COMMUNICABLE DISEASES
Item
- Title
- COMMUNICABLE DISEASES
- extracted text
-
RF_DIS_1_A_SUDHA
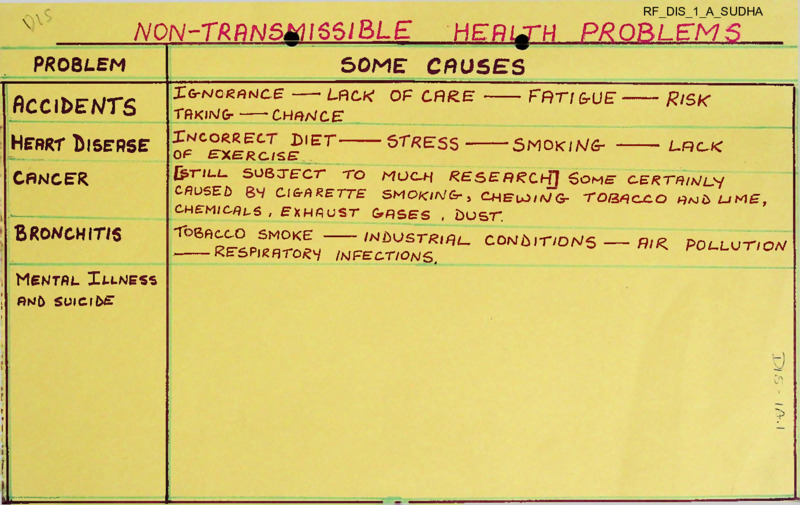
N0N-TRRNSkH65lBLE
x
HERt^TH PROBLEMS
SOME CRUSES
PROBLEM
flCCIbEA/TS
Z^o/ZMCE---- - LACK OF CARE ------ FFtrfGrUE
taking- — chance:
Heart Disease
opCi^Cal^'ET
CANCER
{jp-TIL-L.
Risk
SMOKiWfr ------- L.PKE-K
j-W..,, , ■ ......... ................ ..................
Bronchitis
TO
MOC-H
RESEARCH] SOME C.ERT^/f^l_y/
CAUSED
ClGrRRETTE SMOKlNGr^ C^BuJtN/GCHEMiaRL-S , EKMUST GtRSES , bOST.
1 >----------- ——.................... ..
1
SOBTFCT
i
T bacco smoke
RFSPl^ATC)^^
/ndustt^ial.
/MFEC.TIONS,
TOQ^CjC.O A?ajD LJM£,
comlit/ons__
- A//<
POL.LUT/OA/
i Mental Im-ness
j
AND SUICIDE
I
i
1 1
l
i •
►
! .
r
(
i
E
!l=____
cn
?
HOOK WCRM
HOOK WORM disease is the infestation of very small worms in the
intestines.
The worm is called
'hookworm'.
A hookworm sticks to
the walls of the small intestines with the help of its teeth.
There it feeds mainly on human blood.
The hookworm disease by itself very rarely causes death.
But it makes its victim lazy and lethargic.
Regular loss of
blood may produce serious complications in the patient who may
thus fall a victim to other diseases easily.
Though the disease effects all age groups, it is common
among children. It is prevalent more in areas where people have
the habit of going outdoors for toilet or otherwise bare-footed.
Symptoms:
Hookworms, if present in any significant number, produce
continuous loss of blood in the human body. This condition
is responsible for the commonly observed symptoms like laziness,
muscular weakness, dull skin, dry hair and a constant feeling of
being hungry.
Children having hookworm are pale and thin.
They get
tired easily and do not feel like playing. They will not grow
as they should.
If it is a serious case, the child may have
dull eyes and pale gums.
Some parts of his body may swell.
The doctor can make sure whether the patient is really
suffering from hookworm disease or not through laboratory examina
tion of the patient's stool.
How the Disease spreads?
The actual organisms that cause the disease are the
thousands of eggs laid by the female hookworm in the intestines of
the person suffering from this disease. A female hookworm can lay
up to 15,000 eggs a day. These eggs pass out along with the stools
of the natient and are deposited on the soil where the patient
defecates. These may be scattered to nearby soil by rains and wind.
Where the soil is particularly sandy, moist and warm, these eggs may
develop into larvae within 24 hours.
These larvae usually find their way back into the human
body through the skin of the bare-foot of the person who goes to
defecate in the open or walks bare-foot.
The retention of wet
soil or mud in the toes greatly favours the larvae's entry into the
human body.
... 2
2
When the larvae bites the skin in an effort to enter the
body, it sets up an intense itching and inflammation known as
’ground itch'. The hole made is so small that the victim never
knows that a hookworm larvae is entering his body. Once inside
it makes its way through the flesh to the blood veins and eventually
into the lungs.
Here it may produce lung inflammation which is
often mistaken for pneumonia.
From the lungs, a hookworm may crawl up into the throat
of the victim to rest, but is swallowed back into the small
intestines, where finally, it stays and grows into adult hookworm
capable of laying eggs.
Sometimes, the larvae may also enter the body through
contaminated food and water.
But mostly, it enters through
the skin. It takes about six weeks for the larvae that have
entered the body to become egg-laying adult hookworms. They
excrete a poisonous substance which tends to make the tiny
blood vessels, to which they are attached, swell up and burst.
They move from one place to another in the intestines, having
bleeding sores behind. This chain of the hookworm's life may
continue unless it is broken.
Treatment:
Regular practice of sanitary measures is the only successful
way of getting rid of hookworm disease. This will break the chain
of the hookworm's life-cycle. Houses should be fitted with
sanitary latrines. Defecation in the open should be avoided.
Children should not be allowed to play bare-footed. They should
always wear shoes before going out. Thus, when infestation cases,
the worms will disappear from the intestines.
eradication may take up to seven years.
But their complete
The patient must consult the doctor immediately when
hookworms are suspected. He should not treat himself.
Drinking water should not be taken from a doubtful source.
It should be boiled before drinking.
Foods should be protected
from contamination.
Remember
* Hookworm enters the body through the bare-foot.
* Hookworm mainly feeds on human blood.
* The eggs of hookworm are passed out along with the stools
of the patients. They are hatched when deposited on a
sandy, moist and warm soil.
* Do not defecate in the open.
Use of sanitary latrines will
break the chain of the hookworm's'life-cycle.
* Do not go outside bare-foot.
Make children wear shoes
before going out.
* Get stool examined for hopk worm disease.
* Take ■treatment qq doctor’s advise nnb'
FOUty-BORNF DISEASES
1. ...Diarrhoea
2. Dysentry
J. Typhoid
4. Paratyphoid
5. Cholera
6- Food poisoning
7. Tuberculosis
8. Brucellosis
9. Undulant fever
10. Worm infestations, eg. round warns,
thread worms, trichandua spiralis etc
11. Leptospira haemorrhagica
12. Poliomyelitis.
1J. Lathyrism
14. Epidemic dropsy
15. Ergotism
Food allergy : occurs among some persons due to acquired or inherent, dissynchhracy. Usually the allergic manifestations eg. gastrointestinal upset, uoticui-lu
or asthma are due to protein in the food and therefore foodstuffs which cause
allergy are mostly fish, eggs,- prawn, milk, cheese etc.
food may serve as a vehicle in transmission of diseases.
Food sanitation :
1.
Milk hazard.
excellent food and ideal culture I’icd-inn.
Dirty milk a major health
Warm surrounding favour : growth of-Bacteria. In Urban areas, where the milk is
pooled from various.sourecu before distribution. Contaminated milk samples from
a single source may contaminate the complete stock of milk.
Milk borne diseases are
1. Those due to salmonellae organism
2. Those due to ahigellae organism
3. Those due to staphylocci organise
4, Those due to streptocci eg. sorethroat, scarlet fever.
5. Diphtheria
6. Tuberculosis
7. Poliomyelitis
. 8. Undulant fever
Sources of milk borne diseases ,
--------------------------------------------------Dirty udders of cow
Dirty fingers of milker
Dirty utensils and bottles
Flies
Droplet infection from Milkman otc.
Milk sanitation :1.
2.
Animal should be; clean and healthy as certified by vetemary doctor.
Dairy farm to be clean. 3. Milker free from illness eg. open T.B.,
typhoid, sorethroad or staphylococci eg. boils and abscesses + clothing,
personal cleanliness and nails. 4.Utensils - for storage and transportation
clean + sterilized. 5. Pasteurization - destroys most organisms. Does not
destroy spore forming organisms.
Meat and: fish -
uncovered and left meat.■ Growth of
1. gangrene causing organisms
3. worm infestations
Sanitation :-
3. Oysters - typhoid
4. Infection due to fingers and flies
1. Animals
2. Inspection of cut meat & fish
3. Rapid transportati.on
•Fruits and vegetables
4. Proper storage
5. Correct preservation
6. Ad equate cooking
If eaten raw - poor culture media -
1. Choebic dysentry; . 2. Worn infestations - round worms + thread worms.
proper washing preferably in the KHNO.. Steaming if necessary.
Droppings of rats and mice - leptosp.ire. haemorrhagica.
Prevention of dietary infections
1.
2.
3.
4.
5.
Choice of food -fresh, free from infestations
Storeage and transport. + Preservation, cool dry place protected from relents-.
Kitchen staff
strict hygienic practices free from illness and i-ifecr.iohs.
Water - Boiled
’
7. Use of effective pesticides.
Sanitary conditions
work place + utensils. 8. Row to use only approved
HeaxtH. .educa i~ ion
cl'enic- ls for Vreservi ng or
■ so. addi'i i.y«r.
FOOD POISONING
Injurious offset of food may he due to different causes and gives use
to symptoms of Acute Gastro-Enteritis.
I.
Chemical :
a)
b)
c)
d)
e)
f)
Antimony in Enamel, wore in contact with fruits/acids dissolves out
Zinc from galvanised articles.
As from harmful colouring matter.
Pb (lead) from soldered utensils
Insecticides in food grains
Commercial acids used in manufacture of Bees.
II.
Parasites or their Cysts like Tape-worm Cysts
III.
Bacteria : 1. Salmonella Group causing Salmonellosis or Acute Gastro
Enteritis e.g. a) Entoritidis
0
from
. S-. Typhimurium Q Ducks, eggs & partially cooked meats
b)
. •'v : - '
e.g. Sausages.
Thcco organism are nonsporing and Thermolabile. The symptoms appear after
about 8 hours as severe pain, vomiting, diarrhoea and collapse.
B, Morgan! and Proteus
Bact. Flexneri
B. Coli
Stapphylococcus which may contaminate Food,. Milk, Milk
Products Cakes, etc., due to Staphylococci from the skin,
nose or throat or from the cow's udder if some lesion is
present. This is usually due to an Exotoxin which
multiplies in.the food/milk before ingestion and sometimes
known as Toxin Type, or poisoning.
6. Cl. Botulinum giving rise to Botulism. It produces a potent
toxin and contaminates, fruits and vegetables. Canned and
pickled foods are sometimes the source as Cl. Botulinum is an
anaerobic sparing organism. Symptoms mat be immediate or
delayed after 12-24 hours and are very serious like nervous
disorders or vision and dysphagia to be differentiated
from Belladonna poisoning. Paralytic iteus may occur and
then failure of the heart and respiration.
2.
3.
4.
5.
IV.
Food poisoning may be also caused by poisonous fungi e.g. toadstools
mistaken for mushrooms.
Investigations to be carried out in an outbreak of food poisoning.
Source of infection. Food, milk, cakes etc. to be determined. Food sample,
of suspected--.food to be taken and examined bacteriologically also aerobic and
anaerobic cultures to ba made and examined. Stop further consumption of
suspected food and sale of the same food/milk.
2. Note time interval. When F.P. is caused bv living Infective Bacilli the
incubation period is longer since time for the Bacilli to multiply.and
cause sign. If symptoms appear rapidly, it is due to be preformed Toxin
the food e.g., tinned foods.
3. Agglutination tests may be positive with known culture.
4. Examination of Vomit/Faeces in the acute stage for Bacteria.
1.
Prevention of Food Poisoning
Prompt refrigeration of sliced meats, pastries, custards and cream fillings
to prevent any staphylocci from multiplying.
2. Exclusion from food handling of persons suffering from pyogenic infections
of the hand or skin.
3. Education of food handlers, cook otc, in hygienic standards in preparation
and. storage.
4. Extermination of Rodents from kitchens and stores.
5. Prevention of human carriers e.g. in Salmonella infections.
6. Food should be covered. Left overs avoided.
7. Proper canning and Preservative methods of food.
1.
I I f,
'i.''
ii
ORAL DEHYDRATION
CHOLERA, Gastro-enteritis and other diarrhoeal diseases
lead to much loss of fluid and salts from the body.
This
condition is called dehydration and it often leads to
death if not treated promptly.
One can easily identify a case of dehydration.
The
following are the signs:
The patient has extreme thirst, sunken eyes, shrivelled
finger-tips. He has also rapid pulse and breathing.
In infants, sinking of the soft spot on the head is a
sign of extreme dehydration.
In a case of dehydration, it is necessary to replace the
lost fluid and salts from the body as early as possible.
This
process of replacing the lost fluid is called rehydration.
This can be done by giving early the rehydration solution.
The development of this oral glucose electrolyte
solution therapy for rehydration marks a major achievement in the
treatment of all diarrhoeal diseases. The solution can be prepared
with the following ingredients, in amounts indicated against each
item.
Sodium chloride
3.5 gm
Sodium Bicarbonate
Potassium chloride
2.5 gm
1.5 gm
Glucose/anhydrous
20.0 gm
Drinking water
1 litre
Caution: The solution should not be heated or boiled.
Infants and younger children should be given small
quantities of the solution-two to three tea-spoon-fuls by mouth
after every five to ten minutes.
Older children and adults should
be given as much fluid as they like. Infants should also be
given their usual diet, such as breast milk, cereals, etc.
There is no need to wait for diarrhoea to stop.
Normal feeding
should be continued.
The child should never be starved.
Rehydration solution prepared once should not be used
longer than 12 hours.
In case of need, the solution should be
prepared afresh and this can be kept for use for the next 12 hours
only.
If a patient shows such symptoms as suppression of urine,
cramps in the joints and loss of consciousness, he should be
immediately referred to the nearest health centre or a doctor for
advice and treatment.
2
REMEMBER
A patient of cholera ant4 other diarrhoeal diseases loses
a lot of fluid and salts from his body. This might be a danger
to his life. This can be prevented by giving the patient
rehyc’ration fluid along with normal feeding.
Rehydration solution should be prepared from items
purchased only from registered pharmacists and approved
medicine stores.
The solution once made out of these items
should not be kept for more than 12 hours.
The ingredients used for making the solution can also
be had from the Primary Health Centres.
Source: Swasth Hind - August 1979
‘
ft • "3
CHW-C 1
CHAPTER 2
Smalioox
2.1
Identify cases of fever with rash and report then to the Health
Worker (lale)
Srallpox is an infectious disease in which the rain symptoms are
fever accompanied by a characteristic rash. This rash a.ppears mainly
' on the face, upper limbs and lower limbs end is scanty on the trunk
(see slide S ,F. 1)
The rash must be distinguished from that of chickenpox which is
mainly found on the trunk (see slide S .P. 2)
Srjallrox spreads rapidly from person to person by direct contact
and by contact with articles which have been infecte--’ by small pox cases.
In India smallpox has been eradicated, but you must be alert and
inform the Health Worker (hale) immediately whenever you see any case
which resembles smallpox.
2.2
Inform, the Health Worker of infants aged zero to one year requiring
primary vaccination as follows:
•l-n t'oc intensive area inform the Health Worker (Female)
In the twilight area inform the Health Worker (lale)
lipox can bo prevented by ensuring that every infant is
protected by vaccination as early as possible after birth.
If you come across any infant in your area who has never been
vaccinated against smallpox, inform the Health Worker (lale/F'eraale)
so that he/she can arrange for giving vaccination.
2.3
Assist the Health Worker (riale/Female) in arranging for primary
vaccination
You can assist the Health Worker in arranging for primary vaccination
in the f oilowing ways:
1. Tell the mothers that their children need to have primary
Vaccination to protect them against smallpox.
I
•
2.
Instruct the mothers to bathe their babies before bringing
them for vaccination.
3.
Collect all unprotected infants at a central place at the tine when t
the health Worker is to visit the area.
4» Follow any instructions given by the Health Worker during the
vaccination.
2.4
Follow up cases who have been given primary vaccination.
You should visit each infant or the day after it has been
vaccinated to reassure the mother if the child has fever and to ensure
that nothing is applied on the vaccination site. Visit the child again
4 to 9 days after vaccination to see whether the vaccination has been
successful. The usual course of a successful vaccination is as follows:
1 . Between 3rd to 5th day
2. Between [.th to 9th day
* Between 11th to 12th day
3
4- Between 14th to 21st day
- Blister forms
- Blister becomes larger and pus forms in
blister
- Scab forms
- Scab falls off.
Noto: If the vaccination is progressing normally, do not. interfere
.with it. If it .is infected or there'are any unusual roadt? or.S; refer the
infant to th.
• ir
*" "
,
ft
- 2 -
Educate the cornunity about the importance of primary vaccination
2.5
In your talks with the people in the community, stress the follow
ing points:
.
1.
It is important for every person to be protected against
smallpox by vaccination.
2.
Vaccination is harmless and practically painless.
3
• The vaccination site should, be eared for as follows:
a) Leave it uncovered
b) Do not wash it for 24 hours
c) Do not apply anything to it, eg., ointments, herbs, oils, etcd) Prevent the. child from scratching the site and make sure that
the child’s finger nails are cut short.
4« If there is no reaction by the 6th day the vaccination will have
to be repeated.
/////////
ms
: 15 :
2.
The occurrence of a disease which, is rurally absent fror.i
the area, c.g., if cholera ncroally doos not occur in an
area-and one case of cholera occurs, then a cholera epidemic
is on.
.............................
EFH®ilCiTY- -IS, THEREFQE,- RELAT-IVE- -TO THE USUAL FREQUENCY- CF L DISEASE- ■
III THE ARSA.________ __________________________________________________________
Vigilance against the canon conrunicable and infectious diseases
is an essential component of public health, particularly in areas where those
infections prevail. It is, therefore, necessary that you keep accurate records
of the occurrence of those diseases to be able to know when their incidence
increases or decreases.
.
IT IS ESSENTIAL THAT YOU KNOW THE SIGNS WHICH INDICATE A DISEASE OUTBREAK SO THAT YOU CAN MOBILIZE l£> EARLY LS POSSIBLE PREVENTIVE MEASURES
TO LIMIT- THE SPREAD OF TIE DISEASE. IT IS ALSO -VITAL THAT YOU KNOW HOW
THE FAJTICULAK DISEASE Sil EAES.____________________________________________
Certain diseases are listed as notifiable, i.c. their occurrence
rust be immediately notified to the Medical Officer of the Rrir.’ajy Health
Centre'.
Make sure that you arc familiar with the list of notifiable
diseases in the State in which you are working.
■THE -MAIN FURKSE CF NOTIFICATION IS TO JUT INTO OPERATION AS SOON AS
ICSSIBLE MEASURES TO PREVENT THE DISEASE FROM SPREADING.
7.1
CHOLERA.
Cholera is a notifigtlc disease and as soon as a case is detected
it r.iust be notified immediately to the Medical Officer cf the Primary Health
Centre.
7.1.1
IDENTIFICATION
Cholera is a serious acute intestinal disease.
following signs and symptoms:
i.
ii.
iii.
iv.
Lock for the
Sudden onset of profuse watery stool (rice water stool).
Vomiting
Rapid dehydration (loss of elasticity of the skin).
No fever
”
v. Collapse.
REMEMBER -THAT- BOTH TJ® STOOL AID- THE -VOMIT- ARE INFECTIOUS AID MAY TRANSMIT
THE DISEASE.
7.2
STALL-IOX
Smallpox in India is under control but vigilance r.ust be
maintained to detect any new cases. The disease is characterized by a
skin rash and lias been described in section 18.2.2.
According to current standing instructions, every case of
suspected s: allpox must be seen b. senior experienced Government and World
Health Organization staff.
7.2.1
INDErZTIFI CATION
The patient develops a characteristic rash cn the skin. The
skin r.-sli is preceded by signs and syr’.ptor.is winch reach be on attack cf
’
’
Veho. oevt--.
c’-'.c'a
■'
: "16 :
When the. skin rash appears after two to four days, it is identi
fied ly the following characteristics:
The rash is r?.orc abundant on the face and lihbsthan on the
trunk, i.o. the rash effects aostoly the uncovered parts
(see fig? 7.1a and I).
ii • Fever•
iii. Sore threat.
iv. Backache and 1 cdy ache.
v. Frontal headache.
vi. Restlessness end1 doliriun
i.
Chickenpox rash
S-, 'adlpox ■ rash
Fig: 7.1a:. Srallj'ox rash and cliickcnpcx rash
BEMEMBER THAT THE DISEASE 'IS TRAI'felffTT®-BI CLISE COMTACT WITH THE
RESPIRATORI- DISCHARGES- OF- -FATIE1ITS a© THROUGH MATERIALS WHICH HAVE ■
BEER COIiTAMIHATED BI IUS ARD SCABS FROM THE SKIN LESICUS.
7.2.2
CCUTFfL MEASURES
As scon as you see a patient with a rash suspected to l.o
srallpcx take the following steps:
Ropirt the suspected case i "cdiately to the Medical Officer
(IHC)
ii. Infor.’, your Supervise r ir odiatcly.
iii. Isolate the patient- Tf th< -r.ti"V.t is seen in his ?’ -'.e, 1
i.
: ?7, :
Chickenpox rash
Smallpox rash
Fig. .7»1b: Srallpox rash and chickenpox: rash
..................
GET THE CCQJERATION OF THE COMMUNITY LEADERS TO HELF YOU. On HO ACCOUNTS
MOST ANYBODY ENTER OR T.E/.VE THE HOUSE AID THE FAT1ENT MUST BE CONFINED
TO THE HOUSE ._________________________________________________ _________________
With the help of the Health Worker (Fc- ale) and your supervisor
vaccinate all the vil logo co: "unity.
v. Assist in the disinfection of all the -.’atorials which have been
in contact -wt-th the patient.
e .■_____________________________________________________________________________
FCLLCW THE -EISTRUCTIOIIS -OF- THE DOCTOR- AID- -KRT-ICUA^E -FULLY- MET-H THE
CCIUAIiiMEliT TEAM TO LIMIT THE SPREAD OF THE DISEASE . ____________________
iv.
vi.
With the help of the Health Worker (Fo/alo), carry cut a health
education program: o to increase awareness about the incidonee
of st allpox in the cor. r unity.
At the end of Voluro II of this Manual j'flu will find a card
showing a baly with s:'allpox rash. Show this card tc people in the
octiamity and ask if there is any case like this in the village.
THE EIC-rT TC ERADICATE SMALLFCK IS STILL GOING OH AID HAS HEALED ITS
FI UAL STAGES.
niBLICIZE WIDELY THE INCENTIVE OF Rs.1,000 WHICH THE GOVERNMENT LAYS TO
ANYBODY RETORTING L CASE CF SMALLFCX TO THE AUTHORITIES . THIS INCENTIVE
■IS COHSIDERE> -I-MFORTANT- -III THE -FINAL EF-FOFT- -TO ERADICATE SMAILFCX -IN - ■
■INDIA..____________ ___ .______________________________________________ __
PLAGUE:
7.3
ELa.guc is an infectious disease transmitted tc human icings through
the 1 itc of a flea which lias icon infected by a plague-infected rat cr other
rodent. In rural areas, wild rodents trans;it the infection tc each other
through file 1 ites and, therefore, keep a focus of plague infection alive.
These infective rodents "ay puss the infection onto the domestic rats which
live in cr near houses. From then the infection spreads tc human Icings.
PLAGUE IS TRANSMUTED BY THE BITE CF All INFECTED FLEA, HA1DLIIIG OF TISSUES
CK- HJS OF -INJECTED RATS, AID- BY INFECTED- DROPLETS- CR- SPUTUM FROM -PATIEIJTS
SUFFERING- FRCI-1 I1EUMC1EC HAGUE .i
7.3.1
IDEITIFIGAEIGn
The sings and symptoms ef plague arc'nth local and general.
fcr the following.
i.
ii.
iii.
iv.
v.
Lock
Swelling of the glands in the groin cr armpits.
Small skin haci ’.orrhagos which lock like red spots
Fever.
Restlessness, : cntal confusion and, in sone cases coma.
Staggering gait which : akes the patinet walk like a drunken person.
VERY OFTEN THESE SYMPTOMS, .ESPECIALLY III THE EARLY STAGES, ARE MISSED AID
THE PATIENT IS TREATED FCR A GLAND. INFECTION. THEREFORE, ENQUIRE AS TO
WHEE-EF. OTHER CASES WITH SIMILAR SXMtfW ^MuTHE-SAME AREA HAVE CCCURED.
IF SC,
PLAGUE MUST BE SUSPECTED .
vi.
‘ '
. .
■
Signs of jncui'lohia'develop as the disease progresses.;----
WHEN PNEUMONIA- DEVELOPS THE SPREAD OF THE DISEASE IS RAPID AND SEVERAL ■
CASES OCCUR III A SHORT THE WITH SIGHS AID SYMPTOMS OF PNEUMONIA.________
The confirmation of plague can be i ado only ly laboratory investi
gations. It is, therefore, very important to fenfirm. the presence of plague
early in orlcr tc take emergency ■ .ensures and start treatment. Early treat
ment reduces the mortality rate, which is very high in pneumonic cases.
7.3.2
COUROL MEASURES
As so'-n as you. sec a patient suspected ti ho suffering from plague,
proceed as follows:
' ' '
i. Notify the bfedical Officer (IHC) im:odi?.tely.
ii'. Infer.’, ycur supervisor•
j.-ii . Isolate the patient. The isolation rust ho very strict in cases
of pneumonia and no person should bq allowed near the patient
until the dcctcr secs him and gives further instructions.
iv. Collect all sputum and other discharges in containers, if possible
in a disinfectant solution.
v. Girthing which has- Loen in contact with the patient should bo
disinfected.
vi. Educate the community and tell them hew the disease is spread,
particularly stressing the importance cf the flea in transmission
- -of the disease
CARRY- ‘CUT ALL £HE -INSTRUCTIONS
VISOR III CCHTAIIilRG THE SPREAD OF HAGUE.
vii.
DCCTCR -AID HELP YOUR SU-IER....
Usually the area is closed for travellers and people are not
allowed to leave or enter the area for about a week from the last
confi Tv.ncl daHC •
: 19 :
Iiriunization with plague vaccine should Le carried cut to
contain the infection and protect the local co;r:unity.
ix.( Measures to control the rat population arc carried cut.
x. Destruction of fleas Ly spraying with DDT is an important
........................... c-cntrol- measure-.-................• •
- ■
• -................................................
viii.
BOTH YOU AID THE HEALTH WORKER (FEMALE) HAVE A ROLE TC ILAY FARTICUL/J1LY
•El HEA-ITB -EJUG/.-TIC1L H-MUIJIZA-T-IC-I-!■ RAT 'CONTROL - A-HD DDT- STRAYING OIERATIQITS.
REMEMBER, IF All UNUSUALLY LTxGE NUMBER OF DEAD RATS ARE SEEN AROUND
HUMAN HABITATION'S. YOU SHOULD NOT ALLOW lEOHE TO TOUCH THE'I. RETORT
THE FACT- -TC- YOUR- SUIERVISCR- -WHO WILL ARI ANGE FOR THE DEAD RATS TC- BE EXAMINED FOR LEAGUE.___________________________________________________
■
7-4 POLIOMYELITIS (INFANTILE IARALYSIS)
Pclioryclities affects minly children ’ ut adults gf any age
got the disease. The virus which causes the disease is transmitted 1 y direct
contact with the throat secretions of infected persons, and.pcssi1 ly by the
cental’ination of food with infected faeces •
OVERCROWDING A1!D BAD SANITATION ARE, THEREFORE, THE MAIN FACTORS IN THE
SIREAD CF rCLIOMYFITIS .
’
__
7-4.1 IDENTLET CATION
It is difficult to detect the- disease in its early stages
V&eeusc the signs and" symptoms resemble those of an attack- of influenza.
However, when the paralysis sets in and the child is unallc to move the
affected limb freely, medical advice is usually sought. When the disease
affects the upper part of the spinal...cord, thepationt is unable to breathe
and unless quick treat:.ent is given in a hospital, death results.
The disease is identified Ly the following signs and symptoms.
Icralysis of a litb (arm or leg), usually on one side only.
The paralysis is accompanied l.y wasting of the v.uscles so
that the limb looks thinner and is colder then the other one.
iin. Headache.
iv. Sono stiffness of the neck Int not complete rigidity.
v. Fever and slight sore throat .
. .
i.
ii.
THE SIGHS A® S-YMITOMS MAY-A.-PIEAR- -IN -ISOLATED CASES (R- A NUMBER CF CASES
MAY ATIEAR AT SHORT INTERVALS.__________________________________________
7.4.2
CC1TRCL MEASURES
When you sec a child with paralysis of a lirl and symptoms
which resemble a cold, poliomyelitis should bo suspected. Rrococd as fellows:
i. Send the child to the Fri: ary Health Contie without delay.
ii. Keep a very close watch on the other children who have Loen
in contact with the child j especially schccl children.
iii. Inform your supervisor.
iv. Inform the school teacher that the child is suspected to have
poliomyelitis and request him. to inform, you immediately if
any child is absent from school because of sickness.
IT IS NOT USUAL TO COSE THE SOICCLS UNLESS THE EITDEI-ilC IS K SEVERE CHE.
IT IS EASIER TC WATCH TIE CHILDREN AT SCHCCL AID DETECT EARLY SIGNS CF
DISEASE THAN TC- IET- -T-HHI MIX- -AID FLAY TOGETHER- AWAY- -FROM SCHCCL -WHERE CLOSE
SURVEILLANCE IS 1’CT ICSSIBIE,
CHUI—C I
CHAPTER 3
Commuficable Diseases.
Communicable diseases are those which are transmitted from man to
man or animal to man directly, through infected materials or through
insects. Seme of the common communicable diseases include cholera,
typhoid, smallpox, malaria, filariasis, leprosy, tuberculosis, measles,
common cold, trachoma and sexually transmitted diseases.
3.1
Inform the Health Worker(Male) immediately an epidemic occurs in
his/her area
When a disease occurs in an area where it does not normally occur or
when there arc more than the usual number of cases, an epidemic is
established.
Be alert to err, increase in the number of cases in your area with
the following sig s and symptoms?
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
Diarrhoea, vomitting, jaundice and passing worms
fever with or without rigors
Rash with fever
Cough and cold
Disch irgirrg eyes
Discoloration of skin with loss of sensation
Stiffness of neck
Lockjaw
Paralysis or weakness of limbs in children
Sore on the genital organ with or without discharge
Report epidemics immediately to the Health Worker(Male) so that
the recessary action can be taken to prevent spread of the disease.
3.2-
Take immediate precautions to limit the spread of disease
While waiting for the Health Worker(Male) to arrive you must yourself
take certain measures to limit the spread of disease.
These irrlude the following?
Precaution to be taken
Signs/Symptoms
3.2.1
Diarrhoea, vomitinn, jaur.-.'ice
and passing worms
>
1. Where sanitary latrines are nut
available sec that the stool &
vomit are buried so that flies
do not settle on them.
2.
See that any soiled clothing or
linen of the patient is washed,
boiled and dried in the sun
3.
Tell the community members to boil
water and milk before cf 1 king
4.
Chlorinate all drinking water
sources
5.
Those caring for the patient
should not handle the food of the
family and should wash and dry
their hands after caring for
the patient
6.
See that all food is covered to
protect it from flies
7.
Hands should be washed aftor
defalcation and before handling
food
8.
Sec that all eating utensils
especial!' those used by the
°
c 2
the patient
3.2.2.
fever with or without rigors
1. Isolate
3.2.3
Rash with fever
1. Isolate the patient
2. Keep the patient in bed
in a darkened room
3. See that any dressings which
have been in contact with
the patient arc burned or
buried
4. See that soiled clothing
or linen of the patient
is washed, boiled and
dried in the sun
3.2.3
Cough and cold
1. Isolate the patient especially
from young children
2. Teach people not to spit or
clear the nose indiscriminately
3. Teach people to cover the
nose when sneezing or coughing
3.2.5
Discharging eyes
/
\•
1. Ensure that no one else uses
the patient's towel,
handkerchief or surma stick
2. Teach people not to allow
flies to settle on the
eyes and face
3.2.6
Discolouration
3.2.7
atiffness of neck
1. Isolate the patient
3.2.8
Lock jaw
1. Keep the patient in bed in a
quiet place
3.2.9
Paralysis or weakness of limbs
in children
1. Keep the patient in bed
2. Where sanitary latrines do
not exist, see that the stool
is buried so that flies do
not settle on it«
Sore on the genital organs
with or without discharge
1. Tell the patient to avoid
sexual intercourse until
cured
3.2.10
skin with loss
1. Isolate the patient especially
from children
Start treatment of those signs and symptoms which arc within your
competence to treat. Soe Chapter 11 for details.
3.3.
Educate the community about the prevention anti control of communicable
diseases
There are certain steps which can be taken in order to prevent communicable
diseases from occurring. You should educate the community about the need for
taking the following measures!
1.
Immunization against tuberculosis, diphtheria, uhoopin ■'ough,
tetanus, poliomyelitis, smallpox, cholera and typhoid
2.
Proper disposal of solid waste, liquid waste and refuse
3.
Safe drinking water
4.
Latrine construction
5.
food hygiene
♦
-
8 3 s
6.
Control of mosquitoes, flies and other insects
7.
Control of rats
8.
Destruction of stray clogs
9.
Prevention of overcrowding
10.
Personal hygiene and clean habits
In addition you should tell the community to inform you immediately
there is a case with any of the signs or symptoms mentioned. You should
teach them what speci ic precautions they should take to control the spread
of disease.
pc
////////
V Main, IBIlgk
X Koramcngala
Bangalore-5fifJ34 -/
India
.
'Dr-"J. A.54
INSURING ONE ANOTHER AGAINST DISEASE.
THE RAHA EXPERIENC E.
-z
V v’
The Need
India has the highest mortality rate (1
Asian countries,
and the infant mortality rate
39/1000) among all
is still around 129/1000,
Although there is a significant improvement in the health situation,
accompanied by a substantial growth in manpower and instiutions,
inequalities between geographical areas,
the
social classes and between
urban and rural populations remain unacceptable,
The 'initials are one of the most neglected rural populations, and
serious sickness does not only mean an almost unimaginable degree of
human suffering, but also economic ruin since they'll often have to sell
or mortgage cattle and fields in a belated, mostly ineffective effort
to save their relative.
The underlying causes of this situation need to be analysed, but
this is not our purpose here.
Rather than curse the darkness, let us
Right a candle.
Can the poor ensure themselves?
T'rom our past experience in RAHA,
we are. inclined to answer-this
question with a clear "YES",(if the scheme is built on THREE PILLARS.
These three basic prerequisites can be listed as follows:
1
~ A great number of people must take part.
This is easy to understand.
a
burden which will crush a few, can
be carried more lightly by many.
2--
There must be a great stress on prevention.
All effective means must be used,
and everybody's cooperation
enlisted to prevent people from falling sick.(60% of diseases are
preventable).
Every group that takes part, must be actively engaged
"
in preventive and protective measures under the guida,nce of the nurse
and village Health Promoters.
3-
A spirit of solidarity should be the main motive.
This last element is often over-looked, but it is as essential
as the previous two.
worth,
If everybody tries to get back his money's
irrespective of his medical need,
to fail.
the whole scheme is bound
Every group that can develop a minimum of mutual trust
and an attitude of service,
should be able to do it.
solidarity is not the monoply of Christians,
A spirit of
although it may
imply Christian values.
How is it done in RAHA( Raigarh ^wbikapur Health Association)?
RAHA was started in 1969 but remained rather dormant.
onwards,
i'rorn 1974
it develped itself into a. community based, preventive-
oriented health service.
It serves a population of predominantly tribal people in Surguja
and Agigaxh districts of ^astern Madhya Pradesh.
It tries to
coordinate the work of 3 base-hospitals and 47 rural Health Centros
(2-8 Bed facilities)
staffed by trained nurses-midwives..
2
t
The most characteristic development has been the Village Health
promotors '1'raining Programme.
-^uring the past ten years,
been trained for more than 1000 villages,
approximately 400,000 people.
and work as volunteers.
VHPs have
serving a population of
,
They were selected by the villages,
^very health centre has two to four supervi
sors who act as liasion between health centre and VHP, play a support
ive role and also assist with protective and educational, health
activities(immunizations, mother-child clinics,
etc.)
The nurses conduct monthly follow-up meetings for all the VHP of
their catchment area.
(For further details, kindly refer to the report of 198J "Tribal
Community health")
The Medical Insurance acheme of R/iH/jM.I. S. )
Historical ■development.
It is important to note that the M.I.S. began only after a very
intensive compaign towards community health with stress on educati^
More than 5 years of training village Health Promotors
and prevention.
together with motivation and orientation of the nursing staff preceded
the start of the M.I.S.
^ven then we made the initial mistake of focussing on insurance for
hospitalisation,
since that was the most crucial problem.
There was
very little or no response because nobody wanted to be hospitalised.
proposal for " local treatment" insurance scheme got a better
response.
Our ability to
"double" the contributions of the people
was a strong incentive to both health staff and people.
In the beginning however people did not have the slightest ideal
wah.t "insurance" could moan for them,
and how it had to function.
Therefore the membership fee was kept extremely low.
■“fter three years of operation, most people have began to seeWie
.tremendous bonef its( they were regularly kept informed), and now they
also begin to sec the practical requirements to come toasel%upporting
scheme.
The fees could gradually be raised,
f.iG value of "rice",
and have now been linked with
so that there is no longer need to change every
year.
How does the M.I.S. function at present?
The first thing to understand is that we work"in a two-tier system.
The "local insurance" fund at health centre level is called the
Samaritan Fund.
purpose:-
’
to finance all preventive, protective and curative expenses
of the health centre,
and
to foster early treatment,
independent of economic condition
( when the patient does not have to pay at the time of
treatment he/shc will bo inclined to come earlier)
Collection:
1.
Chiefly from membership fees
- once a year to be paid two months in advance
3
31st January when on 1st April MIg starts(late-comers •.
e.before
i.
pay double)
through the village health promoters who record the names of all
the members,
and forward them to the nurse in cash or kind.
the value is fixed, but they can pay in any form
per person
unborn children are insured together with the mother.
abuse,
the whole family should become members.
To avoid"
i»hen there are
more than six persons ina nuclear femily~(parents, children,grandparents)conccssions can be given to those in excess of six.
2.
incidental other sources
from
donations,
3.
campaigns,
fairs, lotteries etc,
even the members p-.y a nominal Rs.0.50 to
Registration foes:
avoid abuse.
nount
i*
of membership fee
each health centre can decide for themselves,
In principle,
practice,
in
they all want a common directive.
Repeatedly changing the fee is disturbing and not favoured.
Therefore the fee is fixed in relation to a common market
the value of two kilos of rice per person per
commodity e.g.
year.
This allows for minor local, variations,
fosters early collection
and will show a yearly increase in real value.
h’.B.
To ea^ the psychological parting,
part in the scheme,
every family that this year take,
can receive a small bottle pf iodine free of
cost(which in turn can prevent a lot of infectaH
wounds)
Eligibility
Those who belong to the economically weaker section,
of caste or religion,
solidarity,
measures.
irrespective
but who can be trusted to join in a spirit of
and are ready to take part-in the proposed preventive
The presence of an active VHP is therefore essential.
Management of the fund.
The fund are kept at health centre level, but the members are
regularly informed through the VHP.of expenses incurred/income received.
For the first-few years, RAHA has been able to double every rupee
that is collected by fees.
If the fund is insufficient to last a whole year, restrictions can
be agreed upn (
EXCLUDE tonics,
vitamins or part /full payment for
injections)
The Samaritan Fund is not just an insurance schemes.
a catalyser for community participation.
It acts as
It is the change-over
from the old system of health care where everyone pays for himself and
consequently was limited to those who can pay,
to a self-reliant
community health care system which includes the poor because each -one
pays for the other,
and the others pay for him.
In the old system,
those who had enough,
there was no end to the line of sick and only
could afford to pay for our services while the
4
poor either got ruined by these services or had to be satisfied with
Now through the Samaritan Fund we see the sick
lesser services.
diminish in number and the poor can benefit equally because all share th
It is an implicit invitation towards concern for one another
burden.
and gives our health institutions the opportunity to serve those for
whom they originally started.
Central Fund/Hospital -deferral Scheme.
This forms the second tier, because without this the M.I.3. would
not be complete,
the top of the broad-based pyramid would be missinp
Part of the money collected at the health centre level (Samaritan Fund)
is paid into the Central Fund from which under certain conditions the
major share of the hospital bills of members can be paid.
Conditions for referrals
1.
Only those who have paid their contribution to the Samaritan Fund,
2.
two months earlier, can
. benefit from the
scheme.
Besides being a member, there must be an active VHP in the villfOl
who regularly attends the follow-up meetings and has to fill in a
form showing the care that has been taken to prevent the disease,
if applicable.
3.
The health centre has to have a sufficiently qualified and experi
enced nurse who effectively takes care of both preventive and
curative needs.
method of Acferral?
Normally a sick person first reports to the VHP who,
"rises,
when the need
informs the nurse or sends the patient to the health centre.
depending on the case,
the nurse has then to decide whether the patient
need's to be referred to the doctor.
The patient comes to the OPD of the hospital, with a RZJiA
a
referral form on which the nurse has written the essential data of the
case' + treatment given.
hand.
The patient also comes with k-s.100/- in
In case the patient is too poor to collect this amount,
the
nurse who refers has to pay or advance the money from Saneritan Fund.
If treated in OPD only,
the patient pays up to Jxs.100/-,
the
balance above this is paid by the Central Fund.
If admitted by the doctor,
as his share of the bill.
the patient pays also only ^s.WO/-
Ridin pays the rest up to Ks.1000/-
No individual acquires the right to be
referred or to be admitted.
■“nd only the doctor decides when and how long the patient shall be
admitted.
The patient arranges for his own food and shall be
accompanied by a companion who sees to this and other needs.
Limitations;
No case, resulting from a criminal action(abortion, fight)should
be given a RAHZ. referral form.
Individuals already covered by another Insurance Scheme( v. g. Govt.
servants)- should apply to that scheme and not to RAHn.
5
Ko case, older than one month,
should bo givei/a RAHA referral form.’.
(i'.B. Patients are covered by another supplementary programme)
K.B.
as anyone will realise
These regulations are not yet perfect,
but they
provide a framework which is sufficient to operate.
Pan the M.I.S, become self-supporting?
-
at the health centre level
with a competent nurse, who enjoys the confidence of the people
there is no real problem if the patients pay individually.
Our question is: can it be done if people pay collectively?
The answer, based on our experience in RAHA,
is yes,
if you build
on the throe pillars mentioned earlier.
The real cost of treatment for the whole community can be kept low,
if people take an active part in prevention
If they report early, or are detected early
If treatment is started
without
*
delay
If nurses and people are gradually educated towards, .a low-cost and
rational drug therapy
If all protective mep.sures( immunizations,
etc)are used
If herbal remedies/inexpensive home-remedies are used judiciously
~t the hospital level
here I can give accurate figure of the last three years(see appendix)
although the last few months,
we have seen a rather sharp decline in
the number of patients referred(due to a growing awareness among
doctors and nurses), we can rightly assume to get about 500 referral
cases per year(in the J base-hospitals) a,t an average cost of h.s.400/
per patient.
This means we need a yearly collection of Ks.2,00,000/-
"t the present rate of contribution from the Samaritan Fund
(Rs.2/- per person), we therefore aim at 100.000 members.
Given the number of VHPs(approx.1400),
we need only an average of 71.
members to be recruited per VHP(or 12 families).
■* is time passes, people begin to realise the enormous benefits and
numbers are increasing quite satisfactorily.
Here again,
very much depends on
- the understanding and the cooperation of the doctors and hospital
authorities
- the smooth relations between hospital and health centre staff
- the increased diagnostic skills of the health centre staff which
makes early referral possible.
- whether the transport expenses to the hospital can be subsidized.
THE RAHA INFRASTRUCTURE
Village Health Promoters
RAIGARH
DISTRICT
SURGUJA
DISTRICT
TOTAL
983
44-4
1,42.7
VnP Supervisors
59
21
80
Reg.Nurses, RM
31
5
36
"UX.Nurses, M
16
19
35
Dioc.Hoalth Coordinators
2
2
4
100 Beds , . . _n
f‘nbi 1 20
50
"
IcaPur
3
Hospitals
1
Kunkuri
Raigarh
JMJ
Population covered
by RAHA
Total Population of
the district
300,000
100,000
400,000
1,250,000
1,250,000
2,500,000
MEDICAL INSURA NCE SCHEME
Membership total:
•
2000
1980/1
1982
-
10000
1983
-
37000
1984
-
45000
1981 *
RAHA patients referred
-
1982
1983
300
551
-
1984
711
594
2156 Total
BIAAS PAID BY R.JiA
HC-KUNKURI
HC-AMBIKAPUR
RAIGARH JMJ
50,487.95
26,477.25
15,081.00
1982
1,17,076.40
38,694.75
27,336.00
1983
1,76,904.05
79,889.65
29,780.00
1984
1,33,365.50
34, 293.29
16,493.00
4r77r823x2Q
1x72x254x24
88^690^00
1981
TOTAL:
RS:
•
pi.s •' j.a-io
SRI CHINNASWAMY MUDALIAR MEMORIAL TRUST
ENDOWMENT LECTURE
ON
11TH MARCH 1990
"HEART DISEASE - AN OVERVIEW"
BY
DR.V.PARAMESHVARA *
BANGALORE
Mr President, Mr. V.C.Ramachandran, Ladies and Gentleman,
I appreciate the significant honour that the trustees of Sri Chinnaswamy Mudaliar
Memorial Trust hav$ bestowed on me by inviting me to deliver the endowment
lecture this evening, I am proud of the fact that I belong to the band of illustri'tis orators who have preceded me.
The Late Sri Chinnaswamy Mudaliar was a distinguished son of the soil, who has
contributed tremendously towards construction, growth and development of Banga
lore.
Lofty and prestigious buildings bear testimony to his vision and stateman
ship as well as his involvement in the health and welfare of the people. Hence, 1
thought it appropriate to speak on the subject which has become number one
killer in all age groups.
The subject is "Heart Disease - An Overview".
India has the dubious distinction of having the disease and health problems
of both developed apd developing countries.
The case in point is the modern
epidemic of heart diseases.
Rheumatic fever and rheumatic heart disease are
major causes of mortality and morbidity especially in young people.
It has been
estimated that rheumatic fever is the most common cause of heart disease in the
5-30 years age group.
Its prevalence amongst children between 5-15 years is
in the range of 6 per thousand with regional variations.
It is common knowledge
that rheumatic heart disease is typically associated with poverty, poor housing
and overcrowding and the disease has declined throughout the century in indus
trialised societies.
The prevention of rheumatic fever is certainly possible
by early effective treatment, which makes it one of the most preventable cardio
vascular diseases.
The Government should commit itself by appointing a National
Programme Co-ordinator for rheumatic heart disease and also make necessary
budgetary provisions.
Ischaemic heart disease (Heart attacks) is emerging as the most important heart
disease in recent times. Unchecked, the epidemic is threatening to engulf the
whole society in the very near future resulting in incalculable damage.
It is
estimated that by the turn of the century, life expectancy of an average Indian
will be in the range, of 64 years and no doubt, at the rate of demographic tran
sition it could assume an alarming public health dimension.
It is feared that
if present conditions persist, every second person born alive, will die from heart
disease.
The disturbing trend is younger age groups
are
being affected by
coronary artery disease (Heart Attack).
....2
*
54, Kumarakrupa Road, Bangalore - 560 001.
2
Economic advance and changing life styles appear to be primordial causes.
The
sheer size of the problem, the early onset and insiduous development of narrowing
of arteries, provide sufficiently strong reasons to mandate the taking of immediate
steps towards prevention.
The prevention
towards
of
ischaemic
Heart
Disease
(Heart
Attack)
should
be
directed
1. Population Strategy : For altering the life style and environmental charac
teristics .
2. High Risk Strategy : For bringing preventive care to individuals at special
risk.
3. Secondary Prevention : For averting recurrences and progression of disease in
those already affected.
4. Primordial Prevention : Preventing the emergence of predisposing conditions
in regions in which they have not appeared.
The problem has to be seriously tackled by adoption of healthier life style
and environment, screening to identify the disease in its early stages, bringing
preventive care to individuals at special risk and secondary prevention in known
cases.
The Government
responsible for the health of the public, should straight away
garner adequate information on current life styles and prepare time bound action
goals.
It is imperative to formulate a national plan for prevention and control
of heart diseases and also to establish appropriate communication and co-ordination
with other departments, particularly those dealing with food policy, education
and public information.
Government and national medical and voluntary associations should declare a joint
committment towards a tobacco smoke free society.
The whole problem has to be tackled on a war footing and an approach that
emphasises the intervention to change the whole community by health education
and matters such as nutrition and eating patterns, low fat dairy products, changed
diet in institutions, prohibition of smoking, physical activity at work and leisure,
and special training of health personnel.
Use of mass media in health education is an important cost effective method
to enhance community participation.
Mass media experts learned in behaviourial
sciences and health communication skills must be included in this programme.
The need of the hour is better doctors than more doctors, better health education
than more education, better health care than more health care delivery, a politi
cal will, involvement of non-governmental organisations, a dedicated profession
and a motivated community.
" PREVENT DISASTER
§§
§§
PROTECT COMMUNITV"
§§
§§
§§
more than two hours previously. The management of young
children is more difficult—most episodes are poison scares
rather than true poisonings. Rather than give young children
charcoal immediately on presentation, we suggest confining it
to the few who develop symptoms—in a dose sufficient to
increase elimination of the drug.
Repeated doses of oral activated charcoal have not yet been
shown to reduce morbidity and mortality. Further studies are
required to establish its place and the dose to be given. Until
these data are available, severely poisoned adults should be
given 150-200 g through a nasogastric tube over 4-8 hours
with the aims of achieving a maximum reduction in elimina
tion half life and an improvement in the clinical state. The
total dose given is probably more important than the fre
quency of dosing.
] A VALE
Director
National Poisons Information Service (Birmingham Centre),
West Midlands Poisons Unit,
Dudley Road Hospital,
Birmingham B18 7QH
AT PROUDFOOT
Director
National Poisons Information Service (Edinburgh Centre),
Scottish Poisons Information Bureau,
Royal Infirmary, Edinburgh EH3 9YW
1 Neuvonen PJ, Vaniainen M, Tokola O Comparison of activated charcoal and ipecac syrup in
prevention of drug absorption. EurJCIin Pharmacol 1983^4:557-62.
2 Dane! V, Henry JA, Glucksman E. Activated charcoal, emesis, and gastnc lavage in aspinn
overdose. BMJ 198R;296:1507.
3 Scolding N, Ward MJ, Hutchings A, Routledge PA. Charcoal and isoniazid pharmacokinetics.
Human Toxtcolofy 1986;5:285-6
4 Olkkola KT, Neuvonen PJ. Do gastric contents modify antidotal efficacy of oral activated charcoal?
BrJChn Pharmacol 1984;18:663-9.
5 Tenenbein M, Cohen S, Sitar DS. Efficacy of ipecac-induced emesis, orogastric lavage, and
activated charcoal for acute drug overdose. Ann Emerg Med 1987;16:838-41.
6 Neuvonen PJ, Elfring SM. Elonen E. Reduction of absorption of digoxin, phenytoin and aspinn by
activated charcoal in man. EurJCIin Pharmacol 1978;13:213-8.
7 Curtis RA, Barone J, Giaoina N. Efficacy of ipecac and activated charcoal/cathanic: presention of
salicylate absorption in a simulated overdose Arch Intern Med 1984,144:48-52.
8 Neuvonen PJ. Elonen E. Effect of activated charcoal on absorption and elimination of
phenobarbitone, carbamazepine and phenylbutazone in man. Eur J Clin f*
harmacol 1980,17:
51-7
9 Scheinin M, Virtanen R, lisalo E. Effect of single and repeated *
dose of activated charcoal on the
pharmacokinetics of doxepin Ini J Clin Pham Ther Toxicol 1985;23:38-12.
10 El-Bahie N, Allen EM, Williams J, Routledge PA The effect of activated charcoal and hyoscine
butylbromidc alone and in combination on the absorption of mcfenamic acid. Br J Clin
Pharmacol 1985;19:836-8.
11 NcNamara RM, Aaron CK, Gemborys M, Davidheiser S. Efficacy of charcoal cathartic versus
ipecac in reducing serum acetaminophen in a simulated overdose. Ann Emerg Med 1989;18:
934-8.
12 Um DT, Singh P, Nounsis S, Cruz RD Absorption inhibition and enhancement of elimmanon of
sustained-release theophylline tablets by oral activated charcoal. Ann Emerg Med 1986;I5:
1303-7.
I 3 Neuvonen PJ, Olkkola KT. Activated charcoal and syrup of ipecac in prevention of cimetidine and
pindolol absorption in man after administration of metoclopramide as an antiemetic agent. Clin
Toxicol 1984;22:103-1 I.
11 Cordonruer J, Van den Heede M, HeyndricJoc A. Activated charcoal and ipecac *
ymp in prevention
of tilidine absorption in man. let Hum Toxicol 1987;29(suppl 2)105-6.
15 Underhill TJ, Greene MK, Dove AF. A comparison of the efficacy of gastric lavage, ipecacuanha
and activated charcoal in the emergency management of paracetamol overdose. Arch Emerg Med
1990;7:148-54.
16 Swartz CM, Sherman A. The treatment of tricyclic antidepressant overdose with repeated charcoal.
] Clin Ptychophamacol ) 984 ;4:3 36-40
17 Neuvonen PJ, Elonen E, Manila MJ Oral activated charcoal and dapsone elimination. Clin
Pharmacol Ther 1980;27:823-7
18 Lalonde RL, Deshpande R. Hamilton PP, McLean WM, Greenway DC. Acceleration of digoxin
clearance by activated charcoal. Clin Pharmacol Ther 1985;37:367-71.
19 Pond S, Jacobs M, Marks J, Gamer J, Goldschlager N, Hansen D. Treatment of digitoxin overdose
with oral activated charcoal. Lancet 1981 ,ii: 1177-8.
20 Mauro LSj Mauro VF, Brown DL, Somaru P Enhancement of phenytoin elimination by multiple
dose activated charcoal. Ann EmergMed 1987;16:1132-5.
21 llkhanipour K, Yealy DM, Krenzclok EP The comparative efficacy of various multiple-dose
activated charcoal regimens. Am J Emerg Med 1992;10:298-300.
22 Goldberg MJ. Pack GD, Spector R, Fischer LJ, Feldman RD. Lack of effect of oral activated
charcoal on imipramine clearance. Clin Pharmacol Ther 1985; 38:350-3.
23 Mayer AL. Sitar DS, Tenenbein M Multiple-dose charcoal and whole-bowel irrigation do not
increase clearance of absorbed salicylate Arch Intern Med 1992;152:393-6.
24 Boldy DAR, Heath A, Ruddock S, Vale JA, Prescott LF Repeated oral activated charcoal in the
treaiment of carbamazepine poisoning. Lancet 1987;i: 1027.
25 Neuvonen PJ, Elonen E, Haapancn EJ. Acute dapsone intoxication: clinical findings and effect of
oral charcoal and haemodialysis on dapsone elimination. Acta MtdScand 1983;214:215-20.
26 Boldy DAR, Sman V, Vale JA. Multiple doses of charcoal in digoxin poisoning. Lancet
I985;ii: 1076-7
27 Boldy DAR, Vale JA, Prescott LF. Treatment of phenobarbitone poisoning with repeated oral
administration of activated charcoal Q J Med 1986;61-997-1002.
28 Weidle PJ, Skiest DJ, Forrest A. Multiple-dose activated charcoal as adjunct therapy after chronic
phenytoin intoxication. Clin Pham 1991 ;10 71 -1
29 Sessler CN, Glauser FL Cooper KR Treatment of theophylline toxicity with oral activated,
charcoal. Chat 1985;87:325-9
30 Hillman RJ, Prescott LF. Treatment of salicylate poisoning with repeated oral charcoal BMJ
1985)291:1472
31 Hell KF, Hackett IT, Dusci LJ, P.uerson JW Disposition of dothiepin afte- overdose: *
effect of
repeated-dose activated charcoal Ther Drug Monti 1991 ;13:485-9.
(FROM BMJ VOL. 306 9 JANUARY 1993, 78-79,
The cervical spine in rheumatoid arthritis
Needs careful assessment
Rheumatoid arthritis commonly affects the cervical spine,
causing several well defined deformities.' Damage to the
cervical spine from rheumatoid arthritis has been noted in
30% to 46% of necropsy studies and is second in frequency
only to that seen in the metatarsophalangeal joints.3! One in
four inpatients with rheumatoid arthritis and between 17%
and 86% of all patients with ffiis disease have radiological
evidence of instability of the cervical spine.’1
These high rates reflect the anatomy of the cervical spint
and the dynamic forces that act on it. Each of the apophysial
and ligamentous articulations of the cervical spine is suscept
ible to the same inflammatory changes as those in peripheral
joints of patients with rheumatoid arthritis.3 Furthermore,
the cervical spine is constrained between a somewhat rigid
thoracic spine and a skull weighing 6 kg; movement of the
head, which has been estimated to occur around 600 times
each hour, adds to the forces on the articulations.’
Any segment of the cervical spine may be affected by the
rheumatoid inflammatory process, but destructive changes
are most prominent at the occipitoatlantoaxial junction.
Atlantoaxial subluxation is the most common deformity and is
due to destruction and resultant laxity of the transverse
ligament. This allows the atlas to move forward relative to
4
the odontoid process of the axis when the neck is flexed.
In radiographs this is seen as a widening of more than 3 mm
in the space between the anterior arch of C1 and the odontoid.
The corresponding reduction in the space posteriorly
restricts the canal available for the spinal cord. By contrast,
posterior subluxation of the atlas is infrequent and is seen only
in the presence of severe erosion and dislocation of the
odontoid."
Recent studies using magnetic resonance imaging in
patients with atlantoaxial subluxation have shown an inflam
matory mass of granulation tissue around the odontoid arising
from the synovia! lining of the articulations. This periodontoid mass is not visible in patients who have had surgical
fusion of the first two cervical vertebrae or in whom deformity
has progressed to that of atlantoaxial impaction (see
below).’10 The bulging of this mass may further reduce the
space available for the spinal cord and cause -eurological
deficits in patients with only a moderate degree o: _;.<mtoaxial
subluxation.
When the disease affects one of the occipitoatlantoaxial
articulations (termed lateral mass) it may produce the syn
drome of non-reducible rotational tilt of the head, the main
clinical features of which are occipital pain, tender points in ■
SELECTIONS FROM BMJ
VOL. 9
march 1993
the neck, and tilting of the head towards the affected side." If
both sides are affected collapse of the lateral masses allows the
skull to descend on to the cervical spine and the odontoid to
enter the foramen magnum. This deformity has been termed
cranial settling, superior migration of the odontoid, or
atlantoaxial impaction and is seen almost exclusively in
association with atlantoaxial subluxation.”" Subaxial sub
luxation is a late development; it often affects several verte
brae, leading to a “stepladder” deformity. Extensive rheuma
toid disease of the cervical spine results, then, in a combined
deformity of atlantoaxial subluxation—subaxial subluxation
and atlantoaxial impaction—a devastating complication and a ,
truly formidable therapeutic challenge.
Deformities of the cervical spine are seen most often in
patients with rheumatoid arthritis of more than 10 years’
duration. They are usually associated with severe destructive
peripheral arthritis, rheumatoid nodules, a high titre of
rheumatoid factor, and treatment with corticosteroids.’11
Progression of the deformity is unpredictable in a given
patient, but follow up for five to 10 years has shown worsening
of the instability in 16% to 41% of the patients.”" These
percentages may be too low: with progression of the deformity
to atlantoaxial impaction the magnitude of the atlantoaxial
subluxation may seem on radiography to be reduced, giving
the false impression radiologically of improvement."
