DRUG ISSUES INFORMATION RESOURCES
Item
- Title
- DRUG ISSUES INFORMATION RESOURCES
- extracted text
-
INFANT
FORMULA
PROMOTION
RF_DR_8_SUDHA
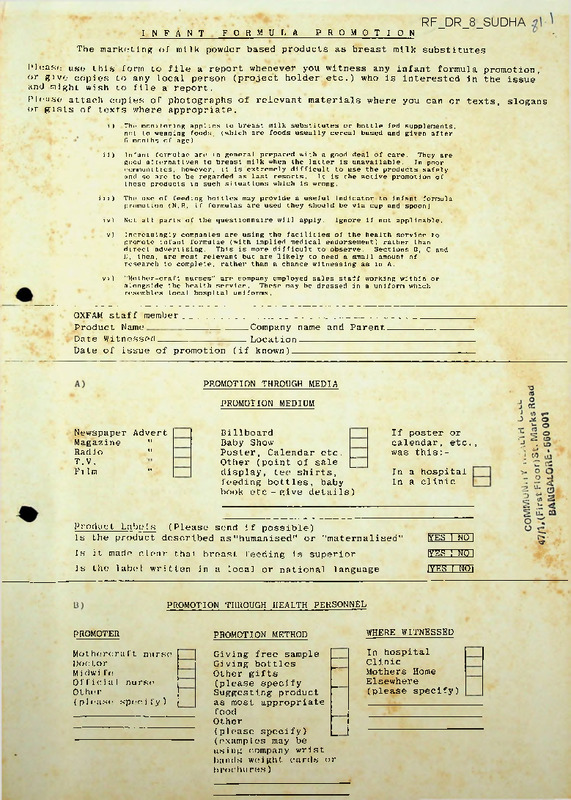
The marketing of milk powder based products as breast milk substitutes
Please use this form to file a report whenever you witness any infant formula promotion,
or give copies to any local person (project holder etc.) who is interested in the issue
and might wish to file a report.
Please attach copies of photographs of relevant materials where you can or texts, slogans
or gists of texts where appropriate.
i)
The monitoring applies to breast milk substitutes or bottle fed supplements,
not to weaning foods, (which are foods usually cereal based and given after
6 months of age).
ii)
Infant formulae are in general prepared with a good deal of care. They are
good alternatives to breast milk when the latter is unavailable.
In poor
communities, however, it is extremely difficult to use the products safely
and so are to be regarded as last resorts.
It is the active promotion of
these products in such situations which is wrong.
iii)
The use of feeding bottles may provide a useful indicator to infant formula
promotion (N.B. if formulas are used they should be via cup and spoon)
iv)
Not all parts of the questionnaire will apply.
v)
Increasingly companies are using the facilities of the health service to
promote infant formulae (with implied medical endorsement) rather than
direct advertising.
This is more difficult to observe.
Sections B, C and
D, then, are most relevant but are likely to need a small amount of
research to complete, rather than a chance witnessing as in A.
vi)
"Mother-craft nurses" arc company employed sales staff working within or
alongside the health service.
These may be dressed in a uniform which
resembles local hospital uniforms.
Ignore if not applicable.
OXFAM staff member_____ ________________________________________________
Product Name
Company name and Parent
Date Witnessed
Location
Date of issue of promotion (if known)
PROMOTION THROUGH MEDIA
PROMOTION MEDIUM
Newspaper Advert
Magazine
"
Radio
"
T.V.
Film
"
If poster or
calendar, etc.,
was this:-
Billboard
Baby Show
Poster, Calendar etc. _
Other (point of sale £
display, tee shirts,
feeding bottles, baby
book etc - give details)
In a hospital
In a clinic
Product Labels (Please send if possible)
Is the product described as"humanised" or "maternalised"
Is it made clear that breast feeding is superior
Is the label written in a local or national language
[YES I NO I
IYES I NO'I
[YES I NO I
PROMOTION THROUGH HEALTH PERSONNEL
PROMOTER
PROMOTION METHOD
Mothercraft nurse
Doctor
M i dw i fe
Official nurse
Other
(p1 ease speci fy )
Giving free sample
Giving bottles
Other gifts
(please specify
Suggesting product
as most appropriate
food
Other
(please specify)
WHERE WITNESSED
_
_
_
_
_
(examples may be
using company wrist
bands weight cards or
brochures)
In hospital
Clinic
Mothers Home
Elsewhere
(please specify)
Dih’S
the promoter receive any inducements (commission,gifts etc. ) [YES | NO)
Can you s p o < ■ i I' y___________________________ _ _______ —----------------------------------------------------II Company employee, does promoter wear a uniform
IYES | NQ|
|YES f CONSIDERABLY 'I 'SLIGHTLY I NCj
If YES doos l his resemble a
hospital nurses' uniform
PROMOTION IN INSTITUTIONS
C)
Institution name------------------ ---------------------------------------------------------------- —---------- (hospital/clinic/other------------------------------ )
Does the institution automatically give newborns infant
formula
Is there a cheap infant formula sales point (milk bank)
Is the mother offered infant formula at a lower price than
local shops
When infant formula is used, does the institution recommend:
feeding bottles/cup and spoon
IYES I NO~1
IYES I NO~I
IYES I NO~1
IYES I NOl
ADDITIONAL INFORMATION The following details would be useful to have
but might prove difficult to obtain and so are not essential. It
might be that there is an appropriate local person - interested in
this issues, who would research this section.
Product Name
Company name and Parent---------------------------Date Witnessed
Name of institution
Location____________________________ (village/town/country wide)
D)
PROMOTION TO HEALTH SERVICE (HEALTH PERSONNEL)
(i.e. promotion to rather than promotion by doctors)
PROMOTION METHOD
TO
Free sample for distribution
Free sample for personal use by health
personnel
Commission on sales
High discount for monopoly product use
Gifts or grants (please give details)
Hospital
Clinic
Doctor
Nurse
Midwife
Pharmacist
Administrator
E)
COMPANY SALES PERSONNEL
In the country, how many 'mother care nurses' does the company
em p1oy
Are there ex-nurses and if not do they receive appropriate
training
Are mother care nurses' wages significantly higher than
hospital nurses'
Do Company Sales Personnel earn commission on sales
Are there other company sales staff
Do sales staff have contact with:
hospital - administrators
Do sales staff work in:
|YES | NOl
|YES | NO]
IYES I NO]
Numbers
doctors/nurses/midwives/pharmacists/
hospitals/clinics/mothers home/other
What local laws govern sales promotion personnel
Other Comments: ( Please write seperately and attach to this form.) Such as results of
medical studies on the prevalence of bottle feeding, or on the health status of bottle vs
breast fed babies. Details of breast feeding promotion programmes. Availability of
. infant formula and cost relative to average wage of a poor family. Marketing of products
other than infant formula (such as sweetened condensed milk) as a breast milk substitute.
1,
A'a-c:
2)
Occdpeitibn:
3)
Drugs Recomended:
4)
Prescribed:
1)
2)
3)
4)
5)
6)
OTC
i) Patient
ii) Chemist
5)
Cost of drugs:
6)
Treatment duration:
7)
When were drugs brought last:
8)
Frequency of illness at home:
9)
Money spent on drugs last year:
10)
Family Income
Salaries:
Agriculture:
Mi sc.:
11)
12)
Annual Expt.'on drugs
as % of Income.
Mi sc.:
f
VJ
urixCTH c£tb
.
commons
Group Discussion on Prescribing Policy - Groups Bl & DI
Questions to be pondered about
1.
Can a Hospital devise a formulary of good quality,
cost medicines?
low
Can this be common for all Voluntary Hospitals?
2.
How can prescribers' compliance be ensured or is freedoja.
of prescribing likely to make this impossible?
Can we ensure Health Workers' compliance with their
formulary (medicine list)?
Will doctors also prescribe from this list?
Is it possible to prevent prescriptions to medical shops
being given?
3^
Where simple low cost drugs will not be sufficient, how do i_
we subsidise to all or those who need help most?
Should all patients contribute to the cost of medicines?
- -If -so, how?
,
4.
Will a Pharmacy Committee, including Doctors, Administrators
and Pharmacists help in implementing cost control or
quality control policy? (in most Hospitals medicines are
the second largest item of expenditure'.)
5.
Have we asked our pharmacists to research costs?
does he know how to do so?
Have we provided tools for the job?
If so,
If so,
what tools?
Are bulk drugs purchases possible on a group of Hospitals-base?
What methods can we devise for obtaining low cost drugs
either for one or many Hospitals?
7.
Do we consider proper stock control, record keeping and
auditing of medicines, purchase and distribution:
unnecessary expenditure
b) essential?
What are our reasons for our attitudes?
9.
Is the production of medicines in the Pharmacy :
a)
too time consuming
b)
too costly in terms of personnel or equipment
c)
uneconomic?
(Broadly thinking of two types: non sterile prescriptions
and sterile prescriptions)
How would you advise your
Hospital Management?
s v o iv s n v g
In many Hospitals the Pharmacy is an important income
producing section.
Will a switch to low cost drugs raise
cost or make it instead a burden on the Institution?
- ig ( jo o |- | js n - j]
8.
10(5 005 -
a)
peoy
5.
Group Discussion on Prescribing Policy - Groups Bl & DI
Questions to be pondered about
1.
I
Can a Hospital devise a formulary of good quality,
cost medicines?
low
Can this be common for all Volun-tary Hospitals?
2.
Hou can prescribers ' compliance be ensured or is fraarlnm
of prescribing likely to make this impossible?
Can we ensure Health Workers' compliance with their
formulajry (medicine list)?
Will doctors also prescribe from this list?
Is it possible to prevent prescriptions to medical shops
being given?
3.
-
Where simple low cost drugs will not be sufficient, how do u .
we-subsidise to all or those who need help most?
Should all patients contribute to the cost of medicines?
.If -so, how?
4>
Will a Pharmacy Committee, including Doctors, Administrators
and Pharmacists help in implementing cost control or
quality control policy? (in most Hospitals medicines are
the second largest item of expenditure'.)
5.
Have we asked our pharmacists to research costs?
does he know how to do so?
Have we provided tools for the job?
If so,
If so,
what tools?
6.
Are bulk drugs purchases possible on a group of Hospitals-base?
What methods can we devise for obtaining low cost drugs
either for one or many Hospitals?
7.
Do we consider proper stock control, record keeping and
auditing of medicines, purchase and distribution:
a)
unnecessary expenditure
b) essential?
What are our reasons for our attitudes?
8.
In many Hospitals the Pharmacy is an important income
producing section.
Will a switch to low cost drugs raise
cost or make it instead a burden on the Institution?
9.
Is the production of medicines in the Pharmacy :
a)
too time consuming
b)
too costly in terms of personnel or equipment
c)
uneconomic?
(Broadly thinking of two types: non sterile prescriptions
and sterile prescriptions)
How would you advise your
Hospital Management?
ewsfrom oxfam • news from oxfam • news fro
rom oxfam • news from oxfam - news from o>
m- news from oxfam • news___from
oxfam • nev
- - -- ------- -----Telephone (0865) 56777 - Telex 83610
Press Office ■ 274 Banbury Road ■ Oxford 0X2 7DZ
EMBARGO 11,00 am THURSDAY, 25 NOVEMBER 1982
THE POOR SUFFER THROUGH MULTINATIONAL DRUG COMPANIES' MARKETING PROFITABLE BUT
INESSENTIAL DRUGS IN THE THIRD WORLD, ARGUES NEW BOOK FROM OXFAM
The uncontrolled sale and promotion of drugs in most poor countries means that they
often do little good and can be positively harmful.
Major manufacturers are acting
irresponsibly in the Third World by ignoring the needs of the majority and not taking
responsibility for the safe use of their products.
Dangerous double standards have resulted in anabolic steriods being promoted as
appetite stimulants for malnourished children; an antidiarrhoeal drug banned in
Britain, because of possible crippling side-effects, is freely marketed in the
Third World and sold without warnings.
Antibiotics are sold on market stalls like
loose sweets, encouraging misuse and drug resistance.
For the Third World poor, the cost of basic life-saving medicines is astronomical.
The price of just twenty tablets of the top-selling antibacterial drug in Mexico
would provide a family of four with their basic diet for two weeks.
A small bottle
of an antibiotic syrup costs a poor Bangladeshi family the equivalent of £35 to a
British family earning £135 a week.
In Bitter Pills, Medicines and the Third World Poor, published by Oxfam on
November 25, Dianna Melrose investigates these alarming facts from the perspective
of the poor, drawing on her own field research, evidence from the manufacturers
involved and Oxfam's wide experience of poverty and ill-health in the Third World.
The poor suffer disproportionately from ill-health.
A few dozen essential
'generic' drugs could be used to save millions in the poorest countries from
unnecessary suffering and death.
The know-how to make these key generic drugs
has been available for decades.
We take them for granted in Britain, but the
majority of the Third World poor are denied them because drugs are produced and
sold for profit rather than on the basis of real need.
The rich world dominates
2
drug production.
Aggressive promotion means that the most expensive brand-name
drugs usually sell best.
The poor are therefore forced to pay unnecessarily high
prices and subsidise new drugs for the rich.
Bitter Pills documents the abuses caused by weak controls and reveals that some
manufacturers - including some based in Britain - are not as scrupulous as they
should be in ensuring that Third World patients and prescribers get full information
on their products.
Some even resist moves to introduce tougher controls in the
Third World that they must comply with in Britain.
The book describes some of the positive initiatives taken at local, national and
international levels to rationalise the use of drugs as part of a broader strategy
for better health - recognising that disease which is rooted in poverty can only be
combatted by an onslaught on poverty itself.
It documents the major obstacles that
Third World governments face in trying to crack down on the drug market.
Rich
world manufacturers and their governments have lobbied to block changes that
would benefit the poor.
Practical suggestions for change are addressed to three groups:
Firstly, if the
poor are to benefit, Third World governments must give priority to preventive
and primary health care rather than to costly hospital services.
The private
drug market should be controlled to safeguard health and priority given to purchase
and manufacture of essential drugs.
Rich world governments should actively encourage Third World governments to adopt
the WHO recommendations which, in theory, they have supported.
They could help
Third World governments make informed choices about drug risks and benefits by making
more information available at little cost, and introducing controls to discourage
exports of dangerous and inessential drugs.
Official health aid should not be tied
to purchases of expensive products and high-technology medical services; and
voluntary agencies should strengthen community health projects which do not rely
on imported drugs.
Manufacturers should take full responsibility for ensuring that their products are
used safely and effectively in the Third World and respond to the real health needs
of the poor by marketing low-priced essential drugs.
3
Dianna Melrose, 30, the author of Bitter Pills, was born in Zimbabwe and grew up
in Latin America.
She holds an MA in Latin American studies from the London
School of Economics and worked as a translator for banking and insurance firms
in the City before becoming an administrator for the British Council.
She joined
Oxfam's Public Affairs Unit in January 1980 and has carried out field research
in Bangladesh, India and the Middle East.
She conducted research for a film on the
marketing of baby milk and medicines in North Yemen and is the author of the
associated book, The Great Health Robbery.
Bitter Pills - Medicines and the Third World Poor, by Dianna Melrose, is
published by Oxfam on November 25 at £4.95.
Distributed by Third World Publications.
Review copies are available on request from the Press Office, Oxfam,
274 Banbury Road, Oxford.
Tel:
Oxford (0865) 56777.
For more information contact Derek Warren, Oxfam Press Office on Oxford
(0865) 56777.
8th November, 1982
BITTER PILLS •
MEDICINES AND THE THIRD WORLD POOR
by Dianna Melrose
Published by Oxfam on 25th November, 1982
Distributed by Third World Publications
151 Stratford Road, Birmingham, Bll 1RD
INTRODUCTION
Throughout the Third World millions of the poorest have no access to life-saving
drugs, while drugs are wasted and misused worldwide.
In poor countries those
that are most needed are often the hardest to obtain, at least at prices the
poor can afford.
Through their uncontrolled sale and promotion in most poor
countries, medicines often do little good and can be positively harmful.
1.
A PILL FOR ALL ILLS?
The poor in the Third World - as in Britain - suffer disproportionately from
ill-health.
Disease that is rooted in poverty can only be attacked by an
onslaught on poverty itself.
But a small number of essential drugs could be
used to save millions of the poor from unnecessary suffering and death.
2.
UNEQUAL DISTRIBUTION
The Third World has three-quarters of the world's population but accounts for
b
little more than 20% of total drug sales.
In the poorest countries, annual drug
expenditure averages only 50p per capita, compared with £35 in the rich world.
Yet this money may represent a crucial proportion of a poor family's income.
Moreover, the distribution of health services is often grossly weighted in favour
of the rich town-dwellers at the expense of the majority of people living in rural
areas.
The poor are therefore forced to rely on untrained drug-sellers offering
potentially dangerous drugs at extortionate prices.
3.
PRODUCER'S MARKET
Throughout the world, drugs are largely produced and sold by private businesses
whose interests are primarily commercial rather than medical or social.
Third
World countries are almost totally reliant on importing finished drugs and so are
subiect to the dramatic price increases which follow inflation.
Inappropriate
patterns of drug consumption are adopted, thanks to the producers' aggressive
COMMUNITY HEALTH CELL
47/1,(First Floor)St. Marks Road
BANGALORE -560 001
2
promotion tactics.
In North Yemen, non-essential drugs, tonics and vitamin pills
account for an estimated 65% of total pharmaceutical imports.
Only 1.3% of
imoorts are of drugs to combat the prevelant and crippling diseases of malaria,
bilharzia and TB.
4.
POOR VALUE FOR THE POOR?
DRUG PRICES
In Third World countries, the cost of drugs in real terms is anything up to 20
times higher than in the producing nations.
Expensive brand name drugs are
marketed instead of far cheaper generics.
Hefty overheads for promotion and
research and development into new drugs are passed on to the poor.
Meanwhile
only a fraction of total research spending (equivalent to half the cost of
developing one new drug) is allocated to poor world diseases.
Poor people are
therefore subsidising new drugs for the rich.
5.
INFORMATION OR DISINFORMATION?
DRUG PROMOTION
Drug promotion helps to ensure that 90% of drugs prescribed by GP's in Britain are
brand-name products.
But at least, in drug-producing countries, advertising is
monitored and doctors are supplied with objective information about cost-effectiveness.
Over-the-counter sales are also strictly controlled.
Such restrictions rarely
apply in poor countries, where misleading or inaccurate promotional literature
goes unchecked and where company salesmen may offer free samples and other sales
inducements to doctors and nurses on a lavish scale.
very intense:
Commercial pressure can be
in Nepal, Brazil and several Central American countries, there is
one doctor to every three salesmen (compared to eighteen doctors for every one
salesman in the UK).
6.
BUYERS BEWARE - UNCONTROLLED SALES AND PROBLEM DRUGS
All too often there is a cruel contrast between advertising claims and the reality
of drug use in developing countries.
Powerful drugs with toxic side-effects
are dispensed by illiterate traders - even by children.
accentuated by irresponsible marketing practices.
The dangers are
Amabolic steriods have been
promoted as appetite stimulants for malnourished children.
have been marketed to treat infants with "common diarrhoea."
Powerful antibiotics
Uncontrolled
marketing and sales has already led to epidemics of drug-resistant disease.
- 3 -
7.
TRADITIONAL MEDICINE
Traditional medicine is still the major source of health care for three-quarters
of the Third World population.
ancient herbal remedies.
Some important modern drugs are derived from
WHO has urged Third World governments to plan their
health systems so that modern health-workers work alongside traditional healers -
with each learning from the other, encouraging patients to visit the health
centres more readily.
8.
TRAIL-BLAZERS - SMALL-SCALE SOLUTIONS
A number of pioneering projects have attempted to tackle ill-health in poor
communities with paramedics providing preventative and curative care.
The
People's Health Centre in rural Bangladesh goes beyond the confines of health
care to try to solve the underlying problems of landlessness, inequality and
powerlessness.
Other projects in a range of developing countries are specifically
aimed at finding imaginative solutions to the problems of lack of vital drugs and
misuse of medicines.
9.
HEALTHY SOLUTIONS - THIRD WORLD NATIONAL AND REGIONAL POLICIES
Sri Lanka, Mozambique, China and other developing countries have adopted national
drug policies to cater for the health needs of the majorities.
A wide range of
policy options are open to Third World governments to improve the use and
availability of drugs.
The key element needed is political will.
Increasingly
developing countries are exploring the advantages of strength in numbers and
pursuing joint pharmaceutical policies to improve their bargaining power with the
rich world producers.
10.
HELP OR HINDRANCE? - THE RICH WORLD'S RESPONSE
Drug-producing nations have a controlling interest in UN agencies such as WHO
that could do more to assist developing countries.
The British and other rich
world governments adopt different standards for drugs for export and give little
active support to Third World governments attempting to implement bold new drug
policies.
They back home-based manufacturers' interests - sometimes at the expense
of the poor.
Leading drug manufacturers have made concessions to the special needs
of developing countries, but they also bring powerful pressure to bear (even
involving their governments) in blocking positive new controls on the drug market
- 4 -
in developing countries.
This concerted industry lobby is active now in
Bangladesh trying to get the government's new drug policy reversed.
11.
HEALTH NOW - ACTION FOR CHANGE
The principal recommendations are addressed to three groups:
Firstly, if the
poor are to benefit, Third World governments must give priority to primary
health care rather than to costly hospital building projects.
Drug imports
and sales should be brought under central control, and purchases made in
accordance with health needs.
Training for health workers should concentrate
on methods appropriate to their countries' needs and resources
Rich world governments should take steps to ensure that the WHO recommendations
with which they have, in theory, agreed are implemented.
They should
reappraise the need for export controls and publish all available information
on drugs and their safe use.
Official health aid should not be tied to purchases
of expensive products and high-technology medical services; and voluntary
agencies should strengthen community health projects which do not rely on
imported drugs.
Manufacturers should be consistent in the standards they apply worldwide and
adopt higher ethical procedures in disclosing full information and marketing drugs
that are essential to the needs of the poor.
o KiizedfA.KaxlaisMorehoUBa,Ward;and Shaikh, Rashid
"For Srport Only:The International trade in
Toxic Substances." Development Forum, January
1982.
o UN Economic and Social Council. Exchange of
information on Banned Hazardous Chemicals and
Unsafe pharmaceuticals. Report of the Secre
tary General E/1981/ 11 February 1961.
o Castleman,Barry I."The ’Double Standard’ in
Industrial control of Health Hazards." Paper
presented to the New York Academy of Sciences,
4 February, 1981.
o UN Commission-on Transnational Corporations.
"Hole of the Information System on Transnat
ional Corporations regarding the exchange of
information on banned hazardous chemicals and
unsafe pharmaceuticals." E/C 10/90 18 June 1981.
o Concern Inc. "Hazardous waste:A community action
guide," May 1981.
» Dowie,Mark."The Corporate Crime of the Century"
Mother Jones, November 1979.
o Fazal, Anwar. "Testimony before the Subcommittee
on International Economic Policy and Trade,
Committee on Foreign Affairs, US House of
Representatives 6 June 1980" IOCU Newsletter,
June 1980.
• Harris, Robert.H. Keynote Address, Special
Open Session on the Dumping on Hazardous
Products, Processes and Wastes, 10th IOCU
World Congress, The Hague, June 1981.
® Weir, David, and Shapiro, Mark. "Circle of
Poison: Pesticides and People in a Hungry
World." San Francisco: Institute for Food
and Development Policy, 1981.
o Wyrick, Bob. "Hazards for Export" Newsday,
Special Report December 1981.
COMMUNITY HEALTH CELL
^/1,(FjrstFloor)St. MarksSoad
BAMGALO.Tc - sSu 001
* Health Action International. Hew "Iniematf...'
. ■'
‘
Consumers By Multinational Drug Companies"
Geneva, 27 to 29 May 1981.
e IOCU Regional Office for Asia and the Pacific.
"Forty Four Problem Drugs - A Consumer Resource
and Action Kit." Hay, 1931.
i
.
.' .
into the Marketing and Advertising of British
Food and Drug Products ir. the Third World. "
Social Audit, Ltd., 1979.
o Newman,Barry. "Co:isumer Protection is Underdeve
loped in the Third World." Wall street Journal,
S April 1980.
o Scherr,S.Jacob. Natural Resources Defense
Council Statement to the Subcommittee on Inter
national Economic Policy and Trade of the
Committee on Foreign Affairs, US House of
Representatives, Concerning the Reagan Decision
of the US Hazardous Substances Export Policy.
