DRUG ISSUE MEDIA COVERAGE
Item
- Title
- DRUG ISSUE MEDIA COVERAGE
- extracted text
-
RF_DR_17_SUDHA
Multinational drug companies a
Third
producing only two major or essen here would cost Rs 15 in Bangladesh,
tial drugs. Today we produce 100. In just across the border. This is because
1952 the value of annual essential the profit margin for drug traders in
drug production was Rs 1 crore. India cannot be more than 12.5 per
Today it is 66 crores — a 66-fold in cent. Other governments allow it to
crease.
be upto 33 per cent.”
And yet the scope for further
Reduction in drug prices in itself,
growth is unlimited. The annual per says Mr Kapadia, may not help much
capita drug consumption in India, ac- to solve India’s health problems. “At
dording to World Health Organisa the moment our per person drug
tion (WHO) statistics, is hardly Rs 8. consumption is around Rs 8 per year.
Over 75 per cent of the population is Even if the drug prices are slashed
beyond the reach of modern medicine. by as much as 25 per cent, which is
“Common man today cannot afford hardly possible, the per capita con
medicines,” claims S. K. R. lyangar, sumption would go up to Rs 10 per
who for the last 20 years has been a year which by world standards is still
leader of the pharmaceutical workers miserably low.
“Drug prices are really a non-issue.
and is the Deputy President of the
Maharashtra Shramik Congress. “The What percentage of your medical bill
by Bhanu Kale
drug 'firms have made ieven simple is spent on medicines? That is a more
things like cotton or bandage or tinc pertinent question. Pathological inTravelling through seemingly un ture of Iodine very expensive. The . vestigation, X-rays, surgery, doctor’s
changeable rural India, along a situation is so bad that if there is a charges, hospitalisation etc. forms
the largest part of one’s medical ex
kachha road surrounded by rice fields train accident passengers hesitate to penses.
and muddy shacks, one is often struck come out and buy the first-aid.”
"The low. consumption of drugs is
According
to
Mr
lyangar,
“
The
by a sign of modern times. One secs
of the general poverty of
a smart young man sporting a nice tie drug prices are exorbitant solely be aourreflection
people. People don’t have enough
cause
with
the
producers,
the
profit
despite sultry weather and carrying
money even to buy food. Is it surpris
motive
comes
first.
Take
the
case
of
an elegant leather bag. The fingers of
ing that they don’t buy drugs?”
turbaned natives, all pointing in dif lodex. In several homes this ointment
ferent directions, do not confuse him. is used to cure simple pain, cuts or
It is macle in the traditional
Confidently he reaches his destina burns.
Comparative
minimum
mouthy
tion; the local chemist or .a doctor. He Ayurvedic way using mostly inexpen
wages (in rupees)
sive
herbs.
I feel it should not cost
is a medical representative of some
more
than
one
rupee
a
.bottle.
Yet
pharmaceutical firm.
Peon
Clerk
In many ways that medical repre it is sold for around Rs 3.50.”
In 1952 Prime Minister Nehru in
sentative symbolises the drug indus- vited
drug
multinationals
to
India,
State
Government
268
340
A-.ry in today’s India. With sophisticat- sparking the growth of an Indian drug (Maharashtra)
*1- ed marketing techniques he has pene industry almost from scratch. Ever
trated even remote villages. Yet the since it has been criticised, perhaps
Central Government
337
445
vast majority of villagers are left un more so than any other industry. The
(Railways)
touched by him. He is selling what Jaisukhlal Hathi Commission's report
•146
561
most people need but only a few can on the drug industry, tabled in Parlia Semi-Government
afford. His appearance suggests aliena ment this year, gave this criticism a (Port Trust & Docks)
tion. His efficient, dynamic way of new fervour. Is the accusation of
550
350
working, ironically, confirms it. His profiteering right? Does the drug in Banks
nicely documented brochures do not dustry bribe doctors-, buy politicians?
inspire trust among those around. The Are drug prices unjustifiably high? Is Textiles
420
520
desperate poverty of the latter is not that the reason for drugs being out
of his making, yet an observer is of the reach of most Indians?
650
Engineering
550
tempted to wonder.
(Mukand Iron & Steel)
High Prices
Growth : Enormous but Inadequate
“No,” asserts B. V. Kapadia, since
753
923
Pharmaceuticals
If growth is a test of worthiness the 1941 chief distributor for East India (Pfizer)
drug°industry comes out with flying of CIBA, the renowned Swiss drug
per capita National Income : Rs 50
colours. In 1948, according to a re multinational. “Our drug prices are
per month.
port of the Organisation of Pharma among the lowest in the world. For
example
nasal
drops
costing
Rs
5
ceutical Producers of India, we were
COMMUNITY HEALTH CELL
Hi mm at Sep I
47/1,(First Floor)St. Marks Roan
14
noou^ssG.
M(@£smg
ffflDLT
ipa^n11
>il
HI A
J -IQ .
• 5G0
Multinational drug companies ajnd the
Third | World
Il '
mixed
blessing
for
psxmr
Rations
by Bhanu Kale
Travelling through seemingly un
changeable rural India, along a
kachha road surrounded by rice fields
and muddy shacks, one is often struck
by a sign of modern times. One sees
a smart young man sporting a nice tie
despite sultry weather and carrying
an elegant leather bag. The fingers of
turbaned natives, all pointing in dif
ferent directions, do not confuse him.
Confidently he reaches his destina
tion; the local chemist or .a doctor. He
is a medical representative of some
pharmaceutical firm.
In many ways that medical repre
sentative symbolises the drug indus
try in today’s India. With sophisticat
marketing techniques he has pene
trated even remote villages. Yet the
vast majority of villagers are left un
touched by him. He is selling what
most people need but only a few can
afford. His appearance suggests aliena
tion. His efficient, dynamic way of
working, ironically, confirms it. His
nicely documented brochures do not
inspire trust among those around. The
desperate poverty of the latter is not
of his making, yet an observer is
tempted to wonder.
ed
Growth : Enormous but Inadequate
If growth is a test of worthiness the
drug industry comes out with flying
colours. In 1948, according to a re
port of the Organisation of Pharma
ceutical Producers of India, we were
producing only two major or essen
tial drugs. Today we produce 100. In
1952 the value of annual essential
drug production was Rs 1 crore.
Today it is 66 crores — a 66-fold in
crease.
And yet the scope for further
growth is unlimited. The annual per
capita drug consumption in India, acdording to World Health Organisa
tion (WHO) statistics, is hardly Rs 8.
Over 75 per cent of the population is
beyond the reach of modern medicine.
“Common man today cannot afford
medicines,” claims S. K. R. lyangar,
who for the last 20 years has been a
leader of the pharmaceutical workers
and is the Deputy President of the
Maharashtra Shramik Congress. “The
drug 'firms have made .even simple
things like cotton or bandage or tinc
ture of Iodine very expensive. The
situation is so bad that if there is a
train accident passengers hesitate to
come out and buy the first-aid.”
According to Mr lyangar, “The
drug prices are exorbitant solely be
cause with the producers, the profit
motive comes first. Take the case of
lodex. In several homes this ointment
is used to cure simple pain, cuts or
burns. It is macle in the traditional
Ayurvedic way using mostly inexpen
sive herbs. I feel it should not cost
more than one rupee a .bottle. Yet
it- is sold for around Rs 3.50.”
In 1952 Prime Minister Nehru in
vited drug multinationals to India,
sparking the growth of an Indian drug
industry almost from scratch. Ever
since it has been criticised, perhaps
more- so than any other industry. The
Jaisukhlal Hathi Commission’s reporton the drug industry, tabled in Parlia
ment this year,' gave this criticism a
new fervour. Is the accusation of
profiteering right? Does the drug in
dustry bribe doctors, buy politicians?
Are drug prices unjustifiably high? Is
that the reason for drugs being out
of the reach of most Indians?
High Prices
“No,” asserts B. V. Kapadia, since
1941 chief distributor for East India
of CIBA, the renowned Swiss drug
multinational. “Our drug prices are
among the lowest in the world. For
example nasal drops costing Rs 5
here would cost Rs 15 in Bangladesh,
just across the border. This is because
the profit margin for drug traders in
India cannot be more than 12.5 per
cent. Other governments allow it to
be upto 33 per cent.”
Reduction in drug prices in itself,
says Mr Kapadia, may not help much
to solve India’s health problems. “At
the moment our per person drug
consumption is around Rs 8 per year.
Even if the drug prices are slashed
by as much as 25 per cent, which is
hardly possible, the per capita con
sumption would go up to Rs 10 per
year which by world standards is still
miserably low.
“Drug prices are really a non-issue.
What percentage of your medical bill
is spent on medicines? That is a more
pertinent question. Pathological in
vestigation, X-rays, surgery, doctor’s
charges, hospitalisation etc. forms
the largest part of one’s medical ex
penses.
“The low consumption of drugs is
a reflection of the general poverty of
our people. People don’t have enough
money even to buy food. Is it surpris
ing that they don’t buy drugs?”
Comparative
minimum
mouthy
wages (in rupees)
Peon
Clerk
State Government
(Maharashtra)
268
340
Central Government
(Railways)
337
445
Semi-Government
(Port Trust & Docks)
446
561
Banks
350
550
Textiles
420
520
Engineering
(Mukand Iron & Steel)
550
650
Pharmaceuticals
(Pfizer)
753
923
per capita National Income : Rs 50
per month.
COMMUNITY HEALTH CELL
47/1.(First FloorlSt. Marks Roadl
Disturbing Wage Differences
According to some, fat salaries paid
by the drug firms also amount' to
bribing the emploj'ecs. Drug compa
nies certainly pay better than most
(see box on page 14). An unskilled
worker in Pfizer, for example, in his
first month can draw a minimum wage
of Rs 753 whereas a headmaster in a
In the minds of many people, high municipal school might retire after 35
prices and high profits in the drug years of service on a monthly wage
industry go together. The fact is that of just Rs 650.
the drug industry in India operates
Certain drugs can be lethal. And
under a straightjacket of price con
trol. Since January 1, 1974 the fixa 100 per cent quality control is im
practical.
So there is always a danger
tion or revision of prices has been
done by the Bureau of Industrial Costs of sabotage. Even one defective bottle
and Prices - which is directly under gone into the market, if detected by
the public, can spoil the firm's name
the Central Government.
A comparative study of commodity and the entire product may have to
prices and drug prices over the last be abandoned. Therefore drug firms
several years makes interesting reve always have a policy of.keeping their
lations. The wholesale price index of workers satisfied by paying handsome
essential commodities (food, cloth salaries. Perhaps they also reckon
Iwpin 1957 was 105.3 (base; 1952 = that it is better to pay their own em
I 00), while that of drugs was only ployees than to let the Government
88.7. In 1969 when the former rose to take away the same money in taxes.
Whatever the justifications for
211.6, the drug price index was only
about 136.9. Thus while the prices of high wages, Mr lyangar feels "this has
essential commodities rose by about created bitterness among workers
IF2 per cent, the rise in drug prices from different industries. In my
was only about 40 per cent. Again
the commodity price index spiralled
to 252 by August 1973; but the price
index for drugs stood only at 148.7.
It seems clear that the budget of an
average consumer has been eroded
more by the commodity price rise
than by the drug price rise.
Free Samples
It is a common practice for all the
drug companies to distribute freely
some of their products to doctors. At
least a few doctors sell these free
samples, illegally, to the patients. This
'^F-r has personally come across one
such case. Many feel that this free
distribution amounts to bribing.
Some feel that as much as 25 per cent
of production goes into sampling,
which, they claim, is largely respon
sible for “high prices” of drugs.
A.'K. Bahl, now financial director
of Cadbury, but who has held a simi
lar position in a drug multinational,
contradicts this opinion. “The distri
bution of samples is not as wides
pread as it is generally believed to
be. And in any case sampling is na
tural jri a competitive society. You
have to let the doctors know about
your product. Samples are given so
that the doctors can make their own
independent assessment of tfee medi
cine and its efficiency. I feel that this
is a very healthy practice.”
Himmat September 15, 1978
DRUG 4s
INDUSTRY,
the monopoly over drug production
.in India. In a developing country like
India, where the health service is lar
gely contained in the private sector,
the multinationals account for 56 per
cent of basic drug production. In a
developed country like Britain the
same figure is 63 per cent, despite the
fact that the health service there is
nationalised (see box on page 17).
Moreover the share of the multina
tionals is decreasing. Many indigen
ous companies are coming up. For
example, Alembic and Sarabhai, both
indigenous, are today among the five'
biggest drug manufacturers in India.
Yet it is a fact that the multina
tional drug firms make high profits.
In India 25 top drug multinationals
made a profit of Rs 11.57 crores in
1973 bn the investment of 32.5 crores.
The Swiss multinational Roche quot
ed Sri Lanka a price for the tranqui-
I.ARGE SCALE PENICILLIN MANUFACTURING :
clean surroundings, strict quality control
union, for example, there are work
ers from pharmaceutical as well . as
from engineering industries and I
have seen the tension among them.
When the workers see that someone
with the same or even less qualifica
tion gets more, they feel jealous. They
too demand more, which their own
industries cannot afford. The result
is confrontation and bitterness. It
also leads to vicious cycle of wage
rise and price rise. The real sufferer
is the average consumer.”
Multinationals
Facts do not support a widespread
opinion that the multinationals have
User valium which was 70 times
higher than the price charged by an
Indian company. Five United Na
tions agencies (WHO, UNCTAD.
UNIDO, UNDP and UNICEF) are
collaborating in an undeclared war on
the multinational drug firms. This
month they are meeting in Buenos
Aires, Argentina, to plan their stra
tegy, They are fighting what WHO's
director-general calls "drug colonia
lism”.
But there is another side to the coin.
At least some people weigh the deci
sion of the United Nations with cauCONTINUED ON NEXT PAGE
15
DRUG
INDUSTRY
MIXED BLESSING — from page 15
lion. They feel the UN has become
■an instrument of ideological warfare.
The third world countries possess" an
overwhelming majority and the ma
jority does not always spell the truth.
Mr Kapadia, for, instance, strongly
defends the drug multinationals.
"They pay Government taxes more
honestly than the local firms. They
pay their workers better. They pay
their shareholders handsome divi
dends — that is why their shares are
so high. And if after doing all this
.they make high profits then I think it
is creditable to them. It shows their
efficient management. What is wrong
with making profit? It is true that like
power profitability can be abused. But
do you abolish power? Do you abo
lish the prime ministership because at
times it is abused? Then why this hue
and cry about the profits of drug mul
tinationals? What is the point in com
plaining that these firms buy Indian
officials and politicians? It is common
sense that you can buy only that
which is for sale. As long as a per
son is ready to be sold, he will be
bought by someone, X or Y.”
Research
The drug industry justifies its pro
fits by saving that much of it is re
invested in research. The Western
drug industry, which includes practi
cally all the drug multinationals,
•f/a;
cash prizes
for slogans/slides/
short films
ON FIRE PREVENTION
Competitive entries are invited by the Government of India,
Ministry of Home Affairs, for slogans/slide designs/short films
on fire preventlon/protection against fire to highlight any of
these important aspects for inculcating sense of fire safety
among the public. The material can be in Hindi, English or any
regional language. Attractive prizes as detailed below are
offered to the best entries:
Prizes
for
slogans
for slide
designs
for short
films
super'8', 16 mm
or 35 mm
sound
First Prize
Second Prize
Third Prize
Rs. 500/Rs. 300/Rs. 200/-
Rs. 1.500/Rs. 500/Rs. 250/-
Rs. 5.000/Rs. 3.000/Rs. 1,500/-
Further details may be obtained
Last date for
from the Fire Adviser. Ministry
of Home Affairs. 2nd floor.
receipt of
Indian Express Building.
Bahadur Shah Zafar Marg.
entries is
New Delhi-110002.
October 31, 1978
davp 78/239
16
spends about half its profits on re
search. Some successful innovators
like Roche spend even more.
Multinationals have contributed
greatly to the development of modern
medicine. In the words of Sir Derrick
Dunlop, former Chairman of the Bri
tish Medicines Commission, "The re
volution (of increase in life expect
ancy) has been very largely due to
the pharmaceutical industry. Some
years ago Sir Ernst Chain said that of
the 66 most valuable drugs introduc
ed since aspirin in 1899 only nine had
been discovered in the Universities
arid research institutes. But all the
other 57 had been discovered by the
scientists working in the laboratories
of an industry devoted to the profit
motive.” It is said that the multina
tionals spend only a fraction — less
than four per cent — of their total
research budget on tropical diseases.
Over a billion people from the third
world are exposed to tropical dise^'p
Though one would wish multinationals
to be more humanitarian in this mat
ter it seems hardly likely that they
would like to be dictated to about
what they should do. Ultimately eac.h
country is responsible for meeting its
own specific needs.
In the absence of the multinationals
could Indian companies take on the
research that is necessary? In the
words of John S. Baker, Managing
Director of Pfizer Limited, “on a
worldwide basis Pfizer spends annu
ally about Rs 20 crores on research
and this has been found as a neces
sary sum for research with a substan
tia! content. The company can afford
to do this because it operates in a
world market. The Indian operation
alone, which constitutes a mere two
per cent of Pfizer’s worldwide total
sales, could never contemplate a l’~I\
lar research venture.”
1
Again to quote from “The Econo
mic Times” : “The growth of the in
dustry in the past decade was mainly
due to the contribution of the private
sector. Some of the bulk drugs which
JDPL .(Indian Drugs and Pharameceuticals Ltd., the public sector firm)
manufactures now were introduced in
the country by the private sector. The
same is true about Hindustan Anti
biotics Ltd. another public sector
company. Judging from this experi
ence, the country has'to depend upon
the expertise of Western European
Nations to keep itself abreast of
changing technology.”
The present Indian Government,
like past ones, is committed to en
courage small scale industries. What
Himmat September 15, 1978
are the chances of small scale drug
units taking over the larger share of
the market? Fortunately remote.
Most doctors hesitate to prescribe
drugs made in the small scale units.
They are often sub-standard and are
produced without the necessary clini
cal conditions.
It is worth quoting, at some length,
from the report of the Committee on
Drug Control appointed by the Cen
tral Government. It states, “By and
large, the smaller units, being housed
in residential buildings, are not de
signed with the necessary layout for
PUBLIC SECTOR :
growth due to private firms
Perhaps the time has come when
we need to decide clearly whether it
is possible or right to refuse what the
multinationals have to offer. As Mr
Bahl puts it, "We cannot take the
benefits of what they offer and still
continue to abuse them.” They are
not running a charity and would cer
tainly like to make maximum profit.
But the profit they make is strictly
within the limits set by the Govern
ment of India — which at most times
has been left of centre. What they
take out of the country as profits is
much less than what they bring in by
exports. In 1973-74 against a remit
tance of about Rs 5 crores made, the
foreign exchange earnings of these
companies were over Rs 12 crores;
thus making a net gain of Rs 7 crores
for the country.
The pharmaceutical industry, by
its very nature, has to have a multi
national outlook. Like diseases, medi
cines also do not know national boun
daries.
The rhetoric of “exploitation by
drug multinationals” is not likely to
recede even if they distribute all their
products free of charge. There are
people who call outright charity as
an instrument of “colonial, capitalis
tic exploitation”. Those who accuse
and those who defend the multina
tionals both have their own argu
ments. One is free to accept either
side. One fact however deserves to be
noted : Soviet Russia, which in theory
1
pharmaceutical manufacture. Except
in a few units attention was not paid
to the hygienic conditions in the
plants as well as in the surrounding
areas...For example emulsions were
being manufactured using a simple
s*f. Bottles were not properly
washed and sterilised before filling. In
one vaccine laboratory bottles wete
not cleaned at all but directly filled.
In a number of units the raw mate
rials were not tested before use while
in others they were partially tested
xand the important tests for arsenic,
lead, heavy metals etc. were not per
formed. In the course of visits to fac
tories, the Committee came across
many instances of fake records and
cooked-up results...... ”
If this is. the report of the. official
Government committee, is there much
virtue in allowing these units to cap
ture a larger share of the rharket by
deliberately restricting multinationals?
Should such a lifeline industry be en
trusted into unclean hands just be
cause they happen to be brown?
Himmat September 15, 1978
DRUG
4
INDUSTRY,
expect the Government to be pater
nalistic. Z. F. Lashkari, who has work
ed in a pharmaceutical firm for nine
years, has some suggestions.
“The Government can set up drug
industries in basically rural areas.
Certain drugs can be reserved' for
manufacture in these rural areas.
"Secondly, it can. change the pricing
policy so as to motivate companies to
reduce costs. According to the pre
sent policy higher the costs, the higher
is the mark-up, and hence the higher
are the profits. This policy gives no
incentives to reduce the costs.
“Thirdly, it can put restraints on
expenditure for advertisements. Sam
ples given can be restricted, too.
“Fourthly, a fairly good proportion
of drugs produced are irrelevant —
like cough-drops, cold remedies, etc.
It is known that these drugs do not
cure and to a certain extent are also
addictives. They sell mainly because
of good marketing techniques and do
not require high technology. The
Government should step in to cut
down such false demands, and restrict
the manufacture of these drugs to
small scale sectors which can easily
produce them.”
Structure of the drug industry in India
Name of sector
Production value in
crores of rupees
!
Production value
percentage-wise
Basic drugs
18
Formulations
28
Basic drugs
27
Indian private
sector
6
80
9
20
Small scale sector
5
80
8
20
Multinationals
37
220
56
53
Total
66
408
100
100
Public sector
,
should be most staunchly opposed to
any multinational exploitation, has
allowed, or rather welcomed, 200 outof top 400 multinationals to operate
within its borders.
Government’s Role
What should the Government do?
The question is of particular relevance
in India where many people almost
formulations
7
Not everybody is content with
Government playing such a moderate
role. Mr lyangar, for example, feels
that “the. Government should take
over the production of essential drugs
and make them available to people at
cheap rates.” Quite a few people
genuinely believe that nationalisation
CONTINUED ON PAGE 23
17
DRUG
INDUSTRY^Jj
down9
‘“Says SZ. jSi\ zfl bush sail!
Dr. R. K. Anand, 44, is a child spe
cialist from Bombay. He also works
as a honorary Associate Paediatrician
and Associate Professor at NairMedical College Hospital, Bombay.
Q: The drug companies distribute
a part of their production as free
samples to the doctors. Do you
think it is a healthy practice?
I personally feel it is not. They
give three reasons to justify this
sampling: to inform us about their
products; to enable us to. evaluate it;
and to enable us to help poor
patients.
All these are only partially valid.
Firstly, they can inform us about
their product by just giving literature
about it. Secondly, most of the drugs
they give have already been tried out
and evaluated. Various papers have
been published on them. We know
their properties well. Thirdly, if a
particular doctor genuinely wants to
help poor patients there are many
ways in which he can help. In most
cases he has enough resources to help
the needy ones.
Actually it is a subtle way of brib
ing a doctor. Right from student
days these drug firms try to win over
the doctors. When you accept their
samples, almost' unconsciously you
feel obliged to prescribe their medi
cines. And samples are not all they
give. They also give generous gifts.
Doctors too are to be blamed for
this wrong practice. Some doctors
actually demand .samples. Unless the
samples are given they don’t prescribe
medicines of that firm. Many doctors
sell these samples, though it is ille
gal. Personally I have decided, nine
months ago, not to accept these free
samples from the drug firms.
18
Q: Do you support a recommend tured mainly for children of a very
ation made by the I lathi Commis young age who can take a medicine
sion that the brand names of vari best in that form. Many parents
ous drugs should’be abolished and nowadays have started in ignorance
that they should be sold only under to give tetracycline to their children
their generic names?
below seven. Is it not the fault of
Yes, 1 do. According to the world the drug firm which manufactures
Health Organisation (WHO) we need .these drops?
In case of baby foods, which are
o.nly a little over 11)0 drugs. The
large majority of the drugs in the now abundant in the market and
market are not necessary. No doubt which make great profit for the drug
the' same medicine manufactured by firms, the consumer is again made to
different companies can have different suffer. Actually even if a mother is
degrees of effectiveness, called, bio malnourished, for the first six months
availability. In smaller units it can she can provide enough milk for her
be less.
child. But because of the advertising
But I think this factor is often by these drug firms, many poor
exaggerated by the drug firms. The mothers too are turning to milk
difference that bio-availability makes powders and are neglecting breast
in curing a patient is not all that feeding. Finally the child comes to
significant. True, there is a danger depend just on often-contaminated
of spurious drugs coming up in the outside milk. It has been proved that
market under the same generic bottle-feeding, especially in a country
names as those of reputed firms. But like ours where good hygiene is no:
maintained, can be harmful wljajks
that danger exists even now.
The abolition of brand names breast-feeding is the ideal food^Wr
would also help reduce the prices of the child and costs nothing.
drugs. No firm would then have a
1 would like to clarify one importmonopoly over a particular drug. ’ant point. When I say ‘‘drug firms”
There would be more competition and I do not just refer to multinationals
hence the consumer would benefit.
which are regularly criticised for
One factor which must be noted such practices. I also have in mind
is quality control. If the existing findian drug flints who also adopt
regulations can be strictly enforced, exactly the same practices.
drugs manufactured even by small
Q: Some people believe that the
scale units will gain credibility. This
real answer to the health problems
factor is important even if brand
of India is not to lower the prices
names are not abolished. Even for
of drugs but to reduce the costs of
big firms strict enforcement of quality
doctors, hospitals, X-Rays, patho
control regulations is necessary. And
logical investigations etc. Do you
it is not too difficult to achieve. In
agree?
Maharashtra, for example, thp Food
and Drug Control Authority is very
There is, no doubt that some doc
tors practise medicine as a business.
efficient.
A lot can be said on that. That is
Q: Do you feel there are many why Gandhiji has included debars
drugs in the market which are sold in the three enemies of pcopleP'^^e
not because of their necessity but said that a doctor would give pills
because they make good money?
to a patient suffering from indigos]
Yes, there are many. For example tion and cure him. But he will not
many tonics contain only some iron try to cure the habit of overeating
and vitamins which are also available which is the root cause of indiges
in food. Ordinary people are taken tion. ‘
in by effective advertising. But for'
We have to train people to remain
much less money they could buy healthy with the minimum of drugs.
nutritious food which will give them Most illnesses can be cured without
all that the tonics promise.
any drugs. We need to get enough
Q: Would you say that the prac fresh air, clean water, nutritious food
tices of the drug firms amount to and exercise.
But all that does not go to say that
profiteering?
Yes. Let me give a couple of exam the lowering of drug prices is an
irrelevant
issue.
Drug prices have
ples. Tetracycline is not meant to be
given to those less than seven years of to be lowered and after having work
age. It harms their bones. But now ed as a consultant to a drug firm I
some firms are manufacturing tetra feel that the drug firms can affprd to
— B. K.
cycline drops. Drops are manufac do so.
Himmat September 15, 1978
cx-^"^ #*& /itv,
^.ocn^/n^ Q tf'
‘Bun On Mmufacture Of
Drug Unjustified9
',U'
c'
CVbv^ .
-'[(M
/oL/AzC^
Wl~
Iz)
' ^cf^MUAr
for reasons other than pregnancy)
By a Staff Reporter
similar gynaecological dis
npi-IE Union Health Ministry’s de- and
orders.
-L- cision in June banning the
The association, the statement
manufacture of all oestrogen-pro- said, was of the view that misuse
gestogen formulations (other than of drugs should be no cause for
those used as oral contraceptives banning them outright. The Indian
in low doses) from December 31 Council of Medical Research also
next and their sale from June 30, was not in favour of banning the
1983, may come as a surprise to drugs, Dr Ghothoskar said.
the pharmaceutical industry and
The Drugs Controller said that
many obstetricians and gynaecolo
the manufacturers were not at
gists in West Bengal.
The Drugs and Appliances Stan fault as the drugs prominently
carried
the warning label : “Nob
ding Committee of the Indian Me
dical Association, Bengal State to be taken by pregnant woman”.1
branch, at a recent meeting said There would not have been a.
that the Drugs Controller of India problem if women took it on a
should consult appropriate scien doctor’s advice. When the stop
tific bodies and experts of specific page of bleeding was not due to
discipline before imposing a ban. pregnancy, these combination drugs
It felt that the withdrawal of such would help restore menstruation.
a “valuable” drug from the mar
The Organization of Pharmaceu
ket would not be justified, as it tical Producers of India, represen
was used gainfully in many gynae ting the industry, in its memoran
cological .disorders.
dum
to the Drugs Controller of
The Union Health Ministry, In India disputed his claim that si
Its circular dated June 25, said milar drugs had been banned in
that medical experts in tTie coun many countries. It quoted some
try had noted that there had been documents to show that these
misuse of these preparations. It drugs
marketed all over
also stated that many countries Europe,were
Britain and the USA.
had banned these . preparations Even if it was misused, the alleg
and that their substitutes were ed problem could not be solved
available in India.
by banning them.
The IMA committee in its re
solution made it clear .that there
There was no drug which could
was no difference of opinion over not be misused by unqualified
the fact that a combined oestro practitioners. The remedy lay not
gen and progestogen preparation in banning the drugs but by tak
should not be used for diagnosis ing appropriate action against the
of pregnancy, because if it was persons misusing them.
used for this purpose there was
The OPPI said that the Drugs
the possibility of “congenital mal Controller had taken the decision
formation”.
against the advice of his own ex
This, it was pointed out. did not perts and that of the Federation
mean, that a fixed dose of the of Obstetricians and Gynaecolo
combination of these two drugs gists of India. The Union Health
had no beneficial tise in other Ministry was not correct in claim
gynaecological
conditions.
The ing that there were non-hormonal
committee recommended that the substitutes available in India for
law should be enforced strictly to :the treatment of a host of mencurb misuse of the drug and pro- «t-rual
1
disorders, a spokesman of
hibit its sale without the prescrip- 1the organization said in Calcutta
tion of registered doctors.
<on Friday.
Dr S. S. Ghothoskar, Drugs Con- rj
troller of India, in a recent Press ■
statement in Delhi, reportedly ; d- [j
mltted that the All India Associa- 3
tion of Obstetricians and Gynae-1
cologists was opposed to the ban a
as the drug was useful in manag- fl
Ing secondary amenorrhoea (stop-fl
page of bleeding among women®
Are we in some danger of drug Drugs we can easily make in our country are being imported
production falling short of demand?
Let us examine the trends.
*1978-79 Import df major bulk drugs which arc also
indi&anousiy manufactured
The Government estimates the
country's requirement of bulk drugs
Cult Druy
Unit
Production
Imports
in 1982-83 at Rs. 625 crores. This is
Qty
Value
(Rs lakhs)
to be met by production within the
1. ANTIBIOTICS
country (Rs. 475 crores) and imports
Streptomycin
225.0
280 1
Tonnes
76.1
(Rs. 150 crores).
95.0
38 5
117 5
T etracyclmc
244.0
96 5
233 0
The production of bulk drugs to
584 6
10.3
92 0
day is about Rs. 200 crores. Consi
1215 2
2. SULPHAS
derable expansion has to take place
Sulphsmeihox J sole
Tonnes
22.0
61 9
143 9
if the target of Rs. 475 crores is to
J. ANTI-MALARIAL
be met.
Chloroquin
Tonnes
45.0
304 0
791.0
The Government's present policy
ANALGESICS
is likely to achieve the exact oppo
Aspirin
Tonn#i^
1303.0
319 4
47 3
Oxyphonyl Buiirono
25.0
site. Several companies are to be
42 9
16.0
95.6
39 6
asked to curtail output.
129 7
.
STEROIDS
If this is persisted with, produ
Prednisolone
869 0
1070.0
69 2
kfl
ction targets will not be met. The
. VITAMINS
gap between production and demand
39 4
MMU
60.0
15.0
will widen. There will be more shor
Vnamm Bi
201 9
29.0
78.710.0
(MU)
tages.
Vitamin R>
Tonnes
28,338.0
109 7
,,
(MU)
Our import bill will then go up
Vitamin 8 i z
165.0
55 1
190.0
kfl
further. This is in spite of expertise
406 1
and experience available to produce
GRANO TOTAL
2755.1
these bulk drugs within the country.
SOURCE : Production figures. ■ Annual Report of the Ministry of Petroleum. Chemicals
Cut in production when the need
1
b Fertilisers. tor 1978-79 Import : ■ Data compiled by the Directorate
is to increase production:
General of Health Services. Ministry ot Health
When more production of drugs 1 .......... .
is the paramount need, we have the
anomaly of drug companies being from Rs. 82 crores in 1976-77 to on several units. Government alloca
asked to curtail production. This stems Rs. 147 crores in 1977-78 (landed tions are not need-based and fall
from the Drug Policy announced in
cost). With belter planning we can short of requirements The question
early 1978 under which companies cut
comes up again: are we planning for
down our import bill.
whose production exceeded the lice
nsed capacity are to peg their output
The table alongside shows figures shortages?
The policy now being followed
at the highest level achieved in the of some major bulk drugs imported in
three years prior to March 1977.
1978-79. It is clear from the table has to be viewed against the needs
the country. The Planning Com
The Drug Policyxis being imple that these drugs are already being of
mission
has laid down production
produced
here.
The
know-how,
the
mented in 1980. The spirit of the
and the capability are all targets for the Sixth Plan. India is a
policy demands that a production experience
signatory
to the Alma-Ata declaration
available
within
the
country.
Yet
freeze, if still deemed necessary.
the goal of primary health
should be at the highest level in the wp are importing these drugs because affirming
care for all by 2000 AD and medi
three years prior to 1980. This would the existing units are not allowed to cines
are a part, however small, of
take into account the normal growth expand.
in production brought about by
If the objection is to expansion this long-term objective.
improved processes and practices
Our per capita availability of
by companies in India with foreign
capital
participation, how does one modern medicines was only Rs. 11 in
If several units in the industry justify imports
from totally foreign- 1976-77, compared to Rs. 79.2 in
have to go back to 1977 levels of owned
Venezuela, Rs. 54.9 in Brazil, Rs. 31.5
companies
abroad?
production, a cut-back of up to 25
in Argentina, Rs. 27.6in Egypt, Rs. 17.1
per cent in bulk drugs and drug for
Today the position is that with in the Philippines, Rs. 15.3 in Thai
mulations is likely. The current output all the licences issued put together land and Rs. 12.6 in Pakistan.
of formulations is around Rs. 1000 the production targets set for 1982Yet we are wasting a valuable
crores. This may shrink to Rs. 750 83 cannot be met. It would seem that
national asset—production capability
crores. Which means that Rs. 250 we are planning for shortages.
already existing within the country.
crores of production will just not be
The
issuing
of
a
licence
does
not
available to consumers. There will be automatically ensure production. A more forward-looking policy is
further shortages, necessitating more Monitoring of the progress of licens urgently called for. We ought to plan
for plenty, not for shortages.
imports.
ed units’ alone will reveal whether
We can easily make the drugs we the licences are being "converted"
/imed in the public interest by
into production.
are now importing:
ORGANISATION OF PHARMACEUTICAL
Imports are already showing an
The non-availability of imported PRODUCERS OF INDIA
alarming trend upwards. They rose raw materials is a major constraint Cook s Building. Dr O N Road. Bombay 400 001
15
DRUG INDUSTRY I THE DOLDRUMS
Tile drugs and pharmaceutical industry
in the country has yet to come of age. In
1948. the value of drugs and pharmaceuticals
manufactured was only of the order of
Rs. 4,200 million. In 1964. the number of
units manufacturing drugs and pharmaceuti
cals was about 1,200; it is now over 2,500.
comprising 119 units in the organized sector'
and the rest in the small scale sector. The
value of bulk drugs produced in 1964 was
Rs. 170 million; it has now risen to
Rs. 4.2 billion. The capital investment in the
industry has also increased from about
Rs. 250 million in 1952 to about Rs. 2.5 billion
in 1974-75.
Of the 119 units in the organized sector.
64 units produce formulations only and 7
have been recently issued industrial licences.
There are 14 units manufacturing pharmaceu
tical auxiliaries, like gelatine capsules.
sutures, etc. In the organized sector, of the
119 units, 24 units have foreign equity
exceeding 50 per cent, 14 have foreign equity
between 40 to 50 per cent and nine units
have foreign equity between 26 and 40
per cent.
During the fifth plan, it is proposed to
increase production of drugs from Rs. 3,700
million in 1973 to about Rs. 5,000 million
al the end of 1978-79. This will require
manufacture of bulk drugs of about Rs. 1.500
million per annum and investment of Rs.
1,500 million for bulk drugs and Rs. 1.000
million for formulations. Production of bulk
drugs in the public sector, which is of the
lune of Rs. 300-350 million at present is
expected to be increased to Rs. 750 million,
contributing about 50 per cent of the total
bulk drugs production in the country. Simi
larly. in the field of formulations the public
sector is expected to contribute about 20
per cent of the total requirements with only
two more years left for the fifth plan to be
over, the investment gap in the industry was
about Rs. 1.8 billion
Nearly 613 million people in India
means as many cases for medical treatment.
But only about 25 per cent of the country's
population has access to modern medicines.
Even within that percentage, the availability
of drugs shows disturbing disparities in
relation to levels of income and urban-rural
distances. The rest of the population depends
on native medicines and folk treatments.
It is in this context that the drug industry
in India has to be viewed and its social
obligations and business viability balanced.
Government's current concern is medicine
for the millions. A drug policy, which is on
the anvil aims at providing at least a few
essential medicines to the common people
at reasonable prices. While implementing
it, economic factors, management inadequa
cies, vested interest back-lashes and the
sheer magnitude of numbers and distances
are bound to counteract. The solutions.
18
Dr Madan is a senior scientific officer
in the Indian Drugs and Pharmaceutical
Limited, a public sector drug company.
IDPL is the largest pharmaceutical complex
of its kind in Asia and the middle cast. Its
share of India’s bulk production of essential
basic drugs and antibiotics is around 40 per
cent. It has two plants, one each at Hyderabad
and
Rishikesh.
They
manufacture
48 products, including 38 drugs, vitamins,
sulphas, analgesics, anti-pyretics, anthelmin
tics, anti-tuberculars. etc. IDPL has plans
to double its output by 1978-79, adding
25 new products. Two new units are to
come up in Bettiah, in Bihar, and Gurgaon,
in Haryana.
According to Madan, the drug industry
has seen a phenomenal growth in the last
25 years and the public sector has had an
important role to play in this. Il started from
scratch. Now the private sector and foreign
companies consider it a viable competitor.
The public sector works under several
constraints. While foreign and private
companies make the high-profit items known
as formulations like multivitamins, cough
syrups and compounds, the public sector
makes low-profit bulk drugs. That explains
why, Dr Madan says, profitability of the
company is low. On lop of it is the responsi
bility of making drugs in short supply.
IDPL is making Chloroquin phosphate
needed for malaria, which no private
company is willing to manufacture since it
is a cheap product. Similarly, when foreign
companies refused to make Aidmat, we
made it from imported raw materials
from Hungary. Again, a company producing
pethidine hydrochloride was shut down
lor three months and IDPL was asked to
step in. We did, but then such things do
cut down our efficiency and profits, Dr
Madan bemoans.
Al limes, he continues, we come under
pressure to discontinue manufacturing
existing drugs. Sulpha Guanadine. a drug
used in control of cholera, was almost
banned because it was believed to be toxic.
We make 1,000 tonnes of it. We approached
the government saying that the number
of people it saves are far more than the
number it "harms” due to its toxicity.
The role of the public and private
sectors and foreign companies is not yet
complementary. The other two sectors con
centrate on high profit and non-essential
drugs like multivitamins, etc. It is not true
that foreign companies bring in technology
otherwise unavailable to India except in
a few cases like insulin. Moreover, they
can much more easily manipulate costs
and prices. Our prices are strictly controlled.
This inhibits the effort we should make in
research and development.
"The public sector as yet has no preferen
tial treatment with regard to licensing.
T'k-
pricing or anything else. In fact, because
we have no lobbyists working for us, we
often get step-motherly treatment from the
government
Yet the foreign companies cannot be
nationalized or their operations stopped.
They run about 40 units which cannot be
shut down as there is no organization to
lake them over. If that comes to pass even
IDPL will incur a loss of Rs. 40 million
in the bulk drugs we supply to them. Also,
some of the essential drugs they make
would go off the market. But. we feel, that
these companies should be made to manu
facture raw materials, stopped from bringing
doctors and prohibited from making slight
changes in formulations with a view to
charging higher prices.
We have been trying to help in the
distribution of drugs to people in rural
areas by designing a bit of household
remedies. But essentially it is the job of the
state governments to allocate more funds
for drugs. Similarly we do not think it is
our task to do research on tropical diseases.
We do industrial research not basic
research. The latter should be done by
national laboratories.
According to Madan, the change-over
to generic terms instead of brand names is
impractical and is not likely to bring down
prices of medicines in any way. Doctors do
not have time to write long formulas. So
they devise other ways. They specify the
drug or the manufacturing company.
Dr S. S. Gothaskar is the Drug Control
ler of India. His job is to enforce the Indian
drugs and cosmetics act and the drug and
magic remedies (objectionable advertising)
act. The first act is aimed at ensuring a high
standard of drugs as well as for weeding
out substandard drugs. The second act is
meant to ensure that no claim for any drug
for curing certain diseases such as cancer
or sexual inadequacy can be advertised.
Apart from this, Dr Gothaskar is charged
with the task of ensuring the quality of
imported raw materials for the drug industry.
He also sees to it that the standards of drug
quality are the same all over India. Besides.
he is secretary to the committee on drug
addiction.
Dr Gothaskar said that the law is com
prehensive but enforcement is not effective.
Some state governments like Maharashtra,
Mysore and Madras are good al enforcing
quality, others are far from it. Partly this
is due to lack of money and manpower but
largely owing to a lack of appreciation of the
importance of this subject. Moreover, drug
control is a state subject. The Centre can do
little in the matter. The drug controller’s
office has only 24 inspectors to cover the
whole country.
Spurious drugs are also checked by
CCMM'drelTY HEALTH CELL
47/1,(First FlaorlCt. Marks Road
india today, june 30. 1976
the drug control office. They are made by
unlicensed and unscruplous operators in
garages and in unhealthy surroundings. Such
units, if they come to the notice of the drug
controller, are raided, the culprits arrested
and their goods seized. But the punishment
meted out to manufacturers of such drugs
is too light compared to the enormity of
their crime. The jail term, according to him.
should be a minimum of three years.
He. however, admits that spurious
drugs are not very prevalent in cities. A
survey of drugs, sold in Delhi, was made and
about 200 samples were taken. None of them
was found to be spurious. In another survey'
of some 60-65 mofussil towns in northern
India some 300 samples were taken of which
40 per cent were spurious. This shows
that the problem of spurious drugs exists
much more in the rural areas than the cities
because enforcement is not very effective
there.
He said that sometimes strict enforce
ment of laws on drugs tend to keep
medicines out of the reach of the rural
^population. So drug schedules are being
revised every ten years. Some of the shorter
acting sulphas like guanidine, analgin, antitistamine will no longer require prescriptions.
In the case of penicillin this cannot be done
because its excessive intake will make the
people immune to it and when they really
require it. it will not be effective on them at
all.
Dr Gothaskar said that there are no
reliable statistics about drug addiction in
the country. There have been random surveys
but nothing comprehensive has been done so
far in this regard. Opium, charas, etc.
have been used in the country for centuries.
What is perturbing the health ministry
right now is the use of drugs by students.
But according to him. the problem is restric
ted to the elite in the cities. So far the problem
of abuse of psychotropic substances has
not yet assumed an alarming proportion in
the country at large except in some areas
of Punjab. This is apparent from the fact
rihat the import of materials for making
barbiturates by anphetaminives and tranquallizers has not gone up significantly in
the last four years. In India hallucinogens
can be imported only under special licence
from the government and hence are, not
available easily for misuse.
But the problem with making too
stringent laws for psychotropic substance
distribution is that it will become extremely
difficult for bonafide users to procure them.
The chemists will stop stocking them because
of the cumbersome rules and procedures.
And the drug addict will be able to gel them
somehow or the other from other channels.
Perhaps the solution to the ticklish problem
is to put in a new schedule and to monitor
their sales more carefully.
If the drug controller finds that the
drug habit is miniscule it will be ignored.
Otherwise they will have to arrange detoxi
fication centres for treatment of drug addicts.
Today, there are no such centres in the
country. The addicts are treated in psychiatric
wards and other such places.
“Nationalization of the foreign drug
companies, the much maligned multinatio
nals is not in the national interest,” said
soft-spoken 52-year-old Champak Zaveri,
who heads the MAC Laboratories Pvt. Ltd.
and also leads the Drugs and Pharmaceuticals
Sections of the All India Manufacturers’
Organization. “If we ever take the step of
curbing the activities of the multinationals,
we would be at a loss and disadvantage. No
doubt the Indian sector has made tremendous
progress in the last 10 to 20 years, but
much remains to be done.
“Without the benefit offoretgn technolo
gy we shall never be able to advance and
make sizeable progress in the field of making
sophisticated drugs. Mr Zaveri asserts that
even countries like Switzerland, Germany
and the U.S.A, have to import, acquire and
adapt raw materials, know-how and techni
que. “In the interview of the Common Man’s
health, the so-called “Sector War", the
Formulation Production
1974
Rs. crores
Public Sector
Organized Sector
—wholly Indian
—with foreinn
participation*
Small-Scale Sector
—wholly Indian
1978-79
%
Rs. crores
Growth
contribution
P-a. %
.28
7
104
.30
13
30
20
160
15
20
220
53
352
10
44
80
20
184
18
23
408
‘Includes also small-scale units with foreign participation
INDIA TODAY. JUNE 30. 1976
800
jealousy between the multinationals and the
Indian sector, must be forgotten and all
should take up the task of nation building.
Of course, the Indian sector is undertaking
research; but, not basic research, which
requires Government's collaboration, as it is
loo expensive.
“When the industry is in a position to
mass-produce drugs, then alone will it be
possible to reduce the prices of drugs—
that will be the only guarantee of cheaper and
quality drugs. Not a single Indian Company
has adopted mass production technique of
drugs. After all. that is our responsibility
and ultimately we shall have to fulfil it.
for the good of our countrymen, he added.
Talking of drug prices, he observed
the general attitude is that a man will
readily and willingly pay Rs. 1.25 for a bottle
of coke; but when it would come to paying
Rs. 1 for a glucose saline 25 ml. amp. he would
demur and dither about the price of drugs.
Zaveri would not like to run down
the Ayurvedic system. It, too. has a
hoary lore and vast literature and some
wonder cures. But. over the centuries the
Ayurvedic Drug have had to be a “standard
ized”.
Reverting to his pet theme with a
quotation from Rigveda: “Let the wind of
knowledge come freely from all directions,”
Mr. Zaveri said, the western countries have
a vast storehouse of advanced medicinal
and physio-chemistry, and we should not
hesitate to drink at this fountain.”
therefore, will have to be based on pragmatic
approaches, awakening of social conscious
ness and assertion of the political will.
The policy under review relates to
licensing and expansion, technology transfer.
pricing, supplies to hospitals and research
and development. Several studies, including
the now well-known Hathi Committee Re
port, offer the data and specify the parameters
for the evolution of a workable policy. A
commitment not to take a dogmatic stance
has been evident both on the part of the
government and the industry. However,
there are differences of opinion.
The government’s view is that foreign
companies will be allowed expansion only in
high-technology areas, and a list of drugs
where expansion will be considered is being
drawn up. Twenty-eight drugs for the public
sector and 10 drugs for Indian-owned com
panies have been reserved. The residuary
list, consisting of about 40 drugs—including
items like chloramphenicol, vitamins A,
Bl2, D-2, and D-3, insulin, steroids and
hormones, aspirin, and chloroquin phos
phate—is left to the others.
The organised sector, comprising foreign
subsidiary companies and Indian firms with
international collaboration, feel that in view
of the large requirement, all those with
technological and management competence
should be allowed to expand and produce
19
the maximum to reach higher levels of
economy of scale and socially relevant
price levels. The organized sector now has to
give 50 per cent of its bulk drug production
to non-associated formulators. It feels that
expansion of foreign companies, on the
condition that all future liabilities in terms
of profit remittance are fully covered by
export earnings, is a reasonable proposition.
The small-scale sector, on the other
hand, asks for a rather rigid stance in
relation to the organized sector. The small
scalers say the foreign companies should be
allowed to expand only in bulk drug
production. They should not be allowed to
formulate their enhanced bulk output, and
their formulating capacities should be frozen
at the present levels. While calling for a cut
back on production above licensed capacity
by the organized sector, the small companies
feel that products involving no major techno
logy should be reserved for their own
expansion.
The government’s wish to avoid respec
tive import of know-how is welcomed by
one and all. That imported technology and
know-how should not be for captive use by
firms—both private and public—is also con
sidered sound. However, unless the condi
tions are congenial for horizontal transfer
of technology from company to company,
including economic incentives for such trans
fer, the growth of the drug industry along
healthy fines cannot be envisaged.
On pricing, the government’s stance is
that the industry should agree to produce on
a large scale, non-profit basis a selected list
of drugs required for mass consumption,
whereas higher prices will be permitted for
other products. The organized sector calls
for realistic incentive pricing to encourage
bulk drug production. It feels a 14 per cent
post-tax return on net worth (equity plus
reserves) as compared with 15 per cent on
capital employed as allowed at present could
induce productive enthusiasm, which has
been sagging for some time in the industry.
The small units say that those with a turn
over of up to Rs. 10 million should be exemp
ted from price control.
On the question of distribution, one
and all agree that the drugs should reach
the customer and the hospitals within the
specified time of their potency and under
hygienic conditions. The government wants
industry to make drugs available in bulk
packings at concessional prices to state
hospitals for distribution in rural areas. The
industry by and large is agreeable to such
supplies, provided bulk purchases are made
through centralized authorities. The smallscale sector, however, has expressed a pre
ference that the government purchase from
its members only.
It is a well-established fact that the
advent of modern drugs and their application
have been the result of constant research
and development, much of which is confined
to developed countries. In India, research
and development in the field of drugs has
20
laboratory which is recognized by National
Council of Science and Technology. One
of the reasons why Ranbaxy has moved
ahead so fast is the emphasis that it places
on R&D. Ranbaxy’s research efforts are
directed towards developing life saving dings
besides drugs relavent to tropical environ
ments.”
Bhai Mohan Singh is Managing Director
of Ranbaxy Laboratories and President of
the Indian Drug Manufacturers' Association.
“The private sector of the pharmaceutical
industry in India,” he said, "has been growing
satisfactorily in the past few years. Efforts
on the part of both the Indian private and
public sector have been very substantial."
“The public sector will play a dominant
role in the manufacture of bulk drugs and
will provide raw material to the private
sector, both Indian and foreign. The govern
ment's decision to earmark areas for the
public sector is indeed commendable. I
do not agree, however, with the Hathi
committee recommendations. Its implemen
tation will hamper the growth of the pharma
ceutical industry in India. Besides there
are a number of hazards and pitfalls in
its implementation. One simple result will
be that chemists will sit on judgement over
the doctor. Pakistan is a glaring example
of the mess which followed the switching
over to generic names. What is needed is
a liberal licensing policy as far as the drug
and pharmaceutical industry is concerned.
The present system is a great impediment in
the way of the Indian sector. Being a latestarter it had to face many difficulties
because of the anomalies of the licensing
system. As the sector has now come of age.
it deserves better consideration. Recom
mendations of the Hathi committee in this
regard need to be implemented at the
earliest.
"Another hurdle in the way of the
development of the Indian sector is the
statutory price control on the industry.
