CHAI BACKGROUND PAPERS
Item
- Title
- CHAI BACKGROUND PAPERS
- extracted text
-
,,
COMMON.™
RF_NGO_3_SUDHA
Z^'1
«n.(H^H"X‘5soo«l
The Catholic Hospital Association of India
C. B. C. I. Centre, Goldakkhana, New Delhi- 110001
Tel. 310694, 322064
Ref. No.
COUNSELLING : TECHNIQUES & METH&ppLOGY.
'Councelling is an enabling and helping relationship, in
which the person seeking help is encouraged for positive growth,
and also to take counsel with oneself. The result of counsell
ing understood in this way would be that the client can get
back to the main stream of life as a normal human person.
Thus a new behaviour in the person counselled is the overall
aim of counselling.
In broad terms we can say that there are two approaches
in counselling:
The first one is called Dispensary approach, and it is
characterised by monologue on the part of the counsellor. Cnee
the problem of the counselee is shared the counsellor prescri
bes solutions and readily provide them, instead of enabling
the counselee to go deeper into the problem by himself/herself,
and arrive at a decision to solve it. Sympathy towards the
counselee is the predominant feeling here. When this approach
is used it can hardly be called a counselling session.
The second, approach is called Bartender approach. Instead
of sympathy, the counsellor displays feelings of empathy
towards the counselee. Companionship is offered to the
counselee in his/her distress situation and not advise. The
counselee is re-assured by the counsellor's attitude of 1 I
am with you', 1 I care about you', towards him/her. Here the
entire attention is focused on the counselee. The counsellor
never takes responsibility of the counselee's problem, but
rather (s)he encourages and enables him/her to take the
responsibility.
The person who comes for counselling is apparently in a
state incongruence. In other words (s)he has lost the equili
brium in his/her inner personality. The measure of happiness
or unhappiness a person has is often determined-by the level
of congruence (s)he enjoys within his/her personality. When
a person is not properly settled within oneself (s)he falls
into a state of incongruence. According to Kasl Rogers this
happens because of the disharmony between:
The real me: How I view myself ( at this present moment)
The possible me: How I view myself that I could be.
Ideal me: How I view myself that I should be.
The counsellor's role is to enable the counselee to
attain the state of congruence. This in practical terms means
helping the counselee to become aware of his/her inner
feelings, to accept them and also to communicate them
if appropriate.
YOUR ATTITUDES & YOUR EFFECTIVENESS
Personal Attitudes: Before we start counselling others, it
is very important to know and realize about our own personal
attitude towards people. The check list given in Appendix I
will help us to see what we ARE in relation to our attitudes.
Answer them with 'Yes', 'I think so' and 'No'. Your answer
should be based on what you ARE and not what you should be.
If you are doubtful about the answer of any question ask
your friend. (Please refer the check list and do the exercise
before you proceed further)
....2..
- 2 If the majority of the answers are 'Yes' or'I think so1
you have the disposition, and the potential to become a good
counsellor. The 'NO's’ are indicators for you to know where
you need to make most efforts to become a good counsellor.
Personal Effectiveness:
The ability to handle ones own problem is important for
the counsellor. 'Johari Window' as designed by Joseph Luft &
Harry Ingham may help us to increase our own personal effect
iveness.
!
1
}
2
?
I Area of ;
, I
free acti-j Blind sPot ;
| vity______ |_____________ ;
j
3
|
mask
I
’+
j unknown
j
I //////////\//////\
\///////////M///// !
I///////////4//ZZZZ1
\///////////\////// i
izzzzzzzzzzzzzzzzzil
I
I
I
I
I
I
I
I
I
I
I
I
I
1st Quadrant:
Information about myself shared by me and others. Close
friendship takes place here. ' I know and you know'. In this
area one feel comfortable with others. And others are also
confortable with us.
2nd Quadrant:
I
Data not known to us, but known to others ( eg. mannerisms
certain unconscious gestures etc) Unless others are free with
us they will not feed us with these things.
3rd Quadrant:
Information about myself, which I know too well, but
unimown to others. We keep it hidden from others. Very often
it is tie wrong self image that prevents one from revealing
them to others. They wear masks and it is very difficult to
deal with such people.
b-th Quadrant:
Information not known to us and others. We must have
heard people telling that ' I never know that I had so much
strength in me' Usually these ' Unknown' manifests itself if
emergency situations.
One measure of uur personal effectiveness is the size of
our 1st quadrant. Because it is in this area that we are most
effective as persons. The interesting thing is that, we
ourselves hold the key to increase this area of our personality
This is possible only through self disclosure and openness
to feed back.
....3..
- 3 a.
Self disclosure;
This means opening ourselves to others as we are. Normaly,
we dont do it for fear of boasting(false humility) or because
we are afraid to show ourselves to others as we are, and thus
we prefer to beat around public facts or things known to every
body. Lack of self awareness also can hamper self disclosure.
To talk freely arid openely about myself, I need to have
a healthy image of myself. Very often we experience tension
within ourselves between the 'real me, but not acceptable to
me;'
and the 'Acceptable me, but not the real me'. At
least the awareness of this will go a long way in helping a
person for self disclosure.
Love and acceptance are essential ingredients for human
growth. We can love and accept ourselves only when some one
loves and accepts us. VJe must give them a chance to do so.
b.
Feed back;
Feed back means the remark, comments, or responses we rece
ive from others about ourselves. It is not easy to be open to
feed back.. But it is important for our own personality
development. Very often acceptance of this feed back depends
also on how it is given. (eg; feed back given in an accusing
and hurting way) Because emotions play an important role here.
The feed back given to us need not be necessarily cent
percent true or valid. Nevertheless, it gives us an indication
as to how others see us. And this is important.
To conclude this section, we may say that to function
as an effective counsellor, we must improve our own personal
attitudes towards others, and also increase our effectiveness
through opening ourselves for more self disclosure and feedback.
THE ART OF COUNSELLING
The constituent elements of counselling are LISTENING &
RESPONDING. In other words the art of counselling means
listening with a sensitive ear and responding with an understand
ing heart. God has given us two ears, but one tounge, so that
we may listen double than we talk!
Listening doesn't mean listening of the verbal experessions
alone, but a clear observation of non verbal communications
(Body language), eg. Facial expression, tone of voice, body
position, gestures etc. When you attentively listen you are
telling the person that 'you are important to me'. The
following points are important for better listening.
- sitting position - to be able to look at the other
directly close enough.
- There should'nt be any external distraction.
- Avoid any internal distraction eg; Frankly admitting the
feeling in the beginning itself, structuring of the
interview in terms of time etc.
- Being sensitive to emotionally charged words.
- Listening also includes proper clarifications at the
right tine .
- Silence; (reflective and not empty-head silence)
...A..
- 1+ -
At this stage one thing the counsellor should keep in
mind is to remain free from any prejudices of his own. Very
often we wear 'eye glasses' made up of our own experiences,
background etc. These eyeglasses may not help us to help the
counselee. Another point otjkeep in mind is the danger of
'filtering out'. This means our tendency to listen and see
what we want to hear and see, and thus we stand to miss the
wholeness of the picture, which the counselee is trying to
present.
•Through sensitive listening and accurate responding, the
counselee enters into the internal frame of reference of the
other; the counselee's experiences is felt as if his/her
(councellor) own experience This 'As If feeling is called
Empathy. Here the counsellor feels with the counselee and..-./;
not feel FOR him/her.
At this stage we have to check our own attitude towards
the counselee. Three attitudes that seem to manifest are
authoritarian, Paternalistic and Companionship. Needless to
say that the companionship attitude is the one we should
nurture in a counselling session.
It is genuineness, understanding and acceptance that
characterises the real helping relationship in a counselling
situation. Genuineness of the counsellor (True to oneself,
and fearlessness in expressing it) wins the respect, trust and
confidence of the counselee, and also it serves as a model for
the counselee to be genuine himself/hers elf. It is und er standing
that helps the client for self exploration. When (s)he feels
correctly understood (s)he is encouraged to explore deeply
into the source of his/her trouble. The counsellor's underst
anding of the counselee is communicated through responses.
The responses should PARROT response. ACCEPTANCE attitude
of the counsellor creates a condusive atmosphere for the
counselling session. However, this does'nt mean that the
counsellor agrees with everything that isbeing said by the
counselee.
The counsellor should'nt take the responsibility for the
counselee and his/her problems. (S)He should be an enabler of
the counselee to take care of his/her problems. The possibi
lity of confrontation in a counselling session can't be ruled
out fully. It takes place normally when discrepencies are
observed in the client in the following areas (a) The ideal
versus the real (b) verbal expression and behaviour (c) what
onesays about oneself and the counsellor's experience of
him/her. These confrontations may hurt the client, but this
hurting is meant to heal, (eg; surgery) However, this must be
based on reality (eg. X'ray). Experiences have shown that
this sort of confrontations help the counselee to be more
genuine in the session and after.
For an effective counselling session, the following skills
are required on the part of the counsellor.
A. Attending; Attending to the counselee has various aspects.
They are 1. Attending contextually J
a+tpntlon
2. Attending personaly
J Physical attention
3. Attending through the posture
U. Attending through visual contact.
- 5 1.
The physical setting of the counselling room should be
pleasing, welcoming and relaxing.
2.
Personal attendance would mean attending to the personal
needs and requirements of the counselee.
3.
The posture we display in a counselling session is also
important, since that too communicates the attitudes and the
internal feelings of the counsellor.
*+.
Visual contact means the proper use of our eyes in a
counselling session. It also includes the use of all our
senses to grasp fully what the counselee is trying to express.
Psychologists are of opinion that only 25% of
is communicated through oral communication.
the message
The energy level of the counsellor as well as the counselee
is also a deciding factor of the effectiveness of the counsel
ling.
The degree of congruence also should be thoroughly
observed, by the counsellor. What people say and how they say
it reveals the depth of problem as well as how they see it
by themselves.
Attending also means listening. listening is an art, which
everybody can develop, but at the same time, which all of us
tend to practice less and less in our day-to-day life. Proper
and careful listening is the key factor which determines the
success of a counselling session. Attention should be focused
not only on the words, but also on the tune and how one says
it. Who, What, When, Where, Why and How (5W H) should be
throughly listend to.
Responding:
Adequate, appropriate and timely responding by the
counsellor, encourages the counselee to bring out more of
himself/herself and also increases his/her confidence. This
responding should be.characterised by the empathy (experiencing
of another person's world 'AS IF' you were there)
B.
The counsellor should:
1.
Respond to the content; eg; You are saying
(or) In other words
2.
Respond to the feeling: The feeling can be understood
through observing the behaviour and presentation. (If the
counsellor feels blank, (s)he can ask himself/herself: How
would I feel rayself in such a situation?)
eg: you f eel
................
(for examples of different feelings ref. Appendix II)
3.
Respond to the content and feeling:
eg: You feel
because
(5W H)
Proper responses, as mentioned earlier, helps the
counselee to explore his/her experience more deeply.
Personalizing:
The counsellor should help the counselee to go beyond the
experiences (s)he is sharing. ’ (S)He should be enabled to put
together the various experiences to get a better understanding
C.
....6..
- 6 -
of his/her own situation. Personalizing in the counselling
context means enabling the counselee to understand where
(s)he is and where (s)he wants to be.
Personalizing has to be done in three areas, viz,.
1. Personalizing the problem: It means helping the counselee
to understand what (s)he cannot do, that has led to his/her
experience. In other words, what is the counselee, that is
contributing to the problem? (counselee deficit)
Personalizing the feeling: eg., you feel
because
you can't
3. Personalizing the goals, eg., you feel..... because you
cant..... and you want to
(In personalizing the goals
the counsellor^ own experience can contribute a lot)
‘2.
Personalizing helps the counselee for an understand of
his/her problem in a better way.
1.
Initiating
This means finding direction in life. Through this skill
the counsellor enables the counselee to operationalize the goal;
identified in the personalizing process, eg., You want to....
as indicated by....... Your first step ihcul;.P (The
counselee should decide what his/her first step should be)
At this stage the counselee should be helped to initiate a
schedule for action, (with different steps and actions)
Initiation enables the counselee for action which will
ultimately led him/her towards a state of congruence and
integrated personality. This ofcourse is the ultimate goal
of counselling,
(Ref: Appendix III)
Counselling a Group in Tension
It is not uncommon that interpersonal conflicts and
breakdown of communication takes place in a team or group of
people working together towards a common goal. Counselling
can be an effective instrument in resolving the conflict in
such situations.
In such a group counselling session, the counsellor will
have to display atmost restraint and balance, so that each
member of the team can build trust in him/her and thus feel
free to express himself/herself fully.
The most important task of the counsellor in a situation
like this is to get the people concerned together in a place.
Once they are collected together thus, the counsellor should
ensure that each one listens to the other, with out inter
rupting the one who speaks. Very often when feelings run
high, people tend to fail to see other's views. And during
the session it might be possible that each one dwell in his/
her own views, trying to articulate his/her stand. To over
come such a situation Rogers suggests a methodology called
'echo game' to ensure proper listening from each other.
According to this methodology each one is made to repeat
what the previous speaker has said, before (s)he start speaking
hirns elf/her s elf.
- 7 The physical setting for the session should be arranged
in a semi-circle way, through which each one faces the counsellor
and sits at an equal distance. It could be in the following
way.
Counselee
X - Counsellor
The counsellor should show acceptance to each individual
attention should be paid, as in an individual counselling session.
The counselees should get the feeling that they are individually
attended to. This is possible only when the consellor can
enter into each one's frame of reference. (S)Hfe should never
show favour to any one, for get baised. The counselees should
be asked to direct the communication to the counsellor and
not to any one in the group. This is important especially
in the beginning of the session.
Through adaquate responses of the counsellor to each
one's point of views, every one else in the group gets a chance
to hear twice his/her own and other's views. This facilitates
better understanding of the other's standpoint for more effect
ive interpersonal relationship in future. It is worth mentioning
here that the experience of many groups have proved that
conflicts and tensions in a team or group can lead to strong
interpersonal relationship, if worked out properly. The skills
required by the counsellor in group counselling and tension
management and the processes are the same as that of individual
counselling.
Conclusion
Nobody can overemphasize the importance of counselling
techniques for personnel involved in people based health
and development programmes. The techniques and methodology
for individual and group counselling described about is not
exhaustive. This paper is meant to be a supplementary
reading after the course on counselling.
prepared by
community health department
catholic hospital association of
India
b.c.i.
c.
centre, goldakhana p.o.
new delhi 110 001 (phone 31069^)
ref: 1. "Barefoot Counsellor" by Er. Joe Currie S.J.
2. "The Art of Helping - III" (Robert R. Carkhuff, Ph.D)
tj:ka/5/8?/ 200.
Appeal J-
CHECKLIST
( From Barefoot Counsellor by Fr. Joe Currie, S.J. )
1 . De I find, ether people interesting?
2. De I find it easy te like others - even those whe are quite
different from me?
3. Am I enthusiastic about others' chances for wellbeing and happiness
4. Can I trust others to take decisions and assume responsibilities?
5. Do I generally relate freely and easily with others?
6. Do I have a deep and open relationship with at least some others?
7. Am I consistently trustworthy and dependable?
8. Can I identify with the feelings and private personal meanings of
others without becoming excessively weighed down by their problems,
"downcast by their depression, frightened by their fear, or
engulfed by their dependency"?
9. Are people important and significant to me?
10. Can I let others be as they are, even when I don't agree with them
nor approve >of their be iiaviour?
11. Do. I -have confidence in my own abilities?
12. Do I'dislike dominating and controlling others?
13. Can I accept my own weaknesses and shortcomings?
14. Am I ready to accept help from others when I myself am emotionally
upset?
15. Do I find it generally easy to listen, to give my full attention,
to others?
16. Am I convinced that I am an important person?
v V.\-\ \\ >
17. Do I encourage others to stand on their own feet, and fight 'the
temptation to take them under my wings? .
:
18. Can I accept myself ai I am, without undue anxiety about fulfilling
the expectations of others?
19. Am I open to new and better ways of doing things?
20. Can I be a good follower as well as leader?
^1. Do others generally find me a warm and loving person?
22. Do people find me approachable and easy to talk to?
23. Can I talk easily and frankly about myself, without'on the one hand
boasting and, on the other, feeling embarrassed?
24. Do I treat each person as an individual, giving him a chance to
prove himself before fitting him into a category?
25. Can I communicate warmth toward people and sensitivity to their
needs without being uncomfortable myself, or making the others
uncomfortable?
APfiMV* jj.
' CATEGORIES OF
FEELINGS
(From tl^e Art of Helping- III.
By Robert R. Carkhuff,Ph.D.)
Happy
Sad
’Angry
Sacred
Strong
Excited
ElatSd
Overjoyed
Hopeless
Sorrowful
Depressed
Furious
Seething
Enraged
Fearful -Bewildered.” Potent Overwhelmed
Panicky Trapped
Super
Impotent
Afraid
Troubled
Powerful Small.
. mild.
Cheerful
Up
Good
Upset
Annoyed ’Threatened Disorganized Energetic Incapable
Distressed Frustrated-' Insecure
Mixed-up
Confident Helpless
Down
Agitated
Uneasy
Fgggy
Capable
Insecure
Levels of Intensity
•
*•
'
Woak
*
X
•
••
Weak
Strong
Confused
Glad
Content
Satisfied
Sorry
Lost
Bad
Uptight
Dismayed
Put Out
*
Timid
Unsure
Nervous
Bothered
Sure
Uncomfortable Secure
Undecided
Durable
Shaky
Unsure.
Soft
7//
I.
1.
2.
3.
4.
5.
6.
7.
8.
9.
(From Barefoot Counsellor by Fr. Joe Currie,_S.J.)
CHECKLIST
General attitude toward the counsellee:
Do I respect his independence?
Do I feel responsible for him and want to protect him?
Do I look forward to seeing him?
Do I tend to over-identify with him?
Do I feel resentment or jealousy toward him?
Am I bored with him?
Am I afraid of him?
Am I overly impressed by him?
Do I want to punish er get rid of him?
II. MY behaviour during the interview:
1 . Do I tend to tighten up and feel uncomfortable?
2. Do I select certain material to dwell on?
I 3. Do I get angry at him for not responding the way I want?
4. Do I discover that I dislike him without reason?
5. Am I vulnerable to his criticism of me?
6. Do I try to impress the other and make a favourable impact?
III. In between interviews:
1 . Do I dream about the other?
2. Do I find myself preoccupied with fantasies about the other?
3. Do I plan the course of future interviews? .
IV. At the end of counselling:
1 . Am I reluctant to let the other go when it is clear that he has
reached as far as he can with me?
TEN
D 0'S
1 . Be yourself.
2. CJncentrate, but in a relaxed way.
3. Listen *
o the full message of the other.
4. Respond adequately and creatively.
5. Communicate interest, warmth and understanding.
6. "Prize" the ether.
7. Confront, if and when necessary, responsibly and sensitively.
8. Help the other te sort eut and clarify his problem.
9. Use simple and direct language.
10. Help the ether to take charge of himself.
*********************
TEN D 0 N 'T. S
1 . Don't advise or look too hastily for a solution.
2. Don’t question from curiosity or from uneasiness.
J. Don't moralise or i’htellectualise
*
4. Don’t make the other depend on yo&.
5. Don't oategorise or pre-judge the other.
6. Don’t be falcely re-assuring or supportive.
7. Don’t evaluate the other or his behaviour or attitudes.
8. Don’t talk tod much, or project yourself into the interview.
9. Don’t look for, or encourage, long narratives.
10. Don’t use technical jargon.(terms).
THE CATHOLIC HOSPITAL ASSOCIATION OF INDIA
Community Health Department
Post Box 2126
CEEHAI
SECUNDERABAD 500 003
Telephones : 8482 93, 84 84 57
Telex
: 0425 6674 CHAI IN
Grams
:
157/6 Staff Road
SECUNDERABAD 500003
MINISTRY OF THE CHURCH IN HEALTH SERVICES
Introduction :
"Action on behalf of justice and participation in the transforma
tion of the world fully appear to us as a constitutive dimension
of the preaching of the Gospel".
- Synod of Bishops 1971
"Behind the revolutions of our day, is man's struggle for human
dignity. Christ is at work here and we cannot proclaim Him to
contemporary man if we do not participate in this struggle. In
such participation we have to work with men of all faiths and
no faith. Christian living is, in this sense, living in response
to the WORD and to the world. It demands the conscious
transcendence of our limited groups solidarities and moving
towards the new humanity which is free from all discriminations".
- National consultation on the
role of Church in contemporary
India, 1966.
"If we wish to be faithful to Christ and take up this attitudes
with regard to our fellowman, we must work for the over all
development of each man, and focus on the sick person more than
oh’his sickness. Since development also means solidarity we
must necessarily turn our attention towards the human community
of the patient, his family first, but also his neighbourhood or
village. This means we must practice community medicine" .
- Pontifical Council Cor Unum,
Document on Primary Health
Care Work, 1978.
"The mission that we have given is a call for a true conversion
of our hearts and also of our methods. Secularization is spreading
in people's hearts from the industrialized and technological
world to the developing world countries. We need to be converted
all the time in order to bear witness as Christians to the sick
who, through our work, will discover the love of Christ. The
rapid development in the field of health service technology has
often meant installing expensive equipment in the hospitals,
requiring a large number of staff for a relatively low number
of patients, while in many of the same countries in the world,
upto 80% of the population are still without health care services.
2
2
Since Christians are the leaven, we must reach out towards the
masses by providing simpleaccessible and'-promotional health
care according to our own possibilities, modest as they are,
or in conduction with the public services, where this is
allowed.
Let us ever be mindful of the fact that service to the sick
begins and continues to operate through the patient's human
environment. COMMUNITY HEALTH CARE IS THEREFORE PART OF THE
COMPREHENSIVE PASTORAL WORK OF THE CHURCH".
- Cor Unum Document, 1978.
"Presently, despite the constraint of resources, there is,
disproportionate emphasis on the establishment of curative
centres - dispensaries, hospitals institutions for specialised
treatment - the large majority of which are located in the urb®
areas of the country .... A dynamic process of change and
innovation is required to be brought in the entire approach to
health man power development ensuring the emergence of fully
integrated bands of workers functioning within the "Health
Team" approach".
- New National Health Policy,
1982.
"The demand for justice has been one of the dominant notes
of this half of the country. Perhaps no other period in
History has witnessed a greater denial of justice also
'The Church, bearing within itself the pledge of the fullness
of the Kingdom, views with joy the present concern for justice^
and with.anxiety the grave threats to justice, all around us.
It is her endeavour to interpret the implications of the Gospel
message of justice and peace in the varying situations being
unfolded in the course of the human pilgrimage on earth. She
has to be the 'Leaven' and the 'salt' of the earth in the con
fusion likely to prevail in the search for justice".
- CBCI, 1978.
"The Church should give its whole hearted support to the peace
ful social changes taking place in the country by verbalising its
support of any efforts made for bridging the gap between the
rich and poor.
"The Church should actively involve itself in removing concrete
cases of injustices happening in the society in which it exists".
- CBCI, 1972.
3
3
"We want our health services to take primary health care to the
masses, particularly in the rural and urban slums. Catholic
Hospitals and dispensaries should stress the preventive and
promotive aspects of health care. Specifically, we would urge
them to join hands with the civil authorities in their
programme for the eradication of leprosy.
Our health outreach programmes may demand a change in the
routine especially of religious communities of men and women
involved in this work, and their formation should prepare
them to meet the new spiritual challenges that are posed".
- CBCI, 1978.
" The commission being conscious of :
a the situation of massive poverty of over 6C% of our people;
b the unjust structures which maintain and perpetuate it;
c the injustices perpetuated on the weaker section o£ the
people;
considers it imperative to reaffirm our commitment to the poor
in imitation of Christ’s preferential option for the poor.
The creative struggle of the people to bring about a new society
invites us to enter into critical collaboration with people of
all religions, ideologies and agencies who strive after a just
society.
A meaningful participation in this struggle calls for :
a.
b.
c.
a serious analysis of society with the tools of social
sciences and in the light of faith;
taking definite and unambiguous stand on various issues;
initiating concrete action programmes for change.
As a credible sign of this process the Church initiates action
for justice within its own structure. In this context partici
pation of all sections of people especially of the laity is
of vital importance".
- CBCI,' 1983.
"With this orientation in view the Commission proposes the
following priorities of work, in the field of health :
1
2
Promote Community Health Programmes on the Priority basis;
Train health care personnel with a bias to rural health
programmes. In this connection it is of utmost importance
to reorient doctors, nurses & para-medical personnel in
our institutions and programmes with Christian values.
4
- 4 -
3
A commission could be set up to study the prevailing conditions
and problems, attitudes and values of doctors, nurses, oaramedical, personnel and other employees.
- CBCI, 1983.
The relevance of quotations cited above can be viewed by different
people differently depending on the concept of health one has.
One thing is getting more and more clear that health is no more
an isolated factor and it is not merely the absence of sickness
but the total well being social, physical, mental and spiritual
of individuals, families and communities. It is in this sense that
the above quotations have their relevance when dealing with
ministry of the Church in Health Care.
Health care is a field in which the Church in India has been
busy for over a hundred years. With more than 2000 health care
institutions all over the country run directly by the dioceses
.
or rej.igious congregations, the volume of work done by the
church is enormous. With ohe well established medical college and
more than hundred nurses' training institutions we train every
year an. army of health care personnel and add to the already
existing ones in the field. With the emphasis since some years
on the field of community health, a new army of village level
health workers (called under different names) are trained and they
are in the field. We have also national organisations, under the
auspices of the Church, dealing with various aspects of health
care i.e. the Catholic Hospital Association of India, Catholic
Nurses' Guild, Catholic Doctors' Guild, Natural Family Planning
Association of India etc. This certainly shows the richness of
the resources at our hand. The question will have to be asked is (
are all these properly utilised for the best interest of the
people of God in India particularly the bast majority of them
living in rural areas and urban slums.
1.
COMMUNITY.HEALTH :
CHAI has definitely committed to this cause for the coming years.
And we do hope to do something thereby contributing our share
to achieve the goal set by WHO and accepted by our country, i.e.
Health For All by 2000 A.D. This we hope to achieve through
our member institutions and others, and with the cooperation,
help and guidance particularly from the members of the CBCI and
CRI. We have now an eight member team for the promotion of
Community Health. The team 'has worked out a philosophy and
vision for our community health programme and a broad plan of
action.
5
2.
- 5 Promotion of Pro-Life Activities :
Efforts will have to be made by all concerned, to bring an aware
ness about the seriousness of this all important aspect of life.
CHAI will be taking some definite steps in this regard in the
c oming years.
3.
Pastoral aspect of health care ;
This is a field rather neglected by the Church. Complaints about
even rude behaviour by the Staff towards patients in -our health
care institutions are not a rare phenomenon. Then the question
is, have we given them the necessary training and orientation ?
Keeping this in mind CHAI organises seminars for health care
personnel from time to time. It is our plan to develop a separate
department in CHAI to meet this crying need' in our country.
We also plan to organise regular residential course for Chaplains
etc. in the future.
Against all what has been mentioned, particularly the various
documents mentioned, the following suggestions are put forward
for Justice,-. Development and Peace in General and the health
section in particular. In this connection, it was very meaningful
to have put the health section with commission for justice,
development arid peace.
1.
To have an evaluation of our existing institutions for
education, training and services in the field of health
in accordance with the present concept of health mentioned
in the documents ( of also the CHAI documents )
2.
Community Health Programme accepted as a priority should be
promoted in all the Dioceses. The members of the CBCI and
CRI should accept this end and make it known to all our
health care institutions.
3.
In order to implement this, St. John’s Medical College,
National Organizations like CHAI, NEPAI, CARITAS INDIA,
IGSSS etc. will have to plan together in collaboration with
other organisations in the field such as VHAI, CMAI, ISI etc.
4.
Possibility of organisations like, CHAI, Catholic Nurses'
Guild, NEPAI to work together will have to be explored, for
better effect and to avoid any unnecessary duplications.
5.
The teaching of the concept of Community Health based on
the various documents dealing with the subject should find
a place in the Curricular in Seminaries and Religious
formation houses.
6
- 6 -
6.
In this connection this comfnission- will' have to work in
collaboration with the commission on Seminary Training etc.
7.
This commission should also work in collaboration with the
commission for Laity and Family.
These are a few suggestions, however practical they may be
which came to my mind. The implementation of them may be
difficult but necessary if we want to respond to the needs of
the time. We all agree that making statements (for which we seem
to be experts in this country) alone will not solve the
problems. We need to translate them into action, which is by
far difficult. But we are left with no choice but to do if if
we want to be meaningful to the society today and faithful to
the gospel message.' Let me conclude this with another quotation
this time from Ashok Menta.
"We must reclaim 900 million people (the number is more now)
of ths world who are today in a state of abject depression.
This human reclamation requires a peculiar type of social
engineering. This is to my,mind the big challenge that all
people, all men of religion, all men of God have to face.
And if it is the proud claim of t^he Christian Churches that
they have that spiritual understanding, that spirited agony and
that spiritual out glow is greater than that of other men of
God, it has to be proved, as I said in the crucible of life
itself. If it is the claim of Christians that even to this
day they feel the agony of Christ on the Cross whenever
humanity suffers as it were, it has to be proved, in action and
not by statement".
Fr John Vattamattom svd
Executive Director
Catholic Hospital Association
.of India.
23-11-87/200
mm/
DIFFERENT APPROACHES TO DEVELOPMENT
In India, especially after the independence, we see thousands
of individuals and groups engaged in the field of development
either full time or part time. To be a social worker or
development worker, to some extent adds to ones status and
position in society today. In spite of all these countless
efforts we hardly see any significant changes in the life of
the nation as a whole, A national net work for a concerted
effort in the field of development is yet to be evolved.
A close look at these groups and individuals in the field of
development will show us thatftheir understanding of poverty
and the corresponding approaches to development varies and in
certain cases diametrically oppose each other. Though one cann't
question their good will and sincerity of purpose, we should know
that, mere good will arid, a sense of sacrifice and committment
do not indeed suffice to make our contribution to development
and social justice meaningful.
The approaches commonly adopted by different people in the
development field can be classified into three. They are :
1)
2)
3)
Welfare approach;
modernization approach
social justice approach
All these approaches proceeds from a clear and definite analysis
and understanding of poverty/or underdevelopment, however
scientific or unscientific the analysis may be.
Before we proceed further, let us be clear about certain
initial facts.
1 . Our ability to identify factors and. forces that create wealth
and poverty determines our ability to tackle the problem.
2
Each one of us has an understanding of poverty and under
development, whether at the conscious or sub»conscious
level. We may have never formulated it, but a cloSer look
at our work will reveal it to us. Always the solutions and
methods adopted, follows from our analysis.
3
Our understanding of underdevelopment and analysis of the
problems are largely influenced or conditioned by our own
-economic
*
soci
background.
- 2
2
Our preception of reality is conditioned by our position in the
society. Thus the causes of poverty identified by the rich may
not be the same as those indicated by the poor.
1)
The 'Welfare Approach :
This approach is deeply rooted in the mentality of religious
minded people and humanists and is favoured by many private
agencies and governments in both developed and *
in developing
countries. The fabulous investments in men and money that
welfare enjoys, compels us to reflect seriously on whether
it deserves it or not.
In this approach, development and under development are
considered as two parallel realities that have always co
existed, and that will always co-exist. Here, poverty is
accepted as a normal result of forces outside the control
of man. These forces are identified as natural and super
natural. Here the symptoms are treated with a rather fata
listic approach, rather than the root causes of the problem
with a critical analysis. Natural forces are seen as
disasters, 'epidemics, earthquakes, cyclones, floods, '
draughts, 'etc. over which man has no control. In the < ■
supernatural sphere, man's status in life is seen as predet
ermined. It is his fate, it is in the plan of God, and'
explanation of poverty reflects a religious tone. Development
workers with.this understanding regrets poverty, but accept
it as fate.
People who see poverty as created by forces outside the
control of man, see little possibility for change. The
solution is seen as a sharing of material gbods and talents
by the blessed and privileged, and the acceptance of these
goods and services by those who are in need of them. The
disposition advocated is a basic contentment with one's
state of life. Work for the poor assumes the nature of
alleviating the suffering of the poor rather than eradi
cating poverty itself. Development work here becomes an
ongoing relief or charity, characterised by 'dolling out'
benefit to the-poor people according to. their needs.
(Giving the man the fish) It is often a spontaneous response
to a situation with little effort made to identify and tackle
the root causes of the problem,.
*
- 3
- 3 -
And in the recipients, it often develops attitudes of depen
dence, laziness and passivity and sometimes creates division
among the poor. It always diverts the attention of the poor . "
from the real issues and anaesthatizes them.
Even a limited study of the history of the welfare approach
and a superficial analysis of the functioning of society
reveal that most of the evils treated by the welfare approach
are the inevitable by products of certain forms of social
organization.
2)
Modernization approach
Like the previous approach modernization too rests on a certain
understanding of poverty and under development. The cake,
they say has to be bigger before it can be shared. So in this
approach increased production and economic growth is stressed,
to remove poverty. Here it is implied that people are poor
because- there is not enough production of goods. Modernization
approach relies on industrialization and on rather sophisti
cated and capital intensive technology. Family planning
compaigns are also of prime importance to keep down the birth
rate and thus to promote economic growth.
Here-,- development is seen as the successful utilization of
resources, natural and human. Such an understanding stresses
the need for patience, hard work, self descipline, sacrifice
investments and quality education, needed for the production
of bigger cake. Under development is seen as the result of
the slow and inadequate establishment of the system of
production and consumption present in the developed countries.
To a great extent modernization then means westernization following closely the methods and patterns of the developed.
The advanced countries become the guides of the developing
countries. On the cultural level it leads to the acceptance
of the ideals of western countries and the adoption of
their attitudes and values.
Those, who can produce more are. encouraged to the level best,
with the contention thaVthe benefits will 'trickel down' to
all. This method of 'Backing the strong’ (green revolution)
is easily recognizable in our five year plans, government
policies ana in the projects run by voluntary agencies.
- 4
-4Even though impressive statistics can be given on the growth
of agricultural and Industrial production, on the number of
students enrolled in educational institutions, education and
public services, a question could be asked : who progresses?
The rich, who only posses the purchasing power, with their
demandscommand .and control the market, and often fund to
imitate western standards of living. Industrialization
responds to this demand, and produces luxury articles which
give higher rates of profit. The production is done at the
minimum cost often introducing sophisticated and capital
intensive technology, thus increasing unemployment. Poverty
and unemployment place the workers at the mercy of the land
lords and industrialists, with low wages, and miserable and
inhuman conditions of work. The state accentuates the situation g
by limiting.or forbidding strikes. Whenever the labour force
is so large and employment so scarce, favoritism and corruption
unavoidably prevail. Extreme poverty drives poeple to borrow
for their subsistence and social needs; money lenders prosper,
for no bank or credit society would lend money in such
circumstances. All this creates a vicious circle.
In a society where serious inequalities already exist a
technological advance leading to increased productivity is
likely tc be limited to those endowed with superior wealth and
social status to the exclusion of the poor majority’ says the
United Nations research institute for social development,
Geneva.
The modernization approach, therefore, ends with the abundence
of luxury articles and' the scarcity of basic goods; with
sophisticated technology and unemployment, low wages, debts and
bonded labours. It produces the wealth of the few and the
poverty of the many^ The limited resources of the nation are
thus used by a small groups for their selfish interests.
3)
Social Justice Approach
The Failure of the modernization and welfare approach lead some
to evolve a different approach to development based on a critical
analysis of the various forces and dynamics at work in the
society. It examines the organization of society and it's
functioning at both micro and macro leyels,
- 5
■'
- 5 There is the conviction that non-economic factors that is the
overall social context of society with its institutions and
structures - Play a very important role in development. It
tries to tackle the root causes of poverty and pays great
attention to the proper distirbution of wealth. It does not
accept mass poverty or under development as a fate.
Moderrfization becomes important only when fare shares to the
masses are possible. The root causes of under development accord
ing to this approach is injustice. If 85% of Indian population
are below or just above poverty line, it is because 15% un
justly enjoy the results of the labour of the 85%.
In this approach one is convinced that deprived groups and
nations_can develop only in the context of a direct attack on
poverty and a move for just distribution of wealth and power.
Instead of depending dis'propotionately on capital formation
and move modern attitudes and values, development ultimately
depends on land ownership, land utilization, employment, wages
and the level of food comsumption. What would development
mean in this historically created condition of under development.
It means the restructuring of society! Efforts in this direction
can be seen in Trade Union, (Balance of power in the production
sector through collective bargaining) marketing co-operatives
(challenge to the unscruplous exploitation of middleman) credit
unions, (against money lenders) Mahila mandals (against low
status of women). Always it was the awareness of injustice
and exploitation in these cases that resulted in the organi
zation of people at various levels. So in this understanding
of development, the approach one would adopt will be awareness
building which will definitely culminate in action.
Genuinely effective development work will have to challenge and
re-organise the relations between the substructures in the
society. The wealthy are the socially privileged, and the
politically powerful. Power and privilege proceed from economic
standing. Culture and religion seem to reinforce the inter
relationship by providing sanctions andjustifications. A
total transformation of these structures and support, is in
evitable. In the economic sphere, this would mean policies •;
geared to serve the needs of the people and not as at present,
for the profit of a few. This woul 1 require that the means of
production, land and capital be socially owned. On the social and
cultural levels, this would mean relationships of equality
between groups of people;
- 6
New ways of thinking feeling and acting, collective promotion
rather than individual promotion. On the political level, to
evolve an organizational set up that makes possible real and
effective decision making power for the people. Thus this
approach aims at a socialist society.
Unlike the previous two approaches to development, this one is
•_d rather distributing
approach,
*
as it demands a commitment to
struggle, and a struggle against the powerful, dominant group;
and it is no easy task. As development workers, what options
does our above understanding leave us with? Can our sincere
desire to alleviate the wretched misery of our countrymen
express itself in meaningful actions that contribute to this
process of collective awareness, collective organization
and collective struggle?
Community Health Department
CHAI, Post Box 2126
157/6 Staff Road
Secunderabad 500 003 A.P.
THE CATHOLIC HOSPITAL ASSOCIATION OF INDIA
Community Health Department
Post Box 2126
Grams
:
CEEHAl
SECUNDERABAD 500 003
Telephones : 84S293, 84 84 57
Telex
: 0425 6674 CHAI IN
157/6 Staff Road
SECUNDERABAD 500003
'
GUIDELINES FOR COLLECTING INFORMATION ABOUT A VILLAGE
Most of us do not belong to the village where we actually
work and therefore, it is most important for us that we
learn as much as we can. These guidelines meant to help
you in collecting information on the village where you
live or where you intend to develop a community health
programme.
THESE GUIDELINES ARE NOT MEANT FOR YOU TO
CONDUCT A FORMAL SURVEY
Most of this information should be got through informal dis
cussions with groups or individuals in the village. Observe as
much time as you can with the people in your visits. When
people come to know you better they will be more Willing to
talk openly about the real problems facing them.
There are two types of information we need to collect. One is
facts. Eg; Location, population, number of schools, number of wells
etc. The other is related to what people think and feel. Eg :
what do people and feel and think about the schools, drinking
water facility etc. We also need to know how people relate to each
other in the village.
It is important to collect both types of information. Facts
are easier to collect. It will take longer to find out what
poeple feel and think. Therefore., it is essential to build a
good'relationship with all the people in a village.
INFORMATION TO BE COLLECTED
Read these guidelines carefully and. remember what you should
find out when you go to the village. Do not take these guide
lines with you when you go to the village. If you do, people
will think you are conducting survey. These guidelines are by
no means complete. You may want to collect more detailedinformation on some of the points given below :
1 .
LOCATION
- Name of village/block/tehsil/district/state.
2
2
-
Distance of village from block x>ffice/tehsil office/district
head-quarters and nearest town.
-
Are there any important rivers, forests, dams, factories,
markets etc. nearby?
2.
GEOGRAPHICAL SET-UP
- Type of land(sandy, rocky, hilly etc)
- . Rainfall, floods, drought etc.
3.
COMMUNICATION SYSTEM
-
-
How do people travel?
What is the condition of roads (kutcha, pakka)?
Frequentcy of transport (buses, trains etc)
(goods trains & passenger trains)?
What are the links with the outside (Eg. information
through people working in towns, radio, TV, through
extension workers visiting the village etc.)?
a
"
What do people think and feel
-
4.
ABOUT THE POPULATION
-
5.
About the transport facilities
About information from outside (Do they feel isolated,
do they feel the need for more information on outside
happenings etc.?)
Total number of people, number of households, hamlets etc. )•
Caste, religions
EDUCATIONAL FACILITIES
-
-
Schools (primary, secondary, technical etc.) and where
are they located, who runs them?
Are they for boys and girls, if not where do girls study ?
Do teachers come regularly ?
How many students in village school and who are they ?
How many adults know how to read and write ?
Was this village included in the National Adult
Education Pregramme ?
What do people feel
-
Is school education important for children - for boys,
for girls ?
What would they like their children to learn ?
Do adults feel the need to know how to read and write ?
3
-3-
6.
ECONOMIC LIFE
A) What is main occupation in the village (agriculture,
looking after animals, local craft, quarry workers)?
AGRICULTURE ;
-
-
Total land in village available for cultivation
Any land not being cultivated in village (if yes, how many
acres and why ?)
How much land is irrigated ?
Source of irrigation(river, canal, dam, tube well etc.)
How many crops grown in a year and what is grown ?
How much is produced per acre on the average (for wet-land
and dry land)?
Does village get any agricultural help from BDO ?
LAND HOLDING.
-
-
-
:
Who owns most of the land in the village, is it irrigated ?
How many families cultivate land belonging to others'? '
How many families work ds labourers in fields belonging to .
others ?
How muoh land would a family., of six require to produce
enough food for themselves for the whole year ?
EMPLOYMENT :
For how many months do families work oh land ?
How many families migrate, for how many months and where
do they go ?
What are the wages per day for agricultural labour in the
village and whenthey migrate ?
Are the wages different for men, women and children ?
What do people think
-
About land distribution
About irrigation facilities •
About help from the block development office
About wages
About employment
LIVESTOCKS, POULTRY ETC
-
Are there buffaloes, cows, goats, sheep, pigs, hens, etc. in
the village ? (is it the main source of income ?)
Who owns the majority of these animals ?
Is there any organized dairy, poultry in the village ?
Is there any potential for developing this ?
4
- 4 -
-
What do people think
-
Is there possibility of expanding this craft ?
Is there need to start some village craft ?
B.
ECONOMIC RELATIONSHIPS
-
To when does a small farmer sell his products ?
When does he sell it ?
How much does he sell it for ?
How much does he have to pay, when he needs to buy it back ?
Who are the money lenders in the village ?
How many acres does the money lender own ?
What rate of interest d,o they charge ?
What happens if the person is not able to repay the lean ?
Which group of people .are mainly borrowing money ?
What do they borrow the money for ?
What is the approximate amount borrowed by an average family ?
What govt, facilities are available for loans (eg. banks,
cooperatives) ?
Who uses these facilities ?
-
-
What do people feel and think
What do people feel about the money lender’s system ?
Are they satisfied with the selling and buying rates ?
Do people think it is possible to have grains/seed/
fertilizer banks ?
-
7.
SOCIAL - POLITICAL FORCES
A.
Social forces :
-
What are the main castes in the village ?
Which caste has the most power ?
How does the caste feeling affect the day to day lives of
the people ?
Do different caste groups live separately from each other ?
Is untouchability practiced ?
Is everyone allowed to take water from the same well ?
b.
Political Forces :
-
Who makes the decisions affecting the village ?
Who is the Sarpanch and what is his economic status ?
What castes does he belong to ?
Who are the panchayat members ?
-
'
■'
'
5'
- 5 --
What is their economic status and what caste do they
belong to ?
Who are the other leaders in the village ?
What influences do they have in the village ?
In what ways do the different leaders influence the
community ?
8.
CULTURAL PATTERNS
-
What are the main festivals in the village ?
What are the customs related to marriage, childbirth,
death etc. ?
How much money do people spend to perform such rites ?
What are some of the important beliefs of people
regarding religion, superstition etc. ?
-
9.
-
-
10.
-
-
SERVICES AVAILABLE '
Drinking water facility and cleanliness of drinking water.
Bank services
Government services like development of agriculture,
irrigation, animal husbandry, welfare activity like
anganwadi etc.
Health services - PHC, sub centres, Malaria workers etc.
HEALTH AND NUTRITION
What is the diet of an average family , poor family ?
What are some 'f the beliefs related to nutrition of infants, small children, pregnant mothers, in specific
diseases ?
Where do people go when they fall sick (local healers, ANM
PHC, private doctor etc;)
Who conducts deliveries in the village and what are the
practices followed during delivery ?
What are the common diseases in the village ?
What is general sanitation in the village ?
What do people think
-
Is health important ?
About the causes of ill-health ?
When do they consider themselves sick ?
Are health services adequate ? '
About cost of health services (local healer, dai, ANM,
private doctors)
- 6 -
11.
-
ORGANIZATIONS IN THE VILLAGE
Are there any farmers clubs, youth clubs, mahila mandals,
ccperatives etc. ?
Who are the members and leaders ?
What do these organizations do ?
Were there any such Organizations which have ceased to
exist ?
What do the people think
-
Are they satisfied with tthe organizations existing in the
village ?
What are some of the problems faced by these organizations
Is there need for such organizations ?
CONCLUSION
As already stated, the points mentioned above are only
GUIDELINES. Once you start discussing these points with
people, many more questions will come to your mind. It is up
to you to find out more about the life of pedple in the
village. It is also important to know if people have taken
any initiative whatsoever in changing their life situation
and with what result.
Do you and the people think that some action can be taken.
for bringing about change for the better ?
■Prepared by ; •
Community Health Team
VHAI
40, Institutional Area
South of IIT
■New Delhi 110 016
14-11-87/200
y
cThe Catholic Hospital Association of India
C. B. C. I. Centre, Goldakkhana, New Delhi- 110001
a
,
Tel.
310694, 322064
CRITICAL ANALYSIS OF THE INDIAN REALITY
India is a great nation having a democratic system of
government, which is a great industrial economy and a country
which rias made much headway in Agriculture.
nuclear community and is in the forefront of
nations in space research.
Today, India is in the
other developing
Since Independence, India has been
making rapid increase in the production of Iron, Aluminium, Electri
city ,Fertilizers, cement etc.
India’s export industry is remarkable
In 1978 it was worth Rs. 3,156 crores, while it was only Rs. 1535
crores in 197O-’71«
Growth rate of Agricultural production in
1977-'78 was about 11 to 12% and the stock of food grains was about
20 million tonnes.
India exports grains to USSR and Bengaladosh.
Food corporation of India is finding it extremely difficult to
provide enough space to store up the stoclc.
This however, is only
one side of the coin
On.the other side we see that more than 48.4% of our countrymen(govt. calculation) live in a constant state of starvation,
nakedness and disease; and that they do not have money.to spend
for a day on food even for survival.
There are.68%, i.e.,
465 million who can not read and write.
70% (i.e. 478 million)
of rural people live in one room huts and 1.90 lakh villages
Diarrhoea kills 3 children every
exist without drinking water.
minute.
There are 3.2 million.leprosy patients and 9 million
bling people in our motherland.
■
Why this contradiction?
of 36 years of land reform?
Why are people landless inspite
Illiterate inspite of about
Rs. 1350 crores being sponfc annually on education?
inspite of massive plans?
Unemployed
Unhealthy inspite of huge budget
allocations on health?
It is not enough to see what is the state of the majority
of Indians, we have to ask also wliy?
A socio-economic .and
political analysis of the Indian reality is necessary to find
out the.causes of such massive poverty, misery and to answer
the WHY.
It is an investigation into the laws which govern
and direct the interaction among different groups in the society.
We analytically observe and percievo even the invisible
elements in a given society and this analysis given us the total
and overall picture of the society in all its dimensions, for .
we analyse the society with reference to its social structures,
2/-
2
the ways and processes of decision making, tho forces behind those
decisions, the real beneficiaries of this decisions, etc.
Our country and for that natter any society, has a parti
cular manner of socio-economic and political organisation, which
in general could be termed as the organisational system.
This
organisational system is maintained and sustained by the values
that the society promotes.
These values are provided by- the
culture, religion and ideology - which together could be called
the meaning system.
in detail.
Social analysis studies both these systems
To understand the Indian reality, we have to study
in detail, how the Indian society is organised and how this
organisation is maintained.
The reflections of Julis Nyerese, the President of Tanzania^
can help us to grasp the various structures and systems that
contantly contribute to the miserable state of affairs of our...
people.
"Poverty is not the real problem of the modern world.,,
The real problem - the thing which creates misery, war and.hatred
among men - is the division of mankind into rich and poor...,.
The reality and depth of tho problem arises because the man who
is rich has power over the lives of those who are poor, and
the rich.nation has power over the policies of those which are
not rich."
As a consequence of this the rich get ever richer
and more powerful, while the poor get
relatively everpoorer and
less able to control their own future.
Sometimes this happens
through the deliberate decisions of tho rich, who use their
wealth and their power to that end.
it happens
’naturally
*
But often or perhaps usually
as a result of the normal working of.the
social and economic systems men have created for themselves.
To group it better,take the case of a landlord and his tenants
or coolies,
Even if as an individual the landlord is the most
generous, just and considerate person, who becomes richer as the
years passby?
The landlord or his tenents or coolies?
If we
take the case of factory owner and his workers, who will be
richer at the end of the year?
So irrespective of the qualities
of the persons concerned, the system functions automatically
*
the rich will becomes richer and the poor becomes poorer and
the gap widens.
This also illustrates that the moral transfor
mation of individuals does not suffice to profoundly alter the
conditions of life of our people, unless structures and systems
must are radically changed.
3/-
3
With this brief introduction let us again go ’Bfeoklu bin
*
organisational and meaning systems existing in our society.
As
stated earlier, economic, political and social systems forms
the organisational system and religion, culture and ideology
forms the meaning system of any given society.
ORGANISATIONAL SYSTEM
Economic system
Every individual and society has to satisfu certain
physical and psychological needs or wants, as for example food,
.
clothing, shelter, medicines, art, entertainment, ceremonies etc.
In the process of producing and circulating the material goods
that meet those needs man relates to nature through certain techno
logical tools called in&trunents of labour.
They also relate
to one another and form certain relations,
Every society thus
posses an economic organisation or system.
There are two widely a ccepted approaches to economics!
The capitalist and socialist.
The former takes for granted the
private ownerwhip of the moans of production, the existence of
wage, labour and the unequal distribution of income.
Such an
economic approach is divested of its real purpose, namely the
satisfaction of the needs of all people and aims at private
profit for the capitalist, who owns the means of production and
employ wage labour.
The socialist approach follows from a stand
in favour of social justice, equality and solidarity.
The.economic system comprises of four basic.structures:
Production, distribution, exchange and consumption.
In the
production structure we can identify the productive forces
(man-nature) and the production relations (man-man), Land Labour
(instruments of labour - tools, mechines, infrastructures) and
capital (money, raw materials) are the means of production and
it gives birth to particular types of social relations and .
organisations and forms particular types of social classess.
The instruments of labour play a significant role in the pro
duction process and to a great extent determine the level of
........V-
4
production.
The social relations are transformed with the
development of the productive forces especially the division
of labour.
So in the economic analysis of a given society, it
is important to study the overall development of the productive
forces and the existing social relations and the mutual relation
and influence between the productive forces and production rela
tions. eg. Are the existing social relations an exploiters -
exploited relation or a collaboration - solidarity relation of
production?
What types of relations are the productive forces
fostering?
The distribution structure - is intimately connected with
the production structure, especially the ownership of the means
of production.
Through this structure, the social product or
national income is distributed.
In the structural analysis of
the economic system, this income distribution ad well as the
growth or reduction of inequali»j»ties, in relation to tho owner
ship pattern of the means of production, has to be studied.
In a natural or subsistence economy, whore production was
for use, there wasnot hardly any oxchange.
The development of
the productive forces and in particular the division of labour
rendered exchange necessary, first through baster — exchange of
goods and later on through money, the general equivalent..
Production for exchange or commodity production increased.
With
the use of money and commodity production, the market progressi
vely developed. In fact commodity production is geared to the
market.
Though most often externally peaceful, market transact™
ions and relations are conflictual.
The interests of the buyers
and sellefs indeed oppose.one another, conflicts also exist
between different traders.
In a market people meet as.commodity
buyers and sellers and class relations are in evidence.
In a
developed economy, trade is not mainly carried out in view of
exchanging goods, but of acquiring profit.
In analysing the
exchange structure, one has to relate it to the production and
distribution structures to uncover this exploitation of the
dominated classes.
Consumption means the purchase and.utilization of a good or
service for the satisfaction of a need.
Though man’s needs are
conditioned by subjective and cultural factors, there exists a
certain objective hierarchy of needs.
Without the fulfilment
of primary needs such as food, clothing, shelter and health,
5/-
5
life itself becomes impossible.
The secondary needs as for
example education, transport, recreation, security etc. arc some
what less essential while tertiary needs could be classified as
Man certainly possesses the right to satisfy his
luxuries.
primary and if .possible his secondary needs, both quantity-wise
ant/qualitywise.
In the analysis of the consumption structure the
quantity and quality of the primary, secondary and tertiary needs
consumed by each social group or class should be calculated and
related to the income, exchange and wealth patterns.
The political system:
Politics constitutes an inescapable dimention of human
It plays an ever greater role in day to day life.
existence.
With the existence of Atomic Weapons, the very survival of
mankind is now in the process of being determind by politics and
politicians.
Political analysis helps one to understand the world
he lives in.
There are two basic approaches to politics: The
capitalist and the socialist.
The capitalist approach takes
for granted and judges inevitable
the internal division of.
society into.two groups or classes the rulers and the ruled.
On
the contrary, the socialist approach introduces the ideology of
In the capitalist approach there are different schools
equality.
of thought on politics.
One sees politics as the
of government 1 while the other considers it as the
power'.
'art and science
’science of
The first theory focusses on the state as nationa and
government, to protect the interests of the nation in relation
to other states and to govern its territory, maintain law a-nd
order etc.
For this, the state has certain machinery:
The Army,
the police, the judiciary and the administrative apparatus.
According to .this, politics is the study of state and its v
institutions.
The second theory looks at politics at the exercise
of power at different levels, especially in the society at large.
According to this, political system is understood as a ny persisted;
pattern of human relationship that involves, to a significant ■.
extent, power rule, or authority.
History thus becomes a
struggle
for power; and the state and its institutions have to bo analysed
in the light of this phenomenon of power.
(Capitalist scholars.have place the basis .or source of power
in different realities: e.g. physical.strength, personal charis
matic leadership, natural superiority, technical competence,
...... >6/-
-
6
-
the military, industrial and political complex, professional
political expertise etc.)
Here the state will only safeguard the interests of the
dominant class.
