CAHP HANDOUTS & RESOURCE MATERIALS
Item

- Title
- CAHP HANDOUTS & RESOURCE MATERIALS
- extracted text
-
RF_NGO_2_SUDHA
CAHP - 203
Reprinted from Journal of the Food Marketing Centre, Xavier Institute,
Jamshedpur, Volume 1, Pages 158-1632 September 1973.
FEEDING AMD MEDICAL CARE FOR 10,000 PRE-SCHOOL CHILDREN
S.N.'Chaudhuri
Professor of Nutrition
Food Marketing Centre, Xavier Institute, Jamshedpur, Bihar
and
Malnutrition among pre-school children is being tackled on a
national level and in this direction the Special Nutrition
Programme of the Government of India has made a singal
contribution. Under this Programme, the Government provides
18 paise daily for a nutrition supplement to pre-school
children in tribal areas and urban slums. The Food Marketing
Centre found that this is economically possible if large
numbers are fed. To this has been added effective Under-Fives
Clinics for as little as 5 paise per day per child under care.
This paper discusses the administrative aspects of the
nutrition programme and stresses on the importance of medical
auxiliaries in running an Under-Fives’ Clinic.
INTRODUCTION
^7yioo;)3i. M arks 3oad
B .M .Laugesen
Community Health Consultant
Co-ordinating Agency for Health Planning, New Delhi.
J
J
-E
■’
~:l
C
0
Nutrition surveys among pre-school children, carried out all over
India under the auspices of the Indian Council of Medical Research,
have revealed a high incidence of protein calorie malnutrition (PCM),
anaemia and vitamin A deficiency as some of the major problems among
this vulnerable segment of the population (1-4). Recent clinical ’ studies comparing malnourished with well nourished infants indicate
that one of the immediate effects of early severe malnutrition may be
an inability to process in-coming stimuli (5). Early severe malnutri
tion, therefore, affects learning and behaviour as well as brain size (6.) .
Nutrition deficiency is directly or indirectly responsible for high
proportion of deaths under 5 years of age, excluding neonatal deaths.
The deaths are principally due to the synergistic effects of malnutrition
and infection (7). Malnutrition in children, as judged by low weight
for age, is associated with a greater frequency and severity of infectious
diseases in India (8).
Malnutrition amongst pre-school children is being tackled on a national
level, and in this direction, the Special Nutrition Programme of the
Government of India has made a signal contribution. Under this programme
which is being administered through District Welfare Officers, the
Government provides funds'to distribute a supplementary meal to pre
school children and pregnant/lactating mothers in tribal areas and
in slums of metropolitan cities. They are often glad to locate res
ponsible voluntary agencies, capable of running this programme effectively.
This was how the Food Marketing Centre, Xavier Institute, Jamshedpur,'
stepped into this programme. The Centre is now feeding 10,000--pre-schpol
children daily in the slums of Jamshedpur.
The infrastructure which is built up to provide an effective delivery
system to serve a hot cooked meal to each of the 10,000 children can
contd/-
be quite extensive. Providing an additional input of health care by
means of an Under-Fives' Clinic through the existing network of services
of the feeding programme and vice versa produces a multiplying, rather
than a purely additive, effect on the health of these children. The
Food Marketing Centre has devised methods to deliver the package of health
care and nutrition to the pre-school child cheaply and simply.
ORGANISATION OF THE PROGRAMME
Overall Administration
Economy of scale is basic to the low-cost requirement of this programme.
The central staff includes one Project Director, one Dietitian and
four young graduate Field Supervisors. The Government allocation of
18 paise per day gives them a sum of Rs.1.800 daily for buying food and
meeting administrative, transport and cooking costs. The central godowns
are used to store bulk items with smaller store rooms attached to all
cooking centres. A Jeep with trailer is used as the main medium of
transportation for distribution of food to the 13 cooking centres
situated in slums.
Cooking Centre
There are thirteen cooking centres under the care of the field
supervisors, each centre is staffed by 1 cook (salary Rs.70.00 per
month) 2 helpers (salary Rs.20.00 per month) and one water carrier,
wherever needed. One food carrier (salary Rs.30.00 per month) takes the
food from the cooking centre to the feeding points. Each cooking
centre cooks for about 1,000 children and is equipped withs1.
One hanging pan balance for weighing food
2.
Big wooden stirring spoons
3.
Very large dekchis (24 inch diameter), each capable of holding
50 kg of cooked food, which can be served to 200 children.
The food is cooked over coal-fed mud chula such as the one used
by local people. A small store containing ration and fuel for 6 days
is situated near each cooking centre.
Feeding Point
There are fifty feeding points. Each feeding point catered from
the cooking centre by rickshaw or handcart, feeds 200 children each
morning and is staffed by one volunteer. On seeing the rickshaw coming,
the children with their own plates converge from every direction, alone
or brought by the mother or elder sister. After the first few months
identity cards had to be issued in order to exclude children of school
going age. Since then, house to house encouragement has been given to
mothers to bring their youngest child for feeding.
The Food
Three menus are being rotated round the week, and one of them is
"khichri". A typical mixture of khicheri for 200 children- isi-
Rice
Masoor dal
Chana dal
Onion
Vanaspati
Masala
..
..
..
..
..
..
..
..
..
..
..
..
6.920 kg.
4.610 kg.
4.036
0.576 kg.
0.576 kg.
To taste
Contd/-
3
This gives 83 gms of mixture per serving, containing about 300 calories
and 12 gms of protein.
IMPACT OF THE SUPPLEMENTARY FEEDING
The children fed are mostly tribals, poor slum dwellers. A nutrition
survey of these children showed that the incidence of protein
calorie malnutrition was 52.7 per cent and that of vitamin A deficiency
25 per cent while anaemia affected half (9). This programme, like all
supplementary programmes, runs the risk of becoming substitute meal for
some children. However, the general impression of the workers in the
programme is that severe malnutrition and vitamin A deficiency have been
greatly reduced after one year of providing this single daily supplement.
THE UNDER-FIVES' CLINICS;
The Food Marketing Centre has opened an Under-Fives' Clinic recently.
It is a mud-wall titled-roof clinic attached to the chulas of one
of the cooking centres. This community-donated clinic is 12 x 15
feet and contains tables and chairs given by the community and one
locable trunk for medicines. One register is'kept for the names and
numbers of new children. Parent retained child health weight records
enable easy record keeping (10).
COST OF MEDICAL SERVICE;-
DPT, BCG, smallpox and typhoid vaccines are obtained free from
Government. Polio vaccine is considered too expensive at present.
Simple inexpensive medicines ne dispensed and twice a week the doctor
visits the clinic to see those children referred by the clinic worker.
Simple standing orders such as those developed at Narangwal and
Jammalamuddugu are being developed. Medicine costs are Rs.300 per month.
Cost breakdowns so far show that expenditure will be about Rs. 15 per
pre-school child-in-the-area per year or easily within 5 paise per day
per child,
ROLE OF INTERMEDIATE TECHNOLOGY;The concept of an appropriate technology for health care recognises
that all countries are subject to limitations in their ability to provide
health care. No country in the world makes available, all of the existing,
most advanced medical techniques, to all of its citizens. Physicians
are scarce almost everywhere and the cost of their training is soaring
as biomedical knowledge expands. Maternal and child health care can be
best, if not only, carried out close to or within the home environment of
the woman and her child - that is mainly within the village. Medical
auxiliaries can effectively fill the' vacuum of health delivery care in
developing countries (11). They do not replace doctors, but they may
substitute for them in a simple Under-Fives' Clinic setting-weighing
children, immunising them and advising mothers on nutrition education.
CHILD HEALTH WORKER CONCEPT;-
Child Health Worker (12) providing health care to under fives should
be a female worker. She may be a school leaver awaiting marriage as in
Jamshedpur, or a widow a in the Okhla programme, or a respected dai as
in the Jamkhed (Maharashtra) programme. The child health worker'can be
taught for some hours each week or be given a 3 months full time course.
In Jamshedpur, half of the course content is for nutrition, one
quarter for pediatrics, and one quarter for elementary nursing skills.
Choosing the child health worker from the same village eliminates the
difficulties of appointing an outsider - the cost of renting or building
accommodation, the problem of loneliness in a strange place far from
4
the nearest tov.m and the difficulties of recruitment for remote localities.
The disadvantages mainly relate to the lower educational standard that
might have to be accepted in recruiting girls from such localities.
Hov;ever local middle aged woman with leadership even though only of 4th
or 5th standard education, can be trained’ to carry out repeated weighing
of children, collection or children for immunisation, nutrition education,
collection of birth and death information, advising on family planning,
referrals of sick children and deworming programmes.
It should be noted that the Jamshedpur concept is quite different
from the practice of Government which rents accommodation in the village
and has a statewide system of transfers within the auxiliary nurse cadre.
It is also different from the practice of Mission Hospitals to build
expensive difficult-to-staff branch dispensaries. The practice’of bringing
in trained staff from outside the serviced area; as at present, does have
serious cost complications, which the child health worker concept avoids.
BIBLIOGRAPHICAL REFERENCES
1.
Dutta Banik (ND) and others. Study on epidemiologic basis of
malnutrition in pre-school children in slum areas in Delhi.
