MEDICINE
Item
- Title
- MEDICINE
- extracted text
-
RF_MP_1_SUDHA
British
np i i
man sags:
Plant trees today, or repent j
by David J. Davidar
'j'HE mighty Himalayan rivers,
the Ganga and Brahmaputra
along with other major rivers such
as the Ghagra, Gomti and Barak have
cauesd widespread damage again this
year, due to flooding. In Uttar Pra
desh, Assam, Bihar over 700 lives
have been lost with no signs of re
lief from the ravaging floods. The
present situation could have been
averted if warnings by numerous en'onmentalists had been heeded. A
^77 Special Report by Time maga
zine tipped India, particularly the
foothills of the Himalayas, as the re
gion where the worst soil erosion in
the world has occurred. British Eco
nomist Barbara Ward gives further
credence to that report by her obser
vation that because the Himalayan
uplands can no longer retain water
there will now be “a fatal alternation
of droughts and floods ”.
ing threatened and so he is slowly be
ginning to respect the soil more,” says
Dr Baker.
His chequered career, replete with
its victories and defeats, shows the
measure of the man. Born in Hamp
shire, England, the son of a parson
who took up horticulture and culti
vating tree nurseries, Baker as a small
boy found himself responsible for the
care of tens of thousands of trees in
his father’s nurseries. “I reckon I
could not escape my love for trees
because it seems to run in the fami
ly”, Baker muses. His great grand
father who married a wealthy land
owner’s daughter spent £ 12,000 (a
lot of money in those days) planting
trees. Another grandfather used to
walk the quiet country lanes of sou
thern England, his pockets full of
acorns, strewing them wherever he
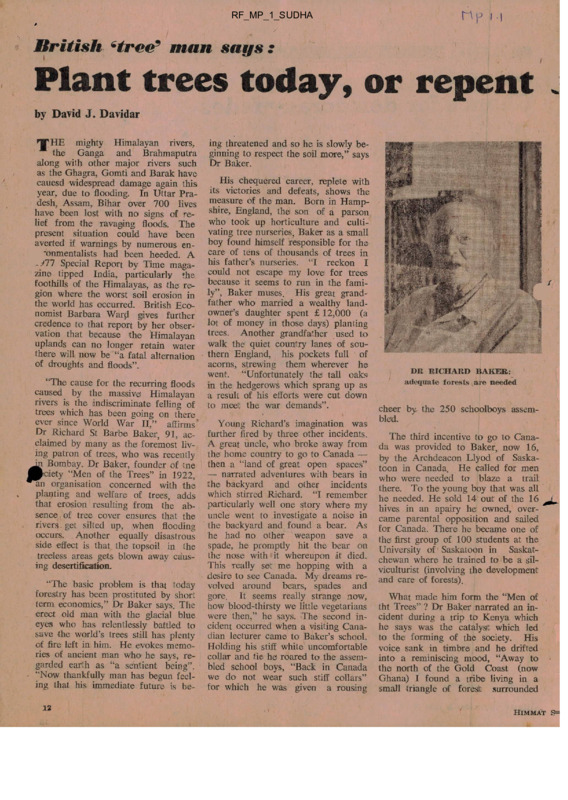
DR RICHARD BAKER:
went. “Unfortunately the tall oaks
adequate
forests are needed
“The cause for the recurring floods in the hedgerows which sprang up as
caused by the massive Himalayan a result of his efforts were cut down
rivers is the indiscriminate felling of to meet the war demands”.
cheer by the 250 schoolboys assem
trees which has been going on there
ever since World War II,” affirms*
Young Richard’s imagination was bled.
Dr Richard St Barbe Baker, 91, ac further fired by three other incidents.
The third incentive to go to Cana
claimed by many as the' foremost liv A great uncle, who broke away from da was provided to Baker, now 16,
ing patron of trees, who was recently the home country to go to Canada — by the Archdeacon Llyod of Saska
dn Bombay. Dr Baker, founder of tne then a “land of great open spaces” toon in Canada. He called for men
|P»ciety “Men of the Trees” in 1922, — narrated adventures with bears in
who were needed to blaze a trail
•an organisation concerned with the the backyard and other incidents
there. To the young boy that was all
planting and welfare of trees, adds which stirred Richard. “I remember he needed. He sold 14 out of the 16
that erosion resulting from the ab particularly well one story where my hives in an apairy he owned, over
sence of tree cover ensures that the uncle went to investigate a noise in came parental opposition and sailed
rivers, get silted up, when flooding the backyard and found a bear. As for Canada. There he became one of
occurs. Another equally disastrous he had no other weapon save a the first group of 100 students at the
side effect is that the topsoil in the spade, he promptly hit the bear on University of Saskatoon in Saskat
the nose with it whereupon it died. chewan where he trained to be a sil
treeless areas gets blown away caus
This really set me hopping with a
ing desertification.
viculturist (involving the development
desire to see Canada. My dreams re and care of forests).
“The basic problem is that today volved around bears, spades and
forestry has been prostituted by short gore. It seems really strange now,
What made him form the “Men of
term economics,” Dr Baker says. The how blood-thirsty we little vegetarians tht Trees” ? Dr Baker narrated an in
erect old man with the glacial blue were then,” he says. The second in cident during a trip to Kenya which
eyes who has relentlessly battled to cident occurred when a visiting Cana he says was the catalysft which led
save the world’s trees still has plenty dian lecturer came to Baker’s school. to the forming of the society. His
of fire left in him. He evokes memo Holding his stiff white uncomfortable voice sank in timbre and he drifted
ries of ancient man who he says, re collar and tie he roared to the assem into a reminiscing mood, “Away to
garded earth as “a sentient being”. bled school boys, “Back in Canada the north of the Gold Coast (now
- “Now thankfully man has begun feel we do not wear such stiff collars” Ghana) I found a tribe living in a
ing that his immediate future is be- for which he was given a rousing small triangle of foreslt surrounded
12
f
HlMMAT S=
—— - »
ASIA
South Korea:
Chance for democracy fades
A FTER the assassination of Presi
dent Park in October 1979, a
new democratic era for South Korea
was promised by the newly-elected
interim president, Choi Kyu Hah.
Instead a purification drive aimed
at wiping out corruption and errant
thought has been launched by the
small group of generals who seized
power after Park’s death. President
Choi Kyu Hah has been pressurised
into resigning, paving the way tor
another military-led authoritarian re
gime, with General Chon Doo Hwan
at its head.
The purification drive which was
launched three months ago is one of
the main political, goals announced by
the military rulers who have taken
near-total control of government func
tions. The purpose of this campaign
is apparently to restore the people’s
trust and confidence in the govern
ment and to promote unity between
the people and officialdom. Among
measures taken is the cancellation of
the licences of 172 periodicals. Al
though some of them were reportedly
unethical and vulgar, and therefore
their closure met with public appro
val, not so palatable, was the enforc
ed closure of a number of serious
magazines.
The purge has also included the
dismissal of “detrimental elements”:
8500 civil servants and officials of
1212
state governments,
trade
unionists, 400 journalists and 70
college professors. They have been
accused of corruption, inefficiency or
disloyalty. About 30,578 “hooligans,
racketeers and gamblers” have also
been rounded up. Of these more than
20,000 have been sent to military
reeducation centres where they rise
at dawn, run four miles, lift logs and
write “confessions” of past misdeeds.
On July 31 a set of reforms was
announcd — private tutoring, which
was considered to be a factor in
widening the gap between the rich
and the poor, was banned, as were
college entrance exams. Chon also
called for comprehensive medical,
but did not specify when they would
come or how they would be paid for.
Most of the political opposition to
Chon’s presidential aspirations has
been wiped out. Kim Young Sam, the
president of the New Democratic
Party, has resigned (under pressure)
after 11 weeks of house arrest. Kim
Jong Pil, leader of the Democratic
Republican Party, was arrested on
charges of corruption and freed only
after he had pledged to abandon poli
tics and restore to the state most of
his personal fortune.
‘vL...
C. \
Himmat
September 5, 1980
Kim Dae Jung, a leading opposition
figure, and a man widely seen at
home and abroad as a symbol of
hope for a greater degree of demo
cracy in South Korea, has been
arrested and is facing a trial on,
among others, charges of sedition and
communist activities. When Kim was
arrested earlier this year, there was
an armed uprising in Kwangju —
Kim’s home province. The military
authorities believe that this uprising
was planned by Kim rather than be
ing a spontaneous reaction. South
Korea’s military rulers obviously see
Kim’s arraignment as part of their
effort to restore stability to the coun
try. Foreign observers and quite a
South Koreans are more inclined
fear instability arising from his trial
and from the military’s effort to
restore the kind of authoritarianism
practised by President Park.
On August 27, when Seouls’s elec
toral college, the National Conference
for Unification, elected Chon Doo
Hwan as the fifth President of South
Korea, it was the culmination of
about seven months of Chon’s behind-the scene manoeuvring initially,
and then outright agressiveness in
consolidating his hold on the coun
try’s politics.
Although interim President Choi
Kyu Hah was expected to stay on in
power until a more democratic system
was established, he was forced to
resign and make way for Chon. Chon
and his colleagues seized on
chance timing of an interview
ween the commander of US forces in
South Korea, General John Wickham,
and a visiting foreign correspondent
to link Chon’s name with the presi
dency first time. A judiciously edited
version of the wire service report was
published in the totally censored daily
newspapers giving the impression that
Washington fully supported Chon’s
bid to “legitimately” become Presi
dent.
Chon had made it clear that strong
leadership was the main qualification
he was offering in support of his presidental ambitions. He called on the
people “to realise that this is the last
chance for saving the nation” from
confusion and disorder. Now it re
mains to be 'Seen how successful he
is; and just how low democracy
comes on his list of priorities.
11
/
omorrow
on all sides by the rapacious Sahara
desert. I knew that in a short while
their remaining trees would be cut
down, they would be decimated.
However there was nothing I could
do about iit then. When I came back
in 1952 with an expedition to the
Sahara I saw that my worst fears had
been realised. Their final tree cover
had been almost destroyed and there
was no escape for them. Their wo
men
uld not bear children as they
did nut want them to suffer, if they
moved to a different place. That in
dent made a terrific impact on me.
aid not want it to happen in other
parts of the world because of an in
discriminate felling of trees. That’s
what started a lifelong commitment
to trees and their welfare.”
This commitment has led Dr Ba
ker to many outstanding achieve
ments in the environmental field. Be
sides founding the Men of the Trees
in 1922, he was instrumental in con
ceiving and leading a trip to the Sahara
to survey 14,400 kilometres of desert
v land in Africa, He started the Sa
hara Reclamation scheme in 1964
asserting that the deserts when re
claimed would prove the granaries
of the world.
Iso initiated the “Save the
F
Rorlwuods” campaign in California.
n The forest giants which were slowly
-^■heing destroyed owe their present
Wffumbers to Dr Baker. Because of
his campaign 26 trillion trees . were
planted. He has also promoted af
forestation in India, Pakistan, Ku
wait, Lebanon, Iran, UAE, Tunisia,
Spain and New Zealand.
A country he has a lot of admira
tion for is China, where he says the
tree cover has been increased from
seven per cent to 27 per cent. Dr
Baker had started sending seeds to
m China 47 years ago.
■
The patriarch of trees has 30 books
on trees and land reclamation to his
credit. One book “I planted trees”
' sold 32,000 copies in its hardback
edition. Currently he is working on
his “magnum opus” (as he calls it)
—ptember 5, 1980
— a book called “Tall Timber” which
will chronicle his life and that of the
250 famous world figures who have
been associated with him and his work.
As this is not his first visit to India
(he first came here is 1931) I asked
him what he felt India ou^ht to do to
prevent increasing deforestation and
enviromental exploitation. “First a
change of thinking must come about.
Why should India follow obsolete
Western ideas and cut down its fore
sts to, prop up the economy? In the
Himalayas tree cutting first started
during World War II when timber
was needed for the war effort. But
even in peacetime the denudation of
forests goes on for paper, matchsticks
etc If you need the wood for econo
mic purposes it is imperative that
enough treees are planted to make up
for those cut,” Dr Baker says. Also
all the workers who would lose their
jobs if the timber industry was halted,
could be given alternative employ
ment in. afforestation programmes.
On one of his earlier visits to
India, Dr Baker had requested the
Bombay Municipal Corporation to
plant a five kilometre belt of trees
all along the city to preserve the oxy
gen content in the atmosphere and
provide a green belt for the city. His
advice went unheeded. “Yet there is
still hope,” he asserts, pointing to
movements like the Chipko movc-
ment near Nainital, UP to preserve
trees. “The peasant too is waking up
to the fact that adequate forests are
needed if his existence is not to be
threatened, which is a good sign,” he
says.'
Dr Baker has accumulated ac
colades in his fight to preserve the
environment. In 1978 he was awarded
the Order of the British Empire
(OBE) and earlier the University of
Saskatoon made him an Honorary
Doctor of Laws. However he counts
higher than these honours the victo
ries he has won over governments and
others vested interests in his fight to
save trees.
Dr Baker’s concern for trees comes
at a vital period in history. In the
last half century an estimated 250,000
square miles of farming and grazing
land have been swallowed by the
Sahara alone. In Rajasthan, sand
cover has increased by about eight
per cent in eight years. The liyes of
about 630 million people are threa
tened by desertification. With these
grim statistics around us Dr Baker
fixes the issues at stake. “One indivi
dual on earth needs 16 acres of tree
cover to fulfill basic needs like re
plenishment of oxygen content in the
air, adequate rainfall etc per year.
Imagine the consequences when the
trees are all gone ”. Quite a scarifying
prospect by any reckoning.
Every student should plant and nurture a
tree...
A plan for the
‘greening9 of India
b
by Niketu Iralu
< RECENT pronouncement by the
** World Wildlife Fund in India says
that in a decade or so an acute “fire
wood famine” would overtake vast
areas of India. A direct consequence
of this crisis wlil be an enormous .in
crease in the use of cow dung for
cooking in rural India. An estimate
states that at present annually 60 to
65 million tonnes of dry cow dung
are used for cooking, equivalent to
eight times the total production of the
fertiliser plant at Sindri a year. The
economac, political and ecological
disaster that can result from pro
longed shortage of firewood for
millions of people is not hard to ima
gine.
r
Public awareness
of the desperate
situation is
~:t developing. Urgently
t !ffast
needed are imaginative policies and
schemes for afforestation on an ex
tensive scale that will be appealing
enough to masses of people. Here are
a few suggestions.
CONTINUED ON NEXT PAGE
1&
t
GREENING — from page 13
For students
The high school students of India
can become the most effective agents
for a national scheme of afforestation.
Why not make the “greening” of
India part of the school curriculum ?
It should be easy to introduce a
scheme whereby every high school
student is required compulsorily to
start growing at least one tree sap
ling in the seventh standard. By the
time of completion of high school the
student would have taken care of a
growing tree for about five years.
Quite apart from the splendid con
tribution he makes to his nation, the
student will learn some precious
lessons about taking total responsi
bility in seeing a thing through and
also involve himself in some manual
labour. Tending a young sapling for
several years will involve disciplined
watering, construction of a small bu
but secure protective fence around
the young tree and some weeding.
Such a scheme could help in the buil
ding of national character and the
breaking down of barriers between
those who work with their hands and
those who do not.
The State will need to finance the
scheme to some extent. The setting up
*
iiiii
A TREELESS PLAIN:
acute ‘firewood famine’ imminent
of forestry nurseries all over the coun
try will be an item of expenditure. But
why not scrap altogether the National
Cadet Corps Scheme which India can
surely do without and use the money
instead to finance an every-student-atree-scheme ? India’s defence capa
bility does not depend critically on
the existence of the NCC.
For politicians
HIMMAT AIR MAIL RATES
Indian
Sterling or
•
other currency Rupees
75.00
Sri Lanka
£ 5
Burma and
Afghanistan US $ 13
All Asia except US $ 14
Japan & Korea
119.00
U. K., Europe,
East Africa, ‘
Japan, Korea,
North Africa,
Southern Africa £ 10
152.00
A $ 16
152.00
New Zealand NZ $ 19.50
165.00
Americas, W. Indies,
South Pacific,
Central Africa,
West Africa,
Rhodesia
US $ 25
212.50
Australia
14
111.00
It may not be a bad idea for some
states in India to start a tradition
whereby MLAs and MPs take on to
grow trees; 10 trees for an MLA and
20 trees for an MP, to mark the
tenure of their representation of the
people. Such a tradition will have the
effect of every MLA or MP leaving
something beautiful behind for their
people.
Years ago Israel adopted a sensible
way of commemora'ing her national
heroes by bestowing trees in their
honour instead of medals or stone
monuments. It must be admitted that
most stone monuments end up by
merely conveying the sense of the per
son honoured being doubly dead and
gone. Whereas trees evoke something
of hope and gratitude in the hearts of
those who behold them. In a country
of India’s size with a bulging number
of heroes needing to be honoured,
the potential from such a scheme is
enormous.
In Israel the number of trees plant
ed to honour those they love and res-
pect are classified into various group
ings. A garden has 100 to 999 trees;
a grove has 1000 to 2499 trees; a
wood has 2500 to 9999 trees and a
forest has more than 10,000 trees.
In considering any scheme to res
tore to India a green mantle of new
trees what the late Dr E. F. Schuma
cher had to say is instructive: “One
of the greatest teachers of India was
the Buddha who included in his tea
ching the obligation of every good
Buddhist that he should plant and see
■to the establishment of one tree at
least every five years. As long as this
was observed, the whole large area of
India was covered with trees, free of
dust, with plenty of water, plentv of
shade, plenty of food and ma'ei
Just imagine you could establish an*
ideology which would make it obli
gatory for every able-bodied person in
India, man, woman and child to do
that little thing — to plant and see to
the establishment of one tree a year,
five years running. This, in a fiveyear period, would give you 2000
million established trees It could be
done without a penny of foreign aid;
there is no problem of savings and
investment. It would produce food
stuffs, fibres, building material, shade,
water, almost anything that man
really needs . . . The really helpful
things will not be done from the Cen
tre; they cannot be done by big orga
nisations; but they can be done by the
people themselves.”
Himmat
September 5, 1980
. k
rip- /-a-.
Kody Medical Electronics Ltd.
NO. 2, 12th EAST STREET,
KAMARAJ NAGAR,
THIRUVANMIYUR.
MADRAS • 600 041.
T.N.G.S.T, No. 170466
C.S.T. No. 53144 Dt. 28-7-80
Telephone : Off. : 410764
FAC : 415960
Telegram : KODYELEC
Telex : 41-21046 KODYIN
KODY VERSASTIM
INTRODUCTION :
I
"Kody versastim" marks the heights of Electrical muscle stimulation
stimulation modes.
After intensive research, 'Kody versastim' has come out with various
found to be beneficial in treating various physiological problems.
Added to the salient features, 'Kody Versastim'
makes the instrument a class of its
technology
stimulation
provides a terminal to carry out
by
providing
settings
various
which
Iontophoresis,
are
which
own.
FEATURES :
Kody versastim offers three stimulation modes, namely the Faradic stimulation mode, the Galvanic stimulation
mode and Iontophoresis.
FARADIC STIMULATION MODE:
The faradic stimulation mode can be further classified into two different modes, namely the continuous
faradic mode and the surge or interrupted faradic mode.
The continuous faradic mode is deemed to be tetanizing ie., producing a constant contraction of normally
innervated musculature. This mode is used to obtain relaxation with muscles in spasm.
The surge or the interrupted mode of faradic stimulation causes a brisk response in the muscles.
faradic current is often used in the management of athletic injury.
Interrupted
GALAVANIC STIMULATION MODE:
The Galvanic stimulation mode can be further classified into two categories namely, continuous Galvanic
mode and interrupted Galvanic Mode.
The Galvanic stimulation mode is found to be beneficial in cases .where R. D. (Reaction to Degeneration)
is present.
It is observed that Faradic stimulation is ineffective in case of patients with R. D., thus making Galvanic
stimulation, the only alternative for symptom R.D.
It is observed that the only mode for stimulation to be used in denervated musculature is the interrupted
Galavanic mode.
IONTOPHORESIS :
Iontophoresis also termed as ion transfer is the introduction of
purpose by means of Galvanic current.
substance
into body
for
therapeutic
Therapeutic results depend on ion introduced, and the pathology present on the desired effects.
Care should be taken on ion selection as there can be contraindication to individual ions
patient sensitivities, a I lergies and complicating factors in specific i nstances.
based on
2
A completely non-invasive concept of iontophoresis is made even more attractive to clinicians because
of the minimal ionic concentration required for effective administration.
Research has shown that the low level ampearage are more effective*as a driving force than high
current intensities
Thus iontophoresis necessiates a low-mill.i ampearage and low percentage of ion
source.
The Kody versastim provides speical electrodes which are designed to carry out iontophoresis with minimal
irritation which is obviously due to the nature of Galvanic current.
PHYSIOLOGICAL RESPONSES OF VERSASTIM .
1.
Relaxation of spasm
2.
Monitored contraction of muscles stimulating active exercise.
3.
Relatively weight-free exercises depending on patient position and electrode
4.
Increased fiber recruitment since most if not all fibers
placement.
will respond to stimulation, differing from
normal, active motion which may recruit only a percentage of fibers.
5.
Circulatory stimulation by the 'pumping action' of the contracting musculature
6.
Enhancement of reticuloendothelial response to clear away waste products.
INDICATIONS :
Electrical stimulation is indicated whereever the above physiologic responses are desired, Most often,
electrical stimulation is employed to provide excercise patterns when patients are unable to perform
them due to pain, restrictions in ranges of motion or other dysfunctions of the neuromuscular system.
Electrical stimulation is not limited, therefore to the musculoskeletal system, but may be utilized in
gynecologic, urologic and ocular musculature problems and most recently, temporomandibular joint (TMJ)
and other dental problems.
CONTRAINDICATIONS :
The patients general health as well as the specific diagnosis will determine the advisability of electrical
stimulation. The presence of the following conditions would preclude electrical stimulation as a treatment
modality.
1.
Fresh fractures to avoid unwanted motion.
2.
Active haemorrhage.
3.
Phlebitis.
4.
Demand - type pacemaker - newer types may suggest extreme caution, rather than
prohibition-
TECHNICAL STECIFICATIONS :
1.
Power supply
2.
Output voltage wavefrom for faradicstimulation mode :
Rectangular/ monophasic.
3.
Maximum output parametres
:
Maximum output current: 140 MA (rms) at 500 Q
load, for faradic and 80 V for galvanic stimulation
mode,
4.
Pulse frequency range for faradic
:
125 Hz.
5.
Pulse width range for faradic
:
230 V A.C. mains
550 micro seconds
3
6.
7.
Interrupted/surge interval for faradic & galvanic with
equal ON & OFF time
:
Interrupt galvanic pulse widths
!
1, 2, 3, 4, Er 5 seconds.
100 & 500 microseconds 20, 40, 60, 80 100 & 300
milliseconds.
CONTROLS :
7. MAINS ONfOFF: This pushbutton control is provided at the back of the Instrument. By pressing
this the mains 230 V AC is connected to the instrument and this is indicated by a Red neon lamp
noted as "Mains" in the front panel. While the mains button is pressed, the Red lamp will glow.
2 AUDIO ONfOFF: This pushbutton control is provided at the back of the instrument,
this audio is switched on. By releasing this pushbutton, audio is switched off.
By pushing
3
VOLUME: This control is provided at the back of the instrument,
volume of the beep sound generated by the instrument.
control
This is
used
to
the
4 AMPLITUDE : This amplitude control is used to vary the intensity of the stimulation.
There are
three LEVEL controls available in the front panel. One for faradic stimulation mode the second for
galvanic stimulation mode, and the third one for iontophoresis. Clock-wise rotation will incr sase the
intensity and vice-versa. Before starting the operation, this control has to be kept in the counter
clockwise direction fully. The adjustment of one amplitude will not alter the other.
5. OUTPUT: The output sockets provided in the front panel is used to connect the patient electrodes
to the instrument. Electrode plugs should be inserted in the sockets before switching on the equipment.
CHEMICALY TO CARRy OUT IONTOPHORESIS :
1.
Chemical - Hydrocortisone :
1
perecent ointment, Pole - positive pole (anode)
Indication - anti-inflammatory used for arthritis, tendenitis, myositis & bursitis.
2.
Chemical - Mecholyl : Mecholyl ointment, Pole - positive po|e (anode)
Indication - Vasodilator, analgesic, used for neuritis, neurovascular deficits, sprains,
3.
Chemical - Acetic acid - 2 Percent,
Pole - negative pole
edema.
(cathode)
Indication - used for calcific deposits, myositis ossificans and frozen joints.
4.
5.
Chemical - Iodine - from lodex (with methyl salicyclate) Pole - negative pole
(cathode)
Indication - sclerolytic, antiseptic Analgesic used for scar tissue, adhesions,
fibrositis.
Chemical - Salicyclate - 10 percent salicyclate, preparation or Iodine with methyl salicyclate.
Pole - negative pole (cathode).
Indication - Decongestant, analgesic :
6.
Chemical - Magnesium :
used for myalgias, rheumatoid arthritis.
2 percent Magnesium sulphate (Epsom salts) Pole - Positive Pole
Indication - antispasmodic, analgesic, Vasodilator, used for osteoarthritis, myositis,
7.
Chemical - Copper :
(anode)
neuritis.
2 percent Copper sulphate
Pole - positive pole (anode)
Indication - Caustic, antiseptic antifungal :
8.
used for allergic rhinitis, dermatophytasis
(atheletes foot).
Chemical - Zinc : 20% Zincoxide ointment
Pole - positive pole (anode) Indication - Caustic, antiseptic, enhances health : used for otitis, ulcerations,
dermatitis, other open lesions.
4
9. Chemical - Calcium : 2 percent calcium chloride.
Pole - positive pole
Indication - stabilizer
of irritability threshold : used for myospasm, frozen joints.
- Trigger fingers, mild tremors.
10. Chemical - Chlorine : 2 percent table salt.
Pole - negative pole (cathode) Indication - Sclerolytic : used for scar tissue, adhesions,
11. Chemical - Lithium : 2 percent lithium Chloride or lithium carbonate.
Pole-positive pole (anode) Indication . specifically for gouty tophi.
GENERAL INSTRUCTIONS
A.
FARADIC STIMULATION :
1.
Select channel - 1 for faradic stimulation.
2.
Select the correct motor points for stimulation.
3.
Secure the electrodes on the right motor points using gel pad and velcro strap.
4. Connect the electrodes to Versastim CH-1. Output point using the recommended cihle.
5.
Select the mode (continuous / interrupt) and also select the required burst interval.
6.
Increase the faradic level for required
7.
Bring the faradic level to the minimum position before disconnecting the cable from Versastim.
8.
Please see figures displayed in the annexure for more details.
stimulation.
STIMULATION SITES FOR FARADIC ELECTRICAL STIMULATION
1. Stimulation of Median Nerve
Ref. Fig. 1. The wrist stimulation site is at the distal wrist crease between the palmaris longus. The
proximal stimulation site is at the distal elbow crease, medial to the biceps brachial tendon, I n obesse
patients the nerve is made more accessible to stimulation by bending the elbow.
2.
Stimulation of Ulnar Nerve
Fig.
Fig. 2.
2. The wrist stimulation site is at the distal wrist crease, lateral to the flexor Carpi Ulnaris
tendon. The below elbow stimulation site is located by placing the stimulator electrode on the lower
border of the medical epicondyle. The above elbow stimulation site is 10 cm. proximal to the below
Ref.
elbow stimulation site when elbow bent at 45 (degree)
3.
Stimulation o Radial Nerve
Ref. Fig. 3. The lower forearm stimulation site is along the laterial aspect of the head of the ulnar
and approximately 3.4 cm proximal to it.
The lower arm (above elbow) stimulation site is approximately
5.6 cm proximal to the lateral epicondyle between the brachialis and the branchioradialis muscles. Abduct
the arm 10 (degree), keep forearm pronoted and bend elbow at 10-15 (dagree)
4.
Stimulation of Peroneal Nerve
Ref. Fig. 4.
The ankle stimulation site is about 8 cm. proximal to the extensor digitorum bevis Muscle.
The below knee stimulation site is at the neck of fibula.
of the knee medical to the tendon of the biceps femoris.
The above knee stimulation site is at the bend
5
5.
Stimulation of the Sural Nerve
Ref. Fig. 5. Mark a point one cm lateral to lateral border of the tendon
achillis.
is approximately 14 cm proximal to the above marked point.
6.
The stimulation
site
Stimulation of the Tibial Nerve
Ref. Fig. 6. The ankle stimulation site is about 8 cm. proximal to proximal phalanx of the
great toe.
The knee stimulation site is at the distal knee crease approx. 1 cm
lateral to the midline of the popliteal fossa.
-------------1
7.
Problem and Remedies
a. Isolated cases of skin irritation may occur at the site of electrode placement following
long term
application. If the electrodes are insufficiently moistened or are in poor contact with the body
the result
may be a pricking pain, skin irritation or electrode burns. To avoid this apply electrode jelly before
J placing
the electrodes over the pain area and make sure that the electrodes are correctly in contact with the body
b. When the instrument is used for the first time it will give the feeling of being kneaded
when the
controls are at maximum. To avoid this. Level control should be kept at minimum so
as to give weak
stimulus, then slowly increase for optimum effect.
B. GALVANIC STIMULATION :
1.
Select channel - 2 for therapeutic galvanic stimulation.
2.
Select mode (continuous/lnterrput)
3.
Select the interrupt width and the burst interval for interrupted galvanic stimulation.
4.
Choose the correct motor points for electrode palcement.
5.
Spread a wet piece of lint cloth (approximately the size of the electrode)
electrodes and secure them using velcro strap.
6.
Increase the galvanic level for a comfortable stimulation.
7.
The galvanic level should ba brought to the minimum level before disconnecting the electrons at the
over the skintnder the
end of therapy.
IONTOPHORESIS :
C.
1.
Choose the right electrode placement.
2.
Prepare the skin under electrodes (to be cleaned with
3.
Choose the right ion for treatment
4.
Apply a thin layer of the ion (if it is in the fform of ointment) on the skin under the
electrodes and place a piece of wet lint cloth over it.
5.
If the ion is in the form of solution, soak a small piece of lint cloth in the
measured amount of
the solution and spread it on the skin under the appropriate electrodes.
6.
Place the electrodes in the correct position (the medicated part
appropriate electrodes) & the eiectrodes
---------1 also be wet.
-- should
7.
8.
lukewarm water)
appropriate
of skin must be right under
Use a velcro strap or light weight sandbags
to secure the electrodes in position.
Select channel 3 to carry out Iontophoresis
the
6
9.
Connect the electrodes to
Versastim CH-3, output point (the iontophoresis level
set
at minimum).
10. Increase the iontophoresis level gradually until a light irritation under the electrodes is reported by the patient,
11. Minimize the iontophoresis level in small steps until no irritation is reported by the patient.
12. Carry out treatment for 20 minutes.
v
13. The iontophoresis level must be brought to minimum position before
dioconnecting the electrodes
at the end of the therapy.
14. The skin under the electrodes must be washed with lukewarm water.
powder is also recommended for the skin under the electrodes.
ELECTRODE
1.
2.
A fina dusting
of talcum
PLACEMENT
Treatment for problems associated with the knee, (figure - 7)
Treatment of scapular condition (figure - 8).
The patient should be in the sitting position leaning
forward on to a pillow.
3.
Treatment of cervical/dorsal - lumbosacral condition (figure - 9) lying position is recommended for this
treatment.
4.
Treatment of sciatic neuritis (figure - 10)
5.
Treatment of gouty tophi (figure - 11)
6.
Treatment of calcific deposits in the deltoid legion
7.
Treatment of peripheral vascular deficit (figure - 13)
8.
Treatment of hyperhidrosis (figure - 14)
1.
The details of the chemicals
recommended
for
(figure-12)
different
pain
syndrome
is
recommended
in the
General Pamphlet.
2.
You have to select the correct chemical appropriate to the pain.
3.
The cathode electrode is larger in size indicated by
a
black
wire.
Anode
electrode
is indicated
by a red wire.
4.
5
6.
The selection of pain areas must be done after detailed discussions with the patient.
Selection of the electrode to be decided based on the recommendation in the pamphlet.
Placement of the electrode other than the eight location shown in the pamphlet must be done as follows.
One electrode to be placed in the pain area,, the other electrode to be placed on the end of
Treatment will be successfull only if the placement is done properly.
the nerve root associated with the pain. --------------
FARDIC
STIMULATION
©1
L. ELBOW STIMULATION SITE
©J
BELOW
ELBOW
STIMULATION SITI?
©J
WRIST
STIMULATION SITE '
FIG-1
©1
ELBOW STIMULATION SITE
OJ
-©J-
WRIST STIMULATION SITE
o
FIG-2
o
- PROXIMAL STIMULATION SITE
©
DISTAL STIMULATION SITE
G
FIG-3
ANKLE
©
* STIMULATION SITE
ABOVE
KNEE
STIMULATION SITE
BELOW
KNEE
STIMULATION
FIG 4
SURAL
STIMULATION SITE1
FIG 5
a NKLS
STIMULATION
SJTJe
•}
f|G-«
KNEG
STIMULATION
SITE
Fig
Fig.
8
7
Fig
Fig.
10
Fig.
11
Fig.
12
Fig.
13
Fig.
14
e
]
12
KODYS PRODUCTS RANGE:
ECG, ECG Simulator Cardiac Monitor, Foetal Heart
Rate Monitor,. Foetal
Doppler,
Vascular
Doppler
Diagnostic Doppler Recorder, Vascular Doppler Recorder, Electronic Pain Killer-TENS-Various Models, Stroke,
Rehabilitation
therapy
equipment-FNMS,
Versastjm.
Electronic
Muscle
Stimulatcr,
with
Provision For
Iontophoresis, Digital Pulse Monitor.
ACCESSORIES :
Pressure cuff recorder
8 MHz Pencil Transducer
2,
3.
5,
and 8 MHz Transducers.
SPARES :
ECG Paper Rolls, ECG Gel, Ultrasound Gel, Clipp-on Electrode, Limb Electrode, ECG Disposable Electrodes
Paediatric Electrode, Reusable Rubber Electrodes.
KODYS SALES & SERVICE NETWORK :
Agra, Ahmedabad, Bangalore, Bombay, Calcutta, Coimbatore, Cuttack, Hubli. Hyderabad, Indore, Kanpur,
Madurai, Nagpur, New Delhi, Pune, Salem, Trichy, Visakapatnam.
VI
— O—
MURTHY. E,
hyansgar,
9th hl
BANG.;LORE-560 069,
752
EXPERIMENTAL METHODS
three weeks after inoculation of the spleen cells, but not on animals tested
in a similar way after one and two weeks from the inoculation. HA anti
body titer does not rise in animals simply transfused with microfilariae,
as stated previously, but it rapidly rises when spleen cells from infected
animals are inoculated into clean animals, and stays at high levels for
periods of over four weeks. Therefore, this is interpreted as another piece
of evidence that the presence of circulating antibodies is not the essential
factor for the release of action of DEC. Also, injections of 0.5 ml of im
mune sera collected from infected animals twice a day for five days into
animals thus passively inoculated with microfilariae were not effective in
reducing the microfilaremia levels, such as seen in groups injected with
the spleen cells from the infected animals. This and previously stated
evidence suggest that release of the activity is not primarily dependent
on the circulating antibodies, but could be a cell mediated response, if
immunity is ever involved.
Treatments with some immunosuppressive measures were found to be
effective in inhibiting the action of DEC at least in certain cases. For ex
ample, the effect of DEC given at a dose of 100 mg per kg was apparently
inactivated in infected cotton rats after treated with prednisolone at daily
doses of 120 mg per kg for 4 days, but administration of 200 mg per kg of
DEC to the same lot of animals caused a significant reduction of micro
filaremia. Previous treatments with 6-mercaptopurine and cyclophospha
mide at similar doses were apparently ineffective in view of the inactivation
of DEC. However, the inhibitory effects of antilymphocyte serum (ALS),
and antithymus serum (ATS) on the release of the microfilaricidal action
oi OEC in infected animals are apparently conspicuous. ALS was prepared
by injecting 107 to 108 lymphocytes isolated from lymph nodes of cotton
rats into two rabbits, once a week for three weeks. The titers of ALS
measured by the cytotoxicity test were 1:60 and 1:120. Ten clean cotton
rats were treated continuously with injections of 0.5 ml of ALS three times
a week, and L. carinii was infected to the animals by the standard method
of the mite bite one week after commencement of ALS treatments. Only
two cotton rats survived through these intensive ALS treatments, and
microfilariae became detectable from seven weeks after the infection. No
antibody as measured with the HA test was detected and DEC was also
ineffective in reducing microfilariae during the period of continous treat
ments with ALS. However, production of antibody began soon after the
ALS treatment was suspended, and in another test of administration of
DEC one month after the ALS treatments had been suspended, the drug
was shown to be still ineffective, while the HA titer of the serum rose to
1:4000. This again suggests that the mere presence of humoral antibody is
not sufficient for disclosure of the action of DEC.
Another interesting aspect of the mode of action of DEC was disclosed
through experimental filariasis in jnds. As stated previousIyT microfilariae
^oTTJrwiteTin Libyan jirds were shown to be refractory to DEC (Worms
et al. 1961). Since the Mongolian jird is susceptible to both D. witei and
JI
EXPE
L. carinii, they were infected with ei
In mixed infections, microfilariae of
blood samples, but can be easily diffe
in morphology. So far as observation
parently ineffective against microfilar
12C. Experimental immun
12C.1 Natural and acquired
reference to certain groups of filariae.
especially when a filarial species have
ffiada £°
natUtral h°St’ SUCh aS
filaria L. carina, to rat, mouse, or ha
sistant the growth of infective larvae t
retarded, and production of microfilar
However, development of acquired
host .s susceptffile to infection of a fila
of large numbers of filariae during lon
events in both human and animal filar
acquired resistance at repeated infectio
aspects, such as the retardation of grow
development to adults, reduction or cl
ing blood, and finally the death of ad
conducted by several groups of worke
acquired immunity with cotton rat fila
reviewed by Scott et al. (1958) and Be
12C.2 Immunodiagnosis of fi
J™/? °‘°g'C s udlesJ" human and
number of difficult problems, and altho
noPX Cf f i" th‘S fieud’ lhe rellablllt* of im
nosis of filanasis has been much debate
'
754
'I
EXPERIMENTAL METHODS
EX
sensitivity. Kagan (1963) presented an excellent review on the immuno
logic studies in the diagnosis of filariasis reported up to 1962. Altogether,
148 papers were available for the skin test, complement fixation test, pre
cipitin test, hemagglutination test, bentonite flocculation test, or PrausnitzKiistner test of filarial infection. The reviewer suggested, “with standard
ization of techniques, immunologic methods can in future be made to
furnish a reliable means of diagnosis, notwithstanding the past unrelia
bility of such methods.”
The essential weak point of the immunodiagnosis of human filariasis is
the difficulty in obtaining the homologous antigen, especially in wucher
eriasis, and the antigens were prepared mostly from animal filariae, such
as Dirofilaria immitis in dogs. However, it is questionable how far filariae
possess group-specific antigens independent from other commonly occur
ring parasites. In this connection, the common occurrence of other nem
atode parasites causes another difficult problem in the diagnosis of
filariasis.
sensitivity. There was no significan
adult worms found in the hosts and
the logarithms of microfilanal den
iXtoanonlvn20“/dith
T
ry 204 f 75 lnfected co
A St.udy for Pur,fication and recov
extracts was reported by Tanaka e
genized lyophilized, delipided, extr
and centrifuged The supernant was
filtered on Cephadex G-200. The qu
were measured by the HA tes‘. and th
bv
by the ratios of antigen unit to prot
demonstrated that the antigen was n
12C.2.1 Antibody response in experimental and human filariasis
r
L u
of antl8
e tnfugation, but about half of the a
Litomosoides carinii infection in cotton rats is considered to be an ideal
model for the immunologic studies is filariasis, since large numbers of in
fected animals with.different history are available, the infection can be
easily controlled, the hosts are free from other nematode infections, the
homologous antigen can be amply supplied, and the reaction of the hosts
are immunologically not unusual. Recent improvements in immunological
techniques, especially the introduction of microtiter method, had made
repeated examinations from such small hosts feasible. A series of experi
mental studies were carried out in this author’s laboratory in order to clari
fy the mode of development of antibodies in the cotton rat filariasis. The
principal methods used were hemagglutination (HA), complement fixation
(CF), immunodiffusion (ID), and fluorescent antibody test (FA). A portion
of the results were reviewed by Tanaka et al. (1970b).
12C.2.1.1 Hemagglutination test
The method applied for the indirect hemagglutination test of cotton rat
sera was described by Tanaka et al. (1968a). A buffered saline extract of
adult worms was used as the antigen. Rabbit sera, collected after immuniz
ing with adult Litomosoides extracts, were used as the standard for deter
mining the optimum condition of the HA test. Formalinized and tanned
sheep red blood cells were used as the indicator, and the test was made
usually in microtiter wells. Sera which showed 3-plus agglutination at 1:32
dilution were regarded as positive. In a series of preliminary tests conduct
ed with stock sera collected from cotton rats with a known history of in_____ fection, 8^5 49274%^of^sanTptes'frdmlnfected rats were positive with the
highest titers over 1:16384 in 8 animals, while all of 68 clean rats were
negative. The test was shown to be excellent in specificity, and good in
I
i
12C.2. 1.2 Complement fixation test
A method of the complement fixa
1970aldTh L,totmosoid^ antigens wa
tha^with^ hC ff 1C1 7th C0Cu’S solutl
that with buttered saline or the alcoh
tTter?!11! 6 ?
fOllOW'"g ™odified t
Of 116cott . 8
Wlthnhe describe
112 (96 6 »/\
C01lectked 11 w
112 (96.6/0) were positive, while only
rats were positive. There was a signific
s oht °f he Sam<; Sera’ W‘th a corre
slight or no correlation was seen betw
parasitizing adults, the number of fem
So far as the Litomosoides infection in
andsp^cifictty
alS° Sh°Wn
12C.2.1.3
Fluorescent antibody test
were used as the antigens. Since trem
prepared w.th this method, the FA tes
over other immunologic tests if it tur
specificity and sensitivity, especially i
756
EXPERIMENTAL METHODS
human filariasis. The antibody against cotton rat globulin was produced
by immunizing rabbits with the antigen purified from 37 cotton rat sera
and the adjuvant. The globulin fraction of the immunized rabbit serum
was labelled with fluorescein isothiocyanate, and purified on cephadex
G-25 and on DEAE cellulose following Kawamura’s method. The FA
test was conducted first by exposing the test sera at various dulutions on
the frozen section antigen, and after washing, by demonstrating the conju
gated antibody with the fluorescent antibody.
When the infected cotton rat sera were applied on the sections of adult
worms, specific fluorescence was most conspicously seen on subcuticular
muscle layers, and also on lateral glands, and on the contents of digestive
canal. Of 7 cotton rat sera collected 11 weeks after exposure to infection,
all showed positive reactions at titers 1:125 to 1:3125, while the titers were
up to 1:25 in clean cotton rat sera, with an exception of a sample which
was positive to 1:125. On the other hand, the antigenicity of the micro
filariae and infective larvae was much weaker than the adults, especially
in the latter, and the highest titer seen with the microfilariae was 1:64.
The results of the FA test reported in these papers have provided im
portant information on the distribution of antigens in tissues of various
stages of the parasite, but its use in diagnosis of filariasis still awaits further
improvements in the technique, because with the present technique, certain
grades of false positive reactions were seen even with sera from clean ani
mals, probably due to the presence of cotton rat antigen in the section of
the worms.
More recently, Barbosa er al. (1972) carried out indirect immunofluorescent tests using fragments of adult O. volvulus from a nodule as antigen.
Tests were made on seven sera from loiasis cases, seven from onchocer
ciasis cases, five from bancroftian filariasis cases, and one from tropical
eosinophilia case. When reactions at 1:40 or higher dilutions were taken as
positive, the test was positive in 19 of 20 sera. In sera from 50 ancylostomi
asis or stronglyloidiasis and those from 50 healthy control subjects were
all negative.
Rombert et al. (1972) also conducted similar indirect fluorescent anti
body tests with eggs of D. immitis and L. loa as the antigens. The results
with D. immitis eggs were rather doubtful in diagnosis of human filariasis,
but with the eggs of Loa all of nine loiasis cases were positive at 1:160
dilution, and ten normal sera and four from ancylostomiasis were nega
tive.
Ambroise -Thomas & Truong (1974) reviewed recent advances in the
immunodiagnosis of human filariasis with various techniques, and also
reported on results of a indirect fluorescent antibody test carried out on a
frozen section of Dipetalonema witei adults.
12C.2.1.4 Immunodiffusion test
—Among various methods of precipitin tests so far proposed, the double
diffusion test by Ouchterlony’s method is considered to be simplest and
theu ge|-d‘frusion tes
ed Precipitation band
^t,gen’
o?2 bZ5 “m 35
and bands. However 15 serum
and 38 samples from filariasis c
TntLen6
a.nti8en>and
t hg T nC pre.cipit,n test Wlth
to be excellent in specificity an
thpt,d°dy syste7.°f the cotton r
the diagnosis of heterologous or
Further analysis of the spec
infections Kv f'Annzwf
workers
'
/ ziAy
(*96
12C.2.2
Since it has been established f
tonSrCa?fi^ detected ,wlth various
from
32
the lnfec
p, week®,af‘eruthe mfection,
the CF test, all of the three uninfe
I
e HA test were more sensitive, a
thronah3innd lh.e
tlter ca
^eeJs after exposure
u/ic
was observed after ten weeks, suc
h Vf51 T dhOgS in*ected with Diro
igh levels throughout the life spa
758
EXPERIMENTAL METHODS
The sequential appearance of 19S and 7S antibodies in cotton rats after
exposure to L. carinii infection was confirmed by Fujita & Kobayashi
(1969a). Altogether, 49 four-week-old cotton rats were exposed to in
fection of about 80 infective larvae by the mite bites, and were sacrified at
intervals of three or four days during the period from 2.5 to 51 weeks from
the infection. The serum samples were fractionated by gel-filtration on
Cephadex G-200, and the HA titer of each fraction was examined for all
the sera. Identification of 19S and 7S globulins was made with ultracentri
fugation, and also by simultaneous gel-filtration with l31I-labelled 7S
immunoglobulin. The HA activity of the infected cotton rat sera appeared
first in the 19S fractions from six to seven weeks after exposure to infection,
lasted until about the 12th week, and then disappeared in most cases, while
the activity in the 7S fractions became detectable later from about the tenth
week, and persisted for long periods thereafter. This was also confirmed by
treatment of the sera with 2-mercaptoethanol.
The development of antibodies in cotton rats after transplantation of
adult L. carinii into the peritoneal cavity was also observed by Fujita &
(1969b). In this case, production of antibodies began much
Kobayashi
earlier than the exposure to infection with the infective larvae, and HA
activity appeared first in the 19S fractions in the sera collected ten days
after transplantation, while the 7S antibody became detectable somewhat
later, gradually increased, persisted thereafter, and became dominant over
19S from about 18th day. As stated previously, the effect of DEC on
microfilariae in the transplanted animals also became active from about
two weeks after the adults were inoculated, roughly coincident with the
appearance of antibodies.
12C.2.3 Immunodiagnosis of filariasis with heterologous
antigens
The above series of studies with the homologus antigen-antibody sys
tem have shown that so far as L. carinii infection in cotton rats is concern
ed, the infected animals can be clearly differentiated from uninfected ani
mals by various immunological methods. It should also be mentioned that
the animals tested were free from other parasites. However, similar tests
with heterologous filarial antigens were more or less unsatisfactory either
in specificity or sensitivty, or in both. As stated previously, immunodiffu
sion test was poor in sensitivity, and usually failed to show positive reac
tions with L. carinii or Dirofilaria immitis antigen when tested on sera from
cases infected with other filarial species, at least using the present meth
od. On the other hand, the HA test is too sensitive in general, and false
positives have been obtained with nonfilarial sera. As reported by Tanaka
et al. (1970a), more promising results were obtained with the CF test.
Among various methods of preparation of antigens from adult worms com
pared, Chaffee’s antigen was shown to be most satisfactory in the pattern of
the block titration and in sensitivity. Antigens extracted with this method
E
from L. carinii, D. immitis, and S
cats with B. ma/ayt, jirds and Apode
immunized
and"
sera
■'«<!•
™"
h““ with L. carinii
tltween rh Oth^ Cases’ varlous gr
.cervijind D. witei, fair for L. c
was fJrWforaJDFP7D4 “d'8"" frafcti
infeclmns
VV/'fc’
t
t'^p-Zxvf
7^ a-
**• • *
3.1 Assessment of clinical manifestations in surveys
In the first report of the WHO Expert Committee; on Filariasis 1 a large
The present Comnumber of different clinical manifestations were listed.
1‘
mittee believes that the manifestations to be reported m any survey should
depend on the training of the staff concerned.
(1) When only auxiliary medical personnel are available the clinical
observations should normally be restricted to recording: (a) enlargements
of limbs; and (b) swellings of testes and scrotum (only to be attempted
when the examination is culturally acceptable).
(2) When a medical officer is a member of the team more detailed
clinical information can be obtained. An interview should be held to
determine the patient’s medical history and symptomatology. Questions
should be asked to obtain information on the following : whether the patient
believes he is suffering from filariasis (using the local term) and whether he
has a history of filarial fever, lymphangitis, chyluria, abscesses, lympha
denopathy, asthma, epididymitis and funiculitis, and scrotum swelling. In
view of the evidence suggesting that filariasis affects reproduction, questions
should be asked about the patient’s reproductive history. The interview
should be followed by, a standardized physical examination as shown in
Annex 3.
t
I
i
3.2 Parasitological and immunodiagnostic procedures in surveys
None of the immunodiagnostic methods now available is sufficiently
sensitive or specific to give reliable estimates of the prevalence or intensity
of filarial infections. Therefore, only parasitological methods are considered here.
The Committee noted that recent investigations have shown that con
siderable numbers of microfilariae are usually lost during the processing and
staining of blood films. Therefore, if conventional methods are to be used,
scrupulous care must be taken in the preparation of the films (see Annex 3,
section 1). An alternative technique is to use a counting chamber; this has
been shown to be a rapid and sensitive means of detecting and enumerating
microfilariae (see Annex 3, section 2). If neither permanent films nor differ
ential species diagnosis are required, this technique may be the method of
choice for examining finger-prick blood specimens.
A recent development that has shown great promise for epidemiological
studies is the use of membrane filter concentration methods. (More detailed
information on these methods is to be found in Annex 3, section 3.) A
further development that has greatly facilitated the examination of persons
1 Wld tilth Org. techn. Rep. Ser., 1962, No. 233.
infected with the nocturnal per
mazine as a provocative measu
peripheral blood in the daytime
The comparative sensitivity
microfilaraemia using examinat
membrane filter concentration ha
treated populations in endemic
indicate that microfilaria rates a
example, it was shown in a hype
filaria rate as diagnosed by the
children than had been anticip
5-9-years age group had micro
detected by the examination of
age group approximately 8 time
concentration technique as by
technique detected 1.5-3 times
in hyper- and hypoendemic are
blood films. A few microfilaria
gross elephantiasis although the
Following mass chemotherap
between 3 and 6.5 times as ma
were diagnosed by 60-mm3 thic
possible importance of low-grad
successful control campaigns, th
concentration methods to supp
studies.
It is recognized that for most
be too costly and time-consum
films remains the routine metho
rates. Whenever possible, a subs
by a concentration technique to
factors for adjusting the prevalen
For this purpose, special attentio
of age since this age group wi
continuing transmission after co
3.2.1 Precontrol surveys
In precontrol examinations it
be taken from the entire popul
the identity and periodicity of an
films should be taken at night
For quantitative studies, measu
individual and examined under
either stained or in a counting c
3.2.2 Post control surveys
Mass chemotherapy. The Committee recommends that when control
has been effected by chemotherapy blood surveys should be performed as
follows:
Six months after the completion of treatment the entire population
should be examined by the same technique as in the precontrol surveys, and
all those found positive should be re-treated. Surveys should be repeated
every 2 years for up to 10 years after the completion of the initial treatment.
A concentration technique should be employed for these examinations
with a sample of the adult population and all the children born since the
start of the campaign. Clinical examinations should be made at the same
time as the blood surveys. Special attention should be paid to individuals
who are considered to be the high risk age group for clinical manifesta
tions.
If the treatment of only individuals showing microfilaraemia has been
the practice then all those treated should be examined by a concentration
technique ; a sample of the rest of the population should be examined by
means of blood films or a counting chamber, and a subsample of this popu
lation, together with a representative sample of children from the last
treatment campaign, should be examined by a concentration technique.
f
TABLE 2.
A DIRECT METHOD O
A HUM
Microfilaria
density per
2|mmJ unit
bloodmeal <*
(D
Probability of
unit volume of
bloodmeal being
infective
(2)
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
1.1
1.2
1.3
1.4
1.5
1.6
1.7
1.8
1.9
2.0
2.2
2.4
2.6
2.8
3.0
3.2
3.4
3.6
3.8
4.0
4.2
4.4
4.6
4.8
5.0
> 5.0
0.0952
0.1813
0.2952
0.3297
0.3935
0.4512
0.5034
0.5507
0.5934
0.6321
0.6671
0.6988
0.7275
0.7534
0.7769
0.7981
0.8173
0.8347
0.8504
0.8647
0.8892
0.9093
0.9257
0.9398
0.9502
0.9592
0.9666
0.9727
0.9776
0.9817
0.9850
0.9877
0.9900
0.9918
0.9933
0.998 +
Vector control only. In campaigns that have employed vector control as
the sole method against filariasis the Committee recommends that the
methods for epidemiological follow-up should be as follows :
(1) 2 years after the start of the campaign a sample of the youngest age
group found to be infected in the precontrol survey should be examined by
a concentration method ;
(2) this examination should be repeated thereafter every 2 years ,
(3) 6 years after the start of the campaign a representative sample of the
total population should be examined by a concentration technique.
3.3 Parameters for an analysis of the dynamics of transmission
In order to obtain the parameters necessary for estimating the intensity
of filariasis transmission in an endemic area that could be used in mathe
matical models for monitoring control programmes and for making pre
dictions, the following factors, at least, need to be observed in field and
laboratory studies.
(1) Parameters relating to the human population
_—---------------(a) the proportion of persons showing microfilariae at a certain
time of the day in unit volume (e.g., 20 mm3) of blood sample ;
(b) the frequency distribution of the number bf cases showing the
Total
No. of people examined
Microfilaria rate (%)
Infectivity index (%) of microfilaria
positive persons (IIP)
Infectivity index (%) of total population (IIT)
no,, j
inde)fis
exPression Pf the In
population, or, in other words, the theo
SiS?on ^e.P^sum
ai Klar,aJ larv?,e a*?d mosq
.CH!at OnJ8 b.a8ed.on blood survey
Samoa , the pretreatment survey was made
taUken korm^he0peop^erexmn%Uend^*OOd^^
b People found positive for microfilari
TABLE 3.
bl.crolilaria
density
per
2 mm*
unit
blood
meal
Prob
ability
of unit
volume
of blood
meal
being
infec
tive (p)
0.1
method
AN indirect
OFo Af m^c ^ofilarun
for calculating
Vensity among
the
carrie
infectivity
Br Us T'-0N
pretreatment (1965) a
!
Tahiti
Western Samoa
Western Samoa
posttreatment (1967) a
pretreatment (1964)«
d(%)
pxd
c (%)
d (%)
pxd
c(%)
d (%)
pxd
c(%)
6
6
0.57
32
32
3.05
6
6
0.57
0.0952
5
0.91
49
17
3.08
1.09
11
6
0.1813
12
).2
16
5
2.66
1.18
0.2952
4
0.3
16
20
4
1.32
64
6
1.98
1.32
0.3297
4
0.4
20
4
1.57
69
5
1.97
23
1.18
0.3935
24
3
0.5
27
3
1.36
73
4
1.81
3
1.36
0.4521
26
0.6
28
2
1.01
30
2
1.10
1.19
1.48
58
9
1.51
76
3
1.51
79
3
1.65
0.7
0.5034
30
3
0.8
0.5507
33
3
1.65
0.5934
2
I. 19
81
2
1.19
32
0.9
35
2
2
1.26
83
2
1.26
1
0.63
0.6321
37
33
1.0
16.
II. 97
90
7
9.73
53
13
0.7484
46
1.1-2.0
5.24
3
2.72
6.34
62
93
7
0.9057
8.15
53
2.1- 3.0
9
6
5.80
0.97
5.80
3.1- 4.0
68
6
0.9660
59
4
3.95
3.95
0.9875
63
4.1- 5.0
72
4
>
100
27.91
37
0.9967
28
36.88
Total: infectivity index
(°o) of microfilaria
positive persons (IIP)
Microfilaria rate (%)
infectivity Index (%)
otal population
)
Natural (observed)
vector infection
rate (%)
94
95
100
1
1
5
0.99
100
4.98
19.1
35.05
1.63
13.5
0.60
8.35
0.61
70.60
(2) Parameters relating to th
(a) the infectivity potenti
the method given in Tab
(b) the amount of blood
(c) the rate of ingestion
microfilariae are ingested
density in the blood, or
during feeding;
(d) the biting density of v
changes) ;
(?) the proportion of vec
index);
(/) the circadian biting
index
(3) Parameters relating to th
(a) the rate of developm
conditions in a vector st
(b) the time required for
local conditions ;
(c) the gonotrophic cycl
(d) the survival rate of
estimated by the age dete
(e) the proportions of
mature larvae (including
each infected host that sh
a year).
I
73.32
30.9
(4) Parameters relating to th
(a) the number of infec
(b) the rate of transfer o
22.7
1
13.2
le of microfilaria-positive
regression line of the cumulative Percentagi
a+b log
x (see Wld Hlth Org.
• Calculated using the ‘i
r density in the log-probit scale, y-a+b
It
cases against the microfilaria
.
techn. Rep. Ser.t No. 359, p. 44, rig. 1).
; d-difference between the cumua c-Cumulative percentage of mlcrofilaria-poslUve cases
lative percentages, or percentage of each class.
(5) Parameters relating to th
in man:
(a) the susceptibility of
(b) immune responses o
(c) measurements of mi
respective microfilaria counts per unit volume of blood sample
arranged according to an appropriate method ;
- (c) the microfilarial periodicity of the local filaria strain,
r
by the method described by Sasa & Tanaka.
I
i Wld Hlth Org. techn. Rep. Ser., 1967, No. 359, p. 44 (Ftg. 1) ^d p.
^le 2).
> Sasa, M. & Tanaka, H. (1972) S.E. Asian J. trop. Med. publ. Hlth. 3, 518-536.
I
1 Detinova, T. S. (1962) Age-gr
Geneva, World Health Organization
2 Meillon, B. de, Hayashi, S. & S
'1
rip, i-s;
Febrile convulsions
MH
r
Further reassuring news about prognosis
pt
i I
1
i
i
■L
1
Among children in the United Kingdom 2-7% have at least
Kecendy, a joint working group of the Royal College of
one febrile convulsion, meaning a fit associated with fever in
Physicians of London and the British Paediatric Association
infancy or childhood and without evidence of intracranial ■
produced guidelines for managing febrile convulsions." The
infection or defined cause (other than infection outside the
working group was convinced that long term <drug procentral nervous system). Just over one third will have at least
U_ used
______l in
•
was rarely indicated, and though it may be
one further febrile convulsion, but the majority slop having
the child with frequently recurring febrile convulsions, there
seizures of any kind, and only 2*4% of those who were
wa? "o^v,d^ncc 1118111 would prevent later epilepsy. Verity
previously normal develop epilepsy (defined as two or more
and Golding s paper suppons this view.
seizures without fever). In the few children who develop
The outcome is usually good for children who have had a
epilepsy there is little evidence that this has been caused by
icbnle convulsion, but two questions remain. Firstly, how do
the febrile convulsions. These are the reassuring findings
we now interpret the earlier repons suggesting that febrile
reponed by Verity and Golding on p 1136. They are based
convulsions might cause later temporal lobe epilepsy? The
on the cohort of nearly 15 000 children in the British birth
cohon studies.suggest that this sequence, if it occurs at all, is
survey, who were born in one week in April 1970. Two other
rare. Ihe earlier studies were retrospective, and though they
large cohort studies in the United States reached remarkably
demonstrated
a s^uence of events, they could not show how
similar conclusions.2'* The new study, based on an unselected
often it happened or that it was necessarily causal. They were
nationwide cohort of children, removes any doubts that the
also based on children whose febrile convulsions had hap
American studies are applicable to British children.
pened at least 40 years ago, when seizures may have been
Febrile convulsions were traditionally regarded as benign,
allowed to continue much longer than would be the case now
so the news from this study may appear welcome but
Very prolonged seizures, lasting much more than half an
unsurprising. Its importance lies in the context of the
hour, may indeed be damaging."'»
changing views and controversies which have surrounded this
Secondly, why are children who have had a febrile
common disorder in the past 20 years. In the 1970s concern
con'
71,10" mo7 P™110 ,0 laler epilepsy than those who have
arose that febrile convulsions were less benign than had been
not? All the cohon studies show the extra risk to be small,
.thought. Prolonged febrile convulsions might cause brain
diough it may increase to 7% with follow up to the age of 25 4
damage, particularly in the temporal lobes, leading much
They also show that the risk is greater if the child has had a
later to temporal lobe epilepsy (now more usually called
complex febrile convulsion (lasting more than 15 minutes,
complex partial epilepsy) as well as to other neurological
or focal, or repeated in the same illness), if there is a family
problems. Patients with temporal lobe epilepsy frequently
history- of epilepsy, or if the child had a pre-existing
had a history of a prolonged febrile convulsion in early
neurological abnormality (though many would not regard this
childhood’; and in those undergoing temporal lobectomy for
as consistent with the label of febrile convulsion). The most
intractable temporal lobe epilepsy the commonest pathologi
probable explanation is that among children who have febrile
cal lesion was mesial temporal sclerosis, again frequently
convulsions there is a small minority with either an inherited
associated with a history of a prolonged febrile convulsion in
predisposition to epilepsy or pre-existing minor cerebral
early childhood.6 A view developed that it was important to
abnormalities, such as focal cortical microdysgenesis," which
prevent febrile convulsions, particularly those which might
predispose both to complex features in the febrile convulsion
become prolonged, and that regular anticonvulsant treatment
and
also to later epilepsy.4" In Verity and Golding’s study the
should be given, at least to selected groups of children who
complex feature most strongly associated with later epilepsy
had had a febrile convulsion.7
particularly with complex partial seizures, was a focal febrile
Three factors ended the phase of enthusiasm for anticon
fixaiI abnTrJnalityb
m0Sl
l°
8 pre’exislin8
vulsant prophylaxis, about which some paediatricians had
always remained sceptical. Firstly, the United States collab
1 hree practical messages emerge. Parents should be re
orative perinatal project, a large cohort study, showed that the
assured about the generally excellent prognosis of febrile
majority of children did well following febrile convulsions,
convulsions. Prolonged convulsions should still be prewith only a slightly increased risk of later epilepsy compared
Ynted,” and to this end parents may give rectal diazepam,
with children who had not had them.2’ Secondly, regular
diough
the working party did not resolve whether this should
anticonvulsant prophylaxis had questionable benefits. The
be done as soon as a convulsion begins or only after five
two most promising drugs, phenobarbitone and sodium
minutes." Prophylactic anticonvulsants are rarely needed
valproate, both have appreciable unwanted effects, and their
and there is no evidence that they have any long term benefit
efficacy in preventing recurrences is uncenain when trials are
in febrile convulsions.
analysed, as they should be, on an intention to treat basis.**
EoKn.u.PnrfenoeorP.edi.uic
ROGER J ROBINSON
Thirdly, even if they did reduce the risk of further febrile
convulsions there was no evidence that they reduced the small ’
London TCIH 9] R
risk of later epilepsy—a limitation which also applies to rectal
‘ 'ZlSV
f
tf'" 'fhnk
cohon Mudy. BMJ
diazepam given at the time of fever to prevent convulsions.
SELECTIONS FROM BMJ
I
VOL. 7
FEBRUARY 1992
1085
F-
s
i■
!
Io
rip M
SI
Vol. v14. No. 3
International Journal of Epidemiology
© International Epidemiological Association 1985
Hdemic of Investigation!
I I l6 L-piVI Vrl
RES PALMER
I
practice the majority of patients in most countries can
be so treated, effectively and efficiently. Infections,
including parasites, and trauma are the major
problems. Trauma is usually relatively easy to diagnose
and treat on clinical grounds alone, or alternatively
beyond the facilities of the hospital, either diagnostic
ally or therapeutically. Nevertheless, routine radiology,
without fluoroscopy, would materially assist the
management ot the majority of patients while, and the
thesis holds good, the additional x-ray facilities needed
for the minority (in developing countries the last 5% or
10%) would be so expensive that they would jeopardize
the supply of antibiotics and anthelmintics. An angio
graphy suite or CT scanner may almost equal in cost the
total health budget of the whole region, yet they have
become a normal part of medical practice in the more
developed countries.
The World Health Organization (WHO OMS) has
started to tackle the problem in several ways, with ideas
and equipment which, while arising from the needs of
the developing countries, are eminently applicable to
even the most developed. Money is not limitless any
where and, even more difficult to accept in countries
where lawyers hover like vultures, absolute diagnost c
accuracy is a goal which not everyone or every countiy
can afford even if it is attainable and desirable.
In imaging the major need worldwide is lor a
straightforward reliable x-ray unit which can examine
all aspects of trauma and provide really good chest at d
abdominal radiographs, including the kidneys and gall
bladder. Adding fluoroscopy trebles not only the initial
cost but subsequent maintenance. It also trebles l ic
patient radiation and without really skilled and
experienced users is a method with a high level ol error.
Because any diagnostic equipment must be correlated
with the clinical services available, tluoroscopy in
WHO terms means a hospital at district (provinci il.
county, or canton) level, where there is a specialist
radiologist. E\en in the most advanced hospitals in
Europe or North America less than 20% of all imaging
procedures need fluoroscopy.
So WHO has now produced specifications foi a
Basic Radiological System, the \\ HO BRS. the
specifications come from a group ol advisors who.
It used to be very easy. Listen to the patient’s chest
using that marvellous invention the stethoscope: look
at the eyes, tongue, fingernails, and feel the pulse.
Sniff, then taste the urine delicately with the tip of the
tongue and make the diagnosis. Then Roentgen dis
covered x-rays, there were ECG’s and EEG’s and a
whole host of other possibilities recently made better,
or worse depending on one’s philosophy, by computers
and electronics. The search for the ultimate accuracy in
diagnosis and therapy has become so complex that the
alternatives are now quite beyond the capacity of the
average physician and the cost is becoming too much
for the individual or the insurance or health service
responsible. Can this epidemic be brought under
Ahntrol? There is no doubt that it must, because
"moving from reasonable diagnostic accuracy to near
100% certainty is so expensive that the business creed
of cost-effectiveness is of major importance and
already clashing with the physician’s ethical wish to do
the best for each individual, regardless of income. That
last 10% of accuracy often accounts for 90% of the
cost and does not necessarily bring an equivalent
benefit to the patient. Even in the most advanced
countries these financial facts of life cannot be ignored,
nor are all diagnostic investigations free from risk.
This dilemma exists in every medical specialty but to
attempt to discuss every aspect would be to fall victim
to the very epidemic which must be recognized and
treated. However, ‘imaging’ provides a good model.
Already there is reason to use a more comprehensive
phrase than ‘x-rays’, but before complaining of the
difficulty in making the correct choice between ultra
sound, radiology, CT scanning, radionuclide or
magnetic resonance imaging, with all the possible
nermutations within each, there^s need to pause and
iden our perspective. About 70% of the people in the
world cannot have the benefit of even the most simple
x-ray examination. Their doctors face no investigative
puzzle: the probable fracture, the chest complaint, the
abdominal pain must be treated on the basis ol the
clinical examination. And it should be added that in
Kenyalta National Hospital, Department of Radiology, PO Box 30588.
Nairobi, Kenya, and the University of California, Davis. USA.
359
360
INTERNATIONAL JOURNAL OF EPIDEMIOLOGY
although the majority are now working at major
European or North American universities, were chosen
because all have many years of practical experience in
countries ranging from the snows of Greenland to the
tropics. Units meeting these requirements are now
available from many of the major x-ray equipment
manufacturers. The system is ‘Basic’ only in terms of
its ability to provide more than one hundred of the
most commonly needed radiographic projections,
which will certainly provide 95% of the needs of small
hospitals anywhere, be they in developing or developed
countries. Technically it is very sophisticated, yet easy
to operate and maintain. The quality of the radio
graphs is as good (and often better) than those now
accepted in major centres. It can work from an
ordinary good electrical supply, or from a battery
pack which can be recharged from any 5 amp source at
any voltage. Should the electrical supply be inter
mittent it can examine 300 or 400 patients before
needing a recharge. It is almost completely radiation
safe, and can be used after minimal training because
part of the ‘System’ is a series of manuals with step-bystep illustrations covering all radiographic and dark
room techniques. When used by a fully trained radio
grapher the results are spectacular and the range of
examinations much wider. It has been tested, it works,
it produces excellent films, and it costs much less to
purchase and install. The money saved can, in
developed countries, be used towards rooms of angio
graphic, CT, U-S, MRI, and other equipment desig
nated by a few initials: these tend to minimize their
enormous cost in capital expenditure, maintenance,
and the often overlooked radiologist and staff time.
WHO has not forgotten the isolated practitioner,
and there is a new manual of x-ray diagnosis to help him
or her interpret the beautiful radiographs provided by
the BRS. Altogether WHO estimates that about 70000
of these BRS units are required worldwide to provide
adequate diagnostic x-ray services: it is to be hoped that
the temptation to purchase (or request from donor
countries) larger and apparently more prestigious
equipment can be resisted. Most of the imaging equip
ment currently used in small hospitals worldwide (when
it works, which is not often) is excessive when related to
the clinical needs and complex to operate and
maintain. One large x-ray room donated to a
developing country may make good publicity, but the
same sum of money would provide radiology for a
much larger slice of the population (and reduce patient
transport costs) if spent on BRS units. Of course it is
possible to buy cheaper x-ray machines, and already
there are imitations which do not meet WHO specifica
tions, but none are as good for the patients and the
doctors, and certainly none are so cost-effedtive.
If that level of imaging has been solved,, w^at nexL
Another WHO scientific group has recently drawn up
specifications for Ultrasound and CT scanners, scare ing through the maze of often conflicting extras an
programmes, each claiming to be better and more
essential than the last. There can be no doubt of the
benefits of ultrasound, but for all practical purposes its
usefulness, outside specialist centres, will be restricted
to obstetrics and abdominal diagnosis, with he thyroid
and neonatal head as fringe benefits. The WHO
specifications are therefore at two levels, the GeneralPurpose (GP) and the Special Purpose (SP) pltrasound
Units. The special purpose specifications differ little
from those now available at major centres where the
potential is limited only by the skill and experience of
the ultrasonologist. [The terminology multiplies with
the equipment: one looks forwared (with apprehen
sion) to magnetic resonators, or will they bi content to
be magnetic personalities or resonating imagers?] The
less expensive and much less complex W|TO—GPUS
provides a very high quality image which will satisfy the
diagnostic needs of all but the most highly trained
specialists. In as yet unpublished trials of a prototype
(equal in size to a 6-inch portable television set), the
fetal heart could be recognized at six weeks|: examining
an unselected consecutive series of over 2( ) patients at
a large teaching hospital there were about o/o in whom
the diagnosis would have been improved by the eight
times more expensive SPUS. It was less easy to be sure
that the treatment would be similarl I improved
(Wachira and Palmer, for WHO, 1983). Again, the
thesis holds good: more than 90% of ultrasound
examinations can be carried out effectively on relatively
inexpensive equipment. Physicians can tie trained in
about one month in a busy department py examining
several hundred cases.
But for those buying diagnostic imaging equipment
for small hospitals and clinics, a word of caution is
necessary. The GPUS costs about one-thirfi of the BRS
and therefore is attractive when money is short.
However, its usefulness is also about one-third, as
ultrasound has no part to play in skeletal di:iseases or
trauma, and is little help in the chest. The WHO-BRS
must be the first choice: ultrasound is an added luxury,
except in a dedicated maternity hospital.
CT scanners have been specified in tie same two
levels, and the WHO group has also provi ied details of
the essentials in clinical specialist support, buildings,
maintenance, training, and recurrent expenditure
before a CT scanner can be justified. Th very understandable aspirations of specialists must be tempered
by the realities of finance and usefulness. \ CT scanner
)
THE EPIDEMIC OF INVESTIGATIONS
in a hospital without neurosurgery, for example, is an
expensive luxury few developing countries can afford:
moreover, about 10 patients per day will benefit from
CT scanning, and this must be compared with the 400
or more who could be examined daily by the 20 BRS
units which can be purchased with the same funds.
In providing such advice and specifications WHO
have been very careful not to sacrifice quality, either in
the resulting images or in the construction of the equip
ment. If money is to be saved, it cannot be at the
expense of diagnostic efficiency or in long-term
maintenance: both would be false economies. Rather,
as the reports make clear, cost effectiveness has been
reached by recognizing that 100% diagnostic accuracy
may not yet be attainable or necessarily desirable.
But equipment design is not the end of the task; there
must be proper choice of the correct investigation from
the ever-increasing range of imaging possibilities.
Ordering a battery of tests can no longer be justified,
nor can physicians continue to add investigations and
blame them all on the risk of malpractice suits. In fact,
as ionizing radiation carries a known risk, and ultra
sound and magnetic resonance imaging are not yet of
>ven safety, it may well be argued that over
investigation is positively risky. There is an unfortunate
correlation between the sophistication of medical
services and the number of investigations per patient,
but as yet too few studies which show a similar
increasing benefit to the patient. There is similar
correlation with the number of malpractice cases and
physicians must accept some of the blame for this.
While lawyers continue to believe that doctors are not
human and may therefore not err, the medical associa
tions have spent too much time on advising their
members that, to stay out of trouble, this AND that
investigation must always be done. In practice that
approach seldom works and more time should be spent
on proving in court that there would have been no
patient benefit by overinvestigation and that, on the
contrary, harm may result. The doctors’ associations
should also press for more intensive review of the ethics
of malpractice suits: the size of the financial gain to the
patient (and lawyer) is no indication of the benefit to
-'ciety. The line between genuine error and true
ilpractice is often distinct and not blurred by over
investigation. There is a very real need for careful study
of this aspect of medical practice with ‘patient benefit’
being the guiding principle. Lawyers can, and often
should, be sued for malpractice also.
Again WHO has made a start. In 1983 the report of
another scientific group was published. ‘A Rational
Approach to Radiodiagnostic Investigations’ was
issued after a comprehensive review of the world’s
361
medical literature, together with reports of previous
seminars and conferences, the recommendations of
various specialist colleges of many countries, and
organizations such as the United States Bureau of
Radiological Health. Many who have read the WHO
report have criticized the conclusions as being too
cautious and conservative, but they are well docu
mented and if adopted everywhere would have a
significant effect in lowering both radiation dosage and
cost. Few will argue with this report, but the major
problem will be to get any physician to follow its
advice. Altering the established habits of conservative
doctors is very difficult and most of us are well estab
lished in our conservative habits! Perhaps the report
should be required reading (with examination?) for all
medical students and housestaff in the hope that they
may gently educate their teachers? Certainly all medical
teachers should also read it, recognizing that one
should never learn medicine in a teaching hospital
because it is too remote from the real world. Patients
always have to be ‘properly worked up’, a requirement
synonymous with ‘over- and unnecessarily investi
gated’. The yardstick should be therapeutic effec
tiveness and cost, which requires the teacher to have
knowledge of the usefulness of each investigation. As
the WHO report emphasizes, the choice of the mos
appropriate diagnostic imaging procedure should b<
made in close consultation between clinician ant
clinical radiologist. This means that an experiencec
radiologist should be on each teaching ward-round:
that would probably mean more radiologists, but the
unnecessary investigations saved might well prove to be
a cost effective investment, disregarding the more
important aspects of patient safety and comfort which
seldom appeal to administrators.
The thesis is easy to propose and defend, and the
principles are as applicable to all types of investigation
as they are to diagnostic imaging. Equally important, ii
would be tragic if physicians in developing countries
who so often come to major centres for further training
and experience, should believe that the present
epidemic of overinvestigation is good for the patient’s
health and well-being. Every specialist group should
study this WHO report at their major medical con
ferences, dissect the conclusions applicable to their own
needs and adopt or disagree with them. Strict criteria
could be formulated, which would be of medical, legal,
and financial importance. Ihe process needs to be
continuous, with every new investigation or test studied
to determine what old investigation it replaces or,
equally likely, whether and when the extra cost is
justified in terms of patient care. At the same time the
legal profession, especially in North America, should
1
1
362
INTERNATIONAL JOURNAL OF EPIDEMIOLOGY
be made aware of these recommendations and their
ethics should be put as clearly under the microscope as
the physicians they prosecute. Society may not be able
to afford the rising cost of health care, but much of it is
associated with the fear of legal action and this cannot
be afforded without restriction either. There has to be a
limit to both.
