LAWS AND ACTS ON TOBACCO
Item
- Title
- LAWS AND ACTS ON TOBACCO
- extracted text
-
RF_PH_5_SUDHA
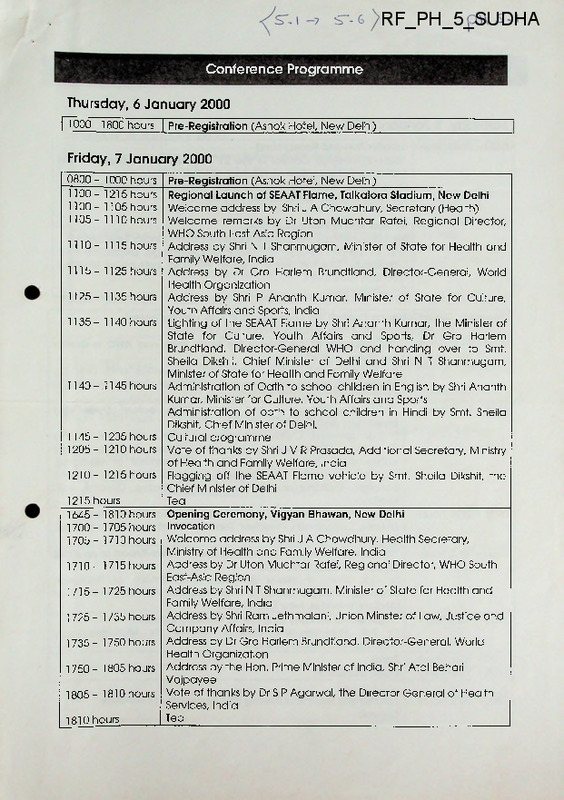
Conference Programme
Thursday, 6 January 2000
| 1000 -1800 hours | Pre-Registration (Ashok Hotel, New Delhi)
Friday, 7 January 2000
0800- 1000 hours
1100- 1215 hours
1100 - 1105 hours
1105 - 1110 hours
1110 - 1115 hours
1115- 1125 hours
1125- 1135 hours
1135 - 1140 hours
1140- 1145 hours
1145- 1205 hours
1205- 1210 hours
1210- 1215 hours
1215 hours
1645- 1810 hours
1700 - 1705 hours
1705- 1710 hours
1710- 1715hours
1715- 1725 hours
1725- 1735 hours
1735 - 1750 hours
1750 - 1805 hours
1805- 1810 hours
1810 hours
Pre-Registration (Ashok Hotel, New Delhi)
Regional Launch of SEAAT Flame, Talkatora Stadium, New Delhi
Welcome address by Shri J A Chowdhury, Secretary (Health)
Welcome remarks by Dr Uton Muchtar Rafei, Regional Director,
WHO South East-Asia Region
Address by Shri N T Shanmugam, Minister of State for Health and
Family Welfare, India
Address by Dr Gro Harlem Brundtland, Director-General, World
Health Organization
Address by Shri P Ananth Kumar, Minister of State for Culture,
Youth Affairs and Sports, India
Lighting of the SEAAT Flame by Shri Ananth Kumar, the Minister of
State for Culture, Youth Affairs and Sports, Dr Gro Harlem
Brundtland, Director-General WHO and handing over to Smt.
Sheila Dikshit, Chief Minister of Delhi and Shri N T Shanmugam,
Minister of State for Health and Family Welfare
Administration of Oath to school children in English by Shri Ananth
Kumar, Minister for Culture, Youth Affairs and Sports
Administration of oath to school children in Hindi by Smt. Sheila
Dikshit, Chief Minister of Delhi.
Cultural programme
Vote of thanks by Shri J V R Prasada, Additional Secretary, Ministry
of Health and Family Welfare, India
Flagging off the SEAAT Flame vehicle by Smt. Sheila Dikshit, the
Chief Minister of Delhi
Tea
Opening Ceremony, Vigyan Bhawan, New Delhi
Invocation
Welcome address by Shri J A Chowdhury, Health Secretary,
Ministry of Health and Family Welfare, India
Address by Dr Uton Muchtar Rafei, Regional Director, WHO South
East-Asia Region
Address by Shri N T Shanmugam, Minister of State for Health and
Family Welfare, India
Address by Shri Ram Jethmalani, Union Minster of Law, Justice and
Company Affairs, India
Address by Dr Gro Harlem Brundtland, Director-General, World
Health Organization
Address by the Hon. Prime Minister of India, Shri Atal Behari
Vajpayee
Vote of thanks by Dr S P Agarwal, the Director General of Health
Services, India
Tea
Conference Programme (confd.)
Saturday, 8 January 2000
0830 - 0845 hours
Introduction and Background
"Global Tobacco Control in the 21s' Century and Update on the
Framework Convention on Tobacco Control"
Dr Douglas Bettcher, Coordinator, Framework Convention on
Tobacco Control, World Health Organization
0845 - 0900 hours
Introduction to Methods of Work
Ms Indira Jaisingh, Advocate, Supreme Court of India, New Delhi
and Dr Srinath Reddy, Professor of Cardiology, Department of
Cardiology, Cardiothoracic Centre, All India Institute of Medical
Sciences, New Delhi
Co-Chairpersons
Plenary 1: Global Tobacco Control: The Economic and Agricultural Context
Co-chaired by Ms Indira Jaisingh and Dr Srinath Reddy
0900 - 0915 hours
“An overview of the Role of the World Bank and WHO in Global
Tobacco Control”
Professor Iraj Abedian, Professor of Economics and Director,
Applied Fiscal Research Center, University of Cape Town, South
Africa
0915-0935 hours
“Role of multinational and other private actors: Trade and
Investment Practices”
Dr Luk Joossens, Centre for Research and Information for the
Consumer Organisations, Brussels, Belgium, Professor Prakit
Vateesatokit, Professor of Medicine, Department of Medicine,
Mahidol University, Ramathibodi Hospital, Medical School,
Bangkok, Thailand and Ms Bungon Rithipakdee, Director, ASH
Thailand
0935 - 0950 hours
“Ownership of Tobacco Companies and Implications on Health”
Dr Hatai Chitanondh, President, Thailand Health Promotion Institute,
Bangkok.
0950 - 1005 hours
"The Cost of Tobacco Related Diseases in India-Report of an ICMR
Task Force Study 1990-1996”
Dr G.K. Rath, Professor & Head, Department of Radiation
Oncology, Institute Rotary Cancer Hospital, All India Institute of
Medical Sciences, New Delhi, India
1005- 1020 hours
"Agricultural Diversity as a Tool of Tobacco Control”
Dr P.R. Panchamukhi, Director, Centre for Multi-disciplinary
Development Research, India
1020- 1035 hours
Break______________________________
1035- 1300 hours
Open discussion_______________
1300- 1400 hours
Lunch/Press Technical Briefing (The Economics of Tobacco
Control)_______________________________
Conference Programme (contd.)
Saturday, 8 January 2000
Plenary II: Industry Challenges and Public Health Responses
Co-chaired by Ms Indira Jaisinah and Dr Srinath Reddy
1400- 1420 hours
“Media and Global Responsibility”
Ms Ambika Srivastava, Media Consultant New Delhi, and Mr
Ross Hammond, Hammond and Purcell Consulting, San
Francisco, USA
1420 - 1440 hours
“Industry Lobbying of the Public Sector and other Tactics"
Dr Y. Saloojee, Executive Director, National Council Against
Smoking, Johannesburg, South Africa, and Dr Elif Dagli, Professor
of Medicine, Marmara University Hospital, Istanbul, Turkey
1530 - 1545 hours
"Case Study in Consumer Protection from Tobacco in South East
Asia”
Dr Sri Ram Khanna, Managing Trustee, VOICE, New Delhi, India,
and Ms Mary Assunta Kolandi, Media Officer, Consumers
Association of Penang, Penang, Malaysia
"Multisectoral and Intersectoral Approach to National Tobacco
Control"
Dr Kishore Chaudhry, Deputy Director, Indian Council of Medical
Research, New Delhi, India
“Women, Children and Tobacco"
Dr Mira Aghi, Consultant to WHO and other UN Agencies, New
Delhi, India
Break
1545- 1800 hours
Open discussion
1440- 1500 hours
1500- 1515 hours
1515- 1530 hours
Conference Programme (contd.)
Sunday, 9 January 2000
Plenary III: Global Tobacco Control Law: Towards a Legal and Regulatory Framework
Co-chaired by Ms Indira Jaisingh and Dr Srinath Reddy
0900 - 0915 hours
0915-0930 hours
0930 - 0945 hours
0945- 1000 hours
1000- 1015 hours
1015- 1230 hours
“International Legal and Policy Framework for WHO Framework
Convention on Tobacco Control”
Mr William Onzivu, Fellow, WHO Geneva
“Regulation of Tobacco Products”
Mr Mitchell Zeller, US Federal Drug Administration Rockville, USA
“The Prospects for Globalizing Tobacco Litigation”
Ms Roberta Walburn, Senior Fellow, WHO Geneva
“The Application of International Law into National Law, Policy
and Practice: Lessons for the Framework Convention on
Tobacco Control"
Ms Judy Obitre-Gama, Lecturer, Faculty of Law, Makerere
University, Kampala, Uganda
Break
Open Discussion and
Introduction to the Working Group Process
1230- 1330 hours
Lunch/Press Technical Brieting/Legal Implications of Tobacco
Industry’s Arguments vis-a-vis the FCTC
1330 - 1630 hours
WORKING GROUPS
Chairpersons, Facilitators, Rapporteurs, and Panelists to be
announced
Working Group 1- “Economic Implications of Tobacco
Production and Marketing”
Working Group II - “Towards establishing National Institutions for
the FCTC: Legal, Policy and Practical
Options”
Working Group III - “Addressing Industry Tactics”
Working Group IV - “The Prospects for Globalizing Tobacco
Litigation”
Plenary IV: Conference Recommendations and Chairs’ Summaries
____________ Co-chaired by Ms Indira Jaisingh and Dr Srinath Reddy
1645- 1745 hours
Working Group Recommendations - Reports by Rapporteurs
1745- 1755 hours
Chairs’ Comments
1755 - 1805 hours
Adoption of Declaration
1805- 1825 hours
Conference Synthesis
Dr Derek Yach, Project Manager, Tobacco Free Initiative, World
Health Organization
Closure
1825 - 1845 hours
e
e
pH S-T-
WORKING GROUP I
ECONOMIC IMPLICATIOINS OF TOBACCO
PRODUCTION AND MARKETING
1. KAMAL KABRA
INDIA (CHAIRMAN)
2. DR G. WOELK
ZIMBABWE (RAPPORTEUR)
3. DR SETH KORANTENG
GHANA
4P.R. PANCHAMUKHI
INDIA
5. R.N. TRIVEDI
INDIA
6. DR BABU MATHEW
INDIA
7. DR G.K. RATH
8. MATHEW ALLEN
9. DR GAJA LAKSHMI
10. DR MANGUELE
INDIA
NEW ZEALAND
INDIA
MOZAMBIQUE
ll.PEMA UDON
BHUTAN
12. S.K. OJHA
INDIA
13. K.K. MARWAHA
INDIA
14. DR INDIRA CHAKRAVARTY
INDIA
15. ANTHONY SO
16. MS MAI YA RANJITKAR
USA
NEPAL
20. BYAKUTUIGA TANEFU
UGANDA
21. JUDY OBITRE-GAMA
UGANDA
22.DR K.N. SHAFIUL ALMA
BANGLADSH
23. DR NISHI RANJAN TALUKDER
BANGLADESH
24. AKHTARI BEGUM
BANGALDESH
25. DR FATIMA EL-AWA
WHO/EMRO
26. YOUNG-JOO JIN
SOUTH KOREA
27. DRD.M. KIIMA
KENYA
28. PROFS.K. VERMA
INIDA
29. HECTOR SOLIMAN
PHILIPPINES
30. SAIFUDDIN AHMED
BANGLADESH
31. ATIE W. SOEKANDAR
INDONESIA
32. YUSINIAR N. DARWIN
INDONESIA
33. DR TIN WIN MAUNG
MYANMAR
34. MR MIFUNDU DU BILONGO
35. KATUALA
RDC
RDC
36. DR F N. ENYINE
CAMEROON
37. MR WIN MYINT
MYANMAR
38. ZEWDIE BELAY
ETHIOPIA
39. MRS KRISSANA TREEYAMANERATANA
THAILAND
pH S’. p
WORKING GROUP III
ADDRESSING INDUSTRY TACTICS
. '
g •
h
1. E. DAGLI
TURKEY (CHAIRMAN)
2. DR SRI RAM KHANNA
INDIA (RAPPORTEUR)
3.DRS.G. VAIDYA
INDIA
4. Y. SALOOJEE
5. J. MBATIA
MALDIVES
6. D. Me CARGO
7. A. AFAAL
MALDIVES
8. AGHIMIRA
INDIA
9. P.C. GUPTA
INDIA
10. S. CHANTORNVONG
THAILAND
11. MARY ASSUNTA
MALAYSIA
12. DR SRI RAM KHANNA
INDIA
13. ROSS HAMMOND
USA
14. THELMA NARAYAN
INDIA
15. JEFF COLLIN
UK
16. MIMTA MOLINARI
ARGENTINA
17. DEBRA EFROYMSOiN
BANGLADESH
18. GARRETT MEHL
19. MAG ARETHA HAGLUND LUK JOSSENS
USA
BELGIUM
20. S,. HONG TIY
FIJI
21. NAIMUL HAQ
BANGLADESH
22. BUNGON RITHIPAKDEE
THAILAND
Working Group IV
THE PROSPECTS FOR GLOBALISING TOBACCO
LITIGATION
1. ELANA MAYSHAR
2. JOSE MARIA OCHAVE
ISRAEL (CHAIRMAN)
PHILIPPINES (RAPPORTEUR)
3. PRAM I LA PATTEN
MAURITIUS
4. LOUISE DELANY
NEW ZEALAND
5. PROF R.K. NAYAK
INDIA
6. T. OBIDAIRO
NIGERIA
7.FILOMENA WILSON
ANGOLA
8. V.S. REKHI
9. YASANTHA KODAGODA
INDIA
SRI LANKA
10. RANI JETHMALANI
INDIA
11. AISEA TAUMOEPEAU
TONGA
12. ZEEBA HIRJI
13. MANOHARAN DE SILVA
14. LINDA BAILEY
15 LULAMA MNUMZANA
INDIA
SRI LANKA
USA
SOUTH AFRICA
TERMS OF REFERENCE FOR WORKING GROUPS.
I: ECONOMIC IMPLICATIONS OF TOBACCO PRODUCTION AND
MARKETING.
Objective:
To present the World Bank Report on the economic effects of tobacco production and
marketing and to discuss the arguments advanced by the Bank.
Expected Outcome:
In view of the World Bank Report;
The economic implications of the report for global and national tobacco control
would have been ascertained.
2.
Practical guidelines for implementing the World Bank Report in Developing
countries would have been compiled for the FCTC.
1.
II: “TOWARDS ESTABLISHING NATIONAL INSTITUTIONS FOR THE
FCTC: LEGAL AND POLICY OPTIONS”
Objective:
To explore various options using law', policy or practice to establish national
institutions for development of the FCTC/national tobacco controls in states of the
developing world.
Examine any difficulties that may be encountered, suggesting feasible and practical
solutions to the problems.
Expected Outcome:
1. All relevant issues relating to establishment of these institutions and and
countermeasures would have been identified.
3.
Develop short practical guidelines for establishment of national Institutions
in the developing world to further FCTC process and later implementation.
zlil: ADDRESSING INDUSTRY TACTICS.
.
(.-----------
"
-————
----------—------------- _
Objective:
To discuss and document the nature of tactics used by the tobacco industry to promote
its products in the developing world. To determine the impact of industry tactics on
tobacco control policies.
Expected Outcome.
1. In view of the complexities of the problem, effective options to counter industry
tactics would have been documented.
2. A short practical guideline on effectively countering the industiy tactics
w ould have been developed.
IV: THE PROSPECTS FOR GLOBALIZING TOBACCO LITIGATION.
Objective:
To discuss and identify all conditions and factors for ensuring successful transnational
claims against the tobacco industry by or for the developing world.
Discuss any obstacles involved and solutions to these problems.
^pected Outcomes:
1. All prerequisites for successful transnational claims against the industry would
have been ascertained.
2. A set of short guidelines would have been developed to undertake litigation
against the industry.
Table 1: An outline of Tobacco Industry Tactics
Tactic
-*
**
^j^c
r c >5
1. Intelligence gathering
Monitor opponents &jSocial trends to anticipate future
challenges.
5
fL°~
~ H
2. Public Relations
To mould public opinion using the media to promote
pro-industry positions. —
3. Political Funding
Use donations to win votes and legislative favours from
politicians.
Cut deals and influence political process.
4""Jv- (G- A-fV
c. U \
5. Consultancy programme
To produce “independent” experts critical of tobacco
control measures.
6. Smokers Rights Groups
Creating impression of spontaneous, grassroots public
support.
7. Creating .Alliances
Mobilising farmers, retailers, advertising agencies to
influence legislation.
8. Intimidation
Using legal and economic power to harass and frighten
opponents.
9. Philanthropy
Buys friends and social respectability-from arts, sports
and cultural groups. +f
s■
'
10. Litigation
Challenges laws.
11. Bribery
Corrupts political system. Allows industry to by-pass
laws
12. Smuggling
Undermines tobacco excise tax policies and increases
profits.
13. International treaties
Using trade agreements to force entry into closed
markets.
j-A ,-J C-A
PROJECT PROPOSAL
Introduction
Tobacco is a major cause of deaths the world over.
3.5 million people around the
world die due to consumption of tobacco in some form or the other. By the year
2020. it is predicted that globally, 10 million people would die as a consequence of
tobacco comsumption and 70% of such deaths would occur in developing countries.
Every year around 630,000 people in India succumb to death due to consumption of
tobacco in some form or the other. Her/His treatment of the various diseases as a
result of tobacco consumption, thus imposing a heavy burden on the family
financially, psychologically as well as socially. The effects of passive smoking on
side stream smoke being immensely potent would have deliterous effects on the
health of the citizens which is highly compromised by the highly polluted towns and
cities. Respiratory diseases occupy a major stake in the disease circle in Bangalore,
the capital of the state of Karnataka, India surpassing all other cities. Therefore the
need to study the tobacco problem in this state. Tobacco indeed contributes to the
economy of the state and to the country in turn, through taxes and duties. The area
under tobacco cultivation in the year 1997-1998 in the state of Karnataka was 69,500
hectares from which 60,800 tons of tobacco was produced or approximately
875kg/hectare. The revenue of the state/country spent on treating tobacco related
diseases far outweigh the revenue earned from it by roughly three to three and a half
times. This puts an additional burden on the economy of the country. Each worker
gets paid about Rs.80 /- (i.e., less than $2) for a day’s work. Their working as well as
housing conditions being deplorable drastically affects their health. They generally
cannot put their children in schools which are usually very far away. Mother’s cannot
nurse their infants at regular intervals, because they are left behind in their homes to
be looked after by another sibling and the distances from their homes to their work
C:\OFFICBTobaxo\PROIECT PROPOSAL - totaocadoc
places ranging from nearly a kilometer to more which they cover by foot. God forbid
if one of the family members get sick! Hospitals are very far away. The sick person
being too sick to walk, neither take a bus which again would be far away and not
punctual, nor take a bullock cart to the hospital would prefer to rest at home till
she/he is in a condition to reach the hospital. Again the loss of pay from the number
of days off work in addition to the hospital bills constantly haunting the sick person.
Therefore for every bit of tobacco consumed, some poor worker somewhere would be
suffering.
As a result, a substitute to the tobacco crop ought to be found as an
alternative for the poor workers and fanners concerned in our attempts to phase out
the crop.
Unfortunately, youth in the age groups of 12-22 form the major percentage of people
taking up this habit. This is of serious concern to the nation as the popular saying
goes, “Today’s youth, tomorrow’s citizens”.
On the contrary, some stem measures
need to be taken to tackle this global problem due to the export chains and hence it
would be necessary to use the Framework Convention for Tobacco Control
developed by the WHO to counter this issue globally.
Genera! objectives
i)
To analyze the public health, economic and social dimensions of the tobacco
problem in the state of Karnataka, India.
ii)
To study the biddy industry in the state of Karnataka, India, its economic and
social dimensions and its global outreach through exports.
CAOFFICE\Tobaooo>PROIECT PROPOSAL - tatexo <fcc
Specific objectives - To study the bidi industry in the state of Karnataka, India.
i)
its economic contribution to the state,
ii) The working conditions of its employed workers
iii)
Its tax exemption
iv)
Its turnover
v)
Local sales in India, and
vi)
Its global outreach through exports and its marketing strategies.
Methodology - Collection of data from (i) Primary, and
(ii) Secondary sources.
Time frame - 1st October 1999 - end of February 2000.
Budget -
Q\OFHCE\Tol«co\PROJECr PROPOSAL - tobacco,doc
pH S’-8
1
’ v*'
WHO International Conference
on Tobacco and Health, Kobe—
“Making a Difference to Tobacco and Health:
Avoiding the Tobacco Epidemic in Women and Youth”
ADOPTED
18 November 1999
Kobe, Japan
14 to 18 November 1999
http://www.wlio.int/toh
KOBE DECLARATION
We, women and youth leaders, non-governmental organization representatives, government delegates, media
professionals, academics, health professionals, scientists and policy-makers, gathered in Kobe, Japan in
November 1999 at the WHO International Conference on Tobacco and Health, are gravely concerned that:
1.
The tobacco epidemic is an unrelenting public health disaster that spares no society. There arc already over
200 million women smokers, and tobacco companies have launched aggressive campaigns to recruit women
and girls worldwide. By the year 2025, the number of women smokers is expected to almost triple. Tobacco
is the one product that kills its consumers when used as recommended. There arc four million deaths per yea
11,000 per day, related to tobacco. If current trends continue, the world will see a growth rate that turns
tobacco use into the single largest cause of death and disability. It is urgent that we find comprehensive
solutions to the danger of tobacco use and address the epidemic among women and girls. Tobacco has been
identified as a contributing factor to gender inequity and undermines the principle of women and children’s
right to health as a basic human right.
2.
The scientific evidence has shown conclusively that both smoked and smokeless tobaccos contain
toxins that cause multiple fatal and disabling health problems throughout the life cycle. Women who
smoke have markedly increased risks of cancer, particularly lung cancer, heart disease, stroke,
emphysema and other fatal diseases. Women experience gender-specific risks from tobacco and
Environmental Tobacco Smoke (ETS) such as negative impact on their reproductive health and
complications during pregnancy.
3.
Tobacco-related diseases lead to high morbidity rates worldwide, contrary to the goals of sustainable
development and well being for all. The use of tobacco results in a net loss of US $200 billion per year
to the global economy, with half of these losses occurring in low-income countries. There arc
immeasurable personal, social and economic costs to women and children particularly those living in
poverty in low-income countries and in rural settings.
4.
Transnational tobacco companies have implemented well-formulated and deliberate strategies to
expand tobacco markets among women and children, particularly in populous and developing
countries. The tobacco industry is manipulating the process of globalisation for profit. The tobacco
industry promotes the false association of tobacco with images of health, liberation, slimness and
.modernity. Multinational tobacco companies have extended their reach into low-income countries at a
time when structural adjustment policies are often resulting in economic hardship and severely
limiting the health and educational resources of these countries.
5.
There is an urgent need for governments and the international community to develop effective gender
specific tobacco control strategies and to allocate sufficient funds for tobacco control programmes that
also reach poor women and girls. Although there are some countries that have implemented effective
strategies against tobacco, such as increased taxation and legislation to ban tobacco advertising, many
governments still have a direct association with the tobacco industry as producers, exporters or
subsidizers.
•
fVe are resolved to:
6.
Demand that the Framework Convention on Tobacco Control incorporate gender-specific concerns
and perspectives and include a women’s protocol; require the active participation of women delegates
and NGOs in the development and monitoring of the Convention and its related protocols; and
demand that the Convention and its related protocols are ratified by all member states without
reservations that are incompatible to the spirit and the letter of the Convention.
7.
Recommend that the governments and the private sector refrain from supporting the tobacco industry
and restructure financial policies to raise taxes ad valorem on all tobacco products to a minimum level
of 2/3 of the price of tobacco; promote policies that broaden employment opportunities for women and
farmers and provide for transitional programmes beyond the tobacco industry; and require that
increased tobacco revenues be used for tobacco control programmes as well as for public sporting and
cultural events previously sponsored by the tobacco industry.
8.
Demand a global ban on direct and indirect advertising, promotion and sponsorship by the tobacco
industry across all media and in all forms of entertainment; and demand public funding for counter
advertising that disconnects women’s liberation and tobacco use and that reaches women and girls in
all cultural contexts. The use of a tobacco-registered brand name, logo, or trademark on non-tobacco
items as well as vending machines that dispense tobacco products should be banned globally.
9.
Ensure that gender equality in society becomes an integral part of tobacco control strategies and
promote women’s leadership which is essential to success.
10.
Develop gender-specific strategies, with regard for diversity and the needs of women and girls in
different cultural contexts. These should include the creation of smoke-free environments, the
reduction of exposure to Environmental Tobacco Smoke (ETS); gender-sensitive cessation methods;
and the adoption of effective strategies to raise public awareness and to reduce tobacco initiation and
use.
11.
Mobilize NGOs, communities, religious groups, media, women’s and youth organizations, and the
scientific communities in the fight against tobacco products through a multidimensional approach.
Monitor the media to ensure accurate and balanced image of tobacco in reporting women’s health
issues.
12.
Call for effective health education in tobacco use and control including media literacy, at all levels of
formal and informal education; invest in overall education in women and girls as a mechanism for
development of skills, empowerment and for improving their capacity to fight against tobacco.
Education and training programmes in tobacco control should be implemented for health care
professionals.
13.
Increase public funding for research and advocacy on women and girls and tobacco; and improve
dissemination of research results to the general public.
14.
Ensure devolution of the tobacco control strategy of WHO and UN agencies and their regional and
country offices; demand that WHO develop and disseminate tobacco control information and
guidelines for best practices worldwide especially in transition and low-income countries.
15.
Incorporate recommendations to combat the negative impact of tobacco in sections dealing with
“women and health” and “the girl-child” in the UN General Assembly Special Session on Women
2000; and similarly incorporate environmental aspects of tobacco control in the review of the Earth
Summit in 2002, and in other relevant UN follow-up sessions to international conferences.
x6. Uphold the principle of women and children’s right to health as a basic human right and build on the
progress made at the Children’s Summit; the UN Conferences on Environment and Development;
Human Rights; Population and Development; the Social Summit; the Fourth World Conference on
Women; Habitat; and the Food Summit. Build on existing documents such as the Convention on the
Rights of the Child; Convention on the Elimination of All Forms of Discrimination Against Women;
Human Rights Covenants; the Draft Declaration for the Rights of Indigenous Peoples; and WHO
Assembly resolutions highlighting gender, health and development; Declaration of ALMA ATA and
the Ottawa Charter on Health Promotion.
January 6, 2000
THE TIMES OF INDIA
Tobacco consumption worries WHO planners
Th« Times of India News Service
NEW DELHI: The health costs of
tobacco-relatcd diseases are far
greater than the income generated
from tobacco as a cash crop, says a
new study by the Indian Council of
Medical Research (ICMR).
The average cost of one case of to
bacco-related cancer is Rs 3.5 lakh.
Last year alone, 1.63 lakh people de
veloped cancer due to tobacco use,
says the study conducted by
ICMR's deputy director general,
Kishorc Choudhary.Tic study was
conducted at two centres, Delhi and
Chandigarh.
As it is, says the World Health Or
ganisation (WHO), India may be
heading for a tobacco epidemic.
One-fifth of the 2.8 million people
who die each year the world over
from tobacco-related diseases are
Indians. Nearly 50 per cent of Indian
males over the age of 15 are smok
ers, it says.
Therefore, to check the increasing
cigarette consumption in develop
ing countries, WHO is using interna
tional law for the first time to reduce
damage to health caused by tobacco
products. An international treaty is
being drawn up for tobacco control.
To discuss these issues, a three-'
day international conference is be
ing organised in Delhi from Friday.
Tie conference is being sponsored
by the Indian government and
WHO.
WHO says in the next two to
three decades seven million people
will die of tobacco-relatcd illnesses
in the developing countries. Tie to
bacco pandemic is dcscrilied as “one
of the major public health disasters
of the 20th century".
However, policy-makers realise
that reducing tobacco consumption
will not be easy. Union health secre
tary J A Chowdhury says curbing
the consumption of tobacco-based
products is a complex issue as tobac
co cultivation is very remunerative.
Therefore,strategies will need to be
worked out for providing alterna
tives to farmers. Tie conference
here will examine issues from the
perspective of a developing country.
What is little known to people is
that there arc about
chemical
substances in tobacco smoke, of
which -138 can produce cancer, the
most dangerous being nicotine, to
bacco tar and carbon monoxide.
Nicotine is an alkaloid that affects
the central nervous system mid is
probably the cause of smokers' de
pendence on the habit.
Details at www.tlmosonndla.com
Inauguration Ceremony
Please note that all the delegates should carry their invitation cards and the
badges for the inaugural ceremony. Due to security reasons no other personal
items such as hand bags or equipment such as celluar phones and lap top
computers are allowed into the hall. Please read the instructions given at the back
of the invitation cards for more details.
Travel inquires and ticket re-confirmations
Our official travel agents, M/s INDTRAVELS will be available to assist you with your
ticket reconfirmations. Travel desks at Ashok Hotel and Vigyan Bhawan, will be set up at
the following times.
Date
Venue
Time
Friday, 07 January 2000
Ashok Hotel
Saturday, 08 January 2000
Vigyan Bhawan
09.00 - 17.30 hrs.
Sunday, 09 January 2000
Vigyan Bhawan
09.00 - 17.30 hrs.
09.00 - 17.00 hrs.
Kindly note that most airline offices close for the weekend by 13.00 hrs. on Saturday
through Sunday. So please contact the INDTRAVEL desk on Friday 07 January to
avoid any inconvenience.
pH SHO
WI-IO/DG/SP
Dr Gro Harlem Brundtland
Director-General
World Health Organization
WHO’s International Conference on Global Tobacco Control Law:
Towards a WHO Framework Convention on Tobacco Control
New Delhi, India, 7 January 2000 (17h35)
Mr Prime Minister,
Distinguished guests,
It gives me great pleasure to be in India today - this is a country and a people close to my heart. I am
especially pleased to be speaking to an audience of some of the world’s best legal and public health
experts.
We come from a wide range of backgrounds, such as public health, medicine, law, media, economics
and social sciences. What has brought us here to Delhi is our common resolve to highlight the grave
problems arising from tobacco in the developing world. This meeting will explore possible means to
address these problems, taking into account developing country perspectives. It will be one of many
important contributions over the next months and years towards a strong international legal tool to
fight tobacco, the Framework Convention on Tobacco Control.
Ladies and gentlemen,
India, with its myriad of cultures and its complex economic and social realities, in many ways mirrors
our new globalized world. But despite its diversity, its disparities and its conflicts, a strong sense of
unity - has kept this immense nation - which harbors nearly one sixth of humanity - together in a
viable and vivid democracy.
The rest of the world is only slowly waking up to this realization that all of us, no matter the physical,
cultural or economic distance, are dependent upon each other. One region’s poverty is another region’s
lost opportunity. One area’s industry may be another area’s environmental disaster, and one country’s
disease outbreak today, may be another country’s epidemic tomorrow.
In 1987, the World Commission on Environment and Development, which I had the privilege to chair,
came up with the concept of ‘’sustainable development” on the basic premise that development needs
of nations must be met in a way that allows future generations to fulfill their own aspirations.
Enshrined in this concept was the whole notion of solidarity, the right to knowledge and access to
basic life-sustaining information for all nations and people. That idea is now institutionalized globally
in a series of environmental treaties. It has entered the vocabulary of policy makers.
We will add health to that illustrious list.
The importance of the role of health in overall development is being rapidly embraced by governments
around the world. It is a conceptual shift not unlike that which took place with the environment 25
years ago. Increasingly, governments realise they need to integrate health into the broader context of
development. They are also beginning to look at investments in health as more than simply a mere
consumption expenditure. Instead, health is increasingly being seen as a major opportunity for growth,
productivity, human progress and poverty alleviation.
My point of departure is a broad reading of the role of health in development. WHO is indeed the
specialised agency on health - but the purpose of our work is not only to combat ill-health - although
WHO/DG/SP
that remains key - it is also to promote healthy populations and communities - and indeed to
demonstrate how wise health interventions can spur development.
There was a period in development thinking - not so long ago - when access to public services, such as
health and education, would have to wait until countries had developed a certain level of physical
infrastructure and achieved a certain level of economic strength. Once countries had become fully
industrialised - large outlays on health care seemed appropriate and necessary. Indeed, it was seen as a
sign of national prosperity and success.
Experience and research over the past few years have shown that such thinking was at best simplified,
and at worst plain wrong.
We have seen that developing countries which invest relatively more on health in an effective manner
are likely to achieve higher economic growth. In East Asia, for example, life expectancy increased by
over 18 years in the two decades that preceded the most dramatic economic take-off in history. A
recent analysis for the Asian Development Bank concluded that fully a third of the Asian “economic
miracle” resulted from these gains.
We have also observed how health spending in some of the world’s richest countries can reach very
high levels and still not provide necessary and quality health services to all their citizens.
Health is not only an important concern for individuals, it plays a central role for the society in
achieving sustainable economic growth and an effective use of resources. And health is even emerging
as an important element of national security.
With globalization, all of humankind today paddles in a single sea. There are no health sanctuaries.
Diseases cannot be kept out of even the richest of countries by rearguard defensive action. The
separation between domestic and international health problems is losing its usefulness as people and
goods travel across continents. Two million people cross international borders every single day, about
a tenth of humanity each year. And of these, more than a million people travel from developing to
industrialized countries each week.
This is not only an issue of infectious diseases. With an explosion of international trade, travel and
media, new cultural influences spread faster than ever before, driven by economic aspirations,
entertainment and advertising. Many of the effects are positive, but we also see drastically negative
effects, such as unhealthy changes in diet - and the rapid spread and increase of tobacco-use.
Disease and death do not stop at national borders, but still our efforts to fight them are far from being
sufficiently international. The time has come for both health and foreign policy to reflect the needs of
the world’s public with greater emphasis on international health security and its contribution to world
peace. Foreign policies and international business practices must acknowledge transnational threats of
disease, the dangers of trade in products and technologies that are harmful to health, economic and
health disparities between and within countries and population growth. Countries must collaborate to
develop strategies that ensure sustainable human security.
As the world’s leading health agency seeking value for our constituents we have chosen our setting we will play an active role in this work; as a facilitator, as a provider of evidence and best practices and as a moral compass.
Ladies and gentleman,
One of the most important political legacies of this century has been the universal ideal of human
rights that are now irreversible as tenets of international law. The past 30 years have seen the birth of
2
WHO/DG/SP
undreds of organizations around the world that have given a voice and a focus to issues that affect
our lives on a daily basis. Our search for justice is as old as we are. Our search for life in harmony
with laws - whether they be natural laws or those that have developed over centuries - is as old as
humanity himself. Access to basic health is, in the final analysis, a search for justice.
It is my firm belief that where there is no vision, there is no progress. The success of our vision lies in
the hands of our Member States.
As nations feel increasingly compelled to co-operate with each other to solve their problems, the
development of binding global public health norms and commitments will become crucial. Although
international health law is still in a nascent and dynamic stage of development, it must address both
the positive and negative health impact of globalisation. Consequently, health development in the 21st
century is likely to make wider use of international legal instruments to take advantage of the
opportunities afforded by global change and to minimize the risks and threats associated with
globalisation.
Today, our focus is tobacco. But the work we do on tobacco has wider consequences. As the
composition of the global burden of disease changes, so must the emphasis of our work. In addition to
continue with the past century’s very successful effort to limit or eliminate infectious diseases, the
work we are doing on a Framework Convention on Tobacco Control stakes out the way disease must
increasingly be fought and prevented in this brand-new century. This is the first time WHO is
exercising its constitutional right to negotiate a set of globally binding rules. The Framework
Convention is a product and a process and a public health movement.
Turning principle into practice is not an easy task, but we will lead the way and as I said, I am
counting on your help. Our task is not to produce worldwide regulations. It is to build a International
legal framework which will assist and support countries in their national regulation process.
The success of our approach will depend on political commitment, capacity building in public health
law and economics, public support and effective enforcement. Legislation and regulation have to
strike a balance between individual freedom and public needs and interests.
For the next few days, you will hear about the science, economics and politics of tobacco control. We
know that tobacco use is a risk factor for some 25 diseases. It was here in India in 1964 that the first
link between oropharyngal cancer and chewing tobacco was identified. Studies from eastern India
were the first in the world to link palate cancer to the chewing of tobacco.
As the recent report of the World Bank has clearly documented, the risks to health and health systems
from tobacco are widely underestimated. So are tobacco industry tactics. When I first looked into the
issue of tobacco use world-wide I was unprepared for what I was to learn about the extent and manner
in which the tobacco industry was marketing a product that killed half of its consumers. I was appalled
to see how the tobacco industry had subverted science, economics and political processes to market a
lethal and inherently defective product that imposed a massive burden of disease and death on
countries.
I am outraged by what I learn with each passing day about the tobacco industry from previously secret
documents that have now come to light mainly due to court cases in the United States, in particular
Minnesota. I want to use this platform to call on national and international public health experts to
work with their Constitutions as well as their countries’ international commitments to help prevent and
combat this man-made epidemic. Let us craft the world first truly viable public health Convention.
Tobacco is freely allowed to kill one person every eight seconds. That is four million preventable
deaths per year. Today in India, tobacco kills 670,000 people every year. In China, if present smoking
patterns continue, about a third of the 300 million Chinese males now aged 0-29 will eventually be
3
WHO/DG/SP
killed by tobacco. Countries like Canada and Sweden that had long bucked the tobacco epidemic now
see it reappearing again. No country and no people are safe from the to acco men
I have occasionally heard comments to the effect that smoking is mainly an industrialized country
problem and that WHO should focus its energies on fighting the traditional peases of poverty, such
as malaria, tuberculosis and childhood diseases. Such comments are understan
e u mism orme .
If unchecked and unregulated, by 2030, tobacco will kill 10 million people each year Seventy percent
of those deaths will occur in the developing world, with India and China in the lead, If nations do not
act individually and together, in the next 30 years, tobacco will kill more people than the combined
death toll from malaria, tuberculosis and maternal and child diseases. Every tobacco related death is
preventable. That is our message. That is our challenge.
Fifty years ago the world found a solution for polio. Today we are on the verge of eradicating it. Fifty
years ago scientists and researchers linked tobacco to cancer and other diseases. I wish I could tell you
that the world has risen to the tobacco challenge as vigorously and unequivocally as it fought polio.
The unacceptable reality about tobacco is that the health community has lost out to the tobacco
industry aggressively seeking new markets and newer victims. The world will have little cause to
rejoice over the health gains of the eradication of polio if we continue to remain unprepared for, and
indifferent to, new challenges such as the one posed by tobacco.
One of the first things that I did at the WHO was to ask our Member Countries to give us a mandate to
negotiate the Framework Convention. This new legal instrument is expected to address issues as
diverse as tobacco advertising and promotion, agricultural diversification, product regulation,
smuggling, excise tax levels, treatment of tobacco dependence and smoke-free areas.
The Framework Convention process will activate all those areas of governance that have a direct
impact on public health. Science and economics will mesh with legislation and litigation. Health
ministers will work with their counterparts in finance, trade, labour, agriculture and social affairs
ministries to give public health the place it deserves. The challenge for us comes in seeking global and
national solutions in tandem for a problem that cuts across national boundaries, cultures, societies and
socio-economic strata.
An early ally has been UNICEF and the Convention on the Rights of the Child. While the Convention
on the Rights of the Child does not explicitly include tobacco, several of its articles address over
arching values essential to safe and healthy development of children and as of this year, the States’
reporting guidelines have now been amended to include tobacco.
For tobacco, this means that the interests of the child take precedence over interests of the tobacco
industry. Later as I share with you some tobacco industry tactics to promote tobacco to children, you
will see why this is important.
Within the United Nations Family, The World Bank is an essential partner in global tobacco control.
Their 1999 report effectively shows that over the long term economies will benefit from tobacco
control. They highlight a basic economic fact. If people stop spending on tobacco, they will spend on
other goods and services that will generate more jobs and revenue than those from tobacco.
We also have a close working relationship with FAO. Together, we are reaching out to tobacco
fanners to ensure that when successful tobacco control reduces demand for tobacco the economic
consequences will be minimized.
Our decision to use legally binding mechanisms to circumscribe the global spread of tobacco on the
one hand, and to regulate the product itself on the other, is based on sound science and irrefutable
documentary evidence. The science that underpins our work is unequivocal - a cigarette is the only
WHO/DG/SP
freely available consumer product which, when consumed as intended by manufacturers, kills. Let us
never forget that.
Nicotine is addictive. A cigarette is not just tobacco leaves rolled in a strip of paper. It is a highly
engineered product. The tobacco industry has studied our saliva and central nervous systems to
determine the right dose of nicotine to deliver so that addiction occurs and is sustained. Other tobacco
products, whether they be beedies, snuff, gutka or spit tobacco, are no less addictive - nor lethal.
Imposing international norms on a global industry that seemingly without qualms can make huge
profits from a product that kills is not an easy task. It is our firm belief that to develop a truly
meaningful global treaty to control tobacco, our Member States must have a clear understanding of the
tobacco industry and its tactics.
Fifty years is a blink of time in a millennium, but fifty years is a long time to sustain a deliberate
deception that causes death and disease. For almost fifty years, the tobacco industry has known that
tobacco products cause deadly diseases. I am speaking to an audience of lawyers and public health
experts - I chose my words carefully. The tobacco industry which acts as a global force is in the
business of selling deception. Deception in science, public health and economics. Internal tobacco
industry documents that have now become public bear eloquent testimony to this.
Tobacco litigation began in the United States 1954. But the major breakthrough came in the 1990s - in
the States of Mississippi and Minnesota - with the revelations of millions of pages of documents
forced from the files of the tobacco industry and with the framing of different types of legal theories
that focused on the conduct of the tobacco industry.
For us, these documents show how and why the tobacco industry has been so successful in defeating
public health objectives in the past and provide valuable lessons into how the public health community
must come to terms with the tobacco industry to make progress in future. We believe the tobacco
industry has fractured the tobacco issue by playing different tunes in different countries. In one it is
labour, in another it is farmers, in a third it is marketing rights. We believe that through our
Constitution and that of our Member States, we can restore the global and national picture so that the
truth can emerge to benefit public health for all.
Consider this internal tobacco industry discussion. A document written by a tobacco industry lawyer
in 1980 sets out some of the reasons for the tobacco industry’s refusal to publicly admit that smoking
causes disease. The document was written at a time when the British and American Tobacco Group
companies were considering changing their public stance on the issue of causation of disease. The
lawyer opposed such a change, and wrote:
“If we admit that smoking is harmful to 'heavy ’ smokers, do we not admit that BAT has killed a lot of
people each year for a very long time? Moreover, if the evidence we have today is not significantly
different from the evidence we had five years ago, might it not be argued that we have been wiljully
killing our customers for this long period? Aside from the catastrophic civil damage and governmental
regulation which wouldflow from such an admission, Iforesee serious criminal liability problems
Tobacco companies also denied for decades that smoking was addictive. In private, they recorded in
the fifties that smoking was addictive. In 1961, a top industry scientist wrote, "... smokers are nicotine
addicts” In 1963, an industry lawyer wrote, “(NJicotine is addictive. We are, then in the business of
selling nicotine, an addictive drug ...” In 1979, a tobacco executive considered the hypothesis that
“high profits ... associated with the tobacco industry are directly related to the fact that the consumer is
dependent upon the product”
The internal documents also demonstrate that the tobacco industry intentionally designed cigarettes to
exploit their addictive potential. While nicotine is a naturally occurring component of the tobacco
5
WHO/DG/SP
plant, the modem cigarette is a highly engineered and sophisticated product in both manufacture and
design. Decades ago, the tobacco industry began to control and manipulate the level and form of
nicotine in cigarettes in a variety of ways.
Publicly, the tobacco industry’ maintains that it does not want youth to smoke. Privately the tobacco
industry' has long recognised that the preservation of its market depends upon recruiting youth. As one
document stated, “Younger adult smokers are the only source of replacement smokers ... If younger
adults turn away from smoking, the industry must decline, just as a population which does not give
birth will eventually dwindle” The tobacco industry documents are replete with discussions of
marketing to youth and the need to increase market shares by enlisting youth.
The documents are an underused public health tool. But that is about to change.
There is some type of tobacco litigation underway in at least 15 countries ranging from personal injury
class action litigation in Australia to health cost recovery in Canada to public interest petitions in
India.
Last October I called for a preliminary inquiry into whether the tobacco industry has exercised undue
influence over UN-wide tobacco control efforts including interfering with WHO’s work. Later this
year I have called for a meeting of international regulators to set in motion the process of regulating
tobacco. The jigsaw is falling into place.
One of the primary' objectives of the tobacco industry is to frame tobacco use as an individual and
behavioral decision. Adults can chose for themselves if they have full access to information. The same
does not apply to children and adolescents. On a given day, between 82,000 and 99,000 young people
- sometime as young as 8 - start smoking or chewing tobacco. Over eighty percent of smokers started
before they were 18. By the time they find out, it is too late. The addiction has taken control.
The good news is that we can buck and reverse the global tobacco trend. We know what works and
how. Taxes work and the young are especially susceptible to increased prices. Advertising and
sponsorship bans work. Smoke free policies work.
Such policy interventions could, in sum, bring unprecedented health and economic benefits. WHO’s
message is that there is a political solution to tobacco and it is routed through policy interventions and
political vision.
The Framework Convention on Tobacco Control is a pathfinder in public health. It will assist in
placing health at the top of national and international agenda and will create a debate on the wider
issues and solutions to health problems.
We owe this to ourselves. We owe this more to future generations. Let us never forget that public
health is a search for equity, solidarity and justice.
Thank you.
6
Ph s', i
Inaugural Session of the
WHO International Conference on
Global Tobacco Control Law :
Towards a WHO Framework Convention
on Tobacco Control
7-9 January 2000, New Delhi, India
Address by
Dr Uton Muchtar Rafei
Regional Director, WHO South-East Asia Region
World Health Organization
Regional Office for South-East Asia
New Delhi
Inaugural Session of the
WHO International Conference on
Global Tobacco Control Law :
Towards a WHO Framework Convention
on Tobacco Control
7-9 January 2000, New Delhi, India
Address by
Dr Uton Muchtar Rafei
Regional Director, WHO South-East Asia Region
World Health Organization
Regional Office for South-East Asia
New Delhi
Your Excellency, the Honourable Prime Minister of India
Honourable Minister of Health and Family Welfare
Honourable Minister of Law, Justice and Company Affairs
Secretary of Health and Family Welfare of India
Director-General of Health Services
Director-General, World Health Organization,
Distinguished
gentlemen,
experts,
dear
colleagues,
ladies
and
In the century that just passed, humanity has, without doubt,
witnessed
tremendous
achievements.
Unprecedented
scientific advances have greatly enriched human life. The
discovery of antibiotics has made a significant difference in
the treatment of diseases and in enhancing longevity of life.
New frontiers have been explored. Formidable health
and economic problems have been surmounted. Global
barriers have been broken and nations have come much
closer to one another and have become interdependent.
Yet, in the midst of all these achievements, there are a
few dark spots. For example, mankind is yet to take
concrete steps to negate the severe health and socio
economic impact of tobacco. As we welcome the dawn of
the new millennium, the world faces a formidable public
health challenge posed by tobacco.
WHO International Conference on Global Tobacco Control Law
Inaugural Session
Already, 800 million of the estimated 1.2 billion
smokers in the world live in developing countries. In 25
years, 75% of the world's smokers will live in these
countries. They will account for seven million of the global
10 million tobacco-related deaths by the third decade of
this century.
Today, 80% of the global tobacco production comes
from developing countries. Four countries, including India,
account for two-thirds of the world's production.
Developing countries, in fact, are virtually sitting on a
time bomb I The question is : can we afford such a man
made calamity in the 21” century ?
The answer is an
obvious NO.
Excellencies, the South-East Asia Region contains one
fourth of the world's population, and carries an even larger
percentage of its disease burden and the poor. Yet, the
Region has the unenviable distinction of having the second
highest annual per capita growth in tobacco consumption
among the six WHO Regions.
The large populations and rapid economic growth in
some countries are an irresistible magnet for the tobacco
industry. Multinational companies and national tobacco
monopolies are expanding
Indonesia and Thailand.
their
business
in
India,
As a result of the powerful advertising and marketing
strategies of these companies, over one million children in
India and Thailand alone take to smoking every year. The
Region also reports not only one of the highest smoking
WHO International Conference on Global Tobacco Control Law - Inaugural Session
rates among women but also oral cancers caused by
tobacco. Cardiovascular diseases, chronic obstructive lung
diseases and lung cancers are already major killers. Every
year, tobacco kills an estimated 580,000 people in the
Region.
We must adopt legal instruments to control tobacco or
our children will accuse us of having wasted the
opportunity. This is one epidemic of several illnesses which
we can control and we must take action now.
For many decades, the tobacco industry has used the
argument that tobacco control will lead to unemployment
and revenue loss for governments. But this is not true. World
Bank reports clearly state that most countries will not face
any significant economic repercussions or job losses if
tobacco
consumption
is
reduced
or eliminated.
For
example, in Bangladesh, which is a net tobacco importer,
elimination of tobacco consumption will
increase
employment by over 18%. Also, a rise in tobacco taxes, in
fact, increases, rather than diminishes government revenue.
In
the
South-East
Asia
Region,
tobacco
disproportionately affects the poor and the most
vulnerable. Over 80% of the workforce in the tobacco
industry comprises women, the poor and children. It is they
who till the land, pluck the tobacco leaves, cure thousands
of metric tonnes of leaves in smoke-filled curing units, and
spend hours in bidi rolling and gutka packaging cottage
industries.
It is they who suffer from numerous occupational
hazards. Their vulnerability is accentuated by the very low
WHO International Conference on Global Tobacco Control Law - Inaugural Session
wages they earn from tobacco. Working in tobacco
production, keeps the poor in poverty.
In many countries of the Region, about 25-30% of a
poor man's income is spent on tobacco. The expenditure
on diagnosis and treatment, travel for treatment, and loss
of income due to absenteeism goes far beyond the means
of most families.
Poverty alleviation programmes are being eroded as
beneficiaries spend larger proportions of their income on
tobacco products than on food, shelter, education and
health. In fact, the government spends more on tobacco
than it receives as revenue.
In the final analysis, it is the tobacco industry which
grows richer, leaving the poor poorer.
Today, the link between TB and tobacco needs no
elaboration. Already, this region accounts for about 40%
of the world's reported tuberculosis cases.
The danger facing a majority of communities exposed
to the TB bacilli and now to smoking or chewing tobacco is
too serious to be ignored.
Excellencies, the time has come for us to respond to
the urgent call to disinvest tobacco in order to enhance the
future welfare of our nations. Today is the hour, tomorrow
will be too late.
The litigation against the tobacco industry in the USA
holds valuable lessons for all of us. The industry cannot be
allowed to continue to sell hazardous and addictive
WHO International Conference on Global Tobacco Control Law - Inaugural Session
products. Nor should it be permitted to continue to lure
millions of innocent children into tobacco use under the
garb of trade liberalization and the right to freedom of
speech. The tobacco industry knows the health hazards of
tobacco and skillfully markets death. With the power of this
information, we must ensure our children understand the
dangers they face.
We also need international laws and regulations to
curb this deception, particularly in developing countries.
Laws that will protect the most vulnerable and ensure that
what is not allowed in developed countries is not allowed
in developing countries either.
This Conference presents a unique and timely
opportunity for developing countries to shape the elements
of a Global Tobacco Control Law. A law that will not only
protect their economic interests but also save the lives of
millions who are, and will be, enslaved by tobacco.
The challenge is obviously daunting, but it is definitely
not unsurmountable. With focused commitment and the
determination of all governments, the world can become
tobacco-free.
Let us enter the new millennium with the determination
and vision to liberate society from the bondage of tobacco.
We owe this to posterity. Together, we can make a
difference. Together, we can make it happen.
Thank you.
WHO International Conference on
Global Tobacco Control Law: Towards a
WHO Framework Convention on Tobacco Control
7- 9 January 2000, New Delhi
World Health Organization
Government of India
Messages
President, Republic of India
Tobacco represents a paradox. While its use has, over the ages, received societal
acceptance, it is not disputed that tobacco whether smoked or chewed, is harmful to
human health. Similarly, the production of tobacco has major social and economic
implications for developing countries in terms of the employment of people on farms
and factories. At the same time, the profit margins from tobacco go to industry and
advertising rather than to small growers and workers. Tobacco control policy has
therefore, to address the negative effects of tobacco in a manner that is imaginative,
weaning people away from the use of tobacco, without hurting any vulnerable segments
of society.
I congratulate the WHO for initiating the development of the Framework Convention on
Tobacco Control. By hosting this conference jointly with the WHO, India has affirmed its
support to the need for global action for tobacco control.
I wish the deliberations all success.
K.R. Narayanan
President, Republic of India
Prime Minister, Government of India
I am happy to learn that the Ministry of Health and Family Welfare and the World Health
Organization are jointly hosting an international conference on "Global Tobacco Control:
Towards a WHO Framework Convention on Tobacco Control" in New Delhi.
The conference represents an emerging global consensus on the need for state
intervention to control the use of tobacco products. Governments all over the world
are beginning to adopt a pro-active role in curbing addiction to tobacco products as
it poses a serious threat to public health. These measures need to be adequately backed
by community participation in disseminating information about the harmful effects of
tobacco products.
It is a matter of concern that the consumption of tobacco products has been steadily
increasing in developing countries. Therefore, the developing countries need to evolve
a common approach on how best to tackle this problem.
The Conference on Global Tobacco Control will provide an opportunity to participants
to discuss this and other related issues as well as exchange information on measures
being taken by various Governments to check the use of tobacco products.
I wish the Conference all success.
A.B. Vajpayee
Prime Minister, Government of India
Chief Justice of India
I am happy to learn that the World Health Organization and the Ministry of Health and
Family Welfare are jointly organising an International Conference on "Tobacco & Law"
at Vigyan Bhavan, New Delhi from January 7-9, 2000.
Health hazards associated with use of tobacco both by the user as well as by the passive
smoker have been highlighted from time to time but precious little appears to have
been done to meet the challenge. India is a party to various resolutions adopted by
the World Health Organization, including the one adopted in 1986 which urged member
countries to formulate a comprehensive national tobacco control strategy. No significant
follow up action, except banning smoking in public places and public transport and
that too in certain cities and localities only and printing of the statutory warning on the
packets of cigarette and in the advertisements relating thereto, has been taken.
Considering that in India alone almost one million tobacco-related deaths take place
every year, the hosting of the International Conference is a timely step in the right
direction. The existing law apparently has not made much impact because of its poor
enforcement and other inadequacies. Causes need to be identified and remedial
steps taken.
The experts, scientists and other delegates taking part in this Conference would have
an opportunity to focus upon the harmful effects of tobacco consumption on public
health and generate community awareness about various harmful aspects of the use
of tobacco. If the Conference can formulate a framework for tobacco control, devise
some effective strategy and propose measures for dealing with the menace, it would
have served a very useful purpose.
I wish the Conference every success.
Dr Adarsh Sein Anand
Chief Justice of India
Minister of Finance, Government of India
General awareness about the detrimental effects of tobacco consumption has been
increasing over the years. Yet there has always been a somewhat hesitant approach in
launching any tangible anti-tobacco programmes in developing countries. This could
be attributed to apprehensions about the undesirable economic and social
consequences of any such measures. In a pre-dominantly agrarian economy like India's
such apprehensions have to be resolved before any meaningful programme can be
made in the direction of tobacco control. There will have to be consultations with
various interest groups before the dream for a tobacco-free society can be realized in
real life.
Any law must necessarily reflect the aspirations of society. If social evils could have
been curbed by legislations alone, this world would have been a veritable Eden.
Therefore, without sanction from society, no law can be effective. It is therefore, very
necessary for the eminent participants of this conference to gauge the mood of society
and appropriately mould the legislation. In this task, a very onerous responsibility has
been cast upon them. They have to carry the global society with them. If they do not
succeed, dur future generations will not forgive us for having missed at the very beginning
of the new millennium, the crucial opportunity while trying to launch a crusade against
tobacco use. I wish the Conference all success.
Yeshwant Sinha
Finance Minister, India
Minister of Law, Justice and Company affairs. Government of India
I am indeed thankful for your invitation to participate in the WHO International
Conference: Tobacco Control Law to be held in New Delhi in the first week of the new
millennium.
The deleterious effects of tobacco consumption on health of smokers, both active and
passive smokers, and on public health in general is well established. I understand that
for developing countries in particular, the Conference will provide a unique opportunity
to devise strategies and framework for international legal instruments necessary to
regulate and control the consumption of Tobacco. I am certain that with the wide
participation of delegates from 55 developing countries, the Conference shall generate
enormous community awareness of the menace posed by the evil habit.
In India, we have made compulsory the printing of a statutory warning on every packet/
package containing Tobacco. We are committed to generate a still wider awareness
of the harmful effects of tobacco especially amongst our young people.
I wish the Conference all success and on behalf of the Law Ministry, I assure you that
every possible effort shall be made to facilitate the widest possible collaboration between
the concerned parties (NGOs, Social Welfare/Health Ministries, etc.) in this crucial matter
of public health.
Ram Jethmalani
Minister of Law, Justice and Company Affairs, India
Minister of Health and Family Welfare. Government of India
There is an urgent need to stem the habit of tobacco consumption. It is now proved
that tobacco is a risk factor for about 25 diseases. Estimates suggest that in India, the
number of persons affected with tobacco related diseases is very high. Out of the
estimated three million tobacco related annual deaths in the world, about 0.8 million
deaths take place in our own country. All this calls for more concerted action to restrict
and eventually eliminate consumption of tobacco.
The government of India has taken a number of steps for discouraging smoking and
intake of products which are tobacco addictive:
it is mandatory to display a warning that smoking is injurious to health on all cartons/
packets of cigarettes.
advertisements relating to tobacco and tobacco related products are not permitted
on state sponsored electronic media.
iii)
smoking is also prohibited in public places like hospitals, dispensaries, education
institutions, conference rooms, the domestic air flights etc.
i)
ii)
There is a growing demand for enacting a comprehensive legislation for control of
smoking and tobacco consumption to reflect the positive commitment of the
Government of India on this subject. This international conference has therefore come
at the most opportune time for us. We look forward to helpful inputs not only for our own
legislation but also for laws having global relevance. Even a slight reduction in the
incidence of tobacco consumption, if brought about by State intervention, will transmit
the right signal to the community and lead to a positive impact on public health. I,
therefore, look forward to the pragmatic outcomes of this Conference, and wish its
mission all success.
[4 • I •
-----
N.T. Shanmugam
Minster of State (Independent Charge)
Health and Family Welfare
Government of India
ty)
Director-General, World Health Organization
At the dawn of the new Millennium, it is appropriate that I visit one of the most populous
countries to urge world leaders to act decisively this century against tobacco. I wish to
thank the host, the Government of India, for actively supporting WHO to hold this meeting.
This conference focuses on Global Tobacco Control Law and offers developing countries
the opportunity to establish their unique perspective on the creation of a viable Framework
Convention on Tobacco Control. The burden of disease resulting from tobacco consumption
is increasing steadily and at an alarming rate in developing countries. It is projected that
developing countries will contribute 70% of tobacco induced deaths if current smoking
patterns continue.
This conference is very timely and important for several reasons. First, developing countries
need to have their views articulated on the issue of global tobacco control. They need to
be fully involved in the Framework Convention's creation and its future implementation. The
Convention will enable developing countries to adopt a collective response to combat the
tobacco epidemic.
Secondly, this meeting will help create a multi-sectoral approach to tobacco control in
developing countries. The evidence of the increasing burden of tobacco-related deaths in
Africa, Latin America and Asia calls for a multifaceted global response. Tobacco is not only
bad for health but, it is also bad for the economy at large. A multi-sectoral approach to
tobacco control is needed if the Framework Convention shall be an effective tool for all
areas of governance which have a direct impact on people's lives and health in poorer
countries. Therefore, the development of the Framework Convention calls on the participation
of other Governmental Ministries in addition to the Health Ministries, such as finance, justice,
trade, agriculture and education.
The conference is also a point of departure for collecting the necessary technical and public
health expertise from developing countries to support WHO efforts for tobacco control. I
hope this conference builds consensus, strengthens the hands of parliaments and
governments participating in this process and gathers the political backing necessary to
control the global spread of tobacco.
Tobacco claims one victim every 8 seconds. Tobacco now kills four million people a year. In
about thirty years, that figure will rise to 10 million, more than the total deaths from malaria,
maternal and childhood illnesses and tuberculosis combined. Globally, between 82,000 and
99,000 young people, some as young as 12 years old, start smoking each day. In India
alone, about 630 000 people die annually from tobacco.
Future generations will recall and judge this conference as one where developing and
least developed countries made a major contribution to health through their efforts to control
the tobacco scourge and reduce deaths.
Dr Gro Harlem Brundtland
Director-General, World Health Organization
Regional Director, WHO South-East Asia Region
Every minute of the day, everyday, someone, somewhere in the world succumbs to a
ruthless killer: Tobacco. The global toll is 4 million lives every year. By the 2020s or early
2030s, based on current smoking trends, the figure could well rise to about 10 million.
Nearly 70% of these deaths would occur in developing countries. This would make
tobacco consumption the leading cause of disease burden in the world.
Keeping this grim scenario in mind, the World Health Assembly, in 1996, requested the
WHO Director-General to develop a Framework Convention for Tobacco Control. For
the next few years concerted efforts were made towards this end. In July 1998, the
Director-General launched the global Tobacco Free Initiative expressly aimed at
reducing tobacco consumption and the burden of tobacco-related diseases globally.
The World Health Assembly, in 1999, in Resolution WHA52-18 also outlined the mechanism,
process and milestones for the development and negotiation of the Framework
Convention. Once in place, the Convention will be an international legal instrument
designed specifically to control the global tobacco pandemic, especially in developing
countries.
The WHO International Conference on Global Tobacco Control Law: Towards a WHO
Framework Convention on Tobacco Control is, therefore, of vital importance. It will add
momentum to the Tobacco Free Initiative. The.Conference will also provide a good
opportunity to consider issues that may be encountered by countries in formulating the
Convention. The focus, of course, will be on developing countries and to consider
mechanisms to foster the widest possible collaboration between health and healthrelated Ministries with regard to implementing the various clauses of the Convention.
I am confident that the Conference will provide a good opportunity for useful interaction
between the participants representing diverse disciplines and to develop a Framework
Convention that will stand the test of time. Most of all, I hope that the Conference will
set in motion mechanisms for sustained action eventually leading to our goal of a
tobacco-free world.
Dr Uton Muchtar Rafei
Regional Director, WHO South-East Asia Region
Project Manager, WHO Tobacco Free Initiative
This International Conference concentrating on global tobacco control law provides an
opportunity for developing and least developed countries to participate effectively in the
formulation of the WHO Framework Convention on Tobacco Control.
The development of tobacco control laws at national and global levels are greatly needed
to deter the highly detrimental impact of tobacco on health today and in the years to
come. The participation of developing countries is central to the effectiveness of this process
since they stand to face the greatest percentage of death and disease caused by the
tobacco epidemic in the future. Institutional capacity for tobacco control in most countries
is weak. Technical and financial resources need to be devoted to improving it. This conference
will help raise political support and promote intersectoral co-operation for tobacco control
in developing countries.
It is hoped this conference will set the foundation for full participation of developing and
least developed countries in the development of a Framework Convention on Tobacco
Control and simultaneously accelerate tobacco control in their countries.''By doing so the
burden of disease and death from tobacco will be curbed.
W-
Dr. Derek Yach
Project Manager, WHO Tobacco Free Initiative
Why control tobacco?
According to WHO estimates, there are currently 4 million deaths a year from tobacco, a
figure expected to rise to about 10 million by the 2020s or early 2030s. By then, based on
current smoking trends, tobacco is predicted to be the leading cause of disease burden in
the world, causing about one in eight deaths. 70% of those deaths will occur in developing
countries. The sheer scale of tobacco’s impact on global disease burden, and particularly
what is likely to happen without appropriate interventions in developing countries, is often
not fully appreciated. The extremely negative impact of tobacco on health and economies
now and in the future is the primary reason why tobacco control on a world-wide basis
should be strongly supported.
What is this conference about?
In 1996, the Director-General of WHO was requested by the World Health Assembly by its
resolution WHO 49.17 to develop a Framework Convention for Tobacco Control (FCTC), in
accordance with Article 19 of the WHO Constitution. Technical work on the feasibility and
the possible form of the Convention was done between then and July 1998. Two resolutionsEB103.R8 (January 1999) and WHA 52.18 (May 1999) - outline the mechanisms, the process
and the milestones for the development and negotiation of the Framework Convention.
Once in place, the FCTC will be an international legal instrument designed to circumscribe
the growth of the global tobacco pandemic, especially in developing countries.
This conference is one of several technical meetings planned by the Tobacco Free Initiative
of WHO, to obtain inputs for the Working Group, which is currently drafting the elements of
the Framework Convention. The focus is on developing countries' perspectives, particularly
from South-East Asia and Africa.
In 1998, WHO launched its global Tobacco Free Initiative (TFI) with the express aim of reducing
tobacco consumption and the burden of tobacco related diseases. Developing a global
Framework Convention for Tobacco Control, therefore, is a cornerstone of the TFI.
Objectives of the conference
•
From a developing country perspective, to consider issues that they may encounter in
formulating the proposed WHO Framework Convention on Tobacco Control.
•
To consider particular difficulties that developing countries may encounter in enacting
tobacco control measures.
•
To propose measures for ensuring that developing countries are able to implement the
Convention, and build capacity to participate in global and national activities for
tobacco control.
To mobilize technical and political support for tobacco control in the developing world.
To consider mechanisms for stimulating the widest possible collaboration between
ministnes of health, foreign offers, trade, finance, environment, justice and education
for the development and future implementation of the Convention.
Expected outcomes
Recommendations on which public health issues and economic considerations
especiaHy from the perspective of trans-national economies and developing countries'
protocol '
''
development and negotiation of the FCTC anS related
Background (contd.)
•
Recommendations regarding the establishment of FCTC national commissions where
appropriate, and how these bodies may facilitate national action in support of the FCTC
and related protocols.
•
A Declaration in support of the FCTC process, as a vehicle of raising political awareness
amongst other sectors and ministries.
•
Recommendations on how the increasing experience with tobacco litigation may be
used as a vehicle for global tobacco control.
Organization of the conference
This conference is jointly organized by the Ministry of Health and Family Welfare, Government
of India and the World Health Organization. Two committees are involved in matters relating
to organizing the Conference.
International Advisory Committee
Chairperson: Justice B.P. Jeevan Reddy, Chairman, Law Commission, India Co-Chairperson:
Dr N.K. Ganguly, Director-General, Indian Council of Medical Research Members: Dr S.P.
Agarwal, Director- General of Health Services, India, Dr Kishore Choudhary, Deputy
Director-General, Indian Council of Medical Research, Prof G.K. Rath, All India Institute of
Medical Sciences, Dr. P.C. Gupta, Tata Institute of Fundamental Research, India, Dr K.S. Reddy,
All India Institute of Medical Sciences, Dr J.N. Pandey, All India Institute of Medical Sciences,
Mr Soli Sorabjee, Attorney-General of India, Mr T.R. Malakar, Deputy Director-General,
Doordarshan, India, Prof Judith Mackay, Director, Asian Consultancy on Tobacco Control,
Hong Kong, Dr Steve Tamplin, WHO Regional Office for Western Pacific, Philippines, Mr A.
Salahi, WHO Office for Eastern Mediterranean, Egypt, Dr Yussuf Saloojee, National Council
Against Smoking, South Africa, Prof (Mrs.) S.K. Berma, Director, Indian Law Institute, Prof. V.S.
Rekhi, Director, National Law Institute University, Bhopal, India, Prof D.N. Jauhar, Punjab
University, Chandigarh, India, Mr R.N. Trivedi, Additional Solicitor-General of India.
Organizing Committee
Chairperson: Shri J.A. Chowdhury, Secretary (Health), Govt, of India Members: Dr S.P. Agarwal,
Director-General of Health Services, India, Dr N.K. Ganguly, Director-General, Indian Council
of Medical Research, Shri J.V.R. Prasada Rao, Additional Secretary, Ministry of Health and
Family Welfare, India, Shri G.R. Patwardhan, Additional Secretary, Ministry of Health and Family
Welfare, India, Shri T.K. Vishwanathan, Additional Secretary, Ministry of Law, India, Shri R.R.
Shah, Additional Secretary, Ministry of Information and Broadcasting, India, Smt Renu Sahni
Dhar, Joint Secretary, Department of Health, India, Ms K. Sujatha Rao, Joint Secretary,
Department of Health, India, Dr K.S. Reddy, All India Institute of Medical Sciences, Dr Kishore
Choudhary, Deputy Director- General, Indian Council of Medical Research, Dr Imam S.
Mochny, WHO South-East Asia Regional Office, New Delhi, Ms Martha R. Osei, WHO SouthEast Asia Regional Office, New Delhi Dr Robert Kim-Farley, WHO Representative India, Shri A.
Gopinathan, JS, UN Division, Ministry of External Affairs, India, Shri Vinay Kumar, Joint Secretary
(Security), Ministry of Home Affairs, India, Shri Gurucharan Singh, Joint. Secretary (Imm. &
Foreigners Div.) Ministry of Home Affairs, India, Shri Ashok Pradhan, Director-General of Tourism,
India, Shri Sanat Kaul, Joint Secretary, Ministry of Civil Aviation, India.
Conference Programme
Thursday, 6 January 2000
117:00 - 21:00 [ Pre- Registration (Ashok Hotel, New Delhi)
Friday, 7 January 2000
19:00-13:00
| Registration (Sign up for Working Groups, Ashok Hotel, New Delhi)
11:00- 12.35
Lighting of SEAAT Flame, Talkatora Stadium, New Delhi
Welcome remarks by Regional Director, WHO South East-Asia Region
Address by Minister of State for Health and Family Welfare, India
Address by the Director-General, World Health Organization
Address by the Minister of State for Culture, Youth Affairs and Sports, India
Lighting of the SEAAT Flame by the Minister of State for Culture, Youth Affairs
and Sports, Minister of State for Health and Family Welfare, Director-General
WHO and Regional Director WHO, South East-Asia Region
Administration of Oath to school children
Cultural programme
Vote of thanks by the Additional Secretary, Ministry of Health and Family
Welfare, India
Flagging off the SEEAT Flame vehicle by the Chief Minister of Delhi
17:00-18:40
Opening Ceremony, Vigyan Bhawan, New Delhi
Welcome address by Health Secretary, Ministry of Health and Family
Welfare, India
Remarks by Regional Director, WHO South East-Asia Region
Address by Minister of State for Health and Family Welfare, India
Address by Minster of Law, Justice and Company Affairs, India
Address by Director-General, World Health Organization
Inaugural address by the Hon. Prime Minister of India
Vote of thanks by the Director General of Health Services, India
Saturday, 8 January 2000
8:30 - 9:00
—- n
Introduction and Background—"---------------------------------
Seo cXr'Cen,u,y
on the Frame:
on Tobacco
Introduction to Methods of Work
Ms Indira Jaisingh, Advocate, Suoreme
.h <> _•
and Dr Srinath Reddy, Profess™
of lndia- New Delhi
Cardiothoracic Centre All Indin ineh
*
10 °9y' DePartment of Cardiolc
Co-Chairpersons
,ndla lnstltute of Medical Sciences. New Dell
Conference Programme (contd.)
Sunday, 9 January 2000
Plenary III: Global Tobacco Control Law: Towards a Legal and Regulatory Framework
_________ Co-chaired by Ms Indira Jaisingh and DrSrinath Reddy
9:00 - 9:30
“International Legal and Policy Framework for WHO Framework Convention
on Tobacco Control”
Mr William Onzivu, Fellow, WHO Geneva
9:30-10:00
"Regulation of Tobacco Products"
Mr Mitchell Zeller, US Federal Drug Administration Rockville, USA
10:00-10:30 “The Prospects for Globalizing Tobacco Litigation"
Ms Roberta Walburn, Senior Fellow, WHO Geneva
10:30-10:45 Break
10:45- 11:15 "The Application of International Law into National Law, Policy and Practice:
Lessons for the Framework Convention on Tobacco Control"
Ms Judy Obitre-Gama, Lecturer, Faculty of Law, Makerere University,
Kampala, Uganda
11:15-12:30 Open Discussion and
Introduction to the Working Group Process
| 12:30-13:30 | Lunch
13:30-16:30
1
WORKING GROUPS
Chairpersons, Facilitators, Rapporteurs, and Panelists to be announced
Working Group I - “Economic Implications of Tobacco Production and
Marketing"
Working Group II - “Towards establishing National Institutions for the FCTC:
Legal, Policy and Practical Options"
Working Group III - “Addressing Industry Tactics"
Working Group IV - “The Prospects for Globalizing Tobacco Litigation”
Plenary IV: Conference Recommendations and Chairs' Summaries
Co-chaired by Ms Indira Jaisingh and Dr Srinath Reddy_______________________
Working Group Recommendations - Reports by Rapporteurs
16:45-17:35
17:35-17:55 Chairs' Comments
Adoption of Declaration
17:55-18:05
Conference Synthesis
18:05-18:25
Dr Derek Yach, Project Manager, Tobacco Free Initiative, World Health
Organization
_______________________________________________
Closure
18:25-18:45
Chairman of the Law Commission, Justice B.P. Jeevan Reddy
Conference Programme (contd.)
Plenary 1: Global Tobacco Control: The Economic and Agricultural Context
Co-chaired by Ms Indira Jaisingh and Dr Srinath Reddy-----------------------------------"An overview of the Role of the World Bank and WHO in Global Tobacco
9:00 - 9:30
9:30-10:15
10:15-10:30
10:30-11:00
11:00- 11:45
11:45-12:15
12:15-13:00
Professor Iraj Abedian, Professor of Economics and Director, Applied Fiscal
Research Center, University of Cape Town, South Africa___________________
"Role of multinational and other private actors: Trade and Investment
Practices"
Dr Luk Joossens, Centre for Research and Information for the Consumer
Organisations, Brussels, Belgium, Professor Prakit Vateesatokit, Professor of
Medicine, Department of Medicine, Mahidol University, Ramathibodi Hospital,
Medical School, Bangkok, Thailand and Ms Bungon Rithipakdee, Director,
ASH Thailand
Break
"Ownership of Tobacco Companies and Implications on Health"
Dr Hatai Chitanondh, President, Thailand Health Promotion Institute, Bangkok
"The Cost of Tobacco Related Diseases in India-Report of an ICMR Task Force
Study 1990-1996"
Dr G.K. Rath, Professor & Head, Department of Radiation Oncology, Institute
Rotary Cancer Hospital, All India Institute of Medical Sciences, New Delhi,
India
"Agricultural Diversity as a Tool of Tobacco Control"
Dr P.R. Panchamukhi, Director, Centre for Multi-disciplinary Development
Research, Dharwad, India
Open discussion
| 13:00-14:00 | Lunch
Plenary II: Industry Challenges and Public Health Responses
_________Co-chaired by Ms Indira Jaisingh and Dr Srinath Reddy
14:00-14:45 "Industry Lobbying of the Public Sector and other Tactics"
Dr Y. Saloojee, Executive Director, National Council Against Smoking,
Johannesburg, South Africa, and Dr Elif Dagli, Professor of Medicine, Marmara
University Hospital, Istanbul, Turkey
14:45-15:15 r?^epSfud/'n Consumer Protection from Tobacco in South East Asia"
A«nnS?nlJaH-n M
TrUSteS' VOICE' NeW Delhi- lndia- and MS Mary
Matay2aK
dl' Med'a ° f'Cer' Consumers Association of Penang, Penang,
15:15-15:45
D^KishJmCha?^^e'5ect°ra'APPro°ch to National Tobacco Control"
New Shijndia
P Y
Ct°r'lndian Council of Medical Search,
15:45-16:00
16:00-16:45
Break_______________
16:45-17:15
17:15- 18:00
Media and Global Responsibility"
.Hammond and PurceluSnsun^
MrRossHammonci‘
‘Women, Children and Tobacco"
-Dr-Mira Aghi, Consultant to WHO and other UN Agencies New Delhi Indic
---------------—•---------- ----------- 5 rVl
INcW UGlllI, lllUlUi
Open discussion
-----------------------
Contact Numbers
Ministry of Health and Family Welfare, Government of India
Nirman Bhawan, New Delhi 110011
Tel: 301-9579
Contact:
Mr Vineet Chawdhry, Director, Public Health.
E mail: <vineet@hub.nic.in>
WHO South-East Asia Regional Office
World Health House, Indraprashtha Estate, Mahatma Gandhi Marg, New Delhi
110002
Tel: 331-7804 to 331-7823
Contacts:
Mrs. Martha R. Osei, Regional Advisor, Health Promotion and Education
(Extensions: 501, 502, 525,526) E mail: <oseim@whosea.org>
Ms. Harsaran Bir Kaur Pandey, Information Officer (Extensions: 424, 401)
E mail: <pandeyh@whosea.org>
Office of WHO Representative for India
Room 533-35, “A" Wing, Nirman Bhawan, New Delhi 110011
Tel: 301-8955, 301-7993, 379-2179, 331-9170
Contact:
Dr Robert Kim-Farley, WHO Representative for India
E mail: <kimfarleyr@whosea.org>
Ashok Hotel
50 B, Chanakyapuri, New Delhi 110021
Tel: 611-0101
Contact:
Ms. Rita Shah, Executive Manager, Front Office.
E mail: <ashoknd@ndb.vsnl.net.in>
The WHO International Conference on
Global Tobacco Control Law:
Towards a WHO Framework Convention on Tobacco Control
7
to 9 January 2000, Hew Delhi, India
Paper
Women, Children and Tobacco
Author
MiraB.Aghi
This paper is commissioned by, and produced for the World Health Organization, Geneva
Women and children are the two most vulnerable groups who become affected by
tobacco - not necessarily by consuming tobacco themselves but also by being around
people and in environments which are filled with tobacco smoke. Then there are those
women and children who work on tobacco plantations and those who work for the bidi
industry. In either of the cases, they get affected, they suffer and many die. In many
countries there is very little political will focusing on this problem. WHO is going to
draw the attention of politicans and governments all around the world with the
Framework Convention on Tobacco Control which is going to strengthen these
governments and NGOs, as well as individuals who wish to take legal actions against
tobacco and pursue policies which will protect people against tobacco. This is to be
viewed as a very serious step towards recognizing the comprehensive rights of women
and children.
This paper will present patterns and dynamics of tobacco use among women and
children and the intervention attempts to weane them away from this potent weed. Also it
will report on the involvement of women and children in the “Bidi Industry” in India to
point out how they are exploited by the tobacco industry.
THE EUROPEAN CHARTER AGAINST TOBACCO SAYS “EVERY CHILD
AND ADOLSCENT HAS THE RIGHT TO BE PROTECTED FROM ALL
TOBACCO PROMOTION AND TO RECEIVE ALL NECESSARY
EDUCATIONAL AND OTHER HELP TO RESIST THE TEMPTATION TO
START USING TOBACCO IN ANY FORM”.
Ample evidence exists to show that the tobacco industry has been targeting
women and children to lure them to the addictive substance. There is a growing concern
that the number of women and children taking up the tobacco habit is going up in the
majority of the countries all over the world. For example in the regions of America and
Europe, the prevalence of smoking for women is the highest at over 20% especially in
Denmark, Norway, Czech Republic, Fiji, Israel and Russian Federation.This is true in
developing countries also where people do not even have the advantage of health
education which includes the ill effects of tobacco. On the contrary the tobacco industry
puts up attractive ads which give the impression to women and children that tobacco is
the “In” thing and that they should not be left behind.According to one African study in
1973 fewer than 3% of Nigerian females students smoked but by 1982, the figure had
increased to 24% among female university and polytechnic students and 52% among
female trainee teachers.
Children
In the developed world cigarette smoking has been the major habit among
children both boys and girls. They usually take to the habit while in school before the age
of 18.
vpar olds in ten developed countries, 1986
Prevalence (%) of smoking among 15- year oios m
“
e
Country
—
All
countries
Do not
smoke (have
tried)
39.9
36.2
Have
never
smoked
34.2
36.3
No. of ~
subjects
4.4
5.6
Smoke
less than
weekly
6.5
8.0
11.8
13.1
6.5
7.1
10.3
11.8
43.3
39.1
28.2
28.9
476
381
Boys
Girls
16.6
13.5
5.0
6.2
5.1
5.6
32.7
29.4
40.6
45.3
603
502
Finland
Boys
Girls
29.1
20.1
6.3
7.4
6.3
10.1
39.9
36.8
18.4
25.6
539
543
Hungary
Boys
Girls
20.4
14.1
5.9
6.8
8.2
8.2
39.9
42.2
25.4
28.7
562
704
Israel
Boys
Girls
5.7
4.1
3.5
3.4
3.5
6.3
30.9
21.3
56.4
64.9
402
559
Norway
Boys
Girls
16.2
17.6
4.1
6.3
9.1
14.4
45.2
35.6
27.4
26.1
627
568
Scotland
Boys
Girls
14.7
15.6
2.6
4.5
3.6
6.7
39.8
40.0
39.2
33.3
771
711
Sweden
Boys
Girls
8.7
10.9
5.7
5.6
7.6
7.1
47.0
37.6
31.1
38.8
541
521
Switzer land
Boys
Girls
9.5
10.5
3.6
4.4
10.2
11.3
35.8
29.3
40.9
44.4
279
341
Wales
Boys
Girls
13.1
15.1
2.4
5.2
4.4
4.4
41.9
41.2
38.2
34.1
954
1104
Smoke
daily
Smoke
weekly
Boys
Girls
15.0
13.8
Austria
Boys
Girls
Belgium
5754
5934
Source : WHO Gross National Study on Children’s Health Behaviour.
It has been observed that smoking prevalence among 11 to 16 year olds in many
Western countries has historically followed adult patterns. In fact teenage prevalence has
changed relatively little in many countries despite concurrent declines in adult
prevalence.
2
Looking at the incidence rate the youth is smoking today the problem is serious
enough to be taken up on a war footing. The matter of special concern is that young girls
have become equal partners and in many cases they surpass young boys in their habit.
Young people both boys and girls take to smoking of cigarettes to conform to their group
of friends. Peer pressure and parental smoking are often quoted reasons for young taking
up the habit. Boys are attracted by the macho image - smoking projects and they report to
feel good, cool, smart, independent, sexy, attractive to girls, sportive free spirited while
smoking. Girls often mention that they smoke because their boy friends, best girl friends
or mothers and older sisters smoke. They report to smoke to be confident, sophisticated,
care free and in control of themselves.
The South East Asian Region, produces and consumes tobacco in many forms.
SMOKING TOBACCO: Like everywhere else in the world, cigarette smoking is
the most prominent form of tobacco use in most countries in South East Asia. In India
however, tobacco is smoked more in the form of bidi, a cheaper product made by hand by
rolling a small amount of flake tobacco (about 0.2 g) in a tendu leaf (Diosyros
melanoxylon). In Indonesia the most popular type of cigarette is the kretak or clove
flavoured cigarette, strong in flavour, nicotine and tar. It is smoked by 80 percent of
current smokers. Imported cigarettes represent a small but significant part of tobacco
consumption in the Region. There are several other ways of smoking tobacco which are
prevalent in specific areas of the Region, such as various forms of pipes (wooden, clay,
metal etc.), the hookah (also known as the hubble bubble or water pipe), cheroots (or
chuttas) and dhumtis.
SMOKELESS TOBACCO: The use of tobacco in various smokeless forms is very
common in India and to a small extent in Bangladesh and Nepal. The tobacco may be
used in raw, processed mixtures and pyrolised forms. The raw forms that are generally
sun-cured or air-cured, consist of flakes of plain tobacco leaves mixed with other
ingredients especially lime, areca nut and I or other condiments. The pyrolised forms
(mishri, bajjar etc) are used as dentifrice. Oral use of snuff is also practiced in some
specific areas.
Within each country of the region there is great variation in consumption patterns.
Rural populations tend to use tobacco more heavily than urban ones.
Bangladesh reports smoking of 16 percent among male students between the ages
of 11 to 16.
In India - The National Sample Survey Organisation (NSSO) has provided
smoking data for 1993 - 94.
The prevalence rates of any form of tobacco use among male rural youth aged 1014 and 15 - 24 years were found to be 1.6 and 21 percent respectively. For females, the
3
corresponding rates were 1.1 and 5.1. In Urban areas, prevalence rates among male
youths in the age groups 10-14 and 15-24 years were lower: 0.5 and 10 percents,
respectively. Among girls, the corresponding values were 0.3 and 1.4.
Specific studies on tobacco use have been done in India demonstrating very high
rates of tobacco use among student (30 to 50%) and non - student youth in Urban and
rural areas. Not only that smoking among medical students has been observed to be 20 40% in some areas.
Indonesia - Survey data of 1993 reports indicate the prevalence of smoking for
males age 10-19 years to be 27.7 percent and for females, 0.6 percent. In a study
conducted on 71 fourth year medical and dental students, 5.6 percent were current
smokers and another 5.6 percent were ex-smokers. Three different studies on child street
vendors showed that well over half were smokers.
Nepal - A household survey of the hilly district of Jhumla, found that smoking
was by far the predominant form of tobacco use in this area. Prevalence of smoking (both
cigarettes and bidis) among youth, was found to be highest between 16 and 19 years for
both boys (39 percent) and girls (16 percent).
Thailand - The National survey conducted in 1996 showed that smoking
prevalence for boys aged 11-14 years was 0.4 percent, which jumped to 18.3 percent and
47.7 percent in the age groups of 15-19 and 20-24 years respectively. In girls, the
corresponding figures were much lower, 0.3, 0.3 and 1.1 percent in the three successive
age groups.
The South East Asia Region thus presents a varied picture with Thailand currently
having the lowest prevalence rates.
The teenage years are the most important period in which decisions about tobacco
use are first made. A lot of experimentation occurs and at this time many occasional users
become regular users. Singapore has taken strong action and has implemented a strong
tobacco control policy. Due to this there has been an overall decrease from 20% in 1984
to 15% in 1998. Of concern is the smoking among young women aged 18-24. There has
been a twofold increase from 2.8% in 1992 to 5.9% in 1998..
The scene is very similar in Africa as well as in countries of South America where
young are observed to smoke. The incidence though not available in many countries,
small studies undertaken have shown that they are starting early, many before teens and
there are equal if not more girls than boys smoking. Also there are reports on out of
school children who have been observed to be addicted to nicotine very early on in their
lives and do not show any signs of changes.
What makes them take up the habit?
Almost everywhere the young smokers seem to take up the habit because they are
in an environment where the significant people in their lives smoke and chew.
Bangladesh - Peer influence and parental smoking habits were found to be major
factors influencing urban high school students to start smoking.
India - Studies of high school students in Patna and college students in Mumbai
showed that tobacco use usually started at the suggestion of friends. In a study of student
tobacco users in Maharashtra, in 1998, two thirds of the addicts to pan I masala / gutka
were introduced to the products by friends.
A few studies seem to indicate that tobacco use is more common among youth
who are living away from their parents (college students, street children), have poor
parental supervision or whose elders use tobacco.
Reasons for starting (and/or using) tobacco use among youth often included a
warm feeling of sharing among friends. Forcing by friends or relatives, a direct form of
peer pressure, was found in two out of eight studies. Other important reasons were
fun/enjoyment or to remove boredom and to pass time. Some young smokers said they
smoked to relieve feelings of anxiety / stress / failure. The desire to enhance one’s image,
adding to one’s status, appearing grown up or macho were reasons cited by many.
Working children also included the necessity to keep awake as a prominent reason.
Children generally started with experimentation and occasional use but with appearance
of withdrawal symptoms, addiction soon took over.
In one study of over 300 college students conducted in Mumbai in 1999, 40
percent admitted to be influenced by advertisements and said that sports and film
personalities (for boys) and stylish lifestyles (for girls) were the most influential factors
in these. Children in a large study in Uttar Pradesh (Mainpuri) were impressed by
advertising depicting a high lifestyle, which included smoking, drinking, good clothes and
affluent surroundings.
Indonesia - Cigarettes are usually offered at social gatherings in both urban and
rural areas. Tips are called “Cigarette money”. Young people are thus influenced by their
elders and by society. A 1995 study of 250 street vendors (below 14 years of age) of
whom 20 percent also sell cigarettes reported on the reasons why they smoke. Reasons for
starting were for fun, the taste, to feel proud to be a smoker and to be macho.
Nepal - The youth reported taking up smoking for fun and recreation. The adults
were a great influence as well, since smoking was highly prevalent among them (> 60
percent).
Thailand - The national Survey showed that male youth, smoked for fun and due
to peer influence. Females often smoked out of lonliness or insecurity.
5
Thus whenever surveyed, young people in developed and developing countries
cite boredom, curiosity and wanting to feel good (or better) or a part of a group as the
main reasons for use. Other functions served by substance use are: to relieve hunger, to
adopt a rebellious stance, for peer / social acceptance, to relieve pain, keep awake or get
to sleep, or to dream.
The pathways for young people who develop patterns of regular and problematic
or harmful use appear to differ from those who merely experiment or maintain irregular
habit or do not smoke. Personality characteristics, individual differences in vulnerability,
family difficulties, association with substance using peers, differential exposure to
substances, shared and non-shared environments, and accumulations of social
disadvantage all play a role.
WHAT CAN BE DONE?
Today there are many experts who believe that it is not easy to weane youth away
from tobacco even though in principle it should be easier since they have not been long
under the influence. It seems like youth have no desire, no motivation, no urgency to give
up the habit. If you tell children that they should not smoke because it will affect their
health, you are telling them the wrong thing. They could care less about lung cancer and
stroke.
A great variety of interventions have been tried on children and young adults
which have met with varied success. Some prominent ones are presented:
SMARTER THAN SMOKING
THE WESTERN AUSTRLIAN SMOKING PREVENTION PROJECT
Objectives:
•
To deglamourise smoking and encourage young people to question the social
desirability of smoking.
•
To make the immediate and short term consequences of smoking more personally
relevant to 10-14 yr olds.
.
To increase the awareness amongst the target group of the social factors that influence
their decision whether to smoke or not.
The strategy mix of mass media advertising, school based resources advocacy
activities, sponsorship of youth oriented activities, research, and evaluation formed the
basis upon which the project has built its brand image and personality.
6
The project has involved young people in all stages of its planning and development.
It has steered clear of traditional ‘just say no’ smoking prevention messages and
acknowledged that many young people may experiment with smoking and therefore other
strategies are needed to communicate to this group. It endeavors to educate and skill
young people to make more informed choices conducive to health.
BE smoke FREE
THE NORWEGIAN SCHOOL-BASED INTERVENTION PROJECT
BE smoke FREE is school-based intervention program targeted at children aged 1215 and based on social skills training. The main idea is to show pupils what it means to be
a free and independent person. The goals were:
•
o
•
•
to be free and independent.
consciousness about making their own decisions.
other ways to reach their goals.
exposing and resisting manipulation.
The training focuses on freedom and independence. Students learn to see that they
largely can choose their own behaviour and that they also can have influence on others.
Students discuss alternative ways of reaching their goals - if a girl wants to stay slim
how can she achieve that with means other than tobacco? If a boy wants to feel more
secure how can he become that without tobacco?
The ban on advertising of tobacco products has had a marked and beneficial influence
upon tobacco consumption and young people’s smoking rates in Norway. However, the
effect of legislation could have been even better if the ban had been accompanied by a
much more active and offensive use of other smoking control measures, in particular,
health information and education.
SMOKING CONTROL PROGRAMME AMONG YOUNG PEOPLE IN SINGAPORE
Based on the following:
1.
DEVELOP PERSONAL SKILLS TO INCREASE RESILIENCE.
2.
STRENGTHEN COMMUNITY PARTICIPATION.
3.
PROVIDE AND IMPROVE SMOKING CESSATION SERVICES.
4.
CREATE SUPPORTIVE ENVIRONMENT.
There is a need for a concerted effort to encourage young people to stay smoke-free.
A co-operative, collaborative, co-ordinated and continuous effort among various sectors
of the society is needed for successful smoking control among young people.
COMMUNITY INTERVENTIONS:
7
STRATEGIES FOR REDUCING YOUTH TOBACCO CONSUMPTION.
ASH
THAILAND
ASH tries to work to empower people to campaign themselves (rather than run all
projects ourselves) but ASH does support these campaigns with media campaigns and a
high profile for tobacco control in the Thai press. Young people are not only targets but
also change agents. All of ASH’s successful youth campaigns reinforce the fact that
young people are effective community educators and that the most effective way to
influence young people is to put them in control.
Besides these interventions there were also those which were school based and
child /youth centered.
Experts feel that these have not been very effective in bringing down the rates
though they are aware that in the absence of these the rates might have gone up much
more than they are today.
Why do school- based, youth-centered smoking interventions have little effect on
behaviour?
•
•
•
•
•
•
•
•
•
•
Smokers and potential smokers are most likely to be absent from school.
Many smokers reject school values.
Children learn remarkably little from school lessons.
Those who learn best are academic and least likely to smoke.
The needs of small specific groups are not met in a general classroom context.
Social influences are very strong.
Waming of risk and also sales restrictions can make smoking seem even more
attractive.
smoking education is affective and does not fit an examination-oriented
curriculum.
Teachers are often unfamiliar with the theories and methods needed.
Teachers modify the programmes.
How can school-based interventions, if they are used at all, be made more effective?
•
•
•
•
•
•
Involve the young people in planning.
Target small specific groups.
Use social reinforcement approaches.
Train teachers in theory and methods needed.
Involve parents for younger children.
Involve peers.
8
•
Develop school “no-smoking” policy for staff and students.
PREVENTING TEENAGE SMOKING - WHAT HAVE WE LEARNT FROM TWO
DECADES OF ACTION?
8
•
8
8
8
8
°
School health education programs have generally proved ineffective in practice.
Comprehensive smoking control programs aimed at all age groups are more likely
to reduce teenage smoking than programs aimed at youth alone.
All mass campaigns are more likely to be effective in the absence of tobacco
advertising and sponsorship.
Price increases reduce adult prevalence and may also have favourable effects on
teenagers.
Efforts to prevent the sales of cigarettes to under - age youth have proved
generally ineffective and do not necessarily reduce prevalence.
Programmes decline in effectiveness when taught in schools remote from the
original developers.
Few schools are willing to provide sufficient time in the curriculum for the
sophisticated methods required for optimum effect.
Schools can probably contribute more to tobacco control by concentrating on
comprehensive approaches, such as “Health Promoting School” programs, which involve
complete bans on smoking in schools, among many other measures. Furthermore, since
smoking is linked with poor educational performance and alienation from school, schools
may have more effect by attending to the needs of their weakest performers than by
promoting intensive programs focusing solely on smoking.
After twenty years of research and development, we still do not have a simple, costeffective method for reducing teenage smoking on a large scale. Comprehensive multi faceted strategies aimed at all age groups seem to offer the best prospects for successalthough even this cannot be guaranteed.
Sophisticated methods requiring extensive time commitments, such as the more
advanced school programs and cessation courses, are unlikely to reach large numbers of
teenagers. The focus should always be on large-scale methods such as publicity and tax
increases, which can influence on whole society’s behaviour and attitudes related to
smoking.
A growing body of research clearly demonstrates that macro level policies and other
interventions lead to reductions in tobacco use in all segments of the population. Some of
these policies, particularly tobacco tax increases and, possibly, comprehensive bans on
tobacco advertising and promotion have their greatest impact on youth and young adults.
Despite the difficulties described above there are ways to reduce uptake of smoking
among adolescents, but they are oblique and they involve behavioural change in adult
smokers. First, parents and family members of pre-teens and teens need to stop smoking.
9
It has been known for a long time that parental and sibling smoking is a risk factor for
smoking in adolescents. It now seems that quitting by parents reduces the likelihood of
offspring taking up smoking.
Conclusion:
The experts in tobacco control are beginning to warn that even where the trends had
started to lower down, it has the tendency to come up or at best to plataeu. Does it mean
we cannot do anything ? No, this is not what the conclusion is. The conclusion should be
to understand that there are several fronts on which the efforts have to be made and that
too almost side by side.
1.
We have to publicise what the tobacco industry is doing to people. We have to show
how it hooks us on a product which harms us when we use it the way they
recommend it. Also we have to be vigilant at all times of their new tricks and efforts.
The U.S anti tobacco lobby is becoming very concerned about
the new trend among some of the young who have started smoking bidis imported
from India. They believe bidis are not harmful like cigarettes and find them very
exciting because of the way they are made and presented.
2.
Price increase - This has been demonstrated effectively in the World Bank report.
Children /youth are sensitive to it and it truly deters new enterants.
3.
Ban smoking in all public places. What is important is not only the ban but its
implementation or carrying out. The ineffective implementation in reality confuses
people and might lead to contrary of what we want.
4.
A complete ban on direct and indirect advertising and promotion. This includes
banning it from TV programmes and films. It has been seen that in many countries of
the developing world children especially boys in urban slums smoke not so much
because the father smokes (they do not want to immitate or follow the father because
he is no good. He comes home drunk and beats the mother and takes away all the
money to leave them starving). Also these same boys do not want to immitate their
peers for they are just like them with no hopes and dreams. They want to immitate
their TV and movie heroes.
5.
Last but not the least helping children to grow up with life skills necessary to face
challenges not only from tobacco but from anything else which weakens their
energies to become slaves and dependent. Life skill which gives them power to think,
to problem solve, to be assertive, to negotiate and to be themselves.
Further they should be given information that they need, counseling that they require
and guidance which makes them wiser. The long term sustainable action will come when
they see the significant people in their lives inspiring them with themselves staying away
10
not only from tobacco but all those lifestyles that harm children in their right
development and obstructs the actualization of their potentials.
WOMEN:
Smoking among women is also of a great concern because of the resultant
morbidity and mortality. The advertising and promotion of tobacco directly influences
women because it is so specifically targetted to their needs and desires. “You have come a
long way baby” - appeals to her so well. The smoking woman in ads looks so confident
carefree and cool. These ads create a special space which the woman lacks when she
cares for the children, the elderly, the busy husband and the household chores. Smoking
relieves the boredom from her life, she so strongly believes. It perks her up, rejuvinates
her and gives her energy, she reports. In her desire to be free and in control of herself, she
forgets the terrible consequences of these habits - not only disease, disabilities and death
but also her slavery to the habit because of its addictive nature. She wants to leave it but
she cannot because of the strong withdrawal symptoms attached to it and because of her
belief that she will put on weight and loose her charm. Thus fostered, encouraged and
motivated by the persistent effort of the tobacco industry by their slick advertising, many
many young girls and women have fallen a prey to the habit of smoking cigarettes.
The tobacco industry spends a lot of money and time devising strategies to get
women to start smoking and maintain this habit.
The internal documents of the tobacco industry reveals that it is overjoyed at finding
that women smokers are likely to increase as a percentage of the total. The industry is
happy to find that women are adopting more dominant roles in society, they have
increased spending power, they live longer than men and they seem to be less influenced
by anti-tobacco campaigns.
•
The industry proceeds by identifying views and desires of women who according to
them appear more driven by lifestyles and image campaigns. It tries to develop a
clearer understanding of attitudes, values and motivations of women as it stands now
and how the social changes are going to impact them. The industry does much to
identify trends among women as consumers, which could relate to lifestyles and
purchase behaviour.
•
The industry feels women respond well to tender imagery in advertising, imagery
which reflects intimacy and closeness, tenderness and gentleness, loving, caring and
sharing. Women who are not working outside the home respond better to escape and
factasy and career women react positively to imagery associated with elegance and
success.
•
The industry feels they know why women smoke - it is started as a social thing. It is
like a forbidden fruit and every daring person wants to taste it. Young girls feel more
mature if they smoke.
O
11
•
The industry still sees a lot of work ahead especially to woo the women in the
developing world. It has brought two new brands of cigarettes for women in China. It
is also luring women in Sri Lanka by offering them free cigarettes.
Large amounts of money are spent by the tobacco industry to promote the use of its
products. This is done not only by promotion through the traditional media like TV, radio,
newspapers and billboards, but also by giving allowances to retailers by direct-mail
advertising, free samples and sponsorships. Though the industry claims loudly that the
advertising and promotional activities are not to initiate smoking among young girls and
women and to increase sales, but simply to encourage competition and to promote brand
choice of adult smokes.
Women in particular have been strongly targeted by the tobacco industry as a
potential growth market and the media campaigns have been geared towards presenting
smoking as a liberating, socially acceptable, sophisticated, sexy and slimming. Cigarette
companies have also portrayed smoking as a “torch of freedom”, a “tool of beauty” and
sign of progress. Advertising in women’s magazines not only encourages smoking
among women but also determines whether these magazines will report on the risks
of smoking to women’s health. Women’s magazines that accept cigarette advertising
have significantly fewer articles about health hazards of smoking and cessation than
magazines that do not carry ads. Cigarette companies have other ways of targeting
women, such as through female sports sponsorship and support of women’s organizations
and funding other activities. There is now considerable evidence from developed
countries that children are aware of tobacco advertising, that tobacco promotion influence
whether young people start and continue to smoke. Young people experiment with
smoking and become regular smokers. Advertising and promotion also reduce the
willingness of current smokers to quit, on the contrary it is likely to serve as a stimulus to
increase their daily consumption. Additionally advertising and promotion could induce
former smokers to resume their smoking behaviour by reinforcing the attractions of
smoking.