(Ind.Pediat.10; 1973; P 19).
2.
Ghai (OP) and others, Nutrition assessment of pre-school children
of a rural community. (Ind J Med Res.58; 1970; P 162).
3.
Rao (NP) and others. Nutritional status of pre-school children of
rural communities near Hyderabad City. (Ind J Med Res.57;1969; P 213).
4.
Chowdhury (MK) and Ramakrishnan (NR). Nutritional status of rural
pre-school children in West Bengal: 1 Nutritional authoropometry
(Ind Pediat. 9; P 136).
5.
Klein (RE) and others. Cross-cultural evaluation of human intelli
gence. (in Lipids, malnutrition and the developing brain. (Ciba
Foundation Symposium). Associated Scientific Publishers, Amsterdam
1972.p.268.
6.
World Health Organization.
1972.P 23.
7.
Joint FAO/WHO Expert Committee on Nutrition (1970).
1971, P 45.
8.
Interaction of Nutrition and infections A prospective field study
on children in selected villages of Punjab: Final Report to ICMR.
Rural Health Research Centre, Narangwal 1972. P 32. (Mimeographed).
9.
Chaudhuri (SN) and Chacko (L). Nutritional status of pre-school
children; A survey in Jamshedpur (J Food Marketing Centre, 1; 1973;
Paper J).
10.
Morley (David). Under-Fives Clinic,
countries by Maurice King and others.
Nairobi. 1966. Sec 16 : 7).
11.
Gish (Oscar). Towards an appropriate health care technology,
Health, manpower and the medical auxiliary, ed by Oscar Gish,
1971. P. 32).
12.
Ghai (OP) .
p 1-4).
Human development and public health.
Eight report
(in Medical care in developing
Oxford University Press,
(in
Health planning for children (Ind. Pediat. 10; 1973.
common ;tv
47/1,(First
cell
Marks Hoad
BAWGAlOBE - 560 001
CAHP 205.
PANJEERI FOR MALNUTRITION.
S. Kapoor P.H.N., B.M. Laugesen F.R.C.S., Shakuntala Nayyar B.Sc.
Community Health Department
Frances Newton Hospital, Ferozepur, Punjab.
SUMMARY;
Panjeeri, a well known traditional Punjabi food for young children,
can be made, packed and prescribed at reasonable cost for the treat.
ment of malnutrition. It should be given along with repeated doses
of advice and encouragement to the mother to feed more food to the
child.
INTRODUCTION;
The Morley weight card in Ferozepur, Punjab allows grading of mal
nutrition in pre-school children into two grades of good nutrition
and three grades of malnutrition (l° II0 and III*) as laid down by
the Nutrition Sub-committee of the Indian Academy of Paediatrics.
But having diagnosed malnutrition, the doctor or the auxiliary must
be able to treat it. And because the cost te community and family
of in-patient treatment is so great, some method of treating such a
common condition is essential.
In protein calorie malnutrition ignorance and poverty both prevent
the child getting enough to eat. By teaching the early use the
cheapest foods, we try and overcome ignorance and lessen the effect
of poverty on the child. Panjeeri is prescribed along with the
teaching
as a food supplement
as a teaching device.
PANJEERI AS A FOOD SUPPLEMENT; .
A supplement to treat protein calorie malnutrition should contain
some extra protein, and enough calories to help prevent such protein
being burnt for caloriAs by the body. And it should be reasonably
priced. A comparison with other products on the market shows that
most of these concentrate on providing protein, and to have a long
shelf life they are packed, in expensive tins, thus only a small
quantity is provided or the price is high. Panjeeri can be made by
any hospital pharmaay or the by the nursing staff, and only enough
need be made to last a week or so.• Thus problems of weevils.or
expensive packaging are avoided.
COMPOSITION OF PANJEERI;
Table 1.
Wheat, or wheat flour (atta)
Bengal grams kabuli channa
Groundnuts
mungphali
Skim milk powder
Unrefined brown sugar shakkar
Cooking oil or clarified butter (Vanaspati or ghee)
47 Gms.
16 Gms.
8 Gms.
g Gms.
16 Gms.
5 Gms.
100 Gms.
contd...page 2,
2
This contains 14 Gms. of protein and supplies 405 Calories.
The above formula is similar to the 'Hyderabad mix' described by
Reddy and other workers at the National Institute of Nutrition,
Hyderabad and it so happens that this is quite similar to the food
known in the North as panjeeri.
COMPARISON OF PANJEERI WITH OTHER FOOD SUPPLEMENTS.
Table 2 shows that panjeeri has few . rivals as a source of low cost
protein and nc rivals if we consider it also a supplier of calories
at.low cost.
>
Table 2.
BRAND NAME.
RETAIL PRICE
FOR 100 Gms
IN RUPEES &
RAISE.
Panjeeri
Cow's milk
Casilan
Egg
Lactogen Milk powder
Trophex
Complan
Hepovite
0.41
0.15
2.88
.... »*U
1.45
2.86
2.60
5.28
Proteinules
4.71
COST PER
100 CALORIES
IN PAISE.
■
10
.. 22
80 ■
31
66
53
Calories nut
given
Calories not
given
COST PER
GRAM OF
PROTEIN
SUPPLIED
IN PAISE.
3
41/2
3
6 '
6 1/2
7
8
10 1/2
10
Other.brand names were either unavailable or did not supply information
on calories or protein content, on the package. The high cost of pack
aging in tins accounts for some of the high cost of well known brand
name s.
PANJEERI AS A TEACHING DEVICE;
For teaching the mother.
We cannot rely on packaged food alone to prevent or treat malnutrition!
Instead we tell the mother tos-
(a)
(b)
(c)
(d)
(e)
feed solids from 4 months of age.
use low cost readily available solids such as potato, kicheri,
banana, dalia.
double the food intake and the number of meals per day.
enrich these solids by adding panjeeri to porridge laddu or
paratha every day.
bring the child regularly for reweighing, more panjeeri, and more
feeding advice.
The mother can be taught and persuaded in conversation, by flash cards
in groups or by feeding' demonstration. Feeding the mal-nourished child
on the spot proves to the mother that small babies can be fed solids.
Also in giving panjeeri, we also include in the packet a pamphlet explain
ing to the mother how to prepare the panjeeri simply and cheaply in the
home.
Each reweighing of the child should tell the mother if she is on the
right track. She is congratulated if successful. If the weight has
oontd...page 3
3
not improved much it usually means that she has not really accepted
the teaching given. Panjeeri keeps her coming hack enough times to
eventually be convinced to 'feed more food1.
For teaching staff.
If nurses can be taught to make the panjeeri, they learn something
practical of great value in treating one of- the commonest diseases,
and what they learn can be taught to the mothers whether they work
in city or village afte'r training. The doctor also, if Panjeeri is
stocked in the pharmacy, or if the mothers know how to make it any
way, will always have a ready answer to a common prescribing problem,
the problem of malnutrition. By studying the response on the weight
chart, the doctor will see'that the best results cpme when he has
persuaded the mother to not only feed the child the panjeeri he pres
cribed, but when she also increases the quantity and frequency of the
child's meals. The fact that he has something in his formulary that
is logical and effective, will encourage the doctor to look out for
malnutrition with an attitude of hope that will transfer itself to
the mother.
PREPARATION AND PACKING.
I. Roast wheat, bengal grams and groundnut separately in a pan till
brown.
II. Separately grind wheat, bengal grams and groundnut while still warm
along with sugar in a home grinder and mix and add milk powder.
(if soyabeans are used instead of milk powder, soak it for 24 hrs
and dry in sun for three days and grind).
Pack
III.
and heat seal 70 gms of mixture into 250 gauge plastic bags
of 3" width and pack 7 such bags into a larger stronger bag
11 cms x 27 cms of 350 gauge plastic along with explanatory pam
phlet .
The net weight of a weeks supply of mixture is-thus 490 gms.
When the panjeeri is made by hospital staff in quantity, it is easier
to use wheat flour than whole wheat. Groundnut can be bought roasted.
Or roasting can be done in hospital kitchens without using any extra
fuel.
COST OF MAKING PANJEERI.
Panjeeri as traditionally made in the Punjab contains almonds, „>
but at much less cost groundnut can be substituted.
Table 3.
Current rate par Kg.
Rs.
Wheat or wheat flour
1.00
Bengal gram
3.00
Groundnut
4.00
Skim milk powder
12.00
Unrefined brown sugar
2.25
Cooking oil’or clarified
butter
7.00
Plastic bags for packing 11.50
Explanatory pamphlet
15 per■ 1000
Roasting, grinding^
packing, supervision &
labour
1.00 per hour
Amount for
490 gms.
(one week's
supply)
Cost for
(one week's
supply)
230 gms
78 gms
39 gms
39 gms
78 gms
Rs.0.23
Rs.0.24
Rs.0.16
Rs.6.47
Rs.0.17
24 gms
10 gms
one
Rs.0.17
Rs.0.12
Rs.0.02
Cost price
Selling price for calculation of comparative -cost
in Table 2
Rs.0.25
Rs.1.83
Rs.2.00
4
Soya bean can be used in place of skim milk if desired, with
considerable saving of cost. If the panjeeri is made at home,
whole wheat can be used instead of wheat flour with slight
saving of cost and improvement of taste-.
