal
gin, oxyphenbutazone
and
cortico-steroids are the
who
commonest examples (Refer ‘‘The physician
A to Z of Drug use - page 31) sets about to treat a
iv
Drugs promoted for indica disease without know
tions that are not clinically
proven or are potentially dan ing anything about it is
gerous, eg., promotion of EP to be punished even if
Forte combinations for preg
he is a qualified physi
nancy testing and induction of
abortion even when there is cian; if he does not give
well documented evidence proper treatment, he
that risk of foetal deformity is
increased by the use of these is to be punished more
preparations, (now banned severely; and if by his
since 1988 June 30.)
treatment the vital
v
Costly Drugs: Drugs which
are inflated in cost by inclusion
of costly, additional, often un
necessary ingredients or by
cosmetic embellishments in
manufacture and packaging.
Tonics and high protein foods
especially baby foods are good
examples.
functions of the pati
ent are impaired, he
must be punished most
severely.”
- Koutilya
Arthashastra
* Wrong Priorities
There is over-production of un
important drugs or drugs for the
rich while drugs for some com
mon health problems are in short
supply. T onics, vitamins, hormone
preparations and high protein
substitutes are being produced in
wasteful abundance while drugs
for leprosy and tuberculosis (two
major public health problems) are
produced at one third and one
fourth of actual requirements.
Similarly Vitamin A and many
vaccines urgently required for
child care programmes are fre
quently in short supply.
6 • HEALTH ACIION AUGUST 19HB
★ Escalating Prices
Price control policies have been
both inadequate and ineffective
and hence the cos. of drugs has
been constantly escalating. With
liberalization policies of the pre
sent government this is bound to
increase further. The purchasing
power of majority of our patients
is limited. With increasing prices,
patients are forced to buy only
part of a prescription or go in for
sub-standard alternatives pro
moted by the drug shops.
B Irrational Drug
Prescribing
Doctors, nurses ano health
workers often prescribe or adminis
ter drugs irrationally. The types of
irrational drug prescribing has been
classified as follows: (4)
Type of
Occurs if a drug is
irrational
prescribed when:
drug use
1 Extravagant - A less expensive
prescribing
drug would pro
vide comparable
efficacy and
safety
- symptomatic
treatment of
mild conditions
divert funds from
treating serious
illness
- a brand name is
used where less
expensive equi
valents are
available.
2
Over- the drug is not
prescribing
needed
- the dose is too
large
- the treatment
period is too long
- the quantity
dispensed is too
great for the
current course
of treatment
3
Incorrect
- the drug is given
prescribing
for an incorrect
diagnosis
- the wrong drug
is selected for
the indication
- the prescription
is prpnared
impt erly
- adjustments are
not made for co
existing medical.
genetic, envir
onmental or
other factors.
4
Multiple
- two or more
prescribing
medications are
used when one
or two would
achieve virtually
the same effect.
COVER STORY
- several related
conditions are
treated when
treatment of the
primary condition
will improve or
cure the other
conditions.
5
Under
- needed medicaprescnbing
tions are not
prescribed
- doser is
inadequate
- length of treat
ment is too brief.
□rug:
Caution against use
USA
Mexico
Brazil
Argentina
There are many background fac
tors which lead to such prescribing
practices.
By infants, children;
during pregnancy: liver
or kidney impairement
[latter can be fatal) or
if overly sensitive to
light.
By infants, children.
during pregnancy or if
overly sensitive to
light.
By infants, children,
during pregnancy
None
Inadequate continuing
education
The doctor, pharmacist, nursa or
health workers in field practice
are inadequately supported by a
process of continuing education
by their professional associations
and training institutions. Once
graduation is over, there is little
opportunity to refresh one's
knowledge of drugs and medical
matters through unbiased sour
ces of information.
vomiting, diarrhoea,
nausea, stomach
upset.
vomiting, nausea,
stomach upset,
rashes
None
.
..■.M.-Z'..'
time to make a good clinical
judgement often results in an
irrational prescription including
drugs for all eventualities.
"Physicians prescribe
medicine of which they f Inducements by medical
companies
know little, to cure
Misinformation is not the only
diseases of which they
method by which doctors are
made
to prescribe irra^iaualiy by
know less, in human
medical companies. Sales promo
beings of which they
tion includes a host of practices
know nothing. ”
such as unethical trade dis
counts, bribes, gifts, sponsorship
- Voltaire
for conferences and travel. The
commercial proposition induces
18th century
many doctors
unethically.
to
prescribe
Unauthorised prescribing
d
Prescribing
power
for
prestige/
Doctors especially often pre
scribe extravagantly as a sign of
'prestige' and 'power'. In India
people often consider a good
doctor to be one who gives a long,
costly prescription, in keeping
with his list of degrees. Many
doctors succumb to this cultural
status symbol. A vicious cycle is
maintained thereby.
wcUnethical medical
advertising
Medical advertising of drugs has
been more often than not. found
to be full of unproven claims of
efficacy. In addition, promotional
literature all over the world by the
same company for the same drug
has been found to be vastly dif
ferent. Facts are withheld or mod
ified. Statistics are used in a
biased manner. Drug company
sponsored misinformation is not
uncommon.
Adverse reaction
publicized
Vomiting, diarrhoea,
nausea, stomach
upset, rashes, kidney
poisoning, can poison
fetus.
Courtesy: Mother Jones, USA
Inadequate training
Doctors, nurses, pharmacists
and health workers may be
inadequately trained in the use of
drugs. The training may be theo
retical and not geared to the
practice of prescribing in the real
life situation. Technical minutiae
may be stressed at the cost of
information on cost, social con
text and hazard.
b
Tetracycline (antibiotic used against various
infections; Lederle Laboratories)
How does such prescribing take
place?
a
RATIONAL DRUG THERAPY
e
Busy outpatients
Many of our institutions are
understaffed especially those run
by the government. The queues
at the out-patient clinic are long
and there is a heavy rush. Lack of
Health workers and practitioners
of other non-allopathic systems
of medicine are often by virtue of
their training unauthorised to
prescribe all the drugs in the med
ical armamentarium. Health
workers may be trained to pres
cribe only a few drugs. Too often
theygetalarger number of drugs
and dispense them to get the
community's approval and get
greater prestige. Many tradi
tional medicine practitioners,
dispense allopathic drugs with lit
tle background training or
knowledge.
□ rugs as a substitute for
caring
□rugs have become a symbol of
the new medical culture, where
HEALTH ACTION AUGUST 1908 • 7
COVER STORY
treatment is primarily drug
oriented and all other aspects of
'caring' and nursing of the patient
are relegated to the back ground.
When simple home remedies like
hot water gargles and nursing
procedures can provide relief to
many symptoms of the patients,
doctors prefer to prescribe
symptomatic drugs instead, thus
increasing drug consumption
irrationally.
i
Commercialisation
medical profession
of
the
There was a time not so long ago
when the doctors' profession
was a vocation. Aspirants to the
profession saw service to the
sick and ailing as more important
than the financial rewards they
would get, if at all, from their
grateful patients. Today the
situation has changed drastically.
Parents are willing to pay lakhs to
get their children into medical
school. No such investment
would be made if the returns
were not equally rewarding. Aspi
rants today therefore see medi
cine as a business investment. In
such a social ethos ‘irrational
prescribing' for pecuniary bene
fits would not at all be frowned
upon. In fact it may even be seen
as a stepping stone to success.
c
Drug use by Consumer Pub
lic - irrational dimensions
i
Self-medication
Medication by patients them
selves is not an uncommon
problem. Either they are too
poor to consult doctors or
because of the easy availabi
lity of drugs they medicate
themselves, encouraged by
the pharmacists, advertise
ments, peer group informa
tion or advise of family
members. A survey con
ducted by the National Insti
tute of Nutrition in the twin
cities of Hyderabad and
Secunderabad covering 10
percent of the 330 retail
Pharmaceutical shops sho
wed that self-medication rate
was an alarming 46 percent.
I
'
ii
take a medicine, not as the
doctor has directed but just
enough to feel better. This is
often the case with antibio
tics and particularly for child
ren. Unused medicine is kept
in the home pharmacy and
given to one or other of the
children or family member
who gets the same symp
toms, next. Unused or unuti
lized portion of prescribed
medicine is often kept beyond
expiry date. If proper storage
Use of unutilized drugs
It is a very common habit
among the consumer public to
Children may have access to
it and this may lead to acci
dental poisoning.
iv
v
vi
■
precautions are not taken, it
may also get denatured. Use
of such medicines is a major
cause of untoward reactions.
iii
Inadequate labelling
storage of medicine
or
Medicines prescribed by doc
tors are often inadequately
labelled by the dispensing
pharmacist. Storage instruc
tions are not very clearly
explained to the patient The
medicine cupboard is often a
source of irrational drug use.
Multiple consultations
Patients often go to many
doctors seeking quick relief of
their symptoms. The doctors
are not often aware that con
sultation with them is one of
many such concurrent events.
Generalists and Specialists
may both be consulted. Prac
titioners of different systems
may be consulted simultane
ously. Different medicines
given by different doctors are
then consumed with the hope
of getting relief. When relief
does occur it is not easy to
decide which medicine brought
it about
Multiple prescriptions then
become a way of life when
symptoms recur. Many drugs
may potentiate one another.
Others may work at cross
purposes. When the consul
tation is of plural systems the
confusion is worse.
usa
-
Status-symbol drugs
Capsules, injections, and
tonics have become status
symbol drugs. They are
thought to be more effective
and also being costlier are
considered to be of greater
prestige value. Patients often
demand or pressurise their
doctors to prescribe one or
more of these and doctors
often comply with the request
to retain the patient and fam
ily in their practice.
lity or need or in other
words improperlypre
'
Peer-group exchange
Consumers of drtigs often
advise relatives, friends and
neighbours about the benefits
a particular prescribed drug
has given them. They are
advised to take these drugs
for what is thought to be a
similar complaint or disease.
This peer group exchange is
often the cause of much irra
tional drug use by. the lay
public.
“The incidence of dis
ease cannot he manip
ulated and so increa
sed sales volume must
depend at least in part
on the use of drugs
unrelated to their uti
scribed, Human frailty
can be manipulated
and exploited and this
is fertile ground for
anyone who wishes to
increase profits,”
- Kefauver Committee
Hearing’on Drugs,
RATIONAL DRUG THERAPY
vii
Inadequate Consumer
Awareness
Probably one of the key fac
tors for irrational drug use by
HEALTH ACTION AUGUST 1988 • 9
COVER STORY
RATIONAL DRUG THERAPY
consumers is the absence of
awareness of drug use, mis
use and the effects of over
use. Consumer education is
next to absent in India. Due to
loopholes in the existing laws,
precautionary product infor
mation is not supplied with the
medical products. The media,
the medical profession, the
educational system and the
social welfare agencies con
centrate on the misuse of
psychotropic substances and
drug abuse. Misuse, overuse
or abuse of commonly pre
scribed drugs is not consi
dered to be an adequately
serious problem for consumer
education. The problem is
further compounded by a
large illiterate population and
the need of such efforts to be
in multiple languages when
they do get organized.
Rational Drug use - Principles
The irrationalities and predispos
ing factors promoting unsafe drug
use in our country have been des
cribed. The challenge that faces all of
us today is: How to counter this
phenomena9 Health for All by 2Q00
AD would be an empty slogan if we
did not join and participate actively in
a consumer and professional move
ment to tackle the 'irrational drug
use' problem. In the absence of
prompt efforts in this direction, we
would probably arrive at a situationover abundant drugs and ill-health for
all by 2000 AD,
What could be our prescription for
action?
A thorough understanding of the
situation would lead us to appreciate
the following principles. (3)
Rational Drug Use
■k means practice of socially con
scious, relevant and scientifically
sound medicine
•A- emphasises the selective use of
drugs based on
- essentiality
- efficacy
- safety
- easy availability
- low cost
- ease of administration
- adequate quality
- preferably of indigenous produc
tion
10 • HEALTH ACTION AUGUST 1986
★ recognises the concept of essen
tial drugs and the concept of
graded lists for different levels of
health personnel
★ recognises the non-role of drugs
in certain conditions, the role of
alternative systems of medicine in
some other conditions and recog
nises the overall limitations of
allopathic medicine in our eco
nomy , social and cultural context.
★ accepts a conscious decision to
boycott certain drugs which are
hazardous or bannable or banned
and use all others only when they
are really needed.
★ means prescription with aware
ness, to avoid as far as possible
iatrogenesis (doctor induced dis
ease) which includes - drug induced problems
- drug interactions
- adverse drug reactions
- emerging drug resistance
* recognises the rights of health
personnel and consumers to un
biased drug information and its
effective communication,
★ understands the role of drugs in
the emerging health movement.
For al! of us concerned about the
increasing medicahsmg of health
action and the ‘over abundance of
drugs'becoming a ‘vestedinterest in
ill health' there is a phenomenal
challenge in making the above
principles of Rational Drug use
- common knowledge
- common practice
- commom commitment.
In conclusion, drugs have allayed
pain and suffering over the centuries.
They have helped many live more
comfortable, productive and mean
ingful lives. All of us committed to the
health movement must ensure that
drugs should continue to play their
limited but useful role in medical ser
vice. However, the use of drugs L nowingly and unknowingly, to make profit
out of human health must stop.
And it will only if
Governments;
drug industries;
planners;
health professionals;
medical colleges;
pharmacy colleges;
nursing colleges,
drug controllers;
pharmacists;
journalists and media persons;
teachers and educators;
social development activists;
consumer groups;
and
the public
commit themselves to promot
ing a Rational Drug Use.
References
1
2
3
4
"
5
6
ICMR/ICSSR (1981)
Health for All-An alternative
Strategy.
VHAK1986)
Banned and Bannable drugs
Shiva Mira (1985)
Rational Drug Therapy
Medical Service, Vol. 42, No. 1,
January 1985.
Management Sciences for Health
(1982)
Managing Drug Supply
Boston, Masachusetts, USA
Narayan Ravi (1984)
Consumer Alert - Consumer
Action
Medical Service, Vol 41, No. 9,
October-November 1984
Werner David 8. Bower Bill
(1982)
Helping Health Worker's Learn
Hesperian Foundation, USA.
Dr J.B. Chandramoujleswara Rao
B.Sc., M.8.B.S
Physician and Surgeon
and
Dr. Mrs. Krishna Kumari
M.e.B.S. O.GO.
Gynaecologist
uuith ten years experience in
their respective fields seek
appointment in hospitals of the
Tuuin cities of Hyderabad and
Secunderabad.
Address:
M.I.G.-l, SRTHRAMPRDU
ELURU 534 006
WEST GODRVRRI DT.
DRUG POLICIES - GOVERNMENT OF INCIA 1978
The Hath! Committee Report
The Government of India set up on February 8, 1974 a
Committee under the Chairmanship of Shri Jaiskhlal Hathi ano
other members of Parliament along with various officials and
non-officials, to enquire into the various facts of the crug
Industry in India.
The Hathi Committee submitted its report to Government
in April 1975. The Eport was laid on the tables of both houses
of Parliament in May 1975. /vfter several inter ministeral
discussion, and discussions with representatives of drug industry,
the views of the cabinet committee was put in February 1977, but
could not be considered. Final decisions of Government based on thereports were made on 29th March 1978.
Broad objects of the 'New Drug Policy
(i) To develop self-reliance in drug technology;
(ii) To provide a leadership role of the public sector;
(iii) To aim at q ..ick self-sufficiency in the ourput
of drugs with a view to reduce the quantum of
import s;
(iv) To foster and encourage the growth of the Indian
sector;
'
(v) To ensure that the drugs are available in abundance
in the country to meet the health needs of our people;
(vi) To make drugs available at reasonable prices;
(vii) To keep a careful watch on the quality of production
and prevent adulteration and mal-practices;
(viii) To offer special incentives tO' firms which are
engaged irz Research and Development; and
(ix) To provide other parameters to control, regulate
and rejuvenate this industry as a whole, with parti
cular reference to containing and channelizing the
activity of foreign companies in accord with national
objectives and priorities.
The new drug policy aims at promoting the Indian Drug
Industry. At first the Hathi Committee also recommended that the
Multinationals should be taken up by Government, however, since this
was a drastic change, this view was not adopted.
If nationalisation
takes place Government would also take over Indian companies above
a certain size. Certain stringencies were, however, laid down with
rc-garo to foreign companies like Small Scaie Sector will be a
prombitec area, formulation licences for foreign companies will be
given only if they.are linked with the production of ohioh technology
bulk crugs from the basic stage.
'
Jy
Another important policy adopted was with regard to Brand
names.
n^m?5 shall be abolished in the first instance in
respect of the following five drugs ;. . .2
COVER STORY
Oipug use
Dr Ravi Narayan, MBBS MD DIH
Community Health Cell Bangalpjje
doctors to over-prescribe glam
orous and costly drugs with
limited medical potential. It is also
unfortunate that the drug pro
ducers always try to push doc
tors into using their products by
all means - fair or foul. These
basic facts are more responsible
for dispbtjions in drug production
and consumption than anything
else. 4?
Eternal vigilance is required to
ensure that the health care sys
tem does not get medicalised,
that the doctor-drug-producer
axis does not exploit the people
and that the abundance of drugs
does not become awested interest hi
|n in
di-health
Sst
—i icaici i. ■■
UnJ rugs are the hallmark of Modern
Medicine. The 'healing professions'
throughout the ages have always
used 'natural' or 'synthetic' products^’
for their medicinal value, to treat var
ious common ailments of people.
Drugs, however, have never in the
the medical
scene
■past, dominated
,
,
.
, ,
as they have done in the second half
_ 5 are a serious
of this century. Today, the 'pill for*W
wanwigs
indictment of the medical profession
every ill culture is well established. It
has ensured that we are probably
the most 'drugged generation' of all
times. Not a very healthy thought!
Throughout the centuries, philo
sophers. social activists and con
cerned doctors have warned against.
the dangers and problems of overuss*
or misuse of drugs by doctors and
the people.
-
The Indiarf.^ituatioh
"There are two types
of physicians - those
who promote life and
attack diseases; those
who promote diseases
and attack life."
- Charaka Samhita
The Indian Council of Me*dical
Research-.and the Indian Council of
Social Sciences ResearcH’set up a
joint study group to study the health
situation in India and evolve an alter
native strategy for our commitment and the drug industry in the country.
to 'Health foe All by 2000 AD." This It confirms the growing evidence
high powered expert committee had that drugs are being pushed on an
some very interesting things to say unsuspecting public by devious
about the present situation of drugs methods which masquerade as
t ‘saies
sales piuiiiuuuii
promotion’ ui
of unug
drug companies
and prescribing practices, in thei&t
Report published in 1981. (1)
.and ‘professional prescribing prac* “There is now an over-production
doct°rs anc*health workers.
of drugs (often very costly) meant«?™^f us who are committed tb
for the rich and well-to-do whil^-/ Healthjpqqd to be concerned about
the drugs needed by the poor this situjjwon. The promotion of a
'Flationaiy^jnjg Use’by the medical
people (and these must be cheap)
are not adequately available. This profession "igjd health workers and
ultimately
by the consumers - the
skewed pattern of drug produc
tion is in keeping with our inequi- patient community and the public, is
tous social structure which an important item on the agenda of
stresses the production of luxury HEALTH ACTION.
goods for the rich at the cost of Irrational Drug Use - some
the basic needs of the poor.:...
dimensions
★ One of the most distressing
To understand the principles of
aspects of the present health Rational Drug Use, one needs to first
situation in India is the habit of identify and appreciate the elements
RATIONAL DRUG THERAPY
of irrationality in the present situa
tion A spate of reports appearing in
our newspapers and periodicals high
light these elements. Of all of them.
however, the report of the recent
'Lentm Commission' and its shocking
findings are the most telling.
Irrationality in drug use arises out of
three sets of factors:
A Irrationality in drug production.
marketing ?"d availability
B Irrationality in prescribing practi
ces of doctors and health
workers
C Irrationality in drug use by the
consumer public.
All these taken together result in
the situation we find ourselves today.
A Irrationality in drug produc
tion, marketing and availa
bility
Industrial Policy
Drug policy continues to be part
of the industrial policy and not
;part of the health policy. Indus
trial growth and profit margins
determine the policy and not
heajjh needs of the people.
- Over abundance
' There is a plethora of drugs pro
ceed in the country. The Hathi
Committee recommended 116
as essential and the WHO says
ROGhare necessary. At present
there are over 60,000 formula
tions in the country.
Quality of drugs
Twenty percent of the drugs
available in the country are sub
standard and spurious. Many are
adulterated. Many arq^old and
being sold after thegjipiry dates
are over.
Turmeric powder ^^tetracy
cline capsules and^pqor quality
intravenous fluidsS^^e been
reported. The substandard ‘gly
cerol’ in J J Hospital highlighted
by the Lentin report is another
example.
Unwanted Drugs
The formulations available include
the following:
i Banned drugs: Drugs which
have been banned in many
countries such as Lomotil and
Clioqujnol.
HEALTH ACTION AUGUST 1988 • 5
COVER STORY
ii
RATIONAL DRUG THERAPY
Irrational
combinations: ★ Over-the-counter sales
Formulations which have
combinations that are anta
gonistic or irrational The
Hathi Committee had sug
gested weeding out of atleast
23 such groups of prepara
tions. These were finally
banned by a gazette notifica
tion in July 1983 but continue
to be available.
iii
Hazardous or Bannable
drugs: Hazardous drugs
Sale of drugs over-the-counter
without doctor's prescriptions or
the necessary statutory checks
are not at all uncommon. This
results from inadequate drug leg
islation and even more inade
quate drug controls. Over-thecounter unauthorised sales of
prescription drugs, which now-adays do not even have the pre
cautionary product information
make the situation even more
hazardous.
which should not be available
without prescription or ade
quate medical supervision.
Preparations containing anal
gin. oxyphenbutazone
and
cortico-steroids are the
who
commonest examples (Refer “The physician
A to Z of Drug use - page 31) sets about to treat a
iv
Drugs promoted for indica disease without know
tions that are not clinically
proven or are potentially dan ing anything about it is
gerous, eg., promotion of EP to be punished even if
Forte combinations for preg
he is a qualified physi
nancy testing and induction of
abortion even when there is cian; if he does not give
well documented evidence proper treatment, he
that risk of foetal deformity is
increased by the use of these is to be punished more
preparations, (now banned severely; and if by his
since 1988 June 30.)
treatment the vital
v
Costly Drugs: Drugs which
are inflated in cost by inclusion
of costly, additional, often un
necessary ingredients or by
cosmetic embellishments in
manufacture and packaging
Tonics and high protein foods
especially baby foods are good
examples.
functions of the pati
ent are impaired, he
must be punished most
severely. ”
- Koutilya
Arthashastra
★ Wrong Priorities
There is over-production of un
important drugs or drugs for the
rich while drugs for some com
mon health problems are in short
supply. T onics, vitamins, hormone
preparations and high protein
substitutes are being produced in
wasteful abundance while drugs
for leprosy and tuberculosis (two
major public health problems) are
produced at one third and one
fourth of actual requirements.
Similarly Vitamin A and many
vaccines urgently required for
child care programmes are fre
quently in short supply.
6 • HEALTH AC I ION Al IGUS1 19HB
★ Escalating Prices
Price control policies have been
both inadequate and ineffective
and hence the cos. of drugs has
been constantly escalating. With
liberalization policies of the pre
sent government this is bound to
increase further. The purchasing
power of majority of our patients
is limited. With increasing prices,
patients are forced to buy only
part of a prescription or go in for
sub-standard alternatives pro
moted by the ding shops.
B Irrational Drug
Prescribing
Doctors, nurses and health
workers often prescribe or adminis
ter drugs irrationally. The types of
irrational drug prescribing has been
classified as follows: (4)
Type of
Occurs if a drug is
irrational
orescribed when:
drug use
1 Extravagant - A less expensive
prescribing
drug would pro
vide comparable
efficacy and
safety
symptomatic
treatment of
mild conditions
divert funds from
treating serious
illness
a brand name is
used where less
expensive equi
valents are
available.
2 Overthe drug is not
prescnbing
needed
the dose is too
large
the treatment
period is too long
the quantity
dispensed is too
great for the
current course
of treatment
3 Incorrect
the drug is given
prescribing
for an incorrect
diagnosis
the wrong drug
is selected for
the indication
the prescription
is preoared
tmpi erly
adjustments are
not made for co
existing medical.
genetic, envir
onmental or
other factors.
two or more
4 Multiple
prescribing
medications are
used when one
or two would
achieve virtually
the same effect.
COVER STORY
- several related
conditions are
treated when
treatment of the
primary condition
will improve or
cure the other
conditions.
5 Under
- needed medicaprescribing
tions are not
prescribed
- dosag is
inadequate
- length of treat
ment is too brief.
□rug:
Caution against use
US.A.
Mexico
Brazil
Argentina
There are many background fac
tors which lead to such prescribing
practices.
By infants, children,
during pregnancy: liver
or kidney impairement
(latter can be fatal) or
if overly sensitive to
light.
By infants, children,
during pregnancy or if
overly sensitive to
light.
By infants, children,
during pregnancy
None
Inadequate continuing
education
The doctor, pharmacist, nurse or
health workers in field practice
are inadequately supported by a
process of continuing education
by their professional associations
and training institutions. Once
graduation is over, there is little
opportunity to refresh one's
knowledge of drugs and medical
matters through unbiased sour
ces of information.
vomiting, diarrhoea,
nausea, stomach
upset.
vomiting, nausea,
stomach upset,
rashes
None
time to make a good clinical
judgement often results in an
irrational prescription including
drugs for all eventualities.
"Physicians prescribe
Inducements
by
medical
medicine of which they f companies
know little, to cure
Misinformation is not the only
diseases of which they
method by which doctors are
made to prescribe irraJorialiy by
know less, in human
medical companies. Sales promo
beings of which they
tion includes a host of practices
know nothing."
such as unethical trade dis
counts, bribes, gifts, sponsorship
- Voltaire
for conferences and travel. The
commercial proposition induces
18th century
many doctors
unethically.
to
prescribe
Unauthorised prescribing
d
Prescribing
power
for
prestige/
Doctors especially often pre
scribe extravagantly as a sign of
'prestige' and 'power'. In India
people often consider a good
doctor to be one who gives a long,
costly prescription, in keeping
with his list of degrees. Many
doctors succumb to this cultural
status symbol. A vicious cycle is
maintained thereby.
