BASIC INFORMATION ON ALCOHOL
Item
- Title
- BASIC INFORMATION ON ALCOHOL
- extracted text
-
I
Page 1 of 3
Chapter 1, Medical Students' Handbook - Medical Council on Alcohol RF_MH_2_C_1_SUDHA
THE MEDICAI. COUNCIL ON ALCOHOIUS
■
'9
MEDICAL STUDENTS’ HANDBOOK: ALCOHOL & HEALTH (3rd Edition
ii
Introduction
1. Facts about Alcohol Content of Drinks
1. Facts about alcohol content
of drinks
The Unit System
2. Alcohol metabolism
3. Predisposition to harm
4. Alcohol-related physical
harm
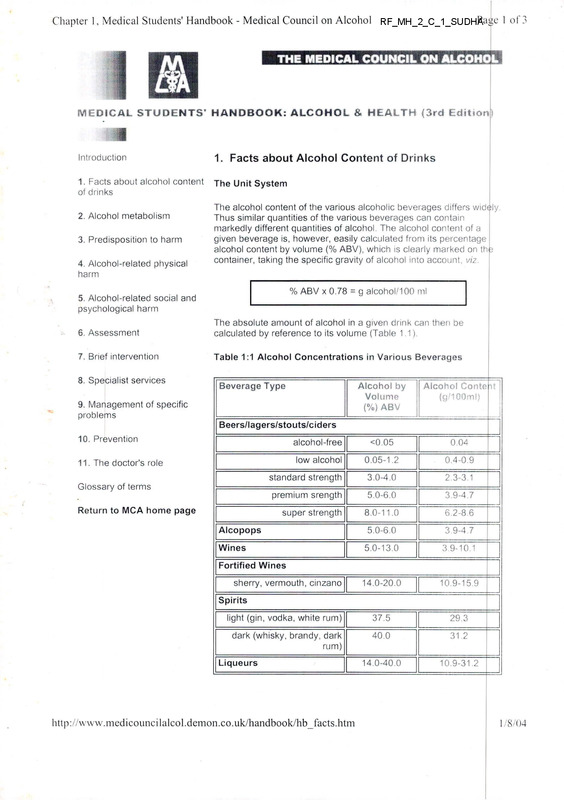
The alcohol content of the various alcoholic beverages differs widely.
Thus similar quantities of the various beverages can contain
markedly different quantities of alcohol. The alcohol content of a
given beverage is, however, easily calculated from its percentage
alcohol content by volume (% ABV), which is clearly marked on the
container, taking the specific gravity of alcohol into account, viz.
% ABV x 0.78
5. Alcohol-related social and
psychological harm
g alcohol/100 ml
6. Assessment
The absolute amount of alcohol in a given drink can then be
calculated by reference to its volume (Table 1.1).
7. Brief intervention
Table 1:1 Alcohol Concentrations in Various Beverages
8. Specialist services
Beverage Type
9. Management of specific
problems
Alcohol by
Volume
(%) ABV
Alcohol Conte it
(g/100mlj
Beers/lagers/stouts/ciders
10. Prevention
alcohol-free
<0.05
0.04
11. The doctor's role
low alcohol
0.05-1.2
0.4-0.9
standard strength
3.0-4.0
2.3-3.1
premium srength
5.0-6.0
3.9-4.7
super strength
8.0-11.0
6.2-8.6
Alcopops
5.0-6.0
3.9-4.7
Wines
5.0-13.0
3.9-10.1
14.0-20.0
10.9-15.9
light (gin, vodka, white rum)
37.5
29.3
dark (whisky, brandy, dark
rum)
40.0
31.2
14.0-40.0
10.9-31.2
Glossary of terms
Return to MCA home page
Fortified Wines
sherry, vermouth, cinzano
Spirits
Liqueurs
http://www.medicouncilalcol.demon.co.uk/handbook/hb_facts.htm
1/8/04
Chapter 1, Medical Students' Handbook - Medical Council on Alcohol
Page 2 of 3
In order to simplify the quantification and hence to facilitate
assessment of alcohol intake, a system, based on defining quanti ies
of beverages containing equivalent amounts of alcohol has been
devised for use in Great Britain. A 'unit' of alcohol is the amount
contained in 1/2 pint (284 ml) of beer, a single glass (125 ml) of tsble
wine, a single glass (50 ml) of fortified wine, for example sherry, or a
single measure (25 ml) of spirits; it approximates to 10 ml or 8 g of
absolute alcohol.
■........................................................... )
o
X
. -E,
half pint
beer
glass
wme
glass
sherr/
L.J
single
measure
spirts
uni’
Inaccuracies of the Unit System
This system is now used widely by the lay public, by 'alcohol
agencies' and by physicians alike. As currently publicized, however,
it is greatly over-simplified.
• the alcohol content of beers and lagers varies considerably
(see Table 1.2) so that a pint of beer (568 ml) may contain
from 2 to 5 units of alcohol depending on its strength
• second, beers and lagers, particularly for off-licence
consumption, are sold in cans, in volumes varying from 330 to
440 or 500 ml, which bear little relationship to the pint
measure
• there is no standardized measure for wine; a 'glass' may
contain from 4 to 12 fluid ounces (114 to 342 ml) and so,
depending on the alcohol content of the wine, from 0.6 to 4.5
units
• until recently the standard 'pub' measure of spirits varied from
1/6 to 1/4 gill (24 to 37 ml) by region; European Community
directives have now ensured that the measure is standardized
to 25 or 35 ml
• measures of drinks consumed at home differ from 'standard'
measures; beer is consumed from bottles or cans in varying
volumes, wine measures tend to be larger while measures of
spirits tend to exceed optic measures by a factor of 2.5 to 2 .0
• the unit system is essentially parochial and does not lend itself
to international comparisons; thus, in Australia and New
Zealand, a 'standard' drink contains 13 ml or 10 g of absolute
alcohol while in the United States of America, a 'standard'
drink contains 15 ml or 12 g of absolute alcohol.
Improving Accuracy
http://www.medicouncilalcol.demon.co.uk/handbook/hb_facts.htm
1 /8/04
Chapter I, Medical Students’ Handbook - Medical Council on Alcohol
Paue 3 of 3
The accuracy of the 'unit' system can be improved by taking
differences in beverage strengths and volumes into account. Thus,
the exact number of units of alcohol in a given beverage volume can
be calculated from the % ABV using the information that 10 ml of
absolute alcohol is equivalent to 1 unit of alcohol. Thus the number
of units of alcohol in a given volume of beverage equals:
% ABV x volume (ml)
1 000
A half-litre can of 8% ABV lager contains 4 units of alcohol
( % x 500 V likewise, a 750 ml bottle of 13% ABV wine contains 9.8
1000
units of alcohol 1 3 x 750 (Table 1.3).
1 000
Newer Drinks
In recent years new ranges of fortified wines, such as MD 20/20 and
Mad Dog, strong white ciders, such as Diamond White and Ice
Dragon, fruit-flavoured lagers and ciders, such as Desperados and
Maxblack and alcoholized soft drinks, the co-called 'Alcopops'. such
as Hooch alcoholic lemon, have been marketed. The fortified wines
have sweet fruit flavours such as cherry, banana and strawberry and
a % ABV of between 13 and 21%. The white ciders, which are
filtered to remove colour and some flavours, have a % ABV of
between 8 and 9%. The lagers and ciders which are additionally
flavoured with citrus fruits or blackcurrant and the 'Alcopops' which
are essentially soft drinks which have been 'fortified' with alcohol
have a % ABV of between 5 to 6%. These drinks are attractively
packaged, often in small volumes, which may nevertheless contain
several units of alcohol. Their obvious appeal to young people has
become a focus of public concern.
© MCA, 3 St Andrew's Place, Regent's Park, London NW1 4LB. Registered charity no 265242
Tel: + 44 (0)20 7487 4445 Fax: + 44 (0)20 7935 4479 e-mail: mca@medicouncilalcol.demon.co.uk
Webmaster: Dr Guy Ratcliffe Website design: Karen Widdowson
http://www. medicounci lalcol. demon, co. uk/handbook/hb_facts.htm
1/8/04
Chapter 2, Medical Students' Handbook - Medical Council on Alcohol
F I
Page 1 of4
THE MEDICAL COUNCIL ON ALCOHOL/]
jt ‘J *
MEDICAL STUDENTS’ HANDBOOK: ALCOHOL a HEALTH (3rd Edition)
*■
Introduction
2. Alcohol Metabolism
1. Facts about alcohol content
of drinks
Once ingested, ethanol is rapidly absorbed from the upper
gastrointestinal tract. The majority is then oxidized, primarily in the
liver; only 2 to 10% is eliminated in urine and breath. Hepatocytes
contain three pathways for ethanol metabolism: the alcohol
dehydrogenase (ADH) pathway in the cytosol; the microsomal
ethanol oxidizing system (MEOS) located in the smooth endoplasm c
reticulum and the catalase pathway located in peroxisomes (Figure
2:1).
2. Alcohol metabolism
3. Predisposition to harm
4. Alcohol-related physical
harm
Figure 2:1 The Metabolism of Ethanol
5. Alcohol-related social and
psychological harm
Ethanol
6. Assessment
7. Brief intervention
8. Specialist services
▼
MEOS
(CYP2EI)
9. Management of specific
problems
ADH
M
Catalase
Acetaldehyde
10. Prevention
11. The doctor's role
ALDH
Glossary of terms
Return to MCA home page
Acetate
Carbon dioxide
ADH
ALDH
MEOS
(CYP2E1
Water
- alcohol dehydrogenase
- a cet aide h yd e d e h yd r o g e n a se
- rni c ro s o rn a I eth a n o I o x i d i zi n g sy st e rn
- cytochrome P450 isoform)
ADH, which exists in multiple molecular forms, catalyses the
conversion of ethanol to acetaldehyde. An 'atypical' ADH has been
http://www.medicouncilalcol.deiTion.co.uk/handbook/hb_meta.htm
1/8/04
Chapter 2, Medical Students' Handbook - Medical Council on Alcohol
Page 2 of 4
identified in between 5 to 20% of Europeans but in 90% of Mongoloid
individuals. Although this isozyme shows a 7-fold increase in activity
in vitro its presence is not accompanied by an acceleration of ethanol
metabolism in vivo.
MEOS activity has now been attributed to CYP2E1, an isoform of
cytochrome P450. Its role in ethanol metabolism in non-habitual
drinkers is probably small, at least when circulating ethanol
concentrations are low. Catalase does not appear to play a major
role in ethanol oxidation, at least under physiological conditions.
Acetaldehyde dehydrogenase (ALDH)
Acetaldehyde is oxidized to acetate by the activity of the enzyme
acetaldehyde dehydrogenase (ALDH). Two major isoforms of ALDH
have been identified which play a major role in hepatic acetaldehyde
metabolism; of these the mitochondrial form (ALDH2) is the more
important. The ALDH2 gene is of considerable interest because it
occurs in two polymorphic forms; the 'wild' type gene encodes the
active enzyme whereas the 'mutant' form encodes an inactive
enzyme. The mutant allele is rarely observed in Caucasians but is
found in some 40% of Orientals; it is inherited as an autosomal
dominant. Individuals carrying the mutant allele have a markedly
reduced capacity to metabolize acetaldehyde and the resultant
increase in circulating acetaldehyde concentrations produces
general vasodilatation with a striking facial flushing response. The
acetate produced as a result of acetaldehyde oxidation is rapidly and
safely metabolized to carbon dioxide and water.
Blood ethanol concentration
Peak blood ethanol concentrations are attained approximately one
hour after ingestion. A number of factors influence the levels
attained, including the speed at which the beverage was drunk,
whether it was consumed together with food, the rate of gastric
emptying and body habitus.
Women attain consistently higher blood ethanol concentrations than
men following a standard oral dose of ethanol because their body
water, and hence the compartment in which the ethanol distributes,
is significantly smaller than in men (Figure 2.2).
Figure 2:2 Gender Differences in Ethanol Metabolism
http://www.medicouncilalcol.demon.co.uk/handbook/hb_meta.htm
1/8/04
Chapter 2, Medical Students' Handbook - Medical Council on Alcohol
Page 3 of 4
90 -i
so
70
•— Males (n=10)
!
i 60
Females (n=9)
o
E!
O
E 50
o
G
ts
£
’E
40
I
o 30
5
20
10
0
0
2
1
3
4
Time (hours)
Blood ethanol concentrations following a standard dose of ethanol
of 0.5g4tg body weight in healthy men and women
source: Marshall at al, Hepatology 1983; 3:701-706
Ethanol is eliminated from the body at a rate of 7 to 10 g (1 unit) an
hour. Blood ethanol concentrations may, therefore, remain elevated
for considerable periods following ingestion. Thus, if an individual
imbibes 6 pints of premium strength beer (18 units) during an
evening, then ethanol will still be detectable in their blood at 11.00
a.m. the following day (Figure 2:3).
Figure 2:3 Time Course of Ethanol Elimination
http://www.medicouncilalcol.deiTion.co.uk/handbook/hb_meta.htm
1/8/04
Page 4 of 4
Chapter 2, Medical Students’ Handbook - Medical Council on Alcohol
300 -I
cn
E
200
3
c
W
£
•o 100
Q
E
0 1----12
2
4
6
8
10
midnight
12
midday
Time (hours)
Ethanol elimination in a non-habitual drinker following ingestion of
150g in the four hours before midnight
The rate limiting factor in the metabolism of ethanol is the
dissociation of the NADH-ADH enzyme complex. The ADH-media ed
oxidation of ethanol results in transfer of hydrogen to the co-factor
NAD converting it to its reduced form NADH. The rate of ethanol
oxidation is, therefore, determined by the capacity of the liver to re
oxidize NADH. Chronic alcohol misuse is associated with an
increase in the metabolic rate for ethanol as a result of induction of
the MEOS system; under these circumstances this alternative
pathway can account for up to 10% of ethanol oxidation.
The oxidation of ethanol generates an excess of hydrogen
equivalents in the liver, primarily as NADH. If the ability of the
hepatocyte to maintain redox homeostasis is overwhelmed, then r
number of metabolic disturbances may arise including hypo- or
hyperglycaemia, lactic acidosis, ketoacidosis, hyperuricaemia,
abnormalities of hepatic lipid metabolism and alterations in the
metabolism of galactose, corticosteroids, serotonin and other
amines.
© MCA, 3 St Andrew’s Place. Regent's Park, London NW1 4LB. Registered charity no 265242
Tel: 44 (0)20 7487 4445 Fax: + 44 (0)20 7935 4479 e-mail: mca@medicouncilalcol demon.co uk
Webmaster: Dr Guy Ratcliffe Website design: Karen Widdowson
http://www.medicouncilalcol.demon.co.uk/handbook/hb_meta.htm
1/8/04
Chapter 3, Medical Students' Handbook - Medical Council on Alcohol
1
Page 1 of 8
THE MfzDICZAL COUNCiL ON ALCOHOL |
MEDICAL STUDENTS’ HANDBOOK: ALCOHOL & HEALTH (3rd Edition
li
Introduction
3. Predisposition to Harm
1. Facts about alcohol content
of drinks
The aetiology of problem drinking can be usefully understood by
employing the classical medical constructs of agent (alcohol), host
(the drinker), and environment. Although the relationships within this
pathogenic system are not fully understood, they do provide pointe rs
to causation, early recognition and prevention of alcohol-related
problems.
2. Alcohol metabolism
3. Predisposition to harm
4. Alcohol-related physical
harm
5. Alcohol-related social and
psychological harm
6. Assessment
7. Brief intervention
8. Specialist services
9. Management of specific
problems
10. Prevention
11. The doctor's role
Glossary of terms
Return to MCA home page
Alcohol, the Agent
Alcohol taken in any amount may be harmful if the time and situati sn
are inappropriate, for example, when driving. Indeed, the risk of
sustaining alcohol-related injuries begins to increase with blood
ethanol concentrations as low as 20 mg/100 ml (4.3 mmol/l). It is
impossible, therefore, to identify a level of alcohol consumption the t
can be described as 'safe'. In the 1980s, however, the Royal
Colleges of Psychiatrists, Physicians and General Practitioners
sought to define more clearly the relationship between levels of
alcohol consumption and the development of alcohol-related physical
harm, excluding injuries. The consensus opinion was that, in men.
intakes of alcohol of 21 units a week or less and, in women, of 14
units a week or less are associated with a 'low risk'. Intakes of
between 22 and 50 units a week in men and between 15 and 35
units a week in women, described as hazardous drinking, are
associated with an 'intermediate risk', while intakes of >50 units a
week in men and of >35 units a week in women, described as
harmful drinking or alcohol misuse, are associated with a 'high
risk' (Figure 3.1). The differences in threshold levels between men
and women reflect the fact that blood ethanol concentrations in
women, following a standard oral dose, are approximately one-third
higher than in men. Intakes in pregnancy should be reduced to 1 tD 2
units, once or twice a week.
Figure 3:1 Alcohol Consumption and the Risk of Physical Harm
http://www.medicouncilalcol.demon.co.uk/handbook/hb_harm.htm
1/8/04
Page 2 of 8
Chapter 3, Medical Students' Handbook - Medical Council on Alcohol
WOMEN
MEN
Sly
50
35
Units
(400g)
per week
Units
(280g)
p e r we ek
( L
21
Units
(■188g)
per week
14
Units
(112g)
p e r we ek
For pregnant women either abstinence or no more than
1-2 unite, once or twice weekly is recommended
Sources:
Roya! College of Psychiatrists, 1986
Royal College of General Practitioners, 1986
Royal College of Physicians, 1987
Sensible drinking
In late 1995, the Government published a review of the scientific and
medical evidence on the health effects of drinking alcohol. The report
set benchmarks for sensible drinking, stating that regular
consumption of 3 to 4 units of alcohol a day for men and 2 to 3 un ts
a day for women will not accrue a significant health risk, whereas
consistently drinking 4 or more units a day for men or 3 or more units
a day for women would be associated with progressive risks to
health. The review also recognised that alcohol conferred protection
from coronary heart disease in middle-aged men taking 1 to 3 units a
day and in post-menopausal women taking 1 to 2 units a day.
This report has been interpreted as 're-setting' the 'low risk' levels to
28 units a week for men (4 x 7) and 21 units a week for women (3 x
7) but these are also the levels at which health risk is said to
increase. Many medical and alcohol agencies were unhappy with
these recommendations although recognising the benefit of setting
daily limits. In consequence, there does not appear to be any
compelling reason, at present, to change the low-risk thresholds from
those originally set by the three Royal Colleges.
The availability of the stronger beers and lagers has made it more
http://www.medicouncilalcol.demon.co.uk/handbook/hb_harm.htm
1/8/04
Chapter 3, Medical Students' Handbook - Medical Council on Alcohol
Pag - 3 of 8
difficult for individuals to be sure how many units of alcohol they are
consuming. However, the inclusion of % ABV on beverage labels
may allow a more accurate assessment (Table 3:1).
Table 3:1 Number of 440ml Cans of Beers Containing 14 and 2 I
Units of Alcohol
Beverage
ABV (%)
Number of 440ml Cans
14 Units
21 Units
Standard
3.6
9
14
Premium
5.0
6
9
Super
9.0
3.5
5
”1
Alcohol consumption in Great Britain
In 1998, the average weekly consumption of alcohol by men aged 1 6
years and over, in Great Britain, was 16.4 units, while women dran<
on average 6.4 units. Overall, 27% of men and 15% of women drank
in excess of the recommended 'low risk' levels of 21 and 14 units a
week, while 6% of men and 2% of women drank in excess of 50 ar d
35 units a week respectively (Figures 3.2 and 3.3)
Figure 3:2 Level of Alcohol Consumption in the Adult
Population, Great Britain, 1998
Men
Women
unitslWeek
□ None
□ <1
6%
□ 1-10
4%
□ 11-21
□ 22-35
ii 36-50
■ >51
unitsiweek
2%i
8%
6%
I
21 %o
3%1(
8%.
1
□ Norn?.
14%
□ <1
10%X
□ 1-7
16%
19%
□ 8-14
□ 15-25
□ 2b-j 5
..Z37%
36%.
ffl >36
Source: ONS - General Household Survey, 1998
Figure 3:3 Percentage of Adults Drinking Over Weekly
Threshold Levels, Great Britain, 1998
http://www.medicouncilalcol.demon.co.uk/handbook/hb_harm.htm
1/8/04
Page 4 of 8
Chapter 3, Medical Students' Handbook - Medical Council on Alcohol
Men
E >21 units/wk
□ >50 units/wk
10
o >14 units/wk
Women
□ >35 units/wk
20 -1
10
0
IHllII
84
86
88
90
92
94
96
98
Source: ONS - General Household Survey, 1998
The Host
Personality
There is no typical personality which predisposes to alcohol
problems. Some problem drinkers undoubtedly have damaged
personalities but it is difficult to know whether this is the
consequence or cause of heavy drinking. Evidence suggests that
younger male problem drinkers are more likely to have severe
personality disturbances; they may drink excessively as a means cf
holding on to a precariously-held image of masculinity, and may
have fathers who were themselves delinquent or problem drinkers
Individuals who are anxious, including those with phobic anxiety
states, appear particularly vulnerable to alcohol misuse, and the
association between depressive states, particularly in women, and
alcohol dependence has long been recognized. Individuals with a
psychopathic personality, characterized by impulsiveness, an
inability to defer gratification and an inability to form close emotional
ties, also appear to find alcohol rewarding and are immoderate in
their drinking, as they are in many other aspects of their lives.
Thus, despite decades of research, no evidence has emerged to
support the belief that there is a typical addictive personality. The
characteristic features so frequently encountered in problem drinkers
are more likely to be the consequences of years of excessive
drinking rather than the cause. Certain traits, particularly associated
with anti-social personality disorder, are however conspicuously
common in the life histories of patients with alcohol problems.
Inheritable Factors
It is now generally accepted that 'alcoholism' runs in families. Indeed,
http://www.medicouncilalcol.demon.co.uk/handbook/hb_harm.htm
1/8/04
Chapter 3, Medical Students' Handbook - Medical Council on Alcohol
Pag35 of 8
it has been estimated that one in three 'alcoholics' have at least one
parent similarly afflicted. Those individuals with a positive family
history, who themselves misuse alcohol, tend to drink earlier in life
and to experience more alcohol-related problems than their
counterparts without a family history. However, simply because a
trait is familial does not mean that it is genetically inherited as
environmental cues may be necessary for its expression.
Twin studies can be used to assess the relative strengths of the
genetic and environmental components of phenotypic variance.
Monozygotic twins (MZ: identical) are genetically identical whereas
dizygotic twins (DZ: fraternal) share only half their genes. Thus, if a
trait has a genetic component the concordance rates will be greate;
amongst MZ twins than DZ twins. In the majority of twin studies on
alcohol-drinking behaviour and 'alcoholism' greater concordance has
been observed in MZ twins. Hereditability estimates of about 0.3 to
0.6 for the amount and frequency of alcohol consumption have bee i
obtained by most investigators where a factor of zero indicates no
genetic influence and a factor of one indicates total genetic control
The results of twin studies do not completely exclude environmental
effects. Identical twins may, for example, have a higher frequency cf
social contact than fraternal twins but when controls are exercised
for this variable the higher concordance observed for drinking
behaviour in MZ twins remains.
Adoption studies can also be used to separate genetic and
environmental factors in phenotype variance. Such studies have
shown that the frequency of 'alcoholism' in later life is three to four
times greater in adopted-away children who have at least one
'alcoholic' biological parent. Studies on adopted men suggest the
existence of at least two different types of 'alcoholism' based on the
clinical features of the parents.
Types of alcoholism
• Type I 'alcoholism' affects both men and women and is more
common than Type II 'alcoholism'. It is 'milieu-limited' as its
expression requires both a genetic predisposition and
environmental provocation; if both these factors are present
then the risk of 'alcoholism' is doubled. Type I alcohol abuse
begins after the age of 25 years; it is generally classified as
mild and legal problems are only infrequently encountered. I
is associated with a history of mild alcohol misuse in either
biological parent.
• Type II 'alcoholism' is male-limited. Environmental factors
appear to play little role in its expression; genetically
predisposed men have a nine-fold increase in their risk of
developing 'alcoholism'. Type II alcohol misuse begins in
adolescence; it is classified as serious and is associated with
frequent encounters with the law. The personality of these
individuals is characterized by impulsivity, excitability, brash
and uninhibited behaviour, and disturbed social relations. It is
associated with severe 'alcoholism' in the biological father
Genetic studies in the future
http://www.medicouncilalcol.demon.co.uk/handbook/hb_harm.htm
1/8/04
Chapter 3, Medical Students' Handbook - Medical Council on Alcohol
Page 6 of 8
Thus, twin, adoption, family hereditability and genetic transmission
studies indicate that genetic factors play a role in the predisposition
to 'alcoholism'. However, a number of important questions remain,
viz-, (i) what are the heritable traits that influence susceptibility to
'alcoholism'?; (ii) what are the genes that control the traits? and; (iii)
could reliable trait markers be found that, would be predictive of the
development of 'alcoholism'?
Unlike disorders with simple Mendelian modes of inheritance,
'alcoholism' is likely to have a much more complex mode of
transmission. Moreover, the ultimate phenotype might be influenced
by environmental factors. This complexity, compounded by the
likelihood that there is more than one genetic type of 'alcoholism' will
make the task of identifying the genetic component extremely
difficult. Nevertheless, this line of research is being actively pursued.
Genetic studies may, in addition, help to differentiate subtypes of
problem drinkers who may respond differently to treatment and
hence may have different outcomes. For example, some 'types' may
respond better to specific drug treatments than others, perhaps
reflecting differences in the neurochemical responses to alcohol
misuse.
An ability to identify individuals genetically predisposed to alcohol
problems raises the possibility of targeting educational and
preventive approaches. The ethical dilemmas posed by such
information require careful consideration.
The Environment
A variety of environmental factors impinge on the individual and
influence their consumption of alcohol. These include the availabil ty
of alcoholic beverages and the prevailing climate of expectations,
traditions and customs.
Culture
Alcohol is proscribed in certain cultures, for example Islam. Under
these constraints, any drinking is in a sense deviant and there is
some evidence that those who do drink in a predominantly abstinent
culture are more likely to be disturbed and to drink abnormally. Some
cultures, for example, the Irish, are intensely ambivalent about
alcohol and combine a high level of traditional condemnation of
drinking and a high prevalence of abstainers with an acceptance c nd
even the promotion of widespread alcohol use.
Parental Influence
The double standard whereby parents and other authorities often
endeavour to prohibit drinking amongst young people, while
conveying by their actions that it is acceptable 'adult' behaviour, o ily
serves to make alcohol seem more attractive to young people as a
means of marking their own transition to adulthood.
Parents pass on their beliefs and attitudes to their children. These
include their drinking habits and views about alcohol. Adolescents
who grow up in a home where alcohol is assigned disproportionate
significance are more likely to drink abnormally themselves.
http://www.medicouncilalcol.demon.co.uk/handbook/hb_harm.htm
1/8/04
Chapter 3, Medical Students'Handbook - Medical Council on Alcohol
Pcge 7 of 8
Paradoxically this holds true both when the parents are strongly 'anti
drink' and where one or both parents have a drinking problem. It
seems that in such homes drinking becomes part of the emotiona
currency of the family. One consequence of this, coupled perhaps
with a degree of biological vulnerability, is that alcohol addiction is
four times more common among the sons of problem drinkers than in
the general population. The family doctor is obviously particularly
well placed to try and prevent the tragedy of alcohol misuse passing
from one generation to the next by educating those at risk and by
early detection of alcohol problems should they arise.
Peer Group Influences
The peer group becomes increasingly important in adolescence and
this can have a major effect on the pattern and quantity of alcohol
consumed as well as the choice of beverage.
Availability
If alcohol is readily to hand, it is more likely to be drunk. Cost is also
very important. In relative terms alcohol has become cheaper in
recent years. Thus, between 1950 and 1976 the length of time a
manual worker needed to work to pay for a pint of beer fell by 48%
from 23 to 12.5 minutes; the work time to pay for a bottle of whisk /
fell even further from 6.5 to 2.5 hours, a 68% reduction. The time
needed to pay for a loaf of bread, on the other hand, increased by
22% during this period. Individuals with high disposable incomes and
those who have easy access to alcohol, or whose drinking is
subsidized, are more at risk of developing alcohol-related problems
(Table 3:2).
The origins of a harmful drinking pattern are. therefore, multifactorial
(Figure 3:4). The influences interact and may promote or diminish
the likelihood of problem drinking.
Figure 3:4 Aetiological Factors in Problem Drinking
Alcohol
Dose pattern
Genetics
Occupation
>•
Personality
Availability
Individual
4
Advertising
Peer Group
4
t
Biological vulnerability
P fry sig ue/He altfr/G en de r
F amity
4
Religion
Tradition
http://www.medicouncilalcol.demon.co.uk/handbook/hb_harm.htm
Culture
1/8/04
Chapter 3, Medical Students' Handbook - Medical Council on Alcohol
Page 8 of 8
© MCA. 3 St Andrew's Place, Regent's Park. London NW1 4LB. Registered charity no. 265242
Tel: + 44 (0)20 7487 4445 Fax: + 44 (0)20 7935 4479 e-mail: mca@medicouncilalcol.demon.co.uk
Webmaster: Dr Guy Ratcliffe Website design: Karen Widdowson
http://www.medicouncilalcol.demon.co.uk/handbook/hb_harm.htm
1/8/04
Chapter 4, Medical Students’ Handbook - Medical Council on Alcohol
Fade 1 of 13
THE MEDICAL COUNCIL ON ALCOHOL
MEDICAL STUDENTS’ HANDBOOK: ALCOHOL & HEALTH (3rd Edition)
Introduction
4. Alcohol-Related Physical Harm
1. Facts about alcohol content
of drinks
The possibility that acutely intoxicated individuals may suffer
abdominal discomfort and may injure themselves, intentionally or
otherwise, is generally recognized; less well-recognized is the fact
that they may develop gastrointestinal bleeding, cardiac arrhythmias,
cerebrovascular accidents and respiratory depression, all of which
may prove fatal. Equally, while it is generally acknowledged that
individuals who chronically misuse alcohol may develop, and indeed
die from cirrhosis of the liver, the fact that they may develop damage
to every organ system in the body and that they are just as likely, f
not more likely, to die as a result of suicide or injury, is generally nlot
appreciated. Thus, while both acute and chronic misuse of alcoho
are associated with the development of physical disorders and harm
(Table 4:1), the association between the two is often missed or
ignored.
2. Alcohol metabolism
3. Predisposition to harm
4. Alcohol-related physical
harm
5. Alcohol-related social and
psychological harm
6. Assessment
7. Brief intervention
Table 4:1
Acute and Chronic Effects of Alcohol Misuse
8. Specialist services
Acute
9. Management of specific
problems
Acute
Accidents
and injury
Acute alcohol poisoning
Aspiration
pneumonia
Oesophagitis
Mallory-Weiss syndrome
Gastritis
Pancreatitis
Cardiac arrhythmias
Cerebrovascular
accidents
Neurapraxia
Myopathy/rhabdomyolysis
Hypoglycaemia
10. Prevention
11. The doctor's role
Glossary of terms
Return to MCA home page
Chronic
Accidents and
injury
Hypertension
Peripheral
neuropathy
Oesophagitis
Cardiomyopathy
Myopathy
Gastritis
Cerebrovascular accidents
Osteoporosis
Malabsorption
Coronary heart disease
Skin disorders
Pancreatitis
Brain damage:
Malignancies
Liver damage:
• dementia
http://www.medicouncilalcol.demon.co.uk/handbook/chapter_4.htm
Infertility
1/8/04
Chapter 4, Medical Students' Handbook - Medical Council on Alcohol
• fatty
change
• hepatitis
• cirrhosis
• Wernicke-Korsakoff
syndrome
• cerebellar
Page 2 o f 13
Foetal damage
degeneration
• Marchiafava-Bignami
syndrome
• central pontine
myelinolysis
These deleterious physical effects may be produced by alcohol per
se, by its metabolites, or by the consequences of alcohol metabolism.
However, an individual's susceptibility to develop alcohol-related
physical harm varies considerably. Thus, for example, only between
20 to 30% of individuals who chronically misuse alcohol will
eventually develop cirrhosis. The determinants of susceptibility have
yet to be identified but genetic, constitutional and environmental
factors are all likely to be important. Equally, habitual drinkers who
have sustained alcohol-related harm may remain asymptomatic for
long periods of time or else may present with florid symptoms and
signs at an early stage.
Alcohol-related physical harm is entirely preventable. Thus, every
effort should be made to identity individuals at risk at an early stage.
Once harm has developed in an habitual drinker, it may still be
reversed, to a large extent, by long-term abstinence from alcohol
Even individuals with established alcohol-related physical harm may
benefit significantly, in terms of outcome, if they cease drinking
alcohol completely.
General Features
Individuals who chronically misuse alcohol may develop a number o
cutaneous, and other superficial signs, irrespective of whether they
have sustained major alcohol-related organ damage (Table 4:2). The
mechanisms by which these develop are unknown, but with the
exception of Dupuytren's contractures, they may all regress, at least
partly, following abstinence from alcohol.
Table 4:2 Cutaneous and Other Superficial
Signs Suggestive of Alcohol Misuse
(Click the link for illustrations of each feature)
Spider Naevi
Telangiectasia
Facial Mooning
Parotid enlargement
Palmar erythema
http://www.medicouncilalcol.dernon.co.uk/handbook/chapter_4.htm
1/8/04
Chapter 4, Medical Students’ Handbook - Medical Council on Alcohol
Page 3 of 13
Dupuytren's contracture
Gynaecomastia
Some of these signs may occur in association with other disorders,
for example, spider naevi and palmar erythema in non-alcoholic
chronic liver disease and Dupuytren's contracture in individuals who
sustain repeated, minor hand trauma, but the signs, in constellation,
occur most frequently in association with chronic alcohol misuse aipd.
as such, are extremely important diagnostic features Clubbing of t ne
fingers may also occur. This may occur in any cause of cirrhosis a;
well as in other non-hepatic conditions.
A number of laboratory test abnormalities may occur in chronic
alcohol misusers including elevation of the serum aspartate
aminotransferase (AST) and gamma glutamyl transpeptidase (GG ")
activities and an increase in the erythrocyte mean corpuscular
volume (MCV). These abnormalities arise as a result of alcohol abuse
perse and do not necessarily reflect the presence of significant
alcohol-related organ damage.