PRESCRIPTION:
One small packet daily for infants; 1-2 teaspoons
three times a day in milk or food from fourth month.
Two small packets daily for Antenatal women, in last
fourth months of pregnancy; 4-6 teaspoons three time
a day after food, and for two months after delivery.
REFERENCES:
Reddy V. etal. Arch Child Health II. 4. 189 - 194
Further copies available from:
Co-ordinating Agency for Health Planning,
C-45, South Extension Part II,
New Delhi - 110049.
CAHP - 206
PROTEIN CALORIE MAI.NUTRITION REDUCED BI A
------
Murray Laugesen * F.R.C.S. and S. Nayyar, B-.Sc’, Community Health
. Department,■Frances Newton Hospital,'Ferozepur, Punjab.
* now at'Co-ordinating Agency for-Health Planning, 0-115, South Extension,
Part II, New Delhi—11001i9'. '
' '
SUMMARY:
;
j,
' ■
Of 11;2 clinic■attenders out of 320 urbanypoor under-five year olds,
the proportion with second or third degree malnutrition.fell from one half
to one third, when followed from first clinic visit for periods up to 20
months. These free clinics were held for one hour in each place weekly, and
early and adequate feedings were stressed.
883 of. parent retained child health records were recovered for inspe
ction at the door, despite panic evacuation during all of December 1971 due to
shelling of this border town. Costs and benefits are discussed. The main bene
fit is that once mothers are taught how to control malnutrition through feeding,
they will not let it recur and mothers and health workers can focus on other
health problems. '
METHOD:
RESULTS:
' •
. In February 1973, a house to house collection of patient retained
child health-records was made. The clinic was visited by half the children
in the-area. These came to the clinic 6 times on average but malnourished
children came 9 times in 20 months.
table i: present nutrition status of all’children under 5 found in
SHEKHAN AND DIHARIAN RASTIS IN FEBRUARY^MARCH 197T7
Attended clinic
Health record . <
recovered
Nutrition good
better than 803 of
1)5
Harvard standard
Malnutrition
li9
Grade 1.71-803 of ..
Harvard standard
Grade 2.01-Y0% of
32”
Harvard standard
Grade 3.603 or less
of Harvard Standard
1U
Not at home, or
refused to have weight 2
taken or resented visits
No. of children
1U2(UU%)
Attended Clinic
record lost
,
Never
attended
h
5h
' 8 -
li5
5
28
Don't
know
Totals
103(32*)
.
-
102(323)
65(203)
2
7
23( 73)
0
25
27( 83)
19 (63)
159 (503) -
320(1063)
peoy
A weekly under fives clinic was started in twp of Ferozepur Citv’s
poorest bastes, in May 1971. The team comprised a doctor, sister, health
educator, laboratory technician,, trained dai, and registration clerk cum
dispenser cum..driver. Medicines and vaccines and all services were provided
free for one hour'-in each place, each week. Weights were recorded at each
cl-inic visit on a Morley health record using's '25 Kg English Salter hanging
scale. Rome visits and feeding .programmes were not part of the programme,
.but effort was made at each visit~T>o encourage the mother to feed more food
to her child-, and-to-start solids from the fourth month. Most children were
treated"fnr. anaemia, and this was treated with iron and folic acid. Illnesses
were treated with a formulary of1' some 50 simple but effective medicines, and ■
vaccines-were given when illnesses allowed. Seven milk biscuits were riven
out each visit in cases of malnutrition.
2
Statistical analysis-of Table 1. shows"no-significant nutritional status difference between previous clinic, a't'tenders and previous non-attenders in
March 1973. ■
.■
.
This table shows that half the children used the free weekly clinic
some time 'during its first 20 months. . And half of the serious or severe
malnutritioned children used.the clinic. At time of review 11.895 of cards
issued were not produced on- asking at the- door, giving an 88% recovery
rate in a very poor area. Many of these records were lost during December
r'1971 when due to shelling of the city, all women and children evacuated to
the country side.where they had to live in grass huts for 1 month. One in
lour of these children were still suffering from serious or severe mal
nutrition after 20 months of a free weekly under fives clinic service
within a few hundred yards of their door.
TABLE 2: • FINAL NUTRITION GRADE COMPARED WITH NUTRITION
GRADE at FIRST CLINIC VISIT----------------------
Shekhan and Diharian bastis. Final nutrition grade as noted
February-March 1973, First clinic visit occurred any time between
May 71 and January 73.
Original nutrition grade
at first clinic visit.
Final nutrition grades.
Nutri
tion
■ .good..
good.
Malnut. Malnut . Malnut.
Grade 1 Grade 2 Grade 3
Do not
know.
Total
■, 30
7
0
0
0
37
Malnutrition
Grade 1
8
23
2
.1
0
3b
Malnutrition'
Grade 2__________
2
17
23
b
0
b6
Malnutrition
Grade 3
b
2
8
9
0
23
2
2
2
lb2
.
'
Original grade
unknown
Total number of
children
-
■
hh"
■
__33.
Table 2 shows that there is*a significant improvement from original to
final (March 1973) nutrition grade in those who attended the weekly
clinic- ( X2
=92.6 for d.t.b) This is highly significant.
.
O.Ol(obs)'
The most frequent nutrition grade in,first clinic visits was 2nd
.degree malnutrition and at review the commonest grade was first degree
malnutrition. Overall the figures showed a 22 in 71_reduction in
moderately serious and very serious .malnutrition. (30.9% reduction in
grades 2 and 3), among those attending the clinic. .
contd.....Page 3.
3
TABLE 3: CHANGE IN FINAL NUTRITION GRADE ACCORDING TO
ORIGINAL NUTRITION GRADE IN CtMC ATTEO'RS:
Final Nutrition Grade.
Shekhan & Diharian
Bastis Ferozepur City
Worse
30
7
0
37
8
23
3
0
3h
19
23
ll
0
115
111
9
0
21i
Nutrition good at first
visit
Malnutrition Grade 1
at first visit________________
Malnutrition Grade 2
at first vis?t
Malnutrition Grade J
at first visit
Total
Do not
know
Same
Better
'
-
2
2
Ill
2
1112
■Original weight not known
No. of ch:ldren
111
85
This table shows that of every 10 clinic attenders, 3 improved,6
stayed the same and 1 worsened his nutrition status from first clinic visit
to time of review.
TABLE li: FINAL NUTRITION GRADE ACCORDING TO SEX:
Final Nutrition Grade.
Worse
Do not
know
Total
Malos
17
li2
8
1
66
Females'
2IT~
li3
6
1
Total .
-- - ----------------
111
85
ill
———==—-
2
Improved
Same
Vli
~TTF2
=========
This table shows" that female children have responded as well as the
male children to the health education and clinic services, and are ?ust
as likely to be brought for-medical care as male children. There is no
relationship between the sex and the attainment of final nutrition grade
The value of x2 = i.,23 (d.f.2) is not significant.
TAELE 5: FINAL NUTRITION GRADE ACCORDING TO AGB WHEN FIRST SEEN.
improved
Year, of age when
first seen
1st
12
2nd
10
.
?
,
Same
Worse
37
io ■
23
1
Original
. Total
weight not
known
59
0
‘
31i
3rd
9
9~
1
0
19
Uth
■6
10
2
“ S
18
Sta
n
6
0
3
Age not Known
0
o
0
2
in
2
Total
HI
85
111
2
■ :iii2
- u This table shews no relation' between agn When first geerr and final
nutrition grade.
- The percentage improvements in nutritional grades in 1st to £th year
of life were 20.3%, 29.h7.b%, 33-3% and b.0.0% respectively for each
year. In comparison for the improvements between two successive years,
these differences are statistically insignificant (P ranging from 0.30 to
0.70). The difference between 1st year and 2 to 5 years taken together
is also statistically insignificant (P=0.20).
POSTS & BENEFITS OF AN UNDER FIVES CLINIC IN REDUCING MALNUTRITION:
1.
The Cost: What is the extra cost of giving a nutritional empnss..
to a weekly clinic? The cost of the health educator at Rs. 200 per mon'
for 2 hours weekly for 20 months and the cost of 1190 Gms of Panjeeri giv^n
six times to each child seen meant a cost of Rs. hli per child actually
improved in nutrit’m grade.'
2.
The benefits: This weekly under fives clinic working in these slum
areas improved about one third of the children with second and third degree
malnutrtition who were seen at the clinic.
3.
Half of all the malnourished children in the area had been seen at
the clinic. (Daily food would attract a much higher percentage, but even
free food did not ensure a d,’ily ''endance of much over 60% even during
the acute food scarcity in. Maharashtra this year.)
U. Education of the Mothers by the Staff: Our experience was that the
advice given.to the mothers to feed their children was more important than
the small food supplements given to encourage attendance among the ..
ed children. Further attendance ensured more exposure to health educau.
5. Education of the Hospital Staff by the Community: The weekly clinic
.exposed the hospital staff to the severe malnutrition found only U Km fr~ i
the hospital. As a result daily feeding centres have' since been establi- ->•’
and’are running smoothly. Further results from this extension approach a -j
..air awaited with interest.