It is quite unnecessary and is not conducive
to its development, particularly when we
want to raise the per capita consumption
of drugs. It is rather strange that, on the
one hand, the government is anxious to
increase the per capita of consumption of
drugs and on the other it continues to impose
new levies on the drug industry or raise
he existing ones.
"Some extremist politicians are demand
ing that the foreign companies should be
nationalized as recommended by the Hathi
committee. This is a policy matter which
can have wider international implications.
However, it is known that a number of
countries have nationalized foreign concerns
for boosting their national industry and
enterprise.
"As far as research and development
efforts by the industry are concerned, I
can take pride in the fact that we have a
well-manned and well-equipped research
Sisir Mitra. President of the OPPI said:
"The Government's accent on health
programmes, during the past four five-year
plans, is to a large extent responsible for the
remarkable improvement in health stan
dards. The pharmaceutical industry has also
played its part more than adequately byt
manufacturing and distributing a wide range
of prophylactic and therapeutic medicines.
"In the fifth plan, an outlay of Rs. 796
crores has been proposed on health pro
grammes. The plan envisages a minimum,
uniform availability of public health facilities.
covering preventive medicine, family plan
ning and nutrition services, especially in the
rural areas. The pharmaceutical industry’s
role in this challenging task is the important
one of making available, in the quickest
possible time, adequate supplies of essential
drugs. Fortunately, the industry has the
capability—technological, financial and
managerial—to undertake this task
"To appreciate the magnitude of the task
let us look at the dimensions of growth
required of the industry. Current production
of drugs in the country is of the order of
Rs. 4.5 billion a year, which works out to
a per capita availability of drugs of Rs. 7.50
per annum. The demand for drugs at the
end of the fifth plan is estimated to be
around Rs. 8 billion or double the present
output. In other words, if this demand is to
be met, the industry would have to double
its production by 1978—79, This is a formid
able challenge which nevertheless has to be
met if the country’s growing requirements arc
to be fulfilled. Assuming that we succeed in
this, the per capita availability of drugs in
1978 -79 would still be less than a mere
Rs. 15 per head per annum, for the country’s
population would by then have increased to
655 million.
"The task of doubling production is so
enormous and so formidable that every
sector of the industry—the public, the large,
medium and small scale must work together,
and complement each other to achieve the
goal. There is enough scope and more for
every sector because the country’s require
ments are so large and rapidly expanding.”
INDIA TODAY. JUNE 30. 1976
remained a weak point when compared to
the rapid expansion of the industry. Even
among the largest companies, including the
foreign subsidiaries, only a few do funda
mental research which is basic to the dis
covery of new drugs. Most of the laboratories
attached to production units do developmen
tal research related to raw materials, quality
control, process improvement and packag
ing. The excuse offered is that basic research
is expensive and profits are not big enough to
support it. There is a tendency to reap the
technological spin-ofl' from advanced re
search done elsewhere in the world. The
performance of public sector companies.
like the Indian Drugs and Pharmaceuticals
Ltd (IDPL) and Hindustan Antibiotics in
the field of research is far from satisfactory.
The small scale sector units pass the res
ponsibilities to government laboratories and
the bigger units. Barring a few. the small
outfits do not even have testing facilities or
trained chemists to supervise production.
The government's stand is that the
industry should spend more on R&D and
undertake research in tropical diseases, nutri
tion and isolation of plant materials. The
present investment of 1.5 per cent of the
turnover on research is far too insignificant.
The industry spends nearly six per cent of the
turnover on sales promotion. The industry’s
argument, “the higher the profits, the higher
the amount available for R&D". goes on
indefinitely. What they forget is that some
"mother companies" which started with
insignificant investments have made fabulous
fortunes by developing new medicines
through dedicated research.
In the modern context, research involves
large investments and an element of risk.
A new chemical, even after identification
for its pharmacological effects, takes nearly
ten years to go through animal tests and
clinical trials before being passed. The ex
perience of the Central Drug Research
Institute has established the cost and time
involved in developing a drug. But research
must go on and the companies which make
profits by manufacturing and selling medi
cines cannot wash their hands off it. The
government’s plan to consider a cess on
research has encouraged some large compa
nies to set think of setting up R&D labora
tories. It may be worthwhile for the
government to encourage cooperative R&D
efforts on drugs as it has done in the case of
other industries.
The question whether drugs should have
brand or generic names has been raised
every now and then, and conclusive answers
are yet to be reached. Studies conducted, in
India and abroad, and the experience of
some countries which adopted generic names
for drugs have shown that it is impractical
to give up brand names. Pharmaceutical
manufacturers in Russia in the early sixties
used generic names exclusively. But, follow
ing studies by the Central Pharmacological
Research Institute to Moscow which showed
that 50 to 75 per cent of drug specimens
INDIA TODAY. JUNE 30. 1976
For the last five years J. B. Mody has
been actively associated with the Indian
Drug Manufacturers’ Association (IDMA)
as a Joint Hon. Secretary' and now as Hon.
Secretary.
"We would not have grown to this
stature without the confidence reposed in
us by the medical profession and the public,”
he said.
The Hathi Committee has accepted most
of the ideas he submitted to it. Apparently,
he was able to convince the Hathi Committee,
that the profits of the drugs and pharmaceuti
cals manufacturers are not very high, as
they have to sink a large sum in research.
For instance, Unique spends Rs. 300.00040.000 annually in research over import
substitution.
"This is a product-mix industry and
it should be permitted a reasonable mark
up of 70 to 80 per cent on the prices. Some
profitability for the firms must be essentially
there." He was all praise for the role of the
small scale sector. "We should develop
more lechnocrafts," he explained, “if we
want our industry to grow."
About the distribution of canalized
items through government agencies. Mody
said that the system was to provide the
items on the best of the last two years'
consumption plus 15 per cent (on more than
Rs. 10 million turnover): or, 30 per cent
on less than Rs. 10 million turnover, for all
new-comers or for new items for existing
units. An ad hoc quota of canalized items
of 5 kg. to 150 kg. was not sufficient for
production purposes.
Explaining this, he said: “The govern
ment should review and then revise the
policy and give canalized items on the
basis of production capacity, so that it will
help al! deserving units to grow faster."
He hoped that the government would
soon implement the recommendations of the
Hathi Committee, especially those pertaining
to the growth of the Indian sector. "That
would be a unique contribution of the govern
ment to this most vital of industries."
submitted were substandard, Soviet drug
houses were allowed to identify their goods
by brand names from the mid-sixties on
wards. The Chinese similarly have returned
to the practice of trade names after trying Q
out generic or chemical names. Most drug g
products have three names—chemical, generic and brand. The first is far too complicated co
for any doctor to prescribe, and a chemist Q
to dish out. The generic name is shorter but 5
lacks the guarantee of exact therapeutic
response, tested dosage, and quality control,
all of which are offered by the branded
product.
Another controversy arising in the public
mind is over the multinational companies
making and selling drugs in India. Some of
them are here due to historical accident,
others were invited to invest in the country
because they brought with them technological
know-how. It is now a well known fact that
no nation is completely self-sufficient in the
field of drug technology. The Hathi Com
mittee acknowledged the role of foreign
capital and technology as follows: "An
important reason why the continued presence
of multinational corporations under appro
priate surveillance is desirable is because
it provides the most effective and economical
method for the transfer of technology in a
field in which technological and product
obsolescence is quite significant. Units in
this industry can be—and indeed, should be—
used for subserving national interests. In
particular, the international character of
operations can be utilized to increase exports
of formulations to a much greater extent
than at present". The accent, therefore.
should be on surveillance (for fair trade
practices and subservience to national
interest.
Whatever decision taken now as a
national policy on the drug industry is
bound to have long-term implications. The
desired growth cannot be achieved with the
present pattern of three-tier control on
licensing, capacity and pricing. Incentives
have to be built into policy directions
towards producing medicine for the millions
at reasonable prices.
The success of a drug policy inevitably
also depends on expansion of medical services
for barring a bunch of broad spectrum
drugs, as modern medicines have to be
administered under doctors’ prescription.
There cannot be relaxation on standards of
manufacture and administration of highly
potent modern drugs. Here, the drug control
machinery will have to be expanded and
streamlined to play the watch-dog function.
The magnitude of India’s population
offers vast opportunities and challenges to
the drug industry. However, these challenges
are common to both manufacturers of medi
cines and administrators of health services.
In the ultimate analysis, the success of a
drug policy will depend on the social purpose
and dynamism of all concerned—the govern
ment, the industry and the medical profession.
Medicine is a matter of ethics and trust.
Trust may yet beget trust. Ethics presupposes
discipline.
— Hz. S. Titus
21
India Today: What is the government's deci
sion on the Hathi committee report?
P.C. Sethi: The Hathi committee report was
submitted to the government in April 1975.
Since then it has been examined in the
Ministry and we have solicited the views of
the planning commission, the Finance
Ministry, the industries ministry, the health
ministry and the concerned ministries. Now
the matter has been referred to a cabinet
sub-comrmttee which is headed by Bansi
Lal, the Defence Minister. We will be able
to take a final decision when this committee
meets........
India Today: Does the government want to
develop the indigenous drug industry? What
is the priority in the government’s thinking
as far as dealing with the problem is con
cerned?
P.C. Sethi: Well, the Hathi committee
recommendations are there. But even without
that there are certain areas where the govern
ment’s thinking is very clear. We want the
drug industry to catch up with the research
and development which has taken place all
over the world. It is not only a question of
producing life-saving drugs or important
drugs today but also of keeping pace with
research and development activities. At pre
sent our total production caters to no more
than 20 per cent of the population. I n terms of
money, hardly six rupees are being spent per
person per annum on medicines. So this is not
an area where we have reached a stage where
we can close our doors to the development
that is taking place in other parts of the world.
India Today: Will the government or the
drug industry have enough financial resources
for research and development?
P. C. Sethi: The drug industry in India
ought to spend more on research and develop
ment than it is. The minimum I would consi
der worthwhile is 20 per cent of the gross
turnover. Apart from that we have several
research institutions financing research work
but they should upgrade the existing techno
logy. But such vast technological develop
ments are taking place in some parts of the
world that where we are not able to catch
up we will have to continue to import
technology. But the main thing is that the
technology which we import should not
be a captive technology of a particular
company but should be on the basis of
national property and should be passed on
horizontally to a private sector, public
sector or joint sector unit.
India Today: How will you ensure that you
will get enough scientific talent and that
you can pay it enough and provide the
requisite equipment to enable it to do proper
research?
P.C. Sethi: The main thing is that the
most advanced and developed countries
are spending so much on R&D that in spite
of the fact that we would be spending two to
three per cent we can’t match the total expen
ses that they put in. But at the same time we
have got technical people and the equipment
and we can certainly do some R&D work.
22
VIEW
TOP
P. C. Sethi,
Minister for
Chemicals and
Fertilizers
For encouraging R&D work in the pesticide
industry, we have imported a cess which
will be pooled and used for R & D activity.
So for the time being we will have to continue
updating Indian technology in the field of
drugs and manufacture of basic drugs and
intermediaries.
India Today: Has there been any significant
reorientation in the government’s policy—
towards manufacture of drugs and pharma
ceuticals apart from recent thinking about
change of foreign brand names and the
monopoly of multinational companies?
P. C. Sethi: The broad principles which will
govern the future drug policy of the govern
ment are: Firstly, to ensure that drugs are
available in abundance in the country to
meet the health needs of our people. Secondly,
to achieve self-suffiency in the next few
years and progressively reduce the quantum
of imports and to develop self-reliance in
drug technology. Thirdly, to make drugs
available both to hospitals and to the
common man at reasonable prices and for
this purpose the system of price control may
have to be continued; to ensure reasonable
return on the capital employed by the
industry. And lastly, to give a leadership role
to the public sector in the drug industry.
India Today: Why is it that some life-saving
drugs are not available or easily available
in India?
P.C. Sethi: There is wide variety of life
saving drugs available in the country and
by and large we are not receiving any com
plaints of shortages. But in working out
our production strategy we propose to
concentrate on the manufacture of 117
essential formulations identified by the Hathi
committee.
India Today: Since it is primarily a question
of importing intermediaries for manufactur
ing some essential drugs, why does not the
government compel companies, especially
multinationals, to manufacture life-saving
drugs by drawing up a list of the essential/
ones? And, also, why does not the govern
ment force multinational companies to mar
ket at the earliest intermediaries of basic
drugs which they have been either allowed
to import or manufacture?
P. C. Sethi: I fully agree. It is our intention
to achieve self-sufficiency in production of
drugs within a few years time. For this
purpose, we are encouraging all the three
sectors of the industry to make investment
for the manufacture of drugs. It is my hope
that imports will progressively go down
over the years.
As a part of our production policy,
the public sector has been given the leading
role to ’Tndianize” the manufacture of bulk
drugs. So far as the multinationals are
concerned, we are now insisting that they
should not remain solely in the formulation
business and that they must also manufacture
bulk drugs. They are also expected to
dilute their equity holding to 40 per cent
in case they have not brought in the latest
technology or are not export-oriented.
India Today: Has the government conducted,
any survey of the price structure of impor
tant antibiotics and broad spectrum drugs
in relation to the purchasing capacity of
patients? Who needs them?
P.C. Sethi: The prices of drugs in India
are controlled under the Drugs (Prices
Control) Order and companies are not
allowed to charge what they like. While
allowing price increase, we have to take
into consideration the cost of production
and give a reasonable margin to the pro
ducers. As things stand the retail prices of
drugs in India are perhaps the cheapest in
the world. It is, however, true that drugs are
largely consumed in urban areas and it will
be our duty to ensure availability and con
sumption of drugs in the poor rural regions.
It must not be forgotten that large sections
of society are, in fact, getting medical
attention including drugs free of cost. These
include government servants at all levels
and industrial workers. You must alsq
remember that medical attention is not
merely a question of drugs, there is the cost
of hospitalization and doctors’ fees which
are also beyond the capacity of the poorest
sections.
India Today: Some of the inexpensive drugs
for relief in cases of common ailments are
constantly being improved or fortified in
the west. For instance, aspirin tablets have
been available for the last three years in
Europe with an admixture of Vitamin C.
But even these simple improvements do not
find their way into products marketed by
our companies.
P. C. Sethi: You will widely appreciate that
there is a wide diversity of drugs available in
the country and almost every year new
formulations are being produced. I do not
think it would be correct to say that simple
improvements do not find their way into
the Indian market.
Unia Fasudev
INDIA TODAY. JUNE 30. 1
Drugs ban
/^waiting th© verdict
3~ tr.any d if’erent brands of clioquinol r :commended
for the prevention or treatment of non-specific
■i larrnoens. How does a doctor choose between them?
A brand of clioquinol from an unknown local firm?
Or hexaform or Hntero-Vioform - world leading brands
from a trustee’. Swiss name, CIBA?
*
an harmful drugs or ban
the ban? For far too long
this three-cornered contro
versy, between concerned
doctors, the government
and drug companies has gone on,
beyond the ken of ordinary mortals
compelled to reside in a world where
faith still heals. Anyway, as the saying
goes, there are too many dangers to life
and limb in the Third World to justify
the import of “foreign” consumerist
phobias. Even the government has not
been above deploying this logic, which
the drug industry itself has used to
good effect to justify the marketing of
questionable formulations.
The fate of the government’s succes
sive attempts to ban certain drugs is an
eye-opener. Precious little has emerged
by way of weeding out harmful or su
perfluous brands since 1975 when the
government-appointed Hathi Committee
delivered its report. Following in the
footsteps of the World Health Organisa
tion (WHO), the committee ruled that
116 essential drugs sold under their
generic names were all that was needed
to replace the 15,000 odd brands cur
rently thriving in the market. But the
government came a cropper by trying
its hand at imposing generic names for
just five! The Delhi High Court ruled in
favour of patented brands - the corners
tones of free enterprise - and the matter
inevitably landed at the doorstep of the
Supreme Court, where it is currently
sub judice.
In a fresh attempt, on October 19,
1981, the Drug Consultative Committee
(DCC) recommended the ban of 23 fix
ed dose combinations (FDCs) on the
basis of its sub committee’s findings. On
December 31, 1981, this was pared
down to a list of 18 by the Drug Tech
nical Advisory Board (DTAB). Both the
DCC and the DTAB are empowered under Sections 7 and 5, respectively, of
the Drugs and Cosmetics Act, 1940 - to
advise the Drug Controller of India
(DCI) on matters related to the produc
tion and sale of drugs.
Taking the cue, the DCI directed the
state drug controllers to ban the manu
facture of amidopyrine (either singly or
in combination) by February 3, 1982;
COMMUNITY HEALTH CELL
The Herald Review August 12 1984 Dummy
(!7/13 (First Floor)St. Marks Road &
Feature
anskits s?le by November 1, 1982; as
weil as the manufacture of phenacetin
and hydroxyquinoline by April 30,
1982. But then, by an order dated Au
gust 3, 1982, following an appeal by
the Indian Drug Manufacturers’ Asso
ciation (IDMA), he chose to extend the
grace period before the ban on the sales
of these to March 31, 1983.
Again, by an order dated June 26,
1982, the deputy drug controller ban
ned the manufacture by December 12,
1982 of FDCs of oestrogen-progesterone
(EP Forte contraceptive pills, whose use
for pregnancy tests was known to lead
to foetal abnormalities). In all, some 10
manufacturers and 19 brands were no
tified in this order and their sale was
banned by June 30, 1983. The manu
facture of all the remaining 15 on the
list was banned by September 30, 1982
and their sale by March 31, 1983.
Unbelievable as it may seem, it took
the Central Government close to one
year to realise that it had no powers
under the Act to act upon the advice of
its committees and ban a drug that had
been found injurious to the health or
lives of its citizens. Since health is a
state subject, Section 18 in Chapter IV
of the Act empowered the state govern
ment to prohibit the sale and manufac
ture of only those drugs that were eith
er not of standard quality or misbrand
ed or adulterated, etc.
teresting features. For a list which was
seeking to undo longstanding harm, it
was surprisingly worded loosely enough
to give scope to various interpretations.
It did not contain all the combinations
earmarked by the DCC; and yet it added
some five others without providing the
reasons for these (See Misguided ban).
Other drugs such as Lomotil and EP
Forte - which had been banned by earl
ier notifications but which were not
Lax controls
All this has meant that while some com
panies have adopted a brazen disregard
for previous government orders, others
have adopted shrewd dodges to exploit
the laxity in governmental drug control
and licensing agencies. For example, Lo
motil - widely used in the treatment of
diarrhoea for the paediatric age group was banned earlier since “it could mask
signs of dehydration and cause fatal to
Beating the ban
Meanwhile, making hay while the sun
still shone on (heir commercial for
tunes, several companies got stay ord
ers fmm the high courts. For instance,
the Bombay-based Unichem Labs and
Nicholas Labs; as well as Organon now known as Infar (India) Ltd, Calcut
ta - all saved their rights to market
brands of EP Forte drugs. Nicholas also
saved its brand Mycropyrin-C (aspirin
and vitamin C) which fell in the banned
combination of vitamins and analgesics.
Only on November 15, 1982, in a
late attempt to remedy this anomalous
situation, was the Drugs and Cosmetics
Act amended. With the newly incorpo
rated sections 10A and 26A, the Cen
tral Government assumed the powers of
banning the import, manufacture, sale
or distribution of any drug which was
likely to involve risk to human beings
or animals; or which lacked its claimed
therapeutic value; or contained ingre
dients in a quantity for which there was
no therapeutic justification.
The Act came into effect on February
1, 1983, and on July 23, 1983, a gazet
te notification was issued by the Central
Government banning 22 single drugs or
FDCs of drugs. This list had many in
The Herald Review August 12 1984 Dummy
Strepto paraxin: unnecessary combination
part of the DCC’s list - did not number
here either.
Quick off the mark, EP Forte manu
facturers had managed another lease of
life by filing writ petitions before the
same high courts, challenging the new
sections 26A and 10A on grounds of
lack of objective criteria for the ban.
The matter was again sub judice.
When the Voluntary Health Associa
tion of India (VHAI) offered to coope
rate with the government on this case,
DCI Dr Gothoskar refused to disclose
either the contents of the petitions filed
by the companies against the govern
ment or an outline of these or even the
names of the government advocates
handling the matter.
Vis-a-vis the ambiguities pervading
the list, Deputy DCI Dr Das Gupta told
VHAI, quite candidly, that since this
was their first attempt at banning
FDCs, they had not foreseen the lacu
nae. Further, that the sudden withdra
wal of many drugs would have created
much greater resentment than it alrea
dy had; hence the decision to conscious
ly wittiidraw only a few.
xic reactions”; manufacturer Searle
reacted with stickers on each silver foil
packing, warning against its use below
the age of six. Last week, not only was
it available over the counter in Banga
lore but the sticker had vanished.
Amidopyrine was banned since it re
tarded the production of infection
fighting white corpuscles in the blood;
recently, in a low key reaction, manu
facturers Ciba-Geigy quietly replaced it
with propyphenazone in their formula
tion but mysteriously managed to retain
the same licensed brand name: Cibalgin. The same thing happened to
Roche’s Saridon, where again the old
formulation was deftly altered.
FDCs of steroids were also banned;
but the May 1984 issue of the Current
Index of Medical Specialities (CIMS)
continues to list the brand Butacort,
minus, however, the steroid predniso
lone (1.5mg) which the producers PCI,
in the most bizarre exchange, replaced
with diazepam or Calmpose (2mg). How
a steroid was allowed to yield place to a
tranquilliser of the same potency, in the
same branded formulation, is amazing.
35
Feature
The modus operand! has been repli
cated several times over. Pfizer current
ly markets the banned tetracycline pae
diatric syrup as oxytetracycline syrup.
It is freely available without prescrip
tion; yet Dr Gothoskar believes that sin
ce it is banned, nobody buys it over the
counter. Its overuse, according to the
VHAI, has led to high incidence of
mottling of teeth at the Rajghera mines
in Dttrg district.
Even the public sector IDPL has not
been above substituting atropine by ho
matropine in its banned combination
with analgesics/antipyretics. All this has
been made possible by the government
ban order, which did not spell out that
chemical equivalents of the banned
generic categories were also prohibited.
But how the licensing authorities have
equally allowed the marketing of chang
ed formulations under the same brand
names is another matter.
Some others, of course, continue to
be marketed quite legitimately since
they have been specifically exempted
from the ban order. Among the EP For
te drugs, the most recent one to catch
the public eye is a brand called Cycle
norm, which was administered by se
nior doctors in a government hospital
in Cauiianore to a housewife Shobna
f ■ delayed periods. Shobna died subse
quently, but the reason for her death is
not known; nor is it known whether the
drug was intended for hormonal pregn
ancy testing or for inducing abortion. A
damning confession was, however,
made in the subsequent court hearing
by Dr V. Sasikumar, secretary, Kerala
State Health Services, Cannanore.
Said he: "The sad thing about the
banned or banning of drugs is that doc
tors are left to understand about this
decision from incomplete reports in
newspapers. Who should inform the
doctors in government and private hos
pitals about these drugs? Nobody has
done it. As with other government deci
sions, initial decisions are widely pu
blished and then come amendments,
court orders, stay orders, vacation of
stay, etc. Ultimately' leave everyone
guessing."
In this guessing game being played
with increasing dexterity, the compa
nies argue glibly that misuse of a drug
is no reason for banning it; they place
the onus on the government. The Drug
Controller has, in turn, thrown up his
hands, saying “I cannot inform
everyone" and shifted the responsibility
onto "those involved in health
education” and the voluntary health
sector. The latter, in any case, are
starved of information and floundering
in the mire of technicalities.
Since this wheel continues to turn
full circle several times over, its con
sequences are not difficult to illustrate.
For example, Lut-Esteron Forte - a high
dose EP drug manufactured by Mac
Labs - continues to be listed for pregn
ancy testing in C1MS. This in turn influ
ences the prescription practices of doc
tors who consult it. Again, diarrhoea
continues to contribute to high infant
mortality rates, while anti-diarrhoeal
packs still go without consumer caution
embossed on them.
In fact, in a recent development, me
dical literature specifying contraindica
tions which earlier used to be inserted
into packs of medicines has by and lar
ge been stopped altogether. Remarks Dr
Ravi Narayan, convenor, Medico
Friends Circle, a voluntary health ac
tion group: “Some companies are now
claiming that this is being done to pre
vent self-medication! But nowadays,
even their own medical representatives
are often not taken into confidence and
are caught unawares by sudden changes
in formulations.”
nufacture and sale.” It ordered the <
Union of India to give “due publicity ”
to this list “not later than two months”
- from March 28, 1983.
How much heed the government paid
to this order was clear in May 1983,
when The Eastern Pharmacist reported
that the Retail and Dispensing Chem
ists' Association had filed a writ petition
in the Bombay High Court demanding
the same information. This court also
directed the government to notify by ga
zette, the list of generic combinations
proposed to be banned under the
amended Act, along with their formula
tions. Nevertheless, the July 23, 1983
ban notification does not contain this in
formation. Till today, nobody - least of
all the DCI - seems to know which
brands are really involved.
One plausible explanation, provided
by the VHAI, is that the drug compa
nies got another stay order, this time (
prohibiting even the publicising of
brands or the names of their manufac
turers. Another is, of course, the sheer
logistics involved. Since most of these
First challenge
drugs were registered by state drug
control authorities more than 20 years
ago, and since outside Maharashtra,
West Bengal and Kerala, such authori
ties are virtually non-existent, even a
willing government would have had its
back to the wall. Despite this daunting
task, Dr Das Gupta is reported to have
told VHAI that a banned brand list will
be available in approximately three
months.
A little earlier, on April 7, 1983,
Panikulangara filed another petition,
this time before the Supreme Court. In
view of the changed circumstances und
er the amended provisions of the Act,
he prayed for:
■ A writ of mandamus from the
court, commanding the government to
cancel all licences and ban forthwith
the import, manufacture, sale and dis
tribution of all 18 drugs recommended
by the DTAB, as well as EP Forte.
It is in the context of this general back
ground that the first public interest peti
tion placed by Vincent Panikulangara,
an Ernakulam-based advocate, before
the Kerala High Court must be viewed.
Since it came before the Drugs Act was
amended, it challenged the DCI’s provi
sion of cut-off dates for the 18 drug
combinations which had been found
“injurious to health”. It prayed that the
court quash all such orders and demand
a fresh notification banning their manu
facture and sales forthwith.
However, given the peculiar circumst
ances in which the court found itself
(See Box), it could only order that "the
brand names corresponding to these 18
formulations must be made known to
the public so that they are alerted to
give a wide berth to such drugs even
before the government comes up with
any steps enforcing a ban on their ma
The Herald Review August 12 1984 Dummy
k
Feature
.. ..
follow defence
Delivered on March 28, 1983, the Ke
rala High Court's judgement was com
pletely overtaken by events. Vincent
Panikulangara’s petition was filed be
fore the Drug and Cosmetics Act was
amended in November 1982. There was
then, no provision under existing law
whereby the court could order the gov
ernment to enforce its drugs ban with
immediate effect. By the time the judge
ment was delivered, however, the
amended act had come into effect, leav
ing the court with no other option than
to record the changed situation and ad
vise the petitioner to await the renewed
efforts of a government freshly armed
with powers.
Nevertheless, the text of the judge
ment delivered by acting chief justice
P. Subramonian Poti and justice K.S.
Paripooman, provides many illuminat
ing insights into the hollowness of cer
tain official actions and their justifica
tion in the government’s counter affida
vit. Especially because, since then, the
government’s arguments have been cit
ed with approval in the counter affida
vit currently placed by the Indian Drug
Manufacturers’ Association for conside
ration before the Supreme Court. Some
highlights:
The main plank of the government's
defence against the charge of lackadaisi
cal enforcement of its own order ban
ning 18 drugs was that these drugs had
in fact been banned “not because they
were injurious to health. But most of
these formulations were banned on the
consideration of therapeutic irrationality,
benefit-risk considerations, consideration
of local condition, toxic effect in
■ A writ of mandamus, commanding
the government to set up a high power
authority to study the damages wrought
by such drugs on the health and life of
citizens; and to pay prompt compensa
tion to such victims.
■ A writ of mandamus commanding
the government and the DCI to frame
and rigorously enforce rules pertaining
to the quality and standard of drugs.
The grounds on which he based him
self were two: Articles 21 and 47 of the
Constitution of India. Article 21 assures
that no citizen “shall be deprived of his
life or personal liberty except according
to procedure established by law”. And
Article 47 that, “The State shall regard
the raising of the level of nutrition and
standard of living of its people and the
improvement of public health as among
its primary' duties and in particular, the
The Herald Review August 12 1984 Dummy
animals". It added that merely because a
preparation has side effects, it cannot be
banned; and that "it may also be rele
vant to point out that all these 18 catego
ries of combinations have not been ban
ned throughout the world and continue
to be marketed in some countries”. It
concluded that "unless the toxic effect is
of a very serious nature, it has been the
practice to allow a certain period" for
stopping production and sale "to avoid
hardships to the manufacturers, dealers
as well as to patients who are taking
these drugs”.
Official bias
In a scathing comment, the judges said,
“One fails to appreciate the hardship to
the patients”; “As between the lives of
the citizens of this country on the one
hand and the loss that may result to the
manufacturers and traders by the imme
diate ban on the manufacture and sale
on the other, the government has chosen
to view the latter as of more concern."
Picking on amidopyrine as an example,
they pointed out that “Even though Gov
ernment of India had realised as early as
in February 1981 of the danger of the
use of this drug consequent on which its
import and manufacture had been ban
ned in India, the Government seems to
have been powerless in effectively en
forcing this ban...”.
Despite official awareness - reflected
in the DCI’s correspondence with state
drug controllers (SDC) - of continued
sales of the drug and its formulations as
late as February 3, 1982, the judges ob
served that "action taken by the SDCs
had not been uniform”. Even this had
not restrained the government from en
tertaining the IDMA’s plea for an exten-
sion of the cut-off date for FDCs of ami
dopyrine, phenacetin and hydroxyquino
line. "Nothing short of prohibiting ma
nufacture as well as sale with immediate
effect would be justified”; "There is no
case that if they are withdrawn from the
market, there would not be effective sub
stitutes, assuming that again is a justifi
able reason,” they said.
Demolishing the difference between
"injury to health" and "therapeutic
irrationality”, the judges held that, “A
drug may be injurious by reason of side
effects, by its adverse reaction on certain
types of patients, by such reactions und
er certain conditions, by its irrational be
haviour in relation to the consumer and
even by its impotence in the matter of ef
fecting a cure for the ailment for which
the consumer is treated with
it...Therefore, whatever may be the way
in which the idea is expressed in the
counter-affidavit the plea reduces itself
to this that, drugs which ultimately are
found injurious in the matter of treat
ment of patients are being
banned...(then) the overriding considera
tion must be the lives and health of the
consumer public.”
They concluded that in a number of
recent cases (such as People’s Union for
Democratic Rights v. Union of India,
AIR 1982 SC 1473 and Maneka Gandhi
v Union of India, AIR 1978 SC 597),
the Supreme Court had read Article 21
of the Constitution in a wider and more
meaningful perspective. “There can be
very little doubt that a person is entitled
to protection of his life and liberty and
any serious encroachment upon the
health of the citizen would call for pro
tection by invoking Article 21 of the
Constitution of India."
State shall endeavour to bring about
ly negated, violated and by-passed”. Its
goals of self-reliant technology, selfprohibition of the consumption, except
sufficiency in production and the lea
for medical purposes, of intoxicating
drinks and of drugs which are injurious dership role of the public sector in the
to health.”
drug industry, had all proved elusive.
Second assault
In fact, he felt that since there was
Inter alia, Panikulangara sought to high “not yet a comprehensive legislation to
prescribe the quality and standards of
light the general situation of the drug
drugs", their reliability was “a matter
industry with a few very broad spec
trum observations. For instance, he
of charity of the manufacturer and des
tiny of the patient”. He alleged that a
pointed out that the recommendations
of the Hathi Committee had not been
fifth of all samples tested were sub
accepted by the government. The com
standard; and three-fifths of all drugs in
mittee had highlighted the havoc played
India were non-specific or pharmacolo
on the Indian drug industry by transna gically irrational.
tional corporations (TNCs) and pleaded
On November 7, 1983 - ie, after the
for its nationalisation. Not only had the
final gazette notification - Panikulangara
Drugs and Cosmetics Act, 1940 allowed
filed an amendment to this petition to
profiteering by TNCs and their dumping bring it further up to date. In this he
of harmful drugs here, but the new
has prayed that the court:
drug policy, 1979, “had been repeated
□ Direct licensing authorities to neith
37
Feature
er grant new licenses nor renew old
ones, for the import, manufacture and
sale of any drug except the 116 recom
mended by the Hathi Committee.
G Direct the government to stream
line the licensing policy, administrative
acts and statutory functions so that use
less, injurious and harmful drugs are
weeded out and essential and life-saving
drugs are easily made available through
the public sector undertakings.
12 Ban the import, manufacture and
sale of those drugs not yet covered by
the recent order of the government.
El Direct the government to appoint
an expen committee to report on the
drug industry and the market after the
period covered by the Hathi Committee.
Achilles heel
The Achilles heel of this petition lies in
its appeal to fundamental rights and its
reliance on Articles 14 and 47. As the
petition itself admits, "a constitutional
mandate to bring about prohibition of
drugs that are injurious to health" can
not “be enforced by a directive of the
court". But it has argued that since the
import, manufacture and sale of such
drugs casts a “backward” dimension to
the Directive Principles of the Constitu
tion, this “can and must be prevented
by judicial action" - ah argument that,
in itself, could prove to be tenuous.
The second weakness of the petition
lies in its largely rhetorical attack on
TNCs’ dominance of the Indian drug in
dustry, which is, strictly speaking, no
longer true and part of the older reality
of the seventies when they controlled as
much as 60 odd per cent of the total
production. No doubt, the larger ones
continue to figure prominently among
the top 20 even today; but they have
been eclipsed in overall terms by the
growth of smaller local units. To illu
strate, in 1982-83, the national sector
(both private and public) produced for
mulations worth Rs930 crore; the fore
ign sector, Rs615 crore. In fact, other
than their tussle for hegemony over lo
cal markets, the opposition of both to
gether to any consumerist public inte
rest litigation is equally trenchant. To
fail to assess the significance of the one,
is serious.
These points are borne out by the
counter-affidavit filed by the Indian
Drug Manufacturers' Association before
the Supreme Court in July 1983. Al
though an amended version of this must
certainly have been filed after the gazet
te notice banning 22 drugs, the original
document is representative enough of
the organisation’s final stand. There are
two major highpoints: firstly, it focuses
very firmly on statute books - ie, the ex38
oxytetracycline: finding the loophole
tant laws which provide “sufficient”
levers for official control of all aspects
of the drug industry - and not on the
applied reality of these laws. For any
laxity or misuse in day to day practice,
it thus blames the government's inabil
ity to extract the maximum potential
out of available laws. Secondly, it fo
cuses - with a great deal of medical ob
fuscation - on defending some of the
banned FDCs.
Not only does the affidavit assert that
the prices of Indian drugs are
“effectively controlled by the govern
ment under the Drug Price Control
Order, 1979", but that the various
Drug Acts “contain sufficient and effec
tive provisions for prescribing the qual
ity and standards of drugs as well as for
regulating their manufacture, distribu
tion, stocking, sale and also the use of
such drugs.” The obverse is then used:
“Prima facie, therefore, any drug which
has been so approved or accepted can
not be regarded as harmful or
injurious"; especially since, if all these
drugs, which have been marketed and
consumed over long periods, continue
“to be administered within the paramet
ers prescribed for each of them...". And
again, that if these drugs have not al
ready been, but “can be effectively re
gulated and controlled” under various
statutory provisions and controls, then
they should not be banned.
Manipulated prices
Three examples would suffice to inject a
modicum of reality into these asser
tions. Firstly, in a paper on drug pric
ing circulated at the voluntary Drug Ac
tion Network meet at Wardha last
week, Dr W.V. Rane and Dr A.R. Pat
wardhan cited the prices of two drugs
with identical ingredients - the*on'i,with
half the contents of the other cost al
most the same. 100 tablets of Corbutyl
(containing Dextropropoxyphene-65ing;
Paracetamol-650mg) manufactured by
Roussel, cost Rs35.83. But 100 tablets
of Norgesic (with 32.5mg and 325mg
respectively of the same ingredients)
produced by Cipla cost Rs31.10. How
does the DPCO, 1979, make this possi
ble?
Then, the 64th report of the Esti
mates Committee, Ministry of Health
and Family Welfare, tabled in the last
session of Parliament, highlighted that
from 1977-78 to 1981-82, the percent
age of substandard drugs was between
14.5 to 21.6 per cent. In 1981-82, 18.3
per cent of drug samples were found to
be substandard. In 1982-83, 60 out of
2,540 were again substandard. It furth
er observed that no information regard
ing the percentage of locally produced J
drugs which were subjected to testing "
by either Central or state drug control
authorities was available. No statistics
related to the number of manufacturers
whose licences were suspended or can
celled were available. No machinery ex
isted to prevent the entry of spurious
and substandard products into the
market.
Further, a recent survey conducted
by the National Institute of Nutrition in
cooperation with the Directorate of
Drug Control Administration and the
Andhra Pradesh Chemists and Drug
gists Association, covering 33 retail
pharmaceutical outlets in Hyderabad
and Secunderabad, discovered two
alarming trends. Not only was the self
medication rate an alarming 46 per
cent; but 58 per cent of the self medi
cated drugs were schedule ‘L’ and ‘H’
drugs, which are not normally meant tri
be sold or consumed because of asso- I
ciated major side effects and toxicity.
To return to the affidavit, annexure
III deals with 'banned' FDCs. In the
opening general comments, it is stated
that FDCs are important “if two or
more drugs are concurrently indicated
for total patient care”. According to Dr
Ulhas Jajoo, the Wardha-based associate
professor of medicine, this practice was
definitely discouraged in modern thera
peutics, especially “when the drugs
were available individually or there was
likelihood of the combination being
misused”. He cites the now banned
category of steroids as a drug of last re
sort, whose doses also need to be indivi
dualised.
In support of the combination of chlo
ramphenicol with vitamin C or Bcomplex, it is urged that the misuse ol
such combinations is unlikely (probablv
The Herald Review August 12 1984 Dummy
Feature
MHMF..:...
r^e). I< added that “an impression is
gaining much clinical ground that the
symptomatic improvement occurs much
more readily in patients with enteric
fever treated with this combination”.
But then no medical references are cit
ed for this cleverly worded rumour.
Playing safe
The affidavit has many other interesting
sidelights. It rigs up an impossibly ela
borate structure of procedures, labs and
tests, to be followed to prove that the
known substitutes for the banned drugs
are as cheap, have comparable availabil
ity and have fewer side effects, etc. Ho
wever, it is easily forgotten that such
tests were never conducted on many of
the banned categories of drugs which
were licensed decades ago. Indeed, the
affidavit itself has been incapable of
such rigour in its defence of FDCs.
In addition, a whole range of incredi
ble assertions cover virtually every
possibility. On the one hand the testi
HARMFUL
DRUGS
Misguided Hogic
If in less than three years, 23 drugs of
ficially recommended for banning are
inexplicably transformed into 22 diffe
rent drugs, after adding five new ones
and subtracting 10. it proves two logi
cal assertions. First, that the original
list was not comprehensive; and second,
that the final one isn’t either.
On October 19, 1981 the Drug Con
sultative Committee (DCC) evaluated the
therapeutic rationale, possible irratio
nality and harmful effects of 34 single
or combination drugs. After specifying
contraindications or simply the useless
ness of some of these, it earmarked 16
of them for immediate ban, as well as
seven for weeding out over a period of
time.
But by December 31, 1981 this list
had been truncated (with some qualifi
cations and some entirely new names)
into the Drug Technical Advisory
Board’s (DTAB) list of 18 undesirables.
Yet again, on July 23, 1983 the list was
incarnated anew with further changes
in the gazette notification banning the
manufacture and sale of 22 drugs issu
ed by the Union Ministry of Health and
Family Welfare.
The minutiae of detailed confabula
tions in the corridors of wisdom and
power are not known: the gazette ex
traordinary mentions no medical rea
sons whatsoever for any of the drugs fi
nally itemised in it. If “Health for All
by 2000 AD” (India is a signatory to
the WHO Alina Ata charter committed
The Herald Review August 12 1984 Dummy
mony of (he Deputy Drug Controller be
fore the Kerala High Court (See box) is
bandied about, with some approval for
his arguments against immediate ban,
especially since, in his opinion, the
drugs were not injurious to health but
were therapeutically irrational. On the
other hand, it is “denied that all these
drugs are lacking in therapeutic ratio
nale or justification...”.
Simultaneously, it is urged that
“merely because a drug of proven the
rapeutic utility, produces side reactions,
or is harmful or injurious to health or
involves any risk to human beings, it
need not be prohibited under Sections
10A or 26A”. Indeed, “Often, it may
be necessary and in the interest of the
country and consumers to permit con
tinued use of a drug despite some harm
ful effects observed in some cases, and
its ban abroad.”
Descending from the perilous to the
superfluous, it is argued elsewhere that
drugs should not be banned “merely on
to this objective) was the general idea,
then there could have been no more
mysterious way of going about it. Osten
sibly the government's efforts are di
rected towards guaranteeing the funda
mental right to life and conservation of
scant per capita earnings (by eliminat
ing dangerous and superfluous drugs
respectively). Especially since it is sug
gested that the use of the impugned
drugs is likely to “involve risk to hu
man beings or the said drugs do not
have the therapeutic value claimed or
purported to be claimed for them or
contain ingredients and in such quantity
for which there is no therapeutic
justification”.
Nevertheless, the wording of various
combinations is loose enough to have
more than one interpretation in court
a lever the affected pharmaceutical com
panies are bound to exploit. In any
case, since only generic categories
(which have several chemical equiva
lents and hundreds of brand identities)
are employed in the notification, the
cause of consumer awareness could
hardly have been furthered.
Loosely worded
The list is stricken by an unusual
‘best of-three, winners-lose-it-all' syn
drome. For instance, it is not clear
whether “combinations of strychnine
and caffeine in tonic" indicts the pres
ence of either or both in a given pre
paration. Other examples in the same
genre are “combinations of yohimbine
and strychnine with testosterone and
vitamins"; and “combinations of iron
the ground that such drug combinations
do not offer any special advantages”. In
fact, drug control authorities “should
intervene only if there? are harmfid el
feels, and leave? the matter of usefulness
of the? drug to the discretion of doctors
who are the best judges.
f inally, of course, in a direct rebuttal
of Panikulangara’s petition, it denies
“that the Petitioner’s fundamental
rights under articles 14 and 21 are? in
any manner affected whether as alle?ged
or otherwise. There is no question of
any deprivation of the? Petitioner’s life
or liberty, firstly because the drugs in
question are not poisons as alleged by
the Petitioner, anti secondly because,
there? is no compulsion on the Petitioner
or any other citizen to take any of these
drugs.” Is this to be taken to mean that
the IDMA in its moment of triumph has
unwittingly acknowledged widespread
self-medication, which is precisely what
has made some? of (he banned combina
lions so dangerous? Jugnu Kamaswamy
with strychnine, arsenic and yohimbine
Then again, as the editorial in the
September 1983 issue of the Monthly
Index of Medical Specialities (MIMS)
pointed out, “Ban on the combination
of ‘atropine with analgesics and anti
pyretics' does not legally bind a maun
facturer to stop or not to introduce •
the combination products of other bella
donna alkaloids or substitutes such as
hematropine with analgesics and
antipyretics.” It added. “Ban on com
binations of ‘tetracycline with, vitamin
C is meaningless if one can market a
combination of doxycycline with vita
min C.” And as the Low Cost Drugs
and Rational Therapeutics Cell of the
Voluntary Health Association of India is
quick to expose, some preparations of
the banned paediatric tetracycline are
now being labelled and palmed off as
oxytetracycline syrups.
Vanishing act
Equally damning is the list of seven
‘also rans’, recommended for immediate
weeding out in the DCC’s original list.
which do not figure in the gazette notifi
cation. In the category of analgesics/
antipyretics, while amidopyrine stands
banned, it is puzzling why analgin
(dipyrone) has been excluded. Dipy
rone, which is the sodium sulphenate of
amidopyrine, shares its propensity for
causing fatal agranulocytosis (marked
reduction or complete absence of white
blood cells), stomach cancer and bone
marrow suppression. Quite logically,
the DCC’s list had banned both simulta
neously.
39
Feature
Medical Association pronounced:
"There is evidence that dipyrone, a de
rivative of atninopyrine that shares its
potential for toxicity, unfortunately is
still being misused. That is probably be
cause it is available in injectable form
and because physicians probably do not
recognise its similarity to atninopyrine
since it is marketed under various trade
marks. Its only justifiable use is as a
last resort to reduce fever where safer
measures have failed. Because dipyrone
may produce fatal agranulocytosis and
other blood dyscrasias, its use as a gen
eral analgesic, anti-arthritic or routine
antipyretic cannot be condoned.” By
1980. without any formal ban proceed
ings. these drugs had vanished from the
drug list and the American therapeutic
scene.
Currently, amidopyrine is banned in
over 20 countries. Analgin sales are
prohibited in Australia, Sweden, UK,
Bangladesh: and severely restricted in
Japan, Philippines, Denmark and Italy.
Neither of them figure on the WHO's
list of essential drugs. In India, leading
brands of amidopyrine like Cibalgin
continue to be marketed despite manu
facturer Ciba Geigy’s 1980 assurance of
replacing it worldwide with propyphenazone. And analgin, without prescrip
tions or bills (in well known brands
such as Hoechst's Novalgin and
Baralgan), continues to gross Rs7 crore
annual sales and ranks among the lar
gest selling analgesics. Novalgin is sold
as a “patent, non-salycilate, analgesic,
antipyretic, antispasmodic, anti
inflammatory, anti-rhemnatic agent for
all kinds of pain, rheumatic fever, rheu
matoid arthritis, relief of colics”.
Hoechst literature suggests that though
the danger of agranulocytosis is remote,
it should be borne in mind and a white
cell count done if necessary.
What's the difference
If Dr S.S. Gothoskar. Drug Controller
of India, and Arvind Nair, communica
tions manager of the OPPI, are to be
believed, the government is awaiting
the outcome of individual toxicity stu
dies of analgin being done by Hoechst,
the University of Boston and West Ger
many. But if amidopyrine coidd be ban
ned, why not dipyrone, especially when
risks outweigh any benefits of their use
and safe substitutes like aspirin are
available.
Other notable omissions are:
■ Fixed dose combinations (FDC) of
ayurvedic and allopathic drugs like stilboestrol, which the DCC felt could be
very harmful since there is no adequate
evidence of the safe interaction of these
two systems of medicine.
40
Fresh lease of life
□ FDCs of chloramphenicol and peni
cillin with streptomycin, notable brands
being Chlorostrep (Parke-Davis),
Strepto-Paraxin (Boehringer-Knoll) etc.
It is however known that quite unrelat
ed to its dose, chloramphenicol can cau
se thrombocytopenia (drop in blood pla
telet count) and aplasia (retardation or
lack of growth) of bone marrow which,
in the DCC's opinion, can result in al
most 100 per cent fatality if not careful
ly monitored. On the other hand, care
less prescription of streptomycin, well
known for its toxicity by itself, can cau
se vertigo and sometimes permanent
blindness. Besides in 1969, a UK study
had found it to be ineffective in such
FDCs.
The indiscriminate use of these drugs
in FDCs has been known to lead to
drug resistance, making them useless in
diseases where they are essential: strep
tomycin for TB and chloramphenicol for
enteric fever (typhoid and paratyphoid).
In Mexico, some 10,000 people died in
a typhoid epidemic when the over
prescribed chloramphenicol failed to
act. In fact, in India there could be no
better argument for discriminate use
than the fact that in 1980, 10 million
were afflicted by lung TB and 0.3 mil
lion by enteric fever, while licensed
production capacity remained underuti
lised. In 1980-81, the production of
only 238 tonnes of streptomycin and
108 tonnes of chloramphenicol
(Ministry of Petroleum, Chemicals and
Fertilisers estimates) had necessitated
imports of 44.1 tonnes and 165 tonnes
respectively (Directorate-general of
Health Services data). As things stand
today, leading manufacturers Glaxo and
Pfizer have virtually stopped streptomy
cin production which is far less remu
nerative than tonics and vitamins.
□ FDCs of steroids, which, the DCC
had stated, could lead to adrenal insuffi
ciency. More specifically, according to
the VHAI, in 1980, the DTAB had pro
hibited their combination with either
bronchodilators or anti-histaminics or
tranquillisers. Only by a sleight of hand
could this have been transformed into
Clause’ 14 of the gazette: “FDCs of ste
roids for internal use except...with oth
er drugs for the treatment of asthma."
Says the September 1983 MIMS:
“Since combinations of steroids with
anti-histaminics.can, at least technically,
be used in the treatment of
asthma...legally, the manufacturers can
claim that in future they will indicate
such products for asthma only, though
in the past such products have been vi
gorously promoted for all types of aller
gies, food poisoning, insect bites and 4
what not. Who will go to the nation’s
206,000 doctors and tell them to forget
all past detailings on, say a branded for
mulation of dexamethasone with cypro
heptadine, and use it in future for as
thma only? No one."
□ FDCs of both analgin and tetracy
cline with vitamin C had been banned
by the DCC since such combinations
lacked in rationale. For instance, vita
min C was supposed to help the absorp
tion of tetracycline in the blood stream ■
an unproven suggestion. Analgin has
been exempted from this category too.
□ FDCs of more than one antihistaminic were banned since the differ
ence between their actions was margi
nal. But this was obviously not suffi
cient reason for the government to en
force this.
Other runners-up FDCs which the
DCC had felt should be weeded out
over a specified period are:
1
□ FDCs of anti-histaminics and tran
quillizers, which the DCC felt might
cause unwanted sedation and interfere
with the patient’s reflexes.
□ FDCs of anti-histaminics, tranquil
lizers and analgesics. Except for injectables which were “not likely to be
misused”, it was felt that these would
also cause unnecessary sedation, espe
cially since “there may not be many cli
nical situations which would need a
FDC of these three categories”.
□ FDCs of paracetamol, antihistaminics and tranquillizers which, ac
cording to the DCC, were hardly justifi
ed by any clinical situation but may be
allowed if the formula contains adequa
te doses of each ingredient.
But the most serious distortion has oc
curred in FDCs of hydroxyquinoline,
which had not featured in the DCC’s
The Herald Review August 12 1984 Dummy
Feature
list a J«ll*Although these are now in
cludc-.l. the use of such preparations in
diarrhoea and dysentery - where widely
used market leaders such as Mexaform
and Enterovioform have caused greatest
harm - is exempted. Drug Controller
Gothoskar clearly believes in setting a
personal example. He is known to have
told VHAI that “this is a safe drug. I
take it myself”. Reacting to Nepal's
decision to ban it, he is reported to
have said that we would have done the
same had we also been an importing
country. But since we manufacture it
ourselves, we haven’t.
Like the Hathi Committee before him,
he is known to have justified this argu
ment on two grounds. First, lack of
equally cheap substitutes (a genuine
problem): and second, absence of docu
mented evidence of victims.
(Unfortunately, since meticulous case
histories are virtually non-existent in
India, such proxy assessments of
benefit-risk ratios can be - and indeed
are - used to justify anything at all.) The
WHO obviously disagrees, since in
1977 it felt that the risks of treatment
outweighed potential benefits and ex
cluded it from the essential drugs list.
But because an Indian Council of Medi
cal Research expert committee had se
conded these opinions in 1978, and sin
ce Gothoskar has stated that he would
not re-evaluate this product but was
willing to consider alternative expert
opinions, the government is clearly con
tent to put the onus on concerned vo
luntary health agencies.
