Treatment of tuberculosis by private general practitioners in India
Item
- Title
-
Treatment of tuberculosis by private general
practitioners in India - extracted text
-
Tubercle
Tubercle (1991) 72, 284-290
© Longman Group UK Lid 1991
Treatment of tuberculosis by private general
practitioners in India
M. W. UPLEKAR and D. S. SHEPARD1
Foundation for Research in Community Health, Bombay, India and 1 Department of International Health,
Harvard School of Public Health, Boston MA, USA
Summary — Early detection and optimal treatment constitute the most important measures in
the control of tuberculosis. This study of prescriptions for tuberculosis recommended by 102
private doctors, practising in the slums of Bombay, shows a lack of awareness among doctors who
treat tuberculosis patients in their own clinics about the standard drug regimens for treatment of
tuberculosis recommended by national and international agencies. While there are a few standard,
efficient, recommended regimens, 100 private doctors prescribed 80 different regimens, most
of which were both inappropriate and expensive. The study highlights the need for effective
communication between those implementing national tuberculosis programmes and the practising
private doctors, continuing education of these doctors for updating their knowledge and their active
participation in at least those national disease programme for which their curative .functions could
contribute significantly to control of a disease.
Introduction
India has about 10 million cases of tuberculosis, the
largest number in the world, and it is estimated that
nearly 400 000 persons die of the disease every year
[1], While there arc pockets of high endcmicity in
some rural areas and urban slums, the prevalence rate
is similar all over the country [2].
Respiratory tuberculosis remains the third major
cause of death in Bombay where 45% population
lives in the slums [3]. Health care services in Bombay,
including the slums, are provided by a mixture of pri
vate and public health care providers and institutions
and it is estimated that about 60% of the people of
Bombay arc cared for by the private medical practi
tioners [4].
Early detection and optimal treatment leading to
the complete cure of patients constitute the most im-
portant measures in tuberculosis control [5]. Effec
tive treatment of an infectious patient helps to pre
vent spread of the disease by breaking the chain of
transmission and reducing the pool of infection [6].
Among the major advances in the past 25 years re
sulting from controlled clinical trials has been the
demonstration that admission to hospital is not nec
essary to treat tuberculosis effectively [7]. The focus
of research in tuberculosis in India for over 3 decades
has been on chemotherapy of the disease and various
combinations of available antituberculosis drugs have
been tried and advocated for use under the National
Tuberculosis Programme [8].
This article attempts to examine prescribing pat
terns of private medical doctors practising in low
socioeconomic areas of Bombay, Drug regimens for
pulmonary tuberculosis recorded by these doctors are
presented, analysed and compared with those recom-
Corrcspondcncc to: Dr M.W. Uplekar, Foundation for Research
in Community Health, 84-A, RG Thadani iMarg, Worli, Bombay
400018, India.
This article is an outcome of a Research Fellowship awarded to Dr
M.W. Uplekar under the Takcmi Program in International Health
at Harvard School of Public Health for the year 1988-1989.
284
285
PRESCRIBING BY PRIVATE GPS
mended by the National Tuberculosis Programme of
India. The paper highlights the need for effective in
volvement of private medical practitioners in disease
control programmes of national importance so that
they may be more effective.
Materials and methods
Analysis
EPI-INFO, a software package developed by Centers
for Disease Control, Atlanta, Georgia, was used for
analysis of the doctors’ prescriptions. The retail con
sumer costs of the drug regimens prescribed by indi
vidual doctors were computed by means of a program
written for the purpose which also converted Indian
rupees to US dollars at an exchange rate of Rs. 15
per dollar (January 1989). Current consumer prices
of antituberculosis drugs were taken from the January
1989 --------------issue of MIMS, India — a privately published\
monthly drug index which provides retail costs of
most of the drugs available in the market [9]. The doc
tors’ rprescriptions
were compared
with those recom,
.
mended by the National Tuberculosis Programme of
India. The costs of recommended regimens were also
computed using both the retail prices of drugs applied
t0 doctors’ prescriptions and the bulk prices at which
<drugs arc made available to the peripheral tuberculo*
sis clinics of the Bombay Municipal Corporation run
under the National Tuberculosis Programme,
A list of all doctors practising in a large low-income
settlement of Bombay was prepared by making visiblc additions to an existing list obtained from the
local medical association. The doctors practising here,
including the members of the local medical association, are a mixture of those qualified in Western
medicine, who are called allopaths, and those qualified in one or more of the indigenous systems such
as ayurveda, homoeopathy and unani, who are called
non-allopaths. All non-allopaths included in the study
had had some'exposure to the Western practice of
medicine, either during the formal training in their
respective systems of medicine or thereafter, before
commencing private practice, usually in the form of
an apprenticeship at private hospitals or dispensaries.
A simple random sample of 143 doctors was selected Resuits
from the list of 287, irrespective of their ages, quali> non
fications or years of practice. The sample included 79 31 doctors (22%), including 22 al
allopaths,
refused
participation
in
the
study
without
allopaths and 64 non-allopaths.
All the doctors included in the study were visited giving any specific reason for their refusal. All those
individually in their clinics and provided a slip with who completed the slips indicated that they treated
a request to ‘write a prescription for a previously un tuberculosis patients in their clinics. The final analyii vujv
j —tu sis included prescriptions of 102 private doctors, obtreated adult
case w.
of osputum positive rpulmonary
we'ighTng about 50*kg.’ Thc' slip included tained from 48 allopaths and 54 non-allopaths.
berculosis '
„
■
Table 1 shows the drug regimens recommended by
three columns for writing the drugs used,■ dosages
and•
the
National Tuberculosis Programme of India [10,
durations. They were asked to mention the total du11].
All except two of the doctors reported they cmration of treatment for the drug regimen prescribed
indicatc
whether
they
treated
tuberculosis
ployed
modem chemotherapeutic agents for treatment
and also to i-------patients in their clinics. The completed slips were col of tuberculosis. The drugs used by the doctors were
lected on the spot by the investigator and later com among those included in the list of essential drugs
of WHO: streptomycin (S), isoniazid (H), rifampicin
piled.
Table 1 Current (1989) short-course regimens in National Tuberculosis Programme in India’ and their costs in US dollars
No.
Doses
Bulk costs
(US dollars)***
Consumer costs
Regimen •*
1.
2.
3.
2EHRZ/6EH
2EHRZ/6TH
2HRZ/4H2R2
2HRZ/6TH
2S2H2R2Z2/4H2R2
2H2R2Z2/4H2R2
240
240
94
240
52
52
32
23
22.5
17
16
13
52.9
40.7
38.3
35.6
20.4
16.3
4.
5.
6.
S = streptomycin, H = isoniazid, T = thiacetazone, R = rifampicin, E = ediambutol.
:ighing 50* kg. ••The'numbcr before the first letter of a regime is the duration in
• Using dosage schedules for patients wei^._ o
’ of'an intermittent regime. •••Bulk and consumer
months of the phase. The number in subscript is the number of doses each week
costs respectively of the drugs in January 1989.
286
UPLEKAR AND SHEPARD
(R), pyrazinamide (Z), ethambutol (E) and thiacetazonc (T).
Drugs used and dosages
None of the private doctors cither reported thiacetazone as a component of the drug regimens they used
or employed any of the recommended intermittent
drug regimens in their prescriptions.
Streptomycin. 70% of private doctors preferred strep
tomycin which is the only injectable antituberculosis
drug available. For an adult weighing 50 kg, 0.75 g or
1 g of streptomycin per day is considered adequate.
Dosages employed by 58 doctors were correct, 10 did
not specify dosages of streptomycin while 2 doctors
prescribed inadequate doses (0.5g). No doctors used
streptomycin intermittently, all advocating it for daily
use for the first 2-3 months.
Rifampicin and isoniazid. These drugs arc also avail
able in a combination form. All except 3 doctors in
cluded these two drugs in their prescriptions. Seven
did not specify the dosages and 2 used excessive
doses of rifampicin and isoniazid — 900 mg and
600 mg daily respectively — but most of them (88)
employed these drugs correctly in doses of 450 mg
and 300 mg a day respectively. No doctor prescribed
intermittent use of either of these drugs.
Pyrazinamide. 34 doctors did not prescribe pyrazinamidc. Of the 66 who did, 43 used it in correct
dosages (1.5-2 g per day), 13 prescribed an inade
quate dose (1 g per day), 2 employed excessive doses
(over 2 g per day) while 8 could not specify the dose
of pyrazinamide.
Ethambutol. 75 doctors used cthambutol as one of
the antituberculosis drugs in their prescription. 55 em
ployed conect dosages (800 mg or 1 g), 10 used it in
excessive doses (over 1.5 g), 3 prescribed inadequate
doses (400 mg) and 7 did not specify the dose. All
used the drug continuously throughout.
Indigenous drugs. Two doctors used indigenous drugs
exclusively for treating their tuberculosis patients:
one employed homoeopathic drugs and the other ad
ministered ayurvedic preparations. These prescrip
tions were not analysed further.
Drug regimens used
L 11 & -
100 doctors using 2 or more of the 5 major antituber
culosis drugs prescribed 80 different regimens. Only
4 of these conformed with one of the 6 standard rec
ommended regimens. All the others varied with re
gard to one or more of the aspects of a drug regimen,
including the drugs used in the initial intensive phase
and in the continuation phase, dosages employed and
durations recommended. The different regimens pre
scribed by private doctors are classified in Table 2
according to the drugs and durations of the regimens.
Table 2 Drug regimens with durations reported by private
doctors
Number of
doctors
Duration
in months
SHRZE
13
12
4
2
2
SHRZ
5
4
12
9
18
6
12-18
9-12
6
9
8
12
18
12
9
<6
6
9-12
12-18
18
24
12
6-9
9-12
12-18
12
6
6
9
Regimens*
3 li
1
1
SURE
HRZE
IIRZ
HRE
SHR
SHE
SRE
HR
__L- —'Z
7
4
3
1
1
1
1
_L_
8
6
8
6
3
1
1
2
• All doctors using streptomycin employed it for the
initial 2-3 months only. Use of pyrazinamide in the initial
phase of 2-3 months was advocated by 67% of doctors
employing the drug; the remainder recommended continuous use.
