WOMEN'S SPECIFIC PROBLEMS-MENOPAUSE/MENSTRUATION/BREST CANCER/WOMEN & MENTAL HEALTH
Item
- Title
- WOMEN'S SPECIFIC PROBLEMS-MENOPAUSE/MENSTRUATION/BREST CANCER/WOMEN & MENTAL HEALTH
- extracted text
-
RF_WH_5_SUDHA
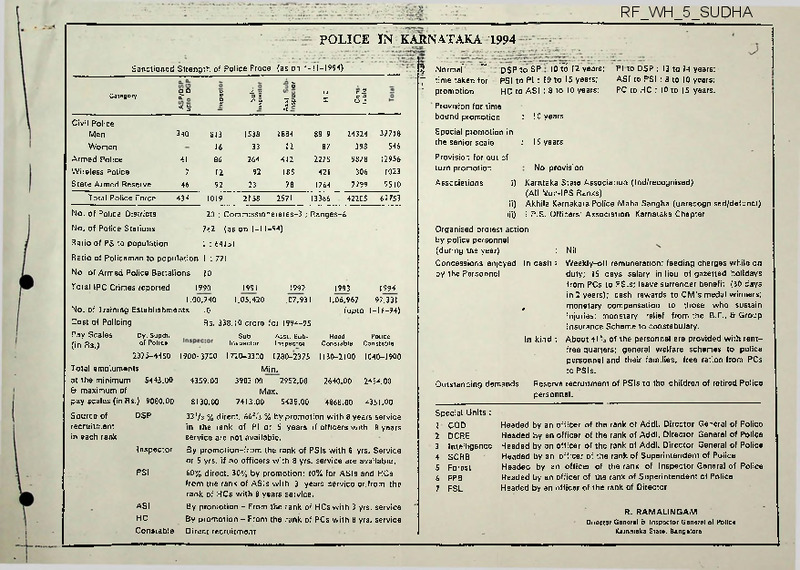
POLICE IN KARNATAKA 1994
Sanctioned Strength of Police Froce (as on l-l 1-1994)
Category
5
DO
XJ o
q
|
£7
< §■
Civil Police
Men
Women
Armed Police
Wireless Police
State Armed Reserve
Total Police Force
340
41
7
46
434
12
92
1019
Provision for time
bound promotion
:
10 years
:
IS years
306
7299
Provision for out of
turn promotion
231
421
1764
12956
1023
9510
Associations
2158
2571
13366
42205
1 : 64151
61753
(as on l-l1 -94)
10
1990
1991
1992
1.00,740
1.05,420
1.07,931
No. of Training Establishments
10
Cost of Policing
Rs. 338.10 crore for 1994-95
Pay Scales
Dy. Supdr.
Sub
Asst. Sub
inspector
Inspector
(in Rs.)
o’Poli«
2375-4450 1900-3700 I720-33C0 1280-2375
Total emoluments
Min.
at the minimum
5443.00
4359.00
3983.00
2952.00
& maximum of
Max.
pay scales (in Rs.) 9080.00
8130.00
5438.00
7413.00
ASI
HC
Constable
ASI to PSI : 8 to 10 years;
PC to HC : 10 to 15 years.
9878
Ratio of Policeman to population 1 : 771
PSI
PI to DSP : 13 to 14 years:
DSP to SP
2275
12
Ratio of PS to population
Inspector
10Y6 12 years:
PSI to PI : 10 to 15 years;
HC to ASI : 8 to 10 years;
412
185
78
742
DSP
"
37718
546
No. of Police Stations
Source of
recruitment
in each rank
time taken for
promotion
24324
398
20 ; Commissionerates-3 ; Ranges-6
No. of Armed Police Battalions
Normal'
7
'
8819
87
1884
No. of Police Districts
Total IPC Crimes reported
5
Special promotion in
the senior scale
1538
33
264
92
813
16
86
||
c 2.
c X)
02
o
—
—
1994
1993
1,06,967
97,331
. (upto 1l-l1-94)
Head
Constable
Police
Constable
1130-2100
IC40-I900
2640.00
2454.00
4868.00
4351.00
33’/s % direct, 662,'s % by promotion with 8 years service
in the rank of PI or 5 years if officers with 8 years
service are not available.
By promotion-from the rank of PSIs with 8 yrs. Service
or 5 yrs. if no officers with 8 yrs. service are available.
60% direct. 30% by promotion; 10% for ASIs and HCs
from the rank of ASIs with 3 years service or.from the
rank of HCs with 8 years service.
By promotion - From the rank of HCs with 3 yrs. service
By promotion - From the rank of PCs with 8 yrs. service
Direct recruitment
No provision
i)
ii)
iii)
Karntaka State Association (Ind/recognised)
(All Non-IPS Ranks)
Akhila Karnakata Police Maha Sangha (unrecognised/defunct)
I.P.S. Officers' Association Karnataka Chapter
Organised protest action
by police personnel
(during the year)
: Nil
Concessions enjoyed In cash : Weekly-off remuneration; feeding charges while on
by the Personnel
duty; IS days salary in lieu of gazetted holidays
from PCs to PSIs; leave surrender benefit (30 days
in 2 years); cash rewards to CM’s medal winners;
,
monetary compensation to those who sustain
injuries; monetary relief from the B.F., & Group
Insurance Scheme to constabulary.
In kind : About 41 % of the personnel are provided with rentfree quarters; general welfare schemes to police
personnel and their families, free ration from PCs
to PSIs.
Outstanding demands
Reserve recruitment of PSIs to the children of retired Police
personnel.
Special Units :
I
2
3
4
5
6
7
COD
DCRE
Intelligence
SCRB
Forest
FPB
FSL
Headed by an officer of the rank of Addl. Director General of Police
Headed by an officer of the rank of Addl. Director General of Police
Headed by an officer of the rank of Addl. Director General of Police
Headed by an officer of the rank of Superintendent of Police
Headed by an officer of the rank of Inspector General of Police
Headed by an officer of the rank of Superintendent of Police
Headed by an officer of the rank of Director
R. RAMALINGAM
Director General & Inspector General of Police
Karnataka State, Bangalore
IsJxzYl
b;
d)
WOMEN’S GRIEVANCE REDRESSAL CELL
OR
CRISIS CENTRE
m^]0AL LMK0EIHE
MULTI^CmARYPRO^
(MULTI-DEPARTMENT; MULT!-A GENCY)
rDEPT OF WOMEN &CWLD DEVELOPMENT
1. WELFAR^DFPT. OF SOCIAL WELFARE
COMPONENTS:
“—DIALLER SYSTEM ("HELPLINE")
- ----- &-
COUNSELLING CENTRE
(FACE TO FACE COUNSELLING)
SHELTER (INDEPENDENT/HOUSES)
'-WOMENS DEVELOPMENT CORPORATION
„
p
vCORPS. OF DETECTIVES [DOWRY SELL)
-WOMENS POLICE STATIONS
Zpoue£--city police
-POLICE HEAD QUARTERS
... OPTIONAL:
SECRETARIAT/RESEARCH CELL
TO CO-ORDINATE WITH
GOVT. DEPTS-oS-SW DEPT
-POLICE DEPT
-LAW DEPT
-COLLEGES
-HOSPITALS etc....
(b)
NGO’s AND
^WOMEN’S
VOLUNTEERS [ ORGANISATIONS
H>SERVICE ORGANISATIONS
U>U.NJCOMMON WEALTH
I AGENCIES
^INDIVIDUAL VOLUNTEERS
LkCCHDI C’C
REPRESENTATIVES
•MEDIA PERSONS
rLAW DEPT
AXA, -LEGAL AID BOARD
^'LAW --LAWFEARS
'-NATIONAL SCHOOL OF LAW
-N! MNANS
~UTY DEPT.
4.PSYCW'-CLINICAL PSYCHOLOGISTS
Q^pp^yMARRIAGE COONS ELLERS
'-PRACTICING PSYCHOLOGISTS
-WOMEN& ORGANIZATIONS
S.NGQs -rlNDimUAL'vDLUNTEE^S
-GROOFS W0RHHV6 FOR WOMEN
STRUCTURE
|
(A)
ADVISORY COUNCIL
(B)
CORE GROUP (MONITORING BODY)
(C)
RESOURCE PERSONNEL
(experts to analyse DATA and ADVlS;7also
for FACE TO FACE COUNSELLING)
(D)
PRIMARY COUNSELLORS
(Trained volunteers to receive call and for
I
CONFRONTING DOMESTIC VIOLENCE
(DOWRY RELATED & OTHERWISE)
STAGE AND NATURE OF INTERVENTION
CATEGORY-1 WORSTPOST INCIDENT
‘POLICE
INVESTIGATION
OF CRIME CASE
(FACILITY ALREADY
IN POLICE)
CATEGORY-II
stage counselling)
* Ambulance (or Link with Ambulance
facility)
Shelter (or link with facility for Shelter^
Rehabilitation)
By
Way
of
CATEGORY - III HOPEFUL - WOMAN UNDER
EXTREME STRESS
4 Counselling cubicles
* Record maintenance system
SOURED RELATIONSHIP
* INTERVENTION
i)
COUNSELLING
ii)
LEGAL AID
iii)
SHELTER
IV) POLICE HELP
SNFRA STRUCTURE
* Telephones & cabins
BAD -
(INTERVENTION MOST BENEFICIAL
PERHAPS LIFE
SAVING)
A SPONSORED CRISIS
CENTRE
MULTI - DISCIPLINARY
MULTI - DEPARTMENT
MULTI - AGENCY PROJECT
HERBAL MEDICINES FOR GYNEACOLOGICAL PROBLEMS
l-J H "
COMMUNITY HEALTH CELL, BANGALORE
I
MENSTRUATION:
1.
Amenorrhoea-
* Grita Kumari (Aloe barbadensis)- Take the fleshy part of the
Iraves; wash it in water few times,, mix with jaggery and eat
in empty stomach in the morning for five days.
* Papaya (Carica Papaya)- Take papaya milk from the fruit; add
2-3 drops with misri (sugar candy-'kalla sakkare').
Consume
it for seven days continuously twice daily.
* Jamun (Euginia; Jambolana)- Take the juice or decoction of
Jamun bark after diluting with water twice daily for about
seven days continuosly.
Cotton plant- Take a decoction of 20 grams each of flowers aid
leaves of the Cotton plant (500 ml. of water boiled to half
its quantity) mixed with 20 grams of jaggery to induce menstrual
flow.
" 125 grams of each of the following ingredients
skb
like sesame
seeds, tender shoots of the cotton plant and tender shoots of
bamboo plants and 220 grams of aged jaggery are to mixed with
the powder and pea-sized pills are prepared.
Take these pills
one at a time with warm water every morning and evening .
■ A good simple formula is shatavari and ashwagandha taken two
parts each, and turmeric and ginger one part each, using one
teaspoonful of the powder per cup of warm water.
Neem- Drink 1 tola of the juice of the tender leaves of neem
for about a month.
A decoction of the bark is also useful.
Onion- Eating the bulbs raw has been noticed to bring about a
desirable regularity in menstruation among women.
It ife is
a case where menstruation does not occur or is obstructed five
I
tolas of onion are cooked in one ser of water till the latter is
reduced to about ten to twenty tolas.
jaggery.
Then add 3 tolas of
This is to be made hot and drunk by the patient for
a few days.
Other reciepes are: three tolas of onion juice
are made luke warm and drunk before going to bed at night.
Or, ten tolas 1 of onion are cut into small pieces, garam
masala is added to it and the whole is roasted in ghee and
eaten.
The obstructed menstruation will become rectified.
2.
DYSMENORRHOEA;
* Kumari-asava which is a given to the patient in a dose of 6 tea
spoonfuls, twice daily after food with equal quantity of water.
* Raljah pravardhani which contains borax in bhasma form, asafoetida- ./>
and kumari, is also an effective drug.
Two tablet
I
* Add sufficient quantity of asafoetida to the food of the patient
which can be given in powder form.
For this it can be fried with
fixisd ghee or butter in a big spoon over fire, this makes it brittle
and powder can be made out of it conveniently.
This powder should
be taken in a dose of 1 teaspoonful twice daily along with food.
It should be followed by hot water.
Because of the pungent smell
it emits, some people do not like to take it alone.
It may be
added with butter milk or vegetables or rice or bread and taken
by the patient.
* Grind the leaves of bitter gourd with some pepper and garlic.
Take this once a day for three days.
* Take the juice of 'karaila'or hacjala kayi loz, once a day for
7 days.
* Make a decoction of somph, avala and jaggery of about 1/2 a cup
twice a day for 30 days.
* Boild the leaves of Arusha(Adathoda Vasica) in a glass of water
and reduce it to half.
From the first day of menses drink in the
morning in empty stomach for 5 days.
* Boil few leaves of Babul TulsiC'nayi tulsi")
in a glass of water
and drink thrice a day.
* Give the powder of the tneder leaves of tamarind 1 tsp with honey
twice a day for 7 days.
3.
MENORRHAGIA:
* Seeds of unripe mango fruit is cut into pieces, fried in ghee,
mixed with sugar and the whole stuff is made into a pill mass.
Several pills are made out later and these are given in stipu
lated doses.
The kernel of the seed is powdered and given in
stipulated doses of 20 to 30 grains with or without, honey.
Fluid extraction of the Park or an infusion of the bark is
•
curative too.
* A drink of the juice of plantain flowers mixed with curds acts
as a curative to young girls suffering from excessive bleeding.
* Burn some amount of coconut coir into ashes- Take a teaspoonful
of the ash, mix it well in tender coconut water, add small
auantity of sugar candy and administer this drug twice a' day
for young girls.
* .Asoka and lodhra are popularly used for the treatment of this
condition.
Thepowder of the bark of these drugs,
is given to
the patient either separately- or in a compound form in a dose of
one teaspoonful four times a day, with cold water.
* The tender leaves of pomegranate along with seven grains of rice
are made to a paste and given to the patient twice daily for a
month.
This works both as a preventive as well as curative
medicine.
* Two grams of each of these ingredients are taken and ground
together: dry (stone) ginger,-gum from the bark of a nemm tree,
ajwan seeds, tamal patra, and equal amounts of the five parts of
the Tulsi plant.
The powder so prepared is boiled in 100 grams
of water till one-fourth of the water remains.
be taken regularly.
The extract should
If excessive flow accompanies dizziness.
Tulsi juice mixed with honey will give quick relief
OLA^
Mx)C
<u_AdZatL
CL
V^v-voouiy
CO^v/zaJ-^
• 5>«o.
2_ ^LjSLcji.^
po rv-^y-VioLf-^^
-4Za£cHu
G^ZZ^
i^zvcZjL
cLdj-i ■
C)^2-2.-
Joouncu^L
^QlcJC
£t<fl
CLVO<Qtad ■
Zf^GO^WOM :
jjJ.■
Oi^Apj^
€ul>-
xUClcLa
cow
ex.
• K^-rvyjVOve.
4^1
'L^JcJL. J<Z-Z.C<2-
uli^cL
,
UajjCL AVvQL-UIX
-ZjO
Acb(_^-
, Cl/\gL
“ZZve
■CLlCLOCHC^,
EVy^'
^O\JLC>UC^
<'
aetF\JL (^GiaJLUXZ AjIOl/V-^
DCU_.UCt2A
, _
O>xZ
-^ci,
YY'^i_a.L-i
'T^e.
.
04
cLsJ
Cucjojjq
<2
£L
cUCl6l<
cQiZxo'
c<fioLc> oict
u
a>AC/
*u.a5jv)
-CK£.
COlcac/gC
<0? lAe.
%
Cl
JJLlzLo.
Zkn'XtM-/
<XOloCaoL '/rj
, >-tXo.. LocveXi •
^CldL?
cLtCa
o^o)
- CJCJduccu ^oea)
i^oZAl
XciQ<ix, •
c^uiook-vie,,
J^jud^Vd^ooa. ■
c<j-A
T^\a3
Zs.
UjOQiJJj
cLucU^o,^ $
''Ikj.i cRoa-ii ©
^■oJJ ‘
Qth&r. rkoQUS
UJG, obibcuc-Ko
0'--Uo+Aj2x
HERBAL MEDICINES FOR GYNEACOLOGICAL PROBLEMS
COMMUNITY HEALTH CELL, BANGALORE
I MENSTRUATION:
1. Amenorrhoea-
* Grita Kumari (Aloe barbadensis)- Take the fleshy part of the
l&aves; wash it in water few times, mix with jaggery and eat
in empty stomach in the morning for five days.
* Papaya (Carica Papaya)- Take papaya milk from the fruit; add
'
2-3 drops with misri (sugar candy-'kalla sakkare').
Consume
it for seven days continuously twice daily.
* Jamun (Euginia; Jambolana)- Take the juice or decoction of
Jamun bark after diluting with water twice daily for about
seven days continuosly.
' AxdHSOKfcisnxsfxSBxgxaniBX
Cotton plant- Take a decoction of 20 grams each of flowers ard
leaves of the Cotton plant (500 ml. of water boiled to half
its quantity) mixed with 20 grams of jaggery to induce menstrual
flow.
125 grams of each of the following ingredients kkh like sesame
seeds, tender shoots of the cotton plant and tender shoots of
bamboo plants and 220 grams of aged jaggery are to mixed with
the powder and pea-sized pills are prepared.
Take these pills
one at a time with warm water every morning *^nd evening .
A good simple formula is shatavari and ashwagandha taken two
parts each, and turmeric and ginger one part each, using one
teaspoonful of the powder per cup of warm water.
Neem- Drink 1 tola of the juice of the tender leaves of neem
for about a month.
A decoction of the bark is also useful.
Onion- Eating the bulbs raw has been noticed to bring about a
desirable regularity in menstruation among women.
It it is
a case where menstruation does not occur or is obstructed five
tolas of onion are cooked in one ser of water till the latter is
reduced to about ten to twenty tolas.
jaogery.
Then add 3 tolas of
This is to be made hot and drunk by the patient for
a few days.
Other reciepes are: three tolas of onion juice
are made luke warm and drunk before going to bed at night.
Or, ten tolas 1 of onion are cut into small pieces, garam
masala is added to it and the whole is roasted in ghee and
eaten.
The obstructed menstruation will become rectified.
DYSMENORRHOEA:
Kumari-asava which is a given to the patient in a dose of 6 tea
spoonfuls, twice daily after food with equal quantity of water.
Ratyah pravardhani which contains borax in bhasma form, asafoetida ■/.
and kumari, is also an effective drug.
Two tablet
!
Add sufficient quantity of asafoetida to thg food of the patient
which can be given in powder form.
For this it can .be fried with
fried ghee or butter in a big spoon over fire, this makes it brittle
and powder can be made out of it conveniently.
This powder should
be taken in a dose of 1 teaspoonful twice daily along with food.
It should be followed by hot water.
Because of the pungent smell
it emits, some people do not like to take it alone.
It may be
added with butter milk or vegetables or rice or bread and taken
by the patient.
,
>
5 /
* Grind the leaves of bitter gourd with some pepper and garlic.
/Take this once a day for three days.
'
* Take the juice of *karaila’or hagala kayi loz, once a day for
7 days.
* Make a decoction of somph, avala and jagaery of about 1/2 a cup
V
twice a day for 30 days.
* Boild the leaves of Arusha(Adathoda Vasica) in a glass of water
and reduce it to half.
From the first day of menses drink in the
morning in empty stomach for 5 days.v
* Boil few leaves of Babul Tulsi('nayi tulsi')
in a glass of water
and drink thrice a day.
* Give the powder of the tneder leaves of tamarind 1 tsp with honey
'/ twice a day for 7 days.
3. MENORRHAGIA:
* Seeds of unripe mango fruit is cut into pieces, fried in ghee,
mixed with sugar and the whole stuff is made into a pill mass.
Several pills are made out later and these are given in stipu
The kernel of the seed is powdered and'given in
lated doses.
stipulated doses of 20 to 30 grains with or without honey.
Fluid extraction of the Park or an infusion of the bark is
curative too.
*,.A drink of the juice of plantain flowers mixed with curds acts
as a curative to young girls suffering from excessive bleeding.
* Burn some amount of coconut coir into ashes- Take a teaspoonful
of the ash, mix it well in tender coconut water, add small
nuantity of sugar candy and administer this drug twice a- day
for young girls.
* Asoka and lodhra are popularly used for the treatment of this
condition.
Thepowder of the bark of these drugs,
is given to
the patient either separately- or in a compound form in a dose of
one teaspoonful four times a day, with cold water.
* The tender leaves of pomegranate along with seven grains of rice
are made to a paste and given to the patient twice daily for a
month.
This works both as a preventive as well as curative
medicine.
* Two arams of each of these ingredients are taken and around
X
together: dry (stone) ginger,-gum from the bark of a nemm tree,
ajwan seeds, tamal patra, and eaual amounts of the five parts of
the Tulsi plant.
The powder so prepared is boiled in 100 grams
of water till one-fourth of the water remains.
be taken regularly.
The extract should
If excessive flow accompanies dizzin&ss.
Tulsi juice mixed with honey will aive guick relief
-to
ok(.o(.+f'pn.
J+lJ^Asd
<kj\cl
'■LI'ka. P<jl>..\cLqa.
T
‘tca^ iS ku^zu; Jii tA^.^o'^oa. t •
v-Cka
U j^LCAUu vjQLLLe
o^XG.c tf'.o^
■Zh.Q
pAj4-C£> t-\J
ZOnAjjj
^.'d_i.c.c. ■
<_ CuJ tea •
oui
<l‘^lcA.
CW
DLU'V.a.
rJrLi./y
(. ist'.'l th
-a
aguxZ.
lCJLu
V||| ■k&J’-
u '^> b<i.
Q.
^Xol.d.tld. drj
''t ^J~l
xt-tL^x<iJ.a.l£.( -Clu.
-U.o ttx..-0/A.
\(
tuo^ z pv-o^zvo&s
ol^e.e-A(b^
V
^dJ-C^
AP^-cZaZ/J"
V
Qth&r,
Qj-v-vO
55
ozxo ce.Acoxf-
<S)rv • l^bkt
AJdPQSQjd
yOaxj/tLuJAA vU /Uyoycxjced
lZ©
Cuajl pcvC^uUL pcU,
kJ H
HERBAL MEDICINES FOR WOMEN— CHC, BANGALORE
I MENSTRUATION
1.
Excessive Bleeding:
.
* Amarantus Spinous(Kannada- •mullu dantu', Telugu- 'attamullu
goranta, nalla doggeli') is used in checking excessive
menstrual flow.
* Drinking of 1 tola of the juice of the tender leaves of neem
are helpful.
* Fried Hibiscus (’dasavala'
in Kannada) in ghee is helpful.
* Seeds of unripe mango fruit is cut into pieces, fried in
ghee, mixed with sugar and the whole stuff is made into a
pill mass.
Several pills are made out later and these are
given in stipulated doses.
The kernel of the seed is powdered
and given in stipulated doses of 20 to 30 grains with or w
without honey.
Fluid extraction of the bark or an infusion
of the bark is curative too.
* A drink of the juice of plantain flowers mixed with curds
acts as a curative to young girls suffering x from excessive
bleeding.
* Xa Burn some amount of coconut coir into ashes- Take a
teaspoonful of the ash, mix it well in tender coconut water
■1s '
add small quantity of sugar candy and administer this drug
twice a day for young girls who suffer from excessive bleeding.
4% mashas each of the gum and marking nut(geru)(Kikar or
Gum Arabic, Acacia Arabica*:jali, karijali, bauni in Kannada)
should be given grinding them along with water.
Asoka and lodhra are popularly used for the treatment of
this condition.
The powder of the bark of these drugs, is
given to the patient either separately or in a compound form
in a dose of one teaspoonfijl four times a day, with cold
water.
Asoka-arista and
•
Asoka-arista and lodrasava are given to the patient in a dose
of one ounce twice daily after food with an equal quantity of
water.
, *zThe tender leaves of pomegranate along with seven grains of•
raice are made to a paste and given to the patient twice
daily for a month.
This works both as a preventive'as well
as curative medicine.
* Pravala and mukta are used in acute attacks of this disease.
They are given in a powder form which is called pisti.
One
grain of the powder of this drug is given to the patien four
times a day. '
* Diet: Old rice, wheat, moong dal, milk and ghee can £>e 'given.
Sugarcane juice, grapes, jack-fruit, banana, amalaki, pome
granate, are very useful.
Hot and spicy things are to be
strictly avo.tdedj
Two grammes of each of these ingredients are taken and ground
together: dry (stone) ginger, gum from the bark of a neem
tree, ajwan seeds, tamal patra, and equal amounts of the
five parts of the Tulsi plant.
The powder so prepared is
boiled in 100 grammes of water till one-fourth of the water
remains.
The extract should be taken regularly.
If excessive
flow accompanies dizziness, Tulsi juice mixed with honey will
give quick relief.
■ * Equal weights of Pathani Lodh, Ochre(Ger) and Oak Galls(Mazu)
should be finely powdered and four grams of it taken in the
morning and evening with milk.
* Half ripe fruits of the country Fig tree(Gular) shduld be
dried in the shade, powdered and mixed with an equal quantity
of sugar.
Six grams of the powder taken with-milk in the
morning and evening gives.
Alternatively, three grams of
Rasaut and an equal quantity of Shellac should be finely
-2-
ground together and made into two dosffs, one to be taken with
milk in the morning and evening.
* Dry Amla should be soaked in juice of green Amla for three
days and then ground into powder.
Six grams of this powder
taken with cow's milk for some days cures the condition.
Other remedies recommended afe:
10 grams each of Selkhari
(Talk) and Geru(Red Ochre) ground together should be taken
in three grams doses thrice daily.
Multani Mitti(Bole
Armeniac) steeped in water and the supernatant water drunk
in the morning is also good for excessive bleeding from the
womb.
Five' grams of bark of £ Kurchi and raw Sugar mixed
together taken' in the' morning and evening is also an
effective’remedy.
* Grind t'ogether the leaves of Mehandi(Lawsonia alba), Bhumi
avala(Phyllantus Niruri) and the rind of the anar fruit
(Punica granatum) and make pills.
stomach in the morning.
Dose: 1 day in empty
The' juice or decoction of the same
also' can be used.'
* Cut a ripe banana at the centre and put one small spoonful
of alum powder and eat in empty stomach in the morning for
2-3 days.
* Half a cup of the Jamun Ju'ice, to be taken twice daily for
five to seven days.
Mix one teaspoonful of dhania' powder in the water in which
rice has been washed.
Dose: 1 glass for a day.
I HERBAL MENSTRUATION
DYSMENORRHOEA- Painful
2.
* Fresh mint chutney or mint decoction is given to decrease
menstrual cramps.
For very severe dysmenorrhoea a decoction
of •Brahmamanduki• leaves is used in rural India.
These
leaves rich in Vellarin is a known sedative and anti
A fist-ful of the leaves boiled in a pint of
spasmodic.
w't'er, and given as a decoction in doses of an ounce «
thrice a day helps to relieve the discomfort in menses.
p Kumari-asava, which is an given to the patient in a dose of
6 teaspoonfuls, twice daily after food with equal quantity
of water.
Rajah pravardhani which contains borax in bhasma
form, asafoetida and kumari, is also an effective drug.
Two tablets of this medicine are given to the patient, twice
a day for about 7 days,immedietly before the due date of
menses.
It relieves congestion in the pelvic organs, works
as a laxative and thus keeps the patient free from any pain
during menstruation.
Add sufficient quantity of asafoetida to the food of the
patient which can be given in powder form.
For this it can
be givEnxtBxthexpatiHHtxxixxaxpHw fried with ghee or butter
in a big spoon over fire, this makes it brittle and powder
can be made out of it conveniently.
This powder kh should be
taken in a dose of 1 teaspoonful, twice daily along f with
food.
It should be followed by hot water.
Because of the
pungent -sSMre it emits, some people do not like to take it
alone.
It may be added with butter milk or vegetables or
rice or oread and taken by the patient.
*/
Grind the leaves of bitter gourd with some pepper and garlic.
Take this once a day for three days.
One hundred grams of juice of green leaves of Bleak Night-
*
shade( Mako) and leaves of Chicory (Kasni) should be placed
on fire and when it coagulates, it should be strained and
drunk after mixing 20 grams of Gur with it.
*
Twenty grames of the leaves of the following eight herbs are
boiled in water: ±k
i)
Sambhalu (Indian Wild Pepper);
Sahinjana(Horse
ii)
iii)
Radish);
Bakayan (Indian Lilac);
iv)
Kasni (Wild Chicory);
v)
Mako (Black Nightshade);
vi)
Khatmi (Marsh Mallow);
vii)
Narma Kapas (Cotton Plant);
viii)
Soya(Dil).
When the leaves are cooked and the water evaporated, they should
be fried in Sesame Oil like any vegetable and tied to the
lower abdomen like a pultice.
It will deal effectively with
inflammation.
* A decoction of root of Cotton Tree(18 grams), Telia Geru
(6 grams), leaves lof Rose Bush (6 grams). Root of Chulai
(6 grams), Gur (24 grams) boiled in 750 ml. of water till one
eight is left.
The decoction should be taken for three days
continuously.
v/*'rake the juice of ‘karaila* loz l/dayx7days.
/■'"Ta Make a decoction of spmph, aval a and jaggery.
cup
2/day x 30 days.
^/Boil two leaves of Arusha (Adathoda Vasica) in a glass of
water and reduce it to half.
From the first day of menses
drink in the morning in empty stomach for 5 days.
Boil few leaves of Babul Tulsi (Occimum basilacum) in a
glass of water and drink 3/day.
* Heat in mustard oil 5 tender leaves of Kujur (Malkanguni:
Celastrus Paniculata). Take 1 tea sp ful 2/day for 21 days.
* Root decoction of Kapas (Gossypium'indicum) 4 oz. 3/day x
7 days.
* Take Kujur oil 3 drops in Honey 1/day x 21 days.
frGive the powder of the tender leaves of imli (tamarind) 1
tsp with honey 2/day x 7 days.
-3I MENSTRUATION:
3. Amenorrhoea- Absence
*prita Kumari (Aloe barbadensis); take the fleshy part of the
leaves; wash it in water few times, mix with jaggery and eat
in empty stomach £ in the morning for 5 daiys.
* XakexanyxsfxkhExstHnsKaixKiadiEiMHsxniEFitiHnEdxxH
Pappaya milk
(Carica Pappaya) from the fruit 2-3 drops with misri (sugar
candy) 2/day x 7 days.
* The juice or decoction of Jamun bark (Euginia; ffJambolana)
Juice after diluting with water 2/day x 7 days.
■ Prepare a paste of the tuber of Kalihari (Gloriosa superba)
and apply over the supra pubi'c region for two hours.
Apply
same paste on the forehead also for the whole night .
* Give the decoction of the seeds of gajer with jaggery 1
tabj.e sp ful 1/day x 7-15 days
* The infusion or decoction of the root of Kapas (Gossypium
Indicum) is given with honey or jaggery in the morning in
empty stomach, and in the evening Dose:
2-4 oz.
A week before theperiods of a woman are due, a decoction of
six grams of Fl^j Seeds (about 250 mi. of water reduced to
half through boiling) mixed with 20 grams of jaggery and 20
grams -of ghee should be taken daily.
Alternatively, a decoc-
tion of ten grams of seeds of Carrots and jaggery should be
taken for about a week. ^Another remedy is to boil six grams
of Baberang (Emoelia Ribes), three grams of dyry
Ginger and
20 grams of Jaggery in 500 ml. of water till half of it is
left.
The decoction should be taken for some days before
it shows its effect
*/ A decoction of 20 grams each of flowers and leaves of the
Cotton Plant (500 ml. of water boiled to half its quantity)
mixed with 20 grams of Gur is also effective in inducing the
menstrual flow,
* Another remedy is to steep 10 grams of Black Sesame seeds
and an equal quantity of small Caltrops (Gokhru) in 250 ml.
of water and to ’grind them in the same water.
It should be
sweetened with sugar, and drunk.
* Treatment with -the seeds of Tulsi ground and suspended in
water for three days beginning from the first day of the
menstrual flow will help the woman to conceive, as this treat
ment is purifies the uterus.
If this treatment is given to
any infertile woman for a year, she is sure to conceive.
* One gramme of each of the following ingredients is taken:
Tulsi s’eeds, naagkesar, ashwagandha, and palash peepal.
These are then ground to a powder that is fine enough to pass
t through cloth.
To this powder are added 10 grams of cow's
milk^ and some sugar.
Administration of this preparation will
restore regularity of menstruation within two months, even
in the case of a woman who has stopped menstruating for some
reason.
e,
125 grams of each of the following ingr^die^nts are seasame
seeds, tender shoots of the cotton plant and tender shoots
of bamboo plants.
220 grams of aged jaggery are mixed with
the powder and pea-sized pills are prepared.
These pills
taken one at a time with warm water every morning and
evening will also restore regularity of periods, even in
cases of women with amenorrhoea.
* Myrrh by itself is often good for amenorrhoea, particularly
„
taken as a tincture.
An anti-Vata or toriiifiying diet is
paKtxEMiaKkyxkxkexxasxaxk±H<skuxHX primarily indicated using
dairy, meat, nuts, oils, whole grains arid other nourishing
foods.
Iron supplements.or Ayurvedic iron ash preparations
Warm seasame oil can bp, applied to the ower
are important.
abdomen or used as a. douche.
A mild laxative can be taken
such as Triphala, aloe gel or castor oil in lower dosages.
* For. amenorrhoea due to cold, many spicy herbs can be usedginger, turmeric, black pepper, cinnamon, rosemary, or the
formula Trikatu.
Fresh ginger and pennyroyal in equal parts,
ounce per pint of water, 1 cup three times a day, is good
Western herbal treatment for this condition, whisk
* Ayurvedic herbs for Vata type delayed menstruation include
asafoetida, cyperus, myrrh, ashwagandha, shatavari, kapika-
,
cchu, black and white musali.
*
A good simple formula is shatavari and ashwagandha two parts
tz each, and turmeric and ginger one part each, using one
teaspoonful of the powder per cup of warm water.
.
* Kapha (water) type delayed menstruation is die to congestion
x/\and- sluggishness in the system.
It can also be treated by
strong warming spices-ginger, cinnamon, cayenne, black pepper
or Trikatu or Clove combination formulas.
* P_itta_-(-fire) type delayed menstruation is usually mild and
can be treated by turmeric or saffron in warm milk.
Other
good herbs are rose, cyperus, dandelion and other cooling emeenagogues.
c
* Drinking of 1 tola of the juice of the tender leav^fe of neem
is effective.
A decoction of the bark is also useful.
* Pumpkin^: Kadu hire, nagadali bali in Kannada; adavibira in
Telugu- their seeds correct the absence of menstrual flow.
* Apium Petroselinum or Parsley: Apiol a green liquid distilled
from the root is much recommended in absent or disturbed X
menstrual flow:
is given then in doses of 2-3 minims given
in sugar or in capsules.
In cases of arrested menstruation
accompanied with fever and malaria, pills made of 2 grains
of quinine suislphate, l/3rd grain of apiol,
a grain perma
nganate of potash are given beneficially.
* Onion: Eating the bulbs raw has been noticed to bring about
a desirable regularity in menstruation among the ladies.
If
it is a case where^ menstruation does not occur or is- obstru
cted five tolas of onion are cooked in one ser of water till
the latter.is reduced to about ten to twenty tolas.
3 tolas of jaggery.
Then add
This is to be made hot and drunk by the
patient for a few days.
Other recipes are: three tolas of
onion juice are made luke warm and drunk before going to
bed at night: Or, ten tolas of onion afe cut into small ,
pieces, garam masala is added o to it and thewhole is roated
in ghee and eaten.
rectified.
The obstructed menstruation, will become
I MENSTRUATION:
4.
Leucorrhoea - White discharge
A regular douching of the genital tract with a decoction of
the bark of the Banyan tree, or the potassium permaganate is
indicated..
Douching pwith decoction of bark of the Banyan of Cig tree
keeps the tissues of the vaginal tract healthy
* The dried and powdered bark of the Muisari (Mimusops Elengi)
tree mixed with an equal weight of raw Sugar should be taken
in nien grams doses every morning with water.
Alternatively,
equal weights of the leaf-sghoots of Bastard Teak (Dhak)
and Banyan tree should be tried and powdered. An equal quant
ity of raw sugar should be mixed with them and nine gram
doses should be taken with 250 ml. of milk thrice daily.
Theroot of the Silk Cotten tree (Sembhal) is another specific
for this condition. Seven grams of its powder with an equal
weight of raw Sugar should be taken with a glass of milk.
* Dry Amla and Liquorice in equal quantities and powdered and
mixed with thrice the quantity of honey make an effective
drug against the disease.
Six grams of the linctus should
be taken in the morning and evening with milk.
* The patient should chew betel nut after meals as it has
curative effect.
* Cumin seeds ground in Tulsi juice and mixed with fresh milk
/of a cow have a beneficial effect in leucorrhoea, and they
also improve the general health of the wonjan.
* 20 grammes of Tulsi juice with rice water, meanwhile restri-
^/cting the diet to rice and milk, or rice and ghee for the
duration of the treatment.
* One teaspoonful of the powder of the banyari tree and fig tree
should be boiled in one litre of water and reduced to half.
The decoction is then filtered and the powder thrown away.
When it is slightly warm, douching should be performed.
This
decoction keeps the tissue cells of this area healthy.
-The-"
* popular medicine used by Ayurvedic physicians in this condi
tion is 'pradarantaka lauha'.
of iron.
This drug contains some bhasmas
For the peeparation of this medicine, the ingre
dients are triturated with the juice of 'kumari'.
Four
grains of this drug is given to the patient three times a
day, with honey,
* When the outer skin of the leaf of this kumari is removed,
a fleshy pulp comes out which is used for the extraction of
juice.
One ounce of this is to be given to the patient
twice daily with a littlye honey added to it, preferably on
an empty stomach.
This juice stimulates the liver, promotes
digestion and regulates the bowels.
* Lodhra is also used for the purpose of douching.
The bark of
this tree is used and the decoction of the bark is prepared
on the lines suggested above.
The medicine is also used
in the form of lodhra asava.
* Tankana or alum is also used both externally and internally
for the treatment of this condition.
Alum is fried in a
vessel over fire and then powdered.
One teaspoonful of the
powder is added to the decoctions described above and used
for the purpose of douching.
* Two grains of this powder are mixed with two grains 01L p
pradarantaka lauha and given to the patient twice daily on
an empty xebkh! stomach mixed with honey.
* Alongwith all the medicines described above tanduledaka
(rice-wash)
is given as a means to accelerate their action.
Rice-wash alone is also useful for the cure of this disease.
* Take the leaves of Drum stick tree in any form as soup or
sagH or chatni.
Take the juice of arhar (Cajanns Indfcus) leaves.
cup with sandha namak (rock salt)
1/day x 30 days
Dose:
1
-2-
* Take thS inner part of the leaves of Gritha Kumari with
1/day in the morning in empty stomach x 5 days.
jaggery.
* Grind the tuber of 4' o'clock plant (Gulavas; Mirabilis jalpa)
in empty stomach.
Mehandi seeds-1 kg. Triphala-250 grams each, grind all these
together; add little bit of the powder of jira, ajwain, and
somph.
Make pills mixing with the syrup
of jaggery. Dose:
1 each 3/day x 30 days.
* Grind and give a handful of Brahmi (Centella asiatica) 1/day
x 30 days.
* Dry and powder separately raw Banana, rice (ara rice, and
4-. Triphala) .
jaggery.
Mix all in equal amount end prepare lehyam in
Dose: 1-2 teaspoonful 2/day x 30 days.
* Grind the leaves of Kena grass anddrink with a glass of
cow's milk.
g
1/day x 3-7 days.
* ^oil few cut pieces of ginger and few flowers (Better buds)
L of arhul (hibiscus Rosa) in a glass of cow milk adding equal
amount of water and reduce it to half.
with sugar.
Strain and drink
2/day; morning and at bed time x 21 days.
* Fluid extraction of the bark or an infusion of the bark of
V mango tree is curative in h leucorrhoea.
* Prepare a tincture or an alcoholic extract of the powder of
betel nut and employ it but freely diluted with wat^r- 1
drachm of the tincture in 4 ounces of water.
This is used
locally or as an injection to stop water discharge from the
vagina and also in checking the hydrosis of water rash of
^pregnancy.
Hdre, a sudden flow of acid fluids from the
stomjph to mouth occurs and an outbreak of burning sensation
(heart burn) in the gullet, as well.
I MENSTRUATION;
5.
Other Problems:
* Drinking of 1 tola of the juice of the tender leavjss neem is
advised even in the aDsence of menstrual flow or the obstru-
ction of such a flew because this is a good corrector of
menstrual irregularities.
This is also used in cleaning
the Uterus.
* The juice of the flowers "is given regularly upto six'mashas
in dosaae to be licked along with hone^. -(-neEOTh
* Bitter gourd; hagala kayi in Kannada; kakara, tellakakra
in Telugu is given internally to cure disorders of menstr
uation (freshly extracted juice).
* rhe seeds of raddish are regarded to be possessing emenago-
guic properties viz. they regulate menstrual cycle among
women and are therefore used in the related disturbances.
The external application of the seeds promotes menstruation.
A teaspoonful of the seeds of raddish is to be ground into a
smooth paste.
then drunk.
This is to be mixed well with buttermilk and
This will commence menses that had become
obstructs.
* If the flow is too little or is accompanied with pain, heat
water, mix mustard powder with it andplace the patient in
such a water upto the waist.
Such a hip w bath for an hour
would render the flow to become normal and pain free.
* Betel nut is regarded as a nervine tonic and an emenagogue
or that which brings about regulation in menstruation and
its cycle.
Gingel ly decoction is given to girls to bring about quick
A pinch of saffron well crushed in a tablespoonful
px)
puberty.
J
of milk is another useful prescription for underdeveloped
girls.
effect,
In adolescence saffron has an overall stimulating
* It is a practice among certain communities in south India to
give the girl who has newly come of age a combination of a
teaspoonful of gingelly oil with a teaspoonful of overnight
soaked urad dal, a few grains of whole Bengal gram and the yolk
of one egg.
girl.
This 'egg nog.' helps in the full maturity of the
In addition, chutney made with coriander leaves, curfy
leaves, mint or fenugreek leaves all help in the full growth
of the adolscent girl.
come on.
Anaemia is checked, regular periods
Mint in particular is supposed to cure painful
periods xsm by acting as an uterine tonic.
* A tasty drink is
raade by mixing in milk egg yolk, four almonds
crushed, a little gingelly powder and a teaspponful of honey.
v This
could be given for sexually underdeveloped girls as well
as for those with undue delay in the onset of periods in
adolscence.
* Green unripe papaya is considered to be a more effective
J emenagogue which brings on the periods quickly.
the flow of periods.
It also increases
Pineapple has similar qualities too.
* Cumin and gingelly decoction sweetened with palm candy is
supposed to help the onset of menses and the free flow of blood.
i
* A modification of the above is to make sweet rolls with jaggery
black cumin and dry turmeric powder and take one or two a day
to help onset of periods.
* Boil pieces of the fig root(Anjeer, Dumeer, Athi pazyam) in
, water and make a decoction.
Filter and drink the decoction
/
for a few weeks to set the cycle normal.
* One gramme of each of the following ingredients is taken:
$ Tulsi seeds,^ naagkesar, ashwarfjandha, and palash peepal. These
are then ground to a powder that is fine enough to pass
through cloth.
To this powder are added 10 grammes of cow's
-2-
milk and some sugar.
Administration of this preparation will
restore regularity, of menstruation within 2 months, even in the
case of a woman who has stopped menstruating for some reason.
* Fry the kernel of the seeds of Neem in til oil and powder it.
Dose:
1 tspfull with sugar candy 2/day in empty stomach x 3-5
days.
* Prepare the decoction of the barks of Jamun tree.
Mango tree
, and shimal tree (Bombax Malabaricum)-silk cotton tree in 2 ltrs
of water reducing it to half. Dose:
1 cup 2/day x 1 day.
- S’-3
HERBAL MEDICINES
AMARANTUS Sr'INOUS( Kannada-'mullu dantu’, Telugu-1 ettamullu
1.
goranta, nalla doggali)
Used in checking excessive "mdnstrual
blood flow and its
( consumption by ladies Soon after childbirth
milk content.
gonorrhoea.
The root
increases their
is regarded as specially medicinal
in women)
laxatibe and galactagogue
(promoting milk production
Its decotion i’s beneficial
in curing urinary retention and
gonorrhoea.
in
In Madagascar a the root is considered diuretic,
The root ground in water is apolied over chancres
(the hard swellings that constitute the primary lesions in
syphilis) that are also infected with fungi,
in addition.
(LEAFY VEGETABLES-Traditional Family
Medicine)
NEEM
1 .
(TFM)
IN LABOUR PAIN:
In Maharashtra, neem is called balantnimb viz the after labour
neem,
the use of neem here is so m^uch reputed.
If the midwife
administers fresh m juice of leaves even before the labour,
contraction of the uterus is facilitated.
The flow will
the
be
clear, the swellings of the uterus and the surroundings get
lessened and the patier^starts getting hunger.Faecal matter
becomes clear, there will not be any fever and even if fever
arises its violence is much less.
Drinking water in which neem bark has been boildd whenever she
feels thirsty after the labour is over,
/
will keep the patient
healthy.
Washing the uterus with warm neem water will relieve the uterine
pains due to delivery and ia also the morbid swellings if
apy.
The wounds will heal and dry up and the orifice becomes
clean and contracted.
V
Fermentation with the inner bark of old
neem trees is highly recommended for all diseases following
delivery.
The fresh juice of neem leaf
after the birth of the child.
meals.
is given for the first three days
This is given before the principl
Such a measure improves the general health of the mother
and also increases the. milk yield.
This is also given to the
cows so as to increase the yield of milk.
s
2.
LEAF PREPARATIONS:
Hysteria in Ladies- Taking fresh leaf juice or leaf decoction
for three to four months will relieve such a hysteria which is
due to the abnormalities of uterus.
If there is ixcess menstrual flow, a drinking of 1
the juice of the tender leaves is resorted to.
tola of
This is advised
even in the absence of menstrual flow or the obstruction of such
a flow because this is a good corrector of menstrual irregulari
ties.
3.
This is also used in cleaning the uterus.
BARK PREPARATIONS:
Amenorrhoea(Absence of Menstrual Flow)- A decoction of the bark
is given as a drink for sarrsstiapixxiR the same.
4.
FLOUER PREPARATIONS:
After Labour Pain- Flowers are ground and applied over the head
or the stomach to relieve the pains at the head or the stomach
following delivery.
Menstrual Irregularities- The juice of flowers is given regu-
V]
larly upto six mashas in dosage to be licked along with hone£.
I
GOURDS AMD PUMPKINS
Sore kayi, halu kumbala
gubba kaya
(TFM)
(the milky pumpkin)
(a bloated vegetable),
The io sweet fruit variety
in Kannada; alaburu,z
sorakaya in Telugu.-
is wh olesome to the developing foetus
and therefore well advised for the pregnant women, as a very
salutary diet.
Kadu hire, nagadali balli in Kannada;
adavibira in Telugu- their
seeds correct the absence of menstrual flow in amenorrhoea.
Bittef Gourd;
hagala kayi in Kannada; kakara,
in Telu’’
tellakakra
is given internally to cure disorders of menstruation.(freashly
extracted juice).
Kadavanchi in Marathi and Kannada are tubers used to procure
abortion.
Bitter Apple; pavamekke kayi,
klaaRmMfctixc chittipapara,
tumati kayi
in Kannada; pey
etipuccha. in Telugu is useful
in
rectifying abnormal presemtation of foetus and also in atrophy
(or non-development and growth.) of foetus.
-2-
vegetables(tfm)
CARROTS: Ths seeds of carrot are emenagoguic
(regulating men
strual cycle), cleaning to uterus and abort ifacient
(i.e. causes
abortion of the f.oetus).
RADDISH:
The seeds of b
raddish are regarded to be possessing
emenagoguic properties viz. they regulate menstrual
cycle among
women and are therefore used in the related disturbances.
The
external application of the seeds is promotes menstruation.
A teaspoonful of the seeds of radish is to be ground into a
smooth paste.
then drunk.
HIBISCUS ;
This is to be mixed well with buttermilk and
This will commence menses that had become obstructs
dasaval
in Kannada-are fried in ghee and given in
menorrhagia or excessive menstrual flow.
FRUITS (TFM)
MANGO: Tind of unripe fruit
is cut into pieces, fried in ghee,
mixed withs sugar and the whole stuff
is made into a pill mass.
Several pills are made out later and these are given in sti
pulated doses in case of menorrhagia or excessive menstrual
flow.
The kernel of the seed is powdered and given in doses of
20 to 30 grains with or without honey i-n—many-af-f-l-ict-i-on's-:—i~i‘ke
excess-menstrual flow.
kernel
For dysentry in pregnant women the
is fried in ghee and given for e ting.
Fluid extraction
of the bark or an infusion of the bark is curative in excessive
menstrual flow, white discharge.
BANANA:
Pregnant ladies will find nashBdxwB consuming ripe
,
banana fruits regularly would nourish their food well and will
als@ pave way to a safe delivery.
A drink of the juice of
plantain flowers mixed with curds acts as a curative to young
girls suffering from excessive haemorrhage during and after
menses.
The relief obtained is quite quick.
PAPAYA: The major use has been in correcting menstrual disorders
or as an emenagogue.
There is a popular quite strong particu
larly in Tamil Nadu that they may cause abortion.
In central
and South America, the seeds are used as anthelmintic and
emmenagogue to normalise mensus troubles.
Juice of the green
fruit is applied in—r-ingworm and as a sure remedy for scorpion
locally as a pessary to uterus to induce abortion.
However,
it is better that pregnant ladies aboid eating paoaHa,
□r ripened,
till the thi^d month.
abortion then.
A fruit salad
raw
For, there would Be a risk o
of honey, milk and paoaya
fruit is an excellant tonic-ideal for children,
feeding mothers
and pregnant ladies(after their third month).
SPICES(TEM)
-PEPPER-:
In Kerala an infusion of the root
is prescribed after/
childbirth to cause an expulsion of the placenta, almost as a
regulars household remedy.
PIPER BETLE-Betel leaf vine in English;
pan,
tatobuli in Kannada
Used for child bearing in' Orissa.
The slender roots with black
pepper are used to cause sterility
in womdn.
PEPPER; /nennasu in Kannada- facilitiates menstruation.
CLOVE: lavanga in Kannatja;
lavangamu, karavappu in Telugu.-
Take a masha of .tie powder of cloves, mix
sugar candy or pomegranate juice.
it with a syrup of
This is to be taken by the
pregnant by licking, teo get rid of the repeated vomitings andthe agitation thereof.
An infusion of cloves also serves the
same purpose but this should not be given if there is an
accompaniment of fever along with vomiting.
CINNAMONUM TAMALA:
dalchini, lavangada pattai,
kadu dalcljini in Kannada;
It
lavanga patri,
talisha patri in Telugu.
is promotive of menstruation and a lactagogue-promoting
milk secretion.
CINNAMOMUM MACROCARPUM:
bhringa, dalchini, lavanga pattre in
Kannada has a reputatijawxaR ed application
in menorrhagia
and also in difficult labours that are due to defective uterine
contractions.
The distress of the labour pain.after child
birth will get
greatly relieved by a drink of the cinnamon
decotion.
<By'consuming a pinch of cinnamon powder daily at
night for a'"month altogether would postpone the reappearance
of menstrual flow as much as possibleTJ^.
CARDAMOMS:
elakki
in Kannada a can cause mm abortion.
Chewing these grains well and gulping in, will ward off stomach
upsets, dizziness of the head and oozing of water in the mouth
as well as the tendency to vomitting.
Another measure to over
come dizziness and avoid vomitting tendency is
to take the
cardomom powder in a glassful of lemon juice.
Drop three to
-3-
four pinches of cardomom powder into a cupful of tender cocoanut
juice, add two spoonfuls of honey to it and take in.
stop vomitting.
In case however,
This will
vomitting is too violent,
adopt this measure thrice a day for two to three days.
SEASONING HERBS(TFM)
MUSTARD:
sasive
in Kannada; avalu in Telugu-
To expel dead foetus:
rattis of fried
3 mashas of mustard and 4
hing are mixed with soury conjee or wine and given as a drink.
Menstrual flow:
If the flow is too little or is accompanied
i
with pain, heat water, mix mustard powder with it and place
the patient
in such a water upto the waist.
Such a hip bath
for an hour would render the flow to become normal and pain
free.
CUMINUM:
women,
jeerige in Kannada; jeeraka
in Telugu- For pregnant
/
seeds are ground and mixed with lime juice and given
in cases of bilious nausea.
Intake of cumin seeds soon after
child birth will increase milk secreation.
■CORIANDER: kottambari,
haveeza
in Kannada; kotimiri
Take a teaspoonful of coriander seeds, powder,
in Telugu-
grindtit smoothly
in water, mix this paste homogeneously in water in which rice
has been washed, add sugar and administer.
This measure can
be continued twice a day till, the vomitting tendency comes
under full control.
APIUM PETROSELINUM OR PARSLEY:Apiol
from the root)
menstrual flow;
(a green liquid distilled
is much recommended in absent or disturbed
it
is given then in doses of 2-3 minims given
in sugar or in capsules.
In cases of arrested menstruation
accompanied with fever and malaria,
pills made of 2 grains of
qui-nine sulphate, l/3rd grain of apiol,
ganate of potash are given beneficially.
1/2 a grain perman
When the leaves are
applied several times a day to the breasts,
it will arrest milk
secfeat ion.
ASAFOETIDA
OF HING: hingu or ingu in Kannada;
inguva in Telugu-
' Hing at the child birth stimulates uterine wall,
render it clean
and stops the terrible disease of makkalla characteristic of
child birth in many women.
To prevent abort ion:Habitual abortion is treated in the foil
manner.
Six grammes of hing are made into 60 pills
■yi^ain). Directly the pregnancy
is given twice a day.
(each,
of
is suspected one such pill
The dose is-then slowly gx increased to
ten pills a day and then ^gradually reduced till confinement.
Such a procedure has proved sutcessful in cases having three’
to five abortions,
or complications of premetritis
ammation of the outer layers of the uterus)
(the infl
or catarrhal
endometritis(discharge from the inner walls of the uterus)
and also in cases in which abortion at sixth month was threatnin<
* Taking a teaspoonful of the decoction of clo'tae to which a
j
little bit of hing is added and doing so thrice a day
'
is bene-
ficial to feeding mothers for this will ensure greater milk
production.
* Keeping a bit of hing enclosed within a piece of cotton
in the ears will ensure freedom from catching cold after child
birth.
DILL-EUROPEAN AND INDIANzsabbasige in Kannada;
sompa in Telugu-
The herb is particularly invaluable for women after child birth.
Consuming its preparations regularly will promote rich secretion
of milk and more imoortantly it also acts a good family planning
measure.
For,
by this procedure, the interval between child
birth and the next menses period gets greatly prolonged so
that both the mother and the child can secure ample time for
halthy and proper nourkshment.
* However as this stimulates abortion,
it is better that the
pregnant ladies should totally avoid eating it during the
first three months.
* Sowa or the Indian Dillis useful otherwise too.
Take fresh
fruits of sowa, powder and keep in a fresh and greased vessej-
One should get up in the early morning at Srahmi muhurta
(3.30)
and lick up 1,2 or 4 tolas of the powder along with ghee.
Or,
one can determine the quantity as per one’s own digestive a
ability and take that amount every day.
After this is fully
digested one should take a meal of milk and rice as much as
desired.
A person who thus consumes 400 tolas fof shatapushpa
can get a progeny of whatever quality he desires.
barren woman can become fertile by this procedure.
■^feftP-Q-NUT-
Even a
COCONUT, BETEL NUT etc
(TFf*l)
COCONUT: Abortion- Take fresh flowers, the fruit of gular
(Ficus Glomerata) and nagar motha-all in equal parts.
Prepare
a decoction which can be given to reduce the chances of abortion
* If pregnant ladies find that there is an excruciating pain
during urination, they are best advised to consume as much of/
tender coconut water and barley water as they desire.
always proves greatly relieving.
This
Another simple recipe to
get rid of the burning sensations during the passing of urine
is to consume tender coconut water twice a day adding to it
a little bit of jaggery and half a teaspoonful of coriander /
powder.
* Coconut oil is an ideal medium for massaging.
month of pregnancy,
it
In the 7th
is quite frequent to suffer from back
Massaging the back with coconut oil or castor oil and
pain.
then taking bath in^hot water will lessen this pain much.
* The coconut coir has been used medicinally.
of this coir into asheswell
Burn some amt
Take a teaspoonful of the ash,
mix it
in tender coconut water, add a small quantity of sugar
candy and administer this drug twice a day for young girls
who suffer from excessive discharge during menstruation.
BETEL NUT: Prepare a tincture or an alcoholic extract of the
oowder and employ it but freely diluted with water- 1
of the tincture in 4 ounces of water.
drachm
This is used locally
or as an- injection to stoo water discharge from the vagina
and also in checking the hydrosis or water rash of pregnancy.
Here, a sudden flow of acid fluids from the stomach to mouth
oECurs and an outbreak of burning sensation (heart burn)
in
the gullet, as well.
* The nut is regarded as a nervine tonic and an emmenagogue II
or that
which brings about regulation in menstruation and
its cycle.
II
’
* The young green shoots are utilised to bring about abortion
in early pregnancy.
KIKAR OR GUM ARABIC,ACAC IA ARABICA:jali, karijali, bauni
ini}'
Kannada- Gum of Babul-This is usually given to ladies after ,
child birth.
Its water removes the pains at' the stomach and__
the intestines.
In excessive menstruation 4-1/2 mashas each
aTrd~-m-a-r-k-i-n-g—n-ut-(~ge-jru--j------
v
of the gum and marking nut
(geru) are given,
grinding them
and along with water.
KATHA,CATHA,KHAIR OR ACACIA CATECHU:
Decotion of the heart
wood of khair is excellent to prevent excessive haemorrhage
For leucorrhoea due to uterine debility,
at child birth.
bleeding and uterine laxedness, pills of kattha and myrrh
in equal ia proportion are useful.
A mixture of these two
drugs is given for strenghthening after child bieth and to
incr§ase milk
secretion.
An aqueous injection of kattha is
given for lircorrhoea and the blood flow at the uterus and
also in gonoorhoea.
A tincture of kattha is an excellant
application for suspected bed sores and also cracked nipples.
GINGER AND TURMERIC (TFM)
31
If \Q
GINGER: To cure vaginismus or spasmodic contractions of the
vagina,
powdered dry ginger is well mixed with castor oil or
castor root powder or paste and then applied to the painful partU
concerned.
TURMERIC:
During labour and as long as the child is young and
breast feeding,
it is advised for the ladies that they should
be regularly taking turmeric-for ex
in milk.
This is an ex
cellent practice as this l$ill stimulate the uterus and will
also porify milk secretion.
CURCUMA ZEDOARIA ROSE: kachora in Kannada; kicchili gadda
in Telugu- The root is an ingredient in some of the strength-
y
ening conserves taken by women so as to remove weakness
,after childbirth.
It is given 3 times a day to women during
the first two weeks following child birth.
ONION AND GARLIC(TFM)
ONION: Eating the bulbs raw has been noticed to bring about
a desirable regularity in menstruation among the ladies.
If
it is a case .where menstruation does not occur or is obstructed
(amenorrhoea or ruddhartava), five tolas of onion are cooked in
one set of water till the latter is reduced to about ten to
twenty tolas.
Then add 3 tolas of jaggery.
This is to be made
-5hot and drunk by the patient fora feu days.
Other recipes
are: three tolas of onion juice are made lake warm and drunk
before going to bed at night:
small pieces,
Or, ten tolas of onion are cut int
garam masala is added to it and the uhole is
roasted in ghee and eaten.
The obstructed menstruation will
become rectified
GARLIC:
Useful in difficult menstruation..
In cases where
much pain is felt at the loins during menstruation,
garlic
juice is given internally and crushed garlics are applied
externally as a massaging material.
* In shooting pains at the loins: Proprietary garlic preparation
called rasona paka helpful.
Garlic and salt are to be ground
together, made into a poultice and bound over the regions
of injury,
sprain,
spasms,
twisting pains and the like.
Mt NS T£ (Ja T)OM.
).
cp
y ■
t
” <3
^fy&T- t'JA TA) L Ca £6
ptoccwto_
-iutfe 1 (0
—/^LCjZgLl'^O
--- .SCCL'U'uty
—^7
C
XjXCt
-7’
cCtAct^uA^Q •
g•
&GrOyC0)'CAL
•
I.
3 .
■
>
1. -Cjek,
<2- <c^C\£x.C wzcc
2>- 'TtU.
4 Pb.vu
,
’-C&jl
^JLIoqz'cclC
9
b~^cLi, ,
i
—S>
.
■
' S7■ Lf85
'the LANCET, JANUARY 14, 1989
Community Health
diseases in rural women; (2) awareness and perceptions of
the women about their gynaecological and sexual disorders;
and (3) die proportion of women who have access to
gynaecological care.
HIGH PREVALENCE OF GYNAECOLOGICAL
DISEASES IN RURAL INDIAN WOMEN
R. A. Bang
M. Baitule
S. Sarmukaddam
A. T. Bang
Y. Choudhary
O. Tale
SEARCH, Gadchiroli-442 605, India
A population-based cross-sectional study
of gynaecological and sexual diseases in
rural women was done in two Indian villages. Of650 women
who were studied, 55% had gynaecological complaints and
45% were symptom-free. 92% of all women were found to
have one or more gynaecological or sexual diseases, and the
average number of these diseases per woman was 3-6.
Infections of the genital tract contributed half of this
morbidity. Only 8% of die women had undergone
gynaecological examination and treatment in die past.
There was an association between presence of
gynaecological diseases and use of female methods of
contraception, but this could explain only a small fraction of
the morbidity. In the rural areas of developing countries,
gynaecological and sexual care should be part of primary
health care.
Summary
INTRODUCTION
Maternal and child health care is one of the eiglit basic
components of primary health care in the Declaration of
Alma-Ata? In some programmes, a more focused approach
has been advocated and promoted—termed selective
primary health care2 or child survival revolution.3 There is
new concern about the health care of women during
pregnancy and childbirth,4 and prevention of maternal
mortality has been identified as a priority.5 By contrast, little
attention has been given to the reproductive health of
non-pregnant women. In third-world countries, such
women tend to encounter the health care system only when
they are the target of family planning programmes.6
The term gynaecological diseases is used in this paper to
denote structural or functional disorders of the female
genital tract other than abnormal pregnancy, delivery, or
puerperium. One reason for the relative neglect of
gynaecological care is a failure to appreciate the extent of
unmet needs in rural areas. Most of the data are from
hospitals or clinics and are highly selective; they give no idea
of the rates in the population.7,8 The few population-based
studies have focused only on specific disorders—ie, cervical
cancer9*16 (chosen for study because of hospital experience),
vaginal discharges,17 and genital infections18 (based on
family planning clinic data). We are unaware of any
population-based study of the whole range of gynaecological
diseases in developing countries. An additional reason for
lack of information on these disorders is the extreme scarcity
of female doctors in the rural areas of developing countries.
Traditionally women from these areas are very reluctant to
talk to or be examined by male doctors for gynaecological or
sexual disorders. Nurses and paramedical workers are not
trained to deal with gynaecological diseases; so the result is
near total absence of care.
In the present study we sought to determine: (1) the
prevalence, types, and distribution of gynaecological
SUBJECTS AND METHODS
Study Area and Sample Population
Gynaecological inquiry and examination is a very sensitive matter
for rural women in India. One cannot randomly select a few women
from a large population and descend upon them. Hence it was
decided to make villages the units of study.