Accidents and Injury
Accidental injury constitutes the largest public health problem in the
United Kingdom today for individuals aged 1 to 40 years, and
accounts for more deaths in adolescents than all other causes
Alcohol is a major factor in road traffic and other transport accidents,
industrial and domestic accidents and accidental drownings and fire
injuries. Alcohol is also a major factor in parasuicide, suicide, violent
assault and homicide. Alcohol-related accidents and injuries are
associated with greater morbidity and mortality than all other alcoholrelated disorders (Figure 4:1).
Figure 4:1
Alcohol Consumption and Relative Risk of Death
1.8
1.6 —
I
I
1.4 —
»
All causes
Accidents and violence
Cancer
— Cerebrovascular disease
Coronary heart disease
1.2
........ '
.....
0.8
0.6 -I—
None
<1
1
2
3
4
5
>6
Humber of drinks / day
American Cancer Society prospective study of 276,802 men aged
40 to 59 years followed for 12 years.
http://www.medicouncilalcol.demon.co.uk/handbook/chapter_4.htm
1/8/04
Chapter 4, Medical Students' Handbook - Medical Council on Alcohol
Page 4 of 13
Mortality ratios for the four most common causes of death from all
causes adjusted for age and smoking habits. 1 drink - 12g of
absolute alcohol (1.5 units)
Source: Boffeta and Garfinkle, Epidemiology 1990; 1:342-8
Gastrointestinal System
Oesophagus
Alcohol reduces the sphincter pressures at both ends of the
oesophagus and impedes oesophageal peristalsis. In chronic alcohol
misusers the resultant motor dysfunction may lead to the
development of gastro-oesophageal reflux, oesophagitis, Barrett's
oesophagus and distal mucosal ulceration. Vomiting occurs
frequently and may result in a Mallory-Weiss tear in the mucosa of
the cardio-oesophageal junction; this is associated with
gastrointestinal bleeding, often profuse. There is a strong association
between alcohol misuse and carcinoma of the oesophagus,
particularly in heavy smokers.
Stomach
Acute alcohol misuse may result in the development of acute
gastritis; individuals may complain of nausea, vomiting and epigast'ic
pain but the symptoms settle quickly after 48 to 72 hours abstinence
from alcohol. Sometimes after alcohol acute gastric erosions develop
which may produce severe haemorrhage. Habitual drinking is
associated with the development of chronic gastritis which may be
asymptomatic or else accompanied by a number of non-specific
digestive symptoms. Chronic alcohol misuse is not, however,
associated with an increased prevalence of peptic ulceration; indeed,
alcohol misusers tend to have a lower prevalence of infection with
Helicobacter pylori than non-habitual drinkers; it has been suggested
that alcohol might have an important ami-Helicobacter pylori effect.
Small Intestine
Both acute and chronic alcohol misuse are associated with the
development of diarrhoea; this probably reflects changes in small
intestinal permeability and motor activity. Habitual alcohol misuse is
also associated with defective absorption of a number of nutrients
including glucose, amino acids, vitamins and minerals.
Further information on alcohol and the gastrointestinal tract can be
found in the MCA Newsletter 19 (5).
Pancreas
Click the links to view illustrations
Alcohol misuse may result in the development of chronic pancreatitis.
Some individuals may develop this condition with alcohol intakes as
low as 1 to 20 g/day (< 2 units); others may need to drink in excess Of
200 g/day (25 units) before evidence of the disease develops, while
some individuals never develop this condition no matter how much
they drink or for how long. In susceptible individuals the longer the
http://www.medicouncilalcol.demon.co.uk/handbook/chapter_4.htm
1/8/04
Chapter 4, Medical Students’ Handbook - Medical Council on Alcohol
Page 5 of 13
duration of drinking the greater the risk.
Alcoholic pancreatitis is a disorder mainly of men in their 3rd to Sth
decades. It may present as an acute episode of abdominal pain,
nausea and vomiting and in severe cases can be accompanied by
profound metabolic abnormalities and circulatory collapse which may
be fatal.
These acute episodes may recur, often precipitated by an increase in
alcohol intake. Complications such as pressure on the common bi e
duct, localized leakage of pancreatic fluid and pancreatic exocrine
and endocrine insufficiency may develop resulting in jaundice,
pseudocyst formation, malabsorption and diabetes. In some
individuals, however, the clinical course is insidious with progression
to pancreatic insufficiency without acute inflammatory episodes
Withdrawal of alcohol at an early stage may arrest the process and,
even when the condition is established, may reduce the number o'
inflammatory episodes and allow for better control of both the
exocrine and endocrine insufficiency.
The diagnosis is made using pancreatic function tests and imaging. A
straight X-ray of the abdomen may reveal pancreatic calcification and
endoscopic retrograde cholangiopancreatography (ERCP) will shew
the typical picture of an irregular and attenuated ductal system.
Management is directed at relief of the pain and correction of both the
exocrine and endocrine insufficiency.
Liver
Click the links to view illustrations
Men drinking equal to or greater than 60 g (equal to or greater than
7.5 units) and women drinking equal to or greater than 40 g (equal to
or greater than 5 units) of alcohol daily are at increased risk of
developing alcohol-related liver disease. Alcohol produces a
spectrum of liver injury but only a minority of individuals misusing
alcohol, some 20 to 30%, develop cirrhosis; of these, approximate y
15% will develop hepatocellular carcinoma as a terminal event; the
factors which determine an individual's susceptibility to develop
significant alcohol-related liver injury are unknown
The majority of individuals misusing alcohol will develop fatty change
in their liver; this is an adaptive lesion which arises because of
changes in hepatic fat metabolism linked to the excess hydrogen ion
generated during ethanol oxidation. This lesion is not in itself harmful
and quickly reverses when alcohol is withdrawn. Individuals are
usually asymptomatic and generally present incidentally.
Individuals who develop alcoholic hepatitis may remain asymptomatic
and escape detection unless they present for other reasons.
Alternatively they may present with clear evidence of chronic liver
disease such as jaundice, hepatomegaly and fluid retention.
The outcome in individuals with alcoholic hepatitis is determined by
their subsequent drinking behaviour, their gender and by the
histological severity of their liver lesion. Thus, in men with mild to
moderate alcoholic hepatitis, the liver injury is likely to resolve
http://www.medicouncilalcol.demon.co.uk/handbook/chapter_4.htm
1/8/04
Chapter 4, Medical Students' Handbook - Medical Council on Alcohol
Page 6 of 13
completely with abstinence from alcohol, whereas in women, and in
individuals of both sexes with severe disease, the liver lesion is like y
to progress to cirrhosis, even if they abstain from alcohol long-term
The mortality rate in individuals presenting with severe alcoholic
hepatitis may be as high as 40%. Certain of these individuals might
benefit, in terms of outcome, from a short course of corticosteroids.
Individuals who develop alcoholic cirrhosis may remain asymptomatic
and come to attention only if inadvertently identified, for example, a
an insurance medical examination. Alternatively, they may present
with features of hepatocellular failure and portal hypertension such as
jaundice, fluid retention, blood clotting abnormalities, hepatic
encephalopathy and haemorrhage from oesophageal varices.
The outcome for patients with cirrhosis is determined largely by the
degree of decompensation at presentation and by the subsequent
drinking behaviour. Thus, a middle-aged man who is identified
incidentally and who subsequently abstains from alcohol has a 6O°/8
chance of being alive in 10 years, whereas a similar individual who
presents with variceal bleeding, who survives the initial presentation
but who continues to drink is unlikely to survive a year. The presence
of superimposed alcoholic hepatitis and the development of
hepatocellular carcinoma significantly reduce survival.
The most important management aim is to ensure long-term
abstinence from alcohol. Complications such as fluid retention and
variceal bleeding are treated symptomatically. Orthotopic liver
transplantation has a place in the management of patients with
decompensated alcoholic cirrhosis who have failed to improve
despite well-documented abstinence from alcohol and expert medical
treatment for a period of at least 6 months. Survival rates are simile r
in these patients to those observed in patients transplanted for non
alcoholic disease. However, recidivism rates are still unacceptably
high in some centres.
Further information on alcoholic liver disease will be found in the
article by C Day in issue 21 of The MCA newsletter.
Cardiovascular System
Both acute and chronic alcohol misuse can affect the cardiovascul ar
system.
Haemodynamic/Electrophysiological Effects
Acute alcohol ingestion may be associated with depression of left
ventricular function and the development of ventricular premature
beats even in individuals with ’healthy’ hearts. These acute effects
may be more pronounced and of greater clinical significance in
individuals with pre-existing heart disease.
Further description of the effect of alcohol on the heart will be foun 1
in the article by Obel and Camm, MCA Newsletter Alcoholis. 1998
Volume 17 (3).
Blood Pressure
http://www.medicouncilalcol.demon.co.uk/handbook/chapter_4.htm
1/8/04
Chapter 4, Medical Students' Handbook - Medical Council on Alcohol
Pag? 7 of 13
Alcohol consumption is associated with increases in both systolic and
diastolic blood pressure which appear to be dose-related. Thus,
systolic blood pressure is increased by, on average, 2.7 mmHg in
individuals drinking 4 to 6 units of alcohol/day and by 4.6 mmHg in
individuals drinking equal to or greater than 7 units/day. These
increases in blood pressure reverse when alcohol is withdrawn, at
least in a percentage of individuals.
Heart Muscle
Alcohol-related heart muscle disease or alcoholic cardiomyopathy
develops in a proportion of individuals who have consumed in excess
of 60 g (> 7.5 units) of alcohol/day for a minimum of 10 years.
Individuals with this condition may be asymptomatic and remain
undetected unless discovered incidentally; they may present with
non-specific manifestations of heart disease such as fatigue,
palpitations or breathlessness especially when the heart is stressed
or else may present with frank heart failure manifest as arrhythmias,
raised central venous pressure, cardiomegaly, pulmonary and
peripheral oedema.
The findings on ECG and chest X-ray are non-specific. The
echocardiogram can, however, be used to identify and quantify
chamber dilatation and ventricular function. Confirmation of the
diagnosis is obtained from cardiac catheterization studies and
histological examination of cardiac muscle biopsies.
The cardiac changes in individuals in whom the disorder is subclinical
will reverse entirely with subsequent abstinence from alcohol Death
occurs within 2 to 4 years of the onset of cardiac failure in individu als
who continue to drink; the course of the illness may, however, be
terminated at any stage by the onset of ventricular arrhythmias
particularly in association with an acute episode of drinking.
The most important management aim is to secure life-long
abstinence from alcohol. Symptomatic individuals are managed with
diuretics and with antiarrhythmic agents, as indicated. This form of
low-output heart failure is quite distinct from the high-output heart
failure observed, albeit rarely, in problem drinkers with thiamine
deficiency; this so-called beri-beri heart disease responds well to tie
prompt administration of high doses of thiamine
Coronary Heart Disease
Daily alcohol intakes of 1 to 3 units protect middle-aged men from
coronary heart disease. Much less information is available in womsn,
but daily intakes of 1 to 2 units may similarly protect those who are
post-menopausal.
Cerebrovascular Disease
Both acute and chronic alcohol misuse increase the risk of stroke,
acute alcohol misuse possibly increases the risk of strokes overall
whereas chronic alcohol misuse more especially increases the risk of
haemorrhagic stroke. Individuals who abuse alcohol are at increased
risk of sustaining head injuries and hence of developing both
subdural and extradural haematomas.
http://www.medicouncilalcol.demon.co.uk/handbook/chapter_4.htm
1/8/04
Chapter 4, Medical Students' Handbook - Medical Council on Alcohol
Page 5 of 13
Nervous System
Alcohol misuse can have profound effects on both the central and
peripheral nervous systems; the damage may be caused either
directly, or indirectly as a consequence of thiamine deficiency.
Central Nervous System
Alcohol intoxication, alcohol withdrawal and fitting are described in
Chapter 10. Chronic alcohol misuse is associated with the
development of several organic brain syndromes. Although these are
traditionally described, as here, as distinct entities their clinical
presentation is often heterogeneous and as such they are best
considered as a spectrum which includes minimal cognitive
impairment, amnesia and dementia.
Alcoholic Dementia
Specific cognitive deficits are demonstrable in some problem dnnkeis
which may or may not be accompanied by mild non-progressive
impairment of intellectual capacity. Non-invasive neuroimaging shows
evidence of cortical atrophy or shrinkage with reduction in the volume
of the cerebral white matter. These changes in mental state and
cerebral appearance reverse, to a variable degree, following
prolonged abstinence from alcohol. The term 'alcoholic dementia' with
its connotation of progression has been applied, somewhat
unsatisfactorily, to this condition.
Wernicke-Korsakoff Syndrome
The Wernicke-Korsakoff syndrome develops in problem drinkers who
are thiamine deficient. However, other as yet unidentified factors
must be important in its genesis as thiamine deficiency, in this
context, is not invariably associated with the development of this
syndrome. Wernicke’s encephalopathy comprises a triad of global
confusion, eye signs and ataxia; the confusional state is
accompanied by apathy, disorientation and disturbed memory, but
drowsiness and stupor are uncommon. The ocular abnormalities
include nystagmus, gaze palsies and ophthalmoplegia, while the
ataxia predominantly affects the trunk and lower extremities. The
clinical abnormalities may develop acutely or evolve over several
days. The cerebral lesion is characterized by degenerative changes
in the structures surrounding the third ventricle and aqueduct,
particularly the mamillary bodies. Korsakoff’s psychosis is an
amnesic state in which there is profound impairment of both
retrograde and anterograde memory but relative preservation of other
intellectual abilities; confabulation may be a feature. The cerebral
lesion is characterized by changes in the dorsomedial thalamus.
Korsakoff's psychosis generally develops after an acute episode of
Wernicke's encephalopathy. However, some patients develop a
combined syndrome from the outset, with memory loss, eye signs
and unsteadiness but without confusion; others do not develop either
the eye signs or ataxia.
Treatment with high-dose parenteral thiamine should be instituted
immediately the diagnosis is suspected and prophylactically in
patients at risk (Table 4:3). The Wernicke's encephalopathy resolves
rapidly but resolution of the Korsakoff's psychosis is less predictable:
some residual memory deficit is observed in approximately 50% of
http://www.medicouncilalcol.demon.co.uk/handbook/chapter_4.htm
1/8/04
Page 9 of 13
Chapter 4, Medical Students' Handbook - Medical Council on Alcohol
individuals.
Table 4:3
Treatment of the Wernicke-Korsakoff Syndrome
A presumptive diagnosis of the Wernicke-Korsakoff
syndrome should be made in patients with a history
of alcohol misuse and one or more of the following
otherwise unexplained symptoms: ataxia,
ophthalmoplegia, nystagmus, confusion, memory
disturbance, comatosed/ unconscious,
hypotension, hypothermia
Give two pairs of IV high potency Pabrinex® t.d.s.
for 2 days; dilute ampules 1 and 2 with 50 to 100
ml of normal saline or 5% glucose and infuse over
15 to 30 minutes
No Response
Discontinue and
reassess
Response
One pair of IM
high potency
Pabrinex® o.d. for
5 days or until no
further
improvement is
observed. Use IV
route in patients
with liver disease
and deranged
blood clotting.
Recommendations of the
Committee on Safety of Medicines
Severe allergic reactions may occur during or
shortly after administration of IV Pabrinex®.
• Restrict use to patients in whom parental
administration is essential
• Administer slowly over 10 minutes plus
• Facilities for treatment of anaphylaxis should
be available
http://www.medicouncilalcol.demon.co.uk/handbook/chapter_4.htm
1/8/04
Chapter 4, Medical Students' Handbook - Medical Council on Alcohol
Page 0 of 13
Treatment of Wernicke-Korsakoff Syndrome was further deesribed m
the MCA Newsletter 19 (4)
Cerebellar Degeneration
A cerebellar syndrome characterized by varying degrees of ataxia,
predominantly affecting the trunk and lower limbs, may be observed
in problem drinkers; the upper limbs are little affected and dysarthria
is not a feature. Non-invasive neuroimaging shows atrophy of the
cerebellar cortex mainly in the anterior and superior vermis. The
condition improves following prolonged abstinence from alcohol.
Marchiafava-Bignami Syndrome
This condition, which is characterized by demyelination of the corpus
callosum, is rare. Affected individuals present with dementia,
spasticity, dysarthria and an inability to walk; the clinical presentation
may be acute, subacute or chronic. No treatment is available,
patients may deteriorate very quickly, lapse into coma and die or else
may survive, profoundly demented, for many years; occasional
individuals who present acutely recover completely.
Central Pontine Myelinolysis
This rare demyelinating disorder of the cerebral white matter is often
rapidly fatal. It manifests clinically as progressive quadriplegia,
pseudobulbar palsy and paresis or paralysis of horizontal eye
movements. Its exact aetiology is unknown although its development
is often associated with rapid correction of hyponatraemia.
Peripheral Nervous System
Individuals who misuse alcohol may develop focal peripheral nerve
lesions when heavily sleeping or stuporosed. These lesions develcp
as a result of nerve compression; 'Saturday night palsy' of the arm
which results from radial nerve compression, is the best example cf
this type of neurapraxia; recovery is inevitable
Individuals chronically misusing alcohol may develop a symmetrical,
bilateral, mixed sensory-motor, peripheral neuropathy, predominar tly
affecting the lower limbs, most likely associated with thiamine
deficiency. Individuals may be asymptomatic or else present with
numbness, pain and burning in the feet and hyperaesthesia; muse e
weakness and diminished tendon reflexes may be observed.
Abstinence from alcohol and supplementation with thiamine may
result in improvement in the condition but this is often slow and
incomplete.
Skeletal Muscle
Skeletal muscle damage may develop in association with both act to
and chronic alcohol misuse; its prevalence is unknown as many
individuals remain asymptomatic; for this reason its presence is often
overlooked.
http://www.medicouncilalcol.dernon.co.uk/handbook/chapter_4.htm
1/8/04
Chapter 4, Medical Students’ Handbook - Medical Council on Alcohol
Page 1 of 13
Acute Myopathy
Acute alcoholic myopathy develops in association with an episode o
acute intoxication or binge drinking. The spectrum of the disorder is
wide; some individuals may be asymptomatic and only detected
because of elevation of their serum creatinine kinase activity, whilst
others may develop an acute toxic rhabdomyolysis with
myoglobinuria, acute tubular necrosis and fatal renal failure. The
majority of individuals, however, present with some combination of: < i
myalgia or muscle pain, typically around the hip and shoulder girdles
and in the calves; (ii) muscle swelling and; (iii) progressive weakness
particularly in the legs and most noticeable on climbing stairs. Once
alcohol is discontinued the symptoms resolve over days or weeks.
Symptoms may recur after further episodes of heavy drinking.
Chronic Myopathy
This condition occurs in individuals with a long history of chronic
alcohol misuse. It develops as a progressive and usually painless
wasting and weakness of the proximal limb muscles. Patients tend io
complain of difficulty climbing stairs, rising from a squatting position,
opening windows and combing their hair; signs of a peripheral
neuropathy may coexist. Abstinence from alcohol results in
considerable improvement over a period of 2 to 12 months
Bone
Chronic alcohol misuse is associated with an increased incidence of
trauma and injury, particularly bone fractures. Indeed, the term
'Battered Alcoholic Syndrome' was coined to describe the presence,
on radiological screening, of multiple bone fractures, at different
stages of healing. Although repeated trauma is an important
aetiological factor in fracture development, these individuals are
particularly vulnerable to trauma because they have an increased
prevalence of osteoporosis; they show a reduction in bone mass
which is thought to reflect a direct effect of alcohol on bone
remodelling and mineralization but other factors, such as nutritional
deficiencies and cigarette smoking may also play a role. These
effects of alcohol on bone metabolism are, at least in the early
stages, reversible.
Skin
Alcohol misuse is associated with the development of a number of
cutaneous abnormalities such as spider naevi and linear
telangiectasia, and is specifically associated with the development of
discoid eczema. Alcohol misuse can also precipitate the development
of psoriasis in genetically predisposed individuals or else exacerbate
existing lesions. In general the psoriatic lesions observed in alcohol
misusers are more severe and more inflamed than in non-drinken
and occur in atypical flexural sites. Alcohol misuse is also associated
with the development of seborrhoeic dermatitis and cutaneous
bacterial and fungal infections. Abstinence from alcohol will help
ameliorate these conditions and, where appropriate, render treatment
more effective.
Malignancies
http://www.medicouncilalcol.denion.co.uk/handbook/chapter_4.htm
1/8/04
Chapter 4, Medical Students’ Handbook - Medical Council on Alcohol
Page 12 of 13
There is a strong association between chronic alcohol misuse and the
development of cancer of the mouth, pharynx, larynx and
oesophagus; smoking has an associated effect. Individuals with
alcoholic cirrhosis are at risk of developing hepatocellular carcinomc
but alcohol misuse per se is not a risk factor for the development of
this tumour. Alcohol, if taken regularly, even in moderate amounts, is
a risk factor for the development of breast cancer in women.
More information on alcohol and breast cancer will be found in the
article by Kemm, MCA Newsletter Alcoholis. 1998 Volume 17 (3).
Fertility
Alcohol misuse may have significant effects on sexual function and
reproductive capacity in both men and women. However, alcohol can
have significant effects on fertility, if taken on a regular basis, even n
moderate amounts. Thus, in susceptible men, alcohol intakes of 4 to
6 units/day can result in a significant reduction in the sperm count; in
many such individuals abstinence from alcohol is associated with
restoration of fertility. Women who drink alcohol in excess of 3
units/day may be subfertile; no information is available on the
reversibility of this effect. Women who consume alcohol in excess of
1 unit/day during the first trimester of pregnancy double their risk of
spontaneous abortion in the second trimester.
Foetal Damage
Regular consumption of alcohol, at any level, during pregnancy may
potentially harm the foetus. The abnormalities observed range from
growth retardation to development of the 'Fetal Alcohol
Syndrome' (Table 4:4, Figure 4:2). The more severe forms of foeta
damage are observed in women misusing alcohol but even these
women may produce infants that are seemingly unharmed. However,
over time, some apparently unaffected infants may develop both
cognitive and behavioural abnormalities; they tend to perform poor y
at school and up to two-thirds show hyperkinetic, emotional, eatinc
and speech disorders. The most vulnerable period for the foetus is
from 4 to 10 weeks gestation but alcohol-related damage may occ jr
throughout the pregnancy. Thus, benefit to the infant can be obtained
if alcohol is withdrawn at any stage of the pregnancy. It is
recommended that women avoid alcohol during the first trimester and
then limit their intake to 1 to 2 units once or twice a week for the
remainder of their pregnancy.
Table 4:4 Fetal Alcohol Syndrome
• Pre and post-natal growth retardation
• CNS abnormalities including microcephaly,
mental retardation, irritability, hypotonia,
inco-ordination, hyperactivity
• Craniofacial abnormalities including short
palpebral fissures, ptosis, strabismus,
epicanthic folds, mid-facial hypoplasia,
smooth philtrum, short upturned nose, thin
upper lip, lower jaw hypoplasia
• Associated abnormalities including
congenital defects of eyes, ears, mouth.
http://www.medicouncilalcol.demon.co.uk/handbook/chapter_4.htm
1/8/04
Chapter 4, Medical Students’ Handbook - Medical Council on Alcohol
Page 13 of 13
cardiovascular system, genitourinary tract
and skeleton and an increase in the
incidence of birthmarks and hernias
Figure 4:2 Schematic Diagram of the Facial Features of the'
Fetal Alcohol Syndrome
Short
palpebral
M icr oc ep h a h/
__----- f es ur e
/
J r
j-A
/
Epicanthic y
Folds -
■l
Thin
upper lip
lJ ptu r ne d
\ nose
$
i
%<■>
5
S m o oth
p hiltrum
Hypoplastic
| JAI
We would like to thank Dr Ruth Mayall, Consultant Anaesthetist, North Manchester
Healthcare NHS Trust, for her assistance in obtaining the medical illustrations included
along with this chapter.
© MCA, 3 St Andrew's Place. Regent's Park, London NW1 4LB. Registered charity no 265242
Tel: + 44 (0)20 7487 4445
Fax: + 44 (0)20 7935 4479
e-mail: mca@medicouncilalcol.demon.co.uk
Webmaster: Dr Guy Ratcliffe Website design: Karen Widdowson
http://www.medicouncilalcol.demon.co.uk/handbook/chapter_4.htm
1/8/04
Chapter 10, Medical Students’ Handbook - Medical Council on Alcohol
Page 1 of 3
THE MEDICAL COUNCIL ON ALCOHOL |
MEDICAL STUDENTS’ HANDBOOK: ALCOHOL & HEALTH (3rd Edition)
Introduction
10. Prevention
1. Facts about alcohol content
of drinks
There is good evidence that, within any population, the level of
alcohol consumption is closely linked to its availability and cost.
Regular access to drinking and pressures to drink, for instance from
advertising and other inducements, promote increased drinking.
Efforts at primary prevention should, therefore, focus on reducing
both average per capita consumption and the quantities consumec
by individuals. The principal approaches adopted are: control of
availability, public education about sensible use, decreasing the
incentives to drink and providing alternatives.
2. Alcohol metabolism
3. Predisposition to harm
4. Alcohol-related physical
harm
5. Alcohol-related social and
psychological harm
6. Assessment
7. Brief intervention
Controls usually take the form either of taxation or legislation aime J
at reducing availability, for example by restricting the time of sales,
and the number and location of licensed premises. These measures
are often unpopular politically but are probably the most potent wa/s
of affecting the overall level of alcohol-related harm in the population
Surveys show that the public accepts the need to restrict access to
alcohol and appreciate the harm associated with unfettered
promotion.
8. Specialist services
Alcohol education
9. Management of specific
problems
10. Prevention
11. The doctor's role
Glossary of terms
Return to MCA home page
The effects of education and social controls on alcohol consumption
is more difficult to assess. In general the effects of education
campaigns have been disappointing in that while they may increase
knowledge of the potential hazards of excess alcohol consumptior
they usually have little or no effect on drinking behaviour. Campaigns
focused on increasing knowledge about alcohol, such as
understanding the units system for measuring alcohol consumptm
and appreciating the patterns and levels of consumption which are
likely to cause harm, are generally useful. Education focused
specifically on certain behaviours such as drinking and driving, or
minimising drinking during pregnancy, can be particularly effective.
In recent years, educational programmes have been devised to
broaden information on all aspects of health, not just the effects oi
alcohol. These aim to inculcate individuals with a sense of
responsibility for their own health and safety and that of the
community. They are designed, for example, to assist individuals :o
decide whether to drink, under what circumstances, and in what
quantities, clear in the knowledge of the consequences of their
actions. It remains to be seen whether this new approach will be
more effective in bringing about change. Peer group education
seems more effective in influencing young people than outside
experts lecturing on alcohol use.
Society imposes its own subtle controls on drinking behaviour wh ch
are difficult to identify and even more difficult to quantify. In recen
http://www.medicouncilalcol.demon.co.uk/handbook/chapter_10.htm
1/8/04
Chapter 10, Medical Students' Handbook - Medical Council on Alcohol
Pag22 of 3
years, for example, attitudes to drinking and driving have changed
dramatically and individuals who indulge in this sort of behaviour are
now considered socially unacceptable. This change in attitude has
occurred gradually over time and cannot be attributed to any specif c
event or series of events. Whether social attitudes to other aspects
of excessive or irresponsible drinking will change over time, and
influence behaviour, remains to be seen.
Advertising
Every year the 'drinks’ industry spends vast amounts of money
advertising and promoting their wares. In recent years, however,
they have been involved with Government in establishing an ethical
code of conduct in relation to advertising and sales promotion, and ;a
number of voluntary 'watchdog' organizations are involved in
monitoring performance to ensure conformity to the agreed
regulations and codes.
Attempts have been made to ensure that advertising does not target
teenagers and to enforce more effectively laws prohibiting sales to
underage drinkers. From a public health and clinical perspective, it is
noteworthy that the early onset of drinking correlates closely with
smoking and other forms of drug misuse.
At a local level, many communities are now examining the part they
can play in reducing the level of alcohol-related harm, for instance by
encouraging alternatives such as non-alcoholic drinks and not linking
social and sporting activities too closely with drinking. In some cities
new bye-laws have been introduced creating zones in which public
drinking is prohibited and attempts made to reduce the level of
drinking at sporting events by banning alcohol sales before and
during the game.
Efforts at secondary prevention are usually directed at high-risk
groups and are aimed at early diagnosis and intervention. High-ris\
groups would include persons who consume amounts of alcohol
known to be harmful and individuals who, for a variety of generic,
social or constitutional reasons, appear to be either unduly
susceptible or else are unduly exposed to the effects of alcohol, for
example, women, the young, Asian Indians, the those in occupaticns
which allow them free or easy access to alcohol. As the risk of
developing alcohol-related physical harm increases significantly wth
daily intakes of alcohol in excess of 40 g (5 units) in women and 6) g
(7.5 units) in men, large proportions of the adult population, in many
countries, fall into these high-risk categories. Therefore the efforts of
secondary prevention, in this context, largely overlap with those of
primary prevention.
A number of campaigns have been undertaken, for example,
National Drinkwise Days, designed to increase awareness among
the public at large and among individuals in the high-risk groups, of
the levels of alcohol consumption associated with the developmei t
of physical harm. These are repeated at intervals and certainly
increase awareness and knowledge, but the effects on behaviour are
less well documented. Health-care screening is becoming more
popular in many countries and as these schemes address several
aspects of health they tend to be more appealing and less
threatening than schemes designed to screen selectively for excess
alcohol consumption. All patients registered with a general
http://www.medicouncilalcol.demon.co.uk/handbook/chapter_10.htm
1 /8/04
Chapter 10, Medical Students' Handbook - Medical Council on Alcohol
Page 3 of 3
practitioner undergo regular health-care screening. Individuals who
are found to be drinking in a hazardous or harmful way can be
alerted and given simple advice about reducing intake either by the
general practitioner or by a practice nurse. Many industrial
companies operate an alcohol policy aimed at the early detection of
alcohol-related problems and early and effective intervention aimed
at preserving the work force. Other companies, while not operating
an alcohol policy as such, arrange for middle and senior
management to undergo comprehensive health screening medics Is,
usually on an annual basis, thereby providing opportunities for ea1y
detection of alcohol-related problems.
Tertiary prevention is, more or less, synonymous with treatment iit
is aimed at ensuring future abstinence from alcohol and preventing
the development of further social, emotional, psychological and
physical harm.
© MCA, 3 St Andrew's Place, Regent’s Park, London NW1 4LB. Registered charity no 265242
Tel: + 44 (0)20 7487 4445 Fax: + 44 (0)20 7935 4479 e-mail: mca@medicouncilalcol demon.co.uk
Webmaster: Dr Guy Ratcliffe Website design: Karen Widdowson
http://www.medicouncilalcol.dernon.co.uk/handbook/chapter_10.htm
1/8/04
Chapter 7, Medical Students' Handbook - Medical Council on Alcohol
1i
Page 1 of 5
THE MEDICAL COUNCIL ON ALCOHOL
MEDICAL STUDENTS’ HANDBOOK: ALCOHOL & HEALTH (3rd Edition)
Introduction
7. Brief Intervention
1. Facts about alcohol content
of drinks
There is good evidence that many patients benefit from
straightforward, focused advice about their drinking behaviour.
Despite this, doctors seem reluctant to discuss drinking behaviour
with their patients, even though in the majority there will be no
particular cause for concern.
2. Alcohol metabolism
3. Predisposition to harm
4. Alcohol-related physical
harm
5. Alcohol-related social and
psychological harm
6. Assessment
7. Brief intervention
8. Specialist services
9. Management of specific
problems
10. Prevention
11. The doctor's role
Glossary of terms
Return to MCA home page
If the patient reports drinking at a hazardous or harmful level then the
doctor is well-placed to offer timely advice about changing these
habits to a less damaging level. The patient's current view of their
own drinking and their attitude towards making change must be
taken into account. This crucial stage is often best addressed by an
approach known as motivational interviewing. This is a technique
which assists the patient to arrive at their own decision about
changing their habits. The clinician should always be positive about
the changes envisaged, stressing the benefits and offering
suggestions for strategies for change. Some patients seen in hospital
and primary health care will respond well to simple advice and it is
always worth using this as a first approach. Other patients will
require more help in making a commitment to change.
It is important to remember that while it might be clear to everyone
else concerned that the patient needs to change their drinking
behaviour, they may not share this point of view. Often, patients w II
acquiesce to a doctor's opinion while not truly incorporating the
advice they are given. The patient's own views of their drinking
habits and problems must be elicited. They may be at a 'precontemplative' stage and may not have thought seriously about
changing their drinking behaviour. In these circumstances the first
task is to provide information and feedback about the risks
associated with their current alcohol intake and to discuss any
associated health problems which may have already arisen. At this
stage it is helpful to make it clear that the onus lies with the patient to
make the necessary change, and only when they are willing to
accept this first step is it appropriate to give advice about strategies
for cutting down and achieving a less harmful level of drinking. The
essential components of motivational interviewing and brief
interventions of this kind have been summarized with the acronym
FRAMES (Table 7:1).
Table 7:1
The Essential Components of Motivational Interviewing and
Brief Intervention.
FRAMES
http://www.medicouncilalcol.demon.co.uk/handbook/chapter_7.htm
1/8/04
Chapter 7, Medical Students' Handbook - Medical Council on Alcohol
Page 2 of 5
• ■ eedback about the risk of personal harm or impairment
D
• Stress personal ■^esponsibilty for making change
A
• ^^dvice to cut down or, if necessary, stop drinking
• Provide a ^"enu of alternative strategies for changing
drinking patterns
F
• l—mpathetic interviewing style
• Se|f efficacy: an intuitive style which leaves the patient
enhanced in feeling able to cope with the goals they have
agreed
Source: Bien et al, Addiction 1993; 88; 315-36
Habits are difficult to change. Many problem drinkers will find that,
much of their life is dominated by the need to drink and many
barriers to change (Table 7:2) will have to be confronted including:
Table 7:2 Barriers to Change
.. Physical
Dependence <’
Psychological
Intra psychic
Stress
Interpersonal
Environment
Habit
Psych iatric
I lln ess
~ Physical
Influence of others
P ess imism/ste re otyp es
Dependence: May be physical or psychological; those physically
dependent will have to be carefully withdrawn from alcohol (Chapter
9); those psychologically dependent will need to identify triggers to
drinking and find new ways of dealing with craving and alternative
ways of coping.