Many patients with rheumatoid disease of the cervical spine
remain asymptomatic for years, but they are at risk of a range
of neurological complications and even sudden death from
medulla.-- compression. Neurological abnormalities may be
subtle and difficult to establish in the presence of deforming
arthritis, muscular atrophy, and the neuropathy that may be
associated with rheumatoid arthritis. Patients may complain
of intractable pain in the neck or the back of the head. They
may have symptoms of vertebrobasilar insufficiency with
vertigo or drop attacks and may have signs of myelopathy.” '*
Myelopathy, once it develops, is usually rapidly progressive.
In patients with subaxial subluxation myelopathy may occur
with only slight subluxation because of the narrower diameter
of the spin canal below, the axis. Profound and complex
neuro!c~:::. deficits may be found in patients with the
co— . .-.d deformity ofatlantoaxial subluxation—subaxial subluxanon—atlantoaxial impaction. Atlantoaxial subluxation
with subluxation of less than 9 mm carries the least risk of
neurological damage, while atlantoaxial subluxation of more
than 9 mm, atlantoaxial impaction, subaxial subluxation,
non-reducible rotational tilt of the head, and combined
deformities are all associated with a higher risk of neurological
*
deficit.
”
Plain radiographs of the cervical spine in flexion and
extension will allow recognition of atlantoaxial subluxation
and subaxial subluxation. In patients with atlantoaxial impac
tion, however, odontoid erosion and osteoporosis may make
plain radiographs inadequate for assessing the extent of
cranial settling and resultant penetration of the odontoid .into
the. foramen magnum. Various, measurements have been
advocated to define the extent of cranial settling. McGregor’s
line, which assesses the protrusion of the odontoid process
above the foramen magnum, is widely used in clinical
practice. Because of its superior contrast capabilities magnetic
resonance imaging is the current first choice technique for
assessing instability of the cervical spine.”17
Patients with a minor degree of atlantoaxial subluxation or
with subaxial subluxalion need treatment only with a soft
cervical collar—which provides symptomatic relief, acts as a
reminder to patient and doctor, and may provide some degree
of protection from trauma. In the presence of intractable
cervical pain, neurological deficits, or myelopathy, or combi
nations of these, the recommended procedures are halo
stabilisation and surgical arthrodesis. The place of surgery in
the early stages of instability of the cervical spine is less
certain, nor is there any consensus on whether progression
can be retarded by early surgery. In a retrospective study of
110 patients with rheumatoid arthritis who had surgical
treatment we found recurrence of their cervical instability
after a mean interval of nine years in 5-5% of patients with
atlantoaxial subluxation who required only atlantoaxial fusion
—but a 36% recurrence rate after a mean interval of 2-6 years
in patients with atlantoaxial subluxation and atlantoaxial
impaction who required fusion from the occiput to C3. No
patient with atlantoaxial subluxation and fusion of C1 and C2
progressed to develop atlantoaxial impaction." '*
Many patients with substantial deformities remain asymp
tomatic, but they are at increased risk of neurological damage
with the passage of time. They are also at risk if they need
surgery or induction of anaesthesia for any other reason. In
one recent study 60% of patients with rheumatoid arthritis
having total hip or knee replacements had radiological
evidence of instability of their cervical spine, and nearly half
of these had no symptoms referrable to their necks.” Patients
with rheumatoid arthritis undergoing any major surgical
procedure should be assessed by having radiographs taken of
the cervical spine in flexion and extension. Indeed, all patients
with rheumatoid disease of the necks, even though asymp
tomatic, should be followed up carefully for evidence of
neurological deficit, and all should undergo periodic radio
graphic monitoring.
AMRIT K AGARWAL
Medical Center,
Beaver, PA 15009
USA
WALTER C PEPPELMAN Jr
Central Pennsylvania Orthopedic and
Spinal Associates,
Harrisburg, PA 17109
DAVID R KRAUS
St Margaret Memorial Hospital,
Pittsburgh, PA 15215
CARL H EISENBEIS Jr
The University of Pittsburgh,
Pittsburgh, PA 15215
l Bland JH, Rheumatoid arthritis of the cervical spine J Rheumatol 1974;1:319-42,
2
Euldcrink F, Meijen KA. Pathology of the cervical spine in rheumatoid arthritis: a controlled study
of 44 spines, JPurhof 1976;120:91-108.
3
Bland JH, Davis PH, London MG, VanBuskirk FW, Duane CO. Rheumatoid arthritis of cervical
4
spine. Arch htm Med 1963;112:130-6.
Conlon PW, Isdale IC, Rose BS. Rheumatoid arthritis of the cervical spine—an analysis of 333
5
cases. Ann Rheum Dis 1966^25; 120-6.
Mcikle JA, Wilkinson M. Rheumatoid involvement of the cervical spine. Radiological assessment.
6
Ann Rheum Dis 1971 ;30:154-61.
Smith PH, Benn RT, Sharp J. Natural history of rheumatoid cervical luxations, Ann Rheum Dis
7
1972;31:431-9.
Konttinen YT, Santavina S, Kauppi M, Moskovich R. The rheumatoid cervical spine. Current
8
Opinion in Rheumatology 19913:429-40.
Weissman BN, Aliabadi P, Weinfeld MS, Thomas WH, Sosman JL. Prognostic features of
9
atlantoaxial subluxation in rheumatoid arthritis patients. Radiology 1982;144:7.45-51.
Larsson EM, Holtas S, Zygmunt S. Pre- and postoperative MR imaging of the craniocervical
10
11
junction in rheumatoid arthritis. AJR 1989;152:561-6. ,
Milbrink J, Nyman R. Posterior stabilization of the cervical spine in rheumatoid arthritis: clinical
results and magnetic resonance imaging correlation. Journal of Spinal Disorders 19903:308-15.
Halla JT, Hardin JG Jr. The spectrum of atlantoaxial facet joint involvement in rheumatoid
12
arthritis. Arthritis Rheum 1990;33:325-9.
Matthews JA. Atlanto-axial subluxation in rheumatoid arthritis. A 5-year follow-up study. Ann
13
Rheum Dis 197433:526-31.
Nakano KK. Neurological complications of rheumatoid arthritis. Orthopedic Chnia of North
14
America 1975;6:861-80.
Kraus DR, Peppelman WC, Agarwal AK, De Leuw HW, Donaldson WF HI Incidence of subaxial
subluxation in patients in generalized rheumatoid arthritis who have had previous occipital
15
cervical fusions. Spine 1991;16(suppl):S486-9.
Agarwal AK, Kraus DR, Eisenbeis CH Jr, Stolzer BL, Balk PM, Barkley TA. Anatomical and
neurological characteristic of cervical spine involvement in rheuma'oid atthnts. J Onhop
16
Rheumatol 19893:77-89.
Kauppi M, Sakaguchi M, Konttinen YT, Hamalainen M A new method of screening for vertical
17
atlantoaxial dislocation. J Rheumatol 1990;17:167-72.
Bell GR, Steams KL. Flexion-extension MRI of the upper rheumatoid cervical spine. Orthopedics
18
1991;14:969-73.
Agarwal AK, Peppelman WC, Kraus DR, Pollock B, Stolzer BL, Eisenbeis CH, et al. Recurrence
of cervical spine instability in rheumatoid arthritis following previous fusion: can disease
19
progression be prevented by early surgery? J Rheumatol 1992;19:1364-70.
Collins DN, Barnes CL, FitzRandolph RL. Cervical spine instability in rheumatoid patients having
total hip or knee arthroplasty. Clinical OrtlttfiJi. < and Related Research 1401 ;272:127-35
(FROM BMJ VOL 306 9 JANUARY »».
l**
SELECTIONS FROM BMJ
VOL. 9
MARCH 1993
to sn.
5
322
CLINICAL NEUROSURGERY
a location not approachable from other techniques. Destructive proce
dures yield best results for cancer pain, but our feelings are that they are
contraindicated for benign generated pain, and stimulation techniques
should be reserved for these patients.
CHAPTER
18
Stimulation of the Peripheral Nervous
System for Pain Control
REFERENCES
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
Akil, H., Richardson, D. E., Hughes, J., and Barchas, J. D. Enkephalin-like material
elevated in ventricular cerebrospinal fluid of pain patients after analgetic focal
stimulation. Science, 201: 463-465,1978.
Akil, H., Richardson, D. E., Barchas, J. D., and Li, C. H. Appearance of beta-endorphin
like immunoreactivity in human ventricular cerebrospinal fluid upon analgesic
electrical stimulation. Proc. Natl. Acad. Sci. USA, 75(10): 5170-5172, 1978.
Basbaum, A. I., Marley, N., and O’Keefe, J. 0. Spinal cord pathways involved in the
production of analgesia by brain stimulation. Adv. Pain Res.: Then: 511-515, 1976.
Hosobuchi, Y., Adams, J. E., and Turkin, B. Chronic thalamic stimulation for control
of facial anesthesia dolorosa. Arch. Neurol., 29:158-161, 1973.
Khachaturian, H., and Watson, S. J. Some perspectives on monoamine-opioid peptide
interaction in the rat central nervous system. Brain Res. Bull. 9(1-6): 441-462,1982.
Richardson, D. E. Auto-inhibition in the sensory system of the cat. Surg. Forum, 21:
447-449, 1970.
Richardson, D. E. Brain stimulation for pain control. IEEE Trans. Biol. Med. Eng.,
23: 304-306, 1976.
Richardson, D. E., and Akil, H. Pain reduction by electrical brain stimulation in man.
Part I. Acute administration in periaqueductal and periventricular sites. Part II.
Chronic self-administration in the periventricular grey matter. J. Neurosurg., 47:
178-194, 1977.
Richardson, D. E. Long-term follow-up of deep brain stimulation for relief of chronic
pain in the human. In: Modern Neurosurgery, edited by M. Brock, pp. 449-453.
Springer-Verlag, Berlin, 1982.
Ruda, M., Allen, B., and Gobel, S. Ultra structure of descending serotonergic axonal
endings in layers I and II of the dorsal horn. J. Physiol. (Paris), 77(2-3): 205-209,
1981.
Watson, S. J., Barchas, J. D., and Li, C. H. Beta-lipotropin: Localization of cells and
axons in the rat brain by immunocytochemistry. Proc. Natl. Acad. Sci. USA, 74:
5155-5158, 1977.
Yaksh, J. L., Hammond, D. L., and Tyce, C. W. Functional aspects of bulbospinal
monoaminergic projection in modulating processing of somatosensory information.
Fed. Proc., 40(13): 2786-1794, 1981.
I
I
DONLIN. M. LONG, M.D., Ph.D.
INTRODUCTION
It has now been 10 years since electrical stimulation of the peripheral
nervous system was reintroduced into medicine for the control of pain
(12, 28, 29, 37). In that period of time our understanding of the anatomy
and physiology of nociception has undergone dramatic change. The
separation of pain (nociception), suffering, and pain behavior has oc
curred, and our understanding that human pain is a complex issue with
physical, psychological, and social aspects is developing slowly. It is
impossible to discuss the therapy of pain without considering the multi
plicity of factors which may influence the complaint (36, 38). In order to
present this summary of afferent stimulation for pain control, it is
necessary to place the stimulation procedures in appropriate historical
context and to discuss current concepts which are important in under
standing human pain. Then it is possible to collate the many publications
dealing with pain control through transcutaneous electrical stimulation
and to place the techniques for stimulation of the peripheral nervous
system appropriately in the therapeutic armamentarium of the physician
interested in treating pain.
Stimulation-induced analgesia was a reality in classical times, and the
description of the use of naturally occurring electrical sources, the electric
fishes for pain treatment, is well documented (32). It was appreciated
centuries ago that electrification of acupuncture needles seemed to im
prove the results in pain control. Benjamin Franklin was an enthusiast
for the value of electricity in medicine and described the effective treat
ment of trigeminal neuralgia with electrical stimulation. This medical
literature over a long period of time is a curious mixture of fact and
fancy, valid scientific observation, and quackery (42). Throughout the
latter half of the 19th century, there were many electrical stimulators on
the market which were freely available to both the medical profession
and the lay public. During this time, it was generally assumed that the
electricity had some special properties, and only rarely is there any
323
324
•
CLINICAL NEUROSURGERY
indication that it was the stimulation of the nervous system which was
beneficial. This, in spite of the fact that Althaus (2) in 1856 had clearly
described sequential paresthesia, hypalgesia, analgesia, and anesthesia
occurring with electrical stimulation of major nerve trunks. Anecdotal
reports correlating nerve stimulation, analgesia, and pain control ap
peared but were not collated or evaluated in any meaningful way. The
rise of surgery, neuroanatomy, and pharmacology, coupled with the
application of the scientific method to medicine, combined to virtually
eliminate the use of electrical stimulation of the nervous system for any
purpose in the early 20th century. One major observation was made when
it was determined that the application of a large electrode around the
upper abdomen seemed to decrease postoperative discomfort and ileus in
abdominal surgery, but this was erroneously attributed to warming the
liver.'The 1965 publication of the gate theory of pain perception rekindled
interest in pain as both a laboratory and a clinical problem (43). By that
time, only one American manufacturer was continuing to make an
electrical stimulator-massage device for sale on the open market.
It would be nice to be able to say that those stimulated by the MelzackWall theory began an orderly progression of research investigating the
cutaneous application of stimulation and then progressing centrally with
more elaborate and potentially dangerous applications. In fact, the clin
ical research centered on the production of an implantable dorsal column
stimulator was based somewhat loosely on the concept that stimulation
of this collection of large afferents would produce the desired effect
without serious concern for the mechanism of action. The fact that
stimulation of the spinal cord was related to the published gate theory
in the most nebulous way did not stop the surge of enthusiasm for spinal
cord stimulation (30). The primary emphasis for the development of
cutaneously applied electrical stimulation as a therapeutic tool came
from the failure of spinal cord stimulation to relieve many patients with
chronic pain (31). The original applications of spinal cord stimulators
were of the phase 2 type, in which a wide variety of painful states were
treated with a single modality of therapy and then analyzed retrospec
tively with regard to pain control. Little was known about the chronic
pain neurosis from which the majority of these patients probably suffered
(35). It was the failure of pain control in large numbers of such patients
that led to a search for a way to predict efficacy of the implanted
stimulators. Shealy first employed the commercially available device (the
Electreat stimulator) and was probably the first to recognize that some
patients found these devices to be adequate therapy and did not need to
progress to implantable stimulators for pain control. The unpredictable
nature of the stimulation provided by this device, its erratic wave form
which could not be studied, and the lack of parameter control led Long
PERIPHERAL NERVOUS SYSTEM AND PAIN CONTROL
325
and Hagfors (30) to design and test a stimulator utilizing a modified
square wave pulse width and controllable amplitude and frequency. This
device went into clinical testing in 1971. At approximately the same time,
the Medtronics Company began to provide a complicated transcutaneous
stimulator for testing purposes. Both prototypes were utilized in survey
studies (phase 2) (Fig. 18.1). Long presented initial data at the organi
zational meeting of the International Society for the Study of Pain in
1973. With the availability of several models of devices, a number of
.other investigators began study, and a series of survey reports supported
efficacy in pain control (Fig. 18.2).
These initial studies were all of the phase 2 type. They represented
broad surveys of an unselected group of patients referred to specialists
for pain control. In general, little attempt was made to modify drug
utilization or influence behavior. Although the studies were organized in
a prospective fashion, the analysis of subgroups was carried out retro
spectively. In 1975, Long and Hagfors reviewed the current literature
and surveyed a group of physicians interested in chronic pain who used
transcutaneous electrical stimulation for their opinion of efficacy. The
results were remarkably consistent. Approximately one-third of this
unselected group of patients achieved satisfactory pain control, a sur-
Fig. 18.1. A prototype stimulator. Vintage 1972 with which the original studies were
done.
326
CLINICAL NEUROSURGERY
» ■
Fig. 18.2. A collection of some of the more commonly used modem stimulators, illus
trating the significant improvements in engineering design.
prising figure in view of the fact that the patients treated were generally
intractable for any other form of therapy. Furthermore, some groups of
patients seemed to do significantly better than others. Those with pe
ripheral nerve injuries responded much more frequently. Other patients
were never improved. Those with central nervous system injury or major
psychological problems were generally not helped by the technique (30).
CONTROLLED INVESTIGATIONS WITH TRANSCUTANEOUS ELECTRICAL
NERVE STIMULATION (TENS)
Following the demonstration that electrical stimulation might have a
beneficial effect upon pain in these survey studies, a number of individ
uals have undertaken controlled investigation of the modality. The
largest controlled series contains 300 patients treated at the University
of Minnesota or Johns Hopkins between 1973 and 1978 (34). The initial
evaluation compared transcutaneous stimulation with sham therapy and
subliminal stimulation. Patients actually using the stimulator achieved
pain relief significantly more frequently than those receiving sham or
subliminal stimulation (who responded at an expected placebo rate). A
prospective analysis of the response of patients to stimulation with regard
to diagnosis was then undertaken. Patients with peripheral nerve injuries
of various kinds responded more than 70% of the time. Patients with
relatively acute musculoskeletal syndromes and postherpetic neuralgia
also benefited regularly, although not as predictably. About one-third of
patients with chronic back pain from the failed back syndrome were
PERIPHERAL NERVOUS SYSTEM AND PAIN CONTROL
327
helped, irrespective of the cause of the disability. The use of stimulation
was beneficial in the treatment of chronic pain in these selected groups
of patients in a situation where most had exhausted virtually every other
form of pain therapy. Some patients were found not to benefit at all.
Those without obvious physical problems who were thought to have
concurrent psychological difficulties were not helped for more than a
short period and frequently claimed to be worsened by the technique.
They were extremely intolerant of the stimulation. Patients with meta
bolic peripheral neuropathies characterized by hyperesthesia or serious
sensory loss were generally not helped. Central pain states such as spinal
cord injury or thalamic syndrome did not benefit.
Over this same period of time, a large number of controlled studies
clearly demonstrated the value of electrical stimulation to be greater
than that expected from nonspecific factors in pain control (so-called
placebo). Stimulation was investigated with peripheral nerve injury, as
contrasted with acupuncture and placebo, and was investigated in an
inpatient and an outpatient in a physical medicine setting. All reported
studies have demonstrated greater than placebo responses and variability
of response between diagnostic groups (1, 3, 23, 46, 51, 60, 62). The
results in peripheral nerve injury are spectacularly good, and many other
forms of chronic pain are benefited (10, 39). Considering the fact that
most of these patients have exhausted other forms of pain control and
that the techniques have been employed without strict attention to
related factors, such as drug misuse, anxiety, or depression, it is probable
that transcutaneous electrical stimulation represents the single most
effective physical entity yet introduced in the management of chronic
pain (11).
RESEARCH AND IMPROVEMENTS IN THE TECHNIQUE
Since the late 1970s, when phase 3-controlled studies demonstrated
the specific value of transcutaneous electrical stimulation for pain con
trol, there have been a large number of studies detailing technical
advances and the exploration of parameter changes which may make the
technique more effective (9, 41, 52, 59). The original stimulation tech
niques used spike or modified square wave pulses with pulse widths in
frequencies ranging from approximately 40 to several hundred and in
voltages which were quite variable but were sufficient to provide longlasting discernible stimulation. The devices were all battery powered.
The original stimulating machines were large, but successive improve
ments led to rapid miniaturization. Solid state circuitry has led to even
more impressive advances, and small programmable devices are now
available. The original manufacturers were Stimulation Technology (see
Fig. 18.1) and Medtronics Incorporated. Since the design and manufac
328
329
CLINICAL NEUROSURGERY
PERIPHERAL NERVOUS SYSTEM AND PAIN CONTROL
turing concepts are relatively simple, many manufacturers rapidly en
tered the field, and today there is a tremendous diversity from which to
choose (see Fig. 18.2). In general there is no evidence that one device
works better than another, and the important factors in choosing a
stimulator of the conventional type are (a) price, (b) the reliability and
stature of the company, (c) the quality of the manufacturer, (d) available
software, and (e) ease of service support. The initial enthusiasm which
brought large numbers of manufacturers into the field has now subsided,
and a smaller number of reliable devices now dominate.
Major advances have occurred in the software. Appropriate electrodes
were an early difficult problem. The original devices utilized simple
electrified stainless steel plates covered by plastic and sponge to provide
stimulation. Now several natural and artificial adhesives which are
hypoallergenic and reusable have been developed to make the devices
increasingly user-friendly. These electrodes have reduced skin irritation,
improved contact and stimulation, and made life much simpler because
of their ease of application. However, they have the disadvantage of
significantly increasing the cost.
Important new research has been carried out in the modification of
parameters to provide better pain relief. It has been suggested that low
frequency trains or bursts of stimulation may be more useful. There is
evidence that patients who do not respond to conventional parameters
of stimulation may be benefited by this low frequency burst mode. The
reverse is also true, but at present it is not possible to accurately
characteriz^patients who would respond to one form or the other most
*.'Otherwise,
predictably
the majority of recent studies relate to clinical
usefulness of transcutaneous electrical stimulation in a wide variety of
pain control situations. The greatest emphasis has been placed upon the
use of stimulation techniques in the alleviation of acute musculoskeletal
syndromes, although chronic pain has also been studied further (5, 8, 20,
21, 26, 27, 44, 55, 61, 65). There has been much discussion of optimum
techniques for general use (7, 13, 24, 45, 64). More recently, some have
explored stimulation of specific nerves, particularly the sympathetic
system for therapeutic blockade affects. Such techniques are not in
widespread use and remain the province of individual investigators
interested in specific pain states. For example, Jenkner and Schuhfried
(24) have described temporary electrical sympathectomy from blockade
of the stellate ganglion for both diagnostic and therapeutic purposes (24).
degree of postoperative pain, these investigators initially ignored pain
control and studied other more measurable factors in the postoperative
period. In a survey study, they demonstrated decrease in ileus, decrease
in atelectasis, improved pulmonary function, decreased intensive care
stay, and decreased hospital stay in a series of patients undergoing
abdominal and thoracic operations. A number of uncontrolled studies
appeared, substantiating these observations and indicating that there
was a reduction in the need for narcotics in these same patients. Even
(hough those are not controlled studies, it appeared possible to conclude
from them that postoperative pain is controlled by electrical stimulation.
The reports available for review indicate that patients achieve satisfac
tory pain control which satisfied them and those caring for them while
using significantly smaller amounts of narcotics than patients who were
not treated with electrical stimulation. A few controlled studies have
appeared (1, 8, 47, 48, 56, 63). Those studies consistently demonstrate
major reductions in narcotics use when postoperative electrical stimula
tion is utilized. Pain control is satisfactory. Long and Solomon (58) have
also shown that transcutaneous stimulation is not useful in patients who
were using narcotics routinely before surgery. However, the same group
of patients denied significant pain relief with any dose of postoperative
narcotic utilized.
Postoperative pain is a difficult phenomenon to study. There is good
evidence indicating that for the same operation carried out by the same
surgeon, the experience will be quite different from patient to patient.
Thirty to forty percent will complain of severe pain, an equal number
will have moderate pain, and a smaller percentage (20%) will virtually
have no pain at all and have little need for narcotics. For this reason it
is very difficult to quantify the pain experience in any reasonable way.
Applying the criterion of satisfactory pain control is more productive,
although it does not allow the comparisons of degrees of pain relief.
When pain relief is considered as the goal, electrical stimulation of the
area surrounding the incision will be satisfactory in the majority of the
patients and will markedly reduce the need for postoperative narcotics.
There is excellent evidence that postoperative complications of intraab
dominal and thoracic surgery can be substantially reduced as well. The
effective use of stimulation for postoperative analgesia will not be real
ized, in spite of its apparent advantages over many current techniques
for postoperative analgesia, until an accessible system of delivery of this
service is available to surgeons.
TRANSCUTANEOUS STIMULATION FOR POSTOPERATIVE PAIN
Shortly after the introduction of stimulation techniques for chronic
pain, Hymes et al. began to explore the possibility of achieving relief
from incisional pain with electrical stimulation. Their preliminary obser
vations were reported in 1973. Because of the difficulty in assessing the
PRACTICAL USE OF TRANSCUTANEOUS STIMULATION (Tables 18.1-18.4)
Pain As A Medical Problem
It is not possible to utilize transcutaneous electrical stimulation effec
tively for pain control without understanding the complaint of pain and
330
•
CLINICAL NEUROSURGERY
PERIPHERAL NERVOUS SYSTEM AND PAIN CONTROL
Table 18.1
Evaluation of Patients for TENS Use
- Accurate physical diagnosis. You can’t just treat a pain.
1.
2. Careful psychosocial evaluation. At least half of patients who arrive at the doctor’s office
complaining of pain have primarily psychiatric problems.
3. Correction of drug misuse or abuse.
4. Treatment of associated problems such as depression.
5. A thorough trial of TENS by trained personnel.
ment of pain as a symptom is likely to fail more often than it succeeds.
If an entity such as electrical stimulation is applied without selection to
a large number of patients, simply treating the complaint of pain, then
the physician will be disappointed with the technique. It is common for
doctors confronted with this new technique to send a few patients for
trials of stimulation. Those patients are usually the most recalcitrant of
their practice and the most likely to suffer from a major psychiatric
problem. Failure of the technique to relieve the pain is interpreted by
the physician to mean that it is valueless for pain control when the error
has been in patient selection. Transcutaneous stimulation has been
available for 10 years and is now a proven technique for the treatment
of chronic pain. It is not ubiquitous in its action, nor is it a panacea. It
is a useful adjunct in pain therapy whose success depends upon accurate
diagnosis and the selection of appropriate patients for trials of treatment
(4). In order to do this effectively it is important to understand pain as
a complex problem and to have a reasonable way to approach the patient
who comes complaining of disabling pain.
Over the years, we have evolved a practical scheme for evaluating
patients with chronic pain. This scheme is based on extensive studies of
more than 2000 patients. This is not the place to present the data upon
which we. base these concepts. However, it is important to summarize
them because they allow a framework within which all forms of pain
therapy may be employed (36, 38).
Table 18.2
Clinical Situations in Which Use of TENS Rarely Helps
TENS rarely helps in the following situations:
1. Psychosomatic pain
2. Drug addiction
3. Situations in which secondary gain is important
4. Metabolic neuropathies
5. Spinal injury
6. Pain of central origin
Table 18.3
Clinical Situations Warranting the Use of TENS
The uses of TENS are (in order of efficacy):
1. Acute, musculoskeletal injury
2. Acute postoperative pain
3. Phantom, stump, and nerve injury pain
4. Chronic pain of musculoskeletal injury
5. Chronic pain in the multiply-operated low back patient
6. Chronic pain of other causes
a. Visceral
b. Sympathetic dystrophies
c. Postherpetic neuralgia
1.
2.
3.
4.
5.
Table 18.4
Effective Use of TENS
Thorough trial (30-60 min) by experienced personnel.
Patient education in device use.
Reasonable number of return visits for reevaluation and reeducation (1 or 2).
One month trial at home using a prescribed schedule.
The decision for purchase and long term use should be between physician and patient,
NOT between TENS therapist and patient.
the various factors which may influence both the complaint and the
success of therapy. While it is not possible in this discussion to elaborate
the psychodynamics of pain and the multitude of factors which are
important, it is necessary to provide a background against which the
physician can choose appropriate pain therapy. The indiscriminant treat
331
Pain as a Symptom of Disordered Thinking
There are a small number of patients who present to the physician in
whom the pain is purely a psychiatric problem. The pain exists in the
mind of the patient, even though it is described in very real, often florid,
terms. Typical patient diagnoses in this group include conversion hys
teria, depression, paranoid schizophrenia, and manic depressive disease.
Conversion hysteria and masked depression are the most likely diagnoses
to be missed in our experience. The key to the conversion hysteric is
often the multiplicity of organ systems involved in the complaints without
evidence for significant demonstrable disease. Masked depression often
presents with intractable headache or back pain which cannot be modified
by any therapy until the depression is recognized and treated. It is
obvious that if transcutaneous stimulation is utilized in such patients in
lieu of appropriate psychiatric therapy, it will fail. Most of these patients
will claim to be aggravated by the treatment.
The Magnified Pain Syndrome
There is another group of patients most important for the physician
to recognize. Many patients, particularly those complaining of low back
pain, have a typical syndrome characterized by the lack of any major
332
CLINICAL NEUROSURGERY
physical abnormalities, complaints of disability which are beyond any
physical findings, a fixation upon physical abnormalities, denial of any
psychosocial problems, and a fixation upon the pain, which easily be
comes a true neurosis. There is usually a history of psychosocial dys
function which antedates the injury, and the complex is frequently
associated with drug-seeking behavior and a desire for disability. Since
many of these patients suffer from apparent musculoskeletal abnormal
ities, transcutaneous stimulation is reasonable to try but most will not
respond to any therapies without attention to the entire symptom com
plex. It is reasonable to treat whatever physical abnormalities can be
identified, but the most important approach to such patients is behav
ioral, and any treatment which neglects the behavioral aspects will
undoubtedly fail.
Pain of Physical Origin
The other large group of patients are those we have termed “objective.”
Such individuals have clear-cut physical reasons for pain, normal premorbid personalities and, generally, the psychosocial influences are
otherwise negligible. It is important to recognize that depression and
anxiety over the chronic disability are very real parts of the chronic pain
syndrome for all patients and are likely to be present in this group.
Attempting to treat pain in the presence of unresolved depression is
futile, and even in this well-demarcated group of patients, it is necessary
to treat depression and anxiety effectively before relying upon any
modality of pain therapy. These patients are the ones that have a
reasonable chance of responding to physical techniques for pain control.
Patients in the other two large groups are really candidates for psycho
therapy, and techniques such as electrical stimulation are at best minor
adjuncts in their management.
The first step in effective use of .any pain therapy is an-accurate
diagnosis with a decision about the physical modalities should be utilized.
An important part of this diagnosis is assessment of psychosocial factors
and the understanding that for large numbers of patients, therapy for
the complain of pain is useless unless appropriate psychiatric and'behavioral therapies occur concomitantly. The successful therapy of pain
depends upon a clear-cut diagnosis of its cause; equally clear-cut differ
entiation of the sensation and suffering purely dependent upon nocicep
tion from suffering; and pain behavior modified by personalities, psycho
logical, or social factors. Electrical stimulation is a technique to treat
pain and will not influence drug addiction, personality disturbance,
personal problems, or the desire for secondary gain (25, 53, 54). Failure
to differentiate pain of an ongoing nociceptive input from suffering and
behavior induced by these other factors will lead to failure of any physical
PERIPHERAL NERVOUS SYSTEM AND PAIN CONTROL
333
modality of pain therapy, including transcutaneous stimulation. The key
to successful use of this therapy is an adequate diagnosis and application
of the technique to those patients who can be expected to benefit from
it. If the complaint of pain is accepted at face value and pain therapies
are uncritically applied, then both patient and physician are likely to be
disappointed with the result.
Even recognizing the complexity of the complain of pain, it is another
matter to evaluate all of its factors. When the syndrome is severe enough
or has gone on long enough, a multidisciplinary approach is mandatory
to assess all the psychosocial components of the pain syndrome and treat
them before proceeding to trials of therapy for the pain (16).
There is now abundant evidence for those situations which are most
likely to respond. Incisional pain will be well controlled anywhere the
electrodes can be placed to surround the incision. Adequate stimulators
and electrodes are available. Since all evidence suggests that pain could
be alleviated, postoperative side effects reduced, hospital stay shortened,
and nursing time saved, it is difficult to understand why electrical
stimulation has not achieved more prominence in incisional pain control.
The major difficulty is that no easily accessible method of delivery has
evolved in most places. In a few hospitals where interested individuals
have established the technique, it is used extensively, but it is not a
system which has been freely available to most patients. This pain control
method certainly deserves further exploration and in all likelihood wider
utilization for postoperative pain (58).
The studies involving acute musculoskeletal pains and the use of
transcutaneous stimulation in physical therapy programs are less con
trolled than those which define its value in postoperative pain and in
several chronic pain states (50). Nevertheless, these reports suggest that
transcutaneous stimulation can play an important role in pain relief from
soft tissue injury. It has been used extensively for athletic injuries and
applied to acute low back and neck pain syndromes. Its effectiveness in
all of these injuries is often dramatic, and transcutaneous stimulation is
now a regularly employed modality in physical therapy units. Again, the
lack of a simple way for the physician to prescribe stimulation in these
acute situations has limited the effectiveness of the therapy.
Transcutaneous stimulation still finds its greatest use in chronic pain
states (4, 34). It is most effective in situations in which the pain is clearly
of peripheral nerve injury origin. Neuroma pain in stump and phantom
limb, at least early in its development, and virtually all types of traumatic
nerve injuries will respond to peripheral stimulation. The stimulation
must be delivered proximal to the site of injury, in the area surrounding
the denervated part, and hyperesthetic areas must be assiduously avoided.
It has been my personal experience that pains of these types will fre
334
CLINICAL NEUROSURGERY
quently relent after long periods of successful control by stimulation.
After one year, many such pains will disappear. The minor reflex sym
pathetic dystrophies also will respond. In general, it is best to place
electrodes over injured nerve trunks proximal to the site of injury or over
the plexus to the involved limb. The success in pain of this kind is well
documented.
Patients with chronic back pain, uncomplicated by multiple operations,
are also benefited in a significant percentage. This varies from report to
report but, in general, such patients find stimulation a useful adjunct in
an aggressive nonoperative program. When coupled with the usual factors
of weight control, exercise, and modification of activities, stimulation is
very effective in providing analgesia, particularly for the occasional more
severe flare-up. The patient suffering from chronic back and leg pain
secondary to multiple operations represents a more difficult problem.
The new diagnostic studies available now allow identification of many
more correctable abnormalities than in the past have been assumed to
exist. When no surgical correction is possible, then electrical stimulation
plays an important part in the conservative management. Stimulation
provides pain relief and reduction in muscle spasm in a significant
number of these patients. The figure has been constant at about onethird in a 10-year experience (11). Considering the fact that these patients
rarely have adequate therapy with anything but an aggressive multidis
ciplinary approach, the number that can be successfully treated with
transcutaneous stimulation becomes significant. Most of those patients
use their stimulators indefinitely.
Abdominal pain from visceral disease responds predictably. The pain
of chronic pancreatitis has been especially treatable. Stimulation takes
place posteriorly over the splanchnic outflow and in the celiac area. Most
patients respond rapidly (32).
It is equally important to be cognizant of those patients who have little
or no chance of benefiting from afferent stimulation. Patients with major
psychological or psychiatric components to their complaint will not be
helped (48). They may demonstrate short-term response, but that is
usually no more than a few days, and is unusual. Patients with these
psychosomatic factors often claim to be worsened by the stimulation or
find the added sensory input intolerable. It is important to remember
that patients with hyperesthesia are temporarily worsened by stimula
tion. The general experience with patients suffering from pain of central
nervous system origin has also been poor. There is no evidence that
patients with pain of spinal cord injury or thalamic syndrome are bene
fited from stimulation. The pain of metabolic peripheral neuropathies
usually will not respond, although some, reports indicate successful ther
apy. There has been no consistency in the reports of the use of stimulation
PERIPHERAL NERVOUS SYSTEM AND PAIN CONTROL
for migraine headache, although an occasional investigator finds the
technique useful. Tension headache, on the other hand, will respond
promptly to paracervical muscular stimulation.
Stimulation is an adjunct in the overall management of the patient
complaining of chronic pain, and like any such technique its use is
optimized by trained personnel, patient education, and adequate support
for both the physician and the patient. It is not a technique that is likely
to be used personally by a busy neurosurgeon. The physician s initial
involvement is in diagnosis and the appropriate selection of patients for
trials of stimulation. Unless the physician is a pain specialist or physical
therapist, it is unlikely that he/she will personally use the device or
supervise the trial. The techniques can be utilized by nurses, physical
therapists, or trained technicians who are experienced in stimulation use.
The first step is the appropriate application of stimulating electrodes in
areas which are most likely to relieve the particular complaint of pain
(Fig. 18.3A-O). This is very important; all too frequently the patient is
simply sent to a supplier of the device and instructed only through the
manufacturer’s advertising material. Stimulating electrodes are not
properly placed, and the patient does not know how to use the machine.
The results of such an approach are obvious. Appropriately, the first
meeting with the patient includes the accurate placement of electrodes
for the most likely successful relief of pain and' then an educational
session with the patient to demonstrate the use of the device. This should
include a schedule by which the patients will try stimulation. These
sessions should be repeated once or twice to be certain that the patient
understands the use of stimulation. Then, the patient can use the
stimulator while going about a normal daily routine so as to accurately
ascertain its value. In general, it requires several weeks to 1 month to be
certain of the effect. Many patients are enthusiastic about pain control
in the first few days, only to discover that it is less effective as their
enthusiasm wanes. There is little excuse for repetitive returns, and there
is no reason at all why a patient has to come to a physician’s office or
some other facility for regular treatments. These devices can be used at
home effectively, and it is much less expensive to do so. If pain relief
persists after an adequate trial, the patient can be instructed to buy the
device. Here again, the physician’s assessment becomes important. Pur
chase of one of these devices should occur only when adequate trials
suggest both to the patient and to the doctor that the stimulator will be
of real long-term use in pain control. This decision should not be made
by manufacturers or distributors of the hardware or software and it
certainly should not be made without a trial of stimulation adequate to
establish efficacy. Even though stimulation has become a commonly used
entity, it is unfortunate that few facilities for its appropriate application
336
CLINICAL NEUROSURGERY
PERIPHERAL NERVOUS SYSTEM AND PAIN CONTROL
Fig. 18.3. (A) Trial stimulation of the sciatic nerve in a patient with sciatica. (B)
Stimulation across an arthritic knee. (C) Stimulation across the brachial plexus in a patient
suffering from brachial plexus injury following mastectomy. (D) Stimulation across the
wrist in a patient with pain of median nerve injury.
Fic. 18.3C and D
337
338
339
CLINICAL NEUROSURGERY
PERIPHERAL NERVOUS SYSTEM AND PAIN CONTROL
exist, except under the direction of a relatively small number of pain
specialists. This makes it difficult for the average physician to refer a
patient for a trial of stimulation. The availability of responsible programs
which will provide this service to physicians and their patients will
undoubtedly increase the general utilization of stimulation (7).
Optimal use of electrical stimulation for pain control requires that the
physician establish a reasonable diagnosis for an ongoing nociceptive
input that is likely to respond to this modality. Pain of peripheral nerve
injury origin and musculoskeletal pain problems are most favorable for
treatment. If the patient’s complaint is complicated by important psy
chosocial factors, then stimulation is likely to be useful only if these
factors are approached at least simultaneously with pain therapy. The
majority of such patients do not need any physical modality but will
respond best to behavioral techniques. The stimulation must be applied
by well trained personnel who will educate the patient and service his
needs during therapeutic trials. Long-term support for maintenance of
hardware and supply of software is required. When these goals are met,
electrical stimulation is a valuable adjunct for pain control. When it is
applied uncritically to the complaint of pain, it is unlikely to benefit
significant numbers of patients (33, 40).
low frequency burst stimulation effects were reversible by naloxone
administration. While the studies to date do not prove tnis sensitiv.ty
with certainty, they certainly are suggestive that some forms of electrical
stimulation are reversible by naloxone. Freeman et al. (15) nave clearly
demonstrated that traditional stimulation is not, and they nave also
shown that stimulation of the spinal cord and peripheral nerves by the
available implantable stimulators is not influenced by naloxone either.
These data prove that the stimulation techniques which have tradition
ally been utilized for pain relief are not dependent upon an opioid system.
No information is available concerning the anatomical patnways or the
neural transmitters which may be involved.
MECHANISM OF ACTION
Given our current understanding of the pathways arid mechanisms
wherein nociception is appreciated as pain, there are four general possi
bilities for a locus of action for electrical stimulation of the nervous
system. The first is in the periphery at the receptor level. It is possible
that the stimulation changes the sensitivity of the receptor (14, 51, 56).
There is no evidence for this, and the mechanism remains a source of
speculation. Another possibility is blockade of transmission of impulses
along nerve trunks. Campbell and Long (11, 44, 66) have suggested that
there is some evidence for a potassium block induced by stimulation. The
experimental evidence for this is far from solid. A third site of potential
inhibition is the dorsal horn. The stimulation activates nonpain-carrying
fibers exclusively, at least as much as can be measured by the perception
of the patient. (It is very important that stimulation not cause pain if it
is to be effective.) Inhibition at the dorsal horn level by interactions
between large and small fibers is certainly possible, but supporting
evidence is not ygt available. A fourth possibility is activation of the
descending inhibitory system. This is quite possible and could occur at
any level, and there are no data which help us to accept or reject this
hypothesis (6).
The relationships of electrical stimulation to the opioid system have
been studied. Sjolund and Ericksson (57) were the first to suggest that
COMPLICATIONS
The complications reported with electrical stimulation have been mi
nor and very few. Skin irritation from the tape, gels, or electrodes is
probably the most common. Burns can occur but are rare. The usual
problem is contact dermatitis. Generalized allergies have developed but
are extremely uncommon. Occasionally, hyperpigmentation will occur
under sites of chronic electrode placement, and neovascularization of the
skin may also rarely occur. There have been no instances of serious
injury -of any kind, and no effects upon other body organs have been
reported. The devices should not be used in the proximity of demand
pacemakers but can be employed elsewhere in the body in these patients.
It is probably wise to monitor the patient in the hospital for a few days
when the devices are to be used in this circumstance. As a precaution, it
has been recommended that they not be used in patients with serious
cardiac irregularities. There is no evidence that they would have any
effect upon the heart and, in fact, stimulation has been used successfully
to treat angina. They should not be used over the eyes. The question of
pain relief followed by resumption of activity with reinjury is very real
(19). This is particularly possible in acute athletic injuries, but no such
instance has been reported. The technique is basically free of side effects
which are of significance.
SUMMARY
Transcutaneous stimulation is a proven effective way to relieve pain.
Its optimal use requires an accurate patient diagnosis. Treatment of pain
as a symptom only is likely to fail. There must be a carefill psychosocial
evaluation, for the majority of patients who come to the doctor complain
ing of pain have major psychological, social, or behavioral factors that
are most important in the genesis of the complaint. Drug abuse must be
corrected. Related symptoms, such as anxiety and depression, must be
treated. Then, a thorough trail of transcutaneous stimulation is manda
340
tory. A desultory use will undoubtedly lead to failure. This trial must
begin with patient education by experienced personnel. Then the elec
trodes must be properly applied, and there must be a regular follow-up
of stimulation to be certain the patient is utilizing it correctly. The
patient must be supported through an adequate trial which should extend
over 2-4 weeks before purchase of the device is contemplated. Further
more, all related nursing and physician personnel must be educated in
the proper use of the technique. The uninformed professional who
denigrates the therapy is a very effective deterrent to appropriate use. In
this situation, transcutaneous electrical stimulation will be of great value
in the treatment of acute musculoskeletal injury and acute postoperative
pain. It will be effective in the treatment of peripheral nerve injury pain,
chronic musculoskeletal abnormalities, chronic pain in the patient who
has undergone multiple operations upon the low back and neck, visceral
pain, some of the reflex sympathetic dystrophies, and postherpetic neu
ralgia. Stimulation will not help a complaint which is psychosomatic in
origin. It will not influence drug addiction. It is not likely to be useful in
any situation where secondary gain is important. The metabolic neurop
athies, pain of spinal cord injury, and pain from cerebrovascular accident
will not respond frequently enough to warrant more than hopeful trials.
The technique is inexpensive, places the patient in control of his own
pain, and has no known serious side effects. Its widespread application
awaits the development of reasonable systems to provide this service to
physicians and patients. Stimulation-induced analgesia deserves a place
in the armamentarium of every physician dealing with the complaint of
pain.
REFERENCES
1.
2.
3.
4.
5.
6.
7.
8.
PERIPHERAL NERVOUS SYSTEM AND PAIN CONTROL
CLINICAL NEUROSURGERY
Ali, J., Yaffee C. S., and Serrette, C. The effect of transcutaneous electric nerve
stimulation of postoperative pain and pulmonary function. Surgery, 89(4): 507-512,
1981.
I
Althaus, J. A treatise of medical electricity, theoretical and practical and its use in the
treatment of paralysis. In: Neuralgia and Other Diseases. Trubner, London, 1859 and
1970.
Andersson, S. A. Pain mntrol by sensory stimulation. Adv. Pain Res. Ther. 3: 569-585
1979.
Aronoff, G. M. The use of non-narcotic drugs and other alternatives for analgesia as
part of a comprehensive pain management program. J. Med., 73(3): 191-202, 1982.
Avellanosa, A. M., and West, C. R. Experience with transcutaneous electrical nerve
stimulation for relief of intractable pain in cancer patients. J Med., 73(3): 203-213
1983.
■
Basbaum, A. L., and Fields, H. L. The origin of descending pathways in the dorsolateral
funiculus of the spinal cord of the cat and rat. J. Comp. Neurol., 187: 513-531, 1979.
Baxter, K. G. Transcutaneous nerve stimulation. Efficacy of clinical applications. J.
Kansas Med. Soc., 1: 18-26, 1983.
Bundsen, P., Peterson, L. E., and Selstam, U. Pain relief in labor by transcutaneous
electrical nerve stimulation. A prospective matched study. Acta Obstet. Gyn
Scand., 60(5): 459-468, 1981.
TFNS bv
Birkhan, J., Carmon, A., Meretsky, P„ and Zinder, H. Modi ica i
‘ and
constant-energy stimulation delivered through multiple electro es.
evaluation. Adv. Pain Res. Ther., 3:607-613, 1979.
10. Campbell, J. N„ and Long, D. M. Peripheral nerve stimulation in the treatment o
intractable pain. J. Neurosurg., 45:692-699, 1976.
11. Campbell, J. N., and Long, D. M. Transcutaneous electrical stimulation lor pain.
Efficacy and mechanism of action. In: Diagnosis and Treatment of
rOn^At> °in'
Chap. 8, edited by N. H. Hendler, D. M. Long, and T. N. Wise, pp. 77-96, 1982.
, 12. Erickson, D. L„ and Long, D. M. Ten-year follow-up of dorsal column stimulation.
Adv. Pain Res. Ther. 5: 583-589, 1982.
13. Frampton, V. M. Pain control with the aid of transcutaneous nerve stimulation.
Physiotherapy, 68(3): 77-81, 1982.
14. Francini, F., Maresca, M., Procacci, P., and Zoppi, M. The effects of non-pain u
transcutaneous electrical nerve stimulation on cutaneous pain threshold and mus
cular reflexes in normal men and in subjects with chronic pain. Pain, 7 7(1): 49-63,
1981.
15. Freeman, T. B., Campbell, J. N., and Long, D. M. Naloxone does not effect pain relief
induced by electrical stimulation in man. Pain, in press, 1984.
16. Fields, H. L. Pain. II. New approaches to management. Ann. Neurol., 9(2): 101-106,
1981.
17. Fox, E. J., and Melzack, R. Transcutaneous electrical stimulation and acupuncture:
Comparison of treatment for low back pain. Pain, 2: 141-148, 1976.
18. Kessler, M., and Struppler, A. Relief of phantom pain following modification of
phantom sensation by TNS. Adv. Pain Res. Ther., 5: 591-594, 1983.
19. Griffin, J. W., and McClure, M. Adverse responses to transcutaneous electrical nerve
stimulation in a patient with rheumatoid arthritis. Phys. Ther., 67(3): 354-355,1981.
20. Hansson, P., and Ekblom, A. Transcutaneous electrical nerve stimulation (TENS) as
compared to placebo TENS for the relief of acute oro-facial pain. Pain, 75(2): 157165, 1983.
21. Hay, K. M. Control of head pain in migraine using transcutaneous electrical nerve
stimulation. Practitioner, 226(1366): 771, 773-775, 1982.
22. Hymes, A. C., Raab, D. E., Yonehiro (Young) E. G., Nelson, G. D., and Printy, A. L.
Electrical surface stimulation for control of acute postoperative pain and prevention
of ileus. Surg. Forum, 24: 447-449, 1973.
23. Jeans, M. E. Relief of chronic pain by brief, intense transcutaneous electrical stimula
tion. A double-blind study. Adv. Pain Res. Ther. 3: 601-606, 1979.
24. Jenkner, F. L., and Schuhfried, F. Transdermal transcutaneous electric nerve stimu
lation for pain: The search for an optimal waveform. Appl. Neurophysiol. 44(5-6)330-337, 1981.
25. Johansson, F., Almay, B. G„ and von Knorring, L. Personality factors related to the
outcome of treatment with transcutaneous nerve stimulation Psychiatr Clin
(Basel), 14(2): 96-104, 1981.
26. Keravel, Y„ and Sindou, M. Anatomical conditions of efficiency of transcutaneous
electrical neurostimulation in deafferentation pain. Adv Pain Res Ther 5- 763767, 1983.
'
.
27. Kumar, V. N„ and Redford, J. B. Transcutaneous nerve stimulation in rheumatoid
arthritis. Arch. Phys. Med. Rehabil., 63(12): 595-596, 1982.
28. Long, D. M. External electrical stimulation as a treatment of’chronic pain. Minn. Med.,
9.
342
'
CLINICAL NEUROSURGERY
PERIPHERAL NERVOUS SYSTEM AND PAIN CONTROL
Long, D. M. Recent advances in the management of pain. Minn. Med., 57: 705-709,
1974.
3Q. Long, D. M., and Hagfors, N. Electrical stimulation in the nervous system: The current
status of electrical stimulation of the nervous system for relief of pain. Pain, 1:109123, 1975.
31. Long, D. M. Cutaneous afferent stimulation for relief of chronic pain. Clin. Neurosurg.,
21: 251-268, 1984.
32. Long, D. M. Cutaneous afferent stimulation for the relief of pain. Prog. Neurol. Surg.,
7: 35-51, 1976.
33. Long, D. M. The comparative efficacy of drugs us. electrical modulation in the
management of chronic pain. In: Current Concepts in the Management of Chronic
Pain, edited by Piere LeRoy, Symposia Specialist, Miami, pp. 53-61, 1977.
34. Long, D. M., Campbell, J. N., and Gucer, G. Transcutaneous electrical stimulation for
relief of chronic pain. Adv. Pain Res. Then, 3; 593-599, 1979.
35. Long, D. M. Surgical therapy of chronic pain. Neurosurgery, 6(3): 317-328, 1980.
36. Long, D. M. A comprehensive model for the study and therapy of pain: Johns Hopkins
Pain Research and Treatment Program. In: New Approaches to Treatment of Chronic
Pain: A Review of Multidisciplinary Pain Clinics and Pain Centers, edited by K. Y.
Lorenz and M. D. Ng, pp. 66-75, 1981.
37. Long, D. M., Erickson, D., Campbell, J., and North, R. Electrical stimulation of the
spinal cord and peripheral nerves for pain control. A 10-year experience. Appl.
Neurophysiol., 44: 207-217, 1981.
38. Long, D. M., Rehabilitation of patients suffering from chronic pain. In: Rehabilitation
of the Neurological Patient, edited by L. S. Illis, E. M. Sedgwick, and H. J. Glanville,
pp. 282-311. Blackwell Scientific Publications, 1982.
39. Long, D. M. Pain of peripheral nerve injury. In: Neurological Surgery, Vol. 6, edited by
J. R. Youmans, Chap. 128, pp. 3634-3643, 1982.
40. Long, D. M. The evaluation and treatment of low back pain. In: Diagnosis and
Treatment of Chronic Pain, Chap. 4, edited by N. H. Hendler, D. M. Long, and
T. N. Wise, pp. 31-42. W.B. Saunders, Philadelphia, 1982.
41. Linzer, M., and Long, D. M. Transcutaneous neural stimulation for relief of pain. IEEE
Trans. Biomed. Eng., 23(4): 341-345, 1976.
42. MacKay, C. Extraordinary Popular Delusions and the Madness of Crowds. Richard
Bentley, London, 1841.
43. Melzack, R. A., and Wall, P. D. Pain mechanisms: A new theory. Science, 150: 971979, 1965.
44. Melzack, R. et aL Transcutaneous electrical nerve stimulation for low back pain. A
comparison of TENS and massage for pain and range of motion. Phys. Ther., 63(4):
489-493, 1983.
45. Meyerson, B. A. Electrostimulation procedures: Effects, presumed rationale, and pos
sible mechanisms. Adv. Pain Res. Ther., 5: 495-534,1983.
46. Moritz, U. .Physical therapy and rehabilitation. Scand. J. Rheumatol. (Suppl.), 43: 4955, 1982.
47. Neary, J. M. Transcutaneous electrical nerve stimulation for the relief of post-incisional
surgical pain. AANA J., 49(2): 151-155, 1981.
48. Nesheim, B. I. The use of transcutaneous nerve stimulation for pain relief during labor.
A controlled clinical study. Acta Obstet. Gynecol. Scand., 60(1): 13-16,1981.
49. Nielzen, S., Sjolund, B. H., and Eriksson, M. B. Psychiatric factors influencing the
treatment of pain with peripheral conditioning stimulation. Pain, 13(4): 365-371.
50. Nordemar, R., and Thorner, C. Treatment of acute cervical pain—A comparative group
study. Pain, 10(1): 93-101, 1981.
51. Procacci, P., Zoppi, M., Maresca, M., and Francini, F. Hypoalgesia induced by
cutaneous electrical stimulation. A physiological and clinical investigation. • . . ■' >
rosurg. Sci., 4: 221-228, 1977.
52. Rao, V. R„ Wolf, S. L„ and Gersh, M. R. Examination of electrode placements y.d
stimulating parameters in treating chronic pain with conventional transcutaneous
electrical nerve stimulation (TENS). Pain, //(I): 37-47, 1981.
53. Reynolds, A. C., Abram, S. E., et al. Chronic pain therapy with transcutaneous e.e<-'■<«■
nerve stimulation: Predictive value of questionnaires. Arch. Phys. Med. ftehao:.
64(7): 311-313, 1983.
54. Richardson, R. R., Arbit, J„ Siqueira, E. B., and Zagar, R. Transcutaneous eiectr.ca
neurostimulation in functional pain. Spine, 6(2): 185-188, 1981.
55. Rizk, T. E„ Christopher, R. P„ Pinals, R. S„ Higgins, A. C„ and Frix, R. Adhesive
capsulitis (frozen shoulder): A new approach to its management. Arch. Phys. .Med.
Rehabil., 64(1): 29-33, 1983.
56. Schomburg, F. L., and Carter-Baker, S. A. Transcutaneous electrical nerve 3timulat.cn
for post-laparotomy pain. Phys. Ther., 63(2): 188-193, 1983.
57. Sjolund, B. H., and Ericksson, M. B. E. Endorphins and analgesia produced ty
peripheral conditioning response. In: Adv. Pain Res. Ther.: 587-592, 1979.
58. Solomon, R. A., Viernstein, M. C., and Long, D. M. Reduction of postoperative pain
and narcotic use by transcutaneous electrical nerve stimulation. Surgery, 8712': 14'2146, 1980.
59. Stamp, J. M. A review of transcutaneous electrical nerve stimulation (TENS . 7. MedEng. Technol., 6(3): 99-103, 1982.
60. Sternback, R. A., Ignelzi, R. J., Deems, L. M., and Timmermans, G. Trazscutanecus
electrical analgesia: A follow-up analysis. Pain, 2: 35-41, 1976.
61. Taylor, P., Hallett, M., and Flaherty, L. Treatment of osteoarthritis of the knee with
transcutaneous electrical nerve stimulation. Pain, 7/(2): 233-240,198L
62. Thorsteinsson, G., Stonnington, H. H., Stillwell, G. K., and Elveback. L- F_ Tramrutaneous electrical stimulation: A double-blind trial of its efficacv for -n-- a —
Phys. Med. Rehabil., 58: 8-13, 1977.
63. Tyler, E„ Caldwell, C., and Ghia, J. N. Transcutaneous electrical nerve aemuiacum
An alternative approach to the management of postoperative pain A-wsc (Cleve.), 6/(5): 449-456, 1982.
64. vanDorn, J. N., and Spierdijk, J. Transcutaneous electrical nerve stinnu r <-• ■'■>.- - of pain. Acta Anesthesiol. Belg., 32(1): 21-31, 1981.
65. Winnem, M. F„ and Amundsen, T. Treatment of phantom limb rail- « - ■> 'XVt
(letter). Pain,/2(3): 299-300, 1982.
' ' *
’
"
66. Zcppi, M., Francini, F., Maresca, M., and Procacci, P. Changes of cvtx-ieeus
thresholds induced by non-painful transcutaneous electrical ne-ve
'• ?
normal subjects and in subjects with chronic pain J Neuro' \ ' ' ’
44(8): 708-717, 1981.
‘
>W»«S- rXvw..-.,....
29.
more than two hours previously. The management of young
children is more difficult—most episodes are poison scares
rather than true poisonings. Rather than give young children
charcoal immediately on presentation, we suggest confining it
to the few who develop symptoms—in a dose sufficient to
increase elimination of the drug.
Repeated doses of oral activated charcoal have not yet been
shown to reduce morbidity and mortality. Further studies are
required to establish its place and the dose to be given. Until
these data are available, severely poisoned adults should be
given 150-200 g through a nasogastric tube over 4-8 hours
with the aims of achieving a maximum reduction in elimina
tion half life and an improvement in the clinical state. The
total dose given is probably more important than the fre
quency of dosing.
J A VALE
Director
National Poisons Information Service (Birmingham Centre),
West Midlands Poisons Unit,
Dudley Road Hospital,
Birmingham B1S 7QH
AT PROUDFOOT
Director
National Poisons Information Service (Edinburgh Centre),
Scottish Poisons Information Bureau,
Royal Infirmary’, Edinburgh EH 3 9YW
1
2
3
4
5
6
7
Neuvonen PJ, Vartiainen M, Tokola O. Comparison of activated charcoal and ipecac syrup in
prevention of drug absorpnon. Eur J Clin Pharmacol 1083^4:557-62.
Danel V, Henry JA, Gtucksman E. Activated charcoal, emesis, and gastnc lavage in aspirin
overdose. BMJ i<>8R;2%:1507.
Scolding N, Ward MJ. Hutchings A, Routledge PA. Charcoal and isoniazid pharmacokinetics.
Human Toxicology 1986;5:285-6.
Olkkola KT, Neuvonen PJ Do gastric contents modify antidotal efficacy of oral activated charcoal?
BrJ Clin Pharmacol 1984;18:663-9.
Tenenbein M, Cohen S, Sitar DS. Efficacy of ipecac-induced emesis, orogastric lavage, and
activated charcoal for acute drug overdose. Ann Emerg Med 1987;16:838-11.
Neuvonen PJ, Elfvtng SM, Elonen E. Reduction of absorption of digoxin, phenytoin and aspinn by
activated charcoal in man. Eur J Clin Pharmacol 1978;13:213-8.
Curtis RA. Barone J, Giacona N. Efficacy of ipecac and activated charcoal/cathartic prevention of
salicylate absorption in a simulated overdose. Arch Intern Med 1981,144:48-52.
Neuvonen PJ, Elonen E. Effect of activated charcoal on absorption and elimination of
phenobarbitone, carbamazepine and phenylbutazone in man. Eur J Clin Pharmacol 1980J7;
51-7
9
Scheinin M, Vinanen R, lisalo E. Effect of single and repeated doses of activated charcoal on the
pharmacokinetics ofdoxepin. hlJ Clin Pham Ther Toxicol 1985;23- 38-42.
10
EJ-Bahie N, Allen EM, Williams J, Routledge PA. The effect of activated charcoal and hyoscine
butylbromide alone and in combination on the absorption of mefenamic acid. Br J Clin
Pharmacol 1985;19:836-8.
11
NcNamara RM, Aaron CK, Gemborys M, Davidheiser S Efficacy of charcoal cathartic versus
ipecac in reducing serum acetaminophen in a simulated overdose. Ann Emerg Med 1989;18:
934-8.
12
Um DT, Singh P, Nounsis S, Cruz RD. Absorption inhibition and enhancement of elimination of
sustained-release theophylline tablets by oral activated charcoal. Ann Emerg Med I986;15:
1303-7.
I
3 Neuvonen PJ, Olkkola KT Activated charcoal and syrup of ipecac in prevention of cimetidine and
pindolol absorption in man after administration of metoclopramide as an antiemetic agent. Clin
Toxicol 1984;22:103-14.