In the developing countries advertisements influence young girls even more as
they may have little to no knowledge about the harmful effects of smoking. At present
tobacco advertising in the developing countries tends to be directed at the general public
although there are attempts to make women as special like in China, Sri Lanka and the
Philippines.
A lot of advertising and promotion is done for chewing tobacco in India where it
has attracted young and old, men and women. Women especially take to it for it is much
more socially acceptable than smoking. It does not bode well for women for very soon
the habit gets addictive. Villages do not have much advertising but the tobacco companies
have very clever ways of doing a lot but doing little. They put posters of famous movie
and TV personalities in a prominent place in a village showing him / her chewing
12
tobacco. This is enough to girls and women take up the habit or practice it without feeling
bad.
As public awareness of the health effects of tobacco has grown in many countries,
the tobacco companies have responded by increasing the amount and variety of tobacco
products and promotions that are targeted specifically at women. A common
characteristic of these efforts is an attempt to allay health concerns by introducing
cigarettes with lower tar and nicotine yields: which do not actually lower the risk of many
tobacco diseases. Informed women who switch to low nicotine cigarettes often
compensate for the reduction by inhaling more deeply or smoking more often. The
tobacco industry lures women by introducing “women only” brands and by presenting
cigarette in beautifully coloured packets and tastes to give women the impression that if
they smoke they will be successful, youthful, happy and healthy. This marketing is often
complemented by tobacco sales in places frequented by women, such as dress shops,
beauty parlours and also where women go to play cards, etc. Some attempts have been
made to appeal to women by selling cigarettes in packages containing fewer cigarettes.
All these efforts by the tobacco companies are not only limited to developed countries but
developing as well. In India, a woman ‘brand’ was promoted in 1990 (which failed due to
the pressure of anti-smoking lobby especially of women). The tobacco companies are
doing the same in China presently and promoting cigarettes by distributing free samples
to young girls at disco houses. In India and Pakistan they sell chewing tobacco in
colourful pouches and boxes which women can put in their purse to be readily accessible.
In the world today there are 200 million women who smoke reports WHO. This
does not include the number of women in South East Asia who practice habits other than
cigarette smoking like smoking bidis and chhutas and chewing tobacco with other
ingredients or alone, rubbing burnt tobacco on her gums and teeth and plugging tobacco
quid under her tongue or in the cheek.
The consequences of tobacco use affects the health of a woman and her children
through out her life cycle. From birth, girl hood, womanhood, pregnancy and birth again
as a mother, tobacco harms the health of the girl, woman and baby.
Evidence is beginning to come out that the health consequences of tobacco are
indeed more serious in women. Lung cancer has been reported among women smokers as
among men smokers but now it is coming out that women smokers develop lung cancer
earlier than men despite starting smoking at a later age and smoking fewer cigarettes or
bidis than men.
The risk of lung cancer among women smokers increases with the number of
cigarettes / bidis smoked per day, duration of smoking behaviour, degree of inhalation,
age of starting to smoke and amount of tar in the smoking material. While the number of
cigarettes smoked per day and the duration of smoking behaviour both leads to risk; the
effect of duration of smoking is greater than that of daily consumption.
13
Lung cancer is over taking breast cancer as the commonest malignancy of women
in the parts of the world where smoking is increasing like in countries of central and
Eastern Europe and also in Western Europe whereever women have not refrained from
smoking the weed. Although women who smoke cigarettes and bidis are likely to die of
lung cancer, those who smoke bidis and chutas and chew tobacco will end up getting
many cancers such as mouth, lip, tongue pharunx, larynx and oesophagus. This is because
when you smoke, you smoke through your mouth and after the mouth, the smoke goes to
larynx, pharynx and oesophagus, the back of the throat, the windpipe and ultimately you
breathe smoke into your lungs. Whereever the smoke goes, it can cause cancer there. The
highest reported incidence rate in the world for cancer of the mouth is among women in
Bangalore, India where women have considerably higher rates than men; this pattern is
also found in Madras again in India.
From the lung toxic by products of smoking such as nicotine go into the blood
system and circulate around through the liver into the other parts of the body, increasing
the risk of carcinoma of the liver. Ultimately the kidneys will remove the by-products
from the blood, which will go through the urine, also increasing risk for cancer of the
bladder where urine is held. In addition there are cancers of renal pelvis and renal body,
which are the two components of the kidney plus a number of other sites, such as the
pancreas and stomach. Though these sites are away from the lungs evidence has shown
that smoking contributes to these diseases. Also there is solid evidence that once women
cease to smoke, their risk of these diseases starts to decrease and with total abstinence the
risk can be reduced to that of a lifetime no-user.
Women, just like men, or even more, suffer from bronchitis, emphysema and
ischaemic heart disease and other diseases of the vascular system. The more they smoke
the higher the rate of getting these diseases. However if they give up their habit, there is a
sure respite from these diseases.
Pregnancy is vulnerable to smoking. The more a woman smokes the greater the
risk for her to develop ectopic pregnancy. Since women who smoke are susceptible to
infections of the reproductive track, they could have problems conceiving and in fact may
not be able to conceive at all.
It has been firmly established that expectant women who smoke are prone to
spontaneous abortions. This is because tobacco smoke contains nicotine, carbon
monoxide and minute amounts of cyanide. Nicotine being a vasoconstrictor renders the
blood supply to the foetus through lack of blood in the placenta. The carbon monoxide,
which ends up in the blood when one smokes a cigarette, reduces the oxygen carrying ’
potential of haemoglobin and as a result reduces oxygen supply to the foetus. If a woman
smokes over intense period, she may build up enough cyanide to cause damage to the
nervous system of the foetus through depletion of Vitamin 12. The risk of spontaneous
abortion is 80% more in women who smoke than those who do not. Due to the same kind
of mechanism a smoking mother is likely to deliver a low birthweight baby. Smoking can
cause growth retardation of the foetus. Research carried out in India is of special
14
significance because of the habits of not only smoking bidis but also chewing tobacco.
This reasearch has confirmed that babies bom to women who smoke bidis during
pregnancy are on an average 200 g low in body weight. A dose response relationship has
also been established i.e with increase in maternal smoking during pregnancy a
corresponding decrease has been observed in baby’s birthweight. Further more all
parameters of foetal growth with head and chest circumference, body length etc. are
reduced in babies of women who smoke. In fact the child’s development up to 11 years is
adversely affected by maternal smoking in pregnancy. Women who chew tobacco gave
birth to babies weighing anywhere from 100 to 400 g less than those delivered by women
with no habit. The crude still birth rate per 1,000 births was 50 in women who chewed
tobacco as compared to a rate 17.1 who did not use tobacco.
Also in India women exposed to passive smoking has been reported to deliver low
birth weight babies with a proportion of 1.8 to 1 who are not exposed. Women who
chewed tobacco during pregnancy were more prone to still birth as compared to women
who did not.
In Bangladesh women who were passive smokers of “biris” (as the bidi is called
in Bangladesh) during pregnancy had twice the number of perinatal death than those
women from similar background characteristics but companion with no tobacco habit. A
study in Osaka, Japan reported that the rate of low birth weight increased with the
intensity of exposure to tobacco smoke. The prevalence was 3.8 % for women whose
partners were non-smokers but 5.6 % for women whose partners were smokers. All this is
reported to be associated with a decrease in mean gestation period. However the good
news is that if an expectant mother is able to give up smoking or / and chewing, she
stands a chance of having normal delivery giving birth to a normal healthy child!
Fewer male foetuses were bom to women who chewed tobacco (50 males for 100
females) compared to women who did not (109 per 100 females). Similarly women who
had the habit of oral application of burnt tobacco had fewer male new boms (81 males per
100 females) compared to women who did not (106 males to 100 females).
France, Germany and the United Kingdom have reported 20 - 25 % of all infant
deaths due to smoking.
Young girls who smoke have problems with their menses. It can be erratic. Also
women who smoke go through menopause earlier. This leads to oestrogen deficiency
resulting in osteoporosis. Smoking leads to weaker, mineral deficient bones by reducing
blood supply and the number of bone- forming cells. If the risk of bone fracture in a nonsmoker is 1.0, the risk rises to 1.5 in a smoker and the fractures are more severe.
In smokers the risk of periodontal disease is 2 to 3 times higher than in nonsmokers. The periodontal disease in smokers is not only higher but also more severe. It is
also likely to result in bone loss. Smoking produces bad breath, gum disease, dental
diseases, tooth erosion and gingival recession. This contributes to loss of good looks in
15
women which they value so much and which the tobacco advertising misleadingly shows
to be related to smoking.
Nicotine reduces the circulation of blood and the uptake of oxygen affecting
women’s hair, skin and eyes. Skin wrinkling is found to be enhanced and occurring
earlier in women who smoke. THERE SEEMS TO BE NO POSITIVE EFFECTS OF
SMOKING.
Once again as in the case of children and youth intervention efforts are not terribly
successful. The studies carried out report the following.
•
•
•
•
•
o
•
•
•
Women are less likely to plan to quit smoking than are men.
Women are likely to smoke for tension reduction and weight control.
Women quit smoking at the same rate as men but are less able to maintain cessation
long-term.
Physicians are as likely or more likely to intervene with female smokers as compared
to male smokers.
The Clinical Implications of these Research Findings Are the following:
Smoking interventions for women may need to emphasize strategies to help them to
develop confidence to stop smoking, to make a commitment to cessation and to
develop strategies for maintaining cessation for long periods of time.
Smoking interventions for women should emphasize tension reduction techniques.
Smoking interventions for women should emphasize weight control techniques.
Physicians need to tailor their interventions for women by targeting concerns of
tension reduction and weight control.
These when combined with the following elements
1)
Legislation
2)
Total bans on advertising whether directly or indirectly (ban and strict implimentation
3)
Smoking in public places
4)
Increase in prices
INVOLVEMENT OF WOMEN AND CHILDREN IN THE BIDI INDUSTRY
I now want to report on an industry which utilizes women and children as if they
have no rights - including the most basic right to live decently in an environment which
does not threaten their health and well being. This is the bidi industry in India. India takes
pride of running an industry which employs so many people to give them livelihood, who
will otherwise starve as they will have no jobs and a source of income - we are reminded
again and again.
Child Labour is one of the burning problems of our society. The fruit of
development has spread unevenly, giving rise to pockets of intolerable poverty. Child
Labour in bidi industry is one such industry where inspite of legislation, there seems to be
16
no justice. The industry though export oriented; because of its low inputs of technology
and its low requirement of technical skill has remained within the purview of unorganised
sector, though the figures of the earnings in the export market makes it difficult to think
of it as an unorganised one.
It is aptly stated that the state of children in any society is an indicator of its level
of development. A country in which many children have no childhood cannot be regarded
as one to be looked up to. It is indeed a grim social reality that even today as we approach
the 21st century, we have not gotten rid of many ills that should have been eliminated
from the face of the earth long time back. Child Labour is one such ill that need to be
done away with. Attempts have been made by producing legislation which prohibits
employment to children but it has not produced as desirable results as deemed necessary.
0
India is the major producer of bidis in the world. It is very difficult to estimate the
number of children working in the bidi industry as only a few of them work in bidi
factories,
Bidi is mostly a home based industry and all children are required to help out.
There are fewer factories and because of labour regulation, the factory owners are
careful to employ children below 14.
3)
Girls are almost never sent to factories - unless they are with their mothers.
1)
2)
Bidi industry is like no industry so intriguing, so conniving, so ruthless. The industry
is the largest employer after agriculture and construction sector, at times the biggest and
occasionally the only employer in the area. About 40 million men and boys are engaged
in collecting ‘Tendu’ leaves used as wrappers for the bidis. Another 60 million are busy
rolling bidis. These are mainly women and girls though also boys women comprising
65% and children around 15 to 25%.
It is very important to understand the functioning of bidi industry in order to
appreciate the role of women & children in this industry.
ft
The production process and relations
Bidi production is labour intensive and is in various stages at various levels. As
said before a factory employs very few workers while a major portion of the bidi
production is typically outside the factory in the workers’ homes.The factory owner who
is the principal employer operates through a number of branches of the company within a
state or across a number of states. Each branch has a specific geographical jurisdiction
marked for operation. A typical branch has two major functions: first, getting bidis rolled
by workers in villages through contractors or sattedars; and secondly, collecting, sorting,
grading, roasting, labelling and packing of bidis that are produced. Each branch of a
company has a manager and a number of employees who perform the activities of
distribution of raw materials to sattedars, checking finished products and all other related
activities.
17
At any given time a branch has a number of sattedars attached with it. Each
sattedar has a specific area to operate, this may be just one village or a cluster of
adjoining villages. It is also possible that in a village there may be more than one sattedar
each for a different bidi company. The converse of this, namely one worker rolling bidis
for different sattedars at the same time, does not usually happen. Often large villages with
a concentration of bidi workers have more than one sattedar.
The branch supplies the raw materials namely, tendu leaves, tobacco and yam in
large quantities to a contractor, to supply back rolled bidis proportionate to the amount of
raw materials supplied. The sattedar in turn distributes the raw materials in smaller
quantities to several workers who take these to their home for rolling the requisite number
of bidis specified by the sattedar.
The worker brings the raw materials home and shares the work with other
members in the family including children. This is necessary because the process of rolling
bidis involves several stages all of which are time consuming and it is not possible for
one worker to perform all the work alone, to produce the required number of bidis in a
day.
First the tendu leaves are cleaned and cut as per the size required by the brand of
bidis to be rolled. The cut leaves are then soaked in water for a few hours to make them
more malleable. At the next stage the bidi is rolled using tobacco and leaf, after which
the edges of the rolled bidis are turned in and tied with yam. Finally, the rolled bidis are
tied in bundles of 12 Or 24 as per the requirement of the sattedar. Thus, the raw materials
are converted into a final product and returned to the sattedar. After checking the quality,
the sattedars stack the bidis of each worker separately and sends the day’s collection to
the branch office through a carrier known as ‘Relaiwala’. The worker in turn collects the
raw material for the next day’s production. Thus, the process goes on.
In the branch the bidis brought by the relaiwala are first checked for quality. Each
bundle, consisting of 12 or 24 bidis, is thoroughly checked for size and quantity of
tobacco filled. The defective bidis are removed and discarded. Then the bidi bundles are
counted and stacked in mesh trays. This is taken as the final production of the contractor
for that day.
The process of production outlined above appears to be simple, but is in fact a
complicated one. The complications arise primarily because of the informal relations of
production at every level and the unorganised nature of the workers involved in
production. Given this, there is widespread exploitation at each level in various forms.
Thus, any discussion on the production process in the bidi industry would be incomplete
without an understanding of the dynamics of exploitation involved therein.
18
Exploitation takes place at both levels of production - the branch exploits the
sattedars and they in turn exploit the workers mercilessly. However, it is the worker who
has ultimately to bear the brunt.
Explotation of Workers by the Sattedar
1)
A common practice adopted by the sattedar is wetting the tobacco prior to
distribution to workers. This is done in order to make the tobacco heavier. Thus, in
reality the quantity of tobacco given to workers is less than what is needed for rolling
bidis. The contractor in this way earns on the tobacco saved.
2)
It is an accepted fact that 800 gms of tendu leaves and 240 gms of tobacco are
required to roll 1,000 bidis, provided the tendu leaves are not defective. Usually tendu
leaves are given to workers without checking their quality. Poor quality or damaged
leaves in the bundle given to the workers would necessarily mean shortage of leaves
to roll the bidis. In addition to this, shortage of tobacco may occur due to one or more
of the following reasons:
a)
the sattedar takes a fistful of tobacco after weighing it, as parampara - a
traditional practice.
b)
the tobacco which was wet at the time of distribution dries up and thus weighs
less in the final check; and
c)
a sudden gust of wind may blow away some amount of tobacco from the open
trays the workers use while rolling the bidis.
Shortage of tobacco and tendu leaves as outlined naturally results in a reduction in the
bidis rolled and the worker is held responsible for this. A reduction in the bidis rolled
leads to a cut in the wages. This wage cut is supposed to be proportionate to the shortage
in the number of bidis produced. However, there is no standard norm observed in cutting
wages and it is as per the whims and fancies of the contractor.
In order to avoid a wage cut arising due to shortage of raw material, the workers often
resort to purchase of raw material on their own to replenish the shortage. The inherent
advantage of this practice is that it would work out to be cheaper compared to the wage
cut. Unfortunately, in many villages workers have to purchase raw material from sattedars
as there would be no other alternative source.
The price that the workers pay to purchase the raw materials from the sattedar is also
quite high compared to the market price. The only person who benefits in this whole
transaction is again the sattedar.
19
3)
About 10 percent of the bidis rolled by a worker are taken away as ‘standard
deduction’by the sattedar, to replace defective bidis. This is done regardless of the
number of bidis rejected during the checking process or ‘chant’ done in the branch.
4)
Bidis brought by the sattedar to the branch are again subjected to checks for quality.
During this process, if one bidi in a bundle turns out defective, then at least one bidi
each in all the bundles are rejected. The rejected bidis are not given back to the
workers but retained by the branch. The sattedar in turn cuts the cost of that many
bidis form the workers wages. The workers would not know the exact number of bidis
rejected on any particular day. Thus, there are usually at least 20 to 25 per cent of
rejects in a day per worker.
5)
The amount of work that a worker receives depends on whether or not he or she is in
the good books of the sattedar. The sattedar distributes the quantum of work to each
worker depending on his will. This situation proves to be very vulnerable for the
workers. This is purposefully done so that no worker can lay any claims on the
contractor to benefits of any kind. Further since bidi production is suspended during
the monsoon, all workers are laid off for a period of two months or so. Apart form
this, the sattedar resorts to devious means to show impermanency of worker’s tenure
by either changing the names in the register every three months and / or by excluding
the names of women workers which in turn affects children who work for their
mothers. Children are never in the sattedar’s register.
6)
The worker does not keep as a practice accounts of work done and wages paid. The
sattedar generally maintains two registers one pukka register in which the proper
details of 10 to 20 workers are noted and another kuchha register in which all the
workers names are entered. However, no pass book is maintained by the sattedar, as
required by law for each worker separately.
7)
In most of the villages, the sattedar, plays multiple roles, He is also generally the
village moneylender, sometimes the local grocery shopkeeper, the village landlord or
the Sarpanch. These roles enhance his hold on the workers, and provides him with
several avenues to exploit the workers. The workers have no option but to accept the
situation.
8)
The sattedar makes weekly payments to workers. Sometimes he charges an interest
claiming that he has borrowed money to pay them because the branch has delayed the
payment to him. This may or may not be true. However, the sattedar often uses this
excuse as a source of additional income. The workers are compelled to accept the
arrangement since they have no alternative. Apart from this, at some places the
sattedars charge a sum of Rs. 1.50 per week as ‘manageri’ from each worker for
running the establishment.
Relations between Branch Office and the Sattedar
20
Thus goes the relationship between the sattedar and the worker in which the
former takes undue advantage of the situation. The roots of this exploitative relationship
lies not merely in the contractors need to appropriate more but also in his nebulous
position vis - a - vis the employer. It is precisely the relationship between the two which
determines to a large extent what follows. He is treated extremely shabilly by the
establishment and is reprimanded for anything going wrong.
Bidi industry is a cottage industry no matter whether it is in rural or urban area.
Every year 900 billion bidis are made by approximately 10 million workers. The majority
of these are poor and illiterate women and children/ Bidi workers are not an organized
group. Because of being illiterate and unaware of their rights, they get amply exploited.
They are unfamiliar with the welfare schemes that the government has launched. Not only
that some of them are so pathetically ignorant that they do not even know the name of
their employer. The managers remove or change the names of the bidi workers in their
registers every 2 months so that he does not have to pay the welfare that the government
has fixed.
The only positive thing that can be said about bidi industry is that it does not
discriminate either on the basis of sex or religion. The rolling is mostly done by children
and women. Many Muslim women who would not work at all, work in this industry
because it allows them to work at home. Only 10% of bidis are made in the factories The
rest are made at home. As of April 1999 the government of India states that there are an
estimated total of 43,99,644 bidi workers but the unofficial figures are more like
100,00,000 (6 million rolling bidi, 4 million collecting leaves). A big chunk of these are
belonging to backward classes & castes. Since it involves working at home it includes
children especially girls. Only a proportion of them are registered workers who are issued
identity cards. It is not in the interest of bidi employer to get their workers cards because
then they will have to give them work benefits and welfare facilities. Like out of
43,99,644 official workers 35,85,018 have ID cards.
0
At present in bidi industry minimum wages are fixed separately for each state and
region resulting in disparity.
Rs. Per 1000 bidis
Rajasthan
Bihar
U.P
M.P
Maharashtra
Gujrat
Tamil Nadu
West Bengal
Kerala
Karnataka
Rs. 22
Rs. 26
Rs. 35
Rs.22.50
Rs.20.35
Rs.18.50
Rs. 16.25
Rs. 14.50
Rs.25.20
Rs. 16.25
21
Andhara Pradesh
Rs.17.85
Employers tend to shift the industries to states or even across borders into Nepal
and Bangladesh where they have to pay less to the workers. Thus the threat of shifting
industry always looms large for the workers are likely to loose jobs.
In the present existing system of contract the bidi workers are exploited due to the
absence of direct relationship with the employer. As the middle man takes a share each
time, the workers lose.
The government has introduced welfare schemes but the rules are so crooked as
well as they lack any reference to ground realities. For example for the entitlement of
almost all the welfare schemes the total family income cannot exceed Rs. 3,500/- per
month, which is extremely absurd. The workers are to observe a small family norm viz
will not have more than two children. This condition does not make sense to them as all
children contribute in making bidis.
All bidi workers are eligible for medical and health benefits. But the dispensaries
are not located according to their conveniences. Also many dispensaries do not have
doctors. Even the medicines are not available in the quantity required and many TB and
cancer patients do not get proper care. Only Rs. 70/- are paid towards prescription glasses
which is far from realistic. Rs. 250/- are paid towards delivery and Rs. 50 as an incentive
for sterilization.
Loans for building or repairing houses are inadequate to say the least.
There is a proposal that the bidi workers be given a loan of Rs. 10,000 and be also
given Rs. 3000/- as ‘gratis. However it has been next to impossible to secure these loans
as the rules get twisted and manipulated.
The government has also made a provision that the children of the bidi worker be
given scholarship to go to school. The following has been approved.
1 -4
5-6
7-10
11 - 12
For degree course
For medical, engineering
Class
Rs. 125 per year
Rs. 250 per year
Rs. 450 per year
Rs. 700 per year
Rs. 1000 per year.
Rs. 3000 per year.
There is also provision to show films, arrange other entertaining activities for the
bidi workers especially children however this works mostly for those areas which have
cooperatives formed by the workers .
22
As pointed out before, the workers are illiterate and because of being continuously
°lted> get timid. In most of the cases they do no understand their rights. Even if they
i t ey get so discouraged because they are required to go to different authorities for
redressal of different grievances.
Provision for the education of the children of the bidi workers was made way
back. Evidence exists that the children of the bidi workers have been harnessed to the
gruelling process of bidi making instead of being sent to school. As most of the women
are being kept out of official registrations children are doubly exploited - first by the
industry and the state because their mothers are not recognized as workers, secondly by
the family by engaging them for long hours whereby they can neither go to school nor
Play.
The tyranny of the household gets multiplied when the home becomes the work
place, its arbitrariness and flexibility making it into a machine of exploitation. Women
continue to be cheated by all the tiers of this industry and but worse they end up
sacrificing the lives of their children to the unhealthy dreariness of bidi industry for hours
on end that stunts their future growth and aspirations.
The workers who sat on the floor are surrounded by trays containing tobacco and
cut or uncut, wrapper leaves, the latter soaked in water emits a peculiar odour while the
tobacco leaves have a characteristic smell too. The mixture of these smells pervades the
whole house. Women and children, heaps of waste, remnants of wrapper leaves and tin
trays stuffed with tobacco or newly made bidis, dirty and tom mats here and there present
a picture almost unbearable and unforgiveable.
In a landmark judgement passed in November 1991 the Supreme Court ordered that a
survey should be conducted to identify the actual workers who rolled bidis so as to ensure
provident fund and other benefits conferred upon the adult worker. This was ordered as a
pass book that should rightfully be kept under the names of women workers. Also
a. The government should examine abolishing the contract system.
b. Child Labour should be prohibited.
However it seems like this directive was never followed as the evidence in the field
shows.
The exploitation of both women and children continues.
The women and children in the bidi making are prone to occupational diseases - like
T.B. caused by continuous inhailing of tobacco. They also have other rheumatic
syndromes resulting from long hours of continuous sitting cross legged in an unhealthy
atmosphere doing a monotonous job. They also suffer from chronic asthma, allergies,
backache, stomach troubles and piles. Also sitting together for hours a T.B patient or one
suffering from chronic cold passes on germs to her fellow workers.
23
As pointed out before in almost all setups of bidi workers 65% happen to be women
while there are 15% children mostly girls. Women are paid less than men and children the
least of all for the same work. Children have no wage structure of their own. It is the
adult male who securs orders on behalf of their females and children as the latters are
utilized as helping hands only. In most cases, neither the women, nor the children have
any mention of them in the employers registers. Raw material and wages are paid to the
male head of the family, providing ample scope for the dishonest employers and their
agents to deny the existence of child labour. There is no mention of I.D cards of children.
Though many of the children join school, the drop out rate is very high and very often the
children are used as farm hands as well in addition to rolling bidis.
Including major trade unions nobody has done any work in organising children in the
bidi industry.
There is never any sound rationale presented for paying lower wages to women and
children. It comes down to plain gender bias. Some male bidi workers remarked “women
and girls’ lack skill and their production is not up to the standard. Bidis produced by a
man taste much better, the tobacco is evenly distributed throughout the length of the bidi
and the leaves are evenly cut“.
However this is not borne out as the majority of the rollers in each and every area are
women and girls they are preferred as well. This is also because women and girls being
illiterate, the employers can take advantage of them. Also the fact remains that they are
not organized as a group to fight back and protect their rights. Also they are reluctant to
join openly in any movement. When women themselves were asked why they are paid
less, the majority said that it was a ‘convention’, only a handful remarked that the
employers were taking advantage of their ignorance. In addition even when women do
realize that an injustice is done to them they said they have no choice. If they did not roll
bidis they and their families will starve. There are examples of cooperatives formed here
and there by the bidi workers and in such cases, there is no discrimination. Not only the
women and children get paid the same amount as men but they are able to avail of the
welfare benefits. The cooperative enables them to have ID cards as one women said ID
card is a must for any bidi roller especially if the roller is a women. Without it she will
not get any maternity benefit, any house building loan or medical benefit. If she is a T.B
patient she would not be provided any free treatment. When a roller without EDC dies her
nearest relative or dependent is denied the stipulated compensation. Inspite of this many
rollers stay without IDC.
Apart from poverty, ignorance and illiteracy, there are some other factors which
enables the employers to exploit women and children rollers of bidi. Though Hindu
women might be shy to deal with the men contractors in the beginning, they get over it
and start working and interacting with them. This is not true of Muslim women and girls
who have to stay under Purdha (in vail) as soon as she starts mensturating which
imposes restrictions on her to deal with men who are non relatives. It is because of this
24
that many cannot secure ID cards in their own names. Not only that they are also absent in
the ledger books of the contractors. This adds to exploitation.
Forming cooperatives have been a hopeful factor because the trickaries of the
contractor has no place here. There is higher pay, no rejection, no stealing raw material
and no abuses. Inspired and empowered by the society the rollers working in a noncooperative set up next to the cooperative ask for equal wages and they end up getting
those. The difficulty is that a lot of money is needed to set up cooperatives. Also the
management of funds is not easy and corruption is likely to crept up. But the fact remains
that a cooperative society can pressurise the concerned agencies for the issuance of the ID
cards. The block administration is the authority to issue cards and the trade unions have to
recommend it to get all the benefits. But the machinery is so complicated.
Prolonged hours at bidi making in an enclosed place which is also their living
quarters, pervaded by a noxious smell of the Tendu leaves and raw tobacco, children end
up suffering often from many diseases. When children get sick they go to private clinics
or traditional medicine practitioners because the welfare health centres are somehow not
within their reach. Also because of shortage of medicines and absence of doctors the
health center is rarely frequented by the bidi rollers.
Playing in childhood is almost taken for granted. Very few bidi rolling children have
an occasion to play outdoor, some play in door but the majority has no time to play. In
most of the settings 2/3 of the children never watch television, only 1/3 occasionally.
Cinema is a rare thing to experience though radio listening is much more common than in
average Indian house. The major source of entertainment is visiting relatives or friends or
occasionally going to the village fair.
Mankind owes to the child, the best it has to give. The child shall enjoy special
protection and shall be given opportunities and facilities by law and by other means, to
enable him to develop, physically, mentally, morally, spiritually and socially in a healthy
and normal manner and in conditions of freedom and dignity. The child shall be protected
against all forms of neglect, cruelty and exploitation. We have to aim for it and nothing
short of it will have to be acceptable.
Child Labour regulation (1956) prohibits employment of children in hazardous
occupations. The distinction between child work and child labour has a lot of loopholes.
Section 3 of legislation exempts employment of children in home based work. There is
high incidence of child work in families on piece rate basis formed out to them by the
production units to circummnent the laws that prohibits children to work. Stringent laws
are required. Employment of children should be uneconomical to bring about an end to it.
Work that denies children education and childhood, needs a holistic regulation
suitable to strengthen enforcement machinery, enhanced access and improved quality of
primary education, an effective nonformal education program, strengthening socio
25
economic development program, participatory efforts by different partners including
government, NGO and civil society.
For a long time we have been hearing the wise say “If you have got your health you
have got everything”. Now all of a sudden we are told that the opposite is true as well. If
you have got just about everything, you probably got your health as well . What about its
flip side namely if you have nothing and are poor, can you have even the remotest
possibility that you might enjoy good health. By coincidence you might but as a rule no
possibility say the poor. What would happen if in addition to being poor you are also
rolling bidis. It is a hopeless situation tells the Medical Officer working in a primary
health center in Andhra. He has seen healthy women turning sickly, children losing their
luster and simply vegetating.
It is important to indicate that if tobacco exploitation has to be put an end to we
have to come up with policies that are gender specific not only for adults but for children
and youth as well. It is recognized that we understand the needs of women and children,
not only needs but their rights to health, well-being, knowledge and protection from the
tobacco industry. The Convention on the Rights of the Child (CRC) and the Convention
on the Elimination of Discrimination Against Women (CEDAW) are potent tools for
children and women to exert and demand that the tobacco industry put an end to its
efforts to make tobacco so attractive to women and children, and to stop exploiting them
both as consumers and workers.
Full implementation of these two conventions necessarily entails implementation
of effective tobacco control measures in every country. Governments must ensure that
the best interests of the child and woman override the power and influence of the tobacco
industry and recognize that the long term economic and social costs of tobacco use
outweigh the immediate political and financial costs of controlling it.
Both these conventions include articles indicating access to health education and
interventions which can form a powerful framework within which women and children
have the right to seek, receive and impart information and ideas. The links between the
rights to information and tobacco control are most obvious with regard to the portrayal of
tobacco in the media including advertising. Media influences that lead to the
development of positive attitudes to tobacco use and misleading information and a lack of
objective information about the dangers of tobacco use pose serious threats to women’s
and children’s rights as provided for in the two conventions.
It is helpful to use both the conventions as a tool to force change in institutional
structures at the national level, i.e. using an international legal instrument to challenge
governments to correct unjust situations at national level. This way it is possible to take
the global and make it local to enforce it. This is particularly important when a
government is unwilling to address human rights issues.
26
WHO can strengthen the role of women in global tobacco control by linking the
Framework Convention against Tobacco (FCTC) with CEDAW. Both CEDAW and
CRC are going to prove helpful to strengthen FCTC as well. FCTC will inspire each
country to fight for its rights to be protected from tobacco through policies and
legislation. “We need an international response to an international problem” as Dr
Brundtland has said. These three conventions can also capitalize on the Beijing Platform
for Action and the United Nations Declaration on Violence Against Women, the
International Covenant on Economic Social and Cultural Rights and help fight the
industry to uproot the dangerous consumable artical which harms when used as
recommended.
27
The WHO International Conference on
Global Tobacco Control Law:
Towards a WHO Framework Convention on Tobacco Control
7 to 9 ianuanf 2000, New Delhi, India
Paper
Multisectoral and bbwswmmD Approach a®
Tobacco Control
Author
Dr. Kishore Chaudhry,
Deputy Director General, Indian Council of Medical Research,
Ansari Hagar, Post Box No. 4911, New Delhi -110 029, India
This paper is commissioned by, and produced for the World Health Organization, Geneva
The magnitude of global tobacco epidemic has tremendously increased since 1950s,
despite of wide reading and acknowledgement of the mounting evidence of the association of
tobacco use with more than 25 diseases1. Tobacco is responsible for death of an estimated 3.5
to 4 million persons each year. However, frightening are the projections for the decade 2020-
2030, when it is expected to kill about 10 million people annually. About 70% of these deaths
would occur in developing countries, where the epidemic is currently on the increase and where
the efforts for its control are not optimal. Despite of clear description and understanding of
modalities for tobacco control, more than one billion people around the world use tobacco and
this will continue to increase due to increase in third world population, poor knowledge of health
risks in many populations, increased prevalence of tobacco use, intensive marketing by
transnational tobacco companies, poor funding for control programmes and difficulties in
implementation.
Although the important role of sectors other than health has been realized for a long
time, the tobacco control has largely been restricted to a public health initiative. Over the 20th
century, tobacco production has seen tremendous systematic growth. This has resulted in a
complex relationship and dependence between the tobacco growers, processors, product
manufacturers, transporters, traders, advertising agencies, users and the regulatory authorities
like agriculture experts, governments, etc. (Fig. 1). These sectors considered the immediate
economic effect as positive contribution to the society. On the other hand, the delayed health
effects were given a backseat with health sector struggling to manage the ever increasing load
of patients of tobacco related diseases. While health sector tried various modalities for tobacco
control, tobacco manufacturers adopted various measures for promotion of tobacco use, often
with active support of sectors other than health. The lobbying by tobacco industry has resulted in
conflict between objectives of different sectors connected with tobacco. Although, the argument
of health sector regarding tobacco’s role in increased morbidity and mortality is quietly accepted
by all, agricultural experts continue to improve the yield of tobacco and provide facilities to
growers; commerce and trade sector continuously harps on the economic contribution by
tobacco; mass media does not wish to loose its earnings by banning tobacco advertisements;
and educational institutions often express inability to provide wider coverage on tobacco
education on account of already heavy curriculum. Clearly, the priority of different sectors is
limited to the boundaries of their respective expertise, and the need for a social change and
action for tobacco control as a social cause has not been realized by them.
Fig. 1
Multisectoral Connections of Tobacco
Other Connected Industries
Tobacco Trade
Farmers
Paper________________________
Wholesalers
Agriculture Labourers
Tendu Leaf__________________
Retailers________
Arecanut________ ____________
Sales Managers
Tobacco Industry
Fertilizers
Irrigation
Match Box
Tobacco Nurseries
Cigarette Lighter
Tobacco Curing
Advertising Media___________
Tobacco Processors
Transportation
Tendu Leaf Collector
Health Services
Bidi Rollers
Welfare Services
Betel Leaf Growers
Revenue Agencies
Tobacco Factories
Customs & Excise
Trade & Commerce
Consumer Affairs
Labour
International Trade
Law & Justice
Education
Environment
Global Concern and Initiatives for Intersectoral Approach for Tobacco Control
There have been some good collaborative efforts between health and other sectors on
tobacco control. Educational efforts through mass media are an excellent example of
intersectoral activity for tobacco control. In some developed countries, no other health topic has
received consistent and diverse media coverage2. In USA, after the Fairness Doctrine in 1960s,
the Public Service Announcements on tobacco had high frequency, extended reach and long
duration, but later were reduced to smaller number of spots often at odd times, due to increased
competition from other areas and consideration of the issue as old by the media managers. This
2
resulted in more anti-tobacco messages being transmitted as paid advertisements rather than
as collaborative activities between sectors. Anti-tobacco awareness through educational
institutions has also been a successful example of intersectoral and even multisectoral
collaboration (also involving mass media) in some countries. Multisectoral approach adopted in
Bangladesh for substitution of tobacco crop (described elsewhere) involved religion, education,
health and other social set ups.
Collaboration with sectors like agriculture and commerce has been at the other end of
the spectrum, where any major tobacco control activities by health sector has often been
resisted. These sectors have actually been using taxpayers’ money to subsidize the tobacco
industry, in developed as well as in developing countries3. Law sector requires a special
mention. Its role cuts across most of the strategies for tobacco control. Through appropriate
legislation, it can not only control tobacco usage by the community, but also would indicate the
policy direction of the government and create a positive social environment for tobacco control.
World Health Organization (WHO), since its inception recognized the importance of
intersectoral action in health protection and included this aspect in its constitution. The concern
on tobacco is reflected by adoption of resolutions by World Health Assembly on national and
international tobacco control measures. The resolutions call on member states to implement
comprehensive tobacco control strategies, including actions related to protection of nonsmokers, educational efforts, elimination of social & behavioural incentives promoting tobacco
use, prominent warnings on tobacco products, promotion of viable economic alternatives to
tobacco production, etc. Intersectoral action for health was also an important component in
achieving the goal of “Health for All by the Year 2000 AD”. The need for intersectoral action in
O
health has been emphasized in many conferences4. Intersectoral Action for Health (IAH) was
established at WHO headquarter in 1996 in support of the renewal of the policy of “Health for All
in the 21s1 Century”. Intersectoral work in health (including tobacco) at the local, national, and
global level was extensively reviewed5,6' This background work provided a frame of reference for
the International conference on “Intersectoral Action for Health”, in Canada in 1997. This
conference defined intersectoral action for health as “a recognized relationship between part or
parts of the health sector with part or parts of another sector which has been formed to take
action on an issue to achieve health outcomes (or intermediate health outcomes) in a way that is
more effective, efficient or sustainable than could be achieved by the health sector acting
alone”7. On the basis of current experience and research in various fields, including reduction of
tobacco use, the conference validated the partnership approach and recommended that the
success must continue to be documented and analysed more systematically to determine what
works under which political, social and cultural conditions. Benchmarks and best practices must
3
be established (including measurements and evaluation models) and the results communicated
better and more widely. The experts felt that analytical framework and tools are needed for more
quantitative indicators, instead of reliance on anecdotal descriptive accounts.
International health community has recognized that tobacco control efforts must come
from all sectors and a partial solution to this problem is not enough. The key elements for
tobacco control recommended by World Health Assembly, for comprehensive tobacco control
programmes include measures from various sectors, such as, health, finance & treasury,
customs & excise, trade & commerce, consumer affairs, agriculture, external affairs &
international trade, law & justice, labour, transport & public service, education, environment,
defense, culture & sports, and religion (WHO Fact Sheet No. 159. Governments for a tobaccoFree World. May 1998).
Religion is a comparative arena for collaborative work on tobacco control. As most
religions preach promotion of healthy lifestyle and religious preaching have a tremendous
following, tobacco control efforts through religious organizations is likely to be effective. Despite
of moral injunction underlying almost all religion, most representatives of institutional religions
have been relatively silent on issue of investments on tobacco8. Potential of religion in tobacco
control is increasingly being realized during the recent years. It is probable that the ancient
scriptures from various religions may not mention about tobacco, as the substance was probably
not known at that time. However, tobacco use is prohibited among Sikhs on account of religious
sanctions. Discussions during the WHO meeting on Tobacco and Religion9 in 1999, indicated
that most religions would promote healthy lifestyle and tobacco use would not be compatible
with religious preaching and therefore, religious communities have a significant role to play in
tobacco control. The meeting recommended collaborations with religious organizations on
evidence-based education programmes.
Increasing use of tobacco products in any society would result in greater social
acceptance of the tobacco use. While health sector people may be more enlightened about the
health hazards of tobacco and may have actually seen the patients’ suffering due to tobacco
related diseases, other sectors although aware of the hazards, may not perceive it as a real
threat due to its social acceptance. Also due to the common observation of frequent use of
tobacco product, they may conceive it as an uphill task and often a utopian dream. Thus, many
sectors other than health, agree with the health hazards due to tobacco and the need for its
control, but lack a drive to carry out intervention programme as an activity of their own Often
such collaboration would turn out to be short-term passive actions by these agencies A greater
interaction between different sectors, the understanding of the problem, and comprehensive
planning and execution by all the concerned sectors, seems to be the only practical strategy for
''
an effective and long-term control of tobacco. The attempt in this communication is to identify
the role and scope of intersectoral and multisectoral approach for tobacco control, with specific
examples from India on past efforts as well on scope for future collaboration. Law sector does
not find its mention in the specific strategies, because when these strategies get implemented,
often a legislative change has already taken place. Therefore, interaction of law with other
concerned sectors is extremely important before as well as after the promulgation of any
legislation for its appropriate framing and implementation.
Indian Experience on Multisectoral and Intersectoral Collaboration in Tobacco
Control
Like many other countries, India also faces a conflict of objectives of various sectors
connected with tobacco10. The Ministry of Health & Family Welfare is convinced about the need
for tobacco control measures, and has taken many administrative steps for reduction of tobacco
use. However, other sectors in view of their mandate have often resisted some of tobacco
control actions or have actually been working for promotion of tobacco use. The Directorate of
Tobacco Development, in collaboration with State Departments of Agriculture, primarily aims at
planning, coordinating and supervising development and marketing programmes of tobacco at
national level. The Indian Tobacco Development Council, constituted in 1966, serves as an
advisory body for this purpose. This Directorate is implementing programmes on production and
distribution of pure seeds and seedlings of tobacco, and on training in improved methods of
tobacco cultivation to the farmers. The Central Tobacco Research Institute is conducting
research on improving the yield and quality of tobacco. A multicentre project by Indian Council of
Agricultural Research helps in agronomy, plant breeding, soil chemistry entomology and plant
pathology, as related to tobacco. The main functions of Tobacco Board, constituted in 1976 are,
regulation of production of Virginia tobacco, ensuring fair and remunerative prices to the
growers, maintenance & improvement of existing markets, and development of new markets for
Indian tobacco outside the country. While the Tobacco Board is concentrating on Virginia
tobacco, the interests of non-Virginia tobacco are being looked after since 1983, by the National
Cooperative Tobacco Growers Federation Limited.
Agriculture is not the only sector in India that resists major tobacco control initiatives. The
labour sector points out the prospect of millions of bidi rollers loosing their job due to major
tobacco control actions, the upheaval in unemployment among farmers is expressed by
agriculture sector, and the prospect of reduced revenue in slow economic conditions is not
considered practical by the financial sector. While there have been dialogues between health
and other sectors on tobacco control measures, there has been a limited progress towards
„
tnhareo control and for development of a national
development of a concerted programme for tobacc
policy on tobacco.
The need for intersectoral and multisectoral collaboration for tobacco control in India has
been realized for more than a decade. Realizing the potential of edcational institutions, the
Indian Council of Medical Research (ICMR) carried out a research project in Goa, from 1986 to
1992, on anti-tobacco community education through school children. The project tested the
feasibility and efficacy of educating school children in empowering them for non-initiation of
tobacco use and the effect of this education on the tobacco use prevalence in the community,
through children-parent interaction. The prevalence rates of tobacco habit were determined
through baseline survey, mid-term survey and a final community survey. The overall reduction in
the prevalence of tobacco usage among men was 11.8% & 13.4% in two experimental areas
and 2.0% in control area. Decrease in prevalence of tobacco use among women was 9.1% and
13.3% in two experimental areas and 10.2% in control area. Based on the experience of this
project, Ministry of Education, Goa, agreed to include an 8 hour course on tobacco as a part of
co-curricular activities for standard five and above.
Agricultural experts participated in a workshop organized by health sector on tobacco
and health in 1987, and presented their experiences on alternate substitutes of tobacco by other
crops and alternate uses of bidi tobacco11. Comparison of net realization from tobacco in Gujarat
with other crops grown in Middle Gujarat revealed that irrigated castor and irrigated cotton
fetched better per hectare profit than tobacco. Rotation of tobacco crop with other crops also
provides more remuneration than producing only tobacco crop in the field. The anticipated
problems in substitution of tobacco with other crops included, advantage of tobacco crop against
theft and stray cattle; specialized facilities created for tobacco processing which can not be used
for any other crops; increased chances of pesticide residues with other crops; the difficulties of
finding a substitute crop in rain-fed area in view of the drought resistant nature of tobacco crop;
and the dependency of millions of people on bidi rolling and tendu leaf collection. Alternate uses
of bidi tobacco included extraction of nicotine sulphate to be used as pesticide in orchards;
pharmaceutical grade organic acids and solanesol; food grade tobacco leaf protein; and
pentosans for production of ferfural, an industrial solvent.
During an ICMR meeting on tobacco related health hazards in 1989, agriculture experts
informed that technology for lowering the tar and nicotine levels in tobacco did exist in the
country. The newly developed technique of bright air curing would decrease the problem of
deforestation. The tobacco crop can also be used for production of vegetable oils More
remunerative alternate crops did exist in different areas, but excess production of these crops
was likely to bring down their prices, thus, rendering them non-remunerative.
6
A major success in intersectoral approach for tobacco control was the collaborative
project between ICMR and All India Radio, the state owned and only radio network in India. The
acronym DATE stood for Drugs, Alcohol, and Tobacco Education. The radio programme was in
the form of 30 weekly episodes of 20 minutes each. Ten episodes focussed on tobacco, eight
each on alcohol and drugs, and two episodes on legal aspects12. The introductory and
concluding episodes touched all the three themes. The episodes were broadcast from 84
stations of All India Radio (out of 104 existing at that time) at prime time, simultaneously in
sixteen languages. The Hindi prototype was sent to selected radio stations of All India Radio for
translation in regional language, as per the specified guidelines. The broadcast was during a
specified time (between 8.00 A.M. and 9.00 A.M. on Sundays, with a repeat broadcast during
the week, generally in the evening). The reach and effect of the tobacco component of the
programme was evaluated through two community based surveys, carried out after the
broadcast of tobacco episodes (which was the first topic to be covered), in areas not having any
organized anti-tobacco programmes. The surveys showed that the potential listeners of radio
comprised 80.4% of the population in Goa and 59.1% of the population in Karnataka. In
Karnataka 31.6% of the potential listeners and in Goa 26.7% of the potential listeners, heard at
least one of the first eleven episodes (on tobacco). Most of the listeners considered the
programme to be very good or good, and felt that it would have effect on the tobacco users to
quit their habit as well as on children to prevent the initiation of habit. About 4% tobacco users in
Goa and about 6% users in Karnataka quit their habit after hearing the programme. About 98%
to 99% of the listeners expressed that such programmes should continue.
The major impetus for multisectoral approach for tobacco control occurred in 1995, with
submission of the twenty second report of the Indian Parliament’s committee on sub-ordinate
legislation (Tenth Lok Sabha), the recommendations of which have also been briefly reported by
Chaudhry & Unnikrishnan13. The committee consisted of Members of Parliament and considered
the information and views of various ministries, departments, experts and unions/ associations,
connected with tobacco control as well as tobacco promotion. Considering the issue of tobacco
in totality, the committee made wide-ranging recommendations, including, strong & rotatory
warning in regional languages on tobacco products; ban on direct as well as indirect
advertisements of tobacco products; prohibition of smoking in public places; initiation of
measures for awareness on tobacco through health infrastructure, educational institutions and
mass media; and initiation of efforts for persuasion of farmers to switch over to alternate crops.
The recommendations of Parliament’s committee, although not binding on the government, are
considered in high esteem and the government makes efforts towards their implementation. The
subsequently heightened "political and bureaucratic will" on tobacco control did see some
actions from various ministries/ departments on tobacco control. The Ministry of Agriculture
requested major tobacco growing states to consider actions for reduction in production of non-
FCV tobacco. Efforts were initiated in the states of Andhra Pradesh, Tamil Nadu, Orissa and
Karnatka. The Department of Agriculture and Cooperation and Indian Council of Agriculture
Research in a joint meeting decided to explore the potential of alternative crops like, medicinal
plants, soybean, sugar cane, waxy type maize, oil palm, vegetables, etc. It was considered that
the schemes for assistance to tobacco system should be discontinued. Research efforts should
concentrate on development of low-tar low-nicotine FCV tobacco crop, and on alternate uses of
tobacco. A scheme be chalked out for weaning away of farmers from cultivation of non-FCV
tobacco. Follow up discussion on implementation of these recommendations with various
concerned ministries showed that various concerned sectors are conducive to drastic measures
for tobacco control, but also pointed out their fallout on Indian economy and trade.
The Government of India realizes that the problem of tobacco in India is complex in view
of varied nature of tobacco use, many sectors being unorganized and under control of different
agencies. The control of tobacco can effectively be carried out, only with a multisectoral
approach involving various concerned sectors. A number of meetings have been organized
between health and other sectors to impress upon the urgent need for tobacco control in the
country and to find out effective modalities in different sectors for this purpose. Strategies for
different sectors are being identified for effective tobacco control in the community, which would
help in planning the national strategy for tobacco control in India during the new millennium.
Workshops on tobacco control are proposed for sectors other than health to stimulate them for
undertaking control programmes as an activity of their own. While major breakthroughs in
multisectoral approach for tobacco control have not yet been achieved in India, it is likely that
the background efforts made in this direction during the last few years would yield good
dividends in the form of different sectors taking the issue of tobacco control as a social
responsibility and not merely endorsing the actions by the health sector.
Major Modalities of Tobacco Control and Scope for Multisectoral and Intersectoral
Approach
Government Policy on Tobacco
Like in many other countries, India is also facing a paradox, wherein some government
agencies are working towards promotion of tobacco, while other departments are working for
control of tobacco use. It is important that the government considers the priorities and takes a
policy decision for unified direction of working for control of tobacco use. Generation of such
“political will” may seriously open the possibility of consideration of the most crucial but so far
neglected issue of crop substitution. Availability of a policy framework is likely to help in
promulgation of legislations, which is an important tool for tobacco control. Legislation may not
only force people to reduce or quit their tobacco use, it can also help in creation of a social
environment, wherein tobacco use would be considered as a deviant behaviour. Such a
situation would be useful for achieving the goal of a "Tobacco Free Society".
Generally, it is believed by the scientists that the money spent for the treatment of
tobacco related diseases is much more than the revenue generated by tobacco. In order to
collect authentic figures on it, the ICMR initiated a project for studying the tobacco economics in
the country. Under the project, the data on cost of management of tobacco related diseases, is
being collected. The information on tobacco economics and the education of politicians and
administrators is likely to increase their will to initiate more anti-tobacco activities.
However, in view of the contradictory objectives of different sectors, a policy decision on
tobacco would not be easy. The policy-makers in different sectors are also influenced by the
societal norms related to tobacco. A regular interaction and discussion of issue between sectors
is important to enable them to identify the enormous magnitude of the diseases associated with
tobacco use, get convinced about the need to take drastic actions, search and plan strategies
for tobacco control related to their area of expertise and execute the plans as their social and
humanitarian duty.
Economics of Tobacco
An often-quoted reason for governmental inertia in taking strict tobacco control actions is
the economic implications of tobacco use. The direct expenditure on treatment of tobacco
related diseases and as well as its indirect cost, both are to be considered while calculating the
costs due to tobacco14. It would however, be useful to consider the economics of tobacco from
the point of view of merit and demerit goods, which means that any revenue or income related to
unacceptable products should also be considered as unacceptable to the society, irrespective of
the quantum of its contribution to the economy. The studies on economics of tobacco generally
indicate that the costs incurred by society due to tobacco use more or less match the benefits
received by the society3. However, most of these studies have considered only the direct
expenses on treatment of tobacco related diseases. The indirect cost of tobacco use, the
ecological effects of tobacco production and use, have generally not been used in models for
computation of economics of tobacco. The models have also not considered the alternate use of
money by community, if it is not spent on tobacco. Similarly, the revenue provision by an
alternate crop (in place of tobacco) also needs consideration in an economic model on the
subject.
The studies related to economics of tobacco are important to convince the decision
makers about the need to initiate more strict measures for control of tobacco. In a review of the
9
■■ i n
orfh ncMR) it was observed that data on cost of
subject at the Indian Council of Medical Research (IC
),
„ . owoiiahip in India. Studies on cost of
management of tobacco related diseases were not ava
heart disease (CHD); and chronic obstructive
management of tobacco related cancers, coronary hear
lung diseases (COLD) were carried out by ICMR. The study collected data from patients of
these diseases on the expenditure incurred by them on diagnosis & treatment of their disease,
expenses incurred on travel for their treatment/ diagnosis, additional expenses for lodging &
food during the treatment period, loss of wages because of the disease, and expenses incurred
by their relatives/ friends. The expenditure incurred by the treating institution on management of
these patients was also collected. In case of premature death, the cost imposed upon the
society (due to premature death) was calculated. The average cost due to a case of tobacco
related cancer was observed to be Rupees 134,449 (discounted at 1990 level - the year the
study began)15. The patients in the cohort spent an average of Rupees 17,965 (including loss of
income due to absenteeism), with another Rupees 4,009 being contributed by the institution in
the form of various services. The loss due to premature deaths of patients of tobacco related
cancers amounted to Rupees 112,475. Using discounting methodology as applied in the study,
the average cost of tobacco related cancers for the year 2000 would be approximately Rs.
350,000 per case. The report on cost of CHD and COLD in India is likely to be available shortly.
Taxation on Tobacco Products
Price of tobacco products vis-a-vis the income level of the community is one of the major
factors influencing the extent of its use by the society. Relative variations in the price of tobacco
products through increase in taxation or through changes in paying capacity of the people has
one of the clearest and most immediate influences on tobacco use. In order to adjust for the two
variables, real price of cigarettes (current price/ price of all goods and services) at different time
periods have been compared with the consumption of cigarettes. Such comparisons in UK,
Canada, and South Africa over the last 2 to 3 decades have shown counter movements of
smoking with relative cigarette price16. This data indicates that if prices are increased the
smoking rate declines, but it tends to increase with a decrease in price of cigarettes in
comparison with the inflationary trends. Thus, a sustained increase in price, which is more than
the inflation rate is necessary for the optimum effect of this measure.
The effect of price increase due to taxation is not uniform over all strata of the
community. The most price sensitive smokers have been found to be women and men aged 2560 years. Variable results have been reported from USA nn
»
h
u irom usa on effect on younger population, who
generally has low incomes but a high proportion available for hh
p < non available for discretionary expenditure. In some
countries low-income groups tend to smoke more, but also red, ire th •
, ,
uiaiso reduce their smoking in response to
tax■ increase. Conversely, they are also
likelv
o encouraged to smoke by a reduction in real
aisollk
ely tn
to h
be
price. UK data does suggest that. Price responsiveness tenHct u
s tends to be particularly high among
10
people in disadvantaged circumstances, and they reduce consumption and expenditure on
cigarettes in the wake of a price rise. In many societies, the price elasticity of demand for
cigarettes by the adult population is around -0.5, i.e. a tax rise which increases the price by 10%
is likely to reduce smoking by 5%. However, taxation rate on other tobacco products would also
determine if sensitive people are likely to quit tobacco use or they may shift to other related
products. This suggests that although increased taxation would be a good modality for tobacco
control, each country would need to examine it closely in their own circumstances to develop an
optimum strategy and fall outs and consequent actions indicated for other sectors.
A wide variety of tobacco products are sold in India. It is smoked in the form of bidis,
cigarettes, hookah, chilum, cheroot, chutta, etc. The common forms of smokeless tobacco use
include betel quid, pan masala, chewing tobacco, khaini, misheri, etc. About 19% of tobacco in
India is consumed in the form of cigarettes, while 53% is smoked as bidis. Remaining tobacco is
used mainly in smokeless forms. Different modalities do differ in terms of quantum of tobacco
per unit consumption. An average cigarette has about 1 g tobacco while an average bidi has
about 0.2 to 0.25 g of tobacco. The unit quantum used for chewing purposes is also smaller than
a cigarette. However, analysis shows that the levels of tar and nicotine in a bidi are comparable
or higher than Indian cigarette, which in turn are higher than their levels in developed countries.
/
The central government tax structure on tobacco products is as complex as its available
variety. Unmanufactured tobacco (which is mainly used for chewing purposes) not bearing a
brand name does not have any excise duty on it. Chewing tobacco and snuff with a brand name
attracts 50% excise duty (ad valorum) on it. Till the year 1994-95, 40% tax was being levied on
chewing tobacco. There is no tax on cigars and cheroots. Smoking mixtures for pipes and
cigarettes has a tax rate of 300% ad valorum. Bidi manufacturers producing less than 2 million
O
pieces annually do not have to pay tax. Bidis (other than paper rolled) produced without the aid
of machines needs to pay Rs. 5 per thousand pieces. Other bidi manufacturers are currently
paying tax of Rs 15.5 per thousand pieces. Currently pan masala is taxed at 40% ad valorum
(24% basic duty plus a special duty of 16%). Majority of tobacco taxes is from cigarettes. During
the financial year 1997-98, the cigarette industry contributed an estimated Rs. 55 Billion. In
1987, the excise structure on cigarettes was changed from ad valorum to specific duty rates on
the basis of length. The current excise rates applicable on filter cigarettes vary from Rs 1,470
per thousand pieces on cigarettes longer than 85 mm to Rs 550 per thousand pieces for
cigarettes smaller than 70 mm (Table 1). The excise on non-filtered cigarettes is still less, being
Rs 370 per thousand pieces on 60 to 70 mm long cigarettes and Rs 110 per thousand on
smaller cigarettes. During the financial year 1999-2000, excise duty was increased by 10% on
non-filtered cigarettes smaller than 60 mm. Taxes on all other cigarettes remained same as last
decreased sales, the sale during 1998-99 being 13% less than the sales in 1997-98 (extract
from speech by Mr. Y.C. Deveshwar, Chairman, ITC Limited at the 88th Annual General Meeting
of the Company on 30.7.99. The Times of India, New Delhi, 7th August 1999, page 19).
An account of tobacco taxation policy of India suggests that it has not been governed by
health hazards of these products. The rates of taxation have been generally in line with the
guiding government concern that the people in the lowest strata of community should pay lesser
taxes. The smokeless tobacco products, common among rural masses, are not taxed. Bidis,
which are known to be used by people in lower economic strata, were not taxed till early 1990s,
- but currently are being taxed lightly. The non-filtered cigarettes attract a much lower tax than
filtered cigarettes, and cigarette companies aim the sale of highly taxed cigarettes towards the
higher socio-economic groups of the society. The Ministry of Finance tried to keep the prices of
certain tobacco products cheaper for low-income groups. The fact was never considered that a
higher tobacco use rate among lower strata would also result in higher occurrence of tobacco
related diseases in this strata. It is important to note that the total amount spent by patients (as
well as by the government) on treatment of tobacco related cancers in India, does not differ
significantly according to socio-economic strata15.
A reason for no tax on unmanufactured tobacco has invariably been that this is an
unorganized sector and it would not be practical to impose tax on this sector. However, bidi
industry also belongs to a scattered small industrial sector. The operational problems related to
tax collection would remain the same irrespective of the taxation level. Thus, the rationale for a
low tax on bidis may not be associated with logistics. There has been no interaction of financial
experts with tobacco experts from other specialties, including health, regarding taxation on
tobacco products. The limited pleas from non-governmental organizations active in the field of
tobacco so far have not yielded the desired effect. It may not be entirely correct to blame the
financial experts for a disproportionate tobacco taxation policy. Often specialists in a field
concentrate on the aspects related to their sphere of expertise. In case of tobacco taxation, the
Ministry perhaps had been using the general principles as applicable to other products. A
greater interaction with specialists from other sectors like, health, commerce, agriculture, labour,
welfare, police, border security force, foreign affairs, etc., would help them assess the real
magnitude of hazards due to tobacco use and the positive influence which can be generated by
a rational taxation policy.
A well conceived taxation strategy should assess its likely implications and intersectoral
or multisectoral plans should be prepared to match the imbalance likely to result from it. For
example, if an increase in taxes on bidis is implemented, likely implications may be a shift of
tobacco users from bidi smoking to smokeless tobacco use, cessation of bidi smoking, a
13
a long time may not be conducive to generation of interest among the target popu.at.on to
explore more on the issue. On the contrary, it may lead to habituation, which means that the
warning is no longer noticed or read. The limitations of the current warning are: (.) the warning
still does not cover many tobacco products, most important being bidis; (ii) The printed warning
is in English, thereby reducing its reach only to persons knowing English; (iii) It is repetitive; (iv)
The colour combination of many cigarette packets does not permit its reading; (v) The size of
the warning on many hoardings and advertisements is very small in relation to its overall size;
and (vi) There was no monitoring regarding its implementation, and no action has been taken
against defaulters.
In view of these limitations, the Government of India proposes a comprehensive
legislation wherein a health warning would figure on all tobacco products and it would be in the
form of more telling slogans, like, "Tobacco can cause cancer", etc. The existing warning labels
in India are inadequate in many respects, including the language used. The Indian Parliament’s
committee on sub-ordinate legislation considered the issue in 1995. Its recommendations
included major changes in warning on all tobacco products, including, expanding the scope to all
tobacco products; warning being bilingual (English and local language); need for pictogrammes
indicating danger due to use of tobacco; coverage of at least 25% of package area for warnings;
colour combinations and legibility; and periodic rotation of warnings.
It has often been stated that bidi manufacture in India is a cottage industry where it is
supposedly difficult to enforce legislation. This may not be correct. Bidi rolling may be carried out
by people in their home or in a factory, but the next step in preparation of bidi (heating of the
rolled bidis and its packing) is carried out in comparatively smaller number of units, which can be
considered as small scale industries and can be brought under legislation. Moreover, the
packets of bidis do have their brand names and other information and printing of a health
warning on these packets is a distinct possibility. The Parliament’s committee on sub-ordinate
legislation on tobacco recommended printing of a warning on individual cigarettes as well.
Although some feel that it may not be possible, the fact that each cigarette has its name or logo
at exactly the same spot on individual cigarette suggests its feasibility.
In the past the enforcement of warning on tobacco products has not been at a desired
level. For optimum effect, it is necessary that the rules be enforced seriously. The rules for such
warnings could be framed by the Ministry of Health, or by other Ministries with the help of health
sector. However, enforcement of these measures is likely to be possible only with a social
awakening. Some deficiencies in enforcement of warnings in terms of legibility, hoardings not
providing lighting on warning part at night, the colour combination on cigarette packets, etc., had
been observed by many people, but they did not report the matter to concerned authorities.
16
Education is necessary about existence of such rules, its provisions and mechanism for
redressal, for optimum enforcement. Support from education, mass media and health sectors is
necessary for this purpose. Support from the enforcing authority (generally police) would also be
needed. The drafting of legislation on warning on tobacco products may be carried out by one
sector, but its enforcement does require a multisectoral approach. Non-governmental
organizations (NGOs) can play an important role in monitoring the implementation of legislative
measures.
Reduction of Tar and Nicotine Levels of Cigarettes and Bidis
The literature suggests that chance of development of lung cancer increases with high
concentration of tar in the smoked cigarettes20. Similar risk pattern has also been observed for
cancers of mouth, larynx and urinary bladder. A time trend analysis of the lung cancer incidence
"1
and reduction in levels of tar in cigarettes also suggests that the burden of lung cancer in the
community is likely to decrease by reduction in tar levels in cigarettes21. Benefits of reduction in
tar and nicotine levels in cigarettes have also been observed for coronary heart disease22.
However, benefits on respiratory symptoms or peak expiratory flow rates have not been
observed following reduction in tar and nicotine levels of cigarettes, mainly due to self
adjustment of smokers for nicotine delivery23 24. Self adjustment by smokers to maintain their
nicotine levels, has also been observed on changing to low-tar low nicotine cigarettes, either by
increasing the number of cigarettes smoked per day or by increasing the toxin yield to the body
through vigorous puffing25,26. While the effect of reduction of tar and nicotine levels of cigarettes
(and bidi) to a very low levels may need further studies, its reduction to medium or low levels
may be useful in Indian context, where the general level of tar in cigarettes or bidi is above 20
mg per piece. It may be emphasized that technology for reduction of tar & nicotine levels in
tobacco is available in India. Measures for this endeavour require active support from agriculture
sector to ensure adequate availability of tobacco with low levels of tar and nicotine and
development of curing/processing methodologies, which yields lower toxins.
The goal of tobacco control programme would be the cessation of habit by as many
people as possible. However, many people who can not quit the habit, but get enlightened about
reduced risk by smoking low tar & nicotine cigarettes, may prefer to choose a product with lower
levels of toxins. Therefore, it would be useful if the tar and nicotine levels are displayed on
cigarette and bidi packets. The considerations for implementation of this measure are similar to
those of warnings on tobacco products and those for reduction of toxin levels in tobacco. Labour
and commerce sectors would need to be convinced about its feasibility, since these sectors are
concerned about welfare of bidi industry, which may plead non-availability of resources.
Resources for testing levels of toxic in tobacco may be required to be set up, either by
agriculture or health sectors.
17
report would have been to find methods of rehabilitation and restructuring of agriculture
practices and economy, rather than merely painting of an imaginary gloomy picture. Education
of the community and interactive workshops involving various sectors would not only help in
acceptance of tobacco control measures by policy-makers and public at large, but also help in
quick identification of redressal mechanisms. The Delhi example clearly indicates that ban by
only one state government on tobacco advertisements helps only to a small extent, because
they do not control many other channels of tobacco advertisements. The problem of tobacco
advertisements through satellite channels requires intervention by the Ministry of Information
and Broadcasting. It would also require contact with other countries through sectors dealing with
.external affairs, in order to develop a unified policy on broadcasting ethics and regulations from
various soils. Effective implementation of the ban would invariably be from sectors other than
health, generally through police and NGOs.
Sponsorship of sports or cultural events by tobacco companies is considered as
surrogate advertisements of tobacco products. The decision-makers in India generally accept it
as a form of advertisements of tobacco products. However, concerned sectors plead the
availability of limited resources for undertaking sports and cultural events. However, they need
to realize that the tobacco industry sponsoring a sports event is only one of the bidders for the
purpose. For the purpose of intervention, one should not consider the quantum of money
provided by the tobacco company, but the gap between the bid by the concerned tobacco
company and the second highest bidder. For the Dhaka triangular cricket series of 1998, Wills
Sports provided a sponsorship fee of Rs. 350 million to the Cricket Board. The ITC Limited does
not consider it advertisement of their cigarette brand, but advertisement of their sports gear
company. However, the statement at the annual General Body Meeting of the company in 1999,
does not even mention it as a subsidiary of the parent company, despite of spending a large
amount on advertisement. It is only a continuous interaction between various sectors, which is
likely to highlight the discrepancies and provide solutions to such issues.
Ban on Smoking in Public Places
Public places are to be visited by all persons of the community and the ambient ’
environment is same for all. So far the tobacco smokers had the right to pollute the ambience
with tobacco smoke. However, the increasing knowledge about the harmful effects of passive
smoking has changed the scenario and many countries have imposed ban on smoking in public
places. In India, such a ban exists only in the states of Delhi and Kerala. The comprehensive
legislation from the central government, which includes provision for a ban in public places, has
so far not been placed before the Parliament. The ban in Delhi was promulgated on 26th Jnauary
1997 after discussion in Legislative Assembly. On the other hand, the ban in Kerala was after a
directive from its High Court and was implemented from 12th July 1999. The Delhi legislation
19
provides for ban on tobacco advertisements, smoking in public places, sale of tobacco smoking
substances to minors, and sale of tobacco smoking substance within an area of one hundred
meters from educational institutions. Some public places, like hospitals, dispensaries,
educational institutions, restaurants, public vehicles, etc, have been defined in Delhi notification,
but the government may, by notification in the official gazette, declare any place of public work
or use in Delhi to be a non-smoking place under this act. A major difference in the legislation in
two states is the definition of public places. While Delhi permits smoking in open spaces, Kerala
considers sidewalks, etc., also as public places and prohibits smoking there. The ban does not
seem to be getting implemented seriously in Delhi, but initial newspaper reports in Kerala
indicate a 30% reduction in sale of cigarettes during the first month of implementation. The
police is taking initiative in effective implementation of the legislation in Kerala. This clearly
indicates the need for an intersectoral and multisectoral approach for tobacco control.
Involvement of education and mass media sectors would further help in better acceptance of the
changing scenario by the community at large.
The Government of India, in 1990, issued an administrative order prohibiting smoking in
select public places like hospitals, dispensaries, educational institutions, conference rooms,
domestic air flights, air conditioned coaches in trains, sub-urban trains and air-conditioned
buses, etc. While the prohibition was successful in certain areas like domestic air flights,
implementation of the order in other areas is not complete and varies with implementing
authorities. Interestingly, it may alone not be the health sector to take such a lead on this issue.
Recently, Railways in India, banned sale of tobacco on Railway platforms. This directive was on
environment grounds and was announced on the World Environment Day in June 1999, which
was less than a week after the World No Tobacco Day on 31st May 1999. Ministry of
Environment initiated the legislation for tobacco control in Goa, which includes provision for
banning smoking and use of smokeless tobacco in public places. However, the bill has been
referred to the President of India for opinion and is still pending. This again indicates the
potential and possibility of other sectors in initiating effective tobacco control measures.
Community Education
Tobacco use has become an established habit all over the world. The eradication of
tobacco related diseases, therefore would not only require political actions but also a social
change. This change can be brought about by education of the community regarding health
hazards of tobacco. Anti-tobacco education would be required to be targeted at decision
makers, professionals and the general public, especially the youth.
In India, a prospective behaviour intervention study on feasibility and effectiveness of
primary prevention of oral cancer, through anti-tobacco education, was a pioneering step by
20
Tata Institute of Fundamental Research, Bombay. The study was conducted in three areas. The
study showed that after an intervention of ten years, a significantly higher proportion of persons
in the intervention group stopped tobacco usage as compared to a control cohort28. Initial efforts
by the government of India on anti-tobacco education were through the implementation of
National Cancer Control Programme, in view of the fact that half of the cancers among men and
about one fifth of the cancers among women in India related to tobacco related sites. The anti
tobacco community education activities have been initiated in 39 districts through district level
projects for control of cancers. The Indian Council of medical research (ICMR) carried out
studies on anti-tobacco community education through involvement of existing infrastructures.
The studies involved radio, health infrastructure, schools and community volunteers. The results
showed that all these infrastructures can reduce the tobacco prevalence, if motivated
adequately.
Covering a large population for educational purposes would be a formidable and
unthinkable job without the support from mass media. The experience suggests that such
programmes would be most cost-effective, if media managers consider it as their own
programme and not take it as a liability to be fulfilled since a directive was received from a
government agency. They however, need support from health sector for availability of reliable
and impartial information on the subject. They invariably wish to feature experts from health
sector in their programme/ write up, to increase its authenticity.
Support from education sector is also paramount in providing information on tobacco and
its hazards to children and youth. Literature from India indicates that a large number of children
start experimenting with tobacco around the age of 10 years or earlier. Many of them tend to
turn regular tobacco users about the age of 15 years. Therefore, earlier the provision of
education on tobacco, better would be the expected results. Proper education at this
impressionable age would help them in developing a personality empowered with courage to not
only refuse the temptation for initiation of tobacco products, but also advise tobacco users to quit
their habit. Such an effect has been observed in ICMR’s study on the subject in Goa.
Ban on Tobacco products
In response to a directive from Jaipur High Court, a committee on health hazards of pan
masala containing tobacco was constituted by the Directorate General of Health Services. The
committee examined the data related to this newer tobacco mixture (about 2 decades old) and
other related mixtures being used in India. The committee’s report was considered by the
Central Committee on Food Standards in November 1997, and recommended a ban on chewing
tobacco in the country. An inter-ministerial meeting called by the Ministry of Health & Family
Welfare discussed the feasibility of such a recommendation. A major problem in decision-
21
making at such times is the logistics involved in implementation of such bans. Example of
another ban, which does not find implementation also, exists in India. The government has
banned the addition of tobacco in toothpaste and toothpowder. The appeal by manufacturers in
the Supreme Court was rejected in 1997, and the ban was notified. However, toothpastes
containing tobacco are still freely available in the country. Social awareness is of paramount
importance in effective implementation of such a ban. Implementation in a ban on chewing
tobacco would require consideration of aspects related to crop substitution by tobacco farmers,
rehabilitation of certain people connected with processing & trade, and support to existing
tobacco users to empower them in quitting the habit so that they don’t shift to other tobacco
habits. Only a concerted action by various concerned sectors can help in effective
implementation of such a ban.
Substitution of Tobacco with Alternate Crops
Literature on tobacco cultivation indicates that for profitable production, tobacco
cultivation does require proper inputs like watering at appropriate times, fertilizers, etc. In many
areas, tobacco cultivation has been shown to be more profitable to the farmers as compared to
other crops grown in the same area. However, such comparison may be artificial, as tobacco
crop may be enjoying certain facilities, which helps in increased yield of the crop and thus bigger
margin of profit. It has been often projected that due to higher remuneration, farmers are not
willing to shift to other crops. This indeed is true in many parts of world, including India. It is
logical to conclude that the farmers are growing tobacco for a monetary return and not for any
loyalty to any crop. Thus, if facilities for cultivation, and the confidence of a minimum support
price at which their produce would be bought by the government or private traders are
withdrawn, the farmers may be willing to shift to alternate crop cultivation.
The Canadian Department of Agriculture carried out a programme for tobacco
diversification in 1987, through provision of incentives to tobacco farmers. The plan was
developed in response to decreased demand for tobacco. Under the Tobacco Transition
Adjustment component of the plan, the farmers were provided cash payment to those agreeing
to stop growing tobacco. The Alternative Enterprise Initiative component provided financial
assistance for specific alternatives to tobacco farming. A 55% decline in number of farms was
observed from 2,916 farms in 1981 to 1,326 farms in 1992. Tobacco Transition Adjustment
Initiative was found to be more successful, with many of the farmers shifting to manufacturing
and service sectors29.
The Bangladesh Cancer Society carried out a demonstration project on tobacco crop
substitution through locally generated funds. About three-quarters of adults in the 15,000 rural
population were found to be tobacco users, with most of the men using bidi or hand rolled
22
cigarettes and women using chewing tobacco. Tobacco growing was also wide spread in the
area. Intervention was through convincing religious leaders, teachers, health care workers, and
other opinion leaders of the importance of discouraging tobacco use by the community.
Agricultural extension workers advised the local tobacco farmers on how to switch from tobacco
production to other food crops such as bananas, okra and maize. Preliminary evaluation after
three years’ intervention showed a dramatic decline in tobacco use. Crop substitution could be
carried out successfully. Okra production was yielding farmers four times more money than they
had earned through tobacco. Local sale of okra helped in enhancing the nutritional status of the
community30.
The Canadian tobacco crop substitution experiment was carried out at a time, when their
tobacco market was at a decline and could not support all the farmers. Therefore, rehabilitation
7
of these farmers had become more or less a compulsion for the agriculture sector. However,
such situations would generally not exist in most countries. Bangladesh also had an advantage
that many alternate crops grown in the area were known to be more profitable than the tobacco
farming31.
Currently in India, tobacco is grown over 0.4 million hectare land, which is less than 1%
of the total cropped area of the country. The maximum land allocation for tobacco cultivation
was in the years 1977 and 1982 (0.5 million hectares). However, the years following these
bumper crop times had also seen the maximum decline in land allocation in the history of
tobacco cultivation in India. A reduction or increase of about 2 to 6% in the area used for
tobacco cultivation has been a usual feature, but there have been three instances of more than
10% reduction in land allocation for tobacco cultivation during the last three decades. The
highest reduction over the preceding year, was seen in 1978 (18%), followed by 16% in 1974
'7
and 12% in 1983. The data suggests that a reduction up to 10% in land allocation for tobacco
cultivation may not have any perceivable effect on agriculture practice, and with well conceived
tobacco crop substitution strategies, even a reduction of about 20% should also be feasible.
About 80% of the Indian tobacco crop is for consumption within the country. The country
has not experienced major reduction in tobacco consumption, which could create urgency for
tobacco crop substitution. Agriculture sector is actually supporting tobacco farming through
provision of tobacco seedlings to farmers, assurance of a minimum support price for their
produce, provision of platforms for auction of their crop, etc. Research by the Indian agriculture
sector has resulted in availability of higher yielding varieties of tobacco. This along with
availability of good seeds and better irrigation facilities has resulted in increase of average
national per hectare tobacco yield from 731 Kg in 1950-51 to 1,501 Kg in 1994-95.
23
Indian agriculture sector has not embarked on to any systematic experiment for
substitution of tobacco crop by some other crop. Comparisons have been carried out on profit to
the farmers from growing tobacco or other crops commonly grown in that area. The comparison
does indicate that many other crops can be grown in that soil and also that some of the crops
can be more remunerative than tobacco. Some of the alternative crops identified and suggested
by Tobacco Board of India are, groundnut, sunflower, mustard, soybean, maize, coriander,
cotton, Bengal gram and some medicinal plants. The argument by agriculture experts is that
these crops may not remain remunerative if the quantum of their produce increases. However,
this argument would be true for any crop, including tobacco. A very high production of tobacco
on two occasions (1977 & 1982) has seen maximum reduction in the land used for tobacco crop
in immediately succeeding years. Such phenomenon by farmers is expected because the
returns from tobacco during the high production year would be lower than anticipated. The
comparative profitability of crops also keeps changing from year to year. The data on cost of
cultivation of tobacco from Central Tobacco Research Institute indicates that the cost of
cultivation of tobacco does not differ significantly, but the profit to farmers may vary depending
upon the unit area yield of the produce. For example in 1994-95, net return to a tobacco farmer
in Bihar growing a high yielding variety (2,500 Kg per hectare) of Pusa chewing tobacco was Rs.
49, 432 per hectare, compared to a return of Rs. 22,010 per hectare for a farmer growing Bandi
variety of tobacco. The input cost for these farmers was comparable, at Rs. 25,568 for Pusa and
Rs. 22,990 for Bandi.
In today’s scenario, agricultural scientists would not consider the gradual substitution of
tobacco crop as practical. However, it must be realized that easy availability of tobacco products
may defeat the very purpose of legislative and educational action towards of control of tobacco
use. Therefore, it is important that the issue of tobacco crop substitution is taken seriously. It is
important that the agriculture scientists consider this measure as a distinct possibility. The fear
of dependency of a large number of persons on tobacco cultivation and trade has often been
projected as a major hindrance for major tobacco control steps. A closer look at the agricultural
practices shows that tobacco farmers may not be dependent solely on tobacco crop. They do
grow other crops in between the tobacco-growing season. A majority of agricultural force
dependent on tobacco is in the form of labourers, who would still find their job intact (with same
wages) if the tobacco crop were substituted with any other crop. Today many alternate crops are
not as remunerative as tobacco, due to the fact that over a period of time the soil has been
conditioned to suit tobacco cultivation. Such a situation is likely to change in a few years if a
serious effort for tobacco crop substitution is initiated. A large number of retailers, especially in
rural areas do not sell tobacco products alone, but it is one of the many items being sold by
them. Thus, gradual reduction of tobacco use would not finish their income, but at the maximum
may result in small gradual reduction of income.
24
While decreased demand of tobacco may force the tobacco farmers to seek alternative
crop cultivation, the reduced tobacco cultivation can also result in reduced availability of tobacco
leading to price escalation and thus, reduced consumption. However, agriculture sector may not
consider a major action of crop substitution on its own. It is important that the steps for demand
and production are suitably planned and matched. Agriculture sector needs to be convinced
about the necessity of tobacco crop substitution and reassured that major educational activities
would be initiated to reduce the demand of the product. The health sector could also advise on
the choice of alternate crop, so that its availability in specific areas could help in correcting
- nutritive deficiencies found in these areas. Besides this intersectoral collaboration, support from
education sector and mass media would also be useful in spreading the anti-tobacco message.
The commerce and transport sectors would need to ensure that the excess alternate crop does
not accumulate in the experimental area and it reaches in time to its identified destination. The
Q
agriculture scientists may identify other crops which are not generally grown in the area but can
be consumed locally. Substitution of such crops would not result in reduction of their prices due
to higher product availability. Sectors like labour and welfare would need to identify proper
strategies for rehabilitation of bidi workers. Although the bidi roller families are entirely
dependent on this work, their low remuneration suggests that there would be no resentment
among these workers on provision of alternate vocation.
Mechanism for Multisectoral Approach for Tobacco Control
The root concept of multisectoral approach aims at initiation of and carrying out the
activities related to tobacco control, by all connected sectors on their own. This ensures that
individual sectors consider it their social responsibility to initiate activities for tobacco control as
related to their sector. The inherent advantage of this approach would be that these sectors
'
would look for budget for these schemes within the sector. Having the expertise in the area, the
plans developed by them are also likely to be more cost-effective.
It would be ideal that every sector takes actions and periodically reviews the activities in
their areas of expertise. However, such expectations are not likely to be practical and an office
for coordination of tobacco control activities would be necessary. Since health is currently the
leading argument for tobacco control, an office under this sector should be acceptable to other
sectors, in all countries.
Currently in most societies, health sector seems to have accepted a self-imposed
responsibility for tobacco control, with the result that other sectors as well as community at large
also tends to associate tobacco control with health. For optimum benefit through a multisectoral
25
intervention, the health sector would also need to change its approach. Tobacco control would
need to be projected as a social cause, wherein a social change is anticipated following which
the societal norm would predominantly be towards non-usage of tobacco. A repeated request
would need to be made to various sectors to apply their mind and plan activities for tobacco
control through their sector or through collaborative actions by many sectors. It can be expected
that the ''will" to carry out an activity and resultant efficiency by specific sector would be higher if
the activity is considered as their own. This was evidently clear in the project "Radio DATE"
between All India Radio (AIR) and Indian Council of Medical Research (ICMR) which has been
described earlier. The degree of possessiveness about the project was so high that AIR team
insisted on calling it an AIR-ICMR project rather than ICMR-AIR project. The will and efficiency
was reflected in indulgence of AIR team in a thorough understanding of the tobacco before
preparation of the programme; meetings by AIR team among themselves, with ICMR team and
with other experts for formulation of the programme; modification of the episodes if not found
appropriate by them; and sometimes adopting an authoritarian role to complete the episodes
within the timeframe.
To change the current scenario on tobacco control from a health-oriented-activity to a
social-activity is not easy. This should also not be taken as dissociation of responsibility by
health sector, but should be considered as a method of adopting a broad-based approach. It is
needless to say that health sector would have to adopt a leading role even for accomplishing
this change. Approach of mutual respect is absolutely necessary for fruitful accomplishment of
collaborative multisectoral or intersectoral activities. Catalysts for this change may differ from
society-to-society, and also from time-to-time. The following suggestions may however, provide
some initial impetus.
a) Office on Tobacco Control: The activities related to tobacco control are many and the
coordinators can not be expected to do full justice if it is one of their responsibilities. Planning of
cost-effective programmes does require full-time thinking and complete dedication on all aspects
of tobacco. Therefore, creation of an office on tobacco control with adequate facilities under
Ministry of Health is highly desirable. The office may monitor the tobacco use status, tobacco
production & trade practices; plan and evaluate cost-effective intervention programmes; interact
with sectors associated with tobacco and undertake.liaison work for initiation of their activities;
initiation & coordination of intersectoral (not necessarily with health sector) and multisectoral
programmes for tobacco control; undertake/ commission research in support of tobacco control;
prepare periodic reports; etc
b) Workshops on Tobacco for Various Sectors: In many situations, different associated
sectors may not be aware of the magnitude of the problem and possible solutions for tobacco
26
control. It would be necessary that programmes are organized in consultation with and after full
involvement of different sectors, which inform them of different facets of tobacco and its control.
The faculty for such programmes would necessarily have to be inter-disciplinary, carefully
selected from fields of health, economics, media, education, sports, youth affairs, agriculture,
finance, law, labour, etc. Such stimuli should be followed by periodic interaction and seeking
their cooperation to initiate activities related to that area.
c) Discussions within Parliament: Parliament or legislative assembly can be considered as
top-most plank for any multisectoral activity. Appropriate discussions highlighting multisectoral
approach and pointing out the specific roles of different sectors are likely to result in maximum
benefit. Discussion of the issue in any Parliament committee may also result in
recommendations for various sectors. The main advantage at this forum is that it could question
any sector and their decisions are acceptable to every sector. Another advantage of such
discussions is the sensitization of members who hitherto have not been taking active interest on
the subject. Indian Parliament’s committee on sub-ordinate legislation, which discussed the
existing cigarette act relating to warning on cigarettes in 1995 (describe earlier), could be
considered as a milestone for the country for multisectoral approach for tobacco control. Follow
up meetings by health sector resulted in appreciation of tobacco problem by other sectors and
initiation of internal discussions to consider remedial measures. While this in itself resulted in
limited activities by these sectors, but their approach towards the issues definitely changed,
which would be useful in development of future interventions.
d) Inter-Ministerial Discussion on Tobacco Control: Most governments would have an
existing mechanism to discuss inter-ministerial issues. Tobacco definitely is a suitable candidate
for such discussion. Such meetings would have a useful purpose for discussion of specific
tobacco related issues, as well as to stimulate various sectors for action on tobacco control.
Such discussions are important in view of the fact that the success or failure of intersectoral
strategies is often a matter of redressing the power gaps between different sectors and
ministries. Quite often follow-up meetings for certain recommendations may catalyze initiation of
control programmes by other sectors. Such efforts between specific government departments
may also serve a similar useful purpose. An example of this approach is the development of the
current health awareness programme for tobacco control, wherein Directorate of Audio-Visual
Publicity (Government of India) was requested to be on the selection board for deciding the
agency for media campaign against tobacco. The experience stimulated the Directorate to offer
conduct of the campaign along with its Song and Drama Division at concessional rates, which
was agreed by the Ministry of Health & Family Welfare. However, even before the funds could
be released for this purpose, the Directorate prepared few anti-tobacco messages in the form of
posters and initiated a print media campaign through newspapers. Under this campaign readers
27
were asked to send their opinion for the best poster. The poster with maximum votes would be
the winner. The persons sending the opinion on best poster would be eligible for an award
selected through lots. While sending the entry form, the readers need to write out a millennium
pledge for not smoking during lifetime (for non-smokers) or to do everything within the person’s
power to give up smoking (for smokers). Within first three days, the Directorate had received
1,500 entries. The Directorate spent the required funds for this campaign.
e) National Tobacco Advisory Committee: Setting up a multi-disciplinary advisory committee
on tobacco would help in holistic understanding of tobacco scenario and planning of control
strategies. Experts from various fields would inform each other of their sectoral problems as well
as initiatives within the sectors. They would also take back the message and suggestions for a
multi-pronged action on tobacco control, from experts in other sectors. This approach may also
result in contribution of funds by non-health sectors, which would represent their commitment.
f) Combination of Tobacco Control with Other Programmes: Sometimes it may be easier to
initiate programmes on tobacco control by combining it with other existing or proposed
programmes. A common example of intra-sectoral collaboration (health) is combining tobacco
awareness programe with education on alcohol & drugs. This has been successfully achieved in
the collaborative programme “Radio DATE”, between All India Radio and Indian Council of
Medical Research’2. Such combinations may become cost-effective and sometimes may be
more acceptable to programme managers or to the community. One example of such continuing
collaboration is the Sri Lanka’s coordinated programme for promoting a healthy drug-free
lifestyle. Recommendations from a workshop in 1996, paved the way for formation of a national
coordinating committee on alcohol, tobacco and other substances, with representatives from all
major organizations working in the area of prevention32. The coordinating committee has been
meeting monthly for the task of formulating a national programme. Country profile for Sri Lanka
has been prepared on alcohol and tobacco. The suggestions and guidelines provided by this
committee have been helpful in gaining support for tobacco control from different sectors.
Combination of tobacco education as a part of healthy lifestyle programmes for cardiovascular
diseases has also been popular in certain countries, including Finland and India. Opportunity for
tobacco awareness may be available while educating about deforestation or religion or even
general hygiene.
g) Networking by Non-Governmental Organizations (NGOs): The NGOs have an important
role in various activities related to tobacco. Besides health-related NGOs, it is important to tap
the potential of NGOs working in non-health sectors. A network of NGOs could discuss & plan
various activities for tobacco control and assign specific duties to NGOs working in specific
sectors for their cost-effective implementation. Different NGOs could take up the responsibility
28
for advocacy for their respective sectors. In view of their great potential, support to these NGOs
from governments or international agencies like WHO, would be a good investment for tobacco
control.
Evaluation of Multisectoral Approach
Evaluation aspects related to multisectoral or intersectoral approach have not been
documented. For logistic reasons, it would be difficult to set up a randomised experiment.
Comparisons of efficacy of similar intervention, through a unisectoral or intersectoral/
multisectoral approach would perhaps only provide an indication of its usefulness. This is likely
in view of the presence of confounders in the form of societal perception over time or location at
different areas, presence of other tobacco control programmes, legislations, etc. So far,
perhaps evaluation of this approach has not been considered while planning intervention
strategies for tobacco control.
Sb
However, few advantages have been observed while undertaking Radio DATE
programme in India. In collaborative programmes, the involved non-health agencies do not need
to be followed for implementation of the programme. On the other hand, at certain times this role
seemed to have been taken over by the AIR team. This was due to the fact that the team
accepted it as their responsibility. The effect lasted not only during the period of programme
implementation, but also for the next few years. This was evident by comparing the number of
tobacco educational programmes broadcast by Delhi station of AIR, before, during and after the
year of broadcast. Such number was very small before the Radio DATE programme started; a
sudden increase was observed during the year of broadcast, which lasted at the same level for
the next two years, after which a decrease was noticed. Another observed advantage was the
cost-effectiveness of the programme. The entire budget spent by ICMR on this project lasting 30
weeks (20 minute episodes broadcast twice a week) broadcast from 84 stations in 16
languages, was approximately US $30,000. An approximately equal amount was spent by AIR
on this programme. There was no profit involved for any agency. The actual broadcast timings
were not even considered by either agency, because it was taken as an opportunity cost. It was
felt that some programme or the other had to be broadcast by AIR during this time and these
programmes were considered as good candidates for prime-time broadcast.
While no clear-cut results or parameters exist for evaluation of multisectoral approach for
tobacco control, the experience suggests this measure is likely to be cost-effective, if not more
effective than unisectoral approach.
29
Recommendations for Framework Convention on Tobacco Control
Exact mechanism for initiation and continuation of intersectral or mltisectoral
programmes for tobacco control would vary from country to country, and also from time to time
depending upon the specific requirements and local circumstances of a country or any area
within a country. However, some suggested measures are likely to work for most countries and
inclusion of such aspects in WHO’s Framework Convention on Tobacco Control are likely to
hasten the process of tobacco control. Importance of these measures in national tobacco control
programme has been described earlier in this paper. These mechanisms may also help in
meaningful negotiations on elements related to Framework Convention on Tobacco Control.
These measures are:
a.
Development of National policy on tobacco.
b.
Establishment of an Office on Tobacco Control.
c.
Establishment of a multisectoral advisory committee for tobacco control.
d.
Networking of health and non-health NGOs interested in working on tobacco control.
Conclusion
For a long lasting and permanent reduction in tobacco use, it is necessary to create
social awareness, which would result in acceptance of non-usage of tobacco products as a
social norm. Many modalities for reduction of tobacco use have been identified, like taxation on
tobacco products, protection of non-smokers from tobacco smoke, ban on tobacco
advertisements, warning on tobacco products, etc. The effective implementation of all these
strategies warrants action from more than one sector. Health being the most powerful argument
for tobacco control, this sector would need to adopt a major role in tobacco control, in terms of
implementation, in providing information related to diseases caused by it, and support to
tobacco users in cessation. However, the role of other sectors can not be discounted. For any
strategy to be cost-effective, all the concerned sectors need to work in tandem. This requires
understanding of the tobacco problem in its entirety and not merely consider the effect of any
intervention in isolation. Greater interaction between different sectors connected with tobacco,
would help them understand the need for taking urgent steps for tobacco control, realize
important predicaments, identify practical and feasible strategies for solving the identified fall
outs or implications of a specific control measure. This approach would help in developing an
attitude of problem solving rather than resist the advent of any intervention by any other sector.
One must expect that changing the scenario of tobacco use would entail major actions affecting
a large segment of the society. However, the solution to this gigantic problem is not to ignore it,
but to collectively find a solution, which would cause minimal upheaval. Multisectoral and
intersctoral approach for tobacco control is thus, the need of the time and deserves utmost
consideration.
30
References
1.
WHO. Guidelines for controlling and monitoring the tobacco epidemic. World Health
Organization, Geneva. 1998.
2.
Erickson AC, Mckenna JW, and Romano RM. Past Lessons and New Uses of the Mass
Media in Reducing Tobacco Consumption. Public Health Reports, 1990, May-June;
105(3): 239-44.
3.
4.
Chaudhry K. Economics of Tobacco. ICMR Bulletin, 1995, May; 25 (5): 55-60.
Kreisel W, and Von Schrinding Y. Intersectoral action for health: a cornerstone for health
for all in the 21st century. World Health Statistics Quarterly, 1998; 51(1): 75-8.
5.
Bettcher DW. Think and act globally and intersectoral! to protect national health. World
6.
Von Schrinding Y. Intersectoral action for health: addressing health and environmental
Health organization, 1997; WHO Document WHO/PPE/PAC/97.2.
concerns in sustainable development. World Health organization, 1997; WHO Document
WHO/PPE/PAC/97.1.
7.
Intersectoral action for health. A cornerstone for health-for-all in the twenty-first century.
Report of the international conference, 20-23 April 1997, Halifax, Nova Scotia, Canada.
World Health organization, 1997; WHO Document WHO/PPE/PAC/97.6.
8.
Crosby M.H. Religious Influences on tobacco investments. Abstract Book of the 1Cfh
World conference on Tobacco or Health. Beijing, 24-28 August 1997. Abstract no. S9/3,
page 21.
9.
Report of the meeting on Tobacco and Religion, 3 May 1999, Geneva. World Health
Organization. Document No. WHO/NCD/TFI/99.12.
10.
Chaudhry K. Control or Promotion - The Paradox. Tobacco Control, SAARC Edition,
1994; 1 (1): 41-6.
")
11.
Jaisani BG. Possible Substitutes and Alternate Uses of Bidi Tobacco. In: Sanghvi LD &
Notani P (eds.). Tobacco and Health - The Indian Scene, Tata Memorial Centre,
Bombay, 1989; page 207-15.
12.
Chaudhry K, Prabhakar AK & Shah B. Report of a Joint Project of All India Radio and Indian
Council of Medical Research on Integrated Broadcasting (1990-1992). ICMR, New Delhi,
1998.
13.
Chaudhry K, and Unnikrishnan K.P. Tobacco Control In India - A Perspective. In:
Proceedings of the 11th World Conference on Tobacco and Health, Beijing, China, in
1997 - under print.
14.
World Health Organization. Controlling the Smoking Epidemic. Report of the Expert
Committee on Smoking Control (WHO Technical Report Series No. 636), WHO, Geneva,
1979.
31
15.
Rath GK, and Chaudhry K. Estimation of Cost of Tobacco Related Cancers Report of an
ICMR Task Force Study (1990-1996). Indian Council of Medical Research, New Delhi,
16.
1999.
Townsend J. The role of Taxation Policy in Tobacco Control. In: Abedian, van der Merwe
R, Wilkins N, and Jha P. The Economics of Tobacco Control - Towards an optimal policy
mix. Applied Fiscal research Centre, University of Cape Town, 1998; p 85-101.
17.
Malouff J, Schutte N, Frohardt M, Deming W and Mantelli D. Preventing smoking:
Evaluating the potential effectiveness of cigarette warnings. The J Psychology, 1992;
126 (4): 371-83.
18.
Basu A, Ganguly SK, and Datta SK. Demographic survey of opinions towards smoking: a
pilot study. J Indian Med Assoc, Nov. 1992; 90 (11): 292-4
19.
Kumar A, Mohan U, and Jain VC. Academicians’ attitude and beliefs towards anti
smoking measures. Public Health, 1996; 110: 241-6.
20.
Stellman SD. Cigarette yield and cancer risk: Evidence from case-control and
prospective studies. In: Zaridze D, and Peto R (eds). Tobacco a major international
health hazard. I ARC Scientific Publication no. 74, Lyon, 1986; 197-209.
21.
Peto R. Overview of cancer time-trend studies in relation to changes in cigarette
manufacture. In: Zaridze D, and Peto R (eds). Tobacco a major international health
hazard. IARC Scientific Publication no. 74, Lyon, 1986; 211-26.
22.
Parish S. Cigarette smoking, tar yields, and non-fatal myocardial infarction: 14,000 cases
23.
Peach H, Hayward DM, and Shah D. A double-blind randomized controlled trial of the
and 32,000 controls in the United Kingdom. Br Med J, 1995; 311:471-7.
effect of a low- versus a middle-tar cigarette on respiratory symptoms - A feasibility
study. In: Zaridze D, and Peto R (eds). Tobacco a major international health hazard.
IARC Scientific Publication no. 74, Lyon, 1986; 251-63.
24.
Withey CH, Papacosta AO, Swan AV, Fitzsimons BA, Ellard GA, Burney PG, Colley JR,
and Holland WW. Respiratory effects of lowering tar and nicotine levels of cigarettes
smoked by young male middle tar smokers. II. Results of a radomised controlled trial. J
Epidemiol Community Health, Jun 1992; 46(3): 281-5.
25.
Benowitz NL, Hall SM, Herning Rl, Jacob P III, Jones RT, and Osman AL. Smokers of
26.
Kolonen S, Tuomisto J, Puustinen P, and Airaksinen MM. Effects of smoking abstinence
low yield cigarettes do not consume less nicotine. N Eng J Med, 1983; 309:139-42.
and chain smoking on puffing topography and diurnal nicotine exposure. Pharmacol
Biochem Behav, Jun 1992; 42(2): 327-32.
27.
Warner KE, Goldenhar LM, and McLaughlin CG. Impact of cigarette advertising
revenues on US magazine coverage of smoking and health. In: Gupta PC, Hamner JE
III, and Murti PR (eds). Control of tobacco related cancers and other diseases International symposium. Oxford University Press, Bombay, 1992- 323-8
32
$
28-
Gupta PC, Mehta FS, Pindborg JJ, Bhonsle RB, Murti PR, and Aghi MB. A 10-year
follow-up study for primary prevention of oral cancer among Indian villagers. In: Gupta
PC, Hamner JE III, and Murti PR (eds.). Control of Tobacco-related Cancers and Other
Diseases. Oxford University Press, Bombay, 1992; page307-13.
29.
Tobacco or Health: status in the Americas: a report of the Pan American Health
30.
Crop substitution: a success story. In: Tobacco Alert, Special Issue, 1995, Geneva,
Organization. Washington, DC, Pan American Health Organization, 1992, pp.94-95.
World Health Organization, 1995.
31.
Karim Z, Islam N, and Chowdhury MA. Rehabilitating Tobacco Growers in Bangladesh.
In: Slama K (ed.). Tobacco and Health, Plenum Press, New York, 1995; page 915-8.
32.
Profile of Alcohol and Tobacco - Sri Lanka. Sober Sri Lanka, Colombo, Sri Lanka, 1997.
33
pyi S’- 24-
The WHO International Conference on
Global Tobacco Control Law:
Towards a WHO Framework Convention on Tobacco Control
7 to 9 January 2000, Hew Delhi. India
Paper
Regulation of Tobacco Products
Author
Mitchell Zeller
Director
Office of Tobacco Programs
United States Food and Drug Administration
This paper is commissioned by, and produced for the World Health Organization, Geneva
B
Good morning. Thank you for this opportunity to talk about the need for effective
regulation of nicotine-containing tobacco products.
I want to share some thoughts with you about why I believe regulation of tobacco
products should be part of any comprehensive effort to reduce the death toll from tobacco
- and in particular, to reduce the number of young people who use tobacco products.
My message to developing countries that are pondering their role in the creation
of the WHO Framework Convention on Tobacco Control is simple — we are talking
about products deliberately designed by their manufacturers to deliver nicotine, an
addictive drug. This inescapable fact should compel all of us to collaborate in the
Framework Convention process to ensure that effective regulation of tobacco products is
a key element of our work.
As many of you know, in 1994 the U.S. Food and Drug Administration launched a
historic investigation of the tobacco industry, and the role of nicotine in the design and
manufacture of cigarettes and smokeless tobacco products.
To help developing countries benefit from some of the regulatory lessons learned
in the 1990’s, I thought it would be helpful to describe how and why FDA launched our
tobacco investigation back in 1994; what we learned; and how we used our legal findings
related to nicotine to create a regulation to reduce young people’s use of tobacco. This
will hopefully give you a better understanding of the regulatory perspective that my
agency brings to any consideration of nicotine and tobacco products.
In the United States, and in many of your countries as well, normal drug
companies want to make drug claims for their products. So they submit applications to
regulatory agencies to get their products approved so that they can make claims on
labeling and in advertising.
But tobacco companies are not your normal drug companies. They are definitely
in the drug delivery business, but they are not your normal drug companies. In fact, they
ordinarily do not make express drug claims. So, how was FDA going to regulate their
products as drugs if the companies did not make explicit drug claims?
Well, it turns out under our statute — the Federal Food, Drug, and Cosmetic Act - that if you can prove that the companies intend their products to deliver drug effects —
like addiction, for instance - then you have a legal basis for regulating.
But, you’ve got to have proof.
So, that’s why we began an investigation into the role of nicotine in the design
and manufacture of cigarettes and smokeless tobacco products. Because if we could
prove the industry’s real intent, then we could regulate.
We began our investigation with many questions and concerns. We wondered
about certain products developed by the companies in the late 1980’s and early 1990’s
that raised important questions about nicotine.
Philip Morris had test marketed a product called Next that had no nicotine in it
whatsoever. Next proved that the companies had the capability to remove all of the
nicotine, if they wanted to. So why did they leave it in? And why did they leave it in at
the levels that occurred in the products?
R J Reynolds had test marketed a product called Premier. Premier was a truly
revolutionary product. There was a little tobacco-like material in it for show. The key
component inside Premier was an aluminum cylinder. Inside the cylinder were dozens of
tiny green pellets. The pellets were coated with nicotine and glycerin. The smoker lit and
heated a carbon tip on the end which, in turn, heated the aluminum cylinder, which
released the nicotine and glycerin from the pellets.