It is well known that leading manu
facturer Ciba Geigy was held liable by
Japanese courts for failing to pass on
information about the dangers of the
drug which caused sub-acute myelo op
tic neuropathy (SMON), resulting in
pain, paralysis, blindness and some
deaths for 10.000-30,000 Japanese in
the seventies. In 1977, the organised
boycott of Ciba products by Swedish
doctors protesting against the continued
promotion of this drug in the Third
World had lost the company 25 per
cent of its Swedish market share, a total
loss of some 75 million kroner.
According to Dr Ole Hansen, who
spearheaded this campaign, in 1935 it
self, when Ciba of Switzerland started
marketing this drug, the company had
received a report from Argentinian doc
tors describing exactly the same side ef
fects as the Japanese cases; and in
1939, experiments with dogs and cats
had proved fatal. In 1977, a Cibafunded study in Bombay emphasised
that “it would be imprudent totally to
ignore the Japanese experience", since
it cannot be proved that SMON in its
The Herald Review August 12 1984 Dummy
--------------------------------------------------------------------------------------------------------------------------------------------
HOW CAN I BAN THIS DRUG?
IT HAS DONE ME WONDERS.
epidemic form is genetically localised to
Japan.
While the company has consistently
managed to “hide facts, deny facts" (Dr
Hansen’s words), hydroxyquinolines
continue to be marketed in more than
100 countries. Yet in 1972, the Journal
of the American Medical Association
stated that clioquinol was “no more ef
fective than a placebo" in preventing
travellers’ diarrhoea; and in 1977, the
UK Committee on the Safety of Medi
cines held that there was “inadequate
evidence” to support its claimed effica
cy in the treatment of diarrhoea.
Limited efficacy
More specifically, the WHO Drug Infor
mation Bulletin, January-March, 1978,
stated: “Hydroxyquinolines are active
only on organisms present within the
intestinal lumen. Used alone, therefore,
they are active only in the absence of
significant tissue invasion - a develop
ment that cannot be excluded with cer
tainty even in patients with asymptoma
tic amoebiasis.” According to Dr P.G.
Pandiya, one-time president of the Phar
macy Council of India, the dramatic re
lief associated with Mexaform was in
fact due to “oxyphenonuim which re
duces the spasm of the intestines and
bowel movements and thus markedly
reduces abdominal pain and
discomfort".
Understandably, it has been placed
on restricted prescription in Australia.
Denmark, Venezeula, Norway, West
Germany, Finland, France. In the US,
the maximum dose of clioquinol for
amoebic dysentery is restricted to 22.5
gms for 10 days. In UK, although avail
able on prescription, it has vanished
from the market. It is actively banned
in Japan, Sweden, Bangladesh. In India,
although theoretically these are pre
scription drugs, they continue to be
freely sold over the counter as cure-all
remedies for all kinds of stomach dis
orders.
In the absence of a ban, appeals by
voluntary health activists lor warnings
on anti-diarrhoeal packs have been in
vain. They had proposed that each pack
should state: "These drugs are known
to cause blindness, paralysis of the legs,
burning and pain in the limbs and loss
of bladder control"; and again, in keep
ing with WHO recommendations, that
“Anti-diarrhoeals are not enough; oral
rehydration is the main treatment
diarrhoea”. But Dr Gothoskar has per
ceptively observed that he cannot ima
gine drug companies doing this. Since
he is also known to have professed hel
plessness in the face of unrestricted
sales, what is the alternative to ban?
Jugiiu Ramaswarny
41
~r
<■
-t-
-23/3/62-
Unreali®ffe pricing
hits drag production
.and investment
VU«<y*ir '->■
sw??- >« »;
Drug prices are under Government control for the
past .two decades. And since the East 10 years they
are fixed according to a clearly defined, rigid pricing
formula. Not only the prices off all bulk drugs but also
the price and profit margins off each and every fin
ished formulation are controlled. On top of this,
there is a ceiling on the overall profit a company can
make. This three-tier control ensures that no com
pany can overcharge or make exorbitant profit or
increase prices without the prior approval of the
K
Government.
>
prices are revised, costs have increased;
further, rendering the approved
prices uneconomic.
While drug prices are rigidly controlled
there is no control whatsoever on
costs of raw materials and packing
materials. Their costs have increased
phenomenally. Costs of other inputs and
services have escalated too —
electricity, water, freight, wages and
salaries..
There are inordinate delays in dealing
with applications for price revision. As
input prices are continuously escalating,
by the time prices are approved
they become uneconomic.
The approved prices are inadequate and,,,
in several cases, even below cost of
production. This is because actual costs 1
are not taken into account; several
.legitimate costs are arbitrarily disallowed.
Unprecedented cost escalation without >
timely price adjustments has sharply
eroded margins to levels well below those
prescribed by the Government.
very few companies are able to get even
a modest return. Some established
units are already in the red; others are
moving rapidly in that direction.
New investment and production have
slowed down while demand is rising.
Result: shortages of several medicines..
The drug policy does not encourage
investment and production. Nor does it
permit optimum utilisation of productive
capacity. It has pushed up the country’s
import bill for drugs to a record
Rs. 113 crores last year.
This policy is crippling a vital industry.
Another look at it is imperative
and long overdue.
No control on cost
Although prices are controlled, there is
no control on the costs of inputs which
have escalated sharply (see table).
The price control order provides
for periodic revision in drug prices
on .the basis of increases in cost of
production, but there is no adequate
administrative machinery to deal
expeditiously with hundreds of price
revision applications. And by the time
COST ESCALATION OF INPUTS
Unit
Price in Price in Percentage:
1976
1981
increase
(Rs.)
(Rs.)
(%)
Rew
materials
Lactose
7.15
14.75
kg
Gelatine
31.09 55.99
kg
Sugar D30
kg
2.15
7.49
Salicylic acid
15.78 32.96
Alcohol
8.86 18.54
kg
(isopropanol)
Packing
material*
Vial 5 ml white 1000
107,07 204.24
Glass bottle
1000
233.60 378.47
(amber) 50 ml
PP caps
1000
140.40 185.76
.Tubes 5 gm
1COO
326.27 656.29
Aluminium foil kg
45.73 69.55
(printed)
Utilities
Electricity
KWPH
0.24
0.45
Furnace oil
Litre
0.96
257
106.29
80.09
248.37
108.87
109.26
90.75
62.02.
32.31
101.15
52.09
87.50
167.71
Inordinale delay
Inordinate delay-in price-revision-Is-not ~
the only problem. What is even worse
is that when prices are finally approved
they are inadequate and far below
what is warranted by the cost of
production and even the Government’sown pricing norms. This is because
actual costs are not taken into account;
several legitimate costs are arbitrarily
disallowed.
Furthermore, the mark-up allowed is
inadequate and unrealistic. Under the
pricing formula the consumer price
of a drug is arrived at by adding a
percentage mark-up to its factory cost.)
Mark-up is not profit; it is to cover
costs not included in factory cost, such as
freight, distribution charges, trade
discount, selling expenses and
manufacturers’ margin.
Under the old formula mark-up was a
maximum of 75% of factory cost for
certain drugs and 150% for others. This
has now been reduced to 40% for
some drugs, 55% for a second category
and 60%-100% for a third, although in no
area have costs gone down. The break-,
even mark-up for most companies is
around 75%. When costs are going up
and prices all round are rising,drug prices
cannot remain the same without
adversely affecting investment,
production and availability of drugs and
medicines.
Sharp decline in profitability
The drug industry, like any other
industry, must have a fair return to enable
it to pay a reasonable dividend and to
plough back for new investment and
increased production. But cost escalation
without timely price adjustments has
sharply eroded margins to levels
well below those prescribed by the
Government. The position today is that
very few companies are able to get
evena modest return.Obviously,there is
something basically wrong with the
policy itself.
The impact of cost escalation'on the
profitability is clearly demonstrated by a
•A
study of the balance sheets of 20
leading companies by the Economic
Times Research Bureau. These 20
companies together account for a total
drug sales of Rs. 474 crores in 1980-81 or
about 50% of the entire production of
the organised sector of the industry. The
study showed (hat although sales
increased by 9.5% in 1980-81 over 1979-80,
profit before tax dropped as much as
25.2%. Retained profits for the year
recorded a sharp decline of 22.5%.
Tire financial viability of several
companies has been severely hit. Some
established units are already in the red;
others are rapidly moving in
that direction.
Shortage
.Naturally, this has adversely affected.
j investment and production. New
■ investment has slowed down. Shortages
of several essential medicines, which
were occasional in the past, have now,
become frequent and wide-ranging.
Other factors have aggravated the
situation: scarcity of critical raw materials':
and packing materials; inadequate arid.
irregular supply of canalised drugs;
power cuts and labour unrest.
ilOW DRUG PRICES COMPARE WITH
OTHER PRICES
- Wholesale price index
All
Drugs &
commodities
medicines
IGO.O
100.0
1970-71 (base)
1975-76
118.7
172.9
186.4
136.1
1973-79
212.3
1979-80
135.2
1980-81
256.9
137.6
A poSacy for growth, not
stagnation
The aim of the policy-makers was to
encourage investment and production.
But the policy has produced the opposite
effect. Our Prime Minister has recently
called for removal of all policy constraints
and procedural handicaps that prevent
optimum utilisation of the country’s
productive potential. But the drug policy
does not encourage more production
to prevent shortages.
Another look at the policy is long
overdue. It is crippling a vital industry. It
has caused shortages and hardships to
the consumer. It has also pushed up the
country’s import bill.
In the year of productivity we need a drug
policy that encourages growth, more
production and greater availability
of drugs and medicines to the consumer
MARK-UP IS NOT PROFIT
Mark-up is meant to cover costs not included in
factory cost: namely,freight, marketing and
distribution costs, trade discount and manufacturers’
margin. The mark-up which was 75% for some
drugs and 150% for others in 1970 has been slashed to
40%, 55% and 60%-100% under the DPCO 1979,
although in no area have costs come down.
ORGANISATION OF PHARMACEUTICAL
PRODUCERS OF INDIA
Cook's Building, Dr. D.N. Road, Bombay 400 001
“Unintended profits” on for^kilations at a time of falling
of imported bulk drugs.
fc dre® pxclq? waaMSoSd?
R. VASANT SATHE, Union Minister
for Chemicals and Fertilizers, was
grilled in Parliament again for his
Ministry's helplessness over the profiteering
from the sales of essential medicines by
their manufacturers. It was again Dr. Joseph
Leon D'Souza. Rajya Sabha member of the
ruling party, who caused acute embarrass
ment to Mr. Sathe and the issue this time
was the "unintended profits" made from the
sales of formulations.
The charge against the Government Is
that it has permitted drug companies to
appropirate for themselves instead of mopp
ing up the "unintended profits” from the
sales of medicines made from bulk drugs
like rifampicin given for treatment of both
leprosy and tuberculosis.
While the drug companies have take a
different view of this matter, it is true that
the fall in the international prices in recent
months of rifampicin and other drugs im
ported for the manufacture of furmulations
have led to the companies making profits
which have not been mopped up by the
Government under procedures laid down in
the Drug Prices Control Order (DPCO)
1979.
Similar charges have been made of unin
tended profits having been made in formula
tions from the bulk drugs, metronidazole for
.treatment of dysentery and dapsone and
lamprene for treatment of leprosy.
Though the Government has granted
licences for the manufacture of rifampicin
to seven companies including the Stateowned Indian Drugs and Pharmaceuticals
Ltd., indigenous production has not com
menced. The country's needs, therefore, are
being met only by imports, which went up
from 8.95 tonnes in 1980-81 to 16.07 tonnes
in 1981-82 and 36.90 tonnes in 1982-83.
Downward trend
For reasons which will be explained here
the international prices of rifampicin which
the drug companies In India had been Import
ing from different countries had been show
ing a downward trend, the prices hovering
between Rs. 1,800 and Rs. 1.675 a kg. The
Government,
however,
allowed
the
companies to charge the prices for formula
tions made from rifampicin on the basis of
a price of Rs. 2,404 a kg. for the bulk drug.
As many as 17 drug companies including
theJDPL have been making "unintended pro
fits" on the sale of these formulations.
The same situation prevails in respect of
a number of other drugs. The most glaring
case seems to be that of the formulations
M
made from metronidazole, the major pro
ducer of which in India is Metroni Drugs
Private Ltd., licensed to manufacture 120
tonnes of metronidazole a year. It com
menced production in October 1981 and the
total production in 1982 and 1983 amounted
respectively to 34.42 tonnes and 45.67
tonnes. The price fixed by the Government
for metronidazole is Rs. 497.98 a kg. and
Rs. 600 for metronidazole benzoxylate.
And yet It has been brought to the notice
of the Government that these two drugs are
available In the market at prices ranging
between Rs. 290 and Rs. 325 a kg for
metronidazole and Rs. 310 and Rs. 347 for
metronidazole benzoxylate. As a result of
the Government having allowed the formulators to use the higher prices as the base.
buyers of these formulations have been pay
ing as much as Rs. 14 for a 60 millilitre bot
tle while it should not be more than Rs. 4,
according to Dr. D'Souza.
Price formula
The DPCO lays down a formula for arriv
ing at the prices of formulations made from
the bulk drugs providing for appropriate
mark-ups for packaging, transport and
marketing. Formulators who make the
medicines from imported bulk drugs which
are cheaper than those produced indigen
ously are required to deposit the profits
worked out on the basis of pooled and reten
tion prices into the Drug Prices Equalisation
Fund account. The Chemicals and Fertilizers
Ministry seems to lack the will to defend
Itself effectively. It has pleaded that it has
issued notices to the companies to provide
details about the unintended profits to help
the Government mop them up.
Apart from the 17 companies which have
been issued notices relating to rifampicin
formulations, notices have also been issued
to as many as 113 companies for a number
of other drugs from the sales of which unin
tended profits have resulted. These drugs
include, apart from metronidazole, dox
ycycline. ampicillin trihydrate, salbutamol,
dapsone and chloroquin phosphate.
The Government should blame only itself
if the spiritlessness of its defence has
spread suspicions about it being hand In
glove with what Is called by its strident
critics as the mafia of the drug industry.
Why the declining trend?
Since the Government has assumed ma
jor regulatory functions for ensuring that the
drug industry does not overcharge the
buyers, particularly those belonging to the
poorest in the community vulnerable to dis
ease. it has undoubtedly the duty to see.
that the benefits of a fall in the international
prices of bulk drugs are promptly passed
on to them. At the same time there has to
be some understanding of why the interna
tional prices of bulk drugs like rifampicin
■have shown a significantly declining trend.
This did suggest that there had been some
efforts at dumping but lately the interna
tional prices of refamplcin are reported to
be climbing.
Rifampicin has beert known as an ef
fective drug for treatment of leprosy. But
only during the last five or six years has
it become widely known as effective for
treatment of tuberculosis as well The result
of this discovery has been that the overseas
manufacturers of the drug have stepped up
production because of the increase in the
.demand, particularly from the developing
countries. ■
While this did effect a downward pre
ssure on price, the overseas suppliers have
a vested Interest in seeing to It that the ef
forts of countries like India to produce the
drug indigenously are either frustrated or de
layed to preserve their own market. This
is best done by making the drug available
at ever cheaper prices since this could rob
them of the Incentive to make expensive
investments on indigenous production.
However present indications of a rising
trend show that international suppliers could
not indefinitely persist with their efforts to
sell the drug cheap to India.
Selectivity given up
The case of the drug companies Is that
the charges of their having made unin
tended profits arise from those who have
focussed their attention on one or two
formulations made for imported drugs availa
ble at lower prices and not on their whole
range of production and profitability. This
merits some attention.
The Government does indeed keep track
of the movements In international prices of
imported bulk drugs but by the very nature
of things the machinery cannot move as fast
as it should. The Bureau of Industrial Costs
and Prices (BICP) has to call for data relat
ing to prices and determine what should be
the selling price and there is inevitably a
time-lag before the benefits of a fall in
international prices can materialise for the
buyer.
The situation in which the Government
finds itself is in fact far more difficult than
what has just been indicated. This is
because of its own earlier draconian but un
imaginative efforts to overregulate the drug
industry without a proper awareness of the
magnitude of the task.
When the Government announced the
drug policy in 1978, it did take a practical
view of wnat could be attempted by way
of regulation. It was decided that a watch
should be kept over the prices of some
selected imported drugs and the Govern
ment should ensure that the benefits of any
fall in their prices should be passed on to
the buyers by the formulators.
However when the Drug Prices Control
Order was issued in 1979, this policy of
selectivity was given up and the order pro
vided for a watch being kept over the im
ports of all raw materials and for the regula
tion of prices on the basis of the
recommendations by the BICP. The result
of this has been to push matters relating
to drug prices into the stickiest mess one
could have thought of.
Wide ranging
It will be interesting to find out whether
there is an entity like the BICP anywhere
in the world being asked to recommend sell
ing prices for such a large number of items
on the basis of price movements influenced
by a variety of factors. The BICP is being
put on an endless run on the trail of prices
of raw materials and bulk drugs to recom
mend what should be fair selling prices and
how much unintended profits should be
mopped up. If the prices rise — as they
do very often — it will have to compute
the new selling prices to save the producers
from the unintended losses too. How much
efficiency and speed can an official agency
bring to a job of such dimensions to ensure
a fair deal both to producers and buyers?
This brings one to the case put forward
by the drug companies. There are not many
producers making only a few formulations
from the bulk drugs. The range of produc
tion of most of them covers quite a large
number and the mix is generally such that
while there may be unintended profits in the
case of one or two formulations, they may
be making losses or just breaking even in
the case of the others.
Though the Government has a respons
ibility to see that there is no unconscionable
profiteering In the case of essential and life
saving drugs and formulations, its task
would be a lot easier if it focusses its atten
tion on the overall profits being made by
the drug companies to ensure that they are
not enriching themselves by fleecing those
who are ill and who can least afford to pay
the prices demanded.
C. V. Gopalakrishnan
tteplacing the
multinationals
ENDING
by Anil Agarwal
Under the political leadership of the Third World, five UN agencies
(WHO, UNCTAD, UNIDO, UNDP and UNICEF) are collaborating in
an undeclared war on the multinational drug companies. They are
fighting what WHO’s director-general calls "drug colonialism”.
A basic drugs list, bulk buying, new patents laws, small-scale
manufacture and traditional herbs are the weapons they have chosen.
Taken separately, the policy of each UN agency is a powerful
lever for change. Taken together they build up into an integrated stra
tegy which could transform the world pharmaceutical scene. This is
the first coherent step taken by the UN towards translating the New
International Economic Order from rhetoric into reality.
_(THE UN agencies seem finally to
have found an answer for Asian
^■pharmaceutical problems. Nearly 90
■■per cent of the world's drug output
comes from the developed countries,
and within these countries, most of it
comes from the giant multinationals.
These firms exploit Asian countries
in every possible way. According to
the UN agencies, they indulge in
excessive profiteering and tax-evasion;
they sometimes sell harmful products;
when their position is challenged by
a budding local industry, they often
try to force it out of business or to
buy it.
At first sight, the monopoly of the
giant multinational drug industry
looks virtually indestructible. Yet the
UN agencies have made some re
markable progress — without any of
the huge and lavishly-funded inter— national projects and conferences for
B which the United Nations is now inB famous. The UN has a workable
■Strategy to help Asian countries boost
their bargaining power against the
drug multinationals, and move to
wards the establishment of their own
drug industries.
The UN strategy is still unofficial
and unwritten. This is because it is
composed of varying strands of think
ing in the different UN agencies. The
opportunity for them to cooperate
came not from within the UN system
itself, but the Government of the
South American state of Guyana. Act
ing on behalf of the non-aligned na
tions, Guyana set up a task force on
pharmaceuticals, consisting of experts
from the World Health Organisation
(WHO), UN Industrial Development
Organisation (UNIDO), and the UN
Conference on Trade and Develop
ment (UNCTAD).
16
This task force is a unique arrange
ment within the UN system. A
number of UN agencies are working
towards a single objective, under the
political leadership of the developing
countries themselves.
This task force is currently visiting
Afghanistan, Indonesia, Pakistan and
the Philippines, as well as nine other
countries in Africa and Latin America
to advise them on an integrated
national policy for drugs. If funds
permit, the task force will also visit
India and Vietnam. Later, the UN
will try to identify concrete pro?
grammes to increase regional coopera
tion within Asia and the rest of the
Third World. The underlying theme
of the UN strategy is simple : drug
use within a country must reflect the
real health needs of the majority of
its population.
There are five main reasons for this
theme. First, the number of essential
drugs needed to meet the health needs
of the majority within a country is
amazingly small — one or two per
cent of the thousands of different
branded drugs at present marketed in
most Asian countries. WHO has pre
pared a list of essential drugs for the
Third World, which consists of only
220 items.
Second, the sources of supply for
most of these essential drugs range
from large multinationals to small,
local manufacturers. By centralising a
country’s purchases and making all
these companies compete for orders.
many essential drugs can be obtained
at much cheaper prices. Sri Lanka,
which pioneered many of these ideas,
bought the tranquiliser diazepam in
1973 at one-seventieth the price
charged by its previous multinational
supplier.
C' “XVTJ?’.".-.'
“mim
COLOmiLISM”
Third, the technology needed to
manufacture many essential drugs is
within the reach of even relatively
small developing countries. UNIDO
now looks upon . pharmaceutical
manufacture as a key area for techni
cal cooperation among developing
countries.
India has a large number of smallscale multipurpose plants, each of
which produces several chemically re
lated drugs in successive batches.
Through UNIDO, India recently sup
plied Cuba with a single plant to
manufacture 15 drugs (including para
cetamol, aspirin, diazepam and vita
min B base), for a mere $ 500,000.
Fourth, the Third World can pro
duce drugs for many essential health
needs from local medicinal plants. The
experiences of China and Vietnam
shows that herbal drugs can be pre
pared in the villages themselves, using
local labour and resources, and sub
stantially reducing the demand for
imported synthetic drugs. A recent
meeting in Lucknow, India brought
together experts from Burma, India,
Nepal, Pakistan, Thailand and eight
other countries to discuss the Third
World production of herbal drugs.
Fifth, as the essential drug lists of
neighbouring countries should be
quite similar, regional cooperation
should become easy.. Countries could
collaborate in joint drug purchasing,
joint market intelligence, joint qua
lity control, joint research and deve
lopment, and possibly even joint pro
duction of drugs and vaccine which
cannot be produced economically by
small countries.
Many of these ideas are already
being.adopted by various Third World
countries. Sri Lanka, for instance, now
restricts its purchases to a basic drugs
list, and Afghanistan is also taking
an interest in centralised drug pur
chasing. The Caribbean Community
CONTINUED ON NEXT PACE
Himmat September 1, 1978
?®8iragiiag
GENERAL MANAGER KINI :
“some achievements to our credit’’
has to be supervised by senior offi
cials. There are umpteen people in
volved down the line. A number of
actions have to be taken like cable
pair allotments etc and records are
made of each action. Anything done
out of the wav is easily found. One
problem is probably there. After the
equipment is available and when a
release is made, a man who has this
information can go to the people con
cerned (who he knew are already
sanctioned a phone) and say. I can
get you a connection. The subscriber
doesn't know 'this. To plug this possi
bility, whenever we decide on a
release, we send an advertisement
immediately to the press, and a small
card to the party concerned.
Q: Shortages of telephones and
equipment encourage corruption
How can funds be made more
.
readily available to avoid this?
For production to increase, it will
take time. A factor which will change
the. situation is our present process of
supplementing indigenous production
I
with import. Telecommunications was
not given core priority in the past,
both for funds and for the plant. For
cable or equipment we depend on our
own production or surpluses. We
largely reinvest what we earn from
our revenue. On the equipment side
we depend on what our own factories
in the country can produce. Very
little was imported except against
World Bank loans because of foreign
exchange difficulties. In the case of
telex, we had to design our own.
.• Which developing country has done
pier 1, 1978
This may be partly true. But the
this? This is the major constraint that
has limited production. Because of question of corruption does not
the improvement of the foreign ex depend on a salary alone. Our salary
change situation, larger imports are scales are the standard Centra! Gov
planned sc we can aim at larger ex ernment scales. It is certainly lower
than public sector undertakings,
pansion than in the past.
Q: Why has the Department not banks, etc. As I said before, the
taken action against the so-called public has a great deal to do with it.
“telephone consultants” who ad You can go on feeding people with
vertise with complete details, assur money to keep your line going and
ing phones within 15 days? There naturally, the man will keep on de
is not even a verbal public disso manding more.
Q: What arc the steps that you,
ciation from them.
as General Manager have taken to
We have issued press notices tn the
improve efficiency?
past and we will issue them again if
I am the last person to say that
it is of any use. We cannot take steps
against anyone from publishing such Bombay Telephones are in perfect
notes. What action can we take? He working order. But I think that we
is not- a subscriber. We do not have have some achievements 'to our
police powers. What offence is dis credit. The service has improved. The
closed? Many of these problems arise complaints on 198 services has shown
a steady downward trend. The written
from shortages.
Secondly there Is a lack of infor complaints per 100 telephones has^K
mation for the public. 1 have studied gone down — from 8.12% in 1976 to BL
this problem and made comprehen 7.19% in 1977 and 2.91% till June this^B
sive proposals for a public relations year. The rate of provisions of new
office. It is not in my capacity to telephone connections have been
sanction this. It has gone to Delhi very sharply stepped up. In the last 2
and will have to be favourably consi years — 1976 to 1977 — the annual
dered by the P & T Department. increase was more than double the
Something may happen soon.
average rate in the previous five years.
The International Subscribers' Dial
Q: What are your proposals?
I would like to do the following : ling service was introduced to London
1. Have some place where the for the first time. After considerable
subscribers can come and get toutine preparation major steps were taken in
information at a counter and not 1977-78 for decentralisation of the
waste the time of senior officers.
organisation and setting up area tele-.
2. I would like to have the phone offices. Five of the six area
counters and the staff specially select telephone offices which were planned
ed.
(
■ are now functioning in different
3. I would like to have print parts of the city and suburbs. Earlier
ed leaflets — with certain points people from Ghatkopar had to come
that people commonly ask. These can here (to Colaba).
Q: According to the rules of the
be used at the counters and for
answering correspondence.
contract signed between the Department and the subscriber, it is illegal JK
All this is something novel for the
Department. It requires organisation.
to charge rental on dead phones.
Q: Perhaps then complaints and
Why does the Department do so?
other correspondence will be
I cannot find any such rules. We
acknowledged?
have sent a reply in a letter to the
It is not enough to merely acknow press to those who say they exist.
ledge correspondence. It has to be'
Q: Why are lines cut without
warning? According to the con
handled. You must not underestimate
the effort involved in keeping things
tract, you must serve at least seven
up to date. There is a big difficulty
days’ notice.
about handling correspondence. It
This notice does not apply to cut
fills a volume. When people are ting off the lines for non-payment of
waiting, they keep on writing. My dues, within the prescribed dates.
officers do not have stenographers. About 45% of the subscribers do not
We have 50 posts vacant. At the pay within the due date. The accounts’
salary we offer, we cannot get the office start ringing up the people who
necessary speed. The officers cannot have not paid and make a record of
the conversation. Of course errors
handle, their own letters.
Q: Is the corruption within the can occur. We issue about 1.2 lakhs
Department so rampant because of
CONTINUED ON PAGE 20
low salary scales?
15
A
strategy
for
Third
World
nations
drug production is largely controlled
by Western multinationals, through
licensing arrangements or local sub
sidiaries.
Forty-five developing countries have
no drug manufacturing facilities
whatsoever, and drug production in
43 others is restricted to packaging
and formulation of imported drugs
into tablets and capsules.
Developing nations which do have
their own drug industry increasingly
complain that foreign-controlled sub
sidiaries indulge in a variety of im
proper trade practices. They are
alleged to charge excessive prices for
their products; to be least interested
in producing those drugs which are
most needed by the bulk of the popu
lation; and generally to impose condi
tions on the transfer of technological
know-how which restrict the growth
of locally-owned industry.
DRUG
INDUSTRY*
Around 1000 million people, most
ly the world’s poorest, are exposed
to mainly infectious and communic
able tropical diseases. Until the mid1970s the total global annual research
expenditure on these tropical diseases
amounted -to about $30 million —
less than one fiftieth of the annual
expenditure on cancer research, and
the equivalent of the cost of build
ing a few miles of motorway.
Anil Agarwal
High drug prices
Thirty years after the formation of
an article “Replacing the multi
the
World Health Organisation, and
nationals” (Himmat, September 1),
Anil Agarwal outlined a combined after massive investments by develop
move by five United Nations bodies ing countries in hospitals, medical
—
WHO,
UNCTAD, UNIDO, colleges and drug factories, modern
UNDP and UNICEF — in an as yet health services are still beyond the
unofficial strategy to combat what reach of the great majority of Third
WHO’s director general calls “drug World people. The use of modern
drugs in the Third World remains
colonialism”.
The following article comprises confined to a small urban elite. In
extracts from a pamphlet “Drugs India, for instance, the consumption
and the Third World", written by of modern drugs in 1973 was only
Anil Agarwal and published by Rs 6 per person, and only 20 per cent
With the end of the colonial era,
Earthscan, which deals in detail with of the population used them, despite interest in the developed world in
the situation as it is and the remedy the fact that India has the most communicable diseases has declined,'
sophisticated drug industry in the
proposed by the UN.
with the result that very few new
Third World.
drugs or vaccines against tropical
HE UN drugs strategy forms
There are enormous differences in diseases have been developed in re
part of a new. approach to deve
lopment within the UN agencies. drugs expenditure between develop cent years. Also the global demand
This aims at increasing production ing and developed nations. For ins for tropical disease drugs is not
^itfrin developing countries through tance in 1967 per capita consumption thought sufficiently large to make
i^^ocess of self-reliance. Wherever of pharmaceuticals in the US was their production and research eco
possible this self-reliance should be over $20, in Japan $15. and in Europe nomic. Those who suffer from these
achieved on a national basis, by the $14, while in Latin America it was diseases are poor, and the drug com
use of appropriate technologies and $4 and in Asia and Black Africa only panies say they find it hard to market
rational utilisation of local resources. $1. Drug costs often represent 40- tropical drugs profitably.
Where this is not possible, effort 60 per cent of the total health care A basic drugs list
should be made to become self-reliant expenditure in developing countries,
The markets of both developed
on a collective Third World level, compared with only 10-20 per cent in
and developing nations are flooded
through cooperative action among the developed ones.
The prices of many drugs sold by with a wide variety of brand medi
the developing countries themselves.
western drug companie.s to the deve cines. Most of these are merely dif
The Third World drug industry
loping countries are often higher ferent combinations of ,a small number
Large-scale commercial drug pro than the prices a<t which they are sold of drugs, presented in different
duction is restricted to a very small at home. For example whereas Bri dosage forms.
number of developing countries. tain paid US firms $2.40 per kg of
The contrast between branded
Brazil, India and Mexico account for Vitamin C in 1973, India had to pay drugs (eg Aspro) and generic drugs
about 50 per cent of the Third nearly $10- Tetracycline antibiotics (eg aspirin) is central to the concept
World's drug production cutside which cost $24-30 in Europe were be of a basic drugs list.
ing sold to India, Pakistan and
China.
CONTINUED ON NEXT PAGE
But even within these countries, Colombia for $100-270.
'J'
Himmat September 15, 1978
19
DRUG
INDUSTRY
same firm than a developing coun substance.
try.
In India the ancient medical sys
UNCTAD therefore strongly re tem of Ayurveda has a materia
commends that developing countries medica containing over 8000 herbal
should centralise their purchases via recipes. The plant Rauwolfia ser
a single state buying agency to the pentina, from which most modern
Several countries have tried to maximum extent politically possible. tranquilisers were developed, came
identify those drugs which are essen Essential prerequisites for centralised from Ayurveda.
tial for the needs of the majority of drug buying are the preparation of a
The Centre for Scientific research
their patients. They have found that basic drugs list and the prescription into Plant Medicine in Ghana has
only a very small number is required of generic drugs only.
found excellent herbal preparations
— in the case of the developing Traditional herbs
against guinea worm and shingles for
countries often just 1-2 per cent of
which western medicine has no effec
Both UNIDO and WHO see the tive remedy. Herbs under investiga
all those on the market.
Even developed countries like use of traditional herbal remedies as tion for diabetes mcllitus and bronSweden and Norway, which provide an important part of the Third World cial asthma appear to be far more
the most advanced forms of therapy strategy for drugs self-reliance, com effective and less risky than modern
to their populations, deal with a ing as they do into the category of drugs.
restricted list of about 2000 drugs in “remedies used on the basis of long
Towards the end of 1978, WHO
their state-run drug distribution sys experience”. All over the world peo will organise a meeting to identify
tems. In West Germany, by con ple have used locally available na and most widely used medicinal
trast, there are 24,000 drugs on the tural drugs for centuries. These pro plants and then establish a network
ducts are trusted by the consumer, of collaborative research centres to
market.
The total drug purchases of indivi and can be assumed safe since no study their effectiveness.
Quality control
The multinational pharmaceutictu
industry has always claimed that the
local manufacture of drugs and the
abolition of brand names will lead
to a deterioration in quality. Deve
loping nations must set up their own
quality control systems if they wish
to undertake generic prescribing and
local manufacture. This is necessary
not only to ensure quality control but
also to set at rest the doubts of the
medical establishment.
Small-scale manufacturing can lead
to problems, where lack of adequate
instrumentation and control can lead
to substandard products.
Few Third World countries possess
adequate drug testing facilities at the
moment. But the central problem of
quality control in developing coun
tries is usually the lack of skilled pe_r_sonnel.
Political will
For the UN policies on drugs to
work, developing nations will above
all need a strong political will.
They- will need this political will at
the national level, to develop and en
LARGE SCALE DRUG MAKING IN INDIA:
but 45 Third World Linds have no facilities at all
force their national drug policies des
pite local professional and commer
dual developing countries are usually toxic effects have been recorded dur cial opposition, and to reform their
existing
health services to serve the
small compared to the worldwide ing widespread use. In .any case many
sales of the large drug companies. modern medicines come from plants primary health care needs of their
The bargaining power of most Third which have , been used in traditional peoples. Without a relevant health
World countries is therefore also medicine through the ages. Today policy based firmly in priinarj’ health
inevitably small. It is further reduc more than half the prescriptions care, there can never be a proper
ed if a country has several importers. written by American physicians are drug policy.
Developing countries will also need
Bulk purchasing usually substantially estimated to contain a plant-derived
reduces the cost of drugs. This is drug — one cither extracted directly a strong political will on the interna
tional
level, to cooperate among them
from
plant,
or
one
synthesised
to
one reason why a developed country
is able to buy drugs cheaper from the duplicate (or .improve on) a plant selves.
20
Himmat September 15, 1978
DOCTORS COMMENT — from page 17
“If doctors had any idea of the
to the politicians. We have no execu
basic problems of rural health care,
tive powers.”
they could campaign effectively in
What alternative plan, if any, has various fields,” stressed one IMA
this association to offer for rural member. “They can campaign for
health problems? An ex-President of better roads in certain areas which are
the IMA had put forward a compre quite inaccessible to health services.
hensive health scheme not dissimilar Naturally, no doctor will want to go to
in principle to the present one. This an area where he has to splash
was not accepted by the Govern through knee deep mud. Doctors can
ment. Nor was it accepted by the also campaign for better agricultural
IMA who thought it was a “personal incomes. Poverty is the root of ill
scheme” and so refused to endorse health. Here it is not the question
of the right kind of diet, but lack of
it.
any. We can influence the agricultu
ral crop pattern of the villages by
pointing out the crops that can im
prove nutrition. Doctors can also
think of ways in which intermediate
technology can be developed so that
specific care can be taken to the
village. At present health camps can
not be held in areas where there is
no clean, tiled floor to lay patients
on.”
fc art of
B
good
wmamgemesit..
moulding
our varied resources —
human, natural,
technological—for the
common good.
Though there has been little feed
back on how the programme is doing
after a year, reports of those work
ing in the field point to areas where
there is room for improvement. For
a start more imagination could be
shown regarding the scheduling of
programmes according to the conveni
ence of the villages rather than of the
functionaries. There could also be
greater flexibility about teaching tech
niques and adopting a more non-formal approach. “There is no point
This doctor takes a band of taking a poster to villages showing a
young doctors twice every month to milk bottle when they don’t get bot
an area in the Uran Taluka in Maha tled milk. The techniques have to be
rashtra. They have just released a based on their ethos”, commented
batch of fish into the village pond. one worker.
Every villager suffers from guinea
worm and the fish will feed on and
Over the distribution • of the kit
destroy these worms. “Doctors do promised to the CHWs there have
go into the backward areas and treat been difficulties. Not all of |:hem
people. But we need mote doctors have received them. Moreover re
concerned with preventive and not plenishing of supplies requires an
just curative measure in the rural effective machine which does not
areas.”
exist. Consequently medicines have
Are there enough concerned with been in short supply.
either?
CHWs — from page 15
Shrlram seminars and courses are part of
this moulding process... which Involves
executives In a ceaseless Interchange of
ideas, discussion of modern techniques,
evaluation and reconsideration of policies.
So that the Shrlram organisation is const*
antly Infused with fresh dynamism... and
our resources are utilised to the optimum.
SHR1RAM CHEMICALS
cines — now even chloromycines are
to be found in the villages along with
aspirins — and more often than not
prescribe them have come to the pri
mary health centres and demanded
certificates for CHWs. “We have
anyway been doing this work, so now
you can give us the certificate,” is
their argument.
In effect the CHWs are meant to
complement and supplement the ser
vices of intermediate health workers
operating at the tehsil and district
level. Even for services like immuni
sation, child and maternity care, they
need supervision of the public health
nurse and the health supervisor.
The nursing staff has to play a
vital role in their supervision and
Himmat November 3, 1978
training because there are too few
doctors and those who arc there spend
95 per cent of their time treating ill
nesses. They are not in a position
to handle the whole gamut from train
ing dais to coronary specialisation.
That is one reason why health care
has been, given secondary importance.
The responsibility of prevention and
promotion of health care should be
shifted to the next cadre of health
workers, that is the nurses. This
aspect of the programme needs
thought.
The programme of CHWs is dove
tailed into the Government’s earlier
scheme of multipurpose workers,
initiated in 1974, under which there
is a female and a male health worker
looking after each subcentre.
The community health worker
scheme is a move in the right direc
tion. It envisages an infrastructure
where health care is made accessible
to people through their own efforts.
What requires the thought of the
medical community as well as of nutri
tionists, social workers and private
agencies is how to improve its imple
mentation. Certainly doctors who
are not prepared to go to rural areas
themselves should not block the
efforts of those trying to provide a
semblance of health care to people
long forgotten — imperfect though
the plan may be.
21
A T first reading, you may be
A tempted to feel that the title of
this book is not comprehensive enough
for the range of subjects covered. The
broad scenario includes the growing
economic imbalance, the dangers of
nuclear energy, alternative to oil,
food, preventing cancer, population,
slum resettlement and changing
philosophies necessary to meet the
crisis and challenge of the second
half of the 20th century'. Geoffrey
Lean argues that all these are vitally
linked to the rich world-poor world
struggle and that indeed solutions to
most of these problems will only be
found through a new attitude towards
the imbalance of the rich and poor
worlds and a world embracing out
look.
From experience
Lean brings to his research know’ledge gained from experience. He
was environment specialist on the
"Yorkshire Post” for eight years. He
is credited with initiating changes in
attitudes and the law which brought
radical solutions to that area of indu
strial England. He now works for
"The Observer”
Union was in the lead with 27 per
cent. Each citizen in the rich world
consumes up to about a tonne of grain
every year — the equivalent of more
than six loaves of bread each day.
This, of course, is not literally true.
What happens is that 90 per cent is
fed to live stock to produce meat,
milk, cheese and eggs when a great
deal of this could be avoided through
more intensive grazing on grassland,
otherwise unproductive for agricul
ture. Animals in the rich world eat
about 1/3 of the world's crop of
food.
More serious still is the fact that a
good deal of some of these products
are imported from poor countries,
many of whose people need the food
themselves.
In the Far East alone some 100,000
children lose their sight every year
through lack of vitamin A — blind
ness which could be prevented at a
cost of about seven paise per child
per year.
These and other facts vividly
underline the gross imbalance in the
world. Aid can go part way to meet
the need but in the long term, all are
The book under review is the pro agreed, more radical answers are re
duct of nearly three years intensive quired. We have to create a new
research, 24,000 miles of travel and pattern of food production and con
interviews with hundreds of people sumption which will include the
— authorities and the man in the ability of developing countries to
street. It is a mine of statistics for grow more of their needs, and an eco
the researcher but readable for the nomy whereby their people can buy
layman. The issues discussed have the food that is produced.
normally been regarded as technical
The potential for increasing food
ones, the province of experts, but
more and more they must become the production in the poor world is en
ormous.
Of the world’s total land
concern of everyone. Lean’s approach
is refreshing in that he discusses solu surface, less than 11 per cent is cul
tions rather than merely outlining tivated out of a possible 24 per cent
crises and proclaiming disaster. He arable land. It is estimated, for in
is realistic but gives us a book of stance, that India could produce at
least 230 million tonnes of grain a
hope.
year in place of her present 105
The author opens with a world sur million tonnes.
vey of the food situation. Although
15 million children die before they Bridging the gap
are five each year, caused mostly
The staggering imbalances and the
through malnutrition and 3/5 of all
developing countries do not get growing economic gap between the
rich
and poor nations calls for a new
enough food to give each, person a
minimum subsistence diet, Lean economic order. Lean examines on
a
basis
of world cooperation, trade
asserts that there is enough food for
all or the potential within easy reach. agreements, stabilising of raw mate
rial prices, the present pro and con
At the beginnnig of the 1970s the practices of multinationals and the
people of Western Europe, Australia, fascinating possibilities of exploiting
and Japan were consuming 23 per cent the resources of the sea bed. It is not
more calories than they required, generally known that at least i of
North America was ahead with an the world’s recoverable oil is thought
excess of 26 per cent, and the Soviet to be beneath the sea bed besides
22
an® 2D®
aiasl
<ifl®
mix
RICH WORLD, POOR WORLD by
Geoffrey Lean : Georage Allen
Unwin; 352 pp; £ 7.95, paper ^rck
£ 4.50.
Mfd
large quantities of “nodules” con
taining manganese, nickel, cobalt,
copper, molybdeum, aluminium and
iron.
In the realm of economic power,
Lean points out that the dice is no
longer completely loaded in favour of
the rich nations. He instances the
vulnerability of rich country econo
mies by the fact that the oil price
hike of 1973 set in motion deep trou
bles when in actual fact the hike only
represented a transfer of two per cent
of the income of developed nations to
OPEC countries. An overlooked
significance of the OPEC countries'
action is that it challenged the
seemingly impregnable old econonrip
order and showed that change
come and come rapidly.
Similarly he argues that there may
be other areas in which the poor
countries can improve their bargain
ing position. He cites the possibility
that the African countries could, for
instance, decide to buy only Volvo
cars and trucks because of Sweden's
record of support for a new econo
mic order.
Lean also advances the idea that
poor countries could reduce their
dependence on rich ones by increas
ing trade and cooperation among
themselves. However he issues a
warning. “The gap between the rich
and poor in the poor world itself is
as great as it is between nations.
Until this is changed increased wealth
Himmat November 3, 1978
High cost of a doctor’s cure for illness
tant part of the treatment of^liar- application is better.
WARDHA
come to a doctor, he feels obliged to
EVERY time a patient goes to a
The simple conclusion is that the prescribe some drugs even if not
rhoea is oral rehydration, which is
doctor, he goes with an element of
Dr Ulhas Jajoo
totally missing. One glass of water prescription is "mainly" to provide necessary.
faith. He expects two things from the
Most doctors do not charge consult
with a pinch of salt, sodium bicarbon <fbremL5Tid~butter” to the prescriber
doctor: one, diagnosis of his prob
ing fees separately. They dispense
ate and two teaspoons of sugar is all and tb~TKe^njg^YTdusEry. The real
lems; two, prescription of medicine from first day; no fever, no abdominal
that is required. A nd it is available to therapy"^repeateffsaline gargles or drugs from their dispensary at an
for treatment.
pain and no vomiting; and, passed
everybody at home. Most diarrhoeas 'steam inhalation — is totally forgot exorbitant cost, which includes their
But do doctors always prescribe
ibe ”
urine
*ine five times in first 12 hours
hours.tjt
< this type are self-limiting and get ten. The repetition of the same drug consulting charge. The charge de
of
right? Do they sometimes overpre
re- ( The treatment given is Lomomycin | cured
<
by the third day. The cost of in different forms has increased the pends on the paying capacity of the
scribe?
person. The name of the drug dis
Jsyrup, two teaspoons six-hourly; / such
f
a minor ailment has been cost of treatment.
Trials have been conducted in US /Lomotil tablet, one with each stool; / ialarmingly raised by visiting a doc
There are innumerable such exam pensed is never told to the patient
in which the prescriber was informe
ied<X Pecto-Kab, two teaspoons six-hourly; \1tor. ,_______ ____ ”___ _______—------ ples. The observations from the pre because if the patient knows it, he
that the prescription would Ibe I Baralgan, twice a day; Flagyl syrup, 7f Case 2. The complaint is common scription can be summarised as fol may try to compare the cost with the
screened for inappropnateness of
__ / two teaspoons three times a day; and ( <cold. The history of illness is running? Afthe:
v market
mark rate.
dr^^rescribed or the doctor would
uld / Pentaimine, one tablet twice a day \ nose
i
for two days; cough for one day;; / 1. Unscientific prescribing. Many / /The
The more drugs prescribed, the
beWS^i to fill in a form justifying]
ngl for three days.
Itthroat pain, one day; and mild fever,, ) prescriptions reveal combinations of/ /•
f
bigger
the profit. The long list of
als
Let us analyse this prescription^7 one
(
the use of antibiotics. These trials
day.
4/ incompatible drugs. Many times the\L
drugs,
revealed a reduction in antibiotic use
)
doses
of
the
drugs
prescribed
are
/
I
g thus, is a mechanism to earn
ise First, most acute diarrhoeas are self- I
The treatment given is tablet Sepmoney
without the patient being <
of as much as a quarter.
limiting. They do not require anti
anti- tran
t
twice a day for seven days;; | inadequate. This reflects the poverty \ 1 iware.
I
Another study published in a lead biotics (Lomomycin).
Otrivin nasal drops three times a day/ I of the knowledge of the prescriber. —' ^Doc
Doctors
have conditioned the
ing US journal reports that in a case
ndly, Lomotil is a drug of the
for seven days; tablet Cosavil, one»2. The prescription is aimed at') I . ,
linds of the people to drugs so much
where doctors were asked to write
orphine group which may reduce
tablet three times a day for seveni / early relief of symptoms even if it is I f?Lrl now if a doctor does not prei ( likely to harm the patient in the long / Ia
the diagnosis along with their p
the frequency of motions but hides
ays; tablet Crocin, one tablet twice al
ibe, the patient starts demanding
scription, it was found that antibio
e fluid loss which continues within
day for seven days; Benedryl coughi \ run. Doctors have a shotgun therapy, I 7^n
ics had been prescribed without an
L™
the gut. In the false security of syrup, one teaspoon three times ai I Their prescription covers all possible
evidence of infection in 62 per cent o
-/ causes for a particular clinical symp- /
.. le* pressure is on the pocket of the
diarrhoea being controlled, a child
day; injection B-c<unplex; throat lo-,
prescriptions. No such studies are
zenges; and syru j B-complex, one 1 tom so as to avoid efforts required for patient — in India, usually a poor
person
— who spends all that he has
available in India or from other
a careful diagnosis. This tendency
teaspoon twice a d?y.
in blind faith.
Thirdly, u ^r-uth kaolin (Pectodeveloping coantr’.ec, but i.u.ny doc
Common cold js a self-limiting ’exposes a patient unnecessarily to
It is not the doctor alone who earns
tors would not be surprised if over iKab) has no role in treatment of viral infection which responds within j many drugs and their side-effects. It
in this business, but also the pharma
prescribing was true in 80 to 90 per diarrhoea. It creates a false impres a week if treated and takes a full I reflects the failure of a doctor to
cent of cases.
sion of diarrhoea being controlled as
week if not treated. The use of al diagnose properly the cause of ill/ ceutical industry. A doctor’s knowl
edge
is enriched from time to time by
In a country like India with an. it solidifies stool.
potent antibiotic hke Septran which \ ness.
extremely low per capita drug conA
Fourth, unliss pain is severe,
can sometimes har n the patient can u 3. Potent drugs have been used pharmaceutical agents, who try to
convince
him that his company’s
sumption — about Rs 15 a year — it is I Baralgan-like drugs do not have any not be justified. Otrivin contains when they
should
normally
be
pre„
„
roduct is the best availably________
only reasonable to expect thahKiocJ use. They should never be given in
ephedrine nasal drops to dry the / served for desperate situations. For
heap of physician’s samples is?
tors will prescribe more carefully and twice-a-day doses but only as a single
nose. It is the costliest such prepara example: use of broad-spectrum po
usually enough to convince those
rationally. This will not only bentffii dose, when required, to relieve pain.
tent antibiotics even for an illness
tion in the market here.
the society as a whole by diverting'
Fifth, Flagyl ris a drug used for
Cosavil contains aspirin and an which does not require them, exposes who are hesitant. The free samples
dnu^expenditure away from un: amoebiasis and giardiasis. Unless antihistaminic drug which also helps the population to the problem of are then sold. It is unusual to see a
_ /
nek^yrrymedi ci nesfoward 1 ife-sgiv- stool examination reveals these
in drying the rose. Prescribing developing resistance against these doctor \vho refuses this bribg.
irig
buVwjll
also help
Crocin — a pain and fever relieving drugs. With drug companies oversell
—
o preparations
-r—'-------------— --- to-I1 organisms, addition of this drug to a
cUt716wn'^Me=effeCts^hd tfiusbenefit \ prescription for bacterial diarrhoea
drug — when aspirin is already being I ing and doctors overprescribing anti doctor hardly ever knows anything!
the individual patient.
(antibiotics are being given already) given is not justified. To suppress the I biotics, disease-causing bacteria are
about the ingredients in the brand
irritating cough of common cold, one already resistant to antibiotics. This
drug that he is prescribing, nor does
is not ethically justified.
consumption is just Rsl5 a year, it is
he have knowledge of other similar
Sixth, Pentaimine is a drug used does not need a Benadryl syrup poses a serious public health problem
obvious that prescribing should be against worms 'It is the costliest (which has antihistaminic drug as an to developing countries.
brand drugs which may be cheaper.
biased toward life-saving drugs and wormicide available in the market ingredient). Adding Benadryl syrup
Corticosteroid preparations like
Why is all this happening in a
not unnecessary drugs like tonics. here. The rationale of adding this
to the drug list only helps in increas Betnelan and Wymisone, though
rofession that is concerned with
Let us study a few prescriptions drug to the prescription cannot be ing the cost of the prescription.
uma
good drugs, can be double-edged
usually given by qualified doctors. explained without carrying out a . Use
injection -------B-complex
and swords. If not used at a proper time
---- ..vof
,-------------1----- —
e root of the malady lies in bur
The following are actual prescrip stool examination.