-"-cUnethical medical
advertising
Medical advertising of drugs has
been more often than not. found
to be full of unproven claims of
efficacy. In addition, promotional
literature all over the world by the
same company for the same drug
has been found to be vastly dif
ferent. Facts are withheld or mod
ified. Statistics are used in a
biased manner. Drug company
Sponsored misinformation is not
uncommon.
Adverse reaction
publicized
Vomiting, diarrhoea.
nausea, stomach
upset, rashes, kidney
poisoning, can poison
fetus.
Courtesy: Mother Jones, USA
Inadequate training
Doctors, nurses, pharmacists
and health workers may be
inadequately trained in the use of
drugs. The training may be theo
retical and not geared to the
practice of prescribing in the real
life situation. Technical minutiae
may be stressed at the cost of
information on cost, social con
text and hazard.
b
Tetracycline (antibiotic used against various
infections; Lederle Laboratories)
How does such prescribing take
place?
a
RATIONAL DRUG THERAPY
e
Busy outpatients
Many of our institutions are
understaffed especially those run
by the government. The queues
at the out-patient clinic are long
and there is a heavy rush. Lack of
Health workers and practitioners
of other non-allopathic systems
of medicine are often by virtue of
their training unauthorised to
prescribe all the drugs in the med
ical armamentarium. Health
workers may be trained to pres
cribe only a few drugs. Too often
they get a larger number of drugs
and dispense them to get the
community’s approval and get
greater prestige. Many tradi
tional medicine practitioners,
dispense allopathic drugs with lit
tle background training or
knowledge.
Drugs as a substitute for
caring
□rugs have become a symbol of
the new medical culture, where
HEALTH ACTION AUGUST 1988 • 7
COVER STORY
treatment is primarily drug
oriented and all other aspects of
'caring1 and nursing of the patient
are relegated to the back ground.
When simple home remedies like
hot water gargles and nursing
procedures can provide relief to
many symptoms of the patients,
doctors prefer to prescribe
symptomatic drugs instead, thus
increasing drug consumption
irrationally.
Commercialisation
medical profession
of
the
There was a time not so long ago
when the doctors' profession
was a vocation. Aspirants to the
profession saw service to the
sick and ailing as more important
than the financial rewards they
would get, if at all, from their
grateful patients. Today the
situation has changed drastically.
Parents are willing to pay lakhs to
get their children into medical
school. No such investment
would be made if the returns
were not equally rewarding. Aspi
rants today therefore see medi
cine as a business investment. In
such a social ethos 'irrational
prescribing' for pecuniary bene
fits would not at all be frowned
upon. In fact it may even be seen
as a stepping stone to success.
□ rug use by Consumer Pub
lic - irrational dimensions
i
Self-medication
Medication by patients them
selves is not an uncommon
problem. Either they are too
poor to consult doctors or
because of the easy availabi
lity of drugs they medicate
themselves, encouraged by
the pharmacists, advertise
ments, peer group informa
tion or advise of family
members. A survey con
ducted by the National Insti
tute of Nutrition in the twin
cities of Hyderabad and
Secunderabad covering 10
percent of the 330 retail
Pharmaceutical shops sho
wed that self-medication rate
was an alarming 46 percent.
ii
take a medicine, not as the
doctor has directed but just
enough to feel better. This is
often the case with antibio
tics and particularly for child
ren. Unused medicine is kept
in the home pharmacy and
given to one or other of the
children or family member
who gets the same symp
toms, next. Unused or unuti
lized portion of prescribed
medicine is often kept beyond
expiry date. If proper storage
Use of unutilized drugs
It is a very common habit
among the consumer public to
Children may have access to
it and this may lead to accidential poisoning.
iv
i.c;:■ V'-f.-...■ :
<.. -f !
. .
:
Inadequate labelling
storage of medicine
vi
Multiple consultations
Patients often go to many
doctors seeking quick relief of
their symptoms. The doctors
are not often aware that con
sultation with them is one of
many such concurrent events.
Generalists and Specialists
may both be consulted. Prac
titioners of different systems
may be consulted simultane
ously. Different medicines
given by different doctors are
then consumed with the hope
of getting relief. When relief
does occur it is not easy to
decide which medicine brought
it about
Multiple prescriptions then
become a way of life when
symptoms recur. Many drugs
may potentiate one another.
Others may work at cross
purposes. When the consul
tation is of plural systems the
confusion is worse.
..
or
Medicines prescribed by doc
tors are often inadequately
labelled by the dispensing
pharmacist. Storage instruc
tions are not very clearly
explained to the patient. The
medicine cupboard is often a
source of irrational drug use.
Status-symbol drugs
Capsules, injections, and
tonics have become status
symbol drugs. They are
thought to be more effective
and also being costlier are
considered to be of greater
prestige value. Patients often
demand or pressurise their
doctors to prescribe one or
more of these and doctors
often comply with the request
to retain the patient and fam
ily in their practice.
precautions are not taken, it
may also get denatured. Use
of such medicines is a major
cause of untoward reactions.
iii
Peer-group exchange
Consumers of drugs often
advise relatives, friends and
neighbours about the benefits
a particular prescribed drug
has given them. They are
advised to take these drugs
for what is thought to be a
similar complaint or disease.
This peer group exchange is
often the cause of much irra
tional drug use by. the lay
public.
v
“The incidence of dis
ease cannot be manip
ulated and so increa
sed sales volume must
depend at least in part
on the use of drugs
unrelated to their uti
lity.or need or in other
words improperlypre
scribed,.Humanfrailty
can' be manipulated
and exploited and this
is fertile ground for
anyone who wishes to
increase profits.”
- Kefauven Committee
Hearing on Drugs,
""USA
RATIONAL DRUG THERAPY
vii
Inadequate Consumer
Awareness
Probably one of the key fac
tors for irrational drug use by
HEALTH ACTION AUGUST 1988 • 9
COVER STORY
RATIONAL DRUG THERAPY
consumers is the absence of
awareness of drug use, mis
use and the effects of over
use. Consumer education is
next to absent in India. Due to
loopholes in the existing laws,
precautionary product infor
mation is not supplied with the
medical products. The media,
the medical profession, the
educational system and the
social welfare agencies con
centrate on the misuse of
psychotropic substances and
drug abuse. Misuse, overuse
or abuse of commonly pre
scribed drugs is not consi
dered to be an adequately
serious problem for consumer
education. The problem is
further compounded by a
large illiterate population and
the need of such efforts to be
in multiple languages when
they do get organized.
Rational Drug use - Principles
The irrationalities and predispos
ing factors promoting unsafe drug
use in our country have been des
cribed The challenge that faces all of
us today is: How to counter this
phenomena9 Health for All by 2000
AD would be an empty slogan if we
did not join and participate actively in
a' consumer and professional move
ment to tackle the ’irrational drug
use’ problem. In the absence of
prompt efforts in this direction, we
would probably arrive at a situationover abundant drugs and ill-health for
all by 2000 AD.
What could be our prescription for
action?
A thorough understanding of the
situation would lead us to appreciate
the following principles. (3)
Rational Drug Use
■k means practice of socially con
scious, relevant and scientifically
sound medicine
* emphasises the selective use of
drugs based on
- essentiality
- efficacy
- safety
- easy availability
- low cost
- ease of administration
- adequate quality
- preferably of indigenous produc
tion
10 • HEALTH ACTION AUGUST 198B
pharmacists;
* recognises the concept of essen
tial drugs and the concept of journalists and media persons,
graded lists for different levels of
teachers and educators;
social development activists;
health personnel
consumer
groups;
★ recognises the non-role of drugs
in certain conditions, the role of and
the public
alternative systems of medicine in
some other conditions and recog commit themselves to promot
nises the overall limitations of ing a Rational Drug Use.
allopathic medicine in our eco
1 ICMR/ICSSR (1981)
nomysocial and cultural context.
Health for All-An alternative
* accepts a conscious decision to
Strategy.
boycott certain drugs which are
hazardous or bannable or banned
2
VHAK1986)
Banned and Bannable drugs
and use all others only when they
are really needed.
■3 Shiva Mira (1985)
Rational Drug Therapy
* means prescription with aware
Medical Service, Vol. 42, No. 1,
ness, to avoid as far as possible
January 1985.
iatrogenesis (doctor induced dis
ease) which includes 4
Management Sciences for Health
(1982)
- drug induced problems
Managing Drug Supply
- drug interactions
- adverse drug reactions
' Boston, Masachusetts, USA
- emerging drug resistance
5
Narayan Ravi (1984)
Consumer Alert - Consumer
* recognises the rights of health
Action
personnel and consumers to un
biased drug information and its
Medical Service. Vol 41, No. 9,
October-November 1984
effective communication.
Werner David S. Bower Bill
* understands the role of drugs in 6
(1982)
the emerging health movement.
Helping Health Worker's Learn
For all of us concerned about the
Hesperian Foundation, USA.
increasing medicalismg of health
action and the ‘over abundance of
drugs ’becoming a 'vestedinterest in
ill health' there is a phenomenal
challenge in making the above
principles of Rational Drug use
- common knowledge
- common practice
- commom commitment.
In conclusion, drugs have allayed
pain and suffering over the centuries.
They have helped many live more
comfortable, productive and mean
ingful lives. All of us committed to the
health movement must ensure that
drugs should continue to play their
limited but useful role in medical ser
vice. However, the use of drugs l nowingly and unknowingly, to make profit
out of human health must stop.
And it will only if
Governments;
drug industries,
planners;
health professionals;
medical colleges;
pharmacy colleges;
nursing colleges;
drug controllers;
Dr. J.B. Chandramowlesujara Rao
B.Sc., M.8.B.S.
Physician and Surgeon
and
Dr. Mrs. Krishna Kumari
M.8.B.S.. D.G.O.
Gynaecologist
uuith ten years experience in
their respective fields seek
appointment in hospitals of the
Twin cities of Hyderabad and
Secunderabad.
Address:
M.I.G.-1, SRTHRRMPRDU
ELURU 534 006
WEST GODRVRRI DT.
PLUG POLICIES - GOVERNMENT OF INDIA 1978
The Hathi Committee- Report
The Government of India set up on February 8, 1974 a
Committee under the Chairmanship of Shri Jaiskhlal Hathi ano
other members of Parliament along with various officials and
non-officials, to enquire into the various facts of the crug
Industry in India.
The Hathi Committee' submitted its report to Government
in April 1975. The Eport was laid on the tables of both houses
of Parliament in May 1975. Zvfter several inter ministeral
discussion, and discussions with representatives of drug industry,
the views of the cabinet committee was put in February 1977, but
could not be considered. Final decisions of Government based on the'
reports were made on 29th March 1978.
Broad objects of the 'New Drug Policy
(i) To develop self-reliance in drug technology;
(ii) To provide a leadership role of the public sector;
(iii) To aim at q..ick self-sufficiency in the ourput
of drugs with a view to reduce the quantum of
imports;
(iv) To foster and encourage the growth of the Indian
sector;
’
(v) To ensure that the drugs are available in abundance
in the country to meet the health needs of our people;
(vi) To make drugs available at reasonable prices;
(viij To keep a careful watch on the quality of production
and prevent adulteration and mal-practices;
(viii) To offer special incentives to' firms which are
engaged it/ Research and Development; and
(ix) To provide other parameters to control, regulate
and rejuvenate this industry as a whole, with parti
cular reference to containing and channelizing the
activity of foreign companies in accord with national
objectives and priorities.
The new drug policy aims at promoting the Indian Drug
Industry. At first the Hathi Committee also recommended that the
Multinationals should be taken up by Government, however, since this
was a drastic change, this view was not adopted. If nationalisation
takes place Government would also take over Indian companies above
a certain size. Certain stringencies were, however, laid down with
regaro to foreign companies like Small Scale Sector will be a
prombitec area, formulation licences for foreign companies will be
given only if they.are linked with the production of ohioh technology
bulk crugs from the basic stage.
'
'
Another important policy adopted was with regard to Brand
names. Brand names shall be abolished in the first instance in
respect of the following five drugs ;. . .2
The Drug Industry in India—
What our experts say
The Industry
Pattern of Prescribing
The total output of’the industry increased
hundredfold-from Rs. 100 million in 1947
to Rs. 10,500 million in 1978-79. This was
due to expanded production, especially of
an ever-increasing number of sophisticated
drugs, and rising prices...
One of the most distressing aspects of the
present health situation in India is the habit
of doctors to over-prescribe glamorous and
costly drugs with limited medical potential.
It is also unfortunate that the drug producers
always try to push doctors into using their
products by all means—fair or foul. These
basic facts are more responsible for distortions in drug production and consumption
than anything else.
The drug industry has enjoyed a higher
man-average profitability so that investment
therein has increased substantially from
Rs. 240 million in 1952 to Rs. 4,500 million
in 1977.
There are about 125 large and medium
factories and nearly 3, 000 small scale sector
units engaged in this industry which pro
vides
employment to
about 100,000
workers.
Pattern of Drug Production
There is now an overproduction of drugs
(often very costly) meant for the rich and the
well-to-do while the drugs needed by the
poor people (and these must be cheap) are
not adequately available. This skewed pat
tern of drug production is in keeping with
our inequitous social structure which stresses
the production of luxury goods for the rich
at the cost of the basic needs of the poor.
Out of a total production of Rs. 700
crores in 1976, 25 percent is taken away by
vitamins, tonics, health restoratives and enzy
me digestants, mostly consumed by the
relatively well-fed urban population. Twenty
percent is covered by antibiotics, only 1.3
percent by sulphonamides (a very cheap and
useful anti-infective) and 1.4 percent by anti
tuberculosis drugs...
6
Structure of the Industry
The existing drug policy rightly emphasi
ses the attainment of self-sufficiency in the
production of drugs, in increasing the share
of the Indian producers and in giving a more
significant role to public sector.
The foreign companies account for about
40 percent of the total drug production in
the country; their share in the production of
basic drugs was about 28 percent and that in
formulations, 44 percent (1978-79). This is
still high.
Price Control
The drug prices are high and continue to
rise. In some instances, Indian prices are
even higher than the international ones.
Packaging increases the cost of drugs
very greatly because the trend is to make it
attractive and highly elegant and to add
cosmetic embellishments to promote sales...
There may indeed be a glut of applications
for the introduction of 'Me-too Drugs' which
will not attract new legislation for another
five years in regard to price control...
Medical Service
Genuine
'breakthrough'
declined in recent times.
research
has
Existing prices of drugs including those
of essential drugs of everyday use is highly
inflated. For example, the cost of analgin
sold over the counter is 30 times the cost of
production.
Prices are often inflated by the use of
brand names.
Very often, prolonged controversy over
the price of a drug has resulted in stopping
its production.
The bill for import of bulk drugs, inter
mediates, solvents etc., has jumped from
Rs. 53.77 crores in 1976-77 to about Rs. 119
crores in 1979-80.
Quality Control
The standards prescribed are unrealistic...
are mechanically copied from books., and not
uniformly enforced in all parts of the country.
Consumption of Drugs
At present the supplies of drugs to urban
and rural institutions within the health care
system is very uneven. In an urban hospital,
for instance, the drug cost is Rs. 6 per patient
October-November 1984
per year while in a Primary Health Centre, it
is about 40 paise per patient per year.
An Overview
We recognise the value and significance
of drugs in the health care system. We fully
support the policy that all the essential drugs
should be produced in the country, preferably
in the Indian sector, and that they should be
made available to the people at reasonable
prices. To realize these objectives, it is
essential to lay down and vigorously imple
ment a national drug policy which will
ensure that the pattern of drug production in
the country (barring drugs meant for export)
should be geared to its actual needs. While
the supply of drugs should be adequate,
eternal vigilance is required to ensure that
the health care system does not get medicalized, that the doctor-drug-producer axis
does not exploit the people, and that the
'abundance' of drugs does not become a
vested interest in ill-healthSource :
Health for All—An alternative Strategy :
report of a study group set up jointly by the
Indian Council of Social Science Research
(ICSSR) and the Indian Council of Medical
Research (ICMR).
7
Misuse and overuse of medicines—Why ?
Some Reasons
1.
2.
3.
8
it proved more dangerous, more
costly, and' generally less effective
than penicillin. The following year,
thanks to massive advertising, Linco
cin became the best selling drug in
Mexico!
Big business The production and
marketing of modern medicines is
one of the biggest, most profitable
business in the world. Drug compa
nies are continually inventing new
products to increase their sales and
profits. Some of these medicines
are useful. But
atleast 90% of
medicine on the market today are
unnecessary.
Doctors
prescrible
them and people buy them, because
the drug companies spend millions
on advertising.
False advertising
Especially in
poor countries, much of the adver
tising, and even the information
published in 'pharmaceutical indexes',
is misleading or false. Information
on dangerous side effects is often
not included. Risky medicines are
frequently recommended for illnesses
less dangerous than the medicines.
(For example chloramphenicol has
often been advertised as a treatment
for minor diarrhoea and respiratory
infections).
Dumping
Drug
companies
in
wealthy countries sometimes produce
medicines that do not sell well in their
homelands. Or the use of certain
medicines is restricted or prohibited
because they have been proved un
safe. It is a common practice for
drug companies to ‘dump' these
medicines on poor countries—often
with a great deal of false advertising.
For example, several years ago the
U.S. government restricted the use
of Lincocin (lincomycin) because
Lack of adequate controls. Poor
countries, especially, have inadequate
laws controlling the production and
sale of medicines. As a result, many
poor countries sell up to 3 times as
many different medicines as rich
countries do. Most of these medi
cines are a waste of money. Many
are completely unreasonable combi
nations of drugs, yet they are widely
prescribed by doctors. For example,
in both Latin America and Asia, a
popular injectable medicine is tetra
cycline combined with chlorampheni
col. This is a senseless combination
because the two drugs are 'incom
patible' and should never be used
together.
5.
Bribes
and
corruption. Drug
companies in rich countries pay
millions in bribes to officials in poor
countries so that governments will
Duy their products. (A major US
Pharmaceutical
company
recenty
admitted to having spent millions of
dollars on bribes to advance its
products in poor countries).
Sale of prescription medicines
without prescriptions This
is
common in many countries (partly
because poor people cannot afford
doctors' fees). Most people who
'self-medicate' try to use the medi-
Medical Service
7.
cines well, so they follow the patterns
set by doctors. Unfortunately, this
often leads to incorrect use.
For
example, in Latin America atleast
95% of doctors, prescriptions for
Vitamin Bn injections are among the
most widely used self-prescribed
medicines in Latin America—at a cost
of millions to a people too poor to
eat well!
8.
Health Workers not adequately
informed In spite of the tremen
dous amount of self-medication in
most
countries, many programs
still do not teach health workers
much about the use—or misuse—of
commonly self-prescribed medicines.
As a result, many health workers to
meet popular demand, secretly pur
chase and administer a wide range of
medicines they know little about.
People not adequately informed.
Neither doctors nor the people are
adequately
informed
about
the
correct use of medicines. Most
doctors rely on the information given
in misleading 'blurbs' supplied with
sample medicines, while villagers
who self-prescribe often receive no
information at all. In Mexico, for
example, upto 70% of prescription
drugs are sold without prescription.
Yet the packaging of these medicines
generally contains no information
about use, dosage, or risks.
9.
Use of medicine to gain prestige
and
power. Another reason for
medicine overuse is that many pro
fessionals use their ability to medicate
as a sort of magic to make people
grateful and dependent. This way
they gain special privilege and power.
In the same way. health workers
may be tempted to give injections
or expensive drugs when home
remedies or kindly advice would cost
less and do more good.
From Helping Health Workers Learn
— David werner and Bill Bower
This rare Himalayan herb will cure your headache. If it doesn't I'll give you a
pill prepared by a famous multinational drug house.
October-November 1984
11
Medication as a Substitute for Caring
Perhaps the biggest reason for over
use of medicines, however, is that doctors
and health workers often find it easier to
hand out medicine than to give the time and
personal attention that people need.
About 4 out of 5 illnesses are self limi
This means people get well whether
ting.
doctor or health worker. They like to believe
that "there is a medicine for everything".
They are disappointed if the doctor or health
worker does not give them any, even when
medicines will do no good and the health
worker carefully explains why.
However, many doctors
and health
workers get into tne habit of giving everyone
medicine—for any and every problem they
have. The less curable the problem, the
more medicines they give!
So a 'vicious circle' results in which the
doctor always gives medicine because the
'patient' always expects (or demands) it,
because the doctor always gives it. The
prescribing of a medicine becomes both
the symbol and the substitute for
human caring. This problem especially
common in places where doctors, nurses, and
health workers are overworked. The result
is not only a costly overuse of medicine, but
a failure to meet human needs on human
terms.
At the same time, people have come to
expect medicine every time they visit a
—Helping Health Workers Learn
David Werner and Bill Bower.
they take medicine or not. Most health
problems can be better managed with
out medication. What often will help
people most is friendly advice and
understanding support.
"The physician who sets about to treat a disease without knowing anything about it
is to be punished even if he is a qualified physician; if he does not give proper treat
ment, he is to be punished more severely, and if by his treatment the vital functions of
the patient are impaired, he must be punished most severely."
—Koutilya Arthashastra
12
Medical Service
'If there are no side effects, this must be Argentina
DRUG COMPANY SPONSORED MISINFORMATION OF DOCTORS
In countries with less well-organized drug control mechanisms, studies have shown
that the same drug manufactured by the same multinational company is sold for more
indications.
with less contra-indications
less side effects
as compared to the information provided in U.S.A.
The following comparison of promotional literature for three drugs bears this out
only too well.
Drug :
Tetracycline (Antibiotic used against various infections; Lederle Loboratories)
Caution Against Use
Adverse reactions publicized
U.S.A.
By infants, children; during
pregnancy : Liver or kidney
impairement (latter can be
fatal) or if overly sensitive
to light.
Vomiting, diarrhoea, nausea, stomach
upset, rashes, kidney poisoning, can
poison fetus.
Mexico
By infants, children; during
pregnancy or if overly sensi
tive to light.
Vomiting, diarrhoea, nausea, stomach
upset.
Brazil
By infants, children, during
pregnancy.
Vomiting,
rashes.
None
None
Argentina
Drug :
nausea,
stomach upset,
Ovulen (birth control pills : GO Searle Co.) in US used for contraception only.
In some Latin countries, Searle recommends it also for regulating menstrual
cycles, premenstrual tension, menopausal problems.
Caution against use
Adverse reactions publicized
U.S.A.
If patient has tendency to
blood clot, liver dysfunction,
abnormal vaginal bleeding,
epilepsy, migrain, asthma, heart
problem.
Nausea, loss of hair, nervousness,
jaundice,
high
blood
pressure,
weight change, headaches.
Mexico
If patient has tendency to
blood clot, liver dysfunction.
Nausea,
Brazil
If patient has
blood clot
None
tendency
to
weight change.
(Contd. to page 30)
22
Medical Service
(Contd. from page 22)
Argentina
Drug :
If patient has tendency to
blood clot.
None
Imipramine (Anti-depressant, Ciba Geigy) In U.S. used for depression only. In
some Latin American countries, Ciba Geigy recommends it also for senility,
pain and alcoholism
Caution against use
Adverse reactions publicized
U.S.A.
If patient has heart disease,
history of urinary retention,
history of seizures, manic
disorder or is on typhoid
medication.
Not
recom
mended
for
children
or
during pregnancy.
Hypertension,
stroke,
stumbling,
delusions, insomnia, numbness, dry
mouth, blurred vision, constipation,
itching, nausea, vomiting, loss of
appetite, diarrhoea
Mexico
During first
pregnancy
Dry
mouth,
sweating
Brazil
If patient has heart disease;
not
recommended
for
children or during pregnancy
None
Argentina
May exaggerate response to
alcohol
None
trimester
of
constipation
itching,
(Taken from the Mother Jones. Courtesy—Health and Society, also mfc bulletin 73-4. Jan-Feb 1982).
30
Medical Service
The Crazy World of Tonics
Mukarram Bhagat
'Health' tonics are a craze with the afflu
ent in the cities with their supposedly hectic,
energy-consuming life-styles. Feeling tired?
Pop a pill or gulp down a spoonful and it will
keep you going (nobody knows where!)
The most commonly used tonics are
multi-vitamin preparations with highly exce
ssive quantities of vitamins.
Incremin C, the famous growth tonic with
the Giraffe logo, contains an important amino
acid lysine which the human body cannot
synthesise by itself. However, a teaspoon
of Incremin contains only about 300 millig
rams of lysine when just a handful of peas
contains about 1800 milligrams of lysine.
The advertising slogan that Incremin turns
"extra eating into extra growth" is medically
unsubstantiated and at best a half-truth.
The quantities of vitamin constituents of
Incremen are absurd: 10 times more vitamin
B1, 25 times more vitamin B12, 2 times
more vitamin B6 than required by the body
daily. (1)
The daily requirement of the human body
of vitamin C is about 50 milligrams, of
vitamin B1 one milligram and some others
in minute quantities of a few micrograms.
Against these well established norms, most
tonic preparations contain between 10 to 50
times the minimum requirements (2) which
are simply excreted away by the body—a
colossal waste of valuable nutrients in a poor
country. Further, most vitamins are needed
in small amounts to stimulate the processes
of normal metabolism, they are not energy
giving in themselves.
28
It is almost certain that the high-potency
multivitamin formulations consumed by the
well-fed are almost wholly rejected by the
body. For example, the daily requirements
of vitamin C can be obtained from a single
fruit or a salad helping. Vitamin A, supplied
by green, leafy vegetables, is stored in large
amounts by the body for proper vision.
Vitamin D is naturally synthesised by the
skin from daily sunlight. Despite all these
simple facts, the craze for 'health' tonics
continue unabated. (2).