And, political power is the capacity of a social
class to realize its specific objective or interests even utilising
the state apparatus.
And the state doos everything to safeguard
the capitalist mode of production and ensures the law a-nd order
in a manner which would not jeopardise this foundation.
In both capitalist or socialist understanding of political
power the state is not and cannot be neutral.
This also holds
good for the whole state apparatus - the police, the army, the
judiciary, the administrative machinery, etc., as well as for-the
ideology prompted through mass.media and the education system. A
In spite of a certain autonomy, all those subsystems fundamentally
serve the state and its objectives.
Only when power is distributed among the individuals and
groups of a society, maximum freedom can be ensured.
Men are
free to the extent to which power is distributed and organised
so as to prevent or at least minimize its abuse.
And only
through the diffusion and distribution of both economic and
political power can be present exploitative political system
can be changed.
The social system
In every society, there is a social system or set of
interactions between social actors or groups.
This concept
implies a certain distribution of social prestige and status,
or in other words a certain social stratification, understood
as the diiferentia 1 ranking .of human individuals, their treatment
as superior and inferior etc.
Various factors do, or can con
tribute to form tills social stratification in different types of
s'.-cieties: Physical or military power, a ge, sox, birth, religion,
certain moral or spiritual qualities, profession, education,
wealth, political power etc.
In fact those factors are usually
combined.
Apparently in-India, the social inequalities are rather
passively accepted.
But this is an important aspect of the
organisational system of the society, and should! be seen a-s a
structure of exploitation.
........ 7/~
An analytical study of the economic, political and social
systems of cur country using the above guidelines will reveal
the shocking fact that it is about 20$ r,f the Indians who con
trol the resources of the country; the production is geared to
cater to the needs of this minority, education health care etc.
are meant for them.
It is they who influence the decisions;
and these decisions do take care of their interests.
minority which has power, which has voice.
It is this
There is a caste
class combination which controls and dominates each aspect of
Indian society.
In other words, such a study will disclose the
fact that there is unequal and unjust distribution of wealth
and income - with its consequences.
Lack of accessaries for the
majority, and abundance of luxuries for the minority.
It will
also be seen that the majority of villages and people exist to
cater to the needs of a handful of cities and minority of
people.
There is a division in the Indian society into a
minority of owness of the means of production (dominatiny,
exploiting and powerful) and a majority of non-owners.
(The
Such a
poor, dominated, the illiterate and the powerless).
division, such an unjust organisation of the society is the
basic or the rootcause of hunger, disease, unemployment, mal
nutrition, illiteracy etc.
The functioning of the dominent
groups, in this systems, seems to be normal, legal and within
the constitutional rights - for the socio economic and politico
legal systems are the creation of this minority.
Meaning systems
The questions that should be asked now are:
'why don't
people change the unjust organisation of the society?'
they accept such inequalities?
social life differently?
Why did
Why did they not strucutre their
Because, they have been the prisoners
and victims of a wrong understanding of society that privileged
the dominent groups and classes.
In the past, men have been as
much exploited by the meaning systems - Religion culture and
ideology - as by the organisational systems.
All human beings, whether religious-minded or secularised
need a comprehensive meaning and explanation for their existence
'why do I live?
Where do I come from?
destiny?
Why suffering and death?
ctions?
Why am I poor or rich?
What is my ultimate
Why these social contradi
Powerful or powerless?
8
Why
meaning to majiv.
(in this context, we focus attention only on
the social functions of religion and culture and on ideology).
The whole meaning system is sometimes called ideological systei.
also.
The inter dependence of the organisational and meaning sys
is very much striking although they enjoy a relative autonomy.
Experience shows that men's understanding of the world is pro
foundly shaped by their socio-economic position in society.
Th
The meaning system influences the organisational system in
two ways: through values (value system) and ideologies.
The is
pact of values on society is rather indirect and progressive.'
Religious or secular ideologies on the other hand, influence
society much more directly and immediately.
Their impact can
either maintain the status quo or promote change.
Every meaning system, whether religious or secular, ultima
tely tends to adjust itself to the existing politico-economic
organisation of society and to legitimize it.
Consequently
in a capitalist system, it becomes on instrument of explotntion
in the hands of the dominant class.
It tends to maintain the
privileges of the class by justifying the order or by diverting
or transforming feelings which might otherwise subvert it.
Religion and culture
All religions unavoidably exercise a social function.
It
is distinguished from other meaning systems by its emphasis on
ultimate.
It offers a systematic message capable of giving a
unified meaning to life, by proposing a coherent vision of the
world arid of human existence, and by giving them t.:?.o means to
bring about the systematic integration of their daily behavious
This message is always situated in a precise historical context
and provic.
believers, reasons
it is in a given social position.
justifying their existence ns
The social position of the
privileged is justified as being part of an order fixed and
-9-
ordained by a divine will, while the promist of better condi
tions in an afterlife is offered to the under privileged as a
compensation for their present position.
Thus if supernatura
lizes the relations between the dominant and dominated, since
each group finds in its religious beliefs and action the justi
fication of its own condition.
In history, religion has played two functions,
(l) Prophetic
or revolutionary function (Protest against politico-economic
injustices and plea for a new society) (2) submissive function
(Legitimization in supporting the statusquo; Rationalization in
explaining the statusquo; compensation in offering other worldly
rewards for the oppressed; social control, in influencing social
behaviour promising afterlife rewards and punishments).
Religion
often plays a rather nagative role in the structural transfor
mation of societies (eg. the caste system; divine right of kings,
slavery, colonialism, and capitalism)
Far from being apolitical and neutral, .religions are often
conservative forces in the society.
They often preach various
human values without translating them into the socio-economic and
political organisations of society.
The meaning system which the
religions provide often moulds the culture of a particular
society influencing their way of thinking, feeling, and acting.
Religion and culture often promote inequalities and oppose social
changes, and thus become ideological instruments of exploitation.
Ideology
The term ideology, was first used in 1797 hy Claude de Tracy
as ’the science cf ideas'.
Most contemporary sociologists,
understand ideology as 'an explicit and generally organised
system of ideas and judgements which serves to describe, explain
interpret, or justify the situation of a group or collectivity
and which largely inspired by values proposes a precise orien
tation to the historical action of this group or collectivity'.
Houtart speaks of ideology 'as a system of explanations bearing
on the existence of the social group, its history and its pro
jection into the future, and rationlising
of power relationship' .
a particular type
The legitimafcioai that an ideology provides
-10to a social group ’is never absolutely logic."!, but contains
emotional elements which are capable of motivating men and giving
them a feeling of security1.
Ideology is thus a fundamental
element in the culture of every human,
religious group.
ethnic, social or even
In this modern sense, ideology always includes
in a more or less explicit manner an understanding (analysis)
of society, a vision of the future, and a choice of strategies
and tactics.
Understood in this way, the concept of ideology
can be used for both a small gloup (trade union,. political
party etc) and a whole society or nation.
They foster the inter
ests of a particular group in society, and promote a specific
socio-economic and political organisation.
They can be classi
fied as Reactionary (turned towards the joast), conservative
(supporting the statusquo), Liberal (proposing minor and gradual
changes), and revolutionary (aiming at radical changes in society).
In socio political analysis of a given society, it is important
that one should critically examine all ideologies and evaluate
the' exact role they play in each society and social group.
As study of the rolt of the mehning system in the present
day India will reveal that it makes
most, if not all;,, of the
poor blind, though have eyes; deaf, though they have ears.; and
dumb, though they have tongues.
We realize that lack of power
economic, political and social . re inforced by the meaning
system, makes them live in a ’culture of silence
.
*
The meaning system is used for socialization.
Socialization
is process, through which a person all through his life, espe
cially in his early years, learns and internalises the socio
cultural elements of his society under the influence of experi
ences and of social agents and, consequently integrates them in
his basio personality and adapts himself to his social environ
ment.
One needs to become critical towards the socialization
process to become free and capable of objectively looking at
the impact of the meaning system on ones thought and action.
The poverty and misery.- we .see in India today is the result
of an unjust social organisation supported by an unjust meaning
system; and development would mean the creation of a more just
society.
1
The following facts and figures will enable us further to
understand the reality we are living in today?
AT THE NATIONAL LEVEL.
Health
20% of urban population have 80% doctors, and 90% hospital
beds, 80%-engineers, administrators and executives, where as
80% of rural population have only 20% doctors, 10% hospital beds
and 20% engineers, administrators and executives.
Life expect
ancy at urban areas is 65 years where as in rural area is only
50 years.
India's percapita consumption of drugs -is one of the
lowest, Rs. 7.50 per annum, compared to
Rs. 310 in USA
Rs. 233 in WEST GERMANY
Rs. 252 in JAPAN
Rs. 78
in UK
- 8 out of every 10 Indians have little or no access to modern
medicine.
- India has the highest mortality rate 139/1000, among
the Asian countries.
- There are about 60 million children malnurished.
- Tn India diahrroea kills 3 children every minute or 1.5 ''
million each year.
Every second an Indian child is exposed
to it.
- while vitamin A defficiency blinds 30,000 children annually
and vit D. defficiency affect 15% of Indian children, the
combined sale of vit A &D account for only 3% of total vitamin.
sales.
- There are an estimated 3.2. million leprosy patients in India.
- Tuberculosis is the number one killer disease and it accounts
for about 3% of the 1
crore annual death in India.
- 20% of the maternal death is due to anaemia.
The mortality
rate among the infants weighing less than 2r$ k.g. is as high
as 75% because of anaemia.
-12- Severe degree of anaemia have been detected in 12$ of pre
school children.
- 90 million are supposed to be in the polio danger zone and
13 million are added to this figure every year.
80% victims
are below 3 yejr^and 15% below 5 years.
- There are 2.5 lakhs totally blind children, about 1.8 are
partially blind and 2.5 are deaf.
- 9 million blind persons in the country,
Out of this 5 million
could be cured by proper surgical interference.
- 40 lakhs suffer from impaired hearing.
- 5 lakhs are orthopaedically handicapped.
mentally retarded (Indian express.Sept 9,
20 lakhs are
1983)
- In 1979 the doctor population Ratio was 1s4400 in India.
But the actual ratio- in the rural area was 1j20,700 and
in urban Is 1,300.
Hospital bed population ratio is 0.49
for 1000 population.
- A student of medicine spends a total of Rs.
studies.
1
lakh for his
In the meantime the government spends 1.5 lakhs
on the same student.
When a doctor leaves the country for
better wages he deprives India of 1.5 lakhs of rupees.
- The number of doctors in 1947 was 47,500 and in 1980 is
2,53,631.
- 90% of the Indian women do not have maternity facilities.
- Out of the annual health budget,
1/5 of the total goes to the
rural sector, while 4/5 goes for maintaining sophisticated
facilities.
Out of the total budget outlay, 75% goes for
salaries and maintenance, 12% towards transport, 12% towards
drugs and 1% for innovative experiments.
- According to a study done by world council of churches
(WCC) on 6000 outpatients in different parts of India on
one particular day in 1973, it was revealed that, out of
this 6000 patients, only 5% needed a doctor,
15% needed auxiliary health personnel's
help
15% needed home care
65% needed no medical care.
Only self curing diseases.
-13-
- According to the latest UTTICSF study (Dec.
1983) ir. all
the developing countries taken together, one lakh children
die every three days.
- In 1980, out of 5>76,OOO villages in India only 97,000
villages were provided with safe drinking water.
Poverty
According to 1981 price scale a person who doesn't have
Rs. 3 for a day is considered to be under poverty line.
The
value of one rupee was 100 paise in 195^-, hut 0.2k paise in
In 1983, according to the Reserve Bank of India the value of
According to the 1981
one rupee is 0.18 paise.
census, in
1979-80, 48.44% of the Indian population was under poverty 1
In 1983 it is calculated that 52% will be under poverty line
However, 75% of. the rural population is under poverty line,
according to a study done by Reserve Bank.
- The poverty line expenditure per persons per month:
In 1961-62 was
Rs.
18 to 20
It
73-7^
11
1978
Rs.
62
11
1980
Rs.
75 to purchase the following items.
35 to 40
4 ounes of grain
3
"
pulses
4
"
milk
1.5
"
sugar
1.2
"
oil, exclusive of expenditure on
health care education and housing.
This moans that,
wj>h>
itself accepts the facts that in 1981 there were 331 million
people in our country who didn't have Rs. 75/- a month!(govt.
The average wage of the agricultural laboures is less than
4/- A world bank survey says India, Pakistan, Bangladesh, Sri
Lanka, 1-ialasya and Thailand has stepped to the position of
a fourth world.
..14-..
-14Land distribution Pattern
Besides incone inequality, another structural feature
common to underdeveloped countries is a general lack of progress
in redistributing the land.
- According to the report of the government 1977-78,
22 million.
the potential surplus acres of land is
Out of this declared surplus is
"
41
taken possession of
and distributed 18.3 lakh aeras to 13
22
*
lakh
26.5 lakh.
lakh beneficiaries.
- The marginal farmers constitute 73$ of all farmers and
cultivate only 23$ of land.
- Large farmer operating over 10 hecters of land are 3$ and
cultivate 26$ of the land.
- The top 5$ of our rural families own 40$ of land where as the
bottom 50$ own only 4$ of the land.
In the overall picture
of our country, the top 10$ own 65$ of the land.
They'.are
politically the most powerful group.
- 85$ of the politicians come from agricultural background,
but 2/3 of them own above 10 acres and 38$ of the politicians
’•
more than 25 acres.
- More than 50$ of the assets in 1971 belonged to the toi> 10$
of the rural populace, ownership of assets enabled them
grabbing of the lions share of agricultural inputs.
The
top 23.3$ who account for 70$ of the land could take 68$ of
the expenditure on agriculture; 82$ of improved machinery,
64$ of investment in wells, 78$ share of other forms of
irrigation and 67$ of fixed capital of farms etc. in 1971
(sixth plan).
Education
The literacy rate - 32.1$ (1981) 20$ of children in India
do not go to school 50$ who join the school leave it in the first
standard. 60-75$ abandan it before Std. V & VIII.
class
15$ reach
.XII.
Less than 1$ finishes college degree.
are not attending schools.
illiterate.
Over 70$ of girls (l1-l4yrs)
78$ of women in the country are
The absolute number of illiterate women rose from
161 million in 1951
to 251 million'in 1981
(Census 1981)
..15...
-15-
More than 50% of the studer.ts in -professional colleges
c;ae from the top 10%
60% of the UGC funds go to 7 elite
ciivarsitios, and only 40% for other 99 universities.
There are also socially disadvantaged groups such as the
economically poor, scheduled castes and scheduled tribes, whose
children are on the periphery of the schooling system.
About
30% of SC children (Boys 20% and girls 56%) and 56% of
ST
children (Boys 49% and girls 70%) are yet to receive elementary
education.
Despite a net work of over 6.5 lakhs schools and colleges,
the employment of over 3 million teachers and an annual budget
of the order of Rs. 3000 crores it has not been possible so far
The real benefits of our school system go to the top 30%
of our population.
They occupy 70% of the places at the seconder
stage and 80% at the university level.
Employment
Unemployment and under employment is a major problem of
the people of Asia.
40% is un or underemployed.
time unemployment is almost unknown.
Tn India full
Our poor are the working
poor, but their works doesn't lend to gainful employment.
Un
employment at the end of the,
53 lakhs
71
"
96
"
176
"
From 1960-69 the daily wages for casual male labourer in Pubjab,
Haryana, Delhi, Himachal Pradesh went up by 89%, but the consumer
retail price went up by 93%.
The top 10% get 33% of the total national income.
bottom 50% get 7.8% and .the. lowest..20%..g_et. _0.,.8%.._
The
-16-
nre owned and controllel by the private sector.
1972
(in crores)
Assets Profits
Assets
1976
Profit,
Tata-
641 .9
48.9
980.7
56.1
Birla
539.4
45.8
974.6
11.8.8
Mafatlal
183-7
14.6
256.5
25.9
Kirlcskar
86.46
4.03
152.4
13.09
% of all Qua? IAS, IFS, and IPS come from the rich est 10%
the people
Housinf;
- It is said that 70% of the rural people live in huts, with
grass, leaves or r eeds roofing.
- According to the annual report of the works and housing ministr
(1881-82) the number of families requiring housing was 12.5
million families.
The' entire outlay for construction assist
ance in the VI plan is Rs. 186 million aimed at benefitting
3.6 million families.
- In all the metropolitan cities, especially Calcutta, thousands
of people lives on pavements.
- In Bombay the cost of a luxury flat is Rs. 40 to 90 lakhs.
Sven bunglows costing not less than 3 crores, with swimming
pool, bar, banquet room,. confoi’yncn hall
ofcc. nvv nr>t mrn her--.
Tax system
1947
19_5_1
•1983
direct tax
52.7%
36.4%
■25%
indirect tax
47.3%
63.6%
75%
Only 0.8% of the people in India pay dxx-oeb taxes.
Big and
middle income groups largely evade paying taxes.
According to dnstur, when you drink a cup of tea costing
20 paose, you pay an indirect tax of 14.5 paise.
At the International Level
Widespread malnutrition is a common feature in all the
Asian countries.
15/1OO born every minute in developing countries
will not live to see their first birthday.
MediCal care will be
available to only 10 of the 85 who survive.
25% of the survivors
-17-
will suffer from malnutrition during the weaning period.
20% <>f the population are seriously under nourii
30% Vfithout safe water or health care
40% xme.iployod or underemployed.
- The developing world has 75% of the world's population,
but only 10 % of the world's wealth.
- 11% of world education spending.
- 30% of the food grains.
- 17% of the world's G1IP.
- 13% of the world's energy consumption.
- 18% of the world's export earnings.
- 8% of the world's industry.
- 6% of the world's health spending.
- Hove infant mortality 50 times higher.
- Every second victim claimed by death is a child below 6 yrs.
Consume only 12.5% of world's produced wealth.
-
Get only 20% economic growth of the world and 2%
of world's research.
- Rich nations dominate International trade, international
policies, International organisations, international judiciary
institutions,
- nutritional studies have shown that in 1939, 39% of the world
had less than 2000 calories per day.
than this.
In 1972, 60% had loss
Practically all these were in the developing
countries.
ARMS RACE
Economists have calculated that in. the united states the
rate of profit is between 8 and 12% in civil Indus ti-y; wlmvw
in Military industry it is between 30 and 40%.
But a U.S.senate
committee which looked at the turnover of 131 monopolies in the
military industrial complex, found that 57 of them had a rate
of 50%> 48 more than 100%, 3 approximately 500, and one company
to a rate of 2000% of profit over the capital invested.
"Every gun that is made, every warship.launched, every rocket
fired, signifies in a final sense, a theft from those who hunger
and are not fed, from those who are cold and are not clothed".
(Dwight D.Eisenhower)
-18-
"The build-up of arms in large parts of the third, world itself
causes growing instability and.undermines development
more
arms do not make mankind safe,, only poorer (The Brandt Commission
1930).
"There must be a way coming down the hill, of de scalating,. . . .
The only solution is not to give us more arms for our security,
but give us more security so we can have less arms.
(Moshe Dayara 1976)
The largest major weapon exporting countries 1977-1980.
Germany
1 ,712
USA
24,893
USSR
15,755
Norway
724
France
6,21 3
Netherlands
536
UK
2,141
Brazil
421
Italy
2,273
Israel
367
The 10 largest major weapon importing countries 1977-80
Iran
3446
Libya
2107
S.Arabia
3133
S.Korea
Jordan
2558
Greece
1987
1900
Syria
2311
Italy
.2167
Iraq
2172
On an average it costs about _t_he_ s age
To arm and train one soldier
to build 1 modern bomber
as it does to
to wipe out small-pox over
10 yrs period.
educate 80 children
to build 4,50,000 modest homes
- The world health organisation spent around !»83 million over
10 years to eradicate small pox in the world.
That amount is
less than two hours oi' global military expenditure.
- To eradicate Malaria - the killer disease that claims the lives
of one million children every year.
needed.
Some 3.500 million are
That amount is less than half of what is spent every
day fear military purposes.
- The United Nations declared the 1980 is the International
Drinking Water supply and sanitation decade.
The aim is to
achieve adequacy in clean water supply and sanitation for
people in the developing countries by the year 1990.
This
requires some 80 million a day for Wyiears, equivalent to
80 days of military expenditure over a 10 year period.
..19..
-19-
- Asian countries in general spend more for their military
forces than for health and education combined.
An international team of specialist commissioned by the
United Nations has con
that the low-income countries of
Asia could improve their per capita consumption by as much as
4-7.6$ with an even a partial reduction in military expenditures
through out Asia.
All these studies show that the gap between the rich
nations and the poor nations is widening as time goes on.
That is why Don Holder Camera said: Today 85/°, tomorrow 90$
rot in misery to make it possible for the conomic comfort of
15$ today and tomorrow 10$ of the world's population.
COMMUNITY HEALTH DEPARTMENT
CHAI
1.
Extent of inequality in the world today:•
a.
In 1850,
world's wealth.
3/4 of the world's population possessed 5/8 of the
In 1975,
2/3 of the world's population possessed 1/8 of the
.
world's wealth
b.
Whence came this uneven distribution of the world's resources?
"The tilting of the balance in favour of the (Jest has come about
in the last 130 years
..through the gun, through colonial plunder,
slave trade, slave labour, child labour, racial discrimination, the
creation of a dispossessed proletariate, and the destruction of the soul
and life-style of many peoples."
(S-Rayan)
c.
The growing gap between the rich nations and the poor had
already been, pointed out by Barbara Ward in the 1950's but the gap
continues to widen:
"Today 85% and tomorrow 90% rot in misery to make possible the
economic comfort ofi 15% today and 10% tomorrow"
(Heder Camara)
d.
The result of this inequality is the ABSOLUTE POVERTY- of
millions in the "fourth" world:
- 1/3 to 1/2 of the two billion human beings in A.sia, .Africa
and Latin America suffer from hunger and malnutrition.
- 1/5 to 1/4 of their children die before their fifth birth
day, and millions of those who do survive lead impeded lives, due to
brain damage, stunted physical growth and sapped vitality due to
undernourishment.
- The life expectancy of the average person is twenty years
less than his counterpart in the affluent world; that is, he is
denied 30% of tho life-span of one born in the developed nations:
he is condemned at birth to an early death.
- 800 million of these people arc illit erat e and, despite
continued expansion of educational opportunities, even more of their
children are likely to be so.
e.
Julius Nyerere, President of Tanzania, has warned the rich
nations: "Poverty is not tho real problem of the modern world, for
we have the knowledge and the resources wbioh will enable us to over
come poverty.
The real problem of tho modern world, the thing which
creates misery, wars and hatred among men, is the division of mankind
into rich and poor".
f.
It is not so much the question of some having more to eat or
better clothes to wear, while others cannot provide even the basic
requirements; it is rather the power that this wealth gives.to some
to dominate, to oppress and to exploit the others.
in so .doing,
the rich and powerful justify themselves: "We deserve this wealth
and power; we have put our God-given talents to use and have worked
hard.
If the rest of the world is lazy, shiftless and ignorant,
w~ can't help that."
-2-
2.
Extent of inequality in India today:
a.
While we often and with some justification, blame all our
problems on the greediness of the affluent, developed nations, the
same ever-widening gap between the "haves" and the "have-nots"
appears here even
b.
Within'our population of upwards 600 millions of people,
roughly 250 million live below the "poverty line", that dividing
line that demarcates bare minimum of survival for an individual.
This is the bottom 40 per cent,
another 250 million live just
above the"poverty line" of human survival, the remaining 15-20
per cent, in an ascending pyramid represent the wealthy, dominant
classes with power, position and quality education: the raw mate
rial for further exploitation of the others.
c.
in rural India, the top ten per cent own 50% of the land,
while the bottom 50 per cent own 4%; top ten per cent get 1/3 of
annual income of the nation,while the bottom 50% get less than
this amount for all of their numbers.
0.1% of the population owns
more than half the wealth of the area.
d.
The poor are organised, without political power, and are
taken advantage of.
A slum dweller admits: "Even to get a
sweeper's job, we have to pay a bribe of Rs.200/-"
e.
The very poor (bottom 40 percent) have less than ft.<>4o/~ per
month to spend.
Most cannot read or write.
I
\ THE CATHOLIC HOSPITAL ASSOCIATION OF INDIA
'•
Community Health Department
CEEHAl
SECUNDERABAD 500 003
Telephones : 848293, 84 84 57
Telex
: 0425 6674 CHAI IN
Grams
:
C0AW«!'?i''°
Post Box 2126
HEALTH CELL
Marks Road57/6 Staff Road
5C0 001
SECUNDERABAD 500003
FEW GUIDELINES TOWARDS SOCIAL ANALYSIS AT MICRO LEVEL
Fr Yvon Ambroise
If one is engaged to develop society, one should first of all
be able to identify the forces operative in the society, to see
how they are operating, the linkages they have and the poten
tial forces they would gain in several areas of life. This
process can be realised by an analysis of the society in a
critical way to unveil the hidden mechanism in it. Very often
society looks on the outside something else than what it is
really in its core. A simplistic outlook can easily say that
society is O.K. while there are several negative forces operat
ing within it to upset the s ciety. All these can be unearthed
only by a process of social analysis.
If a social worker does not have recourse to a critical social
analysis due to his ignorance, he is likely to undermine the
positive forces and join hands with the negative ones without
his knowledge and even against his own intention. Hence the
socigl analysis is a must.
Social analysis can be equated with a diagnosis done by a doctor.
In order to find out the cause of any disease the doctor asks
questions on the several parts of the body and links the data
obtained into a logical explanation. The cleverer the doctor is,
the more connections he knows between several parts and hence
asks pertinent questions about those parts, similarly, a
social Analyst tries to find out the data on the different
parts of society and links them with a logical explanation to
find out the underlying problems in a society. The different
parts of society can be said to be :
Economic system, social system, political system, ideological
system, religious and cultural system, educational system,
health system, etc. To make a social analysis all these systems
must be looked into and analysed. We take each system and see
a certain frame work to analyse the system.
Economic system can be defined as one which contains all
activities pertaining to the immediate survival of man. In
order to analyse these activities, first of all the main
source of economic activities must be identified.
2
:2:
The main sources could be agriculture, fishing, animal husbandry,
industry and hunting. One must identify whether there is one or
more than one source cf income for the particular group we are
Loalin" with. After identifying these sources one must go to a
detailed analysis of each one of them. For example, we shall
take agriculture and analyse it.
Agriculture has land as the basis. Hence one should find out;
the structure of ownership, the structure of the interaction of
different groups arising out of the ownership and the structure
of the distribution of the produce. These three would reveal
the economic dynamics present within the system.
Taking the structure of ownership we may find that there are
three major groups :
- The group that owns maximum land;
- The group that owns enough land; and
- the group that owns nothing at all.
While trying to describe these groups vague or relative and
comparative terms such as many persons, some persons, a few., more
should be avoided. One should give the approximate numbers in
every category, e.g. 5 families owning 50 to 100 acres, 10
families owning 10-50 acres, 50 families owning 1 - 10 acres,
50 families owning no land. This gives one a picture as to who
is the biggest group in the village.
As for the structure of interaction between these groups, we
must try to see the mechanism used by cne group over the other.
Let us take a person owning fifty acres. With the physical
labour of his own family and without hiring workers he may
cultivate himself only around three acres of paddy cultivation.
The rest of the 47 acres are there. In order to cultivate
these 47 acres he needs the collaboration and work of the land
less- labourer. Hence he is actually dependent on the landless
workers who are free to go to another man or to migrate outside
or to undertake any other work such as road-making.
In order to ensure his cultivation the rich man devises
mechanism to see that the landless labourer would depend on him.
Hence he tries to absorb all the surplus from the landless by
several mechanisms to make him dependent on him. Low wages,
:3:
giving loans with exhorbitant interest (120% to 300%) a year
bonded labour, having liquor shops in the workers' area,
celebrating festivals and encouraging people to spend, are
some of the mechanisms of the rich class to absorb the surplus
from the landless and make him dependent on landlord and be
obliged to come for work. This is what we call exploitation.
In this way the cultivation of the 50 acres are assured for
the rich class. By these mechanisms the landlord makes the
landless iepend on him thereby reversing the original position.
As for the structure of distribution of the produce we go into
the analysis of the wage system, how it is given, in what form
and at what seasons. A comparison could be made to different
places and to the rate fixed by the government. If tenancy
system is followed the terms of division of the produce along
with the terms of help rendered during the cultivation have to
be analysed. ■
After having analysed it one must go into the system of marketing
and transport. The role of intermediaries, the money lending system
with reference to marketing, the time of sale of produce, etc.
have to be analysed here. Thus all these when analysed gives
one an idea of how the economic system is functioning.
Taking the social system one has to analyse how the society
is stratified as high and low. Here two logics are operative;
the class logic and the caste logic. The notion of class,
presupposes the equality of man as the base and that inequality
came out in the social process. The notion of class is based on
achievement which today would include moeny and education.
Hence social mibility in terms of the upward one as well as the
downward one is possible. Competition and grouping of the
members of the same class into a solidarity group are characterictics of the class system.
Caste is based on birth and has the philosophy that man is
born unequal and dies so. Everything is determined by one's
birth. Upward or downward mobility is possible only after one's
death i.e. in the succeding lives.
These two systems operate together intermingled. Hence one
has to find out which element : the caste or the class one, that
4
: 4 :
is dominating in a particular society and go into the analysis
of its causes.
The political system represents the collective decision making
One has to examine the way a representative is selected
from the grassroot level to make collective decisions and laws.
Thus this system can be legislative wherein the laws are made,
Judiciary which clarifies whether the law applies to a particular
case or not and the executive.- The executive ordinarily functions
through the government officers in charge of executing these
laws and decisions. In extra-ordinary circumstances when they
cannot do their functions Police is provided to do so. This
political system of representation could be handled by some
groups with a specific ideology promising people that they
would exercise that power to their benefit. This is the political
party. When the representation is 'done by political party or
parties it becomes party politics. All these elements have to
be analysed.
The cultural system would be analysed when one analyses the
system of values. Thus when we make a critical analysis of all
such systems and link the data obtained into a logical expla
nation, there is a social analysis of a particular social reality.
It pin-points the forces and mechanisms operative, the way they
are operating, the groups who enter into operation in an
advantageous or disadvantageous way, the ideology used, etc.
One is able to get a picture of the society along with its main
problems.
Social analysis cannot be learnt only by theoretical means but
by a practical field work. Social analysis is an ongoing exercise
and that one should not feel complacent at the very first attempt.
The first analysis only opens new questions and data to be
searched for. Thus the finding in-depth of new data can even
change the analysis one made before. One should always keep
searching. This develops critical consciousness.
20-11-87/100
mm/
The Catholic Hospital Association of India
C. B. C. I. Centre, Goldakkhana, New Delhi - 110001
Tel. 310694, 322064
DEVELOPMENT
COMMUNITY health CELL
<7/1. (First FloorlSt. Marks Road
CH1T/P-4-A
BANGALORE - 560 001
Development can and for too long I-- been understood
as economic development alone, where the main emphasis is on
increased production and income. According to this’ definitinn
the main objective? of development is to increase the f'Tp with
out bothering to sec who is benefitting from this increase.
In most of our countries, this is the kind of development^
which has been going on. The emphasis has been on increasing
production. As a result of this emphasis production has
increased in many of our countries through green revolution,
or industrialisation. The benefits of this development have,
however, not occured to everyone equitably. In many developing
countries the rich have become more rich and the poor have
either remained where they were or at times have et >n become
poorer. This trend is quite visible at the village level. The
above concept of development is very narrow and thus unacce
ptable.
Development has many aspects - economic, social, cultural
and political. There should be equal emphasis on all these
aspects. Along with economic development, there should be
better distribution of resources and means of production.
The decision making power should not be in the hands of a
few people only. Participation of the majority in all aspects
of development is necessary in this concept of development.
The word 'development' can be divided into "Develop'
'Men' 'T'; Develop men or women to think together to under
stand the reality and to grow fully. Growth of individual
alone is detrimental to society.
Development is a continuous process of change leading
the awareness of one's present state of life and bringing
him to a higher level of life. It is a growing activity
between persons who feel the necessity for development, and
persons who want to work for their own development. It is
also said that development is a continuous process towards
complete humanization by loving one another without selfish
motiveness.
7.'hat is de-vclopment;
Development is a process by which both persons and soc
ieties come to realize the full potential of human life
in a context of social justice, with an emphasis on selfreliance, economic growth being seen as one of’the means for
carrying forward this process".
1.
Prom this it is implicit that development
(a)
is of people and can bo achi^ied only by them. Others can
only be enablers.
(b)
is of people in community with the direction and control
in the hands of local leadership
(c)
is a process in the context of relationships and a total
2
life style consciously evolving towards growth.
(d) is sustained through funtional indigenous institutions
developed from and responsive to the local situation of
the people.
(e)
is an integrated process requiring harmony between people's
and between people afid nature; between the present and the
future; between’the social, economic and political factions.
(f)
is interdependent; the fulfilment of all people depends on
the development of all.
2. Development is: - growth with redistribution
- awareness of people of their problems,
power and the potential they have in
working together.
— to 'de-envc-lop' people from the bonds of
oppressions and powers that suppress them.
- being our brother’s brother and not only
his keeper
- respect for the individual's dignity,
self image and self esteem.
In development we are looking for;
participation by all people
equitable distribution
effective and efficient utilization of human as well as
natural resources.
(d) The growth, in dignity, of the individual in the context of
his family, environemnt and community.
(a)
(b)
(c)
Development is therefore a continuous and dynamic process
that brings about structural and institutional changes.
It must through these changes provide an equal oppor
tunity for all to participate in decsion making in the eco
nomic, social, cultural and political spheres.
A question of power
This consept of development with emphasis on distribution
and social justice requires some funds, mental changes in the
social, economic and political power structure in our societies.
It requires changes in social relationships. It requires re
ducing the power of some and increasing the power of others.
The elite in our societies is not interested in Jshis kind
of development, because it would mean reduction in their pro
perty and power. The elite is ofcourse not willing to give up
its power and position to others.
The kind of development we have in mind cannot avoid con
flicts. However, structural change might not necessarily mean
shedding of blood. In fact fundemontai change should be tried.
in a peaceful way. But it might not always be possible. Vio
lence is almost always star.- d by those who do not want funda
mental change. They violently resist reduction in their power,
privilege and property. The poor have to resort to violence
often in self-defence. Development would mean struggle and wo
cannot avoid it.
- COWWsITY WLTH WAHTMMNT
PECPIE's PARTICIPATTON IN HEALTH
Some decades ago, development of undeveloped communities meant doling
out food, clothes, .medicines and money to the poor who were just passive
recipients. Gradually a realisation came that this'was a bottomless pit
which would never fill. So dame the concept that 'people' should work for
their own improvement. However it was soon realised that people could not
be made to work unless they were involved in the process of development.
Thus came the idea of people's participation.
There are three questions I want to. ask I
»
• 1. What do we mean by people's participation?
2. Who are the 'People'?
3. Is people's participation passible in community health?
Different people have different meanings for people's participation.
Some project workers say that there is overwhelming people's participation
in their peojects; thereby meaning that the people are taking benefits of
the programme. Does merely taking benefits of the programme or,participating
as beneficiaries mean people's participation?
Some call it people's participation when the people are receiving
benefits not as'charity but are paying or rather are forced to pay for the
benefits. Does such payment for services mean people are participating?
Then people are very actively participating in the whole of the commercial
system today where everybody pays for whatever he or she gets. Then can
compulsory payment for the benefits, which is glorified as 'economic
contribution of the people to the programme' be a hallmark of people's
participation?
A very successful community health project claims that 'the villagers
collectively constructed a road from our hospital, to the village so that our
health team would reach the. village', and foreigners are much impressed by
this 'people's participation'. One however finds that' the road was
constructed-by the labourers of the village in 'food, for the work'
programme and the villagers were mainly, paid labourers.
The same community health project says, "our village health workers
have.been selected by the people of the village and our project has a
people's committee as advisory board. 'Though this is meant to be
participation by the poopId in decision makingon closer enquiry, one
finds that almost every 'VEH.W.was'selected by the head of the village
and two or three influential persons and the project staff. The people's
committee consists of established leaders and the rich people of that area.
Toes the decision making power given to the few rich and established leaders
of the village and mutely followed by the rest of the villagers mean
people's participation? By this definition the whole political system
today has vary wide people's participation.
Obviously all these are not examples of people's participation.
The last point takes us to the next, question, 'who are the people'?
This is quite a tricky and political question. A big power invades a small
nation and nuts its 'yes man' in power and says people of this nation
have invited us to liberate them. Do mere heads of government mean people?
A rich man who
also heads the Gram Panchayat takes a decision as to who
should be the VHW from that village. Is he the people?
The male head of the' family says 'the tradition of our family requires
women to remain in purdah and all people approve of this tradition'. Is he
the whole family or are the males alone, the people?
...2
2
No
In all these instances decision nakingdoes not represent the
desire of all the people, definitely not of those who have no voice and
freedom to speak but who very badly need an opportunity to take part in
the decision making to ensure that it is in their interest and not to
oppress them.
Thus I have tried to show what is not people's participation and who
are not 'the people': If this is not people's participation then what
is it?
Who are> the people?
Probably everybody born as a human being has a right to bo included
in the 'people', be it the oppressed or the oppressor.
But for operational purposes, we will have to say that the oppressed,
the exploited and the needy should have priority in the comprehensive ' f.
definition of the people.
When those people understand the situation and issues by critical
consciousness and take part in decision making, implementation and evaluation
of programmes and take the responsibility of the work as well as share
in the benefits....it becomes people's participation.
There cannot be genuine people's participation without a proper political
atmosphere and educational, process. Even then true people's participation
'
may be a distant goal.
Prerequisites of people's participation
Today's political and socio-economic system is directly opposed to real
people's participation. How can there bo a true people's participation when
women have no equality, the poor have no strength to assert and the oppressed
have no opportunity to participate in the decision making of the political
system? When we, the enlight.ered elite citizens of the society have no
scope to participate in the affairs of the nation except to vote for the
best of the available bad choices once in 5 years or to write a letter
to the Editor once in a while, how can those who are weak, poor, oppressed
and ignorant, rea'ly participate?
It is obvious that the real people's participation is a distant dream
to be achieved by a process of economic, political and cultural liberation.
When one ■'.dews the objectives and the claims of people' s participation g
in community health projects one cannot help but laugh. The present system o!
anti-participatory. Moreover there are more vital fields in which people
would prefer to participate first. Health is a low priority issue.
The expectation that people will participate in a real sense in a mere
community health programme is unrealistic. This conclusion is also supported
by the experience of numerous workers in community health who have learnt it
the hard way that people cannot be mobilised and organised through and for
health work. It does not mean that there should be ho efforts towards
people's participation in health programmes, All efforts to involve the-people
the peonle, especially the needy and the oppressed in making decisions and
their implementation should be made. This will marginally help a
participatory culture to be created. But it must be realised that people's
participation is essentially an objective ofApolitical and educational
process, and health work has only weak political implication^. If community
health work is a part of political activity, it will get it's backing
and advantage. But without a proper political context, not much of genuine
people's participation can be achieved in community health work alone.
Hence people's participation per sg,cannot be a primary objective of a.
community health programme.
..3
- : 3 : -
If people.' s participation is real-and genuine, one should not. talk
• of people's participation, in the-project's health programme but of the
project's.participation in the people's health programme. But realistically
this cannot happen through the health process alone.
Sane workers use another misguiding term, 'community participation'
in community health programmes. There are two'obvious fallacies. One,
there is ho organised-entity as 'community' in the villages today. There are
individuals, families, castes, classes, political groups and one cannot
create canmunities out of such individuals and groups for the purpose of
and through mere, community health work (though community health work might
marginally help this process)• Secondly, though claims are made of having
achieved community participation, in reality only the existing social
. organisations (Panchayats, etc,) and established leadership are involved in
decision-making, We have already seen that such leaders alone are not the
people and hence they cannot replace the■community,
W
Economic self-reliance: Why ?
Another popular fashion-word is 'economic self reliance', commonly
used as a criterion of evaluation and boasting feature by many agencies
and. projects in community health; How did this come to be given such an
importance that it has almost become an important objective of canmunity
health programmes?
The workers keep on desperately running after this
objective, forgetting that economic self-reliance is not the purpose of their
work and. they cannot afford to.sacrifice their original purpose i.e. to improve
the .health of the vulnerable people.
With growing realisation in the developed (exploiter) world that mere
doling out of food, and clothes cannot permanently^ improve the life of the poor in
the undeveloped (exploited) countries, a concept was born that people should
be given such economic nrogrammes which can generate income for themselves
and hence they don't-have- to depend^ on outside help eternally.
Self-reliance Logic
Fine'. Good policy'. But then this has to be an objective of economic
programmes -to be achieved, through economic activities. This has been
implicitly accepted in the field of community.health also. This has caused,
■ tremendous diversion and confusion and a time, has come -to challenge this
. assumption. There are many reasons.- When a community health project tries to
■ become economically self reliant, it adopts two methods.
(a) It starts charging the rich to. gain more income, (the so called
'Robinhood' method). Ultimately this results in the community health
project becoming dependent on rich clientele for it's economic selfreliance. To satisfy this clientele comes the sophistication, X-rays,
E.C.G., more indoors, more specialization, and more and more workers and
time to cone up with all this. Also come in the unscientific, unethical
practices like giving unnecessary injections, tonics, mystifying the
symptomatic- relief etc. to draw and retain the paying patients.
The rich class is much more shrewd than community health projects.
It is almost never dependent on this community health project alone for its
own health care (though occasionally individuals may need and seek such
curative services, such examples don't prove that the whole class is
dependent on community health projects). They almost always get their
health needs fulfilled through the commercial nrivate health system.
,-..4
Only in very remote places,:persbns from such, class might depend on community
health projects. Thus the community, health-'project becomes dependent on the
rich class.for its income arid, survival rather than otherwise
.
*
This brings
gradual changes in the priorities, strategies,■methods, behaviour^ and
relationships of the '.community health project and it ends in serving
primarily the needs and priorities of the rich.
An analysis of the clientele of most of the mission hospitals, who
in an attempt to become economically self reliant started charging the cost
of the treatment to patients,1shows that ultimately they ended with two
maladies. . They were' underutilized, and were.utilized predominantly by the
rich class.
...
Sathyamala from vHAI.has described. (Health For The Millions,
February 1980) how she saw atnany places voluntary -hospitals half
*
empty, beds
occupied by the rich, who only could pay the charges:, and the next door •
Government hospitals and dispensaries-inefficient, low quality, corrupt but
still overburdened, full of poor patients. What an irony '. fhen why should
dedicated missionaries run such hospitals ? Even the private commercial
health care system (eg. Jaslok Hospital) can do and-does-.the same; role.
Then where is the difference?
(b) To raise incane, the.second strategy adopted is to charge the poor
more and more in an attempt to make them pay at least the cost.of the
treatment. ..We have already seen how it results in elimination of the'poor
from the curative health care. 60% of admissions in.a .hospital of.a'
famous community health project which claims to be economically self reliant
project. Remaining include rich and poor from the project area but again
in what proportion ? The hospital is mainly utilized by the rich
*
An argument forwarded is that the pocr are1'given primary health
care through VHWs financed by the income generated from the rich in the
hospital. It means the VHWs give lielementary care in the village to the .
poor and rich also but doctors and hospitals are mainly for the rich. Such
discriminatory strategy becomes inevitable when community health .project
accepts the objective of economic self reliance and tries, to raise the
income through health programmes.
.
. ..
It is true that the poor also should be.charged a little for health
care so that they do not become? objects of charity , and'pity.. Also, if they
arp charged they feel that they have paid for health care and so the care
must, be of some quality, earned by them. It is. concn experience that
the poor also value-such treatment and advice/for which they have paid.
But this logic is then taken to, it's extreme that the poor should pay the
whole cost of treatment^ .ijHhich is pretty high in the present system. The
poor, already exploited by the present economic..’system' hatsevery little
resource^ on which community health project further puts its claim.
An argument is often put forward that' the poor also have the
capacity to pay for curative services. They manage to mobilise- the 'resources
when you make it compulsory for them to. pay. ■ This is the philosophy of. the
private doctors. Once, when I put this argument before a poor man, he
.said "Look Doctor Sahabl. If:I am ill and dying and if you press me for
charges'T shall sell my house ." My family shall starve arid then, only I
will be able to pay your money. But. if I-do it does it mean I had the
capacity to pay■you ? "
5 : When this objective of economic self reliance is almost thrust on
the community health projects in .the voluntary sector by funding agencies
let us ask a few questions.
Who is self-reliant today ?
Is the government self-reliant in the sense it generates all its
necessary income by productive activity ? No
It depends on squeezing the
■people by taxes, direct and indirect.. ' None of the welfare programmes of the
government are selfsufficient.
Are the funding agencies-self reliant ? In spite of decades of
working, all of theta continually depend on donations from people in the
developed countries. They do not generate their own income by an economic
programme run by themselves, even though their main field of work is fund
raising.
Funding agencies can raise money through Western capitalism. However
this capitalistic system depends, at least partly on the developing countries
for its market, and'remember, the market is the source of income for capitalism.
It ’is unrealistic to expect in such a situation that community health
projects should be able to generate enough income to become economically
self sufficient.
Health and education are the responsibilities of the state and society,
as is law and order. ■■ Voluntary agencies enter in it because the government
cannot do it adequately for the people. The government gives free health
care to all, specially to the. poor. Then why should the. voluntary community
health projects charge poor patients to whose rescue they claim to have come ?
Many community health.projects tacitly accept this objective of
economic self reliance under increased pressure by funding agencies and they
are forced to either deviate from their primary objectives or to do various
manipulations and show that they are economically self-reliant. This includes
artificially swelling the health income, (some times by selling the
donated drugs or by including the farm income) or by hiding certain
expenditures of health programme. Some projects reduce the expenditure
by underpaying their staff. All these compulsions come because of the
acceptance of the criterion of economic self-reliance.
Having observed closely many community health projects in India and
abroad, and following our own experience. I wish to say that no community
health project which is predominantly preventive and educative in nature
and which serves mainly the poor can become econcmically self-reliant. All
such claims need to be reexamined because they create illusions.
Projects should try to generate income either through economic
programmes or from committed supporters who have money to donate for the
cause. Such income generation will make it less dependent on outside aid.
This cannot howevor be the primary objective of community health work.
6
: - 6 - !
F/iSE LIMITATIONS
Another aspect which community health projects should not uncritically
accept is trying to see that the per capita health expenses in their community
health programme is equal to that of the government. • .Government spends a lot
of money on wrong priorities and al_uocatos- meagre, resources for health due to
which the. poor mainly suffer. Voluutaiy health projects heed not take it as
their responsibility to show ways to fulfil health objectives within the false
limits set by the government. It usually means deprivation of the poor.
What voluntary agencies could.be doing is to decide the minimum health
care every person should get and try to show the ways of doing it at the low
cost level whatever that cost should be compared to the government's per capita
health expenditure. This is the way by which one can press a system to mend
its ways.. Voluntary health projects should not try .to fit into the system's
false limitations. While deciding the minimum health care, the nation's
economic standard (GNP or per capita average income) should be taken into
consideration but not' the per capita health expenses by the government. Otherwise
•we land up with the solutions and ways of community health care which are less
than .minimum to the real needy.
(This is a ■'■lightly abridged version of an article that first appeared
in MFC Bulletin, April 1981. Reproduced-here courtesy MFC-Ed. HFM. MFC is to
publish this and. other important articles in a book form. For details
contact MFC or us).
Source : Health for the Millions, Vol,VIII, No.3, June 1982
£
The Catholic Hospital Association of India
C. B. C. 1. Centre, Goldakkhana, New Delhi - 110001
Tel. 310694, 322064
INVOLVING LOCAL LEADERS
COMMUNITY HEALTH CELL
47/1, (First Floor)St. Marks Hoad
BA.NGAlO.1E - 560 001
In tlie workshop, we have often discussed the importance of invol
ving local leaders in our Community Health Programme. Let us
briefly review who these leaders are, why it is important to
involve them in our programme and how to recognize them in the
community.
WHO ARE LEADERS?
There are two kinds of leaders- formal and informal leaders.
Formal Leaders are persons who have been appointed or elected
to fulfil certain administrative responsibilities for the whole
village. They hold a recognised post and may or may not be
paid for it.
*
Examples
(i)
Sarpanch, Panchayat Members, Tehsildars or
Revenue Collector etc. These leaders are part
of the government's administrative structure.
(ii)
In certain tribal areas each village may elect
its own headman and committee members to help
the headman. These may or may not be a part
of the government structure.
Informal leaders are people whom the community respects and
trust s. People go to such leaders when they have a problem
or need advice.
Examples5
- The people may go to the pujari for all religious
matter s
- The people may take the opinion of certain village
leaders when there is a family dispute
- The people may goto the faith healer (Bhuva, Badwa)
when there is some illness in the family
- The people would take the' advice of the dai in
matters related to pregnancy and child birth
It is thus clear from the above that informal leaders have a lot
of influence in all important matters in the community. The
people look upon them as knowledgeable and having a sound
judgement.
WHY SHOULD WE INVOLVE ALL THESE LEADERS IN OUR PROGRAMMES?
Both formal and informal leaders have a lot of power in the
community and are able to influence the decisions of the people.
In some cases people simply follow a trusted leader, in others,
leaders can get people to participate in an activity by creating
awareness.
leaders arealso capable of forcibly getting the participation
of the people by threats and in extreme cases by actual violence.
It is important for us to work with both kinds of leaders.
Formal leaders may or may not have (EgS Vishalnagar Case) the
trust of the community. But it is important that they be
informed of, and if possible involved in all our activities
because these leaders are usually the most powerful in that
they could have a strong economic hold on the people.
2
Informal leaders, on the other hand, may he more trusted by the
community and can be of great help to us if their cooperation is
sought. They can also influence the community against our
work if their involvement is not sought.
let us now look at some of the ways in which local leaders can
help or hinder our work.
1.
Gaining the trust of the people
When we enter the community as outsiders, it is natural that
the people may question and be suspicious of our motives.
Here, if the local leaders, especially the informal leaders.,
understand our reasons for wanting to work with the community
they can help us to gain acceptance with the people. This
way, they will also help us get more information about the
people, finding out the needs of the community etc.
- A Team of Health Workers wanted to start a Leprosy
Control Programme and cover a whole block. All the
team members were new in the area. At first, the people
of the nearby villages looked at them with distrust.
The team, realising that they needed the trust of the
people to achieve the aim of their programme, made
an effort to contact all the village Sarpanches of
the block before starting their work. They also tried
to find out who were the influential people in the
most important villages, started to befriend them and,
in the process explained their reasons to be there
and what they expected to achieve. In no time the
team felt that people started to look at them in a
different way and came forward to help the programme.
One of the most important local informal leaders became
a strong supporter of the programme, considering himself
as part of the team and helping them in their numerous
difficulties.
2.
Help in specific activities
There are many ways by which local leaders can help us in
our activities. They can be very helpful in planning and
implementing all our programmes. For example, they can be
most useful in involving the community in collecting
information for the baseline survey, getting the community
to decide on a particular plan of action and in helping
to evaluate the success of our programmes. leader's can
help to raise resources from the community for programmes
and can take on a great deal of responsibility to see that
programmes are run smoothly.
- A group of health workers in a tribal area had been
doing health and. development work for 5 years. They
had built up a good relationship with the people
during this time. In the third year, a severe drought
occured in the area and a funding agency gave them
funds for a drought relief programme. The money was
used to buy seeds which did not require much water
to grow.
A committee of 4 persons chosen by each village took
the responsibility for the proper implementation of
the scheme in each of their villages. Within two
days the committees had drawn up an impartial and
3
accurate list of beneficiaries with their land
holdings and the quantity of seeds required by
each. The committee members along with the health
workers purchased the seeds. The distribution
was done in a systematic manner and proper records
were maintained by each committee. Twenty five
villages (with 900 families) benefitted from this
programme.
Just as local leaders can be a great help, not involving
then can also hurt our programme. We have seen that
their support can help us gain community acceptance and
participation. Several case studies which we have discussed
in the workshop have shown the harmful effects of non
acceptance by the community. However, it is important
for us to take into accounu the various factors in a
village situation and not be completely taken in by
whatever a leader says ( remember the case study Hidden Motives).
HOW TO RECOGNIZE INFLUENTIAL LEADERS?
In your visits to the village, you will probably find
that certain people's names are often mentioned in answer
to questions likes
1.
2.
3.
4.
5.
6.
Who are the important people in the village?
Whose opinion do you respect?
Whose advice do you follow?
Who settles arguments within or in between families?
When there is an illness in the family, whom do
you go to?
Who are the first persons to do something when
there is serious trouble in the village?
These people whose names you hear often are probably those
with leadership qualities and respected by the community.
You must remember that you must ask the above and related
questions in different sections of the village otherwise you
may not get a complete picture. Thus, in a village with
different caste groups it is most likely that each caste
group has its own elders and leaders who influence that
caste group more than the leaders belonging to the other
groups. This is an important point for you to remember.
Keeping ones ears and eyes open i.e. by listening and obser
ving people, events, situations, during village visits, you
can identify informal leaders and also check the infoxmcrt ion
you have on individual leaders.
- In a village of south India, a team of health workers
identified very quickly the formal leaders. It was
also easy for them to. find out the informal Caste
Leaders. But it took them several years to realise
that the Hari.jans of the village had great trust
in one of their young men and that, in fact this
young man was one of the most powerful leaders of
the Harijans. This fact came to light when the
Hari.jan colony was burnt down and help had to be
organised to rebuilt it. He was the only one who
could control the grief of the people and encourage
them to rebuild the colony altogether, those who
had not suffered from the fire helping those who
had lost everything.
..4/-
TO SUMMARIZE :
Vie have seen that it is important to involve local leaders
in our Community Health Programme because they are powerful
and can make decisions that result in the success or failure
of a programme. Community participation, so essential for
the success of our programmes, is usually decided by the
community leaders.
***************
Prepared by;
chtt:rrJ 29.3.84
J
Community Health Team
Voluntary Health Association of India
C-14, Oomriunity Centre, S D A
New Delhi-110 016
ANALYSIS OF THE PRESENT HEALTH CARE DELIVERY SYSTEM
_____________________ IN INDIA
To start with, let us examine the rationale and relevance
of an analysis of the existing health care delivery system.
Let us have a look at the following statements based on
authentic statistical information:
Indianas the highest mortality rate - 15.5/1000, among all
the Asian countries.
In India diarrhoea alone kills 3 children every minute or
5
1.
million each year. Every minute an Indian child is ex
posed to it.
Infant mortality rate of India is 125 (1978).
There are about 60 million children in India who are mal
nourished.
There are an estimated 3.2 million leprosy patients in India.
Tuberculosis accounts for 3$ of the 1 crore annual death
in India.
Severe degree of anaemia has been detected in 12$ of pre
school children.
90 million children are supposed to be in the polio danger
zone and 13 million are added to this figure every year.