/Ysyrup _B-complex
is unwarranted
ex- J and in proper conditions, they can
value system. The medical professior/
___ r________
___________
The conclusion is that this is “shot- ) (cept
cept to help pharmaceutical firms oi
on harm the patient in the long run.
tions for two common problems for
has unfortunately been commercia
doctor
earn money—out of an'
which we often visit doctors.
gun” therapy. All the drugs against ‘\ jthe
**u'' J
—*— *to------------------lised. If this goes on too long, the
4. Many prescriptions are aimed at
Case 1. The disease is acute diar the common causes of diarrhoea have Vinjection. Throat lozenges are costly. earning money. Most illnesses that a
faith in the healer may cease to exist.
rhoea. The history of illness is loose been prescribed. Some drugs are not \They help only to suppress the cough private practitioner deals with are — Centre for Science and Environ
ment
_ _____ __ *---- ____ x'
/
motions three or four times a day ethically justified. The most impor- by their local action. Throat paint self-limiting. Once a patient has
*
The
©S
Calcutta: The’ visual shows a
traveller armed with suitcases
rushing to catch a train or plane. The
copy, in large letters, reads: “Got the
runs? Don't forget your Entero
vioform.” This high visibility street
hoarding has been reproduced in the
August issue of South, the Third
World magazine, to illustrate a fea
ture on unscrupulous drugs promo
tion in developing nations. Entero
vioform is an anti-diarrhoeal, ban
ned in the West.
The South article is by Charles
Medavvar of Social Audit, a very
|fe:al and effective British pressure
|Rup, who says: “One important
Third World concern is supply and
promotion of inappropriate and
sometimes positively undesirable
products.” He goes on to add that
three-fourths of all anti-diarrhoeal
drugs sold in developing countries
could be classified “as undesirable
preparations.”
The April 1982 issue of World
Health (the WHO journal) has the
theme ‘Travel and Health.’ An arti
cle on ‘Travellers’ Diarrhoea’ says:
“The best way of preventing di
arrhoea is to avoid exposure to the
infective agent (i.e. in food and
drink). If you do contract diarrhoea,
the mainstay of the treatment is the
use of oral rehydration fluids.” The
message of the article is: if you are
travelling and eating out, keep oral
rehydration salts handy; not Entero
vioform or any other anti-diarrhoeal.
In fact, the article goes on to add,
“There is no evidence that drugs
much part in curing travellers’
^■rhoea except under specific condmons... A vast number of commer
cially available anti-diarrhoeals are
on the market. It is doubtful whether
any of these really cure diarrhoea
although they may temporarily re
duce its severity and relieve symp
toms.”
Because of self prescription of
anti-diarrhoeals, in addition to un
necessary prescription of these pro
ducts by doctors, the Medico Friends
Circle (MFC—a group of activist doc
tors) has launched an educative cam
paign to inform the public about the
principles of modern ‘diarrhoea
management.’ This was decided
upon after the successful protest
movement (by various groups includ
ing MFC) against the hormone pre
gnancy test (Sunday 11 April 1982)
which resulted in its being banned
this June.
MFC’s background paper, ‘Opera
tion Anti-Diarrhoea’ aims ar dispell
ing current diarrhoea myths in
medical practice and promoting the
use of oral rehydration therapy
which is often all that is needed in
the treatment of common diarrhoea.
Here are some facts documented in
the paper which has been prepared
by a team of MFC doctors with
support from- Dr Raj Anand of the
Consumer Guidance Society:
“It is now scientifically estab
lished that in the majority of cases of
acute diarrhoea, antibiotics have no
role to play. About half of such
episodes are caused by virus, against
which no antibiotic can help. Out of
bacterial diarrhoeas only some are
cut short by antibiotics. Antibiotics
should be prescribed only in the
following cases along with rehydra
tion therapy: bloody stools with high
fever; suspected cholera in endemic
areas; when lab investigations are
positive for bacterial infections.”
Besides being expensive and in
effective against common di
arrhoeas, antibiotics unnecessarily
taken can result in drug resistance,
undesirable changes in bowel flora
as well as toxic side effects. Much
misuse of anti-diarrhoeals stems
from their ready over-the-counter
availability, even though many are
Schedule L drugs. The MFC paper
stresses a number of hazards which
self-prescribers are largely unaware
of: Anti-diarrhoeals containing
neomycin not only cause renal dam
age but make dehydration worse and
interfere with absorption of -oral
salts. Binding mixtures containing
kaolin or pectin, merely solidify
■stools without fighting infection.
They give nothing beyond a ‘^false
sense of security” but do not control
’
fluid lost. In cases where antibiotic
therapy is indicated, these prepara
tions interfere with drug absorption.
The paper comes down heavily on
anti-motility agents which are widely
self prescribed. “These drugs have
no role to play in acute diarrhoea.”
The body gets rid of the organisms
that cause diarrhoea by ejecting
them through stools. Anti-motility
agents, by reducing the frequency of
stools, ironically cause the organisms
to remain longer in the gut without,
in anyway, fighting them. One of
these, Lomotil (G. D. Searle) has
. 1
come in for severe criticism the
world over. Since the margin be
tween the therapeutic and the toxic
dose is small, this product could be
very dangerous for children.
Again, the MFC paper says that
there is no evidence that the clioquinol drugs (Enterovioform and
Mexaform by Ciba-Geigy as well as
other brands) are effective against ,
diarrhoea. Because some of these'/ .
’;
brands also contain an anti-motility
. '
agent, they give the impression that
. sll
clioquinol controls diarrhoea. Die- ,
spite being banned in the west for
. , ‘Ji
causing optic nerve damage, these
drugs continue to be promoted iff the j
J
Third World as a preventive for
./
‘travellers’ diarrhoea, Though the
'<
manufacturers argue that the drug is
harmful only if consumed/in large
quantities, since it is widely self- \/
prescribed there is really no way of
•
keeping its consumption down at a
‘safe’ level.
Sales promotion of both anti
motility agents and clioquinol drugs
has attracted sustained protests
from doctors and pressure groups in
the West. In 1977 Swedish, doctors
began a boycott of all Ciba-Geigy
products because of their continued
'
sale of Enterovioform and Mexaform
in Third World countries. With veter
inary doctors also joining the
boycott, an effective dent was made
in this firm’s sales in Sweden. Yet,
both products continue to be sold
and even promoted to the lay public,
as the Lagos hoarding shows.
Last June, Social Audit published
a leaflet listing various kinds of
misuse of Lomotil in childern. Since
1973 the product has been contra
indicated in the USA for children
below two. The Lancet reports that
in Thailand and the Philippine^prescribing information recommends
the product for infants over three
months. Even in the UK.it was being
recommended for children below
one until strong protests from the
Social Audit compelled the firm to
revise its label. The firm has agreed
under pressure even
to contra
indicate the product for children
below two years in all countries
“where the regulating authority per
mits such limitation.”
This means, however, that if the
regulating authority is not vigilant
coRKismr xw-W «u._,
49
enough, the onus is not on the drug
firm. Tablets of this Schedule L
product, easily available without
prescription in Calcutta, have the
dosage indicated for children from
one to three. Lomotil drops have no
adequate warning except “keep out
the reach of children.” Nowhere is it
stated that the medicine should not
be given to children below two.
Literature accompanying the drops
is in complicated medical language
and the jargon about dosage accord
ing to body weight is unintelligible
to the lay person and is a poor
substitute for a clear warning which
ought to be on the outer label. In
terestingly. last December a ques
tion on Lomotil was raised in the Lok
Sabha but no action has been taken.
Health Action International has
been particularly active in raising
public awareness about the clioquinol drugs and Lomotil. Such
efforts are important, considering
the extent to which the multination
als go in sales promotion. The Lagos
Warding is innocuous compared to
inis tailpiece from a back issue of the
MFC Bulletin: “Lomotil, the power
ful anti-motility drug is sold only by
prescription in the US as it is fatal in
amounts slightly over the recom
mended doses. But it is sold across
the counter in Sudan by advertising
that it was used by the astronauts
during Gemini and Apollo space
flights.”
In order to educate selfprescribers. the MFC has listed the
brand names of commonly sold and
misused anti-diarrhoeals: Those
which contain neomycin are: Kaltin.
Renokab and Combactin. Products
containing chloramphenicol which
should be reserved for typhoid and
should never be used for ordinary
diarrohea are: Chlorostrep. Ifistrep
and Enterostrep. Common brands of
binding mixtures are: Pectokab.
Pecklin. Linopec and Chlorambin
suspension. Anti-motility agents be
sides Lomotil are Imodium. Imosec.
Lomofen and Loperamide. While
these are the commonly consumed
brands of anti-diarrhoeals a number
of other brands also are sold and
prescribed. Intrestingly nearly all
these are listed in the popular pre•cribers’ guide. Monthly Index of
Medical Specialities, without all con
tra-indications adequately, de
scribed. Which explains why doctors
continue to prescribe them.
Vimal Balasubrahmanyan
MARRIAGE RACKETS
as bysted
Calcutta: Close on the heels of thebusting of a marriage racket in Sri
nagar (Sunday, 25 July) the West
Bengal police has rounded up
another gang which specialised in
abducting girls and selling them in
other parts of north India and also to
^iiekhs from the Gulf. With this, two
• the biggest girlrunning rackets in
north India have been busted.
The police first started tracking
down the gangsters when they re
ceived a complaint from Abdul Sekh
Police officer interrogating the culprits
Karim of Sikandarpur village,
Hooghly, that two of his daughters
had been taken away by a man from
Aligarh who called himself Osman.
His eldest daughter, Jahanara (16),
was married to Osman while his
younger daughter Farida (12) was
taken away by him on the pretext
that Jahanara was longing to see her.
Another complainant was Sekh Ainaluddin of Kantagarh, Dadpur, who
said that his wife’s sister was taken
away by the same “Osman from
Aligarh.”
Osman and six other members of
his gang were arrested on 15 July
from Dadpur, where they had gone
to arrange a ‘marriage’ for one of the
gang members. Kalyan Mali alias
Kallu. The police raided Osman’s
house in Borotha village, Aligarh to
rescue Jahanara and Farida but
neither of them was there. However,
the police did learn that Farida had
been sold to a man called Sushal
Khan in Haryana for Rs 1.500. Soon
afterwards, the West Bengal and
Haryana police jointly raided Khan’s
house in Faridabad district and Fari
da was rescued from there. The 12year-old girl, who was terror-stricken
after the experience she had been
through, told the police that Sushal.
Khan was planning to sell her to yet
another man for Rs 5.000. The
Haryana police have been requested
to continue the search for Jahanara.
Farida, now in custody, told Sun
day that during her stay with Osman,
she would get only one chapati in the
morning and night and that both
Osman and Sushal Khan used to
torture her as she refused to sleep
with them. Asked how she was sold
to Sushal Khan she said: “Osman
took me out on the road, put me into
a bus and jumped out of it. I felt
someone in the bus holding me from
behind—it was Sushal Khan.’’Os
man, the principal convict, states
however, that Farida was never sold
to Sushal Khan but to another man
called Noor Mohammed of Langloi
near Agra. He has confessed that he
had married many girls with a view
to selling them afterwards. When
this correspondent asked him
whether he, a Muslim, had organised
Hindu weddings, he replied in the
affirmative.
A confidential police report says
that in West Bengal also, 126 adult
and 161 minor girls were missing in
1981. During the first six months of
1982. 76 adult and 66 minor girls
were missing. Another 59 girls have
been ‘married’ to unscrupulous
gangsters, who later traded them.
Clients—according to Osman who
has made big money by trading
girls—are no problem. He comes to
West Bengal because there are not
many girls ‘available’ in UP'. Normal
ly, poor parents are delighted when
they hear that there are boys willing
to marry without asking for dowry.
What is more, these ‘grooms’ bear all
the wedding expenses too. From the
marriage pandal the girls are taken
away and sold in the flesh markets of
north India.
Hopefully, with the arrest of Os
man, the situation can be expected
to improve. Intelligence sources
have said that a large number of girls
were sold in and around Bankunia
village of UP alone. With the busting
of two major rackets in girl running,
perhaps the exploitation of innocent
women will be reduced.
Devaprosad Purokayastha
57
Flood relief work
stepped up
Mrs. Gandhi must take a moral
decision: CS
MLAs have' been present in both
Hyderabad at the same time? It was
had been impersonation in Hyderaba
Could the President and the Prii
on August 15 he was satisfied Mr. Rama Rao allow a person facing charges of im
MADRAS, Aug. 23.
Whether Mr. N. Bhaskara Rao be allowed had lost his majority in the Assembly as Mr. and forgery to continue in off
to continue as Chief Minister of Andhra Bhaskara Rao had presented to Mr. Ramlal a criminal and immoral acts disqt
Pradesh even for a single day should immedia- list of 91 MLAs who were supporting him. It Bhaskara Rao for the rest of hi
tely be decided by the Prime Minister on the was also claimed that he took these 91 MLAs occupying any public office, leave
basis of the moral, ethical and legal issues in to the Raj Bhavan. While the Governor was Ministership, observed Mr. Subrama'
volved in the dismissal of the N. T. Rama Rao very particular about the Chief Minister enjoy
Even as Congress-1 president, N
Government and the installation of the new ing majority and. on that basis, dismissed the
Ministry. Mr. C. Subramaniam, former Union Rama Rao Government, it was incumbent on would have to take a moral decis
him to be sure, while swearing in Mr. Bhaskara her party should support such a
Minister, said today.
Delivering the K. Santhanam memorial Rao. that he commanded the majority dubious character. Without Congre
lecture here, he said even assuming Mrs. support.When Mr. Rama Rao was called upon ing, Mr. Bhaskara Rao could not
Gandhi had not been aware of the happenings to resign, he was conferring with 163 MLAs even for a day. The Prime Minis!
in Hyderabad and that she had come to know (out of the total strength 195 in the Assembly). pected to rise above party and politf
of them only from a news agency, it was her But without going through the legitimate pro rations and ensure that the politics <
bounden duty to go into the moral, ethical and cedure. the Governor hurriedly swore in a was not polluted by such immoral a
legal aspects of the episode, now that she had Chief Minister, whose majority was doubtful, conduct of public men.
to say the least.
with her all facts.
It was alleged there was impersonation of
Impersonation had occurred in Hyderabad.
Communicating with subs
So. apart from the issue of majority or MLAs when Mr. Bhaskara Rao claimed to have Newspapers to get ad
NEW DELHI, Aug. 23.
otherwise, if'was a case of allowing a person produced 91 supporters at the Raj Bhavan. Not newsprint for elections
An underwater grenade to be dropped ini who was prepared to commit .impersonation only that, charges were made that the names
NEW DELH
by helicopter to communicate with submerged1 and forgery to continue as Chief Minister and of many MLAs had been forged in the list sub
The Government has decided t<
submarines has been developed by scientists> take decisions not only on matters of day-to- mitted to the Governor. Wien such serious
criminal allegations were made against Mr. newspapers additional newsprint
at the Armament Research and Developmentt day administration but policy.
Establishment (ARDE), Pune. The grenade re
Mr. Subramaniam strongly pleaded for im Bhaskara Rao, the Governor, instead of ascerta connection with the next general ele
places a similar device now being imported.
mediate investigation of the charges of imperso- ining whether there was no basis for them,
The decision was taken at
When dropped into the sea the grenade gets> nation and forgery which had been prima entrusted the governance of the State to him.
between the Information and Ei
energised by a sea water battery. Electronic: facie established against Mr. Bhaskara Rao.
At the time when Mr. Rama Rao presented Minister, Mr. H. K. L. Bhagat, Fjnar
relays make the device explode under water
Mr. Subramaniam also charged that the Gov- in Delhi 162 MLAs with identification cards Mr. Pranab Mukherjee and me
giving a loud sound which can be heard by< emor, Mr. Ramlal "had observed double stan from the Speaker. Mr. Bhaskara Rao claimed Minister Mr. V. P. Singh.
dards
the submerged submarine.
... ... first in dismissing
„ the Chief
- Minister
- - and to have paraded before the Governor 95
The meeting, held at the initia
User trials have been successfully carried' secondly by bringing the new incumbent". It Telugu Desam MLAs, 36 of whom were pro
out and it is likely to be introduced into service, was claimed on behalf of the Governor that duced before the President. How could 36 Bhagat. reviewed the indigenous a
newsprint situation. It has also t»
that newsprint import will be ii
ensure there is no shortage.—UNI.
MIDNAPORE. Aug. 23.
Relief and rescue operations were stepped
up in West Bengal's flood-ravaged Midnapore
district even as all major rivers — the Silabati,
the Kangsabati and the Keleghai — were reced
ing last night.
The flood water which had entered 85’
villages under Moyna sub-division, was being!
drained out by cutting the embankment near
Dheubhanga. The 60 feet-wide breach near
Ejmalichak was also being repaired.
(
Thousands of people have been rescued by'
speed boats. Army boats are also standing by.■
The district authorities have so far spent Rs.
50 lakhs to combat the floods.
Police said two people died of snake bites!
■ yesterday. Meanwhile, two more persons suc’
cumbed to gastro-enteritis in the district
hospital sources added. — PTI.
Editorial on page 8
(aw*)
/motorised
valves^
FOR
TEXTILE
PROCESSING
INDUSTRY
USING
HOT
THERMIC
FLUID
ALSO
FOR
WATER
• OIL
• AIR
• STEAM
•CORROSIVE
LIQUID ETC.
AVCON CONTROLS
PVT LTD.
@1
once
Oil & Natural Gas Commission
I
I
OFFICE OF THE DY. SUPTDG. ENGINEER (CIVIL)
KRISHNA GODAVARY PROJECT, RAJAHMUNDRY-533 103.
TENDER NOTICE
-> •
Deputy Superintending Engineer (Civil), Oil & Natural Gae Commission, Krishna Godavary Project,
12-59, Prakash Nagar, Rajahmundry, invites on behalf of the Oil & Natural Gas Commission, sealed item
rates tenders from approved and eligible contractors having experience in similar types of works in
CPWD/PWD/RAILWAYS/MES ETC., upto 15-00 hrs. as dates shown below:
SI.
No.
Name of work
Estimated cost
EMD
Cost of
Last date
tender
of receipt
>er non- of a i di-
Date of
opening
tender
Time of
comple
tion
BAKELITE
SANAT1
HYDERAB
The advertiser is intere
basis PROCESSED
COTTON FABRICS. *1
approximately 12 Lakh
may reply with full deta
yiiiiiiiiiiiiiliilliiiilliiiiiiliililillliiiiililiifiiiii
&
dWi® abuse
&
Multiplicity of laws
The addition of a new schedule to the
Drugs and Cosmetics Rules to exercise
stricter control over import, manufacture
issue of who should function as the nodal and sale of psychotropic substances is
agency was reopened by his successor in another action claimed to have been taken
the Health Ministry and it was felt that the by the Health Ministry. This has been
Ministry of Social Welfare should handle it. welcomed to the extent it controls the use
This was endorsed by Mr. Shankaranand. of one type of drugs but this is not the main
Evidently, he forgot— or was it not brought recommendation of the committee which
to his notice—that he himself had given .wants a single law to be enacted to deal
approval in 1980 for the subject being under 'with the prevention and control of abuse
the charge of the Health Ministry. The of both narcotic and psychotropic drugs.
Health Ministry's revised stand was not re
At present there are several laws dealing
ceived favourably by the Social Welfare with one aspect or the other of drug abu^e.
Ministry which was ready to play the role These include the Opium Acts of 1857 and
assigned to it under the scheme but not 1878. the Dangerous Drugs Act of 1930,
shoulder the full responsibility.
the Drugs and Cosmetics Act of 1940, the
Medicinal and Toilet. Preparations Act of
Delay In Implementation
1953 and the Customs Act of 1962. In addi
It contended that all along the Health tion there are State laws. The multiplicity,
Ministry which had set up the committee according to the committee, results in lack
to go'Into the problem of drug abuse had of focus on prevention and control of drug
dealt with it. Its officials participate in the abuse. But the drafting of a single law is
meetings of the WHO concerned with drug yet to be done.
abuse and go on WIO fellowships to study
A disturbing aspect is that as the Govern
the problem in other countries.
ment is dragging its feet in enforcing the
control scheme, the incidence of drug abuse
The Social Welfare Ministry finds no justifi is on the rise. Prior to 1980. the Psychiatry
cation for the Health Ministry declining to Department of the Ali India Institute of
function as the nodal agency for implement Medical Sciences had not received any
ing the drug abuse control programme. It case of heroin addiction but in 1982 there
has conveyed its stand to the Health were at least a dozen patients, according
Ministry and the issue is now before a coordi to Prof. Devendra Mohan.
nation committee comprising the Health
Secretary, the Education Secretary and the Easy heroin availability
Social Welfare Secretary.
In the first six months of this year. 46 pa
tients have been admitted and 180 are being
It Is anybody's guess how soon the issue treated as outpatients. Prof. Mohan noted
will be settled. But the resultant delay in that in 1982. the addicts were mostly stu
iving effect to the recommendations or the dents but now most of the addicts are
iopalan Committee is viewed with concern autorickshaw drivers, businessmen and
by all those who have been associated with those working in hotels in the age group
the problem. The Health Ministry's claim of 20-30. He attributes this to easy availab
that action has been initiated to implement ility of heroin at a low price. According to
the recommendations has not cut any ice him. the price has dropped from Rs. 250
with them.
a gram in 1982 to Rs. 20i a gram at present.
One of the measures claimed is that the He does not think that the trend will be any
c
attention of the Ministries of Education and different in other metropolitan centres.
Social Welfare. Finance. Home Affairs and
Another distressing feature is that the de
Information and Broadcasting, has been lay in deciding which Ministry should handle
drawn to specific paragraphs in the report the subject has hampered the formulation
for necessary action. Where is the need for of the control scheme for the Seventh Plan.
this when representatives of these ministries
were on the committee and as such had
S. Padmanabhan
Lack of focus on prevention and control
HE Union Deputy Minister for Health,
Miss Kumudben Joshi said in the Rajya
Sabha recently that the question
whether the subject of drug abuse should
be dealt with by the Ministry of Education
and Social Welfare or by the Ministry of
Health was under consideration. It may
seem an innocuous statement but behind
it lies a story which not only does not re
dound to the credit of the Government but
also exposes its skin-deep interest in pro
blems of social welfare.
The growing use of intoxicating drugs,
particularly among students, has been a
cause for concern for quite some years and
in 1976 the Health Ministry set up a commit
tee of experts under the chairmanship of
Dr. C. Gopalan, then Director General of
the ICMR, to go into the extent of drug
abuse and suggest remedial measures. The
committee presented its report in 1977 and
its recommendations were broadly In three
categories: legal and penal measures, educa
tional programmes and social action.
The recommendations under the first
category included the setting up of a na
tional advisory board of drug control, enact
ment of a single central law to deal with
the abuse of all intoxicating drugs except
alcohol, evolution of a national policy on
alcohol, removing inadequacies and plugg
ing loopholes in existing laws, more
stringent punishment for drug pedlars.
establishment of a registration service .for
drug addicts and enabling those who re
gister to get the needed supplies of drugs.
Deaddlctlon centres
The educational programmes con
templated creation of awareness of the drug
problem among all social groups and in
clusion of the subject in health education.
Ths social action envisaged involving youth
in challenging programmes and a social
transformation that will reduce the need for
using drugs. It was also recommended that
as part of the general health services.
deaddiction centres should be set up in dif
ferent institutions with Central financial sup
port and utimately there should be one such
centre in each State.
T
The committee noted that though drug
abuse among the general population was
limited, there was a shift from abstinence
to non-abstinence among students particu
larly in the use of alcohol and tobacco and
that the situation was likely to deteriorate
and get out of hand if adequate measures
were not adopted to curb addiction.
The Janata Government which was then
In office lost no time in accepting the
recommendations and
formulating
a
scheme. But before the scheme could be
enforced, the Government fell and the suc
cessor Congress (I) regime took it up in
earnest in 1980.
A scheme for inclusion in the Sixth Plan
was drawn up which envisaged the setting
up of a national advisory board comprising
representatives of all the interests and the
Ministries concerned and the starting of
one deaddiction centre as a pilot project
at the All India Institute of Medical Sciences
In Delhi. It was approved by the Planning
Commission and a financial provision of Rs.
85 lakhs was made for it.
Nodal ministry
The choice of the nodal ministry for the
implementation of the scheme came up
even at that time and it was decided that
the Health Ministry should be entrusted with
the responsibility, at a joint meeting of the
then Health Secretary, the Social Welfare
Secretary and the Chairman of the Drug
Abuse Committee, Dr. Gopalan.
The Health Minister. Mr. B. Shankaranand
not only gave his approval but also got a
resolution passed by the Central Council
of Health seeking effective Implementation
of the control scheme. Following this, the
All India Institute of Medical Sciences was
advised by the Health Ministry to go ahead
with the establishment of the deaddlctlon
centre. But till now neither the national
board has been “set up nor the deaddiction
centre come up.
Enquiries show that the scheme suffered
a setback In 1983 when the Health
Secretary, Dr. S. S. Sidhu was posted as
Adviser to the Punjab Government. The
a hand in making these recommendations?
IF the national advisory board had been set
up comprising representatives of these
ministries, action programmes to control
drug abuse could have been taken by now.
g
H
B
K
£
IS
a
is
it
B
ti
R
K
k
U
B
s
V
6
■
*
B
B
I
*
k
is
I
k
k
i
DECCAN ftaHERALD
M on to; main grouse
Bangalore, Monday, July 23, 1984
Medicmes for masses
WITH AN ELEMENT of gimmickry. Chemicals and
Fertilisers Minister Vasant Sathe announced a 10 to 15 per
cent reduction in the prices of seven essential drugs last week.
The announcement was made at a function at the Indian Drugs
and Pharmaceuticals Limited. Hyderabad, in an apparently
spontaneous response to President Zail Singh's plea to make
available drugs at cheap prices to the poor. Mr. Sathe. who has
been swearing by the slogan “Medicines for Masses" went on
to add that the Government was considering a further price cut
of 15 to 20 per cent. The fact is that the prices of several drugs
have been reduced on a piecemeal basis during the past year,
the cumulative cut being as high as 70 per cent in one or two
cases. Yet. the index numbers of wholesale prices of bulk drugs
and formulations in May this year show an increase of 11 per
cent and 5.5 per cent respectively over the figures for the
corresponding month of 1983.
Mr. Sathe said a new drug policy would be introduced in
two months with a view to realising the twin objectives of
good-quality drugs and “medicines for masses." It remains to
be seen w'hether he can make good this promise, for there is a
good deal of confused thinking in his Ministry and powerful
elements in the drug industry are seeking to impose their own
views. A 14-member steering committee set up by the National
Drugs and Pharmaceuticals Development Council in March
this year is still grappling with the problem of “synthesising”
the reports of its three working groups which dealt with
planning and development, industrial approval, and pricing
policy and procedure. There is a fear, by no means unfounded,
that the recommendation of the working group on pricing to
decontrol 75 per cent of the drugs may open the door for the
big units to manipulate the markets to the detriment of the
interests of both the small units and the general public. While
decontrol is a desirable objective, it should be done in Such a
way that the consumers are not left to the tender mercies of the
captains of industry. The way official members of the working
group agreed to the recommendation and have been trying
since to mitigate its effects indicates that they are not clear
how best to go about the task of achieving the Government's
objectives. The efforts to formulate a new drug policy are
taking place against a complex background. On the one hand,
there is over-production of non-essential drugs and on the other
production of bulk drugs and formulations has fallen short of
targets. The major lesson which emerges from the working of
the previous policy, laid down in 1978, is that a policy is good
only to the extent it is implemented effectively.__________
will hit
vital drug supply
yj^Express News Service
BANGALORE. July 17
Lifesaving drugs will be ‘cho
ked off’ hl the private outlets
for three days following the de
cision
of the Karnataka Che
mists’ and Druggists’ Association
to go ahead with the bandh be
ginning July 27 as part of the
nation-wide
closure of
retail
shops.
An imminent spectre will haunt
the accident victims and emergenev patients being rushed to
hospitals where they might not
receive timely supply of life-sav
ing drugs with only a minisule
government outlets selling them
during the
three
consecutive
days.
The State Drug Control De
partment. is hopeful of meeting
the contingency by dispensing the
drugs through the
government
shops in janatha bazars, coopera
tive stores and medicine counters
in the hospitals. Besides, doctors
are being requested lo keep ex
tra stocks of medicines for emer
gencies.
Ejokfar the tiny official net^’O^^.ould manage to handle
the near-crisis situation during
who have spotted the bandh notiboggle the minds of the people
pes prominently hung in all the
the 3 day closure has begun to
retail medical stores in the city.
State Drug Controller S S
Kattishettar said the Directorate
of Health Services was also be
ing requested
to instruct the
primary health centres and units
in towns and rural areas to keep
enough
stocks in view’ of the
bandh, Efforts were being made
to persuade the retailers to adopt
other forms
of protest other
than the closure.
The Central Drug Controller at
Delhi, Dr S s Gothoskar. who
is in the city on a visit said that it
would be for the stale governments
to
arrange similar
measures
to meet the situation, prompted
by the closure notice. In Delhi
he said drugs would be dispensed
through the super bazars.
The nation
wide strike call
was given by the All-India Or
ganisation of Chemists and Drug
gists to protest against the alle
ged apathy of the government to
settle their demands.
Two of the demands common
to all the states relate to the
postponement of implementation
of Sec 42 of the Pharmacy Act
and removal of the life-saving
drug ‘phenobarbitone’ from Sch
edule ‘X’ which strictly regulated
its sale through special laws and
licences.
The Act which was passed in
1984 and amended in 1976. stipu(Continucd on page 9 Co! 3)
Turn to page 1
get them
from other
states
which had a
_ ___
___
surplus.
lates that only a registered phar
Mr. Kattishettar, who Is also
macist will be allowed to dis
the
vice-president
of
the
Phar
pense drugs. Sec 42 of the Act,
macy Council of India, said that
enforcement of which has been
there were
4-lakh
registered
kepjtf^ abeyance and now come
pharmacists in the country and
into^^ce from Sept 1 this year,
1.25 drug dealers and as such
has given rise to apprehensions
there was no shortage of quali
that it will lead to large-scale
fied persons to handle the drug
closiu-e of medical shops run by
business.
unqualified pharmacists all over
the country.
Association sources however
contend that in states
like
The proposed bundh demand
Gujarat Uttar Pradesh Orissa
ing further
postponement of
and Maharashtra there is
an
the enforcement of Sec 42 will
acute shortage
of pharmacists
not affect the pharmacists in
and colleges and these
states
the state since there is no dearth
will be worst affected when the
of aualfiied
pharmacists here,
according to Karnataka Chemists Act comes in to force. They
fear, that several hundred shops
and Druggists Association Seo
~
in these states will be closed and
retary D.A. Gundu Rao.
hence Karnataka Association is
The Drug Controller
also
extending its support to the de
agreed that this would not pose
mand. though it is not affected
any problem to Karnataka as
as such.
the state turned out 2,000 pha
Yet another demand common
rmacists a year from its 33 col
to all the states is the removal
leges and with another 17 col
from
schedule
‘X
the drug
leges coming up this year there
phenobarbitone, which is exten
would be a surplus of qualified
sively used in treating epilepsy
pharmacists. As far as the un
JonS“drawn periods. At the
qualified pharmacists running
y
moment only
the g0Vernmen|.
the shops, the government held
drug stores doctors and a few
special coaching camps and conshops
are allowed
ou sell cn
to
thee
duc^k an examination certifydrug and the laws governing its
ing|^B those with four years of
are "stringent and cumexpeffene in running the shops
bersome”.
as qualified. This would protect
Dr. Gothoskar said phenobar
tho existing unqualified
phar
macists from losing their business bitone though an essential drug
and widely needed.
was also
he said.
prone
to potential
abuse by
Dr Gothoskar
on the other
youth <isd addicts. Hence it was
hand
contended
that it was
included
in the Schedul
‘X
high time that an element of
along with 17 other habit for
professionalism was infused into
ming drugs marketed
in the
the drugs sale involving human
country. Besides, India being a
Jives unlike other business Espe
signatory to the Geneva
Con
cially, in the wake of widespread
vention simulating the trade of
reports about malpractices and
such
‘barbiturates
could not
negligence in the sale of dan
contravene
the
international
gerous medicines by unqualified
agreement by removnig it from
pharmacists eht enforcement of
the Schedule.
Soc 42 was inevitable to pro
Dr Gothoskar contended that
fessionalise the trade.
stringent laws dealing with rhe
Dr. Gothoskar said eight years
sale and manufacture of barbi
was a long time for the State
turates were inevitable in view
of the country’s name figuring
government to set up an ade
quate number of colleges
to
train enough pharmacists. If
some states
faced dearth
of I
qualified pharmacists, they. could I
in smuggling
of such drugs.
Phenobarbitone was accessible to
patients and the doctors them
selves could administer it with
out
any restriction.
Besides
some shops were given licence to
market the drug.
This being so. the demands of
Karnataka
pharmacists
boils
down to other issues—abolition of
turnover tax on retailers and abo
lition of rural development cess
on medicines. Association Secretery Gundu Rao said in addition
to the 4 per cent Central sales
tax and 8 per cent surcharge
sales tax there was another 10
cent ruraI development cess
(RDC) on the sales tax aU amontmg to 13.6 per cent tax in total.
This would be a burden on the
consumers who would have to
pay 48 parse as taxes and other
Invisible cost
factors on each
rupee they spent on drugs. These
taxes, did not affect the seller in
aj1? way sil?ce they were allowed
to oe passed on to the consumer.
What affected the retailer was
the .5 per cent tax over the to
tal turnover of the shopg which
was not allowed to be passed on.
Mr Gundu Rao said the tax had
been in force since 1931
and
despite representations, the gov
ernment did not
concede to
scrap it.
He argued that a medical shop
owner with an average annual
turnover of Rs 2 lakhs
would
have to pay Rs 1.000 as TOT.
In view of the low profit margin
(about 10 per cent), he lamented
that this
further eroded their
earnings. The profit margin, he
claimed, was not
revised since
1962. According to estimates, the
net revenue to the government
J?
at
stcod
T>_ 2.78
n r-n crores.of TOT
wholesale
Rs
The wholesale
dealers, however, were not sub
ject to the tax.
The other demand of the bandh is abolition of sales tax on
life-saving drugs as was done by
West Bengal. Orissa and Maha
rashtra. This is one of the de
mands being projected by the
pharmacists as a humanitarian
one for the public good.
tiie banning of at least 23 of day thousands of doctors
FTr\'HE
REALISATION
at the expense of poor
' H ’that public liealtn pu tho many irrational drug com > trained
Indians are allowed to man
ff Jicies of developing binations?
These are disturbing ques the public health services of
countries
like India
The answers are obvious England and Arab countries
had been — wittingly or un tions.
just because the country gets
to anyone
with some social
wittingly — Mortgaged to the consciousness.
some foreign ex-change.
Why did not
giant multinational companies
Says Dr Chowdhury, who
who should be most
which control th a pharmaceu doctors,
recently visited
Bangalore:
concerned with these issues,
tical industry and the national
Colonialism has left much of
companies
following
their ask these questions so far — the
developing
world with
or answer them?
techniques is not new.
health
systems
largely
irre
“
Doctors
are
‘
tremendously
What is new is the feeling
that doctors in India and coun ignorant people,” says Dr. Zaf- levant to their conditions.”
The functions of medicine are
tries like it have become rullah Chowdhury of Bangla
social — fulfilling the social
pawns in the game — at the desh. a medical doctor himself
cost of the health of the mil by training. The young project needs to promote good health
coordinator and co-founder of
prevent diseases, treat those
lions.
Gonoshasthya
Kendra
(peo
affected when the preventive
That the multinationals have ple’s health centre) at Savarmeasures fail and rehabilitate
been making astounding pro thana in Bangladesh, says: ’ them. And yet the whole app
fits (some times more than
“Doctors and money are. for roach of medical education is
2000 per cent)
has been most part, safely ensconed in not that of a social science It
known for decades.
Several institutes designed to serve the
is presumed that the body is
feeble attempts at controlling rich. From there they produce machine. Most of the treat
the “mark up” of prices by their scholarly papers saying ment is symptomatic and not
them have been made. When that the poor also have pro prophylactic.
Dr. Triguna Sen became the
blems,
but not problems for
Medical education is open
Minister for Petroleum ana which treatment is available to only
to the rich, who mostly
Chemicals in 1967, he initiat
have their values based on
ed the move :o: abolishing them.”
Several seminars have been money. A student who pays
brand names for some popu
a capitation fee of Rs 1.5
lar formulations and make held in the last one decade in lakh
to 2.5 lakh to undergo
drug companies sell them un tlie country. Lengthy, academic
der generic names. Could it papers have been read by the
be just a coincidence that mi doctors calling for a medicare
nistry (which controls the system that is more suited to
the needs of the majority.
pharmaceutical industry) was
taken away from him and the From time to time there is
talk of evolving a system of
proposal scuttled?
Could it be the normal red “barefoot doctors" and creat
“paramedical
cadres”.
tapism and official lethargy ing
ap
that prevented the Govern Frequently impassioned
ment from considering the re peals are issued asking doc
commendations of the Jaisukh- tors to go to rural areas. There
are
occasional
threats
to
make
lal Hathi Committee which,
among other things, sought rural service compulsory for.
And yet a vast majority of |
the doctors produced at the!
the costly and prolonged
course of studies is not going
to spend all that money with
out deciding in advance who
quickly it could be recovered
and how the investment could
be multiplied over the years.
One need not
expect the
medical practitioners to do
social work
sacrificing their
self interests. All n-’e would
expect from them is not to be
racketeers, not io sacrifice the
interests of public health to
make a fast buck, not to be
come willing tools of com
panies trying to make money
on the sufferings of the mas
ses. Racketeer may be a verystrong word to use, but what
else would you call “general
practitioners" who would send
their patients to half a dozen
specialists unnecessarily- to
get a commission from them,
who would prescribe costlynew brand names just because
the medical representative of
the company had given a good
gift? How many- doctors really
keep abreast of the recent
developments
in
medicine
The only books most
doctors read today are the
bank (pass)
and the
cheque book," says a wag.
The way some °f the mod
ern general practitioners
function now s'1 that they
heed. to know is a list o£
broad spectra® antibiotics.
Even before 'oU comPlete
telling the serf01118’ a Prel
scription willbe scribbled
and the pal| extended -
expense of the tax-payers’ money E
(the Government
spends
on|
training a doctor many times
more than the amount paid by
n medical student as fees) pre
fer to stay in cities even if
they have to live on a meagre
practice or take to teaching
physiology in schools.
But
they would not go to villages
where they would be treated
as demi-gods, where they can
have a thriving practice and
also job-satisfaction.
The result is that even to
day thousands of quacks and
half-baked doctors have a
roaring practice in villages.
Even today various unscien
tific. “systems of medicine”
and “witch doctors” have a
field day. in villages. Even to
BITTER,
PILLS: Medicines
and the Third World Poor by
manna Melrose, Oxfarm publi
cation pPt 277 4.95 sterling Can
"c had from Oxfarm, 59, Miller
Hoad, Benson Town Bangalore560Q46 For payment in rupee
equivalent
other than
___ wt
,____the„ ^rug
—„
firms’ literature tells them?
many question those
How
claims or verifvthem?
continuing
“Doctors need cc:
education. Nowhere in
i India
have I come acWSo arrangei------ oments made bribe State for
providing refresher courses,
for the doctors Rost doctors
are too busy earoing money
to read anythief" Dr Chowd
hury says.
By Someswar
for money Anytbing a httlel’
complicated'will always bc<
referred to specialists. Most!
‘he knowlfe a private'Practitioner i®"' acquires
after nasc;iY,„ «ut of the mecii.cal collegA tfiwt the me
dical renvA .ntat*ves
dole
^onP3 freeSampieS
Does increased life expectancy
in the Third World mean — at
least for the poor — more years
of pain and suffering? With Po
verty itself the main cause Tor
ill-health, most developing coun
tries have, with their mixed-up
priorities , not been
able to
evolve health policies that meet
the conditions
and needs of
their own communities.
There has been a growing sus
picion for long that these poli
cies are influenced to a large
extent by the multinational com
panies or their national counter
parts which have a vested in
terest in continued ill-health of a
majority of the people. Another
doubt
that has been gaining
ground in recent times is whe
ther modern
— by which is
meant Western — drugs offer a
solution at all to the health Pro
blems of the Poor countries
Oxfam, which has been doing
commendable work as a British
Voluntary
agency
promoting
health — as a positive concept
of higher quality oY the life ra
ther than absence of disease —
has brought out this book by
Mrs. Dianna Melrose, based on
field experiences of Oxfain acti
vists.
The book has a fund of use
ful information on health Pro
blems and services available, in
developing countries. It pinpoints
the main problem: the medicare
system is so drug-based and doc
tor-oriented that poor people of
ten buy unnecessary
Western
medicines they cannot afford, be
lieving that they hold the key
to good health. ‘Bitter Pills’ ex
plodes this myth carefully nur
tured. It highlights the work of
organisations like Gonoshasthya
Kendra in Bangladesh crusading
against false claims of multina
tionals.
The book comes
at a time
when there is a growing aware
ness of the need to evolve a
broader
strategy for
better
health in the Poor countries, bas
ed more on preventive measures
and inexpensive, easily accessible
remedies and systems. This book
will go a long way towards co
ordinating the efforts of several
groups in different countries to
evolve this alternative strategy. M
makes valuable reading for every
one who feels concerned anti
wants to bring about the socio
economic changes necessary t°r
such a policy.
■
guts
, ft is ver,. e< to con
demn doct v, but it IS to be
realised
t< only re
flect ihA
in the society,
itself Tt rot ’, also be an
exaSgerati"ol?o
Lhat aU
doctors faun.„to thls category. The, 1 1 e exceptions
from thA^0.^ and more j
s°ciallv e yoU%ils doctors
themJb, ConSfC are today
^arlyeieris- Organisations
of dor+1 Oze”. scientists,
Which rs
ng ,0 evolve
a new a?k6
t"0 medical
Professin h°s fgive a new
direct i<mU
1 he orSa'
hisatin,?’ SoiaLedico Friend
Circle0"8 are:}‘e V°luutary
Health a1
°C india,
Hew D0iiSSoCia!i ^ost Drugs
and Thelhil
s Cell of
;t?aP(’llA<i1111, Arosya
n..
. 11> col d
icasso of India
view. He cracks the boiled
egg he has ordered for
breakfast and tells me that
he “is not in a' good mood
J? talk-” The interview is
men fixed for next morn
ing. I find him at the gal
lery giving some finishing
touches to his paintings.
Greetings over, I ask if
we can now sit down and
talk, but to my utter sur
prise, even with out an
‘excuse me”, Husain walks
away from the gallery. 1
wait another
45 minutes
wondering where he
has
gone. Someone in his room
informs me he is at the
gallery — another helpful
hotel stuff member tells
me he saw Husain going
out of the hotel! Puzzled
by this strange behaviour I
decide to leave the hotel,
only to find Husain coming
in a' car up the drive. I ask
him if he is interested in
the Interview. He renders
no apology for his absence
but effusively leads me to
the poolside and orders Coffee as a prelude to the in.
terview.
Close friends tell me that
he is “very forgetful” anj
I Jet that be an explanation
for his odd, if not rude, be
haviour.
If Husain canvases arc
large, so is his story. He
punctuates his- talk with co
lourful imagery and emer
ges as an ageless figure
with amazing vitality. -j’wo
hours quickly slip by as he
By Aban R. A. Lal
Maqbu! Fida Husain
Photo: G. Narayanaswamy
» S DAWN breaks over aware that his bizarre looks
>ld Delhi, a tall, boy- may sometimes earn him talks of imporant landmarks
Tlishly slim, white-hair- the label of a ‘tramp’. If the in his 50-year-olcl career as
, ed
figure,
quietly price of fame is instant re painter extraordinary’.
Born into a relatively I
. brings his Fiat car to cognition, in his case it has
halt at one of the Dhabas lead to some very funny poor family living in Guja- |
Nizamuddin. With quick experiences and he likes to rat, Husain was one of eight ?
ig-strides he slips inside have a good laugh talking children. His father was an I
is crowded, noisy, place about it. A few years back, accountant. His mother, a' |
■d sips his strong morning on a visit to New York city, Gujarati woman, died when
'■ha”, listening to the talk he w'ent into a 24-hour res Husain was a mere baby of
those who struggle from taurant after a late night one and a half years.
Husain’s childhood was
twn to dusk for sheer exis- movie. He found himself a
nce.
corner seat and as he wait spent at Baroda and Indore
In this milieu of the hum- ed to place the order, he He learnt Persian in school
e, his bare feet and long moved aside a box of ciga and dreamt of being a poet
wing white beard raise rettes he found lying on like his maternal uncle. “I
> curiosity. In fact, he the table top. His
move thought I might one day be
ems to be so well accept- ment was noticed by the come a poet or an art di
", that a fellow stranger manager who was quick to rector for films, but I never
lestions, “Do they pay you confront Husain with a thought of becoming a pain
He claims however.
ell?” to which the old man rude yell: “Out, get out of ter.”
olitely answers: “Yes, my this place.” They thought that he started painting as
a
child
and was eleated
Jss is good to me”. He is him to be a tramp out to
when two of his landscapes
istaken as some
Sahib’s steal the cigarettes!
were
sold
for Rs 10 each,
Getting
this
celebrity
river, since he always
painter to talk about him way back in 1932. “I felt
>mes driving a car.
very
confident
paint
This is Maqubul Fida' Hu- self wasn’t easy. Husain pro ing when I foundabout
that some
iin narrating to
you a mised to be interviewed on one was prepared to pay
ase of his mistaken iden- a Sunday morning during twenty rupees for them. In
ty. India’s Piccasso,
the his recent visit to Banga those days a whole family
been could live on twenty five
tan who might well be des- lore where he had
ribed as the Number One specially invited to display rupees a month. It was a
a
selection
of
his
works
by big sum”. When asked what
modern artist of this counWhen I was price range of Husain
ry, Husain has a piquant a five-star hotel.
ense of humour and thor- tapped on the door of his paintings today, he parried
ughly enjoys the lighter suite at th e appointed hour, the question by saying that
moments of life. He
was a' young 1 ady informed me the paintings he sold for in
mazed when a young cou- that Husal n was out and 1952 for about Rs 500 would
le spotted him at Connau- would retu,rn an hour later. today fetch over Rs 40,000.
?ht Place and he overheard Much later■ I located him at
hem say: “He looks like the hotel’s coffee shop and
On pflge 11, col I
lusain!
Husain is well reminded him of my inter
Tractor run
For a people-based drug policy by
the sun
to India recently.
in six montlis and the '.bird
742 locally manufactured
and 526 imported drugs.
Tlje last category either had
little or no proven therapeu
tic value or could easily be
manufactured by local com
panies, instead of the multi
nationals. at, much lower
costs. . The- report of the
committee. submitted on
May 12, 1982, was approv
ed by the Chief Martial Law
Administrator mi May 29 _
perhaps a speed record In
governmental action. On
June 12, the Drug Control
Ordinance was promulgated.
America exterted maxi
mum pressure on behalf of
1he US companies and was
joined in by
the British,
French, German and Dutch
governments. The US .-.dministration xn Washington d:d
its best 1o have the ban lift
ed. It succeeded in getting
some changes made.
Says Dr. Chowdhury: “Se
venty per cent of the an
nual
drug sales in my' coun
By P. S. Sharma
try are of drugs described as
useless or therapeutically in
significant by the British
ill victims of this energy crun- be that this firewood gives
National Formulary, the Na
he ch: as adults are busy earn- us less energy than is spent
tional
Research
Council.
iil- ing a living or doing house- by trucks in transporting it.
USA and the Federal Drug
Rs hold work, the children come Ultimately, it comes down
Administration,
USA
”. He
er- in handy to be assigned the to so much energy wasted.
said out of the 51 products
a.
fuel-gathering work. Their
Sensibly, firewood is meant
of
Glaxo
sold
in
his
coun
ice education, and mental deve- for local consumption. Its
try, only 17 were marketed
>ur lopment suffer irretrievably. transportation to the cities
in UK and just one-third of
'n,d
The position is much is both uneconomical and
them listed as ‘essential’
worse in villages, especially wasteful, and it should,
drugs by the WHO.
>
in the desert and in the hilly therefore, be completely
xuxuma,
.. —
alSO
Sri Lanka,
which
areas where long distances banned. The alternative so
adopted a similar drug poli
have to be traversed and urces of liquid petroleum
cy buckled under the Ame
lilong hours to be spent on gas available to the urban
tinn
getting drinking water too. Population is highly restrict rican pressure. Pakistan was
too preoccupied with Isla
Farmers with large herds of ed so that the vast majority
mic fundamentalism to bo
cattle have set up biogas has still to deper*d on coal
ther about such progressive
plants and big landlords °r kerosene ®ut suPPlies of
measures. The ‘failure’ of
have started using crop re- coal and kerosene are also
these two countries to ban
sidues as fuel. But the pro- 'united, and "’e kave '° find
blems of those who own no out newer and newer sour these drugs and 1 he fact
that India, considered more' "
land have grown manifold. ces of energy f°r industrial,
advanced, had not bothered
s
When they hardly have en agricultural0 and transportato ban any of these drugs
ough money to buy food, 11011 Purposes- Bydro-eectri.
including the acknowledged
Pra- where is the question of Clty is one sodrce’ )108as is
harmful enterovioform and
1977, their buying firewood? It another Then t'iere ai'e the
maxaform are held out by
5 disseems that millions of rural ocean and tidal
«
pro-American lobby and
ering men and women have got ’’uelear eneJ-gy a, d the lh
mthe multinationals as proof
mine, entangled in a vicious ener- exhaustibie so9rC®,0of.. s°lar
that the Bangladesh policy
e of gy crisis. They eat food, to ®ner8y. The p"mn,tlal 15
sts in produce energy and then
was wrong.
but we d0
,lave as
d dis- spend this human energy — ;vvasl,
et ’he renuisite echnolo8y
■■What is probably the
'ears.
all of it — in producing food "> exploit6^
m„st humiliating comment
lachal an(j gathering fuel to cool
,
he social consciousness
jeono- jt And so on and on tn a .. Even thPn t',e ^'r’sl essen°? India health
personel
treats, circle like the proverbial
°
i n the Indian drug pof for- bullock
going round a
>? , is quoted by the multiicidal, ‘kolhu’.
“CT-nn-ils to condemn the
reCk1’
The firewood crisis ha;
n!*
deskban. Drugs which
Put
oh
d
m
r
an
S
e
s.
w.
hit the city dwellers too. Ac,
been banned in En«limcn- cording to reliable statistics,
11 ? in the 30s and even In
land in recent years
energy nearly three quarters of fire,
available across Hie
-aste a wood and about half of th;
freely ‘,v‘
Jn(Ua.
in this dung used in urban India I;
counter
.
them in jjanillages, purchased. A substantia
U'akeS, moe difficult as
is to part of it Is brought fron,
lif,, u l)f r tl’e '.U,ral P°°r
Sladelnfei‘ our country from
hours the villages on head, in but Ifhe the
ne0?rit’li-n tG “one
they en,L . Chowdhury says.
nee of lock carts or in trucks. Moq
India. consciousness ol
gather wood stoves or chulhas hav;
The s°c“ ie(jjcal coinmutecome an efficiency of only five ft,
thc Indiai
becn arous.