Why ? Manohar S Kamath in his article
in THE DAILY MAGAZINE provide the ans
wers :
"The real culprits behind the 'tonic craze'
are the manufacturers of such formula
tions. The principal reason for their hard
selling of such products that the tonics
and vitamins fell in 'category four' of the
Drugs Price Control Act, which means
that there is no limit on profits made on
these preparations. With easy pickings and
a readymade market, no wonder then that
every new company entering the pharma
ceutical world wants to market its own
brand of tonic rather than any life-saving
drug;" (2)
Explaining how the 'tonic craze' is the
result of systematic campaigns of the large
companies, . ie says :
"The first part of the plan was the mount
ing of an intensive sales campaign to
influence doctors on the need for tonics
in their day to day practice. This was
followed by free sampling" (2)
Medical Service
"The other part of the marketing gimmic
kry in selling tonics was by directly adver
tising in the mass media, to catcl the
public eye. Slogans like "Do you feel tired
at the end of the day? You need..." or "A
woman needs iron every day" gradually
made a deep impact on the people until
many were psyched into believing that
they could not do without a tonic."(2)
Waterbury's Yellow Label Tonic, a
brand leader in the Indian tonics markets,
contains only 3 milligrams of iron per teas
poon just 1/10 of which may be absorbed
by the body. The Indian Council of ledical
Research (ICMR) recommends at least 10
milligrams for women. The producer claims
that this tonic stimulates appetites and builds
bodies. But chemical analysis has revealed
that it has 10% alcohol content which is the
real appetite-stimulant : (1),
We have noted that these tonics are not
consumed by the poor but mainly by the
relatively rich whose ordinary diet adequately
meets their vitamin and other requirements.
In recent years,'evidence has grown that the
excessive vitamins may not simply be dis
charged by the body but may even cause
severe disorders. Prolonged consumption of
excessive vitamin C may form kidney stones,
excessive vitamin A may cause diseases of
the hair, skin and liver and vitamin D in
excess may cause disorders of the kindneys
and bones. (2)
Take this further example from South East
Asia. In the U K„ Sanatogen is marketed
as a 'nerve tonic' for old women who
believe in its doubtful ability to tranquilise. But Sanatogen Powder is marketed to
stuaents in Malaysia who believe in its
ability to stimulate their minds. "Worried
about exams?" says the advertisement. San
atogen will give you "Greater energy and
concentration". Can a drug both stimulate
and sedate? (3)
A person who eats well does not need extra vitamins.
THE BEST WAY TO GET VITAMINS:
Thus, the sheer irrationality and deliber
ate exploitation of consumers through this
sinister "tonic racket" is obvious. The fact
that many such, rackets' continue unabated
is a measure of the enormous influence and
power of the large pharmaceutical corporat
ions not only in India but in many other
countries, particularly the developing ones.
More than 20 years ago, the following
words were spoken before the Kefauver
Committee hearings on drugs in the U.S.A.:
"The incidence of disease cannot be
manipulated and so increased sales volume
must depend atleast in part on the use of
drugs unrelated to their utility or need, or in
other words, improperly prescribed. Human
frailty can be manipulated and exploited and
this is fertile ground for any one who wishes
Source’. Aspects of the Drug Industry in India
C E D.
to increase profits. The enormous sales of socalled tranquillisers are only a small part of
the crop reaped from this ground. The phar
maceutical industry is unique in that it can
make exploitation appear a noble purpose "
(4)
References:
1.
Health for the Millions, VHAI, AprilJune 1981
2.
"Some Boost, and at what price?".
The Daily Magazine, 7 May 1981.
3.
The Impact of multinational corpor
ations on Health in Developing Countries, by
Charles Medawar, Seminar on Health, Food
and Nutrition, Consumers Association of
Penang, Malaysia, 15-20 Sept 1977.
4.
Drugs and the Common Man, Science
Today, November 1970.
COVER STORY
Antidotes to the Drug
The
10 Commandments Industry
of Drug Companies
Thou shaft have tens of 1
thousands of drugs.
2 Thou shaft not question 2
the price of a drug.
1
3
Thou shaft not tamper 3
with nature’s garden.
4
Thou shaft respect thy 4
doctor more than thy
self. He knows best.
Let there be an essen
tial drugs fist.
Let people know the
difference between the
essentia! and nonessential drugs.
Let there be enough of
essential drugs availa
ble and produced with
in the country.
Let there be plenty of
herb gardens, cata
logues and clearing
centres.
Let people know howto
treat their doctors.
Towards a
rational
Drug Policy:
Initiatives in
the country
1
Thou shaft betray thy 5
people and thy nation
for petty rewards.
6 Thou shaft not covet, 6 Let there be a link-up
of conscientious doc
court or subscribe to
tors/ like minded
any other system of
people.
medicine.
7 Thou shaft not reveal 7 Let there be a boycott
of all products of the 2
company secrets.
companies who violate
the code of ethics.
8 Thou shaft first seek 8 Let there be quick
exchanges of informa
remedies for "Ameri
tion on marketing pra
can and European”
ctices / banned pro
ailments.
ducts / cautions.
9 Thou shaft be a dump 9 Let there be counter
advertisements
and
ing ground for banned
quick exchanges of
drugs.
information
among
journalists
and
educators.
10 Thou shaft be a guinea 10 Let there be an awak 3
pig for new and untried
ening of the people to
the rational use of
drugs.
drugs.
5
Augustine J Veliath
Presented at the National Convention of CHA! on Rational Use of Drugs, Nov. 1984.
RATIONAL DRUG THERAPY
Arogya Dakshata Mandal,
Pune has been raising aware
ness about drug related issues
among medical professionals
and the lay public since the past
8 years. They publish a monthly 'Pune Journal of Continuing
Health Education’ - on drug
issues and have also brought out
a book 'Rational Drug Therapy’ in
December 1984.
They launched a movement
called 'Operation Medicine' in
1977 against irrational pres
cription of vitamins, tonics and
tinned foods.
All India Drug Action Net
work: A number of groups have
been working in the field of drug
related issues at various levels
during the past 3-4 years. They
have been in contact with each
other and have been working
informally together sharing infor
mation, putting forward a mem
orandum (demanding a Rational
□rug Policy), participating in
campaigns, lobbying with govern
ment etc. In August 1984, they
felt the need to have a more
organized base and have formed
the All India Drug Action
Network.
Lok Vigyan
Sanghatana,
Maharashtra, or the People's
Science Movement have laun
ched campaigns about anaemia
and irrational anti-anaemia drug
preparations and also about over
- the - counter drugs. They
organize jathas, hold district/
town seminars, write in the
mass media etc.
HEALTH ACTION AUGUST 1988 • 47
COVER STORY
4
RATIONAL DRUG THERAPY
government organization con
sisting of scientists, doctors,
engineers, social scientists,
teachers, students, workers,
peasants, technicians who are
committed
to
popularising
science and channeling it for
social revolution. The KSSP has
recently decided to take up the
□rug issue and initiate a big
campaign to expose the anti
people and exploitative tactics of
the Multinational Drug Compa
nies. The question of essential
versus non-essential and dan
gerous drugs, the inadequacy of
drug safety control measures,
the rising prices of life saving
drugs and the non-implementation of the Hathi Committee
recommendations are the high
lights of the programme.
5
LOCOST or Low Cost Standard
Therapeutics ■ is a collective
voluntary enterprise for rational
therapeutics. LOCOST aims to
promote low cost, scientifically
tested medicine under generic
names. LOCOST is a response
to a growing demand and chal
lenge of the voluntary health
sector to meet the needs of the
deprived sectors of the society
for not only low priced but also
good quality medicine. LOCOST
includes procurement, quality
testing and control, distribution
and educational efforts, and is
located in Gujarat.
6
Bangarapet Mission Tablet
Industry in Karnataka is a suc
cessful small scale venture pro
viding low cost, good quality for
mulations to some mission
hospitals in the country.
7
8
viduals, interested in the health
problems of our people. Through
their monthly bulletin, they dis
cuss drug issues among others.
They have formed a Rational
□rug Policy Cell and have
launched a campaign on antidiarrhoeals.
Kerala Sastra Sahitya Parishad is a voluntary non
Low Cost drugs and Rational
Therapeutics Cell of the
Voluntary Health Association of
India, New Delhi, has been
instrumental in bringing together
various groups in India on the
issue of drugs. They have been
providing informational backing
to these groups, organizing
meetings, informally coordinat
ing some action etc.
Medico friends circle is a
group of socially conscious indi
48 • HEALTH ACTION AUGUST 1988
9
The Kurji Holy Family Hospi
tal Formulary is the result of
the accumulated experience of
the hospital over the last 10
years. It gives a comprehensive
list of drugs to treat 98°/o of the
hospital admissions. It also gives
the generic name, dosage, indi
cations, contra-indications and
side effects of these drugs.
Information about comparative
cost of treatment is also
provided.
10 State Forums: During the past
year drug action forums have
been active in Andhra Pradesh
and West Bengal. Drug Action
forums are also being initiated in
Gujarat and Orissa.
11 The Pharmacology Depart
ment of the Post-Graduate
Institute of Medical Educa
tion and Research, Chandi
garh, provides un-biased tech
nical informtion on drugs and
therapeutics through a monthly
publication ‘The Drugs Bulletin'.
from page 14
To frustrate the move (i.e„
introduction of schedule X)
owners of the retail drug shops
under the leadership of their pow
erful Association had protested
by closing their shops for three
days and subsequently many of
them stopped storing drugs under
Schedule X (even such essential
drug like phenobarbitone to the
great inconvenience of millions of
epileptic patients!). The only plea of
the shop owners being that the
introduction of this schedule
would increase their clerical
burden as they have to maintain
proper inventory. Their plea
seems to lack substance in as
much as legally drugshop owners
are supposed to keep inventories
of all items of prescription drugs
coming under different other
schedules. Could it be that their
real difficulty lies elsewhere? It is
wellknown that majority of the
drugshops in our country are run
without a qualified staff (i.e., a
pharmacist) Only a pharmacist is
eligible to record his signatures on
the prescriptions while dispensing
a drug under Schedule X as
required by the Rule.
Courtesy:
□ rug Disease Doctor
Vol. 2 No. 4/1987
12 Others: The following organiza
tions have also been involved in
drug related issues and are part
of the All India Drug Action
Network:
Consumer guidance Society of
India, Bombay
Comsumer Education Research
Centre, Ahmedabad
Federation of Medical Repre
sentatives Association of India
Health Services Association,
Calcutta
Delhi Science Forum, New Delhi
People's Participation in Science
and
Technology,
Madras/
Bangalore
Centre for Science and Environ
ment, Delhi
Centre of Social Medicine and
Community Health, J N Univer
sity, New Delhi.
What can we do?
- Support them
- Join them
- Keep them informed
about what you are doing
RESOURCE MATERIALS
People, Pills and Prescrip
tions, column in MEDICAL SERVICE
since May-June 1984.
Understanding the Drug situ
ation in our Hospitals, a check
list.
Towards a
People-Oriented
Drug Policy, Special Convention
Issue of MEDICAL SERVICE (Octo
ber-November 1984)
Prescribing Drugs
Questions to ask yourself before writing a prescription.
1.
Need
Is this drug really necessary ?
Is it being given to make the patient feel that something is
being done ?
2.
Aim
What aim is to be achieved by this drug ?
What disorder of function is to be corrected ?
What symptom/s have to be relieved ?
3.
Knowledge
What is the approved or generic name ?
What class does it belong to ?
What are its characteristics ?
Do I have the requisite experience or knowledge to use it ?
Have I weighed
benefit ?
the
toxic
potential
against the
effects
4.
Route and Dosage
By what route, in what dose and at what intervals is the drug
to be given and why ? In what form/s does the drug come ?
5.
Alternatives
Have I selected the
purpose ?
best agent available for this particular
What other remedies might have been chosen ?
How do these compare in efficacy, safety, cost ?
6.
Duration
For what period of time, days, weeks or months will it be
advisable to continue therapy ?
7.
Observations
What observations can be made to judge whether the aim has
been achieved ?
When and how could a decision be made to stop ?
When should they be made and by whom ?
What laboratory
assessment ?
8.
Elimination
investigation
if
any would
help
in
this
How is the drug eliminated ?
Will the patients illness change the usual pattern of distri
bution, effects or elimination of the drug ?
9.
Unwanted effects
What are the side effects or toxic effects of the drug ?
Are they acceptable ?
How frequent are they ?
How can they be modified/managed ?
14
Medical Service
10.
Precautions
Have I checked for the following :
a.
possible allergic risks
b.
possible idiosyncratic reactions
c.
patients drug diet which may interfere with the drug
What precautions can I take to ensure continuation of therapy.
11.
Contraindications
Are there any conditions in which this drug is contraindicated ?
Are these 'absolute' or 'relative' ?
Are there any drugs which should
patient takes this treatment ?
be avoided when
the
Which and why ?
Patients point of view What does the patient believe about the drug ?
12.
What has he been told about it ?
And what has he remembered ?
Does he need additional information ?
Patient reliability
13.
Does his relative need additional information ?
Is the patient reliable for this type of therapy ?
Will he need'get proper supervision by relatives or attendants ?
Cost
14.
1 5.
Is the drug the cheapest drug of that type ?
If not could a cheaper drug do the job as well ?
Finally is there anything else I need to know about this drug ?
Adapted from :
The Lancet II 1186-1187, 27th Nov 1976
i.
A Herxheimer :
ii.
Formulary and Therapeutic guide—Kurji Holy Family Hospital
iii.
Prescribing drugs — MNAMS Handout, Dept of Pharmacology, St John's Medical
College, Bangalore
October-November 1984 (Suppl)
15
7
What Can We Do ?
1.
Educate ourselves
We should make an effort to
available materials on drugs.
avail ourselves of
all
the
We should purchase some of the books and subscribe to some
of the journals and bulletins mentioned in 'widening
horizons' to keep ourselves upto date.
2.
Share and
Disseminate
information
We should circulate all the information and resources to all
our staff and to other colleagues and centres through all
possible channels of communication. We could share our
own initiatives and experiences.
3.
Adopt essential
drug list
We should draw up an essential list for our institution in
which cost, efficacy, safety and quality will be important
criteria (refer to WHO's suggested list)
We could purchase and stock drugs in accordance with this
list.
4.
Adopt generic
We could use/adopt the generic drug concept during pur- J
chasing, prescribing or dispensing drugs.
5.
Stop Irrational
prescribing
Could stop prescribing drugs whose only advertised values
are :—
a.
cosmetic embellishments
b.
elegant packing
c.
irrational combinations
d.
imitative drugs
e.
inadequate evidence of greater value
We could weed out 'banned drugs' as well as restricted
drugs.
We could stop 'injection and tonic' practice.
6.
Avoid Drug
We could refuse to take gifs and physician samples
Industry Linkages
We could avoid allowing drug companies to sponsor events/
meetings
We could beware of unethical trade discounts or other forms
of inducement
7.
16
Adopt Rational :
We could adopt bulk purchasing
Drug Purchase
Support cooperative purchasing or production endeavours
Produce drugs in your hospitals'dispensaries.
Medical Service
8.
Adopt open
policy to nonallopathic systems
and non-drug
therapies
We should be open to other forms of treatment. Seek informa
tion and be willing to incorporate it in our work
Share our experience with others
Send our staff for training in these forms of treatment if
necessary.
9.
Support networks/
organization/
consumer
movements taking
up drug issues.
Find out about all such groups at local, regional, state level
or national level
Support and participate in their activities.
10.
Promote'Health for
all' priorities.
We should actively promote the following in our work :
a.
simple home remedies
b.
herbal remedies and herbal gardens
c.
health education and patient awareness
d.
training of village level workers
e.
community health initiatives
f.
development programmes
g.
awareness building.
Reporting in 1956 on the excessive amount of space taken up by advertisements in
Indian newspapers, the Indian Press Commission commented :
"The largest field of
objectionable advertising which we feel should be put down
by law is of drugs and proprietary medicines
The volume of advertising of such
commodities ranks next only to the volume of advertising of cosmetics.
—Use and Misuse of the Media
Sumanta Banerjee, World Health, Feb-March 1983
October-November 1984 (Suppl)
17
Consumer Alert - Consumer Action
Ravi Narayan
The Problem
The Indian Council of Medical Research
(ICMR) and the Indian Council of Social
Science Research (ICSSR) have, in a joint
study group report entitled "Health for All —
an Alternative Strategy" warned that 'eternal
vigilance is required to ensure that the
health care system does not get medicalised,
that the doctor-drug producer axis does not
exploit the people and that the abundance
of drugs does not become a vested interest
in ill-health'. This warning is a serious
indictment of the drug industry and the
medical profession in the country. It con
firms the growing evidence that drugs are
being pushed on an unsuspecting public by
devious methods which masquerade as
'sales promotion' of drug companies and
'professional prescribing practice' by doctors.
A spate of reports have been appearing
in our newspapers and periodicals of late,
on drug related issues and a review of these
highlight that many of the following practices
are not at all uncommon in India.
(i) Sale of drugs banned in other
countries eg: Lomotil and Clioquinol
preparations.
(v)
Promotion of drugs for indications
that are not clinically proved and are
often
potentially
dangerous
eg:
Promotion of EP forte combinations
for pregnancy testing and induction
of abortion. There is well documented
scientific evidence that risk of foetal
deformity is increased by the use of
these hormonal preparations.
(vi)
Sale of spurious, adulterated or poor
quality drugs eg: Turmeric powder in
tetracycline capsules and poor quality
and reaction producing intravenous
fluid preparations have been reported.
(vii)
Sale of old, expired and unused
drugs. There is the double danger
of effects of denatured drugs as also
of inadequate dosage.
(viii)
Over-prescription and
misuse of
tonics, high protein foods, hormonal
preparations and baby foods that
are both superfluous and a drain on
the family economy.
(ix)
Production of drugs for profits rather
than health needs of people eg: The
ICMR/ICSSR report highlights that
drugs for diseases like leprosy and
tuberculosis which affect millions
are produced at one third and one
fourth of the actual requirements
while tonics, vitamins and high
protein substitutes are being prod
uced in wasteful abundance.
(x)
Sale of drugs over the counter with
out doctors' prescriptions or the
necessary statutory checks.
(i) Sale of irrational combinations and
formulations eg: Hathi Committee has
suggested weeding out of atleast 23
such preparations.
(iii)
Sale of drugs without adequate pre
cautionary product information.
(iv)
Sale of drugs at highly inflated costs
eg: it is reported that Analgin is
being sold at 20 to 30 times the cost
of production.
October -November
33
It is evident then that what is needed in
the country today is a consumer awakening
and awareness building process that will
sensitise people to the realities of the drug
industry, mobilise public opinion, sensitise
policy makers, confront the medical esta
blishment and challenge the drug industry.
This process’ will have to the initiation,
promotion
and sustenance of consumer
action to ensure that the drug policy in India
is more 'people' and 'health' oriented. Is
there any evidence of such an awareness ?
Consumer alert and action
Beginning in the late seventies, there is
an increasing number of organisations,
associations, projects and action
groups
who have begun to create an awareness of
drug-related policy issues.
These groups
are predominantly if not exclusively urban
based, consisting of young professionals and
intellectuals
from
different
ideological
backgrounds.
Since the Medical Profession is the
'instrumental consumer' ie., they prescribe
the drugs, many of these groups have
directed their efforts particularly towards
them. Many others are health or develop
ment
associations,
science popularising
movements and consumer associations who
are increasingly taking up drug-issues as one
of their many activities.
The main types of action they have been
involved in are :—
1.
Meetings :
* ‘The Drug Industry and the Indian
People' organized by Delhi Science
Forum, Society of Young Scientists,
Federation of Medical Representatives
Association of India (FMRAI) and
others in Delhi, November 1 981.
34
* ‘Drug Issues and Feasible Alternatives'
by Voluntary Health Association of
India (VHAI) at Pune, January 1982.
* 'Drug
use and Abuse' by medico
friend circle (mfc) of Tara, June 1982.
* At the AH India Convention of People's
Science Movements at Trivandrum,
organised by Kerala Sastra Sahitya
Parishad (KSSP). A health group was
formed to coordinate joint
action
programme specially on drug issues.
♦ Seminar on 'National Health Policy'
by VHAI, Concern for Correct Medicine
(CCM), All India Women's Conference
(AIWC) and others in Delhi, April 1983.
Drug issues were also discussed.
* Meetings on ‘Drug Policy Issues' were
held in Pune, Bombay, Trivandrum,
Madras, Bangalore and Delhi during
Dr Zafarullah Chowdhury's (of Gonoshasthaya Kendra) whirlwind tour of
India in November-December 1983.
These 'galvanised everyone into more
action'. National and local press gave
coverage right along the tour.
* FMRAI Annual Convention in New
Delhi, December 1983 made a 27 point
charter of demands which included
demands for Rational Drug Policies
relevant to the health needs of the
country effective drug control, ban on
irrational and hazardous drugs.
* Misuse of Drugs — Seminar organised
by the Andhra
Pradesh
Voluntary
Health Association at Hyderabad in
. February 1984.
vs.
People' — A Seminar
organised by West Bengal Voluntary
Health Association at Max Muller
Bhavan at Calcutta in February 1984.
* ‘Drugs
* ‘Low Cost — Cost effective health Care',
one day symposium organised
Kerala Voluntary Health Services.
by
Medical Service
2.
liberties grievances, health professional
associations.
Educational Campaigns
* Arogya Dakshata Mandal (ADM) Pune,
launched a movement called 'Operation
Medicine' in July 1977 against irra
tional prescription of vitamins, tonics,
and tinned foods.
* KSSP launched a campaign for a
'People's Drug Policy' on April 7th
World
Health Day.
District level
Seminars were held in all the 13
districts of the State. On October 2nd,
the Sastra Kala Jatha was launched
with signature campaign. Slide shows,
art forms etc.
Two seminars—“The
Indian Drug Industry' and the People's
Needs" and 'A Drug Policy for Kerala'
are planned for November 1984.
* VHAI along with many associates
launched a campaign in March 1982
(International Women's Day) against
the misuse of hormonal preparations
for pregnancy testing.
* National Alliance for Nutrition of
Infants (NANI) was formed to promote
breast feeding and prevent/control of
promotion of commercial milk foods
and substitutes.
* mfc launched campaign for rational
management of diarrhoea with ORT,
and prevent misuse,'abuse of available
anti-diarrhoeals.
* Lok Vidnyan Sanghatana, Maharashtra
(PSM) launched a campaign about
anemia in women and irrational anti
anaemia drug preparations is the
market, in May 1983.
* FMRAI
have launched a separate
campaign against irrational practices
and role of multinational corporations
in pharmaceutical industry in India.
* KSSP has organised jathas (Science
and Cultural Marches) through the
villages
and
towns of Kerala in
October-November 1983 on 'War: the
war against unscientific practices in
the field of drug industry.
* Drug Action Network launched a
nation wide signature campaign in
April 1984 to demand for a Rational
Drug Policy. This campaign involves
activist and consumer groups civil
October-November 1984
3.
Publications
* mfc published two anthologies — 'In
Search of Diagnosis' (1977) and
'Health Care Which Way to Go' (1982)
which included many articles on drug
issues.
* VHAI published special issue of their
bimonthly—Health for the Millions—in
1981.
Thematic issue was entitled
'Medicine as if people mattered'.
* Centre for Education and Documenta
tion (CED), Bombay, published an
exhaustive well researched book called
'Aspects of Drug Industry in India'.
* Indian Social Institute (ISI) New Delhi,
brought out an Indian edition of the
book 'Insult or Injury' by Charles
Medawar of Social Audit (UK) which
is a study of practices of British
Pharmaceuticals and Food Industry in
Asia.
* 'Taste of Tears'is a recent publication
of VHAI on problems of diarrhoea and
its management.
* Consumer Education and Research
Centre, Ahmedabad, prepared a well
documented report on Analgesics and
submitted it to the Drugs Controller.
35
This report deals with hazardous and
irrational combinations.
* Rational Drug Therapy — first volume
of
the book by Arogya Dakshak
Mandal, expected in December 1984.
4.
Bulletins'Journals
* Pune Journal of Continuing Health
Education, by Arogya Dakshata Mandal.
sensitises its readers to the half truths
of medical advertising apart
from
providing reliable scientific information.
* 'Drugs Bulletin' — of
Pharmacology
Department of Post-Graduate Institute,
Chardigarh is a authentic and authorita
tive resource on drugs in India.
* Handouts of the Low Cost Drugs and
Rational Therapeutic Cell of VHAI
have covered an extensive range of
drug prescribing and policy issues.
5.
Low cost Drugs venturs
* Bangarapet Medical Mission Tablet
industry is a successful small scale
venture providing low cost, good
quality formulation to a limited group
of mission hospitals in the country.
* LOCOST a collective voluntary end
eavour in Gujarat for rational thera
peutics through the promotion of low
cost, quality generic medicines.
It
also plans an educational effort for
minimum use of drugs and increased
awareness of
the
socio-economic
implications of irrational therapeutics.
6.
Public Interest Litigation
* Vincent Panikulangara, a lawye> from
Kerala, filed a writ petition in the
Supreme Court, regarding the ban of
the import, manufacture, sale and
distribution of drugs identified as hazardous
Source :
36
and or irrational by the Drugs Consultative
Committee of the Government of India. This
was done on behalf of the people of India.
7,
Networking
* All these groups have now come toge
ther to form the All India Drug Action
Network. Regional and State level net
work are also forming up, eg : West
Bengal Drug Action Forum, Hyderabad
Drug Action Forum. DAN also bring out
the Drug Action Network Newsletter
which keeps the network up-to-date on
activities and ideas of all the groups.
DAN meets twice a year to plan and
coordinate its activities.
Towards a People's Movement
All the above efforts are small steps to
wards a much more wide based consumer
movement against drug u^e and abuse and
profit oriented drug policies. However, it must
be remembered that in a country like ours
when a very large percentage of people are
below the poverty line and when more than
75 percent of the people have little access to
basic health science a consumer action pro
gramme only on drug matters will continue
to be cut off from the needs and aspirations
of the majority.
Dr Norman Bethune, Famous for his work
in China, wrote ‘The best form of providing
health care and health protection would be to
change the economic system whica produces
ill health-to liquidate ignorance, poverty and
unemployment'.
One hopes that eventually drug related
issues will become part of a much wider
people's campaign for health, development
and socio-political change because at the
root of the entire problem of drug production
and availability lies what Ivan lllich has aptly
described as ‘Social-iatrogenesis-ie., health
policies reinforcing an industrial organisation
which generates ill-health'.