The investigation was conducted in Gadchiroli district, a
backward district of Maharashtra state. Two villages were selected
on the following criteria: socioeconomic composition similar to that
of the average village; leaders who could understand the nature of
study and would persuade the women to participate; prevalence of
gynaecological diseases not known to be atypical.
Village A had a population of 1400 and village B 2200. They were
located 20 km from the district town and from each other. Both had
perennial roads. A primary health centre with two male doctors was
located in village B while a small mission hospital run by the nurses
was located in village A. 'Phus both the villages had good access to
primary health care, though the nearest gynaecologist was at the
district town.
Female social workers, village leaders, and volunteers invited all
females who were age 13 years and above or had reached menarche
to participate in die study, whedier or not they had symptoms.
Investigations
A field camp was set up in the village, first in A then in B, with
facilities for interview in privacy and pelvic examination, pathology
laboratory, and operating theatre. A base pathology and
bacteriology laboratory was established at the project headquarters
20 km away. The study team (a female gynaecologist with 10 years’
experience as consultant, a physician, a pathologist, a laboratory
technician, a nurse, and female social workers) visited the field camp
and conducted the study. The women who were found to have
disease were offered treatment.
First, information was obtained on personal details,
socioeconomic status, perceptions and practices as regards
gynaecological symptoms, past experience of care, and obstetrical,
gynaecological, and sexual history. The women then had a general
physical examination including speculum examination and
bimanual examination of the pelvis; unmarried girls with an intact
hymen had rectal rather than vaginal examination. The following
laboratory investigations were done (apart from vaginal specimens,
omitted in the never married): urine and stool tests; haemoglobin
(cyanmethaemoglobin method); peripheral smear for typing of
anaemia and for parasites; VDRL test (slide flocculation test using
antigen from Government serology laboratories with positive and
negative controls for quality control); sickling test with 2% sodium
metabisulphite; urine culture and antibiotic sensitivities when
necessary; vaginal smear microscopy and gram staining; vaginal and
cervical cytology with Papanicolaou stain (method of Hughes and
Dodds19); culture and antimicrobial sensitivity of vaginal swab
(after transport to base laboratory in nutrient broth, primary
inoculation was done on McConkey and blood agar and growth was
observed 24 h later; motility and gram staining were studied, with
biochemical reactions; specimens were not incubated in carbon
dioxide atmosphere for Neisseria gonorrhoeac, or for anaerobes);
blood biochemistry, when necessary; husband’s semen analysis,
when indicated;20 and cervical biopsy, dilatation and curettage, and
radiological examination when indicated (all histopathology slides
of biopsy or uterine curettage material and suspicious cytology
slides were reviewed by senior pathologists at the nearest referral
laboratories at Nagpur).
Diagnostic terms and entities were those in the International
Classification of Diseases, 9th revision.21 Vaginitis was diagnosed
when the vaginal wall was visibly inflamed and the vaginal smear
showed at least 5 pus cells per high-power field. When smear
THE LANCET, JANUARY 14, 1<
86
TABLE I—COMMON GYNAECOLOGICAL AND SEXUAL COMPLAINTS
(n = 650)
Complaint
Frequency
(%)
88
60
36
82
45
32
132
98
43
63
135
92
Vaginal discharge
Burning on micturition
Childlessness
Scantv periods
Irregular periods
Profuse periods
Amenorrhoca
Dysmcnorrhoea
Dyspareunia
Other
12-6
6‘ 9
•/■9
203
66
9-7
microscopy, gram staining, or culture revealed no pathogenic
organisms, it was labelled vaginitis of unknown origin. Syphilis was
diagnosed when the VDRL test was positive in 1:8 dilution or
more.- Pelvic inflammatory disease was diagnosed when adnexac
were palpable and tender on vaginal examination, with or without
restricted mobility of uterus. Jcffcoate’s criteria2-' were used for
various other gynaecological conditions.
Anaemia in females was defined as a haemoglobin of 11 -5 g'dl or
less.34 Iron deficiency was diagnosed on the basis of hypochromia
and microcytosis in peripheral smear. Vitamin A deficiency was
diagnosed by identification of conjunctival xerosis or Bitot’s spots.
Sickle cell disease was diagnosed by the sickling test, but
homozygous disease and trait, could not be distinguished, in the
absence of electrophoresis.
Because of the sensitive nature of the survey and the cultural
norms of these traditional societies, we aimed conservatively at 50%
coverage of the eligible women. In the event, 654 out of 110-1(59%)
turned up to participate and the investigations were completed in all
but 4. Although every effort was made to persuade both
symptomatic and symptomless women to participate, selection
might have arisen. We therefore visited a 25% random sample of
non-partidpanr. women at home to record their personal,
obstetrical, and contraceptive histories, presence or absence of
gynaecological symptoms (vaginal discharge and menstrual
disorders), and reasons for non-participation.
The data were analysed by use of the SPSS-PC package on a
RESULTS
The mean age of the 650 women was 32-11 years (SD
13-46). 92 (14%) were unmarried, 462 (71%) were married
and living with husbands, 28 (4%) were separated, and 68
(11%) were widows. Thus 558 women were married at the
time of study or had been in the past. 281 (44%) were
farmers, 149 (23%) were landless labourers, 93 (14%) were
housekeepers, 21 (3%) had regular jobs, 46 (7%) were
students, and 55 (9%) were in other occupations. 436 (68%)
were illiterate; 84 (13%) had schooling up to 4th standard,
52 (8%) up to 7th standard, and 65 (10%) up to 10th
standard, and 8 (1 %) had college education.
299 (46-0%) belonged to middle castes and 123 (18-9%)
to lower castes; 138 (21-3%) were of tribal origin and 28
(4-3%) from nomadic tribes; and 62 (9-5%) were of other
castes or non-Hindu.
28 (4%) of the subjects had not reached menarche, 468
(72%) were menstruating, and 154 (24%) had reached
menopause. The mean gravidity was 3-99 (SD 2-77) and
mean parity was 3-75 (SD 2-74). 48 women were pregnant at
the time of study. Out of462 women who were married and
living with their husband, 254 (55%) were using one of the
following contraceptive methods: condom 5, ‘Copper-T’ 7,
withdrawal 2, safe period 2, pills 5, abdominal tubectomy
24, laparoscopic tubectomy 58, vasectomy 151; thus female
contraceptive methods were used by 94 at the time of study
and had been used by a further 29 in die past, total 123.
TABLE II—CHARACTERISTICS OF PARTICI PANTS COMPARED WITH
25% RANDOM SAMPLE OF NON-PARTICIPANTS
Characteristic
Mean age (yr)
Gravidity
Gynaecological symptoms
Vaginal discharge
Scanty periods
I rregular periods
Profuse periods
Dysmcnorrhoea
Bad obstetric history in ever-ntarried
Current use offemale contraception in
Participants
(n = 650)
Non-participant
sample (n = 105)
34 3
3-84
3 99
8-25%
16-4%
149%
13-5%
12-6%
69%
4-9%
15-1%
37-6%
13-4%
51 1%
18-2%
11-36%
A total of 360 women (55-38%) had one or more
gynaecological or sexual complaints (table I). In addition,
many complained of two non-specific but related
symptoms—low backache (197) and lower abdominal pain
(86). The characteristics and symptoms of those who
participated did not differ greatly from diose of the random
sample of non-participants (table 11). The main reasons for
non-participation were: no gynaecological complaints
27/105; “I am too old for such tilings” 17/105; frightened of
gynaecological interview or examination 16/105; out of
village at time of study 15/105; unmarried, so did not want to
be examined 4/105.
The gynaecological and sexual diseases found in the
survey are summarised in table in. The 650 women had a
total of 2344 gynaecological diseases—ie, an average of 3-6
TABLE III—GYNAECOLOGICAL AND SEXUAL DISEASES (n = 650)
Diagnosis
Primary amenorrhoea
Willi mullerian duct aplasia
Without mullerian duct aplasia
Secondary amenorrhoca
Functional uterine haemorrhage
Olrgomcnorrhoea/hypomcnorrhoea
Polymenorrhoca
Menorrhagia
Dysmcnorrhoea
Irregular periods
Primary sterility
Secondary sterility
Frigidity
Dysparcunia
Vaginismus
Senile vaginitis
Trichomonas vaginitis
Candida vaginitis
Bacterial vaginitis
Vaginitis of unknown origin
Cervical erosion
Cervicitis
Endoccrvicitis
Pelvic inflammatory disease
Ovarian cyst
Cystic ovary
Cervical dysplasia
Cervical metaplasia
Cervical polyp
Syphilis
Leucprrhoca
Lcucoplakia of vulva
Gonorrhoea
Cystocelc
Vulvitis
Fibroid uterus
Carcinoma of cervix
Other gynaecological diseases
No
%
4
3
99
105
4
71
269
60
20
57
43
47
20
78
190
347
23
255
272
67
157
6
15
10
68
22
4
9
3
2
1
0
52
1
(01-07)
(00-61)
(00-46)
(0470)
(01-28*)
(22-44*)
(00-85*)
(15-17*)
(57-48*)
(12-82*)
(03-07)
(03-69)
(12-341)
(9-311)
(10171)
(10-991)
(13-98$)
(34-05$)
(62-19$)
(0412$)
(45-70$)
(48-74$)
(12-01$)
(24-15)
(00-92)
(02-30)
(01-07)
(01-23)
(01-53)
(10-50)
(03-38)
(00-61)
(00-30)
(00-46)
(00-30)
(0015)
—
(08-00)
*Oui of468 menstruating; t out of462 living with husbands; tout of 182 over
‘10 yr; §out of 558 ever married.
’’THE LANCET, JANUARY 14, 1989
87
TABLE IV—PREVALENCE OF GYNAECOLOGICAL DISEASES AMONG
WOMEN WITH AND WITHOUT GYNAECOLOGICAL SYMPTOMS
(EXCLUDING PAIN IN LOWER ABDOMEN AND BACKACHE)
Total
With diseases
Without diseases
559
650
per woman. 559 (92-2%) had one or more gynaecological or
sexual diseases.
Premarital sex among the unmarried was diagnosed when
the hymen was tom and the vagina easily admitted two
fingers (girls and women in this area do not use tampons).
On this evidence 43 out of92 (46-7%) of the unmarried girls
had had sexual intercourse.
The most common non-gynaecological conditions found
in the survey were anaemia (in 91%), iron deficiency
anaemia (83%), sickle cell disease (7%), vitamin A
deficiency (58%), filariasis (12%), pulmonary tuberculosis
(2%), leprosy (10%), and urinary tract infection (4%).
History of gynaecological examination was used as an
indicator of professional gynaecological care in the past.
Only 51 (7-8%) had ever had such an examination.
Table IV gives die prevalence of gynaecological diseases in
women with and without symptoms. As an indicator of
gynaecological disease, a gynaecological symptom had a
sensitivity of 59%, a specificity of 90%, positive predictive
value 99%, negative predictive value 16%.
Table v indicates that gynaecological diseases were more
frequent in women with a contraceptive history. Of the 82
who had had tubectomies, 54 (66%) attributed symptoms to
this procedure compared with 16 of 151 blaming their
husband’s vasectomy. The numbers with intrauterine
devices (7) were too small for comment.
DISCUSSION
In this cross-sectional survey, the prevalence of
gynaecological or sexual diseases (92%) and the average
number of such diseases per woman (3-6) were remarkably
high. Infections constituted 50% of the burden—vaginitis,
cervicitis, pelvic inflammatory disease—and the rates would
doubtless have been even higher if we had used more refined
tests. Menstrual disorders form another big group and
infection of the genital tract may be a contributory cause
here. Fibroid uterus was very rare, and not a single case of
carcinoma was found.
The very high prevalences of iron deficiency anaemia
(83%) and vitamin A deficiency (58%) were due to the poor
economic status of this area in general and of women in
particular. The area is endemic for filariasis and leprosy.
One noteworthy finding was that even symptomless
women were very likely to have reproductive tract disease
(table IV). Symptoms arc thus an insensitive tool for
screening, in the presence of a high prevalence rate. The
negative predictive value is also very poor. The
gynaecological complaints volunteered by women during
history-taking were often underestimates —especially with
regard to vaginal discharge and menstrual troubles—
because of the concepts of normality. Thus only 98 women
complained of excessive pain during menstruation, but on
careful inquiry 269 were found to experience
dysmenorrhoea.
There was some trutli in the women’s perception that
contraception causes gynaecological troubles—there was a
statistically significant association between certain
gynaecological diseases and past or present female
contraception. But this can explain only a small proportion
of the morbidity since 78% of the ever-married women had
never used any such contraception, yet had a high
prevalence of disease.
Unfortunately the diseases that do not kill tend to be
neglected. The non-neoplastic gynaecological diseases come
in tliis category, but they could give rise to: difficulty in
occupational and domestic work because of chronic
backache (present in 30-3% women); fetal wastage due to
abortions and stillbirths; neonatal infections from birth
canal infections; anaemia due to menorrhagia; marital
disharmony due to sterility and dyspareunia; anxiety and
stress; and harm to the reputation of family planning
methods due to aggravation of pre-existing gynaecological
disease (this probably accounts for the very low use of
intrauterine devices, despite intense promotion by the state
government).
Nearly half the unmarried girls had had sexual
intercourse. This rather unexpected finding in a traditional
Hindu society indicates that there is a need to provide
adolescent sexual health education and care even in the
villages.
AIDS has not been reported from this part of India. But
when the infection arrives, what will be the effect of high
prevalence of vaginitis and cervical erosion on the
transmission of infection? Will these lesions facilitate the
entry of virus by the vaginal route? This aspect needs
looking into.
Only 7-8% of the women had ever had a gynaecological
examination in the past, even though 55% were aware of
having gynaecological disorders. Obviously there is a large
gap between the need and the care. Similar epidemiological
studies are needed in other areas, with closer attention to
aetiology and women’s perceptions. Finally reproductive
care to women needs to be broadened beyond maternity care
and family planning.
This study was supported by grants to SEARCH (Society for Education,
Action and Research in Community Health) from the Indian Council of
Medical Research, New Delhi, the Ford Foundation, New Delhi, OXFAM
(India), and the Ashoka Foundation.
We thank the women, volunteers, and village leaders of Wasa and Amirza
who participated in the study and made all arrangements; Shri Lambe Guruji
and die mission hospital who allowed their buildings to be used; Sister
Sharma, technician Nandu, and social worker Jamana who helped in
conducting die study; Dr A. V. Shivade, Dr N. M. Munshi, and the late Dr
Vivek Kulnami of Nagpur for reviewing the histopathology and cytology
slides and for guidance in the microbiological work; and Prof Carl E. Taylor
and Dr R. L. Parkar of the Johns Hopkins University, Baltimore, for
guidance in development of the protocol.
Correspondence should be addressed to Dr Rani Bang and Dr Abhay
Bang.
„,
,
References alfoot of next page
THE LANCE T, JANUARY 14, 1989
Occasional Survey
PATIENTS’ PREFERENCE IN INDOMETHACIN
TRIALS: AN OVERVIEW
Peter C. Gotzsche
Liver Unit, Hvidovre Hospital, Hvidovre, Denmark
Summary
Meta-analysis was used to study patients’
preference in 37 crossover trials that
compared indomethacin with newer non-steroidal, anti
inflammatory drugs (NSAIDs). 3 reports did not present
numerical data. Patients who withdrew from the trial were
included in the analysis. The difference between the
proportion of patients who preferred the new drug and the
proportion who preferred indomethacin (the therapeutic
gain) was 14%. After exclusion of 2 unreliable studies the
therapeutic gain was only 7%, and when 4 preliminary
reports were also ignored, the gain was 5% (95% confidence
interval 0 to 10%). In two additional analyses in which the 2
outlying results were excluded, the gain was also 5%. The
findings do not support the trend to replace indomethacin
with newer NSAIDs.
INTRODUCTION
INDOMETHACIN, marketed in 1963,’ is still an important
drug with which the newer non-steroidal, anti
inflammatory drugs (NSAIDs) are compared.2 Superiority
of the newer drugs is usually claimed, but I have
demonstrated severe bias in the analysis and interpretation
of these trials.2 To study whether the newer NSAIDs are
preferable to indomethacin, I have done a meta-analysis34 of
patients’ preference in crossover trials.
METHODS
Details of the literature searches have been published.21 collected
reports on crossover trials, said to be double-blind, that compared
two or more of the seventeen NSAIDs marketed in Denmark with
indomethacin. The trials had to be of tablets or capsules, given in
repeated doses to patients with rheumatoid arthritis, and published
before 1985 in any language. A ‘MEDLINE’ search covering 1966
and onwards was done in May, 1985, and the thirteen companies
that marketed the proprietary products were contacted. The
reference lists of the collected articles were scanned. In the case of
repetitive publication, the most informative report was chosen.
The reports were searched for data on overall patients’ preference
for one of the drugs. When more than one NSAID had been
compared with indomethacin, the newest was selected. Preference
for drugs other than these two was recorded as “no preference”.
The main author and the pharmaceutical company were
contacted for clarification of uncertainties (eg, blinding and
randomisation methods, patients who withdrew, and missing da$?).
For reports without preferences I asked whether such data had been
recorded but omitted from the report.
Under the null hypothesis of no difference between the drugs, an
equal number of patients would be expected to discontinue therapy
on the two drugs. If numbers are different, it is reasonable to give
credit to die drug with fewest discontinuations.2 Therefore,
according to a protocol written beforehand, three analyses were
done of which I considered “B” the most decisive:
(A)
The preferences as stated in the reports were accepted
(participants who withdrew were disregarded)
(B)
Patients who withdrew were included as follows: (a) drug not
stated = no preference; (b) discontinued trial drug = preference for
other drug (unless this drug also discontinued, then = no
preference); and (c) discontinued third drug or placebo or wash-out
period = no preference (unless trial drug also discontinued, in which
case [b] applied)
(C)
To assess the sensitivity of the analysis to preferential
reporting of the offending drug, patients who withdrew were
included as above except for B(a), which was now construed as
indomethacin preference.
The “therapeutic gain” was calculated as the difference between
the proportion (PA) preferring the new drug and the proportion (Pn)
preferring indomethacin.5 For example, if 35 of 100 patients
preferred the new drug, 25 indomethacin, and 40 had no preference,
the therapeutic gain would be 10% (35 - 25%). The variance of the
gain was calculated as (PA-l-PI|-[PA-Pn]2)^-n, where n = total
number of patients in the analysis. The average gain was calculated
by weighting the gains by the inverse of the variance (three
additional weighting schemes are discussed in the results section).
For estimation, 95% confidence intervals (CI) were used. The
binomial distribution was used to calculate the probability of
withdrawal.
RESULTS
50 reports were collected. Nine of ten companies and
seventeen of fifty authors or their colleagues answered the
requests for further information. Details of randomisation
were requested for 47 reports and of blinding for 14. The
answers were usually of little use, such as “the company did
R. A. BANG AND OTHERS: REFERENCES
1.
2.
WHO and UNICEF. Primary health care: report of the International Conference on 13.
Primary Health Care, Alma-Ata, September, 1978. Geneva: WHO, 1978.
Walsh JA, Warren KS. Selective primary health care: an interim strategy for disease
control in developing countries. N EnglJ Med 1979; 301:967-74.
Grant JP. The state of the world’s children, 1984. Oxford: Oxford University Press,
Yajima A, Hisaschwai H, Sato A, et al. Mass Papanicolaou screening for cervical
cancer in Miyasi prefecture. Gynaecol Oncol 1979; 8:131—10.
269-73.
3.
Asia. Baltimore; University Park Press, 1976.
4. Conablc BB. Safe motherhood. WHO Forum 1987; 8:155-60.
16. Grech ES, O’Dowd xMJ, et al. Cervical cytology in Zambia. Med J Zambia 1977; 11:
5. Sai FT. Safe motherhood initiative; a call for action. IPPF Bull 1987; 21: no 3.
112-17.
6. Bang RA. Counselling and choice in family planning. Paper presented at international
17. Bali P, Bhujwala RA. A pilot study of clinico-epidcmiologic investigations of vaginal
conference on Better Health for Women and Children through Family Planning,
discharges in rural women. Ind J Med Res 1969; 5:7-12.
Nairobi, October 5-9,1987.
7. Lilienfcld AM, Lilienfcld DE. Foundations of epidemiology. New York; Oxford
countries: experience in a family planning clinic. Bull WHO 1973; 48:581-86.
University Press, 1980: 133-36.
19. Hughes HE, Dodds TC. Handbook of diagnostic cytology. Edinburgh: Livingstone,
8. MacMahon B, Pugh TF. Epidemiology: principles and methods, Boston: Little,
1968.
Brown, 1970:90.
20. Henry JB, ed. Todd, Sanford and Davidson’s clinical diagnosis and management by
9.
Wahi PN, Lulhra UK, Mali S, Shimkin MB. Prevalence and distribution ofcancer of
laboratory methods. 17th ed. Philadelphia: WB Saunders, 1986.
uterine cervix in Agra district in India. Cancer 1972; 30:720-25
10.
Garud MA, Saraiya UB, Lulla xVt, Khan S, Paraskar M, Daftary D. Cytology
Geneva. WHO, 1975.
screening programme in an urban and rural community in India. Acta Cytol 1983;
22.
Holmes KK, Lukehart SA. Syphilis. In: Braunwauld E, et al, eds. Harrison's
principles of internal medicine. 11th cd. New York: McGraw Hill, 1987; 646.
11.
Aleleya JA. Gynaecological cytology in family planning services in Nigeria. 5 Afr Med 23.
Tindall VR, cd. Jeffcoatc’s principles of gynaecology 5th cd. London: Butterworth,
71975; 50:611-15.
1987.
12.
Wykew W, Muller CJ. Cancer screening and cancer education in rural western Cape. 24.
Penington D, Rush B, Castaldi P, eds. De Gruchy’s clinical haematology in medical
S Afr MedJ1977; 51:821.
t, .ffssio^^o
rwxort soaaoQsd sdart4iwg d,daas>
ertd. doda dg daios? zsart^dvan 3^
d?Ju dado, dad^d daed laoJaod/a
sapscan daad, nzprrJ ^eato edaa?^
SatpaDSeSa -5&.S Sdaaa dzsa.artsb
^©Oe.
sradnas. e$>rs oadrarwa daa'd,
wed, ipisRraa^s oadrarWaa Sd dagy
*sdd4.
oadradaAd. tad. na,£atro'
S,dedrW© acSjVS^ dfddatfartwran
za«daa*>d djd^oiood wd da^
ddaSdaa dfdd.Sd?,
Soard
edada
d»O4aw?a,d
rtprjadaaeporws^ acaSA d^djOAodeaa
djdSddaA SoarO ^CljdJ, tsSjS/Wj
t03Sa3,d. ^oBOjjRS* B^e* «?»
daQ4©f OSJ^F. N^SiSO*
tsp5 ^d~a4daea dasa, SoUjC’ d,ir
OSafr
“F? L'U/a^rWa
rtprjadaajpdrW
art
Sodjafpd
3,d. e, . ^rt rWa ad.ijijCB5',
Toad®'
w3Jsscs'
droauo
dots’.
cdaa.ds’.dip5'. da3,dd oa^rtCod pd
Ssacda Sdotoo3,da«3dDod daS,ddg
rtpradawpSd art d? Sort rW aeade
z^daAd. ^dd SodjaepdoSa d^pda
rtao
Saas
□asSjrts’
rtpradaatps
drta,rW rtodaupF^
eodaadjda.
add. 3? Sort rttfaa ddat Kdad^O
dadda. ^3d craa^rW SradartnaA ad
Sraa dad^da,
wfidSadaASdadoda
ddCoia -sat©" datova So^urt d^
sdootog 3?m3,
zSeOoSoe z>cte...
Soard dada, dded ftadfcrW dt^-pd,
| a33S4,rtConan i.;dodaa 4rVdo3d
I
urtjjfi d4douad d^Oodde <Sdojoa3,d.
| d,3 ddd4daa 3d. daaeAoia «daafrt4,
| z-^z
art
dodSapidd
, a^Baa; aodo Sadaou,
arta^da. ^rfe^od daaodd epda
TOarwcrad daJo'stoJa ■ SatfVa enad
ds^dd^ edatiJOSadda.
rtzprri s/olad adawr^oda ddr44
c^ortdda/, adrasdo,,. . i990d©
. nOjdoziiaaAd; '"'oJjaeKjfafo . dai^odd
4aai?a,3,d.
— -• --*-.._■
tsdaat^ -—
^oaaJ
dtfaartododd —
oacdor
. aipdrieonan S^djS saa^d efi tsaort
aodda. ,
ddo' ; -.3addod . / vpO>- JdarSOTAda,.
20O0dg • daanofcad & ■ odjwartoaog
■' daJotfrt sadjsdif da4oia, Sadjd dao3a,S
ftde
djadsgda, ■ daanacoa
aidar
daodod-'e^dasdaa^ideoad aodrttfda,
daaoddaa
natfa,
add . ' edaxr^
SaipaOSi,a4d4 4.
d,doaad4od ■ usort" . darSepoaada, ■■•, , ,•.
SozaoQsd Sdort4 dado, ■ saaj' dd,d.
A;’-" ..oSptssJrt^- . Sdaqlrdan
dd,xia)d, rtaatoSa, ed^jsa^d O?doi>
cx^yard? dada, eo^dQ dqsadd©
rtprsrad ' dado, Sort, ^pjrtfod . doda . dwdda, ■ dsirdaa^rt .: tosg dedrtda
saQsd. .viraasbrtrt ^{wooadt? i950d
Sodaaeprt odsd. wd oas^rttfg &4d
^djd.dda, d4,!o?dd, da«3?odiiadodan
ddddg d,d eg dafctoadj 555 daoo
rtprcioJad sap; SopdSad,©d.
s3J>neaartad,§a, eddd,d ddBdg 239
rtzprrioJad adaae^ 4; de a rtprrirt
daofi ■ dada, „doad,d ddddg edd
Wdadnane. edort Sau^d dartaOS
Soa3d
954; . ^OOdi.d,
u^dg
dateaa SS dOroada dtdadoddada. '. eo^dp dtpadrtvad
Sort
dada,
aadoaa^rtV Sadaada doua da©oiadf
. dadajjd
oacdard^dd,
■ MaiWa t-oda ddrdaaVrtt braa^
oa^dat^d eduK^’aei, Sdaanaoia«4
^5^
zpart,
dddrt doda
ddaoad ddarttfa naddaatfrt TO05aa3,rf.
daddd 4aadd, d^djieoia S^e^i-W
4aadd. SortoJa dedoiafi aaartdaadd
^rtCod
■ 2>da
dadra ' So.-,;'
OJrtafSdarta3,d.
djaeX dow epraaS,'-. Kdddda,
ddda urtoiag aoiao^SudarfodnaFJ.
d^doJa Sda ao5aod,ra ■ a.odadd,
daaSd daadd SeaJ aodaod,fOrtV5.
d,Sa,d, Soardd pawdrt ' .3, dddaa
poJaOrW Sdaddgd..
1
sadrolj Wd?4, igra, tsgddodjaodrt
Sja^s ajEaddda/ ad dafcsfafcort
wudddan, aeda^da; dort a^rtV
So^oJada,
OjrtarartjaCSa^da;
di
fcodod daJo$?o3aort 3«d«4 atda^da;
dada, da2o$toaOrt SoaoQSdcd aQrtf,
TOdaadd . sa4o5a, .
. sa Sdaaddda^
vod,dartja«Sa^da.'. edda * adaSdxd
dtpadri*
S/UOffO ZTO^cS "
v
r.
4
,, _,
dodo, ^seow rod^rte:. 'ri^rriodod,
sa^i,
rtawas
Ro3oo3,ra
dado,
rtzprrioiad ■
Sadlddrrart .
aoda
^odd ' art«d.' SedrtiWaK
aecdsJd?<So tfajjde. add, ddafc Soard,
daaddSr^d oaao3,
4aadd,
-, uaKoadrirWrt
o?nnaoE9nwi. . oasoQaF3,Q
«c^3d, - daoart. .^dddodan
dga
Sdart4rt«ia
enwdaa^d. ,^d?
• S&rt4rtvaAo5a?
o^ioSae Sadgd
3ao55,Sd.Sdart4o3aaa 4aad. 1
wdea,
SSd^
I doled aardSdartadcd daada^nad,
a«io rtaatd4d3A, d4d4 Sdaaaao d,3
ddr dOSjdo aoOcdo?? daktfosada
rtp.-44 Souopsd daaoddrt seatfadod
daada3,dad.
|
taUj
^3).
I ZvCljO CjOcjrt &5je)3,eSO
rJ&ljilcSjJj
I sdjS^oUo daadadoddada. Soard e
rsaJodoja 2>gra, tsdaatr^L aaoiraensd
Xfa du^ja dodsadod. aodo dortoSa
i epro eaacj;^ ^ddod dan dod
Sopa, 21 #J0,dO '999
5JU 51
49
50
Bryant, p.48.
Hirsch and Warden.
51
53
54
Winona La Duke, “The Struggle for Cultural Diversity," Race, Poverty and the
Environment 1 no. 2 (July 1990).
Hirsch and Warden.
Zeff, Love, and Stubs,.p.4.
Ibid.
55
Ibid.
52
56
Penny Newman. “Killing Legally wkh Toxic Waste: Women and the Environment in
57
the USA" (Paper delivered at the conference, "Women and the Environment" India,
1992).
Ibid., p.24.
ROBERT GOTTUEB
A QUESTION
OF CLASS
the workplace experience
58
Penny Newman, 77w Environment An Issue of Health, Safety and Social Justice 8,
no.l (Summer 1992), Action-Gram, Riverside County Department of Community
Action.
When Larry Davis was a boy, living in the
unincorporated town of Wheeler, IN, population 400,
59
Penny Newman, "Cancer Clusters Among Children: The Implications of McFarland,"
he loved to go into the woods by an old farm near
60
Journal ofPesticide Reform 9 no.3 (Fall 1989): pp.10-13
“Political Difficulties Facing Waste-to-Energy Conversion Plant Siting" (Los Angeles:
Cerrell Associates, 1984).
the edge of town. With his buddies, he'd play in the
creek, wade through the marsh, and camp out under
61
See Cynthia Hamilton, “Women, Home and Community: The Struggle In an Urban
Environment," in Diamond and Orensteln.
62
Ruth Perry, “Engendering Environmental Thinking" (Paper delivered at the University
of California, Santa Cruz, Feb. 24, 1993).
63
Lee.
64
Bob Ostenag, ‘Rose Marie Augustine: School of Hard Toxics," MotherJones (JanV
Feb. 1991): pp. 49-50.
Lee.
Alston, interview.
65
66
67
For discussions on the critical and constructive discourses of science and technology
emerging from the environmental justice movement, see Adeline Levine, Love CanalScience, Politics and P«y)Ze(Lexington, MA: Lexington Books, 1982); Susan MastersonAllen and Phil Brown, Public Reaction to Toxic Wastes Will Collette and Lois Gibbs,
“Experts: A Users Guide" (Falls Church, VA: CCHW Publication, 1985); S. Krimsky,
“Beyond Technocracy: New routes for citizen involvement in social risk assessment,"
in Citizen Participation in Science Policy, ed. J. Peterson (Amherst, MA: University of
Massachussetts Press, 1964.
68
Magdalena Avila, “David vs. Goliath," Crossroads/forward motion 11 no.2 (April
1992): pp. 13-15.
the stars in the summer. When he was in high school,
he began noticing tanker trucks passing over the old road on the way
to the farm, but didn’t think much of it. It wasn’t until later, after being
laid off from Bethlehem Steel’s Bums Harbor plant in northern Indiana
that he had the opportunity to look into the matter of the old farm in
Wheeler.
While laid off, Davis began to follow the growing scandal about the
Midco sites in the city of Gary. Located in former dune and swale areas
near Lake Michigan and the Grand Calumet River, the Midco dump was
Indiana’s version of the Love Canal. Problems at the site had first come
to the community’s attention in 1981, when hazardous wastes, already
leaking from several thousand 55 gallon drums, had been spread
through town by the floods from a major storm. During the next several
days, kids who’d been playing in the puddles left by the storm received
chemical burns, as did workers exposed to the flood waters. Local
residents could also smell chemical odors drifting through their neigh
borhoods. As a result, residents formed a new antitoxics group and
their protests ultimately forced the Environmental Protection Agency
INVIROHMINTAL JUSTICE
26
27
28
29
30
Indicators: Women speak out on the challenges of national grassroots leadership,"
Alston, interview.
Alston, Transforming a Movement," p.31.
Alston, interview.
Ibid.
Gibbs.
31
32
Lee.
Alston, interview.
33
See larry Wilson, “Moving Toward A Movement," Social Policy 19 (Summer 1989):
pp. 53-57.
Alston, interview.
34
35
Likewise, these critiques suggest that essentialist positions Ignore the ways that some
women contribute to environmental problems and to the culture of militarism, and the
ways that some men fight against gender oppression and work foe the environment.
In terms of political strategy, however, some feminists suggest that esaenttaUsm must
be used “strategically" because the destructive discourses and Institutions that
associate women and nature still persist in many societies. See Vai Plumwood,
“Beyond the Dualistic Assumptions of Women, Men and Nature," Ecologist 22, no.l
37
The Roaring Inside Her (New York: Harper Colophon Books, 1978); Carolyn
Merchant, The Death of Nature: Women, Ecology and the Scientific Revolution (Son
Francisco: Harper and Row, 1980); Judith Plant, Healing the Wounds: The Promise of
Ecqfemtnism (Philadelphia: New Society Publishers, 1989); Karen Warren, The
See Karen Stultz, "Women Movers: Reflections on a movement by some of Its
leaders," Social Policy20 (Winter 1990): pp. 36-37; Barbara Israel el.al., “Environmental
Activists Share Knowledge and Experiences: Description and Evaluation of STP
Schools at the Highlander Research and Education Center," PCMA Working Paper
Power and Promise of Ecological Feminism," Environmental Ethics 12 (Summer
Series, no.29 (Ann Arbor: University of Michigan, 1991); Barbara Ruben, “Leading
1990); Rosemary Radford Reuther, New Woman, New Earth (New York: Seabury
Environmental Action (Summer 1992): pp. 23-25. According to the three women I
Press, 1975).
interviewed, the issues of gender and leadership were critically discussed at the
Leadership Summit. The decision was made to appoint, on a rotating basis, one
woman and one man who would act as cochairs for each of the regional network
38
39
leadership skills in the process of their work. According to Israel et.al., some women
Publications, 1991); Lee Quinby, “Ecofemlnlsm and the Politics of Resistance," In
who attended the Highlander Center's STP (Stop the Pollution) schools (workshops
Diamond and Orensteln; Marla Mies, The Lacemakers ofNarsapun Indian Housewives
that bring together environmental justice grassroots activists from around the country
36
feminists ask. Are women who protest “as women" against the bomb or against
environmental destruction engaging in an effective use of society’s own values
against itself or are they accepting society's ideological definition of themselves as
inherently more caring’ Many feminists suggest that the adoption of the historical
association of “women and nature" or “women and environment" by some ecofemlnlsts
is essentialist (that is “naturalistic," it posits a natural, universal woman's essence) In
that it reproduces the age-old gendered relations of power where women and nature
Producefor the Worldmarkel (London: Zed Books, 1982).
40
41
42
43
44
Agarwal, p.127.
Leonle Caldecott and Stephanie Leland, eds., Reclaim the Earth: Women speak outfor
life on earth (London: Women's Press, 1983), p.6.
I am using rhe expression “unmarked" to connote that these environmental justice
activists do not necessarily Identify themselves as engaging In “women's movement."
However, In another sense, clearly these women activists are marked In the dominant
culture by their racial, class, and ethnic backgrounds.
Gibbs.
Interviews conducted byGreenpeace activists from the video, First National People of
Color Environmental Leadership Conference, directed by Karen Hlrsch and A.C.
45
46
Warden, 1991.
Lee.
RobbinLee Zeff, Marsha Love, and KarenStults, eds., fmpoavHngOursafoes.- Women
47
48
Wastes, 1989), p-5Ibid., pp. 5-6.
Hlrsch and Warden.
and Toxics Organizing (Falls Church, VA: Citizen’s Clearinghouse for Hazardous
are once again relegated to secondary status. Many argue that this essentialist use of
the women/nature connection maintains and perpetuates the genderdualism that also
esseruializes men as naturally warring and violent and destructive of the environment.
Alston, Interview.
For example. Bina Agarwal, The Gender and Environment Debate: Lessons from
India,” Feminist Studies 18 no.l (1992): pp. 119-158; Brinda Rao, Dominant
Constructions of Women and Nature in Social Science LiteruturvCNew York: Gullford
gatherings. In this way, many women would gain the opportunity to develop
for leadership development and political strategizing) were not so convinced about
the “gender sharing" approach to leadership training. Instead, they have requested
the implementation of a women's STV school. For these women, confronting the
specificities of gender and empowerment In their activism may best be accomplished
in a “women-only" space.
The notion that women possess a unique consciousness of caring for the eanh and Its
inhabitants creates a point of tension within ecofeminist movements—e.g., some
(Jaru/Feb. 1992): pp.8-13.
See Diamond and Orensteln, Reweaving the World; Elizabeth Dodson Grey, Green
Paradise XodCWellesley: Roundtable Press, 1979); Susan Griffin, Women and Nature:
iNvr
4
organizations In the US, the importance of addressing the complexities of "urban
Robert BuUard and Beverly Wright, "Environmentalism and the Politics of Equity,"
Mid-America Review of Sociology 12 (Winter 1987>. pp. 21-37; Robert Bullard.
Dumping in Dixie: Race, Class and Environmental QutatoyfBoulder: Westview Press,
8
environments" and “urban ecologies" has appeared in some mainstream environmental
discourse. Organizations such as Greenpeace, Sierra Club, and Earth Island Institute's
1990); R.F. Anderson and M.R. Greening, "Hazardous Waste Facility Siting: A Role of
Wanners," Journal cf the American Planning Association 48 (Spring 1982): pp. 204-
Urban Habitat Program have begun to link Inner-city needs with environmental
concerns. These projects construct the awareness of urban areas as “multicultural
ecosystems" that require specific environmental knowledges to ensure sustainable
and socially and ecologically sound development. For example, Sustainable Cities:
Urbanization and the Environment in International Perspective, cd. Richard Siren,
Rodney White, and Joseph Whitney (Boulder? Westview Press, 1991). In addition,
some environmental historians have expanded their objects of scholarly attention to
include cities and metropolitan areas as rightfully “environmental." A good example is
William Cronon’s Nature's Metropolis: Chicago and the Great West (New York: W.W.
Norton, 199D.
5
6
Author's interview with Dana Alston at the Public Welfare Foundation, Washington,
DC, Dec. 22, 1992.
18; US General Accounting Office, Siting of Hazardous Waste landfills and their
Correlation with Racial and Economic Status of Surrounding Communities (US
General Accounting Office, 1983); Sue Pollack and Joann Grozuczak, Reagan, Toxics
and Minorities (Washington, DC: Urban Environment Conference, Inc., 1984).
9
10
11
12
Authors interview with Pam Tau Lee at the University of California’s Labor and
This “blaming the victim" approach is evident in both domestic and international
lobbying campaign for a low-income community that was fighting a major polluting
corporation. The mainstream groups
don’t understand grassroots people and they don’t have much respect
for them either. There was also something else in this debate, they
said, “people who live in industrialized areas, like Niagara Falk,
make a decision and make a tradeoff." I thought well I lived in
Niagara Falls but that wasn’t a conscious decision that I wanted to live
in a polluted area. They say, “well if people wanted a clean
environment they wouldn’t live there." God, they don’t get it.
14
Karl Grossman, "From Toxic Racism to Environmental Justice," E Magazine (May/
15
June 1992): p. 31.
Richard Moore, "Confronting Environmental Racism." Crossroads/forward motion 11
no.2 (April 1992): p. 7.
16
Ibid., p.8.
17
18
19
Alston.
Pat Bryant, Toxics and Racial Justice," Social Policy 19 (Summer 1989): p. 52.
Sharon Noguchi, "Blrkenstockers Meet Ethnic Activists," San Jose Mercury Neus, Feb.
20
21
22
5.1993, p.9B.
Alston.
Gibbs.
The Clinton administration's pro-environmental and social justice rhetoric has, to
some exterc, encouraged many environmental justice activists. A number of prominent
Author’s interview with Lois Gibbs, al the Citizen’s Clearinghouse for Hazardous
Wastes in Falls Church, VA, Dec. 22,1992.
Similarly, people living in developing countries are often accused of being the
major perpetrators of overpopulation, deforestation, and the poaching of endangered
species in their efforts at daily survival in the context of postcolonial or neocolonial
23
24
Dana Alston, "Transforming a Movement: People of Color Unite at Summit Against
'Environmental Racism'," Sojourner's Tl, no. 1 (Jan. 1992): p. 30.
Redclift, Sustainable Development: Exploring the Contradictions (New York: Methuen,
1987); Gita Sen and Caren Grown, Development, Crises and Alternative Visions: Third
analysts of environmental racism In the US, Including Robert Bullard, professor of
sociology at University of California, Riverside, were enlisted to the transition team as
environmental policy experts In order to develop recommendations to Improve the
EPA's regulatory practices and their effects on communities of color (from Lee).
The title of one of the early texts produced on the emergence of the environmental
Justice movement, We Speak for Ourselves.- SocialJustice, Race and Environment, ed.
by Dana Alston (Washington, DC: Panos Institute, 1990).
global capitalism. For more detailed analyses of this argument, see Vandana Shiva,
Slaying Alive: Women, Ecology and Developmenl(London: Zed Books, 1989); Michael
Commission for Racial Justice, "Toxic Waste and Race In the United States: A National
Report on the Racial and Socioeconomic Characteristics of Communities with Hazardous
Waste Sites" (New York: United Church of Christ, 1987).
arenas. For example, Lois Gibbs, director of Citizen’s Clearinghouse for Hazardous
Wastes, recounted an attempt to work with an unnamed "Big Ten" group on a
Alston.
Lee.
Alston.
A slogan coined by Richard Moore, the codirector of the Southwest Organizing Project
and cochair of the Southwest Network for Economic and Environmental JuMke.
13
Occupational Health Program, Berkeley, CA, Jan. 25, 1993.
7
H Ml NT AL JUSTICE -127
World Women's Perspectives (New York: Monthly Review Press, 1987).
In recent years and in response to the exhortations of many people-of-color
25
Ibid.
and actions of the people struggling for local environmental conditions
in marginalized communities. Activists from the environmental justice
movement criticize this top-down, paternalistic approach that charac
terizes many prominent national and international environmental orga
need to regulate and design more advanced stack technologies or to
determine the minimum habitat requirements of a particular organism,
but that “everyone deserves to live in a healthy and safe environment’
nizations and argue persuasively that it is not working. The favorite
regardless of race, class, gender, culture, or species. Organizing for
environmental justice against toxic poisoning is relevant to “everyone’s
international environmental catch-cry “think globally, act locally" should
perhaps be modified to something like, “think locally (with knowledge
backyard’ and that includes the entire planet. Women activists from
diverse backgrounds are simultaneously challenging and redefining
of global linkages), act locally, and global transformation can be
negotiated and realized." Not a terribly catchy revision, yet it empha
sizes the significance of organizing from the grass roots, from the
multiple, local, historically and culturally specific contexts in which
(and in the process, reinventing) discourses and practices of unjust
environmental decision making, gender, racial and class stereotyping,
women (and men) are working to improve the social and environmen
tal conditions of their lives. From these localized, community-driven
and dominant notions of scientific expertise. These women’s voices
from the environmental justice movement speak loudly and clearly and
it’s time to listen.
efforts, a larger “movement" is being forged. As one activist has put it,
NOTES
the environmental justice movement’s grassroots political culture is not
1
an effect of the self-interested NIMBY (not in my backyard) phenom
enon but the critical invention of new forms of coalition politics.68
The phenomenon of the predominance of women, specifically “marginalized”
women, in environmental justice organizations has been documented by various
sources. See, for example, Lin Nelson, The Place of Women in Polluted Places," In
Reweaving the World: The Emergence ofEcofeminism, ed. Irene Diamond and Gloria
People moving in their local communities and neighborhoods are
transforming into “people movement" on a larger scale.
The leadership of the mainstream environmental movement, pre
dominantly white, middle-class men, could learn a lot from listening to
the multiple voices of the “courageous women” and “hysterical house
Orenstein (San Francisco: Sierra Club Books, 1989), pp.173-188; Susan MastersonAllen and Phil Brown, "Public Reaction to Toxic Waste Contamination: Analysis of a
Social Movement," InternationalJournal ofHealth Services 20, no.3 (1990): pp.485500; Anita Light, “Hysterical Housewives or Committed Campaigners", Ecologist 22,
no.l (Jark/Feb. 1992): pp.14-15; Paula DiPema, “Women and the Environment: Truth
vs. 'Facts’," Ms., (Sept./Oct. 1991): pp.21-26; Jane Kay, “Women in the Movement,"
wives" who constitute the majority of people working for change in the
Race, Poverty and the Environment 1, no.4 (Winter 1991); Barbara Ruben, “Leading
expanding network of grassroots environmental justice organizations.
Indicators: Women speak out on the challenges of national grassroots leadership,"
These activists show that by single-mindedly focusing on slogans such
as “save the whales" or “extinction is forever,” the mainstream groups,
perhaps inadvertently, but nonetheless, conceal or ignore their own
accountability in perpetuating the discriminatory and even genocidal
effects of environmental racism. The multiple struggles for material and
cultural survival that these activists and their communities have been
engaged in for years, in the face of massive social and environmental
assaults, illustrate a commitment to addressing the fundamental prob
lems underlying the “environmental crisis." The issue is not that we
Environmental Action 24, no. 2 (Summer 1992): pp.23-25; Anne Wine Garland,
Women Activists: Challenging the Abuse ofPower (New York: Feminist Press, 1988).
2
3
See Robert Gottlieb and Helen Ingram, The New Environmentalists," Progressive,
Aug. 1988, pp. 14-15.
Discourses of environmental preservation, protection, and the conservation of the
“aesthetics of nature" dominate the environmentalism of mainstream groups, especially
the “Group of Ten", which is also called the “Big Ten," and Includes Friends of the
Earth, Wilderness Society, Sierra Club, National Audubon Society, Environmental
Defense Fund, Natural Resources Defense Council, National Wildlife Federation,
Izaak Walton League, National Parks and Conservation Association, and the Nature
Conservancy.
1
2 2 • S O C I A L I ST IIVIIW
study a lot,"64 and for her community organization, Tucsonans for a
as well."67 To this end, many grassroots organizations have recruited a
Clean Environment (TCE!), it pays off. Similarly, neither Rose Marie
Augustine nor Marta Salinas in MacFarland, CA reject the valuable
possibilities of scientific expertise, even though both have come face to
face with its destructive deployment. Augustine is currently working
with doctors and medical professionals to try to establish a health clinic
in south Tucson for the many residents who have been seriously
wide array of scientists, lawyers, university researchers, toxicologists,
and policy experts who can bring their expertise to bear on the many
issues involved. One significant alliance between grassroots anti-toxics
activists and “scientists” is the National Toxics Campaign’s indepen
dently managed laboratory in Boston that is available to any commu
nity group that needs corroborative testing alongside the CDC’s health
contaminated by TCE poisoning. Salinas continues to struggle against
and environmental toxins inspections.
pesticide poisoning in the MacFarland area and is hoping to organize a
CONCLUSION: ENVIRONMENTALISTS LISTEN!
community-led health study in collaboration with sympathetic environ
mental health experts.65
The mainstreaming of US environmental politics since the first Earth
Productive partnerships and new alliances between grassroots orga
nizations and the scientific/medical establishment are able to emerge
as activists shore themselves up with scientific, legal, corporate, eco
nomic, and legislative expertise. Alston discusses the level of impact
that she and others were able to have on the new head of the National
Institute of Health’s (NIH’s) environmental health division.
The N1H tests one chemical at a time and determines whether it is
carcinogenic, but our case to him was that we were contaminated by
multi- sources, lots of different toxics and that this type of testing
really doesn’t speak to this....At first he was very rigid like the rest of
the scientists are, and he kept saying that there’s no protocol, there’s
no model. We kept saying but that's the point, we need for you to go
back to basics. .. About two months later, he had gone down to
Cancer Alley; he was sitting in this woman’s kitchen and he looked
out the front door and saw this one plant spewing out, then he looked
out another window and he saw something else spewing out, and
then he looked out the back window and there was something else
from a different plant So it was so clear to him that the one chemical
exposure model was just ridiculous. Now he says that they have to go
back to the very basic science that they were at 25 years ago when
they were trying to figure out how to test for one chemical. There’s
been a lot of resistance within the agency.66
In this way, environmental justice activists, like Alston, attempt to have
some influence on the theory and practice of science. Others, like
Gibbs, argue that "science is political and we need to use it politically
Day demonstrations in the early 1970s has resulted in its steady de
radicalization and capitalization. This has occurred largely at the ex
pense of low-income communities of color who live, work and play in
marginal "environments" and have never been considered part of the
“mainstream" of US culture. Thousands of people living in these
environments continue to be threatened by the dumping of industrial
toxins in their communities and by the racist "environmental" policies,
often “scientifically" justified, that support these hidden externalities of
capitalist production. Moreover, numerous environmental indicators
have demonstrated that the life-sustaining conditions of the global
environment are deteriorating at an alarming rate. As Lee has argued,
the mainstream environmental movement has not produced a “win
ning strategy" for social and environmental change. The mobilization
of new forms and strategies of grassroots politics being set into motion
by the movement for environmental justice represent powerful inter
ventions into the possibilities of creating such “winning strategies.’
Myriad voices of women activists from communities of color and
low-income neighborhoods, only some of whose words I have in
cluded in this essay, foreground the importance of thinking and
working from the grass roots to effect social and environmental trans
formations. Mainstream environmentalism constructs highly “globalized"
discourses and policies and, in the process, obscures the experiences
1 20 • SOCIALIST RIVIIW
■ NVIRONMINTAL JU CT I Cl • 121
viewed as unsophisticated and unprofessional by high-level
tion; rural: employed by facility; sees significant economic benefits;
conservative; free market orientation; above middle age, high school or
less education; nature exploitative occupations, Le., farmer, mining,
low-income.’60 Women activists in South Central Los Angeles repudi
policymakers. It has been the so-called "experts’ invoking the "neutral
ity" of science who have sanctioned the poisoning of thousands of
people in targeted communities throughout the country and the globe.
Newman contends:
Those of us that live near toxic dumps, "treatment facilities," “sanitary"
landfills, residual repositories, and other such “state-of-the-art" sites
are the true experts on the issue through first hand experience. While
others gather their information from textbooks and reports, we live,
breathe and die this issue....We're the ones that have watched as our
communities have become devastated; we’ve seen homes disappear.
We're the ones that must lie awake listening to our children struggle
to breathe; who comfort the young woman who has suffered her 6th
miscarriage....We're the ones that know the pain of parents whose
beautiful babies die in their arms and the agonizing feeling of
helplessness at not being able to stop it Yes, we know the issue
better than anyone!58
Community self-reliance has become one of the primary strategies in
the grassroots movement for environmental justice because “you can’t
count on the agencies to ‘prove’ there’s anything wrong." They have
learned repeatedly that “the studies produce statistics to be analyzed
away; that the tests produce numbers to be classified into safe levels or
standards; and that 'experts’ can find ways to explain away anything."59
Resource and training organizations such as CCHW and the Southwest
Network’s newly constituted “grassroots training institute" offer com
munity groups technical assistance, leadership training, and organiza
tional development. The level of organizational sophistication and
strategizing emerging in this movement seriously counters the “expert"
ated this ‘expert’ diagnosis. For example, in 1986
Robin Cannon successfully blocked the construction
of LANCER, a 13-acre waste incinerator that the Los
Angeles city council attempted to build in a poor
residential black and Latino community.61 The stereo
types of “unaware," "unconcerned," and “compliant"
poor communities were also expelled by the “Las
Playas Housewives," a women’s organization in
Tijuana, Mexico, that led a successful campaign to
revoke the operating license of a US-owned (Chemi
cal Waste Management, Inc.) toxic waste incinerator
located, not surprisingly, south of the US border.62
Women activists in environmental justice organi
zations possess not only ‘experiential knowledge’ of
the effects of toxins in their environments and bodies
but also extensive understanding and ability to apply
“scientifically" generated knowledges of ecosystem
dynamics, chemical production processes, and the specific uses of a
variety of industrial technologies. For instance, Lee described the
relentless library research that Robin Cannon and her sister undertook
to leam about toxic incinerators in South Central, LA. Lee asserts, “If
you want to know about incinerators, just ask Robin." Similarly, in
opinions of social research institutes such as Cerrell and Associates
Tucson, AZ’s mostly Latino south side, Rose Marie Augustine, a 54-
who provide the State of California and private corporations with
sociological criteria for targeting communities that are “least likely to
year-old “ignorant housewife," can discuss ‘everything there is to
know about TCE (trichloroethylene)."63 Augustine’s research into TCE
resist" the incursion of potentially dangerous industries. Not surpris
ingly, the profile of such a community looks something like the
following: “least resistant: small communities, under 25,000 popula
emissions produced by numerous defense contractors located in south
Tucson, including a Hughes missile plant, has resulted in the corpora
tions’ forced installation of a $33 million air stripper and emission
controller. She contends, “even though we don't have diplomas, we do
discharges. The law permits corporations to kill as long as they stay
within set limits.56
The norms and disciplining of gender, race, and class are foregrounded
and confronted by these environmental justice activists even though
most do not explicitly take on a feminist agenda. By showing up in
In the process of her research on these “scientifically" devised indus
trial standards, she discovered that women and children are not
places considered by the dominant culture to be “unnatural" for
considered in calculations of “acceptable risk." She learned that these
women of color and low-income white women, they challenge the
limitations of oppressive stereotypes. When these women assume
leadership positions in the community and demand changes in family
calculations are determined by the CDC and other local health depart
ments and “are based on occupational exposures for healthy males
working an 8-hour day, 5 days a week, wearing safety equipment in
expectations and responsibilities as they “leave the house and enter the
controlled settings." In many low-income communities, specifically
trenches,” they break down traditional constructions of gender, race,
communities of color located near toxic sites, “children, pregnant
and class and construct new empowered identities and political agen
cies. A number of activists have identified a critique of gender and
sexism as a central organizing skill and have produced a handbook,
Empowering Ourselves: Women and Toxics Organizing, which addresss
issues of community organization that specifically pertain to women’s
women and the elderly are often exposed for 24 hours a day, 7 days a
week with no protective clothing.” Newman’s political strategy, there
experiences of gender.55 These confrontations with the ideologies and
materialities of gender, race, and class also produce new theories about
the workings of power and oppression within environmental dis
courses. For example, in her work fighting the Stringfellow Acid Pits
dumping site, Penny Newman—an anti-toxics activist who, until re
fore, incorporates the effects of environmental racism in low-income
communities of color simultaneously with an analysis of the differential
impact of toxic exposure on women. She refers to this phenomenon as
the “feminization of pollution. ”57
Finally, women activists in the movement for environmental justice
not only produce new understandings of the relationships of “gender
and environment,” they also, in the process, challenge government and
corporate power structures and notions of “professionalism” and scien
cently, served as the western region field organizer for Citizen's Clear
tific expert knowledge. These grassroots organizations do not merely
inghouse for Hazardous Wastes (CCHW)—has gotten her first-hand
seek to reallocate resources (for example, in Superfund disbursements,
knowledge about the supposedly “objective” technocratic rationality
that governs much decision making around issues of the risks of
hazardous substances. She details her critique of the “environmental"
workman’s compensation payouts, or medical expenses), but to trans
discourse of “acceptable risk.”
When we allow discussions about an “acceptable risk" of 1 in 1,000 or
1 in 10,000 we are accepting that it is all right to kill one person In
every 1,000 or 10,000. We have allowed the premise to be that it is all
right for an additional person to die so that a facility can operate.
These calculations are made for each individual chemical under
perfect operating conditions. No calculations are made for the effects
of people being exposed to two or more chemicals simultaneously,
and of course the “kill rate" increases during accidents or “illegal"
form the hierarchical social relationships and fixed boundaries be
tween popular, community-based experiences and the scientific/medical knowledge production industry. It has become overwhelmingly
obvious to the activists in the environmental justice movement that the
notion of the “professional" or the “scientific expert" is highly problem
atic. This criticism embraces both the “experts’ who come from govern
ment, industry, universities or scientific laboratories, and also the
“professional" mainstream environmentalists who are reluctant to take
on the ‘radical’ agendas of grassroots organizations for fear of being
ENVIRONMENTAL JUSTICE* 1 17
the same culprit, white American capitalists. So the cycle has to stop,
somebody needs to develop an interest48
White Earth reservation, also cites culture and sovereignty issues as the
Reveilletown, a post-Civil War community founded by ex-slaves had,
until recently, sustained its residents through an agricultural economy
based on sugar cane production. The residents of the community were
poisoned by vinyl chloride emissions produced by
the Georgia Gulf petrochemical company, and were
relocated in an out-of-court settlement in 1989.59 For
Janice Dickerson, therefore, the environmental conse
key reasons for her participation in the environmental justice struggle.51
She also serves as president of the Indigenous Women’s Network and
argues that “what people really have to understand is that indigenous
people have always resisted and we are still engaged in resistance, and
that we are alive and we intend to remain that way.'52
For whatever reason women In this movement make the decision to
become politically active for environmental justice, they often find that
their work makes them visible or identified as “women,' particularly
quences of Georgia Gulf’s activities destroyed not
only the health of many people of Reveilletown (as
eccentric women. Cora Tucker talks about the time that she was
accused of being a “hysterical housewife’ as she lobbied the state
well as its land, air, and water), but also the integrity
legislature in North Carolina as an activist for voting rights in the early
of a particular African American culture’s way-of-life.
In explaining her current commitment to fighting for
civil rights movement. TYicker and other women who are considered
the soao-environmental rights of her community,
Dickerson continues,
the petrochemical industry in Louisiana is not only
destroying the health of the people, it’s destroying the
environment, the air and the water, it’s destroying the
quality of life that people were accustomed to in the
area, what we are talking about is just plain old survival
for everyday people. From the perspective of the Afri
can American, it’s a civil rights matter. Civil rights and
the environmental movement are both interwoven because again we
are the most victimized. There is no difference from a petrochemical
industry located 2-3 hundred feet from my house and killing me off,
than there is when the Klan was on the rampage just running into
black neighborhoods hanging black people at will. I feel at this point
in my life, there's so many basic issues that need to be confronted and
dealt with from the basic survival of the African American, along the
petrochemical line here in Louisiana, that you can’t really do it on a
part-time basis. There are so many issues that you need to deal with,
somebody needs to get out and do It full time, so I've decided to do
this with my life.50
Winona La Duke, director of the White Earth Land Recovery Project
and a member of the Mississippi band of the Anishinabe from the
“oddities in their communities’ have self-consciously appropriated the
derisive and sexist slur of “hysterical housewife’ as a political term and
have redefined it as a powerful identity.
I’ve learned that’s a tactic men use to keep us in our place. So when I
started this stuff on toxic waste and nuclear waste, I went back to the
General Assembly...and I said, "You're exactly right. We’re hysterical,
and when it comes to matters of life and death, especially mine, I get
hysterical...if men don’t get hysterical, there’s something wrong with
them."55
Tucker and other activists in the environmental justice movement
recount that when they first enter the political arena they are con
fronted with the perception of themselves as being women outside of
their “natural" elements as mothers, housewives, ladies, etc. Tucker
expresses this experience clearly:
If you’re out of the norm they say, “what’s wrong with this woman?"
They think you’re crazy. Most of your mommas would never have
gotten up at a board meeting and say anything about toxic waste
because they were trained that "ladies' didn’t act that way. Ladies
don’t take on an issue. I don’t know if “lady" is a compliment or not.
I really don’t like to be called a lady because my momma used to tell
me that a lady was a woman who didn’t know which way was up.54
■ Nviro HMENTAL JUSTICE •
my community and my family, specifically, could be sacrificed and
that people who were in charge, whether they were health authorities
or local government or state or federal authorities, all knew that my
family was being poisoned and they still made a conscious decision
that it was OK because of the cost involved in cleaning up. That just
totally flipped me out, because I had always believed what was in
your high school civics books. It was my children who motivated me
dearly. I just got really outraged, nobody can say that there is a price
on my children’s heads, nobody can say that based on cost-benefit
analysis, risk-benefit analysis, or whatever weird stuff they use, that
they can justify the killing, the murdering of people/3
ment will, to some degree, assert that they are acting on behalf of the
well-being of their children, their identity as simply “mothers' is by no
means always the central focus of their activism. For instance, Cora
Tucker, who works for environmental justice in her organization
Likewise, Marta Salinas, former resident of MacFarland, CA, a predomi
nantly Latino agricultural community, talks about her reasons for
are not only a question of women’s connection to children but also
confronting the dangers faced by farmworkers and their families due to
the widespread and uncontrolled use of pesticides in the local cotton
and citrus industries.
One afternoon when I heard my little daughter crying inside the
room, I walked over and she had a shoebox with some flowers that
she put in it. She said that her Barbie doll died of cancer, and she
came up and told me, ‘Mom, I know I’m going to die some day, but I
do have a wish, my birthday wish is that I want clean water and dirt
and I want to be in my own home so that I can play. If I die of cancer
I want to die with my kittens so I can die hugging them.*44
Her children and others in the community were not only becoming
sick but also overwhelmed and obsessed with thoughts of cancer,
death, and hopelessness—not the average worries of healthy young
children. Salinas and other mothers in the community have identified a
so-called “cancer cluster" in the MacFarland area, where at least 16
children have contracted a wide variety of deadly cancers since 1983.
Her visibility and activism for the health of her children and community
have taken a toll on her and her family. They have been forced to
move seven times and to relocate the children in different schools due
to the ostracization and local political pressure against her antipesti
cides work.45
Although most of the women in the environmental justice move
“Citizens for a Better America," explains that women’s activism contrib-
wp
utes to an organization because “we go at it from the point of view of
how it affects our children, we see the effects on our children more
than anyone else in the community...women are the first people to
make those connections."46 However, she also insists that these issues
“bread and butter issues."
People don’t get all the connections. They say the environment Is over
here, the civil rights group is over there, the women’s group is over
there, and the other groups are here. They say, "now Miss Tucker,
what you really need to do is go back to food stamps and welfare,
environmental issues are not your problem." And I said to him, “Toxic
wastes, they don’t know that I’m Black." [Most white people) say that
Black people are only interested in bread and butter issues. But
nothing in the world is more bread and butter than clean air to breath
or having good water to drink.47
me
flit
ff|<
OV
The question of community survival in the face of cultural imperialist
attacks by the dominant, white male, industrial complex figures conspicuously in many women of color’s involvments in environmental
justice work. Women in many communities and cultures have custom
arily been seen to be the repositories of or given the responsibilities for
maintaining local, cultural traditions and histories. Janice Dickerson, a
former resident of the now-relocated African American community of
Reveilletown, LA and current director of the Gulf Coast Tenants
Association, speaks to this issue of cultural survival.
I think that Reveilletown might be a focal point for a lot of [black
people! to start looking and begin to realize what can happen to our
history. I mean we lost our history once when we were shipped to
America, and here we are, we’ve been settled here for over a hundred
years and we are uprooted again, and we are uprooted by basically
art
the Nevada Test Site in 1987.
During those same years, other women in the US, not specifically
identifying themselves as feminists or even activists per se, organized
around issues of the environment and the survival of their communi
ties. At the same time that “ecofeminists’ convened the “Women and
the US. Instead, the ecofeminist efforts to theorize and strategize
Life on Earth’ conference, Lois Gibbs was waging her now-famous
and environment" movement, continues to expand and develop its
strategies, organization, and commitment to the grass roots on a
national and, paradoxically, international scale.