.elpless ten per cent. So it may juq
pity "as fih‘"ly
From page 9
The Gonoshasthya Kendra
hi Science Forum; Society founded by Dr. Chowdhury
of Young Scientists, New and his associates in 1972
Delhi; Concern for Correct created history last year and
Medicine, New Delhi; Consu gave the lead to organisa
mer Education & Research tions in the developing coun
Centre, Ahmedabad; Centre tries including India, by
for Education and Documen successfully campaigning for
tation, Bombay; LOCOST, a" ban on liazzrxlous and ir
Baroda; Federation of Medi rational drugs. A eight-mem
cal Representatives Associa ber expert committee of
tions of India', Patna and po which Dr. Chowdhury was a
pular science movements member, recommended . ban
like Maharashtra Lok Vig- on 1707 products of tiiedical
nyan
Sanghatan,
Shas- and pharmaceutical compa
tra Sahitya Parishad of Ke nies in three categories. The
rala and Science Circle of first included 265 locally
made and 40 imported drugs
LI.Sc.
It is at the invitation of regarded as positively ha
some of these groups that zardous which were recom
Dr. Chowdhury,
the one- mended for immediate ban
man crusade against exploi and destruction. The second
tation by multinational com category included 134 orugs
panies, which has grown in which required reformula
to a movement now, came tion and were to be banned
dug
Soviet engineers have desi
gned a prototype oi: a solar
powered tractor. On the out-'
side it differs
from a con
ventional tractor by a bread
visor above
the
cabin.
This
visor is
actually
a
solar
cell
assembled.
of flat-shaped direct solar
energy converters. The maxi
mum capacity of the cell is
400-600 watts. This is too little
and then generate public
activate, the ifactor but
opinion in favour of cheap to
sufficient for recharging stor
alternatives to the modern age batteries. Tractors never
drug-based health system., operate non-stop. Some time
In an article in the forth they idle, while energy ac
coming issue of the Bulletin cumulation is a continuous
which does not stop
of Sciences published by the process,
even on a cloudy day. The
Popular Science Movement cells are sensitive enough to
and the Science Circle, Dr operate by scattered light.
The development of this
Narayan says that practices
does not mean that
which needed to be checked prototype
tomorrow it will go into serial
in India are:
production. Solar cell produc
i. Saie of drugs banned tion is a very costly business.
in other countries, ed. Lo- This tractor, however, can be
motiland cliquinol prepar effectively used for improving'
the design and systems of the
ations.
machine. As soon as the cost
ii. Sale of irrational com of solar cell production comes
binations and formulations down to an acceptable level,
iii. Sale of drugs without the tractor will immediatelv
adequate precautionary pro go into massive production.
ed., Dr., Ravi Narayan ol
SI John's Medical College,
who is actively associated
by Medico Friends Circle,
VHAI and another similar
organisation ‘search’ is wor
king with groups like the
Science Circle to first mobi
lise the science community
duct information. '
iv. Sale of drugs as highly
inflated costs. For example,
Analgin is being sold at 20
to 30 times the cost of pro
duction .,
, Promotion of drugs for
v.
indications that are not cli
nically proved and are of
ten potentially dangerous.
or example, pregnancy test
ing drugs which
induced
abortions were freely sold,
till a campaign was launch
ed against them, despite
well - documented scientific
evidence that the risk of fo
etal deformity is increased
by the use of these haimonal preparations.
vi. Sale of spurious, ad
ulterated or poor quality
drugs Eg. turmeric powder
is sold as
tetracycline in
capsules.
vii. Sale of old, expired
and unused drugs
viii. Over - prescription
and misuse of tonics, highprotein foods,
harmonal
preparations and baby foods.
ix. Sale of drugs without
prescriptions and
x. Production of drugs fox
profits rather than health
needs.
Quoting the Indian Coun
cil of Medical Research
(1CMII) and Indian Council
of Social Science Research
(ICSSR), Dr. Narayan says
that while drugs for dise
ases like leprosy and tube
rculosis are produced at onethird or one-forth of actual
requirements, Ionics vita
mins and high protein sub
stitutes are being produced
in wasteful abundance.
A joint report by ICMR
and ICSSR has warned ag
ainst the emergence of a
•'doctor-drug producer axis”
to exploit the people.
Can India not do what
even Bangladesh could do?
Dog hails
master out
A persistent clojr won the
hearts of the police in
rai and jrot his master a 28
ye?r-old hawker, released 'on
bail. J. Jeevanandam, th"
hawker, was arrested for his
involvement in fisht
’
placed in lock-up at the Tai
laknlam
police station 1st
dog's fidelity the Inspector aI,
not leave till touched by the
dos s fideity the Insnector an
proached the legal aid cell to
get Jeevanandam released
bail.
011
Sold blood
800 times
Madan Lal, 40, father of
five-year-old boy. is one of the
estimated 60.000 people Uho
live on selling their hloosl
Over the last 20 years Madan'
Lal has donated blood about
800 times — at times thrioo
a day
and his rare ‘O’
group with negative Rh fac
tor fetches him customers
from far
off areas.
These
people haunt blood banks at
New
Delhi and put
their
blood on sale for a measly
amount.
Solution to Word Sleuth
Plug In
c? th
Win*
; v.
?;t. -. nty-d > r-:r--K-I-Ifl', 'ilfty*
pri '.■•■><■■ Ono rn- f.pr-'VchFibl ijK’ ovum
fpr-’Vb.A a 5)jr.i'J>'.r <d f?v urn may in??ty
tfrn RCi-r^vkm nf p:"-'?•• an;.'! v. heim’f or not pn rnj^'City
h’rc.o‘e tx iQtUntoiu^d and Oier$ yJ.11 occur wdtettr-ty
< hffore bn no Ghrddintf. mnl.tm or In />:
tatlon wkh
’?'?•/ tho d!.-^p«p.ianco of blred- other &oyint*Ue<' •• etnong
Jris; ivir-.y not iudients pregneney arc hM^.htnry
pi fxhjgxwltkm^
flb.U’Iut^iy. Normally, the urine doif! tc:‘,purer, ynd preetyj
enmple tniicn catty morning cr,x?. of tha liwli."
P>O'jfty a good teat. In itr. phicn,
MMCs have begun to punh VJP
One f.onid think thftt tl?5
r.dtl\ Given orp.Pv, or by tntycf'.on. toMropbe of children «• r,bverety
thtso subaUncc-'S miso ths favet of maimed and hnndlcanped dun
»rhb two honnonf-r. in the blood. the urimlnlpt’ d.ion of a
dnrj
■ c/lihln n
however, both n.ro Bko thuHdnmidn would
hav®
c'jib^lhxi rapidly through th§ bx ought about an appredatkrid
bluddor. The sudden drrhpe Indu and ftwawsB of the dangers of
ces “withdraw.?’ bleeding ftp iA administering drugs to pfrgnmri
lbs nc-nn?4 cyx-ie and tho women women, but Ih.tr. tiM happened
may, aec.otdimi to tho prevailing only in tiw West, where MNC-a
popular
not bo pjqtfjpnl;, are Jloble to be mwl for intlliom
if she in pretnaht. the wcn-iicn Vi
- ... —
<>’ dollars »„»
for wo tiro Impscta
<\ l«YF;v 'iterrmo . v-JU
.znnin- City. ^\.<tymr,cnntnlty:7. .‘n fv-^.
; ■
■'■■'■.•• •■• •••.(•■.: • • fto'f ■ ./ : '• ■•
Weed. ■
■ • -- ■ •'
......... •
jxety of druvs bclnd wllhclvfWa
Tm)
Jonmcl ft? for unnyanngeable . \ldo
Oyn-’i’colouy fuh.l 'OhM^tytys ‘’■f.te- fiom Western mrk£»t&
gorlcally atates that, “hormonal
i.■.-■fs .for pjeynFwy Are» hot reliIn ui&dkinft, tho rclov&nc®
6
i
T1i<? tent te fr-.ln?. positive in prhielfrto such c?; the one ths$
rou,' out of five women. There te abi.nirv; in inw •— the boricfit ctf
■ eJn-? an increased z'.*.h of feetoI i.hn doubt — brcr.me« tnotycrotIVO.
•-bnonnaiitiec.”
In no drcoinstftttcoc c?;n
The ponsibto teratosfiidc notion drug today be given tha beneftfc
eV the honnon;-?; has cl';;/ convjn- of tno doubt. Drug compaiu^ pa-5
; c?d the wlmiifte gronp of tho th<? werKt cuidt’3 tn the jmttsr.
4 \y i«> thtd ’.hc.ty k-;ty r-ho’.J j no The Dintllters’ Company in Bri*
Iony<?k ty- done and they have t'.vi.u t.hfct mankf’tya thalidomide,
sunii® this recommendation in for v^ampte. continued to e:htheir report on 'The Fffcct o; Fs- plvwt'jo in It ’ mlvertteemezr-z; thn^
t-r.>?te £?r?;i Korman os on FaetM tbo drug 7/a.r> rc.fo, ov-ha nfU?
R toyetepsnenn and Tru'emt
jtyAT'-tivo reports beian jyourtng
in, ruid the Brh'tyh A'fc-ii’c.'.'i Jour*i Tho Phy?iotenn. Desk S-tofer^ucs?, rjl supported th? company fci
' which Is the nfllctel text of phur- Ite editorialfl for ‘"omo tlr- %
mno-utk-:’’ coRV’p.nlc.s bi America
? for Arnt’rJcfm doctors, ob>-?.rvcs
OPINION
t strictly: “The uve of orngesintb*
Whfct: have all our Mrthwttfef
, no? HRcnte during tho find, four l<;/-n
in tho meanttyns und
» months of pregnancy is not re- ,-h?.t doing
te thn prevailing mtdkkd
SECRETION
I
■ ^XV'1V;^"?0'E
■
'
.
x
■
"pini™
Kur
’thi-y&u^
Moat enlightened
nieiUoai
jyr&euofj-; iv’t? aox’io of tjoiusi j;
. ilL
/ ’■■■■•':
but thoefl $x»
-f drugs*
:'£« E
..•/,...XV
: uanoj- or II ahe becomes prr cnnnt, <’!™}
.fc rxhl'J tftbiw those toik sh-. ,7 ' «VX'o vo oDla Iro ®; ikTllzl-i-,,t$PSP:''fX’"'’ Atoui ^'0 PlH.-'too nnc! should OT®
UJUWiW "U
tm.u,
VI
i should not be used during pred- has become pregnant by accident,
■- nancy. The u.i& of Psmalo ;?e.v ty&cn tho rteo nr« th® sam
hormones, both ajiroRens and
Fromty..,,..;.,,
the cirouirustancee
®
5 progesterones during early pregybvteus
th® task cd
n nancy may mlously cternagft ths ftehting
n
A1,t that
tho
deadly ignora^ice
1 ofitepiW*
flaht.iiur «j€
nun ouiidirw homonal BP drug)
on« for womeu'e group# silane.
A cursory look nt th^ latest !s
The day h not far a.wc.y whfcp
aSkup/j of MITvW Ind if- (December.
r/ornra, like Ralph Nader's “rat198.1) arul CITdS (September. 1981) ck
’.t" will have t<> militantly con
would conflim that certain multi- front
mnc nmr^
aziis
cJiemfets, over
MNC
otEtess
1-^
to'^4™^SP^"?«'Onpr”Ug! dm eoXleb
rjuSp. -to
nsucy luting without znentloHlus WJ.
J^anteed^sXfete
that this involves u much greater
A'
Sr iwfHh
risk of congenital birth defects to nV^rs V\J.h(lr
of tho children they will bear.
tbu baby in the mother's womb. Kvervona
elso Imo been found ro
Certain firms recommend ire turn rtour.ly wanting
or Ineffective.
irt tho “diagnosis of proKnancy’*.
■white others who had till very
recently advocated ity usq, as 6
prelaw test mention its n::e In
’‘Recondfiry ammenorrhoaft". That
those agents ara contraindicated
In prc-^fmj^cy is still not men
tioned. The drugs publicised in
tliiK category &ro Lut-E«tron
Forty (Mp.c), E.P. Forte tUnichem), Geotsplon fKhandelwal).
Secrodyl (Allcuburya). Cyclenorm
(MPI) and Lynorol (Organon),
Keane firms have cleverly put
under “indications*', “see litera
ture’. Examples: Duoluion (Ger
man Remedies) and Oestrone
(Lyka).
Preparations such as Dteecron
Forte (Nicholas*.
Menst-rogen
(Organon).
Norleetvln (ParkeDavin), Grusecron Forte (Nlcholau), Orgaluten (Organon), Frlinolut-N (German Remedies), Voldy» 21 (Glaxo) have in their llaj
of contraindications
included
&-2Wnancy. Firn/s like Pir.rke-Dw.vid
in triclr contraindications have
olfio included the phrase, “therd
is ecwo evidence t<i show that!
honvnptftl preparation when used
during pregnancy may lead w
xiormallttey
foot a
------- ’•••— *"
dist tubing phenomeu i IO thr.'Mj drugs
*k
folium* U-U* hr indu-
b’ssd tsfi; jfetiy
of thalidomide
By Claude Alvares
& and;
O N C K R N ED
Dnkshata-
f
IMJC
L&
chemic/lls
KfwJTf.’drei/bctorc i
SECRETION
tcrone in maintained and there will occur aa ft discrete malfur-will therefore be no shedding mid [rm or tn association with
But the disappearance of bleed other anomalies - among these
ing may not indicate pregnancy are hereditary pr.wllspusitloiA
absolutely. Normally, tire urine MuxMi
~
dose respou o and tprecise timing
Ilin
Inr-ilU.?’
sample taken early morning can oj y
w jncalt?
provide ft good test. In its place,
MNCn' have begun to push EP
o,
w would think that the <v»One
cftpills. Given orally, or by injection. tae,ophe of children .•><» severely
. 'J-•'.•li these BUbr.tanccs raise the level of nwimed and handicapped duo to
drug
ft ri«m the two hormones in the blood. qJ0 admlnirtration
a,.unmL.ir«v,V“ of ~
J—
i.,Q would —
have
*o
Within a week, however, both uro pKo thalidomide
- ’
expelled" rapidly through the. brought fdwut an appreciation
Iflv in expelled
ft* v-jui bladder. The sudden decline indu- and awareness of the dangers of
oca "wilhdruM•ftl'
•’withdrawal”, bleeding s.n
ss in administering drugs to prcgw»nt
CC3
th* normal cyelo and Iho woman women, but thte has happened
fra •% jnay. according to the prevutlln^ oniv In the West, where MNCa
lie; •.:**. popular windom, not be pregnant. nr0 Hable to do sued for mlllloiu
inrih g If she te pregnant, the secretion Of dollora for negative impacts.
>ely in of progesterone wilt b« main- quc tlWU ^rug contivHvrg, in tact, .
tained naturally, and alw will not coJitinuij to dunk that wo fihcrilw
Weed.
'■ :nnt be unduly alarmed about
’;-A‘ ‘ ■
■
'ports of druys being witttdraftia
..The IntemtisnaV^urnat
for. uninaxiateabio..Mela offwta
fndla
7.0 o'?■ Cent
>. ijico: ijply
.j'Cd
- i the
t’> was
BhopaFs deformed children
Flea For SifcrroF.
By D. C, Jain
HE environmental
pollution {New Jersey Supremo Court has
caused by MIC gas leakage in. held
that even Individuals who
Bhopal last year has resulted in the are Incapable of exercising tho
birth of about 100 deformed and right to die have such a. right In
birth-defective infants till April re Quinlan (1976) the Court allow
this year to the gas victims. About ed Quinlan’s parents to e-?rciso by
1,500 such women are pregnant and proxy her right not to have her
there is every possibility of their life extended by artificial means.
children also being birth-defective Extending the Quinlan analysis it
or deformed.
could be said that an incompatenii
1 am not a prophet of doom but infant lias a right to die that also
with the rapid industrial growth could be exercised by proxy. Karen
and tile scant regard for tho law Quinlan was irreversibly eomatosa
controlling environmental pollution, and in a
persistent
vegetative
we are destined
to suffer recur stale. In many ways her condition
rences of tho Bhopal tragedy and could bo characterized as uufcacb
tho number of deformed children ble. The Court held that the cops.
will multiply. 1 wish to suggest tltutional right to privacy is broad
how to deal with such a problem enough
to encompass a patient's
legally.
decision to
decline
treaWont
When a severely birth defective
certain circumstances.
infant enters a family, its parents under
The
courts
In India could
are faced with
an excruciating
dilemma — should they provide articulate a right Vo privacy that
In certain aspects of the
medical treatment for the child or inheres
terminate treatment when it is un family relationship, ranging from
feasible, medically or economically. the decision to conceive children
to
tho
right
to raise children ac
There are moral and ethical prob
lems associated with the agonizing cording to the parents' values. It
decision of life and death. Some of lis reasonably expected that our
these infants have been born with courts will protect parental deci
out the cognitive part of the brain, sions concerning children’s ralfeisome iiave mental and physical ous and educational upbringing. If
handicaps that although not neces the non-trentmenl decision can be
sarily fatal will severely impair characterised as one that concerns
too,
even minimal functioning. It will an infant’s upbringing, It,
make life miserable for them and may be protected under the Xndlan
their poor parents. The parents may Constitution.
sacrifice everything they possess
If tho parents were without tha
and keep tho infants marginally economic
resources to treat th-s
alive without curing the underlying child, or If the available medical
defects. But to what gain?
treatment
could not benefit fho
be
If these Infants die, their death child, the medical care could
as
an impossible
may result from the decision for characterized
non-lreatment. Non-treatmenx deci duly. A standard for non-treatment
should satisfy
three
sions challenge fundamental atti decisions
tudes towards life and death. The criteria: (1) The standard should
th-®
right to life is the basis of all other project tho best interest of
righits. The United States Supreme child and accommodate tho Into
Court has held that, within limits, rests of tho other participants in
noth abortion and contraception .*o far as they are compatible with
-ecislons should be made according those of the child. (2) The system
To one’s own moral views (Roe V. should provide certainty and consi
VVado (1973) 410 U.S. 113). The de stency of application . in lino with
cision to terminate treatment for a present legal doctrine, .vet retom
birth-defective new-born presents a enough flexibility to handle an un
parallel moral-dilemma.
foreseeable. situation. J") Ths
un’derwdr.e
Medical decisions concerning se standard should riot
verely blrth-defectlvc Infants in widely held moral values of our
volve three primary parties — the society: th<s sanctity of life, tho
child, tho parents and the State.
equal right of all e'Mzens to llfo
An infant’s needs and interests and medical treatment, and tho
are important to any decision con duty of society to protect the weak
cerning its well-being, because the and the helpless.
infant is the focus of the decision.
On tbeso premises, tho standard
Yet defining those needs and inte assumes that (a) whenever tl-.c?
rests is difficult. They are unable infant’s potential quality of life- Is
to express their desires or interests. extremely poor, death is preferable
Inevitably, parents will make the
continued
existence.
(b) A
final determination. Medical caro to
treatment is unfeasible if it cannot
will not always serve the child’s benefit the infant, i.e., if the treat
interest. An infant with a severe ment Inevitably will prove futile.
birth defect will never have an
awareness of the outside world. Medical treatment is unfeasible If
The defect may be Incurable and the child will die within a brief
he may never leave the hospital. period, regardless of any attempt
When a child with severe birth to save the life. When an Infant Io
defects is born, the parents may Irreversibly unconscious, as when
decide that the family should avoid the cognitive part of the brain is
the medical feasi
the financial and psychological dis non-existent,
In
ruption that the infant will create. bility standard would apply.
Parents of the deformed children. such a situation, the physician can
who are themselves victims of the restore breathing through a res
Bhopal tragedy, acting as Indivi pirator but can never restore brain
functioning. The infant at beat
duals will face similar conflicts.
Tho potential satisfaction to be will be able to breathe and per
derived from raising a birth-defec haps to blink and swallow; it never
tive child
must
be juxtaposed will be able to see, feel, think, or
against the necessary sacrifices in otherwise relate to the outside
the parents’ lives. Parents with de world. Under such circumstances,
formed child will often disregard few- wm 1171 argue ‘hat the available
friendship, forgo job opportuni •treatment" -actually benefits tho
physician
ties and spend their life savings in child. As suon as the
an
extra-ordinarily
short time can determine, that the child has
and
for
nothing in
return. no chance to regain consciousness,
Some
parents
will believe treatment can be withdrawn.
that these actions will run directly
On the basis of the above dis*
counter to their personal welfare, cu it is suggested that the
others will gladly make the sacri non-tr atment decision should bo
fice. But still a large number of legalised
in
certain
carefully
parents will feel torn by so many limited
circumstances by legisla
conflicting interests that they will tive enactment. As a first step, tho
find any decision difficult to make. physician must determine that tho
The State is the
guardian of child's condition is medically infea
society’s basic values. One of the sible. Next, the
parents
must
basic values protected by it is the decide whether they wish to con.
sanctity of human
life. For this tinue or withdraw treatment.
If
reason the state has an interest in the
parents decide to terminate
protecting the lives and welfare of treatment, a court will review the
its citizens. When the citizen
in decision. Procedural
review
by
question is an infant, the state in a Court will safeguard the State’s
terest may
be
specially strong, ■interest In the integrity of the de
because an Infant Is unable to care cision-making
process.
for and protect itself. But the state
All this may sound like a chimera
has limited
resources. A birth
defective new-born may drain the to many readers, but at the advent:
state’s resources and yet never of 21st century, India will
need
become a productive citizen. In such
a legislation, to make tho
such a case, the state’s interest in lives of unfortunate persons like
protecting a birth-defective Infant's Bhopal gas victims and their pro
life would be minimal or perhaps geny, less miserable.
What Vic
nonexistent
tor Hugo said has relevance In this
The 14th Amendment to tho context: “There is one thing stron
all the
armies in
US Constitution
Indicates
that ger than
and that Is an Idem
life l.s a
fundamental Interest the world:
which economic interests are not whose time has come.”
strong enough to override. Never
theless, there are decisions which
The author owes gratitude to
recognize that continued medical Elizabeth S MacMillan for her
care may not always serve the beet article “Birth Defective Infants’’
J^rests of every patient.
The Stanford Law Review Feb. 19KJ.
T
Beuer rural-health.:
Paramedics’ role cited
gap. Most community health pro
By Our Staff Reporter
blems like diarrhoea,
skin dis
Bangalore, Dec. 1 — The most eases. chest infections and malnu
practical way to improve rural trition can be tended by a train
health service is to integrate pre ed paramedic, he said.
ventive programmes
with other
Paramedics should
be drawn
areas of health care such as nu from among the community so
trition, agriculture
and family that they
can communicate at
, planning.
that level acceptable to that com
This can be enforced with the munity.
help of para-medical workers as
"Doctors”,
he said, “fail to
envisaged by Dr. Zafarullah Chow reach most patients because they
dhury.
stick to textbooks.” Paramedical
Chowdhury, reknowned for en workers, on the other hand, arc
gineering the ban of 1,707 hazar- able to communicate in more ac
I dous and irrational drugs in Ban- ceptable and
traditional
ways.
' gladesh, told medical students at and with proper training.
can
■ St John’s Medical College, here handle 60 per cent of the ail
today that a doctor's role in a ments in rural areas - without un
rural health
could be fulfilled dermining the role of doctors.
with the help
of trained para
Regarding the
drugs situation
medics. In most third world coun in India, Chowdhury said it was
tries. ihcrce-i'ourths of the health sad that despite ^so many drug
budget is urban-orient^d^ resulting manufacturers
in
the country,
in adverse health conditions in ru they are unable to supply even
ral areas where the masses live. one third of the leprosy and tu
On the con
In India and other developing berculosis drugs.
countries.
only 16 per cent of trary, many useless and danger
the population can afford modern ous formulations are being manu
medicine. Chowdhury said.
In factured and marketed.
Education would be the most
such adverse
conditions, doctors
alone cannot deliver health care effective means of bringing about
to all. The concept of parame a reversal in the deteriorating si
dics could evolve to bridge this tuation, he added.
£
O
to
r.
sZ
J
Hyderabad: A majority of the
analgesic preparation or pain
killers being used as medicine
in the country have been found
scientifically not justified,
according to a study done by
the rational drug policy cell of
the Pune based voluntary
medical group - Medico Friend
Circle.
Analgesic is a substance used in
medicine to relieve pain and is
monly referred to as a pain
T. The 50 analgesic prepa
rations were listed in the
monthly index of medical spe
cialities (MIMS) that gives stan
dard preparations currently
promoted by the pharmaceutic
al industry, the authors of the
study. Dr Jamie Uhrig and Dr
Penny Dawson said in their re
port.
The group using a rigorous
procedure graded the 59 pain
killers into four categories — A,
B,C,D It recommended the im
mediate withdrawal of the pre
parations falling into the B, C,
and D categories. Use of prepa
rations found good and justi
fied according to the study are
plain paracetamol, aspirin, cro
cin, dispirin, mazetol, paracin,
calpol, for twin, curepar, molin,
par von, predimol, pyrigesic.
W
Press Trust of India
sosegon, tylenol and tapal ing analgesics and antipiratics
junior numbering 14 in group to be immediately banned for
they
contained
analgin.
Anadex, avaforton, baralgan,
The group listed apidin, ava- codolsic, dolopar, neogene,
mol, beserol, betaflam, bral, novalgin, novalgine quinine,
cariaspirin, corbutyl, dolopar pamagin, promalgin, sedyn-aplus, equagesic, fortagesic cyc- forte; spasmizol, ultragin,
1‘opan, norgesic, mahdens, ultragin syrup, ultragin injec
parvon-N, proxy von r ralcidin, tion, sirnalgin-A. Analgin, a
spasmo proxyvon, tysyne, minor analgesic, enjoyed wide
sudhinol, tapal, treupel, vega spread popularity in India. It
nin, walagesic be withdrawn.
was an unnecessary and
The group wanted the follow- dangerous drug that had safe
and inexpensive substitutes.
The doctors group said it
Minister to open should be banned. A World
Health Organisation expert
\ meeting
committee had established a list
\
Newstoday
of essential drugs for all coun
Hyderabad. The Minister for tries that include a list of
Small ^cale Industries, Mr S analgesics and antipyretics like
Ramacnander Reddy, will inau aspirin, paracetamol, codeine,
gurate \the 31st Regional pethidine and morphine injec
Purchaser Advisory Council tion.
meeting \of the DirectorGeneral of Supplies and Dispos Pain is a universal phe
als. Government of India, on nomenon and the development
Monday. In vhe meeting, issues of drugs to relieve pain is one of
relating to ' he problems of the few remarkable achieve
small scale in
tries located in ments of modern medicine. It is
southern zone nil be discus necessary to make a j udicious
sed. Central
vernment offi decision on the relevant drugs
cials and officia from Tamil to relieve pain, the doctors said.
Nadu, KarnatakaX Kerala, Pon The Medico Friend Circle with
dicherry, and
hwadeep doctors and socially conscious
will participate ii
meeting. members from all parts of the
killers
country urged for a govern?
ment policy with provision of
all , essential analgesics and
antipyretics at low cost and the
banning of ineffective prepara
tions as a first healthy step in
forming a rational drug policy
in the country.
Mills policy
condemned
Newstoday
Hyde
ad- The policy of the
management of Vijay Spinning
Mills, Vi
awada,
’
in asking
women wo ers seeking reg
ularisation
job to submit eli
vorce cqrti
tes or bonds
promising tha\ they.would not
marry has
n .vehemently
condemned b
the general
secretary of th state Textile
Workers Federa
lak Ram. He ur
the Labour
and the Social Welfare Depart
ments to take appropriate steps
to stop such practi
Television
12.45 Higher education programme
4.00 Higher education programme
oeeds
rose so ©^“daf
From Our Special Correspondent
NEW DELHI, Nov. 21.
The launching of a "universal immunisation
programme" to protect all children against six
specific diseases before the age of one. in
troduction of continuing financial benefits for
acceptors of terminal methods of birth control
and 100 per cent achievement in the establish
ment of primary health centres and sub-centres
are some of the targets the Union Health Mini
stry has set for the Seventh Plan to reach the
goals of "health-for-all" and "net reproduction
of one" by the turn of the century.
The Ministry's proposals, recommended by
the steering group of the Planning Commission.
will require” Rs. 10.329 crores to imple
ment—Rs. 8.138 crores for family welfare, in
cluding maternal and child'health programmes.
and Rs. 2.191 crores for health schemes—in
the Central sector, and Rs. 3,337 crores on hea
lth schemes in the State sector.
This is an eight-fold increase on the Sixth
Plan outlay of around Rs. 1,400 crores but hea
lth planners and administrators feel that unless
resources of this order are provided, the goal
of health for all by 2000 cannot be achieved.
Should not be grudged: It is contended that
an increase in productivity—one of the three
main aims of the Seventh Plan—is not pos
sible unless people are healthy, both physically
and mentally. Hence, these inputs are neces
sary and should not be grudged. The outlay
sought is a little over five per cent of the pro
posed total Plan outlay of Rs. 180,000 crores,
compared to 3.3 per cent in the Sixth Plan.
Though no new strategy is envisaged, the
thrust will be shifted to prevention and the
strengthening of the rural health infrastructure.
The “universal immunisation programme"'
.seeks to immunise babies against diphtheria,
whooping cough, tetanus, polio, tuberculosis
(part of the present programme) and measles.
To achieve this, the existing capacity for vac
cine production will have to be increased.
Already, production facilities have been crea
ted for DPT and BCG vaccines, and a unit to
produce measles vaccine is proposed to be
set up. The Health Ministry expects to get
technology from abroad and set up the unit
by 1988.
Stronger ‘cold chain': Another important re
quirement is an effective ‘cold chain (centres
to store vaccine under refrigeration)., Inter
national assistance is expected for this. Re
cently. there was a meeting In Italy of inter
national donors interested in strengthening the
‘cold chain'. They felt Columbia, Senegal and
India could be helped. If the assistance comes
through, facilities for transport of vaccine in
refrigerated containers from the manufacturer
to the district headquarters, and" for cold
storage at the district and PHC level, will be
created.
For effective implementation of this and
other programmes, the rural health infrastruc
ture will be strengthened at an estimated cost
of Rs. 1.665 crores. The idea is to have one
PHC for every 30.000 of population—in hilly
and tribal regions one for every 20,000—and
one sub-centre for every 5,000 of population
(3.000 in hilly and tribal areas). So far, targets
in this regard have not been achieved. The Se
venth Plan will also try to ensure that the num
bers of 'auxiliary nurse midwives' (AN^I)
(multi-purpose workers) are in accordance with
targets.
100 per cent Central funding: It has been
noticed that States have not appointed male
ANMs as this expenditure has to be borne by
them. The female ANM is fully funded by the
Centre. It is proposed to make the sub-centres
scheme 100 per cent Centrally sponsored.
About 500,000 are expected to be set up with
the full complement of two ANMs.
‘Continuing benefit’ for terminal acceptors:
As regards population stabilisation, acceptors
of terminal methods will be provided attractive
incentives under the "continuing benefit" sche
mes. One envisages a monthly allowance of
Rs. 50 for five years to every such acceptor
after two children.
Another scheme envisages presentation of
a cash certificate, not less than Rs. 50,000. enca
shable after 20 years, only for acceptors of
terminal methods after two female children. It
has been found that such couples disfavour
terminal methods as they want a mate child
to provide for old age. This cash certificate
will provide an assurance of financial support.
About Rs. 3.800 crores are proposed to be
spent oh these schemes, from the proposed
outlay of Rs. 3,138 crores for family welfare.
Can be attained: Official sources are con
fident that if resources .are provided the de
mographic goals set for 1990 can be achieved.
These aim at reducing the crude death rate
from the present 12.5 per thousand to 10.7 per
thousand, the birth rate from 33.3 per thousand
to 27 per thousand, increasing life expectancy
at birth from 55 to 57.5 years and reducing
the infant mortality rate from 114 per thousand
live births to 87.
This will call for an increase In the couple
protection rate, from the present 29.3 per cent
to 42 per cent.
II —
II
Assassination fiasco
may noft deter Oadhafi
From Sashi Kumar
ton which Libya is seen as taking a more ex
treme posture than the other radical. State in
BAHRAIN. Nov. 21.
the area. Syria), his ambition to be acknowle
The Libyan leader, Colonel Muammar Qadha- dged as the ideological and political leader of
fi's' resentment at Cairo's public expose of the the Islamic world had only succeeded In isola
tolled bid to assassinate the former Libyan Pre ting him from most moderate States.
mier. Mr. Abdel Bakoush. and the forms it
Union with Arab States: Union with one or
could take have become a major ponderable more of the Arab States Che made unsuccessful
in diplomatic circles here. The whole affair—in attempts to enter into union pacts with Syria,.
which Egyptian undercover agents posing as Sudan. Tunisia, besides Egypt) has been his
mercenaries undertook to do the Libyan-com constant theme and bugbear. After starting out
missioned hit squad's (two Britons and two Mai- as a passionate follower of Nasser he fell out
tenese) work for them, then faked a with Egypt when Sadat sidestepped his long,
photograph showing the intended victim lying nurtured plans of bringing the two States unden
dead with blood gushing out of a bullet wound a common political banner. The rupture de
on the forehead and fooled Tripoli into announ epened when Egypt signed the Camp David
cing a successful execution—was more illustra peace accord with Israel and ever since there
tive than illuminating, because it was already have been frequent allegations by Cairo of
a wellknown and acccepted fact that terrorism Libyan-sponsored subversion in its territory.
is a centrepiece of the Libyan leader's foreign
The former Egyptian President had branded.
policy.
Qadhaffi "one hundred per cent mad" and his
When the cover on the operation was blown successor, Mr. Mubarak, held.hlm responsible
Libya, far from being abashed or embarrassed. for the Red Sea mining scare that led to an
poured vitriol on the Egyptian leadership for international scouring of those waters, a plot
aborting its mission to eliminate "stray dogs" to blow up the Aswan dam and plans to hijack
(the stock phrase for opponents of the Qadhafi a U.S.-built war plane to Libya. Mr. Mubarak
regime) and ridiculed the Egyptian President. has also accused him of an air raid on
Mr. Hosni Mubarak, for doubling as a sleuth. Omdurman in Sudan- this year, while the
From the interrogation of the four would-be as Sudanese President. Mr. Jaafer Nlmierl. has
sassins now in Egyptian custody it appears, been crying wolf against a Qadhafi scheme
moreover, that the death net cast by Tripoli to overthrow him.
included several other world leaders, among
Israeli colony:' Jordan's resumption of re
them the West German Chancellor. Mr. Helmut lations with Egypt made it an "Israeli colony"
Kohl, the French President. Mr. Francois Mit in Col. Qadhafi's eyes and when his latest shot
terrand. the Saudi King Fahd and—-although at Maghreb unity (of northern African States)
it is not yet clear whether Libya had anything under his leadership was challenged by
to do with it after all—the late Prime Minister, Algeria, he promptly shook hands and sealed
Mrs. Indira Gandhi.
an accord with Morocco over and across and
Overtures suspect While it may be neces against that country. He had then put out
sary to make some allowance for the pro ^tersto Saudi Arabia that was seen as the
Uh kled
■
MEXICO CITY: Army troops dug on Tuesday through the remains of a working class
neighbourhood flattened by a series of gas ex
plosions that authorities say killed at least 544
people and left 10,000 homeless. Some 1.500
people were injured in the fire that raged
through the northern suburb of San Juan Ixhuatepee when a gas tanker exploded on Monday
near a distribution centre, sparking at least 12
other earth-shaking blasts. The blast levelled
houses and factories nearby. The fire, which
survivors said fried birds in the air, began before dawn when 80.000 barrels of liquefied gas
exploded at the distribution centre. Many
houses made from petrol barrels in the poor
suburb simply melted in the immense heat of
the
fire.
killing
their
occupants
in
seconds—UPI.
-j
<1
. 1
/?
1
J
..
Limits on loan
*
WASHINGTON: The IMF has announced a
reduction of "enlarged access" borrowing
options for its member countries next year. The
“enlarged access" borrowing, designed to aid
countries with balance of payments problems,
was reduced to 95-115 per cent from 102-125
per cent of each country's quota in the IMF.
The limit on borrowing over a three-year period
was also reduced to 280-345 per cent from
306-375 per cent of each country's quota. The
IMF also stipulated that a member's total
foreign debt must not surpass 408-450 per cent
of its quota, down from 500 per cent at present.
The limit on loans to compensate for reduced
export earnings Stays at 83 per cent of the
quotas.—AFP
|Tc
vs
Pa
?.
sc
th
cl
o
tf
p
a
Boat tragedy
DHAKA: More than 100 people were, feared
drowned when a boat capsized in a river on
Tuesday In southern Bangladesh. The "Sihangal" turned upside down with more than 500 r
passengers on board in midstream on the Sipl
ton Hola river near the town of Barisal. Many/
passengers swam to safety but more then
......... and
children.
wcr^^J . .
r
I,
\
[
y
|
k units are not interested in producing
‘bulk drugs in countries like India. In
Europe and USA. the multinational
units produce bulk drugs in a spirit
of collaborative relationship. In the
developing countries such produc
tion is avoided by them and where it
is done, the host country pays dearly
for such drugs...The multinational
units operationg in India produce
only a small fraction of bulk drugs.
The main thrust of multinational
units continues to be towards capita
lising on drug formulations and non
drug items like cosmetics and luxury
goods where technology and capital
inputs are much lower and which
permits promotion of aggressive
salesmanship and brings in much
higher returns on investments.”
Even when^ there is a reduction in
production costs, there is no reduc
tion in prices. For example, the price
of Betnelan , manufactured by M/s
Glaxo Laboratories, was fixed taking
into account the cost of production at
^•irticular time. Thereafter, though
^^cost of production came down,
the price was not proportionately
reduced. This was brought to the
notice of the government by the
workers of the company in 1977.
Ultimately, the company was forced
to reduce the price of rhe product by
Rs seven per 100 tablets in February
1979. Again, despite the increase in
sales, the number of workers em
ployed by these companies has not
increased. (Refer table)
‘Drive out harmful drugs’
SYED KAMALUDDIN reports on the Dacca government's
new drug policy which bans the manufacture of a number
of drugs produced by multinational corporations
rPhe new drug policy recently cy said, “are mainly engaged in for
JL announced by the Bangladesh gov mulation. And they procure their raw
ernment, banning the manufacture materials by import, involving an
and import of 237 pharmaceutical pro annual expenditure of more than Taka
ducts with immediate effect and res 60 crores in foreign exchange.” While
tricting the activities of the multina these raw materials produce finished
tional drug manufacturers in the coun drugs worth three times, an additional
try has prompted immediate and quantity of finished products worth
angry reaction from them. The policy Taka 30 crores are also being imported
has also outlined that another about annually.
1,500 pharmaceutical products would
According to the policy statement,
have to be withdrawn in the next nine the Drugs Act of 1940 which is the
months.
basic drug legislation, is outdated and
What particularly annoyed them grossly inadequate. The outdated legal
was that the new restrictive drug poli procedure hinders rather than helps’
cy has followed the most liberal New prompt prosecution and penalties.
Industrial Policy (NIP) which virtually Much of the unethical practices in
denationalised all industries and pro manufacture and trade has been possi
vided all possible facilities to the pri ble because of the weakness of the
vate sector, to play an increasingly existing legislation. Further, the con
important role in national economy. cept of drugs and medicines as an
The NIP has reduced the reserved list essential component of healthcare is
for industries in the public sector to missing.
six: armament and defence related
The statement said: “In the present
industries, atomic energy, air trans drug laws, there is no provision for
port, telecommunication, generation regulation technology transfer and/or
and distribution of electricity and licensing agreement with foreign col
mechanised forest extraction. All laborators. Similarly, there is neither
other industries, including jute and provision for protecting consumers
Again, to simply earn profits, some textiles, can now be owned by both the against drug hazards nor is there any
multinationals are marketing drugs, public and private sectors either protection of national interest in re
spect of patent rights for phar
which are totally or partially banned sepaerately or jointly.
While the industrial policy aims at maceutical substances. The present
in their parent countries. Some of
these drugs are Penicillin and Sulfa “a new dimension and greater thrust government is committed to health
combinations, Penicillin and Strep to industrialisation of the country,” and welfare of the people. As a mem
tomycin combinations, combinations the drug policy’s objective is to ensure ber of the World Health Organisation
with Chloramphenicol and drugs be the supply of life-saving drugs and (WHO) we are committed to health for
longing to the Esgapyrin group. medicines at a reasonable price to the all by the year 2000. Being conscious
These are the drugs which have been people. Multinationals based in Dacca of this responsibility the government
totally banned in the parent coun and Western observers here feel that was anxious to discover the pitfalls in
prospects for the promotion of foreign the national health policy as a whole
tries.
investment in Bangladesh which and the drug policy in particular. As
addition to these, some drugs brightened up with the new industrial the two were inseparably linked, the
ii have been partially banned in policy have largely been diminished government was pleased to constitute
• countries are being marketed due to the drug policy.
an eight-member experts committee to
in our country. These are EstropThe local pharmaceutical industries evaluate all the registered licensed
rogyn, Estrois Forte, Lynoral, Men- would
pharmaceutical products presently
be
particularly
affected
as
the
strogen, Orasecron Forte, Norles- new policy stated that “no foreign available in the country and to formu
train, Secrodyl, Premarin, Disecron,
medicines will be allowed late a national drug policy consistent
Disteron,DuogynonForte, Duogynon proprietary
with the health needs of the country,”
Oral and Amenoron, known as pre to be manufactured under licence in it added.
gnancy test drugs which cause de any factory in Bangladesh if the same
Production or importation of nearly
formation in unborn children. These or similar products are available 2,000 brand names has been banned
drugs have already been either ban manufactured in Bangladesh as this ■under the drug policy.
ned or withdrawn in at least six leads to unnecessary high prices and
The Chief Martial Law Administra
countries during the last nine years payment of royalties. In the light of
policy, all existing licensing agree tor (CMLA) has already promulgated
following the reports that they can this
should be reviewed.”
the new “Drug Control Ordinance of
damage babies in pregnancy, ments
The drug policy, announced by the 1982” to administer the new drug
Sweden was first to ban them in health
and population minister Maj- policy and monitor the functioning of
1970, followed by Finland (’71) USA
and Singapore (’75), Belgium (’77) Gen M. Shamsul Haq, said that a total the pharmaceutical manufacturers as
of
4,140
brands of drugs are available well as others involved in the field of
and the United Kingdom (’78).
in the country now as against only 182 healthcare. The ordinance, prom
Some multinational drug com drugs that the government had earlier ulgated on 12 June came into immedi
panies even reintroduce banned selected as essential. Only about 90 of ate effect. The government has also
drugs under different labels. Duogy these essential listed drugs and medi prepared a list of 150 essential drugs
non, manufactured by M/s German cines are locally manufactured. “All considered" “adequate for most ther
Schering, though banned in India pharmaceutical companies,” the poli apeutic purposes.”
was marketed as Cumorit.
»
35
THE HINDU, Tuesday, September 18, 1984.
17
forum for readers on topics, ideas,
'developments of current interest
Waited a ouaHoroa!! drag poiioef_
[for posativ® heaDth
RUGS and the related chemical industry
form an integral part of the infrastructure
of any National Health Service. To have
a proper and effective “people’s drug policy”
we must have a "people’s health policy"
Without knowing the common or major dis
eases prevalent in our country, we cannot plan
what must be produced and how much of that
to be produced.
Even after 36 years of independence India
could not formulate an effective ‘national health
policy' and medicare programme. The formulatioiv^ a national health policy depends on
soi^P^ng more than building hospitals and
blaming the medical profession for not going
to the villages where 80 per cent of the popula
tion live. Proper health care for the entire
population could not be achieved even in de
veloped countries like the U.S. and the U.K.
But the socialist countries like U.S.S.R. and G.
D.R. could achieve total health care, while the
health care of the people Is nearing completion
In other developing countries like China, Cuba
and North Vietnam. The social structure of the
countries and the class character of its ruling
section on every sphere of life are the reasons
for this achievement.
Proper health of our population could be
achieved if we can eradicate 'communicable
diseases' and for that the Government has set
apart Rs. 36 crores a year Hardly the cost of
a warplane it is planning to buy.
Common diseases and essential drugs
We know the common diseases and the
drugs to be produced to treat them. But if you
study the production pattern during the last few
years you will learn that the Government ad
ministrative machinery is not at all serious to
impj^tent its own decisions nor has the drug
indiw^ taken the Planning Commission re
ports seriously. There are about seven com
mon diseases and 10 drugs termed as essential
drugs. The production of these drugs has
suffered due to the manipulation by the drug
manufacturers and the total negligence on the
part of administration.
The diseases are malaria, filariasis. T.B.,
leprosy.
typhoid,
dysentery,
hepatitis.
hookworm and rabies. These diseases account
for 22 per cent mortality and 18 per cent
morbidity and 80 per cent of the population
is at risk The people of the Third World
countries who are suffering from these tropical
parasitic diseases were compelled by the drug
industry to purchase vitamins and tonics
marketed in very attractive bottles and cartons.
The share of tonics in Indian market is 12 per
cent while in the developed countries it is just
-three per cent.
Obsolete formulations
In India we have 5,000 pharmaceutical firms
producing about 60,000 formulations. Seventy
per cent, that is 42,000 of these formulations
are obsolete and useless. 5,000 are useful and
another 2,500 are of marginal use. The rest may
be included in the harmful group. The Hathi
Committee identified 117 as essential drugs.
The World Health Organisation says 200 of
these are enough to take care of 90 per cent
of the existing health problems. Finally to save
the 80 per cent of the population at risk in India,
we need only 10 drugs, termed the essential
D
drugs. I hey are chloroquine, diethyl carbama- promotion ot health, prevention of diseases, pro
zlne, streptomycin. INH. PAS. thiacetazone mpt diagnosis with treatment and proper rehabil
dapsone, chloramphenicol, metronidazol anc itation in all stages of life from womb to tomb.
piperazine.
In the sphere of drug policy we must see that
This year the drug industry will sell aboul no person dies of any illness for want of
Rs 3.115 crores worth ot formulations, of medicines, irrespective of social and economic
course, mainly tonics and vitamins. The Govern conditions and remoteness of his habitation
ment itself admits that five per cent of that wll Medicines, chemicals and equipment required
be spurious. While there are millions of sepoys for the protection of health, prevention of dis
and policemen, and thousands of officials, eases, restoration of health and rehabilitation
MLAs and MPs. the whole of India has hardly should be freely made available to each and
500 or so drug inspectors to monitor the affairs every individual of the society without any
of 5.000 registered pharmaceuticals and double social, political, economic or geographical con
that number of unregistered firms and straints.
The import monopoly of the State Trading
thousands of chemists and druggists. To test
6Q.000 formulations we have hardly five or so Corporation with its top heavy, and unhealthy
bureaucratic set-up have made things worse.
drug testing laboratories
Out of 5.000 registered firms. 45 are multina The irony is that while it—the STC—could
tional companies. 118 are in the organised In reduce the price of 15 per cent of the imported
drugs, it helped to increase the cost of
dian private sector and six are the chronically bulk
losing public sector firms. Of these 1,500 firms 75 per cent.
Hathi
Committee’s recommendation
are based on loan licence and 3.500 are the
The Hathi Committee recommended nationa
so-called manufacturing units. Hardly 200 are
actually engaged in production and the rest lisation of the drug industry and out of 15 mem
are tablet-making, capsule-filling and tonic bottl bers in the committee nine gave it in writing,
ing plants. Fifteen big concerns produce 80 per to nationalise all the foreign-owned drucj
cent of the drugs and five among them are companies without paying compensation. But
Indian and the rest multinationals. Even after our rulers joined hands with the four bureauc
36 years of freedom, we still import 50 per rats in it who differed. The report as such
cent of the raw materials at stupendous prices. vanished totally right from the Government print
The 45 multinationals market 78 per cent of ing press without a trace. The one presented
the formulations, while the Indian private sector before Parliament is there for you and the na
has a 16 per cent share and the public sector tion to express profound sorrow and the deep
sense of shock and to weep at times and offer
six per cent.
"We are businessmen and not bishops,” said homage.
Eacn patient was found to have received an
an executive of a pharmaceutical firm, to Mr. average
of 10 to 14 drugs for simple ailments.
Hathi. So to be in the drug business profession We generally
a temptation to treat each
profitably, they produce more and more; much new symptom have
as it emerges with a new drug.
more than their rated production capacity. The
avoidable. Osler a great physi
firms have so conveniently and mystically something
tuned the medical profession to go in for the cian—you may not agree his great
completely imported and costly third genera ness—stated in 1901, "One of the first duties
tion rifampicin and ethambutol replacing all the of a physician is to educate the patient not
other cheaper group of drugs for TB. I am sure to take drugs." This may be true a century
back, during his stone age. Now nothing pre
that no medical man has heard of streptomycin. vents
us from choosing a’dozen or so for- every
INH. PAS or Thiacetazone during the last five
years or so and thus they have lost complete patient from 60.000 formulations at our di
sposal.
at a reasonable profit. Most of us have
faith in these drugs. The firms have so conveni
hand information about the length of prescri
ently made these as useless and old-fashioned first
first line of drugs, thereby creating a lack of ptions. It is polypharmacy that we practice now
it is the physician who needs to be blamed
demand for this cheaper group and to project and
it as an excuse to cut down drastically the and censured and not the pharmaceutical firms.
More than 50 per cent of the patients after
production and to increase the import of the
costly rifampicin and ethambutol, and the the first visit to a doctor are treated on hunch.
multinationals have christened these as the intuition, experience, etc. rather than on
‘Third Generation' drugs, yes for the Third established certainty. The evils and dangers of
practising habits by us is very difficult to
World.
Likewise. I may warn you that 'Phenoba estimate and there is no method to determine
rbitone' a cheap life-saving drug required by it in India. There is no secrecy in modern
millions here to save them from epileptic and medicine and if the people are educated to
febrile fits will soon disappear from the Indian take some more care in their health problems
market to be replaced by costly imported sub and if they are willing to carry a notebook
stitutes. Please don't conclude that all the drugs whenever they visit a doctor and demand a
Included in the First generation by the true copy of the case sheet every time from
Americans are harmful. Most of them became their doctor. I am sure that most of the evils
amongst the allopathic practi
first generation because of the manipulation by can be prevented
Let the patient keep his health record.
the multinationals, and just because they are tioners.
If the poorest man can safely maintain a ration
cheap. That is the case with the drugs men card,
what prevents him from keeping his own
tioned above.
health card?
With these details just outlined I may say
Dr. K. Kishore Kumar,
that national drug policy is the part and parcel
of national health policy, which is com
Secretary. IMA. Mavehkarabranch.
Kayankulam (Kerala).
prehensive positive health care and that is
Fight against MPT StilB On
VIMAL BALASUBRAHMANYAN
'The campaign against the horm-
one pregnancy test {Mains
tream, April 10, May 8, July 24),
which seemed to have yielded
results, is not yet over. The fight
is still on. Although the Health
Ministry note on June 30
announced a ban with a defer
red cut-off date, less than a fort
night later, Deputy Minister of
Health Kumud Joshi told the
Lok Sabha that the products
have not been banned. She
merely repeated that the manu
facturers had already been told
to include warnings on the lables.
How these warnings are worded,
their low visibility, ambiguity,
the continued availability of
these drugs over the counter,
and their continued prescription
by doctors for pregnancy testing
have all been outlined in the
previous Mainstream articles.
The campaign against HPT
misuse, initiated — in March by
the Voluntary Health Associa
tion of India, the Medico Friend
Circle, Arogya Dakshita Mandal
and the People’s Science Move
ment, and subsequently joined
by women’s groups and journa
lists all over the country, is the
first such mass protest aimed at
combating the pernicious in
fluence of the drug industry on
the Government and on a large
section of the medical profes
sion. Whether or not the
Government is willing to admit
it, it was this mass movement
that resulted in the ban announc
ed in June. Obviously the drug
industry’s machinery has not
been idle meanwhile. How else
does one explain Kumud Joshi’s
unabashed announcement barely
two weeks later on July 15?