12 March 1981.
’
hail
i .ch, Michael R. "Haphazard
Policy On Hazardous Exports. " The Lancet, 3
October 1981 s 740-42?
s> Silverma.' ,Milton,Dee,Philip. R. and Lydecher,
Mia."The Drugging of the Third World." Paper
presented at the loth IOCU World Cor gross, The
Hague, June 1981.
o "The Penang Declaration on the Export of
Hazardous Substances .and Facilities." Consumer
Currents, February 1981.
IOCU
The Internationa) Organ! sat Ion of Consumers Unions (IOCU) (inks .he activities <consumer organi
zations In some 50 countries. An Independent, non-profit end non-po:11ice I foundation, IOCU prc.v.ctes world-wide co-operation In consumer protection, information and education. The Headquarters of
IOCU are at 5 Emmastraat, The Hague, N^iherlands. Phone '->3’70) -.7633’, Cable interocu Haag. Telex
33561, The Regional Office for Asia and Pacific Is at P.O. Box lOA'5, Penang, "■■liaysla. Telephone
885072, Cable interocu Penang. It lex HA A0i6k> APfOCU.
FURTHER READING
i,
HAT HI COMMITTEE* REPufiT OF T.-8E COMMTTEE ON DRUGS AND PHARMACEUTICAL
INDUSTRY
Ministry of Petroleum & Chemicals, Government of India: April 1975
(Rs.17.00)
2.
MEDICINE AS IF PEOPLE BATTERED
Special Issue of HEALTH FOR THE BILLIONS.
Voluntary Health Association of India
New Delhi
April-June 1981
3.
(Rs.5.00)
ASPECTS OF THE DRUG INDUSTRY IN INDIA
Bukarram Bhagat
Centre for Education and Document
Bombay
February 1982 (Rs.
4.
)
HEALTH CARE-bJHICrl ti!AY TO GO
Medico Friend Circle (Anthology) 1982 (Rs.10-00)
Available from Voluntary Health Association of India, New Dalhi.
5.
HEALTH FOR ALL—AN ALTERNATIVE STRATEGY
ICWyiCSSR Study Group
Indian Institute of Education, Pune (ICSSR, 1981).
Available at Voluntary Health Association of India, New Delhi.
6.
INSULT OR INJURY'
Charles Meds war
Social Audit, England: 1979
(Rs.
)
Available from Indian Social Institute, New Delhi
*
2
j2j
7.
DRUGS ANO THE THIRD WORLD
Anil Aggarual
Earthscan, 10 Porcy Street
London W1 PO DR
1978
8.
(§5,00)
POOR HEALTH, RICH PROFITS
Tom Heller
Spokesman Books
Bertrand Russel Peace Founoation Limited
Gamble Street, Nottingham, England
197? (
9.
)
DRUGS DISINFORMATION
Charles Fledauar
Social Audit Ltd
England
1980
10.
(
)
BITTER PILLS; MEDICINE AND THE THIRD WORLD POOR
Dianna Melrose
OXFAM, 274 Banbury Road
Oxford 0X2 70Z
U.K.
(£4.95)
11.
DRUG DIPLOMACY
Charles fledauar & Barbara Freese
Social Audit Ltd
PO Box 111, London NX1 8XG
1982
12.
(£3.95)
PRESCRIPTIONS Fm DEATH? THE DRUGGING OF THE THIRD bJORLD
Milton Silverman et al.
University of California Pr.ss
2223 Fulton Street, Berkeley CA 94720
1982
13.
(819.95)
DRUGS THAT DON'T WORK
Sidneyuolfe, Christopher Colely and Health Research Group ; 1980
Available from Public Citizen Health Research Group, Dept AC 2000
P Street N.W., Washington DC 20036, USA.
......3
|3»
14.
.tl1* Problem Drugs — a cansuiner action and resource kit on pharmaceuticals
Play 1981.
International Organization of Consumers' Union Registered Office for
Asia and Pacific
PO Box 1045, Penang, ffalaysia.
P-iq/344
LCB/a/28.2.84
Recommended Reading
For Self Education in Drugs Issue - for Social .-.•Lion
1. /Insult or injury?
Charles Jledawar
Social Audit
1980
139PP
Ms. 18
2. ^Bitter Pills
Dianna Melrose
Oxfam Public aff-1982
airs Unit
277ps
Rs.SO
5.
A.
5.
6.
7-
Drugs fc the Third
Anil Aggarwal
World
There is gold in
Alan Klass
bhan Pills;
an enquiry untc the
medical Industrial
Poor Healt&^iicfi. Profits. Tom Keller
Limits t-. Medicine, Ivan Illien
Medical nenesis
jhe Health ,:f
Lake Muller '
A nmj. oxi south Investi
gation
Earthscan
1978
Penguin Special
1975
Spokesman Books
1977
Bertrand Russel
Peace Foundation Ltd
Nottingham, UK.
1980
lulican Bocks,
London.
Faber & Faber Ltd 1982
8.
Pills against poverty. Goran Djurfeldt Oxford IBK,Pub.Ccl9?6
(a study of the intro- Staff an Linelberjfew Delhi.
auction of western
medisine in a Tai-iil
9.
Pills Profits &
Politics
Highlights marketing and sales of British
food and drugs products. Illustrated,
easy reading.
A very well documented convincingly
written book about the tragic drug scene
in the third world and existing courageous
initiatives. Initiatives that are possible
around the world are highlighted, which
gives us a sense of solidarity.
i\ very comprehensive overview cf the drug
situation in the 3rd acrid and the.’;..rc tier? and
Discloses how suppression of unbiased drug cau:
information, and the or ethical marketing
practices by MNC's have repeatedly taken '
place-fnr greater profits.
Describes malpractices cf UNO's in the 3rd
world.Very helpful ir. understanding practices
likes tied purchase, patent laws etc.
.in excellent critical analysis of contemprory medicine.
The book deals with the disparities and the
real causes of illhealth and the existing
health «are in thj third world countries.
Shows hew results of capital intensive western
medical care were in no way superior to the
i. ligenous traditional, medical care- generally
ccnsi'derc-d inferior and unscientific.
2$6pp
Village)
Milton Silverman Lee Berkeley University 1974
California Press
40jpp
Highlights malpractices indulged in by Drag
Companies & the rile of medical personnel in
propagating irrational drugs by irrational
prescribing.
2
10. Prescription for Death
Milton Silverman
Dragging of the 3rd world.Philip R Lee &
Mia Lydecker
i
Berkeley, University
of ’California Press
1982
186pp
11. Drag Disinformation
Charles Medawar
Social Audit,London
1980
49pp
12. Drug Diplomacy
Charles Medawar & Social Audit London
Barbara Freese
1982
119pp
15- The People's Pharmacy I Joe Graedon
a consumers guide to pre
scription drugs dangerous
drag interactions brand
name medications & money
saving home remedies.
‘
14« The People's Pharmacy II joe Graedon with
15. Geneva Press Conference
on Si.lON Proceedings
16. Drug induced suffering
(Proceedings of the Kyoto
Conference)
A very systematically — done analysis
of drag promotion & Irug sales practices
of MNC1 s in the 3rd roil d gives suggest
ions as to what can be none, the bock
is convincing enough to demand action
with its contents.
Shows the double standard of drag ISJC's
as regards the drag information given to
Doctors in UK and Ir jlancv .-fhis- is a study
of MIMS UK & MIMS Ir ilond. gross disparit
ies in the informati m between MIMS UK &
MIMS of a 3rd world, country can very
well be imagined.
Describes vividly the battle between G D
Searle (the American drug company producing
Lomotil) with Social Audit a public interest
group; demanding consumer caution & warning
for use of lomotil in children .A lesson
in courage/', perseverence & systematic scru
tiny cf so called scientific studies.
A very informative bouk.fcr consumers, dele
ted of mystifying medical jargon. Unfortunately
deals with American. brands, though the drug
information is applicable in our context too.
Avan Book, USA
1977
Avon Press
1980
Consumer guide for choosing reliable drugs,
information on arthribes medications,•vita
mins, wiliura.
y.
Japan
I960
Discloses some of the less known facts about
the SMON problem, presents the drug industry's
response, its apology to L.i« SMON victims in
Japan. .
An impressive book sb iut drug induced suffering,
covering pharmacological, clinical & research
studies. Valuable us an exposure of the medi
cal graduates to drug related issue.
Organizing Committee
Japan
■fi-10/344
LCD/a/28.2.84
Recommended Reading
For Self Education in Drugs Issue - for Social A. lion
1. /Insult or Injury?
Charles iviedawar
Social Audit
1980
lJ9pp
Rs. 18
2. ABitter Pills
Dianna Melrose
Oxfam Public aff-1982
airs Unit
277ps
Rs.80
Anil Aggarwal
Earthscan
1978
Alan Klass
Penguin Special
1975
T>
<T"
5.
4-
Drugs & the Third
world
There is gold in
than Pills:
an enquiry untc the
medical Industrial
5«
Poor Health-b-icfi Profits. Ton Seller
6.
Limits t- Medicine, Ivan Illich
Medical neiaesis
The Health ,;.f potions: take. Miller '
A xivj. tn south Investi- '
’
gation
7-
Spokesman Books
1977
Bertrand Russol
Peace Foundation Ltd
Nottingham, UK.
Pelican Bocks,
1980
London.
Faber & Faber Ltd 1982
8.
Pills against iw.verty. Gcrari Djurfeldt Oxford IBH,Pub.Ccl976
(a study of the intro- Staffan Linelberjfew Delhi.
auction of western
medisine in a Tamil
9.
Pills Profits &
Politics
Highlights marketing and sales of British
food and drugs products. Illustrated,
easy reading.
A very well documented convincingly
written book about the tragic drug scene
in the third world and existing courageous
initiatives. Initiatives that are possible
around the world are highlighted, which
gives us a sense of solidarity.
Zi very comprehensive overview of the drugsi tuaticn in the 3rd .rarId and the.’prc I Icre and
Discloses how suppression of unbiased drug cau:
information, and the or ethical marketing
practices by MNC13 have repeatedly, taken
place-for greater profits.
" ”
Describes malpractices of UNO's in the 3rd
world.Very helpful ir. understanding practices
likes tied purchase, patent-laws etc.
An excellent critical analysis of contemprory medicine.
The book deals with the disparities and the
real causes of illhoaltii and the existing
health «are in th? third world countries.
Shews how results of capital intensive western
medical care were in no way superior to the
i. ligeneus. traditional, r'edical care- generally
considered inferior and. unscientific.
256pp
Village)
Milten Silverman Lee Berkeley University 1974
California Press
40Jpp
Highlights malpractices indulged in by Drag
Companies & the role of medical personnel in
propagating irrational drugs by irrational
prescribing.
oG
■7^//
)
17.x Prescriptions for Change Virginia Beardshaw
an
18. Selection cf Essential
Drugs
Expert Committee
19. Therapeutic guidelines
Upunda Yudkin et al
i’/HO Technical
series 615 - 1977
641 - 1901
685 - 1985
African Medical
Research & Edu
cation Foundation
Nairobi Kenya. 1981
■' j
1983
A stimulating book cf acti >n, ideas for drug
campaigners.
These deal with the basic principles of
Rational drug therapy and technical Repor-t
series'- 685 gives the modified essential drug
list.
An excellent guideline for rational therapeu
tics giving special emphasis or 4-he drug cost
as criteria for choice cf drug, diagr?.ma.tic?J.ly
shewn. Practical,simple and. highly recommended
for doctors and trained middle level workers.
A pack of drug related infirnative. Articles
and bibliography on drugs uid the third world.
20. Pill-fering the poor:Drugs Produced by Inter- 475 Riverside
and the 3rd world, an
fith Centre on
Drive,Room 566
information & action pack Corpcrate Respon- New York, N Y
sibility.
USA 10115.
21. UNCTAD na.ic-r issues in Tra
United Nations
Deals with issues related to transfer of tochnsfer ..f Technology to Deve
Conference on
1975 63pp nolcgy, their impact and choices left to the
loping countries./, case of
Trade& Develop
third world countries.
the pharmaceutical industry
ment
td/b/c 6/4
22. Phari-Aceutical a Health
Blum,Andrew
Holmes & Meier
Policy;International perspe Herxheimer
Publishers
1981 267pp Role cf MNC, drug policies, essential drugs
ctives on Provision & control
economies dealt within an authoritative way in
of Medicines.
a collection c.f excellent articles.
23. Pills that don't work
Sidney Vfclffe & International
Coley
Research group
for Drug Legis
lation & Frogs.
New York Farrar,
— Extr< ely informative book, deals with ineffeStraus girauy 1981 223pp ctive highly promoted drugs in US Market itself.
24- 44 Problem drugs:a consumer
Very methodically gives information about 44
I 0 C U
May 1981
action & resources kit on
problem drugs along with articles by some of the
Pharmaceuticals.
leading drug campaigners.
For Reference on Drugs and Pharmacology
1. Kartindale-Tne extra pharmacopeia - 28th Edition
The Pharmaceutical Press. Rs.700 The world's most comprehensive source
of drug information in a single velum
2. Go.cdran gillman. - Macmillan Publishing Co. Inc, 866,5rd Avenue,New York 10022.
3. Physicians.desk reference - Medical Economics co. Inc, Oradell, N J 07649,USA.
4. _Family Medicine. Book - Orient Paperbacks, 36 C,Connaught Place, New Delhi 110001. Rs.30
5. Drug Interactions.
For deeper understanding of ths Indian Drug Scene
l.x Ha±hl_G2Kmittee. Benor-D 1975 Government of India
2.
Sone aspects of the
Indian Drug Industry
. Mukarram Bhagat
’’ “ .
(Hot available.Reprinting J... ’-I for public availability should be
demanded as Hathi CoMiiittee Recommendations, the Hathi Committee
essential drug list would provide the foundation for a demand for
a Rational National Drug Policy.
CEB Bombay. Rs. 19 (3 Sulaiuian Chambers, 4 Battery Street,
Behind Regal Cinema, Bombay 4r'^n39-
1981 IPSSK‘& ICMRastudy Report Highlights the gap between peoples health needs & cur health
'
care'delivery systems and shortages .of essential drugs eg.anti
leprosy .and anti TB drugs.
4- The Indian Pharmaceutical
P L Naravana
360pp A study conducted by the National Council of applied economic
industry; probl eras ana
Research undertaken as a response to 01FI's request to assess
prospects
the present drug status, identification of factors..unpending
growthneeds. Other aspects covered are the Indian and Inter
national pharmaceutical industry, technology trends, price-control
and their impact on production and profitability
,
*
5-v Statement of the National
Ministry of Health
A philosophical statement criticizing its own earlier hospital,
Health Policy
1983 Govt, of India.
curative care centred health policies. It discusses all the pri
ority health issues including drugs. An important tool for the
people to ensure inplemonta'tion of governments own statement of
the National Health Policy.
6. Pharmaceuticals!a third 1978 Available from Dean, ,
4pp.
Rs.10/£1/82
world experience"Seneka
Faculty of Medicine °
A tribute by his friends to this architecht of a courageous phar
Bibiles the Ma«- and his
Colombo campons
work.
University of SriLanka maceutical policy in Sri Lanka, brought out in ccLmiemc-ration of
his death on 29th September '77 in George Town Guyana where he
Colombo & Sri Lanka.
had gone as UNCTAD pharmaceuticals advisor to help in the prepa
ration of a Regional drug policy. His survival would have ensured
major changes in the third world drug and health policies. SriLanka
experience was not a failure as made cut to be by the critics of
rational drug policies- if there were problems they 'were created
purposely by the vested interests. Sri Lanka experience helps us
to identify them.
3.
Alternative Strategy
Health for all
5
Brut; Related lGricdi«uls
Drug Infcrmuti-.n Bulletin 1 H 0
The Medical Letter ._n Drugs 56 Harrison Street,New Rcchell,
and Therapeutics
New Ycrk, USA 10801.
3- Drugs & Therapeutits Bulle
tin U K
Consumers Association London
Health ..ctim International IOCU, P 0 Bex 45, Penang, Malaysia.
Kai News
5. The Rational Health Campaign Rational Health, Oxfam,274 Banbury Road
newsletter
Oxford 0X2 7D2, UK.
Consumer currents
IOCU, Penang, Malaysia.
7. Consumer Interpol
8. Contact
Geneva
An unbiased drug infer ration bulletin.
Very informative newsletter covering
world drug news of special relevance for
us in the third world.
Gives information about the drug action
groups in UK.
Covers consumer issues, specially focus
on MNC's.
Christian Medical Commission
Available from V1IAI
■Jorld Council of Churches
lune Journal of Continuing
Yrogyn Dakshata Mandal,2115 Sadshiv Peth -monthly-Subsciption Rs.lO/yr.
Health Education
rune, Maharashtra.
10. Medico Friends Circle Bulle- 50 LIC Quarters, University Road
tin
lune, Maharashtra.
monthly- Rs. 15/yr.
11. Drug Action Network newsletter. Low Cost Drugs & Rational Therapeutics Cell
Voluntary Health association of India
C-14, Community Centre,SDA New Delhi-16 -bimonthly-so far complementary for Drug Action
network only.
Health for the Millions
April-June '81-special issue
on drugs-"Bungladesh drug Policy'
VHAI address as above.
1}. Counterfact
CEB Bombay.
3 Suiainan Chambers,4 Battery Street
Behind Regal Cinema, Bombay 3914. Eastern Pharmacist-Independent
507 Ashok Bhavan,93 Nehru Place,
organ of pharmaceutical industry New Delhi 19.
trade and profession.
15. ilealtn and Society
P-31, Raipur, Garia, Calcutta-84 .
bimonthly - Rs.l2/yr.
Issues like hormonal pregnancy bests, depoprovera, blood trade etc have bean covered.
Rs.100 annual subscription. Deals with the
industry related issues as well those dealin.
with the policyand rational drug use. Rocoamended for Drug Documentation centres.
...6...
16.
Monthly Index..of. MelicaL.Spficialit Lea
MIL'S India,. 90 Neha-u Pin
./
*
Hew Delhi 19-
17-
Current Index, of Monthly.speciality,
Bic-Gard Jiedi
al
*
Services
88/1,10 Cross, Post Box J18
Bangalore,56OOOJ.
(Prepared specially for the Drug Action Network
and state V il A’s)
Subscription Rs.6o/yr .Relevant for Drug Action
. Documentation centres.
.for scrutinizing the
Subscription Rs.58/yr. as well as the drugs
indicluded in iOS and
CIMS, the drug informa
tion, made available
by the drug Industry»
to comment on their
rationality of drugs
and drag cisinformaticn
if^^ny.
.1 ./'/"'-g'X-—
Dr Mira Shiva, Coordinator,
Low Cost Drugs & Rational Therapeutics
Voluntary Health Association of India
28/2/1984
tor further information please contact
1.
Medico Friend circle
50 LIC Quarters
University Riad,
Pune 411016
2.
"Voluntary Health Association of India
C-14 Community Centre, Safdarjung Development Area
Nev; Delhi 110016
3-
Low Cost Drugs & Rational Therapeutics Cell (VHAl)
105 Rajpur toad
Dehrad un 24oOOi
4.
Arogya Daks hat a M and al
1913 Sadashiv Pt th
Pune 411030
5« Delhi sci nee Forum
J-55 Saket P.Box 4002
New Delhi 110017
6.
Society of Young scientists
All India Institute of Medical Sciences
Ansari Nagar, Nev; Delhi 110016
7.
Concern for Correct Medicine
G-16/8 Rajouri Gardens
New De.thi 110027
8.
Consumer Education and Rest arch Centre
Near Law College, Ellisbridge
Ahmedabad 380006
9.
Centre for Education and Itocumentaeion
3,
Suleman Chambers, 4 Battery Street
Bombay 400039
••.contxl
IO.
LOCOST
C/o GVHA
P.O.
G.
Box 7,
Baroda 390001
11.
Federation of Medical Representatives Association of India
J.S. Majundar, General secretary,
1-E, Rajendra Najar
Patna 800016
IO.
liOCOST
c/o GVHA
G.P.O. Eox 7,
Baroda 390001
11.
Federation of Medical Representatives Association of India
J.S. Majumdar, General secretary,
1-Ej Rajendra Nag ar
Patna £00016
--------- --77^— - -7 -7- 777 7—777--” -■ -77 777_^__ 7: 7 7_ 7 7 1
Pharmaceuticals: Resources, Information
___ 9_ 1
■.. The Bureau d’Etudes et de Recherche pour la Promotion
de la Same has published NOTIONS DE PHARMACOLOGIE, a
handbook for nurses. Copies are available for Z4.00,
CFA1200, or $5.00
Write: Bureau d’etudes, BP 1977. Kangu-Mayombe, Republique du Zaire.
.. . The April-June 1981 issue of the magazine HEALTH EOR
THE MILLIONS carries a discussion of drug therapy, drug
colonialism, the excessive cost of brandname drugs, bulk
purchasing, and other topics. Copies cost Rs. 6; $ .75.
| Write: Voluntary Health Association of India, C-14 Com
munity Centre, Safdarjung Development Area, New Delhi
110016. India.
. .. MANAGING DRUG SUPPLY is a valuable handbook on the
selection, procurement, distribution, and use of pharmaceut
icals. The 592-page, illustrated book costs $22.50, including
seamail postage; airmail by special request. French and
Spanish editions are planned.
Write: Drug Logistics Program, Management Sciences for
Health, 165 Allandale Road. Boston. MA 02130, USA.
... The May 1981 issue of world health magazine is
devoted to essential drugs. Articles include background, an
essay on quality control, and a model list of essential drugs.
The magazine is free and available in Arabic, English, Ital
ian, Persian, Portuguese, Russian, and Spanish.
Write: World Health, WHO, Av. Appia, 1211 Geneva 27,
Switzerland.
. Widespread misuse of drugs is leading to increased inef
fectiveness of many antibiotics. If the trend continues, treat
ment of a number of common infectious diseases will be
jeopardized and lives will be lost through ineffective medica
tion. Medical costs will soar because of the high cost of
alternative treatment. Alarmed at this prospect, the Interna
tional Alliance for the Prudent Use of Antibiotics, a group of
more than 200 medical scientists from 30 count ties, is seeking
data on misuse of antibiotics in developing countries.
Send materials to: Dr. Stuart B. Levy, Dept, of Molecular
Biology and Microbiology, Tufts University Medical School,
136 Harrison Avenue, Boston, MA 02111, USA.
.. . The World Health Organization (WHO) provides infor
mation and training on quality control and drug regulation.
For more information write: Pharmaceutical Unit, WHO,
1211 Geneva 27. Switzerland.
The Canadian Pharmaceutical Association (CPhA) is
developing single sheet package inserts for patients. The
sheets are called "SIMS" (Supplementary Information on
Medication), explain in clear language how and when to take
a drug, what to do if a dose is forgotten, the side effects and
precautions, and other essential information. Sample SIMS in
French and English are available free on request. A full set of
the 100 each of the first 12 SIMS and a filing cabinet cost
$59.95, including mailing costs.
Write: CPhA, 101 - 1815 Alta Vista Drive, Ottawa. Ontario
KI G 3Y6, Canada.
TETRACYCLINE
Ellccts on normal activities:
sunburn If your skm becomes sensitive, ten your doctor, wear protective
clothing, sunglasses Ask your pharmacist about sunscreens Some types of
tetracycline can cause lightheadedness dizziness loss of balance or fainting.
1 hour before or 2 hours after eat>ng Your doctor or pharmacist will tell you if
Liquid tetracycline should be WELL SHAKEN before eacn dose
Stomach upset, vomiting loss of appetite may occur if stomach upset does
effects get worse, call your doctor
A SIMS patient information card on tetracycline.
If you FORGET a dose.
Take your medicine as soon as you realize that you have missed a dose Then
immediately He will tell you if you should still take this drug
ALWAYS REMEMBER:
' Tell your doctor and pharmacist what other drugs you are taking
down the toilet OUTDATED TETRACYCLINE CAN BE HARMFUL
April 1980
... el INFORMADOR, the monthly newsletter of the Asociacion de Servicios Comunitarios de Salud (ASECSA), publishes
information on drugs in its “fichas informativas” column.