Bulletin of Science December 83 Jan. 84 (up dated
Medical Service
Drug Utilisation Survey Report
This survey was conducted by the National Institute of Nutrition
(NiN) in cooperation with the Dir ctorate of Drug Control Administration
and AP Chemists and Druggists Association, Hyderabad in the
twin cities of Hyderabad and Secunderabad covering 10% of the 3 30
retail pharmaceutical shops.
Some of the findings of the survey are as follows:
—
self medication rate was an alarming 46%.
-
27% of the doctors* prescriptions were for 3 to 4 drugs
Only 4.3% of prescriptions were for more than 4 drugs.
—
the maximum number of pres riptions were for Nutritional
Products (tonics, enzymatic preparations and vitamins), then
antiinfectives (antibiotics and sulfas) and then analgesics.
—
58% of the self medicated drugs were schedule 'L* and 'li*
drugs which can ot be sold without prescription, nor should be
consumed without medical supervision, because of the associated
major side effects and toxicity.
-
amongst self administered drugs analgesics, nutritional
products and antibiotics topped the list.
Analgesics, antipyretics and anti-inflammatory drugs:
-
30.2% of the self prescribed analgesics, antipyretics- anc
anti-inflammatory agents
were
scheduled drugs. These were
mainly analgin, phenylbutazone (with or without corticosteroid: )
and ibuprofen.
—
an earlier survey by the CERF (Consumer Education and Research
Centre, Ahmedabad) h.id shown that of 13 over-the-counter brands
of these drugs, 11 did not provide any information. The 44 doctors
interviewed reporte d s eing or: an average 8 to 10 cases of drug
,,,,,, 2
2
drug poisoning per month.
Vitamins and Tonics:
only 31% persons surveyed had a correct concept regarding
nutritional supplements. The majority held the erroneous view
that daily consumption of tonics was essential for health!
The credit for this false belief goes to advertising pr .ssure
as well as doctors’ prescription practices.
-
16% of the doctors had pr scribed simultaneously more than
one vitamin preparation having the same ingredientsin various
dosage forms.
—
iron deficiency anemia, B2 deficiency, were the commonest
deficiencies in the population but sales of B Complex
(Bl, B2, B6 B12) combinations and other vitamins topped
the list of sales figures.
Antibiotics:
-
over 30% of the doctors’ prescriptions contained antibiotics.
-
approximately 12.8% of self—prescribed drugs were antibiotics.
-
most antibiotic prescriptions were for sulfa and trimethoprim
combinations, tetracyclines and penicillin, in that order.
-
tetracycline, sulfa-trimethoprim and penicillin were the
most popular self-prescribed
-
drugs.
30% of the antibiotics purchased for self medication were for
less than a day. Only 18% were purchased for a full course of
five days. Only 40% of prescriptions for antibiotics were bought
for five days.
3
3
The findings of the NIN and CERC surveys indicate the urgent need for
public education where disease and drugs are concerned.
Sources The Drug Action networks Newsletter of the Low Cost
Drugs and Rational Therapeutics Cell, VHAI, New Delhi.
Minutes of the Third Meeting of the Drug Action Forum
Karnataka held on 4th December 1988.
The Drug Action Forum-Karnataka met on the 4th
December 1988 at the office of the People's Trust at
10.30 AM. The meeting was attended by the following
members :
1.
Mr N C Nanaiah
2.
Dr Satish Kumar
3.
Mr R B Hiremath
4.
Dr Vanaja Ramprasad
5.
Mr K Gopinathan
6.
Dr Gopal Dabade.
The agenda taken up for discussions were s(1)
Objectives of the Forum.
(2)
Structure/Members of the Forum.
(3)
Dissemination of information.
(4)
Mobilisation of funds.
PROCEEDINGS
1. Objectives of the Forum
(At the second meeting held on 6th November 1988, it was
decided to register the DAF-K as a Society and the
Co-ordinator has been given the necessary consent to
go ahead with the preliminary work of registration.)
The members discussed this item in great detail and
suggested the following as the likely objectives of the
Society ;
1.
To build awareness amongst general public with regard
to the usefulness/uselessness/benefit-risk ratio of
various systems of medicine in practice.
2.
To undertake studies both in rural and urban areas to
focus on issues around rational use of drugs, use of
banned drugs, economics of prescribing generic Vs brand
names and other similar studies which would help the
government authorities in formulating a people oriented
drug policy.
3.
To disseminate information on the findings of the study
and ot er related matters through newspapers, educative
magazines, journals, exhibitions, films, slides and
TV coverage.
.... .2
2
4.
To dialogue with physicians through the IMA and similar
bodies on rational drug therapy.
5.
To conduct training programmes, workshops and seminary
on matters related to drug issues.
6.
To interact with the voluntary organisations involved
in health and development in Karnataka in regard to
the importance of practice of rational drug therapy.
7.
To co-ordinate and collaborate with national and
international bodies working in a similar direction.
8.
To function as a pressure lobby and initiate steps for
enforcement of ban of any drug.
9.
To bring out a newsletter in course of time.
10.
To initiate centres of Drug Action at district level
and co-ordincte with them.
2.
The structure/members of the Forum
A decentralised structure with an apex body located in
Bangalore was thought appropriate.
To initiate the district
based network of the forum it was suggested that voluntary
organisations based in different parts of Karnataka and
preferably with doctors involved in these programmes have to
be identified and these individual centres work independently
and in union with the apex body.
In order to promote this
idea end co-opt members into the apex body, it was proposed
that discussions have to be held individually and collectively
with the following members and to invite their suggestions
and reactions on the above aspects.
1. Dr C M Francis
2. Mr Premanand Shetty - Ex-Drug Controller, Karnataka
3. Mr Shanbaug - Ex-Drug Controller, Karnataka
4. Dr Mira Shiva
5. Mr Jagadeesh Mundaragi
6. Dr Ravi I'arayan
7. Dr H Sudhershan
8. Dr Gerry Pais
9. Dr S B Maheshwara
10. Dr Anand Kabbur
11. Dr Shyama Narang
12. Mr f! B Joshi
13. Dr Dhruv Mankad
14. Mr B V Sesha
and those who were present at the meeting.
3
3
The address for the registered office is still being
considered.
3.
Dissemination of information
Dissemination of information to the public was given
enough thought during the meeting. Having an independent
bulletin either in English or in Kannada or in both though
may be necessary in the long run, it was considered more
economical to use other bulletins or journals that are
already existing to disseminate information.
The use of
the T.V. through the Bangalore Doordarshan was contemplated
and it would be explored by Dr batish Kumar and Mr Hanaiah.
4.
Mobilisation of funds
To begin with, the forum will not depend on any assured
source of funds for the conducting of the LAF-K activities.
It was suggested by the members that the Forum approach
various agencies in India including Karnataka Rajya Vignana
Parishad as also appeal to individuals for donations, for
specific projects.
The next meeting
The next meeting was fixed for the 4th of January
1989 at the office of the People's Trust at 2 PM.
5.
Minutes of the Third Meeting of the Drug Action Forum
Karnataka held on 4th December 1988.
The Drug Action•Forum-Karnataka met on the 4th
December 1988 at the office of the People's Trust at
10.30 AM.
The meeting was attended by the following
members :
1.
2.
3.
4.
Mr N C Nanaiah
Dr Satish Kumer
Mr R B Hiremath
Dr Vanaja Ramprasad
5. Mr K Gopinathan
6. Dr Gopal Dabade.
The agenda taken up for discussions were
(1)
Objectives of the Forum.
(2)
Structure/Members of the Forum.
(3)
Dissemination of information.
(4)
Mobilisation of funds.
PROCEEDINGS
1. Objectives of the Forum
(At the second meeting held on 6th November 1988, it was
decided to register the DAF-K as a Society and the
Co-ordinator has been given the necessary consent to
go ahead with the preliminary work of registration.)
The members discussed this item in great detail and
suggested the following as the likely objectives of the
Society ;
1.
To build awareness amongst general public with regard
to the usefulness/uselessness/benefit-risk ratio of
various systems of medicine in practice.
2.
To undertake studies both in rural and urban areas to
focus on issues around rational use of drugs, use of
banned drugs, economics of prescribing generic Vs brand
names and other similar studies which would help the
government authorities in formulating a people oriented
drug policy.
....
3.
To disseminate information on the findings of the study
and of er related matters through newspapers, educative
magazines, journals, exhibitions, films, slides and
TV coverage.
2
3
The address for the registered office is still being
considered.
3.
Dissemination of information
Dissemination of information to the public was given
enough thought during the meeting. Having an independent
bulletin either in English or in Kannada or in both though
may be necessary in the long run, it was considered more
economical to use other bulletins or journals that are
already existing to disseminate information.
The use of
the T.V. through the Bangalore Doordarshan was contemplated
and it would be explored by Dr tatish Kumar and Mr Hanaiah.
4.
Mobilisation of funds
To begin with, the Porum will not depend on any assured
source of funds for the conducting of the DAF-K activities.
It was suggested by the members that the Forum approach
various agencies in India including Karnataka Rajya Vignana
Parisha-1 as also appeal to individuals for donations, for
specific projects.
5.
The next meeting
The next meeting was fixed for the 4th of January
1989 at the office of the people's Trust at 2 PM.
Minutes of the Third Meeting of the Drug Action Forum
Karnataka held on 4th December 1988.
The Drug Action Forum-Karnataka met on the 4th
December 1988 at the office of the People's Trust at
10.30 AM. • The meeting was attended by the following
members :
1. Mr N C Nanaiah
2. Dr Satish Kumar
3. Mr R B Hiremath
4. Dr Vanaja Ramprasad
5. Mr K Gopinathan
6. Dr Gopal Dabade.
The agenda taken up for discussions were
(1)
Objectives of the Forum.
(2)
Structure/Members of the Forum.
(3)
Dissemination of information.
(4)
Mobilisation of funds.
PROCEEDINGS
1. Objectives of the Forum
(At the second meeting held on 6th November 1988, it was
decided to register the DAF-K as a Society and the
Co-ordinator has been given the necessary consent to
go ahead with the preliminary work of registration.)
The members discussed this item in great detail and
suggested the following as the likely objectives of the
Society ;
1. To build awareness amongst general public with regard
to the usefulness/uselessness/benefit-risk ratio of
various systems of medicine in practice.
2.
To undertake studies both in rural and urban areas to
focus on issues around rational use of drugs, use.of
banned drugs, economics of prescribing generic Vs brand
names and other similar studies which would help the
government authorities in formulating a people oriented
drug policy.
3.
To disseminate information on the findings of the study
and ot er related matters through newspapers, educative
magazines, journals, exhibitions, films, slides and
TV coverage.
2
2
4.
To dialogue with physicians through the IMA and similar
bodies on rational drug therapy.
5.
To conduct training programmes, workshops and seminars
on matters related to drug issues.
6.
To interact with the voluntary organisations involved
in health and development in Karnataka in regard to
the importance of practice of rational drug therapy.
7.
To co-ordinate and collaborate with national and
international bodies working in a similar direction.,
8.
To function as a pressure lobby and initiate steps for
enforcement of ban.of any drug.
9.
To bring out a newsletter in course of time.
10.
To initiate centres of Drug Action at district level
and co-ordinate with them.
2.
The structure/members of the Forum
A decentralised structure with an apex body located in
Bangalore was thought appropriate.
To initiate the district
based network of the forum it was suggested that voluntary
organisations based in different parts of Karnataka and
preferably with doctors involved in these programmes have to
be identified and these individual centres work independently
and in union with the apex body.
In order to promote this
idea and co-opt members into the apex body, it was proposed
that discussions have to be held individually and'collectively
with the following members and to invite their suggestions
and reactions on the above aspects.
1. Dr C M Francis
2. Mr Premanand Shetty - Ex-Drug Controller, Karnataka
3. Mr Shanbaug - Ex-Drug Controller, Karnataka
4. Dr Mira Shiva
5. Mr Jagadeesh Mundaragi
6. Dr Ravi Earayan
7. Dr H Sudharshan
8. Dr Gerry Pais
9. Dr S B Maheshwara
10. Dr Anand Kabbur
11. Dr Shyama Narang
12. Hr N B Joshi
13. Dr Dhruv Mankad
14. Mr B V Sesha
and those who were present at the meeting.
.3
3
The address for the registered office is still being
considered.
3.
dissemination of information
Dissemination of information to the public was given
enough thought during the meeting. Having an independent
bulletin either in English or in Kannada or in both though
may be necessary in the long run, it was considered more
economical to use other bulletins or journals that are
already existing to disseminate information.
The u'se of
the T.V. through the Bangalore Doordarshan was contemplated
and it would be explored by Dr tatish Kumar and Mr IJanaiah.
4.
Mobilisation of funds
To begin with, the forum will not depend on any assured
source of funds for the conducting of the DAF-K activities.
It was suggested by th° members that the Forum approach
various agencies in India including Karnataka Rajya Vignana
Parisha'1 as also appeal to individuals for donations, for
specific projects.
5• The next meeting
The next meeting was fixed for the 4th of January
1989 at the office of the People's Trust at 2 PM.
minutes of the fourth - dialogue with the network group held
on 05.12.1988 at ashirvad. .
Members present
1. Gopal Dabade (GD)
2. Joseph Panackel (JP)
3. Gerry Pais (GP)
4. KV Sridharan (KVS)
5. H Sudarshan (HS)
o. BS Paresh Kumar (BSPK)
7. Maria Zillioli (MZ)
8. Uma Sridharan (US)
9.
10.
11.
12.
13.
14.
15.
Vanaja Ramprasad (VR)
V Benjamin (VB)
Sujatha D'Magrey (SDM)
G Gururaj (GG)
S P Tekur (SPT)
K Gopinathan (KG)
Ajith Lalwani (a medical
student from UK)
KG welcomed the members and briefed the new members the
idea of getting together of various individuals involved
in health and development work, in such a platform, where
the views and experiences of each of them could be shared
for the benefit of one another. He then requested the
members especially those who have started new experiments
to share their experiences.
GD
He had started his community health programme in a
place called KULAVALLI (cluster of 7 villages) in
Kittur, 30 kms away from Dharward. This is an area, where
the Government has entered into an agreement with Messrs
Karnataka Pulpwood Limited for eucalyptus plantation. In
his experience it was found that eucalyptus cultivation
was not at all an issue for the villagers. Their need was
for land, school, power supply and so.on. The villages
are not accessible by motor transport. People use cycle,
bullock cart etc. The village belonged to one Inamdar
(area being 1700 acres). The land was a gift to Inamdar
by British, for helping them catch one Sangoli Rayanna.
This land is occupied by poor people without obtaining
the legal rights. There is a nationalised bank, the services
of which are not utilized by the villagers; they consider
the bank employees "Englishmen". The villagers, however,
frequent a bank called "Boot Bank", who charges 250%
interest. The bank got this peculiar name because the
defaulters are dealt with their 'boots'.
The total population of these villages is 2777. Forest
dwelling is the main occupation. Two community health
guides attached to Kittur PHC visit these villages.
General Practitioners visit these villages, spending an
hour a day in each village. Muslims and Nayakas are the
communities.
2
2
GD's modus operand! is to stay overnight in these
villages and meei the people discussing with them to
find out their felt needs. One of their felt needs was
education and they wanted a school and they agreed to
contribute whatever they have (like bricks, wood, leaves
etc.) to build a shed. But the question was what sort of
education they should give. Anyway the school started
functioning on a non-formal basis, in the evenings.
It was decided that no health programme would be initiated
till the villagers asks for it.
JP; He explained about his involvement with a research
study on "Community Participation in Mental Health
Care" being undertaken by his department at NIMHANS. The
area covered is under Jugani with a 75000 population,
where' the people contribute to a Health Fund. Although
the study is titled as "Participation", there exists
only "quasi participation", due to ICMR wanting their
"conventional project protocol". JP started interviewing
the people to know what they are wanting in the health
field and to identify their priorities. The method of
getting these information was by recording the discussion
using a tape recorder (without the knowledge of the
interviewee.)
KVS/US; During the past few months they were visiting
various projects in Andhra Pradesh, Tamilnadu and Orissa
in connection with training/evaluation. They were recently
at the Association for Sarva Seva Farms, an off shoot
of Vinobhaji's Bhoodan at Madurai. KVS spent sometime
at Deena Sewa Sangha, looking through the files and
brought out a book called "Continuing Story of the Social
Workers Brotherhood". Uma had been involved in conducting
’Workshops on "Communication and Education" for various
projects including Anganwadi Workers under the ICDS
programme. Changes needed in the educational materials
and evolving new methods in communication are" looked into.
He now wishes to get back to health/medical field
after years of involving in non-medical work. Presently
he is in search of an institution where he could get an
attachment to work in this area. A Consumer Service Society
has been started at Hunsur where issues related to drug use/
abuse are also dealt with. On the request of some of. the
members, he shared his African experience to the group.
GP;
3
■3
HS;
He is involved in documenting tribal knowledge on
different species of trees in the surrounding areas
of BR Hills including their knowledge on astronomy. A
vocational training centre with a view to imparting
employment oriented trade/skills on social forestry,
sericulture etc., is planned.
She is involved with the School' Health programme
of Deena Sewa Sangh, Bangalore. Behavioural Sciences/
holistic health, children needing attention are .covered
in this programme with the help of Dr Malavyka Kapoor
of- NIMHANS. Has attended Workshops, meetings on various
issues in the recent past. She is now in the process of
collecting materials on development of human beings.
MZ;
SDM? She briefed the group about her .training programmes
in Health and Development. Two 10 weeks training
programmes per year are conducted—6 weeks class room
teaching and 4 weeks at the field. After the training
follow, up visits and Workshops/participatory evaluation
are conducted in the field. Topics includes health and
community development; drug action; indigenous medicine;
nutrition; legal aid; cooperation; leprosy; teaching
methodologies; cost analysis; accounts. Every 18 months
a Core Group Workshop is conducted. The participants in
this Workshop being the best trainees in the proceeding
training programmes. The course fee is subsidised.
VB;
He is involved with a Leprosy Project at Karigiri.
While interacting with the members, he gave an account
of how the government, can topple the initiatives of
volags as also how they can influence the same volags.
He told the group, an incident whib took place in Tamilnadu
involving an activist group (he did not want to divulge
the name of the group). The activists were working with
a group of women, building awareness. One one occasion
this group of women marched to'the Primary Health Centre
and gheravoed the staff for their inaction; they also went
to the DHO asking him to look into the issue in question.
The situation improved. Having gained confidence, when
there was draught in the area, they approached the
Sub Collector demanding arrangements for water supply.
4
4
The Sub Collector ordered for immediate remedial action.
The Government ac Madras were surprised to learn of the
effectiveness of the Women’s group and asked the
authorities to conduct an enquiry into the happenings
to find out -who was behind the group. Under "law and
order" problem, the activists records were confiscated
and the staff except, the Director (who was not in statici)
were taken to police custody. After the incident, the
staff arrested by the polic left the organization and the
Director continues his work in accordance with the wishes
of the government officials, with government assistance.
VB also mentioned about a funding agency who refused
to continue supporting a project on the ground that
"the work of the project was in line with the government
policies".
There was some discussion .on the following broader
issues arising out of points mentioned by those of the
participants who shared about their work;
1.
Government initiatives often overlook the interests
and needs of the people.
2.
The general masses have recognised the importance
of education/literacy.
3.
The conventional approach to various studies being
followed by the government establishments does not .
allow the researchers the necessary freedom to
evolve their own methodology. Actual participation
of the community in the governmental programmes and
or its research activities, therefore, remains only
in paper.
4.
■ New methods are to be evolved in communicating
health messages to the people. Changes are to be
made in the educational materials, presently
available, for their effectiveness.
5.
The voluntary organizations may sometime have to
succumb to political pressures in order to avoid
the authorities branding them as anti-government.
6.
Some funding agencies do not support NGOs collaborating/
supplementing government programmes.
ooooooooooooo
r r xr* r v zr v r v tt r v
ft?—)
z.
■■■ ■■ z
H E
COURT
or
RECORD OF PROCEEDINGS
I N U 1 -T
WF(C)No.698/93
DRUG
ACTION FORUH AND ORS
Petitioner (s)
VERSUS
UNION OF INDIA AND ORS
Respondent
( With Appln(s). for impleading party and intervention and Impleading party )
With
W.P(C1v11)No.422/95
Cate : 24/02/97 These Petitions were called on for hearing today,
CORAH :
HON’BLE HR. JUS72CE
HON’BLE HR. JUSTICE
J.S. VERMA
B.N. KIRPAL
For appearing partle- : Hr. Anil B. Diwan, Sr. Adv. with Hr. Shaukat
Merchant, Ms. Bins Gupta, Hr. Ramesh Singh and
Hs. Rakhi Ray,--Advs,
- —
Hr. VR Reddy, ASQ.
Hr. S. Waslra Qadrl, Adv. with Hr. A.D.N.
Rao and Hs. Ani1 Katlyar, Advs.
Hrs. Sushm'a sur1, Adv.
Mr. KK Laroia, Adv. and Hr. Prashant Bhushan.Advs.
Hr. PH Parekh, Hs. B1na Hadhavan and
Hs. Indu Verma, Advs.
Hr. FS Nariman, Sr. Adv. with Mr. Subhash Sharma
Hr. BP Singh and Mr. Abhljeet Chatterjee,Advs.
Mr. S. Sukumaran and Hs. Ural la Narang, Advs.
for M/s. J.B.D. & Co.
Hr. PB
Agarwala and Hs.Praveen Gautam,Advs.
Dr. HP Raju, Hr. TU Ratnam, Hr. KS Mary and
Hr. MKD Namboodry, Advs.
Hr. C. Hukhopadhyay, Mr. RajlvRey and Mr. Rakesh
Sharma, Advs.
Hs. BIna Gupta, Hs. T. Sudha and Hr. Ramesh Singh,
Advs.
Hr. Hukul MudgaK Adv.
Ms. Vim la Sinha and Mr. Gopal Singh, Advs.
M/s. mj Pau 1,
Jana Kalyan Dc>?,
D3
S.A. Vorma,
■e.:- sn;. >;ur ,ui
Cc-irt hx.rfn the following
■:> ! 1; t n
learned Additional Solicitor General Informs
Tlie
us that the
Core Group has Indicated that the period
of
three months would be adequate for completion of the task
dated
12th
Accordingly, we request the Core
Group
by them as
required ^2^ the earlier
February,
1997.
to complete
the
latest by
the
order
task as expeditiously as
31st ' May,—i9SKSr_The_- learned
of
end
and
possible
Additional Solicitor General will give this Intimation to
the Core Group through Its Convenor.
We
are also Informed by learned counsel that the
drugs
particulars
of
manufactured
prior to 17th December, 1996 as required by
the earlier
order
the
stock
existing
the
of
dated 12th February, 1997
been
have
the manufacturers and the same 1s
in
furnished
by
process of
certification
The learned
Additional Solicitor General also states
by the competent
the
authorities.
on
instructions
that there is no objection by the concerned
authorities
to the export of fixed dose combinations
Analgin known
Spasgan and
have been
by the brand na«»s - Baralgan
which
manufactured by somu of the companies prior to
1996
consumption
the same 1s not banned of
of
duly certified
by
to some foreign
countries
the
the competent authorities;
wherein
quantity
and
that
Government through its agencies will monitor
the saiwi ensuring that no part
of
these banned drugs would be utilised
for
strict compliance
such stock
(Baralgin),
Trlgan Injection (k Trlgan E Tablets -
17th December,
the Central
of
of
of
Internal consumption within th» ccwtry.
In view of this
statement of the learned Additional Solicitor General) we
allow those
mannft*'
■■■
'■
authorities
to allow them to export the certified
stock
of such drugs
manufactured prior to 17th December,
1996
to the foreign
countries wherein consumption of the same
1s not banned
1n accordance with the Government’s Export
Policy.
The Central Government would be responsible for
ensuring
that
the
certified stock of
these
utilized on1/ 1n this matter.
List on 14th April, 1997.
[4
drugs
1s
K E
COURT
or
RECORD OF PROCEEDINGS
c. o ■ . ■
I N U Ji .-7
WP(C)No.693/93
DRUG
ACTION FORUH AND ORS
Petitioner (3)
VERSUS
UNION OF INDIA AND ORS
Respondent
( With Appln(s). for impleading party and intervention and Impleading party )
WI th
W.P(C1v11)No.422/95
Cate : 24/02/97 These Petitions were called on for hearing today.
CORAM :
HON’SLE MR. JUSTICE
HON’BLE HR. JUSTICE
J.S. VERMA
B.N. KIRPAL
For appearing partie- : Hr. Anil B. Diwan, Sr. Adv. with Hr. Shaukat
Merchant, Hs. B1na Gupta, Hr. Ramesh Singh and
Hs. Rakhi Ray,-AdvB. — —
Mr. VR Reddy, ASG.
Hr. S. Wasim Qadrl, Adv. with Mr. A.D.N.
Rao and Hs. Anil Katlyar, Advs.
Mrs. Sushm'a sur1, Adv.
Mr. KK Larola, Adv. and Hr. Prashant Bhushan.Advs.
Hr. PH Parekh, Hs. B1na Nadhavan and
Hs. Indu Verma, Advs.
Mr. FS Nariman, Sr. Adv. with Mr. Subhash Sharma
Hr. BP Singh and Mr. Abhljeet Chatterjee,Advs.
Mr. S. Sukimaran and Ms. Urmila Narang, Advs.
for H/s. J.B.D. & Co.
Hr. PB
Agarwals and Hs.Praveen Qautam.Advs.
Dr. HP Raju, Mr. TU Ratnam, Mr. KS Mary and
Hr. MKu Namboodry, Advs.
Hr. C. Mukhopadhyay, Mr. Rajiv Rey and Mr. Rakesh
Sharma, Advs.
Ms. Blna Gupta, Hs. T. Sudha and Hr. Ramesh Singh,
Advs.
Hr. Hukul Mudgal^ Adv.
Ms. Vimla Sinha and Nr. Qcpal Singh, Advs.