Other drugs were reported to be used throughout the duration of
regimens prescribed.
Among doctors prescribing 4-drug regimens, only
26% advocated use of all bactericidal drugs: strep
tomycin, isoniazid, rifampicin, and pyrazinamide.
Ethambutol was a part of 4-drug regimens in 73%
of prescriptions as compared to pyrazinamide which
appeared in 58% and streptomycin in 69% of pre
scriptions.
I
PRESCRIBING BY PRIVATE GPS
I
287
Use of all bactericidal drugs was noted among 57%
of 3-drug prescriptions: 28% of these contained strep
tomycin, replaced in the rest by pyrazinamidc. Ethambutol and pyrazinamide were employed in equal pro
portions of 42% among 3-drug regimens which con
stituted 19% of all prescriptions.
If continuous or appropriate intermittent use of 2
bactericidal drugs for a duration of 9-12 months or
3 bactericidal drugs for 6-9 months or 4 bactericidal
drugs for 6 months is considered adequate, regimens
prescribed by 87% doctors were more than adequate,
those of 8% were adequate and half of these matched
one of the recommended regimens, while 5% doctors
prescribed less than adequate regimens.
least expensive regimen recommended by the Na
tional Tuberculosis Programme is $13 "while that of
the least expensive but adequate regimen prescribed
by a private doctor was $427 Costs of the 6 standard
recommended regimens varied from $13 to $32, with
a mean of $21 while the costs of 80 regimens pre
scribed by 100 doctors varied from $7 to $260 with a
mean of $104.' Thus, besides being less than optimal,
the regimens used by private doctors for treating their
patients with infectious pulmonary tuberculosis were
much more expensive than those considered effective
and recommended under the National Tuberculosis
Programme.
Costs of drug treatment
Comparison between drug regimens prescribed by
allopaths and non-allopaths
The costs of treatment mentioned here do not in
clude doctor’s fees or fees for administering strep
tomycin injection whenever prescribed. Most doctors
practising in these low income areas prescribe ex
pensive drugs and supplement them with vitamins
and tonics. Information about medication prescribed
to the patients other than antituberculosis drugs was
not collected for the present study. The patients buy
prescribed medication from the pharmacists at retail
prices which arc, on average, more than doublccompared to national as well as local bulk prices at which
drugs arc made available to the peripheral tuberculo
sis clinics of the Bombay Municipal Corporation [10,
12].
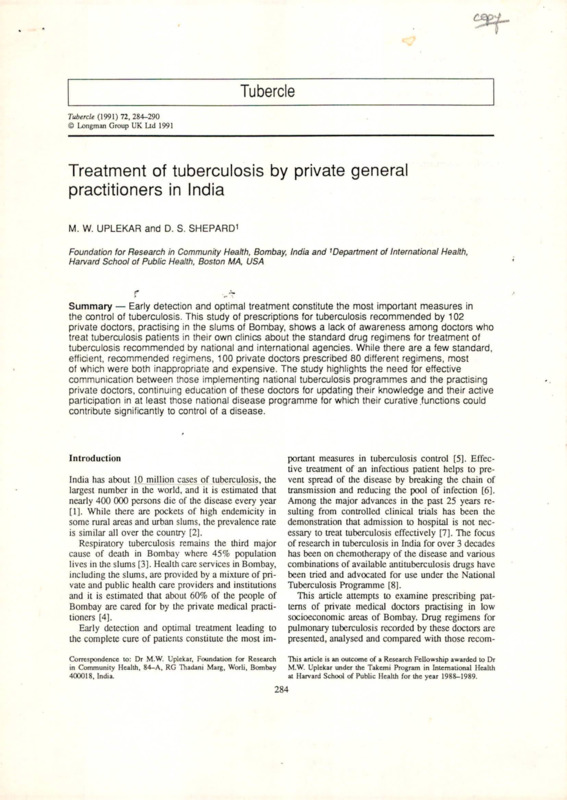
The costs of drug regimens prescribed by the doc
tors varied greatly, as did their prescriptions (Fig. 1).
The costs of standard recommended regimens com
puted after applying the consumer prices and the bulk
prices are shown in Table 1. The total cost of the
50
Figure 2 compares the drug regimens prescribed by
allopaths and non-allopaths.
Drug regimens used. Of the 70 doctors who preferred
regimens containing streptomycin injection, 40 were
non-allopaths. 27% of allopaths chose 5-drug regi
mens and 4 of them prescribed it for over 1 year
while 40% of non-allopaths prescribed 5-drug regi
mens, 15 recommending their continuous use for over
1 year. 38% of allopaths advocated 4-drug regimens,
all prescribing it for less than a year. 52% of non-allopaths also prescribed 4-drug regimens, 2 of them
recommending its duration to be over 1 year. 31%
of allopaths and only 8% of non-allopaths preferred
drug regimens containing 3 drugs. No non-allopath
prescribed a 2-drug regimen though 2 allopaths did.
Costs of drug regimens. 45 of 52 (86%) non-allopaths
and 35 of 48 (72%) allopaths prescribed drug regi-
Number of Prescriptions
40
36
27
30
20
10 4
■
0 -■ w
<50
27
IS
iiih
50-75
12
-L 2
4
o ri
76-100 101-125 126-150 151-175 176-200
US dollars
MB allopaths
LZ3 non-allopaths
Fig. 1 Costs of doctors’ prescriptions. A comparison of allopaths and non-allopaths.
2
>200
&
/OJ|
X it>'
i ; b 0 -
288
UPLEKAR AND SHEPARD
Number of Prescriptions
40
30
■
I
27
20
18
15
13
10
2
0
__ ■■ 0
Two Drugs
Three Drugs
Bi Allopaths
Four Drugs
Five Drugs
Non-allopaths
Fig. 2 Drug regimens used. A comparison of allopaths and non-allopaths.
mens more expensive than the most expensive stan
dard recommended regimen. Prescriptions of 56% of
non-allopaths were more expensive than the mean
cost of all private doctors’ prescriptions as against
those of 33% of allopaths.
Discussion
Very few studies have taken into consideration the
role of private doctors in tuberculosis control [13,
14]. Private doctors are often considered an obstacle
and arc said to have a negative impact on the im
plementation of national disease control programmes
[15]. India has both the largest number of tuberculo
sis patients and a large private health sector. More
over, people tend to prefer private doctors to free ser
vices offered by the government health services [4,
16, 17], Among the poor urban populations, private
doctors are usually the first contact of a patient seek
ing treatment and, since hospitalisation of tuberculo
sis patients is not only expensive but has also been
shown to be unnecessary, the role of a private doctor
who provides domiciliary treatment so convenient to
a patient becomes even more important [7].
It is agreed that the present exercise is a test of
knowledge of a general practitioner about treatment
of tuberculosis rather than a test of his actual practice.
The lack of knowledge and awareness among doc
tors practising in the slums of Bombay about the cor
rect and nationally recommended drug regimens to be
used in the treatment of lung tuberculosis reveals their
ignorance about important advances in the treatment
of a very highly prevalent disease and an absence of
communication between those involved in the imple
mentation of disease control activities and the prac-
tising private doctors. The magnitude of the problem
of tuberculosis in India is such that it is incumbent on
every doctor practising medicine to be able to detect
and treat a case of tuberculosis appropriately. It is
difficult to find a scientific rationale for each of the
80 different regimens employed by private doctors.
The use of correct dosages of rifampicin and iso
niazid in comparison with other drugs may be at
tributed to the availability of a correct type of combi
nation which most doctors prescribe. This highlights
the advantages that drug combinations may offer, if
made available in a form suitable for easy administra
tion, in improving both the patient and the physician
compliance in treatment of tuberculosis. Fox, how
ever, cautions against premature use of triple combi
nations widely available and promoted in this country
in the absense of indisputable data about their pos
sible deleterious effects on the bio-availability of the
constituent drugs [10].
Continuous use of pyrazinamidc was advocated by
33% of those doctors w-ho included pyrazinamidc in
their regimens although efficacy of pyrazinamidc in
the continuation phase of a short-course regime is yet
to be established. This too exhibits ignorance of doc
tors about the scientific rationale of the drug regimens
they were using and their tendency to overmedicatc.
Most doctors used more drugs than required for
treating a case of tuberculosis. Clearly, patients of
most doctors included in the study could receive un
necessarily prolonged chemotherapy if they would
comply. Is there any possibility of the private doctors
using excessive drugs intentionally to achieve rapid
cure for patients, many of whom frequendy change
their doctors? It seems unlikely if the suggested dura-
289
PRESCRIBING BY PRIVATE GPS
lions of the regimens they prescribed are considered.
59 of 77 doctors who prescribed 4 or more drugs had
recommended that their regimens be continued for
over 6 months. About half the doctors were indiscrim
inately using drugs meant for short-course therapy for
long durations of 12 months or more, as advocated
for the conventional drugs used in older standard regi
mens. For most regimens that the private doctors were
using, there is no point in prolonging well organised
chemotherapy beyond 6 months.
An important outcome of research in chemotherapy
of tuberculosis has been the demonstration that inter
mittent administration of drugs, in specific dosages
and intervals, is as effective as giving them contin
uously [18-20]. None of the doctors in this study
used any of the, recommended or other intermittent
regimens. This finding is consistent with Fox’s ob
servation on physicians in the UK who hardly ever
used intermittent treatment as a routine even for the
cases for which it would have proved advantageous
[13]. The reluctance of private general practitioners
to prescribe the much researched and recommended
intermittent regimens needs further investigation.
A general notion is that since they are not ade
quately or as much exposed as allopaths to the prac
tice of Western medicine and judicious use of chemo
therapeutic agents, die non-allopaths tend to overmedicatc and use injections excessively. This is apparent
in drug regimens used by non-allopaths. However,
a closer comparison (Fig. 2) between prescriptions
by allopaths and those by non-allopaths with regard
to drugs used, dosages and durations does not show
any better performance of one group over the other,
both being equally unsatisfactory. It is felt that nonallopaths too must be considered in any attempts to
involve private doctors in tuberculosis control activi
ties.