The full-pagesheets offer information in Spanish on dosage,
dangers, contraindications, storage, and expiration dates.
For a sample write: ASECSA, Apdo. 27, Ciudad de Chimaltenango, Guatemala.
SALUBRITAS
July 1982 5
NOTES
ORT in Egypt
Your front page article for January 1982 ("Egypt: Mothers
cut diarrheal deaths in half with homemade treatment")
makes a critical omission: the group of mothers making ORS
(oral rehydration salts) at home with salt and sugar had
Oralyte (full-formula) packets available to them through the
nearby rural health clinics. Sufficient numbers of ill children
were referred to the clinics after salt and sugar ORS was tried
to have accounted for at least some of the reduced mortality in
that group.
Homemade ORS is clearly an important element in
community-based rehydration efforts, but many of the child
ren at high risk of dying will require referral and more
rigorous therapy if they are to be saved.
Norbert Hirschhorn, MD
The John Snow Public Health Group, Inc.
210 Lincoln Street
Boston, MA 02111, USA
. . . "Health education methods and materials in primary
health care” is the theme of the December 1981 issue of the
newsletter, APPROPRIATE TECHNOLOGY FOR HEALTH. Items
include a health game for children (Togo), a teaching
calendar to help eradicate rats (Barbados), theater for spread
ing health messages (Zambia), and a discussion of illustra
tions in health literature. For a free copy of the newsletter,
write: The Editor, ATH Newsletter, World Health Organiza
tion. 1211 Geneva 27, Switzerland.
. . . The London School of Hygiene and Tropical Medicine
has published the results of field testing of its weight-forheight chart (Cf. SAI.UBRITAS, vol. 5, no. 1). Fora copy of the
report write: Julia Verney, Department of Fluman Nutrition,
London School of Hygiene. Keppel Street (Gower Street).
London WCIE 7 FIT, UK.
... A recent issue of HAITI SANTE, a new quarterly magazine
published by the Cent red’Hygiene familialede Ha i'ti. carries
an article entitled, "Your child and his dentist.” The article
explains the special dental problems of children: teething,
oral hygiene, baby teeth, and other subjects. For a free copy
(vol. 1. no. 4), write: Centre d'Hygiene familiale, 10. lere
Impasse Lavaud, BP 430. Port-au-Prince, Haiti.
. . . “Women. Health and Development" and "Women and
Disability” are the titles of a new series of information kits
distributed by the World Health Organization (WHO). The
kits contain articles, guidelines, bibliographies, and other
information aimed at making the public aware of women’s
needs. For a free copy in English (French and Spanish edi
tionswill beavailable later this year.). write: The Division of
Public Information. WHO, 1211 Geneva 27, Switzerland.
. . . The World Health Organization (WHO) is field-testing its
new manual. TRAINING THE DISABLED IN THE COMMUNITY:
An experimental manual on rehabilitation and disability
prevention for developing countries. The manual contains
training material for the disabled and their families, for
policy makers and planners, local supervisors, community
leaders, and teachers. If you wish to obtain a copy for fieldtesting purposes, write: Dr. J. Krol. Medical Officer. Rehabil
itation Programme. WHO, 1211 Geneva 27, Switzerland. For
others the manual is available from who for S20.00
. . . "Diarrhoea Management" is the title of a slide set that
presents new ideas about oral rehydration. The set. which
includes a detailed instruction sheet, is intended mainly for
community nurses, hospital nurses, and other health
workers. For information write: Foundation for Teaching
Aids at Low Cost (TALC), Instituteof Child Health. 30 Guil
ford Street. London WC1N 1EH, UK.
Ethiopia: Holding her health record, a mother waits in lute to have
her child vaccinated. Photo: Blair Seitz, UNICEF.
6 SALl'BRITAS
July 1982
Voluntary Health Association of India
C-14, Community Centre
Safdarjung Development Area.
New Delhi-110016
Telegrams : VOLHEALTH
New Delhi-110016
t
I elepnones .. 668071
OUR OON CERICABOUT DRUGS
Inspite of the green revolution, white revolution, industrialization,
modernization and development, the country's increase in GLP(O.aas-Kational
Profits), most of these things, have not touched that man who hangs helplessly—
below the poverty line.
The irony of al 1 .our great development is that
the number of such people who are becoming destitutes is increasing.
From 27 we can now boast of 229 Medical Colleges (Karnataka.is planning-to
make a humble contribution and add/to that list).According to
WHO's reco—..
mentations our doctor population ratio is above the requirement. Our
Pharmaceutical Industry is amongst the best in the Third World. The state
spends Rs. 9 per person per year on health. Why then do we still have such
a high incidence of malnutrition? high infant mortality?
Why are there
sti 11 10 mi711 on TB patients when we have crores being spent on the National
IB Programme.? Why do 27 mil 1 ion Indians get Typhoid every year? 6 out of
100 children, are in potential danger of becoming blind with Vit. A deficiency....
Why is it that the great majority
of our population has no access- to basic
health care? 80$ of our do ctor s'11 our health budget cater -to the needs of a
small minority.
Drug costs represent 10-60$ of the total health care-expenditure in the
developing countries (compared ;with 10—20$ in the developed ones).
The rural urban disparity when it comes to health man power allocation
expenses on drugs, vaccines and other health senices is in simple words
UNJUST. Only a very meagre percentage of Rs. 9 alloted per person for
health expenditure reach him, who forms our 'Millions'.
VHAI believes in making health care available to those, who need it most.
Orientation towards "appropriate use of drugs" and non drug therapies is not
merely for those who are given the prescriptions, but also for those who do
the prescribing.
A prescription written with the high medical standards in
mind, may be highly inappropriate in a social context where the patient
cannot afford to buy the drugs, or where buying these drugs for the family
members means being in and out of debt with money lenders.
Our prescript
ion practices have to be modified according to the needs of the people, our
choice of drugs for stocking the pharmacy have to keep this in mind and
most of all the emphasis has to be on people taking self responsibility for
their health and avoiding these drugs as far as possible and using those
non drug therapies that have been recognized to have good therapeutic effect.
Education and awareness as to how to-avoid disease and then how to handle it__
appropriately at the lowest possible cost is the crux of our approach in
low cost appropriate health care.
DRUGS:
The marketing of most brand named drugs specially by the multinational in the
Third World works against the Health of the poor: (l) Most critically -.. because Health Care-priorities are distorted by pressure to buy expensive
inappropriate drugs, which cream off limited resources, and (2) Drugs freely
....promoted in the absence of distribution controls can be dangerous.
(l)
*
-
The effect of promoting th expensive, branded drugs for which generic
equivalents are availnble ^at a fraction of the cost (semetimes as
low as 10$), is to drain limited Health Budgets unnecessarily.
OXFAM PUBLIC ■AFFAIRS UNIT (21.4.'8o)
■ CCMNlUNl i ’ i '■■■■■• c'-tL
47/1, (First Ploo?)^-w!arksRoad
BANSALORc - 560 001
2
-
Third World countries spend a disproportionate amount on Drugs,
often as much as 55% of the total health budget (compared to 11%
of NHS budget on drugs here). Bearing in mind the very 1 i mited
effectiveness of drugs and curative medicine in general in tackl
ing the major health problems - malnutrition, infectious and para
sitic diseases - public funds would be far better spent on prevent-ive health measures arid the basic Primary Health Care infrastruct--ure. For this, WHO estimate that 200 generic drugs would be more
than adequate to meet
Health needs
*
The promotional practices of drug companies, aimed at maximi si ng
profits, run directly counter to the health needs of the poorest.
Drug company salesmen (Glaxo has 500 in India alone) concentrate
their premotion on encouraging doctors to prescribe the most
expensive, latest patented drugs, claiming they are great improve
ments on far cheaper, well-established drugs.
When Beecham's and
Wellcome’s antibiotics and antimalarials are prescribed at public.
expense, instead of penicillin and chloroquine, the drug~budget is
rapidly exhausted. Because of existing imbalances in the .he.alth
services, reinforced by marketing, the brunt of wasteful spending
invariably falls on the poorest, as the rural dispensaries run
short of vital life-saving drugs.
(2)
-
Apart from promotion of unnecessarily expensive , but necessary
drugs, doctors are also encouraged into wasteful overprescribing /
of non-essential- tranquilisers, sympton-allaying drugs, arid tonics.
Onceagain, the indirect effect on the poor, is that Valiui^ being
doled out in hospitals on public funds, can mean shortages' of first
line drugs in the village dispensaries. Where medicines have to
be paid for, .(particularly when the doctor is remunerated for
prescribing rather than consultation) - sales talk may lead him
to prescribe unnecessary drugs e.g. several courses of antibiotics
and vitamins for a sick child, costing anything up to a months
wages.
/
-
Drugs freely promoted in the absence of distribution controls can'
be dangerous,
-
The tr^cl<-’-G-down effects of uncontrolled drug marketing in |he .ab
sence of an adequate health infrastructure, trained health:workers
and controls cn over-the-counter sales can seriously endanger the '
health of the poor. They are most vulnerable through ignorance of
dangers and the misconception that a medicine - any medicine., -.-win
do the trick.
/
-
When under attack for unethical marketing practices in the Third
World, the drug companies argue* that they stick to the letter of
the law. Quite true - But, they demonstrate a total' lack of
social responsibility in promoting potent, potentially dangerous
drugs, in countries .where they know they win be' freely available
over-the-counter,prescribed by local practitioners and traders
with little knowledge of medicine - let alone' sophisticated, drugs.
(Whilst deaths from adverse drug reaction gp unreported in the Third World - in the USA they are estimated at 30,000 per year.) ■■
-
The net effect is that the poor' are encouraged to buy drugs'-far
totany inappropriate uses and irrational self-medication -.parti
cularly of antibiotics leading to serious problems of drug resist
ance - can be fatal. First line antibiotics given io children with
diarrhoea could mean they will die later if they gei IB, because
there will be no way of obtaining or paying for bl second line drug.
BRIEF OUTLINE OF VHAI'S H)LE IN LOW O3ST APPROPRIATE HEALTH CARE
Regarding Dru&_rel^ted_Legislaiion_qt nqiioiijlJLeveJj.
___
-
Forming a lobby against unethical practices of drug, companies.
-
Building awareness regarding WHO endorsed code of conduct as
against that drawn up by multinationals
Seeking information and analysing national policies which may-"
have detrimental implications, specially where drug market- is
concerned.
-
Linking up with medical units of various consumer societies,
other groups and individuals working cn similar lines: eg. Medico
Friends Circel, Centre for Studies in Science and Eivircnment
etc. to form pressure group.
-
Use different seminars, workshops, medical and. nm-medin-ai. journals
to disseminate relevant information.
-
Questioning drug advertisements, giving incorrect information and
malting false claims.
Iteg^rding Production—o_f Generic name drugs:
-
Collect information of experience regarding production of drugs
and low cost health care from other voluntary groups and pro
grammes: eg. Savar in Bangladesh, Guatemala, Philippines, SriLanka, Medicus Mundi/Intcrnational Organisation and seeing
applicability in our Indian context.
-
Encourage or collaborate in production of generic name drugs.
-
Conscientize people regarding quality control and demanding it
- to prevent involuntarily having turning to the sophisticated
drug companies.
-
To identify non allopathic drugs : eg. de Chanes, Homeopathic etc.
of cheaper and more effective to inform others.
Regarding Distribution of_drugs2 (which is the biggest problem for develop-ing countries)
(See appendix-l)
- Encouraging bulk purchase at regional levels
-
Helping to organize distribution channels
-
Help col 1 ee.t background information based' on epidermiological
studies, other field studies
ItegaEding Management—of Ph^rma£iesj_
-
Encouraging formation of pharmacy and therapeutics committee
( See appendix 2)
-
Stocking with appropriate drugs - low cost, generic, avoiding
combinations trade nanes as far as possible
-
Encouraging local preparations of liniments, ointments, syrups
and mixtures (as done by compounders earlier)
■.
.-2/
2
-
Helping in appropriate pricing of treatment (registration,
consultation and cost of drugs)
-
Availability of information on all drugs dispensed vdth.
Regarding Dispensing, of .drugs:
-
Limiting range of drugs in the pharmacy to essential
drugs
-
Use of formulary
-
Ihcouraging use of Physicians' Desk. Reference on extra
phaTmacepea and not relying on the information given by
drug advertisements and drug representatives.
-
Helping in standardization of diagnostic and prescription
procedures ( to avoid unessential and limiting procedures
to the most appropriate)
Regarding ^.Educ^tion_aid_gaining pf_Health Personnel:
-
Collection, analysis and dissemination of relevant inform
ation to health professionals ( and public) regarding use of drugs and their substitutes - role of drug industry
in health services - use of non drug therapies : eg.
• massage, acupressure, acupuncture - investigation and use
of heme remedies and other indigeneous herbal medicines
known to be cheaper and giving good therapeutic results.
-
local preparations of commonly used ointments, syrups etc.
-
planting of medicinal plants in hospital vicinity vdth
specific therapeutic value.
Re^ar ding Health_Education_ qf_P^tients :
-
Enphasis on the concept of..self responsibility regarding
he al th
' -
Special coverage to methods of prevention of common
diseases, eg: those due to poor hygiene, sanitation and
nutrition.
Information about the various govt, health programmes:
- National IB Programme
- MCH & FP
- For Blindness etc.
- Immunization Programmes
Information regarding functions of PHC doctor, sanitary
inspector, ANN etc. for people to know their rights.
Sharing information vdth the people about therapies used
by them
Ihcouraging medically sound customs and cultural practices
- eg. use of Dathun instead of eblgate tooth paste and
discouraging the harmful ones by giving appropriate
information, eg: branding a child on the abdemen, not
breast feeding a child for 3 days..
Giving information about the misuse of - injections tonics - steroids, bottle feeds.
---------------
3/
BRIEF OUTLINE OF VHAI'S K)LE IN LOW COST APPROPRIATE HEALTH CARE
Regarding Orug_rel^,ted_Leasla£ion_gIt nation^l_levelj_
------
-
Forming a lobby against unethical practices of drug, companies..
-
Building awareness regarding WHO endorsed code of conduct as
against that dram up by multinationals
■.
-
Seeking information and analysing national policies which may-'
have detrimental implications, specially where drug market, is
concerned.
<
-
Linking up with medical units of various consumer societies,
other groups and individuals working on simil ar lines: eg. Medico
Friends Circel, Centre for Studies in Science and Environment
etc. to form pressure group.
f
j
-
Use different seminars, workshops, medical and non-medical. journals__ 1
to disseminate relevant information.
-
Questioning drug advertisements, giving incorrect information and
malting false claims.
Re_ga£ding Production_of Generic name drugs:
■>
Collect information of experience regarding production of drugs
and low cost health care from other voluntary groups and pro
grammes: eg, Savar in Bangladesh, Guatimala, Philippines, SriLanka, Medicus Mun di/International Organisation and seeing
applicability in our Indian context.
-
Ph courage dr collaborate in production of generic name drugs.
-
Conscientize people regarding quality control and demanding it
- to prevent involuntarily having turning to the sophisticated
drug companies.
-
To identify non allopathic.drugs : eg. de Chanes, Homeopathic etc.
of cheaper and more effective to inform others.
Regarding Distribution pf_drugs£ (which is the biggest problem for develop-ing countries)
(See appendix-1)
- Encouraging bulk purchase at regional levels
-
Helping to organize distribution channels
-
Help collect background information based on epidermioLogical
studies, other field studies
Re_ga£ding M^jiqgement_of Pharmacies^.
-
Encouraging formation of pharmacy and therapeutics committee
( See appendix 2)
-
Stocking with appropriate drugs - low cost, generic, avoiding
combinations trade names as far as possible
-
Encouraging local preparations of liniments, ointments, syrups
and mixtures (as done by compounders earlier)
2/
j
1
j
i
i
-
Helping in appropriate pricing of treatment (registration,
consultation and cost of drugs)
Availability of information on all drugs dispensed with.
Regarding Dispensijig_of drugs:
-
Limiting range of drugs in the pharmacy to essential
drugs
-
Use of formulary
-
Ehcouraging use of Physicians' Desk. Reference on extra
pharmacepea and not relying on the information given by
drug advertisements and drug representatives.
-
Helping in standardization of diagnostic and prescription
procedures ( to avoid unessential and limiting procedures
to the most appropriate)
Regarding ^Educailpn_and_Training ofjfealth Personnel:
-
Collection, analysis and dissemination of relevant inform
ation to health professionals ( and public) regarding use of drugs and their substitutes - role of drug industry
in health services - use of non drug therapies : eg.
massage, acupressure, acupuncture - investigation and use
of heme remedies and other indigeneous herbal medicines
known to be cheaper and giving good therapeutic results.
-
local preparations of commonly used ointments, syrups etc.
-
planting of medicinal plants in hospital vicinity with
specific therapeutic value.
Regarding Heglth_Education_ pf_Pgtiente :
-
Bnphasis on the concept of,,self responsibility regarding
health
■ -
Special coverage to methods of prevention of common
diseases, eg: those due to poor hygiene, sanitation and
nutrition.
Information about the various govt, health programmes:
- National IB Programme
- MCH & FP
- For Blindness etc.
- Immunization Programmes
Information regarding functions of PHC doctor, sanitary
inspector, ANM etc. for people to know their rights.
Sharing information with the people about therapies used
by them
Encouraging medically sound customs and cultural practices
- eg. use of Dathun instead of Colgate tooth paste and
discouraging the harmful ones by giving ajjpropriate
information. eg: branding a child on the abdanen, not
breast feeding a child for 3 days..
Giving information about the misuse of - injections tonics - steroids, bottle feeds.
---------------
3
Other Activities to_d£crease he^lth_cgre costs:
-
Training of different levels of health personnel to be able
to handle common problems as effectively and as cheaply as possible
-
Investigate role of health insurance schemes in different parts
of India and their feasibility.
-
Preparation of reccmmended reading list of books and material
related to low cost appropriate health care.
-
Formation of linkages with groups working on the same lines
eg: MFC, Centre of Science and Environment
-
Collaborating with groups to do scientific field studies on local
remedies, their utility value and optimum methods of preparation
(Solidarity, SIRTDO, Ranchi)
This background paper is for discussion.
-------------0O0-------------
,
-
Appendix 1
Distribution of Essential drugs in Developing Countries
Drug distribution was identified as a critical factor in health care and the
accomplishment of a comprehensive national drug policy at the consultation
and WHO technical Discussion in 1978.
It appeared that the types of distribution systems or patterns depend
.largely on the political and economic system and the administrative system
under which the Govt, is operating, (effective distribution of resources
depends on nation's politi cal will).
'
•;
Following were the relevant factors to be considered for any system of
distribution of drugs:
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
Health Care System, Demography, Health Indicators
Morbidity pattern
' List of essential drugs and medical equipment
Adequate storage facilities
Administration, personnel forecasting and inventory control
Transportation facilities and maintenance service.
Packaging material standardization and labelling
Quality surveillance and inspection
Education and regular training of staff
Drug utilization studies
;
ta
Appendix 2
The Primary purposes of the Pharmacy and Therapeutics Committee
a.
Advisory
b.
Educational
Functions and Scope
The following list, which is not necessarily ccmprehensive, is often
aS a guide:
A.
To serve in an advisory capacity to the medical staff and hospital
administration in all matters pertaining to theuse of drugs.
B.
To serve in an advisory capacity to the medical staff and the pharma
cist in the selection of choice of drugs which meet the most effecitve
therapeutic quality standards.
C.
To evaluate objectively clinical data regarding new drugs ar agents
proposed for use in the hospital
D.
To prevent unnecessary duplication of the same basic drug or its
combinations.
E.
To recctnmend additions and deletions from the list of drugs accepted
for use in the hospital
F.
To develop a basic drug list or. formulary of accepted drugs for use
in the hospital and to provide for its constant revision.
G.
To make recommendations concerning drugs to be stocked in hospital
patient units or services.
H.
To establish or plan suitable educational programmes for the profess
ional staff on pertinent matters related to drugs and their use.
I.
To recommend policies regarding the safe use of drugs in hospital,
including a study'of such matters as investigational drugs, hazardous
drugs, and others.
J.
To study problems involved in proper distribution and labelling of
medications for inpatients and out patients.
/
K.
To study problems related to the administration of medications,
L.
To review reported adverse reactions to drugs administered.
M.
To evalutate periodically medical records in terms of drug therapy.
list of relevant reading material dealing with drug problem
1.
Drugs and the Third World
Anil Aggarwal
Ear’hsc.rPublication
International Insti--tute for Ehvirc'ric "t
& Development
10 Percy Street
London - August 1978
2.
There is Gold in them
tharpills
Alan Klass
Penguin Special
1975
3.
Poor Health-Rich Profits
Dr. Tom Heller
Bertrand Russel
Peace Foundation Ltd.
Bertrand Russel “sue
Gamble Street
Nottingham
1977
4.
Social Audit
Insult or Injury ?
Charles Medawar
Social Audit Ltd.
9 Poland St.
London W1V3DG
1979
5.
Social Audit
Drug Disinformation
Charles Medawar
Social Audit
Public Interest
Research Centre Ltd.
November 1980
6.
Medicus Mundi Internationales
International
General Secretariat
Organization for
of Medicus Mundi
Cooperation in
Internationalis
Health Care.
Mozartstrasse 1980
Documentation of
D-5100
the General Assembly
Aachen, BRD
(17-19 May 1980)
7.
Essential Drug List
8.
Drugs and PharmaceuticalChapter from "Health for
All - An alternative strategy"
WHO Technical Report 1979
series No. 641
ICMR & ICSSR
New Delhi
August 1980
9.
Hathi Commission Report
001
1974
10.
Food First
Lappe Francis
Moore and Collins
1980
11.
Medical Nemesis
Ivan Ulich
—
2
12.
Confessions of a Medical Heretic
- Dr. Robert.S. Mendelsohn
Contemporary Books
■13.
The Medicine Men
- Vernon Coleman
Arrow Books Ltd.
Essex
1975
- Pharmaceuticals for
Developing Countries
National Academy of
Science, Washington DC
1979
Information Sources on the
Pharmaceutical Industry
- UNIDO Guides to Info.
Sources No.23
UNIDO,VIENNA
1976
Pills Against Poverty
(A Study of the introduction of
western medicine in a Tamil
village)
- Djurfeldt, Goran
Lindberg, Staff an
Oxford, IBH
Pub. Co. New Delhi
17.
In Search of Diagnosis
- Ashwin J.Patel
Medico Friends Circle
Gujarat
13.
Planning Pharmaceuticals for
Primary Health Care
(The supply & utilization of
Drugs in the Third World)
- Oscar jish
Loretta Lee Feller
19.
Drugging the Indian
(Article in"Debanoir'')
- by Shivanand Karkal
July '30
20.
The Ethics of the Drug Industry
(Article in "Business India")
- by Dilip Thakore
July '80
14.
15.
16.
Conference Proceedings
1979
1976
1977
CO^f^or
^01
THE PHAF MCOFOEIAS
DEFINITION :
Pv a pharmacopoeia is meant a book published under
the authority'of a recognised body, generally constituted by law^
for the purpose of securing uniformity of composition and strength
of medicines used in the treatment of disease.
This book^describes
most of the drugs of therapeutic usefulness and pharmaceutic
necessity, withdirections for their preparation, physical or.
chemical characteristics, standardisation and dosage.
The first
B.P. was published in 1864, and the last in 1958.
Other countries,
as the United States, Germany, France, India, etc., also publish
their own pharmacopoeias.
In the year 1955 Government of India published the
first Indian Pharmacopoeia (l.P. ) which includes not only all
useful drugs but also many vegetable drugs of proved therapeutic
value, which grow or can be made to grow in India, with definite
chemical compositions and standards, and other chemical and
synthetic compounds prepared in India.
The current United States pharmacopoeia (U.S.P.) was
issued in 1955 and the first volume of International Pharmacopoeia
was published in 1951.
The Council of the Pharmaceutical Society of Great
Britain periodically publish a book called "The Pritish Pharma
ceutical Codex" (B.P.C. ) which contains not only all the drugs
and preparations of the British Pharmacopoeia but also many
other preparations not contained in it.
National Formulary (N.F.')
and New and Non-official Drugs (N.N.r.') are other recognised
publicat ions.