Wishful thinking? Yes, but those early days have
passed and investigations more accurate than the tip of
the tongue are available. Perhaps this is the problem: if
physicians were more personally involved they might
not request the tests with such gay abandon. As a
radiologist I deplore, but cannot always prevent, the
waste of radiation, money, and my time represented by
many unnecessary investigations. Nor would I like to
give the impression that the problem exists only in
diagnostic imaging. This epidemic is unfortunately
pandemic, but unlike most major outbreaks somewhat
underinvestigated. Yet, even with the knowledge
already available the diagnosis is obvious and the cure
self-evident.
Physician, heal thyself, but preferably without a
battery of further investigations.
BIBLIOGRAPHY
WHO. The Report of the WHO Scientific Group on the Future Use
of New Imaging Technologies in Developing Countries (1984).
WHO. Geneva (In Press), 1985.
WHO. A Rational Approach to Radiodiagnostic Investigations.
Technical Report Series 689. WHO, Geneva, 1983.
WHO. Specifications for the Basic Radiological System. Obtainable
from Radiation Medicine, WHO, 1211 Geneva 27, Switzerland.
■
‘ ofF the Netherlands
Radiology in the Developing World. Journal
Society of Radiodiagnosis Diagnostic Imaging, 1)82. 51. pp 117200.
WHO. The Manuals of Radiographic and Darkroom Technique for
BRS Operators. WHO, Geneva (In Press), 1985.
WHO. Radiodiagnostic Manual for General Practitioners. WHO,
Geneva, 1985.
J
i
Editorial Staff and Board
Editor
Charles du Ve Florey,
Department of Community Medicine,
Ninewells Hospital and Medical School,
Dundee DD1 9SY
UK.
Editorial Assistant
Angela Wainwright,
Collingwood,
New Road,
Wormley,
Surrey GU8 5SU,
UK.
Associate Editors
E Russell Alexander,
Research and Operations Branch,
Venereal Disease Control Division,
Centers for Disease Control,
Atlanta Ga 30333,
USA
H R Anderson,
Department of Clinical Epidemiology
and Social Medicine,
St George's Hospital Medical School,
Cranmer Terrace,
London SW17 ORE,
UK
Dr C Buck (Past-President)
Department of Epidemiology and Prever tive Medicine,
Faculty of Medicine,
London,
Ontario,
N6A 5B7.
Canada.
Dr K Aoki,
Department of Preventive Medicine.
Tsurumai-Cho, Showa-Ku,
Nagoya 466,
Japan.
Dr A R J Aromaa.
Research Institute for Social Security,
Social Insurance Institute,
PO Box 920,
00101 Helsinki 10.
Finland.
Dr T Ayele,
Department of Preventive Medicine anc Public Health.
Faculty of Medicine,
Addis Ababa.
Ethiopia.
Dr U A Gomes,
Department De Medicina Social,
Hospital Dos Clinicas,
14.100-Ribeirao Preto,
Brazil.
Michel F Lechat,
Department of Epidemiology,
Ecole de Sante Publique,
Clos Chapelle aux Champs 30,
1200 Bruxelles,
Belgium.
Dr M Khogali,
Faculty of Medicine,
PO Box 24923,
Safat,
Kuwait.
Editorial Board
Dr H P Lee,
Department of Social Medicine and Pu )lic Health.
University of Singapore,
Outram Hill 0316,
Singapore.
Dr J Mosbech (President)
Copenhagen County Hospital,
St Elisabeth,
2300 Copenhagen,
Denmark.
Dr W M Carraway (Secretary)
Department of Community Medicine,
University of Edinburgh,
Usher Institute,
Warrender Park Road,
Edinburgh.
Scotland.
Dr R Detels (Treasurer)
School of Public Health,
University of California.
Los Angeles,
CA 90024,
USA
Dr S R Leeder,
Faculty of Medicine,
University of Newcastle,
Newcastle NSW 2308,
Australia.
Dr C R Rumeau-Rouquette.
Epidemiology Research Unit on Mothe and Child,
INSERM.
78 Le Vesinet,
France.
Dr R N Srivastava,
Department of Social and Preventive Medicine,
MLB Medical College,
Lucknow,
India.
nr i -t
CHEST RADIOGRAM. IN ITS PROPER PERSPECTIVE
- Dp.S.P.Kalantri
INTRODUCTION
g-jgiwr-j • .■».:
UKJ.’gxa
A modern medical student, born and brought up in an era of
increasing radiological sophistication has started turning a
Nelson’s eye to the traditional bedside methods of making a
diagnosis. Perhaps he should not be blamed, fhe current culture
in the academic institutions and private practice is steadily
reducing his confidence on the utility of bedside signs. Even quite
a few postgraduate teachers have seriously been toying with an idea
of providing chest X-rays to the examinees in their long and short
cases. Patients are also sharing the belief that short of being
radiographed, their examination is highly incomplete. This overuse
of diagnostic radiology, almost global now, the undue popularity of
the Roentgen’s rays and a gradual erosion in the faith on the
Laennec’s tubes should call for concern.
Wg made an attempt to go through the available literature and
to put the chest X-ray in its proper perspective so far as chest
diagnosis is concerned. In this task we have greatly been helped
by a technical report series published by WHO in 1983, its basic
theme centres on the rational use of radiology in all disciplines
of medicine. In the preparation of this article, this report has
extensively been referred to. The questions to which we sought
answers were•
(i) Is routineCXR helpful in screening asymptomatic subjects?
(ii) What is the utility of CXR in the overall assessment of
respiratory diseased
(iii) Why chest X-rays are being overutilized?
(iv ) How reliable are bedside physical signs in the diagnosis
of chest ailments?
The criticisms that appear in parenthesis after some of the
recommendation of WHO Expert Committee are our own.
ROUTINE CHEST X-RAY IN ASYMPTOMATIC POPULATION
2
• Routine chest X-ray on admission to the, hospitals Feingold
surveyed 39000 hospital admissions, the majority of patients were
elderly, chronically ill, poor and came from a population with a
high incidence of tuberculosis. He concluded that if there were
no symptoms referable to chest and no fever, no tuberculosis was
: 2 :
2.
The WHO Expert Committee
thinks that.unless there is high incidence of clinically silent
chest disease, routine CXR. has no role whatsoever in pregnant women.
In support, it quotes a massive study of 12000 women by Bonebrake?
in which not one patient with clinically unsuspected disease
could be detected.
3. Prepperatiw.j^hesX^-ray; Do preoperative chest X-rays, as is
commonly believed, affect the decision to operate, change the
type of anaesthesia, and provide a useful baseline fil± before
operation? Yes, says Sane, who studied a series of children and
found that in 3.8% the results of preoperative chest radiography
changed either the anaesthesia or the type of treatnent. Mi 1 u.e5
also considers.them essential for comparison with a postoperative
film, if a patient develops a postoperative complication. There
are, however, some large studies, which do not share this belief.
The Royal College of Radiologists, in a survey carried out in
England, VZaies and Scotland concluded that CXR should be used
as an adjuvant to careful clinical evaluation of the patient
and^should only be done when it is thought that they will provide
additional useful information.
.7 where patients were drawn
Lloyd Rucker recently did a study^
almost all major surgical specialities. He proposed that certain
risk factors would increase the likelihood that a patient’s preoperative CXR would demonstrate a :serious abnormality. These
were: history of cardiac or lung disease, cancer at any site,
smoking, asbestos exposure, fumes, dusts,
serious systemic disease,
recent thoracic surgery,, abnormal physical findings in the chest,
heart, abdomen and age older than
--- 60 years.
(Unfortunately these
recommendations are so comprehensive and cover
so many aspects that virtually every patient needing surgery might
end up with a chest X-ray. Though a number of other studies have
failed to find usefulness of preoperative chest ray independent
of complete clinical evaluation,> ■’'
the more recent and widely read
surgical texts have avoided the issue entirely,
making no specific
recommendation.
^ags Phest,^r^y... styiy^ pXjjasglected population^
The following are the recommendations from the WHO Expert
Committee on Tuberculosis(l974)^
"Mass miniature radiography is a very expensive screening
1
: 3 :
significant effect on the occurrence of subsequent smear positive
cases, as they usually develop so radpily that they arise
between the rounds of mass radiography examinations.(3) it
requires the services of highly qualified technicians and
medical staff, who could be better used in the other health
service disciplines,0 (4) the apparatus and the vehicle used to
transport it, are often out of service... the committee concluded
that the policy of indiscriminate tuberculosis case finding
should now be abandoned.”
SSil’tphest X-ray survey of selected population:
The Expert Committee opined that the chest X_ray is only
justified in s
Subjects occupationally exposed to respiratory hazards.
(i)
(ii) Countries or areas where there ishigh prevalence of tuber
culosis and similar infections.
( What about Bhopal population then?
Should every subject with
respiratory symptom be radiographed there, or will pulmonary
function testing be a suitable alternative! And should every
subject from endemic zones of tuberculosis be radiographed,
irrespective of physical signs?)
CHEST X-RAY IN DISEASE
1. Tuberculosis:
The WHO Expert Committee suggested three criteria for doing
in patients of tuberculosis:
(i)
tuberculous patient: on chemotherapy. Periodic CXR at
intervals that should be dependant on thqclinical condition
and diagnostic assessment.
(ii) Tuberculous patient: treatment completed,
only if clinically indicated.
Periodic CXR
(iii) Tuberculous patient: defaulter. r.urther CXR if patient das
failed to complete drug therapy.
( Tjqese guidelines are rather vague and it is difficult to
interprete them exactly. Our* criticisms are: (i) How pre wisely
do we define clinical dontion: based on symptoms or
appearance of new signs$ either or neither? (ii) if structural
damage caused by tuberculosis can be picked up by physical
r
; 4 :
lesion, (iv) In defaulters the rational approach should be tto stop
the previously used drugs and start fresh chemotherapy with atleast
three new drugs. Won't further CXRs ddd to the cost of chemotherapy?)
oa^ic^bsase s
The Expert Committee considers clinical evaluation better than
CXR m periodic assessment of COPD. In childhood asthma, however,
it sounds a note of caution and tells us that severe asthma and
repeated attacks, may be an indication for chest radiography, even
m the absence of other clinical findings, h recent study published
in 198?^ also confirms that routine spirogram and chest films have
little role in the management of clinically stable patients.
3• Lyilg. £ancer:
(i) A number of studies have proved that CXR
is useless in picking
up asymptomatic lung cancer and offers no benefit in early
detection of lung cancer.
(ii) Routine follow iup CXR for patients with lung cancer should
only be dictated by clinical
— evaluation and natural history
of cancer.
4.
The Expert Committee
suggests that if there, is no fever and
clinical evidence of chest disease,
CXR. offers no benefit in the
clinical evaluation(Two situations, we feel
, defy this generalisation,
In patients with miliary tuberculosis
and meningitis, where fever
could be absent due to low immunity and the chest signs are minimum
9
CXR is an important diagnostic tool,
j
Similarly in patients with
persistent weight loss without fever and chest symptoms/signs,
CXR often uncovers an hitherto
unsuspected tuberculosis).
S^^^^^ch^t^r^io^rap^Xor. acute pneumonia;
teXtb0Ok °f “,edi01ne sees n° potat in doing .erli
CSfa to know whether the shadow has disappeared.
.TO report agrees
entirely. The later regards clinical deterioration as the only
indication for further CXRs in pneumonia.
(Hqw about this ideas If history and bedside
physical signs strongly
suggest community acquired pneumonia why not do
away even with
an initial CXR? More cost-effective
approach should be to treat
the patient with penicillin, reserving CXR only if the patient
does not respond).
\
: 5 2
OVERUTIL^fION_OF. CI^.oTJC-RAYS
Overutilization of X-rays has been defied as excessive
diatinn per fUm, excessive films per exposure and excessive
exammatrons per patient1.0 Since the first two factors defend
asrcally on the over use of radiology, we decided to find out
why x-rays are being overused. The reasons could be grouped
under three broad categories: the physician factor
9 the pttient
factor and the social/economical/legal factors.
ZhA.>y^cianls_role:
1• Lack of knowledge 2 ’Every patient with
chest pain needs a
CXR!.
2. Undue dependance: How else can I follow
pneumonia, tuberculosis or lung cancer? my patient of
3. Powerless Radiologist: 'How .can
can I stop a Physician getting
his patient’s chest X-ray?
p
4. Striving for perfection:
’The medical record should look
complete.’ ’ I should not miss anything. !
5. CXR as a gold standard: ’I know it’
s pneumonia , but am 1
right?
Busy OPD° No time to think; ’1 had better buy time,
CXR first,
physical examination can wait.’
Peer pressure: 'If they corner me in hospital death
II.
meeting...1
Zh.e_£atlent' s contributi on:
1. Undue demands: 'I ought to have a CXR for
my annual chec^ up.1
2. Reimbursement policies: rBut I am
not paying from my pockets...
3. Reassurance: 'There is something deep within my chest.
why
not rule it out?'
III. Spcial/Economic/LegaJ fadtors:
1 . Institutional requirement: 'Every patient admitted
in medical
service must be radiographed.1
2. Defensive Medicine: 'If someone pulls
me up in the court of
law?1
3. Money matters:
’I scratch your back, you scratch mine *j
reminiscent of the link—cum—cut practice.
4. Cuitural influence: 'When everybody/around is doing the same
thing, why shouldn’t I?’
5. Down to earth logic: I invested 5 lacs in this
!
: 6 :
HOX. RELIABLE . ARE BEDSXPiL,ZHYSIc AL - SIGNS IN. THE p IAGNOSIS
OF CAKpIAC Pa SJA^E?
We came across one article, on the reliability of bedside clinical
signs in cardiac diseases. Though this article on the utility of
cardiac signs appeared in 1978,11 the collective experience of authors
in clinical cardiology(over 60 years), and their critical assessment
of these signs makes us quote some of their views in verbatim.
On the.^rterjal _gulsg.!
■
* Superflouous terms such as dichrotic, anachrotic, bisferiens and
water hammer should be avoided. These abnormalities are diffimilt
to recognise, unreliable and contribute'nothing to diagnosis. They
should better be replaced by description of type of the pulse based on
pulse volume and character; The large volume and sharp upstroke pulse.
the large golume and blunt upstroke pulse, the small volume and blunt
upstroke pulse and the small volume and sharp upstroke pulse.
* These pulse abnormalities are found only when the valve lesion is
at least moderately severe•
* Evaluating the state of the radial artery wall contributes nothing
of value to an assessment of the state of the circulation locally or
in more important vascular beds.
OJL-Jugular_venous Pulse*
*
Apart from the systolic surge(V wave) in tricuspid incompetence,
and ’a’ wave or cannon waves, other abnormalities in JVP are difficult
to recognise, and rarely provide information that can not be more
readily obtained by other means.
Qn Apex Beat:
*The term ’tapping ’ apex beat causes confusion, since it does not
represent right ventricular hypertrophy but a loud and palpable first
heart sound.
*
No attempt should be made to teach students to recognise a right
ventricular apex, because even the trained cardiologist can not
recognise it.
.Left-.parasternal impulse;
ti
* Differe rating between the parasternal impulse of mitral regurgi
tation and that of a right ventricular abnormality requires exceptional
experience.
i 7 :
2,11 Jinrmera s
Although the classic distinction between ejection and pansystolic
fliurmers should be taught, it should be made clear that it is impossible
to categorise all systolic murmers in this way at the bedside.
Other jdoints :
hese are often of little value and
•’ ‘^
J-hese
are often reported
erroneously by students.
Eercussr^n: Ihis is of such limited value that it has
no place in
the routine cardiac examination.
The authors conclude that in the basic teaching of students,
and in
revision courses for non-cardiologists, the emphasis should be
placed
on^those signs which are of the greatest value. To go much be^oOd
this is likely to be counterproductive.
Instead of using a chefct X-ray as a gold standard to assess
reliability of clinical signs, we xdx decided to examine how far an
echocardiogram influences diagnosis and management. The following
are
the conclusions from 3 different studies:
(1) The influence of echocardiogram is greater for diagnosis than
for patient management.2
(ii) The value of echocardiogram is obvious when assessing the
patients for invasive investigations or when proper treatment
or adequate reassurance are impeded by diagnostic doubt. ^hen
the aim is to rule out disease, however, an expert cardiologist's
opinion would often be more appropariate than an echocardiogram. 13
(iii)lf an echocardiogram is used blindly, i.e.
as a primary means
of diagnosis rather than of confirmation of clinical impressions
9
very few positive results will be obtained. ■^he’ investigation
rarely reveals totally unsuspected information. It is in the
assessment of known cardiac disease that the investigation
is more likely to be of greater value in the future. It pan
cut short the bumber of routine cardiac catherrisations of many
patients with known valvular diseases']^
DIAGNOSIS .^£_B^,PIRATORY DISEASE?
Inter-observer variation in detection of respiratory signs is
well known. rhe value of a sign in reaching a clinical diagnosi
s
is dependent on whether its presence, often in conjunction with .
other
signs, discriminate beteen diseases5 and on the consistency with
which observers agree on its presence or absence. An attempt to
rank
the orner of reliability with which chest signs are elicited was
: 8 :
findings(History of patient was not considered) with the true diagnosis
confirmed by chest radiography, pulmonary function tests, arterial
blood gas measurements and CT scans. Their conclusions were?1. The complete agreement about particular respiratory sign was found
55% of the time, ^'he amount of agreement was greatest for
percussion note, wheezing, pleural rub, clubbing and reduced
breath sounds, where as signs such as whispering pectoriloguy was
rated totally unreliable.
2. Tn 28%, clinical diagnosis was incorrect.
However, this study does not tell us whether incorrect structural
diagnosis(say fibrosis, pleural effusion, pneumonia, cavity etc)
necessarily lead to incorrect etiological probability and thus to inco
rrect management. Nor it tells us when should we rely on bedside
diagnosis and what are the guidelines for investigating patient
further.
16
We did a study at M.G.I.M.S. ,Sewagram^ comparing bedside
diagnosis with chest radiograph''in lower respiratory tract diseases
with aim to tailor the utility of chest radiography, Our conclus ions
are *1 . When the diagnosis of respiratory disease rests on interpretation
of crepitation as the only detectable sign, chest radiograph
offers suseful clue to the etiological probability. With other
florid signs, bedside diagnosis correlated very well with chest
radiography. In such circumstances chest radiography does not
add much to etiological diagnosis.
2. Those patients where symptoms strongly suggest respiratory
tract disease but there are no bedside signs demonstrable,
chest radiograph is indicated.
5. Tn a case of pleural effusion where chest radiograph is non
committent about etiological probability, intercostal tenderness
was a definite sign of empyma.
4. In absence of respiratory sign and symptoms, chest radiography
helps in detecting etiological probability in systemic disorders
like P.U.0(5%) and T.B.M.(33%).
WEK£NCES_:
1. WHO Technical Report Serics No.689? 1983(-^ rational approach to
radiodiagnostic investigations: V/HO scientific group on the
indications for and limitations of major X-ray diagnostic
investigations).
2. Feingold, .0; Routine chest roentgenograms on hospital admission
do not discover tuberculosis. Sotrtharn Medical Journal 1977$ 70:579-80.
3. Bonebrake, OR et al: Routine chest roentgenography in pregnaricy.
JAMA 1978240: 2747-48.
4. Sane SM et al: Vaiue of pre-operative chest X-:ny examinations in
children. Paediatrics 1977$ 60: 669-672.
5. Milne. Surgical clinics of North America, 2: 1979$ 2- 83-86.
6. Preoperative chest radiography.e National study by the Royal
College of Radiologists. Lancet 1979$ 2; 83-86.
7. Lloyd Rucker et al. Usefulness of screening chest roentgenograms
in preoperative patients. 1983$ 250: 3209-3211.
8. WHO Technical Report Series No.552, 1974(Ninth Report of the WHO
Expert Committee on Tuberculosis).
9. Michael Owens et al. Influence of spirometry and chest X-aay oja the
management of pulmonary outpatients. Arch.Int,^ed.1987;147:1966-70.
10. O’Abrams, HL. The * overutilization ’ of X-rays. New Hng.J.^d.
11.
12.
1J.
14.
15.
16.
1979; 300: 1213-1216.
Finlaysin, JK et al. Cardiac signs for students: separating yheat
from chaff. BMJ 1978| 1: 1471-73.
Goldman et al. Clinical impact of echocardiogram. Am.J.Med.1983,
75s 49-56.
McDonald et al. J.Clin.Epidemiol. 1988^ 4: 151-161.
Grimmer etal. Lancet. 1982^ 1: 440-41.
Spiteri M.^. et al: T^g Lancet: 1988$ 1: 873-875.
Subhodh Mohan: Efficacy of clinical evaluation and role of chest
radiography in the diagnosis of lower respiratory tract disorders:
Post-graduate thesis 1987,Nagpur University,Nagpur.
I
Is
Tropic^ medicine
|ManageJnent
[convulsions
0400
of febrile
■nires with fever, but
xiety by informing them
Unless risk
non-fatal and gig^nature reassured about^subsequ^^
Shy of
2“^x« >« '“X’
ther^e^ric''appro^hes nra^be,^ ^tsens
ay^he
I months and 5 ^/complex seizures are, 1<
simple and co^Pj or muitiple (2 seizu ■
easlly
I (> 30 nuns), f^a , simple febrile selz^recShildhood and are
cause of seizures in
anxiety
Lest are Sroup
I the most comm
un years
ting tremendous
I S3 «
H have witnessed a large
I S“
»“p-» of this
es imProve^n„uroose
around should be^pre
|on and the airway
one side to pre
ous diazepam is the
IB
of choice
Ja
I
Current approach to
i children with febni
tion and is
intravenous diazep
-potion and by
disadvantage w> h‘
1£ for its admini tr
nQt the
trained and q
reach hospital more
development
and self.
■ have Provlded is much better than pr
the time the Par^ea^js fa£ has led ‘o^ofMaze
II febrile seizures is ,m
are totally bemg^^ {act is
, convulsion has abat_ed.
,he admm strano
S while simple
elae, the even m
izUres have a
of an alternative app^ rhis routejs^imp
■ '‘m’ting "Children W.th complex febnlese^
Ptm by and practical and can be^
forli of
B that even m
prognosis. h
al sequeiae;
effective an P
instruction. T
.
diazepam
permanent neu
® u ctUal dys■ very good 1O“8
personnel after .
suppository an^
t indicated
■ connection with seiz^^.^ difficuitles or mt, seizures. A
Mazepam are P^izure suppositones ar^ntrol are
in solution- Omi 8 a concentration and se administration.
since effectiv pl
20 minutes a
intravenous
not achieve
solution (5 mg/m
^nd its
hi&hly
ed for u
Rectal diazepam m so^
TwQ
studies place the m* .n those th convex
preparation ca
anticonvulsant
use IS
Ki simple {ebnl^t higher between 4 an
subsequent
absorption is f «
4 minUtes. Diazepa
o{ Lss or
i U risk is
prognostic factors mfluenc 8^.^ and
obtained with
pre-packed reCta! fnr intravenous use
q { a famlly history
■I other important p g
lar
meanmtrav^
callable abroad ^pr
■I epilepsy are the prese
tal status. Contrary
bS*ed recU^’wchKd maybe placed o n
i
abnormal neurod J, P^ younger age a^
predictive
power for
The moi
seizure is subsequei
of children vonset, the L
pr’edisposed
to subsequent febr
complex seizure,
or
disorders are 1
Bi
Br
Managenicnt
This consists
^nts- The trei
a1! Education of par
that febrile convuL. any one
deeply distressed dunng^^^^
are weh xiio-^n » any
■
being und
eduCation
cases. Even m
always
WOUld
Firstly al'aymg their
of two aspects.
IW9
I
with a 4 to 5
S°bUuocks should be ^ueeZeThe dosage is
the side and tbMsnation to avoid spillag^
t years
minutes after adm
2 to 4 mg.ted after 5
sSsssSiS3 “““ 'f"" ’
hand is indicated.
M This consists of
; This consists
no the
1 u against febrile setanres-’raising
the conVUl.
con’
a combination of
are equally
s'«°'
■**’**'
tf the child
67
I
using tepid sponging is an excellent method of bringing
down the temperature especially in combination with
antipyretics. Tap water may be used. Ice or very cold water
are unpleasant and generally not tolerated ^ell. A common
error is to cover and thereby overheat febrile children and
this should be avoided.
Anticonvulsant prophylaxis which has been practised so
far has been intermittent prophylaxis using phenobarbitone.
This method though unscientific and di'sproven by convinc
ing pharmacologic evidence unfortunately continues to be
practised widely. In conventionally used doses phenobarbi
tone does not achieve blood levels of significance so rapidly.
By the time anticonvulsant blood levels are achieved most
acute febrile episodes have passed over. Continuous
orophylaxis using phenobarbitone or valproic acid though
effective has also been virtually abandoned owing to the
high risk of using these drugs on a long term basis in contrast
with the benign self-limiting nature of the disease. This form
of therapy is now indicated in only a small group of patients
with a high risk of recurrent seizures or epilepsy in whom
intermittent diazepam has failed.
A new concept in the prevention of febrile seizures is the
use of intermittent diazepam therapy. This reduces the
number of new febrile seizures and allays the family’s
anxiety though it does not alter the occurence of subse
quent epilepsy. The treatment is safe, can be used by
parents after brief instruction and reduces the frequency of
long-lasting recurrent seizures.
Rectal oiazepam
and diazepam suppositories are
the forms of administration most commonly used and have
been studied most extensively. Conclusive studies on oral
diazepa*n are lacking. (Table 1).
^ophyUx>»ualnfld»az#p<mth^pyW^
Route and Dosage
preparation
Indication Efficiency/
___________Comments
Rectal,
diazepam
solution
5 mg/ml
< 12 months
Rectal temp Good.
2-4 mg 12 hrly. > 38.5°C
May also be used
12-48 months
during seizures.
5 mg 12 hriy.
> 48 mths
7.5 mg 12 hrfy.
maximum of 4
doses i.e. 48
hours.
Rectal,
diazepam
suppository
5 mg 8 hriy
Rectal temp Good.
38.5°C
For younger
children 2 doses of
5 mg at 8 hr
intervals during the
1st 24 hrs. If
dosage reduction
required split
suppository
longitudinally.
The side effects of intermittent diazepam prophylaxis are
few and harmless. Sedation and ataxia are the commonest
but are very short lasting and respiratory depression is
extremely rare.
Prophylaxis may be given for 12 to 18 months or to the
age of 3 years whichever comes first.
Approach to various patient categories
1) First attack of simple febrile seizure (low risk gr oup) —
No prophylaxis recommended. Acute anticonvulsant
therapy if future episodes.
2) First attack of simple febrile seizure (high risk group or
complex febrile seizure) — Intermittent diazepam
prophylaxis and acute anticonvulsant therapy if prophy-
68
laxis fails.
3) Children with recurrent simple seizure — Intermittent
diazepam prophylaxis if prophylaxis fails then try pheno
barbitone failing which try valproic acid.
4) Children with simple or complex febrile seizures at a high
risk for epilepsy — Intermittent diazepam prophylaxis as
long term prophylaxis does not confer any extra ther
apeutic benefit in most cases.
5) Children with first attack of seizures during fever in
whom diagnosis points to epilepsy triggered by fever —
Intermittent and long term prophylaxis.
Dianese, G (1978) Archives of Disease in Childhood 54, 224
Hirts, b G, Lee, Y J, Ellenberg, J H, Nelson, K B (1986) American
Journal of Diseases in Children 909, 140
Knudsen, F V (1988) Drugs 36, 111
Knudsen, F V (1977) Acta Paediatrica Scandinavia 66, 563
Knudsen, F V (1979) Archives of Disease in Childhood (1979)54,
855
Knudsen, F V (1985) Journal of Paediatrics 106, 481
Muntho-Kaas, A W (1980) in Antiepileptic therapy advances in
drag monitoring, ed Johannesen et al Raven Press New York, 1980
Nelson, K B, Ellenberg, J H (1976) New England Journal of
Medicine 295, 1028
Ross, E M, Peckham, C S, .West, P B, Butler, N R (1980) British
Medical Journal 280, 207
I
Views and reviews
L
Breast feeding — when to stop
Prolonged breast feeding is a common practice in Ghana
and other developing countries. 202 children visiting a
hospital in Ghana were found to be breastfed beyond the
age of 19 months. All these children showed signs and
symptoms of malnutrition. 15 such children were selected
and given weaning,feeds. Before the study these children s
protein and energy intakes were exactly half those of normal
children’. 10 of the malnourished children were weaned and
breastfeeding totally stopped. These children showed in
crease in intake and their levels slowly rose to that of normal
children. The 5 children who continued to breast feed
maintained their low intakes of weaning foods. These
results indicate that prolonged breast feeding can reduce
total food intake and thus predispose to malnutrition. This
also suggests that in developing countries the proper
weaning age may be about 18 months.
Lancet (1988) ii, 416
r
t
■
Human insulin may mask hypoglycemic signs in diabetes
According to the authors of this study insulin dependent
diabetes mellitus patients who switch from beef/porcine to
human insulin may experience less pronounced sympathetic
adrenal symptoms (tremor, sweating etc) at a given level of
hypoglycemia so that there is less warning of impending
unconsciousness. Neuroglycopehic symptoms as early man~
ifestations of hypoglycemia appear more common in pa
tients on human insulin and the authois main concern is a
change in the quality of insulin reactions with the same
insulin dose. Although the classic early warning signs of
insulin hypoglycaemia viz sweating and tremor may arise
late, patients have very little time to act between onset of
symptoms and severe hypoglycaemic. i eactions.
Calling this phenomenon hypoglycaemia unawareness,
they argue that this disadvantage of human insulin is an
argument for continued availability of beef/porcine insulin.
Lancet (1987) ii 382
Journal of Applied Medicine January 1989
f
t
1 I
'■
1
■
B Y
GARY
TAUBES
’F;
AN ELECTRIFYIN
POSSIBILITY
H ' * "W
s
-
1
-
Any physician « ho had hi hi tred to learn I he academic lantmaiics and had become i he
disciple of some cmincni professor ol medicine had a heavy vested interest in die
traditional loic and the accepted dogmas. . . Io attack this citadel demanded a h IIinimcss to del(he canons ot respectability. to uproot oncsell Irom the imiicisiti
community and Irom tlic miild
'•
Ihniicl BiKiislni. tn Ih> />/m Mtcztv'v.
<»n ilic slate <>l medicine Ik I«h
Wilh.im H.n « .
desciibed the circnluiof'. sysicm in Mi?X
W ’W’ ‘T’ niching Bjorn Nordenslronl opcnile
■ A / will give you sonic idea of the nature
*/■/ of die problem. Unorthodox, io say
W W the least.
li sa winter morning in Stockholm;
V
T
still dark, although well into the day. An old man
lies on the operating table, his chest quilted wi :h
scars from previous cancer operations. He has a
new tumor in what the surgeons have left him of
his lungs. Nordcnstiom has been given permission
to treat him, because the old man doesn't have
■
■
W-W
'M
A Swedish radiologist posits an astounding theory:
W^
the human body has the equivalent of electric circuits
OS
•
•^r
'r
■.
111> .!• / •i-Aiir.i'.. '
..■—
-h .tim »up,Hi»r.ik.-it- xi '.im iiw-1 ( aivip
;'fv
Jft. ' ‘.<
•<
w
I
■t
23
■M
'-V; >
i
1
Region of
injury or
muscle use
Conducting
cable
Electrodes
II
SO
i
■I
Barrier
permeable
to ions
ii v
^X^Oppositely
/
charged ions z
drive circuit
HORDEKSYROm’S CIRCUS’S:
A BIOLOGICAL BHTERY
According to Nordenstrom’s theory, the
H mechanism of the body electric can be
compared to that of a battery. In a bat
tery, the circuit is driven by the separation of
oppositely charged ions. Once the circuit is
closed, long-distance current flows through
he conducting cables; within the battery, ions
BUiLDBN® ELECTRIC
POTENTIAL IN Till BOOY
Injury or even normal muscle use
0
will result in a build-up of positively charged ions in the affected
tissue. In relationship, nearby tissue ap
pears negatively charged. This separa
tion of charge sets the stage for the long
I
distance flow of electricity.
rift across the permeable barrier.
enough lungs left to remove,
and if something isn’t done
hell be dead in a year. Still, the
old man. prepped with Valium,
.s conscious and smiling.
Nordenstrom is tall and
greying, with a military bear
ing; the deep lines under his
eyes are signs of both his 65
years and his propensity to
overwork. Beneath his surgical
gown he wears a rubberized ra
diation vest. He takes hold
of a foot-long needle and stares
down at the old man’s chest.
Guided by x-ray equipment of
his own design—which gives
views of the patient’s chest
from front to back and side to
side—Nordenstrom inserts the
needle, with a slight jerk to get
it through the chest muscle, di
rectly into the center of the tu
mor. He takes up another nee
dle and slips it in ten inches be
low the first. The needles are
24
•
—.O.'ER • A'r-RIL . '96c
platinum electrodes. He hooks
wires to each, then turns to his
assistant and hods. The assis
tant twists a dial on an orange
box, and the treatment begins.
Nordenstrom asks his pa
tient if he feels any pain, and
the old man says no.
A few minutes later. Nordenstrom doffs his gown and
radiation vest and settles down
on a chair next to the operating
table. One of the nurses brings
him and the old man coffee and
cookies. All the while, electric
current courses through the
old man’s chest.
@ o there Bjorn Nordenstrom
sits, calmly sipping his cof
fee while he tries to save the life
of another man with a tech
nique that looks as if it has been
cooked up by a maniacal elec
trician with delusions of gran
deur. But Nordenstrom is no
quack. Not by a long shot: his
track record, as a physician and
researcher, is as good as any
one's. In the 1950s he pioneer
ed a series of remarkable inno
vations in clinical radiology
that seemed radical at the time
but are now' routinely em
ployed at every major hospital
in the world. In the 1960s he
was promoted to the most re
spected position in his field:
head of diagnostic radiology
at Stockholm’s Karolinska In
stitute, then the pre-eminent
radiological research labora
tory in the world. In 1985
he served as chairman of
Karolinska's Nobel Assembly,
which chooses the laureates in
medicine. He is. in the words of
Morris Simon, the director of
clinical radiology at Boston s
Beth Israel Hospital, “a bril
liant. very innovative, very
imaginative scientist, who has
made significant contributions
to radiology and medirine.”
In 1983 Nordenstrom pub
lished a 358-page book cover
ing more than two decades of
experimental work. It’; endtied Biologically Closed Elec
tric Circuits: Clinica . Experimental, and Thecretical
Evidence for an Adcitional
Circulatory System, and it’s
potentially revolutionary . Nor
denstrom claims to have dis
covered a heretofore ur known
universe of electrical activity
in the human body—the bio
logical equivalent of electric
circuits.
As Nordenstrom d ascribes
his body electric, the circuits
are switched on by an injury.
an infection, or a tumor, or
even by the normal ac tivity of
the body’s organs: voltages
build and fluctuate; electric
currents course through arter
ies and veins and across ca-
*
Vessel acts as
conducting cable
Blood
flow
Tissue acts
as barrier
permeable
to ions
Capillary
Charged membranes
act as electrodes
■40
I
r
"1
Enzymes
/
allow
electron
exchange
ip
I
Capillary membranes
furct’on as electrodes
Oppositely
charged ions
drive circuit
-T
I II!ft't
Pores and
gates allow
local ion flow
—
I
-
i*
Area of
detail at right
Vesicles
ferry ions —
through cell
HOW CURRENT FLOWS
THROUGH THE BLOOD STREAM
The biological circuits are driven by the
accumulated charges, which, unlike those
Wr in a battery, oscillate between positive
and negative. The larger vessels act as insulat
ed cables, blood plasma as the conductor. In the
permeable tissue, the fluid between cells con
ducts ions. A key component of the circuit: the
natural electrodes in the capillary walls.
pillary walls, drawing white
blood cells and metabolic com
pounds into and out of sur
rounding tissues. This electri
cal system, says Nordenstrom.
works to balance the activity of
internal organs and, in the case
of injuries, represents the very
foundation of the healing pro
cess. In his view, it’s as critical
to the well-being of the human
body as the Bow of blood. Dis
turbances in this electrical net
work. he suggests, may be in
volved in the development of
cancer and other diseases.
The idea that electric cur
rents can stimulate bodily re
pair. alert defense mecha
nisms. and control the growth
and function of cells is not a
new one in medicine. Bioelectromagnetics dates back at
least 200 years. But the field
picked upa dubious reputation
at the turn of the century, when
researchers who had proposed
electromagnetism as a panacea
were proved wrong, and the
stigma has lingered ever since.
Enter Nordenstrom. His
book is neither an esoteric
piece of theorizing nor the re
sult of a single isolated ex
periment. He backs up his
statements, theories, and con
clusions with a wealth of me
ticulous and ingenious experi
ments, with one clinical ob
servation after another, with
theoretical proofs, and with
known facts. He makes a
strong case, and, at least as far
as he’s concerned, he has
proved it.
Nordenstrom doesn’t spare
his medical colleagues from
the jab of his needles. To him
their attitude toward elec
tricity in the human body is al
most medieval. Knowing of
the “enormous importance of
Ion flow
Peres and
gates close,
creating
long-distance
circuit
of ion flow
CAPILLARIES CLOSE THE CIRCUIT
4^
The membranes of the cells of the capil-
W
lery walls are known to be charged,
causing ions to circulate through the
cells, via gates and vesicles, and between the
cells, via pores. Electrons cross an enxyme
bridge (yellow) through the capillary wall to
close this local circuit. Nordenstrom discovered
that arterial capillaries contract when subject
ed to an electric fie!4 like that caused by the
accumulation of charge at a site of muscle use
or injury. As a result, the pores and gates
close, blocking the local ionic current so that
the ions flow through th- blood stream
and along the capillary walls instead. Thus the
long-distance circuit is switched on.
2S
Leaking venous
. capillary
Closed arterial
capillary
breast tumors. Consid
ering the immaturity of
his science, he has had
remarkable success.
concepts that a review was
deemed desirable .. The importance of the concepts pre
sented in Dr. Nordenstrom’s
book cannot be overempha
In the two hours be
sized.” The reviewer v ent on to
fore Nordenstrom un
call the book “remarkable” and
hooks the electrodes and
“a seminal work.”
sends the old man home, he
A year later, a seco id article
sips his coffee and talks about
appeared, this one in the Amer
J the complete lack of impact his
ican Journal of Roer tgenolowork has had. He's talking less
gy. The AJR is one o ' rhe two
about his cancer treatments
most important journals in the
than about his basic research,
field. The article was i rewrite
and there he’s a little perplexed.
of a Nordenstrom lec ure, and
.Medical researchers have bare
it. loo, came with ar editor’s
ly acknowledged Nordenstrom
note: the publication c f the pa
or his book.
per, it said, was unconventional
"If I m right.” Nordenstrom
and required an exp anation.
is saying, "time works for me.”
THE GATEWAY TO THE
The work was unique. the ediHis voice is raspy: though
lor wrote: unlike the r tulti-auSITE OF AH INJURY
heavily accented, his English is
thor publications common in
good. He tells of years of care
journals, it was all the work of
Venous capillaries don’t contract in an
ful experimenting—hypothe
one man—Nordenstrom. “He
electric field. Attracted or repelled by the
sis and test. Classic scientific
alone is responsible for the orig
electric potential of an injury, ions
method.
inal concepts, the experiments,
and charged cells, e.g., white blood cells, mi
MWhen I had the whole ma
the analysis and the ext. Al
grate through the pores of a venous capillary
terial ready” he says, “nobody
though employing modern terms
near the injury. Because the injury’s elec
wanted to publish it. ‘To whorn
and
instruments, his perfor
tric potential oscillates, it creates an ebb and
should we direct the message9’
mance has been in the tradition
flow of charged cells and ions, critical to healing.
they asked. I said to every
of the pioneer scientist: combody—to biologists, to all doc
plete and isolated immersion in
tors. They should know about
the research.” The journal said
closed electric circuits in mod
this picture is incomplete. As
this. Then they said, ‘We don’t
that a final judgment \/as pre
em electronic technology.”
he sees it, medical research has
dare to publish it.’ If I had done
mature, but that, at the very
asks Nordenstrom in the con
provided a descriptive view of
only one experiment, they
least, the work was “i naginaclusion of his book, “is it seri
the chemical and physical pro
would probably very easily ac
live. experimentally ingenious.
ously plausible that biology'
cesses at work in the human
cept it. But to prove my theory
and provocative” and Reserved
can ‘afford to ignore’ the ex
body, but hasn’t explained
I had to do so many things
serious examination by the
ceedingly efficient principle of
how they’re interrelated. It’s
based on the same principle
medical community.
transporting electric energy’
a picture of effects without
and they [the medical commu
M o such examinat'|on has
over closed circuits?”
causes. In Nordenstrom’s
nity] say it’s crazy because I say
™yet been made, a though
Classical medicine certain
view, the cause behind many
it explains everything. I under
four small groups of research
ly doesn’t deny that there are
pf the effects is the ebb and
stand,
but this is the difficult
ers—one each in Frarce and
myriad electrical forces at
flow in his biologically closed
thing for me. It’s so basic and
Italy, two in Japan— ire bework within the body, in addi
electric circuits.
so important because it plays
ginning to replicate Nortion to chemical ones exerted
| f Nordenstrom is right, these
so many roles in every biologi
denstrom’s experimenis. “His
by hormones and enzymes,
3 circuits may explain many
cal
reaction. It's not my fault.”
work is far too origina says
and physical ones like the pres
fundamental regulatory pro
Nordenstrom laughs.
John Austin, a Columbia Uni
sure of the blood in the arteries
cesses in the human body, and
versity radiologist, who helped
and veins. Every human
even the seemingly inexplica
In 1984. a full year after his
edit the book. “It’s far too wide
thought and action is accom
ble therapeutic effects of acu
book came out (he first review
ranging. Nobody in thi, coun
panied by the conduction of
puncture and of electromag
appeared in the njedical press,
try is beginning to touch what
electrical signals along the fi
netic fields.
in the journal Investigative Ra
he’s doing.”
bers of the nervous system. In
To prove that his theory is
diology. The journal doesn't
Some of Nordenstrom’s
deed. life wouldn’t exist at all
more than just an academic cu
usually print book reviews,
American
colleagues—highly
w ithout a constant flow of ions
riosity, Nordenstrom has
the editor wrote, but Nordenrespected men in the world of
across the membranes of cells.
put his ideas to work, using
strom’s work presented such
medicine—say his worl is unYet Nordenstrom argues that
electricity to treat lung and
“fundamental and far-reaching
deniably revolutionary. If it’s
White blood cells
attracted to positively
charged tissue
L i'C,’. :< • A.-/ . •
ft
CAHCER !S AN INJURY
THAT CREATES A CIRCUIT
si
Interior
cells die
Positive charge
arises in tumor
BUILDING A POSITIVE CHARGE
As o tumor grows, the inner cells are cut off
from the circulatory system and slowly die.
This cell death leads to chemical changes and,
initially, the build-up of « positive electrical
potential in the tumor.
Long-distance circuit
switches on
ACTIVATING THE CIRCUIT
The tumor’s positive charge polarizes
nearby tissue, turning on the long-distance
circuit. Ions flow through bic-od vessels
linked to the tumor, as well as percolating
through the tissue around the tumor.
30
University of Michigan on a
one-year fellowship. At Michi
gan he was an innovator in tl e
use of both radio-opaque
chemical dyes and a method
known as balloon catheteriza
tion. for producing more dis
tinct x-ray images of the hea’t.
blood vessels, and lungs,
gn the autumn of 1956 N'orS denstrom returned to Sto< kholm and began searching for a
way to determine, without cut
ting open the chest and lungs,
whether a lung tumor was ma
lignant or benign. He had an
ingeniously simple solution:
under x-ray guidance. Stic < a
needle through the chest wall
and into the tumor and remove
a tissue sample, then examine
it under a microscope--"a
practical, valid approach to the
thing.” he calls it.
Nordenstrom had pionet red
what’s now known as perc itaneous needle biopsy, a diagnos
tic technique used in even ma
jor hospital in the world. But
before he could put it to use.l he
had to redesign the biopsy leeNordenstrom was born in
dles employed to peneirate
1920 in Ragunda. a village in
deep into the body, and the
central Sweden, and was raised
x-ray equipment needec to
in the city of Bolinas. v> here his
steer them to the tumor. His
ancestors have lived for three
colleagues showed the usual
hundred years. He studied at the
hesitation: much too danger
University of Uppsala, and fin
ous a procedure, they said;
ished his medical training in
Nordenstrom was much too ag
Stockholm. After World War II.
gressive. And it was nearh two
he joined the Swedish Red Cross
decades, not until the 1 >70s,
and spent three months touring
before Nordenstrom’s b opsy
southern Austria with another
technique finally caught >n in
doctor, immunizing orphans
America. Says Richard G 'eenagainst TB. He estimates they
span. head of radiology ai Yale
had inoculated 25,000 children
Medical School. ''Before Nor
by the time his wife called to tell
denstrom came along, if omehim she was pregnant (with the
body had told me you :ould
first of their three boys).
lake a needle and shove it into a
Back in Stockholm, in 1949,
lung and biopsy' a turner, I‘d
he began a career in radiology.
have been shocked.”
He picked his speciality the
Nordenstrom referstc these
way many people do—some
innovations
as the first waves
one offered him a job that paid
of his career. The latest wave
well, and it turne4 out to be in
is his theory’ of biologically
teresting. He also apprenticed
closed
electric circuits. which
for a year with the Swedish sur
building in the
also
began
geon Clarence Crafoord. one
1950s. when his curiosi y was
of the pioneers of open heart
piqued by a subtle phenomesurgery, before going to the
right, it's important not only to
medicine but to all of biology.
(They’ll compare it to Haney's
1628 treatise on the circulatory
system, but they don't want to
have such claims attributed to
them.) And if it's wrong, they
say. the experiments them
selves are brilliant in any case.
What Nordenstrom desperate
ly needs, says Beth Israel s Si
mon. “is to have people per
suaded that it's worth making a
major effort to prove or dis
prove what he says.”
The mystery is why the
medical community has barely
noticed that Nordenstrom’s
theory exists. If you were to ask
radiologists at random about
Bjorn Nordenstrom. you'd be
lucky to find one who knew his
name. If you asked cancer ex
perts. or biophysicists, or
pathologists—scientists whose
disciplines are the heart and
soul of Nordenstrom's book— .
you’d probably get a blank
stare. Bjorn who?
I
TREATING CANCER WITH ELECTRICITY
a
i
i
i
J
)
1
j
non he observed in his prac
tice. Every so often he would
see in his x-rays the forbidding
mass of a tumor nestled within
the lung, and around it a halo of
light-colored streaks radiating
from its edges. Because the im
age reminded him of the rays of
the sun. he called it a corona.
He looked at thousands of
tumors, but only some were
surrounded by coronas, while
others—of the same size, shape,
and location—had none. More
puzzling, a corona might show
up in one x-ray and then fail to
appear in a later one. When
Nordenstrom showed his
x-rays to other radiologists, they
seldom spotted the coronas.
When they did. they consid
ered them trivial and wondered
why Nordenstrom cared.
For nearly ten years he
tracked the coronas on his
x-rays, but found nothing that
could explain their origin or
significance. Even when he
used his biopsy needles to sam
ple tissue from tumors with
and without coronas, he dis
covered no consistent differ
ences between them.
Finally, in 1965. he decided
to perform what he calls a sys
tematic exploration, and began
to lest the electrical properties
of the tumors. This was as much
by necessity as by choice. First,
he had little else left to try: a
tumor in the body is inaccessi
ble to the resources of a labora
tory. but take the tumor out of
the body and you may destroy
the conditions that created
the corona. Second, because he
was working with human can
cer patients, it was one of
the few experiments he could
perform without increasing
the risk to the patient beyond
that already entailed in doing
a biopsy. Nordenstrom says.
“I thought to myself. ‘Isn’t
this silly, just to introduce
a needle to take out samples
of materials? Perhaps I could
see something more, study
something more when I’m in
INSERTING THE ELECTRODES
Negative
electrode
A corona arises naturally during the tumor’s
electropositive phase: spikes appear on
he surface of the tumor, and water (blue)
moves into the surrounding tissue, dehydrat
ing the tumor and forming a series of ra
diating structures and arches. Nordenstrom in
serts a positive electrode into a breast tumor
and a negative one into normal tissue near by.
Dehydrated
zone
Corona
structures
Pcsitive
electrode
ATTACKING THi TUMOR
By running current into the tumor, Nordenstrom amplifies and prolongs the electro
Water
accumulates
positive phase of the already existing cir
cuit. According to him, the current will trigger
a variety of tumor-fighting effects, among
them producing acid in the center of the tumor
and attracting white blood -ells. Water accu
mulates at the negative electrode.
White blood
cells
attack tumor
31
At Karolinska, Nordenstrdm
(left, below) applies his
unorthodox treatment to a
breast cancer patient.
there with my instruments.’ ”
So Nordenstrdm turned his
needles into electrodes and
combined the sampling of tisue with the study of the electri
al properties of tumors in the
body. He measured the electric
potential of the tumor com
pared to that ofsurrounding tis
sue—the voltage, in essence—
and found that tumors with co
ronas were frequently associat
ed with an electric potential.
Moreover, he noticed that in
many of these tumors the inner
most cells had begun to die.
Such tissue death, or necrosis,
occurs when the cells at the core
of a tumor are cut off from the
blood stream as the outer cells
continue to proliferate.
These experiments absorbed
Nordenstrdm almost totally.
"By the late 1960s he was no
longer doing conventional ra
diology; instead he was slowly
32
3 LCOVER • APPfl • 1986
e refused
to take on
an assistant; he
wanted to do every
experiment himself
moving, experiment by experi
ment. into physiology, oncolo
gy, and pathology. He had cre
ated his own field of science,
and had left the establishment
behind.
To understand the electric
potentials in the tumors, Nor
denstrdm measured the poten
tial of blood as it slowly deteri
orated. Blood was the only tis-
sue he could extract from the
body without worrying about
damaging it in the process. He
found that the electric charge
in the decaying blood was first
positive, then negative; over
the course of days it oscillated
slowly between the two states
until all the blood cells had
died off. These results could
explain the variations in volt
age he had discovered in the tu
mors, and became the basis for
one of the key points in his the
ory: any injury to the body cre
ates a voltage that continuous
ly fluctuates between positive
and negative until it finally
reaches electrical equilibri
um—a stale Nordpnstrom be
lieves is associated with heal
ing. Nordenstrdm later found
that the release of energy by in
jured and dying cells could be
the driving force—the bat
tery—of his electric circuits.
Next, Nordenstrdm careful
ly measured the electrical prop
erties of veins, arteries, capil
laries, and blood in living ani
mals. He found that the
electrical resistance of the wails
of the veins and arteries was at
least 200 times that of blood. In
effect, he claimed, these v ;ssels
were acting as insulated c ibles,
and the blood flowing within
them conducted electrici y be
tween the tumor and th: sur
rounding tissue. That muc h was
high school physics.
Then he designed experi
ments to test his theory. He
hooked his electrodes to the
blood vessels of dog* and
showed that the current f owed
preferentially through the veins
and aneries. When he a spiled
an electric current to the blood
vessels, while blood cells, which
carry negative charges oi their
surface, were attracted to the
positive electrode. Blood clots,
loo. would form in the vessels
in response to the current. The
attraction of white blood cells
to injuries isn’t well understood
by scientists, yet Nordenstrom
seems to have demonstated
that a simple, fundamental
principle underlies it.
Nordenstrom spent most of
his waking moments on his re
search. He made mistakes; he
repeated experiments again
and again. He worked absurd
hours for the laid-back Swed
ish life style. He got to bed by
ten but woke up to do his cre
ative thinking between three
and five in the morning: he
would lie in the dark, review
ing his problems from the pre
vious day and planning his ex
periments for the next. He re
fused to take on a junior
researcher, because he wanted
to do every' experiment him
self. so that he would have first
hand information and would
know how best to proceed.
By 1978 Nordenstrom had
completed his basic research:
he had identified all the ele
ments of an electric circuit in
the body. In the vascular inter
stitial closed circuit, or VICC.
as he called it. necrosis in a tu
mor functioned somewhat like
an AC power source. Il built a
fluctuating potential, driving
the circuit with a slowly alter
nating curreni. The blood ves
sels served as electric cables
between injured and healthy
tissue. The blood served as one
segment of the conductor in
the circuit; the fluid between
the cells of tissue—called in
terstitial fluid, it's as conduc
tive as the blood—served as
the other. Enzymes in the cells
of the capillary walls formed
the system’s electrodes. Says
Nordenstrom. “When you have
found all the elements that cor
respond to an ordinary' electric
circuit, and each element per
forms its defined function, it
must work.”
By then the medical estab-
lishment and Nordenstrom had
lost touch. He had given few
lectures on his research and
had published only a handful
of papers. When he began
writing his book in 1979, he
was convinced he had proved
his thesis of biologically closed
electric circuits. But even the
handful of colleagues who
knew of it didn’t seem to care.
When he finished the book
in 1983, medical publishing
houses refused to take it seri
ously. so he raised $50,000 and
published it himself. Of the
2,000 copies printed, only 400
were sold. What he considered
the most important work of his
life languished in obscurity.
Nordenstrom was as much
to blame as anyone. He had
committed one of the cardinal
sins in research: he rarely both
ered to publish in the medical
journals, the traditional net
work of information in this
branch of science. Instead he
chose to pack two decades of
effort into a single tome. (Al
though Nordenstrom has pub
lished 140 papers in his life,
only a few are on his biological
circuit research.)
Researchers hesitated to buy
a book about a seemingly bi
zarre new field—even more so
because Nordenstrom was ask
ing $ 135 per copy to cover his
publishing costs. Moreover,
the book hadn’t been subjected
to peer review, as articles in a
lop journal would have been.
Says Melvin Figley. a professor
of radiology and medicine at
the University of Washington,
and recently editor of the AJR,
“It’s conceivable that it’s all
very solid, but it’s not present
ed in the conventional way.”
Nordenstrom responds that
he did publish three papers,
one in 1971, one in 1974, and
one in 1978. “But there was
no response whatsoever,” he
says. “I published and I talked
about it with my colleagues,
and they didn't understand.
They just said it was a crazy
idea, nothing of importance.”
After that, he insists, he was
more interested in pursuing his
research than in publishing it,
which isn’t quite as rebellious
as it sounds. Most researchers
write up their experiments to
earn promotions in academia’s
highly competitive publish-orperish climate. Nordenstrom
needed no promotions; he was
already at the pinnacle of his
field.
Nordenstrom might not even
have written the book if it
hadn't been for a minor stroke
in 1979 that knocked him out
of action for half a .year. “I was
so scared when I was ill.” he
says, “and I was so afraid that
maybe I would get a heart at
tack. I had to write it down so it
wouldn't be forgotten.” Al
though both his parents are
1
ordenstrOm
resigned as
a Karolinska
administrator to
devote himself to
his research
aliveand in their nineties, Nor
denstrom insists that his life
has been more stressful than
theirs. He began the book
while he was recovering, and
now that it’s out, he doesn’t
want to repeat what he’s al
ready written. “At the mo
ment," he says, “the primary
scientific work is the most im
portant to me. Later on I can
publish. When I have exhaust
ed myself in the sc entific field,
and for various rec sons cannot
do my job, then I can write up
things in articles.''
Figley, an old fr end and col
league, says he had to ask Nordenstrom to submit the article
on his work to the AJR. The
two belong to the Fleischner
Society, an international group
of prominent-radologists and
other medical specialists inter
ested in lung diseases. The arti
cle came from a lecture that
Nordenstrom gav : to the society. (Nordenstrom says that af
ter the talk those present raved
about his work, but only five of
the 62 members bought the
book.) It was Figk y who added
the AJR editor’s n Die, which al
though overwhel ningly com
plimentary of Nordenstrom,
struck some researchers as a
not-so-subtle disclaimer that
said, in effect, that because the
experiments hadn't been repli
cated or review ec by other sci
entists, the article shouldn’t be
construed as representing the
journal’s usual standards for
new- research.
There’s obviot sly confusion
over NordenstrorTs work even
among those co leagues who
know something about it. They
acknowledge thst his experi
mental observatons may be
right—no one fas yet come
forth to point out a mistake—
but suggest that his overall syn
thesis may be a little farfetched. Norden nrom himself
is convinced of the validity of
his basic thesis, c ven if hejnay
have erred in a few particulars.
But when he goes on to assert
that electric crcuits in the
body can explair so many puz
zles, from subtle x-ray findings
in lung cancer, to accumulalion of white blood cells, to
acupuncture, it mly increases
suspicions of quackery among
the more traditionally minded.
That uneasiness was comDISCOVER • APS . • I'.'Bo 33
mem you can see a reactioa
body of existing knowledge.
and large, can’t understand it.
pounded by Nordenstrom s
around the tumor of some f i
Some, like Boguslaw Lipinski,
In their field, learning means
resignation from his adminis
brous scar tissue. After seven
an associate editor of the Jour
keeping up with the explosion
trative duties at Karolinska
months it starts to disappear. I
nal of Bioelectricity, say Norof new technology—CT and
Hospital in 1979. He wanted to
only treated her once. It took
denstrom’s
findings
are
fasci
PET scans, magnetic reso
devote himself to his research,
about .• hour, then she we it
nating
and
original,
and
seem
nance imaging—not returning
he says, and leave behind the
home after the treatment. Af
to fit perfectly into what’s
to the biochemistry and bio
burden of paperwork—of pre
ter five years she still had no re
already known about bioelec
physics they studied way back
siding over a department of
currence. Then she died from
tromagnetism.
Lipinski
goes
in medical school. Yet it’s just
250 people, including 48 full
the recurrence of her ovarian
even
further,
saying
Nordensuch basic scientific knowl
time doctors. The hospital ad
tumor, but I'm sure the luig
strom’s research is the first to
edge that Nordenstrbm’s book
ministrators, who prefer their
tumor would have killed t er
make the scattered theories
demands. Says John Doppdepartment chiefs to concen
first."
and
experimental
results
ac
mann. head of diagnostic radi
trate on patients and manage
His second case: "A young
ceptable
and
understandable
ology at the U.S. National In
ment, not on research, were
girl,
nineteen years of age. She
in the total context of the hu
stitutes of Health (NIH), “1
happy enough to let him go.
had
an
unusual kind of maligman body. If Nordenstrom can
doubt whether a dozen radiol
Outside observers hearing
bring
the
field
recognition,
he
ogists have read it. because
umors of Nordenstrom’s resPerhaps the key obstacle ts
adds, "that is the most impor
they wouldn't be able to evalu
ation could only wonder if
the
acceptance of Nordentant thing that he can do.” In
ate it anyway.”
i nad been subtly encouraged
strcHTi’s
thecrry is its challeng
other words, bioelectromagneThe few experts in bioelecby the Karolinska administraing interdisciplinary nature.
tists may be able to ride to re
tromagnetics who’ve heard of
■ ors because they fell he had
spectability on Nordenstrom’s
ost touch with reality. As one
coattails.
U.S. researcher put it, “The
On a drizzly afternoon,
question in everybody’s mind
Nordenstrom is sitting in his
s whether he has become such
office, talking about cancer
a recluse that it has interfered
treatment and leafing through
with his ability to do science.”
his book. He stops to point out
Nordenstrom, who seems
before and after x-rays of tu
•quiet and stoic by nature, adds
mors: he's talking about his
o the doubts by coming off as a
successes and his failures. And
t of a zealot on the subject
he’s talking about the danger of
’ his work. He admits that
talking at all. Several years ago
,e sometimes feels like' a
his work was written up in the
nineteenth-century missionary
National Enquirer, and he was
working in darkest Africa. Figplagued with telephone calls
ley says that when he went over
for months afterward. He real
Nordenstrom’s manuscript be
izes. however, that his theory,
fore publication in the AJR,
if it’s of any value, must also
ordenstrom was unreceptive
provide routes for therapy. ‘T
Nordenstrom and might be
to any other views of his work,
needed something that would
able to evaluate his work
even serious criticisms. He
attract people’s interest,” he
submit
conflicting
testimony.
seemed satisfied with his own
says, "and cancer treatment is
For instance, when W. Ross
verifications, and that was that.
always interesting. It’s for the
Adey of the V.A. Hospital in
Says Figley, “Nobody doubts
layman or the ordinary doctor
Loma Linda, Calif, reviewed
his sincerity and integrity, but
who wants to know what this is
the
current
state
of
his
field
he has an almost religious fer
good for.”
in The Sciences, he never
vor about this that I think ob
Then he begins to talk about
mentioned Nordenstrom s re
scures his objectivity.”
some
of his cases, pointing
search. He later explained
Perhaps the key obstacle to
them out in his book. His first
he
that
although
owned
Northe acceptance of Norden
was in June 1978.
denstrom’s book, he hadn’t yet
strom’s theory is its challenging
“This patient was too old to
read it. Andrew Bassett, a pro
interdisciplinary nature. Al
be
operated on,” he says. “She
fessor emeritus of surgery at
though it takes off from Nor
was 66. She hadjnetastasis in
Columbia
who
has
used
elec
denstrom’s own discipline of
the lung from an ovarian cancer.
tricity to help heal bone frac
radiology, it quickly veers into
I introduced very tiny elec
tures, criticizes Nordenstrom
biophysics, biochemistry, pa
trodes into the lung, and I gave
has
placed
as
a
newcomer
who
thology, and tumor physiolo
this current here. This is the re
too
much
importance
on
his
gy, to say nothing of elemen
sult—one month after treatown results, and ignored the
tary physics. Radiologists, by
lai e admits
,U ik dial he
sometimes feels
like a missionary
working in
darkest Africa
&
&
s
34 DISCOVER • APRIL • 1986
nancy of the uterus. Surgeons
cut out the uterus. Two years
later she had four metastases in
the lungs: two in the right, two
in the left. The largest one was
four centimeters in diameter.
These tumors do not respond
to radiotherapy—it’s useless.
The surgeons refused to oper
ate, because she had tumors in
both lungs. She got chemo
therapy, but the tumors con
tinued to grow. She lost her
hair. Il was bad. Then they said
to me, ‘Well, you can try.’ I im
planted electrodes, I treated all
four tumors, one at a time.
They all regressed. She's still in
good health seven years after.”
Nordenstrom began think
ing about treating tumors back
in 1965 when he first linked
necrosis in a tumor with a
change in electric potential.
That internal necrosis repre
sented half the process of
healing, but only half, because
the external tumor continued
to grow'. Nordenstrom con
sidered what would happen if
he stuck his electrodes into
the tumor and added some ex
ternal power to the electric
circuit that had been switched
on by the necrosis. If the cir
cuit was related to the pro
cess of healing, he ought to be
able to stimulate it further. It
was all speculative, but ...
By 1978, when he was ready
to treat his first tumor, he had
created a list of expectations of
what his electricity ought to do
if his thesis was right.
First, he figured that be
cause white blood cells, the
primary tumor-fighters of the
body, carry negative electric
charge, he should be able to at
tract more of them to the tumor
by placing a positive electrode
directly in it—the physiologi
cal equivalent of luring more
troops into the battle.
Second, although cancer
cells multiply faster than nor
mal cells, they are also more
vulnerable. The theory behind
chemotherapy is to change the
environment sufficiently to kill
the cancer cells without doing
in the healthy ones. The elec
tric field should likewise create
changes in that environnment,
one of which would be a chem
ical reaction around the elec
trode. like the acid build-up in #
an old battery.
Third, around the outside of
the tumor, the acidic reaction
would kill some of the red blood
cells, or at least damage their
hemoglobin, preventing deliv
ery of oxygen to the tumor.
Fourth, the positive electric
field should move water out of
the tumor, shrinking it and
causing the surrounding tissue
to swell, putting pressure on
the blood vessels and thereby
blocking the flow of blood to
the tumor.
Finally, the chemical reac
tions at the electrodes would
produce a pocket of gas, which
could create a high-pressure
cavity that might actually
break the tumor mechanically,
from the inside out.
Nordenstrom’s tumor-kill
ing tactics sounded plausible.
But he would need permission
to try them on patients. The
only ones the ethics committee
at his hospital would allow him
to treat were those who had re
fused. or failed to respond to,
all other treatment. “I got only
very, very poor cases, where no
other therapy was available—
large tumors growing every-
where,” Nordenstrom says.
Many patients were in such
bad shape that even if he had
been able to destroy Itheir lung
tumors, their cancer w as spreading so fast they woulc probably
have died soon anyway.
Nordenstrom pui his elec
trodes in 20 patients in his first
series of tests. He tre ated them
for up to three hour , and then
they w'ent home. The: treatment
was as experimental as it could
be. Even after testin|g it on ani
mals, he was still uessing at
how to administer ie electric
ity and in what d ages. And
still, in ten ofhis pat ents the tu
mors regressed, and in seven
they disappeared entirely or
simply died, remaining a lump
of harmless tissue . Nordenstrom had achiived what
doctors call clinica and thera
peutic success.
I n his next 25 pa :ients, NorBdenstrom stepped up the
voltage from 10 volts to 20, but
his success rate fell. He now' be
lieves that when 1 e raised the
voltage, he created a short-cir
cuit between the two elec
trodes, w’hich foci sed the elec
tric field on only a small portion of the tumor In his latest
series of patients, he’s starting
with a low er voltage again, and
building it up sbwly. So far
he’s treated 80 patients, with
no fatalities. If no hing else, the
treatment is safe, and it seems
to be a lot more t lan that.
Nordenstrom’ ► Swedish col
leagues are impressed. Folke
Pettersson. chief of gyneco
logical oncolgy at Karolinska
Hospital, has referred half a
dozen patients tc Nordenstrom
over the years, all cases that
w’ere either bey ond hope or
and
had refused surgery,
s
Nordenstrom’s electricity has
killed the turne rs in most of
them. “We are a few here who
think he’s a genilus.” Pettersson
says. Elisabet Bjorkholm and
Ingemar Naslund, both cancer
specialists at Karolinska, have
also sent patients to Norden,1 • 1986
35
Hordenstrom and his wife,
Gerd, live near Stockholm in
the village of Ronninge.
strom. have seen his treat
ments, and are now believers.
But both stressed that they did
not want to raise false hopes.
For now. at least. Nordenstrom’s electric therapy works
only on isolated tumors; the
largest have been four centime
ters across, and most smaller.
It's not a miracle cure.
In the U.S., Nordenstrom's
cancer treatments still haven’t
brought him the attention he
would like. Once again, the
fault may lie in the lack of
available information. Nor
denstrom has only published
the results from his first 20
patients, and that was in the
seccnd-to-last chapter of his
book. Greenspan of Yale, who
says he has read the book, is
at best cautiously optimistic:
“I’ve seen pictures of some of
his cli lical results where tu
mors have diminished in size,
but I haven’t heard him present
a statistical study. As you
know, occasionally tumors will
decrease in size by themselves.
My gut feeling is that’s not the
case here.”
Figley has more reserva
tions. “He’s treated lung nod
ules with low-voltage continu
ous electricity and some have
responded. That can hardly be
the approach to the overall
prob’em of it: ng cancer. It's an
almost exhibitionist kind of
way to go at it.”
Nordenstrom is probably
more aware than anyone else
of the shot-in-the-dark aspect
of his work. Even he seems a
little surprised that he has had
any successes. He compares his
electrical treatment to radiotherapy: “Radiotherapy has
been practiced for eighty-five
years at least, all over the
world, extensively, every day.
year after year. Still we don’t
know how to optimize that
technique. And that’s a fairly
simple principle. With elec
tricity you can play with an
enormous number of parame
ters. In order to make sense of
26
).ER • APfi'l • !936
ES
!
V
• !
'
■
'I
I:
«‘v
'
*
.rm
- ??
A '■
I
I- -.o
I
'i.
V ..,: .
V2
..
. I#
■■
A.
: J
;•
I
■
'/"
’..............- . .
. .
..
.
■
__ kC-. . .n' . . _
it, we ought to have large num
bers of comparable tumors,
sizes, treatments, total cur
rents, locations, etc. It would
take years and years, even if we
start to work now all over the
world.”
M t present. Nordenstrom is
JHa treating only lung and
breast cancers, because he’s
most familiar with them. But
he sees no reason why electric
ity shouldn't work on tumors
elsewhere in the body. He’s
also developing techniques for
combining electrical treatment
with chemotherapy, using the
electrode^ to concentrate the
chemical around the tumor.
So far, he has used the treat
ment on only two patients.
Both have responded well.
Nordenstrom also has a
backlog of basic research wait
ing for him. He’s working on
measuring the potentials creat
ed in bone fractures—one of
the classic areas in which re
searchers have attempted to
speed healing with electricity.
Backed by his studies of the
physiology of fractures. Nor
denstrom hopes he'll obtain
belter results than his prede
cessors. “Everybody can show
that they have a case here and
there where electrical treat
ment seemed to Have acceler
ated the healing.” he says,
“but it’s like shooting into
the woods. They hit something
by chance. You must be able
to predict what's happming.
That’s science.”
Without some kind cf dra
matic coup, acceptance of Nor
denstrom's work could take
decades. Traditionally, a researcher of his statire is
expected to take on and
train young post-docs— fresh
ly minted Ph.D.s or M.D.s—in
his methods and his ideas,
These disciples then go out
into the scientific world and
spread the word. But urtil his
book was published Norden
strom had no disciples, ' Now
he says he's working with a
number of researchers in the
Stockholm area, and Aould
welcome more if they we re am
bitious and talented eno igh.)
. A
I I
i
l|
|
-
While the pay-offs for fol
lowing Nordenstrom may be
enormous if his theory turns
out to be correct, few young re
searchers are ready to risk
their careers by running off to
Sweden to pursue anything so
far out of the mainstream of
medicine. Even if Norden
strom is right, taking up his
work could still lead to a career
of fighting the establishment.
For an ambitious young radi
ologist. working on a new tech
nology like magnetic reso
nance imaging, by compari
son, offers a guarantee of
publishing papers and making
a name in the field. (At one
point Nordenstrom tried to
talk his eldest son. a surgeon.
into helping him with his ex
periments. The son replied, “If
I become a radiologist and suc
ceed. it will be your merit. If I
fail, it will be my fault.” He
stayed in surgery.)
If young researchers are hesi
tant to join Nordenstrom, their
elder colleagues are even more
so. Few established researchers
are ready to give up everything
on which they’ve built their rep
utations in order to duplicate
another researcher’s work. Even
Nordenstrom’s admirers, like
Greenspan, are reluctant to
commit themselves. Asked why
he hadn’t taken aside a post
doc in his department and sug
gested he study biological cir
cuits. he replied vaguely. “I
don’t kjpw; maybe I should.”
When Judah Folkman, a worldfamous cancer researcher at
the Children’s Hospital in Bos
ton. read Nordenstrom’s book
and heard him lecture, he
thought the results were tanta
lizing, and had extraordinary
potential But, he said, “we
didn't start working on it, be
cause we were so busy with our
own things, and we’d have to
train somebody, and we as
sumed other people would get
into it” When Bernard Wat
son, a professor ofapplied med
ical electronics at St. Bartholo
mew's Hospital in London,
tried to get clinicians interested
in using Nordenstrom’s cancer
treatments, they all turned him
down. They seemed afraid to
go before the ethics committees
with a treatment that was so
difficult to understand.
Phillip Chen, associate di
rector for intramural affairs at
|| eoplewho
JL have learned
something as truth
don’t particularly
like to hear that it
may not be correct
NIH, says that Nordenstrom
has to become an entrepreneur
if he expects to get his work
accepted. “If I were NordenStrom,” says Chen. “1 would
stan padding around talking to
administrators at NIH. at the
American Cancer Society, at
foundations. At this point it’s
more a matter of salesmanship
than just being a quiet author
somewhere.”
At 65. however. Norden
strom isn’t about to become a
salesman. Although he’ll give
up his remaining administra
tive duties next year, he in
tends, in his w’ords, to continue
his research until te drops.
Those who are optimistic
about the long-ter m survival of
Nordenstrom’s tt eory tend to
be pessimistic ab yut the mal
leability of the minds of their
colleagues. “Pet haps,” says
Greenspan, “after he’s long
gone and I’m lor g gone, he’ll
be proved to be c jrrect.”
Pettersson poi its out, cyni
cally, that medical researchefs,
like everybody else, tend to
move in faddish flocks—es
pousing interferon one year,
magnetic resonajnee imaging
the next—and f something
isn’t backed by in enormous
flow of money and a good
press, they tend to ignore
Greenspan poin s out that
Nordenstrom is fight—if bio
logically closed electric circuits do exist in the body and
play as key a rcle as he says
they do—there will be quite
a few red faces among medi
cal researchers. “People who
have learned something as the
truth,” he says, ‘ don’t particu
larly like to hear that they’ve
based a large pa rt of their ca
reers on things that were either
incomplete, or r ot completely
correct.”
While Nordepstrom tries to
play down his cancer treatments, his entire theory is likely
to live and die by how the medi
cal community chooses to re
ceive them. NIH’s Doppmann
points out that when Steven
Rosenberg, a researcher at
the National Gincer Institute,
cured a seem ngly hopeless
case of cancer v ith a new drug
called interleuk n-2. he made it
onto the cover of Newsweek
within weeks. “People are
looking for cancer cures,”
Doppman says, “If Nordenstrom is really making tumors disappear that haven’t re
sponded to anything else, he’s
going to be not: ced.”
D
DISCO'. E? • APS It • 1986 37
■
■
.
toward explaining the world around us. Now researchers
suspect it may also explain the world within US.
BY GARY TAUBES
F
human brain is like a hurri- ity.” A relaxed person’s brain gives off
mysteries of turbu
for instance, the mysteries
M ’ cane or the rings of Saturn. It a stream of alpha waves, somewhat like tor
lence
and
the
unpredictability
of the
I is like a dripping faucet. It is, in heartbeats, but the alpha hum is not
the
enigmatic
weather,
stability
of
Sat■ a word, chaotic. At least that’s perfectly steady; the intervals between
rings,
the
and
the
odd
wobble
in
urn’s
what Paul Rapp has concluded voltage peaks and troughs vary slightly.
cases
orbit
theme
of
Pluto.
all
the
is
In
after several years of watching And in a person counting backward by
fluc
in
same:
natural
the
the
systems
people think. Rapp, a physiologist at sevens, these variations become even
the Medical College of Pennsylvania, more erratic, unpredictable, and com tuations that are unpredictable and
seemingly as random as the helterhooks his subjects to an electroen plex. They become more chaotic.
skelter
rattling around of oillions of
cephalograph and monitors their brain
That doesn’t mean the subjects molecules are sometimes repealed at a
at a
waves—the electric signals produced themselves are breaking down, think
by the firing of neurons. He does so ing random, frightened thoughts under higher level of abstraction to have sim
twice for each subject: once with the the pressure of the experiment. On the ple patterns.
So far most applications of chaos the
w subject relaxed, not thinking about
contrary, they may be thinking quite ory have come in the physical sciences.
s anything in particular, and again with
s
clearly. And although their EEGs look In the last few years, however, a scattere2 the subject counting backward from
like graphs of random noise, the rap- ing of brave souls have started applying
700 by sevens. “It’s important to use pearance is deceiving. The “chaos’'
sevens,” says Rapp, “because tens, Rapp observes is different from chaos the theory to the mysteries of life it
| fives, and twos are almost automatic, in the vernacular sense of total disor self—to living organisms rather than to
f
r Rapp is
g and you don’t have to think about the der. It is a mathematical type of chaos: planets or storms or faucets.
mulAdiscipli:
one
of
this
new
breed
of
,
‘
t ing arithmetic.”
it has a hidden order.
researchers,
who
that
in
orary
believe
| When Rapp forces people to think,
Rapp’s search for order in disorder der to understand the brain,
___
7
the
heart,
| he gets an interesting result. The EEG is part of a burgeoning movement,
| registers, as he puts it, “a very dra- loosely called chaos theory, that has of and other physiological systems, they
of
| matic, reproducible increase in the dy- late been cutting a wide swath through have to understand the mathematics o?f
i namical complexity of the brain activ- the sciences. Chaoticians have probed. chaos. To these researchers chaos the
ory offers hope; for its essent al insight
<
i
’
discover
• mat • 1969 63
I
this nonlinear frontier. It’s true that a
computer can’t solve a system of non
linear equations any better than a hu
man being can, at least in the ^ense of
finding a general formula that, would
predict the state of the system at some
arbitrary time in the future, but it can
apply brute force. It can get to [the fu
ture step by tiny step, plugging num
bers into the equations, calculating the
result for a short time after the initial
state, and then repeating the process
thousands of times. In fact, that is how
weather forecasts are done today; the
weather is a nonlinear systerh par
excellence.