Of these, 80$ victims are below 3 years and 15$ below 5 years.
There are 2.5 lakh totally blind children. There are about
8
1.
lakh partially blind. There are another 2.5 lakh who are
deaf. Of the 9, million blind persons in the country, 5
million could be cured by proper surgical interference.
All these are certain important indicators of the health
*
status of India's 70 cyrore population. India adobes tenth
place among the industrialized nations of the world. Pla
nners and leaders narrate success stories of various deve
lopment programmes and the progress achieved in various
sectors. But the lot of the common man and the labourer
continues to be the same and becomes worse even. The illhealth and the high death rate are but the manifestations
of the miseries that majority of the population undergo in
this country. Here it rightly follows that development and
health are integrally related. At the very outset of this
discussion let us try to situate the sick man in the context
of this socio-economic situation prevailing in India.
Development means the satisfaction of the basic needs of the
poor who constitutes the world's majority; at the same time,
development also means ensuring the humanization of man by
the satisfaction of his needs for expression, creativity,
and the capability for deciding his own destiny. Here
again the stress is on the poor man - the satisfaction of
his needs and ensuring the removal of all dehumanizing
forces and enabling him to be master of his own destiny.
Health forms one of the basic needs of man; and more than
-2-
that. sound, health is primary for human existence. The first
part’of this paper presented few instances showing the grave
denial of this right to existence. The 'Alma-Ata' declara
tion of the International Conference on Primary Health Care j
(organised by WHO, Sept. 12,1978) also reaffirms the import-j
ance of health and goes even further to state that health isj
essentially a state of complete physical, mental and social !
well-being and not merely the absence of disease ©r infir
mity. If viewed against this background, provision ofhealth
for all" which is a declared objective of WHO and that of the
Government of India, demands of comprehensive state of
national welfare based on equity of distribution in which
none denies the right of the other for health. Hence health
demands the good harmony of social, economic, political,
cultural, and religious forces conducive to the promotion of
healthy existence of man.
In the existing society, the health care system is part of
the wider social, politi-cal and economic system. The social,
political or economic capability is not equally distributed.
According to the 1931 census, 48.44% of the Indian population
are below the poverty line. Unofficial calculations, which
often picture the real state of affairs, suggest the figure
to be 75%. This figure goes on increasing. According to
1981 price scale, a person who does not have Rs. 5/- a day is
considered to be under poverty line. This phenomena is due to
the anomalies of the distribution system which prevents the
poor from meeting his needs. In the wider economic and poli
tical relations, the health system alone cannot be thought
of as being isolated. Unequal distribution of health care
facilities denies the right to sound health to the majority
of our population. Social and economic inequalities and
powerlessness prohibit the people from the knowledge and the
capacity to afford the health care of their family-the pre
gnant, the children, the adult and the aged. Hence, inequ
alities exist at two levels - (a) in the distribution of the
health care service (b) in the capacity of the people to
afford to maintain good health. Precisely^ these two areas
constitute the central theme of this paper. We shall follow
a sequence and order based on the points given below:
'a. The present health c^re delivery system in India
and its distribution in the rural and urban centres.
b. Availability of these facilities to different econo
mic classes and medication pz'actices.
c. Problems of medical personnel in rural areas.
d. Manufacture and distribution of drugs.
Prior to the discussion on the above let us have a brief
look at our national health policy.
Our National Health Policy
The constitution of India aims at the elimination of poverty,
ignorance and ill-health and directs the State to regard the
raising l§vel of nutrition and the standard of living of its
people and the improvement of public health as among its
primary duties, securing the health and strength of workers,
meh and women, specially ensuring that children are given
.3/
-5opportunities and facilities to development in a healthy
manner. Hence with a view to providing health for all by
2000 AD., the Government of India has revised its health
policy in relation to the economically under-previleged
sections of the Indian population, and especially those in
the rural areas who constitute 80$ of the total population.
The revised statement on the National Health Policy covers
areas as population stablization, reorienting medical and
health education in relation to the hea.lth needs of the
rural and urban poor, need for providing primary health care.
with special emphasis on the preventive, promotive and the
rehabilitative aspects, reorientation of the existing health
personnel, promotion of indigenous and other systems of
medicine, etc. The policy statement considers the problems
of nutrition, food adultration, quality of drugs, water
supply and sanitation, environmental protection, immuniza
tion programme, Mother and Child health service, school.
health programme, occupational health service, medical indu
stry and medical research as areas deserving urgent attention.
All these are geared to providing all the citizens of India
■ sound health, especially those in the rural areas who forms
India's majority of population.
Yet alarming statistical figures glare at us. We have to
admit that the existing health care delivery system does not
cater to the needs of the majority of the people. The poor
and the under-previleged, especially those in the rural areas,
form the majority of the victims of ill-health. We have to
admit that based on this status-quo we have to implement one
by one the meaningfully laid down policies of our National
Health Policy. Now let us pass on to discussions on the
various points mentioned already.
(a) Health Care Delivery System in India:
i.
Administrative set up at the Centre,
State and District levels
The official organs of health at the national level consist
of (1) The Ministy .of Healthand Family Welfare (2) The
Directorate General of Health Services (3) The Central
Council of Health.
The functions in the union list for the ministry of health and
family welfare are international health relations and admini
stration of port quarantine, administration of Central in
stitutes, promotion of research and resea.rch bodies, regu
lation and development of medical,pharmaceutical, dental and
nursing professions, establishment and maintenance of drugs
standards, immunisation & emigration, regulation of labour
and working of mines and oil fields, co-ordination in the
States and other ministries for promotion of health. For
functions in the concurrent list both the Central and State
ministries are jointly responsible. They are prevention of
extension of communicable diseases, prevention of adulter
ation of food stuffs, control of drugs and poisons, vital
statistics, labour welfare, etc. Both Centre and State
Governments have simultaneous powers of legislation.
..4/-
-4The Diroctorc.te General of health services is the principal
advisor .o the union Government in hoth medical end public
health matters. The functions are surveys, planning, co
ordination, programming and appraisal of all health matters
in the r'.cnm.tr'
In brief, the specific functions are inter
na?:. :ua_ __;alth relations and quarantine, Control of drugs
standards, management of medical stores depots, post
graduate training, medical education, medical research,
Central Gove. cal th Scheme, national health programmes,
Central Health Education Bureau, health intelligence, and
maintenance of National Medical Library.
Since many health subjects fall in concurrent list, continuous
consultation, mutual understanding and cooperation are" nece
ssary between Centre and States. The Central Council of
Health, constituted of the State ministries of health with
the union minister as the chairman, looks into these. Briefly
the functions are - to consider and recommend broad lines
of policy in ma.tters related with health, to make proposals
for legislation, to recommend to Central Government for dis
tribution of grants-in-aid to States and to review the uti
lization of that, to establish organisations for promoting
cooperation between State and Central health ministries.
II.
-4t the State Level
The health subjects generally fall in three headings federal, concurrent and state list. The state has complete
autonomy for the functions prescribed in the State list.
Generally, this includes the provision of medical care,
preventiv health services and pilgrimages within the State.
And, the State is the ultimate authority responsible for all
the health services • perating within its jurisdiction.
Tn a'.Z
;/,es tne management of health sector comprises
of the State Ministry of health and-the directorate of health.
The State Ministry of health is headed by a minister of
health and family welfare.
some States the Health Minister
is also incharge of other portfolios. •
The Director of Health Servicds (known in some States as
Director of health and medical services) is the chief tech
nical advisor to the Government on alp. matters relating to
medicine and public health. He is also responsible for the
organisation and direction of all health activities.
With the advent of family planning programme, in some States,
the designation has been charged to Director of health and
family planning. In some States a separate'Director of
medical education is also appointed tq be in charge of medical
education. The Director of health and family planning is
assisted by a suitable number of assistant director, whose
appointment may be either on regional (.basis or functional
(specialists in different branches of public health) basis.
III.
District Level
There are wide differences in the pattern of district health
organisation. The following types are seen (a) One district
chief, one District Medical officer of health, assisted by
two or more deputies. (b) Two district chiefs - in this set
..5/-
-5-
up the civil sugeon/District Medical Officer looks after the
district hospital, and sometimes all medical facilities in
the district', and the District health Officer is incharge of
public health.
People's Participation
The rural local self Government of India, 'Panchayati Raj 1
institutions are meant to ensure people's participation for
the various welfare programmes including health
*
Panchayat!
Raj institutions are elected bodies. It functions at three
levels:
1.
2.
3.
Panchayat - at the village level
Panchayat Samithi - at the block level
Zilla Parishad - at the district level.
The appointed persons of the Government infrastructure at
the district and the block level are the implementing agen
cies. The local self Government functions as a supervisory
and coordinating body.
ii.
Hee.lth Care System - distribution
The health care system of India may be defined as the" industry
which provides health services (health activities ) so as to
meet the health needs and demands of individuals and the
community." It operates in the context of the socio-economic
and political system of the country. It is represented by
the 5 major sectors or agencies which differ from each other
by the health technology applied and by the source of funds
for operation. These are:
I.
Public agencies
1. Primary Health Centres
2. Hospitals - Rural hospitals
- District hospitals
- Specialist hospitals
- Teaching hospitals
3. Health Insurance Schemes
- Employees State Insurance
- Central Govt. Health Scheme.
4. Other agencies
- Defence Services
- Railways.
II.
III.
Private agencies
1. Private hospitals, Polyclinics, Nursing homes and
dispensaries.
2, General practitioners and clinics.
Indigeous Systems of Medicine
- Ayurveda and Sidha
- Unani & Tibbi
- Homeopathy
- Unregistered practitioners.
..6/
-6IV. Voluntary Health Agencies.
V. Vertical Health Programmes.
I. Primary Health Centres: The primary health centre is defird as an “'Institution for providing comprehensive (i.e.
preventive, promotive and curative) health care services to
the people living in a defined geographic area. It seeks
to achieve its purpose by grouping under one roof or coor
dinates in some other manner all the health work of that area."
It is the minimum infrastructure for the delivery of health
care services to the rural people. The scheme started in
1952. The Centre is usually located at the headquarters
of the Block, and serves the population of the Block coining
upto 80,000 to 1,20,000 spread over in about- 100 villages.
To bring the services closer to the people 'sub-centres'
are established at the rate of one sub-centre for every
10,000 population. At present there are 5372 PHC.'s and
37,775 sub-centres (1979). The PHC provides accommodation
for an outdoor dispensary, a consultation room, accommo
dation for MCH/FP services, minor surgery, a small laboratory
and a ward of at least 6 beds, out of which 4 are maternity
beds. Since the PHC is not equipped to deal with compli
cated medical, surgical and obstetric and gynaecological
cases, it is linked up with the subdivisional and district
hospital in the region whore X-ray, laboratory and specia
list services are available.
Function of PHC:1. Medical Care
2. MCH and Family Planning
5. School health
4. Improvement of environmental sanitation with priority
for providing 'safe drinking water and disposal of human
wastes.
5. Control and Surveillance of Communicable diseases.
6. Collection and reporting of vital statistics.
7. Health Education
8. National Health Programmes - as relevent
9. Referrel Services.
Health•Team
PHC:
Medical Officers - 2
Compounder
- 1
Sanitary Inspector-1
Health Inspectors 2
Extention
Educator
,
1
(F.P)
Computer
Auxiliary Nurse
midwife
Driver
Ancillary staff
.7/
-7-
Svib Centre:
Health Worker Female (HWF)
Health Worker Male
(HWM)
Health Assistant (Male)
Health Assistant (Female)
- 1 (for 4 HWM)
- 1 (for 4 HWF)
The PHC thus provides a team work to the health problems
of the oonmiuni'by.
The sub-centres are established at the rate of one per 10000
popula-tion. Health Planners visualise one sub-centre for a
population of 5,000 or even less, in the near' future, when
resources permit.
A sub-centre with a population of 10,000 would yield?
i. Target population for family planning
- 1,500
ii. Deliveries
400
iii. Infants
400
iv. Pre-School children
- 1,500
v. School children
- 2,500
2, Hospita-ls:
Apart from primary health centres, the present organisation
of medical care by the Govt, sector consists of Rural Hospital
International hospitals (2 to 5 lakhs population), District
hospitals (1 to 2 million), specialist hospitals (eye, TE,
leprosy, cancer etc. ) and Teaching Institutions.
In addition mobile hospitals are also under trial.
Difference between Hospitals and PHC's:
Hospitals
- Curative
- No particular
catchment area
PHC's
- Curative, preventive, pro
motive and all integrated
- Catchment area - 80,000 to
1,20,000 people of about
100 villages
- Only curative staff
5. Health Insurance
Limited only to Govt, employees, eg., ESI. , Central
Health. Scheme.
Govt.
4. Other agencies: Medical services to employees of Rail
ways, Defence personnel etc.
II.
Private agencies
There are private hospitals, clinics, dispensaries and private
medical (allopathic) practitioners.
.8/-
-8-
III. Indigenous system of medicine; The practitioners of
indigenous system of medicine - Ayurveda., Sidha, Homo
eopathy, etc., provide the bulk of medical care to the rural
people.
Voluntary health agencies; They occupy an important
place in Community Health Programmes. They supplement
and guide the work of official agencies. Eg. - Indian Red
Cross Society, T.B. Association of India, Family Planning
Association of India etc.
IV.
V. Health Progra.mmc in India; Since India became free,
several measures have been undertaken by the union gover
nment to improve the health of the people. Prominent among
these are a number of vertical health programmes known as
National Health Programmes which have been launched by the
Centra.1 Govt, for the control/cradication of communicable
diseases, improvement of environmental sanitation, nutrition
and rural health. Eg. - National Malaria Eradication Pro
gramme, National T.B. Control Programme, VD Control Programme
National F.P. Programme etc.
The following table gives the number of hospitals and PHC's
in India.
1. Number of hospitals and disicnsaries
2. Number of PHC's
3. Number of Subcentres
4. Hospital Beds
- 17607 (1977)
- 5372(1979)
- 37775(1979)
-449212 (1979)
This table represents the totals at the all India level.
Those do not, however, represent the rural and urba.n split
up figures.
In spite of all the schemes briefed in the previous para
graphs, eight out of ten Indians have little or no access to
modern medicine. The number of doctors in 1980 was2,53,631.
A WHO study mentions that India has sufficinet number of
doctors. But the problem is the lack ofadistribution system
which equally gives importance to rural and urban areas.
Thus the existing health personnel can hardly meet the needs
of the people. The ratio of the hospital bed and population,
is 0.49 pe^
*
1000 population. The doctor population ratio
is 1:4400. When taking split up figures for the rural and
urban areas, rural area has the ratio 1;20,700 and the urban
area has 1:1,300. Thus the rural folk suffers seriously
from lack of enough number of doctors. 80$ of the Indian
population live in villages. But 80$ of our health care
facilities and personnel are in the urban entres catering to
the needs of a minority of the Indian population (20$ of
population). This fact explains the ill-health of the
majority of Indian population. The very same fact explains
the high incidence of infant mortality, spread of communi
cable diseases and high death rate. The Indian child succ
umbs to death due to some diseaseswhich are generally
preventive if sufficiently cared for at- the proper time.
9/
-9Horo again, the reason could be attributed to the general
inaccessibility of the Indian population to the health care
facilities in spite of continued establishment of hospitals
both in tho government and private sector.
(b) Availability of health care facilities to the Poor;
We have already seen tho disparity in the distribution of
health care facilities and the doctor population ratio for
tho rural and urban areas. As mentioned already, this
disparity its.If is one of the main reasons as to why majo
rity of our population - poorer sections of the society
dwelling mostly in rural areas - are denied the right to
adequate health care.
Government a.nd private health care services are available in
India. As already mentioned the Government has started some
rural health programmes. But certain impediments stand in
the way as:a. lack of participation of the people - which develops
a certain apathy and disinterest towards the Govern
mental programme, thus affecting seriously the desired
objective of being of help to tho very sarnie people.
Co-operation of tho people and the health personnel
is vital.
There
b.
is a. certain attraction to work in the urban
areas and the health personnel lack tho motivation to
work in the rural areas. This is a very clear phenomena
found everywhere. This problem is dealt with under
a separate heading. Hence when -the medical officer
or health worker is placed in a rural area he will not
commit himself fully but will try for a transfer to the
more convenient urban centre.
c. In the annual budget allocation, sufficient funds are
not available to the rural centre for the purchase of
medicines and the maintenance of other facilities of
the health centre. Lack of follow up thus gravely
affects the health programmes. 75$ of the budget allo
cations are for maintaining staff, 12% for transport,
12% for drugs and 1% for innovative experiments. When
we take rural outlays it is seen that they are remar
kably lesser when compared with the corresponding
urban allocations.
The Constitution of India has considered health care as a
basic need of the citizens and has assured that it should
reach to the people. But the people cannot expect good
service from the Government health centres. Boor maintenance
and lack of facilities are two main reasons. Health care
centres as LHC's and sub-centres present a very poor show.
District hospitals also do not come upto to tho mark.
Medical colleges and sophisticated Governmental institutions
are generally equipped with- all the modern medical access
ories with specialists for each branch. Medication at
these Centres are, however, controlled by money power.
Corruption has eroded' public life and health care insti
tutions are a.lso no exception to this phenomenon. Private
..10/
-10-
practice of Government doctors worsen the situation still.
All these form a vicious circle in which the poor man is
denied of his'right to proper health care. Thus proper
medical care remains unaccessiblo and unapproachable to the
poor. This is the case of the subsidized Government run
medical institutions.
Another area for health care is the private sector. Differen
private agencies are running hospitals though out the country
As a non-state-supported system this has to be self-support
ing. It has to make its own funds to have enough stock of
the rapidly progressing varied modern drugs, to give high
salary to the doctors and to maintain the large buildings
and sophisticated equipments. High costs of institutionali
zation, sophistication and specialization have to be met
from its own resources. They cannot help but adopt a comm
ercial line. The private sector offers efficient service.
But this works only with money. Depending upon the serious
ness of the disease and the use of medicines, .specialists and
modern equipments the service cha.rges go up. 'Comfortable
and hygeinic accommodation is assured on payment of suffici
ent money. The poor, who is handicapped with the lack of
money, is denied the services of this efficiently working
private health care centres.
The treatment provided to the patients right from diagnosis
and the medication practices followed in our health institu
tions are far from the real life situations and economic
conditions of the poor. The diagnosis process itself grabs
whatever little earning the poor may have. Then the poor
finds it impossible to afford the highly priced prescriptions
that follow. It is sad to note that little effort is made
to research on a treatment and medication process that suits
this poor nation. The present medication practices cater
to the benefit of the drug industrialists and the commerci
alized hea.lth care institutions and not to the care of the
people.
Apart from these economic factors there are certain social
and cultural factors which prevent the poor from giving su
fficient attention to their health and approaching health
care institutions. Their concept of health and disease
are very much misleading. They are not health conscious.
Rural experiences of various health teams suggest that a
villager considers himself sick only at a later stage when
the disease has made its full appearance. Again certain
diseases are taken for granted that they will not create
serious threats to the general physical well being. In
certain remote villages their first resort is 'Hoja',
certain superstitious practices based on 'Manthra' and
'Magics'. Modern medicine is the last and final resort,
often due to the compulsion of few who had had some exper
ience with modern medicine. Certain diseases as chicken
pox are considered to be the blessing of certain goddesses.
Lack of awareness regarding hygiene, food preparation, sani
tation, drainage, care during pregnancy, conducting deliverty, care of infants are only a few instances which show
how certain cultural practices and lack of education seri
ously affect the life of the poor. Coupled with this socio
cultural factors' are the economic incapability of the poor
..11/-
-11to approach the corniercializcd modern medicine. Distance
to the nodical centres and lack of enough competent medical
personnel in backward areas make the situation still worse.
Problems connected with the dearth of competent personnel
are being dealt with under the next heading.
c.
Problems of medical personnel in rural areas:
*
The training and motivation of the health personnel is very
important as regards' rural health work.- Speaking of training,
just like any other branch of education, medical education
also should be sensitive to the social environment of the
community which it seeks to serve, and constantly adapt it
self to the changing requirements. The motivational part
of the person is greatly influenced by the content and value
orientations of the training. In the paragraphs that follow
the descriptions are mainly about doctors, since, in the
present set up, even in the rural areas, the graduate doctor
remains the chief person as regards health care.
The present medical educational system is strictly hospital
based and westernized and hence tho doctors do not inher it
an aptitude or attitude to work in the circumstances and
atmosphere of rural India. Tho doctors also lack an under
standing of the social, cultural and religious concepts of
health and disease in rural India as well as the attitudes
and practices concerned with food, child-birth, child care
and general health care. Similarly there have been very
many traditional systems of medical care. The modern system
of medicine takes much time to gain acceptance in Indian
villages. ‘It is a basic question of cultural difference.
Also it should be noted that certain traditional ways of
health care are .advisable for certain diseases. Thus it
counter acts the many adverse effects of modern medicine.
The modern medical education does not consider these cultural
factors in health care. And also, generally a modern doctor
has but contempt for tho "uncivilized, uneducated" villager
in the place of respect as an individual.
Apart from these, a doctor working in rural area is exposed
to the following problems:- Inadequate living conditions and inability to maintain
an urban standard of living which most medical students
become used to.
- Poor or relatively poor financial remuneration and/or
allowances/compensation.
- Problems of adjustment when accompanied by wife and
young children, especially the education of tho latter.
- Objection of families to rural work especially because
of a lower social status in the profession.
* This part of the paper was prepared after closely
referring 'Trends in under-graduate medical education
in India', prepared by Dr. Ravi Narayan.
12/
-12- Social isolation, because of an inability to fit in with
the simple rural way of life, (more pronounced when the
doctor comes from a predominantly urban background)
--apport and contact between urban and rural commu
nities to an extnnt, which ma.kes a doctor feel complete
ly 'out of place' or 'cut off' in the rural areas.
- Intellectual isolation and inadequate opportunity to
maintain professional compontence or to gain post gra
duate experience under supervision.
- Problems of political interference in work and often
poor relations with local government officials, leading
to frequent transfers.
- Problem of interpersonal relationships with other members
of the team, especially when many are older to him and
have had longer contact with the local people.
- Presence
and, often, professional competition with
practitioners of other indigenous systems of medicine.
- Another major obstacle to attracting doctors to rural
areas is the attitude of the medical profession to rural
work, especially in the light of the present day 'ideal
*
of specialist practice in the large cities. This reflects
a general trend towards an intensely materialistic orien
tation of the medical profession. Consequently, the
preparation and motivation for rural work in the medical
college curriculam has always been inadequate.
Now, Wath this we shall pass on to another important ares
of concern 'DRUGS'.
(d) Manufacture and Distribution of Drugs:
ihe structure of drug industry embodies all the essential
features of the industrial economy of India. Thus, like in
the case of any other industry, profit orientation, monopo
lization, promotion of multi-national corporations, compli
mentary role of public sector etc., are seen hero also.
Drug costs represent 40-60$ of the total health care expen
diture in developing countries like India. In developed
countries the corresponding figure is only 10-20$.
Let us have an enquiry into the reasons for such an unde:. sirable state. Let us now examine some of the evil effects
the industrial and commercial nature of drug manufacturing
brings in:
Production for profit;- Just like any other industry here
too production is based on demand and hence profit. Since
majority of the Indian people are below the poverty line they
find it hard to purchase medicine. The per capita consum
ption of medicine in India is only Rs. 5/-. According to
1973 calculation, 80% of the drugs produced in India are
bought by 20%. The rest of the population shares only the
remaining 20%.
Monopolies:- According to 1973 calculation, out of Rs.370
crores worth of drugs produced by 2300 firms in India.
Rs. 296 crores/of drugs were produced by 110 firms (4% of /worth
the total). Of these 110,'28 are foreign owned or
..13/-
-13collaborated firms and they account for 40% of the total
production. Always production is meant for profit. Artifi
cial scarcity is created by few monopolies coming together.
This is to increase the price. If the full capacity of the
factories are utilized the common man would have got medi
cines at a comparatively low price. The monopolies decide
the price which doos not at all correspond to the real cost
of production.
eg: Bulk soiling price of chloramphenicol is 3 times
its production cost.
Tetracycline it is 2.7 times.
Retail price will be still higher
Chlord^henicol - Bulk selling price - $s. 400/- kg
Retail price
- Rs. 3,050/- kg
For Vit. B.|2 the retail price is 20 times the
bulk selling price.
For Vit. 0
the retail price is 5 times the
bulk selling price.
Corresponding figures for Folic acid & Tetracycline
are 9»2 and 4.5 times respectively.
Multinational corporations:for 40% of total production.
As stated earlier, they account
In pricing they are still worse,
Eg. while we import Librium at Rs. 312/-kg it is\
produced by a Swiss firm in India for Rs. 5555/r- kg.
Another foreign firm was charging Rs. 60,000/-kg for Dexame
thasone which was later reduced to Rs. 16,000/-kg.
Another usual practice is that the subsidiary of the foreign
firm in India buys the penultimate product from its parent
company at high rates, makes the final product, stamps it
as made in India and sells it at fantastically high rates.
The aim of production and resea.rch cither in India or abroad
remains that of maximizing profits.
Public Sector:- The public sector do not. curb the fraudulent
practices of the private firms but they compliment it. One
example could be that Hindustan Antibiotics Ltd. sell Stre
ptomycin at Rs. 345/- kg in retail, whore as the same medicine
is sold to private sector at Rs. 195/-kg which in turn takes
the profit.
Another public sector firm sell 54% of its bulk production
to private firms. Just like other fields of industry here
too public sector sells its semi-finished products to the
private firms which take huge profits on the finished pro
ducts. Thus the people's taxes arc used to make profits to
few giants. All these are some of the examples to show the
fraudulent practices in drug industry. The data regarding
the pricing had been of 1973 - 1974 period. After that the
14/
-14situation night have become worse or in few exceptional cases
improved little. It has.yet to be found out. The data pre
sented above are a few indicators as to how the drug industry
exploits the common man. With the development of pharmacology
and chemical engineering it is possible to distribute com
paratively cheap drugs on a la.rge scale to all needy. But
the social organization of our economy is such that the aim
of production becomes profit oriented.
Advertisements: The advertisements cheat the people misera
bly. Evon medical practitioners are deceived by attractive
advertisements of different medicines. A case of deception
of the common man by advertisements could be "breast-feeding”.
The people arc attracted by baby-foods and there had been
instances to show that while a poor man had even no sufficient
income to feed his family ho resorted to baby-foods thinking
of breast feeding as socondory.
Use of Drugs: The promotional practices of drug compa.nies,
aimed at maximizing profits, liave been directly counter to the
health needs of the poorest. The brunt of wasteful spending
falls on the poorest, as.the rural dispensaries run short of
vital life saving drugs. Apart from promotion of unnecess
arily expensive, but necessary drugs, doctors are also encour
aged into wasteful over prescribing '0£ non-essential tranqu
ilizers, symptom^ allaying drugs and tonics. Similarly
drugs freely promoted in the absence of distribution controls
can also cause serious dangers.
The existing system of qua.lity control of drugs is not
satisfactory. 600 drug inspectors in India. ha.ve to check
30,000 drug formulations. The beurocratic defects worsen
the situation still-decision making, implementing decisions,
etc. The marketing of most brand - named drugs especially
by the multinationals in the third world works against the
health of the poor. Also, drugs banned in the west or used
under severe restrictions always continue to be liberally
used in India eg. anabolic steroids, analgin etc.
Bearing in mind the very limited effectiveness of drugs and
curative medicine in tackling the health problems - mal
nutrition, inf ections and parasitic diseases - public funds
would be far better spend on preventive health measures and
the basic primary health care infrastructure. For this,
WHO estimates that 200 genuine drugs would be more than
sufficient to moot the health needs.
Orientation towa.rds "appropriate use of drugs" has to yet
bo developed. Our proscription practices have to bo modi
fied according to the needs of the people. Our choice of
drugs for stocking in the pharmacy should be according to
this. Most important of all, the emphasis has to be oh
people taking responsibility for their health and avoiding
those drugs as far as possible and rrieg those "non-drug
therapies" that have boon recognized to have good therapeutic
effect. Education and awareness as to how to avoid disease
and then, how to handlo it appropriately at the lowest possi
ble cost is the crux of our a.pproach in low cost appropriate
health care.
..15/-
-15Conclusion:- A brief enquiry has been made into the general
edistribution of health care facilities and health personnel
in India. Availability of service to tho rural (poor) popu
lation has been the c_ore of the discussion, since the
problens of villa.ges represent the problems of the entire
country. Health care in India is being situated in the
context of the existing socio-politico-ccononic realities.
Problems and issues have been raised in this context. It
is hoped, these would serve as certain indicators in the
search for the right type of health services for this under
developed country.
Certain references:
Patil Ashwin J- In Search of Diagnosis.
Indian Council of Social
5
Science Research and Indian5 Health for all - An
Council of Medical Resca.rchJ alternative strategy
The National Health Policy
of India.
Volun+': yyHealth Association^
of India
$
Information (Journal)
PREPARED BY: THE CATHOLIC HOSPITAL ASSOCIATION OF INDIA
C.B.C.I. CENTRE
ASHOK PLACE, GOLDAKKHANA
NEW DELHI 110 001.
Voluntary Health Association of India
Telegrams': VOLHEALTH
C-14, Community Centre
Safdarjung Development Area
New Delhi-110016
New Delhi-110016
, ,
668071
Telephones :
ODoO/Z
0-9/248(a)
*RR:m:10.10.85
HEALTH STATUS OF INDIA
After almost thirty-five years of planning, we may ask
whether, end how much, India has progressed. Only true facts
can answer this question. Achievements and failures should be
neither magnified net played down, as it is often done.
This handout therefore uses the available data . and gives
an overall picture of the present health situation, taking
into consideration both the achievements and the failures in
their f naked forms.
TABLE I
Health Indicators & Birth/Pop. Growth Rates.
Year
Birth
Rate
Death
Rate
IMR
Life
expectancy
at birth
32.1
41.3
45.6
52.1
Pop.
Growth
Rate
12.5
18.9
22.2
20.9
1941-51
39.9
27.4
134
1951-61
41.7
22.8
146
41.2
19.00
138
1961-71
1980
33.3
12.4
127
Mortality Rates
India's health standards are still extremely low.
Compared to developed countries and. several developing
countries, the death rate and IMR of cur country remain
quite high, and its life expectancy rather low. On all these
grounds, the health situation of India is far below the
Asian and world average.
TABLE 2.
International Comparisons Around 1978
Country/
Continent
Life
exp ectancy
at birth_______
Africa
49
46
142
29
17
58
Asia
31
93
19
12
Brazil
61
37.1
77
8.8
28.3
China
65
45
26,7
10.2
16.5
Cuba
73
28.9
19.3
5.9
22.1
53
Egypt
37.6
101.3
10.5
27.1
India
52
33.3
127
20.9
14.2
Malaysia
53
31.8
30.7
6.3
24.4
Pakistan
50
46.8
126
16.7
30.1
Srilanka
65
29.9
7.8
45.1
22.1
USA
74
15.3
8.8
14
6.5
USSR
18.1 . 9.6
70
27.7
8.5
World
29
61
11
18
91
12. Compiled from HS 1982., P.24; HS 1981, PP.l 89-91;
"1982 World 's Children Data Sheet", Population Reference
Bureau Inc. & UNICEF; and World Bank., "Health" , PP.72-3.
Birth
Rate
Death
Rate
Pop.Growth
Rate
IMR
contd
C-9/248(a)
; 2 :
ARR:m:10.10.85
The importance of environmental hygiene is recognized
by all. It has even beenestimated that 60 to 70% of Indians
health problems would disappear withks safe drinking water
and sound sanitation. Following table tells us how
deplorable and alarming is the situation! About 83% of
the urban population has some provision for protected
water supply, but "cnly about 64,000 (10.4%) villages have
adequate water supply of acceptable quality (40,000 of them
have been provided with these facilities during the plan
periods). About 21s,000 (34.7%) villages have adequate
but unprotected sources; and 153,000 (24.9%) are problem
villages (i.e. villages with inadequate water supplies or
infested with endemic cholera, guinea-worm and other health
hazards)."
TABLE 3
Water Supply & Sanitation
Protected Water supply
Sound excreta disposal
Rural
Urban
Rural
Urban
Population %
10
80
2
34
Tuberculosis; About 9 Mn.people suffer from active T.B.
out of which 2.24 are infectious.
1980 - 6.1 lac tuberculosis cases and 8,962 Deaths on an
average. About 5 lac Deaths every year.
Leprosy
- 1/3 of world's Leprosy is in India.
50% ofthe population of India is at risk.
1971 - 3.35 million Leprosy cases
1981
4
"
"
"
25% infectious, 25% have deformities.
Fialaria
1953
1976
25.9 million
236.13 million
174 million live in villages.
Sexually transmitted .disease ; - 20 million suffer from it
and number is increasing.
Mentally retardeds 20 million'
Mentally ill 4-5 million out of which 1.5 million need
Institutions , 3 million need tratment.
contd..
C-9/248(a)
ARR:m:10.10.85
.
'
J *
Blind
9 million
6 million need surgery
1 million new .cases of catract added each year.
25,000 children become blind every year, on
account of vitamin A deficiency. 2-150% of/children
/all
suffer from milder form of Vitamin A deficiency.
Women & Children
Below 15 years - 265 millions in 1983,40% of total population.
Children under 5 year,
15% of total population , 1/3 of total deaths is in children.
50% of infant deaths'occur below one month of age.
Only 20-30% babies are born with the help of trained doctors
& Midwife.
30% of the new born in Inda have less than 2.2 kg weight
at birth. Average weight at birth .
in poor families
2.8 kg in rich class it is 3.2.kg. 75% of pre school children
are below 75% of s :andard weight of well nourished children.
60,000 women die every year in India due to childbirth.
20% suffer from aneamia. 6 million abortion takes place
annually. 4 million of them are induced.
No.of children born on art average to an
Indian women are
4.8
USA
1.9
Cuba
2.3
USSR .
"
2.4
China.
•2.5
Malnutrition 65% of Indian in lower income group suffer
from malnutrition.
1973-60 million are badly malnutraised.
Infants
- (0-1 yr)
P.E.M. - 1.5%
Vitamin A deficiency 0.55%
Vitamin B.complex deficiency not reported.
Preschool
P.E.M - 0.23%
Vit,A.Deficiency 4.0%
B.Complex
"
4.6%
School Children .
.. ’*
P.E.M.
0 - 40%
Vit.A Deficiency ; 10.0%
B.Complex "
11.7%
Womens
Vitamin A deficiency s 5.99%
B.Complex
“
3.8%
Aneamia
30%
P.E.M. : Protien - Energy - Malnutrition.
contd,
. 4 .
C-9/248(a)
ARR:m:10.10.85
HEALTH CARE PYRAMID
Specialis«
from outside
the
community
------- Expe5^es?f 2
Med.students/new .doctors 3
N'urses/paramedics 4
auxiliaries 5
Within th
community
Primary health
6
workers
Mothers &s choolchiId ren7
Communitv 8
David Werner;
Contadt/Aug 1980/57
HEALTH CARE CONTINUUM
12-3
-4
3
6
7
8
primary health
workers
mothers & school
children
community
THE CATHOLIC HOSPITAL ASSOCIATION OF INDIA
Community Health Department
Grams
Post Box 2126
CEEHAI
SECUNDERABAD 500 003
Telephones : 848293, 84 84 57
Telex
: 0425 6674 CHAI IN
:
157/6 Staff Road
SECUNDERABAD 500003
ANALYSIS OF THE PRESENT HEALTH CARE DELIVERY SYSTEM IN INDIA.
Forty years after independence India on the road to development
is now facing a serious crises, India's population continues to
grow at an alarming rate' and the health conditions of the masses
remain distressingly low. Our health services are manifestedly
inadequate and ineffective, especially in rural areas and fail
to cover 70 to 80% of our population,
India is the 11th poorest country in the world with the 2nd
highest population of 762 crores (1986). India's infant mortality
rate is still a deplorable 105/1000. 1.5 million children lives
are taken by diarrhoea alone. There are more than 60 million
children in India who are malnourished; four million cases of
leprosy of which 15% are children less than 14 years. Tuberculosis
amounts for 9-10 million cases of which 2-3 million are
open cases. 50% of all lactating and pregnant mothers suffer
from anemia. Children affected by polio are'on the increase;
more than120,000 are affected of which 80% are below 3 years of
age and despite the efforts towards universal immunization the
numbers keep growing. One million (11,18,948) and more of the
population is disabled due to one reason or the other. All these
are important indicators of the Health Status of the Indians.
And after 4 decades of post Independence planning we may ask
whether and how much India has progressed. Only true facts can
answer this question. Achievements and failure should be neither
magnified or played down as it is often done. The institutional
and manpower growth of our health care system is impressive.
We now have a ministry of Health and Family welfare at the
centre and in the states, large departments of public health
and medical organisations and institutions. Excellent specialized
facilities are available for cardiac diseases, cancer and
neurological and nephrological disorders, A huge infrastructure
of hospitals, dispensaries, subsidiary centres, community health
centres, Primary Health centres has been built. The number of
health professionals and paramedical workers have remarkably
increased. The number of institutions and practitioners in the
Indegenous system of medicine indicate a considerable though
less striking growth. Though many of these health institutions
and personnel serve the upper and middle classes in todays'
society, they could be put to better use. We have every right
to be proud of these achievements. Yet one must also look
at the negative side of the health situation and acknowledge
that "our failures are even more glaring than our successes.
Inside our big hospitals and private nursing homes, we find
modern amenities, highly qualified experts. Outside their
walls, poverty and disease march bleakly over the landscape."
A deeper study of martality rates, disease patterns and conditions
children and women reveals a distressing situation. The poor
coverage and inbuilt inequalities of our health system are
other key elements of this deplorable and unjust situation.
Every human being possess the right to life and health and to
the necessities of life, including proper medical services.
With its commitment to justice, liberty, equality and
fraternity, the Constitution of India clearly recognizes the
Governments' responsibility for health.
2■
2
The world at l^rge and India in particular continue to experience
"the poverty of health in the midst of scientific abundance" and
glaring inequalities in health resources. While basic health
services remain inaccessible to more than the two thirds of
humanity and millions of poor die of easily preventable diseases,
the rich enjoy even more specialized facilities. Most villages
hu.-o no proper health personnel and services, while cities are
saturated with doctors and medical centres, Health which is
claimed to.be right of every individual is in reality a
privilege of the relatively few wealthy.
The Alma Ata delegates at the International conference in Sept.
1978 saw health as a fundamental human right and stated that
"The attainment of the highest possible level of health is a
most important world-wide social goal whose realization requires
the action of many other social and economic sectors in
addition to the health sector. It strongly affirmed the need
of primary health care to achieve an acceptable level of health
by all people by the year 2000 and to reduce todays gross
inequalities which are 'politically, socially and economically
unacceptable'.
According to the 1984 statistics 37.4% of India's population is
below the poverty line, unofficial calculations however suggest
a much higher figure. Dr. Mahler gave the call "Health for all by
the year 2000 A.D." at the 1977 WHO. According to him 'the
present realities of the 3rd world are simply unacceptable.
There is little joy in life now nor any kind of justice for a
child condemned to disease or early death because of the accident
of birth in a developing country... There is no rationale that
can defend a system that withholds the gift of health and care
from nine tenths of a nation's population
.
*
'Resources distri
bution in the medical sector is such that 80 to 90% of the resources
go to meet 10 - 15% of the health problems. Social and economic
inequalities and powerlessness prohibit the people from the
knowledge and the capacity to afford the health care of their
family. In equalities exist at two levels :
1.
2.
—
In the distribution of the health care services
In the capacity of the people to afford to maintain good
health. These two areas make up the central theme of this
paper. We shall follow a sequence and order based on the
following points".
a.
The present health care delivery system in India and its
distribution in the rural and urban centres.
Availability of these facilities to different economic
classes and medication practices.
Manufacture and distribution of drugs.
b.
c.
Our National Health Policy :
The Government adopted a new "National Health Policy" in August
1983 and recomitted India to "the goal of 'Health for all by
2000 A.D! through the universal provision of comprehensive
Primary health care services".
The policy confirms the trend in favour of restructuring the health
services emphasising community, preventive and promotive health
linked to a hierarchy of referral services and integrated with
human development and poverty alleviation programmes. People
must be required to take health into their own hands
3
- 3 through community health volunteers, traditional birth attendants
and practitioners f indegenous medicine, all of them trained
and equipped to make appropriate interventions at given livels
backed up by supporting services. The efforts must be to move
from expensive hospital, drug based curative services, largely
confined to the middle and upper urban strata, to reaching
health to the people where they are and in particular, to
vulnerable segments and backward regions
An analysis of the National Health Policy reveals some striking
difference with the 'Health for all documents'. First the
Government emphasis is much more on poverty alleviation that: on
the reduction of inequalities and the organization of the
oppressed to defend their rights. The policy does not speak
even once of social justice in health and in other fields.
The essential pre requisites to attain the goal 'Health for
all' are completely bypasses, there is no definite and far
reaching programme to promote community participation in important
matters. There is no radical change in the health budget, while
insisting on Primary Health Care, the policy is concerned with
private practice, paying clinics and the establishment of
specialist centres. The attainment of 'Health for all' is
intimately related to the eradication of poverty, inequality
and ignorance. There can be no lasting solution to the country's
health problems, unless and until the illnesses affecting
the society at large are tackled side by side.
Health care delivery system in India °
The challenge that exists today in many countries is to reach
the whole population with adequate health care services and to
ensure their utilization. The large hospital which was chosen
for the delivery of health services has failed in the sense that
it serves only a small part of the population. Therefore it has
been aptly said that these large hospitals are more ivory
towers of disease than centres for the delivery of comprehensive
health care services.
Administrative set up at the Centre, State, and District level :
The health system in India has 3 main links i.e Central, State
and Local.
I.
At the Centre :
The official organs of the health system at the national level
consists of :
1. The Ministry of Health and Family Welfare
2. The Directorate General of Health Services
3.
The Central Council of Health and Family Welfare.
1.
The union ministry of health and family welfare is headed
by a cabinet minister, a minister of state and a deputy health
minister. There are political appointments. The union ministry
has the following departments :
i
ii
Department of Health
Department of Family Welfare
The functions of the Union Health Ministry :
a
International Health relations and administration of post
Gurantine.
4
- 4 b
c
d
e
f
g
H
Administration of central institutions
Promotion of research through research centres and other
bodies
Regulation and development of medical, pharmaceutical,
dental and nursing professions.
Establishment and maintenance of drug standard.
Census, collection and publication of other statistical data.
Emigration and Immunization
Coordination with states and with other ministries for
promotion of health.
It is-the responsibility of both the centre and state for
1
2
3
4
5
6
7
8
Prevention of extension of communicable disease
Prevention of adulteration of foodstuffs
Control of drugs and poisons
Vital statistics
Labour welfare
Ports other than major
Economic, and social planning
Population control and family planning
2.
Directorate General of Health Services :
(
The director general of health service is the principal advisor
to the Union Government, in both medical and public health matters.
The General functions are survery, planning, coordination,
programming and appraisal of all health matters in the country.
The specific functions are :
.
a International health relations and quarantine
b Control of drug standards
c Medical stores depots
.
d Post-Graduate training
e Medical education
f Medical research
g Central Government Health Scheme
h National Health Programmes
i Central education Bureau
j Health Intelligence
k National Medical Library
3. Central Council of Health : A large number of health subjects
fall in the concurrent list which calls for concurrent list which
calls for continuous consultation, understanding and cooperation
between the centre and the states.
The functions of the Central council of Health are :
a To consider and recommend broad lines of policy in regard
to matters concerning health in all its aspects.
b To make proposals for legislation in fields of activity
relating to medical and public health matters
5
- 5 c
d
II
To make recommendations to the Central Government regarding
distribution of available grants-in-aid for health purposes.
To establish any organisations invested with appropriate
functions for promoting and maintaining cooperation
between the central and state health administration.
At the State Level : There are 25 states in India. In all the
states the management sector comprises the state ministry of health
and a Directorate of Health. The State Ministry of Health is
headed by a Minister of Health and Family Welfare and a Deputy
Minister. The Director of Health service is the chief technical
advisor to the State Government on all matters relating to
medicine and public Health. He is also responsible for the
organisation and direction cf all health activities. A recent
development in some states is the appointment of a Director of
Medical Education in view of the increasing number of medical
'colleges.
II At the District Level ; The principal unit of administration
in India is the district under a collector. Most districts in
India are divided into two or more subdivisions each taken care
of by an Assistant or Sub Collector. Each division is again
divided into taluks. Since the launching of the community
development programme in India in 1952, the rural areas of the
district have been organised into community development blocks
each with approximately 100 villages and a population of about
80 to 1,20,000 under a block development officer. Finally
there are village panchayats which are- institutions of rural
local self-government. The urban areas of the district are
organised into the following ;
Four area committee
- Municipal boards
Corporations
Under the multipurpose workers scheme, it has been suggested to
the states to have an intergrated set-up at the district level
by having a chief medical officer with three deputy CMO's.
The recent working groups on health for all by 2000 A.D.
recommended that the District Hospitals should be converted into
district health centres each centre monitoring all preventive,
promotive and curative services of one million population.
The Panchayat Raj is a 3 tier structure of rural local self
government in India.
1 , At the village level the Panchayate Raj consists of
a) The gram Sabha
b) The Gram Panchayat
c) The Nyaya Panchayat
2.
At the block level the Panchayate Raj consists of Panchayat
Samithi. The Panchayat Samithi consists of all Sarpanchas.
3.
The Zila Parishad is the agency of rural local self government
at the district level.
Health Care cf the Community :
The frontiers of health extend beyond the narrow limits of
medical care. Health care covers a broad spectrum of personal
health services ranging from health education and information
through prevention of disease, early diagnosis and treatment
and rehabilitation.
6
- 6 Two major themes have emerged in recent years in the delivery of
health services :
a)
b)
Health service should be organised to meet the needs of
the entire population and not merely selected groups. Health
services should cover the full range of preventive, curative
and rehabilitation services.
The best way to provide health care to the vast majority of
rural people and urban poor is to develop effective
Primary- Health care services supported by an appropriate
referral system.
Levels of Health Care :
P£ima£y_Level.
The first level is usually the point of
con?6ct""5efween the individual and the health system, where
primary health care or 'essential health' is delivered. The
primary health care insitutions in rural India are the
primary health centres and their subcentres. Although there
is a vast network of primary health centres and subcentres in
the country, experience over the past three decades has
shown that PHCs and their subcentres have not been able to
meet effectively the minimum health need of the vast majority
of the rural population. In orderto remedy this, defect,
the government of India in 1977, under its new Rural Health
Scheme, adopted an alternative strategy of delivering primary.
health care through the agency of village health guides
(community health workers). The CLW is a volunteer from the
village itself and is selected by the village community. Besides
providing, primary health care, the village health guide or ■
CLW bridges the cultural and communication gap between the
rural people and the organised health sector.
1 .
2.
Intermediate level : At this level more complex problems are
dealt with. The sub divisional/district hospitals mainly
constitute the second level. They also provide support to
the primary health care institution.
3.
Central Level : This comprises 'Tertiary Care' or super specialist care. This is provided by the central level insti
tutions (e.g. Regional Hospitals, Medical College Hospitals)
They not only provide highly specialized care but also
sustain primary health care as part of a comprehensive
national health system.
Health Care Services :
Thehealth care system is intended to deliver the health care
services. It operates in the context of the socio economic
and political framework of the country. It is represented
by five major sectors.
1.
Public Sector
1. Rural Health Scheme
Primary Health Centres
Sub Centres.
2. Hospitals/Health Centres
Community Health Centres
Rural Hospitals
District Hospital/Health Centre
Specialist Hospitals
Teaching Hospitals
3. Health Insurance Scheme
Employees State Insurance
Central Govt. Health Scheme
- 7 -
4.
Other agencies
Defence Services
Railways
II. PRIVATE SECTOR :
1.
Private Hospitals, Polyclinics, Nursing Homes
and Dispensaries
2. General Practitioners and Clinics.
Ill
Indigenous systems of medicine :
1. Ayurveda and Siddha
2, Unani and Tibbi
3. Homeopathy
’ Unregistered parctitioners
IV. Voluntary Health Agencies
V. Vertical Health Programmes.
PRIMARY HEALTH CENTRE |
Health planners in India have visualised the primary health
centre and its subcentres as the minimum 'infrastructure' for
the delivery of health care services to the people in rural
areas.
FUNCTIONS OF THE PHC :
a.
b.
c.
d.
e.
f.
g.
h.
i.
Medical care
MCH and Family Planning
Improvement of environmental sanitation with priority for
providing safe drinking water, disposal of human waies.
-Control and surveillance of communicable diseases
Collection and reporting of vital statistics
Health education
National Health Programmes
Referral services
Training of village health guides, health workers and
health assistants.
Health team at PHC :
Medical ifficers
- 2
Compounder
- 1
Sanitary Inspector
- 1
Health Inspectors'
- .2
Extension Educator (FP) - 1
C omputer
- 1
ANM
- 1
Driver
- 1
Ancillary staff
- .2
8
- 8
At each sub.centre
Health worker (f)
Health worker (M)
Health assistant (M)
Health Assistant (f)
- 1
- 1
- 1
- 1
The PHC thus represents a TEAM approach to the health problems
of the community.
Community Health Centres : A few PCH's have been upgraded to
CHC's which has been established for coverage of '-ne lakh
population with 30 beds and specialized medical care services in
gynaecology and obstetrics, pediatrics, surgery and medicine.
It has been recommended that one of the doctors at the community
centre level may be from one of the locally acceptable traditional
systems of medicine and one of them must possess public health
qualifications and experience.
2) HOSPITALS : Apart from the primary health centres, the present
orgination of health services by the Government Sectors consists
of rural hospitals, district, hospitals, specialist hospitals
and teaching institutions.
/
a. Rural Hospitals :
It is now proposed to upgrade the rural dispensaries (allopa
thic/ traditional systems of medicine) to primary health
centres. At present a good number of PHCs are located at
tehsils/taluka head quarters which also have hospitals.
Such PHCs may be shifted to the interior rural areas.
b. District Hospitals : There arq/joroposals to convert the
district hospitals into District health centres. Hospital differs
from a health centre in the following respects.
Hospitals
Health Centre
1
Curative services
Preventive, promotive and
curative
2
No catchment area
Has a definite population 80,000
to 1,20,000 to cater to
3
Curative staff
’Mix’ of medical & Paramedical
workers.
3)
HEALTH INSURANCE :
There is no universal health insurance in
India. At present it is limited to industrial workers and their
families. The Employment State Insurance Scheme provides compre
hensive medical care to industrial workers. The central Govt.
Health Scheme provides comprehensive medical-care to central
Govt, employees. The above two schemes cover two large groups
of wage earners in the country. '
4) OTHER AGENCIES :
1 Defence services have their own organization for medical care
to defense personnel. The railways provide comprehensive health
care services through the agency of Railway hospitals, Health
units and clinics.
2 Private Agencies ; Private practice of medicine provides a
large share of the health services available. The general
practitioners constitute 70% of the medical profession. They
provide mainly curative services. Most of them tend to congre
gate in urban areas. The private sector of the health care
services in not organized. ■
9
- 9 -
3
4
5
Indigenous systems of medicine : The practitioners of indi
genous systems of medicine eg. Ayurveda, Siddha provide the bulk
of medical care to the rural people.
Voluntary Health Agencies : The voluntary health agencies
occupy an important place in community health programmes.
The type of service rendered by voluntary health agencies
have been classified as :i Supplementing the work of official agencies
ii Pioneering - new ways and means of doing new things.
Research is one form of pioneering.
Vertical Health Programmes in India ;
Since India became free, several measures have been undertaken
by the government to improve the health of the people. Most
of the programmes have been aided by the International Health
Agencies such as the WHO, UNICEF, USAID, Rocketeller
Foundation etc. These vertical health programmes have been
launched for the control /eradication of communicable diseases,
improvement of environmental sanitation, nutrition and rural
health, e.g. The National Malaria eradication programme,
Diarrhoeal Diseases, Control Programme, National filaria
Control Programme, National T.B. Control Programme etc.
Availability of Health Care Facilities to the Poor
Widespread poverty, malnuturtion and ignorance, insufficient
and or unsafe water supply and many other evils still plague the
countryside. Our health services do not cover the 70 -,80% poor.
The prevalent model of health care is irrelevant for several
reasons. Instead of responding to the specific problems, needs
and aspirations of Indians and being attuned to their customs
and traditions, and taking into account their local medicines
and practitioners, the western system mainly responds to the
1- ^^OxxO^lc conditions and disease patterns of developed
countries| It neglects the indigenous systems of medicine and
uses, highly specialised personnel, sophisticated technology and
c ostly drugs.
The following table gives the quantitative aspect of available
health facilities :
No.
No.
No.
No.
No.
No.
of hospitals
of hospital beds
of community health centresof PHC's
of dispensaries
of subcentres
7474
535735
711
8496
26842
94918
(1986)
(1986)
(1986)
(1986)
(1986)
(1986)
This table represents the total at the all India level - besides
there has been a definite increase in number over t he past 5-6
years, these do not represent the urban and rural split up, nor
does it indicate its functioning and availability to the poor
masses. Eight out of ten Indians have little or no access to
modern medicine. -The number of doctors in 1984 was 2,97,228. A
WHO study mentions that India has sufficient nurhber of doctors.
But how equally are they distributed and how many doctors are
available to the rural population ? The doctor population ratio.
in the urban areas is 1;1;300 and in the rural 1 :20,700.
10 .
- 10 -
The rural population who make up 80% of India's population are
deprived of health facilities while the 20% of the urban
population enjoys 80% of medical care and facilities. This
.partially explains the widespread ill-health prevailing in the
villages. The reason for this disparity in medical facilities
may be due to
Lack of participaticn and cooperation by the people in
Government health programmes.
Improper allocation of funds; 75% of the budget is allocated
for maintaining staff; 12% for transport; 12% drugs and 1%
for innovative experiments. The budget allocated for the
rural areas would be even less.
Medical personnel, especially doctors are reluctant to serve
in the rural areas for more than one reason. Most often due to:
Inadequate living conditions in the rural centres.
Family problems, education of children etc.
Want of social life.
-
Intellectual isolation and inadequate facilities for maintaining professional competence.
Problems of political interference by local government
officials etc.
Presence of and unhealthy professional competition by local
practitioners and those practicing indegenous systems of
medicine.
The present trend of privatization and commercialization of
the medical profession is too strong a temptation to the
young medico, made worse by a lack of motivation for the
right values in life.
Annually 12,000 or m're fresh doctors are added to the already
e^slsLliig. number of doctors so unequally distributed among the
rural and urban population. The medical profession has become so
commercialised that manyayoung student would use any means,
pay any am-’unt of capitation fees to get into medical college
with the feeling that one has got into one of the best money
making ventures of today. And to make matters worse the training
and motivation given in today's mediqal colleges is strictly
hospital based, case -'•riented and not patient oriented,
westernised and sophisticated. The Indian trainee doctor is not
exposed to a real understanding of the social, cultural and
religious concepts of health and disease in rural India and
the many traditional systems of medical care. The attitude
of most doctors towards anything Indian would be one of contempt
with unconcern for the uneducated poor village. The motivation
given to a person depends on the content and valuer orientations
of the training given to them.