Pharmacopoeial Preparations
Few drugs can be administered in their natural state.
They
are either too nauseous, too bulky, or contain some principles
which are injurious to life of health.
They are, therefore,
submitted to certain processes prescribed by the pharmacopoeias,
in order to render them fit for administration, and also to help
their preservation and storing so as to maintain an uninterruoted
supply during all seasons of the year.
The International Pharmacopoeia
is published by the W.H. 0.
The National Formulary is another recognised publication.
The
inclusion of drugs m the National Formulary is based on their
therapeutic merit rather than the extent of use.
The National
Formulary.includes many formulae for pharmaceutical preparations
like elixirs, solutions, tinctures, pills and powders, which are
in common use.
National Formulary (N.F. ) of India is published
by the Government of India.
The British Pharmaceutical Codex
r .. c British Pharmaceutical Codex is the British counterpart
of.N.F. and is published by the Pharmaceutical Society of Great
Britain.
•
: 2
The Physicians's Desk Reference
:
(P.D.R.)
This is an America! body.
The'Indian counterpart is the
CIMS & MIMS.
Financing of this project is done by the drug
companies who buy space to list their products.
The information
in this volume is supplied by the drug companies and is not subject
to critical and objective review, although in recent years most of
the descriptions are similar to the package inserts which are
reviewed.
One deficiency is the tendency to list or to describe
more- fully only new products.
The publisher and the drug companies
do not advocate the use of any particular product, nor is there
any overt attempt to influence the therapeutic practice of the
physician.
On the- other hand, it is only natural that a physician
seeking information in this volume will be attracted to a large
number of nc-w products.
Che of the sections lists products by
therapeutic indications. The superficial and careless physician
might easily fall prey to the dozens of products listed for a
particular disease or symptom without having real knowledge of the
actual therapeutic possibilities or dangers and toxicities.
The a
volume is useful and handy for finding what drugs are available,
what dosage forms are made, and what drug companies manufacture t’H^p
item.
In the final analysis, it must be recognized that this volume
represents a form of advertising.
The Merck Index
For those more scientifically inclined and desirous of
knowing more of the.chemistry and physical characteristics of drugs,
the Merck Index is invaluable.
It is not intended for therapeutic
use.
mcu
. I Y HEALTH CELL
47/1. (First Floor)St. Marks Hoad
BAfUGAJ.03E-66G001
- 0MER
POL
now
you ■ ■
do
not
have
to
take
all
these
hands
down
WHAT IS
CONSUMER INTERPOL?
Consumer Interpol - If you think the name
refers to a force assembled by consumers
to fight international corporate crime,
you are right. Rampant dumping of hazard
ous products, dangerous technologies and
toxic wastes; countless victims (many of
them disabled, dying or dead); the absence
of any comprehensive effort to bring about
a solution.... These have given rise to
an acute sense of impatience among consumer
groups and prompted action against the un
conscionable deeds of some transnational
corporations and 'aid' agencies. Consumer
Interpol, set up by the International
Organization of Consumers Unions (IOCU), is
a dynamic entity incorporating an alert
system, safety campaigns, advocacy for re
gulations, research and training. It aims
to organize citizen action against an
intolerable problem.
HOW DOES IT WORK?
it's global. Consumer Interpol, as the
name suggests, is global. At the core of
the network are members of the IOCU group
numbering more than 120 organizations
located in some 50 countries and represent
ing every continent. The Consumer Interpol
is developing regional centres to support
THE THIRD
FORCE
"The lack of controls on the exports of
toxic substances that are banned or
restricted poses an undue burden on the
'inner limits ' of man; it poses an undue
burden on the 'outer limits ' of our en
vironment; it poses an undue burden on
developing countries that have not yet
the skills and resources to deal with
the problem adequately. The '3rd system,'
the citizens ' groups in developing and
developed countries, must act together
because we cannot rely on the '1st
system, ' the governmental system or the
'2nd system] the commercial network, to
deal adequately with this problem.
We
are concerned here with a major health
issue, we are concerned with a human
rights issue, and we are concerned with
the protection of the environment. "
— Anwar Fazal, President of IOCU,
Keynote address to an NGO Seminar on
the Export of Toxic Substances, New York,
November 20, 1981.
activities in every part of the world.
Each of these centres will have a wide net
work of correspondents; the aim is to have
at least one in every country. Correspond
ents are drawn from consumer, health and
environmental groups and a wide range of
knowledgeable people including journalists
and scholars.
IT'S PARTICIPATORY■ This information-and
-action network encourages participation;
it calls for a cooperative response to a
shared problem. All components of the
Consumer Interpol are two-way systems they GIVE help and they TAKE help. The
'alert' system, for example, welcomes information on hazards from all quarters.
9
Whatever vital information it receives will
be channelled out as warnings to those who
need it. Regional centres, the collection
and dissemination points, will assess in
formation received with the help of some
experts.
IT'S AN ADVOCACY NETWORK. The Consumer
Interpol does not stop at issuing 'alerts.'
It also takes action from time to time to
ensure that the hazards are removed through
legislation and other means. What the
network will do is flexible and it depends
on the issue at hand. A localised problem
may only need a localised response with
help from a few other organizations. For
a global problem, Consumer Interpol may
mount a campaign involving every concerned^
group that wishes to combat the problem, w,
IOCU is not new to such international cam
paigns. It is playing a key part in those
involving infant formula and pharmaceuti
cals through the International Baby Food
Action Network (IBFAN) and Health Action
International (HAI).
IT S Supportive.
The supportive arm of
Consumer Interpol is aimed at making sure
the action-information balance, vital to
any international campaign, is wellmaintained. Research will feed the system
with detailed information while training
ensures that gathered information is well
stored and efficiently used. A data bank
with links to other documentation centres
will be maintained. There will also be
active links with programmes like: o the
International Register of Potentially Toxic
Chemicals (IRPTC) of UNEP; o the Inter
national Programme on Chemical Safety of
ILO, UNEP and WHO; a the ILO International
Occupational Safety and Health Hazard Alert
System and o UNEP's Global Environmental
Monitoring System (GEMS).
DID YOU
KNOW?
• At least 25% of US pesticide exports
in I960 were products that were banned,
heavily restricted, or have never been
registered for use in the United States.
o About 1.5 million people are being
poisoned by pesticides every year, with
half of the cases in poor countries.
Some 30,000 deaths a year - three quar
ters of them in the Third World - are
believed to be due to pesticide poison
ing.
o Several million children's, garments
treated with a cancer-causing fire
retardant called Tris were shipped
overseas after being forced off the US
market by the Consumer Product Safety
Commission.
ACTION
o Many pharmaceutical companies fail to
label their products adequately regard
ing proper use and dosage. Often even
doctors are deprived of crucial infor
mation like potential side effects.
should you receive information on any of
the following...
o In India, the subsidiaries of major
British and American asbestos companies
operate facilities that are 50 years
behind the standard of practice the
firms observe in their home countries.
o marketing of dangerous consumer goods
like toxic foods and dangerous toys
• export of hazardous wastes
o plants that expose workers to serious
health hazards
o adoption in exporting countries of new
bans or strict controls over hazard
ous consumer goods, drugs, pesticides
or industrial chemicals (this is to
alert the network to the possibility
of dumping)
o The US Environmental Protection Agency
estimated that in 1980 at least 57
million tons of hazardous waste was
produced in the United States. There
are not enough safe, secure disposal
sites to handle a fraction of it.
o newly reported outbreaks of illness or
death due to previously known
hazardous agents
...inform the International Organization
of Consumers Unions (IOCU) and we will
take the appropriate action.
(Our
addresses are on the back page.)
: The Corjo/oF* C^irnc. of the Ctn-Klrj
Mothv Toa/5 vctWi't
RESOURCES
• Ahmed,A.Karim;Morehouse,Ward;and Shaikh, Rashid
"For Export Only:The International Trade in
Toxic Substances." Development Forum,January
1982.
© UN Economic and Social Council. Exchange of
information on Banned Hazardous Chemicals and
Unsafe Pharmaceuticals. Report of the Secre
tary General E/1981/ 11 February 1981.
© Castleman,Barry I."The 'Double Standard' in
Industrial control of Health Hazards." Paper
presented to the New York Academy of Sciences,
4 February, 1981.
o UN Commission - on Transnational Corporations.
"Role of the Information System on Transnat
ional Corporations regarding the exchange of
information on banned hazardous chemicals and
unsafe pharmaceuticals." E/C 10/90 18 June 1981.
© Concern Inc. ''Hazardous waste:A community action
guide/' May 1981.
© Dowie,Mark."The Corporate Crime of the Century”
Mother Jones, November 1979.
© Fazal, Anwar."Testimony before the Subcommittee
on International Economic Policy and Tradej
Committee on Foreign Affairs, US House of
Representatives 5 June 1980" IOCU Newsletter,
June 1980.
o Weir, David, and Shapiro, Mark. "Circle of
Poison: Pesticides and People in a Hungry
World.” San Francisco: Institute for Food
and Development Policy, 1981.
O Wyrick, Bob. "Hazards for Export" Newsday,
Special Report December 1981.
o Harris, Robert.H. Keynote Address, Special
Open Session on the Dumping on Hazardous
Products, Processes and Wastes, loth IOCU
World Congress, The Hague, June 1981.
o Health Action International. New "Internat
ional Antibody" Will Resist "III Treatment of
Consumers By l^ultinational Drug Companies"
Geneva, 27 to 29 May 1981.
o IOCU Regional Office for Asia and the Pacific.
"Forty Four Problem Drugs - A Consumer Resource
and Action Kit." May, 1981.
© Medawar,Charles."Insult or Injury? : An Enquiry
into the Marketing and Advertising of British
Food and Drug Products in the Third World."
Social Audit, Ltd., 1979.
© Newman,Barry."Consumer Protection is Underdeve
loped in the Third World." Wall Street Journal,
8 April 1980.
© Scherr,S.Jacob. Natural Resources Defense
Council Statement to the Subcommittee on Inter
national Economic Policy and Trade of the
Committee on Foreign Affairs, US House of
Representatives, Concerning the Reagan Decision
of the US Hazardous Substances Export Policy.
12 March 1981.
• Shaikh, Rashid;and Reich, Michael R. "Haphazard
Policy on Hazardous Exports." The Lancet, 3
October 1981 : 740-42.
_
• Silverman,Milton,Lee,Philip. R. and Lydecher,
Mia."The Drugging of the Third World." Paper
presented at the 10th IOCU World Congress, The
Hague, June 1981.
• "The Penang Declaration on the Export of
Hazardous Substances and Facilities." Consumer
Currents, February 1981.
rincu----------------------The International Organization of Consumers Unions (IOCU) links the activities of consumer organi
zations in some 50 countries. An independent, non-profit and non-politica1 foundation, IOCU promo
tes world-wide co-operation in consumer protection, information and education. The Headquarters of
IOCU are at 9 Emmastraat, The Hague, Netherlands.
Phone (+3170) 476331, Cable Interocu Haag. Telex
33561, The Regional Office for Asia and Pacific is at P.O. Box 1045, Penang, Malaysia. Telephone
885072, Cable Interocu Penang. Telex MA 40164 APIOCU.
(ppsB) PHOENIX PRESS SDN. BHD.. r<’
appendix
MEDICAL SERVICE
Dead line;
OCT-NOV 1984
20th Sept 1984
SPECIAL ISSUE;
Drug pushers or healers?
A list of possible article/reprints‘ A final selection will
be made based on receipt of articles within deadline as well
as coordination with special issues of Health for the Millions
and the mfc bulletin,,
1, Editorial
2. Drugs and the
Healing Process
:: A theological perspective : Fr Samuel Ryan
or
Fr Cedric Rebello
3. Drugs and the
CHAI vision
:: the social relevance
Fr Thomas Joseph
4. Drug situation in
India
:: an overview
A summary from
Health for All
-ICMR/ICSSR
Aspects of
Drug in India
5. A to Z of
Drug issues
;: the how- and why of the
drug situation
Community Health
Cell, Bangalore
6. Misuse/overuse
;: factors/reasons
David Werner
7. Drug prescribing
:: the ethical dilemma
Fr George Lobo
8, A to 8 of Drug
prescribing
;: Banned and hazardous drugs: Community Health
Cell, Bangalore
9. Medicine as a
substitute for
caring
David Werner
10.A people's view of
drugs
David Werner
11.To inject or not
to inject
Janet Aitken
12.The crazy world
of tonics
Mukkaram Bhagat
13,Learning to use
antibiotics wisely
David Werner
14.Diarrhoea
Earthscan/VHAI
15.O.R.T. Options
;: from dependence to
autonomy
David Werner
2
2
16o Drugs and
Pharmacy
regulation
: the legal aspects
Fr P D Mathew
17. In the news
; an Indian media review
Community Health
Cell, Bangalore
18. Consumer AlertConsumer Action
: Drug Action in India
Ravi Narayan
(bulletin of
Sciences)
19. The Kur j i Case
Study
20. LOC’OST
^21. The CPA
: A mission hospital's
efforts towards rational
therapeutics
Tom Kai Hath
: A low cost drug
distribution service
S Sreenivasan
: the CHAI experience
CHAI report
22. Drugs in other
systems
23. Non-drug therapies
24. What can we do? Some suggestions for action
25. Widening horozons and contacts
a) books and journals
b)
education material
c)
other contacts
I
I Community Health
I Cell
I Bangalore
I
medico friend circle
[organization & bulletin office]
326, V Main, 1st Block
Koramangala, Bangalore-560 034
Health
Safety and the
ConsLimeB’
Proceedings of the
IOCU Seminar,
Ranzan, Japan
Dangerous drugs, unfit food and unsafe
products — these are what gave birth to the
consumer movement. Angry at such threats to
their health and safety, consumers in the
United States around the turn of the century
organised themselves and fought back. Today,
consumer organisations are found in most
countries, and some 120 groups are members
of the International Organization of
Consumers Unions (IOCU).
But safety is no longer a national concern.
The global market place brings new problems,
including the irresponsible export of banned
or dangerous products to countries where
government protection of the consumer is
slack. This IOCU seminar which brought more
than 300 consumer leaders, researchers and
scientists together at Ranzan, Japan from
April 6-9, 1983, was therefore timely.
Consumer activists and observers of the
consumer movement will find this publication
a useful collection of papers representing
current views of the consumer movement on
various aspects of product safety such as
legislation, education, information and
trade. The seminar also focused on two
specific groups of chemicals, drugs and
pesticides.
ISBN 967-9973-00-X 118 pages
including surface mail postage
ORDER FORM
Send your order to:
IOCU Regional Office for Asia and the Pacific
P.O. Box 1045,
Penang, Malaysia.
I would like to order
copy/copies of the Proceedings of the
IOCU Seminar on Health, Safety and the Consumer
Please send me my order by surface mail/air mail
The price of US$15.00 a copy covers surface mail postage only.
If you wish your order to be airmailed please add for eacy copy
US$ 7/- for the Americas
6/- for the Europe, Middle East, Australia and the Pacific
4/- for Asia
I enclose my bankdraft (drawn on any bank in Malaysia) for $
made out to the International Organization of Consumers Unions
Name:
Organisation, if any:
Address:
US$15.00
mcu
INTERNATIONAL ORGANIZATION OF CONSUMERS UNIONS
fflate
»tera Freese
Decoding the send uct of a multinational
pharmaceutical company and the Failure of a
western remedy for the third world
0^0©
OrL©OWCY
0C@v wwfe
multinational
corporation—pharmaceuticals
and public health—developing
countries and development—
international
regulation
of
business—marketing medicine
—science: serious abuse of
—corporate social behaviour
—consumer group pressure—
corporate public relations—
international health action—
»
Key Bssues: People are increasingly worried about the
damage done by US and other multinational corpor
ations in developing countries. There isspecial concern
about the pharmaceutical industry — because double
standards in marketing, and other industry practices
are seriously undermining public health in the third
^/orld. There is no effective control over this — though
pressure is now mounting for a World Health Organisa
tion code of pharmaceutical marketing practice.
Drug Diplomacy shows how important these issues are
by looking at the way in which a major US drug corpor
ation has promoted one of its best-selling products in
the third world. The story starts as a small British public
interest group pillories the corporation for promoting
this drug for the treatment of infants in developing
countries. In the US and in other industrialised coun
tries, the law forbids this: this drug is of no value for
children, and may seriously harm them.
Drug Diplomacy explains why the dangers of this drug
pire much greater in developing countries — and then it
describes how the corporation which makes it re
sponded under attack. After an initial public relations
failure, the corporation weighs in with its top scientists
— and with all the scientific evidence — to defend its
position and attack back. The Social Audit report
analyses and demolishes the company’s evidence. It
shows also how the company’s senior scientists consis
tently misinterpreted it.
In the end, the corporation capitulates, and changes its
marketing policies worldwide. But has anything really
changed at all?
DRUG DIPLOMACY:
Decoding the conduct of a multinational phar
maceutical company and the failure of a Western
remedy for the third world.
Status and date of
publication:
New book: ISBN 0-9503392-9-6
Spring 1982
Extent and format:
128 pages. Approx, 180 g. 210mm x 148mm (A5
size). In soft cover only.
Readership and level:
Lay readers. Students — especially of develop
ment and business studies, international
relations, sociology and related disciplines. Also
for students and practitioners of medicine
(tropical, paediatrics) and pharmacology. For
corporate managements: marketing, public
relations, business strategy. Also for government
regulatory agency officials and senior health
policy advisers.
To order:
If there is a distributor's name in the box below, it
would be much more convenient for you to order
through them. If the box below is blank, please
send cash with order to: Social Audit Ltd., 9
Poland St., London W1V 3DG.
Drug Diplomacy can be obtained at £3.95 per copy, plus postage and packing
charges. Add 35p in the UK; or 55p for surface mail to all other countries. For
airmail post, please add 90p per copy to Europe, and £1.80 elsewhere. Please
send cash with order. Payment must be in £ Sterling, and drafts should be
drawn on GIRO or on a London bank.
Please send me
copy/copies of DRUG DIPLOMACY by surface/air
mail. I enclose payment of
(to include post & packing charges as
shown above).
Name and address
Order No./Ref.
Date
If box is blank please order
from Social Audit, 9 Poland
Street, London W1V 3DG.,
UK
(S.1/2/82)
cW
gP PILL-FERING^
o
DRUGS AND THE
THIRD WORLD
o
Why do drug companies spend only 1% of
their annual research budgets on tropical
diseases which affect hundreds of millions of
the third world poor, and have as yet no safe,
cheap and effective drug therapies?
o
Why can Africans buy over the counter, a
pain killing drug, dipyrone, made by a US
company, when this same drug has been
banned in the United States because it is
considered too dangerous for US citizens?
□
Why is the real cost of drugs in third world
countries often much higher than in the
industrialized world — sometimes as much as
20 times more than in Europe or the United
States?
Modern drugs have brought tremendous relief of
suffering around the world. Research-based
multinational pharmaceutical companies have made
some important contributions towards improved
health, discovering drugs to treat a wide range of
illnesses.
Yet thousands of people die every year in the third
world as a result of dangerous, ineffective or inap
propriate drugs, promoted by the pharmaceutical
industry.
PILL—FERING THE POOR, an Information/Action Pack
provides an overview of the problems related to drug
marketing in the third world. It contains articles on the need
for essential drugs, on the suffering wrought overseas by
some US made drugs, and on the high price the third world
poor have to pay for their medicines. The pack includes an
extensive annotated bibliography, basic facts and figures
about the transnational drug industry, and an outline of
suggestions for action on how you can get more involved in
helping to stop abuses.
To order PILL—FERING THE POOR send $4.00 (+ $1.50
for postage) to: Interfaith Center on Corporate Responsibility,
International Health Program, 475 Riverside Drive, Room 566
New York, NY 10115.
PILL—FERING THE POOR
Order Form: Please send me
pack(s) @ $4.00 each. I
enclose a check/money order, payable to ICCR for $
(Include postage. $1.50 domestic, $2.70 overseas surface and
$4.70 overseas airmail.) Bulk order rates available on request.
Name:
Address:
Date:
V i s u a 1 s
SI No
Theme
1.
The World
s
*
2.
Living in two Worlds
3.
Best Medicine
Dumping
Source
Suggested positionin-.;
UNICEF
After editorial
Church & Social
With CHD team * s
Justice (CSA)
article
Helping Health
With article
Worker Learn
Misuse/overuse of
medicines
4.
Rare Himalayan herb
Laxman cartoon
and multi-national
Health Care
Misuse/overuse of
pill for headache
Which way to
medicines
Go
5.
(mfc)
Vicious cycle of
medicine overuse
6. Expensive yes
7.
With article
Not to be taken
worthless
With medication as
Helping Health
a substitute for
Workers Learn
caring
Laxman Cartoon
Health Care
Which Way to Go
_(mfc) _____
With or before Drug
HAI News
June 1932
With "If there are no
misuse in our hospitals
side effects this must
be Argentina"
8.
Who says lomotil has
Social Audit
Before "Crazy world
no value
Handout
(first page
of tonics"
only)
•ss—ss.. a—ss—
—=—=—=:—s=-.s=—s=
COMMUNITY HEALTH CELL
47/1,(First Floor)St. Marks Hoad
BANGALORE -560 001
2
2
Source
Suggested positioning
Doctor, I have taken
Health Care
With "Crazy world of
the tonic
Which Way to
tonics"
Theme
S1_NO
9.
Go? (mfc)
10.
11.
person who eats
Health for the
With "Crazy world of
well does not need
Millions
tonics"
extra vitamins
April-June 1981
What is so new about
sugar-salt solution?
Health Care
Which Way to Go
A
With ’ORT - what are
the options"
(mfc)
12.
Judge with
The Herald
pharmacology book
Review, Oct 14,
. With legal education
1984
13.
Bad information means
Social Audit
bad medicine
(Health for the Alert—Consumer Action"
Millions, April-
With or before "Consumer
June 1981)
14.
Remember medicines
Helping Health
With "Towards a Rational
can kill
Worker Learn
therapeutics".
c^i
Voluntary Health Association of India
C-14, Community Centre,
_£4Q/.M4
LCD/a/24.2.84
Safdarjung Development Area.
New Delhi-110016
Telegrams ': VOLHEALTH
New Delhi-110016
T
668071
Telephones : 668Q72
Drug Information - for Drug Action
The material produced by various individuals is being listed in the
following pages. Most of it has been disseminated from VHAI for specific
purposes namely the drug workshops, the drug campaigns, visits of Drug
Campaigners eg. Dr Oils Hansson, Dr Zafrullah Chowdhury,etc.
Dissemination of the material from VHAI has in the past been limited
to individuals personally known and directly involved in 'Drug Action’. With
wider demand of drug material, the need to categorize, to give the date of
preparation, the Central handout Code number, and authorship has been felt.
The dates are important for certain handouts - eg. the Black Lists of the
brands of irrational and hazardous drugs prepared in August '82 based on
MIMS and CIMS enteries of that time which would have obviously subsequently
altered somewhat.
Specific questions related to particular handouts can be addressed to
the individual who has prepared them, many of whom are not VHAT staff.
List cf Drug related material produced by Medico Friends Circle,
Arogya Dakshata Mandal, Kerala Sahitya Sastra Parishad, Consumers Education
Research Centre, Centre for Education and Documentation, Central Government
Health Service, Lok Vigyan Sanghatna is being compiled likewise for the
Benefit of the newer organizations joining the Drug Action Network.
Dr Mira Shiva
Coordinator .
Low Cos>t 'Drugs & Rational Therapeutic
2
Date
K
VHAI and the Drugs Issue
Our Concern about drugs
2^ The Voluntary Health Association of
India - its activities and its role
in low cost drugs.
1-
2.
3.
4.
The Indian Drug Scene
The Drug Situation in India
& Study of Prevalent diseases .in India
sftd
g£ some essential drugs.
Community Health needs and Indias drug
Industry.
Drugging the Indian.
5.- Drugs-As if people mattered special
issue of Health for the Millions
-s
Bational Drug Therapy
xauioiiax Drug Therapy
tode
Hathi Committee's Essential Drug List
5.
Lists of Essential drugs- a comparison.
(Hathi Committee, WHO Sri Lanka, PGI,
Echo, Action Medior and Pune Workshop)
6.