Stress: For some patients this is a major barrier to making change;
they regularly use alcohol to deal with difficult situations in their lives.
Counselling and other forms of psychological help may be necessary
to overcome this problem.
http://www.medicouncilalcol.demon.co.uk/handbook/chapter_7.htm
1/8/04
Chapter 7, Medical Students' Handbook - Medical Council on Alcohol
Page 3 of 5
The patients' environment can be a barrier to change; for example
they may have a job where selling or entertaining brings them into
regular contact with alcohol, or their social life may be constructed
around drinking occasions.
Habit: Never underestimate the force of habits. The patient needs :o
identify occasions when they have been 'in the habit' of having a
drink: for example at particular times of day, in particular company or
situations. Keeping a regular diary (Figure 6:1) is often a good
means of identifying these risky times. The patient and doctor can
together agree a plan for dealing with these situations and then
review how successfully they have been overcome.
Occasionally alcohol will have been used as a form of selfmedication to cope with psychiatric or physical illness. In these
circumstances, the underlying condition must be identified and
treated along with the alcohol problem so that the patient gains
confidence in coping with the symptoms without recourse to drinking.
■
>
The influence of others is a powerful factor for many. This may
either be of a positive nature, supporting and encouraging the patient
during times of potential relapse, or a negative influence by
encouraging and cajoling them to drink, for example, by saying 'one
won't do any harm', or repeatedly asking why they have given up
drinking and become 'a killjoy'. It is often helpful to rehearse dealing
with such pressure, either at individual interviews or as part of a
social skill management group.
A final barrier to change is a sense of hopelessness or pessimism
The drinker may feel that it is impossible for them to change their
drinking habits. Equally, the doctor may feel pessimistic about the
likelihood of a given patient succeeding in attaining this goal or mere
broadly about their own ability to effect change in any of their
patients. These feelings are often based on a few unrewarding
experiences; it is easy to forget that the majority of problem drinke s
respond well to help and advice.
Aim to enhance the patient’s self esteem and sense of being atde
to cope before they leave the interview.
Set Goals: Goals should be specific, attainable, short-term, and
preferably immediately rewarding. They should be defined and
agreed by the patient.
Involve the family: Family distress is common and encouraging
family members to join in the interview is a useful way of reinforcir g
the decisions made.
Often the patient will respond very well to the advice given and on y
brief follow-up will be necessary. If the interview has taken place in
hospital, then the general practitioner should be told what advice lias
been given so that it can be followed up at a later stage.
In some circumstances the patient will be unable to make the
anticipated changes and may need further help. This may be
because some of the barriers to change have proved insurmountable
in the first instance and will require more detailed attention. Patierts
who are physically dependent on alcohol may need help to withdraw
http://www.medicouncilalcol.demon.co.uk/handbook/chapter_7.htm
1/8/04
Chapter 7, Medical Students' Handbook - Medical Council on Alcohol
Page 4 of5
from alcohol before any changes are possible.
Abstinence or Controlled Drinking: To drink or not to drink is on e
of the earliest questions likely to be raised. Most patients will hope
that they can regain controlled social drinking.
Abstinence from alcohol is the preferred aim in older individuals,
those who have exhibited serious physical dependency on alcohol,
those with significant alcohol-related physical injury and those who
have previously failed to modify their drinking behaviour despite
advice. If the family is very strongly against attempting controlled
drinking, or if the environment is such that relapse seems extremely
likely, then again abstinence is the preferred aim. For some patients,
particularly those who are younger and those who have little
evidence of physical harm, controlled or modified drinking may t»e
appropriate.
Whichever goal is adopted initially, it may have to be modified by
experience and events. It is often helpful to draw up a balance sheet
to help the patient agree their goals and look at the problems which
are likely to arise in making changes. Balance sheets and a diary for
self-monitoring review are very helpful aids (Table 7:3). It is very
important to encourage even modest but realistic gains in the early
stages. Changing habits is never easy and even small gains shou d
be applauded.
Table 7:3 Sample Balance Sheet of Drinking
Likely consequences of drinking
PROS
of
chosen
course
Continuing
Reducing
Stopping
Forget my
worries (for a
time)
Be like others
Family want me
to
Keep my
drinking friends
Not be a kill
joy at
business
lunches
Doctor says it is
the only way my
liver will recover
Save a lot of
money
CONS
of
chosen
course
Partner may
leave
Children very
upset
Lose my job
Liver failure
Didn’t work
when I tried
before
Could I cope
with business
lunches?
Partner
would'nt
believe me
Feel
uncomfortable
with my friends
Liver damage
persists
Further description of managing alcohol problems in general prac ice
will be found in the article by Noble and McLean, MCA Newsletter
Alcoholis, 1998 Volume 17 (4).
http://www.medicouncilalcol. demon, co.uk/handbook/chapter_7.htm
1/8/04
Chapter 7, Medical Students' Handbook - Medical Council on Alcohol
Page 5 of 5
© MCA, 3 St Andrew's Place. Regent's Park, London NW1 4LB. Registered charity no 265242
Tel. 44 (0)20 7487 4445 Fax: + 44 (0)20 7935 4479 e-mail: mca@medicouncilalcol.demon.co.uk
Webmaster: Dr Guy Ratcliffe Website design: Karen Widdowson
http://www.medicouncilalcol.dernon.co.uk/handbook/chapter_7.htm
1/8/04
*
Page 1 of 5
American Council on Alcoholism
Alcoholism
Treatment
HeipLine
..■O^
. . Wife
. .W.wX’.v.w.'.v.waw. ' '
%
i_Qnn_
■ w
.#'A
ox t
AilMfH on ALCOHOLISM
HmfcKitAh tvjufitil
F reci us nth/ Asked Questions
«■
ali
A
^hy do people drink alcoholic beverages (beer, distilled spirits, or wine)?
Positive reasons for drinking alcoholic beverages include:
Celebrating significant occasions with friends or loved ones.
Enhancing enjoyment of social activities and relaxation.
Complementing certain meals.
Participating in religious ceremonies.
Enjoying the taste as a beverage of choice.
Negative reasons for drinking alcoholic beverages include:
Escaping from tension or worries.
Blocking out painful feelings such as fear loneliness, and self-doubt
Attempting to relate better to people.
As a substitute for meaningful relationships with people.
Finding courage or strength to face certain situations.
miat are symptoms of alcoholism?
Only a qualified professional can determine if an individual is alcoholi c. Howe
following warning signals may indicate the presence of alcohol-related problem
these signals involve later stages of alcoholism and involve symptoms that may
to time periods and drinking patterns.
Drinking increasing amounts of alcohol and becoming intoxicated often.
Being preoccupied with drinking, to the exclusion of other activities.
Making, but readily breaking, promises to quit or control drinking,
Experiencing "black outs", Le., unable to remember what he/she said or did
http:!!ww aca-usa.org/acafaq. htm
12/15/03
American Council on Alcoholism
Page 2 of5
drinkins.
Experiencing personality changes, j. e., tense, irritable, denies or conceals dri
wide mood swings.
Milking excuses lor drinking.
Drinking alone, in the morning or before a party.
Refusing to admit to excessive drinking and becoming angry if someone mei
Having Trouble on the job or at school i.e.. misses work or school, is frequer
has conflicts with coworkers or fellow students.
Changing jobs frequently and/or is usually demoted, rarely promoted.
Losing interest in personal appearance or hygiene.
Suffering from poor health, e.g., loss of appetite, respirator/ infections, neiv
Having several arrests for drunken driving or other alcohol-related incidents.
Suffering from family, marital, academic., and/or economic hardships.
Spending a great deal of time overcoming hangovers.
In final stages, experiencing grave social, financial, and personal damage.
Is the person who regularly takes a cocktail before dinner an alcoholic?
1i
Menu
Home
About ACA
AC'A Membership |
About Alcoholism I
FAQ’s
College Drinking |
PUT Courts
Programs
Pvecover/
Selected Readings
Links
Board of Directors
Chairman’s Comer
Not necessarily. Drinking every day - in and of itself - does not indicate alcoho
people drink evert' day for a variety of reasons with no subsequent problems. I
askis: "Do I need that drink?” If the answer is ”No” and you can control the an
alcohol you drink, then more than likely you are not an alcoholic
is there such a thing as a weekend alcoholic?
Yes. Alcoholism is a complex illness and involves symptoms that man be unrcl
periods and drinking patterns. Not everyone exhibits the same symptoms.
What is social drinking? How much does a social drinker drink?
Social drinking is not based on - nor defined by - a certain number of drinks. Vv
an exact definition, social drinking usually takes place with two or mo -e partici]
satisfying to the drinker and participants, and docs not impede the drinker’s heal
interpersonal relations, or economic fimetioning
A social drinker respects alcohol and its effect on the body, consumes alcohol a
familv and social customs, and realizes that alcohol complements the pleasures
the social drinker, drinking is not an end in itself but an accompaniment to othc;
What distinguishes a social drinker from an alcoholic?
Loss of control. A social drinker has control over when, where, and how much
drinks. An alcoholic has lost tins ability and after beginning to drink, usually di
intoxication.
What type ofperson is an alcoholic?
There is no typical alcoholic. Anyone can abuse alcohol and become and alcoh
studies show an increasing number of alcoholic women, teenagers, and children
young as 10 years old. There is also a rising number of alcoholics among senio
http://wv\rw.aca-usa.org/acafaq.htm
12/15/03
American Council on Alcoholism
1 age 3 of 5
is estimated that as many as one out of ten people over age 60 have a cohol-rcla
What is denial?
Denial occurs when a person refuses to believe that alcohol-related sy mptoms a
excessive drinking. Demal is a major obstacle to alcoholic recovery.
What Is the difference between denlai and rationalization?
With denial, the alcoholic believes that drinking has nothing to do with his/her ]
With rationalization, the alcoholic attempts to find logical reasons for c rinking.
drinking to certain occasions - e.g.. 'TH drink because it's my birthday" or "rif e
it’ll help me unwind" - without the ability to control drinking during an / of thus
WTty do alcoholics refuse to recognize their problem with alcohol?
The effects of chronic intoxication interfere with thinking and impairs attitude,'
personality. The alcoholic is incapable of recognizing the serious barn caused
repeated use of alcohol. Until drinking stops, the brain does not function normr
effects may last for weeks or months, but they arc mostly reversible.
How can you help an alcoholic who does not want help?
First, learn as much about alcohol, alcohol abuse, and alcoholism so that you m
able to deal with the problems of alcoholism and some of your own feelings ab<
problem. Next, talk to the person about their behavior changes that result from
firm, considerate, single-minded, and focus on the drinking behavior, r ot the re;
drinking. Some alcoholics always find a reason to drink. Be specific: point out
drinking interfered with the person's life
Offer hope. Alcoholism is a treatable illness. Between one-third to two-thirds (
who seek help actually recover from alcoholism when the first step is taken to s
consumption. Since many alcoholics lapse again into heavy drinking, patience
encouragement can help the alcoholic regain sobriety.
Finally, remember that the worst thing to do is to ignore the problem aad hope t
away.
What is an intervention?
In the book Intervention^ Vernon E. Johnson describes intervention as a "proces
the harmful, progressive, and destructive effects of chemical depender cy are ini
the chemically dependent person is helped to stop using mood-altering chemica
alcohol] and to develop new, healthier ways for coping with Ills or her needs an
The ultimate goal of an intervention is to get the alcoholic into a treatment prog
How does an intervention work?
Intervention occurs when the alcoholic person is in denial or does not seem io v
any help and loved ones, relatives, and even employers decide that it is time zz
io :<
http://www. aca-usa. org/acafaq. htm
12/15/03
American Council on Alcoholism
Page 4 of 5
lake action. Phcy do this to help the alcoholic to recover a sober and icalthy lit
Under the guidance of a professional, an intervention team forms, made up of t\
people who are concerned and close to the alcoholic and who have first-hand kr
the alcoholic's symptoms or behavior.
The team meets and. in an objective and caring way. the alcoholic is confronted
about his/her drinking. By using specific examples of the alcoholic's drinking k
team attacks the alcoholic s wall of defenses, the alcoholic meets heac-on with t
the effects of alcoholism. This process causes discomfort and upset. The alcoh
out ot demal and tins may lead to agreement to seek help.
Wiiai attitude should I have toward a problem drinking spouse?
Don't blame yourself for your spouse's alcoholism. An alcoholic can be \ cry cl
shifting the responsibility for drinking to others and may use your feelings of ca
feelings of guilt within you. You are not responsible for the illness that affects;
and you cannot control or change alcohol-related behavior. Seek professional h
spouse, yourself and other family members.
How do you handle children experimenting with alcohol if one or both pareni
recovering alcoholic ?
One way to prevent alcohol abuse is to give children accurate informat on abou
properties, and its effects on the body. If a child is well informed about the imp
of alcohol and has a feeling of self-confidence, chances of abusing alee hoi are £
reduced "Scare tactics" should not be used to change undesirable beh< vior. Cl
expectations and rules arc important and discipline should be consistent if rules
Finally, seek professional help.
What if Im rhe child of an alcoholic?
Just remember that you are not the cause of your parent’s drinking; it is an illnes
not responsible for their actions. It does not mean that you are a "bad” person a
not feel guilty. If you are really upset about a parent’s drinking, you should try
professional help.
How does an alcoholic recover from alcoholism?
Alcoholism is a chronic progressive illness. While there is no medical cure for
many alcoholics do ’‘arrest" it; te,. stop its progress with medication and trainin
Home AboupACA ACA Membership About Alec holism
FAQ's College Drinking DUI Courts Programs Recovery
lected Readings Links Board of Directors Chairman s Corn
http: .-'/tov. aca-usa. org/acafaq. him
American Council on Alcoholism
This page was last updated on 7-23-2003.
9/1 C/H9
Page 5 of 5
>
Page 1 of2
Saliva Clinics
•A
WAV.
HGG.X..
•"■•v
a.\i.
r<>:: :s :’i€
A/.: 1\VV;.VO:'0-
j
'yUv-3'S
/. vv'-V.Vy"..X7.
v2acSB80^,,,‘ VW&WA.
W/ :W
........................................ J-™.™,.. ......................................
"There is the strange and constant fact that it is only after a pious journey to a di
. ...
whiffy
■ ■
of our mysterious inner voyage to us must himself be stranger, of another faith a
SV/W. 7 ■'."TOv' ••...•
-mm -
• yvav. •;.. ■< y.w;v. a>-
.wiw:vA'.-
- "•
region, in a strange land, that the meaning of the inner voice can be revealed to
to that strange and constant fact there is another: that the person who 'eveals tf
race"
Why India?
••amA-,-. - ■■■■
Global travelers, when they return home, often
are confronted with a riddle; why is it that so
many people in the wealthiest countries seem
so stressed, worried, overweight, angry,
spiritually bereft, and, - in a myriad of ways unhappy?
%•
wx-.--'-" ■
VAWz--
-
IWuV. -
•• ......
.wji:
-
AVWMM'• • •
«««••"
XU,.
"MA...................ww
<wiw*wvw1 • ' •A'.....
■.••■•S'V
WAW-’yA"'"
..... ...........
.. . ... . .,
................... • vr........... •■■■• ■ • • ■
'WWW'.-.-'- •
■
...
■
-X
•
......
•,W®f'W
........
-.w
■?v>> yWXX^
’ Xv-.-.w' ’ X-X-’ww.'wJamaw. . •••<«•■
• 7(w.-.,;.x.v
•••
You see, we create our culture, and are in turn
rrca^ed by it, unless we are able to receive a
LT: perspective. There are many
• •ayX,,WSW.11.-.v.v,7M.
•
i ■.
..... A-
.................. TSxl-:
■...... .-•••awaS
■v
•
Conversely, in a city like Bombay, -where over
70% of people are what we would call
homeless, amidst the most crowded conditions,
seeming chaos, and unspeakable poverty, one
can sense an incredible generosity of spirit and
peace amidst outward turbulence and squalor.
How is this? The answer is, of course, culture.
We iive in culture as a fish iives in water, so
permeated by it that we hardly notice It.
•........... .
<-
...................... .
-MAV,
common-sense reasons why people in the west
feel impoverished amidst relative gluttony,
empty in the middie of opulence, and
victimized despite being given unlimited
» r\ iMz^c
PRICE:
India provides the cppc
charge affordable price
providing treatments th
expensive to be offeree
American treatment clii
J
healthcare professional
J philosophies =nd reiigic
traditions of India, ado,
modified by over hair tl
population, have produ
wealth of peooie who a
psychologically and spii
knowledgeable, with in
qualities. Anyone famili
India is aware, of the tn
resource that is the Inc
* THE CULTURAL COS
i One of the breakthroug
in this treatment plan i:
and explore the culture
H dete rm i n a nts of com pu
I ncreas i n g Iy, *0/4
understand that compu
A
addictive behavior floui
western, American cuit
consequence of distinct
attitudes, which has cn
epidemic of depression
disorders.
■
U L/1-> U i I u ii 111 v. 5.
. ..A.
■
QUALITY of PERSC
India has a huge surpk
educated and experiem
Many Americans are fat, angry, depressed,
dissatisfied, addicted to a variety of drugs or
activities mainly because it is a tall order to
make sensible choices in a culture where you
are exposed to hundreds of advertisements
every day, most of which follow the same
formula: create dissatisfaction and therefore a
no.
ar! than offor
s
colt
if ion far » nnn_
i i vU/
c* i i k. i V4 i i iu kk* I iu i
w i u li ky if i vi O i i ky i i
material need. More dissatisfaction follows.
But this much Is clear: our culture In the west
has reached the stage where the majority of
j;
* MOTIVATIOH:
1 he smqie most import
treatment outcome is t
motivation, regardless
treatment modality, bu
you gauge a client’s me
level? One way is to se^
person is willing to trav
across the world to a p
which he or she will nd
to smoke, drink, or con
caffeine and refined su<
month. Thousands of A
already go to India eac
spiritual renewal and
transformaticn. The pre
1 inrlar*-olzinr> :i ha^linn -j
http:"wvvw. sattvaclinics. coni7why India, him
12/15/03
Page 2 of 2
Saliva Clinics
health problems are self-inflicted, related to
uiiugi vuimiim
ii^swiniy J
crrnnfi niitiiroi anrorofi
*
iifestyie choices. Most peopie iiving in western
culture have the means and the opportunity to
live lifestyles which lead to vibrant health. Most
peopie in the west have shelter, enough money
to eat vegetables and fruits, time to meditate,
and have access to free information about how
to transform the quality of one s life beyond
one’s wildest dreams.
But most peopie do not. In fact, even children
in America are becoming obese and depressed
at Increasing rates.
to
, ,,Prescriptions
,
, antldepressants for cnlldren - unheard or ten years
. western and eastern tn
* COMBINING TRAD’
: TREATMEN 1 WITH
"Ti:
alternative care:
Meditation, acupunctur
; bodywork, and yoga ar
> utilized in selected host
: American in t'eating ac
: disorders and other ailr
: proven result!?. Americ?
? spend more money on
! health care treatments
i not covered by insuren
? they do on traditional t
I India has anc ent tradit
: alternative health care
ago - are skyrocketing. While there are obvious
aimed at preventive m«
optimum health, traditi
reasons why Americans and their children live
v steadily gaining accept;
unhealthy lifestyles - essentially spending lots
< American market.
of time eating processed foods and/or
X
ingesting drugs, immobile In front of an
electronic screen - its also obvious that in
*
order to change the quality of one's health and
one's life that you have to change your
lifestyle.
•
• I
■
.
You know what you have to do: create your
own regimen for exercise, healthy diet, sleep,
and self-reflection, stick to It, and reap the
rewards.
Home I
?:
Long Term Care I Location / Cost / Staff I Faq I Treatment Philosophy
Customer Profile I Contact I What Is Sattva?
s'te
by "TM Gerie's Wif1'" - •••../i*..n?ni?iUinU.ro'T»
I
http: z/www. satt/aclinics.corn/whymdia.htm
2/15/03
IMDiversity.com - Traditional Methods Used to Help Navajos Stop Drinking
Page 1 of 4
CiSIMiJlVERStTY
■a,
awViKe-Ejj-iV- £V- •
________ •
VH-CAoe:
.... . _
WatTXtfS A-•’
VXtXAZ&»”
ivi, howwCi
........ vxtx
home | search jobs j my account | employer profiles ; career center; about us»j heip j employ^03
DAILY NEWS
Traditional Methods Used to Help Navajos Stop
Drinking
by APf The Associated Press
By Leshe I inThicuny Albuquerque .Journal
Gallup. N.M. (AP) As lire smolders and sweet smoke hangs thick in the air. Harrison iim
shakes the rattle of the Native American Church while a couple dozen people sit shoulder=to»
shoulder and sing peyote songs in the dark.
The world outside is cold and wet and fraught with dangers: beer, wine and hard liquor iind
fears that disappear only when they arc drowned in drink.
Inside the drumming circle at the Na’Nizhoozhi Center, Jim offers blessings of cedar smoke
to fortify the spirit and Navajo words to kindle memories of the past.
Recognizing that alcohol Treatment programs that succeed in rhe white world often fail m
Indian country, counselors here-are looking to the past the songs and stories that have
sustained Navajo people for centuries to help Navajos in their battles against alcohol today.
A 6-year-old program immerses Indian alcoholics in 24 days of corn pollen ceremonies,
sweat lodges, drumming, talking circles and tutorials with medicine men in the snug coniines
of cedar-log hogans outside the Na’Nizhoozhi doors.
The program, known as Hinn’ah Bits’os (or Eagle Plume) Society, has shown remarkable
results, with 40 percent of its 1,800 graduates sober two years later.
find it has won Jim. one of its founders, a three-year public health grant io take the concept
nationwide.
Under a $75,000 grant from the Robert Wood Johnson Foundation. Jim will work with
others in the field of substance abuse counseling to try to incorporate traditional elements
into programs for Native American addicts.
http: dwww. imdiversity. com•'Article_Detail. asp?Article_ID= 13858
nvlDiversiiy.com - Traditional Methods Used to Help Navajos Slop Drinking
12 15/03
Page 2 of 4
j!i!« is a roau man wilm me iNativc Aihcncari i nutcn. a iNavajo ncanng pTaciiiidncr aiio <•
recovering alcoholic. An eighth-grade dropout who had his first drink at age 7, he has Studied
modem, scientific approaches to treating alcoholism. But he has found the strongest
medicine in Navajo spirituality.
"Our purpose is not to take people back to the old ways," said Jim. "Our job is to guide them
back to the teachings of the Holy People. To say, ’This is who you are and this is where you
come from so you can carry on in your life, in your job, with your family, with this strength
lo guide you.' ”
The dozen people who took part in the residential program that ended last week included a
silversmith, a sand painter, a heavy equipment operator, a fast food clerk and unemployed,
chronic alcoholics, among others. Many were there by court order after too many arresls for
drunken driving or public intoxication. Others were there by choice, try ing to kick a ha nt
that has cost them jobs and family relationships.
"Having dial Tirsl drink, it's just like lighting a lire,” said Norbert Peshlakai. a noted
silversmith from Crystal, who has tried without success to stop drinking through Christian
based programs and through Alcoholics /anonymous.
"This is working,” Peshlakai said. ”It feels good to get back to the old ways.”
Matthew Kelley, clinical director ofNa’Nizhoozhi, said the center is the largest
detoxification facility in the nation and, at S45 per day for each client, one of the cheapest.
While one or two dozen people are enrolled in die specialized Eagle Plume program at any
time, the main business of the center is more basic to pull intoxicated people off the street
and into a safe place for a few days while they get sober
This is a high-volume, low-cost program," said Kelley.
t he center was built 10 years ago to address Gallup's notorious problem with wandering
street drunks. Nearly 40,000 people a year were cycling through the Gallup jail on public
intoxication arrests before Na’Nizhoozhi opened to replace it with a different approach.
In its first year it saw 24,000 admissions. That has been cut to about 17,000 clients today as
some repeat offenders have graduated to sober lives.
Most of the centers clients are picked up on the streets or dropped off by relatives. They stay
for two to five days before heading home nourished, rested and with encouragement to get
help for alcoholism.
(
Most don’t.
Sixty percent of the admissions each year involve the same 700 people a core gr oup of
chronic drinkers who sometimes spend 200 nights each year sobering up on a Na’Nizhoozhi
cot.
About 95 percent of the clients are Native American mostly Navajo.
http: //www. imdiversity. comCArticleDetail. asp?Article_ID= 13858
12/15/03
IMDiversiiy.com - Traditional Methods Used to Help Navajos Stop Drinking
Page 3 of 4
When the center replaced the drunk tank at the Gallup jail it began offering a standard 12step Alcoholics Anonymous program.
Jim remembers leading Alcoholics Anonymous meetings and watching the disconnect.
”TKpv v. oiilrln'f lUtFi. ir* it ” TiiVi c-zvirt ’’TUpv’d /L ift
th^tn u;nirM tzJI
Drawing on brain wave research Kelley had done on the effects of drumming and other
Native American traditions on relaxation among Navajos and on Jim s personal experience
with getting sober through the old teachings, Jim and other counselors changed their
meetings in 1996.
“Wc started talking about what our grandfathers and grandmothers used to talk about
traditions, having self-respect and responsibility, teachings put forth by the Holy People,”
Jim said. ’’ They started sitting up straight and listening because we were using our own
language.”
Counselors began introducing themselves by using their clan identifications and talking
about the kinship system that ties all Navajos together. Instead ot calling the people receiving
treatment “clients/* they called them "relatives.” lhey built a traditional healing center on a
patch of land next to the center that includes four hogans and four sweat lodges and found
room inside the center for a dormitory for the “relatives'1 enrolled in the program.
Il was a gamble on a developing approach io lire treatment of alcoholism among American
Indians known as the “red road to recover/.”
And n worked.
Six years into the program, four out of 10 people who go through the Eagle Plume program
have quit drinking entirely and maintained their sobriety for two years. Seven out of 10 have
shown significant improvements. That compares with less than a 30 percent sobriety rate for
those who follow AA programs Through The center
lhe wind blows cold outside, but the big metal drum inside the hogan is burning warm with
cedar logs.
The 12 members of the Eagle Plume Society sit in a circle, talking about their lives and
learning the history of the hogan, the eight-sided traditional Navajo dwelling.
Russell Kaye, a sand painter from the Navajo community of Pidon, reflects on his life and
his days in the program.
“Somewhere along the way/* says Kaye. “I have made some mistakes. I am learning wsys to
bling myself back into harmony.**
He hopes to go home sober, stay sober and begin filling orders for artwork that have been
piling up.
Jerome Curley, from the Navajo community of Wheatfields. speaks for the group.
http: Vvawv. imdiversity. com/Article_Detail. asp?Article_ID= 13858
IMDiversity.com - Traditional Methods Used to Help Navajos Stop Drinking
1-7/1 ^.'03
Page 4 of 4
"Wc want to change, to be better men, to be the men we should be,” Curley says.
Jim uses the example of the warrior twins of the Navajo creation story and their encounters
with monsters to teach the importance of maintaining a “warrior mentality” when “relat ives”
leave the center and return io their lives in modem times.
“Our people are still going tlirough these hardships/’ Jim says, “but the monsters are different
now.”
The fire sits in the middle of the one-room log building and visibly glows from the east
facing door.
"Wherever you go,” Jim says, "it guides you home.”
[Back to AP News for Members of the birsi 'Nations]
[Back to the Native American Village]
[Wc welcome youi comments and suggestions...]
"M
■F'
Copyright by The Associated Press. All rights reserved.
JMDiversiry.com is committed to presenting diverse points ofview. However, the viewpoint expressed
this article is the opinion of the author and is not necessarily the viewpoint of the owners or employees
1MD.
IMDivarslty, Inc.
Contact Us
©2003 IM Diversity Inc. All rights reserved.
Privacy Statement
http: zVvn'av. imdiversity. com/Artic leDetail. asp9ArticlelD^ 13858
12/15/03
W h y D o W e Do W hat W e Do?
The D iffu sio n o f A lui h o Ihm T re a rm e n ! M e th o d s in to f rar tit e
Heidi Erickson '’ricliard ,\l .S.,an(. W illiini R. tf Ter.PrD.
Cfnle’t.i .1 Icoh'lisw . Siibi/jiite 4 Jose, ai4 A <1 d ic lie n s (C.dS.Gij, 'i'lit L itiieriily ofNe-A W enco, 'J SR
ABmACT
Hrs da clir.ie.aiH tori: <■ lo athp the pkliculjr Irealcenl
n. cthods that taey ise?
A survey of 70 ekoh ilisir.
p rafest o na r. •juiit title if la in n siip jeKeen irettoiis of
p r.ictice and yeats of ed jca-io a losread e id on tn ent nf a
Iraduional disear - r.odel rf akoholisr. predicted several
aspects of p aetier mevior, including the use if a larger
mi ir. ter ol differerl tieatir.eLt n. elhods, kclisiHi oflte ’.in ih
in Ire a it en, and re: c ir. t: ci d.niir. ol twelve step irngrairs.
P R'-'titir ntrs rtprrted learning mu ireairr. -n appioachee
pr.ir. ar ily through info nr. al ir. ?th id 5, rn r .through st rkshops
aril seir. inars. Endorseir ent ofa r< Hi anal disease t. ndel was
asfoeiaiet with using less e r.denee -base i l eatn: eni n: e ho .Is.
The contindn’ gaj lieisun stiote rnd practice in Ike
ar licliin field r: .q be ie ; to J r.oi lo a i o ur I o f educat.ot, but
rath er lo ra u es in d n: a dels atq ir.re d j u ring mfessio n a
li-i ining th al de- n: scietlific i11'ide nee to hr irrelevant :o practice.
C on la dec ? ] program di re-: tors
E .k h n j id in ited 2 -] cl in c i.m s tc ink 'view
!
O f "2 non in a led. 7f (97% ) partie ipa cd
22.3%
1 WiffiiKK
1 iff
.ft B.2%
&uur£«w»rk 1' .4%
A c ib i o i < te.e d th e U n d e ■ s t.i n d i n g o f 41 •: <: h li > m S c r 1
(Moyers .1 Miller. 1 9 9 3.1 to askss cliuicia.i s;
en do rse i en l o f d ise.1 sc aid p sy <:i o so eial m <: de s
Tri'ir. CoSlvnQUMi 1<).01
I?8
i M’ £ 8’.
iaxprriisnt:n 3333%
Iwo raters developed qualitative categories of
nerhods of diffn Hou. then used th ese to classi .y all
narratives.
Inkr-irte' .ig eement ■ 92 5%. win
discrepancies dec ded iy a th d rate:
% Of
t-ml
18%
18%
18%
11 %
9%
’%
THE IV'IE.RVIEW El) SAMPLE ;X
gi V/ jr
[8.U!
PR EDICT CHS OF PR ACT IE B JHAVIOR
o f 4; ri eihods group ed by 11 c. pric <• i <.ateg oiies
Surveyed al substrnce abuse ireairjeit programs in the
A buquerq jt m e ropolit.in aka
!
A c ra in isle red a qua la rive interview to identify w lai
new .ilcohoIrsm ireainent methods clinician; hoc
lerned since the r inilia train ing. me 10s jey had
ler ned ihem
NEW TREATMENT M ETHODS LEAINEC
JEXTII’Y AG TH S SAMPLE
I
HOW DID THEY LE ARN?
MET30DS
?i):
i (' % worn e n
18.4 y ? ar s o f e d u c a I io n
2.Wi min-nii.es
14.8 years ofcounseliag experience
77% -v liking in o jipat ent-on ly settings
64% m aster. degree, 20% ■fcelora. deg ree
6%
5%
4%
3%
0%
N ?w ly acqu ired ri eih -: <]
‘R claim in ’ lo ha’-e
lerrned i anew
lAliernative! te.apies
C dpiui! siill irrining
0 lher eogaitiv e-be liar- io raI
B fief in le ven lion s
T radii •m.d'staa da rd m elhod s
U ;.e of n ediealic ns
M arilal-f.ini ily ther.ip K'S
P >y cho ih /rap ie s
Spiritor.l appro a chi';
Self-ielp .sp nc aches
A version therapies
70%
70%
69%
43%
3 6%
27%
21%
17%
16%
13%
0%
On areirge. clinicians claimed io ie cur en ly u-ing 32
(M % ) of the 4 • diffeient t.her.ip?uiic m ethods n ruling
their die nts for alee holism
3 i ly c n iciaa sire ng ill •) f be lief i i ihe disc ise m cde I o f
.d'.’oh olisn (not yea's of du ;a it n or ex : e riend < pre die led
praciice behavior. C linic ia is n ore siro ig ly endoriing ihe
diserse n odel w ere r.l:H nr ore likely !<::
I
I
!
I
1
use r. larger nim her ofdiffereal treaini eal m etiods
em [ ha >i.?e A A and ab Mil eie e
■ in vc Ive the fa r ily in ire atm e it
be ni ore direciive in counseling style
u se it elhods w ilh le ss scie a lific evidence of
ef:ic acy (koi M i ler e. ah. 1 9 5 5 )
M .Iler, W . R , A c diev$. N . R . vV ibc irr.e, P& B er. -eIt.
'd E i'JilSj A -.veHtf of alteTr.allves: Effecti.e ire Km er. is for
.rlrok J pro )1?m s. k '5 . R.M ill?: i N . H ealter (Ms I I '.erin;.
idc-kth?
ilr-1 ed. I. M3 Ei. New Y 1.' P l< r. urn Pc-ss.
Moyers I. B„ k .V Ller. ft . R. iJ93j. T eKpMs'
■ o r. ce i lux Ika tor. sofa .co t o lisn:: M easi rem it land lai p lie a li-; r. <
o • tr Tlmei I deciiot?$Fih jJogp of 4 dc'lcfir s B r.*iarhirs Z '38
US.
I Pis •;esear-:P s is s ipporled ir. part h jRi fs T ;2 A •3/ ’ 6f
ard KOi-AAOJ.H from NIXAA.
Teaching of Stress Management
Page 1 of2 ■
Learning Theory for the Teaching of Stress Management
■■■
1. Identify the needs of the audience (individual or group).
2. Establish appropriate goals and specific learning objectives for
specific training sessions.