Much has been written about the cost of tubercu
losis control. In fact, one of the major impediments
in controlling tuberculosis in developing countries is
said to be inability of these countries to earmark
enough funds for mass application of the short-course
chemotherapy [20, 21]. Clearly, the findings of this
study demonstrate the inefficient use of scarce avail
able resources on patients cared for by private doc
tors. This is illustrated by regimens prescribed by pri
vate doctors in this study which, besides being incor
rect, were several limes as expensive as the average
cost of the recommended regimens.
Patient non-compliance is another major hurdle in
effective control of tuberculosis. Estimates in India
indicate that, of every 100 cases in the community,
30 are identified, about 10.5 remain under treatment
for an adequate length of time and that only about 8
arc cured [22]. To the best of our knowledge, studies
on compliance of tuberculosis patients taking treat
ment in private clinics are non-existent It has been
well documented that, in general, doctors’ prescrip
tions are often inappropriate, unnecessary, contain too
many drugs and are unaffordable, leading to partial
filling of prescriptions. The insufficiently informed
health professionals prescribe a number of different
drugs in the hope that one will be effective [23]. The
medical implications of these practices, particularly
in case of diseases like tuberculosis, become apparent
only years later. Studies from many parts of the world
including India show that indiscriminate prescription
of these useful drugs leads to high levels of initial
rifampicin resistance, in addition to high levels of
isoniazid and rifampicin resistance [24], The conse
quences of irregular drug intake and misuse of the
available potent and powerful drugs could be serious.
The important issue is of establishing a meaningful
communication between the private doctor and the
public health services. It is well known that patients
in India mostly report first to a private doctor [2].
Efforts could be made to sec that the private doctors
treat their patients with appropriate regimens and also
that they make reasonable charges. It appears from
tliis study that the private doctors are aware neither
of the recommended less expensive but efficient con
tinuous regimens nor of more suitable and effective
‘supervised’ intermittent regimens that help to ensure
compliance. Doctors could give good treatment for
the initial few months and then, if the patients cannot
afford therapy, they should send them to the public
health service which, in turn should willingly accept
them and be prepared to continue appropriate chemo
therapy rather than turning away the patients as hav
ing had previous chemotherapy. This will, of course,
require input from private doctors as well as from the
public health professionals.
Conclusions and possible interventions
The private doctors serving the urban poor in the
slums of Bombay who treat patients of pulmonary
tuberculosis in their clinics do not consider standard,
cost effective drug regimens in the treatment of pul
monary tuberculosis, including those employed by
the National Tuberculosis Programme of India. This
shows ignorance among private doctors about the effi
cient treatment of a highly prevalent disease of major
public health concern as well as the lack of com
munication between those implementing the National
Tuberculosis Programme and general practitioners. In
290
Ko
light of this, it is important to educate private medical
practitioners to bring and keep their knowledge of
treatment of tuberculosis up to date.
Most private doctors, irrespective of their back
ground and training, use modem chemotherapeutic
agents in the treatment of tuberculosis. Those who
arc trained and qualified in the practice of Western
medicine, as well as those trained in the indigenous
systems, tend to prescribe excessive drugs often in in
appropriate combinations and for periods longer than
necessary. Mere dissemination of information about
drug treatment of tuberculosis may not ensure its im
plementation. Ways need to be considered, such as
adopting national drug regimens, making the neces
sary drugs available to all at uniform prices, and,
at least for the major national disease control pro
grammes, providing appropriate incentives and im
posing sanctions to make private doctors participate
in effective implementation of a programme of public
health importance.
The drug regimens used by private doctors, besides
being less than optimal, were several times as ex
pensive as the standard recommended regimens. This
inefficient use of scarce resources may be avoided
both by continuing the education of private doctors
by experts and by effective use of media and other
possible modes of communication to educate lay peo
ple about the disease, the importance of regularity of
treatment, and the efficient drug regimens to be taken
under a doctor’s supervision. This may also facilitate
effective case finding and ‘case holding, so important
in Die control of tuberculosis, by both public and pri
vate health sectors.
Acknowledgements
The first author deeply appreciates the support of Dr N H Antia,
Director, and Mr Madhu Rokle, Research Investigator, of the Foun
dation for Research in Community Health, Bombay, in designing
and conducting the study. Excellent comments on the earlier ver
sion of the manuscript by Professor Wallace Fox were extremely
useful in revising the paper. We are most grateful to him for his
contribution.
References
1. Health Atlas of India. Central Bureau of Health Intelligence,
Directorate General of Health Services, Ministry of Health and
Family Welfare, New Delhi 1986: 24.
2. Defeat TB: now and forever. Booklet issued by Directorate
General of Health Services, New Delhi, on Silver Jubilee oc
casion of National Tuberculosis Institute, Banglore 1985.
3. Ycsudian CAK. Primary Health Care planning in big cities
with particular reference to Greater Bombay: Published by
Unit for Extramural Studies, Tata Institute of Social Sciences,
UPLEKAR AND SHEPARD
Dconar, Bombay 1984 : 76.
4. Revankar CR, Jha SS, Dongre VV, Deshpande SS, Ganapati
R. Integration of leprosy into general health services in an ur
ban area — a feasibility study. Lepr Rev 1982; 53: 297-305.
5. Workshop Report: International workshop on ‘Research to
wards global control and prevention of tuberculosis with
an emphasis on vaccine development’ Bethesda, Maryland,
November 1987.
6. WHO technical report scries No. 671, 1982: 12.
7. WHO expert committee on tuberculosis. Ninth report. WHO
technical report series No. 552, 1974.
8. Fox W. Compliance of patients and physicians: experience and
lessons from tuberculosis-I. Br Med J 1983; 287: 33-35.
9. MIMS INDIA: Monthly Index of Medical Specialties. New
Delhi 1989; 8(10).
10. Fox W. Tuberculosis in India. Past, present and future. Indian
J Tuberc 1990; 37: 175-212.
11. Chaudhari K. Introduction of short course chemotherapy un
der National Tuberculosis Programme. NTI Newsletter 1987;
23: 104-106.
12. Fox W. Short-course chemotherapy for pulmonary tuberculo
sis and some problems of its programme application with par
ticular reference to India. Lung India 1984; 11(2): 161-173.
13. Fox W. Compliance of patients and physicians: experience and
lessons from tubcrculosis-11. Br Med J 1983; 287: 101-105.
14. Hong Kong Chest Scrvicc/British Medical Research Council.
Survey of the previous investigation and treatment by private
practitioners of patients with pulmonary tuberculosis attending
government chest clinics in Hong Kong. Tubercle 1984; 65:
161-171.
15. Roemer MI. Private medical practice: obstacle to Health For
All. World Health Forum 1984; 5: 195—201.
16. Roth, Gabriel. The private provision of public services in de
veloping countries. Published for the World Bank. Oxford:
Oxford University Press, 1987, 122-157.
17. Uplckar MW. Private doctors and public health: the case of
leprosy in Bombay, India. Nat Med J India 1990; 3: 162-166.
18. WHO collaborating centre for Tuberculosis Chemotherapy,
Prague. A comparative study of daily and twice weekly con
tinuation regimens of tuberculosis chemotherapy, including a
comparison of two durations of sanatorium treatment 1. First
report: the results of 12 months. Bull WHO 1971; 45: 573-591.
19. WHO collaborating centre for Tuberculosis Chemotherapy,
Prague. A comparative study of daily and twice weekly con
tinuation regimens of tuberculosis chemotherapy, including a
comparison of two durations of sanatorium treatment 2. Sec
ond report: the results from 12 to 14 months. Bull WHO 1973;
48: 155-165.
20. WHO collaborating centre for Tuberculosis Chemotherapy,
Prague. A comparative study of daily and twice weekly con
tinuation regimens of tuberculosis chemotherapy, including a
comparison of two durations of sanatorium treatment. 3. Third
report: the results to 36 months. Tubercle 1976; 57: 45^8.
21. Grzybowski S. Cost in tuberculosis control. Tubercle 1987; 68
(supplement): 33-37.
22. Radhakrishna S. National Tuberculosis Program: relative mer
its of enhancing the operational efficiency of different compo
nents of treatment programme. Indian J Tuberc 1983; 30: 3-8.
23. World Health Organization. Report of the conference of ex
perts on the rational use of drugs. Nairobi, 25-29 November
1985. Geneva: WHO, 1987.
24. Trivcdi SS, Desai SG. Primary anti-tuberculosis drug resis
tance and acquired rifampicin resistance in Gujarat, India. Tu
bercle 1988; 69 37-42.
i
i
I
- •
•'
Tubercle
PRESCRIBING BY PRIVATE GPS
Tubercle (1991) 72. 284-290
© longman Group UK Ltd 1991
mended by the National Tuberculosis Programme of
India. The paper highlights the need for effective in
volvement of private medical practitioners in disease
control programmes of national importance so that
they may be more effective.
Treatment of tuberculosis by private general
practitioners in India
Materials and methods
M. W. UPLEKAR and D. S. SHEPARD'
hUMmbar‘
""
o'
H.M,
Summary — Early detection and optimal treatment constitute the most important measures in
tne control of tuberculosis. This study of prescriptions for tuberculosis recommended by 102
Pr'^,8^OCIors,.Prac,isin9 in the slums of Bombay, shows a lack of awareness among doctors who
treat tuberculosis patients in their own clinics about the standard drug regimens for treatment of
tuberculosis recommended by national and international agencies. While there are a few standard
emcient recommended regimens, 100 private doctors prescribed 80 different regimens most
oLwhjChjfltef^JL'O.^
expensfye. The study highlights the needi fbFeffebfive
communication between those implementing national tuberculosis programmes and the practisinq
Private doctors, continuing education of these doctors for updating their knowledge and their active
participation in at least those national disease programme for which their curative funEtFons could
contribute significantly to control of a disease.
ft' (b
Introduction
o
India has about 10 million cases of tuberculosis, the
w“ld-and '* is “a<ed that
m
pcrsons dlc of
discasc every year
, fl
(1).1 Wh.ls.
While .Ivr.
there .ro
arc pockets of high endcmicily. ..inn
I some rural areas and urban slums, the prevalence rate
•
II is similar all over the country (2).