Selection of appropriate analgesic and
antiinflammatory drugs. '
Jrgr ni^.tion
Dr Mira Shiva
1981
4.1.82
D-10.343
Mira Shiva
5.1.82
D-IO.343
Mira Shiva
VHAI
’
. VHAI
JO.8.82
Dr J S Mazumdar
L N Chakravorty and
S Chatterjee
FMRAI
5.12.85
Dr D Banerjee
Dept.of Social
Medicine JNU
Dr Shivanand Karkal
(Reproduced from -Debonair
1981)
'
'•
April-June g2
Guest editpr-Mira Shiv-?. -VHAI
April 82
D-10/341(d)
(reprinted 22.11.83)
Mira Shiva
WHO'
2.^- WHO List of essential drugs for Primary
Health Care.
3. Alphabetical list of Essential and.
complementary list.
4.
Author/Prepared by
>.
V™!
■
WHO
Xerox from WHO’s Te«hni- WHO
cal Report Serios 615
Xerox from Hathi Committee
Report.
. 1? 82
19.10.81
D-9/334(k)
Mira Shiva
VH1I
Dr Ullhas Jajoo
iiQjC
'
.3...
Date
1.
Dumped Drugs and Banning of Drugs
Banning of Drugs
26.8.82
Cede
Authcr/Prepared by
Organization
D-1O.34O
Mrs Chandra.. Kannapiran
VHAI
2. ^-Statement showing the categories of fixed
x dose combinations recommended by the sub
committee of the Drug Consultative Committee
for being weeded out.
5»
Categories of fixed dose combinations reconw^deu-to oe weeded out by the Technical
^Advisory Board(DTAB).
^•^"Scme instances of drug dumping
Drug Consultative CommitteeRecc.mmendations
11.8.82
A-4/119
Drug Controller of India
Nirraan ’Bhawan 25.5.82
Jan. 82
D-IO.343
Mira Shiva
VHAI
5-^ Information on some-o'f the unwanted drugs
baftjied ab
*ea<i
end duaped in the -third world
*
Jan. 82
D-IO.343
Mira" Shiva~
VHAI
6^-—Gazette Notification of the Drug Ban.
14.12.83
D-9/329(a)
Drug Controller of India
Nirman Bhavan, 23,July 83
5.1.82
19.8.82
D-lO/343
Dr Ullhas Jajoc
D-9/354(a.l^ Dr Mira Shiva
MFC
VE.il
Jan 82
£4.8.82
D-IO/342
P-9/334(s)
Dr A K Phadke
Dr Mira Shiva
MFC
VHAI
£5.e.82
25.8.82
D-9/534(h)
D-9/334(i)
Dr Kira Shiva
Dr Mira Shiva
VHAI
VHAI
2^.11.83
D-10/341(d)
Dr Mira Shiva
VHAI
Irrational and Hazardous Drugs
■ J-.-" Misuse of antibiotics
The Clicquincl Controversy
Scientific Scrutiny cf some over the counter
Drugs
4« Why amidopyrines must go
Hsing Tetracyclines for children and
Pregnant women
-6-Z^W^y not to prescribe anabolic steroids.
7*
Some painful facts about a painkill#?
called amidopyrine.
4...
1.
2.
3.
45.
6.
7
Bate
The Black Lists of Irrational and Hazardous Drugs
Brands containing anabolic steroids
25.8.82
Brands containing diphenoxylate(lomotil)
25.8.82
Brands containing Paediatric Tetracyclin
25.8.82
Brands containing analgin and phehacelin
26.8.82
Brands containing hydroxyquinolines(Clioquinals)25.8.82
■ Brands containing combinations of
i) Chloramphenical and streptomycin
August'82
ii) Penicillin and streptomycin
Brands containing irrational •oiibinations of
steroids and antiinflammatory agents
25.8.82
Female Hormones and Hormonal j^eg^gnty- Tests
1,.^ Are hormonal pregnancy tests safe?
Pear Sister letter for the E P-Campaign
11.2.82
References on Oestrogen-Progesterone tests for
•_ . .
Pregnancy
32
*
16.2
4^^"Bear Doctor/Chemist letter
11.2.82
"5. Review of supportive hormone therapy in
Obstetrics 5- 8.82
6.,--Brief Review of present situation of estrogen
‘ progestero.ne drug campaign
15.12.82
7. A letter seeking immediate ban on high dose
Estrogen Progesteron combination drugs
1.7.82
8. Warning Poster against hormonal Pregnancy tests
10.
Amniocentesis- for Sex determination
A world without women
Sex' determination tests- a technology which
will eliminate women
Author/Prepared by
B-1O-34O
B-1O-34O .
D-1O-34O
B-1O-54O
B-1O-34O
Pr Kira Shiva
Dr Kira Shiva
P-10-540
P-9/531(a)
2.
3.
. 9.^The case against E P Forte- a review of the
v
Controversy
Code
Organisation
VHAI
VHAI
II
u
11
If
II
II
II
II
P-10.544(g)
Dr C Sathyamala &
Dr Kirs Shiva
Jh: C Sathyamala
"
"
P-10.341(c)
P-10.344(c)
Dr C Sathyamala
' "
>9/331 (c)
P-10/341(c)
it
it
Dr Kira Shiva
Dr C Sathyamala
"
HCA-P.10
Dr C Sathyamala
"
Dr C Sathyamala with
Saheli Women’s group.
1.11.83
P-10/341(t)
Dr lira Shiva ’&
Aspi Mistry
7«9.82
P-10/342(b)
Dr Sathyamala &
Amrita Chachi
■
it
"
Seheli
Date
Bangladesh Drug Policy
.l./' In support of Bangladesh's Drug Policy
26.8.82
2. Drug Control Ordinance promulgated
}., The Bangladesh ban on hazardous and irrational
drugs, its review and present status.
21.10.82
4.
Bangladesh War
6.
Criteria for recommended withdrawal of
2.11.8}
products from Bangladesh market
Bangladesh: Finding the right prescription
Essential Drugs for the poor-a myth or reality
'82
1.
-2,
Towards Rational Drug Policy
People Oriented Drug Policy - Mozambique
Memorandum-demand for a Rational Drug
Policy for India.
2.11.8}
22.4.8}
Jan.'84
Organization
D-9/}}4/j:l)
Dr Mira Shiva
D-10/}41(d)
Dianna Melrose
Oxfam
(extract from working pap ar
medicines and the poor in
Bangladesh)
Claude Alvares
RUSTIC
with- VHAI
Extract from Expert Committee
report Bangladesh
%dy Chetiy
WPr on Want
Dr Zafrullah Chowdhury &
Dr Suzanne Chowdhury
Gcaosasthya
Kendra
Dr Mira Shiva
VHAI
- Part I and Part II
fj. Goncsasthya Kendra-Peoples Health Centre
10. Bangladesh Drug Policy(Special issue of
Health for the Millions)
Author/prepared by
Dr Mira Shiva
VHal
(Reprint from The Bangladesh Observer)
National Drug Policy for1 Bangladesh from
expert Committee report
5-
7.
‘.8.
Code
D-9/3}4(j)
D-10/}41(d)
B-2.98
VHAI
Health for the Millions
Editor:S.Srinivasan
VHAI
Dr lira Shiva
VHAI
On behalf of Drug Action Jetwork
...6...
1.
2.
3.
45.
6.
7.
;■
Rational Diarrhoea Care
Causes of Diarrhoea
■
Diarrhoea and significance of the problem '
Diarrhoea and malnutrition
Ifermigenent of acute diarrhoea
Low Cost drugs managing diarrhoea
Drugs in the treatment of Diarrhoea
Cost Effectiveness of the different options
available and situations in which they may
be appropriate.
Pate
13.8.82
11.8.82
11.8.82
6.8.82
6.8.82
11.8.82
~>'
Code
Author/Prepared by
D-9/334(f)
D-9/334(d)
D-9/334(e)
D-9/534(b)
D-9/334(n)
D-9/334(c)
Dr Mira Saliva
D-9/334(a)
liable Reproduced from
Committee on International
Nutrition Programmes National
academy Press, Washington.
D-9/334U-2)
Dr Mira Shiva
Organization
II .
II
• lu
ll
It
8.
Antidiarrhceals-their misuse
Focus on clicquinols eg. Mexafcrm enteroviofcrn
and their side effect SMON
7-4.83
9. VHAI's role in diarrhoea Care
June 83.
U^/Special issue of Health for the Millions on
Dec.>83
Diarrhoea.
Drug Industry and Consumer Action
’ 5.1.82
1. 10 Comiranduients of the Drug Companies •
5.1.82
2. Antidotes to Drug Industry
3. ’o’hat consumers can do-Social action by
23.2.82
Consumers to deal with the drug problem
Drug Codes
/iow Cost Drugs and Rational Drug Therapy
l.
International Codes and you
Dec.81
Dec.81
2j/''IFPl',iA Code of Pharmaceutical marketing
Practices
3 ./International Codes and you (HAI reprint)
Dec.85
Dr lira Shiva &
Aspi Mistry
D-10.345
D-10:345
Augustine J Velliith
D-10:340
Dr lira Shiva
D-10/343
D-1O:343
Compiled by lira Shiva
"
IFPMA Code reproduced from
HAI document
HAI
HAI reprint
ill
Pate
1.
2.
Towards Rational Drag Economy
General administration of the Pharmacy
Medicines Procurement and stock Control
Purchase of Medicines
3.
Lew Cost Medicine Project'LOCOMP'
21.12.82
Code
D-9-556
'LOCOST..Project'-the Gujarat initiative in
Bulk Purchase
5. Vffi VHA Genfcral Drug Marketing Unit-Initiative . •
in Bulk Purchase
6. Experience.'of a 'Hospital Pharmacy'
Author/Prepared by
Organisation
Mr Alan Grammer. MPS(GB)
CMAI
NotesPlease contact
Mr Alan Crammer ClL'iI
Holdsworth Memorial Hospital
ity sore, Karnataka, for these
as well as other material or
Pharmacy management.
Dr Ashwin Patel' &
S Srinivasan
VH/I
4-
Dr Ashwin Patel
...
UB VHA
Fr Mullers Hospital ■
Mangalcre(study by Mr 2d Kaebert
VEaI
7.
.
Tablet Mission Industry B.eng^rpct-Pornulation
of Essential Drags
Lev,- Cost Altem.ativ.wjHone remedies ond their rcle in reducing
dependence cn institutionalized medicine
4.1.82
’lucerculosis
11.6.82
Rational TB Care- a priority
11.6.82
VHAI's rcle in TB Care
Seeking information regarding anti TB drag
25.5.82
shortages.
Drags - Legal Action
1. In the Supreme Court of India -Civil writ
7-4.83
Petition No 3492 of 1985, Under Article 32
of the Constitution of India
2. Amendment of the above public writ petition 7.11.83
3. A note on the legal aspects of health issues
and VHAl's intervention
Nov.83
.J?.
3.
study by Mr S' Srinivasan VHAI
(contact 'sources directly)
D PjPandey
D-10:343-
ItlT
D-10
D-10
Dr Mira Shiva
"l
ft
Dr Vincent Panikulangara
II
Mr Aspi Mistry
Concern for
Correct Medicine
VHAI
u
■>
Public Litigation
Centro,Co chin.
II
VH..I
...e...
Date
1.
2.
3-
4.
5•
6.
7-
Workshop Reports
Report of Drug Workshop I
Workshop on Drugs Issues- seeking feasible
alternatives - Pune 8-10th Jan.82
Summary of the above report
Report of Drug Workshop II
Jaipur August 3O-51st, 1982
’Hazardous and irrational Drags'
Drug 'Workshop follow up Information sharing
Report of the Drug sub group at the National
Health Policy Seminar
Report ci Rational Drug Policy discussion
Detween Drug Activists and Policy Kiskers
Drug Action Network
(.Newsletter I
Code
■
Authen/Prepared by
Organization
16.2.82
24.2.82
D-lO/543
D-lO/543
7.10.82
D-1O/545(R11)
11
it
D-10.344
11
t!
4.2. 85
April 83
Dr Mira Shiva
11
THAI
ti
Mr J S Mazumdar &
Dr Mira Shiva
FMRAI
Jan. 84
Dr. N N Mahrotra
nistads ' i
Nev. 8 5
Lot; Cost Drugs Cell
‘-Newsletter II
25.I.84
For Drug Action Networkers ffiily
Minutes of the -ioating with Drug Controller of
Indi'
Nov. 85
"
L«puty Drug Controller
i
of Delhi
I"
"
"
Mr Vasant Sathe,Minister
of Chemicals & Fertilizers 5»1-S4
Meeting of the Drug fiction Networkers at VHAI
1
in Delhi
Jan.84
"
"
"
at CINI Calcutta
50.6.84
Dr Kira Shiv?. f:
■.ispi Kistry
vhai
VHAI
..
ACTION SHEET
WHAT YOU CAN DO
OBJECTIVES:
*
To draw attention to the problem of Lomotil as
outlined in the Social Audit leaflet;
To demonstrate that Lomotit illustrates the wider
issues of activities of drug TNCs in developing
countries.
KEY GROUPS:
*
The medical and other health care professionals;
Your drug and health authorities;;
Other social action groups, particularly those
with special interest in health and development
issues.
METHODS
:
Some suggestions *
Write to the medical and pharmaceutical associa
tions or to the editors of their newsletters and
journals;
Write to the editors of major newspapers;
Call for a press conference.
WHAT WE HAVE DONE HERE
Included in this pack for you:
a
The Lomotil leaflet by Social Audit.
way you can.
Re-print it.
Use it any
Translate it to the
language best suited to your needs.
Or more (in
English only) can be obtained from the HAI
Clearinghouse - US? 6/=- per 20, including airmail
postage);
•
A sample press statement.
If you like, you can
use it as a basis for your letters to the press,
medical and health care groups, etc.
(S.1/12/81)
Lomotil Action Pack
HA I
NEWS No.
2
December 1981
AN ENEMA FOR LOMOTIL ?
THE
STORY
SO
FAR.■■■
In May 1981 a British action research group released a 4-page leaflet
with the words "WHO says LOMOTIL has NO VALUE" across the front page.
At
a glance, it looks like one of the millions of promotional leaflets the
multinational drug companies send each year to doctors all over the world.
It warns doctors by quoting numerous authoritative
But it is different.
medical sources that Lomotil "no value".
(WHO, 1976.)
Lomotil used in the treatment of diarrhoea in children is dangerous.
the US, it is contraindicated for children under two years.
In
Yet as the
leaflet points out, Lomotil is indicated for children of 3 months old in
Hong Kong, Thailand and the Philippines.
Following the release of Social Audit's Lomotil leaflet, a US based drug
multinational launched a counter-attack.
In a statement published in
Scrip (June 3, p. 4) they claimed that the leaflet "does not present a
balanced evaluation of the benefits and risks of Lomotil (diphenyoxlate),
nor
does it accurately portray the manner in which the product is
marketed by Searle.
The statement went on to say that "...standard
medical information has been developed by Searle for all its products
worldwide..." and that Searle supplies up-to-date information to doctors
and other health care professionals "...regardless of whether required by
local laws or government health authorities."
It all sounds very slick
except that in September, at a meeting in London, Searle told Social Audit
that it was reviewing its labelling to indicate that Lomotil was not
recommended for use by children under two-years old anywhere.
A victory, BUT, the issue remains - that Lomotil has no value for
treatment of diarrhoeal diseases in developing countries.
a costlier choice; at worst, a fatal mistake.
drug.
At best, it is
It is an inappropriate
Should not a product like this be demarketed?
*
WHAT MORE
CAN
BE
DONE?
Turn overleaf for some suggestions.
*
"Demarketing refers to corporate decisions - taken because of manage
ment initiative, public pressure, or government regulation - to reduce
or stop completely efforts to sell a particular product because of
risks to the health, safety, or welfare of users." (From 'Demarketing
Infant Formula: Consumer Products in the Developing World' by
James E Post and Edward Baer, in Journal of Contemporary Business,
Vol. 7, No. 4.
Widening H°rizons_£_on_Drug_issues
JJ-
Periodicals
1. Pune Journal of Continuing Health Education
Presents scientific information and opinion on drugs and health
issues to stimulate thought and further investigation.
Annual subscription Rs,10,00 or a five year subscription for Rs.45.00
from Arogya Dakshata Mandal, 1913, Sadashiv Peth, Pune 411030
2.
Drug Bulletin
An informative monthly giving unbiased technical information
on drugs and therapeutics.
Annual subscription ^s.10.00 from Dr VS Mathur, Professor,
Depart ent of Pharmacology and Editor, Drugs Bulletin, PGI of
Medical Education and Research, Chandigarh 160012.
3.
medico friend circle bulletin
A monthly which discusses issues regarding health problems, the
health care system, medical education, drug issues etc., from
the point of view of relevance to the needs of the majority in our
country.
Annual subscription Rs.15.00
Write to Convenor, medico friend circle, 326, V Main I Block,
Korumangala, Bangalore 560034.
4.
HAI News
A very informative bimonthly of the Health Action International
(HAI), covering world drug news of special relevance for the
third world.
is an informal network of health consumer
and development oriented associationsand professionals
concerned with health and pharmaceutical issues, particularly thos'
that adversely affect the poor.
j
2
Annual subscription : US$10.00 from HAI Clearinghouse,
regional office for Asia and the Pacific, International
Organization of Consumer Unions (I0CU), PO Box 1045,
Penang, Malaysia.
—
A number of journals have brought out special issues on
drugs. These may be available
on request
for back issues.
1. Contacts from Christian Medical Commission,
World Council of Churches, 150 route de Ferney,
1211 Geneva 20, Switzerland or VHAI, Nev/ Delhi.
a. August 1981 No.63s ’Getting Essential Drugs
to the People
*
with a model list of essential
drugs.
b. June 1983, No.73s ' Strengthening^and r-gulating
the supply, distribution and production of
basic pharmaceutical products’.
2. Health for the Millions
From Publications Department, Voluntary Health
Association of India, '"-14, Community Centre,
SDA, New Delhi 110016.
a.
Medicines as if people mattered - April-June 1981
b. Special Issues on diarrhoea and tuberculosis
3.
The Journal of the Christian Medical Association
of India
From: ^’he CMAI Office, Christian Council Lodge,
Nagpur 1, Maharashtra.
Sept 1983, Vol LX, No.9, Drugs—Fact, fallacy and fraud.
3
4.
World Healths The magazine of the World Health
Organization, Avenue Appia, 1211 Geneva 27, Switzerland.
July 1984,
Essential drugs for the World.
WIDENING HORIZONS - on DRUG ISSUES
Books
1. Hath! Committee: Report of the Committee on the Drugs and
Pharmaceutical industry.
Ministry of Petroleum and Chemicals, Govt of India,
April 1975, Rs.17.00.
The essential drug list suggested here could
provide the foundation for a demand for a
Rational National Drug Policy.
2. Health for All - an Alternative Strategy
ICSSR & ICMR, 1981, Rs.18.00 Available from VHAI.
In focussing on a comprehensive national policy of health and
a new operational strategy, the report is intended to be
a basic document to initiate a nation wide debate on the
subject as well as positive action towards certain radical
changes to correct the present imbalances in our health
caresystem. Has a very comprehensive chapter on drugs and
pharmaceuticals.
3.
Aspects of the Drug Industry in India.
Mukarram Bhagat, Feb 1982, Rs.19.00
From Centre for Education and Documentation (CED),
3,
4.
Suleman Chambers, Battery Street, Bombay.
Insult or Injury
Charles Medawar, 1980, Rs.18.00, 139 p.
Social Audit, England. Available from : Indian Social Institute
Lodi Road, New Delhi 110003. Highlights marketing and sales
of British drugs and food products. Illustrated easy reading.
.2
2
5.
Health Care Which Way to Go
Medico Friend Circle Anthology II, 1982,
Rs.10.00
from : medico friend circle office, 326, 5th Main, I Block
Koramangala, Bangalore 560034
Raises relevant issues regarding peoples health. Questions why is
there a lack of political will to solve pressing health problems
of the country. How detrimental is the alliance between
medical professionals and the drug industry to people’s health.
6.
Under the lens: health and medicine
III Anthology of medico friend circle is due shortly and will
be available from VHAI and mfc office (above).
7.
Kurji Holy Family Hospital: Formulary and Therapeutic Guide.
January 1983, Rs.12.00
Available from VHAI.
It is the result of the accumulated experience of
senior medical staff of the hospital over the last 10 years. It gives
a comprehensive list of drugs to treat 98% of hospital admissions it also gives the generic name, dosage, indications, contraindications
and main side effects in the same page. Information about comparative
cost of treatment is also provided.
8.
Drugs and the Third World
Anil Agarwal, 1978, $5.00
From Earthscan, 10 Percy Street, London W1 PO DR
A very comprehensive overview of the drug situation in the third
world and the problems and causes.
3
3
9.
Prescription for change
Health Action Internationals guide to rational health projects,
Virginia Beardshaw, November 1983, 85pp
US$10.00
from Health Action International Clearing House
PO Box 1045, Penang, Malaysia.
Gives more than 40 ideas for action research projects on drugs s
- a summary of the main elements of the rational health issues
and suggestions about how to campaign on it;
- advice on how to talk to drug companies and the powers that be
- a reference section that lists the main materials you need to
research on drugs.
10.
Pill-fering the poor: Drugs and the third world.
An information/action pack on drugs and the third world from
Interfaith Center on Corporate Responsibility, International
Health Programme, 475 Riverside Drive, Room 566, New York, NY 10115.
US$4.00 plus postage surface mail $2.70/air mail $4.70.
It provides an overview of the problems related to drug marketing
in the third world. It contains articles on the need for essential
drugs, on the suffering wrought overseas by some US made drugs
and on the high price the third world poor have to pay for their
medicines, ^his package includes an extensive annotated bibliography
basic facts and figures about the transnational drug industry and an
outline of suggestions for action on how you can get more involved in
helping to stop abuses.
11.
Therapeutic guidelines: A manual to assist in the rational
purchase and prescription of drugs.
Upunda, Yudkin et al 1981, pp. 166, Rs.35.00 African Medical and
Research Foundation. Available from VHAI.
4
4
An excellent guideline for rational therapeutics, giving special
emphasis on drug cost as criteria for choice of drug diagramatico
format.
12.
Managcient schedules for dispensaries: A manual for rural health
workers
Peter Petit,
19S3,
Rs.35.00
African Medical and Research Foundation..
Available from VHAI.
13.
44 problem drugs: a consumer action and resources kit on
pharmaceuticals.
IOCU, May 1981.
Available from HAI Clearing House (see 9)
Gives information about 44 problem drugs, 'ftlong with articles
by some of the pleading drug compaigners.
14.
A number of interesting papers to keep you upto date
about the drug issue is availabb from Low Cost Drugs and
Therapeutics Cell, VHAI, C-14, Community Centre, Safdarjung
Development Area, New Delhi 110016.
(write to them for a list)
-Sc^iPT
----------AUDIO -/VISUAL ON THE
CGzVri'/yj:'J
" DPZdG POLICY OF INDIA "
a ,’ '
(First Flocr.I...
•' Q.
>t3
BAftlGAtOAE- 560001
produced
bangalore
BY CENTRE for non-FORM. L & CONTINUING EDUCATION
560 001
“
Slide No
visual
Audio
r»
';'G°
: -'C l-'3WVS
PB°ys^WJSUooHJSJI;j).l/zfc
033
AllfJDbWOO
1.
2.
Sun rise
A villager ploughing
in the field
Music
Music
3.
Paddy fields along
the road side
Villages ... India is the land of
villages... housing 80% of the people
of our country. India has 7i lakh
villages.
4.
A woman working in the
paddy field
Mahatma Gandhi said,’ Indies hopes lie
in the villages. Villages have been
an inspiration to many a poet and seer.
5.
A boy and a girl
looking at us
Yet this 80% of the population are
struggling to find their means for
their existence.
6.
Barli village
name board
Barli is one such village hamlbt in
Karnataka.
7.
Huts
Consisting of only the scheduled castes
.. the deprived section of the people.
8.
People washing
their vessels
The awakening dawn is disturbed by
•tl-ie women doing their daily routine
of preparing their meals.
9.
Children tending
the goats
the children tending the cattle and
sheep of the landlord.
10.
Ramakka preparing
ragi balls
Ramakka too gets ready the ragi balls St
for the family before she goes to the
landlord’s field for work.