R J Reynolds even published studies showing the concentration of nicotine in the
blood of users of Premier, to prove that the nicotine delivery in this product was similar
to conventional cigarettes.
Our question about Premier — why go to so much trouble to completely redesign
the inside of a cigarette, but then make sure that the one thing that you haven’t changed is
the nicotine content? And then publish nicotine blood data to prove it.
, .
.^v .
°
t
We also began our investigation with enormous public health concerns. Let me
give you a few of the facts and figures.
5 million children in the United States alive today will die prematurely because of
their use of tobacco
Take any group of 1,000 20 year-olds who smoke in the United States; here’s
what will happen to them later in life; 6 will be murdered; 12 will die in car
accidents.. .but 250 will die in middle age from smoking, and another 250 will
die in old age from smoking
12 percent of the entire male population in the U.S. under the age of 35 will be
killed by smoking before reaching the age of 70
The U.S. has only 5 percent of the world’s women, but we have 50 percent of the
world’s deaths related to smoking among women
And nicotine addiction is incredibly powerful. It’s so powerful that after surgery
for lung cancer, almost half of all smokers start smoking again. It’s so powerful that
among smokers who suffer a heart attack, 38 percent start smoking again when they are
stiU in the hospital. And it’s so powerful that when a smoker has had his or her larynx
removed, 40 percent still try to smoke again.
J
So these were some of the reasons we started our nicotine investigation.
When we started our investigation 5 years ago, the tobacco companies were
2
fending off charges that they “spiked” their cigarettes with outside sources of nicotine.
There was a lot of media coverage of this “spiking” issue, and we have come to believe
that many in the tobacco industry believed that FDA’s investigation was aimed at trying
to prove the spiking charge.
In fact, when we visited Philip Morris, R J Reynolds, and Brown and Williamson
in the spring of 1994, the companies seemed to go out of their way to prove to us that
they did not spike. In the process, however, they gave us an invaluable lesson in how they
actually blend tobacco leaves.
Blending turns out to be one of the principal ways to manipulate and control
nicotine levels in finished cigarettes. What we learned about blending destroys any notion
you may have had that a cigarette is just some tobacco leaves ground up and surrounded
by paper and a filter.
The typical American cigarette is comprised of 3 types of tobacco. Tobacco leaf
buyers pay close attention to something called “stalk position”., .the location of each leaf
on the tobacco plant. The 10-15 stalk positions in the middle of the plant are the most
highly prized because of their bigger size and higher nicotine content. Tobacco leaf,
being an agricultural commodity, is usually blended over a 3 to 6 crop year period.
The tobacco manufacturers use sophisticated technology to measure nicotine
levels as part of the blending process. Near-infra-red technology enables the companies
to measure nicotine content twice a second for incoming deliveries. Computers typically
store the nicotine content of every 2,000 pounds of tobacco in storage. At any given time,
each company owns hundreds of millions of pounds of tobacco.
So do the simple math. And do it conservatively. Multiply 3 varieties by 10 stalk
positions by 4 crop years. That company computer will give you 120 nicotine different
nicotine levels to pick and choose from.
So, in reality, you have all the nicotine you would need from the naturally
occurring levels in tobacco leaf. The industry didn’t seem to realize the incredible lesson
they were giving us on this important method for carefully controlling nicotine levels.
Through our investigation we discovered several other methods by which the
companies address the blending issue as they carefully manipulate and control nicotine
levels.
If traditional blending of tobacco leaves does not give you the desired nicotine
levels, then do what Brown and Williamson did and invent a new type of tobacco with
double the normal nicotine content. This little project - called “Y-l” by Brown and
Williamson_--_was intended by the company to be, quote, “a blending tool,” so that they
could maintain higher nicotine levels in lower tar products.
We also learned that all of the companies address the nicotine issue in “light” and
“low tar” cigarettes in a more old-fashioned way.. .they simply use a higher proportion of
higher nicotine leaves in the blend of “light” and “ultra light cigarettes.
And we also discovered what I would call “better nicotine manipulation through
chemistry.” The companies do this by adding ammonia compounds into the tobacco.
This has a “free-basing” effect on the smoke chemistry. It alters the pH level of the
smoke and converts the nicotine from a bound chemical state to a more potei^t^ep^^^^
chemical state.
e-KwJfc.
Aaox.<U
•- .
P
|
In addition to what we were learning on our own, early on in the investigation we
began to see the floodgates open as thousands of internal industry documents poured out.
Some of the documents made clear that, at least privately, the tobacco industry knew
many decades ago that nicotine was addictive, and that nicotine was the reason why
people smoke.
I have four documents I want to share with you that speak volumes for the
f)
industry’s knowledge of nicotine’s drug-like effects.
Let me take you back to 1963. This was one year before the first U.S. Surgeon
General’s report on the dangers of smoking, and 25 years before the Surgeon General
concluded that the nicotine in cigarettes was addictive. But in 1963, the top lawyer for
Brown and Williamson wrote, “We are, then, in the business of selling nicotine, an
addictive drug.”
Move forward to 1969. A top research executive at Philip Morris goes to New
York to speak to the company’s board of directors on why people smoke. He writes,
“Long after adolescent preoccupation with self-image has subsided, the cigarette will
even preempt food in times of scarcity on the smoker’s priority list... We are of the
conviction...that the ultimate explanation for the perpetuated cigarette habit resides in the
pharmacological effect of smoke upon the body of the smoker, the effect being most
rewarding to the individual under stress.”
In 1972, a Philip Morris executive wrote a memo that has since become quite
notorious. He wrote, “Think of the cigarette pack as a storage container for a day’s
supply of nicotine.. .think of the cigarette as a dispenser for a dose unit of nicotine.. .think
of a puff of smoke as the vehicle of nicotine.. .smoke is beyond question the most
optimized vehicle of nicotine and the cigarette the most optimized vehicle of smoke.”
And in the early 1970’s a Reynolds executive wrote, “In a sense, the tobacco
industry may be thought of as being a specialized, highly ritualized, and stylized segment
of the pharmaceutical industry. Tobacco products uniquely contain and deliver nicotine,
a potent drug with a variety of physiological effects.’!.
Now young people around the world are the tobacco industry’s new
customers.. .the replacement customers, if you will, for the adults who die or quit each
day. Let me read a few other quotes from industry documents that show their recognition
4
rr
°^-°W 'mPortant young people are to the industry, and just how aware they are that the
addiction to nicotine takes place at a young age:
If the last ten years has taught us anything, it is that the industry is dominated by the
companies who respond most effectively to the needs of younger smokers.”
Evidence now available...indicate^] that the 14 to 18 year old group is an increasing
segment of the smoking population. RJR must soon establish a successful new brand in
this market if our position in the industry is to be maintained over the long term.”
However intriguing smoking was at 11, 12, or 13, by the age of 16 or 17 many regretted
their use of cigarettes for health reasons and because they feel unable to stop smoking
when they want to.. .Over half claim they want to quit. However, they cannot quit any
easier than adults can.”
f
All of the evidence I have described — on the manipulation and control of nicotine
That assertion of jurisdiction enabled us to issue a regulation that will limit the
availability and appeal of tobacco products to young people. Our overall goal is to reduce?
the number of young people who use tobacco products in the United States by 50 percent
within 7 years of our rule going into effect.
—'
And we are going to reduce the number of kids that use tobacco by limiting the.
J
supply of the product to them through access restrictions, and by limiting the demand for
the product by them through restrictions on the advertising, marketing, and promotioDLof -/
the product to kids.
Only two of the access restrictions in our rule are currently in effect - those
establishing 18 as the minimum age of sale for tobacco products, and requiring anyone
under the age of 27 who wants to buy cigarettes or spit tobacco toshow aphotoJD,
We are enforcing these provisions through contracts we sign with the States who
choose to join us in an enforcement partnership. In 1998,41 states plus the District of
Columbia and the Virgin Islands have signed contracts with us. In 1999, we arranged for
the rule to be enforced in all 50 states"plus three territories.^The principal activity under
these contracts is unannounced inspections of retailers we calLcomgli.ance_q^ecks, to see
if retailers will sell a tobacco product to a minor.
b7’
x
Despite the legal uncertainty surrounding our program, we have conducted more
than 150,000 compliance checks and collected more than $700,000 in penalties from
retailers who repeatedly violate the rule. And that legal uncertainty will be resolved in
the next 6 months. The case filed by the industry was heard by the U.S. Supreme Court
last month, and we expect a decision between now and June.
With my remaining remarks I would like to shift gears and talk about the need for
an adequate scientific base to support the evaluation of a new type of marketing by both
tobacco companies and pharmaceutical companies. This scientific base will also support
the kind of global collaboration on tobacco regulation that is needed.
Tobacco companies are testing and marketing so-called “reduced risk” tobacco
products. R.J. Reynolds has the next generation of Premier, which I talked about earlier.
It is called Eclipse.
Philip Morris is test-marketing a battery-operated product called .Accord that uses
a cell-phone-like charger, and another device with computer chips and heating blades.
Eclipse and Accord purport to reduce thejdsk to the smoker and to greatly reduce the
amount of secondhand or sidestream.smoke so that non-smokers will be less annoyed by
those who smoke.
Pharmaceutical companies are interested in using nicotine replacement products
like the patches to reduce a smoker’s daily consumption of tobacco. The theory is that
rather than getting a smoker to quit, nicotine replacement products can help smokers
smoke less. The^assumptionJis that this reduction in exposure to tobacco will lead to an
bverall feduction in harm to the smoker.
I'
It is true that tobacco companies have historically enjoyed an easier and quicker
path to market than the makers of nicotine gums and patches. But as the agency that may
have to evaluate claims for either the tobacco or drug products, FDA has many questions
and - at this point - few answers.
The last thing we need with these new products and claims is to repeat the
mistakes that were made over the last 30 years by governments and the public health
communities in developed countries. Mistakes that have allowed “light” and “low
nicotine” cigarettes to be marketed to smokers under the misimpression that such
products are safer and less addictive.
So we need to be sure that a reduction in exposure to tobacco, or to substances in
tobacco smoke, translates into some meaningful benefit in terms of actually reducing
harm. And the only way we can be sure is if there is an adequate scientific base; first to
demonstrate a reduction in exposure; and then, to provide that critical linkage establishing
that exposure reduction leads to a meaningful reduction in harm.
To help the scientific process along, FDA is funding a new expert committee that
has been convened by the Institute of Medicine in the United States. Their charge is to
study these issues and make recommendations to FDA about the appropriate scientific
and regulatory framework we should have in place to address these complex questions
related to the appropriate regulation of tobacco products and cessation aids.
In conclusion, all of the disclosures over the last 5 years have forever changed the
way the American public views both tobacco products and the tobacco industry. I hope
6
$
\ > c,
the same is true around the world.
I look forward to our victory in the Supreme Court and to working with all of you
in the years to come on this most important of public health issues. And I look forward to
the day when comprehensive global efforts — including strong regulation, stiff price
hikes, and effective prevention and cessation activities - begin to drive down the number
of young people who smoke.
Our goal should be twofold. First, to deprive the tobacco industry of their new
customers — our children — and grow up the next generation of kids not addicted to
nicotine. And second, to help addicted smokers either quit or reduce the harm associated
with their continued use of tobacco in a significant and meaningful way.
Thank you.
C
pH
The WHO international Conference on
Global Tobacco Control Law:
I
Towards a WK Framework Convention oh? Tobacco ContraD
7 to 9 January 2000, Hew Delhi, India
Paper
international 1® aaO awl Wfea ffranewwl te WHO
Framework
Tobacco 0®maro8
Author
William Onzivu
Global Health Leadership Fellow, Tobacco Free Initiative
World Health Organization
This paper is commissioned by, and produced for the World Health Organization, Geneva
EXECUTIVE SUMMARY:
The international legal and policy framework for the development of a global tobacco
control Convention is based on the need to curb the global tobacco epidemic.
Tobacco continues to claim millions of human lives and developing countries will be
hit harder in the next millennium. The basis of this effort stems from Article 19 of
WHO Constitution which empowers WHO to initiate the development of Conventions
to protect public health. Many provisions of WHO Constitution also support this
process. The WHO Executive Board and World Health Assembly have in the past
made various resolutions urging States to recognise and curb the tobacco problem. Of
importance is Resolution 52.18 of the 52nd World Health Assembly in May 1999
which urged member States to prioritise tobacco control. It also laid framework for
establishing a working group, an inter-governmental negotiating body and affirmed
need for support for developing countries during this process.
The legal framework considers application of the World Trade Organisation
(WTO) Trade law and policy, International human rights law, and drug law. These,
expressly and implicitly have provisions to protect public health. Thus, under WTO
law, article XX (b) of GATT 1994 permits trade restriction and control of a product
in a country if it will harm public health. The qualification is that this must be
necessary to protect health and shouldn’t be discriminatory. The need to curb the
tobacco problem is already a necessity. The WTO trade law and policy also
recognises the authoritative guidance of WHO in protection of public health. WTO
trade decisions such as the Thai Cigarette case affirm this. It means the development
of a global treaty on tobacco control poses no conflict with World trade rules. In
addition to tobacco, other areas of interaction between WHOs public health work and
WTO trade regime include the International Health Regulations, food safety,
pharmaceuticals and vaccines and trade in health services. The WTO recognises the
authoritative guidance of WHO in standard setting in these aspects of world trade.
Various WTO agreements provide areas of synergy with these aspects of WHO work.
International Human Rights law offers a viable basis for tobacco control.
The WHO Constitution provides the right to health as a fundamental human right.
Many UN Instruments such as Convention on Economic, Social and Cultural Rights,
the Convention on Elimination of Discrimination Against Women (CEDAW) and UN
Convention on the Rights of the Child among others stress the need to ensure health
for all. Committees of these Instruments have singled out tobacco as a major affront
to health which requires curbing among vulnerable populations such as developing
and least developed countries, women and children. Women and children are being
increasingly targeted by tobacco countries in low income countries. Involvement of
poorer countries in global tobacco control is not only crucial as protection of public
health, but that of human right in developing and least developed countries.
Drug law provides a good example for global regulation of tobacco. Drug
law in developing countries has been used to regulate harmful products such as
poison, quality of drugs etc. It is now well established that there are over 1000
harmful products in tobacco. Drugs and food products and quality are regulated
around the world. We shouldn’t continue to allow tobacco to escape regulation.
Some countries are already using food or poison laws to regulate tobacco. Thus, the
legal and policy aspects of drug regulation offers a good basis for the development of
the WHO framework Convention on tobacco control.
Therefore, it is important that developing countries get involved in the global
tobacco law making process. Existing WHO mechanisms need to be used to enhance
technical support in legal and policy aspects for developing and least developed
countries. The role of increased partnerships between the various UN agencies should
be encouraged and existing legal structures in developing countries should be applied
to further this law making process and future implementation.
I.
INTRODUCTION,
Background
-
This paper is an attempt to expose the legal and policy basis for the
development of a WHO Framework Convention on Tobacco control. It describes the
state of the law that has enabled WHO to undertake this lawmaking. The core of the
paper expounds other justifications that support the development of the Convention.
This complements the increasing global burden of disease from tobacco as the central
reason for developing the Convention. Indeed, the developing world will be hard hit
due to absence of viable tobacco control infrastructure. The development of the
Convention is a necessary vehicle for tobacco control in these countries.
I have considered the following areas of International law, the institutional
law of WHO, the WTO law, Human rights law and Drug law. These are important for
the following reasons. These areas of law justify the development of a legal
instrument that seeks to protect Public Health via a tobacco control convention.
These areas of law are a departure point for a Convention to protect public health. A
convention to control tobacco will in fact strengthen and enhance the field of
application of these laws . Finally, these laws can be the basis of dispelling any
misunderstanding that may arise in the making and implementation of a tobacco
control Convention. Thus, this paper aims to establish that the development of WHO
framework Convention on tobacco control has a sound basis under existing
international legal and policy framework.
The Case for an International Legal Instrument.
C)
The tobacco problem requires multi-pronged strategy to fight it. While national
programmes offer direct means of combating the epidemic, an international strategy
becomes imperative. This is because tobacco industry tactics have been extremely
elusive. Because the industry and the tobacco problem transcends national frontiers,
international regulation offers a stronger tool to avert the tobacco problem.
International action creates a vehicle for concerted action towards containing the ever
rising statistics of tobacco related deaths today.1 Dr Brundtland, WHO Director
General stated that tobacco control cannot succeed solely through the efforts of
individual governments, national NGOs and media advocates. We need an
international response to an international problem2.
The making and implementation of the Convention, the central strategy in the fight
against tobacco depends on continuous political and other support of national
governments, global institutions and civil society. The special importance of
Conventions in International law scarcely need emphasis. The multilateral treaty
remains the best medium available at the moment for imposing binding rules of
1 See Options for the Preparation of an International Framework Convention and Related Protocols for
Tobacco Control, Public Health and International Law Considerations. WHO Geneva 1997.
2 The Director-General of WHO, during the seminar on Tobacco Industry Disclosures, WHO Geneva,
20lh October 1998.
3
precision and details in the new areas into which international law and concerns is
expanding, and for codifying, clarifying and supplementing the customary law already
in familiar settings.3 Protection of public health by controlling tobacco is one where
international law is crucial in addressing the multilateral nature of the problem.
What is a Framework Convention:
Conventions are legally binding international agreements, concluded by States in
written form, and governed by International law. A Framework Convention refers to
a variety of legal agreements, which establish a general system of governance for a
specific area such as tobacco control. The Framework Convention/Protocol approach
allows States to proceed incrementally. The instrument that embodies these specific
commitments is known as a Protocol.4 Examples are the 1976 Barcelona Convention
for the Protection of the Mediterranean Sea against Pollution, which was negotiated
under UNEP, and now has protocols concerning the dumping of hazardous wastes,
land based sources of marine pollution, emergency response to oil spills, and specially
protected areas. The 1979 Convention on Long range Transboundary Air Pollution
which addresses the problem of acid rain in Europe and North America, has seven
Protocols establishing specific obligations relating to the various sources of
transboundary air pollution, including sulphur emissions, nitrogen oxides, volatile
organic compounds, heavy metals and persistent organic pollutants. Other examples
are the 1985 Vienna Convention for the Protection of the Ozone Layer and the 1987
Montreal Protocol on Substances that deplete the Ozone Layer.5
This approach is the most feasible option for global tobacco control. It offers the
advantage of dividing the negotiation of separate issues into individual agreements
rather than trying to resolve all substantive issues in one document, is more politically
acceptable than any other binding approach to global tobacco control, creates a forum
for co-operation and negotiation for implementing detailed protocols, and offers a
model for a continuous and dynamic process of law making.6
II: WHO LEGAL FRAMEWORK
WHO Constitution
WHO is legally empowered to develop Conventions. The development of a tobacco
control Convention is well founded under WHO Constitution, which applies to all its
members which includes all developing and least developing countries. However,
this is the first time that WHO is activating its constitution to develop this treaty’
Article 19 of the Constitution states that the Health Assembly shall have authority to
adopt conventions or agreements with respect to any matter within the competence of
the Organization. A two-thirds vote of the Health Assembly shall bind a member
when accepted by it in accordance with its constitutional processes. It is important to
note that Article 2 of the Constitution endows WHO with several functions that
directly or indirectly require the application of legal principles. These include, to act
3 D.J Harris (1998): Cases and Materials on International Law, Fifth Edition London Sweet *
Maxwell 1998., pages 765-857.
’
’
4 The Framework Convention/Protocol Approach: Framework Convention on Tobacco Control
Technical Briefing Series, Paper 1. Tobacco Free Initiative, WHO 1999.
5 See Birnie and Boyle, Documents in International Environmental Law for these and other
Conventions.
6 Taylor and Roomer, 1996
0
as directing and co-ordinating authority on international health work, to propose
conventions, agreements and regulations, and make recommendations with respect to
international health matters and to perform such duties as may be assigned thereby to
the Organization and are consistent with its objective, and to develop, establish and
promote international standards with respect to food, biological pharmaceutical and
consumer products. Tobacco control is within this ambit. Articles 20, 61, 62, 63, 64
and 65 of the WHO Constitution are also relevant. They provide that members report
annually to the Organization on its action taken to improve its peoples health and on
action taken with respect to recommendations, conventions, agreements and
regulations by the Organization. Members shall communicate promptly to the
Organization important laws; regulations, official reports and statistics pertaining to
health which have been published in the State concerned. Thus, the development of a
WHO convention on tobacco control is legally mandated and based on WHO
Constitution. This constitution governs actions of the Organization and has a binding
or persuasive effect on States who are members of WHO.
Resolutions WHA49.17 and EB103.R11
The idea to develop a global tobacco control treaty evolved since 1975. Gaining
momentum in 1990s, was affirmed in 1995 by the Ninth World Conference on
Tobacco or Health. The World Health Assembly in Resolution WHA49.17 requested
the Director General of WHO, to initiate the development of a Framework
Convention in accordance with Article 19 of the WHO Constitution.
In January 1999, the WHO Executive Board adopted Resolution EB 103.R11.
This charted the course of pre-negotiation and negotiation phases for developing the
Convention. The Resolution suggested 2 key decisions for the 52nd World Health
Assembly to consider:
To establish a Working Group on the Framework Convention on Tobacco
Control, open to all member States.
To establish an inter-governmental negotiating body open to all member States,
to draft and negotiate the proposed WHO Framework Convention on Tobacco control.
This body will prepare a draft text of the Convention.
The adoption by the World Health Assembly of the Resolution commenced the
pre-negotiations phase for the convention. Formal negotiations of the Convention and
its protocols commences with first meeting of the intergovernmental negotiating body
expected in from May 2000. It is envisaged that the Framework Convention and its
related protocols would be ready for adoption by the year 2003.7 The content, inertia
and timing of the Convention and related protocols will depend upon the political
will and sustained commitment of States determined to protect public health from the
scourge of the tobacco pandemic. The interests of governments are paramount in
treaty making and this should be reflected in the process of developing the content
and implementation of the Convention and related protocols. States must perform
these acts in good faith8. As was stated by Judge Gros in the WHO Agreement Case
“in the absence of a super State, each international organisation has only the
competence which has been conferred on it by the States which founded it, and its
powers are strictly limited to whatever is necessary to perform the functions which
its constitutive Charter has defined. The WHO competence is thus that which is
7 Outline of projected activities as endorsed by WHO Executive Board in EB 103.11, 1999.
8 See Article 26 of the Vienna Convention on the Law of Treaties. It provides that a treaty must be
performed in good faith.
attributed to it by States. Specialised agencies of the UN have special competence
which they have received from member States for well-defined tasks.” Treaty
negotiation being a prerogative of States, key governmental ministries will be
involved such as Foreign Affairs, Justice, Finance and Foreign Trade, Environment,
Education, Agriculture and Labour. The role of WHO Secretariat in this is pivotal
and involves the following; Facilitating the activities of the Working Group with
technical support and briefing sessions, assistance in the planning of inter
governmental consultations on the Framework Convention, promotion of the
participation of the least developed countries in the treaty-making process and
technical support to member States to advance the adoption of the convention.
This conference fall within this role. Technical standards on tobacco control are
being established and maintained by WHO, a primary specialised agency in the field
of public health. The authoritative work of the WHO in this field has a binding effect
derived from the WHO Constitution.910 In WHA Resolution WHA49.17, member
States recognised the unique capacity of WHO to serve as a platform for the adoption
of the Convention.
Resolution 52.18
The 52nd World Health Assembly of May 1999 is a landmark for the development of
the WHO Framework Convention on Tobacco Control. The Resolution established
an inter-governmental negotiating body for the Convention, which is open to all
member States. The body’s role is to draft and negotiate the proposed WHO
framework Convention on Tobacco Control and possible protocols. It also agreed to
establish a Working Group on the Convention open to all member States in order to
prepare the work of the Inter-governmental negotiating body. The working group will
prepare proposed draft elements of the Convention. The Working Group will report
on the progress to the Executive Board at its 105th session. It will complete its work
and submit a report to the Fifty-third World Health Assembly.
The Resolution urged member States to give high priority to accelerating work
on the development of the Convention and possible related protocols, to provide
resources and co-operation necessary to accelerate the work, promote
intergovernmental consultations to address specific issues, for example, public health
matters and other technical matters relating to negotiation of the proposed Convention
and possible related protocols, establish where appropriate, relevant structures such as
national commissions and mechanisms to examine the implications of a Framework
Convention on Tobacco Control within the context of health and economic issues,
especially its effects on the economy of agriculturally dependent States, to facilitate
and support the participation of non governmental organizations, recognising the need
for multisectoral representation.
The Resolution urged the Director-General to do the following:
To promote support for the development of the Convention and possible related
protocols among member States, organizations of the United Nations system, other
inter-governmental, non-govemmental and voluntary organizations and the media, to
complete the technical work required to facilitate negotiations on the Convention and
possible related protocols, to convene the working group on the Convention and the
intergovernmental negotiating body on the basis of progress achieved by the working
9 1980 ICJ Reports at page 103.
10 C.F. Amerasinghe, Principles of the Institutional Law of International Organizations 1996 pages
200 - 201.
6
group, to provide the working group and the intergovernmental negotiating body with
the necessary services and facilities to the performance of their work, to facilitate the
participation of the least developed countries in the work of the working group, in
intergovernmental technical consultations, and in the inter-governmental negotiating
body.
It can be noted from this resolution that due consideration has been given to the
role of developing countries in the negotiation and implementation of the Convention.
The Resolution enjoins the international community to facilitate the participation of
developing countries in the work of the Working Group and Intergovernmental
negotiating Body of the Convention. It also calls for due attention to agriculturally
dependent States which largely comprise the developing countries. The call for
multisectoral approach to the process and involvement of NGOS is even more
relevant in developing and least developed countries where the need for tobacco
control is crucial. This conference is also covered under this resolution. This
Resolution is thus a pivotal framework for the participation of developing countries in
the development and implementation of the Framework Convention on Tobacco
Control.
Ill: INTERNATIONAL TRADE AND TOBACCO : THE WORLD TRADE
LAW
Article XX of GATT
The GATT was adopted in 1947 as the main international arrangement to
encourage trade between States. It currently has 135 contracting parties and is
designed to encourage trade between the parties to the agreement, by reducing tariffs
and preventing trade barriers. The World Trade Organization, formed at the end of the
Uruguay round of GATT in 1994 is the primary international institution governing
international trade. GATT 1994 strengthened international trade regime by
broadening WTO’s status, dispute resolution mechanism and jurisdiction. The 1994
agreements are a single package except the plurilateral agreements. The GATT has
provisions for protecting human health. Relevant GATT agreements include
Agreement on Trade in Goods and others such as the Agreement on the Application
of Sanitary and Phytosanitary Measures, Agreement on Technical Barriers to Trade,
Agreement on Agriculture, Agreement on import licensing Procedures, Agreement on
Trade Related Aspects of Intellectual Property (TRIPS) and Agreement on Import
Licensing procedures. The legal framework of the World Trade Organisation is
relevant to the development of the Framework Convention on Tobacco Control.
GATT Article IH (1) prohibits the application to imported or domestic products of
internal taxes and other internal charges, laws, regulations and requirements so as to
afford protection to domestic products. Article III (2) prohibits the application,
directly or indirectly, of internal taxes or other internal charges of any kind in excess
of those applied directly or indirectly to like domestic products or in a manner
contrary to Article III (1) which emphasises non-discrimination: Under Article XI,
prohibitions or restrictions including quotas, import or export licences or other
measures, on the import or export of any product from or another contracting party
are prohibited. Article XX permits exceptions to these limitations. It provides interalia,
“ Subject to the requirement that such measures are not applied in a manner
which would constitute a means of arbitrary or unjustifiable discrimination
7
between countries where the same conditions prevail, or a disguised restriction on
international trade, nothing in this Agreement shall be construed to prevent the
adoption or enforcement by any contracting party of measures...., necessary to
protect human, animal or plant life or health, relating to the conservation of
exhaustible natural resources if such measures are made^ effective in conjunction
with restrictions on domestic production or consumption.’
By 1991, the GATT Secretariat had 17 agreements, which required certain >
products to be subject to import or export restrictions. The important agreements
listed are the Convention on International Trade in Endangered Species of wild fauna
and flora 1973, the Montreal Protocol on Substances that Deplete the Ozone layer,
and the Basel Convention on the Control of Transboundary Movements of Hazardous
Waste and their Disposal. 11
12 WHO Framework Convention on Tobacco control will
be one of many such conventions aforementioned. The GATT has always recognised
that free international trade is not the only relevant policy goal for nations. In fact, it
has many exceptions that give equal or greater weight to other policy goals. In
consideration in these conventions is the exception under Article XX, that justifies
among others trade controls for health reasons.
In addition to Article XX of GATT, there are other side agreements of the WTO
relevant to the development of the Framework Convention on Tobacco Control.
WTO Dispute Settlement Body Decisions on Article XX
GATT Jurisprudence is scarce in the area of public health but decisions in the area of
environmental law can be interpreted for International tobacco control since tobacco
control is a means to protect health, the interpretation of provisos to Article XX can
be applied to the exception relating to human health under the Article. The following
are the four important GATT decisions relevant to the development of the Framework
Convention on Tobacco Control.
Thai Cigarette Case (1990)13
This case concerned prohibitions on import and export of tobacco and tobacco
products by Thailand. Thailand sought to justify the trade prohibitions under Article
XX (b) of the GATT, on the grounds that it had adopted measures to control smoking
which could only be effective if cigarette imports were prohibited and because
chemicals and other additives contained in US cigarettes might make them more
harmful than Thai cigarettes.
The GATT panel held and accepted that “smoking constituted a serious risk to
health and that measures designed to reduce the consumption of cigarettes fell
within the scope of Article XX (b) of the GATT.” It meant that the measures to
protect human health can be applied if necessary to achieve health policy
objectives. On the basis of recommendations adopted in resolutions of the fortythird assembly of the World Health Organisation, the Panel held that other
measures consistent with the GATT were reasonably available to Thailand to
11 See the World Trade Organisation; The Results of the Uruguay Round of Mnltilnr»r,t t
Negotiations: The Legal Texts. 1994, page519
8 Y
1 Mull,lateral Trade
Jackson and Davey, Legal Problems of International Economic Relations, 3
* Edition, 1995, Pages
13 Thailand - Restriction on Importation of Internal Taxes on Ci™rP1t»<. d
on 7 November 1990, BISD/37/S/200.
garettes, Report of the Panel adopted
8
control the quality and quantity of cigarettes smoked, including nondiscriminatory regulations. These must be implemented on a national treatment
basis (such as requiring disclosure of ingredients), a ban on unhealthy
substances, and a ban on advertising and information campaigns. These could
achieve Thailand’s health policy goals.
In fact GATT upheld the advertising ban, stating that various tobacco control
measures could be adopted both to domestic and imported tobacco and still be
consistent with GATT. The case implies that member States of GATT can adopt
strong tobacco control legislation so long as the measures are aimed at protecting
health and do not discriminate between domestic and imported tobacco. Thus, it
would be possible to design stringent tobacco control measures to alleviate tobacco
control deaths without violating GATT commitment. The Panel provided a general
mechanism for tightening tobacco control without breaking WTO rules. For example,
following the decision, Thailand maintained its advertising ban and has upheld other
strict measures to control tobacco use. The future harmonization of tobacco control
policies, including price increases, ad valorem taxes, advertising bans can be adopted
as long as these policies do not discriminate between foreign and domestic products.
It can be concluded that the development of WHO Framework
Convention on Tobacco Control is compatible with GATT law and policy. The Thai
case demonstrates that measures to protect health by control of smoking comes
within the ambit of exceptions laid under Article XX (b) of GATT Agreement. The
panel moreover recognised the authoritative resolutions of a WHO body on the
harmful effects of cigarette smoking. This means that inclusion of trade related
measures in the Framework Convention should be seen as complementing the
law and policy of the WTO especially regarding Article XX of the GATT. Many
commentators have in fact concluded that the Thai Cigarettes case is a victory for
public health. It implies the WTO recognition of the need to inculcate public health
protection goals into international trade. Thailand’s response in adopting and
enforcing strong multifaceted restrictive legislation is a model of what countries can
do when faced with invasion by multinational companies and their advertising.14
The Tuna-Dolphin Case.15
This dispute arose over regulations adopted under the US 1972 Marine Mammal
Protection Act. It regulates the harvesting of tuna by fishermen who are subject to
the jurisdiction of the US. The law limited catch of dolphins to 20,500 per year in this
part of the Ocean. It required the US Secretary of State “ to ban the importation of
commercial fish or fish products caught with commercial fishing technology resulting
in incidental kill or serious injury of ocean mammals in excess of United States
standards. The law meant US environmental standards should be applied to all
countries in respect of their fishing activities. It obliged country of registry of vessels
to satisfy that its regulatory regime was comparable to that of US. US also prohibited
import into its customs territory of yellow-fin tuna products from Mexico, which were
caught with purse seine nets with documentary evidence of this.
14 Ruth Roemer, Legislative action to combat the world tobacco epidemic, 2nd edition, WHO Geneva,
page 78.
15 GATT document. DS21/R, 3 September 1991 (30 LL.M) (1991) 1594).
9
In January 1991, Mexico requested the GATT contracting parties to establish a
panel to examine the compatibility of these US laws with the GATT. The panel
examined the compatibility with GATT under among others Article XX.
At the heart of the case was the question whether these import prohibitions
were permitted under Article XX (b) and XX (g). The panel noted that US was
entitled to invoke Article XX, but noted that, “the practice of panels has been to
interpret Article XX narrowly, to place the burden on the party invoking Article
XX to justify its invocation. The main issue was whether it covered measures
necessary to protect human, animal or plant life outside US jurisdiction. The Panel
concluded that the drafters focused on the use of measures within the jurisdiction of
the importing country. It also held that measures taken under Article XX (b)
must be necessary and should not constitute a means of arbitrary or
unjustifiable discrimination, and that Article XX (b) was intended to allow
restrictions to pursue overriding public policy goals to the extent that such
inconsistencies were unavoidable.
US had not shown that its measures were necessary, or that it had exhausted all other
options reasonably available to it to pursue its dolphin protection objectives in a
manner which was compatible with the GATT especially through the negotiation of
international co-operative arrangements. The conditions adopted were too
unpredictable to be regarded as necessary to protect the health or life of dolphins.
However, the legislation regarding labelling was not discriminatory as it did not
distinguish between products originating in Mexico and those originating in other
countries.
This case supports the development of an international tobacco control
convention because the measures can be argued as necessary (basing on the scale
and evidence of the tobacco problem), is not discriminatory since the subject
matter here is protection of health and national measures will emanate from
international mutual arrangement and each nation will enforce the agreed
measures within its boundaries and report to an international body.
From the face of it, the GATT panel adopted an approach, which seems to make it
difficult to justify trade restrictions, which give effect to national health protection
measures relating to activities emanating beyond the jurisdiction of parties adopting
such measures. Under the GATT, trade restrictive provisions under WHO framework
Convention will have to be proved to be necessary and must be non-discriminatory.
The evidence base of the tobacco problem is so grave that it has become necessary to
have its trade circumscribed. The measures shouldn’t be viewed as discriminatory.
This case encourages use of international co-operative arrangements and the
Framework Convention on Tobacco control is such arrangement. The decision of the
GATT Panel seems motivated by policy considerations, including concern at the
prospect of the adoption of unilateral measures and growing disparities in national
environmental standards, and a desire to encourage an international regulatory
response to trade problems posed by national environmental disparities.16
We can conclude that the Tuna-Dolphin decision was decided on the premises that
nations were taking unilateral measures without a proper international regulatory
framework. The decision encouraged adoption of such frameworks. Thus, the
Framework Convention on Tobacco control will provide an international legal
mechanism so that individual State actions towards tobacco control will be legitimate
16 Philippe Sands, Principles of International Environmental Law, London, 1995 Page 698.
10
0
but not unilateral. Actions for tobacco control will emanate from an international
arrangement. These are justifiable from this decision.
The Shrimp Turtle Case 17
The United States issued regulations in 1987 under the Endangered Species Act of
1973 requiring all United States shrimp trawl vessels to use approved Turtle Excluder
devices or tow time restrictions in specified areas where there was a significant
mortality of sea turtles in shrimp harvesting. These regulations were extended to areas
with likelihood that shrimp trawling will interact with sea turtles with certain limited
exceptions. Certification was granted to countries with a fishing environment, which
does not pose a threat of incidental taking of sea turtles in the course of shrimp
harvesting. It was also granted to nations that provide documentary evidence of the
adoption of a regulatory program governing the incidental taking of sea turtles in the
course of shrimp trawling that is comparable to the United States program. Under
1996 Guidelines, all shrimp imported into the United States must be accompanied by
a Shrimp Exporter’s Declaration form attesting that the shrimp was harvested either in
certified waters under Section 609 or under conditions that do not adversely affect
sea turtles. The 1996 Guidelines extended Section 609 to shrimp harvested in all
foreign countries from May 1996. The US justified the law under Article XX that
among others provides for trade restrictions on health grounds. India, Thailand,
Pakistan and Malaysia applied to the GATT Panel. On appeal, The Appellate Panel
held that US import ban on shrimp and shrimp products cannot be justified under
Article XX of GATT 1994.
This ruling is relevant to tobacco control. First, any trade regulation
measures must not be applied in a manner, which would constitute a means of
arbitrary or unjustifiable discrimination between countries where the same conditions
prevail or is a disguised restriction on international trade. The body also held that a
wider interpretation be accorded to the exceptions from Article XX (a) to Article XX
(g). For example, exhaustible natural resources were defined to mean both non-living
and living resources. A wider interpretation is given to tobacco control if any party
wishes to contest it as a discriminatory measure. The Panel recognised the recent
acknowledgement by the international community of the importance of concerted
bilateral or multilateral action to protect living natural resources and the explicit
recognition by WTO members of the objective of sustainable development in the
preamble to the WTO Agreement. This principle finds expression in protection of
public health by global tobacco control. The protection of human health is arguable as
sustainable development.
It further held that invoking of Article XX (g), if abused or misused, will to
that extent erode the treaty rights of other members. However, because the GATT
1994 makes available the exceptions under Article XX, in recognition of the
legitimate nature of the policies and interests embodied, the right to invoke one
of those exceptions is possible. Article XX is a limited and conditional exception
from the substantive obligations contained in other GATT provisions and the ultimate
availability of the exception is subject to the compliance by the invoking member
with requirements of the chapeau (opening statement). The chapeau is an expression
of good faith. It’s a principle of law, especially in International law, which controls
17 United States - Import Prohibition of Certain Shrimp and Shrimp Products.
11
the exercise of rights by States. The principle Proh^^^^^^^moTnResonle field
State’s rights and enjoins that whenever the assertion of a r ht^mg^ on thefield
covered by a treaty obligation, it must be exercise ona i
furthering the
which is appropriate and necessary for the purpose of the right, in ^rthen"Sthe
111 1
‘*PP iyP“aic
}
chnnld he fair and equitable as between the
interests which it is intended to protect. It should o
H
parties and not one to procure unfair advantage for one or some o
’
,,
The development of a global tobacco control convention would conform to all the
requirements described above. It is an act been done in goo ai . is an evi ence
based action, stemming from the enormity of the global tobacco problem. Thus the
convention will be compatible with the WTO law and policy and practice.
The Beef Hormones Case18
This case relates to a complaint against the European Communities relating to an EC
prohibition of imports of meat and meat products derived from cattle to which either
the natural hormones: oestradiol-17, progesterone or testosterone, or the synthetic
hormones: trenbolone acetate, zeranol or melengestrol acetate (MGA) had been
administered for growth promotion purposes. The EEC law maintained the
prohibition of the administration to farm animals of substances having hormonal or
thyrostatic action. It prohibited marketing, or import from third countries, of meat
and meat products from animals to which substances, including the six hormones at
issue in this dispute were administered..
The Appellate Panel of the World Trade Organisation made a ruling relevant to
protection of human health. Any future dispute between tobacco and trade can be
resolved in reliance of this case since global tobacco control is protection of human
health.
An SPS standard must derive from an objective assessment of the matter
before it, including an objective assessment of the facts of the case and the
applicability of and conformity with relevant agreements. Any measures taken to
protect human health must be based on the agreement. This does not relieve States of
application of customary international law in interpreting the treaty. Precautionary
principle of law though applicable shouldn’t override the Agreement.19
The GATT Appellate Body also held that harmonisation by members of
the SPS measures to international standards, guidelines and recommendations is not
legally binding perse but as in international law, these need to be adhered to in good
faith. The assessment of risks to prohibit trade under the agreement are not a closed
list, i.e. The risk to be evaluated in a risk assessment, is not only risk
ascertainable in a science laboratory under strictly controlled conditions, but
also risk in human societies as they actually exist, like “the actual potential for
adverse effects on human health in the real world where people live, work and
die . The body acknowledged that governments tend to base their legislative
measures on mainstream scientific opinion. It is legitimate so long as it is done in
EC Measures Concerning Meat and Meat Products (Hormones)
The core of the Precautionary Principle, still evolving is reflected in
■
Declaration, which provides that where there are threats of serious nr '
?£ e 15 of lhe Rl°
scientific certainty shall not be used as a reason for nostnonino r
‘[reversible damage, lack of full
environmental degradation. See among others P Sands Prine' °S "e fecUve measures to prevent
Law, Vp] I (Manchester University Press 1995) nage 2|’Pr!nClple8 of Inlernat>onal Environmental
Interpreting the Precautionary Principle (1994) 262
”
Cameron and T.O’Riordan (Eds),
12
good faith and signals a reasonable relationship between the SPS measure and the risk
assessment, especially where the risk involved is life-threatening and is perceived to
constitute a clear and imminent threat to public health and safety. Determination of
this relationship can only be done on a case to case basis, after account is taken of all
considerations rationally bearing upon the issue of potential adverse health effects.
Moreover, without undertaking a risk assessment as a minimum procedural
requirement, members States can still proceed to regulate products under the SPS
Agreement, provided the measures are not arbitrary, discriminatory or amount to
disguised restriction on international trade.
For the development of the Framework Convention on Tobacco control, the use
of evidence supplied by various scientific researches from WHO and member States
is overwhelming. This will constitute a satisfactory and legitimate risk assessment of
the harm tobacco causes to human health. Thus, the SPS Agreement is in fact a
strong basis to assert that WTO law and policy considers the protection of public
health as an important component of its International trade work.. Moreover, this
ruling has widened circumstances for the application of rules under the agreement.
For example, the use of reasonableness as a standard, the dispensing with procedural
requirements for a risk assessment, the acknowledgement of scientific evidence from
International organisations such as WHO, the objective assessments of issues and the
fact that States rely on mainstream scientific evidence to effect legislation to protect
human health all support the development of a global tobacco control Convention.
Relevant GATT Agreements
These agreements attest to the fact that GATT 1994 is not only an arrangement solely
for trade objectives but does have health protection goals in the provisions of the
various agreements.
Technical Barriers to Trade20
The Agreement on Technical Barriers to Trade (1979 TBT Agreement) was
negotiated during the 1973 to 1979 Tokyo Round and adopted in 1979. The
agreement ensures that technical regulations and standards, including packaging,
labelling and marketing requirements and methods of certifying conformity with
technical regulations and standards, are not adopted or applied so as to create
unnecessary obstacles to trade. All products are subject to the agreement. It provides
for use of labels on products such as tobacco.21 The Agreement allows restrictive
technical regulations, as an exception necessary to fulfil a legitimate objective. One of
these is the protection of human health. In assessing such risks, relevant factors of
consideration comprise scientific and technical information, related processing
technology or intended end use products. The scientific evidence on the harm caused
by tobacco is well established. The escape clauses such as “where necessary”,
20 See fully in Ibid. 1994, page 138.
21 See this further in Jacques H.J.Bourgeois, Frederique Berrod & Enc Gippini Fournier (eds) (1995)
The Uruguay Round Results: A European Lawyers perspective, College of Europe, Bruges, European
interuniversity Press. Brussels., page 311
13
“except when” and “wherever appropriate” provide good arguments as tobacco
Control is now a public health necessity for the international community. The
Agreement further states that where urgent problems of health arise, members may
omit procedural requirements for the adoption of the technical regulation. This
expedites global tobacco control by restricting tobacco advertising, packaging, labels
and regulation of nicotine levels in cigarettes. The provision that such actions be
based on scientific evidence is relevant. WHO as the most authoritative world body
on health matters has a wealth of scientific evidence on the lethal nature of tobacco
products and trade."
The Agreement seems cumbersome in application of the health exception
but it is possible for a global tobacco convention to provide the impetus to enable
States fulfil conditions for enforcement of technical regulations relating to health.
Thus, the TBT Agreement is compatible with the development of the Framework
Convention on Tobacco Control.
Agreement on Sanitary and Phytosanitary Measures.22
23
The Agreement provides that WTO members have the right to take sanitary and
phytosanitary measures necessary for the protection of human, animal or plant life or
health. These measures are to be based on scientific principles and shouldn’t be
maintained without sufficient scientific evidence. Evidence from International
organisations is recognised.
Members shall ensure that their sanitary and
phytosanitary measures do not arbitrarily or unjustifiably discriminate between
members States. These measures shall not be applied in a manner to restrict
international trade. They should conform to the agreement and GATT 1994 measures
relating to sanitary and phytosanitary measures especially Article XX (b) of GATT.
Member States shall harmonise these measures based on international standards,
guidelines or recommendations, where they exist. However, members may introduce
or maintain measures which result in a higher level of sanitary or phytosanitary
protection than would be achieved by measures based on the relevant international
standards, guidelines or recommendations, if there is a scientific justification, or if
appropriate for a State. Further, sanitary or phytosanitary measures shall be based on
assessment of the risks to human, animal or plant life or health, taking into account
risk assessment techniques developed by relevant international organisations. In this,
account shall be taken of available scientific evidence, testing methods, ecological
and environmental conditions and or treatment.
On the relevance to tobacco control, the Agreement allows restrictions to
protect human health. Tobacco control is protection of human health. The agreement
enjoins international organisations to provide information as a basis for sanitary or
phytosanitary measures. WHO is such organisation and the fatality of tobacco trade is
well documented by the organisation. WHO provides global guidance in the field of
public health. It promotes technical co-operation in this area and carries out
programmes to control and eradicate disease. The International Health Regulations
ensure maximum security against the international spread of diseases The work of
FAO in setting food standards in the Codex Alimentarius is also another acceptable
standard. WHO effort to develop the Framework Convention on Tobacco Control is
thus legitimate , compatible with WTO law, policy and practice
22 Article 2 of the WHO Constitution grants these powers.
23 See the World Trade Organisation: The Results of the Uruguay Round of Multilateral Trade
Negotiations: The Legal Texts. 1994 page 69.
14
Agreement on Trade related Aspects of Intellectual Property Rights (TRIPS)
a
The TRIPS agreement provides minimum standards for governing the use of
intellectual property, including medical technologies and pharmaceuticals. It
guarantees product and process patent protection. All WTO members are given a year
to fulfil obligations under the agreement, excepting developing nations have a 4 or 5
year grace period. Least developed countries have a 10-year transitional period.
TRIPS like GATT, contains an exception for measures necessary to protect public
health. Australian and South African health warnings of 25% of the packet fall under
this category and these have not been challenged under TRIPS.
In the WTO Dispute Settlement Panel Decision on India-Patent Protection for
Pharmaceutical and Agricultural Chemical Products, the United States complained
that India was in breach of its obligations under the TRIPS Agreement. The Panel
concurred with the US that India had failed td ensure adequate mechanisms for
ensuring product patents for pharmaceutical and agricultural chemical products and
processes. 24 This decision and TRIP calls for harmonisation of intellectual property
standards could help curb counterfeit unregulated cigarettes that flood developing
country markets and increase the risks of the tobacco problem. This could help
control smuggling of these products.
Agreement on Import Licensing Procedures
This provides for licensing of controlled goods such as tobacco and certain dutiable
commodities, such as liquors and methyl alcohol. Hence restriction of tobacco using
licensing poses no conflict with WTO rules provided the procedures laid are followed.
International Convention on the Simplification and Harmonization of Customs
Procedures, Kyoto 1974
c
This has provisions relating to duty free sales in its Annex. The procedures to take to
trade in duty free sales is laid down and this is compatible with the public health
objective of controlling duty free sale of tobacco around the world which has
increased tobacco use.
World Trade Rules and Health: Concurrence or Conflict.
There may be various views on the impact of International trade on the
quality of health. A theory is that increase in per capita income does not necessarily
damage health. A country with a stagnant economy will be under pressure to improve
its health. The opportunity for countries to trade in world markets for goods and
technology facilitates the implementation of needed health programmes at home.
Paradoxically, an expansion of trade can produce negative health effects so large that
they outweigh the conventional benefits from open markets, resulting in an overall
decline in national welfare. The trade in tobacco is a typical example of this
phenomenon.25 In case of tobacco, its no longer possible for developing nations to
24 John H Jackson: The World Trading System: The Law and Policy of International Economic
Relations. Second Edition, 1997, Page 310.
25 See World Bank: Curbing the Epidemic: Governments and the Economics of Tobacco Control,
1999, Pages 67-78.
15
, i ^oiir-v entirely on their own. Unilateral tobacco
create appropriate tobacco control policy e
‘y
rs What are thus needed are
control policies may lead to frictions
™
P^bacc0 controls. When a health
multilateral rules to guide countries in formU]lah g
°
alternative to unilateral
problem involves a transborder physical spih-o
Y^
actions based on economic and political power is
.
design, implementation and enforcement of an appropriate muItilaltera1 ^nient for
dealing with the problem at hand. The contribution of multilateral co-operation is to
reduce the possibility that solutions to the tobacco problem are affected by differences
in the economic and political strengths of the parties involved. Given the justifiable
basis for a diversity of tobacco control standards among countries, it is important to
minimize the risk of solutions being imposed by larger or richer countries. Thus, this
conference is timely and will involve the developing countries in seeking solutions to
the tobacco problem.
Protection of health through tobacco control has promised to be important for the
benefit of future generations. International tobacco control will involve rules of
international co-operation, sanction or both, so that government actions to protect
health of its population is not undermined by actions of other governments, for
example smuggling of cigarettes. Such rules may involve trade-restricting measures.
Secondly, free trade is important for enhancing world economic welfare and
trade restrictions may decrease achievement of this goal. These two theories of free
trade and trade restrictions may seem conflicting. Indeed, there is evidence that health
policy and trade policy are complementary in that increasing world welfare can lead
to citizen demands and governmental actions to improve protection of health. The
poor developing nations may not have effectual citizen demands for tobacco control.
Hence forth, a framework Convention of this nature becomes imperative.
Conclusion
A stronger case exists for the development of the Framework Convention on
Tobacco control. The fact that various WTO Agreements and Panel Cases have
recognised the protection of human health and regulation of products give credence to
the conclusion that a WHO global WHO Tobacco control convention is consistent to
WTO law, policy and practice. What is needed is further elaboration by WTO of
these rules relating to protection of human health. Any future disputes between trade
law and protection of public health using the framework convention may be referred
to the WTO dispute settlement mechanism. As can be seen from the decisions above,
the WTO Dispute panel strongly bases its arguments on general International law.
The WTO Rules on Dispute Settlement provides that member states recognise it as
central to the multilateral trading system. Any provisions of the agreements are to be
interpreted in accordance with customary rules of interpretation of public international
law. Indeed the WTO Appellate Body affirmed this position in the case of United
States - Standards for Reformulated and Conventional Gasoline
Thus, if there is a conflict between WTO obligations and the implementation of
a global tobacco control convention, the later Framework Convention on Tobacco
TJnd
My 199.4 PrOViSiOnS if a state is
top both treaties.
Under Article 30 of the Vienna Convention on the Law of Treaties , “when all the
parties to an earlier treaty are parties also to the later treaty..., the earlier treaty
hSr If he
extent *at ltS Provisions are compatible with those of the later
treaty. If the provisions of two treaties are in conflict, the later in time prevails, as
16
between the parties to both, unless one treaty specifies otherwise. Under Article 30 (4)
(b), if a State is a party to only one of the parties to both, only that treaty governs. It’s
a different matter if both States are parties to GATT and only one, a party to a global
tobacco control convention.
Finally, it must be stressed that international law develops with pace of
global changes, concerns and issues. The WTO trade regime is not averse to
changing global concerns.
Since 1970s and increasingly in 1980s, the fast
deterioration of environment led to global concern on protection of the environment.
This hastened GATT formation of a Body on the environment in 1991. In 1994, WTO
adopted a Decision which established a Committee on Trade and environment to
raise and recommend to the WTO issues relating to the environment. Therefore,
while environment issues have become an aspect of WTO trade regime due to global
concern for the environment, so has increasingly become public health concerns
which WTO needs to enhance it its work. Tobacco is a major aspect of this global
public health concern There should be no conflict between WTO trade regime and
the development of a global tobacco control convention.
IV.
INTERNATIONAL HUMAN RIGHTS LAW AND PUBLIC HEALTH.
Overview
Global control of tobacco is an important facet of protection of public health. Public
health is the science and art of preventing disease through organised community
efforts for the sanitation of the environment, the control of community infections, the
education of the individual in principles of personal hygiene, the organization of
medical and nursing service for the early diagnosis and preventive treatment of
disease, the development of the social machinery which will ensure to every
individual a standard of living adequate for the maintenance of health, and organising
these benefits in such fashion as to enable every citizen to realise his birthright of
health and longevity. Grad, a leading United States expert in health law, has noted
that “the reach of public health law is as broad as the reach of public health itself.
Public health and public health law expand to meet the needs of our society” (Grad
1986). Thus, we can assert that international public health law is as broad as the reach
of international public health itself as both expand to meet the needs of society.
The development of the Framework Convention on Tobacco Control is a mechanism
to attain public health as defined. According to Jonathan Mann26, “The goal of
linking health and human rights is to contribute to advancing human well-being
beyond what could be achieved through an isolated health or human rights based
approach.... The health and human rights perspective offers new avenues for
understanding and advancing human well-being in the modern world.”
A strong link exists between human rights and the tobacco problem.
The increasing deaths resulting from tobacco consumption is a denial of human
rights. The personal freedom of individuals to smoke (which too affects their health )
must be balanced against the freedom of others to live in a smoke-free environment,
and the responsibility of the State to protect public health of citizens and the expenses
incurred by the State arising from tobacco use and problem. The argument by the
tobacco industry that legislation to curtail the industry restricts the right to freedom
26 Jonathan Mann and others, Health and Human Rights in Health and Human Rights, Fall 1994.
17
cannot be accepted. In the US in 1989, Philip Morris launched a US$ 30 million
campaign associating the company with the 200th anniversary of the Bill of Rights.
Commenting on this effort to convey the image of the tobacco company as a great
defender of the peoples liberties, John F. Banzhaf III, Professor of Law at George
Washington University and Executive Director of Action on Smoking and Health
(ASH) in the United States, said “It’s ironic that the manufacturer of the only legal
product that enslaves most of its users is associating itself with freedom.
A powerful argument is advanced against this scheme by the industry to
potray itself as defenders of human rights. In all countries, the government has the
responsibility to protect the health of the people, particularly of the youth, to preserve
the quality of the environment, to regulate trade and commerce, and to promote the
public health, safety and welfare of its citizens. Government action for the welfare of
society as a whole is generally upheld as valid even if it runs counter to the interests
of some individuals, especially when there is compelling necessity for such action.
Thus, the right of States to protect the health of its people by controlling the tobacco
industry through the development of tobacco Control instrument takes precedence
over the freedom of the tobacco industry to promote its harmful product. The lethal
nature and deaths arising from the industry activities need not be overstated.27
Health is not simply the absence of disease. It is something positive, a joyful attitude
to life, and a cheerful acceptance of responsibilities that life puts upon the individual.
According to Stampar, President of the First World Health Assembly, the goal of
medicine is social. It is not only the care of disease, the restoration of an organism.
This became the notion of social responsibility for health as a whole, and the
corresponding duty of individuals to care for their health.
According to Theo Van Boven, formerly Director General of UN Human Rights
Office,
Three aspects of the right to health have been enshrined in the
International human rights instruments. These include, the
declaration of the right to health as a basic human right, the
prescription of standards aimed at meeting the health
needs of specific groups ofpersons, and the prescription
of ways and means for implementing the right to health.
It is important to note that the global human rights movement and Human Rights
Instruments stress the protection of vulnerable groups. These includes women,
children, populations of developed and less developed countries and less educated
segments of the population. The negative health effects of tobacco among these
populations is well documented and the development of a global tobacco convention
will conceptualise the realm of international human rights law.
Applicable International and Regional Human Rights Instruments.
There are various provisions for health in international human rights law
Foremost, the language of the Constitution of the World Health Organization endows
the right to health. It states that:
” See Ruth Roemer, Legislative Action to Combat the World Tobacco Epidemic, Second Edition,
18
The enjoyment of the highest attainable standard of health
is one of the fundamental rights of every human being
without distinction of race, religion, political belief,
economic or social conditions.
The Universal Declaration of Human Rights(1948) provisions on health is
fundamental. Paragraph 1 of Article 25 provides that, everyone has the right to a
standard of living adequate for the health and well-being of himself and his family,
including food, clothing, housing and medical care and necessary social services, and
the right to security in the event of unemployment, sickness, disability, widowhood,
old age or other lack of livelihood in circumstances beyond his control. Motherhood
and childhood are entitled to special care and assistance. The WHO efforts to protect
health of persons especially those of women and children from the scourge of the
tobacco epidemic finds support here.
Article 12 of the International Covenant on Economic, Social and Cultural
Rights (1966) provides that, the States parties to this Covenant recognise the right of
everyone to the enjoyment of the highest attainable standard of physical and mental
health. The steps to be taken by the States Parties to the present covenant to achieve
the full realisation of this right shall include those necessary for: the provision for the
reduction of the stillbirth-rate and of infant mortality and for the healthy development
of the child, the improvement of all aspects of environmental and industrial hygiene,
the prevention, treatment and control of epidemic, endemic, occupational and other
diseases and the creation of conditions which would assure to all medical service and
medical attention in the event of sickness.
Human Rights law has increasingly placed responsibility on States to control
non-State actors28. Thus, a State’s obligation to protect and promote economic and
social rights includes the obligation to prevent non- state actors such as tobacco
companies, advertising agencies and sports activities from promoting tobacco
products which kill. The UN has already developed a code of conduct for
multinationals violating environmental and labour standards especially in poorer
countries. Holding tobacco companies for misleading advertisements targeting minors
and fraud is now based on existing international practice. A global tobacco control
law will further these aspects.
Article 24 of the Convention on the Rights of the Child (1989) provides that
States Parties recognise the right of the child to the enjoyment of the highest
attainable standard of health and to facilities for the treatment of illness and
rehabilitation of health. States parties shall strive to ensure that no child is deprived of
his or her right of access to such healthcare services. States Parties shall pursue full
implementation of this right and, in particular, shall take appropriate measures: to
diminish infant and child mortality, to ensure the provision of necessary medical
assistance and healthcare to all children with emphasis on the development of primary
healthcare, to combat disease and malnutrition, including within the framework of
primary, through, inter alia, the application of readily available technology, and
through the provision of adequate nutritious foods and clean drinking water, taking
into consideration the dangers and risks of environmental pollution, to ensure that all
segments of society, in particular parents and children, are informed, have access to
education and are supported in the use of basic knowledge of child health and
nutrition, the advantages of breast-feeding, hygiene and environmental sanitation and
2S See Andrew Clapham, Human Rights in the Private Sector, Clarendon Press, Oxford, 1993.
19
the prevention of accidents, to develop preventive health care and guidance for
parents. States Parties undertake to promote and encourage international co-operation
with a view to achieving progressively the full realisation of the right recognised in
the present article. In this regard, particular account shall be taken of the needs of
developing countries.
Although the Convention on the Rights of the Child does not contain any
explicit right to protection of harms of tobacco, interpretation of the Convention by
the Committee on the Rights of the Child and state practice demonstrates that tobacco
is a human rights issue. The Committee has thus identified the issue of tobacco
consumption as within the scope of the Convention. Under the State Party Reporting
Guidelines established by the Committee, States are requested to,’’...provide
information on legislative and other measures taken to prevent the use by children of
alcohol , tobacco and other substances which may be prejudicial to their health and
available with or without restrictions to adults, and on any evaluation made of the
effectiveness of such measures, with the data on use of such substances by children.
The Plan of Action from the 1990 World Summit for Children also identified tobacco
use as a problem requiring action, especially preventive measures and education
among young people. Carol Bellamy, UNICEF Director has stated, “ Children have
a right to be protected from tobacco’s collateral effects—they have a right to health
and development and their use of tobacco is frequently a consequence of denial of
those rights. The main violators of children’s rights are the easily obtained legal
substances, tobacco and alcohol”.
The Convention on the Elimination of All Forms of Discrimination against
Women also makes provisions for protection of health of Women. Article 10(h)
makes a provision for health education and information for women and their families.
Article 11 provides for the right to protection of health and to safety in working
conditions. It further provides that protective legislation relating to matters covered in
this article shall be reviewed periodically in the light of scientific and technological
knowledge and shall be revised or extended as necessary. Article 12 provides that
States shall take all appropriate measures to eliminate discrimination against women
in the field of healthcare in order to ensure access to healthcare services. Drug
addiction and tobacco fall in this area. This is relevant for a global tobacco control
law. Recent research in many parts of Africa and Asia has shown the tobacco industry
is increasingly targeting women. A 1992 WHO Publication on Women and Tobacco
showed 10% of women in Africa smoke and the figure is rising. Smoking and
involvement of women in tobacco production all harm their health. The scientific
evidence of the lethal nature of tobacco products justifies the development of the
Convention to protect health of women and this finds support in CEDAW. Indeed the
UN Committee on the Elimination of Discrimination Against Women in its General
Recommendation 24 was on Article 12 covering women’s health throughout their life
cycle. It has stressed increased expenditure for women’s health services.
Article 16 of the African Charter of Human and Peoples Rights provides
that every individual, shall have the right to enjoy the best attainable state of physical
and mental health. States parties to the present Charter shall take the necessary
measures to protect the health of their people. A Protocol to the American Convention
on Human Rights (1969), the Additional Protocol in the Area of Economic, Social
and Cultural Rights (1988) makes a provision on the right to health. Article 10
provides that everyone shall have the right to health, understood to mean the
enjoyment of the highest level of physical, mental and social well being. In order to
ensure the exercise of the right to health, the States Parties agree to recognise health
20
as a public good and, particularly to adopt the following measures to ensure; primary
healthcare is made available to individuals and family in the community, extension of
the benefits of health services to all individuals subject to the State’s jurisdiction,
universal immunisation against the principal infectious diseases, prevention and
treatment of endemic, occupational and other diseases, education of the population on
the prevention and treatment of health problems and satisfaction of the health needs of
the highest risk groups and of those whose poverty makes them the most vulnerable.
Of importance is that many of these international human rights standards can be
found in various constitutions and legislation in various States.29
The ICESCR, CEDAW and Convention on the Rights of the child are usually
grouped as Economic and Social rights. Developing countries usually complain they
are unable to implement these rights due to lack of funds. Recognising the need for
some financial support, the prohibition of advertisement, increased taxes on tobacco
sales and mass education on the dangers of tobacco will be less costly to implement.
These international human rights instruments can only be effective in enhancing
the health of individuals, families, nations and communities if further implemented
through national legislation. However, in case of tobacco, national legislation has not
been effective due to the nature of the tobacco epidemic whose tenets are
transnational. For example, internet advertisement, standard setting in tobacco
products, smuggling and taxation issues and the fact that the industry is multinational
have undertaken years of calculated deceit, national legislation is essential but
insufficient. Thus, the development of the Framework Convention will help realise
aspects of human rights law. Most of the instruments emphasise protection of health
of the youth, mothers, massive health information and education. They provide for
preventive/primary healthcare and also treatment of disease. These provisions are an
ample legal basis for the development of the WHO Framework. Convention on
Tobacco Control. This is because its objectives will help realise health goals provided
in the various human rights instruments.
In conclusion, quoting Dr Jonathan Mann of Harvard University, “ The recent
discovery of inextricable linkages between human rights and health is one of the
great advances in the history of health and society...the major causes of
preventable illness, disability and premature death around the world are caused as
much by societal discrimination, inequity and injustice as by viruses or
parasites....How many preventable cancers result from marketing of tobacco in the
third world while violating the right to information about its dangerous
consequences. ?”
V.
DRUG LAW AND GLOBAL TOBACCO LAW.
World Health Organisation has been instrumental in guidance in the development of
standards and regulations relating to drugs at country level. These include special
reference to the Ethical Criteria for Medicinal Drug Promotion, endorsed by the
World Health Assembly in a Resolution in 1988. Recently, WHO has prepared
Guidelines for Good Clinical Practice for trials on pharmaceutical products. WHO has
been actively involved in the so called ICH process, the convening of a series of
International Conferences on Harmonisation of Technical Requirements for
29 See for example, articles 39(e) (f), 42 and 47 in part IV of the Constitution of India which all
provide for protection of health of men, women and youth. Chapter III of Constitution of Uganda
makes a similar provision.
21
Registration of Pharmaceuticals for Human Use which provides a forum for
regulatory authorities and experts from the pharmaceutical industry of the EU, Japan
and the US to discuss scientific and technical aspects of the marketing authorisation
of pharmaceutical products. WHO has also being able to play a major role in the
Organization of a series of international conferences of drug regulatory authorities,
the recent one in Berlin in June 1999.
The UN Drug Conventions are relevant to global tobacco control. Article 2
of the Single Convention on Narcotic Drugs, 1961 as amended in 1971provides that
drugs specified in its schedules are subject to control and regulation. Under Article 3,
where States or World Health Organisation in its opinion requires amendment of the
schedules, it may recommend adding of such substance to be controlled either under
schedule I or II. This means WHO has an international mandate under the Drug
Conventions to opine that tobacco is a drug subject to regulation. WHO action to
develop a global tobacco control Convention is thus a furtherance of existing
international drug law. Article 32 (1) of the 1988 UN Convention against illicit traffic
in Narcotic Drugs and Psychotropic Substances provides for dispute settlement among
others by way of conciliation, negotiation, inquiry, mediation, conciliation, judicial
process or other peaceful means of their own choice. Oversight monitoring functions
have been granted to the International Narcotics Control Board. This can be applied
for the monitoring of a global tobacco control Convention.30
The European Union has adopted instruments that make provisions related to
drugs. Article 129 contained in Title X of the Treaty on European Union provides
that the community shall contribute towards ensuring a high level of human health
protection by encouraging co-operation between the member States and if, necessary,
lending support to their action. Community action shall be directed towards the
prevention of diseases, in particular the major health scourges, including drug
dependence, by promoting research into their causes and their transmission as well as
health information and education.
The European Free Trade Association (EFTA) has been active in the field of
pharmaceuticals, having been responsible for the development of the Convention for
the Mutual Recognition of Inspections in respect of the Manufacture of
Pharmaceutical Products (Pharmaceutical Inspection Convention (PIC) and for the
Scheme for the Mutual Recognition of Evaluation Reports on Pharmaceutical
Products (PER Scheme). This Convention, originally signed in October 1970, has
been joined by many countries that are not members of EFTA, while a number of
additional countries have shown an interest in accession.
Currently, the deadly forms of nicotine delivery-tobacco products, are the most
widely available and least stringently regulated, while the safest forms of nicotine
delivery-medicines designed to help those addicted to tobacco to quit smoking are
strongly regulated. This amounts to preferential treatment of tobacco products°over
treatment products. This state of affairs even in the developing world has led to calls
for levelling of the playing field between the regulation of medications for treating
tobacco dependence and the regulation of tobacco products.
See Jimmy Gurule, The 1988 U.N. Convention Against Illicit Traffic in Narcotic Drugs and
Psychotropic Substances - A Ten Year Perspective: Is International Cooperation merely Illusory'’
22 Fordham International Law Journal, 1988; David P Stewart, Internationalizing the War on DrugsThe UN Convention Against Illicit Traffic in Narcotic Drugs and Psychotropic Substances 18 Denver
Journal of International Law and Policy, 387/8, Spring 1990. These have further discussed the
implementation of the UN Drug Conventions.
22
It should be noted that tobacco products are the only dangerous products that are
not regulated. Many products including medicinal drugs, food and toxic chemicals are
often regulated. During the Ninth International Conference of Drug Regulatory
Authorities (ICDRA), the Director of the WHO, Dr Gro Harlem Brundtland had this
to say. “ Cigarettes are inherently dangerous products. One of the largest transnational
tobacco companies opposes tobacco content regulation. Yet this company has a food
products division whose contents are regulated. How can we justify that the contents
of food products, made by a company are regulated but that the contents of cigarettes,
another of its products, are not.
It needs to be noted that in order to protect health of consumers;
governments have the general responsibility of restricting distribution of dangerous
products. This usually covers pharmaceutical products as well as toxic chemicals and
addictive drugs, usually given to drug regulatory authorities. Drug and food regulation
usually exist to protect health. Marketing of pharmaceutical products should be
regulated so as to ensure not only the safety but also the efficacy of the product.
Many developing countries have been slow to recognise that legislation
constitutes an important input in the health sector and that the formulation of policies
must be followed by an appropriate legislation to give effect to such policies. There
are other reasons to develop global regulation of contents of tobacco especially
nicotine. Recent research has shown that there are about 4000 other dangerous
substances found in cigarettes.
In many countries including developing nations, many legal systems are
structured on the premise that what is not prohibited by law is permissible. By
sanctioning certain activities, subject to various rules and conditions, and by
prohibiting other activities, a law clarifies what individuals or corporate bodies may
and may not do. Laws on regulation of cigarette content may for example proscribe
dangerous products in cigarettes. To permit control policies to be implemented, there
is need to have an authority whose powers and duties are laid down by legislation. For
example, they can have the power to cancel, modify and suspend a licence.
Legislation in developing world has also helped to ensure that the pharmaceutical
products are of acceptable quality, safety and efficacy. These applicable standards
must be laid down in a legal instrument or other document having the force of law,
and non-conformity with such standards must entail appropriate penalties. Some of
these standards are enforced through registration, certification and information
dissemination. These lay strategies for the assurance of drug quality, safety and
efficacy.31
Registration is usually based on information, which comprises administrative
data, toxicological, pharmacological, pharmaceutical, and therapeutic and clinical
data. Developing countries have prescribed varied grounds for which registration of
drugs may be denied. For example, in Kenya, a certificate may be suspended or
revoked if new information has been discovered by the Pharmacy and Poison Board
indicating that the drug is unsafe or dangerous. Other conditions may include:
procurement of the registration by fraud or misrepresentation, violation of the
conditions subject to which the drug was registered, public interest, misleading
advertisement etc. Tobacco products fall in this category and could be regulated.
Thus, there is an imperative justification to regulate tobacco products and
contents like by legislation. The Framework Convention on Tobacco control will lay
threshold standards and different States can then enact national legislation to
31 See D.C Jayasuriya; Regulation of Pharmaceuticals in Developing Countries, Legal Issues and
Approaches, WHO Geneva, 1985.
23
I
implement this to attain the objectives of national tobacco law. Regulation of tobacco
would be a two pronged approach. First is the regulation of tobacco pro uc s
especially nicotine and other many harmful contents of tobacco. Secon aspec is e
regulation of products that reduce tobacco dependence. This will involve for example
fast track requirements aimed at hastening the approval and use of cessation products.
Existing legal framework in developing countries for regulation of drugs or
pharmaceuticals could be amended to cater for regulation of tobacco products. For
example in New Zealand, the Poison Act has been utilised to regulate tobacco
products. The second option is to develop entirely new Statute law to specifically
address regulation of tobacco products. In this way, the role of the Framework
Convention on Tobacco Control will be instrumental in setting basic framework and
setting the problem clearly in a trans-national context.
VI.
CONCLUDING REMARKS AND RECOMMENDATIONS
The International legal framework for the development of WHO Framework
Convention on Tobacco Control is well established. WHO Constitution provides an
adequate legal basis. There is concurrence between international trade law and
international human rights law on protection of health, from tobacco epidemic. The
intensity of the tobacco problem on developing countries calls for their full
participation in this international law making and implementation process
if tobacco related deaths are to be controlled. Salient recommendations in the legal,
policy and institutional area should include the following:
Developing countries should establish national institutions to support the
development of the WHO Framework Convention on Tobacco Control. This can help
establish a national framework for tobacco control within the States. These could
utilise international legal standards relating to health and support the development of
the Convention.
Developing Countries and the International Community should work with
WTO and its member States to establish a Committee on Trade and Health. This
could be similar to the one established by GATT on the Environment in 1971 and
strengthened in 1994. It could examine upon request any specific matters relevant to
the trade policy aspects of measures to protect health with regard to the application of
the provisions of GATT taking into account the particular problems of developing
countries. The current negotiations in Seattle could be a starting point for this.
Developing countries should harmonise their strategies for tobacco control
and use the Framework Convention on Tobacco Control as a vehicle for tobacco
control. Technical consultation such as this could serve to develop a solid base for
the participation and implementation of the Framework convention in Develonins
States.
F 5
The International community especially WHO should use the Convention to
address the specific problems of developing countries on tobacco control. WHO
should increase technical support to developing countries for the negotiation and
implementation of the WHO Framework Convention on Tobacco Control
WHO should enhance collaboration with the larger international and
regional Human rights machinery. The joint study by WHO and UNICEF on tobacco
and children’s right and a WHO study on CEDAW is a good start. WHO focus on the
tobacco problem should involve the human rights community concerned with the
right to health. This would enable for example, the ECOSOC to emphasise dialogue
with representatives of ratifying States on the right to health and the necessity for
24
,
C
governmental action to curb tobacco use and problem. The chairing by WHO of the
Adhoc UN Task Force on Tobacco control is a positive step in that direction which
needs to be strategically used for this purpose.
25
The WHO International Conference on
Global Tobacco Control Law:
Towards a WHO Framework Convention on Tobacco Control
7 to 9 January 2000, Hew Delhi, India
Paper
Role
MMwafe art Nta w»a® actors: Wrt®
ffionoO annw@s8UBD®DDa Practices
Authors
Lukloossens
Ms Bungon Ritthiphakde
Consultant to the International Onion against
Cancer
Rue de Pascale 33, B-1050 Brussels
Belgium
Email: <Joossens@globalinEcorg>
Tel: 32-2-5470611
Fax: 32-2-5470601
Director
action on Smoking and Health Foundation of
Thailand
Website: <http://www.ash.or.th>
Email: <ashthai@asiaaccess.netth>
Tel: (66-21619 6259
Fax:166-216196258
This paper is commissioned by, and produced for the World Health Organization, Geneua
Abstract: In 1998, around 98% of the world cigarette market is accessible to some
degree to foreign tobacco companies compared with just 50% over a decade ago. This
change resulted from a number of factors, namely the dismantling of state monopolies,
the introduction of free market economies, the establishment of trade pacts and the
gradual removal of global trade barriers. While in the eighties domestic tobacco for the
largest international tobacco company, Philip Morris, was far more profitable than
international tobacco, international tobacco became more profitable in recent years. In
1998 for instance international tobacco generated US$ 5 billion profit and accounted for
almost three quarters of the total tobacco operating profit of Philip Morris. Faced with a
difficult “business” environment in the USA and the falling demand of cigarettes in
Western countries, there has been fierce competition among major multinational tobacco
companies to expand sales in emerging and developing markets in Africa, Asia, Latin
America and Eastern Europe. At the same time, mergers and acquisitions made a few
tobacco companies to be even more dominant actors on the world cigarette market. The
merger of British American Tobacco and Rothmans, the acquisition of RJR International
by Japan Tobacco and the merger of the French Seita and the Spanish Tabacalera in 1999
have dramatically changed the face of the world wide industry. The list of the world’s
top cigarette manufacturers now has four companies at the top which dominate more than
e
70% of the market.
Considering the treat posed by smoking to global health in low-income and middle
income countries and the emphasis of the marketing efforts of international tobacco
companies on developing countries, an international regulatory strategy, such as the
proposed WHO framework convention on tobacco control, is more than urgently needed.
1 Identification of various multinationals and private actors
involved
A feature of the global cigarette market during the present decade has been falling demand in
Western countries, coupled with fast growing demand in other parts of the world, in particular
the emerging countries of Eastern Europe and Asia. As a consequence, there has been fierce
competition amongst major multinational companies to establish a foothold in markets where
cigarette sales are continuing to grow and this has been accompanied by a drive towards
internationalise brands.1 At the same time, mergers and acquisitions made a few tobacco
companies to be even more dominant actors on the world cigarette market.
The merger of British American Tobacco and Rothmans, the acquisition of RJR International
by Japan Tobacco and the merger of the French Seita and the Spanish Tabacalera this year
have dramatically changed the face of the world wide industry. The list of the world’s top
cigarette manufacturers now has four companies at the top which dominate more than 70% of
the market.
Table 1: Classification of the major tobacco companies
(based on 1997 sales, but taking into account the mergers and acquisitions of 1999)
billion units
l.CNTC (China)
2.Philip Morris (USA)
3.BAT/Rothmans (UK)
4.Japan Tobacco (including RJR International)
(Japan)
5.RJR (USA)
b.Reemtsma (Germany)
7.Altadis (Seita + Tabacelera: Spain and France)
8. KT&G (Korea)
9. Tekel (Turkey)
Total sales world wide
1.1
1 700
947
899
487
136
119
99
94
74
5600
China National Tobacco Corporation
Number one is China National Tobacco Corporation, which is a monopoly that produces
around 1 700 billion cigarettes a year or 30% of the world’s cigarette output, but supplies only
the domestic market.
The other three manufacturers are privately owned companies, which improved their position
on the international cigarette market strongly the last decade.
1 World Tobacco file 1998, Market Tracking International Ltd, London,1998 p.1055
2
1.2
Philip Morris
Philip Morris Companies Inc is the largest international tobacco company, which sold 944
billion cigarettes in 1998 or one out of every six cigarettes smoked around the world.
One of Philip Morris key strengths is the Marlboro brand, which is by far the most sold
cigarette brand in the world.
Table 2: The most sold cigarette brands in the world in 1997 (billion pieces)
Marlboro (PM)
Mild seven (JT)
L&M (PM)
Winston (RJR and JT)
Camel (RJR and JT)
Derby (BAT)
Cleopatra
B&H (BAT)
Philip Morris (PM)
555 (BAT)
Source: Maxwell report
485
127
92
70
59
54
50
48
35
35
Philip Morris remains by far the most profitable tobacco company, generating US$ 6.8 billion
tobacco division operating profit in 1997. BAT’ s operating profit amounted to US$2.5
billion, with RJR generating US$1.7 billion and Rothmans US$1.3 billion. Japan tobacco
does not give separate profit figures for tobacco operations.2
While in the eighties domestic tobacco for Philip Morris was far more profitable than
international tobacco, international tobacco became more profitable in recent years. In 1998
for instance international tobacco generated US$ 5 billion profit and accounted for almost
three quarters of the total tobacco operating profit of Philip Morris.
Table 3: Philip Morris tobacco profits 1988-1998: domestic versus international
(US$ billion)________________________________________________________________
year
1988
1990
1992
1994
1996
1998
Domestic tobacco profits
3.1
4.2
5.2
3.3
4.2
1.5
International tobacco profits
0.8
1.4
2.0
2.9
4.1
5.0
Source: PM annual reports
According to the PM annual report 1998, its share of the international cigarette market,
excluding the US, was 13,9% in 1998. While sales of cigarettes on the domestic market
almost didn’t increase during the last 10 years, the international volume more than doubled
from 335 billion cigarettes in 1988 to 717 billion in 1998.
2 World Tobacco file 1998, Market Tracking International Ltd, London, 1998 p. 1061
3
Table 4: Philip Morris cigarette sales 1988-1998: domestic versus international sales
(billions cigarettes)
year
Domestic sales (US)
1988
1990
1992
1994
1996
1998
Source: PM annual reports
219
221
214
221
231
228
International sales (excluding
US)
335
368
421
536
660
717
In the 1998 annual report, the company admitted on the one hand problems on the domestic
market. The cost of the US tobacco settlement and litigation claims was high and ” a bitter pill
to swallow” (p.4), as it reduced its domestic operating profits by more than two thirds.
On the other hand, the company was much more optimistic about the perspectives on the
international market: “ We account for only one out of every seven cigarettes sold outside the
US, leaving considerable room for growth. We are planning for still more volume, share and
income gains in this enormous market.” (p.9)
Faced with a declining domestic market and a difficult “business” environment in the US, it
seems evident that Philip Morris will continue its strategy of expansion overseas for the next
decade, in particular into emerging and developing markets.
1.3
British American Tobacco
British American Tobacco is the second largest private tobacco company and sold 714 billion
cigarettes around the world in 1998. Major brands include Benson & Hedges, Derby, Lucky
Strike, Kent, Kool and State Express 555. According to the 1998 annual report the aim is to
become “the world’s leading international tobacco group (...). We will continue to grow our
existing markets organically, enter new markets quickly and effectively and seek financially
attractive acquisitions.” (p.3)
On 11 January 1999, it was announced that an agreement has been reached on the terms of a
proposed merger of British American Tobacco and Rothmans international. The merger in
May 1999 brought together the second and fourth largest cigarette companies in the world,
with a combined volume in 1997 of over 900 billion cigarettes and a world market share of
over 16%. According to the 1998 BAT annual report, “the proposed merger with Rothmans is
entirely consistent with our strategy, especially as it brings us leading positions in more
markets, strengthens our share in the premium segment and provides further significant cost
savings. The enlarged British American Tobacco will be the clear market leader in the
emerging markets, where most of the future growth is expected.” (p.3)
The strategy behind this merger- the most important in the history of the world cigarette
industry- is in the first place to concentrate the marketing efforts in new markets to promote
BAT internationals brands at the expense of the local companies. Another objective is to
reduce costs, to focus on fewer, larger factories to make more profit.
4
Already in the 1998 annual report BAT is proud “ to have made considerable progress in
moving towards having fewer larger factories. We closed factories in Germany, Panama,
Mexico, Hong Kong, Uzbekistan and Malawi; and made announcements concerning the
closure of factories in Spain and Singapore and part of the factory in Belgium. This move to
larger factories will lead to economics of sale and costs savings in the future.” (p. 12)
Operating profit in 1998 was £1 011 million, compared with £ 1303 M, in 1997. The decline
in pre-tax profit in 1998 was mainly due to initial costs of US tobacco settlements, which
were much higher in 1998 (£613 million costs in 1998 and £258 million in 1997).
According to the trade report World Tobacco 1998, “BAT is the world's most international
cigarette manufacturer and the breadth of its brand portfolio could be said to give the
company an important marketing advantage over its competitors, although in some respects
the plethora of brands could be thought to be a disadvantage. BAT has more cigarette brands,
more factories and lower profit margins than Philip Morris and RJ Reynolds and as a result is
fundamentally less profitable than its main two rivals”, (p. 1083)
World Tobacco concludes: ’’Although the rise in anti-smoking sentiment in major western
markets has posed problems for almost all major tobacco companies, BAT has benefited from
its early initiative to enter emerging markets in Africa, Asia and Latin America.” (p.1084)
1.4
Japan Tobacco
A state monopoly until 1985, Japan Tobacco is now, after the acquisition of RJR International
in 1999, the world's third largest international manufacturer, with combined volumes of 487
billion cigarettes in 1997 (JT: 288 billion and RJR International: 199 billion)
The privatisation in 1985, with the government as sole shareholder, paved the way for more
aggressive marketing of the company’s products as well as for diversification into non
tobacco business. Until 1994, the government remained the sole shareholder but since then
one third of the shares have been sold, with the residual two third being retained.
In 1997, nine of the top ten cigarette brands in Japan were produced by Japan Tobacco. The
flagship brand is Mild Seven, the world’s second most sold cigarette, with a domestic market
share of 36%. Domestic volume sales rose by 2.6% in 1996-97 to 270.6 billion units.
International sales fell during the year by 17.5% to 17.7 billion units.
While Japan Tobacco has limited international experience, RJR has adopted a strategy
of international expansion, in particular into Eastern Europe. International volume of RJR has
grown by 14% from 175 billion units in 1993 to almost 200 billion units in 1997. RJR core
brands -Camel, Winston and Salem- are among the best selling international cigarettes world
wide.3
3 World Tobacco file 1998, Market Tracking International Ltd, London,1998 p.l 161-5
5
2. Trade and investment practices
In 1998, around 98% of the world cigarette market is accessible to some degree to foreign
tobacco companies compared with just 50% over a decade ago. This change resulted from a
number of factors, namely the dismantling of state monopolies, the introduction of free
market economies, the establishment of trade pacts and the gradual removal of global trade
barriers. 4
2.1
Acquisitions and joint ventures
During the 1990s, there has been an increase in the number of acquisitions and joint ventures
word-wide, in particular, in a number of regions and countries formerly closed to
multinational companies. This has been particularly marked in Eastern Europe and in Asia.
This occurred at a time when consumption has been stagnant or declining in developed
countries and as a consequence, multinational companies have been quick to establish
themselves in the newly opened markets.
Since 1990 the list of acquisitions by the three major companies is rather impressive: Philip
Morris made acquisitions or expanded its activities in Hungary, Russia, Czech Republic,
Lithuania, Ukraine, Kazakhstan, China, Poland, Portugal and Mexico; BAT in Hungary,
USA, Uzbekistan, Russia, Poland, Cambodia, Mexico and Turkey; RJR in Russia, Ukraine,
Kazakhstan, Azerbaijan, Turkey, Poland, Hungary, Tanzania, Finland and Romania.5
Local companies tend to lose market share, when multinationals enter the market. In the 1998
BAT annual report, the company stated with some pride: “ British American Tobacco and its
main international competitors are being increasingly successful at the expense of the local
companies.”(p. 5)
2.2
Trade liberalisation and trade pacts
The new face of the tobacco industry includes the disappearance of monopolies in a more
liberalised world. With market liberalisation, agreements like GATT and the appearance of
the World Trade Organisation, monopolies have started to break down. Since the fall of the
Berlin Wall in 1989 for instance, most factories in Central and Eastern Europe have been
taken over by trans-national tobacco companies. No government in these countries
complained about this evolution, as they were eager to have access to western technology and
know-how. There was a need for modernisation of tobacco manufacturing and no funds
available. The preferred solution for new funds was joint ventures.
Health experts were sceptical and were convinced that the privatisation would lead to more
aggressive marketing practices and to a widespread increase in the number of smokers.
Already the opening of the cigarette markets in Japan, Taiwan, South Korea and Thailand to
American cigarette companies in the mid-and late 1980s resulted in an increase of 10% in
tobacco consumption in these countries over and above any expected increase.6
Even the 1999 World Bank report “Curbing the epidemic” admitted that “the removal of trade
barriers tends to introduce greater competition that results in lower prices, greater advertising
and promotion, and other activities that simulate demand.”(p,14)
4 World Tobacco file 1998, Market Tracking International Ltd, London,1998 p. 15
5 World Tobacco file 1998, Market Tracking International Ltd, London, 1998 p. 1058-9
6 Chaloupka F J, Laixuthai A, US Trade Policy and Cigarette Smoking in Asia, NBER Working Paper No.5543,
Cambridge, Mass.: National Bureau of Economic Research, 1996.
6
The first aim of trans-national companies in taking over old fashioned factories is not to
provide help, but rather to penetrate a new market and to sell more of their products. In
Belgium, for instance, the company Welltab was taken over by Philip Morris in 1974 and the
Belgian company Gosset was taken over by RJ Reynolds in 1982. Despite the fact that the
market share of Philip Morris increased from 9% in 1982 to 30% in 1993, the factory was
closed in 1994 in order to transfer its production to a new plant in the Netherlands, where
Philip Morris produces 80 billion cigarettes with less than 2000 workers. (Joossens, 1995)
The Gosset factory was closed in 1990 and its production transferred to a RJR factory in
Germany, which produces more than 30 billion cigarettes a year. Philip Morris, Reynolds,
BAT or Rothmans have all the same production strategy which is to close down the small
factories and to maintain only a limited number of plants at strategic places where they can
produce huge amounts of cigarettes. The labour force is reduced in these plants as the new
machines are extremely powerful and produce 10,000 to 12,000 cigarettes per minute.7
One can wonder why RJR took over a company in Belgium, modernised the infrastructure
and closed it down 8 years later. For TTC’s the take over is a way to penetrate a market and
to promote its brands. In the Belgian example, RJR decreased gradually the advertising
expenditure for the local Gosset brand "Saint Michel" and promoted more and more its
"Camel" cigarettes. Saint Michel was an important cigarette brand in the seventies in
Belgium, but no longer in nineties.
In the case of manufacturers who have gone into growth markets, their immediate strategy is
to improve the local brand because that’s got the market, but their real objective is to find a
prominent place for the own international brands. In fact promotion expenditure for
internationals brands will almost always exceed promotion of local brands and the market
share of international brands will steadily increase at the expense of the domestic brands.
More international brands will be produced at the local factory and eventually exported to the
surrounding countries. For example, Reemstma went into Kyrgyzstan and Kazakhstan in
1998 with the following strategy: first to improve the local brand, then to produce their own
brand West and then to export those brands into the other central Asian markets.8
When the internationals brands are well established in the region, the TTC headquarters may
decide to rationalise production, reduce costs and close down the smaller factories. Only cost
and marketing considerations will be taken into account to maintain or to close a factory.
Another aspect of the dismantling of monopolies is the increase of imported tobacco. World
wide the main cigarette blend types are American-blend, Virginia-blend, Oriental/Turkish
blend, Menthol and Dark/Black blends. Trans-national tobacco companies have mainly been
promoting “American blend “ type of cigarettes, such as Marlboro and Camel. Consumption
of American-blend cigarettes has increased from 25% of world volume sales in 1990 to some
40% in 1997 due to rising sales in the Asia Pacific, Eastern Europe and Latin American
regions.9 The continued shift to American-blend cigarette remains an important global trend.
American blend cigarettes - which use a lot of flue-cured tobacco - have proved to be
extremely popular in markets with a traditional strong uptake of oriental blend or dark
cigarettes such Turkey, Bulgaria or Poland. The uptake of American-blend cigarettes led to a
7 Joossens L, Finding and using information about activities undertaken by tobacco interests to defend
themselves, in : Strengthening Tobacco Control In Central & Eastern Europe: proceedings of a training seminar,
Warsaw, Poland, 20-25 October 1995, World Health Organisation, p.79-84.
8 World Tobacco file 1998, Market Tracking International Ltd, London,1998 p.1269
9 World Tobacco file 1998, Market Tracking International Ltd, London, 1998 p.988
7
strong demand for flue cured tobacco and caused severe problems for the tobacco growers in
these countries. The share of tobacco produced by Polish growers fell for instance from 92%
in 1990 to 50% in 1992, due mainly to a Polish factory which produces Marlboro under
licence and imports its leaf tobacco.10
10 Joossens L, Finding and using information about activities undertaken by tobacco interests to defend
themselves, in : Strengthening Tobacco Control In Central & Eastern Europe: proceedings of a training seminar
Warsaw, Poland, 20-25 October 1995, World Health Organisation, p.79-84.
8
Box 1: The privatisation process in Thailand and the Asean Free Trade Area (AFTA)
Privatisation
As part of the conditions attached to the IMF-led $17.2 billion economic bailout package for
Thailand, some of Thailand’s 70 state owned enterprises must be privatised. One of the
agencies being considered for privatisation is the Thai Tobacco Monopoly. In fact, in its fifth
letter of intent to the International Monetary Fund, the government has set the TTM
privatisation as one of its goals for the first quarter of 1999.
Thailand Finance Minister Tarrin Nimmanahaeminda said the aim of selling shares in state
companies is to make them more competitive. But local and international tobacco control
activists have severely criticised the move on the grounds that a more efficient TTM is not
beneficial to Thailand. But the IMF may not be the only agency pushing for the privatisation
of the TTM. It is known that the monopoly began considering joint-venture possibilities
before the government accepted the IMF-backed bailout. In fact the state enterprise has been
in talks about various ventures for more than a year with several international tobacco
companies, including Philip Morris Co., RJR Nabisco Inc.'s R. J. Reynolds Tobacco
International Inc. (now owned by Japan Tobacco) and British American Tobacco.
TTM executives say that regardless of the outcome of privatisation, changes in their business
model are required now to survive increased competition from overseas. Greater incentives
to retailers will be offered to encourage stronger promotion of local products. If the
monopoly's 275-strong distribution network fails to expand sales in line with targets, a
separate company could be set up to handle marketing directly.
As far back as 1993 Philip Morris had been trying to relocate its operations. In an article
published in July 1993 it is stated that Philip Morris had approached the TTM to have them
produce Marlboro locally. The TTM rejected the offer but Philip Morris then went on to look
into the possibility of setting up a manufacturing plant in Singapore for regional sales. The
article reported that the Philip Morris offer included an offer to set up suitable machinery and
equipment. “Marlboro would pay for the operations adding further revenue to the Thai State
enterprise.” The article stated that “The aim of Philip Morris is to produce cigarettes
competitively with RJ Reynolds, which has stopped exporting Winston from the US and
instead is producing them out of Hong Kong.” The TTM knocked back the offer saying that
the cost of producing Marlboro in Thailand would be much lower and subsequently lead to
higher sales at the expense of TTM brands. The TTM also noted that they were afraid of
being criticised by Thai anti-smoking campaigners and the Ministry of Public Health. The
article quoted a source from the TTM as saying “... we have been scolded enough times by
the Public Health Ministry.” At the time this was occurring the TTM held 97% of the total
Thai cigarette market. 11
ASEAN forum and Asean Free Trade Area (AFTA)
Since the tobacco industry in Thailand is a monopoly, other foreign companies cannot
manufacture tobacco products in Thailand. Also, Thailand’s domestic cigarette market is
protected through high tariffs and central distribution channels. Although the Thai cigarette
market opened in 1991 to foreign brands, cigarettes imported into Thailand are charged a
‘US cigarette war spreads to SEAsia', The Nation, Jul 21st 1993, pg. Bl.
9
22.5- percent tariff from ASEAN countries and a 60- percent tariff from non-ASEAN
countries.
In 1998, at ASEAN summit in Vietnam, the member nations of the ASEAN (Brunei
Darussalam, Indonesia, Malaysia, the Philippines, Singapore and Thailand) agreed that AFTA
would be implemented by 2002. And they also agreed to apply tariffs of 0 to 5 percent by the
year 2000 on 90 percent of their total dutiable items. This would account for about 90 percent
of intra-ASEAN trade. When it comes into force on January 1, 2003, AFTA will impose its
tariff reduction scheme on tobacco products as well. They will then be given a 7-year
adjustment period but import duties are required to be reduced gradually to 5% by 2001.
Sources report that the ASEAN pact makes it far more advantageous for multinational
cigarette companies to produce in one of the member countries. Therefore, Malaysia is
replacing Hong Kong as the Asian hub for cigarette manufacturing due to its cheaper labor
and to more favorable trading arrangements/2
British American Tobacco relocated its Hong Kong manufacturing plant to Malaysia in July
1998. Malaysian Tobacco Company Bhd (MTC) chief executive Russell Cameron said the
move to Malaysia was part of a strategic plan by BAT to consolidate its manufacturing base
in the region. “
Currently, manufacturing for export make up nearly half of the MTC’s total volume and with
the transfer of the Hongkong operations this will increase significantly.” 12
13
12 http://www.fas.usda.gov/tobacco/circular/1999/9907/thailand.html
13 BAT relocating HKplant to M’sia, Singapoer Business Times, 25 April 1998, p 7
10
3 Smuggling
Between 1997 and 2001, the world market for cigarettes is forecast to remain stable, falling
by 0,2% to reach around 5,163 billion pieces. This total does not include the smuggled sector,
which is estimated to account for over 350 billion pieces in 1997.14
The trade in contraband sales world wide grew by more than 110 % between 1990 and 1997.
Markets with a high level of smuggling include China, Taiwan, Hong Kong, Brazil, the
Russian federation and Pakistan. Smuggling remains a world problem, which deprives
governments of revenue but at the same time, has helped to promote some of world’s leading
brands in markets which had previously remained closed to foreign imports. Demand for
western cigarette brands remains high.15
The tobacco industry benefits from smuggling in several ways:
<
smuggling stimulates consumption both directly (through the street sale of cheap cigarettes)
and indirectly (through pressure to lower or keep down taxes)
the threat of smuggling has also been used to avoid trade barriers or to force open new
markets
There is no doubt that the industry benefits from smuggling. The UK tobacco companies even
admitted it in their annual reports. At page 13 of the 1996 Corporate Report of the Imperial
Tobacco Group, the report says: “ In the hand rolling sector, Imperial Tobacco ‘s Golden
Virginia brand is exported to many European countries. In particular, sales to Belgium have
risen substantially, reflecting the growing legal and illegal cross-border trade in re-imports
into the UK.” The annual report 1997 of Gallaher says on page 16 /'Increased tourist
demand from the Canary Islands and higher shipments to Andorra contributed to an increase
in sales to Iberia of around 37%.
Gallaher believes that the gains in Andorra, coupled with a sharp increase of some 13% in
handrolling sales to Belgium and Luxembourg, relate to increased bootlegging trade into the
UK".
There is debate, however, about whether there is evidence of direct tobacco industry
involvement in smuggling. The line of the multinationals is that they sell their cigarettes
legally to dealers and that their responsibility ends there. In a BBC programme on smuggling
in Andorra, a spokesperson of Gallaher defended the policy of his company in the following
way:” We will sell cigarettes legally to our distributors in various countries. If people, if those
distributors subsequently sell those products on to other people who are going to illegally
bring them back into this country, that is something outside of our control...” 16
Exports from the UK to Andorra increased from 13 million cigarettes in 1993 to 1520 million
in 1997. Taking into account that almost none of these cigarettes were legally re-exported,
that Andorra only has a population of 63,000 habitants and that smokers in Andorra don’t
prefer British brands, it is hard to believe that the British companies didn’t know that they
were supplying to smugglers.
14 World Tobacco file 1998, Market Tracking International Ltd, London, 1998 p.1322
15 World Tobacco file 1998, Market Tracking International Ltd, London, 1998 p. 1246-7
16 BBC Money Programme, 8 November 1998.
11
According to the chief EU fraud investigator, Per Knudsen, « British tobacco manufacturers
must have been aware that the sudden increase of the brands to Andorra could not be
explained by the normal market. Neither in Andorra, nor in any of the neighbouring countries.
Simply because these brands are not widely sold outside the UK and Ireland. »
Since 1997, there have been several court cases and official investigations in differents part of
the world which accused the industry of supplying the smuggled cigarettes and/or at least of
being aware of the illegal destination of their products.
B&W and Canada: a former Brown & Williamson executive pleaded guilty to trafficking in
contraband cigarettes between the US and Canada. The cigarettes were sent from a warehouse
in Alabama to a private warehouse in Louisiana, were marked for offshore vessels and thus
tax free, and were then sold to a Vietnamese organisation that smuggled them into Canada.
BAT and China: a former BAT executive was found guilty by the Hong Kong’s High Court
of taking US$2.24 million in bribes in return for ensuring that distributors Giant Island
received huge quantities of duty-free cigarettes earmarked for the mainland. The Judge, Mr
Justice Yeung, said the companies had failed to explain evidence that suggested they knew
vast quantities of their cigarettes were being sold to smugglers. “A leading international
tobacco company sold large quantities of duty-not-paid cigarettes, worth billions and billions
of HK dollars, with the knowledge those cigarettes would be smuggled into China and other
parts of the world.” According to the judge, “ it is also an open secret known to everyone in
Hong Kong that some of these cigarettes would find their way back on the local black
market.”18
19
17
20
RJ Reynolds and Canada: In 1998, for the first time, a major tobacco company was
convicted for actively breaking the law to assist in a smuggling operation. An affiliate of RJ
Reynolds International pleaded guilty to charges of helping smugglers illegally reroute export
cigarettes into Canada. The affiliate, Northern Brands, Inc., has agreed to pay $15 million in
criminal fines and forfeitures for its involvement in these illegal activities.2’
RJ Reynolds and Europe: Spanish authorities seized a ship in October 1997, carrying more
than 120 million Winston cigarettes bound for the contraband market. The mastermind of this
operation, was Michael Hanggl, who says he has been a Reynolds customer for 15 years and
has frequently been a supplier to smugglers who bring Reynolds cigarettes into Spain.
According to The New York Times of May 8 1998, the Reynolds spokesman denied that the
company knowingly sold to smugglers, but also said that Reynolds decided to keep Mr
Hanggl as a customer even after Mr Hanggl told The New York Times in 1997 that he sold to
clients he knew to be smugglers. European authorities say that they believe that the
manufacturers routinely sell American cigarettes to traders who immediately resell them into
black markets set up to evade taxes and offering leading brands at a discount.22
17 BBC Money programme, 8 November 1998
18 Former B&W executive convicted of cigarette smuggling. Associated Press. October 16 1997.
19 Buddle C, Tobacco chief guilty in $33m bribes case, South China Morning Post, June 12 1998
20 Buddle C, Judge blasts tobacco firms as Jerry Lui sentenced. South China Morning Post, June 26 1998.
21 Dow Jones Newswires, RJR affiliate To Pay S15M For Acting As Smuggling Front, December 22,1998.
22 Bonner R. Europe turning to US to fight illicit cigarettes, The New York Tunes, May 8 1998. Bonner R, Drew C. Cigarette makers are
seen as aiding rise in smuggling. The New York Times, August 25 1997
12
RJR and Tanzania: Tanzania’s main tobacco company (TTC) evaded tax amounting to Tsh6
billion ($12 million) between 1995 and 1997 by offloading billions of shillings worth of
export cigarettes into the local market, investigations have revealed. The massive racket was
carried out by a crime ring involving senior Tanzania Cigarette Company (TCC) officials,
police and Tanzania Revenue Authority (TRA) officials.
The racket was first detected by senior company staff who suspected that some of their
colleagues were offloading cigarettes in Mwanza and Moshi ostensibly intended for export to
Sudan.
Formerly state-owned, the TCC was privatised in 1994 and taken over by Geneva-based RJ
Reynolds. The take over was acclaimed as Tanzania's showcase of privatisation because it
earned the country billions of shillings in revenue.