A
The private sector has an important part in the country's health care
system of which the Church's role is of significance. Initially
the Church launched out in caring for the health needs of the
people especially the poor and with funds from abroad etc. most often free medication and care was available to the really
poor’ but through the years with increasing privatization and
commercialization of medical care with increasing price of
modern drugs; higher salaries to doctors; maintenance of massive
buildings; sophisticated equipment etc. a shift in priorities
has-'taken place and today the Church's health care is by and
large no longer for the real poor but only for those who can
afford to pay.
11
11
Apart from the economic factors, the poor are also illiterate
and hence not health conscious. Thar concept of health and
disease is masked by their superstitions and wrong beliefs that
prevent them fr ?m accepting and availing for themselves existing
health facilities.
Drug and the Health Care System
The drug industry in India today is like any other industry,
profit oriented, with monopolization and promotion of multi
national corporations^ The role of drugs in the eradication of
disease is limited. Modern medicines and drugs cover only a
small minority of the people in the poor societies.. It is known
fact in India that among the marketed 60,000 drugs, more that
60% of them are either irrational, unscientific, useless, harmful
or banned.
Essential drugs, which can cope with the overwhelming problems
even in relatively sophisticated societies, number around 200.
But for the villages and the urban slum-dweller great miracles
can be achieved with fewer than 30 well chosen drugs,.- But this
is precisely where the interest of the drug industry wanes.
The drug industry is concerned with profits first, like any
other business, not with the health needs of the majority.
An analysis of the marketed drug formulations show that vitamin
preparations accounted for 15% of the total number of formulations
- the largest single group of drugs marketed. 9% were tonics or
deficiency drugs; 5% tranquilizers and sedatives; expectorants 5%.
All these items together are vigorously sold under popular brand
names with high pressure advertising and sales promotion campaigns.
Most of the basic ingredients required for these preparations
have to be imported eg: in the case of cough syrups and tonics,
none of the basic ingredients in these formulation is produced
in India.
While anti-infections and antibiotic drugs account for 21% of
the total, their production generally falls short of the quantities
required to treat the widely prevalent diseases cured by them.
There is also a growing suspicion that the people of the third
world are .infact being used as 'guinea pigs' for extensive
testing of certain drugs which is now virtually impossible to do
in the developed countries. The reason why these blatant mal
practices continue may be due to :
i)
ineffective, inadequate and corrupt drug machinery facilitating
easy introduction of harmful drugs in the market. Every state in
India has its Food & Drug Administration. With a few exceptions,
most of these are badly managed with poor testing facilities and
lack of trained personnel. They are alos subject to administrative
interference and political pressure.
ii) The enormous power and influence wielded by the drugs
industry enables it to. stall, tone down and even overcome the
orders and regulations proposed by' several organizations, committees
and individuals.
iii) The pharmaceutical industry in India does not have to face law
suits and pay damages to the affected parties. The principal
reason for this is the poor level of consumer awareness and
absence of well organised consumer protection movements.
12
iv) In a situation likethis, one would expect doctors to play
a critical role in controlling the excesses of the drug firms,
but the close ties between the medical profession and the
pharmaceutical industry in such that they feed each others
pockets. Probably the single most important part of drug
promotion is sampling : free samples to doctors which has been
lavish and 'degenerated into a rat race among manufacturers.
Sample drugs are lispensed by most GP’s and may be azen charged
- through acquired free - Roomfull's of drugs have been
acquired by some doctors and later sold to wholesalers. Doctors
also accpet substantial gifts from drug companies. Most doctors
after leaving medical collqge depend on medical representatives
for information about drugs. A large number of people resort to
self-medication and almost all drugs are easily available over
the counter.
With such a situation existing in the medical world, what- about
those destitutes numbering hundreds of millions below the poverty
line probably accounting for more than half of the Indian
population ? Most likely they will simply be bypassed. But
everything will continue to be done in the name of the poor,
the deprived and.the weak»
In conclusion :
x
Our efforts should be towards humanized health care, humanised
living and humanized development of people. We are a country with
the World's third largest medical man-power. We are signitatory
to the Alma Ata Charter of 1978. We are acknowledged as a Third
World Leader - yet
It is here where more than half of its people live below the
poverty line; where 80% ormore children are malnourished; where
half of the world's T.B. patients are; one third of the world's
leprosy patients are struggling to survive; where 1.5 million
children die of diarrhoea and 40,000 children go bling
annuaxly due to lack of Vit A! What has gone wrong and where ?
" You know sometimes it feels like .this. There I- am standing by
the shore of a swiftly flowing river and I hear>the cry of a
drowning man. So I jump into the river, put my arms around him,
pull him to shore and apply artificial respiration. Just when
he begins to breathe, there is another cry for help. So I jump
into the river, reach him, pull him to shore, apply artificial
respiration, and then just as he begins to breathe, another
cry for help. So back in the river again, reaching, pulling,
applying, breathing and then another yell. Again and again,
without end, goes the sequence. You Know, I am SO' bust jumping
in, pulling them to.shore applying artificial respiration, that
I have not time to see who the hell is upstream pushing them
all in " .
Irwing Zola.
23-11-87/200
Im: mm
Prepared toy:
Community Health Department
of the Catholic Hospital
Association of India
157/6 Staff Roa.d
Secunderabad 50'd? 003
BOOK OF NUMBERS
-■--------------------- ■'
c°^u7tf'°
-e-^00
Chapter I
Every 3rd person in the world without safe and adequate
water supply is an Indian
54% of India's population has access to drinking water. Pf
these 80% are urban; 47% are rural
Every 3rd leprosy patient is an Indian. Of the 1.2 crore
leprosy patients in the world, India accounts for 4t lakhs.
The prevalence rate per'1000 population is 5.7
Every minute 3 children.(die of diarrhoea.
One child in ten dties. of dehydration
ORT saves the lives of 500,000 children a year
Every 7th person in the world -is an Indian
India’s population is 762 m.
Every year 13 m population added, r?
1-^:1
To maintian present levels India requires :
127,000 extra schools every year
65,00# new houses and
3.5 m
new jobs every day.
One in every 3,000 children in India contract diabetes
Chapter II
12.5% Death rate in India - Rural 13.7; Urban 7.8
33.8% Birth rate
-
Rural 35.6; Urban 27.0
54 Average Indian’s life - expectancy - Female 54.7; Male 54.1
1 05 infants out of lt)OC die in infancy
IMR in urban areas
66
IMR in Rural areas 113
Out of 100 infants who die, 13.7 die of acute respiratory
illness.
131 of 1000 girl infants born die in .infancy
418 Mothers die for every 100,000 liv-e births
40,000 Indian Children go blind every year due to Vit A and
protein deficiency.
- 2 -
India has the world's highest figures for child labour
17.36 m child labourers - according to Planning Commission
20 nr . according to Unicef (44 m Unofficial fig.)
6C% gpf. them are below 10 years.
0
Chapter III
For every 1000 males there are 935 females.in India, except
in iterala where for every 1000 males there are 1032 females
An average Indian woman walks 1400 kms a year for firewood
Percentage of Central Government expenditure allocated to :
Health
2.4
Education
1.9
Defence
20.0
Percent of population below absolute poverty level :
Urban 40; Rural 51
------ Unicef figures
Urban 27.7; Rural 39.9
-------- Govt. Figures
106
8496
297228
*
170880'
8000
45,000
7474
Medical Colleges
Primary health centres
Doctors
Nurses
Pharmaceuticals companies
Drug formulations in Indian market today (Unofficial
Hospitals
fig. 63,000)
4093
3381
Government Hospitals .
Private hospitals
0
Indian Systems of Medicines(ISM; Ayurveda, Unani; Siddha)
2.91
13,294
1,665
18,179
97
18
1
lakh regular practitioners
dispensaries
Hospitals
beds
Ayurveda Colleges
Unani College js
Siddha College'
>
- 3 Chapter IV
1.5
million die of diarrhoea in India every year
1.5
million are born with genetic disorders
2.5
million infectious tuberculosis cases any given day
2.5
million fresh cases of T.B. every year
2.5
million people in India are affected by hook worm
3420000 Blind / partially blind
5430000 Locomotor disabilities
7500000 affected by mental disorders
12 million disabled in India
85% of children in India suffer from some degree of mal
nutrition
1.2 billion: annual turnover of drug companies in 1981 is
1.2 billion rupees
Source :
1
Health Information of India 1986 - Central Bureau of
Health Intelligence
2
The state of the World's Children - Unicef 1987
3
Newspaper clippings
Catholic Hospital Association of India
C. B. C. I. Centre, Goldakkhana, New Delhi - 110001
Tel. 310694, 322064
„cvV
isst, it lias, been reduced to curative, ar. urban-biased, top-down
'.id an elite-oriented approach.
This improvements have to be nc le
:o combate 3LX1DIT3SS, iiAL/dtlA, DIaRIIHOEAL DISEASES, LEPkOSY, T3
stc .
Besides tnese aspects, attention to be paid in the other
spects such as a well developed distribution of low cast food,
f acceptable quality, available to every person especially to
he rural poor, prevention of food adulteration and maintenance
f the quality of the drugs, safe drinking water, proper environental sanitation, immunization programme, a well planned n.-.Lt. ■■■•
nd child health sex-vices to reduce norb.idil y, <*■
..>x- tn 1 i t i es so as Lu px-o>->tn H.-.i. i
i ■> *
-i or mid
hAnl.th.
Production of life saving drugs u. .der their generic names
specially for the treatment of T3 and leprosy are to be within
he reach of the rural poor who suffer mostly from these disna"..?.
he use of low cast and no cast indigenous and herbal medicines
re to be encouraged.
Nevertheless, when we critically analyse this statement,
e see that very little efforts have been made in the promotion
f low cast drugs for example, nearly 40 to 60 million people
uffer from endemic GOITRE through its prevention is so cheap by
sing iodized salt which is not available to the people i.: need
*
n the same way, more time and money are spent to produce exp er. -
ive drugs than the production of Vitamin A, 'the deffie.'.cy of
hich lead to blindness as 30,000 million children suffer from
I?
Piepa:«l
Community Health Team
Voluntary Health Association of India
(. -14, l ommunity Centre, S.D k
New Delbi-110 016.
b^Nga,
,
/ " ’ • sgo qOi
:-ll/263(a)
..RJ /m/26.9.85
SOME VITAL STATISTICS OF INDIA
AND SELECTED STATES
ANNUAL LIVE BIRTH RATES
1.
The Crude Birth Rate
The Birth Rate is defined as "the number of live births
during a year per 1,000 estimated mid-year population.
"It is given by the formula:
Birth Rate
a
Number of live births during the year
x .1,000
Estimated Mid-year population
India
1980
1981
1982
Combined
Rural
Urban
Andhra
Pradesh
C
R
U
Orissa
C
R
U
Utter
Pradesh
C
R
U
Kerala
C
R
U
33.7
35.1
27.8
33.9
35.6
27.0
33.6
35.3
27.6
31.0
32.0
26.9
31.7
32.7
27.5
30.8
31.7
27.4
31.6
31.9
29.0
33.1
33.4
29.3
33.4
33.6
30.8
39.4
40.3
33.0
39.6
40.8
31.5
38.6
39.9
32.5
26.8
27.0
25.5
25.6
26.0
23.5
26.0
26.4
24.2
contd,
C-ll/263(a)
ARR/m/26.9.85
ANNUAL DEATH RATE
:
2
;
2.
Death Rate
Death rate is the most important of all vital statistical
rates pertaining to mortality. . It is defined as the
number of deaths per 1,000 estimated mid-year population,
in one year.
Number of deaths during the year x 1/100
Death Rate =
Mid-year Population
1981
1982
India
1980
Combined 12.6
12.5
11.8
Rubai
13.7
13.7
13.1
Urban
7.9
7.8
7.3
Andhra
Pradesh
C
11.3
11.1
10.4
R
12.4
12.2
11.6
U
6.8
6.5
6.0
Orissa
C
14.3
13.1
13.0
R
14.9
13.5
13.5
U
7.9
7.9
7.9
1
Utter
Pradesh
C
16.3
16.6
15.1
R
17.3
17.6
16.3
U
10.3
9.9
9.4
Kerala
C
7.0
6.6
6.6
R
6.7
7.1
6.6
U
5.8
6.5
6.2
3.
Infant Mortality Rate
It is the number of infant deaths under one year of age
per 1,000 live births in any population in one year
I.M.R.
=
Number of deaths under one year of age
x 1,000_______________________
'lotal Live Births in the Year
contd
.1/263(a)
l/m/26.9.85
;
3
s
Infant Mortality Rate
India
1980
1981
Combined
127
120
114
Rural
137
130
124
Urban
74
72
65
C
R
U
117
127
66
106
114
65
92
103
40
Orissa
C
R
133
137
149
154
143
150
U
80
86
62
Utter
Pradesh
C
R
U
177
184
114
162
168
104
159
167
99
42
45
29
43
45
30
40
41
34
1982
Andhra
Pradesh
Kerala
C
R
U
****
Reference: Health Statistics of India
1984,
Ministry of Health & Family
Welfare, Nirman Bhawan, New Delhi
4
C-ll/263(a)
ARR/m/26.9.85
2?
~
~
1980
',il. (PER 1000 LIVB BIRTHS)
INFANT miTALITY HATSS ALL INiJlA
(1971 to 1980)
SHS BSTUiATcS
,c 11/263(a)
? RR/m/26.9.85
BIRTH & DEALTH RATES IN INDIA
1901-10 to 2000
References
YEAR S
1. Joseph George, John Desroch
Health Care in India.
2. Kenneth W. Newell Health by the people
WHO Publication 1975
/
Park J.E & Park K.Text Book of
Pr!E<<«erst±sE5B &Z: Social Medicine
4.
HealtJ? Statistics of 1984Ministry of Health & Family Welfare,
Nirman Bhawan, New Delhi.
+ •’— demographic
Goals
The Catholic Hospital Association of India
C. B. C. I. Centre, Goldakkhana, New
Tel. 310694, 322064
** .
CO
DECLARATION OF ALMA-ATA
The International Conference on
meeting in Alma-Ata this twelfth day of
Nineteen hundred and seventy-eight, expressing the need for urgent
action by all governments, all' health and development workers, and
the world community to protect and promote the health of all the
people of the world, hereby makes the following Declaration;
I.
The Conference strongly reaffirms that health, which is
•a state of complete physical, mental and social wellbeing, and
not merely the absence of disease or infirmity, is a fundamental
human right and that the attainment of the highest possible level
of health is a most important world-wide social goal whose reali
zation requires the action of many other social and economic
sectors in addition to the health sector.
II.
The existing gross inequality in the health status of the
people particularly between developed and developing countries as
well as within countries is politically, socially and economically
unacceptable and is, therefore, of common concern to all countries.
III.
Economic and social development, based on a New Inter
national Economic Order, is of basic importance to the fullest
attainment of health for all and to the reduction of the gap
between the health status of the developing and developed countries.
The promotion and protection of the health of the people is
essential to sustained economic and social development and con
tributes to a better quality of life and to world peace.
IV.
The people have the right and duty to participate indi
vidually and collectively in the planning and implementation of
their health care.
V.
Governments have a responsibility for the health of their
people which can be fulfilled only by the provision of adequate
health and social measures.
a
main social target of governments,
international organisations and the whole world community in the
coming decades should be the attainment by all peoples of the world
by the year 2000 of a level of health that will permit them to load
a socially and economically productive life.
Primary health care
is the key to attaining, this- target as. .pant. of. development in the
spirit of .social justice.
-
-2VI.
Primary health care is essential health care based on
practical, scientifically sound and socially acceptable methods
and technology made universally accessible to individuals and
families in the community through their full participation and
at a cost that the community and country can afford to maintain
at every stage of their development in the spirit of self-relian
ce and self-determination.
It forms an integral part both of the
country's health system, of which it is the central function
and main focus, and of the overall social and economic develop
ment of the community,
It is the first level of contact of indi
viduals, the family and community with the national health system
bringing health care as close as possible to where people live
and work, and constitutes the first element of a continuing health
care process.
VII.
1.
Primary health care:
reflects and evolves from the economic conditions and
socio-cultural and political characteristics of the country
and its communities and is based on the application of the
relevant results of social, biomedical and health services
research and public health experience;
2.
addresses the main health problems in the community,
providing promotive, preventive, curative and rehabilivtative services accordingly;
3.
includes at leasts education concerning.prevailing health
problems and the methods of preventing and controlling them;
promotion of food supply and proper nutrition; an adequate
supply of safe water and basic sanitation; maternal and child
health care, including family planning; immunization against
the major infectious diseases; prevention and control of
locally endemic diseases; appropriate treatment of common
diseases and injuries; and provision of essentiosral drugs;
4.
involves, in addition to the health sector, all related
sectors and aspects of national and community development,
in particular agriculture, animal husbandry, food, industry,
education, housing, public works, Communications and
other sectors; and demands the coordinated efforts of all
those sectors;
-35.
requires and. promotes maximum community and individual
self-reliance and participation in the planning, organisation,
operation and control of primary health care, making fullest
use of local, national and other available resources? and to
this end develops through appropriate education the ability
of communities to participate?
6.
should be sustained by integrated, functional and mutually
suportive referral systems, loading to the progressive im
provement of comprehensive health care for all, and giving
priority to those most in need?
7.
relies, at local and referral levels, on health workers,
including physicians, nurses, midwives, auxiliaries and
community workers as applicable, as well as traditional pra-»
ctitioners as needed, suitably trained socially and techni
cally to work as a health team and tc respond to the expre
ssed health needs of the community.
VIII.
All governments should formulate national policies, stra
tegies and plans of action to launch and sustain primary health
care as part of a comprehensive national health system and in
coordination with other sectors.
To this end, it will be necess
ary to exercise political will, to mobilize the country's resources
and to use available external resources rationally.
IX.
All countries should cooperate in a spirit of partner
ship and service to ensure primary health care for all people
since the attainment of health by people in any one country
directly concerns and benefits every other country.
In this con
text the joint WKO/UIJICEF report on primary health care constitu
tes a solid basis for the further development and operation of
primary health care throughout the world.
X.
An acceptable level of health for all the people of the
world by the year 2000 can be attained through a fuller and better
use of the world's resources, a considerable part of which is now
spent on armaments and military conflicts.
A genuine policy of
independence, peace, detente and disarmament could and should rele
ase additional resources that could well be devoted to peaceful
aims and in particular to the acceleration of social and economic
development o;f which primary health care, as an essential part,
should be allotted its proper share.
The Catholic Hospital Association of India
C. B. C. I. Centre, Goldakkhana, New Delhi - 110001
Tel. 310694, 322064
cars
•Since the health care services were first organised by the
British administrators, they totally ignored-the indigenous
belief systems, life styles and health care institutions as well
as the practices which formed an organic unity,
eg. indigenous
medicine and its practices.Hence instead of building on these
foundations and evolving a new system more suited to the life
and needs of trie people with the help of modern science and tech
nology, they decided to make an abrupt and total change by intro
ducing the western system of medicine.
This created a wide
gulf between culture and tradition of the people on one hand and
the health services on the other.
It also prevented the valuable
contributions which the Indians could have made.
Nevertheless, this type of health care system first began
to provide health care services to the people who lived in the
towns and the cities and mainly they were profitable for the
tne
rich and^/elite of the Indian society.
Moreover, this urban
biased, top down and elite oriented approach of the British
period still continue to dominate the health services in spite of
the introduction of primary health centre
during the past JO yrs,
which extents it services to the rural areas though may be in
theory to a great extant.
Moreover, the British
with px-oviding
■■
tv<> services by concentrating on putting up
or constructing hospitals, dispensaries and medical colleges
as well as in training doctors and nurses.
They did introduce
programmes to improve environmental sanitation in towns and
cities•
The urban biasedset up also resulted in the concentration
of hospitals in the towns and cities as there are over 6,168
hospitals in India and about 4,50,000 beds which consume enormous
amount of the national budget mainly for the salary of the
health personnel eg. 755° °f the national income is spent for
the salary and maintenance.
-2-
Hospitals and Primetry Health Centres
1950-51
1'96O-61
1971-72
1979
Hospitals and
dispensaries
8,600
12,000
14,438
17,607
Primary Health
Centres
-
2,800
5,195
5,423
-
Sub-centres
-
Hospital beds
1 , 13,000
Medical colleges
Doctors registered
Dental colleges
Dentists
1,85,600
32,218
40,124
2,98,304
4,49,212
194.7.
1980
29
106
47,500
2,53,631
4
15
1,000
7,419
Outlays on Health Sector
5 yrs plans
Total (in million of Rs)
#of total plan outlay
I
1,009.0
4.98
II
2,378.2
4.58
III
2,255.6
2.60
TV
4,335.3
2.14
V
7,960.0
2.13
Moreover, the system depends too much on doctors who have
received western type of training which is not suitable to our
Indian situation and who are’ not wiUlng' to work in rural areas.
In~jections and drugs are becoming status symbols of a consumer
society.
The cultural alfiiation of the medical profession has
led to over sophistication.
This also led to over production of
drugs and doctors which has led.to expansion of ill-health.
Population
Doctors
Doctorspopnlation ratio
660 million(1979).
.
Rural 80#
-233, .63.1
20#
1:4500
1 :20,700
Urban 20#
80#
1 ; 1,300
• .3.
-319J5O
Ih.-.iber of hospitals
19L7.
6,168
17,607
1 ,13,000
4,49,212
1,20,401
Humber of nurses
Distribution
Urban
90%
Rural
10%
J.P. Naik in his book on "An alternative system of Health
Care services in India" says that the unfortunate aspect of the
post independence administration is the over emphasis on burea
ucracy and failure to involve the people intimately in developmen
From 1921-47 Mahatma Gandhi had mobilized the people and involve
them not only in the national struggle for freedom but also in
several constructive programmes like removal of untouchability
and promotion of village industries and handicrafts.
Hence, if
this type of involvement have been continued in post independent
era, our development would have taken definitely a different
dimention.
We find also that the largest segment of the population
does not earn enough to have purchasing power to provide them
selves with even 1500 calories per day per head.
1980 report
says that Rs. 660/ - /head/annum and various surveys by various agen
cies show that the largest majority in rural area live on about
50 np./day/hoad.
This has resulted therefore in medical care
being out of the reach of the common man and the forces which
cause ill health are primarily socio-economic factors.
Hence, are the present health care plans including "Health
for all an alternative strategy" relevant to the needs of the
country?
References
What is cur response?
(1) Health for all an alternative strategy
(2) An Alternative system of health care services
in India by J.P. llaik.
COMMUNITY HEALTH DEPaRTMEHT,CHAI
EVOLUTION OF THE HEALTH CARE SYSTEM IN INDIA
The Indian tradition of State intervention in health care is
quite old. During the reign of As oka .in 3rd Century BO, the
state established medical centres for man and animals, undertook
planting of medicinal herbs and trees, and supply of potable water
through wells along the highways. In modern times a major role
of the State in health care service has universally been
recognised and accepted.
Historically, modern health service owes its beginning to the
British presence. The first legislation, the Quarantine Act,
was introduced in 1825. But real concern for a state operated
health service appeared after the 'Indian Mutiny1, of 1857, when
the Safeguarding of the health of the troops and the European
civilians became a political necessity. All health meas'.ures
had only this objective. But the prevalance of endemic and
epidemic diseases eventually forced the government to do something
for the Indian civil population which relied on traditional
indegenous forms of medicine.
In the health sector the British did not leave any significant
legacy of an infrastructure. Therefore, a beginning from scratch
had to be made after independence. What was left by the British
was an exhaustive plan called the Bhore Committee Report, a small
network of civil hospitals, a few medical colleges in premier
cities and a network of military and railway hospitals. No
rural health infrastructure of any significance existed at the
time of independence. The expenditure of the British state
was meagre.
In 1947 India had :
17654
*1
2987
7000
750
5000
75
1000
Medical graduates
Licentiates
nurses
health visitors
midwives
pharmacists
dentists
The Government of independent India was faced with the choice of
either expanding the existing health services along the pattern
set by the British or to make radical changes so as to meet the
- 2 needs of the ordinary masses. During the freedom struggle, the
National leaders.had recommended "a National Health Scheme which
would provide free treatment and advice to all those who require
it and to pay special attention to the health needs of the vill
agers" . But the old colonial tradition of having an urban,
curative and privileged class orientation of health service was
perpetuated.
The Indian constitution in its 'Directive Principle of State
Policy1 has vested the state with responsibility for providing
free health care services to all citizens. Article 47 clearly
states the State’s responsibility to raise "the level of nutrition
and the standard of living of its people and the improvement of
public health as among its primary duties". But the VII Schedule
allocates almost all responsibilities to the provincial govern
ment. But health care includes adequate nutrition, safe water
and sanitation, healthy environment, education, employment etc.
Solution of these is necessarily dependent on the economic system "
and political programme of the Union Government.
Health Planning in India :
Health planning in India is part of
socio economic planning. The guide-lines were provided by a
number of Committees dating back to the Bhore Committee in 1946.
Bhore Committee, 1946': In 1943 the Government of India appointed
a Committee, known as Health Survey and Development Committee
(popularly known as Bhore Committee after its chairman Sir Joseph
Bhore). The Committee submitted its report in 1946 and put
forward, for the first time, comprehensive proposals for the
development of a national programme of health services for the
country. The committee proposed preventive wsrk as the "founds- I
tion" and the "countryside as the focal point", and emphasised the
importance of PHCs for providing curative and preventive health
services to the rural areas. The report stressed the need to
develop the Primary Health Centres in two phases in the short
term programme i.e. 10 years, it recommended a PHC for every
40,000 population ant' the long term programme a PHC with a 75 bed
hospital for every 10,000 to 20,000 population. The recommenda
tion included intergration of preventive and curative services
at all administrative levels and introduction of preventive and
social medicine in all medical colleges. The committee also relied
on western medicine and gave no importance to Indian system of
Medicines (iSMfe). The committee's report continues to be a major
national document and has provided guidelines for national
health planning in India.
3
- 3 Mudaliar Committee, 1962 : found the quality of services
provided by PHC's inadequate and recommended strengthening of
the existing PHCs before new centres were established.
Ohadah Committee 1963 : was appointed to study the arrangements
necessary for the maintenance, phase of the National Malaria
Eradication Programme.
Mukherji Committee, 1963 ° was appointed to review the strategy
for the family planning programme.
Jungalwalla Committee, 1967 : studied the problem of integration of
health services and elimination of private practice by Govt.
doctors.
Kartar Singh Committee, 1973 : To 'study and make recommendations
on i) the structure for integrated services.
ii) the feasibility o'f having multipurpose, bipurpose workers.
Shirvastav Committee 1975 : to derive a suitable curricular for
training a cadre of health assistants so that they can serve as a
link between qualified medical practitioners and multipurpose
workers' and to .suggest steps for improving existing medical
education. The most important recommendation of this committee
was that primary health care should be provided withing the
community itself though specially trained workers sp that the
health of the people is, placed in the hands of the people
themselves. This led to the launching of the rural health scheme.
and the programme of training community health workers during
1977-78.
Unicef|WHO joint health policy termed "Basic health service as
"a network of ‘coordinated peripheral and intermediate health
units capable of performing effectively a selected group of
functions essential to'the health -f an area and assuring the
availability of competent professional and .auxiliary personnel
to perform these functions". National health planning in India
was based on the Bhore Committee and the UNICEE/WHO health
policy. So a petwork of primary health centres and sub-centres
was established throughout the country.
Five year Plans : in the'•first xplan period the state spent an
average .of Rs. 39-40 crore per year which was only 2.2% of total
Govt, expenditure. Much less than what the British Govt, had
been spending. At the end-of the first plan, besides 725 PHCs
there were 3307 hospita'ls,. 7100 dispensaries in India, the
4
- 4 majority of hospitals belonging to the State.
In the II five year plan the expenditure on medical and public
health more than doubled and this pattern continued in each
subsequent plan, except during the (plan holiday) and the IV
plan when growth rate of health expenditure showed a drastic
decline. Health facilities too; increased but they were biased
in favour of urban areas. With the launching of the Minimum
needs programme, from the IV Plan onwards rural health infra
structure began to receive some significant attention.
HEALTH PLAN OUTLAYS & PRIORITIES
(Rs. in Cr. & % in brackets)
1
4
5
1
FYP I
FYP II
FYP III
(1951-56) (1956-61) (1961-66)
PHCs & Rural
health,
Hospitals &
Dispensaries
25
(17.86)
Control of
Communicable
diseases.
23.1
(16.5)
Education, Tr- 21.6
aining &
(15.43)
Research
ISM
.4
(.29)
20.2
Other
(14.42)
FYP IV
FYP V
FYP VI
(1969-74) (1974-79)(198C-85)
9k
_
.
121.3
(5.44)
132.75.
OO^J
Ta,ble (I)
64
(28.44)
127.01
70.5
(20.63) (10.99)
265.09
(12)
524
(7.76)
36
(16)
56.3
(16.47)
98.22
(8.5)
111.16 (5.06
4
(1 .78)
6
(2.67)
9.8
(2.87)
11.2
(3.27)
15.83
(1 .37)
28.19
(2.4)
25 .07 _
(1.13)
27.29
(1.23)
23
(10.2)
‘13
(5.8)
■61.7
(18.05)
76.49
(6.6)
89.29
(7.7)
72o 09
67)
*
(10
6
Water Supply
& Sanitation
90.3
(64.5)
49
(35)
146
(64.89)
'76
(33.78)
1821 .
*
209.5
435.03 ■ 681.66
(26.97)
(61.29) (37.64) (30.86)
3922.02
1030.68
5.3
*
1
407
(42.64) (58.08)
(30.81 ) (35.22)
7
Family Planning 7
(.5)
Health total
140
(100)
Plain total
2356
3
(1.33)
225
(100)
4800
27
(7.9)
341.8
(100)
7500
497.36
315
(27.26). (22.5)
1155.53 2209.7
(1.00)
(100)
39322
15902
101
*
(14.95)
6753,07
(100)
97500
Health to
plan
(5.94)
(4.69)
(4.56)
(7.27)
(5.62)
(6.93)
1 1 .. Health suit total to plan
(3.83)
4)
*
(3.
(2.79)
(2.74)
(1.73)
(1.87)
He:alth sub-total
8
9
10
5
- 5 Table (I) gives plan outlay in the Health Sector and Table (JI)
gives Health facilities in India. However, looked at in terms of
percentages the share of health in the total plan has decreased
consistantly from plan to plan with 3.83% in the 1st plan to 1.87%
in VIth plan I Family Planning, water and sanitation always got
a high priority and even gained more importance in successive plans
whereas control of communicable diseases received much lower priority
from the IV plan onwards in terms of percentages spent. The total
expenditure on water - sanitation from I to IV plan was 855 crores.
Out of this 566 crores was spent in urban areas and 289 crores in
rural ie. 66.2% in urban and 33.8% in rural areas. This an a country
where 80% of the population live in villages i
(Refer table II
on page 6)
Health infrastructure is very pour even today, especially in rural
areas as seen from table 2. The best indicator of health care fa
cilities is the number of hospital beds per population. The
earliest year for which this break-up is available is 1956 when
28% of all hospital beds (Govt, and Pvt.) we re located in rural
area that had 80% of the-population. This declined to 13.7% in
1974 clearly showing that rural areas had been neglected grossly
in terms of investment in health sector. Even where gHCg^added
over the years has not been adequate for the rural population.
. .
Between 1966 and 1984 the ratio of PHC to population has remained
constant at one PHG for 80,000 population. There has been a
similar stagnation in hospital - population ratio also.
Health
for An by 2000 A.D.
The GOI endorsed the WHO target of ’’Health for All By 2000 A.D."
which called for the following intermediate goals :
1985
1986
>1990
-
Providing right kind of food for all;
Providing essential drug for all;
a) Providing adequate basic sanitation for all;
b) Providing adequate supply of drinking water for all;
c) Immunization of children against six common
dise,ases namely, measles, whooping cough,
tetanus, diphtheria, polio and T.B.
The targets for 1985 and 1986 remain unrealised, 'food for all’
was already a goal of the Indian State since adoption of the
Constitution. 3 1/2 decades has not brought that goal anywhere
nearer. Regarding medical intervention the facts are as
follows : (see page 7 )
g
/ are concerned it is clear that the nuiaber
- 6 TABLE II : HEALTH FACILITIES IN INDIA
(selected years)
Y ear
No of
Hospitals
1951
1956
1961
1966
1971
1974
2694
3307
3094
4147
3976
4014
1 .3
1.2
1 .4
1 .2
1.4
1 .5
-
-
725
2565
4631
5112
5283
4.4
1 .4
0.8
0.8
0.8
1982
6805
1
5739
1984
7181
1
7210
Popula
tion
Per
Hospital
(In lakhs)
No of
PHCs
Popula
tion Per
Bed
Percent
of Rural
Beds
Percent
of Hos
pitals
Owned
by the
State
Percent
of Beds
Owned
by the
State
No of
Dispen
saries
Percent of
Dispen
saries
Owned by
the State
117000
157000
230000
304000
331000
355461
3199
2554
1930
1628
1673
1668
NA
25.0
NA
NA
NA
13.r
NA
NA
NA
NA
NA
NA
504538
1405
17.2
0.8
536370
1378 '
17.43
NA
NA
NA
NA '
NA
69.5
(16.2)
68.1
(26.7)
68.1
(26.7)
6515
7100
9406
10236
0.9
NA
NA
NA
NA
NA
62.6
(16.0)
.8
*
5
(44.3)
49.3
(45.3)
Rural
Popula
tion Per
PHC
(In lakhs)
No of
Beds
10897
10200
16754
60.9
(14.1)
21780
51.8
(29.6)
(Figures in brackets are percentages in private'sector; the remainder is facilities owned by local bodies)
1.
3.
- 7 State medicare is practically free to all without discri
mination from millionaire to pauper5
There exists a strong and ever growing private sector: of
medicare consisting of hospitals, nursing homes, clinics,
dispensaries which constitute 3/4ths of the medicare field.
State medicare institutions are disproportionately concen
trated in urban areas and rural institutions meant ostensibly
for comprehensive health care, have mostly turned into
curative agencies.
Medicare is provided to the industry workers through the Bmploye< ■ ' State Insurance (Medical Benefit) Scheme financed jointly
by the workers and the employers, Union and Provincial Govt. and
medical profession, and operated by the provincial govts.
Services are rendered for sickness, maternity and employment
injury. This scheme can be viewed as a forerunner of national
health service.
The health of a community is measured by certain parameters Eg :
infant mortality rate, death rate, life expectancy at birth,
sanitation, per capita consumption of food and safe water. In
the context of such parameters, India has made steady progress in
the post independence period. But in terms of international
standards the health situation is still precarious' and alarming.
References 5
1
Health Care in India.
2.
Radical Journal of Health Vol I No. 3, December 1986.
30-11-87/100
rs Jmm
■m- * * * -it * *
,l'
47/l,(Firstfi -
w^rka
BANGAL0B6 - 560'001
AN OVERVIEW OF VARIOUS SYSTEMS OF MEDICINE IN INDIA
All ancient civilizations developed their own systems of
medicine : Ayruveda, Arabic, Egyptian, Greaeco-Roman, Chinese,
etc... Most of them have been practiced in India tosome
degree. While western medicine or allopathy has been bn the
scene in India for only about -200 years it has entrenched
itself and grown. But now there is a growing awareness of
traditional systems like the ayurveda.. The Indian system
starts with the rigveda in 2000 B.C. and is known as Ayurveda.
Ayurveda in Sanskrit means "the science of life" . According
to ayurveda there are three constituents in the psylological
system called 'doshas'. They are 'vayu'(wind), ’pitta'(bile)
and'kapha'(phlegm). Good health results from an ideal balance
between the three factors. The ayurvedic physician evaluates
the patient and sets right the balance by means of drugs,
diet and practices.
There is a predominant 'dosha' in one's constitution and this
decides which foods and activities are suited for the person.
Ayurveda teaches exercising the highest care in selecting
what is wholesome in the matter of food, conduct and behaviour.
It does not treat a person in parts. The body is dealt with
as an integral unit.
In India today there'are
24J153 practitioners of ayurveda
1452 ayurvedic hospitals
11100 ayurvedic dispensaries
97 ayurvedic colleges,.
Sidha
The Sidha system which resembles ayurveda is said
to have originated from the sage Agastya with its records
in Tamil and is practised almost only in Tamil Nadu and
Kerala.
There are
11509 Sidha practitioners
2
- 2 105 Sidha hospitals
311 Sidha dispensaries
1 Sidha college.
Unani Unani Tibb came to India as early as the 13th century
with the Persian scholars fleeing from Persia and Central Asia.
With the support of the Mughal emperors, this system of Arab
medicine took root.in India under the name ’Unani' which is
derived from the Sanskrit ’yavana’ meaning Greek. It was the
Greek ’father of medicine’ Hippocrates who laid the foundation
of the Unani.system more than 2000 years ago. It is based on
the. Hippocratic theory of-humours. Each person is a combination
of four humours -blood, phlegm, yellow bile and black bile.
One’s temperament is sanguine, choleric, phlegmatic or melan
cholic depending on which of these humours' predominates. The
Unani physician treats a person's body as one unit and not the
symptoms.of the diseaseIt holds that’the human body has its
own regenerative powers. Medicine-is given to help these rege
nerative powers to surface.once again. There are in India today
28021. Unani practitioners
98 Unani hospitals
860 Unani dispensaries
17. Unani college's.
Homeopathy . Unlike other indigenous systems of medicine.,
there is controversy on whether homeopathy can be classified
as’traditional medicine'. It is neither ancient as ayurveda
or Unani nor is it native to India. But it has been so widely
practised in India that the government recognises it as a
traditional system of medicine. In the 18th century, Hahneman
a German physician founded the principles of homeopathy. A
basic principle of homeopathy is 'like cures like'. To
strengthen the patients' reative powers, he is given a drug
known to imitate the particular symptoms observed. In homeo
pathy it is not the disease that is cured but the symptom
it generates in a particular individual.
In India there are today
. m
122173 homeopathic practitioners
121 homeopathic hospitals
2163 homeopathic dispensaries
112 homeopathic colleges;
•
3
- 3 -
Naturopathy
Holds that good wholesome food, enough sleep,
exercise and no tension are prescriptions for good health.
The main aim of nature cure is to prevent disease. It teaches
a person the principles of balanced living. The body has
natural ways to counter the onset of disease. The aim of
treatment should be to assist nature in eliminating toxins
from the blood. Suppressing the symptoms by medicine, only
results in the basic disease becoming chronic.
In India today there are
97 naturopathy practitioners
10 naturopathy hospitals
26 naturopathy dispensaries.
Yoga Therapeutic yoga is basically a system of self-treatment.
In any medical system the primary reliance is on medicine. In
the yogic system this external agent is not needed at all
rather, it is the patient himself whose personal understanding,
practise and care cures his disease. It ensures health by
physical and mental purification through control of mind and
body.
In India today are
3 yoga hospitals
6 yoga dispensaries
Acupuncture is a system of treating disease by penetrating
needles to know points of the body selected according to the
disease. Like the traditional Chinese medicine system, the
principles of acupuncture are based on the concepts of Yin
and Yang, the universal-opposites. Ill health is due to an
imbalance between Yang(male, sun, sharp, strength, warm, positive)
and Y-in (female, moon, dawn, quiet, cold, negative) and
acupuncture is designed to restore the balance. The art of
acupuncture is widely known for its pain relieving abilities.
Acupuncture was introduced to India in 1959 at Calcutta by the
late Dr. B K Basu a member of the Dr. Kotnis Medical Mission to
China.
Allopathy
The allopathic system of medicine was introduced into
South India by the Portuguese in the early 16th century. It
was spread by the doctors of the East India Company & European
Missionaries. The allopathic system made' major breakthroughs
in-acute infections, immunization and surgery.
4
However its costs are high, it makes people dependent on drugs
the side effects of its drugs and abuse of drugs are all draw
backs of this system
Today in India there are
297228 medical practitioners
7474 hospitals
26840 dispensaries
106 ijiedical colleges
Modern medicine had brought hope for everybody once. But now
people all over the world are looking for alternatives :
In the west there is a growing demand for "alternative" herbal
remedies and in the Third World it is now accepted that
cheap readily available remedies should replace expensive
western drugs on the market. Almost 70% of our people cannot
afford/S5|h cost of drugs and diagnostic proceedures of
allopathy. Traditional medicinesare being recommended as an
added component to India's health care system because they
are cheap and do not have the side effects associated with
allopathic treatment.
Sources
1
2
3
4
5
Health Care in India by George Joseph, John Desrochers >
and Mariamma Kalathil.
Health for the Millions (VHAI) June 1987 Vol. XIII No. 3.
Manorma year Book 1987.
Yogic Cure for Common Diseases by Dr Phulgenda Sinha.
Health Information of India, 1968.
1 4-11-87/100
rs :mm
SOO 003.
^t.’flarks Ro
,/'?'/". sscooi
AN OV»RVX.W Ol< 1-IFPEHENT COMMUNITY HEALTH PROGRAMMES TN INDIA
(models and approachesJ
1•
INTRODUCTION
Community health approach to health care has been widely reco
gnised as the right alternative, for ensuring-health to the
poor millions in developing natij^as.
In India too, governmen
tal as well as voluntary efforts are mac.e for. the promotion of
community health.
In the evolution of health care system, this
approach has emerged through a process of dialogue between the
medical and the social sciences in an effort to make the
health care system relevant and responsive to the socio-politicoeconomic realities in the society.
Again., in the process of
evolution and formulation of community health in terms of its
principles, -,1 llo~aphiss and methodologies^ various models
have been proposed and practised.
1> this paper an attempt
is made to catagoxiEe these models into four, each with its
own
.c features.
Further, each model. with its characteristics could be explained
as followirj a certain approac1' in community health.
approaches are broadly divided into three.
These
Am understanding
of these three approaches could give us a frame work to assess
<Ap,;.5foacli each models folio s. .Another interesting
correlation is that each of these.tbrea approaches reflects
a certain philosophy of development work-,In the following paragraphs an intrcc. lotion is made into such
an analytical over - lo-..-.
In the latts.-i- part of this paper the
four models with their characteristic;, are listed out.
Under
each model, the particular approach into which it fits into it
is also given with certain indicator- of assessment.
2.
-DIFFERENT MODELS IN CQMMUlItTY HEA 1TH
A study of tie ongoing projects ...nd + he literature available
on them reveal.s that in India there exists different models/
typos of community health products.
major categories.
They fall under four
Each one is run b r different types of insti
tutional set ups as big hospitals, s sail hospitals, rural
dispensaries, or run by non structur si voluntary health/action
groups. Again, each model is unique
In terms of infrastructure,
services rendered, needs met, and th b results achieved.
would be de?.? from
fc -/booming . ti bio «-
'
-
...
It
3•
- 2 DIFFERENT AP. ROACHES IN COMMUNITY HEALTH
Three approaches have been identified in community health.
They are : Medical approach, health extension approach,
Comprehensive approach.
a)
Medical approach ;
Considers health as the absence of diseases brought about by
medical intervention based on modern sciences and technology and
sees the role of the community (the people) as responding
to the directions given by the medical professionals. It
has its roots in the medical model of health care which beli
eves that the eradication of ill health depends on doctors and
medicines.
b)
Health extension approach :
Based on a critique of medical approach. It accepts WHO
defination of health as the total physical, mental and social
well being of the individual. Mere advancement of medical
technology and the sophistication of services would not
bring health to the majority of the people - especially the
poor - and that the approach should be a planned re-distri
bution of health care facilities to reach the vastness of the
society. The approach also advocates other socio-economic
uplift programmes to enable people to benefit from health
care facilities. Preventive care is also emphasized.
c)
|
Comprehensive approach :
Views health, the concept of total well being in the context
of the situational realities of the individual. This concept
is elaborated by stating that health, the state of total
well being, is also a human condition which does not imporve
either by providing more services or mobilizing the community
for providing more health services. It improves only by
having the community take control and responsibility for
decisions about how to mobilize, utilize and distribute
services and resources,, Here community is the subject, decision
maker. It is a process of fconscientization
*
organisation and
capacitation of the coromunity for action. It has bearing on
the social, economic, political and cultural dimensions of
human life, in the sentse that the approach strives to bring
about changes in them -50 that there would emerge a society
where human life would be more healthy in the complete sense
of the word.
3
k
4.
- 3 COMMUNITY HEALTH AND. •-EIE DIFFERENT APPROACHES^ IN DEVELCBjIMT :
Development work is based on certain analysis of the backwardness
of the people. According to the.analysis, different philosophy of
development work are arrived at, They are mainly three approaches ;
Modernisation approach, welfare approach, and social justice
approach. In the context of speaking about different approaches
in community health work, it would be worth mentioning these
approaches. It is interesting to note that reflections of these
approaches are found in the three community health approaches.
a)
The modernization approach analyses poverty as the lack of
enough production and it'makes efforts to gear up production
through advanced technology’in the field of agriculture and
industry. It believes that the results of modernization
would trickle down to the lower strata of- society.
b)
The welfare approach recognizes different classes and castes
existing in the society, ^t is due to the co-existence of
development and under
*
development in the society. This state
is accepted as a normal reality. Efforts are made to alleviate
the sufferings of the poor through organizing relief and
charity work. People are passive receipients here. Recently
there has been some changes in this approach and it recognizes
the participation of the people and the mobilization of their
resource. Programmes also have improved remarkably from
relief work to development programmes aimed at the uplift of
the poor, through income generating programme, literacy
programmes, vocational training etc. The poor continues to
exist and the disparity between the rich and the poor also
continues as a reality. Statusquo is not disturbed.
In social justice approach a critical analysis of the society
employed and poverty and backwardness are understood as man
made historical reality. The reasons are attributed to the
various forces' and the dynamics at work in the society.
Poverty is pregipitated as a result'of injustice. Justice
could be brought in only through a restructuring of the
society. It could be achieved through empowering the people
.. through awareness building and organization. Ultimate
development of the poor would mean fair distribution of the
means of production, living wages, consumption of good food,
availability of public amenities, practice of human values
as love, cooperation and unity.
c)
4
- 4 It becomes clear that the analysis and approaches of development
work has co-relation with that of, community health work,
characteristics of modernization approach are reflected in
medical approach and features of welfare approach find expression
in health planning approach. Social justice approach goes well
with, comprehensive approach in terms of its analysis and
approach.
5 • HIE FOUR. MODELS AND THREE API ROACHES IN COMMUNITY. HEALTH
As mentioned already the community health programme existing
in the country could be classified into four based on the
characteristics. The following table would give that. Under
each programme a note is made as to which approach of community
health it belongs to. To make it clear six indicators are given
based on which this assessment is made. These indicators are :
- role of health services
- role of professional
- role of community worker
- Community participation
- Evaluation & Financial support.
For each approach these indicators show different explanations.
* Conscientization is "an awakening of consciousness, the
development of a critical awareness of a person's on identity
and situation, a reawakening of the capacity to analyse the
causes and consequences of one's own situation and to act
logically and reflectively to transform that reality"
(David Millwood)
5
5
model
Type of institution/
inlrasjEructure^
Capital intensive, highly
sophisticated and insti
tutionalized big hospitals.
Mobile medical team with
doctor & medicines
A
- , CHARACTERISTICS
Nature p f~J5ervices
Rendered
Needs met
- Treatment of minor
- Extensive service from
physical ailments.
hospital.
- Curative care
- Referral and' free
- Running village clinics.
transportation to the
- Referral service, free
hospital.
medicines.
- Weekly or fortnightly visits.
Result
.Qualititatty e
changes
- People become more conscious
about sickness and «icuicines.
- more patients in the hospital
- feeling of dependence in the
people, demanding free
services.
- Shift from home remedies and
indigenous medicines.
B - JTHE~ APPROACH FOLLOy/ED
The approach followed is medical approach- The following are six indicators which would help us to make an
assessment on that ;
Explanation
Indicators
a) Role of health service
- means to improve the health status of the people
b) Role of Medical Professional
- Key to the programme - manager, planner, problem solver, coach, consultant,
clinicianj leader, teacher, evaluator.
c) Role of community health
- a means by which medical advances could be applied more rapidly and effectively.
worker
d) Community participation
- A means to ensure more acceptibility and utilization of services.
e) Evaluation
- Based on analysis and interpretation of statistics which reflect the scope
and results of applied medical science and technology.
f) Financial support
- needed to create, expand and maintain the service.
6
6
RACTERISTICS
MppEL_.II
Type, cf institution/
infrastructure
Needs, met
Nature of service s, rendered
Capital intensive, sophisticated - Extension services.
- Curative and preventive
and institutionalised small
. care
hospitals. ■
- Village clinics
- Referral services
Medical team with or without
- Medicines at reduced rates •
doctor.
- weekly or fortnightly
visits.
- Health education
- MCH programmes/immunization
- Village health workers
with medical kit.
- Treatment of minor
ailments
- referral and free
transportation to
the. .hospital- ■
'i- personal and envi
ronmental hygeine.
itative
~~~ changes
- People meeting in groups
- Leaxn soffit .preventive
methods
- Mopg patients in the
hospital
- Learn that they can do
something about health..
Re sult_
B “ APPROACH FOLLOWED
The approach followed is Medical approach-? But there are certain changes, in the sense that it is not
strictly Medical approach. "There" is an inclination towards Health Extension Approach.
Indicators
Explanation
a Role of health services
- Means to improve the health status of the people
b Role of medical professional
- Medical professional continues to be the key personnel. But, para medicals gain
a role here.
c Role of Community Health
Worker (CHW)
- Along with being a person to ensure more community acceptability for medicines,
CHW also imparts preventive health education.
d Community participation
- a means to ensure more acceptability to medicines as well as a means to disse
minate ideas of preventive health education.
- Based on analysis and interpretation of health statistics that shows the scope
and result of applied medical science as well as the effectiveness of preventive
health education.
- needed to create, expand and. maintain the service.
7
e
Evaluation
f Financial support
KODEL.III
Type, of institution/
infrastructure'
Rural health centres
manned by nurses, not
institutionalised, still
very much structured.
- 7 A ~ CHARACTERISTICS
Nature of services rendered
Needs., met
Kesuits-Qualitative changes
- People become aware of the
- Better environmental
- Preventive, promotive and
importance of preventive
sanitation.
curative
medical care.
- M C H Services
- Community health workers
- Less patients to go to the
- Supplementary income
with simple medicines.
hospital
for a section of the
- Health .Education, Adult
- Better child care
population.
Education
A team composed of a
- People try to see health in
- Small income generating
nurse and social
relation to economic back
worker.
projects
wardness.
- Kitchen garden
- Develop more interaction among
- KCH
the groups, mahilamandals.
4 Collaboration with Govt.
- People became aware of their
and ether agencies
collective strength.
- village meetings and
discussions on diff
erent problems
- promotion of collective
action.
B - APPRuAC H FOLLOWED
The approach followed is health extension approach. The following indicators would make it clear.
Indicators
Explanations
a Role of health services
- as it views that good health isthe result of planned health services, experts
from other fields as economists, social workers, etc., are also involved to
make services effective.
b Role of medical professional- The medical professional is viewed as a component rather than key. further,
experts from ether disciplines are also involved - economists, social workers,
etc. Attempts are also made to include community leaders.
c Role of Community health
- CHW is considered as an agent of change - and works as a multi purpose
Worker
worker which include medical services, prevention, public health work, health
education, nutrition education, food production and housing improvements.
d Community Participation
- Participation of the community is considered important because it provided
a resource base, a means to mobilize more resource - personnel, money and
material. Mainly it involves the community leaders.
8
8
e
.^valuation
f
Financial support
MODEL IV
Type, of institution/
infrastructure
Rural health centres/
action groups
Flexible and non
structured.
One team composed of a
nurse and activitist.
- Concerned with assessing whether a programme with a variety of activities (ranging
from health to economic development programmes) provides the most benefits in
terms of health improvements for the least amount of resources.
- Used to build small health centres and to generate community resources man power, moeny and material. The programme has to be made self supporting.
A - CHARACTERISTICS
Nature of service, rendered
- Services aimed at building healthy
communities.
- Community diagnosis
- Critical understanding of health &
its relation to unjust social order. ■
- Awareness building through nonformal education programmes.
- Organising the people for collective
action.
- Exposing social illness
- Formation of Action groups, Mahila
manuals, youth clubs, village
committees, farmer's club, Trade
unions.
- Demanding services from the Govt.
from health as well as other
departments.
- Identifying and training village
animators.
- Promotion of low cost and simple
home remedies.
Needs met
Results-qualitative changes
Basic needs met by - Participation and collective
action of the people to build
the people through
up a healthy community/
their organized
society.
efforts.
Better services, from - Increased self confidence and
. independency
the Government.
- Faith in their own power to
fight for a healthy society
- Health is considered as a
right and duty and at the
same time seen as a pclitical
issue.
“ People struggling against
social injustices.
- Cooperation among the people
based on critical understanding
of social realities.
- New forms of politics and new
forms of people's movement.
- Alternative indigenous medical
system developed.
9
9 -
B - APPROACHES FOLLOWED
In this model the comprehensive approach is followed.
The following explanation would make it clear.
Explanations
- The concept of health is totally integrated into the socio-political fabric
of the community. Hence health services are a part of a strategy (or an entry
point for development and a tool in process of community growth,
b Rcle of medical
- Since the role of health service is t o enable change in the existing social
professional
structures (to bring about equity of opportunities and services/, the profession
is viewed as a resource - an enabler, educator and a stimulus. The community is
the decision maker which defines the role of the professionals and the
professional is accountable to the people.
c Rcle fo community
- Community health worker\.CHW; is an agent of change, an educator, a volunteer
health worker.
selected by the community. Uses health work primarily as a means of bringing
about change in the attitudes and behaviours, and in the long run, social
structures through health and development activities. Thus, CHW works towards
social justice and social, political and economic equality as well as carrying
out the health and traditional community development tasks. CHW could be better
called community level worker (CLW) since the work is total development work.
d Community participation - Community participation in health is a step w.iich will help people gain control
over their own lives by collectively working towards making the socio economic
and piitical structures compatible with and conducive to health and development of
the poor. It starts with awareness building and organisation. Community is the
decision maker in the community programme and through such involvements they go
through a process of learning to live together, think together and work together
and take control of policies which affect their lives.
e Evaluation
- The community is the evaluator - it is participatory evaluation methods-community
decides on the objectives, priorities and methcdLologies of the process. The dcvelopr
ment worker, as an enabler helps the Community and works with them. The evaluation
itself is the tool and a method for community awareness, self determination and
growth. In the entire process, stress is laid on the qualitative aspects of the
people and the effort at bringing about changes in the existing health delivery
system and the establishment of alternative models of the people.
f Financial support
- To spark off a programme finance is needed. But the goal is to start a programme
which is able to be sustained through community contribution and commitment not
through outside finances. The investment is in education, rather than technology
and expanded services. It also means money to identify and develop indigenous
resources in terras of man power, materials and support. In terms of health aid,
/for it looks/seed mv.ney. Maximum efforts are made to make use of Gcvt. funds
no-g
at the cost of allowing them tc dictate- terms. It should never hamper the community
in its process of growth towards awareness and organisation.