To return to the question of the salience of the “gender and
environment" debate, I want to consider some implications for social
movement theory and strategy that an understanding of the gendered
battle against the Hooker Chemical Company (Occidental Petroleum
Corporation), which had dumped 20,000 tons of toxic waste on the
neighborhoods of Love Canal in upstate New York. It was also the
same year that Penny Newman was leading the battle against the State
of California and a group of private corporations, including McDonnell
Douglas and Rockwell International, for siting and dumping over 34
million tons of carcinogenic, hazardous chemicals in the Stringfellow
around a “women and environment’ connection has remained almost
exclusively within the realm of the production of theory. On the other
hand, the movement for environmental justice, widely recognized as
being driven and energized by women, yet not marked as a “women
nature of the environmental justice movement may suggest. To get at
this question, it is important to look at the different struggles over
Acid Pits, a state-licensed disposal site (now California’s top priority
Superfund site) overlooking the rural community of Glen Avon in
environmental “resources and meanings’ that these women undertake
southern California. In the early 1980s, while thousands of women,
women active in the environmental justice movement, I have learned
about the many ways that they contest and redefine discourses and
practices of not only environmentalism but also of gender, racial, and
class stereotyping. They also question and reconstruct the concepts of
“objectivity’ and the “validity" of scientific expertise.
For example, many women in the movement evoke deep concerns
predominantly white and middle-class, were encircling the Pentagon,
weaving symbolic webs of containment made of yam, flowers, and
children’s photos through its barbed wire fences, Cora Tucker, a
longtime civil rights activist and resident of rural Halifax County, VA,
was organizing against a local uranium mining project and the pro
posed siting of high-level nuclear waste repository near her commu
in this “unmarked”42 women's movement. Listening to the voices of the
nity.
These stories of women’s “environmental” activism represent very
different modes of organization and strategy; one distinguished by the
production of national, large-scale, often symbolic demonstrations and
about the health and future survival of their children and communities
when explaining their initial or continued involvement in fighting for
environmental justice. The identity and experience of being a “mother,"
and the outrage at watching local corporations and government offi
cials exhibiting total disregard for the lives of their children, have
direct action and the other by local, community-based, networking
significantly motivated many women to become politically active. Lois
style activism. At the time, the continuities between these different
levels of women-led actions for the “environment” were not obvious
(although Gibbs did present a speech to the Amherst conference),
Gibbs explains her distress at the serious illness of her one-year-old
son and the rare blood disease that her young daughter developed
when her family moved to Love Canal.
even though they showed evidence of the existence of different
women struggling for many of the same socio-environmental issues. In
the ’90s, there is no visible, active, explicitly “ecofeminist" movement in
It was like what tire hell’s going on here, I did everything right, I
prided myself in being a responsible mother, and then I found out
about the dump. What really got me Involved was the realization that
1 1 O * >O Cl ALIST RE VII W
INVIROMklNTAL JUSTIC1* 111
these gendered roles of “mother” and “nurturer” have included child-
critiques, I am less interested in attempts to answer the question, “Why
rearing, food production, and the overall responsibility for the health
and survival of the community, women’s social location affords them
women?", as I am in understanding the “struggles over both resources
and meanings"40 of gender, race, and class relations and environmental
specific knowledges and investments in issues of the “environment."
conditions that the women in the environmental justice movement are
Both of these arguments, and multiple combinations of the two, are
waging.
represented in numerous ecofeminist writings and actions that have
appeared since the late 1970s.37 How are women activists in the
environmental justice movement situated in these “ecofeminist" de
bates around gender and the environment? I found Alston’s interpreta
tion of the political usefulness of these debates enlightening.
AN “UNMARKED" WOMEN'S MOVEMENT
There may be some truth to both of these theories but I've just found
that women, plain and simple, have a lot of courage...offering them
selves and stepping forward when there is a problem and there are
things to be done. As far as all the intricate, motivating forces behind
this, we can have all kinds of theoretical discussions about that from
now until forever, but I always find that when there is a man who has
distinguished himself in a particular way he’s usually surrounded by
very dedicated, hardworking, courageous women who made it all
work. We have a lot of issues to get over, understand, and deal with
as to why it’s not the woman who was projected forward or who has
gotten the visibility or the credit that she deserved.... Personally, I like
spending my energy trying to change how we are perceived and how
we move forward than analyzing why we’re there in the first place.38
In other words, to what extent do these ecofeminist theories help to
inform movement organization and strategy? The focus, by many
ecofeminist theorists, on the question, “why women?", has been criti
Many ecofeminist writings construct theories as to why women would
organize as women in their struggles for socio-environmental change.
Such theories, as I mentioned earlier, suggest that women possess
unique knowledges about the connections between human health and
survival, the environment, and their ever-increasing destruction by the
“capitalist-militarist-patriarchal complex." These theorists claim that by
virtue of these “innate" or experiential knowledges, women come
together in political solidarity. “Womanist" or “motherist" organization
around issues of militarism and the material conditions of survival is
not something new in the US. However, the late 1970s and early 1980s
marked a particular historical moment in which many, predominantly
white, middle-class women explicitly linked feminist and environmen
talist concerns. The proliferation of the nuclear industry, specifically
the Three Mile Island crisis, prompted women in the US to come
together in 1980 at a conference in Amherst, MA, entitled, “Women and
Life on Earth: Ecofeminism in the 1980’s." Ynestra King, one of the
organizers of the conference and a prominent theorist and activist in
cized as being ethnocentric (i.e., positing the existence of “woman" as
a unitary category whose experiences of patriarchal oppression are
universal) and overly ideological (i.e., locating the domination of
“woman" solely in the realm of consciousness—that is, women are
oppressed because of the ideologies of hierarchy and control—instead
of looking at the material, economic, and political structures through
the movement, declared in the opening address: “We’re here to say the
which these ideological constructs are produced and transformed) by
numerous feminist critics writing on women's organization and struggles
catalyzed a series of now famous nonviolent, direct actions, including
the Women’s Pentagon Actions of 1980 and 1981, the Seneca Women’s
for the environment.39 In agreement with the intentions of these
Peace Encampment in 1983 and the Mother’s and Others Day action at
word ‘ecology’ and announce that for us as feminists it’s a political
word—that it stands against the economics of the destroyers and the
pathology of racist hatred. It’s a way of being, which understands that
there are connections between all living things and that indeed we
women are the fact and flesh of connectedness."41 The conference
IRONMENTAL JUSTICE • 109
1 O S » SOCIALIST MVIBW
This is not, I am convinced, a calculated act on the part of movement
activists in order to construct the appearance of solidarity in the
interests of controlling the movement’s representation. Instead, the
narratives of broadly based consensus and political unity that have
emerged from my interviews and various movement literatures, indi
cate the conviction and insights that come from years of hard political
and organizational work. The women with whom I spoke were re
freshingly candid in their expressions of relief and hopefulness that the
decision was made at the Leadership Summit to remain a grassrootsdriven movement.
One of the effects of the collective commitment to decentralized
grassroots politics that the Leadership Summit established has been a
change in the way the media represent the environmental justice
movement. The image emanating from the summit of an expanding
network of multiple grassroots organizations actively working together
enabled a more complex analysis and portrayal of the movement’s
objectives and activities. Alston asserts that
the media attention previous to (the summit] concentrated on the
tensions between people of color and the environmental movement
as the main issue. The summit helped to broaden the message that
was getting out to the general public...it has broken away from just
the conflict between the two. The media thought what was most
exciting was that people were calling the environmental movement
racist, and that made great headlines. The media has changed because
they started covering the more complicated debates about what
people were facing in environmental degradation—was it race or
class that was involved?...We’re talking about something that’s far
more fundamental than just the dumping of hazardous wastes In our
communities. And (die medial have also shown that there was a lot of
work going on, these people are not just victims, they’re people who
are taking substantive action to try to change die conditions in their
lives and to create something different54
As in many environmental and social justice movements in the US and
internationally, women comprise the majority of “people taking sub
stantive action" in their communities and local organizations. Accord
ing to numerous accounts by activists, women make up about 90% of
the active participants in the environmental justice movement, yet they
are not well-represented in highly visible leadership roles.35 This
situation indicates one of the key challenges for the environmental
justice movement that has emerged from the summit’s principle of
democratic and diverse leadership. How to simultaneously address
issues of gender, race, and class in shaping new forms of leadership
and organization in this new movement for social and environmental
change?
WOMEN AND ENVIRONMENTAL
JUSTICE: SITUATING THE GENDER
AND ENVIRONMENT DEBATES
One of the major commonalities between the environmental justice
movement and other environmental and social justice movements in
the US (and internationally) is the high representation of women
working in the rank and file. The apparent historical pervasiveness of
this phenomenon has inspired a spate of academic and feminist
theorizing about the underlying reasons for the high involvement of
women in movements and struggles for social and environmental
change. Much of this discussion revolves around the question of the
extent to which women’s observed connection to nature and to
environmental concerns has essentially biological or social origins. The
biological explanation contends that women have an innate knowl
edge of the interconnectedness and value of all life on earth due to
their reproductive capacities. Consequently, their experiences of preg
nancy and childbirth compel them to fight for life-affirming policies
and clean, healthy environments as mothers in defense of their chil
dren and families. This position is criticized as being overly “essentialist'36 and deterministic by those theorists who argue that women's
heroic struggles for social and environmental justice must be under
stood as emerging from the gendered socio-cultural roles they have
been expected to fulfill as a result of patriarchal oppression. Since
1 06 • SOCIALIST REVIEW
tai problems- They reject the top-down approach as disempowering,
paternalistic, and exclusive and instead are committed to developing a
more democratic, locally and regionally based, decentralized organiza
tional culture. A commitment to such values, they argue, will build a
movement that truly works. Alston remarks:
amenim action
I think that those of us who study the history of social move
menu have learned so much from other movements that we
made a commitment to spend the next two years building local
and inter-regional structures and to strengthen those, and to
then come back together and see...We didn’t want one person
to emerge as the 'spokesperson" because we have worked too
long and too hard to have the bonds between us destroyed. The
media and the EPA were pushing for this spokesperson, so it’s
been a real struggle. I’m really glad that we made that deci
sion.29
Referring to the issue of the traditional tendencies toward
movement centralization, Lois Gibbs explains:
in the Southeast, as the New Orleans Conference on Labor and the
Environment showed, real live grassroots organizations coming in and
starting from a strong foundation and building up. There was jua a
meeting in Chicago of the Midwest organizations, so the approach is,
I feel, one that's going to win. It's a winning strategy, the top-down
strategy is not a winning strategy.31
Alston expounds further on the movement's organizing strategies by
noting that
the Southwest has been meeting regionally for many years and has
representative leadership, reservation, urban, and rural....Several weeks
ago the Southeast had their first regional meeting in New Orleans,
sponsored by the Southern Organizing Committee. They were expect
ing several hundred people and they had over 1500 show up. I’ve
been to many meetings in the south and they are usually all black or
black and white but to see the indigenous people, the Haitian and
Latino farmworkers, it was unbelievable. I'm going to a planning
meeting in January for the Northeast regional meeting, the Midwest
already has had one meeting that brought together African-American
organizers out of Chicago and Detroit to meet with the Plains
Indians.32
At the People of Color Leadership Summit, one of the things
was the struggle about who was going to take leadership. This
was a real test to see if people really believed that we have
more strength in numbers of groups, as opposed to one, and
when the issue came up about, do we want to centralize, do we
want to develop a key leadership for this thing, people ada
mantly said, "No!” It was one of the first tests of this issue, the
question is how do you keep this together, how do you make it
happen? Every time we see somebody who looks like they're going to
be a leader, we’re biting our fingernails and thinking “media, please
don’t start naming them leaders."30
An interactive environmental justice network has emerged as the most
identifiable structure organizing the movement. Pam Tau Lee describes
this strategy.
What I see is a wonderful phenomenon...the development of net
works. Those networks are based on actual work that is coming out of
the grass roots. You've got the Southwest Network, 40 organizations
that are doing real live work, who have joined a network to create “a
net that works," as Richard Moore puts k. And you've got another one
As one concession to a form of centralization, a steering committee was
established to facilitate a national network. Given that foundations are
notoriously reluctant to support amorphous structures like networks,
preferring the instinitionalization of an “entity," what will become of
the national environmental justice network is yet to be seen. The three
activists I interviewed noted the tensions between the desire to remain
faithful to the imperatives of “direct democracy” by working locally and
on a small-scale, and the impulsion to centralize and “go national” in
order to gain more clout or to “look more like a movement.” The
“parochialism” of many grassroots groups and the political limitations
of failing to link local struggles to national and global ones, have
circulated as internal criticisms of the environmental justice move
ment.33 However, as a social movement in the early stages of its
evolution, the environmental justice movement is intentionally por
trayed, by many of its members, as constituting a solid political front.
ENVIRONMENTAL JUSTICE • 105
America, Puerto Rico, and the Marshall Islands to develop a process for
ees articulated key issues of environmental justice movement building
framing the contours of a “multiracial movement for change" founded
that Included environmental problem-definition, leadership and orga
on the political ideology of working from the grass roots. Conference
nizational strategy, and creating the conditions for coalitions and
participants heard testimonies and reports of the persistence of the
effects of environmental racism in their communities, including exten
partnerships. The participants convened “policy groups' that drafted
recommendations (presented at the United Nations Conference on
Environment and Development gathering in Brazil the following year)
focusing on “the ecological impact of war, underground nuclear test
ing, the international waste trade, and US foreign aid and trade
policies."27 In addition, the Leadership Summit produced, through a
consensus process, a set of 17 organizational principles that would
serve to guide the emergent political process. These “Principles of
Environmental Justice," which were distributed at the summit, con
sive poisoning of air, water, and land that continues to disproportion
ately devastate their environments and health. These discussions also
provided a supportive context for people of color to “reaffirm their
traditional connection to and respect for the natural world," which was
collectively understood as “including all aspects of daily life.” Environ
ment so defined addresses environmental problems in terms such as
“militarism and defense, religious freedom and cultural survival, energy
and sustainable development, transportation and housing, land and
sovereignty rights, self-determination and employment.”25 Dana Alston
describes how the Leadership Summit helped to bring people of color
together in a spirit of political solidarity.
The most important thing that came out of the summit was the
bonding. Many people might think that because they’re nonwhite,
that they’re going to come together, but the society is built on keeping
people divided and we all know about the tensions between African
Americans and Asian Americans and Latinos and Native Americans but
it’s the history, the culture, the society that’s keeping us divided....That’s
how the power structure stays in power, by keeping us separate. So
from the very beginning we had to put together a set of principles
from which we were going to relate to each other.... All decisions
were going to be based on those principles, and that all cultures
coming to the table would be respected; there would be equity as far
as participation and voice, across gender, race, ethnicity, and region. I
think that bonding was important, the idea that there was more that
we shared in common as far as our oppression than there were things
that divided us.26
struct the profile of a broad and deep political project that specifies
environmental justice as “securing our political, economic and cultural
liberation that has been denied for over 500 years of colonization and
oppression, resulting in the poisoning of our communities and land
and the genocide of our peoples." They also function as guidelines to
assist and inform collective actions and decision making. Alston ex
plains that at difficult moments during the Leadership Summit, “we
would go back to the principles and often the answer to the question
would be really very obvious.”28
All of the women activists with whom I spoke maintain that the
a sampling of “professionals' such as lawyers, academics, and
most promising achievement of the Leadership Summit was, not sur
prisingly, its commitment to the construction of diverse, egalitarian,
and nonhierarchical leadership and organizational processes and struc
tures. In contrast to the technocratic rationality and top-down
managerialism that the mainstream environmental organizations have
adopted by mimicking the decision-making approaches of the very
corporations that they oppose, the participants at the Leadership
Summit insisted on something different. As grassroots activists working
in direct response to the threats of pollution, resource exploitation, and
land-use decisions in their communities, they realize that the decision
policymakers. Engaging in critical discussions and debates, the confer
making process is itself a primary issue in the debate over environmen-
The composition and program of the second day of the Leadership
Summit shifted with the arrival of another 250 participants from a
variety of environmental and social change organizations together with
■ NVIRONMINTAl JU1TICI* 103
Justice and Sustainability,’ convened in January of this year and
brought together groups as varied as the Japanese American Citizens
them, whether it’s the Southwest Research Organization or the South
ern Organizing Committee, or Greenpeace, these are organizations
that could help and there’s only a small pool of money. Now these big
bluechip organizations are coming In and foundations are saying,
“Oh, good they've been around for a hundred years and now we don’t
have to take the risk.’ If media people have a choice of tracking down
the Southern Organizing Committee or the Environmental Defense
Fund, you know who’s in their Rolodex. I find it very frustrating
because we’ve built this wonderful movement and it’s almost like
being victimized one more time.21
League, the Environmental Defense Fund, the Latino Issues Forum,
and Citizens for a Better Environment.19
And with a touch of irony, Pam Tau Lee remarks that former EPA chief,
of color organizations has recently formed. EDGE: The Alliance of
Ethnic and Environmental Organizations provides a forum for multira
cial dialogue around issues of sound economic development in light of
California’s rapidly changing demographics and ethnic composition.
Their first conference, “Redefining the California Dream: Growth,
the importance of race and class in organizing for truly effective
environmental change. Most of the women activists I interviewed,
however, were still cautiously watching to see what may come of these
changes. They are particularly suspicious and critical of the ways that
William Reilly, consistently refused to utter the words “environmental
racism" during his tenure. However, toward the end of his term he
became more comfortable with the notion of environmental justice and
referred to it in EPA memos and reports.22 These activist’s criticisms of
the unacknowledged “paternalism" inherent in the “Group of Ten’s’
approach to dealing with the issues of environmental justice illustrate
some “Big Ten’ organizations are choosing to respond to the chal
the importance of the movement’s insistence on self-representation
lenges put forth by the movement. Alston explains that
and self-definition, best signified by the movement phrase “We speak
for ourselves.”23 This unequivocal rejection of a “partnership based on
Such examples provide evidence that the environmental justice
movement has intervened, at least to some extent, in foregrounding
some now see that there are a lot of organizations that have made
[environmental justice] a priority, and you see these same organiza
tions going to set up programs...like the National Wildlife Federation
has a grant proposal out for 1.4 million dollars to work with people of
color...and they are notorious for having terrible relationships with
people of color. They have Waste Management, Inc. on their board of
directors which engages in supreme environmental racism. They will
dump some of the most hazardous materials known in people of
color’s communities. To watch NWF raising all this money to deal
with people of color is very difficult to see.20
paternalism’ with the mainstream environmental movement explains,
in part, the overwhelming enthusiasm surrounding the First National
People of Color Environmental Leadership Summit, which convened in
Washington, DC in October 1991-
PRACTICING ENVIRONMENTAL
JUSTICE: LEADERSHIP AND
DIVERSITY FROM THE GRASSROOTS
Similarly, Lois Gibbs, director of Citizen’s Clearinghouse for Hazardous
Waste, argues that
some of these “Big Ten” groups have put in proposals to the tune of
5 million dollars to do community organizing and outreach to low1.
income community groups, and people of color groups. I look at that
and I know that these people are adopting the rhetoric for foundation
purposes. They use it in their newsletters and their PR pieces, but all
they’re doing is taking away from support groups that could help
Accounts of the proceedings of the Leadership Summit describe the
occurrence of a history making event in which the way “environmental
issues are debated and resolved is changed for good. And for the
better."24 This momentous event brought together 300 African AmeriI
can, Native American, Latino, and Asian American delegates from the
US and a number of conferees from Canada, Central and South
excluding people of color from leadership in the environmental move
ment.”14 The process of “naming” and articulating the specificities of
are never full participants in the decision-making which leads to
them.16
z
nizations. The expression of this new political concept also provided
an organizing tool that could galvanize into action the multiple and
diverse communities and constituencies for whom “environmental
Responses to these challenges have been varied, according to the
activists with whom I spoke. At worst, some of the “Group of Ten’
have expressed outrage and denial and have all but ignored the
invitation to “come to the table as equals.” On the other hand, some
have begun to enter into discussions about building “multicultural and
multiracial organizations,” to share resources such as technical exper
racism" was a painful reality. The extent to which the discourse of
tise, legal assistance, and funding, and to seriously modify their
environmental racism has been engaged by the mainstream media and
organization’s structure and mission. Dana Alston cites the transforma
environmental groups is another question.
tion of the National Toxics Campaign (NTC) as evidence of
How have the appearance of the UCC-CRJ report on toxics and race
and the public naming of the existence of environmental racism
affected the national environmental agenda? By 1990, a variety of
coalitions of minority environmental justice organizations had emerged,
including the extremely dynamic Southwest Network for Economic
such engagements.
environmental racism by movement activists firmly established it as a
significant object of political scrutiny and as a serious critique of the
theory and practice contradictions of mainstream environmental orga
and Environmental Justice (SNEEJ). In January and March of that year,
representatives from many of these coalitions of grassroots organiza
tions composed two recriminating letters to the “Group of Ten” na
tional environmental organizations “calling on them to dialogue on the
environmental crisis impacting communities of color, and to hire
people of color on their staffs and boards of directors."15 The final
letter focused on an analysis of environmental racism and the ways that
the primarily white, mainstream organizations have been complicit in
supporting it.
There is a clear lack of accountability by the “Group of Ten" environ
mental organizations towards Third World communities in the South
west, in the U.S. as a whole and internationally. Your organizations
continue to support and promote policies which emphasize the clean
up and preservation of the environment on the backs of working
people in general and people of color in particular. In tile name of
eliminating environmental hazards at any cost, across the country
industrial and other economic activities which employ us are being
shut down, curtailed or prevented while our survival needs and
cultures are ignored. We suffer from the results of these actions, but
Some organizations, like the NTC, have been transformed by
the environmental justice movement because they allowed
themselves to open up; they made a commitment to get 50%
people of color on the board, to be driven by grassroots
groups. They are really committed to making just partner
ships and not paternalistic partnerships. Now it’s the only
national multiracial environmental organization in the coun
try. They still have their problems....! see them as an ex
ample of a real transformation of a national environmental
organization....They were basically a white organization.17
[living Wl
!
POLLUTIO
1 rovunn inert far
Other promising signs of multiracial coalition building
include the series of “Great Louisiana Toxics Marches”
initiated in 1988 by the Gulf Coast Tenant's Project in New
Orleans. These massive demonstrations (some lasting up
to 11 days and spanning a distance of 100 miles) sent
marchers through Louisiana's “Cancer Alley" and were
organized by a diverse group of grassroots civil rights, church, labor,
and tenant’s organizations together with a number of national bodies
like the Sierra Club and Greenpeace. “The Toxics marches’ have helped
put race on the environmental agenda and to put the environment on
Third World communities’ agenda.”18 In the San Francisco Bay Area,
another coalition between mainstream environmentalists and people
INVIRONMINTAL JUITICI*99
The results of an exit poll conducted by one of the “Big Ten” environ
mental organizations on last year’s presidential election day support
Lee’s observations. According to Alston, the poll reports that
in the white population, 28% said that the environment was one of the
key factors that helped them determine who to vote for, but when it
came to African Americans or Latino Americans it was close to 48%.
Before, when you asked a black person what were the important
issues they would say, "Oh the air smells terrible, the water tastes
terrible, my child has asthma, there’s lead poison
ing in the apartments* but they hadn’t defined
those as “environment" because how it was being
defined by others was whales and ancient forests
and national parks, etc. Now that gap in definition
is being closed, but we always said that people of
color were much more Interested and invested in
these issues than what was being said about us,
that is, that “we’re not Interested, we’re too busy
surviving* even though the Black Congressional
Caucus has had the best voting record on the
environment in the past 20 years.11
Obviously, the notion that these grassroots, com
*WE DON'T HAVE THE COMPLEXION FOR
PROTECTION"”: THE POLITICS OF
ENVIRONMENTAL RACISM
Although people living nearby toxic waste facilities have known for
many years about the detrimental effects to their health and their
environments that industrial pollution generated, it was not until the
publication of a landmark report sponsored by the United Church of
Christ Commission for Racial Justice CUCC-Ciy) in 1987 that an aware
ness of the widespread existence of “environmental racism* entered
into the mainstream political consciousness.
The UCC-CKJ report, “Toxic Waste and Race in the United States,*
compiled the results of a national study that demonstrated a demo
graphic pattern that indicates race as the leading factor in the location
of commercial hazardous waste facilities. The study, presented to the
National Press Club in Washington, DC that same year, found that
people of color suffered a “disproportionate risk" to the health of their
families and their environments, with 60% of African American and
munity-based, social and racial justice-driven or
Latino communities and over 50% of Asian/Pacific Islanders and Native
ganizations are composed of “new environmental
ists’ is contested terrain. Questions of the impor
tance of self-representation, definitional clarity,
and the agency inherent in “speaking for our
selves" are key issues for movement activists. What
is “new" about the environmental justice move
ment is not the “elevated environmental consciousness* of its members
but the ways that it is transforming the possibilities for fundamental
social and environmental change through processes of redefinition,
Americans living in areas with one or more uncontrolled toxic waste
site. The report also disclosed the statistic that 40% of the nation's
landfill capacity is concentrated in three communities—Emelle, AL with
a 78.9% African American population, Scotlandville, LA with 93%
African Americans, and Kettleman City, CA whose inhabitants are
78.4% Latino.13
The concept of 'environmental racism' entered into political dis
course around the environment in 1987 when the Rev. Benjamin
Chavis, the commission’s executive director, formulated the term.
reinvention, and construction of innovative political and cultural dis
According to Chavis, environmental racism is 'racial discrimination in
courses and practices. This includes, among other things, the articula
environmental policy making and the enforcement of regulations and
tion of the concepts and materialities of “environmental justice* and
laws, the deliberate targeting of people of color communities for toxic
waste facilities, the official sanctioning of the life-threatening presence
'environmental racism* and the forging of new forms of grassroots
political organization.
of poisons and pollutants in our communities, and the history of
INVIRONMINTAL JU1TICI-97
ho merging of
•la! [ustico and
snvlronneental
latorosts.
yforo, auumet
people are ait
tfegral pari of
shat should bo
entood as tho
•rnvironuoent.”
you're talking about lead and where people live, it used to be a
housing struggle, if you’re talking about poisoning on the job it used
to be a labor struggle, people being sick from TB or occupational
exposures used to be separate health Issues, so environmental justice
is able to bring together all of these different issues to create one
movement that can really address what actually causes all of these
phenomena to happen and gets to the root of the problems.*
The merging of social justice and environmental interests, therefore,
assumes that people are an integral part of what should be understood
as the “environment.’ The daily realities and conditions of people’s
lives have not been at the center of mainstream environmental dis
course. Traditional environmental arguments have commonly con
structed the relationships of society and “nature," and urban vs. wild/
natural as hostile, even incommensurable dichotomies. Arguments
based on such dualisms often end up blaming the people who have to
live with the consequences of the externalities of unchecked industrial
ization.7 Numerous studies have demonstrated that it is primarily lowincome communities of color that are often targeted for industrial and
toxic waste disposal sites.8 Dana Alston discusses how the environ
mental justice movement’s redefinition of “environment" to account for
the presence of people reflects one of the primary discrepancies
between it and the mainstream movement.
I think you can get at the heart of the difference if you look at the
relationship problem that people of color have with the environmen
tal organizations, for example, the Nature Conservancy, which defines
itself as the “real estate’ arm of the environmental movement and as
being about saving nature, pristine areas, sensitive ecosystems, en
dangered species, and rainforests. But the reality of the situation is
that there is hardly anywhere in die world where there aren’t people
living, no matter how remote you get, and the most vulnerable
cultures are in the areas that are most remote, whether you are talking
about here in the US or In Latin America or wherever, so immediately,
it puts us in confrontation with the Nature Conservancy. We continue
to raise these issues not only in the international arena but here as the
Nature Conservancy goes to buy large tracts of land in New Mexico or
out west where indigenous and Chicano people have lived for
decades and have sovereignty or land-grant rights...with total disre
gard for how these real estate dealings affect the social, political, and
economic life of our communities. We feel that many of these
communities are just as much endangered species as any animal
species...so, we don’t lift up one aspect of the ecosystem over
another.9
Consequently, activists in the environmental justice movement are
unlikely to identify themselves as the “new environmentalists" because
they do not view themselves as an outgrowth of the “old" environmen
tal movement together with its “save the whales and rainforests’
sloganeering. The “old" vs. “new" binary analytic casts the “new"
grassroots, low-income and community-of-color-based activist as “other*
to the normative referent of the mainstream, white, middle-class,
privileged environmentalist. It would be more accurate to regard
environmental justice activists as the “new" civil rights or “new" social
justice activists, since many of the prominent organizers affirm their
roots in and political continuities with the social justice movements of
the sixties, including the civil rights, welfare rights, and labor and
farmworker movements. Moreover, the term “new environmentalists"
suggests that the members of these emerging grassroots organizations,
who come from predominantly African American, Latino, Native Ameri
can, and Asian American communities, are only recently becoming
interested in or aware of the importance of “environmental" concerns.
Pam Tau Lee contests this characterization of communities of color.
If you come into Chinatown, you'll see that recycling didn’t just come
from this new yuppie environmental scene, or if you go into different
African American communities, you’ll see that people have been
recycling and reusing for a really long time. Last summer, I worked on
a project with kids in Chinatown on the environment and they said,
“We called the city and we wanted a recycling program for Chinatown,
and they wouldn’t let us participate in it They said that the trucks are
too big and the streets in Chinatown are too narrow, and they cant
come in."...Some other kids said, ’I think they're prejudice, they dont
care about us!"...If you go to my mother-in-law’s, everything is
washed and hanging to dry, she probably has every styrofoam
container that she ever had from any restaurant, and you’ll find that in
all these communities.10
INVIRONMINTAL JUSTlCi-95
distinguishes it from that of the “mainstream” environmental move
species protection. Issues pertaining to human health and survival,
ment whose constituents have historically been white and middle
class. As someone with high stakes in the transformation and invention
community and workplace poisoning, and economic sustainability are
generally not considered to be part of the “environmental’ agenda.
of feminist and multicultural environmental coalitions, I am particularly
Additionally, the activists I spoke to perceived much of mainstream
environmental discourse to be either fixated on anti-urban develop
ment campaigns (read as "no jobs for city-dwelling people’), or utterly
indifferent to the concerns of urban communities altogether. Many of
interested in the political culture being shaped in this movement. I
have spoken with many activists involved in the environmental justice
movement and have been struck by the stories they tell about the
processes and challenges of configuring and forging this multi-issue,
grassroots movement for the nineties. These women activists, together
with men in their communities, actively produce the conditions for
social and environmental change, locally and nationwide, by reinventing
socio-environmental terms and definitions, constructs of gender, race,
and class politics, forms of leadership, strategies for coalitions, and
the community organizations that comprise the environmental justice
movement are located in low-income and working-class communities
in and around industrialized urban centers throughout the country.
Crucial issues in these communities include lead and asbestos poison
ing in substandard housing, toxic waste incineration and dumping, and
widespread unemployment. Until relatively recently, these are prob
notions of social movement history. Drawing heavily on personal
lems that the mainstream organizations have located outside the do
interviews with three prominent women in leadership roles and a
main of “environment.’4
Clearly, the concept “environment’ is highly problematized in the
variety of movement literatures, I will discuss some of the critical issues
and innovations articulated by the voices of the environmental justice
movement.
SOCIAL JUSTICE: A NEW SPELLING
OF "ENVIRONMENT"
The question of the “newness” of a social movement is often a subject
of debate, at least for some social movement theorists and political
analysts expounding on the emergence of the so-called “new" social
movements. Social movement historians have occasionally referred to
environmental justice activists as the “new environmentalists,’2 a term
that I find misleading. Many of the grassroots activists I interviewed are
reluctant to call themselves environmentalists at all, much less newly
convened ones. In part, this is due to the dominance of the mainly
white, middle-class, and uncritically “preservationist" political culture
from which much of the mainstream environmental discourse has
developed.3 In these mainstream terms, what gets to count as environ
ment is limited to issues such as wildland preservation and endangered
environmental justice movement. The activists I spoke with define
environment as “the place you work, the place you live, the place you
play.’ Moreover, Dana Alston, director of the environment program at
the Public Welfare Foundation and former director of the Environment,
Community Development and Race Project at the Panos Institute,
argues that environmental justice must be
seen through an overall framework of social, racial and economic
justice, and the environment is just one piece in a whole linkage...it
calls for a total redefinition of terms and language to describe the
conditions that people are facing and to come up with solutions.5
Pam Tau Lee, the labor coordinator for the Labor and Occupational
Health Program at the University of California, Berkeley, and a board
member of the National Toxics Campaign Fund and the Southwest
Organizing Network, elaborates further to say that environmental
justice
is able to bring together different issues that used to be separate. If
s ociaXt’yfSOCIALIST RIVIIW
rk on UNCED," written by sotne of the more grawroots-orierted members of
zen’s Network Steering Committee, Aug. 5, 1992.
GIOVANNA DI CHIRO
Dolan, ‘Strong Treaties Elude Even Activists at Earth Summitt," Los Angela
lune 11,1992.
emative treaties are easy to get. Many are posted on the "UNCED treaties
-nee" on ficonat The set Is available for $10 from the U.S. Citizen’s Network on
> (300 Broadway *39, San Francisco, CA 94133). An annotated edition is under
nion and will be published by Commonweal.
> inspired a number of attempts to synthesize and stale this agenda as a whole.
table examples, bah of which will be worth reading for years lo come, are
•eace's Beyond UNCED (available from local offices) and WTrcee Common
DEFINING
ENVIRONMENTAL
JUSTICE
women's voices
and grassroots politics
The language used by activists to represent the
development of a contemporary movement for “en
vironmental justice" in the US abounds with political
conviction, dynamism, and hope. Phrases such as,
“transforming a movement," “reclaiming the land
scape," “empowering ourselves," “reshaping our com
munities," speak to the power and promise that motivate this historical
moment of social movement building. The environmental justice move
ment has materialized within the last decade as a US social movement
that both challenges dominant discourses of environmentalism and
produces new constructs of environmental theory and action. The term
“environmental justice,” which appeared in the US sometime in the mid
1980s, problematizes popular notions of “environment" and “social
justice’ and discursively produces something different. In this essay, I
want to examine some of those differences as they are articulated
through the voices of women activists in the movement.
The vast majority of activists in the environmental justice movement
are low-income women and predominantly women of color.1 From the
start, the gender, race, and class composition of movement activists
Giovanna Di Chiro is writing
on women's environmental-health
octivism that critiques ond
transforms issues of science ond
technology She is in the History
of Consciousness Program of the
University of Californio at
Santo Cruz.
( AIDS' <w
NY'ACT-Uf^ 1^8^ .
,
®
What the Numbers Mean
RISA DENENBERG
ACT UP demonstration 'Wall Street II' in March 1988 marking ACT UPS second birthday and
protesting the lack of money spent on AIDS.
Photo by Miriam Lefkowitz
Why do women die from AIDS so much faster than do men?
Why are so many women with HIV illness of African descent or Latina?
Why is the research on women with HIV disease so limited? How can
we understand what all the statistics mean?
Numbers can be alarming but also revealing. In order to get
answers, we need to ask the right questions and take a hard look at
the available data. The growing number of women with HIV disease
parallels a rise in cancer, drug use, homelessness, incarceration, and
poverty among women.
Epidemiology is the science that studies epidemics and de
scribes the occurrence and distribution of disease in a given location
or population. Its goals include explaining how a particular disease
is affecting people, how it is transmitted (passes from person to
person), and how it can be prevented or controlled.
In the United States it is estimated that health care workers
report 80 to 90 percent of all AIDS cases to local health departments,
who then report them to the Centers for Disease Control (CDC). The
CDC places each case in a category of exposure (the way the person
is presumed to have gotten the virus) and generates statistics and
predictions based on these data. In August 1989, the number of AIDS
cases reported to the CDC reached 100,000.
While the number of AIDS cases is monitored, the number of
people who are HIV positive is only estimated. The U.S. Public Health
Service estimates that 1 to 1.5 million people are HIV positive at
present. An international estimate from data collected by the World
Health Organization suggests that 5 to 10 million people worldwide
have been exposed to HIV. Many people who are HIV positive are
well and may never get AIDS.
With a world view, epidemiologists have suggested that there
What the Numbers Mean
1
are three distinct patterns of HIV transmission geographically. In
pattern type 1 (which includes the United States, some western
European countries, some Central American countries, Canada, New
Zealand, and some countries in southern Africa) cases are dis
proportionately male (10 to 15 male cases for each female case), and
perinatal transmissions (from woman to fetus during pregnancy and
delivery) are low. In pattern II (including many central, eastern, and
some southern African countries, and most of the Caribbean) the ratio
of male to female cases is approximately equal, as are transmission
rates from male to female and female to male. Perinatal transmission
is high. Pattern III includes countries where there have been relatively
few AIDS cases to date (including eastern Europe, northern Africa,
much of Asia, and the Middle East).
The interval between diagnosis of AIDS and death from AIDS
varies in different populations and may have to do directly with access
to health care services. Survival times are shorter in African and
Caribbean countries than they are in the United States. The little data
we do have show clearly that in the United States survival times for
women are shorter tlian those for men. Worldwide this means that
people of color, poor people, and especially poor women of color
are dying faster.
The number of AIDS cases in U.S. women reported to the CDC
was 10,611 as of December 1989, representing 9 percent of the
117,781 cases. This represents a steady increase in the percentage of
women diagnosed over the years of data collection (3 percent in 1981,
6.8 percent in 1983, and 9 percent in 1989). The geographic distribu
tion is similar to that for men—New York, California, Florida, and New
Jersey being the states with the greatest numbers of both men and
women diagnosed with HIV.
The CDC has constructed a hierarchy of exposure categories.
For example, a gay man who has had a blood transfusion would be
recorded as exposed by homosexual/bisexual contact because it is
listed first in the hierarchy. A bisexual woman who has sex with a gay
man would be listed as exposed by heterosexual contact. And a
lesbian intravenous drug user would be categorized as exposed by
her IV drug use. This system assumes likelihood of transmission based
on a U.S. model where AIDS was seen first in gay men. It does not list
woman-to-woman contact as an exposure category and is probably
inadequate to explain all the modes by which women get HIV. In the
period from January 1989 to December 1989, the CDC listed women
as having been exposed to HIV by intravenous (IV) drug use (52
percent), heterosexual contact (31 percent), receipt of blood transfu
2
Women, AIDS, ond Activism
sion (10 [^ent), and unknown (7 percent). The category of homo
sexual/bisexual contact, which accounts for 67 percent of men listed,
excludes women. The next most numerous categories in men are
intravenous drug use (18 percent), combined risk of IV drug use and
homosexual/bisexual contact (8 percent—another category that ap
plies only to men), heterosexual contact (3 percent), receipt of blood
transfusion (2 percent), and unknown (3 percent). The most signifi
cant difference in the statistics for women is that the rate of unknown
causes is more than double for women what it is for men. This
highlights the concern that transmission of HIV in U.S. women is not
fully understood.
A significant trend is the rapidly increasing rates of heterosexual
transmission in women (any contact with a man is considered hetero
sexual, regardless of the man’s sexual identity). These rates increased
from 14 percent in 1982 to 17 percent in 1984, to 26 percent in 1986,
and to 31 percent in 1989.
Ethnicity statistics for women, as of December 1989, break
down as follows: Black (52 percent), white (27 percent), Latina (20
percent), Asian (0.6 percent), and Native American (0.24 percent).
Seventy-three percent of women with AIDS are women of color, while
40 percent of men with AIDS are men of color (the U.S. population is
approximately 25 percent people of color).
Epidemiological statistics do not account for all AIDS cases. An
AIDS diagnosis is made after meeting the CDC’s definition of AIDS,
which was developed from the infections first observed in gay men
in the United States in 1981. It was revised in 1985 and 1987, but is
still based on the infections that gay men get. In brief, AIDS is
diganosed in an HIV-positive individual when a predetermined set of
unusual (opportunistic) infections or cancers are discovered and can
be medically documented or when either a wasting syndrome (large
weight loss) or HIV dementia (change in mental alertness) are iden
tified. Rarely, an AIDS diagnosis will be conferred on an individual
who is not HIV positive if one of the opportunistic infections or
cancers associated with a compromised immune system is diagnosed
definitively. HIV-positive people may be quite ill for months or years
before meeting the definition of AIDS.
Since the CDC definition for AIDS was developed from obser
vations of men, women often die of an opportunistic infection before
they are even considered eligible for an actual AIDS diagnosis.
Women are thus excluded from the total statistical picture. They not
only won’t get counted, they also won’t get treated; they won't qualify
for health benefits, child care, rent subsidies, or other support services
What the Numbers Mean
3
PWAs (People with AIDS) and AIDS activists have p^Pured the
government to provide, and they won’t be provided with information
on how to take care of themselves and how to protect the people with
whom they are having sex or sharing needles. Statistics, in other
words, only count women who already fit into die CDC’s narrow
definition for AIDS; all the other women just remain invisible. Many
women (and of course there are no statistics for this) are diagnosed
with HIV infection only after they have died.
There are many questions that could be answered by epidemi
ologists that would promote a better understanding of women and
AIDS. Woman-to-woman transmission must be studied, and homosexual/bisexual exposure categories must include women (of all
sexual identities) who have been exposed to HIV through contact
with gay and bisexual men. For men as well as for women, unknown
exposure categories must be investigated, and a better understanding
of the risks associated with specific sexual acts must be reached. The
information currently available certainly suggests that more women
are at risk in the United States than has been previously projected.
The rising number of women with AIDS is alarming and must be
heeded by activists, researchers, and public policymakers. The lives
of women who are already ill and those who may be at risk depend
on a greater understanding and a more effective response to women's
experience of AIDS.
4
Women, AIDS, and Activism
How Do Women Live?
KIM CHRISTENSEN
The impact of the AIDS crisis differs dramatically in various
communities. Differing access to medical information, early interven
tions, and treatment, and differing abilities to take time off to take care
of oneself, combine to make HIV infection a radically different
experience for a wealthy, white, childless man than for a low-income
Latina mother. HIV infection tends to worsen already existing forms
of inequality and oppression based on gender, race and ethnicity,
class, sexual orientation, and ability/disability level.
In order to understand the impact of the AIDS crisis on women,
we need a realistic picture of where women are economically, polit
ically, and medically in the United States today. Any group’s access
to resources, public attention, and power is critical in determining
how well they fare in the AIDS epidemic.
Compared with men, women enter the AIDS crisis with fewer
resources and support systems, and yet are responsible for more
people. Our greater vulnerability to rape, battering, and other forms
of sexual violence not only directly increases our chances of contract
ing HIV, but also places women in an inferior "bargaining position”
when negotiating for safer sex.
The medical establishment's view of men as “the norm" further
complicates HIV prevention, detection, and treatment for women. On
the one hand, women are often invisible to medical researchers, and
the AIDS research establishment is no exception. For example, many
experimental AIDS drug trials completely exclude women. On the
other hand, women are often treated as potential “fetus incubators”
whose reproductive capacities are valued more than our lives, or as
guinea pigs for the latest hormonal or surgical intervention. The
traditional invisibility and powerlessness of women vis-A-vis the
medical establishment mean that thousands of women are dying of
How Do Women Live?
5
AIDS before a doctor even recognizes that our symptoms are related
to HIV infection. Our inferior social status also makes it unlikely that
treatments will be developed with our needs in mind.
Heterosexism, racism, and sexism are perhaps the three main
forces that have fostered government inaction and allowed AIDS to
reach pandemic proportions in the United States today. This chapter
paints a statistical picture of U.S. women’s current economic, political,
and medical position. We need this foundation if we are to plan and
organize actions that successfully address women's specific needs in
the AIDS crisis.
Sexism and Women's Position in the AIDS Crisis
Sexist attitudes have had an enormous impact on tire treatment
of women in die AIDS crisis by the medical profession, public policy
officials, and even some AIDS activists. Even more important than
sexism—a set of bigoted attitudes about gender—has been the insti
tution of patriarchy, which perpetuates male control over women’s
labor time, sexuality, and reproductive capacities. This male control
may be exercised by an individual man, as in the case of a battering
husband, or by male-dominated institutions, such as the Supreme
Court, Congress, the New York Stock Exchange, the governing bodies
of any of the major religions, or the medical profession
Violence against women, including legal/societal toleration of
this violence, is one of the most blatant aspects of patriarchal oppres
sion. One out of three women in the United States will be raped during
her lifetime.1 The figures are even higher for African-American and
Latina women.2 Yet, because of the horrendous treatment raped
women receive from police and medical authorities, less than ten
percent of women who are raped report the crime.’ Forty percent of
all American wives are battered at some time in the course of their
marriages.’ The vast majority of women working outside of the home
report being sexually harassed at least once on the job.’ Reliable
estimates of sexual abuse range from one-tenth to one quarter of all
female children.0
Women learn very early that violence can be the price for
“stepping out of line," for insisting on our opinions, our right to
unrestricted mobility, our choice of dress or profession. This violence
(and the constant threat of such violence) constricts our actions,
reduces our aspirations, and distorts our self-images. A woman’s
exposure to HI V, and her ability to take care of herself if she becomes
ill, may be largely determined by her exposure to male violence and
the social supports she can use to defend herself.
6
Women, AIDS, ond Activism
Wo A’s inferior economic status is another fundamental as
pect of patnarchy. While women’s participation in the paid labor force
has increased by oyer 20 percent in the past three decades,’ women’s
wages have not risen comparably. For example, white women who
worked full time in 1988 earned about 65 percent of what white male
full-time workers did.’ Black and Latina women’s incomes are even
lower than those of white women, averaging 59 percent of what white
men make.’
While women’s earnings are generally two-thirds of men’s,
women are often responsible for more dependents. More than half of
all marriages with children now end in divorce;10 women get child
custody in the vast majority of the cases;" only 23 percent of divorced
mothers receive any child support payments at all;12 and for those
lucky enough to receive child support, the average amount is only
$1,200 per year.1’ Many women, especially women with children,
have to be financially dependent on men—either an individual man
(father, husband, ex-husband, etc.) or the male-dominated state. The
alternative, for many women and their children, is grinding poverty.
In the context of the AIDS crisis, women’s inferior economic
status means that we are less likely than men to have health insurance,
less likely to be able to afford the consistent and high-quality medical
attention necessary for early detection of HIV infection and opportu
nistic infections, and less likely to be able to afford quality treatment
for ourselves and our children. For example, AZT, the only antiviral
drug currently approved by the Food and Drug Administration for
HIV infection, can cost up to $8,000 per year.1’ Since this is almost half
of the average U.S. woman's annual earnings, it is unlikely that the
many women without health insurance can afford it.
Since we live in a patriarchal society, women bear dispropor
tionate responsibility for household labor and child care. A fall-time
working woman performs an average of 35 hours of physical house
work labor per week, in addition to her 40-hour paid job.1’ The
average woman who does not work outside the home performs 55
hours of such labor per week, more if she has more than two
children.16 The average husband and father performs less than a third
of that labor time, which does not increase when his wife gets a paid
job.1’
This labor, although vital to the continued smooth functioning
of the economy and the society, is not calculated as “work," nor does
it count as part of the GNP. It does not provide the woman with health
insurance, Social Security, or any independent income. Shouldering
the burdens of the “double day” significantly reduces women's time
How Do Women Live?
7
for (among other things) basic self-care activities such as cs^^sc and
rest.'" For an HIV-positive woman with children, this lack of self-care
time can significantly reduce life expectancy.
Patriarchy also ensures women's lack of control over our sexu
ality and our reproductive capacities. In 1990, there is still no 100
percent effective and safe method of birth control. The tiny percent
age of medical research devoted to this project speaks volumes about
this society's lack of respect for women’s health and autonomy, not
to mention sexual pleasure. The medical establishment abhors the
idea of experimenting on the male reproductive system, despite its
being physically less complex and more accessible. It displays no
such aversion to hormonal and other experimentation on women,
particularly women of color in the United States, and women in the
Third World."
Increasing state control over abortion in the wake of the Su
preme Court s 1989 Webster decision, combined with increasing
forced abortion and sterilization of HIV-positive women (overwhelm
ingly women of color), threatens to steal away the fragile gains in
control over reproduction for which women fought so hard in the
1960s and 1970s. In addition, lesbians encounter enormous obstacles
in obtaining alternative insemination, in adopting or providing foster
care for children, and in retaining custody of their biological children
in cases of contested custody.
Reproductive freedom must mean real freedom of choice for
lesbians, poor women, HIV-positive women, and women of color to
avoid or terminate unwanted pregnancies, as well as to have or adopt
children, to retain custody, and to raise them in safe and economically
viable environments.
Control over sexuality and sexual choices is impossible without
accurate information. Unfortunately, the majority of U.S. youth still
do not receive sex education that is nonjudgmental regarding sexual
choices and that deals with AIDS in a medically accurate way. Heated
controversies have taken place in numerous school districts over
informing students about condom use or distributing condoms, de
spite the fact that 70 percent of high school students are sexually
active.”
In addition, the “double standard" for male and female sexuality
is unfortunately still alive and well, with young women being held
responsible for "controlling" and “harnessing" male sexuality, and for
both birth control and safer sex negotiations. Yet all of the inequalities
cited above (the threat of violence, economic dependence, etc.) often
make negotiating sex, including safer sex, problematic for young
8
Women, AIDS, and Activism
women in heterosexual Wltionships
The institutional supports for heterosexuality, and the threat of
discrimination and violence against women who choose to express
their lesbian sexuality, make “compulsory” heterosexuality the norm
in the United States today. No woman can have sexual autonomy until
she has the option of freely, and without fear, choosing to be sexual
with another woman.
The dominant media bring patriarchal ideas and imagery into
every U.S. household: from the virtual invisibility of lesbianism, to the
romanticized sexual violence in scores of major films, to the absence
of discussion of most of the major issues affecting women’s lives.
Heterosexism is often used (in the media and by individual
men) to reinforce sexism, and to scare heterosexual women into
traditional sex roles. (For example, women in nontraditional occupa
tions, or women who aggressively pursue our rights, are often called
“dykes,” regardless of their actual sexual orientations.) Sexist and
heterosexist ideas and imagery serve to rationalize, perpetuate, and
render invisible the physical, economic, sexual, and political oppres
sion of women. They also make women, especially lesbians, almost
totally invisible in the AIDS crisis.
Oppressed not just by patriarchy and sexism, most HIV-positive
women are also subjected to racism, class oppression, heterosexism,
and ableism. To draw an accurate picture of women’s status, we need
to examine briefly these forms of oppression.
Racism and AIDS
White supremacy is a set of institutions (supported by a set of
racist ideas) that ensures that white people continue to have access
to the labor and other resources of the various communities of color.
Political, economic, and cultural control of these communities is often
necessary for this to occur. Violence against people of color and
official tolerance of and/or initiation of such violence remain institu
tionalized practices that perpetuate racism. Violence against people
of color is not only perpetrated by young white men on the street, it
also reaches into the highest levels of our government. For example,
despite undisputed statistical evidence that a Black person is four
times as likely to receive the death penalty as a white person convicted
of a similar crime, the U.S. Supreme Gourt found that the death penalty
is “not inherently racist" and does not violate the equal protection
provisions of the Fourteenth Amendment.21
The U.S. government’s drug policy is yet another example of
institutional racism. Despite the "just say no" rhetoric, the government
How Do Women Live?
9
has tolerated and often actively participated i^Tie flooding of com
munities of color with addictive drugs. This strategy was widely
employed in the late 1960s in an attempt to “cool out” die Black
Panther Party and other radical Black organizations.22 It has continued
into die 1980s, as CIA shipments of cocaine have been used not only
to fund the anti-Nicaraguan contras, but also to quell domestic un
rest.2’
Continuing economic exploitation of people of color is anodier
key aspect of institutional racism. As in the case of white women, diere
have been some significant changes in the economic status of people
of color in the past three decades. Yet, at the same dme that employed
Black men have been making higher wages, a smaller and smaller
proportion of all Black men have been able to find jobs at all.2' While
Black women have experienced gains in terms of employment and
income, they have increasingly gained sole financial responsibility for
their children. This is, of course, related to the fact that more Black
men are unable to find jobs, and are therefore unable to contribute
to family income. As of 1985, over 44 percent of Black families with
children were maintained by women.” As a result of this combined
racism and sexism, more than halfthe African-American children in
this country are currently being raised in poverty.11' The implications
for these women and their children, in terms of receiving quality
health care for AIDS, are devastating.
Racist imagery in educational materials and the media continues
to indicate the institutional nature ofU.S. racism. Crimes that victimize
people of color often are not deemed “newsworthy” (whereas crimes
with white victims are). Events that primarily or disproportionately
affect communities of color (such as the AIDS epidemic) are not
thought to be of interest to the “general reader," who is assumed to
be white and usually male. The illness and deaths of people of color,
women, and lesbians and gay men are simply not deemed to be
“important” enough to report.
Class Oppression and AIDS
In addition to the issue of unequal access to treatment, this
country's response to the AIDS crisis in general is profoundly influ
enced by its class structure and its profit-driven economy. For exam
ple, treatments that will not be profitable simply are not explored by
major drug companies and are undertaken rarely by the government.
Personal and financial connections between major pharmaceutical
companies and the government agencies responsible for regulating
these companies' AIDS research programs further complicate the
10
Women, AIDS, and Activism
problem.
This is particularly important in the case of women, intravenous
drug users (IVDUs), and others with lower incomes. A drug company
can’t make a profit on a drug if many of the people who need it are
too poor to pay a high price for it. Research and drug trials tend to be
concentrated among those people with enough money to make an
experimental drug “profitable."
Attention to profitability, rather than to saving lives, also leads
to “turf wars” and patent battles that further delay experimental drugs
and even proven treatments from reaching patients who need them.
For example, in 1986, Michael McGrath of the University of California
at San Francisco found that trichosanthin (“Compound Q”) killed
HIV-infected immune system cells in the test tube. However, he
waited two years to announce his discovery, until he and his pharma
ceutical sponsor, Genelabs, could obtain a patent on the product and
sell its licensing rights worldwide. Compound Q may or may not
prove to be an effective treatment for AIDS, but the research on this
vital question was delayed for two years for purely financial gain.22
Heterosexism and AIDS
As with sexism, heterosexism refers not just to the attitudes of
individuals. Rather, a pressure towards heterosexuality is built into
most of our major social, economic, and political institutions.
Violence against lesbians, bisexuals, and gay men is often
tolerated and/or initiated by police. A recent survey showed that 90
percent of lesbians and gay men interviewed had experienced
heterosexist violence, or the threat of such violence, during their
lifetimes.28
Lesbians, gay men, and bisexuals suffer from institutional forms
of economic discrimination in addition to direct housing and job
discrimination. Gay men and lesbians lack spousal health care bene
fits for ourselves and our children, marital tax breaks, “family" status
in rental agreements, the legal right to make decisions for our lovers
in emergencies (including medical emergencies), and even inheri
tance rights in the case of the death of a lover.
As discussed earlier, lesbians and gay men are frequently denied
reproductive rights, including alternative insemination for lesbians,
adoption and foster care, and child custody rights in contested cases.
The heterosexist imagery and ideas put forth in the mass media
and by religious and educational institutions, among others, perpet
uate lite notion that heterosexuality is the only “natural" or “moral”
sexuality. The authorities of many major religions also state or
How Do Women Live?
11
strongly imply that homophobia and heterosexism are i^Rptable,
even divinely sanctioned. Some even claim that AIDS is God's “pun
ishment'' for sexual or other behaviors that they consider to be
unacceptable. This propaganda has a major impact on federal, state,
and local governments' AIDS policies and funding.
Ableism and AIDS
Ableism consists of the practices, behaviors, and attitudes that
deny disabled people, including people with AIDS (PWAs), access to
all or most of the major institutions of this society. One in six Ameri
cans is disabled,” but our visibility, earning ability, and political clout
are far smaller than our numbers. Violence against the disabled
happens throughout our society, yet the media totally overlook the
existence of such violence. Visibly disabled women are often per
ceived to be "easy prey,” and are significantly more likely to be
assaulted than able-bodied women.” In addition, violence against
PWAs (or those who are believed to have AIDS) is on the rise in most
urban communities.”
Economic and insurance discrimination is another major aspect
of institutional ableism. The incomes of employed disabled people
are significantly lower than those of the able-bodied; disabled women
earn only 36 percent of what nondisabled men make.” Direct em
ployment discrimination against the disabled is often compounded
by inaccessibility and discrimination on the part of schools and
universities. Despite the existence of Section 504 of the Rehabilitation
Act (which mandates appropriate education for all cltildren, regard
less of ability level), many disabled children still do not receive the
special education they need to become economically self-sufficient
adults.
In addition to lower income, disabled people often have higher
medical costs than the able-bodied, and are, ironically, much less able
to get health insurance. It is perfectly legal for insurance companies
to deny policies to those with HIV illness, or other “preexisting
medical conditions," and to refuse to pay benefits if people conceal
their disabilities to get insurance. The combination of lower incomes,
higher medical costs, and lack of insurance often results in very low
standards of living for the disabled, especially disabled women and
disabled people of color.
Ableism also perpetuates discrimination in the accessibility of
buildings and transportation. This society was literally not built for
the disabled. The vast majority of streets and sidewalks, apartment
buildings, stores, and offices are totally inaccessible to wheelchair
12
Women, AIDS, and Activism
users. Until recently, fedeWlaw did not require chair lifts on publicly
funded buses, drastically limiting many disabled people's mobility. In
public facilities it is still unusual to find hearing interpretation or
Braille, which would greatly increase mobility and autonomy for the
hearing- and sight-impaired.
Disabled people are often denied control over their reproduc
tive capability. In the early 1900s, as a result of the eugenics move
ment and Social Darwinism, most states had laws on the books
requiring sterilization for the physically disabled, epileptics, and the
“feebleminded.” Although by and large these laws are no longer
enforced, involuntary sterilization of the disabled continues, espe
cially among the developmentally disabled and disabled people of
color.”
Despite being supposedly “nondirective,” many genetic coun
selors continue to "direct” women with genetically passed disabilities
to seriously consider sterilization or abortion. Pregnant HIV-posjtive
womenare often coerced into abortions, despite the fact that only 20
to 50 percent of their children will actually receive the virus. Even
some feminists defend abortion on the grounds that women must
have tlte right to abort “defective" fetuses, including those that have
a chance of being HIV positive. These arguments assume that no
woman would choose to give birth to a disabled fetus, and that
disability is a “personal tragedy," rather than a political and social
problem of accessibility and funding for services and health care.
Rarely, if ever, are PWAs and other disabled people portrayed
as normal and productive members of society. When we're not totally
invisible, disabled people are usually portrayed in the media as pitiful,
childlike victims. We're portrayed as asexual and unable to cany on
personal or romantic relationships, whether heterosexual or lesbian
or gay.
Hie media and the medical profession share the notion that
disability is something to be overcome, that we must “strive to
overcome our disabilities" rather than learn to live within our capa
bilities. Tlie underlying assumption, of course, is that there is some
thing terribly wrong with the disabled person, rather than with the
social structure in which she or he lives.
All these types of oppression reduce women's access to the
information, resources, and political clout necessary to fight AIDS.
Women in general enter the AIDS crisis from a more vulnerable
position than do men. Women who face additional forms of oppres
sion are that much more vulnerable. Solving the AIDS crisis for
everyone means combating the powerlessness and marginalization of
How Do Women Live?
13
many of the oppressed people in this country: women, people of
color, the poor, and the disabled. As AIDS activists, we have a
responsibility to plan our actions in ways that take account of lite
differences among women, as well as our similarities. The informa
tion in the rest of this book will help us all to do that.
Notes
Federal Bureau of Investigation, Uniform Crime Report: Crime in the
United States, 1980, p. 15. The FBI adds the following footnote to their
. statistical estimate "Even with the advent of rape crisis centers and the
improved awareness by police dealing with rape victims, forcible rape,
a violent crime against a person, is still recognized as one of the most
under-reported of all Index crimes...Victims’ fear of their assailants’
return and their embarrassment over tire incidents are just two factors
which can override their decision to contact law enforcement."
2.
Audre Lorde, "An Open Letter to Mary Daly,” in This Bridge Called My
Back: Writings by Radical Women of Color, Cherrie Moraga and Gloria
Anzaldua.eds. (Albany, NY: Kitchen Table: Women of Color Press, 1983),
p.97
3.
Uniform Crime Report, p. 15.
4 Lenore Walker, The Battered IFommr (New York: Harper and Row, 1979),
p. 14.
5.
Ronnie Sandroff, "Sexual Harassment in the Fortune 500," in Working
Woman, December 1988, pp. 69-736.
Sources for varying estimates:
• Susan Forward and Craig Buck, The Betrayal ofInnocence. Incest and
Its Devastation (New York: Penguin, 1978), p. 3.
• Judith Herman and Lisa Hirschman, "Father-Daughter Incest," in Signs
A Journal of Women and Culture, Vol. 2, no. 4, Summer 1977, pp.
735-756.
• Kee MacFarlane, "The Sexual Abuse of Children," inJane Chapman and
Margaret Gates, eds., The Victimization of Women (Beverly Hills, CA:
Sage Publications, 1978), pp. 81-109
7.
Economic Report ofthe President, 1989, Table B-37.
8.
Derived from "Money Income of Households, Families and Persons in
the United States: 1986,” U.S. Department of Commerce, Bureau of the
Census.
9.
“Money Income of I louseholds.. ” Bureau of the Census
10.
“Divorces and Annulments, Rate and Percent Distribution, by Sex and
Age, 1985,” in Statistical Abstract ofthe United Stales, 1989(US. Depart
ment of Commerce, Bureau of the Census), p. 87.
11.
RuthSidel, Women and Children Last (New York: Penguin, 1986), p. 18.
12 Nancy Folbre, Field Guide to the U.S. Economy (New York: Pantheon
Books, 1987), Graphs 3-11.
13- Folbre, Field Guide.
14.
John Bohne, Tom Cunningham, Jon Engbretson, Ken Fornataro, and
Mark Harrington, T+D Handbook: Treatment Decisions, ACT UP/New
York, unpublished, 1989, p. 32.
15.
Joseph Pieck, Working Wives, Working Husbands (Beverly Hills, CA:
1.
14
Women, AIDS, and Activism
Sage Pu^Jnions, 1985).
Pieck, Working Wives, p. 121.
Pieck, Working Wives, p. 123.
Arlie Hochschild, The Second Shift: Working Parents and the Revolution
at Home (New York: Viking, 1989), p. 4.
19.
Susan Davis and CARASA (Committee for Abortion Rights and Against
Sterilization Abuse), Women UnderAttack Victories, Backlash, and the
Fightfor Reproductive Freedom (Boston: South End Press, 1988), p. 22.
20.
Ann Northrop, Hetrick Martin Institute, personal communication.
21.
William Brennan, Dissenting Opinion in McCleskyv. Kemp, U.S. Supreme
Court Reporter, Vol. 107,1987, pp. 1756-1794.
22.
Leslie Cockburn, Out of Control (New York: Viking, 1988).
23.
Cockbum, Out ofControl.
24.
Kimberly Christensen, "Political Determinants of Income Changes for
African-American Women and Men," submitted for publication to Review
ofRadical Political Economics in June 1990.
25.
Folbre, Field Guide.
26.
Sidel, Women and Children Last, p. 3.
27.
Bohne et al., T+D Handbook Treatment Decisions, p. 44.
28.
Survey conducted by National Gay and Lesbian Task Force, New York,
1988
29.
Barbara Mandell Altman, “Disabled Women and the Social Structure," in
With the Power of Each Breath: A Disabled Women's Anthology, Susan
Browne, Debra Conners, and Nanci Stern, eds. (San Francisco: Cleis
Press, 1985), pp. 69-76.