14
Cordonmer J, Van den Heede M, Heyndrickx A. Activated charcoal and ipecac syrup in prevention
of tilidine absorption in man. Vet Hum Toxicol 1987;29(suppl 2): 105-6.
15
Underhill TJ, Greene MK, Dove AF. A comparison of the efficacy of gastric lavage, ipecacuanha
and activated charcoal in the emergency management of paracetamol overdose. Arch Emerg Med
1990;7:148-54.
16
Swartz CM, Sherman A The treatment of tricyclic antidepressant overdose with repeated charcoal.
J Clin Prychopharmacol ) 984 ;4:336-40
17
Neuvonen PJ, Elonen E, Manila MJ Ora) activated charcoal and dapsonc elimination. Clin
Pharmacol Ther 1980;27:823-7.
18
Ijlonde Rl, Deshpande R, Hamilton PP, McLean WM, Greenway DC Acceleration of digoxin
clearance by activated charcoal. Clin Pharmacol Ther 198537'367-71.
19
Pond S, Jacobs M, Marks J, Gamer J, Goldschlager N, Hansen D. Treatment of digitoxin overdose
with oral activated charcoal. Lancet 198l,ii:l 177-8.
20
Mauro LS; Mauro VF, Brown DI, Somaru P. Enhancement of phenytoin elimination by multiple
dose activated charcoal. /Inn EmergMed 1987;I6:1132-5.
21
Ilkhanipour K, Yealy DM, Krenzclok EP. The comparative efficacy of various muluple-dose
activated charcoal regimens./fm J EmergMed 1992;10:298-300.
22
Goldberg MJ, Pack GD, Spector R, Fischer LJ, Feldman RD. Lack of effect of oral activated
charcoal on imipramine clearance Clin Pharmacol Ther 1985; 38:350-3.
2
3 Mayer AU Sitar DS, Tenenbein M. Muluple-dose charcoal and whole-bowel irrigation do not
increase clearance of absorbed salicylate. Arch Intern Med 1992;152:393-6.
24
Boldy DAR, Heath A, Ruddock S, Vale JA, Prescott LF. Repeated oral activated charcoal in the
treatment of carbamazepine poisoning. Lancet 1987;i: 1027.
25
Neuvonen PJ, Elonen E, Haapanen EJ. Acute dapsone intoxication: clinical findings and effect of
oral charcoal and haemodialysis on dapsone elimination. Acta MedScand 1983;214:215-20.
26
Boldy DAR, Smart V, Vale JA. Multiple doses of charcoal in digoxin poisoning. Lancet
1985;ir. 1076-7.
27
Boldy DAR, Vale JA, Prescott LF. Treatment of phenobarbitone poisoning with repeated oral
administration of activated charcoal QJMed 1986;61:997-1002
28
Weidle PJ, Skiest DJ, Forrest A Multiple-dose activated charcoal as adjunct therapy after chronic
phenytoin intoxication. Clin Pham 1991;10:71-4.
29
Scssler ON, Glauser FI, Cooper KR Treatment of theophylline toxicity with oral activated,
charcoal. Chen 1985,87-325-9.
30
Hillman RJ, Prescott LF. Treatment of salicylate poisoning with repeated oral charcoal. BMJ
1985391.1472.
3) Helt KF, Hackett LP, Dusci LJ, Paterson JW. Disposition of dothiepin after overdose: effects of
repeated-dose activated charcoal The'Drug Monit 1991,13:485-9.
8
(FROM DMJ VOL 306 9 JANUARY 1993, 78-79)
The cervical spine in rheumatoid arthritis
Needs careful assessment
Rheumatoid arthritis commonly affects the cervical spine,
causing several well defined deformities.1 Damage to the
cervical spine from rheumatoid arthritis has been noted in
30% to 46% of necropsy studies and is second in frequency
only to that seen in the metatarsophalangeal joints.2 ’ One in
four inpatients with rheumatoid arthritis and between 17%
and 86% of all patients with this disease have, radiological
evidence of instability of the cervical spine.’-1
These high rates reflect the anatomy of the cervical spine
and the dynamic forces that act on it. Each of the apophysial
and ligamentous articulations of the cervical spine is suscept
ible to the same inflammatory changes as those in peripheral
joints of patients with rheumatoid arthritis.2 Furthermore,
the cervical spine is constrained between a somewhat rigid
thoracic spine arfd a skull weighing 6 kg; movement of the
head, which has been estimated to occur around 600 times
each hour, adds to the forces on the articulations.’
Any segment of the cervical spine may be affected by the
rheumatoid inflammatory process, but destructive changes
are most prominent at the occipitoatlantoaxial junction.
Atlantoaxial subluxation is the most common deformity and is
due to destruction and resultant laxity of tht transverse
ligament. This allows the atlas to move forward relative to
4
the odontoid process of the axis when the neck is flexed.
In radiographs this is seen as a widening of more than 3 mm
in the space between the anterior arch of Cl and the odontoid.
The corresponding reduction in the space posteriorly
restricts the canal available for the spinal cord. By contrast,
posterior subluxation of the atlas is infrequent and is seen only
in the presence of severe erosion and dislocation of the
odontoid.'
Recent studies using magnetic resonance imaging in
patients with atlantoaxial subluxation have shown an inflam
matory mass of granulation tissue around the odontoid arising
from the synovial lining of the articulations. This periodontoid mass is not visible in patients who have had surgical
fusion of the first two cervical vertebrae or in whom deformity
has progressed to that of atlantoaxial impaction (see
below).’10 The bulging of this mass may further reduce the
space available for the spinal cord and cause neurological
deficits in patients with only a moderate degree of atlantoaxial
subluxation.
When the disease affects one of the occipitoatlantoaxial
articulations (termed lateral mass) it may produce the syn
drome of non-reducible rotational tilt of the head, the main
clinical features of which are occipital pain, tender points in ■
SELECTIONS FROM BMJ
vol. 9
march 1993
the neck, and tilting of the head towards the affected side." If
stabilisation and surgical arthrodesis. The place of surgery in
both sides are affected collapse of the lateral masses allows the
the early stages of instability of the cervical spine is less
skull to descend on to the cervical spine and the odontoid to
certain, nor is there any consensus on whether progression
enter the foramen magnum. This deformity has been termed
can be retarded by early surgery. In a retrospective study of
cranial settling, superior migration of the odontoid, or
110 patients with rheumatoid arthritis who had surgical
atlantoaxial impaction and is seen almost exclusively in
treatment we found recurrence of their cervical instability
association with atlantoaxial subluxation."”-’ Subaxial sub
after a mean interval of nine years in 5-5% of patients with
luxation is a late development; it often affects several verte
atlantoaxial subluxation who required only atlantoaxial fusion
brae, leading to a “stepladder” deformity. Extensive rheuma
—but a 36% recurrence rate after a mean interval of 2-6 years
toid disease of the cervical spine results, then, in a combined
in patients with atlantoaxial subluxation and atlantoaxial
deformity of atlantoaxial subluxation—-subaxial subluxation
impaction who required fusion from the occiput to C3. No
and atlantoaxial impaction—a devastating complication and a , patient with atlantoaxial subluxation and fusion of Cl and C2
truly formidable therapeutic challenge.
progressed to develop atlantoaxial impaction.” '*
Many patients with substantial deformities remain asymp
Deformities of the cervical spine are seen most often in
tomatic, but they are at increased risk of neurological damage
patients with rheumatoid arthritis of more than 10 years’
with the passage of time. They are also at risk if they need
duration. They are usually associated with severe destructive
peripheral arthritis, rheumatoid nodules, a high titre of ■surgery or induction of anaesthesia for any other reason. In
one recent study 60% of patients with rheumatoid arthritis
rheumatoid factor, and treatment with corticosteroids.611
having total hip or knee replacements had radiological
Progression of the deformity is unpredictable in a given
evidence of instability of their cervical spine, and nearly half
patient, but follow up for five to 10 years has shown worsening
of these had no symptoms referrable to their necks.” Patients
of the instability in 16% to 41% of the patients.'
*
12 These
with rheumatoid arthritis undergoing any major surgical
percentages may be too low: with progression of the deformity
procedure should be assessed by having radiographs taken of
to atlantoaxial impaction the magnitude of the atlantoaxial
the cervical spine in flexion and extension. Indeed, all patients
subluxation may seem on radiography to be reduced, giving
with rheumatoid disease of the necks, even though asymp
the false impression radiologically of improvement.12
tomatic, should be followed up carefully for evidence of
Many patients with rheumatoid disease of the cervical spine
neurological deficit, and all should undergo periodic radio
remain asymptomatic for years, but they are at risk of a range
graphic monitoring.
of neurological complications and even sudden death from
AMRIT K AGARWAI
medullary compression. Neurological abnormalities may be
Medical Center,
subtle and difficult to establish in the presence of deforming
Beaver, PA 15009
arthritis, muscular atrophy, and the neuropathy that may be
USA
associated with rheumatoid arthritis. Patients may complain
WALTER C PEPPELMAN Jr
of intractable pain in the neck or the back of the head. They
Central Pennsylvania Orthopedic and
may have symptoms of vertebrobasilar insufficiency with
Spinal Associates,
Harrisburg, PA 17109
vertigo or drop attacks and may have signs of myelopathy.” "
Myelopathy, once it develops, is usually rapidly progressive.
DAVID R KRAUS
St Margaret Memorial Hospital,
In patients with subaxial subluxation myelopathy may occur
Pittsburgh, PA 15215
with only slight subluxation because of the narrower diameter
CARL H EISENBEIS Jr
of the spinal canal below the axis. Profound and complex
The University of Pittsburgh,
neurological deficits may be found in patients with the
Pittsburgh, PA 15215
combined deformity of atlantoaxial subluxation—subaxial sub
luxation—atlantoaxial impaction. Atlantoaxial subluxation
with subluxation of less than 9 mm carries the least risk of
1 Bland JH, Rheumatoid arthritis of the cervical spine. J Rheumatol 1974;!. 319-42.
2 Eulderink F, Meijers KA Pathology of the cervical spine in rheumatoid arthritis: a controlled study
neurological damage, while atlantoaxial subluxation of more
of44 spines. J Pathol 1976;120:91-108.
3
Bland JH, Davis PH, London MG, VanBuskirk FW, Duane CC Rheumatoid arthritis of cervical
than 9 mm, atlantoaxial impaction, subaxial subluxation,
spine. Arch Intern Med 1963;112:130-6.
non-reduc.j.e rotational tilt of the head, and combined
4
Conlon PW, Isdale IC, Rose BS. Rheumatoid arthritis of the cervical apine— an analysis of 333
deformities are all associated with a higher risk of neurological
cases. Ann Rheum Du 196635:120-6.
5
Mcikle JA, Wilkinson M Rheumatoid involvement of the cervical spine. Radiological assessment.
*
deficit.
”
Ann Rheum Dit 1971;30:154-61
6
Smith PH, Benn RT, Sharp J Natural history of rheumatoid cervical luxations. Ann Rheum Du
Plain radiographs of the cervical spine in flexion and
197231:431-9.
extension will allow recognition of atlantoaxial subluxation
7
Konttinen YT, Santavirta S, Kauppi M, Moskovich R. The rheumatoid cervical spine. Current
Opinion in Rheumatology 19913:429-40.
and subaxial subluxation. In patients with atlantoaxial impac
8
Weissman BN, Aliabadi P, Weinfeld MS, Thomas WH, Sosman JL. Prognostic features of
atlantoaxial subluxation in rheumatoid arthritis patients. Radiology 1982;144:745-51.
tion, however, odontoid erosion and osteoporosis may make
9
Larsson EM, Hollas S, Zygmunt S. Pre- and postoperative MR imaging of the craniocervical
plain radiographs inadequate for assessing the extent of
junction in rheumatoid arthritis./1JR 1989;152:561-6
10
Milbrink J, Nyman R. Posterior stabilization of the cervical spine in rheumatoid arthrius: clinical
cranial settling and resultant penetration of the odontoid into
results and magnetic resonance imaging correlation. Journal of Spinal Disonlen 19903:308-15.
the foram'm magnum. Various measurements have been
11
Halla JT, Hardin JG Jr. The spectrum of atlantoaxial facet joint involvement in rheumatoid
arthritis. Arthritis Rheum 1990;33:325-9
advocated to define the extent of cranial settling. McGregor’s
12
Matthews JA. Atlanto-axial subluxation in rheumatoid arthritis. A 5-year follow-up study. Ann
line, which assesses the protrusion of the odontoid process
Rheum Dit 197433:526-31.
13
Nakano KK. Neurological complications of rheumatoid arthritis. Orthopedic Clinics of North
above the foramen magnum, is widely used in clinical
America 1975;6:861-80.
14
Kraus DR, Peppelman WC, Agarwal AK, De Lcuw HW, Donaldson WF HI. Incidence of subaxial
practice. Because of its superior contrast capabilities magnetic
subluxation in patients in generalized rheumatoid arthritis who have had previous occipital
resonance imaging is the current first choice technique for
cervical fusions. Spine 1991;16(suppl):S486-9.
15
Agarwal AK, Kraus DR, Eisenbeis CH Jr, Stolzcr BL Balk PM, Barkley TA. Anatomical and
assessing instability of the cervical spine.1'12
neurological characteristic of cervical spine involvement in rheumatoid arthrits. J Orthop
Patients with a minor degree of atlantoaxial subluxation or
RAmworo/19893:77-89.
16
Kauppi M, Sakaguchi M, Konttinen YT, Hamalainen M. A new method of screening for vertical
with subaxial subluxation need treatment only with a soft
atlantoaxial dislocation. J Rheumatol 1990;17:167-72.
17
Bell GR, Steams KL Flexion-extension MRI of the upper rheumatoid cervical spine. Orthopedics
cervical collar—which provides symptomatic relief, acts as a
' 1991;14:969-73.
reminder to patient and doctor, and may provide some degree
18
Agarwal AK, Peppelman WC, Kraus DR, Pollock B, Stolzcr BL Eiscnbeis CH, et al. Recurrence
of cervical spine instability in rheumatoid arthritis following previous fusion: can disease
of protection from trauma. In the presence of intractable
progression be prevented by early surgery? J Rheumatol 1992;19:1364-70.
cervical pain, neurological deficits, or myelopathy, or combi
19
Collins DN, Bames CL FitzRandolph RL. Cervical spine instability in rheumatoid patients having
total hip or knee arthroplasty. Clinical Onh^pedn < and Related Reieareh 1001 ;272:127-35
nations of these, the recommended procedures are halo
{FROM BMI VO[
SELECTIONS FROM BMJ
vol. 9
march 1993
.106 9 JANUARY |9«l3 70 »i.
5
'T7lS- J./V. i3
Diabetes anti its. LLiamuzsJji
Health Committee
Lok Vidnvan Sanghatana. Maharashtra
What is diabetes? Why does it occur?
When
sugar in our blood can not be utilised adequately by the cells
in
the body, the level of blood sugar increases beyond
the normal
limit and this is diabetes.
In diabetes, not only the sugar in blood
but the metabolism of carbohydrates, proteins and fats gets disturbed
and a complex disease process sets in.
The iood we eat ultimately gets converted in our body into a sugar
called glucose.
This glucose provides the energy required for the
bodily functions.
A hormone called “insulin" is essential for
the
utilisation of the glucose by the cells.
Insulin is produced by some
special cells
in the organ called "pancreas".
In diabetes,
this
insulin
is either not produced in adequate quantities or does not
get utilised properly, due to which the cells cannot convert
the
glucose
into energy.
Instead, it keeps accumulating in
the blood.
This results in an increased level of glucose in blood.
The exact
reason
as to why insulin is not produced or utilised
properly
is not
known.
To some extent diabetes
is hereditary.
However, obesity, lack of exercise and improper food habits are known
to
interfere
in the action of insulin. This is seen from the
fact
that Indians
settled
abroad with affluent,
sedentary,
Western
lifestyle show a higher pe-reentage of diabetes.
What are the ill effects of diabetes?
If the level of sugar in blood increases beyond normal limits, it has
several ill effects.
The fine blood vessels called "capillaries" get
damaged
due
to high blood sugar.
This may cause blindness due
to
bleeding
from the capillaries in the retina of the
eye.
Diabetes
increases
the chances of cataract or glaucoma
(increase
in
the
pressure in the eye-ball).
Diabetes also affects the capillaries in the kidneys, heart, skin
or
nerves.
It also increases the proportion of fatty substances in
the
blood which
in turn leads to a condition
called arteriosclerosis
(hardening of blood vessels called the arteries).
A fatty substance
called cholesterol gets deposited on the inner lining of the arteries
and
thus increasing the resistance to the flow of blood through
the
arteries. This causes high blood pressu
UlZitaG.
Increased
b’lood sugar
increases the chances of
infection as the
sugar
itself is a good nutrient medium for the infectious agents to
grow.
Therefore, the chances of fungal infection of external genital
organs,
or of urine infection or T.B. are more in diabetic persons.
The prevalence of impotence in diabetic men is higher. In diabetic
women,
if the disease is not kept under check during pregnancy,
the
chances of still birth or of a deformed foetus are more. In
fact
a
diabetic
women should
keep diabetes
under control before
she
conceives.
When should diabetes be suspected?
Diabetes usually occurs after the age of 30 or 40 years.
There
is
the
other, more severe form of diabetes in which the production of
insulin is almost stopped. This can happen in childhood or in young
age
also.
In
this juvenile diabetes, the patient becomes weak,
despite eating frequently. The person remains ever
hungry because
despite having
lot of sugar in the blood, the body
cells cannot
utilise
it (i.e. they remain starved).
The muscles and fats in
the
body get broken down into sugar in an attempt to provide sugar to the
cells.
However, it is of no use due to lack of insulin.
This break
down
of muscles, fat causes loss in weight,
tiredness and . excess
sugar gets filtered down into the urine.
Th$>sugarjafso absorbs more
water
from
the blood into the urine.
This
results
in frequent
urination
and persistent thirst.
If this is not attended to,
the
young diabetic falls seriously ill and may develop coma.
The
symptoms of diabetes in older age are relatively minor.
These
patients have frequent hunger and thirst,
frequent urination and
tiredness as in juvenile diabetes but in a milder form.
The patient
has
to get up at night for urination.
Delayed healing of wounds,
tendency to develop pus,
itching due to fungal
infectionj ami
premature dimness of vision, feeling of tingling, numbness in
hands
and
feet, impotency -in men and unsuccessful pregnancy
in women....
all these symptoms can be due to diabetes.
If close blood
relatives
are/were diabetic,
one should be more suspicious about
these
symptoms.
However, absence of these symptoms does not necessarily
mean absence of diabetes.
Nearly 50% of diabetics do not show these
symptoms. Diabetes can be diagnosed with certainty only through blood
test.
Therefore after the age of forty years, blood sugar- should be
tested at least once in five years.
How is diabetes diagnosed?
As mentioned above, diabetes can be correctly diagnosed only by blood
sugar test.
Test
for only urine sugar does not give
a certain
diagnosis.
This is because in some cases urine may show sugar with
the blood sugar being normal or in some case blood sugar may be high
but sugar may be absent in urine.
2
The blood sugar may be examined after the person
remains without
food,
drink (except water) for 10-12 hours.
This is called as
the
"fasting"
sugar.
If it is more than 140 mg per 100 ml of blood
it
means the person has diabetes.
However, if it is less than 140 mg it
does not necessarily indicate absence of diabetes.
Therefore in such
persons, a test called post-glucose blood sugar is done. In this test
the person is asked to take 75 gram glucose in water after fasting
for 10-12 hours.
The patient is advised not to take anything
except
water,
not to smoke or to exert for two hours after taking glucose.
Exactly after 2 hours? another blood sample is taken ,to test the blood
sugar level.
If the person has diabetes then
b.Lwd'- would be more than 200 mg/100 ml of blood two hours after the
glucose meal.
Some time instead of giving glucose, the patient
is
asked
to have normal food and the blood is tested two hours after.
The test performed by giving glucose is more reliable
for correct
diagnosis because we are giving measured quantity of glucose.
If
the sugar level is found to be 115 to 140 mg in fasting sample or
between 140 and 200 mg in the sample after glucose/food the diagnosis
becomes uncertain.
Under such circumstances further testing or
frequent
testing or
testing after controlling diet and
doing
exercises may be done on the advise of the doctor.
Besides blood sugar what other tests are required?
If diabetes
is confirmed by blood-sugar test a thorough physical
examination
of
the patient
including weight,
blood
pressure,
examination
of the heart, blood vessels, nervous system,
retina is
carried
out because diabetes can affect these systems.
Any problem
of
kidney function can be detected by simple urine examination.
If
any problem is detected in this urine-examination, further test can
be done to know its extent and severity.
Urine sugar is also tested.
Although, test for blood sugar is must for the diagnosis of diabetes,
once
it is'diagnosed urine can be tested every week at home by the
patient himself/herseIf to get a rough idea as to whether the disease
is under control or not.
Initially the urine is also tested for the presence of substances
called "ketones". The presence of ketones indicates that the persons
is suffering from severe diabetes.
This calls for
'immediate
treatment.
Once diabetes is detected tests for blood fats (lipids)
and electrocardiogram of the heart are also done.. Diabetes is
known
to
induce abnormal changes in blood-fat and in the ECG. These
tests
are therefore helpful to decide -pfr the line of treatment.
3
Can it be cured?
What is the treatment for diabetes?
Diabetes
can not be completely cured and once acquired it stays for
life.
However, with appropriate exercise, diet control and drugs
it
can
be
kept under check.
Mild diabetes can be kept under control
without
taking medicines with the help of proper diet and exercise
alone.
In addition to diet control and exercise,
some patients have
to take antidiabetic drugs. In some, only tablets are needed, but
in
some patients, insulin injection is to be taken daily.
Diet:
Indian, especially Maharashtrian traditional balanced diet
is
mainly based on cereals and pulses.
There is no qualitative change
required in this diet for a diabetic person.
One has to avoid sugar,
consume only very limited quantities of oil, butter, ghee, etc., take
only limited quantities of food to maintain weight within prescribed
limits.
The formula for prescribed limit of weight is height
in
cms minus one hundred = weight in kg.
If your weight is more than
this limit, with the help of following simple guidelines change your
diet to reduce weight.
To
reduce 1 kg weight in a month through dieting, one will
have to
reduce
7200 calories from diet (about 240 calories per day).
One
hundred
calories are provided by the
following food
items and
accordingly the calories can be controlled by appropriate
reduction
in
consumption.
Cooked ri.ee - 1 cup - 30 grams of dry
rice);
one
chapati of 6“ diameter (made out of 30 grams of wheat);
one sada
dosa; two idlis; two slices of bread; one cup (katori) liquid dal (in
the form of sambar, amti, etc.); one egg; one banana; 2.5 spoons of
butter, 2 spoons of oil or ghee.
The, following can be. consumed in. liberal quantities as they have low
calories e.g. carrot, cucumber., onion, tomato, lavaki (dudhi bhopla),
radish, clear vegetable soup, etc.
The following should
ke. taken only in moderate quant i4 ies:
(The
calories contained in the oil used for cooking have not been
taken
into account.
Oil should be used to the minimum).
Vegetables
like
cabbage,
cauliflower, ladies finger, brinjal, etc.
Fruits such as
papaya,
sweet lime, oranges, figs, etc.
Fluids such as butter milk
and milk without cream, tea without sugar, fish, lean chicken, etc.
1
The
fol lowing sliuuld. Lifi. Lakeu. in very email
sweet potato, yam, sago, green peas, guava, banana,
apple, etc.
mango,
potato,
custard
gud or
The
following should tie. avoided as. Lar as. possible: Sugar,
ice-cream, jams,
pastries,
cream,
ghee,
jaggery,
honey,
sweets,
They
butter, fried foods, oi.ly pickles, groundnuts, almonds, cashew.
are calorie-rich substances.
Alcohol also has calories like sugar. It should be avoided.
This is
particularly so when the diabetes is severe and not under control or
when
other complications are present.
Eat a little at a time,
four
times a day so that the sugar level in blood does not rise suddenly.
Use only limited quantity of oil for cooking.
Daily 20 grams of oil
per
head
i.e. about 0.
kg per head per month is the
limit.
Other
fats particularly animal fats such as ghee, butter should be
avoided
as they are much more likely to increase cholesterol
in diabetics.
Home made ghee may be used but it should be restricted^only one tea
spoon in a day (10 grams).
Diabetes may also result in other problems relating
to heart and
kidneys. If this happens, this would need further diet control, which
should be done under appropriate medical advice.
There is a general
misconception that diabetic should not eat rice.
As a matter of fact
rice has
less calories as compared to chapati or roti
(weight for
weight).
However, since rice has less fibre content its digestion is
quicker which may increase blood sugar.
There is no harm in
eating
limited amount of rice.
Exercise: Exercise reduces the amount of insulin required to control
blood sugar.
With' the
help of proper diet and
exercises
it
is
possible for some diabetics either to avoid use of drugs altogether
or reduce its dose. Therefore diabetics must do some light exercises.
Hany diabetics are overweight and exercise
helps
to
reduce
it.
Walking
is
the simplest and the safest exercise.
One
should
walk
briskly for at least half hour to stay fit, and for longer time to
reduce weight.
To reduce 1 kg in a month one
has to burn
7200
calories through exercise. Keeping in mind the need to reduce weight
to the desired level within 3-6 months, the diet and exercises have
to be planned.
T;ype.s. of. activities and. calorie consumption ■ p±;r minute:
Cleaning
household utensils, mopping, gardening, painting - 2 to 5 cal;
works
like masonary - 4 to 5 cal; brisk walk, climbing
stairs,
cycling,
tennis, carpentry - 5 to 10 cal.
2
In fact
exercises
are of three types and
the exercise programme
preferably
should
include
all
the three.
Please
refer
to the
separate booklet by the Health Committee on this subject.
Diabetics
should consult doctor before starting these exercises,
and
also
observe the following precautions.
A patient taking insulin should eat 25 to 30 gms
of carbohydrates
(half a banana or guava, half cup milk or butter milk) before
exercise.
Otherwise exercise may induce sudden drop in
sugar
level
causing giddiness.
If
the person also has
hypertension or heart
ailment, only such exercises which can be easily tolerated should be
done
in
consultation with the doctor. However there is no need
to
consult a specialist if one chooses only brisk walk as exercise.
If
there is a problem in the retina of the eye, exercises which include
jerky movements and lifting of weights should be avoided since they
may trigger bursting of already weakened capillaries. Exercise causes
quicker absorption of insulin injected on arm or thigh. If the time
of exercise coincides with that of the injection, the injection may
be taken under the skin on the abdomen.
Medicines: The prescribed medicines should be taken at the right time
in correct dosages and should not be changed without medical advice.
Diabetes cannot be cured and therefore diet control should always be
properly observed. In some cases insulin is needed only for temporary
reasons such as during stress like pregnancy or during illness.
Once
the stress is over, insulin can be replaced with tablets.
Diabetes may cause symptoms such as tingling and numbness or burning
or pains in hands and feet. Sometimes 'B' vitamin is prescribed
to
treat these symptoms but its utility has not yet been
scientifically
proved.
However,
due control on the blood sugar can
reduce
these
problems in some patients.
How to know whether diabetes is under control or not?
Symptoms of diabetes
recede as diabetes is controlled.
The
true
indication
of control of diabetes is level of blood sugar which to
some extent can be gauged by testing urine sugar, brine sugar can be
tested
at
home but it is not very dependable. Its utility
for
a
particular patient is determined by the doctor depending upon factors
like the severity of diabetes and patient's attitude.
If
the patient does not have to take .nsulin it is good to test
the
blood
and urine sugar every month (however, if the patient
cannot
afford it, then at least every three months) to know whether diabetes
is under control. If the patient is on insulin then
more frequent
testing
for blood-sugar is required depending upon the
severity of
the disease.
The usual blood sugar test indicates whether the sugar has
increased
beyond
normal
limits on
that particular day.
A test
called
Glycosylated Hemoglobin' shows the control on blood sugar during the
preceding
3 months. Since this test is more expensive costing about
Ks.
150
to 200, doctors do not advice it
to all
the diabetics.
However,
if the doctor suspects that Die patient does not
take
the
necessary
precautions related to fad’d, exercise and medicines,
this
test becomes quite necessary.
.D(
In the initial stages of the treatment when there is a need to reduce
15
weight,
the patient should keep a note of his/her weight every
days for a^few months and if the progress is satisfactory, a monthly
check-up weight is enough.
Once in a year it is necessary to do a general physical check up and
examination
of
eyes,
urine, blood
cholesterol,
ECG
as diabetes
increases
the possibility of certain problems in the eyes,
kidneys,
and
the heart. These^diseases.are symptomless in the initial stages
and
hence they aggravate silently. These tests are therefore needed
to detect
these diseases at an early stage. This is more so
for
certain retinal problems which otherwise could cause blindness.
This
blindness can be prevented by timely check up and treatment of
the
disorder at an early stage.
What other care is required?
Any increase or recurrence of symptoms of diabetes should be reported
to the doctor and be properly treated. Any infection should also not
be
ignored
and a prompt, proper treatment for that infection
is a
must,
as any
infection can quickly become serious in
a diabetic
person .
Specific time
table for for food and medicines should be strictly
observed.
An
excess dose of insulin or a powerful oral drug
in
relation to diet may cause a sudden drop in the level of blood sugar.
If this happens, the patient may get profuse sweating,
giddiness,
uneasiness
and even unconsciousness. In this situation 4-5 spoonful
of sugar should be taken. A patient on insulin or powerful oral anti
diabetic drugs should carry a small plastic packet of sugar (about
5
spoonful) in his/her packet. Patients taking insulin should carry an
identity card with a drug chart indicating the drug used and dosages.
tt
W
Diab- tics should avoid all forms of tobacco as it increases risk of
heart diseases. They should avoid walking barefoot, should cut
their
nails properly and do proper early dressing for all kinds of injurie
including small cuts as diabetics are more prone to get their wound
infected fast and develop a septic.
4
pi s ■ i fuS"
NATIONAL CAMPAIGN
ON
DUST RELATED LUNG DISEASES
UPDATE
Dear Friends,
It was not long ago that you received the last update. During this period two major tragedies struck our nation;
one was the earthquake in Maharashtra and the other, fire at New Kenda Colliery at Asansol, West Bengal.
We had human loss in both of this, but only difference is, whereas earthquake was natural and unpredictable,
accident in New Kenda Colliery was man-made and predictable. Who ever works or gets opportunity to visit
coal mines of our country knows in what hazardous conditions miners work in them. Many significant and
important safety operations are neglected. The inquiry reports of Chasnala and Mahabircollieries accidents had
already named management for failure in safety standards. Past records also show that there has been twenty
five percent increase in the accidents in the coal mines in the country. But this astonishing fact has not opened
the eyes of either the managements or the policy makers. We express our deep sorrow and solidarity with the
Trade Unions of Asansol and the family members of those who have sacrificed their life in this race of blind
industrialisation.
1. A significant development for NCDRLD, is the announcement of shifting its secretariat to Baroda. If you
remember in the last National Convention which we had in Delhi in December 1992, it was said to shift
secretariat rotation wise so that issues and problems can be highlighted. This will also give this campaign a
true national character.
2.On December 17, 1993, a meeting of the active partners of NCDRLD was convened at Baroda. 25
participants from Trade Unions, Non-Governmental Organisations, Government and Research Institutes and
activists attended this meeting. Mr. Jagdish Patel introduced the agenda to the participants, which was followed
by the presentation of the report of last year's activities of the Campaign by M r. Harsh Jaitli. Most of the activities
are reported in the previous update.
3.
Mr.H.P.
Mishra of MKSS Mandal, Ahmedabad discussed at length about the movement for compensation
and prevention of byssinosis, which is going on in Ahmedabad. While appreciating the efforts made by ESI
Scheme of Gujarat for identifying cases of Byssinosis, he criticised ESI Corporation for delaying the process
of disability assessment and compensation payment to the sufferers. According to Mr. Mishra - workers are
waiting fortheirturn to get compensation. He also expressed the need forspreading the same type of movement
in the areas like Bombay and Kanpur, where textile industry is concentrated.
4. Mr. Jagdish Patel and Mr. Aman Vyas shared their experiences of working with Silicotic workers at Khambhat
(Gujarat). Mentioning about the difficulties faced by them he said that, in Khambh at the employers pressurised
the sympathisers of the movement not to adopt safe technology. The employers lobby used Government
officials in their efforts to stop safety measures. The Co-operative employees were dragged to the court on
flimsy charges, for which court fined them. “ We had our limitation of providing defense to the sympathetic
employers. These were the problem faced by activists in early studies” he said. One of the Semi-Government
organisations has developed the safe-technology upon request by the campaign but this machine still requires
some modifications in design before it becomes acceptable to polishers of different shapes. The machine now
prepared, is useful to only one for type of shape. It was also felt that the polishing work is spreading to the other
new regions where the campaign activities are needed to be initiated. Last year, these agate workers were given
coverage of life insurance under scheme for rural workers by Life Insurance Corporation. JANPATH, an
Ahmedabad based NGO worked as nodal agency. Its representative Aman Vyas informed that among 900
workers covered under this insurance scheme, 25 had already died of silicosis. The LIC felt that this death rate
is very high and so they hiked the premium rates. Which was double of the original rate of Rs.15. JANPATH
is busy negotiating. Ms. Rani Advani of CERC, Ahmedabad, offered her help for litigation against LIC, on this
issue.
SecretariatPTRC : 63, Snehsmruti Society, (Behind Nutan Maheshwar Society)
Shubanpura, Baroda - 390 007, Gujarat
5. Com. Rajkumar Singh, AITUC, Baroda, expressed a need to form a local committee on ESI In Baroda to look
after the problems. During discussion ESI was frequently attacked by the participants. So, In order to clarify
the stand Dr. CharulataShah, Dy. Director, ESI Scheme, Gujarat State, gave details of the working of ESI. She
informed that the most of the criticism of ESIS is for monitory problem, which is handled by ESI Corporation.
She informed delegates that the ESI Scheme gets money from corporation. The amount, the scheme gets from
corporation is too less. The State Government spent Rs.4-5 crore in excess and the State Government is now
asking the Corporation for more money.
6.Dr. J.R. Parikh of N1OH gave details of his recent research on Bysslnosls. His research Is now focused on
prevention part and not on identification. He has reached to the conclusion that, it is the leafy part of the cottonplant which is responsible for the disease. He further informed that if better quality of cotton is used and process
of cotton-picking is modified, the dust level can be reduced. He also explained the design of the training
programme on Byssinosis. He mentioned about the administrative problems during the training of the first
batch, which was taken care of by the arrival of the subsequent batch. All the members supported this strategy,
and requested the secretariat to circulate a copy of his lecture.
7.In the later half of the meeting a budget and activity plan was charted out. It was unanimously agreed to raise
funds for NC-DRLD, through contribution. Major activities included publication and distribution of four updates
every year. In order to motivate and support activities on dust related lung diseases, traveling was also
suggested.
All these activities, along with other expenses like postage-photostat and other administrative assistance would
amount to Rs.1,00,000. This does not include salary of the Co-ordinator and office rent. So need was felt to
raise fund through appeal. Accordingly we are sending you herewith an appeal for the contribution and look
forward for your active involvement.
Role of Secretariat was also discussed. It was clear from the discussion that partners find the role of Secretariat
as a major linking force. Secretariat will not only publish Updates, but also disseminate, information and create
adata bank with the help of PRIA and other Research Organisations. It will also assess the needs of the partners
and link them with the available facility.
The meeting concluded with a note of thanks for the AITUC, Baroda who, provided its office for this meeting.
We look forward to your continued support and involvement in the campaign and your suggestion for making
it more effective.
With best wishes
Yours sincerely
APPEAL FOR SUPPORT
National Campaign on Dust Related Lung Diseases was Initiated in 1990. PRIA, Delhi nurtured the campaign
since its inception by providing secretarial support. The major activities undertaken by the NCDRLD during that
period were National convention, poster competition, and research studies and popular publications. The
campaign has achieved very positive results so far in some areas. Yet it has to go a long way to achieve its
objectives. During all these years, Trade Union and NGOs, doctors, lawyers and Government institutions have
become partners in our struggle to achieve dust free working environment. The campaign needs to be
strengthened further. You have been involved in the campaign activities for quite sometime, now this update
comes to you with an appeal for your contribution.
Jagdish Patel, PTRC, 63, Snehsmrutl Society, (Behind Nutan Maheshwar Society)
Shubanpura, Baroda - 390 007, Gujarat
The cheque/draft should be in favour of NC-DRLD A/C
Med. Res., 52, 6, June, 1964.
K. R. P. Singh, Khorshed M. Pavri, and C. R. Anderson.
\NSM1SSION OF KYASANUR FOREST DISEASE VIRUS
Il.-EMAPHYSALIS TURTURIS, H sEMAP HYSAL.IS PAPU
ANA KINNEARI AND HAEMAPHYSALIS MINUTA.
K. R. I’. SINGH’, KHORSHED M. PAVRI
,
*
and C. R. ANDERSONf.
drum lhe Virus Research Centre, Poona, lndia.)t
;Received fur publication, April 8, 1964.]
in ihc Kyasanur
i disease (KID) epidemic area (Trapido et al., in press), isolations of KFD
Lave been made from seven : 11. spinigera, 11. lurluris, 11. papuana kinneari,
i ['/Jala, ll. kj aumirensis, 11. niinula and 11. Wellington! in that order of frey (Virus Research Centre, unpublished data). Of lhe above, laboratory
.mission ol KI'D virus has so far been reported for 11. spinigera (Varma et al.,
')i i id 14 species of licks of the genus llamaphysalis found
1 he present communication deals with the studies on experimental trans
al transmission of KFD virus by //. lurturis, //. papuana kinneari and 11.
.a and transmission of lhe virus by bile to susceptible animals. These three
. ■> were selected because they have been successfully reared in lhe laboratory.
..ipts to rear other species have not yet been successful.
Materials and methods.
< j 11338 strain of KFD virus, originally isolated from a mixed pool of larvic
nymphs of llama physalis sp. collected in the Kyasanur Forest, was employed
nghoul. Il had undergone three iniracerebral adull mouse passages and five
imuscular passages of infected blood in one-day old while leghorn chicks.
All oflhe species of licks in this study were obtained by ‘Hag dragging' or
iicct picking from leaves in lhe foresl of llillemarur, Shimoga District, Mysore
India. 11. lurluris and 11. papuana kinneari were collected as unfed adults
//. minuia as unfed nymphs and subsequently reared in the laboratory. After
lying the adull females were tested individually for presence of virus as desJ below. Progenies from licks found uninfected were employed in these
i imcnls.
I he ticks were infected as 10 io 15-day old larvic on two-day-old white
h n chicks which had been inoculated intramuscularly 24 hours before with
oximalcly 1O'J LD5U of KFD virus. Some of the freshly engorged larva: were
.itcd and the suspensions inoculated into mice to assure that they had ingested
while feeding ; the remaining fed larva: were kept in desiccators maintained
.c.irch Officer, Virus Research Centre, Poona, India.
ii Member, l he Rockefeller Foundation, Virus Research Centre, Poona.
Virus Research Centre is jointly maintained by the Indian Council of Medical Research
I lhe Rockefeller Foundation.
566
567
al 25°C. to 28°C. and 90 to 95 per cent relative humidity (R.ll.) and allowed to
moult into nymphs.
When lhe nymphs were ready for feeding, some were tested for lhe presence
of virus. The remaining nymphs, in pools of five, were released on one-day-old
chicks to determine their ability to transmit virus by bite. Most of the nymphs
released on chicks allached within 24 hours and became fully engorged in three to
four days. Some, which did not attach, died very soon and were discarded. Blood
from the chicks was drawn into heparin on the third day and on the fifth day after
thp release of the nymphs, and was tested for lhe presence of circulating virus.
Suspensions of lhe fed nymphs from each chick were also tested for virus.
Other nymphs, in groups of 20 lo 30, were fed on one-day-old chicks. These
fed nymphs were not tested for virus but kepi al 25 C. to 28 C. and 90 to 95 per
cent R.H. for moulting into adults. The chicks were bled into heparin on lhe
fourth day after lhe release of the nymphs and lhe bloods were tested for circula
ting virus.
Only the adults of 11. niinula were fed on one-day-old chicks lo determine the
transmission of virus by bile since lhe adults of lhe other two species of licks did
not feed on any KFD susceptible laboratory animal. Because of an acme shortage
of mice it was not possible io test for circulating virus, therefore, lhe chicks on
Which adults of 11. minuia had fed were bled 22 days afier lhe release of ticks and
their serum tested for lhe presence of antibodies. The adults of //. papuana kinneari
and H. lurluris were processed and inoculated into adult mice in order to deiecl
lhe presence of virus.
Suspensions of ticks were prepared by grinding larva: and nymphs in 1-0 ml.
to 1-5 ml. and adull licks in 2-0 ml. of 0-75 per cent bovine albumin in phosphate
saline (BAPS), pH 7-2, containing 1,000 units of penicillin and 1-0 nig. of strepto
mycin per ml. The suspensions were centrifuged at 2,000 r.p.m. for ten minutes.
Al) search for and titrations of virus were done in adull mice inoculated intra
cerebrally. Titres of virus have been expressed as LD5U per 0-03 ml.
Serological confirmation of the virus present in tick suspensions and chick
bloods was made sufficiently often at all stages of lhe experiments to provide reason
able assurance that lhe agent being transmitted was in fact KFD virus. The virus
was identified by complement-fixation tests employing a crude 10 per cent suspen
sion of infected mouse brain as antigen. Immunity in chicks was tested by hiemagglulination inhibition (111) technique (Clarke and Casals, 1955).
Results.
A.
Hannaphysulis lurturis i
(i) Trans-siadial transmission of virus.—The titres of lhe circulating virus on
the fourth Pl day of the four donor chicks fed on by larval tick batches 65, 66,
67 and 68 were 10E,s ^105,1 ^105'6 and 105,0 LD60 for adull mice, respectively
(Table 1). Suspensions prepared from each batch consisting of live fed individual
Kyasanur Forest Disease Virus.
S68
I.uvx and three pools of live larvx each, were tested for virus soon alter dropping
lioni the host All were found to contain virus.
569
A-r<
K. R. P. Singh, Khorshed M. Pavri, and C. R. Anderson.
A#
Table 11.
Transmission of KFD virus to chicks by bile of infected nymphs of Fl. turturis.
Table I.
Trans-siailial transmission of HFD virus in H. turturis.
Balch
number.
(.5
(,(,
67
68
total
Fed larvae :
Circulating <
virus litre
of donor
Indivi
5 larvx in
, chicks on
dual
a pool.
4th PI day.
larvx.
IO1-' I.D4i,
> 10' ‘ I D.o
>!0's I.D,b
10“ I.D..
Unfed nymphs:
|
Unfed adults ;
5 nymphs
in a pool.
Individual
nymphs.
Individual
females.
Indivi
dual
males.
5/ 5
5/ 5
5' 5
4/ 5
11/13
10/15
9/15
5/15
19’20
20/30
15/30
3/ 3*
3/ 3
3/ 3
3/ 3
5/ 5
5 5
5/ 5
3/ 3
3/ 3
3/ 3
3/ 3
1212
15/15
12/12
• Numerators are the number positive for KFD virus ; denominators arc the number tested.
Similarly, suspensions prepared from each batch consisting of five unfed
individual nymphs and three pools of five nymphs each were tested for the presence
of virus 13 to 17 days after moulting and 25 to 30 days after the termination of the
infective feed as larva:. KFD virus was isolated from all the individuals and all
of the pools of the first three batches. In batch 68 all three pools and four out of
live individual nymphs were positive for KFD.
Twenty to 30 days after the emergence of the adults, 90 to 95 days after the
end of the infected blood feed in the larval stage, the ticks from only two batches,
(>5 and 68, were tested for the presence of virus. KFD virus was isolated from ten
out of 15 males and from 11 out of 15 females of batch 65, and from five out of 15
males and from nine out of 15 females of batch 68.
(//) Transmission of virus by infected nymphs io chicks. — Unfed nymphs in
groups of five from batches 65 and 68 were released on nine one-day old chicks
(Table 11). Transmission of virus by bite was accomplished in all cases ; fed
nymphs from each were also shown to contain virus following inoculation into
adult mice. In a second series, groups of 20 to 40 nymphs from both batches were
released on nine one-day old chicks. KFD virus was isolated from the bloods of
all the chicks.
lla-maphysalis papuana kinneari :
(i) Trans-stadial transmission of virus.—Larva: from batches 112, 113, 114
and 115 were released on four infected chicks. The titres of the circulating virus
on the fourth PI day of these four chicks were 10G'°, 105,a, IO1,7 and 103,8 LD60 for
adult mice respectively. Suspensions prepared from each batch consisting of five
fed individual larva: and three pools of five fed larva: each were tested in adult mice
for the presence of virus. All of the individuals and pools of freshly engorged
larvx in batches 112, 113 and 114 and four out of five individual larvx and two out
of three pools in batch 115 were found to contain virus (Table III).
B.
From among the nymphs which emerged from the remaining larvx, suspci
sions were prepared from each batch consisting of five unfed individual nymphs an
three pools of five nymphs each and were processed for virus isolation 15 to 22 da
after moulting and 33 to 35 days after finishing their larval feed. KFD virus v>
detected in four out of five individual nymphs and two out of three pools of nympl
from batch 112 and two out of five individual nymphs and one out of three poo
of batch 113. No virus was detected from either individual nymphs or pools
nymphs of the other two batches.
No virus was isolated from the unfed adults emerging from the three batchv
113, 114 and 115, when individual suspensions of 15 males and 15 females fro
each batch were inoculated into adult mice 78 to 80 days after the termination
K. R. P. Singh, Khorshed M. Pavri, and C. R. Anderson.
Kyasanur Forest Disease Virus.
their larval feed and 12 lo 17 days after moulting. No adult could be obtained
from batch 112 in this part of the experiment as very few nymphs were obtained
and all of them were used in the earlier part of the experiment.
(//) Transmission of virus by infected nymphs to chicks. — Unfed nymphs in
groups of five were released on 20 one-day-old chicks. Transmission of KFD
virus was successful with all the five groups of batch 112 (Table IV). In batch 113,
. pithough three out of five pools of fed nymphs were found infected, transmission
• copld be shown by only one group. There was no transmission of virus by batches
and U5 and no virus was isolated when suspensions of the fed nymphs were
tested in mice. In the second series of experiments when 15 groups of unfed
; pymphs each consisting of 30 nymphs from batches 113, 114 and 115 (five groups
from each batch) were released on 15 chicks, transmission by bite was accomplished
, in three instances in batch 113 and once only in batches 114 and 115.
■siinsaJ
UOISSllUSUVJJ,
•.sqdiUAU paj ui
smiA jo aauosarj
Z
Z
z z z
a
•p3j i
ju jaquinN
3 3 3
•pOSL'dpJ
5i|duiAUjo jaqiunjq
■laqiunu ^aiqD !
sijnsaj
UOISSILUSUCJ±'
.sqdiUAU paj ui 1
3
Hamaphysalis minuta :
(/) Trans-stadial transmission of virus.— Two batches of lame (69 and 70)
were fed separately on two infected chicks. The titres of the circulating virus on
Jhe fourth PI day of these two chicks were IO13 and IO
* ’3 LD50 in adult mice res
pectively. Suspensions prepared from both batches consisting of live fed individual
■( jaryte and three pools of five fed larva: each were processed soon after feeding, and
a|l were found to contain virus (Table V).
C.
.
Z
siuia jo aouasojj
Z
E
•paj
sqdiuXu jo jaqujnbl j
z
•posuopj
sqdiuXu jo jaqiuntq
£
§ 3
3.
■jaqiunu spiHD 1
3
3
Table V.
Trans-stadial transmission of KFD virus in II. minuta.
3
8
•sqnsaJ ,
UOISSHUSUUJJ. j
-.sqdiuAu paj uj I
|
£
siuia jo aauasa-ij
571
Patch
numbep
Circulating
virus titre
of donor
chicks on
4th Pl day
69
70
10‘‘ LD„
*
«
10
LDtu
•P’J !
Fed larvae:
Unfed nymphs :
Unfed adults :
5 larva: in
a pool-
Indivi
dual
larva:.
5 nymphs
in a pool.
Individual
nymphs.
Individual
females.
Indivi
dual
males.
313
*
313
5/ 5
5/ 5
2/3
3/3
2/ 5
1/ 5
5/10
0/10
7/10
0/10
6/6
10'10
5/6
3/10
7/20
7/20
sqdiuXu jo jaquinu
•paseapi
I sqduiAU jo jaquinM |
3
Total
•joquinu iplMO j
8
E
g
•.sqduHu paj U|
|
•paj
sqduiiCu jo jaquin^q
•pascapi
sqduiXu jo Jaqmnbl
•jaqumu :pii|3
* Numerators are the number positive for KFD virus, denominators are the number tested.
3
•sipisaj i
UOISSIIUSUCJJ. |
siuia jo aauasaij
3 3
§ H
Similarly, suspensions prepared from both batches consisting of five unfed
individual nymphs and three pools of live nymphs each were tested for virus 28 to
30 days after the end of their infective feed as larva: and 10 to 20 days after moul
ting. KFD virus was isolated from two out of five individual nymphs and two out
of three pools of nymphs from batch 69 and from one out of five individual
pymphs and from all of the three pools of batch 70.
The unfed adults (10 males and 10 females from each batch) were processed
for the isolation of virus 80 to 82 days after the end of their infective feed as larva
and 16 to 22 days after moulting. In the first batch live out of ten females and
seven out of ten males were infected ; in the second batch only two out of ten
females contained virus.
.*>72
573
Kyasanur Forest Disease Virus.
K. R. P. Singh, Khorshed M. Pavri, and C. R. Anderson.
(ii) Transmission of virus by infected nymphs and adults to chicks.—In the
in si experiment nine groups of five nymphs each representing the two batches were
icluased on nine chicks. Transmission was successful in two instances, once with
i.»ch batch (Table VI). in the second experiment, groups of 30 nymphs from both
batches were released on ten chicks. KFD virus was isolated from the bloods of
ill the ten chicks.
It was observed that when the infected nymphs were still feeding on the
chicks, the host chicks began io circulate virus in their blood, thus giving the
nymphs a chance to ingest some more virus. Due to this a higher rale of infection
was expected in lhe adulls as compared to lhe nymphs. Contrary to expectations
the rate of infection in adulls was found to be lower in lhe case of II. turturis and
H. papuana kinneari and more or less lhe same as in the nymphs in the case of
H. minuta. At lhe present lime there is no explanation fur this behaviour of lhe
virus in licks.
Summary.
Transmission of Kyasanur Forest disease virus by II. turturis, H papuana
fcl/meari and //. minuta was studied. All the three species became infected in
jhe larval stage by feeding on viremic chicks and in the nymphal stage transmitted
>
yirus by bite to other susceptible chicks.
Taui.l VI.
I ransmission of KFD virus to chicks by bile of infected nymphs of H. minuta.
The authors wish to express their gratitude to Dr. T. Ramachandra Rao,
Director, Virus Research Cenire, Poona, for his critical and helpful advice through
-out the investigation Technical assistance of P.K. Deshmukh, L. D’Lima, M.A.
Jlkal, P.G. Jore, M.N. Patil, MJ. Rebcllo, B. Shaikh, and S.K. Virkar is gratefully
•r acknowledged.
REFERENCES.
Clarke, D.H., and Casals, J. (1955)
Raja-*
Varma,
M.G.R.,
P.K., Singh, K.RT., and
Reuello, MJ.
Varma, M.G.R., Weuu, H.E., and Pavri,
Trapido,
IL,
oopalan,
One male and one female lick were released on each of the 14 chicks which
ic bled on the 22nd day after exposure ; no attempt was made to isolate virus
in the bloods of the chicks. Three out of seven chicks fed on by licks of batch
and one out of seven fed on by licks of batch 70 had HI antibodies to KFD
us (lilies - 7, 3, 3 and 3 lubes).
Discussion.
Il is evident from these results that larva: of //. turturis, H. papuana kinneari
i //. minuta became infected by feeding on viremic chicks and in the nymphal
. transmitted the virus by bite to other susceptible chicks. H. papuana kinneari
tied io be less susceptible to KFD virus than the other two species. Although
mil of four batches of //. papuana kinneari larva: were fed on chicks with the
c or even higher litres of circulating virus than those on which //. turturis and
iiinula larva: were fed, trans-stadial transmission was observed in only 25 per
of the nymphs lesled individually, in 30 per cent of the tested lick pools, and
..me of the adulls. Moreover, only some of the infected nymphs transmitted
iius io the susceptible chicks.
...
K.M. (I960)
Improved methods for hemagglutination
studies with arthropod-borne viruses.
Prue. Sue. Exp: Diol. Med., 88, 96-99.
A guide to the identification of all stages
of the Hirniaphysalis ticks of South
India. Didi. Ent. Res (in press;.
Studies on the transmission of Kyasanur
Forest disease virus by Hannaphysalis
spinigera Neumann. Traits. Roy. Sue.
Trop- Med. Hyg., 54, 509-516.
is prevalent should have a laboratory designated to carry out Y
isolation, rapid detection of antigen, and serological procedures 5^'
as CF, HI, IFA, and lil.iSA tests.
Serological surveys of populations should be carried out in 4$
groups: 0 9, 10-19, 20 29, and 30 years.
Vector population. Vector surveillance is necessary for.
following reasons:
.
(a) to obtain information on the distribution of vectors;
(/>) to determine their ecology, their absolute and relative depj
and their susceptibility to insectipides;
(<■) to demonstrate the presence of virus in the vectors
The virus is maintained in nature by transtadial and transov^
transmission within the tick population and by horiz
transmission between lick vectors and various domestic and)
animals. Mun is infected by the accidental bite of an infected ira
lick, llyalomma spp. licks remain the major vector of the y
Studies should be carried out on this vector particularly pit
populations from areas from which the disease has been repo
earlier and also from areas where Hyalomma licks are abundant
virus isolations have been made from them.
dlj
3.1.9 Prevention and control
Control measures are mainly aimed al reducing the populajj
of tick vectors. This is particularly necessary when new areas ofk
are developed for agricultural, industrial, or housing schem
Labour forces working in such areas arc at a high risk of devejgj
Crimean-Congo haemorrhagic fever. A suitable acaricide shoyM
selected and applied prior to the development of such tick-infe£
areas. HCH has been found to be a suitable acaricide, but olbem
also available, l ick repellents are also of value and should b$j
by workers involved in clearing forest and digging gropMS
construction programmes.'
JI
Control of nosocomial spread. Once a clinical diagnosis
Crimean-Congo haemorrhagic fever virus infection with blgf
manifestations has been made, the patient concerned sho
moved to the isolation area of the hospital. Transporting a b|f
patient is hazardous and may spread the disease, caus
jocomial outbreak. The syringes, needles, and other materials
4 on an infected patient should be thoroughly disinfected by heat
Chemicals after use. Special barrier nursing should be practised.
e*fatality rate is especially high among patients who have caught
g'jpfection through nosocomial spread. When an outbreak has
ttfl confirmed, a thorough clinical, virological, serological, ami
qomologicai survey should be undertaken to assess the extent of
? epidemic area and the source of the index case.
F
immunoprophylaxis. In Bulgaria, an inactivated mouse-brain
jpe has been used to immunize workers. However, no
ftdardized vaccine for Crimean-Congo haemorrhagic fever is
"gble; efforts should be made to develop such a vaccine for use
pg persons involved in the investigation of disease as well as
|th personnel and those occupationally exposed to the disease.
C'rs i ■
lit;'.'.
IQ.j/ieseurc/i needs and recommendations
jTrials of specific immune plasma and/or antiviral drugs should
Juried out in areas where Crimean-Congo haemorrhagic fever
jrimon, when such areas are located.
^/Modern molecular biology techniques should be used to
JpP a candidate vaccine for Crimean-Congo haemorrhagic
|)’P.esearch on tick biology, using modern biological techniques,
^|ji.be encouraged.
STflSjllliur Forest disease
y&Hiq(orical background
Ujiy-ijn 1957 there were reports of fatal epizooties in wild
jjgys in forested areas of Shimoga district, Karnataka (formerly
jftjp) State in India, associated with outbreaks of disease in
IjefS who lived in and around the forest fringe. Local inhabitants
Pthe affliction "monkey disease” because of the known
ftlion with dead monkeys. The disease was later named after
Jppalily—Kyasanur Forest—from where the virus was first
3.2.2
Etiology
/<
■/
Kyasanur Forest disease virus is a member of the Elavivirus go,
of the TogaviridaQ family. It is anligcnically related to other (|
borne fiayiyiruses, particularly the viruses causing Far Eastern (|
borne encephalitis, and Omsk haemorrhagic fever.
3.2.3
Epidemiology
The virus lias a complex life-cycle involving a wide variety of I
species, particularly Haemaphysalis spinigera in its nymphal staj
Man is an incidental host and plays no part in virus transmissi
Small mammals, particularly porcupines, squirrels, and rats pre
main reservoirs of the virus. Birds and bats are less important ho
The silent enzootic situation was perhaps dramatically altered
man’s need for more land, both for grazing and other agricultl
purposes. Cattle were put to graze around the forest and I
provided Haemaphysalis licks with a new and plentiful source
blood meals, which in turn resulted in a population explosion am
the licks. Cattle arc very important in maintaining tick populatj
but play no part in virus maintenance. The ticks Iced on 01
mammalian species such as monkeys, which show marked virae
and an illness from which they may die. The monkeys are rccognj
as amplifying hosts for the virus. Seasonal epidemics of Kyasa
Forest disease have been associated with epizootics in monkey^
most important being the black-faced langur (Presbytis enlellus)
the South Indian bonnet macaque (Macaco radiala).
Ihe disease is restricted to four districts (Shimoga, H
Kanara, South Kanara, and Chikamagaioor) in Karnataka ft
India. The epidemic patterns indicate irregular and unpredict
spread of the virus since its recognition in 1957. Earlier, the di?
was found to be limited mainly to an urea around the original ft
covering about 800 km2. Newer foci have since been recogfl
covering over 6000 km2. The latest outbreak during 1982 83 se
to have been the largest. A part of the Nidlc forest of some
hectares was clear-felled by the forest department to make roofl
a cashew plantation. The labour force brought from the pel
bouring areas and some villagers noticed a few dead monkeys
forest by late October and the first cases of the disease in man?
reported from December 1982 onwards.
2,4
Clinical and clinicopaihological diagnosis
fcilb-
MThe incubation period is estimated to be between 3 and 8 days.
disease appears with a sudden onset of fever, headache, and
Vgre myalgia, with prostration in some patients. The acute phase
gtgo about 2 weeks. Gastrointestinal disturbances and
$P)Prrhagcs occur in severe cases. There is no abdominal pain
£ppt in patients in whom there is gastrointestinal bleeding. The
(gpis not palpable but the tip of the spleen may be fell, most often
pt, patients with generalized lymphadenopathy. Bronchiolar
iYp|vement occurs in some patients and results in a persistent cough
}(j abnormal physical signs in (he lungs, in some patients (with
opd-tinged sputum) serious signs of lung involvement have
jj recorded that were considered Io be the precursors of
ippionia.
[•here is a diphasic disease course in a number of patients. The
jjjd phase is characterized by mild meningoencephalitis after an
Jfjle period of 7 21 days. Il is manifested by a return of fever,
ere headache followed by neck stillness, mental disturbance,
afse tremors, giddiness, and abnormal reflexes.
'Convalescence is generally prolonged lasting for up to 4 weeks.
ie pase-fatality rate has been estimated to be around 5-10%.
■^he virus is extremely infectious and therefore is hazardous for
ipfatory workers; more than 100 persons are known to have
igfed from laboratory-acquired infections. The clinical features
knot significantly different from those described for natural
eplions except that the disease is generally milder and, to dale, no
Has proved fatal.
limited haematological and biochemical investigations have
[) carried out, particularly during the early years. Leukopenia has
m,found to be an almost constant feature of the disease,
Jj^ted in all probability through anlileukocylc antibodies.
;Qinbocytopenia ol variable degree has also been found to be an
IQftant feature. Thromboagglutinins have been found in the
fylption of (he majority of patients. In contrast to the findings in
^Offhagic fevers from the USSR and the Korean peninsula,
is no evidence of gross capillary damage apart from those
gjijpntal to thrombocytopenia.