M/s. mj Paul,
Jana Kalyan Dg",
DS
NdJi<
S.k. Varma,
c.t/irt ss.dn the following
tn«.- ;.;<u ,ti>
o ■ i; t n
learned Additional Solicitor General informs
Tlie
Core Group has Indicated that the period
us that the
of
three months would be adequate for completion of the task
by than as
required
February,
1997.
to complete
12th
Accordingly, we request the Core
Group
task as expeditiously as
the
the
latest by
order
dated
the earlier
31st
of
end
possible
and
Hay, — 199fi£z-_The - learned
Additional Solicitor General will give this intimation to
the Core Group through Its Convenor.
We
are also Informed by learned counsel that the
stock
of
drugs
particulars
of
manufactured
prior to 17th December, 1996 as required by
the earlier
order
the
existing
the
dated 12th February, 1997
been
have
the manufacturers and the same is
in
furnished
by
process of
certification
The learned
Additional Solicitor General also states
Instructions
that there is no objection by the concerned
authorities
to the export of fixed dose combinations
have been
of
which
manufactured by soaxi of the companies prior to
to some foreign
1996
consumption
the same 1s not banned of
of
duly certified
by
countries
the
the competont authorities;
wherein
quantity
and
that
Government through its agencies will monitor
strict compliance
such stock
on
(Baralgin),
Trigan Injection II Trigan E Tablets -
17th December,
the Central
authorities.
by the brand naims - Baralgan
Analgin known
Spasgan and
by the competent
the
of
the sarao ensuring that no part
of
these banned drugs would be utilised
for
of
Internal consumption within thi ctontry.
In view of this
statement of the learned Additional Solicitor Osnaral, we
allow those
ma.nuf.srttimrs
authorities
to allow them to export the certified
stock
of such drugs
manufactured prior to 17th December,
1996
to the foreign
countries wherein consumption of the same
1s not banned
In accordance with the Government’s Export
Policy.
The Central Government would be responsible for
ensuring
that
the
certified stock of
these
drugs
utilized on1/ in this matter.
List on 14th April, 1997.
(S.L. Goyal)
Court Master
Court Master
[4
] i-i
'
is
C 0 U R T
0 f
RECORD OF PROCEEDINGS
jU-.-x.ME
I N U x ;t
WP(C)No. 698/93
DRUG
ACTION FORUM AND ORS
Petitioner (s)
VERSUS
UNION OF INDIA AND ORS
Respondent
( With App]n(s). for Impleading party and intervention and Impleading party )
With
W. P(Civ11)No.422/95
Cate : 24/02/97 These Petitions were called on for hearing today.
CORAM :
HON’BLE HR. JUS72CE
HON’BLE HR. JUSTICE
J.S. VERMA
B.M. KIRPAL
For appearing partie'' : Hr. Anil B. Diwan, Sr. Adv. with Mr. Shaukat
Merchant, Ms. B1na Gupta, Mr. Ramesh Singh and
Hs. Rakhi Ray,-Adv&,
- —
:
Mr. VR Reddy, ASG.
Hr. S. Wasim Qadrl, Adv. with Hr. A.D.N.
Rao and Hs. Anil Katlyar, Advs.
Hrs. Suslina sur1, AdY.
Hr. KK Larola, Adv. and Hr. Prashant Bhushan.Advs.
Hr. PH Parekh, Hs. B1na Madhavan and
Hs. Indu Verma, Advs.
Hr. FS Nariman, Sr. Adv. with Hr. Subhash Shanna
Hr. BP Singh and Mr. Abhljeet Chatterjee,Advs.
Hr. S. Sukumaran and Hs. Urmila Narang, Advs.
for H/s. J.B.D. A Co.
Hr. PB
Agarwala and Hs.Praveen Gautam,Advs.
Dr. HP Raju, Hr. TU Ratnam, Mr. KS Mary and
Hr. HKD Namboodry, Advs.
Hr. C. Hukhopadhyay, Mr. Rajiv Ray and Mr. Rakesh
Sharma, Advs.
Ms. Blna Gupta, Hs. T. Sudha and Hr. Ramesh Singh,
Advs.
Mr. Hukul Mudgal
Adv.
Ma. Vim la Sinha and Mr. Qopal Singh, Advs.
M/s. mj Paul,
Jana Krlyan
D3
S.A, Vorma,
..U! ’•••? I'-r'trt KK.rfn the following
j ■ I; r fl
learned Additional Solicitor General Informs
TIts
Core Group has Indicated that the period
us that the
of
three months would be adequate for completion of the task
by them as
required ^2^ the earlier
February,
1997.
dated
12th
Accordingly, we request the Core
Group
order
to complete the task as expeditiously as possible and
---------- ■
■
latest by the end of 31st Hay, - 199ES_-_The learned
Additional Solicitor General will give this Intimation to
the Core Group through its Convenor.
We
are also informed by learned counsel that the
drugs
the
of
stock
particulars
of
manufactured
prior to 17th December, 1996 as required by
the earlier
order
the
existing
dated 12th February, 1997
have
the manufacturers and the same is
furnished
by
process of
certification
by the competent
been
the
in
authorities.
The learned Additional Solicitor General also states
on
Instructions
that there 1s no objection by the concerned
authorities
to the export of fixed dose combinations
Analgin known
Spasgan and
have been
by the brand naiies - Baralgan
which
manufactured by socxi of the companies prior to
1996
consumption
the same 1s not banned of
of
duly certified
by
to some foreign
countries
the
the competent authorities;
wherein
quantity
and
that
Government through Its agencies will monitor
th* saiwi ensuring that no part
of
these banned drugs would be utilised
for
strict canpl lance
such stock
(Baralgln),
Trfgan Injection II Trigan E Tablets -
17th December,
the Central
of
of
of
Internal consumption within thi ctontry.
In view of this
statement of the learned Additional Solicitor Ganaral, we
allow those
mannfirtiimrs
authorities
to allow them to export the certified
stock
of such drugs
manufactured prior to 17th December,
1996
to the foreign
countries wherein consumption of the same
is not banned
in accordance with the Government’s Export
Policy.
The Central Government would be responsible for
ensuring
that
the
certified stock of
these
drugs
utilized on1/ in this matter.
List on 14th April, 1997.
(D'P. Walla)
Court Master
(S.L. Goyal)
Court Master
(4
06%
Ni
s,?'* Verma,
is
Aspirin May Cause More Harm Than Good 7/2/00
file:///D|/rNFO FROM INTERNET/aspirin cffects-jul2.htm
' 13
Aspirm
Caojs® M@re tnWm TTIhain) ®@©^
Taking low dose aspirin as a preventive measure against
coronary heart disease, which is a very common practice,
may actually cause more harm than good, according to'a
just published study.
Bow.-,Sugar./VfacU.ae
Caiciam Channel
Blockers, Ca,us,e.G?
British researchers identified over 5,000 UK men, aged
between 45 and 69 years, who were at increased risk of
coronary heart disease but had not previously had heart
trouble. The men were randomly divided into four different
treatment groups to accurately establish the effect of
aspirin.
The authors found a greater beneficial effect of aspirin in
men with low rather than high blood pressures, not only for
coronary heart disease but also for stroke, although the
modest benefit does not necessarily outweigh the risk of
bleeding. Men with higher pressures may derive no
protective benefit from aspirin but will risk possible serious
bleeding.
Given the widespread use of aspirin for the prevention of
coronary heart disease, the study's authors suggest that
these findings have important implications, although they
admit that further trials are needed to confirm the results.
Because of the strong correlation between blood pressure
found in this study, the authors also stress the importance
of adequately controlling blood pressure for those in whom
the preventive use of aspirin is being considered. In
addition, men who have previously had heart trouble and
strokes and are taking aspirin should continue to do so,
unless instructed otherwise, since they are more likely to
obtain a greater benefit than the general population.
British Medical Journal Jone 25, 2000; 321: 13-17.
COMMENT: W@DD, Dow sfos® asipotrooTi for Site prewenttoira
©t? Ihiearft (dlosease Ss something) foaft H Ihawa team
wavering) ©m for fo® Dasft fow
E feDft fttat [iff ©m@
lof2
7/6/00 3:28 PM
Aspirin May Cause More Harm Than Good 7/2/00
fi!e:///D|/INFO FROM INTERNET/aspirin cffccts-jul2.htm
wawirmg ©tro for fflte Dasff ff®w years. E foils ffteff off ©on©
MS@(d ©[rD®=ffoffaih ©ff an aspirm ffhir@® ffnm®s a w®@kff ©ira®
©©ate r©e©flw© m©sff ©ff fflte fe@irD@ffnffs ate avoid fflte ©to®
@ffffs©ffs= Intoweveir, off appsairs ffteffy as ff@ir m©sff ©wry
arsa ©ff ©te©m© BOOgdsss^ dlrags ar® trooff ffk® ©©Itofftom E
am ©teirogmg my prevtoansfly IteUdl pasofftoiro ©m ff&uos
SMfojjeeff (s@® fe@O©w) ate advising ©n® sff©p imstog
asporm ff© [tower fflte risk ©ff tearft dloseass ate sffrok®.
Titer© ar® ffar m©r@ @ffff@©ffiiv@ fflterapfes ff© d© ffteffn Tte
dleff iis fflte m©sff ffoMteafftonaHa, teff ®^®r©os® ate
cerffam sypptemeroffs w©(ute mak® ffar m©r® sens® ff©r
m©sff p®©pO@ ffteuD Msmg a dragy @v®od aff tow dtosss.
Related Articles:
Few Heart Risk Patients Taking Aspirin
Long Term Aspirin Use Leads so Cataracts
Aspirin, Ace Inhibitor Combination May Be
Dangerous
&ead ahis first | Subscribe to free newsletter ] Current newsietters ] Articies on
weiljnass I Links to wetness J Search site J Home j E-maih Dr@MercoSa.com
Disclaimer - Newsletters are based upon the opinions of Dr. Mercola. They are not intended to replace a one-on-one
relationship with a qualified health care professional and they are not intended as medical advice. They are intended as
a sharing of knowledge and information from the research and experience of Dr. Mercola and his community. Dr.
Mercola encourages you to make your own health care decisions based upon your research and in partnership with a
qualified health care professional.
2 of 2
7/6/00 3:28 PM
TM-\2
The following model list of essential drugs
is taken from the WHO Technical Report series
770 (WHO, Geneva, 1988 "The use of Essential
Drugs").
MODEL LIST OF ESSENTIAL DRUGS
EXPLANATORY NOTES"'
Since the first report on the selection of essential drugs was
published in 1977, the concept of essential drugs has become widely
applied. It has provided a rational basis not only for drug procu
rement at national level but also for establishing drug require
ments at various levels within the health care system.
The international nonproprietary (generic) names for drugs or phar
maceutical substances should be used whenever available,and presc
ribers should be provided with a cross-index of nonproprietary and
proprietary names.
The concept of essential drugs has been endorsed unanimously by
the World Health Assembly. It is intended to be flexible and
adaptable to many different situations; exactly what is regarded
as essential remains a national responsibility.
The wide applicability of the concept is now evident from exper
ience gained in many countries. Most national lists of essential
drugs are stratified to reflect requirements at different levels
within the health care infrastructure. Typically, a very short
list has been compiled for community health workers while the most
comprehensive lists have been reserved for large urban and regional
hospitals.
One hundred and nine countries have now developed lists of essen
tial drugs and more than 40 countries are making great efforts to
implement programmes based on the essential-drugs concept. The
priorities and approaches differ.from country to country in accor
dance with each country's socioeconomic situation, but the concep
tual basis is the same. The WHO Action Programme on Essential
Drugs provides a platform for a harmonized and collective search .
for suitable and feasible- solutions to the problem of the unavaila
bility of the most essential drugs to the majority of the world's
population.
Many drugs included in the list are preceded by a square symbol(_#)J
to indicate that they represent an example of a therapeutic group
and that various drugs could serve as alternatives. It is imper
ative that this be understood when drugs are selected at national
level, since choice is then influenced by the comparative cost and
availability of equivalent products. Examples of acceptable substi
tutions include :
(#) Codeine : Other drugs for the symptomatic treatment of diarrhoea
such as diphenoxylate or loperamide or, when indicated for cough
relief, noscapinc- or dextromethorphan.
(#) Hydrochlorothiazide : Any other thiazide-type diuretic currently
in broad clinical useT
(#) Hydralazine : Any other peripheral vasodilator having an anti
hypertensive effect.
(#) Senna : Any mild stimulant laxative (Either synthetic or of
plant origin)
(#) Sulfadimidine : Any other short-acting, systematically active
sulfonamide unlikely to cause crystalluria.
Hazardous, Bannable and Dumped Drugs
The issue of dumped drugs has been in the news for the past
few years. The drug companies involved in the manufacture
and sales of such drugs have received their due share of condem
nation. Foreign governments
policies, which provided scope
for exports of such hazardous products have been also condemned,
g.,
e.
the Clayton Amendment Act and the U.S. Regulation.
It is well known that sales of medical technologies and drugs
is a commerical enterprise, the motivation being profit rather
than "service1’ or "welfare work".
Realising all this, the question arises as to how much can we,
as citizens of India, expect our drug control authorities to
safeguard our interests. The pressure from the drug industry
is immense. In spite of knowing this, our expectations from
the drug control authorities is high. After all our pharmaceutical
industry is the most developed in the Third World. According
to UNIDO, it belongs to Category V — developed enough to
be self-sufficient.
We have demanded that our imports, production and sales should
give priority to essential, life-saving drugs over irrational and
hazardous drugs, as per WHO's guidelines for Essential Drugs.
The drug industry and its supporters allege that the concept
of essential drugs is only for struggling, less developed countries
of the Third World and not for a country like India, with its
well-developed industry and its high and advanced level of
medical expertise. However, this same lobby puts India in the
category of less developed countries when it comes to the
issue of banning drugs and drug control. The lobby claims that
consideration of hazards over efficacy is a luxury which we
cannot afford.
However, consumers anywhere in the world have the right to
expect that irrational and hazardous drugs are not issued licences
and that licences of banned drugs should be withdrawn .as soon
as possible, the ban implemented, and that all drugs in the
market are quality - controlled. We have 20 per cent substandard
drugs . One out of every five drugs will not be effective.
With the incereasing number of spurious
drugs floating in
the market, the problem is beginning to take on dangerous
proportions.
: 2 :
Since 1980 we've been concerned about
and hazardous drugs.
SOME
BANNABLE
DRUGS
—
WHAT
this
IS THE
issue of dumped
POSITION
NOW
Under Section 23 P of the Drugs and Cosmetic Act
of 1940, the Central government has the power to
issue such directions to the State Governments as
required to execute the Drug Act. under Section
18 of the Act the State Government has the power
to prohibit manufacture,
distribution and sale of
drugs by a gazette notification.
The sub-committee of the Drugs Consultative Committee,
in its 1980 report, recommended the banning of 23 combinations
of drugs, giving their reasons for such banning, 16 categories
of these drugs were recommended for immediate
weeding
and seven of the categories were to be weeded out over a
specified time. Over 500 brand drugs would be thus affected.
This report was presented to the Durg Consultative Committee
at a special meeting on 10.10.81, and later to the Drug Technical
Advisory Board (DTAB) and the Ministry of Health and Family
Welfare accepted it in 1981.
The DTAB, a Statuatory Body under Section 5 of the Drugs
and Cosmetics Act of 1940 recommended banning of 18 fixed
dose combinations. These drugs were randomly selected from
the Pharmaceutical Guide. Out of the 350 brand names affected,
44 were marketed by the foreiqn sector, 8 by public sector,
and 298 by private sector. Most of these drugs were being
produced by national companies According to the authorities,
"the purpose was to give time limit to firms who may already
have purchased the bulk drugs form manufacturing the formula
ties''. What compassion and consideration for the drug companies!
SOME BATTLES
Halogenated Hydroxyquinoline
Ban of fixed dose combinations of halogenated hydroxyquinoline
: 3 :
was to be effective from 1.11.82. The date of the ban was
extended to 31.3.83 through DO No. X19013/8/81-D dated 13.8.82.
High Doses of EP Drugs
Through another DO. No. 12-48/79 DC dated 26.6.82, the Drug
Controller of India directed the State Drug Controllers to ban
the manufacture of high- dose Estrogen-Progesterone combinations
from 31.3.83 and their sales from 30.6.83.
M/s. Unichem Labs, Bombay (OP 2927/82 of writ petion 2928/82), M/s. Nicholas Labs, Bombay and M/s. Organon (now known
as Infac (India) Ltd., Calcutta filed writ petitions in Bombay
and Calcutta high courts challenging the ban. Their contention
was that the Central Government has no powers to ban the
drugs. The High Court of Bombay and the High Court of Calcutta
have granted stay orders against the ban. Now these products
are available in the market.
Section 10A and 26A of the amended Drugs and Cosmetics
Act (April 1982) empower the Central Government to prohibit
import, manufacture and sale of any drugs considered harmful/
toxic or irrational, etc. Since the matter was in court during
the gazette notification of 23.7.83, this combination of drugs
has not been included in it.
What is absolutely objectionable is the fact that — inspite
of the act of the Drug Controller of India's ban of the production
and sale of EP drugs, M/s. Organon have managed to obtain
extension of licences to manufacture these products for another
two years.
Paediatric Tetracycline
Although this drug is banned in its oral liquid from to discontinue
its being prescribed for children because of its often serious
side-effects, it is being manufactured today as a tablet of
30mg. for children — an example of how a 'company can follow
the letter of law and yet disobey it without any legal
consequences.
: 4 ;
Aspirin and Vitamin C
In October 1982, M/s. Nicholas Labs, Bombay filed a writ petition
in the Bombay High Court against the decision to ban the fixed
dose combinations of Aspirin with Vitamin C. The Court ruled
that the State Drug Controller has no power under Section
18 of the Drugs and Cosmetics Act to stop the manufacture
and sales of this product. However, it would be open to the
respondents as and when the law has been enacted, to pass
any fesh ordef as it is considered necessary in accordance with
the law after following procedures prescribed by the Government.
Subsequent to the Drug Amendment Act of 1.2.83, the manufac
turers have again gone to court challenging the
Central
government and Sections 26 A and 10A on the grounds of "lack
of objective criterion for such ban".
This has resulted in the FDA — Maharashtra (which is supposed
to be having the best drug control mechanism in India) informing
the Drug Controller of India that, in the light of the rul ing given
by the Bombay High Court, "it would not be possible for him
to take any action to stop the manufacture and sale of any
of the fixed dose combinations in question". (Letter dated 9.6.1984
ov the Drug Controller of India to the Voluntary Health Associa
tion of India).
Gazette Ambiguities
It is not clear trom the DO letter banning 22 drugs, whether
some drugs like strychnine and yohimbine, and caffesine are
banned only in some combinations, or in all combinations :
any drug containing yohimbine, or strychinine would be
banned (as neither of the two were considered to have
any therapeutic value and infact could lead to serious
side effects).
or the ban was applicable to drugs containing both yohimbine
and strychnine.
or to yomhimbine
vitamins
and
strychnine
with
testesterone
or
: 5 :
or ONLY to drugs which contained all four : yohimbine,
strychine, testesterone and vitamins.
Bangladesh banned 1742 drugs in June 1982. The time period
given to the drug companies to withdraw these products from
the market, to destroy these products was three to nine months,
depending on the product. They were strictly prohibited from
exporting these products to other countries. But we failed to
ban even a few hundreds, let alone 1742 drugs. The time period
given to drug companies was to complete the manufacture
of their formulation and sell off their stocks.
WHO IS MORE IMPORANT
THE CONSUMER ??
—
THE
DRUG
COMPANY
OR
The drug policy is now on the anvil. It is now that we can
assume the responsibility for putting people's health before
the health of the industry. If Indian people have to become
healthy, Indian Drug Policy needs to be rational. The choice
is ours — and we must make a decision now.
VHAI-AIDAN-NCCDP-RDCC DRUG CONSULTATION
I
ON
, '
IMPACT OF POLICY CHANGES ON DRUG POLICY AND DRUG USE
26, 27 August 1996
RCSCARCH & RUJRR€N€SS CAMPAIGN
Compiled By:
Obstretic Drug Information Cell
Rajasthan Voluntary Health Association
Dr. S.G. Ksbra
Ram Babu
Research Consult;
Off. Executive Secretary
Vinod Joshi
Nitir. Gupta
Ajay Sharma
(Analysis)
(Des c'ing)
(Comp uter Assistance)
_______
OBSTETRIC DRUG INFORMATION CELL AT RVHA TO ALERT AGAINST
HARMFUL DRUGS IN PREGNANCY •
A recent survey by the RVHA of the maternity centers in the
city of Jaipur revealed a very high incidence of still births,
congenital anomalies and of abnormal pregnancies needing assisted
deliveries by caesarean section.One of the possible contributory
factor for the incidence of stil births, congenital defects etc
is the indiscriminate and indiscreet use of the drugs in pregnan
cy.
Prescription and intake of drugs in pregnancy needs much
higher level of awareness and readily available information about
the possible harmful affects of the drugs in pregnancy. In India,
where therapeutic preparations marketed run in thousands, it is
still more difficult to be aware of the possible harmful content
of a specific preparation. Good intentions of physicians to do no,
harm to conceptus, while prescribing to a pregnant woman for her
disease and complaints, are thwarted by the lack of readily
available information about the effect on pregnancy of the other
wise commonly prescribed safe drugs to patients. A pregnant lady
has no way to check if the prescribed medicines for her ailment
are likely to harm her precious child in the womb.
To counter the above mentioned adversities, countries with
better developed and more responsive health care systems, run
obstetric drug information centers that disseminate the required
information to enable rational and non-harmful prescription of
drugs in pregnancy. Rajasthan Voluntary Health Association is
perhaps the first in the country to attempt to establish such an
obstetric drug information cell.
rh t h u
The Obstetric Drug Information Cell at the RVHA has alreadyprepared a computer based data-base of the drugs by their generic
and brand names, in term of their reported and recognised (by
drug control authorities of India) effects on pregnancy. Lists of
the drugs that are either not at all to be given in pregnancy
(contraindicated drugs) and those that have to be prescribed with
special caution ( special precaution) are available both by thei
generic and brand names. Lists are also available for the use o
practitioners of various specialities according to the class o
drugs pertaining to their specialities.
The Obstetric Drug Information Cell will provide information
to any pregnant lady seeking information about the possibility of
any harmful effect, on the child in the womb or the pregnancy, of
a drug prescribed to her. The patient may contact, with the
prescription, personally or by sending a photocopy of the pre
scription by post, the Obstetric Drug Information Cell, Rajasthan
Voluntary Health Association, C-41, Dev Nagar, Tonk Road, Jaipur302018, ( between 11 AM to 1 PM for personal visit). During this
time information will also be available on telephone No.512021.
The Obstetric Drug Information Cell will also mail lists of
the contraindicated and the special precaution lists of drugs in
pregnancy to various doctors and hospitals, and to any one seek
ing such lists, subject to the availability of the funds. ,
OBSTETRIC DRUG INFORMATION CELL
Rajasthan Voluntary Health Association, Jaipur
A large number of drugs, approved as safe in non-pregnant and in
non-lactating women, are known to be unsafe in pregnancy and
lactation. These drugs are either contraindicated or are to be
avoided as far as possible (to be given with caution) because of
their known, or potential harmful effect to a pregnant or a
lactating mother, or to the child in the womb, or to a child on
breast feed.
The drugs that may harm the child or the mother or- adversely
effect the pregnancy outcome, besides being1. drugs taken for pregnancy related conditions
might have been taken for
2. treatment of infertility
or
3. for an acute or chronic condition from which a pregnant
or a lactating woman might suffer.
Potential of harm to foetus is maximum in the first three month^
of pregnancy. The development of the organs in a foetus takd®
place in the first three months of pregnancy. The foetus, during
this period, particularly from 18th or 60th day of conception, is
most vulnerable to the harmful effect of the drugs, which may
cause congenital defects leading either to death of the child in
the womb and abortion, or birth of a child with defects.
Substantial risk in second trimester. During the next three
months, drugs may still cause disorders of growth and function,
especially of the brain and the spinal cord, that are mostly
non-fatal.
In the last
three months of pregnancy, drugs may cause problems in the child
birth, or immediately following it, frequently drug related fatal
respiratory failure in the new born, more so if the child is born
premature.Some drugs may cause excessive bleeding in the mother.
Risk to the child and the mother in late pregnancy.
A variety of adverse pregnancy out-comes, such as, abortion^
still birth, neonatal death, congenital defects, or defects in
functioning of the brain etc, are caused by drugs taken in preg
nancy. Rates of such cut-comes are
much higher in Rajasthan as
compared to other parts of our country, and in the country as a
whole than in the developed nations. Excessive and indiscriminate
prescription and consumption of drugs in pregnancy is one cause
of it..
A child on breast feed is vulnerable to the adverse effect of all
the drugs taken by the mother that are secreted in the breast
milk. ’
»
To prevent this large scale medical violence against pregnant
women and their innocent children in the womb, an Obstetric Drug
Information Cell has been created at the Rajasthan Voluntary
Health Association. It will serve the following functions :-
1
D-rug Information Cell with a
Maintain an Obstetric
data base on drugs, by th-eir generic and brand names,
about the safety status of these drugs in pregnancy and
lactation.
2.
The Cell will circulate amongst doctors a list of drugs
that
are either contraindicated or are to be pre
scribed with special precaution in pregnancy and a list
of similar status of
drugs in lactation . This is to
enhance 'the awareness of doctors about the safety
standards of these drugs in pregnancy and lactation and
to serves as a ready reference.
3.
The information at the Cell will be available to the
patients who seek information about the safety status
of drugs prescribed to them in pregnancy and lactation.
The Cell will attempt to persuade the Crugs Control Au
thorities to ensure printing of easily understandable
icon (pictorial depiction) on the drug pack to warn the
user that the drug is contraindicated in pregnancy.
5.
The Cell will prepare tabulated lists for specialists
practitioners showing safety standard of the drugs used
in a particular speciality if the patient is pregnant.
THE AUSTRALIAN RISK
CATEGORIZATION SYSTEM FOR
DRUGS USED IN PREGNANCY
The Australian categorization consists of five separate categories:
.CATEGORY A
Drugs which have been taken by a large number of pregnant.
women and women of childbearing age without any proven increase
in the frequency of malformations or other direct or
indirect harmful effects on the fetus having been observed.