And it was the weather, or rather our
inability to predict it very well, that MIT
meteorologist Edward Lorenz was in
is that complex behavior may be gener actly when it will hit the genius sitting terested in when he stumbled ohto a
ated by systems that are essentially under the tree and how fast it will be key fact about nonlinear systems: that,
very simple and organized. If the 10 bil moving. What’s more, even if your unlike linear systems, they are ex
lion neurons in the human brain gener measurement of the apple ’s starting tremely sensitive to changes in initial
ate electric chaos, for instance, it might point is a little off, your prediction conditions. In 1963 Lorenz did a commean that the brain’s circuitry is orga won’t be too far wrong. In a linear sys- puter simulation of the weather using
nized along simpler lines than has ever tem, a small change in the initial condi three simple nonlinear equations. He
been imagined.
tions results only in a proportionally found that the equations would cqum
small change in the output.
out entirely different future wea her
/ haos has only recently become
In reality, however, most natural sys- when the initial conditions (air
. ' tem
a buzzword, but chaos theory is terns are not linear. Often they don’t
I
and
differed
pressure,
so
on)
perature,
||
actually part of a larger field of move in a simple straight line from
as
little
as
a
of
a per
by
ten-thousandth
1 j mathematics that has been at- cause to effect but in cycles, with the
cent. (That’s about as small as the per
VZ tracting increasing attention for effect feeding back on the cause and turbation of air produced by the flutterseveral decades now. That field is called perhaps amplifying it. Or their behavior ing of a butterfly’s wings, which is vJhy
nonlinear dynamics, and its rising is marked by abrupt transitions, by ef- Lorenz’s discovery is often called the
popularity among scientists has much fects that are all out of proportion to the butterfly effect.) The smaller the initial
to do with the parallel rise in the cause—the straw that breaks the difference, the longer Lorenz had to
availability and power of electronic camel’s back. To describe such systems run his computer before the simulated
computers.
accurately one has to resort to non weather patterns diverged. But eventu
Nonlinear dynamics represents a de- linear equations, that is, to equations ally they always did. And how they
arture from the classical mathematics that contain exponents. And such would diverge, he could never say; only
on which science has been based since equations are, more often than not, too that they would.
Newton. For physical scientists in par complex to solve.
To a meteorologist, that result was
ticular, the key mathematical tool has
So until a few decades ago, scientists disheartening. After all, it is physically
been linear differential equations— dealt with the nonlinear complexity of impossible to measure conditions in the
linear because the variables, like those the natural world either by approx- atmosphere or in any other part of thp
—
in an equation describing a straight
‘
imating it piecemeal with linear equa real world—with infinite accuracy. The
line, aren’t squared or cubed or raised tions or by ignoring it. “During engi initial conditions fed into nonlinear
to even higher powers; and differential neering school,” says Art Winfree, a equations are always subject to error.
because the equations involve rates of University of Anzona biologist who be- What Lorenz showed was that those erchange.
The great
advantage of a linear
,.ff
his career as an engineer, “you rors will always blow up exponentially
ditierential equation is that it is simple largely take courses about linear ap- and
and inin unpredictable
ways. The
The bad
bad I|
unpredictable ways.
simple
that
even
§
was
nonenoug to e solved. If a mechanical proximations
news,then,
simple
proximationstotothings.
things.Toward
Towardthe
theend
end news,
that
even
nonthen, was
system say an apple dropping from a of
ofthe
thecourses
coursesthe
thenrofessnn;
professors always say linear
systems liVo
Lorenz’s pared- ©
linear cvctomc
like Torao-y’c
tree—can be described by such an that the interesting stuff is the non down weather model could generate I
equation, then the solution predicts linear stuff. It quickly becomes clear unpredictable behavior; chaos is inher- |
how the system will evolve with time.
that the whole world is not linear and ent in these systems and will never be f
In other words, if you know the time the nonlinear phenomena always turn vanquished no matter how much we |
when the apple begins to fall and the out to be the interesting things.”
|
improve our measurements.
height it falls from—the initial condi
The arrival of computers gave re
But the good news was just the flip |
tions, in the lingo—you can predict ex- searchers a tool with which to explore side of the bad: even the most complex I
64
DISCOVER • MAY • I9S9
(
(
1
c
c
I
S
t
a
ti
ti
n
n
Vi
fc
nr
N
th
si
is
w
trt
th
m
be
g da
bi
£ str
o
m<
co wf
§ is i
I
| ch<
| ha'
? chi
a
nuof
Id
le
in
unle
al
ss
w
le
ar
behavior might stem from very simple,
deterministic systems. As Lorenz and
many who have followed him have
shown, it takes only a few equations
with a few key variables—working
parts, in the words of Walter J. Free
man, a neurophysiologist at the Univer
sity of California at Berkeley—to pro
duce chaotic behavior. “That’s the real
eye-opener,” says Freeman. “You al
ways thought that unpredictable ran
dom behavior is the result of so many
variables that you can’t possibly en
compass them all. And it’s not true.”
tir
IT
na
it,
xal
nig
4e
rn
er
n?d
?r?r?r>y
he
ial
to
ed
uey
ily
as
-Ily
he
-he
he
ar
?r.
?r-lly I
adn- §I
d-I
ite |
?r- |
be f
ve S
m
■lip |
ex 1
A new intuition
has set in:
some degree of
chaos seems to be
necessary for the
healthy functioning
of the brain and
ecause chaotic behavior may be
generated by just a few working
the heart.
parts, there is hope of under
standing it at some fundamental
level, even if the future state of
a chaotic system cannot be predicted in Nonlinear mathematics provides a tool
detail. Unlike the randomness gener- to probe that complexity in a new way.
’ ’ scientific
ated by a system with many variables, 'T"
“ ' approach is to
The orthodox
chaos has its own pattern, a peculiar dismantle a complex system and focus
kind of order. This pattern is known on its fundamental components—
whimsically as a strange attractor, be quarks, genes, or whatever. In contrast,
cause the chaotic system seems to be chaoticians concentrate on the dynam
strangely attracted to an ideal behavior. ics of the system as a whole: on what
In the universe of states that a chaotic the parts are doing, not individually,
system could conceivably occupy—in but all together.
state space,” as the chaoticians put
The human brain, with its dense
it the strange attractor delineates mesh of profusely interconnected neuthose states. that are actually...
possible, rons, is a good example of what chaos
as <’determined by the nonlinear equa- enthusiasts see as the limitations of the
tions that govern the system.
orthodox, reductionist approach to sci
Weather has become the quintessen ence. “We have developed tools for
tial example of a chaotic system. It studying the brain down to the cellular
never repeats itself precisely, and in the
not-too-distant future it always di
verges from what meteorologists can
forecast on the basis of the best possible
measurements and computer models.
Nevertheless, one can safely say that
the temperature in Kansas City this
summer will not be 900 degrees, as it
is on the surface of Venus; Earth ’s
weather always stays on the strange at
tractor known as climate. Stretching
the attractor metaphor a little, one
might find another example in human
behavior: it is rarely predictable from
g day to day or even minute to minute,
g but it always hovers around that
§ strange attractor we call character. It
| may seem random on occasion, but
| when you delve deep enough, it usually
| is not.
| Physiology and biology seem to be
“ chock-full of unpredictable, erratic be
havior that can now be shown to be
6
£ chaotic rather than classically random.
level,” says Stephen Foote, a neuro
physiologist at the University of Califor
nia at San Diego. “We can draw ana
tomical maps of how certain chemicals
are distributed in the brain; we can
draw physiological maps of what their
response properties are like, or the ac
tivity of individual neurqns. And we’re
still stumped about how to take those
little atoms and molecules of informa
tion and unify those observations into
a coherent theory of how the brain
works.”
Brain chaoticians like Foote, Rapp,
and Freeman are nowhere near devel
oping such a theory. But they are be
ginning to make some interesting glob
al statements about brain function.
What they are findingt-in Rapp’s
counting-backward-by-sevens experi
ment, for example—is that the level of
brain function seems to bo intimately
linked to the degree of chaos in brain
waves.
Freeman analyzed the electric pat
patterns that emerged from the firing of
neurons in the olfactory bulb—the first
part of the brain to respond to odors—
in rabbits. He inserted 64 electrodes
into each bulb and discovered that
when rabbits are not detecting any
odor, the neurons collectively generate
a low-amplitude, chaotic buzz of elec
tric activity. But when rabbits do react
to an odor, the neurons respond with
an intense salvo. The firing is still cha
otic, but it has a particular Spatial pat
I!
tern: some pans of the olfactory bulb
are more active than others. When rab
bits are again presented with the same
odor, the same pattern occurs, “flicker
ing,” as Freeman puts it, “like shadows
over the chaos.”
This implies, says Freeman, that the
low-amplitude chaotic buzz is the
equivalent of an “I don’t know” state.
Unlike transistors, their electronic
counterparts, neurons die if they be
come inactive. The chaotic firing serves
to keep the millions of nerve cells idling
and alive so that they can be shifted
instantaneously into gear in response
to a stimulus.
Rapp takes the proposition even fur
ther: should that chaotic idling degen- but chaotic—that is, they: are produced
erate into a regular, periodic pattern, he in a deterministic way, by, the? nervous
says, with millions of neurons resonat system. What’s more, the fluctuations
ing together, the result would be a mo seem to be more chaotic in healthy
mentary lapse of awareness, Eke the hearts than in diseased ones.
petit mal seizures that afflict some epi
In effect, says Goldberger, a healthy
leptics. Rapp has monitored the brain heart is continually varying its beat coming
reality. Chaos theory has
waves of epileptics and has found that over a range of frequencies. When a proved itself fascinating, but it is still
they_become dramatically less chaotic heart gets old and sick, however, the struggling, at least in the biological sci
during a seizure, which is the same as fluctuations in the interbeat interval be ences, to prove itself useful. In many
saying that they become more periodic come more regular and periodic; the cases it is not at all clear whether the
and regular. The .discovery. has a poten.
range of frequencies decreases, and a math has any relation to the real wdrld;
tial medical application: by monitoring few frequencies get more pronounced, a mathematical model that mimics
a patient’s brain-wave pattern, a doctor sort of like a knock in a car engine. The complexity in nature does not neces
might be able to adjust medication process culminates, says Goldberger, in sarily explain anything. When some
more effectively in order to prevent cardiac arrest, when some of the peri- one reports that some biological system
seizuresfluctuations in the interbeat inter- or another exhibits chaotic beffavior7it
val become very pronounced.
is still legitimate to ask, “So what?”
he heart, too, appears to be beset
f
Why should the heart need chaos?
That will be a fair question until chawith chaos, although the jury is "To be healthy,” Goldberger says, “you oticians start making more predictions
I still out on exactly what role it need to be able to cope with an envi
about the world—predictions that are
g plays. In the late 1970s, MIT ronment that’s throwing you curveballs
JL physicist Richard Cohen pro and sliders and knuckleballs. And if then confirmed by laboratory experi
ment. “That’s the key,” says Michael
posed that during ventricular fibrilla you’re wrapped up in some periodic,
Shlesinger, a physicist at the Office of
tion, the most common form of heart monotonous dynamic, you’re in no Naval Research who hands out funds
attack, the heart goes from beating shape to contend with the environ
for research in nonlinear dynamics.
regularly to beating chaotically. This ment. Chaos is the only mechanism I “Science is judged by predictability.
was the intuitive point of view, and the know for ogenerating
o that necessary Give me an unknown situation and I’ll
researchers backed it up with nonlinear variability and for doing so in a some- tell you what’s going to happen. If I can
mathematical models. More recently, what controlled manner.”
do that, I have a useful theory.” In the
however, a new kind of intuition has
If the idea that the heart needs chaos meantime, some researchers still dis
set in. /A group of researchers led by Ary is borne out, it has an obvious applicamiss the trend toward finding chaos in
Goldberger, a cardiologist at Harvard. tion in the prevention of heart attacks. every biological closet as a fad.
Medical School, has proposed that Goldberger envisions that someday
Yet it is almost certainly more than
some degree of chaos seems to be nec heart patients might wear a tiny device that, if only because it is part of the
essary for the healthy functioning of that monitors their heartbeat and ra- ’------ -,J--------larger, older movement toward apply- !
the heart, as it is for the brain.
dios the information back to a com ing the mathematics of nonlinear dy- |
For some time it has been known puter in their doctor’s office. The com
namics to biology. Not all researchers |
that a heartbeat is not as constant as a puter would analyze the signal and
who practice nonlinear dynamics are 0
metronome; the interval between beats determine whether the level of chaos in finding chaos; chaos is just one type of |
is always changing by small but mea the heartbeat was getting dangerously
behavior a nonlinear system edn dis- £
surable amounts. Goldberger has re low. If so, it would alert the doctor that play. But nonlinear dynamicists in gen- |
ported that these tiny fluctuations are it was time to intervene.
eral share the view that the reductionist §
not random, as was previously thought.
Such visions are a long way from be- approach to science is ultimately lim- I
- ,
66
DISCOVER • MAY • 1989
i
I
c
c
f
s
d
y
p
st
h
lo
ge
m
de
its
to
pa
leg
str
a c
me
uni
anc
cor
hin
mat
fore
T
one
0^0
S-'i®
• • 1
ent genes, and yet those.genes produce
only about 100 differen types of cells
Although every cell in J given human
not all genes
being
being has
the same
same genel,
has the
genei, not all genes
naVJilTS00 ln eVery ceT the different
patterns of gene activity are what distinguish a muscle cell, say, from
a neu—accepted theory of cell evoluron. The
ion says that each of the various
types in the human bldT^X'
through the?SOrS
rigors of
Darwf man natural
of Darwlni
selection; that is, by conveying some
selection,
^Petitive advantage onE^
competitive advantage on those ,
evolutionary ancestors who had it.
auffman has arriveci at a radi
cally different view, tn his com
puter model, 10,00b genes (a
tenth the number in a human
cell} interact according to simterns of the brain cells thatViriatX pie nonlmear rules that determine
when the genes are turned on and
motion. He believes that the very same
when
th- they 3re noL When puffman
equations that describe the coordina
sets
this system in motion, he finds that
tion of the limbs should work for the
it
settles
naturally into one oil only 100
ited in what it can reveal about a com coordination of the neurons; neurobi- s able configurations-diffenjnt distri
plex biological system. “Science as 0 Ogists have already demonstrated the butions of active and inactive genes—
sumes that by finding the smallest existence of rhythmic behavior and that are analogous to the 100 human
phase transitions in networks of neu
component, it’s done something, ” says
rons.
If Kelso can show that the phe cell types He calls this process "anti
Scott Kelso, the director of the Center
chaos ; whereas a chaotic sysfem
nomena
at these two levels are linked
may
tor Complex Systems at Floridaduce disorder with just a few
Pr°
variAtlantic University. <‘But what under he would end up with a u. - ■
, Kauffman’s antichaotic
-----;l system
standing means should really be ad of motion that, he believes,-mightapply has 10,000 variables
and
—
well
to
as
as
horses.
other
nnrrnranimals
dressed. Does it mean that you have
to generate order.
--yet manages
"People have looked at these neuroyour gene-of-the-week story in the
The implications of this result may
press? Or does it mean that you under nal patterns before,” he says. “They’ve be profound. If Kauffman is right the
been sitting right in front of them, but
stand genes as a dynamical system—
they have never appreciated it. That human genome may be a self-Jrgaoizing system, like his computer
““or
,
--” •-*’ more transparent than model, it may produce the rangelof hnof huKelso has spent the last eight years we ve ever imagined. But that's just a man cell types on its -range
.
interest
start.
Now
we
have
to
ask
the
without
own,
how
put
tolooking at
animals are
benefit of natural selection. '
ing questions: How
do animals
change
gether-specificaUy, how they coordi these
Whafos
WhTt
Cmain
^ot
frlP’sP patterns?
njttornc? Tin,-*
tteaming?
.
°
nate billions of neurons and pounds of i. mpmnnr?”
°
.«
because
of
selection
”
ha
«<i_r
iK'iOn’”
Se
MyS
bec-'
hP'
he
“
is memory?”
muscle to produce movement. How
^"Organizing properties '
For'hat matter—why stop there—
does an accelerating horse synchronize
woE’SyStemS On «“the ^'tfo:
What
is
life?
No
one
would
accuse
the
---- on
its legs when it shifts gears from a trot
new
breed
mathematical
biologists
of
of
to a gallop? in the trot, each diagonal
Without i—
’
worrying
about the nittyPair of legs moves as one; the left fore- setting their sights too low. They are gritty of what
genes' are made of, rely’eg and right hind leg, for example, aiming at nothing less than to under ing solely c- on a mathematical model
strike the ground at the same time At stand the laws that control the behavior of
they
< 3 SyS^m,
rz how
rr
. ' interact
----------f 3S
Pprt018^1^'10" °f livins or8anisms.
a certain point, though, as the legs
Kauffman
•
is
taking
on
a
that]1 has
theory
move faster and faster, the trot becomes Perhaps the best illustration of this am- ke-!n ? bedrock,in biology for a century.
unstable, and the horse shifts naturally
ies the ambiand spontaneously into the next stable
say the hubrisj of
configuration: the gallop, fo which both
Kauffman, a developmental biolo nonlmeardynamicists. Says Kauffmanhind tegs stake the ground at approxiWe may have to rethink the theoryt of
gist—and a nonlinear dynamicist by
ute.
;q
Sgs
metime’f0,1°Wedbythe avocation—
has created a computer
model
the
One
genome.
of
human
of
This abrupt "phase transition" from
he key puzzles abou( (he genome
Contributing
one pattern of motion to another is a i
about
the Stanford Linear Collider in the
inat it contains roughly 100,000 differJanuary issue.
as
till
ciny
he
d;
cs
sen
it
.unS‘heo7 ab,es> i—1Iid
s
e
1
f
o
O
f■
I
I
D
!
1
1
D'SCOvej
. MAY •IJs?
67
I
Hf 1-11
Use of Microscopic Technique in
Neurosurgery
Stephen R. Freidberg, M.D.* and John W. Walsh, M.D*
The most significant development in neurosurgery since the innova
tions of Cushing is the use of microsurgical techniques. Many surgical
procedures, not previously possible, are now feasible. Other preexisting
operations have been significantly refined.
Microsurgical principles, however, are not different from those laid
down by Cushing.10 He stressed the delicate handling of tissues and the
necessity of meticulous hemostasis. The microscope with its associated
instrumentation allows careful separation of the most delicate tissues,
coagulation and division of the smallest vessels, and suturing of tiny
nerves and vessels. We can now adhere more adequately to Cushing’s
precepts.
Otologists and ophthalmologists began using microtechniques far ear
lier than neurosurgeons.44 Kurze and Doyle,45 in 1962, reported removal of
an acoustic neuroma with microtechnique. Soon afterward the publica
tions of Jacobson et al.,29 Donaghy and Yasargil,13 and Rand52 confirmed
its value. Today new applications of microtechniques in neurosurgery are
constantly reported, and their use is limited only by the imagination of
members of our speciality.
The Zeiss Op Mi I, introduced almost 30 years ago, has provided
surgeons with clear binocular stereoscopic magnification adjustable from
6 to 40 x with brilliant illumination. This same instrument is used almost
without alteration by most surgeons today. Alterations of this basic model
have not been sufficiently adaptable to gain popularity. New instruments
are improvised and manufactured commercially almost daily. The de
velopment of bipolar coagulation by Malis48 was of major importance. It
has allowed coagulation on and immediately adjacent to vital
structures without danger of injury to them, which would be present with
spread of energy from a conventional electrical cautery. The manufacture
of 9-0 and 10-0 monofilament nylon sutures has made possible the sutur
ing of vessels and nerves of less than 1 mm in diameter.
We have been using the Op Mi I microscope for four years and, like
’“Department of Neurosurgery, Lahey Clinic Foundation, Boston, Massachusetts
Excerpt from The Surgical Clinics of North America,
Copyright © 1976 by W. B. Saunders Company.
2
Stephen
R. Freidberg
and
John W. Walsh
others, find that our applications enlarge constantly. This article discus
ses our current views on microtechniques.
BRAIN TUMORS
Microtechnique has proved useful for tumors of all sizes in difficult
locations. Large cerebral hemisphere gliomas are still approached
through an appropriately large craniotomy and removed with low power
loupe magnification. We have not attempted to remove these tumors
through a trephine opening with a microscope, although Wilson64 has
reported this. Large supratentorial meningiomas, whether parasagittal,
flax, sphenoid ridge, or even convexity, are reduced in size without the
microscope. The microscope is brought into the operation only when the
tumor is of convenient size.
Colloid cysts of the third ventricle are w611 suited to microsurgical
removal. After the cyst has collapsed, small vessels going from the
choroid plexus and ependyma to the cysts can be coagulated and divided,
and the posterior aspect of the third ventricle can be inspected. Little
retraction on the fornix is necessary.
We have not yet had the opportunity to treat posterior third ventricle or
pineal tumors with aid of the microscope. The subtentorial approach
above the cerebellar hemisphere, recommended by Stein,60 is the most
direct approach and avoids the major venous structures that lie above the
pineal tumor. Tumors in the posterior fossa, especially extra-axial
tumors, are ideally suited to removal with microtechnique. Masses in the
fourth ventricle (for example, ependymoma, medulloblastoma, and as
trocytoma) can be reduced in size and have their connections with the
cerebellum or brain stem divided so as to protect the fourth ventricular
floor.
Cerebellopontine angle tumors (for example, meningioma, choles
teatoma. and, most commonly, acoustic neuroma) should be operated on
with microtechnique.49,56,67 Dissection of the mass from the attachments
with underlying cranial nerves and the brain stem is much easier with
magnification (Fig. 1). Large acoustic neuromas, however, remain a
difficult problem. We have been unable to preserve facial nerve function
in the five patients Operated on with microtechnique, although we have
not produced any cerebellar or brain stem dysfunction. Because we prefer
to use controlled hyperventilation anesthesia, resection of cerebellar tis
sue has not been necessary. In one patient with a small acoustic tumor, 2
cm in diameter, the facial nerve was preserved. We have not seen any
intracanalicular tumors suitable for the translabyrinthine approach as
described by House and Hitselberger.28
Chordomas, like cerebellar pontine angle tumors, are intimately at
tached to the brain stem and cranial nerves and should be approached
with the microscope either subtemporally or transclivally as has been
suggested by various surgeons.21,50,61 We had no experience with the
transclival approach. Rand et al.3 reported removal of a chondrosarcoma
from the base of the skull.
Microscopic
Technique
in
3
Neurosurgery
B
Figure 1. A, Left cerebellopontine angle meningioma prior to removal (16x). B, After
microsurgical removal (16x). Arrow points to facial-acoustic nerves.
Pituitary tumors with large suprasellar extension should be aproached transfrontally. 16 Tumor bulk is reduced, and great care should be
taken to separate the mass from the optic nerves and chiasm. Intrasellar
pituitary tumors and those with moderate suprasellar extension can be
removed by way of the transsphenoidal route. Guiot19 has shown how the
suprasellar portion falls into the sella as the intrasellar contents are re
moved, leaving a layer of arachnoid between the tumor and optic appa
ratus. We have not removed any small functioning pituitary micro
adenomas. Hardy22 and others1,63 have shown that these tumors can be
removed while preserving or restoring normal pituitary function in
acromegaly, Cushing’s disease, and galactorrhea with amenorrhea.
Large suprasellar craniopharyngiomas are best approached through
a transfrontal craniotomy.6,40 Microtechniques allow more satisfactory
tumor removal from the hypothalamic area and from the optic nerves and
chiasm. Smaller tumors can be approached transsphenoidally.21,23
HYPOPHYSECTOMY
Transsphenoidal hypophysectomy, as described by Hardy,21 is the
ideal method of ensuring total removal of the pituitary gland for treatment
of breast or prostate carcinoma. The potential complications of this proce
dure, cerebrospinal fluid leak, meningitis, and cranial nerve injuries, are
very real. For the experienced surgeon, the incidence of these complicaI
I
4
Stephen
R. Freidberg
and
John W. Walsh
tions should be minimal. If no complications ensue, the transsphenoidal
route is far less stressful than the transfrontal approach.
CRANIAL NERVES
Microsurgical operations on the trigeminal nerve have been per
formed for classic tic douloureux. A variety of surgical approaches have
been developed over the past several decades for relief of trigeminal
neuralgia; several of these have been refined by the introduction of in
traoperative magnification.66 Initially, the microscope was used to gain
better illumination and visualization during sectioning of retroganglionic
trigeminal fibers through the middle fossa approach. A much clearer
distinction between portions of the trigeminal nerve roots could be
obtained. In 1967, Jannetta and Hand30,33 described their experience with
transtentorial selective posterior root section. They stated that individual
fiber groups could be sectioned more reliably With use of the surgical
microscope, and they achieved better relief of pain with less sensory
deficit or involvement of other trigeminal divisions.
Dandy11 developed trigeminal rhizotomy through the posterior fossa
approach in 1932. A frequent finding in his studies was compression of the
trigeminal nerve root as it exited from the brain stem by adjacent arterial
vessels. Jannetta32 refined this approach by introducing microsurgical
techniques and confirmed the occurrence of neurovascular compression
in all instances. This compression is caused most often by a branch of the
superior cerebellar artery, but occasionally its cause is a branch of the
anterior inferior cerebellar artery. Separation of the compressing vessel
from the nerve root provided dramatic relief of pain in all patients in
Jannetta’s series.
We have had extensive experience with the middle fossa approach.
Here, the increased illumination provided by the microscope has been
especially useful. With better visualization, we can perform root sections
with precision. Recently we began using Jannetta’s posterior fossa proce
dure and we find this approach promising (Fig. 2).
Jannetta et al.31,34,57 recently described vascular compression of the
facial nerve in patients with hemifacial spasm, ^nd he advocates treat
ment by a similar procedure. In all of his patients good relief from facial
spasm has been achieved with this method.
A variety of procedures for other cranial nerye disorders have been
reported. Fisch18 in Yasargil’s monograph described selective interrup
tion of the cochlear or vestibular nerves for intractable tinnitus or
Meniere’s disease. Jannetta 31 believes that these conditions may result
from vascular compression of the cochlear or vestibular nerves at the
brain stem. Microsurgical techniques have also been described for rhi
zotomy in glossopharyngeal neuralgia, for accessary and cervical nerve
rhizotomy in spastic torticollis, and for facial hypoglossal nerve anasto
mosis.
B
Figure 2. A, Right trigeminal root entry zone. Trigeminal root (black arrow) grooves
by superior cerebellar artery (curved arrow) and basilar aneurysm (white arrow) {16x).
B, Polyvinyl chloride sponge (open arrow) between trigeminal root and compressing ves
sels (16x).
5
6
Stephen
R. Freidberg
and
John W. Walsh
CEREBROVASCULAR DISORDERS
Aneurysms
The value of microsurgery in management of intracranial aneurysms
is now so obvious that some authors advocate intraoperative magnifica
tion as an essential part of the surgical procedure. 43,68 The operative
approach to the circle of Willis requires dissecting at considerable intra
cranial depths. Before intraoperative magnification, aneurysmal surgery
was difficult for neurosurgeons because of poor illumination and a re
stricted operative field. To circumvent these problems, large craniotomies
were fashioned, and considerable brain retraction was necessary. This
resulted in occasional cortical trauma and rupture of aneurysms. With the
surgical microscope, smaller craniotomies with less retraction are used,
and, with magnification, surgeons are astounded by the perforating ves
sels and other perianeurysmal structures not previously appreciated.
Once the region of the aneurysm has been explored, the arachnoid
membranes investing the aneurysmal neck and adjacent parent vessels
can be dissected away. This was previously carried out with blunt dissec
tion, but careful sharp dissection is now possible. Less traction or pulling
on the aneurysm itself results, and the likelihood of intraoperative rupture
is reduced. Finally, when the aneurysmal neck is explored and separated
from the now more clearly visualized perforating arteries, a clip or liga
ture can be placed with precision accuracy. The clip may be replaced
safely several times until optimal occlusion of the neck is achieved (Fig.
3).
Using these technical improvements, Yasargil et al.,68 from 1970 to
1974, attained an operative mortality rate of 1.9 per cent on 373 patients
, with aneurysms with a comparable decrease in morbidity. Hollin and
Decker26 reported similar findings with improved postoperative angio
graphic evaluations. Their results and those of others clearly established
the surgical microscope as an essential instrument for management of
intracranial aneurysms.
Arteriovenous Malformations
Fewer reports have appeared on the value of using the surgical micro
scope for resection of arteriovenous malformations. Yasargil,66 in his
excellent monograph, described 14 instances of cerebral and cerebellar
arteriovenous malformations and indicated several advantages obtained
by intraoperative magnification. He stated that when feeding arteries
have been located (usually at a distance from the malformation), they can
be followed toward the malformation and ligated or clipped just outside
the arteriovenous malformation, thus preserving many uninvolved arte
rial branches. Certainly, dissection of feeding vessels arising from the
region of the circle of Willis or the basilar artery is more easily and safely
performed.9-38-39 Here again, the powerful illumination of the microscope
is indispensable. In excision of arteriovenous malformations from deep
intracranial critical brain structures (for example, the brain stem or in
traventricular regions), the microscope is almost essential. Drake’s re
Microscopic
Technique
in
Neurosurgery
B
Figure 3 A, Large multilobulated internal carotid-posterior communicating artery
aneurysm extending under the free edge of the tentorium (white arrow) (16x). B Neck ot
aneurysm occluded with large Drake clip (13x). Black arrow points to proximal internal
carotid artery.
15 are recommended for a review of microsurgical techniques in
ports14’15
posterior fossa malformations.
Microvascular Reconstructive Surgery
Over the past two decades, considerable progress has been made in
surgical management of occlusive cerebrovascular disease.17 Until re-
8
Stephen
R. Freidberg
and
John W. Walsh
cently, the Joint Study of Extracranial Arterial Occlusion4 defined “inac
cessible lesions” as those occlusive or stenotic foci located in the carotid
siphon or within the cranium and those vertebrobasilar lesions situated
above the entrance of the vertebral arteries into the intervertebral canals.
In their studies,25 “inaccessiblelesions” were found in 39.3 per cent of the
patients who have had a stroke. Frequently, multiple sites of focal
atheroma are present. Before the advances in microtechnique, these in
accessible lesions could only be managed medically.
The first significant development for management of these predomi
nantly intracranial lesions was reported separately by Donaghy12 and
Yasargil et al.70 They introduced the surgical microscope into the field of
reconstructive intracranial vascular surgery and described their experi
ences with superficial temporal artery-middle cerebral artery (STA-MC A)
bypass anastomosis and with middle cerebral endarterectomy and em
bolectomy. In Yasargil’s experience, the STA-MCA bypass proved to be a
better anastomosis, providing good clinical results more frequently. Since
then, more than 250 STA-MCA bypass procedures have been performed,
and a large collaborative prospective study has been organized. 54,55 In
addition, several other bypass procedures for intracranial vascular dis
ease have been developed.62
The indications for microvascular reconstruction have been the sub
ject of considerable discussion. 7,8,37,46,62 To date, two basic groups of
stenotic or occlusive lesions have been considered. The first group in
cludes those foci that are located in the inaccessible areas. Examples of
this group are symptomatic middle cerebral artery stenosis or occlusion or
a stenotic lesion of the carotid siphon or intracranial segment of the
internal carotid artery.
Because recanafization of chronically occluded internal carotid ar
teries has not proved feasible, a second group of lesions requiring microvascular operation are present in patients with symptomatic, chronic,
extracranial internal carotid artery occlusion, either unilateral or bilater
al. The key word is symptomatic; the purpose of cerebral revasculariza
tion is to prevent development or enlargement of cerebral infarction. As is
well known, totally occluded vessels may occur in patients who have been
asymptomatic for many years, and operation on these patients may have
no protective benefit. Over the past seven years, revascularization has
provided beneficial results in patients with giant aneurysms when defini
tive clipping or trapping of the lesion would jeopardize the adjacent arte
rial circulation. 62 Similar problems are present in patients with
moyamoya disease.41
Most microsurgical bypass operations have been performed by con
structing an anastomosis between the frontal branches or the parietal
branches, or both of the superficial temporal artery and one or more
branches of the middle cerebral arteries. Occasionally, when the tem
poral artery is hypoplastic, the occipital artery is a suitable substitute.59
Arteries of at least 1 mm in diameter are required for a significant likeli
hood of long-term patency. For most of the extracranial-intracranial revascularizations, an end-to-side anastomosis, using 10-0 nylon suture
material, is constructed to minimize the risk of stenosis. The procedure is
carried out under 16 to 25x magnification (Figs. 4 and 5).
Microscopic
Technique
in
Neurosurgery
j|
Figure 4.
(16x).
Completed STA (black arrow)—cortical artery (white arrow) anastomosis
Recently, alternatives to this STA-MCA bypass appeared in the litera
ture. These procedures were first confined to laboratory animals, but, in
the past two years, several clinical experiences have been reported.
Lougheed et al.,47 Khodadad,35 and Tew62 described a bypass procedure
joining the common carotid artery to the intracranial portion of the inter
nal carotid artery, and thus a greater collateral blood supply could be
mobilized and supplied to the hemisphere at risk. Initial attempts using a
segment of saphenous vein for the bypass graft proved unsuccessful be
cause of postoperative thrombosis. Tew,62 however, reported success with
this technique. More recently, saphenous artery bypass in dogs and radial
artery bypass in humans have proved successful. Studies of long-term
patency, however, have not been reported.
Ausman2 reported revascularization of vessels in the posterior fossa.
In most instances, the occipital artery was anastomosed to the posterior
cerebral artery or the posterior inferior cerebellar artery. Postoperative
patency and disappearance of transient ischemic symptoms occurred, but
long-term follow-up is needed to establish these results. Direct internal
carotid artery-vertebral artery and mammary artery-vertebral artery
bypass procedures in laboratory animals have also been reported. 51
Data on long-term patency and clinical improvement are available for
STA-MCA bypass anastomosis. Reichman et al.54-55 stated that approxi
mately 250 operations have been reported worldwide; they reviewed re
sults in 70 patients who had follow-up studies for a maximum of 27
months (average, 10 months). In their series, 80 per cent clinical im
provement was found in patients presenting with transient ischemic at
tacks and 90 per cent patency rate of the anastomosis. In patients with
10
Stephen
R. Freidberg
and
John W. Walsh
Figure 5. Superficial temporal-cortical
anastomosis. A, Preoperative retgrograde
right brachial angiogram showing total
occlusion of internal carotid artery at bi
furcation. B, Right carotid angiogram four
months after operation showing wide
spread arterial filling of cortical arteries
through STA-MCA anastomosis. C, Late
arterial-capillary phase showing extensive
right cerebral revascularization including
major middle cerebral artery and intra
cranial internal carotid artery.
progressive and completed strokes, the clinical improvement rate drop
ped to 62 per cent; however, that improvement in similar untreated pa
tients is reported as 30 per cent. Comparable results have been reported by
other neurosurgeons. These findings are encouraging and should be
evaluated by a prospective collaborative study.
SPINE
Because of the very limited space available in the spine and the
extreme fragility of the compromised spinal cord, great care must be used
in removing tumors of the spine.53 Microtechnique is useful for small,
Microscopic
Technique
in
Neurosurgery
11
laterally placed, extra-axial tumors (for example, meningioma or
neurofibroma), or for well-encapsulated tumors of the cauda equina, such
as ependymoma. Microtechnique is mandatory, however, for extra-axial
tumors that are more ventral or that seriously displace or adhere to the
cord or cauda equina, such as pseudomucinous ependymoma. Removal of
intramedullary tumors, such as ependymoma or astrocytoma, is ex
tremely difficult without microtechnique. After dorsal myelotomy is per
formed, a tissue plane can be found, and the tumor can be separated
carefully from the cord after its bulk is reduced.
Arteriovenous malformations of the cord are extremely difficult to
excise without a microscope.27’42,69 Despite their formidable appearance,
they can be removed successfully by carefully coagulating and cutting the
attachment to the cord vessel by vessel. The dissection can be performed
in a basically gliotic plane. Two of our patients with midcervical lesions
(one with arteriovenous malformation and one with ependymoma) had
excellent preservations of long tracts with good motor and sensory func
tion in their legs but had central gray matter dysfunction which has
persisted. The patient with arteriovenous malformation had only sensory
disturbance while the patient with the tumor had motor and sensory
disturbance in both arms.
We have performed few lumbar disk operations with the microscope
and have not found it more useful than the loupe and the head light. Our
standard approach to cervical disk disease is the posterior approach.
However, in the few patients in whom a cervical root has been approached
anteriorly for both disk and tumor problems, the microscope has been very
useful in helping to define the limits of the root.20 We have not performed
cordotomies by the anterior approach as described by Hardy et al.24
PERIPHERAL NERVES
Microsurgical technique has greatly improved results of peripheral
nerve surgery. 36,58 With the aid of the surgical microscope, the matching
fascicles within the nerve can be aligned carefully permitting maximal
accuracy when the nerve fibers regenerate. With 16 to 25x magnifica
tion, sutures of 7-0 to 10-0 monofilament nylon can be used to suture the
perineurium perfectly to reduce neuroma formation. This holds true not
only for the small nerves, such as digital nerves, but even on the major
nerve trunks. When neurolysis of a neuroma in continuity is indicated,
each fascicle can be dissected free individually from the surrounding scar
tissue, ensuring maximum potential for return of function.5 Neural
tumors can be resected safely, preserving the nerve fascicles (Fig. 6).
LABORATORY
The operating room is not the place to learn microsurgical techniques.
Initially, the surgeon may be clumsy, and the chance of contamination is
great. Yasargil ’s book65 is recommended for instruction in laboratory
12
Stephen
R. Freidberg
and
John W. Walsh
Figure 6. Neurofibroma of the median nerve in the upper arm during dissection. A. Micro
instruments are freeing the plane between tumor and nerve (6x). B. Tumor removed and
lying adjacent to nerve. Arrows point to nerve proximal and distal to tumor (16x).
Microscopic
Technique
in
Neurosurgery
13
techniques. A well-equipped laboratory in which dissection and suturing
on preserved material and live animals can be practiced is essential for
development of skills that can be transferred to the operating room.
REFERENCES
1. Atkinson, R. L., Becker. D. P., Martins, A. N., et al.: Acromegaly—treatment by trans
sphenoidal microsurgery. J.A.M.A., 233:1279-1283 (Sept. 22) 1975.
2. Ausman, J. T.: Brain stem revascularization. Presented at the Symposium on Micro
neurosurgery, Cincinnati, May 29-31, 1975.
3. Bakdash, H., Alksne, J. F., Rand, R. W.: Osteochondroma of the base of the skull causing
an isolated oculomotor nerve paralysis. Case report emphasizing microsurgical
techniques. J. Neurosurg., 31 -.230-233 (Aug.) 1969.
4. Blaisdell, W. F., Clauss, R. H., Galbraith, J. G., et al.: Joint study of extracranial arterial
occlusion. IV. A review of surgical considerations. J.A.M.A., 209:1889-1895 (Sept. 22)
1969.
5. Brown, B. A.: Internal neurolysis in traumatic peripheral nerve lesions in continuity. Surg.
Clin. North Am., 52:1167-1175 (Oct.) 1972.
6. Carrea, R.. and Mora, H.: Microneurosurgical intracranial radical removal of
craniopharyngiomas. In Handa, H. (ed.): Microneurosurgery. Baltimore, University
Park Press, 1975, pp. 161-172.
7. Chater, N., Mani, J. Tonnemacher, K.: Superficial temporal artery bypass in occlusive
cerebral vascular disease. Calif. Med., 119:9-13 (Aug.) 1973.
8. Chater, N., Spetzler, R., Mani, J.: The spectrum of cerebrovascular occlusive disease
suitable for microvascular bypass surgery. Angiology, 26:235-251 (March) 1975.
9. Crowell, R., and Yasargil, M. G.: Arteriovenous malformations of the posterior fossa.
Presented at the Symposium on Microneurosurgery, Cincinatti, May 29-31, 1975.
10. Cushing, H.: Instruction in operative medicine: with the description of a course given in
the Hunterian Laboratory of Experimental Medicine. Yale Medical Journal ,12:855-879,
1905-1906.
11. Dandy, W. E.: The treatment of trigeminal neuralgia by the cerebellar route. Ann. Surg.,
96:787-795 (Oct.) 1932.
12. Donaghy, R. M. P.: Patch and by-pass in microangeional surgery. In Donaghy, R. M. P.,
Yasargil, M. G. (eds.): Micro-Vascular Surgery. St. Louis, C. V. Mosby Co., 1967, pp.
75-86.
13. Donaghy, R. M. P.. Yasargil, M. G. (eds.): Micro-Vascular Surgery. St. Louis, C. V. Mosby
Co., 1967, 171 pp.
14. Drake, C. G.: Surgical removal of arteriovenous malformations from the brain stem and
cerebellopontine angle. J. Neurosurg., 43:661-670 (Dec.) 1975.
15. Drake, C. G.: Surgical removal of arteriovenous malformations of the brainstem: A report
of three cases. In Handa, H. (ed.): Microneurosurgery. Baltimore, University Park Press,
1975, pp. 21-25.
16. Fager, C. A., Poppen, J. L., Takaoka, Y.: Indications for and results of surgical treatment of
pituitary tumors by the intracranial approach. In Kohler, P. O., Ross, G. T. (eds.):
Diagnosis and Treatment of Pituitary Tumors. New York, American Elsevier Publishing
Co., 1973, pp. 146-155.
17. Fields, W. S., Maslenikov, V., Meyer, J. S., et al.: Joint study of extracranial arterial
occlusion. V. Progress report of prognosis following surgery or nonsurgical treatment for
transient cerebral attacks and cervical carotid artery lesions. J.A.M.A., 211:1993-2003
(March 23) 1970.
18. Fisch, U. P.: Oto-neurosurgical operations: trans-temporal extralabyrinthine operations
on the internal auditory canal, the eighth and the seventh cranial nerves. In Yasargil, M.
G. (ed.): Microsurgery Applied to Neurosurgery. Stuttgart, Georg Thieme Verlag, 1969,
pp. 195-210.
19. Guiot, G.: Transsphenoidal approach in surgical treatment of pituitary adenomas: general
principles and indications in non-functioning adenomas. In Kohler, P. O., Ross, G. T.
(eds.): Diagnosis and Treatment of Pituitary Tumors. New York, American Elsevier
Publishing Co., 1973, pp. 159-178.
20. Hankinson, H. L., Wilson, C. B.: Use of the operating microscope in anterior cervical
discectomy without fusion. J. Neurosurg., 43:452-456 (Oct.) 1975.
21. Hardy, J.: Transsphenoidal hypophysectomy. J. Neurosurg., 34:582-594 (April) 1971.
22. Hardy, J.: Transsphenoidal surgery of hypersecreting pituitary tumors. In Kohler, P. O.,
Ross, G. T. (eds.): Diagnosis and Treatment of Pituitary Tumors. New York, American
Elsevier Publishing Co., 1973, pp. 179-194.
14
Stephen
R. Freidberg
and
John W. Walsh
23. Hardy, J.: Discussion. In Kohler, P. O., Ross, G. T. (eds.): Diagnosis and Treatment of
Pituitary Tumors. New York, American Elsevier Publishing Co., 1973, p. 198.
' 24. Hardy, J., LeClercq, T. A., Mercky, F.: Microsurgical cordotomy by the anterior approach;
technical note. J. Neurosurg., 41:640-643 (Nov.) 1974.
25. Hass, W. K., Fields, W. S., North, R. R., etal.: Joint study of extracranial arterial occlusion.
II. Arteriography, techniques, sites, and complications. J.A.M.A., 203:961-968 (March
11) 1968.
26. Hollin, S. A., Decker, R. E.: Effectiveness of microsurgery for intracranial aneurysms.
Postoperative angiographic study of 50 cases. J. Neurosurg., 39:690-693 (Dec.) 1973.
27. Houdart, R., Djindjian, R., Hurth, M., et al.: Treatment of angiomas of the spinal cord.
Surg. Neurol., 2:186-194 (May) 1974.
28. House, F., Hitselberger, W. E.: The middle fossa approach for removal of small acoustic
tumors. Acta Otolaryngol., 67:413-427 (April) 1969.
29. Jacobson, J. H., 2d, Wallman, L. J., Schumacher, G. A., et al.: Microsurgery as an aid to
middle cerebral artery endarterectomy. J. Neurosurg., 19:108-115 (Feb.) 1962.
30. Jannetta, P. J.: Arterial compression of the trigeminal nerve at the pons in patients with
trigeminal neuralgia. J. Neurosurg., 26 (Suppl.): 159-162 (Jan.) 1967.
31. Jannetta, P. J.: Paper presented at Congress of Neurological Surgeons, Atlanta, Georgia,
October 1975.
32. Jannetta, P. J.: 1. Microvascular decompression of the facial nerve in treatment of hemi
facial spasm in 30 cases. Abstract. 2. Microvascular decompression of the trigeminal
nerves in treatment of tic douloureux. Abstract.ln Handa, H. (eds.): Microneurosurgery.
Baltimore, University Park Press, 1975, p. 123.
33. Jannetta, P. J., Rand, R. W.: Vascular compression of the trigeminal nerve at the pons in
patients with trigeminal neuralgia. In Donaghy, R. M. P., Yasargil, M. G. (eds.): MicroVascular Surgery. St. Louis, C. V. Mosby Co., 1967, p. 150.
34. Jannetta, P. J., Hackett, E. R., Ruby, J. R.: Electromyographic and electromicroscopic
correlates in hemifacial spasm treated by microsurgical relief of neurovascular com
pression. Surg. Forum, 21:449-451, 1970.
35. Khodadad, G.: Extracranial-intracranial bypass grafts. J. Neurol. Neurosurg. Psychiatry,
35:522-526 (Aug.) 1972.
36. Khodadad, G.: Microsurgical techniques in repair of peripheral nerves. Surg. Clin. North
Am., 52:1157-1166 (Oct.) 1972.
37. Khodadad, G., McLaurin, R. L.: The role of microsurgery in treatment of occlusive cere
brovascular disease. Ohio State Med. J., 69:507-511 (July) 1973.
38. Kikuchi, H.: Surgical treatment of arteriovenous malformation. Abstract. In Handa, H.
(ed.): Microneurosurgery. Baltimore, University Park Press, 1975, p. 26.
39. Kondo, A., Kubo, S., Makita, ¥., et al.: Surgical treatment of infratentorial arteriovenous
malformations. Abstract. In Handa, H. (ed.): Microneurosurgery. Baltimore, University
Park Press, 1975, p. 28.
40. Koos, W. T., Bock, F. W., Salah, S.: Experiences in the microsurgery of craniopharyn- .
giomas.ln Handa, H. (ed.): Microneurosurgery. Baltimore, University Park Press, 1975,
pp. 151-160.
41. Krayenbiihl, H. A.: The Moyamoya syndrome and the neurosurgeon. Surg. Neurol.,
4:353-360 (Oct.) 1975.
42. Krayenbiihl, H. A., Yasargil, M. G., McClintock, H. G.: Treatment of spinal cord vascular
malformations by surgical excision. J. Neurosurg., 30:427-435 (April) 1969.
43. Krayenbiihl, H. A., Yasargil, M. G., Flamm, E. S., et al: Microsurgical treatment of
intracranial saccular aneurysms. J. Neurosurg.^ 37:678-686 (Dec.) 1972.
44. Kurze, T.: Microtechniques in neurological surgery. Clin. Neurosurg., 11:128-137,1964.
45. Kurze, T., Doyle, J. B., Jr.: Extradural intracranial (middle fossa) approach to the internal
auditory canal. J. Neurosurg., 19:1033-1037 (Dec.) 1962.
46. Lazar, M. L., Clark, K.: Microsurgical cerebral revascularization: concepts and practice.
Surg. Neurol., 1:355-359 (Nov.) 1973.
47. Lougheed, W. M., Marshall, B. M., Hunter, M., et al.: Common carotid to intracranial
internal carotid bypass venous graft. Technical note. J. Neurosurg., 34:114-118 (Jan.)
1971.
48. Malis, L. I.: Bipolar coagulation in microsurgery. In Donaghy, R. M. P., Yasargil, M. G.
(eds.): Micro-Vascular Surgery. St. Louis, C. V. Mosby Co;, 1967, pp. 126-130.
49. Malis, L. I.: Microsurgical treatment of acoustic neurinomas. In Handa, H. (ed.): Micro
neurosurgery. Baltimore, University Park Press, 1975, pp. 105-120.
50. Mullan, S., Naunton, R., Hekmat-Panah, J., et al.: The use of an anterior approach to
ventrally placed tumors in the foramen magnum and vertebral column. J. Neurosurg.,
24:536-543 (Feb.) 1966.
51. Osgood, C. P., Dujouny, M., Weir, V. P., et al.: Mammary vertebral microsurgical anas
tomosis. J. Surg. Res., 18:531-538 (May) 1975.
52. Rand, R. W.: Microneurosurgery. St. Louis, C. V. Mosby Co.; 1969, 224 pp.
Microscopic
Technique
in
Neurosurgery
15
53. Rand, R. W.: Microneurosurgery. St. Louis, C. V. Mosby Co., 1969, pp. 210-220.
54. Reichman, H.: Extracranial-intracranial arterial anastomosis. In Whisnant, J. P., Sandok, B. A. (eds.): Proceedings of the Ninth Princeton Conference on Cerebral Vascular
Disease. New York, Grune and Stratton, 1975, pp. 175-185.
55. Reichman, O. H., Anderson, R. E., Roberts, T. S., et al.: The treatment of intracranial
occlusive cerebrovascular disease by STA-Cortical MCA anastomosis. In Handa, H.
(ed.): Microneurosurgery. Baltimore, University Park Press, 1975, pp. 31-46.
56. Rhoton, A. L., Jr.: Microsurgery of the internal auditory meatus. Surg. Neurol., 2:311-318
(Sept.) 1974.
57. Ruby, J. R., Jannetta. P. J.: Hemifacial spasm: ultrastructural changes in the facial nerve
induced by neurdvascular compression. Surg. Neurol., 4:369-370 (Oct.) 1975.
58. Smith, J. W.: Microsurgery of peripheral nerves. Plast. Reconstr. Surg.,33:317-329(April)
1964.
59. Spetzler, R., Chater, N.: Occipital artery-middle cerebral artery anastomosis for cerebral
artery occlusive disease. Surg. Neurol., 2:235-238 (July) 1974.
60. Stein, B. M.: The infratentorial supracerebellar approach to pineal lesions. J. Neurosurg.,
35:197-202 (Aug.) 1971.
61. Stevenson, G. C., Stoney, R. J., Perkins, R. K., et al.: A transcervical transclival approach
to the ventral surface of the brain stem for removal of a clivus chordoma. J. Neurosurg.
24:544-551 (Feb.) 1966.
62. Tew, J. M., Jr.: Reconstructive intracranial vascular surgery for prevention of stroke. In
Wilkins, R. H., (ed.): Clinical Neurosurgery. Proceedings of the Congress of Neurological
Surgeons. Baltimore, Williams & Wilkins, 1975, pp. 264-280.
63. Williams, R. A., Jacobs, H. S., Kurtz, A. B., etal.: The treatment of acromegaly with special
reference-to transsphenoidal hypophysectomy. Quart. J. Med., 44:79-98 (Jan.) 1975.
64. Wilson, D. H.: Limited exposure in cerebral surgery. Technical note. J. Neurosurg.,
34:102-106 (Jan.) 1971.
65. Yasargil, M. G.: Experimental microsurgical operations in animals. In Yasargil, M. G.
(ed.): Microsurgery Applied to Neurosurgery. Stuttgart, Georg Thieme Verlag, 1969, pp.
60-81.
66. Yasargil, M. G.: Cranial nerve lesions. In Yasargil, M. G. (ed.): Microsurgery Applied to
Neurosurgery. Stuttgart, Georg Thieme Verlag, 1969. pp. 164-167.
67. Yasargil, M. G., Fox, J. L.: The microsurgical approach to acoustic neurinomas. Surg.
Neurol., 2:393-398 (Nov.) 1974.
68. Yasargil, M. G., Fox., J. L.: The microsurgical approach to intracranial aneurysms. Surg.
Neurol., 3:7-14 (Jan.) 1975.
69. Yasargil, M. G., DeLong, W. B., Guamaschelli, J. J.: Complete microsurgical excision of
cervical extramedullary and intramedullary vascular malformations. Surg. Neurol.,
4:211-224 (Aug.) 1975.
70. Yasargil, M. G., Krayenbuhl, H. A., Jacobson, J. H., 2d: Microneurosurgical arterial
reconstruction. Surgery, 67:221-233 (Jan.) 1970.
Lahey Clinic Foundation
605 Commonwealth Avenue
Boston, Massachusetts 02215
1
Printed and published by Jay W. Gildner for United States Information
Service, New Delhi, and printed at Pauls Press, New Delhi - 110028.
n
1■ 1
Newer Developments
in Pacemakers
I
Robert G. Hauser, M.D.* and Verlin W. Giuffre^'
Artificial cardiac pacemakers have been implanted in over 120,000
patients since the first unit was employed clinically in 1958. The major
ity of these patients are alive today, and long-term artificial cardiac pac
ing has been shown to improve as well as prolong the lives of individu
als with complete heart block and Stokes-Adams syncope. Moreover,
permanent cardiac pacemakers have been found to be valuable in the
management of other potentially lethal or disabling rhythm disorders,
including intermittent and second degree heart block, sick sinus syn
drome, drug related conduction abnormalities and certain supraventri
cular and ventricular arrhythmias. Accordingly, in terms of patients
treated and results achieved, the cardiac pacemaker is the only totally
implantable medical device with a self-contained energy source that is
accepted and commonly available for widespread clinical application.
Despite its notable success, the artificial cardiac pacemaker always
fails’; that is, the useful life of all pulse generators is limited by the
energy source which powers its sensing and pulse-forming circuitry.
Consequently, most patients with pacemakers have had to be readmitted
to the hospital every IV2 to 3 years for replacement of pulse generators.
Although the mortality and morbidity associated with replacement of
pulse generators is low, the discomfort and inconvenience to the patient
and the cost to the health economy are substantial. Information gathered
during a recent survey of physicians 8 and data derived from information
supplied by manufacturers of pacemakers indicate that 50 to 60 per
cent of patients are alive 5 years after the initial implantation, and 30
to 40 per cent will live 10 years or more. Hence, the major thrust in the
development of pacemakers is to produce a family of pulse generators
that will include pacemakers with a minimum useful life of 7 to 10
years and extending up to 20 or more years.
In addition to long-life energy sources, independent investigators
and the pacemaker industry have focused on: (1) reducing the weight
’’Assistant Director, Section of Cardiology, Department of Medicine, Presbyterian-St. Lukes
Hospital; Assistant Professor of Medicine, Rush Medical College; and Clinical Research
Advisor, Division of Medical Sciences and Engineering, IIT Research Institute
**Research Engineer, Division of Medical Sciences and Engineering, IIT Research Institute
Chicago, Illinois
Reprinted from The Medical Clinics of North America, March 1976.
Copyright © 1976 by W. B. Saunders Company.
2
Robert
G. Hauser
and
Verlin
W. Giuffre
and physical dimensions of pacemakers; (2) improving the pacemaker ’s
resistance to environmental electromagnetic interference (EMI) and
non-cardiac bioelectric signals; (3) devising techniques for atrial pacing
without thoracotomy; (4) application of pacing modes for the control of
supraventricular tachycardias; (5) fabrication of more durable, corro
sion-resistant, and stable pacemaker lead-electrodes; and (6) expanding
the numbers and types of non-invasively programmable pacing modali
ties.
The purposes of this article are to review the more recent trends in
prolonging the longevity of pacemakers; to describe innovations in
design, fabrication, and application; and to present a forward look into
advances in cardiac pacing which are now in phases of research and
development or early clinical vahdation.
REVIEW OF CONCEPTS
The implantable cardiac pacemaker has at least three components or
subsystems: pacemaker electronics (Fig. 1), consisting of the timing cir
cuit, which determines the pulse period, and the output circuit regulat
ing the output energy contained in the impulse stimulus; the energy
source, which is self-contained; and the lead-electrodes, which deliver
the output energy to the heart and sense intracardiac potentials. The
pulse generator consists of the pacemaker electronic circuitry and the
energy source. The pulse generator housing which encloses the pace
maker electronics and energy source may be an encapsulating medium
such as an epoxide resin, or a stainless steel or titanium metal can.
Additional circuits and design features are incorporated into spe
cific types of pacemakers. For example, demand or standby noncompeti
tive pacemakers contain a sensing circuit. The sensing circuit employs
an amplifier that responds to cardiac electrical activity and, in turn,
modifies the output frequency so that the pacemaker does not interfere
or compete with intrinsic cardiac electrical activity. The electronic cir
cuitry alone or the entire pulse generator may be hermetically sealed
under a dry helium and air mixture to maintain a totally isolated inter
nal pacemaker environment.
TIMING
CIRCUIT
>
OUTPUT
CIRCUIT
>
AMPLIFIER
Figure 1. Pacemaker electronics.
> ELECTRODES
Pacemakers
3
A number of different pacing modes are available for permanent
stimulation of the heart. The modes may be grouped into two categories:
(1) fixed-rate (asynchronous, parasystolic); and (2) noncompetitive (nonparasystolic)—ventricular-inhibited (demand), ventricular-synchronous
(standby or ventricular-triggered), and atrial-synchronous.
The completely implanted cardiac pacemaker introduced by Char
dack and Greatbatch, Zoll, and Kantrowitz between 1960 and 1962 were
fixed-rate asynchronous pacemakers that delivered impulses without
regard for the underlying cardiac rhythm. With fixed-rate asynchronous
ventricular pacing, the re-establishment of atrioventricular conduction
or the appearance of ventricular extrasystoles may result in competition
between paced beats and the intrinsic cardiac rhythm. Since the advent
of noncompetitive pacing, fixed-rate pacing is employed only when a re
turn to normal sinus rhythm is highly unlikely. The electronics of the
fixed-rate pacemaker are simple and drain less current than noncompe
titive units. Asynchronous pulse generators have been less prone to
premature failure and have exhibited greater longevity than noncompe
titive pacemakers.
The atrial-synchronous cardiac pacemaker,7 the ventricularinhibited (demand) pacemaker,5 and the ventricular-synchronous
(standby) pacemaker 2 are noncompetitive pulse generators introduced
between 1963 and 1966. Noncompetitive pacemakers were developed to
avoid competitive rhythms and the possible hazards of ventricular ec
topic beats and tachyarrhythmias.
The ventricular-inhibited (demand) pacemaker2 stimulates only
when the patient’s ventricular rate falls below the preset rate of the
pacemaker. If a rapidly rising intracardiac signal or R-wave develops a
potential difference between the pacemaker electrodes of 1 to 2 milli
volts (precise values varying between models), the sensing amplifier
alerts the blocking circuit to inhibit the pulse output circuit and resets
the timing circuit. The bifocal ventricular-inhibited (demand) pace
maker1 has been introduced for use in patients with disturbances of
sinoatrial and atrioventricular conduction and in whom it is desirable to
retain the normal sequence of atrioventricular contractions. The bifocal
ventricular-inhibited pacemaker senses ventricular depolarization and
sequentially paces the atrium and then the ventricle on demand. In the
presence of bradycardia and normal atrioventricular conduction, the
atrium is paced while the ventricular pulse output circuit is inhibited.
The bifocal system requires two bipolar lead-electrodes which are posi
tioned in the atrium and in the ventricle.
The ventricular-synchronous (standby) pacemaker2 avoids compe
titive rhythms by sensing the intrinsic intracardiac potential and triggers
the pulse output circuit to discharge a pulse stimulus which falls in the
absolute refractory period of the cardiac cycle. In the absence of sponta
neous ventricular depolarization, the ventricular-synchronous (standby)
pacemaker will discharge impulses at its preset automatic rate. The
pacemaker is designed to have a refractory period of 300 to 400 msec to
prevent rapid cardiac stimulation or firing after an early premature beat.
After each pulse stimulus, the pacemaker does not sense or emit an im-
4
Robert
G. Hauser
and
Verlin
W. Giuffre
pulse for the duration, of its refractory period. Therefore, the maximum
rate of the R-wave triggered pacemaker is }50 beats per minute. Atrialsynchronous pacing7 also requires an atrial electrode to sense the Pwave and a ventricular electrode to pace the heart after a suitable
atrioventricular delay designed in the electronic circuitry. This form of
pacing permits physiologic changes in heart rate and maintains a nor
mal sequence of atrioventricular contraction. A long refractory period
prevents rapid ventricular pacing in the presence of rapid atrial rates.
The maximum ventricular-paced rate is 125 beats per minute; if the
atrial rate exceeds this rate, 2:1 pacer block ensues. The major problem
inherent in atrial or coronary sinus pacing has been the lack of easily
positioned and stable atrial or coronary sintls lead-electrodes.
Since 60 to 70 per cent of patients with implanted cardiac pace
makers have intermittent rate or conduction disturbances? the majority
of pacemakers implanted in this country at the present time are of the
noncompetitive R-wave inhibited demand or R-wave synchronous
standby type. Although physicians have indicated interest in atrial pac
ing? the absence of suitable, commercially available endocardial leadelectrodes and the lack of adequate clinical information have restricted
the application of atrial and atrioventricular sequential pacing.
Methods of Direct Cardiac Stimulation
There are three types of direct pacing electrodes: (1) epicardial; (2)
myocardial; and (3). endocardial. The electrode is the uninsulated por
tion of a lead in contact with body tissue. Unipolar electrode systems
have an intracardiac electrode which is the stimulating or cathodal elec
trode. The anode or indifferent electrode is remote from the heart and
may be a large metal plate on the surface of the pulse generator or on
the metal casing enclosing the pacemaker electronics and battery.
Bipolar electrode systems employ two electrodes in contact with or near
responsive cardiac tissue; the distal or stimulating electrode is the
cathode. Electrodes may be shaped in the form of a hemisphere, ball,
cylinder, helical-tapered or screw-in coil. While the unipolar electrode
system is more suitable for R-wave sensing than bipolar electrode con
figurations, it is also more sensitive to external electromagnetic radia
tion interference (EMI). Hence, although unipolar systems provide the
most reliable noncompetitive mode function, especially in the presence
of small intracardiac signals, they are approximately 10 times more
likely to sense non-cardiac signals such as those arising from adjacent
skeletal muscle or from sources of EMI fields.1"
Each intracardiac electrode is connected to a lead wire which is
usually composed of steel, cobalt nickel alloys, or platinum iridium and
is most commonly shaped in the form of a helical coil. Unipolar leads
are smaller in diameter than bipolar, and the unipolar electrode configu
ration provides superior intracardiac signal detection. Moreover, unipo
lar pacemakers may be less likely to cause life-threatening ventricular
arrhythmias that have been associated with both anodal stimulation and
bipolar pacing. The actual incidence of pacemaker electrode fracture is
not known, but a 10 year retrospective examination of the fate of leadelectrodes revealed that 6.7 per cent of pacemaker leads were fractured.
5
Pacemakers
Despite improved design and metallurgical techniques, wire fracture
continues to occur at a rate of approximately 1 to 2 per cent per year.
Energy Source
The standard energy source for cardiac pacemakers has been the
Ruben-Mallory mercuric oxide-zinc certified cell. Previously the RM-1
certified cell had a useful life of IV2 to 3 years. An average of 4 to 6 such
cells (range 2 to 9) have been incorporated in various pacemaker
models. Each cell had a rated voltage output of 1.35 volts which re
mained nearly constant until the battery approached the end of its
useful life. Near depletion the cell’s voltage dropped off rapidly. Further,
internal losses caused by microshorting between the anodal and catho
dal elements lead to premature battery failure. More than 80 per cent of
pacemakers have been removed or replaced because of actual or im
pending battery failure or depletion.9 Therefore, the primary pacemaker
subsystem that has limited the operating lifetime of pulse generators is
the RM-1 zinc-mercury cell, which had been used by all the major pace
maker manufacturers until 1973 when new energy sources were re
leased for limited clinical trials.
Characteristics of Pacemaker Output
The pacemaker’s electrical output stimulus must be sufficient to
depolarize the ventricles or atria. The minimum energy contained in the
output stimulus should be twice that of the chronic cardiac excitation
threshold. Since the acute post-implantation increase in the threshold of
stimulation may be 3 or 4 times the value obtained at the time of
implantation, fixed output pulse generators must be designed to de
liver impulses whose amplitudes are approximately fourfold that re
quired for long-term pacing. After 1 to 2 months, the early rise in the
threshold of stimulation decreases and plateaus at a constant level about
twice that at implantation.
The amount of energy contained in the pacemaker pulse is deter
mined by the current and voltage output, the physiologic load, and the
duration of the pulse stimulus. Since the required stimulation threshold
current may increase fourfold during the first month after implant, the
minimum acceptable threshold current at the time of implantation must
be no more than 25 per cent of the implanted pacemaker ’s available
stimulus pulse current. Generally, the current thresholds should not
exceed 1.5 milliamperes at the time of implantation. Because the
strength of the impulse is related not only to its current and voltage
characteristics but also to pulse duration, the threshold of stimulation
should be determined using an exemal pacemaker whose output pulse
characteristics match those of the implanted pulse generators.
INCREASING PACEMAKER LONGEVITY
Two fundamental approaches have been taken to prolong pace
maker life. The first is conserving the amount of energy drained from
the battery by the use of small surface area electrodes, the use of adjust-
Robert
6
G. Hauser
and
Verlin
W. Giuffre
able variable output pulse generators (voltage, current, and pulse dura
tion), the development of low-current drain electronic components, and
the maximization of useful pulse generator life by replacement of the
unit immediately prior to battery exhaustion rather than at the average
time of failure recommended by the manufacturer.
The second approach is the development of longer life batteries
capable of powering existing and future pulse generator models for 7 to
20 years. Some of these longer life batteries include: improved mercury
cell, rechargeable nickel-cadmium battery, radioisotope cell, and solid
state lithium battery.
The current trend in manufacturing is to incorporate both ap
proaches into the designs of pacemaker models which will be intro
duced commercially in 1975 and 1976.-It is important to examine both
approaches and to differentiate accomplished fact from overly optimis
tic projections of pacemaker longevity.
Energy Conservation
The proponents of energy conservation for the prolongation of pace
maker life using existing mercury batteries have focused on measures
which tailor energy expenditures to myocardial requirements and on
design and technological advances which minimize losses caused by ex
cessive drain of current by the pacemaker electronics. All pacemakers
contain circuitry for generating the stimulating pulses at a controlled in
tensity and rate. A low power dissipation by the electronic circuitry is
required for chemical battery-operated devices in order to extend the fi
nite life of the battery to the greatest extent possible. For implantable
pacemakers, where the batteries are not replaceable, the stimulus
pulses should be generated at the lowest usable intensity and narrowest
pulse widths without compromising pacemaker performance.
Pacemaker Electronics
Pacemaker stimulus pulses may be voltage-limited or current
limited. Those units that control the voltage output operate in the range
of 5 to 15 volts. Where current is controlled, the stimulus pulse may
range in values up to 20 milliamperes. Early pacemaker design saw
fixed parameter pacemakers such that once the electronic circuitry was
enclosed in the pulse generator the stimulus pulse characteristics were
fixed. During the past 2 years, the programmable pacemakers have been
introduced by several manufacturers. One system, the Omnicor* series
of cardiac pacemakers, allows the physician to change the pacemaker
rate and current output non-invasively using an external programmer
which generates a pulsating magnetic field (Fig. 2) that is detected and
decoded by the implanted pacemaker (Fig. 3).
Sophisticated electronic circuits for implantable pacemakers have
become practical with the development of the integrated circuit. In
tegrated circuit technology has expanded along more than one avenue.
Accordingly, a brief discussion of the components comprising an in
tegrated circuit is appropriate for describing advances in pacemaker
electronic design and fabrication.
’Cordis Corporation, Miami, Florida
7
Pacemakers
Body
Reed Switch
* I■Pacer
Programmer
-------- ——
Magnetic Field
Figure 2. Diagrammatic representation of external programmer delivering train of
electromagnetic pulses which are detected by the pulse generator’s reed switch.
Fundamental to the electronic design of a pacemaker is a solid struc
ture of semi-conducting materials called a transistor. A semi-conducting
material conducts electrical current better than an insulator but not as
well as copper wire. Semi-conducting materials are formed from pure
elements by adding small amounts of impurities to alter their conduc
tion properties. Two classes of materials are used to form semi-conduc
tors: (1) those having an excess of electrons, called n-type material, and
(2) those having a deficiency of electrons, called p-type material. A
sandwich of these materials is made in the form of n-p-n or p-n-p. A
transistor is constructed so that one end of an n-p-n type is called an
emitter (of electrons) and the other end, a collector. The current passing
between the emitter and the collector may be made to vary by the p-type
material in the center of the sandwhich by applying a small amount of
current. The current entering or leaving the p-type material, called the
base, is substantially less than the collector current but it is able to
maintain control over the main current stream. The use of a base and
collector current identifies this type of current control device as a
bipolar transistor.
Unipolar, transistors, on the other hand, require less current for
operation because this type is voltage-controlled rather than currentcontrolled. The unipolar transistor is also referred to as a field-effect
transistor and is constructed with a single p-n junction. A belt of p-type
alloy is used to encircle a bar of n-type material. The main current
stream is solely through the n-type material. Current control is obtained
8
Detecting
circuitry
pulsations
Rate
Counter
Decoder
Pacer
output
circuit
Current
Figure 3. Programmable pulse generator decodes signal train from external programmer
and sets new pacemaker rate and/or current output.
8
Robert
G. Hauser
and
Verlin
W. Giuffre
by an electrical field present from a voltage applied to the encircling
belt. Since the unipolar transistor does not require a control current for
the main current stream, energy is conserved in the operation of the
device.
A further development in the field-effect or unipolar transistor is the
use of a controlling electrode that is insulated from the main body of the
transistor rather than forming a p-n junction. Transistor operation is
still unipolar and it is current-controlled by voltage applied to the
insulated electrode called the gate. The gate is usually composed of metal
but may also be made from polycrystalline materials. The insulated gate
transistor is usually referred to as MOS, or metal-oxide-semiconductor.
Typically, pacemaker electronics have been constructed of many
separate components, including transistors, resistors, and capacitors,
which are mounted on a printed circuit board (Fig. 4). When all these
components are fabricated on a single block of silicon, the result is called
an integrated circuit. The elements of an integrated circuit are fabri
cated in combination to provide interconnected components that are all
contained on or within a single substrate. Although an integrated circuit
contains many elements inseparably joined, its use approaches the sim
plicity of applying a single transistor.
As noted above, MOS transistors provide unipolar operation. The ex
ample cited employed a bar of n material for the main current stream.
MOS transistors are also constructed using p-type material which
requires a polarizing voltage of the opposite polarity. The p-type is com
plementary to the n-type. Hence, when both types are combined in a
single integrated circuit, the result is called a complementary MOS or
CMOS integrated circuit. The advantages of CMOS integrated circuits
include: very low power dissipation, circuit performance insensitive to
wide variations in voltage supply, and excellent noise immunity. When
CMOS transistors are used for digital pacemaker electronics, very low
power dissipation is achieved since the circuit does not contain any
direct paths from one side of the battery supply to the other. The circuit
dissipation is the lowest of any integrated circuit technology.
One disadvantage of any device in a small package is the lack of
control over some parameters that may be necessary for certain applica
tions. For example, it is difficult to make large inductances and capaci
tances in a small volume. When such components are contained within
the same housing as the integrated circuit chip and connected by lead
wires, the total configuration is termed a hybrid integrated circuit (Fig.
5). The term “hybrid integrated circuit” is actually more general and
may be extended to include combinations of two or more integrated cir
cuit types or discrete elements combined with an integrated circuit in
one housing. Hybrid integrated circuits are used for many purposes.
Special functioning circuits are easily constructed by using commonly
available integrated circuit chips of proven performance along with
discrete components that optimize or fine tune the overall performance.
In pacemakers, two integrated circuit types may be combined for the
sensing circuit and for the output pulse generating circuit with the final
composite circuit being termed a hybrid integrated circuit.
Pa CEM/XKERS
o
*’2’
■
-I
Figure 4 Pulse generators with printed circuit electronics (right) and integiated cir
cuits enclosed in a sealed metal case. Though smaller in size, the integrated circuits perform
programmable functions while the printed circuit performs conventional R-wave synchron
ous function at one rate and one output pulse current.
i 3$ ’
1
I> r*
o
O’
I
r.
©
ip
Figure 5.
Hybrid pacemaker circuit containing numerous integrated circuits.
10
Robert
G. Hauser
and
Verlin
W. Giuffre
The trend in pacemaker integrated circuits is towards CMOS in
tegrated circuits. They may be smaller with greater component density
because, with low power CMOS, negligible heat is generated. CMOS
circuits are also less dependent on battery voltage than those using
bipolar transistors.Consequently, as the battery voltage declines, circuit
operation is unaffected and pacemaker performance is maintained. This
characteristic is particularly important for pacemaker circuits whose
sensing function requires a high degree of discrimination and when
complex single or multiple output circuits are required for sequential
pacing. Such circuits are especially important for programmable pace
makers and for future pacemaker models which may be capable of per
forming complex functions.
The transition of pacemaker electronic circuitry from discrete com
ponents to integrated circuits will not only decrease the current drain
from the energy source but it will also improve reliability and reduce the
overall size of the pacemaker. The advantages gained by the use of in
tegrated circuits include the following: the number of connections be
tween dissimilar materials can be reduced; internal chemical reactions
that may occur when individual components are connected can be
eliminated; components within a circuit will exhibit similar changes in
characteristics because of their close proximity; redundancy of circuits
may be employed to increase the reliability without compromising per
formance or increasing costs.
Some of the factors which unfavorably affect reliability of inte
grated circuits include the following: the possibility of flaws during fab
rication is increased because of the small size of the component; a fail
ure in one part of an integrated circuit affects another part which can
lead to catastrophic failure; the skill required to manufacture integrated
circuits is substantial and rigid quality control measures are required.
Hybrid electronics circuitry must be protected from the intrusion of
body fluid, and so they are commonly sealed in a metal enclosure (Fig.
4). The quality of the seal is extremely important since entry of fluid
may lead to short circuits and catastrophic failure of either the sensing
or output circuits or both. For this reason, it is important for the
physician to examine closely the qualifications of a pacemaker manufac
turer before.he decides to use new models clinically. A hospital which
implants cardiac pacemakers should be staffed with physicians and
biomedical engineers or other qualified individuals who are familiar
with the engineering aspects of cardiac pacemakers. Unless this exper
tise is available and used, hospitals should not implant a new pacemaker
model until it has been proven both efficacious and reliable elsewhere.
It is difficult to estimate the number and degree of environmental
hazards that may affect the operation of pacemakers, but electromagne
tic interference with normal operation has received a great deal of pub
licity in previous years. Accordingly, pacemaker manufacturers and
researchers at private institutions have performed extensive studies to
identify potential sources of electromagnetic interference which may
pose a hazard to the patient. Improved shielding and filtering tech
niques have been incorporated into late-model pacemakers to reduce the
probabflity of malfunction from electromagnetic radiation.
Pacemakers
ir
Future trends in pacemaker design will include continued minia
turization of the electronic circuit which will contribute to further
decreases in the size of the pulse generator. Newer integrated circuits
will feature less power consumption with more complex function so that
the battery energy requirements will be used almost totally for stimulus
pulse energy. Pacemakers that are more nearly tailored to each patient’s
requirements will become the rule rather than the exception. Pace
makers capable of autoprogramming will usher in a new era of pace
maker applications. One example is a pacemaker that will track ectopic
ventricular beats and which will then automatically increase its rate to
achieve overdrive suppression of the irritable myocardial foci. Paroxys
mal supraventricular tachycardias likewise will be terminated by an
atrial pacemaker that senses and correctly identifies the tachyarrhyth
mia and which then delivers a sequence of rapid stimuli to the atrium to
terminate the episode. An implantable atrial pulse generator which is
patient-activated has already been shown to be effective in a limited
clinical trial. The pulse generator in the future may also be capable of
tracking the threshold of stimulation so that its impulse amplitide will
be automatically increased or decreased according to minimum energy
requirements needed to pace the heart. Eventually, we will have a uni
versal pacemaker whose function, as well as pacemaker parameters,
will be programmable. Other typical developments may include remote
programming. It is now commonplace to monitor pacemaker patients
remotely by means of a telephone follow-up surveillance system. It is
not unreasonable that the transtelephone mode will permit physicians to
optimally reprogram implanted pacemakers by the same means.