10
Indicators
a Role of health services
- 10 CONCLUSION :
Community health is a term understood and interpreted in
different ways by different people. This is due to the
differences in the analysis of the ill health. Based on one's
analysis the programme that is initiated would confirm to a
particular approach and philosophy.
This paper, we think, would help the implementors of community
health programmes as well as these who intend to start one to
develop a still more reflective understanding. This understanding
blended with our commitment to the poor would help us all to
make our involvement more meaningful.
16-02-88/200
mm/
$
an
I.
OVERVIEW OF DIFFERENT COMMUNITY HEALTH PROGRAMMES IM INDIS
(MODELS AND APPROACHES)
INTRODUCTION
Community health approach to health care has been widely reco
gnized as the right alternative for ensuring health to the poor
millions in developing natives. In India too, governmental as
well as voluntary efforts are made for the promotion of
community health. In the evolution of health care system, this
approach has emerged through a process of dialogue between the
medical and the social sciences in an effort to make the
health care system relevant and responsive to the sociopoliticao- economic realities in the society. Again, in the
precess ofevolution and formulation of community health in
terms of its principles, philosophies and methodologies, various
models have been proposed and practised. In this paper an
attempt is made to categorize these models into four, each with
its 'own characteristic features.
Further, each model with its characteristics could be explained
as following a certain approach in community health. These
approaches are broadly divided into three. An understanding
of these three approaches could give us a frame work to assess
as to which approach each models follows. Another interesting
correlation is that each of these three approaches reflects
a certain philosophy of development work.
g
In the following paragraphs an introduction is made into such . 'ij 3
an analytical overview. In the latter part of this paper the;
g
four models with their characteristics are listed out. Under
' ?
each model, the particular approach into which it fits into
is also given with certain indicators or assessment.
II.
DIFFERENT MODELS IN COMMUNITY HEALTH
'
•■
A study of the ongoing projects and the 1 iterature available
■ ■on them reveals that m India thede exists different models/ '
types of commuhity health products. They fall under four
major categories. Each one is run by different-types of insti
tutional set ups as big hospitals, small hsopitais, rural
dispensaries, or run by non structured voluntary health/ action
groups. Again, each model is unique in terras of infrastructure,
services rendered, needs met,and the results achieved. It
would be clear from the forthcoming thble.
III.
DIFFERENT APPRQACHESIN COMMUNITY HEALTH.
Three approaches have been identifyed in community health.
They are : Medical approach, health extension approach,
Comprehensive approach.
.
(a)
Medical approach; Considers health as the absence of
diseases brought about by medical
interventions based on modern sciences and technology and sees
the role of the community(the people) as responding to the
directions given by the medical i. rofessionals. It has its
roots in the medical model of health care .which b elieves tlitrt the
eradication ofiill-health depends on doctors and medicines.
(b) Health extension ap-rouch; Based on ac critique of medical
approach. It accepts WHO
defenition ofhcaith as the total physical, mental and social
well being of the individual. Mere advancement of medical
2
technology and the sophistication of services would not bring
health to themajority of thepconle
especially the poor - and
that the approach should be a.'planned redistribution of health
care facilities' to reach the' vastness of the society. The
•approach also advocates other socio- economic uplift programmes
to enable people to benefit from health care facilities.
Preventive care is also emphasized.
Viev/s health, the concept of
total well being in the context of
the situational
realities of the individual. This concept
is. elaborated by stating that health, the state of tctnl well
being, is also a human condition which does not improve either
by providing more services or mobilizing the community for
providing more health services. It improves, only by having the
community take control and responsibility for' decisions about
tr how tomobolize , utilize and distribute services and resour
ces. Here community is thesubject, decision maker, It is a
process of conscientizationf organization and capacibation of
the community for action. J-t has bearing on the social,
economic,; olitical andcultural dimensions of human life, in the
scnce that the approach strives to bring about changes in then
so that there would emerge a society wheie human life would be
more healthy in the complete sense of the'word,
.
C Comprehensive appraach:
(c)
IV.
COMMUNITY HEALTH AND THE DIFFERENT APPROACHES IN
DEVELOPMENT ;
Development work is based on certain analysis of the backwardness
of the people. According to the analysis , different philosophy
of development vprk are arrived at. They are mainly three
approaches: Modernization approach,“.welfare approach, and social
justice approach. In the context of sneaking about different
approaches in community health work, it w?uld be worth mentioning
these approaches. It is interesting to note that reflections of
these approaches are found in the three community health
approaches.
(a) Themodernization approach analyses poverty as the lack of
enough production and itmakes efforts to gear up product! n
through ad vane ecK .technology in the field of agriculture and
industry. It believes that the result of modernization would
trickle down to the lower strata of society.
(b) The welfare approach recognizes different classes and castes
existing in the society. It is due to the co-existence of
development and under development in the society. This state
is accepted as a normal reality. Efforts are made to alleviate
the sufferingseof the poor.through organizing relief and
charity work. People are passive receipients here. Recently
there has been some changes in this approach and it recognizes
the participation of the people and the mobilization of their
resource. Programmes also have improved remarkably from
relief work to development programmes aimed at the uplift of
the -poor, through income generating'programme, literacy
programmes, vocational training etc. T^eu poor continues
to
exist and the disparity between the rich and the poor also
continues as a reality. Statusquo is not disturbed.
♦Conscientization is"an awakening of consciousness, the
development of a critical awareness of a person’s on identity
and situation, a reawakening of the capacity to analyse the
causes and consequences of one’s own situation and to act 1
logically and reflectively to transform that reality"
(David Millwood)
..3/-
- 3 In social justice approach a critical analysis of the
society is employed and poverty and backwardness are under
stood as man made historical reality. The reasons are
attributed to the various forces and the dynamic at work
in the society. Poverty is . presipitated as a result of
injustice. Justice could be brought in only through a
restructuring of the society. It could be achieved
through empowering the people through awareness building
and organization. Ultimate development of the poor would
mean fair distribution of the means of production, living
wages, consumption of good food, availability of public
amenities, practice of human values as love, cooperation
and unity.
It becames clear that the analysis and approaches of
development work has correlation with that of community
health work, Characteristics of modernization approach are
reflected in medical approach and features of welfare
ap-roach find expression in health planning approach. Social
justice ap-roch goes well with, com”rehensive approach
in terms of its analysis and approach.
V.
THE FOUR MODELS AND THREE APPROACHES
IN COMMUNITY HEALTH
As mentioned alreadyrthe community health programme existing
in the countty could be classified into four based on the
characteristic. The following table would give that.
Under tach ;rogramme a note is made as to which approach of
community health it belongs to. To make it clear six
indicators are given based on which thiso assesment
is made.
These indicators are: role of health services.
role of professional, role of community worker, Community
participation,evaluation and financial support. For each
approach these indicators show different explanations.
MODEL
A ^CHARACTERISTICS
I.
Type of institution/
infrastructure
Nature of Services
Rendered
Capital intensive, highly
- 'Extension service from
sophisticated and insti
- hospital.
tutionalized big hospitals. - Curative care.
-Running
village clinics.
Mobile medical team with
- Referral service, free
doctor a medicines.
medicines.
- weekly or fortnightly vi
Neec£ m et
Result- Qualitative changes.
- Treatment of minor
physical ailments.
- People become more conscious ab-:.
sickness and medicines.
- more patients in the hospital
- feeling of dependence in the
people, demanding free services.
- shift from home remedies and
indigenous medicines.
- Referral and free
transportaion to the
hospital.
B.THE APPROACH FOLLOWED.
The approach followed is medical approach.
assesment on that.
The following are six indicators vhich would help us to make an
Indicators.
Explanation.
a. Role of health service
b. Role of Medical Professional
- means to improve the health status of the people
- Key to the programme- manager, planner, problem solver, coach, consultant,
clinician, leader, teacher, evaluator.
- a means by which medical advances could be applied more rapidly and
effectively.
- a means to e n s uhe.mdre-acceptibility and utilization of services.
- Based on analysis and interpretation of statistics which reflect the scope
and results of applied medical science and technology.
- needed to create, expand and maintain the service.
c. Role of community health worker
d. Community participation
e. Evaluation
f. Financial support.
A. CHARA,CT ERISTICS
MODEL , II
Needs met
Results- Qualitative changes.
Type of institution/
infrastructure.
Nature of services
r end er ed.
Capital intensive, sophi
sticated and institutiona
lised small hospitals.
- people meeting in groups.
- Extension services,
- Treatment of minor
- learn some preventive methods.
- curative and preventive
ailments.
care.
- More patients in the hospital
- Referral and free
- Learn that they can do something
- Village clinics
transporation
- Referral services.
about health.
to the hospital.
- Medicines at reduced
- personal and environ-8,
rates.
mental hygeine.
- weekly or fortnightly
• visits-.- - - -■
- HEalth Education
- MCH programmes/ immunization.
- Village Health Workers with
medical kit,
Medical team with
without doctor.
or
B.APPROACH FOLLOWED
The approach followed is Medical approach. But there are certain changes, in the sense that it is not strictly
Medical approach. There is an inolin-atimtowards Health Extention approach.
Indicators.
Explanation.
a. Role of health services.
b. Role of medical professional
- Means to improve the health status of the people.
- Medical professionalcontinues to be the key personnel. But, para medicals
gain a role here.
- along with being a person to ensure more community acceptability for medicine?,
CHW also imparts preventive health education.
- a means to ensure more acceptability to medicines as well as a means to
disseminate ideas of preventive health education.
- based on analysis and interpretation of health statistics that shows the scope
and result of applied medical science as well as the effectiveness of prevent -;
health education.
- needed to create, expand and maintain the service.
c. Role of Community Health Worker
(CHW)
d. Community ^anticipation
e. Evaluation
f. Financial support
A. CHARACTERISTICS
MODEL .III.
Type of institution/
infr a s tr uc t ur e
Nature of services
rendered.
Needs met.
-Preventive, promotive
- Better environmental
Rural health centres
and curative.
sanitation.
manned by nurses, not
very
Community
health
workers
M.C.H. Services.institionalized, still
with simple medicines.
- Supplimentary income
much st r uc t ur ed.
- Health education, Adult
for a section of the
Education
population.
A team composed of a
- Smallincome generating
nurse and social
proj ects.
workers.
- kitchen garden
- M C H
- Collaboration with govt
and other agencies.
- village meetings and
discussions'on different
village problems.
- promotion of collective
action.
Results - Qualitative changes.
- people become aware of the importer of preventive medical care.
- Less patients to go. to the hospit
- Better child care.
- people try to see health in relatio
to economic backwardness.
- Develop more interaction among the
villages, formation of small info.
groups, mahilamand als.
- peoplebecame aware of their collect
strength.
B. APPROACH FOLLOWED.
The approach followed is Health Extension approach.. The following indicators would make it clear.
Indicators.
Explanations.
a. Role of health services.
- as it vews that good health is the result of planned health services,
experts from other fields as economists, social workers, etc- are also
involved to make services effective.
b. Role of medical professional
- The medical professional is viewed as a component rather than key. Fnrth r
experts from other disciplines are also involved - economists, social
workers, etc. Attempts are also m-ade to include community leaders.
- CHW is considered as an agent of change - and works as a multi purpose w
worker which include medical services, prevention, public health work, h
education, nutrition education, food production and housing improvements.
c. Role of Community Health Worker
d. Community participation.
- Participation of the community is considered important because it provic .
a resourcebase, a means to mobilize more resource - personnel, money and
material. Mainly-it involves the community leaders.
e. Evaluation.
- Concerned with assesing whether a programme with a variety of activities
(raging from(health to economic development programmes) provides the most
benefits in terms of health improvements for the least amount of resour
f. Financial support.
- Used to build small health centres and to generate community resources man power, money and material. The programme, has to be made self
supp; orting.
MODEL . IV
Type of institution/
infrastructure
Rural health centres/
action groups.
Flexible and non
structured.
One team composed of a
nurse and activist.
A. CHARACTERISTICS.
Nature of service
Rendered,
Needs met
- Services aimed at building
- Basic needs met by the
healthy communities.
people through their
organized efforts.
Community diagnosis.
- Critical understanding of
- Better services from
health and its relation to
the government.
tun just social order.
- Awareness building through
non-formal education
programmes.
-Organizing the people for
collective action.
-Exposing social illness.
- Formation of Action groups,
Mahila mandals, youth clubs,
village committees, Farmer's
club, Trade unions.
Results- Qualitative changes.
- Participation and collective acti
of the people to build up a heaitcommunity/ society.
- Increased self confidence and
independency.
- faith in their own power to fight
for a heolty society.
- Health is considered as a right a;
duty andat the same timeseen as a
politicial issue.
- people struggling against social
injustices.
- Cooperation among the people based
oncrticial understanding of soci
realities.
- New forms of politics and new for?
p eoples' mov ement.
- Alternative indigenous medical syst
developed.
$
- Demanding services from
the Govt, from health
as well as other depart
ments.
- Identifying and training
village animators.
- Promotion of low cost and
simple home remedies.
B. APPROACHES FOLLCWED
In this model the comprehensive approach
is followed.
The following explanation would make it clear.
Indicators.
Explanations.
a. Role of health services.
- the concept of health is totally integrated into the socio-political fabric
of the community. Hence health services are a part of a strategy( or an
entry point) for development and a tool in process of community growth.
of
■
....
- Since the role/health service is to enable change in the existing social!
structures(to bring about equity of opportunities andservices), the profess!:.
is viewed as a resource- an enabler . educator and a stimulus.
The communit
is the decision maker which defines the role of the professionals and the
professional is accountable to the people.
b. Role of medical professional
c. Role of communityhealth worker.
- Community Health Worker(CHW) is anagent of change, an educatcr, a volunteer
selected by the community. Uses health work primarly as a means of bringinabout change in the attitudejand behaviours, and in the long run, social
structures through health and development activities. Thus, CHW works toweds
social justice and social, ■. '1 political and bcbnomic equality as well as
carr_ying out the health and traditional community development tasks.
CHW
could be better called, community level worker (CLW) since the wrk is total
development work.
o7
r
d. Community participation.
- Community participation in health is a step which will help people gain
control over their own lives by coldactively working towards making the
socio economic and political structures compatible with and conducive to
health and development of the poor. It'- starts with awareness building and
organization. Community is the decision maker in the community programme,
and through such involvement they go through a process of learning to
live together, think together and work together and take control of policies
which affect their lives.
e. Evaluation.
-The cqmmunityis the evaluator,- it is participatory evaluation methodscommuriity decides onn the obj ectives, priorities and methodologies-of the
process. The development worker, as an enabler helpes the community and
workd with them. The evaluation itself is a tool and a method for
community awareness, self determination and growth. In the entire
process, stress is laid on the qualitative aspects of the people and
the efforts at bringing about changesin the existing health delivery-ig
system and theestablishment of alternate?a models of the people
-To spark off a programme finance is needed. But the goal is to start
a programme which is able to be sustained through community contribution an>
commitment not through outside financesShe investment is in education,
rather than technology and expanded services. It also means money to
identify and develop indigenous resources in terms of man power, materials
and support. In terms of health aid, it looks for seed money. Maximum.
efforts are made to make use of government funds but not at frhe cost of
allowing them to dictate terms. It should never hamper the community
in its process of growth towards awareness and organization.
f. Financial support
CONCLUSION;
Community health is a term understood and interpreted in diff
erent rays by different people. This is due to the differences
in the analysis of the ill health. Based on one's analysis
the programme that is initiated would conform to a particular
approach and philosophy.
This paper, we think, would help the implementorls’.-jii of commun-r
ity health programmes as well as those who intend to start one
to develop a still more reflective understanding.
This
understanding blended with out commitment to the poor would
help us all. to make our involvement more meaningful. '
tow?
id/as
ab:ka 11/85 :100
CHURCH RELATED COMMUNITY HEALTH PROGRAMMES
YESTERDAY AND TODAY (AN QV,. R-Vlgj)
Types of institut
ions engaged in
C.h. Programme
TYPE I
Mobile
Capital intensive,
highly sophisticated medical
and institutionali team with
zed big hospitals
a doctor
and
medicines
TYPE II
Capital intensive,
sophisticated and
i nstitutionaliz ed
small hospitals
TYPE ITT
Rural health centres
manned by nurses; no
institutionzed, stilJ
very much structured
Need s
Infrastructure
Mobile
medical
team with
or -without
a doctor
a team com
posed of a
nurse and
social
workers
met
Result
- Extension services
- Carative care
- Village clinics
- Referral service
free medicines
- weekly or fortnightly visits
- Minor physical
ail ments
- Free transport
ation fiXX the
seriously sick
- people became more conscious
of their sickness
- More patients in the
ho spital
- Feeling of dependence
- Demand for more free
services.
- Shift from homeremedies and
indigenous medicines.
- Extension service
- Curative and preventive care
- Village clinics
- Referral service
- Medicines at reduced rates
- Weekly or fortnightly visits
- Health education
- MCH programmes/immunization
- Village health workers with
medical kit.
- Minor physical
ailment s
- Free transport
ation for the
seriously sick
- Personal and
unviornmental
hygiene
- People meeting in groups
- Learn some prevention
methods
- More patients in the hospital
- Learn that they can do
something about health.
Preventive, promotice and
curative services
VHWSs with simple medicines
- ' ood drinking
w; t er
- People become more
confident in their
power.
...2/-
2
-Health education^,
Better
Adult Education
environmental
- Small income generating
sanitation
projects
- Kitchen garden
M
CH
- M C H
i Collobration with Govt, and
other agencies
- Village meetings and discussions
on different village
problems
- Promotion of eollective
action
-Develop more interaction
among the villagers
- Less pari ents to go
to the hospitals.
- Better child care
- Mahila Mandals
TYPE IV
- Rural health
c entres/action
groups
- Flexible and
not structured
-One team
- Services aimed at building
composed of
healthy communities
a nurse and - Community Diagnosis
activists
- Critical understanding of
health and it's relation
to the unjust social
order.
- Awarness building through
nonformal education
programmes.
- Organizing the people for
collective action
- Exposing social illnesses.
- Basic needs
met by the
people
themselves
- Better services
from the Govt.
- Participation and collective
action of the people to
build up a healthy
community/society.
- Increased self confidence
and independency
- Faith in their own power
to fight for a healthy
society.
...3/-
3
- Formation of; Action groups
: Mahila Handals
; Youth clubs
: Village Committees
: Farmers' clubs
: Trade unions.
- Demanding new services from the
govt, and better services
from the existing govt, health
institutions
- Health is considered as a
right and duty and at the
s ame time seen as a
political . issue.
- People struggling
against social
injustices.
- Co-operation among them
based on critical understanding
of social realities.
- Identifying and training
village animators
- New forms of politics and new
forms of peoples' movements.
- Promotion of low cost and
simple home remedies
- Alternative indigenous medical
systems developed.
Community Health Department
CHAI
CHURCH REU-TSD COIdfUNITY HEALTH PROGRAMMES
yesterday and1 today
Types of institut
ions engaged in
0,H.Programme
Infrastructure
(an ovsr-vtWT
Services
Rendered
Needs net
Result
TIPS I
Capitai intensive,
highly sophisticated
and institutionali
zed, big hospitals
Mobile
medical
team with
a doctor
medicines
- Extension Services
- Carat ive care
- Village clinics
— Referral service
Free medicines
- Weekly or fortnightly visits
- J4inor physucal
ail ments
- People become more con
scious of their sickness
— Free transportat- - More patients in the
ion for the
hospital
seriously sick
- , .
.
- reeling of dependence
- Demand for more free
services
- Shift from horn remedies
apd_indigenous medicines
TYPE II
Capital intensive,
sophisticated and
institutioiialized
snail hospitals
TYPE III
Rural health centres
manned by nurses; not
institutionsod, still
very much structured
Mobile
medical
team with
ar without
a Doctor
a team com
posed of a
nurse and
social
workers
-' Extension service
- Curative and preventive care
- Village clinics
- Referral service
- Medicines at reduced rates
- Weekly or fortnightly visits
- Health education
- MCH programmes/iramunization
- Village health workers with
medical kit
- Minor physical
ailments
- Free transport
ation for the
seriously sick
- Personal and
enviornmental
hygiene
- Preventive,proraotico and curative- Good drinking
services
water
t VHW’s with simple medicines
.. ....TH crLL
47/1,(First Flo-, j jMarks lioarf
BAMGAiOHt - 5(J0 001
- People meeting in groups
- Learn some prevention
methods -
- More patients in the
hospital
- Laa’n that they can
do something about health
- People become more
confident in ther power
. 2/............................
2
- Health educations,
Adult Education
- Snail income generating
projects
- Better enviornmental
sanitation
- .'i>evelopnore inter
action among the
villagers
- M C H
- Less patients to go
to the hospitals
- Better child care
- Mahila mandals
- Kitchen gardens
- K C H
-Collaboration with govt, and
other agencies
- Village meetings and discussions
on different village
problems
- Promotion of collective
action
TYPE IV
- Rural health centres/
action groups
- Flexible and not
structured
- One team com
posed of a
nurse and
activists
- Services aimed at building
healthy communities
- Community Diagnosis
- Critical understanding of
health and it’s relation
to the unjust social order
- Awareness building through
nonformal education
programmes
- Organizing the people for
collective action
- Exposing social illnesses
- Basic needs
met by the
people
~ themselves
Participation and
collective action of
the people to build
up a healthy communit
society
- Better services
from the Govt. - Increased self
confidence and indepo
ency
Faith in their own
power to fight for a
healthy society
s
s
s
s
s
2
Action groups ■
Mahila mandals
Youth, clubs
Village committees
Farmers 1 clubs
Trade unions
- Demanding new services from the
govt, and better services
from the existing govt, health.
institutions
- Identifying and training
village animators
- Promotion of low cost and
simple homo remedies
- Health is considered
as a right and duty
and at the same time
seen as a political
issue
- People struggling
against social
injustices
- Go-operation among
them based on critical
understanding of
social realities
- New forms of politics
and new forms of
po oplc s1 movement s•
- Alternative indigenous
medical systems
developed
Community Health Department
CHAI
COI-irUHITY HEALTH AITD THE HEA_LI_ITG_ MHISTRY OF THE
“
CHURCH
Fr. Joii
i
*
Vattamattom SVD
Executive Director,
1
Introduction
Representatives of 13t nations, including India,
gathered together at Alma-Ata in the USSR on September 12,
1978 and agreed on the terms of’ a solemn declaration pledging
urgent action by all governments, all health and development
workers, and the world community to protect and promote the
health of all the people of the world.
Thus a new era
dawned in the history of health care of mankind.
An ambitious
target of a 22 year plan was announced to achieve HEALTH
FOR ALL by the year 2000 AD.
This major International
Conference, jointly sponsored by WO aid UIIICEF threw open
a challenge, redefining the whole health care system and the
concept of health itself. It also made it very clear that
health is no more an isolated factor and it is not also a
mere a&sense of sickness.
Health, on the other hand, is the state of total well
being of individuals, families and communities - physical,
mental and social.
We need to add yet another aspect i.e. the SPIRITUAL
WELL SBING, an aspect which was absent in the definition
provided by WO.
The declaration alsospeaks about the
responsibilities of all concerned in maintaining .the health
of every one.
In this exercise my attempt is to bring out briefly
the various aspects and implications of this new approach
to health-care.
In doing so I am only taking a layman's
approach as I am also aware of my limitations. Hence what
I am saying is subject to criticism and corrections.
2
Und er st andi ng the Concept
The ter: Community Health is today, perhaps, more
misunderstood than understood. Hence it is necessary to
have a correct understanding of this. For that the term
health itself has to be understood properly.
Since health
is not an isolated factor, it ca not be defined in a few words
It has to b.e understood in its relation to man and his
environment
Since both these are complex and complicated any
attempts to define health or Community Health becomes all the
more difficult.
However I shall try to present how it has
been understood in the recent past at various levels.
A simple way of understanding of the term Community
Health would be by comparison to the definition of democracy
i.e. health of the community, for the community and by the
community.
In this people are not mere passive recipents of
certain services rendered to them but they are active
partners in the decision making and implementation of all
that is required to maintain the health of individuals,
families and communities.
It can be measured by the capacity of the people to
take decisions and their undertaking of the responsibility
for the decisions they make. In other words in positive terms
it is building up of a healthy community, an in negative terms
it is getting rid of
*
social evils, imbalances and injustices
and whatever it is that hampers the growth of a healthy
community.
HEALTH IS SC PRECIOUS A COMMODITY THAT IT CANNOT BE
ENTIRELY. ENTRUSTED TO SOME SPECIALISTS, IT IS THE RIGHT AND
LSSPOrSlIILITI C-F. INDIVIDUALS,FAMILIES AND COMMUNITIES.
oned, earlier
2.2
mentdl and
lisease or infirmity
we need to add also
lout which the def in:
that it isa sta
>eing and not merely
have already mer.tilension of spiritual
,1th Care has a lot to do with com:
ig to the Alma-Ata declaration, it
Pri
.s
.its in
through theij
and the co tin
2.3
made universal
immunity,
it every stage of th
ice and self-determi
.th for all by the year 2000
Dr. H. Mahler, Director General of WHO explins as to
what it means, in relation to Primary Health Care and also
Community Health.
"It is not a single, finite target: it is
rather a process leading to progressive improvement in the
health of All people.
The concept of health for all in this
process will be interpretted and adapted differently by each
country in the light of its social,economic and even political
characteristics, the health status and the morbidity patterns
of its population and the state of development of. its health
system.
It does not, of course, mean that in the year 2000, or
before that, doctors and nurses will provide medical care for
everybody in the world for all their existing ailments; nor
does it “.-ean that in the year 2000 .nobody will be sick or
disabled.
It certainly cannot be envisaged in purely technd^J
cratic terms, such as doctors, nurses, hospitals,? drugs,
"
X-ray equipment and so forth.
Health for all does not mean
just mors af all these.
The idqa that "more of the sgine" will
solve our problems is no longer valid.
What health for all really means is that.health begins
at horns in schorls and at work places. It is there, where
people live and work, that health is created or broken. What
is really means is that people will use better approaches than
they do now for preventing disease and alleviating unavoidable
disease and disability and have better ways of growing up,
growing old and dying gracefully.
It certainly does mean
that there will be an even distribution, of whatever resources
for health are available .and that much greater efforts will bo
made to apply what is already known on the promotion of health
and the prevention and control of disease.
It also means that
essential health care will be accessibloto all individual and
families in a way acceptable to all of them, which they can
afford and with their full involvement.
IT FINALLY MEANS THAT PEOPLE WILL REALISE THAT THEY
THEMSELVES HAVE THE POWER TO SHAPE THEIR LIVE AND THE LIVES
07 THEIR FAM?'. LIES, FREE FROM THE AVOIDABLE BURDEN OF DISEASE
AND ARE .'.WARE THAT ILL-HEALTH IS NOT INEVITABLE"
The Pontifi cal Council, C.°.r. Unurn, on Primary Health.
'fork
2.4
Even '.'afore the Alma-Ata declaration the Church also
has given clear cut directives in understanding the coicspt
of Primary Health Care and community health.
If we wish to be faithful to Christ and take up his
attitudes with regard to our fellow-men, we must work for
the overall develop, .ent of each man, and focus on the sick
person more than on his sickness.
Since development also means
solidarity, we must necessarily turn our attention towards
the human community of the patient, his family first, but ;
his neighbourhood or village.
This means w must practise
com ami ty medi cine .
The mission that we have been given is a call for a
true conversion of our hearts and also of our methods. Secul
arisation is spreading in people's hearts from the industrial
ized and technological world to the developing (world)
countries.
We need to bo converted all the time in order to
bear witness as Christians to the sick who, through our work
will discover the love of Christ.
Th? rapid development in
the field of health service technology has often meant
installing expensive equipment in the hospitals, requiring
a large nu bar of staff for a relatively low number of patients
while in many of the same countries in the world up to 20^
of the population are still without healthcare services.
Since Christians are the leaven, we must reach out towards
the masses by providin ; simple, accessible and promotional
health care according to our own possibilities, mod:st as they
are, or in conjunction with the public services, where this
is allowed
Let us ever be mindful of the fact that service to the
sick begins and continues to op-rate through the patient's
human environment.
Community Health Care is, therefore, part of the
comprehensive pastoral work of the church.
Christians are^citisens just like anyone else, and must
be committed to the struggle- against under development.
The
example and the teaching of Christ and the exhortations of
the Popes shed light on this commitment and serve as a guide
and encouragement to them in their work which they undertake
for ths love of God and their fellow-men. If they work in
the field of medicine and nursing, the evangelical reflection.
mentioned as the beginning will lead them to ongoing conversion
of heart to provide a better service on behalf of a suffering
members of Christ and to awaken the communities of men to
their responsibilities in this ftrea.
While this now primary health care policy is talcing
shape, members of the religious congregation must take a good
hard look at the current conditions under which they are work
ing in order — where necessary— to re-direct them.
It some
times hap?e.-s that as a result of changes which not everyone
is necessarily aware of, too many of them work in hospitals
and health centres that have become too expensive for the
majority of the population, and are only within reach of the
pockets of a certain "elite" who can afford them.
In this
case the leaven is too far removed from the loaf.
2
5
The Hew national Health Policy of Goveri?—-ent of India
As a follow up of the Alma-Ata declaration our country
which was also a signatory of the doclsation, brought out a
new health policy which again gives us sufficient directives.
...V-
= 4 =
The exiting situation has boon lagely- eng; adored by
the al ost wholesale adoption of health man power development
policies and the establishment of curative centres based on
the Wester-. models, which are inappropriate and irrelevant to
the real needs of our people and the socio-economic conditions
obtaining in our country
The hospital based, disease and
cure-oriented approach towards the establishment of medic.nl
services has provided benefits to the upper cursts of society,
specially those residing ±n the urban areas.
The proliferation
of this approach has been at the cost of providing comprehen
sive primary health care services to the entire population,
£
whether residing in the -urban or the rural areas.
Furthcmoa^H
the continue;' high emphasis on the curative approach has led
to the neglect of the preventive, proactive, public health
and rehabilitative aspects of health care.
The existing
approach instead of improving awareness and building up selfreliance, has tended to enhance dependency and weaken the
community's capacity to cope with its problems,
The prevail
ing policies in regard to the education and training of
medical and health personnel, at various levels, has resulted
in the develop..ent of a cultural gap between the people and
the personnel providing health care.
The various health
programmes have, by and large, failed to involve the individu
als and families in establishing a self-reliant community.
Also, over the years, the planning process has become largely
oblivious of th? fact that the ultimate goal of achievinga
satisfactory health status for all our people cannot be
secured without involving the community in the identification
of their health needs and priorities as well as in the
implementation and management of the various health and
related programmes.
Presently, despite the constraint of resource, there isW
disproportionate emphasis on the establishment of curative
centres - dispensaries, hospitals and institutions for
specialised treatment ■■ the large majority of which are
located in the urban areas of the country.
A dynamic process of change and innovation is required
to be brought in the entire approach to health manpower
develop.-.ent thus ensuring the emergence of fully integrated
bands of workers functioning within the "Health Team"
approach.
Statements by the C 3 C I
If the various statements made at the CHCI - Catholic
Bishops' Conference of India level are indicators, the church
in India is also equally aware of the situation.
The
concept of health is very much linked up with those of justice
economic situation etc.
The Church has no ether alternative
than tc upholdcertain values that will recognise human
dignity and fight against all forces that will hamper this.
As early as 1972the C3CI made the statement. 1 The CHURCH
SHOULD ACTIVELY INVOLVE ITSELF III-BEHOVING CONCRETE CASES
OF INJUSTICES rlAPPENEITG 117 THE SOCIETY IN WHICH IT EXISTS".
This was following a statement by the Synod of Bishops in
Rome in 1971:
"ACTION ON BEHALF OF JUSTICE AND PARTICIPATION
TIT THD TlkAlTSF CREATION OF THS WORLD FULLY APPEAR TO US AS
A CONSTITUTIVE DIICSHSION OF THS PREACHING OF THE GOSPEL"
Specifically on the health sector the C3CI stated in
1973.
" We want cur health services to take primary health
care to the masses, particularly in the rural areas and
urban slums Catholic hospitals and dispensaries should stress
the preventive and promotive aspects of health care.
Specifically, we would urge them, to join hands with the civil
authorities in their program.es for the eradication of
leprosy.
,
"Our health cut-reach programmes may demand a change
in the routine especially of religious communities of nan
and women involved in this work, and their formation should
prepare them to meet the new spiritual challenges that are
posed".
Discussing the situation of cur country today, C3C1
Commission for Justice, Development and Peace in which
health is a component, in its meeting in January 19^3 made
our option very clear when it said;
"The Com ission being conscious of:
a.
the situation of -. assive poverty of over 60%
of our people.
b.
the unjust structures which maintain and
prepetuate it;'
c.
the injustices perpetuated on the weaker section
of the people;
considers it imperative to reaffirm our commitment to the
poor in limitation of Christ's preferential option for the
poor.
The creative struggle of the people to bring about
a new society invites us to enter into critical collaboration
with people of all religions, idealogies and agencies who
strive for a just society.
A meaningful participation in this struggle calls for;
a.
b.
c.
a serious analysis of society with tools of social
science and in the light of faith;
taking a definite and un-ambigous stand on various
issues;
initiating concrete action programmes
for change.
As a credible sign of this process the Church initiates
sections for justice within its own structure.
In this
context participation of all sections of people especially
of the laity is of vital importance."
"Wit?, this orientation in view the Commission proposes
the following priorities of work in the field of health;
1. Promote Community Health Programmes on a priority
basis.
2. Train health care personnel with a bias to rural
health prograimr.es. In this connection, it is of
utmost importance to reorient doctors, nurses and
para-medical personnel in our institutions and
programmes in Christian values".
6
2.7. Iji/A
Teachings of Cferj-.st
We are all so familiar -with, this that any elaboration
of it would be unnecessary.
Two outstanding passages among
j.any which "h specifically mentioned about the purpose of
his coming and which have direct reference to our present
context are John 10;10 and Luke 4:1^-20.
2 •/ CJ'W.I ' S Philosophy and Vision of its Community Health
Programme
The Community Health Department of. CEAIalso felt the
need for a correct understanding of its role in the field
of health. All the prints mentioned above were the basis for
its conclusions. Accordingly we believe that 2
1.
In a country like India, sc vast and varied, where
80$ of its population lives in the rural areas and about
90$ of the country's health care system caters to the
need of the urban minority, a new orientation and re
thinking of the whole health care system is the nred
of the hour.
2,
Health is the total well-being of individuals, familie^
and communities as a whole and not merely the absence
of sickness.
The demands an environment in which the^p
basic needs are fulfilled, social well-being is
ensured and psychological as well as spiritual needs
are met.
Accordingly, a new set. of parameters will have
to be considered for measuring the health of a community
such as the people's part in decision making,■absence
of social evils in the co : unity, organising capacity
of the people, the role women and youth play in matters
of health and development etc., other than the tradit
ional ones like infant mortality rate, life expectancy
etc.
The present medical system with undue emphasis on the
curative aspect tends mainly to.be a profit oriented
business, and it concentrates on 'selling health' to
the people, and is hardly based on the real needs of
vast majority of the people in the country.
The root
causes of illness lie deep i.:. social evils and i .baln^^es, to which the real answer is a political end, unda^F
stood as a process through which people are made awai^P
of the real needs, rights and responsibilities, available
resources in and around them and get themselves organised
for appropriate actions.
Only through this process
can health become a reality to the vast majority of the
Indian Ifesses.
The concept of Community Health here should be understood
as a process of enabling people to exercise collectively
their responsibilities to maintain their health and
to demand health as their right.
Thus it is beyond mere
distribution of medicines, prevention of sickness, and
income generating programmes. V
3
- CURRENT SITUATE PIT/ALBAS OF CONCERN
After having considered the various understandings of the
concept of Community Health in relation to man and his envir
onment, I wouli only .ention in brief the current situation of
the health care system, in our country.
For fear of being too
lengthy I shall not elaborate a .y of the points.
There are
a number of areas of concern based on the present situation.
7/-
3.1
Allocation of budgets and health care jeersp nne_l
Today in our country 80$ of the health budget and
nearly SO1/ of the health care personnel are utilised in urban
areas where only 20$ of the population lives while, where
80;.' of the people live, health care facilities are negligible
and in some areas totally absent.
'What about the distribution
of men and money in this field with regard to the Church?
3.2
Total absence of or lack of safe drinkingwater facilities
in ore than 300,000 of our villages, after 37 years of
Independence.
3.3
Imported Health care system still prevailing in our
country.
3.4
Bver increasing cost in health care delivery beyond the
means of any average person ld
t
*
alone the really poor
3.5
-Tver growing unethical practices in health care delivery
system by indiscriminate practitioners and over prescr
iption of drugs, unnecessary investigations and even
performance of surgery etc. merely for increasing income
for the institutions.
3.6
A medical education and nurses' training system which
are imported and geared to taking care of the elite.
Health care personnel, particularly doctors trained
under this system become rather a 'marketable commodity'
than Christ-like apostles to the sick,
3-7
Nuclear Wars a threat to Health
Medical evidence of the possible destruction of our
present civilisation in the event of a nuclear war is
becoming irrefutable.
Nuclear war coulddestroy in a
single stroke the achievements of thousands of years
of human effort.
Could' a commitment to "Health
for all"
include an increasing pro-life, anti-war
commitment ?
4• FHTURB OF E3ALTH CARS APOSTOLATE IN INDIA
From all that has been mentioned above’ a relevent question
may be raised, i.e. what is the role of the Church in the field
of health in India? To answer this question is not easy as
the field itself is so complex.
Health care is a field in
which the Church in India has been busy for over a hundered
years.
With more than 2000 health care institutions all
over the country run directly by the dioceses or religious
congregations, the volume of work being done by the Church
is enormous.
With one well established medical college and
more than hundred nurses' training institutions we train
every year an army of health care persomel and add to the
already existing ones in the fiefld.
With those tremendous
resources at hand the Church in India can bring about a new
revolution in the field of health as it is expected of us
also.
In order to do this we need to commit ourselves to
certain priorities.
If our commitment is similar to that
of Christ i.e. "PREFSRSNTIAL OPTION FOR THE POOR',' The Chruch
will have to take to heart the community Health programme
and make it. a movement.
Any movement is dynamic and to make
community health a movement it has to be motivated by the
complete invoIvement of the people.
The Church will have £o
give the lead through her organisations at various levels.
What is urgently needed is that the Church takes an official
stand on the side of the common man by promoting Community
Health as a movement.
n z
5. COnCLUSIOH
"
"The medical establishment has become a major throat
to health. The disabling impact of professional control
over medicine has reached the proportions of an epidemic"
Wrote Ivan Illich at the beginning of the introduction
to his book "Limits to Medicine".
Though strange to road
it points out to a certain reality that exist today
in the field of medicine and health care. Yet com. ited as
we are to the cause of the people of God especially that
section whom Christ also preferred, we need to bring about
a change in the present system. As Dr. Ravi Narayan wrote
in the May-Juno issue of our journal, Medical Service:
"With the increasing emphasis on .'Primary Health Care1,
we are all in an an increasingly important quest for
PRIORITIES. We have to seek; clean water before antibio tiqg^
food before vitamin pills, vaccination before kidney machi^Js,
mother's milk before powdered babyfoods mixed with dirty
water, and health for villagers and slums before more hospitals
for the affluent suburbs of capital cities".
This is a
commitment to Christ's preferential option for the poor.
This is a commitment to Community Health as a movement. This
is a challenge before the Church in India which we will
have to take if we want to be relevant to today’s situation
in our country..
;-
°§^§° o§|§° °§^§° °8^§° 0§^§0 o§|§° °§^§°
THE CATHOLIC HOSPITAL ASSOCIATION OF INDIA
Community Health Department
Grams
:
Post Box 2126
CEEHA1
SECUNDERABAD 500 003
Telephones : 84 82 93, 84 84 57
Telex
: 0425 6674 CHAI IN
157/6 sta(T Road
SECUNDERABAD 500003
MINISTRY OF THE CHURCH IN HEALTH SERVICES
Introduction :
"Action on behalf of justice and participation in the transforma
tion of the world fully appear to us as a constitutive dimension
of the preaching of the Gospel".
<<
- Synod of Bishops 1971
•
‘
"Behind the revolutions of our day, is man's struggle for human
dignity. Christ is at work here and we cannot proclaim Him to
contemporary man if we do not participate in this struggle. In
such participation we have to work with men of all faiths and
no faith. Christian living is, in this sense, living in response
to the WORD and to the world. It demands the conscious
transcendence of our limited groups solidarities and moving
towards the new humanity which is free from all discriminations".
- National consultation on the
role of Church in contemporary
India, 1966.
"If we wish to be faithful to Christ and take up this attitudes
with regard to our fellowman, we must work for the over all
development of each man, and focus on the sick person more than
on his sickness. Since development also means solidarity we.
must necessarily turn our attention towards the human community
of the patient, his family first, but also his neighbourhood or
village. This means we must practice community medicine".
- Pontifical Council Cor Unum,
Document on Primary Health
Care Work, 1978.
"The mission that we have given is a call for a true conversion
of our hearts and also of our methods. Secularization is spreading
in people's hearts from the industrialized and technological
world to the developing world countries. We need to be converted
all the time in order to bear witness as Christians to the sick
who, through our work, will discover the love of Christ. The
rapid development in the field of health service technology has
often meant installing expensive equipment in the hospitals,
requiring a large number of staff for a relatively low number
of patients, while in many of the same countries in the world,
upto 80% of the population are still without health care services.
2
2
Since Christians are the leaven, we must reach out towards the
masses by providing simple, accessible and promotional health
care according to our own possibilities, modest as they are,
or in conduction with the public services, where this is
allowed.
Let us ever be mindful of the fact that service to the sick
begins and continues to operate through the patient's human
environment. COMMUNITY HEALTH CARE IS THEREFORE PART OF THE
COMPREHENSIVE PASTORAL WORK OF THE CHURCH".
- Cor Unum Document, 1978.
"Presently, despite the constraint of resources, there is
disproportionate emphasis on the establishment of curative
centres - dispensaries, hospitals institutions for specialised
treatment - the large majority of which are located in the urb>
areas of the country «-... A dynamic process of change and £
innovation is required to be brought in the entire approach to
health man power development ensuring the emergence of fully
integrated bands of workers functioning within the "Health
Team" approach".
- New National Health Policy,
1982.
"The demand for justice has been one of the dominant notes
of this half of the country. Perhaps no other period in
History has witnessed a greater denial of justice also
'The Church, bearing within itself the pledge of the fullness
of the Kingdom, views with joy the present concern for justice^
.and with anxiety the grave threats to justice all around us.
It is her endeavour to interpret the implications of the Gospel
message of justice and peace in the varying situations being
unfolded in the course of the human pilgrimage on earth. She
has to be the 'Leaven' and the 'salt' of the earth in the con
fusion likely to prevail in the search for justice".
- CBCI, 1978.
"The Church should give its whole hearted support to the peace
ful social changes taking place in the country by verbalising its
support of any efforts made for bridging the gap between the
rich and poor.
"The Church should actively involve itself in removing concrete
cases of injustices happening in the society in which it exists".
- CBCI, 1972.
3
X
-
3
-
"We want our health services to take primary health care to the
masses, particularly in the rural and urban slums. Catholic
Hospitals and dispensaries should stress the preventive and
promotive aspects of health care. Specifically, we would urge
them tc join hands with the civil authorities in their
programme for the eradication of leprosy.
Our health outreach programmes may demand a change in the
routine especially of religious communities of men and women
involved in this .work, and their formation should prepare
them to meet the new spiritual challenges that are posed".
- CBCI, 1978.
" The commission being conscious of :
a the situation of massive poverty of over 60% of our people;
b the unjust structures which maintain and perpetuate it;
c the injustices perpetuated on the weaker section of the
people;
considers it imperative to reaffirm our commitment to the poor
in imitation of Christ's preferential option for the poor.
The creative struggle of the people to.bring about a new society
invites us to enter into critical collaboration with people of
all religions, ideologies and agencies who strive after a just
society.
A meaningful participation in this struggle calls for :
a.
b.
c.
a serious analysis of society with the tools of social
sciences and in the light of faith;
taking definite and unambiguous stand on various issues;
initiating concrete action programmes for change.
As a credible sign of this process the Church initiates action
for justice within its own structure. In this context partici
pation of all sections of people especially of the laity is
of vital importance".
- CBCI, 1983.
"With this orientation in view the Commission proposes the
following priorities of work, in the field of health :
■1 • Promote Community Health Programmes on the Priority basis;
2 Train health care personnel with a bias to rural health
programmes. In this connection it is of utmost importance
to reorient doctors, nurses-& para-medical personnel in
our institutions and pr-grammes with Christian values.
4
- 4 3
A commission could be set up to study the prevailing conditions
and problems, attitudes and values of doctors, nurses,- oaramedical personnel and other employees.
- CBCI, 1983.
The relevance of quotations cited above can be viewed by different
people differently depending on the concept of health one has.
One thing is getting more and more clear that health is no more
an isolated factor and it is not merely the absence of sickness
but the total well being social, physical, mental and spiritual
of individuals, families and communities. It is in this sense that
the above quotations have their relevance when dealing with
ministry of the Church in Health Care.
Health care is a field in which the Church in India has been
busy for over a hundred years. With more than 2000 health care
institutions all over the country run directly by the dioceses
or religious congregations, the volume of work done by the
church is enormous. With ohe well established medical college and
more than hundred nurses' training institutions we train every
year an army of health care personnel and add to the already
existing ones in the field. With the emphasis since some years
on the field of community health, a new army of village level
health workers (called under different names) are trained and they
are in the field. We have also national organisations, under the
auspices of the Church, dealing with various aspects of health
care i.e. the Catholic Hospital Association of India, Catholic
Nurses' Guild, Catholic Doctors' Guild, Natural Family Planning
Association of India etc. This certainly shows the richness of
the resources at our hand. The question will have to be asked is
are all these properly utilised for the best interest of the
(
people of God in India particularly the bast majority of them
living in rural areas and urban slums.
1.
COMMUNITY.HEALTH :
CHAI has definitely committed to this cause for the coming years.
And we do hope to do something thereby contributing our share
to achieve the goal set by WHO and accepted by our country, i.e.
Health For All by 2000 A.D. This we hope to achieve through
our member institutions and others, and with the cooperation,
help and guidance particularly from the members of the CBCI and
CRI. We have now an eight member team for the promotion of
Community Health. The team has worked out a philosophy and
vision for our community health programme and a broad plan of
action.
5
2.
- 5 Promotion of Pro-Life Activities :
Efforts will have to be made by all concerned to bring an aware
ness about the seriousness of this all important aspect of life.,
CHAI will be taking some definite steps in this regard in the
c oming years.
3.
Pastoral aspect of health care ;
This is a,field rather neglected by the Church. Complaints about
even rude behaviour by the Staff towards patients in our health
care institutions are not a rare phenomenon. Then the question
is, have we given them the necessary training and orientation ?
Keeping this in mind CHAI organises seminars for health care
personnel from time to time. It is our plan to develop a separate
department in CHAI to meet this crying need in our country.
We also plan to organise regular residential course for Chaplains
etc. in .the future.
Agaihst all what has been mentioned, particularly the various
documents mentioned, the following suggestions are put forward
for Justice," Development and Peace in General and the health
section in particular. In this connection, it was very meaningful
to have put the health section with commission for justice,
development’, -and peace.
1.
.To have an evaluation of our existing institutions for
education., training and services in the field of health.
in accordance with the present concept of health mentioned
in the documents ( of also the CHAI documents )
2.
Community Health Programme accepted as a priority should be
promoted in all the Dioceses. The members of the CBCI and
CRI should accept this end and make it known to all our
health care institutions.
3.
In order to implement this, St. John's Medical College,
National Organizations like CHAI, NEPAI, CARITAS INDIA,
IGSSS etc. will have to plan together in collaboration with
other organisations in the field such as VHAI, CMAI, ISI etc.
4.
Possibility of organisations like, CHAI, Catholic Nurses'
Guild, NEPAI to work together will have to be explored, for
better effect and to avoid any unnecessary duplications.
5.
The teaching of the concept of Community Health based on
the various documents dealing with the subject should find
a place in the Curricular in Seminaries and Religious
formation houses.
6
- 6 6.
In this connection this, commission will- have't o work in
collaboration with the commission on Seminary Training etc.
7.
This commission should also work in collaboration with the
commission for Laity and Family.
These are a few suggestions, however practical they may be
which came to my mind. The implementation of them may be
difficult but necessary if we want to respond to the needs of
the time. We all agree that making statements (for whichwe seem
to be experts in this country) alone will not solve the
problems. We need- to translate them into action, which is by
far difficult. But we are left with no choice but to do it if
we want to be meaningful to the society today and faithful to
the gospel message. Let me conclude this with another quotation
this time from Ashok Menta.
"We must reclaim 900 million people (the number is more now)
of the world who are today in a state of abject depression.
This human reclamation requires a peculiar type of social
engineering. This is to my/mind the big challenge .that all
people, all men of religion, all men of God h,ave to face.
And if it is the proud claim of the Christian Churches that .
they have that spiritual understanding, that spirited agony .and
that spiritual out glow is greater than that of other men of
God, it has to be proved, as I said in the crucible of life
itself. If it is the claim of Christians that even to this
day they feel the agony of Christ on the Cross whenever
humanity suffers as it were, it has to be proved, in action and
not by statement".
Fr John Vattamattom svd
Executive Director
Catholic Hospital Association
of India.
23-11-87/200
mm/
our XQCj/rtch
God's.call is
A C AL-L
It signifies choice
re-sly
with all
,ssi
If God calls, it is in order that wo correspond with His
plan of love, to malce known to us His will to stir up in us a
response of love and to send.us on a mission.
It is in response to God's call that we have committed
ourselves to live and to serve
our vocation
The call is a direct command which God addressess to a
person whom he has chosen for Himself, and whom He destines for
a particular work in His plan of salvation.
Gen.
12s1, Ex 3:10-16, Jerl. 4-9
When God calls, He sends; He gives a mission Gon 12s1; Ex 3:4-11,
4^-22; Is 6:9, Am 7:15
Sometimes, seized with fear, the person called trios to
evade the call. Ex 4:1Off; Jr.1:6, 20:7-18, Jn 1-4.
Sometimes acceptance is instantaneous Gen.
12:4, Is.6:8.
But in his fear as well as in his generosity, in his power to
resist as well as to respond, the person called is completely give:
ever to the Lord in all His truth, and for each one, according to
the situation in which he is placed at the time of the call, there
is a personal response to this will of God, setting him apart for
God 1s work.
Como I
Jesus calls many to follow Him. (Mk. 3:13; 10:21;
td 9:59-62) The account of the calling of the Apostles demonst
rates, well the personal character and the supremacy of the choice
of Jesus, taking with Him "those He wanted" to accomplish His
work. Mk. 3:13v
His preaching is also a call to follow Hira in a new way
of which He possesses the secret Mt.
16:24.
The call is a choice
'to be His companions' Mk 3:14, and a sending in His name to be
His witnesses Mk 6:7-13.
2
-2-
How Paul and Peter understand the calls
Rom. 4:17, 1 Pet.1:3:11
S'.’-ery Christian life is a Toeation:
Rom. 8:1 6
Purpose of God's calls
ICoro 1:26,2:5,Eph 4:1 4
Community of this call the church
2Jns1
followers of all ages,- our apostolic identity and spirituality
refer to an act of 'being sent' not as to a mandate, but as to an
invitation to a privileged relationship which bears witness to
intimate friendship and a shared idea.
To follow God is to taka the road by which He led His
people.
At the time of Exodus? to pass through the desert into
the promise land.
This is what fedelity demands.
'o follow Christ is to walk the road of the Paschal Mystery,
the path He trod for us so as to lead us from death to life? it
is to share His destiny.
This is not done without breaking ties
without taking risks.
SEiTT;
The one who is sent is someone entrusted with, a
mission.
After God had sent the Prophets, God sent His Son, who
in His turn, sent His desciples, empowered by the Holy Spirit, to
continue to carry out God's work or plan.
"I am sending you" this phrase is at the heart of every
prophetic calling (Ex 3:10; Jr.
1:7, Ezk 2:3ff, 3;4ff) Each one
responds to the call of God according to his personal temperment.
Isaiah offers himself: "Behold here I am, send me"
(is. 6:8)
Jeremiah accredit his mission (Ex 3s11ff); he tries to refust it.
(Ex. 4:13) he complains bitterly (fix 5:22); but finally, all
obey (Am 7:15).
This consciousness of a personal mission received
from God is an essential trait of the true prophet.
Reflection: Each day the.invitation comes
To find yet deeper meaning in the missionary call;
It urges me to go beyond myself,
To widen the horizons more and more,
To enter into true concunion.
With "the other", my neighbour;
This means embracing His mentality
His language, His culture,
. .3..
(
-3-
His Very Heart. .
. .
Universality means setting self aside,
Putting others first, being open all the time.
Again, each day it also bids me seek
The deeper aspects of that other call:
To live as a true "sister" in community
With all the self-surrender that implies;
The welcoming smile, the sympathetic ear,
Whole hearted acceptance of each one,
The sensitivity to signals; promptness to forgive
With self-effecting love,
Accepting to be overlooked oneself.
Yes, day by day I must confront this challenge,
To seek new depths of union in my life with God
Letting my heart be opened wider yet
To the dimension of universal love
A love that liberates and heals
An all-transforming love
For love is greater for
Than my poor heart.
s.
133 (139).
ong.
Come follow me
COMMUNITY HEALTH DEPT.
CHAI
CATHOLIC HOSPITAL ASSOCIATION OF INDIA
EVANGELISATION MEANS PROCLAMATION OF THE GOOD NEWS OF
SALVATION TO THE POOR.
Its signs are: The Blind see, the Deaf hear, the Dumb speak, the
Lame walk, the Captives are set free and the oppressed are
liberated.
(lK 4,
18; 7,22).
The Blind: The Poor were unable to see the powers and forces which
dominate and exploit then because the Elite, to keep up
their status quo, never let them see the reality of do
mination and exploitation.
They brainwashed them, with
the words of "Humility, service, obedience, blessed are
the poor, the will of God etc..,".
See:
Now they see, because critically aware of these forces
which dehumanise and exploit them and they see also the
ways and means which put them in the path of liberation
f
and progress.
The Deaf:
For the people who were conditioned to live in perpetual
slavery and suppression the words, freedom, equality
justice and human dignity meant nothing because they
never experienced these realities.