CATEGORY B
Drugs which have been taken by only a limited number of
pregnant women and women of childbearing age, without an
increase in the frequency of malformation or other direct or
indirect harmful effects on the human fetus having been observed.
As experience of effects of drugs in this category in humans is
limited, results of toxicological studies to date (including repro
duction studies in animals) arc indicated by allocation to one of
three subgroups:
x
GROUP Bl •
Studies in animals * have not shown evidence of an increased
occurrence of fetal damage.
GROUP B2 -.-
Studies in animals‘arc inadequate or may be lacking, but available
data show no evidence of an increased occurrence of fetal damage.
^GroupbT’^:'
Studies in animals ‘ have shown evidence of an increased
occurrence of fetal damage, the significance of which is
considered uncertain in humans.
--^CATEGORY C
Drugs which, owing to their pharmacological effects, have
caused or may be suspected of causing, harmful effects on the
human fetus or neonate without causing malformations.These
effects may be reversible. Accompanying texts should be
consulted for further details.
' /.'- CATEGORY D
Drugs which have caused, arc suspected to have caused, or may be
expected to cause, an increased incidence of human fetal
malformations or irreversible damage. These drugs may also have
adverse pharmacological effects. Accompanying texts should
be consulted for further details.
CATEGORY X; Drugs that have such a high risk of causing permanent damage to
the fetus that they should not be used in pregnancy or when there
is a possibility of pregnane}'.
■ '
" Animal studies submitted in support of new drug applications
must conform to New Drug Form Guidelines.
Comments on alphabetical pregnancy risk ratings refer to the 1992ADEC “Medicines in
Pregnancy” categorization booklet. These notes are based on that booklet with additional comments
• and clarification as appropriate.
■
NOTES ON SAFETY OF VARIOUS
t DRUGS AND DRUG GROUPS
’
1
Angiotensin - Converting enzyme (ACE) inhibitors:
Captopril and enalapril are rated as D due to reports of fetal deaths in-utero.
Whilst there is no evidence to suggest that these drugs are teratogenic in humans, it
has been suggested that late in pregnancy, these drugs have effects on the fetal '
renin-angiotensin system, which may be potentially harmful. Therefore, they air best
avoided during prcgnancy.'l4A',1For similar reasons the newer drugs Fosinopril and
Lisinopril are also rated D in pregnancy.
2
Acyclovir
During pregnancy there is no evidence that acyclovir prevents transmission of genital
herpes simplex from mother to fetus and administration during pregnancy is usually
contraindicated on theoretical grounds. p> However, its use should be considered in a
primary attack because viraemia occurs and potential damage could result in the
infant’6’
'
3
Aminoglycosides
Gentamicin, kanamycin, neomycin, tobramycin, amikacin, netilmicin.
Gentamicin and other aminoglycosides are known to cross the placenta. There is
evidence of selective uptake of gentamicin by the fetal kidney resulting in cellular
■ damage (probably reversible) to immature nephrons. Eighth cranial nerve damage has
also been reported following in-utero exposure to some of the aminoglycosides.
Because of their chemical similarity, all aminoglycosides must be considered
» potentially nephrotoxic and ototoxic to the fetus. It should also be noted that
' therapeutic blood levels in the mother do not equate with safety for the fetus.
4
Amiodarone
Because of the long half-life of amiodarone and its major metabolite, and the potential
to cause abnormal thyroid function and bradycardia in the fetus, its use is probab.y
best avoided in the. three months before and throughout the duration of pregnancy.
Where exposure of the fetus is unavoidable, thyroid function (including TSH) should
be assessed promptly in the newborn infant.
.
5
Anticonvulsants •
The riskof a mother with epilepsy giving birth to a baby with an abnormality is about
three times that of die normal population. Some of this risk is due to the
anticonvulsant drugs taken. Mothers, taking more than bne anticonvulsant drug,
might have a higher risk of having a baby with a .malformation than mothers taking ,
one drug. Phenytoin sodium, taken during pregnancy, has been associated with
distinctive craniofacial abnormalities, mental and growth deficiency and less
frequently, oral clefts and cardiac anomalies. This clinical pattern is sometimes called'
die ‘fetal hydantoin syndrome’.
Sodium valproate (valproic acid), it taken in the first trimester of pregnancy, is
suspected of causing an increased risk of neural tube defects (especially spina bifida) in
the exposed fetus; Women taking sodium valproate (valproic acid,, who become
pregnant, should bo encouraged to consider routine ultrasound and amniocentesis for
prenatal diagnosis of such abnormalities.(7) Alternatively, pre-pregnancy genetic
counselling is advised.
In practice, if a padent is stabilized on anticonvulsants prior to pregnancy, and the
padent is counselled as to the potential increase in overall risk, and wishes to continue
with the pregnancy, this therapy is usually continued for that patient throughout the
pregnancy, with close serum monitoring where this is possible. I: has also been
suggested that folate supplementation may reduce, the potential fur teratogenic
outcome. This is in line with the general consensus of advice for these patients
during pregnancy, f7-s’. We would strongly disagree with the D rating for clonazepam,
and would place it at a B3 rating since there is no epidemiological evidence of
teratogenicity with die use of benzodiazepines other than studies cf small numbers
with'inconsistent results. For other fetal effects of benzodiazepines, please refer to
benzodiazepine notes (N...iz;.
6
Antihistamines and Anti-emetics.
The Australian categorisation differentiates between some antihistamines and others;
on their chemical basis, namely that some are phenothiazine derivatives, and that
phenodiiazines used late in pregnane)', have caused prolonged extra-pyramidal
disturbances in the child.
•
-
Phenothiazincs are given a C categorisation, whilst meclozine, dcxc.hlorpheniramine.
and the antiemetic mctoclopmnmle are given an A categorisation. The antihistamine:.
azaadine, methdilazinc and terfcnzJine are given a B2 rating.
3
•3
Doxylaminc is no longer available as a single ingredient, but is contained in a
combination product with paracetamol and codeine. This combination productMersyndol (Merrell Dow) may be regarded as safe for short-term use during
pregnancy. Astemizole is given a C rating because of its long (4-month) elimination
half-life. Because of the potential to accumulate, it should probably be avoided during
pregnancy. In practice, we would not differentiate between the older antihistamines
and anti-emetic preparations, but agree that there may be the theoretical possibility of
extra pyramidal effects from phenothiazines, when used late in pregnancy. There are
insufficient data on loratadine and terfenadine use in pregnancy. Therefore they are
not recommended for use at this stage.
<3
7
3
<5
O
Antimalarial Preparations
>3
O
The antimalarial preparation pyrimethamine is given a B3 categorisation.
Chloroquine and related substances arc given a D categorisation. The antimalarial
combination of pyrimethamine and dapsone is given a B3 rating whilst ,
pyrimethamine and sulfadoxine is given a C rating.
0
O
£
The ADEC categorisation booklet notes that the use of chloroquine and related drug?
in the prophylaxis of malaria is accepted because the small risk to the fetus with the
low doses is outweighed by the benefits to the mother and the fetus.
The difference between pyrimethamine-dapsone and pyrimethamine-sulfadoxine is
that sulfadoxine, and other long acting sulphonamides, may cause kemicterus in
babies during the first month of life, by displacing bilirubin from plasma albumin.
; 3
O
O
Q
3
The difference in the ratings reflects, fairly well, the advice that we give, with regard
to these preparations, namely that chloroquine is regarded as being safe if it is used for
prevention of malaria, and that the pyrimethamine-dapsone combination is not
established as being as safe as chloroquine but may need to be given if exposure to
chloroquine-resistant strains of malaria cannot be avoided. Where this is the case,
folate supplementation maybe used, to reduce the theoretical potential for teratogenic
outcome l’’. Mefloquine has been used later in pregnancy. Not recommended for use
in the first trimester, as limited teratogenicity data are available.
Pyrimethamine-sulfadoxine is generally pct recommended during pregnancy.
8
0
~3
0
Antithyroid Drugs
Antithyroid agents may.cause congenital goitre by inhibiting thyroxine synthesis in
the fetus. During pregnancy these products should therefore only be used after
carefully weighing the mother’s needs against the risk to the fetus. Propylthiouracil is
usually preferred to carbimazole because o: suggestions of potential congenital skin
lesions, arising from the use of carbimazole and related drugs during pregnancy'"'
Appetite Suppressants
9
Fenfluramine is rated B2 and others in the group are rated B3. There are no good
epidemiological data on safety of these preparations during pregnancy. They are not
usually recommended for use during pregnancy.
10
Analgesics (including Narcotics)
The opioid analgesics are given a C categorisation on the basis that narcotic analgesics
may cause respiratory depression in the newborn infant. It is stated that during the
last two to three hours before expected delivery, these preparations should only be
used after weighing die ijeeds of the mother against the risk to the fetus. This reflects
die reality of the risk-benefit ratio of these preparations, since morphine, pethidine
and other narcotics have been used in obstetric practice for many years, with the full
realisation that there may be the potential for respiratory depression. Codeine is given
a category A rating. The narcotic antagonist naloxone is rated A Paracetamol is
regarded as safe to use during pregnancy and is rated A
11
Barbiturates
Amylobarbitone, pentobarbitone, methylphenobarbitone
Barbiturates cross die placenta and appear in the fetus. After prolonged continuous
usage during a large part of pregnancy, they give rise to hypotension, reduced
respiratory function and hypothermia in the newborn child. Continuous treatment
during pregnancy and administration during labour should therefore be avoided.
12
Benzodiazepines
These drugs cross the placenta and appear in the fetus and may, after continuous
administration during a large part of pregnancy, give rise to hypotension, reduced
respiratory function and hypothermia in the newborn infant. Withdrawal symptoms
have been reported with this class of drugs. Continuous treatment during pregnancy
and administration of high doses in connection with delivery should therefore be
avoided. Short-term use, such as single night-time hypnotic dosage, is not considered
to be a problem.
13
Beta-adrenergic Blocking Agents
Beta-adrenergjt blocking agents arc rated as C, because of their potential to cause
bradycardia in the fetus and the newborn. Labetalol, metoprolol, and oxprenolol '■
■ have been successfully used, and have not demonstrated adverse effects in this
regard tiM'.u'M<> However, there have been some studies which have shown lower
birthweight in the infants ofatenolol-treated women compared with.altemative
treatments including labetalol. On that basis, the combined alpha and beta blocker,
labctalol may be a preferred option, to using beta blocking agents.
14'
Calcium-channel Blockers
Verapamil and nifedipine are rated C, due to their potential for fetal hypoxia. The
Swedish category for.verapamilis A. There is sufficient evidence to suggest that vera
pamil may be safely used in pregnancy and it would be more worthy of a Bl rating(,S).
15
Corticosteroids
In animal experiments, corticosteroids have been found to cause malformations of
various kinds (cleft palate, skeletal malformations). These findings do not seem to be
relevant to humans. Reduced placental and birth weight have been recorded in ’
animals and humans after long-term treatment.
Systemic corticosteroids, with the exception of replacement doses, arc listed as C
category, since there is obviously the possibility of adrenal cortex suppressions in the
newborn after'long-tcrm treatment.
Corticosteroids by inhalation have been widely used for many years without adverse
effects in pregnancy, up to 1600mcg daily
The short-term use of antepartum corticosteroids for the prevention of respiratory'
distress syndrome, when warranted, does not seem to pose a risk.
It is also documented that internal pulmonary oedema has been reported with
tocolysis and fluid overload.
Topical steroids, including fluorinated steroids, are listed as Category A. They are safe
for short-term use on unbroken skin for the treatment of appropriate dermatological
conditions.
16
Cyproterone
Cyproterone carries the potential for feminization of the male fetus, and therefore
should be avoided during pregnancy.
17
Thiazides and other diuretics
Thiazides, related diuretics and loop diuretics enter the fetal circulation and may cause
electrolyte disturbances. Neonatal thrombocytopenia has been reported with
thiazides and related diuretics. Loop diuretics, like trusemide and bumetamde are
probably also associated with this risk. During the latter part of pregnancy, products
of this type should therefore only be given on sound indications, and then in the
lowest effective dose.
18
. Haloperidol
Although there have been isolated case reports of birth defects following fetal
exposure to haloperidol in combination with other drugs, no definite cause and effect
relationship can be confirmed.
19
Anticoagulants
Coumarin derivatives, including warfarin, are rated D. We agree with this rating, due
to their teratogenic potential as well as the potential for haemorrhage.
Heparin is also given a C rating due to “increased incidence, of human loss and
prematurity associated with haemorrhage”. The Swedish category for heparin is B2.
We disagree with the C rating, as we believe that heparin, effectively monitored, has
been safely used for prophylaxis and treatment during pregnancy over several years
world-wade. We would place its rating at Bl. This is in line vrith clinical experience
and reviews on the subject(IM7). Obviously, with high-dose use of heparin during
pregnancy; considerations such as bone demineralization and other well known
potential adverse effects on the mother, need to be considered.
20
Lithium
X
Lithium enters the fetal circulation and cases of disturbances of thyroid function of
the newborn infant have been reported. Available data also indicatc'that lithium
dining pregnancy may cause malformations of the cardiovascular system.
21
Non-steroidal Anti-inflammatory Drugs
All drugs in this category arc given a C rating, on the basis of their inhibitory effect on
prostaglandin synthesis and, when given during the latter part of pregnancy, may cause
closure of the fetal ductus arteriosus. When given at term, they may prolong labour
and delay parturition
Continuous treatment with non-steroidal anti-inflammatory drugs during the last
month of pregnancy should only be given on sound indications.
Generally sptxiking, indomethacin, ibuprofen, diclofenac and similar preparations are
not withheld during pregnancy. Aside from the precautions noted above,- they do not
present other risks to the infant .
Aspirin is given a C rating, due to its potential for inhibition of prostaglandin
synthesis, which may cause premature closure ot the fetal ductus arteriosus, its
potential of prolonging labour, and its tendency to increase bleeding capacity in the
newborn
Aspirin-containing products should, therefore, be avoided in late
pregnancy.
Low-dose aspirin has been advocated for prevention of pre-eclampsia. However, if
used, it should be discontinued 1-2 weeks prior to expected date of delivery, because
of uncertainty as to the safety of low-dose aspirin and epidural anaesthesia.
The ADEC Classification booklet also notes that animal studies have shown~aspirin to
cause birth defects in animals, but there is ho conclusive evidence that aspirin causes
malformations in humans. This is in accordance with our own recommendations. It
is to be noted that paracetamol is listed as a category A preparation, as it has not
demonstrated any direct toxicity or teratogenicity when used during pregnancy.
22
Nitrofurantoin
Nitrofurantoin was originally given a C rating, in the.1989 classification, on the basis
of the caution required when given at term or to infants under one month, because of
the theoretical possibility of producing haemolytic anaemia due to immature enzyme
systems in the early neonatal period. In fact, this has not been reported to have
occurred in practice l’6’. It is placed in the A category in the 1992 classification.
Nitrofurantoin has been quite, widely and safely used throughout pregnancy for over
thirty years. In both the United States of America and Sweden it is placed in the
category equivalent to category A. An assessment of the literature confirms the view
that the rate of haematological reactions is very law (around 0.0004% of doses given).
We would, therefore, agree with the “A" categorization p72xl.
23
Sex Hormones, including Oral Contraceptives
Animal studies have shown that high doses of progestogens can cause masculinization
of the female fetus. Because of this virilising effect on the fetus, they are rated D.
The results from these experiments in animals co not seem to be relevant to humans.
in the low doses used in contraceptives.
Obviously, the rating with respect to.these hormones is of most relevance
retrospectively, in the case of inadvertent use of a particular drug in early pregnancy, as
these preparations would not normally be prescribed during pregnancy, if it were
known that the patient was pregnant. In this context, low dose progestogens should
probably be a Bl or B2 rating. (See also comments following, with regard to oral
contraceptives.)
We would also advocate individual counselling where appropriate, to the effect that
the inadvertent use ofdMylestranol, dydrogesterane or medroxyprogesterone in early
pregnancy, should not be regarded as a reason fcr interruption of pregnancy, as the
evidence suggests that the actual risk of virilization is minimal. Anabolic steroids are
rated D due to their potential for virilising effects on the fetus. Danazol has also
demonstrated an androgenic effect on the fetus tn several reported cases.
Stilboestrol is rated X.
Oral contraceptives (again, obviously inadvertently used in early pregnancy) are rated
B3. This is a reasonable rating, since there is no evidence that intake of oral
contraceptives during pregnancy represents an increased risk to the fetus. It should be
noted that the studies, indicating links between oral contraceptives and limb reduction
deformities, were all carried out during the years .when oral contraceptives contained
high-strength oestrogens and progestogens, prior to the introduction of the more
modem low-strength preparations, and progestogen-only preparations in the early
1980’s;
Indeed, early formulations, contained in some cases, 10 to 20 times the
equivalent steroid content compared to modem formulations.
3
3
3
3
3
24
<3
1
•3
Oral Hypoglycaemic Agents
In animal studies birth defects have been demonstrated. They should therefore net be
used during pregnancy but should be replaced by insulin.
’3
.
25
Phenothiazines
Fluphenazine, perphenazine, chlorpromazine, pericyazine, thioridazine,
trifluoperazine, promazine, prochlorperazine.
L\
When given in high doses during later pregnancy, phenothiazines have.caused
prolonged extrapyramidal disturbances in the child.
3
26
3
3
Excess vitamin A may cause birth defects. Women should consider their dietary
intake of vitamin A before taking supplements. The Australian diet usually contains
the recommended daily allowance of2500 ILL
27
3
3
3
; 3
•&
Rifampicin
Bleeding, attributable to hypoprothrombinaemia, has been reported in newborn
infants and in mothers after the use of rifampicin during late pregnancy. In animal
experiments, rifampicin, given during organ development, has caused skeletal
malformations. If rifampicin is used during the last few weeks of pregnancy, vitamin
K should be given to the mother and the newborn infant.
28
3
Vitamin A
Sulphonamides
Sulphonamides may cause kernicterus in babies during the first month of life by
displacing bilirubin from plasma albumin. Sulphonamides should therefore be
avoided as far as possible during the last month of pregnancy.
The rapidly-excreted sulphonamide, sulphamethizole, may be regarded as being sue
for use in pregnancy, bearing in mind the concern about the use of sulphonamide; as
group late in pregnancy.
29
Tetracyclines
During the period of mineralisation of a child’s teeth (the second and third trimester
of pregnancy, the neonatal period and the first 8 years of life) tetracyclines may induce
hypoplasia of the enamel and discolouration of the teeth. Tetracyclines also
accumulate in the growing skeleton. These products should be avoided during the
second and third trimesters of pregnancy.
30
Tricyclic antidepressants
Amitriptyline, desipraminc, imipramine, trimipramine, nortriptyline, opipramol,
protriptyline, clomipramine.
Tricyclic antidepressants have not been shown to be associated with an increased
incidence of birth defects. However, there is evidence of interference with central
monoamine neurotransmission in rats. Care should be taken that there are sound
indications for the use of these antidepressants in pregnancy.
31
Vaccines
The ADEC categorisation booklet states:
“Women of child-bearing age should be tested prior to pregnancy. All seronegative
women of child-bearing age, provided they are not pregnant, should be offered
rubella vaccine. As the virus in rubella vaccine can cause fetal infection, it is desirable
that the vaccine should not be administered to any women who may be pregnant
Those administering the vaccine should be careful to instruct women to whom it is
given that they should not become pregnant for at least two full menstrual cycles.
However, to date, there have not been any rubella-like birth defects in the live bom
infants (about 400) of seronegative mothers vaccinated during or just before
pregnancy. Based on this experience, rubella vaccination during pregnancy need not
be the reason to recommend interruption of pregnancy. The final decision must be
made by the patient and her physician.”
We agree with these comments, and they are supported by the recommendations of
the United States Practices Advisory Committee of the Center for Disease Control,
U.S_A.(25). This group further states that “both yellow fever vaccine and oral polio
vaccine can be given to pregnant women at substantial risk of exposure to infection.
When vaccine is to be given during pregnancy, waiting until the second or third
trimester to minimiseAny concern over teratogenicity is a reasonable precaution” 651
Although adverse effects on the fetus have not been repotted, oral poliomyelitis
vaccine should not normally be given to women during the first four months of
pregnancy unless there are compelling reasons.
There is no convincing evidence of risk to the: fetus from immunisation of pregnant
women using inactivated virus vaccines, bacterial vaccines or toxoids t27).
32
Penicillamine
Penicillamine can cause cutis laxa in the human fetus
33
Bismuth Subnitrate
Bismuth is a heavy metal which crosses the placenta. Although there have beenno
reports of adverse effects in the human fetus, use of this preparation is not
recommended during pregnancy.
34
Sodium Nitroprusside
Sodium nitroprusside is used in high risk situations and there may be additional
hazards associated with the drug. It crosses the placenta. Short term use for control
of hypertensive crises may be safe provided die maternal pH and cyanide levels are
monitored.
35
Hydralazine
Hydralazine is used for treating hypertensive crises, where rapid blood pressure contol
is required. However, it is rated C, on the basis that fqtal distress and arrhythmia have
been reported following intravenous use late in pregnancy.
36
Metronidazole
Reviewingall the available animal and human data on the safety of metronidazole in
pregnancy, we may conclude that epidemiological and clinical data accumulated, over
a period of 30 years, has failed to show evidence of teratogenicity. With regard to
mutagenicity, experimentally, chemicals of a class to which metronidazole belongs,
may be shown to be mutagenic. I lowever, there is no evidence that metronidazole has
this effect in human usage.
r
~
Metronidazole is classified as B2 by the AD EC “Medicines In Pregnancy"
classification system.
I Therefore, if metronidazole is the drug of choice, for a particular infection during
i pregnancy, review of available evidence regarding its safety during pregnancy suggests
^that it may be safely used.
n
r
T3
REFERENCES CITED
TO
1
Pipkin FB, Turner SR, Symonds EM. Possible risk with captopril in
pregnancy: some animal data. (Letter) Lancet 1980;l:1256.
2
Millar JA, Wilson PD, Morrison N. Management of severe hypertension in
pregnancy by a combined drug regimen including captopril: case report.
NZ Med J 1983;96:796-8.
3
Duminy PC, Burger PD. Fetal abnormality associated with the use of
captopril during pregnancy. (Letter) S Afr Med J 1981;60:805.
4
Lubbe WF. The use of captopril in pregnancy. (Letter) N Z Med J
1983;96:1029-30.
’ ’
o
5
Acyclovir - Guidelines for use in hospitals. New Solith WalesiADIS pubs.
o
6
Garland, SM. Antibiotic Guidelines: Obstetrics, Gynaecology and Neonatal
Paediatrics. Melbourne; 1990:7.
10
7
Glasgow G. Current Therapeutics. 1980; (21) :11-2.
10
8
Biale Y, Lewenthal H. Effect of folic acid supplementation on congenital
malformations due to anti-convulsive drugs. Eur J Obstet Gynecol
Reprod Biol 1984;18:211-16.
9
Pyrimethamine combinations in pregnancy'. [Editorial] Lancet 1983;2:1005-7.
10
Reynolds B et al. First year of life after the use of atenolol in pregnancyassociated hypertension. Arch Dis Child 1984;59:1061-3.
11
Plouin PF ex al. A randomized comparison of early conservative use of
anti-hypertensive drugs in the management of pregnancy-induced
hypertension. BrJ Obstet Gynecol 1990;97:134-41.
12
Rubin P et al. Placebo-controlled trial of atenolol in the treatment of
pregnancy-associated hypertension. Lancet 1983;1:431-4.
13
Sandstrom B. Anti-hypertensive treatment with the adrenergic beta-receptor
blocker metoprolol during pregnancy. Gynecol Obstet Invest 1978;9;
195-204.
14
Riley AJ. Clinical pharmacology of labetalol in pregnancy. J Cardiovasc
Pharmacol 1989;3(Suppl 1):53S.
15
Zanchetti and Krikler Eds. Calcium antagonism in cardiovascular therapy
experience yvith verapamil. International symposium,Florence 2-4 October
1980:251. Excerpta Mcdica Amsterdam-Oxford-Princeton 1981.
16
Dahlman T, Lindvall N, Hellgren M. Osteopenia in pregnancy
during long-term heparin treatment: a radiological study post-partum.
BrJ Obstet Gynaecol 1990;97:221-8.
iO
I
1
[0
10
0
0
•;0
0
O
>3
0
0
3
3
3
3
3
3
3
3
3
p
ISS>
•I 3
I
! 3
i’
17
Brill-Edwards P ct al. Heparin prophylaxis during pregnancy. Ani J Obstet
Gynecol 1990;162:870-1.
18
Berglund F et al. Drug use during pregnancy and breastfeeding a classification system for drug information. Acta Obstet Gynecol Scand
Suppl 1984; 126:1-55.
19
Synthetase inhibitors in obstetrics and after. [Editorial] Lancet 1980;2:185-6
20
Karim SM. On the use of blockers of prostaglandin synthesis in the control
of labour. Am Clin Res 1973;5:375-9.
21
Collins E, Turner G. Maternal effects of regular salicylate ingestion in
pregnancy. Lancet 1975;2:335-8
22
Stuart MJ et al. Effects of acetylsalicylic acid ingestion on maternal and
neonatal hemostasis. N EngJ Med 1982;307:909-12.
23
Janerich DT et al. Oral contraceptives and congenital limb- reduction
defects. N EngJ Med 1974;291:697-700.
24
Czeizel A et al. An aetiological evaluation of increased occurrence of
congenital limb reduction abnormalities in Hungary. 1975-1978 IntJ
Epidemiol 1983;12:445-9
25
General recommendations on immunization - recommendations of the
Immunization Practices Advisory Committee.
Ann Intern Med 1983;98:615-22.
26
Hailey F.Fort H et al. Fetal safety of nitrofurantoin microcrystals therapy
during pregnancy: a retrospective analysis. J Int Med Res 1983; 11:364-9.
27
Cunha B. Nitrofurantoin: an update. Obstet Gynecol Survey. 1989;44:
399-406.
28
D’arcy PF. Nitrofurantoin. DICP 1985;19:540-7.
29
ADEC Committee “Medicines in Pregnancy” booklet, Canberra, 1992, Aust.
Govt. Publishing Service.