One is tempted to suspect that
even the deferment of the ban
(to come into effect only from
June 30, 1983) was motivated,
probably with the idea of again
citing new ‘experts’ on the
indispensability of the drugs and
thus pave the way for lifting the
ban. However, despite Kumud
Joshi’s announcement, the whole
MAINSTREAM September 11, 1982
thing seems ambiguous and the
drug industry itself seems unsure
of the Government’s attitude:
will it yield to people’s pressure
or will it bow to pressure from
the drug industry? So the next
step from the industry is under
standable: woo the press.
Business Standard (August 27,
1982) published a report, quoting
drug industry sources who have
urged the Government “to
appoint a statutory body to
examine the propriety of the
ban”. The sources criticised the
June 30 directive and said “the
misuse of these drugs by a few
uninformed or ill-motivated per
sons for pregnancy testing ...
did not warrant a total ban on
their use for any other purposes.”
Does that not sound vaguely
familiar?
When pressure was put on the
baby food manufacturers, their
argument was on similar lines.
Unhygienically prepared, over
diluted, and fed in insanitary
bottles, baby food could cause
infection. Not if the manu
facturers’ instructions were pro
perly carried out. So, if the
illiterate and the ill-informed
don’t know how to bottlefeed,
why blame the innocent manu
facturers? Big business philo
sophy is the same, be the pro
duct baby food or combinationhormone drugs.
Anyway, let’s examine the
drug industry’s point of view.
First of all, a large number of
women (and their unborn babies)
affected by HPT are affluent and
literate. A large number of
prescriptions for these drugs
come from doctors who have no
excuse whatsoever beyond igno
rance and indifference. A large
number of chemists who ‘pre
scribe’ these drugs do so because
they know that doctors them
selves recommend their use for
pregnancy testing, despite the
minuscule warning on some of
the packets and despite all the
latest medical findings.
A senior Calcutta gynaeco
logist, who strongly condemns
HPT misuse, told me a few
months ago that just the previous
week a woman patient had come
to him very agitated, saying she
had taken HPT on a general
practitioner’s advice and now
what should she do? What had
made her suddenly aware of
the danger? Probably the articles
in the press, said the specialist.
If the first doctor had been upto-date with medical knowledge,
and if the brand she bought had
a large, bold warning printed on
the outer label, she need not have
exposed her baby to danger. The
industry’s argument about the
‘uninformed’ doesn’t say how
this situation is going to be pre
vented. And the industry also
implies by using the word’ un
informed’ that only the illiterate
are at a disadvantage. Not a
word about the doctors and
chemists whom they are directly
in contact with.
As for the illiterate: if the
reality in this country is that the
mass of the women are illiterate
and ill-informed, should not
Government health policy be
specially formulated to protect
this majority? The small print
ambiguities which pass for ‘warn
ings’ do not even protect the
literate. Even in literate UK and
USA it was not action by the
Government or the medical pro
fession that brought HPT misuse
to a halt but organised people’s
action. What is the logic in
hiding behind the ‘warning’
excuse in a country where illite
racy reigns and when the ranks
of the ‘uninformed’ include
qualified doctors?
I had earlier mentioned that
the Government has a clear duty
to inform and educate the mass
of women on HPT misuse
through posters and films. Only
recently big prizes have been
awarded for TV and radio scripts
on family planning. But it is left
to a women’s group in Delhi,
Saheli, and VHAI to design a
poster, with text in Hindi that
7
aims at warning the semi-literate
never to take any tablet or injec
DRUGS : DACCA’S BOLD MOVE
tion to confirm pregnancy, and
informing them what kind
Health
Action
International
major US companies affected by the
(HAI) has released a briefing paper,
drugs ban — including Wyeth,
of deformed babies could be
The Rational and Economic Use of
Squibb and Smith Kline — at meet
born if they took any such drug.
Drugs in the Third World, which
ings arranged by the US ambassa
But how many women can two
supports the Bangladesh Govern
dor to Bangladesh, Jane Coon.
voluntary groups with slender
ment’s bold move to rationalise
A number of HAI’s members —
resources reach? Our cynical
national drug policies and eliminate
Oxfam (UK), War on Want (UK),
more than 1,700 drugs from the
Government’s priorities are re
and the International Organisation
Bangladesh
market
by
the
end
of
flected in its attitude not only in
of Consumers Unions — have con
1982. The Government’s action was
the case of HPT. It can be seen
gratulated the Bangladesh Govern
prompted by the report of the
ment on its efforts to establish
in its non-action on the baby
Expert Committee for Drugs that an
rational and economic drug use.
estimated one-third of all money
food front, and its token res
HAI’s new briefing paper gives the
spent on medicines in Bangladesh
ponse to the question of female
reasons behind these endorsements
went into ‘useless, unnecessary and
foeticide only after women’s
and calls on WHO to publicly
at times harmful drugs’.
support the new policy. In addition,
groups had made enough noise.
HAI feels strongly that the
it stresses the need for the Organis
What is significant is that in
Bangladesh Government’s important
ation to establish authoritative
each of these instances
of
initiative demands widespread inter
criteria which other Third World
Government cynicism it is the
national support. The new National
governments could use to determine
Drug Policy is a substantial com
female section of the population
inessential drugs.
mitment
to
public
health
in
one
of
that is vulnerable. It is women
WHO has yet to respond officially
the world’s poorest countries. The
who are illiterate but who have a
to the Bangladesh Government’s
Expert Committee has stressed the
initiative. HAI’s attempts to deter
touching faith in what doctors,
pressing need for change: “At
mine the Organisation’s position on
present, not more than 20 per cent
quacks and chemists tell them;
this move to eliminate wasteful and
of the population have access to
Why does a woman take a drug
harmful
pharmaceuticals
from
even the most essential drugs for
to confirm pregnancy except
Bangladesh have so far met with
their health needs and yet the
silence.
A series of direct questions
because it is she who suffers the
market is flooded with hundreds of
to WHO’s Director-General, Dr
useless or non-essential medicinal
greatest anxiety over it? Why
Halfdan Mahler—have gone unans
products”. The policy is designed to
does a woman give baby food to
wered. HAI urges the WHO to
concentrate provision on some 250
her child except because she
dispel the doubts this silence creates
drugs considered essential for health
more than anyone else wants to
about its commitment to rational,
care. By doing so it follows both
economic Third World drug poli
the letter and the spirit of WHO’s
give her baby ‘the best’, believing
Action Progamme on Essential
cies by unequivocal endorsement of
that tinned food is indeed the
the Bangladesh Government’s New
Drugs,
which
was
unanimously
end
best? Or if not for that reason,
Drugs Policy.
orsed by the May 1982 World Health
isn’t it because her working con
Assembly.
Health Action International is a
ditions compel her to leave the
International support for the
network of more than fifty research,
baby with a bottle in the care of
consumer and development action
National Drug Policy is urgently
others? And why does a woman
needed. The policy has come under
groups worldwide who are interest
heavy attack by pharmaceutical
ed in questions of pharmaceutical
need to be so desperate to get
industry interests since its establish
policy and their effect on the Third
rid of a female foetus except
World. An international clearing
ment on June 12. Industry’s protests
because it is her own position
have led to the appointment of a
house for HAI is operated from the
as a woman that tells her that
committee of militaty doctors to re
International Organisation of Con
view the policy. The review commit
sumers Unions’ Regional Office for
female babies are best not born?
tee and health ministers are being
Asia and the Pacific, PO Box 1045,
All these are related themes.
Penang, Malaysia.
lobbied by representatives of the
The HPT ban is the issue at the
moment, but it is not just a drug
which the Government seems to
advanced countries would not
issue. In each of the instances
have banned them. She also
cited, where women are vulner be pathetically willing to accept
at face value. The Hindu in the
quotes the findings of Dr
able, they are the target of an
past few months has published
Palaniappan whose controlled
unholy combine of big business
many letters from doctors,
studies at Kilpauk showed
and medical science. Add to it
condemning HPT misuse, calling
beyond doubt not only that HPT
the policies of an insensitive
for a ban, and welcoming the
is dangerous to unborn babies
Government and it becomes
ban announced in June. One of
but that it use to bring on a
obvious that mass action alone
the letters, by N.P. Bhanumathy
can protect the interests of this
delayed period would only
of Madras, who has been a vocal
further delay the menses. He had
vulnerable section.
protester on a number of drug
One heartening feature about
demonstrated that often the
issues, clearly shows that the
apparent effect of the drug in
the anti-HPT campaign is the
involvement of a number of ‘other uses’ argument, for which
bringing on a delayed period was
the
drug
companies
claim
their
socially conscious doctors. This
psychological. “A majority of
product is ‘needed’, is bogus.
is necessary because scientific
women who were given dummy
She points out that if the pro
and medical expertise is needed
injections had bleeding much
to counter the pseudo-scientific
ducts were really needed for
earlier than those treated with
‘other uses’ then a number of
arguments of the drug industry,
costly hormones.” She also quotes
the WHO Technical mies No.
657 which says: “Women who
are not pregnant will have their
delayed menses further delayed
if hormones are administered.”
Bhanumathy
then asserts,
rightly, that the drugs, being
useless for ‘other uses’, should
be totally banned — “the point
is no more a technical issue
deserving expert view” — and
that the Government should take
a really ‘conscious’ decision
based on therapeutic rationale.
It will be recalled that in March
this year Health minister B.
Shankaranand had said the
Government had taken a ‘con
scious’ decision not to ban HPT
on the basis of ‘expert’ advice.
The above arguments have
been echoed in the August issue
of the MFC . Bulletin, quoting
recent editions of gynaecology
text-books which do not recom
mend the combination hormone
drug for any case of amenorrhoea. The bulletin editorial
says: “There is no indication
for the use of this high-dose
combination and the patient will
not lose anything if these prepa
rations are banned.”
Commenting on the Govern
ment’s ambiguous stand on HPT,
the MFC has urged all those
concerned about the birth of
babies with needless cogenital
defects to join in the campaign
against HPT drugs by rousing
public opinion and by writing
to the Drug Controller of India,
Ministry of Health, Nirman
Bhavan, New Delhi 16, and
urging him not to go back on
the earlier announced deferred
ban but instead to ban this
dangerous drug now.
WOMEN’S WORLPI
The Price of Courage
ANJALI DESHPANDE
O adhu is being made to pay
the price for having challen
ged existing social mores. The
police is deeply interested in
humiliating her into inaction for
her own sake and as an ominous
lesson to future women activists.,,
If the rich colonisers of Agra are
to acquire land occupied by the
poor through some quirk of law,
if the prostitution at Sikandra is
be maintained in peace without
raising hopes of rescue among
its wretched, if the downtrodden
are to be kept at bay, the voices
of Madhu, Anal and their like
have to be muffled. For males,
the new anti-dacoity measures
come handy. For women, their
sex is the source of innumerable
forms of outrage that the police
does not mind resorting to.
Twentyfour-year-old sprightly
Madhu and her young friends
have become an eyesore to the
Agra police for various reasons.
These members of Chhatra Yuva
Sangharsh Vahini insist on stay
ing in the Harijan basti Bapu
Nagar. They have struck roots
among the 250 families there and
the 450 Harijan settlers at J.P.
Nagar. They rescued Gita, an
unwilling prostitute, from the
infamous flesh market at Sik
andra. And with their support
the dalits lay claim to a little
MAINSTREAM September 11, 1983
piece of land legally owned by
Lajjaram Gupta, a rich colon
iser.
What must irk the police most
of all is the rescuing of Gita.
Forced into prostitution at the
tender age of eight, she had
managed to convey to the Vahini
her desire to be free. It was not
an easy job. Five police officers
had to be transferred before Gita
safely reached the Nari Ashram.
Even in choosing the women’s
home where Gita was to be
placed, Vahini had had its say.
They did not allow the police to
take her to a home of their
choice. The very fact that five
police officers had to be put out
of the way to deliver Gita from
the Sikandra brothel, is proof
enough of the powerful hand of
the police in maintaining the
place. It was also a firm pointer
to the growing force and strength
of the Vahini in Agra which
could not be ignored. Most
important of all, it gave hope to
other prostitutes by making it
clear that those who want to be
free cannot be confined against
their will.
In the whole case Madhu had
emerged as a very determined
and efficient worker. In fact she
was against admiting Gita to the
Nari Ashram, and was preparing
to take her away to Vinoba
Bhave’s Ashram at Paunar where
she had hereself had a year-long
stint. On the eve of her intended
departure she was taken into
custody.
Meanwhile Lajjaram had man
aged to obtain a court decree on
2.5 acres of land at Bapu Nagar
which he had bought years be
fore. Despite Agra falling in C
category of the Urban Ceiling
Act which says no person can
hold over 1500 square metres of
land. Probably in dread of local
resentment, Lajjaram, instead of
sending notice to the 20 families
settled on his land to vacate it,
engineered the destruction of the
statues of Mahatma Gandhi and
Babasaheb Ambedkar. In what
reverence the two leaders are
held by the Vahini and the Harijans needs no mention. There
could have been violent outburst
and then it would have been
possible to stow away quite a few
“trouble-makers” behind bars.
But wise counsel of the .non-vio
lent Vahini prevailed. Nothing
untoward happened. On July 23,
Anal was shot at by Parikh, a
known thug of Agra. The bullet
missed the target, but soon Anal
was surrounded and beaten up.
Anal’s FIR was not registered by
the police, who preferred to act
9
on Parikh’s FIR that Anal had
robbed him of Rs 3.50, a watch,
etc. Warrants against Anal were
issued.
The ordeal for Madhu began
on the night of July 25-26, when
the police descended upon the
Vabini office at Bapu Nagar. She
had been charged under Sections
307 (attempt to murder) and 395
(dacoity) on the basis of an FIR
lodged by Parikh, the man who
had taken a pot shot at Anal and
missed. Anal was not there.
Madhu was. She would not allow
the policemen inside the room
where a number of women from
the colony had taken shelter
from the leaking roofs of their
homes in the pouring rain. A
policeman brought up his knee
to kick her in the lower abdo
men. After she fell down the
police switched off the lights and
lathi-charged the women inside
the room. Finally they took
away Madhu to the police
station.
At the police station she was
beaten up and tortured. Her
ankle bone was broken, she was
burnt with cigarettes, she was
asked to urinate in front of a
row of policemen. Even in the
face of such humiliation she
w'ould not reveal the where
abouts of Anal. The police
told her they would make
a ‘Gita’ out of her, that her
mother would be brought to the
police station and tortured in
her presence, if she did not tell
them where Anal was. The cour
ageous Madhu did not yield.
On July 26 a procession of five
hundred proceeded towards the
police
station to demand
Madhu’s release. The brave UP
police, who had protected Chabiram when he held his durbar and
let the Deoli murderers escape
initially, made the mounted
police charge into the crowd of
unarmed men and women with
kids in their arms. Horses ran
amuck. One hundred and fifty
people were injured. An infant
was flung away from its mother’s
arm and died in the diabolic
lathi charge. A bayonet pierced
the knee of a 12-year-old. The
police -was holding Madhu to
ransom, and they were determin
ed to get Anal as the price of her
release. Section 144 was clamped
JO
on Agra. The terror is so much
that private doctors refuse to
examine and treat the injured,
for fear of repercussions.
Tormented by thoughts of
what the police would do to
Madhu, Anal went and surrender
ed. When Madhu told the ADM
that the police had dishonour
ed her by taking away her
dupatta, the ADM is reported to
have asked the ASI to take away
her dupatta once again, to give
her prasad which consisted to
twisting her arm bghind her
back.
She is now recuperating in
Tundla. Her bladder is ruptured,
the ankle shows a fracture. Her
body is full of bruishes. The
blisters on her mind, the trauma
of those held in custody must be
even deeper. If rape is taken in
a literal technical sense Madhu
was not raped. But what she
underwent, was it less than rape,
mental and emotional?
All Opposition parties in Agra
including the CPI, CPI-M, Janata
Party and the Sarvodayis have
lent support to the movement
against repression and police
torture of activists. On their
persuasion Anal broke his indefi
nite fast in jail. He was not
being permitted to see visitors as
a punitive measure. Despite the
impressive number of parties and
groups that have joined hands
with Vahini on the immediate
issue of police atrocities, quite a
few express reservations regard
ing the basic issue of land-grabb
ing by the rich; not many from
outside the stronghold of the
Vahini have either courted arrest
or made their presence felt in
large numbers, barring one mem
ber from the Rashtriya Seva Dal
and three women leaders. The
vicious slander campaign by the
police and the administration
against Madhu is taking its toll.
She is being declared an “un
chaste” girl. And the so-called
educated middle classes do not
pause to consider why an ‘un
chaste’ woman should have taken
the risk of rescuing Gita in the
teeth of opposition from the
police.
Despite the mounted police
and all, a large number of women
joined a 1000-strong dharna in
front of the Collector’s office.
Fortytwo persons were arrestpd ,
including 12 women. On August
23 five hundred women defiedj
Section 144 to demonstrate
against police atrocities and 51
women were arrested that day.
Among them two were minors
and eight women were carrying
infants. The struggle was echoed
in Delhi on August 9. Twelve
Vahini and Samajwadi Yuvajan
Sabha members courted arrest in
support of the fight in Agra. A
joined committee of various
groups including Indian People’s
Front, SYS, PUCL and PUDR,
was set up on August 31. The
newly-formed Agra Jan Sangharsh Sahyog Samiti will carry
on supportive actions like signa
ture campaign, postering, pro
cessions and dharna to highlight
the role of the police in repress
ing political and social workers
and to fight the character assassi
nation of women workers in
particular.
A woman living away from
her family and mixing freely with
men, does not automatically
become unchaste. And even if
her ideas on sex are not as ortho
dox as many would wish them to
be, chastity is not the whole of
virtue. There is compassion,
courage, intelligence and the
will to live not only for one’s
own narrow self but for better
causes that concern society. On
this count Madhu stands far
above those orthodox women
who are scoffing at her. The
Harijans she lives with realise
this and stand by her This is no
small achievement.
CORRECTION
In Mainstream (August 21,
1982), page 25, column 2, line
11, in place of'‘prevent”, please
read “prepare for”. The sentence
as corrected will read thus:
“With the policy of the Tri
lateral Commission of President
Carter (which is still alive des
pite Carter's defeat) which wit
nessed Americans, Europeans,
and Japanese united in an eco
nomic front, there was a bilateral
accord in Italy between the re
actionary Masons, financiers and
Jewish bankers to invite the
Vatican block to collaborate
with them in order to anticipate
and prepare for the efforts of the
Trilateral Commission”.
The error is regretted. —Editor
WHEN Judith M&gid, a legal
•' aid attorney, laarnod in
1978 that
pharmaceutical
companies were testing new
drugs on inmates at the State
Prison of Southern Michigan,
USA, she considered repre
senting the prisoners tn a
: class «action lawsuit against
, what she felt 'Was dangerous
; exploitation.
■
She had to drop her plana in tho
j Jac© of vociferous opposition. The
> resistance came not from th© drug
j companies, but from the prisoners.
Now, five years later, it fe the
federal US Food , and Drug Ad
ministration that wants io atop
? the medical research. This time
» the prisoners have filed & law; suit — against th© FDA, not the
J drug companies.
1
tamates ' oi ths State
Prison of Southern Michi
gan, USA; staunchly
defend their dangerous
role as human guinea
pigs for drag '■ research.
The money incentive!
and the relative comfort
of the research lab are a
welcome chance to
escape the hostile and
unpleasant prison en
vironment, they contend.
ran in 15TO, ft.tound
,
£
nearly unanimjoua in support-of
research programme, with money
'
the clear incentive.
. u .
A major problem for an Inmu.ts
'at Jackson i3 finding a salaried
job of any sort. With 5,COG pri
soners, this Is the largest walled «•
prison in ths world, and many •
inmates end up with*no work.Asked what would happen If /.ir’ig,
testing slopped, Con© onsweroti v
simply, “I'd be out of a job."
Tho four prisoners listed etho?
attractions o' the research pro
gramme; it provides escape Jeon J
prison tension, crowding,’ s’icne-,
ciio'w hall food and boredom;' . it
provides n chance to sC.,- ’and talk
with outsiders whb treat them
better than the guards; it oii’-rs
an education of sorts .In medicine,
diseases and treatment; it -gives >
them a full medical cxsun far. •
more elaborate than what is _sup®
Thf inmates want the drug re
do not deprive them of that right. plied by normal pricon med’cnl
search to continue.
They con Th© elaborate controls, regula care.
tend that their civil rights would tions- and monitoring of tests set
. Tho prisoners' comments mado
be violated by the very FDA re up in recent years have eliminated
gulations designed to protect them. past abuses. A contained prison it. .clear that being- selected for
They are asking for injunctions population is much better suit medical research In . jail is con
against . the scheduled shutdown ed for tho tests than non-prl- sidered a great privilege.
of the .testing as of June I.
fioner groups, because the en
Tho half-million dollar rese.7’.c?3
The lawsuit has focussed atten vironment and activities of pri lab built by Parke-Davis and Up
controlled. Thera john offers clean, quit- elx-iation on two intriguing questiona. soners can be
colour TV, tab's
Do prisoners have tbn right to Is a greater danget from Inade 12-man words,
• c.; x
. •,
volunteer lor the possibly danger quate testing (.hnn there E risk, r-an'-i
ous role’ of human guinea pig? to prisoners; ’ unsafe medicines' of infection disqualifies a prisonerAnd are they volunteering freely?' might be marketed to tho general from drug tests for six, months,
so a high proportion of those
The prisoners say yes. They population.
Ike the money they earn from the
But the National Commission chosen come .from the- p-Jiond
irug companies and the chance for tho Protection of Subjects of two honour blocks.
o 'trade hostile and unpleasant Biomedical and Behavioural Re
Tho National Commission found
arisen
environment for’ the re- search, after listening to hours of
atiye comfort of the research testimony and visiting foqr pri that test subjects arg dispropor
tionately white. Th© prison popu
ab.
sons in 191G, finally took a posi lation is 68 per cent ’black, but
“It's mor© dangerous out there tion against the tests. It con the pool of volunteer subjects
'Ln the prison)
than the worst cluded that “although / prisoners only 31 per cent black.
Volun
experiment they could ever think, who participate in research affirm teers tend to ho older; in prison
ipjn. here (the lab),” one inmate that they do so freely, the con much longer than average and
ditions of social and economic de better educated
9«i- ''J
October 9, 19S2
ECONOMIC AND POLITICAL WEEKLY
Shiv Shankar, subsequentlyu’-ev-oked the whatever partisan angle it may be
suspensions and the OMOA withdrew intended — can only help jhe-yorkers’
its strike notice.
movement for greater .safety in mines.
Meanwhile, as part of its campaign This would be a charige from the usual
to give itself a better image, the «LMOA situation when members of the CMOA,
has come out with a list of collieries with their ruthless implementation of
it considers unsafe. Any such move by government policy towards the workers
the CMOA opposing the government’s besides^their own oppression of them,
ruthless policy of slaughter minrqg — arcx the immediate targets of the work
however fitful and partial, and fr'om"" ers’ movement.
HEALTH
Cheap but Dangerous
Vinial Balasubrahmanyan
LATE
in August newspapers had a
prominent item- on
why India had
asked Ciba-Geigy to continue market
ing of Enterovioform, an anti-diarrhoeal
recently banned by Bangladesh. The
news, based on a Neto York Times
story, seems to be part of a strategy with
the objective partly of discrediting the
new Bangladesh drugs policy but
more substantially of building an im
age for Enterovioform as an ‘essential
drug for Third World countries'. This
latter motive seems particularly like
ly, considering the growing strength
of the attack on this drug in both de
veloped and developing countries.
The Ciba-Geigy
spokesman is re
ported to have cited Enterovioform as
an example where ‘benefits outweigh
risks’. He admitted that it is “possible”
that “not all
patients in developing
countries are informed of the risks or
of the fact that safer, alternative
drugs may be obtained”. The justifi
cation cited for marketing it is that
"it costs barely one-fifth ot what some
of (he other anti-amoebic drugs cost
and is known to be effective as long
as taken
under a doctor’s prescrip
tion”. 'I he spokesman made no men
tion of the fact that the drug is not
only widely sold without prescription
but is actively promoted by the firm
itself to the lay public in some Third
World countries.
Enterovioform is one of the clioquinol drugs that has attracted sharp cri
ticism because it is known to cause
neurological damage. Last year Social
Audit of UK brought out a leaflet on
the dangers
and
misinformation of
clioquinol drugs entitled “Bad
Infor
mation Means Bad Medicine”. Com
menting of its harmful effects a Lancet
editorial in 1976 had said it was
still being sold over the counter in
1642
IGO countries. At a Penang meeting
last October, noted Swedish neurolo
gist Dr Olle Hansson had said that in
serious cases victims could become
completely blind and their legs could
get paralysed. Dr Hansson is active in
the campaign
against Enterovioform
which he says is irresponsibly being
sold in the Third World, the accom
panying ‘cautionary’ literature contain
ing scientific jargon
unintelligible to
the layman.
A very legitimate
question is: if
Enterovioform is widely sold without
prescription, whose responsibility is it
to inform the public of its risks? Also,
when doctors proscribe it unless pa
tients are told of its risks and the fact
that safer, alternative drugs exist,
how can they make an informed choice?
It is claimed that Enterovioform is
a cheap and
effective anti-amoebic,
necessary in a country where amoe
biasis is -rampant.
The fact is that
the drug of choice against this dis
ease is metronidazole, and if the
country’s health needs demand it, the
drug of . choice
ought to be made
cheaply available. It is a strange kind
of health policy that justifies the foist
ing of a harmful drug for a widespread
disease, simply because it is cheaper
than the safe one.
However, one
suspects
that the
amoebiasis
argument is an elaborate
multinational ’double-speak. This drug
is actively promoted to the lay public
in Third World countries not as an
anti-amoebic but as a cure and pre
ventive for “travellers’ diarrhoea” for
which it has shown no evidence of
being effective. An
outsize boarding
in Lagos, reproduced in the August
issue of South, depicts this product as
a ‘must’ in
every
traveller’s kit.
Would the Ciba-Geigy spokesman
care to elaborate on the risks and be
nefits of Enterovioform in Nigeria? In
fact both
Enterovioform and Mcxaforni (also by
Ciba-Geigy and with
the same active principle) are listed
in the. popular
prescribers’ guide,
MIMS, not under
anti-amoebics but
under anti-diarrhoeals. In any case it
is now known that most of the antidiarrhocals, especially the clioquinol
drugs are useless against common vi
ral diarrhoeas.
Clearly Ciba-Geigy
is
trying to
create the image of an ‘essential drug
for amoebiasis’ while actually continu
ing to promote it to tire lay public as
an ordinary anti-diarrhoeal — it has
long been
self-prescribed thus and
will continue to be thus consumed by
the uninformed. Bangladesh, a country
where endemic
diarrhoeal disease is
probably a much more serious prob
lem than in India, has chosen to ban
Enterovioform. So has Malaysia. A cam
paign against it has begun in Indone
sia. The boycott by Swedish doctors
of Ciba-Geigy products because of
the firm’s continued sale of Enterovio
form and
M exaform in the
Third
World has
resulted in
Ciba-Geigy
losing 25 per cent of its share of the
Swedish market. The
new ‘image’
sought to be created for Enterovioform
must be understood against this back
ground.
The case of SMON victims in Japan
where the side-effects (abbreviated as
SMON) were first
observed is well
known. In Sweden a number of En
terovioform victims were paid massive
demages by Ciba-Geigy in an out-ofcourt'settlement. And last February
the Sunday Tinies reported that a Bri
tish woman won huge damages from
another firm whose similar product
had caused her to go blind and partly
paralysed.
Facts quoted in the latest issue of
HAl Netos (newsletter of Health Action
International) place Ciba-Geigy’s new
tactics in perspective. On August 7 the
Malaysian government bannfed import,
supply and sale of clioquinol. The
move came after pressure groups and
consumer unions gathered mounting
evidence against the drug. On August
12 the Social Audit leaflet was launch
ed in Jakarta soon after the Indonesian
Health Minister announced that
the
drug was still ‘needed’ in that country.
It will be observed that in countries
COfwwiunilTY HEALTH CELL
47/1, First
»»- ■> - >
Doctors urged not
to overprescribe
£■
was also to be completed veryF
Express News Service
P j
Bangalore, Nov. 24: Health soon, he said.
'The Minister lauded the nursing
Minister H. L. Thimme Gowda
care
provided
in
the
Catholic
hospw
has appaled to the doctors in the
State to desist from overprescrib- pitals which was far superior to Hi
X
ing drugs as it could prove to be that in other hospitals.
Earlier.
Father
Ferdinand Q
dangerous for the patients in the
Kayavil, President of the CHAI.
long run.
Inaugurating on Friday the 41st said in his welcome address that (J
national convention and work the manufacture of only expenshop organised by the Catholic sive drugs, meant for the rich, had (j)
Hospitals Association of India on to stop. Drugs should be brought
“Towards a People-Oriented within the reach of the poor. The
drug Policy", the Minister drug production in the country'
lamented that overprescribing had had increased hundred-fold, with
become a fashion for most doc nearly 25,000 drug formulations
tors. a\ was the prescription of and nearly 5000 manufacturing'll
‘glamorous’ and expensive drugs. units. Despite this, drugs reMr Thimine Gowda said that in mained largely a luxury itemj£
Karnataka, Rs. 10 crore was being affordable only by the well-to-do.
spent tor the purchase of drugs He felt that consumer awareness
which was more than adequate if programmes and public opinion
spent judiciously. He cited the mobilisation would help people
instance of a district hospital. know the evils of overconsump
which had used drugs worth Rs. tion .
Father Kayavil said that
40.000 in the first three months of
“Health for all by 2000" was an
the year itself.
Mr Thimme Gowda said that at ambitious plan, as the health
present the State had 1.300 prim problems in the country were too
ary health units and 300 primary big to be tackled so soon. Howev
health centres. In another two er. he felt that collective tenacity
years the Government hoped to of the people and the right health
set up 300 more primary health policies framed by the Govern
units. Recruitment of 570 doctors ment could help achieve the goal.
The CHAI had set up 499 hospit
als and 1.274 dispensaries all over
the country to provide health care
to the masses.
Bishop Gilbert Rego. Eccle
siastical Advisor of CHAI, pres
ided. Father John Vattamattom,
Executive Director. CHAI also
spoke. Dean of St John’s Medical
College. Dr G. M. Mascarenhas
welcomed. Later Excise Commis
sioner J. Alexander inaugurated
the exhibition.
Myopic policy on
drugs bemoaned
BANGALORE, November 28:
The 41st annual convention organised
by the Catholic Hospital Association
of India (CHAI) on the theme “To
wards a people oriented drug policy’’,
has expressed deep concern over the
increasing scarcity of essential and life ■
saving drugs as against wasteful1
abundance of non-essential drugs and >
formulations.
The association said that the con
vention, which concluded here re
cently, also discussed the continuous
availability of banned drugs and the
spiralling cost of pharmaceuticals.
The convention has resolved to
appoint an expert body to formulate a
rational drug policy, which is people
oriented, within the context of a
health care strategy and policy.
Nearly 500 delegates including doc
tors, nurses, hospital administrators
and pharmacists attended the conven
tion.
over increasing scarcity
of life saving drugs
From Our Special Correspondent
BANGALORE, Nov. 27.
Over 500 delegates to the four-day 41st
annual convention of the Catholic Hospital As
sociation of India (CHAI) on the theme "to
wards a people-oriented drug policy", con
sisting of doctors, nurses, pharmacists, hospital
administrators and health activists representing
around 1,900 member hospitals and health care
institutions, which concluded here, has ex
pressed' concern over the increasing scarcity
of essential and life saving drugs, as against
wasteful abundance of non-essential drugs and
formulations.
The excessive number of over 30.000 drug
formulations, as against the Hathi committee
and WHO expert committee recommendations
of 116 and 200 respectively, the continued
availability of banned drugs despite the Govern
ment bans, the continued availability of ban
nable and hazardous drugs in spite of the moun
ting scientific evidence and directives of
various courts, the spiralling cost of drugs as
against the decreasing purchasing power of the
people and the continuing domination' by the
multi-national drug industry as against the na
tional policy of self-reliance were the other
areas of concern.
Govt, list endorsed: The convention fully en
dorsed the Union Government’s list of banned
drugs and agreed to implement it in its organlsa- |
tions and urged all sister institutions to do like-. t
wwise.
It asked the member institutions to prepare ,
a list of essential drugs along the lines of the ‘
Hathi/WHO committees for immediate ad- 1
option In all institutions, urgently take steps to :
reduce the present unhealthy and unethical in- .
fluences of the drug industry on the medical
and allied professions and mobilise public
opinion against the apparent lack of concern I
of State Governments and professional and ex
pert bodies on this vital issue.
The convention resolved to appoint an ex- •
,pert body
J to formulate a rational druga ,policy.
J. •
which is people oriented within the context of
—» care strategy
--------------a- •health
and' policy 1benefiting the
national commitment to health for all by 2000
A.D.
At the 41st annual general body meeting, ,
Fr. Ferdinand Kayavil of Benzigar Hospital, ,
Quilon. Kerala. Sr. (Dr.) M. Fernandes. Marianpur. Hospital. Kanpur, U.P., and Fr. Antony- .
swamy.of the Diocese of Ooty, Tamil Nadu.
were qlectd President, Secretary and Treasurer
respectively of the CHAI, for a term of three
,years.
_.
Study for ban on pain killers
Press Trust of India
Hyderabad: A majority of the
analgesic preparation or pain
killers being used as medicine
in the country have been found
scientifically not justified.
according to a study done by
the rational drug policy cell of
the Pune based voluntary
medical group — Medico Friend
Circle.
Analgesic is a substance used in
medicine to relieve pain and is
commonly referred to as a pain
killer. The 50 analgesic prepa
rations were listed in the
monthly index of medical spe. cialities (MIMS) that gives stan
dard preparations currently
promoted by the pharmaceutic
al industry, the authors of the
study. Dr Jamie Uhrig and Dr
Penny Dawson said in their re
port.
The group using a rigorous
procedure graded the 59 pain
killers into four categories - A.
B, C. D. It recommended the im
mediate withdrawal of the pre
parations falling into the B. C,
and D categories. Use of prepa' rations found good and justi
fied according to the study are
plain paracetamol, aspirin, crodispirin, mazetol, paracin,
^Blpol. fortwin, curepar, molin,
parvon. predimol. pyrigesic,
sosegon, tylenol and tapal
junior numbering 14 in group
•A’.
ing analgesics and antipiratics
to be immediately banned forthey
contained
analgin.
Anadex, avaforton, baralgan,
The group listed apidin. ava- codolsic, dolopar, neogene,
mol. beserol, betaflam, bral, novalgin, novalgine quinine,
cariaspirin. corbutyl, dolopar pamagin, promalgin, sedyn-aplus, equagesic, fortagesic cyc forte, spasmizol, ultragin,
lopan, norgesic, malidens, ultragin syrup, ultragin injec
parvon-N, proxy von r ralcidin, tion, simalgin-A. Analgin, a
spasmo proxy von, tysyne. minor analgesic, enjoyed wide
sudhinol, tapal, treupel, vega- spread popularity in India. It
nin, walagesic be withdrawn.
was an unnecessary and
The group wanted the follow- dangerous drug that had safe
and inexpensive substitutes.
The doctors group said it
should be banned. A World
Health Organisation expert
committee had established a list
of essential drugs for all coun
tries that include a list of
analgesics and antipyretics like
aspirin, paracetamol, codeine,
pethidine and morphine injec
tion.
country urged for a govern
ment policy with provision of
all essential analgesics and
antipyretics at low cost and the
banning of ineffective prepara
tions as a first healthy step in
forming a rational drug policy
in the country.
Pain is a universal phe
nomenon and the development
of drugs to relieve pam is one of
the. few remarkable achieve
ments of modern medicine. It is
necessary to make a judicious
decision on the relevant drugs
to relieve pain, the doctors said.
The Medico Friend Circle with
doctors and socially conscious
members from all parts of the
"Mcst pahvkflfers useless
and harmful9
HYDERABAD, May 12.—A. majo Malidens, Parvon-N, Proxywon, Ralrity of pain-killers used in India eidin, Spasmo-Proxyvon, Tyxyne,
are either dangerous or do not pro Sudhinol, Tapal, Treupel, Veganin
duce the desired results and need and Walagesiu among those io be
to be withdrawn, says a study by withdrawn.
Otiier analgesics and anti-pyrea voluntary medical group, reports
tics it said should be banned were:
PTJ.
Avaforton,
Baralgan,
About 59 of these analgesic pre Anadex,
parations were listed in the month- Codolsic, Dolopar, Neogene. Noval
ly index of medical
specialities. gin, Quinine, Pamagin, Promalgin,
Sedyn-A-Forte,
Spasrilizol,
Ultra
(which gives standard preparations
currently promoted by the phar gin, Ultragin syrup. Ultragin in
maceutical industry), according to jection and Zimalgin-A.
Analgin, a minor analgesic en
a study conducted by the ration
al drug policy col) of the
Pune joying widespread popularity in
the country, was unnecessary and
based Medico Friends Circle.
dangerous
and had inexpensive
The group, grading the 59 pain
killers into four groups. A. B. C. substitutes, the study said.
A World Health Organisation ex
and D, recommended the
with
drawal of the B, C. and D cate pert committee had established a
list of essential drugs for all coun
gories.
Paracetamol, Aspirin, Crocin, Dis- tries which included analgesics and
prin. Mazetol, Paracin, Calpol, Fort antipyretics like Aspirin, Parace
and
win, Curepar. Molin, Para ci I, Par tamol, Codeine, Pethidine
von, Predimol, Pyrigesic, Sosegon. Morphine injections.
The study was conducted on a
Tylenol and Tapal Junior fall in
report
by
Dr
Jamie
Uhrig
and
Dr
group ‘A’.
It listed Apidin, Avamol, Bese Penny Dawson.
rol, Betaflam. Bral, Cariaspirin,
Corbutayl, Dolopar Plus, Equagesic,
Fortagesic, Cyclopan, Norgesic,
Other analgesics ’ and anti*
pyretlcs to be banned were.
Anadex, Avaforton, Bnralggn,
Codolsic,
Dolopar,
Neogene,
Novahrin, Novalgine Qqu.iune,
P&nutgin. promalgin, Sedyn-AForte, Spasmlxol, Ultragiri, Ul«
(ragin syrup, Ultragin injection
and Zimalgin-A.
Analgin, q minor analgesia enjnyin# widespread popuJarhy in
Ute country, wus unnecessary
and dangerous and had tn expensive substitutes, the study
Kxid.
j
’
j
;
■
I
i
A world health organhar.on .
expert
hxi
ed a lUt of essential drugs
countries which included
j Asian seminar calls
‘ratioi^F drag policies
By Our Staff Reporter
ulale the drug industry, change laws
A tour-day Asian seminar on relating to registration, supply of
“Pharmaceuticals and the Poor”, complete, unbiased information on
which concluded in the City on drugs to doctors and consumers,
Tuesday noted with concern “the and tor a scheme to monitor adverse
deterioration in the drug supply drug reactions.
situation” in most Asian countries
Luck of deterrent action by the
where governments have adopted governments had encouraged the
“counterfeit substitutes in the name multinationals to argn . i\ch sell
olf phaun.Kculical mdusln policies”
h.tinjhil liuiiml.'ihias which u, >.
instead of formulating comprehen .banned in (he West ami social
sive and rational - hug policies based other countries in the world. Di
Chowdhury said.
on the health needs of the people.
In a ‘Madras declaration’, outlin
This allected the neighbouring
ing its conclusions, the seminar countries; for instance, drugs- ban
urged the governments to totally ned in Bangladesh were being • ■■ hig
ban irrational and dangerous drugs, gled into the country from InJia.
as a first step. Tins was “an urgent
The declaration urged the govern
need which cannot be postponed ments to take action on the resolu
except at the cost of the nation’s tions adopted by the non-aligned
health”.
countries in Colombo and Havana
Organised by the International in 1976 and 1979, by formulating
Organisation of Consumers Unions, drug policies based on the concept
the Voluntary Health Association of of essential drugs being made avail
India and Asian Communitv Health able al reasonable prices to (he
i Action Network.,the seminar was people.
attended by over 30 delegates from
• different health workers’ groups in
Asia who prepared a 11 point model
national drug policy draft.
Asian countries which have
adopted rational policies, banning
The Hindu 7 Dec 85
the unnecessary and harmful for
mulations, witnessed "a remarkable
improvement in the drug supply
programmes
and drug policies of various coun
MADRAS. Doc. 6.
situation”, the declaration noted.
(j
Participants at a seminar on "pharmaceuti tries in the Third World were greatly influenced
4 Briefing newsmen. Co-ordinator
by a few develop*! countries. He was sorry
I
cals
and
the
poor"
today
stressed
that
consumof .the All India Drug Action Net
i er organisations should actively involve them development strategies had not brought any
work, Dr. Mira Shiva, said the
selves in law suits filed by the Government to appreciable benefit to most people.
proliferation of harmful or unneces
/ Some participants said there was an urgent
protect public interest.
sary “drugs” was the worst in India
They pointed out that several socially rele- ’ need to look at the question of non-availability
and Brazil. At least two-thirds of
of essential drugs to the poor and the general
i
vant
measures
initiated
by
the
,
Government
the 40.000 formulations tnanufaC- '
were thwarted by a few individuals and some non-accessibility of the health care system
j lured in India fell into these cate- i
manufacturers tuning the issues to court. "Even which resulted in increased mortality of the
1 gories.
poor, depite high technology.
1 Dr. Zafrullah Chowdhury from i well-meaning litigation had gone against the inDrug policy irrational: Dr. Mira Shiva. Co
S Bangladesh said the medical com- ! i terests of consumers simply because people’s ordinator. All-lndla Drug Action Network.-so id
( views had not been adequately presented."
n munity in most Asian counities had •
India’s drug policy and practice today were ir
they
said.
become totally dependent on the
More than 50 delegates from 10 countries rational. The manufacture of a host of essential
pharmaceutical industry, for pre- '
generic drugs should be taken up in a big way
scribing medicines, doctors relied 1 , are participating in the four-dny seminar organi instead of going in for more formulations.
sed
jointly by the Asian Community Health Acon the literature supplied by the .
Dr. Kumariah Balasubramaniam. Pharmaceuti
. tion Network, Hong Kong, the Voluntary Health
drug companies themselves.
Association of India. N&w Delhi and the Inter cal Advisor to the Caribbean Community Sec
I Tlie governments also were recal
retariat
in Guyana, said redistributing health
national Organisation of Consumers Unions.
citrant in informing the people and i
care among all sections Of society would re
Penang.
the doctors on which of the formula
quire innovative policy measures. Restricting
Charge
against
multinational
companies:
Des
tions were harmful or useless, said
pite a mushroom growth of pharmaceutical tne national formulary to a limited number of es
Dr. Mira.
firms in India and the Third World, a vast major sential drugs, adoption of generic names, elimina
The seminar also noted “with
ity of people still had no access to reliable and tion of the multiplicity of brand name products
distress the alarming decrease in
basic essential drugs. The participants said and removing from the market unnecessary' and ex
recent years in the production and
regretted some multinational companies con pensive tonics and vitamins and replac . g
supply of vital drugs needed to
tinued
to dump in India and other developing these with’a few essential vitamins and mineral
combat diseases such as Malaria,
countries several harmful drugs banned else preparations would meet with considerable re
TH, other infectious diseases and
sistance from the medical profession and the
where.
nutritional blindness”. There was
Dr. Badal Sen Gupta from Bonn said health urban elites, he warned.
no inbuilt mechanism in our drug
policy to check the decline in the
production of essential drugs Dr.
Mira added.
A fall-out of the proliferation of
formulations was the lack of reliabil
ity and quality of “a large propor
tion of medical preparations on the
market”.
it urged governments to make
laws for ensuring strict quality con
Hol and promptly punish those who
Violated such laws.
Supporting the public's right to
’■complete information on drugs and
public accountability of the drug
industry and health professionals
including doctors”, the declaration
called tor concerted action to reg-
' 4No 21C€€£S
j essgoithJ rags staUIT
Indian Express I I Dec
Slulidj bSiSSC
.Ossigiei’CES drug®
gotta n®
-V
^/3/»Vx.
letter, it has pointed out the in- export that the future operations '
discrimmcie use of Oestrogen* would be taken care of. Il is in .
Progc.stri'ne combination of urugs llio knowledge of {he Delhi Ad.in women What is vital Is’ the ministration that within the city.'
need la educate wo men a bout it .elf there is a flourlblnrw cottag«
me dangers mat the use of these
and.
drugs might entail. If cigarelio spt; ions drug makers.
•
packs across the length and
The lowest tender still continues;
D.'uailUi
of
munirj
can
be
sukf.
Al the end of the ritual, they
with
the
warning
that
sim.king
is
p
tab
for
purchmw
y
f
druws.
A
hue.1 led back home to look after
rigoniUb dni:?
control.
W; d.-.i’s -.,r.<il and their children. injurious to health how is it more
that lh.ru :■> ..njth.js-; wrung: that in loo Capital cilj, right thorough e-winiinaiioij and mralyslij
with cookinv one’s meal and look. Under the nose of the Drug Con- to ensure the efficacy of dnjgri Is’
,J
•;c after i.hildi.-n but in a < ity troih r, tnese drugs continue to he dofinifejy r^riulred.
\dn >c the B: al ( ’.uh wirnestts sold without (heir dangers being
r.-r<>:u s;x-.ikirs than weij London's six’ll out Look at the enormity
P.rk and where. you can of effect-i--possible foetal abnorm
udfetl .-rc»wd; □'•curding :‘lo jvur alities in the pregnant -mother,
»
public meetings >.re of !1‘. foetal abnormalities in the child ■
significance except ' (■> ihuse being bream ivd, if the mother •
. b:i
In get an ‘honourable uses these drugs.
(Jf the 15 companies selling
men lion’ in the newspapers ■
Lncs? urui;s under different brand
\ y<)! r. n t i ry,. bp d.\. . ok h... iL’ 5 names, onlj one has listed amongst
l!-dr Ikdlh; Ac^on
did the “contraindications",
saying
•r.its V : io ■ - :
llut “theje i-. some evidence to
fu. us something which should
that hormonal preparation
ei interest to: all women. In a show
when u.-cd during pregnancy may
I itad to foetal abnormalities."
The drugs are a hormuim pre
paration u-ed large I j as a diag
nostic test for pregnancy,
Nut
only is it nut reliable as a
; diugnmUc fesl — for one'out of
five v.ijrm-n who undergo the lest,
•I leads to fhv wrong conclusion—
but many ’women believe that this
is an injection for abortion. Un
th-_- contrary, the woman who re
ceives the injection runs the risk
of giving biilli to a malformed
baby,
ine literature available with the
World Heailh Urgamsalitm (WHU)
or. the subject points out that
utudies sugi-.c-1 “an iisvuciaUwn
between c.irdjil.v3;>cular defects
and i.e.v ?U*n>id honno.iefj ««» •
poiures dur.ng the first trimester.
Ac am “there exists a suspicion
that the hormones used in preg*
hancj' tests may cause birth de
fects especially cony.enitul heart ’
find limb reduction anomalies.1'
With the availability of hn.
mtinuh^rcul U-.l> uhith enablo
c-arlv defection <4 prvgiuncy, thu:
tpa of these drugs, in any can©1
for pregnancy dcti’cliuu, needs to
be aiscourag* <1.
There are doctors who recom
mend that
pregnant
mother.’f
who take Hila Injection should bo
advised to have medical termina
tion «>f pregnancy.
In any event «n»e would tend to
a%jree with the Health Action
India Wat labels of these diuga
^should carry a warning, m b«‘hi
letters 'Not to be used for prerj»■ ucy <’ gnosis “May cause foetal
abnormalities "
• Ono may argue (hat when thera
•4s such caitou distegard for the
present generalloo, how tun Ode
AST Monday was Intemati- ; d
Women’s Day. A h?ndiu.wom?D gathered at various .%_■
in the city to pass resolutions
!
to underline various demands r
the t'ellerment of the status jf
w omen.
L
PP3T NEWSLETTER
Vol.1
No. 9
-
October 1983
■ Modern medicine, in terms of its spread and
cons.ec :ences, has - in a perverse sense - possibly helped
to create as much disruption as the sum total of all the
military aid the third-world has received. The decay
and collapse of traditional systems of medicine which
depended wholly on locally available materials, the
consequent dependence on non-local skills, materials,
alisB concepts and methods are good indicators of the
lack of correspondence between modern medicine and the
social realities of the third world. It is, perhaps,
because of this that the baby food, supposed to help
children obtain nutrients, causes disease due to secondary
effects; fancy programmes to reduce malnutrition cause
further suffering; new forms of disease grow alongwith
claimed 'cures', in the single-minded mad-race in search
for the elimination of human suffering through thoughtless
drugging of the human body. Perhaps, Gandhi’s identification
of modern medicine wnttHa the essence of witch-craft comes
close to a proper characterization of the problem. •
This issue of Newsletter contains some glimpses of
the problem of disease causation.. 'Man and His Environment ’
is abridged from Britannica Perspectives (Vol.1),
'Cleaning up Third World Disease's from the Economist
(Sept.1983) and the last two pieces are from the
New Scientist (June 30, 1983).
-------- xxxxx-------Man and His Environment
Everywhere in nature life is a collective enterprise.
All organisms, primitive or complex, naturally spend much
of their lives in the company of their own kind; but. in
addition, and more interestingly, they always occur’ in
intimate and lasting associations with other forms of
life not genetically related to them. Any measure that
grossly alters natural conditions is likely also to have
direct or indirect unfavourable effects because all
components of nature are interrelated and interdependent,
Man is dependent not only on other human beings and on
the physical world but also on the other creatures - animals,
plants and microbes - that have evolved together with him.
Man will endanger his own survival if he thoughtlessly
eliminates the organisms that constitute essential links in
the complex and delicate web of life of which he is a part.
Please address all correspondence to: J.K. Suresh, 62/2,
Shop-street, Basavanagudi, BANGrALORE-56O 004.
-2-
All natural phenomena'are the result of complex
interrelationships; all manifestations of human disease
are the consequences of the interp’’
y
: c-? body, mind
and environment. Overwhelming evidence indicates that
many forms of disease have emerged or have been disseminated
in the modern world, because ova*, ways of life have created
new ana complex constellations of circumstances favourable
for their spread. .
'■
u
The outbreak of Manchurian plague at- the turn of this
century constitutes a well-documented example of role of
living patterns in disease causation. The plague bacillus
is widely distributed -among the wild -rodents in many parts
of Asia. Manchurian marmots normally harbour this microbe,
but they do not suffer from this infection under usual
circumstances. Around 1910, a charge in women's fashions
in Europe suddenly' created a large demand for the fur of
Manchurian marmots, and a number of inexperienced Chinese
hunters began to hunt this wild rodent. Until then it .h-'.d
been hunted only by Manchurians who had a taboo forbidding
them to hunt sick animals. In contrast, the inexperienced
Chinese ■ trapped. every animal within reach, especially■the
sickest who were slower and easier to catch. As it turned
out, the sick marmots were suffering from plague, and many
Chinese hunters contracted the infection from them. When the
hunters met in the crowded, illventilated Manchurian -inns,
those who had caught the microbe spread it to their neighbors,
thereby initiating a-widespread epidemic of pneumonic plague.
A change in women's fashions in Europe thus indirectly caused
an epidemic of pneumonic plague in Manchuria.
Porphyria, an affliction whi??.
red blood
cells, illustrates how modern innovations can result in new
forms of disease. This hereditary disorder, originated
with a Dutch women who. migrated, to South Africa in 1686.