Longer-Lived Energy Sources
A wide variety of chemical, biologic, and nuclear energy sources
have been explored to power cardiac pacemakers. The standard mercury
certified cell described earlier was improved in 1973 and, based on in
vitro tests under simulated physiologic conditions, the manufacturer
stated that the “new and improved” Mallory battery plus recent design
changes in pacemaker electronics can result in an expected 5 year bat
tery operating life. The General Electric Corporation introduced its mer
curic oxide-zinc battery which it believes will last 5 years. This battery,
which is designed exclusively to power implantable pacemakers, con
tains the same electrochemical system, but has multiple barriers sur
rounding the anode, and a sturdy case and vent to exhaust hydrogen gas
generated by the battery during its lifetime. The size of the new RM-1
cell and the General Electric battery pair precludes significant reduc
tions in pulse generator size.
Although the first pacemaker implanted in a human patient was a
rechargeable nickel-cadmium battery powered pulse generator, prob
lems with this type of power source at body temperature precluded prac
tical application of the rechargeable concept until the Johns Hopkins
rechargeable pacemaker6 was introduced in 1973. The pulse generator is
powered by a modified nickel-cadmium cell which is hermetically sealed
^Mallory and Co., Inc., Tarrytown, New York
12
Robert
EXTERNAL
CHARGER
6^
li
I
G. Hauser
and
Verlin
W. Giuffre
OUTER HERMETIC SHIELD
INNER HERMETIC SHIELD AND ELECTROMAGNETIC SHIELD ~]
INTERFERENCE
DISCRIMINATION
AND REFRACTORY
PERIOD
TELEMETRY
CIRCUIT
J
R-WAVE
AMP
I
I
INHIBIT
POWER
SOURCE
REED
SWITCH
DISABLE
PULSE
TIMING
CIRCUIT
CONSTANT
VOLTAGE
OUTPUT AND
DEFIB.
PROTECTION
. I
•I
I
I
I
J
Figure 6. Diagram Pacesetter rechargeable pacemaker and recharger.
in a metal case. When fully charged, the battery has an initial output
voltage of 1.45 volts, which is stepped up by the electronic circuitry.
Because of the size of the nickel-cadmium battery, the pulse generator
has a low profile and weighs less than pulse generators powered by con
ventional mercury or lithium cells. The power cell is recharged (Fig. 6)
by the patient weekly for one hour by placing a small charger head over the
pacemaker; although the recharging console is line-operated, power cell
recharging is accomplished by an alternating magnetic field and, thus,
no current path exists between the recharging console and the patient.
In our limited experience, the recharging process is both simple and
safe. Reluctance of physicians to use a pacemaker which requires that
the patient comply with a recharging schedule is a valid consideration;
however, charging a pacemaker once a week requires less from the pa
tient in terms of compliance with a management program than many
common medication schedules. Resistance to the recharging concept
would diminish if recharging were required every 6 to 12 months. How
ever, if the rechargeable pacemaker has a longevity of 10 years, a pa
tient will spend less time recharging —at home for 1 hour weekly—than
he or she would spend in the hospital undergoing 2 or 3 pulse generator
replacements. Between 1973 and 1975, more than 1000 patients received
Pacesetter* rechargeable pacemakers. As of April, 1975, one pacemaker
has been removed because of failure of an electronic component and
there have been no power cell failures. However, the long-term fate of
implanted rechargeable batteries can only be determined by real time
testing, and the 10 year life fully guaranteed by the manufacturer is
based largely on the results of accelerated in vitro studies.
The solid-state lithium battery is a chemical power source composed
of solid, inert materials. The problems encountered with the mercury
battery (mercury migration, zinc migration, gas evolution, and weld cor
rosion) occur because of its inherently corrosive liquid electrolyte sys
tem. The solid-state lithium cell employs ionizable crystals that conduct
Pacesetter Systems, Inc., Sylmar, California
Pacemakers
13
charges through an inert solid structure. Although a number of lithium
batteries are produced by several manufacturers in this country, only
the lithium iodide* cell has accumulated significant clinical implant
time. The model 702E lithium iodide cell4 has two anodes, which are
lithium metal, and a single cathode, which is a proprietary iodide. The
cell generates electricity by migrating lithium ions through the salt. Ele
mental iodide is stripped from the cathode via the absorption of an elec
tron. The positive lithium ion migrates through the salt and combines
with an iodine ion at the cathode-electrolyte interface. Open circuit volt
age of the battery is 2.8 volts and the rated current is 30 microamperes.
As lithium iodide accumulates, the internal impedance of the battery
increases, and useful battery life is determined by the rate and magni
tude of the rise of the cell’s internal impedance. Based on accelerated
tests at body temperature, the projected life of a lithium iodide battery
of this design is approximately 13 years. However, recent evidence
suggests that accelerated in vitro testing using highly resistive loads
and temperatures may not provide accurate estimates of longevity. Since
the lithium battery does not evolve gas, it may be enclosed in an herme
tically sealed metal case. This isolates the battery from the potentially
adverse effects of fluids and prevents cross-contamination between the
pacemaker electronics and the power source. By the spring of 1975, over
4,000 CPI pulse generators,** using the model 702E lithium iodide cell,
had been implanted clinically up to 30 months with no reported battery
failures. During 1975, a number of manufacturers plan to introduce a
lithium-powered pulse generator for clinical validation and trial.
Interest in radioisotope-fueled batteries has led to the development
of a number of nuclear-to-electric conversion techniques in this country
and in Europe. Of the numerous types of thermal and non-thermal con
vertors which have been investigated, only the thermoelectric and the
betavoltaic types are available commercially and have been employed
clinically. Betavoltaic cells utilize a beta particle emitter such as pro
methium-147 whose half-life is 2.6 years; the beta particles emitted by
promethium-147 Strike a stack of p-n junctions in a semiconductor to
obtain an electrical output. Promethium-147 is inexpensive but betavol
taic convertors do not appear to have the potential to power an im
planted pacemaker for more than 5 to 7 years. Thermoelectric conver
tors use piutonium-238 whose half-life is 89 years. The thermoelectric
batteries operate by maintaining a temperature differential across the
series-connected thermocouples to develop a voltage via the Seebeck ef
fect. In order to reduce the number of thermocouples required, most
thermoelectric systems have a low voltage output which is subsequently
stepped up by a DC-to-DC convertor to provide the required input volt
age to the pacemaker electronics. In order to reduce thermal losses, ade
quate battery insulation is essential. Effective insulation reduces ther
mal losses and minimizes fuel requirements and radiation exposure.
Wilson Greatbach, Ltd.. Clarence, New York
'Cardiac Pacemakers, Inc., St. Paul, Minnesota
14
Robert
G. Hauser
and
Verlin
W. Giuffre
The Atomcell* is the most efficient of the thermoelectric convertors
requiring less fuel-loading than any other thermal conversion system.
Because no gas is involved, the power supply and electronics may be
hermetically sealed in a metal enclosure to avoid fluid permeation. In
this country, three manufacturers have employed nuclear power
sources for implanted pacemakers since 1972. Several other manufac
turers in the United States have scheduled initial clinical trials for 1975.
The Medtronic** Series 9000 pacemaker uses a Laurens-Alcatel battery
and was implanted in 272 patients between July, 1972, and October,
1974; there has been one pulse generator failure which was not related
to the power source. The same model pacemaker has been implanted in
642 patients in Europe; of these, only one pulse generator malfunc
tioned due to a random failure of an electronic component. Accordingly,
as of late 1974, the Medtronic Model 9000 has accumulated 4488 effec
tive device-months with a random failure rate of 0.04 per cent per
month. Therefore, based on available information, the Model 9000 pulse
generator is the most reliable pacemaker yet to be introduced for clinical
application.
Pacemakers powered by plutonium-238 radioisotope batteries
should last 20 or more years. Although the initial cost is high, the sav
ings in terms of pulse generator replacement based on currently avail
able units would be substantial if a patient could undergo one procedure
and receive one pacemaker during his/her lifetime. The problems as
sociated with the use of radioactive fuels are well-known but not com
pletely elucidated in terms of risks versus benefits to the user and poten
tial radiation dose hazards to non-users. Currently, the United States
Atomic Energy Commission licenses manufacturers to implant a fixed
number of nuclear pacemakers per month. It is anticipated that nuclearpowered pacemakers will continue to be available on a limited basis dur
ing the foreseeable future.
One of the major advantages of longer life batteries as compared to
the mercury cell is the improvement in reliability that may be achieved.
The failure rate of a cardiac pacemaker, or any other device, tends to be
highest in the first few months after manufacture and toward the erid of
its useful life (Fig. 7). If a group of 1000 pacemakers of the same model
were tested in a laboratory for 2 months, the early or infant mortality
may be 2 to 3 per cent or 20 to 30 units. After two months, the random
failure rate declines and remains stable at 0.15 per cent until it rises
near the end-of-useful pacemaker life. Because of the relatively short
life of the mercury cell, pacemaker manufacturers have been restricted
in the time available for testing units prior to shipment. Consequently, a
number of early or infant failures occurred following implantation. The
introduction of longer life power sources will permit manufacturers to
conduct real-time quality control procedures to eliminate the relatively
high incidence of random failures encountered with mercury battery
pulse generators.
Nuclear Battery Corporation, Columbia, Maryland
' ■'Medtronic, Inc., Minneapolis, Minnesota
Pacemakers
z
H
Z
o
s
15
INFANT
MORTALITY
C
0. NORMAL
SERVICE
WEAROUT
PERIOD
LIFE
UJ
I-
<
(T
I
cr
UJ
D
-J
£
RELIABILITY
OBJECTIVE
MONTHS SERVICE
Figure 7. Typical bathtub-shaped random failure curve.
CONCLUSIONS
Advances in cardiac pacemaker engineering and technology have
led to the introduction of smaller pulse generators which promise to be
more reliable and longer lived. As yet, none of the longer lived energy
sources, including the improved mercury cells, rechargeable nickel-cadmium cell, and the lithium and radioisotope fueled power sources have
been shown to operate reliably in the clinical setting for 5 or more years.
Only real time testing and clinical experience with new energy sources
will provide the information required to substantiate analytical esti
mates of useful battery life. Radioisotope batteries, by virtue of the
problems known and yet to be clearly defined, should be used only in the
absence of a comparable non-nuclear power source.
The application of integrated circuit technologies has assisted in the
reduction of pulse generator size and current drawn from the battery.
The advances in engineering design and technology offer the means to
develop new pacing functions and operating modalities. However, basic
medical research is needed to identify the problems and possible solu
tions and to define the requirements, in engineering terms, before the
new technologies can be fully utilized to treat complex rhythm dis
turbances and to develop devices that may be employed to prevent
sudden cardiac death in high risk patient populations.
REFERENCES
1. Fields, J., Berkovits, B. V., and Matloff, J. M.: Surgical experience with temporary and
permanent A-V sequential demand pacing. J. Thorac. Cardiovasc. Surg., 66:865-877,
1973.
2. Furman, S., and Escher, D. J. W.: Ventricular synchronous and demand pacing. Amer
Heart J., 76:445, 1968.
3. Greatbatch, W., and Bustard, T.: A Pu238O2 nuclear power source for implantable cardiac
pacemakers. IEEE Trans. Biomed. Eng., 20:332-340, 1973.
4. Greatbatch, W., Lee, J. H., Mathias, W., et al: The solid-state lithium battery: A new
improved chemical power source for implantable cardiac pacemakers. IEEE Trans.
Biomed. Eng., 18:317-324, 1971.
16
Robert
G. Hauser
and
Verlin
W. Giuffre
5 Lemberg, L., Castelanos, A., and Berkovits, B. V.: Pacemaking on demand in A-V block.
J. A.M.A., 191:12, 1965.
6. Lewis, K. B., Love, J. W., Humphries, O., et al.: Current status of the Hopkins recharge
able cardiac pacemaker. (Abstract.) Circulation, 49 and 50(Suppl. III):III-95, 1974.
7. Nathan, D. A., Center, S., Wu, C. Y., et al.: An implantable synchronous pacemaker for
long-term correction of complete heart block. Circulation, 27:682, 1963.
8. Parsonnet, V. A.: Survey of cardiac pacing in the United States and Canada. In Cardiac
Pacing, Proceedings of the Fourth International Symposium on Cardiac Pacing (Thalen, H. J., ed.). The Netherlands: Van Gorcum and Comp. B. V., Assen, 1973, pp. 41-48.
9. Rockland, R., Parsonnet, V., and Myers, G. H.: Failure modes of American pacemakers:
In vitro analysis. Amer. Heart J.-, 83:481, 1972.
10. Walter, W. H., Mitchell, J. C., Rustan, P. L., et al.: Cardiac pulse generators and elec
tromagnetic interference. J.A.M.A., 224:1628-1631, 1973.
General Reading
Furman, S., and Escher, D.: Principles and Techniques of Cardiac Pacing. New York, Harper
and Row, 1970.
Samet, P., ed.: Cardiac Pacing. New York, Grune and Stratton, 1973.
a
Note: A more extensive bibliography on the subject will be furnished by the authors upon
request.
Rush-Presbyterian-St. Luke’s Medical Center
1753 West Congress Parkway
Chicago, Illinois 60612
*
Printed and published by Jay W. Gildner for United States Information
Service, New Delhi, and printed at Pauls Press, New Delhi - 110028.
np • ;3Transfer Factor
A Potential Agent for Cancer Therapy
Albert F. LoBuglio, M.D.* and James A. Neidhart, M.D.**
More than 20 years ago, Lawrence reported that injections of leuko
cytelysates from donors immune to tuberculin and streptococcal antigens
could transfer delayed hypersensitivity reactions to nonimmune recip
ients.14 Lawrence selected the term “transfer factor” to describe this
biologic activity and demonstrated that it represented a material of small
molecular weight since the activity of the lysates was dialysable.16 Since
then, numerous reports have confirmed and extended these basic obser-,
vations, as reviewed extensively in a recent publication. 15 This review will
attempt to summarize the basic observations which make transfer factor
an exciting and interesting agent for prospective clinical application, as
well as attempt to indicate some of the deficiencies in current knowledge
which limit and frustrate adequate objective trials of clinical efficacy.
BASIC CHARACTERISTICS OF TRANSFER FACTOR
The vast majority of studies regarding the characteristics of transfer
factor have involved models of bacterial or fungal delayed hypersensitiv
ity in man. These studies suggest that the biologically active component
of transfer factor has a low molecular weight since it is dialysable and has
a delayed elution on Sephadex G-25 chromatography.16,21 The activity
appears to resist digestion with enzymes capable of destroying DNA or
RNA and is stable for long periods (years) in a lyophilized state.15 Most
studies have followed the experimental design outlined in Table 1 and
support the concept that this material can transfer specific cellular im
munity from donor to recipient without evidence of transfer of humoral
I
’'‘Professor of Medicine, Division of Hematology and Oncology, Ohio State University, Colum
bus, Ohio
** Assistant Professor of Medicine, Division of Hematology and Oncology, Ohio State Universi
ty, Columbus, Ohio
This work is supported by NIH Grant L-RO1-CA-14327, Contract NO1-CB-43878 and the Stem
Fund. Dr. LoBuglio is an American Cancer Society Professor of Clinical Oncology.
Medical Clinics of North America—Vol. 60, No. 3, May 1976
Excerpt from The Medical Clinics of North America, May 1976.
Copyright © 1976 by W. B. Saunders Company.
2
Albert
F. Lo Buglio
and
James
A. Neidhart
Table 1. Design of Transfer Factor Studies in Man
Donor identification
Donation of leukocytes (phlebotomy or blood cell separator)
Leukocyte disruption (freeze thaw or sonication)
Harvest of low molecular weight components (dialysis, ultrafiltration, or chromatography)
Volume reduction (lyophilization)
Administration (intradermal, subcutaneous, or intramuscular injection)
Documentation of effects (skin tests, in vitro assays, or clinical response)
immunity. Some studies have also suggested that these preparations
have nonspecific effects on the immune system including enhanced lym
phocyte response to mitogens, 8 improved macrophage chemotaxis,5 in
creased response in mixed leukocyte culture,4 and nonspecific improve
ment in skin test reactivity unrelated to the immune reactivity of the
donor.8 Preparations of transfer factor appear to be nonimmunogenic,
lack histocompatibility antigens, and preclude contamination by
hepatitis virus.15 No doubt, the ease of transfer factor preparation, lack of
documented toxicity, and potential of initiating or reinforcing cellular
immune reactivity has led to interest in its clinical application in a variety
of disease states. However, little is known regarding the nature of the
active component of these preparations and two obvious hurdles in basic
studies of structure and mechanism of action are the lack of animal
models comparable to the experiments in man and the inability to define a
reproducible in vitro assay of transfer factor activity. Despite these limita
tions, Burnet has recently attempted to structure a molecular theory to
encompass current observations of transfer factor activity. 2
TRANSFER FACTOR IMMUNOTHERAPY
For many years, transfer factor represented an unusual and implaus
ible observation apparently unique to man with only modest investigative
interest. However, in the past decade, an increasing number of inves
tigators have directed their attention to transfer factor. The impetus to
this research was a variety of case reports indicating that administration
of transfer factor from donors immune to a specific infectious agent could
in fact increase the immune resistance to that agent in patients with
resistant or life-threatening infection.11,22,24 These individual case re
ports then led to clinical trials which suggested that transfer factor im
munotherapy was beneficial in several disorders including congenital
immune deficiency and chronic infectious states (Table 2). The largest
Table 2. Disease States Apparently Responsive to Transfer
Factor Immunotherapy
Wiskott-Aldrich syndrome8-27
Ataxia telangiectasia8
Chronic mucocutaneous candidiasis9-12
Chronic coccidiomycosis3-7
Chronic or disseminated viral infection19-22
Transfer
I
I
Factor
3
group of patients studied for the clinical effect of transfer factor are those
children suffering from chronic mucocutaneous candidiasis.91012-24
Several observations from these studies may be pertinent to the applica
tion of transfer factor to cancer patients. These children frequently have
transient benefit from chemotherapy (antibiotics) but ultimately have
relapse of their disseminated lesions. They have relatively intact humoral
immune function but usually have variable degrees of impairment of
cellular immunity including negative Candida skin tests, absence of in
vitro assays of cellular immunity to Candida, impaired lymphocyte mito
gen responses, skin test anergy, and depressed macrophage function.
Clinical response to transfer factor appears more likely to occur if total
“antigen load” (extent of infection) can be reduced by concomitant
therapy with antibiotics and other modalities of treatment. Beneficial
response, usually measured by prolongation of disease-free intervals, has
been reported in approximately half the patients and is usually accom
panied by improved skin test reactivity or in vitro assays of immunity to
Candida antigen. Therapeutic regimens have utilized variable amounts of
transfer factor usually given repeatedly over several weeks or months. It
is unclear what factors differentiate those patients responsive or resistant
to transfer factor therapy. These reports clearly represent a selected por
tion of the total experience in transfer factor immunotherapy and the real
incidence of clinical efficacy is unknown. However, the occasional
dramatic effects noted have encouraged further studies and the initiation
of transfer factor trials in neoplastic disease.
TRANSFER FACTOR THERAPY IN NEOPLASIA
Early studies indicated that patients with solid tumors were capable
of responding to transfer factor as judged by transfer of skin test reactivity
to streptococcal antigens,26 while patients with Hodgkin’s disease had
impaired response.20 This evidence of responsiveness led to trials of trans
fer factor in cancer patients. However, the unknowns of transfer factor
therapy become more formidable when attempting to interpret or design
trials of therapy in malignant diseases. Selection of appropriate donors of
transfer factor to treat a particular malignancy is difficult. Identification
of donors on the basis of in vitro evidence of immunity to a tumorassociated antigen has been used in therapy of sarcoma17-18 and melano
ma.28 Other investigators 13 have cross-immunized patients with late
stage malignancy although these donors may well have impaired im
munologic reactivity and be poor sources of transfer factor. A population
with a high probability of prior exposure to a particular tumor-associated
antigen is an alternative source as transfer factor donors. Examples of
this approach would be middle-aged women as donors of transfer factor
for treating breast cancer23 or individuals with prior infectious mononuc
leosis for treating nasopharyngeal cancer.6 “Cured” cancer patients have
not been widely used as donors because of some reluctance to submit
these individuals to any potential immunodepressive effect of leukophoresis.
As with most new approaches to treatment of malignant disease,
transfer factor has rarely been used until all other therapeutic alterna-
4
Albert
F. Lo Buglio
and
James A. Neidhart
tives have been tried and failed. Thus, most of the trials have been in
patients with advanced disease and large tumor (antigen) load. This is
likely to decrease chances for successful immunotherapy if extrapola
tions from animal models of other forms of immunotherapy are valid.
Even with these considerations, trials of transfer factor have been under
taken with some encouraging results.
Spitler,28 Krementz,13 Brandes,1 and Smith25 have reported 20 pa
tients with melanoma treated with transfer factor. Donors were selected
either by cross-immunization or positive in vitro assays to melanoma.
Seven of these patients improved clinically with regression of metastatic
lesions but all have subsequently died of tumor. Tumor-specific lympho
cyte cytotoxicity as an in vitro correlate of response was measured in one
patient and was positive following transfer factor. 28
In osteosarcoma, Levin 17 has reported the effects of transfer factor
from family members on in vitro assays of tumor immunity in 13 patients.
This study demonstrated enhanced lymphocyte cytotoxicity following
immunotherapy with transfer factor. Six patients received transfer factor
as an adjuvant to surgical resection of all existing disease and all 6 have
remained disease-free with follow-up from 9 to 26 months (mean of 16
months). Our experience with transfer factor prepared from family mem
bers by dialysis or chromatography is limited to a small number of pa
tients. Five patients with osteosarcoma have been treated with transfer
factor as an adjunct to primary surgical resection and two patients have
developed recurrent disease at 4 and 12 months, and 3 remain diseasefree at 7, 8, and 17 months. In addition, 2 patients with extensive pulmo
nary metastasis have been put into complete remission with combination
chemotherapy (adriamycin and imidazole carboxamide) and then placed
on maintenance therapy with transfer factor alone without evidence of
recurrence for 11 and 28 months. Studies are presently underway to
examine the role of combined chemotherapy and transfer factor as adjuv
ant to surgical resection in osteosarcoma.
The experience in breast cancer has been less encouraging with only
2 of 11 patients with metastatic disease reported by Smith25 and Oettgen23
showing regression of tumor. Donors of “tumor-specific transfer factor”
were either normal women or patients cross-immunized with each other’s
tumor. Even more limited information exists in renal cell carcinoma
although 2 patients reported by Spitler showed “clinical improvement”
following transfer factor.28 Goldenberg6 has reported tumor regression in
1 of 2 patients with nasopharyngeal carcinoma treated with transfer
factor prepared from donors with previous exposure to Ebstein-Barr virus.
We have seen no clinical benefit in 5 patients with multiple relapses of
acute leukemia who were put into complete remission with chemotherapy
and then treated with transfer factor prepared from family members.
These preliminary and largely anecdotal studies only suggest that
transfer factor may have a role in the immunotherapy of malignant dis
ease.
GOALS OF CURRENT AND FUTURE INVESTIGATION
There are several major problems in our basic knowledge of transfer
factor which must be solved if this approach to immunotherapy is to be
I
Transfer
5
Factor
brought to fruition. The three most readily recognized goals of transfer
factor research include: (1) information on the structure and mechanism
of action of the biologically active component, (2) development of a reli
able in vitro assay, and (3) development of an animal model system with
characteristics similar to man. In addition, there are two practical deficits
in the transfer factor literature. First, almost all reports of biologic activity
or clinical efficacy represent uncontrolled trials. A recent publication by
Walker et al.29 on the efficacy of transfer factor in the therapy of 32
children with immunodeficiency secondary to severe malnutrition should
serve as a model for future studies. If this study had been done as an
uncontrolled trial, it would have demonstrated the clinical efficacy of
transfer factor in that the majority of patients developed positive tubercu
lin skin tests and mortality rate was clearly reduced. However, the au
thors had designed a controlled double blind trial of transfer factor versus
saline placebo and the results were identical in both treatment groups.
This study emphasizes the difficulty of interpreting the results of uncon
trolled studies indicating the biologic activity of transfer factor prepara
tions or the clinical efficacy of such preparations. A second area in need of
development is that of preparative techniques for the biologically active
fraction. It is our experience that the classic dialysis preparation or
chromatographic preparation often yields transfer factor preparation's
which cannot be shown to transfer skin test reactivity despite selection of
donors with well defined, intense delayed hypersensitivity to bacterial or
fungal antigens. In fact, serial preparations from a single immune donor
have been variable in ability to transfer reactivity. These problems may
only reflect our own personal experience but they suggest that better
preparative techniques would allow better defined and structured clinical
experiments.
SUMMARY
This review has attempted to describe the characteristics of transfer
factor which make it a very attractive potential agent for immunotherapy.
Preliminary observations suggest that it may be capable of modifying
resistance to a variety of diseases including cancer but considerable prog
ress in basic knowledge regarding this agent is crucial to its successful
application in clinical disease states. Fortunately, a sizable number of
interested and dedicated investigators are exploring these difficult prob
lems and their success may lead to new approaches in immunotherapy.
REFERENCES
1. Brandes, L. J., Dalton, D., and Wiltshaw, E.: New approach to immunotherapy of
melanoma. Lancet, 2:293-295, 1971.
2. Burnet, F. M.: Transfer factor—theoretical discussion. J. Allergy Clin. Immunol.,
54:1-13, 1974.
.
3. Catanzaro, A., Spitler, N., and Moser, K. M.: Immunotherapy of coccidiomycosis. J. Clin.
Invest., 54:690-701, 1974.
4. Dupont, B., Ballow, M., Hansen, J. A., et al. : Effect of transfer factor therapy on mixed
lymphocyte culture reactivity. Proc. Nat. Acad. Sci. U.S., 71:867-871, 1974.
6
Albert
F. Lo Buglio
and
James
A. Neidhart
5. Gallin, J. I., and Kirkpatrick, C. H.: Chemotactic activity in dialysable transfer factor
Proc. Nat. Acad. Sci. U.S., 71:498-502, 1974.
6. Goldenberg, B. J., and Brandes, L. J.: Immunotherapy of nasopharyngeal carcinoma with
transfer factor from donors with previous infectious mononucleosis. Clin. Res., 20:947
1972.
7. Graybill, J. R., Silva, J., Alford, R. H., et al.: Immunologic and clinical improvement of
progressive coccidiomycosis following transfer factor. Cell. Immunol., 8:120-135,
1973.
8. Griscelli, C., Revillard, J. P., Beteul, H., et al.: Transfer factor in immunodeficiencies
Biomedicine, 18:220-227, 1973.
9. Hitzig, W. H., Fontanellaz, H. P., Muntener, U., et al.: Transfer factor. Schweiz. Med
Wochenschr., 102:1237, 1972.
10. Kirkpatrick, C. H.: Chronic mucocutaneous candidiasis: model budding in cellular im
munity. Ann. Intern. Med., 74:955-978. 1971.
11. Kirkpatrick, C. H., Chandler, J. W., and Schimke, R. N.: Chronic mucocutaneous
moniliasis with impaired delayed hypersensitivity. Clin. Exper. Immunol., 6:375-385,
12. Kirkpatrick, C. H., Rich, R. R., and Smith, T. K.: Effect of transfer factor on lymphocyte
function in anergic patients. J. Clin. Invest., 51:2948-2958, 1972.
13. Krementz, E. T., Mansell, P. N., Hornung, M. 0., et al.: Immunotherapy of malignant
disease: the use of viable sensitized lymphocytes or transfer factor prepared from
sensitized lymphocytes. Cancer, 33:394-401, 1974.
14. Lawrence, H. S.: The transfer in humans of delayed skin sensitivity to streptococcal M
substance and tuberculin with disrupted leukocytes. J. Clin. Invest., 34:219-230,1955
15. Lawrence, H. S.: Transfer factor in cellular immunity. New York, Academic Press, The
Harvey Lectures, Series 68, 1974, pp. 239-350.
16. Lawrence, H. S., Al-Askau, S., David, J., et al.: Transfer of immunologic information in
io^anS
dialysates of leukocyte lysates. Trans. Assoc. Amer. Phys., 76:84-91,
1 C7O3.
17. Levin, A. S., Byers V. S., Fudenberg, H. H., et al.: Immunologic parameters before and
^Hngxmmunotherapy with tumor specific transfer factor. J. Clin. Invest., 55:487-499,
i y 75.
18. LoBuglio, A. F., Neidhart, J. A., Hilberg, R. W„ et al.: The effect of transfer factor therapy
m ™ on tumof immunity in alveolar soft part sarcoma. Cell. Immunol., 7:159-165, 1973.
19. Mouhas. R.. Goust, J. M., Reinert, P., etal.: Facteur de transfert de I’immunite cellulaire
Nouv. Presse Med., 2:1341-1344, 1973.
20. Muftuoglou, A. U. and Balkur, S.: Passive transfer of tuberculin sensitivity to patients
with Hodgkin s disease. New Eng. J. Med., 277:126-129, 1967
21. Neidhart, J A., Schwartz, R. S., Hurtubise, P. E., et. al.: Transfer factor: isolation of a
biologically active component. Cell. Immunol., 9:319-323, 1973.
° C°? ueli’ C’ J’’ Karzan’ D; T>’ Barron, A. L., et al.: Progressive vaccinia with normal
non 3 CaSe possibly due to deficient cellular immunity. Ann. Int. Med.,
60:282—289, 1964.
23. Oettgen, H., Old, L., Farrow. J., et al.: Effects ofdialyzable transfer factor in patients with
breast cancer. Proc. Natl. Acad. Sci. U.S., 71:2319-2323, 1974.
24. Schulkind, M. L., Adler, W. H., Altemeir, W. A., et al.: Transfer factor in the treatment of a
c "T °\C?r??1C rnucocutaneous candidiasis. Cell. Immunol., 3:606-615, 1972.
5. Smith, G. Y Morse,, P. A., Deraps, G. D., et al.: Immunotherapy of patients with cancer.
Surgery, 74:59-68, 1973.
26. Solowey, A C., Rapaport F. T., and Lawrence, H. S.: Cellular studies in neoplastic
disease. In Curton, E. S., et al., eds.: Histocompatibility Testing, 1967. Copenhagen,
Ejnar Munksgaard, 1968, pp. 75-78.
27. Spitler L. E„ Levin, A. S., Stites, D. E., et al.: The Wiskott-Aldrich syndrome: results of
transfer factor therapy. J. Clin. Invest., 51:3216-3224, 1972.
28. Spitler, L. E., Wybran, J.. Fudenberg, H. H., et al.: Transfer factor therapy of malignant
melanoma. J. Clin. Invest., 51:92a, 1972.
29. Walker, A. M Garcia, R.. Pate, P., et al.: Transfer factor in the immune deficiency of
oo 0116 rnalnutrition: a controlled study with 32 cases. Cell. Immunol.,
15:372-381, 1975.
Ohio State University Hospital
410 West Tenth Avenue
Columbus, Ohio 43220
Printed and published by Jay W. Gildner for United States Information
Service, New Delhi, and printed at Pauls Press, New Delhi - 110028.
Hp
XKUS
J
I
CARE
IN
Life and death statistics, reports of diseases conquered or
still being battled tell a portion of the health care story in
America. But there is much more. How available is medical
treatment to the average U.S. citizen? How much of it can he
afford? How good is the care he receives? These are questions
that are matters of great public attention and concern in
the United States today as the traditional private enterprise
system of providing for the nation's health slowly evolves
toward a partnership among the medical profession,
the patient and the federal government.
The following pages in
clude a survey of the sig
nificant new trends in U.S.
health care, a look at how
standards are being main
tained, and separate report
on the latest progress in
medical research and t|echnology. Concluding this
section is a bibliography of
recently published books
on health care and services
in the United States.
■
Charles H. Phillips
/
/.
./■
w®-?®
lp4fe
4
1
4
A.
SssiMBr
Kim
! Ife®
Se
.
a
T
<■/
dK
'
to
■
O'
J//L_
4-W
■ .K-7-
U.S. health care industry employs 4.5 million people.
PROBLEMS
AND
PROGRESS
Across the entire spectrum of U.S.
medical services and research, a
reevaluation has been going on in
recent years from the standpoint ofthe
patient and his doctor, researcher and
his project, the person who pays the
bills and government which often
hdos him pay those bills. U.S. News
orld Report,a Washington, D.C.,
i
newsmagazine which keeps a watchful
eye on the relationship between
government and the private Citizen,
looked into these broad-ranging
subjects and filed the following report
in its June 16, 1975, issue.
Never before have so many Ameri
cans enjoyed such good health care.
Yet, never before has this country’s
medical system been in such turmoil,
or complaints so rife about the way it
provides for the health of Americans.
No industry that affects everybody
so deeply, that employs 4.5 million
people and accounts for eight percent
of the gross national product can ex
pect to escape criticism at a time
v
i all the country’s major institu
tions are under fire.
Few segments of the economy, how
ever, are under as intensive scrutiny
as are the doctors, hospitals, scien
tists, health professionals and others
who make up the medical industry.
The achievements of American
medicine are impressive.
Many diseases that once were killers
—smallpox and polio for example—
have virtually been eliminated. So
have diseases that once killed or
maimed children.
There are heartening signs of prog
ress, too, against heart ailments and
Copyright 1975 U.S. News& World Report, Inc.
many forms of cancer. Infant mortality ical system can do to levels that many
is declining steadily and, at the other health authorities believe are ur real
end of the scale, Americans are liv istic. Many people have come to nsist
ing longer.
that physicians never err—and tend to
By most standards, America’s sue when they think they do.
330,000 practicing physicians, on the
Specialization in medicine is having
whole, are a match for those anywhere other far-reaching effects. The prolif
in the world. They are trained in top eration of medical knowledge has led
flight medical schools and have access to 20 recognized medical specialties
to good hospitals. At their disposal, today—each dealing with one pyrt of
too, are drugs, surgical procedures the body or one set of disabilities.
and diagnostic devices that have rev
For doctors, specialization can offer
olutionized medical care.
greater challenges than general prac
Potent new drugs, sophisticated tice—and usually more financial reequipment and imaginative surgical wards. But specialization has cortribtechniques are saving or prolonging uted to a shortage of general prac
millions of lives or alleviating the dis titioners. Family doctors, as a result,
are harder and harder to find—and
comfort of the afflicted.
Too, more Americans than ever when they are found, long delays in
have access to quality care. Medicaid their outer waiting rooms are routine
and medicare now enable millions —and maddening.
to afford a level of treatment once
What’s more, specialization tsnds
to concentrate doctors in big medical
beyond their means.
Finest care—with problems. In centers where the most advanced
the view of Dr. C. Arden Miller, equipment—and prestige—are lopresident of the American Public cated. The result is a shortage of doc
Health Association: “The U.S. is tors in rural areas and, often, in the
capable of providing its citizens with inner city.
People are angered—and frightened
medical care unsurpassed anywhere
—at the soaring cost of medical care.
in the world. ”
But, Dr. Miller adds: “A host of There are charges that much of the
problems, inside the medical system $115,000 million now spent on health
and out, prevent all Americans from each year is squandered on unneces
getting the benefits of what we know sary hospital stays, surgery.and drugs.
Moreover, many of the advance:;s in
and what we should produce.”
It is the gap between the actual and medicine -----have their darker
seem to 1-----Ja|r
the potential that is at the heart of the side. Powerful drugs that help millions
cause adverse reactions that kill thou
turmoil in health care today....
People want the best medical care, sands of others. Sophisticated tech
administered in the way of decades nology that saves lives contributes to
ago—by a doctor’s coming to the higher costs.
home, black bag in hand. Patients are . Nor have medicare or medicaid
irritated because physicians don’t Been unmixed blessings. The demand
make house calls—even though treat for health services which these pro
ment is almost always better in office grams engendered has played a role
in driving up doctors’ and hospitals’
or hospital.
Awareness of miracle drugs and ad charges. There are also reports of
vanced technology has raised Amer many abuses—doctors and hospitals,
icans’ expectations of what the med- for example, billing the government
for services not rendered, or “ping
ponging” patients from one specialist
to another, with each getting a “cut.”
The Social Security Administration re
cently said medicare programs have
been overcharged $27 million by doc
tors, hospitals and nursing homes
in the past five years.
The turbulence in medicine today is
3
Payments for personal health care, by source of funds
• MF "
J-
.?
faPublic
*1
■
|i
< I Illi IF
|Pr
1|lr
34.2%
37.6%
21.7%
Philanthropy
Iir3.o%
and industry
2.3%
Private health 8.5%
insurance20.7%
1.5%
24.0%
58.3%
1950
t
25.6%
35.4%
«5.3%
1960
1.4%
1970
^1974
Source- "Reprirtted from the Social Security Bulletin, February 1975
Dfe-partment of Health, Education and Welfare
far more than a matter of patient ver
sus physician. Within the health field
itself there is considerable discontent
and confusion.
Growing militancy of doctors, par
ticularly young ones, shows up not
just in malpractice strikes but also
in demands by interns and residents for
shorter hours and better working con
ditions in hospitals. New York has
already seen a strike by young phy
sicians, and there are rumblings in
other cities. “Wars” on cancer and
other dread diseases ordered at White
House level and endorsed by Congress
are seen by many scientists as draining
resources for other research.
Medical schools are upset by what
they regard as conflicting demands
that they maintain high standards and
quality service, yet enroll more and
more medical students.
Then there are the questions of med
ical ethics that are the focus of grow
ing debate, questions that involve de
cisions on who shall live and who
shall die.
It is against this backdrop of tur
moil that the role of government in
health care is drawing increasing at
tention. To many, it seems inevitable
that Washington’s control of the prac
tice of medicine will tighten.
Already, the impact of government
is a large one. The health industry, in
one way or another, receives more
4
than 10 percent of the entire federal
budget. Close to one third of all
health spending comes from federal
funds—including 70 percent of all out
lays for biomedical research. 60 per
cent of the cost of educating physi
cians, 25 percent of all payments for
health services and supplies.
The fact is that health is one of
the most heavily subsidized industries
in the country. And with money
comes control.
Hooked on government aid. So
dependent on federal subsidies have
medical schools and other training
institutions become that the mere sug
gestion of a reduction in funds is cause
for alarm. Student aid to doctors-intraining these days often carries with
it a requirement that would force med
ical graduates to practice where the
government wants them to—usually
in areas short of physicians.
The government is telling doctors
and hospitals what it will pay for
given services under medicare and
medicaid programs—an indirect form
of price control. It also requires re
view of why doctors send patients
under federal programs to hospitals,
and how long they remain there. Doc
tors are under pressure to prescribe
generic drugs—rather than brand
name pharmaceuticals that are often
higher priced—to medicare and med
icaid patients.
New laws just taking effect will give
the government a large say in the con
struction and equipping of new hos
pitals and will require doctors to set
up review panels across the country
to monitor the care they give under fed
erally supported medical programs.
The Food and Drug Administration,
which is getting more power to watch
over the safety of drugs, has just
proposed new regulations wb^h
would invalidate many state laws d
allow the nation's 50,000 pharmacies
to advertise retail prices for prescrip
tion drugs.
As sweeping as controls already
are, they are bound to grow even
more stringent when a comprehensive
national health-insurance program is
enacted by Congress —an event gener
ally regarded as only a matter of time.
What worries many, including some
in favor of national health insurance,
is that the American health-care sys
tem is not yet capable of delivering the
additional care that, would be demand
ed under such a program.
It is argued that any nationwide
plan, by increasing demand for health
services, would create enormous new
inflationary pressures on medica.
s
—and that this, in turn, would lead to
public demands for even more rigid
controls on the cost of care and the
manner in which it is provided.
Dr. Charles Edwards, former assis
tant secretary of Health, Education
and Welfare, spoke for many when he
summed up the status of health care
this way:
“The health-care system is in a
process of change no less sweeping
and no less profound than that experi
enced over the past several decades in
virtually all the other advanced nations
of the world. And the federal govern
ment is the principal instrument of
that change.”
WHO IS
RESPONSIBLE?
By Jerry E. Bishop
The question of responsibility in the
medical field is one of the most
important ever asked. Who says, and
by what standards, that a doctor is
qualified, a hospital fully equipped, a
patientproperly treated? Whoever has
the responsibility also has the
authority to shape the profession.
Traditionally in America, medicine
I
been regulated by the doctors
themselves with only tangential
supervision by government. Now that
balance may he shifting somewhat, as
Jerry Bishop, senior science and
medical writer for The Wall Street
Journal, explains.
Ordinarily, Dr. James C. would have
heard his last formal lecture and taken
his last written examination as a
student when he graduated from med
ical school in Philadelphia, Pennsyl
vania, in 1971 and was licensed to
practice medicine and surgery by the
state of Pennsylvania. His physician's
license is valid for the rest of his life
and, barring some illegal or grossly
unethical act, he is legally permitted by
tl
tate of Pennsylvania to do any
thing from prescribing a tranquilizer to
transplanting a human heart.
Yet, in a Philadelphia suburb where
Dr. C. and three other physicians
minister to the medical needs of
several hundred families, the 35-yearold physician is again studying intently
for an examination. Within the next six
months, he not only will have finished
attending more than 300 hours of
lectures on new developments of
medicine, but will have submitted to
his peers sample records of his care of
patients and will have taken a rigorous
written examination to test his knowl
edge of the current treatment of a
variety of diseases.
If a special committee of physicians
then decides Dr. C. is, indeed, abreast
of new advances in medicine, he will
be certified a “family physician” by
the American Board of Family Practice
and so listed in U.S. medical direc
tories. More important, to maintain
this specialist designation. Dr. C. will
have to continue attending formal
courses and, each six years, undergo a
reexamination of his knowledge and
his treatment of patients.
For Dr. C., certification as a family
physician is strictly voluntary. The
American Board of Family Practice is a
private group organized by physicians.
It hasn't any power to stop Dr. C. from
practicing medicine even if he should
fail the examinations. Indeed, most of
Dr. C.’s patients will be unaware of
whether he's been certified or not.
Why, then, should he bother to
attend the lectures and take the exam
ination? The main reason, the young
physician explains, is that it provides
an impetus to keep up with the rapid
advances in the burgeoning U.S. bio
medical research program. Not only
does he improve his own ability to
diagnose and treat the ills of his
patients, but he remains aware of
which medical centers can provide his
patients with the most advanced treat
ment of any illnesses that are beyond
his competence.
There is another reason. An increas
ing portion of Dr. C.’s fees for treating
patients is being paid by the federal
government. Certification as a special
ist, the young doctor suggests, will be
one of the standards the federal bu
reaucracy will use to determine how
much, if at all, a physician will be paid
for treating a patient whose bills are
paid by the public treasury.
Thus, Dr. C. puts his finger on a
dramatic change taking place in the
traditionally and still largely nongov
ernment-run American system of med
ical care. As the federal government
sharply increases its relatively new
role in financing that care, particularly
the direct payment of hospital and
physician bills, it also is wielding
power to determine quality standards.
Under just two government payment programs, Medicare for the
elderly and Medicaid for the poor and
near-poor, federal spending for hospi
tal, nursing home and physician bills
has grown from nothing in 1964, when
Congress legislated the programs, to
$17,000 million in 1974. Not only are
these programs continuing to expand
rapidly, but the advent of a proposed
national health insurance program
could add anywhere from $10,000
million to $80,000 million to the federal
government's annual medical care bill.
And this doesn’t include several thou
sands of millions more being spent on
the care of war veterans, biomedical
research, mental health care3 and
scores of other federal programs in the
health field.
Along with the government s increased financial stake in medical care
are coming increasing pressures for the
government to institute controls to
prevent waste and abuse. The taxpayers' money shouldn't be used to
pay for unnecessary or substandard
care, it is argued.
The implication, of course, is clear.
Someone has to determine, almost day
by day, whether a patient's care is
necessary and of the highest quality;
whether, for instance, the surgeon is
qualified to perform the operation
and, if so, whether he’s charging the
government a reasonable fee; whether
the hospital is discharging the patient
too soon or not soon enough, and a
host of other questions relating to the
patient’s care.
Thus, the controversy swirling
around the government’s ro e in
medical care is no longer whether it
should pay for the care, but who
determines the quality of that care.
Debate over just how deeply \yashington should involve itself in setting
5
standards of medical care is being
waged in the public print, the chambers
of Congress and in the meeting halls of
the medical societies. To many, the
newly granted federal powers offer a
chance to correct deficiencies in med
ical care that have developed over the
years. The government, they argue,
could upgrade the medical care of
minorities, encourage physicians to
return to rural areas, weed out the
indolent or incompetent physician,
and speed up the time it takes a new
therapy to emerge from a research
center and go into widespread use.
But, on the other side, there are fears
that a bureaucracy will wield the new
powers with a heavy hand, that a
person sitting in an obscure office who
has never seen a patient may soon be
dictating how, where and how long a
patient should be treated.
For almost a century, the standards
of U.S. medical care have been deter
mined almost entirely by the private
sector. And most Americans would
agree that, over the decades, the medi
cal profession has been remarkably
effective in policing itself and provid
ing high quality treatment. By the early
1900s, for example, physicians were
well organized into local medical soci
eties. The societies not only set and
enforced their own strict codes of
medical ethics but forced the various
state governments to require a high
degree of education before a person
could be licensed to practice medicine.
The societies effectively drove the
incompetents, quacks and charlatans
out of medical practice. As the public
recognized the role ofthe local medical
societies in setting high standards of
medical practice, it became almost
impossible for a physician to practice
medicine without being a member of
the local society. Even today, a physi
cian will find it difficult, if not impos
sible, to have his patients admitted to a
hospital unless he is a member of the
local medical society.
6
The medical societies continue to
exert a powerful influence on the
standards of medical care. A physician
who errs in the operating room, per
forms unnecessary operations or over
charges his patients faces censure and
possible ouster by his medical society.
And with dismissal from the medical
society, he quickly loses his hospital
privileges and his patients.
A similar pattern has been followed
as increasing medical knowledge has
led physicians to specialize in certain
diseases or parts of the body. As each
new medical speciality has developed,
whether it be pediatrics or cardiology
or neurology, the medical profession
itself has set up committees called
medical specialty boards. These
boards, which now exist for 22 medical
specialities, set the strict criteria for
designation as a specialist. To be
recognized as a neurologist, for in
stance, the physician must undergo up
to four years training in brain diseases
beyond his standard medical school
education. And then, he must pass a
rigorous examination by the board of
neurology before he can be ‘ ‘certified’ ’
as a neurologist.
Hospital standards, also, have long
been in the hands of the medical
profession. Although hospitals are
licensed and inspected by various
government agencies, notably state
health departments, one of the princi
pal monitors of the quality of hospital
care is the Joint Commission on
Hospital Accreditation, organized by
four medical groups: the American
Medical Association, the American
College of Surgeons, the American
College of Physicians and the Amer
ican Hospital Association. This group
checks hospitals for everything from
fire hazards and the sterilization of
surgical instruments to the keeping of
patient records and the inspecting of
tissue removed by surgeons.
Recently, for instance, the Joint
Commission began requiring hospitals
to conduct medical “audits” of pa
tients ’ care to see if hospitalization was
necessary or if surgery was really
needed. Such audits can—and have—
uncovered doctors who were doing too
many unnecessary tonsillectomies or
undertaking surgery for ulcers before
medication had been tried. Although
hospital accreditation by the Joint
Commission isn’t required by any law,
it is widely used by the medical
profession tojudge a hospital’s quality,
And adding teeth to the Joint Commission’s powers is the decision by admin
istrators of the federal Medicare pro
gram to accept the commission’s eval
uation in deciding whether the hospital
is eligible to receive payments from the
Medicare program.
The medical profession, however, is'
coming under increasingly strong
criticism from the public. The profes
sion, it’s charged, isn’t organized well
enough to adapt to the rapid changes
taking place in medicine.
New methods of diagnosis and new
therapies are pouring out of the re
search centers at such a pace that ir *h
of what a doctor learns in mec J
school or speciality training is obso
lete within five to 10 years. Too many
physicians, it has been charged, are
failing to keep up with these new de
velopments, with the result their patients are receiving less than the best
medical care possible. One medical au
thority estimated at least five percent
ofthe nation’s 330,000 physicians have
failed to keep up with new techniques.
Moreover, the distribution of physi
cians has apparently gone askew. As
Phillip, Abelson, editor of Science
magazine, explains: “The prolifera
tion of knowledge arising from re
search has made specialization in
medicine seem necessary. Specializa
tion has had the further effec* of
s
encouraging concentration of do
in big medical centers. The result is
geographical maldistribution with rural
areas and the ghettos suffering short
ages of physicians. ”
Medical World News, a magazine
aimed at physicians, reported: “Twice
as many doctors per] capita practice in
cities as in rural areas, and four times
as many in the suburbs as in the inner
cities. Some 140 counties with a total
population of half a million people have
no doctor at all, and hundreds have
only one or two.”
Equally important, as more and
more young doctors have chosen to go
into the various medical specialities,
there has been a decline in so-called
“primary care” physicians. These are
the general practitioners, internal med
icine specialists, pediatricians and
obstetricians-gynecologists—the doc
tors most Americans go to for their
day-to-day medical problems. Where
as 40 years ago almost all the na
tion’s physicians were in primary
care, today less than 40 percent are.
As a result, the waiting rooms in
general practitioners’ offices usually
are overcrowded and the doctors
overworked. At the same time, a
surplus of surgeons exists.
'he medical organizations are at
tempting to remedy these matters. For
example, several medical schools have
established programs involving two
years of additional training for young
physicians in order to qualify them as
“family physicians,” the latest medi
cal specialty. The program includes
considerable study of behavioral sci
ences, such as psychology, as well as a
certain amount of training in each of
the major specialities, such as heart
surgery. The program has been well
received. Among the 1973 graduates of
America’s medical schools, more than
1,700 or about 20 percent elected to
take the additional training for a family
practice specialty. Furthermore, thou
sands of doctors already in private
7tice decided during 1975 to seek
Gw. (ification for this specialty from the
American Board of Family Practice,
which sets up the criteria and estab
lishes examinations. The board has
decreed that certified family physicians
must take at least 300 hours of
additional education, through lectures
and symposia, every six years and then
undergo another rigorous examination
in order to retain certification.
Meanwhile, the problem of maldis
tribution of specialists is being at
tacked. Surgical organizations, for
instance, are calling for a reduction in
the number of surgeons being trained
in an effort to encourage doctors to
move into other fields.
Throughout the 1940s, the question
of the quality of care was regarded
largely as a matter strictly between the
patient and his physician. After all, it
was reasoned, the physician was de
pendent upon the patient for his
income, and if the patient was dissatis
fied with the quality of medical care, he
could take his illnesses and his pocket
book to some other doctor.
In the postwar era, though, as the
cost of medical care began to increase,
community groups, unions and insur
ance companies began turning to
health insurance plans of various types
as a means of paying medical bills.
Basically, individuals or their em
ployers would make small, regular
payments to the plans, and the plans
would then pay the cost of hospitaliza
tion and physician care.
By 1960, a large majority of working
Americans and their families were
covered by some form of such health
care insurance. The fact that many
nonworking Americans, notably the
elderly and the poor, weren’t covered,
however, led in 1964 to Congress
enacting the Medicare and Medicaid
programs. Until then, the federal
government’s role in upgrading the
quality of medical care had been
indirect, via the public health agencies,
attacking infectious diseases through
sanitation and vaccination programs
and producing a broad range of new
techniques and discoveries throughout
the medical field.
Initially, the medical care plans,
whether federal or private, were de
signed only to protect the individual
from large and unexpected medical
bills. The plans and programs paid
physicians a “reasonable and custom
ary” fee for their services and reim
bursed hospitals for their cost in caring
for a plan patient.
But the cost of medical care soared
due to new advances in medicine, ris
ing wages of hospital workers and in
flation in general, putting the medical
care plans under severe financial
stress. In New York City, for example,
the cost of one day’s care in a hospital
has zoomed from around $90 or $100 a
decade ago to close to $250. Co^t of the
Medicare program more than doubled
between 1969 and 1974, reaching
$ 12,000 million a year. But much of the
increase was due to inflation rather
than increased benefits to the elderly.
The skyrocketing costs have
brought cries of financial anguish from
unions and corporate employers who
ate having to pay the higher premiums,
and from the Congress and federal
administrators who see a financial
threat to their promise that Medicare,
Medicaid and other federal programs
would provide the elderly and the poor
with quality medical care.
It is against this background of
demands to control the rising cost of
medical care that the government is
moving into its new role in setting the
standards and determining the quality
of medical care. Although there have
been demands to nationalize the na
tion’s medical care system, as has been
done elsewhere, the U.S. C< ngress
instead has chosen to leave thelmatter
of quality control in the hands of the
private sector. The unusual technique
being used was, in fact, spawned by
physicians themselves.
In the late 1960s, most hospitals
began setting up committees of physi
cians to review the lengths of hospital
stays. But some medical societies
began going even further. In northern
California, for instance, one physi
cians group serving union groups as
well as Medicaid patients launched the
idea of a committee of physicians
monitoring a patient’s care immediate
ly upon hospitalization and almost day
by day afterwards. If the patient’s care
deviated from that normally given for
his particular illness, the patient’s
doctor had to justify it to the committee
or risk not being paid by the patient’s
medical plan.
7
This continuing review of a patient’s
care proved unexpectedly helpful in
holding down costs. And as the Con
gress, casting about for ways to bring
the costs of the Medicare and Medicaid
programs under control, started
threatening to impose rigid federal
regulations on the care of patients
under the federal programs, the idea of
so-called “professional standards re
view organizations, ” or PSROs, began
to spread. The Congress did, in fact,
adopt the PSRO approach by declaring
that the government would pay the
hospital bills of Medicare and Medi
caid patients only if their care had
been monitored by a locally organized
PSRO. It also provided federal funds to
help establish and pay for the cost of
operating the more than 200 PSROs
being organized by the hospitals and
medical societies around the nation.
The PSROs generally are left in the
hands of the local physicians. If there
is any question about whether the
hospital admission was necessary or
whether the doctor might be keeping
the patient in the hospital longer than
necessary, the case is referred to a
committee of doctors selected by the
local physicians themselves. The
committee may decide that a certain
hospital stay was unnecessary or too
prolonged. In that case, a hospital will
not be paid for what the PSRO com
mittee considers unnecessary or substandard care.
Rather than being just a method of
controlling costs, the PSROs are rapidly becoming the arbiters of the
quality of medical care. Although, at
the moment, the PSROs deal only with
Medicare and Medicaid patients, the
advent of a federally supported na
tional health insurance program now
being discussed will undoubtedly
mean the PSROs, with the government
watching closely, eventually will be
setting standards of medical care for
almost all Americans.
■
o
„„
PUTTING
RESEARCH TO
WORK
By Charles Marwick
As a vaccine conquered polio, so one
may someday wipe out influenza,
hepatitis, even cancer. Behind these
breakthroughs will stand an army
of biomedical scientists who have
never taken seriously the word
‘1 impossible." Where U.S.
researchers are today in their quest for
solutions to age-old diseases and
disabilities is the subject of this report
by Charles Marwick, Washington,
D.C., editor for Medical World News.
Medical research in the United
States has always waged a two
pronged attack against disease and
disabilities. One is the basic, or “what
if,” approach that probes the funda
mentals; the other is the applied, or
“how to,“concept that can lead to new
applications and solutions. Both are
vital and equally important. For a
quarter of a century, since the end of
World War II, almost continuous expansion of biomedical research has
been going on and a vast body of
knowledge has been accumulated. Today in the United States, the great push
is toward incorporating it into everyday medical practice.
Among the most widely acclaimed
breakthroughs in the practical application of biomedical research, achieved
early in this period, was the development of vaccines against poliomyelitis,
measles and German measles. With
their use, a significant decline, if not
virtual disappearance of these dis
eases, has resulted. Following success
of this kind, scientists have been turn
ing to other viral diseases for which
vaccines have been either unsatisfac
tory or nonexistent. Examples are
influenza and hepatitis.
Vaccines against influenza have
long left a great deal to be desired. New
types of influenza make their appear
ance periodically and therefore require
new vaccines to combat them. But the
ones available do not offer complete
protection or often cause side-effects
almost as bad as the disease itself.
Today, this situation is changing.
Recent influenza vaccines cause fewer
untoward reactions and, indeed, can
now be used for children—an impor
tant high-risk group for whom the older
vaccines were unsuitable. In addition,
the greater purity of these new vac
cines means that they can be given in
more potent dosages.
One very new vaccine uses labora
tory-made mutations of influenza virus
that are sensitive to temperature. Such
viruses grow readily in the cooler parts
r
of the body, but die in the wa
regions. Thus, this virus will not grow
in the lungs, which are warm, and so
will not cause symptoms similar to the
natural disease. On the other hand, it
multiplies readily in the nose and
throat passages where it does the
essential job of any vaccine—the stim
ulation of protective antibodies in the
vaccinated individual. This tempera
ture-sensitive virus vaccine has been
tested in animals and a very limited
study has been done in humans.
Recent research also has thrown
new light on how influenza viruses
alter their genetic make-up and escape
vaccine protection. Studies by Dr.
Robert G. Webster and his staff at
Jude’s Research Hospital in Memphis,
Tennessee, suggest that these “i
or changeling viruses are recombina
tions of viruses formed as the result of
infection with several different varieties of influenza found in both humans
and animals.
It now appears that this is how
nature enables influenza virus to “sur
vive” and trigger the major influenza
pandemics that we know so well.
Eventually, this knowledge may make
'i
4
possible a one-time, all-purpose in
fluenza vaccine.
Three new types of vaccines have
been developed to treat the liver
disease hepatitis. Two of them were
constructed by Dr. Robert Purcell and
his group at the National Institute of
Allergy and Infectious Diseases in
Bethesda, Maryland; the third by
a U.S. pharmaceutical company. In
animal studies, the vaccines show
evidence of protection, and Dr. Mau
rice Hilleman, the investigator for the
pharmaceutical concern, says that the
vaccine is suitable for human testing.
On another front, increasing atten
tion is being devoted to developing
vaccines against bacteria. Bacteria are
much more complicated organisms
than viruses, the primary target of
most vaccines to date. The quantity of
’
terial organisms needed to im
munize an individual, even if modified
so as not to cause overt disease, would
stimulate serious side-effects. A tech
nique has been devised to use only a
part of the organism. Recently, a
vaccine against one type of meningitis
was licensed by the United States and
another vaccine that protects against a
related type of meningitis is about to be
licensed. Both use only a fraction of
the bacterium that causes the disease.
The same principle is being em
ployed in a vaccine against another
significant bacterial infection which
causes meningitis in infants and young
children. The organism causing this
disease is known as Hemophilus in
fluenzae, although it is not related to
i
'enza. Hemophilus influenzae is
tk»~ leading cause of acquired mental
retardation in the United States and
success of the new vaccine will be a
significant achievement.
A second way of immunizing young
children against meningitis caused by
Hemophilus influenzae is to use a
phenomenon known as cross-reaction.
By the age of six years or so, most
children have developed immunity to
Significant changes in
U.S. death rates from 1960 to 1973
i
41%
lit
o
s
§
Q
o
Ico 2% cn
o
=6
■E
co
o
I
HIT
2
E
JQ
s
E
2
*
70%
100%
Source: National Center for Health Statistics
disease-causing bacteria. It is now
believed that the source of this im
munity is the harmless bacteria that
normally inhabit the gastrointestinal
tract. By stimulating the growth of
these harmless bacteria early in the
lives of infants and young children,
scientists believe that the child could
be protected until he acquires his own
natural immunity.
Vaccines cannot cure all health
problems, however. A variety of new
drugs play important roles in the bat
tle. One, called chenodeoxycholic
acid, literally dissolves gallstones that
once would have needed surgery to
cure. The drug has been tested in a
controlled trial at the Mayo Clinic in
Rochester, Minnesota. In a six-month
treatment of 56 patients, more than half
had a reduction in the size of their
gallstones and in 13 the gallstones
disappeared entirely.
Another new drug, in this instance
for the better control of epileptic
seizures, has recently been licensed by
the U.S. Food and Drug Administra
tion. Called carbamazepine, it is the
first new anti-epileptic drug to be
licensed since 1960, but more impor
tant, it offers relief to those epileptics
who either do not respond to or whose
seizures can only be partially controlled by present drugs such as
diphenylhydantoin. This involves
some 40 percent of all epileptics.
Carbamazepine is not regarded as the
final answer to the control of these
hard-to-manage epileptic seizures, but
it is considered an important addition
to the agents currently in use.
Another major field for biomedical
research involves hereditary diseases.
Recent successes in unraveling the
metabolic chemistry of the cell have
enabled scientists to identify a substan
tial number of genetic diseases that
cause mental retardation and other
vital organ disfunctions that usually
lead to death. In such diseases, there is
an inherited failure to metabolite or
breakdown fatty substances. The re
sult is that when they lodge in such
organs as the kidney and liver or in the
central nervous system, mental retar
dation and organ malfunction follows
and such patients often die, for ex
ample, of kidney failure.
j---
9
Dr. Roscoe Brady of the National
Institute of Neurological Diseases and
Stroke in Bethesda, Maryland, has
managed to pinpoint the specific
defect of 10 presently known heredi
tary disorders as a missing enzyme. In
two of these, Fabry’s disease and
Gaucher’s disease. Dr. Brady and his
associates have succeeded in extract
ing from other sources, such as human
placental tissues, enough of the neces
sary enzyme involved and have given it
to the affected patient to reduce the
accumulations of the fatty substance—
lipid, as it is called. At the moment,
because there are very small amounts
of this enzyme available, he can only
temporarily reverse the accumulations
of these lipids. But the work represents
a significant advance against heredi
tary defects.
Nowhere has U.S. medical research
been more spotlighted than in the bat
tle against heart disease. An estimated
1.25 million Americans experience a
heart attack each year and more than
50 percent of them die. About half of
this number die without warning. With
this in mind, efforts have been made to
prevent heart disease by use of drugs
to reduce cholesterol, the fatty ele
ment circulating in the blood. It was
never clear, however, whether these
cholesterol-lowering drugs would ac
tually influence the incidence of heart
attacks. The final findings of a massive
10-year study of such drugs were
reported in 1975 and they turned out to
be negative. The chairman of the study
said that the results make it clear that
heart disease must be prevented essen
tially by changes in a patient’s life. He
recommends sufficient exercise and
warns against smoking as two exam
ples of the type of changes necessary.
Now experts in heart disease also
have found that, contrary to much
previous thinking, the amount of dead
tissue that results from a heart attack
is not irrevocably determined at the
time of the attack. The extent of injury
10
to the heart muscle can be substantial
ly reduced in a number of ways, even
if steps are taken several hours after
the actual attack.
Measures include the use of drugs
that slow the heartbeat, the use of
nitroglycerin which reduces the mus
cle damage and favorably alters some
of the abnormal heart rhythms, devices
that reduce the amount of oxygen
demanded by the heart and increase
the delivery of oxygen to the heart
muscle, and drugs that widen the blood
vessels and improve the flow of blood.
On another major medical battle
front, war on cancer, the search for a
cure still goes on, so far without
success. But real progress cannot be
measured by the success or failure
of such programs. Rather, progress,
when and where it occurs, is due to
careful and patient work that often
started decades ago. The pressure for
quick results has left scientists in a
difficult position. They have not been
very good at explaining the value of
basic research. In part, this is due to
the uncertainties involved. There can
never be any guarantee that a partic
ular piece of basic work will lead to
practical results. Thus, in retrospect,
support of a study which doesn’t seem
to have paid off can look as if the
scientists involved were merely living
off the public purse. The problem, of
course, is in deciding what is worth
supporting and what is not. It is not
really possible to plan this.
Indeed, in the immediate future,
medical science may be unable to
alleviate many diseases. In cancer, for
example, the problems are highly
subtle, the nature of the disease is such
that it is close to the nature of life
itself—in part, this is the fascination of
cancer research to many scientists.
Solving these problems will not be
easy, but in the field of U.S. health
care, biomedical research is consid
ered an investment in the future that
the nation must make.
■
NEW
ADVANCES IN
MEDICAL
EQUIPMENT
By Penelope Lemov
From x-ray scanners to thumbnail-size
artificial membranes, U.S. medical
technology has steadily made
progress in pointing the way to better
and better diagnostic and treatment
techniques. PenelopeLemov, a writer
for The Washingtonian magazine,
describes the major new medical
equipment now available to assist . .e
hardworking practitioner.
American medicine has, in the last 25
years, been treated with a massive
dose of technology. Where once a
physician carried with him his entire
supply of medical equipment, today he
has in his office and at the hospital a
vast array of highly sophisticated new
tools that can diagnose, treat and
oversee the care of his patients.
“Medicine has made tremendous
advances in the last century as a result
of the work of pathologists and bac
teriologists,’’ notes Dr. Victor H.
Frankel, professor of orthopedic sur
gery at Case Western Reserve Mescal
School in Cleveland, Ohio. “But
a /,
even more startling advances are being
derived from applications of elec
tronics, atomic energy, mechanics and
systems engineering.’’
This medical utilization of technol
ogy, which began in the 1950s, has
created a multimillion dollar U.S.
medical equipment industry with an
annual growth rate of 12 percent. Part
of the growth is due to the applica
tion of space-age technology, but much
of it is also due to the introduction
of more patients into the U.S. health
care system through the federally
funded Medicaid and Medicare pro
grams, which have made in-depth
medical care available in recent years
to millions of elderly and disadvantaged citizens.
The U.S. medical equipment indus
try is producing $4,400 million worth
of equipment a year, of which $525
million is exported. Over 2,000 Amer
ican plants employing about 170,000
workers turn out devices that range
from 50-cent eyedroppers to $200,000
computerized x-ray scanners.
The new equipment has its greatest
use as an aid to the physician, still the
indispensable decision maker, ena
bling him to do things that previously
were difficult, if not impossible, to do.
From the devices in the clinical/experimental stage to items widely diffused
and available to many patients, mod
ern medical equipment holds out drac promise of better medical care
i
for more people.
Described below are some typical
new devices.
were related to oxygen deprivation,
again from problems during labor that
were cord or placental in origin. We
needed a way to continuously monitor
the fetus. It was time to apply new
technology to obstetrics just as we did
in every other discipline of medicine.”
Answering that need, the fetal heart
monitor is a counting device that keeps
track of the heartbeat of the fetus and
contrasts it to the pressure within the
uterus during labor. The fetus heart
beat (an electrical impulse) is picked up
ers who over the years have statis
tically had problem deliveries: diabetic
mothers or older women giving birth
for the first time. The procedure’s
success led to the monitoring of all
expectant mothers.
The Premature Infant Respirator
Between seven and 10 percent of
babies born in the United States are
premature, and of those premature
babies, 15 to 20 percent suffer from
Heart Monitor for Unborn Babies
The fetal heart monitor is a device
that first came into use in the mid-1960s
at a few research-oriented hospitals.
Today, it is available at almost all
major U.S. hospitals that provide
obstetrical (care and treatment
of women in childbirth) services.
The monitors are used during labor
to determine whether or not the fetus
is in trouble.
“About 20 years ago,” reports Jane
O’Kieffe, research associate with the
rtment of obstetrics and gynecol
d
ogy at the George Washington Univer
sity Medical Center in Washington,
D.C., “we found that we had almost
eliminated maternal mortality during
childbirth, but we hadn’t made a dent
in the mortality/morbidity statistics for
the baby. Five out of 1,000 otherwise
normal healthy babies were being born
damaged or dead because of cord and
placental problems during childbirth.
We also suspected that learning dis
orders which surfaced in later years
Fetal heart is monitored during labor.
by an electrode attached to the baby’s hyaline membrane disease, a deadly
head in the birth canal. The electrode condition in which the lungs are too
feeds information into the monitor stiff to breathe. Hyaline membrane
while a catheter inserted into the disease was the cause of de<^th of
mother’s uterus measures uterine President John F. Kennedy’s infant
pressure and feeds this information son in 1963, but progress is finally
into the same counting device. “Uter being made in treating this condition.
Dr. Gordon Avery, head of newborn
ine pressure has a direct effect on
service
department at Children’s Hos
the placenta, and this is the time we
Medical Center in Wash
pital
National
look for cord problems, ” says Mrs.
D.C.,
works with a new tech
ington,
O'Kieffe. “By interpreting the rates
which the monitor has recorded, the nological approach in treating these
physician is able to determine the infants. “It’s sort of a foot race,” he
nature of the problem and what the says. “If, when the baby is bom, his
baby’s tolerance to labor is. Some
times it's necessary to do a caesarian
section, in which the fetus is removed
surgically from the uterus.”
At first, fetal monitors were used for
high-risk pregnancies, for those moth11
X
I * ■
Newborn's lungs are loo stiff lo breathe alone.
lungs are stiff and inefficient, he'll
probably die if he isn’t helped. But if
we can help him to breathe those first
few days, then time is on his side. His
body will start to manufacture surfac
tant (moisture), and it is the absence of
surfactant in the lungs that makes the
lungs stiff and unstable.”
There is no artificial or temporary
way to supply the infant with sur
factant. “Specifically, what we needed
to keep him going,” continues Dr.
Avery, “is enough air pressure to
keep his lungs expanded. Respirators
(machines for artificial breathing)
for adults aren’t right for these ba
12
bies.” So special respirators have
been developed.
Children’s Hospital uses a Bourne
Respirator, which delivers air by vol
ume rather than pressure and can be
set to keep up with the fast rate of
breath of a premature baby. Where
an adult breathes 20 times a minute,
the distressed premature baby may
breathe at a rate of 60 to 80 times a
minute. “The respirator can deliver
tiny volumes of air at rapid rates,” says
Dr. Avery. “It can also hold the
expiration pressure so that the lungs
can keep some oxygen in them. The
expiration pressure is like an air
splint—it holds the lungs open. But
you still haven’t won until you've got
the baby breathing on his own, and
getting him off the respirator can be
horrendous. After all, he is dependent
on the machine for air, and he’s
malnourished because he’s only been
fed with intravenous solution, and now
you’re asking him to breathe for
himself with stiff lungs.”
Weaning the baby is still technically
difficult, but some new additions to the
respirators have begun to work out the
problems. “Our respirator,” con
tinues Dr. Avery, “has intermi;
mandatory ventilation control. With it,
you can allow the baby to be connected
to the respirator but breathe for himself
all he wants. You set how much you
want the machine to do for him—all the
breathing, half the breathing, one third
and on down. By the flip of a switch,
we can progressively give the baby
more and more responsibility.
“We also have the assist-mode
control. If the baby is making an effort
to breathe for himself but the breaths
aren’t deep enough, the machine
makes the breath deeper.
“Hyaline membrane disease was
the single biggest cause of death in a
premature infant,” says Dr. Avery. “If
he can only live through the first week,
he has the potential to be normal.
recovers, his lungs will mature and
grow. With our new respirators, we are
increasing his chances of making it
through that first traumatic week.”
Elongating Catheters
Adults who develop hydrocephalus
(water on the brain) are curable: a
catheter or long slim tube is implanted
surgically to carry the fluid away from
the brain, down the jugular vein in the
neck and then into the heart or abdo
men where it is flushed into the blood
stream. Infants born with the disease
(one in 300) or who develop the disease
as a result of illness (one in 100; have
a tragically high mortality/morbidity
rate. The problem with children suffer
ing from the disease is that the catheter
implanted during surgery is unable to
grow with them. This means replace
ment operations at specified growth
periods. Typically, a child faces about
eight procedures by the time he is 13
years old.
Each surgery brings with it more and
more risk, each procedure being com
plicated by scar tissue from the preced
ing operation. The problem is so great
that of the newborns and infants with
the disease, the survival rate is 75
percent at five years of age with a rapid
• drop in survival after that.
“That challenge," says Dr. Thomas
Milhorat, head of the neurosurgery
department at Children's Hospital,
“has been to develop a system that
g
s with the child." Working with
Dr. James McClenathan, chief chest
surgeon. Dr. Milhorat has developed a
device that appears to be a solution.
Spliced to the catheter normally used
in the surgery is a coil of tubing
enclosed in a plastic bag. As the
child grows, the tube uncoils. The
coiled section is 203 millimeters long,
or enough growing room to allow for a
tall adult.
“We haven't invented the wheel,"
says Dr. Milhorat. “We've simply
screwed the wheel to the axle. Cathet
ers for hydrocephalus have been used
for 20 years. Tubing in a bag to gain
length has been used by heart surgeons
for 10 years. We've used a composite
of two technologies that have been
u
in surgery prior to this and shown
their worth."
Telltale Nail
Dr. Frankel has worked at Case
Western with engineers from the med
ical equipment industry indevelopinga
telltale nail for pinning broken hips
together. A series of electronic gadgets
is packed into a hollowed-out stainless
steel orthopedic nail not much thicker
i
I
Computerized heart monitor never gets bored.
than a thumb and only 152 millimeters
long. Included are a two-channel AMFM radio transmitter, an audio ampli
fier, strain gauges and a battery with a
250-hour life span. The system is
turned on and off by an ordinary
magnet held in a doctor's hand.
While the patient’s broken hip is
mending, a broadcast tone rises as
pressure on the fracture is increased.
This allows strenuous movements to
be identified and avoided—such as
when a patient is lifted into a chair.
"We discovered," reports Dr. Fran
kel, “that shuffling about with a walker
produces much less strain and enables
patients to be up and about or out of the
hospital much earlier than we ever
thought possible or safe.”
who have suffered heart attacks. The
patients in the units are connected by
wires to electrocardiograph machines
(machines that record the electrical
impulse generated by the patient’s
heart) so that their heartbeats can be
monitored constantly. This cardiac
rhythm is displayed on an oscilloscope
or screen, which is in turn watched by a
nurse. She is watching for irregularities
in the beat which may precede ventric
ular fibrillation (cardiac arrest in which
the heart muscles' pumping ection
ceases). Ventricular fibrillation can kill
a patient within 60 to 90 seconds.
The problem with the system is that
Computer-Assisted Monitoring System
Cardiac care units are specially
designed hospital wards for patients
13
Pacemaker’s telephone system lets patient lead a normal life . .
even alert personnel have difficulty
spotting irregularities or abnormal
events if they do not occur often. Now,
American Optical Computer company
has developed a new computer-as
sisted monitoring system (CAMS) to
act as a backup to the usual cardiac
care monitoring. CAMS has the ability
to recognize certain abnormalities in
the heart rate, store up these abnormal
events and write them out whenever
the physician or nurse requests infor
mation. The CAMS at George Wash
ington University Medical Center,
which is supervised by Dr. Joel Gorfinkel, is one of three in clinical use
today. “Humans go crazy watching
the oscilloscope, but the machine is
too dumb to get bored,” says Dr.
Gorfmkel. “When well-trained car
diac-care nurses were tested against
the computer for picking up abnor
malities, we found that if there were
less than 60 events in an hour, there
was a low likelihood of a nurse picking
it up. The machine picks up everything
.. .while electric signals are recorded at distant hospital.
abnormal. It may show up a disorder
that’s irrelevant, but it never misses
anything. It’s left to the human being to
sift out the meaningful data. ”
By checking with the computer
hourly, the physician can see how
many and what kinds of abnormal
events are taking place. “If you see a
patient is having 50 of these events an
hour, you may want to intervene with
therapy,” says Dr. Gorfmkel. “This
way we are able to react to prodromes
—preceding events—rather than to the
actual cardiac arrest.”
What has made a system such as
CAMS available in a hospital setting is
the miniaturization of electronic parts.
“Before miniaturization,” Dr. Gorfinkel points out, “a computer such as
this would have been too big for us to
use. Space technology brought miniaturization, and this is the kind of
benefit we are getting directly from the
space program.”
Telephone Monitoring of Pacemakers
Thousands of heart patients owe
their lives to electronic pacemakers,
whose electrodes rest in or on the-heart
and keep it beating normally when the
heart’s intrinsic pacemaker fails. But
these electronic pacemakers run on
live batteries, and they run out of
energy. Therefore, it is important to
follow pacemaker patients and check
14
that the batteries are live. Since the
pacemaker has a life span of two years,
after one year the patient either comes
in for electrocardiographs (readings of
his heart’s electrical impulses) every
two or three weeks or he has the
pacemaker replaced on a fixed date.
There are distinct disadvantages
with both approaches. With fixed-date
replacement, some pacemakers are
replaced that are still working. But
to wait and run the risk that they will
stop is dangerous for the patient. And
regular monitoring is often difficult
for patients.
Recently a new piece of equipment
.has been developed to keep tabs on
these patients via telephone. It is a
specially designed box that the p
keeps with him at home or when he is
traveling. The box has a cradle for a
telephone receiverand two electrodes,
When the patient is called by a nurse
from a central monitoring unit, he
places the telephone in its cradle, his
hands on the electrodes and the elec
tric signal from his heart is. read by an
J
electrocardiograph machine at the
other end of the line. The reading is
recorded, placed in the patient’s file
and the nurse makes an appointment
for the next reading. Patients who are
not feeling well can call in for a read
ing at any time.