D .
v
Respiratory tuberculosis remains the third major
Bombay where 45% population
population
cause of death in Bjjn^ay
!livesjQUie^lusisJ
——■— i —3i].
’ Health care services ui
in jL^vinuay,
Bombay,
inCllKlinP
an' provided Kxr
including the.
the tlllfTlQ
slums, are
by na mavturn
mixture of pri
vate and public health care providers and institutions
and it is estimated that about 60% of the people of
Bombay are cared for by the private medical practitioners [4].
.■
s
■
Early detection and optimal treatment leading to
the complete cure of patients
constimte the ---------most im--------------------Conetpondence to: Dr M.W. Uplekir, Foundation for Reiearch
Heallh> 84*A- RG 'n'*d*ni Marg, Worli, Bombay
portant measures in tuberculosis control [5J. Effec
tive treatment of an infectious patient helps to pre
vent spread of the disease by breaking the chain of
-------------------------- U1V
transmission
and reducing
the puui
pool Ul
of 1Illcvuon
infection (0J
[6].
Among the major advances in the past 255 years
years re
re-
suI(jng from con[rolled cIinical
285
has ^cn ihc
Analysis
EPMNFO, a software package developed by Centers
for’ Disease Control, Atlanta, Georgia, was used for
analysis of the doctors' prescriptions. The retail con
sumer costs of the drug regimens prescribed by indi
vidual doctors were computed by means of a program
written for the purpose which also converted Indian
rupees to US dollars at an exchange rate of Rs. 15
per dollar (January 1989). Current consumer prices
of antituberculosis drugs were taken from the January
1989 issue of MIMS, India — a privately published
monthly drug index which provides retail costs of
most of the drags available in the market [9], The doc
tors' prescriptions were compared with those recom
mended by the National Tuberculosis Programme of
India. The costs of recommended regimens were also
computed using both the retail prices of drugs applied
to doctors' prescriptions and the bulk prices at which
drags arc made available to the peripheral tuberculo
sis clinics of the Bombay Municipal Corporation run
under the National Tuberculosis Programme.
A list of all doctors practising in a large low-income
settlement of Bombay was prepared by making vis
ible additions to an existing list obtained from the
local medical association. The doctors practising here,
including the members of the local medical associ
ation, are a mixture of those qualified in Western
medicine, who are called allopaths, and those qual
ified in one or more of the indigenous systems such
as ayurveda, homoeopathy and unani, who are called
non-allopaths. All non-allopaths included in the study
had had some exposure to the Western practice of
medicine, either during the formal training in their
respective systems of medicine or thereafter, before
commencing private practice, usually in the form of
an apprenticeship at private hospitals or dispensaries.
A simple random sample of 143 doctors was selected
Results
from the list of 287, irrespective of their ages, qualifications or years of practice. The sample included 79 31 doctors (22%), including 22 allopaths and 9 nonallopaths and 64 non-allopaths.
allopaths, refused participation in the study without
All the doctors included in the study were visited giving any specific reason for their refusal. All those
individually in their clinics and provided a slip with who completed the slips indicated that they treated
a request to 'write a prescription for a previously un- tuberculosis patients in their clinics. The final analytreated adult case of sputum positive pulmonary tu- sis included prescriptions of 102 private doctors, obbcrculosis weighing about 50 kg.’ The slip included tained from 48 allopaths and 54 non-allopaths
---- ---------j
dn]g rcgimens rccommendcd by
three rnlnmnc
columns fnr
for .vo.ina
writing the drugs used, dosages
and
durations. They were asked to mention the total du the National Tuberculosis Programme of India [10,
ration of treatment for the drug regimen prescribed 11], All except two of the doctors reported
1V
U1V emV111.
they
and also to indicate whether they
modem
chemotherapeutic U£VIILO
agents for UV<lUllVllt
treatment
- treated tuberculosis
-------------■ployed
----- —..—...u,..
—■
patients in their clinics. The completed slips were col- of tuberculosis. The drags used by the doctors were
lected on <h„
the spot by, the investigator
and later
com those included in the list of essential drags
u .
among
piled.
of WHO: streptomycin (S), isoniazid (H), rifampicin
demonstration that admission to hospital is not ncc10 trcat tuberculosis effectively [7], The focus
of research in tuberculosis in India for over 3 decades
t_.
'
--------uJ.v.apy ofU1C
has been onv;.v...
chemotherapy
theutscasc
diseasearm
andvanoi
various
combinations of available antituberculosis
drags
ha’
—
-----------I_ J
a ■
. e&o_ ..ave
been tried and advocated for use under the National
Tuberculosis Programme [8],
This article attempts to examine prescribing pat
terns of private medical doctors practising in low
socioeconomic areas of Bombay. Drag regimens for
pulmonary tuberculosis recorded by these doctors are
presented, analysed and compared with those recom-
5.
6.
Hui article i* an outcome of a Reaearch Fellowihip awarded to Dr
M.W. Uplelur under the Takemi Program in International Health
at Harvard School of Public Health for the year 1988-1989.
S = Streptomycin, H = isoniazid, T = thiacetaaxie, R « rifampidn, E = ahmbuioL
•Using douge schedule* for patient* weighing 50 kg. -The
..-Dte number before the first
firn later
letter ci
rf .a regime is
i* the duration in
ctXre^Loi' ? **1 thhednUmberjln
Ihe numbef dowa
week
m,OTnillan regime. •••Bulk md consuner
284
Table 1 Current (1989) short-course regimens in Niuonal Tuberculosis Programme in India* end their costs in US dollars
No.
Regimen ••
Bulk costs
(US dollars)***
Consumer costs
Doses
1.
2.
3.
2EHRZ/6EH
2EHRZ/6TH
2HRZ/4HjRj
2HRZ/6TH
iSj H2R2Z2/4H2R2
240
240
94
240
52
52
32
23
22J
17
16
13
5X9
40.7
38.3
35.6
20.4
16.3
UPLEKAR AND SHEPARD
286
(R), pyrazinamide (Z), ethambutol (E) and thiacctazone (T).
Drugs used and dosages
None of the private doctors either reported thiacctazone as a component of the drug regimens they used
or employed any of the recommended intermiuent
drug regimens in their prescriptions.
Streptomycin. 70% of private doctors preferred strep
tomycin which is the only injectable antituberculosis
drug available. For an adult weighing 50 kg, 0.75 g or
1 g of streptomycin per day is considered adequate.
Dosages employed by 58 doctors were correct, 10 did
not specify dosages of streptomycin while 2 doctors
prescribed inadequate doses (0.5g). No doctors used
streptomycin intermittently, all advocating it for daily
use for the first 2-3 months.
Rifampicin and isoniazid. These drugs arc also avail
able in a combination form. All except 3 doctors in
cluded these two drugs in their prescriptions. Seven
did not specify the dosages and 2 used excessive
doses of rifampicin and isoniazid — 900 mg and
600 mg daily respectively — but mosi of them (88)
employed these drugs correctly in doses of 450 mg
and 300 mg a day respectively. No doctor prescribed
intermittent use of either of these drugs.
4 of these conformed with one of the 6 standard rec
ommended regimens. All the others varied with re
gard to one or more of the aspects of a drug regimen,
including the drugs used in the initial intensive phase
and in the continuation phase, dosages employed and
durations recommended. The different regimens pre
scribed by private doctors are classified in Table 2
according to the drugs and durations of the regimens.
Table 2 Drag regimens with durations reported by private
doctors
Regimes'
SHRZE
SHRZ
SURF,
Number of
doctors
13
12
4
12
9
18
2
2
1
6
12-18
9-12
5
4
6
9
1
1
1
8
12
7
4
3
1
I
1
Pyrazinamide. 34 doctors did not prescribe pyrazi
namide. Of the 66 who did, 43 used it in correct
dosages (1.5-2 g per day), 13 prescribed an inade
quate dose (1 g per day), 2 employed excessive doses
(over 2 g per day) while 8 could not specify the dose
of pyrazinamide.
Ethambutol. 75 doctors used ethambutol as one of
the antituberculosis drugs in their prescription. 55 em
ployed correct dosages (800 mg or 1 g), 10 used it in
excessive doses (over 1.5 g). 3 prescribed inadequate
doses (400 mg) and 7 did not specify the dose. All
used the drug continuously throughout.
Indigenous drugs. Two doctors used indigenous drugs
exclusively for treating their tuberculosis patients:
one employed homoeopathic drugs and the other ad
ministered ayurvedic preparations. These prescrip
tions were not analysed further.
Drug regimens used
100 doctors using 2 or more of the 5 major antituberculosis drugs prescribed 80 different regimens. Only
1
1
HRZE
HRZ
HRE
SIIR
SHE
SRE
HR
Duration
in months
8
6
8
6
3
1
1
2
18
12
9
<6
6
9-12
12-18
18
24
12
6-9
9-12
12-18
12
PRESCRIBING BY PRIVATE GPS
Use of all bactericidal drugs was noted among 57%
of 3-drug prescriptions: 28% of these contained strep
tomycin, replaced in the rest by pyrazinamide. Etham
butol and pyrazinamide were employed in equal pro
portions of 42% among 3-drug regimens which con
stituted 19% of all prescriptions.
If continuous or appropriate intermittent use of 2
bactericidal drugs for a duration of 9-12 months or
3 bactericidal drugs for 6-9 months or 4 bactericidal
drugs for 6 months is considered adequate, regimens
prescribed by 87% doctors were more than adequate,
those of 8% were adequate and half of these matched
one of the recommended regimens, while 5% doctors
prescribed less than adequate regimens.
Among doctors prescribing 4-drug regimens, only
26% advocated use of all bactericidal drugs: strep
tomycin, isoniazid, rifampicin and pyrazinamide.
Ethambutol was a part of 4-drug regimens in 73%
of prescriptions as compared to pyrazinamide which
appeared in 58% and streptomycin in 69% of prescriptions.
least expensive regimen recommended by the Na
tional Tuberculosis Programme is $13 while that of
the least expensive but adequate regimen prescribed
by a private doctor was $42. Costs of the 6 standard
recommended regimens varied from $13 to $32, with
a mean of $21 while the costs of 80 regimens pre
scribed by 100 doctors varied from $7 to $260 with a
mean of $104. Thus, besides being less than optimal,
the regimens used by private doctors for treating their
patients with infectious pulmonary tuberculosis were
much more expensive than those considered effective
and recommended under the National Tuberculosis
Programme.