As far as is known, the gene for porphyria has been transmitted
ever since to all her descendents; although these are now
numerous, the disease itself has become a problem only during
recent years. Under ordinary conditions, the porphyria gene
manifests itself only by the production of mild neurological
symptoms and minor skin blemishes usually overlooked. However,
violent reactions often culminating in. death are likely to
occur if porphyric person takes certain drugs such as sulfas
and barbiturates. The normally mild signs and symptoms or
the. genetic disorder are converted suddenty
into a severearid often fatal response by modern drug8 otherwise considered
life saving.
.While man's nature will remain fundamentally the. same
as it has been since Paleolithic times, the patterns of his
disease continue to change because his physiological responses
to changing environmental situations do not adapt him rapidly
enough to the new conditions. Change itself may constitute
a cause of disease. -Once man is adapted-to certain kinds of
food, weather, housing, microbes, and social habits, he
commonly finds it unpleasant . and traumatic to be uprooted
suddenly- and forced to live under new'conditions even though
these appear more favourable to outsiders. As Hippocrates," „
the father of modern biology and medicine, wrote 2,r~0 years
ago, "It is changes that are chiefly responsible for diseases,
especially the greatest changes., the violent alterations both
in seasons and other things”.
Man is trying to eliminate the unpleasant effects of
envir. rmental forces, by controlling them instead of making
the greater effort required to cope with them through his
own adaptive physiological responses. The environmental
control decreases the need for physiological adaptation.
Man finds it more convenient to air-condition his dwellings
than to adapt physiologically to heat or cold; wherever
possible, he tries to use mechanical devices instead of
depending on his muscles; he invents learning aids to decrease
mental effort; he takes drugs as substitutes for mental
discipline in resisting pain and overcoming fatigue.*
Man's control of environment has gone further than his
biological adaptabilities towards eliminating, many forms of
•
suffering; it has thus constituted one of,the-most influential
determinants of modern civilization. Yet, it is dangerous
error to believe that disease and suffering can be wiped out
altogether by raising still further the standards of living,
increasing our mastery of environment, and developing new
therapeutic procedures-. The less pleasant reality is that,
since the world is ever changing, each period and each type
of civilization will continue to have its burden of diseases
created, by the unavoidable failure of biological and social
adaptation to counter new environmental threats.
Environmental pollution illustrates how many of the
adjustments that facilitate life in a hostile environment
commonly express themselves later in disease and misery.
The inhabitants of industrial areas of northern Europe behave
as if they had made a successful adjustment to massive air
pollution. For more than a century they have functioned
effectively and successfully despite irritating substances
in the air they breathe. However, their adaptation is less
satisfactory than might be supposed. The lining of their
respiratory tracts registers the insult of air pollution.
The cumulative effects of years of constant exposure to
various pollutants have resulted in widespread chronic
bronchitis and other forms of irreversible respiratory
disease. Chronic respiratory disease is now the leading
dause of disability among adults in all the industrialized
parts of northern Europe and is becoming increasingly
prevalent in United States.
As in the.case of environmental pollution, apparently
successful adjustments to emotional stresses caused by
competitive behaviour and crowding can result in delayed
organic and mental disease or at least in behavorial disturbance
Through, the experience of social intercourse, man learns to
control the outward manifestations of his emotional responses.
He usually manages to conceal his impatience, irritations
and hostile feelings behind a mask of civil behaviour. Inwardly
however, he still responds to emotional stimuli by means of
-4-
physiological mechanisms inherited from Paleolithic ancestry
and from his animal past. The ancient fight and.flight
responses still operate in him, calling into play through
autonomic nervous system various hormonal mechanisms that
generate useless and potentially ..dangerous physiological
reactions.
The most disturbing aspect of human adaptation to
various situations is paradoxically that human beings are
so adaptable. They can become adjusted to conditions and
habits that will eventually destroy the values most characteris
tic of human life.
In the final analysis, not physical fitness to environ
mental conditions nor comfort of the body, nor even survival
of the human species, suffice to. encompass the richness of
man's nature. Medical problems posed by the environmental
stimuli and insults of modern civilization have acquired a
critical urgency; most technological and social changes now
achieve their full effects in very short time and affect
simultaneously all parts of the world and all economic classes.
Until recently, the rate of change was generally so slow
as to allow time to make proper conscious and unconscious
adjustments. Many.individuals suffered when conditions changed
for the worse but bulk of mankind slowly and almost unconsciously
adapted. The genetic endowment of population became progressively
altered; phenotypic modifications helped each person to
function in his particular niche, and especially most human.
beings slowly learned to achieve better fitness to their milieu
through technological and social innovations without entirely
sacrificing or jeopardizing the future. Now the rate of
change is so rapid that there may not be-time for orderly and
successful operation of these conscious and unconscious
adaptive processes. For the first time in the history of mankind,
the biological and social experiences of the father is almost
useless to his son.
- Excerpts from
'Man and His Environment'
by Rene Dubos
in Britannica Perspectives, Vol.1.
—-—-xxxxx--------
Cleaning up Third World Diseases
Disease is a part of the land scape-in the Third Word.
In Asia, Africa and South America, one person in ten is in
some way disabled. .-Most of the poor suffer diseases such
as acute diarrhoea and pneumonia during their lifetimes.
Because they are undernourished and therefore vulnerable,
many die of these diseases. During the 1960's and'70S
endemic diseases were tackled with pills, vaccines and
pesticides. Scientists now recognize that providing drugs
to cure diseases is no solution in countries where almost
everyone lacks basic resources like food, clean water and
sanitation. Some third world countries, too, are coming
round to the view that money spent on .glamorous drug programmes
could be better utilized on improving living conditions.
Since improving life-style costs money, concentration
on improvements that directly reflect on health - like water
supplies and saniteition, is necessary (around 80% of infections
in the third world are spread through water). Developed
countii.es have generally been able io eradicate infectious
disease through sanitat ion-rather than chemical remedies that
have been pumped into the third world.
Vaccinations, although effective in the ca.se of smallpox
and measles, are not very successful because; 1) it is
difficult and costly to set up distribution.systems,, especially
in rural areas; 2) some vaccines are too.Specific; 3) animal
host must also be treated. The failure of malaria compaign
in India and elsewhere has be’en' attributed to these causes.
'Water plays an important role, as a carrier of micro
organisms and as a breeding ground for vectors. Some water!
related infections could be eradicated solely by improving
community’s water supply. Other parabites could be eradicated
through provision of an adequate excreta disposal systems.
WHO’s goal is to provide safe water and sanitation to.
all by 1990. Its Director General, Dr. Halfdon fehler, said,
’T am utterly convinced that the number of taps per 1000 popula
tion will be an infinitely more meaningful indicator of
health than the number of hospital beds for 1000 population”.
With less money, careful well thought out action-needs
to be taken to improve health standards. It should be borne
in mind that improper methods of improving health standards
have serious side effects. Unless there is a .general availabilit
of clean water, unless there'is sanitation and hygeine education,
diseases will continue to spread and well-intentioned efforts
will cone to nothing.
(Summarized from the Economist,
Sept.10, 1983).
--------- xxxxxx----------
Tree Chopping releases Virus
Forest cleaning is causing a deadly virus that normally
infects monkeys and other small mammals to attack humans.
The latest outbreak of Kyasanur Forest Disease, better known
as monkey disease, came in January in the Western Ghat
mountains of Karnataka. So far it has affected more than
1000 people and killed 96.
The link between tree felling and the spread of the
disease stems from the virus's transmitters - 16 different
species of tick that live on a wide variety of mammals. As
clearing began in Nidlc State Forest last September, the animals
■■nd. their ticks migrated to nearby forests next to villages
in the Belthangadi area of South Kanara district.
-6-
The Indian National Institute of Virology says the
disease is there^lftt of clearing up 400 hectares of fnrer,t
to make way for cashew plantations. So ±ar, six villages
have been affected but there are fears that it could spread
to others in the area.
Most mammals are unaffected by the virus, but monkeys
fall severely ill and die. Humans experience high fever’
pains, headaches, blood vomitting and noSe bleeding. The
human mortality rate is over 10 percent. The • Institute
first noticed the virus in 1957 in the Kyasanur State Forest,
and so.gave it its name. However, locals call it ’monkey
disease1 because monkey deaths often proceed a' human epidemic.
In the last 27 years, the virus has spread to more
than 400 square kilometers of forest in four districts,
and the Institute suspects these earlier 'outbreaks were ■
.also the result of forest clearing.
(New Scientist 30 June, 1983)
—------xxxxx--------
Strange case of the Disappearance of Morning Sickness
The decision to end the manufacture of Debendox, the
best selling morning sickness pill, marks the end of one
of the more startling cases of a "boom" in a particular
illness tied to drug marketing.
Morning sickness usually begins in the first
months of pregnancy. In 1978, doctors in Britain were
dishing out as many prescriptions for morning sickness as
there were pregnancies. They gave a prescription, to
almost every pregnant woman who complained of morning
sickness. Half the prescriptions issued, during this
period were for Debendox. There were 400,000 prescriptions
for Debendox in 1978, and another 400,000 for other
morning sickness drugs, like Ancoloxin and Avomine, The
recipients were most of the 350,000 pregnant women suffering
from varying degrees of morning sickness who consulted
'their doctors. The British National Formulary, published
jointly by the British Medical Association and the
Pharmaceutical Society and distributed to all doctors
by the Department of Healthy states that nausea and
vomiting in the first three months of pregnancy does
not generally.need drug therapy. And yet three-quart er
of all prescriptions were handed out in the first three
months.
'M'errel, the manufacturer of Debendox, decided to
stop making it after losing a court case in the US
alleging that Debendox caused deformity in a new-born baby,.
Since then the number of women complaining cf morning
sickness has dropped; the number of consultations has
fallen by 35 percent since 1979- Patients, as well e.t:
doctors, have become aware of the danger of using,
and asking for, drug therapy during pregnancy.
(Nev/ Scientist, 30 June, 1983).
-------- xxxxx--------
h’TY HEALTH CELL
[First FloorjEc, Marks Road
BANGALORE-560 001
/» .'1<7J V«:
nfr°^rsy
' -X
[I^?t2^9zW;g
^^mS^SQggSS^SQSQQK
B^Sj^S^MaWiffi^EsKKSiSBIils^
;V<:i\ ;. '/<-'■ ;■ ■.
• ' ■ ;'^/dhud^'i^ <-'W' -R^
l<'i<^. V(^R-'.
-/’W^
(<» $M£’RVv' •’ fe- ■ •
■°Mn
The fourteen pecp/e w::.. died are fourteen
administration to whom these shady people
application submittedtothe Additional Sessions
people who are know.: There eouIJ be many
hive access. The one currently in the news con
Judge by his defence counsel.
who are not — Justice 3. Lendo who led the
cerns the complaint lodged by Mr.S.S.Kataria,
cnquininto foe deaths reported in Bombay's]]
a Delhi based pharmaceutical distributor to the
Hospital thorn /V fluid contamination in an
Drug Controller of India and die Drug Control
inrentewntm Aewstrecfc
ler, Delhi that some 30,000 bottles of contami
nated IV (intravenous) fluids were supplied to
As we were about to go to press it was learnt
that Mr. Jaggi has been released on bail. He
reportedly had to furnish a surilyofRs. 50,000.
~ he message contained in the
him by Oslers Pharma, a Coimbatore-based
verdict could not have been lost
on anyone familiar with the
firm. Its products were subsequendy alleged to
have figured in several deaths in Delhi at the
cell was
deadly events. The Issue had
time, leading to their withdrawal. The complaint
high-powered meeting Last April. The higher
——------i made headlr.es Ln February this
lodged on February 3 this year was taken note of
figures in the break- up that follows indicate the
;
1
The acute undetstaffing in the Drugs Control
brought sharply to the fore ata
yeaf-CSer seven people, including a doctor,
following the publication of a newspaper report
Tied in the Capital on being administered a
a. bain—observe the irony of it — life-saving
on the matter three days tier. A team of officials
lower the existing position Overall — 2689 :
from the office of die Drug Controller of Delhi
669; Delhi — 55 : 19; Karnataka — 105 : 36;
fluid.'And it's even now reportedly around, this
seized 12 samples on February 10 from the
Gujarat—317:65; Maharastra—477:81. (This
in these apparently harmless
godown which significantly, was left unsealed
was the position as on April 1 of this year). In
killer fluid ■
looking bottles which, we were warned, contai
ned not glucose, but death.
despite the distributor's entreaties.
.An even biggersurprise followed two months
number of drug inspectors required, and the
contrast the drug industry itself has rapidly
grown,the revenue recorded by it having shot
up from Rs. 10 crore in 1947 to the current Rs.
3000 crore. •
But let us now take a peek at the fluids’
constituents before resuming the history of the
The five questions
raised on the issue in
Parliament thus far
have failed to shake the
Drug Controller’s
office out of its
apparent slumber
controversy'drat has dogged it since the last few
months. The IV (intravenous) fluids are fre
quently resorted to in all hospitals and nursing
homes for meeting the basic nutritional require
ments of seriously ailing or injured patients, it is
essential in the treaunent of dehydration victims
when normal intake becomes difficult — such
as in accident cases, infections, nausea and
gastroenteritis. The elements intravenously
introduced into the body through the ad
ministering of IV fluids include glucose,
dextrose, normal saline, mannitol, and gastric
replacement fluids.
The malaise is intimately related to our low
later, in April, when the Drug Controller's Office
» .
essrs Osler Pharma Ltd., a
health priorities. Health being a state subject,
cleared the samples. The five questions raised
1'1
cooperative venture of 350
Coimbatore doctors, were quick to
the Centra! authorities totally wash their liands
on the issue in Parliament thus far have failed to
_
off the pharmaceutical licensing policies
shake the office out of its apparent slumber; and
deny Press reports blaming certain deaths on
followed in the states, which continue to
in his interview with Newstrack the Drug
subscribe to widely differing guidelines. Their
intravenous fluids (glucose) manufactured by
Controller of Delhi, by' stating that the presence
diem. Dr. S.G. Rajarathnam, the company's
non-observance alone unites them, and those
of fungas in bottles containing IV fluids need
chairman and a medical practitioner, sated that
such as .Maharashtra follow them not at alLThe
not be all due to the manulacturers' negligence,
die drug controller of Tamil Nadu who had
drugcontrollers in many of these states function
had strangely given the impression of being
visited the factory premises on February 10 had
more as beaurocratic scarecrows than as effec
merely an uninterested passerby.
not given any adverse comments so tar. The
tive counters to these latest merchants of death.
That may not so easily be accomplished now
chairman pointed out that die pharmaceutical.
The recent Lemin Commission report which
with the arrest by the CBI of Mr PKJaggi, a drug
company was floated by about 350 doctors from
enquired into the IV fluid deaths in Bombay'sJJ
inspector in the Drugs Control Department,
Coimbatore and Kerala for meeting their own
hospital had exposed die dubious role played
who is alleged to have 'shielded' Oslers Pharma
requirements. The 50,000 bottles of intravenous
by the Maharashtra government in the tragic
episode equally at die officialjministerial levels.
lid, the suppliers of the contaminated bottles to
fluids manufactured by them were tested over a
Mr Kataria. Several senior drug officials are
period of nine days prior io their marketing, he
What now reportedly is unfolding is a sordid
reportedly still to be traced by the CBI. MrJaggi
claimed.
tale of gross corruption and apathy involving
has meanwhile been remanded in judicial
Mr. O.V. Subramaniam, the firm's fulltime
the erring firms and diose in die drug control
custody following the rejection of the bail
director, said iis products were marketed chiefly
28 neiwoSS a rxc w
in Kerala and Tamil Nadu. Mr Kataria of Eskay
except one, had been given a dextrose solution
The IV fluid bottles manufactured by the
Pharmaceuticals, New Delhi, had sought and
Government - owned Hindustan Antibiotics
was given dealership for the Delhi region. In
manufactured by the Faridabad-based Dhavsons
Pharmaceuticals. The exception was Shanti (50)
August 1988 Mr. Kataria, who is also a share
from Sekhpur Khurza who died within a half
last month-end after Bhopal's Hamidia hospital
holder, sent feelers, according to him, sug '
hour ofbeinggiven ringer lactate manufactured
reported observing 'black spots’ and fungal
gating he be made the company's 'vice-chair
by Prem Pharmaceuticals.
Shanti was admitted to the hospital's ward B
growth in some of them. Two persons who
man', marketing, with a fat takehome packet.
This, he said, the board rejected. 'He then
on September 3 with a superficial stab injury in
rigors, one of
indented for one lakh bottles more and sold
the chest. She developed violent rigors and
enteritis, died the same evening. The hospital
only70,000 - says this version —.and procured
swelling immediately on being administered
authorities said it was not possible to ascribe
a dubious test'repon from a private laboratory
the ringer lactate of batch 89532C. The second
the death to the administering of contaminated
on the unsold 30,000. These reportedly carried
case related to 22-year oldTMbhammed Izhar
no paniculars, batch numbers, the dates ol
who died on September 3 after being put on a 5
saline in the absence of a post mortem, none
theless, the state government had felt im
manufacture and expiry’ etc.
per cent dextrose solution of batch no. 318059.
mediately obliged to order an inquiry in the
Izhar registered in the hospital under No.
matter and the hospital to freeze the HAL stocks
207938 and was a patient of abdominal perito
in its possession. Significantly the fluids were
nitis. Izhar too reportedly started shivering, his
manufactured by the HAL using the imported
face swelling up abnormally on being injected
CORE technology and supposed
with 200 ccs. ofthe fluid The twodeaths were im-
the highest standard so far available in the
The tests carried out by Central India
Pharmacopeia,' Ghaziabad, had earlier declared
the 'seized' samples as being 'of standard
quality'. An agitated and disturbed Mr Kataria in
Delhi alleged that "the drug controller and his
Limited also came in for widespread criticism
were administered their contents developed
whom, a patient of gastro
to
be of
department, as also the government analyst,
were pressured by Oslers Pharma to manipulate
the analysis report and give a clean chit to the
erring company" The tardily conducted tests
on the samples, which normally take only a few
seconds to complete suggested, Mr Kataria said,
Gnat 'politicial pressure' was exerted by the
Oslers to formally obtain a clean chit.
Then, in September, a bottle of a life saving
intravenous drug, Mannitol, which was alxrut to
be administered to a patient at die All India
Institute ofMedical Sciences (Al IMS) was found
In all, eight adverse '
reactions stemming
from the use of
contaminated IV fluids
were reported early last
month
to be contaminated with fungus. The AIIMS
Resident Doctors Association said that an
identical incident had been reported some
months before. In May a doctor in the medical
department had found a bottle of saline
produced by Tablets (India) Limited, to be
contaminated widi fungus.The association
subsequently demanded tiiat die company be
blacklisted and no bottles of the batch no 9RB
767,(manufacturing date June'89, expiry date
May’93 and manufacturing licence No-4) be
issued. Tne association warned that failing such
measures the residents would boycott the
company and ask their patients to bring with
them their own bottles.
medately linked to the fluid as it was the only
drug that had been administered. "We can’t be
country
Storage lapses need to be seriously looked
one hundred per cent sure in the other five
into. According to ALtm'ndi/es Extra Pharrm-
cases, but the circumstantial etidence certainly
cope-J. a pharmaceutical guidebook famed for
points to it. They were quite all right till the
its accurate information. .Anhydrous Glucose
moment the fluid was injected and they all had
exactly the same symptoms," -the'doctors
(BAN) needs to be stored in airtight containers.
added
In all, eight adverse reactions stemming from
be stored at 2° to 25' and must be carefully
the use of contaminated A' fluids were reported
The instructionsfone is informed, are seldom, if
Glucose solutions for intravenous use should
examined for the presence of foreign bodies.
Two people recently died on being injected
early last month. Hie hospital authorities took
ever closely followed — not even, according to
with contaminated intravenous fluids in
official notice of four of these although doctors
experts in the field, in some of our reputed
Safdarjung hospital. Five others developed
had earlier, around September-end, been told
hospitals. Dextrose being a sugar-based
severe complications during the same pedal
to discard the faulty batch. Another mishap was
solution, even very tiny cracks suffered by the
after they were administered die fluids. All
averted when doctors at Safdtrjung hospital
bottles during transportation can result in the
seven of them betrayed identical symptoms —
violent shivering, swelling of (he lace and
seized on October 12 a bottle containing
development of fungus. The guidelines laid
contaminated A' fluid. The bottle of normal
down it) this regard, reportedly, continue to be
sometimes acute respiratory problems — from
administering of die fluid, doctors said. All,
saline base bore once more the label of
flouted.
Dhavsons Pharmaceuticals.
-RAJEEVP.I.
WITH BRAJENDRA SINGH
orc sv o
n
iUHAT Allis C MJLMO
own use since 1977 till production was
tests on IV fluids in the past couple ofyears.
(f) the hospital used to manufacture its own
I i||irjbottles. This is a very hazardous
abruptly brought to a halt in 1981.
It is learnt that (a) the daily consumption
practice. IVfluid bottles have a natural inner
of IV fluid in the hospital averages about
relating to IV fluid contamination were
coating which ensures the fluid's separation
3.000 bottles (b) the purchases are effected
heard at the time The hospital stall has the
from the glass walls. Before the boules are
through annual tenders, cleared by a pur
facilities to manufacture IV fluids in
reused they are sterilised once more in the
chasing committee headed by the Medical
Superintendent, (c) ’the hospital's tender
quantities sufficient enough for its own
regulations have built in clauses seeking to
Al IMS costs could be cut down by 30 to 3p%
i v-. equities reveal trott a good number of
• L j [V fluid manufacturers reuse empty
autoclave causing this coating of natural
chemicals to peel off. The fluid, as a result,
suffers silica contamination.
need'. According to experts within the
ensure the quality of the drugs purchased.
if the fluids were not to be procured from
The sets used for administering IV fluids
Sources reveal, however, that these regu
private firms ' During talks with MIMS
produced by small units, have aroused
lations are not always observed. To cite just
officials, the following points were raised:
doctors' apprehensi t>ns regarding the manu
one instance, tender regulations do not
■ The autoclave used for IV fluid manu
facturers' claim that they are sterilised. These
allow a new unit to bid and the purchase
facture has been in disrepair for years. Ml
sets are packed in thin, unreliable plastic
committee can reject any-tender without
dungs considered the MIMS has no reason
bags vulnerable to punctures.
assigning reasons. It is said that even these
to continue buying IV fluids from private
Mos such hazards could be eliminated if
two clauses are being used arbitrarily to
manufacturers, tn public interest. If this
hospitals developed captive IV fluid plants.
cannot be done immediately, the least it can
This applies, in particular, to medium and
victimise suppliers who do not curry the
committee's favour, (d) despite numerous
large-sized public hospitals where their
complaints regarding the quality of IV fluids
remove such loopholes from them as are
daily consumption runs daily into hundreds
and the recent reported deaths in the hos
likely to promote corrupt practises. The
of bottles.
pitals on their account the hospital au
Defence hospitals usually send the.ir own
thorities have shown no inclination as yet to
quality control officers to the IV fluid
The casualties reported in the A1LMS from
do is to review its tender regulations and
FV fluid contamination have given consi
initiate any action against the erring firms.
suppliers' premises to ensure the fluids
derable fillip to this demand. The hospital
All the MIMS is known to do is to remove
quality at the time of delivery. It should not
enjoys the status of being the premier
the offending bottles, or at most have the
be difficult for an institution like the MIMS
institution for medical sciences in the
to evolve a system of quality control on
country and possesses the basic facilities
Drug Controller’s office take the bottles
away for analysis, (e) the MIMS Inspection
required for tile manufacture of IVfluids. It
Control Unit, although well equipped, is
had. in fact, been manufacturing these for its
understood to have conducted hardly any
MUKDEROUS LACUNAE
Dr. Mira Shiva, winner of the first international Olle
Hansson award for her outstanding
contribution in the field of health
activism, exposes some of the
disturbing half-truths spawned by
the IV fluids controversy in this
interview with RAJEEV P.l.
The Drug Controller of Delhi recently
told Newstrack that if the government
analyst found the samples safe there
wasn’t very much more to he done in the
matter. How did that strike you?
Well if he was talking on the basis of those
reportedly based, without bothering to look at
the rest ofthe stocks, and this with the hospitals
B MC 89
similar lines.
cause death.
Ml right, then what did all those people die
of? The clinical reports dearly say that death
followed shortly after the IV fluids were
administered... and so many others reacted to
the fluids When you put all that together, it
becomes clear that these were not isolated
incidents — just consider the number of
hospitals who have relumed the stocks and
blacklisted their suppliers. One would further
■ like to know why, if these were not unnatural
continuing to chum out adverse reports, such a
deaths, the doctors in these hospitals were so
highly
perturbed? So, obviously, those deaths had
irresponsible. But to say that 50 per cent of the
some connection with the IV fluids that were
stocks would have to be found substandard
administered. 'Hie deaths need not, though,
Ivefore he, as the Drug Controller, could have.
have been due to fungal contamination alone,
them withdrawn —that most certainly was the
there
limit.
contaminants: bacterial or viral or chemical in
remark
comes
across
as
being
eleven samples on which the analysis was
. 30
IV fluids from 1977 to 1981. No complaints
might
well
have
been
other
the fluids.
The Drug Controller had further
observed that fungus-hit TVfluids couldn't
So how does one sort out this mess?
.Its a nationwide malaise and much more
serious than some people would have you
imagine. The manufacture of IV fluids requires
technology
much
compared
with
less
that
complicated
as
in
the
required
POINTS TO FONDER
manufacture of most other drugs and injectable
vaccines. Fungal contamination on such a large
scale as reported in IV fluids is unpardonable.
Keeping a check on the latter is comparatively
much easier as the fungus on be spotted with
the naked eye and the side effects are both
more immediate in their occurrence and easier
to report. This is indicated by the experience of
several hospitals. When a gross thing like
fungus escapes the notice of the people who
handle the fluids at vinous levels — stockists,'
pharmacists, nurses, doctors etc., — it means
the responsibility must needs be shared by
them all. Including the fluids' manufacturers
and distributors. It also speaks volumes on the
sort of drug control system we have and its total
failure in ensuring quality control and the
immediate withdrawal'of substandard stuff
These lacunae were equally obvious when the.
AIDS sero positive Anti D Vaccine and other
blood products continued to be used long after
AIDS sero positiveness had been recognized,
Mr H.D. Shourle, a retired ICS officer
0 The Central and state authorities should
and former Director-General of the Indian
Institute of Foreign Trade, has filed a
re-examine the licences issued to manu
facturers of IV fluids, survey facilities and
petition before the National Consumers
equipment in the licensed units, and cancel
Disputes Redressal Commission urging it to
look into the IV fluids controversy. The'
the licences of those failing to measure up
to the standards laid down with regard to
petition was filed on behalf of Common
their safety. These need to be very stringent
and should under no circumstances be
Cause, a voluntary organisation ofwhich Mr
Shourie is director. Subsequently, on
relaxed regardless of whether the unit
October 20, the Supreme Court asked the
concerned is big or small.
Drug Controller of India and drug control
lers in the states to inform it about the steps
being uaken by their respective offices to
arrest the inflow of spurious IV fluids in the
adhered to while licensing new units.
0 The particulars relating to the licences
them to depatch their replies. The following
issued should always be available 2t the
are some of the important points raised in
the petition:
0 In the Delhi Doordarshan newscast on
October 3 and in Newstrack's presentation
of this problem, the Drug Controller of
Delhi had stated that die fungal develop
up of these patients.
ment appeared to be linked to its transport
They both deserve equal attention The
for the manufacturers should be strictly
market A month’s time has been given to
albeit lairfy late. There is practically no follow
Wirch isthe more striking in yourview
— the negligence of the hospital staff or
the apathetic response to the all round
concern over these reported quality
lapses’
0 Theguidelines and conditions laid down
offices of the drug controllers in the states
and Union Territories, and in the office of
the Drug Controller of India. The latter
should arrange for periodic inspection of
the licensed units by the licencing au
thorities concerned.
and storage, and that the contamination
0 The possibility of contamination during
manufacture should be studied in detail.
need not necessarily be harmful if
These studies should include inter alia the
administered intravenously. This opinion
safety requirements.
was subsequently contradicted by doctors
o Die suppliers of IV fluids need to be
who maintain that IV fluids contamination
thoroughly screened.
can cause serious complications, convul
9 Die Drug Controller of the Government
sions and even death.
of India and the drug controllers of the
0 It is understood that the latter are often
states and Union Territories need to be held
manufacturers' apathy is for all to see, not
not reported by the doctors and nurses
personally responsible for anything going
merely in the present case but in most other
concerned out of fear for themselves, and to
wrong in the manufacture and supply of IV
areas of drug manufacture as well. However, in
protect the reputation ofthe institutions that
fluids to the hospitals. Representatives of
the issue here under scrutiny, I think the
employ them. There have been reports that
consumer organisations should, wherever
hospitals have displayed a matching disregard
attempts were made in Delhi's Safdarjang
in the observance of basic precautions like
hospital to tamper with the history sheets of
possible, be associated with the prescription
and observance of the guidelines relating to
checking of expiry dates and looking for
some of those who were administered
the manufacture, stocking and purchase of
suspended particles in the boules. These
contaminated IV fluids.
the fluids.
obvious reasons. It is only when some
There are a great many people who could be
responsibility of the respective drug controllers
responsible public spirited individual decides
blamed, but it's the manufacturers and the drug
posted there, there remains no control
to take up the issue that the truth gets to be
known. This happened last year too during the
control authorities who must chiefly be held
whatsoever on what happens after the drug is
responsible in cases such as these. Further, one
transported elsewhere. Diis lias particularly
cholera epidemic.
thing has become very. very clear, especially
frighteningimplications for suites such as Bihar.
after the Lemin Commission report on the .[I
MP etc., where the drug control mechanism is
Hiispit.il deaths from contaminated glycerol
so
Drag manufacture in the suites being the
manufacturing norms .ire often net followed.
together might have helped save several lives.
Moreover, quite often deaths from IV fluid
infections are blamed on other factors, for very-
But on whom ultimately does the onus
lief.
abysmally
weak
that
even
basic
c. ('fogthe.
ontr-..-stategovernments
drug manufacture and distribution?
something very wrong with the purchasing
d;■<■<:'■. help. Uitiess the drugadministration at
the c;r.tre is made to ensure drug safety
praj ices. followed by these government
This is one area in which 1 would say the
institutions -- such as going in for the lowest
measures in the states things are not going to
improve at ail. The trouble, you see, is that in
government
lias
shown
seriousness,
it's
shameful.
states like Bihar the budget allocated for dnig
organisations and groups have been at pains to
substandard drugs were allowed to be
control activity in the overall health package is
emphasise that so longasyou don’t regulate the
purchased. What is required is an efficient
so inadequate that ’hey are unable to ensure
dnig flow all sons of people (.even those who
mechanism which will test drug samples for
even baste safeguards through the setting up
absolutely
no
Numerous
tenders regardless of the product's quality
There
have
been
cases
when
known
have no intention of following the GMP) are
their safety, especially in our government
quality control ids, and recruitment of
likely to venture into the business. There is
hospitals and health centres.
efficiently monitored dnig inspectors. The
absolutely no way that dnig safety cart be
result is that when such an issue surfaces there
ensured by the existing overloaded, inadequate
is a general tendency to pass on the buck.
drug control mechanism. On account of the
Unless the Health Ministry decides to become
abundance of trash on sale here, doctors often
more responsible, rather than just shift blame
are unable to decide on the drugs they can
onto others. incidents iike these cannot be
safely prescribe and those they can't And to top
It still strikes one as odd that the
majority of IV fluid-related deaths should
have been reported from government
hospitals rather than private institutions.
It can't all be coincidence...
checked. 1: is our system that at various levels
needs to be streamlined. It's indeed a shame
N'u it can't. You see there is no system in
that it should have been Delhi, with its
the.w places to monitor adverse drug reactions |
somewhat better faculties, to first report deaths
As a result m the case of all these who die of
Bom the administenng of IV fluids. A gross
Iatrogenesis (drug & doctor induced death)
none e\ er gets to know the cause of death.
Any comments on
Commission report...
the
Lemin
How efficient are the death review
committees in our hospitals, and do all
hospitals have them?
It is very important. this being the first time in
the country's history that a commission was set
Mt>st hospitals are expected to have them
up to conduct an in depth prolx.- into dnig
though I'm not informed on their functioning.
related deaths. The repun, thorough and
But then, as we ail by now know, the IV deaths
unbiased, had implicated several people and
came to light because some juntor doctors in
urged the importance of strengthening our
the Al IMS and Safdarjung hospital raised the
drug control set up. Its message was that one
issue,
couldn't-rely on private drug testing labs and it
committees or postmortems. It is also a fact that
and
not
th- ..gh
death
review
exposed the politician bureaucrat nexus in (he
most deaths of this nature are reported simply
process Among other peninent questions
as "cardio respiratory arrests", because that way
raised by it was the one concerning the lives lost
they are able to safely cover up the incident
through the administering of substandard
Starvation deaths for instance. It isn’t written on
drugs. Do die victims' families ever get any
the victim's forehead that he'or she died of
compensation? In the case of the Bombay
starvation.
deaths, the government had ordered Rs. 10,000
resistance to break down making it vulnerable
to be paid to each of chcm.Did anyone check if
tiie amount actually reached those for whom it
was intended? And what about those who
sun ive after being administered spurious drugs
but whose lifespan is shortened all the same —
do they get any compensation? And yet,when
such things continue to occur, one can't help
but conclude that the present drug control
system in die country is inherently, gravely
defective — that if the Industry Ministry
continues to be the architect of the nation's
drug policy, our people's health is Ixiund to be
marginalised
OTiat would you say has been the
Indian government's role in the matter of
32 NTfV/OW a D£C 89
it all licences are being distributed without as
('■-•■k-’s
bu>>mfon
to a host of ailments,’sometimes even trivial
much as considering what is being produced or
infections which, in the normal course, he
how. When life-saving drugs like IV fluids start
would have survived. But here too they almost
doing the opposite...
never tell you what precisely the victim died of
Hfi.it are the immediate steps in th*
case of IV fluid deaths that you would
have the parties concerned foilowl
happened in Rajasthan during 'he drought mH
— diarrhoea, pneumonia or whatever .... It
in Kalahandi in Orissa. Drag reactions from IV
lluids are ■ unlike those induced by, say,
penicillin,
They could probably set up an inquiry
as the
former
require close
monitoring — but then who should be
commission to go into the issue — but then
interested in monitoring it? I should think no
whoever knows how long they will be at it or
what will ultimately come out of the exercise.
doctor or nurse would be particularly keen on
Most deatlis having been reported from
government hospitals, there is a feeling there's
reporting their own negligence.
<0-------
health cell
«7/1,(First Floor)St. Marks Koao
BAWG/alqse - ofiQ 001
THE UNCOMMON COLD
By Our Medical Correspondent
HAT EXACTLY is the common cold?
And how has it come to be so named?
As Sir Christopher Andrewes puts it, “That it is
common admits of no dispute. But why cold?
Is it because we feel chilly when we have a cold,
or because chilling brings it on (or is supposed
to), or because the infection is commoner during
the cold time of the year? Perhaps all three ideas
play a part in conveying the image
W
42
Modern medical texts however refuse to call
it tlie ‘common cold’—they prefer to shroud the
ailment under more impressive terms like ‘acute
rhinitis’ and ‘the coryzal syndrome’. But for
our purpose, Andrewes’ definition will be more
than adequate: “The common cold is one of a
number of virus infections which affect, often
repeatedly, the lining of the nose and other
passages leading to the lungs.”
Imprint, December 1978
WINTER OF ’44
they expecting the boy?” she asked. “Yes,” he
said looking at me again. “But they said he
would be arriving tomorrow.”
“They’d forgotten the date,” said Grand
mother in a huff. “Anyway, you can unpack
and have a wash and change your clothes.”
Turning to the servant, she asked, “Is there
any lunch?”
“I will make lunch,” he said. He was staring
at me again, and I felt uneasy with his eyes on
me. He was tall and swarthy, with oily, jet-black
hair and a thick moustache. A heavy scar ran
down his left cheek, giving him a rather sinister
appearance. He wore a torn shirt and dirty
pyjamas. His broad heavy feet were wet. They
left marks on the uncarpeted floor.
A baby was crying in the next room, and
presently a woman (who turned out to be the
cook’s wife) appeared in the doorway, jogging
the child in her arms.
“They’ve left the baby behind, too,” said
grandmother, becoming more and more irate.
“He is your young brother. Only six months
old.” I hadn’t been told anything about a young
brother. The discovery that I had one came as
something of a shock. I wasn’t prepared for a
baby brother, least of all a baby half-brother. I
examined the child without much enthusiasm.
He looked healthy .enough and he cried with
gusto.
“He’s a beautiful baby,” said grandmother.
“Well, I’ve got work to do. The servants will
look after you. You can come and see me in a
day or two. You’ve grown since I last saw you.
And you’re getting pimples.”
This reference to my appearance did not dis
please me as Grandmother never indulged in
praise. For her to have observed my pimples
indicated that she was fond of me.
The tonga-driver was waiting for her. “I
suppose I’ll have to use the same tonga,” she
said. “Whenever I need a tonga, they disappear,
except for the ones with white ponies. .. When
your mother gets back, tell her I want to see
her. Shikar, indeed. An infant to look after, and
they’ve gone shooting.”
Grandmother settled herself in the tonga,
nodded in response to the cook’s salaam, and
took a tight grip of the armrests of her seat.
The driver flourished his whip and the pony set
off at the same listless, unhurried trot, while
my grandmother, feeling quite -certain that she
was going to be hurtled to her doom by a wild
white pony, set her teeth and clung tenaciously
Imprint, December 1978
to the tonga-seat. I was sorry to see her go.
*
#
*
Y MOTHER and stepfather returned in
the evening from their hunting-trip with
a pheasant which was duly handed over to the
cook, whose name was Mangal Singh. My
mother gave me a perfunctory kiss. I, think she
was pleased to see me, but I was accustomed to
a more intimate caress from my father, and the
strange reception I had received made me realise
the extent of my loss. Boarding-school life had
been routine. Going home was something that I
had always looked forward to. But going home
had meant my father, and now he had vanished
and I was left quite desolate.
I suppose if one is present when a loved one
dies, or sees him dead and laid out and later
buried, one is convinced of the finality of the
thing and finds it easier to adapt to the changed
circumstances. But when you hear of a death, a
father’s death, and have only the faintest idea
of the manner of his dying, it is rather a lot for
the imagination to cope with-especially when
the imagination is a small boy’s. There being
no tangible evidence of my father’s death, it
was, for me, not a death but a vanishing. And
although this enabled me to remember him as a
living, smiling, breathing person, it meant that
I was not wholly reconciled to his death, and
subconsciously expected him to turn up (as he
often did, when I most needed him) and deliver
me from an unpleasant situation.
My stepfather barely noticed me. The first
thing he did on coming into the house was to
pour himself a whisky and soda. My mother,
after inspecting the baby, did likewise. I was
left to unpack and settle in my room.
I was fortunate in having my own room. I
was as desirous of my own privacy as much as
my mother and stepfather were desirous of
theirs. My stepfather was ready to put up with
me provided I did not get in the way. And, in a
different way, I was ready to put up with him,
provided he left me alone. I was even willing
that my mother should leave me alone.
There was a big window to my room, and I
opened it to the evening breeze, and gazed out
on the garden, a rather unkempt place where
marigolds and a sort of wild blue everlasting
grew rampant among the lichi trees.
Lichi trees! As long as there were trees to
climb and lichis to eat, I felt I could cope with
life.
THE END
M
41
THE UNCOMMON COLD
Any honest doctor will tell you that for all the misery that it inflicts on you, there is really nothing
like a remedy for the common cold. But built around this common cold is a multi-million dollar drug
industry which offers a colourful range of syrups, capsules, tablets and rubs backed up by an advertis
ing campaign that makes them irresistible for the man with a running nose. Our Correspondent ana
lyses these drugs and shows how the drug industry takes the common man for a ride.
Cold Causes
OW IS the common cold caused? First, the
viruses responsible have to gain an entry
into the upper parts' of the respiratory tract,
and they usually do so through the nose, trans'tted from another infected person. Viruses
fascinating creatures; each is just a bit of
nucleic acid wrapped in a protein coat, so tiny
that electron microscopes, which magnify some
hundreds of thousands of times, are required to
see them clearly. Disease-causing viruses each
have a specific organ or ‘target tissue’ which
they attack. With ‘rhinoviruses’ (from the Greek,
‘rhino’ meaning ‘nose’), the target tissue is the
mucous membrane of the upper respiratory
H
f
Imprint, December 1978
tract. As soon as the rhinovirus invades the
membrane, penetrating into its cells, it sets into
motion a number of changes that ultimately
culminate in a full-blown common cold.
The virus makes a beeline for the nucleus of
the mucus-producing cell, and virtually
‘captures’ the DNA (Deoxyribose nucleic acid)
molecule that makes it tick. Normally the DNA
directs the metabolism and functioning of the
cell, but the virus stops all that, and instead,
forces it to turn out exact replicas of itself. The
virus thus reproduces itself at the expense of
the cell: the cell ultimately dies and hundreds
of viruses are liberated. These again attack other
cells, and the cycle is repeated.
As a result of viral invasion, the blood supply
43
THE UNCOMMON COLD
to the parts concerned increases tremendously
and the mucous membrane begins to swell. This
is responsible for the first symptom—a stuffiness
or tightness in the nose. Those cells of the mem
brane not affected by the virus produce more
and more mucus because of the increased blood
supply. The death of virus-affected cells and
their rupture releases still more mucus. There
fore, there occurs a discharge—a running of tire
nose—which is initially thin and watery. Soon, as
the dead cells are shed off, the secretions become
more viscous, straining the propelling capacity
of the cilia. Therefore, they tend to accumulate,
giving rise to that ‘blocked’ sensation in the
nose. Further down the respiratory tract, the
accumulation irritates the mucous membrane,
eliciting a reflex called the ‘cough reflex’ which
permits a forceful expulsion of the secretions.
Simultaneously, there is a huskiness of the voice,
a feeling of weakness, a chilling sensation and
rarely, a slight fever.
this, where large funds are essential for the
gigantic scale on which advertising and marketing
campaigns are conducted, multinationals are
doing a roaring trade. The two hundreds or so
rhinoviruses may be the bane of millions all over
the world, but to pharmaceutical companies
exploiting this ‘insignificant’ ailment, they are
an endless bonanza of cold, hard cash. Not only
has a multimillion dollar industry mushroomed
around the common cold, but it is even said
that some firms exist more or less solely because
of their ‘cold’ products!
The ‘cold’ industry initially found it difficult
to get a toehold in India becuase of the impreg
nable position held by “grandmother’s reme
dies”. With time however, the trend is changing
and today, the average Indian is slowly but surd^
approaching his American counterpart who po^r
in a pill for everything ranging from boredom
to Bornholm disease.
Endless Market
N A RANDOM survey conducted among
Cold Is Big Business!
some Bombay stores, this writer discovered
to his surprise that the average druggist sold
ITH any ailment, the pharmaceutical
about Rs.800 worth of just a handful of the
industry has always had a penchant for
most popular cold remedies in a month. Consi
churning out ‘remedies’ in inverse proportion
dering that Bombay has more than a thousand
to the actual number of effective or curative
drugstores, this means that Bombayman spends
drugs available. The gimmicks employed are
at least half to three fourths of a million rupees
many and varied, ranging from the ridiculously
a month on the common cold!
simple to the cunningly devious-juggling with
Pharmaceutical sources estimate that the
a few standard drugs, altering the dosage of one,
Indian cold market, as of now, is worth anything
adding some harmless ingredient here, putting
from five to 10 crore rupees a year-closer to 10
in an ‘attractive’ colour or flavour there, chang if analgesics proper are included, and closer to
ing the shape, the size, the colour of the con five if these are excluded. A large chunk of the .
tainer and the packaging, and so on and so . market—between three and four crores-belones
forth. . . . The sky’s the limit as far as pharma to the ‘cold tablet’ range of products. The
ceutical legerdemain is concerned. Actually, if market—ointments, balms, etc—accounts tor
brand names alone were to be eliminated, our
nearly an equal fraction.
pharmocoepias would shrink to unrecognisable,
How has this market evolved? How are
slender versions of their present tome-like selves!
people manipulated into buying larger and larger
Now, with the.common cold, the pharma quantities of cold remedies?
ceutical industry began with three distinct
Says a media source, “Years ago, before the
advantages—one, the universal nature of the
‘cold’ concept came into the picture, consumers
illness, two, the failure of medical science to
were sold on the ‘analgesic’ treatment of the
come up with any specific drug so far, and three,
common cold. Then, the pharmaceutical indus
the resulting willingness of the victims to try
try decided to devise its treatment along three
‘anything’ to get some sort of relief, however
or four different lines, according to the different
transient or imaginary. No wonder it has spawn stages of the common cold. For stage one, where
ed such an infinite range of tablets, capsules,
all one had was a mild sore throat, ‘drops’ and
drops, lozenges, syrups, ointments and what‘lozenges’ were promoted. For stage two, where
a stuffy nose had to be treated, ‘rubs’ were
have-you!. .
It is also no surprise that in an industry like promoted. It was after stage two, for a ‘full-
I
W
44
Imprint, December 1978
THE UNCOMMON COLD
fledged’ cold, that ‘cold tablets’ came to be
advertised. In fact, the concept of the cold
tablet is not even a decade old in India. Stage
four, of course, is when the infection goes much
beyond a cold and an antibiotic becomes
necessary.
“Promoters of ‘cold remedies’ have been
unwittingly helped by doctors. After all, who
wants to go to a doctor for a ‘mere’ cold? Think
. of the waiting, the cost involved when all one
has to do is pop in a pill or rub something sooth
ing on oneself, or better still, get someone you
love to rub it on you? These feelings have been
assiduously farmed by an efficiently-organised
advertisement campaign.
“Vicks manufacturers were, I believe, the
ACrst to set into motion a campaign of this sort.
^R'hey started a series of ads for the promotion
of two categories of products—one of lozenges
and drops and another of ‘rubs’. For the first
category, they had a series of ads depicting
various professionals—singers, actors, politicians
—suddenly developing a hoarse voice in the
midst of their work. . . . and a helpful guy would
give them Vicks drops and presto! they would
be instantly cured.
“As for the ‘rubs’ products, the personal
factor has always been stressed in advertising
media. For instance, the Vicks Vaporub ad
shows those kids getting wet in the rains, their
mother rubbing in Vicks-and they’re hale and
hearty the next morning!
“In recent years, some of the bigger compa
nies have decided to shift the emphasis from the
urban to rural centres. They’ve realised that the
urban market is getting saturated with products,
while the rural market is still largely untapped.
cities like Bombay, competition is fierce and
advertising is expensive. Therefore they’re con
ducting ad campaigns in less urbanised areas—
showing popular films, with their own ads in
between, and with an accompanying trailer
containing their products. Such mobile cam
paigns have proved very effective in the rural
market.
“The latest trend in advertising is to get the
consumer to associate a certain product with a
certain kind of person. For instance, the Vicks
Action 500 ad shows an ‘executive’ complete
with attache case, suit, foreign car, sumptuous
office, secretary, etc. This kind of ‘status-symbolisation’ of a cold remedy was never attempted
before.”
The advertising outlay on cold remedies is
Imprint, December 1978
Days of isolation
The course of a typical cold showing (shaded) occur
rence of symptoms on different days after inoculation
(arrow), number of handkerchiefs used, and presence
(black square) or absence (white square) of virus in
specimen tested.
estimated to be over two crore rupees, annually.
At present, nearly three fourths, that is about
one and a half crore is expended for the promo
tion of ‘rubs’—Vicks Vaporub apparently with a
lion’s share of about one crore rupees. A ‘mere’
half crore rupees is spent on promoting cold
tablets. “But,” says a pharmaceutical source,
“the scope for tablets is gradually increasing,
with a consequent shrinkage of the ‘rubs’
market.”
Pharmaceutical companies follow a more or
less standard procedure when they decide to
market a cold ‘remedy’. First, it is sold as an
"Ethical’ medication, that is, on doctor’s pres
cription only. Corps of medical representatives
(and multinationals have particularly well-orga
nised and huge ones) ‘sell’ the product to general
practitioners and the like. How this ‘selling’ is
accomplished need not bother us here. After a
few years, the product gets established in the
patients’ minds. Or the introduction of new
products by their own firms, or other firms,
shortens the ‘Ethical’ life-span. After this, the
product is withdrawn from the ethical list and
sold as an “Over-The-Counter”. (OTC) medica
tion. Simultaneously, a massive ad campaign is
launched to establish the product on a firm
footing. The product’s subsequent fate is also
largely determined by the advertising media.
O
The Cold Pharmacopoeia
VER the years, ‘remedies’ for colds have
gone through a number of stages. First,
45
THE UNCOMMON COLD
antihistamines were claimed as a panacea but
were later proved to be useless. After this a
group of chemicals called biflavonoids (collec
tively termed Vitamin P) came to be advocated,
and similarly passed into limbo, when their true
worth was discovered. Later still, tire ‘shotgun’
approach-using multiple ingredients-was ini
tiated by an ingenious pharmaceutical industry
out to make a quick buck from tire common
cold.
As for analgesics, tire ‘traditional’ remedy
for headache and colds, the chart carried with
the article lists some of the vast range of brands,
each generically more or less the same, but with
differing prices. (One single drug-Analginalone has 90 different brands!) Another dis
concerting fact is the addition of phenacetin
(known to have certain toxic effects on the
blood and kidneys after prolonged use in high
doses), and caffeine (in too low doses to be of
any use)
Incidentally, a recent study carried out by
the Abraham Lincoln School of Medicine, Uni
versity of Illinois, pointed out that aspirin does
nothing to reduce infection or illness from
dolds. On the other hand, aspirin relieves the dis
comfort of colds and allows persons who would
have otherwise stayed at home, to go to work.
Thus aspirin treatment indirectly increases ‘virus
shedding’ by the patient, making him a greater
epidemiological hazard in the transmission of
the disease.
Let us now take alilose look at each category
of the cold pharmacopoeia.
Coldarin
E SHALL first consider ‘Coldarin’, appa
rently the most popular OTC cold tablet
on the market. It has been on the OTC market
now for tire last five years or so, before which
it was an Ethical product. Its phenomenal popu
larity is no doubt due to an enthusiastic adver
tising campaign, said to cost the manufacturers
(Boots, a multinational firm) some 20 odd lakh
rupees every year.
A typical Coldarin ad goes this way: “Colds
bring misery, suffering, weakness”—interposed
is a blurred image of an individual very obvious
ly undergoing the torment so familiar to many
of us-then: “Bounce back to normal with
specially formulated Coldarin”—below is the
sufferer all smiles. In tinier print follows tire
message-Coldarin brings prompt relief to all
affected areas because it contains one, “a de
congestant to clear runny nose and sinus”, two,
“caffeine to combat that depressed feeling”,
three, “vitamin C to build resistance” and four,
“aspirin to relieve pain”. Tire customer is exhort
ed to take one Coldarin, preferably after meals,
feriog
misery
suffering
weskmess
ESoiujmce feasEx 8® normal wilefo
specially ffoirmimllasesa (CofldJaata
W
46
.■Coldarin brings prompt relief
-io all affected areas because it contains:
o A decongestant to clear runny nose and sinus
o Caffeine to combat that depressed feeling
o Vitamin C to build resistance
® Aspirin to relieve pain
’ ,-Af the first sign of a cold.