Although it has been taken over by Japan Tobacco Incorporated, the firm has retained RJ
Reynolds as the management company. Senior staff implicated in the multi-billion tax
evasion scam are still on board. 23
Philip Morris, BAT and Columbia: in 1999 Colombia’s provincial governors sued tobacco
companies Philip Morris and BAT for $lbillion, alleging they avoided import duty on
cigarette imports.24 According to a study by the Colombian Ministry of Foreign Trade, 64
percent of the 30 billion cigarettes sold each year in Colombia are contraband, while 26
percent are made domestically and 10 percent are imported legally. The report said that of the
5.5
billion Marlboro cigarettes that entered Colombia in the first nine months of 1997, 4.4
billion came from the free trade zones in Aruba and Panama, meaning that they entered tax
free as contraband. Philip Morris denies any wrongdoing. In a statement the company said
that it would “discontinue our business relationship” with any customer found to be involved
in smuggling, but said Philip Morris had “limits to our ability, alone, to affect the cigarette
contraband problem.”25 Confidential documents of BAT of 1994 showed that the company
was well aware that the duty non paid cigarette market in 1993 was already more important
than the duty paid market and that the company had a different marketing strategy to launch
and support their cigarette brands on the legal and illegal market.26
73 Mwakisyala, The East African , Fake Exports Ring Hits Tanzania for $12m. July 14, 1999
24 Francis D, Colombian smuggling helps drug lords do their laundry, National Post, May 13,1999.
25 Farah D, In Colombia, Marlboro is Smugglers’ Haven, The Washinghton Post, August 30 1998.
26 BAT documents nr 503891624-30,503891718-19,503891649-50.
13
Box 2 Smuggling in Vietnam, Hong Kong and Thailand
Vietnam
In low-income countries, such as Vietnam, where locally-produced cigarettes are cheap,
international brands have swept in with an aggressive marketing campaign based on a simple
logic: even if the people can’t afford the higher-priced cigarettes right away, they can start
wanting them now.
.
.
Over the past decade, Vietnam has tried to build a line of defence against the rising incidence
of smoking. Since 1990, the government has tightened its ban on imports of U.S. and foreign
cigarettes, prohibited tobacco advertising, and banned smoking in many public places including hospitals, meeting halls, theatres, and aboard buses and planes.
Many local bodies have placed additional restrictions on cigarette promotion, and numerous
workplaces, ministries, and local people’s committees have forbidden or regulated smoking.
Statistics on cigarette consumption are elusive in Vietnam. But smoking rates are clearly
climbing. In 1996, Vietnam produced 30 billion cigarettes, up from 24.6 billion in 1992 - and
this, of course, does not include the millions of cigarettes smuggled into the country.
Not only do smuggled cigarettes indirectly funnel sales and profits into the companies’
worldwide operations, but smuggling has an additional benefit: It puts tremendous pressure on
countries such as Vietnam to relax or eliminate their bans on cigarette imports. An estimated
10 percent of Vietnam’s demand for cigarettes is met by smuggled varieties, and they can be
found everywhere. Vietnam’s Ministry of Trade said the country is mobilizing border guards,
police, and a special unit of the Trade Ministry to co-ordinate anti-smuggling efforts, fight
corruption, and patrol highly porous land and sea borders. The smugglers are often
Vietnamese hill country and border peasants who carry illegal smokes across from Cambodia
and Laos, just as, a generation ago, Vietcong soldiers and porters hauled rice, arms, and
ammunition down the Ho Chi Minh Trail. The government is hoping to remove the incentive
for the cigarette traffic by providing capital and employment opportunities to farmers in the
border regions.
Hong Kong
Cigarette smuggling has become a lucrative trade because of the substantial price differential
between Hong Kong and neighbouring areas. The prevalence of cheap contraband cigarettes
in Hong Kong not only erodes duty revenue, but also causes health hazards to the community.
The quantity of duty-paid cigarettes dropped by 43.4% from 6,990 million in 1990 to 3,955
million in 1997. While the decrease may be attributable to the success of the anti-smoking
campaign, the increasing level of cigarette smuggling may be a contributing factor. To contain
the problem, the Customs and Excise Department (C&ED) has stepped up its enforcement
efforts. Between January and September 1998, the Department arrested 1 359 persons
involved in cigarette smuggling and seized 78.2 million cigarettes with a duty potential of
$59.5 million.
J H
The Anti-Cigarette Smuggling Task Force (ACSTF), set up in May 1994 continues its
vigorous enforcement action against syndicated smuggling activities. Between January and
September 1998, the ACSTF seized 55.1 million cigarettes with a duty potential of $41 9
million, representing 70% of the total cigarettes seized during the period
Apart from stepping up enforcement, the Government has taken steps to enhance co-operation
with the tobacco industry and liaison with the Customs Authorities in neighbouring areas to
share information and intelligence on both regular and ad hoc basis. Co-operation with the
14
counterparts in the Mainland has led to significant seizures both in Hong Kong and the
Mainland. Moreover, the public has been encouraged to participate through an incentive
scheme which rewards informers.
Thailand.
In the past, the Thai market was closed to foreign cigarettes. The domestic market was
monopolised by the Thai Tobacco Monopoly. The arrival of US servicemen in large number
in Thailand during the Vietnam War in the late 1960s initially served to stimulate demand for
foreign cigarettes. Before that foreign cigarettes were only available in provinces bordering
other countries where foreign brands have been available. Only well-to-do people and those
who had been abroad smoked foreign cigarettes.
Once the growth in demand accelerated, smuggling cartels began providing the supply. After
the opening of the Thai market to foreign cigarettes in 1990, the smuggling activities
continued to thrive because there is still huge profit to be made thanks to high tax policy of
government. There was a huge price gap between legal duty-paid foreign cigarettes and
smuggled foreign cigarettes. Since the crisis struck in mid-1997 the price gap has narrowed,
despite perceived or actual difference in quality of legal duty-paid cigarettes and smuggled
foreign cigarettes. Many smokers continue to buy smuggled foreign cigarettes even as the
price gap has narrowed now. They insist on buying “better quality” smuggled cigarettes with
blue stamp, which indicates that they are made for the US and European markets.
The problem in Thailand is typical among countries where governments put in place
restrictive law and tax policy to try to control tobacco consumption. The country is
surrounded by countries with more tolerance and lower tax on cigarettes, including foreign
brands that can be easily re-exported. Long and porous borders with neighbours make it
difficult to fight smuggling.
Contraband trade seems to have the tacit approval of a large section of society because it
makes it possible for people to buy foreign products at significantly lower prices than they
would from legitimate outlets. That is to say smuggling is widely accepted by the society.
Law enforcement can only hope to keep contraband trade at a manageable level.
Law enforcement officials say the main reason why smuggled cigarettes continue to be
popular among smokers is that contraband cigarettes are found to be of higher quality than
legitimate duty-paid cigarettes. That is the case when comparing cigarettes of the same
international brands. Possible reasons are that duty-paid foreign cigarettes are produced from
different cheaper blends (mainly produced in Malaysia) than smuggled cigarettes (mainly
from US and Europe re-exported from Singapore). Price difference is not so much a factor
that explains the continued popularity of smuggled cigarettes as the perceived higher quality
of the contraband products.
15
4. Recent and changing trends in the promotion activities of
multinationals
4.1 Internet
Multinational companies such as BAT-owned Brown and Williamson and R.J. Reynolds have
launched web sites to advertise their products including pictures and details of special
promotions. The Internet remains an attractive medium for tobacco brands mainly because it
is an ideal place to reach the youth market- their biggest audience.
4.2
Indirect advertising
In Asia- Pacific, some of the world's largest tobacco companies are planning to circumvent
the European Union-wide ban on cigarette advertising and sponsorship by legally promoting
their cigarette brand names in a new range of coffee products. The idea of linking coffee and
tobacco is being tested in Malaysia by World Investment Company , a private company set up
by BAT explicitly to develop non-tobacco products to be badged with names of its cigarettes.
These include Benson & Hedges Quality Blend coffees, Lucky Strike clothing, John Player
Special whisky and Kent Travel, a travel agency. Total sales in 1997, amounted to US$100
Million.28 The amount of indirect marketing, particularly brand stretching, has been
increasing markedly over the past 3 years in Thailand. The most prominent example is Camel
Trophy clothing (although there is also Marlboro Classic clothing this is not being pushed as
strongly at this point.) Camel Trophy clothes are sold in up-market department stores and in
separate Camel Trophy shops. The clothes are periodically sold at significant discount and
"copies" are also widely available in markets around the city. Camel Trophy wear has become
extremely popular over the past year (1998/9) and is commonly seen. Most people, however,
do not know that the clothes are connected to the industry. Philip Morris registered ‘Marlboro
Classic’ in Thailand as a trademark in 1990.
The ubiquitous Camel Trophy sticker adorns almost every 4x4 sold in Thailand. The
company's close connection with off-road activities extends to the promotion of Camel
Trophy clothes through off-road magazines and ensuring a high profile at 4x4 events. So
'high' in fact that it is hard to believe that the relationship cannot be characterised as
sponsorship. In this the TTC s are not only taking advantage of lax enforcement but also in
legislative loopholes that do not forbid the use of minimally altered tobacco brand names and
images.
All manner of items are produced and either sold or freely distributed including car acessories
(such as seat covers and sun visors) and bumper stickers (particularly Camel Adventure
stickers). Whilst not all the products are produced by the tobacco companies (local
manufacturers at times use the logo's without consent) the result is the same Tobacco
company images have appeared on kites, children's shoes, socks, bags, clothes clocks,
cigarette lighters, stickers, hats, sunvisors, ash trays, money boxes, walkmans, earings and
chewing gum.
” World Tobacco file 1998, Market Tracking International Ltd, London 1998 n 77
World Tobacco file 1998, Market Tracking International Ltd, London J 998 p 77
16
Box 3: Judgements against Camel boots advertising
FRANCE: October 1998 - Camel Boots
RJ Reynolds sued for indirect advertising.
In a landmark, case, French representatives of the US tobacco company, RJ Reynolds, have
been found guilty of indirect advertising. In the first case of its kind in France, the Paris
County court ruled that RJ Reynolds had breached the French law which bans tobacco
advertising. The case was brought by the French tobacco control organisation, CNCT. Until
this case, CNCT had successfully sued the media and advertising agencies for indirect
tobacco advertising but had not been able to prove that the tobacco industry was behind the
advertisements. This situation changed following a complaint about a Winston Spirit ad. The
headquarters of RJ Reynolds were raided and police found a document by the RJR subsidiary,
Worldwide Brands, which set out plans for the circumvention of advertising bans in European
countries by using indirect ads such as Camel Boots, etc. It is expected that RJ Reynolds will
appeal against the ruling but for the moment this is an important victory for CNCT and
tobacco control.
FINLAND: March 1998 - Camel Boots
The Marketing Court in Finland has ruled on 30 March 1998 that the use of the word "Camel"
and the camel picture in conjunction with the marketing of Camel Boots is contrary to the Act
on Tobacco Control. This ruling maintained the earlier decision by the National Product
Control Agency for Welfare and Health (STTV).
The decision prohibits the use of the Camel emblem in a curved form with a similar font as it
is used in the emblem of Camel cigarettes. The decision prohibits also the use of a camel
picture similar to that of the emblem for Camel cigarettes.
The Marketing Court considered that the marketing of Camel Boots has been advertising for
footwear. Trade marks of a tobacco product that have been used for a long time as the Camel
marks and that are well-known by the population have been used in the advertising of the
Camel Boots. Therefore the advertising for boots has also conveyed an image of the Camel
tobacco product. The inclusion of an emblem for a tobacco product as a part of the advertising
for another product is marketing that is prohibited in the Finnish Tobacco Control Act as this
also promotes the sales of the tobacco product. Therefore advertising with the use of the
Camel emblem has been directly against the Act.
This is the first case of prohibition of indirect tobacco advertising in Finland that has been
upheld. It is also the first application of the amended (1995) article prohibiting indirect
tobacco advertising.29
29 For the details of the Finnish legislation go to the Finnish tobacco prevention site
www.tupakka.org (partly in English).
17
4.3
Social Development Support programs
The tobacco corporations in Malaysia usually conduct their lobbying activities through the
Confederation of Malaysian Tobacco Manufacturers (CMTM). While the settlement issue
was being hotly debated in the US in 1997, the CMTM in Malasia pooled together US$
280.000 and launched an anti-smoking campaign in collaboration with the Ministry of
Education in some 15,600 secondary schools throughout the country between May and
August. The campaign theme (as in the US) is “Right Decisions Right Now.
The timing of the campaign was significant in that it took place about the same time the US
settlement issue was released, so that the US tobacco corporations would not have to answer
to charges in Malaysia. It also coincided precisely with the controversial Peter Stuyvesant
KRU concert tour whose advertisements were more aggressive and attractive and contrasted
sharply with the preachy, unattractive anti-smoking ones placed sparingly by CMTM’s
campaign.
Although the launch of the campaign received much publicity in the local press, in the
following months a check with secondary schools in Penang revealed that there was no real
campaign activity on the ground. The public health community criticized this campaign by
the CMTM and the Education Ministry’s endorsement.
The government has been criticized for compromising with the tobacco lobby. The lack of
seriousness in addressing the promotion of tobacco, particularly indirect advertisements and
sports sponsorship has been highlighted many times. The tobacco lobby seems to have found
a support in Malaysia’s minister of information, who has indicated that the government’s
television-radio station cannot do without tobacco money. Hence the contradictions and
compromises continue.
The Information Ministry’s support of the tobacco industry seems to have a direct bearing on
the electronic media’s policy on tobacco. While tobacco-related illnesses are increasing, and
the minister of health has declared that the nation is facing a smoking epidemic, there are no
regular anti-smoking messages aired over radio or television in Malaysia.
4.4
Point of sales advertising
A lack of knowledge about restrictions on point of sale advertising by shop owners, in
conjunction with a lack of enforcement by public health officers, has meant that the amount of
advertising in shops is increasing in Thailand. Giving out display cabinets and shelves with
Camel and Marlboro logos and colors is very common in Thailand. Most sellers have them.
The cabinet featured also features the advertising (on the top of the cabinet) for the new
Marlboro cigarette brand which costs only 29 Baht, undercutting the price of leading brand
Krongthip. The cabinets are free and ensure a neat, eye-catching display for the cigarettes.
Recently ‘Lucky Strike’ and ‘Mild Sven’ have become increasingly active. The cabinets have
also become larger including those which contain shelves below for chips etc.
Another method, which TTC’s used to increase their market, was to increase the profit that
went to retailers. TTM brands normally earned retailers 50 satang (or 0.5 baht) per pack To
encourage retailers to sell foreign brands the TTC’s increased the retailers cut to between 1 5
and 1.9 baht per pack. The TTCs also applied for excise department licenses for the retailers
to encourage them to sell foreign cigarettes.
In the interim period between the opening of the Thai market to foreign cigarettes and the
passing of the 1992 Tobacco Products Act foreign cigarette companies tried to rapidly build*
30 ‘Foreign cigarettes growfaster and stronger than expected’, Siam Rat Weekly, September 1991, pg. 22
18
up their distribution networks. At that time few retailers stocked foreign cigarettes. In an
effort to improve this situation a carton of BAT’s ‘State Express 555’ was offered free every
month to retailers in addition to promotional stickers. During the same period Philip Morris
planned to offer gold to retailers to promote Marlboro but the plan had to be dropped once the
1992 act was passed.31
4.5
Corporate affairs Sponsorship
In 1994 a spokesman from Philip Morris Asia said in an interview that their new marketing
policy in Asia (and particularly South East Asia) would be focused on 'corporate affairs.' That
is, they would promote the company name as opposed to brands. He pointed to arts
sponsorship as one of the avenues, which they would take. He blamed advertising bans on the
need to alter their promotion direction and stated that Philip Morris would be extending this
plan to other countries in South East Asia. Examples of this policy in action include the
Philip Morris ASEAN Arts Awards.32 The Philip Morris ASEAN Arts Awards have been run
from the 28th October to the 2nd November every year since 1994. The region-wide Arts
competition was launched in 1994 to storms of protest. In Thailand the competition was
jointly organised with Silpakom University (Thailand’s most prestigious arts university) and
the ‘Arts and Culture’ Magazine. The magazine helped to discredit tobacco activists
objections to the events staging. Art institutes throughout ASEAN supported the competition
including the Art Society of Brunei, the Indonesian Fine Arts Foundation, the National Art
Gallery of Malaysia, Ayala Museum of the Philippines and the National Arts Council of
Singapore. Despite being allowed to continue, the award is not given much coverage by the
media in Thailand. In 1994 an exhibition of the finalists was held in Singapore. The
Singaporean government gave Philip Morris special exemption in order to stage the event.
In 1995 the Thai Art Awards (Thai judging round for the ASEAN awards) offered cash prizes
of 625,000 baht. Privy Councillor and Statesman presided over the opening of the 1996
competition which was held at the National Gallery of Thailand. With him was the secretary
general of ASEAN Dato Ajit Singh and Peter Barnes, president of Philip Morris Asia.
The Medical Council of Thailand opposed the involvement of Silpakom University in the PM
ASEAN Arts awards. Their secretary-general said that if Silpakom University allowed Philip
Morris to sponsor the event, ”it [would] taint the image of pure arts.” He went on to say that
allowing PM to sponsor the event would do more for the firm - “which wants to create a good
image” - than for the arts.33
4.6
Music and pop concerts
R. J. Reynolds Berhad operates a record shop called the Salem Power Station in Malyasia.
The Salem brand has been prominent in sponsoring live pop concerts in the cities, and music
concerts over television under the “Salem Cool Planet” banner. These events are heavily
advertised over television, radio, and newspapers. The advertisements claim the event is
“where the music comes alive.” RJR sponsors live concerts and bring in international stars
31 ‘Thai cigarettes hurt: TTM tries to survive’, Thansethakij, 17lh-23rd February 1992, p 57,
69.
32 ‘Philip Morris new strategy is to use art sponsorship instead of advertising’, Thamsethakij,
July 20 -21st 1994.
33 ‘Art contest’s sponsorship up in smoke?’ The Nation, 26lh July 1994, p44.
19
popular with young people, such as Alanis Morissette, Hooties & the Blowfish, and Paula
Abdul.
, ,
,
,
R.J.Reynolds chooses entertainers that appeal to young peop e ecause
ey ave
controversial images, defy the conventional, and rebel against acceptable norms. The Salem
concerts, which are usually held in Kuala Lumpur, are well attended by young people.
Aggressive advertising for these concerts, especially on television, starts well before the event
itself and appears many times a day, especially during prime time.
When a concert is organized in Malaysia, R.J.Reynolds also sponsors a radio program
where listeners can call in and answer trivial questions about the pop stars and win free tickets
to their concert. RJR would also sponsor contests through newspaper ads young people are
eager to win a free ticket to see their favorite entertainer. In the past, the winner had to go to a
“Salem booth” to collect the ticket. Free cigarettes used to be handed out to the audience
attending the Salem-sponsored events. The distribution of free samples has since been
outlawed.
R.J.Reynolds also sponsors the “Cool Planet Chart” show on television, which gives
the latest update on international pop music. But not all Malaysian teenagers enjoy Western
pop music. To cater to Chinese youth, Salem also sponsors live concerts or music programs
on television featuring such Chinese entertainers as Daniel Chan and Fay Wong.
Other promotional tactics under “Salem Cool Planet” include the “Blockbuster Spotlight,”
where free tickets to blockbuster movies, such as Face Off, Air Force One, My Best Friend’s
Wedding, Nothing to Lose, The Assignment and Excess Baggage are distributed. All one
needs to do is take the newspaper advertisement for the promotion to the participating
cinemas at certain advertised times and redeem it for two free tickets. R.J.Reynolds also
organizes year-end disco parties under the “Salem Cool Planet” banner, previously called
“Salem Celebrations.” Free tickets to the parties can be won by sticking Salem car stickers
(distributed free at gas stations) in a creative manner on your car. Salem Cool Planet
paraphernalia such as coasters are also found in discos.
4.7
Sports
Like other tobacco corporations operating in Malaysia, R.J. Reynolds is also into sports, and
Salem has found its niche in sponsoring tennis. RJR sponsors tennis tournaments or the
telecasts of major tennis tournaments. This way it gets to associate the Salem brand name
with tennis champions, with intensive television advertising. While tennis may not be the
most popular sport among Malaysians (soccer is the favorite national game and is controlled
by Dunhill sponsorship), nevertheless the advertising mileage on television is phenomenal.
Winston World of Action sponsors television programs on wrestling and boxing. As a sport,
wrestling is not well developed in Malaysia; however, the sport has a large television
audience, including children. In 1997, RJR brought wrestlers from the World Wrestling
Federation to perform in several large towns in Malaysia.
Philip Morris has a long history of Marlboro sponsorship of motor racing in Malaysia. The
nation’s quest to host Formula One racing has certainly given Marlboro a special place in the
development of this event. Meanwhile, Marlboro hosts and sponsors other motor racing
events and its telecasts on television, Every Sunday afternoon Marlboro used to sponsor the
Marlboro Total Malaysian Club Prix. Marlboro’s sponsorship of motor racing has been
endorsed by no less than Malaysia’s King, Prime Minister, and the deputy Prime Minister.
The Prime Minister flagged off the Marlboro Malaysian Grand Prix in April 1997
20
4.8
Youth access campaigns
Youth prevention campaigns are now a well known activity of Philip Morris. In the annual
report of 1998 the company explain : “ We expanded our youth smoking prevention efforts to
include 73 programs in 51 countries, and we have plans to increase these efforts in the near
future.” (p.9)
Already in 1993 Philip Morris approached the Ministry of Public Health with materials for a
program to discourage Thai youth from smoking. This offer was rejected, but Philip Morris
has been slowly introducing the programme alone ever since. Initially ASH noticed the
distribution of stickers stating that selling cigarettes to people under 18 is not permitted. In
1999 the project was extended, when Philip Morris began distributing pamphlets to shop
owners on how to refuse sales to those under the age of 18 years.
This campaign has been run in many other countries under various different guises.
Importantly none have ever shown any reduction in smoking amongst young people nor in the
level of compliance of shop owners to the acts provision. In fact studies have shown that this
type of campaign has actually led to increases in smoking amongst young people.
Health advocates believe that the initiative is a public relations strategy by Philip Morris and
that it may well do more harm than good as it reinforces the association of smoking as a
indicator of maturity.
A study, for instance, looking into retailer adherence to the law banning sales of cigarettes to
minors found in 1995 that 91% of the 773 retailers violated the law banning sales to minors. 34
The study set up a ‘sting’ operation wherein students aged 9 to 17 were sent out to try and
purchase cigarettes in five of Thailand’s major cities. Although the retailers were not asked
whether they knew about the law, there was evidence showing that 10% of these retailers
acknowledged the law by displaying ‘No sales to under 18s’ sticker. These stickers, similar
to the ones being distributed by Philip Morris presently, had no effect on the retailers’
adherence to the law. In fact of the 7 retailers which did refuse sales to minors, none
displayed the sticker.
34 Suriyawongpaisal, P., Tantiked, B., ‘Retailers’ compliance to the law banning cigarette sales to minors, 1995,
Tobacco Consumption Control Institute, Bangkok, Thailand.
21
Box 4: Case study on how multinational companies try to influence the tobacco policy of
Asian countries
A.
US Trade Representative
In the 1980s, the US Trade Representative helped to forced open markets of Japan, South
Korea, Taiwan, and Thailand for the US tobacco corporations, and challenged those
countries’ health measures on tobacco as unfair trade barriers using section 301 of the trade
Act of 1974. US-based transnationals then introduced very sophisticated and extremely
effective advertising and promotion techniques along with their products.
In recent years,
the US Government has shown more sensitivity to health concerns. The Doggett Amendment
now prohibits the U.S. departments of Commerce, State and Justice from using government
funds to promote tobacco products, and prohibits employees from opposing tobacco control
measures in other countries.35
36
B.
US Congressmen
In July 1991 US Congressman Mitch McConnell from Kentucky visited Thailand and met
with then Prime Minister Anand Panyarachun and senior Thai officials. He pushed for what
he called a “real opening” of the Thai cigarette market through adjusting import duties and
excise taxes levied on foreign cigarettes which he said, prevented US cigarettes from
capturing a substantial share of the Thai market. Thai officials resisted the pressure pointing
to the fact that the import and excise duties imposed on foreign cigarettes were consistent with
the GATT ruling.37
C.
Local Politician
In March 1992 a closed-door meeting was held to scrutinise the two proposed tobacco control
acts. With the help of a National Assembly Member, one of Philip Morris (Thailand’s)
managers was given access. Though discovered and quickly asked to leave the two
parliamentarians maintained their objections to the acts and to article 4 (banning sale to
minors) and article 11 (ingredient disclosure) in particular.38
D.
Their Embassies
It took Thailand more than six years for the ingredients disclosure regulation to finally get
cabinet approval in 1997 coming into effect on February 10 1998. In April 1995, when the
issue of ingredients disclosure was first brought up,
Representatives from Rothmans, Japan Tobacco, British-American Tobacco and Philip Morris
petitioned cabinet ministers through their respective embassies and through a joint letter on
the subject to the Ministry of Foreign Affairs. They also wrote a letter to the Ministry of
Public Health voicing the concerns of the tobacco companies about the implications of the
law for the companies.
35 "Trade and Health issues: Dichotomy between U.S.
Tobacco Export Policy and
Antismoking Initiatives, ” US General Accounting Office (GAO), May 1990, p 11
36 Bloom J L, International Interests in U.S. Legislation, Health Science Analysis Project Policy Analysis No 3
April 14, 1998.
3
3
37 ‘Anti-smoking lobby deplores US pressure’, The Nation, 20'h July 1991, p4
38 ‘Marlboro man slips into smoking review’, The Nation, 12,h March 1992, pBlO
A US Embassy official stated, in a letter to the Director General of the Business Economics
Department of the Royal Thai Ministry of Commerce, dated January 22, 1998, that
“Washington has instructed me to offer you the attached information regarding proprietary
information and the disclosure of cigarette ingredients.” Also a source from the Ministry of
Public Health said that the ingredients disclosure issue might be raised during discussions
between Prime Minister Chuan Leekpai and President Bill Clinton in Washington from March
10-17 1998.39
The tobacco industries: Rothmans, Japan Tobacco, British-American Tobacco and RJ
Reynolds, themselves formed an association of tobacco importers and sent a letter to the
Ministry of Health. The letter requested that the ingredient disclosure regulation be delayed
pending an inquiry into Thailand’s intellectual property obligations. It went on to say that
they had donated 1.5 million baht to the Thai King’s ‘Flood Relief fund’ and that they would
become more active in supporting Thai tobacco farmers through the setting up of a ‘Thailand
Tobacco Leaf Foundation’ in their attempt to sway the civil servants.
Many government agencies, including the Prime Minister's Office, received letters
complaining that revealing the ingredients of their products was in violation of the Agreement
on Trade Related Aspects of Intellectual Property Rights, as it would mean revealing the
production secrets of each brand of cigarettes. The tobacco firms attempted to avoid the
regulation by not revealing their ingredients to the ministry. This resulted in a shortage of
imported tobacco products apparently aimed at getting consumers to complain about the
shortage of their products.
In a bid to ease the concerns of TTCs, the International Economic Committee asked the
Public Health Ministry to ensure trade secrets were kept confidential. However, a Commerce
Ministry source claimed the new regulation was too rigid and should be eased by allowing
foreign manufacturers and importers to reveal only important ingredients which endanger
health, such as tar and nicotine. He said he was worried that American tobacco producers
might force the United States to retaliate against Thailand by increasing tax on Thai
products.40
39 Woranuj' Maneerungsee, ‘Concern over trade secrets’, Bangkok Post, March 7, 1998
40 ‘Two firms reminded of deadline: Formulas must be lodged by April 10’, Bangkok Post
March 27, 1998
23
Recommendations
Faced with a difficult “business” environment in the USA and the falling demand of cigarettes
in Western countries, there has been fierce competition among major multinational tobacco
companies to expand sales in emerging and developing markets in Africa, Asia, Latin
America and Eastern Europe. At the same time, mergers and acquisitions made in 1999 a few
tobacco companies to be even more dominant actors on the world cigarette market. In future,
a few powerful groups may work with a few powerful countries to derail tobacco control
regulations and conventions.
Considering the treat posed by smoking to global health in low-income and middle-income
countries and the emphasis of the marketing efforts of international tobacco companies on
developing countries, an international regulatory strategy, such as the proposed WHO
framework convention on tobacco control, is more than urgently needed.
•
•
•
9
Direct and indirect advertising, promotion and sponsorship by the tobacco industry across
all media and in all forms of entertainment should be banned world wide. This should
include a ban on the use of any brand names, logos, images or trademarks associated with
the tobacco industry on non-tobacco products and services.
Regional and international trade organisations should follow the example of the World
Bank and ensure that their activities do not promote or support the tobacco industry and
do not diminish the effects of tobacco control efforts. A section on investments and trade
practises that increase tobacco supply and consumption should be included in the
proposed WHO Framework Convention on Tobacco Control.
National governments should recognise the negative impact that tobacco use has on their
economies and take all positive measures to restrict activities of the tobacco industry.
Cigarette smuggling can be reduced, but action need to be at national, regional and world
level. At international level, the proposed WHO framework convention on tobacco control
should contain a specific protocol on smuggling. This protocol should, for instance,
require record-keeping and tracking systems, which place the onus on the manufacturers
to prove that cigarettes arrive legally in their end-user markets
24
The IMHO International Conference on
Global Tobacco Control Law:
Towards a WHO Framework Convention on Tobacco Control
7 to 9 January 2000, Hew Delhi, India
Paper
Situation Analysis: An Overview of the Role of The
World Bank msS ■ ■ Global Tobacco Control
Author
flraj Abedian tPh.DJ
Professor of Economics School of Economics
Director, Applied fiscal Research Center (AFReC)
University of Cape Town, South Africa
This paper is commissioned by, and produced for the World Health Organization, Geneva
Table of Content
Executive Summary
I.
Introduction: Setting the context
1
II.
Tobacco and Public Health: An Overview
3
III.
Socio-Economic Cost of Tobacco: The World Bank Hole
7
Key Policy Recommendations of the World Bank Report:
9
IV.
Global Curbing of Tobacco Use: The Role of WHO
17
V.
Concluding Remarks
18
Selected References
€>
(i)
20
Situation Analysis:
An Overview of the Role of the World Bank and WHO in
Global Tobacco Control
___ Iraj Abedian (Ph.D.) Professor of Economics, University ofCape Town, South Africa
Executive Summary
This paper is set to provide an overall review of the context and the content of the World Bank’s
new policy position with regard to tobacco control, entitled: Curbing the Epidemic: Governments
and the Economics of Tobacco Control (1999). To this end, the paper focuses on the changing
global pattern of tobacco consumption. It argues that a large array of global developments have
turned the smoking epidemic to a transnational problem with public health and economic
dimensions. Global multilateral institutions such as the World Bank and WHO thus have to
respond
The reality is that tobacco, its production and its consumption, is as much a health issue, as is an
economic issue. In effect, increasingly the global focus of tobacco control needs an economicanalytic approach. Both the industry and the public policy makers express great concerns over
the economic aspects of tobacco control. These concerns need to be addressed effectively. The
paper highlights some of the most common economic issues that the policy makers especially in
the developing world encounter.
The paper argues that tobacco has become a complex global health hazard and needs a co
ordinated multi-prong solution at regional and international levels. WHO’ Framework
Convention for Tobacco Control (FCTC) is thus a logical framework for co-ordinated
international action. While WHO is entrusted with the task of championing the public health
issues of humanity, it is abundantly clear that much support and collaboration is needed for it to
succeed. A prime example of such constructive input is the World Bank’s report that demystifies
the economic issues that so often confront the governments, particularly in the developing
worlds. Other multilateral and regional organisations have much to offer in this regard. Practical
ways have to be found in order to create the effective network needed to deal with the looming
global crisis caused by smoking. The World Bank’s policy stance is thus timely and
complementary to WHO’s FCTC.
Iraj Abedian. AFReC, University of Cape Town
India Conference; January 2000
Situation Analysis:
An Overview of the Role of the World Bank and WHO in
Global Tobacco Control1
I.
Introduction: Setting the context
Over the past few years, there has been an unprecedented and rising level of collaboration
between the World Bank (WB) and the World Health Organisation (WHO) in the field of global
tobacco control. Both institutions have primary concerns in respect of global tobacco
consumption, and production. Their collaboration thus needs to be contextualised against the
backdrop of a rapidly changing world economic order; and in particular in view of a dramatic
shift in global patterns of tobacco consumption. The salient features of the recent developments
in this regard include the following:
(a)
Scientific research has established beyond any doubt that prolonged smoking has startlingly
large health hazards. The developed nations have responded to these epidemiological studies,
and have introduced public health policies accordingly. The level of tobacco consumption in
the developed world has been declining steadily.
(b)
Yet the governments of the poorer nations have by and large ignored these scientific
warnings. Meanwhile, smoking prevalence in the developing countries has been rising
considerably. Aggressive investment and marketing by the tobacco industry, alongside with
passive or inappropriate national public policy responses, have been the main contributing
factors to the phenomenon. The majority of humanity is thus exposed to unprecedented,
albeit preventable, risks. The projected casualties of the present-day global public health
policy paralysis is a staggering 10 million deaths per year by the year 2030. Seventy percent
of such deaths will occur in the poorer countries.
(c)
The prevalence of cigarette (as opposed to tobacco) smoking is positively related to income
levels in the developing nations. This may be attributed to the perceived ‘superior behaviour’
1 would like to thank the participants of the ‘October 99 Meeting of the Experts’ in New Delhi, India for their
constructive comments on the first draft of this paper. All errors and omissions remain mine.
Iraj Abedian, AFReC, University of Cape Town
India Conference; January 2000
2
of cigarette smokers. Whatever the psychoanalytic roots of the phenomenon, the fact is that
this pattern tends to glamorise the habit and entrench the pattern of smoking amongst the
young men and women who are the most productive segment of the workforce with rising
income levels.
(d)
Increasingly, tobacco advertising targets women world-wide. With the rising prevalence of
smoking among women, children and the youth become even more exposed to the habit.
(e)
With the rapid globalization, and the removal of barriers to capital mobility, the tobacco
industry finds it convenient to penetrate the markets in the developing countries. The
tansnationalisation of the industry, in turn, consolidates its relative power vis-a-vis the
national governments of the poorer nations; hence the industry assumes inordinate impact on
public health policies in such countries.
(f)
This is further compounded by the global pressures for privatisation of state monopolies,.
amongst them, the state-owned public cigarette manufacturing companies. In pursuit of
higher production efficiency, and in anticipation of larger foreign investment, governments in
the developing countries have followed privatisation and commercialisation policies that
have further entrenched the tobacco industry’s socio-economic position.
(g)
The tansnationalisation of, inter alia, communication has undermined the sovereignty of
governments in areas such as access to information, advertising control, and even retail
products distribution. In effect, tobacco advertising has become a transnational issue that
requires a global response.
In essence the changing pattern of tobacco consumption together with a large array of global
developments have turned the smoking epidemic to a transnational problem with public health
and economic dimensions. Global multilateral institutions such as the World Bank and WHO
thus have to respond.
In May 1999, the World Bank used the occasion of the World Health Assembly to unveil its new
study, and announced its new stance, on the role of governments in curbing the smoking
Iraj Abedian, AFReC, University of Cape Town
India Conference; January 2000
3
epidemic. Apart from the symbolic significance of the collaboration between the two institutions,
the World Bank’s partnership with WHO fills a much-needed gap in a holistic approach towards
global tobacco control. The reality is that tobacco, its production and its consumption, is as much
a health issue, as is an economic issue. In effect, increasingly the global focus of tobacco control
needs an economic-analytic approach. Both the industry and the public policy makers express
great concerns over the economic aspects of tobacco control. These concerns need to be
addressed effectively. The World Bank’s policy stance is thus timely and complementary to the
WHO’ Tobacco Free Initiative.
Against this backdrop, this paper is set to provide an overview of the World Bank’s policy
document, and highlight the necessity for WHO’s critical championship of a global tobacco
control strategy. The structure of the paper is as follows: Section 2 will provide a brief overview
of the public health dimensions of smoking with special reference to South East Asia. Section 3
will examine the overall thrust of the World Bank’s study and the policy recommendations of
Curbing the Epidemics: Governments and the Economics of Tobacco Control. Section 4 will
briefly summarise the WHO’s role, with particular focus on the need for a global Convention on
tobacco control. The paper will conclude with a summary of key observations.
II.
Tobacco and Public Health: An Overview
Nowadays, it is beyond any doubt that smoking is a lethal habit. Even the tobacco industry no
longer refutes the health hazards of smoking2. Equally true is the fact that smoking is
increasingly a developing country phenomenon. In terms of the 1996 statistics, the three
countries of China, India and Indonesia alone consume 44% of the world tobacco. (Chaloupka
and Corbett 1998) Over the past two decades the rapid rise in smoking prevalence among the
poorer nations has increased their share of smokers to 70% of the total in the world. As
importantly, the level of smoking, as measured by cigarettes per capita, has risen in the
developing countries. Figure 1 below illustrates the overall pattern of per capita adult cigarette
consumption in developed as well as developing countries.
2 For the first time Philip Morris via its website openly admits the ill-health consequences of smoking in October 1999.
Iraj Abedian, AFReC, University of Cape Town
India Conference; January 2000
Figure 1:
Smoking is increasing in the developing world
Trends in per capita adult cigarette consumption
Source: WHO (World Health Organisation), 1997
In response to nearly three decades of anti-tobacco public policies, the developed world is
beginning to experience a decline in smoking prevalence. The public health consequences in
these societies are thus likely to decrease accordingly. Meanwhile, the rise in smoking in the
developing world may be attributed to two sets of internal and external factors. Chief amongst
the internal factors are:
(a)
Illiteracy and Low Literacy: It is generally recognised that consumer’s knowledge is a key
determinant of consumption choice. Moreover, in the case of a hazardous item such as
smoking, the level of literacy and education in general plays a major role in consumer choice.
A case in point is an empirical study in India, as illustrated in Figure 2 below.
Figure 2:
Smoking is more common among the less educated
Smoking prevalence among men in Chennai (India) by education levels
Leng th of schooling
Source: Gajalakshmi and Peto 1997
Iraj Abedian, AFReC, University of Cape Town
India Conference; January 2000
5
To the extent that illiteracy, or literacy, is widespread in the developing countries, it
predisposes the population to higher prevalence of smoking. Rising literacy on its own,
however, does not guarantee lower consumption of tobacco. In fact, in many developing
countries with rising literacy and higher income, smoking prevalence tends to increase. South
East Asia over the 1980s and 1990s is a case in point. This is driven mostly by the ‘income
effect’ and the ‘impact of advertising’; in the absence of an effective public awareness
programme. Low literacy, at the same time, undermines public health campaigns that rely on
health warnings, and other forms of health education that require literacy.
(b)
Lack ofpublic education and awareness. Developing nations commonly lack adequate public
health facilities and in general do not pay sufficient attention to preventive measures in the
form of public education and awareness programmes. In the case of an addictive substance
such a tobacco, this is a major drawback. The challenge is to avoid smoking habits to begin
and prevent addiction to set in. Developing countries are generally least equipped to provide
an effective and sustained public awareness programme. The population is thus left exposed
to the health hazards of a variety of preventable diseases, including tobacco addiction.
(c)
Lack of political will: Societal issues ultimately require political will to resolve. The public
health hazards of smoking are no exception. Much too often the political leadership in the
developing nations ‘politick around’ the health aspects of smoking as opposed to dealing
with the hard choices that would provide effective solutions to the problem. One of the
contributing factors in this regard is the short-term time horizon of political office bearers.
Tobacco control policies pay off in the medium to long run. Meanwhile the politician’s
concern is mostly driven by short run prospects. In part this has to do with the issues of
accountability
and
democratic
governance
as
incorporated
in
the
socio-political
superstructure of the country. In some cases, lack of public resource availability is also a
contributing factor. Whatever the cause roots of the phenomenon, the outcome is disastrous
from a public health perspective.
Amongst the external, or global, factors that have raised the level of smoking in the developing
world are the following:
Iraj Abedian, AFReC, University of Cape Town
India Conference; January 2000
6
i.
Rapid pace of Globalization: Freer transfer of goods and easier availability of cigarettes
have provided accessibility that did not exist before.
ii.
Trade Liberalisation and international Capital Flows: Trade liberalisation has led to lower
than otherwise prices for cigarettes. This in turn increases demand and consumption. Rising
demand in the meantime provides the production scale that is needed for efficient
local/regional manufacturing enterprises. Closely interrelated with this are the pressure for
privatisation and the quest for foreign capital inflows. In a number of the developing
countries, the manufacturing of cigarettes has been privatised, using foreign capital. This
leads to a more efficient production, hence lowering of the price with a concomitant rise in
consumption.
iii.
Lack of Co-ordination among Multilateral Institutions: Historically, the tobacco policies of
the multilateral institutions such as the WHO, the UN agencies, the World Bank and the
IMF have not been co-ordinated. This lack of policy co-ordination has in some instances .
led to contradictory policy prescriptions and investment strategies. Of late, however, there
has been a rising level of co-operation among these institutions. In addition to the close
collaboration between WHO and the World Bank, there is growing recognition that the UN
agencies need to harmonise policies and practices if the massive global human losses of
tobacco smoking are to be averted. To this end, the UN Economic and Social Council
resolution 1999/56 of 30 July 1999 is a critical achievement. In terms of the resolution, A
UN Ad Hoc Interagency Task Force is established as a focal point for global tobacco
control. The WHO leads this task force. This augurs well for not only international policy
co-ordination, but also for the success of the WHO’s Tobacco Free Initiative.
iv.
Communication
Revolution:
Unprecedented
inventions
and
innovations
in
the
communication technology has transnationalised, among others, cigarette advertising.
National controls over the content and other aspects of advertising have diminished. As a
result market penetration is made much easier and cheaper for the tobacco industry.
The above list is by no means exhaustive. Yet it illustrates the fact that the combination of
internal and external factors have created a global social milieu in which tobacco use has reached
Iraj Abedian, AFReC, University of Cape Town
India Conference; January 2000
7
epidemic proportions. In terms of the most recent estimates:
°
At present, over one billion people world-wide are addicted to smoking. This number is
expected to rise to 1.6 million over the next 25 years.
•
Approximately 80,000 to 100,000 young people become addicted daily; the majority of these
•
Within the next thirty years, tobacco is likely to be the single biggest cause of death world
are in the developing countries.
wide, killing about 10 million per year. About half of these death will be in the working age
of35to69.
•
It is estimated that about 500 million people alive today will eventually be killed by tobacco
use. More than half of these will occur among today’s children and teenagers. (The World
Bank, 99b)
The picture is particularly bleak for the developing countries. The estimated casualties of tobacco
addiction are further compounded by the lack of social security systems, adequate public health
facilities, and a pervasive general poverty. What these figures fail to show however, is the sheer
magnitude of human sufferings that afflict not only the addicts themselves, but also their
relatives and family members. It is the sum total of these personal and social costs that create a
near catastrophic situation for the developing nations.
Given its high smoking prevalence ratios and the sheer size of its population, South East Asia
looms particularly large in this global picture. And, ironically, the more this region enjoys
economic growth, the more it is likely that smoking prevalence will rise, due mainly to the
income and ‘perceived prestige’ effects. If unchecked, therefore, smoking is likely to become the
region’s foremost public health hazard in the new century. Combating the problem, for the
reasons mentioned earlier, will require a mix of national and international solutions. Much
regional and global policy co-ordination is needed in this regard.
III.
Socio-Economic Cost of Tobacco: The World Bank Role
Tobacco is no longer a public health issue alone. Given the scale of tobacco production world
wide, the number of people employed directly and indirectly by the industry, and the level of
Iraj Abedian, AFReC, University of Cape Town
India Conference; January 2000
8
income generated by the industry for various sectors including the government, it is a fact that
tobacco has assumed a major socio-economic significance. In addition, its exceptionally high
profit margin has meant that the tobacco industry has command over the necessary resources to
establish a power international scientific, commercial, and marketing infrastructure to protect its
interest. The anti-tobacco strategies have thus had to confront a very sophisticated and well-
resourced network.
By the early 1990s, a two-prong development had emerged. One the one hand, as stated earlier,
tobacco had become largely a developing country issue. As such it had become a global public
health with strong and complex economic dimensions. On the other hand it was increasingly
evident that the industry has lost the arguments related to the health hazards of smoking. The
locus of arguments on the side of the industry shifted to the broader issues of mainly non-health
nature. As such governments and societies in general have been increasingly faced with a set
menu of issues related to economics of tobacco, mostly as a counter balance to the harmful
health effects of smoking. Governments were faced with issues related to potential job losses, .
lower growth, loss of tax revenues, and prospects of lower foreign investment. In the developing
world these issues are amongst the most sensitive, socio-politically. And, the fact was, and still
largely is, that these very issues are among the least researched in the developing countries.
This is the backdrop against which the World Bank’s recent tobacco control policy was initiated,
adopted and made public in May 19993. The policy document is entitled Curbing the Epidemic:
Governments and the Economics of Tobacco Control. It is the subtitle that merits special
attention.
Broadly speaking, the document fulfils two much-needed objectives. Firstly it provides a set of
new research evidence drawn from econometric analyses of not only the developed country
cases, but also from the developing countries including India, Bangladesh, South Africa, and
Zimbabwe. Secondly, and possibly more importantly, it addresses directly the very questions that
3 Prior to 1999, in terms of a 1991 policy decision, the World Bank has had a formal policy of not lending for
tobacco production and encouraging tobacco control. However, in practice this non-lending policy has not resulted
in much, particularly that money is fungible and it has proven hard to enforce the policy consistently.
Iraj Abedian, AFReC, University of Cape Town
India Conference; January 2000
9
governments in the developed and developing countries have to face when considering tobacco
control policies. In assessing the document Professor Amartya Sen, the 1998 Economics Nobel
Laureate, observed that: “ It is a fine balance of information and a timely plan of action.” (World
Bank, 1999a) The emphasis on public policy action makes it a particularly relevant report. In this
regard, it lends a coherent and timely technical support to the WHO’s Tobacco Free Initiative.
Key Policy Recommendations of the World Bank Report:
I
The tobacco epidemic may be curbed from either the supply or the demand side. The supply side
J
pertains mainly to crop substitution, trade restrictions, and even banning of the product. Based on
its research, the World Bank Report does not recommend any of these measures, mainly because
they are neither effective and sustainable, nor feasible in most cases. The Report acknowledges
that in the short term, it is unlikely that many lives will be saved, or considerable public health
gains will be made, from investing in supply side measures to combat tobacco. This is partly due
to the time lags that exist between scientific research and the large-scale operationalization of
research findings. However the Report recognises the need for continued research and
development in order to explore viable substitutes for tobacco in the medium to long run. This is
particularly significant for a number of developing countries such as China, India, Malawi,
Brazil, Zimbabwe and the like. In these countries, tobacco production is so large as to constitute
a potential social dislocation following any abrupt discontinuation of tobacco farming. Clearly,
the transition needs to be managed responsibly, that is with least socio-economic burden.
/■X
The curbs on the demand side of the tobacco epidemic are far more immediate and effective;
particularly in the short term. Here, the World Bank Report makes special contributions and
provides specific and feasible policy recommendations to governments world-wide. Below is a
J
summary of the salient proposals.
•>
The most effective short-term interventions that governments can make are those the: affect the
price of cigarettes. Excise taxes are obvious measures in this regard. In terms of economic theory
and well-established empirical research, there exists an inverse relationship between the price
and consumption of any good; including cigarettes. This negative relationship is further affected
by other factors such as income levels and the degree of addiction. Nonetheless, there is no shortIraj Abedian, AFReC, University of Cape Town
India Conference; January 2000
10
term substitute for this type of intervention. This is particularly important for the poorer
countries, because consumption of tobacco amongst the poor is far more price elastic than for the
rich. This is illustrated by the following summary of international studies as shown in Table 1.
Table 1: Comparison ofprice elasticity estimates for cigarette consumption for selected countries
Dare
Reference
Country
studied
Elasticity
estimate
Comments
Time-series 1929-73
1976 Health Interview Survey gives elasticity by
age and sex
1954-81 sales data
Time-series aggregate data 1954-80
Quarterly aggregate sales data 1965-80
1980
1982
Fujii
Lewi t and Coate
USA
USA
-0.45
-0.42
1984
1985
1985
Leu
Bishop and Yoo
Radfar
Switzerland
USA
UK
1988
1990
Godfrey and Maynard
Chapman and Richardson
1993
Keeler, Hu, Bameit and
Manning
UK
Papua New
Guinea
California
1994
Sung, Hu and Keeler
11 US states
1994
1995
1996
Reekie
Tremblay and Tremblay
Van Walbeek
South Africa
USA
South Africa
1997
Economic of Tobacco Control
Report (1998)
Economic of Tobacco Control
Report (1998)
South Africa
-0.50
-0.45
-0.23 (SR)
-0.39 (LR)
-0.56
-0.71
-0.50
-0.3 to
-0.5 (SR)
-0.5 to
-0.6 (LR)
-0.40 (SR)
-0.48 (LR)
-0.877
-0.4
-0.32 (SR)
-0.53 (LR)
-0.66 (SR)
-1.52 (LR)
-0.57
1997
South Africa
-0.59 (SR)
-0.69 (LR)
1956-84 aggregated sales data
Excise elasticity for cigarettes and for non
cigarette tobacco 1973-86
Monthly time-series consumption data, 1980-90
1967-90 panel data
1970-89 Time-series consumption data
Time-series 1955-1990
1972-90 Tobacco Board data
1971-89 Reekie’s data
1970-95 Time-series consumption data,
simultaneous equation modeling
1970-95 Time-series consumption data, single
equation modeling
Source: Economics of Tobacco Control in South Africa, (1998), Chap. 7
The relatively elastic demand means price increases are likely to reduce tobacco consumption
amongst the poor more proportionately than in the case of the rich. It is important to underscore
that such changes are effective only at the margin. Nonetheless, from a public health perspective
the beneficiaries of higher cigarette prices are likely to be the lower income consumers including
the youth and children. For such policy to be effective, however, it is important that the new
taxes are imposed on all tobacco products simultaneously and equo-proportionately. In other
words, increasing the price of cigarettes and not the price of other substitute tobacco products
will in all probability lead to a ‘substitution effect’ with little or no public health gains.
The use of taxation is particularly relevant for at least two reasons: Firstly, as shown in Figure 3
below, in comparison with the developed countries, on the one hand the price of cigarettes is
relatively low, and on the other hand, the tax proportion of the price is low.
Iraj Abedian, AFReC, University of Cape Town
India Conference; January 2000
Figure 3:
Average cigarette price, tax and percentage of tax share per pack,
by World Bank income groups, 1996
Source: World Bank (1999), p.39, Note: Similar results arrive if adjustment for purchasing power is made.
As shown in Figure 4, with the exception of the US, in most developed countries, the tax
proportion of the retail price of cigarettes is in excess of 50%. By contrast in most developing
countries this ratio is substantially less than 50%.
Figure 4:
International Comnarison of Taxes as % of Retail Cigarette Price
Source: Economics of Tobacco Control in South Africa, 1998; Chap. 7.
Iraj Abedian, AFReC, University of Cape Town
India Conference; January 2000
12
This suggests that governments in the developing countries have ample latitude to increase
tobacco taxation and have gains with respect to fiscal revenues as well as public health insofar as
higher taxes raises the price and hence lowers the consumption of tobacco products. It is this
win-win combination that often scapes the governments in the developing countries. More often
than not the reason put forward for not taxing tobacco products is the potential loss of fiscal
revenues. This is by and large a flawed argument. In almost all countries for which data are
available, increases in tobacco taxes have led to a rise in fiscal revenues. The explanation lies in
the inelasticity of tobacco consumption, caused mostly by the addictive properties of the
substance. Of course, taxes cannot continue to rise indefinitely without affecting consumption at
some point. But given the low base of tobacco taxes in almost all the developing countries, and
taking into account the demand inelasticities, there is much scope for sustained tobacco tax
increases in the developing world.
The second, and no less important, reason for raising taxes on tobacco is to increase fiscal
revenues and have the resources to take care of, inter alia, public health expenses. Often it is ■
argued that tobacco excise tax increases are likely to lead to lower fiscal revenues due to factors
such as increased illegal trade in cigarettes and or other forms of tax evasions. There is indeed a
grain of truth in such arguments. Whether or not governments should worry about it depends on
the following factors:
(a)
The integrity and efficiency of the custom services in the country,
(b)
The exposure of the country to the established smuggling routes,
(c)
The efficacy of the law enforcement systems,
(d)
The availability of a strong and widespread informal trading practices in the country.
(e)
The level corruption in the country, and in the region.
Of all the above-mentioned factors, the most pernicious is corruption amongst the political and
technical office bearers. In countries where corruption exists, it corrodes the governance
institutions and provides a thriving environment for smuggling of, inter alia, cigarettes. Clearly,
for smuggling to be so effective as to undermine fiscal revenues from tobacco taxation, it needs
much more than higher cigarette prices, (see Luk Jossens 1998)
Iraj Abedian, AFReC, University of Cape Town
India Conference; January 2000
13
An increasingly important aspect of tobacco taxation is, in my view, the need for regional and or
international co-ordination. Clearly when one country in a given region substantially increases
the tobacco excise taxes it exposes itself to increased smuggling, larger cross border purchases, a
potential loss of fiscal revenue. And as importantly it stands to gain much less in positive public
health benefits than otherwise. A much superior solution would be a co-ordinated and ideally
proportionate tax increases across a given region such as the South East Asia. In such cases,
there is no increased threat of smuggling, every chance of substantial tax revenue gains, and a
much better prospect in terms of public health. Not only in the case of tobacco taxes, but as I will
argue later also in the case of advertising control regional and global co-ordination renders a
much superior outcome. Such policy co-ordination, however, requires political championship as
well as appropriate institutional structuring.
Following tobacco taxation, the next most important form of government intervention in
reducing demand for tobacco products is comprehensive bans on tobacco advertising. As
documented in the World Bank report, bans on advertising are effective in reducing tobacco
consumption. Partial bans of tobacco advertising, however, are ineffective for a variety of
reasons. The most significant aspect of comprehensive bans on tobacco advertising is the fact it
effectively de-glamorises smoking. This is vital for creating a coherent milieu in which
particularly the children and the youth are given a consistent message about the society’s
perception of smoking. This is a necessary condition for arresting the rise in the current smoking
epidemic. Further reinforcement measures are needed in the form of awareness programmes
based on scientific and educational research.
The debate around cigarettes advertising bans, however, invites a series of associated arguments
related to human rights, the smokers’ rights, and the right to advertise a legal product. Closely
related to these issues is the question on whether smokers know their risks. These issues are
adequately dealt with in the World Bank document and I do not intend replicating them here.
However there are two political economy related aspects of these controversies that are not
adequately covered in the report, and in my view merit amplification.
The most important of these issues relates to an evident ‘double standard’ in socio-democratic
norms across countries. It is often argued that banning tobacco advertising could mark the
Iraj Abedian, AFReC, University of Cape Town
India Conference; January 2000
beginning of government encroaching on socio-democratic norms in the society. The tobacco
industry and its sympathisers make a big issue out of this ideological point in the developing
countries. What is often forgotten is that in the developed countries such arguments seem to arise
in an inverse context. In other words, because of the very democratic norms, espoused by the
society, governments in the developed countries introduce stringent measures to provide a better
living conditions for all; something which may well entail a reduction in absolute individual
freedoms. Such curtailments could range from the speed limits on the roads to ban on smoking in
public places, or a comprehensive ban on tobacco advertising as adopted by the European Union
in 1998 and is to come to full effect by October 2006. Surely, the population of the developing
countries deserves a similar benefit of democratic values.
Allied with democratic values is the overarching issue of human rights. The WHO constitution
states:
“The enjoyment of the highest attainable standard of health is one of the
fundamental rights of every human being without distinction of race, religion,
political belief, economic or social conditions. ” (Leary, p.2)
Linking smoking with human rights is bound to invite numerous controversies. At first glance, it
may be argued that the human rights aspects of tobacco use concern the freedom to smoke
without interference from others including the state. (Leary 1999) However, given the irrefutable
addictive nature of the product, it has to be asked: What happens to the human rights of someone
who has been enticed via sophisticated advertising and led to smoking addiction in a young age?
It is with regard to children and the youth that the ‘human right to health’ is of particular
relevance for the global tobacco control initiatives.
From a policy perspective, another pertinent issue is about the assignment of property rights
within the society. In most countries, by default and due to historic reasons the actual assignment
of property rights is in favour of the smoking addicts. As such an attempt to curtail such
perceived entitlement raises strong objections by the beneficiary interest and business groups. As
a result, the onus has fallen on the non-smokers to re-claim their rights, and in the process bear
the ‘burden of the proof’; i.e. costs of generating the required evidence, lobbying expenses, and
the like. Within an alternative constitutional framework, with clearly defined property rights, it
could well be the addicts who not only bear the burden of the proof but also they may be
Iraj Abedian, AFReC, University of Cape Town
India Conference; January 2000
15
required to compensate the non-smokers for the disutility and social discomfort caused.
Ultimately, therefore, it is the value system of the society that needs to determine which way
property rights should be assigned. In terms of economic analysis, clear articulation of property
rights assignment is needed in order to minimise wasteful resource use by contending claimants
to capture the potential gains from property rights. In this way, the society also reveals its
preference for the attendant income distribution consequences of the constitutional ruling.
A final element of the World Bank Report that I believe is particularly pertinent for the
developing countries, and merits singling out for discussion, is the issue of jobs and tobacco
control policies in the developing countries. Understandably, employment is a matter of top
concern for the poorer nations. And, in the political economy discourse around tobacco control it
is often taken for granted that controlling tobacco is equivalent to job losses. Governments and
societies therefore react accordingly. On the face of it the argument has a strong intuitive appeal,
because it posits that tobacco control will lead to less smoking, less or no advertising of tobacco
products, and thus the industry will shrink, jobs will be lost and incomes will disappear
accordingly. However, such arguments are fundamentally flawed. There are good theoretical and
empirical reasons for this. Here are the two main reasons why tobacco control is unlikely to lead
to any noticeable reduction in employment and or income losses.
Firstly, from an aggregate economic point of view on the expenditure side, when smokers reduce
their consumption of tobacco they spend their money on some other items of consumption. There
is no loss of income on the part of smokers; instead they rearrange their spending patterns. This
is called ‘expenditure switching’. The economy as a whole does not sacrifice any income. The
question therefore is whether the new pattern of spending is more or less job creating? This is
essentially an empirical issue and is dependent on the type of economic structure as well as the
pattern of consumer preferences after they quit or reduce smoking. If the consumers spend their
additional resources (given their less spending on cigarettes) on labour-intensive products and
services this might in fact lead to more jobs and not less. Also, it would matter if they spend the
extra money on locally produced goods and services as opposed to imported items. Empirical
studies conducted in USA, UK, South Africa, Scotland and Canada suggest that no job losses are
likely to result from a reduction in tobacco consumption in the society. Characteristically,
expenditure switching by the smokers results in more spending on recreational, food and
Iraj Abedian, AFReC, University of Cape Town
India Conference: January 2000
16
education outlays. Such production processes are commonly more labour intensive than cigarette
manufacturing. Besides, switching expenditures from tobacco to other consumption items has
some other advantages too. In the case of the developing countries, the majority of whom are net
importers of tobacco products, such expenditure switching reduces the so-called balance of
payments problem.
The second reason why tobacco control is unlikely to reduce jobs is this: in the short term
tobacco control policies are more likely to reduce the rate at which people take up smoking and
not reduce the absolute number of smokers. Empirical analysis shows beyond any doubt that
decline in tobacco consumption is a slow process. At the global level, if the anti-tobacco policies
are well co-ordinated and become effective, the current 1.1 billion smokers will grow at a lower
rate than otherwise. But the current market size is unlikely to shrink over the next few years,
possibly even over the next two decades. A similar argument is generally applicable to each and
every country. Broadly speaking, the increase in population together with a rise in incomes over
time would ensure that the market for tobacco products would continue for another 25 to 30
years, at least. This is further reinforced by the addictive nature of tobacco products.
In general, therefore, the fear of employment losses of tobacco control policies is based on poor
and partial economic analysis. The predominant majority of the countries in the world have
nothing to lose from curbing tobacco products. In the short term no country stands to lose.
However there are a handful of countries that need to manage the long term very carefully. These
are the countries for which tobacco constitutes a major economic activity or a major source of
foreign exchange earnings. Zimbabwe is a case in point insofar as its export is heavily dependent
on tobacco; e.g. nearly 98% of the annual tobacco production is exported earning 25% of the
country’s foreign exchange earnings. The same is true for Malawi where tobacco export is major
source of national foreign exchange earnings. Countries such as China, India, and Brazil need to
take careful measures not so much because of export earnings, but mainly because of the large
number of farmers and their dependants involved in the activities related to the tobacco industry.
Part of the long-term management of the situation for these countries may well lie in a co
ordinated and collaborative international pact in search of a global solution for the problem.
Iraj Abedian, AFReC, University of Cape Town
India Conference; January 2000
17
IV.
Global Curbing of Tobacco Use: The Role of WHO
One of the most startling scientific projections of the World Bank report is captured in Figure 5
below. It suggests that if the current pattern of consumption continues, tobacco is likely to kill
nearly 450 million smokers over the first half of the next century. On the other hand if
government interventions are introduced aiming at halving the number of young people taking
up smoking between now and 2020, then over 20 million lives could be saved. However if a set
of interventions aiming at both young and existing adult smokers is effectively implemented,
nearly 200 million lives could be spared of whom at least two thirds live in the developing
countries. This is an unprecedented public health challenge that needs a co-ordinated and well-
implemented remedial strategy.
Figure 5:
Unless current smokers quit, tobacco deaths will rise dramatically
in the next 50 years
Estimated cumulative tobacco deaths 1950-2050 with different intervention strategies
The international lead agency primarily tasked to take up the challenge is the WHO. In May
1996, WHO’s member states adopted the resolution to initiate the preparatory work for the
establishment of a framework convention for tobacco control (FCTC) world-wide. Towards the
development of FCTC, WHO has initiated a new project entitled, the Tobacco Free Initiative
(TFI). When in place, FCTC would be a global legal instrument to curtail any further expansion
in the current tobacco epidemic, particularly in the developing countries. The FCTC in turn
would pave the way for a series of ‘protocol agreements’ pertaining to specific aspects of
tobacco control.
Iraj Abedian, AFReC, University of Cape Town
India Conference; January 2000
18
There is little doubt that the process of concluding the FCTC and its associated protocol
agreements are likely to be protracted and riddled with country and region-specific complexities.
Yet the political will has to be generated to overcome such procedural obstacles. As I have
argued earlier in this paper, the tobacco health hazard has become a global challenge, needing a
global solution. Like many other areas of post-industrial era, a rapidly integrating socio
economic dispensation has brought mix fortunes for human communities. To deal effectively
with many of these issues, be they related to public health or any other aspect of human welfare,
there is need for a new paradigm in thinking and in social governance. Creating a new
framework for the collective welfare of humanities would need to be driven by a set of basic
principles acknowledging, first and foremost, the oneness of humanity and a collective
commitment to carrying out global social governance responsibly.
With respect to averting a global human tragedy caused by smoking addiction, WHO has taken
the lead. For it to succeed, much support is needed from the politicians, the scientific
community, the multilateral institutions, the NGOs and the social activists around the globe.
V.
Concluding Remarks
In summary then, the World Bank report is a path breaking initiative in putting together a body
of theoretical and empirical research with a view to extract an action plan for governments
world-wide. As importantly, the report has considerable implications for WHO’s TFI. The World
Bank concludes that:
The threat posed by smoking to global health is unprecedented, but so is
the potential for reducing smoking-related mortality with cost-effective policies. The report
shows the scale of what might be achieved: moderate action could ensure substantial health
gains for the 21s' century.” (p. 83) Figure 5, above, provides a quantitative illustration of the
potential gains in public health from tobacco control. Herein lies the prospect for the FCTC to
create a global legal framework that would help countries to adopt and adhere to a set of
consistent action plans for tobacco control with substantial public health gains.
It is increasingly evident that in a rapidly integrating world economic order, a great deal of
policy co-ordination and harmonisation is needed in areas such as tobacco control. Increasingly,
Iraj Abedian, AFReC, University of Cape Town
India Conference; January 2000
19
the systemic requirements of the globalized economy require policy co-ordination and possibly
policy convergence. At the regional level, this is particularly significant. Neighbouring countries
need to establish effective policy co-ordination so as to ensure efficacy in tobacco control, while
at the same time preventing potential fiscal revenue losses.
While WHO is entrusted with the task of championing the public health issues of humanity, it is
abundantly clear that much support and collaboration is needed for it to succeed. A prime
example of such constructive input is the World Bank’s report that demystifies the economic
issues that so often confront the governments, particularly in the developing worlds. Other
multilateral and regional organisations have much to offer in this regard. Practical ways have to
be found in order to create the effective network needed to deal with the looming global crisis
caused by smoking.
I cannot do better than to end this overview paper with a commentary on the World Bank report,
Curbing the Epidemic, from Dr Brundtland, the Director General of WHO. She states: “Tobacco
is a major killer world-wide. The biggest cost from tobacco is the enormous toll it brings from
disease, suffering and family distress. Health, and not economic arguments, are the reason for
controlling tobacco, but economic arguments are raised as an obstacle to tobacco control
policies. This report provides an extremely useful, and timely, examination of claims that often
hinder many governments from acting to curb a global killer. ” (World Bank, 99a)
- ENDIA/WASHINGTON DC/USA/15NOV99
4. For a detailed analysis of systemic issues of a globalising society, see Commission on Global Governance (1996).
Iraj Abedian, AFReC, University of Cape Town
India Conference; January 2000
20
Selected References
Abedian, I (1998): “The Optimal Policy Mix for Tobacco Control: a Proposed Framework”,
Chap. 1 in Abedian, et al, (edit):77ie Economics of Tobacco Control;
Towards an Optimal Policy Mix; AFReC, University of Cape Town, the
South African Medical Association,1998.
Chaloupka, F & M. Corbett (1998): “Trade Policy and Tobacco: an Optimal Policy
Approach”, Chap. 11 in Abedian, et al, (edit): The Economics of Tobacco
Control; Towards an Optimal Policy Mix; AFReC, University of Cape Town,
the South African Medical Association, 1998.
Commission on Global Governance (1996): Our Global Neighbourhood (the Report for the
Commission on Global Governance, Oxford University Press.
Joossens, L (1998): “Tobacco Smuggling: an Optimal Policy Approach”, Chap. 12 in
Abedian, et al, (edity.The Economics of Tobacco Control; Towards an
Optimal Policy Mix; AFReC, University of Cape Town, the South African
Medical Association,1998.
Leary,, V.A..(1999): “Conceptualizing The Right to Health: Tobacco Use as a Human Rights
Issue”, Libor Amicorum, Theo van Boven
World Bank, (1999a): Curbing the Epidemic, governments and the Economics of Tobacco
Control, The World Bank, Washington DC, USA
World Bank, (1999b): Tobacco Control Can Prevent Millions of Death World-wide,
News Release No. 99/2189/S
Iraj Abedian, AFReC, University of Cape Town
India Conference; January 2000
BUSINESS ■ TOBACCO BILL
pH- S'
The controversial bill places a blanket ban on tobacco advertising but it may
prove ineffective in curbing bidi and chewing tobacco consumption
■ by Rohit SARAN
NDIA'S ESTIMATED 20 MILLION
tobacco users may have missed the
mother of all statutory warnings.
On April 9. the Cigarette and Other
Tobacco Producls Bill 2001 was
quietly tabled in the Rajya Sabha and
swiftly passed the same day. For a bill that
was in the making for 11 years—it was
first proposed in August 1992—that was
surprisingly smooth sailing.
On the face of it. the bill is significant.
It bans advertising of all tobacco pro
ducts throughout the country. That's a
giant leap forward from the Cigarettes
Act of 19 75 which restricted advertising
and sale of only cigarettes which
account for less than 20 per cent of
tobacco consumption in India.
The bill, which is likely to be cleared
by the Lok Sabha this month, also pro
vides for bigger and clearer display of
I
48
IMJIATOOAV ♦ AIKII.M.MI1
health warnings, restricts the sale of
tobacco products in most public places
and attempts to end the existing legal
discrimination between cigarette and
other tobacco products (see graphic). For
instance, bidis—which have the largest
share of 4 5 per cent in total tobacco con
sumption—were so far exempt from car
rying the statutory health warning. The
proposed law also puts India among the
front-running countries that have put a
comprehensive ban on tobacco ads. “It is
one of the most progressive public health
laws of recent times in India." says Ambika Srivastava, who has been working
on tobacco related issues with the who.
That is as far as the letter of the bill is
concerned. In its spirit, however, the bill
is softer on unorganised sectors of the
tobacco industry. At least that is what a
section of the Rs 35,000-crore industry
fears. The skepticism stems from the
unique consumption pattern of tobacco
in India. In developed countries, tobacco
use is synonymous with cigarette smok
ing. But in India, an estimated 80 percent
of tobacco consumption is in the form of
bidis and chewing tobacco. That would
not have been an issue if the tobacco in
dustry was organised, making its regula
tion easier. A large chunk of bidi and
chewing tobacco manufacturing is a
small-scale—insome cases even a house
hold—activity. Says Amit C. Sarkar.
director of the Delhi-based Tobacco
Institute of India: “We will fully support
a legislation that is pragmatic. But the
current bill has certain provisions that
are counterproductive in the Indian
context and should be revised."
The cigarette industry claims that by
being stricter on them, the bill will cause
a shift of tobacco consumption from
cigarettes to other forms. Besides provi
sions like declaration of nicotine and tar
content anddisplay of pictorial warnings
WHO's International Conference on Global Tobacco Control Law:
Towards a WHO Framework Convention on Tobacco Control
New Delhi, India, 7 January 2000
Dr Gro Harlem Brundtland
Director-General, World Health Organization
Mr Prime Minister, Distinguished guests,
It gives me great pleasure to be in India today this is a country and a people close to my heart. I
am especially pleased to be speaking to an
audience of some of the world's best legal and
public health experts. We come from a wide
range of backgrounds, such as public health,
medicine, law, media, economics and social
sciences. What has brought us here to Delhi is
our common resolve to highlight the grave
problems arising from tobacco in the developing
world. This meeting will explore possible means
to address these problems, taking into account
developing country perspectives. It will be one of
many important contributions over the next
months and years towards a strong international
legal tool to fight tobacco, the Framework
Convention on Tobacco Control.
India, with its myriad of cultures and its complex
economic and social realities, in many ways
mirrors our new globalized world. But despite its
diversity, its disparities and its conflicts, a strong
sense of unity - has kept this immense nation which harbors nearly one sixth of humanity together in a viable and vivid democracy.
The rest of the world is only slowly waking up to
this realization that all of us, no matter the
physical, cultural or economic distance, are
dependent upon each other. One region's poverty
is another region's lost opportunity. One area's
industry may be another area's environmental
disaster, and one country's disease outbreak
today, may be another country's epidemic
tomorrow.
In 1987, the World Commission on Environment
and Development, which I had the privilege to
chair, came up with the concept of "sustainable
development" on the basic premise that
development needs of nations must be met in a
way that allows future generations to fulfill their
own aspirations. Enshrined in this concept was
the whole notion of solidarity, the right to
knowledge and access to basic life-sustaining
information for all nations and people. That idea is
now institutionalized globally in a series of
environmental treaties. It has entered the
vocabulary of policy makers. We will add health to
that illustrious list.
The importance of the role of health in overall
development is being rapidly embraced by
governments around the world. It is a conceptual
shift not unlike that which took place with the
environment 25 years ago. Increasingly,
governments realise they need to integrate health
into the broader context of development. They are
also beginning to look at investments in health as
more than simply a mere consumption
expenditure. Instead, health is increasingly being
seen as a major opportunity for growth,
productivity, human progress and poverty
alleviation.
My point of departure is a broad reading of the
role of health in development. WHO is indeed the
specialised agency on health - but the purpose of
our work is not only to combat ill-health - although
that remains key - it is also to promote healthy
populations and communities - and indeed to
demonstrate how wise health interventions can
spur development.
There was a period in development thinking - not
so long ago - when access to public services,
such as health and education, would have to wait
until countries had developed a certain level of
physical infrastructure and achieved a certain
level of economic strength. Once countries had
become fully industrialised - large outlays on
health care seemed appropriate and necessary.
Indeed, it was seen as a sign of national
prosperity and success. Experience and research
over the past few years have shown that such
thinking was at best simplified, and at worst plain
wrong.
We have seen that developing countries which
invest relatively more on health in an effective
manner are likely to achieve higher economic
growth. In East Asia, for example, life expectancy
increased by over 18 years in the two decades
that preceded the most dramatic economic take
off in history. A recent analysis for the Asian
Development Bank concluded that fully a third of
the Asian "economic miracle" resulted from these
gains. We have also observed how health
spending in some of the world's richest countries
can reach very high levels and still not provide
necessary and quality health services to all their
citizens.
Health is not only an important concern for
individuals, it plays a central role for the society in
achieving sustainable economic growth and an
effective use of resources. And health is even
emerging as an important element of national
security.
With globalization, all of humankind today paddles
in a single sea. There are no health sanctuaries.
Diseases cannot be kept out of even the richest of
countries by rearguard defensive action. The
separation between domestic and international
health problems is losing its usefulness as people
and goods travel across continents. Two million
people cross international borders every single
day, about a tenth of humanity each year. And of
these, more than a million people travel from
developing to industrialized countries each week.
This is not only an issue of infectious diseases.
With an explosion of international trade, travel
and media, new cultural influences spread faster
than ever before, driven by economic aspirations,
entertainment and advertising. Many of the effects
are positive, but we also see drastically negative
effects, such as unhealthy changes in diet - and
the rapid spread and increase of tobacco-use.
Disease and death do not stop at national
borders, but still our efforts to fight them are far
from being sufficiently international. The time has
come for both health and foreign policy to reflect
the needs of the world's public with greater
emphasis on international health security and its
contribution to world peace. Foreign policies and
international
business
practices
must
acknowledge transnational threats of disease, the
dangers of trade in products and technologies
that are harmful to health, economic and health
disparities between and within countries and
population growth. Countries must collaborate to
develop strategies that ensure sustainable human
security.
As the world's leading health agency seeking
value for our constituents we have chosen our
setting - we will play an active role in this work; as
a facilitator, as a provider of evidence and best
practices - and as a moral compass.
One of the most important political legacies of this
century has been the universal ideal of human
rights that are now irreversible as tenets of
international law. The past 30 years have seen
the birth of hundreds of organizations around the
world that have given a voice and a focus to
issues that affect our lives on a daily basis. Our
search for justice is as old as we are. Our search
for life in harmony with laws - whether they be
natural laws or those that have developed over
centuries - is as old as humanity himself. Access
to basic health is, in the final analysis, a search
for justice.
It is my firm belief that where there is no vision,
there is no progress. The success of our vision
lies in the hands of our Member States. As
nations feel increasingly compelled to co-operate
with each other to solve their problems, the
development of binding global public health
norms and commitments will become crucial.
Although international health law is still in a
nascent and dynamic stage of development, it
must address both the positive and negative
health impact of globalisation. Consequently,
health development in the 21st century is likely to
make wider use of international legal instruments
to take advantage of the opportunities afforded by
global change and to minimize the risks and
threats associated with globalisation.
Today, our focus is tobacco. But the work we do
on tobacco has wider consequences. As the
composition of the global burden of disease
changes, so must the emphasis of our work. In
addition to continue with the past century's very
successful effort to limit or eliminate infectious
diseases, the work we are doing on a Framework
Convention on Tobacco Control stakes out the
way disease must increasingly be fought and
prevented in this brand-new century. This is the
first time WHO is exercising its constitutional right
to negotiate a set of globally binding rules. The
Framework Convention is a product and a
process and a public health movement.
Turning principle into practice is not an easy task,
but we will lead the way and as I said, I am
counting on your help. Our task is not to produce
worldwide regulations. It is to build a International
legal framework which will assist and support
countries in their national regulation process. The
success of our approach will depend on political
commitment, capacity building in public health law
and economics, public support and effective
enforcement. Legislation and regulation have to
strike a balance between individual freedom and
public needs and interests.
For the next few days, you will hear about the
science, economics and politics of tobacco
control. We know that tobacco use is a risk factor
for some 25 diseases. It was here in India in 1964
that the first link between oropharyngal cancer
and chewing tobacco was identified. Studies from
eastern India were the first in the world to link
palate cancer to the chewing of tobacco.
As the recent report of the World Bank has clearly
documented, the risks to health and health
systems from tobacco are widely underestimated.
So are tobacco industry tactics. When I first
looked into the issue of tobacco use world-wide I
was unprepared for what I was to learn about the
extent and manner in which the tobacco industry
was marketing a product that killed half of its
consumers. I was appalled to see how the
tobacco industry had subverted science,
economics and political processes to market a
lethal and inherently defective product that
imposed a massive burden of disease and death
on countries. I am outraged by what I learn with
each passing day about the tobacco industry from
previously secret documents that have now come
to light mainly due to court cases in the United
States, in particular Minnesota. I want to use this
platform to call on national and international
public health experts to work with their
Constitutions as well as their countries'
international commitments to help prevent and
combat this man-made epidemic. Let us craft the
world first truly viable public health Convention.
Tobacco is freely allowed to kill one person every
■eight seconds. That is four million preventable
deaths per year. Today in India, tobacco kills
670,000 people every year. In China, if present
smoking patterns continue, about a third of the
300 million Chinese males now aged 0-29 will
eventually be killed by tobacco. Countries like
Canada and Sweden that had long bucked the
tobacco epidemic now see it reappearing again.
No country and no people are safe from the
tobacco menace.
I have occasionally heard comments to the effect
that smoking is mainly an industrialized country
problem and that WHO should focus its energies
on fighting the traditional diseases of poverty,
such as malaria, tuberculosis and childhood
diseases. Such comments are understandable
but misinformed. If unchecked and unregulated,
by 2030, tobacco will kill 10 million people each
year. Seventy percent of those deaths will occur
in the developing world, with India and China in
the lead. If nations do not act individually and
together, in the next 30 years, tobacco will kill
more people than the combined death toll from
malaria, tuberculosis and maternal and child
diseases. Every tobacco related death is
preventable. That is our message. That is our
challenge.
Fifty years ago the world found a solution for
polio. Today we are on the verge of eradicating it.
Fifty years ago scientists and researchers linked
tobacco to cancer and other diseases. I wish I
could tell you that the world has risen to the
tobacco
challenge
as
vigorously
and
unequivocally as it fought polio. The unacceptable
reality about tobacco is that the health community
has lost out to the tobacco industry aggressively
seeking new markets and newer victims. The
world will have little cause to rejoice over the
health gains of the eradication of polio if we
continue to remain unprepared for, and indifferent
to, new challenges such as the one posed by
tobacco.
One of the first things that I did at the WHO was
to ask our Member Countries to give us a
mandate to negotiate the Framework Convention.
This new legal instrument is expected to address
issues as diverse as tobacco advertising and
promotion, agricultural diversification, product
regulation, smuggling, excise tax levels, treatment
of tobacco dependence and smoke-free areas.
The Framework Convention process will activate
all those areas of governance that have a direct
impact on public health. Science and economics
will mesh with legislation and litigation. Health
ministers will work with their counterparts in
finance, trade, labour, agriculture and social
affairs ministries to give public health the place it
deserves.
tobacco, several of its articles address over
arching values essential to safe and healthy
development of children and as of this year, the
States' reporting guidelines have now been
amended to include tobacco. For tobacco, this
means that the interests of the child take
precedence over interests of the tobacco industry.
Later as I share with you some tobacco industry
tactics to promote tobacco to children, you will
see why this is important.
Within the United Nations Family, The World
Bank is an essential partner in global tobacco
control. Their 1999 report effectively shows that
over the long term economies will benefit from
tobacco control. They highlight a basic economic
fact. If people stop spending on tobacco, they will
spend on other goods and services that will
generate more jobs and revenue than those from
tobacco.
We also have a close working relationship with
FAO. Together, we are reaching out to tobacco
farmers to ensure that when successful tobacco
control reduces demand for tobacco, the
economic consequences will be minimized. Our
decision to use legally binding mechanisms to
circumscribe the global spread of tobacco on the
one hand, and to regulate the product itself on the
other, is based on sound science and irrefutable
documentary evidence. The science that
underpins our work is unequivocal - a cigarette is
the only freely available consumer product which,
when consumed as intended by manufacturers,
kills. Let us never forget that.
Nicotine is addictive. A cigarette is not just
tobacco leaves rolled in a strip of paper. It is a
highly engineered product. The tobacco industry
has studied our saliva and central nervous
systems to determine the right dose of nicotine to
deliver so that addiction occurs and is sustained.
Other tobacco products, whether they be beedies,
snuff, gutka or spit tobacco, are no less addictive
- nor lethal.
Imposing international norms on a global industry
that seemingly without qualms can make huge
profits from a product that kills is not an easy task.
It is our firm belief that to develop a truly
meaningful global treaty to control tobacco, our
Member States must have a clear understanding
of the tobacco industry and its tactics.
Fifty years is a blink of time in a millennium, but
fifty years is a long time to sustain a deliberate
deception that causes death and disease. For
almost fifty years, the tobacco industry has known
that tobacco products cause deadly diseases. I
am speaking to an audience of lawyers and public
health experts - I chose my words carefully. The
tobacco industry which acts as a global force is in
the business of selling deception. Deception in
science, public health and economics. Internal
tobacco industry documents that have now
become public bear eloquent testimony to this.
The challenge for us comes in seeking global and
national solutions in tandem for a problem that
cuts across national boundaries, cultures,
societies and socio-economic strata. An early ally
has been UNICEF and the Convention on the
Rights of the Child. While the Convention on the
Rights of the Child does not explicitly include
3
Tobacco litigation began in the United States in
1954. But the major breakthrough came in the
1990s - in the States of Mississippi and
Minnesota - with the revelations of millions of
pages of documents forced from the files of the
tobacco industry and with the framing of different
types of legal theories that focused on the
conduct of the tobacco industry. For us, these
documents show how and why the tobacco
industry has been so successful in defeating
public health objectives in the past and provide
valuable lessons into how the public health
community must come to terms with the tobacco
industry to make progress in future. We believe
the tobacco industry has fractured the tobacco
issue by playing different tunes in different
countries. In one it is labour, in another it is
farmers, in a third it is marketing rights. We
believe that through our Constitution and that of
our Member States, we can restore the global and
national picture so that the truth can emerge to
benefit public health for all.
Consider this internal tobacco industry discussion.
A document written by a tobacco industry lawyer
in 1980 sets out some of the reasons for the
tobacco industry's refusal to publicly admit that
smoking causes disease. The document was
written at a time when the British and American
Tobacco Group companies were considering
changing their public stance on the issue of
causation of disease. The lawyer opposed such a
change, and wrote: "If we admit that smoking is
harmful to 'heavy' smokers, do we not admit that
BAT has killed a lot of people each year for a very
long time? Moreover, if the evidence we have
today is not significantly different from the
evidence we had five years ago, might it not be
argued that we have been willfully killing our
customers for this long period? Aside from the
catastrophic civil damage and governmental
regulation which would flow from such an
admission, I foresee serious criminal liability
problems".
Tobacco companies also denied for decades that
smoking was addictive. In private, they recorded
in the fifties that smoking was addictive. In 1961,
a top industry scientist wrote, ". smokers are
nicotine addicts" In 1963, an industry lawyer
wrote, "[N]icotine is addictive. We are, then in the
business of selling nicotine, an addictive drug ..."
In 1979, a tobacco executive considered the
hypothesis that "high profits ... associated with the
tobacco industry are directly related to the fact
that the consumer is dependent upon the product"
The internal documents also demonstrate that the
tobacco industry intentionally designed cigarettes
to exploit their addictive potential. While nicotine
is a naturally occurring component of the tobacco
plant, the modern cigarette is a highly engineered
and sophisticated product in both manufacture
and design. Decades ago, the tobacco industry
began to control and manipulate the level and
form of nicotine in cigarettes in a variety of ways.
Publicly, the tobacco industry maintains that it
does not want youth to smoke. Privately the
tobacco industry has long recognised that the
preservation of its market depends upon
recruiting youth. As one document stated,
"Younger adult smokers are the only source of
replacement smokers ... If younger adults turn
away from smoking, the industry must decline,
just as a population which does not give birth will
eventually dwindle" The tobacco industry
documents are replete with discussions of
marketing to youth and the need to increase
market shares by enlisting youth. The documents
are an underused public health tool. But that is
about to change. There is some type of tobacco
litigation underway in at least 15 countries ranging
from personal injury class action litigation in
Australia to health cost recovery in Canada to
public interest petitions in India.
Last October I called for a preliminary inquiry into
whether the tobacco industry has exercised
undue influence over UN-wide tobacco control
efforts including interfering with WHO's work.
Later this year I have called for a meeting of
international regulators to set in motion the
process of regulating tobacco. The jigsaw is
falling into place.
One of the primary objectives of the tobacco
industry is to frame tobacco use as an individual
and behavioral decision. Adults can chose for
themselves if they have full access to information.
The same does not apply to children and
adolescents. On a given day, between 82,000
and 99,000 young people - sometime as young
as 8 - start smoking or chewing tobacco. Over
eighty percent of smokers started before they
were 18. By the time they find out, it is too late.
The addiction has taken control.
The good news is that we can buck and reverse
the global tobacco trend. We know what works
and how. Taxes work and the young are
especially susceptible to increased prices.
Advertising and sponsorship bans work. Smoke
free policies work. Such policy interventions
could, in sum, bring unprecedented health and
economic benefits. WHO's message is that there
is a political solution to tobacco and it is routed
through policy interventions and political vision.
The Framework Convention on Tobacco Control
is a pathfinder in public health. It will assist in
placing health at the top of national and
international agenda and will create a debate on
the wider issues and solutions to health problems.
We owe this to ourselves. We owe this more to
future generations. Let us never forget that public
health is a search for equity, solidarity and justice.
Thank you.
KARNATAKA LEGISLATIVE COUNCIL
NINETY FOURTH SESSION
(ADJOURNED MEETINGS)
THE KARNATAKA PROHIBITION OF SMOKING
AND PROTECTION OF HEALTH OF
NON-SMOKERS BILL, 2001
(L.C. Bill No. 3 of 2001)
A Bill to provide for prohibition of smoking in places
of public work or use and in public service vehicles and
for the protection of health of non-smokers in the State of
Karnataka and to make provision for matters connected
therewith or incidental thereto.
Be it enacted by the Karnataka State Legislature in
the fifty second year of the Republic of India as follows:-
1. Short title and commencement.- (1) This Act may
be called the Karnataka Prohibition of Smoking and
Protection of Health of Non-Smokers Act, 2001.
(2)
It shall come into force from such date, as the
State Government may, by notification, appoint and
different dates may be appointed for different (provisions
of this Act.
2
2. Definitions.- In this Act, unless the context
otherwise requires,(a)
“advertisement” means and includes any notice,
circular, wall paper, pamphlet, display on
hoardings, or any visible representation made
by means of any light, sound, smoke, gas or
any other means which has the effect of
promoting smoking and the expression
‘advertise’ shall be construed accordingly:
(b)
“Authorised Officer” means a person appointed
under section 6:
(c)
“Place of public work or use” means a place
which is visited by general public and includes
Auditorium, Hospital Buildings, Health
Institutions, Amusement centres, Restaurants,
Public Offices, Court Buildings, Educational
Institutions, Libraries, Places of worship and
such other places notified by the State
Government to be a Place of Public Work or use
but does not include any open place:
(d)
“Public Service Vehicle” means a vehicle as
defined under clause (35) of section 2 of the
Motor Vehicles Act. 1988 (Central Act 59 of
1988):
(e)
“smoking" means smoking of tobacco in any
form, whether in the form of cigarette, cigar,
beedis or otherwise with the aid of a pipe,
wrapper or any other instrument.
3. Prohibition of smoking, advertisement, sale and
storage of smoking substances.- No person shall,(1) engage in smoking in any place of public work or use,
3
where smoking is prohibited and such prohibition is
dhnlayed or conveyed through any audio! or visual
medium, or in any Public Service Vehicle.
(2) notwithstanding anything contrary contained in
any other law advertise in any place of Public Work or use
or in any Public Service Vehicle to promote sjmoking or
the sale of cigarettes and beedies:
Provided that
relation to,(a)
(b)
this clause shall not; apply in
an advertisement of cigarettes ori beedies in
or on a package containing cigarettes or
beedies;
advertisement of cigarettes or beedies which
is displayed at the entrance or inside a
warehouse or a shop where cigarettes or
beedies are offered for distribution or sale.
(3)
sell cigarettes, beedis or any other! smoking
substance to any person who is below the age of eighteen
years;
(4)
himself or by any person on his behalf, store, sell
or distribute cigarettes or beedis or any other smoking
substance within the premises of any Hospital, Health
Institution, Public Office, Court, Library, College, School
or other Educational Institution and Place of worship.
4. Notice to be displayed.- For the purpose of clause
(1) of section 3, the owner or manager or persoh incharge
of a place of public work or use shall display! or convey
through audio or visual medium in Kannada and English
languages at a conspicuous place or places in the premises
of place of public work or use prominently slating that
4
the entire place or such part of it is a “No smoking Zone"
and that “Smoking is prohibited in such place or, as ~ ie
case may be, part of it.”
5. Penalties.- Any person, who contravenes the
provisions bf: - (1) clause (1) of section 3 or of section 4
shall be punishable with fine which may extend to one
hundred rupees and in case of second or subsequent
offence, shall be punishable with a minimum fine of two
hundred rupees, but which may extend to five hundred
rupees;
(2) clauses (2),(3),(4) of section 3 shall be
punishable with fine which may extend to five hundred
rupees arid in case of second or subsequent offence, shall
be punishable with imprisonment for a term which may
extend to three months, and with a minimum fine of five
hundred rupees, but which may extend to one thousand
rupees.
6. Authorised Officer.- (1) The State Government may
by notification appoint one or more persons in respect of
any area or areas to be authorised officers for the purpose
of this Act.
(2) Every authorised officer appointed under
sub-section (1) shall be deemed to be a public servant
within the meaning of section 21 of the Indian Penal Code,
1860 (Central Act 45 of 1860).
7. Removal of a person from the Place of an
offence.- Any person who contravenes the provisions of
section 3 arid who is being asked by an authorised officer
or a Police’ Officer not below the rank of a Sub-Inspector
of Police to desist from smoking persists, shall be liable to
be removed from the place of the offence. A person
5
removed from the show house, auditoria, amusement
centre or a Public Service Vehicle shall not be entitled to
refund of any payment made by him for journey or for
admission to the demonstration, exhibition, assembly or
meeting or to any other compensation.
8. Court Competent to try offences under this Act
and take cognizance of offences.- [l]No court other
than the court of a Metropolitan Magistrate or Judicial
Magistrate First-Class shall take cognizance of and try an
offence under this Act.
(2) No court shall take cognizance of any offence
under this Act except on a complaint in writing of an
authorized officer with respect to offences under clause
(1) of section 3 or section 4 and on a report in writing of
a Police Officer, not below the rank of Sub-Inspector of
Police, with respect to offences under clauses (2), (3) and
(4) of section 3.
9.
Certain offences to be cognizable and Bailable. -
Notwithstanding anything contained in the Code of
Criminal Procedure, 1973 (Central Act 2 of 1974) offences
, under clauses (2), (3) and (4) of section 3 shall be cognizable
and bailable.
10.
Offences under the Act to be tried summarily.-
All offences under this Act shall be tried summarily in the
manner provided for summary trial of cases under the
Code of Criminal Procedure, 1973 (Central Act 2 of 1974).
11. Offences by Companies.- (1) Where an offence
under this Act has been committed by a company, every
person, who, at the time the offence was committed, was
in charge. of, and was responsible to, the company for the
6
conduct of the business of the company, as well as
company, shall be deemed to be guilty of the offence and
shall be liable to be proceeded against and punished
accordingly:
Provided that nothing contained in this sub-section
shall render any such person liable to any punishment, if
he proves that the offence was committed without his
knowledge or that he had exercised all due diligence to
prevent the commission of such offence.
(2) Notwithstanding anything contained in
sub-section(l), where any offence under this Act has been
committed by a company and it is proved that the offence
has been committed with the consent or connivance of, or
is attributable to any neglect on the part of, any director,
manager, secretary or other officer of the company, such
director, manager, secretary or other officer shall be
proceeded against and punished accordingly.
Explanation.- For the purposes of this section,(a) “Company” means a body corporate and
includes a firm or other association of
individuals; and
(b) “Director”, in relation to a firm, means a partner
in the firm.
12. Delegation of Powers.- The State Government
may, by notification in the Official Gazette, direct that any
power exercisable by it under this Act, may also be
exercised by such officer as may be mentioned therein
and subject to such conditions, if any, as may be specified
therein.
7
13. Compounding of offences.- (1) The State
Government or any person authorised by the State
Government in this behalf by general or special order,
may either before or after the institution of the proceedings
compound any of the offences made punishable under
this Act.
(2) When an offence is compounded under
sub-section (1), the offender if in custody shall be
discharged and no further proceeding shall be taken
against him in respect of the offence compounded.
14. Repeal and savings.- (1) The Karnataka
Prohibition of Smoking in Show houses and Public halls
Act, 1963 (Karnataka Act 30 of 1963) is hereby repealed
and in clause (y) of sub-section (1) of section 92 of the
Karnataka Police Act, 1964 (Karnataka Act 4 of 1964) the
words “smokes or” shall be omitted:
Provided that the provisions of section 6 of the
Karnataka General Clauses Act, 1899 shall be applicable
in respect of the repeal of the said enactment and the
provisions of the said law and sections 8 and 24 of the
he) said Act shall be applicable as if the said enactment and
provisions had been repealed and re-enacted by this Act.
15. Power to make rules.- (1) The State Government
may by notification and after previous publication make
rules generally for the purpose of carrying into effect the
provisions of this Act.
(2) Every rule made under this Act shall be laid as
soon as may be after it is made, before each House of the
State Legislature while it is in session for a total period of
thirty days which may be comprised in one session or in
8
two or more successive sessions, and if, before the expiry
of the session immediately following the session or
successive sessions aforesaid both Houses agree in making
any modification in the rule or both Houses agree that
the rule should not be made, the rule shall from the date
on which the modification or annulment is notified by the
Government in the Official Gazette have effect only in such
modified form or be of no effect, as the case may be, so
however, that any modification or annulment shall be
without prejudice to the validity of anything previously
done under such rule.
9
STATEMENT OF OBJECTS AND REASONS
In order to protect the non-smoking public from the
hazards of passive smoking it is considered necessary to
prohibit tobacco smoking, to start with atleast in a few
selected places, like places of public work or use and in
public service vehicles, where large number of people are
present for prolonged periods.
Promotion of smoking through advertisements needs
to be discouraged and the health of the younger generation,
particularly children, also needs to be protected from the
ill-effects of tobacco smoking by prohibiting sale of
cigarettes, etc., to persons below 18 years and sale,
distribution or storing of such products within the
premises of any Hospital, Health Institution, Public Office,
Court, Library, Place of worship, College, School or other
Institution.
Hence the Bill.
he)
10
FINANCIAL MEMORANDUM
There is no extra expenditure involved in the
proposed measure.
0
0
11
memorandum regarding delegated
LEGISLATION
Clause 15: Clause 15, empowers the State Government
to make rules generally for the purpose of
carrying into effect the provisions of this Act.
The proposed delegation of Legislative powers is
normal in character.
DR. A.B. MAALAKA REDDY
Minister for Health and family welfare
H.C. RUDRAPPA
Secretary
Printed by: Government Central Press, Peenya Bangalore. - 4422/DPAL/C-7
The Meghalaya Prohibition of Smoking and
Non-Smokers Health Protection Act, 1998
Smoking is harmful to health. So it must be
prohibited especially when it is done in public
places. Awareness among the people and legal
prohibition can help in conducting this vice. The
Meghalaya Prohibition of Smoking and Nonsmokers Health Protection Act, 1998 is given
below as a sample Act. People can persuade
State Governments to pass a similar law in their
respective States.
1.
Definitions
In this Act:
Declaration of non-smoking places of pub
lic work or use
Under this Act the Government of
Meghalaya, by notification in the Official Gazette,
declare any place of public work or use in
Meghalaya to be a non-smoking place.
4.
Power of Government to authorise offic
ers
*
The State Government entitled to authorise
one or more persons as competent officers
to act under this Act.
"
Such an authorised person is to be consid
ered as a public servant.
5.
Prohibition of smoking in place of public
work or use.
Objectives of the Act
This law was enacted on 10th July 1998
for prohibiting of smoking in places of public work
or use and in public service vehicles in the State
of Meghalaya. It came into force on 13th July,
1998.
2.
pipe, wrapper or any other instruments.
3.
a)
No person is permitted to smoke in any
“advertisement” means and includes any
notice, circular, wall paper, pamphlet, dis place of public work or use.
play on hoardings, or any visible represen
tation made by means of any light, sound, 6. Prohibition of smoking in public service
vehicles.
smoke, gas or any other means which has
No person is permitted to smoke in a pub
the effect of promoting smoking and ex
pression ‘advertise’ shall be construed ac lic service vehicles.
cordingly;
b)
“Place of public work or use" means a place
etc.
declared as such under Section 3 and in
No person is permitted to advertise in any
cludes auditoria, hospital buildings, health
place and any public service vehicles which may
institutions, cinema halls and amusement
promote smoking or the sale of cigarettes, ci
centres, restaurants, public offices, court
gars, beedis or any smoking substance.
buildings, educational institutions, libraries
and the like which are visited by general 8. Prohibition of cigarettes, etc. to minors
public but does not include any open place;
No one is allowed to sell cigarettes, cigars,
c)
“Public service vehicles" means a vehicle beedis or any other smoking substance to any
as defined under clause (35) of Section 2 person who is below the age of eighteen years.
of the Motor Vehicles Act, 1988 (59 of
9.
Prohibition of storage, sale and distribu
1988);
d)
“Smoking” means smoking of tobacco in
educational institutions.
any form whether in the form of cigarette,
No person is allowed to store, sell or dis
cigar, beedis or otherwise with the aid of tribute cigarettes, cigars, beedis or any other
)
7.
Prohibition on advertisement of cigarettes
tion of cigarettes, etc. in the vicinity of
LEGAL NEWS & VIEWS : APRIL 1999
nd
38
smoking substance within the area of one hun
dred meters around any college, school or other
educational institutions.
10.
mts.
’• of pub-
’ient of
Gazette.
■ use in
se offic
ii ^k;se
it otffcers
e consid-
of public
;e in any
c service
in a pub-
ligarettes
ise in any
reties, ci-
es, cigars,
■ce to any
.;n years.
< distribu/jcinity of
sej| or disany other
APRIL 1999
Penalties.
* Any person who violates Sections 5, 6 or
10 will be punishable.
* The punishment is fine upto one hundred
rupees.
* In case of second or subsequent offences
the minimum fine is Rs. 200 and maximum
Rs. 500.
* for violating Sections 7,8 or 9 the fine may
extend to five hundred rupees.
* In case of a second or subsequent offence
the punishment is imprisonment upto three
months or a minimum fine of five hundred
and a maximum of one thousand rupees or
both.
14.
Certain offences to be cognizable and
bailable.
Offences under Sections 7, 8 and 9 are
considered as cognizable and bailable.
15.
Offences under the Act, to be tried sum
marily.
All offences under this Act should be tried
summarily (summary trial).
16.
Power to delegate.
* The State Government is empowered to
delegate any of its powers to any specified
officer.
* Such an order to delegate its power must
be notified in the Official Gazette.
17.
Composition of offences.
The State Government or any authorised
officer is entitled to compound any offences made
12.
Ejection of violator of this Act from the
punishable under this Act either before or after
place of work or use.
instituting the judicial proceedings.
Any authorised officer or any police officer
not below the rank of Sub-Inspector may eject 18. Power to make rules.
* The State Government is empowered to
any person from the place of public work or use
make rules under this Act for its smooth
who violates the provision of this Act.
implementation.
13.
ninors
* No court is permitted to admit any case
unless a written complaint is lodged by an
authorised officer regarding any offence
committed under Sections 5, 6 or 10 or any
written report is filed by a Sub-Inspector or
an officer above that rank, with respect to
the offence under Sections 7,8 and 9.
Display and Exhibition of Board.
The owner or manager or in-charge of af
fairs of every place of public work or use should
display and exhibit a board at a conspicuous
place in and outside the premises visited or used
by the general public prominently stating that
the place is a “No Smoking Zone”, and Smoking
is an Offence."
11.
the First Class is empowered to take up
any case under this law.
Court competent to try offences under
this Act and take cognizance of offenc
es.
* Every rule made should be presented in
the Legislative Assembly.
* Only the Court of a Judicial Magistrate of
Yet to act
What is the use of a law if the government does not implement it? In order to obviate the
hardships of accident victims, the Motor Vehicles Act (of 1988) provides for the direct initiation of
compensation case on the basis of a police report. But in reality, the victims or their kin are still
having to chase after lawyers, as the state is yet to initiate cases on claims for victims of motor
mishaps.
LEGAL NEWS & VIEWS : APRIL 1999
15
p H - 3~r
NEWS RELEASE
For immediate release
Contact: Surekha Pillai, IP AN
Phone:233?6200
E-mail: surekha@ipan.com
AFTC appeals to Lok Sabha members for speedy clearance of Tobacco
Control Bill
Mumbai, April 21, 2003: As a prelude to the tabling of the Cigarettes and Other Tobacco Products (Prohibition
of Advertisement and Regulation of Trade and Commerce, Production, Supply and Distribution) Bill, 2001, in
the Lok Sabha next week, Advocacy Forum for Tobacco Control (AFTC) has announced that it welcomes the
Bill and views it as a first important step in saving people’s lives by controlling the consumption of both
smoking and smokeless tobacco. AFTC is a coalition of health professionals, research scientists, NGOs and
like-minded people from reputed organisations across the country.