ACKNOWLEDGMENTS:
People in the U.K,, provided the vehicle through Oxfam. People in
New Zealand supplied milk biscuits through CORSO and the Perozepur Municip''-'
Committee gave most of the running expenses in the first year for these <-•'
clinics. Punjab Government through Chief Medical Officer Ferozepur gav .
thousands of iron and folic tablets and B.C.G. vaccine. '
Thanks are due to Mr. Rao, Holy Family Hospital, Delhi and Mr.
Sadashivaiah of C.M.A.I. Family Planning Project, Bangalore for statisticalanalysis, and to all the clinic staff of Frances Newton Hospital, Feroecj..
who worked hard to convince the mothers to feed more food.
------- oOo--------
«CAH? - 207.
Health Planning - how planning begins with a study of
deaths & diseases.
By
B.M. Laugesen, F.R'.C.S. ,
Co-ordinating Agency for Health Planning,
C-45, South Extension Part II,
New Delhi-110049.
When a hospital decides to analyse the diseases in the'community,
it often has to be content with hospital disease data to start with.
This means that diseases which mostly result in death at home, such as
child malnutrition, will be under-reported. However,if such things
are allowed for, the results still show that the area round the hospital
may not need a bigger and better hospital so much as scores of Sub-.
centres round the existing hospital.
The most reliable statistics will be from:
(1) Deaths.
(2) In-patients.
(3) Out-patients.
The only way to be sure that all records are actually included
is to write out a list of all numbers or names wanted, one per line
with a running "study number" in left hand margin and then have the '
charts stacked in that order for analysis so that any missing can be
noted.
Analysis of Deaths:
sex thus:
Death
charts are natura.lly grouped by age &
(a)
Still births plus first-week deaths (perinatal mortality)
We study the mother's chart at the' same time to deduce cause.
(b)
All other first year deaths upto 11 months.
(o)
All Toddler deaths 1-4 years.
^001
1.
(d)
5-14 years male & female.
(e)
Women 15-44 (all pregnant, or upto 8 weeks post partummaternal deaths)
(f)
Men 15-44 years.
(g)
Men & Women, 45 years and over.
Each group is then analysed into preventability groups.
Perinatal Deaths
For the perinatal group the 'P' code of 100 causes given in the
TEO 1965 revision of the International Classification of Diseases will
be found more useful than the A code . Alternatively, the following
are the main groups derived from the 'P' code.
1.
Chronic maternal disease.
2.
Toxaemias
3.
Maternal Infections
contd....page 2.
2
4.
Difficult Labour
5.
Antepartum Haemorrhages
6.
Congenital
7.
Infections of the baby
8.
Immaturity or low birth weight, cause unknown.
9.
Cause unknown, not immature.
10.
All other known causes.
Some of Group 5 may be possibly prevented with fo.lic acid before
conception and low birth weight may be partly prevented by diet
education for the women 40 kg or less in second half of pregnancy.
Deaths in under fives and older children.
The main 'preventability' groups are
1.
Immunisable diseases (include measles)
2.
Malnutrition - infection- anaemia - combinations including malnutrition-diairhoea.
3.
Other faecal - borne disease in absence of malnutrition.
4.
All other, including burns and accidents.
Then it can be decided which of these deaths could be prevented
by a chain of under fives clinics in a 1 hour radius of the hospital,
and what staff would be necessary for this and how to provide staff
and financially support this. Then it can also be decided whether
more deaths still could be prevented, if a village-recruited child
health worker was put to work to cover every 3000 population, backed
up by a weekly visit from the doctor with laboratory technician and
trained nurse. The most- easily preventable death group of all ages
will be found to be the malnutrition and / or anemia"and infection
group in toddlers. This group responds to simple advice to feed more
food and more solids.
All that is needed is a dedicated worker trained to persuade the
mother, and equipped with a cup and spoon and some semi solid food to
prove that the child can eat. The worker need not be highly educated
provided she has leadership ability and social status.
Professor P.M. Shah of Bombay has refuced death and birth rates
in villages, using illiterate social workers, job trained and perio
dically supervised, to concentrate on the malnutrition among toddlers.
Much of malnutrition is due to ignorance of the importance^-of solid
foods from 6 months of age.
Maternal deaths;
The cause
groups are
1.
Haemorrhage and /.or Anaemia.
2.
Sepsis, post-partum or post abortal
Antesartum or Post partum
3.
Hypertensive diseases of pregnancy
4.
Difficult Delivery
contd...page 3.
3
5.
Other obstetrical causes.
6.
Other non obstetrical causes
Then it can be decided
(a) which could be prevented by having a chain of antenatal clinics
or workers in the district
(b) what other communications and transport is necessary to prevent
most of the remaining deaths, and is it feasible at this stage?
Training programmes can then be aimed at the biggest and easiest
"death targets" and the antenatal record and the antenatal clinic is
geared to aim at selecting the high risk ones for hospital delivery.
Analysis of in-patients.
By taking the in-patient register and the main disease diagnosed
in the last 100 patients, we may divide them into two groups.
(a) admission was avoidable if we had a subcentre within three miles
of her home or had better out-patient facilities in the hospital.
(b) admission was unavoidable.
(Analysis done by hospitals (1973) in different states show that a
third or a half of the admissions were thus avoidable.)
Analysis of out-patients.
Special study of every 10th outpatient can be made till 100 have been
studied and they too can be studied as avoidable or unavoidable, if
a subcentre had been near their home. .
Also it may be studied how many miles they have come, and thus the
intensive service area of the hospital can be worked out (of course
the rich can afford to come longer distances.) Then it can be dedu
ced that for maximum service to the public especially to the poor,
the hospital needs village-recruited workers in a number of subcentres
to serve the people who normally never reach the hospital early in the
disease.
Diseases Tally Sheet (duplicated)
This has been designed to allow extra space opposite the common
diseases. The form may be kept on each doctors table. This is the
150 causes of disease and death of the 'A' list of the International
Classification of Diseases, published by World Health Organization,
as revised in 1965.
CONTD.... page 4.
4
DIAGNOSTIC INDEX CARD (18.5 x 14 cm)
PURPOSE: This card records the unit numbers of patients suffering
from each type of disease. From these disease statistics are easily
compiled.
METHOD»
These cards are kept only in medical records department.
Before the new year begins two sets of cards are prepared one card for each disease; and one set for inpatient diseases; one
set for out patient diseases.
Each disease has a code number taktr from the International
Classification of Disease (ICD) published by W.H.O. (available from
any book-seller). The State Government may require the same coding
for disease statistics - for example the 'A' code of 150 causes of
morbidity and mortality.
All those patients with tetanus will be entered on the
tetanus card. The unit number identifies each patient on this
tetanus card. Patients who die have their numbers entered in red.
At the end of the month or year the number suffering from
the disease is read off, using the running number on the edges of the
card.
Each year fresh sets of cards are prepared. By keeping the
annual sets, all patients records with a particular disease in the
last 10 years can be easily studied.
Thus we can find out which villages, which age group, etc.
suffer from certain diseases, and what the seasonal variation is.
The reverse side of this card is the same as the front side.
Samples of these cards and of Disease Tally Sheet are available from
Coordinating Agency for Health Planning.
Further copies
availably.- froms-
Coordinating Agencyfor Health Planning,
C-45, South Extension Part II,
New Delhi-110049.
IN I
OUT
Patient; Patient
ICD Code
Diagnosis.................
Year
Govt? Code
DIAGNOSTIC INDEX CARD
1
2
3
4
5
6.
7
8
9
1
I
10
11
12
13
1
14
15
16
—
—
17
18
19
i
I20
1
□
—
20
j
40
]
60
i
------!■
80
1
j
100
--------------------
120
140
CAHP-216.
HEALTH EDUCATION - THE MISSING LINK IN MEDICAL CARE.
C.M.E.MATTHEWS,
Department of Community Health.
Christian Medical College,
VELLORE.
Imagine that we are visiting a hospital and that when we ask these
questions we are given the following answers:
TubercUlfosis
LeprosyMalnutrition in children
Diarrhoea in children
Infant mortality
Overpopulation.
Why are they problems? Is it because the medical solution ■
is not known? Is it because medical services are not
available? Or is it because the people do not use the
services properly and do not follow the required behaviour
at home? ♦
■ A tuberculosis patient will take treatment Until he feels
better and then he will see no point in continuing; later he
may become resistant to available drugs and a threat not only
to himself but to the community. A leprosy patient may be
' afraid t« come for treatment at all, or in the early stages
may just not realise he has a serious disease. Malnutrition
although largely due to poverty also could be much reduced if
mothers appreciated the importance of giving their children
more food; vitamin A'deficiency could be- easily prevented by
giving greens with negligible, cost. Diarrhoea could be
prevented by better hygiene but villagers d» not think this is
important; when the child is dehydrated they believe in the
power of mantrams alone and eften do not seek medical care.
B A N G A LO .it . geo Qoi
No, they do not have any special, training, its just
common sense really. Even the medical officer does
■ not have much training because as a student he was
not interested in surgery and so he did not bother to
attend those -classes. Yes, he does regret it a little
now.