30
Mutjtaba O, Burrow GN. Treatment of hyperthyroidism in pregnancy with
propylthiouracil and methimazole. Obstet Gynecol 1976; 46:282.
p
t»
o
!
!*
a
' a
X
X
X
X
X
T
2
DRUG REFERENCE CHAR I’ ACCORDING TO MIMS
<■.. 'vx ■
■.¥’ Ktse:
.. y;-" v!
‘ ............. <
i*'
5 AMINOSAJJCYLICACID
•
i FLUOROURACIL
4
•
CARBIDOPA &
BENSERAZIDE
*
•
*
acebutolol
•
CARB IM AZOLE
ACETAZOLAM IDE
*
CARBOPROST
ACYCLOVIR
4
CARISOPRODOL
•
ADRENOCHROME
4
CEFACLOR
•
*.
CEPADROXIL
•
♦
CEFAZOLIN SODIUM
•
C EFOP ERAZO NE SOD
•
•
CEFOTAXIME
♦
•
CEFLAZIDIME
•
CEFLAZIDIME
♦
CEFLRIAXONE
•
•
albendazole
alfacalcidol
•
ALLO PURINOL
•
ALLYLO ESTRENOL
♦
•
•
♦
♦
ALPRAZOLAM
AMANTADINE
♦
AMIKACIN
•
♦
♦
•
AMINEPTINE
AMITRIPTYLINE
♦
•
AMIODARONE
•
•
•
AMODIAQUINE
AMOXAI’INI’.
•
—- - —
A
. •_______
AMOXYCILLIN
—
♦
AMPHOTERICIN B
*
4
AMPICILLIN C
SULBACTAM SOD
•
•
AMRINONE
♦
•
CEPHALEXIN
♦
CETR1ZINE DI HCL
•
•
•
•
CHLORAMPHENICOL
•
CHLORDIAZnrOXIDF.
•
•
•
CHLOROQUINE
•
•
•
•
CHLORTHALIDONE
*
AMYI-OBARBITONE
•
•
CHLORMEZANONE
CHLORPROPAMIDE
CICLOPIROX OLAMINE
*
•
CIMETIDINE
•
•
♦
•
♦
CENTCHROMAN
CHLORAMBUCIL
•
*
AMI ODIPINE
•
CEFUROXIME
•
•
AMILOR1DE
•
•
•
•
analgin
•
•
CINNAR1ZINE
ANTHRAQUINONES
•
•
CIPROFLOXACIN
•
APROTININ
*
•
CISAPRIDE
•
♦
ASPIRIN
ATENQLOI. *
NllEDU’INE
r
i
11
1
*
CLEMASTINE FUMARATE
•
•
•
— ——
•
BETAMETHASONE
•
BETAXOLOL
•
•
•
CLINDAMYCIN
*
CLODF.TASOI. ACHATE
—
—
...............
CLOBETASOL PROPION AIL
CLOBETASONE -17 BUTYRATE
AZITHROMYCIN
•
♦
CLIDLNIUM
•
A1RACURIUM
•>
•
•
ASTEM1ZOLE
CISPLATIN
♦ ’
•
—
•
CLOFAZIMINE
•
CLOM1PHENE
♦
BISOPROLOL
♦
•
♦
•
CLONOD1NE
♦
BUMOCR1PHNE
•
BUMETANIDE
•
—
•
4
—
•
BUSPIRONE
•
•
CLOPAMIDE
•
_________________
•
•
*
CYCLOPHOSPHAMIDE
•
CYTOSINE ARABINOSIDE_________
CAPTOl’RIL
D-PEN1CILLAMIN__________________
•
4
COLISTIN
•
•
-
•
CLOTRIMAZOLE
COUMARINS 4 INDANEDIONES
BUSULPHAM 31 HAL
C1NONIDE P
•
4
♦
BUPRENORPHINE
•
*
CLONAZEPAM
BROMOCRIPTINE
4
♦
CLOMIPRAMINE
BEZA FIBRATE
BLEOMYCIN
•
DANOZOL^
_
•
—
J,——
1 *
DRUG REFERENCE CHART ACCORDING TO MIMS
♦
♦
DEXAMETHASONE
D EXFENFLURAMINE
DEXTROPROPOXYPHE
DIAZEPAM
•
•
GLICLAZIDE
DILOXANIDE FUROATE
Diphenoxylate
UIHIENYLM ETHANES
Dipyridamole
DiSOPYRAMIDE
♦
♦
«
•
•
♦
1* LX OKU BIC IN____
DOXYCYCLINE
ECONAZOLE
enalapril maleate
EPHEDRINE
ERGOTAMINE
ERYTHROMYCIN
ETHAMSYIJKTE____________________
•
HALCINONLDE
*
HALOPERIDOL
♦
HEPARIN
•
HYDROCHLOROTHIAZIDE
•
HYDROCORTISONES SOD
SUCCINATE
•
IBUPROFEN
•
IFOSFAMIDE
— _2_
INDOMETHACIN
*
•
•
•
•
KETAMINE
•
KETOCONAZOLE
INSULINS
ft
IODINE
ISOSORBIDE 5 MONONTRATE
•
♦
—
—
•_____
—
*
•
•
FENFLURAMINE
ITNOPROFEN
•
•
•
•
*
♦
♦
•
GEMFIBROZIL
KETOTOLAC TROMETHAMINE
♦
•
....
— ——
«
•
£
♦
•
♦
•
*
—•
•
......
♦
•
••
•
•
•
•
•
••
•
1
•
•
•
♦
•
•
•
LANSOPRAZOLE
LEV AM ISO LE AND TETRAMLSOLE
«
LEVODOPA
•
*
LISINOPRIL
♦
•
•
LORATADINE
LORAZEPAM_______________________ *
LOMEFLOXACIN
♦
_•----- —— J______
—
LABETALOL
LITHIUM
FTORAFUR__________ _____________
GjMJ-AMINE _
♦
♦
•
♦
KETOPROFEN
LINCOMYCIN
•
*
FLUPHEN AZINE
FURAZOLIDONE___
KETOCONAZOLE
LIDOCAINE
•
FLUCINOLONE ACETONIDE
FR US EM IDE
2___
KETOTIFEN
•
•
•
♦
FELOD1PINE
FLURBIPROFEN
KETOPROFEN
•
•
♦
•
KANAMYCIN
FAMOTIDINE
FLURAZEPAM
*
•
•
♦
IN DAPAM IDE
•
etoposide
FLUOXETINE HCL
IM 1 PRAM IN E___________
•
•
•
«
•
•*
•
HYDANTOINS
HYOSCINE BUTYLBROMIDE
«
— •
•
LTHOSUXIMIDE
FLUOCORTOLONE
*
HOMATROPINE
•
•
•
•
•
GRISEOFULVIN
•
•
«
I’llilNYLESIRADIOL
FLUCONAZOLE
•
«
*
I1YDRALAZINIVDI HYDRALAZINE *
ESTROGENS
ethambutol
GLYCERYL TRINITRATE
•
DOMPERIDONE
DOXEPIN '
GLUCAGON
GLYCOPYRROLATE
«
♦
DISULFIRAM
DOTHIEPIN HCL
•
•
•
♦
D! LT! AZ EM
DIMEN HYDRINATE
GLIPIZIDE
•
♦
DICYCLOMINE
DIETHYL CARB AM AZINE CITRATE *
DILAZEP
GLIB ENCLAM IDE
♦
D1CLOFENN SODIUM
DIfNOESTROL
••
•
GENTAMICIN
•
LOPERAMIDE
LOXAPINE
LYNESTRENOL
MEBENDAZOLE___________ ________
MEBEVERJNE
•
•
•
♦
*___
• •
_ ___ _ —
•
•
♦
•
•
DRUG REFERENCE CHART ACCORDING TO MIMS
uWS!
♦
MELPHALAN
•
MENOTROPHIN
•
MERCAPTOPURINE
•
METFORMIN
•
•
•
•
*
METHOCARBAMOL
♦
NALIDIXIC ACIDL
•
NAPROXEN
NEOMYCIN
NEDLM1CLN
NIFEDIPINE
NIMODIPINE
NITRAZEPAM
NITRENDIPINE
•
•
•
•
•
•
•
ORPKENADRINE
OXPRENOLOL
OXYMETAZOLINE
OXYPHENBUTAZONE
penfluridol
•
•
*
•
•
•
PENTOXIFYIUNE
RANITIDINE
•
•
♦
♦
•
•
•
•
•
•
*
•
•
•
•
•
RIBAVIRIN
PXOXATLDINE ACTTATE
ROXTTHROMY CIN
•
•
SECN ID AZOLE
SELEGILINE
SOD CROMOGLYCATE
SOD. NITROPRUSSIDE
SOTALOL
SPIRAMYCIN
SPIRONOLACTONE
STRPTO KINASE
SUCCINYLCHOLINE CHL.
•
SUCRALFATE
♦
•
•
•
•
*
•
•
•
♦
♦
•
•
•
SLT-FADOXLNEPYR
CME-THAMINE
SULFAMOXOLE
*
•
•
SULPHACETAMNIDE
•
SOD
TA.MOSIFEN
•
•
•
•
PYRAZINAM1DE
•
PENICILLIN - G
PENTAZOCINE
•
QUINIDINE
SALBUTAMOLE
•
•
•
•
•
•
•
•
SISOMYCIN
•
♦
•
PEFLOXACLN
•
♦
•
*
•
ITASOXACLS
•
«
•
OXYTETRACYCLINE
PANCURONIUM
PYRANTEL PAMOATE
•
•
•
OXAZEPAM
•
RAMIPRIL
OFLOXACIN
ONDANSETRON
PROPRANOLOL
•
•
•
OESTROGEN
PROMETHAZLNETHEOCLATE
PROPANTHELINE
•
NORFLOXACIN
OMEPRAZOLE
PROCHLORPERAZINE
•
•
NORETHISTERONENANTATE
NYSTATIN
PROCAINAMIDE
*
•
'
PROBENECID
•
•
N1TROFURANTODI
NORTRJTTYLLNE
PRAZOSIN
PREDNISOLONE
•
«
•
•
PRAZIQUANTEL
•
NICERGOUNE
NICLOSAMIDE
PRALIDOXIME CHLORID
•
•
MUSTINE HCL
POLYMYXIN B
•
*
♦
•
•
•
•
•
PIROXICAM
•
•
•
PIRACETAM
♦
•
*
•
MJTOMYCIN-C
MOMETASONE FUROATE
•
PINDOLOL
•
•
•
•
•
MINOCYCLINE
MINOXIDIL
•
•
*
PIMOZIDE
*
•
METOCLOPRAMIDE
MICONAZOLE
PHENYLBUTAZONE
•
METHYL TESTOSTERONE
MIANSERIN
PHENOBARBITONE
•
♦
•
♦
PHENYLEPHRINE
MLTHYLDOPA
M EXILETINE
•
PERINODO-RIL
PHEN AZO *YRIDINE
•
methotrexate
METRONIDAZOLE
STATION:
•
•
TENOXICAM
1 •
TERAZOSIN
J----------
•
• ---DRUG REFERENCE CHART ACCORDING TO MIMS
<5
•
♦
•
TERFENAD1NE
J
TESTOSTERONE
<5
TETRACYCLINE
THYROXINE SODIUM
0
1
•
•
•
♦
nno-TEPA
P
P
•
nCLOPtDINE
TIMOLOL MALEATE
TINIDAZOLE ■
•
•
TR.A.SIADOL HCL
TRAZODONE
•
•
TOLBUTAMNIDE
*
*
•
•
TRIAMTERENE
TRJCLOFOS SODIUM
0
i
ERiSLUOPERAZINE
'IWXbUOf’EJUDOL
0
"i
1
TRIFL UPEOMAZINE
TRIMETHOPRIM
! 3
'
A
♦
r i•
SULPHA
TRIMIFRVTNE
VALETHAM ATE
I*
VANCOMYC IN
VERAPAMIL
F*
1
!
[*
‘>3
■3
;s>
e
3
-
■3
3
3
• 3?
4
3
3
•
3
"S
!
Gastrointestinal Drug Use in Pregnancy
Category A •
Group Bl
Group B2
Group B3
Category C
Category D
Category X
Unlisted
antacids
cimetidine
bismuth subcitrate
loperamide
dexamethasone
doxcycline
misoprostol
aza thioprine
bisacodyl
cisapride
cholestyramine
nizatadine
diphenoxylate
neomycin
1
dicyclomine
cascara
famotidine
domperidone
omeprazole
hydrocortisone
lactulose
codeine phosphate
ondansetron
hyoscine salts
spironolactone
interferons
mebeverine
dimenhydrinate
ranitidine
hyoscinc-N-butylbromide
mesalazine
olsalazine
docusate
sucralfate
hyoscyamine
octreotide
panerelipase
f'tangula
metronidazole
prednisolone
peppermint oil
meclozine
phenolphdialeine
prochlorperazine
polyethylene glycol
metoclopramide
propantheline
promethazine
pyridoxine
senna, sennosides
vasopressin
sorbitol
ursodeoxycholic acid
sulfasalazine
vitamin D
Based on Medicines in Pregnancy, Australian Drug Evaluation Committee, Australian Government Publishing Services, Canberra, 1992. Copyright, Commonwealth
of Australia, Reproduced with permission.
M
f C/
O
G '
'&' Ci
€4 &
ANTIMICROBIAL DRUG USE IN PREGNANCY
CATEGORY A
GROUP BI
GROUP III
GROUP B3
CATEGORY C
aminoglycosides
CATEGORY D
amikacin
gentamicin
netilmicin
tobramycin
antifungals
nystatin
miconazole
amphotericin
(topical)
ketoconazole
fluconazole
flucytosine
griseofttlvin
antimalarials
mefloquine
pyrimethamine-
chloroquine
pyrimetha mine-
sulfadoxine
quinine
da psone
anti-tuberculous
cthambutol
pyrazinamidc
rifampicin
isoniazid
clofazimine
< rphAknfuirmt
cephalexin
ccplialothin
oilier crphalotporini
macrolides
clindamycin
roxithromycin
erythromycin
lincomycin
amoxycillin
pcniclillins
amoxycillin/
ampicillin
potassium clavulanatc
benzathine
ticarcillin
penicillin
flucioxacillin
benzylpenicillin
piperacillin
cioxacillin
aztreonam
methicillin
procaine penicillin
penicillin V
nalidixic acid
quinolones
ciprofloxacin
norfloxacin
sulphonamides/
„
dapsonc
trimethoprim
co-trimoxazole
sulphadizine
trimethoprim
sulphadoxine
sulphamethoxazole
miscellaneous
hcxaminc
spcctinomycin
acyclovir
mebendazole
chloramphenicol
nitrofurantoin
praziquantel
metronidazole
thiabendazole
fijsidic acid
vancomycin
tan cyclines
tinidazole
zidovudine
IUm.I nil
Mofi< inr, in I'upnmb v, ?n<! rd. Anu: nliaii Ihiitf I’vnlunilon <'nminitirr, AiiMtAliiin < h>veinmri.it I'ublidilnj; Service, Canberra, 1002. Copyright, Commonwealth of Australia, Reproduced
uh pt iinikbitm
Ci
RESPIRATORY
ERUG USE
IN PREGNANCY
UNLISTED
CATEGORY A
GROUP Bl
GROUP Bl
GROUP B3
CATEGIRY C
CATEGORY 0
adrenaline
amoxycillin/
calcitonin
amantadine
alprazolam
cyclophosphamide
astcrnizolc
potassium
dapsonc
beclometliasone
amitriptyline
doxycycline
aza thioprine
aminophyllinc
CATEGORY X
clavular.atc
amoxycillin
Ijr
metronidazole
ciprofloxacin
aspirin
gentamicin
budcsonide
pseudocplicdrine
flunisolidc
chloramphenicol
medroxy-
dalteparin
co-trimoxazoJc
progesterone
enoxaparin .
dcxamctliasooc
mustinc hydrochloride
loratadine
diazepam
tobramycin
methoxaminc
heparin
warfarin
oxymetazoline
benzylpenicillin
cefaclor
ccphalolhin
cefotaxime
pyrazinamidc
clindamycin
ceftriaxone
tcrfcnadinc
codeine
flucioxacillin
vancomycin
diphenhydramine
ipratropium
erythromycin
hydrocortisone
cthambulol
morphine
pamidronate
O
roxithromycin
fcnotcrol
oxazepam
isoniazid
pentamidine
rtreptomycio
orciprenalinc
pethidine
tissue plasminogen
paracetamol
prednisolone
tramazoline
' phenoxy methyl-
rifampicin
salmetcrol
activator
penicillin
pholcodcinc
streptokinase
procaine penicillin
salbutamol
sodium
cromoglycate
X x
terbutaline
theophylline
Based on Medicines in Pregnancy, Australian Drug Evaluation Committee, Australian Government Publishing Services, Canberra, 1992. Copyright, Commonwealth of Australia, Reproduced with
permission.
1
V V h?
y
“ S3 O
y
GC & 6 &
Q G e 4”3 G G Q G to k
Table 6
Cardiovascular Drug Use in Pregnancy'
Category A
adrenaline
Group Bl
Group B2
Group B3
isosorbide
acetylcysteine
clonidine
Category C
amiloride
indomethacin
Category D
Category X
Unlisted
captorpril
adenosine
dalteparin
enoxapariri
dinitrate
atropine
mexiletirte
digoxin
oestradiol
isoprenalinc
lignocaine
^cholestyramine dopamine
amiodarone
labetalol
enalapril
colestipol
flecainide
amlodipine
metolazone
fosinopril
probucol
disopyramide
gemfibrozil
aspirin
metoprolol
lisinopril
n-3 fish oil
ticlopidinc
dobutaininc
spironolactone
atenolol
minoxidil
medroxypro
concentrate
gesterone
sodium
valerate
melhyldopa
glyceryl
betamethasone morphine
trinitrate
acetate
isosorbidc
bretylium
nifedipine
nicotine
bicarbonote
mononitrate
bumetanide
nimodipinc
perindopril
rt-PA
phenytoin
nicotinic acid
chlorothiazide
oxprenolol
pcrhexilcnc
diazepam
pravastatin
quinapril
prazosin
diazoxide
promethazine
ramipril
quinidine
trandolapril
diltiazem
bisuplhate
csmolol
simvastatin
fclodipine
sodium
frusemide
nitroprusside
heparin
sotalol
hydralazine
streptokinase
hydrochloro
triameterence
thiazide
hydrocortisone verapamil
indapamide
warfarin
‘ Rased on “Medicines in Pregnancy", Australian Drug Evaluation Committee, Australian Government Publishing Services, Canberra, 1992,
Copyright, Commonwealth of Australia, Reproduced with permission.
3
DRUGS CONTRA INDICATED IN PREGNANCY BY GENERIC NAME
ACCORDING TO CIMS
3
3
i ■
(3
I
f
I
3
h
i
£
<3
:3
■3
:3
•3
3
3
3
S)
S.No,.
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
• 41
43
45
47
49
•51
53
55
57
59
61
63
65'
67
69
■ 71
73
75
77
79
81
83
85
67
89
91
93
95
97
GENERIC NAME
5-FLUOROURACIL
ACETYL SALICYLIC ACID
ALPRAZOLAM
AMIKACIN
AMINOCAPROIC ACID
AMLODIPINE
AMYLOBARBITONE
ASPIRIN
ATRACURIUM
AZATADINE MALEATE
BETAXOLOL
BUPRENORPHINE
CAPTOPRIL
CARBIDOPA & BENSERAZIDE
CARBOCISTEINE
CEFAZOLIN
CHLORAMPHENICOL
CHLORPROPAMIDE
CIPROFLOXACIN
CISPLATIN
CLEMIZOLE
CLOMIPHENE
CLOPAMIDE
CYCLOPHOSPHAMIDE
DANAZOL
DEXAMETHASONE
DIAZEPAM
DIENOESTROL
DILOXANIDE FUROATE
DIPHENHYDRAMINE
DIPHENYL PYRALINE
DISULFIRAM
DQTHIEPIN HCL
DOXYCYCLINE
EMBRAMINE
ERGOTAMINE TARTARATE
ETHAMSYLATE
ETOPOSIDE
FENFLURAMINE HCL
FLUOROURACIL
FLUPHENAZINE ANATEMSOL INJ
GLIBENCLAMIDE
GLIPIZIDE
HYDROCHLOROTHIAZIDE
HYDROXYZINE HCL
IODINE
ICHEXOL
KANAMYCIN
KETOROLAC TROMETHAMINE
S.No.
2
4
6
8
10
12
14
16
18
20
22
24
26
28
30
32
34
36
38
40
42
44
46
48
50
52
54
56
58
60
62
64
66
68
70
72
74
76
78
80
82
84
86
88
90
92
94
96
98
GENRIC NAME
ACETAZOLAMIDE
ALBENDAZOLE
AMANTADINE
AMINEPTINE
AMIODARONE
AMOXYCILLIN
ASPARAGINASE(L)
ASTEMIZOLE
AY5-AMINOSALICYLIC ACID
BENZOYL PEROXIDE
BEZAFIBRATE
BUSPIRONE
CARBIDOPA
CARBINOZAMINE MALEATE
CARBOPROST
CHLORAMBUCIL
CHLORDIAZEPOXIDE
CHLORTHALIDONE
CISAPRIDE
CLEFAZIMINE
CLOFAZIMINE
CLOMIPRAMINE
CODEINE
CYTOSINE ARABINOSIDE
DEMOECLOCYCLINE
DEXTROPROPXYPHENE
DICLOFENAC SODIUM
DIETHYL CARBAMAZINE CITRATE
DIMENHYDRINATE
DIPHENYL HYDANTOIN
DISMUTH SUBCITRATE
DOMPERIDONE
DOXORUNICIN
DYDROGESTERONE
ENALPRIL MALEATE
ESTROGENS (CONJUGATED)
ETHINYL ESTRADIOL
FELODIPINE
FLUNARIZINE
FLUPENTHIXOL
FLURBIPROFEN SODIUM
GLICLAZIDE
GRISEOFULVIN
HYDROFLUMETHIAZIDE
INDOMETHACIN
IODOCHLOTHYDROXYQUIN
IRON SORBITOL CITRIC ACID
KETOCONAZOLE
KETOTIFEN
VHAI-AIDAN-NCCDP-RDCC DRUG CONSULTATION
ON
IMPACT OF POLICY CHANGES ON DRUG POLICY AND DRUG USE|
26, 27 August 1996
IRRATIONAL PARACETAMOL FDCs
Dr.W.V.Rane
Arogya Dakshata Mandal
The earliest paracetamol combination was with anti-histaminic and
ephedrine as systemic nasal decongestants. Lately the Drug
Controller of India has banned ephedrine anti-histaminic
combinations and drug manufacturers are changing over to
pseudoephedrine. British National Formulary (BNF, No.29, March
95, page 143) says "These preparations are of doubtful value but
unlike the preparations for local application they do not give
rise to rebound nasal congestion. They contain sympatheminetics,
and should therefore be avoided in patients with hypertension,
coronary heart disease, or diabetes, and in patients taking
monoamine-oxidase inhibitors
Many of the preparations also
contain antihistamines which may cause drowsiness and affect
ability to drive or operate machinery". I have mentioned here
under the FDCs and each FDC could have many brands. For sake of
convenience I have mentioned only one brand.
Paracetamol 500 mg + tripolidine 2.5 mg
+ Pseudophehedrine 60 mg.. Actified-Wellcome
Paracetamol 400 mg + Phenylephrine 5 mg
+ diphenpyraline 2.5 mg Cinaryl-Themis
Paracetamol 500 mg + Pheniramine Mai 12.5 mg Cosavil Hoecht
Paracetamol 500 mg + Phenylopropanolamine 25 mg
+ Chlorpheniramine Mai 2 mg Febrex Plus Indico
Paracetamol 500 mg + Chlorpheniramine mal 4 mg
+ pseudoephedrine 60 mg Rinostat - Searla
Paracetamol 325 mg + Dextromethorphan 10 mg + Phenylpropanolamine
25 mg + Chlorpheniramine maleate 4 mg
+ Caffeine 50 mg Alex-Lyka
Paracetamol 500 mg + Promethazine 10 mg
Crophen-10 Shalaks
Paracetamol 500 mg + Codeine 10 mg + Caffeine 30 mg
+ Chlorpheniramine mal 2 mg Neofebrin-NeoPhar
Paracetamol 125 mg + Dextromethorphan 5 mg + Carbinoxamine Mal 1 rg
+ Pseudoephedrine 10 mg per 5 ml - Pedia 3
Ethnor
Paracetamol 250 mg + Analgin 250 mg + Tripolidine 1.25 mg
- Recofast Ethico
Paracetamol 450 mg + Chlorpheniramine mal 2 mg -r Ephedrine 5 mg
+ Bromhexin* 4 mg + Glyceryl glaicolate 50 mg
- Sudin Group
1
BNF, Physicians' Desk Reference (PDR) and Martindale Extra
Pharmacopoea do not mention the combination of paracetamol and
Ibuprofen. But in India it is one of the most widely promoted
antipyretic and analgesic FDC. Some of the analgesic paracetamol
FDCs contain opioid drugs and BNF (NO.29 March 95 page 182) says
"Compound analgesic preparation containing paracetamol or aspirin
with a low dose of an opioid analgesic are commonly used, but the
advantages have not been substantiated. The low dose of the
opioid may be enough to cause opioid side-effects (in particular,
constipation) and can complicate the treatment of overdose, yet
may not provide significant additional relief of pain.... In
general, when assessing pain, it is necessary to weigh up
carefully whether there is a need for non-opioid and an opioid
analgesic to be taken simultaneously.... Caffeine is a weak
stimulant that is often included, in small doses, in analgesic
preparations. It does not contribute to’ the analgesic or anti
inflammatory effect of the preparation and may possibly aggravate
the gastric irritation caused by aspirin. Moreover, in excessive
dosage or on withdrawal caffeine may itself induce headache".
These are some of the Paracetamol FDCs of analgesics.