The direct benefit to the pacemaker
patient is that he can feel secure—he
can travel anywhere in the world and
still be attached to a monitoring sys
tem. There are indirect benefits as
well: a nurse can call the patient
regularly, and while she records the
data, she can also check on medica
tions and ask the patient how he feels.
Since many pacemaker patients are
elderly and alone, this regular contact
is a form of psychotherapy.
Membrane Lung
“There are a lot of diseases such as
pneumonia, shock lung or fungus
infections,” says Dr. Joseph, “where
the lungs need a rest. We needed
something to take the lung’s place
while the patient recuperated and
while we could do all kinds of things
to the lungs—such as clean them out
or medicate them with antibiotics. ”
The membrane lung looks like, and
is about the size of, a closed accordion.
Venous blood (blood from the veins
that is high in carbon dioxide) is taken
from the patient via a catheter to the
membrane lung, cleansed of its carbon
dioxide, supplied with oxygen and then
returned to the patient. While in the
membrane lung, the blood is filtered
through about 50 envelope-like folds of
a sticky white silicone fabric which
allows the blood to stay on one side
ie membrane lung is an artificial
lung developed for patients whose
lungs temporarily don ’t work. It is in
the very experimental stage. Dr. Wil
liam Joseph, a lung specialist with the
George Washington University Medi
cal Center, oversees the second big
gest clinical experimental program
with the membrane lung.
I
I
X
parts of the body in cross section,
much as they would see them in a
textbook drawing.
At Georgetown University Medical
Center in Washington, D.C., a pro
totype body scanner, the automatic
computerized transverse axial
(ACTA) scanner, has been in use for
two years. Costing $272,00C , the
ACTA scanner was built by the National Biomedical Research Founda
tion, which has pioneered in computer
technology and biomedical science.
With the ACTA scanner, a pencilthin x-ray beam passes through a
“slice” or plane of the body and is
detected by sodium iodide crystals on
the other side. Profiles of the issue
density are received by detectc rs as
the x-ray beam moves across or scans
every point in the object frorJi 180
Ordinary X-Ray
Ribs
Diaphragm
Heart
Lung
Ribs
Lung / Vertebra\
_________Heart
<
\
Lung
Breastbone
ACTA scanner has revolutionized the x-ray.
too*
> 4. 3
Aorta
Spinal Cord_____
while the oxygen and carbon dioxide
flow in and out. This is the same action
the lungs’ membranes perform normal
ly. A patient can remain on the
membrane lung for about eight days.
“We can divert about 85 to 90 percent
of the blood through the artificial
lung,” reports Dr. Joseph. “At the
same time, we use a ventilator to
expand and contract the patient’s
lungs so they don't collapse. The
membrane lung isn’t a panacea—we
are still groping our way.”
different angles. The readings, laken
constantly by the crystal detectors, are
fed into a computer. The computer in
turn is programed to reconstruct the
total object from information received
from up to 25,000 readings. It synthe
sizes and reproduces a cross section of
the object in a computer picture shown
on a television screen. The picture can
be photographed with a Polaroid camera and stored on a magnetic tape for a
permanent record.
ACTA Scanner
Machine gives lungs a rest.
One of the more revolutionary
pieces of new medical equipment in the
field of radiology is the scanner—a
new method of taking x-ray pictures.
The scanner allows doctors to see
15
So far, doctors at Georgetown have
used the scanner on over 400 patients
and have scanned the brain, upper
neck, spinal cord, chest, abdomen,
pelvis, knee and lower legs.
“The new technique is extremely
important in the area of brain disor
ders,” says Dr. Alfred J. Luessenhop,
the director of the division of neuro
surgery at Georgetown. “Such prob
lems have often involved risk and
discomfort in diagnostic methods and
exploratory surgery. The ACTA scan
ner is a quick, painless method to
provide more diagnostic information
withoet risk. It does not ‘invade’ the
body hke certain studies which inject
•
....
foreign
material
into the system, nor
doeslt depend on surgical techniques,
It represents a crucial breakthrough
for brain disease.”
The Ocusert
Theocusertistiny—no bigger than a
University Medical Center: “In order
to control glaucoma, the patient needs
to have enough pilocarpine in his eye
to reduce the ocular pressure for a
reasonable percent of time. That
means the patient must put drops of
pilocarpine in his eye on a strict regi
men of four times a day at regular in
tervals. Here we have a drug, pilocar
pine, that is very effective, but com
pliance is very difficult because, in addition to the inconvenience of the rigid
schedule, pilocarpine applied in drop
form has some unpleasant side effects
for many users, such as blurred vision
for two hours after application and
painful ciliary muscle contractions.”
The
eliminates both the
-— ocusert
—-----------------——
compliance and side-effect problems.
The wafer-like device is slipped under
the eyelid. In between the two porous
membranes are crystals of the drug.
year
eye release the
from
drug automatically, all day long for
seven days. The proportion of amounts
released at any one time is greatly
reduced: from milligrams of pilocar
pine via the eye dropper, micrograms
of the drug are released through the
ocusert. This lowered dosage reduces
X
side effects and, because it provides
!
medication for a seven-day period,
compliance is no longer a problem.
Dr. Armaly is excited about other
uses for the ocusert. “In treating
drachoma, an eye disease prevalent in
countries with hot and humid climates,
we are finding antibiotics can be
placed in the ocusert and used to treat
that condition. This is potentially even
more important because drachoma
often affects children, and the prob
lem of rigid drug application in children
is phenomenal.”
Other physicians are experimenting
Eye fluid releases medicine,
with the ocusert to be used interutero
oval band-aid, but is actually a new to release birth control medication
way of delivering drug therapy. Its —again, reducing the need for a
patient’s day-to-day compliance.
most widespread use is in administer
ing the drug pilocarpine into the eye Ocuserts may also be used with other
drugs. “It opens up a whole area of
of glaucoma patients.
Glaucoma is a chronic eye disease use of drugs we have avoided because
characterized by increased pressure of the toxic side effects from large
doses,” says Dr. Armaly. “The ocu
within the eyeball and, without treat
ment, marked by progressive loss of sert with its small but continuous re
lease would permit us to use the behvision. According to Dr. Mansour
......, head
Armaly,
I of the department of efits from these drugs without sufferphthalmology at George Washington ing from the harmful side effects.” ■
oi
thumbnail and much more flexible.
Made up of two layers of a porous
membrane, the ocusert looks like an
i
16
FROM THE BOOKSHELF
for further reading on health care
Deaton, John G. New Parts for Old:
The Afte of Organ Transplants.
Franklin: Philadelphia,
Pennsylvania, 1974.
The author, a professional
doctor, presents the case
histories of many persons who
have received organ transplants
and describes how medical
specialists are trying to solve the
problems of biological rejections.
Eilers, Robert D., and Sue S.
Moyerman, eds.. National Health
Insurance. Richard D. Irwin, Inc.:
Homewood, Illinois, 1971.
An analysis of various types of
national health insurance
programs, accompanied by
comments of noted health care
leaders on specific proposals.
Halacy, Daniel S. Genetic
Revolution: Shaping Life for
Tomorrow. Harper & Row: New
York, 1974.
A well-written study of what is
taking place in the field of
genetics, particularly the
expanding knowledge of genetic
structure.
Hamburg, Joseph, ed. Review of
Allied Health Ednc.ition. University
of Kentucky: Lexington, Kentucky,
1974.
First in a series, this book
appraises recent developments in
allied health fields, including
dentistry, radiology, physician's
assistance and occupational
therapy.
Larson, Leonard A., and Herbert
Hichelman. International Guide to
Fitness and Health. Crown
Publishers, Inc.: New York, 1973.
This international guide contains
the findings of research that can
be used by the individual seek:
a proper exercise program bat
on scientific study.
Locke, David M. Viruses: The
Smallest Enemy. Crown Publishers:
New York, 1974.
In this authoritative, illustrated
volume, the author describes the
current status of research on
viruses and the diagnosis and
treatment of virus-related
diseases.
Vaux, Kenneth. Biomedical Ethics:
Morality for the New Medicine.
Harper & Row: New York, 1974.
The author, a professor of ethics
and an ordained minister,
outlines the ethical concerns
and moral implications of
medicine in an age of organ
transplants and mechanical
means of sustaining life.
Printed and published by Jay W. Gildner for United States Information
Service, New Delhi, and printed at Pauls Press, New Delhi - 110028.
J
rip IHEART AND PULSE
HISTORICAL ASPECTS
ABSTRACT
is
This
pu1se,
brief
a
wi th
historical review of the study of
r e f e? r e n c e s f r o m a n c i e n t I n d i a n ,
the
Egyptian ,
hear t
and
Chinese
and
as
7th
G r ee k med i c i n e The
Heart
century
and
the Pulse have been mentioned as
ear 1 y
B«C n i n t h e A t h a r v a v e d a 1 o n g b e f o r e W i 11 i a m H a r v e y
the
described
the heart and blood circulation in 1628 A.DO
The Heart
Since
time?
immemorial,
the
heart has been known
important organ in the human body.
severa1
times
as
a
Athervaveda as early as 700 B.C,
thought
that
the
hear t
con sci ousn ess (2,3).
which
was
be?
the
most
It has been considered as the seat
of the soul, the abode of love a n d a f f e ct ion
mentioned
to
"Lotus
(4) M
with
The heart has
n i ne
gates",
S u s h r u t a a n d C h a r a k a (5 O 0
the central
organ
and
i1
the
400B.C.)
the
It is but natural that an organ like the
offers unflinching service from the fourth week of
been
our
seat
of
heart,
:Ln tra--
uterine life till the very last moment, should receive our careful and
considered attention when dealing with human ailments.
It
is interesting to note that the Egyptians, during the
process
of
embaIming, eviscerated all organs except the? heart, which was left ' in
situ within the thoracic cage, probably due? to the belief that it.
was
essential
of
Ebers,
to
an
the?
individual even after- death.
Egyptian
document
on
medicine ,
In
the
written
Pa pyre s
in
hieratic
charac ters, dating back to 3000 - 2500 B.C., there? is a refree tc
heart's
movements
and its importance in diseases; there
1
is
a 1 so
the
a
I
description
breast
the
An g i na
of
probably
and one side of the heart and arm,
receptacle f
Charaka and Sushruta considered the heart as a
pectoris.
i
of an ailment in man’s "cardia" with symptoms of pain
and not as a pumpspeculated
Aristotle ? the Greek philosopher and writer (384-322 B.. C - )
on
the role of the heart, and concluded that it was the body s
ner\ e
Era s i s t r a t u s o -f K e o s (310
2G0
centre
and
the organ of thinking-
B.C, > ,
an
i11ustrious contemporary of Herophi1us and
Chrysippus
of
t he
pupi 1
of
man
co
Cnidus was J, a c c o r d i n g t o F i n 1 a y s o n , the -first
describe
the
whi le
the
he a '-t
contracts
and d i1a tes "1i ke the bellows of a blacksmith",
the
pu 1 se
almost
two
moves
forward
heart as a ’ ’ p u m p " - A c c o r d i n g t o h i m
as
a
wave, a discovery
correct
proved
thousand years later by modern research (4).
Heart
diseases
are
Samhita (400 B-C-)-
considered in one of the
chapters
Sushruta
of
In one of the types of heart disease,
f el t
in the region of the heart in which the heart seems as if
drawn
and
crushed,
pierced and c rac ked,
pricked
and
is
"a pain
being
The
split”-
descriptions fits in fairly well with the symptoms of Angina pec tor. .s»
The Pulse
In
Ayurveda,
over 600 different types of pulse
recognized and dea11 with-
readings
been
have
The pulse is regarded as a "meter",
indicates the state of the "soul", embedded within the body,-
wh ic h
whetler
happy or sad, whether troubled by heat,cold or air (2)n
Although Chinese pulse-lore is usually credited to F'ien Ch'iao (600
SOO B .. C . > , it was Wang Shee—ho (280 A-D-> who popularized the art,
2
by
w r i t i n g a m o n u m e n t. a 1
of
t r e a t. i s e o n t h e p u 1 s e ?
i n ten vo 1 umes -
Diagnosis
any disease in those days depended mainly on a study of the
to
and
lesser extent on the state of the tongue
a
and
the
pu 1 se
•facial
appearance of the patient
In
Greek
Addern
medicine, Hippocrates and his contemporary
(500
Demokrites
of
400 B.C.) h ave been c on s i d e r ed t he ea rlies t aut hors
to
make a mention o-f the pulseHerophi1us
(400 B.C.), born o-f Asia tic-Greek parentage at
ChaIcedon ,
a n d t u t o r e d b y t h e g r e a t F* y t h a g o r a s, is often regarded as the
“Father
o-f
o-f
the
norma1
and
He was also the -first to time the beats o-f
the
Anatomy".
He was the -first to study
the
rhythmical
wave
and described in elaborate terms. t he pu 1 se un d e r
pulse..
c on d i t i on s .
abnormal
pulse with a "water-clock”.
It was Erasistratus, who by detecting a sudden leaping of the pul =>e,
the
so
called "lover's pulse", - w h i 1 e e x a m i n i n g A n t i oc hu s
so "I
o-f
Seleucus„ put down his melancholy to an uncontrollable desire -for
his
step-mother Stratonice (5)u
Ga 1 en
( 120
20O A.D.) described 27 varieties
o-f
pul se
readIngs,
Longmans j,
Bombay
a c c o r d i n g t o t heir 1en g t h,b r ead t h and d e p t h.
REFERENCES
s
Ancient Indian Medicines0rient
1 - KUTUMBIAH,P.
Ca1c u 11a, Mad ras, New De1hi, 1962,p.23.
2, BHATIA,Maj.,Gen »S.L.,:Hi story
of
Med i c i ne s pu b 1 i s hed
Man agemen t Comm i t tee, D r.B.C. Roy National Award Fund,
t he M ed i c a 1 C oun c i 1 o f I n d i a , New Delhi,1977,p.46.
the
by
Office of
3. VAKIL.,R.J. sRomance of Healing and other Essayss
House,Bombay, 1961,pp 6,10,12 18,19.
Publishing
4.. MAJOR,R.J.s
Spr i ng f ie1d
Asia
History of Medicines Charles C- Thomas
111 i n o i s, USA, 1977,pp.46, 50, 70,199.
s
5. BETTMANN,0.L.:
A Pictorial History of Medicine: Charles
Publisher, Springfield, Illinois, USA, 1956, pp 28,96.
3
Publ i si her ,
C. Thomas.,
Mp MG
i
i
1
I
AETIOLOGY OF SPLENOMEGALY
AMONG AFRICANS IN AN AFRICAN CAPITAL
Summary. Two hundred and forty cases of splenomegaly seen in one hospital
from 1962 to 1967 are reviewed. In children below the age of ten years we found the
largest number of cases in any one decade of life. The diagnoses in descending order of
frequency were haemoglobinopathy; portal hypertension from cirrhosis, hepatitis and
systemic venous congestion: leukaemia; malignant lymphoma; idiopathic splenomegaly;
malaria; septicaemia; rheumatoid aithritis; acquired haemolytic anaemia; systemic lupus
erythematosus; hookworm anaemia and multiple myelomatosis. With malaria, splenic
enlargement occurred only in children in the acute phase of the disease. Idiopathic
splenomegaly is diagnosed oniy by exclusion and the prefixes “tropical” and “nontropical” appear unnecessary.
. ’ INTRODUCTION
Splenomegaly in tropical countries frequently presents a diagnostic problem .
•
efore the advent of better medical facilities,sp!enomegaly was often attributed to malaTia or was regarded as “idiopadtic tropic splenomegaly'’, or “big spleen disease” — at best
a vague diagnosis. As far as we know, no attempt has been made to classify the causes and
estimate their relative incidence until we undertook this present study.
I
MA'i ERIALS AND METHODS
We examined the case records of all splenomegaly patients (240) seen in the Departments of Medicine,
Surgery and Paediatrics,
from 1962 to 1967
inclusive, and we reached a diagnosis foi each from tlic clinical manifestations recorded, the results of
laboratory investigations,and the response to treatment.
All cases in which the original diagnosis had been big spleen disease (Hamilton et al., 1966) were
classified under the heading “splenomegaly of undetermined origin*’.
RESULTS
Fig. 1 shows the incidence of splenomegaly in the different age groups: the incidence is
highest in the first decade of life and is very low after the fifth decade.
Tabic 1 shows the aetiological diagnoses in descending order of frequency and Figs. 2 to 5
illustrate occutrence of these diseases in the different age groups.
i
j
/
i
!
1
i
)
50
Of the patients with hacmcx'iobivopathy 33 were male and 30 female. More than onethird were younger than five years old, more than a half were less than 10 years old, and
only one out of every nine patients was older than 20 years. In the 63 cases the distribution of the haemoglobin genotypes was SS 87>'., SC 11 /o and CC 1.5%. The SS genotype was
most commonly found in patients below the age of puberty although it occasionally
occurred in ]patients up to 25 years old. Patients older than this^with one exception^had
the SC genotype. The one exception, the oldest patient (45 years), had the CC genofype.
TABLE I
AETIOLOGY OF SPLENOMEGALY IN
DESCENDING ORDER OF FREQUENCY
1
I
I
r
Number
Percentage
1. Haemoglobinopathy
2. Portal hypertension
3. Leukaemia
4. Malignant lymphoma
5. Undetermined
6. Malaria
7. Septicaemia
8. Rheumatoid arthritis
9. Haemolytic anaemia
10. Systemic lupus erythematosus
11. Hookworm anaemia
12. Multiple myeloma
63
55
28
28
21
27.1
23.6
TOTAL
240
12.0
12.0
9.0
7.7
18
16
6
2
6.9
2.6
0.9
0.4
0.4
0.4
1
1
1
NO. OF CASES ‘
RO-.
80NO. OF CASES
l
70-
28-1
26-
60-
2422-
SPLENOMEGALY
50-
20HAEMOGLO3INOPATHY
18-
40-
1430-
1210-
20-
864-
I
10-
20
5
10
15 20 25 30 35 40
AGE IN YEARS
45 50
Fig. 1. Distribution of splenomegaly by age (240
patients).
i
I
10
20
30 40 50
60
30
90
AGE IN YEARS
Fig. 2. Distribution, by age, of splenomegaly due to
haemoglobinopathy (63 patients).
L.
51
SPLENOMEGALY
i
i
Tlie portal hypertension group consisted of patients with cirrhosis of the liver and
hepatitis with or without hepatoma who showed clinical or radiological or post-mortem
evidence of portal hypertension. It also included patients with systemic venous con
gestion from cardiac failure. For any one decade the incidence of portal hypertension and
systemic venous congestion was highest in the first; but if the third and lourth decades
were taken together the peak incidence occurred at 20 —40 years of age. The youngest
patient was two months old, while the oldest was 81 years and showed at autopsy diffuse
hepatitis and splenic congestion. Males were significantly more predominant in this group
by a ratio of 2.7 to 1.
The incidence of leukaemia was highest in the fourth and fifth decades. Chronic
leukaemia accounted for 71% of patients in this group, and just over half of the chronic
leukaemias were lymphocytic. In the leukaemic group, males outnumbered females 1.7 to 1.
NO. OF CASES
8-]
LEUKAEMIA
H109676-
54321-
flfl
6-
iJi
54-
NO. OF CASES
l2“l
3-
i
Ma ■
■ ■
21-
•
LL a
i Mi
0
10
20
30 40 50 60
AGE IN YEARS
0-
'
’70
J * .*
flfl.
a
MALIGNANT
LYMPHOMA
■Inn
7-
PORTAL HYPERTENSION AND
SYSTEMIC VENOUS CONGESTION
■
'iflfl-ffl
fl J
[.a
76—
5-
UNDETERMINED ORIGIN
mJ
3-
fl
60
90
Fig. 3. Distribution, by age, of splenomegaly
due to portal hypertension and systemic
venous congestion (55 patients).
21-
i“_
0-
0 10 20 30 40 50 60 70
AGE IN YEARS
—
1
SEPTICAEMIA
fl-q
0 10 20 30 40 50 60
AGE IN YEARS
Fig. 4. Distribution, by age, of splenomegaly due to
leukaemia (28 patients); malignant lymphoma
(28 patients); undetermined origin (21 patients);
and septicaemia (16 patients).
NO. OF CASES
6-1
I
I
5-
4-
I
I
3-
2--
I -
to
MALARIA
■ fa
.lf,..flju
01234 5678
AGE IN YEARS
9
10 24 25
Fig. 5. Distribution, by age,
of splenomegaly due to
malaria (18 patients).
!
i
52
I
i
1
5
I
I
■
Tire malignant-lymphoma group included all splenomegaly cases diagnosed :s Hodgkin’s
disease, lymphosarcoma, malignant lymphoma, reticulum cell sarcoma aid Burkitt’s
tumour, with peak incidence in the first two decades of life. Twenty-five percent of the
patients were diagnosed as suffering from Burkitt's tumour. All of the Burkitt’s tumour
cases were in their first decade, apart from one who was eleven years old. O ily three of
the twenty-one patients not suffering from Burkitt’s tumour had no palpable lymph node
enlargement. Males were predominant by 4.6 to 1 in this group.
In splenomegaly of undetermined origin we included all the cases wherei no specific
diagnqsis had been made either owing to lack of adequate investigations or because the
investigations made did not lead to any diagnosis. Males predominated by 1.3 tto 1.
Septicaemia accounted for 16 patients, 6.6%. They had splenomegaly but Ao evidence
other than infection of any underlying cause. Included were cases in which (1) Blood
cultures revealed infective organisms. (2) Blood cultures were negative in the presence or
absence of infection of another organ (for example, the lung) and the fever and spleno
megaly disappeared after antibiotic therapy. (?) Bacterial endocarditis was diagnosed.
Ages ranged from two months to 52 yearSybut the largest group was in the :list decade
of life.
The malaria group included patients whose blood had carried malaria parasites during
their illness and whose splenomegaly regressed after anti-malarial therapy.
Tire incidence was highest at two to four years and in all cases but one tie patients
were younger than 10 years. The male/female ratio was 2:1.
The collagen disease group included six patients from 15 — 56 years (sex ratio equal)
with rheumatoid arthritis, one showed evidence of hypersplenism compatible with Felty’s
syndrome. The seventh patient, a 31-year-old female, had systemic lupus erythematosus,
Acute haemolytic anaemia was diagnosed in two cases — both male. In one the disease
was due to deficiency of glucose-6-phosphate dehydrogenase
(G-6-PD)z in the red blood
..
cells. In the other the G-6-PD enzyme had not been measured, and the cause of his
haemolysis remained unknown.
Hookworm anaemia was found in only one patient, a boy of 14 years, His spleen
enlargement disappeared after de-worming and iron therapy.
The only patient with multiple myeloma was a 50-year-old man who later died.
Autopsy proved that multiple myeloma was the cause of his splenomegaly.
DISCUSSION
I
We realize that the patients reviewed here are a selected group, since many people with
asymptomatic splenomegaly do not report to hospital, and that the figures we give for
relative incidences cannot apply to the population as a whole. Yet a small serie; obtained
to
captoxt olf jjYve cccriVYt}. is more likely to reflect to some degree tie various
causes of splenomegaly in the country as a whole, than is a review of cases made, say, in
a small remote village with its extreme ethnic homogeneity and similarity o 'environ
mental factors.
The prominent position occupied by haemoglobinopathy in our aetiologicil table is
due to the prevalence
of sickle-cell anaemia in children. The frequent crises
associated with this disease force the parents to bring the child to hospital. Most of these
children do not reach adult age,and only few of the survivors continue to show spleno
megaly (Watson et al., 1956).
Of next importance is liver cirrhosis and hepatitis, with resultant portal hypertension.
Mustafa (1965) has found that liver cirrhosis is the commonest cause of gross spleno
megaly in the Sudan.
I
SPLENOMEGALY
I
i
53
The infrequency of leukaemia in children in our series deserves comment. We partly
agree with others (Damaschek et al., 1964), that this is due to an understandable “under
diagnosis”. The high incidence of childhood infections
the maternal illiteracy
and the unwillingness to report promptly to hospital, combine to kill die acutely leu
kaemic child before diagnosis. Mostly the mothers visit the local herbalist, or they
medicate the child themselves until clearly it is /dying, and then they rush the child to
hospital. In defence of the mothers, the inadequate medical facilities lead to very long
queues and do not encourage early visits to hospital. We concur with Davies (1965) and
Gelfand (1967), however, that “underdiagnosis” alone may not be the only factor in the
apparent infrequency of childhood leukaemia in Africans. Racial or genetic factors may
be involved. In childhood leukaemia in the U.S.A, the peak incidence occurring at 2 to 5
years in white children is not obseived in non-whitc children, and tlie mortality rate is
lower in the non-white population than in the white (Court-Brown et a!., 1961).
In our adults/Chronic lymphocytic leukaemia was as frequent as the myelocytic
variety, reminding us that sometimes these types cannot be differentiated on clinical
grounds only. Gross splenomegaly is common with chronic lymphocytic leukaemia in
Africans; lymphadenopathy may be absent or barely noticeable. (Gelfand, 1967 and
Haddock, 1967).
The absence of kala-azar in this scries bears out the experience of many clinicians
working
and confirms the report of Cahill (1968) who found that visceral
leishmaniasis is very rare there^and that even the cutaneous form is only found in the
northern parts of Wes‘ Africa near the Sahara desert.
The splenomegalies of undetermined origin form only 9'/o of our series. It is in this
group that we expected to find cases commonly termed “big spleen disease” or “idiopa
thic tropical splenomegaly”, but the clinical picture was not consistent enough to justify
tlie assumption that all these patients were suffering from the same disease, although 50%
has anaemia. We suggest that a harder and longer search might have led to a definite
diagnosis in some of these cases. For example, a search for schistosoma-ova in stools or rectalmucosal biopsies might have revealed schistosomiasis, since splenomegaly may occur in'
schistosomiasis in the absence of portal fibrosis and consequent portal vein hypertension.
(Mustafa, 1965 and Marsden et al., 1969).
We have diagnosed two cases from
rectal snips since the conclusion of this review.
Our pievious impression that malaria is not a frequent cause of splenomegaly in adults
appears to be confirmed by this series. The true frequency of splenomegaly due to
malaria is much higher than reported here because most people with malaria do not
report to hospital or even to a doctor for treatment. It is useful to know, however, that a
facile diagnosis of malarial splenomegaly in an adult is likely to be wrong, 'flic previously
common practice of laying hands on the enlarged spleen and immediately diagnosing
malaria is dangerous - one of the chronic myelogenous leukaemia patients in this series
was referred to hospital as suffering from malaria even though his spleen was touching his
pelvis. Gross splenomegaly with enlargement beyond the umbilicus must be extremely
rare in malaria. Some enlargement does occur, but mostly in children.
A diagnosis of “idiopathic tropical splenomegaly ” or “big spleen disease” is really a
diagnosis by exclusion. Various attempts to incriminate malaria have not been entirely
convincing. Appearances in the liver of lymphocytic infiltration and Kupffer cell hyper
plasia have been reported (Lowenthal ct al., 1968, Gebbie et al., 1964 and Marsden et al.,
1965) as specific for big spleen syndrome,but many pathologists consider these changes
non-specific and without any aetiological significance. Marsden and Hamilton (1969)
recently classified cases of the syndrome into those with and without hepatic sinusoidal
lymphocytosis, but were unable to attribute any aetiological significance to the presence
54
I
or ;absence of such changes in the liver. They observed that even in malarious areas the
syndrome occurs without hepatic sinusoidal lymphocytosis and that the aetiology
remains obscure. Lowenthal and Hutt (1970) recently described a case of tropical
splenomegaly syndrome in Africa in. a Caucasian female who had never ha j overt malaria,
and who had always taken anti-malarial drugs, yet whose condition they believed to be due
to malaria because she had a raised malaria-antibody litre. Her liver biopsy showed
Kupffer cell hyperplasia with sinusoidal lymphocytosis. Although they state that “the
clinical condition settled with conservative treatment’*, they do not indicate whether the
treatment was anti-malarial or not. In an earlier series with 13 African pa: ients the same
authors reported reduction of hepatic lymphocytosis and splenomegaly in only seven of
the 13 after anti-malarial therapy. In fact, the histological appearance of tl e liver became
more abnormal in three of their six patients who failed to respond to anti-malarial
therapy, and in one closely resembled that found in acute leukaemia.
In a series of ten cases of “idiopathic non-tropical splenomegaly” in England, Dacie et
al. (IPbQ^reported post-mortem evidence of lymphosarcoma for two of the pat’ients.and
remarked that in some patients the great degree of lympho-proliferation suggested the
development of a chronic “pre-malignant” lymphoma predominantly affect ng the spleen.
Idiopathic splenomegaly, whether it occurs in tropical or non-trod)ical areas, is
probably multi-aetiological and demands both a hard search for its true cause and along
J" ....
period of follow-up. We prefer not to use tthe
’ tprefixes "“tropical”
and “nen-tropieal ” as
these have aetiological connotations which at present are not justified.
REFERENCES
Cahill, K. M., Trop. geogr. Med., 20 (1968) 109.
Court-Brown, W. M. and Doll, R., Brit. med. J., 1 (1961) 981.
V Bram, M. Q, Harrison, C. V., Lewis, S. M. and Worlledge, S. M., Brit. 1. Haemat. 17
(jvoy) Ji /.
*
Damaschek, W. and Gunz, F., Leukemia, 2nd edition, Grune and Stratton New York U.S.A., 1964.
Davies, J. N. P., Lancet. 2 (1965) 65.
Gebbic, D. A. M., Hamilton, P. J. S., Hutt, M. S. R Marsden, P. D., Voller.A. anld Wilks, N. E.,
Lancet, 2 (1964) 392.
Gelfand, M., J. trop. Med. Hyg., 70 (1967) 85.
Haddock, D. R., J. trop. Med. Hyg., 70 (1967) 60.
m\d- J- 2 <1966>
“"si's0"’ P' 1 S” Gebb‘e’ D’ A' M” llUtt’ M' S’ R" L°the’ F' a"d W'lkS’ N-
I
••
Lowenthal, M. N. and Hutt, M. S. R.,2?. Afr. med. J., 45 (1968) 100
Lowenthal, M. N. and Hutt, M. S. \l.,Brit. med. J., 3 (1970) 262.
Marsden, P. D. and Hamilton, P. J. S., Brit. med. J 1 (1969) 99
Marsden, P. D., Hutt, M. S. R„ Wilks, N. E., Voller, A., Blackman, V., Shah K. K. ?onnor, D. H.,
Hamilton, P. J. S., Banwcll, J. J. and Lunn, H. F., Brit. med. J., 1 (1965) 89 ’
Mustafa, D., J. trop. Med. Hyg., 68 (1965) 183.
O’Connor, G. T. and Davies, J. N. P., J. Pediat., 56 (1960) 526.
Watson, R. J., Lichtman, H.C. and Shapiro, H. D.,Amer. J. Med., 20 (1956) 196.
- 14
BASIC PRINCIPLES OF EPIDEMIOLOGY
Epidemiology is as old as medicine itself. HIPPOCRATES
(460-380 B.C.), when trying to demystify illness occurrence
as being due to supernatural causes, instead pleaded for
viewing "man in his environment" and suggested in his famous
»
’’’On Airs, Waters and Places” that
"whoever wishes to investigate medicine properly
should proceed thus: In the first place consider
the seasons of the year, then the winds, the hot
and the cold, especially such as are common to all
countries, and then, such as are peculiar to ’each
locality. We must also consider the qualities
of the water..."
can be
as
"the study of the
be defined
defined
as
Epidemiology
and determinants
disease
in
human
of
determinants
of
distribution
populations* and is semantically composed of the Greek “epi”
i .e.
‘'people*' and "logos**
= * among", "demos"
"demos’’ ®- "people”
"logos*’ = "science".
H
it is concerned with what is occurring in the population. it
has
become implicit to mean the occurrence of health
problems, not necessarily medically diagnosed but equally
perceived problems. This also makes
well
subjectivelyj
field, for which it is
epidemiology an interdisciplinary
’•
also characteristic to deal with health problems in the
whole population and not only health problems “taken care
of” (Figure 1}.
In the calendar of his
another milestone, He; i
epidemiology
and in 15
"Natural
and
Political
Mortality" using the ve
PARR, an English doc tormedical statistics in E
r
studied the mortality i
assess the "population
concept (the denominator
(the numerator). He
He con
executed jin .1837 while...
imprisonment
W
\ was 51". Wi
doctor
SNOW, a doctor
in the S*
was an outbreak of a c
systematically mapping t
uneven distribution that
water from certain stand pi
CO
population
i854Ksho;ingeinOb?a
FIGURE 1. Epidemiology, an interdisciplinary branch
studying health problems and its determinants
in the population, (shaded area = health problems known)
PROBLEM IDENTIFICATION
Basic principles
occurred (Source: F
on Community Medici
Scientific Publ.,19
PROBLEM IDENTIFICATION
I
16 -
\\
/
This was obvious when calculating the death rates by water
source area (Table 2).
/
I
TABLE 2. Deaths from cholera per 10,000 houses by
source of water supply, London, 1854. (From:
Lilienfield A.M»: Foundations of epidemiology.
*
Oxford: Oxford University Press, 1976)
Water supply
Number
Deathr.
of houses'^from cholera
Deaths in
each 10r000
houses
Southwark &
Vauxhall Cc
40046
126 3
315
Lambeth Co
26107
93
37
Rest of London
256423
1422
59
These basic calculations, again relating a numerator to a
denominator, is what epidemiology is very it x:h about. Even
though this may seem simple enough, it is aperativ?, and
difficult to assess, that there is no syste Atic selection
of cases for the numerator/is well,
that J.e denominator
is representative of the target population aim at.
Snow’s work has become a model for
‘
epics
..ological wo^k
’’from .a clinical . obsox’vatjon to
scilp
;i • ,t hypothesis
.
testing and intervention", illustra :vng th; jhree levels of
ambition in epidemiology, the DESCP.IITIVF (.-hen? where? and
who?),
the
ANALYTICAL
(why?)
and
t e
*NTERVENTIVE
(what...if?).
<r
PROBLEM IDENTIFICATION
/
DESCRIPTION;
time
piac®
| su
_
pl
hy
ge
person
AIMALYSfS;
I ris
I aa
otlolcsy
j
i
hy
Se
iNTERVENTJON:
benefit
actior.
ev
of
Inf
exp
FIGURE 3. Epidemiolo
Thus, even if’ border? in,es
are not very clear cut
cut
relates to
pxace an
risk factors and the eti
t
"Risk factor " then implie
possible
causality
of.
statistical methods. it i
synthesis and
more of a hypothesis gene
in health planning and f
communityof
anaiysJs
testing of hypotheses and a
The ultimate
i *
goal of epidem
strategic
'—ies for the preven
talk in terms of effects
action, to situdy
*; the impac
need
an
experimental
‘''I
a
"natural** experiments rosy
) sometimes
ethically
unwar
would
be needed to <elimi
: "confounding".
Maybe
the
epidemiology will br on 4.this
task of tmedicine to assess
’’evaluation of health care”.
Basic principles
PROBLEM IDENTIFICATION
- .18 -
STEPS IK ORGANIZING AND CONDUCTING A FIELD SURVEY
One way of strengthening the work of the primary health
workers is to encourage their use of simple epidemiological
methods in their attempts
k j to make a community diagnosis.
The steps in making a community diagnosis arc
are more or less
similar to those when
t’hcn making a patient diagnosis
_ l_s (Table 3) :
Evaluating
action
betian
f
Planning action &
health programme -s^”
T
TABLE 3. A comparison between community and patient
diagnosis
COMMUNITY DIAGNOSIS
1. ]Library
w reconnaissance
___ ______ _
2. Field reconnaissance
3. Survey (a) basic demo
graphic (b} specific
4. Community behaviour
5, Diagnosis
Feedback to relevant
individuals & groups
and obtain their
interpretation
PATIENT DIAGNOSIS
Writing report
1. History taking
Symptoms
(a) basic data,
diagnostic leads,
(b) examination,
investigations
4. Other factors
affecting the
patient
5. Diagnosis
Analysis of
and
thiok ing out the
imp Iicat ions
*
:.
-““!“in9ShouSaSiLrUcipat:n
C°nCept
P?n
comiHunities
evaluation and takeZ^c1" bhe ife?1 Situ*^°n the problem
identification ___
'•aRes Piac« by actions of the community
itself or by health
-- i workers of the community (Figure 4)»
The r..
survey should be planned with the intention of a
subsequent action, planned in cooperation with the
community
representatives,
IhnntmuCh
d£ta as Possible should
should be
‘
collected
comunity; are there sources sources
of
information in--regxs.ers,
m earlier surveys or in other
community statistics; which might be of interest in t-ho
planned
surv^S
Why\ Where' who' «hat and wtens abou^
the r’
thorou9hly discussed with representatives
of the
Why qoin^etoUrh»y1^it!S <S°ne7 Where Wil1 ifc take
Who
are going to be interviewed or
<— measured?
““T.zlzcIc When will
place? What will be covered
covered in
W1*i lt take
in the
the survey?
Executing survey
Sampling
An
Bennett4?
prOcess
Londoni’ M^ina^SlS
Of o“ecoSni.tyS
prX8°f
K J~
s&u
area
of
research
PROBLEM IDENTIFICATION
PROBLEM IDENTIFICATION
Steps in organizing
...!. u; •' .
In
„
I .1111
20 -
XSi*
»lch „„ „
asr*
-
ln #
1” ^rarsnsu.
a
SJVn'-STX'-
rather than being tested in th
SAMPLING is the selection of
At an early stage in the
POPULATION? the group to be s
individuals <or cases that fit
•children under 5 in Mogadi
,Somalia. A .population may be
STRATA.* These
” 2mutually ex
ntare
girls
1- or
' "
and illite
ill
sometimes galled an a2?
ELEMENT
elements, °8Umuly
would
individuals,
r
-.Therefore
a samp
which
ideally
J
is represen
sampling frame
“
is useful.
populationi
elements
or
i
register, list of students
frame
is
it.(
it (
available
reliability.
«
identified problem, than to perform *nfor®ation about the
many questions and measurement^
7 °ne Study with too
descrite ‘itSaS, e“n?s3to?Ctindividhi?h Can be USed to
of the scientific1 2tuiv“a 8;.Concepts form
f5*"?work of
refined through research. iencxtic stu«y and are gradually
A VARIABLE is
fro“
which ChangeE
i
one situation ^“nother! characteristic WWch
as variables, Search/is^S/^/^eP^empiricaUy
concepts
between
°n effects
the relationships
variables.
the
sources and
«F°n?!!ips
and effects
of these
^han^.6
“
relationships, changes er the reason foAa^k
The
when witingnaresMrchitreports ^^Aabouf3 s?ould ** noted
the Gomez *
used to define
result^,
A <good
se of
definition as those
oreviJt rejevairlOf’sr.afcto»*I
the previous
of the
the subject.
relevant,
within
5W° ®ai” t^s of
9 «nd non-probability
based upon the law of pr
non-probability sampling in
, when no adequate sampling fram
reports
An accidental sample includ
met in the street etc. Da
sampling
interviewers
are
characteristics /but
not
Snowball sampling is when
find the next case.
organized in terms
terms of
- if change results from
‘ » this is
our variables,
interest on these
*s change
are
measured
-»
befors the cfepXten t ■ a causal i—
occur
relationship
they
Pf^ence of malnutri? T mvariable, if
| we
we «study the
r the community
- that is our
aependent variable, whet
^aiUbnity
and
nSe
inS
of
independent Visriables, <i;vr-^n-f?CtlOUS Tessas, they are
‘ey
*r®
Part
of
the
caulea
a
Of
change in the dependent
variahXe, nutritional status.
Sometimes we describe
events or situations in our studies
but often we
to
things
want
explain
O
of a disease
or behaviourr We. ««„ kJ. or ioou for P^ictors
may
have a THEORY, e,:g. about
w
diarrhoea in a
population. Our theories suggest
hypotheses which childhood
can
can be tested in a spec i f 1 c re^eax'ch
project.
<
amw inL
and minimize variatio
groups and
in i
on varia
study- In
in cluster sampling ce
aH t
these villages. This meanr,
traveiiihg. Cluste
comp^ed to pure random samp
random selection of clusters wi
•isux.: MKS-S K»-s
^aaiple there will alm
some d*.op-outs due to vario
'-—
control
if
these fitted
• sss as*
Probability
--- ’ <• . — -w.
We
and
PnOBLEM IDENTIFICATION
Steps in organizirsg
t
/ .
samples
PROBLEM XDBWIFICATXON
are
eith
characteristicsf which could bias the outcome of the study.
The selection of methods to be used in research will depend
on the questions to be answered. Our goal is reliable and
valid data, as free from bias as -possible, which will
providej an unambiguous response to the research questions.
are
. Measures
considered
RELIABLE if the results are
consistents if the same people are asked the sa^e questions
again, they will give the same answers. They are VALID if
the answers represent the true position - it measures what
it is intended to measure. A finding may be reliable but
invalid or (less often) unreliable but valid, measures may
be unreliable or invalid (or both) because of:
- defects in the measurement procedures
- the circumstances of data collection
- inadequate methods (sample too small, badly
chosen, answers incorrectly recorded,
analysis, carelessly done etc)
These defects introduce a BIAS into the results. Careful
planning! can help to avoid some of these problems, but their
effect <at all stages of the project must be taken into
account when the report is written. There will also be some
random error
<
which lower the reliability of the findings
somewhat no matter how much care is taken. Nothing can be
done
about randosa error except to observe statistical
safeguards.
we have here discussed some of the steps in the research
process as well as the common vocabulary used. w«? will now in lessons and field work - proceed through these steps from
problem
identification all the way to the preser-tation and
'■"i identification
discussion of resultsf which in PHC-oriehted re-earch will
constitute the basis for health promoting activities
II.
PLAHHING
INVEST
EPIDEMIOLOGIC CONCEPTS AND
Health and ill-health indi
"Health is a state
social well-being
of disease or inju
This definition of heal
its statement, still ta
discussions on epidemiol
Measuring "health”, the
difficult, however, The
easier to quantify than t
why the! suggested indica
measurixig ill-health, na
of death before one ye
death per population an
various
ages. Still, h
inequalities between regio
These ill-health charac
demands on the PKC in
annual natural increase
Health Services- Likewis
indicates a need
of good
j
the MCH activities. Pro
be a better indicator o
the commonly used gross
has been shown that LBW
determining the survival
mil lien born during 197
affluent countries. Twe
weight (less than 2.5
children of the developin
.!
PROBLEM IDENTIFICATION
Steps in organizing
PLANNING AN INVESTIGATION
'Q
£
■SE
K.
g
t"!
•w u>
5?
%
OT fr
ao
£4
8H
‘K*£
g
■~"S
ft
T''
er *%'
-*r
IJ
3
W
-•c Xi' •/:?
rt
f--4
sit
Ci
il &
£.
'}
-,5
»•
I
*■•--, -< S'
<•?
I
f*.
rr it?
m
'£■
Si
tt.
r-.H &
•»-•
3
s.s ii c-§ £pS ■?I I idXJI i
8
&
H
5 & :>
B STI §. 2 ■"5s $a . s ri I
hl
5-.^
4^
<s>
3
ft »tj
a--
rs
•'?
<r-
zt-
• wi
ii>
&
- ST
■JS
Sr
g
2
5
ft
C--'
-.3
<4!5
MX-'
!
r;
X~-
in ’%.'
iS
o
£u
7> x
s“?
&■
gZ s ■
•1»
*&
j /•
’
K 1-*
•
i
?:r
i -r
►-■ rt!
>’• -0
t5*
-et^ •'
o a
»-! .SU
3-a;
Is
e:j
"i
«•-4
1
g
r;
’■ 2-
■.-!r
>
.®
o
c >
♦-• © I
JV.
—
<p-
.1
w c
c*
a.
o
?•'{
5» rt
»s
O'-
SI >-■
n
J. ?*
■r? ->■
i
•Ph
-
O
Cl
i
• - d'S
n
■V
•z.
!
ft;-'
‘4»
W
t'V
utu. i-.rt
%■
Cj
--£ rt
o
ro
aar
a
■
Ci
■ (f.
r >.
]
■t-
'.'t'
a
-•
c- --■
5;:’
!.
•i
g
i
<T »
k
?
£
3?r't-r
r:
X
3-.. -..
C? A -- §
!:G . . &.. >• k <-* S
tc
<-.<■ <?
§
r--
£S£ w--
tl
M
Q
{S
5
S
••“♦ l'rt
ix :r a-
<
*§
£
ac s-
y a »
m- o
cr
■ -
}r>-
g; -
=£
~ iT •> O ft
A*
trt
5tr on
Ki/
O C‘ •■*
(rt f-F» c
o
« it ?
rt V*
v>
fi
0
5«. 0 M-.
rr
fj. H-
r*
'ir- >-'■<-hK'
rt-* in
I &’£
11 l
&
> * Su
I
I%
>’?r t
!*'
-t
*£
•-■■
o
s £5
jn
C
iP £
•■■1 n
vn
ft*
G-.
•5
sr
s
•s
'fi
-j
n
G
t
rod
X
:t i-5
M
-
L^.l-Cri;;_ ____ -^- '-.a-'.
6*
Ct
*n|
'. a#
.s«
.
1
"i
8
I
Is
LL
r ^■
n~
'I ■
H fe fx
U
h
1Si
i
*
<s
75i
■
L?
'»
' 1
o ■
sa
-' <s
:•■*<»
:
cl
Sb
•ifef
ut •* ifc
I
■'
sq
Ias> I
—
J
11 R r
rd
d.
Q
i <r
t-. rt-rt
&>
2!
)1<--
yi
rt «
&
,> ff
ft1
H it
f*
ft
-5
01
3
■hr
5S> s-.i :.-T << &.
tn
(15 in
■”/ r^-
•t?
-
-
■?
’’i?
y;4-
a
’
/.■
-'^
'■' alX
I
S3
«..
- !•
.j
t
1\
j
i
I
witmn |figure oj countries.
fe'ABLE 5. Availability and distribution of health
services in three countries. Source: WHO Statistics,
1979:2,
COUNTRY
POPULATION PER
Tanzania
Kenya
Sweden
■
DOCTOR
NURSE
PHARMACY
19000
fl 500
580
*3030
1000
120
*400000
75000
2130
A
5000
-, 900
.
prsv&Jsnce
350 2:
30<* £
MQRTALiTY
§2 SOO
!i
So 600
•200 £
ft
50* .
11 400
fecovesy
ef de&th
-2
J50 2
.•£
Joo €
IS | 3C© \
200
AHENDANCey
?00
50
c’"~ l—2 *~5—T“s----Distance from clinic in mites
: FIGURE‘ 7. An illustr
I
prevalence and incid
1
Un.^er stable'conditions we h
Prevalence * Incidence * dur
tfsjjjnsu h»r. cSne. ^sadatce «a»e3
end owrths Imm cJartoed dsswta
Dfccbjec O*^
fc^-ads^h. 1977-1978}
From this 4w^ can deduce th
measurei for chronic dis&aae
scute diseases
<
' or acute
etiologic studies, incidenc
do prevalence and inciden
instance
and
a
&
Ti&v
prevalence of the disease m
survival
despite
inciden
• decreases.
FIGURE 6, A long way..from health;
Source: The state of the world's
children. Unicef, 1934.
Some basic epidemic logic concepts
/
The concepts* of prevalence and
PLANNING AN INVESTIGATION
i
epictemiology. Pievalence
1
co
incidence (new- c&ses} on t
on the debet side (Figure 7)
incidence
are
basic
in
Concepts and measures
!
TO
a » large
«
e
extent,
COMPARISONS, For these co
alternative explanations w
PLANNING AN INVESTIGATION
j
I
28
/
■
i
when <—-—
•
mow<?ity between t,_
f^?ar^n?
two areas, one with access
. to water supply
other not, we have to take
--- into account
the fact that
of
the
the
Populations
Lcfr.^CO'’P?Sltion
s may
etcfeCThishanr«S:
^“-eco^ie
structure
mai
not be~equ"ar',
tne socio-economic r*-- that c is aPconfouAdin“T"tLla^.“ed
"confoundi"9"
i"PUeS
/commonly labelled "confounding
between an
n
-f t>.3 association
exposure
factor E
D88^13^0"!^^!?
E and
and a disease8
disease u D itif itit xsis both
both a
uiaease-causina factor
fartnr- <
some way related
suspected exposure"(Picure Bj in
5®late<3 to the
Secondtn/X
directions of these
ependin<5 on the strength and
• Depending
factor may
, a confounding factor
either spuriously strengthen or
or dilute an association.
cc
foTO BREASTFEEDJbfG
PROBLEM: Is 1there
‘
an associ
and breastfeeding in the s
at least 6 months are le
diarrhoea?
MEASUREMENTS: Home-visits e
diarrhoea, A pre- tested ques
SAMPLE: f”
•.11/.__ 1___
All children
born du
in the well-defined
catchment
*
--- j
t
I
I
DESIGN: Prospective
r
cohort (
followed from 6 fto 12 mont
the study is 6 months.
.1
Let’s' divide the 400^chiId
<
those’ who v
were breastfed fo
were not (n=3G0)^
E
*
I
Usually, Confounding
Confounding in epidemiology
is accounted for by
means ox some procedure for —
either be indirect or direct- • : SMWDAHDIZATICN This could
that the observed
nu^r-of^ca^r
observed number
of
outcom*
e vssit) is j-ompared with what could be expected’ had
the sliidy groups J
of sofae other event! < "
I ox
certain reference group. The ratio
. of observed to S???ctei’
expected
nun,t,er
casL is e ned th^
i uandardized
. ...
emorbidity
ratio (SHR). Ait«^tively,
Alternatively
•i comparisons betw^n
mult'
when
■
between multiple categories r“
j
method impliesS that
a
axe
the direct
tnat,a common reference category'is
then, are applied the risks
-y
'
for each of these
calculated
reference
umber
and
the
observed number gives •J so calculated
the so called
estandardized rate ratio"
ratio" (SRR) which is comparable
over
s^ve^al study categories. .
An
example
of
these
j jrocedures is
giyen below. This rexample
also illustrates tl
concept of
’’biologic FRACTION*,> the = number
of cases of a disease
that
can be attributed to a certain 2—
exposure.
}
i
t6:?
I
RESULTS:
/
/
/
I
FIGURE 8. Confounding" the association
between an exposure (S) and a disease ID'
risks <
During the 6-month period,
at least one acute diarrho
111 were not.
Thus f the
Incidence => 148/400
0..37 epi
Since 37/100 « 111/300 « 0.37,
there is obviously no asso
breastfeeding! Or?? Well, w
disturbing factor (confoundex)
H'aisr
quality
\
I
breastloedifK}
t
\
\
\
PI*ANb>IMG AN INVESTIGATION
I
1
Concepts and measures
V
^LANNING AN INVESTIGATION
i
I
i.
iL
As a matter of fact, it is:
BREASTFEEDING
Thus: •
'
\
WATER QUALITY'
Good
Bad
Yes~
No
4G
260
40
Total
soiT
Too
Total
300
"Too
'
- ttose having good water are sore
implying that they give up oroast-feedi^g . •
early 4?)
.
! f
;
How, then, to account for this.in the analysis?
children
BREAST-
feeding
with
diarrhoea
WATER QUALITY '.
Good
Bad
Yes
NO
73
3
"3T
38
Total
TT"
71“
are
^r:xt££Us
either by analysing simultan
analysis) ox by standardizin
•two ways:
- indirect standardiz
' - direct.standardizat
Too
INDIRECT STANDARDIZATION:
,
- those lacking good water are wore aware of the
importance of breast-feeding (4 ?
Those
148
follows:
lb thus seeras '&S
-as if there
breast-feeding groups within
hidden
i more
water. A comparison betwee
must consequently t^.ke water q
In the two breast-feeding
111 children with diarrhoe
taking into account the d
groups?
. .
distributed
.In the breast-fed groups
as
G-26MD * 0.71*80 « 53
. i
SNR®‘’Standardized morbidity
»(37/53)•100 «70%
Total
In. the non-breast-fed group:
"Tr
0.26ft2$0 ♦ 0..71M0 »
ill
148
This gives the following incidences:
so » (iix?w«ioo * ii€%
ON: m
in the brea
INTERPRETATION:
i
-- —
is 30 per cent lower and
cent higher than in the whol
DXRBCT STANDARDIZATION: k
breast
feeding
WATER QtJALi'n'
Good
Bad
Total
Yes
3o
0.28
>57^'
T37TT
Totally» w® have observed
many would there be
TStsr
0.'26
0.71
0.37
- had all children ^
- had no child beet*
0.55
0.37
PLANNING AN INVESTIGATION
Xf all children were breast-fed:
The relative risk is
0.10*300 •> 0 .'55* 100 « 85
RjR » 0.28/0,10
If no child was breast-fed:
SRR = "standardized rate ratio" «
M"Calculated no* / Observed no)
100 *
(35/148)•100 = 57% for breast-feeding
where 0.10 is the ’baseli
(’attributable* risk) is
(0.28-0.10) »- 0,16
0.16 "causing*
0e 18*260 ® 46,5
46, e- “extra" ca
an
ETIOLOGIC FRACTION asionq the
and (179/148)*100 « 121% for non-breast-feeding.
of
0,28*300
J
2.8
0.95*100 « 179
-^
* 46.8/73
64%
(or (RR-D/RR « 1.3/2.8 » 64%
The SRR-figures can be regarded as relative risks for
diarrhoea fin the
“
respective groups relative to SRR * 100 for
the whole group.
They can also be used to adjust the original rates (0.37 and
0.37) sc that we Qet the following adjusted values:
Breast-fed children ; 0.57*0.37 « 0.21
Non-breast-fed children: 1.21*0.37 * 0.45
WATER QUALITY
Bad
Good
Crude
incidence
Yes
No
0.10
0.28
0737
0.37
0.55
0.95
Similarly,
(5.5-11/5.5 « 82%
breastfed group and
shr
SRR
Adjusted
incidence
116
57
121
^71’
0.45
27 c
or
(9.5-11/9.5 - 89.5%
non ’breast-feeding
S08MAR¥:
SREAST
FEEDING
Thus, ’’64% of the children
’caused' by* non-breastfeeding
ar . 34
THUS; OUT GF 148 CASES,
WATER AND/OR NON-BREAST-FEEDI
.cases of dianhses
eo ■
Gut of the 148 cases with diarrhoea, how many are "due to:
bad water and/or non-breast-feeding?
Out of the 73
' cases that have access to good water but a,
not breastfed., how many cases of diarrhoea are due to this
'exposure1?
40
20 -
SH
„„
S
goad goctf ba
yas no
PLANNING AN INVESTIGATION
Concepts and measures
PLANNING AN INVESTIGATION
- 34 -
3
SURVIVAL
It also seems natural
to give some overall measure of the
mortality in * group
(cohort) as
.
for example that age, at
which 50 % of the i___
_
individuals
called the median 'survival
nave passed away. This is
’--1
time, M. Another possibility
would be
give the
mean survival time,/ L, which is the
arithmetic average of
the individual
skew distributions
it is characteristic survival times. For
coincide.
that M and L do not
When calculating SISKS
OCCURS?";; Kve\oEBTAIN
THE EVENT OCCURS,
fAk. i^EtiT or iu‘rE£ By which
we
the risk population from e,K4rj e lnto account the SIZE of
*»!
which
new cases of the event are
emitted”.This1 size
size could be
measured
either in "counts” as
in
a
-ixed'
cohort or
experienced.
ivcu. Sincemore often kb am°Unt °f “r-sk-timeSince
ot‘-en than not,
follow-up time
varies L_
between individuals due
to WITHDRAWAL fr-m the study
individual person-times
Withdrawal can occur
may be * lost to
cooperation, etc. *
under study may
may be r- ••
t^\?$
the
e-StUdy st ^ffere’nt
study” wi 11■ fourth5
r
;onow-"P period'
of
individuals, The j
some
because of medical1
S9n for Wlt^rawal is that,
S' SOR,e individual, may have to
removed from the s^udy!
HS
Once the -V.-NT under scuay nas occurred,
has
of course, no longer study
"at
”st risk" for the the individual is,
multiple «S?«ofre?Ces are studied,
same event, unless
The "event” may be a
are studied.
certain
disease" or c~"~*
vf
cause
of
"death"
rlike "end of jbreast-feedi ngw
or some other outcome
or "first visit’’to
clinic”,
it should,
however, be a well-defined . a health
end-point. This is also the
and unique
basic requirement
LIFE-TABLE analysis.
for the
In
r ’ '
life-table
analysis ^can be US€(3 to
summarize
during a
hri7"f7TABLE)
observed
(current)
time period “ but
also r
b^/lso.Earve
to assess
survival .after a cz
certain
Life^bie
or fcreafcment
diagnosis
(CLINICAL LIFE-TABLE)
analysis "&n _
"events” inot necessarily
rbe U£ed on
dealing with^tfwith matters of
death, it could
of stay in
hospital, where
is
"death” is
hospital and
Life-table
r
applied to
been
as
the
contraceptive Practices,
it can els““s^
or fc-failure of
can also
- -o evaluate
■H.WIFG an
investigation
hea1 th
di
Consider
evabaat^
i?neQ as s
during th^“f
•*
resold in t^”reaydur-na
left and nso^
thejr
fit-R*-
rhiiri st,
' .
o? Stifi^io^^h;^1"^
behaviour,
t
the first
used.
We
f£^“ias i
BREAST-FEEDING
analysis
IN
FICTITIA
In the country <of FICTITIA,
decided that, on tne road t
information about the
breast
and duration)
in ute country.
be children
under one year of
has recently been made,
it s
representative sample,
Since
important
to identify
" i-t?OSe
geographically)
that must be su
For purposes of
the material
_.
.
nt.re, consisting
cross-sectxonal study were asked
!«?> TJ*3
chiK4 to
u e 5^1Id receive
~ didfch^«H« i? not bre
gio. breastfeeding stop?
The
results
showed that, out
out of
of
mu' 50° hSe
?rea9t-
br?^;-*po'h« * 4
stopped.
Age
breastfeeding was given up ar© sh
L
Concepts and measures
PLANNING AN INVESTIGATION
•• '■'■’IT-
1
Background
\ J
IV
medicine and commuriityliealth are at the
bottom of the ladder; a choice inversely
proportionate to their usefulnessun deter
N H Antia
mining the health of the nation. These im
portant subjects in medical education also
suffer from a vicious circle for they by
While the medical profession has played an important role m
and large also fail to attract the best
determining the health status of the country, it has also been
teachers. The fossilised methods and
responsible for the distortions in the health care system. What can nature of basic science teaching combined
be done to change the situation?
with glamorised teaching of technology
in the specialised clinical subjects has
resulted in an increase in the annual pro
resulted in the failure to produce medical
THE aim of professional education in the
scientists and basic doctors. While the vast
field of health must be the production of' duction of doctors from about a thousand
to over 13,000 during this period. The
majority will perforce have to eventually
a cadre of professionals who would have
majority are still government colleges
gravitate to general family practise it is
both the competence as well as the
funded by the public exchequer but lately
anachronistic that there is not a single
motivation to serve the health needs of the
there has been a rapid increase in the
general practitioner as a teacher in the
country and its people as a whole. The
private colleges. The struggle to secure a ' medical college especially when the
number and type of health professionals,
seat in a government medical college is
majority of outpatients are flooded with
their recruitment and training for the
demonstrated by the mark list of th®icansimple common ailments from the local
various functions at various levels and
- Lion* 1UU3L
uu determinedHprimarily by didates and by the high capitation fees
vicinity which are then referred to
locations
must be
' th^actuaiprob'lemrof healthm both the paid in the private co1Ie8'\br^hfns,e^c°
specialists for lack of a family physician.
the government ones.
rural and urban situation, the prevailing
rfail’ to get entry into‘u“
The reorientation of medical education
In both cases the advantage is for the
(the ROME scheme) is a farcical exercise
• pattern of diseases, the available health
children of the affluent. Those few who
in a vain attempt to sensitise the student
technology, all this in keeping with the
are admitted in the seats reserved for the
trained for five years in high tech clinical
human and financial resources available
backward castes are at a considerable
medicine to the entirely different rural
to the country.
disadvantage due to their different
health problems of our people in a period
Unfortunately the production of the
aw v.
cultural and educational background,
of three months. The Lentin Commission
number and various categories
of H
person
training is entirely
Despite this after qualifying they too have
has also demonstrated the chaotic ad
nel as well as their I,.
the same aspiration as the rest. Bar excep
ministrative and bureaucratic manage
disproportionate to the actual needs and
tions the reason for the choice of medicine
ment of these hospitals and their specia
has to a great degree been dictated by the
lised units, revealing that even the soperceptions and needs of the medical pro as a career is the assured high level income
called best medical colleges and hospitals
fession whose values and aspirations are with a high social status.
The values of the medical profession
are mere caricatures of the western model
more in consonance with those of the
are, therefore, determined even before the
they choose to emulate.
prevailing western model rather than the
entirely different needs of the vast student enters the portals of the medical
The aim of the medical student after
majority of our own people. Hence the college. These values arc reinforced
qualifying is to specialise and get theo
year
throughout
the
five
and
a
half
course
larger number of doctors than nurses and
retical if not much practical knowledge
and later during post-graduate specialised
paramcdicals, the emphasis on expensive
with the hope that this may help him/her
training.
While
the
honorary
system
atspecialised curative medicine in large
to secure a job abroad or in a five star
uroan
urban hospitals .v.
for non-communicable tracts the elite of the profession, the train
private institution in a city. Since these
diseases rather than the far more effective ing they impart is
avenues are limited, the majority perforce
yet lower low cost preventive, promotive expensive medical l^hn°,0£yJfh^y
'
gravitate to small private nursing homes
and basic curative services for the rural tise. Even worse are the values of lucrative or general practice for which they neither
private
medicine
that
subconsciously
they
population and urban slums.
have the training nor even basic facilities.
inculcate into the receptive young mind.
The crucial role played by the medical
Over-production has now driven them to
With
disparity
the
increasing
between
the
profession (and especially of the private
seek government posts which were dif
sector which now commands two-thirds earnings of the private and public sector,
ficult to fill a decade ago. Unless posted
oi the
me country’s
counuy , medical
u.cu.^. manpower
-------------where
a surgeon in a single operation in
of
as well
as the health expenditure) in reversing the private practice can earn the equiva ent of in a city or district hospital they perforce
have to serve in a rural primary health
*
one or two months salary of his full-time
health priorities can no longer be ignored.
centre where the requirement is chiefly of
Their influence in determining the type counterpart, it is difficult to retain good
a managerial physician to cater to the
teachers
doctors
especially
motivated
and
and quality of the country’s health
health of a population varying from
in
the
clinical
subjects.
This
has
led
to
a
services, either directly, or indirectly as
30,000 to over 1 lakh with about 30 to 60
physicians to the rich and influential, far further deterioration in both the technical
paramedical staff under their guidance
aspects
medical
education
as
well
as
in
of
outweighs that of those who seek to
and supervision. Besides management
develop the health policy and services the values that are imparted to the
even the medical functions are chiefly of
, .
along rational lines for the good of our student.
preventive, promotive and of a social
The values of the vast majority of
society as a whole. The medical profes
medicine nature, the lowest in the
students
is
reflected
in
the
importance
sion has equated health with illness,
hierarchy of medical education. There is
to
the
various
subjects
and
doctors, hospitals, drugs and westernised they assign
little time and even lesser facilities for
even
more
so
in
the
choice
for
post
medical technology and converted illness
i
clinical medicine for which alone he/she
graduate training. The glamorous high
into a lucrative business and industry.
I
is trained. The most important aspect of
tech
and
lucrative
fields
like
medicine
and
Medical education plays a key role in
:
our health system, the primary health
perpetuating this system. The vast increase surgery and their subspecialities likeL
centre which has to cater for the needs of
first
cardiology
and
plastic
surgery
are
the
in the number and size of medical colleges
1
the 70 per cent of our rural population
from 25 to 125 in four decades has choice while preventive and social
Medical Education: In Need of Cure
Economic and Political Weekl)
1571
July 21, 1990
I
is theretore encumbered with a leader
whose training and values are almost
diametrically opposed to the health needs
of the majority of our people and the
functions to be performed.
Under the circumstances the prevailing
system of medical education is almost
entirely divorced from the health needs of
the majority of our people, both in the
public as well as in the private sector. The
over-production of doctors and of drugs
because of their lucrative nature has
invariably resulted in a form and extent
of malpractice which now poses a new
threat to the health of our nation, both
the poor as well as the rich.
The question arises that if the vast
majority of both the non-medical as well
as the medical functions of health can be
best managed by the people themselves
with the help and support of the para
medical workers then why not concentrate
on this aspect of health and ignore the
medical profession which has gone so
awry. This unfortunate attitude continues
to prevail not because of the failure to
appreciate the needs for the increased level
of skills and facilities which are essential
for certain aspects of technical medical
care, however small it may be of the totali
ty of health, but because of a feeling of
helplessness when confronting the entren
ched and extremely powerful bastion of
the medical profession which it has built
for itself through various means. These
vary from offering the lure of an ex
trcmcly lucrative professional career to th.(
children of the rich and influential ai
public expense, high level of monetar)
gains to both the promoters and the politi
cians who run private medical colleges
under the guise of producing doctors for
the rural poor, a good prospect of emigra
tion so attractive to the elite, by offering
the ‘latest’ western type medical care to
the politicians, bureaucrats and the rich
who believe that ‘West is Best* and that
too often free of cost in major government
and five star private hospitals, by
glamourising expensive technology and
mystifying health into an illness business
1 which the people are told is too dangerous
to be left to anyone but the allopathic
trained medical profession and preferably
those who are specialised..
Unfortunately health is too important
a commodity to be left to the tender mer
cies of a profession whose chief interest,
like most other professions in capitalist
market economy, lies in the maximising
of monetary gain regardless of other
scruples. The nation’s health, both pf the
rich as well as of the poor is now threa
tened by the burgeoning health industry
with its insatiable appetite based on self
created demand and consequent rising
costs without concomitant benefit. The
1572
effect of this on the poor masses in a
country with limited resources is far
worse. The health debate even in the
affluent countries is now centred in the
containment of cost, with control of the
medical profession as the key factor.
Since the profession as it exists today
has failed to shoulder their responsibility
the inevitable result is that society has
perforce to undertake most of these func
tions by itself and define the role of the
medical profession in serving its needs.
This must perforce lead to the control of
the profession in the interests of the
society at large. Since self-regulation is not
a part of this new order in India and since
the people must be provided with
adequate basic health care, alternative
means have to be devised to regulate the
medical profession and define their role
in the health care system of the country.
The regulation of the profession must,
start even before the stage of medical
education by determining the human
power required at each level in a graded
decentralised system based within the
community. The gross distortions in the
present set up where there are more
doctors than nurses, more nurses than
ANMs and more ANMs than community
health workers will have to be corrected
for any meaningful health system. This
will invariably result in limiting the
number of medical schools and the
annual production of doctors. It is clearly
unacceptable that the two-thirds who
enter the private sector be trained at the
cost of Rs 3 lakh per head at public
expense in government hospitals.
Since over-production invariably leads
to malpractice, especially in a field where
consumer resistance is at its lowest, the
opening of private medical colleges can
not be justified on the basis that this does
not involve public funds and that over
production wall automatically provide ser
vices to the rural poor. The majority of .
graduates even of these colleges choose to.
practice in urban areas and even if under
economic duress are driven to rural areas
they practice a form of curative medicine
without even minimal facilities and which
is highly dangerous, like the widespread
practice of giving of unnecessary and even t
harmful injections. This has diverted the
meagre income of the poorest from nutri
tion to such necessary and unethical '
medical expenses with little benefit even
for the actual care of their illnesses.
The present form of medical education
which is based on an ad hoc importation
of western medicine also needs a radical
reorientation to meet the entirely different
needs of our people. The teaching of basic
sciences like anatomy, physiology, bio
chemistry and pathology are outdated
even by the western standards they imitate.
Economic and Political Weekly
July 21, 1990
As a'result of the vast increase and rapidly
z changing nature of knowledge the need
is for the teaching of broad principles,
stimulating curiosity and teaching the
intelligent retrieval of information and
utilisation of the libraries and other
documentation facilities; to inculcate a
habit of continuous self-education not
merely to pass exams but as a lifelong
pleasurable exercise; a process which is
almost entirely neglected in the present
curriculum.
Since public needs demand that the vast
majority of the graduates must undertake
general practice whether in private or at
the primary health centre the emphasis of
under-graduate medical education must
be for this rather than specialised services.
The present clinical training is undertaken
entirely in specialised departments, for
strange as it may sound, there is not a
, single general teacher of family medicine
in our entire medical educational system.
As a consequence the young MDBS
doctor sees the patient as a series of dis
jointed specialist problems rather than a
whole human being in relation with his
family, job and society which is the
essence of family practice. This has con
sciously or unconsciously led to over
investigation, over-medication and overreference to specialists and excessive
hospitalised care. The majority of under
graduate clinical medicine should hence
ideally be undertaken within the com
munity at the primary health centre and
community hospital. Since this is a distant
goal there is no reason why the out
patients of medical colleges, which arc
mainly crowded with thousands of
patients from the adjacent locality with
common family ailments should not have
a number of family physicians with simple
pathology and diagnostic facilities to
attend to these problems who are at
present referred by out-patient clerks to
whichever specialist they feel is the correct
one. This simple practical device would
not only screen the majority of patients
• and save much time and expense of both
patients and specialists but also enable
instruction of the students in the most
essential and relevant part of their under
graduate training namely, general practice.
It would at the same time reduce the cost
of these expensive hospitals where some
of the beds can be allotted to these
k
teachers of general practice.
■
The subject of decentralisation of such
■ large and inappropriate urban hospitals
into community health care institutions
where 95 per cent of all preventive, pro
motive and curative services will be
catered to within the 1,00,000 population
level as recommended by the ICMR/
ICSSR report will need to be dealt with
elsewhere.
Far more important than a reorien.
Econoniic and Political Weekly
tion of the technical aspect of the medical
education are the values that are in
culcated during the entire period of training in the young and receptive mind. As
stated previously the influence of the
dominant values of the society at large
will prevail. The most that one can hope
to achieve within this social system is to
inculcate a desire to combine monetary
with job satisfaction, which has somehow
got lost on the way and has led to much
frustration.
The present method of inducting immafure youth at the age of 16 or 17 years
directly after SSC into medical college
cannot be condemned adequately; for
medicine is a subject which deals ulti
mately with people and the most intimate
aspects of their life. Many if not most of
the problems that modern medicine suf
fers from is the conversion of a science
dealing with life into an exercise in mere
technology. This has resulted in the com
mercialisation of health into an ‘illness
business’, from ‘caring’ to ‘cure’, frustra
tion from loss of job satisfaction and
alienation from the people.
Some corrective measures need to be
taken. Five years of training is unneces
sarily long for the technical training of a
basic doctor for the needs of our society.
Specialists will in any case receive ap
propriate additional training in their own
field. Much more important would be to
provide the first onc-and-a-half to two
years of training in the general as well as
health related humanities and basic
sciences both which stand out by their
absence in the present medical curriculum,
This should include subjects like the
sociology, anthropology, economics,
statistics, demography, psychology, ethics,
documentation and communication. This
may either be undertaken in the medical
college with a suitably inducted faculty or
in the departments of the university. This
would help to produce a more mature and
sensitised individual for a three-year
course of which one year should be in
basic medical sciences and two in ap
propriate basic medical technology and
practice.
Even in the field of specialisation the
largest needs will be for the general
surgeon, general physician, paediatrician
and obstetrician/gynaecologist who can
be trained to carry out the common pro
cedures which comprise the vast majority
of specialised care which have now been
appropriated by the ever increasing
superspecialities today. This would leave
only a few problems for the superspecia
lities located in independent institutions,
preferably isolated from the medical col
leges, and acting as pure referral centres
for the most difficult problems. This will
ensure that in the medical colleges the
students will be exposed to the general
July 21, 1990
practice type of medicine and only to the
four above mentioned basic specialities
and not distracted and diverted by the
glamorous but far less important super
specialities with which they need only
nodding acquaintance. This will also
permit the rejuvenation of the four basic
specialities whose realm has been eroded
by the superspecialities in the present
medical colleges and hospitals.
The present system of medical educa
tion dominated by the superspecialities
has played a crucial role in distorting the
values of medicine not only among the
medical students who will be the future
doctors, but also of the public as seen by
the false demand created by these specia
lities. One of the results of this distortion
is the devaluation of most important sub
ject of preventive and social medicine
which, bar exceptions, fails to attract the
best teachers or students. This vicious
circle has to be broken by raising the
prestige of its teachers and by compulsory
devotion of more time and examination
questions to this subject. There are several
examples'where a good teacher has been
able to create interest in what is basically
an interesting subject which is generally
taught drably and perfunetprily. The most
important aspect of medicine, namely,
epidemiology and communicable disease
control, is a part of this discipline.
The importance of the medical profes
sion in determining the health care of (he
nation cannot be underestimated. They
can be the leaders in orchestrating the
health services if not in health care if they
so choose. On the other hand they can and
have played a crucial role in distoning the
whole system. Motives and values arc far
more important and must precede and not
be subordinated to technology which used
appropriately can transform the health of
our people. Used inappropriately it can be
a powerful tool for their exploitation.
The Medical Council of India as the
apex body responsible for medical educa
tion has failed to fulfil its task. Leave aside
setting an example of high moral and
ethical values it has utterly failed even in
devising a curriculum in keeping with the
needs of our country. Nor pas it been able
to resist the political pressures in the open
ing of new colleges which fail to meet even
the elementary needs of medical educa
tion. A radical change in this outmoded
body with the induction of dynamic
young teachers is an essential prerequisite
for the improvement of medical education
in this country.
All this will undoubtedly require a
powerful peoples’ outcry and through
them the development of political will to
bring about the necessary changes.
Without this health care will remain a
chimera and a mirage for the vast
majorit
our people.
1573
COMMUNITY HEALTH CELL
326, V Main, I Block
Koramongala
Bangalore-560034
India
♦
THE JOURNAL OF THE AMERICAN
SOCIETY FOR PSYCHICAL RESEARCH
Volume
July
71
Numbers
1977
Deathbed Observations by Physicians and
Nurses: A Cross-Cultural Survey
Karlis
Osis and Erlendur
Haraldsson
1
ABSTRACT: Surveys of deathbed observations were conducted in the United States
and in India to replicate the findings of a pilot survey carried out in 1959-60 and to
gather more detailed data relevant to the question of post-mortem survival. Physicians
and nurses filled in questionnaires and subsequently were interviewed concerning 442
cases in the United States and 435 in India. The most frequently reported phenomenon
was that of terminal patients having hallucinations of human figures.
The main findings of the pilot survey were confirmed in the present survey in both
cultures. Again, four-fifths of the apparitions were ‘‘survival related”; that is, they
portrayed deceased persons and religious figures. This is in sharp contrast to the
hallucinations of a normal population. Three out of four apparitions were experienced
as having come to take the patients away to a post-mortem modus of existence, to
which 72% of them consented. More patients responded with serenity, peace, and
elation (41%) than with negative emotions (29%) to this ostensible invitation to die.
The data were analyzed for interaction with various medical, psychological, and
cultural factors which could cause or shape hallucinations. In conformity with the
survival hypothesis, the deathbed visions were found to be relatively independent of
these factors as they were assessed in the population surveyed.
Introduction
At times dying patients “see” persons and visionary landscapes
which others present do not see. Usually such deathbed visions are
1 The American survey was conducted with the support of the late Chester F.
Carlson. The greater part of the Indian survey was funded by the James Kidd bequest.
We are grateful to our Indian collaborators, particularly Dr. J. Prasad and Mr. P.
Dayal, and to our American consultants, especially Dr. Gardner Murphy.
4
238
Journal oj the American Society for Psychical Research
interpreted as mere hallucinations which have no basis in external
reality. In the early years of psychical research, Myers (1903) and
Hyslop (1908) recognized some possibly paranormal elements in a
few selected cases of visions of dying patients. Sir William Barrett, a
physicist of the Royal College of Science, Dublin, was interested in
such cases and presented a number of them in a small book entitled
Death-Bed Visions (1926). While some of his cases were carefully
observed by physicians and nurses, others are of lesser evidential
quality. Barrett was particularly impressed by visions that seemed to
mirror some form of contact between patients who were fully rational
and cognizant of their physical surroundings and their deceased
relatives who, presumably, had passed on to the “other world.’’
Often in these cases the ostensible purpose of the deceased was to
take the patient away to a post-mortem plane of existence. Barrett
emphasized cases in which apparitions ran contrary to the patient’s
expectations, for example, apparitions of persons the patient thought
were still living, but who in fact were dead. In several of Barrett’s
cases the apparitions were experienced either with exalted feelings or
with emotions of serenity and peace. Deathbed visions, Barrett
pointed out, often did not conform to cultural stereotypes, e.g., dying
children were surprised to see “angels’’ without wings.