As a result they
were deaf to them.
hear:
Now they hear, they understand the meaning of human dign
ity freedom, equality, justice and development.
Their
ears are attuned to these realities because they already
experience them in their common discussions and action
programmes and in their co-opera'tive living.
V*
The Dumb:
Centuries of suppression and Domination made them silent
)
They were not allowed to express their opinions.
had only to listen, do and die.
They
As a result they were
afraid to open their mouth, thoughts, ideas and feelings
Others thought for them, spoke for them and decided for
them thus made them Dumb.
Speak:
Now the silent masses are getting organised and have
gained the courage to express their thoughts, ideas and
feelings boldly.
They discuss their life problems above
all take their "own deci'sion'.
The Lame:
The age old master, servant relationship made the poor
depend on their masters for every thing.
Their masters
never let the stand and walk on their own feet.
They
remained as children continuously depending on their
"benefactors" for every thing.,
-2-
Now they are confident to stand and walk on their own
feet independently as adults.
They will never allow
themselves to be crippled by any dominating and explo
iting powers, because now they know that it is in walking
on their feet they and their children are going to achi
eve their development.
The
captives:
The social, economic, political, cultural and religious
systems favoured the Elite and kept the poor in fear,
poverty and illiteracy and made them blind and deaf to
the dehumanising and exploitive factors.
are set
The critical understanding of these systems librate them
free:
in their thoughts and attitudes.and motivates them to
struggle for their liberation and progress with hope.
Thus they are no more passive victims of exploitation
but courageous agents of change and commited architecht^
of their own destiny.
This movement from darkness to light, ignorance to knowledge, slavary
to freedom is called salvation.
ction-action
Through a process of aotion-refle
the poor are already experiencing this reality.
They were blind, now they see, were deaf, now they hear, were dumb
now they speak, lame now they walk.
Thus this action reflection
programme becomes good news to the poor though apparently it is a
bad news to the Elite, the Masters, because the poor challenge their
dehumanising thoughts and systems.
If the Elite are not prepared
to change their evil ways they will never be able to experience the
kingdom of God, the Kingdom of Equality, Justice, Truth and Brother
hood."
They have eyes, but they do not see.
They have ears but
they do not hear..."
-COMMUNITY HEALTH DEPARTMENT
CHAI, C3CI CENTRE
GOLDAKKHANA, ASHOKA PLACE
NEW DELHI - 11000\.
a
CATHOLIC HOSPITAL ASSOCIATION OF INDIA
CSCI CENTHE, GOLDAKKANA
NSW DELHI - 11OOO1
Tel : 310194
theology
or
l i b e: ii a t. i o n
This is not an academic treaties on theology. A pragmatic
and analytical approach will be used in this paper.
For an ordinary man in the street or in the village, theo
logy is not a very respectable word today. This is not because
there.is any misgiving about God - Theos - but because the
theological approach has come to mean a mere recitation of
certain propositions, dogmas and faiths, with out any concern
for their relationship to reality. Theology is not an
experience to them, neither do they turn experience into
theology.
The history of theology, and for that matter Christianity
is well-known for its continued accomodation and adaptation
of the changing historical circumstances and to a large scale
social movements. But today the social transformation and
situations are of a different order than it was in the past.
Now, is it possible and up to us to accommodate and adapt?
In the- socio political environment in which we exist today,
the Church is called upon to fulfil its salvitic mission. This
environment is vastly different from what it was ten years ago.
Latin America. s
The theology of liberation developed in Latin America
during the 1960s, through an outgrowth of both the changing
political climate on that continent, and of the liberalizing
trends which took place in the Catholic Church as a result
of Vat. II. Vat. II sharpened with in the Latin American
Catholic community a concern for the poor. For the Christians
here, the gospel became a revolutionary document. Jesus was
the Liberator, who placed himself squarely on the side of
the poor and the oppressed a ;ainst the forces of injustice
and. exploitation. To follow Jesus for these people was to
identify as He did and to work with the poor for the Liberation
of all, who suffered from injustice.
Although untill recently the church in Latin America was
closely linked to the established order, It is beginning to
take a different attitude regarding the exploitation, oppression
and alienation, which prevails here. Individual Christians,
small communities, and the church as a whole- are becoming
more politically aware and are acquiring a .greater knowledge
of the current Latin Americal reality, especially in its
root causes. The Christian community is beginning to read
politically the signs of the times in Latin America.
The Advoca.tes of the Latin American Liberation theology
vehemently asserts their right to evolve- a theology out of
their own experience. But the traditional and established
theologians are sceptic about it on the ground that theology
is made too much anthropiigical.
Situation in the Chur.ch s
The Church in the first centuries, with its minority
..2/-
status in society and the consequent pressures from the nonchristian world, was very sensitive to the action of Cfcist.
(They shared everything in common .... Acts —4. 32-55)
But this situation of the Christian community changed
in the fourth century. Instead of being marginated. and attacked
Christianity was now tolerated (Edict of Milan - AB 313), end
quickly became the religion of the Roman State (Becree of
The ssalonica., 331 AB). The proclamation of the gospel was
then supported and protected by the political authority.
This 'gradually changed the manner of conceivin'- the relation
ship of -lankind to salvation. By the middle ages, when the
church was co-extensive with the known world of that time
and deeply pervaded it, Christians had the vital experience
of security and tranquility, and that we- proclaimed that
outside the church, there is no salvation. To be for or
against Christ came to be fully identified with being for
or against the church. This still prevails in the church
and that we have fully forgotten the "Mission aspect" of
the church (To be the salt and light of the world). Today
we are more aware of our self .sufficiency, .and that christ
is made to speak what we want him to speak.
The church was more concerned about the number of people
saved? (Hew conversions without giving profound reflection
on salvation) and naturally the church tried to work out the
roles which it has to play in this process.
In the early centuries of the church, theology was
closely linked to the spiritual life (realm)
*
This theology
was monastic, and therefore characterized by a spiritual life
removed from worldly concerns. The Christian spiritual life
in the early centuries was thus characterized by withdrawal
from the world,(world, devil, body) (lack of love not a sin)
and it was presented as the model way-to sanctity.
But with St. Thomas Acquinas, theology began to be
characterized as an intellectual decipline, born of the
meeting of faith and reason, and it was considered as a
rational knowledge.
But gradually, we are realising that salvation is not
something other worldly in regard to which the present life
is merely a test. (The kingdom is among you) Salvation in
this real sense -.leans communion of hen with lod and the
co mnunion of men among themselves. The church must cease
considering itself as the exclusive place of salvation and
orient itself towards a new and : adical service of people.
All the same, can the ch.meh be a prophet in our day,
if she herself is not turned to Christ. She doesn’t have
the right to talk against others, 'when she herself is a
cause of scandal in her interpersonal relations and her
internal structures? We cannot talk of the church of the
poor without being a poor church; and that is just what
we are refusing to be - in our life style, transport
facilities, our homes and the property we own.
The church has for centuries devoted her attention to
formulating truths and meanwhile, did almost nothing to
better the world. In other words, the church focused on
orthodoxy and left orthopraxiz in the hands of non
members and to non-believers.
..3/-
3
The fact thet there is an into--locking of interests
between the institutionalized church and the dominant class
of society constrain her involve ...ent in the wore of genuine
liberation. In order to be more responsive to people’s
aspirations, she n -yds to dissociate herself firom the
dominant class by giving up her interests. She is so luch
linked with such system, almost as partners in a narrate
(Church the sprduse of Christ).
In the 19th and 20th centuries, a new awakening is/
sli-htlv visible in the attitude of the church.
Pope -ius
XII, John XXIII’s’’Mater Et >a;istra'’, ’Paco-i In Terris',
Paul Vi's 'Populor’u 1 Iropfessioin all these develop ment integral development of .-'.an ~ is considered.
Ga.uo.iun ft
Spes^(Vat. II) uses the term 'liberation' on two occasions.
'Populorum Byogre ssio 5 speaks clearly of building a world.
.where everynan, no matter what his race, religion or
nationality, can live a fully human life, freed from
servitude imposed on him by other men or by natural forces
over which he had no sufficient control.
In the words of Copy&r, if the Ch-.r-ch wishes to deal
with, the real questions of the - modern world, it must begin
a new chapter of theolo ico-pastoral Epistemology.
Instead
of using only revelation and tradition as starting points,
as classical theolo ;y has always done, it must start with
facts and questions derived from the world and history.
So theology itself has to be liberated from every form
of religious alienation. A theology v/hich is not up-todate is a false theology.
Theology has to be linked to the praxis, and should
fulfil a prophetic function, in so far as it interprets
historical events-,' .with the intention- of■ revealing and
proclaimin • their profound meaning.
It has to be a theolo -y
whiclj is open in the protest against trampled human,'
dignity, in the' struggle against the plunder of the vast
majority of .people, in liberating love, and in the build
ing of a new, and fraternal society (Kingdom of God).
We believe it to be our ‘right end duty to denounce
as evil and sinful? Inadequate wages, lack of food, -exploitation of the poor, suppression of freedom, etc. It is
here that we often makes the mistake, many of us, of
considerin'-: this a politico! attitude, and therefore outside
pur sphere.. Yet, Christ’®| bun prophetic act'ipn and fidelity
to truth certainly presuppose. an inevitable involvement, in
politics.
The commitment to the creation of a-lust society and,-ultimately to a new -non presupposes faith, hope and love
and confidence in the fat re. (Example of A by aha i, 1'oses ...
Heb. 11)
We have to build a church which is both in its
preaching and practice co.^maitted to the poor, to the weak,
and to the exploited.
God in History»
The God whom we. know in the Bible (history of Bible)
is a Liberating God, a God who destroys myths and alienations.
a God vdio intervenes in history in order to break down the
structures of injustice and who raises up prophets in
...4/-
order to point out the way of justice arid mercy. He is the
God who liberates slaves (Exodus & Egypt) who causes empires
to fall down and raises up the oppressed.
In the dawn of human history, God was seen as a trans
cendental being (Mountain) and then a universal being. Then
the concept of God changes (Exodus - Arch) to localization
and he was seen as linked to a particular people (Israel).
And then it gradually extends to all the people of earth
(Amos’ 9/7; Is. 41s1-7) Is.4O°2O-25, entire book of Joshua).
To love Yehoa (or to know Yehoa) is to do justice to the
poor and the oppressed. Prophets criticizes the worship
that is devoid of the touch of reality. "Though you offer
countless prayers and sacrifices, I will not listen. There
is blood in your hand .... cease to do evil and learn to do
right, pursue justice and champion the oppressed? give the
rights of orphan, plead the widow's cause. (Is. IMO-17)
Our encounter with God occures in our encounter with men,
especially in the encounter with those whose human features
have been disfigured by oppression, despoliation and aliena
tion, and who have 'no beauty, no majesty’."
(Is.5322-5)
This becomes more clear in New Testament. Through
humanity, each man has become the temple of God.(St.Paul)
We meet God in our encounter with mon, we encounter him in
the commitment to the historical process of mankind. In
St. Mathew’s Eschatological discourse, ’the least of my
brethren (2554O) designates all the needy? whoever they may
be, and not only Christians or a particular group of people.
The spirituality of liberation will centre on a conver
sion to the neighbour; the oppressed,. and the exploited.
Conversion t"> the Lord implies the conversion to the neighbour.
This means a radical transformation of ourselves, ie.
thinking, feeling, and living as christ, present in exploited
and alienated man. It means to commit oneself to the process
of liberation with an analysis of the situation and a
strategy of action. The Christian has not done enough
of conversion - ie. commitment to the neighbour, to social
justice, to history.
In the Nev; Testament Christ is presented as the one who
brings us liberation. Christ the saviour liberates man from
sin, which is the ultimate root of all disruption of friendship
end of all injustice and oppression. Christ makes man truly
free, that is tc say, he enables man to live in communion
with him, and this is the basis for all human brotherhood the Kingdom cf God.
In this perspective, sin is not only an impediment to
.salvation in the after life. In so far as it constitutes
a break with God, sin is a historical rea.lity. It is a
breach of the communion of men with each other, it is a
turning in of man on himself, which manifests in the with
drawal from others. Because sin is a personal and social
infra-historical reality, a. part rf the daily events of
human life, it is also, and above a,ll an ■ bstacle to life’s
reaching the fullness we call salvation.
5
Christ came and proclaimed the Kingdom of Cod which
meant a society where, fraternity, justice and love prevails,
e.
i.
complete communion of men with God and of men among
themselves.
The poor of whom Jesus speaks and who surrounded him
are the truly poor, the hungry, the afflicted, the oppressed,
and all those for whom society has failed to provide a placei
Through this solidarity with the poor, Jesus proclaimed his
‘Father’s love'for all mankind — and he was persecuted J
Towards a New Theological approach for Indias
The situation in India as we have seen, is so dehumani
zing that no Christian can idly stand by and. call himself
a follower of Christ. All the same.the traditional response
of the church to this situation is still inadequate. The
young people engaged in social action in India today are
really surprised to find that the kind of Jesus they have
met in homilies and catechism classes becomes irrelevant
in the actual life situations of the people.
The picture of Jesus transmitted through monastic
spectacles, who prefers order and quiet, lots of prayer, and
minimum commitment to dangerous issues,and who feels at
home amidst flowers and incense, and likes to dwell in well
constructed monastic houses surrounded by high walls, is
out-dated for India, and is irrelevant to committed people.
To ~ start theologizing for the exploited, we have to
move out of our institutions - church structure - which
silences the prophetic voice of the Bible.
Theology as a function was always present in society, India and elsewhere - but at a certain moment in history, there
arose a professional class of theologians. It must have been
because the society had reached a stage of surplus production,
when some no longer needed to work with their hands and could
take some gher persuits. Some began t-' use this leisure to
theologise. Without being cohsMous of it, their theology
was bound to be a class theology, because such theologians
depended on the upper class for their maintenance. This is
true not only of theology, but of the social sciences as well.
(In China professors doing manual work).
It is natural that every type -f society produced a
theology to legitimize the position of the new dominant
class. So We had a feudal theology, a capitalist theology,
and now we are trying to produce a socialist theology.
The Church in India has become so much inward-looking
(status, position, institutions) that it can never heal itself.
The ’mission' entrusted by Christ is not found here. We have
to proclaim the gospel - also to the rich, hoping that some
atlaast may’ be converted. In addition, we have to realize
that announcing the’good news’also means announcing the 'badnews’ to some. The ’blesseds' have to be accompanied by
the’woe s’.
As Paulo Freire says, According t~ the oppressed, to
bo a man is to be like the oppressed. This is true in
...6/-
6
theology also. The oppressed have internalized the God of
tlx oppressor - which in fact is n't the real God (Death of
God theology).
For ar authentic theology for India, and Indian situa
tion,
it has t- start from the daily day experiences of the
common man in India. The imported western the 'logy can only
perpetuate and stabilize the situation in India today.
Conclusion*
God acts in history for human liberation, from every
form of oppressive conditi'n - including the opression of
poverty, racism, sexism, and colonialism. liberation
theology is thus a theology --f salvation for the ’.-holo
person. Liberation Techolo.gy takes its roots in the lived
historical experience f a people. It demands an adherence
tc it more than just an intellectual comiitment. It demands
a conversion to a new .way' of life.
Community Health Depti
§P^=QUJ2ELI^E§_QN_W5I_^NP_3^=5D-MAIETAIN_A_yiLIAGE_DIARY
A diary is a note book in which we write down regularly, the
significant happenings in our life. It is a personal account
of our thoughts, feelings and observations of events which we
consider important to us.
Similarly, a village diary is a record of significant events
which we have seen or heard about during our village visits
It is also a record of our own thoughts, feelings and obser
vations about our village.
Why do we need to keep a village diary?
1. It helps us to see the change in our villages over a period
of time. This changes could be:
- in people's attitude towards us
- in people's living habits
- more unity in the village etc.’
Eg:After working for a number of months in a village the
local dai brings a pregnant woman to us for examination.
This could mean that the dai has finally accepted us as
persons who will help per and not try to take away her
livelihood. She has changed her attitude towards us I
2.
It helps us to see the change in our own attitudes and
behaviour towards the people we are working with. Over
a period of time we may have:
- developed greater trust in the people.
- understood the reasons for certain habits in the
village
- learnt how to resolve conflicts in village
meetings etc.
3. The above points are extremely useful in evaluating the
effect of . our community health programme. Changes in
attitude and behaviour are different to evaluate, so making
note of significant events in the village can help us see
the change over a period of time.
h-. A village diary can help a new member of the team familiarize
herself with all that has beerihappening in the village.
It will help her to get to know the finer details of the
village in a shorter time.
How do we maintain the village diary?
1. Keep a separate diary for each village.’
2. Note down the date of the visit.
3. Below the date give a short summary of the visit. This
should include the following:
(a) Any significant event like discussions with the
Sarpanch, village leaders, quarrels in the village
etc.,
(b) Any observation and tentative conclusions drawn
from the observation;
(c) Plan of action if any for the next visit.
h-. All village meeting mustbe recorded even if they are
routine meetings.
COMMUNITY HEALTH CELL
47/1, (First Floor)St. Marks RoaA
BAN.-;' to !S 560001
5. Make it a habit to fill in thevillage diary immediately
after the visit, otherwise you will fbrgetto note down
important points.
6. It is necessary to record every single visit to the village.
Read the sample from the diary of "Bhedia" village on this
page. This will give you an idea of how tomaintain your
village diary.
N.B.;
One of the expectations of the CHIT course is that
each teamkeeps a record of their village visits in
the form:'- of the village diary.
The Diary of a Health Team; Village Bhedia
March Uth
Today Radha and I visited the village. We talked to the
Panchayat President (Name- Ramaiah). Wb met him just as he
was leaving the house. We explained to him about the kind of
work we would like to do in thisvillage. He did not seem
very interesred. I think he was getting late. Any way he
has promised to be in at home ne>t week when we come, We also
met the school teacher. He gave us tea. His wife is quite nice.
She could help us in future with our work.
March 11th
Radha was not well; so I took Shanti with me to visit the
village. We met Mr. Ramaiah, the Panchayat President. He
asked about Radha. He has been interested enough, to reco
gnize us. We talked about our dispensary in Janakpuri.
He wants us to start a dispensary in this village. We did not
promise him anything much. As we were talking some more
people joined us;. One was the school teacher. The other was
the Gram Sevak. The Panchayat President has promised to call
a meeting next month as all the people‘in the village are
busy with the harvest now. We were again invited to the
teacher's house.
Some of the village women came to the house
to see us out of curiosity. They seemed happy to see us.
We noticed a.lot of children with Vtt. A deficiency (Bitots
spot)
March 18th
We went straight to the teacher's house. Some/w8nien were
waiting for us in that house. One of them was pregnant and
had swelling of the feet. We gave her advice and asked her
to come to the health centre or send her husband to get the
medicines. The other women in the group said that there was
no one to take care of them when they had a problem and we
discussed the problems a pregnant woman faces. Quite a good
vi sit.
March 25th
We met the panchayat President to fix up a date .for the
meeting. The date for the meeting is April 1st. -Ve also met
some people in thevillage and told them do out the meeting.
Everyone in the village seems to be in a good mood. They
have had a good harvest.
- 3 April 1st
Meeting at 7 p.m. We had to wait for an hour foi- the people
together« I was getting impatient. But Radha said that
this is the way in the village and the people did not mean
to be disrespectful when they didn't turn up on time. The
Panchayat President said that/they needed a dispensary in
the village and has agreed to let us use the school
buildimg for the clinic. The people will pay for the
medicines but if someone cannot pay the Panchayat President
will stundoguatantee. ( I thinkthe wants to stand for the
next election also). We discussed with them that our alm
in working in the village is to improve the generalhealth
conditon and not for curative work alon99 I dont think
they understood very clearly what we meant but seemed
quite cooperative and open. I think it vail take time.
We did not discuss about a village health worker etc.
April 22nd
Didn't enter the last two weeks' visits. I was very busy.
We are conducting a weekly clinic, but it is getting to be
a problem. We don't have a jeep and there is only one bus that
reaches the village at 7 a.m. and leaves around 8.a.m. The
teacher suggested that we go in the evening stay overnight
and reave the next morning. We will have to discuss it with
the other team members.
April 29th
We have decided to stay over night in the village. We will
try it for a month and see how it owrks , The vist was very
good. We staryed in the village at night. All the women
gathered after dinner and we sang some Bhajans with them.
One problem in this village seems to be the drinking water.
-The women haisre to walk 3 miles to fetch water. We discussed
with the Gfam Sevak. We are planning to meet the BDO this
week. The Gram Sevak will accompany us-
chtt:pt:3.9.'81
From your experience, as well as from the insights you have received during these days
please choose a village from among the 7 villages in this map, for initiating a Community
r.ealbh Programme. On the next page, some more information are available on each village.
The Catholic Hospital Association of
C. B. C. I. Centre, Goldakkhana, New Delhi - 110001
Tel. 310694, 322064
SELECTION OF VILLAGES TO START
A COMMUNITY HEALTH PROGRAMME
Ry now, you and your team would have decided the location of
the Community Health Programme to be attached to your Health
Centre, discussed the staffing pattern and resources needed
for it. Now, you have to decide in which villages to start
the programme and what to do there.
To select villages for the programme we would propose the
following procedures
A.
A.
Study the different villages situated in the
target area, their needs, population, and re
sources;
B.
Select villages for starting the Community Health
Programme.
Study the different villages situated in the target area,
their needs, population, and resources?
Visit all villages situated in the target area.
In each village?
i.
ii.
iiio
iv.
v.
B.
meet all officials and leaders;
find out, informally, the socio-economicpolitico-religious structure;
find out what organisations are already
existing? Mahila Mandal - Youth Clubs etc.;
find out resources which can eventually
be used for the programme;
find out readiness of the people to change.
Select villages for starting the Community Health Programme?
Once we have gathered information on all the villages of
the target area, we will have to decide which are the most
appropriate villages for us to start our programme in. We
must not take too many villages to start with, and, at
this point, it is good to remember that Community Health
Programmes require regular and prolonged village visits.
The number of villages to be taken will have to be
decided according to the availability of staff to be
involved in the programme.
When selecting villages it is important to remember that?
- the chosen villages should be of a manageable size.
This would mean villages with about 1000 to 1500
people. Bigger the village bigger the difficulties
we will find in it. In some area it would perhaps
be difficult to find villages with 1000 people. Then
we would, of course, choose smaller ones. Still when
choosing we must remember that we would like our
services to go to the greatest number of people.
- It is important to choose a village where we will be
almost sure of the interest of the people and where
we find them ready to involve themselves in the
programme.
...2/-
2
- It is important for the programme to have, from the
■beginning, the support of the leaders, informal and
formal ones,
- the choice of first village is important. We should
start in villages where people are more responsive
to our ideas. Such villages may not necessarily he the
most needy ones. If we start in a village ready to
accept.change and if we succeed,...then the nearhy villages
will want- the same for themselves. It will then he easier
.for us to rea&h the very needy villages which .are our
actual target.
Once the.'villages are selected, you must:
i.intensify visit to these villages. They must he visited
regularly at least once a week, preferably on the same day
each week. These visits should he utilized to find out the
real and felt need of the people?
ii. if possible, organise village committees with representatives
of all groups present in the village?
iii.
involve the people in detailed planning - fix up with them
realistic objectives to be implemented.
A
At this stage, these objectives could be
*
- health survey of under five children tofaetermine future
priorities of the under five children programme?
- complete general datas on the village so as to be in a
better position to identify the weakest group or the poorest
families in the community. Thisfetudy would help for
planning activities to solve related problems?
-
selection, by the community, of possible candidates to be
trained as Village Health Workers?
during the weekly visits the professional staff will deal
with
- minor ailments
- ante-natal care
CONCLUSION
•
iv.
During the residency course in Community Health we repeatedly
emphasised the. need of involving the peole in the programme from
its beginning. After all, the problem of a village are the pro
blems of the people living in it. It is, therefore, normal that
the people'should be part of the possible solution of that
problem. It means that5
- we nust know the people’s problem
- we must know the local resources available in the community
- we must be ready to discuss with the people, understand them,
find out their readiness to accept change
- we must plan the programme with the people
. - we must involve the people in the implementation of the
programme
- we must regularly discuss the result of the programme with
the people
The Community Health Programme you plan to have must be a People ’s
Programme, meant to meet the People’s need and. helping People tc
find a feasible solution to solve these need®. It should never
be"your" programme.
Prepared by:
****** * * *
Qomniunity Health Team
Voluntary Health Association of India,
'
COMMUNITY
DIAGNOSIS
of Diarrhoea in Children
No unity
No knowledge about
what is available
from outside
No cooperation
People not
interested
Govt, not
giving enough
importance to
villages
No help
^from outside
the village
Lack of interest
Poor^crops
Lack of education
Soil^gets
zwashed away
TREES ARE
BEING CUT
Rainfall
decrease
Underground
-water
decreases
People poof
Land not
----- " "
^fertile^.----- same kind of crops
Not enough
food
Continuous^'Lack of fertilizers
farming
T
Well is not clean
iUNDER[
INUTRITIONj
!LACK OF CLEAN
iDRINKING WATER
No money
to buy
Not many
animals
Low wages
Dry Area
Too'many
people using the same well
cannot dig
'Mother is_ _
over-worked
She has two jobs
house work plus
other work
POVERTY
Lack of unity
j
!
xN0 _
'J^ELL
People are
Agriculture depends
on' rain, rainfalls
on'rain,
or there is too much
~/ DIARRHOEA
jXs CHILDREN
IN
i
/
;,{FOOD NOT COOKED !■
I PROPERLY
!
! FLIESj
—Bad sanitation
Lack of knowledge about
the spread of disease
Values in
Society
REMEMBER ;
s / HEALTH CELL
(bangalore
‘
Marks Rood
-5go 001
This Community Diagnosis is not complete,
There can
be many more reasons which lead to diarrhoea in
children. Find out the actual reasons from the
people in each of your villages. A complete diagnosis
leads to a complete treatment.
16-11-87/200
mm/
Prepared by ;
Community Health Department
of the Catholic Hospital Association of
India
157/6 Staff Road, Secunderabad 500 003
Voluntary Health Association of
Telegrams : VOLHEALTH
C-14, Community Centre,
DAftIGAl.ORE.560O
New Delhi-110016
Safdarjung Development Area.
, ,. .
668071
Telephones : 668072
New Delhi-110016
STOVE!
BASE LIKE
_____
v
CON’‘^C-‘!‘
cetL
NlarksR°ad
In the process of selecting our target area and then the specific villages
in which we will work, we would have found that the people of each village
live with a number of problems. As a team of health workers, we have to
find out which of these problems are more■important to the community.
A good way to find out this information is by conducting a baseline survey.
Such a survey helps us to determine the initial health status of a popula
tion.
Vlhat is a baseline' survey?
A survey is a systematic way of collecting information about the canmunity.
The baseline survey is done before we start a comprehensive Canmunity Health
Programme. Because this survey gives data about the health status of
people before the programme is started it is called a baseline survey.
The baseline survey is done CNLI ONCE.
Tire baseline survey can help us in:
1.
2.
3.
4.
5.
6.
assessing the health needs of a community
enabling local leaders to become more aware of the health
conditions in their canmunity
increasing the community’s awareness of the health problems
facing them
setting objectives for a comprehensive community health
programme with the community
identifying the 'At Risk' population (that needs special care)
evaluating achievements and draw backs of the programme and
resetting priorities at a later stage.
When to do a baseline survey?
Vfe should do the baseline survey
A.
AFTER VIE HAVE
1.
2.
selected the villages we want to work in
intensified visits to these villages
also
B.
AFTER THE COMMUNITY
1.
2.
3.
4.
'
has had time to understand our motives
has realised the need for a community health programme
has understood the concept of community involvement
has understood why we want to do a survey and know how
we will use the information collected.
When the staff of a health centre does a survey before they know the'
community and the community knows them, people misunderstand the''purpose
of the survey. The people may resist and give false information, distrust
the staff, and ill feelings on both sides can be generated. The staff
may even decide ta discontinue work in the village. - It is therefore very
important that the community be well prepared before doing the survey.
■'
•
............ 2/
2
Who docs the survey?
We are likely to get more accurate information if we ask members of
the community to do the survey. Help of the following groups or indi
viduals can be taken:
1.
•2.
3.
' .4.
5.
School teachers
7.
' '
Members of local youth clubs, Farmers' £?lubs, Mahila Mandals Local leaders? both formal arid informal'
etc.
The’ village health worker ( if the community has already
chosen one):
Any interested member of the canmunity
It is important that the people chosen to do the survey hare a good
relationship with a majority of the people.
What information do we collect?
The health status of a community is reflected in the health of the
mother and child, as these are two of the most vulnerable groups in
the community. Therefore tc begin with we collect information about
these groups. If we want to start a specialized programme such aS
programme for leprosy control, TB control, etc., data can be collected
for these purposes also.
How to record the data?
We can use a note book or register for this purpose. You can record
the:baseline data in the first pages of this register. A sample table
giving the information to be recorded is attached at the end of this
ipaper. (Table I).
The information for each family should be entered under each of the
headings.
Sane Definitions:
House Number is the same as Malaria Surveillance House Number.
Family is a group of people
-
who are blood relatives;
living under the same roof;
and sharing the same leitchen.
If the people are living in the same house, but have 2 kitchens, they are
considered as two separate families. In this case, it should be
recorded as follows:
S. No.
H. No.
Head of Family
4
5
15
1-5
Ganesh Chand
Babulal
.3/
»
Head of Family
3
:
The person who takes all major decisions in the family,
(If in a family the son earns but the father takes the
decisions, the father is still considered head of the
family)
Hew to use the data collected?
1.
Total all the columns at the end of each page. Then make a grand total
for each column so that you have the total figures for the village.
Total of column
Total of column
Total of column
=
Total nutrib. r of households
Total population of village
Total number of married Yemen in the
reproductive age group
Total of column
Total number, of pregnant women at the time
7
of the survey
Total of column
= Total number of children 0-1 years
9
(Total number of births- in the last year)
= Total number of children 1-5 years
Total of column 10
Total of column 9^10 = Total number of under fives
Total of column 11 . =. Number of children already immunized
Total of column 12(a) = Total number of deaths -in children
between 0-1 year in the last year
(infant mortality)
Total of column 12(b) = Total nunber of deaths in children between
1-5 years
"
" 12(a) + I2(b)= Total number of deaths in children between
0-5 years
Total of column 12(c) = Total number of maternal deaths
"
2
5
6
—
=
I2(a)+(b)+(c)+(d)= Total number of deaths- in the village
Guidelines for checking if the collected information, is correct;
If our results differ greatly frem the average figures•given below, it is
because:
either the figures do not tell the whole story which may be due to
unsupervised work
faulty addition of the figures
faulty questions used
•
Harijan quarters or some other part of the village not
visited .
• - ■small village,’ chance variation from the average
-
or
the village is much different from the average which may be
due to
'-
progressive village or block, district or state
previous health work done, in the area
sane other cause
-4/
:
4
:
Average figures for .a population of 1000:'
1.
Number of houses
_
2.
Number of women in the reproductive
age (15 - 45 years)
- '200 (15 - 20%' of.the
population)
3.
Number of children between the ages
of 0-5 years
-
125 to 200
150 ( 15$ of . the population)
This figure may be higher in
areas: where nutrition is- good
or family planning services
are poor. This figure may be
lower in areas where veneral
disease-(which causes sterility)
is high, or where there is
poor nutrition.
4.
-Number of' malnourished children
between the age of -0-5 years .
-
-.
5.
Number of children’born per;year
6.
Number of pregnant mothers in one year .-
■7.
Number of obviously pregnant mothers
at any' one time in a village., (after
6 months of pregnancy)
8.
30 to 40 ‘
45 to 60 ( 1g times the number
of births in the village)
10 to 13 (1/3 of the number of
births in the vill age)
Cases of tuberculosis:
a.
b.
9.
90 to 120 (60 to 80% of underfive population)
Number .of, people with sputum
positive tuberculosis
Number' of .people with sputum
negative tuberculosis
Number of people with leprosy
2 to 8.
_
-■
111 -to.- 17;
-
This may vary from 0 to 25 or
even more.
How to 'set priorities on the basis of baseline data?
Eg.
1.
If there is a high infant mortality due to diarrhoea, then the
priorities would be:
a)
■ b)
Efe.
2.
health education of mothers on the importance of
rehydration.drink;
to improve the'drinking water supply of the tillage.
If 90% of the-married women are in the reproductive age (15 years
to menopause) and the average number of children per family is
four, family planning programme should be a priority.
It is important to discuss the findings of the survey with the community
before any definite strategies are planned. Programmes planned with the
community have a greater chance of success.
Mbt:pt:25.'6.,8l
BASELINE
9JRVEY
C-10.253
S:pt:l8.2.. '82
IMMUNIZATION
In our country diarrhoea is the first major cause of death
in children ■ Co’’runic able diseases like diphtheria, whooping
cuix&y., ucuanuS; polio, tuberculosis and measles, from the second
major cause of death. The tragedy is that the illness and
death due to communicable diseases can be easily prevented.
Immunization is a simple and an inexpensive way of doing this.
A child gets whooping cough only once. When a child gets
whooping cough his body makes a substance called antibodies.
These antibodies fight against the germs of whooping cough
and kill the germs. After these germs die, the antibody remains
in the body Of the child for a long time. Later at any time
if the germs of whooping cough-'
enter this child's body :
again, the antibodies that were produced earlier, fight against
the new germs and kill them. This child does not fall ill
.with whooping cough', again. In ^ther words the <hild had
developed immunity (resistance) for whooping cough'.. In the
same way, our bodies can develop immunity (specific anti
bodies) for each of the communicable diseases listed above.
There are different ways by which our bodies develop immunity:
1. Passive Immunity: The antibodies for a particular disease.
are supplied ready made to the body. This can be done in
two ways:
(a)Natural Passive Immunity: The mother passes her antibodies
to the baby in her womb. The antibodies are also supplied
to the child through the breast milk of the mother.
r'g. ’rtibodies for Tetanus, Measles.
(b)Artificial Passive Immunity: The antibodies are taken
from an immune person or immune animal and injected into
the person who needs it urgently.
Passive immunity is a quick way of transfering immunity from
one person to another. The effect of this king of immunity
does not last for long in the person who receives the anti/
bodies. The is because the antibodies are destroyed quickly
and the body does not know how to'produce its own.
2.
Active Immunity:
The body develops this immunity in two ways:
(a) By getting the Actual disease (infection): In the example
of whooping cough given earlier, we saw that a child' gets
a disease and makes its own antibodies. A well nourished
child will be able to make the antibodies faster than an under
nourished child. This is why the severity of the disease is
less in a well nourished child.
(b) By Immunization: In this a small quantity of the germs of a
disease are injected purposely into a person. The body of the
person responds in the same way as it would to a disese i.e,
by producing antibodies. After this the body has enough anti
bodies to fight against the actual infection.
The germs we inject for immunizing
are
*
called vaccines. These
germs can be killed (dead, vaccine) or made weak (live vaccine)
The met'.
of injecting the vaccines is called Vaccination or
immunization.
: 2 :
Examples of live Vaccines: (Germs that are made weak but arc alive)
Polio,
Measles,
Tuberculosis.
Examples of deal vaccines: (Germs thfit are killed)
Dipht eria
Whooping cough
Tetanus.
In active immunity the body takes a little longer to produce
antibodies but the antibodies last longer as compared to
passive immunity.
POINTS TO REMEMBER ABOUT IMMUNIZATION
a.Age. We must try and immunize children before the usual age
when they have the disease. Eg: Maximun number of children
get diphtheria between the age of two and five years. So
children should'be immunized against diphtheria before they
they reach the age of two. As a general rule we must immunize f
all the children before the age of one. Very young children
below three months of age are not good at making antibodies
and they already have ready-made antibodies from the mother.
So one must not immunize children too early. There is a bestt
age to give every vaccine and we must try and immunize our
village children at the right age. (however, when we start
an immunization programme we might find many older children
who have .not received the vaccines at the right age. We should
still immunize them.
b.The right number of doses: Each vaccine has to be given in
the right number of doses as recommended. If we reduce the
number of doses of the vaccine, its effect is lessened.
Eg: BCG vaccine(for tuberculosis) needs to be given in two
doses whereas DPT vaccine has to be given in four doses.
Wtih each dose of the vaccine the amount of antibodies
produced increases and its effect lasts longer.
c.The right interval between doses: (Time between doses): For
each vaccine the right interval between doses is different.
If the doses of a vaccine are given too soon then the child
will not develop a strong immunity. The interval between
the first and second dose is most important. If the gap
between the first and the second dose is too long, then the
first dose is ineffective. This child should bo considered
as a new case for immunization.
d.Strong the vaccine:Thfes is very important. If the vaccine
not stored properly the vaccine will get spoilt. Spoilt vacc
ines are useless. A spoilt vaccine will not be able to sti
mulate the child's body to make antibodies.
ALL VACCINES MUST BE STORED AT THE RECOMMENDED TEMPERATURE
Live Vaccines get spoilt faster than dead vaccines because the
live germs in the live vaccine die quickly if thecvaccine is
not stored properly.
e.Expiry date: Each bottle of vaccine has an expiry date
vrritten on the lebel. This means that the vaccine should not
be used after the expiry date. Before both buying and using
the vaccine CHECK THE EXPIRY DATE.
f. Preferably do hot immunize children during the rainy season.
3/-
: 3 :
IMMUNIZATION IN CHILDHOOD
1.BCG VACCINE; This is to prevent the child from gettin g
tuberculos'is. There are different ppinions about its effect
iveness. As there is evidence that it is effective in
children we still give it. If is a live vaccine.
When should it be given! The first dose of BCG should be
preferably given at birth or soon after birth. The second
does is given at £ years of age (school-going age)
Preparation:' BCG vaccine comes in ampij es as a Freeze dried
vaccine in a powder form. The powder hd«3 to be dissolved in
saline before it can be used as a vaccine. In our local PHC
we have vaccinators specially trained for giving BCG vaccin
ation. We must get the BCG vaccine and the help of the
vaccinator from our PHC.
Points to remember about BCG vaccination:
-The powder and the solution must be kept in a refrigeratrc.
- The vaccination should not be given in bright sunlight
and should , be preferably given in a room or at least
in shade.
- The ampules and filled syringes should be covered with
black paper when not in use.
- The vaccine must be used the same day it is dissolved
in the saline. At the end of the day, if' any vaccine
is - left, this should be thrown away. It should not
be used for the next day even if kepi in a refrigerator
What happens when BCG vaccine is given:
When che vaccine is given a small lump is formed at the site
of the inlection. This lump disappears after half and hour.
About the 3rd week after the injection has been given, the
siteof injection becomes a little thinkened and the place
is painful to touch. This thicikness slowly increases to the
size of a pea. By the 6th week the thickness becomes soft
arid pus is formed. The pus then escapes leading an ulcer.
The ulcer slowly heals and forms a scar.
de must inform the mother about the changes that occur at the
site of the injection and reassure her. Sometimes an abscess
might from at the site of the injection. This usually heals
on its own. If the abscess does not heal, remove pus with the
help of a needle and syringe (aspiration).
BCG Vaccine Jrou-ld not be given to:
- children who are known to have tuberculosis.
- children who already have a scar on the arm
- severely malnourished children
- children with severe skin disease
- acutely ill children.
* Freeze dried means the live vaccine is froozon so that
germs stay alive. Then it is dried and powdered for use.
... A/-
COMBINED VACCINE FOR DIPHTHERIA, WHOOPING COUGH AND TETANUS
(TRIPLE-.VACCINE OR *DPT VACCINE)
This vaccine is given to all the children below five years
of age. It contains killed germs and so can be kept for a
longer period of time. The advantagesof the combined
vaccin© are:
- more antibodies are produced,
- the effect lasts longer.
- the children are given less number of
injections.
When should it be given:
Four doses- are given ,
The best is if the doses are given
as follows:
First dose
: when the child is 3 months old
Second dose
: 4 to 6 weels after the first dose.
Third dose
: 4oto 6 weeks after the second dose.
Fourth dose
: when the child is 1.1/2 to 2 years old.
(Booster dose)
(In rural areas it may not be ipossible to give all the
four doses. In such areas the first and second dose mutt
atleast be given. The internal between the first and
second dose should be between 8 to 12. weeks. If possible
the booster dose should be given 1.1/2 years after the
second dose) @
Points to remember about DPT vaccine:
- DPT vaccine must be kept in the refrigerator between 4°C
to 10 °C. DO NOT FREEZE THEM SOLID (Dpn't keep in the
freezer.) Also DO NOT KEEP IN THE DOOR OF THE REFRIGERATOR.
This destroys DPT.
_ Shake the bottle before using and leave it for 3 minute.
if the liquid is clear, then the vaccine is useless. Send it
back.
- At room, temperature DPT los'es its value in 4 days.
- Keep the vaccine away from heat and light.
What happens when DPT is given:
Normal Reaction: In children there wL 11 be a slight to
moderate pain at the site of the injection. Some children
also might develop a mild fever. Mothers must be warned
about this pain and fever. You can also give antipyretic
(acetaminopheon) to the children with fever . (for dosage
see page 4i4 of ’Where there is no Doctor)
Abnormal Reaction: Some children might develop high fever
and convulsions. This is due to some unknown factor in the
whooping cough vaccine. THESE children should not be given
the next doses of DPT. --------
*DPT is - D fin? Diphtheria
P for Pertussis or Whooping cough’'
T for Tetanus.
@ World Health Organization recommends that only 2 doses of
DPT be given. The first dose 4- weeks after birth and the
second dose 100 weeks after birth.
f 5 :
DPT vaccine should not be given to a child
- with a history of convulsions or other nervous system
disord er.
-’with fever or infectious disease.
- with allergic disease.
- with skin disease
- getting steroid drugs
3.
COMBINED VACCINE FOR DIPHTHERIA AND TETANUS (PT VACCINE);
Whooping cough- does not affect children after the age of 5
years. So children above the age of 5 years should receive
only Dr vaccine. This comes in bottles containing 10-20 doses.
Only one dose of DT is given at theage of 5-6 years.
Same Precautions to be taken as for DPI' vaccine.
h-. POLIO VACCINE;
This vaccine is given orally (b-.y month). It is a live
vaccine and therefore gets spoilt easily.
When should it be given;
Three doses are given. The best is if the doses are given
as follows.
First dose : when the child is 3 months old.
Second dose ; '+ to 6 weeks after the first dose.
Third dose ; h- to 6 weeks after the second dose.
Children above the age of eight years normally do not require
polio vaccine.
(The latest dosage recommended by CMC Vellore is to giVe
5 doses of polio .vaccine at the interval of
6 weeks between
■ each dose)
Points to remember about Polio vaccine;
This is a live vaccine and has to be stored with extra care.
- The vaccine must be kept at a temperature of <- 20°C.
That means, when the vaccine is transported from the
institure where it is manufactured, it should be kept on
dry ice or a freezing mixture. When it is in a centre,
it should be kept in the freezing compartment of the
refrigerator and when it is taken to the village it
should be kept in a flask containing a lot of ice.
- The vaccine should/5^° frozen and thawed repeatedly,
That means that the vaccine must be taken to the village
only when we are sure that we will get enough children
to finish all the doses in the bottle.
- The vaccine must not be kept near the stove etc.
- Polio vaccine must be preferably given in a room or in
the shade of a tree. (Do not give it in a h»t humid,
crowded room).
- The vaccine can be given by a dropper or a spoon. The
dropper or spoon is sterilized by boiling in water for
20 minutes. It is then cooled■by keeping in ice cold
water. The dropper or spoon should also be carried with
the vaccine in the flask to the village,.
: 6 :
-DO NOT USE CHEMICAL DISINFECTANTS like lyson, dettol,
savalon etc. FOR STERILISING THE SPOON OR THE DROPPER
- The vaccine must not be diluted with water, milk or
honey before giving it to thechild.
-
must advise the mother not to breast feed the child
ail east for U hours before and after the child has been
given polio vaccine.
- The child can be given water and
breast milk during this time.
other food instead nf
-The child MUST NOT BE GIVEN HOT MILK, HOT WATER, OR
HOT COFFEE FOR ATLEAST HALF AN" HOUR AFTER THE VACCINE
HAS BEEN GIVEN.
What happens when polio vaccine is given;
It is an oral vaccine and it does not have any effects like
fever, pain etc.
Polio vaccine should not be given to children with:
- high fever
- vomiting
- diarrhoea
- who are on steroids.
5.MEASLES VACCINE: .
It is a lisze vaccine like polio vaccine. Right now it is not
widely available in India. But we hope thatin a few years
time it wLllbecome as common as DPT and Polio vaccine.
It comes in a powder from (just like BCG va ccine). This
powder has to he kept in the freeaing compartment of the
refrigerator. The. solution to dissolve the vaccine comes
in an ampule and has to be kept inside the refrigerator
but not in the freezing compartment.
To use the vaccine, take the cold solution and the powder of
the measles vaccine to it. THIS LIQUID VACCINE MUST BE USED
WITHIN ONE HOUR.
When should
it be given:
Only one dose is given. This is given between the age of 9
months and one year. (Best time 9 months). It is given as
subcutaneous injection. One dose contains 0-5 ml of vaccine.
Points to remember about Measles Vaccine:
The same points in terms of storage for polio must be followed.
What happens when the vaccine is given:
- the child might develop fever within 8 to 9 days.
- The child might also get mild measles (rash).
Measles vaccine should
not be given to children.
- who have already had measles.
.7/-
: 7 ;
CONCLUSION;
In this pap;er, so far we have discussed the different ways
in which a child's body can fight against communicable
diseases by producing antibodies. In order to effectively
produce antibodies against infection, children need to be
immunized at the right age, given the .right number of doses
of the vaccine and these must be given at the right Intervals.
Details of using each vaccine have also been given.
Communicable diseases spread easily from one person to another.
This means that one child with a communicable disease can
give the infection to many other children in the village. As
our aim is to protect asmany children as possible from comm
unicable diseases, it is important that we immunize as many
children as possible at the same time. In most places
children are immunized as and when they come to the clinic.
This practice does prevent the individual child has been
immunized, but does not protect the other children in the
village. In such a village an *epidemic of a communicable
disease could easily break out. TO PREVENT AN EPIDEMIC,
we must immunize atleast 90% of all children under five
years of a.ge in the village.
Vie may "find that there are many undernourished children
in the village. When a child is undernourished it is more
likely to get a communicable disease. These children also
get a more servere attack of the disease. In fact the child's
life can be in danger because the disease will create
further undernutrition. Therefore undernourished children
must be immunized.
J
------------------
=
==
References:
Primary Child Care by King, King, Mahtodipoero
Manual for Immunization by Mass Mailing unit.
* Epidemic means that an unusually large number of persons
get the same disease at the same period of time.
Prepared by
Community Health Team
Voluntary Health Association of
India, C- 1U, Community Centre
S.D. A., New Delhi 110 016
The Catholic Hospital Association of India
'
C. B. C. I. Centre, Goldakkhana, New Delhi - 110001
Tel.
310594, 322064
LIBERA!IN G.EDUCATION
c0M^W1 ‘
4711.
Marks Aoad
660 001
ban0'-'
■<re observe today a big crisis in the education system. Today
there are in the world .600 million illiterate adults. The ideal
to combat this Illiteracy would be a Lasic and popular education.
Development is not only related, to economy. It also has a
very important social dimension. The goods produced to inrease
the economy of a country cannot belong to only a few. Developmenthas to be considered a political question as it is
necessary to make certain changes in society. Education would
then i?e converted into a political force. The consciousness
of the oppressed nations in awakening, opening new perspectives
for the future. Before this pin-pointed need, "education" as
such cannot be considered but only as a process of liberation.
The perspective of Liberating Education ought to orientate the
educative process as a whole; make objectives concrete; rela
tionship between educator and educated, evaluate and revise a
whole series of existing educative systems.
.Formal Education and Liberating Education ; To understand
better the success of liberating education, we ought to know the
most important features. Objectives of Formal Education to
progressively integrate sectors, each time wider, of the popu
lation in the existing society; to reinforce the existing
structures; the decisions are made by a group which is in power
or at its service. Literacy will not be a process of libera
tion if the ways of carrying it out are not changed.
The consciousness of the•educated will be converted into refle
ctions ana shadows of the groups that hold the power of deci
sion. Formal education does not challenge, it gives ready for
mulas. A confrontation could provoke the risk of awakening the
consciousness of all these who can't say anything.
The educators express their opinion plan, make options. The
educated passively assimilate what the others have created.
Vhat they learn does not help them to awaken in themselves a
critical consciousness or the possibility of creativity. The
teaching does not come from a reality lived by the individual,
group or people. There isn't a transforming action. Formal
education_is paternalistic and passive, not applicable to ..
adults. Formal education is based on a mechanical concept
of the consciousness which has to be"filled because it is'emntv.
Liberating education on the contrary tries to awaken and
develop in the educated a critical consciousness by which they
will be capable of - interpreting and evaluating - dialoguing
and confronting with other groups;- committing themselves to
transform society to get mere liberation. Liberating educa
tion wants to make men capable of critising situations living
in a society created for all, in which man is at the service
of all giving of himself to the maximum. It wants to capa
citate men to make history and live the process of their
liberation. One of the most impor.tc.nt points in the libera
ting education will be to acquire a critical consiciousness
through which man gets a certain perspective of the universe
that surrounds him, discovering himself and seeing himself
capable of living a reality interrogating and' interpellating
it, thus capacitating himself for a global consciousness and
from this point we san synthesize it.
2
To understand well the present reality, it is necessary to be
conscious of the experience and the reality of the personal and
collective past. This return to the sources illustrates much
.the reality in which we live. After the analysis described
previously, the consciousness wants to> go further and transform
an existing reality. for this transformation to be efficacious
j-S is necessary to be aware of the elements that work in the
change. from this awareness, we can concretise the form of
beginning the change and the instruments to attain the objecti
ves and to see that the projection is converted into a reality.
AS we have earlier observed; nobody educates or donsciontizes
himself alone. Conscientization does not consist in communica
ting something elaborate to the others who ought to assimilate
and adopt it. Conscientization signifies confrontation, dia
logue, effort to communicate and collaboration.
from all that we have said, we can resume from a pedagogical
point of view as follows :
1.
Education cannot be communication in one direction. This
pedagogy does not give place to the process of human con
sciousness and in some w.ay bars progress. The educative
problems cannot be elaborated but with the group, from
the experience of the group and of each of its members.
2.
The educator makes himself the animator. The animator
motivates the group or the. community in which he finds
himself that they may be conscious of their experience
•to analyse, to interpret, to systemise, to get a vision
of the while and project it. Without an animator to ini-.. .
tiate the start, it is difficult to get a group moving.
The animator does not impose his point of view -but con
front and dialogues with the group. It should-;not come
from his own experiences but it should be from the felt
needs of the group..
In the beginning, it is advisable that the animator should be
one out of the group. But depending on the rate at which the
group increases this consciousness, a member of the same group
will take charge of the animation. This confrontation can
increase and can be made by one group to.another, one commu
nity -to another, by different cultures and peoples. When
there is an animator in the group, he ought to withdraw the
moment the option is made and he ought to respect the decision
of the group even if their decision leads them to a failure.
Thus, at the moment of evaluation the group will be conscious
of its limitations and errors.
Sometimes an option is not be the best, but the only acceptable
one depending on circumstances. What is important is that
they can play a strategic role in the transformation stage
always looking at the goal. Opting limits us. We cannot
choose all the ways at the same time. Through an option man
recognises his existence in the world, his finiteness and his
limitation. When we opt we run a risk. We decide for a
future that still doesn't exist but our responsibility will be
to make it a present reality.
The option as w.e have said is a risk but at the same time an .•
act of overcoming and freedom. Through an option a man assumes
his responsibility and his realisation.
i
- 3 -
The Transforming Action : Through conscientization we project
a new situation that is above’the present situation but through
action it begins to exist ana becomes a reality.
The transforming action is indispensable for liberating edu
cation. It is~oallcd to .change, the relations ibeWeen men-, ,
structures of group and of society. The action is not always
at the service of liberation. The action ceh limit, dominate
end anual, or it may not be consequent to the conscientization
and the decisions taken. The transforming action may need a
reorientation but it has to be coherent to the conscientization
and the option only in case the elements have changed so much
that they ask for a deepening into conscientization and new
options. It is indispensable to opt for a type of action that
is transforming and that signifies a true commitment. This
newly orientates the existing educa.tive systems. Reflection
and action are necessary in this process. Starting from a
transforming action, conscientization can be more critical and
fruitful.
Summarising - Education is a process of liberation
that consists fundamentally in living with the others - a
critical conscientization, liberating options, transforming
actions, critical evaluation.
COMMCNH'V HfAVTH CSU.
47/1,(FirStF’oor)St.MarksRoad
1•
the banking concept .of education as a means of oppression
A.
B.
It is characterised by narration.
Subject - teacher;
■ Contents are lifeless;
3.
Seniority of word
h.
II
reality is motionless
leading to memorization.
It becomes an act of depositing instead of conmunication
1,
C.
object - student - receptacles
1.
2.
Teacher - knowledgeable; student - ignorant (an
attitude of oppression).
2.
Teacher thinks students are taught about..
3.
Teacher talks, students listen fieekly.
4.
Teacher disciplines, students are disciplined.
5.
Teacher chooses, students comply.
6.
Teacher acts; students have illusion of acting.
It serves the interests of the oppressors because:
1,
It regards men as adaptable, manageable beings.
2.
It minimizes the students creative power.
3•
It does not stimulate critical faculties and its
content with a partial view of reality, for the
oppressors think that the more the oppressed can
be made to adapt to a situation the more they can
be dominated..
4-
It does not trust man, a teacher does not seek to
be a pa.rtner of his stiirlents because doing so
would undermine oppression and serve the cause
of liberation.
5-
It trains men to fit into the World
=
ssors.have created by teaching; that men is a
spectator, not a jero-nreatorT
6.
It is a necrophile or death-loving because it
attempts to transform. men to objects, uncreative
and inorganic. Hence, it condemns sli-i.kos of
workers and uses violence to put down the strike,
Hence, those truly committed to liberation must reject
the banking concept and adopt one which is a concept
of men as conscious beings since liberation is an
action and reflection of men upon the world to trans
form it and cannot.be just another deposit to be
made in men..
PROBLEM OF USING LDUCaTION AS a MEANS OF LIBERATION
It aims to pose men1s problems in their relations
with the world :
1.
It embodies communication not transfer of
information.
2
2.
B.
C.
It is not intent on objects alone.
It breaks the vertical patterns in banking education
through dialogue.
‘1 .
Teachers and students become jointly responsible
for a process in which all grow.
2>
Objects for cognition are the objects of reflection
by himself and. the students.
3.
students are critical co investigators in dialogue
with their teachers.
4.
Teacher presents the materials to the students
for their, consideration and re-considers his earlier
considerations as the students express their own.
5.
The teacher creates together with the students the
conditions for true knowledge.