Q. Are you thinking of getting a.qualified surgeon to come
, arid give you a course on surgery?
Well we might do that sometime, but we are all so busy
that it is difficult to find the time for it.
What,
sort of results do you get"?
Q.
Occasionally it works »ut alright, but sane are very
difficult cases. , The body is very obstinate and ignorant
and just does not know how to heal itself, or deliberately
refuses to do so. So what can we do?
What would we think of a hospital where such a conversation
could take place? It ceuld not happen we say. And yet if
we. substitute "health education" for "surgery" we find
that such a conversation could easily take place in very many
hospitals. Why the difference in attitude? Which is more
important?
Consider the major health problems which affect large .
numbers of people in India. Let us take a few examples:
COMMUNITY HEALTH Ci
Who does surgery here? Do you have a qualified
surgeon?
Surgery? Oh we all do surgery - everyone takes
his turn with the knife, from the medical officer
right down to the most junior attendent. Surgery
is very important.
'1 . (F irs t F looD S t. Marks
Q.
2
Infant mortality could be reduced ■bj^.a .better diet for pregnant
wcman and more antenatal care, but village women do not see the
need for this. Family planning services .are available but they
are not fully used.
So what is needed? It is to change people's behaviour, and thi,s
is difficult to do. We can say as in the conversation above that
people are ignorant and obstinate sb that, nothing can be done.
But this may be Just a way of excusing our own faulty technique.
There is a science of behaviour, and ways of bringing about change
have been extensively studied.
Health education is not just giving talks and showing pictures.
Would that be enough to change your behaviour? Nor is it only
telling facts. Health education is based on- the behavioural •
sciences'!— social psychology, sociology and anthropology.
Insights obtained frcm studies in these fields can be applied
to the problem of changing people's behaviour. Merely to hand
out information by means of talks etc,, is like handing out
drugs without first making a diagnosis, and without relating .
the particular local symptoms to the physiology and pathology
of the body as a whole.
The minds of the .people to be educated are not just like blank
^pieces of paper 4n which we can write what we will. Their minds
are more like an organ of the body which has certain fixed
functions, and whose structure and activities are all related to
these functions. The "functions" depend on a person’s goals
and values. Therefore to chang^ knowledge, attitudes or behaviour
we must understand a person's goals and values and their system
of beliefs. So the first principle of health education is:
1.
Know
the culture,
—
- ----------------------
a
That is we must know the customs, beliefs, goals, values,
and way of life of the people we are trying to educate: Their
culture may be different frcm our own n«t only because of
national, state, or regional differences, • ■
, but because of differences in class, caste,
education, religion, and general background. There is usually
a considerable cultural gap between say a doctor and a villager.
Unless this is bridged in some way there will be little real
communication, since communication depends on shared knowledge
and attitudes.
The doctor may think he has explained everything, but it will
not mean anything to the patient, and the doctor will, wrongly,
conclude that the patient is stupid or »bstinate. We cannot
expect the patient himself to bridge this gap, we must g» t*
meet him by learning about his ideas, before we can effectively
teach him our own ideas.
2.
"otart from where they are."
If we start with ideas that are quite unrelated to anything
the patient already knows, then he will not be able t«
integrate what we are saying into his existing system of
concepts and will probably reject it. We should try to
introduce change gradually by building on What..he has already.
■ This takes us back.to principle(1,)because clearly we cannot
do this without knowing the culture.
3
3.
Give people a learning experience.
Just giving information is usually not adequate to change
behaviour. Doctors know all' about the evidence that smoking
causes lung cancer, but that does not stop them from smoking.
A learning experience is much more effective. If the mother
of a child with malnutrition sees her child improve with a
better diet alone, she will be much more easily convinced •
than if someone merely tells her to give the child more food.
4-
Motivate by linking the required behaviour with goals of groups
and individuals.
The action which we want the person to take must be related to
some goal the person has; the action should be seen as a way
of reaching the goal. The goal may or may not be related to
health. For example people may build a latrine because they
think it will give them more prestige, or to imitate some
important persons, and only afterwards they'may discover its
value for health.
5.
Suggest specific, easily carried out behavioural changes.
Studies have shown that people are more likely to follow
advice given if it is quite specific and precise, and they
know exactly what to do. Also there should not be too many
barriers making it difficult for them to do it. If we say
to a mother, 11 you should have your child immunised", she may
agree but do nothing about it; if we say the following she is
more likely to come; "bring your child to the clinic tomorrow
-.at 3 p.m. to be immunised; it is quite near your house and it
will, hot cost you more than ( a small amount)} your neighbour
is coming and you can go with her".
6.
Work through leaders and use group influences.
Many studies have clearly shown the importance of group
influence on a person's behaviour. A group discussion and
decision is often more effective than a lecture. The social
influence of the other members of the various groups to which
people belong is very powerful. Reference groups, that is
• the groups with which people compare themselves also have an
importanfceinfluence.
Groups may often be influenced through their leaders. Leaders
are people that others will listen to and imitate, they need
not have any official position. They may be people who havemore communication with others than the average, or they may
be powerful because' they- have more resources than others, or
more education. ’ If we do not use them, they may work against
the project and prevent any progress being made. If we can
' involve' them and make them feel it is their own project, they
are more likely to'carry on with it even when we are not there.
7.
Obtain participation of the community at all stages.
The community should be involved even in the planning stages
of a .project. .Only if they are fully involved will they take
a real interest in what is to be done. It has been said that
we cannot give health to people,.they must achieve it for
themselves. We must act as catalysts and stimulate them to
do this. One way is to form a health committee and get them
to discuss their health problems and decide their own priorities
and what help they want from us.
4
8.
Meet felt needs first.
If people do not have enough to eat, e.g. no spare cash
to buy food to-morrow and no prospect of work, they will
not be very interested when we talk to them about long
term preventive measures such as immunisation or family
planning which may only help in the remote future. Health
'programmes and community development programmes should be
much more closely linked so. that felt needs can be met.
There is not enough space in-this paper to describe the
various theories on which health education is based. The
above are just a few principles which will give some idea
of the scope and methods of health education. Those who
are interested and have time for further study can become
familiar with the behavioural sciences, and themselves
try out different ways of applying them; others can use
the services of a qualified health educator.
In my opinion, only when health education becomes as
important a subject in medical practice as for example
surgery is at present, will many of the health problems
of India be solved.
BIBLIOGRAPHY.
1.
Selttcted papers on health education. CHEB Training Series 1,
March I960. Central Health Education Bureau, New Delhi.
2.
Social Psychology.
3i
Havighurst R.J., The learning process.
51, 1694, 1961.
4.
Cartwright 0., Some principles of mass persuasion.
Relations 2, 253,. 1949.
5.
The process and effects of mass communication. Ed. W. Schrammu
University of Illicnis Press, USA 1965 p.116.
6.
Health culture and community.
Ed. B.D. Paul, Russell Sage foundation 1955.
7.
Human problems in technological change.
E.H.Spicer, Russell Sage Foundation, 1952. ■
8.
Lionberger H.F., Adoption of ideas and practices. Iowa State
University Press, limes, (Eowa, USA i960.
9.
Rogers E.M.Difusion of innovations.
New York 1962.
10,
Ranganathan K.V. Srinivasan, K and Mathew B.Role of community
leaders in promoting family planning in rural India. Action
Research Monograph No.l. Inst. Pub. Health and Family Planning
Gandhigram 1965.
11.
Nutrition education .in public health programmes - what we have
learned. Amer.J.Pub. Health 51, 1715, 1961.
12.
Community development in India. B. Mukerji, Orient Longmans, 1961.
B. Kunpuswamy, Asia Publishing House 1961.
Amer.J.Pub. Hlth.
Human
Free Press of Glencoe,
BANGA*-OaE-56DO01
SAHP 209.
From
Indian Paediatrics Vol, 10. P, 347-9, 1973.
Nutrition-Education - «j; Education in Child. Care?
by J.P. Greaves, M.Jl., Ph.D
FAO/UNICEF Nutrition Officer
UNICEF, jlew Delhi.
J£&e Planning*Commission of the Government of India> in diseussing
the problem of malnutrition in its App»©ach to.the Fifth Plan (January
1973), speahs ,of’the need t$. integrate feeding programmes "with'health
.
?are, immup^gatiqh and nutrition edueation to form a package".
lij the
belief that the education competent of the package wo.uld be better des
cribed'as "Education in Child Care", this note gets opt.proposals for
wh$.t this might mean; in particular for what might bes
I.
eight, basic universal messages
(i.e.', ^messages generally applicable throughout India, in
rural and urban situations);
II.
in elaborat+oh of these, twenty universal components of the
packet of messages that need to be communicated to village
women;
III.
local modifications of some of these components, identified
in list II by letters in parentheses.
The "messages" listed represent ideas, and some need more specific
identification.
as possibly.
They have been kept deliberately as few and as simple
The ideas are not expressed in the terms which are suppo
sed to be necessarily th® most appropriate for getting them across.
the ideas themselves have been agreed, this aspeet - part of the
"how" cf communication
will need much thought.