30.
Rebecca Grothaus, “AbuseofWomen with Disabilities," in With the Power
ofEach Breath, pp. 124-128.
31.
Survey conducted by the National Gay and Lesbian Task Force, New
York, 1988.
32.
Altman, “Disabled Women and the Social Structure."
33.
Anne Finger, "Reproductive Rights and Disability," in With the Power of
Each Breath, pp. 292-307.
16.
17.
18.
How Do Women Live?
15
stopped asking, "How are you?" There was a certain relielWuming
myself over to this greater cause, where everything was always about
her_ humidifiers, macrobiotic food, appointments. Even now, we are
friends, and still there is a subtext: will she get sick again, will she die?
I wonder, do I just thrive on drama? Do 1 have a martyr complex,
or a death wish? Did I fall for him because of his status? Do I want to
get infected; is this my most recent and subde form of self-destruction?
Friends and family are anxious, ask me about it. They tell me I’m
crazy, and speak of illness and health in hushed tones.
And 1 have to admit, after all these months, sometimes I’m still
scared. I see an article and I think, could I be the first case of saliva
transmission? Why am I still scared? I forget for weeks, and then when
I get sick, feverish, peaked, HIV is there like a threat. I worry secretly,
and when I tell him, he's angry, defensive.
All around us, his friends, my friends, into the hospital, out of
the hospital, dying. When will it start with him? He gets a cold, the flu.
He’s tired, glands swollen.
I hate this virus.
This started out to be about the joys of safe sex, but I guess it’s
complicated.
I am HIV negative, as of my last test. I’ve learned a lot and had
some really hot sex and lots of flirty, sexy stuff, and there’s been a lot
of love and happiness in this relationship. There’s a difference be
tween rational fears and irrational ones. I try to act on the rational
ones. I try to protect myself and my lover from real threats, and try to
overcome the irrational fears.
You can make decisions about your life and love based on what
you want, and not let illness, or fear of illness, make all the decisions
for you.
30
Women, AIDS, and Activism
Unique Aspects of HIV Infection
in Women
RISA
What Is Not Known
A woman with HIV illness who lives in Newark, New Jersey,
lives an average of 15.5 weeks following a diagnosis of AIDS,' while
a white gay male in the northeast region of the United States with HIV
illness lives an average of 20.8 months following diagnosis? There are
many problems in assessing the number of women with AIDS, as well
as the ways in which HIV disease affects women.
Very little is known about women and HIV disease, and very
little research has been done or can be anticipated. Therefore, it is not
possible to draw conclusions about risk factors, disease progression,
opportunistic infections, or proper treatments. However, by framing
the relevant questions, we can provide a basis for understanding what
we need to know.
In this discussion it is important to remember that women's
bodies are different from men's in significant ways, that women are
rarely viewed as individuals in the health care system and often are
viewed as vectors for disease, and that women rarely see primary
health care practitioners and often receive health care in settings
where public health concerns have more priority than individual
concerns. Additionally, women delay seeking care due to, for exam
ple, a lack of resources, the burden of child care and caring for elderly
or ill family members, our being lesbians and afraid of discrimination,
or the fact that so often our complaints of fatigue, headaches, and
weight loss are assumed by ourselves and others to be “merely”
emotional or stress related.
If we want to understand what happens to a woman after
exposure to HIV, women activists will have to be willing to ask
publicly the relevant questions.
HIV Infection in Women
31
Why Do Women Die Foster than Men?
Approximately 73 percent of women with AIDS in the United
States are women of color, yet people of color comprise only approx
imately 25 percent of the overall population. Of women diagnosed
with AIDS, 52 percent are Black, 27 percent are white, 20 percent are
Latina, 0.6 percent are Asian/Pacific Islander, and 0.2 percent are
Native American. Women constitute nearly 9 percent of the total
number of AIDS cases in the United States reported to the Centers for
Disease Control (CDC) through December 1989. Forty percent of men
with AIDS are men of color.’ The disproportionate representation of
people of color of both sexes, but especially of women of color,
reflects the unique social and economic burdens encountered in
living in the United States, and also explains, in part, the mortality
differences between all women and white men. For example, a Black
woman intravenous drug user (IVDU) with pneumocystis carinii
pneumonia (PCP) has die least favorable survival time of any group
of AIDS patients studied.
Statistics on women and mortality also reflect the reality that
women as a group are undercounted, overlooked, misdiagnosed, and
undiagnosed. Further, women are generally treated inadequately
following a diagnosis.
This occurs in the following ways.
• Diagnosis comes late in the course of a woman’s illness. This
occurs because women do not have access to health care or
because they delay health care due to other priorities such as
finding housing and feeding children. It also occurs because
most health care providers are inadequately trained to identify
HIV disease and don’t even look for it in women. Women with
HIV often die soon after they are diagnosed; often diagnoses of
HIV are not made until after their deaths.
• Women are underdiagnosed. The CDC has specific guidelines
for what constitutes a diagnosis of AIDS. They were last updated
in 1987, and many new cases are currently being identified on
the basis of that revision. Still, both the initial and the updated
guidelines show that AIDS is primarily understood as a white
gay men’s disease. Women simply do not fit into this disease
pattern. Therefore, women often die with AIDS-related com
plex (ARC), which is generally understood as a stepping stone
from asymptomatic illness to AIDS and is usually diagnosed
when someone demonstrates HIV-related symptoms such as
weight loss, swollen glands, and fever, but does not meet the
CDC's definition of AIDS. Since many women die of ARC (the
numbers are unknown because deaths from ARC are not tracked
32
Women, AIDS, and Activism
as arf^iaths from AIDS), it is logical to assume that the CDC
guidelines are inadequate for diagnosing AIDS in women; with
out adequate diagnoses, the quality of treatment offered to
women is undoubtedly compromised. Equally serious for these
women is the fact that, without AIDS diagnoses, they do not
qualify for particular benefits available only to people with
AIDS.
• Women are misdiagnosed. They often die of HIV-related
illnesses that are not recognized as such. Perhaps less time and
money are spent on diagnostic tests or on discovering the causes
of a woman’s symptoms. Again, women are not viewed by
health care providers as being likely to have HIV disease. For
example, between 1981 and 1988, there was an unexplained and
significant increase of deaths from pneumonia and influenza in
women aged 15 to 44 in several urban centers in the United
States.4 Many of these deaths might have been from undiagnosed
opportunistic infections common to HIV iUness.
Women and Men: What Are the Differences?
Biologically, women differ from men in several ways that are
relevant to this discussion. Women are subject to unique organ-spe
cific diseases arid conditions (e.g., pelvic inflammatory disease [PID],
endometriosis, uterine tumors, cervical cancer, and vaginal candidia
sis), a higher incidence of some diseases (e.g., simple urinary tract
infection, breast cancer, human papillomavirus infection [HPVD, and
an increased likelihood of suffering serious consequences arising
from common problems (e.g., gonorrhea, chlamydia).
Women die of complications related to pregnancy and to dis
eases of reproductive organs (e.g., cervical, breast, ovarian, and
uterine cancers). The incidence of ectopic pregnancy (a pregnancy
that grows outside of the uterus, usually in the faUopian tube) has
increased dramatically since 1970. In 1970, one in 200 pregnancies
was ectopic; in 1985, one in 48 was ectopic. This reflects, generally,
an increase in sexually transmitted diseases (STDs). STDs such as
gonorrhea and chlamydia often cause asymptomatic infection in
women who later develop a condition called pelvic inflammatory
disease. This acute problem often leaves scar tissue in the genital tract
and greatly increases the risk of ectopic pregnancy, which in turn can
rupture, causing hemorrhage and death.
Some studies note that women IVDUs experience more medical
problems than male IVDUs. This probably reflects the broad spectrum
of medical, social, and economic differences between men and women.
All of this is important in understanding HIV infection in women.
HIV Infection in Women
33
Women ond Symptoms
"
Are women's symptoms of HI V infection the same as or different
from men's? Since we have little information related specifically to
HIV disease in women, we have to look at other differences that can
give us a basis for forming tentative answers to this question. Looking
at die arena of STDs, we know that there are gendered differences
in presentation (how symptoms show up medically, or “present”).
In gonorrhea and chlamydia there is often a long silent phase in
women (sometimes from three to six months), whereas men frequendy show symptoms much sooner, such as a drip or burning
during urination. Some bacterial infections often ascend to other
organs in women (uterus, tubes), but rarely ascend in men. With
monilia (yeast, or Candida), trichomonas, and bacterial vaginitis,
women frequently experience discharge, odor, itching, and pain
while men often carry these organisms without any symptoms or
medical consequences.
On the odier hand, some sexually transmitted infections seem
to be equally distributed and cause similar symptoms in men and
women. Genital herpes and syphilis seem to have equal incidence
sexually. With odier infections that also cause sores or lesions on the
genitals, the same type of symptoms occur with different frequency.
More women and gay men are treated for warts (called condyloma,
arising from HPV infection), and more men are seen clinically for
chancroid (another ulcer-forming sexually transmitted infection of
which there is increased incidence).
Another important difference is related to the menstrual cycle
and vulnerability to infection. Many women with recurrent genital
herpes report outbreaks with their periods. Other problems asso
ciated with periods include premenstrual syndrome (PMS) and
toxic shock syndrome (which can be fatal). Hormone fluctuations
result in recognizable changes in weight, fatigue, sexual desire,
and so on.
A second issue concerning symptoms is whether or not the same
symptom is viewed similarly in men and women. Are women's
symptoms taken as seriously? It's not likely. Often women don't view
their own health symptoms as seriously as they do others’ symptoms.
Mothers who are obviously ill themselves frequently come to a clinic
or emergency room only when their children become sick. Many
clinicians would probably interpret the same symptom—such as a
headache—differently depending on a number of variables, includ
ing gender.
A review of the most common symptoms listed on health forms
34
Women, AIDS, ond Activism
from various HIV asse^Rent programs that serve mainly male clients
include fatigue, fever, chills, night sweats, weight loss, loss of appetite,
headache, blurred vision, insomnia, confusion, concentration prob
lems, sore mouth, sore throat, trouble swallowing, cough, shortness
of breath, nausea and vomiting, diarrhea, muscle or joint pains,
swollen glands, and skin changes. All of these symptoms could point
to problems other than HIV iUness, and many of them could be
interpreted to reflect depression or psychological factors such as
stress or overwork, which are diagnoses more often attributed to
women. An HIV-positive woman, for example, may be at less risk for
weight loss, because women have more body fat. Certainly weight
loss is often ignored in women or understood inappropriately as
something always favorable. There is simply no information regard
ing which symptoms different groups of HIV-positive individuals are
most likely to experience. To improve early diagnostic capability and
greater treatment availability for women, such studies must be under
taken. It is known that an early diagnosis can help prolong life if
relevant medical services are available.
On the other hand, objective clinical signs that can be discov
ered by medical examination are much more likely to raise suspicion
of HIV disease. Some frequent signs include specific medical condi
tions that can result in skin changes; mouth sores; findings on routine
blood tests; and neurological changes such as problems with balance,
numbness, or subtle changes in mental abilities. Yet practitioners who
don’t already have the eyebrow of suspicion raised often overlook
clinical signs in women, especially since AIDS has, from the begin
ning, been defined as a gay men’s disease. An obstetrician/gynecologist (ob/gyn) might find and treat a vaginal yeast infection after
listening to a woman complain of discharge and itching. It is very
unlikely that this doctor will then look in the client’s mouth for oral
signs of HIV disease such as herpes, thrush (oral yeast infection), hairy
leukoplakia (an unusual growth associated with HIV disease),
aphthous ulcers (canker sores), gingivitis (gum infection), or other
medical conditions.
Male and Female Differences in the Mechanism of HIV Exposure
There are some clear differences between men and women in
terms of sexual transmission of a variety of diseases. Where most STDs
are concerned, women are often at greater risk than are men from a
single episode of vaginal intercourse. For example, the risk of women
being infected with gonorrhea is approximately double that for men.
As repeated unprotected sexual intercourse occurs, the risks of trans
HIV Infection in Women
35
Women ond Symptoms
Are women’s symptoms of HIV infection the same as or different
from men’s? Since we have little information related specifically to
HIV disease in women, we have to look at other differences that can
give us a basis for forming tentative answers to this question. Looking
at the arena of STDs, we know that there are gendered differences
in presentation (how symptoms show up medically, or “present").
In gonorrhea and chlamydia there is often a long silent phase in
women (sometimes from three to six months), whereas men fre
quently show symptoms much sooner, such as a drip or burning
during urination. Some bacteria] infections often ascend to other
organs in women (uterus, tubes), but rarely ascend in men. With
monilia (yeast, or Candida), trichomonas, and bacterial vaginitis,
women frequently experience discharge, odor, itching, and pain
while men often carry these organisms without any symptoms or
medical consequences.
On the other hand, some sexually transmitted infections seem
to be equally distributed and cause similar symptoms in men and
women. Genital herpes and syphilis seem to have equal incidence
sexually. With other infections that also cause sores or lesions on the
genitals, the same type of symptoms occur with different frequency.
More women and gay men are treated for warts (called condyloma,
arising from HPV infection), and more men are seen clinically for
chancroid (another ulcer-forming sexually transmitted infection of
which there is increased incidence).
Another important difference is related to the menstrual cycle
and vulnerability to infection. Many women with recurrent genital
herpes report outbreaks with their periods. Other problems asso
ciated with periods include premenstrual syndrome (PMS) and
toxic shock syndrome (which can be fatal). Hormone fluctuations
result in recognizable changes in weight, fatigue, sexual desire,
and so on.
A second issue concerning symptoms is whether or not the same
symptom is viewed similarly in men and women. Are women’s
symptoms taken as seriously? It's not likely. Often women don’t view
their own health symptoms as seriously as they do others’ symptoms.
Mothers who are obviously ill themselves frequently come to a clinic
or emergency room only when their children become sick. Many
clinicians would probably interpret the same symptom—such as a
headache—differently depending on a number of variables, includ
ing gender.
A review of the most common symptoms listed on health forms
34
Women, AIDS, ond Activism
from various HIV asse^Bent programs that serve mainly male clients
include fatigue, fever, chills, night sweats, weight loss, loss of appetite,
headache, blurred vision, insomnia, confusion, concentration prob
lems, sore mouth, sore throat, trouble swallowing, cough, shortness
of breath, nausea and vomiting, diarrhea, muscle or joint pains,
swollen glands, and skin changes. All of these symptoms could point
to problems other than HIV illness, and many of them could be
interpreted to reflect depression or psychological factors such as
stress or overwork, which are diagnoses more often attributed to
women. An HIV-positive woman, for example, may be at less risk for
weight loss, because women have more body fat. Certainly weight
loss is often ignored in women or understood inappropriately as
something always favorable. There is simply no information regard
ing which symptoms different groups of HIV-positive individuals are
most likely to experience. To improve early diagnostic capability and
greater treatment availability for women, such studies must be under
taken. It is known that an early diagnosis can help prolong life if
relevant medical services are available.
On the other hand, objective clinical signs that can be discov
ered by medical examination are much more likely to raise suspicion
of HIV disease. Some frequent signs include specific medical condi
tions that can result in skin changes; mouth sores; findings on routine
blood tests; and neurological changes such as problems with balance,
numbness, or subtle changes in mental abilities. Yet practitioners who
don’t already have the eyebrow of suspicion raised often overlook
clinical signs in women, especially since AIDS has, from the begin
ning, been defined as a gay men's disease. An obstetrician/gynecologist (ob/gyn) might find and treat a vaginal yeast infection after
listening to a woman complain of discharge and itching. It is very
unlikely that this doctor will then look in the client’s mouth for oral
signs of HIV disease such as herpes, thrush (oral yeast infection), hairy
leukoplakia (an unusual growth associated with HIV disease),
aphthous ulcers (canker sores), gingivitis (gum infection), or other
medical conditions.
Male and Female Differences in the Mechanism of HIV Exposure
There are some clear differences between men and women in
terms of sexual transmission of a variety of diseases. Where most STDs
are concerned, women are often at greater risk than are men from a
single episode of vaginal intercourse. For example, the risk of women
being infected with gonorrhea is approximately double that for men.
As repeated unprotected sexual intercourse occurs, the risks of trans
HIV Infection in Women
35
mission may be about equal. Still, a woman who has few sexual
encounters with many men is at greater risk than a man who has few
sexual encounters with many women; hence the biology of the
double standard.
Exposure to HIV during sex does not always cause infection,
but it is sometimes assumed that women are at greater risk than are
men of exposure by heterosexual intercourse. There is evidence that
in Africa and in the Caribbean the ratio of male-to-female cases of
AIDS is about one to one. In recent studies of adolescents in New
York City, this pattern of equal representation of women is now
emerging. We need to know' what variables increase a woman’s risk
of being infected. A woman with a chronic yeast infection or who is
menstruating is at greater risk of transmitting HIV if she is infected,
but is she also at greater risk of contracting HIV if she is not? It is this
aspect of transmission that has not been studied or even considered,
yet it suggests urgency for teaching risk reduction to women, whether
heterosexual or lesbian. It is likely that a woman with an STD, a genital
ulcer disease (herpes, chancroid, syphilis, lymphogranuloma vene
reum), condyloma (wans), or cervical dysplasia (an abnormal pap
smear result) is at increased risk of acquiring HIV if exposed.
Some HIV transmission risks are equal for men and women,
such as receiving anal sex and sharing intravenous (IV) drug works.
But there are some unique risks when HIV-infected semen is depos
ited into the vagina. It is important to know that, while HIV has an
affinity for T-lymphocytes (T-cells), it also can reside in other types
of cells (other kinds of white blood cells, some types of neurological
cells, and several others). The cells in the cervix are unique in that
they respond to hormonal changes throughout a woman's cycle and
play a significant role in allowing or disallowing different intruders to
have access to the higher organs. An inhospitable cervix would never
allow sperm to penetrate or pregnancy to occur. It is due to the cyclic
change in immune function that these events are allowed to occur.
The uterus and tubes are considered sterile and not to be invaded by
ordinary or pathological germs, although “healthy" germs abound in
the vagina (as they do in the mouth). The cervix, then, is a responsive
organ, which has some power to decide what gets in.
In one small study of cervical tissue from HIV-positive women,
the virus was able to be cultured from endothelial cells (lining of the
cervix) and monocyte-macrophage cells (a type of white blood cell)
as well as from the cervical mucus? So, certain cervical cells actually
become infected with HIV. In this study, die women with infected
cells also had symptoms of an infected cervix (cervicitis). It is possible
36
Women, AIDS, and Activism
that HIV can cWe a local cervicitis before spreading to the rest of the
body. It is also likely that an already infected cervix is at greatly
increased risk of becoming infected with HIV.
Further, in studies of the wart virus HPV, it has been found that,
while tire transmission rate is high for the virus (about 50 percent of
sexually active heterosexuals test positive for HPV), the route by
which viral expression and disease occur is not known. In fact, while
nearly half of some samples are HPV positive, only 1.5 percent of
women show clinical evidence of the warts.
Immune suppression in a woman's genital tract is proposed by
some researchers as the mechanism of this phenomenon, and recur
rent genital fungal and viral infections are associated with transient
suppression of cell-mediated immunity? Another proposed mecha
nism is an allergic response (to sperm, to yeast, to spermicides) inside
the vagina, which may increase the likelihood of developing the
warts. Allergic responses also relate to cellular immunity.
A good bit is known about immunity and women’s genital tracts.
It appears that cancer of the cervix, which is curable when detected
early, often occurs following an invasion of microorganisms, partic
ularly viruses. Whole books have been written on HPV and volumes
regarding the minute details of cervical cancer, which is detected by
routine pap smear screening. As yet, we have no proposed protocols
for the gynecological care of HIV-positive women. Some of the
research has been done; it simply hasn’t been applied to understand
ing HIV infection.
About Opportunistic Infections
We know that HIV causes some life-threatening events as a viral
agent. It is believed to be responsible for certain neurological (ner
vous system) disorders such as aseptic meningitis and AIDS dementia.
But the majority of HIV-related problems occur because HIV
suppresses the body’s immune system: the reduced number and
reduced capacity of lymphocytes make a person less able to fight
infection. Almost all people will get ill when infected with certain
harmful germs such as syphilis. The person whose immune system is
compromised is at even greater risk of disease, complications, and
death from such germs. But germs that are ordinarily harmless also
threaten the lives of people who have HIV disease. Hence die term
opportunistic infection.
Opportunistic infections are also caused by harmful germs that
would normally cause only limited infection. For example, many
healthy people have herpes sores on the lips at times, but when such
HIV Infection in Women
37
herpes is found spreading to die throat or lungs in a pers^^vith HIV,
Chronic vaginitis, ^^ecially recurrent monilia or yer.st infec
it Is considered opportunistic and is indicative of a damaged immune
system.
Opportunistic infections that have been observed in men and
women include coccidiodomycosis, cryptococcosis, cryptosporidio
sis, isosporiasis, mycobacterium avium, mycobacterium Kansasii, M.
tuberculosis, cytomegalovirus, pneumocystis carinii, toxoplasmosis,
and candidiasis. These are the medical names for the bacteria, virus,
fungus, protozoa, and so on that infect a compromised immune
system. Ninety percent of AIDS deaths are attributed to opportunistic
infections, many of which could be treated. Some opportunistic
cancers are also associated with HIV disease, such as Kaposi’s sar
coma (KS, which usually begins as a skin disease) and lymphomas
(which begin in lymph tissue).
The frequency of both cancer and certain infections does differ
by gender, but it has not been studied in relation to HIV disease.
Women are known to have a very low incidence of KS, but are prone
to chronic, persistent vaginitts. Beyond this, little is known regarding
sex differences. There are known geographic differences in certain
opportunistic infection prevalences, and the pattern of opportunistic
infections in HIV disease differs greatly from patterns seen in other
immunocompromised states, such as in people with cancer or on
steroids. Young children with HIV disease get different opportunistic
infections because their immune systems are both immature and
compromised.
But the woman question? Well, it just hasn’t been adequately
studied.
tion, was noted in 24 percent of HIV-positive women in one study.
Of these women, 86 percent progressed to AIDS.’ Some researchers
now suggest that chronic yeast is associated with a frequent incidence
of oral thrush and is a good predictor for development of opportunis
tic infections. Research on whether such women would benefit from
treatment of their vaginitis has not been undertaken.
What about other vaginal conditions? There has been a tremen
dous increase in the incidence of all STDs since 1980 in the United
States, particularly of penicillin-resistant gonorrhea, syphilis, chlamy
dia, and herpes. Many such conditions lead to abnormal pap smears.
Treating the infection often results in the return to a healthy cervix.
Untreated or untreatable infections (such as herpes) often result in
progression to cervical cancer—a known state of immunodeficiency.
Some studies suggest that genital herpes (HSV-2) may be a risk factor
for subsequent HIV infection in exposed men. At least 20 percent of
women with visible warts on the cervix are found to have coexisting,
precancerous changes. HIV infection, too, may be a risk factor itself
for cervical changes that precede cancer. Women with HPV or genital
herpes are told to have pap smears every six months. But we do not
yet have guidelines on pap smear frequency for HIV-positive women.
Current Knowledge of Women's Genital Health Must Be Applied
to HIV Disease
Information that can be obtained from medical texts, self-help
books, and current research can be applied to the issues surrounding
HIV disease.
Transmission issues seem to be related to vaginal health and
therefore, naturally, to the practice of safer sex. Infections that go
untreated probably increase the risk of HIV transmission to women.
Genital tract health is affected by cyclic hormonal changes as well as
by the types and combination of germs present in the vagina. Further
exploration would probably reveal a unique pattern of opportunistic
infection in the genital tracts of HIV-infected women. Some HIV-in
fected women may get sick and die of more ordinary infections such
as chlamydia or monilia.
38
Women, AIDS, ond Activism
Some Speculation about HIV Infection and a Womans Body
Recognizing gender differences and understanding that HIV
positive women are dying without AIDS diagnoses suggest certain
assumptions about what is going on in women who are exposed to
HIV.
First, the mechanism of exposure differs where vaginal inter
course occurs. The cervix, which at certain times of the month allows
sperm to travel into the uterus, is susceptible then in a unique way,
at that time probably only surpassed by direct blood-to-blood trans
mission. So the rate of transmission may be high in a woman having
unprotected vaginal sex with an HIV-positive man. Even in womanto-woman sex, which many consider to be less risky, transmission
risk is likely to be increased according to vaginal conditions. Any
condition affecting the health of the vagina, genital tract, and rectum
undoubtedly affects transmission rates and degree of exposure in all
women.
Further, coexisting untreated infections render the vagina and
cervix susceptible in additional ways.
When immunocompromise first occurs, an increase in STDs is
likely. There is currently a dramatic increase in the rate of STDs,
HIV Infection in Women
39
especially in teenage females who have had vaginal intercourse.
Chronic, recurrent, difficult-to-treat infections are likely the next stage
of early HIV infection Young women without primary health care
providers who arc seen in emergency rooms probably get multiple
doses of antibiotics, are not fully examined physically, and are prob
ably not listened to regarding their complaints or believed when they
say they took their medicine, did not have vaginal sex again, or
whatever. Stereotypes abound among even the best health providers
treating young women, including the assumption that all their patients
are heterosexual, sexually active, unable or unwilling to follow direc
tions, and so on.
In women who have tested positive for HIV antibodies, often a
reversal of the above scenario occurs. The woman may complain of
vaginitis on many occasions and be treated with vaginal suppositories
without being given a pelvic exam. The provider may even know that
candidiasis can occur vaginally in the HIV-positive female but know
little else about the female genital tract. He or she may not be skilled
at doing pelvic exams and may conduct an inadequate exam. Refer
rals are rare or nonexistent. Appropriate lab tests are often unavail
able. This situation leaves an HIV-positive woman exposed to the
continuing risk of the presence of multiple, known, and sometimes
treatable infections and the additional risk of cervical cancer.
On the other hand, a known HIV-positive woman may seek and
receive gynecological care and be treated adequately for gynecolog
ical problems by a provider who knows little about other subtle signs
such as cough, weight loss, or oral thrush that may suggest early
opportunistic infections. A woman with chronic lymphadenopathy
and other signs may be diagnosed with ARC and end up dying of a
pelvic infection that failed to respond to treatment. The failure to
respond may indicate that the organism responsible for the infection
was never identified. Some opportunistic infections that may in fact
invade the upper genital tract include cytomegalovirus, tuberculosis,
disseminated herpes, Candida, and perhaps some of the rarer fungal
infections. Certain other infections such as HPV might spread
throughout the body or at least invade the upper genital tract under
conditions of immunocompromise.
The shorter urethra in a woman exposes her urinary tract to
more organisms from all kinds of sexual activity and even from certain
hygiene practices (the anus, vagina, and urethra are all very close).
Urinary tract infection by common germs and by opportunistic infec
tions may occur more frequently in females than in males and must
be studied. Chlamydia and gonorrhea in the pelvic organs may be
40
Women, AIDS, and Activism
more serious^HlIV-positive women and may require different treat
ment, and opportu nistic infections such as cytomegalovirus, M. tuber
culosis, and salmonella may be involved.
Looking retrospectively at the deaths of women who were IV
drug users or who died of pelvic infections or ectopic pregnancies,
even reviewing maternal deaths to look for possible HIV-related
signs, would probably be very revealing. One similar study in New
York City on the deaths of male IVDUs revealed that a possible AIDS
diagnosis had been overlooked in about half of the death certificates
reviewed.
A Few Words about Research
Obviously much needs to be done. Educational materials need
to be distributed to women and to doctors as well as to activists and
social service workers. Research demands must be framed by activ
ists, and research demands for women need to be framed by feminists.
Women are suffering the medical effects of living in a sexist society.
We are important, we do get AIDS, we are not the same as men,
we need our own place on the research agenda. And equally impor
tant, we must not be afraid to ask questions, undertake our own
research projects, write about our experiences and about what we
know. What we have to contribute to understanding the problem and
having an impact on its solutions should not be underestimated.
Notes
Patricia Kloser, "Women with AIDS: A Continuing Study 1988,” Newark,
NJ- University of Medicine and Dentistry of New Jersey, in VInterna
tional Conference on AIDS: The Scientific and Social ChallengeCOuawa,
Canada: International Development Research Centre, 1989), p. 171.
2.
John Piette, "Regional Differences in Survival with AIDS among Gay
White Males in the United States," Providence, RI: Brown University, in
V International Conference on AIDS, p. 170.
Survival statistics vary greatly and can be difficult to interpret. It is
clear, however, that race, gender, ethnicity, geography, incarceration,
and drug use are all important variables that can affect survival time from
diagnosis of AIDS to death from AIDS-related causes. Confounding these
variables are the additional elements of access to care, appropriateness
of care, adequacy of diagnostic ability, and accuracy of reporting.
3.
Centers for Disease Control, HIV/AIDSSurveillance Report, January 1990,
pp. 1-16.
4.
Chris Norwood, “Alarming Rise in Deaths: Are Women Showing New
AIDS Symptoms?” Afc.,July 1988, pp. 65-67.
5.
R. J. Pomerantz el al., “Human Immunodeficiency Virus (HIV) Infection
of the Uterine Cervix," Annals ofInternal Medicine, 1988, Vol. 108, pp.
321-327.
1.
HIV Infection in Women
41
F. H. Sillman anil A. Sedlis. “Anogenital Papillomavirus Inlection and
* Neoplasia in Immunodeficient Women," ObstetricsandGynecologvClinics ofNorth America. Vol 14, no. 2,June 1987.
7. J I.. Rhoads et al., “Chronic Vaginal Candidiasis in Women with Human
Immunodeficiency Virus Infection," Journal of the American Medical
Association, Vol. 257, no. 22, June 12. 1987, pp. 3105-3107.
6
Additional references:
• T. W. Cheung and F. Siegal, “Kaposi's sarcoma (KS) in Women with
Acquired Immune Deficiency Syndrome (AIDS),” Queens Hospital
Center. Jamaica, NY, and Long Islandjewish Medical Center, New Hyde
Park, NY. Presented at the V International Conference on AIDS, Mon
treal, June 1989
• D. J. Gloeb, M. J. O'Sullivan, J. Efantis, “Human Immunodeficiency
Virus Infection in Women." American Journal ofObstetrics and Gyne
cology, Vol. 159, no. 3. pp 756-768.
• M. E. Guinan and A. Hardy, “Epidemiology of AIDS in Women in the
United States 1981-86." Journal of the American Medical Association,
Vol. 257, April 17, 1989, pp 2,039-2,042.
• V. E Holmes and F. Fernandez, "HIV in Women Cun-ent Impact and
Future Implications," Physician Assistant, May 1989, pp. 53-57.
• K. F. Kelley and S. H. Vermund, “Human Papillomavirus in Women:
Melhodologic Issues and Role of Immunosuppression," in Reproduc
tive and Perinatal Epidemiology. M. Kiley, cd., Boca Raton, FL: CRC
Press (forthcoming), 1990.
• C. Marte et al., "Need for Gynecologic Protocols in AIDS Primary Care
Clinics," Bellevue Hospital. Community Health Project, New York, NY.
Presented at the Fifth International Conference on AIDS, Montreal, [une
1989.
• K. F. H. Miller et al„ "High Rates of Cervical Dysplasias, Cervical
Intraepithelial Neoplasias (CIN) and Human Papilloma Virus in HIV
Infected Female Patients," Univeristy of Munich Women's Hospital,
Munich, West Germany. Presented at the V International Conference
on AIDS, Montreal, June 1989.
• H. Minkoff. “Confronting AIDS: What Every Woman's Physician Should
Know," Female Patient, Vol 12, 1987, pp. 49-64.
• J. L. Mitchell. "Women, AIDS and Public Policy," AIDS and Public Policy
Journal, Vol. 3, no. 2, 1988.
• D, Ribble et al.. "Difference in Stage of Presentation and Presenting
Symptoms Ijetween Women and Men in a Primary AIDS Clinic," Belle
vue Hospital, Community Health Project, New York, NY. Presented at
the V International Conference on AIDS, Montreal, June 1989.
• R. W. Rochat et al., "Maternal Mortality in tire United States: Report from
the Maternal Mortality Collaborative," Obstetrics and Gynecology, Vol.
72, July 1988, pp. 91-97.
• R. Selik et al., “Impact of the 1987 Revision of the AIDS Case Definition
in the United States," Centers for Disease Control, Atlanta. Presented at
the V International Conference on AIDS, Montreal, June 1989.
• M. W. Vogt. D. J Witt, D. E Craven, "Isolation Patterns of the Human
Immunodeficiency Virus from Cervical Secretions during the Menstrual
42
Women, AIDS, and Activism
Cycle of Women at Risk for the Acquired Immunodeficiency Syn
drome," Annals of Internal Medicine, Vol. 106, 1987, pp. 380-382.
C. B. Wofsey, “Human Immunodeficiency Virus Infection in Women,”
Journal ofthe American Medical Association, Vol. 257, April 17, 1987,
pp. 2,074-2,076.
C. B. Wofsey et al., “Isolation of AIDS-Associated Retrovirus from
Genital Secretions of Women with Antibodies to the Virus,” Lancet, Vol.
1, 1986, pp. 527-529.
ACT UP protests of the Nolionol Institutes of Health in Bethesda, Maryland, May 21, 1990. The
‘Invisible Women,” on affinity group, wore gauze to symbolize womenb invisibility in AIDS
research and trealment.
Photo by Donna Binder
HIV Infection in Women
43
-fc±H=S-
Socio-Cultural Implications Of Menstruation And Menstrual
Problems On Rural Women’s Lives And
Treatment Seeking Behaviour
Archana Joshi*
E. Kurien
M. Misra
A. Mehta
M. Rajeshwarii
S. Biswas
Operations Research Group
Baroda
Introduction
This paper describes women's understanding of menstruation and their ability to cope with the associated
rigid socio-cultural norms and practices associated with it in rural areas of Gujarat. The study also bring
forth women’s concern about menstrual problems and factors that guide their treatment seeking behaviour.
It is widely noted that menstruation, which is a mark of "womanhood", has a powerful socio
cultural significance in practically all societies in the world. Attitudes, practices and beliefs vary widely
according to religion and culture.
In developing countries, people are entrenched in deep rooted cultural practices, passed from one
generation to the other. In India, it is believed that most of these practices originated from Vedas. In the
Vedic lifestyle, there are rules for women to follow during menstruation. Some of these rules prohibit them
from preparing food that is offered daily to the Lords as part of the Vedic rituals and ceremonies and
prevent them from performing pujas and rituals.
Over time, as people move away from the understanding of the Vedic rituals, various other beliefs
and practices became prevalent. The theme of contamination has now become prominent in rituals and
practices related to menstruation, particularly in the rural areas. Menstruating women are considered impure
or unholy and are neither allowed to participate in any social or religious functions nor are they allowed to
enter the kitchen. These chores are taken over by other women, older daughters and even men in the family.
Literature Review
A literature search reveals that several researchers in India studied the socio-cultural aspects of
menstruation as early as the nineteen sixties. For instance, Srinivasa has referred to studies conducted by
Rao and by Koshi, to assess the age at menarche and menstrual patterns among school and college girls
(Srinivasa, 1970; Rao, 1963: Koshi et al., 1970). The studies reveal that the onset of menstruation among
girls is at around 14 years. Late onset of menarche evokes feelings of anxiety among parents, a reaction that
seems to be justified considering the observations of Komura and associates (Komura et al., 1992) who
investigated the relationship between age at menarche and reproductive ability in 2278 married women who
started menstruating. They reported that a group of women in after the age of 18 years have a significantly
higher rate of infertility (15.7%) than other women (5%). Irregular menstruation during the first few years
after menarche has been related to decreased reproductive ability. The findings indicate the importance of
menarche before the age of 18 for normal reproductive functioning.
Studies have also indicated that there are misconceptions, ignorance, and incomplete knowledge
about the biological basis of menstruation among young girls. In the USA, sixth grade students who view
themselves as "prepared" for menarche, have incomplete knowledge and possess a variety of
misconceptions. Girls' knowledge of the location and function of reproductive structures have been found to
be faulty', and most did not understand how reproductive structures are interrelated (Koff and Rierdan,
1995).
The socio-cultural norms and practices associated with menstruation have been brought forth again,
almost two decades later, by some of the researchers in India (Van Woerkens, 1990; George, 1994). Despite
the fact that onset of puberty is celebrated in some parts of the country, a menstruating woman is considered
impure and unholy and is not allowed to participate in any religious or social functions. The rules are found
to be more rigid among Hindus than in other communities.
Chaturvedi and Chandra in their study have observed a clear relationship between menstrual
attitudes, physical distress and premenstrual change among college students (Chaturvedi and Chandra,
1991). Those who reported considerable menstrual problems considered menstruation to be "debilitating"
and had an "unhealthy" attitude whereas those who had pre-menstrual well being considered menstruation
to be a " natural event and had a "healthy" attitude. Similar observations have been made among Icelandic
nursing students (Sveinsdottir, 1993). However, most of these studies however have been focussed on
women living in urban areas and little is known about these aspects among rural women.
Several researchers have shown that menstrual disorders constitute one of the major reproductive
health problems (RHP) among women (Bhatia and Cleland 1995; Patel, 1994; George, 1994). A study
carried out by Patel in tribal areas of Gujarat has shown that excessive bleeding during menstruation is
reconsidered a "severe" women's illness, the causes of which have been attributed to heavy workloads,
weakness, consumption of "hot" foods; intercourse during menstruation and side-effects of tubectomies.
Researchers have also studied menstrual problems as a consequence of surgical contraception.
Disturbances such as menorrhagia and dysmenorrhoea have been reported as symptoms resulting from
sterilization (Purkayastha and Bhattacharya, 1992; Lethbridge, 1992). However, it had been argued by
others that these menstrual disorders are not long term (Rulin et al., 1993). A study population of 500 lowincome group women undergoing sterilization were interviewed before sterilization, 6 to 10 months after
2
surgery and 3 to 4.5 years later. An increase in severe dysmenorrhoea which emerged as a disturbing but not
significant trend at 6-10 months did not continue over the next 3 to 4.5 years.
Some researchers have suggested that regulation of hormonal menstrual cycles is beneficial to a
woman's health. For example, Dennis (1992), in his paper on cultural change and the reproductive cycle,
has shown that frequent menstrual cycles are associated with a number of gynecological problems.
According to him suppression of the menstrual cycle with cyclical hormones such as oral contraceptives is
the simplest way to lower the incidence of a number of medical problems including benign breast disease,
ovarian cysts, dysfunctional bleeding and salpingitis (inflammation of uterine tubes). Similar observations
have also been made elsewhere (Moghissi, 1958). It is stated that dysmenorrhoea can also be prevented with
cyclical hormone administration. Thus, the practice of consuming oral pills to regulate menstruation could
aid in lowering the incidence of gynecological morbidities.
Menstrual problems, thus constitute one of the most severe reproductive health problems among
women in India. An association between the use of surgical contraception and menstrual problems too has
been established. Coupled with these medical issues are traditional norms and practices and ignorance about
menstruation that dictate a menstruating woman’s life and restrict her mobility and treatment seeking
behavior. The problems may be worse in rural areas (where nearly 70 percent of the Indian population
resides) where there are inadequate health care facilities and a much more rigid adherence of traditional
norms and practices.
It thus becomes imperative to understand rural women's views on (a) menstruation from its onset to
menopause, (b) the influence of menstruation on their daily lives, (c) beliefs and attitudes toward
menstruation, reproduction and use of family planning methods and (d) menstrual problems and treatment
seeking behavior. The present paper is an attempt in this direction.
The issues discussed in the present paper are part of a larger study conducted by Operations
Research Group (ORG) entitled ’Understanding Sexual Health Problems and Behavior of Women in Rural
Areas of Gujarat'. The study, sponsored by the Ford Foundation, was initiated in the year 1996.
3
The Study Site
The study was conducted in two talukas1 (Padra and Baroda) in Baroda district of Gujarat. In all 8 villages
were selected. In some of the villages (3 out of 8) the researchers had conducted studies on women's work
load and child health and development in the past and the community members were familiar with the
research team and aware of the purpose of their visit. The other five were neighboring villages (See Figure
1). These villages were however not representative of all talukas in the district.
Profile of Villages:
These villages are located at distances of about 20-25 km from Baroda city. The villages are small and the
number of households in these villages range from less than 100 to about 300. The socio-economic profiles
of these villages are similar. The majority of the population belongs to the Hindu community (87%).
Among these, nearly two-fifths (37%) are upper caste Hindus. The proportion of Muslims is significantly
higher in the villages of Baroda taluka (20%) than in the villages in Padra tahika (4%). In both talukas,
people have strong religious beliefs and practices which occasionally leads to communal violence.
Agriculture, mainly on unirrigated land, is the main occupation of people. A little more than 50 per
cent of the households are landless. Most of the men and women earn their livelihood by working as
agricultural or casual labourers. Socio-economic disparity among various caste groups is wide. There is a
high rate of emigration from these rural areas to countries abroad (like the US and UK) among those who
are economically better off. Hence, to a certain extent, there is increasing exposure to western mass media
and life styles.
All the villages have electricity, public transportation and other basic amenities. Most of the houses are
kutcha (mud and thatch) or of mixed type made of brick walls and tin on tiled roofs. Government health
providers viz., auxiliary nurse midwives (ANMs) visit 6 out of the 8 villages. Their roles are limited to
providing family planning services and immunization. Services of health care providers (MBBS/ RMP) are
available within each village or at close proximity. The distance of the nearest primary health center (PHC)
is about 8 to 10 km away. For certain illnesses such as measlesjaundice and infertility, faith healers are
often preferred to providers practising any other system of medicine.
1 taluka : a smaller division of the district
4
*
Research Methodology
To begin with, house listing was done using a detailed checklist to identify married women in the age group
15-49 years suffering from RHPs. Of the 1067 married women contacted in the villages, 262 (25%)
reported a current RHP. Although the major RHPs reported were white discharge (53%) and urino-genital
problems (48%), as many as 24 percent reported menstrual problems. These problems were described by
women as irregular bleeding, profuse bleeding, scanty bleeding, unnatural (black) bleeding, painful
bleeding and prolonged bleeding (>7 days). The other RHPs reported were infertility (4%) and uterine
prolapse (2%).
Community mapping was subsequently done to select women from different socio-economic
clusters (called faliyas) to ensure adequate representation. Among these, women who were willing to
participate in the study and could be contacted during repeat visits were selected. In all, 68 of the 262
women reporting RHPs were selected in the study.
Data were gathered primarily through repeated indepth interviews, (4-6 times) for a period of 6
months from March to August 1996. Interviews were conducted in local Gujarati language by 5 women
researchers, with the help of 5 women field assistants. Informal group discussions were also conducted with
women who did not report RHPs during the study period. Their views and opinions on social norms and
practices prevailing in the community related to menstrual and other related reproductive health problems
as well as treatment seeking behavior were obtained. Group discussions also served as a platform to
"validate" trends and patterns emerging from the repeated indepth interviews.
In the small villages, one group discussion was held per village and in the larger villages, two group
discussions were held per village, one within the high income group and one within the low income group.
Each group comprised of 6-7 married women somewhat with roughly similar socio-economic
characteristics. Nine group discussions were conducted in all.
During the course of the field work, local health care providers including traditional birth attendants
(TBAs. locally known as Dais), private practitioners as well as doctors (MBBS) working with the mobile
health services provided by a non governmental organization (NGO) in the area, were also interviewed.
Key informant interviews were conducted with some of the influential and educated members of
the community. These interviews were conducted both with men and women. Information about general
social and cultural practices in the community, and local terminology used for menstrual problems and
other RHPs was collected. Using the terminology as well as the symptoms described by women during the
5
indepth interviews, the key informants were asked to rank various RHPs with respect to perceived degree of
severity, causes of these problems, preference for treatment, mode of transmission and other related issues.
The exercise also helped to dispel ambiguity regarding various concepts and terms encountered during the
process of data collection. For instance, terms such as 'sitting aside1 (chheti besi) 'dirty hair' (mathu mali),
'date' (tareek) all indicate the duration when a women is menstruating.
As mentioned above, the interviews were conducted by researchers and the field notes were written
in Gujarati. These notes were later expanded and translated in English. While most of the data were
analyzed using the software package ‘dtsearch’, some of the information was also tabulated manually to
facilitate analysis.
Results
Profile of Selected Women
Most of the women selected for study are young: around 35 years of age. The majority (80%) are Hindus,
and live in nuclear families (65%). Hardly any women are educated up to the primary level and more than
two fifths have no formal education. The majority (66%) participate in income generating activities
primarily as agricultural or casual labourers. ( see Table I)
Half of the women reported that they started menstruating by 14 years of age and a significant
proportion (41 %) stated that they attained puberty after their marriages. Age at first conception was reported
to be 18 years or earlier by the majority of women (71 %).
While most (62%) of the women have adopted a permanent method of family planning as many as
18 percent of all women desired hysterectomy to relieve them from their current RHPs. Menstrual problems
constituted about 31 percent of the total RHPs reported.
Throughout the course of data collection, it was observed that women did not hesitate to discuss
menstruation and related problems. This could be attributed, to a certaimextent, to the fact that interviews
were being conducted by women researchers. However it was also observed that the presence of in-laws,
male relatives and/or a husband did not deter them from sharing their experiences and problems openly. At
times, even other community members contributed actively to the data gathering by narrating anecdotes
and customs associated with menstruation. Hence it was felt that open discussion of menstruation was not
taboo in the community.
6
Attitudes Towards Menstruation
Attempts were made to assess the attitudes of women toward menstruation. Past studies have revealed that
personal experiences are likely to influence menstrual attitudes and there is a clear relationship between
menstrual attitudes and physical distress. If women experience pain during menstruation or have had painful
experiences related to menstruation they tend to have a negative attitude toward menstruation. However,
despite the fact that all of the 68 selected women reported some reproductive health problems, the majority
(three-fourths) did not have a negative attitude towards menstruation. Though they were angry, irritated and
embarrassed on the days they menstruated, they perceived that the advantages of menstruation far
outweighed the negative aspects. They believed that it was a natural gift (kudrati bhet).
It is good to menstruate. It is essential for a woman. Without it we cannot have
children
But. sometimes I gel angry and irritated that I cannot do anything.
Even for a small thing I have to ask somebody, so 1feel shy and then get angry.
Many times, ifI have to attend marriages and am menstruating, I curse myself, I
feel bad that I cannot go.
It is so embarrassing when we have our periods. Everybody comes to know about'
it.... Anyway, it is not in our hands, we cannot become a man now. Throughout our
life we will remain women. Infact we should consider it a giftfrom God. It is
important to menstruate, we cannot have children otherwise
Ifa girl does not
menstruate then her parents will start worrying because getting her married will
be a problem.
»
Women in the study areas believed that vitality and good eyesight were related with a menstrual
cycle. Scanty' menstruation and/or menopause, according to them, results in poor eyesight. Overall, the
benefits of menstruation were perceived as maintenance of good eyesight, purification of blood and growth
of the body. Some also believed that it was necessary to deplete the body of excessive heat (garmi) and
disease:
It is good, all the disease in the body comes out. Ifone does not menstruate, the
uterus will become diseased and the body will swell.
Ifeel that it is necessary to menstruate. Ifwe do not menstruate now then we might
lose our eye sight in old age.
However, the most vital function of menstruation was perceived as reproduction. More than onethird of the women stated that it is a manifestation of womanhood and its onset signalled that the girl was
ready for marriage and procreation. The belief that menstruation is a mark of womanhood is reflected in the
following sentences:
It is a gift given by God to women. It is very necessary. It is our body's greatness
that we can become mothers. And, even ifwe get irritated, what is the use ? It is
going to come every month. It is a custom among us, that as soon as a girl becomes
mature (attains menarche), she is considered a burden on this earth. We should get
her married as early as possible.
Around one-fourth of the women expressed a completely negative attitude towards menstruation.
All of them had achieved their desired family size. Most of these women experienced menstrual problems
such as excessive and/ or painful periods. The physical problems caused anger and irritation. Another
opinion regarding menstruation was that it was dirty and a curse to women.
/ get severe back aches. I do notfeel like working. It is really a curse to get periods
for 15 days a month. All those days, I cannot cook, fill the water or do puja. I am
thinking ofhaving my uterus removed
The duration and regularity of the menstrual period was considered to be related to good health and
body heat (garmi). Almost half of the respondents reported that they bled for 4-5 days, a period which was
considered "normal". Scanty periods (i.e. menses for less than 3 days) were believed to result in garmi and
thereby a lower chance of conception. Menstruation for just one day was believed to be "abnormal".
People around me - my parents-in-law and my sister-in-law scare me. They say
that I will not conceive because ofscanty periods. I have been marriedfor 3 years
and have no children. My husband thinks that there is something wrong with me
because I menstruate for only one day.
One woman who menstruated in the form of spotting spoke of the anxiety she and her family
experienced when the doctor told her that she would never conceive as she did not have a regular flow.
However, she later gave birth to three boys.
The doctors are mad. They say anything they want. That doctor told me that 1
would never became a mother.... My husband told me not to worry and to have
faith in God. See, I have 3 sons now.
Onset Of Menstruation
Age at Menarche Most women could not accurately remember the age at which they started menstruating
for the first time. Almost half of them recollected that they attained menarche around by the age of.14 years.
8
Parents were concerned when their daughters did not begin menstruating by the so called 'appropriate' age
of 14-15 years.
In rural areas, though girls are married at an early age (12-16 years) they are expected to stay at
their natal home until they attain puberty. By and large, marriage is consummated only after the girl starts
menstruating. Traditionally, a ceremony called “gauna" is held at the natal home and then the girl is sent to
her husband's house.
A delayed onset of menstruation could delay gauna and the girl's ability to bear children could be
questioned. This, in turn, could jeopardize her marriage.
Nevertheless, in the study areas, early marriage prior to onset of menstruation is perceived to be
auspicious and is expected to bring blessings to the parents. A woman who experienced her first menstrual
periods just one month before her marriage regretfully stated:
»
My parents missed their blessing by one month. Just one month before the wedding
I started menstruating. It is a beliefthat ifparents get their daughters married
before they have started menstruating, then the parents are blessed (punn maleyj.
Awareness ofMenarche-. Though most of the women were unaware of the concept of reproduction prior to
the onset of menarche, all of them gradually learnt of the association between menses and reproduction.
More than half of the women reported that they had absolutely no previous knowledge of the
phenomenon until they attained menarche. A few women (7) who had some idea stated that their knowledge
was limited to the awareness that "women bled from the vagina on certain days of the month". Apparently,
they knew nothing beyond this. Even women who had attained menarche at 16 years or later stated that they
were not fully aware of the implications of menstruation.
Those who admitted to having some knowledge stated that they had observed older relatives
following the social norms and restrictions associated with the phenomenon. About one fourth of those who
knew menstruation was related to a woman's ability to bear children and was an event that happens every
month, learnt about it either through friends or relatives, or from their sisters-in-law belonging to the same
age group.
Due to inadequate prior knowledge among most of the respondents, the first reaction at the onset of
menarche was usually negative and they reported being either scared, puzzled or shocked. The experiences
of two women reflect the effects of their first menstrual periods.
9
1 did not know anything. Things were different in our days. When I got itfor the
first time, 1 was sleeping. It was at night. When I got up in the morning-1 saw
blood all over my skirt. 1 got very scared, ran to my mother and told her, 'Mother,
' somebody came and hit me at night - so much blood is flowing'.
Myfriends knew that women menstruate and they had told me about it - so I knew
a little. When I got my MCfor the first time, I was restless. 1 thought 'What has
happened? " I made a vow to our Goddess and begged her to stop this. I promised
to offer coconuts ifshe heard my prayer. Ifelt shy to tell anyone, butfinally told
myfriends that I had got 'it'.
Finding it difficult to cope with such situations alone, nearly one fifth reported that in these
circumstances, they usually told their sisters, friends or sisters-in-law, preferably of the same age group.
Around one-third reported that they approached their mothers. At times, when the first menstrual period
occurred after marriage at the in-laws house, the women approached the sister- or mother-in-law. One
woman recollected:
Earlier, I was not aware ofmenstruation. When I got married and came to my in
laws ' home, my mother-in law explained everything to me and said that I would not
be allowed to sleep with my husband till I start menstruating. This is how I learnt
about the menstrual cycle (MC).
None of the women stated that they had been informed about menstruation, prior to its onset, by
their mothers. The general belief among women themselves was that girls should not be informed about
menses before its onset and some even considered it a sin to do so. When probed whether they would
inform their daughters in advance, they said that it was unnecessary and improper to do so. Besides, women
also felt that girls now-a days were more aware of these aspects as a result of schooling where they get more
opportunities to discuss things with their peer group than the respondents did when they in school.
Norms and Practices Observed at the Onset ofMenstruation The advent of menarche brought along with
it the restrictions and practices associated with menstruation. The women reported that they were taught
how to make a pad from an old sari or skirt and were shown the manner in which it was to be placed in the
underwear. In certain cases, women were instructed to wear a kachto ( a long skirt locally called chaniya
pulled tightly under the groin and tucked at the back) under another skirt instead of a cloth pad.
10
Almost all the women were told that they were not supposed to pray during the days they were
menstruating nor stand near the area where the pictures of the Gods were placed. They were also instructed
not to attend social occasions (such as weddings) as certain religious rites were performed during such
ceremonies.
While the above norms were common among all women in the community irrespective of religion
and caste, women belonging to the Hindu community were particularly instructed to maintain physical
isolation for the first 3-4 days of the menstrual periods. The idea behind the prescribed isolation was to
prevent the spread of impurity associated with menstruation.
All women reported that they were advised to observe some degree of isolation while menstruating.
Based on the degree of isolation advised, the respondents can be divided into two categories: (1) partial
isolation and (2) complete isolation. The taboos associated with partial isolation included: (a) not filling
drinking water nor touching the earthen pots containing drinking water; (b) not milking the buffalo or cow;
(c) not touching anyone, and (d) not cooking or helping in food preparation. More than half were instructed
to maintain partial isolation at menarche. Reminisced one of the women:
My mother told me, 'You have grown up now and become an adult. ’ She gave me
an old petticoat to wear as a 'kachto' under the skirt I was wearing She told me to
sit asidefor 4 days, not touch anybody, not go near the cooking stove norfill
waler. She said that I would be able to touch everything only after I washed my
hair on thefourth day.
Around one-fifth of the women reported that they were told to maintain complete isolation. In
addition to the above taboos, these women were also restricted from (a) filling water used for washing
clothes or vessels, (b) performing chores both inside and outside the house, (c) going on outings, and (d)
they were expected to sit and sleep outside the house during this period.
Other changes associated with puberty included switching over to wearing saris instead of skirts to
distinguish them as young adults and, in some instances, discontinuation of schooling. Some were also
expected to maintain a certain degree of decorum and told not to laugh loudly or talk with members of the
opposite sex. In this context, one woman recollected:
My parents were very strict. They stopped me from going to school. My mother
said that it was time for me to get married.
The first menstrual period was joyously welcomed by mothers and mothers-in-law as it signalled a
girl’s fertility and hence, her ability to bear children. More than three-fourths stated that a special sweet
11
(normally sheera2) was prepared for them at menarche. A few women recalled that their mothers distributed
sweets to neighbours and friends to celebrate the event.
Implications Of Menstruation On A Woman's Daily Routine
Social Norms and Practices Currently Observed during Menstruation (The taboo behaviour started at
menarche continued to be followed throughout life but with a considerably lower level of rigidity.) There
was a substantial decline in the number of women practicing complete isolation. Just three women reported
observing complete isolation from all routine activities, while the rest maintained either partial isolation
(61%) or restricted themselves only from religious activities (33%). The Reported degrees of restriction,
analyzed by using a Guttman's scale, is shown in Table 2.
Often the type of restrictions observed by these women were influenced by their religion and by the
amount of social support they received during the days they menstruated. Muslim women were relatively
less rigid with respect to these practices than Hindus.
All 13 of the Muslim women continued performing their routine chores. However, all of them
strictly refrained from participating in any religious activities. Apart from being restricted from saying the
Namaz they were also not allowed to touch the Koran, fast during Ramzan or cook the special foods during
festivals.
There was a significant change in the pattern of daily activities among the Hindus. In addition to
refraining from participating in any religious ceremony, women maintained a physical distance from every
one except for their infant children. If they accidentally touched anyone, water was sprinkled on the
’defiled' person, a procedure that is believed to purify him/her. While most were not allowed to touch the
earthen pots containing drinking water, others were also expected to stay away from the copper vessels
containing water stored for washing clothes and utensils. Those who did performed chores such as washing
clothes, refrained from touching them once dry.
All the routine activities were resumed only after the traditional head bath was taken either on the
third or fifth day following the onset of each menstrual period. This was one of the ritual purification
processes adopted to wash away the impurity associated with menstruation. Often menstruation is also
2 A sweet made of semolina, milk and clarified butter (ghee)
12
*
referred to as " her head is dirty (rnathu mailu chey). Symbolically, menstruation is also referred to as "
bathing (nahvan) "as well as "bathing and washing (nahti-dhotl)".
Due to the various taboos associated with the phenomenon, menstruating women often had to
depend on others for routine chores. Meals were generally cooked by relatives in joint families or
neighbours, friends and even by husbands in the case of women living in nuclear households. At times, the
woman herself was served food by others and, in certain cases, in separate utensils specially kept aside. As a
consequence of this dependency, meals were often not served according to the routine schedule. In some
households, meals were not cooked at all, resulting in the family sustaining on an inadequate diet of dry
snacks. Often this situation led to verbal altercations between husband and wife.
Certain women who earlier had lived in joint families became more flexible in their attitude once
they moved to nuclear set-ups. One of the women recalled:
Earlier my mother-in-law took care ofall the chores on the days I menstruated.
After her death, there is no one to do all the work in the,house. My husband does
not know how to cook. So. I have stoppedfollowing all these customs. During the
days I menstruate, I get up early in the morning at around 5 o ’ clock and bathe.
Only then do I start the work. On other days I am not particular about the time I
bathe. But, I do not perform 'puja. We shift the photograph ofour Goddess and
place it behind a curtain so that even my shadow does notfall on it.
Those who observed isolation during menstruation followed the customs strictly as they feared that
non-conformance to the norms would be tantamount to sinning. Of all the Hindu communities, the various
Foolmalis (traditionally cultivators of flowers) were most rigid in their attitudes. Two of our women in the
sample belonged to this community.
One Foolmali woman, reportedly, was extremely drained by the physical violence inflicted on hei*
by her alcoholic husband. This woman menstruated for 10-12 days a month and depended on her husband to
perform most of the household chores as her children were small. The following sentences reflect her
difficult situation.
My husband gets very angry when he has to cookfoodfor 10-12 days. He shouts at
me and says, 'How long will I cookfor you ? You will have this problem all your
life. Get your uterus removed, or go away to your mother's home'. At limes he
does not cookfor 2-3 days, so we have to starve sometimes. Sometimes he gets
angry and beats me up. He does not even talk to me when I have my periods - all
the 11 days.
Once he broke my wrist, I had to have an X-Ray taken
('photo').... he hits me with anything he can get hold of; not just a stick..... He hits
me on the back, pulls my hair and kicks me. At times, he hits me continuouslyfor
an hour.
13
At times, the burden of customary norms is so heavy that it results in economic losses to the
household as well as physical abuse by the husband. The effect is more intense in the case of persons
belonging to the lower socio-economic strata where it is imperative for the woman to work and contribute
her share to the household coffers. One woman lamented:
/ cannot work in the fields [when menstruating]. It is my only way ofearning. Ifwe
do not work in the fields, our income will get affected. God will punish us by not
giving us our meals.
Despite the restrictions observed during menstruation, by and large women reported that there is no
respite from work. Although there is a reduction in activities performed 'inside' the house, this is
compensated for by household chores outside the home such as grazing cattie, collecting fire wood etc.
When the researchers asked the respondents about the rest they should be enjoying during the days they
menstruated, one of them replied sarcastically,
No one will let me rest on those days. Since 1 cannot do any work in the house, my
in-laws tell me, 'Go to the fields, collectfodder and dung. We will take care ofall
the work inside the house. You go and do all the work outside the house.' What
rest are you talking about?
Hygiene and Sanitary Practices The precautionary measures adopted at menarche were usually continued
throughout the later period. The majority of women (87%) used cloth pads made from old, clean saris or
petticoats. However, a few (6) women preferred to wear a petticoat in the form of a kachto in order to
absorb the menstrual discharge. Two women who had scanty periods did not use any precautionary
measures. While one used only underwear, the other allowed the menstrual flow to collect in \\ersalwar (a
type of pyjama traditionally worn by Muslim and Punjabi women) as she was not in the habit of wearing
underwear.
The practice of washing and drying the soiled cloth also reflects the various beliefs associated with
menstruation. Most of the women used soap and water, however, some kept a separate soap exclusively
used for cleaning the cloth in order to prevent the spread of'impurity'. The process was carried out usually
in the backyard and some women who had bathrooms even preferred to wash the cloth away from the
house. Care was also taken to throw the water used for washing the cloth far away from the house. One
woman stated:
/ wash the cloth piece (after each use) with soap and water and dry itfar away so
that no one sees it. 1 take water in a tagara (a semi circular metal container) for
14
washing the cloth and throw the dirty walerfar away. We cannot throw the water
any where because ifa snake smells it. it will become blind and w will be cursed.
Some women (8) went as far as the village pond in order to prevent the soiled ’impure' water from
coming in contact with other members of the family. In addition, the cloth was washed only after all the
other clothes were washed.
Precautions were also taken while drying the cloth. Some covered it with another cloth, while
others dried it far away from the house. A few even maintained a separate clothesline for this purpose.
The cloth was generally reused for 2-3 months. Several beliefs were also associated with its
disposal. The habit of burying or burning the cloth was common. Some stated that if the shadow of a man or
animal fell on it, it was a bad omen. Similarly, if a pregnant woman stepped on a soiled cloth it would have
an adverse effect on her.
Women took adequate measures to maintain personal hygiene. Though all usually cleaned their
genital parts while bathing, some (24) also washed these parts two or more times a day during menstruation
after urinating, or when changing the cloth. Women belonging to the Muslim community were very
particular about washing their genital area throughout the month and not just on the days they were
menstruating. This habit, known as hath path, is part of their religious practice.
Sexual Behaviour Apart from routine chores, menstruation also had a profound effect on the sexual
behaviour of these women. Almost all (94%) maintained sexual abstinence during the days they
menstruated. Staunch beliefs pertaining to ’impurity' deter women from having a sex with their husbands.
As many as three-fourths of them said that their husbands would become ’impure' and thus ’unfit' to
perform religious activities if they had intercourse during menstruation. They even took extreme
precautions to sleep on a separate quilt-like mattress. These mattresses were kept away from the other
bedding used by the family and washed after each menstrual period.
Some women (10) reported that they felt it was ’dirty' to have sex during menstruation, while three
women either said they feared conception or believed that pregnancy resulting from sex during
menstruation could lead to the birth of an abnormal child. Some even stated that the bleeding would become
extremely profuse if they had intercourse during this period.
A fear of negative consequences for the husband was yet another belief that prevented women from
having sex with their husbands during menses. Some were apprehensive about their husbands becoming
15
blind or impotent, while others believed that it would result in sexually transmitted infections if they had
sex with their husbands during menstruation. One woman stated:
Thefirst lime I had sex after my second marriage, I was menstruating. Ifeel that
he (husband) got eruptions (folli) on his penis because ofthis reason. Ifeel that his
body got the heat (garmi) from my body.
Concept of "Safe Period" Though most were aware that there were certain days in a month considered
safer than the rest, during which chances of conception were lower, the majority had misconceptions about
when that safe period occurs.