Comparison between drug regimens prescribed by
allopaths and non-allopaths
Costs of drug treatment
The costs of treatment mentioned here do not in
clude doctor's fees or fees for administering strep
tomycin injection whenever prescribed. Most doctors
practising in these low income areas prescribe ex
pensive drugs and supplement them with vitamins
and tonics. Information about medication prescribed
to the patients other than antitubcrculosis drugs was
not collected for the present study. The patients buy
prescribed medication from the pharmacists at retail
prices which arc, on average, more than double com
pared to national as well as local bulk prices at which
drugs arc made available to the peripheral tuberculo
sis clinics of the Bombay Municipal Corporation [10,
12).
The costs of drug regimens prescribed by the doc
tors varied greatly, as did their prescriptions (Fig. 1).
The costs of standard recommended regimens com
puted after applying the consumer prices and the bulk
prices arc shown in Tabic I. The total cost of the
6
6
9
• All doctor* using streptomycin employed it for the
initial 2-3 months only. Use of pyrazinamide in the initial
phase of 2-3 months was advocated by 67% of doctors
employing the drag; the remainder recommended continuous use
Other drugs were reported to be used throughout the duration of
regimens preschhed.
287
Figure 2 compares the drug regimens prescribed by
allopaths and non-allopaths.
Drug regimens used. Of the 70 doctors who preferred
regimens containing streptomycin injection, 40 were
non-allopaths. 27% of allopaths chose 5-drug regi
mens and 4 of them prescribed it for over 1 year
while 40% of non-allopaths prescribed 5-drug regi
mens, 15 recommending their continuous use for over
1 year. 38% of allopaths advocated 4-drug regimens,
all prescribing it for less than a year. 52% of non-al
lopaths also prescribed 4-drug regimens, 2 of them
recommending its duration to be over 1 year. 31%
of allopaths and only 8% of non-allopaths preferred
drug regimens containing 3 drugs. No non-allopath
prescribed a 2-drug regimen though 2 allopaths did.
Costs of drug regimens. 45 of 52 (86%) non-allopaths
and 35 of 48 (72%) allopaths prescribed drug regi-
Number ol Prescriptions
36
30
20
■60
60-76
76-100 101-125 126-160 161-175 176-200
US dollars
allopaths
fZ_] non-allopaths
Fig. I Costs of doctors’ prescriptions. A comparison of allopaths and non-allopaths.
>200
UPLEKAR AND SHEPARD
288
Number of Preeorlptlon*
40 —------------------------------------
30
20
io
2
0
■i 0
Two Drug*
Three Drugs
■I Allopath*
Four Drugs
Five Drug*
IsjiH Non-allopaths
Fig. 2 Drug regimens used. A comparison of allopaths and non-allopalhs.
using private doctors. The magnitude of the problem
of tuberculosis in India is such that it is incumbent on
every doctor practising medicine to be able to detect
and treat a case of tuberculosis appropriately. It is
difficult to find a scientific rationale for each of the
80 different regimens employed by private doctors.
Discussion
The use of correct dosages of rifampicin and iso
Very few studies have taken into consideration the niazid in comparison with other drugs may be at
role of private doctors in tuberculosis control [13, tributed to the availability of a correct type of combi
14], Private doctors are often considered an obstacle nation which most doctors prescribe. This highlights
and are said to have a negative impact on the im the advantages that drug combinations may offer, if
plementation of national disease control programmes made available in a form suitable for easy administra
[15]. India has both the largest number of tuberculo tion, in improving both the patient and the physician
sis patients and a large private health sector. More compliance in treatment of tuberculosis. Fox. how
over, people tend to prefer private doctors to free ser ever, cautions against premature use of triple combi
vices offered by the government health services [4, nations widely available and promoted in this country
16, 17], Among the poor urban populations, private in the absense of indisputable data about their pos
doctors are usually the first contact of a patient seek sible deleterious effects on the bio-availability of the
ing treatment and, since hospitalisation of tuberculo constituent drugs [10].
Continuous use of pyrazinamide was advocated by
sis patients is not only expensive but has also been
shown to be unnecessary, the role of a private doctor 33% of those doctors who included pyrazinamide in
who provides domiciliary treatment so convenient to their regimens although efficacy of pyrazinamide in
the continuation phase of a short-course regime is yet
a patient becomes even more important [7].
It is agreed that the present exercise is a test of to be established. This too exhibits ignorance of doc
knowledge of a general practitioner about treatment tors about the scientific rationale of the drug regimens
of tuberculosis rather than a test of his actual practice. they were using and their tendency to ovcrmedicate.
Most doctors used more drugs than required for
The lack of knowledge and awareness among doc
tors practising in the slums of Bombay about the cor treating a case of tuberculosis. Clearly, patients of
rect and nationally recommended drug regimens to be most doctors included in the study could receive un
used in the treatment of lung tuberculosis reveals their necessarily prolonged chemotherapy if they would
ignorance about important advances in the treatment comply. Is there any possibility of the private doctors
of a very highly prevalent disease and an absence of using excessive drugs intentionally to achieve rapid
communication between those involved in the imple cure for patients, many of whom frequently change
mentation of disease control activities and the prac- their doctors? It seems unlikely if the suggested dura-
mens more expensive than the most expensive stan
dard recommended regimen. Prescriptions of 56% of
non-allopaths were more expensive than the mean
cost of all private doctors’ prescriptions as against
those of 33% of allopaths.
PRESCRIBING BY PRIVATE GPS
lions of the regimens they prescribed are considered.
59 of 77 doctors who prescribed 4 or more drugs had
recommended that their regimens be continued for
over 6 months. About half the doctors were indiscrim
inately using drugs meant for short-course therapy for
long durations of 12 months or more, as advocated
for the conventional drugs used in older standard regi
mens. For most regimens that the private doctors were
using, there is no point in prolonging well organised
chemotherapy beyond 6 months.
An important outcome of research in chemotherapy
of tuberculosis has been the demonstration that inter
mittent administration of drugs, in specific dosages
and intervals, is as effective as giving them contin
uously [18-20], None of the doctors in this study
used any of the recommended or other intermittent
regimens. This finding is consistent with Fox’s ob
servation on physicians in the UK who hardly ever
used intermittent treatment as a routine even for the
cases for which it would have proved advantageous
113). The reluctance of private general practitioners
to prescribe the much researched and recommended
intermittent regimens needs further investigation.
A general notion is that since they are not ade
quately or as much exposed as allopaths to the prac
tice of Western medicine and judicious use of chemo
therapeutic agents, the non-allopaths tend to overmedicatc and use injections excessively. This is apparent
in drug regimens used by non-allopaths. However,
a closer comparison (Fig. 2) between prescriptions
by allopaths and those by non-allopaths with regard
to drugs used, dosages and durations docs not show
any better performance of one group over the other,
both being equally unsatisfactory. It is fell that nonallopaths too must be considered in any attempts to
involve private doctors in tuberculosis control activi
ties.
Much has been written about the cost of tubercu
losis control. In fact, one of the major impediments
in controlling tuberculosis in developing countries is
said to be inability of these countries to earmark
enough funds for mass application of the short-course
chemotherapy [20, 21], Clearly, the findings of this
study demonstrate the inefficient use of scarce avail
able resources on patients cared for by private doc
tors. This is illustrated by regimens prescribed by pri
vate doctors in this study which, besides being incor
rect, were several times as expensive as the average
cost of the recommended regimens.
Patient non-compliance is another major hurdle in
effective control of tuberculosis. Estimates in India
indicate that, of every 100 cases in the community,
30 are identified, about 10.5 remain under treatment
289
for an adequate length of time and that only about 8
are cured [22]. To the best of our knowledge, studies
on compliance of tuberculosis patients taking treat
ment in private clinics are non-existent It has been
well documented that, in general, doctors’ prescrip
tions arc often inappropriate, unnecessary, contain too
many drugs and arc unaffordable, leading to partial
filling of prescriptions. The insufficiently informed
health professionals prescribe a number of different
drugs in the hope that one will be effective [23]. The
medical implications of these practices, particularly
in case of diseases like tuberculosis, become apparent
only years later. Studies from many parts of the world
including India show that indiscriminate prescription
of these useful drugs leads to high levels of initial
rifampicin resistance, in addition to high levels of
isoniazid and rifampicin resistance [24]. The conse
quences of irregular drug intake and misuse of the
available potent and powerful drugs could be serious.
The important issue is of establishing a meaningful
communication between the private doctor and the
public health services. It is well known that patients
in India mostly report first to a private doctor [2],
Efforts could be made to see that the private doctors
treat their patients with appropriate regimens and also
that they make reasonable charges. It appears from
this study that the private doctors are aware neither
of the recommended less expensive but efficient con
tinuous regimens nor of more suitable and effective
’supervised’ intermittent regimens that help to ensure
compliance. Doctors could give good treatment for
the initial few months and then, if the patients cannot
afford therapy, they should send them to the public
health service which, in tum should willingly accept
them and be prepared to continue appropriate chemo
therapy rather than turning away the patients as hav
ing had previous chemotherapy. This will, of course,
require input from private doctors as well as from the
public health professionals.
Conclusions and possible interventions
The private doctors serving the urban poor in the
slums of Bombay who treat patients of pulmonary
tuberculosis in their clinics do not consider standard,
cost effective drug regimens in the treatment of pul
monary tuberculosis, including those employed by
the National Tuberculosis Programme of India. This
shows ignorance among private doctors about the effi
cient treatment of a highly prevalent disease of major
public health concern as well as the lack of com
munication between those implementing the National
Tuberculosis Programme and general practitioners. In
F
290
UPLEKAR AND SHEPA
r’™S“
Deonar, Bcmbay 1984; 76
R- Integration of Icprosy1mo7eyV’ .I?Csh1pande $$. Ganap.
ban area - a feasib htv n g?Cral heaIth Services a7i
sSSSM- ....