Probably the advice
-*-of those familiar with social customs and beliefs regarding illness,
and with food habits and tabus, should be sought.
Marked regional
variation |n tfcpse respects may pean that basically universal messages
should he communicated i^i different ways in different parts of the
Gauntry.
Valuable assistance in these regards copjd be. given by the
Peni.ral .health Edipation Bureau.
The packet of messages or ideas represents "what every mother
needs to know".
Every father, too. . But all village and blook level
workers with whom she comes in contaOt,including balsevikas, gram sevikas, piukhya sevilcg.s, and also nurses.
ANMs and PHC doctors, who will
/•••
negd. training or at least "qrient^tion" in the integrated package
pregramme, should also be aware of, and sympathetic to, this packet,
so that the messages will be reinforced at various levels and .the
mother wi.X_l. nQt be eub.jegted t-P «*nfli£t.ing advice.
Ip other. words,
THis means that the training given
all should speak with ene voice.
in sp-going.programmes, such as the Applied Nutrition Programme, n^eds.
te be reviewscbwibh this jacket sf messages in jiind.
Based, or. these messages a simple "Manual en Child Care, for '
village level workers", might'-be developed, ’ Suofa a manual shpuld be
written in the loial language.with local modifixations and adaptations
>f thermsssages..
It should be Complemented with a "Manual"on Child——
Care-,- -for-Slonk/Distxi.c.t_.level_^npervisors''r7 and perhaps sne for
Sta&e level coordinators and training institution staff.
Successive
manuals, and training syllabi, should be developed from the bottom up,
by seeking answers to questions such as* "Who will teach the mothers/
supervisors/teapheps?1’
properly?"
"Wh^t ds they need to know in order to de this
However, implementation of tjje training should bf-
oourse proceed from the top down.
Throughout, as much emphasis should*
be placed on bow* messages should be communicated as on what these
messages should be,
Child Care Education
I.
t
Basic universal messages
1.
Breast fe^d as long as possible . .
'
2,. . Introduce ^mi-solid food from 5 to 6 months
II.
3.
Feed young children 5 or 6 times a day
4,
Don't reduce food in
5.
Use the health services available
illness
.•
,
6.
Get children immunized
T,
Keep yourself and your surroundings clean; drink clean w'ater
§.
JJave no more than 2 or
children, 2 te 3 years apart.
Universal components
!.■ Mother-tp-be
(d) . «jat more than usual amount of^cereal
■ -£nd pulse, ajid plenty'pf dark green
: and yellow vegetables and fruits;
(A,)
(ii) visit PHO docter/ANM during last three
months' of pregnancy.
T-Tew baby,
'
(1J
Mother's milk is best „ don't discard
cplfli^irum;
3 • ;
• (ii)
if you feed additional liquids,
use a traditional feeding vessel,
.
-■
3.
never a spoor!
Keep *n breast feeding as lopg' as possible, but this is not
sufficient by itself after the
age of 5--toe 6 ..months.
4,
'While breast feeding the chi^zU
mother sheuld eat ©ore tha^
■ (i)
usual amount of cereal and pulse,
and plenty of”darte-;green and
yellow vegetable and fruits; (a)
(ii)
visit the doctpr/ANM for *heok-up.
Start semi-solii food (local staple .or mashed up ready-to-eat feods)
after 5 to 6 months, and also
undiluted cow's milk if you can.
These foods must be prepared
cafefully.
■
‘
(B).
Give what you would normally give
later, much earlier.
And add
vegetables and fruit,
$•
As the child grows the amount and variety of foods should be increased.
?,.•
By the time he is one
a*
year old he should be fed similar
foods to the rest of the family -
,
cereal, pulses, green vegetables,
perhaps supplemented by processed
yeady-to -eat foods - hut in
•
order to get as much as he needs
hp should be fed these solid
foods 3 or 4 times a day.
V,
(A)
When you are unable to feed the child with your own milk, sokid ■
food (which ©ay include yuppiementary re.ady-.to—eat. .foods)
should be given .5 or 6 times a
•
•
day.
Also, if possible, undilu
ted cow's or hj?ffalo's milk or
.
Mijfone.
■
(Ciltone £s 50 per cent
milk and 50 per cent milk extend
er frtm vegetable sources.)
.
Do not u,se excessive water for booking' rice and vegetables.
8.
If you drain the water after cooking-.
do n»t discard it* it is good far you
and should be consumed. » *
To prevent tfye child getting some diseases he should be immunised*
9?,
This will probably make him a little ill
but will prevent him- getting terrible
i
scars later and perhaps dying.
10» T»- prevent him getting other diseases he should be kept clean and
his surroundings k should be as clean as
possible.
Don't spit cough.
11,. Dq n<?t let excreta lie around where your baby may be playing.
Remove it quickly to a place outside
his reach.
After baby defaecatea wash
him clean with soap and wash your hands.
Your" child may get sick if he puts dirty
hands in his mouth.
12* Hands should be washed before eating and before preparing food,
and before holding and feeding the baby.
ap.d-feeding’utensils should be kept clean and not allowed
'
to attract flies.
Flies mean dirt means .
danger.
1,4. Fo^d should b.e kept covered from flies and dust.
IS*- Only the- safest available water should be drunk.
A child needs
plenty of water.
(C)’
to- recognise signs of pommon diseases* cough, diarrhoea -
dehydration, fever, running ear, skin
diseases, sore eyes and poor sight.
Learn their management ana how to deal
■ -
with accidents in thg home,, and when t«
seek advice from AUM/dqfjtor
(B)
17, When, the ohild is ill with fever or diarrhoea continue to feed him
as before - but you may have to prepare
,the food more appetisingjy. You may have
t«> for»e him a little.
Re will get
better quicker if he eats plenty of
■
.
-
*
^erealj pul.Rg, gsreeji vegetables .(A)
EnjCpurage" the ,ehild to play with simple household articles and
things he can gather in the neighbour-
5
19.
Children cared for in this way are likely to be alert and
20.
Children cared for in this way are likely to survive much better
curious and grow well.
(E)
-t-
than those who are not.
You may not then
want so many children - family planning
can show you how to achieve this, and
and how to space those you do have by
2 or 3 years.
"III.
Some local modifications
(A)
Give examples of particular cereals, pulses and vegetables,
and methods of the£r preparation.
If it is customary to
eat animal foods such- as eggs, meat or fish, and these can
readily be obtained, they should be referred to.
(B)
Give examples of suitable recipes from local-foods.
(C)
Source of this water to be discussed in detail.
(D)
(i)
If there are local schemes for the provision of
Vitamin A capsules, or iron/folic aoid tablets, explain
how these can be obtained, and why.
(ii)z
If rickets
is a problem (parts of central India?)
explain importance of allowing child some exposure to
..
sunlight.
(E)
"Will grow well" - if the mother is likely to come in
contact with a centre using health record/weight charts,
these should be referred to and explained,
.May 1973.
Further copies available from
Coordinating Agency for health Planning,
C-A5, South
Part 2,
New Pelhj.- 110049.
CAHP 218
Reprinted from
Human Rights in Health
Ciba Foundation Symposium 23 (new series)
published 1974 by ASP (Elsevier • Excerpta Medica •
North-Holland), Amsterdam
Personal health care:
the quest for a human right
MAURICE KING
An intervention is merely a convenient
name for one of the acts necessary to provide
personal health care, be it injecting peni
cillin, administering polio vaccine, testing
By adding ‘rights’ to ‘wants’ and ‘needs’
we make a difficult pair into an even
more difficult trio. The right to personal
health care can be considered as a group
of interventions that an individual will only
sometimes need, may not always want, which
are not to be imposed on him, but which
must be available. In view of the present
circumstances of the developing countries,
the interventions constituting this right can
only be a part of the objectively assessed
medical needs of a community. They are
certainly not the same as its total wants,
the relationship between the trio being
conveniently expressed in the form of the
diagram in Fig. 1.
COMMUNITY HEALTH CE
Personal health care is the help in sickness
that one man can give to another by virtue
of his special skill and knowledge. If a sick
man lacks access to it, he is denied the
possibility of being helped by any of a large
number of medical interventions of varying
complexity, cost, and benefit.
If we are
to do anything useful to promote human rights
in this field, we have eventually to specify in
detail which of these interventions constitute this
right.
the urine, or even transplanting a kidney.
Health care, and the interventions of which
it is made up, can be simple or complex,
expensive or cheap, and it is our task to
try to determine what is the minimum
quantity of it which all men everywhere
have a right to enjoy. If this right could
be defined in detail and generally agreed
upon, we could observe it, handle it, cost
it, and above all measure it, both in quantity
and quality, and see who gets it and who
does not. Perhaps, when we have done so,
more people might enjoy it.
47/1, (F irs t H o o rlS t. Marks
■BANGA l O .,- 5 u j 001
Nowhere do we fail more dismally to
apply what we already know for the good
of our fellows than in the provision of
personal health care. It has been estimated
that more than half the world’s people have
no access to the modern means of health
care at all,2 and this is in the Second
Development Decade of the UN, in which
health is being seen, not only as a means of
development, but as one of its ends. Such
is the human condition ■ against which we
search for a human right, our entire purpose
for doing so being to see that no one shall be
denied that right.
be placed on a scale of increasing cost and
complexity, in terms of both the equipment
needed for them and the demands upon
the operator who does them. The detailed
relationships of such a scale are inevitably
somewhat arbitrary and in practice the scale
can only be partial. For example, it is
difficult to know exactly where two closely
similar tests, such as determinations of the
blood urea and of the blood sugar, come in
respect of one another. Nevertheless, a scale
such as that shown on the left of Fig. 2 can be
made out.