Ifone wants children, then one has to have intercourse during those 4 days ofthe
menstruation andfor 3 days after the menses. All my 3 children were conceived
during those days.
Similarly, 4 respondents reported that they maintained abstinence on the days they menstruated in the belief
that they would conceive ifthey had intercourse on those days.
Practices Adopted to Postpone Menstruation. Sometimes menstruating women did not disclose when they
were menstruating to other, in order to be able to participate in social occasions.
Gujarat, a state of varied cultures, celebrates a number of festivals with pomp and gaiety. Marriages
and social functions (for example, the thread ceremony), are held throughout the year. Women look forward
to such functions and festivals for entertainment and social interaction, as well as respite from routine
chores. In view of this, sometimes they resort to ways and means of postponing their menstrual cycles.
Around one-third of the women interviewed, admitted to using oral contraceptive pills to delay
their periods but not as a family planning measure. Almost all were aware that this method could be used to
postpone menstruation. Although some were aware of the names of these pills (Mala-D), others commonly
referred to them as "pills to postpone menses" (masik lambavani goli). A woman stated:
/ wasjust married and was expecting my MC 2-3 days after the marriage. My
sister-in-law got 10 tabletsfor me from the store, 1 took one daily and my MC got
delayed.
Some women procured these pills directly from the chemist's store whereas others requested their
husbands, close friends or relatives to buy them. Women were aware that the ANMs visiting their villages
16
also carried these pills. Health functionaries who were interviewed during the study also supported the fact
that women demanded such pills, not as a measure for birth control, but to postpone menstruation.
Two women consulted their doctors with regard to such decisions. One of them who had consumed
oral pills on an earlier occasion, once again sought help from the doctor prior to her son's babri (a ceremony
amongst Hindus wherein a boy's head is shaved for the first time) to postpone menstruation:
The second time, I took an injection jrom the doctor during the 'babri' ofmy son. This
injection cools (thandak) the body and postpones MC.
Thus, consumption of oral pills or injections to postpone menses seems to be a matter of
convenience and a common and accepted practice in the study area. However, the repercussions of such
behaviour may have long-term effects for some women. Improper utilization or inappropriate consumption
of pills without medical advice may result in delayed and profuse menstrual bleeding and consequently lead
to uterine problems. Such practices may also lead to irregular cycles and the anxiety of suspected
pregnancy. This fear of pregnancy may cause women to seek medical advice or visit local healers to induce
an abortion.
There were several other measures, women adopted to alter their menstrual cycle. Menstruation, as
stated before, is believed to be necessary for depletion of body heat and consumption of "hot food" is
perceived to aggravate the condition. These "hot foods"3 are believed to increase body temperature resulting
in an enhanced blood circulation and thus profuse menstrual flow. Hence, foods termed "hot" or "garam"
were avoided prior to important events. Almost half of the women (44%) avoided consumption of these hot
foods while menstruating. One woman stated:
I avoidfish and brinjal. These increase the heat fgarmi) in the body and thus, heat
generationfrom the private parts
this leads to excessive menstrualflow.
Hot foods:
Brinjal, jaggery, spices, bajri (millet), non-vegetarian foods, onion, chilly, alcohol
papaya seed, dry ginger powder (sonth), Zatpat (flavoured betelnuts) etc.
Another woman added:
/ avoid eating hot and spicyfoods. Ifl consume jaggery, bajri or sukhdt even one
day after the periods, I get spotting the next day because ofthe heat. I have also
reduced eating mutton.
Another belief was that consumption of flat beans (Valor papdi) could lead to tetanus if consumed
during menses and hence it was avoided.
Besides the above, one fourth of the women also avoided sour (Khatu) foods on the days they
menstruated as these also were believed to increase menstrual flow and backache.
Four women stated that making a vow to the tulsi (bcimum sanctum), a plant worshipped by the
Hindus, or to the Mahisagar, a river that flows near the study areas, aided in delaying the next menstrual
period. One of the women recollected:
Once I prayed to the tulsi plant to delay my MC. I made a vow (badha) to get MC
postponed.
We have to offer rice, betel nuts, money and waler to the plant and
pray and afterwards we have to bring these (offerings) back and keep them in a
box at home.
Various measures were also adopted to induce menses when it was overdue. Women were aware
that missing a period when one had not adopted any contraceptive method could indicate pregnancy.
Several incidents were narrated during discussions with community members wherein women (both
married and unmarried) attempted to induce an abortion jyhen they suspected an unwanted pregnancy.
Those who were unmarried often sought an abortion in a covert manner and usually adopted
traditional or home remedies during the initial period (2-3 months) of pregnancy. Some measures tried were
consuming a large quantity' of’hot’ foods such as papaya or a boiled concoction of ground black pepper and
water. Some also of consumed a large dose of an anti-malarial drug (locally called a "chlorine tablet"),
which has a high quinine content. One of the TBAs stated that half a liter of alcohol, if consumed at one
time, would definitely induce menstrual flow.
A brittle sweet made of dry ginger powderjaggery and clarified butter (ghee)
Sour foods:
Curd,.buttermilk, lemon, tamarind, etc.
18
Some women even mentioned that tablets were available at the chemist's store to induce menses.
Taking vows was another measure adopted for this purpose. For unmarried women, medical consultation
was sought onl\ if all the above attempts failed. However, married women were more likely to seek medical
attention immediately as, according to them," they had nothing to hide". Ten out of the 68 women had
attempted to induce an abortion and in fact, one woman had tried it five times. While all five of the women
who sought medical termination of pregnancy (MTP) services from doctors (private and government) were
successful in their attempts, most of those who adopted other measures were unable to abort the pregnancy.
One unsuccessful woman recalled:
I had tried to induce an abortion fmahina padavvaj after the birth ofmyfirst
daughter. We did not want another child so soon. 1 was one and a halfmonths
pregnant. So my husband went to our family doctor and got 3 tablets. 1 took one
tablet each dayfor 3 days, but nothing happened, my periods did not come.
One woman, whose husband stopped caring for her once he discovered that she had had a pre-marital sexual
relationship, recollected her unsuccessful attempt aborting her first pregnancy after marriage.
/ did not want this child. What is the use ofhaving a child when your husband is
not interested in you? I knew that he would not care for the child. So, when one of
our cowsfell sick, I consumed 4 long capsules meantfor her, thinking that heal
(garini) generated by the capsules would lead to an abortion. 1 was 4 months
pregnant at that time.
This woman, who later separated from her husband and resumed her relationship with her pre
marital lover spoke about the anxiety she underwent when she did not menstruate for one and a half months.
Initially, I boiledjaggery, ground pepper and water and drank this 2-3 times, hut it
was no use ......... Then, I told myfriend to get tablets (gollij so that I could get
my periods. The man at the store gave her 2 tablets. Just 2 tablets cost me Rs. 12.1
ate both and got my MC the next day.
Menstrual Disorders and Treatment Seeking Behaviour
Types of Menstrua! Problems: Disorders pertaining to menstruation compose a significant segment of all
the RHPs reported by women in rural areas. Among the 68 women covered under the present study, 21
(31%) stated that they suffered from menstrual problems, the reported symptoms being excessive bleeding,
scanty flow, irregular cycle (reported by 6 women each) and extreme pain during periods (5 women). Other
problems mentioned were prolonged menstrual flow, and black coloured discharge (see Table 1).
19 .
Just two women reported having only menstrual problems and the rest mentioned the incidence of
other disorders such as urinary' tract infections (UTI). white discharge, infertility and uterine prolapse along
with their menstrual problems. Almost half (10 out of 21 women) suffered from UTI and white discharge
along with menstrual disorders.
Some women were worried when they menstruated twice during the same calendar month, even
though their cycles were of the 25-28 days interval. They felt that there was something wrong with them
since their cycle occurred twice a month. Some women shared these apprehensions with an ANM or a local
doctor and asked for medicine to treat this problem.
This practice was also reported by the health providers (ANMs, private practitioners) in the
villages.
Duration and Severity of Problems-. Nine out of the twenty one women reporting menstrual problems said
they had been suffering for more than 5 years, whereas 8 women reported that the onset had been-during the
past one year. The problem was perceived to be "severe" in thirteen cases. The intensity of the problem was
estimated on the basis of description given by the subject. These were subsequently ranked by the
researchers as mild5 and severe6 .
Besides menstrual problems, more than half of the 68 women interviewed complained of other
minor physical discomforts such as body pain or ache, weakness, nausea or dizziness on the days they
menstruated. The most common complaint (reported by 24 women) was body ache on all the days of
menses.
Sometimes the menstrual problems were linked to supposed moral transgressions.
Ifan unmarried girl has had a sexual relationship with a male, she will have
problems such as severe stomach ache on the days she menstruates. Otherwise,
there will be no problem.
5 ‘Mild’: The women suffers from the problem, but does not report that it hampers her daily
routine life (household and economic)
6 ’Severe': The problem reportedly affects the woman to such an extent that she is
only able to perform her normal activities with great difficulty
20
Perceived Causes ofMenstrual Problems: Almost half (10 out of 21) the women reporting menstrual
problems stated that their problems commenced soon after sterilization. A similar observation was made in
the case of other RHPs as well. Several women also linked problems such as UT1 and white discharge to
surgical contraception.
Immediately after the operation I would get my periods every 10 days. It is only
since the past few years that it comes at a monthly interval. Now. my periods stink
a lot and come in clots. Also, initially I used to menstruate onlyfor 4 days but after
the operation, it has stretched to 7 days.
Fear of menstrual irregularities or problems also influences women's use of contraceptives. Most of
the women inter* iewed have used family planning methods at some time in the past. Permanent methods
appear to be more popular (64%) once the desired family size has been achieved (see 'fable 1). Other
women reported that they do not use any contraceptives as they feared that their flow would become more
profuse and/or irregular. This fear appeared to be particularly acute for the use of Copper T.
Several other factors were believed to be responsible for problems related to menstruation:
"excessive" intake of hot (garain) foods or medicines could cause garmi, and result in menstrual problems.
Treatment Seeking Behaviour: Several efforts are made by rural women to get relief not only from
menstrual problems but also from associated aches and pains. While some reported taking home remedies
for their problems, others seek prompt medical treatment particularly if their problems persist.
During the visit to the villages, women gave examples of traditional modes of treatment for
excessive menstruation. One treatment is to consume a mixture of fennel seeds and lump sugar (khadi
sakar) which has been soaked overnight. This is believed to cool the body (bring thandak) and thus reduce
the menstrual flow. Other foods that were perceived as "cooling" are gum of acacia (gundar), milk and
banana. In contrast, those with scanty flow are advised to drink a solution of ground black pepper and water
as the heat (garmi) generated by this spice is believed to enhance the flow.
Some of the women (10 out of 21 reporting menstrual problems) did not seek any treatment. Most
of these women reported recent onset of their ailments. The major reasons stated for hesitating to approach
health providers were 1) fear of a gynecological examination: 2) problems of commuting; and 3) financial
concerns. One woman expressed her hesitation in seeking treatment from a doctor because the provider
misdiagnosed her case as an irregular menstrual cycle, although she was actually pregnant.
My menses had not come for one and a halfmonths. I had consulted a private
doctor at a nearby village. The doctor gave me 1.0 capsules, each costing Ils. 3.
After taking the capsule, the bleeding started. It was so excessive that I was
21
immediately rushed to the SSG Hospital (the districts civil hospital) in the night. 1
was admittedfor 10 days. The doctor told me. 'You are lucky to have come here in
lime. Had you come later, by an hour, it would have been difficult to save you!
When I asked the doctor what the problem was, he told me 'You were pregnant,
who advisedyou to take the capsule ? It is the medicine which caused the bleeding
(abortion).
However, women were more prompt and particular about seeking treatment for problems related to
menstruation than they were for RHPs. This could be because they considered such problems to be more
serious and a threat to their fertility.
*
The remaining 11 women sought treatment from private (6) or government (5) providers. Pour
women sought treatment only once but ignored the problem when it recurred. Others sought treatment
initially as w'ell as whenever the problem reoccurred. Thus, private practitioners (RMP/ MBBS) and
government doctors were equally popular sources while seeking medical treatment for menstrual problems.
However, only two of the women reported that they got relief from the menstrual problems from the
prescribed medicines.
While three women made the decision to seek treatment on their own, five were encouraged by
their husbands to approach health providers.
Hysterectomy
A recent trend is the practice of resorting to hysterectomy as a permanent solution to menstrual problems, as
well as freedom from social norms and restrictions observed during menstruation. At times, the magnitude
of social restrictions is so enormous that a hysterectomy is seen as salvation from all anxieties. Even
women with apparently no physiological problems yearned for a hysterectomy rather than other sterilization
operations once they had achieved their desired family size. During the household survey 22 (2%) of the
1067 married women contacted reported that they had opted for hysterectomies. Besides, several women
enquired eagerly of the possibility' of camps in their villages for this purpose.
In this regard, one of the doctors (MBBS) providing mobile health services for a local NGO said.
There is a great demandfor hysterectomies in rural areas. Only afew women had
a hysterectomy because it is a costly operation and the service is not as easily
available as sterilizations which are conducted during (sterilization) camps at the
village level.
22
Among the 68 women who were selected for the study, 12 wanted to get their uterus removed.
Some of these women viewed hysterectomy as a long term solution and believed that opting for surgery was
more practical than consulting doctors at regular intervals.
On thefirst day ofmy menses, the pain is so severe that 1 roll on the floor.
clutching my stomach
Ifeel that there is something wrong with my uterus, so 1
want to get it removed.
Other women reported that they were tired of the restrictive behaviours and the resultant
dependency on others' help for household chores and hence wanted a hysterectomy. One of the woman
commented.
As ire are born as women. >re menstruate. 1find it very irritating. We have to
follow so many restrictions during that period as we belong to the Foolmali
community. My children are very small, so I have to depend on others to cook the
meals. I wanted to get my uterus removed, my husband had also agreed. But my
mother-in-law did not allow me to. I wish my periods would go away. Do you have
any tablets so that my periods can stop?
Usually, government hospitals advocate hysterectomy only for cases with severe physiological
problems. It has been observed that often wealthier rural women with no physiological problems get their
uteruses removed at private clinics at a fairly high cost of Rs.7000-8000. This amount was unaffordable for
the poor, who reportedly save for months together to have a hysterectomy done.
Only one out of 68 women had undergone a hysterectomy operation. She opted for the surgery due
to post sterilization complications. She said:
After the operation (sterilization), 1 had problems related to my MC. Sometimes it
would reoccur within a span of 10-12 days. The cycle was not regular. 1 suffered
like thisfor one and a halfmonths andfinally got my uterus removed.
By then
I had spent around Rs. 4000-5000 on treatment.
Conclusion And Recommendation
Views and Beliefs about Menstruation
Menstruation is viewed as a natural phenomenon by rural women. It is believed that menstruation is
necessary to dissipate heat (garmi) and disease from the body.. Women arc aware that menstruation signals
that the body is prepared for reproduction and that it is important for procreation. However, they do not
understand the timing of ovulation during the menstrual cycle. In other words, they are unaware of the
periods that are safe and unsafe for conception.
23
Menstrual flow for a period of 4 to 5 days, at a one month is perceived to be normal. Any variation
in this pattern causes considerable anxiety, worry and apprehension among women. Menstrual How for 1-3
days is considered scanty and 'abnormal' by women and is seen as a threat to their fertility. By and large
women do not have a negative attitude toward menstruation despite the fact that all reported having some
RHPs.
Women's Experience At Onset Of Menstruation
Age at onset of menstruation is reported to be around 14 years. The first experience is stated to be
‘shocking1 and ’frightening'. Prior knowledge about menstruation is rarely given to young girls and mothers
do not believe in discussing this matter with their daughters. A peer group is the main source of information
on menstruation for most of girls, and it is from peers that they also gradually learn about the connection
between menstruation and reproduction.
The onset of menstruation is nevertheless celebrated among household members by preparing
sweets.
Effect of Menstruation on Women's Daily Lives
Menstruating women have to maintain a certain degree of isolation because they are considered ‘impure1
and ‘polluted’ Sexual abstinence is observed during the days a woman is menstruating because of the fear of
transmining impurity and disease to the partner. Sex during menstruation is perceived as ’dirty'. While
religious restrictions are followed by almost all women, other social restrictions and norms are observed to
varying degrees. The restrictions are more rigidly practised among Hindus than among Muslims. These
restrictions limit women's abilities to perform domestic chores and have a significant impact on their lives.
Hence, they often resort to the irregular and inappropriate use of oral contraceptive pills to postpone their
menstrual cycles.
Women express a desire to have hysterectomies to relieve them from the social and cultural
restrictions once the desired family size is reached. There is also an increasing trend among women who
prefer a hysterectomy (big operation) to a tubectomy (small operation) for the double advantage of
contraception and ending menstruation.
24
Menstrual Problems and Treatment Seeking Behaviour
Menstrual problems are perceived as 'serious' and women seek prompt medical treatment from private or
government providers. These problems are largely attributed to 'garmi' caused by (a) hot or sour foods; (b)
sterilization and (c) allopathic tablets. Since menstruation is believed to be necessary for dissipation of
'garmi", women who have scanty periods think that the heat gets accumulated in the body. The
accumulated heat (garmi) manifests as eruptions on the body or prevents conception or results in profuse
bleeding. Hence for most of the menstrual problems, women seek treatment (at home or outside) that would
cool the bods' (thcmdak ni data).
An explanatory model showing relationship between causes of'garmi1 and menstrual problems is
shown in Fig. 2.
Recommendation
It is recommended that programmes that aim to address the reproductive health need of women should
focus on:
•
developing a comprehensive information, communication and education (IEC) programme
targeted towards adolescent girls to educate them on issues related to menstruation and
reproduction.
•
preparing a simple procedure to calculate the timing of ovulation to prevent unwanted
pregnancies and the practice of induced abortion.
•
counselling by health care providers on irregular and inappropriate uses of oral
contraceptive pills and unnecessary hysterectomies.
Further research needs to be undertaken to understand the treatment seeking behaviour of women
suffering from reproductive health problems and the process of deciding to seek treatment. There is also a
need to quantify the extent of misutilization of oral pills for postponing menstruation as well as number of
women who have undergone medically unnecessary hysterectomies.
25
References
Srinivasa, D.K. 1977. Aspects of knowledge, attitude and practice related to menarche. J. Family Welfare,
23(3): 28-36.
Koinura, H., A. Miyake, C.F. Chen, 0. Tanizawa and H. Yoshikawa. 1992. Relationship of age at menarche
and subsequent fertility". Eur. J. Obstet. Gynaecol. Reproductive Biology. 44(3):201 -3.
Koff, E. and J. Rierdan. 1995. Early adolescent girls’ understanding of menstruation. Women Health. 22(4)
Van Woerkens. M. 1990. Dialogues on first menstrual periods. Economic and Political Weekly. 25(7): WS7WS14.
George, A. 1994. It happens to us: menstruation as perceived by poor women in Bombay. In: Listening to
Women Talk about their Health Issues and Evidences from India (edited by: Gittelsohn, J., M.E. Beatley,
PJ. Petto, M. Nag, S. Pachauri, A.D. Harison, L.T. Landmark. Har-Anand Publications, pp. 168-183.
Chaturvedi, S.K., P.S. Chandra. 1991. Socio cultural aspects of menstrual attitudes and premenstrual
experiences in India. Social Science Med.. 32(3):349-351.
Dennis, R. 1992. Cultural Change and the Reproductive Cycle. Social Science Med. 34(5):485-489.
Moghissi, K.S. 1988. Treatment of endometriosis with estrogen - progestin combination and progestogen
alone. CH Obstet Gynecol. 31:823-828.
Bhatia, J.C. and J. Cleland. 1995. Self reported symptoms of gynecological morbidity and their treatment in
South India. Studies in Family Planning. 26(4):2O3-2I6.
Patel. P. 1994. In: Listening to Women Talk about their Health Issues and Evidences from India. (Edited by:
Gittelsohn. J.. M.E. Beatley, P.J. Petto, M. Nag, S. Pachauri, A.D. Harison, L.T. Landmark). Har-Anand
Publications, pp.168-183.
Purkayastha, S. and P.K. Bhattacharyya. 1992. Aftermaths of surgical sterilization with special reference to
menstrual disturbances.” J. Ind. Med. Association. 90(2):29-30.
Lethbridge. DJ. 1992. Post-tubal sterilisation syndrome. Image J.Nurs. Sch., 24(1): 15-18.
Rulin, M.C.. A.R. Davidson, S.G.Philliber, W.L. Graves, and L.F. Cushman. 1993. Long term effect of
tubal sterilisation on menstrual indices and pelvic pain. Obstet-GynecolXl(I): 118-21.
26
Table 1: Profile of Selected Women in Rural Areas
Characteristic
Age (years)
£35
>35
Marital Status
Married
Separated
Children (no.)
£3
>3
none
Type of Family
Nuclear
Joint
Religion
Hindu
Muslim
Occupation
Agri/casual labourer
Housewife
Cultivator
Others (petty business, etc)
Education
Illiterate
Primary
Middle & above
Age at Menarche (years)
Before marriage
After marriage
Age at 1st conception (years)
£ 18
> 18
NA (Not conceived)
Attained menopause
No
Yes
Use of Family Planning Method (Current)
Permanent method
Temporary
Women reporting menstrual problems as their major RHP
27
Sample
(N = 68)
N
%
51
17
75
25
67
1
99
48
13
7
71
19
10
44
24
65
35
55
13
80
19
28
24
9
7
41
35
13
II
30
27
I]
44
40
16
40
28
59
41
48
13
7
71
19
10
67
99
7
42
i6
21
62
38
31
Sample
(N = 68)
N
Characteristic
Types of menstrual problems reported*
- irregular bleeding
- profuse bleeding
- scant)' bleeding
- unnatural bleeding (black, stinks etc.)
- painful bleeding
- prolonged bleeding (>7 days)
Hysterectomy
Do not desire
Desire
Undergone
%
6
6
6
5
5
2
55
81
18
1
* Multiple responses
(Other RHPs reported were white discharge 79%. Uriiio genital problems 51%, Uterine disorders 4% and
infertility 7%)
28
Table 2 :
Norms and Practices Observed During Menstruation by Women
Taboo Activity
Religious activities
Sleeping and intercourse with husband
Attending social occasions (babri@/ marriage/ etc.)
Cooking/ filling water
Touching anyone (except infants)
Working inside the house
Sitting/sleeping inside the house
Touching dry clothes
Filling water in copper vessels
Economic activities/ work
Percentage*
97.06
94.12
79.41
58.82
35.29
17.65
7.35
5.88
4.41
1.47
♦Data computed on the basis of using a Guttman's scale exceed 100% due to multiple responses.
@ babri is a ceremony among Hindus where a boy's head is shaved for the first time.
29
FIG.2 : INTERRELATIONSHIP BETWEEN CAUSES OF GARMI’(BODY HEAT) AND MENSTRUALPROBLEMS
Scanty Periods
Poor/Vitality
Intake of
Eyesight
Sterilization
Hot or Sour Foods
Allopathic
Tablets
(Retains Body Heat)
Menopause
Increase
GARMI
(Body Heat)
(NO Menses)
j
Profuse
Menstruation
Poor Chance
of Conception
Eruptions on
Entire Body
Accumulation of
Garmi in
Private Parts
I
I
T---------
Opt for
Less Blood
Sexual Intercourse
Hysterectomy
in body
during MC
I
Transmission of
Weakness
infection to Partner
Seek Treatment
that cools body (Thandak ni dava)
CaJ H
Women's Environment & Development Organization
News & Views
Bo
Vol. 6, No. 1
April 1993
Does the Breast Cancer Epidemic Have Environmental Links?
WEDO and New York's Commission on the Status of Women Hold Joint Hearing
s there a breast cancer epidemic? “If one in eight women now get
breast cancer when it was one in 20 just three decades ago, I would
I
NBC New York reporter Carole JenJdns interviews Dr. Devra Lee Davis, an
. : rvironmemal medicine, at the WEDO-New York City Commission on
the Status ofWomen hearing on breast cancer chaired by Bella Abtug.
WEDO'S FUTURE
An Editorial
call that an epidemic,’’ said Dr. Devra Lee Davis, Visiting Professor in
the Department of Environmental and Occupational Medicine at Mount
Sinai Medical Center in New York and Scholar in Residence at the
National Research Council of the National Academy of Sciences.
“Why are women in their sixties getting more breast cancer than
ever before?" Dr. Davis asked. "They’ve had their kids, they’re not
alcoholics, we can’t explain it by known risk factors. But they were
*Rosie-the-riveters’ during World War H, and ever since they’ve been
exposed to new industrial materials, new household chemicals and pes
ticides." Increased detection by mammography can’t account for it, she
said, for "breast cancer deaths increased 1% a year in the U.S. both
before and since mammography.”
Along with some two dozen other experts and concerned citizens.
Dr. Davis testified at a March 2nd public hearing on possible environ
mental links to breast cancer—focusing in particular on pesticides and
on extremely low levels of radiation from nuclear power plants and
electric power lines (electromagnetic fields).
The hearing was organized and held by WEDO and the New York
City Commission on the Status of Women, both chaired by Bella
ollowing the UN Earth Summit in Brazil last June .and the
Abzug, at City Hall, as part of WEDO’s ongoing Women for a Healthy
tremendous breakthroughs WEDO and the women it support
Planet program.
F
ed were able to achieve there, and with the success of the
Women’s Tent, Planeta Fernet^ at the parallel grassroots Rio ’92
Global Forum, it was time for WEDO to focus on its future and
the tasks ahead for a young, but strong and trend-setting
organization.
The decision was to continue—to grow and expand the net
work of WEDO women so the message and the methodology
could be strengthened for the all-important follow-up to the Earth
Summit and related milestones in the near future: the 1993 World
Conference on Human Rights, the 1994 International Conference
on Population and Development, and the 1995 Fourth World
Conference on Women.
But as we extend our Women’s Action Agenda and advocacy
efforts for sustainable development into related fields such as
human rights, population and democracy, WEDO also recognizes
that it must expand its base by embracing more and more women
activists around the world in its work.
continued on page 2
• This docx not mean you have a one in right chance of breaat cancer now, but
that you may be one of right who could develop the dricase if you live to 85.
better fam fatamfa,
Dear Mrs. WEEK), the letter begins.
The writers live in Comuneros, a squatter settlement not far from the Colombian capital of
Bogotl Seven years ago, 18 families migrated there from the city center. Now, the writers say, there
are 159 members in the compound. They make their living by recycling. (The photos they enclosed
show their situation.) 'The level of life is low and now is tending to get worse.”
“Our principal preoccupation is the environment conditions and the health of children,” who,
they report, suffer from respiratory difficulties, dermatitis, underfeeding and stomach disease.
“We think that the diseases are related to the environmental conditions,” and so, they say, “it's a
community where we can use the WEDO’s report card.”
A group of women, with
support from a local NGO,
are starting to deal with their
problems. They are organiz
ing a cooperative to improve
the recycling process so they
can “reach a better quality of
life.”
They are “Waiting
your news” (see page 4), and
the letter is signed:
.Sm/uc.
and
WEDO-City Hearing Examines the Environmental Links to Breast Cancer
Continuedfrom page 1
Although the causes of breast cancer—
now the most common cancer in women—are
not completely clear, this doesn’t mean we
shouldn’t act. Dr. Davis said: “We know we
can prevent a disease before we know the
cause of it, as we did with cholera in 19th cen
tury England, or lung cancer in this one."
While each expert testified there is a grow
ing body of scientific evidence suggesting a
"There was a 30% drop in breast cancers
when three carcinogenic pesticides were
phased out in Israel." reported Dr. Samuel
Epstein, a Professor of Occupational and Environmental Medicine in the School of Public
Health at University of Illinois Medical Center
in Chicago. Yet, he added, "none of the cancer
establishment’s 5100 million in studies has
focused on organochlorine pesticides."
cess of fission would act very differently from
natural radiation processes or X-rays."
Very small amounts of protracted radiation
are 1,000 times more toxic than a short-term
X-ray, he said, because it affects bone marrow
and the immune system. "Around one nuclear
facility after another, there has been an
increase in cancer," Dr. Slemglass explained.
“But the ‘establishment’ wouldn't accept
epidemiological findings because My
link between breast cancer and avoidable envi
He cited a study of Connecticut women
ronmental contaminants, much more research
on this link needs to be done.
with breast cancer who had 50-60% higher
levels of PCBs and DDT in their breast tissue
“We regret the dearth of research in this
area." Bella Abzug said. “Thar has to change.
We need to find out"
than women without breast cancer. An EPA
study found that U.S. counties with waste sites
were 6.5 times more likely to have elevated
radiation" could cause such effects.
Based on this testimony, findings and rec
ommendations, WEDO and the Commission
will issue a complete report with concrete pro
couldn't understand how a small amount of
One group of women in suburban New
breast cancer rates than coundes without haz
posals for legislative initiatives, public/private
York, concerned about above-average breast
ardous waste sites. An added problem is that
partnerships and other collaborative efforts to
cancer rates in their area, is doing its own
most are sited in poor black or Hispanic areas.
research. The West Islip Breast Cancer Coali
Another factor is radiation, according to
tion is conducting a community-wide study.
They sent questionnaires to every household in
town and, on a detailed map showing every
house and building, have documented every
case of breast cancer. So far, the ongoing study
has found several clusters' of breast cancers,
indicating that the cause or causes may be
environmental.
further investigate the potential causal agents
of breast cancer.
Because these findings show yet another
Dr. Ernest Stemglass, Professor Emeritus of
Radiological Physics at the University of Pitts
connection between women’s and environmen
burgh School of Medicine: “Since the begin
tal issues and in particular how they are nor
ning of the century we have known that radia
tion of all types induces cancer. What was not
being adequately addressed by decision-mak
ers, WEDO will use this information to
known was how nuclear reactors and nuclear
encourage women to set their own health-care
testing would create such sudden, great
priorities and agendas through its Community
changes, that radiation produced by the pro
Report Card project.
10
WEDO Helps Grass-roots Women Get Access to the 4th UN Women's Conference
en years after the end of the UN Decide
T
ing degrees to improve the economic, social
na. local and national meetings are planned by
for Women (1976-85), women from every
and political status of women, to end discrimi
women's groups around the world. Official
part of the globe will gather in Beijing, China,
nation against them and ensure their equal par
UN regional meetings will be held in 1994 in
September 4-15, 1995, for the UN Fourth
ticipation in society.
World Conference on Women: Action for
The Decade's final, comprehensive state
Equality. Development and Peace. Some will
ment, The Nairobi Forward-Looking Strate
come as members of official national delega
tions. composed of men as well as women.
Others will be members of women’s groups to
participate in a parallel forum of non-govem-
gies for the Advancement of Women, later
approved by the UN General Assembly, pro
vided a framework for renewed commitment
by governments and the international commu
mental organizations (NGOs) that, hopefully,
nity to act on the growing worldwide women's
will have a direct impact on Conference
decisions.
movement demands for equality with men.
Although the 84-page document reflected limi
5VEDO Challenges Restriction
In an action alert memo sent to its interna
tional network in early March. WEDO warned
tations imposed by male-led governments, it
was unprecedented for its time, setting forth an
action agenda that ranged across all aspects of
that a policy approved by the UN Commission
social policy, with special emphasis on the
on the Status of Women (CSW). which has
needs of poor women in urban areas and
developing countries.
responsibility for conference preparation,
might severely restrict participation of grass
Conference Goals
roots women’s groups in the 1995 event
In contrast to the open access policy that
The Beijing conference will have three
essential tasks:
allowed broad participation and input by
1. Evaluate what UN member states have done
women into the UN Conference on Environ
to implement the Forward-Looking Strate
ment and Development, the CSW initially
gies. Each nation must present a formal
decided that only organizations accredited to
report; WEDO and other women’s groups
the UN Economic and Social Council
will evaluate what has and has NOT been
done;
(ECOSOC) and interested international NGOs
would be allowed to participate.
2. Update the document with new action rec
WEDO and other women’s groups suc
ommendations to correspond with changing
cessfully challenged this restriction at Vienna
conditions over the last decade;
meetings in March of the CSW and the NGO
Separatory forum. WEDO Co-Chair Bella
3. Develop new strategies for women’s
Abzug, in the action memo, urged women to
For the 20,000 women from all countries
advancement.
press the CSW and their governments to allow
who took part in the 1985 meeting at Nairobi,
full participation by grass-roots women’s
it was an inspiring experience in which they
groups, particularly from the developing
nations, in every phase of the process from
learned from each other, strengthened existing
regional meetings to the Beijing conference
home with hundreds of new ideas and exam
In response, the CSW agreed to follow the
expanded access procedures accepted for the
Commission on Sustainable Development and
the 1994 Population Conference in Cairo.
Decade of Women
networks and built new ones, and returned
ples of what women can accomplish when
they act together.
Preparations for the 1995 World Women’s
Conference are already underway at the UN
Division for the Advancement of Women in
Beginning with the UN International
Vienna. The Conference Secretary-General is
Women's Year in 1975, three world confer
Gertrude Mongella, formerly Tanzania's
ences on women's concerns were held at five-
ambassador to India and an active member of
year intervals: Mexico City in 1975, Copen
hagen in 1980 and Nairobi in 1985. All three
WEDO’s International Policy Action Commit
tee (IPAC).
approved recommendations designed in vary
In addition to the March meetings in Vien
Senegal, Indonesia. Argentina and West Asia.
No official meeting has been scheduled yet for
Europe, the U.S. and Canada.
WEDO’s Objectives
WEDO, as an international network of
women concerned with environment, develop
ment, social justice and an equal role for
women, is making the 1995 conference a
major focus of activity..
Our objectives are to ensure the maximum
inclusion of women in official delegations to
the Beijing meeting and the maximum access
for women from NGOs and grass-roots groups
to present relevant sections of our Women’s
Action Agenda 21 on environment, develop
ment, gender balance and other proposals, par
ticularly in the regional meeting and — morato
ry process, as well as at '
for inclusion in the ftru
document, which will be.
UN General Assembly.
agio.
y the full
The past 10 years have brought tremen
dous changes for women, some positive, some
negative. Women’s movements, nationally and
internationally, are growing in influence and
strength. In the industrialized nations women
continue to break down legal social and politi
cal barriers to their full participation in society,
and grass-roots women’s groups can be found
in almost every developing nation in the
world. But in the aftermath of the collapse of
the Soviet bloc and the rise of ethnic hatreds.
violence against women, attempts to deprive
women of reproductive rights, growing impov
erishment, hunger, homelessness and illness,
the world in many ways has become a more
dangerous place for women and their families.
The new Forward-Looking Strategies that
will emerge from The Fourth World Women's
Conference must reflect women's expanding
needs, and this can happen only if women
from every nation and region are activated to
participate in the decisions that shape their
lives. WEDO expects to have a major role in
informing and mobilizing women for this
effort. If you want to participate, contact
WEDO.
Inside: Looking Back 16 Years
Fivndinfi {acid cfawge. Zivice. /$67
ISSN0897-2613 • Vol.2#4
A Call to Resist Illegitimate Authority
April, 1993
Environmentalists and Breast
mcer Activists Tell New York
Co> mission: ACT NOW!
IA. .ANA SCHREIBER
On March 2nd, the New York
City Commission on the Status of
Women (CSW) and the Women's
Environment and Development
Organization (WEDO) held a public
hearing to address the connection
between breast cancer and the envi
ronment. More than thirty environ
mentalists, cancer activists, cancer
researchers, public health officials and
politicians addressed the commission
ers in the hope that their testimony
could spur legislation and halt the
ferocious pace at which this disease is
killing women.
Bella Abzug (center), Chair of the New York City Commission on the Status of Women, and Dr. Dcvra Ixc
Davis (right), of Mt. Sinai Medical Center, being interviewed by Channel 4, March 2, 1993.
The hearings covered potential
Photo: Lise Beane, Women's Community Cancer Project
risk factors including: pesticides and
earlier issue of the RESIS T newsletter National Womens Health Network,
other toxic chemicals; radiation expo
(#246,
May/June 1992) here we will 1325 C Street, NW. Washington, DC
sure from power plants and nuclear
testing; electromagnetic fields; hor provide edited testimony from a por 20005. or call (202) 347-1140.
tion
of
the
hearing, focusing on infor
mones in food; reproductive technolo
mation that was not in the earlier BELLA ABZUG, Chair of both the
gies such as Depo-Provera; and mam
article. For more details, contact the CSW and WEDO, opened the hearing:
mography. In addition, activists in
CSW, 52 Chambers Street, Suite 209,
Long Island, New York City and
Boston reported on their work and
NY, NY 10007. lei. (212) 788- I am here today as the chair of two
2738. For a report on mammography organizations, one local, the other interupcoming plans. Because we have
addressed many of these issues in an for women under 50, contact the
<
^Hearing________________
\ jbtiond’ but I30'!1 dedicated to making
better world: the New York City
Commission on the Status of Women
and the Women’s Environment and
Development Organization. We have
come together to explore, for the first
time ever in a forum of this kind, grow
ing scientific evidence of a link between
the incidence of breast cancer and envi
ronmental factors.
Our ultimate goal is to bring pres
sure to bear on local, state and federal
public health policy makers to broaden
the parameters of the scientific inquiry
so that more resources, both financial
and scientific, can be redirected toward
^finding causes that will lead to the pre
vention of a disease that is killing
44,000 women every year. This is a
responsibility that society has to face.
Seven out of ten women who will come
down with the disease will have no
dying today than ever before, how can
this not be an cpjdcmic? The word epi
demic comes from the Greek and
means “among the people.” Breast can
cer today afflicts one out of every nine
women by the age of 85. Three decades
ago it affected one in 20. Is that not an
epidemic? Some people have suggested
answer has something to do with the
unusual environments they encoun
tered in the newly industrializing work
place, and then later in those sparkling
clean domestic environments that they
were encouraged to maintain in their
households, with all those brand-new
chemicals that were used indoors, mate
that this epidemic is nothing more than
rials you purchased at the drug store
the fact that we are getting better at
detecting cancer. Let me tell you why
and hardware store, such as pesticides
which are banned today.
We can explain only 30% of the
cases of breast cancer. [I.E., only 30%
of women who get breast cancer are in
this is not likely to be the whole expla
nation. The most important reason is
that we don’t even know how much
mammography is taking place today. so-called high-risk categories such as
There is no national survey of mam having a family history of breast can
mography. The estimates of the rate of cer.] So what accounts for the rest?
the mammography have developed According to several new studies (see
from a Gallop poll conducted for the RESIST ft 246) women with breast
American Cancer Society of its general cancer have increased levels of certain
ly well-educated, upper middle class chemicals (40-50% more residues of
volunteers, most of whom are quite PCBs and metabolites of DDT] in their
health-conscious and almost all of
[breast] fat. This should come as no
known risk factors to explain it. We
whom can get reimbursement for their
think it is time we step up our efforts to
look for causes, without abandoning
our commitment to developing better
and better treatment protocols.
mammograms. For rest of the public,
surprise, as experimental studies in ani
mals have indentified a number of caus
One of the reasons that were in the
situation we are in is that for too long
medical research, and other forms of
scientific research, have often eliminat
ed the participation of women in mak
ing their findings. Now that’s beginning
to change, and the participation of so
many women, many of whom are here
-today, have helped to do that — to cre
ate a public outcry about women with
AIDS, who for a long time were
ignored by the CDC; about women
and heart disease; and now, in the ques
tion of cancer itself.
Why Look at Environmental Risks?
DR. DEVRA LEE DAVIS, a visting
professor in the Dept, of Environmen
tal and Occupational Medicine at Mt.
Sinai Medical Center, and founding
director of the International Breast
Cancer Prevention Collaborative
Research Group:
we really don’t know what the rate of es of breast tumors. We have failed to
mammography is.
pay attention to the animal studies. The
But I can tell you, one reason lively debate about the role of dietary
mammography cannot explain all of the
increases in breast cancer is that the
increase is occuring not just in new
cases, but in deaths, and the increase is
occuring not just in the United States, chemical exposures, the evidence
but in most of the major developed remains incomplete, but is tantalizing
countries of the world, and in some of and growing.
those countries there is no mammogra
All of the known risk-factors that
phy screening of young women.
can be identified for breast cancer can
The two biggest risk factors for be linked to estrogen. But guess what?
breast cancer are sex and age. We can
tell you what women want. We want
better treatments for those of us who
are at risk, which is all of us. We want
safer and. more effective screening tech
Estrogen is not just something that you
make inside yourself. It is influenced by
chemicals. That is to say, those pesti
cides and toxic chemicals that you are
taking into your body — in animals,
niques. For our daughters and their
[were associated with] increased levels
children, we want to prevent the disease
of estrogen. Why should they not do it
in humans? The common link of all of
from claiming as many of them as it
will us. We want to know why relatively
the known and suspected risk factors
more women in Bella Abzug’s genera
for breast cancer could be this: there are
tion, women now in their sixties, are
dying of breast cancer. From all we
compounds we call xeno-estrogens,
which although foreign to the body,
once taken into the body increase the
know about breast cancer, they should
have less of the disease. After all, they
had children earlier in life, and they had
Some of our colleagues have said breast
more of them.
cancer is not an epidemic. I want to
know, if relatively more women arc
So why are these mothers of the
baby-boomers dying more? Maybe the
VaL 2. >4
fat may not be so polarized if the issue
becomes what’s in the fat, not just the
fat itself. As to other causes, such as
electromagnetic fields (EMFs) or other
RESIST New,letter
total amount of estrogen you are
exposed to. That could be the link here.
We are trying to pursue that research.
Why have we paid so little atten-
nntinueJan next page
Page Five
LETTERS
Dear RESIST,
On behalf of the Union of Palestinian
Women’s Associations (UPWA), we wish to
express our sincere appreciation for the con
tinued support we’ve received. [Your recent
grant] to UPWAs Leadership Development
Program will result in expanding and
strengthening this important program
designed to develop the leadership capacity
of Palestinian Arab women community
organizers.
We also wish to recognize the impor
tant and valuable role of RESIST in provid
ing crucial funds and assistance to many
excellent groups working for peace and
social justice; which allows organizations
like [ours] to continue developing its pro
grams while working within the broader
movement for peace, justice, and equality
to effect social and political change.
We feel honored and proud to be a
grantee of RESIST, a truly unique founda
tion whose dedication and commitment to
the struggles of women, and peoples in
communities of color spans a period of over
25 years and continues to be source of cm-
powerment and hope for us all.
Finally, we wish to extend special con
gratulations to the dedicated board mem
bers and staff of RESIST on the occasion
of the foundation’s 25th Anniversary Cele
bration. May our combined efforts con
tribute to a better society for all our future
generations.
I need to get six to ten copies for commit^
members.
Many thanks for the great work you
are doing. It boggles my mind that so few
of you can do so much.
Sincerely,
Virginia Senders, PhD
Shutesbury, MA
Khariyeh Abudayyeh and Mahajarad
Union of Palestinian Womens Associations
Chicago, IL
Ed. Note: Gee thanks! This is what it’s all
about. We’re very happy to provide 10- 20
copies of the newsletter for free for orga
nizing purposes if we have enough extras
Dear RESIST,
available.. For more than that, we may
What a superb newsletter you put out! have to charge for postage, so call or write
It’s always good, and sometimes it’s superb. to ask ifthere are enough and how much
I read the February issue with great interest it will be. For back issues of "Breast Can
and, moved by the call not to accept cer and the Environment, “ (1/246, May/
NAFTA but to organize, took it to my June, 1992) we are charging $1.00 per
church (very main-line Protestant) Peace copy because we had to re-print the issue
and Justice Committee. I proposed that we to fulfill requests. Please write with com
do some study of NAFTA and then perhaps ments, criticisms and suggestions for
move on to action. There was some resis future articles.
tance, but eventual agreement that everyone
would at least read the newsletter, and we
would make further decisions after that. So
ILLEGITIMATE AUTHORITY
Far MraewaMea -4 r>*
ta:
RmW. Oar y«—w 14.. Siwir.M., MA F2J4J
The RESIST Newsletter is published ten
times a year by RESIST, Inc., One
Summer Street, Somerville, MA 02143.
(617) 623-5110. The views expressed in
artidcs, other than editorials, are those
of the authors and do not necessarily
represent the opinions of the RESIST
staff or board.
RESIST Staff.
Nancy Wechsler
Nancy Moniz
Newsletter Editor: Tatiana Schreiber
Typesetting:
W Graphics
Printing:
Red Sun Press
Printed on Recycled Paper
Page Two
RESIST Newsletter
---------
April 1993
Cancer Hearing
eontinueJfrom pagefive
tion to preventing a disease that afflicts
so many women? One reason is that
prevention is less glamorous. But also,
think about this: fewer profit if we pre
vent the disease. More profit from it’s
treatment. Although this country now
spends about 14% of its GNP on
health care, we have devised no new
cure for advanced breast cancer in two
decades. We spend five times more on
chemotherapy than is spent in England,
but we have no better record on cancer
deaths. We cannot afford to keep on
with the same old ways. If we could fig
ure out how to prevent only 20% of all
cases, we will have spared 35,000
k women and their families from the
” sometimes disfiguring, and often dis
abling experience of breast cancer.
[Currently there is debate in
Congress about the value of the
Delaney Clause which forbids the addi
tion of cancer-causing pesticides to pro
cessed foods.) We have had a failure in
this country to regulate pesticides ade
quately and that failure is evidenced by
a number of recent studies. We know
that dogs whose homeowners use resi
dential pesticides die of increased rates
of certain cancers. We know that in
some homes where children have been
exposed to pesticides indoors, those
children have increased rates of brain
cancer and leukemia. We have growing
evidence that there may be an link. The
problem with the Delaney Clause is the
public has come to believe that we are
protected against these exposures. The
Delaney Clause has absolutely nothing
to do with such things. It does not
apply to what you spray in your house
or put on your lawn. In addition it docs
not provide any protection for those
who are at most risk, who are farmers
and gardeners.
We know from more than 20 stud
ies in 8 different countries that farmers
are at increased risk for certain cancers
that we think are associated with their
exposure to pesticides. What we need is
a comprehensive reform of pesticide
regulation in total. It may mean chang
ing Delaney, but not to make it weaken
rather, to make it more comprehensive.
Page Six
Tatiana Schreiber ar the March 2rxl hearing in NYC.
ABZUG: We hope that’s what will hap
pen, but to make sure, those of you
who are interested should write to
Carol Browner at the EPA and let her
know what you think.
Radiation Exposure and Breast
Cancer
DR. JAY GOULD, medical statistician
and economist, and Director of the
Radiation and Public Health Project,
sponsored by the Commission for
Racial Justice of the United Church of
Christ. He is the coauthor, with B.
Goldman, of Deadly Deceit: Low-
Levi Radiation High Level Cover-Up:
In the period between 1935 to 1944,
before the nuclear age began in 1945,
there was an actual decline in breast
cancer incidence; if it had continued
until today, the incidence of cancer in
women between 50 - 74 would have
been half of what you see today. I’d like
to call your attention, as a statistician,
to the data I’ve gathered, based on
information from the National Cancer
Institute. What [my the data show] is
that the increase in breast cancer really
began with rhe nuclear age in 1945.
But you also sec that in 1970 after the
opening of the Millstone reactor [on
Long Island Sound] you had another
increase which is so large it’s impossible
to escape the fact.
RESIST Neunleller
activist group, being interviewed by RESIST editor
Photo: Lise Beaoe, Wotuen'i Community Cancer Project
[In addition,] after 1979, the date
of the Three Mile Island accident, there
was an enormous national increase
which apparently peaked in 1988, seven
years after the accident. The other chart
shows that in the country as a wh-4e,
because civilian nuclear reactc
.e
concentrated .in rhe northeast part of
the country, you have very high per
capita exposures in those regions
[strongly] correlated with very high
breast cancer rates. Whereas in regions
with very few reactors, like the moun
tain regions and places like Texas and
Louisiana, where male cancer rates are
extremely high because of exposure to
petrochemical contaminants in the
environment, the amazing thing is that
because of the relative lack of radioac
tive emmissions from nuclear reactors,
breast cancer rates in those states are
extremely low.
Now the probability that this kind
of effect could be produced by chance is
so small it’s inadmissable. It means that
the scientific community has to find
out: why do we have this correlation?
The Millstone Plant, in particular, is
only 12 miles away from Suffolk Coun
ty. From 1970 to 1975 it had enormous
emmissions of radioactive iodine and
strontium, two of the most lethal
radionuclides, known to be highly car
cinogenic, and which concentrate in
milk and water and other foods. This
kind of exposure simply has to be inves-
April. 1993
■<
'
icer Hearing
^continualJam page seven
Westchester, where they continued to
use the Croton water supply, a few
miles downwind from the Indian Point
Long Island Women Take Action
Abram Pektkau] that the small protract
plant, there has been a continuing and
West Islip Breast Cancer Coalition.
ed radiation emissions over a long peri
od of time produces much greater dam
sharp rise in cancer rates. The same
thing has been happening on Long
age to cell membranes through the
formation of free radicals which attack
Island.
It is my recommendation that we
less than one year ago after I was diag
cell membranes and puncture them in
look immediately at ways to set up a
friends who have this disease, who live
matter of a few minutes to hours; as a
result, very small amounts of radiation
commission to reexamine whole ques
in West Islip. I felt that this was more
than just a coincidence. I needed to
It was not until 1972, 30 years into
nuciear age, that it was discovered [by
are typically 100-1000 times as toxic as
the same [dosage] of a medical X-ray
given in a short time. That’s because
these free-radicals interact and deacti
vate each other, causing them to
become inefficient at high concentra-
^fins but very efficient and deadly at
levels.
Strontium-90 is very dangerous,
because it gives off a very fast beta ray
which can penetrate the bone marrow
and produce an effect on the immune
system of the whole body which
impairs the ability of the body to fight
cancer. These things were only fully
understood in the last 15-20 years.
Over 40 studies in the scientific litera
ture show that around one nuclear facil
ity after another, there has been increase
in cancer, including breast cancer. This
epidemiological evidence is overwhelm
ing, but was not accepted because it was
not understood how a small amount of
radiation could have such enomous
effects.
In fact, the [Petkau effect] causes
)the risk to rise much more rapidly at
low-doses than at high doses, and as a
result, we now find that small releases,
regarded as harmless in the past, are in
fact causing contamination of our milk
and food, and this has never been ade
quately investigated because it was
believed to be too small a dose com
pared to ordinary x-rays or mammogra
phy. We have grossly underestimated
the effects of very small amounts of
radiation added into our drinking water
supply.
Since 1967, New York city has
been able to obtain more than 80-90%
of its water from distant sources in the
Catskills and the Delaware water sys
tion of shutting down Indian Point. We
did not appreciate how dangerous it r
to the water supply of New York City.
And the people of Harlem and the
South Bronx are more heavily exposed
to water from the Croton reservoir than
people from Brooklyn, Queens and
Staten Island, who receive much of
their water from the more distant
sources which are not contaminated by
radioactivity.
We would actually like to see all the
nuclear plants in the country phased
LORRAINE PACE, president of the
Our grassroots organization evolved
nosed with breast cancer. I have twenty
find out what we all have in common. I
must say, living on Long Island is a
delight, but we have one of the highest
rates of breast cancer in the state. Some
how, there seems to be something dras
tically wrong. Risk factors [primarily
being Jewish and affluent] and lack of
education and early detection have been
the explanations we have been given
from our experts. Long Island can no
longer accept these explanations with
out demanding further studies.
[In trying to find out why so many
women were being diagnosed with
out.
ABZUG: OK, well you know this com
mission has limited authority, but we’ll
breast cancer] I discovered that the New
York tumor registry was at least four
work on it.
years behind in their statistics. No one
STERNGLASS: We nbw have an
administration that must show an abili
ty to reduce health costs or it will not
be reelected. We can show that after
could tell me how many women were
diagnosed with breast cancer in 1992.
The statistics quoted were from 1988.
Yet, with one phone call I could find
out who won the New York Stare lot
Three Mile Island was shut down,
infant mortality in Pennsylvania
dropped 30-40% in two years after it
tery, and where their ticket was pur
chased. These priorities are clearly
was shut down. We have an enormous
amount of data, which is ignored by the
military nuclear establishment, which
says that all these health problems have
addressed.
Since there were no current statis
tics available, we decided to do a demo
graphic study of West Islip. Our goal
been vastly aggravated by our refusal to
admit the biological hazards of nuclear
was to locate and visually identify the
bomb testing and nuclear weapons pro
unbalanced and we feel they must be
areas and incidence of breast cancer.
From the beginning we had the assis
tance of Dt. Roger Grimson, a biostatis
tician [at SUNY-Stonybrook], who
duction...
Note: Jay Gould and Dr. Stemglass oversaw the color-coding and mapping
have been asked by members of the process. With the assistance of the Suf
National Breast Cancer Coalition to folk County Health Department and
prepare a report on the role of radio Good Samaritan Hospital in West Islip,
active chemicals in contributing to we have written a single page survey
high breast cancer rates in Long and distributed it to every household.
So far, our response has been over 52%,
Island.
which goes to show that women are
very concerned.
On the map, we have definitely
tem. Since then, the cancer rates in
New York City have declined. But in
continued on next page
RESIST Neuryletter
April. 1993
Hearing
page eight
IRnd certain clusters, consistently on
the whole map. Of about 4500 respon
dents so far, over 300 had malignant
breast cancer, more than 1,000 had
School of Social Work; member of
steering committee of One in Nine, the
Long Island Breast Cancer Action
Coalition; also serves as New York State
grassroots coordinator for the National
ronmental Health to study the relation
ship between the environment and
breast cancer. [The amendment passed
Breast Cancer Coalition [Balaban
in the House by a vote of 283-131, an
recently served as the only Long Island
representative on the panel of the Cen
important victory in this struggle.] We
lies. I think this needs to be thoroughly
investigated. The survey has had anoth
ters for Disease Control which exam
to have an impact on federal legislators.
er effect on West Islip. Nineteen
women who answered our survey said
ined data from a Long Island Breast
Cancer study and concluded that the
high rates of breast cancer in Suffolk
We need support desperately to help
them understand that this is not just a
group of ninny women walking around
and Nassau County were due to
with small cause. This effects every
benign breast disease, and most report
ed other forms of cancer in their fami
they didn’t have breast cancer. Then,
they went for a check-up and found out
they were walking around with malig
nant breast cancer. That’s a lot of
women in one very small little area.
During the Vietnam War, we all
mourned the loss of 58,000 men and
women. During that same ten year peri
od, our nation lost 330,000 women to
breast cancer. They went very quietly,
but it’s time not to be quiet anymore.
[After our first mailing we] went to
our congressman who is from West
Islip. He contacted Revlon, and they
donated $5,000. We did two more
mailings. We’re hoping to get at least a
75% response rate. We'll go door to
door. We’re very determined, we want
to know why we got this breast cancer
and why all our friends got it. We’ve
been working very hard, but we don’t
intend to stop.
We intend to map out where all the
transmission lines are and all the trans
formers, and all the water wells. We
family in this country.
Government officials and their scien
Government sponsored scientists
have told us that we on Long Islai^B
tific representives would have us believe
it’s “the preponderance of women on
Long Island with high risk factors” and
what’s really insulting is that they don’t
think we can do the arithmetic to know
that they still have not begun to look at
the unknown risk factors, those that
cancer cases.
My first suggestion is that we have
to stop referring to “high risk factors.”
These are really the small amount of
known risk factors, which are usually
simply described with no explanation.
There are no studies on why being Jew
One in Nine Convenes its Own
Research Panel
have no place to begin. When I served
on the CDC panel. I raised the ques
would be too expensive. Too expensive
compared to what? The cost of treating
breast cancer? The disruption to a fami
ly? A woman’s life? Too difficult? What
do scientists do when their children tell
them algebra is too difficult? We hope
they aren’t told not to bother, but are
sent back to try harder.
Breast cancer, an epidemic disease
for which every woman is at risk
deserves no less consideration. Today in
BARBARA BALABAN, director of
New York’s statewide breast cancer hot
line and support program at Adelphi's
VoL 2. >4
SPRING
ish or well-to-do causes breast cancer.
Next we have to look seriously at
tion of the environmental impact on
breast cancer incidence. I was told this
was too difficult an area to study, and
stone unturned.
munity support. They then had the
nerve to suggest we redirect our ener
gies toward increasing compliance with
early detection mechanisms, and by
implication preserve the status quo.
continued on next page
what the unknown risks might be.
There’s been a lot of discussion of elec
tromagnetic fields, but as yet, no defini
from EMFs. So far, they have sent a
maybe that’s where these clusters are?
Maybe there’s something else. We don’t
know, but we don’t want to leave one
have done a great job mobilizing com
account for more than 50% of all breast
tion of acceptable levels of EMFs, so we
the addresses, we want to compare,
maybe where there’s a transformer,
need elected officials in every city to try
“known risk factors.”]:
wrote to the Long Island Lighting Co.
and we asked for an address of where
every transformer is, to look ar risk
map, but you have to be a genius to
read the map. I don’t even think they
can read it; we said, please, just send us
I
ammendment calling for a two-year
study by the National Institute of Envi
Washington, a subcommittee is voting
on the National Institute of Health’s
rcauthorization bill. There is a Waxman
RESIST New,letter
Movqs "Project ELF"
located In the
Chequamegon
National Forest In
Northern Wisconsin.
For more information:
Nukewatch
P.O. Box 2658
Madison, Wl 53701
(608) 767-3023
•
Cancer Hearing
cvniiniudfrom page nine
They conveniently forgot that early
detection is not prevention. We still do
not know the cause of breast cancer,
nor do we have a cure.
Well, we women know better than
they what we have to do. On Nov. 1 we
are convening a two-day scientific hear
ing on Long Island. Leading researchers
throughout the country will present
creative ideas on some new directions
we can look to understand more about
the environment/breast cancer connec
tion. [The panel will be headed by Dr.
Devra Davis, and Dr. Susan Love,
director of the Breast Cancer Center at
the University of California in Los
Angeles.] This will be paid for by com^^inity-raised funds, and not one perWn dedicated to the patronizing and
regressive attitudes of previous adminis
trations will be included.
The National Breast Cancer Coali
tion has shown that united, we have a
voice that reaches all segments of the
government. On Sunday May 2nd, we
will rally in Washington, DC to
demand that breast cancer be declared a
national epidemic and be made a top
priority in this country. You, your fami
lies, and your friends are invited to join
us. Together we can make a difference.
We have to, our lives depend on it. In
the time I’ve been speaking, two more
women have been diagosed with breast
cancer. For every two speakers, another
woman dies of this disease. This has got
^^top. Thank you.
0
Looking Back
that you
are
permanently
unable to reproduce instead of
being able to choose the time
when you may have children in
the future.
No existing contraceptive
method is foolproof no matter
how conscientiously used. If
the government and compulsory
pregnancy forces were really
serious about this issue they
would be working day and night
and pouring millions of dol
lars into developing a contra
ceptive method that is both
medically safe and effective.
And even then abortion would
be necessary ip some cases as
a back-up mea.ure. But, of
course, they aren't serious
except about curtailing the
rights of us all. How can we
take a government and a soci
ety's pro-life stance serious
ly when they are the same peo
ple who also brought us the
neutron bomb, a bomb that
kills people and leaves prop
erty intact?
The Supreme Court decision
of 1973
said that it
is
between a woman and her doctor
to decide if she wants to ter
minate a pregnancy. It does
not say that every American
woman must undergo abortion,
it merely says that if she
wants to have an abortion,
as women throughout the ages
have had in a valid attempt to
control their fertility, she
will not have to die in the
attempt.
The Doyle-Flynn bill, the
Hyde Amendment and the Supreme
Court decision are nothing but
sexist and racist attacks on
poor people-. I don't know how
many of you knew Fanny Lou
Hammer, a poor Black woman, a
civil rights activist and
freedom fighter. She died this
year and I just found out this
week that in the early 1960s
she was a victim of forced
sterilization. She used to
say, "I'm sick and tired of
being sick and tired." I think
we're all sick and tired of
being sick and tired. It's
time for the oppressors who
are trying to control us to
get real sick and real tired.
We demand a woman's right to
choose. Defeat the Doyle-Flynn
bill.
O
Barbara Smith is a Black fem
inist lesbian writer and
activist who lived in Boston
from 1972-1981. She currently
lives in Albany, NY.
We hope to publish a "Looking
Forward" article on reproduc
tive rights in an upcoming
issue of the newsletter.
We Thought You Might
be Interested...
Neighbors Talk to be published
this spring...
Boston area writers announce the spring
publication of Neighbors Talk in Roxbury,
Dorchester and Jamaica Plain, a collection of
poems, raps, and stories about Boston com
munities written by those who live there.
All kinds of people come together in
Neighbors Talk, teenagers; women from the
Dominican Republic and Haiti; Native
Americans who live in Dorchester; people
who’ve lived in the communidcs for over 60
years. More than 80 people contributed sto
ries and served on the community editorial
boards that shaped the book.
The images in Neighbors Talk create a
vibrant picture of neighborhoods more often
described by people who live outside them.
Here, residents rejoice in neighborhood vic
tories and Nelson Mandela’s visit; youth
defend rap with a touch of “pizzazz jazz.”
Over half the funds to publish the book
have been raised. The rest will come from
pre-orders, so ordering now will help make
publication possible. For price and postage
info, call Rachel Mr
' ’ 7) 522-6513, or
write Neighbors Ta
Ave., Jamaica
Plain, MA 02130------.ache! Martin, a
long-time friend of RHSIST, guest-edited
“Listen Up: Youth, Writing and Resistance,”(^ES/57]#237,July/August, 1991).
Computers Available for non-profits
in Massachusetts...
The Nonprofit Computer Connection
(NCC) is a technical assistance program
helping nonprofit organizations use informa
tion technology effectively. NCC has several
hundred personal computers it will distrib
ute in 1993 to eligible nonprofits in Massa
chusetts. To be eligible, a group must be taxexempt and have at least one full-time staff
person. Community-based health and human
services agencies, cultural organizations,
co mm unity-based educational organizations,
and housing and economic development
groups will all be considered. Individuals,
churches, schools, and “organizations whose
primary activity is advocacy" are not eligible.
Call the NCC Donation Program
Coordinator at (617) 728-9151. or write
Donation Program Coordinator, Nonprofit
Computer Connection, 30 Federal St., 5th
Floor, Boston, MA 02110.
RESIST Newsteller
April 1993
9
^Lu^vihcc^ - }
OuL
<1
^ cvxe^A.
To
ZIaxl . e^o
o C< C4J2 GUQJ2_ -T'AQ SU T
a
j
j
VLOtccCUJL Aoot
o
MJuJTv
•
IKxsl-- r^o^cljLt^a. - ^cc(q) -To QATACooGe.
-bv'e_axiT rwLUe. ^ecActuo
~
A£,<_O nA>->veAACCec(. •
3) 6v^XXLf
alcCgcTo
Adot
QocucLjla. o>^ +8^ TuTjz."
JbevLoT
^xsT'ACv cou>g uvul6-fe <Ls
^CA^CW^.
bocLu
CcJ^UULlCo V e- .ZOP^oJ)
Cfe.
.£,'-l-pp Y^ iQ >A-> '
p MlU?_ .xtbyDyO'
3$
d^icJ^dCL
3) Pr\
kCcUcd^
jO^po^
U3ll4^ OK1‘O<^
’-k-
*2)
'c- (.]&i Lcwjlu, - <-L-,eni>(
<su. cua. cuxtcp^eAc f <
,d)-o '<i^q_c-Lu1c_ Gt^Cjbv oteXi-i
1 A
^Cq-Co.
ol
z-UcV-CL
ULS-tVCv,
<XIa%cU-CC>ca.