Albuminuria appears in most cases during the acute febrile stage.
gyiular casts have been occasionally observed. In most cases, the
tpbjospinal fluid is clear with no increase in cells or alterations in
proteins, chlorides, or sugar. In patients developing the second ph
with meningeal signs, there is an increase in both cells and protej
I he histopathological lindings from 3 fatal cases in man shot
similarities to the observations reported for other haemorrhs
fevers. Il was concluded that the histopathological changes, in b
man and monkeys, appear to be mild in comparison with the seve,
of the clinical illness. The haemorrhagic phenomena that wcres
in some cases of the clinical disease were not adequately explail
by the histological appearance of the organs or blood ves
examined.
3.2.5 Etiological diagnosis
Unlike many other arboviruses, the Kyasanur Forest dis<
virus has a prolonged viraemia of about 10 days or more. Of the;
collected during the first H days of illness about 95% container)
virus. The serological response of man to infection with this v
was studied in 10-4 fever patients, all of whom had demonslrj
viraemia; the patterns of serological response were not unlike 1)
seen with other flavivirtts infections. The response depended t|
whether the current infection was the first encounter with a flavi^
(primary) or whether there had been a previous infection wilL
or more ilaviviruses (secondary), For secondary infections, spej
serodiagnosis was difficult. Both the neutralization test and thea
gel diffusion test are specific; the latter is also useful in the field. '
agar gel diffusion test is less sensitive than the neutralization lcs|.’i
primary infections, hacmagglutination inhibition tests or s)
radial haemolysis tests seem to be satisfactory.
3.2.6 Treatment
There is no specific treatment for Kyasanur Forest disc
Supportive and symptomatic treatment should be provided, sup
analgesics for myalgia and headache, intravenous fluids'
dehydration, and blood transfusions if there is hacmorrhas
During convalescence, rest and an adequate diet seem to be
major requirements. It is not necessary to isolate the patients.
3.2.7 Surveillance
A surveillance system has been set up by the Karnataka
government that records the number of cases and deaths suspe
t>?ing due to Kyanasur Forest disease, isolation of the virus from
$ (aken during the acute phase is sometimes carried out, but only
small number of suspected cases.
Jhe majority of human infections, with the exception of those
ipped in the laboratory are transmitted exclusively in and around
! forest. During forest clearing operations, rodents and monkeys
,j): their lick ectoparasites migrate to other areas, thus enlarging
jfpeus of natural infection. Attempts should be made to detect the
ys pr antigen in licks and a serological survey of rodents should
gypied out in virgin forest areas that arc to be cleared.
1,8 Prevention and control
Qa forest tracks used by man, the number of licks can be
Jlfolled by spraying with acaricides. This, and the application of
sptive repellents for the personal protection of the forest
’fjyrers, may be implemented in restricted areas where monkey
ttbs occur.
Jpi§ proposed that the population al risk should be immunized
|pjpactivated-killed Kyasanur Forest disease vaccine prepared
&$iipk embryo fibroblast.
/pmsk haemorrhagic fever
. flislorical background
fjfnsk haemorrhagic fever is an acute febrile disease. Ils
Mfterislic features are: viral etiology, natural locality,
jjyorrhagic symptoms in patients, and a relatively benign course.
Pgses of the disease were first reported in 1944 45, although there
Sine evidence that similar cases appeared also in 1941 43, in rural
ys north of Omsk (Western Siberia). In 1945 and 1946 during two
bfpaks of Omsk haemorrhagic fever there were more than 200
|;^00 cases, respectively, and in subsequent years, clinical,
^fpiological, and etiological features of the disease were studied
(('group of medical specialists from Omsk and Moscow. As a
;lt pf these studies it was concluded that Omsk haemorrhagic
j'p'js a specific viral haemorrhagic disease different from other
iwp yiral haemorrhagic fevers.
i/llownig an infective lick bile, the incubation period is ol the older ol 7—12 days..-’)
lilnoss begins abruptly will) fever, chills, malaise, irritability, headache, and severe!^
in the limbs and loins followed by anorexia, nausea, vomiting, and abdominal paim
is continuous but may be remittent and sometimes biphasic, resolving by crisispplji
niter 8 days. The face ami neck are Hushed and oedematous, the conjunctivae and ph,a£)
are injected, and there is oedema of the soft palate. The mouth is dry and the braat^fja
loul odour. Patients are depressed and somnolent. In most cases a fine petechia|;fi
begins on the trunk and then covers the entire body. The liver is enlarged in aboiff
of cases but the respiratory system is unaffected. A haemorrhagic cnanthema appears)
the soli palate and uvula early in the illness and other bleeding manifestations, incly^
huematemesis and mclaena, appear on about the fourth or fifth day in over 75% of patiei
Leukopenia and severe thrombocytopenia me common. Large purpuric areas caused
subcutaneous extravasation of blood occur al times. Bleeding occurs in descending gj
of frequency from the nose, gums, buccal mucosa, stomach, uterus, intestines, anfi-JUJI
Gastric and nasal haemorrhages often lead to death, involvement of tho centrg|ln?jig|
system is seen in 10-25% of cases and usually indicates a poor prognosis; it includ$J:j
rigidity, excitation, and coma. The mortality rale is often as high as 30-50%, usnajly^
to shock, secondary blood loss, or intercurrenl infection. This severe disease is, ip'sh
contrast to the pattern of disease in Africa, where haemorrhagic phenomena apcJ'4PB
are only rarely reported. A recent report “ described an unusual outbreak of haemOffhi
fever in Rawalpindi District, Pakistan where the index case, a farmer, was admitted
hospital with haematemesis and mclaena. A laparotomy was performed following ®j|
four members of the operating team became ill and two of them died. A vims Sifflilaj
^nmean haemorrhagic fever virus was isolated.
’illAsj
KYASANUR FOREST DISEASE
This disease is caused by a llavivirus which, like Omsk haemorrhagic feyef yirt
unligenically related to the lick-borne encephalitis complex but only rarely cgnjesoji
involving the central nervous system. The virus was first isolated in Mysore State/Ipd
1957 and human infections, which still occur, are limited to villages surrounding Kyi?
Forest. The virus is now known to be widely distributed in India but human infectibf
not occur outside Mysore.
After an infectious lick bile, there is an incubation period of 3 7 days before tijgjiU
onset of fever, frontal headache, severe myalgia, and prostration. This is quickly mW
by nausea, vomiting, confusion, and restlessness. The conjunctivae are injeejetj
palate is suffused and often covered with maculopapular haemorrhagic spots. A genefj)
lymphadenopathy has been noted and many patients have bronchiolar inyolvyipenfl
fever generally lasts 5-12 days and sometimes follows a biphasic course; a mild men
encephalitis occasionally occurs during the second phase. Epistaxis, haematerqejjjr
^^loptysis, mclaena, and bleeding gums arc common and sometimes there may bpjuj
^Bleeding. Albuminuria, leukopenia, and thrombocytopenia are usual fipding§. j^?j
« Weekly epldcinlolugicol record, 51: 301-308 (1976).
')• ill
pportion ol patients may die, usually 8 12 days alter the onset of illness, developing
ja or bronchopneumonia prior to death. The majority of patients, however, make an
iypntful and complete recovery.
The virus is transmitted by llaemaphyxalix ticks, especially //. spinigera, and is
stained in small mammals. In Mysore Slate, the silent enzootic situation was drajcftlly altered by man’s need for more grazing land. Cattle were put to graze around
‘forest and provided the llaemaphyxalix tick with a new and plentiful source of blood
(Is, which produced a population explosion among the ticks. The abundant ticks fed
Other mammalian species such as monkeys, and these became infected with Kyasanur
'est disease virus and developed marked viraemia and an illness from which they died.
yks noted in 1957 that human infection was preceded by illness and death in forestjjling Langur ami Macacux monkeys, which acted as amplifiers of the virus.
OMSK. HAEMORRHAGIC FEVER
^epidemic of Omsk haemorrhagic fever occurred in Omsk and Novosibirsk Oblasts
^fria between 1945 and 1948. The virus was transmitted by the tick Dermaceiitor pictux
•j?y contact with infected muskrats (Ondatra zibethica). Most of the more recent
i pf disease in man appear to have been acquired through direct contact with muskrats.
t infections originate in the northern forcst-steppe-lake belt of western Siberia, which
(ins much wet grassland and swamp.
Allowing an incubation period of 3-7 days, the illness begins abruptly with fever
)h often follows a biphasic course), headache, vomiting, and diarrhoea. An enanthema
;e palate, sometimes haemorrhagic, generalized lymphadenopathy, and menmgism
Summon findings. Epistaxis, haematemesis, mclaena, and uterine bleeding may occur,
UMBpied by a marked leukopenia, thrombocytopenia, and albuminuria. The central
ji4§ system is rarely involved. The case fatality rate is low (0.5-3%). Convalescence
J?e prolonged but there uro no sequelae.
jig, precise epidemiology of Omsk haemorrhagic fever is still unknown. There exists
logical cycle of unknown complexity, which may involve rodents and ticks. Muskrats,
1 were introduced into the region some 60 years ago for hunting purposes, are some[jjfected and are capable of transmitting the virus by direct contact.
JUNIN, LASSA, AND MACHUl’O VIRUSES
1 three of these viruses arc members of the arenavirus taxon, a name derived from
clusion-like dense particles seen by electron microscopy that give the virion an
rance of having been sprinkled with sand. The three viruses have rodents as their
| hosts and reservoirs in which they induce a persistent infection: the rodent suffers
pffects and develops no immune response, although during its lifetime the animal
pas to excrete virus, particularly in the urine. The rodents arc presumably infected
tJWO
Oll/O/7
.
l/^Y6 -lcns
fg'Z-L-Z'l
Oengue virus etiology.
A significant and welcome
feature of all these epidemics was the total absence of
the “shock syndrome".
Studies on the distribution and habits of the
mosquito vector of dengue, viz. Aedes aegypti, are being
continued at the Virus Research Centre, Poona and the
National institute of Communicable Diseases, Delhi.
A new finding made last year, i. e. the habit of the
species to breed in tree holes, in South India, was
confirmed by further studies. A study conducted at
Bangalore yielded some pockets in the city where A.
oegypti were found in large numbers and dengue viruses
were isolated from them.
This is a finding of
considerable significance since this disease had not been
reported in Bangalore
viruses in this country. The ICMR Virus Unit at
N.I.C.D., Delhi has been entrusted with the work of
determining the nature of illness it produces in man.
Sandfly Fever
Sandfly fever was hitherto well known to occur in
the and regions of West Pakistan and Middle East
countries. Its occurrence in India was thought to be
doubtful. However, the Sandfly fever virus was isolated
in India in 1967 on two occasions from febrile cases at
Aurangabad (Maharashtra). The follow up studies have
resulted in several more isolations of this virus both
from sandflies and from sera of febrile patients indicating
activity of the virus in this area. As a result of this
significant finding, epidemiological studies have been
initiated at these areas.
Kyasanur Forest Disease (KFD)
This tick-borne virus disease first recognised in
1957, continued to pose a serious problem although
still restricted to a small area in Shimoga District.
Mysore State. Tne last two years witnessed the largest
incidence of human cases so far reported. A collabo
rative venture of vaccination was undertaken by the
Virus Research Centre, Poona, and the Department of
Health. Government of Mysore. Killed KFD vaccine was
produced at the VRC and was administered to a section
of the population, at risk, for a field trial. Efforts such
as these and experiments for controlling ticks have been
intensified but serious attention is still being devoted
to the more basic problem, viz. that of understanding
the dynamics of the natural cycle. The role of certain
species of bats which have beer, found to nave antibodies
to this virus, not only in the KFD epidemic area but
also well outside the limits, is being studied.
Japanese Encephalitis (JE) & West Nile (WN)
Virus Infection
Unlike the dengue viruses. JE virus infects several
extrahuman hosts and thus has a complex natural cycle.
Pigs are now known to be good indicators of the
prevalance of the virus in any given locality. As the
vector mosquito, Culex tritaeniorhynchus, has a predi
lection to breed in paddy fields, it is more than likely
that the changing ecological patterns brought about
by the large irrigation projects undertaken in our
country will affect the distribution of this mosquito,
and hence of the virus that it carries. Intensive compa
rative studies h%ve, therefore, been started in irrigated
and non-irrigated areas in Andhra Pradesh with particular
reference to the Nagarjunasagar Project.
As revealed by serological surveys, West Nile
virus is perhaps the most prevalent among the arbo
ENTEROVIRUSES
Work on entero-viruses is being mainly conducted
at the Enterovirus Research Unit at Bombay; Pasteur
Institute, Coonoor; the Enteroviruses Unit at the
Christian Medical College, Vellore and the Virus Unit
at the K. G. Medical College, Lucknow.
At the Pasteur Institute, Coonoor, large batches
of bulk monovalent oral vaccine (Sabin) for the three
types of polio virus have been prepared and checked
for the absence of SV<0 virus. These are being tested
for neurovirulence at the National Control Laboratory
of the National Institute of Communicable Diseases,
Delhi, before release for public use.
Vigilance for polio cases in Bombay city has been
maintained and no change was noticed in the epidemio
logical patterns of the disease. A collaborative project
has been undertaken with the Directorate of Public
Health and B. J. Medical College, Poona, to study four
rural areas in Poona District to determine (i) the
entero-virus pattern in the child population; (ii) the
extent of natural immunity against polio-virus in the
local community, and (iii)the efficacy of the oral polio
vaccine in this rural community.
During 1969-70, 84 cases of paralytic illness were
detected among the chilaren vaccinated against polio
in Greater Bombay. From 52 cases studied, ten strains
of polio type I and seven strains of polio type 2 were
isolated. This has highlighted the need to review
the lack of efficacy of the vaccine which may be due to
loss of potency at the time of administration or inter
ference by other wild enteroviruses prevalent in the
community.
Preliminary results of a study have
& \b/v|c
195 ZOONOSES
'Tm.rf?oc-ic ci
SoucJ }C(C(.
Control of JE
(a) VECTOR CONTROL : The vector mosquito (s) of JE are widely
scattered and not easily amenable to control. An effective way to deal
with them is to resort to aerial or ground fogging with uftra-lowvolume (ULV) insecticides (e.g..malathion. fenitrothion). All the
villages reporting cases should be brought under indoor residual
spray. The spraying should cover the vegetation around the houses,
breeding sites and animal shelters in theaffected villages Uninfected
villages falling within 2 to3 tan radiusnflhe infected villages should
also receive spraying-as a preventive measure. Villages within the
proximity -of infected villages should be kept under surveillance. The
use of mosquito nets should be advocated.
4b) VACCINATION : Vaccination of population at-risk has .been
recommended^ killed "mouse -brain” vaccine is available For
primary immunization, 2 doses of 1 ml each (0.5 ml for children under
the age of '3 years) should be administered subcutaneously at an
interval of 7-14 days. A booster injection of 1 ml should be given after a
few months (before one year) in order to develop full protection
Protective immunity develops in about a month's time after the second
-dose Revaccinations may be given after 3 years. The vaccine is best
^L.ecJ in the inter-epidemic period It should be offeree to the most
Vulnerable and high-risk groups (8. 9).
-Kyasanur Forest Disease
Kyasanur Forest Disease (KFD) is a febrile disease associated with
haemorrhages caused by an arbovirus flavirirus and transmitted to
man by bite of infective ticks
(c)
(d)
Problem-statement
Earlier the disease was found to be limited mainly to an area
around the original focus (Shimoga distnct)covenng about 800 sq. km
Newer foci have since been recognized. The disease is now restricted
ko four districts (Shimoga. North Kanara, South Kanara and
®Chikamagaloor) in Karnataka State in India covering over 6000sq. km
( 10). Serological surveys in different parts of India revealed antioodies
to KFD or a closely related virus in humansand animals, particularly in
cattle in Kutch and Saurashtra (11).
According to recent reports, the disease continues to be active in
its endemic foci. The latest outbreak during 1983-1984 seems to be
the largest with 2167 cases and 69 deaths, as against 571 cases and
15 deaths during 81. The Karnataka Government has established a
surveillance system which monitors the occurrence of KFD in humans
and mortality in monkeys in known epidemic, as well as neighbouring
areas. Deaths of monkeys are considered as heralders of this disease
in endemic areas.
Epidemiological features
(a) Agent . The agent KFD virus is a member of group B togaviruses
(flaviviruses). It is antigenically related to other tick-borne flaviviruses.
particularly the Far Eastern tick-borne encephalitis and Omsk
haemorrhagic fever. Unlike in many other arbovirus infections, KFD
has a prolonged viraemia in man for about 10 days or more.
(b)
Natural hosts and reservoirs
Small mammals particularly rats and squirrels are the main
reservoirs of the virus (10). Birds and bats are less important hosts.
The monkeys are recognized as ampl'rfing hosts for the virus.
However, they are not effective maintenance hosts because most of
PD infection. Cattle provide Haemaphysahs ticks with
Host factors
(i) Age: Majority of cases affected were between 20 and
(ii) Sex: Attack rate was greater in males than in fen
Occupation The attacked people were mostly cultivators wl
forests accompanying their cattle or cutting wood (iv) Humai
The epidemic period correlates well with the period of greate
activity m the forest, i.e.. from January until the onset of rains
Mode of transmission
The transmission cycle involves mainly monkeys and;
disease is transmitted by bite of infective ticks, especially
stages There is no evioence of man to man transmission!
Incubation period
Estimated to be between 3 and 8 days
History
the virus was first isolated
Vectors
The virus has a complex life cycle involving a wide varietj
species. At least 15 species of hard ticks of the genus Haemal
particularly H. spmigera and H turtura are known to tran<
disease. KFD has also been isolated from soft ticks (12) The
number of human and monkey infections occur during drier
particularly from January to June This period coincides with
nymphal activity of ticks
(f)
KFD was first recognized in 1957 in Shimoga district of Karnataka
State in South India. Local inhabitants called the disease "monkey
disease" because of its association with dead monkeys. The disease
was later named after the locality— Kyasanur Forest — from where
Ecf. /?.
a plentiful source of blood meals, which in turn leads to a p
explosion among the ticks Thus cattle are very imp
maintaining tick populations but play no part m virus mai
(10). Man is an incidental or dead-end host and plays no pa
transmission
(e)
3.
t_/e
Clinical features
The disease appears with a sudden onset of fever, hea
severe myalgia, with prostration m some patients.The at
lasts about 2 weeks Gastrointestinaldisturbancesand hae
from nose. gums, stomach and intestine may occur in sei
In a number of cases, there isa second phase character!
meningoencephalitis after an afebrile period of 7 to 21
manifested by a return of fever, severe headache follow
stiffness, coarse tremors, abnormal reflexes and mentaldis
The case fatality rate nas oeen estimated to be 5 to 10 pe-
/a) Control of ticks: Since KFD is a tick-borne disea:
ticks should be undertaken. For control of ticks in forests, s
can be made by power equipment or by aircraft-mounted eqi
dispense carbaryl, fenthion, naled or propoxur at 2.24 k(
ingredient per hectare (13). The spraying must be carried i
spots", i.e., in areas where monkey deaths have been repod
50 m around the spot of the monkey deaths, besides the erx
Since the heavy tick population in the forest areas is attrib1
to the free roaming cattle, restriction of cattle movement is
bring about a reduction in vector population (5). (b) ^aca'l
population at risk should be immunized with killed KF
(c)Personal protection: Protection of individuals exposed
of infection by adequate clothing and insect repelle”*®
dimethyiphthalate (DMP. DEET) should be encouragedexamine their bodies at the end of each day for ticks and re
promptly. The habit of sitting or lying down on the grou^
discouraged through health education.
4.
Chikungunya Fever
A dengue-iike disease caused by a group A virus, the ch
virus and transmitted by Aedes. Culex and Mansonia me
manifested by high fever and severe articular pains in ’
spinal column (14) The virus was first isolated from
197
Efar during an epidemic in Tanzania in 1952-53. Chikungunya
Ejj-word meaning "doubling up" owing to excruciating pint
fc^ewas an outbreak of this disease in Calcutta in 1963-64
^jhBr in Mudras in 1965, which gave rise to 3,00.000 cases in
jjSty.alone (15). According to reports, the virus has not been
1965 (16).
17.
18
19.
20
*sfihOL: (a) Vector control: The Aedes aegypti mosquito should
Bfeiin target of control activities It requires active community
HjBntto keep water storage containers free of mosquitoes and
Ssjaie the other breeding places of mosquitoes in and around
dwellings (17) The organophosphorus insecticide. Abate
.-joggly being used as a larvicide. It can prevent breeding for up
J>(ths wtie.'. applied on sand granules, does not harm man and
'^•affect the taste of water. Antilarval measures can preventan
-^‘but do not give immediate results when an epidemic has
& broken outJn such cases, antiadult measures alone can bring
KMianid interruption of transmission. A new technique
. -j of aerosol spray of ultra low-volume (ULV) quantities of
. .if or sumnhion (250 ml/hectare) has been found to be
jisyffi interrupting transmission and stopping epidemics of DHF
ji^foplets kill the mosquitoes tn the air as well as on water By
mZ.iJLV treatments at about 10 days apart, the Aedes Research
aftargkok was able to reduce adult mosquito densities by more
. • — rent for several weeks (18. 19) (b) Vaccine. No vaccine has
I®Ba-zsta|ied that is considered suitable for use.
Brucellosis is one of the major bacterial zoonoses, and in humans
is also known as Undulent fever. Maha fever or Mediterranean fever. It
is occasionally transmitted to man by direct or indirect contact with
infected animals. It is caused by different species of the brucella group
of organisms and characterised by intermittent or irregular febrile
attacks, with profuse sweating, arthritis and an enlarged spleen The
disease may last for several days, months or occasionally years
Brucellosis is both a severe human disease and a disease of animals
with serious economic consequences.
jKile'Fei'er
JS’febiile illness caused by a group B arbovirus. Thedisease
igih.Airica, the Middle East. South-West Asia and India, and
i&Jbyi.ertain species of Culex mosquitoes. Clinically, it is
:.d;bya sudden onset of fever, severe headache and malaise
cVeral days. In children, a maculopapular rash of short
pffiappear. In the aged, afatalmeningo-encephalitismaybe
Sever is known to occur in the arid regions of West Pakistan
i;Ea.',t. Its occurrence in. India was thought to be doubtful.
™B67, the Sandfly fever virus was isolated in Aurangabad
tpl'irom febrile cases The virus was also isolated from
“V-.The control of sandfly fever is based on the control of
Diagnosis is established only after detecting the prese
virus in the blood and or serological evidence
Control
BRUCELLOSIS
•
I1D6 2). Tech Rep. Ser.. No. 369
$fj?5j. Permanent Institutes. Nev- Delhi
l&etal (1980). Review of Medical Microbiology. 14thed, Lange
?W?'iblications. California
yT.;il978), World Health Statistics. Quarterly Report. 31 (2) 120
te-and Shah K.V. (1956). Ind. J. Med. Sci.. 10: 582
W75J ICMR Bulletin. March 1975
pfflndia. Ministry of Health and Family Welfare (1987). Annual
1'11)86-87. Department of Health and Family Welfare
Blrliistitute of Virology. Pune (198O)Japanese Encephalitis in
te^lR-'New Delhi
BJH79). Japanese Encephalitis, Technical Information and
BailorTreatment. SEA/CD/79. WHO. New Delhi
S®B5)Tech. Rep. Ser 721
K'l5)-.Manual of Zoonosis
Wli>,’(1971). Indian J. Med. Res.. 59: 312
ro34)Chemical methods for the Control of arthropod vectors
B’pf Public Health importance.
international Organizations of Medical Sciences (1977).
Liveable. Diseases. Provisional International Nomenclature.
|®£h. 0978). Bull WHO, 56 (6) 819-832
lnle,,‘9ence’ Ministry of Health (1974). Annual
Director General 1969 and 1970. Nirman Bhawan, New
WHO (1979). WHO Chronicle. 33 107
WHO (1972). World Health, Aug-Sept., 1972
WHO (1972). WHO Chronicle, 26. 463
WHO (1975) VMdy Epid Rec.. No. 23. 6 June 1975
BRUCELLOSIS
Probelm statement
Brucellosis is a recognized public health problem with world-wide
distribution. It is endemic where ever cattle, pigs, goats and sheep are
raised in large numbers. Important endemic areas for brucellosis exist
m Mediterranean zones. Europe. Central Asia. Mexico and South
America.
Animal brucellosis is reported from practically every State in India.
However, no statistical information is available about the extent of
infection in man m wirious parts of the country (1)
The prevalence of human brucellosis is difficult to estimate. Many
cases remain undiagnosed either because they are inapparent or
because physicians in many countries are unfamiliar with the disease
Agent factors
(a) Agent . The agents are small. Gram negative rod-shaped, nonmotile. non-sponng and intracellular coccobacilli of the genus
Brucella. Four species infect man. B. mehtensis. B. abortus. B. sins.
and B. canis. B. mehtensis is the most virulent and invasive species; it
usually infects goats and occasionally sheep. B abortus is less virulent
and is primarilya disease of cattle B. suis is of intermediate virulence
and chiefly infects pigs. B. cams is a parasite of dogs, (b) Reservoir of
infection: Main reservoirs of human infection are cattle, sheep, goats.
swine, buffaloes, horses and dogs In animals the disease can'cause
abortion, premature expulsion of the foetus or death. Cross infections
can often occur between animal species The injected animals excrete
Brucella in the urine, milk, placenta, uterine and vaginal disenarges
particularly during a birth or abortion The animals may remain
infected for life.
Host factors
Human brucellosis is predominantly a disease of adult males
Farmers, shepherds, butchers, and abattoir workers, veterinarians
and laboratory workers are particularly at special risk because of
occupational exposure. Immunity foliows infection.
Envronmental factors
Brucellosis is most prevalent under conditions of advanced
domestication of animals in the absence of correspondingly advanced
standards of hygiene. Overcrowding of herds, high rainfall, lack of
exposure to sunlight, unhygienic practices in milk and meat
production al I favour the spread of brucellosis The infection can travel
long distances in milk and dust. The envionment of a cow shed may be
heavily infected The organism can survive for weeks, or months in
favourable conditions of water, urine, faeces, damp soil and manure
Mode of transmission
Transmission is usually from infected animals to man. There is no
evidence of transmission from man to man (2). T a routes of spread
are :
(a) Contact infection: Most commonly, infection occurs by direct
contact with infected tissues, blood, urine, vaginal discharge, aborted
Private Circulation to Medical Profession only
August 1993
W OfeWfc F©©t
Inside
capable of feeling any type of sensa
In Greek mythology, there was once
a great warrior called Achilles. When he
was a small baby, the Gods told his
tion.
Thus, he is incapable of feeling pain
mother to dip him in river Styx as this
Page 1
The Diabetic Foot
Page 3
Diabetes among Indians
or other uncomfortable sensations. The
patient may not be aware of any injury
would make him completely safe from
any harm or injury. The mother held him
or infection until it has progressed to a
up by his heels and dipped him com
severe stage, or are pointed out by a
pletely in the river. As Achilles grew up
he became well known as a warrior and
relative or the doctor This makes it dif
ficult to detect injury or infection at an
as nothing could hurt him, everybody
early stage when management would
be simpler. Although diabetic
feared fighting him. Until one day,
another famous warrior called Paris
neuropathy more commonly affects the
shotapoisonedarrowwhich hit Achilles
Page 5
Emergency Surgery in
Diabetes’
Page 7
Pancreatic Transplants
Page 10
Practical Aspects of
InsulinTherapy
in his heel. This was the oart of the body
that had been held in the mother’s hand
when she had dipped him in the river
sensory nerves, the motor nerves
may also be involved. The motor nerves
which innervate the small muscles of
tion nor importance is given to this.
the feet help in maintaining the shape
The poisoned arrow could kill Achilles.
From that day onwards, any vulnerable
To quote a passage from the ancient
chronicles, "In the thirty ninth year of his
reign Asa was diseased in his feet, and
and the "arches" of the foot. When
these nerves are affected, there is a
aspect of a person, has been called as
the "Achilles heel" of that person. This
his disease became severe; he sought
help from his physicians but died in the
could well be applied to the feet of any
forty first year of his reign." (II
Chronicles XVI, 12-14). Some
‘cocked’ up and the area of the sole
to bear most of the weight of the body.
diabetes like eye, kidney and nerve
authorities regard this quotation as one
of the earliest references to diabetic
problems, that we overlook the impor
foot disease and many of the more
bearing may have to bear the brunt of
tance of foot care in diabetes.
The importance of preventing foot
problems in a diabetic should NEVER
sceptical ones feel that there is not
much more that we can do today about
the body weight. This change in the nor
diabetic foot problems compared to
panied by a decrease in the sensitivity
be underestimated. If one were to see
the number of indoor patients in any
what was done for Asa. This attitude is
is one of the most important predispos
unfortunate as foot problems in
diabetes are preventable provided a
ing factors in diabetic foot disease.
specialised diabetic clinic or hospital,
one would find more than half are there
because of some fpot problem. These
few basic instructions are followed and
rarely given its due is the autonomic
proper care taken. Before the "do’s and
don’ts" about foot care can be dis
that have many important functions in
and therefore was not safe from harm.
diabetic. We tend to pay so much atten
tion to the long term complications of
are also patients who need to stay in
the hospital the longest. Whilst with ex
wasting of the small muscles of the feet
and this may change the configuration
of the foot. The toes may become
near the heads of metatarsals comes
Areas which are not normally pressure
mal architecture of the foot accom
One aspect of neuropathy that is
nerve involvement. These are nerves
Editorial Advisors
cussed, it would be worthwhile to con
sider briefly some of the mechanisms
which predispose the diabetic to foot
the body and of these many functions,
cellent management, we are able to
save many a foot, quite a number of
the patients still need to undergo an am
problems. This would enable giving in
□ Dr. S.M. Sadikot
putation. The majority of foot problems
occur in diabetics with insensitive feet,
possibly without adequate circulation
the blood supply to the limbs, deter
structions to the patient in a much more
mine sweating and also maintain the
rational manner rather than just giving
him some "commandments' to ob
normal texture of the skin. Whr ihese
nerves are affected in diabetes, it
Consultant Physician &
Endocrinologist,
Jaslok Hospital & Research
and are PRECIPITATED by infection,
Centre & S.L Raheja Hospital,
Bombay.
are preventable. Even if they do occur,
Director of Medical Sciences,
Boots Pharmaceuticals Ltd.
□ A.D. Paul
Head of Medical Support,
Boots Pharmaceuticals Ltd.
Bombay.
are usually definite precipitating fac
tors, a vast number of the foot problems
□ Dr. J.S. Bakshi
Bombay.
injury, or both. Due to the fact that there
(
it is possible to "catch" them at the ear
liest so that the management is simpler
and the results much better. The
tragedy is that neither adequate attenS. M. Sadikot, Consultant Physician and
Endocrinologist, Jaslok Hospital &
Research Centre & S.L Raheja Hospital,
Bombay
the ones that are especially relevant to
our discussion, are that they regulate
serve.
causes a reduction or even a complete
Neuropathy
absence of sweating in the feet and the
Nerve involvement due to diabetes
is one of the commonest long-term
complications of diabetes. Involvement
of the sensory ne:' 'es going to the feet
brings about many varied symptoms
and signs but many patients have a
marked reduction in the pain sensation
*
lower legs. A reduction in sweating
causes the outer layers of the skin to
become dry and this makes the skin of
the feet, brittle and liable to develop
cracks which may form entry points for
infecting bacteria. The skin also loses
its ability to stretch and therefore any
change in the shape of the feet also
and a significant number of patients go
tends to cause the development of
on to have insensitive feet, and are inf
breaks and cracks in the skin. This ab-
D I A B E T E S--------------------------------
----------------------------
FORUM.____________________ ____
sence of sweating is extremely impor
depend upon the relative severity of the
understand that the aim is to avoid in
formation. Two areas where he should
tant as in one major study it was
two conditions in any individual patient.
fections and trauma to the feet, then the
look very carefully are between the toes
reported that diabetic ulcers only oc
In any case, neuropathy and vascular
significance about foot care is easily un
and at pressure points at the bottom of
curred in those feet that had a sig
disease, in severe forms, presenting
derstood.
the feet.
nificant reduction in or a complete
in the same patient is dangerous be
Inspecting the feet daily
absence of sweating.
The autonomic nerves are also
responsible for regulating the blood
cause the patient becomes prone to
painless ulcers which are resistant to
treatment.
Some patients, especially those that
are obese or have joint pains may find
This is of utmost importance in order
it difficult to lift up the feet for a close
to catch any problem at the earliest
inspection. They can very easily use a
supply to the feet and this supply is af
fected when the nerves are involved.
Surprisingly, feet that are affected with
autonomic neuropathy appear warm
Foot Care for Diabetics
with good peripheral pulsations and
have been shown to have an increased
blood supply. This increase in the
warmth leads many to mistakenly feel
that the circulation in the limb is ade
quate. This is definitely not the true
situation. It is known that although the
total blood going to the leg and feet
Wash feet daily with lukewarm water
and soap, just as washing hands
Dry feet well, also between the toes
Cut nails straight across
Ingrown nails and calluses should
receive expert attention
Keep the skin supple with a
moisturizing lotion, but do not apply it
between the toes
Change daily into clean, soft socks or
stockings which must neither be too
big nor too small
Keep your feet warm and dry
Preferably wear cotton socks or
stockings and leather shoes
Never walk barefoot-neither indoors
nor outdoors
Always wear shoes that fit
This applies also to sandals
Examine shoes every day for cracks,
pebbles, nails and other irregularities
which may irritate the skin
may have increased,most of this blood
is shunted directly from the small
arteries to the veins, bypassing the
capillaries. It should be remembered
that it is at the capillary level that the
real function of the blood circulation
takes place. Therefore, although the
total quantity of blood flow to the feet
may appear to increase in diabetic neu
ropathy, this is of no real use and one
could say that in practical terms there
is a lack of blood supply to the feet.
Peripheral vascular
diseases
The inadequate blood supply to the
limb may be further compromised by
the presence of peripheral vascular dis
ease, which is much more common
amongst diabetics than in non
diabetics. In this condition, the arteries
supplying blood to the legs and the feet
are narrowed down by atheroma forma
tion. The earliest symptom of this could
be pain in the legs whilst walking.
Some patients get pain at night when
they are lying down but this can be
relieved by hanging the foot over the
edge of the bed and is increased if the
Infection and trauma
Failing this, a relative would have to be
ges and peripheral vascular disease
search for any breaks in the skin, scars
instructed in the means of foot care.
predispose the patient to serious foot
and burn marks and any redness that
Washing the feet daily
complications. The majority of these
may be a sign of infection, any punc
foot problems need to be precipitated,
ture or injury marks, any darkening of
This may not seem a common prob
the skin, presence of corns and callus
lem in our country with the habit of
Patients with high risk to
have foot problems
are under the mistaken notion that
1.
Peripheral neuropathy
scrupulously dry at all times so that
2.
Peripheral vascular disease
even when they have a bath, they cover
3.
Severe retinopathy or
their feet with a plastic bag.
In addition to maintaining cleanli
patient gets up and walks around. The
ortriggered by infection, traumaor both.
Therefore, the focus in preventing
and parched, the nails lose their lustre
and the small amount of hair on the toes
serious foot complications would aim at
efforts to avoid trauma and infection to
may be lost. The feet of a diabetic with
the feet or in the least, diagnose their
autonomic neuropathy appear warm
presence in the very early stages so
that adequate measures can be taken
the skin is cold. This may sound con
at a time when management of the
fusing but it should be realised that
patient would be somewhat easier.
diabetics do not have a clear-cut
What are the ways and means to
demarcation between those that have
avoid trauma and infection in a foot
only a neuropathy and those that have
already prone to complications?
only peripheral vascular problems.
If one reflects on the changes
Most of them have varying degrees of
brought about by the neuropathy and
both, and the clinical picture would
the peripheral vascular disease, and
2
mirror to examine the bottom of the feet.
he should be inspecting! He should
feet may feel cold, skin appears dry
whilst with peripheral vascular disease,
stage. But the patient must know what
It is apparent that neuropathic chan
having a daily bath, but some diabetics
nephropathy
diabetic
feet
should
be
kept
4.
Previous foot ulcers
ness (so important to avoid infection),
5.
A foot deformity for whatever
washing the feet daily helps in the skin
reason
6.
Blind or partially sighted patients,
and those living alone
regaining some moisture that may be
lacking because of the neuropathy. The
water thabjs used to wash the feet
shoukflbe tepid, neither very hot nor
(Contd. on pg. 9)
DIABETES
FORUM
Diabetes among Indians
The prevalence of Diabetes Mellitus
lion diabetics in India. This figure, with
varies in different geographic regions
and in different ethnic groups. Although
nosis of Diabetes Mellitus, and there
fore the validity is open to question.
Now that the W.H.O. has laid down
standardised criteria, these will be used
rise to a phenomenal 35 million by the
Epidemiological studies of the prevalence of
many studies have been carried out in
the past (Table 1) to look for the
prevalence of diabetes in india, these
have used varying criteria for the diag
increasing incidence, is estimated to
Table 1
year 2000! This may pose a major
Diabetes Mellitus in India
Year
Author
Place
1971
Tripathy etal
1972
public health problem and impose a
severe burden on the healthcare sys
Prevale ice (%)
tem in our country. This calls for ap
Urban
Hural
Cuttack
1.2
—
Ahuja et al
New Delhi
2.3
—
1979
Johnson et al
Madurai
0.5
—
Risk factors for NIDDM in
Indian population
1979
Gupta etal
Multicentre
3.0
1.3
Diet
1984
Murthy ef al
Tenali
4.7
—
1986
Patel
Bhadran
—
3.8
1988
Ramachandran et al
Kudremukh
5.0
—
propriate and effective preventive
measures to be adopted to curb or atleast delay the onset of diabetes.
by all investigators and it should soon
be possible to compare data from
various regions and ethnic groups.
Epidemiological studies carried out
in different parts of the world brought
With recent urbanisation and mode
out an interesting finding that Indian
~ migrants who were settled abroad had
i high prevalence of diabetes. These
studies, indicate that Indians as an eth
nic group have a high risk of developing
rnisation of living conditions, there has
been a transition from consumption of
natural food rich in fibre content to more
of refined food containing very little fibre.
1989
Kodali etal
—
Gangavathi
2.2
Moreover, lower utilisation of calories by
—
1.6
lack of physical activity leads to un
8.2
2.4
diabetes and the susceptibility may be
genetic in nature.
A survey conducted by the Diabetes
1989
Rao etal
Eluru
1992
Ramachandran et al
Madras
favourable adiposity. The usefulness
of a calorie-restricted fibre-rich diet in
Research Centre in Madras, two
populations belonging to the same eth
the management of diabetes has been
unequivocally proved by the extensive
nic group but of different socio
diabetes are the major factors that
do carry a high risk of progressing into
economic status, living in urban and
rural areas showed different rates of
studies of Professor M. Viswanathan
determine the vast differences in the
overt diabetes. With increasing ur
banisation there would be higher con
prevalence of diabetes (Table 2).
The age-adjusted prevalence of
and co-workers. This diet is similar to
the diet of a common man in India and
the urban and the rural areas. In our
has high fibre content available from
diabetes in the urban population was
8.2% and 2.4% in the rural population.
new to known ratio of 1:2 in an urban
version rate from IGT to diabetes and
this should result in an increase in the
prevalence of diabetes in India in the
area and 3:1 in a rural population
near future.
This study showed the wide difference
in the prevalence of diabetes in urban
and rural India. The prevalence was
8.4% in urban men and 7.9% in urban
r'<omen compared to 2.6% and 1.6% in
-.oral men and women respectively.
Age, body mass index (BMI) and the
waist to hip ratios (WHR) showed posi
known to undetected diabetes between
studies, we have recently reported a
Evidence from epidemiological
The relationship between obesity and
tions are in agreement with data
studies described so far clearly point
diabetes is complex and confounded by
many heterogenous factors. It is general
ly agreed upon that obesity definitely con
reported in several epidemiological
out that Indians as an ethnic group have
studiesof diabetes in urban: rural
a very high risk of developing diabetes.
migrant Indians.
With increasing urbanisation and in
Impaired Glucose
Tolerance (IGT)
Impaired Glucose Tolerance was
was considerably lower especially in
classified as an entity different from
the rural population.
diabetes because long term follow-up
studies have shown that a large
proportion of the subjects with IGT
Nevertheless,
relatively non-obese population.
A study from Orissa state and a mul
ticentric study by the Indian Council of
Medical Research (ICMR) have also
shown that the prevalence of diabetes
is higher in urban areas compared to
of the prevalence of IGT/diabetes
varies in different populations and is
Prevalence of
undetected diabetes
In a developing country like India, il
literacy and a lack of awareness about
A. Ramachandran,
Deputy Director
Diabetes Research Centre and
M. V. Hospital for Diabetes, Madras
creased life expectancy combined with
a rapid growth in population, a
usually around one.
An important observation made in
the Madras Diabetes Survey was that
the prevalence of IGT was almost
similar in urban and rural populations
(8.7% vs. 7.8%) despite a four-fold
lower prevalence of diabetes in the lat
tributes to the unmasking of the disease
in a genetically prone individual. Associa
tion between upper body adiposity and
phenomenal increase like an epidemic
greater risk of diabetes has been shown in
of diabetes in India has been foreseen
several ethnic populations. It is interesting
to note that at Diabetes Research Centre,
Madras, we have observed a similar as
by many epidemiologists. In 1990, it
was estimated that there were 15 mil
Table 2
Age-adjusted prevalence of diabetes and IGT
may remain as such or revert to nor
mal tolerance and the prevalence of
microvascular complications such as
retinopathy is negligibly small. The ratio
that in rural areas.
Obesity
around Madras city. These observa
tive association with diabetes in both
the populations. The mean value of BMI
upper body adiposity and BMI were
found to be positive risk factors in this
natural food sources.
urban & rural populations
Prevalence %
No.
Diabetes
IGT
Urban Total
900
8.2
8.7
Men
457
8.4
8.8
« 7-9
^2.4
8.3
Women
443
Rural Total
1038
ter (Table 2). This observation as
Men
520
sumes significance in view of our
earlier observation that 35% of the IGT
Women
518
7.8
.
2.6
8.7
1.6
6.4
FORUM
ans have a genetic susceptibility to
Familial aggregation of
diabetes
markers of NIDDM. Collaborative
study from our centre and Dr G.A. Hit
develop diabetes which appears to be
man in London has shown no associa
come exposed when they migrate and
Asian Indians are shown to have in
creased familial aggregation of
diabetes with higher prevalence of
tion of NIDDM with the amylin gene, in
achieve improved socio-economic
the South Indians (Dravidians).
status. Present evidence suggests that
diabetes among the first degree rela
tives and vertical transmission through
two or more generations. It was found
Conclusion
that 45% of the Indians compared to
38% of the Europeans had positive
insulin resistance may be a common
feature in Indians leading to the high
To summarise, it may be said that
the probable causal factors in diabetes
in Asian Indians include ethnic suscep
prevalence of diabetes and other me
tabolic disturbances that are possibly
responsible for the high rates of
coronary heart disease.
family history of diabetes.
A recent analysis of family history in
tibility, genetic factors, migration from
the NIDDM patients attending the
Diabetes Research Centre, Madras
change in life style, socio-cultural fac
tors, diet, physical activity, obesity,
in India. This stresses the need for
showed that positive family history was
stress, age, sex, parity and presence
adopting
present in 62% and 53% had first de
gree relatives with diabetes. It was also
noticed by Viswanathan et al that the
of insulin resistance.
measures to curb or atleast delay the
rural to urban areas with a concomitant
There is little doubt that Asian Indi
At the current rate of growth it is es
timated that by the turn of the century,
there will be about 35 million diabetics
intensive
preventive
onset of this disease.
prevalence of diabetes increased with
Glycaemic control:
Can it be achieved?
increasing family history of diabetes.
They noted that the prevalence of
sociation between diabetes and WHR
even in the relatively non-obese South
diabetes among offspring with one
diabetic parent was 36% which in
creased to 54% with positive family his
Advances in the realm of diabetes
diabetes and its treatment should
management have indeed been
constitute a vital part of the health
ly lower degree of obesity in com
parison with theirwestern counterparts.
tory of diabetes on the non-diabetic
parental side also. The cumulative risk
of developing diabetes in the offspring
rewarding. Increasing numbers of
care plan. It is heartening that there
patients have lived for longer years
is evidence linking good control with
In urban South Indians, the body
by the age of 70 years was 41 %-64%
following diagnosis, thanks to the
a favourable effect in reducing late
mass index has been shown to be a
changed outlook about diabetes
diabetic complications such as
strong predictive factor of diabetes in
in these two groups. The prevalence
rate (62%) and the risk (73%) increase
care.
diabetic retinopathy, nephropathy
women, but only of marginal predictive
further when both parents have
The two major objectives of
and neuropathy. Studies in animals
nature in men.
diabetes. The offspring of diabetic
parents are reported to develop the dis
diabetes management are to restore
and humans have also shown that
the deranged metabolism to as
good
ease at least a decade earlier than their
‘normal’ a state as possible and to
ameliorate and possibly help
enable the patient to live a life as
prevent chronic complications of
close to ‘normal’ as possible. While
diabetes. It is therefore, that
Indian population who had a significant
Age, sex and parity
In an urban-rural survey in Madras,
we found that the prevalence of
diabetes was 21% in the group above
40 years and 41% in the age group of
55-64 years.
Majority of the
epidemiological surveys show a male
preponderance among Indian diabetics.
Parity has no independent effect on
glucose tolerance in Indian women un
less it is associated with obesity.
parents.
Genetic susceptibility in
ethnic groups
an important causal role in hyperten
sion, dyslipidemia and upper body
adiposity and may eventually lead to
an increased prevalence of coronary
artery disease.
Genetic component in the
etiology of NIDDM
Epidemiological evidences for a
strong genetic component in the etiol
ogy of NIDDM are many and come from
different sources.
4
ther significance.
The attainment of optimal
note, Indians in Fiji and Singapore are
blood glucose level at all times may
glycaemic control is essentially de
pendent on the ability to monitor the^
be difficult. This however, does not
degree of control achieved. Present
mean that one should give up the
ly, diabetic control can be assessed
goal of glycaemic control. It would
rather effectively with the help of
shown to have higher prevalence of
NIDDM compared to the host population;
This disparity in the prevalence of
NIDDM which gets unmasked by environ
mental influences.
Autosomal dominant
inheritance of diabetes
clearly play an important role in its etiol
ogy. These two factors may also play
glycaemic control has assumed fur
ly normal, it can be made livable and
diabetics, maintaining a normal
out their greater genetic susceptibility for
years before the onset of diabetes and
the life of a diabetic may not be strict
enjoyable. It is true that for some
and Insulin Resistance
sulin resistance may be present many
may
Certain ethnic populations showa high
diabetes in different ethnic groups points
Hyperinsulinemia (a higher level of
control
prevalence of NIDDM. It is interesting to
Hyperinsulinemia
circulating insulin in the blood) and in
diabetic
Autosomal dominant inheritance of
NIDDM with vertical transmission of the
disease through at least three genera
tions is quite frequent in Indians,
Among the South Indians, we and
be futile to set normal glucose levels
laboratory parameters such as test
as a goal of treatment if it were im
ing of urine for sugar and ketones,
measurement of plasma or blood
possible to achieve.
The main treatment modalities in
glucose concentrations and
diabetes are patient education,
glycosylated haemoglobin or al
dietetic
oral
bumin levels. Effective monitoring is
hypoglycaemic agents (OHA s) and
the key to achieving optimal control
adjustments,
insulin-no more, no less. There are
of blood glucose levels and success
no other therapeutic approaches
either. The control of diabetes large
ful management of diabetes.
The development of newer treat
ly depends on the triad of diet, physi
ment regimens including highly
others have reported younger age at
cal activity and insulin or OHAs
purified insulin and human insulin,
onset of the disease compared to the
which are interdependent and must
and increasing awareness about
them, together with effective
This pheno
be balanced properly. Not to forget
menon and the prevalence of NIDDM
the ‘intangibles’ - stress, timing, food
monitoring and patient education
probably suggest the strong influence
absorption, etc., which can also in
of genetic loading in unmasking
fluence the diabetic control.
have made optimal glycaemic con
trol a reality. This means that satis
western population.
diabetes early in life.
The diabetic patient’s involve
A great deal of interest is focussed
ment is crucial for achieving good
on the identification of the genetic
control and hence education about
factory diabetic control is an
achievable proposition in many
patients.
)
D I A B E T E S
FORUM____ _____________________
Emergency Surgery in Diabetes
It has been estimated that one half
of all diabetic patients require surgery.
They are at a slightly inreased overall
risk of operative mortality (3.4%) versus
their non-diabetic counterparts (2.5%).
Of all those cases, about 5% are per
formed on an emergency basis. Sur
geons often encounter either metabolic
catastrophe such as profound hyp
oglycaemia, ketoacidosis (DKA) or hy
perosmolar hyperglycaemic non
ketotic dehydration (NHND) and coma
accompanying an acute surgical condi
not toxic per se, but induce harmful ef
fects by their ionization at body pH. If
allowed to accumulate, these result in
protein catabolism, impaired wound
healing and lessen the risk of infection.
blood sugar level is reduced near 150300 mg/dl, 5% dextrose is given in
saline. If possible, surgery should be
homeostasis, prevent fluid imbalance,
systemic acidosis which has detrimen
Majority of emergency operations are
delayed until after this initial interval of
tal effects on cellular function, eventual
ly inducing cardiovascular collapse.
because of severe infections. These
metabolic correction.__________ ,
acute conditions are frequently con
Major stress induces the secretion of
ducive to DKA. The metabolic distur
Factors favouring metabolic
decompensation
stress hormones that counteract the ef
bances complicate the diagnosis and
fects of circulating insulin. Fever which
management of the underlying surgical
Several factors in the perioperative
is not uncommon during post-operative
problem; for example, DKA can cause
period predispose the diabetic
period leads to increase in stress hor
abdominal pain mimicking surgical ab
patient to metabolic decompensa
mones and thereby rise in blood
domen. Correction of metabolic disor
glucose and ketone concentrations.
tion. These include:
der may alleviate the abdominal
tion. This group carries significant risk.
1.
Some are diagnosed to be having
Absolute or relative
insulin deficiency
frjbetes for the first time during the
operative process. They are at high risk
2.
Stress hormone excess
as well.
3.
Fasting
4.
Dehydration
The frequent association of com
bined surgical and metabolic problems
make diagnosis and management of
diabetes difficult. The surgical problem
Management of ketonuria and hy
may be the result of an uncontrolled hy
perglycaemia require increase in dose
perglycaemic state. Caution needs to
be exercised regarding the reliability of
of insulin whereas concurrent ketonuria
and normoglycaemia require glucose
infusion along with insulin. It is impor
physical findings or laboratory results in
diabetic patients. The paucity of
tant to note that ketonuria may become
symptoms in diabetic patients with
intra-abdominal pathology is seen fre
glucose level before improvement is
more marked despite decreasing blood
quently by general surgeons, a fact at
noted. This is due to conversion of beta
tributed to sensory neuropathy.
The presence of neuropathy may
hydroxybutyrate to acetoacetate during
lead to gastroparesis which in turn can
cause aspiration pneumonitis if timely
the latter is measured in urine ketone
*( ”-sogastric suction is not done or
?. juropathy involving bladder may lead
to urinary retention demanding
catheterization. Patients with cardiac
autonomic neuropathy have an in
herent risk of cardiorespiratory arrest
leading to high mortality rate.
Physiological
considerations
Hyperglycaemia during acute illness
necessitating surgery may be caused
by increased glucose production,
decreased tissue utilisation and
decreased renal clearance of glucose.
Hyperglycaemia causes osmotic
diuresis leading to water and electrolyte
loss, resulting in dehydration. This may
have detrimental effects on vascular
volume and cellular membrane func
tion.
“Ketone bodies”, like acetoacetic
acid and betahydroxybutyric acid are
resolution of the ketonemic state, and
In the diabetic patient, insulin resis
symptoms of DKA or permit more ac
tance also occurs, this calls for adjust
curate localisation of the causative fac
ment of insulin dose on an individual
tors in the surgical abdomen.
Sufficient rehydration and electrol
basis based on blood glucose monitor
ing.
Patients are usually fasted for at
least eight hours prior to surgery so that
yte replacement and insulin treatment
can be achieved within 4-6 hours to im
aspiration does not occur. A decrease
in external glucose results in stimulation
ketogenesis. In the presence of DKA
insulin is infused by pump at a rate of
6-10 units/hour after an i.v. bolus of 6-
of endogenous production of glucose
and through mobilisation of fatty acids
from adipose tissue to enhance hepatic
ketone production to provide tissues
with alternative energy source. A rela
tive deficiency of insulin decreases the
peripheral utilisation of ketone bodies,
prove hyperglycaemia and to suppress
10 units. Saline solution should be
started with administration of 1000 ml
in 1-2 hour followed by 500 ml/hour
thereafter. Potassium chloride/ phos
phate frequently needs to be added to
the second litre of solution. Plasma
incresing their plasma concentration.
Thus fasting sets the stage for the
glucose concentration would decrease
development of ketoacidosis.
result of dilution through fluid replace
Pre-operative
considerations in
emergency surgery
The major objective in the medical
Col J.S. Saini, Endocrinologist,
management of a diabetic during
Army Hospital, Delhi Cantt
surgery is to maintain metabolic
by 80-100 mg/dl hourly as a combined
ment and insulin induced glucose up
take and decreased hepatic glucose
output. For patients in hyperosmolar
non-ketotic state, insulin doses are
generally lower and obese patients
with sepsis have significantly higher
insulin requirements. Where the
test.
The patient presenting with metabo
lic crisis and requiring immediate
surgery represents a substantial opera
tive risk. There are two approaches that
can improve the outcome. The first is
the ability to temporize or delay the sur
gical procedure most often through the
use of radiologic or endoscopic inter
vention. Examples of this include endo
scopic percutaneous transhepatic
drainage of the biliary tree in a patient
with cholangitis or cholecystitis, or
colonoscopic detorsion of a sigmoid
volvulus. The second is the successful
treatment of the metabolic disorder.
However, if metabolic situation is
secondary to a surgical problem and the
patient is responding poorly despite ap
propriate therapy, surgery should not
be delayed further.
Intraoperative
management
In the past, regional anaesthetic
techniques were preferred because
5
D I A B t I t 5
FORUM —
general anaesthetic agents resulted in
sympathetic stimulation leading to
release of epinephrine which ag
on the result of regular plasma
electrolyte
tests.
Dilutional
Calories Chart
hyponatraemia may rarely occur when
GIK infusion is prolonged. This should
gravates hyperglycaemia and
predisposes to DKA. Newer techni
be treated by additional saline infusion
The calories given below are basically for a person weighing around 70 kgs. People
ques however are very safe and without
and if necessary slowing GIK slightly.
who weigh less than this may spend relatively less calories in carrying out similar
these side-effects. Intraoperatively,
hypoglycaemia is most dangerous and
difficult to diagnose. Therefore, fre
Post-operative
management
quent glucose monitoring is important.
The blood sugar and electrolytes are
maintained by using GKI drip and doses
Once metabolic derangement has
been corrected, the post-operative
are adjusted appropriately.
Surgery and patients with
IDDM
In IDDM patients, various methods
have been advocated and these in
cluded giving various proportions of
patient’s usual morning insulin doses
(one half or two thirds) followed by
glucose infusions of various rates and
concentrations. A more physiological
activities whilst those who are more than this weight would spend that much more
calories.
Activity
state is often uncomplicated. Reinstitution of normal pre-operative insulin
regime is usually possible within a few
days. Failure of improvement in meta
bolic status is indicative of infection
which should be treated vigorously.
Oral drugs can be started when the
patient starts taking full meals.
Open-heart surgery, cardiac surgery
with cardiopulmonary bypass requires
Lying down, sleeping, sitting.
1 to 1.25
Standing, strolling (1 mile per hour), playing cards, knitting,
2 to 2.5
sewing, darning, desk work, car driving, electric typing,
using calculators, etc.(NOTE : in many of these activities,
greater amounts of insulin than other
operations because of the fact that
the calories spent may increase if the activity is associated
attractive version is to give the full
glucose containing fluids are used to
with stress, anxiety, anger etc.)
morning insulin dose, followed by a
glucose infusion (usually 10%) at a rate
to match the patient’s usual dietary in
prime the bypass pump. Also, unusual
take.
At present, a system which con
tinuously provides intravenous glucose
and insulin is preferred. One of the
methods is the use of low doses of in
sulin (0.5 - 1.0 U/h) by infusion pump
accompanied by glucose drip. How
ever, glycaemic control using ‘mini
pump’ system is not always good and
degree of surgical trauma, hypothermia
horse-back riding (walking speed), playing musical
settings, GIK system is not very effec
instruments like piano, playing billiards and snooker, golf
tive and a separate line system with
very frequent blood glucose monitoring
using a power cart to move around, manual typing, auto,
is advisable.
T.V. and radio repair.
Walking at 3 m.p.h., cycling at 6 m.p.h., volleyball (6 men
The care of the diabetic patient need
there is some risk of metabolic decom
pensation. Larger doses of both insulin
concentrated towards the correction of
Practically, there are two methods by
2.5 to 4
glucose and electrolyte abnormalities in
4 to 5
non-competitive), horse riding (sitting to trot), playing golf
with lugging around the golf bag, sailing (handling small
boats), badminton (social doubles), cleaning windows.
a planned and controlled manner. The
use of percutaneous drainage techni
Walking at 3.5 m.p.h., cycling at 8 m.p.h., table tennis, golf
delivered. The first is to use separate
ques can be extremely helpful in
diabetic patients with undrained septic
foci during the period of metabolic im
trot), badminton (social singles), tennis (social doubles),
intravenous lines, one to deliver
balance.
glucose (usually 100 ml 10% dextrose
any callisthenics, painting walls, light carpentry (hobby).
thesiologist and intraoperative
solution given per hour) together with a
cardiovascular monitoring can provide
'piggy backed’, infusion of insulin given
best opportunity for speedy and less
Walking at 4 m.p.h., cycling at 10 m.p.h., roller skating,
by a syringe driver (usually at 2-4 U/h).
complicated recovery.
horse riding (trot), gardening (digging).
which insulin and glucose can be
0
Conclusion
ing emergency surgery requires exper
tise. The primary effort should be
therefore preferable.
Level walking (2 miles per hour), level cycling (5 m.p.h.),
and liberal use of inotropic drugs en
hance the demand for insulin. In these
with such low insulin delivery rates
(2-4 U/h) and glucose (5-10 g/h) are
Calories
spent per
minute
An experienced anaes-
5 to 6
(carrying clubs), dancing (at a pace of a dance like the fox
6 to 7
The second ‘combined infusion’
Insulin in surgery
method is now the most popular and
comprises glucose and insulin mixed in a
single infusion bag along with small
amount of potassium to prevent
hypokalaemia. This glucose- potassium-
tent injection of foreign protein
(competitive), tennis (social singles), light downhill skiing,
produces greater antibody
waterskiing.
.
true for unpurified insulins.