Although we cannot, at this symposium,
specify in detail exactly what human rights
in personal health care shall be, we can, I
think, go a useful distance towards deciding
what they should look like, which will be at
least something towards promoting their
fulfilment.
This scale has at least two significant
features. The first is that if a particular hospi
tal laboratory can do a certain test, it can
usually do all the tests below it in the scale.
If, for example, it can measure the haemoglo
bin, it can surely test the urine for protein. If
it can measure the protein-bound iodine, it
can certainly measure the blood sugar.
THE ORDERING OF INTERVENTIONS
Closely associated with this is the fact that,
if
a patient has access to a test at a particular
At its simplest, our human right in
personal health care is but a group of the point in the scale, he probably has access to
appropriate interventions taken from the all those below it. The second significant
totality of medicine. The question is: which feature is that the position of a particular test
group? In making our selection we need on the scale has little relation to its diagnostic
to consider both medical and economic usefulness. Those higher up the scale are not
criteria. In establishing the medical criteria necessarily any more use to the patient or to his
we are assisted by the possibility of ranking doctor than those lower down.
interventions into some sort of order or
technological scale.
CLINICAL
That there is an order among interven
tions is well seen in clinical pathology, for
example. Thus the simplest, cheapest, and
almost the oldest test of all, and still one
of the most useful, is to test the urine for
protein. A little more demanding in equip
ment and skill is the measurement of
haemoglobin. Slightly more expensive and
difficult is the measurement of the blood
sugar. Considerably more complex and
costly again is the estimation of the protein
bound iodine in the blood. Towards the
extreme in sophistication and expense come
such
procedures as radio immunoassay.
Such differences
enable interventions to
PATHOLOGY
radioimmunoassay f
SURGERY
- - heart transplant
increasing
cost and
complexity
protein-bound I
iodine]
thoracotomy
blood sugar"'
blood urea *
hoemog'obin
urine proton..
HUMAN Right i
Caesarian section
• wound suture
An outline of the technological scales
clinical pathology and surgery.
A similar hierarchical scale of inter useful to consider some ‘trade-off’ between
ventions exists in surgery, from the simplest cost and benefit which would allow some
suturing of a wound at one end to the trans particularly beneficial procedures just above
plantation of a heart at the other, with such the human rights threshold to be included,
procedures as Caesarean section and thoraco while some of those of lesser benefit just below
tomy coming somewhere in between. Here it were excluded. In practice, however, such
again, if a hospital can do a thoracotomy, it a re-ordering of the scale might be oversha
can certainly provide a Caesarean section. If dowed by two further peculiarities of the
a patient is in a position to get an operation various interventions —their clustering,and the
higher up in the scale, he can probably also disjunctions between them.
get all those lower down. Here too the benefit
of a procedure may bear little relationship to
its position in the scale.
THE CLUSTERING OE INTERVENTIONS
Similar
scales can be constructed in
other specialities, such as radiology, or even
internal medicine, and to some extent there is
a correlation between them. For example, if
a hospital is just able to provide a Caesarean
section, it will certainly be able to measure the
haemoglobin, but perhaps not the blood urea.
It is significant that these technologi
cal scales can be constructed in terms of what
health units in developing countries are cap
able of doing, and that they are susceptible to
exact measurement. They are also some mea
sure of the way in which these health units
appear to grow, in that they are apt to add
on more complex procedures and so move up
the scale. Even in units showing a very great
imbalance, between, say, excessive surgery
and no child welfare, their development within
specialities is likely to follow such a scale.
Many medical interventions are closely clus
tered or associated in the sense that if one is
available, another can be provided at little or
no extra cost. Thus, if a laboratory can exa
mine a thick blood film for malaria, it can
examine the stools for amoebae at no further
expense. If children are already being
weighed, it is hardly more expensive to chart
their weights. The provision of a health centre
makes it possible to supply a large cluster of
interventions, and a district hospital another
cluster.
The definition x>f a human right in per
sonal health care must take into account this
way in which interventions naturally associate
together. As shown in Fig. 3, the ‘right’
should try to include a cluster rather than
If such an approach is valid it may
help us to define human rights in health care.
Perhaps there is a ‘threshold’ somewhere on
these scales below which everything might be
included as a human right?
But, before going further, more must
be said about benefit. Needless to say, a scale
on which benefit was ranked would look com
pletely different. But, alas, it is, economically
speaking, quite impractical to define human
rights either entirely or even largely in terms
of benefit. However, benefit is an, important
aspect to consider at the ‘threshold’ point on
the technological scale. Here it would be
Fig. 3. The clustering of interventions and the
disjunctions between them.
cut across it. Such clustering means that
there is not much point in deciding whether,
for example, BCG vaccine should be a human
right independently of the means to chart
children’s weights, with which it is so closely
associated. If these are already charted, the
marginal cost of providing BCG vaccine is
not great. One of the most significant asso
ciations is that between the interventions for
child care and those for family planning, the
former providing a most useful vehicle for the
latter.
THE DISJUNCTIONS BETWEEN GROUPS OF
INTERVENTIONS
As a natural corollary of clustering there
are wide gaps or disjunctions between some
groups of interventions. Take, for example,
the treatment of dehydrated children. It is
possible to provide in a mere 20 pages of basic
English a complete account of how to treat
dehydrated children, including some elemen
tary physiology and rules of thumb treatment,
such that 95% of them can be cured at little
cost. To improve on these figures requires a
level of knowledge and an expenditure of at
least an order of magnitude greater. For
example, an understanding of milli-equivalents is required, together with an Astrup
machine. There is thus a clear disjunction or
gap between a group of simple interventions
that are adequate for the vast majority of
children, and a much more costly and sophi
sticated group which are required if a higher
cure rate is to be achived.
There is a similar disjunction in the field
of clinical pathology. US S500 will provide a
microscope and all the equipment and materi
als needed for a wide range of simple but very
useful investigations, appropriate to a health
centre or district hospital? But a sum of money
of an order of magnitude greater is required to
provide the equipment for the next methods
up the technological scale, including such
items as an autoclave and a flame photo
meter.
It is through disjunctions, or natural planes
of cleavage between groups of interventions,
that we must define human rights in personal
health care. Thus the simpler group of pro
cedures described here for the treatment of
dehydration and the simpler set of laboratory
methods have good grounds for being consider
ed as a universal human right.
‘GOOD MEDICINE’ IS MORE THAN A LIST OF
INTERVENTIONS
A list of interventions, however carefully
chosen, can only provide the barest framework
for medicine. It might specify, for example,
that a health worker should be able to examine
the eai- and recognize certain abnormalities in
it, or that he should be able to teach a mother
how to express her breast milk. But many
small details are also important, such as when
during the examination of a child is rhe best
time to examine his ear, and how he should
be held while this is being done, or whether a
mother is shown how to express her breast milk,
or merely told how to do so. These small de
tails, even kindness, are no less a human right
than the intervention itself. Something else
has thus to fill in the detail round the skeleton
provided by a bare list of interventions. Al
though a detailed pattern of practice stems
from the whole tradition and ethos under which
health workers are trained, it is most easily
handled if it is carefully defined in manuals
that are written round the interventions and
so serve to fill them out in detail. Ideally
such manuals should embody a pattern or sy
stem of practice that should be widely accept
ed as ‘good medicine’ under the particular
circumstances for which they are written—a
problem to which I shall return.
PACKAGING THE INTERVENTIONS WHICH
FORM THE RIGHT
Having proceeded so far we find ourselves
with a wide assortment of simple and compa
ratively cheap interventions in the various
fields of medicine which confer great benefit
at little cost, and at least deserve considera
tion as human rights. But lists of interven
tions by themselves
are of comparatively
little use to a health service, even if they are
filled out in manuals. If human rights are
to be realized by the provision of services,
they have to be developed in a form which
encourages health services to implement them.
Some wider concept and more effective health
service ‘tool’ is needed, and it is useful to
think in terms of ‘health care packages’.5
From the point of view of the health ser
vices a ‘package’ is much more than merely
a careful collection of interventions. It also
contains every thing technically necessary to
promote their application. Critically impor
tant is a detailed set of behaviourally defined
educational objectives for the staff applying
a package. These objectives embody the inter
ventions for training purposes, and are in prac
tice the most convenient way of listing them.
Other necessary items, besides manuals, are
teaching aids, curricula, equipment lists and
ways of recording and reporting, together with
methods of evaluating both the knowledge
of trainees and the quality of the services
they provide. A package should also contain
methods of supervising the workers applying
it, and of introducing it on a service scale.