CUxZ£v^2Xy •
■
/Oopfq
>©JtO. '^-s^ pCQXJLZ o2 ^bdjc.. CxcltU CXCC&d CL^C^
XooJc > ■" '
CdLc^L
— T&JcCl
>#)
oAoj-Cil
Cvcd
do L
-dvocdo1 bo.
k-wc Ui • dvci
dz
Q_aa ‘O-A. ULXzttAyot" pyw.ci-tcc.
<-cUxd?
cvxd
@zd
tx9< Ll
txdLL olLgo toujSJy >^dUe.
&U Pooch
bcdZc) - /Q, ol^cecJ-Ce
&) Avv-iZciC MouLLl/cg^P - ^bcuolc’v
+(a£_ «x^vacuGxPi
4<DO'
aoi
■S) P^cclxfit£<C 4gukk£vA£Q_- fxkcu- t)Oo~~ cKLld ti (xp-plx-od.
Ck pcbdJL cJ
IaoxccIxp^x.
olax^
•'"wLCA • <Mr cZcxrt.
^tKL, CCrvv-VUO"tl c '^CuulcL •
l(a,lao/
>2) C Cb^pcctbjzJ) — A
> C<n_7 Jg,u<
Oiv^vVo
n i ,'T-'. I
^vck'oM.
bCxJz^-
) AfrvvGx
cuasL
hSLcccta
vet" -Li
X^v rvvitJX^oeP-Co• •
clas-
ok
^cuxot
^- - -
2> 7°^
Jkod-zol
UdouCu^
CoJuXy
'
'
dx. <^xxSjl^
q^<j2^ cldxvew.
’
'
(3
-/qgcCI'c ~^> Coc^ot^ub' ocl - CLc^^e^. 7
(1jc>CjD^\juJC
cia,
fiflMcn.MWTf-' QGbll^A&g. ctZuc cuaJU^
) hAJZxJk. ^cccCc
Jvv toxit^Ax^ IaJ2JU
CLAzqL vZxcJc
JtAxO.
0<j>u&OQCNl o/
® C1^:C^- CEC&Jc-kA) ~
CotsJ
p-^Qo^a^c^/ po^'cLoA,
cmZtZv yooppoic pow^c^u •'
4-t^
a-Ux^j^
o^ ■e>Gx ulj2jhsUv-u
- it
~
ccotc^ ciM-.k-
^iT€DiLcnAe6,e/&feD/^
H
T U/A L
f}&0 jZj iO N ■
lets
cl
^uX
3 -to S'" cd^ev+wvM^ ©< crji^pttGCcko*^
<Olc^J
.^<Js2gL £X-Iq>^ uO-ei-C^
^^^CUWUAXLcC Q^^jZiocp/
.C\Cljtl,CtLUXt
’OU-AtXv '
0 VvcLouxajlC ^qZo,
($Jb<QAj/-cO vv) <x stcGocAi)^
utbuz-UZy £
J!vOO<^
r\A4Zly /
tcu^h2o^y
c.
cxcW^jX
cooo^t
/j\j'fy&cFic
p=u^
^C^c<x.l^Uvq
®
o^&aac^
/
cU^C
CCmC;<,^
O^
&0
^Uu
eJLf^oC^ cVoou^eC
o< cGxy
<xdcu^
-To et
c< LtttLc
-(Le^ce^l 09
^rrLCVvAcLjA -UjJjXA/e^ •
°
'
V
C)
(2)Poh
i\j/^7c - LV^Cyoo.
obocLC^vx^x
^-xxctc
Pocuclu.
ccu^ gGlcqcL ^oot -O. ^Cv-exv ojp'ctU- >-vvL(J<
©< boCCoot
UJuj-Cv r^JjCA GU> Q^
^0\ LAAaoIkx —
©P/^'
UJO V-^-AJlyC-v •
uZoiaxC ■
S’c?oc^
'7
- B-B-as''5!
■ 7' 7 '' '■ £Bm ■
p^YTGGGoL
pCQ-CJL
OXg.
BcoJl
0/^ lziAJ2lZC BTjBcp
oLoJj^tL^ O>gacJ
x^ppLux
fOGcCr
<+-
Ogg
BB €>V-X
U^Ji- (XLpcJ^cL
07/4€^S-
to aZL
Aaq/m? PteGNANcy.
A
D-nxcutg tJp — Pjcccct ^'cvluq.
@ QvoJxhx Uze
xx a C<^ziA>
tc
p'Yoa-^^kA^t'
-GxU./
4?^ cL V5jX_C.l-vu.Ct / Co VVXl'ty9<LC/<b cv
''rvo^ 7;' " t'-11 - Quuv^c.h
ettut c/jiacc^^Li
ctv<J c-wi't^uix lxa. G£cq_<l<j
CUCae/
cctC^-XVvM-S .
•
U,<A.
*s4o VxzyXcXv •
g) ttetcUlC^CnJcXl) - 2^ CO te>
@ HCixctaoCvg^ — ZIuwCgl— (Ocm
p-y^jLf,A,'^zsd.
<Xt.e,-cv Get boxt ^teww, • £ovcOuvz\ctcx A-uJoJojiiZ
<z.Jx> ex Colo.Lt -<U-occU be, Q^yoUiid -Co
tet
caxx/<2a_
^o^^-cxc).
T 7
0 LlU.QL — ltdw.\D
.£Ia£_
cLua.
GU^cL 4-Uq. Ubv^AO
XeZuiAz\x2x<. J^y' tkJL.
b-clo,L < Cyqldefect -
Okzex
t^X4A.t"
^yd^LOJkOM.
-zodeZctv
odaduc
t>JO^''z'CU-v,
'-ICzjl
cXS
y^cuitC.
/-v-CLx-ts ta,i^ be Cu>ieJ ■
<5 P/ cepsy.
© A^W /VaXU/c^e) - AuaaZ"
^^Ceju-voXiy
•
NAU SPA
.............
'
............... ............
MoAAiON -
HA 0>lTvAL
0/
0^ 72- C^JteA)' ■ /$J2_
rvXjzzx.I
ova
'-ga
ui-i’cA
pCLL
<^i'
oLoio. <-Ci
'-C%aJ2uz<- <-A to VA>-Lo
-GV CCLQVLf
v^OUVHltv^
O<
^pV7OCC_etxAAjL
3
-to
Jt\jXA
P'VOLaqcJ
^UCCQJIA^UuL
'
S’ OjbOVkbvM^ </> co^v-yoltccd-to^
p^ej^y^UAARs C^Cot t^h>w>'x-uxik‘oi4. ©Z"’^
o^CJLj^
JUO V_CVkQ>c\_l
($) KxXa^mxUx. c 3c>iz
<q<-cxJ
J-
ShedsicL
ZAjlZj-0u yOYd-v^o<u
oJj&zA-O^.
<_u-6t2'- »-v^i_.(Jq.
e< '-'tcCU Acov-Cvxy
t^ooLZ
u^ClL^qA-
ca>C4Az
& CtGcbc^e u^^oUAX4
-vCZA CCUL
<ye^l cctoo V<loU <A
V^cIpxujlC A/uZol ^-ov^fa.co(a) - <Iov
aho^ACo^,
,^£cb£ttACc^
JboLLsis^.
CK stccocA.3^ o/)
^du.-^ •
^iAA-Lzbj
j
7^
Bugjy^
—---- ------- — ~
IdONS.
- f/oucJQjv
C
0
^OLCcd <-d-x
c-c'Cc-kX-
CX-AzO1
c-UocUX
COOtszH
^lo(.l'C,V4
o^l-xo1
<4xMxvCLCe^.ok
-t>.u,u^vcx^y
ucv-e^ XUi.A>-xxlty
cbLa.L^a pyoa^^^ccj • ^oi’Ccci
pV'eqL^ovvvco
X.'i-Cfij
^C<eXcAjz^Jo vu_ <ccL
4-oo -JLo^
'ICaX f<o-^^od.
IXtAAlACbL -L-<y^
/<?'>AyDCAAfid ' Joy
vAfi. C O t'v<^vA^x£>Le_o(.
oLmjkJ_v<.'|
Ux
<-U^jo )<.<io>^col
J-o
OVQ5cCX> vv<z
O.t)iAOU^a.-
c<yAc/_ z -dx-tclX Leo 'I (<s^ (~caiJ.
-4oo vzSUXc^ •
,
10
rv
Cqjx.
co_ ^\dLex
(^)
Q C^Q.yp'kjO"
^'YObL^i-^Ji
uR/^oko^
cyyj
CULLUAXekoit.
DCUlU , A’ txcvi
4<,vs o
-Pcag.C^
CU<JL-
o) blood
oh:
ca
■4'0 3
(S) &itU£XQ.viCLli
.(ACCCf
(^QkskxJAO^VV C
JboCLod- c
-O ro -^drnO V) ^;pvXYapQ9r
■TfTTrltfYvry 2*q P^OOt/^xt^ X> /^lOAxmr
Trrrp pnoc/ zrno o-yjon
-poo/<7 TV?j>
■a^T-fra^rp 'bo-xy «)
^r<y*jf >a-i — (y>/
v'io?y^n^Yn-3-<Anf- ^pp-YT^) |
z kv->?
^M-q/
■4
■ v 4 ir /
.
« </{ </» ••
”
zcrx o-j'Yrr TrpYj^v
ff r,
~o^^'pxxyp
*
/1
/
(j *
?)e/;'nn-Y^ _
*•
J
_____________ _—**
- •
no^(Z)
No7a.5^9/o^r/ v5>QH’b'?/l//~z7
Appce( T(x\/ou>^^LX-tj2-
fe'
Izj^A) —
kccyiz
(peZcu. •
Ctvc (cLua-v , 1e2_cttv-\O
Ccx^ls£v
^vO'CXaCUS
Cco3
dTv-VC.) L'Oa/dl" /.oc/_Ccj
\*
^tkfcu. 3y™ v-VAJOvcZ-ep .
(£)
r4^ -
PcnAjdji^ o^
©< betlect
ebuLod. -5/cxo t -ex ^Cv-ex< ck>ctt^ >^Lk
OJU>(\
rvAj^Cfe. GU> GV Q Q>aCA.0< (
CAAAdISA - UAQ^ tct
®pcaj
COO'•■'VACxa. ■
vCLfc^co^
u-LoiaaC ‘
<
&Wci.
J
OF
bcuUL o/ IAA2^_C
<x /3cc.cj2.
5^ fttve
c^ clotx^ cla^vJ yocctr
^oL-
Covxa^^
, 3J I^Lv'e. v<xctac<
cci
lxvLC^
claa,Lu£) io tcc
JJ: Qlz
<4-
ow Hajl, cc^c-c/eX
GcU^m •
0/
-
——------------ -—-——
— <7^
(f) /XtAClXZtk-— A-Goo^y /fclAJL ~ CM^vJbXzt^ ^CLAJ2-
■ C3u<&J,ia. ^ZozjIg
cc
-cotAQCy-co LzU
oltcoukow. <5^ cCujg ^icwajzx/o<x£< <si©o+
ujuJXa,
wudJz.
<-H ^uv'Cag .
© CWkceJ
.- .
llCLu-U - '1'^cUZ - ~n^ a^. be ^ex>UW
p&g.C4<O^
-pYDpQJ<
(£ aK
I
_/«
'
!-...».
n
fo\J ^pYLvdtpp^
"V. I D.rs ?
Z"» I xZ "J
\ZXXV'^'>lztf‘)O
zOC LAOCz1
hJ H - S -
PA IN ■-
ZAbOC/3
- Btvo - '/\J<2J2>n^u
l)
v\^. MxJL.- CL^Llc
OCtizxzUAxZs^lzU
xaJjlLlu
du JciclClZogI-ccI • "rf^s. j^ouJ
<JL&UZ i£&jc ^l-lac-C-CZu^-s lc^ ^ke.
feo.
^guAolcwXZxmjjs:
qeX
' f-<AQ(_CL.l
b&
CLSU.Lt
1^ ^aacx- (Claulu.
0ylvcLl<aO
tcC£
ULA£X-ZeJ_
<-lLl
-tp-bc-LCL -Cl
cx^A
<a
Ll>CcicXc
Ake
C'VNcJLz ■CLCl.tt
^odXlX
<CL<uy ^CA^GJL.
vuoLlcvcc
II’txc •XQ IAC<
Z^et/x J&didd
uZcalU
tx^cJ -tlxx pxbj^t.
QQ-tlMAD
CZCqACjcI r
vtZvJL
t^UZcLujA/y_
bctom. -ICAr. lAcJoolisl, eZZkc.
(Laasa-
ctUic
<3ovvCvxc.sLloll
^C<ACL-Ui
Nb<>J^yZ^Cu'uC'Wj
CCcLLtoL
3^ ZClA.
^e<if< y ccice. v/ te.oiL'QJ.
CLftclt
«-i
(ccbOLCL
<€L
•
«
^-u?cU
Ozv-st/ 4LUCU,
£b Lu< ■
JooaJc Jdsxo
'^LLm
#< Ci -t^isLi-Cy O^ZeXL.Q_C^
-<tuL ^xCl^cC
rkt.c^/'tCcy .
• CU CcO tvcLzio
't’toiZZ.
cLcCi.v'QXy
Gu-cy . "nCc
•■LtCc
CZajc
-cuZLccli
oclaqI
clCoo
COO LLOxc'Cg
CA-y/cUL k)(L<Ac»^u
uckb^
‘AXLe.j-Vx.
-CajlCA.
k-CJ
Cicl-CC—
l-lCCvciic
v'VtZici.'c
uciclv vx_
-XAjc
’^vxxXfoicL
CLLcCL
-kC-CLJ
<a£j2>vi_- (-UclZslX
g/ilo
/kuta
'Lo
A llac.L£Luao^
<Laa£^
clx^ LyO GLiaJ
PJalcl.c^ OA^\oL <LO llClCx. U/-€xX ■
LAjkZXc
^^jZ^vZy
ajajl.
baxlc 1^ old.
■Ac.Coi^-ux-^^-icC.Q.cZ ^£s(L
GL.CC
■ Pro
C\SL
f)
oXJLUj Lgiy
C^
M.<j^ ^Astia^-zd e^ycL^u &o^ ^6eX cUZCv«Ay. ■
j'l'cnc<c\ c?^ U-Uo p'Zppm ^Juuilr -u. <yicu^v,V
1'-v(.£a^v<zCG/
ca_>l.-/-Cv
uXoe-uey. fJz ccttio
«Ll£cla •
Ascco_
Coo toe!
CUCoCoC
O>laJ
p<O^\cLu^
vuv
z&UVACcLI
<1C
CX<Ja
blo©c)
yuOL^ot-C
OVL Llv^z
loa/mj u>a7~
mjm:-/-Ca.
rvvOzY-e.
QLV^La. -Ao '■>
-CUe_-
ciyopctC^S" •
Du/cp)- A- iajcci .fc<s.wr
C^U
^Tuc
ckSLcove
v^xOCt^OL ■
C^\d ^phjP\/ ^L><-CAJiLc4CC4
(X.tAc)
cuxao'
be Qev^,vc -uV/Lce
+&x
p^pQA. <Xva£!> eZRiL kzxZ^
x2a>
M.dcc Qt^r&y^
exp
cZcam^m.
O^viOUMAjt
.C^cLucc
Gtt>ltvM2XU
CetvU^C^bow ’ 2t
•
■
^PvLSiOK1 .iGf
y-A -
- /U-._ Cc^/axx'ow o^^cCkjx, x.oot
P 'Pp
jo-r^tUfood
Qy^^l^icHL
a^lo^
Cl^LlsL&dti^
cu^
<m>
ok
a kc-Ltxu.-
-tvc Io Xs^i^vxaiLy.
CttbicAZ6iL a^<l
$ CU^<ZJ,Ca - kbJcj!_ +ta_ <X.oot
u_t
ova
4C'J2_ <-kJO-C<bt
O'r 10 cut
^U’vQ- ~olZ£Cl€^ •‘Rq>-vxo v*e. <vU
~Ct\£, pla,^L.^L^
.400 <-<
oc-ctr ■
0)tca.cl£co _
yKj^ -‘
aGxbvcv)
cot U\£^
CCeo’
CLJ,
7 t\c.
4<jl
r^oujK^.
bojjy ax'd
kJH'5-
—
•• i
A
^p.6AS>'U.
*
■
0 VxU.CUX'.cJ fVc-lxX A-LO'vUjujl'p - /o C^OULd-ftX. XvUCKi/
&U2. violcuwi Aoot
JOoi-uoK
•'<-&
C v\€xa_ vto
vex£ W-iAe.^ v^a^cLcl t\,iex -
■•$)
•?» vjA.o.1;
^iL<AcpUAj
acJo^ - To
ry\xlAi -Oeoic^co ut.^, ^ollcLcv
J-vxxclc/Zuui. - aCcLx A6OL
A.eco»u-,vcc^wCec(. ■
<IulCv
UjidojUos
JbOtUd
^\djL
XtlpCv ^rvxjtLczu
/vu_Lct4<oL'Zi_t
uJ-CCtv ^vl<A
.£LkC_. j-v-vq Uaila_ '
'-^VCipp^crvxjp<,-v.^-
-ctP c/Cv
I (<&
&a.s\1sx(XJ'')(.e
'CxZn-^. -
toic’i u-vtc/A> Cj
/<aAcW'-z
^sx'^
eXitc >'>vxcClX-'Ai-'VO
Q JJoACU
^ccvocuZGC cLCoJr JcO
d) ZlCo'xotvd
A LWto
^buMcn^-vZ) ^oaJcszdL ov^juxM.Cot'
(X J^CuUjL
k>Mxj2_dI
rvd(A
las-C<€v
y^opycny ULCJicA CO^d VcL&lX’-
WvCtA
clo
clexv1 C4con
vlfiJitbe^yoco v^u /
Qtv'Cj,
£tocu
)o)
la.
' MMaC
ou-Lou-T.
*T) (To 1 iciLQ.eQcl
v-vaocCc.
LU-CMa.
AczJL/ai +o cnCceozae
'
ctilccc vax.cZ dMj boi.lccyy
v. actols
vu
ex uxxhxl JU-Cxyoo.
^)>x aoP ^vCGt /
cv
ex edax-scu.ct6uL
x<yO\j.xjk_ JKoJJ^s do L'TOcexxoc
'
cxJotixXuv y& ■Y^yOOxaZcb w£/ <<.OQO £gA£CLl2co v e .^cyopo)
po^JLcc^ey /blcccL- <xxrvu>u
_Z>-i ccxccdc
<o ecyoj
vxxcUq.
ocvtyovcL
cla.
CcvaxZ
cx>(\j2_cc/
CX-U2. co LL vXLAUL^cU.
vczlxltyCL/
CJU<>
cb-^d:
^tc
oCAuc clMcv-e.Ac.d Luot-Txxn.
Cfe '&^A[Op >~KM Ip vc ■
I / K IcLk
cysyovew o cL
f^k’Crvh. lokvvty
d’o Claxcx-G.xvaXCx ■
Co uuld dx.
ucwltv ex /pLtxcU
lAQZdx
(J cuctlcv
^AciOvtcc
J<Cci^t »ttc
3) f^'ClOGL.ce.
kvclxcd.L
Wlc'/Ca
c<vaJ
OK.COIX
ftxo1
oext- •
Cccocvcct
CtoS
Gcd ‘
Mjxo.ua
d) P~^Lp<x^
v^ivuev ucxCLtc
^Vu-Cc-
JAcLuxcLC
cxALS
>tf) CGjve^^aAZixv^c^) -f^ctccxa
c(ecce4<ocv c?/ ctc^-e
^a<aq cXi
A
ga.
Jjejct^poov^cut
CCu4ZeA
-CeLLCa.
ojac
bci<c^cicx{
Avu
Ac
• -©C4JU.C4D
Q
umLL
W)CLAX CX'vd -40
CX^& A>X2..CLQ.l'
/ <■ t
Cel A >ti-uxt" utkLi./' -SiCvotL^c’
-tl
•UU.LC -
aaAjgcu
ctAAd
camU.
o.Uo
ex
CL-t" ►T^L LZi • 7
4a
^va’1^ <^AcaAa4.l
9 Vc’cW C MvMx
■^tC'Qky
Xoot:
o^Lcej?l
<A.oct xa
X4
^i^wbouhQ -T^uuoGu. ©/
ocvcxa
Co
^cb^L.
^-ckg - ^-Lqu^cLloua
o>cve^v cte.c^
N. ,
^A'..'
Co Cda) - /2>o_cGla
/ ,..
UxbLCe.
cJLS>
QLxCCtcp^J^txc f
CCcv
<i)-o vn/xxclule
pGV-Ow.
CCL«ty -/t*
uj.
Q-<Az^c^
Q CACtxx/xZy
X "> P > n .<■» «.I j . > ZCJ1 ii I A 0
^)/l C\J-oCv.(j
M
fc<>te-A,v
1 C) 1 P i AO let.
>
.....
KZ.
(X-vCt
oLoX.tL'Qxy
^o^-Acyo qaZlLs '
.9^XssL
-,c
rwCJa. &^Iqc>CCqjoL cex^
oLcctii,-
QAX/ .
Ova^L G< 'i-tAJO
WO-LLl
C^Q
f ClAxd °GL
iXJZC’Uu? m. (J
(Lo^Ge_>^JXcuJ^^c) • <4-<
ica.
C^Lccx^c i
bcxtu_ •
Nb'jJ
liM'Iki
{WI-4W7
Gl> Pooch C ■0>>u^UX
- /^.
olt,cocA'o
-cccu^va.C lxLc^y'cecc^<lt co.
<ix,^n^,cCuAjt2_ <2
Al^<v(g<.C ^CuLLt/CS^p - A^UmA^A.
cAxdcbo-cv
44>ML ©J^^CcGxtx ^-LcCt
ML
CxqcCcvc<Y,tT cLuj QJXXULX. •
''''site I^v-
£■' arv^
aj^cebx.
c>h baxlG
ex vpixoto
v-izvulolsu <-U\a_.
<r>t’JCv
b'reev^t
K^x'ictiv •
>p l^<x\,cctx£t£<C Aiuktulv wj2_- Nqaaj - be*.
tu<4A_ ex
duxUjL
eJ. UclxZcLxpjx
ex-'
c ^CculcL •
-CKjg
JLi'c«.
-xiv *(jxCk
c^ ^pp'dbdsL
JerU^APJ-t-'occ
Vo
( tXn •
^JUxcf<jz.cl
cu’fek.
exx-A
bu^tt^-
cle.xA?Uyo
b\s^
vL«xd.
-2./oo)
wm/] p^T? TTrpO
^p-TYY ^T7T)C5YV>OOb
-Tryvj-o a,gq <yy? -pt>
-prYDpQ^
K)^'1
'Vj-rq-' vipfocy _pm h Apocy ttvt- vsao
710 ^3'ro ^rznqop'rsv]
-r^ /CR>7?OCJ'
vrcy
V°
pTn^dc/r)
p-
^Tcr'-'P?'v^t-/ (^
- "5yv^/ (t
.Lot.l>d
') CLlA,
lQ
to^x^x-LiAab
OZ&D
CXcL?
, /-4A z b'J 4AZo
cA/tol
i
OR SUMMARIES
Egypt
Dissemination
Encourage Journalists to
Cover Reproductive Health
OR Summary 15
After Egyptian print journalists attended a series of briefings on
reproductive health issues, their reporting of these issues improved. Health
agencies can improve coverage of reproductive health issues by providing a
regular flow of accurate information to a broad range ofjournalists.
£ Background
To raise public awareness of reproductive health
(RH) issues, the Population Council
FRONTIERS project and the Futures Group
POLICY project jointly organized press
briefings and provided background materials to
key journalists from Arabic newspapers and
magazines. From May 1999 to June 2000,
project staff worked closely with 20 Egyptian
journalists, including editors of women's pages
I
and senior editors. The four press briefings
covered youth, marriage patterns, contraceptive
technology, and menopause. The press kit
prepared for each briefing contained fact sheets,
reference materials, a contact list of key experts,
and an evaluation sheet.
.
2000, one-fifth covered topics featured in the
press briefings. Similarly, one-third of the 127
magazine articles identified covered press
briefing topics.
“The numbers and figures presented ... will
have a more effective impact on public
opinion. ”
-Participating journalist
♦ Journalists attending the press briefings
reported that their knowledge of RH issues
increased and that they planned to use the press
kits to write their articles. Some journalists
shared the press kits with their colleagues.
To assess RH reporting and track coverage
resulting from the intervention, project staff
monitored eight major Arabic newspapers and
nine magazines daily. All articles on RH were
coded according to their topic, length, and use of
research findings.
Findings
I
♦ The press briefings did generate press
coverage. Of the 433 RH articles published in
newspapers from May 1999 through March
^Frontiers
♦ The project did improve the quality of
reporting, but room for further improvement
remains. Roughly one in three articles based on
the press briefings cited research findings or
information included in the press kit. Although
project staff stressed the need to use multiple
sources, most articles were based on a single
source of information.
♦ Of the total pages devoted to RH topics, more
than one in four dealt with safe motherhood.
The second most popular topic was reproductive
RH Topics Covered in Newspapers and
Magazines
tract infections, followed by sexual health,
youth, menopause, and quality of services (see
Figure).
♦ The majority of RH newspaper articles were
news stories. In contrast, more than half of the
magazine articles were feature stories; half of
these articles were one page or longer. Both
media formats are useful for research
dissemination: newspapers are widely read by
policymakers, while magazines tend to be
shared with others and retained for a long time.
Policy Implications
♦ Research dissemination should include
briefings and resource materials for journalists.
Links with both print and broadcast journalists
should be developed.
♦ To broaden the range of RH topics presented,
more local agencies should be involved in media
relations activities. More information about
family planning and female genital cutting*
should be provided to journalists, since these
topics currently receive little press coverage.
la Newspapers
Magazines
♦ Health agencies should seek to improve the
quality of reporting by providing a regular flow
of accurate information and helping journalists
to identify newsworthy stories.
November 2000
‘See OR Summary 14. NGOs Need to Join Forces to End FGC.
Hegazt, Sahar and Mona Khalifa. 2000. Increasing the Coverage of Reproductive Health Issues in the Egyptian Press: Final Report. For
more information or to obtain a copy ofthe English Final Report of this study, contact: Population Council, 6A Giza St.,P.O. Box 115,
Dokki 12211. Giza. Cairo, Egypt. Tel.: 20-2-5725910: Fax: 20-2-5701804; E-mail: frontierspccairo.org.
This project was conducted with support from the U.S. AGENCY FOR INTERNATIONAL DEVELOPMENT under Cooperative Agreement
Number HRN-A-00-98-00012-00.
OR SUMMARIES
Zimbabwe
Reproductive
Tract Infections
RTI Screening Methods for Women Are
Not Cost-effective
OR Summary 1
Existing methods for screening reproductive tract infections among family
planning clients are not cost-effective: laboratory tests are too costly, and
syndromic case management often leads to missed infections and
unnecessary treatment. Health programs should continue to emphasize
preventive measures—changing individual behavior and promoting
condom use.
Background
Reproductive tract infections (RTIs) are common
in Zimbabwe. Many RTIs increase the risk of
human immunodeficiency virus (HIV) infection.
In 1998, the Zimbabwe National Family Planning
Council (ZNFPC) conducted an OR study to
assess the feasibility of adding RTI diagnosis and
treatment services to its menu of services. The
study population consisted of 1,634 clients at
three ZNFPC clinics. Each client was asked about
lower abdominal pain, vaginal discharge and other
RTI symptoms, was examined for clinical signs of
RTIs, and was given laboratory tests to confirm
the accuracy of diagnosis based upon symptoms
W and signs.
Findings
♦ RTI prevalence. Laboratory tests found that 9
percent of all family planning clients had one or
more of the sexually transmitted RTIs (gonorrhea,
trichomoniasis, and chlamydia). These three RTIs
have serious public health consequences. Most
clients with RTIs (26% of all clients) had either
Candida or bacterial vaginosis, which are not
sexually transmitted. Two-thirds of FP clients had
none of the five RTIs assessed by laboratory tests.
♦ Applying clinical guidelines. The study
assessed the use of national guidelines for
diagnosing and treating RTIs when laboratory
tests are unavailable. Referred to as “syndromic
management,” the guidelines direct providers to
treat with drugs all common causes of the specific
syndrome or the combination of clients’ reported
symptoms and clinical signs observed during a
pelvic examination. Identifying RTIs based on the
guidelines was not effective because:
4-Symptoms did not correlate well with
RTIs. More than one-third of the clients with
one or more RTIs (detected by laboratory
tests) had no symptoms, and thus were not
diagnosed as infected using the syndromic
approach. Conversely, 47 percent of the
family planning clients who had RTI
symptoms and clinical signs, and therefore
were identified as infected under syndromic
management, did not actually have any of the
five tested RTIs.
4- Service providers did not always follow
the syndromic management guidelines. They
treated only 53 percent of the women who
complained of lower abdominal pain and 65
percent of those who reported vaginal
discharge and had clinical signs of it. The
rest of the women went untreated (some
were, in fact, uninfected and did not need
treatment).
^Frontiers
IN It C PRODUCT IV t HUUH
♦ Cost of interventions. None of the
interventions studied is affordable to programs in
low-resource settings. The lowest-cost
intervention is to use syndromic management to
evaluate only those FP clients seeking RTI
services (see Table). However, this intervention
has its drawbacks. In the study 75 percent of RTI
cases were undetected and 56 percent of the
women treated were misclassified as infected and
thus received unnecessary treatment. Laboratory
tests provide accurate diagnosis, but they are very
expensive.
Policy Implications
♦ Most health agencies in developing countries
lack the resources required to implement
syndromic management of RTIs on a large scale.
For example, in Zimbabwe estimated per capita
spending on all health care was US$47 in 1998.
Applying syndromic management of RTIs to all
FP clients would cost more than 10 percent of
these scarce resources.
♦ The ineffectiveness of syndromic approach in
identifying women with RTIs calls for a more
concerted effort in advocating for and supporting
the development of simpler and more costeffective laboratory tests.
♦ In the absence of more cost-effective
approaches to RTI management, ZNFPC and
other health agencies need to put greater emphasis
on measures to reduce unsafe and unprotected sex,
including condom promotion and counseling
services to increase clients’ perception of personal
risk and knowledge of safer behaviors.
December 1999
Accuracy and Cost of Four RTI Diagnostic Models for FP Clients
Diagnostic Model
(n = 1,623)
# of Women
Correctly
T rested
# of Women
Given Drugs
Needlessly
Total Cost
of Drugs
and Lab
Tests (US$)
Cost per Clinic
Client (US$)
Syndromic approach for FP clients
seeking RTI services (n = 410)
130
168
4,024
2.48
Syndromic approach for all FP clients
337
298
8,605
5.30
Syndromic approach for all FP clients,
with laboratory testing of clients with
RTI symptoms and clinical signs
337
0
6,722
10.30
Laboratory testing for all FP clients
524
0
41,819
25.77
Zimbabwe National Family Planning Council. 1999. Demand for and Cost-Effectiveness of Integrating RTI/HIV Services with Clinic
based FP Services in Zimbabwe. Formore information, contact: Population Council, P.O. Box 17643, Nairobi, Kenya. Tel. 254-2-713480; Fax: 254-2-713-479; E-mail: pubh'cationsfopopcouncil. or.ke.
This project was conducted with support from the U.S. AGENCY FOR INTERNATIONAL DEVELOPMENT under Contract Number CCP3030-C-00-3008-00 and Cooperative Agreement Number HRN-A-00-98-00012-00
OR SUMMARIES
Mali
Female Genital
Cutting
FGC Excisors Persist Despite
Entreaties
OR Summary 2
Programs to persuade traditional practitioners to discontinue the practice of
Female Genital Cutting (FGC) are ineffective. Interventions must address
the demandfor FGC rather than focusing on the supply.
Background
About 94 percent (DHS, 1996) of Malian women
aged 15-49 have experienced Female Genital
Cutting (FGC). In Mali FGC is associated with
serious gynecological and obstetric complications.
In 1998 the National Center of Scientific and
Technological Research of the Mali Ministry of
Secondary and Higher Education and Scientific
Research conducted an evaluation of programs to
eradicate FGC. The study assessed the work of
three national nongovernmental organizations
Excisors continued to perform FGC.
Most excisors remained unconvinced
that FGC is harmful to women.
(Association Malienne de Suivi et d’Orientation
des Pratiques Traditionnelles/AMSOPT,
Association pour le Progres et la Defense des
Droits des Femmes/APDF, and Association de
Soutien au Developpement des Activites de
Population/ASDAP) working in Bamako and five
regions of Mali. These NGOs had attempted to
persuade traditional practitioners of FGC
(“excisors”) to abandon the practice. Excisors are
typically women from the blacksmith caste who
come from families recognized by the community
as excisors. Family members learn the practice by
assisting excisors.
All three NGOs employed outreach workers to
educate excisors and community members on the
adverse effects of FGC on women’s health. Two
NGOs developed income generation schemes to
provide the excisors with alternative revenues.
One NGO sought to train excisors to advocate
discontinuation of FGC. Researchers interviewed
the heads of the three NGOs, 10 field staff, and
41 excisors. They also conducted 45 focus group
discussions with 380 community members.
Findings
♦Nearly all families practice FGC. Ninety-one
percent of a nonrepresentative sample of 126
women under age 40 said that they had
circumcised their daughters. Nevertheless, the
practice may be declining, since 98 percent of the
134 women over age 40 said that they had
circumcised their daughters.
♦ Major decision-makers regarding FGC are
heads of family groups, religious leaders, the
village chief, and grandmothers. Community
members defended the practice as a means of
continuing cultural traditions, fulfilling religious
obligations, controlling female sexuality, and
preparing girls for marriage.
♦ Community members and NGO staff reported
that the excisors continued to perform FGC,
despite their statements to interviewers that they
^Frontiers
IN ntPKODUCTIVt HEALTH
had abandoned the practice. Excisors who had
truly discontinued FGC did so for two major
reasons: (1) retirement due to advanced age, poor
eyesight, or replacement by their daughter; and (2)
the promise of income from alternative activities.
Most excisors remained unconvinced that FGC is
harmful to women.
FGC eradication programs
must reach diverse audiences,
including men, opinion leaders,
religious leaders, and
traditional midwives.
♦ The strategy of converting excisors was
ineffective because:
4- Parents continued to seek out excisors as
needed. They also found health workers willing
to do FGC.
4-The low social status of excisors does not put
them in a decision-making role to end FGC.
4- Excisors receive community recognition for
their role and thus payments from their work are
not their only source of motivation.
Men Talk about FGC
“The world changes. That’s why we can
now talk about excision with you. Before,
no one would want to come to hear you
discuss such topics.”
“Perhaps our grandchildren will not go for
excision. In any case, abandonment will not
happen during our lifetime.”
— Participants in a focus group discussion
Policy Implications
♦ Programs must focus on reducing demand for
FGC from the community, rather than seeking to
reduce the supply of excisors willing to do FGC.
♦ NGOs must develop broad-based community
education campaigns that promote discussion
about FGC and encourage local leaders to speak
out against the practice. FGC eradication
programs must reach diverse audiences, including
men, opinion leaders, religious leaders, and
traditional midwives.
♦ Research should focus on designing effective
intervention strategies based on reproductive
health and human rights, countering arguments
made by FGC adherents, and documenting NGO
activities.
January 2000
Mali Ministere des Enseignemenls Secondaire, Superieur et de la Recherche Scientijique, Centre National de la Recherche Scientifique et
Technologique. 1998. Evaluation de la Strategic de Reconversion des Exciseuses pour I'Eradication des Mutilations Gdnitales Feminines
au Mali. For more information, contact: Population Council, P.O. Box 21027, Dakar Senegal. Tel.: 221-824-1993: Fax: 221-824-1998:
E-mail: pcdakarGvpcdakar.org.
This project was conducted with support from the U.S. AGENCY FOR INTERNATIONAL DEVELOPMENT under Contract Number
CCP-3030-C-00-3008-00 and Cooperative Agreement Number HRN-A-00-98-00012-00.
Burkina Faso
Postabortion
Care
Upgrading Postabortion Care Benefits
Patients and Providers
OR Summary 3
Training hospital staff to improve emergency medical care for women with
miscarriages and unsafe abortions leads to better patient care, shorter
hospital stays, lower costs, and increased contraceptive use. Local
anesthesia is essential for pain control. Physicians trained to provide
postabortion care have trained other medical teams in Burkina Faso as well
as in Senegal, Guinea and Haiti. Health officials from other West African
countries have expressed interest in PAC training.
Background
At the request of the Family Health Directorate of
the Ministry of Health (MOH), the Reproductive
Health Research Network (CRESAR) conducted a
study during 1996-1998 to introduce emergency
care for women with complications from
miscarriage or unsafe abortion. With technical
assistance from Population Council and
JHPIEGO, CRESAR trained staff at two large
hospitals in Ouagadougou and Bobo-Dioulasso to
provide postabortion care (PAC). Training for
physicians, nurses and midwives covered manual
vacuum aspiration (MVA), family planning
methods, infection prevention, and
communication with patients. Staff also
participated in the development of policies and
standards for PAC services.
To measure changes in knowledge and behavior,
CRESAR interviewed 330 patients with abortion
complications and 78 providers before the
intervention, and 456 patients and 41 providers
after the intervention. Information on hospital
costs was also collected.
Scaling Up
During the pilot study the MOH,
CRESAR, and service providers at the
two study sites drafted national
policies and standards for PAC
services. The standards specify
essential components of quality PAC
services, such as infection prevention
procedures and routine patient
counseling. The MOH has adopted
these policies and standards and has
begun to extend services to regional
hospitals.
The four physicians trained during this
study have trained other medical
teams in regional hospitals in Burkina
Faso. They have also trained
providers in Senegal, Guinea and
Haiti. Health officials from other West
African countries have expressed
interest in PAC training.
^Frontiers
JI IN KtraODUCTIVE HEALTH
nnaiiiyo
♦ Patient satisfaction was significantly higher
after improved PAC services were introduced.
Nearly all patients stated that providers answered
their questions readily and gave clear explanations
and instructions.
♦ Nearly all patients (94%) received family
planning counseling. After counseling, 83 percent
of the patients accepted a contraceptive method,
compared with 57 percent before the intervention.
♦ Verbal reassurance alone is inadequate for pain
control during MVA. Local anesthesia is essential.
♦ Providers swncneo toivivA as tiieirpreferreu
treatment for postabortion care. MVA lowered
costs for both the hospital and patients due to
shorter hospital stays, less use of general
anesthesia, and less staff time, compared with
previous clinical practices.
Policy Implications
♦ During expansion of PAC services, special
attention should be given to quality of care and
linkages to family planning services. Costs for
MVA equipment and other supplies should be
included in hospital budgets.
♦ The hospitals used as study sites can play a key
role as reference, training and study centers for
other practitioners.
Benefits of Improved PAC Services
Before
Training
After
Training
23
Staff time for emergency treatment (minutes)
73
Length of hospital stay (hours)
36
19
Cost to patient (USD)
$34
$15
Patient informed of immediate return of fertility
13%
90%
Patient received FP method
57%
83%
February 2000
Ministry of Health, Burkina Faso, J998. Introduction of Emergency Medical Treatment and Family Planning Services for Women with
Complications from Abortion in Burkina Faso. For more information contact: Population Council, 128 Sotrac Mermoz.P.O. Box 21027,
Dakar, Senegal. Tel. 221-824-1993; Fax: 221-824-1998; E-mail: ncdakar(a)Dc.dakar.ors.
This project was conducted with support from the U.S. AGENCY FOR INTERNATIONAL DEVELOPMENT under Contract Number CCP3030-C-00-3008-00 and Cooperative Agreement Number HRN-A-00-98-00012-00
Senegal
Postabortion
Care
Train More Providers in Postabortion
Care
OR Summary 4
Improving postabortion care (PAC) services benefits patients and reduces
costs. Providing PAC services can result in shorter hospital stays, decreased
patient costs, better communication between providers and patients, and
increased acceptance of contraceptive use by women treated for abortion or
miscarriage. Local anesthesia is neededfor pain control.
Background
Findings
In Senegal, nearly one in five women requiring
emergency obstetrical care has had a nonmedical
abortion. Recognizing unsafe abortion as a serious
health problem, the government adopted a
national health strategy in 1997 that aims to halve
the number of unsafe abortion cases by the year
2001.
♦ After training, providers quickly shifted to
MVA from other clinical techniques.
In 1997 the Center for Training and Research in
Reproductive Health (CEFOREP) and the
Obstetrics and Gynecology Clinic (CGO) at Le
Dantec University Teaching Hospital in Dakar
introduced new clinical techniques to improve
emergency treatment for women with
complications from miscarriage or abortion. The
CGO and two other teaching hospitals served as
pilot sites. Physicians, nurses and midwives at the
three sites received training in manual vacuum
aspiration (MVA), family planning, and
counseling. The United Nations Population Fund
and JHPIEGO Corporation provided equipment,
logistics support and training.
To measure the impact of the training, CEFOREP
interviewed 320 women receiving emergency
treatment and 204 providers before the
intervention and 543 patients and 175 providers
after the intervention. Information on service
delivery costs was also collected.
♦ Changes in service management reduced
hospital stays by nearly half, to an average of 1.2
days. Patient costs dropped by 25 percent,
although the cost (CFA 26,700 or US$46) remains
high for these patients (see Table).
Expanding access to PAC and
improving referral procedures could
save more women’s lives.
♦ Communication between providers and patients
improved. Patients received more information
about the treatment and more psychological
support. However, verbal reassurances did not
reduce the need for local anesthesia for pain
control.
♦ After the intervention, the proportion of patients
who received family planning counseling doubled.
Of those who were counseled, the proportion of
women who decided to use a contraceptive
method increased from 56 percent to 76 percent.
^Frontiers
Policy Implications
♦ Expanding access to PAC and improving
referral procedures could save more women’s
lives. More than two in three of all patients
interviewed had visited two or more hospitals
before receiving treatment, delaying care for up to
4.7 days from the onset of symptoms.
♦ PAC training should be extended to more
physicians, midwives and nurses. Pain control
medication is essential. PAC supplies and
equipment should be included in hospital and
clinic budgets.
♦ FP counseling should be systematically
provided to all postabortion patients.
Benefits of Improved PAC Services
Before
Training
After
Training
Patients admitted immediately for
treatment
55%
69%
Length of hospital stay—2 hospitals
2.3 days
1.2 days
35,800 CFA
(US$61)
26,700 CFA
(US$46)
Patients counseled about family planning
18%
34%
Of patients counseled, those who received
a contraceptive
56%
76%
Cost to patient
February 2000
Centre de Formation et de Recherche en Sante de la Reproduction and Clinique Gynecologique et Obstetricale Chu A. le Dantec, 1998.
Introduction des Soins Obstctricaux d'Urgence et de la Planification Familialc pour les Paticntes Presentant des Complications Lie£s a un
Avortement Incomplet.Fbr more information, contact: Population Council, 128 Sotrac Mermoz, P.O. Box 21027, Dakar, Senegal. Tel.
221-824-1993; Fax: 221-824-1998: E-mail: pedakar a pcdakar.org .
This project was conducted with support from the U.S. AGENCY FOR INTERNATIONAL DEVELOPMENT under Contract Number CCP3030-C-00-3008-00 and Cooperative Agreement Number HRN-A-00-98-0001 2-00
OR SUMM '.RIES
Kenya
Postabortion
Care
Offer Family Planning on
Hospital Wards
OR Summary 5
The most effective way to ensure that women being treated for incomplete
abortion obtain family planning is to offer information and services in
hospital gynecological wards, this study concluded. Having ward staff
provide contraceptives on the ward is more convenient than having regular
family planning providers visit the ward or having patients go to a separate
clinic. Findings from this study have been key in informing the expansion
plan for PAC in Kenya.
Background
In Kenya, more than one in three women
hospitalized for gynecological problems have
complications from miscarriage or unsafe
abortion. These women generally receive no
information or services for family planning or
other reproductive health needs.
During 1996-1997, the Kenya Ministry of
Health (MOH), Population Council and Ipas
collaborated to test three models for providing
postabortion care (PAC) and family planning
(FP) information and services in two areas of
the hospital. The three models are: (1) having
gynecology ward staff provide postabortion FP
services on the ward; (2) having staff from the
maternal and child health/FP clinic provide FP
on the gynecology ward; and (3) providing FP at
the MCH/FP clinic after PAC treatment but
before hospital discharge. Six large district and
provincial hospitals served as pilot sites.
Researchers compared the effectiveness of the
three models by using surveys given before (481
patients and 140 providers) and after the
intervention (319 patients, 92 male partners of
patients, and 106 providers).
^Frontiers
ly
KtrKODUCTlVt HEALTH
The intervention consisted of: (1) training doctors
and nurses in manual vacuum aspiration (MVA)
and postabortion FP; (2) providing equipmentand
supplies; and (3) reorganizing services to better
suit patients’ needs. All pilot sites designated
small rooms for MVA procedures, thus speeding
up patient flow and freeing up the main operating
rooms. The hospitals offering FP services created
private counseling areas on the wards by
converting unused space, adding partitions, or
reorganizing space. They obtained contraceptive
supplies from the hospital’s MCH/FP clinic.
Findings
♦ Model 1 - providing postabortion FP
information and services on the ward - led to
increased adoption of contraception and shorter
hospital stays. Under Model 1, more patients
actually received FP counseling and services than
in the other two models (see graph).
♦ Providers and patients reacted positively to the
improved PAC services offered in all three
models. Providers preferred MVA to pre
intervention clinical treatment methods. Before
the package was introduced, only 7 percent of all
PAC patients received FP counseling, compared
with 68 percent after the intervention.
♦ In all settings PAC services could be further
improved by providing patients with more
information. Only 16 percent of the patients were
told what to do if problems developed. Similarly,
only 41 percent of the patients were warned that
they could conceive again soon after abortion.
Roughly half of the patients were told about the
possible side effects of their chosen method.
♦ Pain control practices remain a problem. Only
3 percent of the patients in both the baseline and
post-intervention groups received pain
medication, and thus nearly all women reported
pain during treatment.
♦ Husbands/partners of patients indicated a strong
interest in receiving more information from
providers. More than 90 percent of the men
interviewed said that they would have liked to
know more about their wife/partner’s condition
and family planning. One hospital began to
counsel couples on the gynecological ward.
Policy Implications
♦ Postabortion FP information and services
should be offered on gynecological wards by ward
staff. Ward staff may need additional training in
FP counseling.
♦ Men accompanying PAC patients should also
be offered information on their partner’s condition
and FP counseling, if the woman consents.
♦ PAC providers must provide medication for
pain control and should not rely on verbal
reassurances alone.
♦ To ensure that PAC services continue, hospital
administrators need to ensure that staff are
adequately trained and that equipment, supplies,
and drugs are available. Both pre-service and in
service training are needed to integrate PAC skills
into the existing health system.
♦ Based on these findings, the Kenya MOH
developed detailed workplans for expansion of,
improved PAC services. These plans have now
been incorporated into a national strategy to
expand PAC throughout Kenya, in both the public
and private sector.
February 2000
Solo, Julie, et al. 1998. Creating Linkages between Incomplete Abortion Treatment and Family Planning Services in Kenya: What Works
Best? Also see Improving Care of Postabonion Patientsin Hospitals, OH Summaries, January 1998. For more information, contact:
Population Council, P.O. Box 17643, Nairobi, Kenya. Tel. 254-2-713-480; Fax: 254-2-713-479: E-mail: publications@popcouncil.or.ke.
This project was conducted with supportfrom the U.S. AGENCY FOR INTERNATIONAL DEVELOPMENT under Contract
Number CCP-3030-C-00-3008-00 and Cooperative Agreement Number HRN-A-00-98-00012-00.
OR SUMMARIES
Peru
Quality of Care
Managers Must Monitor Quality of Care
Regularly
OR Summary 6
Family planning providers at Peru’s government health facilities conform
to national care guidelines in that more than 90 percent of them treat their
clients respectfully and offer them a wide choice of contraceptive options.
Nevertheless, the majority ofproviders couldfurther improve the quality of
care by giving clients more information about correct use and possible side
effects of their chosen method and by screening for contraindications. A
100 percent quality standard ought to be established to avoid violation of
individual reproductive rights.
Background
In the late 1980s, Peru’s National Family
Planning Program within the Ministry of Health
(MOH) assigned method-specific targets to
clusters of health facilities. In 1998 the MOH
changed its policies to ensure that services
responded to individual reproductive health
needs and wishes. It eliminated method quotas,
ended voluntary surgical contraception (VSC)
campaigns, and issued norms to ensure quality
of care and informed choice.
In 1999 the Population Council collaborated
with the MOH to determine whether providers
were complying with the new guidelines and,
secondarily, to develop a monitoring system to
assess compliance over time.
Findings
♦ More than 90 percent of MOH family
planning providers treat their clients with
respect and provide a variety of contraceptive
options without showing bias for or against any
particular method.
♦ Nevertheless, MOH providers can do more to
ensure that every client receives adequate
information about her/his chosen method. For
example, most providers warned simulated
clients about possible menstrual changes
associated with the injectable DMPA, but they
did not mention possible delayed conception
after discontinuation. Actual clients in exit
interviews showed adequate general knowledge
about the pill, condom, injectable and VSC.
However, specific knowledge concerning the
method chosen or used was incomplete.
♦ Most providers in urban health centers did not
check simulated clients for three of the four
medical conditions that are contraindicated for
DMPA use. Few of the providers in health
centers gave information on danger signs
requiring medical attention.
♦ More than 90 percent of clients who had been
sterilized in hospitals stated that they had made
the decision themselves or jointly with the
provider and 98 percent knew its reproductive
consequences.
^Frontiers
RtPKODUCTlVr HEALTH
♦ In urban health centers, simulated clients were
counseled for 2 to 45 minutes. Providers
conveyed 43 percent more information in the 9
to 14-minute sessions compared with 2 to 8minute sessions.
♦ In home interviews, most clients at rural
health posts stated that they had made the
decision to use contraception, and many had
selected a specific method prior to visiting the
health post. Rural clients, however, had limited
knowledge about their chosen method.
Policy Implications
♦ The MOH has produced and circulated new
quality of care norms and strengthened its
provider retraining efforts and supervision
strategies.
♦ MOH facilities and individual providers
should be evaluated on the quality of their
performance and should receive regular
feedback.
♦ Providers should invest as much time as
needed in interactions with clients.
♦ A 100 percent quality standard must be
established to avoid violations of individual
reproductive rights.
♦ Two of the five data collection modes- the
client exit interview and the use of simulated
clients requesting DMPA - proved reliable for
monitoring the quality of care in health centers.
Monitoring tools for hospitals and rural health
posts need further improvement.
February 2000
Study Design
In order to conserve time and funds, the study used Lot Quality Assurance Sampling to draw a
sample of Peru’s 6,589 service delivery points. The study sample consisted of 19 hospitals, 19
health centers, and 19 health posts. Six observations were obtained in each facility. Data were
collected from June through August 1999 as follows:
♦ Hospitals were assessed using reports of simulated clients who requested VSC counseling
and home interviews with VSC adopters.
♦ Health centers were assessed using reports from simulated clients who requested the
injectable DMPA and exit interviews with family planning clients.
♦ Rural health posts were assessed through home interviews with clients who had recently
started using family planning.
For an element to meet the LQAS standard, at least 95 percent of the six clients interviewed at
each facility had to receive specific information or a specific service from the provider in at
least 80 percent of the facilities sampled. Parallel analyses were made on the basis of 95
percent confidence intervals in each sample (N = 114).
Leon, Federico R.. 1999. Peru: Providers’ Compliance with Quality ofCarc Norms.
Leon. Federico R. el al.. 1999. Counseling Sessions Length and Amount of Information Exchange in Peruvian Clinics. For more
information, contact: Population Council, Av. San Borja Sur 676, Lima 43, Peru. Tel. 511-475-0275; Fax: 511-475-0675; E-mail:
pclimafa.amauta.rcp.net.pe or contact: Population Council. Escondida 110, Villa Coyoacdn, 04000, Mexico, D.F. Mexico. Tel. 52-56598537; Fax: 52-5554-1226; E-mail: disemina'u popcouncil,ore.mx.
OR SUMMARIES
Egypt
Access &
Quality of Care
Family Planning Providers Should
Encourage Clients to Discuss Sexual
Problems
OR Summary 7
Both clients and providers welcomed the inclusion of discussions on
sexuality during family planning counseling. Providers who were trained in
sexuality counseling were more likely to discuss sexual matters with clients.
Clients preferred to have the provider initiate the discussion.
Background
This 1999 study, the first of its kind in Egypt,
examined the feasibility and impact of introducing
discussions of sexuality during family planning
(FP) consultations. Conducted by the Population
Council in collaboration with the Egyptian
Ministry of Health and Population (MOHP), the
study took place in four MOHP clinics and two
private clinics affiliated with the MOHP. Nurses
and physicians at all six clinics attended a two-day
training session on contraceptives with an
emphasis on barrier methods.
Providers in the three clinics that had been
randomly chosen as intervention sites also
received three days of training on sexuality,
gender and counseling skills. To assess the
acceptability of sexuality counseling as well as
impact of training, researchers interviewed 25
providers and 503 clients, held five focus group
discussions, and debriefed seven “mystery clients”
(women who posed as clients).
Findings
♦ Family planning consultations with trained
providers were more likely to include a discussion
of sexual matters compared with consultations
with untrained providers (see Table). More than
two-thirds (71%) of the clients who received
sexuality counseling said they were not
embarrassed to discuss such private issues. The
most common sexual problems raised by clients
were loss of sexual desire and pain during
intercourse. Reports of mystery clients showed
that, despite training, providers’ technical
competence in managing such problems was
somewhat limited.
Client Experiences during Family Planning Consultations
Clients who were:
Control (%)
(n = 183)
Intervention (%)
(n = 320)
Counseled on sexual relations
18
44
Encouraged to ask questions
84
95
Counseled on chosen method’s effect on sexuality
22
41
Given a barrier method
2
9
^Frontiers
OL
IS XtrKODUCTIVt HtAtTH
Client Attitudes and
Experiences
“If the doctor asks us those [sexualityrelated] questions we would tell her
about our problems but otherwise I would
be embarrassed to tell her.”
“I often could not have sex with my
husband because of the IUD (bleeding).”
- clients interviewed after clinic visits
♦ Women attending focus group discussions
reported various sexual problems related to
family planning. Expressing their reluctance to
initiate discussion of sexual problems, they said
that they would like the provider to ask some
routine questions about their sexual relations
and indicate a willingness to discuss sexual
topics. As confidentiality is a major concern,
they prefer to talk with a provider they know,
preferably a woman.
♦ Clients at the intervention clinics noticed
improvements in the quality of care. They were
significantly more likely than clients at the
control clinics to report that the provider had
encouraged them to ask questions, had provided
all the information they were expecting, and had
explained how their chosen contraceptive
method could affect their sexual relations.
Policy Implications
♦ Sexuality issues, including potential effects of
contraceptive options, should be incorporated
into family planning counseling. Pre-service and
in-service training for providers should include
instruction on sexuality, sexual problems, and
their relation to family planning methods.
♦ Referrals to teaching or university hospitals
should be established.
♦ Health education messages should encourage
the public to ask family planning providers
about concerns and questions regarding
sexuality.
March 2000
♦ Clients at the intervention clinics were more
likely than those at the control clinics to receive
counseling on the male condom and to obtain a
barrier method, mainly condoms. The majority
of clients using barrier methods planned to use
them for a short time before switching to
another method.
Abdel-Tawab, Nahla et al., 2000. Integrating Issues of Sexuality into Egyptian Family Planning Counseling.Fbr more information,
contact:Population Council, 6A Giza St., P.O. Box 115, Dokki, Cairo, 12211 Egypt. Tel 20-2-571-9252; Fax 20-2-570-1804; E-mail
frontiers@pccairo.org .
This project was conducted with supportfrom the U.S. AGENCY FOR INTERNATIONAL DEVELOPMENT, Office ofPopulation, under
Cooperative Agreement No. HRN-A-00-98-00012-00.
OR SUMMARIES
Indonesia
Institutionalization
of OR
Coordinated Studies Are Needed to
Assess Trends
OR Summary 8
Longitudinal studies with consistent indicators and representative study
populations are needed to identify changes in maternal and child health
indicators.
Background
In 1999 the Population Council/Indonesia
conducted a critical review of 11 Indonesian
surveys and studies that measured various
indicators of maternal and child health (MCH)
between 1996 and 1999. Many of these studies
tried to link these indicators with the nation’s
economic crisis, which began in July 1997.
Council staff sought to explain how these
studies came up with divergent findings.
Findings
♦ The timing of data collection activities and
their geographical coverage are key factors
leading to differences in findings.
♦ Data need to be disaggregated to the lowest
level possible in order to ascertain differential
impacts across regions, among socio-economic
and age groups, and by gender and urban/rural
residence.
|
♦ Attributing changes in MCH indicators to the | fl
economic crisis may be misleading. Health and ; I
nutritional status appears to have been declining H
before the crisis began. The overall impact of
the economic crisis may not be reflected in
MCH indicators for several years.
♦ Family planning services experienced some
disruptions during 1997-1999. The price of
■ B
contraceptives rose in late-1997 and early 1998 I
and fluctuated greatly between mid-1998 and
mid-1999. Clinics reported a significant increase;
in stockouts of contraceptives between 1997 and ■
1998. During October 1998 through July 1999
stockouts in primary health centers and at
^Frontiers
I
midwives’ clinics remained at relatively high
levels (see Figure 1). Nevertheless,
contraceptive prevalence and the number of
health facilities offering contraception did not
change significantly during 1997-1999.
♦ The incidence of sexually transmitted
infections increased from 1997 to 1998, but it is
unclear whether this trend is related to the
economic crisis.
♦ The proportion of urban and rural childrai
aged 6-17 months who were underweight - a
sign of chronic malnutrition - was higher in
1998 than in 1995 (see Figure 2).
Figure 2. Percent of Children Aged 6-17
Months with Low Weight-for-Age,
Policy Implications
♦ Government and nongovernmental agencies,
donors, and researchers need to coordinate the
planning of key research studies to ensure that
comparable and useful measures are developed.
♦ Program planners and other decision-makers
must take into account the limitations of each
dataset before making generalizations to a wider
population or linking health indicators to socio
economic trends. They also need to understand
that the various data collection methods have
different advantages and disadvantages.
♦ To ensure that research findings are useful to
program managers and planners, researchers
should make sure that findings, research
methodology and sample size are reported
accurately and that indicators are comparable in
time-series studies. In order to distinguish new
trends from short-term fluctuations, researchers
should analyze at least three data points and use
trend analysis techniques. Tests of statistical
significance are essential in order to identify true
differences between groups.
March 2000
O' -3OSD □<-2 5SD 1<-2OSD
Gardner. Michelle and Lila Amaliah, 1999. Analysis of Conflicting Crisis-related Research Results. For more information,
contact: Population Council. Sanga Rehana, 53, Lodi Estate, 3rdfloor. New Delhi, 110003, India; Tel. 91-11-461-10912;
Fax 91-11-461-0912; E-mail: frontiersQpcindia.org; or Population Council Indonesia, Menara Dea Building, Suite 303, JI.
Mega Kunigan Barat Dav. E4.3, No. I. Jakarta, 12950; Tel. 6221-576-1011; Fax: 6221-576-1013; E-mail:
pcjktQcbn. net. id.
This project was conducted with supportfrom the U.S. AGENCY FOR INTERNATIONAL DEVELOPMENT, Office of
Population, under Cooperative Agreement No. HRN-A-00-98-00012-00.
OR SUMMARIES
Kenya
Reproductive
Tract Infections
Identifying RTIs Remains Problematic:
Prevention Is Essential
OR Summary 9
More than half of the family planning and antenatal clinic clients in
Nakuru, Kenya had one or more reproductive tract infections (RTIs).
Roughly one-third of these infections were sexually transmitted. Using
syndromic management algorithms based on the woman’s reported
symptoms, providers correctly classified only 5 to 16 percent of women who
later tested positive with laboratory results. Given the limitations of
syndromic management, programs need to stress prevention of sexually
transmitted infections (STIs).
Background
Findings
Since 1990 the Nakuru Municipal Council has
implemented a multifaceted program to reduce the
incidence of reproductive tract infections,
especially those that are sexually transmitted,
including HIV/AIDS. Staff in the Council’s five
health clinics use syndromic management
guidelines, based on clients’ reported symptoms
and clinical signs, to identify clients with RTIs.
♦ Fifty percent of FP clients and 59 percent of
ANC clients had at least one RTI, as detected by
laboratory tests. A relatively high proportion of
clients - 14 percent of the FP clients and 21
percent of the ANC clients - had one or more
sexually transmitted infections (chlamydia,
gonorrhea, and trichomoniasis).
In 1998 the Population Council conducted a study
to assess the accuracy of syndromic management
and determine the best ways to integrate RTI
management into existing antenatal (ANC) and
family planning (FP) services. Sources of data
included: (1) findings from a medical
examination, including a pelvic exam and
assessment of symptoms and clinical signs, of 906
FP clients and 815 ANC clients; (2) clients’ (and
their partners’) risk factors for STIs; (3) laboratory
tests for five RTIs; and (4) interviews with 18
nurses and 195 clients. After an assessment of
existing RTI services, 18 nurses from the five
municipal clinics attended a three-day refresher
course in syndromic management, including
training in using a checklist for client
management.
♦ Vaginal infections due to bacterial vaginosis,
trichomoniasis and candidiasis were more
common (47% FP and 56% ANC clients)
compared with cervical infections due to
gonorrhea and/or chlamydia (7.5% of FP and
9.4% of ANC clients).
♦ Most women found to have an RTI through
laboratory testing were asymptomatic and showed
no clinical signs. Only 23 to 29 percent of ANC
and FP clients with infection reported one or more
RTI symptoms, and 37 to 43 percent of infected
clients were found on examination by a provider
to have clinical signs.
♦ Applying syndromic management guidelines,
providers were able to classify correctly as
^Frontiers
^1N REPRODUCTIVt HEALTH
Prevalence of RTIs among Study Population (%)
infected only a small proportion of the women
who actually had a laboratory-diagnosed R.TI
(5% of the FP clients and 16% of the ANC
clients).
♦ Current syndromic management guidelines for
women classified as having vaginal discharge
syndrome are more reliable for managing women
who have a vaginal infection than for managing
women having a cervical infection. Most women
classified by providers as having a vaginal
discharge syndrome (61% of FP clients and 70%
of ANC clients) did in fact have a vaginal
infection, whereas only 11 percent of FP clients
and 8 percent of ANC clients classified as having
vaginal discharge syndrome had a cervical
infection.
♦ Collecting STI risk assessment information
from clients did not significantly improve
providers’ ability to identify women with cervical
infections.
Policy Implications
♦ Given the poor performance of syndromic
management for women presenting with vaginal
discharge as a symptom of an STI, programs need
to emphasize treatment, by improving providers’
counseling skills and encouraging them to educate
clients about STI symptoms and preventive
measures, especially dual protection.
♦ If programs insist on continuing to use
syndromic management of vaginal discharge, then
women classified by providers as having vaginal
discharge syndrome should be first treated as
having a vaginal infection (i.e. bacterial vaginosis,
candidiasis and trichomoniasis) rather than a
cervical infection. If symptoms persist, treatment
for cervical infection may be advisable.
♦ Algorithms for managing vaginal discharge
need to be reviewed to emphasize treatment for
bacterial vaginosis, which is the most common
RTI and has been associated with increased risk
for HIV infection and pelvic inflammatory
disease.
March 2000
Solo, Julie: Ndugga Maggwa: Janies Kariba Wabur; Bedan Kiare Kariuki; and Gregory Maitha. 1999. Improving the Management of
STIs among MCH/FP Clients at the Nakuru Municipal Council Health Clinics. For more information, contact: Population Council, P.O.