The Bill seeks to put a total ban on advertising of tobacco products and prohibits sponsorship of sports and
cultural events either directly or indirectly, it prohibits the sale of tobacco products to minors, and specifies that
the new warning on cigarette packs should be more prominent in terms of legibility, language, colour and
display. The Bill proposes that the Nicotine and Tar content will have to be specified on packs. Goods without
specified warnings on nicotine and tar will be confiscated and penalties will be levied.
Over the last few weeks, several arguments critical of the Bill have been put forward by certain sections of the
Tobacco industry and AFTC members pointed out that though they are unfounded, they merit reasoned
refutation. AFTC addressed these issues in detail, {detailed background note appended)
Addressing the concern on the Bill leading to unemployment among tobacco workers, the AFTC representatives
pointed out that the Bill primarily involves demand-reduction strategies geared to prevent new entrants to
tobacco habit. Demand reduction Will not be sudden but will be spread over several years, giving sufficient time
U set in motion alternate employment opportunities to anyone dependent on or engaged in tobacco production.
Hence the fears of unemployment among tobacco workers, farmers and retailers are unfounded. Dr K S Reddy,
Coordinator, HRIDAY-SHAN, and a founding member of AFTC, said, “We believe that it will benefit the
farmers, workers and the country as a whole if the government helps the process of diversification wherein
people engaged in tobacco production can be shifted to alternate occupations.”
On the ban on tobacco advertising, Shoba John, Tobacco Control Advisor to PATFI Canada, a public health
NGO and member of ATFC, said “A World Bank Study of 102 countries demonstrates that countries which
have imposed a comprehensive ban on all forms of tobacco advertising have had steeper declines in tobacco
consumption compared to those that had not done so.”
Advocacy Forum for Tobacco Control, V-15, Green Park Extension, New Delhi-110016; Contact no.: 2616
7459, 2617 6230; Fax no.: 2616 7397; Email: info@hriday-shan.org; contact@hriday-shan.org
Renowned behavioural scientist Dr Mira Aghi said, “The Bill is a significant tool to protect the health of the
public which otherwise stands to bear colossal suffering in the form of not only deadly and disabling diseases
but also by falling prey to an addiction which is very hard to be freed from.”
Talking about the ban proposed in the Bill on sale of tobacco products to minors and within 100 metres of
educational institutions, Monika Arora, Programme Manager, HRIDAY, an NGO working with school children
on tobacco control issues and member ATFC, said, “These are measures aimed at restricting easy youth access
to tobacco products. If supplemented with pragmatic implementation procedures, this would prove to be a major
step in preventing early initiation into tobacco addiction. It is well documented that the age at initiation into
tobacco use spans across the teen years and that prevention at these early stages would help reduce consumption
considerably.”
The Bill also mandates effective health warnings that are clear and visible, including provisions for pictures.
Experience of countries like Canada and Brazil which have introduced pictorial health warnings occupying 50
^er cent and more of the package space shows that they are effective not only in discouraging use among
current tobacco users but also extends caution to potential users. Recently, the 14 countries of European Union
and Thailand have enacted laws introducing pictorial health warnings.
“All of these are public health measures which are in public interest and are well founded on evidence. They
need to be supported by every right thinking person who values the health of our people. AFTC looks forward
to an early passage of the Bill and to its effective implementation after enactment,” said Mr Taposh Roy,
Director - Information & Public Affairs, Voluntary Health Association of India. While urging the government
to remain strongly committed to tobacco control, AFTC too assures that the civil society will play a vigorous
role in community mobilization to support such measures.
AFTC has also welcomed the WHO Framework Convention on Tobacco Control (FCTC), the world’s first
public health treaty. “The FCTC bodes well for the Indian Bill, as a natural source of strength and support. It
also provides an opportunity for global coordination. Once the Indian Bill is passed and we need additional
measures, FCTC will be a natural resource to refer to and draw from,” added Dr Reddy.
^^.bout AFTC
^Representatives of the AFTC coalition are experts on various aspects of public health and have worked for
many years among vulnerable sections of society to campaign against the evils of tobacco usage. They include
Dr. P C Gupta & Dr. Surendra Shastri of Action Council Against Tobacco-India; Ms. Alka Kapadia of the
Cancer Patients Aid Association, Mumbai; Alimedabad-based Prof. Manubhai Shah, Managing Trustee of the
Consumer Education and Research Centre; Dr. Mihir Shah, Asst. Professor, Dept, of Periodontia, Govt. Dental
College & Hospital, Ahmedabad; Dr. Rakesh Gupta. Rajasthan Cancer Foundation, Udaipur; Ms. Shoba John,
Tobacco Control Advisor, PATH Canada, Mumbai; Ms. Monika Arora and Dr. K.S. Reddy of HRIDAYSHAN, Mr. Taposh Roy, VHAI, New Delhi; Ms. Padmini Somani and Ms. Devika Grover of the Salaam
Bombay Foundation; Mr. Bobby Ramakant, of Indian Society Against Smoking- ASHA, Lucknow; Ms. Renu
Khanna of Sanrakshan.New Delhi; Dr. Mira Aghi from Delhi and Dr. Dhirendra Sinha from School of
Preventive Oncology, Patna.
Advocacy Forum for Tobacco Control, V-15, Green Park Extension, New Delhi-110016; Contact no.: 2616
7459, 2617 6230; Fax no.: 2616 7397; Email: info@hriday-shan.org; contact@hriday-shan.org
CONCERNS ABOUT THE CIGARETTES AND OTHER TOBACCO
PRODUCTS (PROHIBITION OF ADVERTISEMENT AND REGULATION OF
TRADE AND COMMERCE, PRODUCTION, SUPPLY AND DISTRIBUTION)
BILL, 2001
I. ADVERTISING
The Bill seeks to ban all forms of direct and indirect advertising. It also bans tobacco
sponsorship of sports and cultural events.
What does Advertising do?
o
Increases consumption: Tobacco companies often claim their advertising is aimed
only at brand switching and not at attracting new consumers. It does not appeal to
business sense that an industry that works under tremendous compulsion to
consistently replace half of its committed users (who prematurely die from using their
products), does not want to recruit fresh users. It is therefore evident that tobacco
advertising, as with advertisements for any other products, is geared at increasing
product use.
©
Lures gullible youth and children through glamorous and deceptive promotional
stunts addicting them for a life-time. Advertising, which projects tobacco use in
congenial surroundings or associates the brand name with idolized role models,
legitimizes the habit in these young minds and projects the use of tobacco as socially
acceptable.
Why do we need an ad ban?
o
®
o
o
Tobacco advertising involves the promotion of a product that is proven to cause 25odd life-threatening or disabling diseases and induces life-long addiction amongst its
users.
To protect people from being misled by false images or misleading health claims and
deprived of their right to make a free and informed choice.
To prevent fresh users from picking up the habit and thereby reduce consumption and
resultant morbidity, mortality and economic loss to the community and the nation
To protect children and adolescents from being attracted to tobacco products.
Do tobacco Advertising bans work?
A World Bank Study of 102 countries demonstrates that countries which have imposed a
comprehensive ban on all forms of tobacco advertising have had steeper declines in
tobacco consumption compared to those that had not done so.
Does the ban leave cross border advertising unabated?
The apprehension about the possibility for continued cross-border advertising should be
allayed by the fact that the recently concluded WHO Framework Convention on Tobacco
Control (FCTC) recognizes the right of countries to ban cross-bcirder advertising and
apply appropriate penalties against violators. If we enact suitable national legislation,
such penalties may include marketing bans on products so advertised. The FCTC also has
strong provisions on smuggling. International protocols are soon to be initiated both on
cross-border advertising and smuggling. This would facilitate sufficient marketing and
trade regulation of international brands coming into the country.
Effect on allied industries like the Advertising Sector
Experience from home and abroad reveals that relinquishing a particular brand or a
product does not affect the revenues of this multi-product industry, as alternate products
would replace them.
TOBACCO PACKAGE WARNINGS
II.
The Bill mandates effective health warnings that are clear and visible, including
provisions for pictures.
Experience of countries like Canada and Brazil which have introduced pictorial health
warnings occupying 50 % and more of the package space shows that they are effective
not only in discouraging use among current tobacco users but also extends caution to
potential users. Recently, the 14 countries of European Union and Thailand have enacted
laws introducing pictorial health warnings.
BAN ON SALE OF TOBACCO PRODUCTS TO MINORS AND WITHIN 100
METERS OF EDUCATIONAL INSTITUTIONS.
III.
o
These are measures aimed at restricting easy youth access to tobacco products. If
supplemented with pragmatic implementation procedures, this would prove to be a
major step in preventing early initiation into tobacco addiction.
•>
It is well documented that the age at initiation into tobacco use spans across the teen
years and that prevention at these early stages would help reduce consumption
considerably.
o
It is also well established that persons who started smoking in teens are much more
likely to die early due to tobacco related diseases.
o
The provision is restricted to minors only and does not place any restrictions on the
sale of tobacco products to adults.
WOULD THE BILL LEAD TO MASSIVE UNEMPLOYMENT AMONG
TOBACCO WORKERS AND RETAILERS?
IV.
o
The Bill does not contain any provisions directly regulating tobacco production.
°
It primarily involves demand-reduction strategies geared to prevent new entrants to
tobacco habit. Demand reduction will not be sudden but will be spread over several
years, giving sufficient time to set in motion alternate employment opportunities to
anyone dependent on or engaged in tobacco production.
Hence the fears of
unemployment among tobacco workers, farmers and retailers are unfounded.
®
As the Bill does not ban the sale of any tobacco product, there would not be any
adverse effects on the sale and profits to retailers.
»
With the current rate of population growth in developing countries like ours, there is
not going to be a sudden drop in tobacco consumption even with comprehensive
tobacco control policies, as the actual number of tobacco users in the population
would not fall in the near future. Consequently, the Bill would not have any
immediate effect on tobacco supply side. It would, however, initiate a progressive
decline which will result in a substantial reduction in tobacco consumption over the
next half century. It will also prevent many young persons from becoming early
addicts.
o
On the contrary, increasing mechanisation of the production process and profit
motivated, political maneuvering at the auction floors by large tobacco and leaf
companies are largely responsible for the rampant unemployment and poverty among
tobacco workers and small farmers. When global tobacco demand falls and our
exports shrink, the tobacco industry is quick to abandon the farmers while protecting
its profits and diversifying its investments.
»
We believe that it will benefit the farmers, workers and the country as a whole if the
government helps the process of diversification wherein people engaged in tobacco
production can be shifted to alternate occupations.
V.
IS THE BILL PARTIAL TO SMOKELESS TOBACCO?
The Bill, as reinforced with the Standing Committee provisions and passed by the Rajya
Sabha, encompasses all forms of tobacco products- smoking and smokeless. It thus
provides a level playing ground to all of them. Peculiarities of various segments of the
tobacco industry could be better addressed while drafting Rules under the Bill.
VI.
BAN ON SMOKING IN PUBLIC PLACES
The bill recognizes and protects the rights of non-smokers to remain safe from the
harmful effects of environmental tobacco smoke (passive smoking). Skeptics have
doubted whether this provision can be effectively implemented. We believe that this Bill
confers a much needed entitlement to non-smokers to assert that right. Public education is
also required to raise the consciousness of the ban and its rationale. A combination of
regulation (to confer the right) and community mobilization (to assert and respect the
right) is needed to ensure smoke-free public places.
pH-S^
Responses Io (he hill
cigarettes and other tobacco products (prohibition of
ADVERTISEMENT AND REGULATION OFTRADE AND COMMERCE,
PRODUCHON, SUPPLY AND DIS TRIBUTION) Bil l ,, 2001
Introduction
The Tobacco Control Bill introduced recently in the Indian Parliament has been the suhjccl of
much debate and comment in the media. Some of the opinions expressed rellecl concerns about
(lie Bill's provisions or its effects. These concerns need a reasoned response, AI IC has
attempted to do that below by providing clarifications about key provisions of.the Bill and
addressing other concerns.
I.
W
ADVER HSING
Ute Bill seeks to ban all forms of direct anil indirect advertising. It also bans tobacco
sponsorship of sports and cultural events.
What does Advertisiiif} do?
•
Increases consumption: Tobacco companies often claim their advertising is aimed only al
brand switching and not al attracting new consumers. It docs nolhippeal to business sense that
an industry that works under Iremcndous compulsion to cortsislcnlly replace half of its
committed users (who prematurely die from using their products).aloes not want to recruit
fresh users. Il is therefore evident that tobacco advertising, as with ndvcrliscincnls for any
other products, is geared at increasing product use.
•
Lures gullible youth and children through glamorous and deceptive promotional stunts
addicting them for .a life-time. Advertising', which projects tobacco use in congenial
surroundings or associates the brand mime with idolized role models, legitimizes the habit in
these yoiini1, liniids and projects the use of tobacco as socially acceptable.
117/)' do we need mi nd ban?
•
Tobacco advertising involves the promotion of a product that is proven to cause 25 odd lifethreatening or disabling diseases and induces life-long addiction amongst its users
•
To protect people from being misled by false images or misleading health claims and
dcpiFvcd of their right to make-a free and informed choice.
To prevent fresh users from picking up the habit and thereby reduce consumption and
resultant morbidity, mortality and economic loss Io the community and-.lhc nation
l<> protect children and adolescents from being attracted Io tobacco products.
•
•
Do tobacco hlvei fisiiti; baas work?
A World Bank Study ol I (12 countries demonstrates that voimltics vv.hieh have unpi>a>vd .1
comprehensive ban on all forms of tobacco advertising have had slvcpvi declines in tobacco
consumption computed Io those that had not done so.
Does the halt leave cross border advertising unabated?
I he apprehension about the possibility for continued cross-border adveilismg should be n'H'avffl
by the lad that the recently concluded WHO I'famework C'onvelltiftn on Tobacco Control
(If'l(') recognizes the right of countries to ban cross-border advertising and apply appropriate
penalties against \ iolalors. If we enact siiitabl'e national legislation, such penalties may include
maikcting bans on products so advertised. The l ( ' l (' also has strong pros isipns.on smuggling.
International protocols are soon to be initialed both on cross-border advertising and smuggling.
I his would 'facilitate sufficient marketing and trade regulation of international brands coniine
into the.country.
Effect on allied indtisfl-ies like the .hlvertising Sector
Experience from home and abroad reveals that relinquishing a particular brand or a product does
not affect the revenues of this multi-product industry, as alternate products would replace them.
II.
TOBACCO PACKAGE WARNINGS
The Bill mandates effective health warnings that tire clear and visible, including provisions for
pictures.
Experience of countries like Canada and Brazil which have introduced pictorial health warnings
occupying, 50
and more of the package space shows that' they ate effective not onlv in
discouraging use among current tobacco users but also extends caiilion Io potential users.
Recently, the 14 countries of European .Union and Thailand have enacted laws introducing
pictorial health warnings.
III.
BAN ON SALE Ol TOBACCO PRODUCTS TO MINORS AND WITHIN I ()()
ME TERS OE EDUCATIONAL INSTTI'UHONS.
•
These are measures aimed al restricting easy youth access lo tobacco products. II
supplemented with pragmatic implementation procedures, this would prove lo be a major
step in preventing early initiation into tobacco addiction.
•
Il is well documented (hat the age al initiation into tobacco use spans across lhe teen years
anil that prevention at these early stages would help reduce consumption eonsiderablv .
•■
Il is also well established that persons who started smoking in teens are much more likclv to
die early due to tobacco related diseases.
lhe provision is restricted to minors only and does not place any resliielions on the sale ol
tobacco products to adults.
•
IN.
NNOll.D Illi: BUI. LEAD TO MASSINE
I OB \( ( () WORKERS AND RE JAILERS?
•
I INEMPI ()N MEM
NMONG
I he Hill does not contain any provisions directly regulating tobacco production ■
Il primarily involves demand-reduction strategies geared to prevent new enltanls Io tobacco
habit. Demand reduction will not be sudden but will be spread over several years, giving
sufficient time Io set in motion alternate employment opportunities to anyone dependent on
or■ engaged in tobacco production.
Hence (he fears of unemployment among tobacco
workers, farmersand retailers are unfounded.
•
Aslhe Bill does not bun the sale of any tobacco product, there would not he tiny adverse
effects on the sale and profits Io retailers.
•
With the current rate of population growth in developing countries like ours., there is nol
going to be a sudden drop in tobacco consumption even with comprehensive tobacco control
policies, ;ts the actual number of tobacco users in the population would nol fall in lhe near
future. ( onseqncnlly, lhe Bill would not have any immediate effect on tobacco supply side. Il
would, however, initiate a progressive decline which will result in a substantial reduction in
tobacco consumption over the next half century. Il will also prevent many young persons
from becoming early addicts.
•
On lhe contrary, increasing mechanisation of lhe production process and profit motivated.
political maneuvering at (he auction floors by large tobacco and leaf companies are largely
responsible lot the rampant unemployment and poverty among (ohttcco workers and small
farmers. When global tobacco demand falls and our exports shrink, the tobacco industry is
quick Io abandon lhe farmers while protecting its profits and diversilying ils investments:.
We believe that it will benefit the farmers, workers and the countrv as a whole if lhe
government helps the process of diversification wherein people engaged in tobacco
produelion can be shilled lo alternate occupations.
IS II IE Illi I. PARTIAL TO SMOKELESS TOBACCO?
rfhc Bill . as reinforced with the Standing Committee provisions and passed by the Rajya Sabha.
encompasses all forms of tobacco products- smoking and smokeless. It thus.provides a level
playing ground lo all of (hem. Peculiarities of various segments ol the tobacco industry could be
better addressed w bile drafting Rules under the Bill.
\ I.
BAN ON SMOKING IN PUBLIC PLACES
The hill recognizes and piotcds lhe rights of non-smokers.-to remain sale from the hatmlitl
effects of environmental tobacco smoke (passive smoking). Skeptics have doubted whelhet this
provision can be effectively implemented. We believe that this Bill confers a much needed
entitlement lo non-smokers to assert that right. Public-education is alsb required to raise the
consciousness of the ban and its rationale. A combination of regulation (to confer the right) and
community mobilization (to assert and respect lhe right) is needed to ensure smoke free public
places.
Preliminary Draft, Comments Welcome
26th March, 2001.
Health and Human Rights Aspects of the Proposed Anti-tobacco Bill
Arindom Mookerjee
*
Background Paper on Tobacco presented at the Regional Consultation ofHealth and
Human Rights organized by the National Commission for Human Rights in association
■with the World Health Organization and the Ministry ofHealth and Family Welfare,
Government ofIndia, on April 10-11, 2001 in New Delhi.
* WHO National Consultant to the Government of India on Economics and Policy of
Tobacco Cessation. The views expressed in the article are his personal opinions and in no
way reflect those of either the WHO or the GOI.
Introduction
The validity and sanction of any social legislation has to be rooted in the gamut of human
rights it seeks to protect or promote. The legislation we are referring to here is the anti
tobacco Bill entitled “TAe Cigarettes and Other Tobacco Products (Prohibition of
Advertisement and Regulation of Trade and Commerce, Production, Supply and
Distribution) Bill, 2001.” and the obvious rights issue is the question of public health. At
one level, there may seem to be a contradiction of sorts. After all, human rights as I see
them essentially are rights of individual; they accrue to a person because they are human
and they apply to all people around the world. Notion of public health and social
legislation belong to the community as a whole. The dialectics between the two differ on
a case-to-case basis. An investigation into these issues perhaps raises more questions than
provide answers. Should community rights override individual rights? Shouldn’t
legislation to promote public health in a democratic welfare state have respect for
individual privacy? The paper seeks to address some of these and related issues in the
particular case of tobacco. Section 1 deals with the various linkages between health and
human rights. Section 2 enlists the salient features of the anti-tobacco Bill. Section 3
reviews the provisions of the Bill in the context of the accepted notions of health and
human rights while Section 4 dwells on a broader coalition of law-enforcing agencies,
human rights organizations and other members of civil societies to make a meaningful
impact in this field.
Section 1
The triad of health, human rights and social legislation
To begin with a simplistic relationship between the three can be presented thus: The right
to health is to be recognized as a basic human right. The legislative imperatives of the
same needs to be put in place firmly. Good health then can be seen as a consequence of
the two.
One approach to the study of the relationship between health and human rights is to focus
on the ways in which health policies, programs and practices can protect and violate
rights in ways that they are designed and implemented. The contra-positive approach
would be to study the health consequences of disregarding or disrespecting the basic
human rights. Whatever the approach, the indivisibility and interdependence of rights as
they relate to health cannot be questioned and the promotion and protection of human
rights can be as powerful as a vaccine.
Equally important is the conditions in which these interplays work. Here one needs to
distinguish between the medicinal aspects of private health care and the larger domain of
public health. While the former focuses on health of the individual, public health has
come to be defined as “...(ensuring) the conditions in which people can be healthy.” The
distinction lies in the fact that the latter encompasses a much larger and more general
objective, viz, the health of populations. Clearly, populations cannot be “healthy” unless
the individuals comprising the populations remain so. But individual medical (health)
care, while being necessary, is by no means sufficient to achieve the goal of public
health. There is no mistaking the fact that smokers derive a private benefit from smoking
tobacco and the health costs are bome privately by them. What this does not reveal is that
in so doing the health of majority of non-smokers is affected adversely. More on tobacco
being a “public bad” in a later section.
The role of law - Where the government comes in
Given the objective of public health, enabling conditions need to be created to help
individuals make informed choices, to isolate the changing patterns of vulnerability and
develop effective response mechanisms for combating the same. It is important to realize
that the human rights paradigm cannot operate in a legal vacuum. Some existing authority
needs to enunciate the law and put into place appropriate enforcement and redressal
mechanisms. This is where the government (state) comes in. There ought to be no
confusion of the role of the state. In the past, guns, drugs, alcohol, which have been
2
highly prized by some, and abused by others, have been the object of societal sanctions.
Few have succeeded and the main reason has been that the state has been sucked into the
vortex of a prohibition fever where it wanted to play both doctor and patient. It is
important for the state as well as for the opponents of the state to define its scope in
public action. To be able to respect, protect and fulfill and safeguard its human rights
obligations the government has to bring about well-defined legislation to facilitate the
functioning of the legal systems.
Today, the philosophy of “responsive communitarianism ” is gaining popularity among
wide sections of society. This essentially means balancing individual rights with social
responsibilities, or individuality with community. In many cases (like in tobacco), there is
a basic tension between our individual desire for privacy and our deep concern for public
safety and public health. This is where the government comes in - not for example, as the
arbiter to decide who should smoke and who not and how much etc but to outline the
priorities and the means of achieving the same.
To sum up, the fundamental reciprocity between health and human rights is well
established and the need to put in place a proper regulatory framework to aid and nurture
this synergy should be the guiding lights of policy makers and analysts in this field.
Section 2
Salient Features of the anti-tobacco Bill
The Cigarettes (Regulation of Production, Supply and Distribution) Act, 1975 was
reviewed by the Parliamentary Committee on Subordinate Legislation in February, 1995
and a large number of suggestions was made. The new Bill entitled “7%e Cigarettes and
Other Tobacco Products (Prohibition of Advertisement and Regulation of Trade and
Commerce, Production, Supply and Distribution) Bill, 2001.” has been introduced in the
Rajya Sabha on 7th March, 2001 and has since been referred to the Standing Committee
on 12th march, 2001. The Bill would be effective as far as the provisions regarding
cigarettes are concerned, all over India, but for other tobacco products only to the UTs,
Punjab, West Bengal, UP and Goa. This is because other tobacco products (other than
3
cigarettes) are in the state list, and only these states are have passed resolution in their
state legislatures undertaking to adopt a central law in the matter. The other states could
adopt the law pertaining to other tobacco products merely by passing a resolution in their
legislature. Some of the salient features of the Bill are:
•
To prohibit the advertisement of all tobacco products and to provide for its
regulation in trade and commerce.
•
To prohibit smoking in public places.
•
To prohibit selling of tobacco products to persons below the age of 18 years.
•
Indication of nicotine and tar contents on the packets.
®
Indicating of the warning on the package in English as well as Indian languages.
o
Total ban on sponsoring of any sport/cultural events by cigarettes and other
tobacco product companies.
•
Empowering Sub-Inspectors of Police or equivalent officers of State Food or
Drug Administration of the Central/State Governments to carryout the provisions
of this legislation and confiscation of the goods in case of any violation.
However, the owner of the goods will be given the option to pay a fine in lieu of
the confiscation, which should be equal to the value of the goods confiscated.
•
Imposition of a fine up to Rs.200/- for minor offences relating to smoking in
public places, sale of tobacco products to minors.
These provisions are to be looked in conjunction with certain legislative and
administrative steps already taken by the government. They include:
4
1. The Cigarettes (Regulation of Production, Supply and Distribution) Act,
1975 requires manufacturers or persons trading in cigarettes to display a
statutory warning. Similar warning is required to be displayed on
advertisements also.
2.
Instructions have been issued through the Cabinet Secretariat prohibiting
smoking in hospitals, dispensaries, educational institutions, conference
rooms, domestic air flights, AC sleeper coaches, suburban trains etc.
3.
Direct tobacco related advertisements are prohibited on Doordarshan and
All-India radio. The cable TV regulation Act has been recently amended
prohibiting tobacco advertising on cable TV also.
4.
Under PFA rules, a warning “Chewing of Tobacco is injurious to health”
has also been made mandatory.
Though information is still to be received from all states, the states of Delhi, Goa and
Sikkim have some form of legislation that prohibits smoking in public places and sale to
minors. Such steps are under consideration in Rajasthan and West Bengal also. In Kerala,
the High Court has directed the Government to stop the practice of smoking in public
places by taking steps under the IPC.
Section 3
The Bill through the Health and Human Rights lens
Let us examine what human rights implications the Bill has and what public health
aspects the Bill aims to promote. First a small backgrounder. Patterns of smoking in the
world suggests that the habit is percolating to those with limited access to information
(more so correct information) and education and those who face greater vulnerability to
health risks on account of their socio-economic standing. Particular mention must be
5
made of children smokers and the fact that they are special target groups of tobacco
companies. So what is it about the nature of tobacco that is considered unacceptable?
Is tobacco a ‘public bad’?
Notions of ‘privateness’ or otherwise of tobacco is explained by the fact that while being
“exclusive” in use, it is certainly “non-exclusive” in effect. The tobacco user may be
doing so in his private capacity but he cannot exclude others from the harmful exposure
of tobacco smoke, others bear the harmful effects despite zero risk-taking. Adult non-
smokers face increased risks of fatal and disabling disease due to exposure to other
smoke. Babies bom to smoking mothers are likely to have lower birth weights, face
greater risk of respiratory disease and sudden infant death syndrome. This is over and
above the fact that the use of tobacco represents a health hazard to the user herself. In fact
the uniqueness of tobacco stems from the fact that it a substance that is dangerous when
used the may it is meant to be used unlike firearms or marijuana where instances of abuse
have rendered them harmful.
It is well documented that the use of tobacco carries with it the risks of health hazards
and addiction but private and community perceptions vary when it comes to classifying it
as a “bad” or what economists call “demerit “ good. The consumer must be deriving
certain benefits that explain his revealed preference in repeated use (apart from the fact
that tobacco is addictive). To that extent his marginal disutility is overridden by the
basket of perceived gains that accrues to him. From a societal point of view, the existence
of third party risks and environmental pollution, potential fire hazards etc are defense
enough in clubbing it as an example of a public “bad” or something that is undesirable for
consumption.
The Indian Factsheet
Based on a few community-based surveys in India, it is estimated that 8 lakh deaths could
be attributable to tobacco use. It is estimated that half of the long-term smokers will be
6
eventually killed by the habit and of these half will die during the productive middle age.
As per information given by Indian Council of Medical Research (ICMR), as of 1999, the
prevalence of tobacco related cancer was 163500 cases, coronary artery disease due to
tobacco use was 4450000 and obstructive lung disease cases due to tobacco use were
3920000. The total economic cost of treating tobacco related diseases comes to almost Rs
13,500 crores per annum (at 1990 levels). At today’s rates, the expenditure could exceed
Rs 25,000 crores. This includes components like expenditure on diagnosis, treatment,
loss of wages and expenditure of the treating institution.
Viewed in this light, obviously there is a public health prerogative and what kind of
human rights are being sought to be protected with the introduction of the Bill?
Alternatively, in the event of the Bill not coming into effect, what rights are violated and
what are its health consequences?
First the right to information, and as stressed earlier, the right to correct information.
Consumer sovereignty and rationality of decision-making is aided by informed choice.
By displaying nicotine and tar contents and other health warnings, the right to
information is attempted to be bridged. Prohibiting sale to minors protects Child health.
A non-smoker’s right to clean air is addressed by prohibiting smoking in public places,
where a “public place” is well defined. It has been defined as
“means any place to which the public have access, whether as of right or not, and
includes auditorium,
hospital buildings,
health institutions,
amusement centres,
restaurants, public offices, court buildings, educational institutions, libraries, public
conveyances and the like which are visited by the general public but does not include any
open space "
An important aspect of any legislation is the enforcement and monitoring of the law. A
large part of mainstream opposition and/or skepticism stems from the lack of credibility
of enforcing the law effectively. Special attention has been given in the anti-tobacco Bill
to plug this lacuna. Authorities have been empowered to fine and confiscate offenders. It
7
should however be borne in mind, that any social legislation needs time to take root. The
law prohibiting advertisement in any place or public service vehicle in Delhi was
promulgated in 1996. As regards the ban on smoking in public places in Delhi, it is
reported by the Government of N.C.T. of Delhi that during the year 2000, 1404 raids
were conducted in public places and public conveyances to check smoking resulting in
fines being imposed in 294 cases. In the year 2001, 604 checks have been conducted and
238 people have been fined. This is not to say that the law is being enforced in letter and
spirit, but to suggest that there is nothing that we need to be defensive about when
questions are raised regarding implementation of existing laws. The fact that the laws
exist assures a measure of protection to non-smokers who stand up for their rights.
Imagine a situation where they will have nothing to fall back on when they feel
physiologically and morally violated due to exposure to tobacco smoke.
To sum up, the Bill is to be looked at from the perspective of public health. Its raison
daitre is to protect individual freedom, not curb them. It doesn’t at any point mention that
people need to give up smoking, nowhere is any curb on tobacco production intended to
be put in place. Its strategy is clearly a demand-reducing one. The supply chain is left
untouched. If public health is accepted to be important, the Bill simply reiterates a basket
of human rights that needs to be respected and fulfilled.
Section 4
Envisioning a grand coalition
However noble the intentions, on cannot wish away the presence and operation of
pressure groups. The obvious reference is to the tobacco lobby that in its acutely
erroneous self-justifying means, work towards the perpetration of an ill-informed,
hazardous regime. Their economic rationale is sometimes strong enough to push civil
rights to the background. Unfortunately in a democracy like ours, public policy priorities
get skewed towards areas that are more “lucrative”. Given that the resources are limited
and there is a plethora of public activities that need to be undertaken, the various demand
8
compete for a place in the rooster. Having taken the bold initiative to put a legislation in
place, we cannot allow it to come to naught.
It is here that a broad alliance needs to be formed - to advocate, to educate and to
counter-attack when needed. The National Human Rights Commission (NHRC) is a
watchdog firmly in place but its role lies more in ex-post enforcement of the legislation.
The members of the civil societies, public health activists, academia and sympathetic
sections of the industry should form a broad-based coalition to uphold the dignity of basic
health rights and resist tendencies in echelons of power to fall victim to subversive
attacks from the opponents of individual freedom and liberty. For if they fall, the larger
victim will be the health and state of the citizens of this country.
9
25 September
s SuOve
ivei'iiiOii Wets duuuieu uufiny ine 56th Wofiu nedilii Assemoiy, wnich Look piace from
to 2 c Hay 2uu3, at the Paiais des nations, Geneva. It was opened for signature by aii Members
:ne Wo rid i-ieairh Organization, or Members of rhe united Nations, and by regionai economic
egranon organizations from 10 June zuuo to 22 June 2003 at the vvoric neaitn urqamzation
Headquarters in Geneva, and remains open for signature at United Nations Headquarters in New
York from 30 lune 2003 to 29 lune 2004.
pH-
SACTob
World Health Organization
Tobacco Free Initiative
WHO Library Cataloguing-in-Publication Data
WHO Scientific Advisory Committee on Tobacco Product
Regulation.
Scientific Advisory Committee on Tobacco Product Regulation
(SACTob)
recommendation on tobacco product ingredients and emissions.
l.Smoke - analysis 2.Tobacco, Smokeless - chemistry 3.Tobacco chemistry 4.Tobacco smoke pollution - prevention and control
Tobacco industry - legislation 6.Guidelines I.Title
5.
ISBN 92 4 159054 8
(LC/NLM classification: HD 9130.6)
© World Health Organization 2003
All rights reserved. Publications of the World Health Organization can be
obtained from Marketing and Dissemination, World Health Organization, 20
Avenue Appia, 1211 Geneva 27, Switzerland (tel: +41 22 791 2476; fax: +41 22
791 4857; email: bookorders@who.int). Requests for permission to reproduce or
translate WHO publications - whether for sale or for noncommercial distribution
- should be addressed to Publications, at the above address (fax: +41 22 791
4806: email: permissions@who.int).
The designations employed and the presentation of the material in this
publication do not imply the expression of any opinion whatsoever on the part of
the World Health Organization concerning the legal status of any country,
territory, city or area or of its authorities, or concerning the delimitation of its
frontiers or boundaries. Dotted lines on maps represent approximate border
lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers' products does
not imply that they are endorsed or recommended by the World Health
Organization in preference to others of a similar nature that are not mentioned.
Errors and omissions excepted, the names of proprietary products are
distinguished by initial capital letters.
The World Health Organization does not warrant that the information contained
in this publication is complete and correct and shall not be liable for any
damages incurred as a result of its use.
Printed in World Health Organization, Geneva.
Preface
The Scientific Advisory Committee on Tobacco Product Regulation (SACTob),
established by the World Health Organization, held its first meeting in October 2000.
The committee is composed of national and international scientific experts on product
regulation, smoking cessation and laboratory analysis. SACTob advises WHO about
scientifically sound recommendations to Member States addressing the most effective
and evidence-based means to achieve a co-ordinated regulatory framework for tobacco
products. The work of the committee is based on recent leading edge research on
tobacco product issues and aims to fill the regulatory gaps in tobacco control.
The present recommendation was finalized by SACTob during its Fifth Meeting in 2527 November 2002 held in Brisbane, Australia.
0
Scientific Advisory Committee on Tobacco Product
Regulation (SACTob) Recommendation on Tobacco Product
Ingredients and Emissions
Background
Historically, cigarettes and other tobacco products have been exempt from health and safety
standards for ingredients and emissions that are typically applied to other consumed
products including foods, beverages and drugs (1. 2, 3). Although some countries have
begun to develop and apply standards for allowable ingredients, there are no globally
accepted standards or guidelines (2). Presently limits on emissions from tobacco products
have not been implemented with the exception of estimates of tar, nicotine and carbon
monoxide (2). An important consideration in the regulation of ingredients is that when the
cigarette is used as intended, the ingredients can be modified and emission profiles altered
during the processes of combustion (“burning”) and pyrolysis (“modification by heat").
Therefore, the focus of this document is on the importance of evaluating tobacco product
emissions as well as their ingredients under the conditions in which these products are
actually used. The purpose of the document is to provide recommendations to support the
development of protocols for assessing tobacco product ingredients and associated
emissions with the intent to reduce tobacco caused disease.
The central premise is that tobacco product ingredients and emissions thereof, including
nicotine, should be regulated. Ingredients include all product components, materials used to
manufacture those components, residual substances from agricultural practices, storage and
processing, and substances that can migrate from packaging into the product. [The term
ingredients is preferred to terms such as “additives” and “processing aids”]. Emissions
comprise what is actually delivered to the user and are the product responsible for most
tobacco-attributable death and disease. Emissions are substances that are produced when
the product is used and this is distinguished from "exposure", a term that in this context
refers to the fraction of emissions that is actually absorbed by the user.
In the case of smokeless tobacco products, emissions refer to substances released during the
process of oral use (“chewing”). In the case of the cigarette and other smoked products, the
term refers to the constituents of the smoke. This includes those emissions directly inhaled
by the user of the product (“mainstream smoke”) and those inhaled by nonusers and users
alike (“secondhand tobacco smoke").
The preferred focus for regulation is the emission from the product when it is used as
intended [exceptions may include certain cigarette ingredients such as nicotine and
ammonia,. These principles apply to all smoked products including novel cigarette
substitutes and smokeless tobacco products (4). recognizing that all tobacco products have
ingredients and emissions.
This focus on emissions as the critical point for regulation does not exclude consideration of
allowable ingredients and design features. This is consistent with the emphasis that the
tobacco industry itself places on the nature and acceptability of the emissions in their
product development and evaluation (1, 2. 5. 6). This includes industry research on the
andtheitstobacco
acceptability
to
physical nature of the smoke ( smoke’ ^emist y and
d aooearance) of
product
potentral consumers (5.7). The physical des g
g)
interact with its chemical make-up to influence us iu
.
f a idi,
the size of the cuttings of the tobacco in cigarettes and ^'ess tobacco
'eve' ° acidhy
(pH), and the presence of other substances interact to influence he re ease> ofn.cotme from
the product (3 5). Similarly, physical and chemical charactenst.cs of cigarettes interact to
alter the size distribution of the aerosol particles that convey mcotine and other chemicals
and establish the degree of absorption (5).
The emphasis on both ingredients and emissions recognizes that actual health effects of
tobacco products depend on their physical nature, their chemical make-up and how they are
used (2. 3, 8. 9. 10). For example, more frequent or longer use of a product delivering lower
levels of toxins per unit may result in greater risks to health than less frequent use or fewer
years of use of a product that is more toxic per unit (11. 12. 13). Because the tobacco
industry has a history of marketing its products on the basis of apparent reductions in
toxicity with the intent being to increase consumption of their products, a regulatory strategy
to reduce toxins must be accompanied by oversight of marketing and by surveillance of
consumer use to detect such effects (3, 13).
It should be recognized that tobacco is a unique consumer product which could not be
introduced into the market today under any known consumer regulations if it were not
already established world-wide among a variety of substantially addicted populations.
Therefore, its regulation requires a radical approach that will deviate substantially from the
regulatory norms applied to other consumer products such as foods, cosmetics, and drugs.
Given that tobacco product emissions are known to vary greatly and can consist of
thousands of toxicants, there is no alternative but to establish upper limits for selected
constituents, based on toxicity profiles, as a means of progressive toxicant reduction in order
to begin progress towards reduced toxicity and addictiveness (14, 15).
It is important to note that for many products, regulatory limits are set on the basis of
defining safe limits on exposure. The level of toxicants in tobacco products is so high that
no regulatory strategy could be based on either safe levels or product safety However a
large number of toxic constituents have been identified in the tobacco smoke and substantial
variability exists in the levels of individual constituents across brands of cigarette and other
products. This variability suggests that performance standards for the emissions of tobacco
t b T hy-eSn p
S Upper limitS for individual toxic constituents based on
what appears to be technically feasible.
It is acknowledged that standards for upper limits of ingredients or emissions will not
necessanly result in decreased health risks even though that is the net
These
recommendations must not form the basis for the develonmem „r „ J . \
!
claims that would imply health benefits or claims about the health pFFpT de“nptOrf a"d
.fta. Mod. .» forms of .obrmco-^d d,.X«;X<on
"
2
Observations and Principles
•
Tobacco products have the capacity to cause addiction, due to their nicotine content
and other substances in the emissions.
•
Manufacturing processes can further add to the toxicants and can make nicotine
more readily available for absorption into the body (for example, through the
manipulation of pH, selection of aerosol particle size, the addition of chemicals and
changes in other physical parameters of the materials such as paper porosity and
size of the cut tobacco material).
•
Combustion and pyrolysis of tobacco material in tobacco products, such as
cigarettes [both manufactured and hand-made,, pipes, cigars, and bidis, result in the
formation of additional toxicants and can increase the addictive effects of nicotine
•
Cigarette ingredients and emissions regulation are intended to support tobacco
control efforts to prevent initiation and to stimulate cessation.
•
One of the purposes of this regulation of tobacco products is a progressive
reduction in the level of toxic chemicals in tobacco product ingredients and
emissions, through periodic setting of standards. The upper limits set by the
regulations do not in any way indicate an acceptable level of safety for any tobacco
product and its emissions.
•
The development of ingredient and emissions regulation should aim to reduce
health risks, although there is no expressed or implied measure of disease
reduction.
•
Smokeless tobacco products also produce emissions that are addictive and toxic.
Recommendations
1.
Regulations in terms of setting upper ingredients and emissions limits for toxicants
need to be developed for all tobacco products whether they are intended for
smoking or non smoking methods of consumption. Variation in the ways in which
tobacco products are used needs to be considered in establishing performance
standards.
2.
For tobacco products intended to be smoked, the manufactured product needs to be
differentiated from the product actually intended for consumption which is its
emission (“smoke”), and the critical focus of regulation must be on the emissions.
3
Ongoing surveillance and research must be instituted to assess the consequences of
regulation on initiation, cessation and health effects in order to modify the
regulatory process on a regular basis.
3
4.
With respect to nicotine, it remains uncertain at this time whether public health
would be better served by increased or decreased levels of nicotine per unit (e.g.,
cigarette) and further study of this issue is required.
5.
No health claims can be permitted based on the level of ingredients or emissions or
whether the products meet regulatory standards for ingredients and emissions.
References
(1) Slade J. Henningfield JE. Tobacco product regulation: context and issues. Food and
Drug Law Journal. 1998, 53 Suppl, 43-74.
(2) World Health Organization. Advancing Knowledge on Regulating Tobacco Products.
Geneva, World Health Organization, 2001.
(3) Stratton K. Shetty P. Wallace R, Bondurant S, eds. Clearing the smoke: assessing the
science base for tobacco harm reduction. Institute of Medicine, Washington. DC, National
Academy Press, 2001.
(4) Slade J. Innovative nicotine delivery devices from tobacco companies. In: Ferrence R,
Slade J, Room R, Pope M, eds. Nicotine and Public Health, Washington DC, American
Public Health Association, 2000: 209-228.
(5) Food and Drug Administration. 21 CFR Part 801, et al. Regulations restricting the sale
and distribution of cigarettes and smokeless tobacco to protect children and adolescents:
final rule. Federal Register 1996, 61 (168): 44396-45318.
(6)
Hurt RD, Robertson CR. Prying open the door to the tobacco industry's secrets about
nicotine: the Minnesota Tobacco Trial. Journal of the American Medical Association, 1998.
280 (13): 1173-1181.
(7)
Abdallah F. Tobacco taste. Tobacco Reporter, November 2002.
(8)
Hoffmann D, Hoffmann I. The changing cigarette, 1950-1995. Journal of Toxicology
and Environmental Health, 1997, 50: 307-364.
(9)
Peto R, Lopez A, Boreham J, Thun M, Heath C. Health effects of tobacco use: global
estimates and projections. In: Slama K, ed. Tobacco and health. Proceedings of the 9th
World Conference on Tobacco and Health, 10-14 Oct 1994, Paris, France. New York.
Plenum Press, 1995: 109-120.
(10) Royal College of Physicians of London. Nicotine addiction in Britain: a report of the
Tobacco Advisory Group of the Royal College of Physicians. London, Royal College of
Physicians, 2000.
(11) Doll R. Peto R.
Cigarette smoking and bronchial carcinoma: dose and time
relationships among regular smokers. Journal of Epidemiology and Community Health,
1978,32:303-313.
(12) National Cancer Institute Monograph No. 8. Bethesda. U.S. Department of Health and
Human Services, National Institutes of Health, National Cancer Institutes, 1997.
(13) National Cancer Institute. Risks associated with smoking cigarettes with low-machine
measured yields of tar and nicotine. Smoking and Tobacco Control Monograph No. 13.
5
Bethesda, U.S. Department of Health and Human Services, National Institutes of Health,
National Cancer Institutes, NIH Pub. No. 02-5074. 2001.
(14) Henningfield JE. Zeller M. Could science-based regulation make tobacco products less
addictive? Yale Journal of Health Policy. Law and Ethics. 2003.
(15) Myers M. Regulation of tobacco products to reduce their toxicity.
Health Policy. Law and Ethics. 2003.
6
Yale Journal of
41
“Towards Implementation of
Tobacco Control Legislations
in India”
w yournw
G
Tobacco contains over 4700 chemicals,
60 of them are cancer producing.
©
Tobacco is promoted as a cash crop but it
kills 5 million people worldwide every year.
©
The nation gets Rs.24,000 crores anually
as revenue from tobacco;
spends
Rs.27,000 crores for treating tobacco
A Panel Discussion
related illness.
©
Over 25 serious diseases are directly
associated with tobacco use, including
heart and lung diseases.
©
Chewing tobacco causes oral cancer;
India has highest number of oral cancer in
the world.
©
Tobacco use in men causes impotence
and in women infertility.
G
Tobacco use shortens life by 15-20 years.
C
Tobacco is a major cause of deforestation.
Date :
Tuesday, 30th May 2006
Time :
9.00 am to 1.00 pm
Venue ;
Sri Jayadeva Institute of
Cardiology (SJIC) Auditorium
Bannerghatta Road, Bangalore - 69
Is jointly organized by:
To cure one kg of tobacco 8 kgs of wood is
used.
TOGETHER WE CAN
ELIMINATE TOBACCO
The Consortium For
Tobacco Free Karnataka (CFTFK)
—g
and
Sri Jayadeva Institute of Cardiology (SJIC), >
Bangalore
Supported by Ministry of Health, Govt, of India
and World Health Organisation - Country office
You are invited to the panel discussion which is
organised in view of World No Tobacco Day-2006.
Theme:
“Tobacco: Deadly in any form or disguise”
Tobacco addiction is a global epidemic that is
increasingly ravaging countries and regions that can
least afford its toil of disability, disease, lost productivity
and death. The tobacco industry continues to put
profits before life; its own expansion before the health of
future generations; and its own economic gain ahead of
the sustainable development of struggling countries.
Recognizing the need to curb the Tobacco epidemic the
World Health Organization (WHO) initiated a first ever
public health treaty known as the Framework
Convention on Tobacco Control (FCTC) in 1999. It was
ratified in 2004. India was one of the forty countries that
first ratified FCTC on 27th February 2005. Before
ratifying FCTC, Indian government passed an Act in the
parliament on 1st May 2004; known as “The
Cigarettes & Tobacco Products (Prohibition of
Advertisement and Regulation of Trade and
Commerce, Production, Supply and Distribution Act
2003”. In March 2003, the Karnataka government
passed an Act in the Assembly known as “The
Karnataka Prohibition of Smoking and Protection of
Health of Non-Smokers Act, 2001 .
The CFTFK found that despite the enactment of effective
legislations for tobacco control there exists a gap in its
implementation. Therefore this year during the World
No Tobacco day, the CFTFK is planning to bring senior
government officials who are responsible for enforcing
the Tobacco Act together with civil society
organizations to evolve appropriate strategies for
addressing the gaps in its implementation. Participants
from all the districts in Karnataka and a few participants
from the neighbouring southern states will participate
in the panel discussion.
The Consortium for Tobacco Free Karnataka (CFtW)
was formed in the year 2001 by various health care and
social development agencies and Government
institutions working in the area of cancer, mental health
and cardiology in Bangalore, to achieve the following
objectives.
« To create awareness among the various sections of
society on the ill effects of tobacco consumption
and cultivation.
Application for Registration
(Please fill this and send it to the address given overleaf for communication)
Name:__________________________________
1. Sex :
Male / Female
2. Name of the Organisation, Address with
Telephone and Email ID
To launch educational programmes among the
students community, children and youth including
school drop outs and street children.
To advocate for tobacco control policies that would
address the socio-economic, health and
environmental implications of tobacco use.
The members of the Consortium for Tobacco Free
Karnataka are: Karnataka State Junior Doctor’s
Association, Bangalore Institute of Oncology,
Banashankari Charitable Trust, Indian Medical
Association, Community Health Cell, Cardiological
Society of India-Karnataka, Cancer Patient’s Aid
Association-Bangalore, Christian Medical Association
of India-Bangalore, Indian Red Cross Society,
Bangalore, Sri Jayadeva Institute of Cardiology,
National Institute of Mental Health and Neuro Sciences,
Kidwai Memorial Institute of Oncology, Rotary
Bangalore City Centre, Ambedkar Medical College and
World Vision India.
3. Experience in working for tobacco control
Yes/No
4. If yes, How many years ?_______ ;________
5. How do you think participating in the
programme would help you in your work ?
Over the years, the CFTFK has organized public
awareness programmes in different places, awareness
programmes for students and submitted
memorandums to policy makers to check the trends
both in demand and supply of tobacco.
Address for Communication:
Community Health Cell
359, Srinivasa Nilaya, Jakksandara I Main,
I Block, Koramangala, Bangalore - 560 034.
Phone: 25531518, Telefax: 25525372
Mob : 9448034152, Email: chc@sochara.org
Signature
Date:
zssQrt ddasAcfo
Scdoojra
£d_j-----------dozoado dSod
—
— deTOddra 2006 dodo Ajdojad ddr
ddxrad ddrcdo© qyartd&jsbddort z^odo sfcda
zoadd xldsad dozsado &edcdoe& ddjaedrt ddeoo 2004
zsaSrioa^do. edd «s eadjado zsaori zooao.
d©, z-odo eadjarfdo
eadoacio zsaQrt wdd <adod©od
dozsadd <sbedcdod>c( ddrtwoo
sadjreAo.
w add ddrodo©co & adodo/tedo dz3r
eJ
*o
co
doaddesaAd. ddr e^rdjarafcsariwo aea^ Ajadcdorfo ZodA^desartodd. esddd ad^
zSdcdo^zsaSrt zodd, uadjasd esodrte eroeo^dod epaodoz&rtedo drido, dfsaod dodo,
ate ddxraa^ d^droa da.
eJ
©
d? eaoiodcdodo
«<
^rtdeid5, dodo,doz3ado dna^rrteb (zsa&cado adez^, ss^srod,
dcdjaQd, ddwrozsodododozSdcdoedaodztro^dodd) ioododdodouarios^do.
2003d© zsaort woad (2003 34de acdodo).
roosod esQcdo© SeodwGdrd
#! &?Ad aododorttfdoG< zsaodiaadodd.
; 1. Ajadra^ dtfd©
dotsado
^0
@00
dtdo^jdo. 2. uOcdoOri dotrodo diado^do. 3. dd^d d^^dja^ztreod
dotrodo tsaSouado (dotsado drodod d^d doood
daadodd,
dozrodo
^c^p6,
erootsodjadodd,
esofe&deeartodd). 4. ^^ed
dotsado ajaddoouo
aodo
wdd
ddoed dotsado dsado^jdo
^>c>d
sadjajdo
dtd'^^d'd©, duaddodd. www.fhrai.com/stoppress.htm or www.whoindia.org
adori edd da desad© dd|do dod^ra.
1 Arodraad ds^d© dotrodo x!edc3 aded ddrzsad d^d doa©d ed^a d-dsrodd
ddpaA earaod 60zjS0 So.ao.
es^dcdo ^udd ^?odo t^adodo© todcOo^ ddedcsadd©,
coartoa ?«^rid uodo doo^D. «<s
*d©
adpd! Prided6' jSedzsadd
ddslradedo. « d°dd©
*
Prided
3edod)do t^odo edoad,
0e3 wdaddedo
edoad^ dod
200 dja rt<&. d? eadoado 1 doe 2004 Ood tsadcdo©d2
2. saeoa- saeSetsozte
*
doddoodeo xdde^ wd^a dowado dnadrri^do dsadodjdo
adeddeoaAd. -d? aododod wdcdo sa© saeSecsozte1 adddd (100 rt») ^d©,
dotsaddodoadododo .di acdododed enoSo^d©, 200 doa dod djaddesariodd.
vadjarfo, adobos' 2004 ©od tsaOodoeDd.
3.
Ajdde^' sards dosad dsa^rd^do zsaSooad daxbc^do Prided6, diadod
^d©. ^dded
*
zsaSooa^d zirsedr 90$ 60xio do. e^drt aoedwaddo. 'soddd
addled sgddsaddo ds ^edd©^ "dowa& xiaddootadoadodd. dowaWod ^dp6,
a
_a
enoo&artodd.aodo 'sddesado usaod.
d? ao±>do enjoo^dc^dodo ddr z^oo S^edsa z^odo xiaad djssac£o dod
added a^xJoarbs^do. dodde^p ds Recoded eroeo^d© 5 ddr z|co
sards 5
xiaad dossaod dod a^xJoard^jdo. ds doddo wrixj^i, 2005 Ood zsae«d©d.
4 dotjsvdod dodaOXid dsa^rded SdodOri dsados&cd. Prided6, e$!aa dozrod
dna^rrteed doadod oortdod d»od 18 ddr^od 3ddo dod&d do^?rt daado^do
esdoa$ aodod$od z?adod©60 x>o,£d. 30 do do. as^od ^u^d doe© udadded.
Soddo ert^l, 2005 d© zsaori wodd.
3s Reddort^cd dozjaud sazda dowaad daa^rd
doe© sadua ooa^oaAQ.
dozsaud©, dao5, sards ddrae^es6, ddoara ad^aoed ddo/sdxjuaAe^-ds doddoddo
ewoaxjd© 2 ddrd d,e»
sards sooo djs dod ^jsddesarddd. dodddp
ejwo4?Xjde^5 ddr s^eo g>i.
ddrod© zjrortdSoxbdddrt dod. dowad sadusddo LdO. sadjsdo eroop^dodad©,
ddxbd dod sards doosadd addrt^eo odd©d. ado© sadjsdo enooo^dodad
add xjort&Xj. <a© ddrri aosart ad^sasDdrt^do dd&rdeo edsadddodd.
des^j dortSoXj desad addrteb ( $ao&a dd / ^dd add
1.
© m
xjadrKd^ *xte
d©
dowa& x3edd
2.
xio^pd sdad loo rtacds^rt dowa& doado^do
3.
dosa& zsaEooado, xledeo djse^aSoxbd addrteb, ddrteb
4. 18 ddr^od ^ddo deeded do^rt dowa& djadod)^
ddrte’od wod <awprt dodara
&radoart>d)cd- od^adddo 3e<s? ddedded.
SI. No
“Towards Implementation of Tobacco Control Legislations in India’
Tuesday, 30th May 2006, Convention Hall, NIMHANS
.
PARTICIPANT REGISTRATION FORM
Name (adxJcda):.......................................................................................................................................................
Organisation (xforf):
................................................................................................................
Name of the district (tJedoda adidda):
......................................
Address (Ss>ax>):
Tel. No.(Office) cd/adasarf xJcs5s(d^tO) ......................................................................................................
Mobile
Email (badass?):
Have you confirmed your participation to the organisers earlier in writing (Yes/ No):
Sada& tpartadtoxfoadoda tart adood-aetador?
adaaotd aadadrirfoda adaaaod aaa^ada&daaoa?
(a^cb/^ej:.................................
(Only for out-station participants) Do you require travel support? (Yes/ No)
Sadart root? zd^oda esadaijdid <^tdodae (zdort^.-aOad zdjao’ftadadort adrog)? (a?>cda /
.............................
Have you requested for travel support in writing to the organisers? (Yes/ No)
NOTE: Travel support will be provided for only two participants per district. Priority will be given to
participants who have sent in their registration form (with request for support) earlier.
xdjazdad: aaaort ^odarf^
Sdpda ^ort adaag SeduarfaaScda.
adaaeocsaadrf adgadad^ d'fetoAcdadOrt aaanaad^ djazdeaariaa^tda.
adaaozd xiaort z^odaada
*
daaeo
Framework Convention Alliance
Statement of the Framework Convention Alliance
Tobacco use is the leading cause of preventable death in the world today At present, 4 million people a
year die from a tobacco-related disease. If current trends continue, 10 million people will die cacti yeai by
the year 2030, with the majority of these deaths occurring .in developing countries. If swift action is not
taken, tobacco will soon become the leading cause of death worldwide, causing more deaths than
tuberculosis, pneumonia, diarrheal diseases, and (lie complications of childbirth for that year combined.
The negotiation of the Framework Convention on Tobacco Control (FCTC) represents an historic
opportunity for global action to curtail the tobacco epidemic. The Framework Convention Alliance would like
Io commend .the Member States for their efforts so far and urges them to take bold actions to advance the
FCTC process. Members of Iho Framework Convention Alliance offer the following recommendations for
O the procedures, principles and substance of the FCTC:
On the procedures of the Intergovernmental Negotiating Body (INB), we would urge that: there be full
NGO participation in all meetings of the Negotiating Body, working groups, ad hoc bodies and any oilier
committees that are established by the INB for the purposes of negotiating or implementing the FCTC; and
that tobacco companies and their affiliates should not be an official party to the negotiations and should not
be allowed to serve on any advisory, scientific, enforcement or implementation bodies of the FCTC.
On the principles of (he FCTC, we would argue that: tobacco control policies must be evidence-based using
methods of proven effectiveness and drawing upon international best practice; the principle aim of the
FCTC must be to substantially and quickly reduce death, disease, and disability; the protection and
promotion of public health must be the guiding principle for all the decisions and actions of the negotiating
parties; the Convention itself should include specific obligations on, among other issues, advertising, duty
free sales, product regulation, smuggling, and warning labels, rather than reserving all obligations for
inclusion , in protocols; the public health provisions of the FCTC should take precedence over other
inlmimlioiml ikiioihiiouIs. For oxamplo, moasuros Io protect public health may conceivably conflict with
trade liberalization, but the public health objectives are legitimate and should lake precedence over trade
when lives are at stake; and that, nothing in the FCTC undermine existing tobacco control initiatives or.
regulations in any signatory slate nor prevent, preempt or discourage any party from taking stronger action
than required by the FCTC.
Finally, we would also like to make some recommendations on the substance of the FCTC, which should
include, among other measures: a total ban on all forms of direct and indirect tobacco advertising,
sponsorship, promotion and "brand stretching”; strong measures to combat tobacco smuggling, a ban on
■ tax free sales and tax-free import allowances of tobacco; comprehensive tobacco products regulation,
including but not limited to minimum standards for manufacturing, packaging, ingredient and smoke
composition and disclosure, product content and labeling; prominent picture-based health warnings
. covering at least 50% of the package in the main language of the country in which the tobacco product is to
be sold (and markings on every pack with its origin and the country of final destination); a prohibition on the
pH'-sn-
Page 1 of 1
Goijhnuniiy rivaitfi Ccii
From:
To:
Sent:
Attach:
Subject:
Shoba John" <sjohn_patncan@vsnl.net?’
<sichander@hotmail.com>: "Community Health Cell" <sochara@vsnl.com>
Tuesday, April 22, 2003 2 23 PM
Bill concoms.doc
Response to industry
Hi Chander,
1)
Attached with please find the response to potential arguments against the
Bill from the tobacco industry. You may use it for press release, in press
interviews or to be sent out to Karnataka MPs in Lok Sabha.
2)
Aiso,
please send the Kannada report copy at once io Stivarna by email. She
is awaiting the same from yon.
3)
Can you QUICK!.Y confirm the name in which the printer's cheque is to be
drawn. this is most urgent as I would icavmg town agam und dom. want io
aeiay the cheque any runner.
r hanks and Best
Shoba
4/23/03
RESFONDLNG TO CONCERNS ABOUT THE CIGARETTES AND OTHER TOBACCO
PRODUCTS (PROHIBITION OF ADVERTISEMENT AND REGULATION OF TRADE
AND COMMERCE, PRODUCTION, SUPPLY AND DISTRIBUTION) BILL, 2001
Introduction
The Tobacco Control Bill introduced recently in the Indian Parliament has been the
subject of much debate and comment in the media. Some of the opinions expressed reflect
concerns about the Bill’s provisions or its effects. These concerns need a reasoned response.
AFTC has attempted to do that below by providing clarifications about key provisions of the Bill
anil addressing other concerns
I.
ADVERTISING
The Bill seeks to ban all forms of direct and indirect advertising. It also bans tobacco
sponsorship of sports and cultural events.
Wbat does Advertising do?
•
Increases consumption: Tobacco companies often claim their advertising is aimed only at
brand switching and not at attracting new consumers. It does not appeal to business sense- that
an industry that works under tremendous compulsion io consistently replace half of its
committed users (who prematurely die from using their products), docs not want to recruit
fresh users. It is therefore evident that tobacco advertising, as with advertisements for any
other products, is geared at increasing product use.
•
Lures gullible youth and children through glamorous and deceptive promotional stunts
addicting them for a life-time. Advertising, which projects tobacco use in congenial
surroundings or associates the brand name with idolized role models, legitimizes the habit in
these young minds and projects the use of tobacco as socially acceptable.
tv by do we need an ad ban?
•
®
•
•
Tobacco-advertising involves the promotion of a product that is proven to cause 25-odd lifethreatening or disabling diseases and induces life-long addiction amongst its users.
To protect people from being misled by false images or misleading health claims and
deprived of their right to make a free and informed choice.
To prevent fresh users from picking up the habit and thereby reduce consumption and
resultant morbidity, mortality and economic loss to the community and the nation
To protect children and adolescents from being attracted to tobacco products.
Do tobacco Advertising bans work?
A World Rank Study of 10? countries demonstrates that countries which have imposed a
comprehensive ban on all forms of tobacco advertising have had steeper declines in tobacco
consumption compared to those that had not done so.
Does the ban leave cross border advertising unabated?
The apprehension about the possibility for continued cross-border advertising should be allayed
bv the fact that the recently concluded WHO Framework Convention on Tobacco Control
(FCTC) recognizes the right of countries to ban cross-border advertising and apply appropriate
penalties against violators. If we enact suitable national legislation, such penalties may include
marketing bans on products so advertised. The FCTC also has strong provisions on smuggling.
International protocols are soon to be initiated both on cross-border advertising and smuggling.
This would facilitate sufficient marketing and trade regulation of international brands coming
into the country.
Effect on allied industries like the A dverfising Sector
Experience from home and abroad reveals that relinquishing a particular brand or a product does
not affect the revenues of this multi-product industry’, as alternate products would replace them.
H TOBACCO PACKAGE WARNINGS
The Bill mandates effective health warnings that are clear and visible, including provisions for
pictures.
Experience of countries like Canada and Brazil which have introduced pictorial health warnings
occupying 50 % and more of the package space shows that they arc effective not only in
discouraging use among current tobacco users but also extends caution to potential users.
Recently, the 14 countries of European Union and Thailand have enacted laws introducing
pictorial health warnings.
HI.
BAN ON SALE OF TOBACCO PRODUCTS TO MINORS AND WITHIN 100
METERS OF EDUCATIONAL INSTITUTIONS.
•
These are measures aimed at restricting easy youth access to tobacco products. If
supplemented with pragmatic implementation procedures, this would prove to be a major
step in preventing early initiation into tobacco addiction.
•
It is well documented that the age at initiation into tobacco use spans across the teen years
and that prevention at these early stages would help reduce consumption considerably.
•
It is also well established that persons who started smoking in teens are much more likely to
die early due to tobacco related diseases.
The provision is restricted to minors only and does not place any restrictions on the sale of
tobacco products to adults.
•
IV.
WOULD THE BILL LEAD TO MASSIVE LY EMPLOY MEM AMONG
TOBACCO WORKERS AND RETAILERS?
e
The Bill does nol contain any provisions directly regulating tobacco production.
*
It primarily involves demand-reduction strategies geared to prevent new entrants to tobacco
habit. Demand reduction will not be sudden but will be spread over several years, giving
sufficient time to set in motion alternate employment opportunities to anyone dependent on
or engaged in tobacco production.
Hence rhe fears of unemployment among tobacco
workers, fanners and retailers are unfounded.
®
As the Bill docs not ban the sale of any tobacco product, there would not be any adverse
effects on the sale and profits to retailers.
9
With the current rate of population growth in developing countries like ours, there is not
going to be a sudden drop in tobacco consumption even with comprehensive tobacco control
policies, as the actual number of tobacco users in the population would not fall in the near
future. Consequently, the Bill would not have any immediate effect on tobacco supply side. It
would, however, initiate a progressive decline which will result in a substantial reduction in
tobacco consumption over the next half century. It will also prevent many' young persons
from becoming early addicts.
•
On the contrary, increasing mechanisation of the production process and profit motivated,
political maneuvering at the auction floors by large tobacco and leaf companies are largely
responsible for the rampant unemployment and poverty' among tobacco workers and small
farmers, when global tobacco demand fails and our exports shrink, the tobacco industry is
quick Io abandon the farmers while protecting its profils and diversifying its investments.
•
We believe that it will benefit the fanners, workers and the country as a whole if the
government helps the process of diversification wherein people engaged in tobacco
production can be shifted to alternate occupations.
V.
is THE Bin. PARTIAL TO SMOKELESS TOBACCO?
The Bill, as reinforced with the Standing Committee provisions and passed by the Rajya Sabha,
encompasses all forms of tobacco products- smoking and smokeless. It thus provides a level
playing ground to all of them. Peculiarities of various segments of the tobacco industry could be
better addressed while drafting Rules under the Bill.
BAN ON SMOKING LN PUBLIC PLACES
The bill recognizes anil protects lhe rights of non-smokers Io remain safe from (he harmful
effects of environmental tobacco smoke (passive smoking). Skeptics have doubted whether this
provision can be effectively implemented. We believe that this Bill confers a much needed
entitlement to non-smokers to assert that right. Public education is also required to raise the
consciousness of the ban and its rationale. A combination of regulation (to confer the right) and
community mobilization (to assert and respect the right) is needed to ensure smoke-free public
places.
&
.
AZ<
7 C^SKs
(2) &
Q) __
<7■^^J'
/77e>Co-^J-
O —
'
Qp —
• -■••. '
~
•'•
■ ,JU
■
^h/r~
&
P 7>^.p
(7^) _
CAXI^
. c/’z^5’
^X_
C2vx_<2^_ ,
,
g
4^
7^^
A
2Z
k
_
pl
__
P/Lty
CA#>-^ 'TX!^
WHO Framework Convention on Tobacco Control
Preamble
The Parlies to this Convention,
Determined to give priority to their right to protect public health.
Recognizing that the spread of the tobacco epidemic is a global problem with serious
consequences for public, health that calls for the widest possible international cooperation and the
participation of all countries in an effective, appropriate and comprehensive international response.
Reflecting the concern of the international community about the devastating worldwide health.
social, economic and environmental consequences of tobacco consumption and exposure to tobacco
smoke,
Seriously concerned about the increase in the worldwide consumption and/production of
cigarettes and other tobacco products, particularly in developing countries, as well as about the burden
this places on families, on the poor, and on national health systems.
Recognizing that scientific evidence has unequivocally established that tobacco consumption
and exposure to tobacco smoke cause death, disease and disability, and that there is a time lag between
the exposure to smoking and the other uses of tobacco products and the onset of tobacco-related
diseases.
Recognizing also that cigarettes and some other products containing tobacco are highly
engineered so as to create and maintain dependence, and that many of the compounds they contain and
the smoke they produce are pharmacologically active, toxic, mutagenic and carcinogenic, and that
tobacco dependence is separately classified as a disorder in major international classifications of
diseases,
Acknowledging that there is clear scientific evidence that prenatal exposure to tobacco smoke
causes adverse health and developmental conditions for children,
Deeply concerned about the escalation in smoking and other forms of tobacco consumption by
children and adolescents worldwide, particularly smoking at increasingly early ages.
Alarmed by the increase in smoking and other forms of tobacco consumption by women and
young girls worldwide and keeping in mind the need for fulLparticipalion of women at all levels of
policy-making and implementation and the need for gender-specific tobacco control strategies.
Deeply concerned about the high levels of smoking and other forms of tobacco consumption by
indigenous peoples,
Seriously concerned about the impact of all forms of advertising, promotion and sponsorship
aimed at encouraging the use of tobacco products,
Recognizing that cooperative action is necessary to eliminate all forms of illicit trade in
cigarettes and other tobacco products, including smuggling, illicit manufacturing and counterfeiting.
Acknowledging that tobacco control at all levels and particularly in developing countries and in
countries with economies in transition requires sufficient financial and technical resources
commensurate with the current and projected need for tobacco control activities.
Recognizing the need to develop appropriate mechanisms to address the long-term social and
economic implications of successful tobacco demand reduction strategies.
Mindful of the social and economic difficulties that tobacco control programmes may engender
in the medium and long term in some developing countries and countries with economies in transition,
and recognizing their need for technical and financial assistance in the context of nationally developed
strategies for sustainable development,
Conscious of the valuable work being conducted by many States on tobacco control and
commending the leadership of the World Health Organization as well as the efforts of other
organizations and bodies of the United Nations system and other international and regional
intergovernmental organizations in developing measures on tobacco control,
Emphasizing the special contribution of nongovernmental organizations and other members of
civil society not affiliated with the tobacco industry, including health professional bodies, women s.
youth, environmental and consumer groups, and academic and health care institutions, to tobacco
control efforts nationally and internationally and the vital importance of their participation in national
and international tobacco control efforts,
Recognizing the need to be alert to any efforts by the tobacco industry to undermine or subvert
tobacco control efforts and the need to be informed of activities of the tobacco industry that have a
negativelffipacfori tobacco control efforts,
Recalling Article 12 of the International Covenant on Economic, Social and Cultural Rights.
adopted by the United Nations General Assembly" bri" 16 December 1966. which states that it is the
right of everyone to the enjoyment of the highest attainable standard of physical and menial health.
Recalling also the preamble to the Constitution of the World Health Organization, which stales
that the enjoyment of the highest attainable standard of health is one of the fundamental rights of every
human being without distinction of race, religion, political belief, economic or social condition.
Determined to promote measures of tobacco control based on current and relevant scientific.
technical and economic considerations,
Recalling that the Convention on the Elimination of All Forms of Discrimination against
Women, adopted by the United Nations General Assembly on 18_December 1979, provides that States
Parlies to that Convention shall take appropriate measures to eliminate discrimination against women
in the field of health care,
Recalling further that the Convention on the Rights of the Child, adopted by the United Nations
General Assembly on 20 November 1989, provides that States Parties to that Convention recognize
the right of the child to the enjoyment of the highest attainable standard of health.
Have agreed, as follows:
PART I: INTRODUCTION
Article 1
Use of terms
For the purposes of this Convention:
(a)
“illicit trade” means any practice or conduct prohibited by law and which relates to
production, shipment, receipt, possession, distribution, sale or purchase including any practice
or conduct intended to facilitate such activity;
(b)
"regional economic integration organization” means an organization that is composed of
several sovereign states, and to which its Member States have transferred competence over a
range of matters, including the authority to make decisions binding on its Member Stales in
respect of those matters;1
(c)
“tobacco advertising and promotion” means any form of commercial communication.
recommendation or action with the aim, effect or likely effect of promoting a tobacco product or
tobacco use either directly or indirectly;
(d)
“tobacco control” means a range ofi,supply, demand and harm reduction strategies'that
aim to improve the health of a population by eliminating or reducing their consumption of
tobacco products and exposure to tobacco smoke;
(e)
“tobacco industry” means tobacco manufacturers, wholesale distributors and importers of
tobacco products:
(f)
“tobacco products” means products entirely or partly made of the leaf tobacco as raw
material which are manufactured to be used for smoking, sticking, chewing or Snuffing;
(g)
“tobacco sponsorship” means any form of contribution to any event, activity or individual
with the aim, effect or likely effect of promoting a tobacco product or tobacco use either directly
or indirectly;
Article 2
Relationship between this Convention and other agreements and legal instruments
I.
In order to better protect human health, Parties are encouraged to implement measures beyond
those required by this Convention and its protocols, and nothing in these instruments shall prevent a
Party from imposing stricter requirements that are consistent with their provisions and are in
accordance with international law.
2.
The provisions of the Convention and its protocols shall in no way affect the right of Parties to
enter into bilateral or multilateral agreements, including regional or subregional agreements, on issues
relevant or additional to the Convention and its protocols, provided that such agreements arc
compatible with their obligations under the Convention and its protocols. The Parties concerned shall
communicate such agreements to the Conference of the Parties through the Secretariat.
1 Where appropriate, national will refer equally to regional economic integration organizations.
PART II: OBJECTIVE, GUIDING PRINCIPLES AND GENERAL OBLIGATIONS
Article 3
Objective
The objective of this Convention and its protocols is to protect present and fuhiregeneralions
from the devastating health, social, environmental and economic consequences of tobacco
consumption and exposure to tobacco smoke by providing a framework for tobacco control measures
to be implemented by the Parties at the national, regional and international levels in order to reduce
continually and substantially the prevalence of tobacco use and exposure to tobacco smoke
'
Article 4
Guiding principles
To achieve the objective of this Convention and its protocols and to implement its provisions.
the Parties shall be guided, inter alia, by the principles set out below:
1.
Every person should be informed of the health consequences, addictive nature and mortal threat
posed by tobacco consumption and exposure to tobacco smoke and effective legislative, executive,
administrative or other measures should be contemplated at the appropriate governmental level to
protect all persons from exposure to tobacco smoke.
2.
Strong political commitment is necessary to develop and support, at the national, regional and
international levels, comprehensive multisectoral measures and coordinated responses, taking into
consideration:
(a)
the need to take measures to protect all persons from exposure to tobacco smoke;
(b)
the need to take measures to prevent the initiation, to promote and support cessation, and
to decrease the consumption of tobacco products in any form;
(c)
the need to take measures to promote the participation offmdigenous individuals and
communities in the development, implementation and evaluation of tobacco control
programmes that are socially and culturally appropriate to their needs and perspectives; and
1
(cl)
the need to take measures to address gender-specific risk?) when developing tobacco
*
control strategies.
3.
International cooperation, particularly transfer of technology, knowledge and financial
assistance and provision of related expertise, to establish and implement effective tobacco control
programmes, taking into consideration local culture, as well as social, economic, political and legal
factors, is an important part of the Convention.
4.
Comprehensive multisectoral measures and responses to reduce consumption of all tobacco
products at the national, regional and international levels are essential so as to prevent, in accordance
with public health principles,.the incidence of diseases, premature disability and morialiiy’jdtTeto
tobacco consumption and exposure to tobacco smoke.
5.
Issues relating to liability, as determined by each Party within its jurisdiction, are an important
part of comprehensive tobacco control.
6.
The importance of technical and financial assistance to aid the economic transition of tobacco
growers and workers whose livelihoods are seriously affected as a consequence of tobacco control
programmes in developing country Parties, as well as Parties with economies in transition, should be
recognized and addressed in the context of nationally developed strategies for sustainable
development.
7.
The participation of civil society is essential in achieving the objective of the Convention and its
protocols.
Article 5
General obligations
I.
Each Party shall develop, implement, periodically update and jreview comprehensive
multisectoral national tobacco control strategies, plans and programmes in accordance with this
Convention and the protocols to which it is a Party.
2.
Towards this end, each Party shall, in accordance with its capabilities:
(a)
establish or reinforce and finance a national coordinating mechanism or focal points for
tobacco control; and
(b)
adopt and implement effective legislative, executive, administrative and/or other
measures and cooperate, as appropriate, with other Parties in developing appropriate policies for
preventing and reducing tobacco consumption, nicotine addiction and exposure to tobacco
smoke.
3.
In setting and implementing their public health policies with respect to tobacco control. Parlies
shall act to protect these policies from commercial and other vested interests of the tobacco industry in
accordance with national law.
4.
The Parties shall cooperate in the formulation of proposed measures, procedures and guidelines
for the implementation of the Convention and the protocols to which they are Parties.
5.
The Parties shall cooperate, as appropriate, with competent international and regional
intergovernmental organizations and other bodies to achieve the objectives of the Convention and the
protocols to which they are Parties.
6.
The Parties shall, within means and resources at their disposal, cooperate to raise financial
resources for effective implementation of the Convention through bilateral and multilateral funding
mechanisms.
PART III: MEASURES RELATING TO THE REDUCTION
OF DEMAND FOR TOBACCO
Article 6
Price and tax measures to reduce the demandfor tobacco
1.
The Parties recognize that price and tax measures are an effective and important means of
reducing tobacco consumption by various segments of the population, in particular young persons.
2.
Without prejudice to the sovereign right of the Parties to determine and establish their taxation
policies, each Party should take account of its national health objectives concerning tobacco control
and adopt or maintain, as appropriate, measures which may include:
(a)
implementing tax policies and, where appropriate, price policies, on tobacco products so
as to contribute to the health objectives aimed at reducing tobacco consumption: and
(b)
prohibiting or restricting, as appropriate, sales to and/or importations by international
travellers of lax- and duty-free tobacco products.
3.
The Parties shall provide rates of taxation for tobacco products and trends in tobacco
consumption in their periodic reports to the Conference of the Parties, in accordance with Article 21.
Article 7
Non-price measures to reduce the demandfor tobacco
The Parties recognize that comprehensive non-price measures are an effective and important
means of reducing tobacco consumption. Each Party shall adopt and implement effective legislative,
executive, administrative or other measures necessary to implement its obligations pursuant to
Articles 8 to 13 and shall cooperate, as appropriate, with each other directly or through competent
international bodies with a view to their implementation. The Conference of the Parties shall propose
appropriate guidelines for the implementation of the provisions of these Articles.
Article 8
Protection from exposure to tobacco smoke
1.
Parties recognize that scientific evidence has unequivocally established that exposure to tobacco
smoke causes death, disease and disability.
2.
Each Party shall adopt and implement in areas of existing national jurisdiction as determined by
national law and actively promote at other jurisdictional levels the adoption and implementation of
effective legislative, executive, administrative and/or other measures, providing for protection from
exposure to tobacco smoke in indoor workplaces, public transport, indoor public places and. as
appropriate, other public places.
'—'------------ -
Article 9
Regulation of the contents of tobacco products
The Conference of the Parties, in consultation with competent international bodies, shall
propose guidelines for testing and measuring the contents and emissions of tobacco products, and for
the regulation of these contents and emissions. Each Party shall, where approved by competent
national authorities, adopt and implement effective legislative, executive and administrative or other
measures for such testing and measuring, and for such regulation.
Article 10
Regulation of tobacco product disclosures
Each Party shall, in accordance with its national law, adopt and implement effective legislative.
executive, administrative or other measures requiring manufacturers and importers of tobacco products
to disclose to governmental authorities information about the contents and emissions of tobacco
products. Each Party shall further adopt and implement effective measures for public disclosure of
information about the toxic constituents of the tobacco products and the emissions that they may
produce.
Article 11
Packaging and labelling of tobacco products
1.
Each Party shall, within a period of three years after entry into force of this Convention for that
Party, adopt and implement, in accordance with its national law, effectjvejneasures to ensure that:
(a)
tobacco product packaging and labelling do not promote a tobacco product by any means
that are false, misleading, deceptive or likely to create an erroneous impression about its
characteristics, health effects, hazards or emissions, including any term, descriptor, trademark.
figurative or any other sign that directly or indirectly creates the false impression that a
particular tobacco product is less harmful than other tobacco products. These may include terms
such as “low tar”, “light”, “ultra-light”, or “mild”; and
(b)
each unit packet and package of tobacco products and any outside packaging and
labelling of such products also carry health warnings describing the harmful effects of tobacco
use, and may include other appropriate messages. These warnings and messages:
(i)
shall be approved by the competent national authority,
(ii)
shall be rotating,
(tii)
shall be large, clear, visible and legible,
(iv) should be 50% or more of the principal display areas but shall be no less than 30%
of the principal display areas,
(v)
may be in the form of or include pictures or pictograms.
2.
Each unit packet and package of tobacco products and any outside packaging and labelling of
such products shall, in addition to the warnings specified in paragraph 1(b) of this Article, contain
information on relevant constituents and emissions of tobacco products as defined by national
authorities.
3.
Each Party shall require that the warnings and other textual information specified in
paragraphs 1(b) and paragraph 2 of this Article will appear on each unit packet and package of tobacco
products and any outside packaging and labelling of such products tn its principal language or
languages.
4.
For the purposes of this Article, the term “outside packaging and labelling” in relation to
tobacco products applies to any packaging and labelling used in the retail sale of the product.
Article 12
Education, communication, training and public awareness
Each Party shall promote and strengthen public awareness of tobacc.o..c.oiitiol.issues, using all
available communication tools, as appropriate. Towards this end, each Party shall adopt and
implement effective legislative, executive, administrative or other measures to promote:
(a)
broad access to effective and comprehensive educational and public awareness
programmes on the health risks including the addictive characteristics of tobacco consumption
and exposure to tobacco smoke;
(b)
public awareness about the health risks of tobacco consumption and exposure to tobacco
smoke, and about the benefits of the cessation of tobacco use and tobacco-free lifestyles as
specified in Article 14.2;
I
'
(c)
public access, in accordance with national law, to a wide range of information on the
tobaccoTndustry as relevant to the objective of this Convention;
(d)
effective and appropriate training or sensitization and awareness programmes on tobacco
control addressed to persons such as health workers, community workers, social workers, media
professionals, educators, decision-makers, administrators and other concerned persons;
(e)
awareness and participation of public and private agencies and nongovernmental
organizations not affiliated with the tobacco industry in developing and implementing
intersectoral programmes and strategies for tobacco control; and
(f)
public awareness of and access to information regarding the adverse health, economic.
and environmental consequences of tobacco production and consumption.
Article 13
Tobacco advertising, promotion and sponsorship
1.
Parties recognize that a coptprehensive ban on advertising, promotion and sponsorship would
reduce the consumption of tobacco products.
2.
Each Party shall, jn^accordance with its constitution or constitutional principles, undertake a
comprehensive ban of all tobacco advertising, promotion and sponsorship. This shall include, .subject
to the legal.environment and technical means available to that Parly, a comprehensive ban on cross
borderadvertising, promotion and sponsorship originating from its territory. In this respect, within the
period of five years after entry into force of this Convention for that Party, each Party shall undertake
appropriate legislative, executive, administrative and/or other measures and report accordingly in
conformity with Article 21.
3.
A Party that is not in a position to undertake a comprehensive ban due to its constitution or
constitutional principles shall apply restrictions on all tobacco advertising, promotion and sponsorship.
This shall include, subject to the legal environment and technical means available to that Party.
restrictions or a comprehensive ban on advertising, promotion and sponsorship originating from its
territory with cross-border effects. In this respect, each Party shall undertake appropriate legislative.
executive, administrative and/or other measures and report accordingly in conformity with Article 21.
As a minimum, and in accordance with its constitution or constitutional principles, each Party
4.
shall:
(a)
prohibit all forms of tobacco advertising, promotion and sponsorship that promote a
tobacco product by any means that are false, misleading or deceptive or likely to create an
erroneous impression about its characteristics, health effects, hazards or emissions;
(b)
require that health or other appropriate warnings or messages accompany all tobacco
advertising and, as appropriate, promotion and sponsorship;
(c)
< restrict 'the use of direct or indirect incentives that encourage the purchase of tobacco
products by the public;
(d)
require, if it does not have a comprehensive ban, the disclosure to relevant governmental
authorities of expenditures by the tobacco industry on advertising," promotion and sponsorship
not yet prohibited. Those authorities may decide to make those figures available, subject to
national law, to the public and to the Conference of the Parties, pursuant to Article 21:
o
(e)
undertake a comprehensive ban or, in the case of a Party that is not in a position to
undertake a comprehensive ban due to its constitution or constitutional principles, 'restrict)
tobacco advertising, promotion and sponsorship on radio, television, print media and. as
appropriate, other media, such as the internet, within a period of live years; and
(f)
prohibit, or in the case of a Party that is not in a position to prohibit due to its constitution
or constitutional principles 'restrict!, tobacco sponsorship of international events, activities and/or
participants therein.
5.
Parties are encouragedyo implement measures beyond the obligations set out in paragraph 4.
Parties shall cooperate in the development of technologies and other means necessary to
6.
facilitate the elimination of cross-border advertising.
7.
Parties which have a ban on certain forms of tobacco advertising, promotion and sponsorship
have the sovereign right to ban those forms of cross-border tobacco advertising, promotion and
sponsorship entering their territory and to impose equal penalties as those applicable to domestic
advertising, promotion and sponsorship originating from their territory in accordance with their
national law. This paragraph does not endorse or approve of any particular penally.
8.
Parties shall consider the elaboration of a protocol setting out appropriate measures that require
international collaboration for a comprehensive ban on cross-border advertising, promotion and
sponsorship.
Article 14
Demand reduction measures concerning tobacco dependence and cessation
I.
Each Party shall develop and disseminate appropriate, comprehensive and integrated guidelines
based on scientific evidence and best practices, taking into account national circumstances and
priorities, and shall take effective measures to promote cessation of tobacco use and adequate
treatment for tobacco dependence.
Towards this end. each Party shall endeavour to:
(a)
design and implement effective programmes aimed at promoting the cessation of tqbaccp
use, in. such locations as educational institutions, health care facilities, workplaces and sporting
environments;
(b)
include diagnosis and treatment of tobacco dependence and counselling services on
cessation of tobacco use in national health and education programmes, plans and strategies, with
the participation of health workers, community workers and social workers as appropriate;
(c)
establish in health care facilities and rehabilitation centres programmes for diagnosing.
counselling, preventing and treating tobacco dependence; and
(d)
collaborate with other Parties to facilitate accessibility and affordability for treatment of
tobacco dependence including pharmaceutical products pursuant to Article 22. Such products
and their constituents may include medicines, products used to administer medicines and
diagnostics when appropriate.
PART IV: MEASURES RELATING TO THE REDUCTION
OF THE SUPPLY OF TOBACCO
Article 15
Illicit trade in tobacco products
1.
The Parties recognize that the/eljminatioiVpf all forms of ijlic.it trade; in tobacco products,
including smuggling, illicit- manufacturing and counterfeiting, and the development and
implementation of related national law, in addition to subregional, regional and global agreements, are
essential components of tobacco control.
2.
Each Party shall adopt and implement effective legislative, executive, administrative or other
measures to ensure that all unit packets and packages of tobacco products and any outside packaging
of such products are marked to assist Parties in determining the origin of tobacco products, and in
accordance with national law ancl relevant bilateral or multilateral agreements, assist Parties in
determining the point of diversion and monitor, document and control the movement of tobacco
products and their legal status. In addition, each Party shall:
(a)
require that unit packets and packages of tobacco products for retail and wholesale use
that are sold on its domestic market carry the statement; "Sales only allowed in (insert name of
the country, subnational, regional or federal unit)” or carry any other effective marking
indicating the final destination or which would assist authorities in determining whether the
product is legally for sale on the domestic market; and
(b)
consider, as appropriate, developing a practical tracking and tracing regime that would
further secure the distribution system and assist in the investigation of illicit trade.
3.
Each Party shall require that the packaging information or marking specified in paragraph 2 of
this Article shall be presented in legible form and/or appear in its principal language or languages.
With a view to eliminating illicit trade in tobacco products, each Parly shall:
(a)
monitor and collect data on cross-border trade in tobacco products, including illicit trade.
and exchange information among customs, tax and other authorities, as appropriate, and in
accordanceWith national law and relevant applicable bilateral or multilateral agreements;
(b)
enact or strengthen legislation, with appropriate penalties and remedies, against illicit
trade in tobacco products, including counterfeit and contraband cigarettes;
(c)
take appropriate steps to ensure that all confiscated manufacturing equipment, counterfeit
and contraband cigarettes and other tobacco products are destroyed, using environmentallyfriendly methods where feasible, or disposed of in accordance with national law;
(d)
adopt and implement measures to monitor, document and control the storage and
distribution of tobacco products held or moving under suspension of taxes or duties within its
jurisdiction; and
(e)
adopt measures as appropriate to enable the confiscation of proceeds derived from the
illicit trade in tobacco products.
5.
Information collected pursuant to subparagraphs 4(a) and 4(d) of this Article shall, as
appropriate, be provided in aggregate form by the Parties in their periodic reports to the Conference of
the Parties, in accordance with Article 21.
6.
The Parties shall, as appropriate and in accordance with national law, promote cooperation
between national agencies, as well as relevant regional and international intergovernmental
organizations as it relates to investigations, prosecutions and proceedings, with a view to eliminating
illicit trade in tobacco products. Special emphasis shall be placed on cooperation at regional and
subregional levels to combat illicit trade of tobacco products.
7.
Each Party shall endeavour to adopt and implement further measures including licensing, where
appropriate, to control or regulate the production and distribution of tobacco products in order to
prevent illicit trade.
Article 16
Sales to and by minors
1.
Each Party shall adopt and implement effective legislative, executive, administrative or other
measures at the appropriate.government level to prohibit the sales of tobacco products to persons
under the age set by domestic law', national lawjor eighteen. Thesemeasures may include: ~
(a)
requiring that all sellers of tobacco products place a clear and prominent indicator inside
their point of sale about the prohibition of tobacco sales to minors and, in case of doubt, request
that each tobacco purchaser provide appropriate evidence of having reached full legal age.
(b)
banning the sale of tobacco products in any manner by which they are directly accessible.
such as store shelves;
(c)
prohibiting the manufacture and sale of sweets, snacks, toys or any other objects in the
form of tobacco products which appeal to minors; and
(/I d~)
0-pP
WHO Framework Convention on Tobacco Control
Preamble
The Parties to this Convention,
Determined to give priority to their right to protect public health.
Recognizing that the spread of the tobacco epidemic is a global problem with serious
consequences for public, health that calls for the widest possible international cooperation and the
participation of all countries in an effective, appropriate and comprehensive international response.
Reflecting the concern of the international community about the devastating worldwide health.
social, economic and environmental consequences of tobacco consumption and exposure to tobacco
smoke.
Seriously concerned about the increase in the worldwide consumption and/production of
cigarettes and other tobacco products, particularly in developing countries, as well as about the burden
this places on families, on the poor, and on national health systems.
Recognizing that scientific evidence has unequivocally established that tobacco consumption
and exposure to tobacco smoke cause death, disease and disability, and that there is a time lag between
the exposure to smoking and the other uses of tobacco products and the onset of tobacco-related
diseases,
Recognizing also that cigarettes and some other products containing tobacco are highly
engineered so as to create and maintain dependence, and that many of the compounds they contain and
the smoke they produce are pharmacologically active, toxic, mutagenic and carcinogenic, and that
tobacco dependence is separately classified as a disorder in major international classifications of
diseases.
Acknowledging that there is clear scientific evidence that prenatal exposure to tobacco smoke
causes adverse health and developmental conditions for children.
Deeply concerned about the escalation in smoking and other forms of tobacco consumption by
children and adolescents worldwide, particularly smoking at increasingly early ages.
Alarmed by the increase in smoking and other forms of tobacco consumption by women and
young girls worldwide and keeping in mind the need for full participation of women at all lex els of
policy-making and implementation and the need for gender-specific tobacco control strategies.
Deeply concerned about the high levels of smoking and other forms of tobacco consumption by
indigenous peoples,
Seriously concerned about the impact of all forms of advertising, promotion and sponsorship
aimed at encouraging the use of tobacco products,
Recognizing that cooperative action is necessary to eliminate all forms of illicit trade in
cigarettes and other tobacco products, including smuggling, illicit manufacturing and counterfeiting.
Acknowledging that tobacco control at all levels and particularly in developing countries and in
countries with economies in transition requires sufficient financial and technical resources
commensurate with the current and projected need for tobacco control activities.
Recognizing the need to develop appropriate mechanisms to address the long-term social and
economic implications of successful tobacco demand reduction strategies.
Mindful of the social and economic difficulties that tobacco control programmes may engender
in the medium and long term in some developing countries and countries with economies in transition.
and recognizing their need for technical and financial assistance in the context of nationally developed
strategies for sustainable development,
Conscious of the valuable work being conducted by many States on tobacco control and
commending the leadership of the World Health Organization as well as the efforts of other
organizations and bodies of the United Nations system and other international and regional
intergovernmental organizations in developing measures on tobacco control.
Emphasizing the special contribution of nongovernmental organizations and other members of
civil society not affiliated with the tobacco industry, including health professional bodies, women's.
youth, environmental and consumer groups, and academic and health care institutions, to tobacco
control efforts nationally and internationally and the vital importance of their participation in national
and international tobacco control efforts,
Recognizing the need to be alert to any efforts by the tobacco industry to undermine or subvert
tobacco control efforts and the need to be informed of activities of the tobacco industry that have a
negative unfiact on tobacco control efforts.
Recalling Article 12 of the International Covenant on Economic, Social and Cultural Rights.
adopted by the United Nations General Ass‘embTy-6h 16 December 1966, which states that it is the
right of everyone to the enjoyment of the highest attainable standard of physical and mental health.
Recalling also the preamble to the Constitution of the World Health Organization, which states
that the enjoyment of the highest attainable standard of health is one of the fundamental rights of every
human being without distinction of race, religion, political belief, economic or social condition,
Determined to promote measures of tobacco control based on current and relevant scientific.
technical and economic considerations.
Recalling that the Convention on the Elimination of All Forms of Discrimination against
Women, adopted by the United Nations General Assembly on 18 December 1979, provides that Stales
Parties to that Convention shall take appropriate measures to eliminate discrimination against women
in the field of health care,
Recalling further that the Convention on the Rights of the£hjld, adopted by the United Nations
General Assembly on 20 November 1989, provides that States Parties to that Convention recognize
the right of the child to the enjoyment of the highest attainable standard of health.
Have agreed, as follows:
PART I: INTRODUCTION
Article 1
Use of terms
For the purposes of this Convention:
(a)
“illicit trade” means any practice or conduct prohibited by law and which relates to
production, shipment, receipt, possession, distribution, sale or purchase including any practice
or conduct intended to facilitate such activity;
(b)
"regional economic integration organization” means an organization that is composed of
several sovereign states, and to which its Member States have transferred competence over a
range of matters, including the authority to make decisions binding on its Member States in
respect of those matters;1
(c)
“tobacco advertising and promotion” means any form of commercial communication.
recommendation or action with the aim, effect or likely effect of promoting a tobacco product or
tobacco use either directly or indirectly;
(d)
“tobacco control” means a range of supply, demand and harm reduction strategies' that
aim to improve the health of a population by eliminating or reducing their consumption of
tobacco products and exposure to tobacco smoke;
(e)
"tobacco industry” means tobacco manufacturers, wholesale distributors and importers of
tobacco products;
(f)
“tobacco products” means products entirely or partly made of the leaf tobacco as raw
material which are manufactured to be used for smoking, sticking, chewing or snuffing:
(g)
“tobacco sponsorship” means any form of contribution to any event, activity or individual
with the aim, effect or likely effect of promoting a tobacco product or tobacco use either directly
or indirectly;
Article 2
Relationship between this Convention and other agreements and legal instruments
1.
In order to better protect human health, Parties are encouraged to implement measures beyond
those required by this Convention and its protocols, and nothing in these instruments shall prevent a
Party from imposing stricter requirements that are consistent with their provisions and are in
accordance with international law.
2.
The provisions of the Convention and its protocols shall in no way affect the right of Parties to
enter into bilateral or multilateral agreements, including regional or subregional agreements, on issues
relevant or additional to the Convention and its protocols, provided that such agreements are
compatible with their obligations under the Convention and its protocols. The Parties concerned shall
communicate such agreements to the Conference of the Parties through the Secretarial.
1 Where appropriate, national will refer equally to regional economic integration organizations.
PART II: OBJECTIVE, GUIDING PRINCIPLES AND GENERAL OBLIGATIONS
Article 3
Objective
The objective of this Convention and its protocols is to protect present and futuregenerations
from the devastating health, social, environmental and economic consequences of tobacco
consumption and exposure to tobacco smoke by providing a framework for tobacco control measures
to be implemented by the Parties at the national, regional and international levels in order to reduce 7 &>•
continually and substantially the prevalence of tobacco use and exposure to tobacco smoke.
A
Article 4
Guiding principles
To achieve the objective of this Convention and its protocols and to implement its provisions.
the Parties shall be guided, inter alia, by the principles set out below:
1.
Every person should be informed of the health consequences, addictive nature and mortal threat
posed by tobacco consumption and exposure to tobacco smoke and effective legislative, executive.
administrative or other measures should be contemplated at the appropriate governmental level to
protect all persons from exposure to tobacco smoke.
2.
Strong political commitment is necessary to develop and support, at the national, regional and
international levels, comprehensive multisectoral measures and coordinated responses, taking into
consideration:
(a)
the need to take measures to protect all persons from exposure to tobacco smoke;
(b)
the need to take measures to prevent the initiation, to promote and support cessation, and
to decrease the consumption of tobacco products in any form;
(c)
the need to take measures to promote the participation offmdigenous individuals and
communities in the development, implementation and evaluation of tobacco control
programmes that are socially and culturally appropriate to their needs and peispegtivcs; and
(d)
the need to take measures to address gender-specific risks) when developing tobacco7
control strategies.
3.
International cooperation, particularly transfer of technology, knowledge and financial
assistance and provision of related expertise, to establish and implement effective tobacco control
programmes, taking into consideration local culture, as well as social, economic, political and legal
factors, is an important part of the Convention.
4.
Comprehensive multisectoral measures and responses to reduce consumption of all tobacco
products at the national, regional and international levels are essential so as to prevent, in accordance
with public health principles,, the incidence of diseases, premature disability and mortality due to
tobacco consumption and exposure to tobacco smoke.
5.
Issues relating to liability, as determined by each Party within its jurisdiction, are an important
part of comprehensive tobacco control.
i';.
'
.
’
6.
The importance of technical and financial assistance to aid the economic transition of tobacco
growers and workers whose livelihoods are seriously affected as a consequence of tobacco control
programmes in developing country Parties, as well as Parties with economies in transition, should be
recognized and addressed in the context of nationally developed strategies for sustainable
development.
7.
The participation of civil society is essential in achieving the objective of the Convention and its
protocols.
Article 5
General obligations
1.
Each Party shall develop, implement, periodically update and review comprehensive
multisectoral national tobacco control strategies, plans and programmes in accordance with this
Convention and the protocols to which it is a Party.
Towards this end, each Party shall, in accordance with its capabilities:
(a)
establish or reinforce and finance a national coordinating mechanism or focal points for
tobacco control; and
(b)
adopt and implement effective legislative, executive, administrative and/or other
measures and cooperate, as appropriate, with other Parties in developing appropriate policies for
preventing and reducing tobacco consumption, nicotine addiction and exposure to tobacco
smoke.
3.
In setting and implementing their public health policies with respect to tobacco control. Parties
shall act to protect these policies from commercial and other vested interests of the tobacco industry in
accordance with national law.
4.
The Parties shall cooperate in the formulation of proposed measures, procedures and guidelines
for the implementation of the Convention and the protocols to which they are Parties.
5.
The Parties shall cooperate, as appropriate, with competent international and regional
intergovernmental organizations and other bodies to achieve the objectives of the Convention and the
protocols to which they are Parties.
6.
The Parties shall, within means and resources at their disposal, cooperate to raise financial
resources for effective implementation of the Convention through bilateral and multilateral funding
mechanisms.
PART III: MEASURES RELATING TO THE REDUCTION
OF DEMAND FOR TOBACCO
Article 6
Price and tax measures to reduce the demandfor tobacco
1.
The Parties recognize that price and tax measures are an effective and important means of
reducing tobacco consumption by various segments of the population, in particular young persons.
2.
Without prejudice to the sovereign right of the Parties to determine and establish their taxation
policies, each Party should take account of its national health objectives concerning tobacco control
and adopt or maintain, as appropriate, measures which may include:
(a)
implementing tax policies and, where appropriate, price policies, on tobacco products so
as to contribute to the health objectives aimed at reducing tobacco consumption; and
(b)
prohibiting or restricting, as appropriate, sales to and/or importations by international
travellers of tax- and duty-free tobacco products.
3.
The Parties shall provide rates of taxation for tobacco products and trends in tobacco
consiimptiorunlhelr periodic reports to the Conference of the Parties, in accordance with Article 21.
Article 7
Non-price measures to reduce the demandfor tobacco
The Parties recognize that comprehensive non-price measures are an effective and important
means of reducing tobacco consumption. Each Party shall adopt and implement effective legislative,
executive, administrative or other measures necessary to implement its obligations pursuant to
Articles 8 to 13 and shall cooperate, as appropriate, with each other directly or through competent
international bodies with a view to their implementation. The Conference of the Parties shall propose
appropriate guidelines for the implementation of the provisions of these Articles.
Article 8
Protection from exposure to tobacco smoke
I.
Parties recognize that scientific evidence has unequivocally established that exposure to tobacco
smoke causes death, disease and disability.
2.
Each Party shall adopt and implement in areas of existing national jurisdiction as determined by
national law and actively promote at other jurisdictional levels the adoption and implementation of
effective legislative, executive, administrative and/or other measures, providing for protection from
exposure to tobacco smoke in indoor .workplaces, public transport, indoor public places and. as
appropriate, other public places.
—--------------
Article 9
Regulation of the contents of tobacco products
The Conference of the Parties, in consultation with competent international bodies, shall
propose guidelines for testing and measuring the contents and emissions of tobacco products, and for
the regulation of these contents and emissions. Each Party shall, where approved by competent
national authorities, adopt and implement effective legislative, executive and administrative or other
measures for such testing and measuring, and for such regulation.
Article 10
Regulation of tobacco product disclosures
Each Party shall, in accordance with its national law, adopt and implement effective legislative.
executive, administrative or other measures requiring manufacturers and importers of tobacco products
to disclose to governmental authorities information about the contents and emissions of tobacco
products. Each Party shall further adopt and implement effective measures for public disclosure of
information about the toxic constituents of the tobacco products and the emissions that they may
produce.
Article 11
Packaging and labelling of tobacco products
1.
Each Party shall, within a period of three years after entry into force of this Convention for that
Party, adopt and implement, in accordance with its national law, effective measures to ensure that:
(a)
tobacco product packaging and labelling do not promote a tobacco product by any means
that are false, misleading, deceptive or likely to create an erroneous impression about its
characteristics, health effects, hazards or emissions, including any term, descriptor, trademark,
figurative or any other sign that directly or indirectly creates the false impression that a
particular tobacco product is less harmfill than other tobacco products. These may include terms
such as "low tar”, “light”, “ultra-light”, or “mild”; and
(b)
each unit packet and package of tobacco products and any outside packaging and
labelling of such products also cany health warnings describing the harmful effects of tobacco
use, and may include other appropriate messages. These warnings and messages:
(i)
shall be approved by the competent national authority,
(ii)
shall be rotating,
(iii)
shall be large, clear, visible and legible,
(iv)
should be 50% or more of the principal display areas but shall be no less than 30%
of the principal display areas,
(v)
may be in the form of or include pictures or pictograms.