3. Select appropriate content to match goals, learning objectives and
time available.
4. Select appropriate teaching/learning strategies based on age,
educational level, Occupation, interest of participants, group size,
length of training and training intervals, facilities and
environment.
5. Sequence instructional strategics appropriately.
6. Explain the importance of establishing set, internal transition and
pacing.
7. Provide opportunities for appropriate practice by participants.
8. Explain the importance of modeling.
9. Demonstrate good presentation skills.
10. Analyze group dynamics in simulated situations and identify
strategies for handling specific situation, i.e. slow learners and
resistant group members.
11. Evaluate understanding and skills acquisition.
12. Provide appropriate reinforcement and feedback.
13. Establish appropriate levels of mastery.
http://wvv^7.unl.edu/stress/mgmt/teach.html
Teaching of Stress Management
1/20/04
Page 2 of 2
14. Select appropriate equipment, audio-visuals, instructional
materials and facilities.
15. Evaluate training and modify it based on evaluation.
16. Establish a method for follow-up to evaluate effectiveness of the
program for future development.
17. Explain the role of behavior modification strategies in promoting
life-style change.
18. Apply motivational theory in designing instructional strategies
for use with specific types of groups or individuals.
19. Discuss the importance of feedback and reinforcement in
learning stress management coping skills.
20. Identify how parl/whole learning is important in teaching
relaxation skills.
21. Explain the need for proper timing and progression in teaching
intervention strategies.
22. Explain state-dependent learning.
The Hindu : 'Alcohol abuse a serious problem in State'
Page 1 of 3
THE sM®a.HINDU
|Group Publications
Online edition of India's National Newspaper
Tuesday, Dec 18, 2001
About Js
Contact Js
Southern States
News: Front Page | National | Southern States | Other States |
International | Opinion | Business | Sport | Miscellaneous | Features |
Advts: Classifieds | Employment | Obituary |
Southern States - Karnataka-Bangalore
Alcohol abuse a serious problem in State'
By R. Vijaya Kumar
BANGALORE, DEC. 17. The final report of the Task Force on
Health and Family Welfare, chaired by Dr. H. Sudarshan, has
urged the State Government to take ''responsible action"
towards prevention and control of alcohol abuse.
In an elaborate analysis of the increasing problem in
Karnataka, the task force has termed alcohol abuse as a
major public health problem and a socio-economic issue. The
task force has suggested various measures to reduce the
problem.
Imparting training to all medical officers, especially at the
primary healthcare level on screening patients for alcoholrelated problems, and early detection and intervention for
health-related problems are some of the suggestions.
According to the report, training should include sensitisation
on the association of alcohol use with domestic violence, and
sexually-transmitted diseases, including HIV/AIDS.
Stories in this Section
• BMP to launch project for
removing debris from roads
• Scholarships: CAG indicts
official
• Tight security for cricket
match
• ' Alcohol abuse a serious
problem in State'
• ' NCERT has become an RSS
puppet’
Archives
Yesterday's Issue
Datewise
Features:
Magazine
Literary Review
Metro Plus
Open Page
Education
Book Review
Business
SciTech
Entertainment
Young World
Folio
Though Article 47 of the Constitution states that ' 'The State
shall regard the raising of the level of nutrition and the
standard of living of its people as among its primary duties
and, in particular, the State shall endeavour to bring about
prohibition of the consumption, except for medicinal
purposes, of intoxicating drinks and drugs which are injurious
to health," the State governments have abdicated their
responsibility. The reasons cited are loss of revenue, cost of
policing,
corruption
of enforcement
machinery,
illicit
distillation, hooch-related deaths and, above all, lack of
political will.
According to the report, the alcohol industry contributes a
major part of the revenue of the States. In 1997 it was
estimated to be about Rs. 17,000 crore in the form of taxes
and levies. The rate of liquor consumption in the country is
growing at a steady 15 per cent annually.
In Karnataka, though accurate figures are not available, the
sale and consumption of alcohol and alcoholic beverages is on
the increase. What is worrying is that it is spreading among
http://www.hinduonnet.eom/thehindu/2001/12/l 8/stories/2001121803030300.htm
11/29/03
The Hindu : 'Alcohol abuse a serious problem in State'
Page 2 of 3
sale and consumption of alcohol and alcoholic beverages is on
the increase. What is worrying is that it is spreading among
the youth, including high-school students.
According to the report, alcohol consumption results in a
large number of problems, adversely affecting almost every
organ in the body. While gastritis is an early symptom which
brings the patient to the doctor, it can lead to hepatitis and
cirrhosis. There is also an increased risk of cerebral
haemorrhage.
According to the task force, while alcohol consumption is an
accepted social and traditional norm in many developed
countries, it used to be predominant among males and rarely
among women in India. But this pattern of drinking has
rapidly changed.
''Social drinking" is considered to be synonymous with
''moderate drinking". While this is so in the traditional
''wet" or alcohol-using culture, it is not so in a ' 'dry"
country like India. Now social drinking has come to mean
drinking to intoxication.
In Karnataka, while about one-third of the adult male
population uses alcohol, one out of two people who drink
develop significant problems related to drinking. It has also
been found that alcohol dependence is a recurrent and
relapsing illness which affects one in four drinkers in
Karnataka.
The task force report has said that alcoholism is a disease
which needs intense medical and psycho-social interventions
for the alcoholic and his family.
The report has further said that as a public health issue, the
medical, social and economic costs borne by the larger
population (not just the alcoholic) as a result of alcoholism
are immeasurably greater.
It has also said the lax implementation of regulations and
laws is leading to increased production and wide availability
of alcohol. This stems from the perceived loss of income to
the Government from reduced production and sale of alcohol,
and is compounded by pressure from the liquor lobby.
Unfortunately, this does not take into account the spending
on health and the economic loss due to alcohol-related ill
health.
Quoting a 10-year study conducted by NIMHANS in
Karnataka between 1988 and 1999, the report has said that
Karnataka's installed capacity for beverage alcohol is one of
highest in the country. Production has gone up by 150 per
cent, and per capita consumption by 114 per cent (which
means that the average consumption by an average drinker
has gone up from nine bottles of whisky per year to 20
bottles).
Other findings of the NIMHANS study are: people are
beginning to drink at an earlier age (average age dropped
from 25 to 23 years), and in larger quantities; more than 50
http://www.hinduonnet.eom/thehindu/2001/12/l 8/stories/20011218O3O3O3OO.htm
1 1 29/03
F
The Hindu : 'Alcohol abuse a serious problem in State'
Page 3 of 3
beginning to drink at an earlier age (average age dropped
from 25 to 23 years), and in larger quantities; more than 50
per cent of all drinkers have a problem drinking pattern, and
associated morbidity; early alcohol-related health problems
are under-recognised by the primary healthcare physician;
heavy drinkers far outweigh chronic alcoholics in numbers
and account for substantially more medical, social and
economic problems; the problem is larger and more serious
in rural areas; and the Karnataka Government's alcoholrelated health expenditure and losses due to alcohol-related
industrial accidents was Rs. 975 crore, more than the
earnings from excise on beverage alcohol.
The task force has suggested some measures to reduce the
problem. They are: reduce the supply by increasing the
taxes; increase the minimum age for legal purchase of
alcohol; reduce the number of alcohol outlets; restrict the
hours of sale of liquor; and restrict sales on certain days.
Alcohol use and abuse is associated with violence, especially
against women and children. It is important to actively look
for history of violence in drinkers. Alcohol abuse has a
definite association with serious risk behaviour such as
unsafe sex which will lead to sexually-transmitted diseases,
the report has said.
Send this article to Friends by E-Mail
Southern States
News: Front Page | National | Southern States | Other States |
International | Opinion | Business | Sport | Miscellaneous | Features |
Advts: Classifieds | Employment | Obituary |
The Hindu Group: Home | About Us | Copyright | Archives | Contacts | Subscription
Group Sites: The Hindu | Business Line | The Sportstar | Frontline | Home |
Copyright © 2001, The Hindu. Republication or redissemination of the contents of this screen are expressly
prohibited without the written consent of The Hindu
http://www.hinduonnet.com/thehindu/2001/12/18/stories/2001121803030300.htm
1 /29/03
The Hindu : When images sink in
age 1 of4
THE sMsfeJMHINDU
| Group Publicgtic ns ▼
About Us
Contact Us
Online edition of India's National Newspaper
Monday, Aug 05, 2002
Metro Plus Hyderabad
Published on Mondays, Tuesdays,
Wednesdays & Thursdays
Features: Magazine | Literary Review | Life | Metro Plus | Open Page |
Education | Book Review | Business | SciTech | Entertainment | Young
World | Quest | Folio |
Metro Plus
Bangalore
Chennai
Delhi
Thiruvananthapuram
Visakhapatnam
Hyderabad
Kochi
When images sink in
The recent ban on the surrogate advertisements promoting liquor on
television has opened a fresh round of debate among the talking
heads. SYEDA FARIDA reports.
liffi!
■ I
HHml 'c?
I9
II
r ~
I
PRIDE
I
OlHtUI sponsor
•
Archives
Datewise
•
•
•
•
•
•
•
•
•
•
•
•
•
Classified
Lead
Life Style
Fashion
Music
Personality
Eating Out
Madras Miscellany
Issues
Arts & Crafts
Information Technology
Shopping
Heritage
Miscellany
News
News Update
Front Page
National
Regional:
• Southern States
• Other States
International
Opinion
Business
Sport
Miscellaneous
Index
DRINK DEEP: Packaged water, apple juice anyone? - Photo: P.V.
Sivakumar
HAVE YOU watched this image on television lately? Darts fly and voila,
it hits the bull's eye! It is the slick duel at the darting board commercial
of Haywards 5000. Was it about a darting kit? Or how about this? A cool
dude going high at a glass of sparkling drink -the line says Aristocrat
Apple Juice, one of the bolder commercials to hit the tele tube today.
Advertisement as a popular medium of paid communication has drawn
public ire time and again for moving away from truth andthe consumers
' right to know' to providing false images. Enter the new concept of
surrogate advertisement — the advertisement of the items on the
negative list, those that have downbeat social favour, such as tobacco
and liquor. The masked creatives leave it to the consumer to read
between the lines.
For instance, the Haywards 5000 darting kit, Mera No 1 Me Dowell's
packaged drinking water, ditto for the Kingfisher ' king of good times'
beer going the packaged water way, theWills Lifestyle, ITCGTDs'(Greeting Cards Division) Expression Greetings cards and the Red
http://www.hinduonnet.eom/thehindu/mp/2002/08/05/stories/2002080500700100.htm
1 1 29/03
The Hindu : When images sink in
Page 2 of 4
& White Bravery Awards from the tobacco wing.
Brand managers call it leveraging on the existing equity of the brand,
agencies define it as an exercise in brand recall of products on the
negative list, while the government comes down heavily on the
intriguing concept of surrogate advertising. With the anti-tobacco lobby
going strong worldwide, every country has a negative list of products.
One of the popular examples of surrogate advertisement from Sweden
with a ban on liquor advertising has been the usage of black and white
terriers for the Scottish whisky.
A parliamentary consultative committee on surrogate advertisement,
headed by Additional Secretary Anil Baijal, was set up recently to
deliberate on the determination of advertisements that would fall under
the surrogate bracket. The committee observed that Me Dowells and
Gilbeys Green Label were the cases of surrogate advertisement since
there was clear recall of the actual product, which is liquor in each case
following which the I&B ministry sent show cause notices to television
channels quoting the Cable Television Networks Rules Act 2001
according to which ' no broadcaster is permitted to show advertisement
which promotes directly or indirectly the promotion of alcohol, liquor or
other intoxicants...’ (Rule 7(2) of the Cable Television Networks Rules
Act) and calling for a ban on such commercials. And this fresh ban on
the airing of the surrogate advertisement Aristocrat Apple juice and the
likes on the Indian airwaves - STAR, Sony and Zee TV networks has got
the talking heads get into the debate over society versus financial
figures.
Celebrity endorsements, with Shatrughan Sinha for the Bagpiper soda
to the leading stars such as Akshay Kumar for the Red & White Bravery
Awards, events -- Baccardi Blast which has been a pilgrimage with the
hip youth, Kingfisher - Saurav and Jadeja at the popular jig for a
mineral water, the famous Charminar Challenge and the other sports
promotions -- Gold Flake Open and Royal Challenge, music -- Charms
Spirit of Freedom Concerts and fashion -- the designer collection at the
Wills Lifestyle chain of stores, the face of surrogate advertising has
been ever improvising while the story boards have been reworked and
gone creative.
"Event marketing has benefited sports, fashion and music. For instance
music got quite a patronage with the Charms Spirit of Freedom
Concerts featuring Indian classical music to the Western bands such as
Rock Machine. The companies have an advertising budget maximum of
which is spent on television. And when television does not carry them
where do you spend that to get the visibility?" asks Satish Kocharekar,
director, Livewires Advertising Pvt Ltd.
One essential function that surrogate advertising does is that of brand
recall and not necessarily an exercise in increasing sales. Commodities
such as tobacco and cigarettes are habit-forming with a high degree of
brand loyalty and rely on word-of-mouth product information. Thus, a
strong convincing logic is needed to convert the consumer to the brand
over a sustained period of time, consequently the strong ad appeal.
"They drink the image," says Chandrasekhar, an advertisement
consultant. While it is easy for the teenagers to switch brands, the
consistency and brand loyalty comes at 26-30 years, he observes.
"A brand is a sum total of the product, with the imagery and feeling.
The change in maturity may lead for instance a shift from the front line
http://www.hinduonnet.com/thehindu/mp/2002/08/05/stories/2002080500700100.him
1 1 29/03
The Hindu : When images sink in
I
Page 3 of 4
Navy Cut to chief executive India Kings imagery," says Sandeep Nath,
director Livewires Advertising Pvt Ltd. On one hand is the drive to break
the brand loyalty and on the other the competition from the house of
the global liquor majors and smuggled cigarettes, and the ban on
advertisement.
"Consumers should be given a choice. In the absence of this there will
be bootlegging and adulterated products lining up on the shelves," says
Chandrasekhar.
Observers believe that when the license to set up the industry,
manufacture and sale is given, it would be suicidal for the authorities to
take a high moral ground and stop the advertisement. The tobacco and
liquor industry provide a major chunk to the exchequer in the form of
the Central and State excise and under other tax heads. "There is an
ethical question. The government is keen that surrogate advertising
does not advertise liquor; to that extent the surrogate advertising is
wrong. But manufacturers have every right to sell the product," says
Vishwa Mohan, vice president RK Swamy BBDO.
The industry on its own has demonstrated the maturity and sense of
responsibility to promote instruments of advocacy of restraint and
moderation in consumption of alcoholic products. "Society for Alcohol
Related Social Policy Initiative (SASPI) is a self-evident initiative in this
direction. Me Dowell's and Seagram's have undertaken campaigns for
responsible drinking," says Vijay K. Rekhi, president UB Group Spirits
Division.
Some of the reasons for the ban on the advertising of the products have
been to shield the young and impressionable minds from consumption.
The Tobacco Institute of India (TH) is of the opinion that the freedom of
commercial expression should be permitted since tobacco is a legal
product and that consumption should be an informed personal choice
for adults only.
"Rather than an outright ban on advertising, the government should
endorse the code in operation which specify the timings when the ad
should be aired," says Vijay Rekhi.
Yet another reason why liquor ads in particular face flak has been the
frames being used in the commercial. 'What have women got to do
with the darting kit," says a consumer. Further, can anyone go on a
high on an apple juice?
"You don't want to induce children to smoke and thus remove the
sports sponsorship as in the case of cricket. Fair enough. But then one
tends to question the censorship for other advertisements shown on the
television," says Santha John, director Mindset EYW Advertising Pvt Ltd.
As regard to the debate, the liquor product has shown negative growth
rates plunging to a current 2.5 million cases from a 3.7 million cases in
2000 while there has been a de-growth in cigarette volumes with the
restriction on smoking in public places ever since the Tobacco Products
(Prohibition of Advertisement and Regulation) Bill 2001 called for a ban
on smoking in public places, and on surrogate advertising with a total
ban on sponsoring of sports and cultural events by cigarette and other
tobacco product companies. As a thought forward, the companies have
put their eggs in different baskets 'cashing in on their expertise' in
http://www.hinduonnet.eom/thehindu/mp/2002/08/05/stories/2002080500700100.htm
1 1 '29/03
The Hindu : When images sink in
age 4 of 4
hospitality, lifestyle and more.
As of now, the ban applies to the liquor segment. It is yet to be seen
how soon the axe falls on the tobacco surrogates - lifestyle, retail and
the works. And it would not be long when the companies producing
sports kits, darting boards, sparkling water, ice cubes and greeting
cards would also be known for the liquor and cigarettes they make.
Printer friendly page
Send this article to Friends by E-Mail
Metro Plus Bangalore Chennai Delhi
Thiruvananthapuram Visakhapatnam
Hyderabad
Kochi
Features: Magazine | Literary Review | Life | Metro Plus | Open Page |
Education | Book Review | Business | SciTech | Entertainment | Young
World | Quest | Folio |
The Hindu Group: Home | About Us | Copyright | Archives | Contacts | Subscription
Group Sites: The Hindu | Business Line | The Sportstar | Frontline | Home |
Comments to : thehindu@vsnl.com Copyright © 2002, The Hindu
Republication or redissemination of the contents of this screen are expressly prohibited without the written
consent of The Hindu
http://www.hinduonnet.eom/thehindu/mp/2002/08/05/stories/2002080500700100.htm
1 1/29/03
Page 1 of 5
the right strokes
The Hindu : Parenting
THE fta HINDU
(Group Publications *
About Us
Contact Us
Online edition of India's National Newspaper
Monday, Jul 14, 2003
Metro Plus Chennai
Published on Mondays, Tuesdays,
Wednesdays & Thursdays
Features: Magazine | Literary Review | Life | Metro Plus | Open Page |
Education | Book Review | Business | SciTech | Entertainment | Young
World | Quest | Folio |
Chennai
Coimbatore
Metro Plus
Bangalore
Visakhapatnam
Kochi
Thiruvananthapuram
Delhi
Hyderabad
Parenting — the right strokes
Parenting is a happy experience. But for parents these days, it is
fraught with travails and tensions, what with the rapid transition from
a traditional culture to a more western one. KAUSALYA SANTHANAM
writes...
NO..NO.
V.
\
LEFT
/
•
Archives
Datewise
•
•
•
•
•
•
•
•
•
•
•
•
•
Classified
Lead
Life Style
Fashion
Music
Personality
Eating Out
Madras Miscellany
Issues
Arts & Crafts
Information Technology
Shopping
Heritage
Miscellany
News
News Update
Front Page
National
Regional
• Southern States
• Other States
International
Opinion
Business
Sport
Miscellaneous
Index
"IT IS the duty of the old to feel anxious about the young. And the duty
of the young is to scorn the anxiety of the old," says the elderly
librarian at Oxford in "The Golden Compass", the first of Philip
Pullman's fascinating trilogy. A family friend, the father of two teenage
daughters, quoted these lines with delight when we met him some
months ago.
Parenting, as is pointed out incessantly and rather intimidatingly, these
days, is not an easy road. It has always been an endless one as the
http://www. hinduonnct. com/thehindu/mp/2003/07/14/stories/2003071400050100.him
I 1 29/03
The Hindu : Parenting
the right strokes
Page 2 of 5
anxious years continue; one is never free of the tension and travails
that being a parent means. Balanced of course by the unequalled joy
that it brings. Infancy, childhood, the difficult teens, the uncertain
twenties... it goes on. The turbulent relationship continues with the
squabbles and the serious differences between two generations that can
make the ' gap’ seem a chasm at times and a mere hairline crack at
others.
For the urban parents of today, the rapid transition from a traditional
culture to a strong western influence has brought in problems that their
parents did not face. Apart from the strong consumer lifestyle in a
globalised economy, the differences in attitudes and outlook between
them and Generation Next embrace such a diversity of topics that walls
can come up as quickly, even before you can say ' Berlin’ and then take
as many years to demolish. Teen years begin to assume the
proportions of a lifetime of pitched battles with the "You can'ts" and the
"I won'ts" filling the air with the frequency of rapid fire shots. The
parents-as-ogres and children-as-monsters phase seems to go on
forever. Till suddenly one day, if you are fortunate, the miracle happens
- it's not just truce but ceasefire and before you know it, you are
friends!
Chennai, a conservative society which is registering changes at an
astonishing frequency, has parents grappling with the morphing
scenario — pubs, discos, the more liberal interaction between the
sexes, dating. The academic scene too is fraught with tension for the
parent as everyone around you seems to have a wizard for a child who
can notch up scores with magical prowess minus the Potterian wand.
The urge to have one of these models of academic excellence as your
very own to flaunt makes the 1960s or even the 1970s parent take on
Dinosaurian hues.
With achievement becoming the buzzword, parents are keen to nurture
individualism and enterprise. But when the young who have the West
for their model, turn to western ways, the dilemma sets in as the
balance begins to totter and parents watch with panic the loss of
'traditional values' — respect for elders, the scoffing of traditional
clothes and the ever growing appetite for Western food as the colas and
the burgers take over. Many parents are worried about behavioural
problems.
"My children behave perfectly at school. But the same is lacking at
home. There is a lack of respect for their grandparents," worries Priya,
a mother of two. "I never indulge them but they simply cannot take
rebukes. My ten-year-old takes on much more than she can handle —
debates, girl guides, cycling, games — and then passes on all the
tensions to me. She neglects her food and then has no energy to carry
on with these activities. My children are least health conscious and live
on junk food. When we were young, we did not demand variety on the
menu all the time. Certain things we did not like, certain things we
learnt to like. They don't allow this to happen," she frets.
"When I was a girl, I had just four sets of clothes and was quite happy.
Looks were not a matter of concern while at school. But, my daughter is
worried that she is not fair enough and slim enough to qualify for the
now accepted norms of beauty though I think she is quite pretty," says
Shaiia, mother of a 14-year-old while Priya is afraid that all this
attention on looks is taking her daughter's attention away from her
lessons. The beauty contests and the cosmetic industries advertising
http://www.hinduonnet.eom/thehindu/mp/2003/07/14/stories/2003071400050100.htm
11/29/03
The Hindu : Parenting
the right strokes
Page 3 of 5
blitz have made a difference to how girls view themselves and the time
spent on appearance is inordinate, they both feel.
Communication is a major problem area. "My daughter has told my
husband, 'whatever be the problem, don't talk to me in the early
morning before I go to school, when I come back from school or at
night.' Where does that leave us?" asks Shaila with a helpless smile.
"You don't understand the tensions we face," is a charge that parents
face all the time. Selfishness, a materialistic attitude, lack of sensitivity,
not enough giving and sharing on the part of the young are other areas
of anxiety. More serious are the reckless driving, addiction to alcohol
and experimentation with drugs, for parents of boys. The pub culture
that has begun making its presence in the city has parents fearing "we
are going the ' Bangalore way'." "Parents in Chennai are finding it quite
difficult to deal with the changing scene," says Dr. Vijay Nagaswami,
psychotherapist and relationships consultant. "Parents have always
found their role tough but now they are talking more openly about the
problems they face. Workshops are now being held in the city for
parents, such as the one organised by the voluntary organisation
Nalanda Way recently, on how to deal with a changing world."
The key to good parenting is to bond and spend time with the child
from the infant stage and later share your thoughts with him/her and
become a trusted friend even in the pre-adolescent stage. The focus, he
says should be to share and not find out. "We place too much of a
premium on education and not vocation. If a child wants to be a DJ, he
should have the freedom to become one. These are legitimate career
options, not just engineering or medicine. Unfortunately, we don't
follow the West in the right areas such as freedom of choice and dignity
of jobs."
The therapist says he comes across more single parents now than
before. But Chennai, 'the reluctant metro', has still not become
impersonal; it offers more back-ups and family support for single
parents than perhaps any other metro. Adolescent sexuality is not a
new phenomenon, says the specialist. It's just that now it's much more
open. "When kids are pushed on all sides, they are on the look out for
an escape, a completely different lifestyle which makes them
experiment with sexuality as well." As for the pubs here, "they are very
different from those in the West," he points out. Many youngsters go
there to be seen more than anything else. Alcohol is a different matter
altogether as some youngsters may get hooked on to it. But for most,
pub and disco hopping is just a phase in their lives and if they are
focussed on a career, they will not spend too much time on it. It is only
when children don't have a trusting relationship with their parents they
will keep their world away from them.
"We have to give our children basic values which are never outmoded
such as pursuit of excellence, honesty, integrity and the need to be
forgiving and caring. Then things will work out well."
Sociologist Prema Rajagopalan feels that parents have to modify their
approach to parenting. "Seventy per cent of the parenting problems are
caused by the parents — they are driven by external pressures and
don’t know what they want." There are changes internally within the
family structure such as the break up of the joint family and there are
external pressures such as globalisation. "We are not going either the
Indian way or the Western way. We give our children freedom but
expect something in return. And Indian society has not got out of
http://www.hindiionnet.com/thehindu/mp/2003/07/14/stories/2003071400050100.htm
1 I 29/03
The Hindu : Parenting
the right strokes
Page 4 of 5
kinship ties. We are constantly worried about what our relatives, friends
and acquaintances will say to what our children wear and whom they
are out with. Parents have to make their choices. Every family has its
rules and you should instil these in children. If you reason with the
young, they understand. You have to be firm. One of my colleagues cut
off the cable TV connection when his child spent too much time in front
of the set."
She feels many of the problems are caused because parents act
according to convenience — allowing their children freedom when it
suits them and restricting at other times. Thrusting your ambitions on
the children and fulfilling your unrealised dreams through them is very
unfair. In the joint family system, the child received a lot of love and
less attention, now the child gets a lot of attention and less love as
parents don't accept the child for what he/she is but try to groom the
child according to what they want. Building up trust and giving freedom
with responsibility will work fine, she feels.
"The youngster is stuck between the authority of parents and teachers
on the one hand and peer pressure on the other," says psychiatrist Dr.
N. Rangarajan. "During adolescence, the child is trying to find his own
identity. If authority is too demanding and the peer group is accepting,
he settles in. The parent, however, wants an extension of himself and
his beliefs are driven by society. He wants his identity to be defined by
the fact that his son is in the IIT or in the U.S. If the child can't
measure up, he begins to feel inferior and a sort of ganglord supremacy
sometimes sets in and this can result in delinquency. Disrespect for the
grandparents can arise from the fact that they are often more
conservative than the parent and the youngster is rude in order to
reduce interaction with them."
There is, however, nothing like total freedom for anyone, he underlines,
and a child is answerable to his parents. The level of freedom can be
reached through an interactive process between parent and offspring.
One can't blame parents alone if something goes awry. Parents,
teachers and children are all involved in the process of a child's
development and growth of personality.
Parents are of different kinds — the autocratic, the overindulgent, the
neglectful and the democratic one. The last, of course, is the best, says
counsellor and special educator, Usha Ramakrishnan. He/she lays down
laws, has certain controls, explains them and lets the child develop his
own personality. The ineffective parent is one who does not carry out
the threats and the child does not take him seriously and so continues
in the same vein. Each child has a different emotional intelligence level
and should be handled accordingly. Some youngsters are naturally
good at taking care of themselves and handling others while others just
can't. "We give children negative strokes and we tell them what not to
do. Every parent thinks what he/she does is best; we don't sit back and
think. When children receive emotional warmth, they get strength and
are able to take stress. The emotional warmth begins with touch and
bonding at which Indians are very poor."
The first few years are critical and one can't correct mistakes in
parenting later, is what all the experts stress time and again. Just as it
is important to embrace your children tightly when they are young, it is
also very important to know when to let go when your grasp is
suffocating, says Dr. Nagaswami.
http://www.hinduonnet.com/thehindu/mp/2003/07/14/stories/2003071400050100.htm
1 I 29/03
The Hindu : Parenting
the right strokes
Page 5 of 5
Many parents tend to cling on and this can sour a relationship. When
the child is ready to fly, parents who are not obsessed with fears of the
empty nest, help him replicate the happy home he has left behind and
use their parenting as a model for his own.
The network
THE NETWORK for Information in Parenting (NIP) was created in Tamil
Nadu in 1999 by the Bala Mandir Research Foundation, which is NIP's
Secretariat, as a response to the growing concern for the need to
address early childhood care and development through effective
parenting at home and through institutions.
The NIP is an organisation of like-minded individuals and institutions
committed to parenting and creating the right environment for the
development of children in the rural and urban areas and to promote
child-rearing practices with special focus on children below six years.
"The major intent is to demystify parenting. The activities inspired by
the Hincks Dellchrist Children's Centre in Canada in the U.S. were
conducted with the help of the UNICEF. The Tamil Nadu Government
had been very helpful and the programme has proved useful. We are
now involved in 30,000 anganwadis," says Maya Gaitonde, who
represents the Secretariat. "We are also working with schools. The
Learning Through Play Material is available in Tamil, Kannada, Hindi,
Bengali and Telugu, and is unique as it uses simple pictures to
communicate. Contact address: Bala Mandir Research Foundation, 126,
G.N.Chetty Road, T.Nagar, ph:28214252.
Printer friendly page
Send this article to Friends by E-Mail
Metro Plus Bangalore Chennai Coimbatore
Kochi Thiruvananthapuram Visakhapatnam
Delhi
Hyderabad
Features: Magazine | Literary Review | Life | Metro Plus | Open Page |
Education | Book Review | Business | SciTech | Entertainment | Young
World | Quest | Folio |
The Hindu Group: Home | About Us | Copyright | Archives | Contacts | Subscription
Group Sites: The Hindu | Business Line | The Sportstar | Frontline | The Hindu eBooks | Home |
Comments to : thehindu@vsnl.com Copyright © 2003, The Hindu
Republication or redissemination of the contents of this screen are expressly prohibited without the written
consent of The Hindu
http://www.hinduonnet.com/thehindu/mp/2003/07/14/stories/2003071400050100.him
1 1/29/03
The use and abuseof alcohol, cannabis, opium and other
drugs has a relatively long history in India. In the last two
decades, with the introduction of heroin, the problem has
acquired new a nd alarming dimensions. Today, India is not
only an acknowledged transit country but also has a
significant drug con sumer population. It is clear that India
faces a serious problem of drug abuse, and remedial
measures are urgently required.
Drug abuse ravages society in in numerable ways. It affects
people in their most productive age groups. It imposes an
unimaginable burden on families and often destroys them. It
has a serious impact on public health. Drug abuse is a
recognised risk factorin the spread ofHIV/AIDS.Thereisa
well-established relationship between drugs and crime.
Problems! nthecomm unityareoftenreflectedattheworkplace.
Workplacescan beseriously impacted bysubstancefalcohol
and drug) abuse, through accidents, absenteeism, workplace
violenceand health related problems. Preventive measures
againstsubstanceabuseandplannedassistancefortroubled
employees not only keep such problems in check, but in the
long run a Iso ini prove productivity.
Responses to drug demand reduction need to take into
account factors initiating and maintaining drug abuse.
Problems relatingtosubstanceabusemayariseasa
consequenceofpersonal, family orsocialfactors, orfrom
certain work situations. As itisoften a combination ofthese
factors, multiple approaches to prevention, assistance,
treatmentand rehabilitation are required.
Indiahasbeencognisantofthegrowingproblemofsubstance
use and several agencies, both governmental and non
governmental are engaged in prevention and treatment
activities. Encouraged by the sub-regional experience o i
community drug rehabilitat ion garnered between 1990 an a
1992,a newproject,AD/IND/94/808 titled “Develop ng
Comm unity DrugRehabilitation a nd Workplace Preven tic n
Programmes” wasdeveloped.Thisprojectwasfinanced b
the United Nations Drug Control Programme (UNDCP). will
funds provided by the European Commission (EC), with the
International Labourorganization (ILO) as the executing
agency and the Ministry of Social justice and Em powermen!
(MSJE) as the implementing agency. The project was based
on the ILO Reference Model, which was used a nd adapted in
theearlierprojects.
The 808 Project titled “Developing Community Drug
Rehabilitation and Workplace Prevention Programmes”
focused on training and manpower development,
developmentofcommunitybased rehabilitation programm's
with a focus on Whole Person Recovery, and workplace
prevention programmes. The project demonstrated the
flexibility and adaptability of the ILO model of com mu nity
based rehabilitation in different regionsand culturalsetting,
within India. Human resource development formed the
backbone ofthis project.
Theprojectprovidedagoodexampleofpartnership betwee'
thenon-governmentalorganisations(NGOs),governmentala id
international agencies. It also created another form of
partnership, which facilitates interaction and collaborati )n
betweenemployersandworkers,betweenenterprisesandNGOs
offeringdrugdemand reduction servicesas well as betweer
respective organisations and the community, in addressir g
issuesrelatedtosubstanceabuse.TheAssociationofResourcf
Managers against Alcohol and Drug Abuse (ARMADA) was a
resultof such a partnership, and will attemptto continue the
successfulcollaboration built upduringtheproject.
The project has made a significant impact both at region a I
and national levels. The gains achieved in this project need
projects were based on the ILO model for community based
drug rehabilitation and workplace prevent ion. It emphasises
to be maintained and strengthened in orderto achieve its
long-term objective-the reduction of substance abuse and
its adverse consequences through effective community and
work placein itiativesinacoherentnationalstrategytocom bat
substanceabuserelated problemsin India .
the need for development of integrated services for persons
with addiction, a shift in focus to prevention, and for the
developmentofeffectivepartnershipstodealwiththecomplex
problems caused by drug a nd alcohol abuse in society.
This monograph presents two key experiences. The
experiences of drug treatment and rehabilitation centres
throughout the country in implementing community based
drug rehabilitation, and that of workplace prevention
programmesimplementedindiverseworksettings.Boththese
MinistryofSocialjusticeandEmpowerrfient
Governmentoflndia
UNDCPRegionalOfficeforSouthAsia
International LabourOrganization
European Commission
PARTNERSHIPS FOR DRUG DEMAND REDUCTION IN INDIA
Contents
Sectionsand Boxitems
1.
Introduction
i
2.
ThelnternationalLabourOrganizationReferenceModel
4
4
Addiction Rehabilitation
ThelnternationalLabourOrganizationCodeofPractice
RecognisingandHelpingBeforeAddictionSetsln-"TheTraffic Lights Model
5
5
6
Workplace ProgrammesTowards Prevention -AParadigm Shift
3.