Box 17643, Nairobi. Kenya. Tel. 254-2-713-480; Fax 254-2-713-479; E-mail: miblicalions&nopcouncil.or.ke.
This project was conducted with support from the U.S. AGENCY FOR INTERNATIONAL DEVELOPMENT under Contract Number CCP3030-C-00-3008-00 and Cooperative Agreement Numbers CCP-3050-A-00-4013-00 and HRN-A-00-98-00012-00.
OR SUMMARIES
Burkina Faso
and Mali
FGC
Female Genital Cutting Harms
Women's Health
OR Summary 10
Women in Burkina Faso and Mali who have had their genitals cut are more
likely to have gynecological and obstetrical problems, including bleeding,
internal scarring, vaginal narrowing, and complications during childbirth.
More severe cutting increases a woman’s risk of other reproductive health
problems.
Background
In collaboration with the Ministries of Health
(MOH) of Burkina Faso and Mali, the
Population Council conducted two studies in
1998 to describe the occurrence and severity of
health problems related to female genital cutting
(FGC). This traditional practice entails partial or
total removal of girls' external genitalia.
Study participants were consenting women who
received a pelvic exam during prenatal, family
planning, obstetric, or gynecological
consultations at MOH clinics. Providers were
trained to observe the types and complications
of FGC. In order to assess their potential role as
change agents, providers in Mali also received
training on the health effects of FGC and client
counseling. In Burkina Faso, health providers
recorded information on and interviewed 1,920
women at 21 health centers in the rural
provinces of Bazega and Zoundweogo. In Mali’s
Bamako district and Segou region, providers
recorded information on 5,390 women in 14
urban and rural health centers.
94 percent in Mali had been cut. In Burkina
Faso, Type 1 (removal of the clitoral hood
and/or clitoris) was most common. Nearly three-;
fourths (74%) of the women in Mali had Type 2 ;
(clitoridectomy and removal of the labia
minora). Five percent of women in both groups !
had the most severe form of FGC, Type 3 or
infibulation, which entails partial or complete
removal of the external genitalia with
stitching or narrowing of the vaginal opening.
FGC was found among all ethnic groups.
Gynecological
Complication
Obstetric
Complication
[□Burkina Faso BMaH~[
Findings
♦ The prevalence of FGC was very high - 93
percent of the clinic clients in Burkina Faso and
* Based on client reports in Burkina Faso and actual
deliveries in Mali.
^Frontiers
♦ Fourteen percent of the clients in Burkina
Faso and 5 percent of those in Mali had at least
one gynecological complication related to FGC.
In Burkina Faso, where the majority of women
have Type 1 cutting, keloid scarring and vaginal
stenosis (narrowing of vaginal walls due to
scarring) were the major complications reported
by women. In Mali, where Type 2 cutting
predominates, hemorrhaging from scar tissue
was the major complication observed by clinic
staff, followed by vaginal scarring and
obstruction.
♦ In both countries, women who were
infibulated (Type 3) were almost two and a half
times more likely to have a gynecological
complication than those with a Type 2 cut.
Similarly, women with a Type 1 cut were much
less likely to have a complication than those
with more severe cuts.
♦ FGC was found to be a major risk factor for
complications during childbirth, with risks
increasing according to the severity of the cut. In
Burkina Faso, cut women were three times more
likely to report having had a difficult delivery
than uncut women. Women with Types 2 or 3
cutting were more likely to experience
hemorrhaging or perineal tearing during
delivery.
♦ Among the women in Mali who gave birth at
the clinic, 29 percent of those who had been cut
experienced complications during childbirth,
compared with 7 percent among those who had
not been cut. In Mali, 5 percent of uncut women
experienced complications during delivery
compared with 18 percent of women with Type
1 cutting, 30 percent of those with Type 2. and
36 percent of those with Type 3.
♦ In Burkina Faso, cut women were 1.5 times
more likely than uncut women to show signs of
genital infection, particularly vaginal discharge,
suggesting that FGC may render women more
susceptible to RTIs.
Policy Implications
♦ All health personnel should receive
information on the serious health problems
associated with FGC.
♦ In addition to women’s rights issues,
information on the deleterious health effects of
FGC should be used in community education
campaigns.
♦ People assisting women giving birth should
anticipate the possibility of FGC-related
complications.
March 2000
Diop, Nqfissatou J., el al. Etude de I'EfTicacitd de la Formation du Personnel Socio-sanitaire dans 1’Education des Client(e)s sur I’Excision
au Mali. Bamako, Mali: Population Council, 1998.
Laboraioire de Same Communautaire du Bazega. Evaluation de la Prevalence, de la Typologie, et des Complications Liccs a I’Excision
chez les Patientes Frequentant les Formations Sanitaircs du Bazega. Ougadougu, Burkina Faso: Population Council. 1998.
Jones, Heidi, et al. Female Genital Cutting and its Negative Health Outcomes in Burkina Faso and Mali Studies in Family Planning Vol.
30. No. 3. September 1999. For more information, contact Population Council, P.O. Box 21027, Dakar, Senegal. Tel. 221-824-1933; Fax
221-824-1998; E-mail: pcdakaru ncdakar. org.
This project was conducted with supportfrom the U.S. AGENCY FOR INTERNATIONAL DEVELOPMENT under Contract
Number CCP-3030-C-00-3008-00 and Cooperative Agreement Number HRN-A-00-98-00012-00.
OR SUMMARIES
Mali
Female Genital
Cutting
Empower Health Workers to Advocate
against Female Genital Cutting
OR Summary 11
Health providers are an important potential resource in campaigns to
eradicate female genital cutting (FGC), but a concerted effort is needed to
ensure that they can become effective behavior change agents. After a threeday training course, providers’ knowledge about FGC increased, but few of
them counseled their clients about FGC.
Background
The various initiatives to eradicate FGC in Mali
-public education campaigns and conversion of
traditional excisors - over the past two decades
have had little impact on this traditional
practice. This study assessed the use of health
personnel to combat FGC. as recommended by
the World Health Organization.
Conducted in 1998 by the Association de
Soutien au Developpement des Activites de
Population (ASDAP), a nongovernmental
organization, and the Ministry of Health, the
study covered 14 urban and rural health centers
in Bamako and Segou region. In the eight health
centers that served as experimental sites, 59
health providers, including physicians,
midwives, nurses and aides, attended a three-day
training course on identifying and treating
medical complications related to FGC and
counseling clients about FGC. In the six centers
that served as control sites, 48 providers were
interviewed.
Findings
♦ Nine in ten health providers are opposed to
FGC and are willing to play an active role in
educating their clients about FGC.
♦ Nevertheless, some providers support the
medicalization of FGC. Nine percent of the
providers who had been trained and 29 percent
of those in the control group stated that FGC
presents no health risk if performed in hygienic
conditions. Thirteen percent of the 107
providers interviewed admitted that FGC is
being practiced at their facility. Four providers
said they had performed FGC procedures.
I
«
I
♦ Training did change some providers’ attitudes .
regarding FGC. Before training, 39 percent of
providers thought that an uncut girl had loose
morals; after training, 26 percent still held this
belief. The proportion of providers who thought J
that men prefer to marry women who have been ’■S
cut declined from 32 percent to 28 percent,
while the proportion who thought that FGC
guarantees a girl’s virginity decreased from 14
percent to 9 percent.
♦ Providers’ knowledge of FGC increased
dramatically after training. Roughly three in four 9
trained providers knew at least three immediate
and long-term complications (see Figure).
However, providers were uncomfortable
discussing FGC with their clients and felt too
rushed due to the large volume of clients during
the morning clinic sessions. Group health talks
were held in only two of the eight experimental
^Frontiers
IN HtPHOOVC I l\ I Hl All II
fl
a
2
1
Health Providers' Knowledge of FGC
[□Before Taining El After Training
clinics. Only six of the 1,105 clients interviewed
were counseled about FGC.
♦ The majority of health providers have
provided treatment to girls with complications
following FGC. More than one third had to refer
a client for further treatment of FGC
complications. Nevertheless, providers
acknowledged that they have limited
competence in caring for FGC complications,
even after training.
Policy Implications
♦ Mali’s MOH is using the study results to
develop a new curriculum to promote
standardized, mandatory- training on FGC for all
health providers.
♦ Based on the study findings, the MOH issued
a policy banning the practice of FGC in its
facilities.
♦ The three-day training course was effective in
changing provider attitudes toward FGC, but
additional training in communication skills is
needed to overcome providers’ reticence to
discuss FGC with their clients.
♦ To eradicate FGC, community education
initiatives are needed in addition to clinic
education.
April 2000
Diop, Naftssatou J., et al. Etude de I’Efficacite de la Formation du Personnel Socio-sanitaire dans I’Education des Client(e)s sur
I’Excision au Mali Bamako. Mali: Population Council, 1998 For more information, contact Population Council, P.O. Box
21027. Dakar. Senegal. Tel. 221-82-1-1933: Fax 221-824-1998: E-mail: ocdakara pcdakar.ore.
This project was conducted with supportfrom the CS. AGENCY FOR INTERNATIONAL DEVELOPMENT under Contract
Number CCP-3030-C-00-3008-00 and Cooperative Agreement Number HRN-A-00-98-00012-00.
Egypt
Postabortion
Care
Expand Access to Postabortion Care
OR Summary 12
Training providers and introducing a case management protocol led to
improved postabortion care at ten government and teaching hospitals in
Egypt. Patients reported shorter waits and greater satisfaction with the
medical services they received. Physicians adopted treatment methods
associated with lower complications and provided more health-related
information to patients.
Background
Findings
A 1994 pilot study in two Egyptian hospitals
showed that upgrading postabortion care (PAC)
and training physicians in manual vacuum
aspiration (MVA), infection control and
counseling led to significant improvements in the
care of postabortion patients. This 1997 study,
conducted by the Egyptian Fertility Care Society
with support from the Population Council, sought
to institutionalize improved postabortion medical
care and counseling procedures in ten hospitals seven government hospitals and three university
hospitals.
♦ After their training physicians had significant
gains in knowledge about short-term
complications, adverse health impacts, and the
immediate return of fertility following
postabortion treatment. Physicians were more
likely after the intervention to recognize that PAC
patients should receive information about the
cause of miscarriage and the need to eat well, rest
and use contraception during recovery.
In the 1997 intervention, five senior physicians
from each hospital attended a five-day training
course in MVA, infection control, and family
planning (FP) counseling. The physicians then
supervised four months of on-the-job training of
doctors and nurses at the 10 hospitals. A case
management protocol, including emergency
medical treatment, pain control, and FP
counseling, was also introduced. Researchers
measured the resulting changes in knowledge and
practice by administering surveys before (255
physicians, 311 nurses, and 508 patients) and after
(246 physicians, 263 nurses and 497 patients) the
intervention. Data were also collected from 1,036
medical records.
Care of Postabortion Patients
Postoperative Appointment
FP
Problems__________________________
□ Pre-inlervention 1 Post-intervenlion |
♦ After the intervention, physicians shifted from
nearly universal use of dilatation and curettage
(D&C) to use of MVA in 57 percent of cases
^Frontiers
IN BtPBODUCTIVE HEALTH
requiring emergency medical treatment. More
than three in four physicians reported lower
complication rates with MVA, compared with
D&C. More than half said that MVA is more
effective and easier to use than D&C.
♦ The shift to MVA led to a shift from general
anesthesia to local anesthesia in about 30 percent
of the cases. Following the intervention, the
proportion of physicians stating that mild
analgesia and local anesthesia can reduce patients'
anxiety increased significantly. However, pain
control techniques still need improvement: 18
percent of post-intervention patients did not
receive any pain control medication. Although the
proportion of patients reporting extreme pain did
not increase significantly, reports of moderate
pain increased five-fold (from 5% to 27%).
♦ Nearly three in four (73%) of the post
intervention PAC patients stated that the service
they received at the hospital was excellent,
compared with 44 percent before the intervention.
Post-intervention patients were more likely than
pre-intervention patients to report that the
provider was friendly, that they waited less than
30 minutes for medical services, and that they
received information about possible
complications, their management, and follow-up.
♦ The proportion of PAC patients who said that
they had received family planning information at
the hospital increased from 35 percent to 47
percent. However, only 7 percent of the PAC
patients received a contraceptive method before
discharge.
Policy Implications
♦ Training and protocols for PAC, including
procedures for control of pain and infection,
should be standardized in hospitals as well as
undergraduate and graduate medical schools.
Government and teaching hospitals should include
MVA supplies as standard items in their budget
and should ensure an adequate supply of pain
medication.
♦ Some aspects of PAC still need improvement:
pain control, information given to patients, and
the provision of FP counseling and services.
Nurses should be given a greater role in
comforting, counseling, and informing PAC
patients. Simple guides on MVA instruments and
FP counseling should be developed.
Utilization
♦ The Ministry of Health and Population’s
“Healthy Mother/Healthy Child” project is
training providers in MVA and other elements of
PAC, including pain control and linkages with
family planning services. Ten new hospitals have
introduced improved PAC through the Healthy
Mother/Healthy Child project—five in Aswan,
two in Luxor, and three in South Qena. Expansion
into new sites in Fayoum and Bani Sewef is
underway.
May 2000
Nawar, Laila et al.. 1997. Scaling-up Improved Postabortion Care in Egypt: Introduction to University and Ministry of Health and
Population Hospitals. Formore information, contact: Population Council, 6A Mohamed Bahie Eddine Barakat St.. Ilf1'floor, Giza, Egypt.
Tel. 20-2-571-9252; Fax 20-2-570-1804; E-mail: frontiers'amccairo,ore .
This project was conducted with support from the U.S. AGENCY FOR INTERNATIONAL DEVELOPMENT under Contract Number DPEC-00-90-0002-10 and DPE-3030-Q-00-0023-00.
Peru
Quality of Care
Tell Clients How to Use Their Chosen
Method
OR Summary 13
Family planning providers in Peru need to focus more closely on giving
clients relevant information on their chosen method and asking key
questions in order to make the most efficient use of the time available for
client counseling.
Background
In 1998 the Peruvian Ministry of Health (MOH)
issued quality of care norms to ensure that
family planning providers respond to their
clients’ reproductive health care needs and
goals. In mid-1999 the Population Council
collaborated with the MOH on a study to
determine whether the length of counseling
sessions affects the amount of information
provided to the client.
Using Lot Quality Assurance Sampling, the
study focused on 19 health centers in 10 urban
areas, drawn from a national sample of 172
facilities. Six simulated clients (women posing
as clients) made a total of 114 visits to the 19
health centers during June-July 1999. Each
simulated client was trained to say that she
wanted to switch from the rhythm method to a
more effective method. After counseling, she
chose the injectable Depo-Provera but stated
that she wished to consult her husband before
beginning use.
To assess the quality of counseling, the
simulated clients completed a checklist after
each visit, indicating what information had been
given to them. The checklist consisted of 46
items reflecting optimal information exchange.
It covered: questions to identify factors relevant
to contraceptive options; information on
available contraceptive methods; questions to
screen for contraindications to injectable use;
information about injectable use, side effects
and warning signs; use of barrier methods for
temporary protection against pregnancy; and
follow-up instructions.
Findings
♦ Providers conveyed more information during
sessions lasting nine minutes or longer,
compared with shorter sessions. During the
sessions lasting 9-14 minutes, providers covered
42 percent of the 46 items on the information
exchange checklist, compared with 30 percent
of the checklist items during shorter sessions of
eight minutes or less. However, information
exchange improved only slightly during
counseling sessions lasting 15-45 minutes.
Length of Counseling Session
^Frontiers
IN RiPHQDUcrivr Ht-MIH
fry
♦ Longer counseling sessions did not lead to
more information exchange because the
providers spent the extra time giving clients
more details about methods they were not
planning to use, rather than giving them
essential information on use of their chosen
method and screening for contraindications. In
fewer than 20 percent of the visits, providers
asked about vaginal bleeding, discussed breast
cancer, advised interim use of barrier methods,
or asked whether the client understood.
♦ Nevertheless, providers are meeting many
quality of care goals. In more than four in five
counseling sessions, providers asked standard
questions needed to assess appropriate
contraceptive options, discussed four or more
contraceptive methods, and asked the client to
make a choice of methods.
♦ Providers involved in the study welcomed the
feedback regarding the quality of their
counseling. They cited time constraints as the
major cause of insufficient counseling. Some
visits were clearly too short, but the average
visit lasted 15 minutes, which should have been
sufficient to cover key information. Researchers
concluded that providers could have used their
counseling time more efficiently. Also, they
missed opportunities to provide client-centered
treatment by asking questions to ascertain each
client's situation and needs.
Policy Implications
♦ The MOH should test an alternative model for
client counseling in order to help providers to
give more effective, client-centered family
planning counseling. This model consists of five
steps:
1. A warm welcome;
2. A client-centered diagnosis that
identifies a subset of appropriate family
planning methods;
3.
Provision of appropriate, personalized
information on appropriate methods,
leading to choice of a single method;
4.
Screening for contraindications,
education on use of the method chosen,
and instructions for follow-up; and
5.
Feedback to ensure understanding and
appropriate follow-up.
This model should stress the provider's role after
a contraceptive method has been chosen,
including screening for contraindications, giving
instructions on correct use, and discussing side
effects and warning signs. The MOH should
develop job aids to help providers implement
this model and should undertake operations
research to assess its value.
September 2000
Leon. Federico R. et al., 1999. Counseling Sessions Length and Amount of Information Exchange in Peruvian Clinics. For more
information, contact: Population Council, Av. San Borja Sur 676, Lima 43, Peru. Tel. 511-475-0275; Fax: 511-475-0675; E-mail:
pclima(a>amauta.rcp.net.pe or contact: Population Council, Escondida 110, Villa Coyoacdn, 04000, Mexico, D.F. Mexico. Tel. 52-56598537; Fax: 52-5554-1226; E-mail: diseminatrz popcouncil.ore.mx.
This project was conducted with support from the U.S. AGENCY FOR INTERNATIONAL DEVELOPMENT under Cooperative Agreement
Number HRN-A-00-98-0001 2-00.
Egypt
NGOs Need to Join Forces to End FGC
OR Summary 14
Fifteen Egyptian non-governmental organizations are actively involved in
programs to eradicate the practice offemale genital cutting. To make these
programs more effective, NGOs shouldform coalitions, engage in advocacy,
train activists in communication skills, and evaluate the impact of their
programs.
Background
Until recently, the practice of female genital
cutting (FGC) has been nearly universal in
Egypt. However, a 1998 national survey found
the first signs of a decline in the practice among
adolescents since 1994 (El-Gibaly et al., 1999).
Non-governmental organizations (NGOs)
working in community development, health and
women’s rights have played a leading role in
advocating eradication of FGC in Egypt. To
document and assess the impact of anti-FGC
programs, the Population Council conducted an
assessment from August 1999 to February 2000.
Researchers telephoned numerous Egyptian
NGOs to identify those most actively involved
in anti-FGC programs. Then they conducted indepth interviews with officials of 15 NGOs as
well as staff of the Ministry of Health and
Population, UNICEF and the UnitedNations
Population Fund (UNFPA).
Findings
♦ Most NGOs had no evaluation mechanism in
place to assess the impact of their interventions.
Some NGOs collect information on process
indicators, such as the number of meetings,
attendees, and requests for information. Few
NGOs measure the impact of their interventions
on participants’ knowledge, attitudes, or
practices.
♦ Each of the four basic intervention models
identified in the assessment was useful in
addressing some aspect of the behavior change
continuum, from creating awareness to
increasing knowledge, to talking with others
about FGC, culminating in the decision to take a
firm stand against FGC. The four intervention
models are:
4- Awareness-raising. Many NGOs have
organized large lectures and seminars for
community members, with medical and
religious leaders discussing the harmful
effects of FGC. Such meetings reach large
numbers of people at a relatively low cost.
4- Community members as change
agents. Some NGOs have trained influential
community members or individuals who are
^Frontiers
J| IN RtraODUCTIVC IltALfH
opposed to FGC (positive deviants) to talk
to others in their community. NGO leaders
reported that this approach did lead to
knowledge gains and attitude change
regarding FGC.
■F Community' development Several
NGOs have integrated anti-FGC messages
into literacy classes and a program for
handicapped youth. A few NGOs have
added anti-FGC components to their
comprehensive development programs. This
approach is promising, since it targets the
entire community and reaches individuals
through multiple channels such as seminars,
home visits and literacy classes. However, it
is expensive and labor-intensive.
■F Advocacy. A few NGOs have done
advocacy work such as: organizing meetings
of government officials; providing
information to politicians, researchers and
journalists; building coalitions with other
NGOs; training local leaders in advocacy
skills; and producing radio and television
programs on FGC.
♦ Although most NGO officials recognized the
importance of networks and coalitions for
combating FGC, only two NGOs belong to such
groups.
Policy Implications
At a two-day seminar held in January 2000 in
Cairo, 40 representatives of NGOs, government
agencies, research institutes, donor agencies, "
and Cooperating Agencies discussed the
assessment findings and recommended that:
♦ NGOs should form coalitions to reinforce and
complement each other’s work. They should
involve government agencies, media outlets,
research institutions, and communities in broad
scale interventions.
♦ More advocacy activities, particularly those
that combine media and policy activities, are
needed to create a strong social and political
environment against FGC in Egypt.
♦ Anti-FGC messages should discuss social,
religious and legal perspectives rather than
focusing on the health hazards of FGC.
♦ NGOs should develop partnerships with
research institutions to obtain technical
assistance in evaluation. They should develop
indicators to measure the different stages of
attitude and behavior change.
♦ Outreach workers and community advocates
need training in communication techniques and
problem-solving skills, assistance in defining
their activities, and better supervision.
September 2000
Abdel-Tawab, Nahla, and Sahar Hegazi.2000. "Critical Analysis of Interventions against FGC in Egypt. " Cairo: Population Council. For
more information or to obtain a copy of the English Final Report or the Arabic Condensed Summary ofthis study, contact: Population
Council, 6A Mohamed Bahie Eddine Barakat St., Ilf"floor, Giza, Egypt. Tel.: 202-571-9252; Fax: 202-570-1804; E-mail:
frontiers pccairo.org .
This project was conducted with supportfrom the U.S. AGENCY FOR INTERNATIONAL DEVELOPMENT under Cooperative Agreement
Number HRN-A-00-98-00012-00.
docto^Plavs with the
A
nipple of a woman suffer
ing from breasl cancer
as he discusses Iter case with a
panel of 10 other doctors.
A
58-yenr-old
unmarried
woman, who had never exposed
herself in public, is asked to
strip to her waist to be examin
ed for breast cancer by a team of
specialists.
A mother of three begins sobb
ing hysterically when the doelor
Informs her, without any prior
warning, that she has cervical
cancer.
These are Just three real inst
ances of the insensitivity shown
by doctors while dealing with
cancer patients, says Jyolsna
Govil. president of Cancer
Sahyog (Cancer Aid).
I lers is a Delhi-based volunta
ry group, assisting doctors at
the All India Institute of Medical
Sciences and lhe Rotary Cancer
Hospital.
While harassed doctors in our
hospitals complain they are ove
rextended. having to deal with
as many as 30 patients every
day. patients and their families
feel a little more sympathy
would go a long way in quelling
their fears.
Today breast cancer is the
number two killer of women in
India. Cervical cancer-is also on
the rise, as are king and oral can
cer. And yet the medical profes
sion has done little to inform
women about this dreaded
disease.
Brief information capsules
are a must, especially since doc
tors are tomlomming lhe fact
that unlike the West, where onethird of cancer patients get
cured. Indian survival rates are
low. Too many patients come for
diagnosis when the disease has
entered the third and fourth sta
ges and is too advanced to cure.
The 16th International Can
cer Congress held in New Delhi
recently had specialists focus
ing on the different forms of can
cer and the steps being taken
worldwide lo (real it. A small
adjunct of this huge Congress
was a series of Interactions bet
ween doctors, cancer survivors
and volunteers organised in
support groups.
The support groups attempt.
through sympathetic counsel
ling. to bridge the information
gap currently existing between
doctor and patient.
Several cancer survivors, wor
king as volunteers, spoke about
flow an initial Intervention
would have helped them dispel
their own fears. Mona Saiga), a
cancer survivor living in Delhi.
spoke about how her world alter
ed radically when she learned
she had breast cancer. The doc
tors didn't tell me anything. I
wish someone had helped me
overcome the initial trauma."
"For lhe patient, the doctor Is
God. Most doctors however
refrain from taking on this awe
some responsibility." observed
Mary Goodwill, an American
volunteer.
Govil
spoke
about
the
patients' need to have someone
listen to them so they could
express their Icars.
This refrain was voiced repea
tedly by volunteers from across
the globe, whether they belong
ed to small Slovenia — as does
Vida Zabric. working with the
voluntary group Reach to
Recovery — or giant Canada
where Blossom Stllson works
wtlh a therapy group. The
universal feeling is that psycho
logical
morbidity
decreases
when the patient is better
Informed.
Zabric. a retired engineer.
tells her patients. "I am the liv
ing proof that you can survive.
My husband gave up hope. I did
not and I am still alive."
Dr Robert Macbeth, a retired-
/Ma Tola, head of the
department of occupational the
rapy at theTata Memorial Hospi
tal in Bombay. spokqpf the pio
neering methods her unit has
devised to cope with a whole
range of disfigurements. She
works in tandem with a speech
therapist and physiotherapist.
Several patients come to them
suffering from post-operative
anxiety, having suffered facial
disfigurement or having losi
their voice box ora limb. Il takes
many weeks to make them
come to terms with their new
reality.
"For example, a woman who
has lost her breasl will have to
undergo bra training. We Insist
that a temporary pad be Insert
ed al lhe earliest, so lhat a
woman can go home looking
complete." Tola said.
Earlier women were using
pouches made out of foam. Tola
attended a course in latex tech
nology In Kerala In 1985 to learn
to make breasts of latex. These
cost Rs 150 per piece and last
one year. Today, breasts made
from silicon are also popular
although they cost as much as
Rs 7.000 per piece.
Tola
regrets
that
para
medical workers like her are not
accorded respect within the
medical community. "Unlike In
the West, we continue to be dis
criminated against by doctors.
both financially and in terms of
status. The result is lhat no one
wants to become a para-medical
worker and we face an acute
shortage." she said.
Campaigning
against cancer
The best soldier in the battle against cancer is
someone who has survived the disease.
PADMA TANDON reports on efforts to
educate the public — and the medical
profession
surgeon from Toronto. Canada.
maintained lhat in lhe develop
ed count ries one out of 11 wom
en suffered from breast cancer.
"A large number of these wom
en are married and find it diffi
cult lo cope with this disease."
he pointed out. 'They equate los
ing an intrinsic part of their ana
tomy to losing their sexuality.
Many arc unable to show their
husbands and. if it is a weak
marriage, it simply breaks up
under (his new pressure?
Others just want to return
home and lead a normal life." Dr
Macbeth added.
In India, breast cancer is
more of an urban phenomenon.
prevalent amongst ' belter-off
sections where women do not
breast feed. Cervical cancer is
found among poorer women.
Lack of access to toilets, multi
ple partners, and having too
many children loo early, are fac
tors (hat cause this disease.
Distribution of easy-to-read
material makes people more
aware of the symptoms of lhe
disease, said Dr J Elizabeth of
lhe Armed Forces Medical Colle
ge. Pune, citing her own experi
ence with 200 women who filled
out a questionnaire knowledgea
bly .liter reading pamphlets on
cancer.
If pre-surgery comprises one
traumatic stage in a cancer
patient's life, then post-surgery.
whether It be of lhe breasl.
trachea or limb, requires a con
certed rehabilitative effort.
A major problem facing pati
ents is the sheer cost of treat
ment. While the arsenal of anti
cancer drugs has grown, with
50 chemotherapy drags availa
ble to combat 100 types of can
cer. their prices are sky high.
The wonder drug Taxon for
breast and ovarian cancers is
prohibitive, with a course of six
injections costing Rs 31.000.
Platinum-based drags used to
cure lung and ovarian cancers
are even more expensive.
But there is a world-wide
swing towards more affordable
drugs. Dr J Stjenisward. chief
of WHO's Cancer and Palliative
Care unit in Geneva, is a strong
advocate of morphine-based
drugs for cheaper relief for
patients.
Stjcrnsward cited the exam
ple of Kerala as having brought
down the Incurability rate of
cancer patients from 85 per
cent lo 55 per cent during the
last four years. High education
■ levels plus district-level cam
paigns helped ensure patients
came in for early diagnosis.
Stjcrnsward announced that
a major campaign is to be laun
ched in India, lb create public
awareness for self-detection of
breast, oral and cervical cancer.
In lhe Kerala programme, lhe
proportion of cases detected ear
ly rose from 15 to 40 per cent. as
women informed about the sym
ptoms of the disease reported
immediately lo health workers 4*
Women's Feature Service
IVth Annual Conference of Breast Cancer Foundation - India
Bangalore on 8th, 9th & 10th March 2000
Host: Bangalore Institute of Oncology, Bangalore
ORGANISING COMMITTEE
Date:
Ref.:
Chairman:
Dr. B.S. AJAIKUMAR
Vice Chairman:
Dr. M. GUNASHEELA
To
Dr. Ravi Narayan
Community Health Centre
Koramangala
BANGALORE.
Reception Committee
Chairman:
Dr. B.S. SRINATH
Organising Secretary:
Dr. B.S. RAMESH
^^ance
March 16, 2000
Dear Sir,
On behalf of the organising committee of IVth Annual conference of
Breast cancer foundation-India, Bangalore I sincerely thank you for
sparing us your valuable posters which was exhibited for the
awareness ofpublic
Dr. GANESH NAYAK
Trade Exhibition:
Dr. V.S. HIREMAT
Treasurer:
Dr. SHEKAR PATIL
The valuable message of public awareness for the eradication of
cancer was conveyed to the viewers through each posters, which was
appreciated by and\133^&
Scientific Committee:
Dr. K.S. GOPINATH
Dr. M. UDAYKUMAR
Dr. RAKESH MITTAL
Thanking You,
Travel & Accomodation:
Dr. RAVI B. DIWAKAR
Yours sincerely,
Registration :
Dr. SANJEEV SHARMA
Dr. NARENDRA
Hospitality & Entertainment:
ANALINI RAO
"kannan GHARPURE
Dr.Ramesh S.Bilimagga
OrgfSecretary
Auditorium &
Hall Arrangement:
Dr. V.K. AHUJA
Dr. VIJAYARAM
Public Function:
Mrs. SUBHA E. DASA
Souvenir:
Dr. KALLUR. G.
Dr. MANJUNATH SASTRY
Catering:
Sq. LDR. B.S. SRINIVAS
Address for Correspondence:
Dr. RAMESH S. BILIMAGGA, Organising Secretary
Bangalore Institute of Oncology, 44-45/2, 2nd Cross, R.M.FL Extension,
Bangalore - 560 027. INDIA. Tel: 2225698, 2221723 Fax:91-080-2293862
E-mail: bilimaga@vsnl.com.
Website: angelfire.com/scifi/conference
"'Courtesy: DABUR PHARMACEUTICALS - ONCOLOGY DIVISION
~ m^ACMLu.
^oo^clUoqJ
Q^yovl<iLOt<
ol
-^volb
.
jphcZJUAJjt^
3) ‘/dvLpj-ox< -
- 4^ CmJccoww ol ca^ xoot
Q^lsfc
(XLCCQC
^<Ju^/.(£x^ast
QlAJ^
ocdC
^xCji^JjZ
.
S>^ iAoJrlc
Q)Lq qA£^
f) fcOJL
pC<LGZ
^LsebveC) 03 ok_
ii
r\ a /i<r
cl-vaJ'
ox.
c^ ^ouajl-
I
c'rcle
bulletin
JANUARY-FEBRUARY 1983
Witches, Healers and Gentleman Doctors
The story of the psychomedical experts-the
doctors, the psychologists, and sundry related
professionals-might be told as an allegory of science
versus superstition : on the one side, the clear
headed, masculine spirit of science; on the other
side, a dark morass of female superstition, old
wives’ tales, rumors preserved as fact. In this alle
gorical version, the triumph of science was as
inevitable as human progress or natural evolution ■_
the experts triumphed because they were right.
But the real story is not so simple, and the
outcome not so deary “ progressive. ” It is true
that the experts represented a less parochial vision
than that of the individual woman, submerged in
her family and household routines: the experts
had studies; they were in a position to draw on a
wider range of human experience than any one
woman could know. But too often the experts,
theories were grossly unscientific, while the tradi
tional lore of the women contained wisdom based
on centuries of observation and experience. The
rise of the experts was not the inevitable triumph
of right over wrong, fact over myth; it began
with a bitter conflict which set women against
men, class against class. Women did not learn to
look to an external “ science ’’ for guidance until
after their old skills had been ripped away, and
the ‘ wise women ’ who preserved them had been
silenced, or killed.
In Europe the conflict between female lay
healing and the medical profession had taken a
particularly savage form: the centuries-long witch
hunts which scar the history of England, Germany,
France, and Italy. The witch hunts themselves
were linked to many broad historical developments:
the reformation, the beginnings of commerce, and
a period of pleasant uprisings against the feudal
aristocracy. But for our purposes the’ important
point is that the targets of the witch hunts were,
almost exclusively, peasant women, and among
them female lay healers were singled out for per
secution. It is to this aspect of the witch hunts that
we now turn briefly.
The Witch-Hunts
The extent of the witch craze is startling: in
the late fifteenth and early sixteenth centuries there
were thousands upon thousands of executionsusually live burnings at
stake-in Germany,
Italy, and other countries. In the mid sixteenth
century the terror spread to France, and finally to
England. One writer has estimated the number of
executions at an average of six hundred a year for
certain German cities-or two a day; ‘ leaving out
Sundays. ’ Women made up some 85 percent of
those cxecuted-old women, young women, and
childeren.
The charges leveled against the ‘ witches ’
included every misogynist fantasy harboured by the
monks and priest who officiated over the witch
hunts: witches copulated with the devil, rendered
men impotent (generally by removing their penises
which the witches then imprisoned in nests of bas
kets ), devoured newborn babies, poisoned livestock,
etc. But again and again the ' crimes ’ included
what would now be recognized as legitimate medi
cal acts-providing contraceptive measures, perform
ing obortions, offering drugs to ease the pain of
labor. In fact, in the peculiar legal theology of the
witch hunters, healing, on the part of a woman,
was itself a crime. As a leading English witch
hunter put it:
For this must always be remembered, as a
conclusion, that by Witches we understand not
only those which kill and torment, but all Diviners,
Charmers, Jugglers, all Wizards, commonly called
wise men and wise women....... and in the sanic
number we reckon all good Witches, which do no
hurt but good, which do not spoil and destroy, but
save and deliver .... It were a thousand times
better for the land if all Witches, but especially
the blessing Witch, might suffer death. 2
........ The inquisitors reserved their greatest
wrath for the midwife, asserting :
The greatest injuries to the Faith as regards
the heresy of witches are done by midwives; and
this is made clearer than daylight itself by the
confessions of some who were after-wards
burned. 6
Folk medicine Vs ‘ Scientific ’ medicine
In fact, the wise wcman, or witch, as the
authorities labeled her, did possess a host of reme
dies which had been tested in years of use. Liber
Simplicis Medicinae, the compendium of natural
healing methods written by St. Hildegarde of Bingen
(A. D. 1098-1178) gives some idea of the scope of
women healers’ knowledge in the early middle ages.
Her book lists the healing properties of 213 varie
ties of plants and 55 trees, in addition to dozens
of mineral and animal derivatives. Undoubtedly
many of the witch-healers ’ remedies were purely
magical, such as the use of amulets and charms,
but others meet the test of modern scientific
medicine. They had effective painkillers, digestive
aids, and anti-inflammatory agents. They used
ergot for the pain of labor at a t me when the
Church held that pain in labor was the Lord’s
just punishment for Eve’s original sin. Ergot
derivatives are still used today to hasten labor and
aid in the recovery from childbirth. Belladonna
still used today as an anti-spasmodic-was used by
the witch-healers to inhibit uterine contractions
when miscarriage threatened. Digitalis still an
important drug in treating heart ailments, is said
to have deen discovered by an English witch.
Meanwhile, the male, university - trained
physicians, who practiced with the approval of
the Church, had little to go on but guesswork and
myth. Among wealthier people, medicine had
achieved the status of a gentlemanly occupation
well before it had any connection to science, or to
empirical study of any kind. Medical students
spent years studying Plato, Aristotle, and Christian
theology. Their medical theory was largely restri
cted to the works of Galen, the ancient Roman
physician who stressed the theory “ temperaments”
of men, “wherefore the choleric are wrathful, the
sanguine are kindly, the melancholy are envious ”
and so on. Medical students rarely saw any
patients at all, and no expriinentation of any kind
was taught. Medicine was sharply differentiated
from surgery, which was almost everywhere consi
dered a degrading, menial craft, and the dissection
of bodies was almost unheard of.
Medical theories were'often grounded more in
“ logic ” than in observation: “ Some foods brou
ght on good humours, and others, evil humours.
For example, nasturtium, mustard, and garlic
produced reddish bile; cabbage and the meat of
old goats and beeves begot black bile. ” Bleeding
was a common practice, even in the case of wounds
Leeches were applied acdording to the time, the
hour, the air, and other similar considerations.
Incantations and quasi-religious rituals mingled’
with the more “ scientific ” treatments inherited
from ancient Greece and Rome. For example, the
physician to Edward II, who held a bachelor’s
degree in thelogy and a doctorate in medicine
from Oxford, prescribed for toothache writing on
the jaws of the patient, “ in the name of the
Father, the son, and the Holy Ghost, Amen, ” or
touching a needle to a caterpillar and then to the
tooth. A frequent treatment for leprosy was a broth
made of the flesh of a black snake caught in a dry
land amoung stones.
Such was the state of medical “ science ” at
the time when witch-healers were persecuted for
being practitioners of satanic magic. It was witc
hes who developed an extensive understanding of
bones and muscles, herbs and drugs, while physic
ians were still deriving their prognoses from
astrology and alchemists were trying to turn lead
into gold. So great was the witches ’ knowledge
that in 1527, Paracelsus, considered the “ father
of modern medicine, ” burned his text on ph- r.naceuticals, confessing that he “ had learned from
the Sorceress all he knew. ”
Well before the witch hunts began, the male
medical profesion had attempted to eliminate the
female healer mainly the better-off, litetatc woman
(3)
healer who competed for the same urban clientele
as that of the university trained doctrs. Take for
example, the case of Jacoba Felicie, brought to
trial in 1322 by the Faculty of Medicine at the
University of Paris, on charges of illegal practice.
She was a literate woman and had received some
unspecified “ special training ” in medicine. That
her patients were well off is evident from the fact
that (as they testified in court) they had consulted
well-known university trained physicians before
turning to her. The primary accusations brought
against her were that
...She would cure her patient of internal
illness and wounds or of external absesses. She
would visit the sick assiduously and continue to
examine them in the manner of physicians, feel
the pulse, and touch the body and limbs.®
Six witnesses affirmed that Jacoba had cured
them, even after numerous doctors had given up,
and one patient declared that she was wiser in the
art of surgery and medicine than any master
physicians or surgeon in Paris But these testimo
nials were used against her, for the charge was
not that she was incompetent, but that - as a
woman-she dared to cure at all.
Conflict America
Commercial envy
The regular doctors banded together in 1847
1i form their first national organization, pretentio.isly entitled the American Medical Association,
aid one of the AMA’s first tasks was to survey the
competition the 40,000 regulars plus a “ long list
of irregular practitioners who swarm like locust in
every part of the count, y.’’
The regular doctors were caught in a contr
adiction of their own making. Medicine had once
been embedded in a network of community and
family relationships. Now', it had been uprooted
transformed into a commodity which potentially
any one could claim as merchandise, a calling
which anyone could profess to follow. So long as
medical education was cheap, and medical fees
were not too cheap, there was no limit to the
numbers of regular doctors. Thus the patrician
ideal of the gentleman doctor could never be
realized. And of course, the deeper the doctor
sank into commercialism, and the more they
spawned in this
fertile muck-producing new
doctors simply for profit- the less likely they were
to achieve the status and authority of their collec
tive dreams. Ahead lay nothing but humiliation.
Dr. G. H. Reed of Teledo wrote poignantly in
the Journal of the American Medical Association
about “ a doctor who was found crying because
he was hungry. ”
A great deal- it is impossible to say exactly
how much - of the competition which was reducing
male regular doctors to tears was coming from
women. By mid century there were not only
female lay healers to contend with, there was
a new
creed of middle-class women who
aspired to enter the Market as regular, professional
physicians. Like the women who had become
involved in the Popular Health Movement earlier,
they were motivated by a spirit of reform: they
were opposed to the excesses of heroic medicine
and equally important, they were outraged at the
implicit indecency of the male doctor - female
patient relaionship.
By mid-century the private horrors of mixed
sex medical encounters had become a public issue.
Samuel Gregory, an irregular physician argued in
1850 that male obstericians, by their very prese
nce, created enough anxiety in their patients to
lengthen the process of labour. Gregory’s book
“ Man-midwifery exposed and corrected;" or
"the Employment of men to attend women in child
birth, shown to be a modern innovation, unnecessary,
unnatural and injurious to the physical welfare of the
community, and pernicious in its inf.'uence on Profe
ssional and public morality" was a great success, and
in 1852 “ a few ladies of Philadelphia ” organized
around their belief that “ the BIBLE recognizes
and approves only women in the sacred office of
midwife.”57 And Catherine Beecher raised the
charge of seduction and sexual abuse, taking place
in the practices of the most apparently benevolent,
honorable, and pious doctors
Women doctors and male opp’-sition
Given the tensions and moral compromise
associated with male medical care, the mid-nine
teenth-century movement of women into medical
training took on the aspeccts of a crusade-for
female health, for decency.
It was this sense of being involved in a mor a •
crusade which accounts for the determinetion of
our early female doctors. For example, Elizabeth
Blackwell applied to over sixteen schools before
she found one which would accept her, but, as she
said, ‘ The idea of winning a doctors’s degree gra
dually assumed the aspect of a great moral struggle,
and moral fight possessed attraction for me. ’ In
the same year that Blackwell gained admission,
Harriet Hunt was admitted to Harvard Medical
College-only to have the decision reversed because
the students threatened to riot if she came. (Har
vard had admitted three black male students the
year before and that, according to the white male
majority, was enough ) Undaunted, Hunt went to
seek a medical education at an ‘ irregular ’ school.
Through the efforts of women, there were, by 1900,
approximately five thousand trained women doctors
in the land, fifteen hundred female medical stude
nts and seven medical schools exclusively for
women.
Male doctors recognized that women in pro
fession posed a threat which was far out of proport
ion to their numbers. The woman patient who
considered herself socially superior to female lay
healers, yet was repelled by male medicine, would
naturally welcome a woman professional. Faced
with this threat male doctors responded every
argument they could think of : How could
a lady who was too refined for male medical
care travel at night to a medical emergency ?
operate when indisposed (e. g. menstruating) ?
If women were too modest for mixed-sex medical
care, how could they expect to survive the realities
of medical training-the vulgar revealations of ana
tomy class, the shocking truths about human
reproduction, and so on ? (Elizabeth Blackwell
admitted that she first found the idea of medical
training ' disgusting. ’)
The regular doctors did not rely on persuas
ion alone to discourage women from medical
education. The would-be woman doctor faced some
very solid road blocks at every step of her career.
First it was difficult to gain admission to a ‘ regular’
school (the ‘ irregular ’ sects, descended from the
Popular Health Movement, mantained their femi
nist sympathies and openness to female students).
Once inside, female students faced harrassment
from the male students ranging from ‘ insolent and
offensive language ’ to ' missiles of paper, tinfoil
( and ) tobacco quids. ’ There were professors who
wouldn’t discuss anatomy with a lady present and
textbooks such as the 1848 obstetrics text which
declared, ‘she (woman) has a head almost too
small for intellect but just big enough for love. ’
Having completed her academic work, the
would-be woman doctor often found the next steps
blocked. Hospitals were usually closed to women
doctors, and even if they weren't, the internships
were not open to women. When she did finally
make it into practice, she found her brother regu
lars unwilling to refer patients to her and absolu
tely opposed to her membership in their medical
societies. It was not until 1915 that the AMA. it
self admitted female physicians.
[ Extracted and abridged from the second
chapter of' For her own good-150 years of experts’
advice to women ’ by Barbara Ehrenreich and
Deirdre English, Anchor books, New york 1979.
References have been omitted due to lack of space. ]
The Foundation For Research
In Community Health
requires a full-time
PHYSICIAN
(Preferably with post-graduate qualification)
for a
RURAL COMMUNITY HEALTH PROJECT
in
North Alibag Taluka, Raigad District.
The project covers 35000 population in 31 villages
each with a village health worker, 6 sub-centres
and a 12—bedded health centre with scope for fur
ther expansion.
The job entails providing a comprehensive medical
service to the project area. Knowledge of Marathi
is essential.
Salary equivalent to Government Medical College
scales and commensurate with qualifications and
experience. Housing benefits and allowances as per
the rules of the organization,
Please apply stating previous salary drawn and
complete bio-data to :
The Director,
Foundation for Research in
Community Health,
34-A, R. G. Thadani Marg,
Worli Seaface,
BOMBAY-400 018.
(5)
The Women’s Health Movement
by S. B. Ruzek. Praeger, New York, 1979.
The women’s movement lias been concerned
with many controversial areas in recent years, but
one of the most heated debates has centred on the
health care of women. The Boston women’s health
book collective was an attempt to extract the
health care of women from a profession they have
viewed as sexist and at the care of male dominated
attitudes. The Women's Health Movement is an
effort to deal with this complex and emotionally
charged area.
The book presents a limited area of inform
ation in an eminently readable, flowing style. The
subject matter, dealing primarily with the women’s
movement and health care over the past 15 years,
is absorbing, with many inflammatory issues pre
sented in a factual and unbiased way. It is obvi
ous that the author as a social scientist has taken
great effort to present a detached unemotional
document. At times, this work is more a critique
of the whole structure of society and the organiza
tion of health care than simply a review of women’s
issues in health.
The book presents data on many controversial
issues in women’s health including the Intra
Uterine Device (IUD), Oral Contraceptive
(OC) and the Morning After Pill. The introduc
tion of the IUD was permitted withoutany regu
lation. The subsequent morbidity and mortallity
due to the Daikon Shield (an I U D) was evident
in 1973, yet there was a 3 year interval to the
adoption of regulatory legislation The introduction
of OC was eqully distressing. Limited studies of
132 Puerto Rican women over a year and 718
women for less than a year constituted all the
prior knowledge available before their release on
the mass market. Five deaths went unexamined in
the study. Although this is a blatantly inadequate
trial, it needs to be viewed in the context of its
time. Prior to the scandal over Thalidomide in 1962,
many drugs were being placed on the market with
out evidence of safety or efficacy. The data presen
ted on DES [Diethyl Stilbesterol - one oestrogenic
harmone. ] and the M. A. Pill is also anxiety pro
voking for women. One year after the evidence for
vaginal cancer in the femal offspring of women-who
had taken DES during pregnancy was documen
ted, DES was released as a M. A. Pill, again with
scant evidence of efficacy or safety. That women
should be aware of these issues and demand more
knowledge of potential contraceptives is imperative.
That women should be the sole purveyors of fur
ther research in this field is not so obvious, yet such
a presumption is stated and encouraged in the book.
The book makes some important observations
on drug advertising and exposes many of the
blatantly sexist advertisements which portray
women in stereotyped and unflattering roles. The
book provokes a thoughtful evaluation of women’s
roles and needs in the health system.
[Book-Review published in Social Science &
Medicine, 16 : 1310-1311, 1982.]_________________
Medical laboratory manul for tropical countries
( Volume - 1 )
By Monica Cheesbrough Published by M.
Cheesbrough, 14 Bevills Close, Doddington, Cambs;
England, 1981. 519-f-xiipp. Price-Sterling 5.95
(including postage) for developing countries.
The manual is intended for use as both a
training and a reference work for laboratory techni
cians at intermediate and referral hospitals in
tropical countries, but would be equally useful for
laboratory technicians in temperate countries. It
begins with a section on the organization of a
laboratory service and the place of the technician
within it. This is followed by a very practical sec
tion of 50 pages on anatomy and physiology. The
third section provides comprehensive coverage of
medical parasitology. The section on malaria is
particularly complete, including not only labora
tory diagnosis and details of the life cycle but also
background information on geographical distribu
tion, epidemiology, clinical features, complications,
immunity, prevention and control. There is even
a discussion of drug resistance. Each chapter ends
with a list of references and recommended reading.
The chapter on clinical chemistry is extremely
good and includes some aspects which, although
pertinent, have been neglected in other manuals,
i. e. maintence of laboratory equipment (and even
instructions on how to repair minor faults) and the
preparation of quality control samples using locally
available resources, which will free laboratories
from dependence on commercial products.
Review in World health forum 3 (2): 244-245(1982).
OPPRESSIVE
“SCIENTIFIC”
[ The following is one more page extracted
from the book " 150 Years............. ” “Scientific”
Gynaecology in the nineteeth and early twentieth
century believed that woman’s body was contro
lled by her reproductive organs and consequently
these organs were held responsible for all sorts of
diseases. The following paragraphs give an idea
of the barbaric treatment given for the " disorders
of reproductive organs. ’’]
—Editor
Since the reproductive organs were the source
of dierease, they were the obvious target in the
treatment of diesease. Any symptom-backaches,
irritability, indigestion, etc., - could provoke a
medical assault on the sexual organs. Historian
Ann Douglas wood describes the “local treatments’’
used in the mid-nineteenth century for almost any
female complaint. This (local treatment) had four
stage, although not every case went throhgh all four:
a manual investigation, “ leeching, ’ “ injections,'’
and “ cauterization. ” Dewees (an American
medical professor) and Bennet, a famous English
gynecologist widely read in America, both advo
cated placing the leeches right on the vulva or the
neck of the uterus, although Bennet cautioned the
doctorto-count them as they dropped off when
satiaiecL lest he “ lose ” some. Bennet had known
adventurous leeches to advance into the cervical
cavity of the uterus itself and he noted, “ I think
I have scarcely ever seen more acute pain than
that experienced by several of my patients undei
these circumstances. ’’ Less distressing to a
twentieth century mind but perhaps even more
senseless, were the
“ injections ” into
the
uterus
advocated by
these doctors.
The
uterus became a kind of catch all, or what one
exasperated doctor referred to as a “ Chinese toy
shop ’ : Water, linseed tea, and “ decoction of
marshmellow ... tepid or cold " found their way
inside nervous women patients, The final step,
performed at this time, one must remember, with
no anestetic but a little opium or alcohol, was
cauterization, either through the application of
nitrate of silver, or, in case of more serve infection,
through the use of much stronger hydrate of
pottass, or even the “ actual cautery, ” a “ whitehot iron ” instrument.
PROCEDURES
The most common of surgical intervention in
female personality was ovariotomy, removal of the
ovariesor “ female castration. ” In 1906 a leading
gynecological surgeon estimated that there were
150,000 women in the United Status who had lost
their ovaries under the knife. Some doctors boa
sted that they had removed from fifteen hundred
to two thousand ovaries apiece. According to histo
rian G. J. Banker Benfield :
Among the indications were troublesomeness,
eating like a ploughman, masturbation, attempted
suicide, erotic tendencies, persecution mania, simple
“ cussedncss, ” and dy>menorrhca ( painful men
struation). Most apparent in the enormous variety
of symptoms doctors took to indicate castration
was a strong current of sexual appetitivencss on
the part of women.
The rationale for the operation flowed directly
from the theory of the “ psychology of the ovary
since the ovaries controlled the personality, they
must be responsible for any psychological disorders;
conversely psychological disorders were a sure sign
of ovarian disease. Ergo, the organs must be re
moved.......... ..
The overwhelming majority of women who
had leeches or hot steel applied to their cervicer,
or who had their clitorises or ovaries removed,
were women of the middle to upper classes, for
a'er all these procedures cost money. But it should
not be imagined that poor women were spared the
gynecologist’s exotic catalog of tortures simply be
cause they could'nt pay. The pioneering work in
gynecological surgery had been performed by
Marion Sims on black female slaves he kept for
the sole purpose of surgical experimention. He
operated on one of them thirty times in four years,
being foiled over by post operative infections.
After moving to New York, Sims continued his
experimentation on indigent Irish women in the
wards of the New York Women's Hospital. So,
though middle-class women suffered most from
the doctor's actual practice, it was poor and black
women who had suffered through the brutal period
of experimentation.
UoH \
COMMUNITY HEALTH CELL
47/1, (First H«or)St. MarksRoad
BANGALORE -560 #01
ACTION-ORIENTED RESEARCH ON
ALTERNATIVE MEDICINE & WOMEN’S HEALTH IN INDIA
( a project starting February 1989 )
Introduction :
Out of a national workshop of women's group working on
the field of health, held in Tamil Nadu, it was realised how
little we know about other methods of treatments for women's
complaints than those of the allopathic medicine. This means
a whole popular knowledge on healing is getting lost, while the
methods proposed by modern medicine remains highly inaccessible
to rural India and inefficient to many chronic complaints.
Woman, the primary health giver, is the last to be taken
care of. Many aspects of her health are neglected to start with.
those concerning her specificity as a woman (see ref. 1)
Since women need obviously to take care of themselves,
they need to have in their hands, understanding of their health
and simple methods of treatments relying on what is accessible
to them, like plants and natural elements.
The goal of this project is to gather this information from
as many healers as possible, in all approaches and distribute it,
in order to make it accessible to more women.
The research
will take place in a constant process of exchange, giving whatever
training is needed to make this possible (in basic gynecology
and obstetrics, approach to medicinal plants, basic acupuncture .)
It will give women a chance to take their health into their hands
(see ref. 2).
We are concious we will be confronted to many different
concepts of health, disease and the healing process. Attention
will be given to understand those approaches and to integrate
them into existing practices in a meaningful and culturally acceptable
way. Special attention will be given to stories and myth from
women and their own perceptions of these concepts.
Final outcome :
The outcome of this project will be a publication, initially
in the languages used to collect the information (Bengali, Gujarati,
Hindi, Mahrati. Oreya, Tamil, Telugu) as well as in English. With
the help of organisation active in the field of women s health,
it is expected to make this work available to as many women
as possible and to generate a feed-back.
The research process will increase the networking between
urban and rural groups, as well as between India and other countries.
Finally this process should enable us to get a better under
standing of the adequate use of each method available, and in
what field of problems they give the best results. So that ultimately,
the choice will not be made only because it is the most recent method
one has heard of, or because it is the one selling its services in the
area, but instead for its real indications!
Methodology
It has been decided that since we are going to meet many
different approaches we should to start from the plants themselves
(the mineral or the animal extract) which are common to all. An
information-sheet will be filled up completely for each corresponding
to a specimen. The information-shiet is established after preliminary
interviews done with the first group to start, and after workshops
taking place with the health workers involved with the collection of
the information (basic gynecology and obstetrics, approach to botany,
and other as deseed). The information-sheet has been also discussed
with a computer*so that it will be easy to compile and to draw
conclusions.
The women's life stories, concepts and other methods ■
diet, exercises, acupuncture_will be collected separately and
written down.
2
We are collecting all information on simple remedies, that
women can collect, prepare and use by themselves for their most
common complaints, starting with the one that will come out of
the workshops with health workers and village women.
The field covered is :
1 -problems of the cycle (too long, too short, irregular- absent,...),
the menstruation (painful, too havy, too scanty...) and the problems
of menopause and menarque
2
- infections: urinary, genital and vaginal discharge
3
- tumors : cervix, uterus, breast, benign and malign
4
- pregnancy
(a)
(b)
(c)
(d)
(e)
5
before (infertility, contraception,...)
begining (spontaneous abortions, nausea,...)
advance (contractions, bleeding, anemia,—)
birth (problem of labour, hemorrage, eclampsia, retention,....)
post-partum and breast feeding (infections, engorgement,—)
- neglected aspect of general health (back-pain, joint-pain,
fatigue, depression,...)
*The second phase of this project will be spent in :
-
small scale tests in clinics and groups focussing on primary
health.
analyses (functional and content of plants) when not already
studied,
computer processing,
writing of the first draft of the publication.
3
INITIATORS INVOLVED :
- Devakirubai D. a.n.,SRED, Arakkonam, Tamil Nadu, collecting
info, in Tamil.
SRED trained 20 health workers in villages, has one gynec.
clinic in allopathy and one in siddha medicine and homeopathy.
- Bharati Chaudry ( Action India and JAGORI ) New Delhi
collecting info, in Hindi.
Bharati is working on educational health in a forest area,
botanical help available, acupuncture training has started with^j)
7 village women
- Saswati Roy,SWADHlNA, Calcutta, collecting info, in Bengali
and Oreya.
SWADHINA is an organisation for self reliance of women,
active in W. Bengal, Orissa and Bihar.
- Vd. Smita Bajpai, CHETNA, Ahmedabad, collecting info, in
Gujarati, Hindi, and Mahrati.
CHETNA is a nutrition and health awareness center working
in many villages spread in 3 neighbouring States.
- Umamaheshwari A. (Deccan Dev. Soc. ANVESHI) Hyderabad,
collecting info, in Telugu.
Uma is working in 40 villages in ayurvedic medicine preparing
remedies herself and training women.
r
RESOURCE PERSONS:
- Indira Balachandran, botanist, Arya Sala Herbal
Kottakal, Kerala
Garden,
- Dr. Shyama K. Narang (allopathy and acupuncture) Bangalore.
The coordination is done by the collective of the women directly
involved, plus feminist support groups. The convener is Rina Nissim
from the Geneva Women's Health Center.
4
Possible collaboration with us :
Initially planned for 7 groups, we can still integrate two more
groups who would like to join the venture!
Additionally, other input will be appreciated, like :
- contacts to meet healers, women's groups and research centeis,
- feminist translators,
- help to promote the results,
- creation of plant distribution centers,
- etc ...
If any of this is meaningful to you, contact us quickly!
References :
1 -
"High prevalence of Gynaecological Diseases in
Rural Indian Women", Bang, Baitule, Choudhary,
Sarmukaddam and Tale, The Lancet, January 14, 1989.
2
-
Boston Women's Health Book Collective, Our bodies
Ourselves”, Simon and Shuster Publ. N.Y. USA 1976.
3
-
Rosangela Gramoni and Francoise Chipier, 'The Geneva
Women's Clinic : Promoting Demedicalisation and
Self-reliance in Health', working paper for the WHO
conference on women as providers of health care, March 1982.
• 4 -
5 -
Rina Nissim, 'Natural Healing in Gynecology',
Pandora, London N.Y. 1986.
Sheryl Burt Ruzek, 'The Women's Health Movement :
Feminist Alternative to Medical Control' Praeger
Publishers USA 1978.
Contact Address :
Research-action on alternative medicine and women's health
do. Shyama K, Narang, 93 A II Cross, Indiranagar, 1st Stage,
Bangalore-560 038.
MEASURE
Coiiniuiincntiou
£
Policy
Brief
HOW DOES FAMILY PLANNING
INFLUENCE WOMEN’S LIVES?
mong the many changes that occurred in
the second half of the 20th century,
perhaps the most significant and personal
for women has been the means to choose whether
and when to have children. This “reproductive
revolution” — made possible by the expanded
availability of modern contraceptive methods in
the last 30 years — has helped give women the
chance to pursue new roles and activities outside
the home. These new roles and activities ultimately
contribute to a country’s economic and social
development.
In the less developed world, more than half of
couples now use family planning, compared with
only 10 percent in the 1960s. As countries have
modernized and become more urban, and as
women have become more educated and begun to
marry later, smaller families have become more
desirable as part of a modern lifestyle (see Figure 1).
”1
A
Organized family planning programs have helped
women meet their reproductive goals by making
contraceptives more widely available, even in many
low-income, rural communities. Nevertheless, wide
variations in family planning use still exist within
and among countries.
Research tells us that womens ability to plan
their families has altered their work experiences,
educational prospects, and relationships with their
husbands and families. Whether or not these
changes are beneficial depends on the context in
which women live — in particular, women’s
perceived and actual ability to make decisions
about their own lives, inside and outside the home.
Policymakers and program planners who want to
expand women’s choices and opportunities need to
understand how family planning programs and
other investments can help make women’s aspira
tions a reality.
The effes® ©f family planning ©n
women's lives
Women's desired number of children, selected less
j^reloped countries
Several research efforts in the past decade have
examined the relationships between family plan
ning and women’s lives, using different approaches:
■ The Women’s Studies Project of Family Health
International (FHI) coordinated 26 studies in 10
countries over five years, asking women directly
whether and how they had benefited from family
planning.
■ The International Center for Research on
Women (ICRW) and the Population Council
coordinated studies in less developed countries to
explore women’s perceptions about family planning
and, in particular, why some women do not use
contraception.
■ The Demographic and Health Surveys (DHS)
provide standardized survey data on women’s
desired and actual childbearing collected from
more than 40 less developed countries. These data
have permitted cross-country analyses of the char
acteristics of women and families who use or do
not use family planning.
The data collected from these projects support
the following conclusions.
As women have smaller families, they spend
less time on unpaid work in the home and more
time in paid employment. In Bolivia, for example,
analysis of survey data showed that contraceptive
use was associated with working for pay outside the
home, and that a growing number of women
entered the workforce from 1994 to 1997. The
research did not show whether the change in work
status was due to family planning use — or the
other way around, that work status affected family
planning use. Nevertheless, researchers concluded
that family planning is at least an enabling factor as
women enter the labor force in increasing numbers.1
More time in the work force translates into
greater earnings. A long-term study in the city of
Cebu, Philippines, showed that, among women
who continuously work for pay, women with
fewer children had greater increases in earnings.
Over an 11-year period, the average change in
income for women having between one and three
Figure 2
Contraceptive use among women who say they
would prefer to avoid pregnancy
Percent of married women ages 15-49
so u»cii Demographic and Health Surveys, 1990-95 (Calverton, MD: Macro International).
This group is referred to as having an “unmet need” for family planning.
pregnancies was twice that of women who had
more than seven pregnancies.2
Many women, however, have mixed feelings
about work. While working for pay can increase
womens autonomy and income, it can also carry
additional burdens. The Cebu, Philippines study
showed that longer hours — rather than better jobs
or better pay — contributed to some of the
increase in womens earnings. Many of the women
interviewed said they would have preferred not to
work outside the home. Similarly, FHI studies in
other countries found that working women face
additional stress because they have taken on the
dual responsibilities of working outside the home "
and continuing to manage a household.
Access to contraceptive services can improve
educational prospects for young women, particu
larly those who would be forced to drop out of
school if faced with an unplanned pregnancy. Yet
young women who are sexually active may face
serious obstacles to using family planning services.
A study conducted in three cities in Zimbabwe
found that secondary school students who were
sexually active were discouraged from going to
family planning clinics and had to rely on private
or secret sources for contraception. One woman
explained: “I had tried to get some tablets, but I
was chased from the clinic. I think it was because I
looked very young. ... But now I regret it. I could
have finished school.”3
Whether young women choose to delay
"
childbearing and pursue studies may depend on
the range of opportunities available to them. A
study in Brazil found that for some teens, preg
nancy was a welcome event, even if it meant inter
rupting their studies. Similarly, young women in a
Jamaican study revealed mixed feelings about preg
nancy; the study quoted one girl as saying that a
pregnant teen “would feel happy in a way.”'1 Some
girls will choose motherhood over education if they
believe that it will give them greater status than
pursuing other options, such as school or work.
Still others have no choice but to pursue mother
hood, if faced with an unplanned pregnancy.