5.
*ards global control and preveX^T^V^
arc trained and qualified in thX °S,S' 771050 who
an emphasis on vaccine defel.^
• .! tuberculosis wit
medicine, as well i hnJ •
°f Wcstcrn
November 1987.
opment Bethesda, Marylan.
6. WHO technical report series No. 671, 1982: 12
systems, tend to present cxc^^ '? thC ,ndi£enous
7. WHO
appropriate combination and for^Slf8.0^" 10 in'
UdmirS^^S”Ninlh repon We
necessary. Merc disseminn.- for_p^nods fongcr than
8.
lessons fXtu^rcX^^X^rf/ioa?’8' experience anc
Of information
drug treatment of tubcrculos^X
lnforniadon about
about
9.
MIMS
INDIA- Month!
7 1983; 2S7- 33-35.
piementation. Ways need to bp
nol,cnsurc its imDelhi 1989; 8(10).
Y n cx of Medical Specialties. New
adoptmg nafional £ug regtome^s
mT^ SUCh 35
be considered,
sary drugs available fo all at untfo™"8
Past’presentandfuture-/ndian
at least for the major nafinnni h f
pnC0S’ and’ 1L SrXrional
^motherapy up.
grammes, providing annrnn • d?scasc control pro
23: 104-106. DCrCUj°S,S Pr^mmc.
Newsletter 1987;
posing sanctions to mZX ? ,"Cenljves ^d im<n effective implementation^3 C doctors Participate
sis and some problems ofTu pro3Py
pulmonary luberculohealth importance.
3 proSrammc of public
ticular reference to Ind.a X
*«* parbeing less^nXXS^re^eve^0"’
13. fox W. Compliant of pau^aXyII(2)’ 16,-173‘
lessons from tuberculosis-II li,
' expenence and
287’ 10,-,°514. Hong Kong Chest SeX ce/Srifish M f
Survey of the previous inv«ripa,
\ ReSCarch
practitioners of patients with’
^atment by Private
Pensive as the standard recommend
S aS
inefficient use of scarce re
dcd reg™ens. This
both by continuing the education of™7
aV0'ded
by experts and bv en>cr
f pnvate doctors
possible modes of comm
USe °f mcdia and other
15.
Pie about the disease th Z^'0" 10 CdUCatc
16
b-eatment, and ScPentT^ °f
P«>of
supervision. nuZTv",
under a doctor’>s ;;™™n
^1'?8‘mCnrObC“
'akCn
effective case finding and case holS S° fac,lllalc
in the control of
i
. 0 (,nS> so lrnportant
vate heahh secto rCU,°S,S' by
pnvatc health sectors.
Acknowledgements
'hebS;P'X>" Of Dr N H Anna.
for Rescan in Comm^pf
Fornand conducting the study Excellent
Bomba-V- ,n designing
-on of the manuscript £ PrO7eSso! wT" r 00
Car,’Cr vcr
useful in revising the paper We are
F°X WCrC MIremely
contribution.
P
We are most g^teful to him for his
References
Directorate General of Hedth 5^7“ M nCalth
2 D7,'y -Se'fare’ NeW Dclhl 1’986- 24 ’
°f Hca,th
Un" f“
Judies, Tau
~
clmlcs-
Fe,
-o
122-157.
±,e"^?7
,St
Up,'!kar UMw
,o leprosy
leProsyi„
,n BombaI8'
B*nk' O’f"d:
““ *
19. WHS cXto^g’ce^XXbT^ ’97^^3L597I
riXXreXTS^
bemotheraPy. including a
comparison of two durations of
»dr„ resull,from
Prague. A XpSve^tudyof da^'and^' ChemotheraPy-
report: rhe resold ro
1 ™rd
21. Grzybowski S rL, . ?
Tuher^ 1976; 57: 45-48
(supplement): SS-Sz"
rC °SIS conIr°l- Tubercle 1987; 68
22. Kadhakrishna S. National Tuberculosis Proa
. ■
its of enhancing the operational nfr •
°8ra,T1- relative mernents of treatment programme 7
°f differcnt compo23. World Health Org^iza ™ReX'’f
’983; 30; 3~8Pens on the ration! use of dX N
of e*1985. Geneva: WHO, 1987
8 ‘
25-29 November
UnXdtqXd ri^mXr a”ti’lubercuIos,s dnrg resisbercle 1988; 69 37^2
“ in Gujarat
resistance
Gujarat,- India
India.- TuTu-
i)
Tubercle andLunv Disease < 1993) 74, 332-337
-0 1993 Longman Group UK Lid
Tubercle and
Lung Disease
Planning and Practice
Private doctors and tuberculosis control in India
M. W. Uplekar. S. Rangan
Foundation for Research in Community Health. Worli. Bombay. India
.S' UMMA R Y. Over three quarters of the 8 million registered doctors in India are engaged in private medical
practice. In urban and rural areas alike people prefer private doctors to public health services for their health
care needs. A majority of patients and those with suspected tuberculosis also report first to private doctors.
Nevertheless private doctors seem to be alienated from national efforts towards control of tuberculosis, there
being no well-defined role for them in the National Tuberculosis Programme. This study of private doctors
practising in the low income areas of a metropolis of India reports on the knowledge of private doctors about
diagnosis and treatment of tuberculosis and their awareness and perceptions about the public health services
available for tuberculosis control.
The study reveals gaps and weaknesses in the private doctors’ reported practice of managing lung tubercu
losis. the most important and persistent problem of public health concern in India. The need for organized
efforts towards involving private doctors in disease control programmes wherein their curative functions could
contribute significantly is stressed.
RESUME. Plus de trois quarts des 8 millions de medecins enregistres en Inde exercent en pratique privee.
En region urbaine comme en region rurale les habitants preferent se faire soigner par les medecins prives
plutot que dans les sectcurs de sante publiques. La majorite des patients et des personnes soupgonnes d’etre
infectes par la tuberculose s’adresse d'abord aux medecins prives. Neanmoins, les medecins prives semblent
eloignes des efforts nationaux de lutte contre la tuberculose. puisqu’il n’existe aucun role clairement defini
pour eux dans le Programme National contre la Tuberculose. La presente etude sur les medecins prives
exer^ant dans les regions economiquement faibles d’une metropole indienne analyse leurs connaissances sur le
diagnostic et le traitement de la tuberculose et sur leur information et perception des services de sante publique
disponibles pour le controle de la tuberculose.
L’etude revele des lacunes et des faiblesses chez ces praticiens en ce qui concerne leur prise en charge de la
tuberculose pulmonaire ; ceci constitue le probleme le plus important et le plus tenace de sante publique en
Inde. Est soulignee ici la necessite d’impliquer davantage les medecins prives dans des programmes de lutte
contre la maladie oil leur action therapeutique pourrait etre d’une grande utilite.
R E S U M E N. Mas de las tres cuartas partes de los 8 millones de medicos registrados en India ejercen en
practica privada. Tanto en las areas urbanas como rurales, los habitantes prefieren ser atendidos por los
medicos privados mas bien que por aquellos que trabajan en los servicios piiblicos de salud. La mayoria de los
enfermos y de los sospechosos de tuberculosis ven primero a los medicos privados. Sin embargo, los medicos
privadios parecen estar alejados de los esfuerzos nacionales de control de la tuberculosis, no existiendo ningun
rol deflnido claramente para eilos en el Programa National de Control de la Tuberculosis. El presente estudio
sobre los medicos que ejercen en las areas de bajos ingresos de una metropoli de India informa sobre sus
conocimientos sobre el diagnostico y el tratamiento de la tuberculosis y sobre su informacion y percepcidn
acerca de los servicios piiblicos de salud disponibles para el control de la tuberculosis.
El estudio revela lagunas y carencias en los medicos privados en Io que respecta al manejo de la tuberculosis
pulmonar. el problema mas importante y persistente de salud publica en India. Se hace entasis en la necesidad
de impiicar mayormente a los medicos privados en los programas de control de la enfermedad. en los cuales
sus funciones curativas podrian ser una contribucion importante.
Correspondence to: Dr M. W. Uplekar. Consultant. Foundation tor
Research in Community Health. 8-1—I. RG Thadani Marg, Worli.
Bombay 400 018. India.
Paper received 22 June 1992. Final version accepted 29 March 1993.
332
Private doctors and tuberculosis control in India
INTRODUCTION
Despite the massive proliferation of government health
services after independence, the private health sector in
India is by far the largest medical sector and is responsi
ble for almost three quarters of ail medical care.1 In rural
and urban areas alike, people prefer to pay fees to a
private doctor — modem or traditional — rather than
obtain free care at a Western-type public hospital.2 Not
much, however, is known about the contribution of pri
vate doctors to improving the health of the populations
they seek to serve. How well do they perform their pri
mary function of providing curative services? What is
their role in the national disease control programmes?
In the absence of a truly effective vaccine, early de
tection and optimal treatment — the primary functions
of a practising doctor — are also the most important
measures for tuberculosis control. Tuberculosis thus
provides a classic example for studying the role of pri
vate doctors in controlling diseases of public health
importance. The National Tuberculosis Institute, re
sponsible for designing, launching and monitoring the
National Tuberculosis Programme, has identified the
involvement of private medical practitioners as a key to
the success of tuberculosis control in India.3 Few stud
ies, however, have looked into the extent of their
involvement in tuberculosis control activities.4-5
This paper examines the role of private doctors in
tuberculosis control. The response of private general
practitioners (GP) practising in low income areas of
Bombay to questions aimed at assessing their knowl
edge and practice as regards the diagnosis and treat
ment of lung tuberculosis, their awareness of the
national tuberculosis control programme and their im
pressions of public health services for tuberculosis
control are presented, analyzed and discussed. Such
information may, it is hoped, contribute to a better
understanding of the present contribution of private
doctors in tuberculosis control, help delineate the re
sponsibilities of private medical practitioners and iden
tify possible ways and means to involve them in the
implementation of tuberculosis control activities as well
as other disease control programmes of public health
importance.