Jogging at 5 m.p.h., cycling at 12 m.p.h., basketball,
The fact that most diabetics
simplicity and effectiveness. The com
.
insulin dependent and may re-
sium chloride and 15 units short- acting
■
quire insulin only intermittently
Running at 5.5 m.p.h., cycling at 13 m.p.h., playing squash
insulin infused over five hours. The in
is good enough reason to use
(social level), handball (social level), vigorous game of
sulin content of the infusion is altered
only purified insulin (ideally
by substituting a new bag according to
human insulins) in these
| patients.
potassium content is varied depending
6
8 to 10
vigorous downhill skiing, carrying loads of around 36 kgs.
undergoing surgery are non-
bined GIK infusion generally contains
500 ml 10% dextrose, 10 mmol potas
frequent blood glucose monitoring and
7 to 8
response. The same holds
insulin, or ‘GIK system’ has gained
widespread acceptance due to its
Walking at 5 m.p.h., cycling at 11 m.p.h., badminton
It is well known that intermit
10 to 11
basketball.
|
________ y
D I A B E T E S---------------------------------------------
FORUM________________ _________
Looking [F©^gj^
Pancreatic Transplants
As insulin is secreted by the beta
cells situated in the pancreas, it was but
natural that efforts would be made to try
and transplant a pancreas in insulin de
pendent diabetics who are completely
The supression of the immune system
means that the patient is defenseless
against any infection. Even a minor ill
ness which in normal circumstances
would not even bother most people
Although efforts have been made to see
if half a pancreas can be removed, this
does not seem to have worked in
managing the diabetes in the recipient
improvement in the state of the retina
or the nerves. This does not mean that
good blood glucose control does not
help in managing these complications,
but it could be that the time at which the
being that if the transplanted pancreas
would lead to a major problem in these
patients. There is also a fear that long
and, the safety for the donor has not
really been worked out. Thus, the only
method of getting a pancreas for
does function, then it would secrete
term intake of these drugs may lead to
transplants is from cadavers of people
plications may reach a stage of such
enough insulin to practically “cure" the
malignancies like lymphomas occurring
patient! The first pancreatic transplant
in the patient. Add to this the cost of
who have donated their bodies for such
medical purposes. This is very rare in
time may not be of substantial help.
was performed way back in 1966 at the
therapy and one will realise that
University of Minnesota by Dr. Richard,
pancreatic transplants still have too
our country for social and, importantly,
medico-legal reasons, and one would
Thus, if the aim is to avert or at least
minimise the chronic complications
many problems which need to be sorted
never be able to get adequate organs
then the organ transplant should be
out.
for transplants.
deficient in the hormone. The hope
Lillehei. The initial results were very dis| 'ppointing, but surgical techniques and
transplant is carried out is too late.
Many of these chronic diabetic com
severity that glycemic control at this
done at a much earlier time. The need
for an early transplant, the paucity of
methods to help preserve the
transplanted organ have steadily im
organs, morbidity associated with the
proved since then and Dr. Sutherland,
operation and the cost and side effects
of immunosuppressive therapy, all
leads one to conclude that pancreatic
from the same university who at
present has the greatest experience
with these transplants is optimistic
transplants, presently, are associated
about the future of this operation. Un
fortunately, his optimism is not shared
with too many drawbacks to gain wide
by most other authorities. As of last year
around 2700 pancreas transplants had
But from this concept, investigators
have explored the possibility of
been done worldwide, most of these in
transplanting the beta cells themselves,
association with kidney transplants. In
raising exciting possibilities.
acceptability.
spite of all the advances only half the
pancreas which are transplanted do
show activity at the end of one year, and
Myths and Concerns
about insulin use in
Type II Diabetes
there is still considerable morbidity and
the occasional mortality associated
with this operation.
p. Besides the surgical skill involved,
I Jne of the major problems associated
Once on insulin always on
insulin
with pancreatic transplants is the need
to immunosuppress the patient who
It is assumed that once a
receives the organ. In its absence, as
with all other organ transplants, the im
mune system of the patient s body will
patient is put on insulin he will
continue requiring insulin.
While this is true of Type I
reject the transplanted organ. A major
diabetes, it is not so, in
breakthrough in transplantation
surgery occurred in 1979 with the intro
duction of a drug called cyclosporin. It
Type II diabetes. Itiswrongly assumed that exogenously
administered insulin will lead
helps in immunosupression and now
the use of cyclosprin along with other
to disuse atrophy of the beta
drugs such as imuran and prednisolone
cells. This has never been
do improve the chances of pancreas
survival after transplantation. Last year
shown to occur in practice; on
the contrary, by reducing
may have brought about a new
glucotoxicity, insulin therapy
breakthrough in immunosupression
therapy. A Japanese company has in
troduced a new drug called FK-506,
Even if these problems are ironed
It was hoped that when pancreas
Thus it may be used intermit
derived from soil fungus, which is un
out, there is still a major drawback,
especially in our country, of producing
enough organs for transplants. Unlike
the kidneys, which we have two and one
of which can be safely donated to a
transplants were carried out, the better
glycemic control would improve other
chronic complications like retinopathy
and neuropathy. Unfortunately, studies
from two major centres have shown that
tently during periods of disor
dergoing trials. It is supposed to have
100 times the efficacy of cyclosporin
recipient, we have only one pancreas.
pancreas transplants do not lead to any
without many of its side effects.
The use of immunosupression is as
sociated with phenomenal side effects.
improves beta cell function.
dered control to reverse the
metabolic derangement
quickly.
DIABETES------- - --------------- ---
FORUM__________________________
Mr. P.F. A, a male aged 38 years was admitted
in a comatose condition around 6 a.m. The ac
companying relative informed the resident on
This case report illustrates a rela
tively common dilemma seen when
insulin regimens. The fasting blood
wake him up, and when this failed, he had been
glucose levels tend to be in the unac
The Somo’gyi phenomenon is a
that the relative could give was that the patient
ceptably high range whilst the control
manifestation of hyperglycaemia fol
was a diabetic, taking insulin, and the family
throughout the day may be quite fair!
lowing, possibly unrecognised,
physician had told them that the blood glucose
From a practical viewpoint, there seem
hypoglycaemia. The clinical picture
to be three main causes for this:
here, is one of worsening control in the
1.
face of increasing insulin doses and is
erratic eating habits. The patient was comatose
with a pulse of 110/minute, regular but ’racy'. The
BP was recorded as 180/95. The patient felt cold
and clammy and his clothes were wet possibly
due to sweating. The heart sounds very well
heard, there was no murmur. The examination of
the chest and the abdominal system was normal
except for sinus tachycardia, and the examination
of a catheter specimen of urine showed the
presence of trace of glucose but no ketones. The
A simple waning of the insulin ef
manifested especially by early morning
control over the blood glucose
levels in the early morning period
dosage could lead to i .■ .oqlycaemia,
The Dawn phenomenon
3.
The Somogyi phenomenon
random blood glucose estimation done by pinprick
and the use of a "stick’ showed the blood glucose
It is of greater importance to correctly
to be below 45 mg%. After blood had been col
distinguish between the Dawn and the
lected for other routine tests, 100 c.c. 25% glucose
Somogyi phenomenon, as the manage
was slowly infused and this was followed by a drip
of 5% glucose. The patient gradually regained
ment of these are radically different and
consciousness and in a few hours seemed to be
a misdiagnosis can lead to quite a
back to normal.
catastrophe, as happened in this
At this time, a further detailed history was
elicited. The patient informed us that he had been
diagnosed as a diabetic about 2 months pre
viously and had been put on a single prebreakfast
patient.
Dawn phenomenon
and a week back, when his blood glucose had
been examined, the fasting blood glucose was
found to be 160 mg% whilst the post lunch values
were 172 mg%. Surprisingly, his glycosylated
hemoglobin levels were in mid normal range. In
When insulin dependent diabetics
(cathecolamines, glucagon, growth
hormone and cortisol) rise as a conse
quence of the hypoglycaemia and their
effect on the liver causes the blood
glucose to rise. As there does not seem
to be “fine tuning” of the magnitude of
the counter regulatory responses and
because these hormones also cause
insulin resistance, there is often an
tend to go much higher than normal. In
serves to intensify the nocturnal
they rose and the insulin requirements
units and 3 days later to 40 units. Inspite of this,
increased between 3 a.m. and 7 a.m.
and this increase in the insulin require
that he had been feeling quite unwell, and when
seen by his doctor had complained of tiredness
But the counter-regulatory hormones
continuous subcutaneous insulin in
fusion (CSII), overnight monitoring of
the blood glucose levels showed that
this time, the patient volunteered the information
patient is asleep, may go unrecognised.
creasing the amount of insulin in order
fast dose of the insulin had been increased to 36
trolled, and in fact there was some rise seen. At
which occuring at night-time when the
were closely monitored during intensive
conventional therapy or whilst being on
view of the fasting hyperglycaemia, the prebreak
the fasting blood glucose levels could not be con
hyperglycaemia. Excessive insulin
overshoot of the blood glucose which
dose of 20 units of Lente insulin. This had been
gradually increased to 32 units of Lente insulin
Somogyi phenomenon
fect so that there is not enough
insulin at night-time to maintain
2.
ments and the hyperglycaemia that fol
lowed was referred to as the “Dawn”
phenomenon. Later, this phenomenon
to counter the fasting hyperglycaemia
hypoglycaemia and increase the
counter regulatory response. This may
be seen as a further increase in the fast
ing hyperglycaemia inspite of increased
insulin doses. Too much of an increase
in the insulin dose could of course lead
to a level of hypoglycaemia from which
the counter regulatory hormones may
had been attributed to the uncontrolled diabetes
was also reported in non-insulin de
pendent diabetics and even in people
and the headache to the high blood pressure.
who did not have diabetes.
glucose levels and the patient may
and early morning headache For the first time,
his BP was found to be slightly high. His tiredness
The previous morning, he had been asked to
take his usual dose of 40 units of Lente insulin. In
It is now fairly well established that
not be able to increase the blood
manifest with frank hypoglycaemic
many hormones undergo diurnal varia
coma.
insulin at his pre-dinner time and also to restrict
tions. These changes in hormonal
Waning of insulin effect
his bedtime quota to milk. It was hoped that this
levels occur both, in diabetics as well
would decrease the raised early morning blood
as in non-diabetics, but tend to be more
The third condition which commonly
This case report illustrates a relatively com
pronounced in a diabetic. Soon after the
leads to a fasting hyperglycaemia is a
mon clinical problem wherein the fasting blood
onset of sleep, there is a surge in the
waning of the insulin effect seen over
glucose levels are higher than acceptable whilst
secretion of growth hormone. Cortisol
night. In other words, the amount of in
shows a significant increase between
sulin in the body decreases overnight
addition, he was asked to take 10 units of Lente
glucose levels.
the control throughout the rest of the day seems
to be fairly good.
2
1) What are the common causes for this to occur?
2) How does one differentiate between these
causes?
3) In the case report were there any ‘warnings'
of impending hypoglycaemic coma which
should have alerted the treating doctor?
4) How would you have approached this case, if
the patient had come to you with rising blood
glucose levels inspite of increasing doses?
5) What is the further management of this
patient?
8
a.m. and 4 a.m. and reaches peak
Differential diagnosis
The best way to distinguish between
patients are treated with “conventional”
got up by 5.30 a.m., efforts had been made to
control of the patient was poor, possibly due to
)’
early morning hyperglycaemia.
duty that due to the fact that the patient regularly
urgently shifted to the hospital. The only history
j
sulin requirements and the consequent
the two would be to estimate the blood
glucose levels at different times
throughout the night. The patient could
do self monitoring of the blood glucose
levels at home, or if hospitalised, this
could be done by more conventional
methods. The estimations should be
done before the post-dinner snack (or
bedtime), at midnight and at 3 a.m.
In patients showing the Somogyi
phenomenon, a typical pattern would
be normal or near normal, blood
glucose levels at bedtime and midnight
which decrease appreciably around pf)
a.m. It has been shown that a value oT'
around 70 mg% at 3 a.m. would suggest
the presence of the Somogyi
phenomenon. In patients manifesting
the Dawn phenomenon, the blood
glucose levels at bedtime, midnight and
at 3 a.m. would tend to be similar and
after this time, the blood glucose levels
would increase to reach hyper
glycaemic levels by early morning.
If it is not possible to do the blood
glucose estimations, one method that
may give a clue to the presence of the
Somogyi phenomenon is to do a urine
glucose estimation (in a double voided
specimen) around 3 a.m. and in the
early hours. If the former shows no
glucose but the latter is MARKEDLY
positive, the patient may be experien<p>
ing post-hypoglycaemic hyper
glycaemia. There are several other
clues that may also point to this diag
nosis. Rapid fluctuations in the results
of the urine tests showing negative
results and then suddenly changing to
maximal values. Wide swings in the
and this decreased amount of insulin is
values shortly after waking up. The
not enough to prevent a rise in the blood
catecholamines gradually increase
glucose levels. Fortunately, the
overnight whilst glucagon remains rela
management
tively constant. Growth hormone, cor
phenomenon and the problems of
tisol and the cathecolamines are all
waning insulin levels is basically the
of
the
Dawn
potent insulin antagonists and these
same and therefore, the main clinical
changes in the secretion of the an
problems is the differentiation between
tagonists seen during the overnight
the Dawn phenomenon and the
period could explain the increased in
Somogyi phenomenon.
blood glucose levels which are not re
lated to meal intake is another pointer
to the diagnosis.
Management strategies
Once the diagnosis of the problem is
clear, the management does not offer
any difficulty. In patients with Dawn
phenomenon, one needs to increase
the overnight insulin whilst the reverse
seems to be the case with the Somogyi
phenomenon. How this is done would
obviously depend on the individual
patient. For the management of Dawn
phenomenon, one or more of the fol
lowing could be done:
(Contd. on Pg. 12)
D I A B E T E S-------------------------------------------------------------------------------
FORUM____________________
The Diabetic Foot
(Contd. from pg. 2)
very cold. This means that the patient
should always check the temperature
of the water before pouring it on his
feet. Some authorities advise that the
temperature of the water be checked
by the hands (if the patient withdraws
the hand very rapidly, it is very hot).
However, it needs to be borne in mind
that neuropathy may also affect the ner
the feet are very dry, then one may need
Footwear
different in size or failing this he may
to apply some mild lubricant like "baby"
oil. Conversely, if the skin is moist, then
This is one of the most important
areas in preventing trauma to the feet.
cially for him. This may also have to be
it would be better to apply some mild
Unfortunately, this is an area where one
comes across the most obstinacy. A
powder especially between the toes.
The point to remember is that the skin
should be neither too dry or too moist
diabetic should never walk barefoot.
The use of chappals really offers no
and therefore there should be a fine
protection against trauma and their use
balance between the use of lubricants
is as good as going out barefoot. Un
fortunately, many patients refuse to
and powder.
have to have some shoes made spe
done by others who have special
problems like cocked up toes, high ar
ches of the feet or other structural de
formities.
The shoes should have uppers
made of soft leather. The soles of the
shoes should also be of leather since
rubber (or other synthetic) soles do not
ves going to the hands and these too
Nails
may be relatively insensitive to the heat.
change over from wearing these chap
pals inspite of all persuasion, saying
The best time to manage the nails is
after washing the feet as the nails are
that the use of shoes is not only uncom
fortable but goes against their tradition
al dress style. In such cases, one
have we seen thorns or nails push right
through the rubber soles? The shoes
compromise would be to insist that the
together. The soles and the insides of
chappals should be stitched and not
the shoes must be closely examined
have any nails in them..
Women also rebel against the use of
before the shoes are put on everyday.
One would be surprised by what may
shoes, but this is an argument that does
not hold good especially in urban areas
be sticking out through the soles or
It would be best to check the tempera
ture of the water using the elbows.
patients to soak their feet for a while.
relatively softer at this time. Nails
should never be cut by the patient but
he should only file them so that no
This is especially true in those who use
sharp edge is left. There is no need for
bathtubs and many patients who have
cutting the nails very close to the edge
or trying to shape them by cutting the
side edges inwards. The sharp edge of
There is also a tendency in some
aching feet use tubs or basins to soak
their feet in order to get some relief.
■'torse still, some put a disinfectant
1 fAjtion in the basin, in the misconcep
tion that this will clean the feet better.
One should never soak the feet as this
often allows the patients’ skin to come
into contact with the warm water for too
the scissors tends to cause minute in
juries and infection often starts here.
Medical advice
Many of the patients we see with
serious foot problems seem to have
long. More importantly, this causes the
brought it upon themselves by trying to
skin to become macerated and such a
indulge in self doctoring. Some
skin is very proneto act as an entry point
for infection. The use of disinfectants
patients when they see a corn or a cal
should be discouraged because the
offer adequate protection. How often
should be stitched rather than nailed
where excellent shoes for women are
even be embedded inside the shoe.
All new shoes even if they are spa
routinely available. Another argument
that is used is that the shoes that the
cious, need breaking in. New shoes
should never be worn for mere than an
doctor feels are good for the feet are
hour at a time. What this implies is that
not fashionable enough! This may be
true in many cases as unfortunately, the
arbiters of fashion do not take into con
one should not wait till the last minute
before getting new shoes. It is advisable
for the patients to keep two pairs of
sideration the skin condition of a
diabetic. At the same time decent look
shoes so that the other pair can be com
fortably worn in an emergency. They
should also get some newshoes much
lus are tempted to take a knife or some
ing shoes are available for women
other sharp object and try to remove it.
before they would need to be worn
wrong disinfectant or even a mild one
in a strong solution can damage the skin
Such self-inflicted wounds are often
which may not be in the height of
fashion but are nevertheless quite good
painless and may not be noticed until
looking and suitable for wearing by a
considerably.
Similarly, the soap that is used for
serious infection has supervened. One
diabetic. For those who are too vain to
accept anything but the latest in
fashion, the best thing is to tell them,
while so that they would get gradually
for treating calusses and corns includ
"Think how fashionable you would look
Similarly, many of us have the tenden
ing corn pads and adhesives. In fact,
if you lost a foot by not taking care”.Not
that the problem of vanity is the sole
cy to wear out the shoes completely and
only change them when the soles of the
prerogative of women, I have come
across many men with the same at
titude and have used the same argu
ment with telling effect.
shoes have given way completely. This
Let us now come to the type of shoes
at all!
If these simple guidelines are fol
the bath
or the washing of the feet
should be a very mild one, may be a
baby soap. After all, the skin of a diab
etic should be treated with as much care
and attention as that of a newborn baby!
jj'a practice of using rough stones to
s’crub the feet, especially the soles
should be avoided. It leads to too many
small cracks and fissures in the skin.
Drying the feet
should never use commercial prepara
tions which are available in the market
it would be worthwhile to avoid applying
any medication to the skin unless it is
under medical supervision. Most of
the medicines available for applying to
the skin may turn out to be too strong
for diabetic skin. Strong medicines burn
the skin. Patients often use medicines
like mercurochrome to treat mild infec
The towel used to dry the feet should
be of the soft variety. Coarse towels can
cause as much damage as the use of
tion or injuries. This is not only too
strong but is usually ineffective. The
stones for scrubbing the feet. The feet
colour of such medications tends to
mask the redness that may be the only
should preferably be patted dry rather
sign of spreading infection in the ab
than be rubbed. Often, many patients
give their feet a brisk rub down in the
hope that this would improve the cir
sence of any pain sensation.
culation. This really does not help and
can cause minute breaks in the skin
from where infection can enter. Care
ful attention is to be paid to patting dry
the area between the toes as these
often tend to remain wet and
may
macerate.
After the bath
This is the time that most of the
patients should examine their feet. If
Socks
The best socks to wear are soft cot
ton ones. These tend to absorb moisture but this may end up as an
that should be worn. They should be
made of soft leather rather than of any
other synthetic material. They should
be big enough to accommodate the foot
spaciously, especially, the front part
which should not bunch up the toes.
Many Patients feel that such spacious
shoes make them look awkward and
have a tendency to choose shoes that
are a size too small. The patient should
be advised to make an imprint of his
feet on a piece of paper and the shoes
that he buys should be broad enough
regularly. These shoes can be then
worn at home every day for a short
broken in and so could be worn regular
ly when the old shoes finally wear off.
is obviously a wrong practice as torn
soles provide no protection and may
be as good or bad as wearing no shoes
lowed, the chances of preventing
serious foot problems from developing
would be very bright. Many patients
may feel that this is all getting unduly
finicky about the need for excellent foot
care. But considering so many patients
with serious foot problems and the
morbidity associated with this, one must
understand that there is no better treat
ment than prevention. After all, the old
saying,
‘For want of a nail,
the shoe was lost;
advantage in our country where one
tends to perspire a lot. The socks
and long enough to completely cover
should not have tight elastic top as this
may interfere with the blood circulation
the feet. Often there maybe slight
to the feet. It may be better, under the
circumstances, to allow the top of the
socks to be loose even if they have a
be allright for one foot may cause the
same size shoes to be slightly tight for
the other foot. In this case, he will either
should not come chillingly true for the
tendency to roll down a little.
have to get shoes that may be slightly
patient!
the imprint. This should be done for both
variations in the two feet and what may
For want of a shoe,
the horse was lost;
For want of a horse,
a war was lost’,
9
9^ FORUM----------- ----------------------
Practical Aspects of Insulin Therapy
Storage
One of the most common problems
that patients seem to have is about the
storage of insulin that they are using.
Insulin preparations are temperature
sensitive and require proper storage. It
is recommended that insulin vials be
stored between 2-8°C i.e. in a
refrigerator. If not stored in this way, the
withdraw the insulin through the needle
places where the room temperature
for most of the patients, storing of the
and the vial should be discarded.
The older conventional insulins,
would be high for many months in a
insulin vials should never be a problem.
year. The vials should NEVER be kept
The insulin vial and the accessories
which many still use, are available in
most places in India. This is especially
true for all the cities, towns and district
in the deep freeze or the freezer section
can be carried in the travelling bag. The
places. The newer insulins are also available quite widely. With this relatively
of the refrigerator. In fact, any insulin
patient should carry the vial that is cur
vial that has been kept in this freezer
rently being used in the bag that he will
section should be thrown away. This
carry with him personally rather than
point is, unfortunately, not too well
Guidelines for Storing insulins
Whenever possible, store the
insulin in a refrigerator at the
recommended temperature of 2-8°C
(36-46°F)
Do not use insulin that has been
frozen (be careful not to place the
insulin too near the cooling system of
the refrigerator or the freezer box)
If you cannot store your insulin in
a refrigerator, keep it in a cool
and dark place
Do not subject the insulin to high
temperatures, such as can occur.a) in the glove compartment of a car
b) on a sunny window ledge
c) near a cooking rage
d) on top of electrical equipment,
e.g. tape recorders, TVs etc.
When travelling in aeroplanes, the
insulin should be carried in the cabin
hand baggage and not in suitcases,
etc. that will be transported in the hold
Carry extra vials while travelling
abroad, as you may not get your
brand or strength of insulins
physiochemical characteristics of in
wide availability of insulin, there does
known and many patients do tend to
sulin preparation may be altered and
not seem to be any need for storing a
large number of insulin vials for future
stock the insulin vials in the deep freeze
port. Because it is rather doubtful that
or the freezer section under the mis
the patient and his baggage would ar
preparations should not be exposed
use. It is advisable that the patients only
taken notion that this would ensure that
to heat or sunlight.
keep one extra vial for use in an emer
the insulin would be preserved well. In
rive at the same place and at the same
time! It is also highly advisable that
may affect the potency. Insulin
of the train or checking it in at the air
The newer purified insulins that are
gency like breakage of the vial currently
fact,many chemists keep their stock of
patients should always carry extra in
being increasingly used these days are
in use. At the same time, there are
insulin in the deep freeze and only
sulin vials and syringes etc., to face
even more stable than the older in
patients who stay in villages where the
remove the number of vials which they
emergencies like a stay of longer dura
sulins. This is due to the fact that the
insulin may not be freely available.
feel they would sell during the day, and
tion than expected, breakages, loss
and other similar problems, especially
newer insulins have a neutral pH. Oc-
Under these circumstances, there may
then store these in the non-freezer sec
cassionally, when the longer acting in
be a need to stock insulin vials. How
tion of the refrigerator. Only a few of
sulins are not properly stored, they tend
ever, extra vials, if any, must be stored
the patients taking insulin, would need
if they are travelling to places where re
placements may not be easily avail
to form clumps. It may be difficult to
in a refrigerator, especially in those
to store a large stock of insulin, whilst
able.
L’
D I A B E T E S---------------------------------------------------------------------------------------------------
FORUM_________________________
action may, in some patients, last for a
further 2 weeks. The effect of the drug
often lasts for around 5-7 days after a
severe hypoglycaemic attack in
patients
taking
250
mg.
of
chlorpropamide daily.
l am often asked by my diabetic
patients about the chances of their
children also getting diabetes. Is there
any way one can predict the risk for
such children to get diabetes?
while, I was calledin by the family again
as the patient had again gone into
coma. I again injected intravenous
glucose and the patient became quite
normal. Later a colleague of mine told
There is no way that one can confi
me that he had been called by the family
dently predict the chance of a child of a
in the early morning, as the patient
diabetic parent for getting diabetes. All
would not wake up. Was I dealing with
such children should be considered at
something different from hypo
high risk and be tested yearly, so that
glycaemia, and if so which conditions
the onset of diabetes can be diagnosed
at the earliest. It would be prudent for
such children to maintain ideal body
would make the patient recover with in
travenous glucose and then relapse.
How should such patients be treated?
weight, exercise regularly and treat any
From the history given, surely, you
When intravenous glucose is in
jected, the rise in the blood glucose
levels allows the patient to regain con
sciousness. But the hypoglycaemic ac
tion of the drug may last even after the
effect of this administered glucose is
over. Thus, the patient relapses, and
this sequence may be repeated. The
best way to manage such episodes in
general practice is to inject intravenous
who get a severe hypoglycaemic attack
several days before the effect of the
drug wears off.
Steinberg after studying the family his
whilst on chlorpropamide do have the
What is the lime that should elapse
tories of many patients had charted the
tendency to go into repeated attacks of
between the taking of the injection and
relative probability of a person, with a
hypoglycemia, even though the correct
the subsequent meal. ?
family history of diabetes, for getting
treatment has been administered for
diabetes. This chart is shown below.
the initial attack. The reason for this is
This is a very common problem and
leads to funny situations where the
•
100
Identical twins or both parents
50-80
One parent and a sibling of the non-diabetic parent
One parent and a parent of the non-diabetic parent
One parent, a sibling, and a grand-parent via the nondiabetic parent
patient sits with the food plate in front
of him and then as soon as the injection
is given he starts eating very fast, feel
ing afraid that otherwise he may go into
coma. This misconception should be
removed.
Generally speaking, the patient is
advised that the insulin injection should
be taken about 20 to 30 minutes before
the meal. This is to allow some of the
injected insulin to get absorbed into the
blood stream so that the insulin levels
W
50
One parent and one sibling
30-40
Two grand-parents (not spouses)
One parent and first cousin on the non-diabetic parent’s side
25
20
prevents the post-meal blood glucose
from rising excessively. Even normally,
Two grand-parents (spouses) or one parent
the absorption of the food from the gut.
One grand-parent
Thus, giving the injection 20 to 30
minutes before the food is an attempt
to mimic the normal physiology.
Uncle or aunt
First cousin
hours after the meal, when the blood
glucose is falling, the insulin action
such that the peak insulin activity coin
cides with the period when the
postprandial blood glucose would tend
to be the highest.
Conversely, in “early activators,” the
peak activity may be seen with an hour
and in such cases, there may be a pos
sibility that the patient gets a “hypo” at
this time as the eaten food may not have
been digested and absorbed in this
short period. In such circumstances, it
may be necessary to eat right after the
injection is taken. In severe case, the
injection may need to be given after the
meal although this is quite rare. Thus,
whilst most of the patients may need to
have a gap of about 20 to 30 minutes
between their insulin injection and the
meal, this time interval needs to be in
dividualised in many cases.
have alredy started to rise as the food
is digested and absorbed. This
it has been shown that the insulin
secretion from the pancreas precedes
One sibling
at its peak. This would lead to an ex
cessive rise of postprandial blood
glucose levels. Later, about 3 to 4
it may be necessary to prolong the time
between the injection and the meal
have had a severe attack may require
continuous intravenous glucose for
duced hypoglycaemic coma. Patients
Diabetic relatives
blood glucose is seen at 2 hours after
the food, the insulin action would not be
patients, especially if they are older and
were dealing with chlorpropamide in
the long duration of action of this drug.
in such patients would be that insulin
would not be available in adequate
amounts at the time when required.
When the peak rise in the post food
would be peaking and this may lead to
a “hypo” at this time! In such patients,
associated conditions like lipid
Probability
(Percent)
be seen after possibly 60 minutes, the
peak may be at 3 to 4 hours and the
onset after 8 to 10 hours. The problem
glucose, see that the patient takes a
snack of complex carbohydrates and
then hospitalise the patient. Often, such
rnblems, hypertension, etc.
r At the same time, many years ago,
Such charts may not be directly
levels to rise and have an effect when
the food is absorbed. In slow ac
tivators, the rise inthe insulin levels may
Post
As a part of its activities, Diabetes
Forum has started a Diabetes Post
Line where our panel of experts will
answer all queries which you may
have regarding any aspect of
diabetes management.
All the same, the time period be
tween the injection and the eating
Please send your letters, questions,
problems in management, etc. to:
needs to be individualised. There are
Diabetes Post Line
useful for individual patients. After all,
Although, most books mention that the
the patient who asks this question is not
effect of chlorpropamide lasts for
interested in statistics and probability,
around 36 hours, this is usually after a
a delay in the absorption of the injected
A Division of
but is only interested in the risk for his
single dose has been administered.
insulin, the levels of which start to rise
Boots Pharmaceuticals Ltd
children! Thus, the best answer that
When patients are given 250-500 mg.
much later than expected. Normally,
17 R Kamani Marg, Bombay 400 038
one can give for such questions is that
of the drug daily, a steady state is
when a short acting insulin is injected,
some patients who are 'slow ac
OMAGNUS
tivators'. Such individuals tend to show
all these children should consider them
reached after 4 days. When the drug is
one expects that the effect would start
selves at a high risk for getting diabetes
continued, the duration for which the
around 30 minutes after injection and
at some stage in their lives.
drug stays in the body, and exerts its
that it would peak after 2 hours and
□ / have a patient on chlorpropamide
blood glucose lowering action, is much
have an onset of action after about 6
who recently went into hypoglycaemic
more. Studies have shown that if a
coma. He recovered when I injected in
patient takes the drug for 2 weeks and
travenous glucose but then after a
then discontinues it, the hypoglycaemic
hours.This is why one advises that the
injection be taken around 30 minutes
before the food. This allows the insulin
Replies will be sent individually.
Queries which may be of general
interest to practising doctors will be
published in the issues of Diabetes
Forum with your identity being with
held, if you so desire, We look for
ward to hearing from you.
11
Case Study
3.
(Contd. from pg. 8)
1.
2.
■
3.
Give a small pre-dinner dose of
Decrease the amounts of
intermediate or long-acting insulins
given during the morning
intermediate-acting insulin, if the
patient is not already taking one
viously manifesting the Somogyi
If the patient is taking a dose of an
intermediate-acting insulin before
There were several clues present which
dinner, this could either be
judiciously increased or the timing of
the injection delayed so that the
maximum activity could be seen
around 2-4 a.m. and
A small dose of regular insulin could
be given before the post-dinner
snack
The purpose of all these manipula
The patient, Mr. P.F. A., was ob
phenomenon in the previous days.
could have pointed to the correct diag
nosis. There was a worsening of blood
insulin dose as could be seen from the
increase in the levels of early morning
hyperglycaemia. The patient also com
plained of feeling extremely tired in the
morning and of having a headache. His
BP was found to be high for the first time
tions would be to increase the amount
of insulin available in the body during
the crucial 2-4 a.m. period. It is obvious
An indirect clue would be the midnormal
after the increase in the insulin doses.
that if an additional injection is given or
levels of glycosylated haemoglobin in
the dose of the insulin is increased, cor
responding changes must be made in
spite of unacceptable fasting blood.
the dose of insulin given at other times
in order to prevent day time hypog
lycaemia.
haemoglobin tends to "average” out
The strategies to manage the
Somogyi phenomenon could be:
VIII National Diabetic Congress
December 3-5,1993
organised by
Diabetic Association of India.
glucose control inspite of increasing the
Venue
I.P.G.M.E. & R/S.S.K.M. Hospital/Hotel Taj Bengal, Calcutta
Last date for receipt of abstracts
glucose levels. Since glycosylated
September 30,1993
the ambient blood glucose levels, a
Organising Secretary
midnormal glycosylated haemoglobin
Dr. D. Maji
Department of Endocrinology
S.S.K.M. Hospital/!.P.G.M.E. & R. Calcutta 700 020
Phone: 4785796
estimation along with high fasting blood
glucose and “fair” post-meal values
should have pointed out to the pos
1.
Decrease the dose of the evening
insulin injection
2.
Add, or increase, the amount of
dinner or, preferably, the bedtime
of blood glucose at some time during
snack
the 24 hours.
sibility that the patient may have been
undergoing episodes of very low levels
BOOTS
H
NORDISK
uma nt
INSULINS 11
A new standard in diabetes care
Human
NORDISULIN
TM
Human
INSULATARD
Neutral Insulin
Isophane Insulin (NPH)
• Onset1/? Hour • Max. effect 1-3 Hours • Duration 8 Hours
• Onset Viz Hours *
Max. effect 4-12 Hours •Duration 24 Hours
Human
Human
TM
MONOSULIN
MIXTARD
Insulin Zinc Suspension
Mixture of 30% Human Nordisulin and 70% Human Insulatard
• Onset 2’/? Hours • Max. effect 7-15 Hours • Duration 24 Hours
• Onset 1/2 Hour • Max. effect 2-8 Hours • Duration 24 Hours
Full prescribing information available on request from:
<£> MAGNUS
A Division of
Boots Pharmaceuticals Ltd
[JN9 Nordisk Gentofte AIS
17 R Kamani Marg Bombay 400 038
U\J (Novo Nordisk AIS) Denmark
VIRAL
What is Jaundice?
Jaundice is not a disease. It is a
manifestation of an underlying disease
like the fever in Typhoid or ‘flu’. Although
most often it occurs as a result of an
underlying liver disease, it can occur as
part of various other problems quite
unrelated to the liver. The lesson here is,
when jaundice occurs find the cause for it
and then only a proper treatment can be
given. As many of the drugs taken have
to be metabolised by the liver to make
them effective, excrete or detoxify, do
not blindly take remedial measures which
may infact further harm the already sick
liver.
What is Hepatitis B (HB) ?
It is a virus (HBV) infection which is
highly infectious. It makes the liver swell
and affects the functions of its cells. Most
often it may be a self limited process but
sometimes it can perpetuate the damage
leading to cirrhosis (scarring of the liver)
with an increased risk of developing liver
cancer, in India, we do not know how
many people are affected by this illness
every year due to lack of proper statistics.
When a developed country like U.S.A.,
more than 25,000 people contact
Hepatitis B per year, certainly the figure
must be much higher in our country.
Fortunately, for many people the body’s
natural defences will fight off the virus
and develop immunity to it. However,
about 2-10% of adults infected with HBV
will become carriers or develop chronic
HB which means that they remain
infectious.
How is HBV transmitted?
HBV is 100 times more contagious than
the AIDS virus It may be transmitted
through contact with infected body fluids,
blood, urine, saliva, seminal fluid, vaginal
secretions and breast milk. HBV can be
transmitted through sexual contact (both
hetero and homosexual) as well as through
sharing of razors, toothbrushes IV needles.
tattooing and other sharp instruments.In
this context, 1 must mention that a
preliminary report of a study conducted
by me tends to show that a significant
number of patients could have got infected
by receiving injections with contaminated
needles. It is therefore best to avoid
injections when the same illness can be
treated with oral medications and if
injections are necessary to be used, only
disposable needles and syringes should
be used. It is a myth that a drug given by
injection will be curing an illness more
effectively in all instances.
Anyone who is exposed to blood or body
fluids of an infected person is at risk. The
hepatitis B virus can live outside the body
for upto ten days on a dry surface
Ss there a vaccine for HBV?
There are safe and effective vaccines
against Hepatitis B. Three injections are
required for full protection. The second
injection is given one month after the
first, and the third is given six months
later. The vaccine provides immunity for
ten years or longer. As it will not ‘cure’
a person who is already infected with
HBV it is advisable to check your blood
to see whether you are already infected
before the vaccination. The World Health
Organization
has
recommended
Hepatitis B vaccination to be included in
the routine vaccination of children.
What are the Symptoms?
Very often this illness may have only
minor symptoms and may be mistaken
for an attack of flu and not all may even
develop jaundice. The stronger the
response of the body's immune response
the more severe would be symptoms
including the jaundice. Thus the
chronicity leading to cirrhosis of the liver
may occur more often in perons who had
a milder attack and neglected taking
proper care and rest.
What is a carrier?
When the virus continues .to persist in the
body for more than six months, that
person is considered a carrier. The most
important fact about the carrier is that
this person can pass the virus,
unknowingly to others and yet remain
without symptoms even for a lifetime.
However, carriers have a higher risk of
developing cancer of the liver.
What should a carrier do ?
Carriers should remember that the virus
is present in all body fluids like blood,
semen, vaginal fluids, urine and saliva. A
carrier should never have unprotected sex
unless the other person is immune to
HBV or has received the vaccine. They
should get a check-up every six months
to assess the status of the liver. Alcohol
which is toxic to the liver should be
avoided.
For more information on Hepatitis 8, please contact
Or. Ravi Kootoor MD.DM
Professor and Head of the Department of
Gastroenterology,
St. John’s Medical College, Bangalore
VIRAL
HEPATITIS
What is Jaundice?
Jaundice is not a disease. It is a
manifestation of an underlying disease
like the fever in Typhoid or 'flu’. Although
most often it occurs as a result of an
underlying liver disease, it can occur as
part of various other problems quite
unrelated to the liver. The lesson here is,
when jaundice occurs find the cause for it
and then only a proper treatment can be
given. As many of the drugs taken have
to be metabolised by the liver to make
them effective, excrete or detoxify, do
not blindly take remedial measures which
may infact further harm the already sick
liver.
What is Hepatitis B (HB) ?
It is a virus (HBV). infection which is
highly infectious. It makes the liver swell
and affects the functions of its cells. Most
33 is
VDRL IM PREGN.^CY
Q:
Recently we have started doing routine VDRL for .all antinatal
patients.
Onr.as.qioral 1 y we come across positive cases.
the dilutinn.q are very low eg: 1:2. or 1:4.
Sometimes
Should we treat these
patient?
A:
Routine HLood VDRL done during pregnancy is an excellent practise.
The unfortunate occurence of congenital syphilis can be eliminated if
this is done everywhere.
Ideally VDRL is done at the first antenatal
visit and at 32 weeks to eliminate the possibility cf infection
occuring after the 1st visit.
VDRL must be done correctly and whenever reactive, in higher
dilutions to find the maximum dilutions.
Later follow up
will be
possible only if these dilutions are documented.
VDRL is a non-specific test and can be reactive in conditions
•ther than-Syphilis which includs pregnancy.
So it is not correct
to assume that the person is suffering from syphilis whenever a VDRL co...s
comes as reactive..'
*
•
Please remember that any dilutions is possible in syphilis.
But very high dilutions do not occur in ether conditions.
So high
dilutions like 1:32 and above can be assumed to be duq/syphilis and
to be treated.
The lower dilutions may oy may not be due to.syphilis.
Other factors like history and clinical features should be looked into.
If further drubt exiets it is advisible to do specific test, eg:'TPHA,
But unfortunately very few centres in this country a»e doing
FTAABS etc.
this.
So if it is impossible to rule out syphilis in pregnancy it is
advisible to treat as for syphilis if patient is not allergic to
pencillin.
In such situation it is the duty of the doctor t« explain
to the couple that though the test may be positive due to pregnancy
itself, it is also possible it is due to .syphilis infection.
The
decision of giving treatment should be made only after taking the
consent of the patient.
•
4>ften doctcw-do. not realise the emotional and psychological
reactions when some one is treated for VD.
Occassionally,.this can be a
legal matter.
The'treatment , for early syphilis (ie. all
im rifestations
that
appear during’the first 2 years after the infection) is as f«llcws:
>.
Inj. Benzathene Pencillin 24 lacs (PENIDUKE LA 24) IM as a single
dose.
2.
OR
Inj. PROCAINE Hi.NCTL.1 TNE 8 lacs (PPP) IM daily x 10 days.
If the patient is reliable or admitted, procaine pencillin should
be prefered.
If the patient is allergic to pencillin:
1.
Gap Tetracycline 500 mg 6th hourly on an empty stomach x 15 days. CR
2.
Tab Erythromycin 500 mg 6th hourly x 15 days.
Pregnant woman and children below 12 years should not receive
Tetracycline.
After the treatment V^RL should be repeated once in 3 months x 1 year
and «nce in 6 months till/become Non Reactive.
The VDRL is expected to become non-reactive 3 months -18 months
i.E early syphilis after the treatment.
GENITAL HERPES
Genital herpes is a common sexually transmitted, disease.
It usually occurs for the first time within 2 weeks of sexual
intercourse with a person having active disease.
In some, the
condition keep coming again and again even without further
sexual intercourse.
How often this may take place is difficult
to predict.
The disease starts as one or more water bubble like blisters.
Later these blisters break and small ulcers are formed.
When
these ulcers are present the person can infect the sexual partner
during intercourse.
When the ulcers are not present the person
is not infectious to others.
So it is advisable to avoid
intercourse or use some protective device when ulcers are present.
If the partner also has. the same disease there is no need to '
take any precautions.
Usually this disease does not affect the health of the person.
But it .can be a cause of much guilt, worry and anxiety.
Plenty of research is going oh, to find a permanent cure for
this commonest VD of the world.
Some drugs are useful to cut short
the duration of the ulcers, (eg. Acyclovir)
These are used only
in some special situations.
Many new drugs are being tried all over the world for a
permanent cure.
Till such medicines are available the persons
suffering from the disease must accept the fact that there is not
anything available anywhere in the world which is useful in
stopping the disease coming again and again.
A simple test, usually done only by the skin specialists
(TZANCK Test), can give evidence about the disease, if the patient
comes at the stage of the blisters.
Blood VDRL which is done to detect syphilis will be non
reactive (negative) in this disease.
But it is done as a routine
to rule out associated syphilis infection.
TREATMENT
‘
Only gentle cleaning the area with plain water and soap is
needed and the ulcers will heal within 3-7 days.
If there is much
pain or pus or ulcers take longer time to heal the patient should
consult the treating doctor.
Venereal Diseases
1,
Tnere are about 15 venereal diseases .
Most of them are
easily treatable,
2.
Venereal diseases are only transmitted by intimate and
direct contact (usually by sexual intercourse) with a
patient who is suffering from the same disease.
3.
It is passible, though rare to get VD through unsterile
injection needles and blood transfusion, but not by
using a public urinals or eating strange foods.
b-. It is possible to get more than one venereal disease from
one contact,
Go it is important to complete the follow
up with necessary urine and blood tests before assuming
that one is cured of venereal diseases.
5.
The blood VDRL is done to detect only one veneraal disease
e.
i.
6.
Syphilis.
The usual cost of the test is Jts.10 to 20/-
VDRL can be positive even when there is no syphilis.
Sometimes it is positive in other diseases and occasionally
even in normal healthy individuals,
7.
Blood VDRL can be positive in normal pregnancy without syphilis,
•
and blood VDRL is routinely done in pregnancy
8.
Specific tests (eg.TPHA) are available to know whether the
patient is really suffering from syphilis.
9• Venereal diseases can be present in the body even though
patient do not have any complaints but these diseases can
be detected easily with simple urine and blood tests.
10.
as
a rule a period of 6 months should elapse before one
can be certain of not getting VD after the previous contact.
After this period if tiie patients blood + urine tests are
allright and do not have any external sign of VD it can be
safely assumed that the person is not suffering from any V.D.
11.
Diseases other than VD can affect the genital parts producing
much anxiety and guilt.
It is important to consult a
competent doctor and take an opinion.
12.
Many normal conditions like pearly penile papules, Fordyce
spots,
cutis
ansorina, nocturnal emissions, spermatorrhea
etc. can produce doubts as to the existence of VD.
But a
competent doctor can easily recognise these conditions and
reassure the patients.
13- Pencillin injections are given for only 2 venereal diseases
e.
i.
for syphilis and occasionally for gonorrea.
2. . .
1R. Medication to prevent the development of VD after
suspected contact with the disease is not recommended
at all.
It is virtually impossible to take treatment for all the
1? venereal diseases.
The wrong medication or inadequate dosage often suppress
the manifestations of the VD and produce difficulties in
the diagnosis and treatment of the V.D. later.
1J. Some patients develop fear of venereal disease (Venereophobia)
though tney do not suffer from any VD or sometimes after
getting cured from VD.
In mild forms reassurance by the
doctor is sufficient.
In severe forms medications .and
sometime psychiatric help may be necessary.
16. The V.D. patient is the usual target of unscruplous
laboratories and doctors who scare the patients informing
them they are suffering from VD and offer very expensive
investigations and treatment which sometimes run into
thousands of rupees.
Rarely patients take action about
them due to the social stigma attached to these diseases .
When in doubt, it is always safer to take another opinion
from a reputed institution.
Deutsche
Stiftung
fur
internationale
Entwicklung
German
Foundation
for
International
Development
Fondation
Fundacion
Allemande
Alemana
pour le
para el
Developpement Desarrollo
International
Internacional
THE ORAL HEALTH ALLIANCE
THE BERLIN DECLARATION ON
ORAL HEALTH AND ORAL HEALTH
SERVICES IN DEPRIVED
COMMUNITIES
THE ORAL HEALTH ALLIANCE
THE BERLIN DECLARATION ON
ORAL HEALTH AND ORAL HEALTH
SERVICES IN DEPRIVED
COMMUNITIES
Proceedings of an International Workshop
held at
The German Foundation for International Development (DSE)
Conference Centre, Villa Borsig, Berlin
September 1992
FOREWORD
The oral health is improving in industrialized countries and deteriorating
in developing countries. But within the more affluent countries
improvements in oral health are not occurring in most dcpr.ved
communities Indeed, the oral health of children in many c tveloping
countries is worse than in developed countries and the former cannot
afford the appropriate resources to deal with the diseases. In all countries
the dental profession and governments place most emphasis on the
curative and technological aspects of dentistry rather than promoting
prevention and community programmes for oral health which are more
effective at improving oral health and would have greater impact on the
oral health of dentally deprived communities. The curative methods
cannot be sustained at all levels of development.
Because the German Foundation for International Development (DSE) and
the NGO 'Dental Aid" (Zahnmedizinische Entwicklungshilfe - ZME) were
aware of this problem they invited dentists, health workers, directors of
health service projects and programmes and academics from twenty-eight
countries to an international workshop on "Improving Oral Health and Oral
Health Services for Deprived Communities". The workshop was held from
September 14th to 19th at the DSE Conference Centre at Villa Borsig in
Berlin, before the 80th FD1 Annual World Congress.
The workshop provided an unique forum for people who work in
community- based and community-oriented oral health programmes to
1
exchange experiences' and discuss issues in primary oral health care at an
international level
The objectives were to:
• identify and discuss issues and actions relevant to communityoriented and community-based oral health programmes;
• identify problems and barriers in planning and implementing oral
health programmes for deprived groups and discuss approaches to
overcome them;
• formalize a network between the different groups and projects
represented;
• inform the public and decision makers and raise awareness of
these issues among the dentists by publishing the workshop
proceedings.
During the workshop the need was expressed for better and continuing
communication between oral health workers concerned about improving
the oral health of all people including those who are deprived. Therefore a
new group was constituted which was named the "Oral Health Alliance ".
The group formulated the Berlin Oral Health Declaration and recommended
strategies-based on the principles in the declaration. A newsletter and
periodical critical reviews of current concepts in relation to oral health
issues will be published and widely distributed.
2
THE BERLIN DECLARATION
ON ORAL HEALTH 1992
BACKGROUND
When the Alma-Ata Declaration was formulated in 1978, there were
two developments which were not foreseen or anticipated. These are
the rapid global economic crisis of the 1980s and the AIDS pandemic
with the current problems of its prevention and control. The economic.
social as well as political crises in most developing countries have
adversely affected health in terms of:
. o provision of services
« access and coverage
o financing of services
o quality of services
® status of health
Deprived communities exist at the country level and deprived groups
exist within countries. At the country level it was a description of the
world's poorest nations. Many of these nations have low per capita
incomes and increases in their populations of around 3% per annum.
Their health and oral health services are grossly maldistributed. The
dental caries level is relatively low in the rural poor - a DMFT at twelve
years of age of 1.5 or less, but in the urban poor decay rates are higher
than among the rich. Dental caries is common in poor countries and the
severity is rising. The deprived have a high proportion of their decayed
teeth unfilled or treated by extraction.
For deprived groups within countries the definition is more difficult but
the following characteristics are common: poverty in comparison to the
rest of the country (the poverty line has been set at 370 U.S. dollars
annual income per capita in 1985 purchasing power parity dollars),
marginalization either by geographical remoteness or because they have
been dispossessed of their land/homes or because they feel that the
existing services are not for them. This is often exacerbated by high
levels of illiteracy and a lack of formal education. Frequently they do
not feel a part of the larger group.
The direct problems of poverty are unemployment, low income, limited
education and inadequate diet. This leads to overcrowding, poor
housing, inadequate water and sanitation, lack of land to grow food,
which in turn are related to infectious diseases, pollution, accidents,
stress, alienation, instability and insecurity. The urban poor are at the
3
interface between underdevelopment and industrialization and their
disease patterns reflect the problems of both. From the first they carry
a heavy burden of infectious diseases and malnutrition, while from the
second they suffer the typical spectrum of chronic and social diseases.
Good health of individuals, families and communities requires a decent
environment built on a solid foundation of fairness, respect and
equality. Until recently it was predicted that, by the year 2000, the
number of the people in the world living below the poverty line would
be reduced by 300 million. Now the World Bank suggests that the
numbers in poverty have increased substantially - from 1,051 million
to 1.133 from 1985 to 1990.
In any society, the principles of natural justice are based on equity, on
balancing the scales between right and wrong, between what is fair and
what is unfair "Equity in health implies that ideally everyone should
have a fair opportunity to attain their full potential and, more
pragmatically, that no one should be disadvantaged from achieving this
potential, if it can be avoided." (WHO, 1986, Social Justice and Equity in
Health. WHO Europe, Copenhagen). By definition, inequity means
injustice. Despite efforts in the past decade to make health systems
more equitable, in the poorer countries and communities things are
getting worse in terms of people s health and access to health care. The
first priority is to gel the international community and national
governments to make a commitment, through positive actions, towards
solving some of the causes of poverty. It is a human right to have access
to the basic, necessities for healthy living.
HEALTH IS A BASIC HUMAN RIGHT and oral health is a significant
component of general health. Although oral diseases are not lifethreatening, they are important public health problems. The reasons for
their importance are their high prevalence, public demand, and their
impact on individuals and society in terms of pain, discomfort, social
and functional limitation and handicap and the effect on the quality of
life. In addition the financial impact on the individual and community is
very high and this is going to increase due to the infection control
measures required for the prevention and control of hepatitis and
HIV/AIDS.
Oral health has not been given the attention it deserves. As a result,
people who are poor and living in difficult circumstances, whether in
developing or industrialized countries, continue to be dentally
neglected, a situation that has every likelihood of worsening as the
global debt crisis and privatization of health services occur
4
An important feature of oral diseases is that effective preventive
methods which are simple and cheap are available, but in many cases
these methods are not appropriately applied The development of
dental program mes'incorporating effective simple and cheap preventive
methods and which involve local people and build upon their strengths
and capacities have a better chance of ultimately improving both
services and community oral health. These community-based
programmes are more likely to lead towards self-reliance and self
management of oral health programmes
The purpose of this document is to provide guidelines to health
planners for planning, implementing and evaluating relevant oral health
projects and programmes. This may be accomplished when planners:
• move from a biomedical model to a social development model of
health care and health care education;
o initiate ongoing monitoring and evaluation based upon the
principles of community-based action research;
• involve community members in assessing needs and
project/programme development. The intention is to reduce
dependency, enhance personal autonomy and enable oral health
and well being to occur:
« Prepare and support health workers to work with local people
for health and equity in dentistry.
Oral health projects and programmes aimed at improving oral health
and oral health services in deprived communities should be- developed
recognizing certain issues and principles. These are spelled out in the
remainder of this declaration.
ISSUES TO BE CONSIDERED
It is important for health planners, administrators and all advocates to
be aware of a number of issues that encompass the world of workers
wanting to provide primary care and nurture oral health in dentally
deprived communities.
Underdevelopment:
The recognition that many communities are dentally deprived has
unfortunately produced a number of inappropriate responses. The
worst is that programmes developed in one setting have been
transferred without adaptation to a completely different one. The
5
results of such efforts have been to create or increase the state of
dependency of deprived communities and to reinforce their sense of
powerlessness and their lack of ownership of the programmes. The
fragmentation, within many deprived communities, exacerbated by
poverty. lack of formal education and high illiteracy levels, result in
little participation by the people in such programmes. These problems
will not be resolved by any attempt to put the blame for their existence
on any one community, group or individual.
Ethical values:
Communities frequently resent unsolicited research activities being
carried out in their midst. Similarly, appointment of external
consultants to programmes by outside bodies with neither the
agreement of the communities involved in programmes nor with clearly
defined tasks, results in the disaffection and dissatisfaction of the
com m unity
Health Promotion:
Most present programmes concentrate their efforts on the provision of
curative services giving little attention to health promotion
Goals and evaluation procedures:
Many programmes frequently lack clearly defined realistic goals
developed in collaboration with the community. Seldom are appropriate
socio-dental indicators applied. They take into account the
measurement of well-being and the quality of care. This results in a
lack of well defined appropriate and comprehensive process and impact
measures, which take into account health promotion and community
development activities.
Resources:
There is a misallocation of resources. The majority of the resources are
used by the minority of the population who require the least care.
Eighty percent of the resources are consumed in clinics which serve
twenty percent of the population.
The training provided for many oral health care workers is frequently
carried out in inappropriate sellings. Consequently workers are illequipped to function where they are most needed and thus redress the
imbalance in availability of appropriate care.
6
In many countries the migration of the population to the >rban areas is
resulting in large underserved peri-urban populations
Programme organization and support.
The progress of many programmes is impeded because of frequent
changes in administrations Such situations are often made worse
because the administrative infrastructures are weak. Often morale is
low because of poor training and limited job satisfaction.
Little understanding of these problems and a reluctance within the
dental profession to share and delegate responsibilities for oral health
in the community further inhibits the development of appropriate
program mes.
7
GUIDING PRINCIPLES FOR IMPROVING
ORAL HEALTH
When developing a programme or project to improve oral health by
working with people it is important to take into account each of the
following principles.
The Role of Governments
Article V of the Declaration of the Alma Ata Conference (1978) states,
that “Governments have a responsibility for the health of their people
which can be fulfilled only by the provision of adequate health and
social measures." A main social target should be the attainment of the
world of a level of health that will permit all people to lead a socially
and economically productive life. Primary health care is the key to
attaining this target as part of development in the spirit of social justice.
"
Reducing Inequalities
Principles for action are:
1. Policies should focus on improving living and working conditions, adequate
and safe housing, access to high quality food, control of pollution, safe water
supplies, employment policy, welfare system.
2. Policies need to be directed towards enabling people to adopt healthier
lifestyles. Distribution of cheap and nutritious food, control of advertising of^
health damaging products, provision of clear information, access to leisure 1A
exercise facilities.
3. Policies require a genuine commitment to decentralizing power and decision
making, encouraging people to participate in every stage of policy planning
process
4. Health care based on principle of making high quality health care accessible to
all. Resource allocation in relation to social and health needs, geographical
distribution of services linked to measures of need and access, focus on
acceptability of care from disadvantaged groups.
8
Underdevelopment
Oral health development is not achieved through the unmodified
transfer of skills or programmes, personnel or equipment to deprived
communities. Adaptation rather than uncritical adoption should be the
rule. ’
Dependency
Dependency is disabling. Although it is recognized that most pre ?cts
can not be completely self-financing and require state or institutional
support, they should be deliberately developed and implemented in
ways that ensure continuation by the communities in which they are
located.
Empowerment
Communities must be enabled to obtain and contribute resources to
sustain, self-manage, and satisfy their programme objectives and needs.
Community Involvement
Oral health decisions should always be made collectively with local
people who best know their own problems, needs and capacities, so that
control of dental projects and programmes rests with the community
being served. The right of all communities deprived of oral health care,
to organize services and training programmes should be acknowledged.
Partnerships
Projects should be developed and implemented mutually (by
institutions and persons) on the basis of honesty, respect and
reciprocity in that partners share and learn from each other. Partners
must declare their assumptions and expectations, and decide how to
work together to resolve problems and make decisions.
Consultants and co-operating agencies have an obligation to be
responsive and responsible commitment to project objectives is
essential.
9
Assessing needs
The assessment of needs has to be based on collaborative efforts
between users and providers. This should lead to the agreement of goals
and targets, that reflect people’s needs and to the implementation of
services and evaluations that are based on these set goals.
Epidemiology is a fundamental tool in the development and evaluation
of health plans and programmes. It is necessary to develop indicators
different from those normally used. They should measure social,
economic and health impacts. Socio-dental indicators are more relevant
measures of needs and should reflect pain, discomfort, function and
aesthetics as well as clinical indicators of dental health such as caries,
bleeding gums and pocketing, number and position of teeth. Other
impact measures include loss of sleep, work loss and opportunity costs.
Priorities
Priorities should not be developed solely on the basis of the demand for
treatment. Health promotion can alter a community's perception of the
problems and hence priorities. Priorities should be established through
a partnership between the community and the professional advocates
for oral health.
Goals
The community should be involved in setting goals that are stated in
terms of oral health, oral disease, health promotion, equity, training and
personnel and health service.
Oral Health Promotion
Oral Health Promotion should have the highest priority and follow the
principles as defined in the Ottawa Charter for Health Promotion (1986).
Health Promotion means building healthy public policy, creating
supportive environments, strengthening community action, developing
coping skills and re-orienting dental services. Health promotion policy
must take into consideration: the uneven distribution of health and
disease, the uneven distribution of health hazards in the physical and
social environment and of personal behavioural risk factors and
10
opportunities to adopt a healthier personal lifestyle as well as the
uneven distribution and quality of health care.
Preventive Strategies
Authorities should recognize that the preventive approach is an
essential and inescapable recommendation.
Governments should apply mass preventive measures. Oral health
strategies should be integrated with general preventive approaches
within an overall context of health which lead to improvements in the
quantity and quality of life.
The preventive measures should be simple and effective and not
contradict each other or confuse the community.
Evaluation
Evaluation should not be seen as a mere technical activity but more as
an educational learning process in order to improve social conditions
and human life. It should therefore shift from being autocratic to a
more democratic participatory exercise. The community should be
involved in the formulation and assessment of the impacts of the
programme. Process measures should not only include the number of
procedures performed but health promotion and community
development activities. The results should be discussed and acted upon.
Treatment strategies
The services should be based on the development of local human
resources. Community needs should be defined and mechanisms
established for regionalising services. This should be done on the basis
of levels of care which requires referral and redefines the roles of
different health personnel.
It is also important to ensure that proposed strategies are compatible
with scientific knowledge and technological advances.
11
Ethics
All activities performed should comply with ethical standards accepted
and outlined in the Helsinki Declaration and by a local ethical
committee.
Experts/Consultants
Local people are experts on community life, functions, and potential.
Outside consultants who have a particular expertise should only be
selected after full consultation and at the request of the host
community.
The experience and qualifications of the consultants should be vetted to
ensure that they are suitable for the task on hand.
In all cases local/regional expertise should be given priority before
considering consultants from further afield.
Once the invitation is agreed, the host country and community is to
ensure that adequate facilities are available to enable that the tasks
agreed upon are carried out. The consultant has an obligation to carry
out these tasks and submit a report to the local counterparts before
submitting it to the sponsoring agency.
Resources
Resources (human, facilities, finance) should be shifted from central
offices and hospitals to the communities.
Communities are a very important resource for improving health. They
should be mobilized to play a more active role in promoting health.
These roles include needs assessment, design of appropriate health
programmes, decision making and local generation of resources to
promote self-sufficiency.
Whenever possible, appropriate technology in terms of personnel,
equipment and materials should be used. There are many simple
clinical methods and ways of organizing the provision of services which
are easily sustainable and can be made readily available through the
use of basic instruments and local assembly or production. These should
be chosen in preference to more sophisticated technologies.
12
Personnel Preparation
Preparation of oral health personnel should emphasize both educatio.n
and training. The curricula of all oral health workers should reflect the
major shift from the medical.to the social model of health which implies
the incorporation of social andbehavioural sciences.
...
*arc-
’
r
Personnel preparation should be part.of a process which ensures career
advancement and flexibility. In considering the curricula for oral health
workers the civil service grade of the worker on qualification should be
used in a.positive rather than negative way to ensure more community
orientation as well as adequate remuneration and not merely to prolong
the length of the training unnecessarily to qualify for a higher grade.