Some 30 years later, Barrett’s work inspired one of us (K.O.) to
systematically study deathbed experiences using modern survey
methods and statistical evaluations. In 1959-60, under the auspices of
the Parapsychology Foundation, K.O. conducted such a survey. It
was the first of its kind and will be referred to in this paper as the
“pilot survey.’’ The report on the pilot survey was published by the
Parapsychology Foundation as a monograph, Deathbed Observations
by Physicians and Nurses (Osis, 1961).
K.O. found that deathbed visions which appear to be suggestive of
post-mortem survival tended to be independent of factors known to
cause hallucinations, enhance their occurrence, or influence their
content. Medical factors—such as illness predisposing to halluci
natory experiences, high fevers, medication with morphine, etc.—did
not seem to generate an increase in the frequency of after-life related
experiences. In some instances, such medical factors even appeared
to suppress survival-related phenomena. Moreover, personal vari
ables such as the patient’s sex, age, education, socio-economic
status, and religious affiliation also appeared to be of little
importance.
The contents of the dying patients ’ hallucinations were analyzed
and found to be different from those of hallucinations in the general
population and the mentally ill. For example, hallucinations of the
dying are usually visual, as is the case in most ESP experiences, and
rarely auditory, the predominant mode in mentally disturbed
*
t
239
Deathbed Observations by Physicians and Nurses
persons. Terminal patients were reported to have seen apparitions of
the deceased, rather than of the living, two or three times more often
than do people in the general population. Of all the apparitions of
identified persons, 90% were of relatives of the patient; of these,
90% were close relatives: mother, father, spouse, sibling, and off
spring. This occurs infrequently in the hallucinations of the general
population.
K.O. also performed extensive interaction analyses on the data of
the pilot study. This led to the discovery of many patterns which
supported the post-mortem survival hypothesis. He believed,
however, since most of the findings were post hoc, that without
verification in later surveys the weight of the findings would be rather
limited.
The two new cross-cultural surveys described in this paper were
carried out to replicate the pilot study. The range of questions was
greatly expanded in order to obtain more information which might
either support the evidence for post-mortem survival, or provide facts
contradicting it and thus lend weight to what we have termed the
“destruction hypothesis.” Information from the pilot survey and
other sources was used to formulate a model, or series of hypotheses
concerning deathbed visions. The model is a bi-polar one which
sharply contrasts two mutually exclusive concepts: the survival
hypothesis and the destruction hypothesis.
A Model
of the
Two Basic Hypotheses
Survival
Death is the transition to another
mode of existence.
A.
*
of
Deathbed
Visions
Destruction
Death is the ultimate destruction
of the personality.
Sources ofDeathbed Visions
Extrasensory Perception
1. Extrasensory awareness of
discarnate entities, e.g., de
ceased relatives and religious
figures.
Sick Brain or Delusions
1. Malfunction of the nervous
system and the dying brain.
2. Clairvoyant or precognitive
glimpses of post-mortem ex
istence.
2. Schizoid reactions to severe
stress.
B.
Influence ofHallucinogenic Factors on Deathbed Visions
Independent of Medical Factors
1. The presence of halluci
nogenic medical factors will not
Dependent on Medical Factors
1. The presence of halluci
nogenic medical factors will in-
240
Journal of the American Society for Psychical Research
increase the frequency of visions
related to post-mortem ex
istence.
crease the frequency of halluci
nations related to post-mortem
existence —i.e., the more dis
turbed the brain processes, the
more numerous the “otherworld” fantasies.
2. Conditions detrimental to
ESP will decrease the frequency
of after-life related phenomena.
2.
C.
Content ofDeathbed Visions
Perceptions
1. After-life related visions will
be relatively coherent, and orien
ted to the situation of dying and
the transition to another mode of
existence, including “other
worldly ” messengers and en
vironments.
D.
ESP not involved.
Hallucinations
1. Hallucinations will portray
only memories already stored in
the brain and express desires,
expectations, and fears of the in
dividual, as well as beliefs char
acteristic of his culture.
Influence ofPsychological Factors on Deathbed Visions
Conditions Related to Awareness
ofan “Other World"
Conditions Related to Halluci
nations of This World or
‘ ‘Other- World '' Fantasies
1. Clarity of consciousness and
an intact sense of reality will
facilitate awareness of an “other
world” and its messengers,
while states in which contact with
external reality is absent will
impair such awareness.
1. Clarity of consciousness and
an intact sense of reality will be
less conducive to all kinds of
hallucinations than states in
which contact with reality is
absent.
2. Patients’ expectation of re
covery or dying will not influence
the occurrence of after-life re
lated visions.
2. Patients ’ expectation of re
covery will facilitate this-life
hallucinations, while expec
tation of dying will facilitate
hallucinations of an after-life.
3. Presence of stress will not
increase the frequency of visions
related to an after-life.
3. Presence of stress will in
crease the frequency of halluci
nations related to an after-life.
t
Deathbed Observations by Physicians and Nurses
E.
1.
241
Variability of Content Across Individuals and Cultures
Perceptions
Little variability.
1.
2. Visions involving basic
characteristics of the “other
world’’ will be essentially similar
for men and women, young and
old, educated and illiterate, re
ligious and nonreligious, Chris
tian and Hindu, American and
Indian. Only minor differences
among them will be expected.
Hallucinations
Much variability.
2. Hallucinations are purely
subjective. They will vary widely
with the dispositions, psycho
logical dynamics, and cultural
background of the individual.
Method
We approached physicians and nurses in both the United States
and India in two steps: (a) a two-page initial questionnaire was
distributed concerning the extent and kinds of observations they had
made of dying patients, and of those who were close to death but
recovered; (b) individual interviews were held with respondents on
the details of cases reported in the questionnaires and which fell
within the scope of the survey.
Questionnaires and Procedure
The survey in the U.S. was conducted between 1961 and 1964 in
New York, New Jersey, Connecticut, Rhode Island, and Pennsyl
vania. The second survey was carried out in Northern India during
1972-73.
Although the same basic questionnaire was used in both surveys,
slight adjustments were made in the questions asked of the Indian
respondents —e.g., tropical diseases and the Hindu and Moslem
religions were covered—in order to accommodate them to the cultural
differences.
In the initial questionnaire we asked the medical personnel about
their observations of the following:
1.Hallucinations of human figures experienced by (a) terminal
patients (those not recovering), and (b) by non-terminal patients
(those who were close to death but recovered).
2. Hallucinations of surroundings (landscapes, etc.) experienced
by (a) terminal patients, and (b) by non-terminal patients.
3. Mood elevation (sudden rise of mood to elation or serenity) in
terminal patients.
242
Journal of the American Society for Psychical Research
In the U.S. the questionnaire, with a covering letter, was mailed to
a stratified random sample of 2500 physicians and 2500 nurses. Those
not responding received another letter asking for a reply. A total of
1004 responses was received.
Our Indian consultants advised us not to use the mails to distribute
the questionnaire. We therefore worked mainly in large university
hospitals. Usually the professor of medicine or professor of surgery
arranged meetings with the hospital staff during which we gave a
short talk and distributed the questionnaires to be filled out.
Practically all the physicians and nurses we approached returned the
completed questionnaires (a total of 704).
Interviews
American respondents who reported pertinent cases were inter
viewed by telephone. In India, telephone contacts had to be replaced
by personal interviews, mainly in hospitals but sometimes in the
homes of the respondents.
We developed three separate follow-up questionnaires for the
following types of experience: (a) hallucinations of human figures, (b)
hallucinations of surroundings, and (c) mood elevation. Each of these
questionnaires consisted of 69 questions used to guide the interview.
Open-ended questions were used, e.g., “What was the patient ’s
behavior indicating that he/she was experiencing hallucinations?’’
Questions proposing a set of alternative answers were also used, e.g.,
“Was the patient calmed by the hallucination, did he/she become
excited, or was there no apparent effect?’’
Questions covered (a) characteristics of the patient such as sex,
age, education, religious belief and degree of involvement in it, and
belief in an after-life; and (b) medical factors such as diagnosis,
medical history, medication, temperature, and clarity of conscious
ness. Additional questions elicited information from the respondents
concerning their date of graduation from professional school, degree
received, religious beliefs, belief in life after death, and attitudes
toward hallucinations. The main part of the questionnaire was
devoted to obtaining as many details as possible about the experience
reported, e.g., how the patient described the hallucination. A total of
877 cases, about evenly divided between the U.S. and India, comprise
the main part of the data.
Evaluation of the Data
The interview data were coded and recorded on computer cards.
Each item in the various categories was analyzed for frequency of
occurrence. For example, responses to the question, “What was the
primary diagnosis of the illness?’’ were grouped into basic categories
Deathbed Observations by Physicians and Nurses
243
such as malignancies, cardiovascular disease, respiratory disease,
kidney disease, brain disease or injury, etc. Then the data were sub
mitted to cross-tabulations. Items describing factors that might
influence each other were considered jointly: for example, compari
sons between the number of patients suffering from diseases known
to cause hallucinations (brain diseases, uremia) and the number of
patients suffering from other kinds of diseases were made in terms of
the frequency with which the patients hallucinated living persons,
dead persons, etc. Differences were assessed by chi-square statistics.
We report below only probabilities associated with the chi-square
analyses. We used the significance level of P = .05 (two-tailed).
Results
We completed a similar number of interviews in the U.S. (442) and
in India (435). The vast majority of patients involved were terminally
ill (714). We also had 163 cases of patients who recovered from
near-death conditions. Hallucinations of human figures, or seeing
apparitions, was the type of phenomenon most frequently reported
(by 591 patients). A total of 112 vision cases were primarily of
heavenly abodes, landscapes, gardens, buildings. In 174 cases,
patients did not report seeing anything unusual, but their moods
became elevated to serenity, peace, elation, or religious emotions.
This report covers only cases of apparitions of human figures seen by
terminal patients (471 cases).
Characteristics of Apparitions Seen by Terminal Patients
As noted above, reports of terminal patients “seeing ” persons not
observed by others present comprise by far the largest and most
interesting part of our data. The sample derives from 216 interviews
with American respondents and 255 from Indian respondents.
Duration of apparition. As in most instances of spontaneous ESP,
the apparitional experiences were usually of quite brief duration:
48% lasted for five minutes or less, 17% from six to 15 minutes, and
only 17% for more than an hour (Table 1, Row a).
Timing of apparition. The closer in time the apparition was to the
patient’s death (Table 1, Row b), the more frequently it had
characteristics suggestive of an after-life. The time between seeing
an apparition and losing consciousness was generally shorter than the
time between losing consciousness and clinical death.
Identity of apparition. The apparitions in our sample portrayed
living persons, dead persons, and mythological or historical religious
figures. According to the findings of the pilot study, apparitions of
the living have nothing to do with post-mortem survival. On the other
244
Journal of the American Society for Psychical Research
Table 1
Characteristics
of the Apparitional
in Terminal
Patients
Experience
Variables
Characteristics
Number of Cases
U.S. India Total
Percentage*
U.S. India Total
a.
Duration of
apparition
1 sec.-5 min.
6-15 min.
16-59 min.
1 hr.-l day
Longer
No information
85
17
11
13
4
86
83
43
50
31
10
38
168
60
61
44
14
124
65
13
9
10
3
38
20
23
14
5
48
17
18
13
4
b.
Interval between
apparition and
death
0-10 min.
11-59 min.
1-6 hrs.
7-24 hrs.
Longer
No information
17
7
26
28
117
21
36
59
64
41
52
3
53
66
90
69
169
24
9
4
13
14
60
14
23
25
17
21
12
15
20
15
38
c.
Identity of
apparition
Living
Dead
Religious figure
Combination of above
No information
30
124
22
11
29
38
54
93
7
63
68
178
115
18
92
16
66
12
6
20
28
48
4
18
47
30
5
d.
Sex of
apparition
Male
Female
No information
59
91
66
103
30
122
162
121
188
39
61
77
23
57
43
14
13
28
4
42
17
14
13
14
2
14
6
Purpose of
apparition
Taken for visitor
To comfort patient
To take patient away,
with consent
To take patient away,
without consent
To send patient back
Threatening
Reliving memories
No information
40
102
142
41
50
47
1
0
4
26
118
53
2
13
1
52
54
2
17
27
170
1
0
4
27
26
1
6
1
18
1
6
9
f.
Emotional
reactions,
1st group
No effect or relaxation
Serenity
Elation
Negative
No information
60
46
56
33
21
65
40
32
91
27
125
86
88
124
48
31
23
29
17
28
18
14
40
30
20
21
29
g-
Emotional
reactions,
No effect or relaxation
Negative
Positive, nonreligious
60
33
77
65
91
36
125
124
113
31
17
39
28
40
16
30
29
27
*
245
Deathbed Observations by Physicians and Nurses
Table 1 (Continued)
Variables
Characteristics
2nd group
Positive, religious
No information
Number of Cases
Percentage*
U.S. India Total U.S. India Total
25
21
36
27
61
48
13
16
14
♦Percentages do not include cases about which no information was available.
Figures in some percentage columns do not add up to 100 due to rounding off.
hand, apparitions of the dead and of religious figures may have
characteristics suggestive of life after death. We termed apparitions
in this category “survival-related apparitions,’’ and they comprised
80% of the cases in the pilot survey. The proportion of survivalrelated apparitions in the present survey was remarkably similar to
that of the pilot survey: 83% in the U.S. and 79% in India (Table 1,
Row c).
Could these proportions be characteristic of hallucinations in
general among persons who are not near death? Fortunately, two
British surveys of hallucinations experienced by the general
population provided data for comparison. In the “Census of Halluci
nations’’ (H. Sidgwick and Committee, 1894) it was reported that only
33% of the sample had hallucinations similar to those in our survivalrelated group; D. J. West (1948, p. 190) reported 22% in a “mass
observation’’ survey. (Categories that do not fit our classification
scheme are excluded in the calculation of these percentages.) Thus
we conclude that terminal patients in both the pilot and in the present
survey saw apparitions of the dead and of religious figures about
three times more frequently than the general population sampled in
these two British studies.
While the proportion of survival-related apparitions in the U.S. and
India is remarkably stable, the identity of the apparitions experienced
within this group varied greatly. American patients for the most part
saw deceased persons while Indian patients predominantly saw
religious figures (Table 1, Row c; Table 2, Rows a and b). In a
detailed analysis to be reported elsewhere we were able to trace
some, but not all, of the reasons which might account for these
differences. In the visions of the Indian patients (especially the
males), female figures were extremely rare (Table 1, Row d). This
fact alone could have reduced the total number of apparitions of the
dead, thereby increasing the proportion of religious figures in the
Indian sample (Table 2, Row b). Thus, while the frequency of
survival-related apparitions is the same in both samples, the
characteristics of these apparitions are strongly molded by cultural
forces.
246
Journal of the American Society for Psychical Research
Table 2
Identity
a.
b.
of
Apparitional
Variables
Identity
Secular
Mother
Father
Spouse
Sibling
Offspring
Other relatives, previous
generation
Other relatives, same
generation
Other relatives, next
generation
Unidentified relatives
Friends, acquaintances
Unidentified persons
Totals:
Religious
God or Jesus
Shiva, Rama, Krishna
Mary, Kali, Durga
God of death & messengers
Saints & gurus
Angels, Devi, etc.
Demons & devils
Other religious figures,
unidentified
Totals:
Figures
*
Number of Figures
U.S. India Total
Percentage**
U.S. India Total
60
15
49
27
27
16
16
10
15
17
76
31
59
42
44
28
7
23
12
12
14
14
8
13
14
23
9
18
13
13
5
7
12
2
6
4
2
10
12
1
8
4
0
9
21
25
240
4
14
8
61
178
4
23
29
86
418
0
4
10
3
12
7
1
7
9
13
0
5
0
3
9
1
17
13
4
18
5
17
2
30
13
9
18
8
26
3
42
0
16
0
10
29
3
22
17
5
24
7
22
3
28
12
8
17
8
24
3
2
33
31
107
33
140
♦Totals include cases in which several figures were seen by the same patient.
♦♦Percentages do not include cases about which no information was available.
Figures in some percentage columns do not add up to 100 due to rounding off.
Ninety-one percent of all identified apparitions of persons were
relatives of the patient. (In 20%, the identity of the apparition was not
ascertained.) Of these, 90% were close relatives, i.e., mother,
spouse, offspring, sibling, and father —in that order of frequency
(Table 2, Row a). The religious figures were usually described merely
as an angel or god, or were unidentified. When identified they were
named according to the patient’s religion, e.g., no Hindu reported
seeing Jesus; no Christian a Hindu deity.
Purpose of apparition. Quite often patients told respondents why
the apparition had visited them. In 50% of the cases in the pilot
survey, the stated purpose of the apparition was to aid patients in
their transition to another world: “to take them away.’’ In the present
Deathbed Observations by Physicians and Nurses
247
study this purpose was reported in 65% of the cases (Table 1, Row e).
For further analyses we excluded two somewhat ambiguous cate
gories: that the figure came “to comfort’’ the patient, which could
imply either a “this-life” purpose or a “take-away’’ purpose, and
cases where patients were said to be “reliving memories’’ which, of
course, indicates no contemporary purposes. Thus, after adjusting
the data in this way, the take-away purpose is clearly dominant in all
three surveys: pilot, 76%; U.S., 69%; India, 79%.
Patients' response to apparition. In the pilot survey it was found
that a large majority (89%) of the patients who saw apparitions with a
take-away purpose eagerly consented “to go’’ with them. Although
consent was expressed in 72% of the present survey’s take-away
cases, 28% did not consent, and some patients reacted with fright
and screams for help. Practically all these negative responses came
from Indian patients who refused to consent (Table 1, Row e). In our
unpublished interaction analyses we found that this difference in
consent between the U.S. and Indian samples may be partly due to
the patients ’ religion and partly to their nationality.
Patients were said to have reacted to the apparition with noticeable
emotions in 70% of the cases.2 Many of them reacted with positive
emotions (41%), while a considerable number (29%) had negative
emotions—particularly in cases where the patient did not consent “to
go’’ with the apparition. Of those with positive emotional reactions,
half were serene and peaceful and half were elated (Table 1, Row f).
We also asked our respondents to evaluate patients’ positive
emotions as religious or nonreligious feelings (Table 1, Row g). They
reported that 35% of those positive emotions were of religious
nature. Terminal patients usually suffer from pain and other kinds of
discomfort; consequently their moods are rather depressed. The
elation and serenity that the survival-related apparitions aroused in
most of the patients contrasted sharply against the gloom of dying.
Medical Factors
Drugs. Various medical factors are known to increase the likelihood
of hallucinatory behavior. Medication consisting of certain analgesics
and sedatives, such as morphine and Demarol, might have caused
hallucinations in some of our cases. However, the majority (61%) of
the 425 patients about whom we have such information had not
received drugs which could cause hallucinations. Half of those who
were under sedation had received such small doses or such weak
Patients’ emotional reactions to apparitional experiences were ascertained on an
alternative question scale. For our analyses items registering positive emotions'were
grouped together as (a) either serenity or elation (Table 1. Row f). or (b) either positive
nonreligious emotions or positive religious emotions (Table 1, Row g).
248
Journal of the American Society for Psychical Research
drugs that the respondents did not consider them to have been
psychologically affected. Of the 20% who were influenced, more than
half (11%) were said to be only mildly affected. Eight percent were
moderately affected and only 1% strongly affected (Table 3, Row d).
Thus the evidence indicates that in most cases the apparitional
experiences were not drug-induced.
Temperature. High body temperature sometimes leads to halluci
nations. Only 8% of the patients ran fevers of over 103 degrees
(measured orally) which might have facilitated hallucinatory behavior
(Table 3, Row c).
Diagnoses. Hallucinations may be associated with injury and
diseases of the brain, and with uremic poisoning caused by kidney
malfunction, although many brain-injured patients, especially those
with strokes, do not hallucinate. Only 12% of the patients in our
sample, including stroke cases, had such diagnoses (Table 3, Row a).
In addition to primary diagnoses, we also considered secondary
illnesses, previous illnesses, and any other factors in the patient’s
history which might have been hallucinogenic, e.g., alcoholism or
mental illness. This measure is rather inflated since we included in it
diagnoses only suspected by the physician and diseases which were
not active at the time of the terminal illness. We also included the
primary diagnoses involving the three hallucinogenic categories
discussed above. Only 25% of the patients had secondary diagnoses
which could have been hallucinogenic (Table 3, Row b).
‘ ‘Hallucinogenic index.' ’ It was also important to know how many
patients might have had at least one of the following possible
hallucinogenic factors: drugs, high fever, and primary and/or
secondary diagnoses of a hallucinogenic nature. We therefore
established a “hallucinogenic index’’ which includes every patient
who had one or more of the above-mentioned indices. It should be
noted that we included in this index cases which do not strongly
suggest that the patients ’ hallucinations were of an abnormal origin,
e.g., stroke cases, cases in which medication only slightly affected
clarity of consciousness, etc. Nevertheless, such indices are present
in only 38% of the cases; the majority (62%) are free of them. In the
pilot survey, it was found that deathbed visions are relatively
unaffected by medical factors. The data from the present survey give
the same impression.
Clarity of consciousness. We inquired into the clarity of
consciousness of the patient at the time of the apparitional
experience, a condition which is closely related to medical factors.
We had this information for 457 cases. Almost half (43%) the patients
were in a normal state of consciousness; they were fully aware of and
responsive to their environment. In 29% awareness was mildly
impaired, but the respondents could still communicate with their
249
Deathbed Observations by Physicians and Nurses
patients. Only 17% were in such a severely impaired state of
consciousness that little or no communication was possible. In 11%
clarity fluctuated and could not be accurately determined for the
times the hallucinations were experienced (Table 3, Row e).
Hallucinogenic medical factors are clearly absent in two-thirds of
our data. Could these factors nevertheless have affected the
remaining third of the patients who were included in the “halluciTable 3
Medical
a.
Status
of Terminal
Seeing Apparitions
Patients
Number of Patients
U.S. India Total
Percentage*
U.S. India Total
Variables
Medical Status
79
28
107
37
11
23
61
39
100
29
16
22
Primary
diagnosis
Cancer
Heart & circulatory
disease
Injury & post
operative
Respiratory
disease
Brain injury/disease, uremia
Miscellaneous
No information
10
62
72
5
25
16
9
26
35
4
11
8
28
25
4
26
64
10
54
89
14
13
12
11
26
12
19
b.
Secondary
diagnosis,
possibly hal
lucinogenic
Present
Absent
No information
68
137
11
40
187
28
108
324
39
33
67
18
82
25
75
c.
Body
temperature
(oral)
Less than 100'
100o-103°
Above 103°
No information
128
55
16
17
129
94
20
12
257
149
36
29
64
28
8
53
39
8
58
34
8
None
Medication, no
effect
Mildly affected
Moderately
affected
Strongly affected
No information
94
165
259
49
71
61
39
31
40
18
79
49
20
16
17
8
19
11
22
5
25
10
1
21
32
6
46
12
3
4
0
8
1
Clear
Mildly impaired
Severely impaired
Fluctuating
No information
98
31
36
38
13
100
103
39
12
1
198
134
75
50
14
48
15
18
19
39
41
15
5
43
29
17
11
d. Medication
affecting con
sciousness
e. Clarity of con
sciousness
♦Percentages do not include cases about which no information was available.
250
Journal of the American Society for Psychical Research
nogenic index”? Could they have spuriously enhanced the frequency
of those characteristics which were found in the pilot study to support
the post-mortem survival hypothesis? These characteristics are (a)
predominance of survival-related apparitions of dead persons and
religious figures, (b) their “take-away” purpose, and (c) the patients’
appropriate emotional reactions. Cross-tabulations between the
“hallucinogenic index” and the nature of the apparition (living,
dead, or religious figure) show that there was no significant inter
action. The presence of hallucinogenic factors did not increase the
frequency of survival-related trends such as apparitions of the
deceased, religious figures, or expression of the “take-away ”
purpose. Hallucinogenic factors did, however, significantly affect the
expected emotional reactions of the patients in the American sample
(P = .03). They seemed to suppress serenity, peace, and religious
emotions, and to increase the incidence of negative reactions. This
trend is not significant in the Indian sample. We conclude that the
medical variables ascertained in the survey seem to be relatively
unrelated to the apparitional experiences in terminal patients.
Demographic Factors
Demographic factors such as age, sex, educational level, and
occupation (Table 4, Rows a-d) did not interact significantly with any
aspects of the patients’ apparitional experiences.
Psychological Factors
We analyzed several psychological factors to determine whether
they tended to shape the phenomenological aspects of the main
phenomena: apparitions of the living, the dead, and religious figures;
purpose of the apparitions; and the patients’ emotional reactions to
them.
Stress. Hallucinations tend to occur in situations of severe stress
and social deprivation (Siegel and L. J. West, 1976; L. J. West, 1962).
Not only are visits to terminal patients by relatives and friends often
restricted, but most such patients are going through very stressful
situations, compounded by having to cope with severe pain.
Therefore, could their hallucinatory experiences be due to stress
rather than to extrasensory awareness of “visitors ” from another
mode of existence? We attempted to answer this question by evalu
ating an indirect indication of stress found in the data of the patients
in our sample —their mood on the day before the hallucination
occurred. We assumed that negative moods such as anxiety, anger,
or depression would indicate more stress than would positive moods.
The least stress, we believed, would be indicated by moods
designated by our respondents as “normal ” or “average.”
251
Deathbed Observations by Physicians and Nurses
Table 4
Characteristics
a.
b.
c.
d.
e.
of Terminal
Seeing Apparitions
Patients
Number of Patients
U.S. India Total
Percentage*
U.S. India Total
Variables
Characteristics
Age
1-30
31-50
Over 50
68
97
90
0
87
119
264
1
9
10
81
27
38
35
19
25
56
No information
19
22
174
1
Sex
Male
Female
99
117
175
80
274
197
46
54
69
31
58
42
Education
None, pre-school
Primary
High school
College
No information
13
57
73
45
28
77
59
65
38
16
90
116
138
83
44
7
30
39
24
32
25
27
16
21
27
32
20
56
29
85
41
19
30
Occupation
Professional,
manager, clergy
Clerical, sales,
crafts
Farmer, laborer,
services, house
wife
No information
9
40
49
7
26
17
70
81
83
103
153
184
52
55
53
214
26
12
85
10
5
48
6
3
22
15
3
3
3
214
26
12
97
68
12
14
28
Religion
Hindu
Christian
Moslem
Protestant
Catholic
Jewish
Other or none
No information
97
68
12
14
25
51
36
6
7
f.
Degree of in
volvement in
religion
No involvement
Slight
Moderate
Deep
No information
12
27
44
64
69
3
12
48
65
127
15
39
92
129
196
8
18
30
44
2
9
38
51
5
14
x 33
47
g-
Belief in an
after-life
Belief
No belief
No information
69
6
141
70
6
179
139
12
320
92
8
92
8
92
8
♦Percentages do not include cases about which no information was available.
Figures in some percentage columns do not add up to 100 due to rounding off.
252
Journal of the American Society for Psychical Research
There were no significant interactions between the patients ’ moods
on the day prior to the apparitional experiences and what the
apparition represented. We also failed to find any appreciable
interaction between mood and patients ’ emotional reactions to the
apparitional experience. The purpose of the apparition was not
significantly related to mood in either the American or the Indian
sample taken separately. However, this relationship is significant in
the pooled data from both populations (P = .001), and it is in the
direction opposite to what would be expected on the hypothesis that
stress is a causative factor in apparitional experiences. Patients with
normal moods experienced apparitions with a peaceful “take-away ”
purpose more frequently (54%) than did those who had positive
(31%) or negative (27%) moods. From these data we may infer that
while the stress experienced by the terminal patients might have
caused other kinds of hallucinations, it is unlikely that it affected the
incidence of apparitions which expressed purposes related to post
mortem survival.
Desires and expectations. A patient’s desires, expectations, or
“wishful thinking” might be possible causes of hallucinations. For
example, a thirsty traveler in the desert might have the illusion of
seeing water when none was there. We ascertained from our
respondents the number of patients who had expressed a desire to
have a visit from a living person, such as a spouse or a child, and then
checked on how many of these persons were later hallucinated. We
found only 13 such cases, an insignificant fraction of the total sample.
Furthermore, there were no indications in the data to suggest that
persons who had recently visited the patient appeared frequently in
his hallucinations. Of those visitors, only nine were hallucinated.
Fear of dying. In order to cope with their fear of dying, patients
who expect to die might be motivated to hallucinate “messengers”
from the after-life. (This would not be the case for patients who
expect to recover.) In neither the American nor the Indian sample,
however, were the intentions or identity of the survival-related
apparitions significantly correlated with the patients’ expectations of
living or dying. This is particularly apparent in cases where the
patient did not consent to the “take-away” purpose of the apparition
and screamed for help. Patients’ emotional reactions to the
apparitional experiences also failed to relate significantly to the
motivational variables ascertained in the surveys.
Cultural Factors
We hoped that cross-cultural comparisons would throw light on the
hypothesis that some deathbed visions may portray certain aspects of
a reality external to the patient.
Deathbed Observations by Physicians and Nurses
253
According to our model we assume that some apparitions may in
some way exist independent of the observer. As cultural factors have
a more powerful effect on subjective hallucinatory experiences than
on observations of external reality, the degree of influence of such
factors as religion and belief in post-mortem survival might give a
clue as to the true nature of deathbed visions.
Religion. Our sample population consisted mainly of Christians
(43%) and Hindus (48%). In the U.S. the stratifications were 51%
Protestant, 36% Catholic, 6% Jewish, and 7% unaffiliated or
belonging to other religions. Eighty-five percent of the Indian
patients were Hindu, 10% were Christian, and 5% were Moslem
(Table 4, Row e). This distribution roughly equals the affiliation
proportions among the general population in the areas surveyed,
except for the small unaffiliated group in the U.S. This discrepancy
disappears if we assume that most of the patients whose affiliations
were not reported actually were not affiliated with any religious
denomination. Apparently religious affiliation was not a factor in
determining the phenomena. The question remains, however,
whether the patients ’ religion could have determined the important
core characteristics of the apparitions. Religion did not significantly
influence the purpose or the kind of apparition seen (living, dead, or
religious figures). And both the occurrences of survival-related
apparitions (of the dead and/or religious figures) and their after-life
purposes appear to have transcended the widely divergent religious
ideologies of Hindus, Catholics, Protestants, Jews, and Moslems.
The patients ’ emotional reactions of serenity, elation, and religious
feelings engendered by apparitional experiences were similar among
Catholics and Protestants in the U.S. Unfortunately, we had too few
patients of other religions for effective comparison in the American
sample. Therefore Catholics and Protestants were compared only
with the rest of the patients as a whole—including those who were
unaffiliated, those of other religions, and those whose affiliations
were not reported. This mixed group showed different emotional
reactions such as less serenity (P = .02) and less religions feelings.
(P = .06).
In India the small minority of Christian patients was reported to
have reacted more with serenity and religious emotion than the
Hindus did. Part of this difference was traced to the respondent bias
of Christian nurses and therefore it cannot be interpreted with
reasonable certainty. However, there were more similarities than
differences: like Americans, many Hindu patients responded with
serenity, peace, and religious emotions.
The real difference between the American and Indian reactions to
the apparitional experience lies in the patients’ readiness to consent
254
Journal of the American Society for Psychical Research
to the “take-away” purpose of the apparition: with only one
exception, all the American patients were ready “to go,” while 34%
of the Indian patients were not. Can this be explained in terms of
their differences in religion? There was indeed a difference, though
not a significant one: only 16% of the Indian Christians did not
consent “to go,” as compared to 37% of the Hindu patients. It seems
probable that this no-consent attitude is due to both national and
religious factors. Patients ’ involvement in religion did not signifi
cantly affect the nature of the apparition experienced, its purpose, or
their emotional reactions to it.
Belief in life after death. A patient’s belief in life after death is
important for understanding his ways of coping with approaching
death. Yet surprisingly few (one third) of our respondents were aware
of their patients’ beliefs, or lack thereof, in an after-life. The majority
of them reported that they either did not discuss the matter with the
patients, or did not pay enough attention to remember it (68% of the
cases). It is remarkable that 12 patients who did not believe in life
after death saw apparitions (Table 4, Row g). This, of course, is too
small a sample for detailed interaction analysis. We assumed that
patients whose beliefs were weak or non-existent might have been
more likely to neglect mentioning the matter to their physicians or
nurses than would those who had strong convictions. We therefore
contrasted this “no information ” group with the believers.
Our analysis revealed that belief in an after-life has no significant
influence on the frequency of the kind of apparition seen, though it
did seem to influence the patient’s ostensible communication with it.
More patients in the “believers” group than those in the “no
information ” group experienced apparitions with a “take away”
purpose and consented “to go” with them. This difference is
significant in both the U.S. (P = .05) and the Indian (P = .004)
sample. There was no such difference in Indian patients who did not
consent “to go.” (Since there was only one “non-consenter” in the
American sample, this comparison could not be made.)
Belief in life after death did not significantly affect serenity and
elation in the American patients, but it did increase such feelings at
the expense of negative reactions in the Indian sample (P = .005). In
both countries, belief strongly increased positive religious responses
(U.S., P = .004; India, P = .002).
A number of other variables were ascertained and analyzed—
among them the possibility of respondent bias, as mentioned
above—but they are not discussed here due to lack of space. Reports
on phenomena other than hallucinations of human figures were also
collected and evaluated: visions of scenery, etc., mood elevation
shortly before death, and experiences of patients who were near
death but recovered. We hope to report on these elsewhere.
Deathbed Observations by Physicians and Nurses
255
Discussion
The American and Indian surveys were designed to replicate the
findings of the pilot survey and to provide more detailed data bearing
on the hypothesis of post-mortem survival. While the pilot survey
unearthed many findings which were interpreted as being consistent
with the after-life hypothesis, it had severe limitations concerning the
statistical certainty of these findings. Because the pilot survey was
the first of its kind, previous information was inadequate in helping to
predict many of the trends which emerged in that study. Therefore
the possibility that such unexpected trends were due to chance
variations could not be ruled out. However, most trends in the
present survey are reasonably consistent among themselves and with
those of the pilot survey. This diminishes the probability of chance as
an acceptable explanation.
Our model of deathbed experiences related to post-mortem
survival assumes (a) that survival-oriented apparitions may to some
extent be due to ESP of or from “another world’’ (e.g., deceased
relatives or religious figures) or (b), if this is not the case, are entirely
subjective. Therefore we hypothesized that medical factors which
often cause hallucinations but which are not known to affect ESP will
not increase the frequency of seeing after-life related apparitions. In
all three surveys, the data conformed to this hypothesis. Further
more, we postulated that medical conditions which impede sensory
(and, we presume, extrasensory) contact with the external world also
reduce the incidence of seeing after-life oriented hallucinations. This
was confirmed.
.
.
We carefully considered psychological factors which might have
caused hallucinations. Severe stress, especially in situations of
drastically reduced social contact, can find release in hallucinations.
Psychiatrists suggest that deathbed visions actually are schizoid
episodes through which patients cope with very stressful situations
by hallucinating pleasing fantasies of another world. A careful
analysis of the data revealed no support for this counterhypothesis.
Stress was not significantly related to the core phenomena of
deathbed visions. In both the American and Indian samples, the
trend went in the opposite direction: stress tended to reduce the
survival-related aspects of these experiences. Patients’ desires,
wishes, and expectations also had no significant influence. In a large
number of cases, patients experienced apparitions which appeared to
be in opposition to their own motivations, though consistent with our
hypothesis of post-mortem survival. Some psychiatrists have de
veloped the concept of “latent motivation’’—motivation which is not
expressed verbally or exhibited in behavior. However, this concept
has been severely criticized and generally rejected in scientific
256
Journal of the American Society for Psychical Research
research. We did not find any definite indices in our data of “latent
motivation’’ with regard to the main phenomena of deathbed visions.
The most .viable counterhypothesis is cultural conditioning. In
childhood and youth, cultural beliefs are transmitted to us in various
ways. Could they re-emerge in the visions of the dying—a kind of
playing back of old records? The cross-cultural survey in India was
primarily done with this question in view. Our model assumes that
individual and cultural factors will completely shape deathbed
visions, provided they are caused by these factors. However, if they
are based on perception of some form of external reality, or ESP
glimpses of “another world,’’ we hypothesized that only modest
differences between cultures would emerge, with the main features
remaining the same. An analogy could be found by contrasting a
typically American and a typically Indian painting of a mountain: the
details would be quite different while the basic characteristics of a
mountain would be clearly recognizable.
We found a very close agreement in all three surveys with regard to
the frequencies of survival-related apparitions: dead and religious
figures versus those of the living. The ostensible “take-away’’
purpose of the apparition was also equally present. Absence of
influences by medical and psychological variables was indicated in all
three samples. The core phenomena are the same.
Cultural coloring, however, was present. The sex of the
hallucinatory figure was largely determined by culturally conditioned
preferences which, in turn, seem to influence the proportion of
hallucinations of dead and religious figures. Religion had a
comparably slight influence on the main phenomena, though it did, of
course, determine the naming of the religious figures. We interpret
these modest cultural differences according to our model: they seem
to support the hypothesis that deathbed visions are, in part, based on
extrasensory perception of some form of external reality rather than
having entirely subjective origins.
Each culture develops dominant attitudes or values concerning
what is desirable and meritorious to say or do, and what is
undesirable and degrading. In Western culture, talking about
personal contact with the dead is often felt to be undesirable. In spite
of the fact that 27% of an American sample studied by Greeley (1975)
answered “yes’’ to the question “Have you ever felt that you were
really in touch with someone who had died?’’ only rarely were such
experiences told to professional people. In a British survey, Rees
(1971) contacted 277 widows and 66 widowers in selected localities.
Of this number, 94% were suitable for interview. Forty-seven percent
of that sample reported hallucinations of the presence of a dead
spouse. None of them discussed their experiences with their doctors,
and only one out of 137 did so with a clergyman. The main reason for
Deathbed Observations by Physicians and Nurses
«
4
257
not discussing the experience was fear of ridicule. It is likely that
patients in our survey also had a negative response bias; that is, they
avoided telling medical personnel about “seeing” apparitions of the
dead. If this is so, our sample represents fewer survival-related
apparitions than the number actually experienced.
Another possible way in which cultural conditioning could shape
the data is through respondent bias. The medical observers might
have reported what they believed they were supposed to, according to
cultural norms, and left out what went against the grain of their
particular culture. We found no serious distortion in favor of the
after-life hypothesis. On the contrary, we detected some under
reporting of those phenomena which we hypothesize as being related
to post-mortem survival.
Our data came from interviews with physicians and nurses rather
than with the patients themselves. This could introduce a source of
bias in reporting and sampling. However, some studies by Moody
and Kubler-Ross are based upon interviews with patients. In
Moody’s (1975) account of the experiences of resuscitated patients,
he states that quite a few of these patients, while in a near-death
state, became aware of the presence of deceased relatives as well as
what we have called religious figures “who apparently were there to
ease them through their transition to death” (p. 43). In a personal
communication Kubler-Ross (1976) has on the basis of her experience
with terminal patients confirmed the main characteristics of our own
findings: a predominance of survival-related apparitions, their
“take-away ” purpose, and patients ’ reactions of serenity, peace, and
religious emotion.
The issue of survival after death obviously cannot be assessed
solely on the basis of experiences of dying patients. The entire range
of other phenomena suggestive of an after-life—such as out-of-body
experiences, reincarnation memories, apparitions collectively per
ceived, and certain kinds of mediumistic communications —have to be
considered together with the various explanatory hypotheses (other
than survival) that have been advanced (see, e.g., Hart, 1956, 1959;
Murphy, 1961; Roll, 1974; E. M. Sidgwick, 1923; Stevenson, 1974a,
1974b, 1975; Tyrrell, 1953). Noyes (1972), Noyes and Kletti (1972,
1976), and Garfield (1975) have published surveys of cases which
involve deathbed experiences characterized by altered states,
panoramic memories, and also some phenomena similar to those
covered in the present report, but without having ascribed to them an
after-life interpretation. Discussion of the full range of data and
theories related to the survival question does not fall into the scope of
this paper.
We conclude our report on the cross-cultural survey of the
experiences of dying patients by stating that the main findings are
258
Journal of the American Society for Psychical Research
consistent among the three surveys that have been conducted in the
United States and in India over a 15-year period. The central
tendencies of the data support the after-life hypothesis as it is
formulated in the model we outlined briefly earlier in this paper.
i
References
Barrett
, W. F. Death-Bed Visions. London: Methuen, 1926.
Garfield , C. Consciousness alteration and fear of death. Journal of
Transpersonal Psychology, 1975, 7, 147-175.
GREELEY, A. M. Sociology of the Paranormal: A Reconnaissance.
Beverly Hills, Calif.: Sage Publications, 1975.
HART, H Six theories about apparitions. Proceedings of the Society for
Psychical Research, 1956, 50, 153-239.
ofSurvival. Springfield, Ill.: Charles C Thomas,
^1959^
Hyslop , J. H Psychical Research and the Resurrection. Boston: Small,
Maynard, 1908.
Kubler -Ross , E. Personal communication, 1976.
Moody , R. a ., Jr . Life After Life. Atlanta: Mockingbird Books, 1975.
Murphy , G Challenge of Psychical Research. New York: Harper &
Row, 1961.
MYERS, F. W. H. Human Personality and its Survival of Bodily Death.
London: Longmans, Green, 1903. 2 vols.
NOYES, R., Jr . The experience of dying. Psychiatry, 1972, 35, 174-183.
NOYES, R., Jr ., and Kletti , R. The experience of dying from falls.
Omega, 1972, 3, 45-52.
Noyes , R., Jr ., and Kletti , R. Depersonalization in the face of life
threatening danger: A description. Psychiatry, 1976, 39, 19-27.
OSIS, K. Deathbed Observations by Physicians and Nurses. New York:
Parapsychology Foundation, 1961.
Rees , W. D. The hallucinations of widows. British Medical Journal,
1971,4, 37-41.
ROLL, W. G. Survival research: Problems and possibilities. Theta,
1974, 39-40, 1-13.
SlDGWICK, E. M. (MRS. H.). Phantasms of the living. . .Proceedings of
the Society for PsychicalResearch, 1923, 33, 23-429.
Sidgwick , H., and Committee . Report on the census of hallucina
tions. Proceedings of the Society for Psychical Research, 1894, 10,
25-422.
SlEGEL, R. K., and West , L. J. (Eds .). Hallucinations: Behavior, Ex
perience and Theory. New York: Wiley, 1975.
STEVENSON, I. Twenty Cases Suggestive of Reincarnation. (2nd ed.
rev.) Charlottesville: University Press of Virginia, 1974. (a)
*
Deathbed Observations by Physicians and Nurses
♦
259
Stevenson , I. Xenoglossy: A Review and Report ofa Case. Charlottes
ville: University Press of Virginia, 1974. (b)
STEVENSON, I. Cases of the Reincarnation Type. Volume I. Ten Cases
in India. Charlottesville: University Press of Virginia, 1975.
Tyrrell , G. N. M. Apparitions. London: Duckworth, 1953.
West , D. J. A mass observation questionnaire on hallucinations.
Journal of the Societyfor PsychicalResearch, 1948,34, 187-196.
WEST, L. J. (Ed .). Hallucinations. New York: Grune and Stratton,
1962.
A.S.P.R.
5 West 73rd Street
New York, N.Y. 10023
Department ofPsychology
University ofIceland
Reykjavik, Iceland
SANDOZ (INDIA) UNITED
1.
What does Hydergine contain?
Hydergine contains co-dergocrlne mesylate which consists
of equal parts of hydrogenated, alkaloids of ergot;
dihydroerqocristine? ditydrdergocornih e and dihydroergocryptine (Dihydro- -ergocryptine and dihydro-B-ergocryptine
in the proportion of 2:1) .
2.
What are the indications of Hydergine therapy; Symptoms
and signs of mental deterioration^ notably those related to
ageing: dizziness, headache poor concentration, disorienta
tion, impaired memory, lack of initiative, mood depression^
unsociability, difficulties with daily living activities
and with self care.
Various symptoms in acute cerebrovascular disorders and as
a sequalae of cerebral infarction.
3.
What is the mechanism of action of Hydergine?
Hydergine improves the neuronal cell metabolic activity by.
- inhibiting phosphodiesterase activity, which reduces eyelid
AMP turnover and thus improves cell performance.
- Inhibiting the rate of breakdown of adenosine triphosphate
which is the main energy reservoir of cells.
- Improves protein synthesis thus normalising the enzyme
content of the neuronal cell for improved metabolic activity.
- Experimental studies also indicate that Hydergine modifies
cerebral neurotransmisSiqn by its stimulant effect on dopamine
and serotinin receptors and by blocking effect on L-adrenopeptor
sites. The improvement in neurotransmission is reflected in the
changes in electrical activity of the brain by EEG studies after
administration of Hydergine.
4.
What is the effect of Hydergine on cerebral blood flow?
*
Can it be compared to Vasodilators?
A definite increase in cerebral blood flow occurs after
prolonged Hydergine therapy. This effect cannot be attri uted
to cerebral vasodilatation, but rather to an improvement n •
cerebral metabolic activity. f“
When thcnxironas are functioning
in an Improved manner there is an Increased demand and
utilisation of cerebral oxygen and blood. The local edema is
decreased with
with a secondary improvement in microcirculation.
decreased
Thus Hydergine cannot be compared bo vasodilators, as. it
primarily acts by improving the metabolism of the derange
neuronal cell and as a consequence secondary improvement n
microcirculation by relieving udema.
OOZ (INDIA) LIMITED
5.
-2-
How does Hydergine help in cerebrovascular diseases?
There is no drug, including HYdergine which can reverse
the atheroscelerotic process.' Patients with vascular damage
to the brain have diffuse cerebral insufficiency - the slow
gradual degenration pf neuronal cell. This manifests with
siyns/symptoms of mental deterioration. Hydergine by directly
nnd hL°n the H^abolism of nerve cell improves neurotransmission
and hence gradually restores the activity of the neuronal cell.
Favourable effect of Hydergine on various symptoms due to
r^rovascu^ar disturbances has been confirmed by various
studies.
6.
What is the dosage of Hydergine and nature of therapy?
Hydergine‘is recommended tobe taken orally - 1 mg three .times
a day for a period of 12 weeks, it
cc“ 1—
* * in
• • patient^
r' •
It can
be started
having acute cerebrovascular episodes, as soon as the acute
phase is over and patient can take oral medication.
7.
How does Hydergine compare to Piracetam.
Pfracutam is presumed to improve the metabolic aotivitv
of neuronal cell; but has no effect on neurotransmission.
Hydergine not only improves the metabolism of nerve ceil but
also directly has a stimulant effect on neurotransmitters
dopamine and serotonin.
A comparative study has shown improvement in symptoms and EEG trac
tracings significantly in favour ofHydergine as compared to
Piracetam. •
9.
Can Hydergine improve memory in normal person?
Hydergine has been administered in a dosage of 12 mg. a day
to normal healthy volunteers for a period of two weeks at the
end of which there was a significant improvement in memory
‘
as measured by psychometric tests.
9.
What is the rde of Hydergine inpediatrtc practice?
Hydergine has been tried in'Minltnal Brain CDysfunction1 in
children in. total dosage of 1.5 mg/d.fy withi some success.
Further studies are in progress.
oroarcss.
).
What are the pharmakokenetLes of Hydergine?
Eli1nIln^?inai£n£UtratiOni25%
dt”‘° 19 r->Pldly absorbed
occurs in 2 pha-aeg. with a short C and longer U
halt Lite-°n an awrage, the L-phase half lite is 4 hours after
absorption and beta phase is 12 hours after absorption as
l2t0? £r°m u^lnary excretion. The maximal plasma
concentration is 0.50n<j/ml after Img tablet is taken.
I
ANOOZ (INOIAp'UMITEO
Al.
-3-
What are the SE and CI
■
*
of Hydergine therapy?
§j:.de Effects t Nasal stuffiness, transient nausea and gastric
by
upsets may occur occassionally but are usually prevented by
taking the drug with food. In majority side effects
disappear without specific, measures being taken,
precautions? Caution is required in presence of severe
bradycardia. Blood pressure should be checked following
high dosage, as a drbp in blood pressure may occur owo-i f'
Hydergine should be kept out of reach of childrens
Contra-indications:
APS;ra
30.5.1983
Known hypersensitivity to the drug.
A Comparative Evaluation of
Mebendazole, Piperazine and Pyrantel
in Threadworm Infection
a
Anthelmintic Study Group
on Enterobiasis
(INDIAN PEDIATRICS 1984, 21: page 623 to page 628)
•i
4
VOLUME 21—AUGUST 1984
A COMPARATIVE EVALUA
TION OF MEBENDAZOLE,
PIPERAZINE AND PYRANTEL
IN THREADWORM
INFECTION
Anthelmintic Study Group
on Enterobiasis*
J
ABSTRACT
J
i
3
I
A randomized controlled multicenter trial was
done in 434 patients with threadworm (TW) infec
tion, diagnosed by perianal adhesive cellophane tape
smear, and comprising 2 series of2 groups each, to
compare pyrantel (N=119) with mebendazole
(J4=1O5), and pyrantel (N=109) with piperazine
(^N—101). Response was evaluated 14 days after
treatment by taking perianal smears for TW eggs on
4 consecutive days, cure being defined as all 4 smears
negative. Pyrantel was significantly more efficaci
ous (P<0.05) than both the comparative drugs.
The cure rates were—Series A: pyrantel 94.1%,
mebendazole 67.6%; SeriesB: pyrantel 91.7%,
piperazine 67.3%. The incidence of side effects
was—Series A:pyrantel 3.3%, mebendazole 8.1%;
Series B: pyrantel 5.4%, piperazine 27.3%
(P<0.01).
Key words: Enterobiasis, Pyrantel pamoate.
Mebendazole, Piperazine citrate.
*The investigators who participated in the study
were Joshi RN, Mehta BJ, Ahmedabad: Bhandari
NR, Savant SM, Bhopal: Amdekar YK, Dalal
NJ, Mehta (Mrs) KP, Bombay: Bhattacharjee RC,
Dadina (Mrs) Z, Calcutta: Verma S, Delhi:
Barua AC, Sarmah HC, Gauhati: Ismail M,
Hyderabad: Jain NK, Yadav SC, Lucknow:
Ekambaram S, Muthurajan S, Ranjini (Miss)
MP, Madras: Srivastava SP, Thakur AN, Patna:
Deodhar JN, Navarange J, Pune: Premnaryan N,
Secunderabad: Blah (Mrs) I, Shillong: Balakrishnan V, Phillip (Mrs) E, Trivandram.
The study was coordinated by Arui S. Nanivadekar,
Shrikant D. Gadgil and Vasant V. Apte, Medical
Research Division, Pfizer Limited, Express
Towers, Bombay-400 021.
Threadworm (TW, Enterobius vermicularis) infection is frequently encountered
in practice, especially in children. As the
eggs of TW are rarely found in stools it
is rare to diagnose TW infection by a direct
smear stool examination.
The most
appropriate method for ascertaining the
presence of TW infection is micro
scopic examination of adhesive cellophane
tape (ACT) smears from the perianal
region. Being cumbersome the method is
often neglected and the diagnosis of TW
infection is based on symptoms or on the
mother’s report of having seen little worms
in the child’s stool or crawling around the
child ’s anus at night. Likewise the efficacy
of an anthelmintic in TW infection is
often judged from post-treatment relief
of symptoms.
Review of published literature on the
evaluation of anthelmintics in TW in
fection reveals that several studies suffer
from one or more lacunae in the design,
e.g. small numbers of patients, lack of
control groups, imprecise methods of
diagnosis, inadequate duration of follow
up and inappropriate criteria of cure(l-5)
Pyrantel pamoate (Combantrin, Pfizer)
was investigated in India in the late 1960s
and early 1970s(6) whereas mebendazole
became available later. Although pyrantel
became available in this country in 1982
there has been a paucity of clinical trials
comparing these two drugs in TW infection.
This study was undertaken, therefore, to
evaluate the relative in-practice efficacy of
these two relatively new drugs and also
of piperazine which has been in use for
over two decades.
Material and Methods
The study was carried out between
August 1983 and January 1984. From 12
operational areas in the country (see
623
ANTHELMINTICS IN THREADWORM INFECTION
footnote) 26 investigators were selected:
2 each from 10 areas, and 3 each from
2 areas. Of these, 24 were pediatricians
and 2 consultant physicians. All followed
the same standard protocol.
Each investigator was requested to
select 20 consecutive patients, either male
or female, fulfilling the following criteria:
age 1 to 10 years with suspected thread
worm infection; no anthelmintic taken for
worms during the preceding one month;
perianal ACT smear positive for thread
worm eggs; willingness of parents to take
ACT smears as instructed and to bring the
child for follow-up as per protocol. The
investigators were randomly assigned to
two series, A and B, each containing 13
investigators with at least one from each
operational area.
In series A the patients of each investi
gator were randomly assigned to either
pyrantel or mebendazole; in series B,
to either pyrantel or piperazine.
Before treatment, a perianal ACT
smear was taken from each patient on two
consecutive mornings before he passed
motion. To take these smears a special
perianal ACT device imported from Japan
was used {Fig. 1) which made it convenient
for a child’s parent to take the smears
at home and bring them for examination.
Only patients with a positive perianal
ACT smear for TW eggs were included in
the trial. Presenting symptoms of these
patients were recorded.
The doses of drugs were: pyrantel
pamoate (Combantrin)—a single dose of 10
mg base/kg body weight; mebendazole—a
single dose of 100 mg; piperazine citrate—
50-75 mg base/kg body weight in a single
daily dose for 7 days. All drugs were
administered orally.
Seven days after treatment side effects
were recorded if reported voluntarily by
624
the patient or his parent, or if observed by
the investigator.
Perianal ACT smears were taken on
4 consecutive days, 14 days after treat
ment, but not later than 28 days. If the
smear was negative for TW eggs on all
four days the child was considered as
cured. The microscopist who examined
the smears was kept unaware of the
patient ’s treatment to ensure unbiased
examination.
The differences in cure rates between
groups were analyzed for statistical signi
ficance by chi-squared test. Side effects
were analyzed from all patients, i.e. com
The fre
pleters and non-completers.
quency of a side effect in a group was
compared with the overall frequency in
the study by Poisson’s test.
Results
A total of 453 patients were included
in the study. Of these, 9 were excluded
from analysis: 6 because their initial
perianal ACT smears were negative for
TW eggs and 3 because they received in
adequate doses of trial drugs. A further
10 patients did not complete the study:
3 because of side effects {Table III), 1
because post-treatment perianal ACT
smears were not available and 6 because
they were lost to follow up. Thus 434
patients completed the study and were
eligible for analysis: 224 in series A and
210 in series B.
Table I shows the composition and
characteristics of the patient groups.
Children aged 8 years or less formed 83 %
of all patients (360/434). Likewise, 83%
of all patients (359/434) had body weight
of 20 kg orless. Anal itching was the most
common (81%) presenting symptom,
followed by disturbed sleep (27%) and
worms seen by mothers (19%).
>
5
VOLUME 21—AUGUST 1984
INDIAN PEDIATRICS
Cellophane strip
cellophane strip unfolded to
show its structure and use
£
1
Bas
Blue spot
Day 2
[
- Name
inner
cover
for blue
spot
Blue
spot
I
Day 1
Report
JS§
I
1
~ threadworm eggs.. The
Fig. 1. Cellophane strip device used to take perianal smears for
envelope (left) containing the strip has boxes marked for the patient's name, the
dates of taking smears and the microscopist's report. The strip (right) has two
sticky blue spots with protective covers. On day 1 the cover over one spot is
lifted off, the spot is pressed firmly and evenly over and around the anus, and
the cover is replaced. On day 2 the process is repeated with the second spot,
but now both the protective covers are peeled off the strip folded and the’ two
spots pressed over each other. The eggs, if present, are sealed between the
spots and can be seen directly under a microscope, The blue colour helps cut
off glare.
As shown in Table If the cure rate with
pyrantel was significantly higher (P <0.01)
than that with mebendazole (94.1% vs
67.6%) and with piperazine (91.7%) vs
67.3 %). Besides, the cure rates with pyran
tel in the two series were comparable.
Anal itching, which is considered as a
characteristic symptom of threadworm
infection, was completely relieved in a
majority of cured subjects with all the
three drugs. In series A 88% of children
cured with pyrantel (96/109) were comple
tely relieved of anal itching; the corres
ponding figure was 76% (53/70) for
625
ANTHELMINTICS IN THREADWORM INFECTION
TABLE I—Pretreatment comparison of patient groups
Series A
Series B
Criterion
Sex ratio M : F
PYR
N = 119
MEB
N = 105
PYR
N = 109
PIP
N = 101
55 :45
55 :45
52 :48
57:43
9
11
33
15
38
15
25
39
28
19
34
17
.1
Age
1 — 2 yr
3 —4 yr
48
5 —Syr
8 4- yr
35
8
26
Weight
*=10 kg
6
81
9
23
15
12
70
17
62
10
1
4
5
64
17
4
97
24
96
19
14
21
82
24
20
82
20
23
11 —20 kg
21 — 30 kg
30 +
kg
Symptoms
Anal itching
Disturbed sleep
Worms seen
PYR = pyrantel;
MEB = mebendazole;
PIP
piperazine.
Figures are percentages.
TABLE II—Percentage cure rates
Series
Drug
B
626
pyrantel;
% cured
P*
t MEB
119
105
94.1 1
67.6 J
<0.01
r pyr
X pip
109
101
91.7 I
67.3 J
<0.01
mebendazole;
PIP = piperazine.
r pyr
A
PYR
No. of pts.
MEB
♦X2(l df).
I
VOLUME 21—AUGUST 1984
INDIAN PEDIATRICS
TABLE III—Side effects
Series B
Series A
Nature
PIP
N = 110
PVR
N = 121
MEB
N = 111
PYR
N = 111
Griping pains
1
1
0
5*
Nausea
Anorexia
1
Kl)+
0
2
0
13*
1(1)+
0
1
2
0
14*(1)+
Vomiting
1
0
Diarrhea
0
Giddiness
Urticaria
0
0
0
0
Other
1
4
1
0
2
1
1
2
1
+Dropouts;
Figures are numbers of patients.
♦Significantly higher than overall incidence in study (P<0.05 by Poisson’s test).
I
According to Wolfe(7) a single perianal
ACT smear will detect 50% of TW in
fections, 3 such tests on consecutive days
will detect 90% of infections and 5 con
secutive tests will detect 99% of infections.
A similar observation has been made
earlier by Brown(8). Therefore, a series
of smears taken on several consecutive
days is necessary for properly evaluating
the efficacy of drugs in TW infection.
Although some workers have pre
viously used unconventional technique(3)
and an inadequate number of perianal
ACT smears after treatment(3-5), in the
Discussion
present study ACT smears were taken on
The countrywide extent of this study 4 consecutive days to improve the accuracy
involving 26 investigators permitted a large and reliability of post-treatment efficacy
number of patients to be enrolled within a evaluation. Further, these post-treatment
short period for a meaningful assessment smears were taken on days 15 to 18 to
of the comparative clinical efficacy of the . avoid possible false negative results due
three anthelmintics. The new device used to tempprary suppression of egg produc
for perianal ACT smear (Fig. 7) provided tion or egg laying by the worms.
Since anal itching in threadworm in
a convenient and appropriate method for
detection of threadworm infection in the fection is caused by crawling of female
day-to-day practice situation. In all pro threadworm on the perianal skin, it is
bability it also helped avoid many logical to expect relief of this symptom
when the infection is cured. This was
dropouts.
mebendazole. In series B the respective
figures were 77% (63/82) for pyrantel and
81% (44/54) for piperazine.
In series A the incidence of side effects
was 3.3% (4/121) on pyrantel and 8.1%
(9/111) on mebendazole. In series B it was
significantly higher (P<0.05) with pipera
zine (30/110 or 27.3%) than with pyrantel
(6/111 or 5.4%). The frequency of nausea,
vomiting and griping pains was signifi
cantly more (P<0.05) in the piperazine
group than in the study as a whole.
627
•t
%
*
♦
ANTHELMINTICS IN THREADWORM INFECTION
indeed the case in a large majority of Decision Services, Bombay? Mr. S.
cured patients in the present study.
Nambi’s assistance with logistics was
However, in some patients the symptom
valuable.
was not relieved completely despite cure
of infection, which could possibly be REFERENCES
due to a residual cutaneous effect of
1. Azeez MA, Roguraman R, Suresh S, Ambil S,
threadworm infection or due to secon
Viswanathan J. A comparative study of
dary infections as a result of scratch
pyrantel pamoate (Nemocid) and mebendazole
ing. This was not investigated in the
in helminthiasis in children. Antiseptic 1983
present study.
80: 575-577.
Pyrantel pamoate and mebendazole 2. Singh H, Nath G, Sandhu SS, Paruthi SC.
Clinical trial with piperazine senna combina
were well tolerated but the frequency of
tion. Indian Med Gazette 1969,9: 47-56.
side effects was significantly higher in
3.
Narmada R, Rao MJ, Raju VB. Mebendazole
patients treated with
piperazine,
the
in the management of oxyuriasis in families.
commonest side effects being nausea and
Antiseptic 1977, 74: 627-629.
vomiting.
This may be related to the 4. Fierlafijn E, VanparijsOF. Mebendazole in
enterobiasis: a placebo-controlled trial in pedia
seven day’s duration of treatment and the
tric community. Trop Geograph Med 1973
fact that piperazine is completely absorbed
25: 242-244.
whereas pyrantel and mebendazole are not.
5. Brugmans JP, Thienpont DC, Wjjngaarden IV,
The prolonged treatment schedule of
Vanpari.is OF, Schuermans VL, Lauwers HL.
piperazine recommended for T\V in
Mebendazole in enterobiasis: radiochemical
fection is inconvenient and some doses
and pilot clinical studies in 1278 subjects
JAMA 1971,217: 313-316.
are likely to be missed. Both pyrantel and
6. Chandra H, Akhter J, Mathur YC. Combantrin
mebendazole offer the advantage of a
(pyrantel embonate) in roundworm and thread
single dose therapy with better toleration.
worm infestation in children. Paper presented
However, owing to its significantly higher
at X South East Asia Regional Seminar on
efficacy pyrantel would appear to be the
Tropical Medicine and Public Health, Bangkok
Oct 26-30,1971.
preferred drug for treating TW infec
tion in an individual, family or community. 7. Wolfe MS. Oxyuris, Trichostrongylus and
Trichuris. Clinics in Gastroenterol 1978 7201-217.
Acknowledgements
8. Brown HW. Basic Clinical Parasitology, 3rd
ed. New York, Appleton-Century-Crofts, 1969,
The coordinators are grateful to Dr.
p!32.
R.S. Dayal, Agra, for his critical comments
during preparation of the manuscript.
Data processing was done by Mr. S.S..
Kulkarni, Medical Research Division, Reprint requests : Dr. A.S. Nanivadekar, Medical
Pfizer Limited and Mr. A.R. K.annappan, » Research Division, Pfizer Limited, Express
Towers, Bombay-400 021.
628
e
-
I
Horoscope
1
If Picasso
painted your
toenails...
... would you show them to the
world? Toss off your shoes, take
off your stockings and run
barefoot through the sand?
^Vith Nailtech
.... ....Nail Lacquer you can!
By Michael Lutin
ear readers: Mars is passing through horribly insecure Can
cer all month, so you might find yourself clutching an infant
while getting hysterical with a landlord—and everybody will be
touchy around Mother's Day. Mercury goes retrograde for three
weeks on the 12th, so wherever you're going, leave an extra hour
for gridlock and/or derailment. If a Gemini asks you out, don't
bother to get dressed until you hear the doorbell. Scorpios and
Capricorns are in cahoots to take over the world and Taureans are
out of control again. This will mean certain frenzy on Wall Street
and in mental hospitals. Tensions break on the 20th, and you'll
have to negotiate like mad for anything you want. The trick this
month is to get the other person to offer you the last potato chip.
fAURUS^ “
Dance the night awav.
Wear <iprn s .jik lah
\ I •( I I t |! 11| )|l
i
. i •' 1 ‘
'.H
it '
.i« i ji it i
lor Spring and Suimnei
that last and last and last.
Now you have
Nailtech Nail Lacquer.
Even Picasso couldn't do better!
X
™ ~
April 20—May 20
(
! t.llll | >< I ’I'll' I II’
i. .|.
1 • < 1.1.•/ling sf),k |i", (>i
MP
(i/ <, ■
if.! ’lx .
i| I'l.i.
\ < 'HI ' ,i»
,
u>n
I li, \ I " -v. lx >•' i'' 1'irli < ■ "ii V
• ”i lit
link ,J||4| Bill w Ill'll \ uni uilci < iini.ij ”ii ilx I I rl.i uM
' .
cincigc from the chocolate l akc \ou \c been diowningyoiii >onows in.
relax, open up. and start to communicate again. Success has alwass de
pended on the art of negotiation —ever since Eve sold her first apple.
GEMINI
May21-June21
Expect a few of your other selves to surface. You're unusually tentative
and noncommittal now. Consider providing tranquilizers for anyone
whose fate hangs on your decisions. The Capricorn planets have had you
fretting a lot recently, but with Venus meeting Jupiter in Gemini right now
you’re lucky, gorgeous, blessed, loved, and loving toward all. So blow
one little kiss across the room and warm the world.
CANCER
June22-July22
In recent months, you have become a perfect pretzel of flexibility and
compromise. But now, just when you should be most obedient and com
mitted, the camel’s back has finally gone out and even a chiropractor can’t
fix it. If you could just calmly sit down, say what’s on your mind, talk
truth—but no. You have to sit there stewing until POW! the guy asks you
to pass the butter and gets the whole dish in his kisser.
'NAILTECH
PERFECTCRtME
LEO
July23-August22
After an arduous winter you’re on top of it at last. This is a professionally
rewarding time. OK, so maybe you re not Brenda Starr, but there s a win
dow in your office now, you’ve got some positive feedback from upstairs,
and probably a pay raise. One minor glitch: family life can make you feel
trapped and crazy. In general, though, it’s a good time to enjoy success,
and still have some fun when you pull the shades down at night.
VIRGO
1
NAIL LACQUER .5FL.0Z
NAILTECH
August 23-September 22
You really arc at your advice-giving best when yourdcarest friend is suing
for divorce or your sister is agonizing over a choice between cosmetic sur
gery or a new couch. On a good day. Mother Teresa herself couldn’t be
more compassionate than you. Since you arc professionally secure right
now, you can just sit back on your tuffet. peer through your telescope, and
be your cool, dispassionate, philosophical, wonderful Virgo self. ► 264
Nailtech, Inc. 1989
M
i
Hearth
ars..several states have updated eiist- difficult to tell a partner, ‘ 1 may have in
What keeps people like Olson and
ig STD laws to encompass HlV-infec- fected you with a disease...and you Raev skygoing—so ni etifnesTBF ^To ng
tion, or passed “partner-notification’’ may die.' What a relief to have someone as eighteen hours a day—is a-.strong
laws to deal exclusively with AIDS. say, T will inform your partner for you commitment to,.contact tracing. Says
Raevsky: “ You can' t do. this ’job i f you 5:
They range fromNew.York'sApro^ision and I won't tell her who you arQ.,”’
making contact tracing'available for
Hpw do the, medical dct^tives find /--don’t believe in it, if you. don’t feel
AIDS patients who ask for it, to South the emotional strength to bring this kind you're doing the right?thing.” “It's a
Carolina’s law, which requires that pa of news to people, day after day? Olson depressing job,’’ adds Olson. “But
tients disclose partners’ names.
confesses that after spending weeks try people have a right to know if they come
There is a significant difference be ...6
ing to track someone down, there are in.t.ocontact with someone with HIV pr _
tween contact tracing for AIDS and oth times when she can’t get up the nerve to any STD. And somebody has to warn-^
6
er STDs: with AIDS, tracees, if knock onjLllUQr
them.’’
0
infected, cannot be cured; they can only
be counseled. Some experts question
the relevance of notifying people after
the fact, arguing that monies spent on
tracing programs would be better spent
on educating people to avoid the sexual
habits that make them vulnerable to
HIV in the first place. Those who favor
contact tracing say that even people
who are infected can benefit from
knowing their status, taking steps to
help themselves. “General education
J programs have obviously failed these
people,’’ Raevsky counters. “Many
f
}
people we deal with don’t even perceive
themselves to be at risk. ’ ’ .
Many women find false comfort in
.
the fact that they don’t fall into the clas-;
sic high-risk groups—gay, bisexual, or
1
IV-drug-using men. Though women
represent only about 10 percent of repO.rted AIDS cases, the number of fe|
male cases today is about the same as
\
the number of cases among men just
Hh two to three years- ago. Short of practic
«« w
I
A* ' 4
4
1 1
... L _ . »
'
' '
D •»
■ ■ «« 1 r a > •
44
T
t 1 «a
♦ la a »'a
a « a la
*4
a ■ . a• a
es ing safe sex (which few are doing),
women'can Only pray that partners are
healthy, heterosexual, and monoga
mous,
’
.
Even Women who broach the subject
of AIDS with sexual partners may be
misled. Twenty percent of the men surveyed in a recent College study admitted
they.would lie to a woman about having
had an AIDS-antibody test in order to
get her into bed. Twenty-five percent of
those surveyed at a California testing
site said they would not tell partners if
they tested positive.
Partner notification is a voluntary
process, even in states like Colorado,
where contact tracing is law. The suc
cess of such programs depends on a per
son’s willingness to, in effect, kiss and
tell. “More often than not, people com
ply,’’ says Raevsky. “After all, we of
fer these people a valuable service. It’s
VOG I' E MAY 1989
>
' -sal
Introducing Face Magic and Leg Magic.
The makeups with sunscreen that
conceal imperfections...beautifully.
[YIJI-YO'LEARYj M
LEG MAGIC. *
St
Face Magic conceals facial imperfections. Long
lasting SPF 20 sunscreen. Easy to apply... waterproof...
holds makeup hours longer. So light it comes in a tube.
In many skin tones.
Leg Magic hides spider veins, blotches, even varicose
veins. Moisture-rich, waterproof, with SPF 16 sunscreen.
Glides on, dries in seconds. Sexy shades for all skin tones.
Don’t face another day without a little magic.
LYDIA O’LEARY * FACE MAGIC 8. LEG MAGIC
At Dayton’s and other fine stores. Call 1-800-524-1120. Also, in Canada and Puerto Rico.
Hp
<•
Chaos and Fractals in
Human Physiology
I
■
Chaos in bodily functioning signals health.
Periodic behavior can foreshadow disease
by Ary L. Goldberger, David R. Rigney and Bruce J. West
A medical student monitoring the rhythms of
/\a heart notices that the tempo sometimes
/ jLchanges dramatically from minute to minute
and hour to hour. A clinician maneuvering a bron
choscope into a lung observes that the trachea
branches into smaller and smaller airways. The stu
dent senses that the interval between heartbeats
varies chaotically. Perhaps the clinician recognizes
that the network of airways resembles a fractal.
Physiologists and physidaris have only recently be
gun to quantify such possibilities of chaotic dynam
ics and fractal architectures. Their investigations are
challenging long-held prindples of medicine and are
revealing possible forewarnings of disease.
The conventional wisdom in medicine holds that
disease and aging arise from stress on an otherwise
orderly and machinelike system—that the stress de
creases order by provoking erratic responses or by
upsetting the body’s normal periodic rhythms. In
AIRWAYS OF 'THE LUNG (left) shaped by evolution
and embryonic development resemble fractals gen
erated by computer (below). The bronchi and bron
chioles of the lung (here a rubber cast) form a “tree”
that has multiple generations of branchings. The smallscale branching of the airways looks like brandling
at larger scales. When physiologists quantified ob
servations of the branching pattern, they discovered
that the lung tree has fractal geometry.
1
J
•(
. v> .
-y
1
I
b
w
■■ W
II
’1
•
'/ r I
\
i
1
i
I
i
}
i
14
low-power microscope lens, one can dis
changes in the weather. Under some cir cern asymmetric branches, called den
cumstances deterministic nonlinear sys drites, connected to the cell bodies. At
tems—those that have only a few sim slightly higher magnification, one ob
ple elements—behave erratically, a state serves smaller branches on the larger
called chaos. The deterministic chaos of ones. At even higher magnification, one
nonlinear dynamics is not the same as sees another level of detail: branches on
chaos in the dictionary sense of com- branches on branches. Although at some
• ’ n or randomness.
-V.
regularity and unpredictability, men,
brancnmg of
oi a jieuron
o.v
constrained level the branching
ueuiuu stops,
ldealized fractals have infinite deta±
important features of health. On the
remarkabl
------are er hand, decreased
remarkable
even
remarks
other hand, decreased variability
variability and
and acac kind of randomness
npriori!cities
thePdetails of a fractal at a certain
are associated
assodated may be associated withl fractal geometry. that the^details
cert
periodicities are
centuated periodidties
Fractal structures are often the rem- scale are similar (though not necessarily
with disease. Motivated by these^
identical) to those of the structure seen
at larger or smaller scales. If one saw
for periodic
behavior
that might
T,oko.nnr
.-----that mieht
indicaindicate environment (the seashore, the at
developing sickness (especially diseases mosphere, a geologic fault), fractals two photographs of the dendrites at
two different magnifications (without
of the heart). In addition, we havc begun
any other reference), one would have
to S^e the flexibility'and strength of are likely to
to deciding
dedding iwhich photograph
irregular fractal structures and the iadai>
adapfractaIs developed inde- Sfi^Tty tn
lability and robustness of systems th
dentl of nOnlinear dynamics, and corresponded to which magnification.
exhibit apparently chaotic behavior.
P^nd
coimections between the All fractals have this internal, look-alike
y,
property called self-similarity. I
disciplines are not fully established.
Because a fractal is composed of simihaos and fractals are subjects asA fractal, as first conceived by Benoit
i
sodated with the disdpline of B Mandelbrot of the IBM T. J. Watson lar structures of ever finer detail, its
length is not well defined. If one atVJ nonlinear dynamics: the study of
consists of geometric
swt^nstliat respond disproportionately Research
Research Center,
Center^
len h 0 a fractal
to measure
the past five years or so we and our col
leagues have discovered that the heart
and other physiological systems may be
have most erratically when they are
young and healthy. Counterintuitively,
Increasingly regular behavior sometimes
Wt UJX'-X
£------ / -
tu CLL1CL1/ x-x- xxxx.
---------------t
finer than the ruler can possibly
wx
-----------------
.
uring instrument increases, therefore,
the length of a fractal grows.
Because length is not a meanmgfm
concept for fractals, mathematicians cal
culate the “dimension” of a fractal to
certain chemical reactions and the
.1.
42
the Maccarhusetts Institute of Tecnn
gy
VIGYAN SCIENTIFIC AMERICAN February 1990
jects of classical, or Euclidean, geometry.
c
d
I®
II
■!
i
■ il«
7
7
!> SKI
■
a
H
5>
?
?
9
If
will
, t \ ■, I
e
pas®
■>
X
ill Gai
ait
\
’‘■I'E
■
3)
-A
5
^2
7
r
-S :.
IS
iM
-^-X ;•
-■
7'X
V
Tines have a dimension of one, circles
have two dimensions and spheres have
three. But fractals have noninteger (frac
tional) dimensions. Whereas a smooth
Eudidean line precisely fills a one-di
mensional space, a fractal line spills over
' into a two-dimensional space. A fractal
line—a coastline, for example—therefore
has a dimension between one and two.
Likewise a fractal surface—a moutain,
for instance—has a dimension between
two and three. The greater the dimen
sion of a fractal, the greater the chance
that a given region of space contains a
piece of that fractal.
T n the human body fractallike strucI hires abound in networks of blood
JL vessels, nerves and ducts. The most
carefully studied fractal in the body is
the system of tubes that transport gas to
and from the lungs. In 1962 Ewald R.
Weibel and Domingo M. Gomez and lat
er Otto G. Raabe and his co-workers
made detailed measurements of the
lengths and diameters of tubes in this ir
regular network of airways. Recently two
of us (West and Goldberger) in collabora
tion with Valmik Bhargava and Thomas
R Nelson of the University of California
at San Diego reanalyzed these measure
ments from the lung casts of humans
and several other mammalian species.
We found, despite subtle interspecies
differences, the type of scaling predicted
for the dimensions of a fractal
at
SELF-SP^ULARITYof a system implies that features of a structure or a process look al
at
different scales of length or time. When the structures of the small intestine are obsei
several different magnifications (drawings aboveX the resemblance between the larger and
smaller details suggests self-similarity. When the heart rate of a healthy individual is record
ed for three, 30 and 300 minutes (curves below), the quick, erratic fluctuations seem to vary
in a similar manner to the slower fluctuations.
~
150
LU . .