•
It involves constant unveiling of reality.
1.
it strives to make consciousness of reality
emerge;
2.
it stimulates critical intervention in reality;
3.
it denies that man is abstract, isolated and
unattached to the world;
it develops cto's power to perceive critically
the way they exist in the world with which and
in which they find themselves;
it is set oh demythologizing
it considers dialogue indispensable
it acknowledges nun as a historical being.
4.
5.
6.
7.
D.
It affirms men as beings in the process of becoming as uncompleted beings with a likewise unfinished reality.
E.
It is revolutionary futurity :
1.
2.
3.
4.
5.
it roots itself in the dynamic present and does
not believe in permanence or a well-behaved present
nor a predetermined future;
it is prophetic and hopeful ;.
‘ it looks at the past only to understand as a problem
that can be criticised or transformed. (Any situa
tion in which some men prevent others.from enga
ging in the process of inquiry is one of violence):
it presents the present situation as a problem
that can be criticised or transformed. (Any situa
tion in which some men prevent others from engaging
in the .process of inquiry is one of violence);
it is dironted towards humanization - which is
man's historical vocabi^A
jwinfisg which is
carried out in fellowship and solidarity.
pting to do this inuividually results in having more.
F.
It believes that man subjected to domination must
fight for emenicipation.
G.
It cannot serve the interest of oppressors.
.../3
- 3 -
No oppressive "order allows the oppressed to
question.
H.
revolutionary leaders a.ust use this nethod in the
revolutionary leaders process, they cannot use
oppressive tools for humanization.
Community Health Cell
CHAI Golden Jubilee Evaluation Study
Policy Delphi Method - Response to Question-1'of first round
27th June, 1992.
A SUMMARY OF RESPONSES CONCERNING ECONOMIC, SOCIAL AND POLITICAL
TRENDS IN THE COUNTRY AND THEIR POSSIBLE IMPACT ON THE HEALTH
STATUS OF THE PEOPLE
To facilitate collation and reading we have separated the three
factors, though in reality they are closely inter-related.
There
is therefore some overlap.
I.
ECONOMIC TRENDS ;
These were foremost in the responses and are described first.
Twenty-six panelists (80%) felt that the new economic policy
recently introduced would continue for sometime and would have
an overall adverse effect on the health status of people and
on health care services. A summary of the broader economics
related scenario and health impact is given first and later the
more specific impact on health care services.
A. National and International Economic Scenario
1.
With the new economic order we are now in a unipolar world.
The economically advanced and industralised nations are
coming together and dictating terms. The underdeveloped/
developing nations will keep on seeking grants/aid/loans
and gradually become overdependant and impoverished.
International trade has always favoured the advanced nations
since the Second World War. The situation will be worse in the
unipolar world as there will be no bargaining power at all.
2.
International agencies like the World Bank, IMF, IDA, IFC
and ADB have become tools of exploitation, determining
national policies.
3.
All this has been added on top of our already mismanaged
economy running on deficit financing and with a parallel
economy in black money over which the government has no
controli
4.
These new trends have been variously described as globa
lization of the economy, moving towards a more capitalistic
form of production and distribution, free market economy,
the neo-liberal model of development, the Americanisation
of our economy etc.
5.
There are very few options with the new policy. We will
have devaluation, privatisation, liberalisation, an increase
in exports, a decrease in imports, an increased need for
repayment of foreign loans, and a decrease in government
spending.
Unscrupulous, middle men and women will play
havoc.
2
2
B.
C.
6.
Decreased government spending will occur primarily by a
reduction of expenditure in the services and development
sectors as other changes in government.spending would cause
an upheaval among the organised labour and elite minority.
Thus several panelists felt that subsidies to health,
education, housing and other services will reduce.
There
will be a reduction of budget allocation per person for
health.
7.
This economic process will benefit the business and industrial
community to become richer, with marginal benefit to the
organized sector of labour. There will be a more affluent
middle class. However the majority comprising of marginal
farmers, workers in the unorganized sector, landless labourers
and daily wage earners will not be benefitted. Among them the
children, women and the illiterate will be the sufferers.
Poor people(s) everywhere will lose control more and more
of the ability to determine their livelihood and lifestyles.
Their health status will deteriorate and they will be unable
to avail themselves of the services of privatised health,
education etc.
Poverty
1.
It was widely felt that the gap between the 'haves' and
'have-nots' would increase due to inequitable distribution
of resources.
2.
Impoverishment and the absolute number of the poor would
increase.
Agriculture, Forestry
1.
The agriculture sector will move towards cash crops rather
than essential foods. This would further deplete available
food stuffs for the poor, especially the rural poor, leading
to greater malnutrition.
2.‘ Due to pressures of modernization?deforestation and replace
ment with social forestry programmes using fast growing trees
like Eucalyptus would cause decreased precipitation, decreased
rain, decreased water table, increased droughts and floods
and therefore an increase in water borne diseases. Defore
station would also cause loss of top soil, decreased fertility
of soil, decreased production of food, malnutrition and
starvation.
D.
Industry
1.
The present liberal industrial policy will lead to a
proliferation of all kinds of industries throughout the
country, causing pollution related health problems. The
government would not have adequate machinery, or the will,
to safeguard the environment.
2.
The new economic policy would bring about a growth in
consumer based production geared to the world market.
This would have the following results, namely
a)
ignoring of local needs, which will affect the poor
badly?
.3
3.
E.
growth of large national and multinational agencies,
throttling the small scale industries, resulting in
increased unemployment and breakdown of mental health,
c)
large scale environmental destruction with resultant
health hazards and avoidable deaths.
3.
The technological model of development will be pursued
vigourously to meet middle class needs.
It will have ill
effects on health eg., increasing power (energy) needs will
be met by coal (highly polluting) or dams (dislocating people)
or through nuclear plants (causing hazards.'due to radiation).
4.
The opening of markets to multinational companies will result
in increased availability and consumption of more chemicalised
preserved foods, and artificially flavoured and coloured foods
This will cause dietary imbalance and increased cancers.
Lifestyle Changes
1.
F.
b)
As already indicated above the market economy and growing
consumerism will affect lifestyles of the middle class and
create consumerist compulsions for the poor eg., there will
be a loss of traditional food habits.
Changes in Budgetary Priorities
Changing attitudes to social concerns and the reduced avail
ability of resources for 'welfare*123456 will affect the quality
of nutrition, education etc., and consequently health,
particularly of high risk groups.
2. There will be a diversion of funds from basic needs like
health to the para-military and military sectors.
1.
Comments regarding the impact of these economic forces on health
care services were as follows
G. Commercialisation and Privatization
1. Several panelists predicted an increased commercialisation
and privatization of medical/health services.
2. This is already evident in the rapid proliferation of
private polyclinics and the 'Apollo Syndrome'.
3. There will be further mushrooming of corporate "business
health centres" with expensive, high tech facilities and
consumerist promotion and values.
4. This will be promoted by the leaders of the country at the
cost of basic health services.
5. Health professionals in general and medical professionals
in particular have succumbed to commercialisation of
curative services.
6. Only the profitable services will flourish eg., new drugs
and diagnostics and certain higher specialities.
.4
4.
7.
H.
I.
The affluent middle class will create a demand on the system
for these type of services. They will be mainly urban based.
Accessibility
1.
Medical facilities will marginally increase with little or
no accessibility to specialised or super-specialised services
for common people.
2.
The cost of diagnostic and curative medical services will keep
on going up at a galloping rate. Many services presently
affordable to common people will go beyond their reach in
10-15 years.
3.
Church based groups providing health services will compete
with the private sector to retain "market share".
Overall
less attention will be paid on lower income groups.
4.
There will be an increase in health insurance schemes for
the public.
5.
There will be less money for the health sector under the
government.
This will mean that health care will be neglected.
The poor will suffer the most and have less access to medical
services.
Type of Medical Care
As indicated earlier there will be an increase in the
expensive, technological facilities, benefiting fewer people
at the apex of the pyramid.
These will primarily satisfy
the caregivers. There will be increased dependancy on the
medical system to maintain health, rather than self reliance.
2. Presently, the government health care system is hardly
working, partly because of shortage of funds.
It will be
unable to cope with increased demands and pressures on the
system in the future.
Rural and tribal health care may suffer.
1.
J.
Pharmaceutical / Medical Industry
1.
There will be a sharp rise in drug prices due to unjust
claims of intellectual property rights.
2.
The pharmaceutical industry will now have a greater say in
the setting of priorities and in determining the direction
that health services will take.
3.
There will be increasing dependance on pharmaceutical
multinationals at the cost of indigenous and traditional
.health care systems.
4.
There will be increased large scale experiments of new
drugs on the poor.
:5. There will be an increased pushing of mechanistic procedures
In summary, so far, there will be a greater need for health
services for the poor, while paradoxically, access to health
services will be limited to the privileged groups only.
. .5
5.
aspirations
K,'Health Personnel, their education and
-----
1.
There will be an increasing commercialisation of education
in health sciences, with proliferation of capitation fee,
educational institutions turning out untrained, unmotivated
health personnel. Their education will be inappropriate.
2.
Doctors, nurses and other medical personnel seeking jobs in
India or abroad for a better salary and living conditions
may often fail to maintain/develop a correct attitude to
their profession/association.
I». 1. Three panelists (SP/o) felt that the economic trends at present
and these likely during the next 10-15 years were positive.
It was felt that market economy would increase income and
money flow. More people would be brought above the poverty
line.
There would be an increased production of goods.
There
would be increased and better transportation. All these would
affect the health status positively.
M.
2.
There would be a growth of hospitals in the corporate sector,
greater professionalisation in hospital/health management and
the development of insurance as a means of third party payment.
3.
Communicable diseases would be eradicated or controlled but
there would be an increased incidence of heart diseases,
diabetes, cancer etc.
1. One panelist felt that improvement in education may be the
most important factor affecting health.
Economic improvement
and reduction in population growth are often associated with
improved educational status, particularly of women.
2.
It was felt that urban migration encourages industry, impro
ving the GNP and thus helping in bringing about economic growth.
3.
AIDS could cause a depletion of the workforce with massive
economic losses.
H. 1. Another panelist suggested that health was not totally
dependant on economic, political and social issues alone.
2. It was felt that the questionnaire was not formulated to
find out objectively the causative factors of health and
sickness, so that one can ascertain in which direction to
move in the future.
3.
O.
It was felt that the economic and social status of people
in the world and in India would rise independant of any
political system. However haves and have-nots would
increase.
One panelist did not comment on the economic aspect.
II. SOCIAL TRENDS
A. Urbanisation
1.
The process of increased urbanisation will continue and
will be a major factor affecting the health of individuals.
6
6.
2.
There is an extension of big cities and the urban poor have
a lower health status than the rural population.
3.
Adequate facilitxeshrWiil not be available for this group.
Sanitation problems, garbage piles, over crowding, insuffi
cient civic services lead to degeneration of quality of
environment, subhuman conditions and more ill health.
4.
Slum lords and mafias further deprive families in slums of
their earnings, resulting in further deterioration of health.
5.
Increasing pollution due to industries.
B. Demographic Changes
1.
The health status of women is going to get worse as the sex
ratio over the years is going from bad to worse.
Social
pressures and the low value for women and girl children will
continue for sometime.
2.
The increasing number of the elderly will bring about a major
shift in health service needs.
3.
Further increase in population will put greater pressure on
existing services, with the result that they will be less
efficient.
It will result in deterioration of other' available
resources.
C. Family Types
D.
E.
1.
The single or nuclear family system will be more common.
2.
The breakdown of the family unit would bring most of health
care from homes to the service sectors.
Education
1.
Improvement in education may easily be the most important
factor affecting health, particularly education of women.
2.
However, the quality of education and values promoted by
it could be questionable.
Role of Media
1. Television will play a major role in the social lives of
people leading to greater consumerism.
2. For eg., advertisements will bring about an attitudinal
change with respect to food stuffs,moving people away from
healthy natural foods to junk foods.
3.
F.
With a new culture dominated by TV propaganda, old values
systems will be replaced.
Values / Spirituality / Religion
1.
The sense of community will loose ground and a narrow sense
of individualism will thrive.
7
2.
Several health and related problems stem from common ills
like man's confusion, lack of identity and responsibility,
materialism and humanistic beliefs, false values and lack
of spiritual strengths.
3.
There will be aPrQSrQSSiyerosion of values in social life.
4.
The most disturbing element in the present social condition
is moral degradation.
From the highest offices of the country,
the politicians, the bureaucracy, it has gradually started
lengthening its tentacles to all types of social institutions
and social services. Majority of the so called intelli
gentsia are willing to make any kind of compromise in their
life for personal gain/prosperity.
The system of accepting
"capitation fee" alone has opened up a flood gate of corruption.
Tax avoidance, unscrupulous trade and business practices have
crept into the social service institutions in a significant
manner. Even institutions related to various religious bodies
are not free from dubious practices. The tiny minority who
try to stand against such a wave are labelled as "unsmart"
and "outdated".
Socio economic maladjustment is resulting in increased social
tension and violence of various forms. Mental disorders are
on the increase. Many modern health problems originate from
social problems eg., drug abuse, AIDS, STD etc.
5.
G.
Churches will loose their popularity.
splincer groups of Christianity.
There will be many more
Cultural Changes
1. There will be accelerated cultural alienation eg., leading
to abandonment of traditional system^ of medicine, traditional
food practices.
2. Many will follow a westernised style of life.
3.
H.
There will be a marginalization of sections of the population
including dalits.
Change in Life Styles
1. There will be an increase in smoking, drinking (alcohol), and
an increase in levels of tension.
2. Change in dietary habits and increased use of vehicles.
3.
Need pattern and so health pattern will change.
>
4. Change of life style will change the epidemiological scenario
of the country.
The problem of chronic non-communicable
diseases will increase, while most communicable diseases will
be eliminated or controlled.
I.
Fundamentalism / Separatism
1. Regional, ethnic, linguistic, communal and caste conflicts
will lead to large scale victims.who will have to be treated.
This is already happening in Jammu and Kashmir, Punjab and
other places.
2. Religious consciousness, probably without god-experience as
love, and the consequent communalism could be on the increase
affecting social and individual life and health.
8
3. The associated problems of mental health and adjustment
will need greater attention.
J.
Social Problems
1. Social problems like crime, delinquency and prostitution
will increase.
.
.
2. There will be increased social disharmony end tension.
K.
Awareness
1. The awareness of people will grow and a sort of helplessness
may grow leading to- greater unrest and violence. This will
be exploited by vested economic and political groups.
2. The public are going to be more aware of their rights to
medical services. There is likely to be more litigation in
the health field.
3.
L.
Consumer protection councils will make all government
employees to be more accountable. This may make government
jobs less attractive than now/forcing even currently employed
personnel to leave the government service.
Social Trends
On the positive side
1. Educational level will be on the rise. Therefore need for
freedom and better life style will be on the rise.
2. Science and Technology will be increasingly at the hands of
our people with techniques and skills to improve life.
3.
Focus on ecological and gender issues in public policy.
III. POLITICAL TRENDS
A. International
1. Politically we are not going to be as autonomous as we are today
2. There will be greater neo-colonial exploitation through the
oppressive "new world order".
3.
India will be more and more subject to one new world order,
dictated by the West and Washington, with the cooperation of
the local elite.
4.
The fall of communism in Eurdpe will adversely affect the
concept of national health insurance in other parts of the
world.
5.
There is a chance of a stable government.
Changes in the
Soviet Union will have an impact on political parties.
Relationship with United States will not be very good as our
country tries for self-sufficiency and development.
6.
Another highly disturbing element is that some politicians,
though small in number, serve the interests of the foreign
nations.
. .9
B. National
1, Several panelists raised the issue of political instability
and inadequacy. There is hardly any political party with
the goals of good government based on a policy or direction.
And there is no reasonable chance of continuity. Health will
be one of the difficult areas which cannot be improved in a
developing country without political will and stability.
Unless ofcourse, effective health care is possible outside
the governmental system.
2. There will be greater criminalisation of our politics.
3.
Political power is grabbed at whatever cost.
4.
There will be negative political activities confusing and
confounding the average person at the grass roots level.
At present there are many political parties working in an
aggressive and competitive way, each decrying the other
party and the party in power in a particular state, making
it difficult for constructive and progressive work to be
undertaken to completion in the overall interests of the
people and country. People at the grass-roots who need the
services of health personnel will not get it as there will
be artificially created hurdles.
5.
With political instability at national level and other
seperatist/fundamentalist movements and divisive forces of
language and caste working on a political level, health and
social welfare programmes for the marginalised will be most
affected.
6.
There is a serious fear that communalism is on the ascent.
If by any chance such parties gain control the whole political
life will change. This would seriously affect all volunteer
agencies, especially as foreign money for social services will
be setiously curtailed.
The church will be asked to remain
with the four walls for Sunday worship and not to- enter the
field of health or education.
7.
The principle of "divide and rule" is being used by politi
cians of all ideological colours. Communalism is dividing
the poor also, so that they are unable to get together in
an organised movement and fight or struggle for their rights,
with regard to health and other basic human necessities.
8.
Political support to corruption and dishonesty at all levels
of the government health care’ delivery system, forcing people
to go to non-governmental private agencies.
9.
Politically it will be the moneyed who run the country.
10.
There will be efforts by the marginalised groups to take to
extremism.
11.
The organised might of the organised sections will resist
efforts to mobilise the unorganised million.
12.
A strengthening of the conservative agenda of the current
government will set the climate for national development.
Health budgets will be reduced.
10
10.' ■
13.
Politics and politicians in the country have earned a verynegative connotation because of the degraded form of political
culture pursued since 1947.
Honest politicians interested in
the welfare of common people cannot survive. They will be
attacked mentally and physically even - all under the Gandhian
veil of non-violence. People who protest get labelled as
terrorists and disruptionists. Most nefarious socio-economic
violences are skillfully protected by the guardians of the
country, with no punishment meted out.
14.
The overwhelming majority of politicians are self-seeking.
The
odd idealists here and there cannot give their work the shape
of a movement to bring changes.
15.
The left wing is totally unnerved by recent political changes in
the international scenario.
They never did have a big say in
Indian politics, neither is any significant change expected.
The right wing is divided into two basic group social democrats
and ultraright.
The so called social democrats have substantia]^
lost popularity and power as they could not demonstrate social
interest, they did not try to distance themselves from the
self-seeking (investor class of) politicians. Gradually their
image was tarnished. The emergence of fundamentalist force
could be even disasterous.
But people are more or less tired
with both Gandhian and non Gandhian democrats, they are aware
about all big promises since 1947, and opt for a change in the
coming election.
There is reason to believe that the funda
mentalist group may try to change and adapt to secure their
position in Indian politics.
New forces are not at sight, no
sane person amongst the intelligentia are willing to enter into
politics.
It is the unscrupulous who are jumping into it,
their attraction is big money, big name (may be due to notority),
big position in society, all black deeds, stupidity, failure
could be covered up quickly by the miracle touch of "Money
force".
16.
Indians, as people in Russia and so on will hate violent social
movements and Marxist analysis, separating or focussing on the V
poor or weak alone, creating imbalance in approach to social
issues and so to health issues.
17.
There will be stabilisation of the Government by the Congress
as a political party.
18.
Rightist and-communal forces will be. on the increase. ■ Several,, t
panelists., felt.-that'theflatter wil_l/jaffeet-health services’-.—
adversely. : : i.
-j| ,
19.
Decline of trade unionism - this will make it possible for
hospitals to run without too much labour trouble.
20.
The growing disparity between haves and havenots caused by
inequitable distribution of resources shall result in social
tension, strife, disturbance, de-stabilisation, increased
criminal activities seriously affecting quality of life.
21.
There will be an increasing political consciousness and
literacy. Hospitals will need to give more personalized care.
22.
There will be increased student movements.
11
11
23.
Total absence of a positive national interest by the leaders,
in the public services and the various sectors that contribute
to the health of people.
C. Regional
1. Problems of separatism especially in border states may intensify.
2. Instability of government at the regional level (as is already
happening in the North-East, Punjab and Kashmir) will affect
health care services (government and private) and health status
too.
3.
There will be increasing autonomy to the states.
This will
require hospitals to satisfy local needs and abide by local laws.
4.
There will be increasing consciousness among tribals and dalits.
Assertion by ethnic groups and subgroups,politically and econo
mically, resulting in increased autonomy by/for such groups.
Their demands and needs will have to be satisfied by hospitals/
health services.
5.
There will be greater awakening among the marginalised, espe
cially dalits, tribals, and backward classes.
It would mean
their participation in social, political and economic processes
in the country will become a demand, and justly s®.
People
centred, participatory health care processes will be the demand.
6.
Increased regionalisation will lead to intolerance of people
from other regions in the country.
IV. EFFECTS ON HEALTH/HEAI.TH CARE - due to a combination of the various
factors (other than those already mentioned)
1. Basic Factors
•influencing the health status of the population and contributing to
the quality of life are water supply, sanitation, housing/yfood
(nutrition), environment, education(awareness), overall socio-economic conditions (including safety and security).
Trends in the
different factors are :
2.
Water Supply
Some quantitative improvement in reveraqe (through tube-wells etc.,)
is expected.
But maintenahc. cl quality (safe, potable water) will
not occur in the next ten to fifteen years. Mortality is already
reduced, but morbidity due to water borne diseases will remain high.
The two other views were that due to deforestation and increased
water utilisation for agriculture, the availability of drinking
water will become critical leading to increased water related
diseases.
3.
Sanitation and Housing
Presently committed resources are meagre as compared to the need.
There could be a marginal improvement in this.
However incidence of
air borne diseases will remain high.
. .12
4.
tlua: xtipnal Status
• / ' •
There could be a major breakthrough in food production. However,
chances of improvement in nutritional status of the poor are low.
Withdrawal of subsidies will cause further rise in food prices the impact on pulses and oilseeds has already created havoc.
Production costs are rising disproportionately due to use of
improved farming methods and technology - hybrid seeds, irrigation,
use of chemical fertilisers and pest control. The distribution
system is also faulty. There is increased export of food items to
meet the foreign exchange crisis.
The lot of the common people
will therefore remain unchanged.
5.
Environmental Degradation
Will continue.
The small movements here and there are like ripples
that will not develop into a tide in the near future.. Manifold
effects on health will result.
6.
Education (Awaireness)
There will be improveir.ant in literacy rates, but there is cause
"
for pessimism regarding real "education". The new education
policy and the system promotes mass production of technocrats.
There is a neglect of the humanities and overemphasis on science
and technology, which will produce more technologically knowle
dgeable "inhumans".
Schooling facilities for the poorer sections
will be inadequate. The government schools are already over
crowded and in a poor state.
The holistic approach to health is practicable in an educated
society only.
7.
There will be an increase in tobacco related diseases including
cancer, respiratory tract and cardiovascular disease.
The huge
profit margins of the cigarette manufacturing companies is clear
evidence of this.
8.
The pandemic spread of HIV and AIDS could result in the reversal
of the gains of other health programmes. A conservative estimate A
is that over one million people in India are affected by HIV.
9.
Increased cancers and other diseases due to industrial pollution,
and”dumping of industrial waste including nuclear waste, from
rich countries into the Third World.
10.
The increasingly complex drugs
the market will be used and
prescribed indiscriminately,
that iatrogenic or medicine induced
ilxness will increase, tor
wimple allergies, side effects.
11.
Ethical problems related to the use of modern medical technology
have already surfaced, for example provision of services for
diagnosing and eliminating the female fetus.
12.
Wholesale adoption of allopathy, without critical evaluation, will
create new health hazards and economic exploitation.
The weaker sections will realise that unless they have a signi
ficant say in the running of health services, they will be cheated
of their rights to health as in education.
14. Monopoly in the medical system - in our vast country, there is room
for many levels of health workers, who need to be trained and dep
loyed to do their jobs responsibly and competently. With a strong
support system (up and down and sideways) and with good team lead
ership, the impact on health will be positive. However professional
councils do not want to change with the times, and continue to act
selfishly in isolation, for fear of loosing their monopoly.
13.
u
The Catholic Hospital Association of India
C. B. C. I. Centre, Goldakkhana, New Delhi - 110001
Tel. 310694, 322064
DEVELOPMENT
Development can and for too long
been understood
as economic development alone, where the main emphasis is on
increased production and income. According to this definitinn
the main objectives of development is to increase the r'~r> with
out bothering to see who is benefitting from this increase.
In most of our countries, this is the kind of development,
which has been going on. The emphasis has been on increasing
production. As a result of this emphasis production has
increased in many of our countries through green revolution,
or industrialisation. The benefits of this development have,
however, not occured to everyone equitably. In many developing
countries the rich ha.ve become more rich and the poor have
either remained where they were or at times have et.-n become
poorer. This trend is quite visible at the village level. The
above concept of development is very narrow and thus unacce
ptable .
Development has many aspects - economic, social, cultural
and political. There should bo equal emphasis on all these
aspects. Along with economic development, there should be
better distribution of resourses and means of production.
The decision making power should not be in the hands of a
few people only. Participation of the majority in all aspects
of development is necessary in this concept of development.
The word 'development' can be divided into "Develop'
'Men' ' T' ; Develop men or women to think together to under
stand the reality and to grow fully. Growth of individual
alone is detrimental to society.
Development is a continuous process of change leading
the awareness of one's present state of life and bringing
him to a higher level of life. It is a growing activity
between persons who feel the necessi’y for development, and
persons who want to work for their own development. It is
also said that development is a continuous process towards
complete humanization by loving one another without selfish
motiveness.
V.hat is development;
Development is a process by which both persons and soc
ieties come to realize the full potential of human life
in a context of social justice, with an emphasis on selfreliance, economic growth being seen as one of the means for
carrying forward this process".
1.
I'rom this it is implicit that development
(a)
is of people and can be achivcd only by them. Others can
only be enablers.
(b)
is of people in community with the direction and control
in the hands of local leadership
(c)
is a process in the context of relationships and a total
....2/
2
life style consciously evolving towards growth.
(d) is sustained through funtional indigenous institutions
developed from and responsive to the local situation of
the people.
(e)
is an integrated process requiring harmony between people's
and between people add nature; between the present and the
future; between the social, economic and political factions.
(f)
is interdependent; the fulfilment of all people depends on
the development of all.
2. Development is; - growth with redistribution
- awareness of people of their problems,
power and the potential they have in
working together.
- to 'de-envelop' people from the bonds of
oppressions and powers that suppress them.
- being our brother's brother and not only
his keeper
- respect for the individual's dignity,
self image and self esteem.
In development we are looking for;
participation by all people
equitable distribution
effective and efficient utilization of human as well as
natural resources.
(d) The growth, in dignity, of the individual in the context of
his family, environemnt and community.
(a)
(b)
(c)
Development is therefore a continuous and dynamic process
that brings about structural and institutional changes.
It must through these changes provide an equal oppor
tunity for all to participate in decsion making in the eco
nomic, social, cultural and political spheres.
A question of power
This concept of development with emphasis on distribution
and social justice requires some funds, mental changes in the
social, economic and political power structure in our societies.
It requires changes in social relationships. It requires re
ducing the power of some and increasing the power of others.
The elite in our societies is not interested in jjhis kind
of development, because it would mean reduction in their pro
perty and power. The elite is ofcourse not willing to give up
its power and position to others.
The kind of .development we have in mind cannot avoid con
flicts. However, structural change might not necessarily mean
shedding of blood. In fact fundemontai change should be tried.
in a peaceful way. But it might not always be possible. Vio
lence is almost always star, .d by those who do not want funda
mental change. They violently resist reduction in their power,
privilage and property. The poor have to resort to violence
often in self-defence. Development would mean struggle and wo
cannot avoid it.
- CO^’TINITY |||ZLTH DEPARTMENT
DIFFERENT APPROACHES TO DEVELOPMENT
In India, especially after the independence, we see thousands
of individuals and groups engaged in the field of development
either full time or part time. To be a social worker or
development worker, to some extent adds to ones status and
position in society today. In spite of all these countless
efforts we hardly see any significant changes in the life of
the nation as a whole. A national net work for a concerted
effort in the field of development is yet to be evolved.
A close look at these groups and individuals in the field of
development will show us thatftheir understanding of poverty
and the corresponding approaches to development varies and in
certain cases diametrically “oppose each other. Though one cann’t
question their good will and sincerity of purpose, we should know
that, mere good will and. a sense of sacrifice and committment
do not indeed suffice to make our contribution to development
and social justice meaningful.
The approaches commonly adopted by different people in the
development field can be classified into three. They are :
1)
2)
3)
Welfare approach;
modernization approach
social justice approach
All these approaches proceeds from a clear and definite analysis
and understanding of poverty or underdevelopment, however
scientific or unscientific the analysis may be.
Before we proceed further, let us be clear about certain
initial facts.
1
Our ability to identify factors and forces that create wealth
and poverty determines our ability to tackle the problem.
2
Each one of us has an understanding of poverty and under
development, whether at the conscious or sub»conscious
level. We may have never formula te<) it, but a closer look
at our work will reveal it to us. Always the solutions and
methods adopted, follows from our analysis.
3
Our understanding of underdevelopment and analysis of the
problems are largely influenced oy conditioned by our own
-economic
*
soci
background.
- 2 -
Our preception of reality is conditioned by our position in the
society. Thus the causes of poverty identified by the rich may
not be the same as those indicated by the poor.
1)
The Welfare Approach :
This approach is deeply rooted in the mentality of religious
minded people and humanists’ and is favoured by many private
agencies and governments in both developed and in developing
countries. The fabulous investments in men and money that
welfare enjoys, compels us to reflect, seriously on whether
it deserves it or not.
‘ .
In this approach, development and under development are
considered as two parallel realities that have always co
existed, and that will always coiexist. Here poverty is
accepted as a normal result of forces outside the control
of man. These forces are identified as natural and super
natural. Here the symptoms are treated with a rather.fata
listic approach, rather than the’ root causes of the problem
with a critical analysis. Natural forces are seen as
•disasters, epidemics, earthquakes, cyclones, floods,
draughts, etc. over-which man has nd control. In the
supernatural sphere, man's status in life is seen as predet
ermined. It is his fate, it is in the-plan of God, and
explanation of poverty reflects a religions tone. Development
workers with this understanding regrets poverty, but accept
it as fate.
People who see poverty as created by forces "outside the
control of man, see little possibility for change. The
solution is seen as a sharing of material goods and talents
by the blessed and privileged, and the acceptance of these
goods and services by‘those who are in need of them. The
disposition.advpcated is a basic contentment with one's
state of life. Work for the poor assumes the nature of
alleviating the suffering of the poor rather tha,n eradi
cating poverty itself. Development work here becomes an
ongoing relief or charity, characterised by 'dolling out
*
benefit to the poor people according to their needs.
(Giving the man the fish). It is often a spontaneous response
to a situation with-little effort-made'to identify and tackle
the root causes of the problem.
- 3
- 3 -
And in the recipients, it often develops attitudes of depen
dence, laziness and passivity and sometimes creates division
among the poor. It always diverts the attention of the poor
from the real issues and anaesthatizes them.
Even a limited study of the history of the welfare approach
and a superficial analysis of the functioning of society
reveal that most of the evils treated by the welfare approach
are the inevitable by products of certain forms of social
organization.
2) Modernization approach
Like the previous approach modernization too rests on a certain
understanding of poverty and under development. The cake,
they say has to be bigger before it can be shared. So in this
approach increased production and econoric growth is stressed,
to remove poverty. Here it is implied that people are poor
because-there is not enough production of goods. Modernization
approach relies on industrialization and on rather sophisti
cated and capital intensive technology. Family planning
campaigns are also of prime importance to keep down the birth
rate and thus to promote economic growth.
Herey development is seen as the successful utilization of
resources, natural and human. Such an understanding stresses
the need for patience, hard work, self descipline, sacrifice
lave-stments and quality education, needed for the production
of bigger cake. Under development is seen as the result of
the slow and inadequate establishment of the system of
production and consumption present in the developed countries.
To a great extent modernization then means westernization following closely the methods and patterns of the developed.
The advanced countries become the guides of the developing
countries. On the cultural level it leads to the acceptance
of the ideals of western countries and the adoption of
their attitudes and values.
Those who can produce more are encouraged to the level best,
with the contention thatfthe. benefits will ’trickel down1 to
all. This method of ’Backing the strong
*
(green revolution)
is easily recognizable in our five year plans, government
policies and in the projects run by voluntary agencies.
- 4
- 4 -
Even though impressive statistics can be given on the growth
of agricultural and Industrial production, on the number of
students enrolled in educational institutions, education and
public services, a question could be asked : who progresses?
The rich, who only posses the purchasing power, with their
demands, command and control the market, and often fund to
imitate western standards of living. Industrialization
responds to this demand, and produces luxury articles which
give higher rates of profit. The production is done at the
minimum cost often introducing sophisticated and capital
intensive technology, thus increasing unemployment. Poverty
and unemployment place the workers at the mercy of the land
lords and industrialists, with low wages, and miserable and
inhuman conditions;of work. The state accentuates the situation
by limiting or forbidding strikes. Whenever the labour force
is so large and employment so scarce, favoritism and corruption
unavoidably prevail. Extreme prverty drives poeple to borrow
for their subsistence and social needs; money lenders prosper,
for no bank or credit society would lend money in such
circumstances. All this creates a vicious circle.
In a society where serious inequalities already exist a
technological advance leading to increased productivity is
likely to be limited to those endowed with superior wealth and
social status to the exclusion of the poor majority’ says the
United Nations. research institute for social development,
Geneva.
The modernization approach, therefore, ends with the abundence
of luxury articles and' tl.o scarcity of basic goods; with
sophisticated technology and unemployment, low wages, debts and
bonded labours. It produces the wealth of the few and the
poverty of the many. The limited resources of the nation are
thus used by a small groups for their selfish interests.
) Social Justice Approach
The Failure of the modernization and welfare approach lead some
to evolve a different approach to development based on a critical
analysis of the various j'orces and dynamics at work in the
society. It examines tho organization of society and it's
functioning at both mierp and macro levels.
- 5
- 5 There is the conviction that non-economic factors that is the
overall social context of society with its institutions and
structures. - Play a very important role in development. It
tries to tackle the root causes of poverty and pays great
attention to the proper distirbution of wealth. It does not
accept mass poverty or under development as a fate.
Modernization becomes important only when fare shares to the
masses are possible. . The root causes of under development accord
ing to this approach is injustice. If 85% of Indian population
are below or just above poverty line, it is because 15% un
justly enjoy the results of the labour of the 85%.
In this approach one is convinced that deprived groups and
nations_can develop only in the context of a direct attack on
poverty and a move for just distribution of wealth and power.
Instead of depending dispropotionately on capital formation
and move modern attitudes and values, development ultimately
depends on land ownership, land utilization, employment, wages
and the level of food comsumption. What would development
mean in this historically created condition of under development.
It means the restructuring of society! Efforts in this direction
can be seqn in Trade Union, (Balance of power in the production
sector through collective bargaining) marketing co-operatives
(challenge to the unscruplous exploitation of middleman) credit
unions, (against money lenders) Mahila mandals (against low
status of women). Always it was the awareness of injustice
and exploitation in these cases that resulted in the organi
zation of people at various levels. So in this understanding
of development, the approach one would adopt will be awareness
building which will definitely culminate in action.
Genuinely effective development work will have to challenge and
re-organise the relations between the substructures in the
society. The wealthy are the socially privileged, and the
politically powerful. Power and privilege proceed from economic
standing. Culture and religion seem to reinforce the inter
relationship by providing sanctions andjustifications, A
total transformation of these structures and support, is. in
evitable. In the economic sphere, this would mean policies
geared to serve the needs of the people and not as at present,
for the profit of a few. This would require that the means of
production, land and capital be socially owned. On the social and
cultural levels, this would mean relationships of equality
between groups of people;
- 6
- 6 -
New ways of thinking feeling and acting, collective promotion
.rather than individual promotion. On the political level, to
evolve an organizational set up that makes possible real and
effective' decision making power for the people. Thus this
approacn aims at a socialist society.
Unlike the previous two approaches to development, this one is
a rather distributing approach, as it demands a commitment to
struggle, and a struggle against the powerful dominant group;
and it is no easy task. As development workers, what options
does our above understanding leave us with? Can our sincere
desire to alleviate the wretched misery of our countrymen
express itself in meaningful actions that contribute to this
process of collective awareness, collective organization
and collective struggle?
Community Health Department
CHAI, Post Box 2126
157/6 Staff Road
Secunderabad 500 003 A.P.
The Catholic Hospital Association of India
C. B. C. I. Centre, Goldakkhana, New Delhi - 110001
Tel. .310694, 322064
HON FORMAL EDUCATION
Education today:
Teacher-student relationship: I know; you don’t know
I am active, you are passive.
Content:
Past oriented
Bookish- memmorizing (capacity of de seeming,
criticising etc. are not developed.
Only
intelligence is developed)
-knowledge that is transmitted is the under
standing of the society of the dominant group.
-banking education: You.will be a producer
for the dominant class. Hence education is
given as far as production and consumption
are concerned,
More investment in Higher
education.
Consequences Create conformity: No creativity maintain the
existing pattern of society.
The philosophy and methodology of Paule Freire have
made a profound impact on educational thinking and models,
expecially in the field of Adult Education.-
Paulo Freire dis
tinguishes between a magical or unreflective way in which man may.
confront the world around him and a critical vision of that world.
He wanted to reform the illiterates basic perspective on reality,
which has usually been a prefound pessimism and fatalism, by
enabling him to gain awareness of his capacity to shape his
environment and to acquire the means to do so.
Literacy training
shouldn't immense the pupil in his status, but rather give him the
capacity to overcome it.
There is no education that is neutral.
Education
either functions as an instrument which is used to facilitate
the integration of the younger generation into the logic of
the present system and bring about conformity to it, or it
becomes the practice of freedom, tho means by which men and
women deal critically and creatively with reality and dis- .
cover how to participate in the transformation of tho world.
The present education is for domestication, an instrument for
the maintenance of statusque or a means for imposing the
values and instrests of the dominant class.
In a society that is dominated, people are living in a
culture of silence,
The only way to understand the culture of
silence is to see it as a totality that is itself part of a
larger comples.
We must also know the culture (or cultures)
2/-
2
of this larger
complex, because it conditions the develop
ment of the culture of silence.
Not that the culture of silent
is not something created by the netrapolis (cente-periphery)
in specialised laboratories and then shipped out to the.do
minated; nor is it a spontaneous generation on the spot.
Tn
arises from the interrelations of the oppressed and the oppre
ssor.
They arc the result of structural relations between the
doninator and the dominated.
Wo must first see how dependence
a special sort of relationship that gives tise.to two differed’
way of being, thinking, expressing oneslef etc.
That of the
culture of silence and that of the culture that has a voice.
The relation between the doninator and dominated,
exist in a broad social context.
Some of them come about as "
the dominated assimilates the dominatcrs cultural mytlis.
.
This- dependent society is, by definition a silent society.
Its voice is not.a genuine one, but a simple echo of the voice
of the doninator,. The dependent society’s silence under the
directing society, is repeated in the internal relationships
with in the dependent society.
Its own power elites, who are
silent under the doninator, silence the people too.
Because
the oppressed has internalized the oppressor.
Our education programme will depend very much on
the attitude we have towards the illiterate.
If we think that
the illiterates are marginalized or moved out of ..the centre
of the society.
Our approach.in adult education will be to
bring them back to the centre.
We will see them as stupid
illiterates, who have strayed from the. right path and we want
to make them happy by giving them the gift of the world.
With
an approach like that literacy programmes will never enable
a man to read freedom, becuase they fail to denounce .society
itself, which is depriving him ofhis right to speak.
That
is why it is so-important to demythologise the reality a
person lives in.
The fist phase of the method of education in an on the
spot study of the context in which the illiterates live, in
order to identify the common vocabulary and the probeIm issues
around which the process of reflection could develop,
..... 3/-
Through information conversations^ learn and listen to
their vocabulary; observe the off-repeated.topics of their
conversations;-especially their felt needs.
Observe their
world view i.e. their ideology, their mentality e.g« unemploy
ment, low wages poverty and misery etc..
Develop different'
lists of words, problems and situations for different
villages .(slums etc.).
The second phase involves the selection, words from the
vocabulary that-has been discovered,
’those most changed with
essential—meaning and thus major emotional content, but also
the typical-expressions of the people.
Three'criteria could govern this choice.
The first is
the .capacity of the words to include the basic sounds of the •
language.-
The' seeond is' that vocabulary, when organised should
enable the people to move from simple .letters and sounds to
more complex ones.
The third criteria is that the words are
chosen -for their potential capacity to confront the social
cultural and political reality.
The words should provide
mental and-.emotional stimulation, ...that ..they should suggest
and mean something important,
(eg. the word ’work’ provokes
a range of associations with the nature of human existence,.
economic. . functions, co-operation, unemployment, wages, etc.
The third phase of
*
materials.-
the 'method develops teaching
Paulo yreire speaks of two types of materials.
One.is.a set of cards or. slides which breakdown the words
into parts for more careful analysis.
The. second is- a set of
cards of fictional or real situations^, related to the words, wli
are designed to impress on the pupil.,.,through vision or image of
the word, -and -also' to.stimulate his. -thinking about the situatio
that the word implies.
-The educator role in this is:
- To enter’into dialogue with the illiterate about concrete
situations.
- To offer -him the instruments with which’he can teach himself
to read and write.
- To promote self discovery in the participants through explo
ring the dimentions of the teaching mate-rial used
-To promote dialogue, discussion and not monologue.
4
The livelier the discussion or debate, greater the
number, of ideas and implications drawn and the richer and
move meaningful of the critical insight into the problem as
The educator-Animator tries to
well as memory of the word.
get all the members of the group to participate by directing
questions to them, prologning the discussion so that they
will realize the deeper meaning of what was once for them
an obvious, accepted reality.
The Paulo Fraire method doesn't aim chiefly at liter
training, but at conscientization.
It means an 'awakening of
consciousness1, a change of mentality involving an accurate
realistic awareness of one's place in nature and society; the
capacity to analyse critically its causes and consequences,
achieve a deepening awareness both-of the socio cultural
reality which shapes their lives and of their capacity to
transform that reality.
There is no conscientization if the
result is not the conscious action of the oppressed as an
exploited class struggling
any one else.
for liberation,
lie one oonscienti
The educator and the educatee together conscien
tise themselves.
* * * * *
.4
*
C H D
PZ
TEAM
The Catholic Hospital Association of India
C. B. C. I. Centre, Goldakkhana, New Delhi- 110001
Tel.
310694, 322064
IDUCATIOIT A1TD DSV.TJLO.?: "JUT
?I,3. Julius X. llyerero, Proniclo ,t , UAitod
^public of Tanzania, and ‘.ic-norary Preside;
International Ceuncil *
or Adnl-t Sducation.
?./-
a:
J to do it for the.-.selves
tbe
.catio„i ^ust be seen as o. be
-ritaria;
S'.
11 Coil'
1.976, a-t Ja:
BEYOND SOCIAL WORK
During their summer vacation, a group of students went to a
village to help the villagers complete a well that they were cons
tructing with government assistance.
During their work there, the
students discovered that the villagers were not receiving the
necessary funds that they had been premised by the local Block
Overseer to complete the well.
That official wanted a bribe f>om
the villagers before he would release the money.
But, with stu
dent support and encouragement, the villagers refused to pay the
bribe. The students began to investigate the situation while work
ing side by side with the villagers. They discussed the question
of rights with the villagers and urged them to take steps to seek
payment of the required funds.
The students told the villagers
that if they (the villagers) decided to take action, they (the
students) would accompany and support them in their efforts.
Finally, the villagers got up enough courage to walk seven miles
from their village to the Block Development Office.
An equal num
ber of students joined them.
Villagers -and students together
demanded of the B.D.O. and his superior, the D.D.O., the payment
of public funds owed for the completion of the well. The following
day, both officials, perhaps expecting a pnlite, official welcome,
drove to the village by jeep.
The villagers greeted them with even
stronger demands for the payment of funds owed them for the well.
The following day, the villagers received the funds, and in the
weeks following, further payments were made for tho completion'of
the well.
ELIMINATING THE MIDQ.LE MAN
On the local bazaar day, villagers came from miles arountl into
the central market place to buy and. sell, and to meet their friends.
There are four main roads leading into the bazaar from the surround
ing villagesIt has long been the custom for the town merchants to
send their agents out along these roads to grab the fowl, grains,
vegetables and fruits which village women are carrying into the bazaar
to sell.
By so doing, these agents prevent the women from reaching
the bazaar with their goods, where they can bargain in order to got
the best price possible.
These agents then pay the simple village
women a nominal sum for their wares - far below a fair price - and
head back to town in time to enjoy a considerable profit for their
trouble.
Since this was a practice of long standing, the village
women had grown used to this sophisticated form of stealing.
However, local high school and college boys and girls had
become aware of the injustice in this practice and organised them
selves into teams to patrol the main roads leading into the bazaar
on the weekly market days.
They protected the women from these
agents some »f whom they chased away.
They explained to the vil
lage women that they deserved and could obtain higher prices for
their produce, if they sold their items themselves in the bazaar.
Within two months the roads were cleared of agents sent by the
merchants.
On one occasion, as a result of their work, the students faced
arrest by the police who had been called in by the merchants.
Fpweger, a group of girls challenged the police to put them in jail
for what they were doing.
A crowd of about 200-300 people massed
in front of tho police station and the students had to be released.
-2-
This is an on-going issue, since merchants, often with police
protection, continue to try to send their agents out on bazaar day
to intercept the village women before they reach the bazaar.
And
students and villagers continue in their efforts to protect these
women from being exploited.
Land-GRAB BL I NG
Tribal land cannot legally be transferred, by.sale or otherwise,
to non-triba'ls.
The government can, however, grant authority to non
tribals to take over tribal land if, "in the judgement of the govern
ment,", such a takeover is required for "the national interest".
The area around Chaibasa is rich in natural resources. A mine
owner was working on the edge of a village near Chaibasa.
He dis
covered in his mine a very expensive type of stone.
This stone was
in great.demand and brought a high price in Calcutta, where it was
used in building luxury homes and office buildings
In order fur
ther to increase his profits, the owner decided to expand his mine
and by so doing he threatened the very existence of the neighbouring
village and its inhabitants, many of whom were employed in the mine.
The owner made a trip to Patna where he managed to convince the
officials there and got the stone in question labelled by the govern
ment as "necessary for the national interest".
Returning from Patna
with the required permission, the mine owner frightened a few of the
villagers into selling their land to him for the minimal legal rate
of Rs.400/— per acre, whereas the actual value of the land was closer
to ten times this amount,
gut he succeeded in convincing"the people
that if they would not sell him their land at the minimal rate, the
police would in any case «ome to take their land from them, and they
would receive no money at all.
But other villagers were not so easily hoodwinked.
They orga
nised themselves and, through sit-dowhfe at the site of the mine,
they tried to stop further work and resist the takeover'of their
land and homes.
However, police came and drove them away from the
work site.
The owner, with police protection brought ,:in workers
from other villagers to keep the mine open.
A group from the threatened village informed the students of
their problem and asked them for their help. The village was divided
into various interest groups. . The students decided to visit' tfie vil
lage and study the situation as they spoke with the villagers.
One
of the village leaders, together with the students invited the mine
owner to a meeting at which the issue could be debated.
Even though
the owner had tt/ice warned the students not to interfere in "this
private matter between me and the villagers", he agreed to come to
the meeting.
The students took the opportunity to expose the owner's
tactics in getting the "legal authority" to expand his mine. The
students followed up this meeting by organising a mass meeting of
the entire village during which the villagers, encouraged by the
presence and support of the students, rose one after another to
denounce the owner and warn him against trying to expand his mine
into their village.
As a result of these two meetings, the villagers made it clear
to the mine owner that under no circumstances would they allow the
mine to be expanded into their village.
The owner, despite the
fact that he. had, "t he law" on his side - a law purchased in the
r'
his meeting with the. necessa,'y officials, gave up his
OUTCRY AGAINST NEGLIGENCE
Late one night, a Calcutta-based truck struck a young student on
a Chaibasa street.
The driver fled, but not before another student
noted down the number of the truck and also took a set of the'truck's
keys.
(The driver drove off with a duplicate set.)
The student
immediately gave the number and keys to the officer on duty at the
local thana.
The officer first refused to take any action, only
after public pressure was brought to bear on the poiicewere both
the driver and the truck seized two days later.
In the meantime, the injured student was admitted to the local
government hospital in a conscious condition.
Two days later, how
ever, his condition took'a serious turn and he was operated on.
He
never regained consciousness.
The necessary medicines were not
available in the hospital, so students had constantly to go and buy
what medicine they could find in the local bazaar.
One evening,
the hospital ran out of oxygen and the students had to rush to
Jamshedpur, some,forty miles distant, to bring the needed oxygen.
The student died the next morning.
During the week the student spent in the hospital, the truck
owner never came forward to offer any form of assistance.
the police make any efforts to bring him forward.
Nor did
As a result of this negligence, an application.was submitted
to the D.C. in the name of the students of Chaibasa demanding that
/.that
the s.p. be removed;/that action also be taken against the person in
action be cnarge of medicine and oxygen supply at the government hospital;
taken
that action be taken against the driver of the truck; and, finally^
the police^^ compensation be made by the truck owner to the family of the
officer ondead student.
The application went on to say that should no resduty at
ponse on these points be made within four days, the students would
the time
begin a hunger strike in front of the D.C.'s office.
of the
accident;
,
The D.C. did not respond and so the students undertook a hunger
strike, during which two of the students had to be hospitalised.
They ended the strike only when the D.C., meeting with the students
in his office, promised to deal with all the students' demands
within a one-month period.
At the conclusion of one month, a student delegation went to
meet the D.C. who informed thorn that he had nothing to report to them.
A week later, some 900 students marched on to the D.C.'s office
for the D.C. had as yet done nothing in connection with the students'
demands. The students met again, and contrary to a faction that
wanted to turn•violent, a core group of students decided to detain
peacefully all the trucks of the Calcutta—based company coming into
Chaibasa. That evening, one truck was halted^ A few days later,
the truck owner's son came to Chaibasa to begin negotiations with
the students and with the family of the dead student regarding compen
sation.
Uhen negotiations between the truck owner and the family of
the deceased broke down, a Rs.250,000/- compensation case was taken
out by the family against the truck company.
This case is still
in court.
As a result of the students' actions, the S.P. was trans
ferred and the Civil Surgeon of the government hospital fled and
was replaced by a new man with a new assistant.
I!
PERSISTENCE WINS THE DAY
In a local village high school, with nine out of every ten
students tribals, one hundred and thirty-two tribal students in
classes IX and X and not received their government scholarships for
between two and four years.
Organising themselves with the help of a student leader, two
hundred students of this school marched on the Welfare office demand
ing either payment of their scholarship money or an explanation of
why they were not receiving their scholarships.
The Welfare Officer
refused to speak with him individually.
Finally, the students sent
in a representative to tell the officer that if their scholarship
money was not forthcoming, a larger group of students would be march
ing on his office.
The officer immediately began to bargain with
the student, but the student walked out of his office, refusing to
deal individually with him. The students then went to the D.C.'s
office and made an appointment with him for the following morning.
Next day, the students arrived late for their appointment after
their three-mile walk from the village school. They made another
appointment for the following week, but when they arrived at the
D.C.'s office they were told that he had gone to Delhi.
When they
finally succeeded in meeting the D.C., he tried to give them various
reasons why government scholarship money can be withheld from tribal
students.
However, when scholarship payments were next made, an
additional ten percent of the original number of tribal students in
that school, who had not been receiving their stipends from the
government, did in fact receive the scholarships.
SAMPLE QUESTIONS TO INITIATE DISCUSSION
Would you; agree with the actions taken by the students in these
incidents? Why or why not?
2. Should students get involved to this extent in social issues,
are these imvolvements distractions from their studies?
3. What was the basic driving force behind the students'
actions?
4. Should social awareness stopat/study of a situation or should it
lead to action?
5. Are you aware of similar situations and issues in your own community?
n o, t • ts .sc inji.,-..!.ic',s U'i t”
PRIORITY THRUSTS OF CHAI
DECENTRALIZATION IN CHAI:
The Catholic Health Association of India (CHAI) has membership of 3128 health institutions
spread all over India. More than 70 percent of these institutions are small health centres
located in remote villages and tribal settlements. They were largely involved in institutional
centred curative health care. It was not in line with the vision and mission of CHAI, which
emphasis community based preventive health care. Thus CHAI took the responsibility of
enabling its Member Institutions (Mis) integrating their existing curative care with village
based preventive care. But it found it difficult in extending knowledge and technical support
services to Mis based on their problems and needs as they differ from institution to institution
in accordance with the socio-economic and cultural situation of the area where its is located.
This led to the initiation of a decentralised process in CHAI seven years back.
Objectives
The objectives of the decentralization in CHAI are:
To ensure that all Mis are actively involving in community based preventive health care.
To identify and address region and area specific health issues more effectively through
initiating a system of multi-level planning.
To provide a platform for the Mis at regional and diocesan level for networking with
church bodies like-minded NGOs for the collective action for health promotion.
■
■
■
Achievements
Decentralised Structures:
As part of decentralised administration, eleven regional units (ecclesiastical division) and 98
diocesan units have been created. The table below presents the distribution of the region
wise distribution of the diocesan units and Mis.
REGION WISE DISTRIBUTION OF DIOCESAN UNITS AND Mis
ISI
Regions
States
No
I1
I’
3.
4.
5.
6.
7.
The Catholic Health Association of Andhra Pradesh
Andhra Pradesh (CHAAP)
The Catholic Health Association of Tamil Nadu, Pondicherry
Tamil Nadu (CHAT)
The Catholic Health Association of Karnataka
Karnataka (CHAKA)
The Catholic Health Association of Kerala
Kerala (CHAKE)
The Catholic Health Association of Maharashtra, Gujarat,
Goa, NagarHaveli
Western Region (CHAW)
The Catholic Health Association of
Madhya Pradesh (CHAMP)
The Catholic Health Association of
Bihar (CHABI)
Madhya Pradesh,
Chhattisgarh
Bihar, Jharkhand,
Andamans
Mis
Diocesan
Units
9
319
18
439
9
273
6
468
10
285
6
308
13
271
8.
North Eastern Catholic
Association (NECHA)
9.
Orissa Catholic Health Association
(OCHA)
10.
Rajasthan, Uttar Pradesh Catholic
Health Association (RUPCHA)
11’
West Bengal Catholic
Association (WBCHA)
Health
Health
Arunachal Pradesh,
Assam, Nagaland,
Manipur, Meghalaya,
Mizoram, Sikkim, Tripura
Orissa
10
242
5
129
Rajasthan, Punjab,
Haryana, Jammu Kashmir
& Himachal Pradesh, New
Delhi, Uttar Pradesh,
Uttaranchal
West Bengal
4
284
8
110
98
3128
Total
All the eleven regions have a minimum organisational and administrative. They are
autonomous institutions registered under Societies Act, structure. Nine regions have projects
of their own mobilising resources from different funding agencies. The regional units are
actively involving in enhancing the competency of the Mis in the areas of promoting
community-based health care.