Planning the numbers and types of oral health personnel should not
rely purely on a dental perspective. Training of personnel should occur
when the context can absorb and support the graduates. Oral health
personnel should be trained alongside other health personnel.
Oral health personnel trained at the community's expense should be
encouraged to work in the community. Status and salaries, training,
promotion and position should be equalized to those of general health
personnel.
Rights of Health Workers
Professional bodies must ensure that the human rights of oral health
personnel are guaranteed in accordance with the UN Charter of Human
Rights.
The rights of health workers should be protected so that they can
provide services without sexual, political and professional harassment.
Caring for deprived communities should not be considered a subversive
activity but rather governments are responsible for the human rights of
oral health personnel.
Health workers have a right to be informed about the possible hazards
in their working environment, for example radiation, mercury
intoxication and cross-infection.
Health workers have a right to continuing education. The employer
should actively encourage and assist health workers to acquire
appropriate continuing education and training.
13
Scientific Basis of Oral Health Strategies
Services and oral health promotion strategies should be modified on the
basis of scientific knowledge regarding the effectiveness, efficiency and
cost-benefit of common interventions. This implies a constant review of
the scientific basis for health education methods and messages, training
and education of health workers, life history of oral diseases, oral
pathology, preventive and treatment strategies, infection control,
research and research methods, social science in oral health and
community based programmes.
Research
Research can be beneficial and enabling if it is applied and focuses on
real community problems , includes local people in both its
development and implementation (participatory and educational), and
leads to .immediate feed-back and actions for oral health. It should
contribute to the kind of longer term sociopolitical changes that are
necessary.
14
RECOMMENDED STRATEGIES FOR
DEVELOPING ORAL HEALTH CARE
PROGRAMMES IN DEPRIVED COMMUNITIES
I INTRODUCTION
Although there are sufficient dentists in the world today, the majority
of people do not have access to adequate, affordable and acceptable oral
health services. The following strategies should redress the imbalance in
oral health between the deprived and other citizens.
Because of the wide variation in the circumstances of different
communities and countries, detailed universal prescription cannot be
made. However general guidelines can be outlined.
Two principles of the primary health care approach have to be
considered in almost all programmes if lasting solutions to problems are
to be found. These are community participation and multisectoral co
operation and integration. An important element in achieving equity in
oral health and oral health services is the success of the multisectoral
approach in securing community development. The responsibility of
governments and co-operating and partnership agencies in this respect
must be underlined.
Sothat efforts do not become mere palliatives reinforcing the unjust
structures that perpetuate poor health services, health should be
viewed as inter-related with the problems of unemployment, high
prices and inadequate housing. Oral health care, to be liberating in
action for the poor and deprived, should take into consideration the root
causes of ill-health. The root causes of the health problems of the poor
are poverty and powerlessness.
II STRATEGIES FOR ORAL DISEASE PREVENTION
Prevention should be based on the principles of Health Promotion: re
orienting oral health services, creating supportive environment,
building healthy public policy, supporting community action, developing
coping skills.
15
In addition to the general principles outlined in the Berlin Oral Health
Declaration the following points should be considered in all
program mes.
• The application of preventive measures depends very much on
the socio-economic situation of the country and therefore a
flexible approach to preventive programmes should be taken
which will permit adaptation to suit existing circumstances. Such
adaptation must be undertaken by utilising scientifically tested
methods of health education and prevention;
• In most deprived communities, countries and population groups,
other health problems are much more important than oral health
problems;
• Appropriate technology should be used (eg. chewing sticks) and
people should be enabled to make their own
toothbrushes/toothpaste and self-care should be encouraged.
Families should be enabled to carry out their own set of preventive
activities;
• Some combinations of different fluoride regimens do not always
lead to a clinically significantly better cumulative effect.
Specific Strategies include:
1. FluoridationThe promotion of fluoridated toothpaste is the most appropriate way for
many countries to reduce the levels of caries. The highest priority
should be to make cheap fluoridated toothpaste widely available. In
furtherance of this strategy therefore:
• International companies should be persuaded to sell cheap
fluoride toothpaste in bulk;
• Health education messages about tooth cleaning for caries
reduction should be given less emphasis until people can get
fluoride toothpaste on a regular basis;
• International co-operation agencies should be encouraged to
distribute fluoride toothpaste.
2. Health education:
Health education should be put in a health promotional context. Thus it
should be combined with the provision of curative services for teachers,
16
Iamilies and students and carried out in a supportive environment
where there is clean water and healthy food in stores near to schools.
3. Integration of health promotional activities:
Oral health messages and activities should be included in general health
messages and actions. Integration and a common risk factor approach
outlined below should be the cornerstones of health promotional
activities. The fundamental'concepts are:
• Tackling causes common to a number of chronic diseases;'
■ • Including oral hygiene education as part of general hygiene;
® Developing population rather than high-risk strategies.
The approach can be developed because of risk factors common to a
number of chronic diseases, including dental caries, periodontal disease
and oral cancer. Diets which lead to caries also contribute to obesity,
coronary heart disease and diabetes. Periodontal diseases and oral
cancer are related to smoking. Smoking causes cancers elsewhere in the
body and respiratory diseases. Integrating activities with groups
concerned about those chronic diseases should be more effective than
disease specific activities
Oral cleanliness should be seen as part of grooming and body
cleanliness. It is logical that instead of separating oral cleanliness
education from general hygiene they should be combined. These
programmes should emphasize lay competence, be supportive and non
mystifying, and should not blame the victim.
A population strategy decreases the overall level of disease in the
population and does not concentrate entirely on high risk individuals. It
tackles the underlying causes of the distribution of the disease rather
than the causes of the incidence of disease in individuals.
Ill ORAL HEALTH SERVICES
A basic necessity is a budgeted oral health plan which takes into
account the health situation of the community including an inventory of
its own resources and is developed with the participation of the
community. A national plan can provide a useful framework for local
groups to begin planning their own service. In this respect the advocacy
or facilitator role of the dental public health professional is important in
providing expert information and advice.
In planning oral health services all possible resources should be
considered, including the role of independent practitioners, which
should be complimentary to that of government service staff.
17
The six As should always be considered in order to improve health
services. These are’availability, accessibility, accountability,
affordability, accommodation and acceptability.
The problem of unequal distribution of oral health personnel within the
health service exists in nearly all countries. There have been several
approaches to motivate dentists to work in rural and deprived areas. All
have failed although training, salary and conditions were favourable.
Greater success has occurred with auxiliary personnel. Training more
auxiliary personnel may be an important way of increasing coverage.
But this should not be allowed to lead to the creation of a two-tier
service in respect of appropriateness and quality of care. The important
role that such auxiliary personnel can play needs therefore to be
supported strongly.by governments and professional bodies.
The development of a referral system that is sensitive to the needs and
difficulties of those using it should be part of the planning process. The
importance of such a referral system consists not only in providing for
the necessary treatment for the more complex problems but also in
legitimizing and supporting the role of the primary care level and the
workers providing it. This should be recognized. The referral system can
also act as a barrier to the development of a two-tier system of health
care when seen in this way. It is the responsibility of governments to
ensure a health service which is of equal status and qualitv for all
citizens
How can the inclination of professionals to perform complex clinical
procedures be reconciled with the frequent need for simple care
without causing frustration and sometimes a 'braindrain'? Job
satisfaction could be achieved by:
• Balancing the number of dentists (higher technical workers) in
training with needs. This may well entail the training of more
auxiliaries and many fewer dentists;
• Providing a range of alternative activities which are
demonstrated by role models as being both valid and legitimate;
• Encouraging dental workers to integrate their work with that of
the health team. This implies the socialization or popularization of
the practice of dentistry as is occurring in a number of
community-based projects;
• Utilizing selection procedures for dental students which
emphasize the ability to engage in non-clinical activities as an
important part of their future work;
• Developing career pathways for all oral health personnel
including general practitioners.
18
Job functions need to be clearly stated. For example, suggested functions
and activities of a community dentist are:
Manager
Activities
Leader of primary oral health care team
Monitoring and control 1ing the oral health sot-system
O-rganise/co-ord i nate preventive, treatment, and referral services
Help data analysis research and information dissemination
Help plan, supervise and evaluate the oral activities
Agent of socio
economic.
development
Development of community participation in oral health
Liaison with the public, politicians and other sectors
Participate in community meetings and development activities
Participate in intersectoral projects eg.. food and water
Advocacy of better oral health
Critical analysis of intersectoral plans for oral health
implications
Influence politicians to make healthful decisions
Support appropriate development e g., local food production
Dental officer
Complex treatment of patients
Promotion of oral health at community, family and individual
levels
Educator
Continuing education of colleagues
Training of lower level oral health workers
Oral health education of families and communities
It is essential to develop secure funding for the budget. This can come
from within the community and/or outside it.
Economic constraints will determine the coverage achieved by health
services. Without economic development extensive coverage with oral
health care will not be possible. This leads to rationing where decisions
have to be made concerning strategic teeth- that should receive
priority.
Developing countries may need support to strengthen their health
services, but they do not want or need conditional help. They do not
need operating dentists but rather help in strengthening training
programmes and with clinical and educational materials.
Donor agencies may play unfortunate roles in funding postgraduate
studies in areas which are of no relevance to existing national situations.
Increased responsiveness, sensitivity and responsibility to local
situations in this respect is called for.
Comprehensive planning procedures involve intersectoral co-operation
and integration, frequently involving ministries of health, education,
finance and social-welfare, universities, schools for oral therapists, oral
19
associations professional interest groups and international bodies. The
planning group must involve all these structures as appropriate.
Equally important however, the planning activity must involve finding
out the’needs of the community in relation to oral health. Hence the
planning of personnel training for oral health cannot be carried out
without being built up from a comprehensive community diagnosis. As
such it is best if the planning group is as broadly representative as
possible and that it’should be able to call on the professional skills of a
range of specialist advisers particularly those in the social sciences.
There should be support and encouragement for local initiatives in
developing oral health services, including assistance with the
develop.ment of appropriate technology in the form of personnel,
equipment and materials.
The role of international bodies in calling the attention of the oral
profession to their responsibility in providing for the oral health needs
of the whole population rather than selected groups needs to be
e mphasized.
IV COMMUNITY INVOLVEMENT
Genuine partnership between oral health personnel and the community
depends upon mutual respect and trust. To build such a partnership is
often difficult and may require a variety of contacts with different
groups of the community as there are likely to be different levels of
participation arid interests. It is clear that it will be necessary to
approach the community through local leaders and involve them in the
planning, implementation, and evaluation of the community-oriented
service as a first step. Later this should lead to the development of a
fully community-based service, which is perceived by the community
as their service.
There may be existing health workers in the community. It is important
to include them and to define and develop their advocacy and facilitator
roles within the group.
Neither the scientific basis of community based oral health programmes
nor the capacity of the community to participate in such programmes on
a scientific basis should be undervalued.
For many deprived'communities health is defined in terms like caring,
sharing, belonging and being able to look forward to tomorrow. A
20
I
It
UNIVERSITY COLLEGE LONDON MEDICAL SCHOOL
DEPARTMENT OF EPIDEMIOLOGY AND PUBLIC HEALTH
66-72 Gower Street
London WC1E 6EA
Telephone 071 387 7050
Ext
Fax 071 380 7608
Telex 9312134004 (NPG)
E-mail: A.Sheiham@ucl.ac.uk
Tel: 071380 7601
22nd February 1994
Dr Thelma Narayan
No 376 “Srinivasa Nilaya”
Jakkasandra, 1st Main
1st Block, Koramangala
Bangalore 560 034
Dear Dr Narayan,
I enclose a copy of the Berlin Declaration as requested.
Your pamphlets and newsletter are interesting. There are no easily
transferable materials I can send you. Please come and see me if you
come back to London.
Yours sincerely,
Head of Department and Professor of Epidemiology and Public Health Professor MG Marmot
Professor of Dental Public Health Professor A Sheiham
MEDICAL
SCHOOL
Deutsche
Stiftung
fur
internationale
Entwicklung
German
Foundation
for
International
Development
Fundacidn
Fondation
Alemana
Allemande
para el
pour le
Developpement Desarrollo
Internacional
International
THE ORAL HEALTH ALLIANCE
THE BERLIN DECLARATION ON
ORAL HEALTH AND ORAL HEALTH
SERVICES IN DEPRIVED
COMMUNITIES
DSE
THE ORAL HEALTH ALLIANCE
THE BERLIN DECLARATION ON
ORAL HEALTH AND ORAL HEALTH
SERVICES IN DEPRIVED
COMMUNITIES
Proceedings of an International Workshop
held at
The German Foundation for International Development (DSE)
Conference Centre, Villa Borsig, Berlin.
September 1992
FOREWORD
The oral health is improving in industrialized countries and deteriorating
in developing countries. But within the more affluent countries
improvements in oral health are not occurring in most deprived
communities. Indeed, the oral health of children in many developing
countries is worse than in developed countries and the former cannot
afford the appropriate resources to deal with the diseases. In all countries
the dental profession and governments place most emphasis on the
curative and technological aspects of dentistry rather than promoting
prevention and community programmes for oral health which are more
effective at improving oral health and would have greater impact on the
oral health of dentally deprived communities. The curative methods
cannot be sustained at all levels of development.
Because the German Foundation for International Development (DSE) and
the NGO "Dental Aid" (Zahnmedizinische Entwicklungshilfe - ZME) were
aware of this problem they invited dentists, health workers, directors of
health service projects and programmes and academics from twenty-eight
countries to an international workshop on "Improving Oral Health and Oral
Health Services for Deprived Communities". The workshop was held from
September 14th to 19th at the DSE Conference Centre at Villa Borsig in
Berlin, before the 80th FDI Annual World Congress.
The workshop provided an unique forum for people who work in
community- based and community-oriented oral health programmes to
1
exchange experiences and discuss issues in primary oral health care at an
international level.
The objectives were to:
• identify and discuss issues and actions relevant to communityoriented and community-based oral health programmes;
• identify problems and barriers in planning and implementing oral
health programmes for deprived groups and discuss approaches to
overcome them;
• formalize a network between the different groups and projects
represented;
• inform the public and decision makers and raise awareness of
these issues among the dentists by publishing the workshop
proceedings.
During the workshop the need was expressed for better and continuing
communication between oral health workers concerned about improving
the oral health of all people including those who are deprived. Therefore a
new group was constituted which was named the "Oral Health Alliance".
The group formulated the Berlin Oral Health Declaration and recommended
strategies based on the principles in the declaration. A newsletter and
periodical critical reviews of current concepts in relation to oral health
issues will be published and widely distributed.
2
THE BERLIN DECLARATION
ON ORAL HEALTH 1992
BACKGROUND
When the Alma-Ata Declaration was formulated in 1978, there were
two developments which were not foreseen or anticipated. These are
the rapid global economic crisis of the 1980s and the AIDS pandemic
with the current problems of its prevention and control. The economic,
social as well as political crises in most developing countries have
adversely affected health in terms of:
• provision of services
• access and coverage
• financing of services
• quality of services
• status of health
Deprived communities exist at the country level and deprived groups
exist within countries. At the country level it was a description of the
world's poorest nations. Many of these nations have low per capita
incomes and increases in their populations of around. 3% per annum.
Their health and oral health services are grossly maldistributed. The
denial caries level is relatively low in the rural poor - a DMFT at twelve
years of age of 1.5 or less, but in the urban poor decay rates are higher
than among the rich. Dental caries is common in poor countries and the
severity is rising. The deprived have a high proportion of their decayed
teeth unfilled or treated by extraction.
For deprived groups within countries the definition is more difficult but
the following characteristics are common: poverty in comparison to the
rest of the country (the poverty line has been set at 370 U.S. dollars
annual income per capita in 1985 purchasing power parity dollars),
marginalization either by geographical remoteness or because they have
been dispossessed of their land/homes or because they feel that the
existing services are not for them. This is often exacerbated by high
levels of illiteracy and a lack of formal education. Frequently they do
not feel a part of the larger group.
The direct problems of poverty are unemployment, low income, limited
education and inadequate diet. This leads to overcrowding, poor
housing, inadequate water and sanitation, lack of land to grow food,
which in turn are related to infectious diseases, pollution, accidents,
stress, alienation, instability and insecurity. The urban poor are at the
3
interface between underdevelopment and industrialization and their
disease patterns reflect the problems of both. From the first they carry
a heavy burden of infectious diseases and malnutrition, while from the
second they suffer the typical spectrum of chronic and social diseases.
Good health of individuals, families and communities requires a decent
environment built on a solid foundation of fairness, respect and
equality. Until recently it was predicted that, by the year 2000, the
number of the people in the world living below the poverty line would
be reduced by 300 million. Now the World Bank suggests that the
numbers in poverty have increased substantially - from 1,051 million
to 1,133 from 1985 to 1990.
In any society, the principles of natural justice are based on equity, on
balancing the scales between right and wrong, between what is fair and
what is unfair. “Equity in health implies that ideally everyone should
have a fair opportunity to attain their full potential and, more
pragmatically, that no one should be disadvantaged from achieving this
potential, if it can be avoided.” (WHO, 1986, Social Justice and Equity in
Health, WHO Europe, Copenhagen). By definition, inequity means
injustice. Despite efforts in the past decade to make health systems
more equitable, in the poorer countries and communities things are
getting worse in terms of people's health and access to health care. The
first priority is to get the international community and national
governments to make a commitment, through positive actions, towards
solving some of the causes of poverty. It is a human right to have access
to the basic necessities for healthy living.
HEALTH IS A BASIC HUMAN RIGHT and oral health is a significant
component of general health. Although oral diseases are not life
threatening, they are important public health problems. The reasons for
their importance are their high prevalence, public demand, and their
impact on individuals and society in terms of pain, discomfort, social
and functional limitation and handicap and the effect on the quality of
life. In addition the financial impact on the individual and community is
very high and this is going to increase due to the infection control
measures required for the prevention and control of hepatitis and
HIV/AIDS.
Oral health has not been given the attention it deserves. As a result,
people who are poor and living in difficult circumstances, whether in
developing or industrialized countries, continue to be dentally
neglected, a situation that has every likelihood of worsening as the
global debt crisis and privatization of health services occur.
4
An important feature of oral diseases is that effective preventive
methods which are simple and cheap are available, but in many cases
these methods are not appropriately applied. The development of
denial programmes incorporating effective simple and cheap preventive
methods and which involve local people and build upon their strengths
and capacities have a better chance of ultimately improving both
services and community oral health. These community-based
programmes are more likely to lead towards self-reliance and self
management of oral health programmes.
The purpose of this document is to provide guidelines to health
planners for planning, implementing and evaluating relevant oral health
projects and programmes. This may be accomplished when planners:
• move from a biomedical model to a social development model of
health care and health care education;
• initiate ongoing monitoring and evaluation based upon the
principles of community-based action research;
• involve community members in assessing needs and
project/programme development. The intention is to reduce
dependency, enhance personal autonomy and enable oral health
and well being to occur;
• Prepare and support health workers to work with local people
for health and equity in dentistry.
Oral health projects and programmes aimed at improving oral health
and oral health services in deprived communities should be developed
recognizing certain issues and principles. These are spelled out in the
remainder of this declaration.
ISSUES TO BE CONSIDERED
It is important for health planners, administrators and all advocates to
be aware of a number of issues that encompass the world of workers
wanting to provide primary care and nurture oral health in dentally
deprived communities.
Underdevelopment:
The recognition that many communities are dentally deprived has
unfortunately produced a number of inappropriate responses. The
worst is that programmes developed in one setting have been
transferred without adaptation to a completely different one. The
5
results of such efforts have been to create or increase the state of
dependency of deprived communities and to reinforce their sense of
powerlessness and their lack of ownership of the programmes. The
fragmentation, within many deprived communities, exacerbated by
poverty, lack of formal education and high illiteracy levels, result in
little participation by the people in such programmes. These problems
will not be resolved by any attempt to put the blame for their existence
on any one community, group or individual.
Ethical values:
Communities frequently resent unsolicited research activities being
carried out in their midst. Similarly, appointment of external
consultants to programmes by outside bodies with neither the
agreement of the communities involved in programmes nor with clearly
defined tasks, results in the disaffection and dissatisfaction of the
com munity.
Health Promotion:
Most present programmes concentrate their efforts on the provision of
curative services giving little attention to health promotion
Goals and evaluation procedures:
Many programmes frequently lack clearly defined realistic goals
developed in collaboration with the community. Seldom are appropriate
socio-dental indicators applied. They take into account the
measurement of well-being and the quality of care. This results in a
lack of well defined appropriate and comprehensive process and impact
measures, which take into account health promotion and community
development activities.
Resources:
There is a misallocation of resources. The majority of the resources are
used by the minority of the population who require the least care.
Eighty percent of the resources are consumed in clinics which serve
twenty percent of the population.
The training provided for many oral health care workers is frequently
carried out in inappropriate settings. Consequently workers are illequipped to function where they are most needed and thus redress the
imbalance in availability of appropriate care.
6
In many countries the migration of the population to the urban areas is
resulting in large underserved peri-urban populations.
Programme organization and support:
The progress of many programmes is impeded because of frequent
changes in administrations. Such situations are often made worse
because the administrative infrastructures are weak. Often morale is
low because of poor training and limited job satisfaction.
Little understanding of these problems and a reluctance within the
dental profession to share and delegate responsibilities for oral health
in the community further inhibits the development of appropriate
programmes.
7
GUIDING PRINCIPLES FOR IMPROVING
ORAL HEALTH
When developing a programme or project to improve oral health by
working with people it is important to take into account each of the
following principles.
The Role of Governments
Article V of the Declaration of the Alma Ata Conference (1978) states,
that “Governments have a responsibility for the health of their people
which can be fulfilled only by the provision of adequate health and
social measures." A main social target should be the attainment of the
world of a level of health that will permit all people to lead a socially
and economically productive life. Primary health care is the key to
attaining this target as part of development in the spirit of social justice.
A
*
Reducing Inequalities
Principles for action are:
1. Policies should focus on improving living and working conditions, adequate
and safe housing, access to high quality food, control of pollution, safe water
supplies, employment policy, welfare system.
2. Policies need to be directed towards enabling people to adopt healthier
lifestyles. Distribution of cheap and nutritious food, control of advertising of
health damaging products, provision of clear information, access to leisure aW
exercise facilities.
3. Policies require a genuine commitment to decentralizing power and decision
making, encouraging people to participate in every stage of policy planning
process
4. Health care based on principle of making high quality health care accessible to
all. Resource allocation in relation to social and health needs, geographical
distribution of services linked to measures of need and access, focus on
acceptability of care from disadvantaged groups.
8
Underdevelopment
Oral health development is not achieved through the unmodified
transfer of skills or programmes, personnel or equipment to deprived
communities. Adaptation rather than uncritical adoption should be the
rule.
Dependency
Dependency is disabling. Although it is recognized that most projects
can not be completely self-financing and require state or institutional
support, they should be deliberately developed and implemented in
ways that ensure continuation by the communities in which they are
located.
Empowerment
Communities must be enabled to obtain and contribute resources to
sustain, self-manage, and satisfy their programme objectives and needs.
Community Involvement
Oral health decisions should always be made collectively with local
people who best know their own problems, needs and capacities, so that
control of dental projects and programmes rests with the community
being served. The right of all communities deprived of oral health care,
to organize services and training programmes should be acknowledged.
Partnerships
Projects should be developed and implemented mutually (by
institutions and persons) on the basis of honesty, respect and
reciprocity in that partners share and learn from each other. Partners
must declare their assumptions and expectations, and decide how to
work together to resolve problems and make decisions.
Consultants and co-operating agencies have an obligation to be
responsive and responsible commitment to project objectives is
essential.
9
Assessing needs
The assessment of needs has to be based on collaborative efforts
between users and providers. This should lead to the agreement of goals
and targets, that reflect people's needs and to the implementation of
services and evaluations that are based on these set goals.
Epidemiology is a fundamental tool in the development and evaluation
of health plans and programmes. It is necessary to develop indicators
different from those normally used. They should measure social,
economic and health impacts. Socio-dental indicators are more relevant
measures of needs and should reflect pain, discomfort, function and
aesthetics as well as clinical indicators of dental health such as caries,
bleeding gums and pocketing, number and position of teeth. Other
impact measures include loss of sleep, work loss and opportunity costs.
Priorities
Priorities should not be developed solely on the basis of the demand for
treatment. Health promotion can alter a community's perception of the
problems and hence priorities. Priorities should be established through
a partnership between the community and the professional advocates
for oral health.
Goals
The community should be involved in setting goals that are stated in
terms of oral health, oral disease, health promotion, equity, training and
personnel and health service.
Oral Health Promotion
Oral Health Promotion should have the highest priority and follow the
principles as defined in the Ottawa Charter for Health Promotion (1986).
Health Promotion means building healthy public policy, creating
supportive environments, strengthening community action, developing
coping skills and re-orienting dental services. Health promotion policy
must take into consideration: the uneven distribution of health and
disease, the uneven distribution of health hazards in the physical and
social environment and of personal behavioural risk factors and
10
opportunities to adopt a healthier personal lifestyle as well as the
uneven distribution and quality of health care.
Preventive Strategies
Authorities should recognize that the preventive approach is an
essential and inescapable recommendation.
Governments should apply mass preventive measures. Oral health
strategies should be integrated with general preventive approaches
within an overall context of health which lead to improvements in the
quantity and quality of life.
The preventive measures should be simple and effective and not
contradict each other or confuse the community.
Evaluation
Evaluation should not be seen as a mere technical activity but more as
an educational learning process in order to improve social conditions
and human life. It should therefore shift from being autocratic to a
more democratic participatory exercise. The community should be
involved in the formulation and assessment of the impacts of the
programme. Process measures should not only include the number of
procedures performed but health promotion and community
development activities. The results should be discussed and acted upon.
Treatment strategies
The services should be based on the development of local human
resources. Community needs should be defined and mechanisms
established for regionalising services. This should be done on the basis
of levels of care which requires referral and redefines the roles of
different health personnel.
It is also important to ensure that proposed strategies are compatible
with scientific knowledge and technological advances.
11
Ethics
All activities performed should comply with ethical standards accepted
and outlined in the Helsinki Declaration and by a local ethical
committee.
Experts/Consult ants
Local people are experts on community life, functions, and potential.
Outside consultants who have a particular expertise should only be
selected after full consultation and at the request of the host
com munity.
The experience and qualifications of the consultants should be vetted to
ensure that they are suitable for the task on hand.
In all cases local/regional expertise should be given priority before
considering consultants from further afield.
Once the invitation is agreed, the host country and community is to
ensure that adequate facilities are available to enable that the tasks
agreed upon are carried out. The consultant has an obligation to carry
out these tasks and submit a report to the local counterparts before
submitting it to the sponsoring agency.
Resources
Resources (human, facilities, finance) should be shifted from central
offices and hospitals to the communities.
Communities are a very important resource for improving health. They
should be mobilized to play a more active role in promoting health.
These roles include needs assessment, design of appropriate health
programmes, decision making and local generation of resources to
promote self-sufficiency.
Whenever possible, appropriate technology in terms of personnel,
equipment and materials should be used. There are many simple
clinical methods and ways of organizing the provision of services which
are easily sustainable and can be made readily available through the
use of basic instruments and local assembly or production. These should
be chosen in preference to more sophisticated technologies.
12
Personnel Preparation
Preparation of oral health personnel should emphasize both education
and training. The curricula of all oral health workers should reflect the
major shift from the medical to the social model of health which implies
the incorporation of social and behavioural sciences.
Personnel preparation should be part of a process which ensures career
advancement and flexibility. In considering the curricula for oral health
workers the civil service grade of the worker on qualification should be
used in a positive rather than negative way to ensure more community
orientation as well as adequate remuneration and not merely to prolong
the length of the training unnecessarily to qualify for a higher grade.
Planning the numbers and types of oral health personnel should not
rely purely on a dental perspective. Training of personnel should occur
when the context can absorb and support the graduates. Oral health
personnel should be trained alongside other health personnel.
Oral health personnel trained at the community's expense should be
encouraged to work in the community. Status and salaries, training,
promotion and position should be equalized to those of general health
personnel.
Rights of Health Workers
Professional bodies must ensure that the human rights of oral health
personnel are guaranteed in accordance with the UN Charter of Human
Rights.
The rights of health workers should be protected so that they can
provide services without sexual, political and professional harassment.
Caring for deprived communities should not be considered a subversive
activity but rather governments are responsible for the human rights of
oral health personnel.
Health workers have a right to be informed about the possible hazards
in their working environment, for example radiation, mercury
intoxication and cross-infection.
Health workers have a right to continuing education. The employer
should actively encourage and assist health workers to acquire
appropriate continuing education and training.
13
Scientific Basis of Oral Health Strategies
Services and oral health promotion strategies should be modified on the
basis of scientific knowledge regarding the effectiveness, efficiency and
cost-benefit of common interventions. This implies a constant review of
the scientific basis for health education methods and messages, training
and education of health workers, life history of oral diseases, oral
pathology, preventive and treatment strategies, infection control,
research and research methods, social science in oral health and
community based programmes.
Research
Research can be beneficial and enabling if it is applied and focuses on
real community problems , includes local people in both its
development and implementation (participatory and educational), and
leads to immediate feed-back and actions for oral health. It should
contribute to the kind of longer term sociopolitical changes that are
necessary.
14
RECOMMENDED STRATEGIES FOR
DEVELOPING ORAL HEALTH CARE
PROGRAMMES IN DEPRIVED COMMUNITIES
I INTRODUCTION
Although there are sufficient dentists in the world today, the majority
of people do not have access to adequate, affordable and acceptable oral
health services. The following strategies should redress the imbalance in
oral health between the deprived and other citizens.
Because of the wide variation in the circumstances of different
communities and countries, detailed universal prescription cannot be
made. However general guidelines can be outlined.
Two principles of the primary health care approach have to be
considered in almost all programmes if lasting solutions to problems are
to be found. These are community participation and multisectoral co
operation and integration. An important element in achieving equity in
oral health and oral health services is the success of the multisectoral
approach in securing community development. The responsibility of
governments and co-operating and partnership agencies in this respect
must be underlined.
Sothat efforts do not become mere palliatives reinforcing the unjust
structures that perpetuate poor health services, health should be
viewed as inter-related with the problems of unemployment, high
prices and inadequate housing. Oral health care, to be liberating in
action for the poor and deprived, should take into consideration the root
causes of ill-health. The root causes of the health problems of the poor
are poverty and powerlessness.
II STRATEGIES FOR ORAL DISEASE PREVENTION
Prevention should be based on the principles of Health Promotion: re
orienting oral health services, creating supportive environment,
building healthy public policy, supporting community action, developing
coping skills.
15
In addition to the general principles outlined in the Berlin Oral Health
Declaration the following points should be considered in all
program mes.
• The application of preventive measures depends very much on
the socio-economic situation of the country and therefore a
flexible approach to preventive programmes should be taken
which will permit adaptation to suit existing circumstances. Such
adaptation must be undertaken by utilising scientifically tested
methods of health education and prevention;
• In most deprived communities, countries and population groups,
other health problems are much more important than oral health
problems;
• Appropriate technology should be used (eg. chewing sticks) and
people should be enabled to make their own
toothbrushes/toothpaste and self-care should be encouraged.
Families should be enabled to carry out their own set of preventive
activities;
• Some combinations of different fluoride regimens do not always
lead to a clinically significantly better cumulative effect.
Specific Strategies include:
1. Fluoridation:
The promotion of fluoridated toothpaste is the most appropriate way for
many countries to reduce the levels of caries. The highest priority
should be to make cheap fluoridated toothpaste widely available. In
furtherance of this strategy therefore:
• International companies should be persuaded to sell cheap
fluoride toothpaste in bulk;
• Health education messages about tooth cleaning for caries
reduction should be given less emphasis until people can get
fluoride toothpaste on a regular basis;
• International co-operation agencies should be encouraged to
distribute fluoride toothpaste.
2. Health education:
Health education should be put in a health promotional context. Thus it
should be combined with the provision of curative services for teachers,
16
families and students and carried out in a supportive environment
where there is clean water and healthy food in stores near to schools.
3. Integration of health promotional activities:
Oral health messages and activities should be included in general health
messages and actions. Integration and a common risk factor approach
outlined below should be the cornerstones of health promotional
activities. The fundamental concepts are:
• Tackling causes common to a number of chronic diseases;
• Including oral hygiene education as part of general hygiene;
• Developing population rather than high-risk strategies.
The approach can be developed because of risk factors common to a
number of chronic diseases, including dental caries, periodontal disease
and oral cancer. Diets which lead to caries also contribute to obesity,
coronary heart disease and diabetes. Periodontal diseases and oral
cancer are related to smoking. Smoking causes cancers elsewhere in the
body and respiratory diseases. Integrating activities with groups
concerned about those chronic diseases should be more effective than
disease specific activities
Oral cleanliness should be seen as part of grooming and body
cleanliness. It is logical that instead of separating oral cleanliness
education from general hygiene they should be combined. These
programmes should emphasize lay competence, be supportive and nonmysnfying, and should not blame the victim.
A population strategy decreases the overall level of disease in the
population and does not concentrate entirely on high risk individuals. It
tackles the underlying causes of the distribution of the disease rather
than the causes of the incidence of disease in individuals.
Ill ORAL HEALTH SERVICES
A basic necessity is a budgeted oral health plan which takes into
account the health situation of the community including an inventory of
its own resources and is developed with the participation of the
community. A national plan can provide a useful framework for local
groups to begin planning their own service. In this respect the advocacy
or facilitator role of the dental public health professional is important in
providing expert information and advice.
In planning oral health services all possible resources should be
considered, including the role of independent practitioners, which
should be complimentary to that of government service staff.
17
The six A s should always be considered in order to improve health
services. These are availability, accessibility, accountability,
affordability, accommodation and acceptability.
The problem of unequal distribution of oral health personnel within the
health service exists in nearly all countries. There have been several
approaches to motivate dentists to work in rural and deprived areas. All
have failed although training, salary and conditions were favourable.
Greater success has occurred with auxiliary personnel. Training more
auxiliary personnel may be an important way of increasing coverage.
But this should not be allowed to lead to the creation of a two-tier
service in respect of appropriateness and quality of care. The important
role that such auxiliary personnel can play needs therefore to be
supported strongly by governments and professional bodies.
The development of a referral system that is sensitive to the needs and
difficulties of those using it should be part of the planning process. The
importance of such a referral system consists not only in providing for
the necessary treatment for the more complex problems but also in
legitimizing and supporting the role of the primary care level and the
workers providing it. This should be recognized. The referral system can
also act as a barrier to the development of a two-tier system of health
care when seen in this way. It is the responsibility of governments to
ensure a health service which is of equal status and qualitv for all
citizens.
How can the inclination of professionals to perform complex clinical
procedures be reconciled with the frequent need for simple care
without causing frustration and sometimes a braindrain ? Job
satisfaction could be achieved by:
• Balancing the number of dentists (higher technical workers) in
training with needs. This may well entail the training of more
auxiliaries and many fewer dentists;
• Providing a range of alternative activities which are
demonstrated by role models as being both valid and legitimate;
• Encouraging dental workers to integrate their work with that of
the health team. This implies the socialization or popularization of
the practice of dentistry as is occurring in a number of
community-based projects;
• Utilizing selection procedures for dental students which
emphasize the ability to engage in non-clinical activities as an
important part of their future work;
• Developing career pathways for all oral health personnel
including general practitioners.
18
Job functions need to be clearly stated. For example, suggested functions
and activities of a community dentist are:
Manager
Activities
Leader of primary oral health care team
Monitoring and controlling the oral health sub-system
Organise/co-ordinate preventive, treatment, and referral services
Help data analysis research and information dissemination
Help plan, supervise and evaluate the oral activities
Agent of socio
economic.
development
Development of community participation in oral health
Liaison with the public, politicians and other sectors
Participate in community meetings and development activities
Participate in intersectoral projects e.g., food and water
Advocacy of better oral health
Critical analysis of intersectoral plans for oral health
impl ications
Influence politicians to make healthful decisions
Support appropriate development e.g., local food production
Dental officer
Complex treatment of patients
Promotion of oral health at community, family and individual
levels
Educator
Continuing education of colleagues
Training of lower level oral health workers
Oral health education of families and communities
It is essential to develop secure funding for the budget. This can come
from within the community and/or outside it.
Economic constraints will determine the coverage achieved by health
services. Without economic development extensive coverage with oral
health care will not be possible. This leads to rationing where decisions
have to be made concerning strategic teeth' that should receive
priority.
Developing countries may need support to strengthen their health
services, but they do not want or need conditional help. They do not
need operating dentists but rather help in strengthening training
programmes and with clinical and educational materials.
Donor agencies may play unfortunate roles in funding postgraduate
studies in areas which are of no relevance to existing national situations.
Increased responsiveness, sensitivity and responsibility to local
situations in this respect is called for.
Comprehensive planning procedures involve intersectoral co-operation
and integration, frequently involving ministries of health, education,
finance and social-welfare, universities, schools for oral therapists, oral
19
associations, professional interest groups and international bodies. The
planning group must involve all these structures as appropriate.
Equally important however, the planning activity must involve finding
out the needs of the community in relation to oral health. Hence the
planning of personnel training for oral health cannot be carried out
without being built up from a comprehensive community diagnosis. As
such it is best if the planning group is as broadly representative as
possible and that it should be able to call on the professional skills of a
range of specialist advisers particularly those in the social sciences.
There should be support and encouragement for local initiatives in
developing oral health services, including assistance with the
development of appropriate technology in the form of personnel,
equipment and materials.
The role of international bodies in calling the attention of the oral
profession to their responsibility in providing for the oral health needs
of the whole population rather than selected groups needs to be
emphasized.
IV COMMUNITY INVOLVEMENT
Genuine partnership between oral health personnel and the community
depends upon mutual respect and trust. To build such a partnership is
often difficult and may require a variety of contacts with different
groups of the community as there are likely to be different levels of
participation and interests. It is clear that it will be necessary to
approach the community through local leaders and involve them in the
planning, implementation, and evaluation of the community-oriented
service as a first step. Later this should lead to the development of a
fully community-based service, which is perceived by the community
as their service.
There may be existing health workers in the community. It is important
to include them and to define and develop their advocacy and facilitator
roles within the group.
Neither the scientific basis of community based oral health programmes
nor the capacity of the community to participate in such programmes on
a scientific basis should be undervalued.
For many deprived communities health is defined in terms like caring,
sharing, belonging and being able to look forward to tomorrow. A
20
\ V ' : \lA •
■®§k
RuijU, JL&aUii ■x.uis^.U.u.y.i
JUAjJ UUMillU yiAW-Uj
•-sisluliiaj
W
^LiitUUiair
Si/iviiDy
Wisy
'\'
SyipiUiliuv
-
^zUbty'W^x^Jji'-UiH^iiihfc
;
’
^aswisi®
\w.y.V\iu-y tv ■xi£-ji.ii!.«i
■■•: yy^xfy>?xUh;.
fl S l'-> •
W?
Fluoride : Too Much Can Cripple You
Excess flouride in drinking water can lead to fluorosis, a disease that surfaces in a variety of
symptoms. The sub-mission planned for its control had as its key thrust awareness-raising, disease
identification through village level epidemiological surveys and launching preventive measures
essential for a disease which has no cure. Dr. A.K. SUSHEELA and G.GHOSH describe the
submission’s strategy and warn against misleading publicity recommending fluoride-based
toothpaste for better dental health.
lthough India has had the
A
problem of fluorosis for over
50 years, very little had been
clinical research to understand fluoride
4.
in its totality. Researches in this field
done to mitigate the sufferings of the
are still being promoted by various
afflicted until the National Drinking
national and international agencies.
Water Mission was launched in 1986-
Inspitc of the fact that India has
5.
6.
7.
87. It is estimated that nearly 25
substantial fresh water resources, there
is a chronic shortage of “safe drinking
8.
water” in the country. The shortage
9.
may vary, from mild to acute, depend
Computerized management infor
mation system
^million people arc afflicted with
fluoride poisoning due to environ
mental pollution.
Improvement of maintenance
methods
action on body tissues and on health
Scientific source finding
Continuous monitoring and evalu
ation
Community involvement and
Awareness programmes.
This article focusses on the activi
ing upon geographical, topographical,
ties in the Sub-Mission on “Control of
mental pollution with fluoride unlike
climatic and other factors. The spread
Fluorosis” and the programmes which
In India, the magnitude of environ
in many parts of the world, is greatly
of the disease from four to 13 states
arc on in the various states to remove
enhanced by use of fluoride contami
over a period of 50 years is mainly
fluorosis and associated health prob
nated water, food, cosmetics like
due to population overgrowth necessi
lems. The health problems have by
toothpastes and even drugs. Due to the
tating the use of more and more water;
now attained a magnitude, which is
earth’s crust being extremely rich in
people digging tube wells indiscrimi
roughly estimated to have afflicted 25
fluoride-bearing minerals, the water is
nately anywhere and everywhere; and
million people, perhaps with an equal
naturally fluoridated. The maximum
total unawarcncss of the importance of
number on its way to being affected.
content so far detected is
water quality for human consumption.
The task assigned and the funds
earmarked by the “Water Mission” to
fluoride
38.5 ppm (mg/lilrc) in drinking water.
To tackle the drinking water
problem on a war fooling, the Govern
achieve die objective of the Sub
ranging from 1.5 to 38.5 ppm can
ment of India during 1986, set up a
Mission on “Control of fluorosis" viz.
cause severe health problems. Initially,
Technology Mission on Drinking
to provide safe drinking water, prevent
the health problems were known to
Water and related water management
and control fluorosis within a time
exist in only four states - two in the
kouthem and two in the Northern parts
with the Department of Rural Develop
frame is by no means a casual task. A
ment as the nodal agency. The strategy
total commitment on the part of the
of India and nowhere, else. But to-day,
adopted for visible results is to focus
Public Health Engineers, doctors, para
Drinking water containing fluoride
13 states, nearly fifty per cent, arc
on Sub-Missions, countrywide. The
medical workers, village level func
declared endemic for fluorosis and
major Sub-Missions operating arc:
tionaries and voluntary organizations to
associated health problems as a result
1.
Control of Fluorosis
work in a co-ordinated manner, is a
of drinking fluoride contaminated
2.
Eradication of Guincaworm
unique feature of the programme. The
water. Il has become an urban as well
3.
4.
Removal of Excess Iron
Removal of Salinity and Brackish
available in the field of public health
as a rural health problem, affecting the
poor and rich alike.
Source Finding and Water Manage
engineering, dcfluoridation of water
and health science have been identified
ment.
and brought together to work in an
ness and
5.
Government efforts
What did the Government of India do
The methodologies adopted arc:
to deal with this public health prob
1.
lem? Since the early 1930s, the major
2.
Improvement of technical methods
focus has been to promote basic
3.
Improvement of materials and
researches, cpidcmiolgical studies and
48
HEALTH for the Millions
best scientific talents and expertise
Purification of water
designs
September-October 1990
integrated manner, with the participa
tion of the people themselves.
Control in three phases
The Sub-Mission on “Control of
Fluorosis” has a three phased pro-
practices. It may not be out of place
is low,
gramc specially designed keeping in
view the limitations and the lacunae in
to mention here that some of the text
books on Public Health Engineering in
explored for mixing the water from
educational programmes in the country'.
India still describe procedures to
conccnpation of fluoride to permis
The programme has been implemented
fluoridate drinking water rather than to
in 18 districts in eight states during
defluoridate it. Besides, the doctors
the past three years, covering over
graduating from medical schools in the
Water Mission, we arc accepting
50,00,000 people. The activities of the
country arc not taught about fluorosis
contamination upto 1.00 ppm as
various phases arc based on the
in great detail. Fluorosis is considered
the permissible upper limit as we
following objectives:
a disease which has no treatment or
have no other alternative. However,
Phase-I
To conduct training-cum-
cure and preventive aspects arc often
we do create awareness among the
awareness camps, and
neglected. It is also true in India that
people, that the less the fluoride in
update the information on
the disease was very often misdiag
fluorosis, drinking water
nosed as arthritis, spondylosis or
hase-II
two sources, thereby diluting the
sible levels.
O
Presently in the National Drinking
water, the better the health.
o
We also have data in India to
quality and defluoridation
ankylosing spondylitis. We arc not
suggest that 0.4 ppm of fluoride in
procedures for doctors,
surprised to note the statement in
drinking water is causing mild,
Public Health Engineers,
Chemical Engineering News, (Page 37,
moderate and severe forms of
para-medical workers and
August, 1988) that most doctors in the
dental fluorosis and therefore we
governmental and non
U.S. have not studied the disease and
arc looking for water with less and
governmental personnel.
To launch epidemiological
do not know how to diagnose it. It
survcy(s) in the affected
early warning symptoms of fluoride
of the body’s muscle fiber and
villages, taluks and districts
toxicity/poisoning may not be under
connective tissue including the oral
to assess the exact magni
stood at all.
cavity caused by the use of
therefore emerges that even in U.S. the
tude of the problem as well
Phase-III
possibilities arc also
less fluoride contamination.
o
It is also a fact that due to atrophy
fluoride, people living in endemic
During Phasc-II, the cndcmicity of
as to analyse the quality of
every drinking water source
the villagcs/districts for fluorosis is
areas lose their teeth at an early
identified by visits to schools and from
age; they look much older and
in the area.
dental check-up. White, yellow, brown
those who can afford it, resort to
To introduce appropriate
and black tooth enamel discolouration,
measures to provide safe
either in spots or in horizontal speaks,
the use of dentures.
O
Muscular weakness, loss of muscle
drinking waler as well as to
is the sign of occurrence of dcnpil
power and neurological manifesta
ameliorate, prevent and
fluorosis. In such eases, the water is
tions leading to excessive thirst, a
control fluorosis.
probably contaminated with fluoride
tendency to urinate more fre
and the location endemic for fluorosis.
quently, although the volume of
an update on fluorosis which includes
During the past three years, several
urine is not too large, are not
information on clinical manifestations,
epidemiological surveys along with
uncommon among the afflicted
diagnosis, early warning signs of
water quality testing with a focus on
individuals.
The Phasc-I activities arc essentially
fluorosis and procedures to identify
fluoride have been conducted by
subjects afflicted with fluorosis. Under
professionals, after attending the
intestinal problems viz. anorexia,
conditions, without having to
update camps. Based on the most
pain in the stomach, intermittent
try out sensitive laboratory-based
O
Severe and widespread gastro
recent data, the following observations
diarrhoea, chronic constipation, gas
tests, besides educating the people on
and corrective measures both for
formation and a bloated feeling in
the importance of drinking safe water,
providing safe waler and preventing
the stomach (non-ulccr dyspepsia)
water quality assessment and dcfluori-
the disease have been inPoduccd
caused due to drinking fluoridated
dation procedures (both at the domes
during the Phase-III activities:
tic and community defluoridation
O
In an area endemic for fluorosis, it
water have been confirmed.
Changing the source of water with
installations) arc dealt with. A little
is not necessary that every source
low levels of fluoride (below 1
over 5000 individuals which include
of water is contaminated with
ppm) provides relief from the
doctors, Public Health Engineers and
fluoride. The good sources arc
gastro-intestinal problems within a
village level functionaries have been
identified, labelled and the people
period of two to three weeks.
trained in this Sub-Mission over the
are educated to drink from the
areas endemic for fluorosis, gastro
period of three years. The need for the
good sources only; the fluoride-
intestinal problems alert suspicion
up-date is essential, as doctors and
contaminated sources arc used for
of fluoride toxicity and arc used as
engineers during their paining lay
washing and cleaning purposes. If
early warning signs for preventive
emphasis on western concepts and
the yield of water for consumption
measures to be introduced. The
September-October 1990
HEALTH for the Millions
In
49
A profile of a few districts in India revealing the number of people ailing due to fluoride
toxicity are shown
Name of the districts
Total population and the
Range of fluorid
and state
number of people afflicted with
in drinking
different complaints
water
Dharwad (Karnataka)
Total population examined
--
72,744
0.3-150 ppm
Afflicted with:
B
Raichur (Karnataka)
Dental Fluorosis
-
12,266
Skeletal Fluorosis
—
3,747
Gastro-intcstial problems
—
6,304
-
1,50,215
Total population examined
0.2-7.5 ppm
Afflicted with :
Amreli (Gujarat)
Dental Fluorosis
--
12,933
Skeletal Fluorosis
—
2,999
Gastro-intestinal problems
—
1,882
-
56,189
Total Population examined
1.8-11 ppm
Afflicted with :
Gurgoan (Haryana)
Dental Fluorosis
-
9,919
Skeletal Fluorosis
-
6,762
Gastro-intestinal problems
—
245
—
85,792
Total Population examined
0.2-19.6 ppm
Afflicted with :
Kurnool (Andhra Pradesh)
Dental Fluorosis
—
6,970
Skeletal Fluorosis
-
600
Gastro-intestinal problems
-
200
—
14,91,791
-
43,927
Total population examined
Afflicted with :
Dental Fluorosis
50
HEALTH for ‘.he Millions
Skeletal Fluorosis
-
8,833
Gastro-intestinal problems
—
30,400
Scplcmbcr-Oclobcr 1990
0.1-9.6 ppm
damage caused to the human
intestinal mucosa, due to drinking
fluoridated water is extensive.
Under die Water Mission, in the
affected areas where there arc no
good sourcc(s) of water, domestic
dcfluoridation procedures are being
popularized among lactating
mothers as well as pregnant
(expectant) mothers, besides
erecting community dcfluoridation
tanks for the public. Alternative
sourcc(s) of safe drinking water,
either by bringing it in from a
distance through pipelines (if eco
UNICEF
nomically viable) or through
alternate underground sources arc
also being considered for implem
Credit
entation.
The reports published from India,
_by earlier investigators, have been
^pbstanlially up-dated during the last
Denial fluorosis in child
10-15 years. It is strange to note that
the west invariably quotes Indian
reports on fluorosis which arc out
dated. For example, an Indian report
which appeared in 1970 in a WHO
publication entitled “Fluoride and
Human Health" indicates that one can
get afflicted with fluorosis by drinking
water contaminated with 20 ppm of
fluoride if consumed for 10 years; this
is most conveniently quoted by the
pro-fluoridation experts of the western
world suggesting that water with 2
ppm is safe to drink. The fact remains
that even 2 ppm of fluoride contami
nated water can cause crippling
fluorosis, if the calcium content of the
ter is low and alkalinity high and if
•
isumed for even a couple of years,
leaving aside 10 years.
Harmful publicity
Intermittently, we also face problems
in the country due to the World Health
Organization’s publicity for use of
fluoride in the name of prevention of
caries as “teeth arc for a life time”
(as though other organs arc not!).
WHO’s recommendation to drink
fluoridated water, to use fluoride
toothpaste, use fluoride salts in
cooking and have it available on the
table for use with food which has been
reporting on the unsuitability of WHO
promoted as educational material for
guidelines for fluoride concentration in
the past several years, has come under
drinking water. A recent report from
severe criticism in India.
With the
Netherlands, based on a study in
initiative taken by the Ministry of
Senegal has shown dental fluorosis in
Health and Family Welfare (Govt, of
children where fluoride in water
India) during 1989, WHO has been
ranged from 0.1 to 7.4 ppm, and
asked to refrain from such publicity in
prevalence of mild dental fluorosis is
India as it causes more damage than
68.5 per cent at 1 ppm of fluoride in
good to the people. WHO has also
drinking water. When fluoride ex
been asked to add a footnote to their
ceeded 4 ppm, the prevalence of
pamphlets indicating that it is not
dental fluorosis reached 100 per cent.
applicable to India and other countries
It
where excess fluoride is die problem.
guidelines for fluoride concentration in
has been suggested that the WHO
WHO headquarters in Geneva have
drinking water in Senegal arc unsuit
also been informed through their
able and the upper limit should be
Regional Office at New Delhi of the
reduced to 0.6 ppm (Lancet : 11, 223-
Water Mission’s efforts to dcfluoridatc
225, 1988).
water as well as control fluorosis in
India at massive expenditure. It would
that in India, WHO has extended
It is now quite gratifying to note
be worthwhile if such UN organiza
support to the Waler Mission activities,
tions would adopt a bifurcated policy
particularly the Sub-Mission on
in dental care appropriate to develop
“Control of Fluorosis". WHO, during
ing countries without imposing fluoride
the early 1970s, was fully prepared to
everywhere. In the developing coun
fluoridate India’s water, but, because
tries, to prevent dental caries the need
of the opposition they faced from
of the hour is not fluoride but ade
Indian scientists, the scheme could not
quate awareness of die importance of
be implemented. Perhaps the support
oral health and hygiene besides
that is now forthcoming may be the
improving adequate calcium and
beginning of a new era, when WHO
vitamin C in the diet.
may consider a totally different
Some developing nations arc now
strategy for prevention of dental caries
September-October 1990' HEALTH for lite Millions
51
In reality, by using fluoride for
in India and other developing countries
different depths of the lube, the
instead of promoting the use of
amount of fluoride in the fluoridated
preventing caries, believing that it only
fluoride.
brand of paste is highly variable. In
makes the enamel strong, no longer
none of the so-called fluoridated
holds good because fluoride also
brands of the toothpaste, the quantity
causes demineralization of the teeth
of fluoride in the paste is revealed on
which get pitted, perforated and
the carton or the tube. The expiry dale
chipped. In other words, the damage it
It is unfortunate that the use of
of the toothpaste is never revealed
causes to the teeth is never taken into
fluoride for prevention of caries,
either. These we consider unethical
account as it nullifies the age old
although formulated and brought out
concept that “fluoride is good for
50 years ago by U.S.- based dentists,
practices.
In order to ensure quality control
is still being promoted the world over
procedures in manufacturing, a maxi
without questioning the rationale nor
mum contaminant rale of 800 ppm
the health hazards which have been
may be permitted in Indian tooth
emerging due to fluoride poisoning. It
pastes, but we insist on having a
Toothpaste and fluorosis
teeth.”
Towards heart disease and cancer?
In addition to the above, fluoride
has been show by Indian dentists that
warning inscribed on the carton which
by use of fluoridated toothpaste for
should read: “Excess fluoride is
induces cholesterol production in males
brushing teeth, in young and old, the
injurious to health”. This would alert
and can also lead to blocking/calcifica-
scrum fluoride levels are enhanced
the consumer to look for a paste with
tion of blood vessels, specially in the
within minutes (Rajan et al. Fluoride
least fluoride contamination. We arc
region of the main vessel leading from
in toothpaste : Cause for Concern,
^roridc 21:4, 1988; Rajan et al,
also aiming at curtailing the false
the heart viz. the aorta, causing
publicity for promoting the use of
cardiac problems. This certainly means
Scrum and Urine Fluoride in Tolhpastc
fluoride in the name of prevention of
that Ute toxic effects of fluoride far
Users, J.Ind. Dent. Assoc. 59:137-142,
caries. Although children below the
outweigh its benefits in the Indian
situation.
1987). The oral mucosa, rich in blood
age of six years arc not supposed to
vessels absorb fluoridations rapidly.
use fluoridated toothpaste, as per the
The sub-lingual blood vessels (the ones
recommendation of the Indian Council
below the tongue) drain the stuff
for Medical Research, invariably the
of cancer due to fluoride in the U.S.
directly to the superior vcnccava and
advertisements arc aimed al children,
(Cancer Mortality in Relation to
then to the heart. It is not true that
misguiding the public.
Fluoridation and Population Changes,
toothpaste never enters the body unless
Perhaps due to the brain-washing
There arc reports on high incidence
Data from 140 largest U.S. Cities from
it is swallowed/ingestcd. Fluoride docs
publicity promoting fluoride fob
1940-1980, Burgstahlcr, Int. Confer
enter circulation directly from the oral
prevention of caries on television,
ence of the Fluoride Society, Utah,
cavity through the fine blood vessels
radio and other print media, people do
1986). Data based on animal experi
of the mouth. Fluoride being a persis
not quite realize the damage that
ments from Japan and other parts of
tant bioaccumulator, even small
excess fluoride can do to them. It has
the world, also suggest that fluoride is
amounts that enter through fluoridated
been shown that excess ingestion of
cancer-causing (Mutation Research,
'
toothpaste, are guaranteed entry, not
fluoride leads to the accumulation of a
139, 193-941, 1984; Science of Total
only in children but even among adults
particular chemical substance viz.
Environment 68, 79-76, 1988). These
wl the cumulative or additive effects
^fluoride are causing serious concern.
dermatan sulphate, both in bone and
arc serious problems that a nation
teeth. The substance, on accumulation,
ought to take into account before we
lends to demineralize the area around,
start adding fluoride in massive doses
It has been discovered in India
both in teeth as well as in bone. Such
to drinking water and toothpaste just
recently that there is no toothpaste
demineralized zones in the teeth get
because a few dentists, and of course
marketed which is free of fluoride,
whether labelled or otherwise. The
pitted and perforated in dental fluoro
sis besides being discoloured (Sushccla,
concepts to promote the use of
fluoride.
amount of fluoride arising as a
et al, Arch. Oral Biol., 33 10,765.
contaminant from the raw materials
1987). The belief that cavity formation
the manufacturers, promote
outdated
— Dr. A.K. Susheela is National Co-
used viz. chalk, talc and calcium
occurs only in dental caries is out
carbonate, may be as high as 800
dated. In fact, cavity formation may be
Ordinator for Health Sector Activities,
ppm. It has also been observed in
aggravated in some due to excess
Sub-Mission on 'Control of Fluorosis',
India as a result of extensive labora
ingestion or use of fluoride, leading to
Technology Mission on Drinking
tory investigations that the fluoride is
dermatan sulphate formation and
Water. Dr. G. Ghosh is Director of
not mixed homogenously in the paste.
ensuing demineralization of the tooth
the National Drinking Water Mission.
When the paste is squeezed out from
matrix.
52
HEALTH for die Millions
September-October 1990
01J /-S
Published by the British Fluoridation Society Ltd
with the support of a grant for educational purposes
from the Health Education Council
[FOffiwSiofe
g®ts
odd f g!M agafflgft
TH E best news for dental health in
jtain for years — that is how many
alth authorities are responding
to the Water (Fluoridation) Act,
which received its Royal Assent in
October, 1985.
«
The Act makes it clear that it is
perfectly legal for health authorities
and water suppliers to introduce
fluoridation schemes to prevent tooth
decay. Millions of children in England,
Scotland and Wales stand to benefit
throughout their lives.
Up to now about ten per cent of
Britain has had water supplies fluori
dated. Fluoridation means adjusting
the natural fluoride up to the control
led level of one part of fluoride per
million of water — a safe and highly
effective procedure which has gen
erally halved tooth decay among
children drinking fluoridated water
from birth.
A court case in Scotland two years
ago, whilst totally vindicating fluori
dation as a benefit to public health,
cast doubt on its legality. That doubt
hinged on the precise legal definition
of words in previous Acts of Parlia
tooth decay
ment concerned with the management
of water supplies.
So the government decided to set
the record straight with a new Act
which specifically dealt with the
powers of public bodies to fluoridate
water.
Now that the Act is finally on the
statute book, there is no doubt
whatever. Health authorities are free
to ask water suppliers to add fluoride
to water as soon as detailed guidance
has been issued by the DHSS and the
Department of the Environment.
Most health authorities regard
fluoridating water as the single most
important thing they can do to prevent
the misery and pain of toothache. They
can now go ahead with their plans.
The new Act confirms that it is up to
health authorities to decide whether
to fluoridate local water supplies in the
interests of preventing dental caries —
one of the commonest diseases in the
country and one of the most expensive
for the NHS in treatment costs.
As before, health authorities still
have to request the cooperation of
water suppliers, some of which have in
the past been reluctant to comply
because of possible legal problems.
Those problems no longer apply,
thanks to the Water (Fluoridation) Act.
Once a health authority has decided
to request a particular scheme, it must
publish details in the local press and
consult with local authorities at least
three months before implementing the
proposal.
It must do the same if, for any
reason, seeking to discontinue a
fluoridation scheme.
Separate legislation has yet to be
introduced to cover Northern Ireland.
[tofafflot Gw
dtoffl® fe G©fe
HEALTH authorities now have the best
opportunity they have ever had to
improve the dental health of the
community. That is the view of the
British Association for the Study of
Community Dentistry, which has long
advocated fluoridation as the most
effective way of tackling dental caries.