Com mu nity Based DrugRehabilitation
Institutional Framework
Im piemen ting Non Governmen tai Organisations (NGOs)-A BriefGlimpse
TrainingofNGO Staff
Assistance to NGOs
The Initialstep UnderstandingGround Realities
Community Based DrugRehabilitation Initiatives--Different Organisations Adopt Different Com munities
Mobilising the Community and Motivating Clients for Treatment
Treatment and Rehabilitation-Different Strokes by Different Folks
Workasan Essential Pa rtofRecovery
Extending Economic Supportto Families
The Impact ofCommunity Based DrugRehabilitation
Boxes
Boxl -TheJewelLosesitsLustre
Box2-MiddleClassBlues
Box3-Teaching Livelihood Skills
Box4- Microcredit in theCommunity Based Drug Rehabilitation Project
BoxS-AFutureforSameer
Box6-PrabhaandHerFriends
Box?- Women with Addiction
4.
Workplaceprevention Programmes
Substance Use-WhatdoOrganisationsTraditionallydo?
The Rationale for Workplace Interventions
The International Labourorganization ReferenceModelatthe Workplace
Indian Workplaces-FocusingontheAlcoholand Drug Problem
Workplace Prevention Programmes-BuildingPartnerships
Understandingthe Problem
Trainingand Sensitisation
7
7
7
8
8
8
10
14
15
18
21
23
9
16
18
20
20
22
22
25
25
25
26
26
26
27
28
29
30
PolicyDevelopment
Programme Implementation
Boxes
Box 1-The 12 EnterpriseSurvey
27
29
Box2-AModelPolicy
5.
Boxes
Boxl-Employee’sReactions
Box 2- Perfect Partnerships: TISCOand Calcutta Samaritans
Box3-NonefortheRoad
Box4-DrinkingandDrivingDon’tmix
BoxS-TheFaceOffwithFeni
Box6 -TheMahindraStory
Box7-HittingtheJackpotatHindustan Motors
Box8-AOD Policy HelpsModi Rubbers
Box9-TheHinduPromotesTotal Health
Box 10-Cummins and Muktangan Mitra Partnership
Box 11 -MICOKeepstheGreensGreen
■
32
Workplaceprevention ProgrammeExperience-ImpactandSustainability
32
32
33
35
36
38
39
39
40
40
41
6.
MovingForwardfromtheWorkplacePrevention Programme
Formation ofThe Association of Resource Managers against AlcoholandDrugAbuse
42
7.
DevelopingCommunityDrugRehabilitationand Beyond
43
8.
SourceDocumentsandSelected References
46
ListofMain Abbreviations
48
Introduction
< IcoholanddrugrelatedproblemsarenotnewinIndia.
Overtheyears, however, theabuseofsyntheticand semi
synthetic opiates and and psychotropic substances has
replacedtrad itionalusepatterns.Whilealcoholisstillthemost
widelyusedintoxicantinthecountry.heroin.canna bis,volatile
solventsand pharmaceuticalpreparationslikebuprenorphine,
codeinecontainingcough syrupsand benzodiazepinesare
some ofthe other most commonly abused drugs. The South
Asia DrugDemand Reduction Report(2000) represents the
first major attempt to document the problem and responses
tosubstanceuse(drugsandalcohol)intheregion.Thereport
acknowledges the serious resource scarcity for drug demand
reduction activities and the need for Non-Governmental
Organisation (NGO) involvementand external assistancefor
developingsustainable programmes in thisarea.
In India, demand reduction activities have evolved over the
years. The initial interventions in the 1950’s and 1960’s
consisted predominantly of treatment of medical
com plica! ions. The 1970’s and 1980’ssawthe development
ofmoreintensivetreatment services, initially hospital based,
andtheemergenceofthenon-governmentaltreatmentsector.
In the 1990’s, there emerged multiple treatment approaches
to address these complex problems.
Earlierlnitiatives
TheMinistryofSocialjusticeandEmpowerment(MSJE) earlier
known as theM inistry of Welfare, has been sponsoring NGOs
workingintheareaofdrugrehabilitationsincethemid-1980s.
The focus of these MSjE funded interventions was
predominantlyoncounsellingandmedicaltreatmentofsevere
addictions.Theyfocusedlargelyonclientsduringtheirstayin
the rehabilitation centres.The follow-up was poor, and focus
on important aspects such as social re-integration,
occupational stability, and maintenance of recovery received
scant attention. Recovery was thus incomplete and relapse
rates were high. The need to develop a comprehensive
programme to deal moreeffectively with addiction related
problems, the need to reach the community rather than wait
fortheaddictstoreachthetreatmentcentres.andtoimprove
thequalityofrecovery was felt.
IntersectoralPitarrtnershipslo FackleDn g< r iA 1 CO hoi
Problems-PilotProjects
The Ministry of Social Justice and Empowerment has I ?ng
perceived the need for a coherent national strategy to deal
with substance abuse. While several agencies (bo h in
governmentand in thevoluntaiv sector) dealing with wellare,
health, education, labourhavelong been cognisant of the
problems related to substance use, it is inter-sectoral
partnershipsbetweenorganisationsthathaveledtoaforward
movemen tin the area of treatment and rehabilitation.
Two demonstration projects carried out between 1989 and
1992 involved such inter-sectoral collaboration betwec n the
International Labour Organization (ILO), the Euro pea !
Commission (EC),theMSJEand fourDelhi based NGOs. he
first projecttitled ‘Prevention and Assistance Programme sio
Workers with Drugand Alcohol Related Problems’ focuse Jon
grouptrainingandthedevelopmentofdrugrehabilitationand
reintegrationservicesthroughacommunity-orientedappioach.
Emphasis was laid on recovering addicts being gain :ully
employed. This was done by introducing income generz ting
activitiesthatwere supported by a revolving loan scheme.
Outputs from this project in eluded:
• Formulationoftrainingc u rriculaonaddict ionrehabilitation
• TrainingofNGOstaff
• Production ofa trainer’s manual and practitioner’ s
handbookon addiction rehabilitation
• Video presentation of the demonstration project to other
NGOs
• Experience with rehabilitation of 1000 recovering ad -Jins
The second project “Asian Regional Programmer for
CommunityDrugRehabilitation”addressedworkerswitf drug
and alcohol related problems in India, Philippines, Sri Lanka
and Thai land. In India, this project was implemented bv the
Ministry of Labour in collaboration with employers' a n d
workers’ organisations and a numberofenterprises .Six
enterprises implemented prevention and assis ance
programmes.OverSOOO workers were reached and 400 stall
memberstrained toassist in variousaspectsofworkp ace
in rib'
initiativesto preventand reducedrugproblems. Information
material was disseminated to these enterprises.
Project808: Community Based Rehabilitation and
WorkplacePreventionProgramme
The project ‘808’ titled “Developing Community Drug
Rehabilitation and WorkplacePrevention Programmes” was
the joint initiative of the ILO, United Nations DrugControl
Programme(UNDCP),MSjEandtheEC.Itwasconceivedofin
1994 to last for three years, but was extended by a further
twovears,untilDecemberl999,becauseoftheoverwhelming
responsetoit.
Theimmediateobjectivesoftheprojectwere:
• To establish the capacityat the national level to mobilise
community participation in developingdrug rehabilitation
services and workplace prevention and assistance
programmes throughout India
• To introduce to, and train, key drug rehabilitation
professionalsand paraprofessionalsin a widerspectrum
of rehabilitation approaches and techniques
• To introduce, and train professionals (including NGO
representatives) in developingprevention and assistance
measures at the workplace as well as supportive action in
thecommunity.
*
PhaselXommunityRehabilitation
This involved strengthening selected NGOs in various
componentsofaddictionrehabilitationunderthelLOReference
Model (discussed in Section 2) with a focus on Whole Person
Recovery (WPR).WPRseekstomakea person‘drugfree, crime
free and gainfully employed’.Th is phase included a rapid
situation assessment of substance abuse problems in the
identifiedcommunity.therehabilitationofidentified substance
abusers in that comm unity, with an emphasis on vocational
rehabilitation and aftercare. A major component included
developing income generating activities and supported
employment, as well as training of recovering drug users in
developingeffective work habits.
Phase2.WorkplacePreventionProgranime(WPP)
Workplacesmirrorthecommunity.andthewellbeingofthe
com munityandworkplacesareinextricablylinked.Therefore,
it is imperative that initiatives to rehabilitate a nd prevent
addiction be a joint ven Jure between the community and
theworkplace.
Theexistingsituation
At the time of initiating the ILO Workplace Prevention
Programme, few companies had programmes to deal with
alcoholand drug problems. Even thosethat existed were
initiatedmainlyonafeltneed.andfocusedalmostentirelyon
employeeswithaseriousproblemofaddiction.Relapserates
werehigh.leadingtoapessimisticandrathernegativeattitude
towardssuch programmes.
partnerships for drug DEMAND REDUCTION IN INDIA
TheobjectivesofthelLOmodelofWorkplacePrevention used
inProject808wereto:
• Createand maintain adrugfreeenvironmentatthc
workplace
• Generatean open atmospherewheresubstance users
areabletocomeforward and seekassistancewithout
risk of recrimination or personal consequences
• Laydown systemsand proceduresforidentificalioi ,
motivation and referral to treatment, of persons with
substance use related problems.
TheResults
The project successfully developed and established 1S
community based drug rehabilitation programmes in nine
cities/townsacrosslndia,whereitreplacedthe‘medicarmodel
with the‘community model’. The emphasis was on involving
the family and community leaders in treatment. Focus was
alsoon the inclusion ofvocational rehabilitation and income
generating activities in rehabilitation, with the emphasis on
WholePerson Recovery.
Coverage
Rehabilitation ant
Programmes:
•
•
•
•
■iili I'"
IScommunitybaseddrugrehab'litation programmes
in ninecities/townscovering 25.000 drug users
411 participantstrainedoverl 2 trainingworkshops
12 enterprises and 110,664 employees covered
1420managers, supervisors,worker’srepresentatives
and NGOstaff trained in'localworkshops
Twelveworkplaceprevention programmes were initiated in 8
cities through a partnership between selected NGOs and
enterprises. Treatment and care was extended to employee i
with drugand alcohol problems. The main emphasis was on
preven tionofdrugand a Icoholproblemsat theworkplace.
Several NGO staff and enterprise personnel were trained in
both rehabilitation and prevention to create a large pool of
resourcepersons.Thiswasdonethroughseminars.workshops
fellowshipsand study tours.
AttemptofthlsMonograph
Thereisgrowingworkon theextent, patternsand problems
associated with drugand alcoholusein India. However,the
documentation ofefforts to handle such problems in a
comprehensive manner is completely lacking. Th ■s
monograph attempts to capture the results of such
interventionsacrossthecounty. It isnotjusta reporton
Project 808. It is an attempt to capture the spirit of the
community and workplace programmes and the need foi
partnerships to address the complex problems of drugs an c
alcoholinoursociety.Themonographgoesbeyondnumbers
It provides real life examples ofwho benefited and how. It
narrates the success stories of enterprises that initiated the
workplace programme. It describes programme form illation
and the process of setting up of comprehensive community
based interventions and workplace programmes. The
monograph has been based largely on the reports provided
by the participating organisations, project documents,
evaluation reports (appendixed as source documents) and
site visits by the con tent providers.
Several lessons learnt from the experiences gained during
th is project and the limitations of some of the efforts are
also shared. These rich experiences provide valuable
insights for treatment providers, policy makers,
administrators, trainers and researchers workingtowards
reducing drug and alcohol related problems in the
community and at the workplace.
The project“Developing Community Drug Rehabilitation and
Workplace Prevention Programmes” is referred to a; the
Project808, CBDR (Community Based Drug Rehabilitation)
projectandWPP(WorkplacePreventionProgramme),orsi nply
the Project in d ifferent sections of the monograph. The tc rm
“substance” referstobothdrugsand alcohol. In manyoft he
case illustrations provided, names have been changed to
protectconfidentiality. Alist of the main abbreviations used
in this monograph is provided at the end.
INTRC DUG HON
yet-''*
■
ThelnternationalLabourOrganization
Reference Model
“The ILO Reference Model forms the basisfor both the Com
I munityandWorkplaceinitiatives.Someofthekeyconcepts
of the model arediscussed in this section.
• Commitmenttoadrugand alcohol free life
• Adaptationtoworkand responsibility
• Social re-integration
• Personal growth and self acceptance
• Acceptanceofhighervalues
Addiction Rehabilitation
TheUnitedNations(intheresourcebookon
Measures to Reduce
Illicit Demand for Drugs)definesRehabilitationas “theprocess
of helping individuals to establish a state where they are
physically, psychologically, andsociallycapableofcopingwith
the situations encountered, thus enabling them to take
advantageofthesameopportunitiesthatareavailabletoother
peopleinthesameagegroupinthesociety”.Thecrucialgoalof
rehabilitation is re-entry, readjustment and independent
functioningofthe recovered substance userintosociety.
Rehabilitation asdefined bythelLO relies on the“combined
and co-ordinated use ofeducational, social and vocational
measuresfortrainingorretrainingtheindividualtothehighest
leveloffunctionalability”.
WhoiePersanRecovery
Theaim ofacomprehensivetreatmentprogrammeis not just
togettheaddicted individual off alcohol ordrugs. Itfocuses
on ma king the person ‘drug free, crime free and gainfully
employed’.The keyelementsofWPR include:
lOOEl PROGRAMME DESIGN
/
“THE RECOVERY CENTRE**
ADDICTED
PERSONS
INTAKE
&
I
ASSESSMENT 1
#
VOCATIONAlX
REHABHITATION X
(AKO FUTURE )
.
~Xente»i»«ises^
GROUP
COUHSULING
“THE RECOVERY'
!’70U0W.ut»
I AFTER-CARE
iRt i
GROUP-
INOIVIOUAL
& FAMILY COUSEILIKG I
| ANO CASE MGMT
|
i
PARTNERSHIPS FOR DRUG DEMAND REDUCTION IN INDIA
SEtFH€U» 1
ACTIVITIES ]
(FUTURE |
smo) y
ForpeoplestrivingtoWPR.fourfactors, popularly known as
theFourKeystoChangearenecessary.Theseare:
• Practicalguidanceonwhatneedstobedone
• Caringencouragementforone’sefforts-apowerfuTfuer
for motivating recovery
• Successfulrolemodelswhohaveachieved thegoal
• Apeerlearninggroupworkingtogethertowardsthatgoal
Self-Help
ForWPRtooccur.thecommitmentoftheaddicted in dividual
tochangeiscrucial.Thepowerofself-helpftheideathatby
helping another, we help ourselves) in recovery is well
recognised. One of the best recognised self-help
organisationsistheAlcoholicsAnonymous(AA), which was
initiated in the USA in the 1930’s. Several other forms of
self-help groups, either led by peers (ex-users), or
professionally led peergroups have served as powerful
vehicles for recovery.
After-care
Ithasbeen wellestablished that forrecovery from addiction
to becompleteandthechances of relapse to be minimised,
providing continuous care forthe recovering person beyond
institutionalservices iscrucial.Thisin cludesfosteringsoc ia I
re-integration,helpingfamiliessupporttherecoveringperson,
and ensuringthe ex-user’s adaptation to employment.
Partnerships
Foreffectivetreatment, rehabilitation and aftercare, there
needstobenetworkingbetweendifferentindividuals,agencies
and community organisations. Families of substance users,
ex-users, non-governmental agencies, detoxification ant
treatmentcentres, hospitals, legalandenforcementpersonnel
allplayanimportantpartin recovery.
WorkandRecovery
Productive work is an essential partof recovery. Addicted
individualsoftenneedhelptokeeporgetjobs.toadapttowork
moreeasily.tohandlethedemandsandresponsibilitiesofwork,
togetalongcomfortablywithfellow-workers.tobeacceptedas
trustworthy, and to be able to accept direction and authority
without resentment. This is whatiscalled Workconditioning.
Vocational Rehabilitation refers to train!ng/retraining the
recovering addict for suitable and viable employment,
selective placement, on-the-job assistance and follow-up,
sensitisingkeyemployersandworkers ’groupsto addiction
as a safety and health problem, and forging relationships
with community groups that have a business and
employment orientation.
Where“openemployment”(conventionalworkforanemployer)
is not a viable option, alternatives such as self-employment,
supported work, apprenticeship, and co-operatives may be
• Information,educationandtrainingprograrnmesconcerni ig
alcoholanddrugsshouldbeintegratedwherefeasibleintc
broad-based health and safety programmes
• Principles of confidentiality and non-discrimination shot Id
beensuredtoprotectworkerswhoseekassistanceforsuch
problems
• While it must be recognised that the employer ha<
authority to discipline workers for employment-related
misconduct associated with alcohol and drugs,
counselling, treatment and rehabilitation should be
preferred to disciplinary action
Recognisingand Helpingwith Problems
Before Ad diction Sets In- The Ti
Lights Model
Whatever the nature of employment, work-conditioning
increases the likelihood of successful vocational
rehabilitation.
While addiction is a chronic and potentially relapsing
conditionwhichrequiresintensivetreatment,itisincreasingly
recogn ised that risky (e. g. drunken driving, in travenousdri g
use) and regular patterns of drug and alcohol use art
associated with m a jor p u b I ic h ea Ith, soc i a I a n d wo rk p I a c e
problems. Inthecontextofworkplacepreventionofsubstance
use.thelLOusesthetrafficlightanalogytocategoriselevels
DevelopingSMARTObjectives
ofdrinkingand druguse. Usingthisana logy, person scan be
categorised under three zones: the green, amber and red.
moresuitableforaddicted personsin recovery.
All organisations desire to improve programme effectiveness
and achieve successful results. It is important to develop
SMART objectives for th is. SMART objectives are:
Specific in defining programmeobjectives
Measurable outcomes
Attainablegoalswhichare
Relevantandare
Time-bound.
II
Tftf International Labour Organization
Codeoffffractice
The ILO Code of Practice on the management of alcohol and
d rug related problems at the workplace was evolved in 1995.
The key points in this code ofpracticeincludethefollowing:
• Alcoholanddrugpoliciesandprogrammesshould promote
the prevention, reduction and management of alcohol and
drug related problems in theworkplace
• Such problems should beconsidered health problemsand
dealtwith in anon-discriminatory manner
• Assessment ofthe problem and evolution ofa policy and
programmetoaddressissuesrelatedtoalcoholand drugs
needstobeajointinitiativeofem ployersand workers
• The policy should beclearand unambiguous and apply to
the entire workforce
• job situations that contribute to alcohol and drug related
problems need to be identified and appropriate preventive
orremedialaction taken
IT
The “traffic light” representation of the drug and alcohol
problem at the work place is simple and attractive. Person ;
withanaddictiontosubstancesorseriousproblemsassociated
withitarecategorisedasbeinginthe“red”zone,thoseatrisk
todevelop problems related to use a re in the “amber” zone,
and those with no problems are in the “green zone”. The
philosophyofthelLOapproachistokeepthe’greensgreen'.
shifttheambertothegreenandtheredtogreenoramber.The
ILOmodelthusshiftsthefocusfromtheredzonetogreenand
amberzoneinterventions.ltseekstodevelopacomprehensive
approachtotheproblemattheworkplace.ltspeaksalanguage
comfortable to employees and management, fosters
collaborations with other agencies, focuses on policy
development and guidelines as a key activity, and allow >
flexibility in approaches. These strengths help companiesto
read ilyacceptthe model.
THEINTERNAriONALLABOURORGANIZATIOMREfERENCLMiiijEl
Workplace Programmes
Prevention -AParadigm Shift
Towards
Traditional workplace substance abuse programmes focused
almostexclusivelyon provid ingassistancetoafewworkersin
theredzone.Ashifttoa prevention programmeexpandsthe
focustotheentireworkforce.withanemphasisonworkersin
the green and amber zones. It also focuses on “life-style”
changes by developing lifestyles that promote healthy living,
and replace substance use with healthy alternatives.
I
ManagementLedPragrammes
Substance abuse prevention programmes should be the
responsibility of the management, with the focus on
performance.whichisamanagementissue.Acomprehensive
workplace programme on substance abuse should be
in tegrated intomanagem entstrategies, sue hasoccu pation al
safety and heath, to ensure longterm sustainability.
L
| Programme 1|
I
Workplacepolicy
Fora successful programme, a written policysettingoutthe
objectives and goals ofthe programme, its structure and
elements, coverage, rolesand responsibilities should be
formulated. Guidelines must be available for training,
counselling, assistance and treatment referral, testing, and
consequences of policy violation.
III
I
I. Alcohol
I
| Prevention |
11
IB!
I
I
Total Stafflnwolvement:
Atall levelsofprogrammeplanning, policy Formulation and
programmeimplementation,involvementofbothmanagement
and employee representatives is vital for programme
sustainability. Various levels of staff need to be sensitised
and trained in the programme’s objectives.
GoingBeyondtheWorkplace
A successful workplace prevention programme ensures the
involvement and well being ofthe worker beyond the factory
gates, both at home and in the community. It a Iso involves
actively developing community and family linkages.
EnsuringPrograrnmeSustainability
Thesupportofihetopmariagement.availabilityofresoiircesfor
theprogramme,regularprogrammeevaluation,and integration
PAR INI RSHIPS FOR DRUG DEMAND REDUCTION IN INDIA
J#?
■
Sil
Ib
s
ofthe programmeintoongoing programmesof health, welfare,
occupationalsafety.securityorhumanresourcescanstrengthen
programme sustainability. Networking with local and regional
agenciesforsupporttotheprogramme.andnetworkingacross
enterprisestoshareexpertiseandresourcesareotherstrategies
to ensuresustainability.
Page 1 of 2
."National Centre For Drug Abuse Prevention::.
"I
ARTICLE’S
Article of the month
Charter
RRTCs
Articles
News & Events
Glossary of Terms
Training
Resources
Publications
Links
FAQ
Site map
NGO Profile
Ministry Report
Guest Book
Archives
Article in Mara
COMMUNITY DEVELOPMENT FOR HARM REDUCTION FROM DEPENDENCY TO ENPOWERME
TAPPING THE SOCIAL CAPITAL WITHIN USER NETWORKS
The field of harm reduction has generated considerable interest as a public health res
aimed at reducing and containing the negative impacts of continued substance ijise. One p
reason for the surge in interest in harm reduction was the emergence of the HIV/AIDS epi
and its linkage to injecting drug use. Practitioners in the field are recognising the limitati
specific strategies such as drug - substitution and needle exchange programmes. Ther
need, therefore, to broaden the scope of current harm reduction strategies by incorporating
systemic factors, which directly or indirectly affect the quality of life of user groups.
We need to move away from reductionist paradigms to adopting multi-causal inter
ecological models, which recognise that substance use has a reciprocal relationship betwe
individual and his or her social environment. Harm reduction strategies ought to be di
towards strengthening the adaptive capacities of the users and their networks; enhanci
supportive qualities of their social environment; and improving the relationship between the
components.
The Role of Social Capital in Community Development: One way of addressing the
neglected area of marginalisation of substance users, is through the deployment of partici
community development methods, which have the potential of tapping the social capital o
networks and enhancing their ownership in programme planning and implementation,
capital is the basic fabric or the essential ingredient of communities, and is a prerequis
community development processes.
Within the context of the developing world a multitude of socio-economic and health r
problems impinge on marginalized population, and the depleted stocks of social capital a
these groups have contributed to their relative poverty, and consequently their social excl
The stigmatisation of the drug problem along with the mental health consequence of prol
substance use often results in depleting the already scare resource of social Capital with
group of heterogeneous dependent users. How then do we, as harm reductionist interv
reconstruct social capital amongst deprived networks of substance users9
Biography: I have been working in the area of substance use since 1984 in New Del
Mumbai, India. My focus has been on developing an integrated community based progr
which is accessible to both substance users and marginalized people. Set up an
governmental agency in 1987 called Mukti Sadan Foundation which has its base in two
biggest slum communities of Asia, Jogeshwari and Dharavi. Felt the need to include eco
rehabilitation programme such as an engineering and fabrication factory; for user
marginalized youth in collaboration with UNESCO and DOH, Germany in 1999. Currentl
holding the position of Executive Director of Mukti Sadan Foundation.
Professionally I am a trained Medical and Psychiatric Social Worker. I received my M
Degree and my M.Phil degree in Social Work from the Tata Institute of Social Sciences, M
Currently I am in the process of completing my Doctoral Programme from the Tata Instit
Social Sciences. My area of interest has been the role of social systems in process of ad
h ttp: //w w w. n c cl ap. o rg/a rl i c1 es. p h p
1 1 1 /04
."National Centre For Drug Abuse Prevention::.
Page 2 of 2
and recovery from substance use. Developing qualitative research methods in understandin
seeking behaviour of substance users and network analysis has been another area of inter
me.
Currently I am working as the National Coordinator for the UNDCP for a study on drug
amongst women in India. This has been a major area of interest since 1991 when I worke
the Commonwealth Secretariat, UK, to undertake the first study on women substance us
India. The second area of interest has been the development of community based approac
demand reduction and harm reduction. I have worked with the WHO, UN/EiSCAP an
European Union to develop this approach for Mumbai since 1988 as temporary adviso
consultant.
Shobha Kapoor - Mukti Sadan Foundation,
A-103, eden-3, Hiranandani Gardens,
Powai- Mumbai (India)
E-mail: mukti@bom8. vsnl.net.in
The Use of Acupuncture in Drug Addiction Treatment
- by Judd R. Spray and Sharon M. Jones
Alternative medicine in the United States is a billion-dollar industry. A 1993 study published i
New England Journal of Medicine found that the American public spent almost as much
pocket money on alternative medicine in 1990 ($10.3 billion) as they did on hospitaliz
($12.8 billion). In fact, the study estimated that people made more visits to unconventional th
providers (425 million) than they did to primary care physicians (388 million) Viewed
skepticism by some, and virtually unknown to many, alternative medical techniques de
serious attention
Acupuncture, now one of the most popular forms of alternative medicine, was virtually unkno
the United States until recently. In 1971, James Reston, one of the New York Times'
respected journalists, was traveling in China when he was stricken with acute appendiciti
subsequent article on the use of acupuncture as an anesthetic turned his misfortune int
spark of much Western interest in acupuncture and other Chinese medicines.
Serious medical research and experimentation with the healing powers of acupuncture has
the discovery of a highly promising weapon in the fight against chemical dependency. T
there is a consensus in the medical community that more reliable scientific data on the s
need to be collected, anecdotal evidence and clinical success stories strongly sugges
acupuncture can alleviate many of the serious symptoms of withdrawal, thus facili
detoxification and encouraging acute addicts to continue treatment.
Recent enthusiasm for acupuncture treatment has encouraged some detoxification clini
incorporate it into their programs. Court systems in several major cities have created
courts," in which a program of intensive counseling and treatment, sometimes incl
acupuncture, is substituted for traditional prosecution. The need for more effective approac
dealing with repeat drug offenders, combined with the relatively low cost of maintaining die
drug court programs, makes some law enforcement officials hopeful that acupuncture will
effective part of the solution for addicts who find the lure of substance abuse more powerfu
the threat of incarceration.
This site is designed & developed by I-Edge Solutions Pvt. I td
301. Lloyds Chamber, Bldg. No 2, 409 Mangalwar Peth, Pune 411 011, India 'Tel No 9 ’
http://www.ncdap.org/articles.php
1 11/04
Page 1 of6
fndn'Tedica - Cyber Lectures
...
■
Dental Healthcare & X-ray C
www.fndmedica.com
Cyber Lech
MEDICAL ACUPUNCTURE
DR VINAY VARMA
ACUPUNCTURE IN MODERN MEDICINE Acupuncture is an important prestigious heritage of Chinese
people. Traditional Chinese medicine which includes acupuncture has been largely integrated with Western
medicine in China. Patients entering hospitals and clinics may opt, if they wish, for the whole spectrurh of
antibiotics or other modern drugs, OR they may prefer to take the door that leads to the traditional
Acupuncture department. Western or Chinese, who do we discuss medicines in such isolated and culturally
relative terms, while disciplines like mathematics and physics know no such boundaries. Since traditional &
Western medicines have the same object to cure and help suffering humanity. They should not have to
compete but rather compete but rather complement each other for the ultimate good of the patient. For the
patient whose only wish is to get well as quickly as possible, without any harmful effects, this is all that
matters for the patient.
Considerable controversy has surrounded Acupuncture, on the one hand extravagant claims have been
made for its efficacy while, on the other hand, it has been criticized for its lack of Scientific standing. There
are fake training centers, fake acupuncturists. Unfortunately, every profession has its incompetents, quacks
& confidence tricksters. Acupuncture practitioners may have more than their fair share of these because
there is no agreed standard of training which must be reached before one may practice acupuncture
So what is a Scientific method ? At the close of the last century, T. H. Huxlay defined science as
“organized common sense ” and the method of organization came to be known as “ Scientific method ” The
scientific method consist of observations inference and experiment, followed by the formulation of
hypothesis, theories and laws which in turn are subject to verification or otherwise by further experiments.
Acupuncture was born from keen observations of clinical facts. Aldous Huxley states that a needle stuck
into one’s foot should improve the headache or functioning of one’s liver is obviously incredible, it can not
be believed because, in terms of currently accepted
physiological theory it makes no sense. Within our system of explanation there is no reason why the needle
prick should be followed by an improvement of headache or liver function. Therefore, we say it can’t
happen. The only trouble with this argument is that, as a matter of empirical fact, it does happen, inserted
at precisely the right point, the needle in the foot regularly affects the function of liver, or improves the
headache. What should we do about events which by all the rules, ought not to occur, but which
nevertheless occur ? Two course are open to us, we can either shut our eyes with the hope that, if wp don’t
look at them, they will go away and leave us in peace or alternatively we can accept them - accept them
for time being as inexplicable anomalies and confirm, that is what I have done.
It is believed that acupuncture developed in both India and China, independently of each other. If wq go
back to the Indian medical classics, known as Vedas, said to have been written about 7000 years ago, we
find "needle therapy" mentioned there. The oldest known Chinese book on acupuncture, Nei Ching, did not
appear before fourth century before Christ and historical data indicate that the Nei Ching was probably
written around the second or Third century B. C. One volume of the Vedas, known as Suchi Veda, I
translated as the "art of piercing with a needle," was written approximately 3,000 years ago and deals
entirely with acupuncture, and described 180 points known as "MARMA", which are said to heal or kill. The
whole knowledge of Shalya Chikitsa or acupuncture is arranged in an orderly manner in eight volumes of
the famous ancient CLASSIC SUSHRUTA SANHITA. Nevertheless, one cannot argue the fact that t|he
http://www.indmedica.com/cyberlecl .cfm?clid=45&catid=43
I I 1 /04
. Indmedica - Cyber Lectures
Page 2 of 6
acupuncture was more developed by the Chinese than the Indians, and presented to the World in a mxe
complete fashion. So, WHAT IS ACUPUNCTURE ? The word Acupuncture is derived from Latin. In Lc tin,
acus = needle, pungra = to prick, to prick a needle for treatment is acupuncture. The combination of
acupuncture and moxibustion is known in Chinese as Chen Chiu [ needle & heat therapy.] Acupuncture
treatment is usually carried out by inserting very fine needles at acupuncture points. Acupuncture point
means a specific spot on the body surface where needling is done to get particular therapeutic response.
The practice of cauterizing a part of the ear or body with a hot metal probe is very common in rural India
and many Asian countries even today, is nothing but rudimentary form of acupuncture. The Eskimos cf
instance, are still using sharpened stones for treating their illnesses. The Bantus of South Africa scratch
certain areas of their skin to ally the symptoms of many illnesses, while in Brazil there is a tribe whose
method of treating illnesses is to shoot tiny arrows from a blow pipe on to a specific areas on the surface.
Karate, the martial art of unarmed combat from Japan is yet another variation of acupuncture. Moxibustion
represents a special form of point stimulation and involves burning pieces of drug plants generally the
moxa leaf, either on needle so as to conduct heat into the body, or in some cases actually on the surface of
the skin directly or indirectly by using some kind of barriers like ginger of garlic slices.
MECHANISMS OF ACUPUNCTURE Acupuncture is not a drug, it is a complete science OR healing
system by it self, having several effects to regulate the function of the human body and to increase its
resistance by enhancing the immune system and the anti-inflammatory, analgesic, anti-spastic, anti-siock
and anti-paralytic abilities of the body. So, Acupuncture effects can not be explained by single theory Nor
is acupuncture simply a trigger for releasing endorphins to create a temporary anesthetic effect by blocking
nerves that transmit pain message, as currently maintained in medical circles. It is far more than that.
Originally, the theory of Acupuncture is based upon an ancient Chinese concept of ( w ) holism. This
concept views human beings not only in relation to our own integral totality of body mind, and spirit, b jt
also as microcosmic expressions of a universe whose characteristics are inherent in every organism & in
every process. Health is viewed as the maintenance of harmony between ourselves and this universe while
illness in an expression of disharmony. The most fundamental biologic expression of the relative balahce or
imbalance of that primordial energy which the Chinese called Qi (pronounced Chi ). A free and balanced
flow of Qi in the body expresses harmony and health while a blockage of this energy indicates illness Qi
travels along certain pathways called meridians. There are TWELVE PAIRED & TWO UNPAIRED
meridians, named pertaining to particular organ. Acupuncture points and meridians have been
demonstrated in 1933 by a special technique called by Kirlian Photography ( Kirlian & Kirlian of USSR and
it was confirmed that acupuncture points have low electrical resistance than surrounding skin surface.
Gunn & associates have correlated the acupuncture points with points of accepted anatomical structures.
Most of acupuncture points correspond to motor points of muscles.
YIN & YANG THEORY, THEORY OF FIVE ELEMENTS, ORGAN CLOCK and many more traditional
theories not only explain Chinese Philosophy but dictates the rules to practice the art of acupuncture.
These theories are difficulty to digest by others who are trained in so called Modern Medicine. But some of
these are getting proved to very close to Modern Medicine, for example ORGAN CLOCK & CIRCADIAN
RHYTHM .
Research based on Modern Medicine started in & outside China, only after Mr. Nixon’s visit to China 1971.