MATERIALS AND METHODS
The island city of Bombay, spread over 603 km2 and
housing a population of 9.9 million, was the location
of the study. The city is predominantly a trading, com
mercial and industrial centre which plays a vital role
in the country’s economy. Since it offers better job
opportunities, there is a continuous influx of rural
migrants into the city who gel absorbed into the poor
ly paying informal sector and settle down in shanty
settlements in all kinds of vacant areas. It is estimated
that about 51% of the city's population lives in such
settlements. One such large low income settlement in
Table 1.
333
The Interview Schedule.
1.
2.
3.
Do you come across tuberculosis patients in your clinic?
Do you treat them?
How many patients of pulmonary tuberculosis are under your
treatment at present? (Stale approximate numbers)
4. Is tuberculosis notifiable?
5. Could you name some other notifiable diseases?
6. What are the early manifestations of pulmonary tuberculosis?
7. How would you manage a patient presenting with productive
cough of 3 weeks’ duration and no other symptoms?
8. How do you confirm diagnosis of tuberculosis in adults?
9. Where do you send your suspected tuberculosis patients for
investigation?
10. How much does it cost to diagnose a case of tuberculosis?
11. What investigations do you perform on your tuberculosis
patients during the course of anti-TB treatment, and how often?
12. What percentage of your patients do you think fail to complete
the prescribed treatment?
13. Could you tell us the two most common reasons for default?
14. Do you refer your tuberculosis patients to municipal or
government clinics? When?
14a. If you do what is your opinion about the public health services?
14b. If not. why not?
15. Could you tell us the approximate average cost of medical
treatment for a tuberculosis patient?
16. What do you know about the National Tuberculosis
Programme?
17. Who updates your knowledge about tuberculosis?
Bombay. Dharavi, which has half a million people
living in an area of one square kilometer, was selected
for the study. Apan from an adjacent teaching hospital,
health care facilities available within this area include
an urban health centre. 3 peripheral dispensaries and
outreach services run by the municipality and numerous
private doctors practising in each of its lanes and by
lanes. A small part of this settlement housing an esti
mated 200 000 people was randomly selected. A list
of all the doctors practising in the area, allopathic
(trained in Western medicine) as well as non-allopathic
(Ayurvedic. Unani, Homeopathic, etc.) was made and a
random sample of 143 doctors was drawn from the list
of 287 doctors. A semi-structured interview' schedule
was prepared by the first author — a practising physi
cian himself — and administered to the selected doctors
by himself and a research investigator oriented in rel
evant aspects of TB and trained and experienced in
conducting private doctor interviews (Table 1). The
recorded responses were later compiled and analyzed.
For a question on the treatment of pulmonary tuber
culosis, a slip was provided for the respondent to fill in
a prescription for an adult, infectious (sputum positive
for acid-fast bacilli), previously untreated patient of
pulmonary' tuberculosis weighing 50 kilograms. These
responses were analyzed separately using EPI-INFO. a
software package developed by the World Health
Organization and Centers for Disease Control. Atlanta.
Georgia, and have been published earlier.6
RESULTS
31 doctors refused interviews without giving any spe
cific reason for their refusal, and 10 doctors could not
give enough time to complete the schedule at one
I
334
Tubercle and Lung Disease
stretch. Completed schedules were obtained from 102
doctors — 48 allopaths and 54 non-allopaths — with
an overall response rate of about 70%. There was no
significant difference between the answer rates of
allopaths (90.97%) and non-allopaths (88.27%). Doctors
were given a choice not to respond to any question if
they so wished. While 26.74% of responses from
allopaths fell into the categories of ‘do not know’ or ‘no
response’, those of non-allopaths falling into these
categories amounted to 47.38%.
Tuberculosis patients in private clinics
All private doctors did come across patients suffering
from pulmonary tuberculosis in their practices and
treated them in their clinics. The number of pulmo
nary tuberculosis patients being treated in a private
doctor's clinic at the time of the study varied from 0-20
(Fig. 1). In response to notification^of cases of tuber
culosis, 25 out of 102 doctors did not know whether
tuberculosis is notifiable, 23 said that TB is not notifi
able, 27 felt it may be notifiable but it is not compulsory
to do so, while 7 chose not to reply. When asked to
mention a few other notifiable diseases, 29 could not.
Others mentioned one or more including smallpox,
cholera, food poisoning, meningitis, diphtheria and
tetanus.
cough mixture and wait for the response before investi
gating further; 11 would dispense only cough mixture,
requesting the patient to report if cough persists; 17
would send the patient off with only a course of anti
biotics. and only 20 replied that they would first inves
tigate the case before starting treatment. The practice of
first treating any patient with a long standing cough for
pulmonary tropical eosinophilia was being observed by
11 doctors. In response to the question about confirma
tion of clinical diagnosis of tuberculosis, the necessity
of performing a Chest X-ray, Complete Blood Counts
(CBC) and Erythrocyte Sedimentation Rate (ESR) was
felt by 99 doctors. Three doctors would rely on X-ray
alone, while sputum examination for the diagnosis of,
tuberculosis was mentioned by only 39 doctors.
All. except for two doctors who employed indig
enous drugs in the treatment of tuberculosis, prescribed
drugs used in short-course chemotherapy, irrespective
of the sputum status of the individual. No doctor men
tioned use of thiacetazone or any of the older standard
Table 2.
Drug regimens and durations reponed by private doctors
Regimens*
SHRZE
80-----------------------------------------------------------------------
SHRZ
60
60
o
u
SHRE
■o
“o
40
5
Z
19
HRZE
Number of
doctors
Duration
in months
13
12
4
2
2
1
12
9
18
5
4
I
1
I
6
9
7
4
3
1
1
1
1
1
6
12-18
9-12
8
12
18
12
9
< 6
6
9-12
12-18
18
24
8
12
6
6-9
HRZ
8
9-12
HRE
6
12-18
SHR
3
12
J Patients
SHE
1
6
Fig. 1—Tuberculosis patients in private clinics
SRE
1
6
HR
2
9
20
11
■
10
2
0
0
1-5
6-10
11-15
16-20
Management of lung tuberculosis
All doctors replied correctly about the early manifesta
tion of pulmonary tuberculosis. When questioned about
the management of a patient presenting with produc
tive cough of over 3 weeks’ duration, 43 doctors said
that they would treat the patient with antibiotics and
•All doctors using streptomycin employed it for the initial 2-3
months only. Use of pyrazinamide in the initial phase of 2-3
months was advocated by 67% of doctors employing the drug; the
remainder recommended continuous use. Other drugs were reponed
to be used throughout the duration of regimens presenbed.
S = Streptomycin; H = Isoniazid; R = Rifampicin; Z = Pyrazinamide;
E = Ethambutol.
Source: Uplckar M W. Shepard D S. Treatment of tuberculosis by
private general practitioners in India. Tubercle. 1991; 72: 284-290.
Private doctors and tuberculosis control in India
regimens in the treatment of pulmonary tuberculosis.
While there are several efficient recommended standard
regimens. 100 doctors prescribed 80 different regimens,
most of which were both inappropriate and expensive
(Table 2). A detailed analysis of the reported presenptions of private doctors for pulmonary tuberculosis has
already been published.6
Costs of diagnosis and treatment
Patient compliance in private practice
Only 7 doctors reported that all of their pulmonary
tuberculosis patients completed the prescribed treat
ment. 52 doctors put the treatment completion rate of
their patients at 50%, 22 reported it to be between
25% and 50% and 21 admitted that less than a quar30
25
25
21
i
•o
j
20
4-1
15
12
10
5
I I I I I I I I I . I n
100-133 140-166 173-200 206-233 240-266 273-300 306-333
Cost in USS
recommended regimens
2.
3.
4.
5.
Perception in brief
Number of Doctors sharing
the perception
Patients are illiterate.
They do not realize the
importance of regular
treatment.
Drugs are expensive. Patients
can not afford complete
treatment.
Patients are careless.
They spend all their money on
alcohol, smoking, gambling.
Patients get better very
soon and do not feel the
need to continue treatment.
Patients are ignorant and
do not bother about the
consequences of not taking
treatment.
32
25
22
20
3
Use of public health facilities
The nearest municipal clinic, which offers both diag
nostic (X-ray and sputum examination) and treatment
facilities to patients of tuberculosis free of charge under
the city tuberculosis programme, has one trained doctors
who visits the clinic twice a week, one treatment organ
izer and one health visitor. The clinic has around 500
registered cases, with an average daily attendance of
about 35 patients.
A large majority of the 91 doctors were referring
only those patients who could not afford treatment in
private clinics and those who wished to use public health
facilities for treatment at municipal or government
clinics. When these doctors were asked about their
opinion of the public health service’s treatment of tuberculosis, 38 doctors put it as ‘average’ and 53 doctors
recorded ‘not satisfactory’ on a 5 point scale ranging
from very good to bad.
11 doctors would never refer their tuberculosis
patients to municipal or government clinics for treat
ment. The reasons they put forward included poor
service (4), bad treatment (2), poor quality of drugs (3)
and non-availability of drugs (2).
Awareness of the National Tuberculosis Programme
2
National Programme
USS 66.6
Table 3. Private doctors' perceptions about the common causes of
patient default.
6
5
0
ter of their pulmonary tuberculosis patients complete
the prescribed treatment. The private doctors' percep
tions of some of the causes of treatment default by
tuberculosis patients are given in Table 3.
1.
Patients suspected of suffering from pulmonary tuber
culosis were being sent for investigation by all of the
doctors to either private laboratones or chantable insti
tutions. and none of them referred the suspects for
diagnosis of tuberculosis to the public health facilities
available in the vicinity. Doctors' estimate of the costs
of diagnosis of pulmonary tuberculosis varied from
Rs.50 (USS3.3) to Rs.200 (USS 13.3). 41 doctors were
observing the practice of referring all of their newly
diagnosed cases to private consultants for advice on
treatment, thus adding to the costs. The most expensive/
shon-course chemotherapy regimen recommended by
the National Tuberculosis Programme cost less than
Rs. 1000 (USS66.6) at the time of the study. A wide
variation was observed among the doctors’ estimates of
costs of drug treatment of pulmonary tuberculosis,
from a minimum of Rs. 1500 (US$100) to Rs.5000
(US$333.3) (Fig. 2). 17 doctors could not give an
estimate.