11.
Sidhi, Linga and
Veerabadrappa having
meals
Ramakka family is a happy family ...
they may have lots of trouble when
money is concerned. Yet hardly there
is quarrel in the family.
12s
Veerabadrappa
going to vzork
Veerabadrappa goes to vzork in the
morning at a quarry 2 kins away while
Ramakka vzorks for the landlord.
I?
Sidhi looking
after Linga
Their daughter Sidhi, a 5 year old
would be the second mother of the
child Linga..the son of the family..
the light of the future., the apple of
their eye..
14.
Sidhi and Linga
having food
Sidhi loves to play with her brother
Linga ... she would carry him around..
feed him and put him to sleep singing
songs.
15.
Dev; trickling down
That day it was an unusual cold morning
the dew was trickling down the palms of
the hut...
16.
Linga passing loose
motion
to her surprise..Linga was passing
loose motion .. she cleaned the first
time ... a second time...
but the motion went on. That day -the
child was uncontrolable. He wept
badly.
17.
18.
,,
■she did not know what to do... the chile
would not eat., she hoped that if her
mother comes and breast-feeds the
child that his hunger would be appeased
19.
Sidhi looking for hei'
mother
she waited for her mother... and the
waiting was too long for her.
20.
Ramakka coming
As soon as Ramakka arrived she was
apprehensive..because of the way
Sidhi looking forward to her coming.
21.
Ramakka giving money
to Sidhi
on reaching inside she discovered her
plight and the trouble her dear child
was going through.. She immediately
reached for the end of the saree and
untied the only saving she had.. lOpaise
and gave it to Sidhi to bring the
powder for diarrhoea.
22.
Sidhi coming with the
powder
Sidhi went to the local man and brought
the powder
23 •
-Ramakka mixing
Ramakka mixed the powder with mill? and
fed it to the child. The condition of i
the child remained ths unchanged.
24.
Linga lying near the
harican lamp
she looked through the night keeping
■the vigil... the child remained -the
same.
25.
Ramakka with local dai
Next morning she called on the local
dai Yellamma, the old woman of this
place... when she narrated her the story
of tiie child, Yellamma went round,
pulled a few herbs and said,’Grind this
herbs, pull out the juice and feed it
to the child and report it to me in the
evening.
26. Ramakka working in
the paddy field
Rammaka went dutifully and administered
the medicine. She was already late for
the vzosk that day... the food was not
ready yet. She advised Sidhi to take a
special care of the child and informed
her if anyting serious happens please let
me know and left for work.
27. Ramakka coming back
home
In the evening she hurridiy coming.
anxious about the child and yet hopeful
that the situation would have changed.
28. Linga passing loose
motion
on arrival she found the situation had
not changed.
29. Local dai and
Ramakka
and she rushed to the local dai again
and she advised her to go to temple.
30. Temple
Ramakka went to the local Gangamma
temple and cried out
31. Ramakka crying
’Here is your child Gangamma...open your
eye and take her sickness away... I will
cut a cock and make pooja for you...
please cure him of the malady. Sainakka
wept at the Goddesses feet.
32. Sunrise
Next morming the situation being
unchanged she mused about the wonder
of the modern medicine and asked her
husband to borrow money and rushed to
Bethamangala 5km from this village.
33. Doctor coming
and brought the Doctor Chidambara.
The doctor arrived with wonder medicine
infection...
34. Doctor injecting
He dutifully administered an injection
35. Collecting rupees
collected Rs 7/- and asked Veerabadrappa
to come and collect the liquid.
36. Linga lying and
Sidhi sitting
Indeed the medinine woEked. The baby
did not have loose motion for some time
and the child slept for a little while.
Ramakka was relieved.
37. Linga again passing
loose motion
Yet her satisfaction was short lined.
The child again passed loose motion
and it was unxisxx unabaited. Nov/ the
sense of danger was felt by Ramakka.
38. Ramakka/ and Sidhi
sitting at the door
She had no other go but to go to KGF
big hospital 20km from her village. She
did not have sufficient money nor the
courage to go so far. She never visited
the town.
39. Ramakka getting money
Yet she pleaded with her husband to get
some money from the land lord, to be
paid back after the harvest. She got
the money and ...
40. Ramakka walking
now she wished good-bye and went across
+h<=> « mnrv marshv redd ’ fields
Bin
41. Ramakka coming out of
field
Music
42. Ramakka crossing the
stream
she had to cross streams before she
could arrive in Bethamangala.
43. Bus going
to catch bus to KGF
44. KGF Hospital gate &
hoarding
on arrival at KGF she had to look
around for the hospital, requesting
people hess and there on the way
45. Hospital gates closed/
Ramakkqiooking at it
on arrival at the hospital the sign
board was prohibiting her to meet
the doctor
*
46. Ramakka pleading with
the gate-keeper
she pleaded with the gate-keeper to
let her in. The gate-keeper shouted
’Can’t you see the board?Come tomorrow.
This is not your home to come when
and where you like. Sir, she pleaded •
My baby is very sick. I can not wait
for tomorrow. I have not informed
my people at home. I am coming from
a long distance, please have some pity
and allow me to see the doctor.
"No madam, the rule for everyone is
the same. You should have known about
the timings of the hospital.
She requested again and...
47. Ramakka. giving money
He answered OK. You better pay me
Rs 2/- and I can let you in.
48. Ramaltka with doctor
She entered and met the doctor after
some time. The doctor was too tired
to attend to the patient. Looking at
the condition of the child dehydrated
so long, he shouted at her.
"Don’t you know how to take care of the
child? You people have many children
and yet you' do not know how to take care
of them. Why do you bring the child
at the last moment.
49. Doctor giving the
prescription
Then he furiously wrote out a long
prescription. He requested IV fluids
to be administered and other medicines
for the baby to stop the diarrhoea.
50. Pharmacy
She carried thigfjrescription to the
pharmacy and asked for the medicine, The
pharmacist billed her Rs 60/-. She had
not that much of money. She had spent
enough for the bus, at the gates and at
the counter. She could not buy
all the medicine. •
51. Ramakka coming through
the paddy field
She bought just a few tablets and
went back, picked the baby and was
on her way back home. She did not
meet the doctor with IV fluids as
she had asked her to. Because
she feared another bout of scolding
and another bill for administerin g
the big injection.
52. Ramakka and Linga
(sillohoutte)
on her way back home she discovered
her baby to be limp. By thes time
she reached home the baby&s body
was cold. She screamed on realising
that her baby was dead.
(music)
53. Villagers running to
Ramakka’s hut
The people fi‘om the village came
running to hear what had happened
and sadness was writ large on the
face of everyone.
(music)
54. Villagers Idiking
into 'the hut
The darling of the village was
no more.
After the burial, the whole house
fox- Ramakka was empty.
55. Ramakka cooking alone
There was no cry of the child
whilb at cooking.
56. Siddhi
For Sidhi, she no longer had her
younger brother to cuddle and put
to sleep.
57. Ramakka sitting near
the haricane sai lamp
The nights were no longer
troublesome, nor was it necessary
to light the lamp at evening.
^wwgrfcyy
The light of the house extinguished.
There is no longer joy pervading
the house. Who can fill this vaccum?
(music)
58. Cemetry
on whom shall we place the
responsibility of the child’s death?
IKjRv'
pcVjCviK ;
/
59
cartoon(doctor in the
crowd)
shall we blame the doctors?
There is only one doctor for 14
thousand rural population.
Doctors are trained in big hospital
atmosphere, therefore they feel
inadequate to work in villages.'
60
Ramalcka with doctor
when the doctor spoke to Ramalcka
Ramakka could hardly answer because
for her doctors are big people, they
cannot be countered or counter
answered-they are all lenowing and
omni potent. Indded the doctor’s
culture and the culture of the people
are very different.
61
cartoon( a steth lying
on a heap of rupees)
one can become a doctor only if he is
rich and can afford good money.
How
will then a doctor understand
that rural poor cannot even afford
food.
62
Doctor with Ramakka
The baby could have been saved even
at the last minute-but the long
list of the doctor did the trick.
63
A prescription with lots of
drugs reccomended
While prescribing the drugsspecially to the poor, the doctors
need to look into maximum effeciency
better safety and minimum cost.
64
cartoon
this is a rational drug use.
65
Hospital
can we blame the hospitals?
66
Hospital varanda
It’s set up-it’s distance...
F7
Ramalcka walking
People like Ramalcka cannot afford to
go to cities.
68
sofisticated equipments
operation theatre
It is only in cities that hospitals
are furnished with sofisticated
modem equipment.
70
Budget or cartomn or
statistics
71
Injections
72
Pharmacy
A large percentage of government
health budget goes in putting up
hospitals and maintaining them.
villages which house 8O>5 of the
population get only 40 percent of the
budget allocation.77;4of the villagers
have never used the primary health
centre. How can each centre serve
90 thousand population with two
doctors, minimum amenities and drugs?
can we blame the drug industry?
It’s innumarable verities of drugs?
30,000 fo rmulations...
75
drug packets
music
74
Advertisement
(Babies food)
It’s profit motive...
75
close-up of a women
and the aggressive business
approach...
76
essential drug list
The world healthe organisation
says only with 200 essential drugs
and 45 complimentary drugs all the
deseases can be cured. In India the
I-Iathi commission says we need only
116 essential drugs to cover all
the illnesses.
77
Gifts to the doctors
plenty of money is spent for adver
tisement, propaganda and gifts to
doctors by the durg companies-for
unessential drugs. Here is the
medical representative...
78
medical rep being interviewed
What are your basic job funtion?
15to start with, at t.-e very beginin,.
of the day we plan our work in orde
to achieve our objective-our
objective is to get the maximum
sales...and to get the sales we
have to plan cur day that what is
the people I am going to see during
the day, who can fulfil my require
ment or my achievement for the day.
And after once we leave the house,
we go on planning on our 'way, or
waiting near the particular doctor’ >
chamber, we think in what best way
we can convince the doctor so that
he prescribes maximum for our compar
products for which I am working or
for products specifically I have gon
I may probably talk to ham about 5 c
6 products at a time but my interest
may be to get support atleast for
2 or 3 products.
79
Tonics
Many die because there are not many
essential drugs available or produce
in sufficient quantities in India.
25%
drugs produced are tonics
which do not help in any way the
health of the people.
80
Art work
(statistic circlg)
20% are antibiotics, but only 1.4%
drugs are for IB and 1.3%’ for lapros-
81
TB patients
of the 20 million, Tb patients in th
world, 10 million are in India of
them 500 thousand die every, year.
82
Laprody patients
Of them 10 million leprosy patients
in the world 4 million are from India
S3
Blind people
out of 9 million blind 5 million
are blind because
of the non-availability of treatment
and drugs....
25,000 children go blind every year
because of vitamin A scarcity.
84
Dr.Kulasekaran
Dr.Kulasekaran says, the life of the
baby could have been saved if the
mother administered boiled water,
a pinch of salt and a scoop of suger
mixed, time and again.
<35
a child affected by
diarrehea
Every year 1.5 million die of diarrehea
70% of them because of dehydration...
85
cementry
56% of deaths are avoidable, by the
intervention of medicine, But there
are many more siddis who die unnoticed.
should vze allow them to die?
dont vze have a part in avoiding these
murders?
87
Linga with his mother
music
88
Linga with his grand father
mucic
89
Siddi locking after linga
music
90
Ramakka and siddi sitting
at the door
music
91
acknowledgements
music
92
sound and voice
music
93
photography
music
94
script and direction
music
95
produced by
music
THE END
BITTER PILLS.
Diana Melrose
Oxfam. Some copies of this book
are available with us. The ori
ginal price is Rs 100. However
it can be made available at a
discount for those involved in
drug action.
THE CASE AGAINST E P FORTE - A
Review of the Controversy.
Cyclostyled note prepared by
Mira Shiva and Aspi Mistry.
Review of the campaign and
latest views of Ob and Gynae
experts on the use of these
drugs in secondary amenorrhoea.
HEALTH FOR THE MILLIONS - SPECIAL
ISSUE ON DIARRHOEAWill be out in November. This
issue has been designed and
written by Mira Shiva and Aspi
Mistry as the contribution of
the Low Cost Drugs and Rational
Therapeutics Cell to the Anti
Diarrhoea Campaign.
SUPREME COURT WRIT PETITION
NO. 3492 OF 1983
Petition filed by Vincent
Panikulangara on hazardous and
irrational drugs. Available on
request.
ANY DOCTOR
Will tell
You MAT if YOU ARE TENSE
OR OiSTRAUORF THERE IS
ONE SUKE WAY TO FEEL
NATIONAL HEALTH POLICY SEMINARA REPORT
VHAI
This is a fairly detailed report
of a one day seminar held in
Delhi on this topic. The objective
was to focus the attention of the
authorities on the implementation
aspect of the policy document.
It emphasised the role that the
voluntary health sector should
be playing in policy making and
implementation. At the seminar,
one of the sub-groups had con
centrated on drug related issues.
The conclusions of the sub-groups
are part of the report and the
report of the drug sub-group has
also appeared in the MFC bulletin.
THE WAR AGAINST BANGLADESH
Claude Alvares. Published by
RUSTIC in association with VHAI.
Documents and background material
related to the ban on 1707 harmful
and worthless drugs in Bangladesh;
the new drug policy and events
thereafter.(See also "Bangladesh"
issue of Health for the Millions)
>|HfV ME WITH YouC
HEHD |U YOUK UIRYEK 0ISH.<
TVUS IS HUSHED UY, OF
COURSc 6SCAUS6 it would
CCHi’lETEU' RUihJ ME
DRUG CCHYRNIES.
toutbwj : "
rtMLin "
other activities
In August Mira Shiva and Tina
DeSa conducted a 5 day workshop
in school health for teachers,
headmasters, wardens, community
health coordinators. The emphasis
was on helping school children
develop self-reliance in health
care and guiding them through
their teachers to participate
in health work. We see this as
an important aspect of building
a peoples health movement.
'k The Kerala Sastra Sahithya
Parishad (KSSP) has organised
2 jathas (science and cultural
march) starting on 2 Oct and
concluding on 7 November.During
57 day long march the jathas
will give performances at about
500 centres. The object of the
is1 to translate the slogan
"Science for Social Revolution"
into a practical programme of
action. The 'themes of various
performances in the local lang
uages are based on contemporary
social problems and unscientific
approaches to various issues e.g.
"War : the war against unscientific
practices in the field of the
drug industry".
#-In November Mira Shiva will be
conducting a workshop in Patna
on 1 clinical assessment * . The
participants will be middle level
field workers working in tribal
areas where people do not have
easy access to any other health
facilities. This workshop is int
ended to upgrade diagnostic and
therapeutic skills along the lines
of "low cost drugs and rational
therapeutics." The emphasis would
be on striking a balance between
preventive and curative health
care.
^•Aspi Mistry has also been
working with a citizens group
of Dehradun, "Friends of the
Doon" who are organising against
limestone quarrying in the
Mussoorie hills. The quarrying
activity has been gradually
destroying the water resource
base of the area and leading
to land degradation. Through
intervention in a public interest
petition filed by the Rural
Litigation and Entitlement Kendra,
Dehradun, an interim stay order
against the quarrying has been
obtained from the Supreme Court.
We feel the need for health
groups to be involved in health
related problems.like environmental
problems, misuse of pesticides,
lathyrism, etc.It will be recalled
that such inter-disciplinary action
was the topic of discussion in
April when Mr Etsuro Totsuka
( the Japanese lawyer who had
successfully fought for SMON
victims in the Tokyo court) had
met a number of health, legal aid,
and consumer action groups. A note
on the legal aspects of health
issues has been prepared by Aspi.
Although it has been prepared with
VHAI in mind it is equally applicable
to any other health or activist
group. ( Available on request )
■frow,
II
B3 7.
for 2-5 hours and drying it
detoxifies it. This 'health
education' for those with severe
time and fuel constraints is
meaningless; moreover the res
ponsibility is sought to be
shifted from the state and the
landlord to the labourer.In the
light of Dr Ahmad's study we
seriously question the plans of
the MP Govt to set up two par
boiling plants. The only solution
is to completely ban the cult
ivation of khesari dal in the
country.
The World Health Organization says:
it A number of medicines, which are of
no value and are even dangerous, are often given
to treat diarrhoea. Money and time are
wasted in their use. WSo...
who says lomotil
has NO VALUE?
LOMOTIL (diphenoxylate/atropine) is made by the US
multinational drug company, G.D. Searle; and
promoted to physicians all over the world in terms
such as “established success”, "good tolerance”,
“excellent value” and “ideal for every situation". This
leaflet — prepared and published by Social Audit Ltd.,
and friends
*
— calls into question these claims.
LOMOTIL may be of value in giving symptomatic relief
for non-specific “travellers’ diarrhoea” in adults. But
experts say Lomotil — and other products like it2 —
have iittie or no place in the treatment of young
children — especially in developing countries, where
infective diarrhoeas are the major cause of death in
children aged under three.' Lomotil’s limitations
include:
QQ 0 01)0 OQOQOiJ
Lomotil
StARLE
POTENTIAL DANGERS
“Lomotil, which is widely used in the
treatment of diarrhoea in the paediatric age
group, is dangerous and unwarranted . . .
we urge that all physicians treating infants
and children avoid the potentially dangerous
use of Lomotil for the treatment of
diarrhoea.”
(Clinical Notes [1974])3
“Lomotil can relieve the symptoms of acute
gastroenteritis in children, but it can also
mask the signs of dehydration and cause
fatal toxic reactions . . . use of this
combination for treatment of diarrhoea in
children is hazardous.”
(The Medical Letter [1980])“
“Lomotil is a dangerous combination of
drugs contra-indicated for children under 2
years of age and probably never indicated in
childhood diarrhoea.”
(Pediatrics [1980])5
QUESTIONABLE USEFULNESS
“The use of Lomotil as an antidiarrhoeal
agent in children is difficult to justify . . . we
doubt if it has any place in the treatment of
diarrhoea in children.”
(Arch, of Dis. in Child. [1979])6
“A diarrhoea that needs 4 such tablets to be
cured would probably have been cured
without it too. A more prolonged diarrhoea
needs proper investigation and specific
therapy rather than a blindly harmful
stopcock.”
(Leb. Med. J. [1974])7
ECONOMIC WASTE
Lomotil costs up to 25 times more than other
widely-used symptomatic treatments for
diarrhoea.
(AMREF[1980])a
1
“Lomotil (no value).” (WHO [1976])'
Lomotil
HOW USEFUL . . .
“The management of acute diarrhoea in
childhood is essentially dietary . . .
Unnecessary drug prescription for these
chldren should be vigorously opposed.”
(The Lancet [1976])®
. . . Against Dehydration?
“The cause of death in diarrhoea is
DEHYDRATION . . . Diarrhoea is the most
common cause of death in children under
three years of age. . .”
(WHO [1976])’
LOMOTIL is not a treatment for dehydration. It
may reduce the loss of fluid from the body but
can also allow fluids to accumulate in the
paralysed gut.
“LOMOTIL can mask fluid losses without
diminishing them, and the drug itself can
cause fatal adverse effects . . . there is no
evidence that reduced motility diminishes
the loss of fluid and electrolytes into the
lumen of an inflamed intestine.”
(The Medical Letter [1975])“
The accumulation of the body’s vital fluids within
the intestine can be just as dangerous as the
more obvious dehydration:
“In diarrhoea, life-threatening situations
are reached ... so long as fluid and
electrolytes are excessively lost into the
lumen whether they are expelled from the
lumen to the outside of the body or not. . .”
(J. of Singapore Ped. Soc. [1976])'0
Small feeds of water (or a weak electrolyte
solution) given frequently by mouth is the only
first-line treatment against serious childhood
diarrhoea. If this fails after 24 hours, intravenous
therapy and hospitalisation may be needed.
... Against Infection?
“Acute diarrhoea in children is usually
Infective, but antibiotics and anti-diarrhoeal
drugs rarely help.”
(Drug and Ther. Bulletin [1978])''
LOMOTIL is widely and often successfully used
by adults as a symptomatic treatment of
bothersome, non-specific “travellers’ diarrhoea”
(which is rarely serious). But in children infective
diarrhoea is serious. LOMOTIL prevents the child
from getting rid of the infective agent and may
prolong the period of infection.'2
“In patients with infective diarrhoea, the
use of constipating agents make the carrier
state last longer by stopping the organism
from being excreted.”
(AMREF[1980])s
A comparison between LOMOTIL and a placebo
in treatment of an infective diarrhoea reported
that:
“Febrile volunteers receiving Lomotil
alone experienced over a day more fever
than those in other treatment groups,”
suggesting that “drugs that retard gut
motility may facilitate intestinal
infection...”
(JAMA [1973])’3
HOW SAFE?
“Because of its depressant effects it is no
longer recommended for children.”
(Brit Med. J. [1976])'4
LOMOTIL poisoning in children can include
atropinism, respiratory depression, coma, and
even death. Symptoms can appear even at near
therapeutic doses:
“Lomotil ingestion is a cause of serious
poisoning in young children, especially those
aged under five. It is always hard to assess
the dose in patients suffering from
poisoning, but it seems that young children
may develop pronounced symptoms after
taking only one to five tablets.”
(Brit Med. J. [1977])'5
The difference between therapeutic and toxic
dose is unpredictable:
“We were unable to find a correlation
between the severity of symptoms and the
dose ingested. Because of this it is not
possible to predict what dose will be toxic in
children, and while some may have only the
mildest symptoms with relatively large
doses, others develop severe toxicity on
ingesting an amount near the normal dose.”
(Arch, of Dis. in Child. [1979])6
“There is a very narrow range between
allegedly therapeutic and toxic dosages, and
many cases of toxicity in children have been
reported.”
(Pediatrics [1980])5
“The narrow margin between therapeutic
and toxic doses, and the high incidence of
atropine hypersensitivity, make Lomotil a
potentially dangerous therapeutic agent.”
(Clinical Notes [1974])3
“The dangers of this drug to children have
not been well recognised. The narrow range
between therapeutic and toxic doses, and
also the possibility of a child being
abnormally sensitive ... may account for the
severe toxicity sometimes seen with low
dosage.”
(Clinical Pediatrics [1973])'6
• typically, no adverse reaction reporting systems
exist; and
• drugs such as LOMOTIL (available only on
prescription in the West) are in practice freely
available over the counter.
HOW EXPENSIVE?
The cost of the smallest available size of
LOMOTIL would for many people in developing
countries be equivalent to at least one day’s
income. Other effective preparations for
symptomatic treatment of diarrhoea' 8>'9 cost
much less.
According to the African Medical and Research
Foundation (AMREF), the cost of treatment with
LOMOTIL is about twice the cost of treatment
with codeine syrup orcodeine phosphate.
Treatment with a kaolin mixture, which may also
give relief20, costs about 25 times less.8
DESPITE THE DANGEROUSLY VARIABLE
RESPONSE, SEARLE’S RECOMMENDED DOSES
FOR INFANTS AND CHILDREN AND THE
PACKAGE WARNING INFORMATION VARY
AROUND THE WORLD.
LOMOTIL WITH NEOMYCIN (an antibiotic)
is recommended by Searle for the treatment
of “diarrhoea of bacterial origin.” This is
unacceptable:
In the US, LOMOTIL is contra-indicated for
children under two years old.
“Antibiotic and sulphonamide
preparations should be avoided for the
treatment of diarrhoea even when a
bacterial cause is suspected because
they may prolong rather than shorten
the time taken to control diarrhoea and
carrier states.”
(BNF [1981])2'
“This warning by the manufacturer is not
because there has been inadequate
paediatric testing of the drug but rather
because severe life-threatening reactions
(which are not rare) occur in this age group.”
(Am. Fam. Phys. [1976])'7
In Britain, however, the makers recommend it for
one-year-olds; and in Hong-Kong, Thailand, and
the Philippines it is offered for infants of three
months old.
Special circumstances in developing countries
compound the potential danger of treating
infants with Lomotil in this way. In developing
countries:
• children are relatively lighter than those of the
same age elswhere;
• the amount of medical supervision is greatly
lower;
i
J
•I
I
|
I
9
|
I
H
I
“Neomycin not only can cause renal
damage, but also it makes diarrhoea,
dehydration, and nutritional Josses
worse and could interfere with oral
rehydration therapy.”