Recent research for a mechanism of acupuncture has primarily focused on analgesic effect of
Acupuncture. Analgesic effects of acupuncture may be explained by GATE CONTROL THEORY OF
RONALD MELZACK and P D WALL, LONDON ( 1965 ). This theory believes that all pain impulses are
controlled, modulated and modified by means of a functional gate which is located in the substantia
gelatinosa of the spinal cord, and at higher levels. Normally pain impulses are conducted by small diameter
fibres ( delta & C fibres ) at the speed of 1-2 m/ sec, inhibit substantia gelatinosa cells in turn reduces its
inhibition over firing of T cells to higher levels and thus pain impulses are allowed to pass and pain is felt.
Non-noxious impulses of acupuncture conducted by large diameter fibres ( a beta fibres ) at the speed of
120 m/ sec. activates substantia gelatinosa which in turn inhibits, firing of T cells and thus no impulses are
allowed to pass and thus gate is closed and pain is not experienced even though pain impulses can ravel
up to the level of spinal cord. This theory fails to explain analgesic effect above spinal cord level and
modified theories like “Two Gate Theory” and “Four Gate Theory” have been but forward.
Dr. Bruce Pomeranz, Prof. Of Neurobiology of Toronto University and his co-worker suggest that the
naturally occurring endorphin play a prominent part. Acupuncture analgesia can be explained to a large
extent as being due to the release of a hormone called “Endorphine” during Acupuncture needling.
http://www.indmedica.com/cyberlecl .cfm?clid=45&catid=43
I 1 1 /04
• Indmedica - Cyber Lectures
Pa^e3 of 6
Endorphine is a naturally occurring neuropeptide having a chain of 31 amino-acids and like morphine and
other opiates it has a propensity of binding on to the opiate receptors of pain cells in the brain. The present
evidence suggest that, acupuncture stimulation results in a message to the brain causing release of
Endorphine from the pituitary gland and mid brain raphe system Experimentally it has shown that ablalon
of the pituitary gland & likewise injection of Nalorphine which is a morphine antagonist annuls acupuncture
analgesia. Endorphine takes some time to get release from the pituitary and this may be the reason for
there being an induction period which has to elapse before an operation can commence under acupuncture
analgesia. Chemical Or Humoral mechanisms are also involved in Acupuncture. For instance, if rabbit is
acupunctured its pain threshold is found to rise, & if the blood from this animal is then circulated into a nonacupunctured rabbit, the pain threshold of the second animal also raises, like wise perfusion of spinal :luid
from Acupunctured to non-acupunctured animal results in a similar effect showing that chemical
transmitters are definitely involved in the mechanism of acupuncture. Many acupuncture points have
specific effects on insertion of needles. For instance 1. ZUSANLI (St. 36 ) needling at this point,
Phagocytosis of staphylococcus Aureus by the leucocytes increases by one to two times even in case of
healthy persons. Rise in the phagocytic index from 1.74 to 3.97 and rise in the Phagocytic power from 48.2
to 71.5% have been registered on the second day after acupuncture. 2. A two to eight fold increase in
antibody titre, rise in gamma-globulin a specific immunoglobulins after needling at Quchi (L. I. 11. ) and
Sanyinjiao (Sp. 6) have been reported.
The last of the theories on acupuncture is that of Bio-electrical phenomenon. This theory suggests that
Western medicine deals with body chemistry , the principles of working in acupuncture have to do with
body physics. In 1973 at Yale University School of Medicine Burr and Associated confirmed that all living
things have electrodynamics fields which can be mapped out with fine voltmeters. These fields vary with
physical and mental conditions and thus may be used in diagnosing and treating a variety of disorders..
CLASSIFICATION: Acupuncture may be classified as 1) Symptomatic acupuncture 2) Classical or
Traditional acupuncture 3) Acupuncture Anesthesia. It may be further sub divided into (a) Body
Acupuncture (b) Ear Acupuncture (c) Scalp Acupuncture
Symptomatic acupuncture is mainly practiced by BARE FOOT DOCTORS as first line symptomatic
treatment for non specific short lived illness in rural setup. Classical Acupuncture is based on (W) Hol Stic
Approach. Total person is evaluated before treatment, regardless of the particular treatment. Acupuncture
does not treat named disease but rather the cause of the disease because symptoms are just signals of a
problem in the body. Although acupuncture’s effects are not permanent in treatments for analgesia a id
some pain disorders but they are long lasting. They are permanent when treating disorders from deafhess
to sterility. Acupuncture Anesthesia is one of the most impressive developments of Chinese medicines. It
was in 1958, that the foundations of Modern Acupuncture Anesthesia were laid by first operation under
acupuncture anesthesia at Shanghai and it was a tonsillectomy. The term ‘acupuncture’ anesthesia ‘is
really a misnomer. Although pain impulses are cut off by raising the pain threshold, other sensations like
temperature, balance and vibration sense are found to remain intact. Hence it would be more accurate to
use the term ‘Acupuncture Analgesia’ Advantages: 1) It is absolutely safe, non-toxic and free from adverse
effects like over dosage, side-effects of drugs and hypersensitivity reaction. 2) There are no major
disturbance of physiological functions under acupuncture anesthesia. 3) Hemorrhage too is very much
less, and blood transfusion is less often needed. 4) Post - operative complications are much less as
compared with general anesthesia. 5) Analgesia continues for several hours after the operation and
consequently post-operative pain is very much reduced. 6) Post-operative nausea, vomiting and respiratory
complications are absent. 7) Dehydration, electrolyte imbalance and post-operative debility are
circumvented because the patient can eat or drink immediately after and even during surgery. 8)
Acupuncture anesthesia is simple safe effective and economical. Like any other innovative procedure;
acupuncture anesthesia too has certain limitations and unsolved problems. While pain threshold is greatly
elevated, it may not be always one hundred percent complete, and some patients may still experience
varying degrees of pain during certain stages of an operation. In abdominal operations, difficulty is
sometimes encountered owing to inadequate muscular relaxation and discomfort from traction on the
viscera. So, in recent years ACUPUNCTURE ASSISTED ANESTHESIA is preferred in western countries.
Acupuncture anesthesia (analgesia) has been tried in over 100 different types of operations in over 2
million cases with success rate of about 90% in China. Generally, it is thought to be more effective in head,
neck and chest surgery. In India too, few major surgical operation are performed under acupuncture
analgesia and results are encouraging. Medical acupuncture is relatively recent terminology i.e.
acupuncture approach most commonly integrated by physicians into conventional medical practice
http://www.indmedica.com/cyberlecl .cfin?clid=45&catid=43
1/1 1/04
. Indmedica - Cyber Lectures
Page 4 of 6
INDICATIONS: Theoretically it is possible to help or cure by acupuncture any disease that can be affected
by a physiological process. So, acupuncture can be used in many conditions. The W. H. O. at the
Interregional Seminar, Beijing 1979, drew up the following provisional list of disorders that lend themselves
to acupuncture treatment. The list is based on clinical experience { and not necessarily based on controlled
clinical research }. Upper Respiratory Tract: Acute sinusitis Acute rhinitis Common cold Acute tonsilliti$
Respiratory System: Acute bronchitis Bronchial asthma ( most effective in children and in patients without
complication disease) Disorders of the Eye: Acute conjunctivitis Central retinitis Myopia (in children )
Cataract ( without complications ) Disorders of the mouth: Toothache, post-extraction pain Gingivitis Acute
and chronic pharyngitis Gastro intestinal Disorders: Spasm of the oesophagus and cardia Hiccough
Gastroptosis Acute and chronic gastritis Gastric hyperacidity Chronic duodenal ulcer ( pain relief) Acute
and chronic colitis Acute bacilliary dysentery Constipation Diarrhoea Paralytic ileus Neurological &
Musculo-skeletal Disorders: Headache and migraine Trigeminal neuralgia Facial palsy ( within three to six
months ) Meniers’s disease Neurogenic bladder dysfunction Nocturnal enuresis Interconstal neuralgia
Cervicobrachial syndrome Frozen shoulder, tennis elbow Sciatica, Low-back pain Osteo-arthritis
The only criticism is that this list was drawn up by a panel of Western qualified clinicians. It would have
been more gracious of the W. H. O to have allowed and have this list of disorder set out in their traditional
equivalents as well, in listing these disorders. This list has many drawbacks and is not acceptable to all. In
ancient times, even disease like tuberculosis, malaria etc had been treated by acupuncture. But now iis
proved that in these disease acupuncture cannot play the key role and effective medicines have been
found. One should remember that acupuncture is neither panacea for the disease not it is alternative o
modern medicine. There is nothing like alternative medicine. However a cure depends upon how well the
cause of the disease is understood and in consequences to what extent it can be eliminated and
Acupuncture should be used were it can give better & long lasting results compare to modern medicine.
One should know the limitations of Acupuncture first. Acupuncture will never replace conventional medical
treatment. As we learn more about it, the possibilities of using acupuncture alongside 'orthodox' medicine
will increase. Acupuncture should be practiced as a BRANCH OF MEDICINE Acupuncture is highly
effective in management of musculoskeletal & neuropathic pains by virtue of its well know analgesic
effects, cervical spondylosis low back ache, sciatica, arthritis, trigeminal neuralgia, migraine, pain of
secondary cancer (course of cancer cannot be influenced by acupuncture at present) or any acute or
chronic painful condition. Results are long lasting without side effects which is the main advantage over
modern medicine in case of chronic pains. All most all non-progressive paralytic conditions respond well to
acupuncture treatment. Acupuncture “ HASTENS” the speed of natural recovery and should be combined
with rehabilitation & physiotherapy techniques to improve quality of life. Respiratory ailments potentially
accessible to acupuncture intervention include allergic rhinitis, sinusitis, and bronchitis. Gastrointestinal
ailments include gastritis, irritable bowel syndrome, hepatitis, and hemorrhoids. Gynecological problems
include dysmenorrhea and infertility. Genitourinary problems include irritable bladder, prostatitis, male
infertility, and some forms of impotence. In ophthalmology so called incurable eye conditions like optic
atrophy retinitis pigmentosa, high myopia, skin disorders vitiligo, psoriasis etc. Acupuncture, particularly
when applied to the external ear, has proven valuable for managing substance abuse problems and
reducing prescriptions for narcotic analgesics. One of the most socially visible for acupuncture, this
application has gained the respect of rehabilitation programs internationally. For mental and emotional
disturbances, acupuncture can be useful as a transient aid in early and acute emotional states such as
anxiety, excitability, worry, early stages of depression, and fearful states In malignancies, acupuncture can
be considered as an additional therapy to combat the secondary effects of conventional therapy, and as an
adjunct in pain management. Off late, acupuncture is indicated by N I H, USA to alleviate side effects of
anti malignancy drugs like resistant nausea & vomiting. In recent years, people with HIV have been using
acupuncture to enhance the immune system and reduce pain, to manage HIV-related disorders and
symptoms and the side effects of anti-retroviral therapy , to help in the process of recovery from druc and
alcohol addiction, and to cope with stress and emotional disorders.
COMPLICATIONS: Complications of acupuncture ( acupuncture accidents ) can occur from improper
technique, lack of skill, or failure to observe certain guidelines and are very much PREVENTABLE 1 PAl?
PAIN
on insertion of the needle may be because of a) Bad acupuncturist b) Bad needle c) Bad posture d) pad
patient 2. BLEEDING sometimes occurs on withdrawal of the needle. This may be considered a ben gn
complication 3. FAINTING - uncommon as with any injection 4. THE FORGOTTEN NEEDLE - therapist
may forget to remove the needle after treatment 5. BENT, BROKEN OR STUCK NEEDLE 6. INFECTION
if needles are not sterilized properly. PERSONAL SET of needles are used to take away the fear of AIDS/
HEPATITIS B 7. INJURY TO INTERNAL ORGANS OR VITAL STRUCTURES 8. OVER CORRECTION
OF CERTAIN PHYSIOLOGICAL PARAMETERS, especially if the patient is also on drug therapy or
htlp://www. indmedica.com/cyberlecl .cfm?clid=45&catid=43
1 I 1 /04
. Indmedica - Cyber Lectures
Page 5 of 6
associated with hypertension / diabetes 9. COMPLICATION FROM ELECTRO - ACUPUNCTURE 10
ADDICTION TO ACUPUNCTURE 11. ABORTION certain points in first trimester may induce abortion
RECENT DEVELOPMENTS Electro - Acupuncture, Transcutaneous Electrical Nerve Stimulation (TEN
S ) Sono - Acupuncture, Laser Acupuncture And Homeo - Acupuncture
THE W. H. O. VIEW POINT OF ACUPUNCTURE v Acupuncture should be integrated with western
medicine and included in the medical curricula v Acupuncture analgesia is a “VALUABLE ADDITION” to
the therapeutic armory of the QUALIFIED ANESTHETIST. A western - trained physician may require no
more than THREE MONTHS TRAINING to learn the technique in theory and practice v Special programs
might be organized to reverse the unfavorable at attitudes of medical professionals and to educate this
general public about the safety of the procedure, its indications and its limitations
ACUPUNCTURE AS TODAY In CHINA, 800 DISEASES are being treated with ACUPUNCTURE
THERAPY and at least in 140 countries in the world. Many prestigious hospitals, universities, and m edical
schools around the world have now established departments for acupuncture research, therapy and
analgesia. The Karolinska Institute, Stockholm, Sweden for instance, the Ivory tower which awards Nobel
Prizes annually in Western medicine and allied science, has established a Pain Clinic with Acupuncture
since 1982. SRI LANKA - Best training Centre outside China having separate Minister for Traditiona
Medicines & Acupuncture. US Government - opened the office of Alternative Medicine at the National
Institute of Health and found Acupuncture can help relieve the nausea caused by chemotherapy in a Edition
to analgesia. The FDA approved Acupuncture needles for use by licensed practitioners in 1996 BMJ
2000;321:11 ( 1 July ) issue news is that Acupuncture wins BMA approval and according to Mark Sil|ert,
BMJ, Acupuncture should become more widely available on the NHS and family doctors should be trained
in some of its techniques, a BMA inquiry has concluded. The therapy has proved effective in treating back
and dental pain, nausea and vomiting, and migraine, the BMA's Board of Science and Education has found
after a two year study
ACUPUNCTURE IN INDIA v There is mushrooming of fake acupuncturist because of lack of proper
institutions v Dr. B. K. Basu Memorial Research & Training Institute , Calcutta Recognized By W. B. Govt 1996 v Three Govt. Clinics in Calcutta: ONE MONTH TRAINING: Medical Officers of Bankura, Hoocly &
Nadia Dist. v Dr. Kotnis Acupuncture Medical College, LUDHIANA, Punjab v P. G. I. Chandigarh, few
Hospitals in Delhi, Nanavati Hospital, Bombay Port Trust Hospital, G. T. Hospital & Others at Mumbai,
have Acupuncture Department v S. D. M College Of Naturopathy & Yogic Science - Ujre, Acupuncture for
B. N. Y. S Degree - Mangalore University. ( Rajeev Gandhi University ) v Many qualified Doctors arp taking
up Acupuncture
CONCLUSION: Evidence-based acupuncture is a simple method for no-drug pain control and should be
taught in medical schools and made available to all physicians. ( Evidence-based medicine (EBM) is the
use of the best current evidence in making decisions about the care of individual patients ) Acupuncture is
one of the best of modality for treating the sick, It works, it is great, if it does not work, patient still can get
his surgery done or medical line of treatment as many be the indication. The safety of a technique must be
judged on its results in the hands of competent practitioner who use it properly. If this criterion is accepted,
acupuncture per se must be seen as a very safe therapeutic system, whose complication are very rare and
are easily avoided or rectified. It is does no good, at least it does no harm either. In conclusion it is clear
that research on acupuncture will not be only significant for the health and welfare of the people but also
important for the progress of medical science. As we learn more about it, the possibilities of using
acupuncture alongside 'orthodox' medicine will increase When acupuncture is combined with modern
medicine, the patient benefits. Combining Western medicine and Acupuncture is what DR VINAY VARMA
is practicing to bring smile by relieving pains and thus ADDING LIFE TO YEARS.
TIPS: Where to go for Acupuncture Acupuncture should be practiced as a BRANCH OF MEDICINE; so go
to a practitioner who is fully qualified to treat western medical conditions, as well as being fully trained in
acupuncture.
For LIVE DEMONSTRATION, Or Further Details, please feel free to contact DR VINAY VARMA, Anand
Polio & Pain Relief Centre, Eureka Colony, Op: SBI Zonal Office Sholapur Road, Keshwapur, HUBLI 580023. Phone:283977
http://www.indmediea.com/cyberlecl .cfm?clid=45&catid=43
1 /1 1 /04
. Indmedica - Cyber Lectures
Page 6 of 6
If you want to know more about this topic, please click here
Home | About Us | Public Section | All Specialities | Medical Jobs | Consultation | Medical Admissions | Hospitals | Tenders
Medical/Dental/Pharmacy/Nursing/Homoeopathy Colleges | Equipment Suppliers | Pharmaceuticals | Blood Banks | SID Clinics
Setting Up A Blood Bank | Legal Advice | Grievances/Complaints | Guest Book | News | Humor | E-Greetings | Cor tact Us
Copyright © 2000 Ind Medica Ltd. All Rights Reserved. Terms and Conditions Last updated : 11-Jan-04
http://www. indmedica.com/cyberlec l.cfm?clid=45&catid=43
l/H/04
What is Rehabilitation Treatment or "rehab?"
Rehabilitation programs traditionally have the following basic
elements:
Initial Evaluation
Abstinence
Learning about addiction
Group counseling
AA or other 12 step participation
Individual counseling
A family program
What will "Rehab" accomplish?
Abstinence:
In many cases it seems that as long as the substance is in the blood stream, thinking remains
distorted. Often during the first days or weeks of total abstinence, we see a gradual clearing of
thinking processes. This is a complex psycholmncal and biological phenomenon, and is one of
the elements that inpatient programs are able to provide by making sure the patient is fully
detoxified and remains abstinent during his or her stay.
Removal Of Denial:
In some cases, when someone other than the patient, such as a parent, employer, or other
authority, is convinced there is a problem, but the addict is not yet sure, voluntary attendance
at a rehab program will provide enough clarification to remove this basic denial. Even those
who are convinced they have a problem with substances usually don't admit to themselves or
others the full extent of the addiction. Rehab uses group process to identify and help the
individual to let go of these expectable forms ol denial.
Removal Of Isolation:
As addictions progress, relationships deteriorate in quality. However, the bonds between
fellow recovering people are widely recognized as one of the few forces powerful enough to
keep recovery on track. The rehab experience. \\ hether it is inpatient or outpatient involves
in-depth sharing in a group setting. This kind of sharing creates strong interpersonal bonds
among group members. These bonds help to form a support system that will be powerful
enough to sustain the individual during the firsi months of abstinence.
"Basic Training:"
Basic training is a good way to think of the experience of rehab. Soldiers need a rapid course
to give them the basic knowledge and skills ilk \ will need to fight in a war. Some kinds of
learning need to be practiced so well that you can do them without thinking. In addition to the
learning, trainees become physically fit, and perhaps most important, form emotional bonds
that help keep up morale when the going is hard.
HOME\ Using This Guioe Inpatient Profiles. ' hitpatient PM'iles | Eating Disorder Programs
Internet Resources Manager's Yellow Pages IY^>fessional Resources | Guest Editorial| Info for
\ Facilities | Coiitnany/Aontact Fecillvsick
How To Choose The Right Program
2
Inpatient or Outpatient?
The goals of rehabilitation can often be accomplished without necessarily "going away" to an
inpatient setting. Structured outpatient treatment programs include education, group bonding, work
on more subtle forms of denial, and support in maintaining abstinence. However, since the decision
to go to treatment must be made for each session over a period of weeks or months, there must be a
greater degree of self-motivation.
Who needs inpatient treatment?
The simplest criteria for making this decision arc as follows:
Outpatient treatment requires:
1. Willingness and ability to attend sessions dilligently and regularly.
2. The ability to abstain from all mood alterinc substances for 48 hours at a time with
support.
Those who cannot meet these criteria will probably need to be referred to an inpatient
rehabilitation program.
What if the addicted person doesn't believe he or she has a problem?
External motivation is OK. Many poeple start recovery because of a push from someone else.
All rehab programs are voluntary. (Historical 1\. Rockefeller programs, which were
involuntary, were not a success.) Therefore, the patient must still give his or her consent to
treatment. This level of acceptance is good enough for the beginning of recovery.
For adolescents, we feel that the basic training, even if the patient clearly wants to return to
drug use as soon as possible following treatment, is still worth a great deal. The education and
the experience of what recovery is like may not he utilized immediately, but are likely to be
valuable in the future.
What if the addicted person has been in treatment before'/
It is good to get evaluation and advice about this from a professional familiar with recovery.
Sometimes the individual is at a new stage of recovery, and the experience will be entirely
different than before. Al other limes, it may be repetitious. Some programs have a specialized
"relapse" track, which may be more relevant.
When we evaluate patients who have relapsed. \e look at three areas:
l.Was there ever a full recovery program in place?
2.1s there a source of enabling that is preventing recovery from working?
3.1s there an internal "Stuck Point," (See Terrance Gorsky's writings) that stops the
recovery process at a certain spot?
What if the problem has significant psychiatric aspects?
This is a hard question to address in general. I \ aluation by a professional who specializes in
substance abuse as well as mental health is particularly important. Many mental health
specialists are well trained at recognizing symptoms of psychiatric problems, but may not be
as knowledgable about how emotional symptoms interact with addiction. Addiction specialists
may not be as sensitive to emotional problems and diagnoses. Let's take anxiety for example:
Anxiety can be a result of addiction.
Anxiety can be an accompaniment of addiction.
Anxiety can be a contributor to addiction.
If you think the person you are concerned abom could be "dual diagnosis," put your energy
into getting the best possible initial evaluation and treatmem recommendation.
Where addiction and other psychiatric problem coexist, the options are either to focus on the
addiction first, or both problems at once. It is almost never optimal to focus on emotional
problems before focusing on an active addiction
What kind of program
Freestanding Inpatient Rehabilitation
These programs live by their ability to create a hl’e-changing experience. Many of them do
amazing work in the short time they have.
Hospital Based Rehabilitation Unit
The quality depends on the particular unit and hospital. Some insurance policies may only
reimburse for a unit that is part of a general hospital. Hospital based rehab units may be more
able to work with patients who have complicating psychiatric or physical illness.
Hospital Detoxification Unit
Withdrawal from alcohol and sedative medical ion is the most dangerous, though opiate
withdrawal is extremely intense. Freestanding rehab programs may do detoxification, but the
hospital may have more medical backup for complicated or difficult cases. Increasingly,
detoxification is being done on an outpatient basis.
Watch out for the problem of the patient who finishes the detoxification feeling better than in
years, and is suddenly no longer motivated for ircatment. Before entering a unit that does
detoxification only, be sure that a very strong r nte has been established for follow up
rehabilitation, either inpatient or outpatient.
Long Term Residential Program
Following rehabilitation, many individuals lack the impulse control and sober habits to
successfully maintain a recovery in their community. This ! specially true of young people,
who have maturational work to do as well as recovery.
ke the difference between
For these individuals, long term residential treatment may
success and failure. Professional staff in rehab ; rograms will help evaluate the need and
feasibility of long term residential treatment.
Staff in rehab programs are also a good source > up to date !. nowledge about the quality and
services of long term residential programs.
Therapeutic Community
>ciated with an A A or 12 step
The term "rehab" usually refers more to programs that arc
nanon and such programs
tradition. Therapeutic Communities have then origins with
oriented primarily for heroin abusers. Nowadav many arc much stronger supporters of total
abstinence and the 12 step principles. They ma; encourage ; d require residential stays of up
to 2 years. When the addiction is serious enough io warrant ich a long length of stay, these
programs may offer an approach that is unique! effective.
Should you focus on programs exclusively for a special popu
Special programs for special populations have a drainages .
people have a tendency to think that they are "different" fr>
isolation. If they find themsel\ e.s in a program that is spec
with, that "uniqueness" defense may melt awa\ ()n the o;
member of a special group may acutally strengi in the sen
need to pick and choose among recovery tools and suppoi
good for early recovery.
Criterion: If membership in a special grOqp is likely to be treatment, then do try to find a special program of high qn
program with people of roughly similar background may I
1011?
disadvantages. Addicted
veryone else. That is part of the
d for just the group they identify
..and, feeling like a special
of being different, and with it a
kicking and choosing is not
d barrier to mainstream
. Otherwise, a mainstream
ne helpful.
Matching the program to the person
A major part of recovery is "identifying" with othe; recovbrii
differences may be an impediment to seeing the e>>umonalir
diversity is useful. It is often surprising who an indi\ idual m
>ple. Extreme cultural/educational
addictions. In general, some
ntifies with, on the other hand.
adding culture shock to the stress of rehabilitaiton is not then
sic in itself.
Local vs. Long Distance:
Many insurance companies emphasi:iae local treatment. One ad \ ntage is that family members can
more easily participate in the family program. On ilie other ha
the cost of airfare is a small fraction
of the total outlay, and the program's ability to provide just th Tvices you need may justify travel,
Especially for young people, being awiy from familiar "peop
iaces and things," may be an
advantage. Rehab programs away frommorne may also have
A'ith long term residential programs
in their locale.
\
HOME | Using This Guide | Inpatient Proiiles Outpatieni : . i des | Eating Disorder Programs |
Internet Resources | Manager's Yellow Pages Professional
ources | Guest Editorial | Info for
Facilities | Company/Contact Feedback
Glossary of Terms
Abstinence:
The act of refraining from the use of the subslai . c or substances on which a person has
become dependent.
u
Addiction:
The physical and psychological craving for a substance that develops into a dependency and
continues even though it is causing the addicted person physical, psychological and social
harm. The disease of addiction is chronic and progressive, and the craving may apply to
behaviors as well as substances.
l/ACOA:
Adult Children of Alcoholics. A self-help organ mation for individuals who have suffered and
suffer as the result of the alcholism of one or bmh parents.
Al-Anon:
A self-help organization for individuals whose lives are afl
member.
led by the addiction of a family
Alcoholic:
Someone who as the result of their alcohol com niption, eiiher excessive or habitual, suffers
or has suffered physical, psychological, cmolioi 1. social or occupational harm.
ij
z AA:
Alcoholics Anonymous. A voluntary, anonymous self-hel]
gunization of individuals who
have recognized their chemical dependence and are commiued to living a life of abstinence.
Abstinence is achieved by a 12-Step Program and members of AA support each other by
sharing their own struggles, experiences and hopes.
Alcoholism:
A disease characterized by excessive and liabni. 1 drinking of alcoholic beverages, that causes
the alcoholic, physical, psychological, and soci. ! harm.
Antabuse (disulfiram):
A drug which alters the way in which the body breaks dow . alcohol. Someone who is taking
antabuse and consuming alcohol will have a violent physical reaction to the alcohol, nausea,
vomiting and rapid changes in blood pressure occur. Antab e is sometimes prescribed as a
part of treatment after detoxification is complet io reduce Hm possibility of relapse.
Chemical Dependency:
A general term to describe a-physical or psych
gical reli
? on drugs.
Co-Dependency:
The condition in which people allow the behavior or sickm. •> of another to affect them to the
extent that they lose their own sense of identity and their o
life becomes unmanageable.
1 >r of another and having
Co-dependency is characterized by trying to control the be
unrealistic expectations about the power of lhai ontrol.
Detoxification:
The process of withdrawing a person from an\ idictive si
naturally when the addict cannot get his or her di .ig, and ui
detoxification process can be both uncomfortab. • and daily
supervision, detoxifcation is controlled and safe. Detoxifc.
treatment.
lance. Detoxification occurs
; these circumstances. The
vs, but under hospital
precedes rehabiltation
Dual Diagnosis:
The presence of a substance abuse or chemical dependency
psychiatric disorder.
VCW Vb. Enabling: Caa
iagnosis with a coexisting
Any behavior or aciton that assists the addict in the contim
either intentional or unintentional, and is usually done out <
Enabling allows the addict to continue their desii uctive be!
n of their addiction. Enabling is
ve and misguided concern.
ior.
FA:
Families Anonymous. A self-help organization ■ >r familie
the addiction of a family member.
hose lives have been affected by
Halfway House:
A residence for those who have completed treatment al a i
ready to return to their community. They need daily suppo
of their lives. Often, this includes assistance in vetting a jol
independently.
litation facility but are not yet
assist them in the restructuring
nd gradually living more
Intervention:
When people whose lives are affected by the ad ict. confn
about the addict's behavior and how it has affc > d them. .
the addict to accept help and go into treatment. I he panic!
the arrangements for treatment, transportation t< etc.
im or her with their feelings
ervention is an attempt to get
in the intervention make all
Long Term Residential Treatment:
Station program are still not
A treatment program for those who having completed a re:
ready to return to their communities and maintai a recove . Similar to a halfway house
sturcture often needed to
program, long term residential treatment olfers die suppor:
ind 6 months.
control the impulse to relapse. Programs usual! un betw
Methodone:
A drug used with heroin addicts as a substitute lor heroin,
detoxifcation to ease the discomfort, and it is used in main
it is administered orally under controlled conditions, and i
of rehab program. Like heroin, methodone is addictive.
MICA:
Mentally 111 Chemical Abuser. MICA refers io j ngrams I
Narcotics Anonymous:
A self-help organization of individuals who ha\ > recogni.
are committed to living a life of abstinence.
odone is used both during
nee programs. In maintenance,
illy accompanied by some form
se who are dually diagnosed.
ir dependency on drugs and
Recovery:
The change of attitudes and behaviors that brim about a I
terms of a process not a single event. It is ongoi
andon
Recovery embraces the idea that one lives life ; nively o
e of chemicals. Recovery is in
rs to being "in recovery."
iy at a time.
Relapse:
To repeat the addictive behavior for which an individual 1
eived treatment.
Sobriety:
A life free of chemicals or chemical dependent'
Tolerance:
The need to take increasingly large amounts of iiemicals i
effects; the same effects previously achieved b\ mailer a;
Twelve Step Programs:
The 12 Steps are the philosophical basis of Alcoholics An
der to achieve the desired
its.
i)us and all Anonymous
self-help groups. They are the means by which one can gel
life. The first step is to acknowledge one's powerlessness o
life has become unmanageable.
Withdrawal:
The symptoms experienced by substance abusers when the
they have become dependent. These symptoms are usually i
they may include, nausea, insomnia, anxiety, weakness, tre
convulsions, and dementia.
HOME | Using This Guide | Inpatient Profiles Outpatient I
Internet Resources | Manager's Yellow Pages Professional i
Facilities | Company/Contact I Feedback
0 recovery and achieve a sober
die substance and that one’s
op using the drug upon which
Peasant and uncomfortable;
ling, sweating, dizziness.
'. js | Eating Disorder Programs |
eiirces | Guest Editorial | Info for
%
Back to main
guide homepage How to cut down on your drinking
If you are drinking too much, you can improve your life and health by cutting down. How do you know if
you drink too much? Read these questions and answer ‘yes’ or ‘no’:
Do you drink alone when you feel angry or sad?
Does your drinking ever make you late for work?
Does your drinking worry your family?
Do you ever drink after telling yourself you won't?
Do you ever forget what you did while you were drinking?
Do you ever get headaches or have a hang-over after you have been drinking?
If you answered ‘yes’ to any of these questions, you may have a drinking problem. Check with your doctor
to be sure. Your doctor will be able to tell you whether you should cut down or abstain. If you are
alcoholic or have other medical problems, you should not just cut down on your drinking — you should
stop drinking completely. Your doctor will advise you about what is right for you.
If your doctor tells you to cut down on your drinking, these steps can help you. You might find that some
strategies are more useful than others. Remember you can have the support of your family and/or friends to
overcome your alcohol problem.
1. Write your reasons for changing
Why do you want to drink less? There are many reasons why you may want to cut down or stop drinking.
First think carefully about your reasons for wanting to change. Then have a look at the list below and mark
those that apply to you. If you have other reasons write them and discuss them with your doctor and/or
counsellor.
you will feel better
you will have more energy
you will lose excess weight
you will sleep better
you will save money
you won't have any hangovers
you will work better
your performance at work will improve
your health will improve
your family life will improve
your memory will improve
there will be less conflict at home
you won't be thinking about your next drink all the time
you will prevent serious health problems
2. Set a drinking goal
Choose a limit for how much you will drink. You may choose to cut down or not to drink at all. Talk to
you doctor about what is right for you.
Here are some suggestions about setting goals:
if you are trying to stop drinking altogether, it is important to set a definite 'quit date'
if you are trying to reduce your drinking, it will help if you plan on which days you will drink alcohol and
how many drinks you will have on each of these days. Make sure that you have at least two alcohol-free
days in a week
it also helps to record the number of drinks that you have each day. Keeping a record will remind you to
cut down and it will help you to keep track of whether you are following your goals
Now - write your drinking goal on a piece of paper. Put it where you can see it, such as on your
refrigerator or bathroom mirror. Your paper might look like this:
DRINKING GOAL
I will start on this day ....
I will not drink more than
I will not drink more than
OR
drinks in one day
drinks in one week
I will stop drinking alcohol.
3. Keep a ‘diary’ of your drinking
To help you reach your goal, keep a "diary" of your drinking. For example, write down every time you
have a drink for one week. Try to keep your diary for 3 or 4 weeks. This will show you how much you
drink and when. You may be surprised. How different is your goal from the amount you drink now? U >e
the "drinking diary" below to write down when you drink.
Week:
Number of drinks
Type of drinks
Place consumed
Monday
Tuesday
Wednesday
Thursday
Friday
Saturday
Sunday
Now you know why you want to drink less and you have a goal. There are many ways you can help
yourself cut down. Try these tips.
4. Tips for cutting down
Watch it at home
Keep a small amount or no alcohol at home. Don't keep temptations around.
Change the way you drink
quench your thirst with non-alcoholic drinks before having an alcoholic drink
avoid salty snacks when you are drinking
eat before drinking; It will make you feel more full and then you will drink less
have one or more non-alcoholic drinks before each alcoholic drink
try to take small sips of your drink, avoid gulping, drink slowly
dilute your drinks, e.g. add soda to wine and mixers to spirits
take a break of one hour between drinks.
Take a break from alcohol
Pick a day or two each week when you will not drink at all. Then, try to stop drinking for one week. Think
about how you feel physically and emotionally on these days. When you succeed and feel better, you n ay
find it easier to cut down for good.
beam how to say NO
You do not have to drink when other people drink. You do not have to take a drink that is given to you.