The diocesan units formed are in the process of creating the infrastructure required to
function as autonomous bodies. They have their own programme to meet the needs of the
Mis supported by CHAI and the respective regional units. Development of projects and
mobilisation of resources at the diocesan level is essential for the sustainability of the
diocesan units and now the efforts are in that direction.
Multi - Staged Decentralised Planning
One of the strategies adopted for strengthening the decentralised structure as effective,
responsive and vibrant in meeting the needs and problems of the Mis is the establishment
and activation of multistage decentralised health planning. The five stages of decentralised
health planning of CHAI is as given below.
-2-
Decentralised Health Planning
Networking
The regional units are networking with church bodies and like-minded NGOs for tackling the
issues affecting the functioning of the health centres. They also participated in the People
Health Assembly and signature, Campaign for Universal Accessible to Health Care. The
regions - CHAT and WBCHA - succeeded in bringing together of the different actors of
health, both Government and Non -government organisations for reflecting on the health
issues affecting the poor.
Health Policy
The Orissa Catholic Health Association (OCHA) is developing a health policy for the region.
The Catholic Health Association of Western Region (CHAW) has done a need assessment
study for the region. Based on this study outcome the region is contemplating to evolve its
health policy.
Future Thrust
Decentralisation provides opportunities for the Mis to come together at regional and
diocesan levels for sharing their problems and needs and planning out actions and their
implementation and made networking and collaborative work with church bodies and like
minded NGOs as a reality. Translating these energies into concrete programmes of action
and create a definite positive health impact at the various levels is the future thrust of
decentralisation.
CAPACITY BUILDING:
The creation of the Capacity Building team in CHAI four years ago is the direct result of the
Organizational Development (O D) process initiated. It is based on the finding that mere
training of the participants in selected subject area will not bring the desired change in the
performance of the individuals and their organisations.
What is required more importantly is enhancement of the capacity of the individuals and
organizations in discharging their responsibilities in the areas of their involvement.
Accordingly capacity building is defined as a change in capability of an individual or a team
or an organization and change of capability can be in any one of the combination of the
following areas: behaviour, values and attitudes, know-how, application of knowledge and
experiences and networking.
Objectives:
The objectives of the capacity building team are:
•
•
•
•
•
•
To evolve and strengthen Regional Resource Team (RRT) in all eleven regions.
To enhance the knowledge and skill of the regional and diocesan leaders in the areas of
organizational perspective and governance.
To ensure the active involvement of the regional and diocesan units and member
institutions in health planning and management at their respective level.
To re-engineer the health planning of the congregations so that the active involvement of
the health centres of the respective congregation in community based preventive health
care is ensured.
To enable health professionals updating their knowledge and skill in the areas of health
planning and management and community health promotion through organizing and
conducting national level trainings.
To produce and make available manuals, modules, reading materials and audio-visual
aids for the community health trainers and practitioners.
Activities:
The important activities of the capacity building team are:
•
•
•
•
•
Forming and strengthening RRT through selecting and training community health
trainers and ensuring their availability to regions for organizing and conducting training
related to community health. Presently nine regions have resource team.
Extending knowledge, skill and technical supports to the regional and diocesan units and
member institutions and ensure the evolvement of health planning at those levels. Four
regions, nine diocesan units and 170 member institutions have already made a
significant progress in this direction.
Congregations are enabled to reorient their health plan. The congregations' health plans
are evolved based on the plan of their health centres. The plans of the health centres, in
turn reflect the health problems and needs of the poor people of the villages located in
and around them. This planning practice has been achieved in nine congregations.
Enhancing the knowledge and skill of the board members of the regional and diocesan
units in governance and perspective building.
Member Institutions are extended with technical, operational and organizational skills
required to implement community health programmes.
-4-
•
•
National level trainings in the areas of project planning and management, PME,
community health, perspective building, rational drug therapy, participatory rural
appraisal etc. In the last four years, a total of 532 health professionals have been trained
in either one of the above said areas.
Production of training manuals, booklets and charts. The manual on project planning
and management has been already published. A manual on Making Development
Organisation performing will be published shortly.
Future Direction:
The capacity building programmes, indeed, helped the participants to gain knowledge and
skill in the subject areas of the trainings and enhanced their functional efficiency. However,
the impact of these training the functioning of the organization from which the participants
represented is limited. This problem will be overcome through giving more emphasis to
capacity building of the organisation rather than the individuals. Moreover, a long duration
health management training is thought of, which will meet the health man power requirement
of the congregations.
CHAI’S EFFORT TO DEAL WITH HIV/AIDS;
Involvement with HIV/AIDS work
As HIV/AIDS was becoming a serious health and social problem, there was an urgent cry
from all quarters of the church to respond to this grave situation. Since CHAI is the structural
body responsible for health, everyone looked up to CHAI for guidance and direction on
HIV/AIDS.
Milestones of CHAl’s growth with specific focus on HIV/AIDS
1993
AIDS Desk was formed “Think-tank" group
1994
CHAl’s Policy on HIV/AIDS
1995
CHAl’s Plan on HIV/AIDS
1996-1997
Personnel from the member institutions were trained to plan and initiate
actions in their regions
1998-2001
- Developed human resources in care and support.
- Networking with like-minded organizations for policy lobbying and
advocacy.
2002 - 2004
The quality of life of the persons infected & affected with HIV/ AIDS is
enhanced through a process of specific interventions such as
implementers forum & promoting access to parallel system of
medicine.
Specific Areas of Involvement:
CHAI approached the situation at various levels
Prevention
social
care
Thrust Areas
Prevention
Prevention had been an utmost concern. CHAI had done pioneering
work in the area of school health. Developed modules and innovative
approaches for Life Skill Education in schools ad colleges with the
collaboration of CRI in 1997- 1999.
Now we have been invited by Andhra Pradesh State AIDS Control
Society to be the nodal agency for the school health programme in
the state of AP for the non-govemment schools.
Training
Training of the health care personnel with specific skills on prevention,
counselling, care and management. About 650 persons have been
trained and about 50% of them are directly involved in giving care
while others have initiated activities along with their ongoing work.
Training Programmes &
Participants trained
Networking
Networking with church related institutions, NGOs and Government agencies - such as
APSACS for the school health programmes “Life Skills Education" and Drop-in Centers".
-6-
TB and Malaria Control Programme through the regional units. Training on microscopy
through Government agency.
Collaborating and networking with other Churches for care and prevention Community
Health Watch Groups.
Policy: Consultations were organized at Regional and National level to form policies.
1. Common church policy
Intensive efforts had been taken to network and collaborate with church bodies, church
related institutions and NGO's to bring out a common church policy on HIV/AIDS.
Prevention, care, management, counselling and training of personnel. This policy
would be available in six months.
2.Congregation and institution policy
Policies to be made flexible to ensure that persons infected and affected are cared and
supported. Consultations and discussions with 212 decision and policy makers of the
member institutions were organized.
(St. Ann’s of Luzen sought help in developing the policy and now they have started a center
in Vijayawada, Andhra Pradesh for both men and women with HIV/AIDS).
Continuing Educational Material
Through our interventions, there was a felt need for scientific and updated information
among our membership. Personnel who have been trained by us are updated with the
recent developments with continuing educational material on HIV/AIDS and the concerns
and issues. This material is sent once in four months.
Impact
Nine years into HIV/AIDS work - we stop to look back and see if we have made a dent in the
epidemic. Has our mission of Christian love reached to the forsaken one?
We feel content enough to say YES!! We made a dent in this epidemic through our love,
service, and efforts.
The approaches and strategies used during the past nine years in the areas of prevention,
training, networking, impact on the policies, and disseminating information enabled us to be
instrumental in starting 35 organizations/ institutions in India for the care, support and
management of persons infected and affected with HIV/AIDS.
Organisations working for HIV/AIDS
Research
Oraganisation
Hospitals
Hospice
48%
Integrated
Approach
HIV & TBto
6%
Community
Approach
Back in 1993 when the challenge of HIV/AIDS was hurdled at us, there was not even a
single church related institution for the care and support of these most neglected and
rejected ones. But today we are glad to see 35 institutions giving these services. One
young sister from Mumbai says that she feels it is enough if we can allow them to die in
peace and dignity.
Institutional care has always brought criticism about the sustainability, feasibility and impact
in the long run. However, when we look closely we found the impact the institutions have
made:
The institution facilitates acceptance in the community.
The local community contributes in caring for persons with HIV/AIDS through
volunteering to serve or meet their needs. Thereby through this process remove
stigmatization.
The organization facilitates to build back the lost relationships of the persons with their
family and community.
Promotes dignity of life.
The experiences shared by our member institution working with HIV/AIDS have shown
that institution/ organizations are instrumental in fostering community support in the
course of time. (eg. Jyothi Terminal Care center)
The membership involved in HIV/AIDS works were initiated based on the needs of the
people. The situation differs from state to state thus each organization is a unique model by
itself. Some of them focus on children while others care for men and women.
Few approaches that have made difference.
Integrated Approach
Mukta Jeevan now has an integrated approach to communicable diseases. The pioneer
institution by sisters of Helpers of Mary in Thane was started for the Leprosy patients. After
the outbreak of HIV/AIDS as some of patients also are with HIV. The management adopted
a mainstream approach to patient care. Patients whether with leprosy, TB or HIV/AIDS are
isolated neither among themselves nor from their families and friends. The caregiver and
visitors take universal precaution in the care and management of the inmates who live as a
family there. There are men, women and children with and without infections.
The families are supported to earn their livelihood through various income generation
programmes. The children are sent to the local schools.
Community Involvement
Jyothi Terminal Care Center - A hospice was started two years ago in Mumbai has about 40
inmates. There was a stiff resistance from the local community. They have even requested
the hospice to be shifted. However, over a period of six months, the community observed
that the patients were cared by the caregivers without fear or stigma.
The carers also
started going into the community and sensitizing them. The response was overwhelming.
-8-
The organization is now run solely on local contribution, which even includes food, clothing
and medicine. The local community takes care of the dead. They perform the last rites
according to the patient’s wishes. The women folk of the community volunteer their services
in the kitchens. A place, which was started as a hospice, has generated such a large
community response.
Implementers Forum: A forum of organizations is envisaged at regional level of the
members involved in HIV/AIDS related work. The main aim of the forum is to:
Training and enhancement of skill development
Establishing linkages/network with others working for HIV/AIDS
Collaborate for specific issues such as gender sensitivity, care and support
Updating and sharing of resources - material and man power.
y Support and care of the caregivers.
Some of our learning and challenges over the nine years are:
•
As India is a vast country having different cultural, the problems presents and the
approach needs to different.
•
A significant finding is that the training programme enabled the members to address the
concerns of the HIV/AIDS.
•
There has been an attitudinal change among the membership and a considerable shift in
the policy regarding admission for treatment.
•
Some of the membership has made a shift from institutional care to community based
care, which is foreseen as a positive development towards the mainstreaming of the
persons infected and affected with AIDS.
New initiatives
Based on our learning, the new initiatives envisaged are:
Implementers forums
Integration of HIV/AIDS to communicable diseases
Research and promotion of parallel system of medicine
Training on care and management
Research documentation
Through the initiatives
•
We hope to evolve care and support from the community-based organization and
providing basic care and counselling at home.
•
To establish much stronger network with national and international agencies working
in this field to mobilize a massive effort against HIV/AIDS to meet this challenge
adequately, efficiently and effectively.
-9-
THE DISTRICT HEALTH ACTION FORUM (DHAF)
1. The Concept
The District Health Action Forum (DHAF) is a structure as well as a strategy for bringing
together on a regular basis various stakeholders or actors (the state including local
governments, non-governmental, academic and activist) involved in health for initiating
dialogue and discussions, facilitating consensus in understanding health scenario,
encouraging collective decision making and promoting joint action in health.
2. Objectives
The DHAF is useful in achieving the following objectives.
Effect convergence of resources available in a district for promoting primary health care
Promote a higher degree of utilisation of the existing (government, private and voluntary)
facilities for primary health care.
❖ Activate the PRIs and strengthen them in their endeavours for promoting primary health
care
Create a responsive and responsible civil society to enter into meaningful negotiation
with the power blocks for pro-poor policies and decisions on primary health care
❖ Build up the capacity of the community to deal with health problems
<• Establish and ensure operations of regular arrangements for various stakeholders of
health at different levels to enter into dialogue hold discussions and initiate joint action
programme on health. (The DHAF primarily strives to establish regular arrangements at
district level. Simultaneously or subsequently, similar sub-district level arrangements may
also be brought into being).
❖
Composition and Structure
The composition and structure of DHAF vary from district to district. The district level officers
(DMO or DHSO and district officers for Malaria, TB and Leprosy) of the department of
health, education, rural development, ICDS and public relations, members of CHAI,
members of the Voluntary Health Association of India (VHAI), members of the Christian
Medical Association of India (CMAI), representatives of district level NGOs involved in health
and development, diocesan social service societies and human right movements, and
leaders and functionaries of PRIs are now found as members in different DHAFs. The
number of members in a DHAF is in the range of 20-25 organisations.
DHAFs also have Executive Committees where responsibilities are shared between
government officers and others. The posts of President, Secretary and Treasurer are shared
by NGOs, CHAI members and in some places even by the government officers.
Activities of DHAF
♦
♦
♦
Developed profiles of all actors in the field of health
Worked out a detailed district health profiles.
Dialogues and discussions on health problems
♦
♦
♦
♦
Joint celebrations and campaigns
Interventions to control outbreaks of epidemics
Advocacy with PRIs
Addressing specific health issues
♦
Developing joint plans of interventions in partnership with governments
-10-
♦
♦
Capacity building of health activists and health care providers
Extending support to PRIs in planning and implementing primary healthcare programmes
♦
♦
Awareness building on epidemics and outbreak of other calamities and disasters
Extend mutual support to the member-organisations of the DHAF to improve the
♦
efficiency of their ongoing activities
Encouraging better utilisation of existing facilities for health care
Viability
The DHAF is a viable strategy because owing to the new developments in health sector, the
state alone cannot in future provide health care, which thereby entails the involvement of
others too in this sector. The credibility possessed by CHAI members, the openness of
NGOs to the proposed strategy, the urgent need felt by PRI functionaries to get supported in
many areas of local governance and an overall positive disposition of governments to
collaborate with NGOs are factors favouring the implementation of the project or ensuring
the viability of the idea.
Advantages
A new culture of mutual support and sharing of resources has started to develop among the
stakeholders of health by creating the DHAF. This contributes to the social capital, which will
enhance the efficiency in utilisation of available resources and thereby enable the members
of the DHAF to serve its target population more effectively. Strengthening of PRIs and
enhancing the capacity of both PRIs and village population is a long-term investment in
health care. This will result in increased participation of the community in health care
management and better collaboration of local governments and village community. The
forum, if property managed, can in long run emerge as a point of convergence of interest,
resources and concerns that can create a new equilibrium in power dynamics at grass root
level. The plans of action now being developed by the 14 DHAFs in the northern region aims
at this. This is a contribution of very high order to social infrastructure that can as in the case
of social capital multiply the efficiency of resources invested in promoting health. Similarly,
the forum can function as a district level arrangement for health surveillance. Over and
above, it ensures efficiency of the existing arrangements and systems for provision of
primary health care without demanding more financial investment in this sector. Thus the
DHAF in long-run, will effect changes in the capacity of the local community to manage
health problems, strengthen the health care providers to address more effectively the health
care needs of the population they are serving and increase the level of participation of all
stakeholders in health care management. The ultimate result shall be improved health
condition of the people in the target districts. When both social and material benefit accruing
from DHAF is compared to the cost involved, it may be found that DHAF is a cost-effective
strategy in deed. Besides, it can be a self-financed venture once it emerges as a full-fledged
arrangement. A period of three to five years may be required for a DHAF to reach this stage
of self-sustenance.
-11 -
rJ'Gro ' 3-
Vision & Mission
The Catholic Health
Association
- Bihar and Jharkhand
(CHABIJ)
Catholic Mission in Bihar/Jharkhand
Beginnings of Catholic mission
: 1927
Beginning of organized health care
: 1977
No of Rural Health Centres
: 44
No of Hospitals
: 08
Cunent status
Dioceses
. 14
Health care centres/hospitals. 0-6 bed
- 229
7-30 beds - 23
31-50 beds
- 06
above 50 beds - 06
Origins of CHA in Bihar/Jharkhand
CHAI
CHAP | CHABI | CHAKA RUPCH IWEBCHA |
CHAT CHAKE NECHA CHAMP CHAW
• Birth of CHABI
: 4 May 1993 MIS - 260
• Renamed to CHABIJ
: Jan. 2000
• Dependency on Centre
: 1993-1996
• Independently function
Since June 1996 with the
help ofMEMISA
• Membership
: 282 (as per date)
Vision
Envisage a Hol
transformati
on istic Healthy Society with self- responsibility for Its
Mission
Ensure
self responsibility for their own Health &
Development
Promote people s medicines, Traditional methods of health
promotion treatment
Join hands with people s movements & like minded Institutions
Work In partnership & fellowship with other NGOs
Collaborating with Government s programs & making use of
Major Strategies
1996 - 1999 "HEALTH
: CommunitFOR
y Based
th CareBY MANY MOREMANYHealMORE
1999 - 2001 : ”Empoweri
nHog women,
especi
al y mothers
Har
Mah
Khar
KI
Bal
A Family Doctor " d" " Every Mother Be
2000 - 2003 : Formation of Neighbourhood Healthy Communities ( N H C)
Integrated approch to Health Care
2000-2001 : Net working with Jan Swasthya Antholan - “
HEALTH
AS HUMAN RIGHT “
2000 - 2003 : District Health Action Forum ( DHAF)
2002 - 2004 . " Doctor
Food For AH, Healto tnutri
h FortioAll"
- Moving away from Drugs
nalcipfood,
medicin&esdiwisease
th peoples parti
ations.alternative
IN SEARCH
OF A COMMUNITY
MODEL
OF HEALTH
CARE BASED ALTERNATIVE
Summary of Organisational Development - RU
Continuation of Side No.fl
Achlevemerrts:a. Appoi
ntment of Diocesan Health Co-ordinators (D.H.C.) in 12
Dioceses
b. Regulated quarterly DHU meeting - updating of MIS
c. oriDieonted
cesanPrgs.
Health Policy formulation & Under taking of people
d. Fixing standard Health Care for 0 - 30 bedded institutions
e. Prepared standing order for 0 - 6 bedded MIS
Neighbourhood Health Communitie:i (NHC) 2000 - 2003
Achievements
• No of N.H.C Centres
: 12 Old i 5 New
• No. of Vil ages covered in 12 centre 1125
• No. of Committees formed
: 864
• No. of families profitted
14319
• No. of Dais trained
1178
• No. of Dais Kit given
: 134
• No. of trained Vaids are in practice : 167
• No. of V.H.Ws trained
1575
• No. of S.H. group formed
1131
• Total savings
i Rs. 725717
• No. of schools in Health education are given : 90
• No. of Health Fund formed
: 15
• Total amount from Health Fund : 10540.50
Continuation of Slide 11
* No. of families using Bednets using
: 10000 ;
• Balawadi Centre opened
• No. of Kitchen Garden
• No. of families doing agriculture after training : 125
• No. of families doing veg. Cultivation after trg.: 63
• No. of families making compost after trg.
• No. of families doing fruits cultivation
: 108 •
• No. of girls are studying tailoring
• No. of Trees Planted
: 3639 i
Continuation of Slide 12
• Chanalised from Govt.:
1. Medicines received
30000
2. Immunization
2400 children
3. Polio Vaccination
4200 "
No. of help received from govt, project
a. House constructed
42
b. No. of families received Loan : 108
c. Well digged
124
d. Check Dam
13
e. Bridge constructed
58
2
District Health Action Forum (DHAF) - 2001- 2003
Activities
Health resource mapping by people
zing and
strengthening grass root level organizations for HEALTH
ASOrgani
HUMAN
RIGHT
with Government
atNetworki
districtn&g state
level Health Authorities, Panchayat and Mandals
Survey and surveil ance on health issues
Identifying district specific health issues for action
Cleanliness and environmental protection campaign
Preparing an action plan for a definite period of time
Celebrating health related occasions and festivals
Consultation on participatory action for health
Seminars and workshop for imparting medical knowledge
Control of Communicable Diseases - Malaria, T.B., HIV/AIDs & , Blindness
Organising PEACE COMMITTEES - Vil age, District & State level
Advantages of Decentralization
- MIS strengthened i people oriented
- Beneficiaries are profiting more from activities
- MIS
activiitnievols vement more in community oriented
- More involvement of church authorities
- Better cooperation of Religious superiors.
• Formation of Diocesan Health Unit
• Better coordination among the Nurses
• Col
th other.sectors - such as education,
devellaborati
opmenton &wiPastoral
Major Activities and Achievements
DHAF - Achievements
- Formulation of Jharkhand Health Policy
- ColRellaaborati
tionshionp with NGO & G.O improved
- Better Planning with people at grass root I
- Animation of government personnel &
Resources
- Monitoring & Evaluation
- CHABI - an accepted active NGO by
Jharkhand & Bihar Government
LIVELIHOOD & HEALTH PROJECT ( LWR )
COMPACT PROGRAM
Achievements
• Area of operation-no. of Panchayats . 1
Achievements of R.U
LIVELIHOOD & HEALTH PROJECT ( LWR
Achievements:
# Attitude towards life is getting positive changes
# Secured clean drinking water
# Improved personal & environment hygiene
# Gender
area equity between Men & women in working
# Alfamicohol
liesic problem reduced & better care for their
# 25% improvement in Agriculture - Quality i Quantity
# Self employment increased among women i youth
# Migration of youth to cities controlled
Ro# Formul
writingatiofonBiofharDlStocosan
H. PolHic.yPolicy
# Better understanding between authorities and MIS.
#■ Invol
v
ement
of
Church
Completed Heath Profile authorities in Health Care
•■ Study
of standard
Upgradati
on cofal MIShealth care of MIS in Bihar & Jharkhand
Techni
••• StFunct
ructiuoralnal
Campaign for Health as Human Right
# Participation in Global Health March & People's Health
Assembly in Dakha & Kalkatta
it Formulation of Jharkhand St H. Policy with other team
# Re orientation of Religious Congregations
• Total No. of vil ages
: 12
• Total No. Population under care 4981
• No. of Vaids Trained
: 64
• No. of Dais trained
: 66
No of VHWs trained
No. of Motivational W S
No. of Leaders trained
No. of Farmers trained
No. of TOT participants
No. of S.H. Group formed
No. of Youth Committee formed
No of Farmers Committee formed
No. of children Club formed
Future Directions
• Qual
FunctiityonalUpgradation of members - Structural &
• ofFoodil ness
Security of beneficiaries to ensure Prevention
• HIV/A1DS awareness through schools & colleges
• Open a Voluntary Counseling & Testing .... (VCTC)
• Communicable Disease Control
• Activating Gram Sabhas
Challenges Ahead
• col
Polliatiborate
cal Upheaval
i unwi(Churches)
l ingness of Government to
with NGOs
- HIV/AIDS due to migration and mines
• Malaria Control
- Food security
N<4 o -
Healing Ministry Sunday : Order of Worship
February 13,2005
“Sharing the Abundance of Life”
Theme:
Call to Worship: I will heal my people and will let them enjoy abundant peace
and security. You will have plenty to eat, until you are full, and
you will praise the name of the LORD your God, who has
worked wonders for you.
Joel 2:26 b, Jeremiah 33:6 a NIV
Opening Prayer: God our father, Son and the Holy Spirit. We thank you for your
Son, Jesus Christ, the source of our life who has come into this
world to give it more abundantly. Give us the strength and con
fidence to all your people who put their trust in Thee, through
*"^
the weakness of our mortal nature we can do no good thing
without Thee. Mercifully accept our prayers. Grant us the help
of Thy grace that we may receive this abundance of life in our
family life, social life, and in our life with You, Amen.
Opening Hymn : “The Lord's my shepherd I'll not want”
Praise and Worship
Leader.
Father, we thank you for the abundance of life and healing
available in your name.
All:
Praise you God, our father for you are the source of our
life.
Leader.
We thank you for the abundance that you have shared with
each of us.
All:
Praise you God, the Holy Spirit who gives us this privilege
in our life
Leader:
We thank you for Lord Jesus who has made this possible
for us through His life.
All:
Praise you Lord Jesus, for your springs of life in each of us
Minister.
We thank you God in three persons for the promise of
abundance of life and healing and the promise of restoration fojps,
all of us.
9)
All:
We praise and worship thee, O God the Father, the Son and
the Holy Spirit. Amen.
Confession
Leader:
And now I ask you before God, who searches the heart and let
us humbly confess our sins to the Almighty God who wants us
to have and share the abundance of life.
Do you sincerely confess that you have sinned against God
and deserved His wrath and punishment?
Then declare so by saying:
All:
I do confess
Leader:
Verily you should confess: for Holy Scripture declares: “If we
say that we have no sin, we deceive ourselves, and the truth is
not in us.”
ii
All:
Leader:
Do you heartily repent of all your sins committed in thought,
word, and deed? Then declare so by saying:
I do repent
Verily you should repent, as did the penitent sinners: King David,
who prayed for a contrite heart; Peter, who wept bitterly; the
sinful woman; the prodigal son, and others.
Do you sincerely believe that God by grace, for Jesus’ sake, will
forgive you all your sins? Then declare so by saying:
All.
I do believe
Leader.
Verily you should so believe for Holy Scripture declares: “God
so loved the world that He gave His only begotten Son, that who
soever believe in Him should not perish, but have everlasting life."
Do you promise that with the aid of the Holy Ghost you will
henceforth amend your sinful life? Then declare so by saying:
All:
I do promise
Leader:
Verily you should promise for Christ, the Lord, says: “Let your
light so shine before men that they may see your good works
and glorify your Father which is in heaven”.
Finally, do you believe that through me, a called servant of God,
you will receive the forgiveness of all your sins?
Then declare so by saying:
All:
I do believe
Leader.
As you believe, even so may it be unto you.
Upon this your confession, Almighty God, our heavenly Father,
who has given His only Son to die for us and for His sake for
gives us all our sins, and have mercy upon us. To them that believe
on His name He gives power to become the son of God and has
promised them His Holy Spirit. He that believes in Him and is
baptised shall be saved. Grant this, Lord unto us all. Amen.
The Word:
Deuteronomy 28:1-14
Psalms 147:1-20 (Responsive reading)
Epistles 2 Peter 1:1-11
Sermon:
Topic “Sharing the abundance of life”
Bible Passage St. John 10: 10-18
St. John 10:7-16
Suggested outline for this sermon available on page 6
(The message to be preached preferably by a Health Professional.)
Intercession of Healing (A health professional leads the congregation in intercession)
Healing Ministry Week - Litany 2005
Leader.
Eternal God, our Heavenly Father, we come to you as children
coming to their parent trusting in your unfailing love and asking
you to give abundance of thy blessing and beseech thee to
hear our prayer.
All:
Lord, Hear our Prayer
Leader.
We plead for peace in this world and in our country. Bless the
efforts of all the people and nations who work for peace and
harmony in the world.
Alt.
Lord, Hear our Prayer
Leader.
Lord we pray to remove the barriers of different kind, which keep
the nation and the land divided, broken and wounded. Healer
of the nations, we pray for the churches and its healing ministry
in the whole world. We pray your blessing on healing ministry
week celebration that are being observed in different parts of
the land this year so that it may be fruitful to the society in large.
Alt.
Lord, Hear our Prayer
Leader.
Merciful Father, we humbly beseech thee to enlighten the
rulers of this land so that they may rule the country with just
decision and earnestness. We beseech thee to heal the Wounds
of the nation and countries so that your peace may be felt in the
world of your creation.
.
Alt.
Lord, Hear our Prayer
T
Leader.
Bless the healing service of the governments in different parts
of the world and servants who are looking after the works so
that they may render a fruitful service to the needy people of
the respective area.
All:
Leader:
Lord, Hear our Prayer
Gracious Lord, we pray for your blessings upon Christian Medi
cal Association of India and its service in different regions of
the land for the one hundred years. Heavenly father, we pray for
those who support their work and the help rendered to CMAI in
carrying out its services effectively in needy areas and ask for
your blessing in the years to come.
Alt.
Leader:
Lord, Hear our Prayer
We thank you Lord for the guidance you have given to the CMAI
in the past, when it celebrates its hundred year of service in the
land as an organisation and we thankfully remember all those
who serve in the CMAI in different capacities by your grace. We
pray for the CMAI Central office and officers and others who
are in the services of CMAI in different capacities and ask your
guidance so that they may be true to their calling.
Alt.
Leader.
j
Lord, Hear our Prayer
We pray for your enlightening gifts on mission hospitals and the
staff there, their works and witness in India and help them to
follow the model service rendered by the founding members.
Heavenly father bless our hospitals, medical and nursing
schools, healthcare setting in different parts of India. Heavenly
Father, we ask for your guidance for the institutions that are
facing problems of different magnitude so that they may find a
solution to their problems by your grace.
Alt.
Leader.
Lord, Hear our Prayer
Father, we pray for the doctors that you may grant them the gift
of calm hearing and the gift of healing. Father, we pray for the
nurses that you may grant them the gift of patience and caring
instincts and the gift of healing. Lord we pray for the Allied Healt
iv
Professionals that you may enlighten them to enlighten others.
Master, we pray for the administrators that they may seek and
give heed to the divine guidance in the midst of human man
agement.
Alt.
Lord, Hear our Prayer
Leader.
Gracious Lord, we pray for the Chaplains that they may contrib
ute healing to the suffering and gospel of hope through their
ministry. Loving Father, move our hearts and hands at the sight
of pain, suffering and despair of others so that they may see
you through our actions.
Alt.
Lord Hear our Prayer
Leader.
Lord we pray for all who are in trouble, want, sickness, anguish
of labour, peril of death or any adversity. Specially for those who
are suffering for Thy name and for Thy truth’s sake, comfort, O
God, with Thy Holy Spirit, that they may receive and acknowl
edge their afflictions as the manifestations of Thy will.
p
Alt.
O Lord, we beseech Thee mercifully to receive the prayers
of Thy people. Grant that they may both perceive and know
what things they ought to do and also may have grace and
power faithfully to fulfil the same. Through Jesus Christ,
Thy son, our Lord who is the source of our abundance and
the person to answer our prayers. Amen.
Song:
“All the way my saviour leads me"
(Offertory)
(If the Eucharist is celebrated, kindly continue the liturgy of the communion service.)
Concluding Prayer
t
God, our heavenly Father, the source of our abundance. We
thank you for blessing us through this worship. For the
abundance we have received from you. Help us to go into
the world and share this abundance to a world sick with sin
and suffering, that you may remain in efforts in making our
life meaningful and relevant in the situations where we need
your abundant grace and mercy. May your presence with
us bring about abundance in the contexts we struggle to
bring justice and peace and prosperity. Amen
Benediction
Minister:
The Lord bless thee and keep thee. The Lord make His face
shine upon thee and be gracious unto thee. The Lord lift up His
countenance upon thee.
May Grace and peace be yours in abundance through the knowl
edge of God the Father and of Jesus our Lord, and through the
Closing hymn:
Holy Spirit. Amen.
“Guide me, O thou great Jehovah”
Acknowledgements: Prayer of confession: Lutheran order of worship Pg.48
Benediction: Lutheran order of worship Pg. 14
v
Suggested Outline for Sermon
Topic:
"Sharing the Abundance of Life”
Scripture:
St. John 10:7-16
Aim
To help understand that God in Jesus Christ intention of His coming is to help
us have abundance of life, as He is the source of our life and a God who heals
and restores us to the original status for which we are created.
God in Christ is our source of the abundance of life. He expects us to exercise
our trust in him to have this abundance of life that which is possible in this life
and the life to come.
Goal
• To realise God is the source of the abundance in our life
o
•
I
To help congregation members to know that God in Christ wants us to
have abundance of life by becoming part of His kingdom, thus inviting us to
have a share in the abundance
To understand Jesus and His ministry’s whole purpose is to have and share
this abundance of life with others.
Introduction
The context of this passage in which Jesus claims “I am the Good Shepherd
who is willing to die for the sheep.” And also He says, “All other claims by others
are not sincere but mine is true that you may have life and that life in abun
dance." Nobody has made such claim so far and it is the call of the creator to
look after us with an agenda to satisfy us in this life with abundant life.
•
Abundance in Christ only for His Children
“My sheep, hear my voice, I am the good shepherd. All the promises for the
abundant life is only for His children who abide in Him, and exclusive for His
sheep as the followers of the Good Shepherd. The exclusive status is not avail
able to others except those who accept and follow Jesus Christ.
•
Abundance is a state of mind to experience
Abundance is a state of mind. It comes from the security that we receive from
God. His promises, assurance, salvation, protection, His pastures, nurture and
nourish us to a state of abundance. The Zachaeus, the tax collector, had all1
facilities in life still he was not happy with his life. It is Christ’s entry into his life
that brought a transformation to abundance. He experienced abundance of life
that day.
•
Abundance is possible in this life and life to come
Many times we give up on life after abusing it and then say nothing can be done
about it and eventually we spoil this life and the life to come. But meeting Christ
can bring about a new outlook about God, His love, His concern and care for
each one of us. The story of the Samaritan lady depicts this in John Chapter 4.
Knowing that God loves and cares for us is a great feeling.
Conclusion
Christ, our creator and our source of life, alone can give us abundance. As we
internalise God’s demands and feed on in faith, we will be satisfied and that is
God’s agenda for each one of us whatever may be our status or stature in life.
vi
vii
Jesus could see that everybody looked tired and hungry. He looked at them
and felt very sorry for them. He said to His helpers, “Give these hungry
people something to eat.” His helpers were very surprised. They said to
Jesus, "How can we give them something to eat? There are no shops here,
and even if there were shops, we do not enough money to buy food for so
many people."
One of Jesus' helpers named Andrew said, “There is a little boy here with
some bread and fish, but he only has enough for himself.” “Ask him whether
he will give Me his bread and fish," said Jesus. The little boy was so glad to
share his food. And Jesus took the bread and fish from him, and said, “Tell
everybody to sit down on the grass."
When everybody was sitting down, Jesus said grace, and then He began to
break up the bread and fish. He gave some pieces to each of His friends
and they all gave them to some of the people.
When Peter had given out what he had, he went back to Jesus. Jesus was
still breaking the little loaves and small fishes into pieces. He gave some
more to Peter and Peter gave it to another group of people.
He gave some more to Andrew and Andrew gave it to another group of
people. He gave some more to James and James gave it to another group
of people. He gave some to John and John gave it to another group of
people. He gave some more to each of his helpers and they all gave it to
other groups of people.
They went on and on taking the bread and fish from Jesus and giving them
to the people until everyone had had plenty to eat. The little boy had as
much as he could eat as well. Jesus shared the little loaves of bread and the
few small fish between everyone! Everyone had enough to eat.
Then Jesus said to His helpers, “We mustn't leave scraps of food on the
hillside. Take some baskets and collect up all that is left over." So the helpers
borrowed some big baskets from the people who lived in the country-next
door and they collected all the food that was left over. There was so much
food that the helpers filled twelve whole baskets.
I
At last Jesus said to the people, “It’s getting late now and it’s time that you
all went home." So they did. And as they went, they talked about the all the
wonderful things that Jesus had said and done.
A prayer
“Thank you, Lord Jesus, for the little boy who through his sharing could
satisfy a lot of people who were hungry. Help me to remember that you will
always bring plenty of situations where there is shortage. Help me to share
whatever gift or talent that I have. Amen.”
Activity
t
Share this story with children and ask them whether they would like to offer
their best to Jesus who multiplies and blesses hundred fold. Ask the chil
dren to enact the story.
--- --- viii
-1)
CHRISTIAN MEDICAL ASSOCIATION OF INDIA
Plot No.2, A-3 Local Shopping Centre, Janakpuri
New Delhi 110 058
Invites you to celebrate
The Healing Ministry Week, 2005
And
The Centenary of the founding of the Medical
Missionary Association (1905 - 2005)
On the theme
“Sharing the Abundance of Life”
Bible Studies
Healing Ministry Week Celebrations
February 7-13, 2005
CMAI Day of Prayer
February 9, 2005
Healing Ministry Sunday
February 13, 2005
•To Att'Bishops, (Pastors, (Heads of Institution and Members ofCMAI
Dear Partners in the Ministry of Healing,
reetings to you in the name of Jesus Christ, the name from which every
healing proceeds. It’s my privilege to bring two booklets to you. Six Bible
studies to be used during the week of celebration and an Order of Worship to be
used on the healing ministry Sunday which includes a Sunday School lesson
plan. In the same envelope, you will also find the poster.
G
This year's healing ministry week is special because 2005 also marks 100
years since the founding of the Medical Missionary Association. In the year
1905, missionaries involved in medical work in India came together at Miraj,
Maharashtra to form the Medical Missionary Association (MMA), so that they
could be supported and strengthened spiritually, technically and in fellowship
with one another. It was renamed and formally registered in 1926 as the Chris
tian Medical Association of India.
As we look back over the past century, we are truly grateful and acknowledge
His faithfulness. He has blessed us abundantly, and it is from the abundance that
we have received, we have been able to share with others. Therefore we find, in
this centenary year of the founding of the Medical Missionary Association, that
“Sharing the abundance of life” is the appropriate theme for the healing ministry
week 2005.
The Christian Medical Association of India is celebrating the Healing Ministry
Week along with the Catholic Health Association of India and the Commission
for Health Care Apostolate of the Catholic Bishops’ Conference of India. This
broader partnership will enable many more congregations to learn about the
Healing Ministry.
The week will be celebrated from February 7-13, 2005. February 9 is a special
day of prayer and February 13 will be the Healing Ministry Sunday. Many
institutions, congregations and organisations and individuals have earmarked
the Healing Ministry Sunday collections to be sent to us in the past years and I
take this opportunity to thank you for this partnership.
We would like to record our appreciation to the contributors of these Bible
Studies. Our grateful thanks to Ms Esther David, New Delhi; Rev Al David
Chaplain, Arogyavaram, AP; Rev Fr Alex, Executive Secretary, Commission for
Health Care Apostolate CBCI; Rev Fr Thomas Ninan, CMAI and Rev Fr PA
Philip, Vicar, St. Gregorios Orthodox Church, Janakpuri, New Delhi.
We are interested to know how you celebrated the Healing Ministry Week and
Sunday in your congregations, institutions and health centres. We would appreci
ate your suggestions for strengthening this partnership, so that we can continue
to have meaningful celebrations in the future.
With best wishes and prayers,
Yours in Him,
Rev Sharath David
Sr Programme Coordinator
Chaplain section, CMAI
Monday, 7® February
John 15:1-8
ABUNDANCE BY ABIDING IN CHRIST THE
SOURCE OF OUR LIFE
“ Remain in me, and I will remain in you. No branch can bear fruit
by itself; it must remain in the vine. Neither can you bear fruit
unless you remain in me.”
& ^Israel is a luxuriant vine”, said Prophet Hosea (Hosea 10:1).This rich
and meaningful concept of vine and branches is often found both in the
Old and New Testament. The vine was almost the symbol of Israel.
Jesus says, “I am the true vine.” The Greek word, ‘alethinos’ means real,
genuine and authentic. Jesus is the true source of our lives. He invites
everyone to ‘remain’ or ‘abide’ in Him, like ‘a branch abides or remains in
the vine’, so that we in turn bring out fruit in abundance. Fruitless
branches will end up in disaster! They will be 'cut and thrown into fire’.
Abundance in life means a life that is truly and totally in communion with
Jesus.
When we read this text from John 15:1-10, we notice that there is a
word that is repeated almost 10 times. Can you identify that word? Yes,
the word ‘remain’ or ‘abide’. When school children are trained to write an
essay, the teachers will never be happy if the same word is repeated in a
paragraph over and over again. No good author or journalist will ever dare
to do that either! But a great Evangelist like John does it! Why? What was
the reason?
The root word for ‘remain’ or ‘abide’ in Greek is ‘menain’, and it is used in
two contexts. First, when a branch of a tree attaches itself to its trunk, and
receives everything for its growth and development, especially to bring
..forth new shoots, leaves and fruits, it is total dependence. Not even a
'minute it can remain separate! It is a profound and unique union. Such
should be our communion with Jesus.
Second context is that of a child that is being formed in the womb of a
mother. The child or the embryo truly and totally depends on the mother
for its very being and existence. Like the baby in the womb, and its total
dependence or ‘remaining’ in the mother, we need to remain or abide with
Jesus. The abundance in life is the fruit of our abiding in Jesus.
Question for reflection:
Do I abide in Jesus? Am I in constant communion with him? Have I found
the reason why I lag behind or lack efficiency?
FrAlex
CBCI
John 4:4-38
Saturday, 12m February
LIFE IN ABUNDANCE IS EXPERIENCING
CHRIST OUR HEALER
Life in abundance is received from Christ our source of life. There is no other
source to experience the abundance of life. “If you knew the gift of God and
who it is that asks you for a drink, you would have asked him and he would
have given you living water”
he abundance of life to mankind is a gift from God. This needs to be
requested and received from God who is our source of the abundance
of life.
T
Meeting Christ in our daily life
'
The woman had the privilege of meeting Christ physically and knowing
him spiritually to receive the gifts of God. We need to realise that in
different situations and activities of life we can meet and experience
Christ. He wants everyone to have a taste of Him by meeting Him,
knowing Him and experiencing Him and accepting Him, which is equiva
lent to drinking the living waters.
Accepting Christ as the source who knows our life
Just being aware of situations does not lead us to the source of life. We
need to go deeper in exercising our faith in every situation. Many times we
have no control over situations. But Christ knows and He controls the situa
tions for us. We need to be conscious and ready to recognise Christ and
accept Him in every situation of our life.
Acknowledging Christ through our witness
Knowing Christ results in joy unspeakable which can only be expressed
through our sharing about Christ. God is pleased with our intention to
acknowledge Him in every situation even in the midst of people who do
not know Him. Sharing and witnessing about Christ increases our readiness to live the abundance of life.
Experiencing abundance and healing
Knowing and experiencing Christ leads to healing and wholeness in one’s
life. “Indeed, the water I give him will become in him a spring of water
welling up to eternal life.” There is a sense of satisfaction and fulfilment
when we experience the abundant life.
Question for reflection:
What is abundance of life to someone with a chronic/terminal illness like
cancer/HIV/AIDS?
Rev Sharath David
CMAI
6
j
"
CHRISTIAN MEDICAL ASSOCIATION OF INDIA
Plot No.2, A-3 Local Shopping Centre, Janakpuri
New Delhi 110 058
Invites you to celebrate
The Healing Ministry Week, 2005
And
The Centenary of the founding of the Medical
Missionary Association (1905 - 2005)
On the theme
“Sharing the Abundance of Life”
Bible Studies
Healing Ministry Week Celebrations
February 7-13,2005
CMAI Day of Prayer
February 9, 2005
Healing Ministry Sunday
February 13, 2005
Wednesday, 9,h February
Romans 5:15-17
SHARING THE ABUNDANCE MEANS SHARING
CHRIST HIMSELF
" For if, by the trespass of the one man, death reigned through that
one man, how much more will those who receive God's abundant
provision of grace and of the gift of righteousness reign in life through
the one man, Jesus Christ."
BT” he theme for this day attempts to answer this question in
I Romans :15 - 17, St Paul finds ‘Sin’ as one of the causes for suffer
ings. He talks about the power of sin as it leads to the ‘ultimate death’.
The troubling question remains: Who can deliver us from this sin and
suffering?
Thanks be to God. God shared, in fact, sent His only begotten Son
Jesus Christ to us and through Him, we receive God’s Grace which is
power, strength and comfort to us in our suffering (Rom 5:15-17). The
grace of God makes us strong when we are weak (2 Cor 12:8-10) and
enables us to face the challenges in our journey. How was it possible for
Jesus Christ to share His Grace with us? It is His willingness not to
consider His ‘Being God and equality with God’ (Phil 2:6) but to lose His
very identity.
As the suffering humanity needs this Grace of God, the biggest chal
lenge for us is to choose between these two. Jesus said, “You are the salt
of the World” (Matt 5:13). Salt can be identified in two ways. First it can be
kept in a decorative container and placed on the table. It has a name,
recognition and identity. Second, by the taste of salt in water/cooked food.
b It has no visibility, no name and no identity. But it has its own influence. If
the Healing Community wants to share the abundant grace of God to the
sick and suffering, it has to choose the second one. There is no other way.
We are the answer to the unanswered question of the suffering humanity.
Questions for reflection:
1 .What are the ways that God’s grace can be channelised to the suffering
humanity?
2.What are the sacrifices we need to make to be the Channels of Gods
grace?
Rev Al David
Arogyavaram
Thursday, 10m February
Luke 18:1-8
ABUNDANCE OF LIFE IS JUSTICE NON-COMPROMISED
“And will not God bring about justice for his chosen ones, who cry out
to him day and night? Will he keep putting them off? I tell you,
he will see that they get justice, and quickly."
n the story of creation, God felt good at every stage of His creation. It
was perfect and abundant. The deformation done by evil is reformed by
the salvation work of the Son of God, Jesus Christ. The reformation was
done to appropriate this to each one of us. The real transformation by way
of reformation, which is given to us by Jesus Christ, is lacking in each one
of us. Jesus tells the parable of the judge who did not fear God nor regard
man and the poor widow who pleaded him to grant justice for her. Though
he was unwilling at first he granted her justice later.
I
The wellbeing of a society largely depends upon the dispensation of
justice. We can’t characterise a society as abundant if justice is bruised or
adulterated. Unrelenting and uncompromising justice is the hallmark of
abundance. Affluence and abundance as a result of strangulating justice
is not a healthy Christian approach. The pathetic scene of the contempo
rary world underlines this fact.
God gave Israelites the manna in abundance but He never wanted them
to store the excess for the next day. We need to ask for our daily need and
rest our hope in Him. God gives in abundance and instead of accumulat
ing it for our own benefits, He expects us to share it with those in need.
The psalmist upholds the coexistence of justice and peace in Psalm
85:10-15. The world will be at peace only when justice prevails here.
Amos also speaks about a life in abundance where justice is kept intact
(Amos 5:11-13). “But let justice run down like water, and righteousness
like a mighty stream.” (V.24)
In His maiden speech at Nazareth Synagogue Jesus pleads for justice in
the society. His whole mission is to restore justice and thereby ensure the
establishment of God's kingdom in the world. Therefore, both the Old
Testament and New Testament clearly states that justice is a precondition
for abundance of life.
Questions for reflection:
1. Do you believe in today’s pseudo-affluent society where abundance comes
through sacrifice of justice?
2. What is your action plan for the restoration of justice in the society?
Fr PA Philip
New Delhi
4
Friday, 11“’ February
Luke 18:18-30
SHARING MEANS RISKING AND
VULNERABILITY
“Do not commit adultery. Do not murder., Do not steal. Do not bear false witness.
Honor your father and mother."
he rich man’s reply gives a clue about his familiarity with these condi
T
tions that Jesus places before him. His childhood and youth must
have had a rich religious upbringing through what I would call an exem
plary family atmosphere. Realistically we all are the products of our
parental upbringing and to a large extent we continue to follow them as
examples in most areas of our lives.
It is often the conflicts in life, which draw us towards Jesus. And it is
during such times that He challenges us to take bold steps - steps that
would lead us to life eternal. Here Jesus identifies sharing as one of the
major tools that would help us on the road to eternal life. The greatest fear
in the aspect of sharing is the risk and the vulnerability associated with it.
The Surrendered Life
The life of sharing indeed involves a life surrendered unto the will of God.
It is indeed, a unique experience to realise that all that we are, our body,
mind and spirit and all that we possess are bound by the perfect will of
God. This would mean making oneself vulnerable to some harsh realities
which one would rather not think of. It is a thin line that divides the two
positions and it will always demand a commitment that requires to be
renewed every moment of our life.
Call to Discipleship
There is a unique invitation towards discipleship. The conflict in the rich
ruler is between two forces of discipleship, between his old far too familiar
past and his unknown future - risky and vulnerable indeed, but with a
promise that it would lead him to eternal life. Discipleship indeed is a
journey, filled with conflicts at various points of life but a learning experi
ence where one renews his life long commitment to become a disciple of
Jesus. Sharing our life in Jesus brings us closer to the reality of eternal
life as something that can be sensed and experienced here on earth and
not as something that one needs to hope for.
Questions for reflection:
1. What am I missing in life?
2. Am I contented with life? If not, what is the reason?
Fr Thomas Ninan
CMAI
John 4:4-38
Saturday, 12m February
LIFE IN ABUNDANCE IS EXPERIENCING
CHRIST OUR HEALER
Life in abundance is received from Christ our source of life. There is no other
source to experience the abundance of life, “if you knew the gift of God and
who it is that asks you for a drink, you would have asked him and he would
have given you living water.”
he abundance of life to mankind is a gift from God. This needs to be
requested and received from God who is our source of the abundance
T
of life.
,
Meeting Christ in our daily life
"
The woman had the privilege of meeting Christ physically and knowing
him spiritually to receive the gifts of God. We need to realise that in
different situations and activities of life we can meet and experience
Christ. He wants everyone to have a taste of Him by meeting Him,
knowing Him and experiencing Him and accepting Him, which is equiva
lent to drinking the living waters.
Accepting Christ as the source who knows our life
Just being aware of situations does not lead us to the source of life. We
need to go deeper in exercising our faith in every situation. Many times we
have no control over situations. But Christ knows and He controls the situa
tions for us. We need to be conscious and ready to recognise Christ and
accept Him in every situation of our life.
Acknowledging Christ through our witness
Knowing Christ results in joy unspeakable which can only be expressed
through our sharing about Christ. God is pleased with our intention to
acknowledge Him in every situation even in the midst of people who do
not know Him. Sharing and witnessing about Christ increases our readiness to live the abundance of life.
Experiencing abundance and healing
Knowing and experiencing Christ leads to healing and wholeness in one’s
life. “Indeed, the water I give him will become in him a spring of water
welling up to eternal life.” There is a sense of satisfaction and fulfilment
when we experience the abundant life.
Question for reflection:
What is abundance of life to someone with a chronic/terminal illness like
cancer/HIV/AIDS?
Rev Sharath David
CMAI
.
■
Christian
Medical
Association of
India
Plot Na 2, A-3 Local Shopping Centre. Janakpuri. New Delhi 110 058 Phones : (011) 2559 9991, 2559 9992,2559 9993, 2552 1502
Grams : 'CRISMEDIND' Fax ;(011) 2559 8150 e-mail: cmajdelOvsnl.com cmaiGcmal.org, Visit us at • www.cmai.org
From the General Secretary
Dear friends,
very year, in the second week of February, we observe the Healing Minis
E
try Week. This includes a week of Bible studies, a CMAI day of prayer, and
the Healing Ministry Sunday. It is an opportunity for churches, congregations,
institutions and individuals to be aware of issues related to health, healing and
wholeness, and to be challenged by the need for healing around them. Started
by CMAI in 1986, it is now celebrated jointly along with the Catholic Health
Association of India and the Health Apostate of the Catholic Bishop’s Confer
ence of India as a joint effort to reach the church across the country.
This year's healing ministry week is special because 2005 also marks 100
years since the founding of the Medical Missionary Association. In the year
1905, missionaries involved in medical work in India came together at Miraj,
Maharashtra to form the Medical Missionary Association (MMA), so that they
could be supported and strengthened spiritually, technically, and in fellowship
with one another. It was renamed and formally registered in 1926 as the Chris
tian Medical Association of India.
As we look back over the past century, we are truly grateful and acknowledge
His faithfulness. He has blessed us abundantly, and it is from the abundance
that we have received, that we have been able to share with others.
It is appropriate, therefore, that in this centenary year of the founding of the
Medical Missionary Association, “Sharing the Abundance of Life” is the theme
for the healing ministry week 2005. As we complete one century and enter the
next, let us continue to proclaim and share with all around us, the abundance
of life He has given us.
We invite each one of you to share in this reaffirmation of our calling.
Dr Vijay Aruldas
General Secretary, CMAI
logUtorod Under Societies Regn. Act of 1860 Rog. Na 17 of 1036 33 6 BPT no. h
(N)
ABOUT CMAI
As the official health arm of the National Council of Churches in India (NCCI),
and a fellowship of over 330 Christian healthcare institutions and over 6000
individual Christian healthcare professionals across the country, the Christian
Medical Association of India is the voice of India’s Christian health work, and
the only organisation of its kind in the world.
Started in 1905 as the Medical Missionary Association, and renamed and
registered in 1926 as the Christian Medical Association of India, the CMAI
works to strengthen the healing ministry of the church by working:
• with individual Christian healthcare professionals to make them spiritually
vibrant, technically excellent and socially relevant.
• with Christian healthcare institutions to be ethical, compassionate, techni
cally competent and reaching out the marginalised
® with churches and congregations to be involved in the healing ministry with
those in need
• with the government and civil society as expert advisers and to advocate for
a just and healthy society
• in special interest of need such as substance abuse, HIV/AIDS, women’s
issues, palliative care, involving congregations with needy communities, health
of urban marginalised, community-based health financing.
CMAI brings out eight different quarterly publications: the flagship publica
tion, Christian Medical Journal of India on Christian perspectives in health,
and others on primary healthcare (circulation of 18,000), development, man
agement, rational drugs, substance abuse, palliative care, network news.
Through boards and training committees made up of experts who give their
time voluntarily, CMAI inspects and accredits institutions, conducts examina
tions and certifies candidates in:
• ANM and GNM nursing programmes (under the Indian Nursing Council)
• Nine allied health training programmes such as medical laboratory techno
logy and radiology technology and counselling
• Clinical-pastoral training for chaplains
• PG medical training in multispeciality practice and palliative medicine.
CMAI’s institution members include CMC, Vellore, CMC, Ludhiana, Miraj Medi
cal Centre, MOSC Medical College, CRHP Jamkhed, and other mission hos
pitals and community health programmes in cities, towns and village across
the country. CMAI’s individual members, belonging to health related profes
sions in government, private and mission institutions. It works through 13
regions in the country, and conducts retreats, workshops, conferences,
consultancies etc. to strengthen Christian health work and witness.
We invite all Christian health professionals - Doctors, nurses, allied health
professionals, administrators, chaplains, community health professionals and
others interested in the healing ministry, to join as members. Details are avail
able on the website www.cmai.org, or on writing to: The General Secretary,
CMAI, Plot No.2, A-3 Local Shopping Centre, Janakpuri, New Delhi 110 058;
E-mail: cmaKgcmai.org
- Media
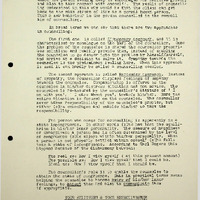 RF_NGO_3_SUDHA.pdf
RF_NGO_3_SUDHA.pdf
Position: 1240 (17 views)