2.
Each unit packet and package of tobacco products and any outside packaging and labelling of
such products shall, in addition to the warnings specified in paragraph 1(b) of this Article, contain
information on relevant constituents and emissions of tobacco products as defined by national
authorities.
3.
Each Party shall require that the warnings and other textual information specified in
paragraphs 1(b) and paragraph 2 of this Article will appear on each unit packet and package of tobacco
products and any outside packaging and labelling of such products in its principal language or
languages.
4.
For the purposes of this Article, the term “outside packaging and labelling” in relation to
tobacco products applies to any packaging and labelling used in the retail sale of the product.
Article 12
Education, communication, training and public awareness
Each Party shall promote and strengthen public awareness of tobacoo- cantrol..issues, using all
available communication tools, as appropriate. Towards this end, each Party shall adopt and
implement effective legislative, executive, administrative or other measures to promote:
(a)
broad access to effective and comprehensive educational and public awareness
programmes on the health risks including the addictive characteristics of tobacco consumption
and exposure to tobacco smoke;
(b)
public awareness about the health risks of tobacco consumption and exposure to tobacco
smoke, and about the benefits of the cessation of tobacco use and tobacco-free lifestyles as
specified in Article 14.2;
!
(c)
public access, in accordance with national law, to a wide range of information on. the
tobacco industry as relevant to the objective of this Convention;
(d)
effective and appropriate training or sensitization and awareness prpgfa.in.uics on tobacco
control addressed to persons such as health workers, community workers, social workers, media
professionals, educators, decision-makers, administrators and other concerned persons;
(e)
awareness and participation of public and private agencies and nongovernmental
organizations not affiliated with the tobacco industry in developing and implementing
intersectoral programmes and strategies for tobacco control; and
(f)
public awareness of and access to information regarding the adverse health, economic.
and environmental consequences of tobacco production and consumption.
Article 13
Tobacco advertising, promotion and sponsorship
1.
Parties recognize that a comprehensive ban on advertising, promotion and sponsorship would
reduce the consumption of tobacco products.
7
2.
Each Party shall, in accordance with its constitution or constitutional principles. undertake a
comprehensive ban of all tobacco advertising, promotion and sponsorship. This shall include, subject
to the legal environment and technical means available to that Party, a comprehensive ban on crossborder advertising. promotion and sponsorship originating from its territory. In this respect, within the
period of five years after entry into force of this Convention for that Party, each Party shall undertake
appropriate legislative, executive, administrative and/or other measures and report accordingly in
conformity with Article 21.
3.
A Party that is not in a position to undertake a comprehensive ban due to its constitution or
constitutional principles shall apply restrictions on all tobacco advertising, promotion and sponsorship.
This shall include, subject to the legal environment and technical means available to that Parly,
restrictions or a comprehensive ban on advertising, promotion and sponsorship originating from its
territory with cross-border effects. In this respect, each Party shall undertake appropriate legislative,
executive, administrative and/or other measures and report accordingly in conformity with Article 21.
As a minimum, and in accordance with its constitution or constitutional principles, each Party
shall:
(a)
prohibit all forms of tobacco advertising, promotion and sponsorship that promote a
tobacco product by any means that are false, misleading or deceptive or likely to create an
erroneous impression about its characteristics, health effects, hazards or emissions:
(b)
require that health or other appropriate warnings or messages accompany all tobacco
advertising and, as appropriate, promotion and sponsorship;
(c)
( reslriqt-'the use of direct or indirect incentives that encourage the purchase of tobacco
products by the public;
(d)
require, if it does not have a comprehensive ban, the disclosure to relevant governmental
authorities of expenditures by the tobacco industry on advertising, promotion and sponsorship
not yet prohibited. Those authorities may decide to make those figures available, subject to
national law, to the public and to the Conference of the Parties, pursuant to Article 21:
<1
(e)
undertake a comprehensive ban or, in the case of a Party that is not in a position to
undertake a comprehensive ban due to its constitution or constitutional principl.es/restrici')
tobacco advertising, promotion and sponsorship on radio, television, print media and', as
appropriate, other media, such as the internet, within a period of five years; and
(f)
prohibit, or in the case of a Party that is not in a position to prohibit due to its constitution
or constitutional principles festricj), tobacco sponsorship of international events, activities and/or
participants therein.
5.
Parties are encouragedjto implement measures beyond the obligations set out in paragraph 4.
6.
Parties shall cooperate in the development of technologies and other means necessary' to
facilitate the elimination of cross-border advertising.
7.
Parties which have a ban on certain forms of tobacco advertising, promotion and sponsorship
have (he sovereign right to ban those forms of cross-border tobacco advertising, promotion and
sponsorship entering their territory and to impose equal penalties as those applicable to domestic
advertising, promotion and sponsorship originating from their territory in accordance with their
national law. This paragraph does not endorse or approve of any particular penalty
8.
Parties shall consider the elaboration of a protocol setting out appropriate measures that require
international collaboration for a comprehensive ban on cross-border advertising, promotion and
sponsorship.
Article 14
Demand reduction measures concerning tobacco dependence and cessation
I.
Each Party shall develop and disseminate appropriate, comprehensive and integrated guidelines
based on scientific evidence and best practices, taking into account national circumstances and
priorities, and shall take effective measures to promote cessation of tobacco use and adequate
treatment for tobacco dependence.
Towards this end, each Party shall endeavour to:
(a)
design and implement effective programmes aimed at promoting the cessation of tobaccp
US.edn.such locations as educational institutions, health care facilities, workplaces and sporting
environments:
(b)
include diagnosis and treatment of tobacco dependence and counselling services on
cessation of tobacco use in national health and education programmes, plans and strategies, with
the participation of health workers, community workers and social workers as appropriate;
(c)
establish in health care facilities and rehabilitation centres programmes for diagnosing,
counselling, preventing and treating tobacco dependence; and
(d)
collaborate with other Parties to facilitate accessibility and affordability for treatment of
tobacco dependence including pharmaceutical products pursuant to Article 22. Such products
and their constituents may include medicines, products used to administer medicines and
diagnostics when appropriate.
PART IV: MEASURES RELATING TO THE REDUCTION
OF THE SUPPLY OF TOBACCO
Article 15
Illicit trade in tobacco products
1.
The Parties recognize that the/eljminationlof all forms of illicit trade in tobacco products.
including smuggling, illicit manufacturing and counterfeiting, and the development and
implementation of related national law, in addition to subregional, regional and global agreements, are
essential components of tobacco control.
2.
Each Party shall adopt and implement effective legislative, executive, administrative or other
measures to ensure that all unit packets and packages of tobacco products and any outside packaging
of such products are marked to assist Parties in determining the origin of tobacco products, and in
accordance with national law aiiTTelevant bilateral or multilateral agreements, assist Parties in
determining the point of diversion and monitor, document and control the movement of tobacco
products and their legal status. In addition, each Party shall:
(a)
require that unit packets and packages of tobacco products for retail and wholesale use
that are sold on its domestic market cany the statement: "Sales only allowed in (insert name of
the country, subnational, regional or federal unit) ” or cany any other effective marking
indicating the final destination or which would 'assist authorities in determining whether the
product is legally for sale on the domestic market; and
(b)
consider, as appropriate, developing a practical tracking and tracing regime that would
further secure the distribution system and assist in the investigation of illicit trade.
3.
Each Party shall require that the packaging information or marking specified in paragraph 2 of
this Article shall be presented in legible form and/or appear in its principal language or languages.
4.
With a view to eliminating illicit trade in tobacco products, each Party shall:
(a)
monitor and collect data on cross-border trade in tobacco products, including illicit trade.
and exchange information among customs, tax and other authorities, as appropriate, and in
accordance with national law and relevant applicable bilateral or multilateral agreements;
(b)
enact or strengthen legislation, with appropriate penalties and remedies, against illicit
trade in tobacco products, including counterfeit and contraband cigarettes;
(c)
take appropriate steps to ensure that all confiscated manufacturing equipment, counterfeit
and contraband cigarettes and other tobacco products are destroyed, using environmentallyfriendly methods where feasible, or disposed of in accordance with national law;
(d)
adopt and implement measures to monitor, document and control the storage and
distribution of tobacco products held or moving under suspension of taxes or duties within its
jurisdiction; and
(e)
adopt measures as appropriate to enable the confiscation of proceeds derived from the
illicit trade in tobacco products.
5.
Information collected pursuant to subparagraphs 4(a) and 4(d) of this Article shall, as
appropriate, be provided in aggregate form by the Parties in their periodic reports to the Conference of
the Parties, in accordance with Article 21.
6.
The Parties shall, as appropriate and in accordance with national law, promote cooperation
between national agencies, as well as relevant regional and international intergovernmental
organizations as it relates to investigations, prosecutions and proceedings, with a view to eliminating
illicit trade in tobacco products. Special emphasis shall be placed on cooperation at regional and
subregional levels to combat illicit trade of tobacco products.
7.
Each Party shall endeavour to adopt and implement further measures including licensing, where
appropriate, to control or regulate the production and distribution of tobacco products in order to
prevent illicit trade.
Article 16
Sales to and by minors
1.
Each Party shall adopt and implement effective legislative, executive, administrative or other
measures at the appropriate, government, level to prohibit the sales of tobacco products to persons
under the age set by domestic law; national law'or eighteen. TheseTneasures may include:
(a)
requiring that all sellers of tobacco products place a clear and prominent indicator inside
their point of sale about the prohibition of tobacco sales to minors and. in case of doubt, request
that each tobacco purchaser provide appropriate evidence of having reached full legal age:
(b)
banning the sale of tobacco products in any manner by which they are directly accessible.
such as store shelves;
(c)
prohibiting the manufacture and sale of sweets, snacks, toys or any other objects in the
form of tobacco products which appeal to minors; and
(d)
ensuring that tobacco vending machines under its jurisdiction are not accessible to minors
and do not promote the"sale'b'ftobacco products to minors.
2.
Each Party shall prohibit or'promote the prohibition'of the distribution of free tobacco products
to the public and especially minors'
3.
Each Party shall endeavour to, prohibit.'the sale of cigarettes individually or in small packets
which increase the affordability of such products to minors.
4
The Parties recognize that in order to increase their effectiveness, measures to prevent tobacco
product sales to minors should, where appropriate, be implemented in conjunction with other
provisions contained in this Convention.
5.
When signing, ratifying, accepting, approving or acceding to the Convention or at any time
thereafter, a Party may. by means of a binding written declaration, indicate its commitment to prohibit
the introduction of tobacco vending machines within its jurisdiction or, as appropriate, to a total ban
on tobacco vending machines. The declaration made pursuant to this Article shall be circulated by the
Depositary to all Parties to the Convention.
6.
Each Party shall adopt and implement effective legislative, executive, administrative or other
measures, including penalties against sellers and distributors, in order to ensure compliance with the
obligations contained in paragraphs 1-5 of this Article.
7.
Each Party should, as appropriate, adopt and implement effective legislative, executive.
administrative or other measures to prohibit the sales of tobacco products by persons under the age set
by domestic law, national law or eighteen.
Article 17
Provision ofsupport for economically viable alternative activities
Parties shall, in cooperation with each other and with competent international and regional
intergovernmental organizations, [promote, as appropriate.'economically viable alternatives for tobacco
workers, growers and, as the case may be, individual sellers.
PART V: PROTECTION OF THE ENVIRONMENT
Article 18
Protection of the environment and the health ofpersons
In carrying out their obligations under this Convention, the Parties agree to;have due regard to
the protection of the environment and the health of persons in relation to the environment in respect of
tobacco cultivation and manufacture within their respective territories.
PART VI: QUESTIONS RELATED TO LIABILITY
Article 19
Liability
1,
For the purpose of tobacco control, the Parties ’■shall considerz?aking legislative action or
promoting their existing laws,(where necessary, to deal with criminal and_civjl liability, including
compensation where appropriate.
2.
Parties shall cooperate with each other in exchanging information through the Conference of the
Parties in accordance with Article 21 including:
(a)
information on the health effects of the consumption of tobacco products and exposure to
tobacco smoke in accordance with Article 20.3(a); and
(b)
information on legislation and regulations in force as well as pertinent jurisprudence.
3.
The Parties shall, as appropriate and mutually agreed, within the limits of national legislation.
policies, legal practices and applicable existing treaty arrangements, afford one another assistance in
legal proceedings relating to civil and criminal liability consistent with this Convention.
4.
The Convention shall in no way affect or limit any rights of access of the Parties to each other’s
courts where such rights exist.
5.
The Conference of the Parties may consider, if possible, at an early stage, taking account of the
work being done in relevant international fora, issues related to liability including appropriate
international approaches to these issues and appropriate means to support, upon request, the Parties in
their legislative and other activities in accordance with this Article.
PART VII: SCIENTIFIC AND TECHNICAL COOPERATION AND
COMMUNICATION OF INFORMATION
Article 20
Research, surveillance and exchange of information
I.
The Parties undertake to develop and promote national research and to coordinate research
programmes at the regional and international levels in the field of tobacco control. Towards this end.
each Parly shall:
(a)
initiate and cooperate in, directly or through competent international and regional
intergovernmental organizations and other bodies, the conduct of research and scientific
assessments, and in so doing promote and encourage research that addresses the/fleTermiiTanis)
and consequences of tobacco consumption and exposure to tobacco smoke as well as research
for identification of alternative crops; and
(b)
promote and strengthen, with the support of competent international and regional
intergovernmental organizations and other bodies, training.atid_support_Jor all those engaged in
tobacco control activities, including research, implementation and evaluation.
2.
The Parties shall establish, as appropriate, programmes for national, regional and global
surveillance of the magnitude, patterns, determinants and consequences of tobacco consumption and
exposure to tobacco smoke. Towards this end, the Parties should integrate tobacco surveillance?
programmes into national, regional and global health surveillance programmes so (hat daTa are
comparable and can be analysed at the regional and international levels, as appropriate.
3.
Parties recognize the importance of financial and technical assistance from international and
regional intergovernmental organizations and other bodies. Each Parly shall endeavour to.
(a)
establish progressively a national system for the epidemiolpgjcal^suryeillance-ol-tobacco
consumption and related social, economic and health indicators?
(b)
cooperate with competent international and regional intergovernmental organizations and
other bodies, including governmental and nongovernmental agencies, in regional and global
tobacco surveillance and exchange of information on the indicators specified in paragraph 3(a)
of this Article; and
(c)
cooperate with the World Health Organization in the development of general guidelines
or procedures for defining the collection, analysis and dissemination of tobacco-related
surveillance data.
4.
The Parties shall, subject to national law, promote and facilitate the exchange of publicly
available scientific, technical, socioeconomic, .commercial and legal information, as well as
information regarding practices of the tobacco industry and the cultivation of tobacco, which is
relevaHt to this Convention, and in so doing shall take into account and address the special needs of
developing country Parties and Parties with economies in transition. Each Parly shall endeavour to:
(a)
progressively establish and maintain an updated database of laws and regulations on
tobacco control and, as appropriate, information about their enforcement, as well as pertinent
jurisprudence, and cooperate in the development of programmes for regional and global tobacco
control;
(b)
progressively establish and maintain updated data from national surveillance programmes
in accordance with paragraph 3(a) of this Article; and
(c)
cooperate with competent international organizations to progressively establish and
maintain a global system to regularly collect and disseminate information on tobacco
production, manufacture and the activities of the tobacco industry which have an impact on the
Convention or national tobacco control activities.
5.
Parties should cooperate in regional and international intergovernmental organizations and
financial and development institutions of which they are members, to promote and encourage
provision of technical and financial resources to the Secretariat to assist developing country Parlies
and Parties with economies in transition to meet their commitments on research, surveillance and
exchange of information.
Article 21
Reporting and exchange of information
1.
Each Party shall submit to the Conference of the Parties, through the Secretariat, periodic
reports on its implementation of this Convention, which should include the following:
(a)
information on legislative, executive, administrative or other measures taken
implement the Convention;
to
(b)
information, as appropriate, on any constraints or barriers encountered in
implementation of the Convention, and on the measures taken to overcome these barriers;
its
(c)
information, as appropriate, on financial and technical assistance provided or received for
tobacco control activities;
(d)
information on surveillance and research as specified in Article 20; and
(e)
information specified in Articles 6.3, 13.2, 13.3, 13.4(d), 15.5 and 19.2.
2.
The frequency and format of such reports by all Parties shall be determined by the Conference
of the Parties. Each Party shall make its initial report within two years of the entry into force of the
Convention for that Party.
3.
The Conference of the Parties, pursuant to Articles 22 and 26, shall consider arrangements to
assist developing country Parties and Parties with economies in transition, at their request, in meeting
their obligations under this Article.
4.
The reporting and exchange of information under the Convention shall be subject to national
law regarding confidentiality and privacy. The Parties_shall protect, as mutually agreed/ any
confidential information that is exchanged.
Article 22
Cooperation in the scientific, technical, and legalfields and provision ofrelated expertise
1.
The Parties shall cooperate directly or through competent international bodies to strengthen
their capacity to fulfill the obligations arising from this Convention, taking into account the needs of
developing country Parties and Parties with economies in transition. Such cooperation shall promote
the transfer of technical, scientific and legal expertise and technology, as mutually agreed, to establish
and strengthen national tobacco control strategies, plans and programmes aiming at, inter aha'.
(a)
facilitation of the development, transfer and acquisition of technology, knowledge, skills.
capacity and expertise related to tobacco control;
(b)
provision of technical, scientific, legal and other expertise to establish and strengthen
national tobacco control strategies, plans and programmes, aiming al implementation of the
Convention through, inter alia:
(i)
assisting, upon request, in the development of a strong legislative foundation as
well as technical programmes, including those on prevention of initiation, promotion of
cessation and protection from exposure to tobacco smoke;
(ii)
assisting, as appropriate, tobacco workers in the development of appropriate
economically and legally viable alternative livelihoods in an economically viable manner:
and
(iii)
assisting, as appropriate, tobacco growers in shifting agricultural production to
alternative crops in an economically viable manner;
(c)
support for appropriate training or sensitization programmes for appropriate personnel in
accordance with Article 12;
(d)
provision, as appropriate, of the necessary material, equipment and supplies, as well as
logistical support, for tobacco control strategies, plans and programmes;
(e)
identification of methods for tobacco control, including comprehensive treatment of
nicotine addiction; and
(f)
promotion, as appropriate, of research to increase the affordability of comprehensive
treatment of nicotine addiction.
2.
The Conference of the Parties shall promote and facilitate transfer of technical, scientific and
legal expertise and technology with the financial support secured in accordance with Article 26.
PART VIII: INSTITUTIONAL ARRANGEMENTS AND FINANCIAL RESOURCES
Article 23
Conference of the Parties
I.
A_Conference of the Parties is hereby establishe.d. The first session of the Conference shall be
convened by the World Health Organization not later than one year after the entry into force of this
Convention. The Conference will determine the venue and timing of subsequent regular sessions at its
first session.
2.
Extraordinary sessions of the Conference of the Parties shall be held at such other times as may
be deemed necessary by the Conference, or at the written request of any Party, provided that, within
six months of the request being communicated to them by the Secretariat of the Convention, it is
supportedby at least one-third of the Parties.
3.
The Conference of the Parties shall adopt by consensus its Rides of Procedure at its first session.
4.
The Conference of the Parties shall by consensus adopt financial rules for itself as well as
governing the funding of any subsidiary bodies it may establish as well as financial provisions
governing the functioning of the Secretariat. At each ordinary session, it shall adopt a budget for the
financial period until the next ordinary session.
5.
The Conference of the Parties shall keep under regular review the implementation of the
Convention and take the decisions necessary to promote its effective implementation and may adopt
protocols, annexes and amendments to the Convention, in accordance with Articles 28, 29 and 33.
Towards this end, it shall:
(a)
promote and facilitate the exchange of information pursuant to Articles 20 and 21:
(b)
promote and guide the development and periodic refinement of comparable
methodologies for research and the collection of data, in addition to those provided for in
Article 20, relevant to the implementation of the Convention;
(c)
promote, as appropriate, the development, implementation,and evaluation of strategies.
plans, and programmes, as well as policies, legislation and other measures;
(d)
consider reports submitted by the Parties in accordance with Article 21 and adopt regular
reports on the implementation of the Convention;
(e)
promote and facilitate the mobilization of financial resources for the implementation of
the Convention in accordance with Article 26;
(f)
establish such subsidiary bodies as are necessary to achieve the objective of the
Convention;
(g)
request, where appropriate, the services and cooperation of, and information provided by.
competent and relevant organizations and bodies of the United Nations system and other
international and regional intergovernmental organizations and nongovernmental organizations
and bodies as a means of strengthening the implementation of the Convention; and
(h)
consider other action, as appropriate, for the achievement of the objective of the
Convention in the light of experience gained in its implementation.
6.
The Conference of the Parties shall establish the criteria fprjhe participation of observers at its
proceedings.
Article 24
Secretarial
1.
The Conference of the Parties shall designate a permanent secretariat and make arrangements
for its functioning. The Conference of the Parties shall endeavour to do so at its first session.
2.
Until such time as a permanent secretariat is designated and established, secretariat functions
under this Convention shall be provided by the World Health Organization.
3.
Secretariat functions shall be;
(a)
to make arrangements for sessions of the Conference of the Parlies and any subsidiary
bodies and to provide them with services as required;
(b)
to transmit reports received by it pursuant to the Convention;
(c)
to provide support to the Parties, particularly developing country Parlies and Parties with
economies in transition, on request, in the compilation and communication of information
required in accordance with the provisions of the Convention;
(d)
to prepare reports on its activities under the Convention under the guidance of the
Conference of the Parties and submit them to the Conference of the Parties:
(e)
to ensure, under the guidance of the Conference of the Parties, the necessary coordination
with the competent international and regional intergovernmental organizations and other bodies:
(f)
to enter, under the guidance of the Conference of the Parties, into such administrative or
contractual arrangements as may be required for the effective discharge of its functions: and
(g)
to perform other secretariat functions specified by the Convention and by any of its
protocols and such other functions as may be determined by the Conference of the Parties.
Article 25
Relations between the Conference of the Parties and intergovernmental organizations
In order to provide technical and financial cooperation for achieving the objective of this
Convention, the Conference of the Parties may request the cooperation of competent international and
regional intergovernmental organizations including financial and development institutions.
Article 26
Financial resources
1.
The Parties recognize the important role that financial resources play in achieving the objective
of this Convention.
2.
Each Party shall provide financial support in respect of its national activities intended to achieve
the objective of the Convention, in accordance with its national plans, priorities and programmes.
3.
Parties shall promote, as appropriate, the utilization of bilateral, regional, subregional and other
multilateral channels to provide funding for the development and strengthening of multisectoral
comprehensive tobacco control programmes of developing country Parties and Parties with economies
in transition. Accordingly, economically viable alternatives to tobacco production, including crop
diversification should be addressed and supported in the context of nationally developed strategies of
sustainable development.
4.
Parties represented in relevant regional and international intergovernmental organizations, and
financial and development institutions shall encourage these entities to provide financial assistance for
developing country Parties and for Parties with economies in transition to assist them in meeting their
obligations under the Convention, without limiting the rights of participation within these
organizations.
5.
The Parties agree that:
(a)
to assist Parties in meeting their obligations under the Convention, all relevant potential
and existing resources, financial, technical, or otherwise, both public and private that are
available for tobacco control activities, should be mobilized and utilized for the benefit of all
Parties, especially developing countries and countries with economies in transition;
(b)
the Secretariat shall advise developing country Parties and Parties with economies in
transition, upon request, on available Sources of funding to facilitate the implementation of their
obligations under the Convention;
(c)
the Conference of the Parties in its first session shall review existing and potential sources
and mechanisms of assistance based on a study conducted by the Secretarial and other relevant
information, and consider their adequacy; and
(d)
the results of this review shall be taken into account by the Conference of the Parties in
determining the necessity to enhance existing mechanisms or to establish a voluntary global
fund or other appropriate financial mechanisms to channel additional financiaPf&SOurces.jis
heeded, to developing country Parties and Parties with economies in transition to assist them in
meeting the objectives of the Convention.
PART IX: SETTLEMENT OF DISPUTES
Article 27
Settlement of disputes
I.
In the event of a dispute between two or more Parties concerning the interpretation or
application of this Convention, the Parties concerned shall seek through diplomatic channels a
settlement of the dispute through negotiation or any other peaceful means of their own choice.
including good offices, mediation, or conciliation. Failure to reach agreement by good offices.
mediation or conciliation shall not absolve parties to the dispute from the responsibility of continuing
to seek to resolve it.
2.
When ratifying, accepting, approving, formally confirming or acceding to the Convention, or at
any time thereafter, a State or regional economic integration organization may declare in writing to the
Depositary that, for a dispute not resolved in accordance with paragraph 1 of this Article, it accepts, as
compulsory, ad hoc arbitration in accordance with procedures to be adopted by consensus by the
Conference of the Parties.
3.
The provisions of this Article shall apply with respect to any protocol as between the parties to
the protocol, unless otherwise provided therein.
PART X: DEVELOPMENT OF THE CONVENTION
Article 28
Amendments to this Convention
I.
Any Party may propose amendments to this Convention. Such amendments will be considered
by the Conference of the Parties.
2.
Amendments to the Convention shall be adopted by the Conference of the Parlies. The text of
any proposed amendment to the Convention shall be communicated to the Parties by the Secretariat at
least six months before the session at which it is proposed for adoption. The Secretariat shall also
communicate proposed amendments to the signatories of the Convention and, for information, to the
Depositary.
3.
The Parties shall make every effort to reach agreement by consensus on any proposed
amendment to the Convention. If all efforts at consensus have been exhausted, and no agreement
reached, the amendment shall as a last resort be adopted by a three-quarters majority vote of the
Parties present and voting at the session. For purposes of this Article, Parties present and voting means
Parties present and casting an affirmative or negative vote. Any adopted amendment shall be
communicated by the Secretariat to the Depositary, who shall circulate it to all Parties for acceptance.
4.
Instruments of acceptance in respect of an amendment shall be deposited with the Depositary.
An amendment adopted in accordance with paragraph 3 of this Article shall enter into force for those
Parties having accepted it on the ninetieth day after the date of receipt by the Depositary of an
instrument of acceptance by at least two-thirds of the Parties to the Convention.
5.
The amendment shall enter into force for any other Party on the ninetieth day after the dale on
which that Party deposits with the Depositaiy its instrument of acceptance of the said amendment.
Article 29
Adoption and amendment ofannexes to this Convention
1.
Annexes to this Convention and amendments thereto shall be proposed, adopted and shall enter
into force in accordance with the procedure set forth in Article 28.
2.
Annexes to the Convention shall form an integral part thereof and, unless otherwise expressly
provided, a reference to the Convention constitutes at the same lime a reference to any annexes
thereto.
3.
Annexes shall be restricted to lists, forms and any other descriptive material relating to
procedural, scientific, technical or administrative matters.
PART XI: FINAL PROVISIONS
Article 30
Reservations
No reservations may be made to this Convention.
Article 31
Withdrawal
I.
At any time after two years from the date on which this Convention has entered into force for a
Party, that Party may withdraw from the Convention by giving written notification to the Depositary.
2.
Any such withdrawal shall take effect upon expity of one year from the date of receipt by the
Depositary of the notification of withdrawal, or on such later date as may be specified in the
notification of withdrawal.
3.
Any Party that withdraws from the Convention shall be considered as also having withdrawn
from any protocol to which it is a Party.
Article 32
Right to vole
1.
Each Party to this Convention shall have one vote, except as provided for in paragraph 2 of this
Article.
2.
Regional economic integration organizations, in matters within their competence, shall exercise
their right to vote with a number of votes equal to the number of their Member States that are Parties
to the Convention. Such an organization shall not exercise its right to vote if any of its Member States
exercises its right, and vice versa.
Article 33
Protocols
I.
Any Party may propose protocols. Such proposals will be considered by the Conference of the
Parties.
2.
The Conference of the Parties may adopt protocols to this Convention. In adopting these
protocols every effort shall be made to reach consensus. If all efforts at consensus have been
exhausted, and no agreement reached, the protocol shall as a last resort be adopted by a three-quarters
majority vote of the Parties present and voting at the session. For the purposes of this Article. Parties
present and voting means Parties present and casting an affirmative or negative vole.
3.
The text of any proposed protocol shall be communicated to the Parties by the Secretarial at
least six months before the session at which it is proposed for adoption.
4.
Only Parties to the Convention may be parties to a protocol.
5.
Any protocol to the Convention shall be binding only on the parties to the protocol in question.
Only Parties to a protocol may take decisions on matters exclusively relating to the protocol in
question.
6.
The requirements for entry into force of any protocol shall be established by that instrument.
Article 34
Signature
This Convention shall be open for signature by all Members of the World Health Organization
and by any States that are not Members of the World Health Organization but are members of the
United Nations and by regional economic integration organizations al the World Health Organization
Headquarters in Geneva from 16 June 2003 to 22 June 2003, and thereafter at United Nations
Headquarters in New York, from 30 June 2003 to 29 June 2004.
Article 35
Ratification, acceptance, approval, formal confirmation or accession
1.
This Convention shall be subject to ratification, acceptance, approval or accession by States and
to formal confirmation or accession by regional economic integration organizations. It shall be open
for accession from the day after the date on which the Convention is closed for signature. Instruments
of ratification, acceptance, approval, formal confirmation or accession shall be deposited with the
Depositary.
2.
Any regional economic integration organization which becomes a Party to the Convention
without any of its Member States being a Party shall be bound by all the obligations under the
Convention. In the case of those organizations, one or more of whose Member States is a Party to the
Convention, the organization and its Member States shall decide on their respective responsibilities for
the performance of their obligations under the Convention. In such cases, the organization and the
Member States shall not be entitled to exercise rights under the Convention concurrently.
3.
Regional economic integration organizations shall, in their instruments relating to formal
confirmation or in their instruments of accession, declare the extent of their competence with respect
to the matters governed by the Convention. These organizations shall also inform the Depositary, who
shall in turn inform the Parties, of any substantial modification in the extent of their competence.
Article 36
Entry into force
1
This Convention shall enter into force on the ninetieth day following the date of deposit of the
fortieth instrument of ratification, acceptance, approval, formal confirmation or accession with the
Depositary.
2.
For each State that ratifies, accepts or approves the Convention or accedes thereto after the
conditions set out in paragraph I of this Article for entry into force have been fulfilled, the Convention
shall enter into force on the ninetieth day following the date of deposit of its instrument of ratification,
acceptance, approval or accession.
3.
For each regional economic integration organization depositing an instrument of formal
confirmation or an instrument of accession after the conditions set out in paragraph I of this Article
for entry into force have been fulfilled, the Convention shall enter into force on the ninetieth day
following the date of its depositing of the instalment of formal confirmation or of accession.
4.
For the purposes of this Article, any instrument deposited by a regional economic integration
organization shall not be counted as additional to those deposited by States Members of the
organization.
Article 37
Depositary
The Secretary-General of the United Nations shall be the Depositary of this Convention and
amendments thereto and of protocols and annexes adopted in accordance with Articles 28, 29 and 33.
Article 38
Authentic texts
The original of this Convention, of which the Arabic, Chinese, English, French, Russian and
Spanish texts are equally authentic, shall be deposited with the Secretary-General of the United
Nations.
IN WITNESS Wl-IEREOF the undersigned, being duly authorized to that effect, have signed (his
Convention.
DONE at GENEVA this twenty-first day of May two thousand and three.
FIFTY-SIXTH WORLD HEALTH ASSEMBLY
Agenda item 13
WHA56.1
21 May 2003
WHO Framework Convention on Tobacco Control
The Fifty-sixth World Health Assembly,
Recalling its resolutions WHA49.17 and WHA52.18 calling for the development of a WHO
framework convention on tobacco control in accordance with Article 19 of the Constitution of WHO;
Determined to protect present and future generations from tobacco consumption and exposure to
tobacco smoke;
Noting with profound concern the escalation in smoking and other forms of tobacco use
worldwide;
Acknowledging with appreciation the report of the Chair of the Intergovernmental Negotiating
Body on the outcome of the work of the Intergovernmental Negotiating Body;1
Convinced that this convention is a groundbreaking step in advancing national, regional and
international action and global cooperation to protect human health against the devastating impact of
tobacco consumption and exposure to tobacco smoke, and mindful that special consideration should be
given to the particular situation of developing countries and countries with economies in transition;
Emphasizing the need for expeditious entry into force and effective implementation of the
convention,
1.
ADOPTS the Convention attached to this resolution;
2.
NOTES, in accordance with Article 34 of the Convention, that the Convention shall be open for
signature at WHO headquarters in Geneva, from" 16 June 2003 to 22 June 2003, and thereafter at
United Nations headquarters in New York, from 30 June 2003 to 29 June 2004;
3.
CALLS UPON all States and regional economic integration organizations entitled to do so, to
consider signing, ratifying, accepting, approving, formally confirming or acceding to the Convention
at the earliest opportunity, with a view to bringing the Convention into force as soon as possible;
1 Document A56/TNF.DOC./7.
WHA56.1
4.
URGES all States and regional economic integration organizations, pending entry into force of
the Convention, to take all appropriate measures to curb tobacco consumption and exposure to tobacco
smoke;
5.
URGES all Member States, regional economic integration organizations, observers and other
interested parties to support the preparatory activities referred to in this resolution and effectively
encourage prompt entry into force and implementation of the Convention;
6.
CALLS UPON the United Nations and invites other relevant international organizations to
continue to provide support for strengthening national and international tobacco control programmes;
7.
DECIDES to establish, in accordance with Rule 42 of the Rules of Procedure of the Health
Assembly, an open-ended intergovernmental working group that shall be open to all States and
regional economic integration organizations referred to in Article 34 of the Convention, to consider
and prepare proposals on those issues identified in the Convention for consideration and adoption, as
appropriate, by the first session of the Conference of the Parties; such issues should include:
(1)
rules of procedure for the Conference of the Parties (Article 23.3), including criteria for
participation of observers at sessions of the Conference of the Parties (Article 23.6);
(2)
options for the designation of a permanent secretariat and arrangements for its
functioning (Article 24.1);
(3)
financial rules for the Conference of the Parties and its subsidiary bodies, and financial
provisions governing the functioning of the secretariat (Article 23.4);
(4)
a draft budget for the first financial period (Article 23.4);
(5)
a review of existing and potential sources and mechanisms of assistance to Parties in
meeting their obligations under the Convention (Article 26.5);
8.
FURTHER DECIDES that the Open-ended Intergovernmental Working Group shall also
oversee preparations for the first session of the Conference of the Parties and report directly to it;
9.
RESOLVES that decisions that had been taken by the Intergovernmental Negotiating Body on
the WHO framework convention on tobacco control concerning the participation of nongovernmental
organizations shall apply to the activities of the Open-ended Intergovernmental Working Group;
10.
REQUESTS the Director-General:
(1)
to provide secretariat functions under the Convention until such time as a permanent
secretariat is designated and established;
(2)
to take appropriate steps to provide support to Member States, in particular developing
countries and countries with economies in transition, in preparation for entry into force of the
Convention;
(3)
to convene, as frequently as necessary, between 16 June 2003 and the first session of the
Conference of the Parties, meetings of the Open-ended Intergovernmental Working Group;
2
WHA56.1
(4)
to continue to ensure that WHO plays a key role in providing technical advice, direction
and support for global tobacco control;
(5)
to keep the Health Assembly informed of progress made toward entry into force of the
Convention and of preparations under way for the first session of the Conference of the Parties.
3
WHA56.1
ANNEX
WHO Framework Convention on Tobacco Control
Preamble
The Parties to this Convention,
Determined to give priority to their right to protect public health,
Recognizing that the spread of the tobacco epidemic is a global problem with serious
consequences for public health that calls for the widest possible international cooperation and the
participation of all countries in an effective, appropriate and comprehensive international response,
Reflecting the concern of the international community about the devastating worldwide health,
social, economic and environmental consequences of tobacco consumption and exposure to tobacco
smoke,
Seriously concerned about the increase in the worldwide consumption and production of
cigarettes and other tobacco products, particularly in developing countries, as well as about the burden
this places on families, on the poor, and on national health systems,
Recognizing that scientific evidence has unequivocally established that tobacco consumption
and exposure to tobacco smoke cause death, disease and disability, and that there is a time lag between
the exposure to smoking and the other uses of tobacco products and the onset of tobacco-related
diseases,
Recognizing also that cigarettes and some other products containing tobacco are highly
engineered so as to create and maintain dependence, and that many of the compounds they contain and
the smoke they produce are pharmacologically active, toxic, mutagenic and carcinogenic, and that
tobacco dependence is separately classified as a disorder in major international classifications of
diseases,
Acknowledging that there is clear scientific evidence that prenatal exposure to tobacco smoke
causes adverse health and developmental conditions for children,
Deeply concerned about the escalation in smoking and other forms of tobacco consumption by
children and adolescents worldwide, particularly smoking at increasingly early ages,
Alarmed by the increase in smoking and other forms of tobacco consumption by women and
young girls worldwide and keeping in mind the need for full participation of women at all levels of
policy-making and implementation and the need for gender-specific tobacco control strategies,
Deeply concerned about the high levels of smoking and other forms of tobacco consumption by
indigenous peoples,
Seriously concerned about the impact of all forms of advertising, promotion and sponsorship
aimed at encouraging the use of tobacco products,
WitA 56./
Annex
Recognizing that cooperative action is necessary to eliminate all forms of illicit trade in
cigarettes and other tobacco products, including smuggling, illicit manufacturing and counterfeiting,
Acknc wledging that tobacco control at all levels and particularly in developing countries and in
countries with economies in transition requires sufficient financial and technical resources
commensurate with the current and projected need for tobacco control activities,
Recognizing the need to develop appropriate mechanisms to address the long-term social and
economic implications of successful tobacco demand reduction strategies,
Mindful of the social and economic difficulties that tobacco control programmes may engender
in the medium and long term in some developing countries and countries with economies in transition,
and recognizing their need for technical and financial assistance in the context of nationally developed
strategies for sustainable development,
Conscious of the valuable work being conducted by many States on tobacco control and
commending the leadership of the World Health Organization as well as the efforts of other
organizations and bodies of the United Nations system and other international and regional
intergovernmental organizations in developing measures on tobacco control,
Emphasizing the special contribution of nongovernmental organizations and other members of
civil society not affiliated with the tobacco industry, including health professional bodies, women’s,
youth, environmental and consumer groups, and academic and health care institutions, to tobacco
control efforts nationally and internationally and the vital importance of their participation in national
and international tobacco control efforts,
Recognizing the need to be alert to any efforts by the tobacco industry to undermine or subvert
tobacco control efforts and the need to be informed of activities of the tobacco industry that have a
negative impact on tobacco control efforts,
Recalling Article 12 of the International Covenant on Economic, Social and Cultural Rights,
adopted by the United Nations General Assembly on 16 December 1966, which states that it is the
right of everyone to the enjoyment of the highest attainable standard of physical and mental health,
Recalling also the preamble to the Constitution of the World Health Organization, which states
that the enjoyment of the highest attainable standard of health is one of the fundamental rights of every
human being without distinction of race, religion, political belief, economic or social condition,
Determined to promote measures of tobacco control based on current and relevant scientific,
technical and economic considerations,
Recalling that the Convention on the Elimination of All Forms of Discrimination against
Women, adopted by the United Nations General Assembly on 18 December 1979, provides that States
Parties to that Convention shall take appropriate measures to eliminate discrimination against women
in the field of health care,
Recallingfurther that the Convention on the Rights of the Child, adopted by the United Nations
General Assembly on 20 November 1989, provides that States Parties to that Convention recognize
the right of the child to the enjoyment of the highest attainable standard of health,
Have agreed, as follows:
WHA56.1
Annex
PART I: INTRODUCTION
Article 1
Use of terms
For the purposes of this Convention:
(a)
“illicit trade” means any practice or conduct prohibited by law and which relates to
production, shipment, receipt, possession, distribution, sale or purchase including any practice
or conduct intended to facilitate such activity;
(b)
“regional economic integration organization” means an organization that is composed of
several sovereign states, and to which its Member States have transferred competence over a
range of matters, including the authority to make decisions binding on its Member States in
respect of those matters;1
(c)
“tobacco advertising and promotion” means any form of commercial communication,
recommendation or action with the aim, effect or likely effect of promoting a tobacco product or
tobacco use either directly or indirectly;
(d)
“tobacco control” means a range of supply, demand and harm reduction strategies that
aim to improve the health of a population by eliminating or reducing their consumption of
tobacco products and exposure to tobacco smoke;
(e)
“tobacco industry” means tobacco manufacturers, wholesale distributors and importers of
tobacco products;
(f)
“tobacco products” means products entirely or partly made of the leaf tobacco as raw
material which are manufactured to be used for smoking, sucking, chewing or snuffing;
(g)
“tobacco sponsorship ” means any form of contribution to any event, activity or individual
with the aim, effect or likely effect of promoting a tobacco product or tobacco use either directly
or indirectly;
Article 2
Relationship between this Convention and other agreements and legal instruments
1.
In order to better protect human health, Parties are encouraged to implement measures beyond
those required by this Convention and its protocols, and nothing in these instruments shall prevent a
Party from imposing stricter requirements that are consistent with their provisions and are in
accordance with international law.
2.
The provisions of the Convention and its protocols shall in no way affect the right of Parties to
enter into bilateral or multilateral agreements, including regional or subregional agreements, on issues
relevant or additional to the Convention and its protocols, provided that such agreements are
compatible with their obligations under the Convention and its protocols. The Parties concerned shall
communicate such agreements to the Conference of the Parties through the Secretariat.
1 Where appropriate, national will refer equally to regional economic integration organizations.
6
Annex
WHA56.1
PART II: OBJECTIVE, GUIDING PRINCIPLES AND GENERAL OBLIGATIONS
Article 3
Objective
The objective of this Convention and its protocols is to protect present and future generations
from the devastating health, social, environmental and economic consequences of tobacco
consumption and exposure to tobacco smoke by providing a framework for tobacco control measures
to be implemented by the Parties at the national, regional and international levels in order to reduce
continually and substantially the prevalence of tobacco use and exposure to tobacco smoke.
Article 4
Guiding principles
To achieve the objective of this Convention and its protocols and to implement its provisions,
the Parties shall be guided, inter alia, by the principles set out below:
1.
Every person should be informed of the health consequences, addictive nature and mortal threat
posed by tobacco consumption and exposure to tobacco smoke and effective legislative, executive,
administrative or other measures should be contemplated at the appropriate governmental level to
protect all persons from exposure to tobacco smoke.
2.
Strong political commitment is necessary to develop and support, at the national, regional and
international levels, comprehensive multisectoral measures and coordinated responses, taking into
consideration:
(a)
the need to take measures to protect all persons from exposure to tobacco smoke;
(b)
the need to take measures to prevent the initiation, to promote and support cessation, and
to decrease the consumption of tobacco products in any form;
(c)
the need to take measures to promote the participation of indigenous individuals and
communities in the development, implementation and evaluation of tobacco control
programmes that are socially and culturally appropriate to their needs and perspectives; and
(d)
the need to take measures to address gender-specific risks when developing tobacco
control strategies.
3.
International cooperation, particularly transfer of technology, knowledge and financial
assistance and provision of related expertise, to establish and implement effective tobacco control
programmes, taking into consideration local culture, as well as social, economic, political and legal
factors, is an important part of the Convention.
4.
Comprehensive multisectoral measures and responses to reduce consumption of all tobacco
products at the national, regional and international levels are essential so as to prevent, in accordance
with public health principles, the incidence of diseases, premature disability and mortality due to
tobacco consumption and exposure to tobacco smoke.
5.
Issues relating to liability, as determined by each Party within its jurisdiction, are an important
part of comprehensive tobacco control.
7
WitA 56.1
Annex
6.
The importance of technical and financial assistance to aid the economic transition of tobacco
growers and workers whose livelihoods are seriously affected as a consequence of tobacco control
programmes in developing country Parties, as well as Parties with economies in transition, should be
recognized and addressed in the context of nationally developed strategies for sustainable
development.
7.
The participation of civil society is essential in achieving the objective of the Convention and its
protocols.
Article 5
General obligations
1.
Each Party shall develop, implement, periodically update and review comprehensive
multisectoral national tobacco control strategies, plans and programmes in accordance with this
Convention and the protocols to which it is a Party.
2.
Towards this end, each Party shall, in accordance with its capabilities:
(a)
establish or reinforce and finance a national coordinating mechanism or focal points for
tobacco control; and
(b)
adopt and implement effective legislative, executive, administrative and/or other
measures and cooperate, as appropriate, with other Parties in developing appropriate policies for
preventing and reducing tobacco consumption, nicotine addiction and exposure to tobacco
smoke.
3.
In setting and implementing their public health policies with respect to tobacco control, Parties
shall act to protect these policies from commercial and other vested interests of the tobacco industry in
accordance with national law.
4.
The Parties shall cooperate in the formulation of proposed measures, procedures and guidelines
for the implementation of the Convention and the protocols to which they are Parties.
5.
The Parties shall cooperate, as appropriate, with competent international and regional
intergovernmental organizations and other bodies to achieve the objectives of the Convention and the
protocols to which they are Parties.
6.
The Parties shall, within means and resources at their disposal, cooperate to raise financial
resources for effective implementation of the Convention through bilateral and multilateral funding
mechanisms.
PART III: MEASURES RELATING TO THE REDUCTION
OF DEMAND FOR TOBACCO
Article 6
Price and tax measures to reduce the demandfor tobacco
1.
The Parties recognize that price and tax measures are an effective and important means of
reducing tobacco consumption by various segments of the population, in particular young persons.
8
WHA56.1
Annex
2.
Without prejudice to the sovereign right of the Parties to determine and establish their taxation
policies, each Party should take account of its national health objectives concerning tobacco control
and adopt or maintain, as appropriate, measures which may include:
(a)
implementing tax policies and, where appropriate, price policies, on tobacco products so
as to contribute to the health objectives aimed at reducing tobacco consumption; and
(b)
prohibiting or restricting, as appropriate, sales to and/or importations by international
travellers of tax- and duty-free tobacco products.
3.
The Parties shall provide rates of taxation for tobacco products and trends in tobacco
consumption in their periodic reports to the Conference of the Parties, in accordance with Article 21.
Article 7
Non-price measures to reduce the demandfor tobacco
The Parties recognize that comprehensive non-price measures are an effective and important
means of reducing tobacco consumption. Each Party shall adopt and implement effective legislative,
executive, administrative or other measures necessary to implement its obligations pursuant to
Articles 8 to 13 and shall cooperate, as appropriate, with each other directly or through competent
international bodies with a view to their implementation. The Conference of the Parties shall propose
appropriate guidelines for the implementation of the provisions of these Articles.
Article 8
Protection from exposure to tobacco smoke
1.
Parties recognize that scientific evidence has unequivocally established that exposure to tobacco
smoke causes death, disease and disability.
2.
Each Party shall adopt and implement in areas of existing national jurisdiction as determined by
national law and actively promote at other jurisdictional levels the adoption and implementation of
effective legislative, executive, administrative and/or other measures, providing for protection from
exposure to tobacco smoke in indoor workplaces, public transport, indoor public places and, as
appropriate, other public places.
Article 9
Regulation of the contents of tobacco products
The Conference of the Parties, in consultation with competent international bodies, shall
propose guidelines for testing and measuring the contents and emissions of tobacco products, and for
the regulation of these contents and emissions. Each Party shall, where approved by competent
national authorities, adopt and implement effective legislative, executive and administrative or other
measures for such testing and measuring, and for such regulation.
Article 10
Regulation of tobacco product disclosures
Each Party shall, in accordance with its national law, adopt and implement effective legislative,
executive, administrative or other measures requiring manufacturers and importers of tobacco products
to disclose to governmental authorities information about the contents and emissions of tobacco
9
HHA56.1
Annex
products. Each Party shall further adopt and implement effective measures for public disclosure of
information about the toxic constituents of the tobacco products and the emissions that they may
produce.
Article 11
Packaging and labelling of tobacco products
1.
Each Party shall, within a period of three years after entry into force of this Convention for that
Party, adopt and implement, in accordance with its national law, effective measures to ensure that:
(a)
tobacco product packaging and labelling do not promote a tobacco product by any means
that are false, misleading, deceptive or likely to create an erroneous impression about its
characteristics, health effects, hazards or emissions, including any term, descriptor, trademark,
figurative or any other sign that directly or indirectly creates the false impression that a
particular tobacco product is less harmful than other tobacco products. These may include terms
such as “low tar”, “light”, “ultra-light”, or “mild”; and
(b)
each unit packet and package of tobacco products and any outside packaging and
labelling of such products also carry health warnings describing the harmful effects of tobacco
use, and may include other appropriate messages. These warnings and messages:
(i)
shall be approved by the competent national authority,
(ii)
shall be rotating,
(iii)
shall be large, clear, visible and legible,
(iv)
should be 50% or more of the principal display areas but shall be no less than 30%
of the principal display areas,
(v)
may be in the form of or include pictures or pictograms.
2.
Each unit packet and package of tobacco products and any outside packaging and labelling of
such products shall, in addition to the warnings specified in paragraph 1(b) of this Article, contain
information on relevant constituents and emissions of tobacco products as defined by national
authorities.
3.
Each Party shall require that the warnings and other textual information specified in
paragraphs 1(b) and paragraph 2 of this Article will appear on each unit packet and package of tobacco
products and any outside packaging and labelling of such products in its principal language or
languages.
4.
For the purposes of this Article, the term “outside packaging and labelling” in relation to
tobacco products applies to any packaging and labelling used in the retail sale of the product.
10
Annex
WHA56.1
Article 12
Education, communication, training and public awareness
Each Party shall promote and strengthen public awareness of tobacco control issues, using all
available communication tools, as appropriate. Towards this end, each Party shall adopt and
implement effective legislative, executive, administrative or other measures to promote:
(a)
broad access to effective and comprehensive educational and public awareness
programmes on the health risks including the addictive characteristics of tobacco consumption
and exposure to tobacco smoke;
(b)
public awareness about the health risks of tobacco consumption and exposure to tobacco
smoke, and about the benefits of the cessation of tobacco use and tobacco-free lifestyles as
specified in Article 14.2;
(c)
public access, in accordance with national law, to a wide range of information on the
tobacco industry as relevant to the objective of this Convention;
(d)
effective and appropriate training or sensitization and awareness programmes on tobacco
control addressed to persons such as health workers, community workers, social workers, media
professionals, educators, decision-makers, administrators and other concerned persons;
(e)
awareness and participation of public and private agencies and nongovernmental
organizations not affiliated with the tobacco industiy in developing and implementing
intersectoral programmes and strategies for tobacco control; and
(f)
public awareness of and access to information regarding the adverse health, economic,
and environmental consequences of tobacco production and consumption.
Article 13
Tobacco advertising, promotion and sponsorship
1.
Parties recognize that a comprehensive ban on advertising, promotion and sponsorship would
reduce the consumption of tobacco products.
2.
Each Party shall, in accordance with its constitution or constitutional principles, undertake a
comprehensive ban of all tobacco advertising, promotion and sponsorship. This shall include, subject
to the legal environment and technical means available to that Party, a comprehensive ban on crossborder advertising, promotion and sponsorship originating from its territory. In this respect, within the
period of five years after entry into force of this Convention for that Party, each Party shall undertake
appropriate legislative, executive, administrative and/or other measures and report accordingly in
conformity with Article 21.
3.
A Party that is not in a position to undertake a comprehensive ban due to its constitution or
constitutional principles shall apply restrictions on all tobacco advertising, promotion and sponsorship.
This shall include, subject to the legal environment and technical means available to that Party,
restrictions or a comprehensive ban on advertising, promotion and sponsorship originating from its
territory with cross-border effects. In this respect, each Party shall undertake appropriate legislative,
executive, administrative and/or other measures and report accordingly in conformity with Article 21.
11
Annex
WHA56.1
4.
As a minimum, and in accordance with its constitution or constitutional principles, each Party
shall:
(a)
prohibit all forms of tobacco advertising, promotion and sponsorship that promote a
tobacco product by any means that are false, misleading or deceptive or likely to create an
erroneous impression about its characteristics, health effects, hazards or emissions;
(b)
require that health or other appropriate warnings or messages accompany all tobacco
advertising and, as appropriate, promotion and sponsorship;
(c)
restrict the use of direct or indirect incentives that encourage the purchase of tobacco
products by the public;
(d)
require, if it does not have a comprehensive ban, the disclosure to relevant governmental
authorities of expenditures by the tobacco industry on advertising, promotion and sponsorship
not yet prohibited. Those authorities may decide to make those figures available, subject to
national law, to the public and to the Conference of the Parties, pursuant to Article 21;
(e)
undertake a comprehensive ban or, in the case of a Party that is not in a position to
undertake a comprehensive ban due to its constitution or constitutional principles, restrict
tobacco advertising, promotion and sponsorship on radio, television, print media and, as
appropriate, other media, such as the internet, within a period of five years; and
(f)
prohibit, or in the case of a Party that is not in a position to prohibit due to its constitution
or constitutional principles restrict, tobacco sponsorship of international events, activities and/or
participants therein.
5.
Parties are encouraged to implement measures beyond the obligations set out in paragraph 4.
Parties shall cooperate in the development of technologies and other means necessary to
6.
facilitate the elimination of cross-border advertising.
7.
Parties which have a ban on certain forms of tobacco advertising, promotion and sponsorship
have the sovereign right to ban those forms of cross-border tobacco advertising, promotion and
sponsorship entering their territory and to impose equal penalties as those applicable to domestic
advertising, promotion and sponsorship originating from their territory in accordance with their
national law. This paragraph does not endorse or approve of any particular penalty.
8.
Parties shall consider the elaboration of a protocol setting out appropriate measures that require
international collaboration for a comprehensive ban on cross-border advertising, promotion and
sponsorship.
Article 14
Demand reduction measures concerning tobacco dependence and cessation
1.
Each Party shall develop and disseminate appropriate, comprehensive and integrated guidelines
based on scientific evidence and best practices, taking into account national circumstances and
priorities, and shall take effective measures to promote cessation of tobacco use and adequate
treatment for tobacco dependence.
12
Annex
2.
WHA56.1
Towards this end, each Party shall endeavour to:
(a)
design and implement effective programmes aimed at promoting the cessation of tobacco
use, in such locations as educational institutions, health care facilities, workplaces and sporting
environments;
(b)
include diagnosis and treatment of tobacco dependence and counselling services on
cessation of tobacco use in national health and education programmes, plans and strategies, with
the participation of health workers, community workers and social workers as appropriate;
(c)
establish in health care facilities and rehabilitation centres programmes for diagnosing,
counselling, preventing and treating tobacco dependence; and
(d)
collaborate with other Parties to facilitate accessibility and affordability for treatment of
tobacco dependence including pharmaceutical products pursuant to Article 22. Such products
and their constituents may include medicines, products used to administer medicines and
diagnostics when appropriate.
PART IV: MEASURES RELATING TO THE REDUCTION
OF THE SUPPLY OF TOBACCO
Article 15
Illicit trade in tobacco products
1.
The Parties recognize that the elimination of all forms of illicit trade in tobacco products,
including smuggling, illicit manufacturing and counterfeiting, and the development and
implementation of related national law, in addition to subregional, regional and global agreements, are
essential components of tobacco control.
2.
Each Party shall adopt and implement effective legislative, executive, administrative or other
measures to ensure that all unit packets and packages of tobacco products and any outside packaging
of such products are marked to assist Parties in determining the origin of tobacco products, and in
accordance with national law and relevant bilateral or multilateral agreements, assist Parties in
determining the point of diversion and monitor, document and control the movement of tobacco
products and their legal status. In addition, each Party shall:
(a)
require that unit packets and packages of tobacco products for retail and wholesale use
that are sold on its domestic market cany the statement: “Sales only allowed in (insert name of
the country, subnational, regional or federal unit)” or carry any other effective marking
indicating the final destination or which would assist authorities in determining whether the
product is legally for sale on the domestic market; and
(b)
consider, as appropriate, developing a practical tracking and tracing regime that would
further secure the distribution system and assist in the investigation of illicit trade.
1 There has been considerable discussion throughout the pre-negotiation and negotiation process concerning the
adoption of an early protocol on illicit trade in tobacco products. The negotiation of such a protocol could be initiated by the
INB immediately following the adoption of the FCTC, or at a later stage by the Conference of the Parties.
13
Annex
WHA56.1
3.
Each Party shall require that the packaging information or marking specified in paragraph 2 of
this Article shall be presented in legible form and/or appear in its principal language or languages.
4.
With a view to eliminating illicit trade in tobacco products, each Party shall:
(a)
monitor and collect data on cross-border trade in tobacco products, including illicit trade,
and exchange information among customs, tax and other authorities, as appropriate, and in
accordance with national law and relevant applicable bilateral or multilateral agreements;
(b)
enact or strengthen legislation, with appropriate penalties and remedies, against illicit
trade in tobacco products, including counterfeit and contraband cigarettes;
(c)
take appropriate steps to ensure that all confiscated manufacturing equipment, counterfeit
and contraband cigarettes and other tobacco products are destroyed, using environmentallyfriendly methods where feasible, or disposed of in accordance with national law;
(d)
adopt and implement measures to monitor, document and control the storage and
distribution of tobacco products held or moving under suspension of taxes or duties within its
jurisdiction; and
(e)
adopt measures as appropriate to enable the confiscation of proceeds derived from the
illicit trade in tobacco products.
5.
Information collected pursuant to subparagraphs 4(a) and 4(d) of this Article shall, as
appropriate, be provided in aggregate form by the Parties in their periodic reports to the Conference of
the Parties, in accordance with Article 21.
6.
The Parties shall, as appropriate and in accordance with national law, promote cooperation
between national agencies, as well as relevant regional and international intergovernmental
organizations as it relates to investigations, prosecutions and proceedings, with a view to eliminating
illicit trade in tobacco products. Special emphasis shall be placed on cooperation at regional and
subregional levels to combat illicit trade of tobacco products.
7.
Each Party shall endeavour to adopt and implement further measures including licensing, where
appropriate, to control or regulate the production and distribution of tobacco products in order to
prevent illicit trade.
Article 16
Sales to and by minors
1.
Each Party shall adopt and implement effective legislative, executive, administrative or other
measures at the appropriate government level to prohibit the sales of tobacco products to persons
under the age set by domestic law, national law or eighteen. These measures may include:
(a)
requiring that all sellers of tobacco products place a clear and prominent indicator inside
their point of sale about the prohibition of tobacco sales to minors and, in case of doubt, request
that each tobacco purchaser provide appropriate evidence of having reached full legal age;
(b)
banning the sale of tobacco products in any manner by which they are directly accessible,
such as store shelves;
14
Annex
WHA56.1
(c)
prohibiting the manufacture and sale of sweets, snacks, toys or any other objects in the
form of tobacco products which appeal to minors; and
(d)
ensuring that tobacco vending machines under its jurisdiction are not accessible to minors
and do not promote the sale of tobacco products to minors.
2.
Each Party shall prohibit or promote the prohibition of the distribution of free tobacco products
to the public and especially minors.
3.
Each Party shall endeavour to prohibit the sale of cigarettes individually or in small packets
which increase the affordability of such products to minors.
4.
The Parties recognize that in order to increase their effectiveness, measures to prevent tobacco
product sales to minors should, where appropriate, be implemented in conjunction with other
provisions contained in this Convention.
5.
When signing, ratifying, accepting, approving or acceding to the Convention or at any time
thereafter, a Party may, by means of a binding written declaration, indicate its commitment to prohibit
the introduction of tobacco vending machines within its jurisdiction or, as appropriate, to a total ban
on tobacco vending machines. The declaration made pursuant to this Article shall be circulated by the
Depositary to all Parties to the Convention.
6.
Each Party shall adopt and implement effective legislative, executive, administrative or other
measures, including penalties against sellers and distributors, in order to ensure compliance with the
obligations contained in paragraphs 1-5 of this Article.
7.
Each Party should, as appropriate, adopt and implement effective legislative, executive,
administrative or other measures to prohibit the sales of tobacco products by persons under the age set
by domestic law, national law or eighteen.
Article 17
Provision ofsupport for economically viable alternative activities
Parties shall, in cooperation with each other and with competent international and regional
intergovernmental organizations, promote, as appropriate, economically viable alternatives for tobacco
workers, growers and, as the case may be, individual sellers.
PART V: PROTECTION OF THE ENVIRONMENT
Article 18
Protection of the environment and the health ofpersons
In carrying out their obligations under this Convention, the Parties agree to have due regard to
the protection of the environment and the health of persons in relation to the environment in respect of
tobacco cultivation and manufacture within their respective territories.
15
WHA56.1
Annex
PART VI: QUESTIONS RELATED TO LIABILITY
Article 19
Liability
1.
For the purpose of tobacco control, the Parties shall consider taking legislative action or
promoting their existing laws, where necessary, to deal with criminal and civil liability, including
compensation where appropriate.
2.
Parties shall cooperate with each other in exchanging information through the Conference of the
Parties in accordance with Article 21 including:
(a)
information on the health effects of the consumption of tobacco products and exposure to
tobacco smoke in accordance with Article 20.3(a); and
(b)
information on legislation and regulations in force as well as pertinent jurisprudence.
3.
The Parties shall, as appropriate and mutually agreed, within the limits of national legislation,
policies, legal practices and applicable existing treaty arrangements, afford one another assistance in
legal proceedings relating to civil and criminal liability consistent with this Convention.
4.
The Convention shall in no way affect or limit any rights of access of the Parties to each other’s
courts where such rights exist.
5.
The Conference of the Parties may consider, if possible, at an early stage, taking account of the
work being done in relevant international fora, issues related to liability including appropriate
international approaches to these issues and appropriate means to support, upon request, the Parties in
their legislative and other activities in accordance with this Article.
PART VII: SCIENTIFIC AND TECHNICAL COOPERATION AND
COMMUNICATION OF INFORMATION
Article 20
Research, surveillance and exchange of information
1.
The Parties undertake to develop and promote national research and to coordinate research
programmes at the regional and international levels in the field of tobacco control. Towards this end,
each Party shall:
(a)
initiate and cooperate in, directly or through competent international and regional
intergovernmental organizations and other bodies, the conduct of research and scientific
assessments, and in so doing promote and encourage research that addresses the determinants
and consequences of tobacco consumption and exposure to tobacco smoke as well as research
for identification of alternative crops; and
(b)
promote and strengthen, with the support of competent international and regional
intergovernmental organizations and other bodies, training and support for all those engaged in
tobacco control activities, including research, implementation and evaluation.
Annex
WIIA56.1
2.
The Parties shall establish, as appropriate, programmes for national, regional and global
surveillance of the magnitude, patterns, determinants and consequences of tobacco consumption and
exposure to tobacco smoke. Towards this end, the Parties should integrate tobacco surveillance
programmes into national, regional and global health surveillance programmes so that data are
comparable and can be analysed at the regional and international levels, as appropriate.
3.
Parties recognize the importance of financial and technical assistance from international and
regional intergovernmental organizations and other bodies. Each Party shall endeavour to:
(a)
establish progressively a national system for the epidemiological surveillance of tobacco
consumption and related social, economic and health indicators;
(b)
cooperate with competent international and regional intergovernmental organizations and
other bodies, including governmental and nongovernmental agencies, in regional and global
tobacco surveillance and exchange of information on the indicators specified in paragraph 3(a)
of this Article; and
(c)
cooperate with the World Health Organization in the development of general guidelines
or procedures for defining the collection, analysis and dissemination of tobacco-related
surveillance data.
4.
The Parties shall, subject to national law, promote and facilitate the exchange of publicly
available scientific, technical, socioeconomic, commercial and legal information, as well as
information regarding practices of the tobacco industry and the cultivation of tobacco, which is
relevant to this Convention, and in so doing shall take into account and address the special needs of
developing country Parties and Parties with economies in transition. Each Party shall endeavour to:
(a)
progressively establish and maintain an updated database of laws and regulations on
tobacco control and, as appropriate, information about their enforcement, as well as pertinent
jurisprudence, and cooperate in the development of programmes for regional and global tobacco
control;
(b)
progressively establish and maintain updated data from national surveillance programmes
in accordance with paragraph 3(a) of this Article; and
(c)
cooperate with competent international organizations to progressively establish and
maintain a global system to regularly collect and disseminate information on tobacco
production, manufacture and the activities of the tobacco industry which have an impact on the
Convention or national tobacco control activities.
5.
Parties should cooperate in regional and international intergovernmental organizations and
financial and development institutions of which they are members, to promote and encourage
provision of technical and financial resources to the Secretariat to assist developing country Parties
and Parties with economies in transition to meet their commitments on research, surveillance and
exchange of information.
17
WHA56.1
Annex
Article 21
Reporting and exchange of information
1.
Each Party shall submit to the Conference of the Parties, through the Secretariat, periodic
reports on its implementation of this Convention, which should include the following:
(a)
information on legislative, executive, administrative or other measures taken to
implement the Convention;
(b)
information, as appropriate, on any constraints or barriers encountered in
implementation of the Convention, and on the measures taken to overcome these barriers;
its
(c)
information, as appropriate, on financial and technical assistance provided or received for
tobacco control activities;
(d)
information on surveillance and research as specified in Article 20; and
(e)
information specified in Articles 6.3, 13.2,13.3, 13.4(d), 15.5 and 19.2.
2.
The frequency and format of such reports by all Parties shall be determined by the Conference
of the Parties. Each Party shall make its initial report within two years of the entry into force of the
Convention for that Party.
3.
The Conference of the Parties, pursuant to Articles 22 and 26, shall consider arrangements to
assist developing country Parties and Parties with economies in transition, at their request, in meeting
their obligations under this Article.
4.
The reporting and exchange of information under the Convention shall be subject to national
law regarding confidentiality and privacy. The Parties shall protect, as mutually agreed, any
confidential information that is exchanged.
Article 22
Cooperation in the scientific, technical, and legalfields and provision ofrelated expertise
1.
The Parties shall cooperate directly or through competent international bodies to strengthen
their capacity to fulfill the obligations arising from this Convention, taking into account the needs of
developing country Parties and Parties with economies in transition. Such cooperation shall promote
the transfer of technical, scientific and legal expertise and technology, as mutually agreed, to establish
and strengthen national tobacco control strategies, plans and programmes aiming at, inter alia-.
(a)
facilitation of the development, transfer and acquisition of technology, knowledge, skills,
capacity and expertise related to tobacco control;
(b)
provision of technical, scientific, legal and other expertise to establish and strengthen
national tobacco control strategies, plans and programmes, aiming at implementation of the
Convention through, inter alia:
(i)
assisting, upon request, in the development of a strong legislative foundation as
well as technical programmes, including those on prevention of initiation, promotion of
cessation and protection from exposure to tobacco smoke;
18
Annex
WHA56.1
(ii)
assisting, as appropriate, tobacco workers in the development of appropriate
economically and legally viable alternative livelihoods in an economically viable manner;
and
(iii)
assisting, as appropriate, tobacco growers in shifting agricultural production to
alternative crops in an economically viable manner;
(c)
support for appropriate training or sensitization programmes for appropriate personnel in
accordance with Article 12;
(d)
provision, as appropriate, of the necessary material, equipment and supplies, as well as
logistical support, for tobacco control strategies, plans and programmes;
(e)
identification of methods for tobacco control, including comprehensive treatment of
nicotine addiction; and
(f)
promotion, as appropriate, of research to increase the affordability of comprehensive
treatment of nicotine addiction.
2.
The Conference of the Parties shall promote and facilitate transfer of technical, scientific and
legal expertise and technology with the financial support secured in accordance with Article 26.
PART VIII: INSTITUTIONAL ARRANGEMENTS AND FINANCIAL RESOURCES
Article 23
Conference of the Parties
1.
A Conference of the Parties is hereby established. The first session of the Conference shall be
convened by the World Health Organization not later than one year after the entry into force of this
Convention. The Conference will determine the venue and timing of subsequent regular sessions at its
first session.
2.
Extraordinary sessions of the Conference of the Parties shall be held at such other times as may
be deemed necessary by the Conference, or at the written request of any Party, provided that, within
six months of the request being communicated to them by the Secretariat of the Convention, it is
supported by at least one-third of the Parties.
3.
The Conference of the Parties shall adopt by consensus its Rules of Procedure at its first session.
4.
The Conference of the Parties shall by consensus adopt financial rules for itself as well as
governing the funding of any subsidiary bodies it may establish as well as financial provisions
governing the functioning of the Secretariat. At each ordinary session, it shall adopt a budget for the
financial period until the next ordinary session.
5.
The Conference of the Parties shall keep under regular review the implementation of the
Convention and take the decisions necessary to promote its effective implementation and may adopt
protocols, annexes and amendments to the Convention, in accordance with Articles 28, 29 and 33.
Towards this end, it shall:
19
WHA56.I
(a)
Annex
promote and facilitate the exchange of information pursuant to Articles 20 and 21;
(b)
promote and guide the development and periodic refinement of comparable
methodologies for research and the collection of data, in addition to those provided for in
Article 20, relevant to the implementation of the Convention;
(c)
promote, as appropriate, the development, implementation and evaluation of strategies,
plans, and programmes, as well as policies, legislation and other measures;
(d)
consider reports submitted by the Parties in accordance with Article 21 and adopt regular
reports on the implementation of the Convention;
(e)
promote and facilitate the mobilization of financial resources for the implementation of
the Convention in accordance with Article 26;
(f)
establish such subsidiary bodies as are necessary to achieve the objective of the
Convention;
(g)
request, where appropriate, the services and cooperation of, and information provided by,
competent and relevant organizations and bodies of the United Nations system and other
international and regional intergovernmental organizations and nongovernmental organizations
and bodies as a means of strengthening the implementation of the Convention; and
(h)
consider other action, as appropriate, for the achievement of the objective of the
Convention in the light of experience gained in its implementation.
6.
The Conference of the Parties shall establish the criteria for the participation of observers at its
proceedings.
Article 24
Secretariat
1.
The Conference of the Parties shall designate a permanent secretariat and make arrangements
for its functioning. The Conference of the Parties shall endeavour to do so at its first session.
2.
Until such time as a permanent secretariat is designated and established, secretariat functions
under this Convention shall be provided by the World Health Organization.
3.
Secretariat functions shall be:
(a)
to make arrangements for sessions of the Conference of the Parties and any subsidiary
bodies and to provide them with services as required;
(b)
to transmit reports received by it pursuant to the Convention;
(c)
to provide support to the Parties, particularly developing country Parties and Parties with
economies in transition, on request, in the compilation and communication of information
required in accordance with the provisions of the Convention;
20
Annex
WHA56.1
(d)
to prepare reports on its activities under the Convention under the guidance of the
Conference of the Parties and submit them to the Conference of the Parties;
(e)
to ensure, under the guidance of the Conference of the Parties, the necessary coordination
with the competent international and regional intergovernmental organizations and other bodies;
(f)
to enter, under the guidance of the Conference of the Parties, into such administrative or
contractual arrangements as may be required for the effective discharge of its functions; and
(g)
to perform other secretariat functions specified by the Convention and by any of its
protocols and such other functions as may be determined by the Conference of the Parties.
Article 25
Relations between the Conference of the Parties and intergovernmental organizations
In order to provide technical and financial cooperation for achieving the objective of this
Convention, the Conference of the Parties may request the cooperation of competent international and
regional intergovernmental organizations including financial and development institutions.
Article 26
Financial resources
1.
The Parties recognize the important role that financial resources play in achieving the objective
of this Convention.
2.
Each Party shall provide financial support in respect of its national activities intended to achieve
the objective of the Convention, in accordance with its national plans, priorities and programmes.
3.
Parties shall promote, as appropriate, the utilization of bilateral, regional, subregional and other
multilateral channels to provide funding for the development and strengthening of multisectoral
comprehensive tobacco control programmes of developing country Parties and Parties with economies
in transition. Accordingly, economically viable alternatives to tobacco production, including crop
diversification should be addressed and supported in the context of nationally developed strategies of
sustainable development.
4.
Parties represented in relevant regional and international intergovernmental organizations, and
financial and development institutions shall encourage these entities to provide financial assistance for
developing country Parties and for Parties with economies in transition to assist them in meeting their
obligations under the Convention, without limiting the rights of participation within these
organizations.
5.
The Parties agree that:
(a)
to assist Parties in meeting their obligations under the Convention, all relevant potential
and existing resources, financial, technical, or otherwise, both public and private that are
available for tobacco control activities, should be mobilized and utilized for the benefit of all
Parties, especially developing countries and countries with economies in transition;
21
WHA56.I
Annex
(b)
the Secretariat shall advise developing country Parties and Parties with economies in
transition, upon request, on available sources of funding to facilitate the implementation of their
obligations under the Convention;
(c)
the Conference of the Parties in its first session shall review existing and potential sources
and mechanisms of assistance based on a study conducted by the Secretariat and other relevant
information, and consider their adequacy; and
(d)
the results of this review shall be taken into account by the Conference of the Parties in
determining the necessity to enhance existing mechanisms or to establish a voluntary global
fund or other appropriate financial mechanisms to channel additional financial resources, as
needed, to developing country Parties and Parties with economies in transition to assist them in
meeting the objectives of the Convention.
PART IX: SETTLEMENT OF DISPUTES
Article 27
Settlement of disputes
1.
In the event of a dispute between two or more Parties concerning the interpretation or
application of this Convention, the Parties concerned shall seek through diplomatic channels a
settlement of the dispute through negotiation or any other peaceful means of their own choice,
including good offices, mediation, or conciliation. Failure to reach agreement by good offices,
mediation or conciliation shall not absolve parties to the dispute from the responsibility of continuing
to seek to resolve it.
2.
When ratifying, accepting, approving, formally confirming or acceding to the Convention, or at
any time thereafter, a State or regional economic integration organization may declare in writing to the
Depositary that, for a dispute not resolved in accordance with paragraph 1 of this Article, it accepts, as
compulsory, ad hoc arbitration in accordance with procedures to be adopted by consensus by the
Conference of the Parties.
3.
The provisions of this Article shall apply with respect to any protocol as between the parties to
the protocol, unless otherwise provided therein.
PART X: DEVELOPMENT OF THE CONVENTION
Article 28
Amendments to this Convention
1.
Any Party may propose amendments to this Convention. Such amendments will be considered
by the Conference of the Parties.
2.
Amendments to the Convention shall be adopted by the Conference of the Parties. The text of
any proposed amendment to the Convention shall be communicated to the Parties by the Secretariat at
least six months before the session at which it is proposed for adoption. The Secretariat shall also
22
Annex
WHA56.1
communicate proposed amendments to the signatories of the Convention and, for information, to the
Depositary.
3.
The Parties shall make every effort to reach agreement by consensus on any proposed
amendment to the Convention. If all efforts at consensus have been exhausted, and no agreement
reached, the amendment shall as a last resort be adopted by a three-quarters majority vote of the
Parties present and voting at the session. For purposes of this Article, Parties present and voting means
Parties present and casting an affirmative or negative vote. Any adopted amendment shall be
communicated by the Secretariat to the Depositary, who shall circulate it to all Parties for acceptance.
4.
Instruments of acceptance in respect of an amendment shall be deposited with the Depositary.
An amendment adopted in accordance with paragraph 3 of this Article shall enter into force for those
Parties having accepted it on the ninetieth day after the date of receipt by the Depositary of an
instrument of acceptance by at least two-thirds of the Parties to the Convention.
5.
The amendment shall enter into force for any other Party on the ninetieth day after the date on
which that Party deposits with the Depositary its instrument of acceptance of the said amendment.
Article 29
Adoption and amendment ofannexes to this Convention
1.
Annexes to this Convention and amendments thereto shall be proposed, adopted and shall enter
into force in accordance with the procedure set forth in Article 28.
2.
Annexes to the Convention shall form an integral part thereof and, unless otherwise expressly
provided, a reference to the Convention constitutes at the same time a reference to any annexes
thereto.
3.
Annexes shall be restricted to lists, forms and any other descriptive material relating to
procedural, scientific, technical or administrative matters.
PART XI: FINAL PROVISIONS
Article 30
Reservations
No reservations may be made to this Convention.
Article 31
Withdrawal
1.
At any time after two years from the date on which this Convention has entered into force for a
Party, that Party may withdraw from the Convention by giving written notification to the Depositary.
2.
Any such withdrawal shall take effect upon expiry of one year from the date of receipt by the
Depositary of the notification of withdrawal, or on such later date as may be specified in the
notification of withdrawal.
23
Annex
WHA56.I
3.
Any Party that withdraws from the Convention shall be considered as also having withdrawn
from any protocol to which it is a Party.
Article 32
Right to vote
1.
Each Party to this Convention shall have one vote, except as provided for in paragraph 2 of this
Article.
2.
Regional economic integration organizations, in matters within their competence, shall exercise
their right to vote with a number of votes equal to the number of their Member States that are Parties
to the Convention. Such an organization shall not exercise its right to vote if any of its Member States
exercises its right, and vice versa.
Article 33
Protocols
1.
Any Party may propose protocols. Such proposals will be considered by the Conference of the
Parties.
2.
The Conference of the Parties may adopt protocols to this Convention. In adopting these
protocols every effort shall be made to reach consensus. If all efforts at consensus have been
exhausted, and no agreement reached, the protocol shall as a last resort be adopted by a three-quarters
majority vote of the Parties present and voting at the session. For the purposes of this Article, Parties
present and voting means Parties present and casting an affirmative or negative vote.
3.
The text of any proposed protocol shall be communicated to the Parties by the Secretariat at
least six months before the session at which it is proposed for adoption.
4.
Only Parties to the Convention may be parties to a protocol.
5.
Any protocol to the Convention shall be binding only on the parties to the protocol in question.
Only Parties to a protocol may take decisions on matters exclusively relating to the protocol in
question.
6.
The requirements for entry into force of any protocol shall be established by that instrument.
Article 34
Signature
This Convention shall be open for signature by all Members of the World Health Organization
and by any States that are not Members of the World Health Organization but are members of the
United Nations and by regional economic integration organizations at the World Health Organization
Headquarters in Geneva from 16 June 2003 to 22 June 2003, and thereafter at United Nations
Headquarters in New York, from 30 June 2003 to 29 June 2004.
24
Annex
WHA56.1
Article 35
Ratification, acceptance, approval, formal confirmation or accession
1.
This Convention shall be subject to ratification, acceptance, approval or accession by States and
to formal confirmation or accession by regional economic integration organizations. It shall be open
for accession from the day after the date on which the Convention is closed for signature. Instruments
of ratification, acceptance, approval, formal confirmation or accession shall be deposited with the
Depositary.
2.
Any regional economic integration organization which becomes a Party to the Convention
without any of its Member States being a Party shall be bound by all the obligations under the
Convention. In the case of those organizations, one or more of whose Member States is a Party to the
Convention, the organization and its Member States shall decide on their respective responsibilities for
the performance of their obligations under the Convention. In such cases, the organization and the
Member States shall not be entitled to exercise rights under the Convention concurrently.
3.
Regional economic integration organizations shall, in their instruments relating to formal
confirmation or in their instruments of accession, declare the extent of their competence with respect
to the matters governed by the Convention. These organizations shall also inform the Depositary, who
shall in turn inform the Parties, of any substantial modification in the extent of their competence.
Article 36
Entry into force
1.
This Convention shall enter into force on the ninetieth day following the date of deposit of the
fortieth instrument of ratification, acceptance, approval, formal confirmation or accession with the
Depositary.
2.
For each State that ratifies, accepts or approves the Convention or accedes thereto after the
conditions set out in paragraph 1 of this Article for entry into force have been fulfilled, the Convention
shall enter into force on the ninetieth day following the date of deposit of its instrument of ratification,
acceptance, approval or accession.
3.
For each regional economic integration organization depositing an instrument of formal
confirmation or an instrument of accession after the conditions set out in paragraph 1 of this Article
for entry into force have been fulfilled, the Convention shall enter into force on the ninetieth day
following the date of its depositing of the instrument of formal confirmation or of accession.
4.
For the purposes of this Article, any instrument deposited by a regional economic integration
organization shall not be counted as additional to those deposited by States Members of the
organization.
Article 37
Depositary
The Secretary-General of the United Nations shall be the Depositary of this Convention and
amendments thereto and of protocols and annexes adopted in accordance with Articles 28, 29 and 33.
25
WHA56.1
Annex
Article 38
Authentic texts
The original of this Convention, of which the Arabic, Chinese, English, French, Russian and
Spanish texts are equally authentic, shall be deposited with the Secretary-General of the United
Nations.
IN WITNESS WHEREOF the undersigned, being duly authorized to that effect, have signed this
Convention.
DONE at GENEVA this [date of month] two thousand and three.
Fourth plenary meeting, 21 May 2003
A56/VR/4
26
)
FIFTY-SIXTH WORLD HEALTH ASSEMBLY
WHA56.2
Agenda item 4.1
21 May 2003
Appointment of the Director-General
The Fifty-sixth World Health Assembly,
On the nomination of the Executive Board,
APPOINTS Dr Jong-Wook Lee as Director-General of the World Health Organization.
Fifth plenary meeting, 21 May 2003
A56/VR/5
FIFTY-SIXTH WORLD HEALTH ASSEMBLY
WHA56.3
Agenda item 4.2
21 May 2003
Contract of the Director-General
The Fifty-sixth World Health Assembly,
I
Pursuant to Article 31 of the Constitution and Rule 109 of the Rules of Procedure of the World
Health Assembly,
APPROVES the contract establishing the terms and conditions of appointment, salary and other
emoluments for the post of Director-General;
II
Pursuant to Rule 112 of the Rules of Procedure of the World Health Assembly,
AUTHORIZES the President of the Fifty-sixth World Health Assembly to sign this contract in
the name of the Organization.
Fifth plenary meeting, 21 May 2003
A56/VR/5
FIFTY-SIXTH WORLD HEALTH ASSEMBLY
WHA56.4
Agenda item 4
21 May 2003
Expression of appreciation to
Dr Gro Harlem Brundtland
The Fifty-sixth World Health Assembly,
Expressing its profound gratitude to Dr Gro Harlem Brundtland for her outstanding and
visionary managerial, political and technical leadership, characterized by integrity, strength, endurance
and determination;
Appreciating her highly successful efforts to place issues of health and determinants of ill-health
at the centre of the global political agenda;
Commending her personal effort to establish evidence of the important role played by health in
economic development and poverty reduction;
Paying tribute to her challenge to society as a whole in her endeavours to achieve a healthy life
for all, with a special emphasis on underprivileged and vulnerable people;
Acclaiming her success in strengthening the role of WHO as the lead agency in health, in
constructive cooperation with others in the international community;
DECLARES Dr Gro Harlem Brundtland Director-General Emeritus of the World Health
Organization as from the date of her retirement.
Fifth plenary meeting, 21 May 2003
A56/VR/5
WORLD HEALTH ORGANIZATION
FIFTY-SIXTH WORLD HEALTH ASSEMBLY
Provisional agenda item 13
A56/8
10 April 2003
WHO Framework Convention on Tobacco Control
Note by the Secretariat
1.
As agreed at its sixth session (17 February to 1 March 2003), the Intergovernmental Negotiating
Body of the WHO Framework Convention on Tobacco Control submits herewith to the Fifty-sixth
World Health Assembly for its consideration the text of the proposed WHO Framework Convention
on Tobacco Control adopted at its final plenary meeting on 1 March 2003.
2.
Information on the proceedings of the Negotiating Body is contained in the report by the Chair.1
Details on the procedure to be followed for adoption, signature and ratification of the Convention is
set out in a separate document.23
ACTION BY THE HEALTH ASSEMBLY
3.
The Health Assembly is invited to consider the following draft resolution which has been
drafted by the Chair as agreed by the Negotiating Body at its final plenary meeting on 1 March, 2003?
The Fifty-sixth World Health Assembly,
Recalling its resolutions WHA49.17 and WHA52.18 calling for the development of a
WHO framework convention on tobacco control in accordance with Article 19 of the
Constitution of WHO;
Determined to protect present and future generations from tobacco consumption and
exposure to tobacco smoke;
Noting with profound concern the escalation in smoking and other forms of tobacco use
worldwide;
Acknowledging with appreciation the report of the Chair of the Intergovernmental
Negotiating Body on the outcome of the work of the Intergovernmental Negotiating Body;4
1 Document A56/INF.DOC./8.
2 Document A56/INF.DOC./2.
3 Document A/FCTC/INB6/PL/SR/4, section 3.
4 Document A56/INF.DOCJ7.
A 56/8
Convinced that this convention is a groundbreaking step in advancing national, regional
and international action and global cooperation to protect human health against the devastating
impact of tobacco consumption and exposure to tobacco smoke;
Mindful that special consideration should be given to the particular situation of
developing countries and countries with economies in transition;
Emphasizing the need for expeditious entry into force and effective implementation of the
convention,
1.
ADOPTS the WHO Framework Convention on Tobacco Control;
2.
CONFIRMS, in accordance with Article 34 of the Convention, that the Convention shall
be open for signature at WHO headquarters in Geneva, from 16 June 2003 to 22 June 2003, and
thereafter at United Nations headquarters in New York, from 30 June 2003 to 29 June 2004;
3.
CALLS UPON all States and regional economic integration organizations entitled to do
so, to consider signing, ratifying, accepting, approving, formally confirming or acceding to the
Convention at the earliest opportunity, with a view to bringing the Convention into force as
soon as possible;
4.
URGES all States and regional economic integration organizations, pending entry into
force of the Convention, to take all appropriate measures to curb tobacco consumption and
exposure to tobacco smoke;
5.
URGES all Member States, regional economic integration organizations, observers and
other interested parties to provide support for the preparatoiy activities referred to in this
resolution and effectively encourage prompt entry into force and implementation of the
Convention;
6.
CALLS UPON the United Nations Ad Hoc Interagency Task Force on Tobacco Control
to continue to provide support for strengthening national and international tobacco control
programmes;
7.
REQUESTS the Director-General:
(1)
to provide secretariat functions under the Convention until such time as a
permanent secretariat is designated and established;
(2)
to take all appropriate steps to provide support to Member States, in particular
developing countries and countries with economies in transition, in preparation for entry
into force of the Convention;
(3)
to continue to ensure that WHO plays a key role in providing technical leadership,
direction and support for global tobacco control;
(4)
to keep the Health Assembly informed of progress made toward entry into force of
the Convention and of preparations under way for the first session of the Conference of
the Parties.
2
A56/8
ANNEX
WHO Framework Convention on Tobacco Control
Preamble
The Parties to this Convention,
Determined to give priority to their right to protect public health,
Recognizing that the spread of the tobacco epidemic is a global problem with serious
consequences for public health that calls for the widest possible international cooperation and the
participation of all countries in an effective, appropriate and comprehensive international response,
Reflecting the concern of the international community about the devastating worldwide health,
social, economic and environmental consequences of tobacco consumption and exposure to tobacco
smoke,
Seriously concerned about the increase in the worldwide consumption and production of
cigarettes and other tobacco products, particularly in developing countries, as well as about the burden
this places on families, on the poor, and on national health systems,
Recognizing that scientific evidence has unequivocally established that tobacco consumption
and exposure to tobacco smoke cause death, disease and disability, and that there is a time lag between
the exposure to smoking and the other uses of tobacco products and the onset of tobacco-related
diseases,
Recognizing also that cigarettes and some other products containing tobacco are highly
engineered so as to create and maintain dependence, and that many of the compounds they contain and
the smoke they produce are pharmacologically active, toxic, mutagenic and carcinogenic, and that
tobacco dependence is separately classified as a disorder in major international classifications of
diseases,
Acknowledging that there is clear scientific evidence that prenatal exposure to tobacco smoke
causes adverse health and developmental conditions for children,
Deeply concerned about the escalation in smoking and other forms of tobacco consumption by
children and adolescents worldwide, particularly smoking at increasingly early ages,
Alarmed by the increase in smoking and other forms of tobacco consumption by women and
young girls worldwide and keeping in mind the need for full participation of women at all levels of
policy-making and implementation and the need for gender-specific tobacco control strategies,
Deeply concerned about the high levels of smoking and other forms of tobacco consumption by
indigenous peoples,
Seriously concerned about the impact of all forms of advertising, promotion and sponsorship
aimed at encouraging the use of tobacco products,
Annex
A 5 6/8
Recognizing that cooperative action is necessary to eliminate all forms of illicit trade in
cigarettes and other tobacco products, including smuggling, illicit manufacturing and counterfeiting,
Acknowledging that tobacco control at all levels and particularly in developing countries and in
countries with economies in transition requires sufficient financial and technical resources
commensurate with the current and projected need for tobacco control activities,
Recognizing the need to develop appropriate mechanisms to address the long-term social and
economic implications of successful tobacco demand reduction strategies,
Mindful of the social and economic difficulties that tobacco control programmes may engender
in the medium and long term in some developing countries and countries with economies in transition,
and recognizing their need for technical and financial assistance in the context of nationally developed
strategies for sustainable development,
Conscious of the valuable work being conducted by many States on tobacco control and
commending the leadership of the World Health Organization as well as the efforts of other
organizations and bodies of the United Nations system and other international and regional
intergovernmental organizations in developing measures on tobacco control,
Emphasizing the special contribution of nongovernmental organizations and other members of
civil society not affiliated with the tobacco industry, including health professional bodies, women’s,
youth, environmental and consumer groups, and academic and health care institutions, to tobacco
control efforts nationally and internationally and the vital importance of their participation in national
and international tobacco control efforts,
Recognizing the need to be alert to any efforts by the tobacco industry to undermine or subvert
tobacco control efforts and the need to be informed of activities of the tobacco industry that have a
negative impact on tobacco control efforts,
Recalling Article 12 of the International Covenant on Economic, Social and Cultural Rights,
adopted by the United Nations General Assembly on 16 December 1966, which states that it is the
right of everyone to the enjoyment of the highest attainable standard of physical and mental health,
Recalling also the preamble to the Constitution of the World Health Organization, which states
that the enjoyment of the highest attainable standard of health is one of the fundamental rights of every
human being without distinction of race, religion, political belief, economic or social condition,
Determined to promote measures of tobacco control based on current and relevant scientific,
technical and economic considerations,
Recalling that the Convention on the Elimination of All Forms of Discrimination against
Women, adopted by the United Nations General Assembly on 18 December 1979, provides that States
Parties to that Convention shall take appropriate measures to eliminate discrimination against women
in the field of health care,
Recallingfurther that the Convention on the Rights of the Child, adopted by the United Nations
General Assembly on 20 November 1989, provides that States Parties to that Convention recognize
the right of the child to the enjoyment of the highest attainable standard of health,
Have agreed, as follows:
A 56/8
Annex
PART I: INTRODUCTION
Article 1
Use of terms
For the purposes of this Convention:
(a)
“illicit trade” means any practice or conduct prohibited by law and which relates to
production, shipment, receipt, possession, distribution, sale or purchase including any practice
or conduct intended to facilitate such activity;
(b)
“regional economic integration organization” means an organization that is composed of
several sovereign states, and to which its Member States have transferred competence over a
range of matters, including the authority to make decisions binding on its Member States in
respect of those matters;1
(c)
“tobacco advertising and promotion” means any form of commercial communication,
recommendation or action with the aim, effect or likely effect of promoting a tobacco product or
tobacco use either directly or indirectly;
(d)
“tobacco control” means a range of supply, demand and harm reduction strategies that
aim to improve the health of a population by eliminating or reducing their consumption of
tobacco products and exposure to tobacco smoke;
(e)
“tobacco industry” means tobacco manufacturers, wholesale distributors and importers of
tobacco products;
(f)
“tobacco products” means products entirely or partly made of the leaf tobacco as raw
material which are manufactured to be used for smoking, sucking, chewing or snuffing;
(g)
“tobacco sponsorship” means any form of contribution to any event, activity or individual
with the aim, effect or likely effect of promoting a tobacco product or tobacco use either directly
or indirectly;
Article 2
Relationship between this Convention and other agreements and legal instruments
1.
In order to better protect human health, Parties are encouraged to implement measures beyond
those required by this Convention and its protocols, and nothing in these instruments shall prevent a
Party from imposing stricter requirements that are consistent with their provisions and are in
accordance with international law.
2.
The provisions of the Convention and its protocols shall in no way affect the right of Parties to
enter into bilateral or multilateral agreements, including regional or subregional agreements, on issues
relevant or additional to the Convention and its protocols, provided that such agreements are
compatible with their obligations under the Convention and its protocols. The Parties concerned shall
communicate such agreements to the Conference of the Parties through the Secretariat.
1 Where appropriate, national will refer equally to regional economic integration organizations.
A56/8
Annex
PART II: OBJECTIVE, GUIDING PRINCIPLES AND GENERAL OBLIGATIONS
Article 3
Objective
The objective of this Convention and its protocols is to protect present and future generations
from the devastating health, social, environmental and economic consequences of tobacco
consumption and exposure to tobacco smoke by providing a framework for tobacco control measures
to be implemented by the Parties at the national, regional and international levels in order to reduce
continually and substantially the prevalence of tobacco use and exposure to tobacco smoke.
Article 4
Guiding principles
To achieve the objective of this Convention and its protocols and to implement its provisions,
the Parties shall be guided, inter alia, by the principles set out below:
1.
Every person should be informed of the health consequences, addictive nature and mortal threat
posed by tobacco consumption and exposure to tobacco smoke and effective legislative, executive,
administrative or other measures should be contemplated at the appropriate governmental level to
protect all persons from exposure to tobacco smoke.
2.
Strong political commitment is necessary to develop and support, at the national, regional and
international levels, comprehensive multisectoral measures and coordinated responses, taking into
consideration:
(a)
the need to take measures to protect all persons from exposure to tobacco smoke;
(b)
the need to take measures to prevent the initiation, to promote and support cessation, and
to decrease the consumption of tobacco products in any form;
(c)
the need to take measures to promote the participation of indigenous individuals and
communities in the development, implementation and evaluation of tobacco control
programmes that are socially and culturally appropriate to their needs and perspectives; and
(d)
the need to take measures to address gender-specific risks when developing tobacco
control strategies.
3.
International cooperation, particularly transfer of technology, knowledge and financial
assistance and provision of related expertise, to establish and implement effective tobacco control
programmes, taking into consideration local culture, as well as social, economic, political and legal
factors, is an important part of the Convention.
4.
Comprehensive multisectoral measures and responses to reduce consumption of all tobacco
products at the national, regional and international levels are essential so as to prevent, in accordance
with public health principles, the incidence of diseases, premature disability and mortality due to
tobacco consumption and exposure to tobacco smoke.
5.
Issues relating to liability, as determined by each Party within its jurisdiction, are an important
part of comprehensive tobacco control.
6
A 56/8
Annex
6.
The importance of technical and financial assistance to aid the economic transition of tobacco
growers and workers whose livelihoods are seriously affected as a consequence of tobacco control
programmes in developing country Parties, as well as Parties with economies in transition, should be
recognized and addressed in the context of nationally developed strategies for sustainable
development.
7.
The participation of civil society is essential in achieving the objective of the Convention and its
protocols.
Article 5
General obligations
1.
Each Party shall develop, implement, periodically update and review comprehensive
multisectoral national tobacco control strategies, plans and programmes in accordance with this
Convention and the protocols to which it is a Party.
2.
Towards this end, each Party shall, in accordance with its capabilities:
(a)
establish or reinforce and finance a national coordinating mechanism or focal points for
tobacco control; and
(b)
adopt and implement effective legislative, executive, administrative and/or other
measures and cooperate, as appropriate, with other Parties in developing appropriate policies for
preventing and reducing tobacco consumption, nicotine addiction and exposure to tobacco
smoke.
3.
In setting and implementing their public health policies with respect to tobacco control, Parties
shall act to protect these policies from commercial and other vested interests of the tobacco industry in
accordance with national law.
4.
The Parties shall cooperate in the formulation of proposed measures, procedures and guidelines
for the implementation of the Convention and the protocols to which they are Parties.
5.
The Parties shall cooperate, as appropriate, with competent international and regional
intergovernmental organizations and other bodies to achieve the objectives of the Convention and the
protocols to which they are Parties.
6.
The Parties shall, within means and resources at their disposal, cooperate to raise financial
resources for effective implementation of the Convention through bilateral and multilateral funding
mechanisms.
PART III: MEASURES RELATING TO THE REDUCTION
OF DEMAND FOR TOBACCO
Article 6
Price and tax measures to reduce the demandfor tobacco
1.
The Parties recognize that price and tax measures are an effective and important means of
reducing tobacco consumption by various segments of the population, in particular young persons.
7
A 56/8
Annex
2.
Without prejudice to the sovereign right of the Parties to determine and establish their taxation
policies, each Party should take account of its national health objectives concerning tobacco control
and adopt or maintain, as appropriate, measures which may include:
(a)
implementing tax policies and, where appropriate, price policies, on tobacco products so
as to contribute to the health objectives aimed at reducing tobacco consumption; and
(b)
prohibiting or restricting, as appropriate, sales to and/or importations by international
travellers of tax- and duty-free tobacco products.
3.
The Parties shall provide rates of taxation for tobacco products and trends in tobacco
consumption in their periodic reports to the Conference of the Parties, in accordance with Article 21.
Article 7
Non-price measures to reduce the demandfor tobacco
The Parties recognize that comprehensive non-price measures are an effective and important
means of reducing tobacco consumption. Each Party shall adopt and implement effective legislative,
executive, administrative or other measures necessary to implement its obligations pursuant to
Articles 8 to 13 and shall cooperate, as appropriate, with each other directly or through competent
international bodies with a view to their implementation. The Conference of the Parties shall propose
appropriate guidelines for the implementation of the provisions of these Articles.
Article 8
Protection from exposure to tobacco smoke
1.
Parties recognize that scientific evidence has unequivocally established that exposure to tobacco
smoke causes death, disease and disability.
2.
Each Party shall adopt and implement in areas of existing national jurisdiction as determined by
national law and actively promote at other jurisdictional levels the adoption and implementation of
effective legislative, executive, administrative and/or other measures, providing for protection from
exposure to tobacco smoke in indoor workplaces, public transport, indoor public places and, as
appropriate, other public places.
Article 9
Regulation of the contents of tobacco products
The Conference of the Parties, in consultation with competent international bodies, shall
propose guidelines for testing and measuring the contents and emissions of tobacco products, and for
the regulation of these contents and emissions. Each Party shall, where approved by competent
national authorities, adopt and implement effective legislative, executive and administrative or other
measures for such testing and measuring, and for such regulation.
Article 10
Regulation oftobacco product disclosures
Each Party shall, in accordance with its national law, adopt and implement effective legislative,
executive, administrative or other measures requiring manufacturers and importers of tobacco products
to disclose to governmental authorities information about the contents and emissions of tobacco
8
A 56/8
Annex
products. Each Party shall further adopt and implement effective measures for public disclosure of
information about the toxic constituents of the tobacco products and the emissions that they may
produce.
Article 11
Packaging and labelling oftobacco products
1.
Each Party shall, within a period of three years after entry into force of this Convention for that
Party, adopt and implement, in accordance with its national law, effective measures to ensure that:
(a)
tobacco product packaging and labelling do not promote a tobacco product by any means
that are false, misleading, deceptive or likely to create an erroneous impression about its
characteristics, health effects, hazards or emissions, including any term, descriptor, trademark,
figurative or any other sign that directly or indirectly creates the false impression that a
particular tobacco product is less harmful than other tobacco products. These may include terms
such as “low tar”, “light”, “ultra-light”, or “mild”; and
(b)
each unit packet and package of tobacco products and any outside packaging and
labelling of such products also carry health warnings describing the harmful effects of tobacco
use, and may include other appropriate messages. These warnings and messages:
(i)
shall be approved by the competent national authority,
(ii)
shall be rotating,
(iii)
shall be large, clear, visible and legible,
(iv)
should be 50% or more of the principal display areas but shall be no less than 30%
of the principal display areas,
(v)
may be in the form of or include pictures or pictograms.
2.
Each unit packet and package of tobacco products and any outside packaging and labelling of
such products shall, in addition to the warnings specified in paragraph 1(b) of this Article, contain
information on relevant constituents and emissions of tobacco products as defined by national
authorities.
3.
Each Party shall require that the warnings and other textual information specified in
paragraphs 1(b) and paragraph 2 of this Article will appear on each unit packet and package of tobacco
products and any outside packaging and labelling of such products in its principal language or
languages.
4.
For the purposes of this Article, the term “outside packaging and labelling” in relation to
tobacco products applies to any packaging and labelling used in the retail sale of the product.
9
Annex
456/8
Article 12
Education, communication, training and public awareness
Each Party shall promote and strengthen public awareness of tobacco control issues, using all
available communication tools, as appropriate. Towards this end, each Party shall adopt and
implement effective legislative, executive, administrative or other measures to promote:
(a)
broad access to effective and comprehensive educational and public awareness
programmes on the health risks including the addictive characteristics of tobacco consumption
and exposure to tobacco smoke;
(b)
public awareness about the health risks of tobacco consumption and exposure to tobacco
smoke, and about the benefits of the cessation of tobacco use and tobacco-free lifestyles as
specified in Article 14.2;
(c)
public access, in accordance with national law, to a wide range of information on the
tobacco industry as relevant to the objective of this Convention;
(d)
effective and appropriate training or sensitization and awareness programmes on tobacco
control addressed to persons such as health workers, community workers, social workers, media
professionals, educators, decision-makers, administrators and other concerned persons;
(e)
awareness and participation of public and private agencies and nongovernmental
organizations not affiliated with the tobacco industry in developing and implementing
intersectoral programmes and strategies for tobacco control; and
(f)
public awareness of and access to information regarding the adverse health, economic,
and environmental consequences of tobacco production and consumption.
Article 13
Tobacco advertising, promotion and sponsorship
1.
Parties recognize that a comprehensive ban on advertising, promotion and sponsorship would
reduce the consumption of tobacco products.
2.