Practice ways ot say no politely. For example, you can tell people you feel better when you drink less.
Stay away from people who give you a hard time about not drinking.
Stay active
What would you like to do instead of drinking? Use the time and money spent on drinking to do someth ng
fun with your family or friends. Go out to eat, see a film, or play sports or a game.
Get support
Cutting down on your drinking may be difficult at times. Ask your family and friends for support to help
you reach your goal. Talk to your doctor if you are having trouble cutting down. Get the help you need to
reach your goal.
Watch out for temptations
Watch out for people, places or times that make you drink, even if you do not want to. Stay away from
people who drink a lot or bars where you used to go. Plan ahead of time what you will do to avoid drinking
when you are tempted. Do not drink when you are angry or upset or have a bad day. Section 5 below
"Dealing with difficult times" will help you with this.
5. Dealing with difficult times
Changing habits like drinking can be difficult. There will be times when you may drink more than what /ou
have planned or there might be times when it is very difficult not to drink or limit your drinking.
Can you think of any difficult times when you had problems in controlling your drinking?
Where were you?
Who were you with?
What were you doing?
What were you feeling?
Now look at the list below. Mark the situations or feelings that tend to make you drink more. If you have
other similar situations, write them below. Then discuss your list with your physician, counsellor, family
member or a close friend.
when I go to a party
when I go to dinner
when I go to the pub
meeting people in social situations
when I am with friends who drink
when I am on my own
when I am feeling in a low mood
when I am feeling anxious
when I am feeling angry
when I am feeling stressed
when I want to relax
when 1 have had a difficult day
when I have had an argument
when 1 am in a celebrating mood
when I invite friends over
Now you have the list of the most difficult times for you to resist drinking. If it is at all possible 1 avoiding
difficult situations will be very useful. Your initial strategy should be to reduce the temptation to drink.
However, in the long term, avoiding difficult situations may not be practical so it is also important to woik
out strategies to cope with difficult situations. Take a look at some of the strategies below and mark those
that would be useful to you:
If you have the habit of going to pubs after work or have the habit of meeting your friends there try to
organise a different social activity, e.g. going to see a film, or going to a gym or a park
If you drink mainly at night try to keep yourself busy, go to places where you cannot drink, e.g., movies
If you drink when you are with friends who drink heavily try to avoid contact with these friends
If you drink when you are alone reduce the amount of time that you spend alone, e.g. join a club or a
support group or increase time doing activities with family members
If you drink when you are bored try to plan enjoyable activities, e.g. shows, movies, exercise, hobbies etc.
If you drink when you are stressed learn relaxation techniques or engage in relaxing activities, e.g.
gardening
If you drink when you feel depressed or if you think that drinking calms your anxiety you must consult
your doctor about it
Make a list of your most difficult times and write below a few strategies to help you In each of these
situations
Difficult times
Strategies
eg, Friday night after work
eg invite a non drinking friend to go and see a movie
6. Important things to remember
Keep your drinking at a level which is within the safe limits
Remember to have two alcohol-free days a week
Be realistic; you may want to plan your drinks for social occasions
Remember not to drink more than your limit.
7. A word about set backs
Most people do not cut down or give up drinking all at once. There may be times when you will find it
difficult to stick to your goals. You might find that you had a few more drinks than you had planned to
drink.
Do not get discouraged — do not think of yourself as a failure. Learn from each occasion. Keep on trying
Remember:
do not give in because you have had a bad experience
take one day at a time and gradually it will get easier
you need your family and friends to support you
every time you stop yourself from doing something as a habit you are one step closer to breaking the habit
the craving for alcohol will go if you mentally occupy yourself with something else
you should consult your physician and/or counsellor concerning your difficulties
Do not give up.
If you cannot achieve your goals it is important that you ask yourself'why not?’ or 'what went wrong?’.
That might help you plan different strategies in the future. Use the diary on the next page to help you
identify factors that are connected to your desire to drink and which need to be dealt with in order to he p
you to reach your goals.
8. About detoxification
If you are physically dependent on alcohol, the first part of treatment is called detoxification. Detoxificat on
refers to a period of time when you stop taking alcohol. As a result your body has to re-adjust to a norma
state without alcohol and you are likely to experience symptoms of alcohol withdrawal. The most common
symptoms include nausea, shaking, sweating, irregular heart beat, anxiety and fatigue. These symptoms
gradually improve over 3 to 5 days. People who have been drinking very heavily for a long time may
experience more serious symptoms such as fits, confusion about the day, time or where they are. They may
experience hallucinations, that is, seeing or hearing things that do not exist. For most people who are
moderately dependent upon alcohol, it is safe to withdraw from alcohol as an out patient or at home. und?r
the supervision of a doctor. Others need to be in a hospital setting. Discuss which is best for you with y )ur
doctor. Medication can help to reduce unpleasant symptoms of withdrawal during the withdrawal phase,
though if you experience only mild withdrawal symptoms, you may need only support, lots of fluids and
nuti ition. There is no medication that will cure an alcohol problem.
When withdrawal is finished, you will need to use the non-drug strategies described in this leaflet. Self
help groups such as Alcoholics Anonymous are also helpful for many people.
Understanding your drinking - diary
This diary will help you identify factors that are connected to your desire to drink and which need to be
dealt with in order to help you to reach your goals. If you have slipped back, it will help you answer the
question "why" and "'what went wrong?" That might help you plan different strategies in the future.
Day. date, times
Where, with, when, what
Thoughts before drinking/drug taking
What did you do?
Behaviours, feelings, consequences
What did you drink/take?
Number of standard drinks or drugs
Further sources of help for alcohol problems
Self Help Groups:
Al - Anon Family Groups UK and Eire
61 Great Dover Street, London SEI 4YF
020 7403 0888 24-hour helpline
Understanding and support for families and friends of alcoholics whether still drinking or not.
Alateen for young people aged 12-20 affected by others’ drinking.
Alcoholics Anoymous
PO Box 1, Stonebow House, General Service Office, Stonebow, York YO1 7NJ.
01904 644026 Administration
Helplines:
020 7352 3001/7833 0022 (London);
0141 226 2214 (Scotland);
01907 6255574 (Mid Wales);
01685 875070 (South Wales);
01639 644871 (Swansea)
Helpline and support groups for men and women trying to achieve and maintain sobriety and help other
alcoholics to get sober.
Drinkline
UK helpline: 0800 9178282 (Mon to Fri 11 am-11 pm)
Asian Line
0990 133 480 (Mon l-8pm) Hindi, Urdu, Gujerati and Pujabi
Confidential alcohol counselling and information service
Northern Ireland Community Addiction Service
40 Elmwood Avenue, Belfast BT9 6AZ, Northern Ireland.
Tel: 01232 664 434
Scottish Council on Alcohol
2nd Floor, 166 Buchanan Street, Glasgow G1 2NH, Scotland
Tel: 0141 333 9677
Suggested Reading
Free information pack: Think About Drink, Health Education Authority Customer Services, Marston Book
Services, PO Box 269, Abingdon 0X14 4YN
The Family Partners Pack, Alcohol Concern, 1996
Drinking Problems: Information and Advice for the Individual, Family and Friends. Chick J and Chick I.
Optima 1992
[1] Adapted, with permission, from World Health Organiazation, 1998, Mental Disorders in Primary Care:
a WHO Education Package and Andrews G and Jenkins R, eds, 1999, Management of Mental Disorders
(UK Edition) World Health Organization Collaborating Centre for Mental Health and Substance Abuse
Download this section - PDF | RTF | Help
Return to the top of the page
Website designed and maintained by CEBMH
Copyright © 1998-2001 World Health Organization
Guide developed by the WHO Collaborating Centre for Research and Training for Mental Health. Institi le
of Psychiatry, Kings College London.
1
Treatment
What is the Issue?
The provision of treatment options for those who develop problems associated with the
misuse of alcohol, including alcohol dependence, or "alcoholism", is an issue of concern to
health care systems. Central to this issue is how to enable individuals with problems of
alcohol abuse and dependence to resume normal function. As defined by the ICD-10
classification system, the alcohol dependence syndrome is characterized by craving for
alcohol, difficulty in controlling the compulsion to drink, withdrawal, tolerance to
increasingly high doses of alcohol, neglect of other areas of life, once important, and
persistent consumption despite clear evidence of harm (WHO 1992).
A number of approaches to the treatment and management of alcohol problems exist,
each with its proponents and evidence to support its effectiveness.
What is the Debate?
Historically, the debate over which treatment options are most effective stems from the
existing and often opposing views regarding the underlying causes of alcohol problems.
One school of thought favors the "disease model" (Jellinek), while others favor a view of
alcohol use, abuse and dependence as part of the same continuum. As a result, the long
term treatment goals of "disease model" approaches is complete abstinence, while other
approaches allow for a return to moderate drinking.
Proponents of the "disease model" have argued for treatment with an emphasis on
abstinence, based largely on the tenets of Alcoholics Anonymous and similar self-help
groups. This model has tended to support the notion that there is something unique in the
physiological, psychological and spiritual makeup of alcohol-dependent individuals, and
that in order for them to lead "normal" lives, complete abstention from alcohol is the only
road to recovery.
The "disease model" with its emphasis on extended residential treatment and long-term
affiliation to self-help groups has been challenged by those who view alcohol use, misuse
and dependence as part of a reversible sliding scale. The emphasis here is on early
identification of potential problems and assisting individuals to change the patterns of th^ir
drinking in order to reduce undesired negative consequences. Inherent in this approach s
the notion that it is possible for individuals to learn to drink responsibly, especially if they
are diagnosed early, but even after they have met the criteria for dependence. The focus
of the treatment modalities offered within this model tends to be community based and
non-residential in nature.
What are the Approaches?
Treatment of alcohol related problems and dependence covers a broad range of
interventions focusing on physiological approaches, psychological interventions, or on
modifications of behavior or milieu. They generally involve three stages, addressed
differently within each approach: detoxification to minimize withdrawal, rehabilitation or
follow-up, and maintenance. Different approaches to treatment can be used individually or
in conjunction with each other, depending on the needs of the patient and on what seems
most appropriate under the circumstances.
In practice, treatment of alcohol problems and dependence ranges from brief counseling to
prolonged treatment or life-long affiliation with self-help groups. The important first step,
however, consists of screening to assess the severity of the problem and to be able to
diagnose dependence, if appropriate. A range of standardized assessment tests is
available, some of which can be applied specifically to populations of adults or youth.
Others, such as the AUDIT (Babor et al., 1992), are applicable across cultures.
For some individuals with alcohol abuse problems, brief intervention, followed by
counseling, has proven effective (Chick et al., 1985; WHO Brief Intervention Study Group,
1996) in modifying behavior.
Group therapy and self-help groups are among the most prominent approaches to
treatment. These include Alcoholics Anonymous, popular mainly in North America and
Northern Europe in which the focus is on the individual and on achieving complete
abstinence as the only effective solution. In contrast, the "club" system, popular in parts of
Central and Southern Europe, focuses on the community, engaging the individuals family
and social network in the recovery process (Hudolin, 1984). A third self-help approach is
"controlled drinking", in which the view of use, abuse and dependence on a continuum
prevails, and where the ultimate goal can be resumed moderate drinking (Davies, 1962;
Kishline, 1994). The appeal of these approaches depends largely on the view of problem
drinking in different cultures and the relationship of the individual and the community within
the different traditions.
Pharmacotherapy offers another treatment option with the goal of assisting individuals to
manage alcohol problems. Among the more commonly used drugs are disulfiram (or
Antabuse), as well as and acamprosate and naltrexone, both effective in preventing
relapse (Kranzler, 2000). Pharmacotherapy is often used in conjunction with counseling
approaches (Barber & O'Brien, 1999).
Other therapies include: aversion therapy; behavioral therapy emphasizing coping and
problem-solving skills, stress management, and social skills training; alcohol education;
and family therapy. Often, these approaches are used in combination with each other.
Pharmacotherapy, for example, may be coupled with behavior modification approaches.
Which of these treatment approaches is most effective is a question open to debate. Much
depends on the circumstances surrounding the individual and the nature of his/her
problems with alcohol. Some have argued that while less dependent drinkers may achieve
"controlled drinking" and moderation, abstinence is more suited to high dependence
drinkers (Sobell and Sobell, 1995).
Research carried out mainly in the United States into the potential value of matching
patients to particular treatment modalities according to a set of criteria has failed to show
any specific advantage for one treatment type over another (Project MATCH, 1997). In
patient treatment for alcohol dependence has been shown to be effective; however the
benefit of this approach over less intensive treatment such as outpatient or day treatment
is not apparent.
Is there a Consensus?
There appears to be mounting consensus that no single approach to the management of
drinking problems or alcohol dependence holds the key to success. There is clear
evidence to support the hypothesis that the capacity of the professionals delivering
treatment is a considerable factor in determining successful outcomes.
There is a growing consensus in favor of evidence-based practice in relation to the
management of alcohol problems. The introduction of harm minimization approaches tc
the management of drinking problems has gained significant currency in Europe, Canada
and Australasia (Plant et al. 1997; Grant & Litvak, 1998). The United States, Asia and
Central Europe continue to have a strong commitment both from funders and treatment
providers to traditional abstinence only approaches.
Suggested Readings
Babor, T., F., de la Fuente, J.R., Saunders, J. & Grant, M. (1992). AUDIT: The Alcohol
Use Disorders Identification Test: Guidelines for Use in Primary Health Care. Geneva,
Switzerland: World Health Organization.
Barber, W.S. & O'Brien, C.P. (1999). Pharmacotherapies. In: B.S. McCrady & E.E. Epstein
(Eds.), Addictions: A Comprehensive Guidebook, New York, NY: Oxford University Press.
Davies, D.L. (1962). Normal drinking in recovered alcohol addicts. Quarterly Journal of
Studies on Alcohol, 21: 94-104.
Grant, M. & Litvak, J. (Eds.), 1998. Drinking Patterns and Their Consequences.
Washington, DC: Taylor & Francis.
Heather, N., 1995. Brief intervention strategies. In: R.K. Hester & W.R. Miller (Eds.),
Handbook of Alcoholism Treatment Approaches: Effective Alternatives. Needham Heights,
MA: Allyn and Bacon.
Hudolin, V.L., 1984. Alcoholism programme at the University Department for Neurology,
Psychiatry, Alcohology and other dependencies: Dr. M. Stojanovic, University Hospital,
Zagreb. Alcoholism: Journal on Alcoholism and Related Addictions, 20(1-2): 3- 51.
Jellinek, E. M., 1972. Disease Concept Of Alcoholism. New Haven, CT: College and
University Press.
Kishline, A. (1994). Moderate Drinking: The New Option for Problem Drinkers. Tucson:
See Sharp Press.
Kranzler, H.R. (2000). Medications for alcohol dependence - New Vistas. Journal of the
American Medical Association (JAMA), 283(23): 1016-1017.
Plant, M., Single, E. & Stockwell, T. (Eds.) (1997). Alcohol: Minimising the Harm. Whqt
Works? London: Free Association Books.
Project MATCH Research Group (1997). Matching alcoholism treatments to client
heterogeneity: Project MATCH post-treatment drinking outcomes. Journal of Studies on
Alcohol, 58, 7-29.
Sobell, M.B. & Sobell, L.C. (1995). Controlled drinking after 25 years: How important was
the great debate? Addiction, 90(9), 1149-53.
WHO (1992). The ICD-10 Classification of Mental and Behavioral Disorders. Geneva,
Switzerland: World Health Organization.
WHO Brief Intervention Study Group (1996). A cross-national trial of brief interventions
with heavy drinkers: WHO Brief Intervention Study Group. American Journal of Public
Health, 86(7): 948-955.
back to top
policy issues.lit
ml
policy issues.ht
ml
■ index.html..\index.html
d
is
C
U
S
si
O
n
/
d
is
C
U
S
si
0
n
Aabouticap/
h .Apublications/p
about icap.ht international.htm.Ainvited/inv t ublications.html
ml
1
ited.html
\publications/p
.Aabout icapZ international.htm.Ainvited/inv 1 ublications.html
about icap.ht 1
ited.html
ml
\d
is
C
U
S
si
Q
n
d
is
C
U
S
Si
Q
n
b
t
00091fe5-sp00
Pi gc 1 ol 2
.Alcohol in India
b’U
THE GLOBE Magazine
vj;
367
tpAAIcohol in India
J BlO''A
r f
.
. ..
Monica Arora. Programme Manager of HRIDAY/SHAN
Prohibition is incorporated in the Constitution of India among the
directive principles of state policy. Article 47 says: "The state shall regard
the raising of the level of nutrition and standard of living of its people as
among its primary duties and in particular, the state shall endeavour to
bring about prohibition of the use except for medicinal purposes of
intoxicating drinks and of drugs which are injurious to health."
■
...
During the pre-independence period. Mahatma Gandhi himself issued
several strong statements against the sale and consumption of alcohol.
The Alcohol Situation in India
Alcohol is one of the commonly consumed intoxicating substances in
India. Il has traditionally been drunk in tribal societies, although it has
won increasing social acceptance among other groups, urban males being
the prime example. It is easily available and widely used, especially at
festivals such as Deepawali and Holi. At the moment the use of alcohol is
infrequent among w omen who also tend to resist the habit among male
family members.
Betw een 15 and 20 per cent of Indian people consume alcohol and. over the past twenty y ears, (he
number of drinkers lias increased from one in 300 to one in 20. According to The Hindustan nines n
is estimated that of these 5 per cent can be classed as alcoholics or alcohol dependent I'his translaics
into about five million people addicted to alcohol.
Of what is actually consumed, the Intake of Indian Made Foreign Liquor (I.MF1.) is growing al the
considerable rate of 15 per cent a year. Again, The Hindustan Times says that 65 per cent of the
Indian liquor market is controlled by whiskey manufacturers. The state of Kerala stands firsi in p<-i
capita consumption of liquor at 8.3 litres, followed by Punjab 7.9 litres.
Alcohol Situation in India among youth
Today in India, the tendency to alcohol consumption has percolated down to the youth. I he media ia .
played a leading role in encouraging the use of alcohol among young people by such means as the
portrayal of drinking in congenial social settings, by associating the habit with glamour and celebrity
status, and by direct and indirect advertising.
O\ er the years, the age al which youngsters begin to consume liquor has come down in Kerala. In
1986 the age was 19. by 1990 it had dropped to 17. and by 1994 the age was 14.
Indian liquor brands
The varieties of alcohol manufactured for consumption in India are:
Beer
Country Liquor
Indian Made Foreign Liquor (1MFL)
Wines
Indian liquor brands have registered significant growth in recent years - some of the top Indian
alcohol brands showing an increase of as much as 50 per cent in sales (1993-97). (’lined Iheweries
registered an increase of nearly 20 per cent in sale in the year 1998-99.
Taxes on alcohol
Alcohol is a significant contributor to government revenues in many states. In most state’- this
accounts for over 10 per cent of total state tax revenues, whilst in the Punjab this accounts for ovci
one third.
file: 'Office\d\abrahani\Alcohol in India.htm
I. I 97
Alcohol in India
Page 2 ol 2
Policy measures in India
Alcohol policy is under the legislative power of individual states.
Prohibition, enshrined as an aspiration in the Constitution, was introduced and then w ithdrawn in
Haryana and Andhra Pradesh in the midi-1990s), although it continues in Gujarat, w ith partial
restrictions in other states - Delhi, for example, has dry days. There was an earlier failure of
Prohibition in Tamil Nadu.
Increasing taxes as a means of reducing alcohol consumption is problematic as it has been shown u
be unresponsive to price change. Tax increases will further add to economic hardship for consumers
and have little or no impact on the reduction in other negative impacts. There would, how ever, be an
increase in corruption, crime, and the production and consumption of illegal liquor.
An important aspect of policy is to delay initiation among youth. One way of doing this is to enforce
age limits. The legal minimum age to purchase liquor ranges from 18 years in some state to 25 ycai s
in others. Delhi has minimum age limit of 25 years. So far, the efficiency of enforcement has not been
studied. It has, however, been shown that an increase in the age of legal drinking from 1 8 years to 2 I
years achieves nearly 60 per cent of the effect of prohibition on alcohol consumption
Legislation: alcohol advertisement
The Cable Television Network (Regulation) Amendment Bill, in force September 8. 2()()(). complelch
prohibits cigarette and alcohol advertisements. The government controlled channel. Doordarshan.
docs not broadcast such advertisements but satellite channels however are replete with them
Efforts to counteract the problem
Ministry of Social Justice and Empowerment has been active in this field. In 1985-86 it urged the
establishment of a reduction programme. The ministry co-operates with media and youth
organisations and collaborates with the Ministry of Health and Family Welfare and with N( i()s
involved in the problem. The Ministry of Social Justice and Empowerment, in partnership with the
I Jnitcd Nations International Drug Control Programme (UNDCP) and the International Labour
Organisation (ILO). has launched three major initiatives for alcohol and drug demand reduction.
Non-Governmental efforts have been led by the Indian Health Organisation (II IO). Youth for Christ
India (YFC), Health Related Information Dissemination Amongst Youth (HRIDAY). and the Student
Health Action Network (SHAN).
THE GLOBE Magazine
file: OITice\d\abraham\Alcohol in India.htm
1 I
Page 1 of?
bnij.com Patel 316 (7141): 1394a
■
Home Help
Search/Archive
P.\IJ 10QS131G: 1394 ( 2 May ) ’
Feedback
1W ..Ml
■\SLS-
t
n
r
Table of Contents
Email ilus article t<> a in ?nd
Respond to this article
\ iews and reviews
IA .!.. responses to llus article
PubMtd citation
Personal view’s
Related articles in Pub \le.i
Dow nload to ( itatioi;
The politics of alcoholism in India
Search Medline loi ariicles b\
At a recent meeting in Goa organised by the National Commission for
Women, its chairwoman, the vibrant and outspoken Ms Mohini Giri,
l^iicl. V.
Alert me when:
\cv\ ariicles cue ihi>
exhorted the women of Goa to join hands with millions of women in
other Indian slates to demand that prohibition be implemented to reduce the appalling damage
resulting from alcohol misuse by men.
The use of prohibition in India has a long history. Gujarat, the home stale of Mahatma Gandlu.
declared prohibition soon after the British left and has stuck to this policy ever since. More recently
however, prohibition became a major vote winner in the states of Andhra Pradesh and Harya ia.
.Alcohol misuse has become such an enormous problem that it is now the main issue on w hie i
elections are being fought and won.
Alcohol misuse is one of the main killers of young men in India today. But its real impact is an the
social and family dynamics that underlie our communities. Domestic violence and an exacerbation o,
poverty have made alcohol misuse the single most important problem for women in India. A rec .'ill
study in Goa showed that women attending primary care clinics were more likely to cite a dr nkinc
relative as a key problem in their homes. They were also more likely to cite problems w ith making
ends meet and to suffer from a depressive or anxiety disorder.
W hat has changed over the past 20 years is that these women are now an increasingly potent electoral
force. Women's organisations have successfully mobilised millions of women and struck a sensiiixe
chord in identifying alcoholism in their families as being a potentially preventable cause of p o\ erty
and abuse. Rather deviously, women have been identified by opportunistic politicians as a \ ole bank.
political parties have thrown all the benefit of hindsight to the wind and made prohibition their prim e
election promise. The result was that the Telegu Desam party won a famous electoral victory.
winning 224 out of 294 seats in Andhra Pradesh. Subsequently, the party which pul prohibition at the
top of its agenda won the elections in Haryana with a large majority.
But has prohibition made any difference to the real problem
that is, drinking by men? IfGujaral is
anything to go by prohibition is a complete failure. Not only is alcohol readily available to tke rich,
but the poor have to resort to illegal brews, with a consequent rise in criminal acli\ ity and deaths
from methanol poisoning. Prohibition has introduced massive problems for the government irca.surics
and caused further hardships for the poor by increasing unemployment. In Andhra Pradesh alcohol
htlp: biiij.bnijjournals.com/cgi/content/full/316/7141/1394/a
10 31 03
bmj.com Patel 316 (7141): 1394a
P igc 2 of 3
breweries were shut with the loss of hundreds of legitimate jobs; the state w as \ irluall v bankrupted.
The government attempted to counter the budgetary deficit by raising taxes and the cost of subsidised
rice, the staple food of millions of Indians. Despite this, the deficit continued lo spiral oul of control
reaching a third of the annual budget outlay. Finally, the Reserve Bank of India threatened to
w ithdraw the overdraft facility to the state. The government then relented and introduced the . \P
Prohibition Act 1997, which effectively removed prohibition in favour of a more regulated alcohol
retailing system.
"There has been no mention of any public health initiatives"
\n amazing feature of all this grassroots democracy is that there has been no mention of an\ public
health initiatives to tackle alcohol misuse. Primary preventive strategies would enable the reduction
of problem drinking in an entire population. Such strategies could include the strict enforcement of
laws on licensing and on drinking and driving, and the provision of peer education on drinking
behaviour in colleges and schools. Secondary prevention would enable the reduction of the effects ol
problem drinking once it had been detected in an individual. How often docs a woman w ho has been
battered by her alcoholic husband receive counselling or a health worker \ isit her home to counsel die
husband? How often does a man who has been in hospital for a bleeding gastric ulcer or after a
drinking and driving accident receive information on the nearest Alcoholics Anonymous mcc mg
place’? Counsellors could work with other organisations, such as Alcoholics Anonymous and he
Indian Psychiatric Association, in a united campaign to help families affected by problem drinking
The policy of prohibition is at odds with an essential ingredient of any community health programme
namely, its participatoryapproach. By identifying drinking in men as the problem, the current
approach alienates and excludes them from participating in finding a solution. Bar owners and
alcohol manufacturers, usually men, see their livelihood destroyed and, instead of empathism e w ith
women on this sensitive issue, they feel threatened.
The current drive by the National Commission for Women is an admirable example of women
uniting in an effort lo make their lives better by forcing the government lo act. Bui in then x ocilcrotis
support for prohibition w omen's groups should remember that it will always be the poor w ho will
suffer the most from prohibition. A community based, participatory public health model lo tackle
alcohol misuse is the only way to reduce the negative impact of problem drinking while safeguarding
the economic benefits of alcohol, avoiding punishing the majority who drink sensible. and pr eventing
deaths and crime which result from the illegal bootlegging industry.
\ ikram Patel
. Siinguth Society for Child Development and Family Guidance.Goa. India
B.VI.I 1998
Rapid Responses:
Read all Rapid Responses
blip: bmj.bmjjournals.com/cgi/content/full/316/7141/1394/a
10 31 03
A Tipsy Liquor Policy
of 12
Page
A Tipsy Liquor Policy
H B Soumya
"And when I'm dead, don't bury me at all,
Just pickle my bones in alcohol,
An amphora of wine at my head and feet,
And then I'm sure my bones will keep"
These lines are from Goscinny and Uderzo's Asterix mid Caesar's Gill.
Tremensdelirious sings these lines on being served with the alcohol
of his choice. But what about Delhi? Are all concerned parties ha :>p\
with the government's excise policy?
Licensing procedure
The Delhi government issues manufacturers an L-l/1 -1A license
every year on the fulfillment of some criteria. An L- l is issued to an
Indian made Foreign Liquor (IMFL), which is given an approval
certificate on meeting a minimum sales figure target, which appl es
to all of India except Delhi. It is also required to undergo quality
checks. An L-l A license is issued to country liquor manufacturers
who have to undergo quality checks that are carried out by the
government laboratories. IMFL brands are sold by government retail
outlets, which have L-2 licenses, like the Delhi Tourism and
Transport Development Corporation (DTTDC), the Delhi State
Industrial Development Corporation (DSIDC), the Delhi State Ci' il
Supply Corporation (DSCSC), and the DCCWS (expansion
unknown) which run various outlets. While country liquor is sold in
Government shops that are issued L-10 licenses sell. These shops also
sell cheap IMFL, priced below Rs. 90.
http://www.ccsindia.org/RP01_ 6.html
1
3/03
A Tipsy Liquor Policy
Page . of 12
applicant in view of the provision of rule 7 of Delhi Intoxicants
license and sale rule, 1976
• Documentary evidence to prove that the alcohol is
manufactured from natural alcohol (double distilled) Extra
natural alcohol
I he IMFL or the beer brand proposed to be sold bv the applicant of
the L-l license should be owned by the distillery and in respect < I the
IMFL brands, excluding wine, the applicant should be in possession
of trade mark certificate in respect to these brands. However if the
brand has been sold in Delhi before 1993-94 the TMC is not
required. For the approval of rum and whiskey brands, the brand
must have sold a minimum quantity in the all India market
excluding Delhi as indicated in the terms and conditions.
Once the license is approved, the applicant has to submit the
following:
• Registration of brands
• Approval of bonded warehouse
• Approval of label
• Fixation of ex-distillery prices
Distilleries and breweries also have a bone of contention with the
liquor policy of the government. According to the Constitution ol
India, under Article 47, it is the
"Duty of the state to raise the level of nutrition and the standari ' o/'
living and to improve public health—the state shall regard the
raising of the level of nutrition and the standard of living of its
people and the improvement of public health as among its prima-i/
duties and in particular, the state shall endeavour to bring about
prohibition of the consumption except for medical purposes of
intoxicating drinks and drugs which are injurious to health. "
However experience of prohibition in other countries has shown that
lutp://www.ccsindia.org/RPO I 6.html
1
3/03
A Tipsy Liquor Policy
Page 2 of 12
The L-l licences are given to a company, society, or manufacturing
firm: partnership or proprietorship firm provided the applicant
owns a distillery. The applications for this are invited through
advertisements in leading newspapers. The prime job of 1 -1 license
holders is to supply liquor to other license holders.
A number of certificates need to be submitted along with ar L-l
license application. These are listed below:
• Solvency certificate from SMD
• Income tax clearance certificate
• No dues certificate from collector (excise)
• No dues certificate from sales tax officer
• Declaration of distillery on affidavit regarding sale and
minimum ex-distillery prices and distance of distillery from
Delhi
• CA certificate for sale and minimum ex-distillerv prices
• Certificate from Excise authority regarding sale figures
• Registered partnership deed/memorandum and article of
association
• Duly audited annual account and balance sheet of distillery
• Attested copy of the license for establishment of
distillery/winery/bottling unit/brewery
• Power of attorney
• Attested photocopies of export passes/EVCs verifying the sale
figures of the whisky and rum brand for which distillery has
applied
• Trade Mark Certificate (TMC)
• Usership agreement under Trade & merchandise Marks Act,
1958
• Certificate from a government authorised laboratory or other
reputed private institution regarding quality of brand.
• An affidavit stating that there is nothing adverse or against the
http://www.ccsindia.org/RP01_6.html
I I '3/03
A Tipsy Liquor Policy
Page z- of 12
the prohibition would be counter productive. Therefore, the Delhi
government grants a privilege to the distilleries with regulations
without granting any right to trade in liquor.
L-2 licenses are given to only select undertakings ol the Delhi
government namely DTTDC, DSIDC, DSCSC, and DCCWS. I he
proposal for opening a vend has to come from these corporations
Individuals wanting to rent out their premises for such a vend have
to approach these institutions, which after looking at the suitabil tv
of the premises approach the relevant offices for the grant of the
license. The premise is required meet the following specifications
• Fhe premise should be a pucca building with a minimum floor
area of 400 sqft and located in a commercial area
• The area MLA should give his positive opinion on the matte ■
• The Collector of excise, the DEO, and the representative ot fl i e
corporations and the area SMD have to inspect the premises.
• The shop shall not be within 75m of the following
Industrial estate or any construction site
.Major educational institution
Religious place
- Hospitals and nursing homes with more than twenty five beds
Colonies of labourers and harijans
The permission of the area's MLA is a must. If approval is not gix en.
then a retail outlet cannot be opened. For instance, in Vasanl Kurip
there is not a single alcohol retail outlet, due to the negative opinion
of the MLA of the area.
If all these qualifications are met by the proposed premise, then the
license is given and the concerned party is required to deposit an
amount of Rs. 60,000 as the license fees. IMFL/beer brands are sc Id
hltp://www.ccsindia.org/RP01_6.html
1/3/03
A Tipsy Liquor Policy
Page 5 of 12
by these vends at rates fixed by the excise commissioner. In the v ear
1999-2000, there were 224 L-2 license holders.
L-3, L-5 licenses are given to hotels, which are approved b\ the
Department of Tourism and are categorised as Budget hotels, The
approval of the department of tourism is necessary for the gra it of
an L-3 license. This license is for the sale of liquor to its residents.
These hotels can also apply for an L-5 license for serving of liqu Tr in
exclusive bars and in the restaurant in the hotel premises, The
following need to be submitted with the application ol an I -5 license:
• Documentary proof regarding legal status of the hotel
• Whether the hotel is in legal possession of the plot.
• Completion certificate in respect of the hotel building.
• Trade license from the Local authority (MCD/NDMC)
• Lodging house license from the local authority
» Certificate of registration of eating house license issued by tl I?
DCP
• Documentary proof regarding applicant being an income tax
assessee and sales tax assessee.
• A layout plan of the hotel, site plan of the license outlet and he
liquor stores.
The application is to be submitted to the Commissioner of Excise.
After scrutiny of the documents, the premises are inspected by the
excise officer as under the excise rules, particularly rule 1 1 of the
Delhi Intoxicants License and Sales Rule, 1976. The premises should
not be within 75m of any of the institutions as were listed in the case
of L-2 licenses.
Once the hotel has been found to be suitable, the views of the
public/residents are invited on the proposal giving 7 days time to
file objections before the licensing authority. If no objection is
received then the authorities proceed with the approval for gran ol
Imp://www.ccsindia.org/RP01_6.html
1 1 3/03
A Tipsy Liquor Policy
Page ( of 12
license. An L-5 license is given only with an L-3 license and the same
requirements apply to an L-5 license. The total number of L -3/1 .licenses given in 1999-2000 was 42.
An L-4 license is given to an independent restaurant approved I a' the
Department of Tourism. Applications are submitted to the
Commissioner of excise with the relevant documents. The restau ant
should be located in a commercial area with adequate parking space-.
The requirements of rule 11 of Delhi Intoxicants License & Sales
Rules 1976 have to be met by the restaurant. The requirements and
procedure are the same as in the case of L-3 and L-5 licenses, t he
total number of L-4 licenses given in 1999-2000 was 81.
i -19 licenses are given for the service of liquor in a club registered
under the Societies Act 1860.The applicant is required to submit on
the letterhead of the club an application along with the following
documents:
• Registration certificate in respect of the club
• Documentary proof in support of legal possession of the plot ol
the club.