But the Association's
President,
Professor Aubrey Sheiham, points out that
health authorities must be prepared to
campaign vigorously for their fluoridation
policies at local level.
MfeD Itofemg
to fe©to
SPEAKERS of all political parties in both Houses of Parliament expressed their
strong support for fluoridation during the successful passage of the Water
(Fluoridation) Bill.
Here are just a few of the important statements made during the debates in the
Commons and in the Lords:
Mr Kenneth Clarke (former Minister of State for Health)
"Water fluoridation has advantages over all these (other) methods in that it is
highly cost-effective, does not require the use of trained personnel or conscious
effort by the recipient and confers a benefit on the whole of a given community".
Mr Michael Meacher (Opposition Spokesman on Health)
"Dental caries is one of the most costly diseases... Its prevention or reduction,
in terms of the individual's health and to the nation as a whole, is a prize worth
striving for. How can one justify not giving the child who lives in Wolverhampton or
Salford the same protection as the child who lives in Birmingham or Watford
already enjoys?"
Mr Michael Meadowcroft (Liberal Spokesman on Health)
"The most telling fact is that during twenty years or more since the argument has
been contested in and out of the public arena ... no professional health body has
changed its mind about the efficacy of fluoridating water".
Lord Winstanley (a former general medical practitioner)
"As a doctor, and as a person who has looked into the issue with great care, / can
say that I am wholly convinced that no public health measure has ever been
subjected to such exhaustive and dose scrutiny and ever been found to be so totally
free of dangerous side effects or risks of any kind".
Lord Colwyn (a practising dentist)
"With the addition of one part per million of fluoride to water, we have the safest,
most widely available method of bringing prevention to patients who do not seek
first-hand advice from the dental surgery as well as the regular attenders".
2
"The new Act reaffirms that it is legal to
fluoridate but it does not deliver
fluoridation on a plate”, said Professor
Sheiham. "Health authorities still neeckkj
receive the cooperation of water supp^ J
and will no doubt find that opposition,
though from a tiny minority, is vociferous
and well-organised".
Professor Sheiham commends health
authorities generally to follow the exam
ples already shown in the West Midlands
and North West, where regional coordina
ting groups have been set up to ensure that
NHS policies are well publicised and
effectively implemented.
Both groups are led by District Health
Authority Chairmen. John Charlton (South
Birmingham) chairs the West Midlands
group and Gordon Legat (South Manches
ter) chairs the North Western group.
The West Midlands group, established
in 1978, has had remarkable success.
Since its inception, fluoridation schemes
have been introduced to serve half a million
people in Coventry, Solihull, Warwickshire
and Worcestershire. Health authorities
have also concluded agreements with
water suppliers for schemes which will
benefit a further 1 J million consumers jn
many parts of the region - schemes wf
can proceed without delay thanks to me
Water (Fluoridation) Act.
"While each District has to decide
locally on the principle of whether to
fluoridate, experience shows that they
need to get together, usually with their
Regional Health Authority, to stand any
serious chance of putting policies into
practice", said John Charlton.
Hot on the heels of the West Midlands
are health authorities in the North West, a
region with no fluoridation at present but a
record of poor dental health.
"We are determined to make sure
children in Greater Manchester and
Lancashire benefit from the new legis
lation", said Gordon Legat. "Just three
schemes could cover the vast majority ot
our population. We must not miss the
opportunity created by the new legis
lation”.
Other regions are known to be actively
considering the next steps to take.
Professor Douglas Jackson, Chairman ot
the British Fluoridation Society, said that
the Society would do everything it could to
see that the vast amount of campaign
expertise built up in the West Midlands
was made available to health authorities in
the rest of the country.
Yet another ‘thumbs up’
©ffl lorarrM©
YET another major report on fluori
dation has given it a clean bill of
health on safety. A special working
party set up to investigate alleg
ations by opponents of fluoridation
about possible links with cancer
found no evidence of hazard.
This conclusion confirms earlier
reports by the Royal College of
Physicians, the US National Cancer
Institute and many other scientific
jfcdies that fluoride in the water Whether present just naturally or at
artificially supplemented levels - does
not cause cancer.
Like the others, the Knox Report
found no cause for concern, either in
terms of cancer in general or cancer of
any specific part or organ of the body.
The working party reached this view
after exhaustive inquiries into previous
allegations and after giving full
consideration to the work of scientists
from all over the world.
The report - "Fluoridation of Water
and Cancer: A Review of the
Epidemiological Evidence" - was
commissioned by the DHSS.
The working party was made up of
individuals eminent in epidemiology,
cancer research, pathology, statistics
and water treatment, and was led by
Professor E.G. Knox of the Universtiy of
Birmingham.
After four years' study the working
party published a report in January,
1 985. In its preface, Dr E.D. Acheson,
Chief Medical Officer at the DHSS,
said: "The wealth of evidence which
has been gathered during this period
(i.e. of 40 years' experience of water
fluoridation) including that presented
in this report, justifies the conclusion
that fluoridation is a safe and effective
method of reducing dental decay".
, SsKOiS MlWfflra® MBH
REJECTED IN KNOX REPORT
THE Knox team had carefully examined the statistics on cancer deaths produced by two
American anti-fluoridationists but rejected their work on the following grounds:
7
A major weakness in the method used by the two
Americans is their failure to make comparisons between
cancer death rates in different populations as fair as
possible — in other words to compare like with like.
2
3
They made many mistakes and inconsistencies in the
handling of data.
They failed to conduct acceptable tests of statistical
significance.
The cancer scare was also firmly knocked on the head recently by Lord Jauncey, the judge presiding over a
court case in Scotland where anti-fluoridation groups were trying to stop Strathclyde Regional Council from
introducing a scheme.
Lord Jauncey dismissed their arguments, concluding in his verdict that fluoridation is safe and beneficial.
3
ANGLESEY X
(fluoridated)
'—
average five-year-old:
1.59 teeth
\ decayed, missing
\
or filled
/>-
ARFON
(non-fluoridated)
average five-year-old:
3.55 teeth
decayed, missing
or filled
ONLY a narrow strip of water
separates the children of Anglesey
from those of mainland Wales. But
where dental health and tooth decay
are concerned, the children of main
land Arfon could be an ocean away.
For in a study of dental decay in both
places, the evidence points conclusively to
the fact that children on fluoridated
Anglesey have many fewer decayed,
missing or filled teeth than their
counterparts in non-fluoridated Arfon.
The study was carried out by resear
chers from Gwynedd Health Authority and
the Universities of Leeds and Birmingham,
who had noted that tooth decay among
English children appeared to be falling.
They wanted to find out if a similar
phenomenon had been experienced in
Wales.
Taking Anglesey - where the water is
fluoridated - and comparing it with the
adjacent mainland area of Arfon - where
the water contains only relatively low
natural levels of fluoride at 0.1 parts per
million-seemed a good way of finding out.
As the diagrams of this page show, the
results were significant. The research team
compared the dental health of children
aged 5, 12 and 1 5 who had been born and
bred in the two areas. The five year-olds in
Anglesey had, on average, 1.59 teeth
decayed, missing or filled while in
non-fluoridated Arfon the figure was over
twice as high at 3.55.
By the age of 12, the Anglesey child,|.'
had 2.59 teeth decayed, missing or filled.
In Arfon the figure was much higher at
4.46.
And for teenagers at 1 5 the compara
tive figures were 4.73 for Anglesey and
7.69 for Arfon - still a very big difference.
Other comparisons of dental health also
put Anglesey in a favourable light. For
every 100 five year-olds in Anglesey, only
one deciduous tooth had been
extracted . . . the figure for Arfon was 45.
The comparative figures for permanent
teeth of the 12 year-olds were 13 and 74
respectively, and for the 1 5 year-olds 48
and 108.
As in England, the state of the children's
teeth is improving in Wales - but with
fluoridated areas showing a better track
record.
Between 1974 and 1983 there was a
drop in tooth decay among five year-olds of
44 per cent in the fluoridated area
compared with 22 per cent in the
non-fluoridated community.
Xr
Five-year-olds:
number of extracted
'milk' teeth per 100
children
Twelve year olds:
number of permanent
teeth extracted per 100
children
4
FLUORIDATED
Anglesey
1
w
Anglesey
13
wwwwwwwwww
WWW
NON-FLUORIDATED
Arfon
45
WWWWWWWWWW
WWWWWWWWQW
WWWWWWWWRW
wwwwwwwwww
WWWW
Arfon
74
WWWWWWWWWW
WWWWWWWWWW
WWWWWWWWWW
WWWWWWWWWW
wwwwwwwwww
WWWWWWWWWW
WWWWWWWWWW
wwww
i
ta@©fes Site te®®
te KBMESWi
MANCHESTER and Newcastle are both large industrial
kities in the north of England. You would have no reason to
Suppose that children living in one or the other enjoy much
better or worse dental health.
But 5-year old Manchester children have two and a half
times as much tooth decay as 5-year-olds from Newcastle.
Why should that be? The answer is fluoridation.
In July, 1 985 a random sample of 245 children in North
Manchester was examined, together with a similar sample
from Newcastle.
The differences were considerable. Manchester
5-year-olds had on average 3.3 teeth decayed, missing or
Five-year-olds:
number of teeth
decayed, missing or
filled per 10
children
filled. Those from Newcastle had only 1.3 teeth decayed,
missing or filled.
Whereas only 30 per cent of Manchester children had
never experienced dental decay, as many as 62 per cent of
Newcastle children had never experienced it.
Newcastle receives fluoridated water. For the moment,
Manchester does not.
Commenting on the results of the survey, the District
Dental Officer for North Manchester, Mrs Jacqueline
Duxbury, said: "Fluoridation must remain a major objective
for Districts like ours, where dental health of young
children still needs to be improved".
FLUORIDATED
Newcastle
13
NON-FLUORIDATED
Manchester
33
WWWWWWWWww
WWW
wwwwwwwwww
WWWQWWWWWW
wwwwwwwwww
WWW
Five-year-olds
% free of tooth decay
FLUORIDATED
Newcastle
62 out of 100
NON-FLUORIDATED
Manchester
30 out of 100
xmmm
mrnxm
xixmxw
xrxtxixw
xrxixtxm
XTXWXW
xi
5
Putting dental mottling
Sit© |JWS[p@©®W@
OPPONENTS of fluoridation, as if
clutching at straws to try to find
something to complain about, claim
that fluoride causes dental
fluorosis, a severe form of dental
mottling. This is not true.
Dental mottling, the white or brown
flecks which occur mainly on second
teeth, is usually caused by damage to
the teeth while they are still developing
in the gums. It results in certain areas
of the tooth enamel being under
calcified.
Most of the mottled areas are not
detectable except to the professional
eye. They have a specific distribution
not only on the tooth surface but
between the teeth.
The number of children with this
form of mottling varies from one
community to another, whether or not
i. TOOK]
the water is fluoridated. In fact, it has
been found that in areas where
drinking water is fluoridated to a level
of one part per million, the number of
children with dental mottling is no
greater than elsewhere and in some
places is less than would be expected.
Dental fluorosis is a far more severe
form of dental mottling which may
appear if the natural level of fluoride is
much higher than that maintained in
fluoridation schemes. It is far more
noticeable than dental mottling, has a
different distribution, affects all the
teeth, and is considered to be the first
sign of possible fluoride toxicosis.
So in their over-enthusiasm to
condemn fluoridation, those who are
opposed to it on principle have wrongly
confused dental mottling - which is
found in its mild forms in all
communities - with dental fluorosis.
6
LORD Avebury, Chairman of the Parliamentary Human Rights
Committee, believes that fluoridation of water supplies is perfectly
consistent with personal liberty.
Writing last year in the "British Dental Journal", he dismisses as
invalid the so-called libertarian arguments used by opponents of
fluoridation.
He said: "Fluoride is a natural constituent of water supplies, as
indeed it is of many foods. The adjustment of the quantity to an
optimum level cannot be compared with the addition to water of a
substance not found there ordinarily.
"Nor can it be described as 'mass medication’, a term frequently
used by opponents, since it is not a means of curing a disease. A
substance which has the effect of maintaining medical or dental
health is more in the nature of a food or nutriment than a medicine.
"The individual liberty arguments against fluoridation are invalid,
as can be judged from the fact that the issue has never been taken
up by the National Council for Civil Liberties.
"No consumer has the right to dictate the chemical composition
of the water supply, a recipe for anarchy. What is at stake is not the
erosion of liberty but, in the words of a former Minister of Health,
'the erosion of millions of teeth and the resultant suffering and
misery of thousands of children which fluoridation would go far to
prevent'."
DISEASES IN THE WORLD TODAY
the foods that prevent them
all kinds of meat, but especially liver
fruits, especially citrus fruits,
mango, pineapple, berries
guava
green vegetables
sea foods,'such as fish, shellfish
algae
and
iodized salt
whole milk, butter and cheese
yolk of eggs and liver
vegetables, especially carrots and
"greens"
yellow fruits, such as mango and papaya
red palm oil
ci man-made disease
Japan. Yields, at 1.6 tons per hectare,
million
Bilateral
of about 7 per cent, in real terms, reach
would be less than half those achieved
assistance programmes of oecd (Organ
ization for Economic Cooperation and
ing $63,000 million in 1973. Their ex
ports of manufactured products have
Development) countries contributed an
been rising at twice that rate and now
additional
represent more than one-third
Japan,
in
Korea,
Taiwan,
Western
Europe and the United States.
Most developing countries will need
substantial external assistance to finance
the heavy
agricultural
investments required
for
development. The recent
alarm about world food prospects has
been useful in
focussing attention
on
to
$
$
2,440
800
million.
million
annually
in
1973 and 1974. Progress is being made
toward the establishment of an Interna
tional Fund for Agricultural Develop
ment, proposed at the World Food
Conference, in which the oil-exporting
tional agricultural research effort, spon
$ 3,000 million at present to $ 6,500 mil
lion in 1985.
■ Finally, there is increasing evidence
that population growth is beginning to
slow down in the developing countries
are
pledged
to
gramme), is under way. The developing
< An Indian scientist demonstrates the dramatic
contrast between ordinary rice and a new
hi^^'ield variety. Modern technology. has
bt^ght about spectacular improvements in
food productivity through the development of
hybrid strains.!Photo WHOlFAOjD. Mason)
Farmers on a communal farm in Peru apply
ing fertilizer to cabbages. Most developing
countries could increase their food production
several fold if only they had access to the
technical advances that have been made in
agriculture. (Photo WHOI FAOIC. Sanchez)
the
example,
rising by over 8 per cent annually. At
this rate, they should increase from
sored by the World Bank, fao and undp
(United
Nations
Development
Pro
have more than tripled, from USS 724
For
contribute
and
organizations
also been growing.
about half of the target of $ 1,000 mil
lion. A major expansion of the interna
countries
multilateral
been lagging behind the more advanced
developing countries, their exports have
volume of exports of manufactured
products from South Asia is currently
this problem. In the past four years,
total commitments for agricultural pro
jects by the ibrd (International Bank
for Reconstruction and Development)
other
of the
total. While the poorest countries have
countries themselves are channelling
more of their own resources into food
production.
There are
other encouraging
signs.
Quite apart from the countries of opec
(Organization of Petroleum Exporting
Countries), many developing countries
have been successful in expanding their
exports and thus improving their ability
as birth rates continue to fall while mor
tality rates are levelling off. Flere agaim
progress has been greatest in some
the more advanced developing coun
tries; but there are indications that the
population growth rate in
India
may
also have passed its peak.'
These developments are coming none
too soon; but taken together they give
to pay for needed food imports. Total
exports of the developing countries, ex
reason for hope that hunger and mal
cluding oil, have been growing during
nutrition may finally be banished from
the past two decades at an annual rate
this earth.
□
\7
BIBLIOGRAPHY
L.R. Brown and E.P. Eckholm, By Bread
Alone. Praeger, New York. 1974.
FAO. Assessment of the World Food
Situation, and The World Food Problem.
Prospects for National and International
Action. Rome. Nov. 1974, US Depar^
ment of Agriculture, Economic ResearaB
Service. The World Food Situation and
Prospects to 1985. Washington. D.C,
1974: International Food Policy Research
Institute. Meeting Food Needs in the
Developing World. Washington. D.C..
Feb. 1976: OECD. Study of Trends in
World Supply and Demand of Major
Agricultural Commodities, 1976: Ameri
can Association for the Advancement of
Science. "Food", special issue of Science.
5 May 1975: "Food and Agriculture",
special isssue of Scientific American,
September 1976.
Fred H. Sanderson, "The Great Food
Fumble". Science. 9 May 1975.
F.H. Sanderson and Shyamal Roy. "Food
grain Demand and Supply Prospects in
India. 1980. 1990 and 2000". Brookings
Working Paper, 1976.
WHO Technical Report Series:
No. 584. Food and Nutrition Strategies
in National Development. 1976
No. 590. Vitamin A Deficiency and Xer
ophthalmia. 1976.
No 593. Methodology of Nutritional
Surveillance, 1976
THE FIVE PRINCIPAL DEFICIENCY
what are they- how to detect them
Insufficient red pigment (haemoglobin)
in the blood (mainly iron deficiency)
Main symptoms: pallor of skin and
mucous membranes, general fatigue.
breathlessness after exertion, palpitation,
loss of appetite (anorexia), indigestion
(dyspepsia)
Enlargement of the thyroid gland result
ing from iodine deficiency
endemic
goitre
Main symptoms: deformity of the neck,
mental retardation and deaf-mutism:
may occur in children born to mothers
with goitre
Severe protein deficiency
kwashiorkor
Main symptoms: swelling (oedema).
apathy and irritability, "flaky-paint" skin,
sparse, straight and dyspigmented hair
Severe calorie deficiency
marasmus
Main symptoms: growth retardation,
wasting, no subcutaneous fat, atrophied
muscles — "all skin and bone"
Severe Vitamin A deficiency
xerophthalmia
Main symptoms: dryness of the eyes
(xerosis), night-blindness (nyctalopia),
corneal ulcerations, leading to blindness
Atmospheric pollution causing dryness of eyes
By Our
Our Staff
Staff Correspondent
Correspondent WP
By
—
BANGALORE. March 5.
Rising levels of atmospheric pollution is cited
as one of the most common factors that cause
dryness of the eyes. With the number of vehicles
increasing annually, air pollution is on the rise,
and the eyes are made to wade through a sea of
highly polluted air leading to evaporation of the
tear film that surrounds the eye.
What is this eye disorder referred to as dry
ness of the eyes? "This is typically characterised
by itching or burning sensation in the eye or
redness of the eye and sometimes heavy tired
and watery eyes,” says Dr. Ram Mirlay, consult
ant ophthalmologist. Dryness is a common
problem worldwide, and he is of the view that all
steps should be taken to protect the eyes from
the dust. “If dryness is not checked, it will lead to
chronic eye disorders”, he cautions.
One of the ways to protect the eyes is to wear
dust protective goggles. "Don't you wear slip
pers or shoes when you walk on the road, simi
larly use this goggles to safeguard your eyes", he
says. However, even this, he points out, may not
give total protection as the eyes are not totally
shielded.The problem
problem of
of dryness
dryness occurs
occurs when
when
shielded.The
the tear film, which is vital for clear vision and
for the eye to remain healthy, begins to evap
orate on account of constant exposure to the
various pollutants including the pollen dust, an
environmental condition peculiar to Bangalore.
Even airconditioned setting and long hours
spent in front of the computer screen can cause
this dryness, ophthalmologists say. According to
them, airconditioners provide cooled dry air
which evaporates the tear film, and those who
work in such surroundings in cities that are dry
and have low levels of humidity, are likely to be
affected most.
As for the computers, research indicates that
up to 75 per cent who work on computers expe
rience one or more reversible eye problems. This
is because when a person focuses hard on a
computer screen, his blinking rate drops and
this facilitates dryness. It is learnt that when
people converse they blink between 18 to 25
times per minute on an average, but when they
read or study the rate drops. When viewing a
computer screen, it drops to about seven times a
minute, it is said. The decreased frequency of
blinking causes the tear film on the eye to evap-
or^r
fasterresulting
resultinginindryness.Dryness
dryncss.E
______
could
be treated by the use of tear substitute or an
artificial lubricant. The artificial lubricant sup
plements the natural moisture of the eye and
offers immediate relief." Polyvinyl alcohol based
solution is the closest substitute to natural
tears." says Dr. Ram Mirlay. However, it is essen
tial to consult a doctor first before using the tear
substitutes. According to him. in the U.S. 50 per
cent of all eye drops are tear substitutes.
Here is some information that could help re
duce eyestrain for computer users. Take breaks
by just looking around the room; wear glasses;
keep the screen free from dust: adjust lighting in
the work area to minimise reflections and glare:
adjust position of computer screen so that the
top of the screen is slightly below eye level, posi
tion your screen so that you are looking down at
As regards computer setting, black characters
on a white background are usually the best, but
other combinations are allright, if there is plenty
of contrast between characters and the back
ground. Dark backgrounds should be avoided.
Lastly, blink more often while working at your
computer screen to check dryness of the eyes.
NSAIDs Cause 1 in 5 Heart Failures 7/2/00
filc.7//D|/INFO FROM INTERNET/nsaids_heart faiiure.htm
C®ms@ 1 m
'sy 2, JOGC
InlfgairS IFaoDiw©®
This recent study found that the use of nonsteroidal
anti-inflammatory drugs (NSAIDs) caused a greater than
3.©=tF©Dd] mcreas® m fite crosEk off s©irof@sfiov@ Ihsairt ffaoDw®
(CHF) in patients with a history of heart disease. In those
without a history of heart disease, the use of NSAIDs still
increased the risk by 60%.
^SAIIXCauifo .sfeart
HiJSwnGeno£S»
Aimgstcsrnntgte
Although previous studies have shown that the use of
NSAIDs could lead to the development of congestive heart
failure (CHF) in some patients, the magnitude of the
association was not fully understood.
Gaesoa
CstoumGiarmel
3lS£^rsCausg^I
Sieatfias
Canada KeiectsOtestrg
The authors speculate that if their results are correct, it
means that NSAIDs are responsible for 19% of all hospital
admissions for CHF.
what.Our.Aneg^ar§
Ate
goirtJina for Arsenic
PojtoaiaS
Strong,.jmrnune
System Kills Ebote
;
Smoking Oama^s
ThytoW '
:;,
CHF, commonly referred to as simply "heart failure", is a
disorder in which the heart loses its ability to pump blood
efficiently, thereby failing to meet the demands of the body.
As pumping action is lost, blood may back up into other
areas of the body, including the liver, gastrointestinal tract,
and extremities (right-sided heart failure), or the lungs
(left-sided heart failure). Some other potential causes of
CHF include:
Testosterone;
Conteibutosta
;
Ateetosdetofis
: corona^ Surgery May i
ngt.be Worth Risk
ttercun/ coisonirt; :
SaatM^teOMSA
iRBhtroSZjtew'HOt,
Raite.Stroke R;sk
StahlSsLW^toess
Vi?ir,5r •<T.‘.ri'i<
'
1 of2
° high blood pressure
° heart valve disease
° congenital heart diseases
° cardiomyopathy
° anemia
° irregular heartbeats (arrhythmias)
° hyperthyroidism
° kidney disease
° infections
In addition to NSAIDS, other drugs such as beta-blockers
and calcium channel blockers have also been shown to
increase the risk of CHF.
7/6/00 3:40 PM
NSAIDs Cvjse 1 in 5 Heart Failures 7/2/00
Archives of Internal Medicine Josie 20©Q; 160:
saaft-xtfemt
* '
„ '
»
"
*-
file:///D|/INFO FROM INTERN ET/nsaids heart failure.htm
777-734.
/ COMMENT: Aowtoer reasom that we
to be carefuS
atoort av®idin® drags. Kt ns iimp©rtairrt to recogirofee
heir® that aspirin), Advil] aired Motrim type drags ar®
iOlllIf avaaOabD® woto©Mt a pr@s©[ropto©ijD amd may cays® toes®
:T serieoos sod® effects. Kt os possobie that toe
widespread nos® ©f toes® drags os contributing to to®
/ "epodemoc” ©tr heart faoOMr® goitmg ©ou (se® artocD®
b®D©w). Ks to© temperary pain refeff pr©vided by
■
toes© medications worth to® risk of this
Doferthreatenong adverse reactoonT
Rela'cec Articles:
NSAIDS deduce Effectiveness of Antihypertensive
Therapy
US Experiencing Heart Failure "Epidemic"
NSAIDS Report
,
Arginine and exercise improve heart failure
NSAIDs May Harm Kidneys of Eideriy
■
IFtetem To Table of Contents Issue #16©
,^MAMAVA.A-/^MAM.M^A<WAWAMA<MAVA<VAMA\kWA>AV.MA<VA^\\MA^:AMAWAMA'.:AMA<SVAWW.VAMAW.WA^«AVAMAWAW.^^
shis firs?: ] Subscribe to free nawsietter J Current newsietters [ Articles on
wellness ] Urates to weiiness I Search site [ Home | E-mail: Dr@Mercola.com
Disclaimer - Newsletters are based upon the opinions of Dr. Mercola. They are not intended to replace a one-on-one
relationship with a qualified health care professional and they are not intended as medical advice. They are intended as
a sharing of knowledge and information from the research and experience of Dr. Mercola and his community. Dr.
Mercola encourages you to make your own health care decisions based upon your research and in partnership with a
qualified health care professional.
2 of 2
7/6/00 3:40 PM
Hygiene Systems To Improve Health
Cle:///D|/TNFO FROM INTERNET/ntercola-allergies,infection & stress.
1 of!
6/21/00 11:57
ALLERGIES, INFECTION & STRESS
The following information is abstracted from
Dr. Kenneth Seaton and the book Prostate Health in 90 Days by Larry Clapp,
Ph.D. J.D.
Respiratory infections and allergies constitute the greatest stress on the people in
most developed societies. Approximately 80% of visits to doctors offices are for
upper respiratory problems. There are two common myths associated with
allergies and common respiratory infections that provide strong clues to their
management: The average adult has 5 colds per year.
Allergies are not caused by allergens such as pollens, house mites, dust or other
such substances. While it is true that these types of tilings trigger allergic
symptoms, the underlying cause is a malfunctioning immune system; "Immunity
gone wrong". The allergen simply triggers an incorrect immune system response.
In a sense, the immune system identifies the harmless allergen and tries to kill it.
The allergic symptoms many of us are so familiar with, runny noses, watery eyes,
etc., are direct signs of our immune systems trying to kill these harmless
substances. This type of immunological mayhem cannot be separated from the
stress put on our immune systems from infections (in many cases sub-clinical
infections). Many auto-immune diseases can be viewed as a severe form of
allergy where the immune system attacks its owner.
Dr. Seaton's studies over the past years demonstrate that the constant
auto-inoculation of the nose and eyes by the fingertip area, leads to an overloaded
immune system and most of the infections of the upper respiratory tract. This
overload of tire immune system through the contact of the fingertips to the eyes
and nose is maintained by our congested urban areas, an environment rich in man
made toxic substances (pollution) and fast, mass transportation which move
microbes from one part of the world to another each day. All of which impacts us
each time we touch our fingertips to the sensitive membranes of our eyes and
nose, overloading our immune systems.
5#
Germs Are Transferred Through Your Fingernails
When we think of diseases being transferred from person to person, we conjure
up images of people sneezing or coughing on each other. We picture germs
hurtling out of people's mouths and noses and rocketing through the air right into
our own noses or mouths to infect us. A frightening picture, but one that we need
not worry about, because relatively few germs become airborne, and fewer still
1 of 13
£ile:///D|/INFO FROM INTERNET/mercola-allergies jnfcction & sires
Hygiene Systems To Improve Health
actually bother us.
Germs aren't hurtled at us by coughs and sneezes. They're handed to us during
routine-and intimate -physical contact. Germs are handed to us because human
hands-especially under the nails-are a cornucopia of germs. If you take samples
from various parts of the hands you'll see that while there are tens, hundreds,
thousands of germs on the backs and palms of the hands and on the fingers, there
are tens of millions, sometimes hundreds of millions of germs under the
fingernails.
The fact that the undersides of the fingernails are a breeding ground and a safe
haven for genns is double trouble. First, the fingernails are not protected by the
"homy" layer of skin, making it easier for genns to enter the body via the
fingernails. Once inside they can get into the many blood vessels that feed the
remarkably sensitive fingertips. Second, it is with our fingertips that we
commonly touch each other-and ourselves. Fingertips touch flesh when we shake
hands, when we caress a lover, when we grab hold of someone's arm to steady
them. Fingertips are involved when we hand someone a pencil or a dollar, when
we touch a computer keyboard or telephone. Fingertips come into play when we
scratch ourselves, floss our teeth, prepare and eat our food.
Once on the hand germs accumulate under and around the fingernails, from
where they hitchhike to the damp membranes of the eyes and nose
(autoinoculation). Surprising, this is the process by which many germs and
allergens affect our metabolism... through the contact of our fingertips to the eyes
and nose.
Autoinoculation
The average person touches their nose, mouth, and eyes many times a day. If you
watch a group of adults for an hour, you'll find that 1 out of every 3 touches their
nose, and 1 in every 2.7 touches their eyes. Even this small amount of innocent
touching is enough to carry germs from the mouth, where they were probably
unable to penetrate the body's defenses, to the nose or eyes, where they have an
easier time causing damage. This passing of germs from one part of your body to
another, unknowingly carrying them to the places the germs like the best, is
called autoinoculation. But whether the germs come directly from others, arrive
indirectly via items we touch, or move from one part of our body to another via
autoinoculation, they're bad news.
Lowering Albumin: the "Hidden" Problem with Infection and Disease
If germs entering the body simply did their damage, that would be serious
enough. But they unwittingly do far more. In order to fight off invading bacteria,
viruses, fungi and other invaders, the body sends the immune system into action.
In no time at all, T-cells, B-cells, macrophages, eosinophils, and other immune
system soldiers are engaged in battle with the enemy. Here's how poor hygiene
can lead to health disasters:
• The battle against genns is a protein-based battle, because the immune
system utilizes many protein-based substances to fight off the invasion.
° The immune system rapidly produces more protein-based substances to
defend the body.
° There can only be a certain concentration of all proteins in the body.
2 of 13
6/21/00 12:1
Hygiene Systems To Improve Health
fHe:///D|/ENFO FROM INTERNET/mercola-aliergies jnfection & stress
° When the concentration of immune system proteins goes up, the
concentration of other proteins must fall.
° One of the proteins that decreases when the immune system is engaged in
battle is albumin, and that's where the trouble lies.
Albumin is an important protein that is found in most animal tissues. Medical
doctors know about albumin, and often measure the amounts found in the blood
with a simple blood test. Standard blood work-ups include albumin, depicting
anything between 3.0 and 5.2 as "normal." Albumin has not been a focus of
traditional medicine despite the fact that albumin levels are the single most
important indicator of health status. If the level of albumin in your blood drops,
your risk of contracting a serious possibly deadly-disease shoots way up.
Statistical reports demonstrate that albumin levels correlate closely with age, but
are not truly age-related. That is, albumin levels tend to drop as we grow older,
but don't necessarily have to.
Albumin is assembled in the liver from more than 500 amino acids. It is the most
abundant protein in the bloodstream, and has many important duties. It:
° Protects easily damaged tissues from the free radicals that can destroy cells
and cause cancer by altering cellular DNA.
° Guards against heart disease by transporting the antioxidant vitamins that
help keep the coronary arteries clean, binding up fatty acids that tend to
clog arteries and stabilizing the ratio between HDL ("good" cholesterol)
and LDL ("bad" cholesterol).
° Binds up waste products, toxins, and dangerous drags that would Otherwise
damage the body and encourage disease. It also detoxifies the fluids
surrounding cells.
° Protects the biological terrain by buffering the blood against pH changes.
° Helps to keep the blood flowing smootlily by preventing red blood cells
and other substances from clumping together.
° Is essential for transporting vitamins, magnesium, copper, zinc, bilirabin,
uric acid, sex hormones, thyroid hormone, other hormones, and fatty acids
tliroughout the body. It regulates the movement of nutrients between the
blood and the body's cells.
° Stabilizes red blood cells and growth hormones.
° Plays a major role in controlling the precise amount of water in various
bodily tissues.
° Plays an important role in transporting and circulating reservoirs of thyroid
hormones.
° Purifies the cerebrospinal fluid, nourishes brain cells, and maintains the
blood-brain barrier.
° Helps to ensure that there are adequate amounts of certain key minerals in
the bones.
« Binds and transports the "stress hormone" known as cortisol, reducing
stress-induced damage to the thymus gland, brain, and connective tissue.
Albumin has been described as a "portable liver" because the liver is the body's
chief mechanism for disarming toxins and other dangerous substances, and
because albumin, which is made in die liver, does the same throughout the body.
It’s as if the liver has sent millions of tiny pieces of itself to every single little cell,
to round up and destroy harmful substances and organisms.
Albumin plays an indispensable role in maintaining the delicate chemical balance
3 of f3
6/21/00 12:
Hygiene Systems To Improve Health
ftle:///D|/INFO FROM INTERNET/mercola-aiiergies,infection & stress
of the nourishing fluids (interstitial fluids) that surround and support the trillions
of cells in the human body. If these fluids are healthy, the cells will flourish. But
if the fluids become polluted, or depleted of certain substances, the cells cannot
heln
fall —
ill,-------and disease,—
willw.,
swe.en
bodv
-- r but
~—-—r —thronoh
—.——-the.
--'-J ■ ‘Albumin
---------- — is
—-■ like,
— a— filter
——
that removes toxins from water, iikefne net that scoops debris out of a swimming
pool, like the dispenser that squirts extra vitamin D into milkalbumin ensures that
bodily fluids are clean, filled with nutrients, and properly balanced. And when
you're filled with health-giving fluid, you cannot help but be healthy.
When Albumin Levels Fall
Ideally, there should be 5.0 g/dl (grams per deciliter) of albumin in the blood.
(Some doctors and laboratories state this figure as 50 grams per liter, which is the
same thing.) Lower levels, around 3.5 or so, are commonly seen in long-time
vegetarians and people suffering from malnutrition, kidney disease, cancer,
severe infections, Crohn's disease, pancreatitis, and other diseases. However,
levels don't have to fall as low as 3.5 before trouble appears.
Low levels of albumin have been linked to all cancers, with the risk of
developing cancer rising as albumin falls. Albumin is low in all people suffering
from cancer. You can track the progress of the disease by looking at the patient's
albumin level-the lower the albumin, the more rampant the cancer. In fact, a low
albumin level may actually cause cancer. Albumin normally neutralizes aflatoxin,
nitrosamines, and other powerful carcinogens (cancer-causing substances).
Without sufficient albumin to keep these and other carcinogens under control,
cancer can flourish.
Back in 1775 we learned that at least one form of cancer could be caused by
"dirt." Chimney sweeps exposed to soot were more likely to develop scrotal
cancer than other people. Simply washing themselves carefully every day reduced
their risk to normal. Few of us are anywhere near chimney soot these days, but
we are exposed to many airborne chemicals, especially if we live in polluted
cities or near certain kinds of factories and plants. We also know that some forms
of cancer are caused by viral infections. That's why it's vital that we regularly and
carefully wash away any germs or chemicals that can cause cancer, as well as
those that can indirectly cause the disease by overwhelming our immune systems
and reducing our albumin, allowing cancer to sneak in the "back door."
Declining albumin also indicates an increased risk of heart disease. A long-term
British heart study found that a low albumin level was a good predictor of heart
disease. Another study stated that the odds of suffering from coronary' artery'
disease doubled when the albumin level fell to 4.4 (that's only about 10% below
the ideal level Of 5).
Low levels of albumin are associated with several other diseases, including
Hodgkin’s disease and HIV, the precursor to AIDS. Indeed, you can use low
albumin levels as a "predictor" of mortality. People with albumin levels below
3.5 g/dl are approximately twenty times more likely to die from all causes than
those with albumin levels of 5.0 g/dl. Many studies have confirmed this fact.
Nursing home residents with albumin levels of 3.5 g/dl had a death rate of about
50%, compared with an 11% rate found in those with higher levels (around 4.0
g/dl). Among men and women over the age of 70, death rates were 40% lower in
those with albumin levels of 4.4 g/dl, compared to those with levels of 4.2 g/dl.
Hip fractures are a serious problem for the elderly, who often weaken and die
4 of 13
6/21/00 12a
Hygiene Systems To Improve Health
file:///D|/INFO FROM INTERNET/mcrcoIa-allergies,infection & sires:
after the break. Among hip-fracture patients whose albumin levels were low
(3.0), the death rate was 70%. But among those with albumin levels 4.0, the death
rate was only 11%."
Why Does Albumin Fall?
Albumin levels drop when the immune system engages in a battle with invading
bacteria, viruses, fungi, and other germs. It also falls when the body is forced to
deal with an onslaught of toxins and other dangerous substances that we inhale,
drink, or eat, or that get into the body through the skin, respiratory system, or
other ports of entry'. The fact that the body mounts a powerful offensive is good,
for otherwise we would die. But the unintended consequence, the shortfall in
albumin, is harmfill in the long run.
Temporary drops in albumin levels are necessary, and not a problem. It's as if we
miss a credit card payment one month because of unexpected medical expenses,
then make the missed payment, with interest, the next month. Our credit takes a
small "hit," then quickly recovers before any permanent damage is done. The
problem comes when we're continually battling infections, parasites, and toxins.
Then our albumin runs low for months on end and, like a person who doesn't
make a credit card payment for several months, our "credit" is eventually mined.
Now we're facing serious illness, and we never seem to have enough resources to
beat the disease and "get ahead."
Increasing Your Albumin Level
It's important to monitor your albumin level and make sure it stays high, since
low albumin has been linked to an increased risk of death from all causes in both
sexes and among all races and age groups." The ideal albumin level is 5.0, but the
average level in the United States is only about 4.2 -too low for optimal health
and low enough to encourage disease. Albumin is produced in the liver, but
there's no way to encourage the liver to make more-no drugs, no diet, and no form
of exercise that will spur production.
Doctors can infuse albumin intn the body, and may do so for patients suffering
from cancer and other serious diseases associated with low albumin.
Unfortunately, "albumin shots" don’t work. When albumin is infused into the
body, it upsets the carefully calibrated concentration of proteins (osmotic
pressure). The liver attempts to get the concentration back to normal levels by
halting its own production of albumin. And if that doesn't work quickly enough, it
starts destroying albumin in a frantic attempt to get things back to normal in the
body. The liver doesn't understand that the extra albumin may be helpful; it only
knows that something is out of balance, and balance must be restored.
The only way to keep albumin levels high is to stay healthy. I know that sounds
like circular reasoning-low albumin causes you to be sick, and the only way to
increase albumin is to not get sick-but it's not. When we have an infection or have
been injured, the total number of antibodies and certain other proteins rise. Since
there can only be so many proteins in bodily fluids at one time, if the antibodies
and other proteins associated with infection or injury rise, then the albumin must
fall. Remaining healthy is the only way to keep the antibodies and other proteins
at normal levels, leaving "room" for plenty of albumin.
Fortunately, we can lower the risk of infection by paying scrupulous attention to
5 of 13
6/21/00 12?
Hygiene Systems To Improve Health
file:///D|/INFO FROM INTERNET/mercoia-allcrgies,infection & stress
personal hygiene. Infection is often caused by the foreign bodies (germs) which
enter our body through the mouth, nose, eyes, and fingernails, as well as through
cuts in our skin. Good hygiene won't prevent cuts, but it can eliminate many of
the germs that are lurking around our eyes, mouth, nose, and fingernails. By
preventing the germs from getting into our bodies and causing infections, we
keep our antibodies at a normal level, allowing our albumin level to rise.
Other Problems That May Be Helped or Prevented with Good Hygiene
Prostate problems, including cancer, are known to be linked to high testosterone,
which is kept in balance by albumin. But it's not just men with prostate cancer
who can be helped by proper hygiene. A great many ailments are caused or
worsened by poor hygiene and the inevitable drop in albumin, including:
Acne. Bacteria can grow in the sebum that abounds in glands just underneath the
skin. Scratching, rubbing, or pinching acne can introduce even more germs to the
infected areas.
Aging. Decreased albumin levels are probably the major cause of accelerated
aging and contribute to most of the dysfunction we see with increasing age.
Decreased albumin levels will increase free cortisol which causes most of the
damage.
Allergies and asthma. Many of the substances carried in the fingernails,
including staph aureus and worm eggs, can trigger allergic reactions or asthma
when we autoinfect ourselves. The facial dips in the hygeine system literally stop
most allergic pollen, dust or mold reactions in minutes.
Alzheimers. Immune system dysfunction seems to be the single most important
reason we develop progressive dementia.
Athlete's foot. Our fingernails can pick up from our feet the fungi that cause
athlete's foot, and then deposit it to other areas of skin, spreading the infection.
Arthritis. Infectious and rheumatoid arthritis can both be caused by invading
organisms which can be kept out of the body with proper hygiene.
Candida. A common problem, especially for women, the fungi and yeast that
cause Candida can produce annoying to serious infections in the vagina,
gastrointestinal tract, and elsewhere. There are women who had suffered with
chronic vaginal yeast infections (for as long as 20 years) who had their problems
disappear in one week on the hygiene program, especially from the baths.
Colds and flus. Although we instinctively flinch when someone with a cold
coughs or sneezes on us (or anywhere near us), most of the moisture expelled
from the mouth during a cough or sneeze does not contain many germs. That's
because cold viruses do not routinely "hang out" in the saliva pools which
comprise most of the droplets shot from the mouth by coughing and sneezing.
Instead, the viruses congregate in the nose, which has the temperature and other
conditions they prefer. Not only do cold viruses favor the nasal environment (the
nasal passages are more hospitable for cold viruses), they also have a better
chance of getting into the body and its cells via the nose. Since vve touch our
noses many times during the day, the chance of carrying germs to and from the
nose is great.
S nf It
6/21/00 1:
Hygiene Systems To Improve Health
fiie:///D|/TN FO FROM INTERNET/mercola-allergies,infection & stres
Diabetes. Recurrent infections are a problem that plagues diabetics. Slopping the
infection autoinfection cycle will help many diabetics avoid needless infection
and allow their bodies to concentrate on healing.
Measles. Although generally harmless when it strikes in childhood, measles can
be a very serious disease for adults. It's very difficult to get people, especially
children, not to scratch or touch themselves when infected, raising the likelihood
of contagion. Excellent hygiene of the hands, especially the fingernails, may help
to keep the disease contained.
Pneumonia. Often called the senior citizen's "best friend" because it leads to a
relatively quick and painless death, pneumonia often strikes after or in
conjunction with other respiratory ailments. This means that a cold or flu can
prepare the way for pneumonia-the same cold and flu that can be prevented with
impeccable hygiene.
Worms. Almost everyone plays host to these tiny invaders at some point in their
life-and perhaps many times. Worm eggs are easily picked up by our fingernails
when we touch various surfaces or other people, and then enter our body via the
mouth, nose, or eyes when we touch ourselves. Worms can be draining and
debilitating, damaging body tissue and robbing of us nutrients and energy. It's
best to wash away worm eggs before they get inside and force us to employ
stronger measures to get rid of them.
And that's not all. AIDS, chicken pox, circulatory problems, cystic fibrosis,
dandruff, ear and eye infections, fat metabolism disturbances, herpes, multiple
sclerosis, sex hormone imbalances, skin diseases of various kinds, and thyroid
disorders can also be helped or avoided by good hygiene, which helps prevent
germs from entering the body and keeps albumin levels up.
Too Simple to Be True?
This sounds like a simple idea, perhaps too simple to be worthwhile. However, it
is no more than an extension of the work of the great Austrian doctor, Ignaz
Semmelweis, who created an incredible uproar in the medical community in the
1840s when he insisted that doctors wash their hands before examining women in
the maternity ward. (The doctors often came right to the maternity ward from the
morgue, where they had been dissecting cadavers, without stopping to wash their
hands.) Pregnant women used to plead to be cared for by the midwives rather
than doctors, because those who were cared for by the midwives (who did not cut
up dead bodies) had a much higher survival rate. But the doctors refused to heed
Dr. Semmelweis’ plea. They were insulted by the very' idea that they might be
carrying germs to tlreir patients and killing them. So they drove Dr. Semmelweis
out of the hospital and into the insane asylum, where he died.
Yes, washing your hands sounds like a very simple solution to an incredibly
complex set of problems, but the simplest ideas are often the best. Sometimes
changing just one thing produces dramatic results. Scurvy used to decimate the
crews of ships sailing the high seas in the 15 , 16 th, and 17th centuries. The
problem was solved when sailors began eating citrus fruits or drinking lemon or
lime juice. Pellagra was a terrible scourge for many centuries in various
countries. It attacked many in the United States, leading to the "Four D's":
diarrhea, dermatitis, dementia, and death. This mysterious and impossibly
7 of 13
6/21/00 12:C
Hygiene Systems To Improve Health
file:///D|/INFO FROM INTERNET/mercola-allergiesInfection & stress
complex disease was eradicated by adding niacin, one of the B vitamins, to the
diet. A solution doesn't have to be complex. It simply has to work. And good
hygiene works!
The Solution
As is often the case in Nature, the solution is astonishingly simple and reliable!
Advanced personal hygiene of the fingertip area, especially under and around the
fingernails, and by the daily cleansing of membranes in the front of the nose and
around the eyes can remove the overload from our immune systems and reduce
the number of clinical and sub-clinical infections of the upper respiratory tract to
levels never before thought possible. This non-invasive, non-pharmaceutical
solution is surprising simple and effective. Advanced hygiene is a more scientific
approach to washing that keeps germs, environmental toxins and allergens away
from our bodies before they can cause any stress or damage to our systems.
Further, once the overload is removed from our immune systems, many allergies
are self correcting. Not only does advanced personal hygiene reduce the amount
of auto-inoculation of allergens, but once the overload is removed from our
immune systems, the allergen that used to trigger allergic responses no longer
causes immunological mayhem to our systems. The allergy is gone. Even though
people may have different genetic predisposition’s to allergies, stress and
frequency of illness, it is an individuals standard of hygiene that determines the
differences between people, not differences such as race, social or income levels.
The Skin
cl/tn 10 Tvrxf mot o
zz>rirvrr r\vpr r\iir Kr\r1»<=»o Tt 10 on rxrnoti
fh/a K/»art liwpr
1 JL1V OIVlll IO 11X71
14. VUVVlHlg V » VI X7X41 C/VJUIVO, 11 10 Uli X71 ii;C4Ll. HXkVz VIIV/ 11VU1 I, 11 » VI
or brain. In fact, it is the largest organ in the body, and one of the most complex.
How would you wash your heart, liver or brain each day? In reality, the skin is an
endocrine organ, part of our immune systems. It is a vital and integral part of the
immune system itself T cells, the master cells of the immune system, after
passing through the thymus, migrate to the skin's surface where, amazingly, they
receive maturation hormones from skin cells. Even tiny traces of chemicals can
interfere with the skin cell's ability to produce these complex hormones which are
vital for maintaining the immune system throughout our lives.
Fingertips
The sense of touch and blood flow and sensitivity of the fingertips is so
extraordinary' that a blind person can read by feeling. The fingertips are a real
extension of our brain. Dolphins, with very large brains, can never build any
civilization or even weapons to protect themselves.
-Our hands, with their opposable thumbs, arc perhaps the most remarkable design
in all of nature.
The area under the fingernail has no dead homy skin layer and is very thin. The
blood flow to the nail bed is about the most complex of tire entire body. Constant
use of chemicals under and around the fingernails can cause those chemicals to
be absorbed directly into the blood stream. One dangerous side effect of
constantly applying antiseptics/disinfectants to the fingertips is the introduction
of chemicals into the delicate tissues of the eyes, nose, skin, hair and food
through touch.
8 of 13
6/21/00 12:
Hygiene Systems To Improve Health
Gle:///D|/INFO FROM INTERNET/mercoia-allergiesJnfection & stress
Further, the skin, particularly of the fingernail area, is teeming with a wide
variety of germs, something like the natural flora of the rain forests in South
America. These germs should be in perfect balance, competing and producing
complex chemicals that prevent colonization by pathogenic microbes.
Amazingly, many people become sick because they do not have enough of the
correct type of germs on their skin. We call this the "natural disinfecting power"
of the skin. Natural oils, waxes and secretions should be on the skin and perhaps
are vital in the production of the hormones that cause T cells to mature.
Antiseptics, Disinfectants & Antibacterial Agents
Over the last 15 years, Dr. Seaton formulated and tested approximately 5,000
different soaps. For years he tried every type of antiseptic/disinfectant?
. antibacterial agents available, t hey ALL failed for the following reasons: (1)
Most are not effective against ALL types of germs, thus some overgrow. (2) The
combination of several different types of these is highly toxic, and causes stress
for the immune system. (3) ALL chemicals that kill germs will kill people, if used
in sufficient concentrations or over many years. (4) These chemicals disturb the
natural balance of healthy microflora. (5) Over a period of time, all substances
applied to the skin are absorbed through it and affect the body's internal
metabolism and (6) the emulsion of the soap, when tiny traces are introduced into
the eyes and nose, sends the immune system into disarray and contaminates the
delicate tissues.
Further, there is grave concern in the medical community about the overuse of
antibiotic medications, which has given rise to all sorts of antibiotic-resistant
bacteria and deadly new infections. Now the overuse of antibacterial soaps is
causing us similar concern. Our common skin flora includes a wide range of
germs that are normally harmless; in fact, they compete with disease-causing
microorganisms and in many cases provide a natural immunity against disease.
Too many germs may pose a threat; too few, and we have an artificially sterile
biological ecosystem in which virulent new organisms may take hold and
flourish.
Fligh Performance Hygiene Facial and Body Soap, by trial and error, enormous
research and scientific design, does NOT disturb the natural disinfecting power of
the skin, does NOT disturb the immunologic function of skin cells producing
these complex hormones and is NOT toxic, no matter how many times it is used,
even on a newborn baby. Dr. Seaton is constantly striving to improve Iris product,
especially in its emulsion so it does not stress the immune system's ability to
recognize self from non-self.
His High Performance Hygiene soap is a natural product. That means it is NOT
made from petroleum products. Many soaps today are. Many manufactures use
the carbon chain from petroleum products to develop a hydrophobic and
hydrophilic carbon chain. For example; many manufacturers of consumer soaps
use a type of ingredient similar to brake fluid called Diethylene Glycol or
Triethylene Glycol. These substances are used to give the soap a smooth
non-drying look, however, they are completely unnatural to the skin. These
detergent-type soaps made from petroleum products are completely unnatural and
remove the essential skin lipids. It is important to note: The skin is an organ, like
the heart and the liver. Ask yourself the questions: "Would you rub brake fluid all
over your liver everyday for 50 years?" "Would you have a healthy liver? "
Q nf 1 a
6/21/00 1
Hxsicno Systems To Improvs Health
file:///D|/INFO FROM INTERNET/mercoia-aiiergies.infection & strei
Ail important test for a soap is: Can you eat a quart of it with no effect? There is a
scale of poisons normally used in the pharmaceutical industry. For example;
Nicotine, heroin and cyanide are S6, this means only a few drops can kill. A
natural soap should be SI, practically non-toxic, because no-one can eat enough
of it to cause any problems. The High Performance Hygiene soap is so safe, that
many people have reported to Dr. Seaton that their cats or dogs have eaten half a
tub. I tell them not to worry. It will do them more good than harm. I have to make
certain that my dog doesn't get near the soap because he tends to eat it as well.
Fortunately, I keep my dog outside. Animals have remarkable sense of smell and
taste and seem to know what is poisonous and what is not.
As many do, making soap with Diethylene, Ethylene, Triethylene Glycol, or even
Propylene Glycol is completely against common sense. To give some idea of the
side effects the world's most prestigious Pharmacopoeia (Martingale, 28th ed.),
published by direction of The Council of the Pharmaceutical Society of Great
Britain slates the following about these chemicals:
Diethylene and Triethylene Glycol; A colorless almost odorless hydroscopic
syrupy liquid with a sharp sweet taste. The toxic effect following ingestion by
mouth are; depression of the central nervous system, degenerative changes in the
kidneys and liver. The symptoms and effects are those similar to those produced
by Ethylene Glycol intoxication. Seven children, aged 6 to 31 months, died
following ingestion of a preparation in which the solvent was found to be
Diethylene Glycol.'
Because the skin absorbs most substances that are applied to it, the soap maker
needs to pay careful attention to these matters. This is particularly important
when substances are applied under and around the fingernails where the skin is
very thin and has no dead skin homy layer and a very high blood flow. In
addition, whatever you apply to the fingertips ends up getting into the eyes and
nose because of the astonishing frequency of self-inoculation (the touching of the
fingertips to the eyes and nose). Further, the skin must contain the oils, fats,
waxes and enzymes plus germs that were designed by Nature. A soap not only
must clean the skin, it must replace the oils that are washed away. It must replace
the oils as close to those designed by nature. The genius learns from nature.
The soap chemist must have a knowledge in immunology, biochemistry,
dermatology, physiology, as well as chemistry. Dr. Seaton spent over 16 years in
full time research attempting to make the world's most scientific soap. His efforts
resulted in a revolutionary Tub Soap. It is the easiest way to clean the fingernails,
hands, skin and hair. Young children and old people cannot handle a bar of soap.
The bar of soap and the liquid pump are totally useless In cleaning under and
around the fingernail area in all ages, which is the most important area with the
highest concentration of germs. lif there are 10 million germs on the hands, it is
estimated that 9.9 million are under and around the fingernails. The bar or liquid
soap totally concentrates on cleaning the palm and back of the hands. This is
equivalent to hunting crocodiles in the Sahara desert. There are none there!
Under and around the fingernails where the germs are is equivalent to the Nile
valley where all the crocodiles can be found.
Further, because we are an animal and have animal fats and oils on our skin, it is
impossible to make a soap from pure vegetable oils that is going to restore the
natural skin lipids, and ensure that the natural disinfecting power of the skin
10ofl3
6/21/00 12:C
Hygiene Systems To Improve Health
fiIe:///D|/INFO FROM INTERNET/mercoIa-allergies jnfection & stress
remains in tact. It is essential to make soap from a combination of animal and
vegetable oils. Many native races living under natural conditions have perfect
skin, and use special soaps derived from plants and animal fats. Remember, you
are as old as your skin! You areas attractive as your skin! Your immune system Is
as good as your skin! Your health can be determined by your skin, and you are
recognized by those who know you by your skin.
Instructions for the Hygeine System
Throughout liistory, people living in cleaner societies have had higher albumin
levels and longer lives. Dirty fingernails, which are indicative of overall
cleanliness, have long been associated with lower albumin levels. Cleanliness is
certainly a path to better health and longer life! Regular washing of the hands and
face-at least five times a day-is an excellent start, but it's only a beginning.
Carefill scrubbing for a full minute, which few of us do, can remove up to 90% of
the germs from most of the body, but not the fingernails. Neither will regular
hand and face washing eliminate the germs hiding in the nose and eyes. And
scrubbing with regular soap is not enough. In fact, washing with some soaps can
actually increase the numbers of germs. Something more is needed.
Here are the instructions for using the various soaps in the hygeine system:
Overall Hygeine
1. Tty to use a bath and not a shower. You could use however shower in the
morning but it would be best to have a bath at night. When you take your bath but
one half to one full cup of salt in the tub. This will help clean the genital tract,
rectum and skin. If you do not have well water and use municipal water it is
likely your water has chlorine in it. In this case it would be best to fill your tub
from the shower head after you have attached a chlorine filter.
2. If you are a man NEVER insert your fingers into a woman's vagina unless your
fingernails are clean with this system. If you are a female do not allow digit
penetration of your vagina. If you break this rule you will greatly increase your
risk for acquiring a vaginal infection.
3. Do NOT bite your nails. This habit should be stopped immediately! One can
go to any pharmacy and obtain a solution that is used to help baby's from sucking
their thumbs. It is non toxic and will work in days to stop you from biting your
nails.
4. If you are a woman with long nails cut them to regular size. It will be virtually
impossible to clean your nails well if they are very long. The other, perhaps more
important issue, is that long nails prevent stimulation of the fingertips. If this
happens for a prolonged time you will actually get brain atrophy. The brain
requires regular stimulation from the fingertips to stay healthy.
5. Tty to get to bed by 9 PM (10 PM at the latest). This will maximize your peak
cortisol levels.
Hand Soap and Facial Dips
1. This system of hvgiene replaces bar, liquid, and hair soaps, as well as skin
creams. You must follow instructions exactly to get the results.
11 of 13
6/21/00 12:
2. If the soap dries out, put the lid back on.
3. Hand washing. It is essential to prod the thumbs and fingernails (with dry
hands) into the soap several times for approximately three seconds. Make certain
to stick your fingers so that the nails is completely covered with the soap. It is
also helpful to rotate the fingers to make certain the soaps is inserted on the sides
of the nail. Use the excess soap clinging to the fingertips to nib all over the rest of
the hands. Then wet, create lather, and rinse. Wash hands at least five times a
dav.
4. Skin cream: These soaps contain their own unequaled moisturizer. For best
results do not use any skin cream. If necessary, we recommend sunflower oil.
5. Face washing. Massage the soap into the skin, lather, then rinse. For those with
acne or other skin problems, use frequently. The facial dip is explained below.
6. Bath/shower. Use the sponge supplied. Wet both body and the sponge. Then
turn off water and create a rich lather using the sponge and soap. Rinse.
7. Hair. Wet hair, use plenty of soap, massage into the scalp for 30 seconds, then
rinse. Use a conditioner only if necessary.
8. Facial Dip A & C. Use Facial Dip A (hydrogen peroxide/zinc/magnesium)
most of the time, preferably first tiring in the morning, because it's very soothing
to the nasal passageway and eyes. Use Facial Dip C (iodine/HOI) especially at the
first sign of any infection (usually if Facial Dip A isn't working). It is safe to use
up to 4 half-eyedroppers of Facial Dip C during infections such as colds, sore
throats, or sinus problems. Do not use Facial Dip C every day month after month.
With Facial Dip A, use a capful in a normal hand basin containing 5 to 8 quarts
of very warm water. With Facial Dip C use between 1 and 4 half-eyedroppers in 5
to 8 quarts of very warm water. It is essential to add 1 to.2 tablespoons of salt
(sodium chloride) at least 80% of the time, yer nor all the time. Do not mix Facial
Dip A and C together. Use the hand basin, not a separate bowl. (The bacteria in
the hand basin are essential to activate the process.) Mix the solution with
running water, never your fingers. Do not draw the water to the back of the
throat. Simply allow the first two inches of the nasal passageway to be cleaned.
10. Bath: Add half a pound of table salt, Plus 5 halfeyedroppers of Facial Dip C
when you are actually in the water. Supervise young children. This bath is good
for very young children who cannot perform the facial dip and to clean the
genital tract in males and females. Do not add any soap for lo minutes because it
deactivates the iodine.
11. Foot soak. Add 4 to 6 half-eyedroppers of Facial Dip C to one gallon of hot
water, plus a tablespoon of salt. Soak feet for 10 minutes, particularly if you have
problems or fungal infections.
12. Vitamin supplement. This system works very well with 1,000 mcg (not
sublingual) of vitamin Bl 2, but not with multivitamins. It is a good idea to fast
one day a week, perform sensible exercise, and go to bed early, around 8 p.m.,
about twice a week.
12 of 13
6/21/00 12:1
Hygiene Systems To Improve Health
fiie:///D|/INFO FROM INTERNET/mercola-aiiergies,infection & stn
13. Please note: Cleaning the fingernails, nasal passageway, and eyes is very
complex. Do not use any other chemicals. Follow these instructions exactly.
Dr. Seaton's soap can be obtained in our office at a reduced rate or you can
contact the distributor directly.
Read this first | Subscribe to free newsletter | Current newsletters | Articles on wellness | Links to wellness | Search site |
Home | E-mail: Dr@Mercola.com
fl
“e b3S“! U.pon 1110 °p™ons of Dr. Mercola. Thev are not intended to replace a one-on-one relationship with a qualified health care
T in,^'U
KenlOl cani professional
J
.nd
Of
4
k .A
j?LS - I A *2-8
THE HIDDEN HAZARDS OF MICROWAVE
COOKING
by Anthony Wayne and Lawrence Newell
Is it possible that millions of people are ignorantly sacrificing their health in
exchange for the convenience of microwave ovens? Why did the Soviet
Union ban the use of microwave ovens in 1976? Who invented
microwave ovens, and why1? The answers to these questions may shock
you into throwing your microwave oven in the trash.