Contraceptive use can improve family
relations. Family planning carries psychological
and other benefits, such as freedom from fear of
unplanned pregnancies and the ability to spend
more time with each family member. In Indonesia,
about 80 percent of women surveyed said that
family planning had enabled them to have more
leisure time and spend more time with each child
and with their husbands. Couples interviewed in
Zimbabwe named family planning as an important
factor in quality of life, and couples in Bolivia felt
that their conjugal relations had improved.5
On the other hand, in communities where
family planning is not socially accepted, women
who use contraceptives can face difficult conse
quences. Some women may fear disapproval or ret
ribution — even violence — from their husbands,
disdain from relatives and friends, or ridicule in the
community. In Bangladesh, women who were the
first in their village to use contraception faced
ostracism by community members. In Mali, where
fewer than 10 percent of married women practice
family planning, researchers found that many
women use contraception secretly and fear punish
ment if their husbands find out.6 In a study in
Zambia, one man interviewed said: “I cannot allow
my wife to become a whore. Women who use
contraceptives cannot be trusted.”7
Remaining needs
In just a few decades, women have made great
strides in their ability to plan their families, yet
progress has been uneven. An estimated 120 mil
lion women in the less developed world say they
would prefer to delay or stop childbearing, but are
not using any family planning method.8 In some
countries, more than one-quarter of all married
women foil into this category (see Figure 2). Several
studies have asked women with an unmet need
why they do not use contraception. The reasons are
numerous, including a lack of knowledge about
family planning methods and services, ambivalence
about wanting a child, opposition from husbands
and other family members (as discussed above),
health concerns, and fear of contraceptive side
effects.’ Many of these reasons overlap and relate
to two underlying issues: the gender-related
expectations that shape womens lives and the qual
ity of family planning services available to women.
Addressing gender inequality. Although women
have long been the intended beneficiaries of family
planning and reproductive health programs, gen
der roles, particularly the unequal power wielded
by men and women, influence the extent to which
women can make decisions about their health and
quality of life. In many societies, women’s autono
my is limited, so that major family decisions —
including whether to use contraception and how
many children to have — are the principal domain
of husbands.
Gender expectations can also limit the benefits
that women are able to gain when they do decide to
use family planning. Some women with fewer
children may find that their opportunities in life
differ little from their peers (or elders) who have had
more children. Population Council studies in parts
of rural Egypt and Bangladesh showed that declines
in fertility were not associated with measurable
changes in gender roles or womens opportunities.10
The international community has identified a
broad range of policy changes and investments to
improve the range of choices and opportunities
available to women — including adolescent
women. They include:
■ improving educational opportunities for girls
and women, and more broadly, making girls’ and
women’s empowerment a specific development
objective;
■ expanding women’s employment opportunities
and child-care options for working mothers;
■ revising laws, such as those on property and
inheritance, that establish or reinforce women’s
inferior position in society;
■ supporting community-based initiatives diat
encourage men and women to discuss changing
gender roles and norms;
■ implementing programs for adolescents, in and
out of school, to help them make better life choic
es and protect themselves from unintended preg
nancies and sexually transmitted infections; and
■ passing and enforcing international treaties such
as the Convention on the Elimination of All Forms
of Discrimination Against Women (CEDAW).
Improving the quality ofservices. Family plan
ning and other reproductive health programs need
to establish and evaluate quality approaches to
providing services. Service quality depends on a
combination of factors, such as a reliable supply of
a range of contraceptive methods, technical
competence of service providers, and offering con
venience, respect, and privacy to those who use
the services. Research shows:
■ Family planning programs should improve peo
ple’s knowledge of contraception and reduce their
fear of methods. Women and men need better infor
mation about how to use contraceptives and what
side effects to expect once they do adopt a method.
□ Programs should make greater efforts to reach
men with services and information, and to
encourage them to adopt or support their partners
adoption of family planning.
■ Health workers should treat people with dig
nity, explain possible problems and how to manage
them, and provide clients with alternatives.
■ Services should make greater efforts to reach
out to adolescents, and at a minimum, not deny
services to young or unmarried individuals who
seek them.
■ Community organizations and women’s groups
should educate women to demand quality services.
Making complementary
investments
Governments and women’s health advocates
increasingly recognize that investments in women
go hand in hand with investments in family plan
ning and reproductive health services. Such invest
ments are not either-or choices, but represent
mutually reinforcing objectives. The vast majority
of the world’s governments endorsed these objec
tives and the specific actions needed to achieve
them at the 1994 International Conference on
Population and Development and 1995 Fourth
World Conference on Women.
Improvements in women’s status can create
favorable conditions for increased use of family
planning, better reproductive health, and greater
POT
contributions of women to development. Family
planning programs should be part of a mutually
reinforcing web of programs designed to give
women greater control over their reproduction and
over other aspects of their lives. Ultimately, these
investments will allow women to contribute more
fully in the social and economic development of
their communities and countries.
^e?es,eireees
1 B. Barnett and J. Stein, Womens Voices, Womens Lives: The
Impact ofFamily Planning (Research Triangle Park, NC:
Family Health International, 1998): p. 83.
2 B. Barnett: 15.
5 B. Barnett: 101.
4 B. Barnett: 28.
5 B. Barnett: (various references).
6 B. Barnett: 21.
7 N. Yinger, Unmet Needfor Family Planning: Reflecting
Womens Perceptions (Washington, DC: International Center
for Research on Women, 1998): 14.
8 A. Gelbard, C. Haub, M. Kent, “World Population Beyond
Six Billion,” Population Bulletin (Washington, DC: Population
Reference Bureau, 1999).
9 C. Westoff and A. Bankole, Unmet Need: 1990-1994,
Demographic and Health Surveys Comparative Study No. 16
(Calverton, MD: Macro International, 1995): 16; N. Yinger,
Unmet Needfor Family Planning: Reflecting Womens
Perceptions: 13-16; and J. Casterline, A. Perez, A. Biddlecom,
Factors Underlying Unmet Needfor Family Planning in the
Philippines, Research Division Working Paper No. 84 (New
York: Population Council, 1996).
10 S. Amin and C. Lloyd, Wfrwewjr Lives and Rapid Fertility
Decline: Some Lessons from Bangladesh and Egypt, Working
Paper No. 117 (New York: Population Council, 1998).
Acknowledgments
Lori Ashford of the Population Reference Bureau
prepared this policy brief with helpful contributions from
Jennifer Adams, Michal Avni, Barbara Barnett, Patsy Bailey,
Barbara Crane, Mai Hijazi, Bessie Lee, Jeanne Noble,
Nancy Williamson, and Nancy Yinger.
This work has been funded by the U.S. Agency for
International Development (USAID) under the MEASURE
Communication project (HRN-A-00-98-000001-00).
POPULATION REFERENCE BUREAU
MEASURE Communication
1875 Connecticut Ave., NW, Suite 520, Washington, DC 20009 USA
Tel.: (202) 483-1100 ■ Fax: (202) 328-3937 ■ E-mail: measure@prb.org or popref@prb.org
Web site: www.measurecommunication.org or WWW.prb.org ©Population Reference Bureau, May 2000
MEASURE
Communication
\ll \-'l \l
<- Ollllllllim illicit
I
Poli c )■
B r i e /
MEETING YOUNG WOMEN’S
REPRODUCTIVE AND SEXUAL HEALTH NEEDS
ith more young people on earth than
ever before, the sexual and reproductive
lives of todays young women will have
a dramatic effect on the health, prosperity, and size
of the worlds future population. Todays young
women are the healthiest and most educated to
date, but they still face obstacles to achieving their
full potential. For example, complications from
pregnancy, childbirth, and unsafe abortion are the
major causes of death for women ages 15 to 19 in
less developed countries. Additionally, young peo
ple ages 15 to 24 have the highest infection rates
of sexually transmitted infections (STIs), including
HIV7AIDS, and teenage women are becoming
infected at twice the rate of teenage men.
Policies and programs that work for the
advancement of women must address the unique
needs of young women in the vulnerable — and
often overlooked — age group of 10 to 19.
In 1994, governments agreed at the
International Conference on Population and
Development (ICPD) “to meet the needs of
adolescents and youth for information, counseling,
and high-quality sexual reproductive health
services,” as a way to “encourage them to continue
their education, maximize their potential, and pre
vent early marriage and high-risk childbearing.”1
The ICPD and the Fourth World Conference on
Women in Beijing in 1995 recognized these goals,
not only as needs of young people, but also as
their rights.
W
The sexual and reproductive
lives of young women
Age at marriage is one of many aspects of
young women’s lives currently in transition.
Overall, marriage before age 18 is less common
than it was a generation ago, but there is regional
variation. Compared with levels 20 years ago, early
marriage has declined in much of Asia and subSaharan Africa2; however, girls are still marrying at
a young age in some countries. In Bangladesh,
average age at marriage is 14.2 years. About half of
15-to-19-year-old women in Mali, Mozambique,
Niger, Chad and Uganda are married, and in
many other sub-Saharan countries, at least onefourth of 15-to-19-year-old women are married.
Marrying later in life has a number of impli
cations for young women. Those who marry later
are more likely to have a basic education and have
fewer and healthier children. However, later mar
riage, combined with increased premarital sex
among adolescents, puts young people at greater
risk of unintended pregnancies, unsafe abortion,
births out of wedlock, and STIs, including
HIV/AIDS.
Premarital sexual activity is common in
many parts of the world and is reported to be
on the rise in all regions.3 In many countries,
young women and men are under strong social
and peer-group pressure to engage in premarital
sex. The average age of marriage has risen in many
Table 1
Age at marriage and age at first sexual
intercourse amoung young women*,
selected countries
Country
Cameroon
Kenya
Niger
Bolivia
Brazil
Guatemala
Haiti
Indonesia
Philippines
Median age
at marriage**
Median age at
first intercourse
18.0
20.2
15.3
20.9
21.0
19.2
20.5
19.9
22.7
15.9
16.8
15.3
19.0
18.8
18.6
18.7
19.8
22.8
«o uI, Demographic and Health Surveys (Calverton, MD: Macro
International).
"Among women ages 25 to 29.
""Includes formal marriage and cohabitation. Median age indicates that
half the women surveyed entered their first union before this age and
half after this age.
Policy
Figure 1
Women giving birth by age 20, selected
countries
sourcexDemographic and Health Surveys, 1995-1998 (Calverton, MD: Macro International).
’ 1995 National Survey of Family Growth (Hyattsville, MD: National Center for Health Statistics).
Figure 2
Unmarried adolescent women who have recently*
received money or gifts in exchange for sex,
selected sub-Saharan African countries
Percent of women ages 15-19
50-i
sour ci .Demographic and Health Surveys (Calverton, MD: Macro International).
•Zimbabwe: within the past 4 weeks; Uganda: last sexual encounter; other countries:
within the past 12 months.
Brief
parts of the world and the age of puberty for
women has fallen, giving young people more years
“at risk” of having premarital sex.
For example, in Kenya, there is more than a
three-year gap between age at first intercourse and
age at marriage, and in Brazil, it is slightly more than
two years (see Table 1, page 1). Surveys show that the
percentage of women having premarital sex by age
20 ranges from 4 percent in the Philippines and 44
percent in Tanzania, to 86 percent in Jamaica.4
Serious risks and consequences accompany
increased premarital sex, particularly when young
people do not have access to adequate reproductive
health services and information. Specifically, these
risks can include STIs, including HIV/AIDS, and
unintended pregnancies. When faced with an
unintended pregnancy, many young women will
seek an abortion, which in many countries is
inaccessible, illegal, or unsafe. Unsafe abortions —
self-induced or done by an untrained provider —
can result in severe illness, infertility, and even death.
Complications from unsafe abortion are the leading
cause of death among teenagers in some countries.5
Adolescent women are less likely than
women over age 20 to use contraceptive
methods. Reasons for this include lack of informa
tion, misinformation, and fear of side effects, along
with geographic, social, and economic barriers to
access and use of contraception. Typically, family
planning services are designed to serve married, j
adult women. Unmarried teens may find service
providers hostile or unhelpful, especially where
strong cultural or religious beliefs condemn sexual
activity among unmarried adolescents. Teens may
be unwilling to disclose their sexual activity to
parents or service providers. Also, the sporadic and
unplanned nature of adolescent sexual activity can
be an obstacle to consistent contraceptive use.
Surveys indicate that 12 percent to 42 percent of
married adolescent women in less developed coun
tries who say they would prefer to space or limit
births are not using family planning. If sexually
active, unmarried adolescents were included in the
surveys, the unmet need percentage would certainly
be higher.6
Of the 15 million young women ages 15 to 19
who give birth every year, 13 million live in less
developed countries.7 Thirty-three percent of women
in less developed countries give birth before age 20,
ranging from a low of 8 percent in East Asia to 55
percent in West Africa. In more developed countries,
about 10 percent of women give birth by age 20;
however, in the United States, the level of teen child
bearing is much higher, at 19 percent. Figure 1 shows
births to young women in selected countries.
Young women and their children face serious
health consequences from early pregnancy and
^childbearing. More adolescent girls die from
^pregnancy-related causes than from any other cause.
Because they have not completed their growth,
adolescent girls are at greater risk of obstructed labor
(when the birth canal is blocked), which can lead to
permanent injury or death for both the mother and
infant. Infants of young mothers are also more likely
to be premature and have low birth weights. In many
countries, the risk of death during the first year of life
is 1.5 times higher for infants born to mothers under
age 20 than for those born to mothers ages 20 to 29.’
All women face higher risks during first births than
in subsequent births; for teens, the risks are greater
still. Because adolescents have less experience,
resources, and knowledge about prenatal care and
childbirth than older women, drey and their children
suffer when obstetric emergencies arise.
exploitation and abuse of
young women
Because sexual violence and exploitation are
abuse of power, young women are especially at
risk, and the violations can have devastating and
long-lasting consequences. Statistics on rape suggest
that between one-third and two-thirds of rape vic
tims worldwide are 15-years-old or younger.’ Since
girls are more likely than boys to be subjected to
sexual violence, girls are at risk of becoming infect
ed with HIV and other STIs at a much younger
age. Other risks include unintended pregnancies,
physical injury, and psychological trauma. Studies
also show that young people who have been vic
tims of sexual abuse are more likely to engage in
high-risk sexual behavior than those who have not
been abused.”
Sexual exploitation of children and adolescents
is a multibillion-dollar illegal industry, according
to UNICEF. Some young people become prosti
tutes in order to make money. In many places,
such as in Bangladesh, Brazil, Nepal, the
Philippines and Thailand, young people are lured
or forced into prostitution.11 Similarly, poverty
leads many young women in sub-Saharan Africa
and elsewhere into sexual relationships with older
men — sometimes known as “sugar daddies” —
who give the young women money and other
necessities, such as clothing and school fees, in
exchange for sex (see Figure 2).
Young women and HIV/AIDS
Half of all people infected with HIV are under
age 25, according to WHO estimates, and about
half of all new infections are among 15-to-24year-olds.12 Ninety-five percent of people with
HIV live in the less developed world.
Young women are particularly vulnerable to
STIs, including HIV/AIDS, for biological and
cultural reasons. Adolescents in general are at
high risk of contracting HIV and other STIs
because they often have multiple, short-term sex
ual relationships, do not consistently use condoms,
and lack sufficient information on how to protect
themselves from HIV/AIDS. Adolescent women,
in particular, are at a biological disadvantage
because they have fewer protective antibodies than
do older women, and the immaturity of the cervix
increases the likelihood that exposure to the infec
tion will result in the transmission of the disease.'3
Moreover, because women often do not show
symptoms of chlamydia and gonorrhea — the
most common STIs — and because having
another STI increases an individuals susceptibility
to HIV, womens risk of contracting and spreading
these infections is especially high. In fact, teenage
women become infected with HIV/AIDS at twice
the rate of teenage men. In addition, sexual
violence and exploitation, lack of formal education
(including sexuality education), inability to
negotiate with partners about sexual decisions, and
lack of access to reproductive health services all
work together to put young women at especially
high risk.
Policy and Program Implications
Meeting young womens needs for reproduc
tive health information and services is vital to their
future. At recent world conferences, governments
committed to a universal agenda for action to
improve the sexual and reproductive health of
adolescents, as follows:14
■ Provide health education to adolescents,
including information on sexuality, responsible
sexual behavior, reproduction, abstinence, family
planning, unsafe abortion, STIs including
HIV/AIDS, and gender roles.
■ Encourage parental involvement and promote
adult communication and interaction with
adolescents.
■ Use peer educators to reach out to young
people.
■ Provide integrated health services for adolescents
that include family planning information and
services for sexually active adolescents.
■ Make health services adolescent-friendly by
ensuring confidentiality, privacy, and respect, and
by providing the high-quality information neces
sary for informed consent.
■ Take measures to eliminate all forms of violence
against women and end trafficking in women.
Research and program experiences suggest that
policymakers and health providers need to remove
legal and institutional barriers that impede young
peoples access to existing family planning and
reproductive health services. In addition, informa
tion and services need to be designed to accommo
date the unique needs of adolescents and young
adults. Examples include providing sexuality edu
cation in schools before teens become sexually
active; providing specially designed services for
youth in clinics or community settings; and using
popular entertainment, mass media, and peer edu
cation — where young people are trained to talk
to their peers — to convey information on sensi
tive topics. Successful programs are usually those
that involve youth in design and implementation.
Sexuality education for youth has long been
hampered by adult concerns that knowledge will
promote promiscuity among unmarried teens.
However, worldwide reviews of studies by the
World Health Organization and United Nations15
conclude that sexuality education does not encour
age early initiation of intercourse, but can delay
first intercourse and lead to more consistent contra
ceptive use and safer sex practices.
References
' United Nations, Programme ofAction ofthe International
Conference on Population and Development (New York:
United Nations, 1994): para 6.7.
2 Alan Guttmacher Institute (AGI), Into a New World:
Young Womens Sexual and Reproductive Lives (New York:
AGI, 1998): 17.
3 Population Reference Bureau, Improving Reproductive
Health in Developing Countries (Washington, DC: PRB,
1997): 5.
4 S. Singh er al., “Gender Differences in the Tuning of First
Intercource: Data from 14 Countries,” International Family
Planning Perspectives Vol. 26, No. 1 (New York: Alan
Guttmacher Institute, 2000): 26
3
J. Senderowitz, “Adolescent Health,” World Bank
Discussion Papers 272 (Washington, DC: World Bank,
1995): 17.
6 B. Shane, Family Planning Saves Lives (Washington, DC:
Population Reference Bureau, 1997): 17.
’ AGI, Into a New World: Young Womens Sexual and
Reproductive Lives.
5 B. Shane, Family Planning Saves Lives: p. 4.
’ L. Heise et al., “Ending Violence Against Women,”
Population Reports, Series L, No. 11 (Baltimore, MD: Johns
Hopkins University, 2000): 9.
Ibid.: 13.
" AGI, Into a New World: Young Women’s Sexual and
Reproductive Lives.
12 Joint United Nations Programme on HIV/AIDS
(UNAIDS), AIDS Epidemic Update: December 1998
(Geneva: UNAIDS, 1998): 9.
13 AGI, Into a New World: Young Womens Sexual and
Reproductive Lives: 34.
14 Family Care International, Commitments to Sexual and
Reproductive Health and Rights for AIL Framework for Action
(New York: Family Care International, 1995).
15 UNAIDS, Impact ofHIV and Sexual Health Education on
the Sexual Behavior ofYoung People: A Review Update
(Geneva: UNAIDS, 1997).
Acknowledgments
This policy brief is adapted from The Worlds Youth
2000, a PRB wallchart and report written by Anne Boyd in
collaboration with other PRB staff
This work has been funded by the U.S. Agency for
International Development (USAID) under the MEASURE
Communication project (HRN-A-00-98-000001-00).
POPULATION REFERENCE BUREAU
MEASURE Communication
1875 Connecticut Ave., NW, Suite 520, Washington, DC 20009 USA
Tel.: (202) 483-1100 ■ Fax: (202) 328-3937 ■ E-mail: measure@prb.org or popref@prb.org
Web site: WWW.measurecommunication.org or WWW.prb.org ©Population Reference Bureau, May 2000
MEASURE
Communication
e
MEASURE
Policy
Brief
IS EDUCATION THE BEST
CONTRACEPTIVE?
he World Bank calls womens education
the “single most influential investment
that can be made in the developing
world.” Many governments now support womens
education not only to foster economic growth, but
also to promote smaller families, increase modern
contraceptive use, and improve child health.
Educating women is an important end in and of
itself. But is education the best short-term strategy
for advancing womens reproductive choice in
low-resource settings?
The United Nations, the U.S. National
Academy of Sciences, the Population Council, and
others have examined the linkages between educa
tion and childbearing to provide a greater under
standing of these issues. This policy brief highlights
key findings from their investigations. The evidence
suggests that a number of factors influence child
bearing decisions, and that both short-term and
long-term policy options need to be considered to
improve womens reproductive health.
T
Werage number of children per woman
by education level
soutci>Demographic and Health Surveys 1995-1999 (Calverton, MD: Macro International).
notii For Mali, Zambia, and Nepal, data include secondary-level education and higher. The
other three countries show secondary-level education only.
The links between education
and childbearing
Women with more schooling tend to have
smaller, healthier families. Throughout the
world, more education is associated with smaller
family size. In a number of less developed
countries, women with no education have about
twice the number of children as women with ten
or more years of school.1 Women with more
education usually make a later, healthier transition
into adulthood: They have their first sexual
experience later, marry later, want smaller families,
and are more likely to use contraception than their
less educated counterparts.
The relationship between women’s
education and family size varies across settings.
The fertility rates of women with similar levels
of education differ from country to country
(see Figure 1). The most highly educated women
in some African countries, for example, have larger
families than do women in other regions who have
only a few years of schooling. Additionally, past
research has demonstrated that modest levels of
education are not always associated with smaller
family size. A 1995 study found that in some less
developed countries, women with a few years of
schooling had about the same number, or more
children, than did women with no education.2
This study concluded that in countries that are
more developed and have higher female literacy
levels, more education is consistently associated
with lower fertility. In the poorest countries, how
ever, a small amount of education may have little
effect on fertility levels.
Steep fertility declines often occur among
women who have had seven or more years of
school. In many of the poorest countries, seven
years of education is the “threshold” level for a
fertility decline of 20 percent or more. Research
indicates that the less developed the country, the
more years of education are required to affect
fertility levels and related indicators such as age at
marriage and contraceptive use.3
Policy
National context is important in influencing
family size, especially when female education
levels are low. The context in which education
takes place is critical in shaping childbearing
decisions. Researchers suggest that several aspects .
of national context are especially important4:
■ Universal education. Fertility levels tend to
decline more rapidly where schooling is wide
spread or primary school enrollment is nearly uni
versal. When a larger proportion of the population
is brought into the educational system, even a
small amount of education may be associated with
fertility decline. Researchers believe that as overall
education levels rise, social norms concerning
childbearing and parenting change. Even those
women without much formal education will be
affected by the changing community norms
regarding smaller family size. In addition, parents
with children in school or with educational
aspirations for their children may choose to have
fewer children. Schooling often increases the costs
of having children?
Figure 2
Average number of years of schooling among
women, selected countries
Brief
■ Exposure to the mass media. In some settings,
research suggests that universal education may be
less crucial to fertility declines than in the past. In
Cote d’Ivoire and Senegal, which have not achieved
universal education, substantial fertility declines
have occurred since the early 1960s. Researchers
believe that a number of factors — including radio
and television exposure — may be fulfilling some
of the role that universal schooling played in the
past?
■ Strength ofthe family planning program. A strong
family planning program promotes smaller, healthi
er families. Even educated women may have a
£
difficult time limiting the number of children they^
have if the services that they need — including
information, counseling, and supplies — are not
available. An analysis of survey data from 31 less
developed countries found that when a country has
a moderate to strong family planning program,
even a modest level of education can be associated
with a substantially lower fertility rate. By contrast,
in countries with a weak or nonexistent family
planning program, the fertility rate of married
women with a few years of education is often
higher than that of noneducated women.7
■ Availability ofemployment opportunities. High
levels of female labor force participation and
higher wages for women are also associated with
smaller family size? A few years of education can
result in smaller family size when they provide
access to a job that offers a promising alternative to
early marriage and childbearing. Working outside
the home may expose girls to nontraditional roles
and values. For working women, children might
represent an “opportunity cost” in terms of lost
earnings or lack of advancement. For these women,
children may also mean a heavier “double burden”
of household and work responsibilities.
Why do eefaseafad women
have smaller families?
At present, no scientific consensus exists about
the exact processes by which education affects
childbearing. Are special skills imparted through
formal education that enable and encourage
women to have fewer children? Theories abound
regarding the different mechanisms involved.
Often, education is associated with characteristics
that might lead a woman to choose fewer children:
literacy skills, greater personal autonomy, and
exposure to new values, ideas, and role models.
Literacy skills — reading comprehension,
in particular — appear to have a pronounced
impact on family size. Among women in South
Africa, one study found that strong reading com
prehension skills, regardless of family income level,
affected family size. The study author suggests that
access to information plays an important role in
decisionmaking. Women with strong comprehen
sion skills are better equipped to access and
interpret information, whether it is provided in
the classroom or through the mass media. More
informed women, in turn, tend to have greater
demand for and be better users of health services.
Are literacy skills more important than years
in school? Research conducted in Ghana also
found that higher female literacy is associated with
lower fertility. This study determined, however,
that the time spent in school had a strong impact
on fertility over and above the effect of literacy
skills alone. Years in school might influence
fertility in different ways: by changing student
values, by making it more likely that a girl will
marry an educated husband who desires a smaller
family, and by improving knowledge through
family life education or other means.9
Young women who are exposed to education,
particularly at secondary levels, may be more
likely to perceive that they have greater
autonomy. They may have a greater ability to make
decisions, to move freely, to earn money, and to
have control over their earnings. Even if they do not
participate in the formal labor force, these women
may bring a sense of autonomy into other areas of
their lives. For example, they may have a larger role
in the decision about the choice of a husband and
the timing of marriage. Within marriage, they may
have better rapport with their husbands, particularly
in relation to childbearing decisions.10
Schooling may make new values and ideas, a
wider social network, and different role models
accessible to students. Similarly, having children who
are in school may change the values and ideas of
parents. Typically, the norms conveyed through
formal education promote the small, nuclear family."
Parents with children in school may also be more
likely to view childhood as a time of growth and
dependency; they may be less likely to view children
as economic contributors to the household.12
The importance of nonschool factors
Women who are more educated usually differ
in many ways from their less educated counter
parts. Often, they are wealthier, reside in urban
areas, and have better access to services. To what
extent do nonschool factors — socioeconomic
status, ethnicity, parental education, individual
goals, later age at marriage, and marriage to an
educated husband — influence childbearing
decisions? The relative importance of different
factors probably varies from one setting to another.
Husbands’ education and household wealth
typically influence fertility; however, most studies
show that womens education has a greater impact
on fertility.13
Kqsjipgsing women to make healthy
childbearing decisions
Efforts to improve educational attainment
must continue regardless of any impact on
childbearing practices. But what conclusions may
be drawn about the connection between education
and childbearing? The research does not provide
any simple formula governing years of education
and family size. The effects of education on
women depend upon a wide variety of social,
cultural, and economic factors. With these caveats
in mind, what are the policy implications?
■ Promote universal education and secondary-level
education. Near universal enrollment in primary
school and in secondary-level education is impor
tant in influencing childbearing decisions. In some
low-resource settings, however, it may not be real
istic to achieve universal education or high levels of
secondary school attendance in the near future.
Relatively few women in many less developed
countries have seven or more years of schooling
(see Figure 2). A study of education and fertility in
sub-Saharan Africa concluded that “most countries
are far from providing mass schooling for their
populations, and as a result of war, economic
austerity, or high levels of population growth,
some have witnessed stagnation or erosion of the
educational gains of earlier decades.”1,1 A key
question for policymakers is whether it is feasible
in the short-term to dramatically raise national
education levels.
■ Expand mass media and population education
programs. Radio and television programs can
heighten awareness, promote new ideas, and
encourage healthier behaviors. Population educa
tion can be incorporated into both in-school and
out-of-school programs, conveying information
about AIDS, gender equality, family planning,
responsible parenthood, and other topics.
■ Improve literacy levels. Comprehension skills
appear to play a special role in influencing child
bearing decisions. Thus, enhancing literacy skills by
improving school quality and by providing educa
tion programs for those not in school may yield
economic, as well as population and health returns.
■ Strengthen family planning efforts. A strong
family planning program provides women with the
services and information required to make healthy
childbearing decisions. Family planning services
are a key ingredient in reducing family size and,
for young people, in encouraging healthier transi
tions into adulthood.
■ Provide employment and earning opportunities for
women with basic education. Research suggests that
when women have promising employment and
earning opportunities they may forgo early
marriage and childbearing. Policies designed to
increase womens employment and wages may
encourage smaller, healthier families.
Kefes'enees
'United Nations, Department of Economic and Social
Affairs, Population Division, Linkages Between Population
and Education (New York: United Nations, 1997): 12.
2S.J. Jejeebhoy, Women’s Education, Autonomy, and
Reproductive Behaviour: Experiencefrom Developing
Countries (Oxford, UK: Clarendon Press, 1995).
3 Ibid.
*1. Diamond, M. Newby, S. Varle, “Female Education and
Fertility: Examining the Links” in Critical Perspectives on
Schooling and Fertility in the Developing World, C. Bledsoe,
J. Casterline, J. Johnson-Kuhn, and J. Haaga, eds.
(Washington, DC: National Academy of Science Press,
1999): 23-45.
’ C. Lloyd, C. Kaufman, and P. Hewett, The Spread of
Primary Schooling in Suh-Saharan Africa: Implications for
Fertility Change (New York: The Population Council,
1999).
6 Ibid.
71. Diamond, M. Newby, S. Varle, “Female Education and
Fertility: Examining the Links”: 32-33.
8 Ibid.: 42-44.
’ P. Glewwe, “School Quality, Student Achievement, and
Fertility in Developing Countries” in Critical Perspectives on
Schooling and Fertility in the Developing World, C. Bledsoe,
J. Casterline, J. Johnson-Kuhn, and J. Haaga, eds.
(Washington, DC: National Academy of Science Press,
1999): 128-131.
,0S.J. Jejeebhoy, Womens Education, Autonomy, and
Reproductive Behaviour: Experience from Developing
Countries.
111.
Diamond, M. Newby, S. Varle, “Female Education and
Fertility: Examining the Links”: 37.
11 C. Lloyd, C. Kaufman, and P. Hewett, The Spread of
Primary Schooling in Sub-Saharan Africa: Implicationsfor
Fertility Change: 6.
13 S.J. Jejeebhoy, Womens Education, Autonomy, and
Reproductive Behaviour: Experience from Developing
Countries: 32.
'* C. Lloyd, C. Kaufman, and P. Hewett, The Spread of
Primary Schooling in Sub-Saharan Africa: Implications for
Fertility Change: 51.
Acknowledgments
Dara Carr of the Population Reference Bureau prepared this
policy brief with helpful contributions from Jennifer Adams,
Lori Ashford, Barney Cohen, Peter Donaldson, Elizabeth
Gould, Carl Haub, Mai Hijazi, and Nancy Yinger.
This work has been funded by the U.S. Agency for
International Development (USAID) under the MEASURE
Communication project (HRN-A-00-98-000001-00).
POPULATION REFERENCE BUREAU
MEASURE Communication
1875 Connecticut Ave., NW, Suite 520, Washington, DC 20009 USA
Tel.: (202) 483-1100 ■ Fax: (202) 328-3937 ■ E-mail: measure@prb.org or popref@prb.org
Web site: WWW.measurecommunication.org or WWW.prb.org ©Population Reference Bureau, May 2000
Cominiin ica tion
I HEALTH
For a woman’s well-being
Menopause is the time in a woman’s life
when menstruation ceases. This can occur
any time between the ages of40 and 52 and
results from the loss of ovarian follicular
activity. The follicles-structures that hold
and release eggs widrin the ovaries — play a
role in the production of female hormones
oestrogen and progesterone, which arc
vital for fertiliry and reproduction. Ar. a
woman ages, hormoneproGuctiondccImrs .
progressively, resulting in irregular inc'.’.strual cycles and finally cess-.rtior of men-
•
expectancy, w:t» note .-.■■J m<>:<. w.rten
living even up to four decades after rhe
onset of menopause, it is imperative that
more attention is paid to the effective med
ical management of menopause. For a
number of years oestrogen was thought of
as the magic hormone for the management
of menopause. Today phyto-oestrogen or
‘plant oestrogen which mimics the action
ofoestrogen in women, are becoming pop
ular. Currendy, around seven phyto
oestrogens have been identified, with
isoflavones - the phyto-oestrogens found
in soya - evincing the most interest.
According to Dr. Adam Carey,
Medical Director, The Centre for
Nutritional Medicine, London, studies
have shown that soya has an impact on a
number of conditions related to heart dis
ease, osteoporosis, menopause symptom
^dief and possibly cancer, and these effects
V' attributed to isoflavones. A trained
obstetrician and gynaecologist, Carey has
co-authored a number of papers and has
over 10 years of teaching experience. He
left clinical practice in the United
Kingdom’s National Healdr Service four
years ago to take up his present appoint
ment. He is currently involved in tackling
a wide variety of clinical problems that
include gynaecology, weight management,
reproductive endocrinology and sports
nutrition.
Carey, 41, is also working on four
research projects, all ofwhich look into var
ious treatment options for menopausal
symptoms. Excerpts from an interview he
gave Ravi Shanna:
► Listening to the talkyou gave to some of
Bangalore's leading gynaecologists, it was
obvious thatyou area great advocate ofthe
84
use of isoflavones to manage menopause.
In layman s tertns, what are isoflavones ?
It has been known for some time that
ifyou are to restrict osteoporosis and build
bones one needs weight-bearing exercises,
building blocks (essentially vitamins and
minerals) and builders (which are known
to be oestrogen). But now there are other
compounds and hormones that are clearly
as effective in building bones as oestrogen.
One of these may be progesterone, the
other being isoflavones. Isoflavones, which
are a compound found in soybean and
other legumes, appear to have a positive
effect on bones. We are also seeing that diet
can have an important effect both on the
in the leg (thrombosis) and cancer of the
womb, and also in the short-term increas
es the risk of heart diseases. These risks
weren’t so clear five years ago. The bal
ance has now changed and during the last
five years there has been a lor of research
on soya and soya isoflavones.
► How did you get interested in
isoflavones?
By listening to my patients. Being
trained as an obstetrician and gynaecolo
gist I was seeing a lot of patients who were
coming with two basic problems. One,
they were scared of traditional hormone
replacement therapy (HRT), given the
(possible) risks of breast cancer associated
with it. They would tell me, “This is some
thing that really troubles me, nonetheless I
would do it”. And second, whilst they were
taking HRT they were concerned about
theside-effects.particularlytheydidn’rlike
to have a cyclical bleed, which occurs for
the first few years post-menopause if the
woman is using HRT. A cyclical bleed is
very much like a menstrual period, the
experience .is similar and it comes every
month, but it is an induced bleed. And
most post-menopausal women would
rather nor have any bleeding. Because of
these two reasons all my patients would tell
me, “I don’t like the side effects of HRT
and I don’t think (a cyclical bleed) is nat
ural.” This is what made me start thinking.
► Are you advocating an alternative?
building blocks and in being a builder.
► How do isoflavones work!
Isoflavoncs are a chemical which have
a structure that is similar to that ofoestro
gen. Hence they bind to the same kind of
receptors that oestrogen binds to. Like
die key of a car. It is not the original key
but it still opens the door. It is a key that
opens the same doors that oestrogen does,
but maybe it doesn’t fit so well. So it
doesn’t open all the doors all the time but
it does most of the time.
► There is a body ofcore research that sug
gests that the community should look at
isoflavones in clinical use and practice.
Yes. Five years ago the climate was
that oestrogen was absolutely good for
everything. That climate has now
changed. Oestrogen has now been found ■
to increase the risk of breast cancer, clots
It is a complement as opposed to an
alternative. I don’t use it as a golden bul
let. It is part of a holistic management.
What I offer only goes hand in hand with
conventional medical practices. My team
works with doctors and dietitians seeing
patients jointly. We then medically
define what the patient needs in terms of
her lifestyle and then the dietitian or
nutritionist will take her through step by
step on how she should change it.
A patient may be on HRT, but her
HRT will be more effective if her diet is
right. Some patients do not want HRT,
so this is better. It may not be as effective
as HRT for reduction of hot sweats, but
then getting your diet right does not have
any side -effects. And when you use thi ngs
like isoflavone the effectiveness improves.
In other words, getting your diet right
improves your symptoms to a degree,
when you add nutritional supplementaFRONTLINE. JUNE 21.2002
development. The NFSIT
seems to lack the technical
expertise to evaluate the pro
posals it receives for funding.
The difference between the
TDB and the new proposals is
that the TDB’s operations are
governed by Acts ofParliament.
There are mechanisms in place
to ensure continuous flow of
funds - though the Finance
Ministry tries its best not to pay
the TDB’s dues fully - as well as
the availability of technical
expertise to evaluate projects,
assess market potential and
monitor progress.
The source of funds for
TDB’s operations is the '• i :
Collections under the R&D Cess Act, 1986
Year
1986-87
1987-88
1988-89"
1989-90 ’
1990-91 _
1991-92
1992-93
1993-94
1994-95
1995-96’
■ ■
■
.nay.c.c
■map uq
Cess collection Payments
(as per CGA's figures) to IDBI
8.84
’ 5.00
16.31
27.20
' 30.12
32.78
44.89
1.00
10.00'"
3.00
"
60.74
71.43
81.41 "
’364.M
80 :3
49
' .AW.
Allocation Payments
to TDB
to TDB
a1-..
BE
RE
27-84' "
30.00 30.00
29.97
70.00 49.93
49.93_
50.00 20.00
28.00
70.00 50.00 ' 50.00’ “
6279
70.00 63.00
220.69
63 00 &Z00_ ’57.00 _
68.00
85:93
made for technolog} :mis
in the form oflump? •.>■:. roy.ri
3ft 91
ties and dividends - as
•:<■< J
767 %
2 t .84
under the R&D Cess A.-t of
1986. This amount is paid into
>02-2003
the Consolidated Fund of India
(CFI) and the "the Central government TDB in 1995. The consequent amendmay... pay to the development bank (the ments to the R&D Cess Act were made in
IDBI’s venture capital fund), from time to
1996. Despite the creation of this new
time, from out of such proceeds... such
mechanism, rhe government’s reluctance
sums of money as it may think fit for being to part with the cess is apparent (seeTablc;
utilised for the purpose of the fund”. The
the figures for the cess collected for 2001R&D Cess Act came into being after the 2002 are not yet available). Budgetary allo
formulation of the Technology Policy in cations to the TDB have always been less
1983. Two years later the Technology dian the amount collected and the actual
Policy
Implementation
Committee payments even lesser. For instance, while
(TPIC) recommended the creation of a
the budget estimate (BE) for 2001-02 was
Technology Development Fund (TDF).
Rs.63 crores, it was brought down to Rs. 57
The cess began to be collected only crores in the revised estimate(RE). The BE
from 1988-89. Imports in.the pharmaceu for the current year is Rs.58 crores, about
tical, ITand biotechnologysectors too con
the same as last year’s RE, 7.9 per cent
tribute to this cess. From this perspective,
down from last year’s BE. The BE has been
too, it does not make sense to create sepa progressively coming down from a mairate boards and funds for these sectors.
mum of Rs.70 crores (see Table).
However, the amount that the government Considering that the Finance Ministry had
thought fit to pay into the IDBI’s VCF was consumed the Rs.283.47 crores that had
only a fraction of the cess collected. For accrued until 1994-95, it would have been
IDBI, funding technology through VCF only appropriate for it to release the entire
was not a priority because the VCF was but cess money every year since then. But this
a small fraction of its overall operations.
is not happening.
This suited the Finance Ministry too The TDB assists technology develop
over the years it seems to have dipped its ment through equity capital or financial
fingers into this fund also as part of its fis assistance (grants and loans at 6 per cent
cal manipulations. Until 1995-96, the gov
simple interest) to industrial concerns and
ernment had transferred to IDBI only other such agencies attempting the com
Rs.27.84 crores out ofthe Rs.364.88 crores mercial application ofindigenous technol
ogy or adapting imported technology for
that had accrued as cess until then.
At the urging ofthe Ministry ofScience wider domestic application; and through
and Technology, which felt that the money financial assistance to R&D institutions
due to industry for technology develop engaged in developing indigenous tech
ment was being wasted, the administration nology or adapting imported technology
of the cess fund was transferred from ■for commercial application. Funding by
IDBI’s VCF to the DST by establishing the the TDB, under the current guidelines,
FRONTLINE. JUNE 21. 2002
covers only half the estimated
project cost and the enterprise
seeking assistance has to pro
duce evidence of provision
made for the remaining
amount.
The strength of the TDB’s
funding process lies in the thor
ough project evaluation and
monitoring mechanisms that
have been put in place. Given
the DST’s access to expertise in
all areas of science and technol
ogy, both within the govern
ment and in the private sector,
its project evaluation commit
tees comprise thebestpersonsin
their fields and their assessment
of technology is bound to be
good. Indeed, financial institu^
tions such as ICICI, IDBI ai^fe
venture capitalists such as the
Gujarat Venture Capital Fund
and
Risk
Capital
and
Technology Corporation Ltd
have begun to realise the bene
fits of the TDB’s evaluation and have
agreed informally to provide additional
funding to any project that the TDB clears.
Already funds in the form of loan repay
ments have begun to flow into the TDB.
In creating the TDB the government
has arrived at a correct mechanism, albeit
belatedly, to fund technology develop
ment. Instead of consolidating and
strengthening the mechanism, the creation
ofa multiplicity ofsimilar agencies is being
attempted. The scope of the TDB’s oper
ations can be expanded easily to include
R&D projects. This is well within the terms
of the Technology Development Board
Act. Its sources of funding can be divers^
fied (though this might call for an amenl^r
ment of die Act) and additional funds can
be earmarked for specific purposes. For
instance, the corpus fund that was
announced for R&D in the pharmaceuti
cal sector can be set apart for the said pur
pose alone.
But if the government has funds to be
allocated in such ways, it is unclear why the
cess collected is not transferred folly to the
TDB. After all, the TDB operates the
TDF, which was created by an Act of
Parliament and is meant to be operated
outside the government’s budgetary mech
anism. In fact, as a first step, the sum of
about Rs.500 crores that is the remainder
ofthe total cess accrued since 1988-89 after
payments made to the TDB, should be
transferred fully to the TDF so that the
TDB is able to net more promising tech
nologies and R&D projects. ■
tion that has a pharmacological action
. similar to. oestrogen, you have an even
bigger effect. For some people it can be
an alternative, for many a complement.
Studies have also shown that they work
together synergistically.
► Getting your diet-right seems to he the
key?
Yes. For example, if an overweight
patient has urinary incontinence doctors
won’t want to operate on them. Because
we know that if they are slimmer the oper
ation is more successful. If they have osteo
porosis doctors prescribe oestrogen. We
now know that if they don’t get their diet
right oestrogen won’t have anything to
work on. So they have to have their diet
corrected.
► Can hotflushes, one ofthe main mani
festations ofmenopause, be controlledby diet?
kYes, studies have shown that you can
W
uce them by reducing caffeine intake.
But only to a degree, though. Dietary
modulation is reasonably effective but
doesn’t cure it. Isoflavones reduce the
occurrence of hoc flushes by 50 to 60 per
cent. Oestrogen by about 85 to 90 per
cent. Another hormone - progesterone may also be useful in the fiiture.
► Isoflavones can he taken naturally in the
form ofsoya. Why a capsule?
Absolutely, I’m all for the eating of
whole foods. But I don’t see a lot of soya
being eaten in India. Dietary changes are
difficult to make. Also bigger, more thor
ough studies have to be undertaken
before a whole nation changes its diet.
And even ifstudies have proved that soya
is as effective as oestrogen and complete
ly safe, I would still question the merit of
changing a nation’s cultural background.
communities notably in the Far
have a soya-rich diet. Are there any
studies showing a lower incidence there of
distressful menopausal symptoms?
Absolutely. If you look at the epidemological studies from Japan, where most
of this work has been done, the Japanese
have the lowest incidence of diseases asso
ciated with menopause, be it breast cancer,
endometrial cancer, cardiovascular disease,
osteoporosis - and in men, prostrate can
cer. Illnesses that are very high risk in the
United Kingdom (U.K.), the UnitedStates
and now increasingly in India. Studies
show that both in the U.K. and the U.S. at
least 80 per cent of post-menopausal
women experience one or more of these
symptoms, one of three women has osteo
porosis and by the age of 80 almost all of
them have had at least one osteoporosisproduced fracture.
In medical journals when they talk of
FRONTLINE, JUNE 21. 2002
Asia they assume that what is happening in
Japan is happening in India. My experience
with Indian gynaecologists clearly shows
that many more Indian women than the 5
to 10 per cent that journals indicate, suffer
menopausal symptoms. A recent study in
Bangalore showed that more than half the
women who go through menopause expe
rience symptoms.
In Japan the very high intake of
isoflavones amongst other things is
reducing the incidence ofall the common
diseases that are killing people in the rest
of the world. Less than 10 per cent of
Japanese women experience menopausal
symptoms. But when they move to the
U.S., within one generation they become
prone to breast cancer, endometrial can
cer, cardiovascular disease and so on. So
it is not the genetics of the Japanese
women that is protecting them, but
something in the environment - either
the air they are breathing or the food they
are eating. We think it is the food.
BOOKS FROM THE left
War Against the Planet
The Fifth Afghan War, Imperialism, and Other
Assorted Fundamentalisms
Vijay Prashad
PP- viii +110, paperback, Rs 75 (Rs 45.00 for Members;
52.50 for Associate Members)/ $ 7 ($ 4.20 for Members)
The Market That Failed
A Decade ofNeoliberal Economic Reforms
in India
C.P. Chandrasekhar and Jayati Ghosh
pp. xiv + 192, hardcover, Rs 275 (Rs 165.00 for
Members; 192.50 for Associate Members)/
$ 18 ($ 10.80 for Members)
Weakening Welfare
. The Public Distribution ofFood in India
Madhura Swaminathan
pp. viii + 140, HC Rs 275 (Rs 165 for Members, Rs 192.50
for Associate Members), P8 Rs 95 (Rs 57 for Members; Rs
66 for Associate Members) overseas HC $ 17 ($ 10.20 for
Members) PB $ 12 ($ 7.20 for Members)
► Can isoflavones reverse these disorders?
You can’t reverse ageing. Heart
attacks cause death, but a fractured hip
does not cause immediate death. But 20
per cent of women who have a break in
die leg will die within the first 12 months
of that fracture. This is because they con
tract pneumonia or whatever else.
Fractures take a lot of money to put right.
Fractured spines, which leave little old
ladies all bent over (the Dowager’s hump),
cause chronic pain and disability.
It is estimated that the amount of
money spent on treating osteoporosisrelated cases in England is £1 billion a year.
Even ifwe can’t stop all the cases, it would
help if we could delay them. Menopause
was never a problem 200 years ago since all
of us died before menopause. It is a prob
lem today because many of us live up to
80. Most women have 30 years post
menopause and they get their fractures in
their 70s and 80s. We are looking to push
the likelihood of these fractures happening
when the women are 90 or 100.
► Do men experience menopausal symp
toms?
Men very rarely, for example, experi
ence hot flushes, only if they are undergo
ing chemotherapy. But men also have
problems associated with changes in their
hormonal levels as they get older. Most
men after the age of 45 experience a fall of
some of the androgens in their bodies.
They also get osteoporosis - about a third
as often as women. They are also at car
diovascular risk and often show abnormal
lipid profiles. Isoflavones improve those
lipid profiles. ■
Depoliticizing Development
The World Bank and Social Capital
John Harriss
pp. vi + 145, HC, Rs 2501 $ 15 (Rs 1501 $ 9 for Members;
Rs 175 for Associate Members)
Local Democracy and Development
People’s Campaign for Decentralized Planning in
Kerala
T.M. Thomas Isaac and Richard W. Franke
pp. xiv + 290, Rs 185 (Rs 111 for Members; Rs 129.50 for
Associate Members) / $ 15 ($ 9 for Members).
Selected Writings ofJotirao Phule
Edited, with annotations and Introduction,
by G.P. Deshpande
crown quarto, pp. xii * 247, hardcover, Rs 450 (Rs 270.00
for Members; 315.00 for Associate Members)/? 40 ($ 24.00
for Members)
Nobodies to Somebodies
The Rise ofthe Colonial Bourgeoisie in Sri Lanka
Kumari Jayawardena
pp. xxx + 412 + 16 pages of 23 black and white
photographs. Rs 650 (Rs 390 for Members; Rs 455 for
Associate Members) / $ 35 ($ 21 for Members)
Islam and Jihad
A.G. Nooram
pp. xii + 115, Rs 75 (Rs 45 lor Members; Rs 52.50 for
Associate Members) / $ 7 ($ 4.20 for Members);
I The RSS and the BJP
I
A Division of Labour
A.G. Noorani
pp. xiv + 112. Rs 75 (Rs 45 for Members; Rs 52.50 for
Associate Members) I $ 7 ($ 4.20 for Members)
I
|
POSTAGE FREE for individual orders in India.
Cheques/drafts should be in favour of LEFTWORD BOOKS, j
Add Rs 45/$ 2.50 to cheques drawn on banks outside Delhi, i
LeftWord Books
12 Rajendra Prasad Road, New Delhi 110001
Phone: (91 • 11) 335 9456,335 6966. Email: leftword@vsnl.com j
85
I HEALTH
A virus lives on
The World Health Assembly decides to retain existing stocks of the
smallpox virus for continued research into new vaccines, without
setting a future date for their destruction.
At its January 14-18 meeting, the
WHO board accepted the advice of its
N a controversial move that could have
Director-General
Gro
Harlem
far-reaching consequences, the 55th Brundtland and the advisory committee
World Health Assembly (WHA) on May for variola virus research that ongoing
18 went back on its six-year-old resolution research would not be completed by end
to destroy the current stockpiles ofsmall 2002 - the deadline set in 1999 for the
destruction of virus stocks. Brundtland
pox virus variola and decided to retain
had said: “The research programme
them indefinitely for international
research. This reversal is a dear fell-out of should be completed as quickly as possi
the heightened fears of bioterrorism built ble and a proposed new date for destruc
up chiefly by the United States in the wake tion should be set when the research
of post-September 11 anthrax attacks.
accomplishments and outcomes allow
Endorsing the recommendation consensus to be reached on the timing of
made
by
the
World
Health destruction.” Given the history of the
Organisation’s (WHO’s) 32-member issue, it is unlikely that consensus would
Executive Board in January, the WHA ever be reached.
decided to retain the existing stocks of
Indeed, in a speech to the board the
variola virus to allow continued research
U.S. Assistant Surgeon-General Kenneth
into new vaccines and anti-viral drugs Bernard said that continued research into
against smallpox “on the understanding improved vaccines was vital in the wake of
the September 11 attacks and subsequent
that steps should be taken to ensure that
all approved research would remain out anthrax scare. “We regard the potential
come-oriented and time-limited and
release ofsmallpox as a critical national and
periodically reviewed”. Since smallpox international security issue... We are curwas effectively eradicated in 1979, stocks rendy making progress in research
of live virus exist only in two high-secu designed to develop new tools against
rity laboratories - the Centres for Disease smallpox... The need for new drugs and
Control and Prevention (CDG), Adanta,
vaccines is particularly acute in parts ofthe
U.S., and the Russian State Centre for world with large populations of immuno
Research on Virology and Biotechnology suppressed people such as those with
HIV/AIDS for whom the current vaccine
(VECTOR), Koltsovo, Novosibirsk.
The last case of naturally occurring would be potentially lethal.” Russia too
smallpox was in Somalia in 1977 and in
echoed these views which found all-round
1980 the WHO declared the disease to support among the 32 members, includ
have been completely
ing Japan, which had
The decision to
eradicated globally. One
been earlier among the
retain current
of the key factors that
front-ranking
oppo
enabled eradication of
nents, along with Brazil,
stockpiles of the
smallpox, the disease
Cuba, India and China,
smallpox
virus
is
a
that
had
afflicted
to the idea of retaining
mankind for centuries fall-out of the fears the stocks.
and has no treatment
China, which like
of bioterrorism
India is not currently a
even today, through an
built up chiefly by member of the board,
intensive
worldwide
the U.S. in
was the lone voice ofdis
immunisation
cam
paign between 1967 and
sent. It wanted a final
the wake of
1979, is the fact that the
deadline for destruction
only known host of the post-September 11
without any excuses for
anthrax attacks.
further
delay.
variola virus is rhe
human body.
Interestingly, in con
R. RAMACHANDRAN
I
86
trast to its the earlier stand on the issue,
the Indian representative to the meeting
apparendy sat quietly through the delib
erations. India’s current disposition
towards the U.S. would seem to have dic
tated its endorsement ofthe WHO’s pol
icy reversal.
Since Edward Jenner discovered it in
1796, the conventional vaccine is based
on live vaccinia, the causative virus of
cowpox. It is estimated that the current
world vaccine stock is about 110 million
doses, including 500,000 doses main
tained by the WHO at its Collaborating
Centre for Smallpox Vaccine in
Bilthoven, the Netherlands. The centre
also holds the seed virus used to produce
the vaccine.
Since the vaccine itself does^fe
require the variola virus, the Gl^El
Commission for the Certification of
Smallpox Eradication recommended in
December 1979 that any remaining
stocks of the virus (isolated from infect
ed blood, tissue samples) should be
destroyed or transferred to one ofthe four
WHO-designated reference laboratories
in the U.S., the U.K., South Africa and
Russia. This was endorsed by the WHA
in. May 1980. However, by the end of
1983, all variola stocks in South Africa
were destroyed and those in the U.K.
were transferred to the CDC.
Consequently, today all known
stocks of the virus have been consolidat
ed at the two WHO collaborating cen
tres at the CDC and VECTOR. The
CDC is a reposi tory of4 51 smallpox virus
samples and the Russian collection con
tains about 150 samples. Of course, tj^e
is no guarantee that somewhere in^e
world there is not another potential
source of virus - the corpse of a person
who died ofsmallpox and is buried in the
Arctic or Siberian permafrost, or a virus
vial unknowingly retained in some labo
ratory, or samples deliberately retained by
some country out of a suspicion of the
motives of the Russian and U.S. govern
ments or out of intentions of biowarfare.
To clear the way for the subsequent
destruction of these stocks, the two lab
oratories
undertook
cloning
and
sequencing of deoxyribonucleic acid
(DNA) fragments ofselected virus strains
under high-containment biosafety level 4
(called P4) conditions. Since 1983 such
clones have been kept in a few laborato
ries in the U.K., the U.S., Russia and
South Africa. Because the cloned DNA
fragments had the potential to create a
FRONTLINE. JUNE 21, 2002
One of the key factors that enabled the eradication of smallpox through an
intensive worldwide immunisation campaign between 1967 and 1979, is the
fact that the known host of the variola virus Is the human body.
smallpox-like virus by recombination
with vaccinia or monkeypox viruses, the
WHO required the registration of all
clones ofvariolaDNA and restricted their
use and distribution. Arguing that the
clones obviated the need for the infec
tious virus for reference purposes, the
WHO Ad Hoc Committee on
Orthopoxvirus Infections resolved in
1986 that the virus stocks be destroyed
“if no serious objections were received
from the international health communi
ty’’:
At the May 1990 WHA, the U.S.
jkclared that technological advances now
^owed the entire virus genome to be
sequenced within three years and offered
to destroy all the virus stocks at the CDC.
In December 1990, the WHO Ad Hoc
Committee on Orthopoxvirus Infections
endorsed the proposal for sequencing ofthe
virus genome joindy by the U.S. and
Russia. It also decided that the remaining
virus stocks be destroyed by December 31,
1993, provided sufficient sequence infor
mation was available and serious scientific
objections were not raised. By December
1993, Russian and U.S. scientists had suc
cessfully sequenced the genomes of two
strains ofvariola major - Bangladesh 1975
and India 1967 - and one strain of vario
la minor - Garcia 1966. (Variola minor is
a milder form of the virus with a much
smaller mortality rate of 1 per cent as com
pared to 30 per cent in variola major.) At
present 10 different strains of variola have
FRONTLINE, JUNE 21,2002
been sequenced completely.
While the larger ethical issue of
whether humanity has the right to exter
minate a living species deliberately does
pose a dilemma, purely from a research per
spective, thescientific community has been
divided on the issue and has debated on it
extensively since 1991. The proposed
destruction by 1993-end did not come
about because of this division of opinion
among researchers and public health spe
cialists. Those supporting destruction
argued that once sequencing is complete,
the virus itself is no longer necessary and,
once destroyed, smallpox ceases to be a
potential threat to public health, be it from
accidents, military use or terrorism. On the
other side of the question, it was argued
that having the virus in its functional form
offers much more information for science
than the mere record of its genetic code can
possibly impart. It was further held that the
smallpox virus has evolved along with its
host, humans, and its strategies to evade the
human immune system are very specific,
but are only beginning to become known.
The 1996 WHAadopted a resolution
recommending that destruction should
take place on June 30, 1999. The threeyear period was given to achieve a broad
er consensus before a final decision was
taken. In 1998, a WHA survey of the
positions of its 191 members revealed
that of the 79 countries that responded,
74 were in favour of destruction. Russia
was against it while the U.S., the U.K.,
France and Italy were undecided.
Between 1990, when the U.S. offered to
destroy its stocks - and so did Russia and 1998 there had been a change in their
respective perspectives. In January 1999,
the Ad Hoc Committee also found itself
lacking in unanimity over the issue.
Two factors were responsible for the
change in the U.S. position. One, a dis
closure by a Russian defector, Ken Alibek,
former deputy director of the Russian
Bioweapons Programme, that following
termination of mass vaccination, and in
the atmosphere of the Cold War, Russia
had developed facilities to produce the
virus in tonne quantities in a month and
had even weaponised the virus. Two, a
1998 report by the U.S. National
Academy of Sciences’ Institute of
Medicine (IOM), which assessed the sci
entific need for live variola virus without,
however, addressing the costs that may be
involved in such research and weighing
the risks of release of the virus arid its reemergence.
“The most compelling reason for
long-term retention of live variola virus
stocks is their essential role in the identi
fication and development of antiviral
agents for use in anticipation of a large
outbreak of smallpox,” the IOM report
said. It also said that live virus would be
necessary for the development of novel
types of vaccine. It also favoured live or
“replication-defective" virus for the study
of variola pathogenesis and the response
ofthe human immune system. The small
pox virus has very different biological
properties. If this could be understood, it
would reveal more about the human
immune system, it was argued.
Accordingly, in April 1999, a month
before the 52nd WHA, President Bill
Clinton sought a delay in the proposed
destruction of the virus. The White
House statement said that the President’s
decision was based on a consensus rec
ommendation of his advisers, reflecting
agreement among all departments, and
also the fact that the administration can
not be certain that destruction of the
declared stocks will eliminate all the virus
in existence. U.S. media reports then
quoting officials said that the U.S.
believed that Iraq, North Korea and
Russia had bioweapon programmes
based on the smallpox virus. Indeed,
Donald A. Henderson, Director of the
Johns Hopkins Centre for Civilian
Biodefence Studies, who directed the
WHO smallpox immunisation cam
paign and who is a former adviser in the
Clinton administration, believes that a
87
desire to be able to retaliate in
on an anti-vaccinial drug,
the event of a biological
which could be more thor
attack was behind the admin
oughly evaluated through
istration’s reversal which he
animal studies^ and such
claimed emanated from the
studies would not require
Defence Department.
retention of the variola virus,
The 1999 WHA, influ
they said.
enced by the U.S. stand,
Running counter to this
agreed by consensus to the
perspective, the WHO com
“temporary retention, up to
mittee on variola virus
but not later than 2002, of
research reported to the
the existing stocks of variola
board that “significant com
virus for the purpose of fur
ponents of this research,
ther international research
most notably refinement and
into antiviral agents and
use ofan animal model devel
improved vaccines, and to
oped in 2001 and the devel
opment of antiviral drugs,
permit high-priority investi
gations of the genetic struc
were unlikely to be complet
ture and pathogenesis of
ed by the end of2002.” It fur
smallpox.” While affirming
ther stated that to study the
that the final elimination of
animal model (cynomola^k
all variola virus remained the
monkey), further access
goal of the WHO and all
live variola virus was neces
member-states, the resolu
sary after the expected 2002
tion said that “any such
destruction date. This the
research shall be conducted
board endorsed, and based
in an open and transparent
on this the Director-General
manner only with the agree
recommended retention of
ment and under the control
stocks without setting a
ofWHO."
deadline.
In a perceptive article
An Indian expert in bio
written in October 2001,
logical warfare,
Kalyan
Henderson
and
Frank
Banerjee, former Director of
Fenner analysed the various
the National Institute of
research priorities identified
Virology (NIV), Pune, and
Gro Harlem Brundtland, Director-General of the World Health
by the expert group and
a former member of the
Organisation, arrives for the opening session of the 55th World
argued why the deadline set
National Security Advisory
Health Assembly at the United Nations in Geneva.
by the 1999 WHA should be
Board (NSAB), is furious
adhered to. They looked at the develop anti-vaccinial drugs or monoclonal anti with the WHA decision. As a dissenting
ment in the research areas identified: the bodies,” they argued.
member
of WHO’s
Ad
Hoc
development of a more attenuated, less
Questioning both the feasibility and Committee, he has reasons to be furious.
reactogenic vaccine; and the develop wisdom of pursuing the development of He feels that continuing research widr
ment of an antiviral drug that could be antiviral drugs, Henderson and Fenner the smallpox virus may enable the U^p
used in the treatment of smallpox. An pointed out the high cost (about $500
military to develop it as a bioweapon. In
associated important area was the evalu
million, which no government was ready the wake of the September 11 events, the
ation of a suitable animal model in the to invest) ofdeveloping a newanti-micro- U.S. proposes to have a stockpile of 286
absence of any known non-human host bial drug and the fact that it would take million doses of the vaccine by the year
for smallpox.
eight to 10 years of research and devel end, enough for every U.S. citizen. ‘So
Two candidate vaccines, which pro opment to bring it to the market. Added
where is the rationale for developing a
duced satisfactory antibody levels but to this would be the large sums of money new vaccine with live virus?" he asks,
that would be required to build up and echoing the point raised by Henderson
produced less side effects in animal tests,
had been identified. But, for obvious rea maintain stockpiles of reasonable size of and Fenner.
sons they could not be tested in an area the drug for possible future use. Secondly,
Criticising the U.S.’ unilateral deci
where smallpox was endemic. Therefore,
here too there would be a lack of proven sion to retain the stocks indefinitely,
an assurance of their efficacy was no efficacy of the drug, however effective it Banerjee accuses the WHO of having
longer possible. From that perspective, may appear in a surrogate host with a sur
become a “cat’s paw” in the issue.
administrations would procure more of rogate virus in the absence yet of a viable “Research does not need the live virus and
the proven vaccine thus foreclosing the variola/monkey model. An anti-viral
there is no justification in retaining the
rationale for further research on modified drug, they argued, might be more useful stocks. The people of the world and the
vaccines, they argued. “It would seem
in preventing the disease in immune- WHO worked hard to eradicate small
appropriate that future research efforts be compromised patients who would be at pox, only to leave the most potent
directed at mitigating the possible effects risk of “progressive vaccinia” disease if bioweapon in the hands of the custodial
of adverse reaction through die use of vaccinated. Research efforts should focus powers," he said. H
88
FRONTLINE, JUNE 21, 2002
- Media
 RF_WH_5_SUDHA.pdf
RF_WH_5_SUDHA.pdf
Position: 875 (25 views)