Norms are needed for costs and output per
worker. Some measure of its epidemiological
impact is also required, where this is observa
ble. The items in this heterogeneous list are
conveniently called ‘components’, and all
relate in some way to the particular group of
interventions forming a package. A health
care package can thus be defined as an inte
grated set of components assisting the application of
a particular group of interventions for the improve
ment of health care under specific socioeconomic
conditions.
‘Health care packages’ are becoming fash
ionable and mean different things to different
people. Very often they are taken to mean
merely a particular mix of services, such as
a certain combination of child care and
family planning, and the idea of several inte
grated components serving a selected set of
interventions is lacking.
The real purpose of a package stems from
the postulate that, although individual com
ponents are useful by themselves, their com
bined effect is likely to be more than merely
additive. Thus a kit of laboratory equipment
or a manual is little use alone, but integrated
with one another and used together they may
be very valuable. Great emphasis is placed
on the components being complete and inte
grated. Thus, if a particular item of equip
ment is described in a manual, it has got to
be in a government’s medical stores list.
The components have also to be complete,
in the sense that a child care manual has to
specify all the knowledge that a worker re
quires in this field.
This is not the place to go much further
into packages from the point of view of the
health services, except to say that their
boundaries are largely a matter of administra
tive convenience and that it is at the bottom of
the scale that they promise to be so useful,
because it is here that such a vast quantity of
services are required. This is also where welldesigned packages can in some measure aug
ment scarce technical, administrative and
educational skills, and help to make up for
limited opportunities for communication.
Higher up the technological scale these cons
traints are so much less severe that packages
lose their point. One of the great opportuni
ties of a package is that it enables great atten
tion to be concentrated on the many small
details upon which successful health care ulti
mately depends —an attention which they
seldom get. Packages promise to be useful
administrative and educational tools that can
save hard-pressed administrators and teachers
much trouble. They also throw into sharp
relief the technical deficiencies which now so
greatly hinder services. For example, one
such deficiency that has come to light in the
attempt to put together a child care package
is that there is still no account in English of
how a medical auxiliary should examine a
child.
Thus cpackages’ have the unique advantage they
that are at the same time both an exact way of defin
ing rights in personal health care, and a valuable
administrative tool for implementing them.
Fig. 4. The access of the population in a develop
ing country to different technological
levels of health care.
WHICH PACKAGES MIGHT BE CONSIDERED A
HUMAN RIGHT?
We are now in a position to consider
which group of packages might be practically
attainable as a human right. In view of the
extreme economic constraints of so many
countries, packages for the delivery of out
patient rather than in-patient care deserve
priority, some of the cheapest and most effec
tive interventions being those for the preven
tion or treatment of infectious disease. Hu
man rights in maternal and child health
should come high on the list. A very strong
case can also be made out for the provision of
simple operating facilities, and such surgical
interventions as should be within the capacity
of a general duty medical officer, especially
those required for trauma and operative obste
trics. Much progress towards the develop
ment of such a surgical package has indeed
already been made. The technical quality
of medicine at this level is greatly increased
by the provision of simple laboratory methods,
and of surgery by the availability of blood
transfusion.
WHO IS GETTING HIS RIGHT AND WHO IS NOT?
Fig. 4 is a graph in which the ordinate is
a composite scale derived from the scales in
Fig. 2, and represents the cost and comple
xity of the interventions available to a patient.
The abscissa is the percentage of the popu
lation enjoying care at a particular level. If
we assume that a patient having access to a
certain intervention also has access to the
interventions below it in the scale, then it is
possible to show the care provided by diffe
rent types of health unit, and that enjoyed by
societies with different health care patterns.
Fig. 4 shows the technological levels of care
ideally provided by health centres and by
district, regional and national hospitalts. It
also shows the hypothetical pattern for a
developing country where a small elite have
access to almost any intervention, if necessary
by going abroad for it, while more than half
the population have no access to the modern
means of health care at all.
Fig. 5 shows what the graph would look
like for two hypothetical countries with highly
Fig. 5
cost and
complexity
industrial country with highly'
egalitarian health care distribution
technological
level of tne
interventions
accessible to
HUMAN RIGHT ?
developing country with highly
egalitarian health care distribution
Percentage of the population having’
access to a particular level of care
Fig. 5. Two egalitarian patterns of distribution of
health care.
egalitarian health care patterns, one industrial
and the other developing, and also where the
human right might come on such a graph.
Percentage of the population having
access too particular level of care
Fig. 6. The use of indices to measure the profile
of access to health care.
If a graph of this kind is to be useful it
has to be obtainable by observation, and for
this indices or markers are required at the
varying technological levels, as shown in Fig.6
—the lower levels being of particular interest
for a definition of human rights. One of the
advantages of defining these rights in terms of
packages is that, if they contain suitable
tracers or markers, it should be comparatively
easy to know who is enjoying them and who is
not. In child care, for example, the possession
of a weight chart is an ideal marker, and all
the less-privileged children in developing coun
tries need one. If the issue of a weight chart
forms part of a mother and child health pack
age, then its possession by a child is good
evidence that he has access to the rest of the
package, should he need it. Data on who
possesses a weight card could readily be
obtained during a census.
Other markers will be required for packages
defining ambulatory adult care, and for in
patient services at The level of the district
hospital.
It would also be useful to have
markers at other points on the technological
scale beyond those which it is realistic at
present to consider as possible human rights.
For example, access to contrast radiography
promises to provide a useful marker for com
paratively sophisticated services. Patients are
referred for it from a wide range of specialist
departments, and if the distribution of income
among the people getting this investigation
matched that of the population as a whole, it
could be assumed that all sections of the pop
ulation had equal access to a wide variety of
sophisticated interventions. The neccessary
data would not seem unduly difficult to
obtain.
Fig. 7 shows the directions in which poli
ticians and the major political factions within
medicine would like to see money spent, the
tension between them being particulary acute
in the developing countries. In many countries
the large, conservative, hospital-based, tech
nologically preoccupied group seek to spend
the money on raising the peak level of care for
the privileged. The smaller, socially committed
and more community-oriented minority would
like to see it spent to enable more people to
attain a minimum level of care, and thus obtain
their human rights.
Fig. 7. The tensions over priorities for development of health services.
RIGHTS IN RESPECT OF QUALITY
FROM PACKAGES TO RIGHTS
In personal health care ‘quality’ is at least
as important as ‘quantity’. Few things are
more difficult to measure but is proba
bly easiest
to measure the comparati
vely simple services with which we are
concerned. If the way things should be done
is completely specified, and a pattern of ‘good
medicine’ defined as part of a package, the
care provided is much more susceptible to
observation in the interests of quality contiol.
If, for example, a package requires that dehy
drated children be rehydrated in a clinic with
an oral rehydration set, then the presence or
absence of such a set is a measure of the quality
of this particular intervention. If the package
requires an auriscope which works, its presence
in a working condition is another measure of
quality. Other and more important indicators
of the quality of care are how many days a
week a clinic is open, and whether the growth
of all children is monitored on a chart. The
use of an objective, weighted quality score
promises to make it possible to arrive at a very
useful indication of the quality of care given by
a particular clinic. It must, however, be closely
related to what is practicable, be decided on
with the participation of the health workers,
and be used more as a ‘team game’ than a
threat of sanctions. The level of a worker’s
knowledge also provides another oblique indi
cation of the quality of his services. Thus, if the
objective examinations forming part of a pack
age show a health worker to have little
understanding of what he is about, then the
quality of the care he provides is likely to be
low. If his understanding is better, his per
formance is likely to be better also. Even
though none of these indicators are absolute
measures of the quality of care, they are all in
some degree an estimate of it. In aggregate
they promise to be useful, but only where
‘good medicine’ has been carefully specified
and packaged.
One of the first steps is the national
recognition by the medical profession of the
technical quality of the Packages that might
constitute a human right. Every sentence in
their manuals and every procedure and drug
will have to be scrutinized. Will it be agreed,
for example, that a combination of penicillin
and streptomycin is to be advised for newborn
children with septicaemia when every paedi
atrician thinks that ampicillin and cloxacillin
are better—and more expensive? The national
adoption of a package requires agreement by
the leaders of the profession and the govern
ment that the package epitomizes good
medicine’under their particular socioeconomic
circumstances. But a national consensus is a
different thing from an international one, and
this is what will have to be achieved if a use
ful definition of human rights is ever to be
widely accepted. Here we are up against the
great cultural variations between different
national patterns of medicine, and any agreed
system of even elementary medicine will be
difficult to reach. As a result, sponsorship
and promotion by the appropriate international
organizations will not be achieved lightly.
Perhaps the continued experience of a number
of countries with closely related packages will
pave the way for the subsequent international
recognition of those representing human rights
in personal health care. It seems likely that
we shall have to proceed from packages to
rights, and not vice versa, because it is only
as packages that rights can be manipulated.
In ten years’ time it will be good to hear a
director of medical services say that his clinics
employ the ‘Human Rights Child Care
Packages, Mark VIT and that 97% of the
children in his country have access to it.
- Media
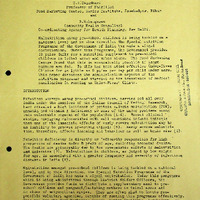 RF_NGO_2_SUDHA.pdf
RF_NGO_2_SUDHA.pdf
Position: 1749 (11 views)