Paracetamol + Ibuprofen
500 mg + 400 mg
Acetofen Masco
333 mg + 400 mg
Brucet Micro Nova
325 mg + 400 mg
Anaflam Albert David
325 mg + 300 mg
Brupal Geno
325 mg + 200 mg
Ibugesic plus Cipla
250 mg + 200 mg
Nopane Jr. Combat
162.5 mg + 100 mg
Combiflam suspn/5 ml Roussel
125 mg + 100 mg
Brupal Kid Geno
250 mg + 400 mg + Dextropropoxyphene 32.5 mg
Bren-PX Kopran
300 mg + 400 mg + Chlormezanone 250 mg
Ibuflamar MX Indico
325 mg + 400 mg + Chlorzoxazone 250 mg
Brenlax Kopran
Paracetamol + Dextropropoxyphene
650 mg + 65 mg
Carbutyl □- Roussel
500 mg + 32.5 mg
Proxytab Wockhardt
400 mg + 70 mg
Dexovon
400 mg + 65 mg
Parvon Jagsson Pal
U.S.V.
2
350 mg + 32 mg
Parvon-N Jagsson Pal
325 mg + 65 mg
Darvocet Eli Lilly
These are types of FDC combinations and each could have hundreds
of brands. There are many other FDCs as follows:
Paracetamol 500 mg + Pentazocin 15 mg Foracet Ranbaxy.
Paracetamol 300 mg + Chlorzoxazone 250 mg Dodil - Duphar
Paracetamol 450 mg + Chlormezanone 100 mg
Dolobak-Brown & Burke
Paracetamol 250 mg + Mefenamic acid 500 mg Longagesic Tata Ph.
Paracetamol 500 mg + Mefanamic acid 500 mg Meftal Forte BlueCross
Paracetamol 650 mg + Ketoprofen 50 mg
Redufen-A
Unique
Paracetamol 500 mg + Phenylbutazone 50 mg Actimol Pharmed
Paracetamol 250 mg + Phenylbutazone 100 mg + Diazepam 2 mg
+ Magnesium, tri silicate Arcure Nulife.
Paracetamol 250 mg + Oxyphenbutazone 100 mg
+ Dextropropoxyphene 32.5 mg
Uniloids
Combigesic.
Paracetamol 500 mg + Oxyphenbutazone 100 mg Flamox forte Glennark
Paracetamol 325 mg + Oxyphenbutazone 100 mg Prestigesic Synthico
+ Phenyl-iso-propylpyrazolone 150 mg
Paracetamol 250 mg + Methocarbamol 350 mg Robinaxol Khandelwal
Paracetamol 500 mg + Metoclopramide 5 mg Metopar CFL Pharma
Paracetamol 325 mg + Codeline 30 ng -TWC Ethnor
Paracetamol 500 mg + Indomethacine 25 mg Idicine-P IDPL
Paracetamol 350 mg + Indomethacin 25 mg
Suract SOL Ph.
Paracetamol 450 mg + Orphenadrine 35 mg Orphanol Torrent
Paracetamol 250 mg + Propyphenazone 150 mg Anafebrin Themis Chem
Paracetamol 300 mg + Propyphenazone 50 mg
+ Caffeine 50 ng Dart Juggat Pharma
Paracetamol 250 mg + Propyphenazone 150
+ Caffeine 50 ng Saridon Roache
Paracetamol 325 mg + Methocarbamol 400 mg Flexinol Protec
3
Paracetamol + Carisoprolol 175 mg + Caffeine 32 mg Carisoma Comp.
- Wallace
Ibuprofen is not only combined with paracetamol, but there are a
few more FDCs of Ibuprofen as follows:
Ibuprofen 200 mg + Pseudoephedrine 30 mg
Arinac Knoll
Ibuprofen 400 mg + Pseudoephedrine 60 mg
Arinac forte Knoll
Ibuprofen 400 mg + Methacarbamol 750 mg Ibugesic-M Cipla
Ibuprofen 200 mg + Metahcarbamol 750 mg Robiflam Khandelwal
Ibuprofen 400 mg + Dextropropoxyphene 65 mg Ibuproxyvon Wockhardt
Ibuprofen 200 mg + Dextropropoxyphene 32.5 mg Subdu U.S.V.
Ibuprofen 400 mg + Colchicin 0.25 mg Kebutacin-I Kee Pharma
Ibuprofen 200 mg + Chlorzoxazone 250 mg Paraflax Ethnor
This paper shows 50 different FDCs of Paracetamol with various
other drugs and in different concentrations. Each type of these
FDCs can have many more brands.
Ref: Drug Today June - August,
AIIMS, July, 1996.
4
'96
:
s
y '
. So/ci
S/^acyJs
ex too lit
&-p>peir‘ Ce
y tc
/1<q.
f'b <^. -v^
>^rc>rm3.e^
L^0b'C\i'l
'
D = /%
t- De
cs-y
i'o.
h-^CSr^z^,
< cj">-zx> cSZ-Cl-o
!<=>>( rs
io)
S>-< pva! CS->O szei.
c5*>t-<2- csf /i-S
ep) SS^XS--- -
■^-h^sple
($[
'fl&e.i'C'J
<2on hi^tedL
<^hi'tasJ'
SAo-iaM
<70
i(PP<^
/^PP
C^X><Xi.a
c^ri^/l^
/PC^dt
L^^lX>,Cj
c~^
fach
l-'-^’-_'-
=>’c-/er L 7^-ve
t~'j<^~>P> ! Cr-,-~>
Zst?
OX-<—j c£
|
u^oc"c;t .
/3j-^-xl^ c-l
do
'^- ~^l
£Z C3>-l^O <_~^v-TJi_-i
^k>-^CJ><^»7C<2.
/A
$/;//
^'crZ'/ZoLx-u^p
i1^£>
c'
P'i — a/; <sx. / o on ,
h^-Z^-yTXXc^^
C+^->cXi
^2^-0
l4-c<)k-ii
Xei <_
£ cr-'v-uvi/'/eii^
2^r7'
C<j
Oxu/^
AavC_
Z? -j /r^€~
zo
<^£r? X-^-
- s^//
Lt
j^kjLj lacfe
a
crp^ce Ye£ >^cn_^
■'
rf-'jzno^'/ -
,
7
(3b
i 1 &?))
;'^
5 fen cncLo
fictyypfestQ
i^oecS
<b{
yC a C fe^
iSt-riCa '^—is:> cr-jd-j n'zk-t-i
d<SZ><z.
C<Z)&
fo&
<S>^C-^j-o /z
y^l'X^,-,'-) fo I_^~d2
crlic^T-e . QFDOi cf
/S-e <z^kr->r'-&^->i'' eyf
o.
,K^>y&-->-ia'r<jp'
v*! k6^,-r^siS)
dx^oc^l Z^t-^-!,!-~i >e g€tz_ ^><_;
S^ca^-icXc^cLl-^ Sl>)c-&
A7oA av<^' I <^.hLa
g —
c>^^f c-^ca-I
c~»->
J^-&
o-tfcQ. /An'
tfUnxS
Z?<i-zz^i_^ c(.
<5e_5T-<2
/--7<^T>-T-^ c“
^A-<S-O^.
^/is<~^x^c-'TC'Ci^ic\K(^-> z>t4?Zest's c\xe?
/'X?<i's <s^ /^-e^o<z- <-^>}^>
<yy>a.ll^-t'<L
&
'1.
<v'
/-)!& r)'—
Cz^l^., ‘o'/JP) ,
MML' iz,3a. |A~
The E P Case
Mira Shiva
High dose combination of Oestrogen and
Progesterone has finally been banned. It is tragic
that the public had to fight for 6 long years for
getting a hazardous drug combination banned, that
too against all odds.
It was the socially conscious health activists
and consumers bodies that had initially raised the
issue in the first place, when the EP campaign was
launched way back in 1982 on Women’s Day on 8th
.March. Due credit goes to the press for keeping
"the issue alive all these years and supporting the
stand of the people.
It was the drug health and consumer groups
who protested when on 2! st July 1982, the ban order
for manufacture was given as December 1982 and
ban for sales as June 1983.
How could a drug
recognized as hazardous be allowed to be manufact
ured and then sold for almost another one year ?
It was not surprising when this was misused by the
manufacturers to challenge the hazardous nature
of the drug, saying that if the drug was hazardous
wouldn’t it have been banned immediately by the
DC authorities and since it wasn't - it was obvi
ously non hazardous 1
|The Legal Battle
The drug companies were quick enough to
| find the legal loopholes and the stay order against
the ban order was obtained from the Calcutta and
Bombay High Courts on
legal technicalities.
The fact that it involved a hazardous drug which
could maim and cripple the unborn foetus when
. consumed by ignorant pregnant women, -did not
appear
to be a matter worth considering.
Even making an attempt to find out the number of
women put at risk, with annual sales of Rs 7 crore
woitb of drugs (majority of them are consu
med for pregnancy tests and for induction of
abortion though on paper the indications permitted
had been only for secondary amenoorrhea) was
not done.
Questions were raised in the Parliament,
repeated requests were made to the Health Ministry
and Chemical Ministry to make attempts at getting
the stay vacated.
In the words of Supreme Court Justice
probably the government never wished to vacate the
stay; this became obvious because the subsequent
events are pointers to scheming.
Again it was due to a writ petition that
Supreme Court took up the issue again. Justice
Ranganath Mishra's comments on banning of
drugs is a telling commentry .
“This court as early as 11.4.1983
directed issue of notice to the Medical Council
of India, The Indian Medical Association,
The Drugs Medical Council of India, The In
dian Medical Association & The Drugs Control
Authorities of the States except that of Kerala,
as it was already made a respondent to the
writ petition. Obviously such notice was given
as in the opinion of the Court, the matter was
one of great importance and the Court looked
for participation of these authorities in the
debate with a view to assisting the Court in
the disposal of the matter. We are surprised
that the notice from the Court has not evoked
response excepting the State of Karnataka
Statutory bodies when called upon by a Court,
in particular the apex Court of the Country, are
duty-bound to respond and join the proceedings
before the Court. These bodies are not litig
ants and do not have the choice of keeping
away from the Court like private parties in
ordinary litigations opting to go ex-parte. The
present matter is certainly one which is suffici
ently important and the stake of the entire
nation is high; when the Court SUO moto
extended the ‘opportunity of being heard and
invited the named statutory or other authori
ties to come forward and place their view
7
points cn relevant aspects, an attitude of
callous indifference cannot be appreciated.
We hope and trust that there would be no
repetition of such a situation'.
The Public Hearings
It was unfortunate for public that the
public litigation case was referred back to the Drug
Controller of India. In its Court Order of Novem
ber 1986 Supreme Court gave direction to hold
public hearings to seek the views of consumers and
health groups and decision be taken by end of July
1987. The drug companies were shrewed enough to
use the professional bodies like FOGSI (Federation
of Obstetrics Gynaecology Society of India) to be
their spokesman FOGSI till the very end continued
to support the stand of the Drug manufacturers
stating that the drug was essential and absolutely
safe. Luminaries such as Dr. C. L. Jhaveri, Dr. C.
S. Dawn, Dr. B. N. Purandare did their utmost to
tilt the balance in favour of the manufacturers. The
role of the WHO expert and the Deputy Drug
Controller who chaired the Calcutta hearing was
not very creditable.
The silence of professional and academic
bodies such as IMA, IMC. at such a time was
unforgivable. It was only the Indian Academy of
Paediatrics that had expressed its deep concern
against the continued sales of high dose E. P. drugs.
The public hearing in Bombay ably proved that
when called upon, the women's organisations can
give a bitter fight for a cause. Even the public
notices for the public hearings were inserted inconspiciously In the papers, the hearings were stated
to be for “formulations of oestrogens and progest
erone”, in the first public notice and “combination
of oestrogen and progesterone” for the second one.
The failure to clearly state that the public hearings
were being held to decide whether or not to ban
combination of high dose Estrogen-Progesteronc, was
too significant to be overlooked as an unintended
errors. The way the 4 public hearings in Madras,
Delhi, Calcutta and Bombay were held on 5th Feb.
10th April, 10th July and 14th July 1987 respectively
is a story in itself. Even when the Drug Technical
Advisory Board met in May 1988, the minutes of
the 4 public hearings were not made available, nor
the summary of the arguments for and against the
drug ban was -sent to Boards members for prior in
formation. The fact that it took 6 long years to issue
a Gazette Notification to ban a drug — shows the
forces working on it. A drug, which is known to be
hazardous - which has been mainly used in pre
gnancy - a drug which was banned by the Drug
Controller of India himself in 1982 - a drug which
ICMR strongly recommended to be banned in 1982
as well as in 1987 - a drug which was not allowed
to be registered or sold in the parent country
Netberlands by Organon Infar. was strongly con
tested by drug manufacturers and they had the aud
acity to challenge the DCl's ban order in India.
Enforce the ban immeditely
The EP case involved a drug which the con
temporary Gynaecological medical literature does not
even mention, as it has no role-and as it is not us
ed by any gynaecologist or a doctor, as safer alter
natives exist. Not merely had several drug regulatory
authorities banned the drug, but several companies
had withdrawn the product themselves. It was du|
to sheer gist and perseverance of the drug activists,
health and consumer groups that the ban order has
come now. Should this be counted as success ?
We have learnt from past experience that
unenforced drug bans are as bad as no bans. The
Gazette Notification was issued on 15th July 1988.
Government media of AIR and Doordarshan should
have been used to inform the chemists, medical pro
fessionals and the ignorant consumers about the drug
clearly stating the brands and their manufacturers 1
The Drug Control Authorities owe this to the nation.
The stocks from the. manufacturers and the market
should be withdrawn and destroyed.
The Health Ministry has had 6 long years to
make available to the medical professionals the reco
mmended alternatives. Safe, low cost simple pregna-|
ncy tests, which basic health workers can use, should
be easily available as part of Mother and Child He
alth Programme. Permitting al this stage the manu
facturer and sales of high dose EP drugs as single
ingredients in the same dose would be ridiculing and
sabotaging the ban. The ban 1ms come 6 years too
late; now the implementation of the ban must be
immediate. The Drug Control Authorities and the
manufacturers must be held responsible if these
drugs continue to be sold. If this could happen for
a drug like high dose EP which the consumers and
health groups considered a watertight case-what wo
uld be the fate of other many hazardous drugs?
Let the government and Drug Controller of India
announce how they are going to make the ban effec
tive.
a a
8
STUDY
OF
PAIN KILLERS
(ANALGESICS & ANTIPYRETICS
ANDNSAIDS)
LISTED IN A COMMERCIAL PUBLICATION
FOR DOCTOR'S USE
By
Dr Gopal Dabade
Drug Action Forum - Karnataka,
57, Sony, Tejaswinagar,
Dhanvad 580 002
Karnataka. India
Tel 0836-2461722
drdabade®sancharnet.in
STUDY OF PAIN KILLERS (ANALGESICS & ANTIPYRETICS AND NSAIDS)
LISTED IN A COMMERCIAL PUBLICATION FOR DOCTOR'S USE.
Pain killers are a group of drugs that are most commonly used. This study is an
attempt to bring to the notice of the consumers regarding the type of pain killers
that are available for ; doctor to prescribe to the patient. Are the drugs promoted to
doctors’ from the list of Essential Drugs by WHO? Are the drugs scientific? And if
L the pricing °_f dr,lg? 's justified._____________________________________________
WHY THIS STUDY?
Pain is perhaps the most common symptom for which patients seek guidance ind
help from doctors Pain killers are a group of drugs that are extensively used both by
general practitioners and consultants.
Drug Action Forum - Karnataka (an independent, non-profit and non governmental organization campaigning for Rational drugs and policies) took up this
study, with an attempt to bring to the notice of the consumer, regarding the type of the
pain killers that are commonly promoted to doctors. A commercial publication used
exclusively by doctors was referred to get the common pain killers that are promoted by
various drug manufacturers.
The study is mainly aimed for consumer groups that are actively involved in
building awareness among consumers by involving in campaigning and lobbying for
rational drugs. It is hoped that the consumer groups would be better equipped to lobby for
rational drugs, when dealing with drug policy makers, w'ith studies of such nature
The study is relevant because in India, doctors after passing out from the medical
colleges have no access to unbiased and scientific information to them regarding drugs.
They are often compelled to depend upon the information that is given to them by drug
companies or at times by information that is supplied to them through company
sponsored seminars. Often drug companies promote irrational drugs to doctors. Using the
case study of pain killers, this study confirms the above statements.
Industry promotion - in the form of direct-mail brochures, journal, displays, professional
courtesies or detail person or pharmaceutical representatives - is intended to be
persuasive rather than educational.
The pharmaceutical industry cannot, should not, and indeed does not purport to be
responsible for the education of physicians in the use of drugs.
j Goodman & Gilman's, The Pliannaccutical basis of therapeutics. IO1*1 edition. Page number 64
The study is mainly under two heads:
i.
ii.
Rationality: - Does the drug listed in the commercial publication (MLMS), match
with the Essential Drug list by WHO? And is the drug rational?
The drug prices: - Comparing the Essential Drug prices set by different companies.
(1) Is the drug Essential and Rational?
For the sake of this study three publications have been used. One is a commercial
publication used by doctors extensively all over India and the other two are scientific
publications. Among the scientific publications one is the well known “WHO mode) list
of Essential Drugs”, first published in 1977 and has been regularly updated every two
years. The other scientific publication is “The Pharmacological Basis of Therapeutics”,
10dl edition by Goodman & Gilman, a standard text book which is used for reference and
study by academic medical professionals all over the globe
a) Monthly Index of Medical Specialities (MIMS)
The commercial publication is “Monthly Index of Medical Specialities” known
popularly by its acronym MIMS (www mims-india com). The June 2004, volume 24,
number 6 issue of MIMS'lists in its index, 90 groups of drugs under different categories.
But for the present study only two categories were selected Firstly Analgesics &
antipyretics and secondly NSAIDs (Analgesics is a term used for all categories of pain
killers. Antipyretics are drugs that reduce fever NSAIDs is an acronym for Non Steroidal
Anti-Inflammatory Drugs, a term used for all categories of drugs that reduce
inflammation and do not belong to the steroid group of drugs) All these analgesics &
antipyretics and NSAIDs are available in various forms (like tablets and syrups etc) and
also different dosage forms. Totally 235 formulations (manufactured by 49 drug
companies and sold under 120 brands) were systematically scrutinised with reference to
World Health Organization (WHO) Model List and a standard text book of
Pharmacology.
b) WHO Model List of Essential Drugs :-
The WHO Model list of Essential Drugs 2003 referred to in this study contains
about 375 drugs in 500 formulations (or dosage forms). These could provide safe,
effective treatment for the vast majority of communicable and non-communicable
diseases. Essential Drugs should be the drugs of first choice, more so in a situation where
financial resources are a crunch. The list was first published in 1977 by WHO and has
proven that most diseases can be managed with few medicines All the 235 drugs in our
study were checked to see whether they are included as Essential Drug or not.
OF THE TOTAL 235 FORMULATIONS LISTED FOR THIS STUDY ONLY 23
(9%) MATCHED WITH ESSENTLAL DRUGS.
Rationality
To assess whether the drug is rational or not, a standard text book of
Pharmacology, titled Goodman & Gilman's “The Pharmacological basis of Therapeutics”
was referred. This is a standard text book, used extensively by teachers and medical
students during medical teaching and training.
The term “ratic nal” is used for drugs that are scientific in nature by being referred
and recommended or mentioned in standard text books. Irrational drugs on the other hand
do not find mention or are not recommended in such text books. So with the help of the
text book the following two criteria were evolved:-
1. Firstly if the formulation is not mentioned in the book (for example combination
like Paracetamol with Ibuprofen) then it is considered as irrational
2. Secondly if the formulation is described but the text book does not advocate it, the
formulation is considered as irrational (for example Analgin or Nimesulide).
If a certain formulation does not fall under both the above mentioned criteria, it is
labeled as Rational drug
What is Rational drug?
If their efficacy is clinically proven and the therapeutic benefits outweigh the risks, they are called as
rational drugs
What is irrational drug?
If there is no good clinical pharmacological evidence on their therapeutic benefit and safety then, such
drugs are considered as irrational drugs.
The presence of irrational drugs is not only an economic burden but also can be harmful. This is truer
for developing country like India.
OF THE TOTAL 235 FORMULATIONS THAT WERE STUDIED A TOTAL OF
95 (40%). THUS THE NUMBER OF RATIONAL DRUGS ARE 140 (60%).
SUMMARY OF THE STUDY (part 1)
Of the total 235 formulations that were screened only 22 (9%) confirmed to the
Essential Drug list of WHO, 140 were (60%) rational drugs and remaining 95 (40%)
were irrational
Only one out of every ten drugs that are promoted to doctors confirm to WHO’s
Essential Drugs. And out of every ten drugs, six drugs are rational. From this it is obvious
that if a doctor prescribes a drug, there is only one in ten chances of prescribing the drug
of first choice. This is not an acceptable situation where financial resources are always a
major crunch.
Some interesting observations:- Following were some of the interesting observations
after the study.
1. A reputed (?) multinational company (Aventis) manufactures and sells the drug
Analgin. This drug is absolute as several safer alternatives exist.
2. Another hazardous (harmful) drug is Nimesulide. It is manufactured by 5 '
companies, and amongst them 4 companies manufacture the drug for use in
children too. This drug has never been allowed in USA and banned in several
European countries.
3. Diclofenac - a pain killer often usee by both specialists and general practitioners
is also manufactured in the form of injectable. The injectable form of this drug is
not mentioned in the standard text book (The Pharmacological Basis of
Therapeutics, 10th edition by Goodman & Gilman), that has been referred for this
study.
4. Aspirin - a popular and most commonly needed pain killer is not manufactured
by any drug company. Aspirin is listed in WHO’s list of Essential Drugs Only
one drug company i.e. Nicholas Piramol manufactures an irrational combination
of Aspirin (Acetyl Salicylic acid) 350 mg with Caffeine 20 mg under the trade
name Micropyrin. So this study observes that some drugs which are on the
WHO’s Essential Drugs list are not promoted to the doctors by any drug company.
In fact Aspirin should have been made available for the doctors’ to prescribe.
5. A combination of the drug Ibuprofen with Paracetamol is perhaps the most widely
used irrational combination. In this study 6 drug companies manufacture this drug
and most of them even have the preparation for use in children (in the form of
syrup). A question often raised by the consumer is that, why do doctors prescribe
such an irrational combinations. As mentioned above one factor is that such drugs
are heavily promoted by the drug companies to the doctors. During medical
education students are taught by the teachers that such combinations are irrational
and that they can be harmful to the patients, but as they start prescribing drugs to
patient, the flood of misinformation by companies overshadows the scientific
information.
(II) Cost analysis of Essential Drugs
The second part of the study analyses the cost of the Essential Drugs listed in
MIMS. This part of the study is important as it gives a picture to the consumer regarding
the cost of the drugs that should have been of top priority for a doctor to prescribe.
WHO’s Essential Drugs list has only three NSALDs viz. Paracetamol, Ibuprofen
and Aspirin. As Aspirin is not manufactured by any drug company we studied the pricing
of only two drugs i.e. Paracetamol and Ibuprofen.
Following are the highlights:a. Paracetamol 500 mg is manufactured by 6 drug companies. Amongst them 2 drug
companies (SKF and Nicholas Piramol, the former being a multinational)
manufacture and sell the same drug Paracetamol under two different brand names
with different pricing. There can be no scientific justification for this.
(For details refer to the chart on next page).
Chart showing the drug Paracetamol being sold by different companies with varying cost
Sn
Trade name
Generic name
Price of the drug
for 10 tablets.
1
Calpol
Paracetamol
500 mg
Rs. 8.78 / 10 Tablets
2
| Crocin
Paracetamol
500 mg
Rs. 7.98/ 10 Tablets
3
Disprin Paracetamol
Paracetamol
' 500 mg
Rs. 9.40/10 Tablets
Paracetamol
500 mg
Rs. 4 88 / 10 Tablets
Paracetamol
500 mg
Rs. 4.21 / 10 Tablets
4
Manufacturer
GSK
| Doliprane
Reckitts
Nicholas Piramol
5
| Molidens
6
1“
Paracetamol
500 mg
Rs. 6.30 / 10 Tablets
IPCA
7
Ultragin
; Paracetamol
500 mg
Rs. 8.80/ 10 Tablets
Wyeth
8
. ............
1
Rs. 13.50 /10 Tablets
East India
b
Paracetamol
500 mg
The lowest priced Paracetamol is for Rs 4.21 and the costliest is at Rs 13.50. A
whooping price difference of 69%. How does one explain such a huge price
difference? Drug companies spend lot of money in promoting a drug to the doctor
and this cost is recovered by hiking the price of the drug. Doctors are neither
taught during their student days nor do the drug companies mention its price (cost)
when they promote the drug to doctors. So doctors tend to prescribe the costliest.
Unfortunately the consumer also believes that a costly drug is better acting. The
consumer is not aware that one could buy the same drug of another company at a
much lower rate. Medicines are the only commodities in the market where the
buyer is not the chooser.
Drug pricing of Ibuprofen 400 mg did not show much variation.
sn
Trade name
Generic name
Price of the drug
for 10 tablets
Manufacturer
1
Brufen
Ibuprofen 400 mg
FG. 5.05
10 Tablets
Knoll
2
Ibugesic
Ibuprofen 400 mg
Rs 5 93
10 Tablets.
Cipla
Drug pricing of Diclofenac 50 mg: - Diclofenac is another common pain killer used
though not in the list of Essential Drugs by WHO This drug has wide variation in prices
from one drug company to another, as shown in the chart below.
sn |
Tradename
■ Voveran
2I
Manufacturer
Generic name
Price of the drug
for 10 tablets
Diclofenac 50mg
Rs 15/ 10 Tablets.
Novartis
Diclofenac 50 mg
Rs. 3 15/ 10 Tablets
Themis
Chemicals
SUMMARY OF THE STUDY (PART II)
Drug prices need to be regulated by governments. But this study shows that
Essential Drug prices show such wide variation. This is an area that needs further studies.
But suffice it to say that drug pricing is not properly regulated by the government. There
is an urgent need for consumer groups to be actively involved in bringing awareness on
this issue.
- Media
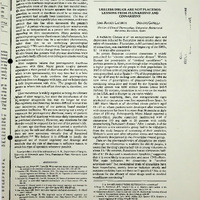 RF_DR_13_SUDHA.pdf
RF_DR_13_SUDHA.pdf
Position: 208 (102 views)