Each Party shall, in accordance with its constitution or constitutional principles, undertake a
comprehensive ban of all tobacco advertising, promotion and sponsorship. This shall include, subject
to the legal environment and technical means available to that Party, a comprehensive ban on crossborder advertising, promotion and sponsorship originating from its territory. In this respect, within the
period of five years after entry into force of this Convention for that Party, each Party shall undertake
appropriate legislative, executive, administrative and/or other measures and report accordingly in
conformity with Article 21.
3.
A Party that is not in a position to undertake a comprehensive ban due to its constitution or
constitutional principles shall apply restrictions on all tobacco advertising, promotion and sponsorship.
This shall include, subject to the legal environment and technical means available to that Party,
restrictions or a comprehensive ban on advertising, promotion and sponsorship originating from its
territory with cross-border effects. In this respect, each Party shall undertake appropriate legislative,
executive, administrative and/or other measures and report accordingly in conformity with Article 21.
10
Annex
A56/8
4.
As a minimum, and in accordance with its constitution or constitutional principles, each Party
shall:
(a)
prohibit all forms of tobacco advertising, promotion and sponsorship that promote a
tobacco product by any means that are false, misleading or deceptive or likely to create an
erroneous impression about its characteristics, health effects, hazards or emissions;
(b)
require that health or other appropriate warnings or messages accompany all tobacco
advertising and, as appropriate, promotion and sponsorship;
(c)
restrict the use of direct or indirect incentives that encourage the purchase of tobacco
products by the public;
(d)
require, if it does not have a comprehensive ban, the disclosure to relevant governmental
authorities of expenditures by the tobacco industry on advertising, promotion and sponsorship
not yet prohibited. Those authorities may decide to make those figures available, subject to
national law, to the public and to the Conference of the Parties, pursuant to Article 21;
(e)
undertake a comprehensive ban or, in the case of a Party that is not in a position to
undertake a comprehensive ban due to its constitution or constitutional principles, restrict
tobacco advertising, promotion and sponsorship on radio, television, print media and, as
appropriate, other media, such as the internet, within a period of five years; and
(f)
prohibit, or in the case of a Party that is not in a position to prohibit due to its constitution
or constitutional principles restrict, tobacco sponsorship of international events, activities and/or
participants therein.
5.
Parties are encouraged to implement measures beyond the obligations set out in paragraph 4.
Parties shall cooperate in the development of technologies and other means necessary to
6.
facilitate the elimination of cross-border advertising.
7.
Parties which have a ban on certain forms of tobacco advertising, promotion and sponsorship
have the sovereign right to ban those forms of cross-border tobacco advertising, promotion and
sponsorship entering their territory and to impose equal penalties as those applicable to domestic
advertising, promotion and sponsorship originating from their territory in accordance with their
national law. This paragraph does not endorse or approve of any particular penalty.
8.
Parties shall consider the elaboration of a protocol setting out appropriate measures that require
international collaboration for a comprehensive ban on cross-border advertising, promotion and
sponsorship.
Article 14
Demand reduction measures concerning tobacco dependence and cessation
1.
Each Party shall develop and disseminate appropriate, comprehensive and integrated guidelines
based on scientific evidence and best practices, taking into account national circumstances and
priorities, and shall take effective measures to promote cessation of tobacco use and adequate
treatment for tobacco dependence.
11
A56/8
2.
Annex
Towards this end, each Party shall endeavour to:
(a)
design and implement effective programmes aimed at promoting the cessation of tobacco
use, in such locations as educational institutions, health care facilities, workplaces and sporting
environments;
(b)
include diagnosis and treatment of tobacco dependence and counselling services on
cessation of tobacco use in national health and education programmes, plans and strategies, with
the participation of health workers, community workers and social workers as appropriate;
(c)
establish in health care facilities and rehabilitation centres programmes for diagnosing,
counselling, preventing and treating tobacco dependence; and
(d)
collaborate with other Parties to facilitate accessibility and affordability for treatment of
tobacco dependence including pharmaceutical products pursuant to Article 22. Such products
and their constituents may include medicines, products used to administer medicines and
diagnostics when appropriate.
PART IV: MEASURES RELATING TO THE REDUCTION
OF THE SUPPLY OF TOBACCO
Article 15
Illicit trade in tobacco products'
1.
The Parties recognize that the elimination of all forms of illicit trade in tobacco products,
including smuggling, illicit manufacturing and counterfeiting, and the development and
implementation of related national law, in addition to subregional, regional and global agreements, are
essential components of tobacco control.
2.
Each Party shall adopt and implement effective legislative, executive, administrative or other
measures to ensure that all unit packets and packages of tobacco products and any outside packaging
of such products are marked to assist Parties in determining the origin of tobacco products, and in
accordance with national law and relevant bilateral or multilateral agreements, assist Parties in
determining the point of diversion and monitor, document and control the movement of tobacco
products and their legal status. In addition, each Party shall:
(a)
require that unit packets and packages of tobacco products for retail and wholesale use
that are sold on its domestic market carry the statement: “Sales only allowed in (insert name of
the country, subnational, regional or federal unit)" or carry any other effective marking
indicating the final destination or which would assist authorities in determining whether the
product is legally for sale on the domestic market; and
(b)
consider, as appropriate, developing a practical tracking and tracing regime that would
further secure the distribution system and assist in the investigation of illicit trade.
1 There has been considerable discussion throughout the pre-negotiation and negotiation process concerning the
adoption of an early protocol on illicit trade in tobacco products. The negotiation of such a protocol could be initiated by the
INB immediately following the adoption of the FCTC, or at a later stage by the Conference of the Parties.
12
Annex
A56/8
3.
Each Party shall require that the packaging information or marking specified in paragraph 2 of
this Article shall be presented in legible form and/or appear in its principal language or languages.
4.
With a view to eliminating illicit trade in tobacco products, each Party shall:
(a)
monitor and collect data on cross-border trade in tobacco products, including illicit trade,
and exchange information among customs, tax and other authorities, as appropriate, and in
accordance with national law and relevant applicable bilateral or multilateral agreements;
(b)
enact or strengthen legislation, with appropriate penalties and remedies, against illicit
trade in tobacco products, including counterfeit and contraband cigarettes;
(c)
take appropriate steps to ensure that all confiscated manufacturing equipment, counterfeit
and contraband cigarettes and other tobacco products are destroyed, using environmentallyfriendly methods where feasible, or disposed of in accordance with national law;
(d)
adopt and implement measures to monitor, document and control the storage and
distribution of tobacco products held or moving under suspension of taxes or duties within its
jurisdiction; and
(e)
adopt measures as appropriate to enable the confiscation of proceeds derived from the
illicit trade in tobacco products.
5.
Information collected pursuant to subparagraphs 4(a) and 4(d) of this Article shall, as
appropriate, be provided in aggregate form by the Parties in their periodic reports to the Conference of
the Parties, in accordance with Article 21.
6.
The Parties shall, as appropriate and in accordance with national law, promote cooperation
between national agencies, as well as relevant regional and international intergovernmental
organizations as it relates to investigations, prosecutions and proceedings, with a view to eliminating
illicit trade in tobacco products. Special emphasis shall be placed on cooperation at regional and
subregional levels to combat illicit trade of tobacco products.
7.
Each Party shall endeavour to adopt and implement further measures including licensing, where
appropriate, to control or regulate the production and distribution of tobacco products in order to
prevent illicit trade.
Article 16
Sales to and by minors
1.
Each Party shall adopt and implement effective legislative, executive, administrative or other
measures at the appropriate government level to prohibit the sales of tobacco products to persons
under the age set by domestic law, national law or eighteen. These measures may include:
(a)
requiring that all sellers of tobacco products place a clear and prominent indicator inside
their point of sale about the prohibition of tobacco sales to minors and, in case of doubt, request
that each tobacco purchaser provide appropriate evidence of having reached full legal age;
(b)
banning the sale of tobacco products in any manner by which they are directly accessible,
such as store shelves;
13
AS6/8
Annex
(c)
prohibiting the manufacture and sale of sweets, snacks, toys or any other objects in the
form of tobacco products which appeal to minors; and
(d)
ensuring that tobacco vending machines under its jurisdiction are not accessible to minors
and do not promote the sale of tobacco products to minors.
2.
Each Party shall prohibit or promote the prohibition of the distribution of free tobacco products
to the public and especially minors.
3.
Each Party shall endeavour to prohibit the sale of cigarettes individually or in small packets
which increase the affordability of such products to minors.
4.
The Parties recognize that in order to increase their effectiveness, measures to prevent tobacco
product sales to minors should, where appropriate, be implemented in conjunction with other
provisions contained in this Convention.
5.
When signing, ratifying, accepting, approving or acceding to the Convention or at any time
thereafter, a Party may, by means of a binding written declaration, indicate its commitment to prohibit
the introduction of tobacco vending machines within its jurisdiction or, as appropriate, to a total ban
on tobacco vending machines. The declaration made pursuant to this Article shall be circulated by the
Depositary to all Parties to the Convention.
6.
Each Party shall adopt and implement effective legislative, executive, administrative or other
measures, including penalties against sellers and distributors, in order to ensure compliance with the
obligations contained in paragraphs 1-5 of this Article.
7.
Each Party should, as appropriate, adopt and implement effective legislative, executive,
administrative or other measures to prohibit the sales of tobacco products by persons under the age set
by domestic law, national law or eighteen.
Article 17
Provision ofsupport for economically viable alternative activities
Parties shall, in cooperation with each other and with competent international and regional
intergovernmental organizations, promote, as appropriate, economically viable alternatives for tobacco
workers, growers and, as the case may be, individual sellers.
PART V: PROTECTION OF THE ENVIRONMENT
Article 18
Protection of the environment and the health ofpersons
In carrying out their obligations under this Convention, the Parties agree to have due regard to
the protection of the environment and the health of persons in relation to the environment in respect of
tobacco cultivation and manufacture within their respective territories.
14
Annex
A 56/8
PART VI: QUESTIONS RELATED TO LIABILITY
Article 19
Liability
1.
For the purpose of tobacco control, the Parties shall consider taking legislative action or
promoting their existing laws, where necessary, to deal with criminal and civil liability, including
compensation where appropriate.
2.
Parties shall cooperate with each other in exchanging information through the Conference of the
Parties in accordance with Article 21 including:
(a)
information on the health effects of the consumption of tobacco products and exposure to
tobacco smoke in accordance with Article 20.3(a); and
(b)
information on legislation and regulations in force as well as pertinent jurisprudence.
3.
The Parties shall, as appropriate and mutually agreed, within the limits of national legislation,
policies, legal practices and applicable existing treaty arrangements, afford one another assistance in
legal proceedings relating to civil and criminal liability consistent with this Convention.
4.
The Convention shall in no way affect or limit any rights of access of the Parties to each other’s
courts where such rights exist.
5.
The Conference of the Parties may consider, if possible, at an early stage, taking account of the
work being done in relevant international fora, issues related to liability including appropriate
international approaches to these issues and appropriate means to support, upon request, the Parties in
their legislative and other activities in accordance with this Article.
PART VII: SCIENTIFIC AND TECHNICAL COOPERATION AND
COMMUNICATION OF INFORMATION
Article 20
Research, surveillance and exchange of information
1.
The Parties undertake to develop and promote national research and to coordinate research
programmes at the regional and international levels in the field of tobacco control. Towards this end,
each Party shall:
(a)
initiate and cooperate in, directly or through competent international and regional
intergovernmental organizations and other bodies, the conduct of research and scientific
assessments, and in so doing promote and encourage research that addresses the determinants
and consequences of tobacco consumption and exposure to tobacco smoke as well as research
for identification of alternative crops; and
(b)
promote and strengthen, with the support of competent international and regional
intergovernmental organizations and other bodies, training and support for all those engaged in
tobacco control activities, including research, implementation and evaluation.
15
A 56/8
Annex
2.
The Parties shall establish, as appropriate, programmes for national, regional and global
surveillance of the magnitude, patterns, determinants and consequences of tobacco consumption and
exposure to tobacco smoke. Towards this end, the Parties should integrate tobacco surveillance
programmes into national, regional and global health surveillance programmes so that data are
comparable and can be analysed at the regional and international levels, as appropriate.
3.
Parties recognize the importance of financial and technical assistance from international and
regional intergovernmental organizations and other bodies. Each Party shall endeavour to:
(a)
establish progressively a national system for the epidemiological surveillance of tobacco
consumption and related social, economic and health indicators;
(b)
cooperate with competent international and regional intergovernmental organizations and
other bodies, including governmental and nongovernmental agencies, in regional and global
tobacco surveillance and exchange of information on the indicators specified in paragraph 3(a)
of this Article; and
(c)
cooperate with the World Health Organization in the development of general guidelines
or procedures for defining the collection, analysis and dissemination of tobacco-related
surveillance data.
4.
The Parties shall, subject to national law, promote and facilitate the exchange of publicly
available scientific, technical, socioeconomic, commercial and legal information, as well as
information regarding practices of the tobacco industry and the cultivation of tobacco, which is
relevant to this Convention, and in so doing shall take into account and address the special needs of
developing country Parties and Parties with economies in transition. Each Party shall endeavour to:
(a)
progressively establish and maintain an updated database of laws and regulations on
tobacco control and, as appropriate, information about their enforcement, as well as pertinent
jurisprudence, and cooperate in the development of programmes for regional and global tobacco
control;
(b)
progressively establish and maintain updated data from national surveillance programmes
in accordance with paragraph 3(a) of this Article; and
(c)
cooperate with competent international organizations to progressively establish and
maintain a global system to regularly collect and disseminate information on tobacco
production, manufacture and the activities of the tobacco industry which have an impact on the
Convention or national tobacco control activities.
5.
Parties should cooperate in regional and international intergovernmental organizations and
financial and development institutions of which they are members, to promote and encourage
provision of technical and financial resources to the Secretariat to assist developing country Parties
and Parties with economies in transition to meet their commitments on research, surveillance and
exchange of information.
16
Annex
A 56/8
Article 21
Reporting and exchange of information
1.
Each Party shall submit to the Conference of the Parties, through the Secretariat, periodic
reports on its implementation of this Convention, which should include the following:
(a)
information on legislative, executive, administrative or other measures taken to
implement the Convention;
(b)
information, as appropriate, on any constraints or barriers encountered in
implementation of the Convention, and on the measures taken to overcome these barriers;
its
(c)
information, as appropriate, on financial and technical assistance provided or received for
tobacco control activities;
(d)
information on surveillance and research as specified in Article 20; and
(e)
information specified in Articles 6.3, 13.2,13.3, 13.4(d), 15.5 and 19.2.
2.
The frequency and format of such reports by all Parties shall be determined by the Conference
of the Parties. Each Party shall make its initial report within two years of the entry into force of the
Convention for that Party.
3.
The Conference of the Parties, pursuant to Articles 22 and 26, shall consider arrangements to
assist developing country Parties and Parties with economies in transition, at their request, in meeting
their obligations under this Article.
4.
The reporting and exchange of information under the Convention shall be subject to national
law regarding confidentiality and privacy. The Parties shall protect, as mutually agreed, any
confidential information that is exchanged.
Article 22
Cooperation in the scientific, technical, and legalfields and provision ofrelated expertise
1.
The Parties shall cooperate directly or through competent international bodies to strengthen their
capacity to fulfill the obligations arising from this Convention, taking into account the needs of
developing country Parties and Parties with economies in transition. Such cooperation shall promote
the transfer of technical, scientific and legal expertise and technology, as mutually agreed, to establish
and strengthen national tobacco control strategies, plans and programmes aiming at, inter alia'.
(a)
facilitation of the development, transfer and acquisition of technology, knowledge, skills,
capacity and expertise related to tobacco control;
(b)
provision of technical, scientific, legal and other expertise to establish and strengthen
national tobacco control strategies, plans and programmes, aiming at implementation of the
Convention through, inter alia:
(i)
assisting, upon request, in the development of a strong legislative foundation as
well as technical programmes, including those on prevention of initiation, promotion of
cessation and protection from exposure to tobacco smoke;
17
A 56/8
Annex
(ii)
assisting, as appropriate, tobacco workers in the development of appropriate
economically and legally viable alternative livelihoods in an economically viable manner;
and
(iii)
assisting, as appropriate, tobacco growers in shifting agricultural production to
alternative crops in an economically viable manner;
(c)
support for appropriate training or sensitization programmes for appropriate personnel in
accordance with Article 12;
(d)
provision, as appropriate, of the necessary material, equipment and supplies, as well as
logistical support, for tobacco control strategies, plans and programmes;
(e)
identification of methods for tobacco control, including comprehensive treatment of
nicotine addiction; and
(f)
promotion, as appropriate, of research to increase the affordability of comprehensive
treatment of nicotine addiction.
2.
The Conference of the Parties shall promote and facilitate transfer of technical, scientific and
legal expertise and technology with the financial support secured in accordance with Article 26.
PART VIII: INSTITUTIONAL ARRANGEMENTS AND FINANCIAL RESOURCES
Article 23
Conference of the Parties
1.
A Conference of the Parties is hereby established. The first session of the Conference shall be
convened by the World Health Organization not later than one year after the entry into force of this
Convention. The Conference will determine the venue and timing of subsequent regular sessions at its
first session.
2.
Extraordinary sessions of the Conference of the Parties shall be held at such other times as may
be deemed necessary by the Conference, or at the written request of any Party, provided that, within
six months of the request being communicated to them by the Secretariat of the Convention, it is
supported by at least one-third of the Parties.
3.
The Conference of the Parties shall adopt by consensus its Rules of Procedure at its first session.
4.
The Conference of the Parties shall by consensus adopt financial rules for itself as well as
governing the funding of any subsidiary bodies it may establish as well as financial provisions
governing the functioning of the Secretariat. At each ordinary session, it shall adopt a budget for the
financial period until the next ordinary session.
5.
The Conference of the Parties shall keep under regular review the implementation of the
Convention and take the decisions necessary to promote its effective implementation and may adopt
protocols, annexes and amendments to the Convention, in accordance with Articles 28, 29 and 33.
Towards this end, it shall:
18
Annex
A 5 6/8
(a)
promote and facilitate the exchange of information pursuant to Articles 20 and 21;
(b)
promote and guide the development and periodic refinement of comparable
methodologies for research and the collection of data, in addition to those provided for in
Article 20, relevant to the implementation of the Convention;
(c)
promote, as appropriate, the development, implementation and evaluation of strategies,
plans, and programmes, as well as policies, legislation and other measures;
(d)
consider reports submitted by the Parties in accordance with Article 21 and adopt regular
reports on the implementation of the Convention;
(e)
promote and facilitate the mobilization of financial resources for the implementation of
the Convention in accordance with Article 26;
(f)
establish such subsidiary bodies as are necessary to achieve the objective of the
Convention;
(g)
request, where appropriate, the services and cooperation of, and information provided by,
competent and relevant organizations and bodies of the United Nations system and other
international and regional intergovernmental organizations and nongovernmental organizations
and bodies as a means of strengthening the implementation of the Convention; and
(h)
consider other action, as appropriate, for the achievement of the objective of the
Convention in the light of experience gained in its implementation.
6.
The Conference of the Parties shall establish the criteria for the participation of observers at its
proceedings.
Article 24
Secretariat
1.
The Conference of the Parties shall designate a permanent secretariat and make arrangements
for its functioning. The Conference of the Parties shall endeavour to do so at its first session.
2.
Until such time as a permanent secretariat is designated and established, secretariat functions
under this Convention shall be provided by the World Health Organization.
3.
Secretariat functions shall be:
(a)
to make arrangements for sessions of the Conference of the Parties and any subsidiary
bodies and to provide them with services as required;
(b)
to transmit reports received by it pursuant to the Convention;
(c)
to provide support to the Parties, particularly developing country Parties and Parties with
economies in transition, on request, in the compilation and communication of information
required in accordance with the provisions of the Convention;
19
A 56/8
Annex
(d)
to prepare reports on its activities under the Convention under the guidance of the
Conference of the Parties and submit them to the Conference of the Parties;
(e)
to ensure, under the guidance of the Conference of the Parties, the necessary coordination
with the competent international and regional intergovernmental organizations and other bodies;
(f)
to enter, under the guidance of the Conference of the Parties, into such administrative or
contractual arrangements as may be required for the effective discharge of its functions; and
(g)
to perform other secretariat functions specified by the Convention and by any of its
protocols and such other functions as may be determined by the Conference of the Parties.
Article 25
Relations between the Conference ofthe Parties and intergovernmental organizations
In order to provide technical and financial cooperation for achieving the objective of this
Convention, the Conference of the Parties may request the cooperation of competent international and
regional intergovernmental organizations including financial and development institutions.
Article 26
Financial resources
1.
The Parties recognize the important role that financial resources play in achieving the objective
of this Convention.
2.
Each Party shall provide financial support in respect of its national activities intended to achieve
the objective of the Convention, in accordance with its national plans, priorities and programmes.
3.
Parties shall promote, as appropriate, the utilization of bilateral, regional, subregional and other
multilateral channels to provide funding for the development and strengthening of multisectoral
comprehensive tobacco control programmes of developing country Parties and Parties with economies
in transition. Accordingly, economically viable alternatives to tobacco production, including crop
diversification should be addressed and supported in the context of nationally developed strategies of
sustainable development.
4.
Parties represented in relevant regional and international intergovernmental organizations, and
financial and development institutions shall encourage these entities to provide financial assistance for
developing country Parties and for Parties with economies in transition to assist them in meeting their
obligations under the Convention, without limiting the rights of participation within these
organizations.
5.
The Parties agree that:
(a)
to assist Parties in meeting their obligations under the Convention, all relevant potential
and existing resources, financial, technical, or otherwise, both public and private that are
available for tobacco control activities, should be mobilized and utilized for the benefit of all
Parties, especially developing countries and countries with economies in transition;
20
A 5 6/8
Annex
(b)
the Secretariat shall advise developing country Parties and Parties with economies in
transition, upon request, on available sources of funding to facilitate the implementation of their
obligations under the Convention;
(c)
the Conference of the Parties in its first session shall review existing and potential sources
and mechanisms of assistance based on a study conducted by the Secretariat and other relevant
information, and consider their adequacy; and
(d)
the results of this review shall be taken into account by the Conference of the Parties in
determining the necessity to enhance existing mechanisms or to establish a voluntary global
fund or other appropriate financial mechanisms to channel additional financial resources, as
needed, to developing country Parties and Parties with economies in transition to assist them in
meeting the objectives of the Convention.
PART IX: SETTLEMENT OF DISPUTES
Article 27
Settlement ofdisputes
1.
In the event of a dispute between two or more Parties concerning the interpretation or
application of this Convention, the Parties concerned shall seek through diplomatic channels a
settlement of the dispute through negotiation or any other peaceful means of their own choice,
including good offices, mediation, or conciliation. Failure to reach agreement by good offices,
mediation or conciliation shall not absolve parties to the dispute from the responsibility of continuing
to seek to resolve it.
2.
When ratifying, accepting, approving, formally confirming or acceding to the Convention, or at
any time thereafter, a State or regional economic integration organization may declare in writing to the
Depositary that, for a dispute not resolved in accordance with paragraph 1 of this Article, it accepts, as
compulsory, ad hoc arbitration in accordance with procedures to be adopted by consensus by the
Conference of the Parties.
3.
The provisions of this Article shall apply with respect to any protocol as between the parties to
the protocol, unless otherwise provided therein.
PART X: DEVELOPMENT OF THE CONVENTION
Article 28
Amendments to this Convention
1.
Any Party may propose amendments to this Convention. Such amendments will be considered
by the Conference of the Parties.
2.
Amendments to the Convention shall be adopted by the Conference of the Parties. The text of
any proposed amendment to the Convention shall be communicated to the Parties by the Secretariat at
least six months before the session at which it is proposed for adoption. The Secretariat shall also
21
A 56/8
Annex
communicate proposed amendments to the signatories of the Convention and, for information, to the
Depositary.
3.
The Parties shall make every effort to reach agreement by consensus on any proposed
amendment to the Convention. If all efforts at consensus have been exhausted, and no agreement
reached, the amendment shall as a last resort be adopted by a three-quarters majority vote of the
Parties present and voting at the session. For purposes of this Article, Parties present and voting means
Parties present and casting an affirmative or negative vote. Any adopted amendment shall be
communicated by the Secretariat to the Depositary, who shall circulate it to all Parties for acceptance.
4.
Instruments of acceptance in respect of an amendment shall be deposited with the Depositary.
An amendment adopted in accordance with paragraph 3 of this Article shall enter into force for those
Parties having accepted it on the ninetieth day after the date of receipt by the Depositary of an
instrument of acceptance by at least two-thirds of the Parties to the Convention.
5.
The amendment shall enter into force for any other Party on the ninetieth day after the date on
which that Party deposits with the Depositary its instrument of acceptance of the said amendment.
Article 29
Adoption and amendment ofannexes to this Convention
1.
Annexes to this Convention and amendments thereto shall be proposed, adopted and shall enter
into force in accordance with the procedure set forth in Article 28.
2.
Annexes to the Convention shall form an integral part thereof and, unless otherwise expressly
provided, a reference to the Convention constitutes at the same time a reference to any annexes
thereto.
3.
Annexes shall be restricted to lists, forms and any other descriptive material relating to
procedural, scientific, technical or administrative matters.
PART XI: FINAL PROVISIONS
Article 30
Reservations
No reservations may be made to this Convention.
Article 31
Withdrawal
1.
At any time after two years from the date on which this Convention has entered into force for a
Party, that Party may withdraw from the Convention by giving written notification to the Depositary.
2.
Any such withdrawal shall take effect upon expiry of one year from the date of receipt by the
Depositary of the notification of withdrawal, or on such later date as may be specified in the
notification of withdrawal.
22
Annex
A 5 6/8
3.
Any Party that withdraws from the Convention shall be considered as also having withdrawn
from any protocol to which it is a Party.
Article 32
Right to vote
1.
Each Party to this Convention shall have one vote, except as provided for in paragraph 2 of this
Article.
2.
Regional economic integration organizations, in matters within their competence, shall exercise
their right to vote with a number of votes equal to the number of their Member States that are Parties
to the Convention. Such an organization shall not exercise its right to vote if any of its Member States
exercises its right, and vice versa.
Article 33
Protocols
1.
Any Party may propose protocols. Such proposals will be considered by the Conference of the
Parties.
2.
The Conference of the Parties may adopt protocols to this Convention. In adopting these
protocols every effort shall be made to reach consensus. If all efforts at consensus have been
exhausted, and no agreement reached, the protocol shall as a last resort be adopted by a three-quarters
majority vote of the Parties present and voting at the session. For the purposes of this Article, Parties
present and voting means Parties present and casting an affirmative or negative vote.
3.
The text of any proposed protocol shall be communicated to the Parties by the Secretariat at
least six months before the session at which it is proposed for adoption.
4.
Only Parties to the Convention may be parties to a protocol.
5.
Any protocol to the Convention shall be binding only on the parties to the protocol in question.
Only Parties to a protocol may take decisions on matters exclusively relating to the protocol in
question.
6.
The requirements for entry into force of any protocol shall be established by that instrument.
Article 34
Signature
This Convention shall be open for signature by all Members of the World Health Organization
and by any States that are not Members of the World Health Organization but are members of the
United Nations and by regional economic integration organizations at the World Health Organization
Headquarters in Geneva from 16 June 2003 to 22 June 2003, and thereafter at United Nations
Headquarters in New York, from 30 June 2003 to 29 June 2004.
23
Annex
A56/8
Article 35
Ratification, acceptance, approval, formal confirmation or accession
1.
This Convention shall be subject to ratification, acceptance, approval or accession by States and
to formal confirmation or accession by regional economic integration organizations. It shall be open
for accession from the day after the date on which the Convention is closed for signature. Instruments
of ratification, acceptance, approval, formal confirmation or accession shall be deposited with the
Depositary.
2.
Any regional economic integration organization which becomes a Party to the Convention
without any of its Member States being a Party shall be bound by all the obligations under the
Convention. In the case of those organizations, one or more of whose Member States is a Party to the
Convention, the organization and its Member States shall decide on their respective responsibilities for
the performance of their obligations under the Convention. In such cases, the organization and the
Member States shall not be entitled to exercise rights under the Convention concurrently.
3.
Regional economic integration organizations shall, in their instruments relating to formal
confirmation or in their instruments of accession, declare the extent of their competence with respect
to the matters governed by the Convention. These organizations shall also inform the Depositary, who
shall in turn inform the Parties, of any substantial modification in the extent of their competence.
Article 36
Entry into force
1.
This Convention shall enter into force on the ninetieth day following the date of deposit of the
fortieth instrument of ratification, acceptance, approval, formal confirmation or accession with the
Depositary.
2.
For each State that ratifies, accepts or approves the Convention or accedes thereto after the
conditions set out in paragraph 1 of this Article for entry into force have been fulfilled, the Convention
shall enter into force on the ninetieth day following the date of deposit of its instrument of ratification,
acceptance, approval or accession.
3.
For each regional economic integration organization depositing an instrument of formal
confirmation or an instrument of accession after the conditions set out in paragraph 1 of this Article
for entry into force have been fulfilled, the Convention shall enter into force on the ninetieth day
following the date of its depositing of the instrument of formal confirmation or of accession.
4.
For the purposes of this Article, any instrument deposited by a regional economic integration
organization shall not be counted as additional to those deposited by States Members of the
organization.
Article 37
Depositary
The Secretary-General of the United Nations shall be the Depositary of this Convention and
amendments thereto and of protocols and annexes adopted in accordance with Articles 28, 29 and 33.
24
A 56/8
Annex
Article 38
Authentic texts
The original of this Convention, of which the Arabic, Chinese, English, French, Russian and
Spanish texts are equally authentic, shall be deposited with the Secretary-General of the United
Nations.
IN WITNESS WHEREOF the undersigned, being duly authorized to that effect, have signed this
Convention.
DONE at GENEVA this [date of month] two thousand and three.
25
www.eu2003.gr
56th World Health Assembly
Geneva, 21 May 2003
Statement
On
The Framework Convention on Tobacco Control
By
Professor Constantines Stefanis
Minister for Health and Welfare, Greece,
on behalf of the European Union
Mr. Chairperson, Director General, Distinguished delegates,
Dear colleagues, Dear friends,
I have the honour to speak on behalf of the European Community and its Member
States. The Acceding Countries Cyprus, the Czech Republic, Estonia, Hungary, Latvia,
Lithuania, Malta, Poland, the Slovak Republic and Slovenia and the Associated Countries
Bulgaria, Romania and Turkey declare that they have aligned themselves to this statement.
Ladies and Gentlemen,
We are moments away from achieving a major agreement, moments away from the
world’s first global Framework Convention on Tobacco Control, moments away from
creating history. These moments we would like to express our most sincere acknowledgement
to all those that helped us to get here. The Chairperson of the last sessions of the
Intergovernmental Negotiating Body, Ambassador Seixas Correa and his predecessor
Ambassador Celso Amorim, the facilitators and the members of the Bureau, as well as the
members of the WHO Secretariat for their dedication and tireless efforts they have carried out
in moving forward the Framework Convention Process. Likewise, we would like to thank the
Director General of WHO Mme Brundtland, for her great work of support throughout this
process. Finally, we would like to thank the Non Governmental Organizations, which had the
interest, the knowledge and the will to contribute in our efforts.
The objective of the Framework Convention on Tobacco Control is the promotion of
public health. Thus, the European Community has been fully committed to a strong and
widely accepted Convention from the beginning. We are determined to protect our citizens
from tobacco consumption and exposure to tobacco smoke and to empower them to live
healthy lives, free from the scourge of tobacco. For us, curbing down the tobacco epidemic is
of great importance.
The European Community has done much to control tobacco consumption through
legislation, recommendations, through EU-wide information campaigns and through support
for networking and smoking prevention and cessation projects. Still, it believes that much
more needs to be done, not only within its Member States, but also all over the world. The
Framework Convention obliges us all, inspires action, sets clear goals, which can be used to
forward the continuous national work, which lies ahead of us. The Framework Convention
can be the catalyst for advancing national, regional and international action and global
cooperation.
The European Community and its Member States are now preparing themselves to be
among the first to sign and ratify the Framework Convention as currently drafted.
Ladies and Gentlemen,
Tobacco consumption and exposure to tobacco smoke are threats to our health. There
is a common understanding of that fact and now, after a long negotiating process, a shared
view of what needs to be done. It is therefore a necessity that we put into force the soonest
possible the Framework Convention, the key instrument to address tobacco control.
Thank you.
2
New Evidence of Escalating Tobacco Industry Activity to Derail
the Framework Convention on Tobacco Control
February 2003
k fact
Challenging corporate abuse
Building grassroots power
Since 1977, Infact has been exposing life-threatening abuses of transnational corporations
and organizing successful grassroots campaigns to hold corporations accountable to
consumers and society at large. Infact is an NGO in Official Relations with the World Health
Organization (WHO).
The Network for Accountability of Tobacco Transnationals (NATT) includes 75 NGOs from
50 countries working for a strong, enforceable Framework Convention on Tobacco Control.
Introduction
n the final stages of drafting the Framework Convention on Tobacco Control (FCTC),
!transnational tobacco corporations are escalating their efforts to undermine the
treaty. Recently released tobacco industry internal documents—made public for the
first time in this paper1—reveal that Big Tobacco has targeted certain African and Latin
American countries in its attempts to subvert the treaty. With the aid of notorious PR
firms, powerful trade associations, and close allies in top-level government positions,
Philip Morris, British American Tobacco (BAT), and Japan Tobacco International are
coordinating a formidable challenge to the world’s first public health treaty.
This report examines the presence of the three largest tobacco transnationals at
the fifth round of FCTC negotiations (INB5) in October 2002—using evidence gathered
from internal corporate documents, news reports, and by representatives of Infact and
other NATT members. The final round of negotiations will determine whether govern
ments seeking to protect global public heath over the profits of the tobacco industry
manage to overcome the efforts of the tobacco transnationals. Infact and NATT will
continue to investigate and expose tobacco industry interference in the FCTC.
Tobacco Industry Groundwork
New Evidence Reveals Extent of PR Firm
Mongoven, Biscoe and Duchin’s Duplicity_____ _ ____________
ccording to Philip Morris internal documents, the corporation has enlisted Jack
Mongoven of the notorious corporate spy firm Mongoven, Biscoe and Duchin
A
(MBD) to advise the tobacco giant on how to thwart the FCTC. In 1999, Philip Morris
commissioned Mongoven to investigate a variety of areas in which the tobacco giant
could influence the FCTC. According to a recently released memo chronicling MBD’s
plan, Mongoven was to identify “priority countries at the WHO and key ministries/names, ”
provide “analysis of prior conventions to identify generic concerns about conventions,”
and prepare “a draft youth smoking prevention protocol.”2
In the same document, Philip Morris states its intention to identify sympathetic
government allies: “our plan will lack teeth until we know those markets where we can
participate in the development of government policy viz (sic) the convention.” Philip
Morris acknowledges that once the idea of a Convention is adopted it “will be able to
discuss views on the Convention in principle and at the national level in those markets
where we have access to government decision makers.”3
MBD has a long relationship with the tobacco industry, and in 1997 advised
Philip Morris “if it could not delay the adoption of the convention it should instigate a
co-ordinated strategy to make it as weak as possible.”4 According to an analysis by
Stacy Carter of the Department of Public Health at the University of Sydney in Australia,
“WHO’s system of regions is also a potential weakness, because each contains at least
one country which is weak on tobacco control and likely to support the interests of the
1 Under the terms of a 1998 settlement with the US State of Minnesota, tobacco corporations are required to disclose documents
related to US tobacco litigation. This responsibility includes maintaining until 2008 a website, onto which new documents are
uploaded regularly.
1 Email correspondence from Matt Winokur, “WHO follow-up,” March 30, 1999, Philip Morris Document ID:2072268126.
3 Email correspondence from Matt Winokur, “WHO follow-up,” March 30, 1999, Philip Morris document ID: 2072268126.
4 Jeremy Laurance, “Tobacco Company Attacked Over its Lobbying Tactics," The Independent (London), 19 March 2002.
Treaty Trespassers - page 2
INFACT, February 2003
industry and it may be this potential portal which MBD were exploiting.”5 These internal
documents clearly illustrate that the tobacco giant has been involved in a detailed plan to
subvert the work of the WHO by exploiting the regional structure of the system.
Philip Morris Internal Documents Reveal Plan for Country Targeting_____________
According to a Philip Morris International Corporate Affairs Action Plan that was
posted on the corporation’s internal documents website last fall, in 1990 the tobacco
giant devised its “Anti-tobacco Network, Question WHO Strategy on Tobacco” plan.
Philip Morris’s strategy included identifying allies in Latin America and Africa while
setting the following action steps:
•
•
•
•
•
Test WHO regional office support on WHO priorities in Latin America;
If WHO regional office strategy is successful in Latin America, apply in Africa,
Philippines and India i.e. encouraging WHO to redirect its priorities to its original
mandate;
Request GAO [US Government Accounting Office] to review US funding priorities
of WHO;
Work with selected journalists to question WHO priorities, budget; and,
Assist smokers groups to join consumers organizations.6
The more recent strategic work of MBD to figure out ways to influence international
regulation builds on the corporation’s own internal planning established years prior.
BAT Documents Illustrate Coordinated Industry Effort________________________
According to internal documents of BAT, it seems the second largest tobacco
corporation was also looking to influence the WHO, especially in Latin America. A
recent report released by the Pan American Health Organization describes the purpose
of BAT’s Public Affairs Research Group (PARG): “to influence the vote of diplomatic
delegations (sic) participation in the International Organizations at Geneva. So as to
counteract proposition against the tobacco industry, specifically the ones proposed at
OMS (WHO) General Assembly.” In the same document the corporation notes that it is
necessary for the industry to work together in order for this plan to thrive. “As in the past,
for this initiative to be successful, it requires the participation of PMI and all BATCo. and
BAT Industry (Souza Cruz [Brazil]) companies in the region.”7 While Philip Morris and
BAT fight for market share in this region, this document illustrates the industry’s desire
to preempt meaningful regulation by the WHO, which prompted these two competing
tobacco giants to cooperate.
Governments with Tobacco Industry Representation:
Big Tobacco’s Plan in Practice
Malawi_________________________________________________________________
s internal corporate documents illustrate, Philip Morris long ago identified Africa as
A instrumental to the priorities of the world’s largest tobacco corporation. For this
5 Stacy Carter, “Mongoven, Biscoe & Duchin: Destroying Tobacco Control Activism Front the Inside,” Tobacco Control, 11,
Issue 2, March 2002.
6 “PMI Affairs Action Plan 1990,” Philip Morris Document ID: 2084339680.
7 “Profits Over People,” Pan American Health Organization, November 2002.
Treaty Trespassers - page 3
INFACT, February 2003
reason Philip Morris set its sights on Malawi, one of the largest producers of tobacco leaf
in the world. According to the 1990 Philip Morris International Corporate Affairs Action
Plan, the tobacco giant wanted to “approach allies in large tobacco growing countries
to raise questions about WHO priorities eg. Latin America Tobacco Council, Minister
of Health of Malawi.”8
In Malawi, it seems that Philip Morris’s strategy has paid off as two representa
tives of tobacco industry trade associations served on the country’s delegation at
INB5—the Chief Executive for the International Tobacco Growers Association (ITGA) of
Africa and the General Manager of the Tobacco Exporters Association of Malawi.9
The ITGA Chief Executive for Africa, Mr. G. Thangathyanga is adamantly opposed
to the FCTC or any efforts to reduce tobacco consumption. In response to the global
convention he said, “Blocking access to international markets as advocated by the
anti-tobacco lobby will kill thousands of people whose lives depend on the crop.”10
While the farming of tobacco is a major source of revenue to Malawi, many studies
have discredited this argument and instead have found the conversion to other crops
would have a positive effect on tobacco dependent economies.11 In addition, Mr.
Thangathyanga’s argument ignores the millions of people who die each year from
tobacco related illnesses.
Another example of a Malawian delegate representing the tobacco industry’s
interests is Mr. Mbale, the General Manager of the Tobacco Exporters Association
(TEAM), a tobacco industry trade group. In 2000, when asked what the objectives and
functions of his organization were, he replied “to represent the interests of the Tobacco
Industry” and “To help co-ordinate activity to minimise the impact of Anti-smoking
lobbyists.”12
This is evidence that the action plan Philip Morris put into place in 1990 has
been effective in allowing the tobacco giant access through the governments of tobacco
producing countries. Despite the targeting of Malawi by the world’s largest tobacco
corporation, the African region has maintained the strongest positions being advocated
by countries negotiating the FCTC.
Tobacco Industry Representation on Delegations of China, Turkey, Japan________
Malawi is not the only country with FCTC delegates closely tied to the tobacco indus
try—many other countries also have tobacco industry representation at the negotiations.
At INB5, China sent the Division Director and an Officer of its State Tobacco Monopoly
Administration, and Turkey sent its Deputy Director-General of the State Monopoly on
Tobacco and Beverages. Japan had five members of its Ministry of Finance—which
owns a 67% stake in Japan Tobacco—on hand, with two of the individuals coming from
the Tobacco and Salt Industries Office of the Ministry.13
• Dr. Judith Mackay and Dr. Michael Eriksen, The Tobacco Atlas. A World Health Organization Publication, 2002; “PMI Affairs
Action Plan 1990,” Philip Morris Document ID: 2084339680.
’“List of Participants,’’The World Health Organization, A/FCFC/INB5/DIV/2 Rev.l, October 21, 2002.
10 “Fanners Say No Economic Life Without Tobacco,” All-Africa.com, August 13, 2001.
" Curbing the Epidemic: Governments and the Economics of Tobacco .Control, A World Bank Publication, 1999.
13 “Prospects for Malawi’s Tobacco Industry,” Traders, Issue 2 April-July 2000, Page 58.
13 “List of Participants, ” The World Health Organization, A/FCFC/INB5/DIV/2 Rev. 1, October 21, 2002.
Treaty Trespassers -- page 4
IN FACT, February 2003
Trade Associations Push an Insidious Agenda
l hilip Morris also had many of its “friends” on hand at INB5. While some tobacco
Ptransnationals had highly visible delegations of top level representatives in Geneva,
Philip Morris seems to have decided to take a more subtle, but no less insidious tack, and
allow trade associations to do its dirty work.
International Tobacco Growers Association__________________________________
In addition to having a place on the delegation of Malawi, the ITGA sent Antonio
Ambrunhosa, the Chief Executive of ITGA worldwide, to attend INB5. The ITGA website
states that the association is “the legitimate voice of millions of tobacco farmers all over
the world. It was formed in 1984 to foster co-operation and information-sharing between
its tobacco-growing members and contribute to the international debate on tobacco
issues.” Also on the organization’s website, the ITGA argues against the establishment
of tobacco control policies because “there are many other health priorities well ahead of
tobacco control.”14 But according to the World Bank, tobacco control is an urgent priority
because by 2030 tobacco will become the world’s leading cause of preventable death
and 70% of all tobacco related deaths will occur in the developing world.15
Even though the tobacco association is an active participant in FCTC talks, in
2001 the ITGA “vowed to continue to fight outside the WHO system by lobbying govern
ments and other United National (sic) and international organizations.” In addition, in
2000 Mr. Ambrunhosa said, “Our experience with the WHO is that it is not interested in
dialogue with tobacco growers, only in pursuing its economically destructive agenda.”16
These statements clearly illustrate that the goals and ideals of the ITGA run counter to
those of the WHO and the FCTC.
International Travel Retail Confederation____________________________________
The International Travel Retail Confederation (ITRC) was established after the
prohibition of duty-free sales in the European Union, and had previously been known
as the International Duty Free Confederation. Keith Spinks, who formerly represented
Rothmans Tobacco on the International Duty Free Coalition, is now the Director General
of the ITRC.17 After the most recent round of negotiations Spinks assessed the current
situation by saying, “We must now enhance our efforts with governments to maintain
the support of those countries opposed to the proposal to restrict or ban duty-free
tobacco sales. We must also increase political activity with those countries that have
not considered the issue fully but in many instances, have merely allowed their health
ministries and tobacco activists to make policy decisions without considering the implica
tions and consequences.” According to the ITRC website, Philip Morris Duty Free is a
member of this organization.18
14 ITGA Home Page, www.Tobaccoleaf.org , Document retrieved: January 8,2003. “Commentary on World Health Organization
Statements,” wwM.Tobaccoleaf.org, Document retrieved: January 8, 2003.
15 Curbing the Epidemic: Governments and the Economics of Tobacco Control, A World Bank Publication, 1999.
16 “Tobacco Growers Condemn Underhand Tactics by the World Health Organization,” www.tobaccoleaf.org/Media/
011031 2.htm. October31,2001; “World Health Organization Leaves Farmers Out ofDebate on Their Future once Again,” ITGA
press release, PR Newswire, March 13, 2000.
17 “ITRC Annual Report Calls for United Approach to Industry Changes,” March 2, 2001, www.travelretailworld.com; List of
Delegates, ‘INFOTAB International Conference, Hong Kong 1989”, Philip Morris document ID: 2021594097.
18 “Conclusions From the Latest WHO Talks: ‘No Time for Complacency,’” October 31, 2002, www.travelretailworld.com.
Treaty Trespassers - page 5
INFACT, February 2003
International Association of Airport Duty Free Stores_________________________
The International Association of Airport Duty Free Stores (IAADFS) had a number of
representatives in attendance at INB5. Thierry Lebeaux, who is the head of the EU
office for Citigate Public Affairs and has represented the IAADFS since 1999, told an
Infact representative that his organization does not represent the tobacco industry. But
according to the IAADFS website Philip Morris is both a member and supporter of the
organization, sponsoring events along with Japan Tobacco in 2002.19
Another representative of the IAADFS in attendance at INB5, Jon Kent, held a
strategy meeting with Philip Morris representatives in 1999. According to Philip Morris’s
internal documents, Jon Kent and a Philip Morris representative met on July 15, 1999.
A week later, the IAADFS drafted a letter to its membership regarding a Philip Morris
proposal.20
The groups present at the negotiations seem to have been very aware of each
other and may even have had a concerted strategy. For example, on October 23,
2002, Keith Spinks of ITRC and Jon Kent of IAADFS presented a workshop together on
the future of duty-free tobacco and were described as “the key drivers in the lobbying
process.” According to the ITRC website, the purpose of the gathering was to "update
the trade on the latest developments in the industry’s campaign against the proposed
global abolition of duty-free tobacco sales” and noted that the workshop was to be held
the week prior to and the week of the negotiations.21
Tobacco Transnationals at INB5: Exerting Influence with
High-Profile Attendance and Backroom Bargains
bat_________________________________________________ ________
ven though many tobacco industry allies were in attendance at 1NB5, representa
Efives of the tobacco giants were also out in full force. The most brazen of
the tobacco transnationals was BAT with at least 12 representatives including the head
of International Political Affairs, the Manager of International Regulatory Affairs and
the Manager of its Legal Division. During the negotiations, BAT representatives were
handing out its position paper on the FCTC, which states:
“...we believe that the need for an international response in the form of a detailed and
binding multilateral convention is much more limited than stated in the Preamble of the
FCTC. Observing the proceedings of the international negotiating body over the last two
years strengthened our view that if there is to be a convention, it should for the majority of
issues be limited to non-binding guidelines for national governments.” 22
BAT’S main objective is to maintain the status quo through voluntary, non-binding regula
tions, which at best will do nothing to curb the tobacco epidemic and at worst will provide
19 Personal communicarion by Infact with Thierry Lebeaux, Citigate Public Affairs, October 14,2002; “Passport To your Global
Village,” www.iaadfs.org, June 2002, Vol. 12, No. 3.
20 Email correspondence from Robert Moore to Karen Chaikin, “IAADFS Meeting in Washington, DC (International Association
of Airport Duty Free Stores)” July 6, 1999, Philip Morris Document ID: 2072356394; Mail Merge letter from the International
Association of Airport Duty Free Stores, July 22, 1999, Philip Morris Document ID; 2072050948.
21 “Tobacco Workshop Planned for Cannes,” September 30, 2002, Travelretailworld.com.
22 Personal accounts by Infact representatives to INB5, October 2002; “British American Tobacco’s Comments On the New
Chair’s Text of a Framework Convention on Tobacco Control,” A/FCTC/INB5/2, August 2002.
Treaty Trespassers - page 6
IN FACT, February 2003
protection for the industry in the future.
In addition to making the views of BAT known through its position paper, these
representatives of the tobacco giant were also eager to engage in discussions with
members of NATT. For example, Akinbode Oluwafemi of Environmental Rights Action
(ERA), a Nigerian NATT member, had a long conversation with Kehinde Johnson, the
Corporate Affairs Director for BAT Nigeria. Johnson shared that the tobacco giant has
done everything in its power to counter what it considers to be the most effective tobacco
control group in Nigeria. Through the conversation BAT confirmed it had engaged in
several tactics to block the media from reporting ERA activities. It has also embarked on
an intensive collection of information on ERA and Oluwafemi.23
Japan Tobacco International____________________________ _
The government of Japan owns 67% of Japan Tobacco International, which gives
the third largest tobacco corporation unparalleled access to governments and the FCTC
negotiating process. Before INB5 began, news reports out of Japan projected that the
country’s delegation would lodge opposition to tobacco consumption reductions because
the ministry was obliged under national legislation to promote tobacco. From the
floor of the negotiations, Japan’s delegation criticized the FCTC’s stated purpose of
reducing tobacco consumption. In addition to the five members of the Japanese delega
tion representing the Ministry of Finance—who were presumably looking to protect
their investment—Japan Tobacco bolstered its presence with at least 12 corporate
representatives. 24
Philip Morris____________________________________________________________
Philip Morris played a more undercover role than the other tobacco transnationals
at INB5. It made inroads through allies and trade associations, perhaps executing plans
outlined in internal documents years prior. According to news reports at the end of the
last round of negotiations, Philip Morris admittedly had representation there, including a
member of its international management.25
Even though Philip Morris took a lower profile than the other tobacco transnation
als, its influence was no less pervasive. Philip Morris may have decided it was not
necessary to send many of its executives because it already has many friends within the
Bush Administration helping to determine the US position on the FCTC. For example,
Karl Rove is a senior advisor to the President and one of the most powerful voices on
the Bush team. This relationship dates back to 1994 when Rove was instrumental in
constructing Bush's winning gubernatorial campaign. After the election, Rove continued
to advise Bush, while continuing his previous career as a lobbyist and consultant for
Philip Morris.26
25 Personal communication by Environmental Rights Action with Kehinde Johnson, Corporate Affairs Director, BAT Nigeria,
October 2002.
24 Green, Shane, “Japan Seeks Extra Mild Treaty in Fear Over Ash and Cash,” vnvxv.SMH.com.au, October 9, 2002; “Japan
to Oppose Tobacco Consumption Cuts,” Japan Today, October 8, 2002; Statement made by Japan during WHO Formal FCTC
negotiations, October 16, 2002; Personal accounts by Infact representatives to INB5, October 2002.
25 Rachel Rivera, “Tobacco Control Treaty Moves Toward Global Ban on Cigarette Advertising,” AFXPress, October 15,2002.
26 Ed Vulliamy, “America in the Grip of Bush’s ‘Iron Triangle’,” The Observer (UK), December 3, 2000.
Treaty Trespassers -- page 7
INFACT, February 2003
In another example of Philip Morris’s access, Bush appointed Tommy Thompson
as the Secretary of Health and Human Services—the cabinet department where the
head of the US Delegation to the FCTC is employed. When Thompson was the governor
of Wisconsin, he maintained an open door policy with Philip Morris, receiving $70,000 in
campaign contributions. During that time, Thompson took trips to three continents paid
for by Philip Morris and even owned stock in the tobacco giant.27
Finally, Dan Troy is the powerful lead counsel for the US Food and Drug Adminis
tration (FDA). He came to this position a year ago after leaving a Washington, DC
law firm where he had argued against FDA attempts to limit tobacco advertising. He
is known as an industry-friendly expert on First Amendment law, having argued that
there is not a difference between commercial speech and political speech, and therefore
corporations should not be held to stricter requirements.28
Bush Administration and the FCTC
) hilip Morris’s close ties to the Bush Administration may be the reason for the
close resemblance between its positions on the FCTC and the positions that the
current administration is taking. In August 2001, US Representative Henry Waxman
submitted a letter to the Bush Administration outlining the similarities between Philip
Morris’s position and the positions taken by US negotiators at the previous round of
treaty talks in April 2001. Waxman identified 11 places where Philip Morris wanted
language removed from the draft text, and the US delegation advocated changes that
bore a striking resemblance to the demands of Philip Morris 10 out of the 11 times.
The tobacco-friendly interventions made by the US continued at INB5 as the delegation
said it could not agree that the tobacco industry should be held responsible for all the
harm caused by its products.29
F
27 “Industries that Backed Bush Are Now Seeking Return on Investment,” The Wall Street Journal, March 6, 2001; David Pace,
“Thompson Has Strong Tobacco Ties,” Washington Post Online, January 10, 2001.
28 Michael Kranish, “FDA Counsel’s Rise Embodies US Shift,” Boston Globe, December 22, 2002.
29 Letter from Henry A. Waxman, Ranking Minority Member of US Congress to President Bush, November 19, 2001; Statement
made by the US during formal FCTC negotiations, October 16, 2002.
Treaty Trespassers - page 8
IN FACT, February 2003
46 Plympton Street
Boston, MA 02118 USA
617.695.2525
Fax: 617.695.2626
info@infact.org
www.infact.org
: fact
Challenging corporate abuse.
Building grassroots power
RE: Input required
Subject: RE: Input required
Date: Sat, 9 Sep 2000 17:57:41 +0100
From: "Sharad Vaidya" <sgvaidya@goatelecom.com><> p
To: <sochara@vsnl.com>
g -
Ii
Dear Dr. Thelma,
I am glad that
The Government of Karnataka is planning an amendment or their bill and have
been in touch with you.
The following are the precautions you have to take:
1.Please be in touch with the secretary in Law department who is charge of
drafting the Bill.
2.After it is drafted it will go the Law Secretary and then to the Chief
Secretary. Once it is approved by him it will be circulated to all the
Ministers.
It is here and at every stage and on every table the tobacco industry would
be active to dilute the Bill as much as possible. The industry people would
be meeting every MLA not to support the Bill.
3.
The farmers lobby supported by Devegauda former Prime Minister would
pressurise the government with all their arguments that the farmers lives
are at jeopardy.
4.
The hospitality industry would send in their objections that tourism will
suffer. .
5.The restaurant's association would send in their representations.
6.
The Kiosk owners would meet the press and pronounce that their business
would suffer.
7.The Tobacco Institute of India would send its representations will all
false claims
The big bosses of tobacco industry would have already met important
bureaucrats and Ministers and the MLAs not to support the Bill.
7. The farmer's lobby is likely to lead morchas strikes etc to the Vidhan
Soudha to protest against the BILL
Therefore you have a lot of work to do.
We did the following:
1.
Meet the press as often as possible with press conferences, letters to
the editor, articles, and press releases. Meet the editors of the
important press and impress upon them the need for such an act. They are
often not knowledgeable about the effects of tobacco. Brief them the changes
that are occurring in the world.
Log on to WWW.WHO and you will have much more information to support your
cause.
If you have contacts on internet on NRI seek their support . Send them
e-mail addresses of the CM, and other important Minister. Please also send
me their addresses and addresses of CS Finance Secretary etc so that when
you go to the press I can support you from other organisations in the
country, and send the Ministers.
2.
Organise meetings of various medical organisations such as IMA and
specialist organisations, women's organisations, Rotarians, Lions Jaycees,
Round Table, Parent teachers Associations and as many organisations as you
can get
publicise views of every meeting to the press and send the
representations to the concerned bureaucrats.
2. Keep the student bodies like NSS to lead morcha to the Vidhan Soudha when
the Bill is being discussed. Bigger the rally, more chances of success.
Iof2
9/1 l/oo
RE: Input required
3.
Dr. B.S.Srinath Director of BIO(Bangalore Institute of Oncology, knows
most of the things we have done.A representation from BIO and KIDWAI
memorial should also send their representations.
4.
Please see that you meet as many bureaucrats and MLAs as possible as well
as Ministers.
-Minister of Agriculture would-be very important.ITG has its factory in
Bangalore. It will use all its power to dilute the Bill.
Have the data about the number of farmers and other data from Kidwai
Memorial Dr. Nandakumar about the increasing deaths from lung cancer in
Bangalore and other tobacco related deaths from Tobacco related diseases.
5.
Dr. Paramesh is an active votary of the Bill.
6.
Do not be afraid of blaming the government for the partnership it has
with the tobacco industry and openly criticise them for being insensitive to
the misery and deaths of the poor.
If you need any more information please free to write.
I am also asking my secretary to send you the data about tobacco use of
Karnataka.
Regards,
Dr. Sharad Vaidya
----- Original Message----From: Community Health Cell [mailto:sochara@blr.vsnl -net.in]
Sent: 09 September 2000.08:05
To: Sharad Vaidya
Subject: Input required
Dear Dr. Vaidya'
We have noted your change of address.
do keep us informed about the
activities of NOTE.
I would be greatful if you could send us a copy of the Goa acts/orders
relating to Tobacco use, e.g. banning smoking in public places and if
you have anything on gutka/chewed tobacco.
hence any inputs that you can
send to us will be useful.
with regards
yours sincerely,
Dr. Thelma Narayan
Coordinator
Community Health Cell
PS : Chitra is visiting Bangalore.
r
*
2 of 2
pH - S'-
its
The World Health Organization
Tobacco & Health
in the
Developing World
A Background Paper
for the
High Level Round Table
on
Tobacco Control and Development Policy
Organized by the European Commission in collaboration with the World Health
Organization and the World Bank
Brussels, 3-4 February 2003
I.
Introduction.
Health impact and burden of disease attributable to tobacco use... 4
II.
Explaining the mortality gap between the rich and the poor - tobacco use
among the less educated and the poor.......................................................... 6
Tobacco use and malnutrition........................................................................ 7
Health and safety of family farmers who grow tobacco................................. 7
Tobacco, deforestation and environmental health implications.................... 7
Child labour.................................................................................................... N
Cost-effective interventions that make a difference...................................... 8
Treatment for tobacco dependence...............................................................9
Research for tobacco control........................................................................ II
III.
Conclusion.............................................................. .............................. 1 -
2
I.
Introduction
Health and education are the basis of economic productivity. Healthy
populations are critical for poverty reduction, economic growth and long-term
development.
In addition to the traditional burden of communicable diseases, developing
countries today are faced with a huge increase in noncommunicable diseases, mental
il ness and violence and injuries. Tobacco is a major contributor to these diseases,
which now account for more than half the disease burden in those countries. This
alarming increase threatens to undermine their economic and social development.
Tobacco is cultivated in many regions around the world and can be legally
purchased in all countries. The dried leaf of the plant Nicotiana tabacum is used for
smoking, chewing or snuff. Contrary to what many believe, tobacco use and its
attributable deaths are not a bane that afflicts developed countries primarily.
In June 1995, representatives of 22 international organizations and other
individuals met in Bellagio to examine the implications of current global trends in tobacco
production and consumption for sustainable development, especially in developing
countries. The meeting participants concluded that tobacco posed a major challenge
not just to health but to social and economic development and environmental
sustainability. The participants recommended that tobacco control be more widely
recognized as a development priority, and expressed concern that it was not on the
agenda of most development agencies.1
II.
Health impact and burden of disease
attributable to tobacco use'
Currently, an estimated 4.9 mil ion deaths per year are caused by tobacco.
Without further action, it is predicted that in 2020 the mortality burden attributable to
tobacco wil increase two-fold. Approximately 70% of these deaths wil occur in
developing countries. Together with HIV/AIDS, tobacco use is the fastest growing cause
of death in the world and is set to become the leading cause of premature death in the
2020s.
The past few decades have seen dramatic increases in smoking in developing
countries, especially among males.2 This contrasts with steady but slow decreases.
mostly among males, in many industrialized countries. Smoking rates are on the rise
in some low and middle income countries, especial y among young people and women,
and they remain relatively high in most of the former socialist economies. Smoking
substantial y increases the mortality risk from lung cancer, upper aerodigestive and other
cancers, heart disease, stroke, chronic respiratory disease and a range of other medical
conditions (see Table 1).3 In populations where smoking has been common for many
decades, tobacco use accounts for a substantial proportion of all mortality.4
Recent epidemiological studies il ustrate the magnitude of the tobacco epidemic
in developing countries. In China, for example, if current smoking patterns persist,
approximately 100 mil ion of the 300 mil ion Chinese males now aged 0-29 wil die as
a result of tobacco use. Significantly, tobacco use was found to be a major cause of the
mortality caused by tuberculosis in China. Tobacco's adverse effects are not limited to
cigarette-smoking. In India, bidi smoking and tobacco quid chewing were shown to play
a significant role in the development of fatal diseases.5
Table 1: Tobacco use related diseases
Principal diseases caused in part by smoking
Cancers of mouth, pharynx and larynx
Cancer of oesophagus
Cancer of lung
Cancer of pancreas
Cancer of bladder
Ischaemic heart disease
Hypertension
Myocardial degeneration
Pulmonary heart diseasea
Other heart disease
Aortic aneurysm
Peripheral vascular disease
Arteriosclerosis
Cerebral vascular disease
Chronic bronchitis and emphysema
Pulmonary tuberculosis
Asthma
Pneumonia
Other respiratory disease
Peptic ulcer
This section is largely based on Chapter 4 of the World Health Report 2002.
Other harmful effects caused in part by smoking
Cancer of lip
Crohn's disease
Cancer of nose
Osteoporosis
Cancer of stomach
Periodontitis
Cancer of pelvis of kidney
Tobacco amblyopia
Cancer of body of the kidney
Age-related macular degeneration
Myeloid leukaemia
Reduced fecundity
Reduced growth of fetus
Smoking also harms others. There are definite health risks from passive
smoking and smoking during pregnancy adversely affects foetal development. In June
2002, the International Agency for Research on Cancer concluded that involuntary
smoking (exposure to secondhand or 'environmental' tobacco smoke) was carcinogenic
to humans.6 Chewing tobacco may lead to oral cancer, as does cigar or pipe smoking.
In industrialized countries, smoking is estimated to cause over 90% of all lung cancers
in men and about 70% of all lung cancers in women. In addition, smoking is responsible
for 56-80% of all chronic respiratory disease and 22% of all cardiovascular disease.
Figure 1 shows the sub-regional burden of disease attributable to tobacco.
Worldwide, it is estimated that tobacco causes about 8.8% of deaths and 4.1% of
DALYs" (59.1 million). The rapid evolution of the tobacco epidemic is illustrated by
comparing the estimates for 2000 with those for 1990. In 2000 there were at least a
mil ion more deaths attributable to tobacco, with the increase being most marked in
developing countries. The extent of disease burden is consistently higher among groups
known to have smoked. For example, mortality due to tobacco-related diseases is
greater in males (13%) than in females (3.8%). Worldwide, the proportion of diseases
caused by tobacco use is as follows: 12 % for vascular disease: 66% for trachea
bronchus and lung cancer and 38% for chronic respiratory diseases.
Figure 1: Burden of disease attributable to tobacco (% DALYs in each subregion)
Source: Doll 1998 Table 11,12 and 13.
Burden of disease attributable to addictive
substances related risks: TOBACCO
Source: World Health Report 2002
* DALYs -Disability Adjusted Life Years- measure the burden of disease in population. It combines ‘Years of Life
Lost’ (YLLs) and Years Lived with Disability’ (YLDs).
Approximately 16% of the global burden of tobacco-related illness occurred in
countries of the Western Pacific Region that experience low child and low adult mortality
such as China, Lao People's Democratic Republic, Mongolia, Papua New Guinea, and
Viet Nam. whereas 20% occurred in South-East Asian countries that experience high
child and high adult mortality (Bangladesh, India, Myanmar and Nepal) Figure 2 shows
the enormous death toll that awaits if effective interventions are not put in place rapidly.
Figure 2: Unless current users quit, tobacco use deaths wil rise dramatically over
the next 50 years
Baseline
500 ’
= -100
g,
If proportion of
young adults
taking up smoking
halves by 2020
If adult
consumption
halves by 2020
I 300 •
3 200'
■§ ioo
0 J-fl1950
Year
Source. Peto et al. 1994, Peto. personal communication
Explaining the mortality gap between the rich and the poor - tobacco use
among the less educated and the poor
The staggering size of the burden of disease attributable to tobacco use in
developing countries justifies in itself significant investments in comprehensive tobacco
control programmes. It is, however, important to note that tobacco use, and its
associated burden of disease, tend to follow a gradient. That is, poorer individuals tend
to use tobacco products more than their wealthier counterparts. Similar patterns exist
with respect to education levels and socio-economic status.7 For example, in China,
individuals with no schooling were 6.9 times more likely to smoke than individuals with
a college degree8 while uneducated adults in Brazil were 5 times more likely to smoke
than adults who had received at least a secondary education.9 Figure 3 il ustrates these
patterns. In a comprehensive review of tobacco use prevalence patterns, The World
Bank concluded that "prevalence in most developing countries is already highest among
the poor, and if these countries experience a similar pattern to the high-income
countries, the gap in smoking between rich and poor groups wil widen over time".
Figure 3: Smoking prevalence among men in Chennai, India, by education levels
Source: Gajalakshmi et al. 2000
6
The aforementioned figures suggest that the poorest socio-economic groups wil
likely suffer the consequences of tobacco use more than the richest. Although few
studies have examined whether tobacco use 'explains' the socioeconomic differences
in diseases that it causes in developing countries, the emerging evidence is clear.
Differences in tobacco use can explain a significant portion of the mortality gap between
rich and poor. In Canada, England and Wales, Poland, and the United States, the
middle-age mortality gap between rich and poor would be reduced by between one-half
and two-thirds if smoking could be eliminated.10
Tobacco use and malnutrition
In addition to its direct effects on health, tobacco use contributes to malnutrition
because money is spent on tobacco instead of food. In Bangladesh, for example, it has
been estimated that if poor people did not smoke, 10.5 million fewer people would be
malnourished.11
The proportion of household expenditures used to purchase tobacco products
is often very high in developing countries. For example, in Bulgaria low income
households with at least one smoker spent 10.4% of their total income on tobacco
products in 1995. In China, smokers surveyed in the Minhang district reported spending
17% of their household income on cigarettes.12 Recent research in India found an
association between tobacco use and low body mass index (BMI) and thinness.
Tobacco use was found to be an independent risk factor for low adult BMI13 and an
independent risk for thinness.14 Being underweight is a major mortality risk factor in poor
countries, causing more than 3.7 mil ion deaths per year 15
Health and safety of family farmers who grow tobacco
Quite apart from the health impacts of smoking or chewing tobacco are the
health hazards of working with tobacco. The nicotine inhaled from smoking or absorbed
from chewing tobacco is also rapidly absorbed through the skin when harvesting
tobacco, leading to a condition called ‘green tobacco sickness' (GTS). GTS has been
reported to occur in 1-10% of US tobacco workers. Younger workers are at higher risk,
which means that the prevalence may be even higher in developing economies where
children play a substantial role in harvesting and processing tobacco.16
Recent reseach in southern Brazil by Christian Aid revealed fundamental
problems in the relationship between a multinational tobacco company and growers.
Farmers were found to suffer from illnesses associated with exposure to pesticides
including depression, anxiety, neurological dysfunction, muscle aches and Parkinson's
disease-like tremors.17
Tobacco, deforestation and environmental health implications
Tobacco cultivation is increasingly being linked to deforestation because wood
is often used as fuel to cure tobacco leaves. A recent study that assessed the amount
of forest and woodland consumed annually for curing tobacco concluded that
7
deforestation related to tobacco constituted an issue of global relevance which could be
found on all continents, on average contributing nearly 5% to overall deforestation in the
respective growing countries of the developing world.18 The Bellagio statement on
tobacco and sustainable development concluded that, in the developing world, "tobacco
poses a major challenge, not just to health, but also to ... environmental sustainability."’9
In addition to its environmental impact, deforestation has been associated with
outbreaks of parasitic and other infectious diseases by favouring the spread of malarial
mosquitos or freshwater snails that spread schistosomiasis and other diseases such as
lymphatic filariasis, dengue fever, leishmaniasis, Chagas disease and bacterial
meningitis.20
Child labour
In the late 1990s, UNICEF concluded that the use of children in tobacco
production was widespread in many tobacco producing countries. Children harvesting
tobacco often experience nausea, vomiting and faintness due to nicotine poisoning, and
frequent heavy lifting and repetitive strain can cause permanent damage to growing
spines.21 The ILO is also actively working to stop the exploitation of children involved
in bidi rolling.22 Tobacco farmers often have no option but to involve their children in
tobacco cultivation because they cannot afford to employ casual labour and cannot
manage all the work themselves.23 Work-related injuries and fatalities in children have
been estimated to reach 6 million and 32,000, respectively, each year.24
Cost-effective interventions that make a difference
In most countries some form of government action, including taxes and
legislation, has been enacted to control tobacco consumption. Countries that have
adopted comprehensive tobacco control policies including a ban on advertising, strong
warnings on packages, controls on the use of tobacco indoors, high taxes on tobacco
products, and health education and smoking cessation programmes have had
considerable success.25
WHO has examined how best to reduce the health burden associated with
specific risk factors such as childhood undernutrition, cholesterol, unsafe sex and
tobacco use by reviewing the cost-effectiveness of selected interventions aimed at these
risk factors."' For tobacco, WHO examined the benefits of various interventions such as
taxation, advertising and sponsorship bans, smokefree policies, information provision
through package and labelling or counter-advertising and cessation programmes for
population health (in terms of DALYs) through the impact of reduced smoking on the
incidence of cardiovascular disease, respiratory disease, and various forms of cancer.
It was found that such interventions, not surprisingly, have a larger impact on population
health in regions with a high prevalence of tobacco use, especial y those in the second
or third stage of the tobacco epidemic (for example, Argentina, Guatemala, Ecuador.
Peru, Georgia, Hungary, Bangladesh, Nepal, Sri Lanka, Cambodia, China and Viet
Nam).
* This section is based on Chapter 5 of the World Health Report 2002.
Taxation was found to be the intervention of choice in all regions. Not only does
it have the greatest impact on population health, it is also the most cost-effective option.
Taxation also raises revenue for governments. Sometimes a portion of revenues from
tobacco taxes is allocated to the health sector to promote health and discourage
smoking behaviours. This in turn can help make other types of tobacco control efforts
both more effective and self-financing. This is particularly important to developing
countries where money to finance new public health initiatives is often scarce. The
combination of taxation, comprehensive bans on advertising, and information
dissemination activities was found to be affordable and cost-effective in the majority of
subregions under study. Adding smoking restrictions in public places increases the
costs, but results in even greater improvements in health.
These results match the findings of a comprehensive review of tobacco control
interventions by The World Bank. The World Bank reaches the conclusion that most
demand-side interventions such as increases in price, advertising and promotion bans,
and smoking restrictions are effective in reducing tobacco attributable mortality and
morbidity. However, while interventions to reduce demand for tobacco are likely to
succeed, measures to reduce its supply are less promising with one exception,
smuggling controls.
For example, the World Bank concludes that on average, a price rise of 10%
would be expected to reduce demand for tobacco products by about 8% in low and
middle income countries.26 Using a model of cohort smokers alive in 1995, it is
estimated that tax increases that would raise the real price of cigarettes by 10%
worldwide would cause about 42 mil ion of these smokers to quit, preventing a minimum
of 10 million tobacco related deaths. A combined set of non-price measures (such as
comprehensive bans on advertising and promotion, bans on smoking in public places,
prominent warning labels, and mass information) would cause some 23 mil ion smokers
to quit and would prevent 5 mil ion deaths.27 These conclusions have tremendous
implications for public health.
Treatment for tobacco dependence
Tobacco dependence is characterized as a long term disorder with high relapse
rates demanding ongoing care 2e. The treatment of tobacco dependence includes
(singly or in combination) behavioural and pharmacological interventions such as advice
and counselling, intensive support and administration of pharmaceuticals that contribute
to reducing or overcoming tobacco dependence in individuals or populations.29
Treatment of tobacco dependence significantly reduces the risk of tobaccorelated diseases in the short and medium term. Meta-analyses show that, along with
price and non-price measures, treatment of tobacco dependence is a cost-effective
policy measure in low and middle income countries30 As tobacco dependence
increasingly becomes a disease of low and middle income countries, getting adult
smokers to quit wil be essential.31
Despite the evidence on the effectiveness and cost-effectiveness of tobacco
treatment, smoking cessation interventions and treatment for tobacco dependence are
scarce in low and middle income countries, where health care providers do not
commonly carry out even minimal cessation interventions.
Treating individuals for tobacco dependence in low and middle income countries
is hampered by a number of factors. These include:
• The lack of a supportive environment to help smokers quit (e.g. smoke-free
places and smoke-free health care systems);
• Lack of integration of tobacco dependence treatment into health care
systems;
• Lack of knowledge and training of health care providers;
• High price of nicotine replacement therapy (NRT) products and cessation
services, and no insurance coverage;
• Regulation of NRT products.
Each of these factors is dealt with below.
Creating a supportive environment
The social environment lies at the heart of smoking cessation. For cessation
efforts to be successful, smoking must be made socially unacceptable. Tobacco
cessation must therefore include a broad mix of interventions that attempt to change the
social climate by, for example, increasing tobacco taxes, banning advertising, increasing
public health information and creating smoke-free public places. The other components
of a tobacco control framework include a health systems approach that promotes clinical
best practice and a surveillance, research and information approach.
Integrating tobacco dependence treatment into health care systems
Currently, tobacco dependence treatments and support to help smokers stop are
rarely integrated into health care systems and are not widely available to the general
public. Ensuring the availability of such support would entail training health care
providers and strengthening the infrastructure of health care systems to enable them to
accommodate, integrate and deliver tobacco dependence treatment services. This wil
require commitment and resources by governments.
Training health care providers
Health care providers who do not have a basic knowledge of the dangers of
tobacco use are less likely to motivate smokers to quit. In a recent WHO survey of
health professionals in Bahrain, Kuwait and the Republic of Korea an average of 17%
of physicians were reported to be unsure about whether or not passive smoking
increased the risk of heart disease in non-smoking adults. Only 22% of physicians in
Kuwait and Bahrain and 2% of pysicians in the Republic of Korea were reported to be
well-prepared to provide brief counselling advice to their patients.'12 Smoking rates
among the general population in these countries range from 23-64%.33 As role models
in many societies, health care professionals need to reduce their own tobacco
consumption in order to set better examples for their peers and patients. In view of the
high smoking prevalence proportions (55%, 53% and 48%) among male health care
professionals in Bosnia-Herzegovina, Bulgaria and Georgia, respectively34 health
professionals themselves would greatly benefit from smoking cessation training
programmes. In a number of countries, a decline in the prevalence of smoking among
physicians has preceded a decline in prevalence of smoking in the general population.
Improving accessibility of nicotine replacement therapy
Currently there are six approved formulations of NRT (gum, patch, inhalers,
nasal sprays, sublingual tablets and lozenges). The use of NRT increases the long-term
rates of smoking cessation and relieves the symptoms of nicotine withdrawal.35 NRT
doubles the smoker's chances of quitting. Despite a number of studies documenting
10
NRT's high safety, efficacy and utility,36 its availability is largely limited to some
developed countries, and its high costs restrict its accessibility. A recent survey on the
availability of NRT products in various developing countries showed that selected NRTs
such as gum and patch were sold over the counter in Venezuela and Qatar, while in
Thailand they were available only through prescription.37 In all countries first-line
pharmacotherapy such as Bupropion SR'V is not reimbursed by the health care system.
Deregulating NRT products
In comparison with cigarettes, NRT products are more stringently regulated and
hence less widely available. Deregulating nicotine products and lowering their price wil
improve their accessibility. Governments should ensure that NRT is at least as
accessible as tobacco products. Private and public partnerships should be fostered in
order to influence policies and programmes that make treatment of tobacco dependence
more available, affordable and accessible.
Research for tobacco control
Current knowledge on tobacco control has never been more comprehensive and
thorough. However, as always, gaps exist and more research is needed. The Research
for International Tobacco Control (RITC) unit of the Canadian International Development
Research Centre (1DRC) has been a leading player in creating a strong research,
funding and knowledge base for the development of effective tobacco control policies
and programme aimed at developing countries. A recently-updated Global Agenda for
Tobacco Control Research concludes that funding for tobacco control is clearly
inadequate at institutional and global levels. Funding levels must be increased and
coordination between existing research initiatives must be strengthened.
' A non-nicotme medication with anti-depresent properties. It is the first non-nicotine pharmological agent to be
approved for use in smoking cessation and has received regulatory approval In both the US and European Union
III.
Conclusion
Each day more than 13,000 people die prematurely because of tobacco use.
This figure is expected to almost double by the year 2020. Countries at all levels of
development are victims of the tobacco epidemic. The health impact alone of tobacco
warrants significant investment in strong tobacco control programmes. However, the
health consequences of tobacco use are only one facet of the tobacco epidemic. The
following factors heighten the importance of acting swiftly:
• The poor and uneducated are more likely to be victims of tobacco use;
• The burden of disease associated with tobacco use is increasingly borne by
developing countries;
• Tobacco use can contribute to malnutrition;
• The growing of tobacco leaves can have devastating health consequences
for farmers, and workers -especially children:
• Tobacco farming has been shown to contribute to deforestation;
There are signs of hope. Just recently the Organisation for Economic Co
operation and Development (OECD) Development Assistance Committee (DAC)
adopted a key Reference Document on Poverty and Health which specifically mentions
the profound effect of tobacco use on poverty and malnutrition in low-income countries,
when poor families purchase addictive tobacco rather than food. In the words of Dr Gro
Harlem Brundtland, the time has come to "involve the highest levels of Government and
the highest levels of opinion leaders in their efforts to build on the present momentum,
secure commitment, and reap the significant health and economic benefits that can be
achieved from a reduction in tobacco use."
1 Bellagio Statement on Tobacco and Sustainable Development, Bellagio, Italy, June 1995.
URL: http://www5.who.int/tobacco/page.cfm?tld=48
’ Corrao MA, Guindon GE, Sharma N, Shokoohi DF, editors. Tobacco control: country profiles.
Atlanta (GA): American Cancer Society; 2000
' Doll R.Uncovering the effects of smoking: historical perspective. Statistical Methods in Medical
Research, I February 1998, vol. 7, no. 2, pp. 87-117(31)
4 Pcto R, Lopez AD, Boreham J, Thun M, Heath CW. Mortality from tobacco in developed countries:
indirect estimates from national vital statistics. Lancet 1992: 339; 1268-78
' Liu BQ, Pcto R, Chen ZM, Boreham J, Wu YP, Li JY, et al. Emerging tobacco hazards in China.
BMJ 1998; 317- 1411-22.
Niu SR, Yang GH, Chen ZM, Wang JL» Wang GH, He XZ, et al. Emerging tobacco hazards in China.
BMJ 1998; 317; 1423-4.
0 Dikshit RP. Kanhere S. Tobacco habits and risk of lung, oropharyngeal and oral cavity cancer: a
population-based case-control study in Bhopal, India. International Journal of Epidemiology 2000; 29:
609-14.
‘ International Agency for Research on Cancer. Involuntary smoking. Summary of Data reported and
evaluation. I ARC, 2002. (Full report in press)
URL: http,//monographs.iarc.fr/htdocs/monographs/vol83/02-involuntary.html
® Bobak et al (2000) Poverty and Smoking inTobacco Control in Developing Countries. Edited by
Prabhat Jha and Frank Chaloupka. Published by OUP for the World Bank and World Health
Organization.
‘ Chinese Academy of Preventive Medicine (1997). National Prevalence Survey of Smoking Pattern.
Beijing: China Science and Technology Press.
’’ World Bank (1990). Brazil; The New Challenge of Adult Health. Washington D C , The World Bank.
1,1 Bobak et al (2000) Poverty and . In: Jha P, Chaloupka FJ, eds. Tobacco control in developing
countries. New York: Oxford University Press, 2000.
Efroymson D, Ahmed S, Townsend J, et al. Hungry for tobacco: an analysis of the economic impact
of tobacco consumption on the poor in Bangladesh. Tobacco Control 2001;10:212-2 17
12 de Beyer et al. Poverty and tobacco, Tob Control 2001 10:210-211
V?
O
Shuklal IIC. Gupta PC, Pcdnckar M. Hebert JR. Tobacco use: an independent risk factor for poor
nutrition -Implications for public health in India. (Unpublished)
Shukla HC, Gupta PC, Mehta HC, Hebert JR. Descriptive epidemiology of body mass index of an
urban adult population in western India. J Epidemiol Community Health. 2002 Nov;56( 11 ):876-80.
15
World Health Report 2002
16
McBride JS, Altman DG, Klein M, White W. Green tobacco sickness. Tobacco Control 1998; 7:2948.
17
Christian Aid. 2002. Hooked on tobacco. Report by Christian Aid/ DESER on British American
Tobacco subsidiary, Souza Cruz
h Geist Helmut J. Global assessment of deforestation related to tobacco farming. Tob C ontrol
1999:8:18-28 ( Spring )
' Bellagio Statement on Tobacco and Sustainable Development, Bellagio, Italy, June 1995.
URL: http://www5.who.int/tobacco/page.cfm?tld=48
Jl World health Organization. 1999. Removing obstacles to healthy development: report on infectious
diseases. Geneva : World Health Organization, 1999. WHO/CDS/99.1
URL: http://whqlibdoc.who.int/hq/1999/WHO_CDS_99.1 .pdf
1 UNICEF. The State of the World's Children 1997 (Oxford, 1997)
22
International Labour Organization. Facts on Child Labour. Sustainable development at work. World
Summit on Sustainable Development. ILO 2002.
URL: http://wwwjlo.org/public/cnglish/burcau/inf/download/wssd/pdf/childlabour.pdf
23
Christian Aid. 2002.
24
Graitcer, Philip L. and Lercr Leonard B. I998. Child Labor and Health: Quantifying the Global
Health Impacts of Child Labor. The World Bank.
URL; http://www.globalmarch.org/virtuallibrary/worldbank/child-labor-health-quantyfmg.pdf
2' World Health. Guidelines for controlling and monitoring the tobacco epidemic . Geneva: World
Health Organization: 1998.
13
The World Bank. Curbing the epidemic: governments and the economics of tobacco control. Senes
Development in practice. Washington DC: The World Bank, 1999.
L'RL: http? www I .worldbank.org/tobacco/rcports.htm
Ranson K. Jha P. Chaloupka FJ, et al. The effectiveness and cost-cffcctivcncss of price increases and
other tobacco-control policies. In: Jha P, Chaloupka FJ, cds. Tobacco control in developing countries.
New York. Oxford University Press, 2000.
■s Fiore MC, Bailey et al., Smoking cessation. Rockville, MD. Agency for Health Care Policy and
Rescrch. US Department of Health and Human Services, 1996 ( Clinical practice guidelines No. 18.
Publication No 960692
■' World Health Organization (WHO) European Partnership Project to Reduce Tobacco Dependence.
February 2001. Recommendations on the treatment of Tobacco Dependence: Evidence based core
recommendations for health care systems in Europe.
World Bank. Curbing the epidemic. Governments and the economics of tobacco control.
Washington. The World Bank. 1999
1 Pcto. R., Lopez, AD., Borcham, J., Thus, M. & Heath, C. ( 1994). Mortality from Smoking in
Developed Countries, 1950-2000: Indirect Estimates from Natinal Vital Statistics. Oxford University
Press. ( Updated 1998)
’ Unpublished data from the WHO Global Health Professional Survey in Bahrain. Kuwait and Korea.
2001.
" Corrao MA. Guindon GE, Sharma N, Shokoohi DF, editors. Tobacco control: country profiles.
Atlanta (GA): American Cancer Society; 2000.
" Corrao MA. Guindon GE, Sharma N, Shokoohi DF, editors. Tobacco control: country profiles.
Atlanta (GA)- American Cancer Society; 2000.
' Rigotti NA. Treatment of tobacco use and dependence. N Engl J Med 2000:346 (7): 506-12
h Cromwell J. Bartosch WJ. Fiore MC. Hasselblad V. Baker T. Cost-effectiveness of the clinical
practice recommendations in the AHCPR
guideline for smoking cessation. Agency for I lealth Care
Policy and Research. JAMA. 278(21): 1759-66, 1997 Dec 3.
Data from Global Health Professional Survey in Bahrain, Kuwait and Korea 2001. Unpublished.
14
I his document Was produced by the World Health Organisation (WHO) for Health & Consumer Protection Directorate
and represents the views of the World Health Organisation (WHO). These views have not been adopted or in any way <i|
by the Commission and do not necessarily represent the view of the Commission or the Directorate General for Hen
accept responsibility for any use made thereof.
Responses to the bill
CIGARETTES AND OTHER TOBACCO PRODUCTS (PROHIBITION OF
ADVERTISEMENT AND REGULATION OF TRADE AND COMMERCE,
PRODUCTION, SUPPLY AND DISTRIBUTION) BILL, 2001
Introduction
The Tobacco Control Bill introduced recently in the Indian Parliament has been the subject of
much debate and comment in the media. Some of the opinions expressed reflect concerns about
the Bill’s provisions or its effects. These concerns need a reasoned response. AFTC has
attempted to do that below by providing clarifications about key provisions of the Bill and
addressing other concerns.
I.
ADVERTISING
The Bill seeks to ban all forms of direct and indirect advertising. It also bans tobacco
sponsorship of sports and cultural events.
IVliat does Advertising do?
•
Increases consumption: Tobacco companies often claim their advertising is aimed only at
brand switching and not at attracting new consumers. It does not appeal to business sense that
an industry that works under tremendous compulsion to consistently replace half of its
committed users (who prematurely die from using their products), does not want to recruit
fresh users. Il is therefore evident that tobacco advertising, as with advertisements for any
other products, is geared at increasing product use.
•
Lures gullible youth and children through glamorous and deceptive promotional stunts
addicting them for a life-time. Advertising, which projects tobacco use in congenial
surroundings or associates the brand name with idolized role models, legitimizes the habit in
these young minds and projects the use of tobacco as socially acceptable.
Why do we need an ad han?
•
•
•
•
Tobacco advertising involves the promotion of a product that is proven to cause 25-odd lifethreatening or disabling diseases and induces life-long addiction amongst its users.
To protect people from being misled by false images or misleading health claims and
deprived of their right to make a free and informed choice.
To prevent fresh users from picking up the habit and thereby reduce consumption and
resultant morbidity, mortality and economic loss to the community and the nation
To protect children and adolescents from being attracted to tobacco products.
Do tobacco Advertising bans work?
A World Bank Study of 102 countries demonstrates that countries which have imposed a
comprehensive ban on all forms of tobacco advertising have had steeper declines in tobacco
consumption compared to those that had not done so.
Does the ban leave cross border advertising unabated?
The apprehension about the possibility for continued cross-border advertising should be allayed
by the fact that the recently concluded WHO Framework Convention on Tobacco Control
(FCTC) recognizes the right of countries to ban cross-border advertising and apply appropriate
penalties against violators. If we enact suitable national legislation, such penalties may include
marketing bans on products so advertised. The FCTC also has strong provisions on smuggling.
International protocols are soon to be initiated both on cross-border advertising and smuggling.
This would facilitate sufficient marketing and trade regulation of international brands coming
into the country.
Effect on allied industries like the Advertising Sector
Experience from home and abroad reveals that relinquishing a particular brand or a product does
not affect the revenues of this multi-product industry, as alternate products would replace them.
II TOBACCO PACKAGE WARNINGS
The Bill mandates effective health warnings that are clear and visible, including provisions for
pictures.
Experience of countries like Canada and Brazil which have introduced pictorial health warnings
occupying 50 % and more of the package space shows that they are effective not only in
discouraging use among current tobacco users but also extends caution to potential users.
Recently, the 14 countries of European Union and Thailand have enacted laws introducing
pictorial health warnings.
III.
BAN ON SALE OF TOBACCO PRODUCTS TO MINORS AND WITHIN 100
METERS OF EDUCATIONAL INSTITUTIONS.
•
These are measures aimed at restricting easy youth access to tobacco products. If
supplemented with pragmatic implementation procedures, this would prove to be a major
step in preventing early initiation into tobacco addiction.
•
It is well documented that the age at initiation into tobacco use spans across the teen years
and that prevention at these early stages would help reduce consumption considerably.
•
It is also well established that persons who started smoking in teens are much more likely to
die early due to tobacco related diseases.
The provision is restricted to minors only and does not place any restrictions on the sale of
tobacco products to adults.
•
IV.
WOULD THE BILL LEAD TO MASSIVE UNEMPLOYMENT AMONG
TOBACCO WORKERS AND RETAILERS?
•
The Bill does not contain any provisions directly regulating tobacco production.
•
It primarily involves demand-reduction strategies geared to prevent new entrants to tobacco
habit. Demand reduction will not be sudden but will be spread over several years, giving
sufficient time to set in motion alternate employment opportunities to anyone dependent on
or engaged in tobacco production.
Hence the fears of unemployment among tobacco
workers, fanners and retailers are unfounded.
•
As the Bill does not ban the sale of any tobacco product, there would not be any adverse
effects on the sale and profits to retailers.
•
With the current rate of population growth in developing countries like ours, there is not
going to be a sudden drop in tobacco consumption even with comprehensive tobacco control
policies, as the actual number of tobacco users in the population would not fall in the near
future. Consequently, the Bill would not have any immediate effect on tobacco supply side. It
would, however, initiate a progressive decline which will result in a substantial reduction in
tobacco consumption over the next half century. It will also prevent many young persons
from becoming early addicts.
•
On the contrary, increasing mechanisation of the production process and profit motivated,
political maneuvering at the auction floors by large tobacco and leaf companies are largely
responsible for the rampant unemployment and poverty among tobacco workers and small
fanners. When global tobacco demand falls and our exports shrink, the tobacco industry is
quick to abandon the fanners while protecting its profits and diversifying its investments.
•
We believe that it will benefit the fanners, workers and the country as a whole if the
government helps the process of diversification wherein people engaged in tobacco
production can be shifted to alternate occupations.
V.
IS THE BILL PARTIAL TO SMOKELESS TOBACCO?
The Bill , as reinforced with the Standing Committee provisions and passed by the Rajya Sabha,
encompasses all forms of tobacco products- smoking and smokeless. It thus provides a level
playing ground to all of them. Peculiarities of various segments of the tobacco industry could be
better addressed while drafting Rules under the Bill.
BAN ON SMOKING IN PUBLIC PLACES
The bill recognizes and protects the rights of non-smokers to remain safe from the harmful
effects of environmental tobacco smoke (passive smoking). Skeptics have doubted whether this
provision can be effectively implemented. We believe that this Bill confers a much needed
entitlement to non-smokers to assert that right. Public education is also required to raise the
consciousness of the ban and its rationale. A combination of regulation (to confer the right) and
community mobilization (to assert and respect the right) is needed to ensure smoke-free public
places.
pH-S.
CIGARETTES AND OTHER TOBACCO PRODUCTS
[PROHIBITION OF ADVERTISEMENT AND REGULATION OF TRADE AND COMMERCE,
PRODUCTION, SUPPLY AND DISTRIBUTION] ACT, 2003
&
Cigarettes and other Tobacco Products (Prohibition of Advertisement and Regulation of
Trade and Commerce, production, Supply and Distribution] Rules, 2004
a
Prohibition ott sale of Cigarettes and other Tobacco Products around Educational
Institutions Rules, 2004
&
Cigarette and other Tobacco Products (Prohibition of Advertisement and Regulation of
Trade and Commerce, Production, Supply and Distribution) Rules, 2005
&
Supreme Court Judgement in Murli S. Deora Us. Union of India & others case
TOBACCO KILLS
THE WHOLE FAMILY
Compiled by: Hemant Goswami
ah
Burning Brain Society
CIGARETTES AND OTHER TOBACCO PRODUCTS ACT, 2003
Compiled by: Hemant Goswami for Burning Brain Society
Cigarettes and Other Tobacco Products (Prohibition of
Advertisement and Regulation of Trade and Commerce,
Production, Supply and Distribution) Act, 2003
SECTIONS
I.
Short title, extent and commencement.
2.
Declaration as to expediency of control by the Union.
3.
Definitions.
4.
Prohibition of smoking in a public place.
Prohibition of advertisement of cigarettes and other tobacco products.
5.
6.
Prohibition on sale of cigarette or other tobacco products to a person below the
age of eighteen years and in particular area.
7.
Restrictions on trade and commerce in, and production, supply and distribution
of cigarettes and other tobacco products.
8.
Manner in which specified warning shall be made.
9.
Language in which the specified warning shall be expressed.
10.
Size of letters and figures.
11.
Testing laboratory for nicotine and tar contents.
12.
Power of entry and search.
13.
Power to seize.
14.
Confiscation of package.
15.
Power to give option to pay costs in lieu of confiscation.
16.
Confiscation not to interfere with other punishments.
17.
Adjudication.
18.
Giving opportunity to the owner of seized packages.
19.
Appeal.
20.
Punishment for failure to give specified warning and nicotine and tar contents.
21.
Punishment for smoking in certain places.
22.
Punishment for advertisement of cigarettes and tobacco products.
23.
Forfeiture of advertisement and advertisement material.
24.
Punishment for sale of cigarettes or any other tobacco products in certain places
or to persons below the age of eighteen years.
25.
Prevention, detention and place of trial of offences under sections 4 and 6.
26.
Offences by companies.
27.
Offences to be bailable.
28.
Composition of offences.
29.
Protection of action taken in good faith.
30.
Power to add any tobacco products in the Schedule.
BURNING BRAIN SOCIETY
#3,
ass Office, Business
Arcade,E-Mai
Shilv:alsoci
ikvieety@burni
w, Sectorngbrai
17-E,nChandi
garh 160 n017gbraiINDIA
Tel:Gl+91-172-5165555,
5185600
.org : www.burni
n.org
2
pi-vS
Guidelines for implementation of Article 5.3 of the
WHO Framework Convention on Tobacco Control
on the protection of public health policies
with respect to tobacco control from commercial
and other vested interests of the tobacco industry
INTRODUCTION
1.
World Health Assembly resolution WHA54.18 on transparency in tobacco control
process, citing the findings of the Committee of Experts on Tobacco Industry Documents,
states that “the tobacco industry has operated for years with the express intention of
subverting the role of governments and of WHO in implementing public health policies to
combat the tobacco epidemic”.
2.
The Preamble of the WHO Framework Convention on Tobacco Control recognized the
Parties’1 “need to be alert to any efforts by the tobacco industry to undermine or subvert
tobacco control efforts and the need to be informed of activities of the tobacco industry that
have a negative impact on tobacco control efforts".
3.
Further, Article 5.3 of the Convention requires that “in setting and implementing their
public health policies with respect to tobacco control. Parties shall act to protect these policies
from commercial and other vested interests of the tobacco industry in accordance with
national law”.
4.
The Conference of the Parties, in decision FCTC/C0P2( 14), established a working
group to elaborate guidelines for implementation of Article 5.3 of the Convention.
5.
Without prejudice to the sovereign right of the Parties to determine and establish their
tobacco control policies. Parties are encouraged to implement these guidelines to the extent
possible in accordance with their national law.
Purpose, scope and applicability
6.
Use of the guidelines for implementation of Article 5.3 of the Convention will have an
overarching impact on countries’ tobacco control policies and on implementation of the
Convention, because the guidelines recognize that tobacco industry interference, including
that from the State-owned tobacco industry, cuts across a number of tobacco control policy
areas, as stated in the Preamble of the Convention, articles referring to specific tobacco
control policies and the Rules of Procedure of the Conference of the Parties to the WHO
Framework Convention on Tobacco Control.
1 “The term ‘Parties' refers to States and other entities with treaty-making capacity which have expressed
their consent to be bound by a treaty and where the treaty is in force for such States and entities." (Source: United
7.
The purpose of these guidelines is to ensure that efforts to protect tobacco control from
commercial and other vested interests of the tobacco industry are comprehensive and
effective. Parties should implement measures in all branches of government that may have an
interest in, or the capacity to, affect public health policies with respect to tobacco control.
8.
The aim of these guidefines is to assist Parties" in meeting their legal obligations under
Article 5.3 of the Convention. The guidelines draw on the best available scientific evidence
and the experience of Parties in addressing tobacco industry interference.
9.
The guidelines apply to setting and implementing Parties’ public health policies with
respect to tobacco control. They also apply to persons, bodies or entities that contribute to, or
could contribute to, the formulation, implementation, administration or enforcement of those
policies.
10.
The guidelines are applicable to government officials, representatives and employees of
any national, state, provincial, municipal, local or other public or semi/quasi-public institution
or body within the jurisdiction of a Party, and to any person acting on their behalf. Any
government branch (executive, legislative and judiciary) responsible for setting and
implementing tobacco control policies and for protecting those policies against tobacco
industry interests should be accountable.
11.
The broad array of strategies and tactics used by the tobacco industry to interfere with
the setting and implementing of tobacco control measures, such as those that Parties to the
Convention are required to implement, is documented by a vast body of evidence. The
measures recommended in these guidelines aim at protecting against interference not only by
the tobacco industry but also, as appropriate, by organizations and individuals that work to
further the interests of the tobacco industry.
12.
While the measures recommended in these guidelines should be applied by Parties as
broadly as necessary, in order best to achieve the objectives of Article 5.3 of the Convention,
Parties are strongly urged to implement measures beyond those recommended in these
guidelines when adapting them to their specific circumstances.
GUIDING PRINCIPLES
Principle 1: There is a fundamental and irreconcilable conflict between the tobacco
industry’s interests and public health policy interests.
13.
The tobacco industry produces and promotes a product that has been proven
scientifically to be addictive, to cause disease and death and to give rise to a variety of social
ills, including increased poverty. Therefore, Parties should protect the formulation and
implementation of public health policies for tobacco control from the tobacco industry to the
greatest extent possible.
2 Where appropriate, these guidelines also refer to regional economic integration organizations.
Principle 2: Parties, when dealing with the tobacco industry or those working to further its
interests, should be accountable and transparent.
14.
Parties should ensure that any interaction with the tobacco industry on matters related to
tobacco control or public health is accountable and transparent.
Principle 3: Parties should require the tobacco industry and those working to further its
interests to operate and act in a manner that is accountable and transparent.
15.
The tobacco industry should be required to provide Parties with information for
effective implementation of these guidelines.
Principle 4: Because their products are lethal, the tobacco industry should not be granted
incentives to establish or run their businesses.
16.
Any preferential treatment of the tobacco industry would be in conflict with tobacco
control policy.
RECOMMENDATIONS
17.
The following important activities are recommended for addressing tobacco industry
interference in public health policies:
(1)
Raise awareness about the addictive and harmful nature of tobacco products and
about tobacco industry interference with Parties’ tobacco control policies.
(2)
Establish measures to limit interactions with the tobacco industry and ensure the
transparency of those interactions that occur.
(3)
Reject partnerships and non-binding or non-enforceable agreements with the
tobacco industry.
(4)
Avoid conflicts of interest for government officials and employees.
(5)
Require that information provided by the tobacco industry be transparent and
accurate.
(6)
Denormalize and, to the extent possible, regulate activities described as “socially
responsible” by the tobacco industry, including but not limited to activities described as
“corporate social responsibility”.
(7)
Do not give preferential treatment to the tobacco industry.
(8)
Treat State-owned tobacco industry in the same way as any other tobacco
industry.
18.
Agreed measures for protecting public health policies with respect to tobacco control
from commercial and other vested interests of the tobacco industry are listed below. Parties
are encouraged to implement measures beyond those provided for by these guidelines, and
nothing in these guidelines shall prevent a Party from imposing stricter requirements that are
consistent with these recommendations.
(1)
Raise awareness about the addictive and harmful nature of tobacco
products and about tobacco industry interference with Parties’ tobacco control
policies. '
..
19.
All branches of government and the public need knowledge and awareness about past
and present interference by the tobacco industry in setting and implementing public health
policies with respect to tobacco control. Such interference requires specific action for
successful implementation of the whole Framework Convention.
Recommendations
1.1
Parties should, in consideration of Article 12 of the Convention, inform and
educate all branches of government and the public about the addictive and harmful
nature of tobacco products, the need to protect public health policies for tobacco control
from commercial and other vested interests of the tobacco industry and the strategies
and tactics used by the tobacco industry to interfere with the setting and implementation
of public health policies with respect to tobacco control.
1.2
Parties should, in addition, raise awareness about the tobacco industry’s practice
of using individuals, front groups and affiliated organizations to act, openly or covertly,
on their behalf or to take action to further the interests of the tobacco industry.
(2)
Establish measures to limit interactions with the tobacco industry and
ensure the transparency of those interactions that occur.
20.
In setting and implementing public health policies with respect to tobacco control, any
necessary interaction with the tobacco industry should be carried out by Parties in such a way
as to avoid the creation of any perception of a real or potential partnership or cooperation
resulting from or on account of such interaction. In the event the tobacco industry engages in
any conduct that may create such a perception, Parties should act to prevent or correct this
perception.
Recommendations
2.1
Parties should interact with the tobacco industry only when and to the extent
strictly necessary to enable them to effectively regulate the tobacco industry and
tobacco products.
2.2
Where interactions with the tobacco industry are necessary, Parties should ensure
that such interactions are conducted transparently. Whenever possible, interactions
should be conducted in public, for example through public hearings, public notice of
interactions, disclosure of records of such interactions to the public.
(3)
Reject partnerships and non-binding or non-enforceable agreements with
the tobacco industry.
21.
The tobacco industry should not be a partner in any initiative linked to setting or
implementing public health policies, given that its interests are in direct conflict with the
goals of public health.
Recommendations
3.1
Parties should not accept, support or endorse partnerships and non-binding or
non-enforceable agreements as well as any voluntary arrangement with the tobacco
industry or any entity or person working to further its interests.
3.2
Parties should not accept, support or endorse the tobacco industry organizing,
promoting, participating in, or performing, youth, public education or any initiatives
that are directly or indirectly related to tobacco control.
3.3
Parties should not accept, support or endorse any voluntary code of conduct or
instrument drafted by the tobacco industry that is offered as a substitute for legally
enforceable tobacco control measures.
3.4
Parties should not accept, support or endorse any offer for assistance or proposed
tobacco control legislation or policy drafted by or in collaboration with the tobacco
industry.
(4)
Avoid conflicts of interest for government officials and employees.