• No objection certificate from the area DCP
• List of members of the club
• List of office bearers of the club
• Registration passed by the management Committee to start the
bar facilitv in the club and also to meet the liability thereof.
Rest of the procedure with regard to the grant of license is the same
as indicated in respect of L-3/ L-5 license.
Liquor, being an excisable article, can not be stored beyond a certain
limit. A consumer is allowed to store a maximum of 20 litres. For
higher possession, an application to the department and the payment
of Rs. 2000 would get the applicant an L-49 license. I he applicant has
to be an income tax assessee to be eligible for the permit. The totr
Imp://www.ccsiiidia.org/RP01_6.htnil
A Tipsy Liquor Policy
Pauc7 oi l 2
number of L-49 licenses given in 1999-2000 was 258.
Status of alcohol industry in India
The alcohol industry is very important for the govern men I. It
generates an estimated Rs. 16,000 crore per annum in spite of the fact
iftatthe per capita consumption of liquor in India is the lowest in the
world. The total liquor industry is worth Rs. 2,000 crore. IMPL
accounts for only a third of the total liquor consumption in India
Most IMFLs are cheap and are priced below Rs. 200 per bottle.
Alcohol sales proceeds account for 45%of the total revenue collection
in the country. Whiskey accounts for 60% of the liquor sales while
rum; brandy and vodka account for 17%, 18% and 6% respective
MNC's share is only 10% and they have been successful only in t io
premium and super premium ranges.
\I
Post WTO the government may have opened India to foreign
distilleries, but the duty has been increased from 222% to 464-706 0
This is due to the fact that there is a 100% customs duty , 150'3
contravening duty, local taxes, distributor's margin, retailer's ma gin
and publicity charges. The cost is finally borne by the consumer.
Though the government claims that this is being done to protect the
domestic liquor industry, the domestic industry accounts for 99lL of
the market share. This protectionist policy could prove to be
counterproductive and lead to smuggling. As of now, onlv 45°. o
the sales are through legal channels and only 25% of this is dutv aaid
tor.
Within India itself, the policy of alcohol retail differs from state to
state. While some states like Maharashtra, Uttar Pradesh, and I a nil
Nadu have a liberal policy, some states like Haryana and Andhra
Pradesh have had very bitter experiences in trying to make these
states dry and have eventually had to withdraw the police.
Method of ordering
htlp://www.ccsindia.org/RPO l_6.html
. 3 03
A Tipsy Liquor Policy
Rase <■ of 12
The L-2 licensed authorities on the basis of the price of the alcohol
place the orders for IMFL. For liquor priced below Rs. 90, the orc er is
equally distributed among all those manufacturers who have been
licensed in this category. For the alcohol priced between Rs. 91 and
Rs. 205, the order is distributed among the L-l holders in this
category depending on the production capacity of the brewer\ I or
the premium brands (above Rs. 205) the orders are placed b\ the
individual vends themselves. Any stock of liquor lying unsold in a
branch of an outlet is transferred to another shop of the same chc in.
When stocks pile up, a committee is appointed to look into the
disposal of the stock of liquor. On a visit to a shop run by the DS DC
in Saket on July 1, 2001, about 15 whiskey, 14 rum brands and 15
beer brands in the under Rs. 90 category, and about 30 brands of
alcohol (whiskey, gin, vodka, rum) in the Rs. 91- Rs. 205 category
were displayed on their board of products with their prices.
1 lov\ ever, there was no beer available in this shop and only aboi I 5
rum brands were stocked in the shop.
The sales figures of alcohol over the various years for entire Del ri is
given below:
G>
Year
Sale of beer in
bottles
Sale of
IMFL
199495
18,797
29,784,767 15,304,848
199596
26,753,113
31,100,383 17,813584
1 Year
Sale of beer in
bottles
Sale of
IMFL
l._
199697
Sale of country
liquor
Sale of country
liquor
1
28,852,880
39,999,614 27,470,904
hup:A wwvv.ccsindia.org/RPO l_6.html
I I 3/03
Paqe9 of 12
A Tipsy Liquor Pol icy
199899
3,657,063
47,567,740 31,920,975
199900
32,111,134
44,707,386 33,513,108
SoLirce: delhigoi>t.nic.in website
(The sale of liquor did not have any units)
fhe revenue growth of the excise department is tabulated below
Year
Revenue (Rs.
crore)
199495
308.45
199596
335.75
199697
446.10
199798
545.00
Year
199899
Revenue (Rs.
crore)
526.50
1999- 566.00
00
Sor/rce: delhigovt.iiic.in website
hltp://www.ccsindia.org/RP01_6.html
I 3/03
A Tipsy Liquor Policy
Page I ( ol' 12
In 1996-97, till October, the total revenue collected b\ the Delhi
government was Rs. 1429 crore. The excise contribution was Rs.
(.9
347.87 crore (24.34%). The cost of collection incurred by the
department was 0.4 crore (2% of the revenue). (All these figures c re
according to the report on the delhigovt.nic.in website.')
As can be seen from the sales figures, there is a lot of fluctuation n
the quantities sold every year. When asked about this, the releva nt
authorities refused to comment.
Area of objection
The Delhi government is the sole buyer and seller of alcohol in Delhi.
I here was Rs. 4 crore worth of liquor of inferior quality lying in the
government retail outlets, according to a report in the Times of Imlin
dated May 29, 2001. What is meant by inferior qualit\ liquor is
something no one knows. On asking, the concerned officials in tl e
DTTDC head office in Lakshmi Nagar said that the liquor was ju A
unsold stock.
The government's excise policy is subject to a lot ol sudden changes
The manufacturers sometimes just need to get their I -1 licenses
renewed and at times they need to apply afresh, like in the year 2.001
In 1993, the L-l license holders were allowed to set up 5 'dedicated
shops in Delhi in which they could sell their approved brands in
addition to having them sold in the government retail shops The
policy was withdrawn in an ad-hoc manner in 1994. On being
questioned about the effects of this policy, an official in one of the
country's leading breweries said that the introduction of this pol cy
had led to an increase in their revenue by almost 30% which the\
have lost out on since the policy got crushed. Recently, the
government's policy to open up 45 private liquor shops was quashed
by the cabinet, because it meant that the MLA's power in the issue ol
a no-objection certificate for the setting up of a retail outlet wouLI bt
questioned. Had this policy been implemented, the government
http://www.ccsindia.org/RP01_6.html
I I 3/03
A Tipsy Liquor Policy
Paye I I ol' I 2
K—*
would have earned Rs. 7.5 lakhs on each vend as license fees
annually.
So, are all the concerned parties satisfied? Apparent!\ not
Customers often complain that they buy the alcohol that is made
available to them and that the brand of their choice is difficult to ^et.
Sometimes the scarcity is real, at other times it may be a case oi
"brand pushing". (The market rate for brand pushing starts al Rs. 30
per case.) Brand pushing depends on which companv is willing to
pay more commission to the man who is at the outlet of the
government liquor vend. For example, a cheap whiskey may can •y a
commission of Rs. 30 per case while a premium brand may carrv Rs.
oO per case. Though some officials of certain firms admitted to the
practice of brand pushing, the DSIDC officials vehementlv denie .1
this practice.) Lines are long, stocks inadequate, and the service
leaves a lot to be desired. More vends; particularly private ones
would be welcome by the customers. The manufacturers would
definitely welcome a change in the excise policy, not just in terms ol
licensing but also in terms of retail. It would mean a cleaner and
clearer system and would eliminate the monopolistic and
monopsonistic power of the government (the cost of which in 2001
was Rs. 4 crore of unsold liquor lying in government retail outlets)
by bringing in efficiency through competition. The government
would definitely not be worse off with the introduction of private
stores. In fact, more revenue, in the form of license fees as well as in
the form of taxes that would accrue to the government from these
vends. The net alcohol consumption would also not increase. Th. 're
would be just a change in the buying pattern of the people. Instead
of stocking liquor as people do now, the same alcohol would be
bought over a period of time in smaller amounts. Studies conducted
by the Fraser Institute of Canada in Alberta, a place where alcohol is
sold privately, have shown that privatization ol liquor retail has not
lead to an increase in consumption or any increase in crimts
1 he only party that would be worse off would be the people wh a
http://www.ccsindia.org/RP01_6.html
I 303
A Tipsy Liquor Policy
Page I 2 of 12
have made this policy—namely the people who are benefiting fro n
the current policy. Whatever benefits they are accruing now would
decrease, perhaps even be eliminated. But it would mean a big st ■P
towards consumer satisfaction. In any case, don't we all believe in
the greatest good of the greatest number?
Sources
• Excise link on the Delhi government website located at
delhigovt.nic.in
• Ajay Jain, Accounts officer, DTTDC
• Shivani Singh, Staff reporter. Times of India
• R P Singh, Area manager, United Breweries
• Shivani Singh, "Saathi's Plan to Privatise Liquor Vends
Scrapped", Times of India, May 29, 200'1
liilp://www.ccsindia.org/RP01_6.html
I I 3/03
• about distillery industry of India
Page I of4
About Distillery Industry of India
The use of alcohol as drink is an age-old story in India
and it appears that the technique for fermentation and
distillation was available even in the Vedic times. It was
then called '' Somarasa" and was used not only for its
invigorating effect but also in worship. To date, not
only has the consumption of alcohol been continued
but it is an integral part of the Ayurvedic system of
medicine.
The First distillery in the country was set up at
Crwnpore(Kanpur) in 1805 by Carew & Co. Ltd., for
manufacture of Rum for the army. The technique of
fermentation, distillation and blending of alcoholic
beverages was developed in our country on the lines of
practices adopted overseas particularly in Europe.
The distillery industry today consists broadly of two
parts, one potable liquor and the industrial alcohol. The
potable distillery producing Indian Made Foreign Liquor
and Country Liquor has a steady but limited demand
with a growth rate of about 8 per cent per annum. The
industrial alcohol industry, on the other hand, is
showing a declining trend because of high price of
Molasses which is invariantly used as substrate for
production of alcohol. The alcohol produced is now
being utilized in the ratio of approximately 52 per cent
for potable and the balance 48 percent for industrial
use. Over the years the potable liquor industry has
shown remarkable results in the production of quality
spirits.
The utilization of Ethyl alcohol or Ethanol, now popularly
known as alcohol, for industrial use is a recent
phenomenon and its importance came into being
towards the end .of the second world war. With
protection being granted to the sugar Industry in 1932,
a large number of sugar factories were established in
http://www.aidaindia.org/aida/about_distillery.htm
I 1,3/03
• about distillery industry of India
Paec2 of 4
the country, particularly in Maharashtra and Uttar
Pradesh where irrigation facilities existed for cultivation
of sugarcane. This increase resulted in accumulation of
molasses, which resultantly, caused unmanageable
environmental problems. At that time the demand for
molasses was almost insignificant and the sugar mills
had to incur some expenditure on removal of this by
product i.e. molasses. For resolving these problems a
joint committee of U.P. and Bihar was constituted to
explore the possibilities of developing alcohol based
industries for the purpose of utilization of molasses. The
Committee
in
its
report
recommended
the
establishment of distilleris for production of alcohol,
utilizing molasses as substrate. They also recommended
that alcohol produced by the distilleries should be
admixed with petrol, to supplement motor fuel. The
production of alcohol did not only help in solving the
problems of disposal of molasses but it also filled up the
gap in the demand and supply of motor spirit. As a
substantial quantity of alcohol after meeting its
requirement for manufacture of gasohol alcohol was
diverted for production of alcohol based chemicals in
different parts of the country. The utilization of alcohol
for this purpose progressed steadily and a substantial
quantity of alcohol produced in the country is now
being utilized for manufacture of solvents and
intermediates. Till a few years back a little more then
50 % alcohol produced in the country was being utilized
for production of alcohol based chemical but after the
decontrol of molasses in the year 1993 the utilization of
alcohol for production of chemical, dye-stuff, synthetic
rubber, polymers and plastics etc. has received a
setback.
Manufacture of alcohol
In this country the bulk of alcohol is being produced
from sugar cane molasses. Molasses is a thick viscous
bye-product of the sugar industry which is acidic in
nature, rich in salts, dark brown in colour and it also
http://www.aidaindia.org/aida/about_distillery.htm
I I 3.4)3
/ about distillery industry of India
Page 3 ol'4
contains sugar which could not be crystallized For
manufacturing alcohol, the Molasses is diluted with
water into a solution containing 15-16 % of sugars This
solution is then inoculated with yeast strain and is
allowed to ferment at room temperature. The fermented
wash is distilled in a series of distillation columns to
obtain alcohol of adequate/ requisite strength and
quality/ specification. This alcohol is used for various
purposes
including
potable
and
industrial
For
manufacture of alcoholic beverages, the alcohol is, if
required, matured and blended with malt alcohol (for
manufacture of whisky)
and diluted to requisite
strength to obtain the desired type of liquor/ Indian
Made Foreign Liquor (IMFL). This is bottled in bottles of
various sizes for the convenience of consumers.
The production of alcohol has been acknowledged since
the earliest recorded history and at least since ancient
Egyptian records of 2000 BC. The modern sciences of
microbiology, enzymology and biochemistry certainly
belong to the twentieth century and these sciences
have added flesh to the empirical knowledge of distillers
m the previous millennia.
Today we have 295 distilleries, which are scattered
throughout the country which
have an installed
capacity for production of 3198 million litres of alcohol.
The requirement of alcohoTTn~country for all purposes
however stands at about 1200 to 1300 million litter of
alcohol in a year. Which works out about 40 percent
licensed capacity. The bulk of capacity thus remain
dormant which can be advantagely utilize for production
of anhydrous alcohol for being used as oxygenate/ fuel.
The utilization of ethanol as oxygenate is the prime
need of the country because the enormous increase in
the population of motor vehicles after emphasize has
been major cause of air pollution in particularly in
metropolises and
big cities. As the air pollution
disposing a serious threat to the health of community it
is absolutely necessary to devise way and means of
http:// vvww. aidaindia.org/aida/aboutdistilleryditm
1 1/3/03
about distillery industry of India
Pane 4 of 4
curbing pollution. Cheapest and best way to alternative
this objective is to utilize ethanol as oxygenates in
admixture with Petrol/ Diesel. The implementation of
this program has been delayed rather inordinately and
it should therefore be implemented as promptly as
possible.
Alcohol is a member of a class of organic compounds
containing carbon, hydrogen and oxygen, considered as
hydroxyl derivatives of hydrocarbons, produced by the
replacement of one or more hydrogen atoms by one or
more hydroxyl (-0H) GROUPS.
http://www.aidaindia.org/aida/about_distillery.htm
1 1/3/03
. Complete health care and medical information from India
Paic 1 of?
Icoholism is a chronic, often progressive disease characterized by excessive and repetitive
consumption of alcohol despite repeated alcohol related problems such as health, social o
economic functioning of the individual. Alcoholism constitutes of symptoms such as
A strong compulsion to drink. This is called craving.
Alcohol is often taken in larger amounts or over a longer period of time than the
person intended
When alcohol use is stopped after a period of heavy drinking, there is development
of characteristic withdrawal symptoms such as nausea, sweating, shakiness and
anxiety.
There is development of tolerance i.e. there is a need for increased amounts of
alcohol in order to achieve a desired effect.
Predisposing Risk Factors
Following risk factors may lead an individual to alcoholism.
1) Age - Men usually develop alcoholism in the third or fourth decade. It develops later in
women.
2) Sex - Alcoholism is more common in males than females.
3) Socio-economic status - Alcoholism is more prevalent in lower socio-economic groups
and less educated class of people.
4) Family history of alcoholism - Children of alcoholics are about four times more likely to
become alcoholics than children of non-alcoholics. Genetic factors partially explain this
pattern.
5) A person's environment such as the influence of friends, stress levels and the ease of
obtaining alcohol may also influence drinking and the development of alcoholism.
Prevalence
About 1% to 10% of the world's population aged 15 years and over are estimated to
consume alcohol at that level, depending on the country of residence.
Surveys conducted in USA on drinking practices reveal that 70% of adults drink alcoholic
beverages at least occasionally and about 12% are heavy drinkers. In USA, the ratio of
male to female drinkers is approximately 3:1.
In India, studies carried out in northern states and in West Bengal show that the
prevalence of alcohol addiction is 10 to 19 per thousand. The prevalence rate of alcoholism
is comparatively low in the southern states of India. In India, it has been estimated that
40-50% of all males drink alcohol as compared to less than 1% of female adults.
In North America and countries in northern Europe, alcohol is frequently taken in
concentrated forms to help in socializing. Alcohol dependence in these countries is usually
characterized by heavy consumption of strong spirits, a tendency to periodic drinking and
by overt drunkenness. In some countries, alcohol is consumed as wine, usually with meals.
Here the alcohol dependence is characterized by a relatively continuous intake of alcohol
and little overt drunkenness. Beer is also used in a similar way.
http://www. medivisionindia.com/addiction/introduction.phtml
If) 31 03
Complete health care and medical information from India
Page 2 of 3
and little overt drunkenness. Beer is also used in a similar way.
Clinical Features
Alcohol does not require digestion and is quickly absorbed into the body. The affects of
alcohol are seen about 10 minutes after consumption and peak at 40-60 minutes after
consumption. The effects of alcohol depend on how much is taken, the expectations of the
drinker and the circumstances at the time. Eating can slow down the effects of alcohol. The
age, size and sex and how quickly people drink makes a difference. The effects appear early
in those who are mentally or physically fatigued, in epileptics, in persons with head injury,
and in those who have taken barbiturates or other CNS depressants. Regular drinkers
develop a tolerance to alcohol and a reduced sensitivity to it i.e. there is a need for
increased amounts of alcohol in order to achieve a desired effect. In addition, some
physiological adaptation occurs so that the alcoholic appears less intoxicated and less
impaired in performance at a given concentration of blood alcohol than is a non alcoholic.
I
Alcohol produces three stages 1) Stage of excitement
2) Stage of incoordination
3) Stage of narcosis.
The symptoms are due to the depressant action of alcohol on the central nervous system
1) Stage of excitement:
Small amounts of alcohol produce a sense of well being and pleasure resulting from
inhibition of higher centres. People may become more sociable, active, self confident and
talkative. The drinker converses well, laughs and smiles more readily or becomes angry
more easily. It relaxes the control of emotions. There is lack of normal restraint and the
drinker may behave in an obscene manner or talk in a vulgar manner. This is called flippant
stage.
The face appears to be flushed and the conjunctivae are injected. The pupils are dilated a id
they sluggishly react to light. The pulse is fast and the breath smells of alcohol. Some
people may retain mental clarity. In this stage the blood alcohol concentration is between
0.05 to 0.1 per cent (50-100 mg%).
2) Stage of incoordination:
The concentration of alcohol in blood in this stage ranges from 0.1 to 0.3 percent (100-300
mg%). This is the stage where offences are most committed. There is incoordination of
thought, speech and action. This stage is sometimes called the stage of confusion because
the person is confused due to incoordination of thought. The speech is slurred and
incoherent and there is difficulty in pronouncing consonants. This is due to incoordination of
speech. There is also incoordination of muscles which leads to staggering gait. There is alio
impairment of skilled movements and the reaction time is increased. A person driving a
vehicle may commit an accident. A person is not fit to drive a motor vehicle with a blood
concentration of 0.1 per cent or 100 mg% and above. The statutory limit for a charge of
drunken driving in UK is 80 mg%.
The eyes appear suffused and the pupils usually dilated. Pupils sluggishly react to light.
There is blurred vision and the person may also experience double vision. There is dryness
of mouth and furred tongue. The breath smells strongly of alcohol. Nausea and vomiting
are commonly present. Vomiting may be dangerous but it may also have. Some sobering
effect as it may relieve the stomach of some alcohol. The person is untidy in his appearance
and may suffer from hiccups. Depending upon the inherent emotions, the individual may
become morose, gay or irritable. On drinking heavily, deep depression can be released with
disastrous results. Under the effect of alcohol, the person may plunge into sexual excesses;.
http: www .medivisionindia.com/addiction/introduction.phtml
1 ) 3 1 03
„
Complete health care and medical information from India
Pa tic 3 ol 3
disastrous results. Under the effect of alcohol, the person may plunge into sexual excesses.
It is said that alcohol kindles the desire but takes away the performance.
Various other accidents are also associated with intoxication including traffic accidents,
falls, burns, drowning and work related accidents.
3) Stage of narcosis:
In this stage the blood alcohol level is 0.3 percent (300 mg%) or above. This is also known
as the stage of coma as the patient passes into deep sleep and responds only to strong
stimuli. Mouth and the tongue are frequently dry. The tongue may be furred. There may □e
excessive salivation. The temperature is low and the pulse is rapid. Pupils may be
contracted. Nystagmus may be present. On stimulating the person by pinching his neck Qr
face, the contracted pupils may dilate initially and slowly return to their original size. This is
known as Macewan's sign. It is helpful in differentiating alcoholic coma from other
comatose conditions.
There is slow, stertorous respiration and the skin is cold and clammy. The pulse is very
feeble. If this stage lasts for more than twelve hours, paralysis of heart and respiratory
centre may occur or pulmonary edema may occur resulting in death.
In this stage, Saturday night paralysis occurs. It is so called as it is seen in workers who
receive their salary at weekends and go on drinking. While drunk, they may assume an
abnormal posture, which may result in pressure on radial nerve and lead to its paralysis.
The common effect of heavy drinking is 'hangover'. In this, the person experiences
headache, nausea, irritability, stomach upset, thirst and tiredness about 8 to 12 hours after
drinking. Headache is due to cerebral edema. Blackouts may be experienced by some
wherein they do not remember all that happened during a heavy drinking episode.
Alcoholism is characterized by psychic dependence on alcohol in all degrees. In milder
degrees, alcohol may be desired if not present at meals or social functions. At moderate
degrees, the individual is compelled to drink in order to work or participate socially. He m
use all means to get his supply of alcohol. In cases of strong dependence, the individual
drinks alcohol far exceeding the cultural norms and also drinks in unacceptable situations
He is so obsessed that he may use unfair means to maintain the supply of alcohol to the
extent of drinking unusual or poisonous mixtures. Tolerance to alcohol may develop. This is
the development of body or tissue resistance to the effects of alcohol so that larger doses
are required to produce the original effect. There may be some cross-tolerance between
alcohol and barbiturates, which is mutual but incomplete.
Another characteristic feature of alcoholism is its physical dependence. If the body develops
dependence to alcohol, a sudden cessation of alcohol intake is likely to produce withdrawal
symptoms. Withdrawal symptoms are manifested by tremors, sweating, nausea, severe
anxiety, inability to sleep, irritability, increase in the pulse rate, rise in temperature, hyper
reflexia and postural hypotension. In severe cases there may be hallucinations, convulsiors
and delirium. The intensity varies with the duration and the amount of alcohol taken. If the
symptoms are severe and proper medical management is not given, the condition could b|?
fatal.
http://www.medivisionindia.com/addiction/introduction.phtml
1 (1/31 '()3
■ Complete health care and medical information from India
Page 1 of?
Various complications can arise due to alcoholism. These are:
(1) Intoxication:
The effect of alcohol is dose-dependent and results in progressive depression of the
reticular activating system of the brain. This is followed by the general depression of the
central nervous system function leading to coma and eventual death through respiratory
arrest. A blood alcohol concentration of 0.1% is considered conclusive of intoxication.
(2) Alcoholic amnesia:
Alcoholic amnesia or blackout is a short term memory loss occurring during period of acute
intoxication with a rising blood alcohol level. The loss of memory is in the short- term range,
beyond the immediate 3 to 5 minutes. Remote memory that is the events prior to the onset
of the rising blood level remains intact.
(3) Withdrawal:
If the body develops dependence to alcohol a sudden cessation of alcohol intake is likel\ to
produce withdrawal symptoms. The earlier and most common features of alcohol
withdrawal are anxiety, anorexia, insomnia and tremor. The patient appears hyper-alert
and has jerky movements, irritability and a tendency to be easily started. Delirium tremens
is most severe withdrawal state. It is characterized by marked tremor, anxiety, insomnia,
anorexia, paranoia and disorientation. The person may attempt self-harm during outburst
of irrational behavior. The state of delirium tremens peaks after about 3 days of abstinence
but can also occur several days thereafter. The delirious state persists 2 to 3 days and
rarely longer and often ends abruptly. Convulsive seizures of grand mal type may occur
during the withdrawal from alcohol. The seizures tend to occur during the first later,
especially if other depressant drugs have been used chronically.
(4) Malnutrition:
Many alcoholics show signs of malnutrition. There is replacement of normal caloric intake
by alcohol. Also the available funds are used to purchase alcohol rather than food. Nutrient
depletion resulting from chronic alcohol ingestion may gradually lead to damage of various
body tissues. The central nervous system and the liver appear to be affected most
significantly. Their dysfunction may further degrade nutritional wellbeing. The effects on
other body tissues are also related to malnutrition such as on endocrine, cardiovascular
hematological and immune system. The alcoholics derive a major portion of caloric intake
from alcohol. These are termed as empty calories as the alcoholic beverages do not contain
significant amount of important nutrients like protein, vitamins and minerals. Over the
period of months, depletion of nutritional stores is inevitable and there is deterioration of
nutritional status.
In alcoholic patients, there are frequent abnormalities in digestive and absorptive abilities.
Maldigestion and malabsorption may seriously compromise utilization of ingested food and
degrade further the already poor nutritional status of the affected patient. The impaired
digestion and absorption is due to the damaging effect of alcohol on the stomach and small
intestines and subsequently on the liver and pancreas.
(5) Disorders of the gastrointestinal system:
Alcoholics show great frequency of symptoms such as abdominal pain, erratic bowel
functions, nausea and vomiting, gastrointestinal hemorrhage and jaundice.
The alcoholic is susceptible to developing esophagitis that is inflammation of the
esophageal mucosa. This is due to increased acid production by the stomach and frequent
vomiting. There is also regurgitation of stomach contents into the esophagus.
Excessive alcohol ingestion leads to inflammation of the pancreas. This condition is termed
as pancreatitis. When there is a single episode, which is reversible, it is termed as acute
pancreatitis. Acute pancreatitis is manifested by upper abdominal pain, nausea and
vomiting, ileus, decreased plasma volume, low blood pressure and serum electrolyte
blip: w \\ w.nicdivisionindia.com/addiction/complications.phtml
10/31 U3
• Complete health care and medical information from India
Page 2 of?
vomiting, ileus, decreased plasma volume, low blood pressure and serum electrolyte
disturbances. When there are repeated bouts of pancreatitis resulting in chronic irreversible
scarring of the gland it is called 'chronic pancreatitis1. It is manifested by longstanding pain,
fat malabsorption leading to weight loss, malnutrition, and foul-smelling bulky stools often
with diarrhoea. It may also lead to endocrine insufficiency that is diabetes mellitus.
(6) Disorders of the liver:
The most common development in alcoholic liver is increased fat in the liver parenchyma
the so called alcoholic fatty liver. In some patients, continued heavy drinking may lead to
necrosis of the liver cells and inflammation. This is termed as alcoholic hepatitis. This
condition is characterized by enlargement of the liver, jaundice, abdominal pain and fever
It may lead to more fulminant form, advancing to death or cirrhosis of the liver. Alcohol c
cirrhosis of the liver is the final part of the spectrum of alcoholic liver disease. In this
condition there is fibrosis associated with disruption of normal liver lobules and formatioln of
nodules.
(7) Neurological disorder in alcoholism:
Excessive use of alcohol may lead to acute and chronic brain and peripheral nerve
dysfunction. Both the acute and chronic stages show alteration in memory, impairment of
intellectual functions such as calculation, comprehension and new learning as well as
impaired judgement and lability or shallowness of affect.
Secondary alcohol related effects may lead to organic brain damage. Blood alcohol levels
may be high enough to induce coma with hypoventilation may cause hypoxia sufficient :o
produce organic damage. Vomiting during alcoholic stupor may lead to aspiration of gastric
contents. Head injury associated with alcohol related trauma. Due to alcoholic
hypoglycemia there may be serious and sometimes fatal damage to the central nervous
system. Condition caused by acute niacin deficiency such as dementia, dermatitis and
diarrhoea may develop rapidly.
Peripheral neuropathy is also frequently reported in the alcoholics. The onset of symptons
is slow over weeks or months. Involvement is usually bilateral and symmetrical. The first
symptom may be pain in the calf muscles or feet or there may be associated burning,
tingling in the lower extremities. Later, these symptoms may occur in the hands and arms.
As the process continues, muscle weakness and wasting also occur. There may be foot drop
gait. Later the legs may become completely paralysed. There is numbness of stocking o
glove type.
Abstinence from alcohol and nutritional supplements may show improvement in some
patients though in advanced cases there may be some degree of permanent disability.
(8) Alcoholic amblyopia:
This is a rare type of eye disorder. In the past it was referred as tobacco alcohol amblyopia
as it was encountered in alcoholics who are usually also heavy smokers and are
malnourished. The condition is characterized by painless, bilateral blurring of vision with
reduced visual acuity and scotomas.
(9) Sleep disturbances:
Sleep disturbances including frequent awakening, restless sleep, insomnia and might
terrors are the most common complaints of the alcoholics. There is marked insomnia when
there is abrupt withdrawal from alcohol.
(10) Hematological disorders:
Anemia is the most common abnormality amongst the blood disorders due to alcoholism.
White blood cell and platelet production and function are also affected. Basically there is
defect in cell proliferation, cell maturation and cell survival.
(11) Disorders of the heart:
htip://w\\ w.mcdivisionindia.com/addiction/complications.phtm I
H) 31 03
>• Complete health care and medical information from India
Page 3 of 3
(11) Disorders of the heart:
Due to excessive ingestion of alcohol, a number of factors indirectly produce effects on the
heart. These factors are decreased potassium levels, decreased magnesium levels, alter 2d
fluid balance, increase in blood lipid levels, alcohol withdrawal reactions, beri-beri heart
disease and beer drinkers heart.
Drinking large amounts of alcohol often leads to lowered levels of serum potassium which is
particularly true in those people who drink heavily and neglect food. Alcohol selectively
increases the urinary excretion of magnesium and lead to lower magnesium levels. Severe
alcohol withdrawal symptoms seen in alcoholics such as withdrawal seizures, nausea and
vomiting and delirium tremens may place a stress on patient's cardiovascular system and
lead to heart failure.
(12) Effects of alcohol on skeletal muscles:
Heavy alcohol ingestion has an adverse effect on the skeletal muscles and the heart
muscles. It leads to acute alcoholic myopathy, chronic alcoholic myopathy and subclinical
alcoholic myopathy.
Acute alcoholic myopathy is characterized by muscle pain, tenderness and swelling. The
proximal muscles of the extremities, the pelvic and shoulder girdle and the muscles of tie
thoracic cage are the most common sites of involvement.
Chronic alcoholic myopathy is characterized by muscle wasting and weakness of the sane
muscle groups as acute alcoholic myopathy.
Subclinical myopathy may be defined as acute myopathy in which patients are seen in with
acute intoxication or withdrawal but symptoms related to skeletal muscles are absent oi
obscured by the presenting symptom.
Treatment in all forms of alcoholic myopathy consists of abstinence from alcohol and return
to a nutritious diet rich in vitamins.
http: ww w.medivisionindia.com/addiction/complications.phtml
10'31'03
Page 1 of 2
Industry Targets the Young
f
alcohol
i
Industry Targets the Young
"Scandal as drink bosses target our children" was the headline in the Daily Expres
article was inspired by the recent Eurocare publication, "Marketing Alcohol to You
People", an eye-catching brochure which brings together examples of advertisem
from all over the world. The text shows how the drink industry cynically sets out t
persuade the young to consume alcohol by making it appear glamourous, fashion
and amusing. The advertisements associate alcohol with sporting and sexual pro
Heroes of the football field play with the logo of a particular beer emblazoned acr
chests. Beautiful young women imply a willingness to surrender to the man who s
particular kind of booze. Perhaps most notoriously, there is the Carlsberg baby of a few months who, in the colours of Liverpool FC, is already a living advertisem
Carlsberg lager.
It was this last image which caught the attention of Gro Harlem Brundtland, the Director G
the World Health Organisation, at the recent ministerial meeting in Stockholm on Young Pe
Alcohol. Holding up the brochure, she said that this was evidence of what governments con
about the well-being of youth were up against.
Besides the Daily Express, other major national newspapers took up the story, as did televi
radio. The industry was perhaps unprepared and could only come up with the comment tha
"Marketing Alcohol to Young People" was "inaccurate and misleading" though the various
spokesmen could hardly deny that the advertisements were genuine and spoke for themsel
"Self-regulation is working," said the industry's Portman Group and it is true that a numbe
complains have been upheld but these have been against such flagrant violations that they
hardly be ignored without the system being totally discredited.
Those working with the problem would say that what is much more insidious is the relentle
pressure exerted by the kind of advertising strategies highlighted in "Marketing A cohol to
People".
The fact is that problems arising from alcohol use among the young are rising, particularly
United Kingdom, and there is a vast consequent cost to the NHS - besides the terrible pers
price many families have to pay. At least the Portman Group is happy with how things are
the self-regulation front.
Ironically on the day "Marketing Alcohol to Young People" was reported in The Daily Telegr
same newspaper announced a "ground-breaking" appointment at Bacardi-Martinij one of t
Portman Group's major funders: a marketing director with special responsibility for "the yo
market" and audiences at musical events.
Alcohol Alert (links to previous issues of Alcohol Alert)
This issue of Alcohol Alert (link to index)
htlp://w\vw.ias.org.uk/publications/alert/01 issue 1/alertO 10 l_p5.html
12/2/03
Industry Targets the Young
F age 2 of 2
This issue of Alcohol Alert (link to index)
Institute of Alcohol Studies)Elmgren House|l The Quay|St Ives
Cambridgeshire PE27 5AR) Tel: 01480 4667661 Contact the IAS
Copyright 2003
http://www.ias.org.uk/publications/alert/01issuel/alert0101_p5.html
*
12/2/03
- Media
 RF_MH_2_C_1_SUDHA.pdf
RF_MH_2_C_1_SUDHA.pdf
Position: 875 (25 views)