(Population Report , 1980)22
j
“Medicines which should not be used
in the treatment of diarrhoeas...
Neomycin ...”
(WHO [1976])'
B
Treatment with LOMOTIL plus NEOMYCIN
costs about three times more than
treatment with LOMOTIL alone.
ji
5
REFERENCES:
1 World Health Organization: Treatment and Prevention of Dehydration in Diarrhoeal Diseases (A Guide for
Use at the Primary Level) (Geneva: WHO, 1976). LOMOTIL is one of 9 treatments not recommended.
The same preparation is sold by Janssen Pharmaceutical Ltd. and known as “Reasec”. Other proprietary
names: Diarsed (Fr.); Retardin (Swed.). (Source: Martindale’s Extra Pharmacopoeia, 27th Edition).
3
Drake M E, & Drake M E Jr.: “Lomotil Intoxication in Pediatric Patients” (in) Clinical Notes (June 1974)
pp. 501-2.
4
“Lomotil for Diarrhoea in Children” (in) The Medical Letter (iss. 25,1975) p. 104.
5
“Delayed Cardiopulminary Arrest after Lomotil Ingestion” (in) Pediatrics (Jan 1980) pp. 157-8.
6
Curtis J A, & Goel K M: “Lomotil Poisoning in Children” (in) Archives of Disease in Childhood (iss. 54,
1979) pp. 222-5.
7
Uthman S M: “Some Complications of Diphenoxylate Hydrochloride with Atropine” (in) Lebanese
Medical Journal (iss. 27/5,1974) pp. 521-2.
8
Upunda G, Yudkin J, and Brown G: Therapeutic Guidelines (A manual to assist in the rational purchase
and prescription of drugs) (Nairobi: African Medical and Research Foundation, 1980) p. 96.
9
“Drugs for Acute Diarrhoea in Childhood” (in) The Lancet (Nov. 20,1976) p. 112.
10 Wong Hock Boon & Michael Toh HoSing: "Lomotil Poisoning" (in) The Journal of the Singapore
Pediatric Society (April 1976) pp. 34-7.
11 “Diarrhoea in Children” (in) Drug and Ther. Bulletin (Jan 6,1978) p. 2.
12
Pittman F E, “Adverse Effects of Lomotil” (letter to editor in) Gastroenterology (Iss. 67/2,1974) pp. 408-9.
13
Dupont H L, & Hornick R B: “Adverse Effect of Lomotil Therapy in Shigellosis” (in) Journal of the
American Med. Assoc. (Dec 24-31,1973) pp. 1525-8.
14
Bell D R: “Diseases of the Alimentary System” (in) British Med. J. (Nov 20,1976) p. 1240.
15
Penfold D, and Volans G N: “Overdose from Lomotil” (in) British Med. J. (Nov 26,1977) pp. 1401-2.
16
Snyder R, Mofenson H C, & Greensher J: “Toxicity from Lomotil” (in) Clinical Pediatrics (Jan 1973)
pp. 47-9.
17
Wasserman G S: “Lomotil Ingestions” (letter to editor in) Am. Fam. Physician (Oct 1976) pp. 27-8.
18
Smits B J: “The Irritable Bowel Syndrome” (in) Practitioner (July 1974) p. 43.
19
Collins C D: “Lomotil in Treatment of Post-Vagotomy Diarrhoea” (in) British Med. J. (Sept 3,1966)
pp. 560-1.
20
Portnoy B L, et al: “Antidiarrhoeal Agents in the Treatment of Acute Diarrhoea in Children” (in) Journal of
the American Med. Assoc. (Aut 16,1976) pp. 844-6.
21 British Medical Assoc. &The Pharmaceutical Soc.of G.B., British National Formulary 1981, No. 1,
(London: The Pharmaceutical Press and the BMA, 1981) p. 40.
22 The Johns Hopkins University, “Oral Rehydration Therapy (ORT) for Childhood Diarrhoea” (in) Population
Reports (Issues in World Health) (Nov/Dec 1980) p. 54.
2
* SOCIAL AUDIT AND FRIENDS
SOCIAL AUDIT Ltd is an independent non-profit making action-research unit, concerned with
improving government and corporate responsiveness to the public generally. Its concern applies to all
corporations and to any government, whatever its politics. Social Audit has reported and campaigned
on a wide variety of public interest issues. Its interest in multinational drug companies and in
development is reflected in this leaflet — with hopefully others to follow — and also in the
publication of Insult or Injury? (An enquiry into the promotion of British food and drug products in the
third world, 1979); and Drug Disinformation (What British and other multinationals tell doctors about
their products at home and abroad, 1980).
This leaflet — for which Social Audit is wholly responsible — could not have been prepared and
published without the generous support given by:
War on Want, 467 Caledonian Rd., London N7 9BE, and The International Organisation of
Consumers Unions, Regional Office for Asia and the Pacific, PO Box 1045, Penang, Malaysia.
SOCIAL AUDIT LIMITED 9 POLAND STREET LONDON W1V3DG
© Social Audit Limited 1981
SMART DRUGS
MINDBOGGLING
Improve your memory
and intelligence with
electric yellow or
neon-blue
brain boosters!
•SANDEEP Khurana and his wife
Sheetal are apprehensive when the
doctor prescribes Piracetam fortheir
four-year-old daughter. They wonder
about the effectiveness of the new
drug and the fact that they had already
tried out similar prescriptions to treat
hheir daughter’s learning disability’
" Thedoctorbrushesawaytheirfears
by reeling off a string of impressive
facts. Clinical studies, he tells the
couple, has proven that Piracetam
can produce dramatic improvements
in verbal learning. Besides being ef
fective in the treatment of dyslexia, it
is found to help people who are re
covering from a stroke and those with
alcoholism, senile dementia and
sickle-cell anaemia. It is also believed
to enhance the brain’s resistance to
various injuries and boost its ability to
recover from injuries.
•HIMANSHU Goyal is a bit nervous.
He has an important meeting with his
American business partner the fol
lowing morning and has several re
ports to prepare, many facts to
memorise and, above all, get some
rest.
He visits the medical store round
Ke block andretums home with bottles
Wf Piracetam, Vasopressin and
Hydergine. After taking the appropri
ate doses ofeach ofthese he goes into
the study to slip on his cranial electric
stimulator along with the light and
sound device. He is sure that the com
bination of chemicals and brain ma
chines has a synergistic effect that will
create the optimal psychobiological
state for the tasks that lie ahead.
An hour later, Himanshu feels different. His
brainwave activity has altered, and an EEG would
show that it has become more regular and has in
creased in amplitude in certain frequencies, causing
him to feel simultaneously profoundly relaxed yet in
a state of intense concentration, loose and creative as
well as mentally quick and alert. He is now in the optimal
state to imprint new memories, to plan new and more
creative strategies, to visually rehearse every detail of
his upcoming meeting.
s
OUNDS far-fetched? Well, both the brain ma
chines and the cognitive enhancement com
pounds already exist in the United States where
drugs like marijuana, cocaine and LSD are fast
losing their glamour—and customers—to the
new breed of brain boosters. Some of the smart
drugs, as these cerebral aids are commonly called, are
being increasingly prescribed by Indian doctors and
demanded by customers, too. If the trend catches on, the
day may not be far when brain boosters become as
THE WEEK ■ JULY 30. 1995
popular in India as they are in the west.
times as powerful as Piracetam.
For now, however, it is the US and Europe that are the
The smart-drug movement is the result of the efforts
biggest markets for the mind magnifiers. Some of the of the American 'Life Extension’ gurus Durk Pearson and
smart drugs are high-powered pharmaceuticals; others Sandy Shaw, who promote the use of nutritional supple
are vitamins and nutrients.andareavailableas beverages ments as a way to optimise mental function and neutralise
at 'smart bars’ in the hippest clubs of San Francisco, Los immunity-destroying, age-accelerating agents known as
Angeles and New York.
free radicals. Hydergine, the brain enhancer discovered
Often called ‘cognitive enhancers’, these drugs are by the Swiss pharmaceutical firm Sandoz, shares a com
not legally available in the US, with the exception of mon source with LSD. the choice drug of the 60s and 70s.
Prozac, the top selling anti-depressant. Many of these are The source is ergot, the same cereal fungus. Surprisingly,
nothing but repackaged medications for treating various it was discovered by the same scientist. Albert Hoffman,
illnesses. Hydergine, for example, is used to treat an age- a man revered as the Daddy of Acid.
related decline in mental capacity.
Hydergine is not theonly IQ-enhancer
Deprenyl is used for the treatment of
available. The list is bigger than the ge
Parkinson's disease, a crippling brain
neric aspirin prescriptions available
Millions of dollars
disorder. Dilantin is widely prescribed
worldwide. The logic behind thecreators
to treat patients with epileptic seizures.
of many of these drugs is that if these
are being spent
The more popular of these smart drugs
formulations can help rejuvenate ailing
on research by
include Piracetam, used in the treat
minds, they can help enhance the per
ment of certain learning disabilities and
formance of the healthy one too.
pharmaceutical
some types of memory loss and
However, theystill have no scientific
giants to develop
Aniracetam, which was developed to
proof to back their claims. Critics of
treat loss of memory in older adults and
smart drugs point out that Hydergine
smart drugs.
attention disorders in children.
and Piracetam have been subjects on
These drugs could
Pharmaceutical giants round the
extensive research and the results are at
world just cannot resist the lure of the
best encouraging in animal tests, and
quickly produce
mindboggling profits that can accrue
dubious in case of humans. "There is no
sales of over a
from the sales of the smart drugs. Mil
conclusive evidence that any drug can
lions of dollars are being spent on re
improve intelligence," says Dr B.
billion dollars
search by these companies, who are
Rajendran, a Kochi neurologist. Agrees
a year in the
locked in fierce competition to develop
Dr Satish Chandra of Bangalore's Na
patentable memory enhancement drugs.
tional Institute of Mental Health and
US alone.
Since the Food and Drug Admin
Neurological Sciences: "We, in
istration of the US is primarily
fact, do not promote the use of
oriented toward treating dis
such drugs."
eases in a medical context, and
Gary’ Wenk, professor of neu
has not shown much interest in
rology at the University of Ari
giving its approval to drugs that
zona, claims that he’s never
simply improve people’s memo
tested a pharmaceutical for
ries or boost intelligence, the
cognitive enhancement that he's
companies have found a way out.
found to be effective. The results.
They are directing their efforts
he says, are minimal at best.
toward gaining approval fortheir
Raymond Bartus. chief scientific
cognition-enhancement drugs as
officer at Cortex Pharmaceuti
treatments for medical problems
cals in California, believes that
such as Alzheimer’s disease,
those with a memory deficit.
dementia and senility. Such cog
particularly in the early stagr‘c
nitive drugs could quickly pro
of Alzheimer's disease, can hr#
duce sales of well over a billion
helped with the use of
dollars a year in the US alone,
nootropics. “They (nootropics)
and ultimately outsell antibiot
are doing something, but not in
ics and tranquilisers.
all patients," says Bartus.
Many of the smart drugs may
The ‘Smart Pill race’ has re
sulted in the creation of a new
also cause minor side effects.
Hydergine and Piracetam, for
drug category called the
instance, can cause insomnia.
nootropics. from theGreek words
noos (mind) and tropein (turn),
nausea and headaches. Diapid
meaning 'acting on the mind' Some of the nootropic can cause runny nose, irritable nasal passages, and
drugs being tested now on humans include Vinpocetine. stomach cramps. "Vasopressin is an alkaloid used in
which speeds up learning, improves memory and seems obstetric practice but is potentially hazardous if
to block the action of substances that disrupt memory; unsupervised," adds Dr Rajendran.
Aniracetam. which appears to be about 10 times more
Critics say that some of these smart drugs make
potent in improving and protecting memory than people forgetful and less alert. These side effects may be
Piracetam; Prainiracetam, which seems to improve even worse if the drugs are taken in large doses over a
learning and memory by enhancing the firing of neurons long period of time, or in combination with other smart
in the hippocampus (a key to the formation of long-term drugs. Dr James McGaugh. director of the University ol
memories), and Oxiracetam, apparently two to three California’s department of psychobiology, believes that
SMART DRUGS
WIDE VARIETY
NOOTROPICS
PIRACETAM: The
original nootropic was
developed by C.E.
Giurgea (who coined
the term 'nootropic') in
the 1960s for the Bel
gium-based UCB labs.
In clinical trials, it has
shown to be effective
for the treatment of
dyslexic children and
memory disturbances
in people undergoing
electric-shock therapy.
PRAMIRACETAM: A
b variation
of the
W’Piracetam moiecule.it
was developed by
Parke-Davis as a treat
ment for Alzheimer's dis
ease.
ANIRACETAM: Devel
oped to treat age-re
lated memory impair
ment and attention
deficit syndrome in chil
dren.
IDEBENONE: A lead
ing nootropic in Japan
where 1990
sales were
upwards of
S300 million, it
is widely pre
scribed for
cognitive en-
hancement as well as
for Alzheimer's.
OTHER SMART
DRUGS
HYDERGINE: It is the
only cognitive enhancer
with FDA approval.
Called the 'ultimate
smart pill', it is claimed to
increase mental ability,
prevent damage to
brain cells and even re
verse existing damage
to brain cells.
the whole smart drugs deal is about as seri
ous as astrology. “Some of the drugs being
promoted as cognitive enhancers are just
the opposite—they are cognitive impairers,”
says McGaugh.
While scientific proof is patchy, there is
no stopping the growing popularity of these
drugs. Many health food stores and mail
order companies in the US sell amino acid
supplements, claimingthat they make people
feel younger, more energetic, and mentally
sharper. Health food bars also mix amino
acid powders into smart drinks, with names
like Power Punch and IQ Booster, which they
claim can make people smarter.
The most popular smart amino acids are
phenylalanine,
tyrosine,
choline,
pyroglutamate, L-carnitine and arginine. The
scientific validation, even in the caseof amino
'ds, is hard to come by. In fact, these aminoWids areabitdangeroustotamperwith. One
amino acid—tryptophan—was taken off the
market in 1990 because its supplements
probably caused 19 deaths and about 1,500
cases of a serious blood disorder.
Even Prozac has been deemed unsafe by
some groups. A widely prescribed anti
depresent drug fluxetine (sold under the
brand name Prozac) may trigger suicidal be
havior in some patients-. According to Dr
Prakash Masand of the State University of
New York, two patients treated with the drug
began fantasising about suicide. One tried to
hang himself and the other kept thinking
about jumping out of the hospital window.
The suicidal thoughts subsided after the drug
had been discontinued for four to 10 days.
Despite the fears about the side effects,
smart drugs is a growing market niche. They
can be roughly divided into two categories:
VASOPRESSIN: De
rived from a hormone
secreted by the pituary
gland and originally de
veloped to treat diabe
tes, It has been widey
researched for its effects
on memory and mental
alertness. A nasal spray.
It goes directly into the
blood stream.
DEPRENYL: Touted as
the anti-ageing aphro
disiac, It was originally
developed to ease
symptoms of Parkinson's
disease. Users claim it
enhances mental func
tions, increasessex drive.
and has an anti-depressant function.
SMART NUTRIENTS
PHENYLALANINE: An
essential amino acid,
one that is obtained from
food or other external
sources. It is converted
to tyrosine In the body
LUCIDRIL: It breaks and stimulates the cen
down to DMAE (a natu tral nervous systrem.
rally occurring nutrient
TRYPTOPHAN: An es
found in sea food) in the
blood stream. Users sential amino acid, pre
cursor
tothe neurotrans
claim it increases alert
ness, improves memory, mitter serotonin which
promotes
feelings of re
helps in brain oxygen
ation and may help de laxation and well-being.
lay the ageing process Users claim tryptophan
because of its antioxi
dant effect.
Side effects can in
clude insomnia and
hyperexcitability.
has anti-depressant ef
fects, and it has been
widely used as a non
addictive sleep inducer.
In 1990, the FDA re
moved it from the mar
ket because tainted
products in Japan re
sulted in 19 deaths.
GLUTIMIC
ACID:
Found in vegetables,
fruits, meat, and dairy
products as well as in the
brain, this acid is be
lieved to have cognitiveenhancing and mood
elevating effects.
L-CARNITINE: An
amino acid that facili
tates the action of the
neurotransmitters
acetycholine (essen
tial for memory func
tion) and serotonin,
and may be related to
the production of
nerve-growth factor in
the body.
ARGININE:
An
amino acid that
causes the pituary
gland to release natu
ral growth hormone, it
is said to aid in the
building of muscle and
the burning of fat.
pharmaceuticals and health foods.
hind Smart Products, Inc., one of
The former, however, are not avail
San Francisco’s premier nutrient
able in the US as readily; one can
companies. (San Francisco, or New
acquire these IQ igniters in Mexico
Brainia, as smarties call it, is the hub
or get them by mail order from Eu
of the smart cosmos.) “When I think
rope through a legal loophole which
of taking smart drugs, I feel like I'm
allows individuals to import three
upgrading a computer. It’s like going
months' supply of their prescription
from a 286 chip to a 386.’’ says Rennie.
pills.
Who are the people who use
The health foods, despite their
these super chargers? Mostly the
name, are more dangerous as they
yuppies who are i n search of an edge
are more freely available in the US,
over their rivals. They treat their
fuelling the so called “smart revolu
brains like their sports cars. But
tion ".Those who wanttosupplement
there are other users too: those
their psyches sans the anti
slogging it out in the Silicon Valley
Alzheimer's pharmaceuticals can
and other high-tech colonies also
consume what are known as nutrients.
indulge in these brain fuels.
Smart drinks have
In their trendiest incarnations, these
However, there is also some good
market friendly.
are packaged as smart drinks. They have
news which has started coming out of the
market
friendly
names—Energy
smart
drugs revolution. A growing bodd
names Energy
Elickshure, Psuper Psonic Psyber Tonic
of research suggests that amino acid?
Eliekslnire or Fast
or Fast Blast—and come in colours which
may provide a non-toxic, non-addictive
range from electric yellow or plain old
Blast and come in alternative for those trying to overcome
mauve to neon-blue.
to cocaine and amphetamines.
colours like electric addiction
These drinks, which seem straight out
Researchers at the Massachussetts In
of Star Trek: The New Generation, are made
yellow and
stitute ol Technology and Harvard .Medi
of a combination of vitamins and amino
cal School have also found that the amino
neon blue.
acids and, occasionally, a sizable dose of
acid—tyrosine—may be effective in
caffeine.
treating depression. And the pharmaceu
As in every other craze, the smart
tical firm Sigma-tau is developing an
revolution has unleashed a new brand of entreprenuers. acetylised version of L-carnitine, an amino acid, to treat
They are led by John Morganthaler who, along with ex- Alzheimer's.
naval geronotologist Ward Dean, has written the move
Hype or hip, the smart drugs are here to stay and
ment bible, Smart Drugs and Nutrients: How to Improve many believe that it is only a matter of time that these find
Your Memory and Increase Your Intelligence Using the more acceptance outside the US and Europe.
Latest Discoveries in Neuroscience.
Traditionalists, though, insist that the best way to
Morganthaler believes that stupidity, like polio, is a reach the lop is by sticking to the safer method of burning
disease and that he has been put on earth to help obliter the grey cells. For, the only side-effect would probably be
ate it. He is not alone in this task. Mark Rennie, a night rising grades.
club owner, attorney and entrepreneur, is the man be—O.P. MALIK
-MFI
THE WEEK ■ JULY 30. 1995
THE WEEK a JULY 30. 1995
Personal Time
YOUR
HEALTH
The Pros and Cons of Botox
Just because the FDA has approved the anti-wrinkle shots
doesn’t mean that they’re for you By Michael D. Lemonick
re you sufficiently
bothered by wrinkles to
stick needles into your
face? That’s the question
millions of Americans will be
asking themselves once the
Botox craze starts in earnest.
Botox injections, as you
may have heard, are the biggest
thing since nose jobs. They are
A
already the most popular cosmetic procedure in the U.S.;
about 1.6 million Americans got
the shots last year—a so-called
off-label use of a drug originally
approved to calm twitchy eye
muscles. The fact that the shots
reduce wrinkles too was an
unanticipated bonus; doctors
were allowed to use Botox for
that purpose, but tire manufac
turer, Allergan, couldn’t adver
tise it to the public.
Now the company can,
thanks to tire U.S. Food and
Drug Administration’s decision
last month to approve Botox for
tire removal of certain wrinkles.
Now clinics are expected to be
inundated by people yearning
to be wrinkle free. Before
scheduling an appointment,
though, you should know what
Botox can and can’t do, and
what the downside might be.
Botox is short for “botu
linum toxin,” the substance that
causes botulism, a sometimes
fatal form of food poisoning. It
sounds scarier than it is; in
small quantities, Botox merely
interrupts nerve impulses to
muscles in the face. The lines
that furrow the forehead when
you raise your eyebrows, the
crow’s feet that appear when
you squint and the creases be
tween the eyebrows when you
frown are all caused by tension
in underlying muscles, which
contract and squeeze the skin
like an accordion. Botox keeps
this from happening.
Fortunately, Botox is so
diluted that serious side
effects like allergic reactions
are rare. If the doctor slips, in
most cases the worst that can
happen is that you will lose
the ability to raise your eyelids
all the way; or, if you’re getting
shots around the mouth, a
mistake could leave you drool
ing. But even a perfectly exe
cuted procedure has conse
quences. Depending on which
wrinkles you go after, you
might not be able to frown or
raise your eyebrows or squint.
Is this a problem? Not
enough to discourage Botox
enthusiasts. In Hollywood,
however, the treatments are so
popular that some directors
complain that their leading ac
tors can no longer convincingly
perform a full range of facial
expressions. The good news is
that even if there’s a little
accident, Botox wears off after
a while (which also means you
have to go back every six
months, at up to $500 per
treatment). Slipups are pretty
rare, however, as long as you
go to someone who knows
what he or she is doing.
That includes knowing
when Botox won’t be useful at
all. Muscles cause some wrin
kles, but many result simply
from the loss of elasticity' that
goes naturally with aging (or,
less naturally, with smoking
and sun exposure), causing the
skin to sag and crumple. There
are treatments for this sort of
wrinkle, but Botox isn’t one of
them, says Dr. David L. Feld
man, director of plastic surgery
at Maimonides Medical Center
in Brooklyn, New York. “I had
a patient recently who came in
asking for Botox,” he says. “It
would have done no good at all.
In fact, she might have ended
up looking worse.”
So Botox isn’t a cure-all,
and it has some pretty odd
side effects. But if you don’t
mind getting shot up with
poison and you don’t mind
paralyzing parts of your
face—well, you’ve got
plenty of company.
n
Botox questions?
E-mail Michael at
michaellemonick@aol.com
TIME, MAY 13 2002
BUBBLE BREAKTHROUGH In
the first clear win for gene
therapy, French doctors report
that they have successfully
treated four boys with “bubble
boy” disease, the immunesystem disorder so devastating
that its victims spend their lives
confined in germ-free isolation.
It was 2% years ago that doctors
first repaired the genetic
mutation that kept the children
from producing healthy
infection-fighting cells, and
today the kids are still thrivin
It was a dramatic coup for a
therapy that has had more
than its share of failures.
FREAKY FROGS All is not well
among the lily pads. Foryears,
frogs with missing legs or extra
eyes have been turning up in
ponds across the U.S. Now sci
entists wonder if trace amounts
of weed killer in rainwater may
be partly to blame. A new report
shows that male frogs exposed
to altrazine—the best-selling
agricultural herbicide—can
develop multiple male sex
; organs or both male and female
' organs. Scientists think that
■ even low concentrations of the
I .weedkiller—one-thirtieth
' 5 level allowed in drinking
! S water—can cause the male
; s hormone testosterone to
1 “ morph into the female hormone
1 | estrogen. Does altrazine
( * affect humans? No one really
i | knows. But as scientists point
• J out, people don't spend as
i ; much time in the wateras
' 2 frogs do. —By Janice M. Horowitz
Ana Figueroa
Lining Up for a
Pinch of Poison
y obsession WITH BOTOX started innocently enough, with
M
a routine visit to my Hollywood dermatologist. I’d always had an un
sightly frown line between my eyebrows, but I used to consider it the
mark of a deep thinker. Living in southern California, I had heard a lot
about die cosmetic uses of botulinum toxin in recent years. Injected just under
neath the skin in tire form of a product called Botox, the toxin relaxes wrinkles by
paralyzing the underlying facial muscles. The effects typically last three to four
months. In high concentra
tions, botulinum toxin is a
deadly poison. But Botox
uses extremely diluted
doses. I confessed my cu
riosity to tire doctor, though
the idea of hating a potential
biological weapon injected
into my face made me a little
queasy. My doctor assured
5
me drat die injection would
take only a second. Just
|
moments after agreeing to
s
it, my forehead was relax|
ing in a state of botulism!
induced bliss.