, takie one .Coldarin,
/preferably after meals.
flWa
with Vitamin C
THE SPECIAL COLD TABLET
Imprint, December 1978
THE UNCOMMON COLD
at the first sign of a cold. The punchline of the
ad, so to speak, is in bold black letters-Coldarin,
with Vitamin C, The Special Cold Tablet.
So much for the ad. Now let’s see what each
tablet of Coldarin actually contains: Phenyle
phrine 10 mg, Caffeine 30 mg, Vitamin C 20 mg,
Aspirin 600 mg, Calcium carbonate 200 mg and
Terpene hydrate 30 mg.
Phenylephrine theoretically causes nasal de
congestion by constricting the blood vessels tn
the nose. But no pharmacological authority
advocates phenylephrine as an oral decongestant
because it is not well absorbed from the gut and
it does not selectively act on the blood vessels
of tire nasal mucous membrane. Even if it were
to be so advised, Coldarin’s 10 mg would be too
little.
’ Consider the next claim “caffeine to combat
that depressed feeling”. Caffeine is a central
nervous system stimulant, and even an ordinary
cup of coffee contains 50-100 mg of caffeine.
We all know how effectively this combats ‘that
depressed feeling’-Coldarin contains only 30
mg of caffeine.
Consider now the third claim-“Vitamin C
to build resistance”—a wonderfully vague state
ment indeed. The content is 50 mg of vitamin
C, which oddly enough happens to be the daily
minimal requirement of a healthy adult. And
since not many of us suffer from scurvy, which
is a sure indication that we’re getting more than
our daily requirement of vitamin C, one can’t
see how a miniscule amount like 50 mg extra
will help. In fact, it will only be washed out of
tire body within 24 hours of so. Probably the
promoters are trying to capitalise on tire “Vita
min C for Cold” controversy. They are, perhaps,
lit aware that Dr Pauling advocates large doses
(and by large he means a dosage in the region of
several hundreds to several thousand milligrams
per day) to fight the common cold... but more
of this later. The Coldarin ad again stresses tire
Vitamin C angle: “Coldarin—with vitamin C—
The Special Cold Tablet” There’s nothing
‘special’ about the 50 mg of vitamin C added—it
merely provides yet another excuse to further
hike up the tablet’s price.
At long last, we come to “aspirin to relieve
pain”, and since aspirin is an established anal
gesic, to be administered orally in the adult dose
of 300-1000 mg, one cannot quibble about it.
It is indeed ironical that the one legitimate claim
tire tablet boasts of—that too of an analgesic—
is mentioned last in the ad.
Imprint, December 1978
Tirus, a careful analysis of this sort proves
that Coldarin is only a glorified analgesic tablet
(which was traditionally used to treat colds any
way) with a few extra ingredients thrown in to
be sold at a price three-four times that of ordi
nary analgesic tablets. The extra ingredients
may be theoretically all that the promoters
claim (or imply) to be—but in the quantities
present, they are more or less ineffective, as any
pharmacologist will tell you.
Vicks Action 500
TT ET US GO on to “Vicks Action 500”, anILj other OTC product believed to be the
‘arch-competitor’ of Coldarin. The manufactur
ers very courageously put it straightaway on
the OTC market, without the usual span of years
as an ‘Ethical’ medication. Though a bare couple
of years or so on the market, Action 500 is
said to be doing extremely well—again largely
due to an intensive ad campaign costing its
manufacturers (Richard Hindustan, another
multinational) around 25 lakh rupees a year.
Action 500 is also marketed in an attractive
‘capsule’-like form, which helps the manufac
turers in two ways. Since the average consumer,
for. some unfathomable reason, always thinks a
capsule is more ‘potent’ than a tablet,.it is bound
toevoke a better response from him, and second
ly, it provides the manufacturers one more
reason to justify their price.
An analysis of Action 500’s formulation
reveals that each tablet contains—Salicylamide
390 mg, phenacetin 242 mg, Caffeine 32 mg,
Sodium Citrate 32 mg and Ephedrine 8 mg.
Salicylamide is a weak, aspirin-like drug and
therefore its dosage should be greater than
aspirin’s for the same effect. This is supposedly
counterbalanced by the addition of phenacetin,
which has a painkilling action of its own. How
ever, as mentioned before, pharmacologists no
longer recommend its inclusion because of its
high toxicity. The next ingredient is Caffeine
32 mg and we have just seen, in the case of
Coldarin, how effective 30 mg were. Sodium
citrate has been added as a ‘filler’. At long last,
we come to Ephedrine, which falls in the same
‘decongestant’ category as Coldarin’s phenyle
phrine. Unfortunately, even if Ephedrine did
work as an effective nasal decongestant when
given orally (a very big if, because usually it has
been administered locally, in the form of nasal
drops, for tills effect). Action 500's dose of
eight mg is just too small.
47
THE UNCOMMON COLD
Ethical Market
S AN EXAMPLE of a cold tablet from the
‘Ethical’ market, we shall consider ‘Vikoryl’
(which for a change, is the product of an Indian
company, Alembic). Each Vikoryl tablet con
tains Aspirin 200 mg, Paracetamol 120 mg,
Phenylephrine five mg and Chlorpheniramine
maleate two mg. Paracetamol has been added
presumably due to its anti-pyretic and analgesic
action, to add to aspirin’s. We have seen above
that 10 mg of oral Phenylephrine is not effective
as a nasal decongestant, so that the efficacy
of Vikoryl’s five mg can well be imagined.
That leaves Chlorpheniramine maleate. This
is an antihistamine, which can hardly be recom
mended for a viral disease like the common
cold. As ‘Drugs of choice, 1978-79”, an inter
nationally
acknowledged pharmacological
authority, says "Despite clinical evidence that
antihistamines do not cure or abort the common
cold, and are indicated only in a few rare
instances of cough, occurring as a manifestation
of allergy, many of these compounds have been
incorporated into popular cough preparations."
Sir Christopher Andrewes also deplores this
in ‘Assessing Cold Cures’ (“The Common Cold”,
Chapter 16, p. 151) “Tire sad thing is that years
after the antihistamines were debunked as cold
cures in scientific journals, they are still being
sold in quantity for this purpose and bringing
in large profits. A new cold-cure is headline
news: debunking a cold-cure does not deserve a
line of even the smallest print.”
We have, in all, considered in detail just
three cold tablets. But it has become obvious
that each is a sort of prototype on which every
other is based. The recipe is very simple: Take
an analgesic or two, a decongestant, an anti
histamine, Vitamin C and any other harmless
ingredient you can lay your hands on easily.
Make a combination after your heart’s fancy,
add an enticing colour and flavour, arm yourself
with the finances necessary for a hectic ad cam
paign, and presto! you will have automatically
joined tire long line of pharmaceutical companies
eager to alleviate the torture of the teeming
millions suffering from the common cold-at a
price of course!
A
Ointments
HAT does the ‘cold’ industry have in
store for us in the shape of Ointments?
Take “Vicks Vaporub” (another member of
W
48
Vital facts about Colds and Flu
and how to fight these ailments
"Ifind
Anaein of
great help",
says Nurse
Angela
Fernandes.
Richardson Hindustan’s ‘Vicks’ ‘family’) for
instance. Till recently, Vicks Vaporub has been^^
striding across the ‘rubs’ market like a Colossusf^P
Reports now indicate that Alembic’s ‘Rubex’ is
making good headway in this lucrative market.
A comparison of the two formulations is inter
esting.
Every bottle of Vicks Vaporub contains
Menthol 2.82%, Camphor 5.25%, Thymol 0.1%,
Turpentine oil 5.57% and Paraffin oils and
essential oils to make the rest.
Every bottle of Rubex, on tlje other hand,
contains Mentisol 2.82%, Camphor 5.25%.
Thymol 0.1%, Turpentine oil 5.6%, and Euca
lyptus and nutmeg oils.
60 grams of Vicks Vaporub costs about
Rs.6.50.
65 grams of Rubex costs about Rs.6.20.
Can the discerning reader perceive any signi
ficant difference in the composition (even the
% composition!!) of the two brands?
Of the various constituents of the ‘rubs’
products, Camphor is what pharmacologists ca^A
a ‘counter-irritant’-a drug, that when rubbe^^
in, increases blood supply and warms the part.
So are menthol and turpentine oils. Thymol is an
anti-bacterial and anti-fungal substance, used
primarily in certain skin creams, lotions etc.
Cold is caused by viral infection; it is not a skin
disease. Paraffin oil is an ‘emollient’—a spreading
lubricating substance that facilitates application
over the skin. Eucalyptus oil is a volatile odorous
oil obtained from Eucalypta plants, also added
as an counter-irritant. Nutmeg oil is another
volatile oil got by distilling nutmeg. It is a
flavouring agent and a mild rubifacient—a drug
that resembles a counter-irritant in effects.
Thus it is obvious that not a single constitu
ent of the ‘rubs’ range has any direct connection
Imprint, December 1978
THE UNCOMMON COLD
with the common cold—notwithstanding the
claims of products like Rubex, which has an ad,
prominently displayed in many drugstores,
depicting a happy mother holding aloft her
child, both bursting with health, and the slogan
reading “Ah-choo. . . .Rubex. . .choo!” (which
could be roughly translated as “Colds? Gone
with Rubex!”) Rubbing these ointments on the
chest, back, etc—even by the most loving of
touches can have little effect on the common
cold.
Syrup Solutions
].\JEXT, LET us go on to the myriad multij.'•! hued, multi-flavoured ‘syrups’ the cold
industry has put out on the market. Take, for
instance, Waterbury’s Red Label. Its ad runs as
Allows—“Recurring Coughs and Colds? Take
Waterbury’s Red Label!” It is claimed to be
‘The Best Remedy for Coughs and Colds’ and
it ‘Builds resistance while it gives relief. A harassed-looking housewife is shown in her kitchen,
and under this, the theme continues—“Colds
and coughs come when your body’s resistance
is low. When they go, they leave you weaker
still. So you get coughs and colds more easily
again. And again. But the work of the house
must be done. A housewife can’t really fall sick;
can she?-The thing to do is to build up your
body’s resistance while you fight your coughs
and colds. Only Waterbury’s Red Label does
both. It has two groups of ingredients—First it
has Creosote and Guaiaicol which relieve coughs
and colds. Secondly, it has ingredients that tone
up your system, restore energy and build up
resistance.
Every 15 ml (about three teaspoonful) of
elixir contains—Creosote 0.0075 ml, Iron 3 mg,
Manganese 0.7 mg, Guaiaicol 0.00035 ml,
sodium salicylate 0.135 gm, sodium benzoate
18 mg, sodium iodide 1.8 mg, potassium phos
phate 22 mg, sodium hypophosphate 18 mg,
malt extract 1.05 mg, and aqueous extract of
cherry, eucalyptus, yerba santa, gentian, etc.
Now Creosote and Guiaiaicol are expectorants
(drugs that increase the output of fluid, facili
tate expectoration or promote the discharge of
mucus, from the respiratory tract). But, accord
ing to ‘Drugs of choice, 1978-1979” there is
considerable controversy regarding their effi
cacy. One experimenter has shown significant
expectorant activity in anaesthetised animals
Wh@ro y©u"re weak,
coughs and colds never
seem to go away.
Coughs and colds come
when your body's resistance
is low. When they go, they
leave you weaker still. So you
get coughs and colds more
easily again. And again. But
the work of the house has to
be done. A housewife can't
really fall sick, can she?
The thing to do is to build up
your body's resistance while
you fight your cough and cold.
Only'Waterbury's Compound
Red Label does both.
Waterbury’s Compound
Red Label has two groups
of ingredients: First, it has
Creosote and Guaiacol which
relieve coughs and colds.
Second, it has unique tonic
ingredients which tone up
your system, restore energy
and build up resistance.
Send coughs and colds away
with Waterbury’s Compound
Red Labol.
Now available in 2 sizes.
Stay strong and healthy with
Waterbwry’s
Compound
RED LABEL
—the most trusted family tonic
A QUALITY WARNER-LAMBERT PRODUCT.
Imprint, December 1978
49
THE UNCOMMON COLD
only when given in toxic doses at certain seasons
of the year. Another has shown that sputum
‘stickiness’ does decrease but only with doses
of 300-600 mg four times a day. Therefore the
amounts of Guaiaicol and Creosote in Water
bury’s Red Label are too microscopic to be
effective.
Second Group
ONSIDER now the second group of in
gredients ‘that tone up your system,
restore energy and build up resistance’.
Sodium salicylate is the sodium salt of salicyclic acid, just as aspirin is the acetylated com
pound of the same. Its uses (Satoskar, Kale,
Bhandarkar-Pharmacology and Pharmacotherapeutics Vol I, p.126) are in the oral doses
of 0.6 to two gm for muscle-pain, joint-pain,
etc and five to 10 gms in acute rheumatic fever.
So much so Waterbury’s 135 mg per every 15
ml cannot even cure these ailments, leave alone
coughs and colds. In fact, one would require
about 10 whole bottles (470 ml each) for the
first use, and about 100 bottles for the second
use.
Sodium benzoate is the sodium salt of ben
zoic acid, and has been added merely as a
preservative.
Sodium iodide is a compound of sodium
and iodine. Iodides are used in therapy as expec
torants, but the minimum effective dose of
sodium iodide for this purpose (Satoskar et al,
p.8O5, Appendix B) is 250 to 500 mg. A little
rough calculation again reveals that one would
need at least four to five bottles of Waterbury’s
to make up this dose!
This writer could not trace sodium hypophosphate and potassium phosphate in any of
the pharmacoepias he consulted, which leads
him to suspect that they have been added as
mere ‘fillers’.
Malt extract is got from barley and contains
a number of sweetening and enzymatic sub
stances, while the aqueous extract of cherry,
eucalyptus,yerba santa, gentian, etc are flavour
ing agents. All these have been possibly thrown
in only to impart that characteristic ‘sweet’
taste to the syrup.
Coming now to the variegated mineral con
tent of the syrup, we must admit that iron,
manganese, sodium and potassium are minerals
we need for normal health. We require at least
10 mg of iron in our diet, of which only one mg
C
50
is actually absorbed, while the rest is excreted.
The daily requirement of manganese is about
350 mg. Sodium comes to us in the form of
common salt, which is mainly sodium chloride.
To quote Orten Neuhaus (“Human Bioche
mistry”) “The usual daily intake of sodium
chloride is about 10-15 gms. This is far greater
than what is required (about 4-6 gms daily) but
the amount is used chiefly because of its flavour.
About 98% is eliminated by way of urine and
2% by faeces. The usual amount of potassium
in the diet is 2.4 grams (about 1.5-4.5 is needed
daily)”
A deficiency of any of these minerals causes
certain disease processes to develop. A defi
ciency of iron for instance causes anaemia. That
of sodium leads to what doctors call ‘hypon^^
tremia’. Similarly a potassium deficit is calld^P
‘hypokalemia’. Medical science has still to
record a single case of pure manganese defi
ciency.
Now each of these deficiency states produces
definite signs and symptoms. Normally all of us
get our required quota of minerals from our
diets-in fact, we get more than is required most
of the time, and the extra is just excreted.
Waterbury’s minerals will also suffer from this
fate. At least, this writer has yet to see Water
bury’s Red Label prescribed for iron-deficiency
anaemia or hyponatremia or hypokalemia!
Therefore, in concluding this discussion of
Waterbury’s ‘second group of ingredients that
tone up your system, restore energy and build
resistance’, one can only ask, “Resistance?” To
What? The cold viruses!?” (Medical science
would indeed hail it as a magnificent break
through in cold research if the assorted minerals
the syrup contains ‘built up’ resistance to ttjAt
cold viruses!) and “How?” (for, as we ha^r
seen, in a healthy individual getting his required
mineral quota from his daily diet, Waterbury’s
minerals will only be taken in from one end and
discarded through the other end of the gastro
intestinal tract!) In the case of a weak person,
it may be good for general deficiency. But that
is as far as it goes.
All in all, Waterbury’s Red Label is a pleasant-tasting mixture. It is largely ineffective as
far as its claim—the best remedy for coughs and
colds’—is concerned. It is therefore a pleasant
surprise to discover that other syrups on the
market, like Glycodin and Vicks Formula 44, at
least contain an anti-tussive (cough-depressing)
drug in effective doses.
Imprint, Etecember 1978
THE UNCOMMON COLD
Drops and Lozenges
E NOW come to the variety of cough
drops, lozenges, etc marketed by the
cold industry.
Take for instance Vicks 44 cough discs.
Each contains—Dextromethorphan 3.65 mg,
Ephedrine 3.76 mg, Benzocaine 1 mg, Cetyl
pyridinium chloride 0.4 mg and Menthol 4.8
mg.
Dextromethorphan is an anti-tussive (cough
depressant) while ephedrine acts as a broncho
dilator (widening the bronchial tubes to facilitate
‘bringing up’ and coughing out the secretions)
but their doses for these uses are 15-30 and
15-60 mg respectively (Satoskar et al). There
fore Vicks’ 3.65 and 3.76 mg respectively are
aaL going to be effective unless you take at
Wst five or six at a time!
Benzocaine is a local anaesthetic, and ‘sensi
tisation’ is a dangerous effect of its use in such
local medications. After repeated use, an allergy
can develop and a fatal swelling of the glottis
can occur (a few such cases have been reported).
Cetylpyridinium chloride is what pharma
cologists call a ‘cationic surfactant’—a drug with
detergent, emulsifying, anti-bacterial and anti
fungal effects. But its concentration and.contact
time in the ‘cough drop’ formulation have not
been proved to be adequate to achieve this
purpose.
Menthol is a substance got from plants-of
the ‘Mentha’ variety. As Drill’s ‘Pharmacology
in Medicine’ puts it, “menthol when applied
locally causes a pleasant tingling sensation and
a feeling of coolness. These changes which are
probably due to the result of an effect on the
sensory nerve or nerve endings have led to the
^^>f menthol in a variety of proprietory nose
drops, liniments and cigarettes.” Menthol too
has obviously got nothing to do with the com
mon cold—the cold industry has merely capitalis
ed on its ‘soothing’ action.
W
66"OrALLS”’ another heavily-advertised proX JL duct, contains two main constituents—
menthol and eucalptus. Menthol has just been
considered. Eucalyptus is a substance got from
a plant of the Eucalypta variety. It has an aro
matic camphoraceous odour and a pungent
cooling taste—neither of which is going to help
the common cold any.
Much has been made of the ‘soothing’ effect
of this class of product—the fact remains that
Imprint, December 1978
gOOOErlCTE3
Glycodin mstta's csa.ll ccsigDi eselEeirs?.
all they actually do is increase the flow of saliva,
and as “Drugs of choice, 1978-1979” says
“Although the use of gargles, lozenges, troches
and cough drops is helpful in stimulating the
flow of saliva and thus preventing the ‘drying
out’ of the pharyngeal (throat) mucous mem
branes, most of the stimuli that give rise to
cough originate in the lower respiratory tract,
which is not reached by demulcent saliva. ”
(emphasis mine) Therefore it can be inferred
that these products are not of much use even in
the relief of cough (not all cases of cough any
way), leave alone the other symptoms of the
common cold.
Mouth Wash
ET US NEXT take a look at ‘Listerine’, the
antiseptic solution, which contains-Menthol 0.04%, thymol 0.06%, eucalyptol 0.09%,
methyl salicylate 0.06%, benzoic acid 0.03%,
boric acid 235% and alcohol 27%.
We have seen what menthol is. Thymol is
classified in a group of chemicals called ‘miscella
neous phenols’ and to quote from Goodman
Gillman’s “The Pharmacological Basis of Thera
peutics” (p 992) “Thymol is both antibacterial
and antifungal. It is promoted for the treatment
of acne, haemorrhoids and tinea pedis.s It is
also present in some mouth washes but in the
concentrations used, it is not effective within
any practical contact time, "(emphasis mine)
L
51
THE UNCOMMON COLD
Have you a cough coming on?
Eat sugar candy ’
RUK SHETH, former ProfessorDirector of the Department of
Pharmacology, KEM Hospital and Seth
G S Medical College, Bombay was asked
his opinion on the plethora of cold reme
dies sold on the market “Most of them
are as good as simple aspirin in adequate
dosage. Colds usually take their own time
to disappear and the ‘remedies’ marketed
I only give symptomatic relief.”
As for the shotgun, multi-ingredient
cold tablets, Dr Sheth said, “These sell
because people believe that aspirin is
meant only for headaches, so that if you
prescribe it for colds, there is an element
of resistance on the part of tire patient.
There are a lot of misconceptions preva
lent—like cold tablets must contain one
drug for drying the secretions, one drug
for cutting down the duration of colds
and so on. Advertising campaigns are
partly responsible for these misconcep
tions.
No multi-drug combination has yet
proved effective in controlled trials. Most
of them contain aspirin, an anti-histamine,
a decongestant and vitamin C. No one has
proved that the secretions in colds are
histamine-induced, so that anti-histamines
can be of no possible use. The deconges* tant dose is too small to be effective—but
if it is increased it can lead to adverse
effects like prolonged wakefulness. Vita
min C as advocated by Dr Linus Carl
D
Methyl salicylate, benzoic and boric acid are
the constituents that justify the name ‘anti
septic’. Alcohol acts as an antiseptic only in
concentrations of 70% by weight (Satoskar et al,
p. 53, Vol I) so that ‘Listerine’s 27% of alcohol
will only produce a sensation of warmth and
increase salivary secretion (This factor no doubt
accounts partly for the popularity of ‘anti
septics’ and ‘tonics,’ to name but two types of
products that cash in on alcohol)
Imprint, December 1978
Pauling has to be in doses of 1 gm, and
more per day—most tablets contain just
25 to 50 mg.”
With respect to ointments, Dr Sheth
says “They’re a good gimmick. People
fall for the warmth, tingling and vapour
that the volatile oils contained in them
generate when rubbed it—after all, when
you take a tablet you don’t feel anything!
Again no controlled trials have ever been
undertaken to prove the efficacy of these
ointments.”
Finally, coming to cough drops, lozen
ges, etc, Dr Sheth said, “A bit of Khadi
Shakhar—which our mothers used to give
us—is as good. The object is to prevent
drying of tire throat mucous membrances
which brings on coughing. This purpose
can be served easily by a piece of sugar
candy, lemon drops, etc.”
How were pharmaceutical companies
allowed to make and get away with their
grandiose claims? “Well, the fact is that
even in the USA it is only now that phar
maceutical companies are being asked to
prove each and every claim they make.
But here, so long as a combination prepa
ration is not harmful, permission is grant
ed by the authorities.”
Asked if he agreed with this writer’s
belief, that the cold industry was taking
the consumer for a ride, Dr. Sheth smiled
and said “Yes, of course it is!”
Listerine throat lozenges are also sold on the
market, and are thought to be very popular.
1 can only close this section on lozenges by
quoting Drill’s “Pharmacology in Medicine”,
p 1881,” Lozengesand troches are flat, variously
shaped medicated candies. Besides the active
ingredients which are mostly antiseptics or anti
biotics, menthol and local anaesthetics, they
contain sugar and mucilage. They are designed
to soothe a sore throat or similar oral infection.
53
GENERIC FORMULATIONS OF SOME COLD REMEDIES (TABLETS)
CONSTITUENTS (IN MILLIGRAMS/TABLETS)
!
■
i
ASPIRIN
PHENACETIN
(may be toxic)
CAFFEINE
(dose too small)
DECONGESTANT
(not effective)
ANTIHISTAMINE
(not effective)
VITAMIN C
OTHERS
(dosage too small)
I,- ■;
I.-
ASPRO
350
20
AVEDAN PLUS
350
30
Acetyl ammo
Phenol-125
8
3.
ANACIN
389
16.2
Quinine 8.1
7
4.
ANALGIN
5.
APIST1N
225
150
6.
CODOPYRIN
250
250
Codeine 8
13
7.
CAFIASPRIN
300
8.
COLITHEN CPA
230
150
9.
CODA LG IN
260
260
90 Brands
(Believed unsafe)
6
2
30
6
30
600
10.
COLDARIN
11.
COSAVIL
12.
DISPRIN
13.
DR1STAN
230
97
14.
DAPRISAL
160
160
4
30
Atropine 0.3
Phenobarb 20
Codeine 8
30
50
10
11.25
15
•
■
HALLS
16.
MICROPYRIN
350
17.
MICROPYRIN C
350
i
17
■!
CaCo3 200
Terpene 30
25
Phenazone
Salicylate 250
14
!
1
12
16
5
10
17
20
5
Amylobarbitone 32
18
Menthol, Eucalyptus
12
7
20
14
25
18.
CECON 500
100
19.
REDOXON
(Chewable)
200
20.
REDOXON
(Tablet)
50 ’
21.
VIKORYL
200
(Salicylamidc)
22.
VICKS
(Action 500)
390
(Salicy lain ide)
242
23.
VEGANIN
250
250
24.
VERIN DON
250
ZEET
15
Soluble
15.
25.
:
8
1.
2.
■
■.
Approx Price
(In Paise)
Sodium Ascorbate 450
12
3
Paracetamol 120
15
32
Sodium Citrate 32
Ephedrine 8
32
32
Codeine
24
Phenobarbitone 16
10
5
2
•
1.5
4
4
■
THE UNCOMMON COLD
They are generally conceded to be of dubious
value and the US Pharmacoepia does not contain
any such preparation" (emphasis mine).This is
the nearest that that august tome comes to
debunking this class of products!
IV—Vitamin C For The Common Cold?
ITAMIN C or ascorbic acid is a chemical
commonly found in citrus fruits, green
vegetables, tomatoes, etc. It is essential for a
number of biochemical reactions at the cellular
and subcellular levels in the body. It is needed
for the synthesis of a vital protein called colla
gen, which is responsible' for the integrity of
blood vessels, bones, cartilage and teeth. Man
seems to be tire only animal whose liver cannot
agjthesise ascorbic acid—most other animals
J^R.roduce it from glucose. In man, deficiency
of this vitamin causes a disease called scurvy,
characterised by bleeding in the skin and sub
cutaneous tissues, muscles, joints, gums, etc.
Vitamin C, as a cure for the common cold,
first came into the news when a paper by
Dr Linus Carl Pauling was published by ‘Nutri
tion Review’ in 1967. Dr Pauling’s paper, coming
as it did from a controversial figure like him,
created a sensation in medical circles.
In the late 1960s, Dr Pauling opened the
Pandora’s box of yet another controversy. Work
ing in close association with two other bio
chemists, Dr Fred Klenner and Dr Irwin Stone,
Dr Pauling became fully convinced of the bene
ficial effects of large doses of Vitamins (‘mega
vitamin therapy’) on ailments ranging from
cancer to tire common cold. Dr Klenner had
observed the ‘curative’ effects of Vitamin C in a
number of viral diseases. Dr Irwin Stone too
l^kworked on Vitamin C for the least forty
yWs. Dr Pauling’s advocation of large doses of
Vitamin C for the common cold was actually
based on Dr Stone’s work, which he admitted
as much in “Vitamin C and the common cold”,
a book published in December 1970.
Shorn of all controversy, what exactly does
Dr Pauling prescribe for the common cold? I
can only quote‘>from his book-“Take about
one-half level teaspoonful of the powder form
of ascorbic acid each day. At the'first sign of a
cold, take about a gram of ascorbic acid each
hour till the symptoms disappear. This usually
occurs within a few hours. For a few days there
after, take a slightly higher doses than normal,
since cold symptoms have a tendency to reappear
if tire dose is dropped to maintenance level all
V
Imprint, December 1978
Trachea
Longitudinal section through a human head showing
the direction flow of mucus backwards through the
nose, downwards from the sinuses, and up and overthe-top from trachen to oesophagus.
too soon. You must not be disappointed if your
physician at first expresses opposition to your
use of ascorbic acid.”
Unfortunately, there is still no conclusive
proof, one way or the other, about the exact
role of Vitamin C in the treatment of tire com
mon cold. No one has yet clearly demonstrated
how exactly Vitamin C prevents, aborts or cures
colds. Its reported beneficial effects in other
diseases like atherosclerosis and cancer have
also to be confirmed.
The author would like to acknowledge the
following sources, on which certain sections of
the ‘Uncommon Cold’ are based:
1) "The Common Cold" By Sir Christopher
Andrewes.
2) "Pharmacology and Pharmacotherapeutics"
Vols I and U By Drs Satoskar, Kale and
Bhandarkar
3) "Drugs Of Choice, 1978-1979” Ed by Dr
Walter Modell
4) Drill’s "Pharmacology In Medicine”
5) Goodman Gillman’s "The Pharmacological
Basis of Therapeutics "
6) Martindale’s "Extra Pharmacoepia"
7) “Current Therapy 1978”
8) “The Indian Pharmaceutical Guide, 1978"
9) Orten and Neuhaus-“Human Biochemistry”
THE END
55
“The discipline of
the world marketplace
is an excellent measure of efficiency
and a force to stability”
John F. Kennedy 1917-1963
Even the world
is getting to be too small
a market for us
at Teksons, Thana
and at Singapore.
Imprint, December 1978
OH^FOTaKsonstlil.
Kolshet Road, Thana.
^jfeading manufacturers of heat exchanger^nponents and hydraulic flexibles.
everest/78/TL/321
Brief Note on 'Antispasmodics - I (Spasmolytics)
Compiled by
Dr.Sagun Desai
Introduction
■">
In the strict sense, all those drugs which can relax the
smooth muscles in the body and thereby abolish the spasm and
associated effects should be defined as spasmolytics. A large
number of agents can be put in this category. But from the
view of clinical application, antimuscarinic drugs like atropine
and a scoporamine and their synthetic and semisynthetic
derivatives are conventionally called as antispasmodic or
spasmolytic drugs. These drugs have actions on the smooth
muscles of Gastro-intestinal system, biliary system, genitourinary
tract etcA and therefore are widely used in treatment of
disorders'of these systems. Besides relaxation of smooth muscles
of these systems, may also have various’other pharmacological
actions which can be used therapeutically or are responsible for
producing undesirable effects.
We shall briefly consider these agents here.
Atropine and Sopolamine
Both atropine and scopolamine are alkaloids »f belladona
plants. Atropine is chiefly found in Atropa Belladona and
Datura Stramonium^ Atropine is also knewn as hyoscyamine.
Scopolamine (hyescine) is chiefly hielded from Hysscyamus
Niger and Scopolia Carniolica. Both these alkaloids competitively
block the muscarinic actions of exogenous and endogenous
acetylcholine by blocking muscarinic receptors in various organ
systems.
Pharmacological actions
a)
Gastro Intestinal Tract :
Atropine and scopolamine reduce both the tone and mobility
of all parts of the gastro intestinal tract. This has led to
their use as antispasmodic adjents for gastro intestinal disorders
and in the treatment of peptic ulcer. Atropine only partially
blocks the effects of vagus nerve stimulation and does not interfere
significantly with normal.
b)
Other smooth muscles
Atropine decreases the normal tone and amplitude of contrac
tions of the ureter and bladder, and often eliminates drug
induced enhancement of ureteral peristalsis. Therapeutic
doses tend to reduce the tone of the fundus of the bladder and
enhance the tone of the trigenal sphincter and hence, tend to
produce urinary retention.
Atropine exerts a mild antispasmodic action on the gall
bladder and bile ducts in man. Atropine alone is not effective
as a biliary antispasmodic.
Atropine has negligible effects on the human uterus.
Scopolamine when used to cause amnesia during labour does not
alter or interfere with uterine contractions or increase the
duration of labour. Both cross the placental barrier, but the
foetus is not adversely affected.
2
Other actions
(1) Belladona alkaloids reduce the secretions of the
exocrine glands except production of milk. They reduce
salivary secretien causing dryness of mouth. Volume
and total acidity of gastric secretions are decreased.
All phases of gastric secretions are partially reduced.
Pancreatic, bile and intestinal secretions are not
significantly affected. They reduce the secretions
of nose, mouth, pharynx and bronchi. Following atropine,
bronchial secretions become viscoid . Even in small
doses, sweat secretion is reduced xaa raising the body
temperature.
(2) Atropine produces mydriasis and cycloplegia resulting
into blurring of vision, photophobia, diplepia etc.
It may precipitate glaucoma in susceptible people.
(3) Conventional doses of atropine produce tachycardia
but blood pressure is not changed significantly.
(4) Atropine in routine doses producer insignificant
stimulation of CNS but in toxic doses it may produce
excitation, restlessness, irritability, hallucinations,
delusions convulsions, etc.
In therapeutic doses Scopolamine produces drowsiness,
euphoria, amnesia and - dreamless sleep. B»th Atropine and
Scopolamine‘are effective orally and are rapidly absorbed from
the gastro intestinal tract*.
c)
Adverse Reactiwns
Adverse reactions to belladona alkaloids are mainly due to
extension of their pharmacological actions. They include dryness
of mouth, difficulty in swallowing, fever, constipation,
blurring of vision, retention of urine in elderly and palpitation.
toss Occasionally they may produce allergic manifestations.
Large doses may produce acute poisoning.
Use of Belladona Alkaloids as Antispasmodics
(1) Gastro intestinal colics ; Both Atropine and Scopolamine
are used to control hypermobility and pain associated
with diarrhoea and dysenteries. Drug induced diarrhoea
(guanetridine, reserpine) and constipation due to spastic
state of intestine (morphine) are relieved by Atropine.
Occasionally they may be useful in treating conditions like
pyloroppasm, cardiospasm or hypertrophic pyloric stenosis,
diverticulitis, etc.
(2) Other smooth muscle colics : Though atropine has a
weak relaxant action on smooth muscles of genito urinary and biliary tracts, it used in combination with
morphins/pethidine to relieve ureteric and biliarycolics. Occasionally Atropine may be useful in
dysmenorrhoea. It is also used to allay the frequency and
urgency of accompanying c/ystitia, It is frequently
employed to control nocturnal ekm eneuresis in children.
Preparations and dosage
1.
Tablets of Atropine Sulphate s 0.5 mg tabs.
Dose 0.25 — 2.00 mg
2.
Atropine sulphate Injection ; 0.5 mg. in 1 ml
Dose ■» 0.25 - 2.0 mg by subcutaneous or intramuscular
injection
3.
Hyoscine (ScopolamineX Injection s 0.4 mg in 1 ml.
Dose : 0.3 - 0.6 mg. by subcutaneous injection.
3
Synthetic and Semisynthetic Substitutes for Bel^adona Alkaloids
Atropine substitutes are developed because of the lack
of selectivity h in action of belladonna alkaloids. Thus, the
dose of Atropine required to produce the therapeutic effects on
gastro intestinal tract, invariably produces numerous adverse
effects. Therefore, drugs have been synthesized to produce more
therapeutic selectivity. Unfortunately, therd is no such ideal
substitute for Atropine.
The spasmolytic atropine substitutes are mainly used in
the treatment of peptic ulcer and colics, The quarternary
ammonium compounds are relatively free from the central effects
of belladoma alkaloids due to poor crossing of blood-brainbarrier. They are poorly and unreliably absorbed from the gut
after oral administration but usually have a somewhat more
prolonged action. Because of their ganglion blocking property,
over and above actions like Atropine, they produce impotence,
urinary retention, postural hypotention and curarimimetic
action (neuromuscular blockade) leading to respiratory paralysis.
There are many antispasmodic Atropine substitutes available.
Commonly used are :
(1) Atropine Methonitrate : Mainly used in opthalmic practice.
But also used orally in the dose of 0.2 - 0.4 mg. orally. 4-6
times daily in the treatment of congenital hypertrophic
pyloric stenosis.
(2) Methacopolamine Bromide : Quarternary ammonium compound.
No CNS effects of Scopolamine. used in peptic ulcer,
renal colic, frequency of micturition associated with
cystitis. Dose 2-5 mg. x 3 times a day orally or 0.25 1.0 mg. by injection. Less potent than atropine.
(3) Methantheline : (Banthine) Synthetic quarternary ammonium
compound with a high ratio of ganglion blocking to
antimuscarinic activity. More potent thnn atropine and
comparatively longer duration of action (6 hr,s.)
Dose 50-100 mgs orally x 6 hrly or 15-25 mg i.m. inj.
(4) Propantheline (Pro-banthine) : Closely related chemically
to methantheline with similar properties but tw« to
five times more potent than it. One of the most widely used
antimuscarinic drugs. Usee] j_n peptic ulcer, for
relieving pain of diverticultitis and in treatment of
diarrhoea. Available as 15 mg tabs. Dose 30-45 mg. x
6 hrly orally or 10-20 mg i.m. inj.
(5) Oxyphenonium (Antrenyl) : Quarternary ammonium compound
with a high ganglionic blocking action. Dose 10 mg. orally.
(6) Adephedrine Hydrochloride (Trasentine) ; Has a weak
muscarinic blocking and a prominent direct relaxant effect
on smooth muscle, used for spastic colon, biliary colic
and dyamenorrhoea. Less potent than atropine.
Dose 75-100 mg x 3-4 times a day orally or 50 mg i.m. inj.
(7) Dicyclomine Hydrochloride (Bentyl) ; A tertiary amine with
antispasmodic action. Decreases spasm of the GIT, biliary
tract, ureter and uterus, without producing characteristic
atropinic effects on the salivery, sweat or gastro
intestinal glands, the eye, or the cardiovascular system,
except in large doses. It appears to be a direct non
specific relaxant of smooth muscle and not a competitive
blocker of acetylchloline.
Thipenamil is similar to dicyclomine and is closely related
to local anaesthetics, with local anaesthetic activity. However,
clinical use of these drugs has been disappointing.
4
Other drugs ;
( i) Homatropine methylbrumide
( ii) Hyoscinc - N - Butylbromide (Buscopan)
(iii) Diphemanil
( iv) Pipenzolate (Piptal)
( v) Poldine
( vi) Clidinium (Quarzan)
(vii) Procyclidine
(viii) Glycopyrronium
( ix) Pavatrine
( x) Isopropamide Iodide
( xi) Emepronium (Cctiprin)
(xii) Flavoxate (Urispas)
(xiii) Oxyphencyclimine
(xiv) Tricyclamol
Many of these drugs in tolerated doses are claimed to be
superior to atropine. None, however, can be considered as highly
effective in action and clinically a effective doses will
evoke some adverse effects.
Certain of the synthetic belladonna substitutes are used
much more extensively than are the natural alkaloids in a
number of clinical conditions. However there are few situations
in which this preference is supported by evidence.
Sources
1.
Goodman and Gilman
The Pharmacological Basis of Therapeutics
* Sixth Edition 1980
2.
Sato’skar, Kale and Bhandarkar
Pharmacology and Pharmacotherapeutics
Seventh Edition 1980
# 3.
Dr. R. Laurence
Clinical Pharmacology
Fifth Edition 1980
Annexure
Inventory on use of Antispasmodics
LOGOST
Name
Qualifications
Profession
Professional standing (in years)
Address
Tel.No.
1.
How often do you prescribe/use antispasmodics. ?
Quite often / Frequently / Occasionally.
2.
For which clinical conditions do you prescribe/use them
(3)
(1)
(2)
(4)
(5)
(6)
(7)
(8)
(9)
3.
Preparations/formulations common ly prescribed/use by you
(You may use brand names if you wish so). Please write
in order of preference.
(3)
(1)
(2)
4.
Route of administration commonly adopted by you :
Oral / Intramuscular / Intravenous
5.
Average duration of treatment with antispasmodics
days.
6.
Reasons for using the drug of first choice;
(4)
(1)
(4)
(5)
(2)
(5)
(6)
(3)
(6)
7.
Commonly encountered adverse reactions/toxieity in your
practice while using drug of first choice.
(2)
(3)
(1)
(4)
(5)
(6)
8.
While prescribing/using the antispasmodics do you
consider the 'cost factor' ?
Yes / No / Not relevant.
Any other information/comments which you wish t* share :
9.
(signature )
THANK YOU
Antispasmodics - III
Inventory on use of Antispasmodics
- Dr.Sagun Desai
- Dr. (Mrs.)Rajul Desai
Introduction
Pharmacologically speaking belladonna alkaloids like
atropine and scopolamine are very effective and reasonably
safe antispasmodics. However a large number of synthetic
and semisynthetic atropine substitutes have been developed
with claims of increased safety, less toxicity, more
specificity and prolonged duration of action. This has resulted
in mushrooming of a large number of marketed antispasmodic
preparations, often in combination with analgesics and
anxiolytics. Obviously this results in increased cost. Their
superiority, over atropine and/or spopolamine is not unequivocally
proved. Still they are widely prescribed and used by medical
profession. The aim »f this small study was to find out various
aspectssix of use of antispasmodics by doctors in Baroda City.
Method
A small questionnaire (Annexure) was evolved incorporating
various aspects of- antispasmodics. This was sent t* 70 doctors
in various categories, doctors working in general teaching
hospitals, charitable hospitals and privately practicing, with
an appeal letter to fill it up and send back. The questionnaire
was sent 5-7 days in advance. A careful thinking and filling up
should not have taken more than 15-20 minutes from the individual.
Active personal follow up was done to collect the questionnaire.
The results are briefly summarised and discussed.
Results
TABLE 1 : Response of Doctors
No.of doctors to whcm
questi onnaire was
_ sent_
Surgeons
15
"Physicians
13
Gynaecologists
10
Paediatricians
10
Resident doctors
12
General Practitioners
10
70
Category
No. of
doctors who
responded
8
6
6
2
6
5
33
%
53.33
46.16
60.00
20. 00
50. 00
50.00
47.14
TABLE 2 ; Qualifications of respondents
M.S. (Gen. Surgery)
7
M.S., M.Ch. (Urology.)
1
M.D. (Medicine)
7
M.D. (Ob. & Gy.)
6
M.D. (Paediatrics)
.
2
M.B.B.S.
10
33
TABLE 3 : Professional standing (experience) in yrs.
Yrs .
0 - 3
4 - 6
7 - 9
10 - 12
Nos.
4
13
3
5
Yrs.
Nos.
13-15
0
16 - .18
1
19-21
3
- 21
3
Not answered 1
2
Of the respondents, seven prescribe/use antispasmodics
quite often, 18 using frequently and 8 only occasionally. The
clinical conditions for which these antispasmodics are
used are varied.
TABLE 4 ; Frequency distribution of use of antispasmodics
in various clinical conditions
Ureteric colic
Intestinal colic
Nonspecific colic
Dysentery
Biliary colic
22
18
13
12
9
Dysmenorrhoea
Peptic ulcer
Gastritis
8
5
4
Infantile colic
1 to 3
Intestinal parasites
-d»Labour
-doPost MTP cramps
-doPelvic inflammatary
disease
-doSalpingitis, post
-dooperative, p«st-I.U.D.
insertion, Episiotomy
Backache, Diffuse
Oesophageal sp^sm
TABLE 5 : Choice of drugs (Frequency distribution)
Drug
First choice
Baralgan
Belladonna (atropine)
Buscopan
Dicyclamine
Spasmindon
Spasmoproxyvon
)
Avafortan, Trigan
)
Colinol, Stelabid
)
Colimox, Cydropam
)
Probanthine
Antrenyl
Maxigan
)
Epidosin
Alternative
12
6
2
4
2
14
4
9
2
10
1 each
varying
from
1 to 6
7
4
3 each
0
> 0
°
P.S.
(1) Brand names are mentioned without comments. One can
refer to composition of several of above in part II and
arrive at own comments.
(2) Several preparations have figured as alternatives
only occasionally, (one or twice) and are not mentioned.
(3) Curiously 2 doctors mentioned paracetamol and 1 pethidine.
Of the 33 respondents, 32 resort to oral route of
administration while using antispasmodics. 11 of them use them
intravenously and 10 resort to intramuscular injection.
TABLE 6 ; Average duration of treatment with
antispasmodics
_ Days___ ____ Respondents, _ _ Days_ _ _ _Resgondents
3
5
1
5-7
1 - 2
4
7-10
2
3
2 - 3
10 - 20
• 1
3 - 4
3
S.O.S.
1
4 - 5
10
Few
2
varying accor
ding to condi- 1
tion
3
TABLE 7 : Reasons for using drug of first choice
1.
2.
3.
4.
5.
6.
7.
8.
9.
Efficacy
15
Less side effects
14
Cheap
9
Easy availability
9
Reputation »f
4
company
Additional anal
4
gesic + antiemetic
action
Absence of sedative 1
Available oral +
1
parenteral route
Specificity
1
10. Orally effective
11. Only drug
12. No combination of
drugs
13. Experience
14. Because of first
exposure information
15. Easy to remember
brand name
16 . No specific
reason
17. Preferred combinaxxtion
18. Quick relief
1
1
1
1
1
1
1
1
1
TABLE 8 : Commonly encountered adverse reactions to
the drug of first choice
No adverse reaction
12
Dryness of mouth
7
Constipation
5
Not replied (? No reaction)
4
Retention of urine and gastro
3 each
intestinal upsets
2 each
6. Abdominal distension, vomiting
allergic reactions
1 each
7. Sedation, leucopenia, decreased
appetite, thrombophlebitis
perspiration (?), pain in abdomen (?)
failure of therapy.
1.
2.
3.
4.
5.
15 respondents consider the factor of cost before using/
prescribing antispasmodics. 14 tnink that factor of cost
is irrelevant. 2 do not think about cost and 2 have kept
mum on the matter. A few interesting comments received have
been reproduced :
(1)
(2)
(3)
(4)
(5)
(6)
(7)
(8)
(9)
In suspected inflammatory pathology of abdomen use of
intravenous baralgan should be restricted since it
decreases guarding and pain making reassessment difficult.
I do not prefer combination of analgin and diazepam with
antispasmodics.
The addition of sedative should be deprecated.
Rationale of combinations with dosages be explored.
Antispasmodics are meant only for symptomatic relief
and therefore, efforts should continue to arrive at a
definite diagnosis
In our experience, isopropamide has highest incidence
of constipation and urinary retention and dicyclomine
has highest incidence of allergic reactions.
For dysmenorrhoea, antiprostaglandin drugs like aspirin
are superior. Reassurance of course is needed every
time especially for post MTP cramps.
We need to use cheap and effective drugs.
Antispasmodics should not interfere with bleeding and
clothing mechanisms directly or indirectly in obstetrics
and gynaecology practice-
-4
(10)
Antispasmodics producing paralytic ileus should not
be used in paediacric practice.
(11)
High cost of medicines of brand names from well known
companies unnecessarily put the burden on poor
patients for better treatment. Medicines of other
compaanies with the same formula cost less. Why
there should be vast difference between the cost of
same medicines of different companies ?
Discussion
No discussion is offered.
The study is open for Jrour own interpretations, comments
criticism, etc.
ANTI
S P A S MOD ICS- II
Compiled by:
Dr. Nayan D. Swad.ia
NS
(Gen. Surgery)
Sr.
No.
Trade Name
(Company)
Composition
Rate at Sheth
Khushalchand
Charitable
Medical Centre
(S.S.G.Hospital)
6
Avai
lable
as
Market
rate
4
5
For 1 0
tablets
2-40
1-25
3-90
5-30
1 0 ml.
tablets
5-10
n.a.
Ampule' 5 ml
Vial JO ml
2-85
14-70
N.A.
N.A4
For 10
tablets
6-00
n.a.
Ampules 2 ml
5 ml
1 -40
2-20
1-50
2-10
Vial — 30 ml
13-25
12-50
Analgin - 500 mg
+ (a)5 mg(b)0.1 mg
1 0 tablets
3-90
5-20
Belladona dry
extract (containing
0.25 mg) active
alkaloids of bello—
donal 25 rrg +
Phenbarb 50 mg.
1 0 tablets
1-75
N.A.
1
2
3
1 .
Antrenyl
(Ciba Gegy)
Tablet
Ocyphenomide
5 mg
Duplex
Qxyphenonjqm
Bromide 1 0 mg
1!
Drops
Ckyphenonium
bromide 1 Ort^/ml
2.
Avafortan
(Khandelwal)
Inject ion
Avapyrazone 24 mg
+ Metamizol
240 mg
Tablet
Avapyrazone 60 mg
+ Nbtamizol 21 0 mg
5.
Baralgan
(Hoechst
Inject ion
Analgin 500 mg +
(a) P-Piperidinoe
thoxy - o-Carb—
methoxy Benzo
phenone hcl-2mg
+
(b) diphenyl pipericlno-clthylacetamidebromo-methylate 0.02 mg
Tablet
4.
Bellaphen
(INGA)
...2.
2
1
2
3
5
6
10 tablets
retard
1-45
n.a.
10 tablets
3-75
N.A.
4
5.
Be Haden al — Tablet
HL (Sandoz)
Hyoscine -0.0.208mg
+ Hyoscyamine 0.2292"
+ Phenobarb 50 mg
6.
Bral
(Micro
Labs.)
Same as Baralgan
Tablets
7
Duscopan
(German
Remedies)
Tablets
Hyoscine-N butyl
bromide 1 0 mg
1 0 tablets
5-55
4-90
Inject ion
Hyoscine N butyl
bromide 20 mg
Ampul 1 ml
1-60
N.A.
Tablets
(a)Hyoscine N
butyl bromide
10 ng +
(b)Annlgin O.25mg
10 tablets
7-10
N.A.
Injection in 5 ml
(a) = 20 mg +
(b) = 2.5mg
Ampule
5 ml
3-50
n.a.
Colimex
(Carter
Wallace)
Suspension per ml
Dicyclomine hcl
10 mg + dimethylpolysiloxane 40 mg
1 0 ml.
bottle
3-85
3-70
10.
Cyclopam
(Indoco)
Dicyclomine hcl
20 mg + Parace
tamol 500 mg +
Diazepam 2.5 mg.
Tablets
10
2-85
n.a.
11.
Max igan
(Unichem)
12.
Prydonnal
(Eskay lab)
3-90
3-70.
8.
9.
Buscopan
Compos itum
(German
Remedies)
Paracetamol 500 mg
+ Hy os ay amine Sulph
0.22 mg + Scopola
mine hydrochloride
0.02 mg + atropine
sulpji 0.02 mg +
Ipherobarb 30 mg
Capsule
pack of
6
..3
3
13.
Pyrispam
(Biddle
Sawyer)
Capsule
Dicyclomine hcl
1 0 mg + Parace
tamol 500 mg +
Chlordiagepox id
5. mg
1 0 Cap
sules
7-55
N.A.
Syrup <per 5 ml.
Dicyclomine hcl
mg + Paracetamol
125 mg
60 ml
bottle
7-05
n.a.
Spalein
(Martel
Hammer)
Ana.lgin - 500 ng
D ihyd r oet have r in e
Chloride 40 ng
Tablets
4-90
N.A.
15.
Spasmolysin
(Standard)
Analgin 500 mg +
atropine methanitrate + O.52 mg +
Paraverine hcl
15 mg + Diazepam
2.5 mg___
Tablet
10
3~35
N.A.
16.
SpasmoProxyvon
(Wockhardt)
Capsules
Dicyclomine 1 0 mg
+ dextropropoxyphene
hcl 65 ng
+ acetaminophen
400 mg
+ chlordiazepoxide 5 mg
6 cops.
5-50
5-50
Papaverine hcl 15 mg
+ bellandona dry
extract 5 mg
+ ana.lgin 500 ng
-I- phenobarb 25 ng
+ caffeine 25 ng
mag.trisilicate
75 mg
Tablets
10
5-20
N.A.
Same as Baralgan
Ampule
2 ml
5 ml
14.
17.
Synalges ix
(Geoffery
manners)
18.
Trigan
Tablet
Same as Baralgan
Viol 50 ml
x 10 tab.
- Media
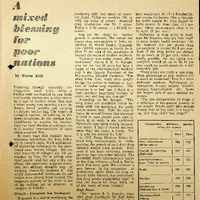 RF_DR_17_SUDHA.pdf
RF_DR_17_SUDHA.pdf
Position: 1437 (14 views)