F
300 MINUTES
■
100
Sg
s
LU
501
150
30 MINUTES
|| .00
in
s 5°.
i
i
i
1 50!
3 MINUTES
100
S
50
VIGYAN Scientific
American
February 1990
43
tv
i
■!
Many other organ systems also appear
to be fractal, although their dimensions
have not yet been quantified. Fractallike
structures play a vital role in the healthy
mechanical and electrical dynamics of
the heart First, for example, a fractallike
network of coronary arteries and veins
conveys blood to and from the heart
muscles. Hans van Peek and James B.
Bassingthwaighte of the University of
Washington recently used fractal geom
etry to explain anomalies in the blood
flow patterns to the healthy heart. Inter
ruption of this arterial flow may cause a
myocardial infarction (heart attack). Sec
ond, a fractallike canopy of connective
tissue fibers within the heart—the chor
dae tendineae—tethers the mitral and
tricuspid \alves to the underlying mus
cles. If these tissues break, there can be
severe regurgitation of blood from the
ventricles to the atria, followed by con
gestive heart failure. Last, fractal archi
tecture is also evident in the branching
pattern of certain cardiac muscles> as
well as in the His-Purkinje system, which
conducts electrical signals from the atria
to the cardiac muscles of the ventricles.
Although these fractal anatomies
serve apparently disparate functions
in different organ systems, several
common anatomical and physiologi
cal themes emerge. Fractal branches or
folds greatly amplify the surface area
available for absorption (as in the intes
tine), distribution or collection (by the
blood vessels, bile ducts and bronchial
tubes) and information processing (by
the nerves). Fractal structures, partly by
virtue of their redundancy and irregular
ity, are robust and resistant to injury.
The heart, for example, may continue to
44
February 1990
VIGYAN Scientific
American
pump with relatively minimal mechani
cal dysfunction despite extensive dam
age to the His-Purkinje system, which
conducts cardiac electrical impulses.
r^ractal structures in the human body
pH arise from the slow dynamics of
JL embryonic development and evolu
tion We have suggested that these proc
esses—like others that produce fractal
structures—exhibit deterministic chaos.
Recent investigations in physiology have
uncovered other examples of apparently
chaotic dynamics on shorter, experimen
tally accessible time scales. In the early
1980’s, when investigators began to ap
ply chaos theory to physiological systerns, they expected that chaos would be
most apparent in diseased or aging sys
tems. Indeed, intuition and medical tra
dition gave them good reason to think
plot appears ragged, irregular and, at
first glance, completely random. But a
pattern emerges from the' heart-rate
data plotted over several different time
scales. If one concentrates Ion a few
hours of the time series, one finds more
rapid fluctuations whose range and se
quence look somewhat like th|e original,
longer time-series plot. At evin shorter
time scales (minutes), one fijnds even
more rapid fluctuations thafc again ap
pear to be similar to the original plot.
The beat-to-beat fluctuationsTn differ
ent time scales appear to be sejf-similar,
just like the branches of a Jometric
fractal. This finding suggests that the
mechanism that controls heart rate may
be intrinsically chaotic. In othdr words,
the heart rate may fluctuate donsiderably even in the absence of fluctuating
external stimuli rather than relaxing to a
homeostatic, steady state.
I
iia
TTl o investigate whether beat-to-beat
| heart-rate variations are indeed
.JL chaotic or periodic, one can com
pute the Fourier spectrum of the time
series plot for heart rate. The Fourier
spectrum of any waveform (such as the
time-series plot) reveals the presence of
periodic components. If a time-series
plot showed a heartbeat of exactly one
beat per second, the spectrum would
show a sharp spike at a frequency of
one beat per second. On the other hand,
the time-series plot of a chaotic heart
beat would generate a spectrum that
showed either broad peaks or no welldefined peaks. Spectral analysis df nor
mal heart-rate variability in fact shows a
broad spectrum suggestive of chaos.
Another tool for analyzing the dynam
BLOOD VESSELS of the heart exhibit fractallike branching. The large vessels (cast at left) ics of a complex nonlinear system is a
branch into smaller vessels (top drawing), which in turn branch into even smaller vessels “phase space” representation. This tech
(bottom drawing).
nique tracks the values of indeperident
variables that change with time. The
number and type of independent vari
so. If one listens to the heart through a meostasis: physiological systems nor ables depend on the system [see “Cha
stethoscope or feels the pulse at the mally operate to reduce variability and os,” by James P. Crutchfield, J. Ddyne
wrist,
' the\rhythm" of the heart seems) to to maintain a constancy of internal funcFarmer, Norman H. Packard and Robert
American , De^embe regular. For an individual at rest the ricin. According to this theory, developed S. Shaw; Scientific
pulse strength and the interval between by Walter B. Cannon of Harvard Medical ber, 1986]. For many complex systems
heartbeats seem roughly constant. For School,
School, any
any physiological
variable, inin all of the independent variables cannot
physiological variable,
this reason cardiologists routinely de- eluding
its be readily identified or measured. For
cluding heart
should return
to its
rate, should
heart rate,
return to
scribe the normal heart rate as regular ““normal
phase-space represehtaafter it
it has
,
has been
normal”” steady
steady state
state after
been such systems
sinus rhythm.
-perturbed.
* ’ ’ The principle of homeostasis tions can -be plotted using the methoci of
More careful analysis reveals that suggests that variations of the heart rate delay maps. For the simplest delay map,
healthy individuals have heart rates that are merely .transient responses
toeach
a fluc
»
point on the graph corresponds to
fluctuate considerably even at rest. In tuating environment. One might
o reason- the value of some variable at a given
healthy, young adults the heart rate, ably postulate that during disease or ag- time plotted against the value of that
which averages about
perbody
min is less able to maintain a
ing the
’ • 60 beats
same variable after a fixed time delay. A
ute, may change as much as 20 beats constant heart rate at rest, so that the series of these points at successive times
per minute every few' heartbeats. In the magnitude of the variations in heart rate outlines a curve, or trajectory, that de
course ofa day the heart rate may vary is greater.
scribes the system’s evolution.
from 40 to 180 beats per minute.
A different picture develops when one
To identify the type of system dynam
For at least five decades physicians carefully measures the normal beat-to- ics (chaotic or periodic), one determines
have interpreted fluctuations in heart beat variations in heart rate and plots the trajectories for many different initial
rate in terms of the .principle
’ / of ho-- them throughout a day. This time-series conditions. Then one searches for an atVIGYAN Scientific
American
February 1990
45
I
11
1
II
I
I!
|
I
(1
i. •
tractor: a region of phase space that at
tracts trajectories. The simplest kind of
attractor is the fixed point. It describes
a system—such as a damped pendu
lum—that always evolves to a single
state. In the phase space near a fixedpoint attractor, all the trajectories con
verge to a single point.
The next most complicated attractor
is the limit cycle. It corresponds to a sys
tem-such as an ideal, frictionless pen
dulum—that evolves to a periodic state.
In the phase space near a limit cycle, the
trajectories follow a regular path, for ex
ample, one that is circular or elliptical
Other attractors are simply called
“strange.” They describe systems that
are neither static nor periodic. In the
phase space near a strange attractor,
two trajectories that started under al
most identical conditions will diverge
over the short term and become very dif
ferent over the long term The system de
scribed by a strange attractor is chaotic.
T A 7e recently analyzed the phasel/V space representations for the
r V normal heartbeat. What we
found was more like a strange attractor
than like the periodic attractor charac-
teristic of a truly regular process. This *
observation was another indication that
the dynamics of the normal heartbeat
may be chaotic.
The mechanism for chaos in the beatto-beat variability of the healthy heart
probably arises from the nervous sys
tem. The sinus node (the heart’s natural o
pacemaker) receives signals from the in
voluntary (autonomic) portion of the
nervous system. The autonomic nervous
system in turn has two major branches:
the parasympathetic and the sympathet
ic. Parasympathetic stimulation decreas
es the firing rate of sinus-node cells,
i
!
I
140 —.
1.0
^130 ■
^120 f||
-8
£
H
2 100 T A- .
.
-
S 80
^70l
- 60 &
0
. i
..
.
300
600
TIME (SECONDS)
’
"
0
’ 900
140
£
50
60
70
80
90 100 110
HEART RATE (BEATS PER MINUTE)
100
h
300
600
TIME (SECONDS)
140
<£9°
r
^130
z
2120
£
“-110
0
.02
.04
.06
.08
FREQUENCY (HERTZ)
’00.
g 90
<
3!
I
gi110 -
o .6
££
900
°oB
'■
90
.04
.06
.08
FREQUENCY (HERTZ)
HEART RATE is shown as time-series plots (left), Fourier spectra (cen
ter) and phase-space plots (right). A heart rate 13 hours before car
diac arrest (top) is nearly constant as indicated by the flat spectrum
and the phase-space trajectory suggestive of a point attractor. A
American
100 -
80
.02
I
:1
«;■
-2 -
£ 70
1
'''
QH
<
VIGYAN Scientific
1
90
100
HEART RATE (BEATS PER MINUTE)
5
120
e Buj
■8 K
80
300600
TIME (SECONDS)
L
80
&• j-
130
\ J
''j- o§
.4 r.
p
£
80
.1
1.0
J
UJ
0
900
I
w
&
.2
70 2f
46
.1
3 -4 -
£ 80 ~
r
.04
.06
.(
FREQUENCY (HERTZ)
8.
co
w 90
60f
.02
0
.6 $
S100
I
90
£~
80
X
.8
H
co
H®-
LO r-
10
60
0
2 S’ 00
.2
^130
z
SI 20
li
si110
.6
UJ 90-.
so
I
O F-
I3 -4
o-i 10K7.
•I
120
EuG?
February 1990
.1
■
1-1
-I
. 1red
90 100 110 120 130 140
HEART RATE (BEATS PER MINUTE)
70r
heart rate eight days before sudden cardiac death (middle) is quite
periodic as shown by the spike and the trajectory suggestive of a
noisy limit cycle. A healthy heart rate (bottom) appears erratic; it has
a broad spectrum and a trajectory resembling a strange attractor.
whereas sympathetic stimulation has the
opposite effect. The influence of these
two branches results in a constant tugof-war on the pacemaker. The result of
this continuous buffeting is fluctuations
in the heart rate of healthy subjects. Re
cently investigators, including Richard J.
Cohen and his colleagues at the Massa
chusetts Institute of Technology, have
quantified the reduction in heartbeat
variability that occurs after heart trans
plantation, a procedure in which the au
tonomic nerve fibers are cut.
Recent evidence from several laborato
ries suggests that chaos is a normal fea
ture of other components of the nervous
system. Gottfried Mayer-Kress of the Los
Alamos National Laboratory, Paul E.
Rapp of the Medical College of Pennsyl
vania and Agnes Babloyantz and Alain
Destexhe of the Free University of Brus
sels have analyzed electroencephalo
grams of healthy individuals and have
found evidence for chaos in the nervous
system. Otto E. Rdssler and his col
leagues at the University of Tubingen in
West Germany have also discovered in
dications of chaos in components of the
nervous system that are responsible for
hormone secretion. They have analyzed
temporal changes in hormone levels in
healthy human subjects and have found
apparently chaotic fluctuations.
Other workers have recently simulat
ed interactions among nerve cells to
show how chaos might arise. Walter J.
Freeman of the University of California
at Berkeley has demonstrated that chaos
can be generated in a model of the olfactory system. The model incorporates a
feedback loop among the “neurons” and
a delay in response times. Earlier, Leon
Glass and Michael C. Mackey of McGill
University had recognized the impor
tance of time delays in producing chaos.
Why should the heart rate and other
,
systems controlled byy the nervous systern exhibit chaotic dynamics? Such dynamirs offer many functional advantages. Chaotic systems operate under a
wide range of conditions and are there-■
fore adaptable and flexible. This plasticity allows systems to cope with the exigendes of an unpredictable and changing environment.
Many pathologies exhibit increasingly
.„
and' a 'loss of" variabili-'
periodic behavior
ty. Early indications that even the dying
heart may behave periodically came
from Fourier analysis of electrocardio
graphic waveforms, during ventricular
tachycardia or ventricular fibrillation, the
very rapid cardiac rhythms that most
commonly cause cardiac arrest. In the
mid-1980’s Raymond E. Ideker and his
colleagues at the Duke University School
of Medicine recorded the waveforms as
sociated with ventricular fibrillation
!
il
NEURON exemplifies fractal structure. The cell body branches into dendrites, whit in turn
branch into finer fibers. This structure may be related to chaos in the nervtxis sys
from the innermost layers of the dog lar pathologies, however, has been shown
heart. They found that the fibrillatory ac- to represent nonlinear chaos—although
tivity inside the heart was a much more the pulse may feel quite “chaotic” in the
peiiodic process than previously thought. colloquial sense.
In 1988 two of us (Goldberger and
Rigney) did a retrospective study of the “ITYjhysiology may prove to fee one
of the richest laboratories for the
ambulatory electrocardiograms of peoJI
well
pie who had severe heart disease. We JL study of fractals and chaos as w
types
of
nonlinear
ics.
other
as
dynamics.
discovered that the pattern of heartbeats
of those patients often became less vari- Physiologists need to develop a better
able than normal anywhere from min understanding of how developijnental
utes to months before sudden cardiac processes lead to the construction of
death. In some cases the overall beat-to- fractal architectures and how dynamic
beat variability was reduced; in others processes in the body genaate ap; irent
highly periodic heart-rate oscillations ap chaos. In the near future, studies c fractals and chaos in physiology may pro
peared and then stopped abruptly.
Somewhat similarly, the nervous sys- vide more sensitive ways to charaqterize
dis
tern may show the loss of variability and dysfunction resulting from agi
the appearance of pathological periodic- ease and drug toxicity.
ities in disorders such as epilepsy, Par
kinson’s disease and manic depression,
FURTHER READING
And
whereas under normal conditions
i
-----------An Essay on the Importance
of Being
white-blood-cell counts in healthy subNonlinear . B. J. West in Ltcture Notks in
jects have been reported to fluctuate
Biomathematics 62. Edited by S. Levjme.
chaotically from day to day, in certain
Springer-Verlag, 1985.
cases of leukemia the white-cell count
Fractals
.and Medic
in Physiology
oscillates periodically.
Ary L. Goldberger and Bnxe J. We? t in
The periodic
Yale Journal ofBiology and Medicine, fol.
.
’ patterns in disease and
60, pages 421-435; 1987.
the apparently7 chaotic behavior in health
Physiology
Dimensions .
in Fractal
do not imply that all pathologies are as
Bruce J. West and Ary L. Goldberger in
sociated with increased regularity. In
hes
American Scientist, Vol. 75. No. 4, pages
some cardiac arrhythmias the pulse rate
354-365; July-August, 1987.
is so erratic that the individual may comNonlinear
Dynamics -in Sodden Car
plain of “palpitations.” Some of these
Syndrome : Heartrate
diac Death
events actually represent oscillations
Oscillations
, a , L.
and Bifurcations
Goldberger, D. R. Rigney, J. Mietus, E M.
that seem irregular but are actually peri
Antman and S. Greenwald m Experient ia.
odic when carefully analyzed. In other
Vol. 44, pages 983-987; 1988.
arrhythinias the heartbeat is in fact unpredictably erratic. None of these irregu-
VIGYAN Scientific
American
February 1990
I
1
I
47
9
MODE OF ACTION
AND
CLINICAL RESPONSE
AQUEOUS EXTRACT
OF HUMAN PLACENTA
Dr.
BISWANATH
ROY
Incharge
Scientific & Medical Department
ALBERT DAVID LIMITED
Reprint from
THE
EASTERN PHARMACIST
Annual issue,
April 1976.
Page 63 - 65
Mode of Action
It is still a subject of discussion, to know the
mode of action of aqueous extract of Placenta.
Prof. V. P. Filatov, observed in his elaborate and
illustrious experiments that tissues when kept under
2° to 4°G for 7 days some vital substances are prod
uced in these preserved tissues. Prof. Filatov defined
these vital substances as Biogenic stimulators.9
Recent clinical response of aqueous extract of
human placenta in different degenerative diseases,
produced interest to evalute the mode of action of
Placenta liquid—water soluble.
It is suggested that the clinical usefulness, as a
result of parenteral use of. placental extract is due
primarily to the presence of Biogenous or Biogenic
stimulators, produced in the extract due to autolysis
under low temperature (2 to 4°G) preservation for 7
days. These vital tissue regenerators exert a broad
spectrum effect through the interaction of substances
such as Nucleotides, Enzymes, Vitamins, Steroids
Aminoacids, fatty acids, trace elements and other yet
unidentified autacoids, the exact mechanism of
action is not yet known, but there is clear and
unequivocal clinical evidence to show that combined
action of these tissue extracts is beneficial in certain
types of conditions, characterised by tissue growth
stagnation, metabolic degenerative condition and
lowered immunity response factors.10
Some authorities think that the action of Place
ntal extract is due to the presence of natural steroid
in the solution. 100 ml of Placenta liquid contains
5 mg of Natural G 17 Ketosteroid (CLR formulation)
and the therapeutic dose is 2 ml Intramuscularly
daily or alternate days. 2 ml Placenta liquid contains
only O. 1. mg which is far below the therapeutic doses
stated in standard books of medicine.
Before the isolation of Cyanocobalamin from
liver extract, the mode of action, of liver extract
was considered, on its clinical response. Liver extract
contains besides Gyanocobalamin, folic acid, folinic
acid, Vitamin B-Gomplex and other unknown
haemopoietic factors. Similarly placenta extract
contains multiple substances for Biogenous stimul
ators along with Index substance and Alkaline
phophatase.
Liver extract contains Histamine, which is isolat
ed to avoid anaphylastic shock to the patients.
Histamine content of Placenta has not been ment
ioned either in Indian or foreign literature,11 so it
can be assumed that either Histamine is solated
during the process or it is destroyed, during the
process of manufacture.
Placenta extract liquid contains nucleotides like
DNA and RNA and enzymes like Alkaline Phospha
tase. Besides the combind effects of all thp vital
substances, Alkaline Phosphatase has an important
role to discharge the therapeutic efficacies of aqueous
extract of human placenta.
It is well known that DNA and RNA have a
vital role for the cell metabolism, specially the
metabolism of nuclei. Adequate Amount of Alkaline
Phosphatase is essential in the body to help DeoxyribonucleicAcid and various transaminase tohave their
functions in the process of metabolism. Deficiency
of Alkaline Phosphatase, leads to infertility in
females.12 Alkaline phosphatase deficiencies may
lead to the diseases of the two systems mainly i. e.
the Skeleton and liver and billiary tract 12A- It may
be presumed when Alkaline Phosphatase level is
maintained in the patient for a longtime, DNA,
RNA and transaminase supplied with Placental
extract and available in the body can take up their
metabolic energies, resulting in better metabolism
of cells. Alkaline Phosphatase of Placenta liquid is
present as natural form, which does not produce
any adverse effect on the body.
Dr. S. Kameswaran13 and Dr. S. Sinha14 had an
elaborate clinical trial with Prostanglandine and
Plancental extract in cases of Atrophic Rhinitis
respectively. In their studies it has been revealed that
the effects of Prostaglandins and Placental extract in
the treatment of Atrophic Rhinitis are very similar.
From this study it can be thought that the mode of
action of Prostaglandin and Placentrex is more or less
similar. These comparative studies are yet to be
done and possibilities are not remote. Alcoholic
extract of Placental tissue contain Prostaglandin16.
Indomethacin inhibits the action of Prostaglandins.
Inhibition of Placenta extract activity with Indome.1 mode
_J_ of
_r _action of ----’icous
thacin may prove the
aqu
extract of human placenta is similar to tha t of
Prostaglandins.
Though aqueous extract of human placenta was
introduced since 1954 in the treatment of Corneal
ulcer with or without hypopyon1, yet it did not gain
attention of the research Scientists and Clinicians till
1967. In 1967, author of this article gave a clinical
trial in cases of leucorrhoea with aqueous extract of
human placenta, combined with nonspecific milk
protein and Cyanocobalamin 2 In 1969 Dr. B. N.
Purandare, President, International Federation of
Obstetrics & Gynecology, alongwifh Dr. C. B.
Purandare and Dr Usha Hirlekar tried aqueous
extract of human placenta combined with nonspecific
milk protein and Cyanocobalamin in cases of primary
and secondary infertility and they got 75% successful
results in their studies3.
Since 1969 various clinical trials have been con
ducted by different workers in different fields of
medicine and most of them got encouraging results.
It has been observed that aqueous extract of human
placenta acts more specifically in the treatment of
degenerative diseases and indolent ulcers like post
radiation burns4.
Aqueous extract of placenta is in use In West,
particularly in Europe. Water soluble placenta liquid
has been extensively used both as injections and oint
ments—in treatment of peripheral circulatory distur
bances. Also in dermatology this is applied in treating
various skin disorders, such as ulcus Cruris, psoriasis
and urticaria. The main application in Cosmetology is
with skin changes associated with inadequate local
circulation and degeneration of cells i.e. aging Skin 6.
In West, animal placental extract is used, collecting
these placentae at 32 weeks gestation, considering
that placcenta contains maximum nutrients at this
time of gestation.
In India aqueous extract of human placenta has
been obtained, placentae are collected after
parturition6. Human placental extract provides
better therapeutic effects as these extracts are
obtained from homogenous placental tissues. Human
placental extracts have a better therapeutic effects on
human beings with practically no adverse reactions
Composition :
Human placental extract contains multiple vital
subsntances in natural form. So far analysis of
aqueous extract of human placenta shows the
following natural substances.
Nucleotides—Ribonucleic acid, Desoxyribonucleic
acid, Adenosinetriphosphate.
Enzymes—Alkaline Phosphatase, Acid Phospha
tase, Glutamate —Oxaloacetate transa
minase, Glutamic acid and Pyruvic
acid transaminase.
Vitamin—Vitamin E, Vitamin Bj, Riboflavine,
Pantothenic acid, Vitamin B2, Nicotinic
acid, Biotin, p-amino benzoic Acid,
Vitamin B12 Choline and Inositol.
Steroids—Natural C17 Ketosteroids.
Aminoacids—Alanin, Asparagine, Asparaginic
acid, Cysteine, Glutamic Acid,
Glycine, Histidine, Larcine, Lysine
Proline,
Serine
Phenylalanine,
Threonine, Tryptophane, Tyrosine,
valine.
Fatty acids —Linolic acid, Linolenic acid, Oleic
acid, Palmitic acid.
Trace element5—Sodium, Potassium, Calcium,
Magnesium,
Copper, Iron,
Phosphorus, Manganese, Sili
con.
Out of these natural substances, Alkaline Phos
phatase is considered as pivotal ingredient, because
standardisation of the product is considered with the
quantum-presence of Alkaline Phosphatase.7 Alka
line Phosphatase is thermolabile and in aqueousex tract
of Placenta, if Alkaline Phosphatase can be preserved,
then all other substances will be present. For this
reason calculation of Alkaline Phosphatase is consi
dered as the index of standardisation of aqueous
extract of human placenta. Alkaline Phosphatase,
present in the solution to the extent of 50 percent is
considered as standard. This calculation is done by
the method of King Armstrong Unit—100 ml of
Solution contains at least 50 K. A. U. Alkaline
Phosphatase.8
References :
Clinical response :
1. Dasgupta, B. K. et al : J. I. M. A., Vol. XXIII. No.
9. June Page 322-385, 1954.
Clinical response of aqueous extract of human
placenta has been proved beyond doubt in various
2. Roy, B., Medicine, Science & Services : Vol, III No. 9,
Page 36-38 March 1967.
chronic degenerative and infective diseases. B. K.
Dasgupta et al16 proved its therapeutic efficacies in
3. Purandare, B. N. et al, The Clinicians, Vol XXXIV,
No. 1. Page 45 48, JAN. 70.
corneal ulcer ond corneal ulcer with hypopyon. B.
The paper was read on 30-12-69 at XV All India Congress
Roy and B. N. Purandare et al have proved its
of Obstetrics & Gynaecology, at Mandogao, Goa.
clinical respone with nonspecific protein and Cyano
4. Mukherjee, A. K., Literature of M/s. Albert David Ltd,.
cobalamin in eases of nonspecific leucorrhoea
Calcutta.
primary and secondary inferlity respectively. S. J.
5. Scientific literature : CLR, Berlin.
Kumbhani tried in paralysis of lower limbs followed
by poliomyelitis.17 M. Mallya has tried acqueous 6,7,8. Scientific literature of M/s. Albert David Limited,
Calcutta.
extract of human placenta parenterally in cases of
9. Filatov, V P.: Tissue therapy, foreign language Publishing
Ischaemic limbs.18 A. K. Mukherjee have received
House, MOSCOW, 1955.
excellent results in the treatment of post radiation
Scientific literatures of M/s. Albert David Limited,
ulcer in 20 cases. Out of 20 cases, he got successful 10. Calcutta.
result in 19 cases.19 P. P. Karnik et al tried Place
CLR, Berlin.
11.
99
ntal extract preliminary in cases of Atrophic
Rhinitis.20 D.S. Shukla had an extensive trial with 12. De, A. K et al : Paper read in XIX All India Congress
of Obstetrics & Gynaecology at Jamshedpur on 28 12-75.
aqueous extract of human placenta in infected burns
12A.Trumper Max, Abraham Cantoraw ! Clinical Bioche
and wounds 21 A K. Mitra tried aqueous extract
mistry 6th Ed. p. 454.
of human placenta in the treatment of suspected
13. Kameswaran, S. et al : Paper read at All India Congress
tubal blockage.22 B. Joseph and her associate tried
of Otolaryagology at Calcutta on 9-1-76.
in pelvic inflammation, tuboovarian masses and tubal
14. Sinha, S. et al : Paper read at All India Congress of
blockage with aqueous extract of human placenta.23
Otolaryagology at Calcutta on 9-1-76.
J. Seetamma and A. Chandrakaladevi tried Placen
15. Karim, S. S. : Brief. Med J. : VOL II page,l 635-40,
tal extract in combination with antibiotics in cases
1974.
1974.
of Pelvic inflammation and the results were very 16 Dasgupta, B. K. et al : J. I- M. A. 1954.
satisfactory.24 P. Brahmyyashastri had a review of
17. Kumbhanis. J : Reprint of his paper by personal com.
different
degenerative
Placental extract in
munication with M/s. Albert David Ltd., Calcutta
diseases.26 S. Sinha and his associates had an
18. Mallya, M. i The Antiseptic, VOL 68, No. 9, Page 655elaborate successful trial with aqueous extract of
661,1971.
human placenta in cases Atrophic rhinitis. S.
19. IVIUMiciji-t,
A .: ividviiai
Personal «.communication with M/s.
Mukherjee, rt
Albert David Ltd , Calcutta
Varadarajan had a clinical trial with aqueous
extract of human placenta in cases of bronchial 20. Karnik, P. P. • The Eastern Pharmacist, VOL XV No.
172, page 113 114.
asthma and different allergic conditions.26
21. Shukla, D S. : Extract of thesis for M. S. (Surgery)
Kanour University 1972.
Conclusion :
From the clinical response, obtained by different
specialists of different branches of medicine, it is
assumed that aquous extract of human placenta has
a wide spectrum of therapeutic activies in different
diseases, specially in cases where immunity is
lowered. Raw materials for this medicine are
abundantly available in the country and detailed
investigations will further prove its worth both in
the field of human and veterinary medicine.
22.
Mitra, A. K.
Associate prof, of Obst. & Gjnae : MCH,
Calcutta Personal communication with M/s. Albert David
Ltd., Calcutta.
23. Joseph, B. et al: J of Rajasthan Medical College, 1972.
” i Cong24. Settamma, J., et al: Paper read atXIX All ’India
24-12-75
at
ress of Obstetrics & Gynaecology on 21
12
Jamshedpur.
25. Brahmyyashastri P. J Paper read in 63rd Ind Science
Congress at Waitair on 6-1-76.
26.
Bharadarajan, S : Personal communication with M/s.
Albert David Ltd , Calcutta.
PRINTED BY COMMERCIAL SUPPLIERS • 53-3563
1 .3)
>•
TENS
X L
TECHNICAL SPECIFICATIONS:
Pulse frequency rate
5 to 125 Hz
Pulse width
50 to 800 Micro second
Pulse shape
Rectangular
Max output voltage
100V (0-100V Variable)
Max current output
38 mA
Burst frequency
x
2 Hz
Timer range
Upto 99 Min.
Power supply
220V AC Mains.
OPERATING INSTRUCTIONS:
1. Connect the Mains plug and switch on the Mains
"ON/OFF"
switch to "ON". Check for Neon glow.
2. Set all stimulation parameters to minimum level.
3. Connect the patient electrodes.
4. Select the •AUTO', MANUAL MODE.
5. Keep the pulse width to 150 to 250 Micro
second range for general
pain symptom.
6. Select the frequency.
7. Press 'SET' switch momentarily and check for beeper sound.
Adjust the sound to optimum effect.
8. Select the amplitude till the patient feels
it.
amplitude for pain symptoms.
Don’t give more
contu...2
contu,..2
9. Once the therapy is over switch OFF the equipment and keep all
controls to minimum positions.
10, Wash electrodes and dry them.
APPLICATIONS:
1. Low back pain.
2. Labour pain
3. Non-united fracture healing procedure.
4. Post-operative pain.
5. Head ache. Migraine headache..
6. Paraplegia & Hemiplegia
7. Diabetic neuropathy
8. Peripheral neuropathy
9. Intractable cancer pain and many more
For applications (1) to (4) - 1 Hour / session, 4 sessions / day
Max therapy timings.
ACCESSORIES:
2 sets of Metal Electrode/ 2 sets of Rubber Carbon Electrode/
4 Nos Velcro strap/ TENS Jelly - 100 gms - 1 No., Instruction Manual
and a Carrying case.
OPTIONALS:
1. Sterilized post-operative electrodes of 9 width.
AMPLITUDE SETTING:
FREQUENCY SETTING:
0
5
1
6-15 Hz, 7
OV, 1
70V, 6
5 Hz, 2
20 Hz, 8
10W, 2 - 20V, 3
80V, 7 - 90V, 8
40 V, 4
100V.
60 V/
6 Hz, 3 - 7.5 Hz, 4 - 9 Hz, 5 - 10 Hz,
33 Hz, 9 - 75 HZ/ -10 - 125 Hz.
PULSE WIDTH SETTING: IN MICRO SECONDS.
1
9
50, 2
100, 3
150, 4
600, 10 - 700/ 11 - 800.
200, 5
250, 6
300/ 7 - 400/ 8
500/
TREATMENT PROCEDURES AND ELECTRODE PLACEMENTS
Probably one of the most controversial topics with TENS is the
question of ideal electrode placement, Many te^chniques are
suggested# based on nerve roots, acupuncture points# and trigger
points. All are valuable but vary with each individual case.
B
f
A
C2
intercostobrachial
cervical
i
supraclavicular
t
^T3
—14
1
-I5
T6
medial &
lateral
T8
T9
C6.
r
thoracic rami
I T10
Til
T2
T3
T4'
Th
T6.
T7
T8
T9
( * '.
L2
C
--
C6
\
S4
S5)J S3
Iliohypogastric
ilioinguinal
ulnar
obturator
fumorjl
branch of
gemtolcnior jl
obturator
median
C8
lateral,
medial. &
posterior
femoral
L3
S2
iL4
ul iar, radial
iC/i
L2
median
%
sacral
radial
L3
I
posterior rami
I 1
C8
N
C5
T12
*-412
IC7
upper
lateral,
posterior,
lateral. 8
medial cutaneous
y
^Tl°
/ I 1
cervical
C4
K
^T2
_J7
•upracla vlculir
auricular ____
upper —
& lower
lateral 1
C3
C4
great &
small occipital
C3
lateral, medial. &
intermediate ----of thigh
cutaneous
saphenous
lateral
cutaneous
L5
saphenous
superficial &
deep peroneal
lateral
cutaneous
SI
medial calcaneal
sural
SI
A
A
B.
Fig.
Dermatome chart—anterior (A).
B
medial &
lateral plantar
Fi9-
-------
1 rZ„tOme
____
1^t
chart-P°st®nor (B). (Figs. A and B from Horn-'
ero-Sierra C: Neuroanatomy:
Contu ••2..
. .2. .
An experienced user with TENS will quickly be able to establish
several key auatomic points to cover most conditions/ however the
following are some recommended electrode placement for common
conditions.
PLACEMENT OF ELECTRODES FOR THE UPPER EXTR EM IT Y s
Flg.
Upper extrenrU, .Ih M. *««•-“
epicondyle, and hoku.
I
"*
*•
)
. .3. .
1. C3 - C7 nerve roots / dermatomes
2. Point of pain
3. Tip of acromion
i
4. Hoku (web space between thumb and forefinger)
5. "Wrist-Watch" position# dorsal wrist
6. Tip of lateral epicondyle
PLACEMENT OF ELECTRODES FOR THE LOWER EXTREMITY :
I
i
i
□
□
f’9Lower extremity
electrode placements: nerve
root, gluteal, popliteal, and
posterior lateral malleolar.
contu . . 4..
V
. .4. .
1. LI - Si Nerve Roots / Dermatomes
2O Gluteus maximus center (’’bulls’ eye”)
3* Popliteal space
4. Posterior lateral malleollus
5. Head of the fibula
6. Specifically for the knee; transartharalt medial / lateral knee.
PLACEMENT OF ELECTRODES FOR THE LOWER BACK :
1. Associated nerve roots / dermatomes
2. Gluteal sites as above
3. Popliteal sites as above
I
4. Crossed pattern : Paravertebral at LI and L5, in a box like
pattern^ with the circuits crossing at L3
GENERAL CONFIGURATIONSs
1. Associated nerve roots / dermatomes
2. Point of pain
3. Acupuncture points proximal to point of pain"
4. Acupuncture point distal to point of pain
I
i
5. If pain can be pinpointed, consider the cross pattern technique,
with the crossing point at the painful site.
6. Bilateral placements are extremely effective with mid-back
and low back pain.
7. Contralateral placements are suggested when the pain site is
not accessible due to amputation, dressings, open wounds and
casts.
RECOMMENDED TECHNIQUES FOR SPECIFIC APPLICATIONS :
1. TENS IN NON-UNITED FEACTURE TREATMENT :
It may be proven that the actual current mode (high or low
frequency), pulse alternating or direct current, or wave form makes
little difference.
The electrical energy and the bone itself may
be the key factors in determining the outcome of non-united fractures.
It is known that bone exhibits piezo electrical qualities and that
currents are generated in low micro amperage range, when the bone is
stressed.
I
contu .. 5 ..
. . 5. .
Application of electrical energy to bone enhances Osteogenesis
(bone formation) and hence TENS fits into this picture nicely,
offering electrical parameters, and low cost, as compared with
the existing devices for this purpose.
a) SELECTING THE PARAMETERS:
1. Frequency / Rate should be as high as 120Hz.
2. Pulse width should be as wide as 300 to 500 micro seconds.
3. Intensity should be the lowest possible, "barely sensed"
by the patient
4. Course of therapy should consist of 1 hour per session#
4 times
daily.
b) ELECTRODE PLACEMENT:1. If tne fracture site is encxosea
a plaster
cast, electrodes
in a
plaster cast,
enclosed in
and distal
to the
should be placed proximal and
the cast; two or four
distal to
electrodes can be used.
Polarity is not important.
2. If the fracture site is free of casting, three basic patterns
are
available.
a) With two electrodes, c..
one placed on the either side of the
fracture site, about 6" apart.
b) With four electrodes. a crossed pattern, about 6M r
the crossing point directly over the fracture site.apart. with
c) With two electrodes.
in between the t.o
pattern' with the
Treatment should continue for atleast 6 months before
it is
discontinued, however follow •up should be done at
every 4 or 6 weeks
to monitor changes in the status of the nonunion.
With man ihade
nonunions, it may take more than 1 year of TENS’Stimulation 4o
produce favourable effects.
contu . .6.
O O 6 • •
2. OBSTETRIC CASES
LABOR AND DELIVERY
X
S
The use of TENS as a form of analgesia for delivery is growing
rapidly. The literature, although mostly from foregin sources,
speaks highly of this procedure and has spurred American
researchers to investigate this apparently safe, non invasive,
non drug method of providing a relatively pain free delivery.
The reluctance to use any new method with pregnant patients is
understandable.
No known or reported untoward effects are
listed in the available foreign literature.
ECTRODE PLACEMENT DURING LABOR :
Place two electrodes at the level of the brassiere strap, one
on each side at the spine, near the nerve roots. Elongated
electrodes (1 x 6" or 1 x 9") are preferred so that several
nerve roots may be covered, extending distally from approximately
T8 to LI.(figure
). This equipment is activated on the
morning of imminent delivery and left on all though delivery.
/
/ r
/
1. Keep the frequency as'higfi*1 aS'possible (100-125Hz)
2. Pulse width should be minimum (150 Micro second)
3. Amplitude should be comfortable, but low.
4. Keep the equipment in "BURST" mode.
ELECTRODE PLACEMENT DURING LABOR CONTRACTIONS :
A second pair of electrodes, may be placed paravertebrally along
the lowest portion of the spine without the patient sitting on
them. (i.e. approximately, at SI and below).
Activate this
circuit with the above parameters already discussed, expect,
change the "BURST'1 mode to "STD" (BOOST) mode with each labor
contraction to block the contraction pain but should not be
left on in "STD" mode when the pain abates.
contu . .7. .
. .7. .
ELECTRODE PLACEMENT DURING SECOND STAGE OF LABOUR :
Take away the distal pair of electrodes from the sacral region
(lower portion electrodes) and relocate them to the anterior
abdomen/ in aV shaped configuration/ diagonal and lateral to
the pubic triangle.
£lcct /oclc
Do not alter the parameters already discussed except that the
amplitude may be slightly increased to block contraction pain but
this should not create any muscle contraction. Continue to do
the stimulation as discussed in the second stage.
USE OF TENS FOLLOWING THE LABOR;
Tens may also be used for postpartum pain. With cesarin sectioned
patients/ the incision and scar discomfort may also be allevated
with TENS application. The placement of electrodes are different.
Place the elongated electrodes (1 x 6” or 1 x 9”) at the level of
the brassiere strap (as already discussed) and place the other
pair of electrodes at both ends of the incision / scar.
DO NOT CHANGE THE PARAMETERS.
contu ..8..
I
!
I
...8. . .
(
USE OF TENS IN POST OPERATIVE PAIN;
Place the electrodes parallel to and approximately 1” from the
incision / scar, using elongated (lHx 9”) electrodes if available;
(figure 1 ) or in a crossed pattern, using four standard square
electrodes (figure 2. ) •
r
I
*•*'
•Tn
a
FIC, - Z
F/6-/
1. Keep the frequency at the higher rating (80 to 125 Hz)
2. Pulse width should be kept at 150 Micro seconds.
3. Amplitude must be minimum but sensed by the patient.
4. Select the "STD” mode.
5. Operate the equipment for 1 hour, four times daily,
is severe/ additional sessions are recommended.
If pain
6. If treatment is necessary for a prolonged period of timer
"BURST” may be selected at times to avoid accommodation.
I
USE OF TENS IN MORNING SICKNESS
TENS has also proved effective in controlling “Morning sickness” and
other forms of nausea keep one electrode on the tip of the right
I
..9...
I
i I
...9. ..
Acromin and the other electrode on the right hoku point. This
technique does not work it electrodes are placed on the left
side. Keep high frequency (80-120 Hz) t pulse width medium
(150 - 250 micro seconds), amplitude minimum but should be
sensed and select the ••STD11 mode. Treat the patients for
3 0 minutes every morning.
I
Mp i~3
TABLE TOP TENS
TRANSCUTANEOUS ELECTRICAL NERVE STIMULATOR
INSTRUCTION MANUAL
j
KODYS SALES & SERVICE NET WORKS AT
Bangalore, Bombay, Calcutta, Coimbatore, Delhi, Ernakulam, Hyderabad.
Madras, Madurai, Nagpur, Vijayawada and Visakhapatnam
M. G. K. Art Printers, Madras-20
CONTENTS
Page
1.
Introduction
2
2.
Specification
2
3.
Controls
4.
Operating Instructions
5
5.
Placement of Electrodes
6
6.
Problems and Remedy
14
7.
Warning
14
8,
TENS I heory and Applications
15
3
2
1.
Introduction
Kodys Table Top TENS is the first Multichannel Transcutaneous Electrical Nerve Stimulator (T. E. N. S.)
available in India with built-in Timer facility. The equipment is mains operated with patient Isolation facility.
2.
Specification-Technical :
Power Supply
230 V ac mains.
Output voltage waveform
Rect-angular variable.
Max output voltage
65V, with IK-ohm load per channel.
Pulse frequency range
2 to 50Hz per channel
Pulse width ON time
400 micro sec (fixed) per channel
Max current output
20mA (r.m.s.) with 500 ohm load per channel
Timer-set Time
1 to 99 minutes.
Patient Isolation built in
3
3.
CONTROLS
(i) MAINS ON OFF: This push button control is provided at the back of the instrment By pressing this
the maine 230V AC is connected to the instrument and this is indicated by a Red neon lamp noted as
** Mains " in the front panel. While the mains button is pressed the Red lamp will glow.
(ii) AUTO/MANUAL
This control is provided at the back of the instrument, When this push button switch is not
pressed, the instrument is set to
AUTO " mode and When it is pressed the instrument is set to
11
Mode.
When
the
instrument
is in Auto, the instrument will be automatically switched off
MANUAL
once the therapy time equals the SET time, In the MANUAL mode once the therapy is over we have
to switch off the instrument manually.
(iii) VOLUME
This control is provided at the back of the instrument,
the beep sound generated by the instrument.
This is used to control the volume of
(iv) SET
To start the operation of the instrument the SET control provided at the front panel has to be
pressed momenterily once.
(v) RESET
Pressing momenterily the RESET button provided at the front panel will reset the time to zero
<0) and the timer will start from zero minute.
4
(vi) TIME SET
The Thumb wheel switch provided at the front panel is used to set the therapy time when the
instrument is used in AUTO mode, When the switch is set to “ 99 " the instument will switched
off after 99 minutes automatically. When it is • 00 ' the instrument will not function in • Auto ' mode.
(vii) MAINS
The Red Neon lamp marked as * MAINS ' in the front panel
OFF switch provided at the back is pressed.
will glow
when the
Mains ON/
(viii) AMPLITUDE
This Amplitude control is used to vary the intensity of the stimulation. There are two ‘AMP’
controls available in the front panel
One for channel 1 and the other for channel 2. Clock wise
rotation will increase the intensity and vice versa. Before starting the operation this control has to
be kept in the counter clock wise direction fully. The adjustment of one amplitude control will out
alter the other.
FREQUENCY
This • FREQ ' control is used to vary the number of pulses/sec delivered from 2 to 50. Turning the
control in clock wise direction will increase the frequency. There are two frequency controls available
and adjusting one control will not alter the frequency of the other, LED's provided in the front will
flash according to the frequency selected.
OUTPUT:
The output sockets provided in the front panel Is used to connect the patient electrodes to the
instrument. Electrode plugs should be inserted in the sockets before switching on the equipment.
5
4.
Operating Instructions :
1.
Place the electrode over the pain area with coupling medium jelly,
sign should be kept on the pain site.
2.
Connect the electrode pluge to the output sockets.
' output sockets.
to the ‘
3.
Check whether
clockwise.
4.
Select the number of pulses per second (frequency) required by adjusting the frequency control.
5.
Press the MAINS ON/OFF switch to ON position and check whether Red neon lamp lights
‘ ON '.
6.
Select AUTO or MANUAL Mode.
7.
Set the therapy time if you want to operate the instrument in AUTO mode.
8.
Press SET switch. Check for Beeper sound, LED flash
the
amplitude
controls
Electrode with
* + ' sign electrode should be connected
are at minimum value position, i. e.,
and
Timer
fully counter
* 0 ‘ (zero).
Now the
instrument is ready for operation.
9.
Adjust the Amplitude from lower rating to higher gradually till the patient feels comfortable.
10.
Press and release RESET switch.
11.
The instrument will switched off automatically if it is in AUTO mode.
This will reset the Timer to zero minute.
6
12, Once the therapy is over turn the Amplitude control to minimum position,
5.
13.
Unplug the electordes from the instrument and also from the patient.
14.
Switch off the Main Switch.
Placement of Electrodes.
Figures and table given in this section provide .he electrode placement for different pain
symptoms but indicated positions are not the exact final placement area. The coiiect pain area
can only be found after a careful study of the symptom.
— ;o.'—
HECK PAM
%
S^JLl>£K
Low
P«^
Neck pain
------- St\fiTl^
Low back pain
KHEE PAM
POSTERIOR
1—.
AMKLE PAM
■j
r
■ 4*
Sciatica
Arm pain
Knee pain
Si.
■-
f ■:
f’
fc
4
Shoulder pain
POSTERIOR
ANTERIOR
ANTERIOR
i
€
o
PAIN 'PATHWAYS LEGEND
A—arm
P—Legand foot
DERMATONE LEGEND
C—Cervial
T—Thoracic
L—Lumbar
S—Sacial
Suggested etectrods placement for some of the most common pain problems
PAIN AREA
RECOMMENDED ELECTSODE PLACEMENT
Headche
A
P
' + ' ON PAIN AREA
Shoulders
A
P. 9
' 4- ' P :
9.8
9 8
Arms
A
P. 7. 5
Waist
B
P
6
6
Legs and Feet
B
P. 2, 1
Hip
B
P. 4
Leg front fatigue
2
2
Leg rear fatigue
2
2
Low back pain
A
B
Phantom Limb
Both probes axial to amputation
Table-1
Electrode Placement for T.E.N.S.
Pain Area
14
6.
Problems and Remedy
1.
Insolated cases of skin irritation may occur at the site of electrode placement following long
term application. If the electrodes are insufficiently moistened or are in poor contact with the
body, the result may be a prickling pain, skin irritation or electrode burns. To avoid this apply
electrode jelly before placing the electrodes over the pain area and make sure that the electrodes
are correctly in contact with the body.
7.
WARNING
1.
Table Top T. E. N. S. is for external use only.
2.
If skin irritation occurs beneath or around the electrode site discontinue use, consult physician.
3.
Should not be used for individuals using demand type cardiac pacemakers.
4.
Avoid abrubt
slowly.
5.
Should not be used over the carotid sinus nerves, laryngeal or pharyngeal muscles.
6.
Should not be used during pregnancy or delivery.
7.
Should not be used by patients with known myocardial disease or arrhythmias without evaluation
by a physician.
changes
in
control
settings.
Stimulater
controls
should
always be adjusted
15
8.
Keep out of reach of children.
9.
Turn stimulator off before applying, removing or changing electrodes.
8. T. E. N. S. Theory and Application :
The following brief details about T. E. N. S. are taken from a Book ° Pain Conirol ’* with T.E.N.S.
by Robert A Ersek. U.S.A. This material is provided only for reference and private use.
Introduction
Transcutaneous Electrical Nerve Stimulation, the basis for this series of discuseions will be examined
as to its evaluation, area of usage and efficacy as a non-toxic, non-pharmacologic therapy for the relief
of a number of acute and chronic pain states.
Its roots lie in the basic concept of electro analegesic. The “ shocking " concept-electricity had its
begining in Socratic times
Seribonius largus claimed to cure arthritis and headaches with the application
of electric torpedo fish in the first century. The therapeutic belief in electro-analgesia continued throughout
the middle ages.
The use of electroshock therapy as a modality of treatment for psychiatric depression is a profound
from of pain modulation by electro-skimulation.
With the proposal of the Gate Control theory by Meizack and Wall in 1965, a rational basis for
electro-analegesia was postulated.
16
In 1967, Wall and Sweet applied the gate control theory clinically using implanted stimulating device
through low voltage, percutaneous electrical stimulation of themselves. This work then led to stimulation
of the peripheral nerves on the posterior cord for pain control. As one might expect the acute and chronic
pain states area the result of a wide spectrum of pathologic conditions, i e., causalgia, polycythemia vera,
peripheral nerve injury, phantom limb pain, lower back pain, bursitis, cervical pain, postherpetic neuralgia,
cord injury, parturition, past operative pain and ilens, and intractable cancer pain. Some of the patients treated
with TENS have reported a marked reduction of such pain.
What is T.E.N.S. ?
It has been well established both by history and experience that such procedures as heat, massage
vibration, and itching are sometimes useful in modulating the symption of pain. These procedures can as a
group, be categorized as pain modulators secondary to counter- irrilation, which ircation the interaction
of the components of the sensory nervous system. The medical diathermies, hydro-collator packs, etc , histori
cally utilized by physical therapists represent pain treatment with counter-irritation. T.E.N S. is also a form of
treatment utilizing counterirritation secondary to the introduction of an electrical current to produce sensory
modulation. Most T.E.N S. unit produce a direct current from a self-contained battery source usually of an
asymmetricial, biphasic wave from with a positive rectangular wave component combiued with a negative,
inverted spike component, or a rectangular, monophasic wave from with only a positive component. The current
frequently generatedjhas a voltage range of 0—9C) volts (60 m. amps.), and ajrate rangeof 0-100 Hertz. The pulse
width which is commonly a third adjustable parameter usually provides a pulse with duration range of 10-100
micro seconds, in the monophasic wave forms, and 150-500 micro-seconds in the asymmetrical biphasic
wave form.
The phasic input provided by the T.E.N S, device is thought to stimulate the large diameter afferent
A fibers. According to the Gate Control Theory (Melzack and Wall. 1965), the stimulation of laige diameter,
afferent A fibers relieves pain.
17
The Gate Cantrol Theory
Its very name suggests that there is gating machanism in the nervous system.
machanism is in lamica II and III (substantia gelationosa) of the dorsal horn.
The location of this
This Gate mechanisam is an intermediate structure between the transmission cell of lamina V, which
must be stimulated in order for a pain interpretation and response to occur AND the sensory fibers which
via the dorsal root, enter the dorsal horn at the surface of the zone of Lissauer and lamina I
Restated, the T-cells must reach their threshold and be activated if pain is to be interupted. The
activity of the A and C fibres has the potential of eliciting a response of the T-cells. Before they can effect the
T-cells the potentials from both fiber types must pass through the substance gelatinosa, i.e.. Gate. Whether
or not pain results is determined by the relative activity in the large diameter A fibers, and the small diameter
C fibrers. High levels of activity in the A fibers, by a negative feed back mechanism, ** close " the Gate by
•• toning down '' the effect of both large and small fiber input to the T-cells. Elevated activity levels in the
C-fibers “ opens ,r the Gate, again by a negative feedback mechanism, which results in the net effect that
input from both the large and small fibers reach the T-calls and create, by spatial or temporal summation,
the excitation of the T-calls with perceived pain as the net result.
Often we see the clinical symptom of pain accompanied by a history indicating the occurance of
some noxious stimulus of an interse or prolonged nature. This type of pain is typified by musculo skeletal
injuries, cuts, burns, herniated disc syndromes, etc. These stimuli are medicated by the C fibers which have
the net effect of faciliating transmission across the substantia gelatinose, resulting in activation of the
T-cells in limina V, yielding pain.
This illustrates pain resulting in C fiber dominance over A fiber secondary to excessive stimulation
of C fibers. Some pain syndromes seen clinically illustrate pain resulting from a different type of neurological
18
Interaction.
In some neurological pathologies, such as neuralgias, there is
myelinsheath destruction and A
fiber destruction, resuting in a decreased functional capacity of the A fibres. Although in this instance
C fiber activity may be unchanged, the C fibers may become dominant over the A fibers, secondary to the
decreased functional ability of the latter fiber group. Thus, the normal
balanced " A-C fiber interaction
is altered by the A fibers becoming
submissive “ to the C fibers.
Approach To The Patient
Because of the potential anxiety people may experience when anticipating
electrical "
stimulation because of the connections of the word “ electrical ", we suggest that the initial contact
with the patient should reflect the use of the word *' Neuromodulation
Once the patient has experienced
the neuromodulation curreut, an additional explanation of its electrical properties may be indicated.
to
It is benefical to emphasize to the patient that one may terminate the treatment at any time
reduce the possible anxiety which may have been created.
Electrode Placement
The efficacy of T.E.N.S tieatment .depends greatly on the proper selection and placement of
electrodes to ensure the most efficient modulation of the peripheral and central nervous system. The basis
for proper electrode placement appears to rest in the proper evaluation of the dermatomes in which the
corresponding spinal cord segment levels to influence the nervous system most effectively.
Random electrode placement has produced random result. It is important to emphasize that each
professional who uses T.E.N.S should duplicate or create a consistent, logical procedure for selecting
electrode placement sites.
19
Application of Tens for Different Pain Symptoms :
Tens in Post Operative pains :
10 hours after the end of the operation, electrical stimulation was applied for the first time. This was
performed by utilizing a stimulator with a frequency of 2, 6 Hz, Two electrodes were located on both thighslateral aspect-and linked with the stimulator by a ''Y" shaped wire. To close the circuit, another electrode was
placed in the lumber region. Blood pressure and pulse were monitored throughout the session of stimulation,
but no appreciable alternations were observed. The time of each session was approximately 15 to 20 min.
Results of the Treatment :
In the Control group,
the average time of a
dynamic ilens until the reappearance of the peristalsis
was approximately 26 hours. In the investigated and stimulated group, the effects are presented in three sets.
In 33 cases, or 65% of the patients, peristalsis appeared following the initial session of electrical stimulation
between the 10th and 11th hour. The intestinal motility was rather weak during that period, and it lasted
for about 2-3 hours.
The second session of electrical stimulations five hours later produced peristalsis in 46 patients, or
9 % of all cases. This was strong enough so that the next, or third sessons was no long necessary for
these patients in the remaining 5 patients, 9% peristalsis appeared after the 3rd and final session, i e., 20 hours
after the end of operation.
Even if the relief from pain is only 50-80% that is enough to enable the patients to move easily in bed
thus avoiding any lung complications. Possibly in major operations many serious complications could be
prevented by using this method even without additional drug therapy.
20
Tens in the Pain management of Spainal Cord Injuries :
Complicating the already paralyzed and devasted individual is the factor of pain. Essentially pain arises
at three different sites, and of course, can be in combinations : at the site of trauma, pain referred from
damaged roots, and pain experienced below the level of injury.
TENS plays a definite role in the conservative management of spinal cord injured patients with pain.
However its effectiveness has been found to vary depending upon which of the three types and sites of the
pain are presant and the psychological states of the patients.
Tens in Chronic Recurrent Headache :
Under this heading we included all types of chronic headache of primary origin. They are classical
migraine (mosty in women) cephalgia vasomotorica, cluster migraine, cervical syndrome (secondary headache)
and combined headache.
Classical migraine seems to be the most refactory for treatment. It is much easier to stop an attack
of migraine than to act prophylactically. If the session is performed during the attack, one is likely to
witness sudden, and even dramatic cessation of the pain. After many sessions in 40 of cases, the attack
diminished in severity, duration and frequency. Another 30 benefit to some degree from the stimulations
althougn their improvement is not so marked, in the remaining group condition remains unaltered.
Cephalgia vasomotorica is the most common type and often called just migraine - The outlook is
much better than in classical migraine, with the possibility of permanent remission, 50 of our patients
responded favorably to TENS treatment.
21
SELECTED CASE HISTORIES FOR DIFFERENT SYMTOMS
Case History-1 Diagnosis : Severe Adhesive Capsulitis
Case History 1 : Diagnosis :
Severe Adhesive Capsulitis
The patient is a 51 year old white female who had complaints of a painful left shoulder and arm for
2 years. She had noted the onset of pain 6-/ weeks prior to her visit to her physician. The area was
injected with cortisone with no apparent relief. She was referred to an orthopaedic surgeon, who made
a provisional diagnosis following x-rays of the shoulder: serve adhesive capsulitis.
Manipulation of the left-shoulder was doneunder general anesthesia. The patient's range of motion
had improved well following surgery. Eight months later she began complaining of increased pain and
difficulties with right shoulder. A diagnosis of early adhesive capsulitis was made. After treatment
of injections of cortisone into the rotator cuff and physical therapy treatments, it was decided that
manipulation of the right shoulder was necessary. This was performed.
Because of considerable pain and restriction of motion over the right greater tuberosity, She was
She continued with therapy
started on T.E.N.S. treatments and began to utilize the unit at home
at home for three months, Then she returned the device since she was free of pain and complete
mobility of her arm.
Case History 2 :
Diagnosis :
Diabetic neuropathy
The patient is a white male, age 50.
eight years.
He stated he had no sensatien in extremities for the past
22
Medications :
Apresoline 10 mg qid
NPH Insulin 80 u qid
Atromid S 500 mg qid
Tegretol (with poor response)
The electrodes were placed at the ulnar and radial nerve sites on the right and left wrists. The patient
had immediate sensation in fingers, and hands were warm to touch.
He was checked regularly by telephone and continued to have good response to T. E N,S., was able to
drive a car.
The results pleased him greatly.
When soon In the office 6 months later, the patient felt he was having less success with T.E.N.S.,
Electrodes were piaced at the ulnar and radial nerves below the elbow at the right and left arms. He had
immediate sensation to his fingers.
Fingers felt warm to touch and color improved.
This particular patient uses the device continuously in order to maintain sensation and pain relief.
(Constant usage is necessary in a small percentage of patients).
Case History 3 :
Diagnosis :
Lateral and Medial Epicondylitis.
The patient is a 42 years old white female who presented herself with complaints of pain not related to
known trauma. The area of pain was in the right elbow, with increasing pain in pressure directly over the
lateral epicondylar area and down iuto the brachial radialis muscle mass.
She was sent to the pain centre for treatment with T.E.N.S. Electrodes were placed at the epicondylar
origin, approximately one and one-half inch below the area on the muscle mass of the medial radialis,
mid portion of the dorsal aspect of the area along the brachil radiails, and the dorsal aspect of the wrist.
23
The patiant responded well on the first reatment, and was able to extend her elbow without pain. She
was anxious to use the instrument at home, and continued to do so with excellent reponse. Her exercise
program was also continued, and she was pleased with the treatment.
Case Histrory 4 :
Diagnosis :
Chronic Plantar Fasciatis and Calcaneal Spur-Right Foot.
Patient is a white female, age 50, first seen in 1969. She was treated conservatively with medications
and injections to the painful site. Butazolidin Alka was prescribed.
July-SX procedure of planter fasciectomy and removal of calcaneal spur on right foot.
continued to improve following this procedure, wearing molded arch supports.
The patient
March, 3 years later. The patient presented herself with acute chest and back pain. Cardiac problems
were ruled out, and a diagnosis of costotransverse facet eyndrome was noted. The patient started on
colbenamid.
February, 1 year later. The patient was seen because she fell on the ice with complaints of pain at
the base of her spine. X-rays show a forward displacement of the last two coccygeal segments.
May of the same year. The patient was having increased pain and marked tenderness and pressure
over the lumbar sacral area at the left side and left sciatic notch : DXL 4-5 intervertebral disc protrusion into
the sciatic nerve. Medications : Tanderil and colbenamid.
24
She was treated with injections to the area and with medications through the following year
when she started T.E.N.S. treatments. The electrodes were placed at L-S site and sciatic notch bilaterally, with
good results.
Alter 1 week of T.EN.S. therapy the patient was elated over relief obtained and was able to
move her left leg without aid. Proper utilization for home use of the instrument was demonstrated to the
patient and her husband to insur proper placement of the electrodes.
She continues to have go< d relief of pain and has become more functional She still continues on her
medications of colbenamid and Naproxyn. The serum uric acid found to be elevated 3.8 mg. consequently
colbenamid was continued.
Case History 5 :
Diagnos:s :
Multiple Myeloma.
Patient is a white female age 58, who fell and broke her left hip 10 years ago.
She had a prosthesis
implanted.
An oithopaedic surgeon saw her with complaints of constantjpaln on the left hip with tenderness from
L-3 to sacrum. She was treated conservatively with medication, brace and injections.
Over the next four years her pain increased over the greater trochanteric bursa and an excision of the
bursa of the left hip was performed The patient continued to have serve pain in the area, and an excision of
scar on the left hip was performed with good results. She continued to do well for the next 2 years. At this
25
Ime she was admitted again for consultation at which time various studies were performed and she was found
to have a high gamma globulin content. An oncologist was called in consultation, who diagnosed multiple
myeloma, placed her on proper medication along with Meprospan and Prednison 5 mg.
The patient continued to have increasing pain in the iow back area over the next 4 years, with pain on
pressure at the left sciatic notch and over the left greater trochanter. She was started on T.E.N.S. therapy with
two bars placed over the left trochanteric site. The first treatment was not successful (as often happens), but
on the second, she found the pain to be less servere and was able to use the device at home. She was closely
followed by telephone contrat. After 6 months of self treatment, she reported she felt better, but her res.
ponse to T.E N.S. was decreasing due to increasing difficulties with pain in the left lower lumbar spine.
Case History 6 :
Diagnosis :
Carcinoma of the bladder
The patient was a white male, age 71. with a diagnosis of bladder carcinoma, and collapse of the 4th
lumbur vertebrae ; ostaoporosis.
He was first seen at home
His appearance and behaviour was that of an acutely ill patient in
extreme pain at right lumber 4, and the right iliac crest The patient appeared very weak and obviously
had suffered a great weight loss. He refused to be hospitalized and was cared for by RN's on a 24 hour
service. He used an electric heating pad constantly with obvious burn, but refused to discontinue to use it.
Medications :
Demerol 75 gm q 4h for pain IM
Dilaudid 2 gm q 4h for pain IM
Phenergan 12.5 gm. q 4h pain IM
Norgesic 4h
Valium 5 gm q 4h
26
T.E N.S. was explained to the patient, his wife, and nurses. He was heavily medicated, therefore, it
was difficult to keep him awake during the procedure. The electrodes were placed at right lumbar 1 and 4 right
iliac crest, and right posterior superior iliac crest.
Foilowing the application of the electordes, the patient was able to be without medication for 7| hours.
The following day he was more lucid and apparently free of pain
The nurses regulated the instrument-
The nurse tried to assure the patient that T.E N.S. would probably alleviate spmass.
The next day the patient ate lunch for the first time and apparently had no need for injections.
One week later the patient's condition deteriorated, and a pelvic scan revealed carcinoma of the
bladder with apparent metastisis.
He expired the following day.
As is demonstrated by the above cited case histories, T.E.N.S. is not the magic cure, What it
does serve to do is reduce dependency on narcotics, and free individuals to return to a fuller life.
—;o:—
The above
usuage of T.E.N.S.
to give more knowledge about the
However tr ere is no guarantee that the same may be obtained by our T.E.N.S,
Applications
and
histories
are
printed
here
KODY'S PRODUCTS RANGE :
i
•
•
Electrocardiograph
Foetal Monitor
•
•
•
Blood Flow Detecters
Electronic Pain Killer-T.E.N.S. (Pocket and Table Model)
Electronic Stroke Rehabilitation Therapy Unit-F.N.M.S.D. (Pocket and Table Model)
•
Muscle Stimulator
•
e
Interferential Therapy Apparatus
Holter Monitor
Spares and Accessories
t
For more information feel free to contact us !
Factory :
KODY MEDICAL ELECTRONICS LIMITED
Type 11-37, Dr. V. S. I. Estate,
Thiruvanmiyur, Madras-600 041.
Phone: 415960
Grams : KODY ELEC
Telex : 41 65 46 KODY IN
9(2 - XL,
Science in Medicine: Too Much or Too Little and
Too Limited in Scope?
LEON EISENBERG, M.D.
Eoston, Massachusetts
Contrary to the common assertion that there is too much science in
medicine, it is precisely the application of the natural sciences in tl te
clinic that has enhanced the diagnostic and therapeutic powers of II le
physician. Much of the criticism of science In medicine mistakes t ie
technology made possible by science, and the way that technology Is
employed, for science itself. What has hampered progress is too
narrow a view of the sciences relevant to medicine. The concepts and
methods of the social sciences must be integrated into medical educa
tion if physicians are to be enabled to respond effectively to illness as a
human experience. Nonetheless, without major changes in the social
context of medical practice, efforts to improve performance through
curriculum reform will be futile.
It has become commonplace to hear it said, not only by the laity, but by
medical students and physicians as well, that there is too much science in
medical education. Indeed, some teachers of basic science believe such
a view underlies Physicians for the 21st Century, the report of the Panel
on the General Professional Education of the Physician and College
Preparation for Medicine. That interpretation was specifically rejected in
the commentary on the report adopted by the Executive Council of the
American Association of Medical Colleges [l], but many academics
remain uneasy. The public seems to yearn for the icon of the physician
portrayed in Sir Luke Hides’ “The Doctor,” a physician, let us remember,
who could do little more than be a comforting presence at the bedside
while his young patient’s illness ran its course.
Still, are those of us who celebrate the contribution of science to
medicine merely deluding ourselves that the recent history of clinical
medicine is one of progress? Why, in John Knowles’ [2] trenchiint
phrase, are we “doing better and feeling worse”?
From the Department of Social Medicine and
Health Policy, Harvard Medical School, Boston,
Massachusetts. This work was presented in part
at a Conference on Biopsychosocial Medicine.
May 13, 1987, Wickenburg, Arizona, and is to be
published as a chaoter in White KL. ed: The task
of medicine: dialogue at Wickenburg. Palo Alto:
Henry J. Kaiser Family Foundation (in press).
Requests for reprints should be addressed to Dr.
Leon Eisenberg, Department of Social Medicine
and Health Policy, Harvard Medical School. 25
Shattuck Street. Boston, Massachusetts 02115.
Manuscript submitted November 12, 1987, and
accepted November 16, 1987.
APPLICATION OF SCIENCE TO THE CLINIC
Paul Beeson [3] undertook the instructive task of comparing the treat
ments recommended in the first (1927) edition of Cecil’s Textbook of
Medicine with those in its 14th (1975) edition. By contemporary stein-dards, Beeson rated the value of 60 percent of the remedies in the f rst
edition as harmful, dubious, or merely symptomatic; only 3 percent
provided fully effective treatment or prevention. In the 48-year interval
between the two editions, effective regimens had increased seven-fdld
and the dubious ones had decreased by two-thirds.
The motor behind these accomplishments has been the systematic
application of the basic biomedical sciences to the investigation Of .■t*. v’-"
disease. Although research in the natural sciences began to exer a
.
l
r
March 1988
The American Journal of Medicine
Volume 84
483
i
... ...
SCIENCE IN MEDICINE—EISENBERG
shaping influence on medical theory in the last half of the
19th century, it did not have a major impact on medical
practice until the 1940s. Today, we have entered an era
in which the rate of advance in fundamental science Is
rapidly accelerating; the time lag between discovery and
application has been remarkably shortened. Consider
only what has become possible through the use of recom
binant DNA methods employing restriction fragment
length polymorphisms (RFLPs) [4]. I cite them to highlight
the continuing fruitfulness of "reductionistic science”—
when that reductionism is applied to appropriately chosen
problems. In 1987, two sets of papers [5-8] reported
important new research on the biologic substrate of (1)
manic depressive disorder and (2) Alzheimer’s disease.
Egeland and co-workers [5] demonstrated, in an Old
Amish kindred, linkage between the major locus for bipo
lar disease and the loci for insulin and the oncogene Ha
ras- 1 on chromosome 11. It is presumably not coinciden
tal that the marker genes on chromosome 11 are also
closely linked to the gene encoding tyrosine hydroxylase,
the principal enzyme in the synthesis of catecholamine
neurotransmitters. In the same issue of Nature, two other
research groups found no evidence for such a linkage in
three Icelandic [6] and three non-Amish American [7]
kindreds characterized by autosomal dominant transmis
sion of bipolar disease. A fourth report [8], appearing a
month later, revealed a close linkage between bipolar
affective disorder and the X chromosome markers for
color blindness and glucose-6-dehydrogenase deficiency
in three Israeli kindreds. What these reports establish is
the heterogeneity of the inherited diathesis for affective
disorders. Furthermore, the genetic evidence from the Old
Amish pedigree, rather than precluding a role for environ
mental precipitants of manic depressive disease, pro
vides new possibilities for their specification. The ability to
detect persons at risk through RFLPs in informative family
kindreds permits the design of studies to identify the
environmental factors that result in expression of a genet
ic diathesis in some patients and phenocopies in still
others.
In the same month, Science published reports of
equally exciting contributions to an understanding of the
biology of Alzheimer’s disease. St. George-Hyslop and
co-workers [9] obtained data tracing the defective gene to
chromosome 21 in autosomal dominant familial Alz
heimer’s disease (FAD). Two other research groups
[10,11] demonstrated that the gene coding for beta amy
loid protein, which accumulates in the brains of patients
with Alzheimer’s disease and of older patients with
Down’s syndrome, also maps to chromosome 21. Pro
vocative as these findings are, the FAD gene may not be
identical with the gene coding for beta amyloid protein;
moreover, the FAD gene proved not to be on the region of
chromosome 21 that, when present in a third copy, leads
to Down's syndrome. Delabar et al [12], using a cDNA
484
March 1988
The American Journal of Medicine
probe to determine the dosage of the beta amyloid protein
gene on chromosome 21 in patients with sporadic Alz
heimer’s disease, with trisomy-21 Down's syndrome, and
karyotypicaily normal Down’s syndrome, reported evi
dence for gene duplication in leukocyte DNA from all
three sets of patients. However, according to Tanzi et al
[13], the genetic defect in FAD is not tightly linked to the
amyloid beta-protein gene; moreover, St. Gecrge-Hyslop
et al [14] found that chromosome-21 genes are not
duplicated in either familial or sporadic Alzheimer's dis
ease. For all the ambiguity in the interpretation of these
findings, they represent a considerable advance in the
' understanding of Alzheimer's disease, a disease whose
incidence is increasing as more Americans survive to the
age of risk and whose prevalence grows even faster as
we become more expert at postponing death. Any hope
of preventing Alzheimer’s disease or controlling its
course rests on fundamental research in neurqbiology.
The very success of biomedicine has exacted a price
in the way it has narrowed the physician’s focus exclu
sively to the biology of disease. However, the remedy
does not lie in abandoning reductionism where it is appro
priate but in incorporating it within a larger sopial frame
work to enable the physician to attend to the patient as
well as to the disease. As an intellectual bridge over the
chasm between molecular biology and social science, let
us turn now to the uses of clinical epidemiology in identify
ing and analyzing contemporary therapeutic dilemmas.
RESEARCH ON MEDICAL PRACTICE
The problem is apparent in everyday medical practice,
during which physicians make decisions to recommend
standard treatments whose effectiveness they take for
granted. The extent of variation in physician judgment was
'
not recognized until the methods of clinical epidemiology
were applied to study the rates at which procedures were
being employed. The findings identified marked variability
that was not attributable to differences in morbidity in the
populations surveyed.
Wennberg and Gittelson [15] documented the extent of
variation in rates for surgical procedures among small
geographic areas with comparable populations. In a sur
vey of the New England states, rates for tonsillectomy
were found to vary seven-fold and those for hysterectomy
and prostatectomy four-fold from one area to another. In .
research on the Medicare population, similar patterns of
variation in the performance of surgery have b*en demon
strated; for example, rates for coronary artery bypass
surgery range from a low of seven to a high of 23 per
10,000 from one region of the United States to another
[16]. There is a remarkable parallel between the number
of surgeons per population and the rates for operative
procedures across countries: both figures are about twice
as high for the United States as for the United Kingdom,
with Canada about halfway between the twq [17]. How-
Volume 84
SCIENCE IN MEDICINE—EISENBERG
.
ever, these data do nor tell us whether the United States is
oversupplied, the United Kingdom undersupplied, or Can
ada about right.
The problem is not simply the pecuniary interest of
physicians working in a fee-for-service system. In a com
parison among Norway, the United Kingdom, and the New
England states, surgical rates showed similar variability
within each country despite the differences in rates be
tween countries and in the methods of organizing and
financing medical care among them [18]. These findings
contrast with relatively small variations in rates for appen
dectomy, regarded as the only acceptable treatment for a
presumptive diagnosis of appendicitis. That there are
differences between surgeons is evident, not only from
geographic variations, but also from second-opinion stud
ies, which have found that about one-quarter of patients
for whom surgery is recommended by one surgeon have
that opinion reversed by a second [19]. If United Kingdom
s for the seven common operations examined by
Wennberg and Gittelson had applied to the United States,
deaths associated with surgery would have decreased by
a third to a half [20].
What options are there to change this unsatisfactory
state of affairs? By having specialty colleges specify the
indications for particular procedures [21] and by feeding
back information to local practitioners on area variations
[22], it has been demonstrated that surgical rates can be
reduced. Yet such steps do no more than reify expert
opinion. Professional consensus can be no better than the
quality of the evidence on which it is based; for many
medical and surgical procedures, the available data are
equivocal. As Vayda and Mindell [23] point out, “the issue
of necessary versus unnecessary surgery wiil not be
resolved until the question of efficacy or effectiveness of
competing treatments (or treatment versus nontreatment)
is answered.” For that we will need: systematic collation
of available information; randomized clinical trials to eval? treatments of uncertain efficacy; and a mechanism
tv change physician behavior to accord with the best
available evidence.
TECHNOLOGY OR SCIENCE?
Some critics conclude from the apparent over-reliance on
technical procedures that medical practice suffers from
“too much science.” That criticism confuses science
with technology and mistakes biomedical science for the
only science relevant for medicine. The misuse of tech
nology stems from such factors as: a medical payment
system that pays doctors more the more they perform
procedures, and the failure of medical education to pre
pare doctors to weigh competing claims.
The current reimbursement scales of the fee-for-service system reward procedures with fees far higher than
those for time spent in clinical assessment. A gastroen-
_
ROLE OF THE SOCIAL SCIENCES
The ultimate measure of the effectiveness of medical
care is its impact on the health status of the population it
serves. Existing patterns of medical practice do not pro
vide information on the denominator; that is, the relevant
population from whom the sample seen in the office is
drawn. The fact is that community surveys regularly identi
fy many more symptomatic persons and many more with ,
abnormal physical findings than are under medical care
[29]. By having persons in the community complete a
daily health diary, Demers et al [30] found that only a small
minority of self-identified illness episodes resulted in going
to the doctor; the vast majority were managed within the
family or by the use of “alternative” practitioners. In the
presence of life stress, symptoms are not only more likely
to be experienced but also more often lead to medical
consultations [31,32]. Moreover, failure to recognize de
pressive syndromes manifested through somatic symp
toms is all too common in medical practice [33]; it re
flects serious inadequacies in the preparation of physi
cians for primary care practice [34].
The education doctors receive is so narrowly focused
on individual case management that they have lost sight of
March 1988
5
■
terologist realizes a net hourly income from endoscopy
that is more than six times greater than from the general
management of the patient's illness [24]. The disproportion between the fees paid for procedures and those for a
thorough history and physical examination is transforming
gastroenterologists into endoscopists [25] and cardiolo
gists into “catheterologists” [26]. The fact that the net
income of technically oriented specialists is much higher
than that of primary care practitioners influences the
career choices of young physicians and contributes to the
disproportion in the ratio between generalists and special
ists.
The second factor leading to the misuse of technology
is the inability of many practitioners to weigh competing
claims. All too many medical graduates have not mas
tered the rudiments of biostatistics and decision theory.
Without reasonable proficiency in the logic of scientific
inference and the methods of statistics, practitioners lack
the tools to assess the conclusions drawn in medical
articles. How else are we to understand the persistence of
carotid endarterectomies or the rush to embrace radial
keratotomies in the absence of evidence to justify their
use? Doctors have an altogether unwarranted faith in the
reliability of clinical methods and tests [27]. How else are
we to explain the indifference to matters of sensitivity and
specificity in ordering tests and evaluating test findings
[28] without weighing a priori probabilities? The fact is
that medical education, far from being “too scientific,”
suffers from too much emphasis on memorizing evanes
cent “facts” and too little on science as a way of framing
questions and gathering evidence.
The American Journal of Medicine
Volume 84
485
■
SCIENCE IN MEDICINE—EISENBERG
their responsibility to the community they serve. Even in
Britain, where all citizens are assured coverage by a
national health service, general practitioners limit their
responsibility to the patients who consult them, and over
look those in their panel who are silent [35], thus missing
the opportunity to promote and monitor the health of the
population. Medical education must be broadened to in
clude the concepts and methods of social epidemiology.
The pattern of disease characteristic of a particular
society is a function of its level of development. Consider
the changes in disease epidemiology in the United States.
In 1900, the three leading causes of death were infec
tious: pneumonia, tuberculosis, and diarrheal disease. By
1940, they had declined sharply and had been displaced
by increasing rates of heart disease, cancer, and cerebro
vascular disease [36], The decline in mortality from infec
tious disease resulted from improvements in sanitary en
gineering, housing, hygiene, and nutrition during an era
when there had been few advances in medical therapeu
tics; the new pattern of mortality arose from changes in
diet, physical activity, smoking, and exposure to environ
mental toxins, as well as from the graying of the popula
tion, as more people live into the age of risk for chronic
diseases.