A few days later I noticed a |
difference: the frown line bei
tween my eyebrows had disap- I
peared! I was hooked. Now mil
lions ofother American women
can be, too; the Food and Drug
Administration recendy ap
proved tire toxin for temporary
wrinkle removal. Mind you,
most women in my part of tire
country couldn’t care less if
Botox had FDA approval or not.
Statistics show drat more titan
1.6 million cosmetic Botox pro
cedures were performed in tire
United States last year, and I’ll
bet that most of tirose were in
Los Angeles. Still, millions of
women in America’s heart
land—not to mention the rest of
tire world—are unfamiliar with
the wonders of a litdc shot of
poison in the face.
Not me. Increasingly com
fortable with die procedure, I
decide to try’ a “Brows and
Botox” event at the trendy
Valerie Beverly Hills cosmetics
46
salon. I arrive fashionably late
and leave my car with die park
ingvalet. Inside, I find dozens of
denim- and Prada-clad women
nibbling finger sandwiches and
sipping Perrier. Alcohol is a
no-no; it's hard to give informed
consent to a medical procedure
ifyou’re tipsy.
First salon owner Valerie
Sarnelle waxes each woman’s
eyebrows into McDonald's
arches. Then Dr. Jessica Wu, a
Harvard Medical Schooltrained cosmetic dermatolo
gist, discreetly shoots up die
women with Botox as diey sit
in a makeup artist’s chair. The
scene is a little jarring, like
finding a Clinique counter in a
mcdiadone clinic.
Like me, most of the women
have been Botoxed before but
have come to sample the doc
tor’s “technique.” The buzz is
tiiat Wu’s gende touch has
earned her a celebrity follow
ing. She wnn’t give names, but
discloses that before this year’s
Oscars, she made house calls to
tiiree female presenters to give
diem Botox shots in dieir
armpits. “It eliminates perspi
ration," says Wu.
After Sarnelle shapes my
eyebrows and graces me with
fake mink eyelashes, I am ready
for Wu. I worry for an instant
that the good doctor might deny
me my fix. After all, my last
Botox shot is still working. But
Wu takes one look at me and de
termines that I am a prime can
didate. “Around die eyes,” she
proclaims. Wu and her two
medical assistants set up tidy
row’s ofgauze, Q-Tips, gloves
and a biohazard-disposal pail.
As an assistant holds an icefilled cloth to my face, I sign a
consent form. The doctor opens
up two small rials, dien hovers
over me, needle in hand. “Smile.
Relax. Smile. Relax,” she in
structs, trying to determine die
exact latitude of my crow’s feet.
Two or three faint pinches on
each side of my eyes, and I’m
done. That’s it—no stinging, no
soreness. Days later I’m not
aware of any new sensations—^
or losing any old ones.
”
The odier women at die
event gather around me for a
look. “You know’, you should
catch the corners of your
mouth before they start to
droop too much more,” one
Rizzo, 39, an Emmy Award
winning makeup artist, frets
about living in a town obsessed
with looks and age. “Our stands
arils are so much higher here®
she says. “I’m sure if I lived on
some farm in Iowa, I couldn’t
care less about Botox.”
By die end ofdie afternoon.
die Browsand Botox event
evolves into one big support
group. I feel oddly close to these
women I barely know, as ifwe
have shared some important rite
ofpassage together and
emerged better—or at least bet
ter-looking—for it. Collectively,
w'e encourage Abbe Hausner,
45, to take the Botox plunge, but
she remains wary.“I think for
my first time. I’d rather do it in
private,” she says.
Not me. From now on, I’m
Botoxing in public.
NEWSWEEK MAY 20. 2002
HEPATITIS
C
THE INSIDIOUS
SPREAD OF A
VIRUS
octors have
unsterilized needles.
Hundreds of used,
Sayyeda Hassan Metwally,
54, remembers a nurse in
millions are jecting
her 11 relatives and
four neighbors with a single
infected
syringe. The campaign end
ed only when an oral drug
with the
came on the market in 1982.
Now the government is
stealth virus. scrambling to control an
epidemic it helped create.
This story would be tragic
Most don’t
enough even ifEgypt were an
isolated case, but it’s not.
know it.
Hepatitis C has become a
global
epidemic. About 170
BY ANNA
million people, 3 percent of
the
world
’s population, suf
KUCHMENT
told
Saeed Taha
The
48-year-old
electrician
is
to
live.
that
he has
only
sprawled on weeks
a Cairo
hospital
bed with tubes connected,
seemingly, to every' major vein
and artery. A decade ago he
was diagnosed with hepatitis
C. Overcome with fatigue, tire
^Jrer ofthree quit his job and
spent his life’s savings on in
terferon, one oftwo drugs ap
proved to fight the virus. But it
didn’t help. “Don’t believe
what is said about medicine
and doctors,” he says. “In this
disease nothing makes a difference.”
On tire next bed lies Abdullah ElShahhat, 70, who was diagnosed four
months ago but already displays the
swollen legs and belly characteristic of liver
disease. The two are among the 15 to 25
percent of Egyptians infected with hepati
tis C—the highest rate of any country' in the
world. Many' contracted it in the same way
as Taha: through a government-sponsored
campaign begun in 1961 to fight tire tropi
cal disease schistosomiasis. Medical work
ers injected millions of Egyptians with
D
40
fer from the disease—four
times more than HIV. Hepatitis C doesn’t
kill with the virulence of AIDS, but it kills
nevertheless. About 15 percent of patients
mount a strong-enough immune response
to completely' throw offthe virus. But the re
maining 85 percent have the disease for life.
Of those, one in five develops cirrhosis,
which can lead to cancer or liver failure.
What really has health officials worried is
what is expected to happen in the next 20
years. Since HCV, the hepatitis C virus, can
lie dormant in the bloodstream for decades,
millions of people who are already infected
ABDULLAH EL-SHAHHAT, 70: The former
minibus driver is among the 15 to 25 percent
of Egyptians infected with hepatitis C
but don’t know it will start getting sick. That
will boost the rate of liver failure around the
world, making organs for transplant even
scarcer than they are now. The demand for
costly drugs to suppress the disease may sky
rocket, putting them even further out of
reach ofpoorer countries, like Egypt, whose
public-health systems are al ready stretched.
Health officials can’t even begin to esti
mate what resources they’re going to need,
because even basic data about hepatitis C are
virtually nonexistent. That’s partly because
scientists identified it only 14 y'ears ago. By’
the time they developed tests to spot the
pathogen, it had been spreading silently for
decades. In Europe and North America,
public-health officials began screening
blood supplies in the early 1990s, at least
eliminating the virus’s spread. Developi
nations, which account for the vast majont^^
of HCV' patients, have only begun to follow
suit. So far only a minority, including
Thailand, South .Africa and Brazil, screen
blood. I n other countries wealthy enough to
perform transfusions, such as China and
India, contaminated supplies may still be
infecting new patients. Carlos Varaldo, a
hepatitis C patient advocate in Rio de
Janeiro, calls it a “viral time bomb.”
In Egypt, it’s already exploded. “We
wish to give free medication to all of the pa
*
tients.
’ says Saeed Aoun, undersecretary'
for preventive affairs at Egypt’s Ministry of
Health. “But this requires billions of dollars
every year.” Already' more than 50 percent
of Egypt’s health-care spending goes
toward treating patients with liver disease,
most of whom have hepatitis C. The major
ity qualify- for vouchers that they can re
deem for free medicine. But to get th^
vouchers, hep C patients, already we.^P
from their illness, must stand in line for
hours outside the Ministry of Health. And
the value of die vouchers is unpredictable—
it varies from month to month, based on a
patient’s persistence, political connections
and what die government has in its coffers.
That puts pressure on doctors. "It is very
difficult to decide what medication co pre
scribe for a patient when you know he
might not be able to get the same [govern
ment] allowance each month,” savs Dr.
Mamdooh Diaa of die Munufcyya public
hospital, just north of Cairo.
In sub-Saharan Africa, which has one of
die highest rates of HC\ infection in die
world (i.mgh g f■»m I. ’ co 6 percent of die
pci? '..don), most patients simply go undia • \sed. “Doctors aren’t iouking tor hepatis C,” says David Heymann of die World
41
LS.cienc.e_
A Viral Time Bomb
NVANSRITOOMMNON, 72: Unlike most hep C
patients, she can afford medication—and a
private room at a Bangkok hospital
Health Organization (WHO). “They’re
looking for TB or malaria.’' And, say many
African physicians, there’s little motivation
to test for a virus they simply cannot afford to
treat. The situation is equally dire in Russia,
where hepatitis C has increased fourfold in
the past decade, due mostly to rampant IV
ding use. “We are already considering this an
epidemic, and there is very little we can do to
stop it,” says Scigey Kolesnikov, a deputy in
Russia’s Duma who is lobbying to start a na
tional program to combat all forms ofhepati
tis. The government, he says, has imported
only a limited amount of medicine, which it
distributes to those who can afford it. “We are
really only curing tlie rich,” he says. Even
Brazil, with one of Ute best health-care sys■ms in the developing world, is struggling.
Up to 5 million people arc believed to be in
fected, but only a small minority have been
diagnosed. As more and more patients devel
op symptoms, the government is concerned
it may simply run out ofdrugs, which it now
distributes free.
The spread of HCV is of particular con
cern for countries with a high rate of HIV.
In the United States, it affects as many as
one third to one half of all HIV patients.
And the presence of one makes tire other
more deadly. Two recent studies have
shown that co-infection with hep C leads to
a more rapid progression from HIV to full
blown AIDS. The reverse is also true. As
HIV knocks out a patient’s immune system,
it undermines the body’s ability to fight off
HCV, making it more likely that a sufferer
will progress to end-stage liver disease. Co
infection also complicates treatment.
“Hepatitis C appears to increase one’s risk
toxicity from the HIV medicines,” says
Dr. Stuart Ray, an expert on co-infection at
the Johns Hopkins University' School of
Medicine in Baltimore, Maryland.
Developed countries are equally con
cerned. Ironically, the virus is more of a pri
ority' in wealthier nations, which have a rela
tively low rate of infection, plenty of
resources and fewer competing health con
cerns. Hepatitis Chas recently grabbed head
lines in the United States as celebrities rang
ing from former “Baywatch” star Pamela
Anderson to country' singer Naomi Judd have
announced they’re infected. “I can’t go to a
social event without meeting someone with
hepatitis C,” says epidemiologist Miriam
Alter of the U.S. Centers for Disease Control
and Prevention. By the end of the decade, the
death toll from hep C is expected to triple in
the United States. In die United Kingdom,
42
Progression
@ INFECTION 15% of patients mount a
Hepatitis C can lie dormant in the body for decades before causing
fatal liver damage. Worldwide, 170 million people suffer from the
disease, and millions more will show symptoms in coming decades.
I
J
successful immune response and clear the
virus from their bodies within the first year.
I
85% of patients retain HCV, becoming
chronic carriers.
© CIRRHOSIS
80% of carriers
harbor the virus for
decades without
suffering adverse
symptoms.
20% develop
cirrhosis within
20 years, which is
marked by the
buildup of scar
tissue in the liver.
□ 5% (high)
L_1 1.1-5,0 (intermediate)
0.1 or less (very low)
Unknown
Who Gets Treatment?
Who Is Most at Risk?
RICH COUNTRIES: Infected patients use
costly drugs like PEG-lnterferon/Ribavarin.
Prevention efforts target IV drug users.
■ IV drug users
POOR COUNTRIES: Unable to afford drugs,
developing nations concentrate on preven
tion. Blood screening and stopping the reuse
of syringes are top priorities.
■ Blood recipients'
■ Infants born to infected mothers
■ Exposed health-care workers
■ People with multiple sex partners
People with infected steady partner
'PRIOR TO 1092 IN DEVELOPED COUNTRIES. SOURCES: MIRIAM ALTER. COC; DR. STUARTRAY, JOHNS HOPKINS SCHOOL OF MEDICINE; JOHN WONG. ET AL .AMERICAN JOURNAL
OF PUBLIC HEALTH. RESEARCH AND TEXT BY JOSH YUUCK ANO JOHN SPARKS. GRAPHIC BY CHRISTOPH 6LUMRICH-NEWSWEEK
roughly 5,000 new cases are being diagnosed 1960s, physicians were seeing liver disease in
each year, and the government is racing to people who didn’t have citiicr of the known
keep up. “The epidemic is growing faster hepatitis viruses. Lacking a better name Tor
than the number we’re treating," says Nigel die syndrome, they dubbed it“non-A, non-B”
Hughes of die British Liver Trust That’s not hepatitis.
To this day, tiiere is no reliable cure. The
because the disease is spreading faster, but
because increasing numbers of Britons who best treatment available is a combination of
were infected as a result of IV drug use in the die protein interferon, which boosts im
1970s—die so-called “flower power genera mune response, and die antiviral drug riba
tion”—are developing symptoms and being virin, a distant cousin of AZT. Thken to
diagnosed. The pattern is similar in die gether, they clear the virus in 50 to 55
United States, where drug use was rampant percent of patients after six months to one
during the ’60s. Why has the C virus come to year. But they cause such severe side ef
light so recentiy, and traveled the world so fects—including hair loss and heart fail
fast? Consider its habitat. Unlike the A virus ure—that, in the United States, one patient
(which spreads via fecal matter) or die B in seven abandons the regimen. Bill
virus (which passes easily between sex part Schwartz, 65, a retired lieutenant colonel,
ners), die C virus can’t spread unless a carri compares his yearlong treatment to “West
er’s blood enters anotiier person’s veins. And Point plebe year and Vietnam combat.” And
the opportunities for such commingling ex it didn't control his infection.
Few people in developing countries can
ploded during die 1940s and ’50s, when
reusable syringes caught on and hospitals be afford treatment. A full course of interferon
costs
about $20,000—the price of a small
gan using blood as medicine. By' the late
NEWSWEEK MAY 20, 2002
house i n Brazil, or about what the president
ofSouth Africa earns in one year. For people
like Nvansri Toommnon, 72, the wife ofa re
tired Thai Air Force colonel, that’s not a
problem. She can afford a private room at
' Bangkok’s Bumrungrad Hospital. But even
Thai doctors would be hard-pressed to af
ford the treatment for themselves. “If 1 had
to be treated, it would be almost impossible,”
says Dr. Sirirung Songsivilai, a professor at
Mahidol University’s school of medicine.
Also, because die medication needs to be
taken regularly over a long period of time
and comes with serious side effects, a coun
try' must havea good public-health system in
place to deliver tire drugs. For these reasons,
the WHO advises developing countries to
focus on stemming the spread of new infec
tions, rather than on treating existing ones.
The best hope of fighting hepatitis C in
the Third World, says the WHO’s
Heymann, is to find a vaccine. That’s a
cause Michael Houghton, vice president of
hepatitis C research at Chiron Corp., who
led a team of scientists in identifying the
virus in Ute late ’80s, is now devoted to. But
he says tire formula is at least five years
away from U.S. government approval.
Improved drugs arc also in tire pipeline.
The market for hepatitis C treatment is
© CANCER 75%
of those developing
cirrhosis suffer no
serious effects from
liver scarring.
25% develop end
stage liver disease,
which can involve
cancer, require a
transplant or result
in death.
now exploding, and drugmakers have sev
eral new compounds in the works. At least
three companies are developing protease
inhibitors, which block a key enzyme that
allows tire virus to replicate. And ScheringPlough, the current leader in hep C treat
ment, is developing molecules that could
be combined with protease inhibitors to
create the kind of multidrug cocktail that
has proved so effective against HIV. “The
parallels between these two [epidemics]
are just phenomenal,” says Dr. Lawrence
Deyton, chief public-health officer for the
U.S. Veterans Administration. “We’re today
in hepatitis C where we were in HIV 10
years ago, where we had only one or two
dings that were very toxic and not very ef
fective. (fa patient’s liver is not in trouble, it
may be perfectly appropriate to watch and
wait for something better to come along.”
In tile meantime, many are turning to
herbal remedies. Even in the United States.
where most people can afford medical treat
ment, roughly 30 to 40 percent of HCV pa
tients prefer alternative medicines. Dr.
Robert Gish, medical director of the liver
transplant program of the California Pacific
Medical Center in San Francisco, tells pa
tients: “I have medicines that can cure you,
but will make you sick. Herbalists have nice;-
CLOCKWISE FROM LEFT: UARKA-CUSTOM MEDICAL STOCK PKOTO, PHOIOTAKE. PROFESSORS MOTTA, NlSfil. FUJITA-SPl-CUSFCM
MEDICAL STOCK PHOTO. CUSTOM MEDICAL STOCK PHOTO
cines that will help with your quality- of life,
but won’t cure you.” For the developing
world, herbal remedies have the advantage of
being affordable. One of the most popular
herbs is milk thistle, or silymarin. which has
been used to treat liver disease, or “bad bile,”
for more titan 2,000 years. Chinese use the
herbs schizandra and licorice root for the
same purpose. Scientists have only begun to
test many of these remedies. So far there’s lij^.
de evidence that they do much more th^
perhaps relieve symptoms such as inflamma
tion. That’s good enough for Haj Hussein,
who goes to die old neighborhood of Bab El
Khalk, just outside the old gates of Cairo.
every couple of weeks to purchase a $3 bag of
herbs. The 62-year-oId, with yellow-tinged
skin and dark shadows under his eves, savs
the herbs work wonders. “When I know that
my enzymes are OK. I can work. I can live!”
For the vast majority of hepatitis C sufferers
around the world, such cheap remedies trill
have to do until scientists and health officials
can offer something better.
WITH i".»'EELA ISMAIt IN CAIRO, KAREN MACGREGOR
0 IAC MARGOLIS IN RIO DE JANEIRO,
EVE Cn / Nt IN MOSCOW JOE COCHRANE IN BANGKOK.
■ tV.NLOt IN LONDON. ANNE VN0ERW000 ANO JOHN
OAVIO SPARKS IN NEW YORK. KAREN SPRINGER IN
CHICAGO ANO PAUL MOONEY IN BEIJING
43
Race for Ruins
Malaysia’s eastern waters are littered with the wrecks
of ancient ships. Who will get their treasures?
COLLECTING THE LOOT:
(From left) a Chinese
era, members of
Sjostrand’s team
sort through
ceramics pulled
from the Desaru, a
Malaysian diver at
the wreckage site, a
salvaged ring-handled jar
from Thailand
BY LORIEN HOLLAND
TEN SJOSTRAND IS OBSESSED
with wrecks. For tire past nine
years, the Swedish marine engi
neer has been scouring tire wa
ters off Malaysia’s east coast for
tije wreckage of ancient trading ships. So
he has uncovered seven vessels, ranging
in age from the 14di-century Turiang to the
Desaru, which dates to around 1830. He
has not only hauled up valuable treasures
but also has helped fuel a rising regional in
terest in just what is resting on Southeast
Asia’s seabeds.
Sjostrand and his team located the
wreck of the Tbriang—which appears to be
of Chinese origin—in 43 meters of water,
more than 100 nautical miles off the
Malaysian coast. Although trawling nets
had seriously damaged the deck, great
stacks of ceramics from China, Thailand
and Vietnam lay below. The cargoes were
packed separately, indicating that tire vessel
had made several ports of call to fill its
hold. And tire fact that the wreck dates from
the mid-14th century’ provides strong evi
dence that Southeast Asian kilns were al
S
44
ready operating and competing with
Chinese kilns before the Ming Emperor
Hongwu banned private trade outside
China in 1371.
There is plenty' more down there. Vessels
from China, Java and India plied their trade
on the region’s monsoon winds from as ear
ly as the I Oth century. They carried every
thing from bowls and flatware to spices and
salted fish. Already more than 30 ships have
been excavated in the region, and there may
be many more still undiscovered. The
wrecks have proved invaluable in filling his
torical gaps, with each one proriding a con
crete glimpse of a specific moment in time.
Indeed, Sjostrand’s seven wrecks proride
strong evidence that regional trade—as op
posed to the great trade routes documented
in Chinese and Arabic records—was an im
portant business. The cargoes of the region
al traders show that Southeast Asians
preferred traditional pale green ceramics
and were far less interested in the blue and
w'hite china that was all the rage in Europe
from the 16th century on.
But marine archeologists may be run
ning out of time. The advances in sonar
technology that have helped people like
Sjostrand—w'ho shares both his treasures
and his knowledge with the Malaysian gov
ernment—find the wrecks mean looters also
have easier access. At the same time, com
mercial fishing in the region—especially
with dragnets diat scrape the ocean floor—
has intensified. The nets shave off tire top of
the wrecks, scattering their precious cargo
and destroying the masts or protruding
hulls that would help divers locate them.
“Someone or something else will get to tire
wrecks if action isn’t taken soon,” says John
Guy, curator of the Indian and Southeast
Asian Department of London’s Victoria and
Albert Museum. “The result is that the pace
ofwreck recovery has increased dramatical
ly, and at tire same time there is an urgency
that wasn’t there in tire past.”
Pulling treasures up from the depths is
NEWSWEEK MAY 20, 2002
easy feat. Visibility at the wreck sites is
3n near zero because of high winds, and
each year there arc only two short periods
when conditions in tire South China Sea al
low for deep-water diving. Merely locating
tire ships is a difficult task. Sjostrand-who
developed a taste for ceramics more than 20
years ago while working as a commercial
marine engineer in Singapore—started
searching in tire early 1990s. He decided
on a 10-mile-by-250-milc corridor down
peninsular Malaysia’s east coast, in what
was once one of the world’s busiest ship
ping lanes. During the first tw'o years, all he
found were rubbish and oil pipes. Still, he
had enough savings and determination to
push ahead. It helped that local fishermen
w'ere often able to point out areas where
diet' had found broken ceramics in their
nets. Eventually, he got lucky. "Once you
«
mow rleft: no credit, stem sjoshuno izi.no credit
decide to do something, then you don’t stop
before you've finished,” Sjostrand says.
To whom do the artifacts belong?
Malaysia’s national museum gets first pick,
since most of tire wrecks are in Malaysian
waters. The museum gets 30 percent of the
haul, while Sjostrand keeps 70 percent—an
arrangement both sides seem happy with.
Sjostrand is training museum stall' in ma
rine archeology', and has helped diem set up
an excellent exhibition at the national mu
seum dtat showcases cargoes from a
total of 10 shipwrecks dating back to the
Tbriang. "Malaysia is at the crossroads of
maritime trade in diis region, but our gov
ernment doesn't have that much money to
spend on underwater archeology,” sa> Adi
Taha, director-general of the Department
of Museums & Antiquities in Malaysia.
Working with people like Sjostrand is da-
only way to get artifacts to the surface.
“Some might say this is commercialization,
but I say it is commissioning,” says Taha.
For his part, Sjostrand funds his under
water archeology by selling to museums and
private collectors a significant proportion of
die plates, jars, bowls, teapots and spoons
brought to die surface. Though he retains a
large collection of ceramics bought from
dealers over the past two decades, the pieces
recovered from die. wrecks are his favorites.
“For me there is far more value in a piece
when you know exactiywhere it comes from,
and you can piece together its history."
The best may be yet to come. In 1511, a
Portuguese ship, the Flor de la Mar, sankin
the Strait of Malacca along with its bootv
looted from the rich Sultanate of Malacca.
An Indonesian salvage team spent several
million dollars trying to locate the wreck in
the early 1990s. and predicted the discov
ery ofseveral billion dollars’worth ofgold.
j.'.'eeio'.’.: ■ '.ones and other artifacts. Thev
found littl. and eventually ended the
s.- arc,,. But div Flor th la Mar ■ still out
there son.:, where, waiting to be salvaged.
Unless looters get thereun
"
45
- Media
 RF_DR_8_SUDHA.pdf
RF_DR_8_SUDHA.pdf
Position: 565 (41 views)