22.
The involvement of organizations or individuals with commercial or vested interests in
the tobacco industry in public health policies with respect to tobacco control is most likely to
have a negative effect. Clear rules regarding conflicts of interest for government officials and
employees working in tobacco control are important means for protecting such policies from
interference by the tobacco industry.
23.
Payments, gifts and services, monetary or in-kind, and research funding offered by the
tobacco industry to government institutions, officials or employees can create conflicts of
interest. Conflicting interests are created even if a promise of favourable consideration is not
given in exchange, as the potential exists for personal interest to influence official
responsibilities as recognized in the International Code of Conduct for Public Officials
adopted by the United Nations General Assembly and by several governmental and regional
economic integration organizations.
Recommendations
4.1
Parties should mandate a policy on the disclosure and management of conflicts of
interest that applies to all persons involved in setting and implementing public health
policies with respect to tobacco control, including government officials, employees,
consultants and contractors.
4.2
Parties should formulate, adopt and implement a code of conduct for public
officials, prescribing the standards with which they should comply in their dealings
with the tobacco industry.
4.3
Parties should not award contracts for carrying out any work related to setting
and implementing public health policies with respect to tobacco control to candidates
or tenderers who have conflicts of interest with established tobacco control policies.
4.4
Parties should develop clear policies that require public office holders who have
or have had a role in setting and implementing public health policies with respect to
tobacco control to inform their institutions about any intention to engage in an
occupational activity within the tobacco industry, whether gainful or not, within a
specified period of time after leaving service.
4.5
Parties should develop clear policies that require applicants for public office
positions which have a role in setting and implementing public health policies with
respect to tobacco control to declare any current or previous occupational activity with
any tobacco industry whether gainful or not.
4.6
Parties should require government officials to declare and divest themselves of
direct interests in the tobacco industry.
4.7
Government institutions and their bodies should not have any financial interest in
the tobacco industry, unless they are responsible for managing a Party’s ownership
interest in a State-owned tobacco industry.
4.8
Parties should not allow any person employed by the tobacco industry or any
entity working to further its interests to be a member of any government body,
committee or advisory group that sets or implements tobacco control or public health
policy.
4.9
Parties should not nominate any person employed by the tobacco industry or any
entity working to further its interests to serve on delegations to meetings of the
Conference of the Parties, its subsidiary bodies or any other bodies established pursuant
to decisions of the Conference of the Parties.
4.10
Parties should not allow any official or employee of government or of any
semi/quasi-governmental body to accept payments, gifts or services, monetary or inkind, from the tobacco industry.
4.11
Taking into account national law and constitutional principles, Parties should
have effective measures to prohibit contributions from the tobacco industry or any
entity working to further its interests to political parties, candidates or campaigns, or to
require full disclosure of such contributions.
(5)
Require that information provided by the tobacco industry be transparent
and accurate.
24.
To take effective measures preventing interference of the tobacco industry with public
health policies, Parties need information about its activities and practices, thus ensuring that
the industry operates in a transparent manner. Article 12 of the Convention requires Parties to
promote public access to such information in accordance with national law.
25.
Article 20.4 of the Convention requires, inter alia, Parties to promote and facilitate
exchanges of information about tobacco industry practices and the cultivation of tobacco. In
accordance with Article 20.4(c) of the Convention, each Party should endeavour to cooperate
with competent international organizations to establish progressively and maintain a global
system to regularly collect and disseminate information on tobacco production and
manufacture and activities of the tobacco industry which have an impact on the Convention or
national tobacco control activities.
Recommendations
5.1
Parties should introduce and apply measures to ensure that all operations and
activities of the tobacco industry are transparent.3
5.2
Parties should require the tobacco industry and those working to further its
interests to periodically submit information on tobacco production, manufacture,
market share, marketing expenditures, revenues and any other activity, including
lobbying, philanthropy, political contributions and all other activities not prohibited or
not yet prohibited under Article 13 of the Convention.1
5.3
Parties should require rules for the disclosure or registration of the tobacco
industry entities, affiliated organizations and individuals acting on their behalf,
including lobbyists.
5.4
Parties should impose mandatory penalties on the tobacco industry in case of the
provision of false or misleading information in accordance with national law.
5.5
Parties should adopt and implement effective legislative, executive,
administrative and other measures to ensure public access, in accordance with Article
12(c) of the Convention, to a wide range of information on tobacco industry activities
as relevant to the objectives of the Convention, such as in a public repository.
(6)
Denormalize and, to the extent possible, regulate activities described as
“socially responsible” by the tobacco industry, including but not limited to
activities described as “corporate social responsibility”.
26.
The tobacco industry conducts activities described as socially responsible to distance its
image from the lethal nature of the product it produces and sells or to interfere with the setting
and implementation of public health policies. Activities that are described as “socially
responsible” by the tobacco industry, aiming at the promotion of tobacco consumption, is a
marketing as well as a public relations strategy that falls within the Convention’s definition of
advertising, promotion and sponsorship.
27.
The corporate social responsibility of the tobacco industry is, according to WHO,4 an
inherent contradiction, as industry’s core functions are in conflict with the goals of public
health policies with respect to tobacco control.
Recommendations
6.1
Parties should ensure that all branches of government and the public are informed
and made aware of the true purpose and scope of activities described as socially
responsible performed by the tobacco industry.
6.2
Parties should not endorse, support, form partnerships with or participate in
activities of the tobacco industry described as socially responsible.
3 Without prejudice to trade secrets or confidential information protected by law.
■'WHO. Tobacco industry and corporate social responsibility - an inherent contradiction. Geneva, World
Health Organization, 2004.
6.3
Parties should not allow public disclosure by the tobacco industry or any other
person acting on its behalf of activities described as socially responsible or of the
expenditures made for these activities, except when legally required to report on such
expenditures, such as in an annual report.5
6.4
Parties should not allow acceptance by any branch of government or the public
sector of political, social, financial, educational, community or other contributions from
the tobacco industry or from those working to further its interests, except for
compensations due to legal settlements or mandated by law or legally binding and
enforceable agreements.
(7)
Do not give preferential treatment to the tobacco industry.
28.
Some governments encourage investments by the tobacco industry, even to the extent
of subsidizing them with financial incentives, such as providing partial or complete
exemption from taxes otherwise mandated by law.
29.
Without prejudice to their sovereign right to determine and establish their economic,
financial and taxation policies, Parties should respect their commitments for tobacco control.
Recommendations
7.1
Parties should not grant incentives, privileges or benefits to the tobacco industry
to establish or run their businesses.
7.2
Parties that do not have a State-owned tobacco industry should not invest in the
tobacco industry and related ventures. Parties with a State-owned tobacco industry
should ensure that any investment in the tobacco industry does not prevent them from
fully implementing the WHO Framework Convention on Tobacco Control.
7.3
Parties should not provide any preferential tax exemption to the tobacco industry.
(8)
Treat State-owned tobacco industry in the same way as any other tobacco
industry.
30.
Tobacco industry can be government-owned, non-government-owned or a
combination thereof. These guidelines apply to all tobacco industry, regardless of its
ownership.
Recommendations
8.1 Parties should ensure that State-owned tobacco industry is treated in the same
way as any other member of the tobacco industry in respect of setting and
implementing tobacco control policy.
8.2 Parties should ensure that the setting and implementing of tobacco control policy
are separated from overseeing or managing tobacco industry.
5 The guidelines for implementation of Article 13 of the WHO Framework Convention on Tobacco
Control address this subject from the perspective of tobacco advertising, promotion and sponsorship.
8.3
Parties should ensure that representatives of State-owned tobacco industry does
not form part of delegations to any meetings of the Conference of the Parties, its
subsidiary bodies or any other bodies established pursuant to decisions of the
Conference of the Parties.
Enforcement and monitoring
Enforcement
31.
Parties should put in place enforcement mechanisms or, to the extent possible, use
existing enforcement mechanisms to meet their obligations under Article 5.3 of the
Convention and these guidelines.
Monitoring implementation of Article 5.3 of the Convention and of these guidelines
32.
Monitoring implementation of Article 5.3 of the Convention and of these guidelines is
essential for ensuring the introduction and implementation of efficient tobacco control
policies. This should also involve monitoring the tobacco industry, for which existing models
and resources should be used, such as the database on tobacco industry monitoring of the
WHO Tobacco Free Initiative.
33.
Nongovernmental organizations and other members of civil society not affiliated with
the tobacco industry could play an essential role in monitoring the activities of the tobacco
industry.
34.
Codes of conduct or staff regulations for all branches of governments should include a
“whistleblower function”, with adequate protection of whistleblowers. In addition, Parties
should be encouraged to use and enforce mechanisms to ensure compliance with these
guidelines, such as the possibility of bringing an action to court, and to use complaint
procedures such as an ombudsman system.
INTERNATIONAL COLLABORATION AND UPDATING AND
REVISION OF THE GUIDELINES
35.
International cooperation is essential for making progress in preventing interference by
the tobacco industry with the formulation of public health policies on tobacco control. Article
20.4
of the Convention provides the basis for collecting and exchanging knowledge and
experience with respect to tobacco industry practices, taking into account and addressing the
special needs of developing country Parties and Parties with economies in transition.
36.
Efforts have already been made to coordinate the collection and dissemination of
national and international experience with regard to the strategies and tactics used by the
tobacco industry and to the monitoring of tobacco industry activities. Parties would benefit
from sharing legal and strategic expertise for countering tobacco industry strategies.
Article 21.4 of the Convention provides that information exchange should be subject to
national laws regarding confidentiality and privacy.
Recommendations
37.
As the strategies and tactics used by the tobacco industry evolve constantly, these
guidelines should be reviewed and revised periodically to ensure that they continue to provide
effective guidance to Parties on protecting their public health policies on tobacco control from
tobacco industry interference.
38.
Parties reporting via the existing reporting instrument of the Framework Convention
should provide information on tobacco production and manufacture and the activities of the
tobacco industry that affect the Convention or national tobacco control activities. To facilitate
this exchange, the Convention Secretariat should ensure that the principal provisions of these
guidelines are reflected in the next phases of the reporting instrument, which the Conference
of the Parties will gradually adopt for use by Parties.
39.
In view of the paramount importance of preventing tobacco industry interference in any
public health policy with respect to tobacco control, the Conference of the Parties may, in the
light of experience with implementing these guidelines, consider whether there is a need to
elaborate a protocol in relation to Article 5.3 of the Convention.
10
USEFUL SOURCES OF INFORMATION
Relevant literature
Brandt AM. The cigarette century. The rise, fall, and deadly persistence of the product that
defined America. New York. Basic Books, 2007.
Chapman S. Making smoking history. Public health advocacy and tobacco control. Oxford,
Blackwell Publishing, 2007.
Callard C, Thompson D, Collishaw N. Curing the addiction to profits: a supply-side
approach to phasing out tobacco. Ottawa, Canadian Centre for Policy Alternatives and
Physicians for a Smoke-free Canada, 2005.
Feldman EA, Bayer R (Editors). Unfdtered: conflicts over tobacco policy and public health.
Boston, Harvard University Press, 2004.
Gilmore A et al. Continuing influence of tobacco industry in Germany. Lancet, 2002,
360:1255.
Hastings G, Angus K. The influence of the tobacco industry on European tobacco control
policy. In: Tobacco or health in the European Union. Past, present and future. Luxembourg,
Office for Official Publications of the European Commission, 2004:195-225.
Lavack A. Tobacco industry denormalization campaigns: a review and evaluation. Ottawa,
Health Canada, 2001.
Mahood G. Tobacco industry denormalization. Telling the truth about the tobacco industry's
role in the tobacco epidemic. Toronto, Campaign for Tobacco Industry Denormalization,
2004.
Pan American Health Organization. Profits over people. Tobacco industry activities to market
cigarettes and undermine public health in Latin America and the Caribbean. Washington DC,
Pan American Health Organization, 2002.
Simpson D. Germany: still sleeping with the enemy. Tobacco Control, 2003, 12:343-344.
Hammond R, Rowell A. Trust us. We're the tobacco industry. Baltimore, Johns Hopkins
University Press, 2001.
World Health Organization. Tobacco company strategies to undermine tobacco control
activities at the World Health Organization. Geneva, World Health Organization, 2000.
World Health Organization. Tobacco industry and corporate social responsibility - an
inherent contradiction. Geneva, World Health Organization, 2004.
Yach D, Bialous S. Junking science to promote tobacco. American Journal of Public Health,
2001,91:1745-1748.
11
Web resources
WHO sites:
Tobacco Free Initiative: http://www.who.int/tobacco/en/
WHO publications on tobacco: http://www.who.int/tobacco/resources/publications/en/
WHO European Regional Office:
http://www.euro.who.int/healthtopics/HT2ndLvIPage?HTCode=smoking
Tobacco control in the Americas (in English and Spanish):
http://www.paho.org/english/ad/sde/ra/Tobabout.htm
Sites with general, regional or national information and topics related to tobacco
control:
Action on Smoking and Health, UK (and special page for the tobacco industry):
http://www.newash.org.uk/ash r3iitasl.htm
Corporate Accountability International and the Network for Accountability of Tobacco
Transnationals: www.stopcorporateabuse.org
Economics of tobacco control: http://www 1 .worldbank.org/tobacco/
European Commission:
http://ec.europa.eu/health/ph determinants/life style/Tobacco/tobacco en.htm
European Network for Smoking Prevention: http://www.ensp.org/
Framework Convention Alliance for Tobacco Control: http://www.fctc.org/
International Union for Health Promotion and Education:
http://www.iuhpe.org/?page=18&Iang=en
Model Legislation for Tobacco Control manual:
http://www.iuhpe.org/?lang=en&page=publications report2
Tobacco industry: http://tobacco.health.usyd.edu.au/site/supcrsite/links/docs/tobacco ind.htm
Smokefree Partnership: http://www.smokefreepartnership.eu/
Thailand Health Promotion Institute: http://www.thpinhf.org/
Tobaccopedia: the online tobacco encyclopaedia: http://www.tobaccopedia.org/
More links to tobacco sites:
Various international and national tobacco control web sites:
http://www.tobacco.org/resources/general/tobsites.html
National tobacco control web sites:
12
http://www.sniokcfrcepartnership.eu/National-Tobacco-Control-wcbsitcs
Centre de rcssources anti-tabac: http://www.tabac-info.net/
Comite National Contre le Tabagisme (France): http://www.cnct.org
Office Fran^ais de Prevention du Tabagisme: http://www.oft-asso.fr/
Latest news on smoking and tobacco control: http://www.globalink.org/news/fr
Ministere de la sante, de la jeunesse et des sports: http://www.sante.gouv.fr/
Latest news on smoking and tobacco control: http://www.globalink.org/news/es
13
pH "S.
W Sasette
snrrw’
Jfefia
EXTRAORDINARY
q>>! II —WJ1
PART 51 — Section t
wiwi it uraiftrtt
<,
PUBLISHED BY AUTHORITY
tF
^W; "if 19, 2002/ W 1923
37]
No. 37]
29,
NEW DELHI, MONDAY, MAY 19,2002' VAISAKHP. 29,1925
ifa qn s Fit? Y3 wasr <fr '^nfr t rzwfc “s v? areni 'trasH >£
*■?<
ft w: 31 wfr i
Separate paging is given to ibis Pari la order that it may he fikd ab a sejnwte oTrnpilatiun.
MINISTRY OF LAW AND JUSTICE
‘'
(Legislative DcpurtHieat)
New Delhi, the 19ih May,2003/ f'ais.Ma29, 1925 (SaM
The following Act of Parliament received the assent of tFe!lPr&ident on the
1 Sth May, 2003, and is hereby published for general information:—
THE CIGARETTES AND OTHER TOBACCO PRODUCTS
(PROHIBITION OF ADVERTISEMENT AND REGULATION
OF TRADE AND COMMERCE, PRODUCTION, SUPPLY
/AND DISTRIBUTION) ACT, 2003
No. 34 of 2003
[18/A May, 2003.]
An Act to prohibit the advertisement of, and to provide for the regulation oftrade
and commerce in, and production, supply and distribution of, cigarettes and
other tobacco products and for matters connected therewith Or incidental
thereto.
Whereas, the Resolution passed by the 39th World Health Assembly (WHO), in its
Fourteenth Plenary meeting held on the 15tli May, 1986 urged the member States of WHO
which have'not yet done so to implement the measures to ensure that effective protection is
provided to non-smokers from involuntary exposure to tobacco smoke and to protect chil
dren and young people from being addicted to the use cf tobacco;
Ako whereas, the 43rd World Health Assembly in its Fourteenth Plenary meeting held
on the 17th May.. 1990, reiterated die concerns expressed in the Resolution passed in the 39th
World Health Assembly and urged Member States to consider in their tobacco control
strategies plans for legislation and other effective measures for protecting their citizens with
special attention to risk groups such as pregnant women and children from involuntary
exposure to tobacco smoke, discourage the use of tobacco and impose progressive restric
tions and take concerted action to eventually eliminate ail direct ami indirect advertising,
promotion and sponsorship concerning tobacco,
THE GAZETTE OF INDIA EXTRAORDINARY
[Part II—
And whereas, it is considered expedient to enact a comprehensive law on tobacco in
the public interest and to protect the public health;
And whereas, it is expedient to prohibit the consumption of cigarettes and other
tobacco products which are injurious to health with a view to achieving improvement of
public health in general as enjoined by article 47 of the Constitution:
And whereas, it is expedient to prohibit the advertisement of, and to provide for
regulation of trade and commerce, production, supply and distribution of, cigarettes and
other tobacco products and for matters connected therewith or incidental thereto:
Be it enacted by Parliament in the Fifty-fourth Year of the Republic of India as fol
lows:—
Short title, ex
(1) This Act may be called the Cigarettes and Other Tobacco Products (Prohibition
1.
tent stnd com of Advertisement and Regulation of Trade and Commerce, Production, Supply and Distribu
mencement.
tion) Act, 2003.
(2)
It extends to the whole of India.
(3)
It shall come into force on such date as tile Central Government may, by notification
in the Official Gazette, appoint and different dates may be appointed for different provisions
of this Act.
Declaration as
to expediency
the Union.
Definitions.
2.
It is hereby declared that it is expedient in the public interest that die Union should
take under its control the tobacco industry.
In this Act, unless the context otherwise requires,—
(a)
“advertisement" includes any visible representation by way of notice, circu
lar, label, wrapper or other document and also includes any announcement made orally
or by any means of producing or transmitting light, sound, smoke or gas;
3.
(b)
“cigarette” includes,—
(I)
any roll of tobacco wrapped in paper or in any other substance not
containing tobacco,
(t'O any roll of tobacco wrapped in any substance containing tobacco,
which, by reason of its appearance, the type of tobacco used in the filter, or its
packaging and labelling is likely to be offered to, or purchased by, consumers as
cigarette, but does not include beedi, cheroot and cigar;
(c)
“distribution” includes distribution by way of samples, whether free or oth
erwise;
(d)
“export", with its grammatical variations and cognate expressions, means
taking out of India to a place outside India;
(e)
“foreign language” means a language which is neither an Indian language
nor the English language;
(/) "import”, with its grammatical variations and cognate expressions, means
bringing into India from a place outside India;
(g) “Indian language" means a language specified in the Eighth Schedule to the
Constitution, and includes any dialect of such language;
(/i) "label" means any written, marked, stamped, printed or graphic matter, affixed
to, or appearing upon, any package;
(i)
“package" includes a wrapper, box, carton, tin or other container;
(/) “prescribed" means prescribed by rules made under this Act;
(k) “production", with its grammatical variations and cognate expressions, in
cludes the making of cigarettes, cigars, cheroots, beedis, cigarette tobacco, pipe to
bacco, hookah tobacco, chewing tobacco, pan masala or any chewing material hav
ing tobacco as one of its ingredients (by whatever name called) or snuff and shall
include—
(i)
packing, labelling or re-labelling, of containers;
(if) re-packing from bulk packages to retail packages; and
(Hi) the adoption of any other method to render the tobacco product
marketable;
Sec.1]
THE GAZETTE Oh' INDIA EXTRAORDINARY
(0 “public place” means any place to which the public have access, whether as
of right or not, and includes auditorium, hospital buildings, railway waiting room,
amusement centres, restaurants, public offices, court buildings, educational institu
tions, libraries, public conveyances and the like which are visited by general public but
does not include any open space,
(m) “sale", with its grammatical variations and cognate expressions, means any
transfer of property in goods by one person to another, whether for cash or on credit,
or by way of exchange, and whether wholesale or retail, and includes an agreement for
sale, and offer for sale and exposure for sale;
(«) “smoking", means smoking of tobacco in any form whether in the form of
cigarette, cigar, beedis or otherwise with the aid of a pipe, wrapper or any other instru
ments;
(o) “specified warning” means such warnings against the use of cigarettes or
other tobacco products to be printed, painted or inscribed on packages ofcigarettes or
other tobacco products in such form and manner as may be prescribed by rules made
under this Act;
(p) “tobacco products” means the products specified in the Schedule.
4.
No person shall smoke in any public place:
Provided that in a hotci having th irty rooms or a restaurant having seating capacity
of thirty persons or more and in the airports, a separate provision for smoking area or space
may be made.
5. (/) No person engaged in, or purported to be engaged in the production, supply or
distribution of cigarettes or any other tobacco products shall advertise and no person
having control over a medium shall cause to be advertised cigarettes or any other tobacco
products through that medium and no person shall take part in any advertisement which
directly or indirectly suggests or promotes the use or consumption of cigarettes or any other
tobacco products.
(2)
Prohibition of
smoking in a.
public place.
Prohibition of
advertisement
of cigarettes
and other to
bacco
pro-
No person, for any direct or indirect pecuniary benefit, shall—
(a)
display, cause to display, or permit or authorise to display any advertisement
of cigarettes or any other tobacco product; or
(4)
sell or cause to sell, or permit or authorise to sell a film or video tape contain
ing advertisement of cigarettes or any other tobacco product; or
(c)
distribute, cause to distributes, or permit or authorise to distribute to the
public any leaflet, hand-bill or document which is or which contains an advertisement
of cigarettes or any other tobacco product; or
(d)
erect, exhibit, fix or retain upon or over any land, building, wall, hoarding,
frame, post or structure or upon or in any vehicle or shall display in any manner
whatsoever in any place any advertisement of cigarettes or any other tobacco prod
uct:
Provided that this sub-section shall not apply in relation to—
(a) an advertisement of cigarettes or any other tobacco product in or on a
package containing cigarettes or any other tobacco product;
(i)
advertisement of cigarettes or any other tobacco product which is displayed
at the entrance or inside a warehouse or a shop where cigarettes and any other to
bacco products are offered for distribution or sale.
(J) No person, shall, under a contract or otherwise promote or agree to promote the use
or consumption of—
(a) cigarettes or any other tobacco product; or
(A) any trade mark or brand name of cigarettes or any other tobacco product in
exchange for a sponsorship, gift, prize or scholarship given or agreed to be given by
another person.
THE GAZETTE OF INDIA EXTRAORDINARY
[Part II—
Prohibition on
mJc of cigarette
or
other
tobacco prod
ucts to a per
son below the
age of eighteen
years and in
particular area.
6. No person shall sell, offer for sale, or permit sale of, cigarette or any other tobacco
product—
Restrictions on
trade
nod
commerce m,
tion P>u
and distributlon of cigstobaccod “T
uc[s
7. (/) No person shall, directly or indirectly, produce, supply or distribute cigarettes or
any other tobacco products unless every package of cigarettes or any other tobacco products produced, supplied or distributed by him bears thereon, or on its label, the specified
warn'n8 including a pictorial depiction of skull and cross bones and such other warning as
maV be prescribed.
(2) No person shall carry on trade or commerce in cigarettes or any other tobacco
Pr<x*ucts un'ess every package of cigarettes or any other tobacco products sold, supplied or
distributed by him bears thereon, or on its label, the specified warning.
(a) to any person who is under eighteen years of age, and
(A) in an area within a radius of one hundred yards of any educational institution.
(3)
No person shall import cigarettes or any other tobacco products for distribution or
supply for a valuable consideration or for sale in India unless every package of cigarettes or
any other tobacco products so imported by hitn bears thereon, or on its label, the specified
warning.
(4)
The specified warning shall appear on not less than one of the largest panels of the
package in which cigarettes or any other tobacco products have been packed for distribu
tion, sale or supply for a valuable consideration.
(5)
No person shall, directly or indirectly, produce, supply or distribute cigarettes or
any other tobacco products unless every package of cigarettes or any other tobacco prod
ucts produced, supplied or distributed by him indicates thereon, or on its label, the nicotine
and tar contents on each cigarette or as the case may be on other tobacco products along
with die maximum permissible limits thereof:
Provided that the nicotine and tar contents shall not exceed the maximum permissible
quantity thereof as may be prescribed by rules made under this Act
Manner
In
which spec!Tied warning
shall be made.
g. (/) The specified warning on a package of cigarettes or any other tobacco products
shall be—
(a) legible and prominent;
(b) conspicuous as to size and colour;
(c) in such style or type of lettering as to be boldly and clearly presented in
distinct contrast to any other type, lettering or graphic material used on the package
or its label and shall be printed, painted or inscribed on the package in a colour which
contrasts conspicuously with the background of the package or its labels.
(2) The manner in which a specified warning shall be printed, painted or inscribed on
a package of cigarettes or any other tobacco products shall be such as may be specified in
Language in
which the
specified
warning shell
be expressed.
the rules made under this Act.
(J) Every package containing cigarettes or any other tobacco products shall be so
packed as to ensure that the specified warning appearing thereon, or on its label, is, before
the package is opened, visible to the consumer.
9.- (/) Where the language used on a package containing cigarettes and any other
tobacco products or on its label is—
(a) English, the specified warning shall be expressed in the English language;
(A) any Indian language or languages, the specified warning shall be expressed
in such Indian language or languages;
(c) both English and one or more Indian languages, the specified warning shall
be expressed in the English language as well as in such Indian language or languages;
(d) partly English and partly any Indian language or languages, the specified
wanting shall be expressed in the English language as well as in such Indian language
or languages;
. EE GAZETTE OF INDIA EXTRAORDINARY
Sk- H
(e)
language;
5
any foreign language, the specified warning shall be expressed in the English
(/) partly any foreign language and partly English or any Indian’language or;''"
languages, the specified warning shall be expressed in the English language as well as"
in such Indian language or languages
(2)
No package of cigarettes or any other tobacco products or its label shall contain
any matter or statement which is inconsistent with, or detracts from, the specified warning. nl
10.
No specified warning or indication of nicotine and tar contents in cigarettes and- Size of letters
any other tobacco products shall be deemed to be in accordance with the provisions of this
and
Act if the height of each letter or figure, or both used on such warning and indication is less
than the height as may be prescribed by rules made under this Act.
II.
For purposes of testing the nicotine and tar contents in cigarettes and any other Testing labotobacco products the Central Government shall by notification in the Official Gazette grant ratorT for nlcorecognition to such testing laboratory as that Government may deem necessary
contents'1
12.
(f)Anypoliccofficer,notbelowtherarliofasub-inspectororany officerof State Power of
Food or Drug Administration or any other officer, holding the equivalent rank being not cn|ry and
below the rank of Sub-Inspector of Police, authorised by the Central Government or by the sealchState Government may, if he has any reason to suspect that any provision of this Act has
been, or is being, contravened, enter and search in the manner prescribed, at any reasonable
time, any factory, building, business premises or any otherplace,—
(a) where any trade or commerce in cigarettes or any other tobacco products is
carried on or cigarettes or any other tobacco products are produced, supplied or
distributed; or
(b)
where any advertisement of the cigarettes or any other tobacco products has
been or is being made.
2 of 1974
(2)TheprovisionsoftheCodeofCriminalProcedure, I973,shallapplytoeverysearch
and seizure made under this Act.
13.
(/) If any police officer, not below the rank of a sub-inspector or any officer of State
Food or Drug Administration or any other officer, holding the equivalent rank being not
below the rank of Sub-Inspector of Police, authorised by the Central Government or by the
State Government, has any reason to believe that,—
(a) in respect of any package of cigarettes or any other tobacco products, or
(5)
products,
Power to
.■’-■f
in respect of any advertisement of cigarettes or any other tobaccd ■
i . ■■
the provisions of this Act have been, or are being, contravened, he may seize such package
or advertisement material in the manner prescribed.
(2)
No package of cigarettes or any other tobacco products or advertisement materiil"^'
.
seized under clause (a) of sub-section (/) shall be retained by the officer who seized the "
package or advertisement material for a period exceeding ninety days from the date of the
seizure unless the approval of the District Judge, within the local limits of whose jurisdiction
such seizure was made, has been obtained for such retention.
14.
Any package of cigarettes or any other tobacco products or any advertisement Cohfiscztion
material of cigarettes or any other tobacco products, in respect of which any provision of' of package.
this Act has been or is being contravened, shall be liable to be confiscated:
Provided that, where it is established to the satisfaction of the court adjudging the
confiscation that the person in whose possession, power or control any such package of...... qq,
cigarettes or any othertobacco products is found is not responsible for the contravention of ,,,
the provisions of this Act, the Court may, instead of making an order for the confiscation of
such package, make such other order authorised by this Act against the person guilty of the
breach of the provisions of this Act as it may think fit.
THE GAZETTE OF INDIA EXTRAORDINARY
opdon 't° 8piy
ls< U) Whenever any confiscation of any package of cigarettes or any other tobacco
costs in lieu of Products is authorised by this Act, the court adjudging it may, subject to such conditions as
confiscation
ma> he specified in the order adjudging the confiscation, give to the owner thereof an option
to pay, in lieu of confiscation, costs which shall be equal to the value of the goods confiscated.
(2)
On payment of the costs ordered by the court, the seized packages shall be re
turned to the person from whom they were seized on condition that such person shall, before
making any distribution, sale or supply of such packages of cigarettes or other tobacco
products, get the specified warning and indication of nicotine and tar contents incorporated
on each such package.
Confiscation
16. No confiscation made, costs ordered to be paid under this Act shall prevent the
not to inter- infliction of any punishment to which the person affected thereby is liable under the.provisions
ofthis Act or under any other law.
Adjudication.
17. Any confiscation of cigarettes or any other tobacco products may be adjudged or
costs may be ordered to be paid,—
(a) without any limit, by the principal civil court of original jurisdiction within the
local limits of whose jurisdiction such confiscation has been made, costs have been
ordered to be paid,
(b) subject to such limits as may be specified by the Central Government in this
behalf by such other court, not below a civil court having pecuniary jurisdiction
exceeding rupees five thousand, as the Central Government may, by notification in the
Official Gazette, authorise in this behalf.
Giving oppor18.
jq0 order adjudging confiscation or directing payment of costs shall be made
own'/r l° 'of “nless tl’e owner or P«rson in possession of the package of cigarettes or any other tobacco
seized pickages.
products has been given a notice in writing informing him of the grounds on which it is
proposed to confiscate such package, and giving him a reasonable opportunity of making a
representation in writing, within such reasonable time as may be specified in the notice,
against the confiscation mentioned therein, and, if he so desires, of being heard personally
or through a representative in the matter
,
Provided that, where no such notice is given within a period of ninety days from the
date of the seizure of the package of cigarettes or of any other tobacco products, such
package shall be returned, after the expiry of that period, to the owner or the person from
whose possession it was seized.
(2) Save as otherwise provided in sub-section (/), the provisions of the Code of Civil
Procedure, 1908, shall, as far as may be, apply to every proceeding referred to in sub- '5 of 1908
section (/).
Appeal.
19. (?) Any person, aggrieved by any decision of the court adjudging a confiscation,
ordering the payment of costs, may prefer an appeal to the court to which an appeal lies from
the decision of such court.
(2) The appellate court may, after giving to the appellant an opportunity of being
heard, pass such order as it thinks fit confirming, modifying or reversing the decision or
order appealed against or may send back the case with such directions as it may think fit for
a fresh decision or adjudication, as the case may be, after taking additional evidence, if
necessary:
Provided that an order enhancing any fine in lieu of confiscation or confiscating of
goods of greater value shall not be made under this section unless the appellant has had an
opportunity of making a representation and, if he so desires, of being heard in person or
through a representative in his defence.
(3)
No further appeal shall lie against the order of the court of appeal.
THE GA2E7TE OF INDIA EXTRAORDINARY
Sec-
20. (7) Any person who produces or manufactures cigarettes or tobacco products,
which do not contain, either on the package or on their label, the specified warning and the
nicotine and tar contents, shall in the case of first conviction be punishable with imprisonment
for a term which may extend to two yean, or with fine which may extend to five thousand
rupees, or with both, and for the second or subsequent conviction,with imprisonment for a
term which may extend to five years and with fine which may extend to ten thousand rupees.
Punishment
for failure to
give specified
warning and
nicotine and
tar contents.
(2) Any person who sells or distributes cigarettes or tobacco products which do not
contain either on the package or on their label, the specified warning and the nicotine and tar
contents shall in the case of first conviction be punishable with imprisonment for a term,
which may extend to one year, or with fine which may extend to one thousand rupees, or with
both, and, for the second or subsequent conviction, with imprisonment for a term which may
extend to two years and with fine which may extend to three thousand rupees.
21. (7) Whoever contravenes the provisions of section 4 shall be punishable with fine
which may extend to two hundred rupees.
2 of 1974.
22. Whoever contravenes the provision ofsection 5 shall, on conviction, be punishable—
(a) in the case of first conviction, wi th imprisonment for a term which may extend
to two years or with fine which may extend to one thousand rupees or with both, and
(A) in the case of second or subsequent conviction with imprisonment for a term
which may extend to five years and with fine which may extend to five thousand
rupees.
Punishment
for advertise
ment of
cigarettes and
tobacco
products.
23. Where any person has been convicted under this Act for the contravention of the
provision of section 5, the advertisement and the advertisement material for cigarettes and
other tobacco products may be forfeited to the Government and such advertisement and
advertisement material shall be disposed of in such manner as may be prescribed by rules
made under this Act.
Forfeiture of
*vemsemcm
«
men(
material.
24. (/) Any person who contravenes the provisions of section 6 shall be guilty of an
offence under this Act and shall be punishable with fine which may extend to two hundred
Punishment
for sale of
ciganttes or
any other
tobacco
products in
certain places
or to persons
below the age
of eighteen
yeirs.
rupees.
(2) All offences under this section shall be compoundable and shall be tried summarily
in accordance with the procedure provided for summary trials in the Code of Criminal
2 of 1974.
Punishment
for smoking in
certain places.
(2) An offence under this section shall be compoundable and shall be tried summarily
in accordance with the procedure provided for summary trials in the Code of Criminal
Procedure, 1973.
Procedure, 1973.
25. (7) Notwithstanding anything contained in any other law for the time being in
force, the Central Government or the State Government may, by notification in the Official
Gazette, authorise one or more persons who shall be competent to act under this Act:
Provided that the person so authorised may, if he has reasonable ground for believing
that any person has committed an offence under section 4 or section 6, may detain such
person unless the accused person furnishes his name and address, and otherwise satisfies
the officer detaining him that he will duly answer any summons or other proceedings which
may be taken against him.
(2) Any person detained under sub-section (I) shall forthwith be taken before
Magistrate to be dealt with according to law.
(3) Any person committing an offence under section 4 or section 6 shall be triable for
such offence in any place in which he may be or which the State Government may notify in
Prevention,
detention and
pl.ee of trial
of offences
under sections
4 end 6
THE GAZETTE OF INDIA EXTRAORDINARY
[Part 11—
this behalf, as well as in any other place in which he is liable to be tried under any law for the
time being in force.
GO Every notification issued under sub-sections (/) and (J) shall be published in the
Official Gazette, and a copy thereof shall be exhibited for information to the public in some
conspicuous place or places as the State Government may direct.
(5) Every person authorised under sub-section (?) shall be deemed to be a public
servant within the meaning of section 21 of the Indian Penal Code.
45 of I860.
Offences by
26.
(/) Where an offence under this Act has been committed by a company, every
companies.
person who, at the time the offence was committed, was in charge of, and was responsible to,
the company for the conduct of the business of the company, as well as the company, shall
be deemed to be guilty of the offence and shall be liable to be proceeded against and
punished accordingly:
Provided that nothing contained in this sub-section shall render any such person
liable to any punishment, if he proves that the offence was committed without his knowledge
or that he had exercised all due diligence to prevent the commission of such offence.
(2) Notwithstanding anything contained in sub-section (/), where any offence under
this Act has been committed by a company and it is proved that the offence has been
committed with the consent or connivance of, or is attributable to any neglect on the part of,
any director, manager, secretary or other officer of the company, such director, manager,
secretary or other officer shall be proceeded against and punished accordingly.
Explanation.—For the purposes of this section,—
(a) “company” means a body corporate and includes a firm or other association
of individuals; and
(b) “director”, in relation to a firm, means a partner in the firm.
27.
Notwithstanding anything contained in the Code of Criminal Procedure, 1973, an2 of 1974
Offences to be
bailable.
offence punishable under this Act shall be bailable.
Composition
of offences.
(1)
28.
Any offence committed under section 4 or section 6 may either before or after
the institution of the prosecution be compounded by such officer authorised by Central
Government or State Government and for an amount which may not exceed two hundred
rupees.
(2) Where an offence has been compounded under sub-section (/), the offender, if in
custody, shall be discharged and no further proceedings shall be taken against him in respect
of such offence.
Protection of
29.
No suit, prosecution or other legal proceeding shall lie against the Central
action taken in Government or any State Government or any officer of the Central Government or any State
good faith.
Government for anything which is.in good faith done or intended to be done under this Act.
Power to add
any tobacco
products in the
Schedule.
30.
The Central Government, after giving by notification in the Official Gazette, not
less than three months' notice of its intention so to do, may, by like notification, add any
other tobacco product in respect of which it is qf opinion that advertisements are to be
prohibited and its production, supply and distribution is required to be regulated under this
Act, and thereupon the Schedule shall in its application to such products be deemed to be
amended accordingly.
Power of
Central
Government
to make rules.
(/)
31.
The Central Government may, by notification in the Official Gazette, make rules
to cany out the provisions of this Act.
(2) Without prejudice to the generality of the foregoing power, such rules may provide
for all or any of the following matters, namely:—
(a) specify the form and manner in which warning shall be given in respect of
cigarettes or other tobacco products under clause (o) of section 3;
Sec. 1]THE GAZETTE OF INDIA EXTRAORDINARY
9
(A) specify the maximum permissible nicotine and tar contents in cigarettes or
other tobacco products under the proviso to sub-section (5) of section 7;
(c)
specify the manner in which the specified warning shall be inscribed on each
package of cigarettes or other tobacco products or its label under sub-section (2) of
section 8;
(d)
specify the height of the letter or figure or both to be used in specified
warning or to indicate the nicotine and tar contents in cigarettes or other tobacco
products under section 10;
(e)
provide for the manner in which entry into and search of any premises is to be
conducted and the manner in which the seizure of any package of cigarettes or other
tobacco products shall be made and the manner in which seizure list shall be prepared
and delivered to the person from whose custody any package of cigarettes or other
tobacco products has been seized;
(f)
provide for any other matter which is required to be, or may be, prescribed.
(3)
Every rule made under this Act and every notification made under section 30 shall
be laid, as soon as may be after it is made, before each House of Parliament, while it is in
session, for a total period of thirty days which may be comprised in one session or in two or
more successive sessions, and if, before the expiry ofthe session immediately following the
session or the successive sessions aforesaid, both Houses agree in making any modification
in the rule or notification or both Houses agree that the rule or notification should not be
made, the rule or notification shall thereafter have effect only in such modified form or be Of
no effect, as the case may be; so, however, that any such modification or annulment shall be
without prejudice to the validity of anything previously done under that rule ornotification.
NothlngcontainedinthisActshallapplytoanycigaretteorothertobaccoproducts
32.
Act
not
to
or package of cigarettes or other tobacco products which is exported:
dgnrcttw or
Provided that nothing in this section shall be deemed to authorise the export of any
package of cigarettes or other tobacco products, not containing the specified warning and
indication of nicotine and tar contents to any country if the law in force in that country
requires that the same or similar warning and nicotine and tar contents shall be specified on
other tobacco
each package Of cigarettes or other tobacco products.
Explanation.—For the purpose of this section, any cigarette or other tobacco products
or package of cigarettes or other tobacco products shall be deemed to be exported before the
commencement of this Act, if the necessary steps for export have already been taken
notwithstanding that the actual export has not taken place.
49 of 1975
33. (7) The Cigarettes (Regulation of Production, Supply and Distribution) Act, 1973,
is hereby repealed.
(2) Notwithstanding such repeal, anyth ing done or any action taken under the provisions
of the aforesaid Act, shall, in so far as such thing or action is not inconsistent with the
provisions of this Act, be deemed to have been done or taken under the provisions of this
Act as if the said provisions were in force when such thing was done or such action was
taimen and shall continue in force accordingly until superseded by anything done or any
action taken under this Act
Repeal
and
HE G AZETTE OF INDIA EXTRAORDINARY
[Part II—Sec. 1)
THE SCHEDULE
[See section 2(p)]
1.
Cigarettes
2.
Cigars
3.
Cheroots
4.
Beedis
5.
Cigarette tobacco, pipe tobacco and hookah tobacco
6.
Chewing tobacco
7.
Snuff
8.
Pan masala or any chewing material having tobacco as one of its ingredients (by
whatever name called).
9. Gutka
10. Tooth powder containing tobacco.
SUBHASH C. JAIN,
Secy, to the Govt, ofIndia.
PRINTED BY THE MANAGER, GOVERNMENT OF INDIA PRESS, MINTO ROAD, NEW DELHI
AND PUBLISHED BY THE CONTROLLER OF PUBLICATIONS, DELHI, 2003.
MGIPMRND—1138QI—20-05.2003.
LAW & POLICY
RESEARCH
POLICY BRIEF
ENDING TOBACCO SUBSIDIES FOR PUBLIC HEALTH
Table of Contents
I.
Introduction
II.
The Tobacco Board Act: Need for Repeal
III.
Subsidies and Incentives for Tobacco growers
IV.
V.
VI.
(i)
Subsidies
(ii)
Tax Cuts
(iii)
Specialized incentive schemes
(iv)
Relaxation of Production Ceilings
(v)
Loans
Phasing Out Subsidies and Incentives for Tobacco Farming
(i)
FCTC
(ii)
Constitutional basis
(iii)
COTPA
(iv)
Order of the Karnataka High Court
Case Studies for Other Jurisdictions
(i)
EU
(ii)
United States of America
(iii)
Australia
(iv)
Bangladesh
The Road Map Ahead & Recommendations
I.
INTRODUCTION
Tobacco is one of the leading causes of death in India. It has been estimated by the
Tobacco Control Policy Evaluation Project that by 2020 smoking will lead to 1.5 million
deaths in the country and deaths caused by tobacco are set to increase by 3% every year.1
Statistics show that more than one-third of adults in India, almost half men and one in
'jhaet. al., A Nationally Representative Case-Control Study of Smoking and Death in India, The New England
Journal of Medicine (2008)
five women are regular tobacco users.23These disturbing figures indicate an urgent need
to reduce tobacco consumption to ensure public health and safety within the country.
In its efforts to combat tobacco use, India signed and subsequently ratified to the
Framework Convention on Tobacco Control (“FCTC”) by the World Health Organization
(“WHO”) in 2005. The FCTC mandates its members to implement control mechanisms
on both supply and demand factors for reducing consumption of various smoke and
smokeless tobacco products. It obliges its signatories to show marked reduction in
production of tobacco and encouraging economically viable alternatives.3 Most
importantly, Article 5.3 created provisions protecting public health policies from
commercial and other- vested interests of the tobacco industry. Articles 17 and 18, oblige
States to promote economically- viable alternatives having due regard to the health of
the tobacco farmers and the environment.
In
2003,
The Cigarettes
and Other Tobacco
Products
(Prohibition of
Advertisement and regulation of trade and commerce, production, Supply, Distribution)
Act was enacted with the objectives to “provide for the regulation of trade and
commerce in, and production, supply and distribution of, cigarettes and other tobacco
products and for matters connected therewith or incidental thereto”, “ to take
concerted action to eventually eliminate all direct and indirect advertising, promotion
and sponsorship concerning tobacco” and “to prohibit the consumption of cigarettes
and other tobacco products which are injurious to health with a view to achieving
improvement ofpublic health in general as enjoined by article 47 of the Constitution.”
The FCTC, COTPA, and the Indian Constitution bestow responsibility upon the
government to protect public health and reduce the use of tobacco. Article 5.3 of the
FCTC requires that members should immune their ‘national health policies from
commercial and other vested interests of the tobacco industry’. This mandates that the
government should not provide any preferential treatment to the tobacco industry.
However, that is not what is happening. The continued existence of the Tobacco Board
established under the Tobacco Board Act, 1975,
and the provision of subsidies for
tobacco farmers with an aim to develop and incentivise the tobacco industry is a direct
2Akansha Singh & LaishramLadusingh, Prevalence and Determinants of Tobacco Use in India: Evidence from
Recent Global Adult Tobacco Survey Data (2014)
3 Framework Convention on Tobacco Control, Articles 15-17
violation of the government’s bligations under Article 5.3 of the FCT and its
constitutional obligations to protect public health.
Tobacco control would not be possible without completely eliminating incentives
that promote tobacco production i.e. supply reduction. It is not viable to expect
reduction in usage of tobacco if the government is actively supporting tobacco growing,
providing incentives to tobacco farmers and encouraging the growing and therefore
consumption of tobacco.
This Brief is divided into three parts. After the introduction, Part II and III
provide an account of governmental support to the tobacco industry. Such support
varies from subsidies, tax cuts, insurance schemes, relaxation of production ceilings and
loans. In Part IV, we will analyse legal basis for phasing out tobacco subsides and other
support programs. We will identify arguments under FCTC, Indian Constitution,
COTPA, and the Karnataka High Court judgment. After this, we will look at various
other jurisdictions such as United States of America, European Union, and Australia to
find out how they phased out tobacco subsidies and other similar programs for the
tobacco producers and finally suggest a Road Map and Recommendations for India in
phasing out subsidies.
II.
THE TOBACCO BOARD ACT - NEED FOR REPEAL
India is the world’s third largest producer of tobacco having around 300 million Kg flue
cured Virginia tobacco in 2014-15.4 In total, India produced 9% of the world’s tobacco.s
This is a result of support to the tobacco industry by the Tobacco Board through
subsidies, schemes and preferential treatment given to the tobacco industry by
governmental agencies. India’s policy towards tobacco production and cultivation is
inherently contradictory. On one hand the government has committed to taking strong
steps to control tobacco use in various treaties while on the other hand different
departments and boards promote, incentivize and subsidize tobacco cultivation. This
«See http://www.ctri .org.in/for_tobaccoEconomy.php
5Ibid
contradiction has the effect of nullifying the incentives taken by the government in
trying to reduce tobacco consumption.
India’s best efforts at tobacco reduction are undermined by the following issues:
i. The existence of the Tobacco Board itself, which is contrary to provisions of
COTPA;
2. The subsidies and incentives provided by the Tobacco Board and other similar
state agencies to encourage tobacco production whichare against the ideals of the
constitution and COTPA.
Much before the COTPA and the FCTC, as early as in 1975, the Tobacco Board Act was
enacted to set up the Tobacco Board. The aim of the Act is to provide for the
development under the control of the Union of the Tobacco industry. The Board was
established to for the overall development of the tobacco growers and the Indian
tobacco industry. The head office of the Board is at Guntur, Andhra Pradesh. The main
functions of the Board is to recommend minimum export price for the Virginia tobacco,
marketing and promotion of Virginia tobacco, disseminate useful information about
tobacco to the stakeholders, purchase produces from the farmers when required and
sponsor scientific research to improve tobacco production. In other words, the function
of the Board is to promote the production and consumption of tobacco.
The Tobacco Board Act, 1975 and COTPA, 2003, have numerous provisions
which clearly contradict each other. The aim of Tobacco Board Act is to provide for the
development under the control of the union of the tobacco industry, while the aim of
COTPA is to provide for the regulation of trade commerce in and production, supply
and distribution of cigarettes and other tobacco products. The Tobacco Board Act aims
at encouraging the tobacco industry while COTPA has been enacted to restrict it.
The Tobacco
Board Act contains provisions
for the
maintenance and
improvement of existing tobacco markets and the development of new markets outside
India67, encouraging the marketing of Virginia tobacco in India? and propagating
information useful to the growers, dealers and exporters.8 On the other hand, COTPA
6 Section 8(2)(c) of the Tobacco Board Act
7 Section 8(2)(e) of the Tobacco Board Act
8 Section 8(2)(f) of the Tobacco Board Act
discourages the use of tobacco and imposes progressive restrictions and requires the
State to take concerted action to eventually eliminate all direct and indirect advertising,
promotion and sponsorship concerning tobacco?. It further prohibits the advertisement
of tobacco products and any such person taking part in advertisement1011
.
The Tobacco Board Act lists the functions of the Tobacco Board which is to be set
up in consonance with the Act". These functions include sponsoring and assisting
research for the promotion of the tobacco industry. Further, the Board can grant loans
to any person for the purpose of this Act1213
. The purpose of these loans can be drawn
*IS
from section 8 of the Act i.e. the growth of Virginia tobacco its marketing and export etc.
whereas, COTPA requires the state to discourage the use of tobacco and impose
progressive restrictions and take concerted action to eventually eliminate all direct and
indirect advertising, promotion and sponsorship concerning tobacco'3.
It must be noted that the saving clause of the Tobacco Board Act, states that "The
provisions of this Act shall be in addition to, and not in derogation of, the provisions of
any other law for the time being in force.1!" This provision of the Act implies that the
Tobacco Board Act cannot be given an overriding effect over the provisions of any other
Act in force. COTPA has no such savings clause. As a result, in the case of a conflict
between the Tobacco Board Act and the COTPA, the provisions of the Tobacco Board
Act cannot derogate from the provisions of the COTPA and all the provisions of COTPA
would prevail.
This view has been bolstered by a judgment of the Supreme Court in the case of
I.T.C. Ltd. v. State Of Karnataka & Ors’s. The Court observed that "Section 31 of the
Central Act [The Tobacco Board Act] makes it clear thht it does not derogate from any
law but enacts something in addition." The Court held that a Karnataka law which was
in contradiction of the Tobacco Board Act (a Central Act) would prevail in light of
Section 31. This was despite a well established constitutional provision that a Central
5 Preamble of COTPA
‘“Section 5 of COTPA.
11 Section 8(2)(i) of the Tobacco Board Act
12 Section 17(c) of the Tobacco Board Act
13 Preamble of COTPA
‘‘Section 31 of the Tobacco Board Act
IS(1985) Supp SCC 476
Act would prevail over a State Act when laws are passed on the same subject.1617
Hence, in
case of a contradiction between the provisions of Tobacco Board Act and COTP A, those
provisions of the former Act that derogate from COTPA must be read down and would
have no effect. The provisions of COTPA will apply.
In addition, when there is a conflict between two provisions it is a generally
accepted legal principle known ‘leges posteriors priorescontraiasabrogant ’ which
means that the newer legislation would overrule the older provision. This is commonly
understood as the concept of ‘implied repeal’. An implied repeal of an earlier law can be
inferred where there is an enactment of a latter law which has the power to override the
earlier and is totally inconsistent with the earlier law i.e. both laws cannot stand
together.‘7
The provisions of the Tobacco Board Act 1974 are at loggerheads with the
COTPA, 2003. In such a scenario it would be wise to refer to the social circumstances
and the purposes of both acts. The COTPA was enacted in 2003 and was amended as
recently as 2015. While the Tobacco Board was enacted in 1975, back in the day when
tobacco was looked at merely as a profitable cash crop. Since 1975, harmful effects of
tobacco consumption have been brought to light through scientific research and
numerous studies. Tobacco is no longer just a cash crop, but one of India’s leading
killers. There is a growing social need to reduce tobacco production. The COTPA is
therefore more in tune with needs of the present society, while the Tobacco Board Act is
now obsolete.
The COTPA is a socially beneficial legislation that embodies the global urgency to
reduce tobacco production. In lieu of scientific research findings regarding the social,
economic, environment and health costs; COTPA can be seen as India’s contribution
towards reducing tobacco-related social costs globally. COTPA reflects the stand of the
National Human Rights Commission of India (NHRC) in collaboration with the
Government of India and the WHO at the South-East Asia Regional Consultation on
‘Public Health and Human Rights’ at New Delhi in 2001; where in addition to the right
l6Article 251 of the Constitution
17 Om PrakashShukla v. Akhilesh Kumar Shukla and others, AIR 1986 SC 1043
to health and the right to clean air, it recognized the rights of citizens to
programs/facilities to encourage tobacco control18.
Further, COTPA is in consonance with the current National strategies for tobacco
control such as the National Tobacco Control Programme (NTCP) which was launched
by Ministry of Health and Family Welfare, Government of India in 2007- 08, with the
objective to control tobacco consumption and minimize its effects; and facilitate
effective implementation of tobacco control. NTCP is implemented on a national, state
and district level. State tobacco control cells (STCC) or Anti- tobacco cells (ATC) and
District tobacco Control Cells have been setup under the programme. Their primary
focus is on the planning, monitoring, implementation of tobacco control activities etc. in
the light of COTPA and FCTC (Framework Convention on Tobacco Control) provisions.
Additionally the Ministry of Health and Family Welfare has published reports
pushing for alternative livelihoods for tobacco farmers and bidi rollers, it has initiated
workshops to train doctors, published a tobacco cessation programme etc. All these
activities point to the fact that the Ministry of Health and family welfare is promoting
the cause of tobacco reduction in lines with the COTPA, while the Tobacco Board’s
activities are contrary to these programmes. There is a clash between the activities of the
Ministry of Health, and family to reduce tobacco use; and central government under the
Tobacco board to promote tobacco production. It needs to be highlighted here once
again that the COTPA being a more recent legislation is in line with the current policies
of tobacco reduction. The objectives of Tobacco Board Act were formulated 35 years ago
and are not only redundant but also in conflict with current objectives of public health
and welfare.
Hence in light of Section 31 of the Tobacco Board Act and the principle of
‘Implied Repeal’, it can be said that, as there is a conflict in the very objectives of both
the acts. However, since the Tobacco Board is an authority established by the Central
government under an Act, its dissolution would only be possible by the act of the
legislature or by the Supreme Court declaring it ultra vires.
18 National Human Rights Commission of India, “Report on Regional Consultation on Public Health and
Human Rights”, New Delhi, 2001
III.
SUBSIDIES AND INCENTIVES FOR TOBACCO GROWERS
In complete disregard of the attempts of numerous tobacco control policies, the Tobacco
Board has been giving out huge subsidies to tobacco growers all over the country. The
Tobacco Board shows a huge annual expenditure of Rs. 454 Lakhs in extension and
development projects.1? This expenditure only adds to the massive economic costs
arising out of tobacco related diseases which has been estimated at Rs 1,04,500 crore.*20
The monetary incentives offered by the Tobacco board keep increasing every year in
complete disregard to India’s international obligation to reduce tobacco use. The
Tobacco Board is allowed to provide subsidies and incentives to the tobacco industry,
while the government turns a blind eye to its activities. The Board provides incentives in
various forms to tobacco growers, and some of these are as follows:
fi)
Subsidies:
The
Board
provides
subsidies
to
SC/ST/Women/Small
andmarginalized farmers for extension of services.
•
In the year 2009-2010, the Board reflects an expenditure of a whopping
Rs 292.40 Lakhs in lieu of subsidies' provided for farm mechanization,
Improving yield & Quality of FCV tobacco and curing practices.
•
In the year 2012-13 the annual report indicates an increased expenditure
•
Additionally, a subsidy of Rs 105 Lakhs towards subsidies for growers of
of Rs. 372.55 lakhs as subsidies to tobacco growers, a growth of 27.4196.21
tray tobacco nurseries was also extended.22
•
Subsidies of up to 30% of the costs of bio-fertilizers to tobacco growers, to
tarpaulins used by barns and workshops eliminating non-tobacco related
products, towards bulking shed, venture furnaces etc.
‘’Tobacco Board India, “Annual Report 2013-2014” at page 35 ■
20 Ministry of Health and Family Welfare, Executive summary, “Economic burden of tobacco related
diseases in India”2Oii
21 Tobacco Board India, “Annual Report 2012-2013” at page 207
“Ibid
•
In 2012-13, loans were provided to 79822 beneficiaries for funds
amounting to RS154 crores at low interest rates, in the states of Andhra
Pradesh and Karnataka, by the Tobacco Board with the help of
nationalized and commercial banks.23
•
The Tobacco Board has also developed the concept of Good Agricultural
Processes or GAP under which it extends subsidies of certain inputs to
farmers in lands identified as “model project areas” in order to convert and
enhance productivity in these lands.
fii)
Tax cuts: In addition to subsidies, Favourable tax cuts have been granted to
the tobacco industry by various State governments. For example the
Rajasthan government slashed the VAT on tobacco. In orders passed in June
2015, the Rajasthan state government reduced VAT on “tobacco and its
products excluding bidi" to 45 per cent, from the existing 65 per cent, saying it
was “expedient to do so in public interest”. Similarly, VAT was reduced to 35
per cent from 65 per cent on paan masala. However, the existing 65 per cent
VAT on bidis has been left unchanged. These orders on tax cuts have been
stayed by the Rajasthan High Court.24Such tax benefits amount to providing
preferential treatment to the tobacco industry under Article 5.3 of the FCTC.
(Til)
Specialized Insurance Schemes: The Government of India has proposed to
implement Crop Insurance Scheme for FCV tobacco, as a plan scheme with
50% subsidy on annual premium. Subsidization of the premium for crop
insurance to the extent of 25% was sought from individual state governments
to reduce the burden of the growers and accordingly. As of 2013, the outlays
of the Scheme involving a premium subsidy of Rs 256.75 crore was prepared.
The scheme proposals are yet to obtain the sanction of the Government for
23Tobacco Board India, “Annual Report 2013-2014” at page 35
24 Rahul Joshi v. Union of India &Ors.,(W.P. No. 8680/2015), Rajasthan High Court, order dated 03.07.2015.
implementation, because of lack of consent from the State governments over
sharing of the premium cost.2s
fiv)
Relaxation of Production Ceilings: The tobacco industry is not only
encouraged through direct monetary benefits of subsidies and incentives. It is
also encouraged by the lenient government rules and non-penal regulatory
measure. Due to its dangerous nature, tobacco production is allowed by
registered producers only and up to a fixed quota set every year. The Tobacco
Board, based on the economic interests of the producers, decides the crop size
of FCV tobacco separately for Karnataka and Andhra Pradesh, announces the
tobacco policy annually. For the year 2014-2015, it was set to 104 million kgs
for the state of Karnataka*2627
. It is now an established norm that growers do not
stick to the limit set. The penalty imposed on growers is usually relaxed due to
pressure from farmer groups and the sale of tobacco products invariably
exceeds the fixed quota. The sale of excess tobacco produced is not limited to
registered owners; unregistered owners too are given permission to allow
excess sale.2? Occasionally when the limits are enforced, non-adherence to
these limits would be merely lead to a penalty by the Tobacco board and the
proceeds from the penalties go to the ‘Tobacco fund’, which is again used to
boost the tobacco industry itself. Hence the markets continue to be flooded
with excess tobacco while tobacco fund keeps getting heavier from the
penalties imposed, perpetuating the cycle of tobacco growth.
(V)
Loans:In addition to incentives provided by the Tobacco Board, because of the
absence of any holistic government policy, while on the one had, the
government professes its commitment to reducing tobacco cultivation by 80
per cent by 2020, the public sector banks are sanctioning nearly 40 per cent
“Price stabilisation fund trust annual report 2013-14, published by the Ministry of Commerce and Industry,
available athttp://commerce.nic.in/psft/Annual_Report_2013-14.pdf
26 See generally http://tobaccoboard.com/propolicy.php
27Tobacco Board circular no: F.No: 1(54)A/2013-2014/PDN/: “2013-14 Crop Season - permission from 20th
January for sale of Excess/Un-authorized tobacco produced by Regd/unregd. growers - Guidelines" on 9.01.2014
of their agricultural loan outlay to tobacco crop alone.In Karnataka there are
nearly 75,000 to 80,000 tobacco cultivators and the crop is grown on 80,000
acres. Even during drought and farmers suicides due to loss of food crops last
year, financial institutions had no issues lending to tobacco farmers. These
loans are given as Agricultural loans, which come under the priority sector in
the District Credit Plan. Out of the agricultural loans, lending to tobacco
farmers accounts for more than 40 per cent of the total crop loan in the
district.
During 2015-16, the total advances made by various public sector
banks, regional rural banks and cooperative banks to tobacco farmers in
Mysuru district was nearly Rs.i,2oocrore out of the Rs. 2,499.72 crore
allocated for agriculture.28
IV.
Phasing out Subsidies and other Incentives for Tobacco
FARMING
In the previous parts of this Policy Brief, our discussion revolved around government’s
failure in fulfilling its obligation in controlling production and consumptionof tobacco
and tobacco related products.Constant direct and indirect Governmental support for
tobacco farming sabotages efforts by civil society to control tobacco’s use and to protect
life, health, and environment. One of the most health distorting government activities is
provision of the subsidies to tobacco producers. Rather than discouraging tobacco
farming, the government, directly and indirectly, encourages it, jeopardizing its
international obligation.
This Chapter builds legal arguments against subsidies provided by the government;
on the line of the FCTC, the Indian Constitution, and the COPTA.While developing
arguments against subsidies, various other jurisdictions will be referred to establish the
feasibility of such arguments.
28 “Tobacco Accounts for 40% of Crop Loans in Mysore” (The Hindu, April 4'h, 2016) Available at:
http://www.thehindu.com/news/national/karnataka/tobacco-accounts-for-4 0-pc-of-crop-loans-inmvsuru/article8430910.ece
(i)
Framework Convention on Tobacco Control: Article 5.3,17 and 18
The FCTC was the first treaty under the aegis of the WHO. It reaffirms the right of all
people to the highest standard of health. It aims at encouraging tobacco control,
especially in developing countries by disseminating knowledge and promoting
economically viable alternatives. The convention focuses on the socio-economic
difficulties faced by developing countries and aims to provide technical and financial
assistance.
Article 5.3 of the FCTC provides for protecting public health policies from vested
commercial interests of the tobacco industry. Article 17 obligates parties to reduce the
supply tobacco by encouraging economically viable alternative crops and Article 18
speaks about protecting the environment. Hereby, a detailed discussion of these Articles
arefollowed:
a. Article 5.3: Restricted interactions with the Tobacco Industry and No
Preferential Treatment
Article 5.3 of the FCTC requires state parties “to protect public health policies on
tobacco control from the commercial and other vested interests of the tobacco
industry, in accordance with national law. ’’Compliance with this Article can mostly be
assessed based on two recommendations in the Article 5.3 Implementing Guidelines2’:
Restricted interactions with the Tobacco Industry and No Preferential
Treatment: The Guidelines require limiting interactions between the government and
the tobacco industry to those that are strictly necessary and ensuring transparency in
the interactions that do occur. Further, the Guidelines also require that state parties to
not give preferential treatment to the tobacco industry.
^Guidelines for Implementation of Article 5.3 of the WHO Framework Convention on Tobacco Control on
the protection of public health policies with respect to tobacco control from commercial and other vested
interests of the tobacco industry, available at: http://www.who.int/fctc/guidelines/article 5 3.pdf
The fear of increasing affiliations between public authorities and tobacco
companies was recognized in the 54,hWorld health assembly meetings0, which urged
countries to control subversive tactics of the Tobacco industry of influencing policymaking. It is stressed that state parties should develop and implement policies and
procedures
for
determining
what
constitute
necessary
interactions,
prohibit
unnecessary interaction and provide clear codes and procedures for the conduct of any
necessary interactions.
An examination of implementation of the guidelines in India clearly reflects the
sad state of affairs. These are due to following reasons: first, the close connection
between the Tobacco board and governmental agencies. Tobacco Board Act, 1975 is
clear violation of the principle of limiting interactions between the government and the
tobacco industry. The members of the Tobacco Board includes elected members of the
Parliament (3), those appointed by the Central Government (8) to represent various
ministries namely Agriculture, Commerce, Finance, and Industrial Development as well
as up to 10 members, appointed by the Central Government from among growers of
tobacco, dealers and exporters (including packers) of tobacco and tobacco products.31
Second, Section 8 of the Tobacco Board Act, 1975 lays down the primary function
of the Board as the promotion of the development of the tobacco industry by all such
measures as it deems fit, under the control of the Central Government. Such measures
include, among other things, the establishment of an auction platform with previous
approval of the Central Government, recommending minimum prices to be fixed for the
purpose of export to avoid unhealthy competition and for the purpose of promotion. The
provision further stipulates that the Board’s functioning be in liaison with Union
agencies, institutions and authorities concerned with the tobacco industry.
Third, Section 16 of theTobacco BoardAct, 1975 provides for payments to be
made to the Tobacco Board by way of grants and loans by the Central Government. The
Tobacco Board Rules, 1976 also allow the Board to associate itself with anybody
interested in the promotion of the tobacco industry, on the basis of representations
3054th
World
Health
Assembly
http://www.who.int/tobacco/framework/wha eb/wha54 18/en/
3> Section 4(4) of the Tobacco Board Act, 1975
meeting,
available
at:
made.32Although no grants have been made in the present financial year, the provision
is open for use anytime.
Fourth, in 2010, the Tobacco Board sponsored theGlobal Tobacco Networking
Forum, which was an international tobacco industry event.
The sponsorship of the
Conference by a Government agency was severely condemned. The Hon’bleKarnataka
High Court observed that the participation and financial contribution of the Tobacco
Board in the conference was an indirect promotion of tobacco and hence ordered the
Tobacco Board to withdraw its sponsorship and participation in the conference.33
Finally, interaction between government agencies and Tobacco industry is not
only restricted to the Tobacco board but also extends to other agencies such as the
Directorate of Tobacco development. Established in 1966, under the direct aegis of the
Department of Agriculture, Co-operation and Farmer welfare. Its main functions are to
maintain
liaison
between
state and central
governments concerning
tobacco
development work, rendering technical advice to the states and central governments
and offering suggestions, compiling and presenting statistics on tobacco production,
area, yield, researching on economics of tobacco production and devising attainable
strategies for various departments. 34
No other industry enjoys such flagship support of the government. As described
in Chapter 2, the Tobacco industry is bestowed with a slew of direct and indirect
monetary incentives as a form of preferential treatment. The Court also directed the
Union Government to consider adopting a Code of Conduct to comply with its
obligations under Article 5.3 of the FCTC. Despite these orders, the Government has not
adopted a Code of Conduct as directed by the Court. Thus strengthening the argument
that Tobacco industry exercises significant influence over policy-making to further its
commercial interest, is prima facie violation of Article 5.3 guidelines.
Article 17
32 Rule 10, Tobacco Board rules, 1976
33The Institute of Public Health v.The State Government of Karnataka (W.P. No 27692/2010)
3«The Directorate of Tobacco development, available at: http://dtd.dacnet.nic.in/organisation.htm
Article 17 requires Parties to promote, as appropriate, economically viable alternatives
for tobacco workers, growers, and possibly individual sellers. Article 18 recognizes that
Parties agree to have due regard to the protection of the environment and to health with
respect to tobacco cultivation and manufacture. While the FCTC aims at tobacco control,
it also realizes that tobacco production is a source of income for poor farmers especially
in developing countries.
In 2014, The Conference of Parties of the FCTC, discussed “Economically
sustainable alternatives to tobacco growing”35, keeping in mind the interests of various
stakeholders of the process. The discussion focused on systematic research and policy
application, not only in terms of economic and social costs but also, eco-friendly and
environmentally sustainable alternatives.
Tobacco subsidies act as an encouragement for farmers to continue or increase
efforts in tobacco cultivation. Instead of educating the farmers about appropriate crop
alternatives, based on weather conditions and land quality. The government is boosting
tobacco production rather that discouraging them. Tobacco subsidies and incentives are
paradoxical to the obligations under Article 17.
Tobacco production also degrades the environment; causing soil infertility; ground
water and soil contamination due to excessive use of pesticides; air pollution and
deforestation from tobacco curing activities etc. (Discussed further in the next section).
Therefore incentivizing tobacco through subsidies would be contradictory to Article 18,
since cultivating tobacco is not only harmful to the consumer but it also to the farmers.
(ii)
Constitutional basisfor phasing out subsidies
The subsidies and other form of incentives and provided by the Tobacco Board are in
direct violation of provisions of the Constitution. These activities of the Tobacco Board
are a threat to the Fundamental right to life under Article 21 and the Directive Principles
of State Policy under Articles 39,47, 48A and 51.
35 COP of The Framework Convention on Tobacco Control, Economically-viable alternatives for tobacco,
farming under Articles 17 & 18” at Russia 2014
Article 21, Right to life and health: Article 21 of the Indian Constitution lays down that
“No person shall be deprived of his life or personal liberty except according to procedure
established by law”. It mandates that no person shall be deprived of his life and personal
liberty except according to the procedure established by law. The Supreme Court in
UnniKrishan, J.P v. State of A.P& observed that the expression ‘personal liberty’ is of
wildest amplitude. The Court expressly recognized ‘Right to Health’ as of the significant
rights protected by Article 21.
Self-preservation of one’s life is the necessary concomitant of the right to life
enshrined in Article 21, fundamental in nature sacred precious and inviolable.37The
Hon’ble Supreme Court inMuraliDeora v. Union ofIndia88, observed that a non-smoker
cannot be afflicted by various diseases including lung cancer or of heart, only because he
required to go to public places. Under Article 21 of the Constitution no one can be
deprive of his right to life unless according to the due process of law, inter alia, a nonsmoker cannot be affiliated with various diseases of lung and heart just because he is
required to go to public places. Every non-smoker was to be protected from the harm of
passive smoking and no doing so would violate Article 21.
The Kerala High Court came down heavily against the inaction of the state
government in preventing smoking in public, it held that “the continued omission and
inaction the part of the respondents to comply with the constitutional mandate to
protect life and to recognize the inviolable dignity of man and their refusal to
countenance the baneful consequences of smoking in public at large has residted in
extreme hardship and injury to citizens and amounts to a negation of constitutional
guarantee of decent living as provided under Article 21 of the constitution of India". 39
Tobacco use violates ‘right to life’ of both passive smokers and that of the tobacco
farmers. Thetobacco farmers are exposed to various health problems due to transdermal
nicotine absorption. Green Tobacco Syndrome is a common ailment amongst tobacco
farmers. The toxicity to the cardiovascular system and carcinogenicity of chronic dermal
nicotine exposure are also likely to exist as non-smoking tobacco harvesters show
similar cotinine and nicotine levels as active smokers in the general population.
36 (1993) 1 SCC 645
37Durga Das Basu, Shorter Constitution of India, 377 (14,hedn., 2010)
3S(2001)8 SCC 765
39K. Ramakrishnan and others v. State of Kerala (AIR 1999 Ker 385)
Exposure to pesticides leads to a host of skin disorders, clinical diseases and others0.
Tobacco farming is harmful and endangers the lives of those involved in its cultivation.
Thus incentivizing the tobacco production through subsidies and other schemes,
with the sole purpose of increasing the tobacco production endangerslives of the farmers
involved in the cultivation of tobacco along with those consume and are exposed to
tobacco products clearly violate Article 21.Encouraging the consumption and production
of tobacco is not only a violation of fundamental rights but also of the Directive
Principles of State Policy (“DPSP”).
Article 47 lays down responsibility on the State to raise the level of nutrition and
the standard of living of its people. Not only does it specifically empower the state to
prohibit the consumption (except medicinal use) of intoxicating and psychedelic
substances (alcohol or other brews, drugs such as cannabinoids or opiods or laboratory
preparations like amphetamines.) Three key responsibilities can be gleaned from this
article - improvement of nutrition of the people, improvement of their standard of
living and prohibition of substances that the State considers harmful to the health of its
citizens.
The provision for prohibition of certain substances in the interest of public health
is one of the most noteworthy features of this Article, as it empowers the State to
infringe an individual’s right to consume such substances. The Article allows for strict
control over the production, possession and trade of such substances. Even an absolute
prohibition on liquor can be enforced by the State so as to fulfil the objective of public
*
health.4
Such a ban can not be protested on the basis of Art. 19 (1) (g) as the right
guaranteed by it is not absolute - it can be restricted by the state under certain
conditions. The reasonableness of limitations on it can be interpreted in accordance
with the DPSPs, that is to say, Art. 47 can be effectively read into Art 19 so as to make
such a ban legitimate.*
2
As already highlighted, the ill effects of tobacco use on health are common
knowledge. Its detrimental effects extend to tobacco farmers as well. It was found that
tobacco use is high among tobacco growers. Tobacco related illness amongst farmers
4°Shabbiret. al., Risk Assessment of Pesticide Exposure on Health of Pakistani Tobacco Farmers, 20
JournalofExposureScienceandEnvironmentalEpidemiology,i96-204 (2010)
41Nashirwar v. State of M.P. AIR 1975 SC 360: (1975) 1 SCC 29
42DurgadasBasu: “Shorter Constitution of India” - 14
* Edition Reprint (2010) - LexisNexis
cannot be brushed as mere occupational hazards, the farmers need to be saved from
these life-threatening situations. Poor farmers indulge in tobacco cultivation solely due
to lack of viable economic alternatives. It is consequently the duty of the state to
facilitate the movement of farmers from tobacco to other crops by disseminating skill
and knowledge. On the contrary, the action of the tobacco board in continuing to grant
subsidies and incentives to tobacco farming amounts to direct promotion of tobacco,
rather than protecting farmers contravenes Article 47.
Article 48A places an imperative constitutional duty on the State to “promote,
protect and improve the man-made environment and natural environment^.” By
reading this provision with Art. 21, the Supreme Court has elevated environmental
protection to the same pedestal as concerns of human rights.44When the social and
economic costs take the center stage, often the environmental costs are ignored. While
allowing incentives towards tobacco production, the state is ignoring environment costs
of tobacco production. The tobacco industry is one of the country’s major pollutants, it
requiring 8 kgs of fuel wood to cure one kg of tobacco, and nearly 70 million tons of
paper to make cigarettes. All this from wood that is sourced from our forests, causing
global deforestation of 2-4%, which is has a considerable carbon footprint.45 Tobacco
also depletes nutrients from the soil faster than other crops,«6 reducing the fertility of
soil. Tobacco production therefore needs numerous external inputs such as fertilizers
and pesticides. Excessive use of pesticides and fertilizers causes soil pollution and
ground water contamination and reducing the fertility of the soil.47 in a country like
India, where millions are malnourished and food security is a major issue. The social
benefits of using the same area for the growth of food crops are greater than tobacco
production.The continued provision of subsidies and supporting environmentally
destructive activities of the tobacco goes against the spirit of Article 48A which is the
constitutional obligation towards protection and improvement of the environment.
■’’GodavarmanThirumalpad T.N. v. Union of India, (2002) 10 SCC 606, 621: AIR 2003 SC 724
'’“ArvindDatar: “Commentary on the Constitution of India" - 2nd Edition Reprint (2010) - LexisNexis
Nayantara S. Nayak, Tobacco curing and fuel efficiency in Karnataka, South Asia Network for development and
Environmental Economics, Working paper No: 77-13, 5(January 2013)
Conference of the Parties to the WHO Framework Convention on T.obacco Control, “Study group on economically
sustainable alternatives to tobacco growing (in relation to Articles 17 and 18 of the Convention)”, 2008 at page 4
Lecours et al., Environmental Health Impacts of Tobacco Farming: A Review of the Literature, 21 Tobacco
Control, 192-93(2011)
Article 51 lays a duty on the State to fulfill its international duties by promoting
peace and security, honouring its international obligations to foster respect for
international law, maintain just and honourable relations with other nations and
encourage the use of arbitration as a pacific means of international dispute resolution.
Article 5.3 of the FCTC requires that members should immune their ‘national health
policies from commercial and other vested interests of the tobacco industry’.
This
means that, the government should not provide any preferential treatment to the
tobacco industry. Such preferential treatment includes providing subsidy to the farmers.
India, who is signatory to the convention, enacted the COTPA to control the use of
tobacco by regulating its production, trade and advertisement among other things.
However, it is interesting to note that the Tobacco Board Act, 1975, which established
Tobacco Board, is in direct contradiction with the India’s international commitments at
WHO and of COTPA. The Tobacco Board provides subsidies for tobacco farming to
develop and incentivise tobacco industry. This establishes a prima facie case of Article 51
violation.
It is thus put forth by this policy brief that the ill-effects on public health, the
environment and the public harm caused by tobacco production are undeniable. By
allowing the subsidies and incentives to boost tobacco cultivation the activities of the
Tobacco board violates ‘Right to life’ under Article 21 and are also contrary to the
Directive policies of the constitution under Article 37, 47 and 48A, requiring us to strive
for an intervention. It therefore urges ending subsidies for Tobacco farming and
supporting alternative livelihoods.
(Hi)
COPTA
The Cigarettes and Other Tobacco Products (Prohibition of Advertisement and
Regulation of Trade and Commerce, Production, Supply and Distribution) Act, 2003
(“COTPA”) was enacted to prohibit advertisement and regulation of tobaccobusiness in
India.The tobacco control policies in India are implemented by different departments of
the government, leaving space for contradictions. On the one side COTPA (Ministry of
Family Affairs) aims to reducing tobacco use in the interests of public health. It
prohibits smoking in public places, sale of tobacco products to minors and places
restrictions on the advertising of tobacco products. On the other side, the Indian
Tobacco Board (Ministry of Commerce and Industry) was constituted in 1975 and still
continues to promote the development of the tobacco industry. This justifies phasing out
of subsidy and other incentives for tobacco production.
(iv)
Order of the Karnataka High court
The Karnataka High Court recently issued an order on tobacco subsidies in a public
interest litigation brought by the Cancer Patients Aid Association that could be a good
starting point for phasing out tobacco subsidies.''8 The petitioner sought the cessation of
subsidies as being in violation of the FCTC, the Indian Constitution and the COTPA; and
instead asked that the State and Central Governments provide support and
rehabilitation for tobacco farmers in switching to alternative crops.
On June 1, 2015, the Karnataka High Court disposed the PIL with an order
directing the relevant Departments of the State and Central Governments to take steps
to (a) reduce the local demand and supply of tobacco products, (b) consider a policy for
the rehabilitation of tobacco growers and related tobacco workers and (c) consider
whether or not to continue direct and indirect incentives and subsidies for tobacco
production. The Karnataka High Court further opined that there is a need for policy
decision and policy framing authorities should draw up a procedure good for the society.
The issue of subsidies and support programs for tobacco farming has long been a
sensitive topic as efforts to stop these programs are fiercely countered by the tobacco
industry with the argument that such measures would end up destroying the livelihoods
of hundreds of thousands of tobacco farmers. However, such arguments overlook the
significant health hazards that tobacco cultivation poses to tobacco farmers as well as
the growing body of evidence that suggests that many farmers are willing to move away
from tobacco farming if given viable alternatives.
It is, thus, imperative to look at the issue of tobacco farming holistically and
ensure that plans to phase out subsidies are accompanied by programs that provide
strong support to tobacco farmers for transitioning to alternative livelihoods. By
considering both these issues, the recent order of the Karnataka High Court provides a
«8 Cancer Patients Aid Association v. State of Karnataka and others, W.P No: 55697/2014
timely opportunity to develop a timeline for phasing out tobacco subsidies and bolster
efforts to support the rehabilitation of tobacco farmers.
V.
CASE STUDIES FROM OTHER JURISDICTIONS
Tobacco entails a very high social cost to the society owning to its harmful effects on
public health and environment. As discussed earlier, tobacco subsidies are contrary to
the provisions of FCTC, Constitution and COTPA. Tobacco subsides have to been
globally recognized as a threat to the health and environment, jeopardizing efforts to
improve public health. Many countries across the globe have phased out the subsidies
they use to provide
Globally many countries and regions have been able to phase out tobacco subsidies
in a systematic manner. The US, Bangladesh, EU and Australia and many others have
been able to successfully phase out subsidies and support programs for tobacco farmers.
Looking at the methods and mechanisms applied by each country to phase out tobacco
subsidies, could help India in developing its out phasing-out plan.
(i)
The European Union
The European Union has been successful in bringing together its member countries and
effectively ending the tobacco subsidies regime. It was no easy feat as the EU member
states are amongst the top tobacco producers in the world. In the early 2ooo’s, the EU
spent up to 1000 million pounds towards tobacco subsidies.49 Countries like Poland and
Bulgaria even continued to demand more direct inputs, as tobacco was a major source of
revenue for these countries. But as health concerns from tobacco use became more
apparent.
The support for tobacco producers in EU began in the 1970s. During the 1970s,
tobacco demand grew many folds in the Europe. This led the European Economic
49
Free Trade versus public health, Health Policy and European Union Enlargement, available at:
https.7/books.googIe.co.in/books?id=yygXw7R7gxsC&pg=PA211&lpg=PA211 &dq=tobacco+subsidies+in+EU&so
urce=bl&ots=BaDK5_fY7q&sig=MZ5JrOmaIdgl5W6_IiSJ0J_N7c&h]=en&sa=X&ved=0ahUKEwj_6NuZ8d_KAhWLB44KHSvTCPQQ6AElTzAI#v=onepage&q
=tobacco%20subsidies%20in%20EU&f=false
Community to establish an organization exclusively for manage tobacco production and
trade. The Common Market Organization for Tobacco (“CMOT”) was established to
implement an intervention policy based system of norm and intervention prices, which
included the obligation to buy tobacco at the intervention price (minimum support
price) and to abolish taxes having effect equivalent to customs duty and any quantitative
restriction or measure having equivalent effect which formed part of a national
organization of the markets in the sector.
However, CMOT failed in regulating demand and supply in the tobacco market,
leading its abolition through the Common Agriculture Policy (CAP) Reforms of 1992.5°
This set of reform established a premium system that allowed for the cultivation
contracts between growers and first purchaser in the supply chain. Further reforms were
introduced in 1998s1 which established an auction system for cultivation contracts to
reflect market conditions and quota buy-back arrangements was introduced to help
producers who wish to leave the sector but find no purchasers for their quotas. Thus, the
CAP 1992 created a system wherein tobacco producers were given minimum support
price and provided a safe exit to tobacco farmers.
However, the pressure from civil society and health groups considerably grew
demanding the removal of support to the tobacco producers. This resulted in 2001
Communication
on
Sustainable
Development
at
Gothenburg
Summit
by
the
Commission, wherein the Commission recommended to “adapt the regime so as to
allow for a phasing out of tobacco subsidies while putting in place measures to develop
alternative sources of income and economic activity for tobacco workers and growers
and decide an early date accordingly” s-
This communication inspired reforms to the Common Agricultural Policy in 2004.53 The
reforms lead to the abolition of production quotas and minimum support price from
production. The Member States were given a transition period to adjust, between 2006
and 2009. During this transition period, Member States could either completely break
50
http://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX%3A31992R2075 (EEC No. 2075/92)
51
http://eur-lex.europa.eu/legal-content/EN/TXT/?uri=celex:3l998RI63 (EEC No. 1636/98)
52
EC Regulation 864/2004
the link between production and the financial aid provided to the tobacco sector known
as "decoupling" or could continue to link part of the provided aid to production.
Decoupling aid from production allows producers to grow other crops while maintaining
stable incomes.54 Since 2010, EU aid has been completely decoupled from production.
The old support system was converted into direct payment systemss and rural
development programss6 in equal portions. The de-coupling allows farmers to shift to
production of other crops should they so desire.
Even though the EU successfully phased out tobacco subsidies, the controversy
still remains. The subsidies can start again if the Members of European Parliament vote
to amend the Common Agriculture Policy. The European Parliaments plenary vote on
22 October, 2014 on the draft budget for the European Union revealed a divided
Parliament but rejected two amendments which aimed to stop EU subsidies for tobacco
production.57
(ii)
United States of America
The US economy experienced the Great Depression in early 1990s wherein tobacco
prices sky rocketed due to low production. To bring the economy out of shambles, the
government introduced various reforms. One of those was reform was targeted towards
tobacco industry, by establishing a Tobacco Program. The Tobacco Program was
established by the Agriculture Adjustment Act of 1938. The program gave producers a
safety net under auction prices and provided manufacturers with a stable crop of raw
materials. The producers were given a support price by which the farmers received a
minimum price for each unit of their production. The support was divided into two parts
viz, direct market purchases and non-recourse loan. Through direct market purchase,
the government bought directly from processors and handlers at the support price and
then disposed the commodities through other “non-competing” outlets. Through non
recourse loans, the government issues government-purchase contracts which enabled
farmers to retain title to their commodity while turning it over to the government with
the option to repurchase within a given time period by repaying the loan. Given the
54http://ec.europa.eu/agriculture/tobacco/
5ihttp://eur-lex.europa.eu/legal-content/en/TXT/?uri=CELEX:32013RI30 7 (EU 1307/2013 )
56http://eur-lex.europa.eu/legal-content/en/TXT/?uri=CELEX:32013R1309 (EU 1309/2013)
57http://www.epha.org/6218
producer’s option to repurchase the commodity; if the market rate exceeded the loan
rate, the loan rate effectively became the price support for the commodity.
Increase in demand for other crops and increased political and economic
pressures in 1980s prompted several changes in the Tobacco Program. As political
pressure to modify or end the Tobacco Program gained momentum, several members of
Congress and opponents of the Tobacco Program questions how the government could
support tobacco production while it simultaneously supported efforts to reduce tobacco
consumption. This change in scenario lead to a new statute known as The No-Net-Cost
Tobacco Program Act, 1982 came into existence.
The No-Net-Cost Act mandated the Tobacco Program to operate at no net cost to
the federal government or taxpayers and to limit increases in support price for tobacco.
This was followed by the Tobacco Improvements Act of 1985, which further lowered
price supports and made annual changes in price support levels and quotas.
This was followed by increasing political pressure demanding less regulations
and freer markets for all of U.S. agriculture, including tobacco. This lead to coming into
effect of The Agricultural Improvements and Reform Act of 1966 which terminated
supply control and price stabilizing programs for most major crops, leaving only the
tobacco, peanut, and sugar programs intact.
Numerous lawsuits from both within and outside the tobacco industry brought
pressure on the Tobacco Program during the 1990s. Lawsuits seeking reimbursement
for Medicaid or other costs associated with the consumption of tobacco products were
filed against tobacco manufacturers by 46 states. These lawsuits were successful in
developing an agreement to settle the existing state Medicaid lawsuits in exchange for
the tobacco industiy’s agreement to change some of their marketing practices and to
make payments to the states in excess of $200 billion over a period of 25 years. These
payments were to compensate state governments for the expenses incurred in the
treatment of tobacco-related illnesses through government-sponsored health insurance.
programs and Medicaid in US.
In addition to political pressure from some non-tobacco advocates and tobacco
companies, growing opposition to the Tobacco Program began to escalate among
tobacco farmers during the latter 1990s and early years of the new century. Internal
opposition to the Tobacco Program was also enhanced by the growing disunity of quota
holders and growers. Despite escalating problems within the tobacco industry and
several initiatives to terminate the Tobacco Program, it remained intact during the 20th
century.
In the 21st century, the political and economic stage was set for a tobacco buyout
and termination of the Tobacco Program due to growing political and economic
pressure. Increased international tobacco production, in addition with improved foreign
quality had narrowed the number of premium tobacco manufacturers who were willing
to pay for U.S. leaf. Furthermore, the price differential between U.S. and foreign
tobaccos had generally widened in recent years, causing further erosion in the U.S.
market share of world tobacco production and trade.
Ultimately, in 2004 an Act called The Fair and Equitable Tobacco Reform Act,
was introduced which established the Tobacco Transition Payment Program (TTPP),
also known as the tobacco quota buyout.The main objectives of the Act were to
terminate the federal tobacco program, compensate tobacco quota owners for
elimination of their government created quota assets. The provisions of this Act
removed support for tobacco from the Agriculture Adjustment Act, 1938. Therefore,
only the part of the Adjustment Act which provided safety net for tobacco farmers were
removed by this new Act. This Act provided for payments to eligible tobacco quota
holder for the termination of tobacco marketing quotas and related price support, as full
and fair compensation for any losses related to such termination.s8This tobacco quota
buyout ended in 2014.
(iii)
Australia
Tobacco was first grown in Australia in 1818 at the Emu Plains in New South
Wales and by 1850's cultivation extended to Queensland and Victoria. Due to the growth
of tobacco cultivation all over the country and the scope for high profits, a large number
of potential cultivators were drawn towards tobacco cultivation at the turn of the 20th
century. Observing that, the Australian Government made large areas of land available
for tobacco cultivation. The number of tobacco farmers grew to over 800 by 1932;
however, since the majority of tobacco was grown on unsuitable soil, the farmers faced
58
immense difficulty in competing with the international market in terms of quality and
quantity of production.
Tobacco product manufacturers in Australia were reluctant in buying locally
produced tobacco and thus relied on imported tobacco for their products. Perceiving
this to be a great threat to the tobacco industry in the country, the Australian
Government began its first of many regulatory measures in 1936. The Local Leaf
Content Scheme (“LLCS”) mandated the Australian manufacturers to use a minimum
quantity of locally produced tobacco in their products. The initial amount of locally
grown tobacco to be used was 7.5%, which was increased to 28.5% in 1966, and 57% in
1970.59 The manufacturers were given incentives like concession on duty of imported
raw tobacco. Such sorts of incentive to the manufacturers are form of indirect subsidy to
tobacco farmers.
The Government also passed the Tobacco Marketing Act, 1965 to deal with the
problems of marketing, pricing and grading cultivated tobacco. The law established the
Australian Tobacco Board (“ATB”), which later became Australian Tobacco Marketing
Advisory Committee in 1990. ATB was an advisory body that made recommendations
regarding domestic and overseas marketing of tobacco at federal and state level.
Another objective of the ATB was administration and regulation of the Tobacco Industry
Stabalisation Plans (“TISP”). TISP worked on a quota basis to ensure strict supply and
price of tobacco. Each year the ATB recommends the national marketing quota for the
next selling season to the relevant ministers. Once the quota was determined, the
aggregate quota was divided among the three tobacco cultivating states (Victoria,
Queensland and New South Wales). The quota committees of the state tobacco boards
allocated quota to individual growers. Therefore, the implementation of the TISP
worked on a two-tier level with ATB at the national level and the state tobacco boards at
the state level. TISP dealt with matters such as setting local price, determining the grade
and minimum price schedule, distribution of quota and allocation among the states,
conversion of quotas to individual growers, arbitration of disagreement of rates of
quotas, sourcing of tobacco bought by manufacturers. Both the TISP and the LLCS were
due to expire on 30th September 1995.
’Tobacco growing in Victoria, available at: littp://www.alpinelink.coni.au/tobaccoproduction/
In 1990, the Industry Commission was of the view that with all the statutory
marketing arrangements, tariff concessions and other measures of government support,
tobacco was by far the most subsidised agricultural activity in Australia, receiving
assistance at around six and a half times the rate of other horticultural activities, and
over 12 times the average rate for all agricultural activities.6o61
Later that year, the
Commonwealth Government agreed with the tobacco manufacturing industry to
restructure its policy on tobacco. This included a package for the winding down of the
Australian Tobacco Marketing Advisory Committee, the Local Leaf Content Scheme and
the Tobacco Industry Stabalisation Plan.
In the final year of TISP (1994) 600 tobacco growers remained and by the end of
1995, the number had gone down to 366. The phasing out of subsidies and the
assistance provided to tobacco farmers were done mainly with two schemes: the rural
adjustment scheme and the voluntary quota retirement scheme. The quota retirement
scheme or the quota buy out scheme was intended to reduce tobacco leaf production
capacity by 1.5 million kilograms. This would be done by incentivising the farmers to
leave the industry. It was implemented in different ways in the three states. In
December 1993 the Victorian Government announced a restructure package which was
built around a $3 million grant, combined with a plan to introduce the Tobacco Leaf
Industry (Deregulation) Act 1994 which repealed the Victorian Tobacco Leaf
Stabilisation Act 1966 and the Marketing of Primary Products Act 1958. As part of this
restructure, a number of quota holders in marginal growing areas voluntarily
relinquished their quotas to the State Government for $2.00 per kilogram and import
tariffs were reduced to zero.6’ The scheme in Victoria was administered through the
Rural Finance Corporation. Payments made under the scheme will be in the form of a
loan from the RFC, which will be converted to a grant at the end of the five-year period.
The loan will be secured by a mortgage over the grower’s property in favour of the RFC,
above which existing mortgages will be given priority. Sale or leasing of the property can
take place provided appropriate security to replace those assets is provided. A
consultancy service was created which was funded by Department of Primary Industries
60 Industry Commission. Annual Report 1989-1990. Canberra: Australian Government Publishing Service, 1991
61 Tobacco growing in Victoria, available at: http://www.alpinelink.com.au/tobaccoproduction/
and Energy to advice growers whether to participate in the quota retirement scheme and
to advice the growers to move to other agricultural options.
The Rural Adjustment Scheme (“RAS”) was established by the Commonwealth
Government to assist the process of structural adjustment within rural industries. The
basic objective has remained the same. In particular, the scheme is intended to help
farmers with prospects for long-term viability to overcome short-term financial
difficulties, and to assist farmers in extreme financial difficulties to re-establish
elsewhere.
The last sales contracts in Northern Queensland were filled in early 2004, and in
Victoria and southern Queensland a majority of growers voted in support of a federal
government and industry-funded buyout of the leaf growing industry announced in
October 2006. The federal Government announced a $40.9 million package to buy out
all the licenses and help tobacco growers to move to non-tobacco alternatives. This
package was known as Tobacco Growers Adjustment Assistance Package. Growers in
Queensland were given up to $23.3 million dollars while British American Tobacco
Australiacompensated growers in Myrtelford for a $10 million with each farmer eligible
for a maximum amount of $150,000. All outstanding sales transactions were expected
to be completed in 2009.
(iv)
Bangladesh
While EU, US and Australia are developed countries, a more relatable case would be
that of Bangladesh. Bangladesh has been successful in ending subsidies for tobacco
production. Such a feat was possible due to the active involvement of Bangladeshi
judiciary, legislation and executive alike. In 1999, the Supreme Court of Bangladesh
passed orders directing the government to take steps:62
i.
Phase-by-phase to stop giving subsidies to farmers to grow tobacco;
ii.
if possible and necessaiy, to produce other agricultural products;
iit.
to rehabilitate tobacco works to other beneficial jobs;
iv.
restrict issuance of licenses for tobacco production, specifying reasonable period.
62Nurul Islam, WP 1825 of 1999, Supreme Court of Bangladesh
Further in 2010, the Ministry of Agriculture of Bangladesh has taken strict
measures to withdraw subsidies, especially those on fertilizers. The Bangladesh
government recognized the need regulate excessive use of fertilizers in tobacco farming
and has made the procurement and use of fertilizers subject to strict conditions.
Additionally, the Bank of Bangladesh, which is the central bank of the country. In 2010,
passed a circular ordering all scheduled commercial banks to refrain from granting any
loan for tobacco farming. 63
Apart from these measures Bangladesh has been actively encouraging alternative
crop farming instead of tobacco. In 2013, it passed an act known as the Smoking and
Tobacco Products Usage (Control) (Amendment) Act, 2013, which discourages all forms
of tobacco production. It also provides technical and educational support to its farmers
to encourage transitioning into alternative jobs.
The numerous measures taken by countries only show us that it is possible to end
the subsidy regime in India too. As tobacco production is a complicated process,
employing various people at different levels. The policies for phasing out should be
implemented in timely and systematic steps over a period of many years. This would
give farmers and processors enough time to smoothly transition into alternative
livelihoods. Apart from time, adequate governmental support through monetary plans
or non-monetary measures such as training, technical education, research etc. are
necessary to effectively implement these policies.
IV: The Roadmap Ahead& Recommendations
One of the main aims of this policy brief is to deliberate on ways to facilitate
rehabilitation
of tobacco
employees
into
‘sustainable’
alternative
livelihoods.
Sustainable not only in economic terms, but also encompassing social and physical
development of tobacco workers. The goal of alternative livelihoods is to address the
problem of poverty and vulnerability of the tobacco workers.
63 Circular dated 18 April 2010, The Bank of Bangladesh
The Tobacco industry being a complex one, involves different personnel at each
level. Tobacco farmers for cultivation; bidi rollers, tendupluckers, factory workers,
processors and others, for manufacturing and processing. Each of these workers have
different socio-economic challenges that this policy brief wishes to tackle.
The FCTC has formulated Guiding principles to ensure sustainable alternative
livelihoods in relation to Article 17 & 18. In fact, one of the aims under the FCTC is to
find viable alternatives for tobacco farmers so that they may be transitioned to other
options in agriculture, which would reduce tobacco growing and, as a consequence,
curb, the increased consumption of tobacco.
Tobacco subsidies and incentives and support to tobacco growers are against the
basic principles and obligations of the Union of India under the FCTCto which India is a
party. Parties to the FCTC adopted guidelines for implementing Art. 5.3’ which relates
to the protection of public health policies on tobacco control from the commercial and
other vested interests of the tobacco industry. In the guidelines for implementing Art
5.3, it is plainly stated under the seventh recommendation, for member states to “not
give preferential treatment to the tobacco industry.”Additionally, the guidelines to Art.
17 of the FCTC obligates member states to promote economically-viable alternatives for
tobacco farmers rather than entrenching them into tobacco farming with subsidies.
Finally, Art. 18 of the FCTC charges members with having due regard to protecting the
health of tobacco farmers and the environment.
Incentivizing tobacco farming through subsidies would be contradictory to Art.
18 since cultivating tobacco has various negative effects on the farmers and the farm
land.Thus, in the interests of public health, the health of tobacco farmers and also the
environment, it is imperative that tobacco subsidies and incentives by the State are
stopped.
The very continuance of the Tobacco Board Act 1975 goes against the principles
of the promotion of public health through the COTP A. The Tobacco Board Act was
enacted in 1975 and it was set up with its stated objective for the development of the
tobacco industry under the control of the Union. The Act set up the Tobacco Board
having its head office at Guntur, Andhra Pradesh.
The functions of the Board are
enumerated under S. 8 and sub section (1) clearly reads “It shall be the duty of the Board
to promote, by such measures as it thinks fit, the development under the control of the
Central Government of the tobacco industry.” These ‘measures’ include providing for the
regulation of the production and curing of Virginia tobacco, keeping a close eye on
national and international tobacco market prices and fluctuations, maintaining and
improving current tobacco markets both in and outside India, prescribing minimum
prices in order to prevent unhealthy competition amongst the exporters, regulating the
Indian tobacco market, providing useful information to tobacco growers, dealers and
exporters, purchasing Virginia tobacco from dealers if it is considered necessary in the
interest of the growers and disposing the same either in India or abroad, promoting the
grading of tobacco at the level of growers, maintaining the registry of tobacco and
tobacco seedling farmers, and finally, sponsoring, assisting, co-ordinating or
encouraging scientific, technological and economic research for the
promotion of tobacco industry.
These objectives of the Tobacco Board Act 1975 are in complete contradiction and
opposition to the new and subsequent legislation, being the COTPA which was brought
about in 2003 for the regulation of tobacco consumption, and aims to protect public
health. The Preamble of the COTPA states that it is “for theregulation of trade and
commerce in, and production, supply and distribution of, cigarettes and other tobacco
products and for matters connected therewith or incidental thereto... AND WHEREAS
it is expedient to prohibit the consumption of cigarettes and other tobacco products
which are injurious to health with a view to achieving improvement of public health in
general as enjoined by Article 47 of the Constitution”.
Recommendations:
(i)
There should be a clear and holistic policy on tobacco control and public
health, which addresses, not only advertising and promotion of tobacco but
also tobacco subsidies, steps to control tobacco growing and a plan for
alternatives for tobacco farmers, as directed by the Karnataka High Court.
This Policy should be framed by all concerned government departments -
ministry of health, agriculture and commerce.
(ii)
One of the crucial policy measures that must be taken by the central
government is to wind up the Tobacco • Board. The Board can no longer
continue, with its aims and objectives of promotion of tobacco when the
COTPA has been enacted for regulation and control of tobacco.
(iii)
All tobacco related subsidies, including subsidies for farming, fertilizers,
agricultures, whether given by the Board or other agencies must be stopped.
(iv)
All other incentives such as crop loans, welfare schemes and measures given
to tobacco farmers must be stopped.
(v)
Instead, benefits and support can be provided for tobacco farmers to get them
out of tobacco and into alternative livelihoods. Farmers are leaning towards
shifting from tobacco to other crops but are unable to do so due to lack of
finances, information or opportunity.
Encouraging tobacco workers to
alternative livelihood does not merely mean, substituting one economic
activity with another. The concept of livelihood diversification is based on the
fact that more diversified a production unit is, farmers have wider choices of
economic and productive activities. Essentially it goes beyond the idea of
substituting tobacco with sugarcane or maize. These alternative should
provide opportunities that would allow farmers to enhance their health and
socio-economic wellbeing6^
Cvi)
It is usually seen in India that tobacco farmers do so because they have been
farming tobacco traditionally. It is seen that these farmers look at tobacco as a
secure option because they lack knowledge to assess the profitability of other
crops. Educational and training programmes will give farmers an opportunity
to look at different crops. It will also assist farmers in adopting farming
techniques that would increase profitability.
(vii)
The Tobacco Board can be used instead to promote alternative livelihoods for
tobacco farmers and to get them out of tobacco growing: In Malaysia for
example, a Tobacco Industry Restructuring Plan was launched in 2005 to
meet Malaysia's commitment to the FCTC and to anticipate the negative
impact expected from the ASEAN Free Trade Agreement. It focuses on kenaf
as an alternative for tobacco growers. More than 15 million euros are being
invested in research and development of the industry as a whole, from crop to
Principle 1 of the Guidelines under Articles 17 & 18
final product. Tobacco growers willing to switch to kenaf have been provided
with cash incentives of 554 euros per hectare as well as seeds, fertilizers,
pesticides and training. The National Kenaf and Tobacco Board is responsible
for promoting the new crop among tobacco growers.
- Media
 RF_PH_5_SUDHA.pdf
RF_PH_5_SUDHA.pdf
Position: 1060 (20 views)