335
cost
less
than
Fig. 2—Costs of drug treatment of tuberculosis (private doctors'
estimates)
When asked whether they had heard about the National
Tuberculosis Programme,/32 doctors replied in the
negative and the rest in the affirmative. All of those
who replied in the affirmative, however, expressed
their inability to elaborate on their knowledge about
the activities under the National Tuberculosis
Programme.
336 Tubercle and Lung Disease
Updating knowledge about tuberculosis
In response to a question about means of updating their
knowledge on tuberculosis. 67 doctors mentioned me
dical representatives of drug companies as their main
source of acquiring new knowledge on drug treatment
of tuberculosis. 24 doctors relied on conventional text
books, 6 updated their knowledge through lectures and
meetings arranged by medical associations, while 5
chose not to reply to this question.
DISCUSSION
In India, it is common knowledge that although doctors
trained in different systems of medicine are enagaged in
private practice, they are not prohibited from practis
ing any other system in which they are not trained.
As Western medicine, identified with quick cures, is
most popular, most non-allopaths practise allopathic
medicine.
One of the major reasons why studies on private
doctors arc few and far between is their reluctance to
cooperate in providing information related to their
practices, in our past experience, attempts at eliciting
detailed personal information reduced answer rates
j considerably. In this study, therefore, no personal de
tails of any kind were requested. Even the names and
I qualifications of doctors were noted from the name
boards always prominently displayed by the doctors.
Also, since the main objective of the study was to assess
knowledge and practice of all practising doctors treat
ing tuberculosis patients, and not to compare the per
formances of allopaths and non-allopaths. the first
questions asked each doctor were whether he came
across and whether he treated tuberculosis patients in
his clinic; the interview proceeded if the answer was in
the affirmative.
Notwithstanding the fact that utilization of peripheral
government health services in urban as well as in rural
areas is poor, most national disease control programmes
are solely run by and through the public health services.
Few attempts have been made to involve private doctors
in implementing disease control programmes. As a con
sequence, some private doctors are unaware even of the
existence of such national efforts of great relevance to
their own sphere of activity. This is clearly demonstrated
in the present study, where about 30% of the doctors had
never heard of the National Tuberculosis Programme
(NTP). while all of them treated tuberculosis patients in
their own clinics.
The importance of the notification of communica
ble diseases cannot be overemphasized. Private doctors'
laxity in reporting notifiable diseases is known for all
such cases and it is not surprising that none of the pri
vate doctors included in the present study ever reported
a case of tuberculosis. When over 60% of tuberculosis^
patients report to doctors of modem medicine,'" it is
imperative that some effective mechanism for the nolifi-
cation of diseases of public health importance by private
health providers be established and implemented.
Banerji puts the blame of the NTP's modest achieve
ments squarely on the health providers, public as well as
private, who send tuberculosis patients home with bot
tles of cough mixture.7 Less than 20% of the doctors
included in the present study were adhering to the prac
tice of first investigating a case of chronic cough before
instituting definitive treatment: the remaining majority
prescribed non-specific symptomatic therapy hoping that
the patient, if he failed to respond, would return.
Overdependence of private doctors on chest X-ray as
the diagnostic tool for pulmonary tuberculosis is note
worthy. Il is likely that this may lead to overdiagnosis,
overmedication and wastage of short-course chemo
therapeutic drugs on patients who may not need such
treatment. This aspect needs to be investigated further.
Use of sputum examination fbr confirmation of clini
cal diagnosis of pulmonary tuberculosis by only 39
doctors highlights not only their ignorance of the value
of this simple test in clinical practice but also their
indifference to the public health implications of the
sputum status of a tuberculosis patient. This is also
demonstrated in their blanket application of shoncourse chemotherapy to all cases of pulmonary tuber
culosis. Another probable reason for most of the
doctors' dependence on X-rays for diagnosis may be
because, being more expensive, the X-ray could prove
to be financially more viable to the referring doctor
than the cheaper sputum examination - especially in
cases where there is some financial arrangement be
tween the doctor and the diagnostic centre. This may
also be the reason why none of them prefer to refer
patients for investigation to the nearby public health
facilities where both these tests are offered free of
charge to the patient.
While the most expensive anti-tuberculosis treatment
regimen recommended by the National Tuberculosis
Programme, applying retail prices of the drugs at the
time of the study, cost less than Rs. 1000 (US$66.6), al)
the private doctors estimated the cost of drug treatment
of tuberculosis to be over Rs. 1500 (USS 100) (Fig. 2).
The observation that most doctors were prescribing
short course chemotherapy for a longer than necessary
duration possibly explains their overestimate of the cost
of tuberculosis treatment (Table 3). This practice is not
only an inefficient use of scarce resources but could also
adversely affect the compliance rates of low-income
patients.
No information is available on treatment completion
rates of tuberculosis patients seeking treatment in pri
vate doctors’ clinics. Il is reasonable to expect improved
compliance from patients taking treatment from their
preferred providers. Estimates of treatment completion
rates of their patients reported by the doctors themselves
are contrary to this expectation, most doctors staling
that very few of their patients completed the prescribed
treatment. The doctors, however, have pul the blame of
default entirely on the patients themselves (Table 2). As
Private doctors and tuberculosis control in India
was to be expected, none of the doctors had any mecha
nism for tracing the defaulters and putting them back on
treatment, since they neither recorded the patients’ com
plete addresses, nor did they utilize their clinic assist
ants, when they had any, to visit the defaulter/.' The
private doctors' concern about the problem of patient
defaulting and the imput they could provide to mini
mize this problem is another area which merits further
investigation.
A tuberculosis:.panent referred by any private doctc/
to the public health service is treated no differently from
anyone presenting to the clinic directly, and no record of
the referral source of patients is mainrainetl. Looking at
the poor utilization of public health services and the low
opinion doctors have of them, no links appear to exist
between private doctors and public health services/
both’ of which on the contrary condemn each other
respectively for money-mindedness and inefficiency.
Much could be written about the training conditions
of doctors in India. The poor performance of private
doctors clearly shows the inadequacy of their under
graduate as well as in-practice training. The content
and quality of undergraduate training with regard to
diseases of public health importance leave much to be
desired, but elaboration on these aspects would be out
of the scope of this paper. One fact deserving mention
here is the total lack of any organized effort at provid
ing continuing medical education for practising doctors./
a situation which is further accentuated by the fact that
no system for the renewal of practice licences exists
here. It is regrettable that many doctors have to depend
on drug company representatives to update their knowl
edge of therapeutics, a task that could be very effec
tively undertaken by their own associations and medical
colleges, as well as by the programme managers of the
national disease control programmes.
It is evident that private doctors cannot be wished
away, as the people themselves opt for their services,
but at the same time they must not be granted total free
dom to act as they see fit without heeding the wider re
percussions of their actions. What can be expected of
private doctors if they do not see any place for them
selves in tuberculosis control activities: if the public
health sendees do not even attempt to reach out to them
and attempt collaborative efforts: and if no incentives
are provided for conducive performance nor sanctions
imposed for actions detrimental to the health of the
people?
In the virtual absence of any collaborative effort be
tween private doctors and public health services, several
specific areas for mutual cooperation could be identi
fied. These include inviting representatives of private
doctors to participate in the planning process of tuber
culosis control activities: involving them in case-finding
activities within the areas of (heir practice; providing
them with free or subsidized diagnostic facilities;
making drugs available, at least for the poorest patients
diagnosed and referred by private doctors, at the public
337
centre, or supplying drugs to individual doctors on sub
mission ot reports and records and perhaps undertaking
the verification of the proper use of durgs; and to
improve case holding, providing them with educational
material and the services of a social worker for impart
ing health education, motivating patients to complete the
prescribed treatments and tracing defaulters. Adequate
orientation and training of private doctors on various as
pects of tuberculosis control, and the vital contribution
they could make in facilitating it. must precede the un
dertaking of any specific interventions and continue on a
regular basis. Unfortunately any attempts at involving
private doctors in tuberculosis control are conspicuous
by their absence today. Pilot experiments employing
strategies aimed al eliciting doctor participation could
provide the much needed information on the strengths
and weaknesses of private doctors in contributing
meaningfully to tuberculosis control.
There is a need for better communication between
private doctors and those implementing disease control
programmes. It is unreasonable to expect private doctors
to follow appropriate clinical and public health practices
without adequate knowledge of the correct ones. The
commercial interests of private practitioners may not
always come in the way of obtaining their cooperation
in a few specific disease control programmes to begin
with. In the case of tuberculosis in particular, where (he
experience of private doctors could significantly con
tribute to disease control, the wider public interest must
take precedence over the narrow concerns of private
doctors.
J
i
l
Acknowledgements
The authors are deeply erateful lor the support of Dr N. H. Antia.
Director, and Mr Madhu Rokle. Research Investigator, of the Founda
tion for Research in Community Health. Bombay, in designing and
conducting the study.
References
1. Duggal R. Nandraj S. Shelly S. State sector health finance — A
Database: All India. The Foundation for Research in Communitv
Health. Bombay 1992: 12.
2. Roth G. The private provision of public services in developing
countries. Published for the World Bank. Oxford: Oxford
University Press. 1987: pp 122-157.
3. Defeat TB: now and forever. Booklet issued by Directorate
General of Health Services. New Delhi. Silver Jubilee of the
National Tuberculosis Institute. Bangalore: 19X5.
4. Fox W. Compliance of patients and physicians: experiences and
lessons from tuberculosis - II. BMJ 1985: II: 161-173.
5. Hong Kong Chest Sen ice/British Medical Research Council.
Survey of the previous investigation and treatment by private
practitioners ol patients with pulmonary tuberculosis attending
government chest clinics in Hone Kone. Tubercle 198465: 161-171.
6. Uplekar M W. Shepard D S. Treatment of tuberculosis by private
general practitioners in India. Tubercle 1991: 72: 284-290.
7. Banerji D. Tuberculosis as a problem of social planning in India
NIHAE Bulletin. 1971:4:9-25.
a
- Media
 RF-TB-2.15.pdf
RF-TB-2.15.pdf
Position: 2806 (5 views)