These statistics only begin the analysis of health needs
within the population. The distressing fact is that morbidity
and mortality are inversely correlated with social class;
persons with the lowest income and the least education
have the greatest need but are allocated fewer resources
for their health care even in a country with a national
health service, such as the United Kingdom [37]. A Task
Force of the United States Department of Health and
Human Services identified a gap of 5.6 years in life
expectancy between whites and blacks and a black mor
tality rate more than 40 percent higher than that for whites
[38] . The most important contributors to the disparity
were heart disease and stroke, homicides and accidents,
cancer, and infant mortality, each of which can be re
duced by public health preventive measures and timely
medical care.
Just as sociology can help physicians to recognize the
role of class and social organization as disease determi
nants at the macro level, social anthropology enables the
physician to understand that illness, patienthood, and
health-related behaviors are social constructions that biol
ogy does not account for. I have elsewhere proposed the
usefulness of distinguishing between "disease" and "ill
ness," terms employed synonymously in ordinary usage
[39] . Physicians are taught to conceptualize diseases as
abnormalities in the structure and function of body organs
and tissues. However, patients suffer illnesses; that is,
experiences of disvaiued changes in states of being and in
social function. Similar degrees of organ pathology can
generate quite different reports of pain and distress; ill-
486
March 1988
The American Journal of Medicine
ness may occur in the absence of detectable disease; the
course of the disease is distinct from the trajectory of the
accompanying illness. A visit to the doctor is more likely,
on average, when disease is present; but having a dis
ease, feeling ill, and becoming a patient are not coterminous [40].
Furthermore, life circumstances have a profbund ef
fect on disease risk through their influence on host resis
tance. When the counties of North Carolina were ranked
on an index of social disorganization, the stroke mortality
rate (disaggregated by age) for black men proved to be
highest in the tier of counties in the highest quintile on
social disruption [41]. Ruberman et al [42] studies! cumulative mortality following myocardial infarction among pa
tients enrolled in a trial of beta-blockers; mortality proved
to be highest among those with the least education, the
most life stress, and the greatest social isolatior.
Nuckolls et al [43] tracked a cohort of white married
primiparae of similar age and social class with measure
ments of life change scores (a proxy for stress) and social
support. Life change and social support each had an
independent effect on the risk for the complications of
pregnancy, with high life change increasing, and high
support decreasing, the risk; in effect, sociall support
buffered the pregnant woman against stress. Brown and
Harris [44] studied the social ecology of psychiatric disor
der among women in London. Rates for depression
proved to be severalfold higher among working-class than
among middle-class women. Moreover, among those in
the working class, depression was found more, often
among those with three or more children under 14 in the
home, with no outside employment, and without an inti
mate or confiding relationship with a husband or boy
friend; that is, one in which feelings were shared, whether
or not sexual intimacy also occurred.
The relevant social sciences include as well: economic
analysis for an understanding of resource allocation; his
tory for an essential perspective on the development of
medical theory and practice; and social psychology for
the illumination of the doctor-patient relationship [45].
WHAT WERE THE VIRTUES OF THE
OLD-FASHIONED FAMILY DOCTOR?
,
Let me return to the question I raised at the outset: is it true
that the "old-fashioned family doctor" was more respon
sive to patient needs than his successors have proved to
be? Mind you, I do not contend that doctors today, or
yesterday, for that matter, are—or were—as aware of
the personal and social issue in patient ca|e as they
should be; to the contrary, it is my thesis that a key
function of systematic instruction in the social sciences is
to address that failing. But were things better once upon a
time? If not, whence stems the belief that they were?
The fact is that complaints about practitioners being
Volume 84
SCIENCE IN MEDICINE—EISENBERG
"too scientific" date from well before applied science had
any appreciable impact on medical practice. Professor
Francis W. Peabody [46] wrote in 1923:
The layman of the older generation . . . who feels that
something has been lacking in the way of warmth, sym
pathy and understanding ... is very apt to hark back to
earlier days. ’What we need,’ he says, ’is a general
practitioner!’ • (p. 7)
The virtues of that general practitioner stemmed from
an intimate acquaintance with patient, family, and com
munity over years of practice, and not from formal instruc
tion received in medical school. Those virtues were inher
ent in the doctor’s role in an America of small towns,
family farms, and multigenerational families, an American
that was disappearing as he wrote. Generalist or special
ist. today's physician no longer has the chance to know
the extended family over several generations, with one in
five American families moving every year; familiarity with
""-e conditions of the patient’s social, business, and
< jestic life" is no longer automatically accessible to
"neighborhood” doctors now that our population has
shifted to a predominantly urban locus, with its anonymity
and fragmentation. The task for contemporary medical
education is to teach physicians to obtain, through sys
tematic and sensitive inquiry, that knowledge of the pa
tient's "social, business, and domestic life” which astute
practitioners once acquired through long acquaintance
with family and community. Preparation for medical prac
tice in an increasingly pluralistic society requires knowl
edge of and respect for cultural differences. Patients differ
in their values, their beliefs about health and illness, and
their expectations of the doctor’s role [47].
It is not enough to mean well. The doctor must know
enough to do well for the patient. That requires as deep an
understanding of the social sciences as of the biologic
sciences.
BARRIERS TO IMPLEMENTATION
at are the barriers to a more widespread incorporation
of humanistic and psychologically responsive care into
medical practice? Those barriers include: acquired insen
sitivity; skepticism about the "reality” of psychosocial
factors; misattribution of therapeutic effects; difficulty in
learning new skills; and the current social context of
medical practice.
Acquired Insensitivity. Certain aspects of proper medi
cal care all agree to be desirable arise from claims that
* Indeed, a century before Peabody, we find in Balzac’s novel
Pere Goriot. written in 1834, a passage that might have been
written today. Bianchon. reassuring his friend Rastignac that he
cares for the dying Goriot, comments:
“Doctors already in practice see only the illness: I can still see
the sick man, my boy.”
are irrelevant to effectiveness in a narrow medical sense.
Treating patients with respect, giving them scheduled
appointments, providing amenities in the clinic, keeping
the clinic open evenings for patients who work, and
allowing time to listen and reflect are right and proper on
grounds of simple decency, whether or not it has been
demonstrated that they lead to disease control. Failure to
disprove the "null hypothesis” in a randomized trial would
not alter their propriety. They stand on their own as dicta
to guide human relationships without requiring pragmatic
justification.
Why is responsiveness to these issues not universal?
The reasons are not far to seek. Responsiveness costs
money. It reduces "efficiency.” It demands that the doc
tor value the patient’s time equally with his or her own.
The dignity of patients is all too often given short shrift in
the large institutions where doctors are trained. The bu
reaucratic structure of hospitals and clinics is organized to
facilitate internal operations and to preserve staff privi
leges. Students mode! themselves on what they see.
Bianchon, the student, can still see "the sick man;”
Bianchon, the doctor, will have learned to see "only the
illness”—in order to get his job done expeditiously. The
flaw is not in the students we recruit; it is in what they learn
from us.
Indeed, a case can be made for the proposition that the
formal content of the curriculum (much of which is forgot
ten by the time of graduation) has less impact on the kind
of physicians students will become than the covert curric
ulum; that is, the values the curriculum implicitly embod
ies (by what is not taught as well as by what is), the
behaviors modeled by the faculty, and the rewards and
admonishments given to students. Taken together, they
constitute a powerful social press for conformity with
extant professional values. Socialization may be what
education is all about. A century later, American medical
schools continue to follow the 1893 Hopkins model of
four years of college, an exacting admissions process,
and four years of medical school1- despite change in the
nominal content of courses. Research by social scientists
offers a penetrating analysis of professional socialization
[49-53]; the findings appear to have had little influence
on medical education, perhaps because social science, a
critical discipline by its very nature, is practiced by "out
siders” without clout in the power structure of medicine.
Skepticism about the “Reality” of Psychosocial Fac
tors. Efficacy is a proper major concern of practicing
physicians. Many psychosocial interventions are advocat
ed on the grounds that they will lead to better outcomes.
r Indeed, the recognition that four years have magic properties for
the production of reliable physicians dates back at least as far as
the medie'val English universities, if not to the first great medical
school, founded in Salerno in the 11th century [48].
March 1988
I
The American Journal of Medicine
Volume 84
487
I
i
i
I
I
SCIENCE IN MEDICINE—EISENBERG
One such is the proposition that a sensitively ascertained
history and a carefully performed physical examination
will often lead to the current diagnosis without depen
dence on an extensive battery of costly, often superflu
ous, and sometimes risky tests [54]. Early recognition and
appropriate management of psychosocial problems yield
better outcomes with fewer visits and less hazard than the
endless search for a biologic will-o’-the-wisp in patients
who somatize distress [55]. Why, then, does such evi
dence not persuade more physicians to modify their prac
tice styles?
There is widespread skepticism among physicians as
to whether psychologic and social factors are as “real"
as biologic ones [56]. Classroom exercises will have
convinced all of them of the power of biologic reductionism. It is not only that so much more time is devoted to the
natural as opposed to the “unnatural" sciences in medi
cal education, but that the elegance of molecular biology
is so much greater. Contrast the detail in which it is now
possible to describe the pathophysiology of the thalasse
mias—from emors in the genome, through variant hemo
globin structures, to clinical manifestations [57]—with
what can be said about the pathophysiologic link between
social isolation and mortality risk.
Berkman and Symes [58] have demonstrated that pa
tients in the lowest quartile on a social network index
experienced more than two times the mortality of those in
the highest quartile during a nine-year interval. That is a
solid fact and a very important one for medical practice,
beause it has relevance for all patients and not merely
those with a relatively uncommon genetic disease. How
ever , the mechanisms by which social isolation translates
into disease risk remain a matter for surmise. To be sure,
that does not alter the power of the phenomenon one
whit. But because being able to describe the pathophysi
ology of disease is so central to the culture of biomedi
cine, physicians continue to be skeptics about social
research, when they are not downright arrogant in their
dismissal of it [59].
Misattribution of Therapeutic Effects. Most patients
treated by most doctors get better most of the time. This
stems in part from the self-limited nature of most illness
episodes, and in part from the positive expectancies
aroused by the medical encounter [60]. However, be
cause transactions between doctors and patients are
mediated by procedures and medications, doctors attri
bute the benefits obtained to the remedies prescribed and
fail to recognize the role of ritual and symbolism in heal
ing. This unacknowledged bonus for medical practice is
treated as “experimental noise" in pharmacologic re
search. Placebos are employed in clinical trials as proxies
for expectancy effects in order to parse out the “specific”
actions of drugs. Because the drug is the focus of inquiry,
equally specific patient and doctor effects are left unac
counted for.
483
March 1988 ’ The American Journal of Medicine
Consider the findings of a randomized double-blind
clinical trial of clofibrate [61]. Among the men in the
“active drug" arm (of....................
the study, those who took their pills
regularly had a significantly lower five-year mortality than
did non-compliers (15.0 percent versus 24 6 percent).
However, among the men receiving a lactose placebo,
those who took their pills experienced an equally large
reduction in mortality as compared to poo' compilers
(15.1 percent versus 28.3 percent). Because the focus of
the study was on the drug, the investigators concluded.
that.
that: These findings . . . show the serious difficulty ....
. . of
evaluating efficacy in subgroups determined by patient
responses . . .“ [61, p. 1038]. How bizarre to downplay
the demonstration of a highly significant mortality effect
associated with compliance, an effect so large it would
have caused the stock of a pharmaceutical company to
soar, had the difference been attributable to the medica
tion! It was precisely the restricted focus of the research
to the collection of data on traditional medical variables
that made it impossible to account for the outcome in
terms of characteristics that may have been associated
with compliance (such as social class, cigarette smoking,
alcohol consumption, diet, exercise, or other health hab
its).
Until the psychosocial context of the encounter be
tween doctor and patient is given explicit attention in
research and teaching, doctors will be as mystified as
their patients about the ingredients of effective medical
care.
Unlearning Old Habits. Psychosocial interventions do
not lead to dramatic changes in outcome that tire immedi
ately evident to the individual physician; they <ire discern
ible only over time and with a large enough patient sampie. For example, as many as 10 percent of patients
counselled by physicians to stop smoking do in fact stop
[62]. It is possible to read the findings as “no tnore than"
10 percent and dismiss counselling as ineffective by the
standard expected of most interventions. Oh the other
hand, once we recall that some 60 million Americans still
smoke, 10 percent amounts to some 6 million persons
who might be spared the hazards associated with ciga
minority took their
rettes if all doctors, rather than just a minority,
public health responsibility seriously. Wheih changing
from one treatment method to another involves unlearning
old habits and acquiring new skills, change is painful and
slow in coming.
Franz Kafka [63] has epitomized the problem in one
sentence in the short story, The Country Doctor. “To write
prescriptions is easy but to come to an understanding with
people is hard." Doctors are trained to “do something.”
They believe [64] that patients expect a consultation to
have a tangible outcome: a pill or a shot. It requires the
disruption of overleamed habits to change from doing to
listening (and to come to recognize that listening is an
important way of doing). It demands a shift in paradigms
Volume 84
SCIENCE IN MEDICINE—EISENBERG
from disease to illness in order to change from prescribing
to attending to meanings and to helping patients to exam
ine options. Despite the fact that it is primary care physi
cians to whom patients with psychosocial disorders turn
and from whom they get such help as they receive [65],
most practitioners report themselves ill-trained for the
task, uncomfortable with it, and reluctant to undertake it.
Social Context of Medical Practice. Robert Ebert [66],
in commenting on the Western Reserve experiment in
medical education, had this to say about the limits to
curriculum reform:
Nonmedical school forces are far more important in
shaping the character and career plans of young physi
cians than anything that happens to them during the four
years of medical school.
The most decisive determinant of physician failure to
incorporate a psychosocial approach into practice stems
from the perversity of current reimbursement schemes.
°hysicians are rewarded disproportinately when they per;rm procedures in contrast to providing “cognitive ser
vices.” One need not suppose that physicians are solely
motivated by economics to recognize that it is difficult to
resist the temptation to carry out a procedure, if only to
confirm a clinical diagnosis, when it yields greater income
and at the same time impresses the patient with its
magical properties. What is needed is a reimbursement
scheme that is technology-neutral, a scheme that leaves
the decision to employ procedures to clinical judgment
rather than to the pocketbook. Even the family physician,
with little technology to command, soon discovers that
taking the time to listen to patients and to explore their
lives with them reduces income sharply. This long-stand
ing problem has been exacerbated by Medicare and Med
icaid fee schedules, which can only be described as
mean, both in motive and in effect for patient and physi
cian [67].
The current emphasis in national health policy on con
trolling costs rather than on enhancing health outcomes
exorably ratchets down on the provision of comprehen
sive care. It can only promote cynicism among our stu
dents if we preach humanism and ignore the realities of
the contemporary scene [68]: admissions policies de
signed to unload the “losers” onto county hospitals;
house officers overwhelmed by more admissions and
sicker patients; “sicker and quicker” discharges dictated
by the bottom line; the deliberate “demarketing” of un
profitable services; the squeeze on outpatient clinics to
increase throughput (i.e., income); and resistance to qual
ity control rationalized in the rhetoric of clinical freedom,
Let me be explicit about our responsibility as faculty
members.
Do we mean what we say when we urge students to
attend to the personhood of the patient? Then, when we
conduct teaching rounds, we must visit the bedside and
ask patients how they feel and what their illness means to
them; we undercut our words when we limit our questions
to lab values and differential diagnosis in conference
rooms off the wards.
Do we want our house officers to care for their pa
tients? Then, let us begin by caring for interns and resi
dents; it is intolerable that we exploit them as cheap labor,
reprimand them for error, but rarely praise them for
accomplishment.
Is informed consent a ritual formula designed to meet
the legal requirements of the record or is it a process
through which we validate the autonomy of the patient? f
the latter, then we must take the time to demonstrate to
our students how the information the patient needs to
have can be presented clearly and more than once, in
order that the doctor can support the patient's right to
choose among alternatives.
Do we really believe in improving standards of care?
Then, we must support quality controls with teeth to them
and be prepared to have our own practices subjected to
close scrutiny.
Do we really mean what we say about the importance
of equity and access for all in health care? Then, we must
become visible to our students as activists in behalf of the
37 million Americans without health care coverage. What
is unconscionable is silence on the matter when the
academic medical centers we serve rationalize retreat
from justice in language and concepts borrowed from the
marketplace [69].
Unless we put as much energy into the effort to change
the social context in which cur graduates will practice as
we do into curriculum reform, we will have betrayed the
very principles we profess. Our patients and our students
deserve better of us.
ACKNOWLEDGMENT
I thank S. J. Adelstein, A. B. Brandt, D. D. Federman, and
A. Kleinman for providing critical reviews of earlier ver
sions of this manuscript, and Mrs. C. Fujimoto for her care
in revising the final paper for publication.
REFERENCES
1.
AAMC Executive Council: Commentary on the Report of the
Panel on the General Professional Education of the Physi
cian and College Preparation for Medicine. J Med Educ
1986; 61: 346-352.
2.
3.
March 1988
Kpowles J, ed. Doing better and feeling worse: health in the
United States. New York: WW Norton, 1977.
Beeson PB: Changes in medical therapy during the past half
century. Medicine (Baltimore) 1980; 59: 79-99.
The American Journal of Medicine
Volume 84
489
J
Kan YW, Dozy AM: Polymorphism of the human beta-globin
structural gene: relationship to sickle mutation. Proc Natl
Acad Sci USA 1978; 75: 5631-5635.
5. Egeland JA, Gerhard DS. Pauls DL. et al: Bipolar affective
disorders linked to DNA markers on chromsome 11. Na
ture 1987; 325: 783-787.
6. Hodgkinson S, Sherrington R, Gurling H. et al: Molecular
genetic evidence for heterogeneity in manic depression.
Nature 1987; 325: 805-806.
Detera-Wadleigh SD, Berrettlni WH, Goldin LR, et al: Close
linkage of c-Harvey-ras-1 and the insulin gene to affective
disorder Is ruled out in three North American pedigrees.
Nature 1987; 325: 806-808.
8. Baron M, Risch N, Hamburger R, et al: Genetic linkage
between X-chromosome markers and bipolar affective
illness. Nature 1987; 326: 289-292.
9. St. George-Hysiop PH, Tanzi RE, Pollnsky RJ, et al: The
genetic defect causing familial Alzheimer's disease maps
on chromosome 21. Science 1987; 235: 885-890.
10. Goldgaoer O, Lerman Ml, McBride OW, et al: Characteriza
tion and chromosomal localization of a cDNA encoding
amyloid of Alzheimer's disease. Science 1987; 235:
877-880.
11. Tanzi RE, Gusella JF, Watkins PC, et al: Amyloid beta
protein gene: cDNA, mRNA distribution, and genetic link
age near the Alzheimer locus. Science 1987; 235: 880884.
12. Delabar JM, Goldgaber D, Lamour Y, et al: Beta amyloid
gene duplication in Alzheimer's disease and karyotypically normal Down's syndrome. Science 1987; 235: 13901392.
13. Tanzi RE. St. George-Hysiop PH, Haines JL, et al: The genet
ic defect In familial Alzheimer's disease is not tightly
linked to the amyloid beta-protein gene. Nature 1987;
329: 156-157.
14. St. George-Hysiop PH, Tanzi RE, Pollnsky RJ, et al: Absence
of duplication of chromosome 21 genes in familial spo
radic Alzheimer's disease. Science 1987; 238: 664-669.
15. Wennberg JE, Gittelson A: Variations in medical care among
small areas. Sci Am 1982; 126: 120-134.
16. Chassin MR, Brook RH, Park RE. et al: Variations in the use
of medical and surgical services by the Medicare popula
tion. N Engl J Med 1986; 315: 1365-1368.
17. Vayda E, Mindell WR, Rutkow IM: A decade of surgery in
Canada, England and Wales and the United States. Arch
Surg 1982; 117: 846-853.
18. McPherson K, Wennberg J, Hovind O, Gllfford P: Small area
variations in the use of common surgical procedures: an
International comparison of New England, England and
Norway. N Engl J Med 1982; 307: 1310-1314.
19. McCarthy EG, Finkel ML: Second opinion elective surgery
programs: outcome status over time. Med Care 1978; 16:
984-994.
20. Wennberg JE, Bunker JP, Barnes BA: The need for assess
ing outcomes of common medical practices. Annu Rev
Public Health 1980; 1: 277-295.
21. Dyck FJ, Murphy FA, Murphy JK, et al: Effect of surveillance
on the number of hysterectomies in the Province of Sas
katchewan. N Engl J Med 1977; 296: 1326-1328.
22. Wennberg JE, Blowers L, Parker R, Gittelsohn AM: Changes
in tonsillectomy rates associated with feedback and re
view. Pediatrics 1977; 59: 821-826.
23. Vayda E. Mindell WR: Variations in operative rates. Surg Clin
North Am 1982; 62: 627-639.
24. Almy TP: The role of the primary physician and the health
care ‘’Industry.” N Engl J Med 1981; 304: 225-228.
25. Spiro HM: My kingdom for a camera—some comments on
medical technology. N Engl J Med 1974; 291: 10701072.
26. Phibbs B: The abuse of coronary arteriography. N Engl J Med
4.
490
March 1988
The American Journal of Medicine
irt
■a
•
27.
28.
29.
30.
31.
32.
. 33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
Volume 84
1979;301: 1394-1396.
Koran LM: Reliability of clinical methods, data and judgements. N Engl J Med 1975; 293: 642-650, 6^6-701.
Casscells W, Schoenberger A, Grayboys TB: Interpretation
by physicians of clinical laboratory results. N Engl J Med
1978: 299: 999-1001.
White KL, Williams TF, Greenberg BG: The ecology of medi
cal care. N Engl J Med 1961; 265: 885-892.
Demers R, Altamore R, Mustin H, et al: An exploration of the
- depths and dimensions of illness behavior. Fam Pract
1980; 11: 1085-1092.
Tessier R, Mechanic D, Dimond M: The effect of psychologi
cal disease on physician utilization: a prospective study. J
Health Soc Behav 1976; 17: 353-364.
Mechanic D: Effects of psychological distress on perceplions of physical health and utilization of i|nedical and
psychiatric facilities. J Human Stress 1978; 4: 26-32.
Katon W, Kleinman A, Rosen G: Depression and somatiza
tion. Am J Med 1982: 72: 127-135, 241-247.
Kleinman A: The cultural meanings and socia uses of illness. J Fam Pract 1983; 16: 539-545.
Hart JT: A new type of general practitioner. Lancet 1983; II:
27-29.
Levy Rl, Moskowitz J: Cardiovascular researcht decades of
progress, a decade of promise. Science 1985:217: 121—
129.
Department of Health and Social Security: Inequalities in
health: report of a research working group. London: De
partment of Health and Social Security, 1980.
The Secretary's Task Force: Report on black and minority
health. Washington: U.S. Department of Health and Hu
man Services, August 1985.
Eisenberg U Disease and illness: distinctions between pro
fessional and popular ideas of sickness. Cult Med Psychi
atry 1977; 1: 9-23.
Eisenberg L: Rudolf Ludwig Karl Virchow, where are you
now that we need you? Am J Med 1984; 77: 524-532.
Neser WB, Tyroler HA, Cassel JC: Social disorganization
and stroke mortality in the black pooulaton of North
Carolina. Am J Epidemiol 1971; 93: 166-175.
Ruberman W, Weinolatt E. Goldberg J, et al: psychosocial
influences on mortality after myocardial infarction. N Engl
J Med 1984; 311: 552-559.
Nuckolls KB, Cassel J, Kaplan BH: Psychosocial assets, life
crisis and the prognosis of pregnancy. Ami J Epidemiol
1972; 95: 431-441.
Brown GW, Harris T: Social origins of depression:study of
psychiatric disorder in women. New York: Free Press,
1978.
Eisenberg l_ Kleinman A: The relevance of social science
for medicine. Boston: D Reidel, 1981.
Peabody FW: Doctor and patient. New Yori : Macmillan,
1930.
Harwood A, ed: Ethnicity and medical care Cambridge:
Harvard University Press, 1981.
Talbot CH: Medicine in medieval England. New York: Ameri
can Elsevier, 1967; 64-71.
Becker H, Geer B: The fate of idealism in medical school.
Am Sociol Rev 1958: 23: 50-56.
Bosk C: Forgive and remember. Chicago: University of Chi
cago Press, 1979.
Mumford E: Interns: from students to physicians. Cambridge:
Harvard University Press, 1970.
Freidson E: Professional dominance. New York: Atherton
Press, 1970.
Freidson E: Doctoring together, a study of professional so
cial control. Chicago: University of Chicago Press, 1975.
Hampton JR, Harrison MJG, Mitchell JRA, et
'■ al: Relative
xdn '
contributions of history-taking, physical examination,
and
laboratory investigation to diagnosis and mai
management of
5t5.
56.
57.
58.
59.
60.
61.
medical outpatients. Br Med J 1975; 1: 486-489.
Mumford E. Schlesinger HJ. Glass GV, et al: A new look at
evidence aoout reduced cost of medical utilization follow
ing mental health treatment. Am J Psychiatry 1984; 141:
1145-1158.
Eisenberg L: Mindlessness and brainlessness in psychiatry.
Br J Psychiatry 1986; 148: 497-508.
Weatherall DJ. Clegg JB: The thalassemia syndromes. Ox
ford: Blackwell Scientific Publications. 1981.
Berkman LF, Symes SL: Social networks, host resistance
and mortality: a nine year follow-up study of Alameda
County residents. Am J Epidemiol 1979; 109: 186-204.
Petersdorf RG, Feinstein AR: An informal appraisal of the
current status of "medical sociology." In: ref 53: 27-48.
Frank JD: Persuasion and healing (revised ed). New York:
Schocken Books. 1974.
Coronary Drug Project Group: Influence of adherence to
treatment and response of cholesterol on mortality in the
Coronary Drug Project. N Engl J Med 1980; 303: 1038-
62.
63.
64.
65.
66.
67.
68.
69.
1041.
Surgeon General: Smoking and health. Publication no. (PUS)
79-5006. Washington: U.S. Department of Health. Educa
tion and Welfare. 1979.
Kafka F: A country doctor. In: The basic Kafka. New Ycrk:
Pocket Books. 1979.
Comaroff J: A bitter pill to swallow: placebo therapy in
general practice. Sociol Rev 1976; 24: 79-96.
Regier DA, Goldbert ID, Taube CA: The de facto U.S. mental
health services system. Arch Gen Psychiatry 1978; 35:685-693.
Ebert R: Cited in Bishop JM: Infuriating tensions: science and
the medical student. J Med Educ 1984; ;59: 91-102.
Berrien R: What future for primary care private practice? N
Engl J Med 1987; 316: 334-337.
Eisenberg L: Health care: for patients or for profits? Arn J
Psychiatry 1986; 143: 1015-1019.
Jonsen AR: Leadership in meeting ethical challenges. J Med
Educ 1987; 62: 95-99.
Reorinted from the March issue of The American Journal of Medicine, A Yorke Medical Journal,
Published by Cahners Publishing Company, a Division of Reed Publishing USA, 249 West 17th Street, New York. N.Y., 10011.
Copyright 1988. All rights reserved. Printed In the U.S.A.
/
NEED FOR CHANGE IN
MEDICAL PARADIGM
“Diseases present through the personality
of the patient" said Sir James Spence - a
leading medical brain of the nineteenth
century. Application of the conventional
Euclidean mathematics to Medicine has
given us a distorted vision of the whole
gamut of man and his illnesses. Modern
fashion and obsession for specialisation
has given a further blow to the holistic
approach to disease. Organ based sub-spe
cialities train people tohave a tunnel vision
to the ultimate detriment of the ailing hu
manity. The new science of “fractals” and
“chaos" looks at man as a whole. A very
small initial deviation in the system may
end up with catastrophic final results. The
conventional medical paradigm of one gene
- one enzyme - one defect-one clinical
syndrome-one drug does not hold good any
longer; not that it has done any good so far.
Even minor changes in other systems will
have significant effect on the outcome of
any system disease. This is true of all
systems in this dynamic universe. Even
after elaborate computer analysis for pre
dicting the weather, I xirenz was amazed to
find its predictability being rather poor. He
propounded the "butterfly effect" i.e.even
if a I utterfly were to swing its wings in
Beijing (with all the other parameters hav
ing been taken into consideration) there
could be unexpected storm tn New York a
month later. This kind of “butterfly effect"
is seen in daily practice of medicine if one
keeps his eyes open.
________________
Doctors have been predicting the unpredictable all these years. The outlook of
the medical fraternity towards health and
disease needs a sea change. Application
of non-linear mathematics to medicine
has clearly shown that all outcomes in
health care delivery depend on the finer
details of the organism(men) to begin
with. As of now it is next to impossible to
fathom all the minutae of variables inside
man to predict the outcomes. Except for
rare uniovular twins, no two individuals
are alike and how can one generalise
anything in human sciences?
When we consider day to day health care,
we are rudely shocked to know the state of
affairs. A good doctor is one who can
understand his patients to the extent pos
sible before labelling him with a disease. A
wrong label may cause irreparable damage
to the victim. Diagnosis of a disease is not
the end in itself; it should be the means to
our end viz of helping the suffering. The
present scenario of specialisation and sub
specialisation (super specialisation in In
dian English) has been cutting at the very
root of this new scientific approach in
medicine of “chaos" and “fractals” where
the knowledge of the whole organism is
more important than the expertise in a
limited field of medicine for proper diag
nosis of man’s illness.
Specialisation in medicine has a very sig
nificant role in health care delivery. A
patient who has had an acute upper
aliementary bleed, or one with acute attack
of asthma or one needing a bypass graft,
should be attended to by a highly skilled
and practising specialist. Even if this spe
cialist has been on a long holiday, his level
of performance may go down temporarily.
This has been shown by studies of occa
sional cardiac surgeons vis-a-vis daily car
diac surgeons. So far so good. Such a
skilled specialist must be free only to do his
job at which he is the undisputed expert.
That, by no means, gives him the right to be
called a good doctor to practice clinical art
on patients. A well trained clinician should
be in charge of all diagnostic work. He is
the one to interrogate, investigate and arrive at the final management strategy. Majority of times this clinician will be able to
finallv
finallydisnose
dispose of
ofthe
the oatient
patienteither
eitherwith
with a
reassurance or drug treatment. If an occa
sional patient has clear cut indications for
further study or intervention then, and only
then, should the speciality trained special
ist be brought into the picture. The latter
may be needed in every upper alimentary
bleed at the earliest possible opportunity or
very rarely needed in a patient with chest
pain which turns out to be due to angina of
left main coronary artery disease.
One of the areas where high tech-medicine
June
1993
MEDICINE UPDATE
93
/
has been palpably advantageous to man is
emergency care. This area needs special
attention. Teams of highly skilled (trained)
and motivated physicians, surgeons,
anaesthesiologists and nurses are in great
demand. Although the outcomes in terms
of mortality are relatively high in this area,
(which sometimes has an adverse
psychologic effect on the members of the
team) the benefits outweigh the draw
backs. Unconscious patients, poisoning,
acute asthma, acute heart attacks, alimen
tary bleeds, accidents, crime victims, pa
tients with burns etc.need the expertise of
these type of teams and special areas in the
hospitals where these unfortunate victims
can be managed. Emergency medicine
should be a definite speciality. These doc
tors and nurses should have no genera!
responsibilities at all.
Let us see the other side of the coin. If a
patient with some chest pain were to land
directly in a unit geared for bypass surgery
both technically and fiscally, there is a
good chance that he will end up on the
bypass table for surgery. This is because
fixed anatomic obstructive lesions in the
coronary arteries(coronary artery blocks)
are many times seen even in young people.
Vietnam and Korean war casualty studies
and studies of young crime victims in New
Orleans have all clearly shown that young
•M
/
people (mean age 20 - 22 years) have had
fairly severe coronary blocks in one, two
or even three vessels. These fixed blocks
rarely kill anyone. We still do not know
the real cause of sudden death or a mas
sive heart attack, although we have theo
ries about a fresh atherosclerotic plaque
(not fixed old block) either rupturing
suddenly or ulcerating initiating a clot on
topwhich finally blocks the flow of blood.
If all those youngsters who died in war
were to be seen in a busy bypass unit,they
would have all been bypassed at the age
of 22 years’!
One cannot understand the gravity and
implications of our present reductionist
attitude in medicine. Even in abstract
sciences like physics, reductionistic atti
tudes have failed to deliver the goods.
How can any such measures work in an
amazingly complex human organism?
We need to change the present medical
paradigm to look at man as a whole and
as a part of this macrocosm.
FURTHER READING
FIRTH F.R.:
CHAOS - Predicting
the unpredictable
Br.Med. ]
1991:303; 1565 - 68
Prof. B.M. Hegde
Dean, Kasuturba Medical College
Mangalore.
0* CO*,,WV»«0 loucanow »0« MIAC'>C>«4
t
UPDATE
LOOK OUT IN JULY ISSUE ...
ENDOMETRIOSIS
URINARY INCONTENTINENCE
AVOIDING COT DEATH
THERAPEUTICS INDEX ON ANTIBIOTICS
94
June 1993
MEDICINE UPDATE
I.
MEDICINE
I
—1
-------
i' 7 ;
py- ♦ i / II'I *.
Worth one’s salt
Biochemic medicine, based on organic salts, is becoming popular
he patient’s face had turned an omi
nous blue. The pulse rale was low.
And he was slowly losing essential
body fluids. But in this case there was no
need for panic, no rushing to the cardio
logist or neurologist. The remedy was
simple — regular doses of Kali
Phosphoricum.
Homeopathy? No. But a similar
school of medicine which is slowly gaining
—
popularity
biochemistry.
There is a growing
belief (hat the most com
plicated diseases strike
because of (he lack of
something very basic in
the human body. And
that these can be diagnos
ed and dealt with at home.
Biochemistry is one
such science that caters to
the concept of (he arm
chair doctor. It works on
the basis that all substan
ces necessary to heal, 3
restore and overcome dis- |
eased conditions, are |
found in the body itself. §
The body holds its own “»
menl in (he human body.
"The cure is so simple, that people do
not even need to visit a doctor to prescri
be the medicines," says Captain V.K.
Ramchandani, a retired naval officer
who has taken up biochemistry as a
hobby. "All one has to do is to pick up a
book, describing not only the nature of
the various salts and (he symptoms of
the diseases, l)ut also the temperament
With biochemistry this question does
not arise. "All one is doing is adding to
the salts, which are already present in
the body," explains Dr Bhandari.
Biochemistry is also less complicated
than homeopathy, since one doeii not
need to go beyond the basic salts to find
a cure. All a layman has to do is to, read
about the various salts, match them
against (he symptoms of his disease and
find out which one descri
bes his condition best.
For instance, in the
case of a stomach ache,,
the symptoms of various
stomach ailments are
described. So,, the person
knows if he is suffering
from cholera or colic. If
indeed a person is stiffen
ing from cholera, then
that is also further divid
ed into different symp
toms of the disease. If the
patient has a red face, dila
ted pupils, etc., he needs
Ferrum
Phosphorica
while a blue face, as men-*
tioned earlier, would call
for Kali Phosphorium.
An Imbalance In the
ratio of body salts Is
the cause of
physiological
problems. Hence, one
does not need to go
beyond the basic salts
to find cures, feels Dr
K.K. Bhandarl
The medicines cost around Rs 20 per
bottle (local brands), and are available at
shops selling homeopathic medicines.
ITET TI FTT
♦
1
W 2J.f< «p.;-
L
I
£
1__ L
.4
L *
'^S
I
I
f-
U )l
cures, provided it has a normal supply of
those elements essential to its well
being. Hence, a deficiency of one or
more of these elements — i.e., tissue
salts — can lead to bodily disorders.
As far back as 1873, Dr Schussler, a
German homeopathic doctor, defined
12 inorganic salts which maintain the
physiological balance.
In due course, the modern biochemist
has added to Schussler’s 12 basic salts,
finding therapeutic use for every ele-
66
A
of the patient, his likes and dislikes."
And unlike homeopathy, there is no
harm done in case of a wrong prescrip
tion. "Homeopathy works on the prin
ciple that likes are cured by likes," opi
nes Dr K.K. Bhandari. "For instance, a
snake bile is cured by taking a bit of the
poison and mixing it in the sweet pills.
So, in the case of a wrong diagnosis, a
person may have a completely different
disease introduced into his system and
end up suffering from it, instead."
Rfl M S
I'rt JUS T 11'
1
£
Biochemistry also claims cures for
nervous afflictions and alcoholism..
Although no cure for cancer has been dis
covered yet, there is a preventive offe
red. "Cancer is caused due to lack of
potassium salts in the body," says Dr
Bhandari. "So, if a person starts taking
potassium salts early, to make up for the
deficiency, it is likely that he won’t suf
fer from the disease."
The obvious advantages of the
method lie in the simplicity and accessi
bility. And of course, the fact (hat it
claims to be as much — if not more —
effective and less harmful to the system
than allopathic medicine, has gone a
long way in making people sit up and
take notice. •
Prlya Sahgal/New Delhi
s
SUNDAY 1—7 AuguM 1OT3
Rod ST' /
READER 'S DIGEST
derlying disorder that is causing inherited neurological disorder
them all,” says Dr Edward Hook, a called Tourene syndrome, and he
correctly diagnosed Ochsman s
professor of medicine.
Leaving no stone unturned is condition.
Now 35. Ochsman is happily
critical — sometimes even when
and the father of two chil
married
it’s the wrong stone. Bruce Ochstakes medication to con
He
dren.
man experienced constant grunt
trol
some
of his symptoms. He be
ing, eye blinking and a dry’ cough,
lieves
his
diagnosis is the result of
symptoms that grew worse when
his staunch refusal to discount any
he turned 16.
Dwtors^insisted his problems possibility. “The best advice 1 can
psychological in nature.
nature. “I offer anyone facing a situation like
were psychological
•
•
-----j mine is to keep looking into every
didn’t believe this,” Ochsman says,
“but I couldn’t rule out the possibil alternative,” Ochsman says. “If
ity.” So at 19, he consulted a psy your doctor doesn’t know the an
chiatrist. Fortunately, the doctor swer, you may’ find it — sometimes
had recently learned about a rare, where you least expect it.”
u
Buzz Words
S1TVE RACE, host of the BBC’s panel game “My Music,” recalls an early
• ^once got caught with a. copyright
,fo’r
Korsakov’s The Flight of the Bumblebee, which I adapted for a 19>7
commercial for honey just a year before Rimsky-Korsakov came out of
00 Aldie publisher's solicitor's letter put it, "We must regretfully sting
you for your share of the honey. ”
-
No Holds Barred
countries are becoming all alike, aren’t they? Well,
and
no Languages still build barriers, and gestures can be more troubleObscene gestures come in so many regional vaneties that tirtualh any
hand motion means something horrendous somewhere.
Desmond Morris, author of The Naked Ape and
Gestures says some of Europe’s hand signals emerged 2000 years ago
— and that details like the single market or the demise of communism
are not about to change things.
142
ii
i
I
t
I
I
1
I
I
READER 5 DIGEST
Fehman
and remain in control of the discusperimental drug saved her life.
Lyon, a founder and now execu- sion, without alienating your doctive director of the American Por tor.
Educate yourself. As a little
phyria Foundation, hopes to help
others avoid her experience. “I girl, Nancy’Rogowski began sufferworry about all the ill people who ing unexplained joint dislocations;
" and‘ may even die because; the
. also
suffer
f slightest ’bumps
’ ’brought*
they may be afraid to press for an- massive bruises. Doctors could find
• • opinion."
• • - •Lyon says.
nothing
wrong. Several even re
other medical
i
Studies suggest that many peo- ported Nancy’s parents for susple feel intimidated by their doc peered child abuse.
Her symptoms continued into
tors. Richard Frankel, a leading ex
jpert on doctor-patient
m
commu- her 20s. Then in 1982. she connication, recently reviewed over suited an oral surgeon about one of
1000 cases of disgruntled patients at her many jaw dislocations. After
a large organization. He found that taking a detailed medical history,
encounters w'ith medical staff often the surgeon suspected a connecleft patients feeling “humiliated"; tive-tissue disease. Since he wasn’t
some doctors were rude; others sure which one it w'as, he referred
didn’t look patients in the eye or Rogowski to a specialist.
Additionally, she set off for a
interrupted their efforts to explain
their complaints; many spoke in university’ medical library' to read
all she could find on connective-tis
confusing medical jargon.
In another study’, Frankel found sue diseases. “It took me tw o years
that physicians, on average, gave to go through the literature, but I
patients only 18 seconds to de finally' figured out 1 had Ehlersscribe their medical complaint be- Danlos syrndrome — or EDS." she
fore interrupting. As a result, the says. This rare group erf genetic disdoctors heard only some of the orders causes the connective tissue
symptoms — and may have missed between joints to become fragile,
vital clues. Some interruptions The disorder also affects skin con
were perceived by patients as in dition and can prolong bleeding.
Rogowski learned jhere is no
timidation. Frankel says.
What can the patient do against known cure or treatment for EDS.
intimidation? If your doctor inter but by taking special precautions to
rupts. Frankel suggests, make cer avoid injury’. EDS patients usually
tain you return to your symptoms live a normal life-span, in 1984.
and complaints. “Make a 1list be- Rogowski organized a foundation
forehand, so you won t forget." he to provide EDS patients with practi- '
• •
~
savs. —
Desiree. cal advice about their illness.
thing.
The important
Ivon stresses is to assert yourself u Knowledge empowers you to take
140
7993
yxyEX YOI R DO
‘ she
‘ says.
charge of your health."
Here are some basic steps to fo
low in educating yourself abo
your illness:
1. Acquire your medical r
cords. Seeking a second or thi
opinion about a medical conditio
is nowr standard practice. To sa
time and expense, arm yourse
with copies of your records, inclu
ing test results. X rays, and phy
cian summaries of your condition
2. Learn your family 's medic
history. When Ida Fees siste
Joann, died of a ruptured abdom
nal aortic aneurysm at the age
42, Fee grew suspicious. H
mother and some other relativ
had also died fprematurely.
Fee, 38. investigated her fam
history, studied death certificate
compared symptoms and, bas
on a lead from her family doct
spoke with experts. After a yea
search, she discovered that
other members of her family h
died of the same condition. Marf
syndrome. a genetic disorder. F
alerted her entire family. Eight
them — herself included — ha
Marfan. Her detective work m
save their lives.
There are roughly 5000 other
netically transmitted diseases.
vou have a medical problem t
doctors can’t diagnose, look
your family’s medical history a
discuss it with your physician.
Don't rule out anythin
When Dr Peter Gross, an inf
tious-diseases expert, first ca
B^ien.
! Your Doctor
Doesn’t g
Knowi|
I
?D0„-t?iveupifyJ
“
"
T^aity Ki Al El IN s medical odyssey began when she was 39.
I'irst came unrelieved itching,
followed by fatigue and pain in her
arms and legs. A hard-working
management consultant and the
mother of a five-year-old boy, she
went to specialist after specialist,
but their examinations revealed
nothing.
Desperate for an answer,
Klafehn visited a major medical
clink*. Aller routine tests, a physi
cian told her that her problems
1’ihKAMs, j Rcadvr'.s DigcM Roving Edi
tor. s |k *cm Iizva in inrdnal topics lie is the author
ol six IxMiks on incdKinc and has won a numlier
ol awards for medical writing
/W
■■
'
-SLS.- 1
were all in her head. She asked for a
CAT scan, a highly detailed X ray of
the Ixxiy, Unwarranted, the doctor
said.
By now, Klafehn had seen more
than 25 specialists. She asked her
own doctor once more for a CAT
scan. Again, she was turned down.
I'hen, almost five years after the
onset of her symptoms, a rock-hard
lump appeared on her neck. A bi
opsy revealed advanced Hodgkin’s
disease, a form of lymphatic cancer.
If the CA'l' scans had been per
formed when she first requested
them, the disease would almost cer
tainly have been detected earlier.
Klafehn is now doing very well, but
she’s still very angry with the
cians who dealt with her
handedly.
v Klafehn is not alone. Man
pie who know something is
with them go from doctor to
in search of an answer. Part
troublesome are the rare,
phan," diseases. In a 1989
the US National Commissi
Orphan Diseases staled tha
than one-third of all peopl
contract a rare disease go on
years before receiving an a
diagnosis.
Even less-rare diseases ca
lify doctors. “Almost no sing
ing in medicine points to o
swer," says Dr Frank Davi
senior vice president of the
can College of Physicians. “S
tors can look at a spot on th
chest X ray and come up w
different opinions of what
ing it. This happens every da
Guessing Game. Mo
says Dr Angelo DiGeorge, a
atric endocrinologist and
recognized diagnostician,
doctors simply don’t want t
they don’t know what’s wro
in effect, they make a gues
happens far more often tha
people realize.
Doctors can also disag
treatment. Paediatric neurolo
Fred Epstein tells of a young
whose brain scan revealed
tumour in his pituitary gland
ommended against surge
cause I thought the tumour
rAf -
THE
INDEPENDENT
COMMISSION
ON HEALTH
IN INDIA
Voluntary Health Association of India
CONTENTS
!
Preface
•;
Members & Associates of The Independent Commission
on Health in India
Chapter I
ws
Current Health Status in India and its
Vulnerable Areas..............................
1
Chapter II
Food and Nutrition Security
15
Chapter III
Perspectives in Medical, Nursing and
Paramedical Training and Education
23
Chapter IV
Health Policy
35
Chapter V
Decentralised Health Planning
45
Chapter VI
Public Health Institutions
55
Chapter VII
Indigenous Systems of Medicine at the
Crossroads..........................................
63
Chapter VIII
Health Services in Rural and Urban Areas
75
Chapter IX
Reorganisation of the Organisational Structure
of Health Services ...........................................
97
Public Health Situation: With Special Reference
to the Countrol of Communicable Diseases ......
115
Environment and Health
A.
Environmental Sanitation and Community
Water Supply...........................................
131
B.
145
2
I p laR
■. J
7
r
■
Chapter X
Chapter XI
,
■K--:
Ecological Degradation and Health
.
Chapter XII
Chapter XIII
.AW; '5
Control and Prevention of Non-Communicable
Diseases
A.
Lifestyle-Related Diseases
151
B.
A Case for Banishing Tobacco
165
C.
Emergency Health Care
173
D.
Preservation and Restoration of Vision ...180
Health of Women
183
w1
Jo
L
W
7 f
: I
■■
If
I
Chapter XIV Health Problems of Specialised Groups
Disability : Issues and Solutions ..
199
208
213
Population Stabilisation: Intervention Strategies
221
A.
B.
C.
Chapter XV
Child Health................................
Elderly Persons..........................
Chapter XVI Dental Health
233
Chapter XVII Mental Health
237
Aw
Chapter XVIII The Voluntary Sector in Health Care: Need
for a New Paradigm............. 245
Chapter XIX The Private Health Sector and Related Issues
251
Chapter XX
259
Medicine, Medical Care and Drug Policy
'1
Chapter XXI Important Issues in Health Financing
A.
Health Expenditures ..........................................
273
B. The Economics of Health Care in India: A Case
Study of Sewapuri Block in Uttar Pradesh........293
Chapter XXII Regulating Medicine and Ethics
307
Chapter XXIII Health Education
319
Appendix
1.
2.
3.
Public Hearings .......................................
Corporate Initiatives in Community Health
References..............................................
tW
This is an Executive Summary of the
voluminous Report of the Independent
Commission on Health in India. The
main report Is available in full or In
sections from Voluntary Health
Association of India
C
337
350
356
...J
Members and Associates
of
The Independent Commission On Health In India
Members
Alok Mukhopadhyay (Convenor): Executive Director, Voluntary Health Association of India.
Former Country Director OXFAM. Editor, State of India's Health Report.
R. Srinivasan: Former Secretary, Ministry of Health and Family Welfare, Government of India.
Former Chairman of the Board, World Health Organisation, Geneva.
Balu Sankaran: Well known Orthopaedic Surgeon; former Director General, Health Services,
Government of India, and Consultant to the World Health Organisation.
“ i book
K.R. Venugopal: Former Secretary to the Prime Minister of India. Author of' the
The Indian Public
Distribution System". Member of the
- ----------"Deliverance From Hunger ---------South-Aslan Commission on Poverty Alleviation.
............i
Harcharan Singh: Former Health Advisor, Planning Commission, Governmentof
India and
Consultant to the World Health Organisation in Nepal. Presently, Consultant to
various national and International health projects.
Ashish Bose: Honorary Professor at the Institute of Economic Growth and formerly Jawaharlal
Nehru Fellow. Former Member of The National Commission on Urbanization and
Advisory Council monitoring the 20 Point Programme.
Raj Arole: Magsasay Award winner and known for his outstanding contribution to rural health
through his Jamkhed project In Maharashtra.
Shanti Ghosh: Eminent Pediatrician; former Professor of Pediatrics at Safdarjung Hospital.
Advisor and Consultant to the World Health Organisation and other international
agencies.
N.S. Deodhar: Former Director, All India Institute of Public Health and Hygiene, Calcutta and
Additional Director General, Health Services, Government of India. Currently,
Consultant to various national and international health projects.
Darshan Shankar: Director of the Academy of Development Sciences at Karjat andI s one
of the founders
-------of
- Lok Swasthya Parampara Samvardhan Samlti and the
Foundation for the Revitalization of Local Health Traditions.
H. Sudarshan: Recipient of the 'Right Livelihood Award' for his outstanding work in the tribal
regions of Karnataka.
Bhaskar Ray Chaudhuri: Noted Neurologist; former President, Indian Medical Association
and former Vice-Chancellor, Calcutta University.
Member Secretaries
Almas All
N.K. Sinha
Associates
★ Centre for Enquiry Into Health and Allied Themes (CEHAT), Bombay
i
★ Commuhity Health Cell (CHC), Bangalore
★ Foundation for the Revitalization of Local Health Traditions (FRLHT), Bangalore
★ South-South Solidarity (SSS), Delhi
★ Vivekananda Girijana Kalyan Kendra (VGKK), Mysore
★ Gramin Vikas Vigyan Samltl (GWS), Jodhpur
★ VHAI (Delhi and North East Offices)
State VHAs:
Assam, Delhi, Himachal Pradesh, Karnataka, Manipur, Nagaland, Orissa,
Punjab, Rajasthan, Tamil Nadu, Uttar Pradesh, West Bengal and other State
VHAs
S.K. Sushlla
Dinesh Mohan
C.R. Ramachandran
Klshore Murthy
Ali Baquer
Sanjoy Ghose
Amlt Shovan Ray
Bhavna B. Mukhopadhyay
RN. Sehgal
R. Srlnlvas Murthy
Ravi Duggal
Jill-Carr Harris
Mira Shiva
Chandra Kannaplran
N.M. Mathew
M.C. Valdya
Pratap Sisodla
Bharat Jhunjhunwala
Amar Jessanl
K.J. Nath
Dr. Therlan
Taposh Roy
Sanjay Kapur
Dipankar Dasgupta
Shrldl Tekur
Rama Baru
Cedric Finch
Indu Prakash Singh
Kaverl Dasgupta
The Commission has consulted widely with people all over the country. We have
listed above, the names of those who have contributed to the formation of our
vision. However, we regret that we might not have been able to record the name
of every person who has been of help to the Commission and we apologise for any
omission or errors in this list.
I
Perspectives in Medical, Nursing and
Paramedical Training and Education
he goals of medical education in India have been
clearly defined and endorsed over the last five
decades since Independence. For instance, the
concept of the social physician (Bhore Committee 1946,
Mudaliar Report 1961), the basic doctor (Patel Report
1970), family and community-oriented general
practitioners with social responsibility (Srivastava Report
1975), the community-oriented physician for
comprehensive health care (ICSSR-ICMR 1981) and the
community physician (NEPHS 1990) have all underlined
the type of doctor required in this country.
However, despite greater clarity in the stated goals
of policy, the phenomenal quantitative growth of the
institutional framework, efforts to qualitatively reorient
the curriculum to match policy goals, and the growing
populist rhetoric of doctors for the villages, medical
education has moved towards greater and greater crisis.
This is illustrated by the fact that a majority of young
medical graduates still opt for urban hospitals and clinical
practice; the trend towards specialisation is high; the
vacancies in rural health centres have reached significant
proportions; and professional interest, both at the level
of the practitioner and educator, continues to be in illness
care at the secondary and tertiary level, rather than in the
challenges of primary health care and public health, which
emphasise primary prevention. The increasing
commercialisation, privatisation and erosion of norms in
medical ethics also underscore the point. In addition, the
problem of full-time teachers being involved in private
practice and the growth of the doctor-drug-producer nexus,
continue to exist.
These distortions are progressively eroding the focus
of health service development, and the nature and goals
of medical education in the country. We shall focus here
on the lack of congruence between the stated goals and
policy formulations and the ground realities.
Diagnosis of the Problem
An overview of the growth and development of
medical education in the country is necessary to effectively
understand the dynamics of change and the emerging
25
w Independent Commission on Health in India
problems in this sector. There has been a massive
quantitative expansion of medical college facilities in the
country since Independence. For instance, the number
of colleges has increased from 22 in 1947, admitting 1,983
students, to 145 colleges in 1995, admitting 16,200
students annually.
commercialisation are negative trends, which are the result
of money power and political patronage becoming more
significant. For instance, the nexus between the capitation
fee college lobby and the political system, through
contributions to party funds, is a well-established
phenomenon.
However, regional variations exist. Based on the
Mudaliar Committee norm of one college per 50 lakh
population, a review of the current situation shows that
the number of medical colleges in some states {such as
Karnataka, Maharashtra, Tamil Nadu and Delhi) is higher
than their entitlement and requirement, whereas states like
Bihar, Madhya Pradesh and Uttar Pradesh have far fewer
colleges than their requirement. Although, at the national
level, the figures even out, the medical education sector
also reflects the overall regional imbalances and disparities
that exist in all aspects of the health system of the country.
The faculty in medical institutions are still poorly
motivated towards broader health and development goals,
and are not sufficiently trained for their role as educators.
In fact, most of them are averse to public health. This
problem is further compounded by the continuing canker
for private practice among full-time teachers, inadequate
selection guidelines that still stress academic qualifications
rather than the aptitude or motivation to teach and
competence, the increasing shortage of teachers in
government colleges due to transfers and lack of job
satisfaction. More recently, the lure of better-paid and
stationary jobs in the private medical education sector,
is an added element.
Admission requirements and selection procedures have
been changing over time. There are now greater
opportunities for the socially disadvantaged sections of
the community and special groups to join medical
institutions. In addition, the trend in admissions for women
has shown a substantial increase. However, in recent years
the ability to pay high tuition fees has become a major
determining factor, both for free and payment-seeking
admission to medical colleges. Even though legally,
capitation fees have been struck down as “unconstitutional,
unreasonable, unfair and violative of the right to
education”, this evil practice still continues unabated at
some places.
Currently, too many doctors are being produced at
the cost of training other members of the health team. If
the production of practitioners of other systems of
medicine is included in medical manpower statistics, this
situation of ‘excess’ becomes worse. Instead of having a
proportion of three nurses to one doctor, we have the
reverse - for every one nurse we have three doctors. There
arc further distortions. Majority of doctors opt for
postgraduation, leaving far less GPs. Clinical specialists
far exceed the pathologists, micro-biologists, radiologists,
etc. The worst situation is seen in the area of public health,
which fails to attract students.
The number of government colleges grew
trcmcndo.usly till 1974. This was followed by the
increasing commercialisation and privatisation of medical
education after 1988, especially in the states of Karnataka,
Maharashtra and Tamil Nadu. Related to this process of
The recommendations of the Medical Council of India
(MCI) for curriculum change have added, since 1954, a
whole parallel structure of a Department of Preventive
and Social Medicine (PSM). PSM or community medicine
as it is called today, was envisaged as a joint programme
with all the departments, thereby permeating the entire
course. However, far from becoming an integral
component of medical education, PSM has only been
marginalised and neglected. At present, the involvement
of all other departments in the process of social and
community orientation is inadequate, at places even
totally lacking. While one department shoulders the entire
responsibility for reorientation, the other departments
continue to focus and draw inspiration from high-tech,
hospital-oriented tertiary and secondary care medicine as
practised in the West. In fact, the gross disregard of MCI
recommendations among medical college authorities and
faculty is perhaps itself a major obstacle for change.
Student wastage at the course level is not significant.
However, there is increasing evidence that the investment
of the taxpayer ’s money in medical education benefits
the private health care sector and the health services of
the established market economies of the world, more than
it supports the state government ’s own primary health care
and hospital services.
Braindrain is estimated to have reached an alarming
30 per cent of annual output in 1986-87. However, this
problem has recently been overshadowed by a new
Medical, Nursing and Paramedical Training and Education
phenomenon - the increasing investment in private, high
technology diagnostic centres by Non-Resident Indian
(NRI) doctors - which is being portrayed as an ‘altruistic
process’. In reality, this is turning out to be a market
economy process, supported by the medical-industrial
complex of the West in search of new markets!
Corruption has become the bane of public and private
life in India. It has crept into all sectors of development
and human endeavour, reflecting an overall decline in
ethics and values. Medical education is no exception.
Apart from medical malpractices at the time of admission
and examinations, corruption has led to a growing nexus
between the medical profession and the medical-industrial
complex, creating vested interests. The mushrooming of
privately-financed colleges and the increasing problem
of private practice among full-time teachers have further
compounded the problem.
Medical students and junior doctors are the only
groups within the structure of medical education who arc
marginally involved in collective efforts to maintain
standards or improve the existing situation. Professional
leadership and the teaching faculty have not shown much
interest, dynamism or the ability to counter political and
other bad influences in various aspects of medical
education.
Postgraduate education has focussed mainly on
secondary and tertiary care and super-specialisation, less
on basic sciences, and the least on public health and its
related disciplines. This trend has to be reversed. Areas
like public health epidemiology, primary health care,
community health, general practice and family medicine
should become the major focus of postgraduate education.
Interaction between medical educationists and the
growing number of well-known projects, institutions, co
ordinating centres and training and research institutions
in the voluntary sector, which have experimented with
alternative humanpower development strategics, is long
overdue. Efforts at continuing education have also been
woefully inadequate, especially in the context of the
massive army of doctors, health workers and health
professionals who need regular and urgent updates and
skill development to provide effective services. The
growing interest in the Open University concept and the
Distance Learning Module should be harnessed for this
task.
While the MCI has been responsive to the suggestions
s 26
of expert committees, it has recommended changes in the
curriculum too cautiously and even incorrectly. At present,
primary health care reorientation continues hand-in-hand
with the traditional emphasis on secondary and tertiary
care. Further, there is total neglect of public health and
primary prevention through IEC (information, education
and communication') in health, etc.
A basic problem in the MCI structure is that, since
education i^a state subject, the MCI has in principle, a
recommending function only, not a regulatory one. In the
absence of actual regulatory teeth and money, the MCI’s
ability to maintain standards has been severely
compromised by state governments/state universities
falling prey to pressure groups and extraneous influences.
At the same time, MCI inspectors have not be^n able to
maintain the high ethical standards expected of them to
ensure the enforcement and maintenance of standards. As
in all aspects of national life, corruption and extraneous
influences of money power and political interference have
managed to circumvent the inspection mechanism.
Issues such as the cost and financing of medical
education have been greatly neglected by policy-makers
and researchers. It is important to note that, over the years,
the cost of medical education and health care has escalated
rather than declined. The trend towards commercialisation
(through donations and capitation fees) is the direct result
of inadequate planning and review of this important
component of health humanpower development.
Preventing market distortions is possible, not just through
legal controls but by seeking greater clarity in Iternative
avenues of support to higher education. The rctent move
at both the central and state level to introduce NRI quotas
in government colleges (based on payment, like capitation
fees) is therefore, an extremely retrogressive step,
encouraging commercialisation rather than responsible
privatisation.
Since the seventies, there has been growing concern
about the nature of medical education in the country, in
terms of its relevance and growth Expert committees and
policy statements have viewed the complexities of the
medical education process in the broader socio- economiccultural-political context. The National Education Policy
in Health Sciences (1989) and the Eighth Plan document
have also endorsed such a broad analysis. The suggested
policy shifts arc:
★
A proper balance between technological and
humanistic medicine.
27
★
★
Independent Commission on Health in India
A more holistic approach, covering the promotive,
preventive, curative and rehabilitative aspects of
medicine.
A proper balance between tertiary hospital-based
education and primary community-based education.
A shift from the use of teacher-oriented to learneroriented methods, which would include self-directed
learning and self-evaluation.
A progressive change from narrow discipline-oriented
teaching to a problem-oriented'approach.
A shift from theoretical teaching to experimental
learning.
A major change in the role of the medical teacher,
from one who imparts a defined quantum of
knowledge to one who facilitates and motivates
community-based student learning.
However, there has been an overall lack of political,
administrative and professional will to actually change
realities at the ground level. While populist rhetoric is
getting more pronounced, the actual development process
is becoming subservient to market forces, much
aggravated since the inception of the New Economic
Policy.
There is, therefore, a growing dialectical tension
between the increasing need to reorient medical education
towards the needs and priorities of the community, and
the increasing trend towards privatisation,
commercialisation and high-tech tertiary care. The current
scenario is, therefore, full of contradictions, challenges,
and ill-disposed.
Experiences in Community
Orientation
The broader contextual issues in which medical
education reform and reorientation have to be situated,
have been emphasised in the foregoing. Although the
reality of medical education described here is disturbing,
the picture is not totally bleak. The growing spirit of
introspection and dissatisfaction has led to some
experimentation and innovation in medical education in
a few institutions all over the country; committed faculty
have gone beyond diagnosing the problem and evolved
alternative approaches to address it. A review of the key
experiments and emerging initiatives follows.
The Kottayam Experiment (1972-76)
The Kottayam experiment was the forerunner of the
integrated teaching approach whereby a student has a
holistic view of medicine, with clear goals of community
medicine as well. In this experiment, the curriculum
content and process evolved from classroom interaction
between the teachers and students, based on feedback from
community experience, beginning from the first semester
itself. A small multidisciplinary core team functioned
as both instructors in all the subjects, and supervisors of
all the learning experiences. This experiment was directed
towards integration and community orientation at all
levels.
Not surprisingly, the established medical education
system did not take this experiment seriously. However,
the government of three southern states adopted the
course outline and elements of the experimental course
for B.Sc. Public Health Nursing (Kerala), Health Assistants
(Tamil Nadu), and B.Sc. Health Sciences (Andhra
Pradesh).
The ROME Programme (1977)
The ROME (Reorientation of Medical Education)
programme was launched in 1977. It was introduced at
the central level to involve medical colleges; the students
were to be given exposure to community health problems
and the direct delivery of specialised health care services
to the rural population. It aimed at inculcating an interest
in the challenges of community health care in students
and faculty members. Medical colleges were to be
involved in the direct delivery of health services in rural
and semi-rural areas. Each medical college was required
to adopt three primary health centres. Three large mobile
clinics were given to each participating college to
provide expertise and specialised assistance to primary
health centres. Guidelines were drawn up by the Ministry
of Health and Family Welfare, aimed at balancing
provisions for the delivery of health services, with
recommendations for teaching and training. The students
were supposed to stay in the primary health centres
complex (hostel accomodation sanctioned) for a certain
period of time, and faculties of various disciplines were
supposed to visit by turn. About 105 medical colleges
participated in this scheme. While the ROME experiment
was, in principle, a good scheme, it lacked flexibility
and suffered from faculty disinterest and inadequate
resource management.
Medical, Nursing and Paramedical Training and Education
Moving Beyond the Teaching Hospital: A wide
range of initiatives have developed to provide
experience at the primary health care/community
level, so that students and the faculty gain a learning
experience beyond the walls of the teaching hospital.
These initiatives are additionally significant because
the process, experience and demands, chal lenge the
established value systems of medicine, the culture
of medical education, the urban middle class
aspirations of the students and faculty, and the
ingrained enthusiasm for high technology oriented
secondary/tertiary level medicine. Community
orientation programmes (COP) in the pre-clinical
years, and community-based postings in the internship
years, have shown great potential. However, these are
too limited to make an lasting impact to loosen the
grip of ‘clinical medicine ’ and surgery.
The Health University (1980s)
Two states, Tamil Nadu and Andhra Pradesh, initiated
a process of bringing together all the medical colleges
in the state under the jurisdiction of a single technical
university (the Medical University). Administrative reform,
and the standardisation of the curriculum, facilities and
examinations arc the primary objectives of this experiment.
State sponsors and policy-makers have, however, not yet
fully explored the potential of this idea, which could lead
to a more integrated approach to health humanpower
development in a state. While the scope of such an
initiative is tremendous, the dangers of centralisation, the
marginalisation of medicine/health from the general
educational system, and the domination of clinical faculty
at all levels needs to be avoided. In brief, the basic
objectives and concepts behind recommending the
establishment of Universities of Health Sciences, has not
been conceived correctly. The idea was not to convert
the Directorate of Medical Education into a ‘University’,
clubbing all medical colleges. It went far beyond - to
developing a full team of health manpower, from
community level workers to tertiary level experts, public
health specialities, researchers, etc.
Widening Horizons: Introducing new concepts and
topics as additional subjects to widen the horizon of
future doctors and prepare them for involvement in
primary health care and community-based situations,
is another important group of initiatives. These include
behavioural sciences, ethics, first aid, nursing, rational
therapeutics, social paediatrics, social obstetrics,
epidemiology, management and health education.
The efforts are, however, isolated and not sustained.
Medical College Initiatives
Over the years, serious efforts have been made by a
few medical colleges to operationalise some of the
recommendations of expert committees. A smaller
number have gone further to evolve a more sustained and
regular community-oriented training strategy within the
overall framework of the orthodox curriculum.
A recent study undertaken by the Community Health
Cell (CHC) has identified 50 initiatives that represent this
strategy. These can be classified into six broad areas which
form an integral part of the reorientation process.
Improving the Pedagogy of Medical Education:
Important areas of innovation and reorientation are the
clarification of objectives at the institutional and
departmental levels, and improvement in the skills of
the staff in modern educational techniques. This has
helped to make the process of education more rational
and meaningful, both for the students (who are clients
of the system) and the faculty (who are facilitators of
the system). However, while improvement in pedagogy
is an important step, it is not sufficient, since it has Io
be balanced with a simultaneous change in content
towards greater social and community relevance.
& 28
★
Improving Skill Development: Greater opportunities
to develop skills have been explored at the student
and internship level by increasing in-service training
through camps, clerkships and special postings. Here,
skills can be acquired through graded responsibilities
in actual procedures. However, these attempts have
remained ad hoc and not found place in the routine
methodology covering all disciplines.
★
Transcending Compartmcntalisation: Attempts
have been made to integrate subjects and phases of
teaching at different levels and go beyond the historic
compartmcntalisation process. These have, however,
been hampered by the orthodox MCI subjcct-wisc
classification of disciplines and the structured
framework of subject-specific examinations.
Promoting Self-Learning: Initiatives to promote self
learning by students have been taken by some
institutions. This is probably the weakest area of
innovation because of the traditional hierarchical
educational system which sees students as passive
recipients rather than active participants.
29
Independent Commission on Health in India
have also been suggested, in which health personnel
go to the people and learn from them rather than being
agents of predetermined packaged programmes.
Graduate Feedback
A recent study conducted by CHC obtained feedback
from young doctors (who had experience in primary
health care/peripheral health institutions) on what they
felt should be the changes in medical education, in the
light of their experiences. This was probably the first time
consumers of medical education were providing feedback
after working in primary health care. Their suggestions
for modifying the curriculum structure can be a useful
guide to curriculum development and the reform process.
The MFC (Medico Friends Circle) anthology of ideas
is an exhaustive formulation of a community-oriented
curriculum framework that focusses on primary health
care service providers.
The alternative track (MCI/GOI/WHO), where the
proposed curriculum is problem-based (like the
McMaster University Model), community-oriented
(like the ROME scheme) and learner-centred. The
curriculum should consist of seven units (of seven
months each) - devoted to human biology, primary
health care and tertiary health care. Interns should
spend six months in rural health care centres and siv
months in clinical departments. The appropriatene.
and effectiveness of both the conventional curriculum
and the alternative track should be compared in the
context of primary health care and Health for All.
Community Health Trainers in the
Voluntary Sector
A large network of community health trainers have
evolved in the voluntary sector in India who have used
innovative approaches and methods in training that are
significant for medical education and reform. These
courses arc more participatory, experimental, actionoriented (using small group techniques) and communityoriented. TrainingDis based on social/ societal analysis
and, in many cases, also explores the affective aspects
of work - value orientation, group dynamic skills,
teamwork and motivation. Case studies, simulation games,
role plays and problem-solving exercises are also
important components. It is time that medical educators
moved beyond their ivory' towers to learn and interact
more actively with these pioneers, and make use of these
experiences towards improving medical education and
making it need-based.
*
The MCI’s alternative, proposed a track that focussed
on general practice, family medicine and maternal
and child hcalth/community health.
The Consortium of Medical Colleges has proposed
an inquiry-driven strategy for medical education
reform, involving a consortium of medical colleges
in India. This group 'has been undertaking small
research projects and building up a framework for
alternative curriculum.
Alternative Tracks and Experimental
Curriculum
Innovative programmes all over the world have
suggested a shift from the orthodox medical education
framework to alternative tracks that are Icarncr-ccntrcd and
problem-solving oriented, which teach integrated human
biology and community-oriented clinical medicine. In India,
only a few' alternative postulates directed towards evolving
such a curriculum framework have been advanced. However,
no actual experiments have been conducted so far. Six such
initiatives arc:
The Jawaharlal Nehru University plea for a new public
health policy, which includes the concept of a
managerial physician, where epidemiological
capabilities, managerial capabilities and social
awareness have been outlined. Approaches for training
The Miraj manifesto is an alternative framework put
up to the Maharashtra government by the Wanlcss
Hospital in Miraj.
These six different approaches and processes illustrate
the growing desire for change that is beginning to be
manifested among a small but critical group of medical
college faculty personnel and health policy activists.
Some broad similarities have emerged. The most
important features of the evolving alternatives for
undergraduate medical education are the following:
★
The medical course should produce communityoriented, socially conscious primary health care
providers.
*
Promotivc, preventive and rehabilitative aspects of
health care and primary prevention and public health
should be given emphasis.
Medical, Nursing and Paramedical Training and Education
Competence and capability in multidisciplinary skills
should be geared to community-based action.
More than 50 per cent of the entire course should be
community-based. The faculty of all departments
should be involved in community-based teaching.
★
★
Social/valuc assessment should be done during
selection. There should be a simultaneous motivation/
orientation towards community needs throughout the
course.
industrial complex (geared to profit-making).
In response to the complex factors that are actively
distorting the role, scope, goal, objectives and context
of medical education today, it is believed that with
collective commitment, this disturbing trend and
distortion can be reversed. The following agenda for action
is recommended.
1.
The setting up of a National Health Humanpower
Development Commission. This will bring together
the apex bodies of all categories of health
professionals (being the central council of all systems
of medicine), representatives of key national health
training centres and the trainers and co-ordinating
agencies of the voluntary sector, to initiate a process
of need-based and data-based integrated health
humanpowcr development planning, responding to
health care needs rather than market expectations.
2.
A comprehensive ban on medical college expansion
till the problem of commercialisation and capitation
fees is adequately monitored and controlled. Mcgacducational efforts (colleges with 150-300 sea's) should
be encouraged to improve their quality and standard
by reducing the number of seats to 100 or less.
3.
Strengthening the Medical Council of India |o control
commercial distortions and any fall in standards by:
including representatives from the social sciences,
voluntary agencies and consumer groups in the
governing body; co-opting professional leadership
from national training and research centres; and
instituting a professional interdisciplinary core team
at the headquarters.
4.
Continuing medical education reform by moving
from just making recommendations to minimum
requirements on issues such as: the formation of
medical education cells in medical colleges, selection
procedures (moving beyond academic merit to the
assessment of social values), faculty development,
improving pedagogy, promoting skill development
and promoting self-learning.
5.
Examination reform, by introducing safeguards that
prevent the operation of money/political influence,
and encourage the proper selection and orientation
of examiners, to prevent irresponsible and unethical
practices in the examination system
6.
Providing creative autonomy within the context of
Problem-solving and integration should take place
at all levels.
Competence and skill should be emphasised rather
than the mere acquisition of knowledge.
Communication management and organisational
skills should be developed for community work.
The conventional curriculum should be changed with
courage, and tempered by flexibility and creativity.
Strategies should be evolved through field-oriented
research and experiments. They should be constantly
evaluated and reviewed by the faculty and students.
All the institutions involved in this alternative search
are premier institutions or well-known policy groups,
conversant .with the existing MCI framework and yet
following an alternative construct. This is a positive
development and, perhaps, the single-most convincing
reason for the concept and framework of creative
autonomy to be considered urgently by both the
government and the MCI, while keeping up the
momentum of reorienting the existing curriculum in the
majority of the colleges. The time has come for the
government to allow a few credible institutions to
experiment boldly and creatively.
Recommendations
Medical education is at the crossroads today. What
has been highlighted here is the complex mosaic of issues
that have determined the structure, content and framework
of medical education that currently exists in the country.
These determinants of change are slowly responding to
the new market economy processes that arc shifting
medical education from the apex of health care and human
resource development (responding to (he needs oj the
large majority of our people) to the apex of the mcdical-
s 30
31
x Independent Commission on Health in India
the Indian Medical Council Act, to allow a few
selected institutions of proven academic and research
competence to experiment with an alternative parallel
curriculum that is more specifically geared to primary
health care, public health, family medicine and general
practice than the present curriculum.
7.
Urgent efforts to initiate distance learning processes
for the continuing education of doctors and all
existing members of the health team, which will
update knowledge, improve skills and link the process
to accreditation, service promotion and career
development. Links with the Open University system
would greatly facilitate this process.
13. Finally, a strong countervailing health-oriented
movement needs to be initiated by health and
development groups, consumers and people ’s
organisations, that will enhance the role of the
community, patients, consumers and the people in
the entire debate on reform in the health and medical
sector. Change has been directed and controlled for
too long by professionals, making the process
subservient to professional needs, rather than people ’s
health needs.
Nursing Education and Training
8.
The reorientation of all postgraduate education
towards the goals of the National Health Policy and
primary health care, and enhanced commitment to
postgraduate training in public health and allied
disciplines. Linked to this would be the development
of an all-India Public Health Cadre to strengthen the
public health services in the country.
Although nursing services are a primary component
in the healing and care of patients, nursing education
started much later than medical education. In fact, in some
parts of India, the training of nurses started only about a
100 years ago. Over the years, nursing services in India
have come a long way to meeting the requirements of
hospitals.
9.
Promotion of research in health systems and in health
manpower development. Pooling the resources of
national organisations like the MCI, Indian Council
of Medical Research and the National Academy of
Medical Sciences, to ensure that reorientation and
reform is practical, field-oriented, etc.
Currently, there are approximately 487 institutions
offering general nursing and midwifery (certificate)
courses, with an annual admission capacity of about
20,000; about 54 colleges offering graduate and
postgraduate nursing courses; and more than 494
auxiliary nurse-midwife (ANM) training schools. In
addition, there are a few institutions with specialised
diploma courses. However, these institutions are unable
to meet the growing needs of the country.
10. Setting up a national think-tank to undertake a detailed
review' of the private sector in health care and medical
education in the country. To identify the means by
which it should be regulated to maintain standards
and technical excellence and enhance its contribution
to the health care needs of the country and the goals
of the National Health Policy.
11. While the medical education sector needs continuing
reform, its domination of the health humanpower
sector should be balanced by a new focus on
environmental health, public health speciality,
nursing, multipurpose community-based health
workers and allied health professionals, encouraging
reorientation and strengthening quality enhancement
in training all these cadres. The emphasis should be
on skill development and social/community
orientation.
12. Establishment of Universities of Health Sciences in
all major states and groups of small states/Union
Territories.
A few Commission members interacted with
experienced nursing personnel to record their perceptions
on the health and health care problems of the country,
with special reference to nursing care and services. Valuable
information was gained during these discussions and
certain deficiencies were pointed out. For instance, there
is no uniformity in the syllabus for nurses - the standard
of education varies from state to state and from institution
to institution; there is a serious shortage of qualified and
competent faculty in various institutions, etc.
Paradoxically, graduate nursing personnel are mainly
involved in supervisory and teaching roles, whereas nurses
qualified in general nursing and midwifery are mainly
utilised for curative care in hospitals and nursing homes.
ANMs are usually posted in community health centres
(CHCs), primary health centres (PHCs) or sub-centres (SCs),
and mainly perform community health services. Many
of them arc also employed by private clinics, nursing
- Media
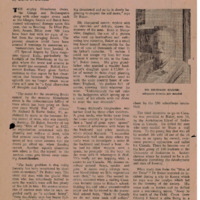 RF_MP_1_SUDHA.pdf
RF_MP_1_SUDHA.pdf
Position: 6442 (1 views)