O’er 90% of American homes have microwave ovens used for meal
preparation. Because microwave ovens are so convenient and energy
efficient, as compar ed to conventional ovens, very' few homes or
restaurants are without them. In general, people believe that whatever a
microwave oven does to foods cooked in it doesn't have any negative
effect on either the food or them. Of course, if microwave ovens were
really' harmful, our government would never allow them on the market,
would they? Would they? Regardless of what has been "officially"
released concerning microwave ovens, we have personally stopped using
ours based on the research facts outlined in this article.
The purpose of this report is to show proof - evidence - that microwave
cooking is not natural, nor healthy, and is far more dangerous to the
human body than anyone could imagine. However, the microwave oven
manufacturers, Washington City politics, and plain old human nature are
suppressing the facts and evidence. Because of this, people are continuing
to microwave their food - in blissful ignorance - without knowing the
effects and danger of doing so.
How do microwave ovens work?
Microwaves are a form of electromagnetic energy, like light waves or
radio waves, and occupy a part of the electromagnetic spectrum of
power, or energy. Microwaves are very short waves of electromagnetic
energy that travel at the speed of light (186,282 miles per second). In our
modem technological age, microwaves are used to relay long distance
telephone signals, television programs, and computer information across
the earth or to a satellite in space. But the microwave is most familiar to us
as an energy source for cooking food.
Every microwave oven contains a magnetron, a tube in which electrons
are affected by magnetic and electric fields in such a way as to produce
micro wavelength radiation at about 2450 Mega Hertz (MHz) or 2.45
Giga Hertz (GHz). This microwave radiation interacts with the molecules
in food. All wave energy changes polarity from positive to negative with
each cycle of the wave. In microwaves, these polarity changes happen
millions of times every second. Food molecules - especially the molecules
of water-- have a positive and negative end in the same way a magnet has
a north and a south polarity.
In commercial models, the oven has a power input of about 1000 watts of
alternating current. As these microwaves generated from the magnetron
bombard the food, they cause the polar molecules to rotate at the same
frequency millions of times a second. All this agitation creates molecular
friction, which heats up the food. The friction also causes substantial
damage to the surrounding molecules, often tearing them apart or
i-
forcefully deforming them. The scientific name for this deformation is
"structural isomerism".
By comparison, microwaves from the sun are based on principles of
pulsed direct current (DC) that don't create frictional heat; microwave
ovens use alternating current (AC) creating frictional heat. A microwave
oven produces a spiked wavelength of energy with all the power going
into only one narrow frequency of the energy spectrum. Energy from the
sun operates in a wide frequency spectrum.
Many terms are used in describing electromagnetic waves, such as
wavelength, amplitude, cycle and frequency:
Wavelength determines the type of radiation,T.e. radio, X-ray,
ultraviolet, visible, infrared, etc.
Amplitude determines the extent of movement measured from the
starting point.
Cycle determines the unit of frequency, such as cycles per second,
Hertz, Hz, or cycles/second.
Frequency determines the number of occurrences within a given
time period (usually 1 second); The number of occurrences of a
recurring process per unit of time, i.e. the number of repetitions of
cycles per second.
Radiation = spreading energy with electromagnetic waves
Radiation, as defined by physics terminology, is "the electromagnetic
waves emitted by the atoms and molecules of a radioactive substance as a
result of nuclear decay," Radiation causes ionization, which is what occurs
when a neutral atom gains or loses electrons. In simpler terms, a
microwave oven decays and changes the molecular structure of the food
by the process of radiation. Had the manufacturers accurately called them
"radiation ovens", it's doubtful they would have ever sold one, but that's
exactly what a microwave oven is.
We’ve all been told that microwaving food is not the same as irradiating it
(radiation "treatment"). The two processes are supposed to use
completely different waves of energy and at different intensities. No FDA
or officially released government studies have proven current microwaving
usage to be harmful, but we all know that the validity of studies can be and are sometimes deliberately - limiting. Many of these studies are later
proven to be inaccurate. As consumers, we're supposed to have a certain
degree of common sense to use in judgment.
Take the example of eggs and how they were "proven" to be so harmful
to our health in the late 1960's. This brought about imitation egg products
and big profits for the manufacturers, while egg farms went broke. Now,
recent government sponsored studies are saying that eggs are not bad for
us after all. So, whom should we believe and what criteria should we use
to decide matters concerning our health? Since it's currently published that
microwaves - purportedly - don't leak into the environment, when
properly used and with approved design, the decision lies with each
consumer as to whether or not you choose to eat food heated by a
microwave oven or even purchase one in the first place.
Motherly instincts are right
On a more humorous side, the "sixth sense" every mother has is
impossible to argue with. Have you ever tried it? Children will never win
against a mother's intuition. It's like trying to argue with the arm appearing out of nowhere - that pinned you to the back of the seat when
your mother slammed on the brakes.
Many of us come from a generation where mothers and grandmothers
have distrusted the modem "inside out" cooking they claimed was "not
suitable" for most foods. My mother refused to even try baking anything in
a microwave. She also didn't like the way a cup of coffee tasted when
heated in a microwave oven. I have to fully agree and can't argue either
fact. Her own common sense and instincts told her that there was no way
microwave cooking could be natural nor make foods "taste they way
they're supposed to". Reluctantly, even my mother succumbed to
re-heating leftovers in a microwave due to her work schedule before she
retired.
Many others feel the same way, but they’re considered an "old fashioned"
minority dating back to before the 1970's when microwaves first
overwhelmed the market. Like most young adults at the time, as
microwave ovens became commonplace, I chose to ignore my mother's
intuitive wisdom and joined the majority who believed microwave cooking
was far too convenient to ever believe anything could be wrong with it.
Chalk one up for mom's perception, because even though she didn't know
the scientific, technical, or health reasons why, she just knew that
microwave ovens were not good based on how foods tasted when they
were cooked in them She didn't like the way the texture of the
microwaved food changed either.
Microwaves unsafe for baby's milk
A number of warnings have been made public, but have been barely
noticed. For example. Young Families, the Minnesota Extension Service
of the University of Minnesota, published the following in 1989:
"Although microwaves heat food quickly, they are not recommended for
heating a baby's bottle. The bottle may seem cool to the touch, but the
liquid inside may become extremely hot and could burn the baby's mouth
and throat. Also, the buildup of steam in a closed container, such as a
baby bottle, could cause it to explode. Heating the bottle in a microwave
can cause slight changes in the milk. In infant formulas, there may be a loss
of some vitamins. In expressed breast milk, some protective properties
may be destroyed. Warming a bottle by holding it under tap water, or by
setting it in a bowl of warm water, then testing it on your wrist before
feeding may take a few' minutes longer, but it is much safer."
Dr. Lita Lee of Hawaii reported in the December 9, 1989 Lancet:
"Microwaving baby formulas converted certain trans-amino acids into
their synthetic cis-isomers. Synthetic isomers, whether cis-amino acids or
trans-fatty acids, are not biologically active. Further, one of the amino
acids, L-proline, was converted to its d-isomer, which is known to be
neurotoxic (poisonous to the nervous system) and nephrotoxic (poisonous
to the kidneys). It's bad enough that many babies are not nursed, but now'
they are given fake milk (baby formula) made even more toxic via
microwaving."
Microwaved blood kills patient
In 1991, there was a lawsuit in Oklahoma concerning the hospital use of a
microwave oven to warm blood needed in a transfusion. The case
involved a hip surgery patient, Norma Levitt, who died from a simple
blood transfusion. It seems the nurse had warmed the blood in a
microwave oven. This tragedy makes it very apparent that there's much
more to "heating” with microwaves than we've been led to believe. Blood
for transfusions is routinely warmed, but not in microwave ovens. In the
case of Mrs. Levitt, the microwaving altered the blood and it killed her.
It's veiy obvious that this form of microwave radiation "heating" does
something to the substances it heats. It's also becoming quite apparent that
people who process food in a microwave oven are also ingesting these
"unknowns".
Because the body is electrochemical in nature, any force that disrupts or
changes human electrochemical events will affect the physiology of the
body. This is further described in Robert O. Becker's book, The Body
Electric, and in Ellen Sugarman's book, Warning, the Electricity Around
You May Be Hazardous to Your Health.
Scientific evidence and facts
In Comparative Study of Food Prepared Conventionally and in the
Microwave Oven, published by Raum & Zelt in 1992, at 3(2): 43, it
states
"A basic hypothesis of natural medicine states that the introduction into the
human body of molecules and energies, to which it is not accustomed, is
much more likely to cause harm than good. Microwaved food contains
both molecules and energies not present in food cooked in the way
humans have been cooking food since the discovery of fire. Microwave
energy from the sun and other stars is direct current based. Artificially
produced microwaves, including those in ovens, are produced from
alternating current and force a billion or more polarity reversals per
second in every food molecule they hit. Production of unnatural molecules
is inevitable. Naturally occurring amino acids have been observed to
undergo isomeric changes (changes in shape morphing) as well as
transformation into toxic forms, under the impact of microwaves produced
in ovens.
One short-term study found significant and disturbing changes in the blood
of individuals consuming microwaved milk and vegetables. Eight
volunteers ate various combinations of the same foods cooked different
ways. All foods that were processed through the microwave ovens
caused changes in the blood of the volunteers. Hemoglobin levels
decreased and over all white cell levels and cholesterol levels increased.
Lymphocytes decreased.
Luminescent (light-emitting) bacteria were employed to detect energetic
changes in the blood. Significant increases were found in the luminescence
of these bacteria when exposed to blood serum obtained after the
consumption of microwaved food."
The Swiss clinical study
Dr. Hans Ulrich Hertel, who is now retired, worked as a food scientist for
many years with one of the major Swiss food companies that do business
on a global scale. A few years ago, he was fired from his job for
questioning certain processing procedures that denatured the food.
In 1991, he and a Lausanne University professor published a research
paper indicating that food cooked in microwave ovens could pose a
greater risk to health than food cooked by conventional means. An article
also appeared in issue 19 of the Journal Franz Weber in which it was
stated that the consumption of food cooked in microwave ovens had
cancerous effects on the blood. The research paper itself followed the
article. On the cover of the magazine there was a picture of the Grim
Reaper holding a microwave oven in one of his hands.
Dr. Hertel was the first scientist to conceive and carry out a quality clinical
study on the effects microwaved nutrients have on the blood and
physiology of the human body. His small but well controlled study showed
the degenerative force produced in microwave ovens and the food
processed in them. The scientific conclusion showed that microwave
cooking changed the nutrients in the food; and, changes took place in the
participants' blood that could cause deterioration in the human system.
Hertel's scientific study was done along with Dr. Bernard FI. Blanc of the
Swiss Federal Institute of Technology and the University Institute for
Biochemistry.
In intervals of two to five days, the volunteers in the study received one of
the following food variants on an empty stomach: (1) raw milk, (2) the
same milk conventionally cooked; (3) pasteurized milk; (4) the same raw
milks cooked in a microwave oven; (5) raw vegetables from an organic
farm; (6) the same vegetables cooked conventionally; (7) the same
vegetables frozen and defrosted in a microwave oven; and (8) the same
vegetables cooked in the microwave oven. Once the volunteers were
isolated, blood samples were taken from every volunteer immediately
before eating. Then, blood samples were taken at defined intervals after
eating from the above milk or vegetable preparations.
Significant changes were discovered in the blood samples from the
intervals following the foods cooked in the microwave oven. These
changes included a decrease in all hemoglobin and cholesterol values,
especially the ratio of HDL (good cholesterol) and LDL (bad cholesterol)
values. Lymphocytes (white blood cells) showed a more distinct
short-term decrease following the intake of microwaved food than after
the intake of all the other var iants. Each of these indicators pointed to
degeneration. Additionally, there was a highly significant association
between the amount of microwave energy in the test foods and the
luminous power of luminescent bacteria exposed to serum from test
persons who ate that food. This led Dr. Hertel to the conclusion that such
technically derived energies may, indeed, be passed along to man
inductively via eating microwaved food.
According to Dr. Hertel,
"Leukocytosis, which cannot be accounted for by normal daily deviations,
is taken very seriously by hemotologists. Leukocytes are often signs of
pathogenic effects on the living system, such as poisoning and cell
damage. The increase of leukocytes with the microwaved foods were
more pronounced than with all the other variants. It appears that these
marked increases were caused entirely by ingesting the microwaved
substances.
This process is based on physical principles and has already been
confirmed in the literature. The apparent additional energy exhibited by the
luminescent bacteria was merely an extra confirmation. There is extensive
scientific literature concerning the hazardous effects of direct microwave
radiation on living systems. It is astonishing, therefore, to realize how little
effort has been taken to replace this detrimental technique of microwaves
with technology more in accordance with nature. Technically produced
microwaves are based on the principle of alternating current. Atoms,
molecules, and cells hit by this hard electromagnetic radiation are forced
to reverse polarity 1-100 billion times a second. There are no atoms,
molecules or cells of any organic system able to withst and such a violent,
destructive power for any extended period of time, not even in the low
energy range of milliwatts
Of all the natural substances - which are polar - the oxygen of water
molecules reacts most sensitively. This is how microwave cooking heat is
generated - friction from this violence in water molecules. Structures of
molecules are tom apart, molecules are forcefully deformed, called
structural isomerism, and thus become impaired in quality. This is contrary
to conventional heating of food where heat transfers conventionally from
without to within. Cooking by microwaves begins within the cells and
molecules where water is present and where the energy is transformed
into frictional heat.
In addition to the violent frictional heat effects, called thermic effects, there
are also athermic effects which have hardly ever been taken into account.
These athermic effects are not presently measurable, but they can also
deform the structures of molecules and have qualitative consequences.
For example the weakening of cell membranes by microwaves is used in
the field of gene altering technology. Because of the force involved, the
cells are actually broken, thereby neutralizing the electrical potentials, the
very life of the cells, between the outer and inner side of the cell
membranes. Impaired cells become easy prey for viruses, fungi and other
microorganisms. The natural repair mechanisms are suppressed and cells
are forced to adapt to a state of energy emergency - they switch from
aerobic to anaerobic respiration. Instead of water and carbon dioxide, the
cell poisons hydrogen peroxide and carbon monoxide are produced."
The same violent deformations that occur in our bodies, when we are
directly exposed to radar or microwaves, also occur in the molecules of
foods cooked in a microwave oven. This radiation results in the
destruction and deformation of food molecules. Microwaving also creates
new compounds, called radiolytic compounds, which are unknown fusions
not found in nature. Radiolytic compounds are created by molecular
decomposition - decay - as a direct result of radiation.
Microwave oven manufacturers insist that microwaved and irradiated
foods do not have any significantly higher radiolytic compounds than do
broiled, baked or other conventionally cooked foods. The scientific
clinical evidence presented here has shown that this is simply a lie. In
America, neither universities nor the federal government have conducted
any tests concerning the effects on our bodies from eating microwaved
foods. Isn't that a bit odd? They're more concerned with studies on what
happens if the door on a micro wave oven doesn't close properly. Once
again, common sense tells us that their attention should be centered on
what happens to food cooked inside a microwave oven. Since people
ingest this altered food, shouldn't there be concern for how the same
decayed molecules will affect our own human biological cell structure?
Industry's action to hide the truth
.As soon as Doctors Hertel and Blanc published their results, the
authorities reacted. A powerful trade organization, the Swiss Association
of Dealers for Electro-apparatuses for Households and Industry, known
as FEA, struck swiftly in 1992 They forced the President of the Court of
Seftigen, Canton of Bern, to issue a "gag order" against Drs. Hertel and
Blanc. In March 1993, Dr. Hertel was convicted for "interfering with
commerce" and prohibited from further publishing his results. However.
Dr. Hertel stood his ground and fought this decision over the years.
Not long ago, this decision was reversed in a judgment delivered in
Strasbourg, Austria, on August 25, 1998. The European Court of Human
Rights held that there had been a violation of Hertel's rights in the 1993
decision. The European Court of Human Rights also ruled that the "gag
order" issued by the Swiss court in 1992 against Dr. Hertel, prohibiting
him from declaring that microwave ovens are dangerous to human health,
was contrary to the right to freedom of expression. In addition,
Switzerland was ordered to pay Dr. Hertel compensation.
Who invented microwave ovens?
The Nazis, for use in their mobile support operations, originally developed
microwave "radiomissor" cooking ovens to be used for the invasion of
Russia By being able to utilize electronic equipment for preparation of
meals on a mass scale, the logistical problem of cooking fuels would have
been eliminated, as well as the convenience of producing edible products
in a greatly reduced time-factor.
After the war, the Allies discovered medical research done by the
Germans on microwave ovens. These documents, along with some
working microwave ovens, were transferred to the United States War
Department and classified for reference and "further scientific
investigation." The Russians had also retrieved some microwave ovens
and now have thorough research on their biological effects. As a result,
their use was outlawed in the Soviet Union. The Soviets issued an
international warning on the health hazards, both biological and
environmental, of microwave ovens and similar frequency electronic
devices.
Other Eastern European scientists also reported the harmful effects of
microwave radiation and set up strict environmental limits for their usage.
The United States has not accepted the European reports of harmful
effects, even though the EPA estimates that radio frequency and
microwave radiation sources in America are increasing at 15% per year.
Carcinogens in microwaved food
In Dr. Lita Lee's book, Health Effects of Microwave Radiation Microwave Ovens, and in the March and September 1991 issues of
Earthletter, she stated that every microwave oven leaks electro-magnetic
radiation, harms food, and converts substances cooked in it to dangerous
organ-toxic and car cinogenic products. Further research summarized in
this article reveal that microwave ovens are far more harmful than
previously imagined.
The following is a summary of the Russian investigations published by the
Atlantis Raising Educational Center in Portland, Oregon. Carcinogens
were formed in virtually all foods tested. No test food was subjected to
more microwaving than necessary to accomplish the purpose, i.e.,
cooking, thawing, or heating to insure sanitary ingestion. Here's a
summary of some of the results:
Microwaving prepared meats sufficiently to insure sanitary ingestion
caused formation of d-Nitrosodienthanolamines. a well-known
carcinogen.
.Microwaving milk and cereal grains converted some of their amino
acids into carcinogens.
Thawing frozen fruits converted their glucoside and galactoside
containing fractions into carcinogenic substances.
Extremely short exposure of raw, cooked or frozen vegetables
converted their plant alkaloids into carcinogens.
Carcinogenic free radicals were formed in microwaved plants,
especially root vegetables.
Decrease in nutritional value
Russian researchers also reported a marked acceleration of
structural degradation leading to a decreased food value of 60 to
90% in all foods tested. Among the changes observed were:
Deceased bio-availability of vitamin B complex, vitamin C, vitamin
E, essential minerals and lipotropics factors in all food tested.
Various kinds of damaged to many plant substances, such as
alkaloids, glucosides, galactosides and nitrilosides.
The degradation of nucleo-proteins in meats.
Microwave sickness is discovered
The Russians did research on thousands of workers who had been
exposed to microwaves during the development of radar in the 1950's.
Their research showed health problems so serious that the Russians set
strict limits of 10 microwatts exposure for workers and one microwatt for
civilians.
In Robert O. Becker's book. The Body Electric, he described Russian
research on the health effects of microwave radiation, which they called
"microwave sickness." On page 314, Becker states:
"It's [Microwave sickness] first signs are low blood pressure and slow
-- • pulse. The later and most common manifestations are chronic excitation of
the sympathetic nervous system [stress syndrome] and high blood
pressure. This phase also often includes headache, dizziness, eye pain,
sleeplessness, irritability, anxiety, stomach pain, nervous tension, inability
to concentrate, hair loss, plus an increased incidence of appendicitis,
cataracts, reproductive problems, and cancer. The chronic symptoms are
eventually succeeded by crisis of adrenal exhaustion and ischemic heart
disease [the blockage of coronary arteries and heart attacks]."
According to Dr. Lee, changes are observed in the blood chemistries and
the rates of certain diseases among consumers of microwaved foods. The
symptoms above can easily be caused by the observations shown below.
The following is a sample of these changes:
Lymphatic disorders were observed, leading to decreased ability to
prevent certain types of cancers.
An increased rate of cancer cell formation was observed in the blood.
Increased rates of stomach and intestinal cancers were observed.
Higher rates of digestive disorders and a gradual breakdown of the
systems of elimination were observed.
Microwave research conclusions
The following were the most significant German and Russian research
operations facilities concerning the biological effects of microwaves:
The initial research conducted by the Germans during the Barbarossa
military campaign, at the Humbolt-Universitat zu Berlin (1942-1943); and,
From 1957 and up to the present [until the end of the cold war ], the
Russian research operations were conducted at: the Institute of Radio
Technology at Kinsk, Byelorussian Autonomous Region; and, at the
Institute of Radio Technology at Rajasthan in the Rossiskaja Autonomous
Region, both in the Union of the Soviet Socialist Republics.
In most cases, the foods used for research analysis were exposed to
microwave propagation at an energy potential of 100
kilowatts/cm3/second, to the point considered acceptable for sanitary,
normal ingestion. The effects noted by both German and Russian
researchers is presented in three categories:
Category' I, Cancer-Causing Effects
Category n, Nutritive Destraction of Foods
Category IB, Biological Effects of Exposure
CATEGORY I
CANCER-CAUSING EFFECTS
[The first two points of Category’ I are not readable from our report copy.
The remainder of the report is intact. J
3. Creation of a "binding effect" to radioactivity in the atmosphere, thus
causing a marked increase in the amount of alpha and beta particle
saturation in foods;
4. Creation of cancer causing agents within protein hydrolysate
*
compounds
in milk and cereal grains [*these are natural proteins that are
split into unnatural fragments by the addition of water];
5. Alteration of elemental food-substances, causing disorders in the
digestive system by unstable catabolism
*
of foods subjected to
microwaves [*the metabolic breakdown process];
6. Due to chemical alterations within food substances, malfunctions were
observed within the lymphatic systems [absorbent vessels], causing a
degeneration of the immune potentials of the body to protect against
certain forms of neoplasties [abnormal growths of tissue];
7. Ingestion of microwaved foods caused a higher percentage of
cancerous cells within the blood serum [cytomas - cell tumors such as
sarcoma];
8. Microwave emissions caused alteration in the catabolic [metabolic
breakdown] behavior of giucoside [hydrolyzed dextrose] and galactoside
[oxidized alcohol] elements within frozen fruits when thawed in this
manner;
9. Microwave emission caused alteration of the catabolic [metabolic
breakdown] behavior of plant alkaloids [organic nitrogen based elements]
when raw, cooked, or frozen vegetables were exposed for even
extremely short durations;
10. Cancer causing free radicals [highly reactive incomplete molecules]
were formed within certain trace mineral molecular formations in plant
substances, and in particular, raw root-vegetables; and,
11 In a statistically high percentage of persons, microwaved foods
caused stomach and intestinal cancerous growths, as well as a general
degeneration of peripheral cellular tissues, with a gradual breakdown of
the function of the digestive and excretive systems.
CATEGORY II
DECREASE IN FOOD VALUE
Microwave exposure caused significant decreases in the nutritive value of
all foods researched. The following are the most important findings:
I. A decrease in the bioavailability [capability of the body to utilize the
nutriment] of B-complex vitamins, Vitamin C, Vitamin E, essential
minerals and lipotropics in all foods;
2. A loss of 60-90% of the vital energy field content of all tested foods;
3. A reduction in the metabolic behavior and integration process capability'
of alkaloids [organic nitrogen based elements], glucosides and
galactosides, and nitrilosides;
4.
A destruction of the nutritive value of nucleoproteins in meats;
5.
A marked acceleration of structural disintegration in all foods.
CATEGORY HI
BIOLOGICAL EFFECTS OF EXPOSURE
Exposure to microwave emissions also had an unpredictably negative
effect upon the general biological welfare of humans. This was not
discovered until the Russians experimented with highly sophisticated
equipment and discovered that a human did not even need to ingest the
material substance of the microwaved food substances: that even
exposure to the energy-field itself was sufficient to cause such adverse
side effects that the use of any such microwave apparatus was forbidden
in 1976 by Soviet state law.
The following are the enumerated effects:
1. A breakdown of the human "life-energy field" in those who were
exposed to microwave ovens while in operation, with side-effects to the
human energy field of increasingly longer duration;
2. A degeneration of the cellular voltage parallels during the process of
using the apparatus, especially in the blood and lymphatic areas;
3. A degeneration and destabilization of the external energy activated
potentials of food utilization within the processes of human metabolism;
4. A degeneration and destabilization of internal cellular membrane
potentials while transferring catabolic [metabolic breakdown] processes
into the blood serum from the digestive process;
5. Degeneration and circuit breakdowns of electrical nerve impulses within
the junction potentials of the cerebrum [the front portion of the brain
where thought and higher functions reside];
6. A degeneration and breakdown of nerve electrical circuits and loss of
energy field symmetry in the neuroplexuses [nerve centers] both in the
front and the rear of the central and autonomic nervous systems;
7. Loss of balance and circuiting of the bioelectric strengths within the
ascending reticular activating system [the system which controls the
function of consciousness];
8. A long term cumulative loss of vital energies within humans, animals and
plants that were located within a 500-meter radius of the operational
equipment;
9. Long lasting residual effects of magnetic "deposits" were located
throughout the nervous system and lymphatic system;
10. A destabilization and interruption in the production of hormones and
maintenance of hormonal balance in males and females;
11. Markedly higher levels of brainwave disturbance in the alpha, theta,
and delta wave signal patterns of persons exposed to microwave emission
fields, and;
12. Because of this brainwave disturbance, negative psychological effects
were noted, including loss of memory, loss of ability to concentrate,
suppressed emotional threshold, deceleration of intellective processes,
and interruptive sleep episodes in a statistically higher percentage of
individuals subjected to continual range emissive field effects of
microwave apparatus, either in cooking apparatus or in transmission
stations.
Forensic Research Conclusions
From the twenty-eight above enumerated indications, the use of
microwave apparatus is definitely not advisable; and, with the decision of
the Soviet government in 1976, present scientific opinion in many
countries concerning the use of such apparatus is clearly in evidence.
Due to the problem of random magnetic residulation and binding within
the biological systems of the body (Category HI:9), which can ultimately
effect the neurological systems, primarily the brain and neuroplexuses
(nerve centers), long term depolarization of tissue neuroelectric circuits
can result. Because these effects can cause virtually irreversible damage to
the neuroelectrical integrity of the various components of the nervous
system (I. R. Luria, Novosibirsk 1975a), ingestion of microwaved foods
is clearly contraindicated in all respects. Their magnetic residual effect can
render the pyschoneural receptor components of the brain more subject
to influence psychologically by artificially induced microwave radio
frequency fields from transmission stations and TV relay-networks.
The theoretical possibility of psycho telemetric influence (the capability of
affecting human behavior by transmitted radio signals at controlled
frequencies) has been suggested by Soviet neuropsychological
investigations at Uralyera and Novosibirsk (Luria and Perov, 1974a,
1975c, 1976a), which can cause involuntary subliminal psychological
energy field compliance to operative microwave apparatus.
FORENSIC RESEARCH DOCUMENT
Prepared By: William P. Kopp
A. R. E. C. Research Operations
T061-7R10/10-77F05
RELEASE PRIORITY: CLASS I ROOIa
'
Ten Reasons to Throw out your Microwave Oven
From the conclusions of the Swiss, Russian and German scientific clinical
studies, we can no longer ignore the microwave oven sitting in our
kitchens. Based on this research, we will conclude this article with the
following:
. Continually eating food processed from a microwave oven causes long
1)
term - permanent - brain damage by "shorting out" electrical impulses in
the brain [de-polarizing or de-magnetizing the brain tissue],
.2) The human body cannot metabolize [break down] the unknown
by-products created in microwaved food.
.3) Male and female hormone production is shut down and/or altered by
continually eating microwaved foods.
.4) The effects of microwaved food by-products are residual [long term,
permanent] within the human body.
. Minerals, vitamins, and nutrients of all microwaved food is reduced or
5)
altered so that the human body gets little or no benefit, or the human body
absorbs altered compounds that cannot be broken down.
.6) The minerals in vegetables are altered into cancerous free radicals
when cooked in microwave ovens.
.7) Microwaved foods cause stomach and intestinal cancerous growths
[tumors]. This may explain the rapidly increased rate of colon cancer in
America.
.8) The prolonged eating of microwaved foods causes cancerous cells to
increase in human blood.
.9) Continual ingestion of microwaved food causes immune system
deficiencies through lymph gland and blood serum alterations.
. Eating microwaved food causes loss of memory, concentration,
10)
emotional instability, and a decrease of intelligence.
Have you tossed out your microwave oven yet?
The use of artificial microwave transmissions for subliminal psychological
control, a.k.a. "brainwashing", has also been proven. We're attempting to
obtain copies of the 1970's Russian research documents and results
written by Drs. Luria and Perov specifying their clinical experiments in this
area.
Click here for another article on Microwave Cooking
Read this first j Subscribe to free newsletter | Current newsletters | Articles on wellness | Links to wellness I
Search site | Home | E-mail: Dr@Mercola.com
Disclaimer - Newsletters are based upon the opinions of Dr. Mercola. They are not intended to replace a
one-on-one relationship with a qualified
health care professional and they are not intended as medical advice. They are intended as a sharing of
knowledge and information from the research
and experience of Dr. Mercola and his community. Dr. Mercola encourages you to make your own health
care decisions based upon your research and
in partnership with a qualified health care professional.
BROCCOLI SPROUTS
Small quantities of fresh broccoli sprouts contain as much
cancer protection as larger amounts of the mature vegetable
sold in food markets, according to researchers at Johns
Hopkins University. Just 5 grams (0.17 ounces) of sprouts
contain concentrations of the compound glucoraphanin equal to
that found in 150 grams (5.2 ounces) of mature broccoli. The
compound is a precursor to sulforaphane, proven in animal
studies to boost cell enzymes that protect against molecular
damage from cancer-causing chemicals.
Sulforaphane has been shown to mobilize, or induce, the body's
natural cancer protection resources and help reduce the risk of
malignancy. Broccoli is the best source of the chemical
precursor to sulforaphane — glucoraphanin. Now, broccoli
sprouts are an ''exceptionally rich source" of inducers of cellular
enzymes for "detoxifying" chemical carcinogens -- cancer
causing compounds. Some of these compounds are potent
enhancers of phase 2 enzymes, which speed the detoxication
of electrophiles and reactive oxygen metabolites. Therefore,
they say, induction of phase 2 enzymes by these compounds
can "...protect cells against mutagenesis and neoplasia."
The researchers attempted to calculate how much broccoli one
would have to eat in order to produce a significant degree of
protection against cancer, based on epidemiologic evidence.
They found that one would have to eat about two pounds of an
average broccoli a week in order to reduce, say, one's risk of
colon cancer by about 50%.
An additional complication is that it is impossible to determine
by the looks of this cruciferous vegetable alone or even with
knowledge of how and where it was grown whether you are
buying the 'high-inducer' or 'low-inducer' broccoli. The
enzyme-inducing abilities of samples taken from 22 varieties of
fresh and 7 brands of frozen mature broccoli vary greatly. Only
concentrations.
But fresh broccoli sprouts offer an alternative. One can get
away with eating 10 to 100 times lower quantities. Three day
old sprouts have the additional advantage that they're far more
uniform in their potency. Broccoli sprouts look and taste
something like alfalfa sprouts, according to the researchers.
The report also notes that small quantities of broccoli sprout
extracts markedly reduced the size of rat mammary tumors that
were induced by chemical carcinogens.
The researchers refer to the concept of "chemoprotection" —
deliberate efforts to increase the body's own defense
mechanisms to reduce susceptibility to carcinogens by
administration of substances that can be precisely identified,
and ideally, delivered in the diet. The interesting aspect of
chemoprotection strategies is that they’re almost never
organ-specific. Chemoprotection produces a general cancer
protective effect which blocks multiple steps - a cascade of
steps — that are common to cancer formation.
INSIGHT: At the present time, broccoli sprouts are not being
grown commercially. However you can grow them yourself quite
easily. You can purchase organic broccoli seeds from Johnny's
at 207-437-4301. Item number 148, four ounces are $9.00 or a
pound for $12.00. Non-organic seeds can probably be
purchased through farm supply stores or other seed catalogs.
You can also call Jaffe Brothers at 619-749-1133 for
instructions on how to sprout. They also sell sprouting lids to
apply to Ball jars which make the entire process quite
convenient. The library or health food store may also have some
instructions on sprouting seeds.
A small amount of spouts go a long way. A pound of sprouts will
probably make over ten pounds of sprouts which from the
researchers calculations translates up to as much cancer
protecting phytochemicals as 1000 pounds (half a ton) of
broccoli! The other major benefit is that the sprouts don't smell
as you don't have to cook them. They are eaten raw, usually as
an addition to salad. I have already ordered my sprouts. I
suspect that there are similar benefits for many of the other
vegetables when eaten as sprouts. From the Proceedings of
the National Academy of Sciences (1997;94:10367-10372)
Sprouting Instructions:
Sprouting Time 5-7 days Temperatures 60-80
Yield 1 Tbs seed=l-l 1/2 cups sprouts
Place seeds in the jar and cover with cheesecloth or other
porous material. Secure the cloth with a rubber band. Fill the jar
full with filtered -water and let soak overnight. In the morning
drain off the water. The cloth will keep the seeds in the jar.
Rinse seeds with water again and let drain. You can also use
reusable plastic sprouting lids (available from Jaffe Brothers at
619-749-1133) which attach to Ball jars. This avoids having to
use new cheesecloth each time. Put the container on its side in
a dark location that stays about 70 degrees. Rinse twice each
day with water and drain. Continue the rinse cycle until
harvested. When sprouts are 1-2 inches long you can put them
in the light to green them up. You can rinse out the hulls or skim
them of the top of the water with a spoon. They are not harmful
to eat but removing them minimizes spoilage when sprouts are
stored. Sprouts are best stored in an airtight container in the
refrigerator and keep for about one week.
Read this first | Subscribe to free newsletter | Current newsletters | Articles on wellness | Links to wellness |
Search site | Home | E-mail: Dr@Mercola.com
Disclaimer - Newsletters are based upon the opinions of Dr. Mercola. They are not intended to replace a
one-on-one relationship with a qualified health care professional and they are not intended as medical
advice. They are intended as a shar ing of knowledge and information from the research and experience of
Dr. Mercola and his community. Dr. Mercola encourages you to make your own health care decisions
based upon your research and in partnership with a qualified health care professional.
Free Newsletter
Read this first
Carbohydrates
Lower Your Grains and lower your insulin levels.
Over the past fifteen years, our dietary establishment has
made a virtual industry of extolling the virtues of carbohydrates.
We're constantly told that carbohydrates are the good guys of
nutrition, and that, if we eat large amounts of them, the world
should be a better place. In such a world, the experts tell us,
there will be no heart disease and no obesity. Under such
guidance, Americans are gobbling breads, cereals, and
pastas as if there were no tomorrow, trying desperately to
reach that 80 to 85 percent of total calories advocated by the
high-carb extremists.
Scientific Evidence of the value of eating few grains
Unfortunately, the debate over the validity of this concept has
primarily been waged in the media and lay publications and
not in the scientific journals. Many of the popular books which
support this position are gimmicky, and often, lack adequate
scientific referencing. Yet, at their core is very important
concept - limiting the intake of carbohydrates, (especially as
cereal grains and starches), will improve human health.
Read this first | Subscribe to free newsletter | Current newsletters | Articles on wellness | Links to wellness |
Search site | Home | E-mail: Dr@Mercola.com
Disclaimer - Newsletters are based upon the opinions of Dr. Mercola. They are not intended to replace a
one-on-one relationship with a qualified
health care professional and they are not intended as medical advice. They are intended as a sharing of
knowledge and information from the research
and experience of Dr. Mercola and his community. Dr. Mercola encourages you to make your own health
care decisions based upon your research and
in partnership with a qualified health care professional.
< "WST'TUTIOfJ.V. f KINDISSASzs
'CONSTTTUTT INA7. S JN DISEASES
Constitutional skin diseases is a common problem.
Left untreated these idseases have a tendency to be chronic.
Often infection enters due to scaratching or due to medications
producing nus discharge and swelling of the affected part.
Usual1y the patient goes from doctor to doctor and
switch from one system of medicine to another.
gets reTief for varying periods of time.
Often patient
The Ahief reason
for their persistence is because the affected person doesn't
understand why these skin diseases occur.
Basically these types of skin diseases are constitutional
and the person is bom with a tendency to develop it.
But
only a small percentage of the oeoal.e who has this tendency
actualTy develop the skin disease and only in a minority it
persist and becomes troublesome.
Some of the factors which aggravate or precipitate
these conditions are dry skin, climate, working enviormment
and psycho'ogical stress.
Psychological factors usually
mean person's inabi1ity to adjust well with his enviornment
which’inc1udes family, friends, work, finances etc.
Very often persons who suffer from chronic skin diseases
become suspicions that they have certain diseases like
cancer, V.D., leprosy, leucoderma etc.
Though a competent
doctor can easily recognise these conditions, he may ask
for some investigationsto confirm, but more often to reassure
the patient.
One of the major symptom associated with constitutional
skin disease is itching.
Scratching is socially embarrasing
and the patient feels very conscious and guilty about it.
tc.
Itching is an into1erblesymotom and the patient scratches
so that the sensation gets converted to tolerable pain or
burning.
Repeated scratching produces skin damage and allow
the skin to become thick and dark.
The nerves underneath
the skin will become irritable and produces Itching on
slight
^revocation.
The best stimulus for itching is
scratching itself and the ■ kin wit1 be irritable for quite
sometime after a lout of scratching.
So unless the scratching
stops the skin disease will always be present.
-2-
Often the person touches the affected part without
his knowledge.
Once an irritable area is touched the area
bcomes very itchy and the person will have to scratch.
Most
of the time the affected area is touched as a matter of habit,
usually when the person is immersed in some mental activity
like reading or thinking,
(Usually long spells of regretting
£he past or worrying about the future).
If the person can ask someone to remind him frequently
he wij.1 be aware of the habit.
Then he could prevent the
itching by applying the prescribed medications and doing
something more active like going for a walk etc.
Sometimes
th- person realises this too late and will be forced to
scratch.
But such episodes will become rarer and stoo if he
concentrates on his problem.
The medications are to reduce the itching.
But medications
cannot help the patient unless the patient understands the
effect of scratching and makes an effort to avoid it.
Applying
the prescribed ointment 10-15 minutes before the usual times
•of itching, eg: after undressing, bed time, etc will help
to reduce the itching.
The person must make very effort to
achieve a cure at the shortest possible time.
As mentioned earlier the person with constitutional skin
diseases has the tendency to get them.
So even after a cure
it is important to avoid the provocating factors which produces
the disease.
If relapse actually takes place it is better
to take treatment again as early as oossible.
n|s ' /a- so
di.(,
i.
LEUCODERMA (VITILIGO)
Leucoderma'is a common skin disease.
It produces white,
patches due to loss of colour producing substance known as melanin.
The exact nature of the disease is still not known.
It is not contagious and usually produces no health problems
except for the appearance.
It has nothing to do with leprosy.
In
India it is definitely a social disease since many believe that
leucorderraa is contagious and is a form of leprosy.
The effect of treatment vary.
In majority very satisfactory
results can be obtained if treatment is taken regularly.
Leucoderma is unpredictable in its course.
It can appear &t
almost any age.
Only a small percentage of the patients get wide
spread patches.
In the majority, the patches are confined to the
covered parts of the body and in such cases doctors rarely recommend
treatment unless the patient is very anxious.
It is important to remember that even after a complete clearance
the white patches can come back any time, and the patient may
have to take the treatment again.
The usual treatment recommended involves exposing the patches
to sunlight after giving local or internal medication.
The ideal
time for the treatment is when the sunlight is brightest ie.
between 10 AM and b- PM.
The following precautions are necessary
while taking the treatment.
1. STRICTLY adhere to the recommended duration of sun
exposure.
Over exposure can produce severe reactions.
Under exposure will delay the response.
2.
Not to exceed the time limit even if the sun is
not very bright for example on a cloudy day.
3.
The patches must be covered to protect them from
sunlight if patient is going out in the sun on the
same day.
M-. Protect the eyes either by covering or with dark
glasses during sun exposure.
J. If any reaction like itching, burning pain or
blister formation occurs, STOP the treatment
and
contact the doctor as early as possible.
COMMON EJJ-E.4 — S S
. .2. .
COMM ON E -\LDN e ss
Common Baldness or loosing hair during adulthood is a
universal problem.
This tendency is purely hereditry and procur
produced by the influence of hormones by certain glands
in the body which becomes active after the perosn becomes
matri^e. (Puberty) .
puberty.
So common baldness starts only after
Though the glands and the hormones are normal the
effect on the hair roots is different in different individuals
and is purely hereditary.
But hereditary factors does not
manifest like a mirror image of the parents.
Often a wide
variations are observed and sometimes the genes carrying the
trait can even skip generations.
in common baldness which affects every one, some of the
hairs which enter the resting phase are not replaced.
The
percentage of the hair could be so low that some will never
have noticable hair loss.
But on the other hand there are
people with strong hereditary tendency to lose hair rapidly
and become almost totally bald in their twenties.
The common baldness follows certain well defined patterns 1'
in men.
But in women it is more diffuse, and obvious thinning
confined to certian areas of the scalp is rare but seen
occassionally.
Since dandruff occurs only on hairy areas and spares
bald areas many will think dandruff is the cause of baldness
which is not true.
TREATMENT
Since common baldness is a physiological response to the
sex hormones, at present there is no modality which will arrest
Removal of the glands (Castration) will certainly
this process.
arrest the further hair loss but obviously cannot be recommended.
Hi_br transplantation gives satisfactory results if done
by experts.
This is very expensive and time consuming.
Well fitting wigs
good remedy for many.
A new drug -
MINOXIDIL is under investigation-.and also being marketted in
United States,
will have to wait and watch about its safety
and effectiveness in common baldness.
cont..3 ..
NORMAL Hair growth
and
common
dai.dness
The hair goes through a cycle known as hair cycle.
These are :
1.
Growing Phase
(ANAGEN);
i -D-dring this phase the hair ’grows continously.
growth rate for scalp hair is about 1 cm/month.
The
The length
of the hair depends on the length of the growing phase which
is largely determined by heredity.
This varies from few months
to sometimes 20 to .30 years.>. which .ej^plaibs ,w))y- some, have .'vcf
*
unusually
long hair .
Du.r^g^,th^.gppwing\p}ias.e.r if ..the. hairJ s;w
is pulled, out,- h.air ropt .will.;te, bal.cK.ifP..- cplpur.. -r
2..
Resting•.Phase> ;(TEL'CG.EN)i-£.w
ew »t>J;~ .0. badinU
s>vp<f
sebnt-r.6'1 sc-mov.n!: ■
:svx ha: i~j fc:.;s
During this phase the root degenerates slowly and become
loose at „-£he attachr'nt.
This last for 1-2 months.
Towards
the end of this phase the hair can be pulled out with gentle
pressure.
The hair root will be white in colour.
About
2O?( of the scalp hair will be in resting phase at any given
time.
3.
Falling Phase (CATAGEN)
During this phase a new hair start growing from the
bottom of the. hair, root to replace the old hair.
fal's off.
Old.hair
The hair is pushed out by the new hair which
takes its place,. . r
This is the normal;hair cycle.
■■
•
- .
-
■
iirf j
The ■ following points aj
are note worthy.
1.
During falling phase hair will come out naturally without
using any force - This should not be taken as loosing hair..
2.
With moderate force the hair in'the resting phase will
come out easily.
seem to fall.
3.
That is why during combing,lot of hair is
-
Usually most of the scalp hair comes out during bath.
is why people who take bath less often complain that they
loose more hair while taking bath,since the accumulated
number of hair is in the resting phase will come out while
putting pressure on the scalp h'air.
4.
People who have thick hair notice more hair coming out
since pr^potionately more hair enter the resting phase
for them.
cont.
That
COMMON BALDN-1SS
COMMON BALDNESS
Common Baldness or loosing hair during adulthood is a '
universal problem.
This tendency is purely hereditry and nfocr
produced by the influence of hormones by certain g.l ands
in the body which becomes active after the perosn becomes
matri^e. (Puberty) .
So common baldness starts only after
Though the glands and the hormones are normal the
puberty.
effect on the hair roots is different in different individuals
and is purely hereditary.
Put hereditary factors does not
manifest like a mirror image of the parents.
Often a wide
variations are observed and sometimes the genes carrying the
trait can even skip generations.
In common baldness which affects every one, some of the
hairs which enter the resting phase are not replaced.
The
percentage of the hair could be so low that some will never
have noticable hair loss.
But on the other hand ttere are
people with strong hereditary tendency to lose hair rapidly
and become almost totally bald in their twenties.
The common baldness follows certain well defined patterns i>
in men.
But in women it is more diffuse, and obvious thinning
confined to certian areas of the scalp is rare but seen
occassionall y.
Since dandruff occurs only on hairy areas and spares
bald areas many will think dandruff is the cause of baldness
which is not true.
TREATMENT
Since common baldness is a physiological response to the
sex hormones, at present there is no modality which will arrest
this process.
Removal of the glands
(Castration) will certainly
arrest the further hair loss but obviously cannot be recommended.
Hifer transplantation
a»t<
------- ■-
-
- I P>~ 3 2-
PSORIASIS
Psoriasis is a very common skin disorder.
About 1-3% of the people
all over the world irrespective of country and race suffer from Psoriasis.
Posriasis is NOT CONTAGIOUS to others and usually does not affect the
perosn's health.
Psoriasis usually affects the skin and occassionally the nails and
very rarely the joints. ' On skin it manifests as scaly patches.; Sometimes
only the soles or palms are affeteted where it is seen as scaly.patches and
cracks-which bleeds often.
Itching is usually mild in Psoriasis.
But in
some it can be severe and disturbing and aggravated by physical and emotional
stress.
Pboriasis has no relationship with food and the effect of certian food
on Psoriasis is only coincidental.
A
.
..
•
'
Psoriasis is due to the production of excessive skin which is shed as
scales.
The basic cause of this, excessive skin production, occuring only
in certain individuals is not known yet.
Extensive reasoarch is going on
all over the world,about Psoriasis.
Psoriasis is unpredictable in its course.
Natural appearance and
disappearance are observed, sometimes even without any medications.
Sometimes the disease clear for many years.
Some patients observe remarkable
improvement and sometimes total clearance of Psoriasis during certian
seasons particularly either in summer ar in winter.
Appearance of Psoriatic patients on the sites of injury is a common
occurar.ce.
This also happen whereever patient scraches.
So it is
important to avoid injuries and avoid scratching.
Various medications are aval 1 ahie for the treatment of Psoriasis.
Though a guaranteed cure even after the stoppage of treatment is not available
at present, in most patients satisfactory clearance of Psoriasis can be achieved
with s;r. pie treatment.
The type of treatment recomended varies according to the severity of
the disease, associated symptoms like itching, the location of the patches}
patient's occupation, social needs etc.
be
Often various modalities, of medicines have to/tried before coming to
the conclusion of what suits one individual patient.
Some of the very effective medications are also sometimes inconvenient,
expensive or toxic, so
is usually reserved for people with severe disease
(eg.PVUA, Methotrexate, Oral Retinoids etc).
Such treatment should be taken
only under strict medical supervision.
cont..2..
.2..
froriasis being a chronic skin disease produces much social and
those..;...
psychological problems. It is observed thajt/wno have well adjusted
personal and professional lives accept the disease and the treatment better.
The following points should be noted in regard to the treatment
(a)
For best results apply the ointment immediately after bath-
(b)
The ointment should be gently rubbed into the Skin.
.(c)
AU ointment should be applied to the minimum to sensitive areas
After
application ointment should not be present on the skin.
like face, armpits, joints, between fingers etc.
(d)« Areas like palms and soles where thick patches produces cracks
*
soaking the parts in warm water for 10-30 minutes before applying
the ointment will be useful for faster relief.’
(e)
The ointment should be apjblied only to all scaly patches old and
new and not to the healed patches with only colour change.
7)lo -
ATOPIC DERMATITIS
Atopic dermatitis (infantile Eczema) is a constitutional
type of skin disease.
It is not contagious to others.
The skin
is very itchy and the child scratches and the disease is the
result of the scratching.
Sometimes large areas of the body
can be affected.
The disease is unpredictable in its behaviour.
Though most
children are free of the disease by the age of 1 year, many many
continue to have the disease for a long period.
Till the disease
disappear on its own it has to be kept at under control.
The following measures are very useful.
tie the childs hands to prevent him/her from
1. Never
*
scratching.
When the child scratches a lot take him and hold
close to your body and talk to him.
Divert his attention.
Gently
rub the area where he was scratching.
2.
Many children have secere bouts of scratching when they
feel insecure.
For eg. when parents have a fight.
Try to
avoid such situations.
3.
Breast feeding the child is a good practice.
It gives
the child a sense of security in addition to all the advantages
of breast feeding.
7.
Your child’s skin is usually dry because of this disease,
It is likely to become worse in a place like Bangalore where the
climate is very dry.
The following measures will help to
reduce the dryness.
a. use minimum amount of soaps and detergents for bathing.
Even better, avoid soap completely.
Gram flour is better.
(Bengal gram or green gram)
b. Immediately after bath when the skin is wet smear a
vegetable oil (coconut oil, olive oil etc) or cold cream
generously all over the body.
The effect will be much less
if applied when the skin is dry.
5.
To cut the nails once in 3 days.
It will be easier
if it is done after bath.
6.
Avoid putting woollen and other rough clothes directly
over the skin.
It will irritate the skin.
. . .2. . .
2
7.
Accept the condition and avoid indulging in long discussion
with friends and relatives about the disease in the presence of
the child.
8.
The child should never be allowed to feel less acceptable
or lovable because of the disease..
It is quite possible that
child will have problems of being accepted by others outside the
house.
9.
But non acceptance in the home will have much worse effect.
Managing a child with atopic dermatitis is not easy.
Good understanding between the parents is essential.
The
temptation of blaming each other for the childs plight should
be avoided.
10.
The medication should be correctly used.
Often more than
what is required is used to produce severe side effects and toxic
effects.
The medication shuuls be used just enought for the
satisfactory control of the disease.
11.
Stop using the ointment once the child develop painful
boils or pus filled boils.
12.
rarely.
Ointment will make the infection worse.
Well managed children will only require medical attention
But never hesitate to consult the doctor.
Doctor is
primarily meant to reassure you and help you to manage better.
J2I-3 - /«-3s
DRY SKIN
The skin problems directly or indirectly due to dry skin
are very common.
The following factors contribute to this condition:
1. Situate: Dry skin is common in a place like Bangalore
where the atmospheric humidity is low throughout the year.
In
addition the dryness of the air becomes more pronounced during
the winter months (November to March ') .
2. Heridity;
Dry skin runs in families and heriditary influence is
pronounced.
3.
Age;
Dry skin becomes worse with increasing age.
Once a person
gets symptoms due to dry skin it can only becomes worse without
treatment year after year.
The dry skin can produce symptoms by itself or it makes many
skin diseases worse.
Treatment ■■
The skin is dry because of lack of moisture.
So unless the
skin is made to retain more water dry.skin will remain.
The most important step is to hydrate the skin.
This can be
done by soaking the body in water for a long time (water tub or
long bath).
Before tne water is allowed to dry apply a vegetable
oil or vaseline to all dry areas of tne body.
The oil has to be
rubbed into the skin, preferably after mixing with a small amount cf
water.
If done correctly the oil will enter the skin rapidly.
(if
applied on a dry skin tne oil will not enter the skin and will
dirty the clothes).
A little amount of Talcum powder can be used to remove the
oily appearance on areas like face and neck.
If any ointment is prescribed for tne associated skin disease,
this can be applied over the skin, after applying the oil or
vaseline.
Soap Soap and detergents should be used to the minimum by people
who suffer from dry skin.
Soaps with high alkali content and
medicated soaps should be avoided.
Gram flour , (eg green gram or
ben ;al gram) is a good substitute for soaps.
The problems associated with dry skin are part of the
person's skin and so cannot be cured, but only be controlled.
After few visits to tne doctor for guidance the patient snould
know how to manage the skin throughout the year.
■
1
High mortality despite good care-seeking
behaviour: a community study of childhood
deaths in Guinea-Bissau
M. Sodemann,*1 M.S. Jakobsen,1 K. Molbak,2 I.C. Alvarenga Jr.,3 & P. Aaby4
The care-seeking behaviour of mothers of 125 children deceased aged 1-30 months was investigated by
verbal autopsy in an urban area of Guinea-Bissau. A total of 93% of the children were seen at a health centre
or hospital during the 2 weeks before death. In a previous survey covering the period 1987-90 we found that
78% of the children who died had presented for consultation (8); despite this increase in care seeking, infant
j&rtality had not decreased. Comparison of elapsed time from disease onset to first consultation between
^pdren who died and matched surviving controls indicated that the interval was shorter for children who died
man for those who survived (odds ratio (OR) = 0.7; 95% confidence interval (Cl): 0.5-0.99). Of the 125
terminally ill children, 56 were hospitalized. A total of 20 children died on the way to hospital or while waiting
in the outpatient clinic. Lack of hospital beds resulted in 15 mothers being refused hospitalization for their
child. Of hospitalized children. 42% were discharged as improved or recovered during the 30 days preceding
death. These results reveal a need for improved hospital admission criteria, improved recognition of the
symptoms of serious illness, better discharge criteria, and the implementation of quality assurance systems
for health services.
Introduction
Many studies have reported a significant decrease in
child mortality following general improvements in
primary health care (PHC) (J. 2). Such decreases are
mainly the result of improvements in antenatal care
and vaccination coverage: the effect of diarrhoeal
disease programmes is less unequivocal. However, as
vaccines and antenatal care cannot entirely eradicate
the problem of excess childhood mortality in devel
oping countries, better case management of severely
ill children is clearly needed.
Improvements in the management of severely ill
children are often based on audits of case histories
with fatal outcomes (3). However, few studies in
developing countries have investigated care-seeking
l^haviour prior to death in serious childhood illness
^Bder to improve case management (4-6). Mortal
1 Department of Epidemiology and Social Medicine, Universily ol
Aamus. Hoegh-Guldbergsgade 10, DK-8000 Aarhus C. Denmark;
and Danish Epidemiology Science Centre. Statens Seruminstitut.
Copenhagen, Denmark. Requests for reprints should be sent to Dr
Sooemann at the former address.
1 Danish Epidemiology Science Centre, Statens Seruminstitut.
ity surveys have found large variations in the propor
tion of children seen at a health facility before dying
(7-10). It is important to explain why mortality re
mains high among under-5-year-olds in settings with
easy access to health care facilities. For example, in a
rural area of the Gambia, where 80% of children
were fully immunized and PHC programmes had
been active for 10 years, infant mortality was still
120 per 1000 live births in 1990 (11). In the Bandim
suburb of Bissau. Guinea-Bissau, we previously re
ported that the infant mortality was 94 per 1000 and
under-5-year-old mortality 215 per 1000. despite the
presence of two health centres, a mother-and-child
health clinic and an outpatient clinic (3).
We conducted the present study on patterns of
care-seeking behaviour prior to a child's death to
investigate child mortality on the basis of the moth
er’s experience The aim was to obtain individual
case histories that could be used to improve patient
management in primary health care programmes
and thereby lower childhood mortality in developing
countries.
Subjects and methods
Copenhagen. Denmark
•' Ministry of Health, Bandim. Bissau. Guinea-Bissau.
* Danish Epidemiology Science Centre. Statens Seruminstitut,
Copenhagen. Denmark, and Projecto de Saude, Bandim. Bissau.
Guinea-Bissau.
Reprint No. 5771
Of me Wond Hoatth Organization 1997 75 (3). 209-212
Study area
The study was carried out in the suburbs Bandim 1
and Bandim 2 of the capital Bissau Guinea-Bissau.
The population of approximately 25000 persons
S' World Heann Organization 1997
205
M. Sodemann et al.
is served bv two local health centres (with senior
nurses consulting), one mother-and-child health
clinic (with physicians consulting) as well as an out
patient clinic at the paediatric ward of the national
hospital (with hospital paediatricians consulting).
All inhabitants live within 1km of a health centre
and within 3km of the mother-and-child health clinic
and outpatient clinic Apart from a small one-time
charge levied for a child's vaccination chan, no fees
were"charged at health facilities in Bissau during the
study period. Since 1979, the area has had a demo
graphic and health surveillance system that covers
the following: registration of all pregnancies and
births: and for children less than 3 years of age, rou
tine collection, by means of 3-monthly visits to all
houses, of information on vaccinations, infections.
nutritional status, migrations, and deaths. Morbidity
and care seeking are monitored by weekly house
hold interviews. Traditional remedies for severe dis
eases are not generally the first treatment choice.
Study population
The cohort followed in the present study consisted of
all 1347 children born in Bandim 1 or 2 between 1
May 1992. and 30 April 1993. Deaths were ascer
tained by means of the routine surveillance system.
Two additional rounds of data collection were car
ried out in 1993 and 1994; furthermore, a census of
the entire population was performed in 1994. Verbal
autopsies were conducted by two of the authors
(MS ICA) and a specially trained Guinean mid
wife. Interviews were carried out from July 1992 to
November 1994. by which time the youngest children
in the study cohort were 18 months of age and the
oldest children 30 months of age. Median time from
death to interview was 7 months (25-75th percentile.
6-9 months). The immediate cause of death was
determined by combining information from the
verbal autopsy, the morbidity survey, and a reeister
of hospital diagnoses Morbidity information was
considered valid if the child had been followed up
until death, and hospital diagnoses were considered
valid when the child had been hospitalized for more
than 24 hours. Hospital records were available for 43
of 56 hospitalized children (76.8%) A probable
cause was determined for 93% of all deaths. In this
study, hospitalization" was defined as hospitaliza
tion at any time during the 30 days precedinc death.
regardless of subsequent discharge from hospital.
Households with deaths were divided into two
socioeconomic status groups: group 1 (50 mothers)
consisted of households with two or more of the
following; corrugated iron roof television, inside
toilet, and electricity: group 2 (75 mothers) consisted
of households with less than two of these charac
206
teristics. Socioeconomic information was obtained
from the health surveillance system.
Statistical methods
Sample means were compared with the Student's itest for normally distributed data, but the KruskallWallis test was used when sample variances were
significantly different. In bivariate analyses, back
ground factors were controlled for by means of a
Mantel-Haentzel stratified analysis of two-by-two
tables. A nested case-control study was earned out
by matching a control to each fatal case, The couqol
was chosen from among children in the study A ilation participating in a weekly morbidity survey.
age-matched (rl month), had experienced an epi
sode of disease within the same month as the fatal
case, was seen at a health centre or a hospital, but
survived at least 3 months following the episode.
Time to consultation was measured as the number
of days between the onset of illness and the first
consultation. The odds ratio was calculated as the
ratio of discordant pairs, and 95% confidence inter
vals (CI) were calculated with Miettmen's test-based
approach (72)
Results
Childhood mortality in the study group
All deaths of live-born children (248/1347) were in
vestigated by verbal autopsies with the mother, or
the nearest relative if the mother was absent The
circumstances, timing, and location of each contact
with health care personnel during the fatal illness
were recorded during the interviews. The proportion
of stillbirths was 55 per 1000 births, perinatal morta itv was 81 per 1000 births, and infant mortality 91 p^r
1000 live births. However, only post-neonatal deaths
(125/1347) were included in this analysis.
Of the 125 such cases. 114 had verifiat^ *’
formation on care seekinc. Of these. 106 children
(93%) were seen by a health professional during
the 14 days preceding death. Of the eight other$•
two died on the way to consultation, three *e
suddenly and unexpectedly, and three from >
eases ascribed to traditional ceremonial caus
Compared with our previous mortality surve)
the same city, the behaviour reported here
presents a significant reduction in the risk of n^
beinc brought to a health facility (risk rano f
0.3: 95% Cf: 0.2-0.7) (8). Moreover. 33 (26-4 °
the deaths occurred tn hospital, whereas in
previous survey 45% of deaths occurred in hospit .
A total of 23 children (18.4% of deaths) 1
WHO Bul'eun QMS vol 'o
vol 75 199"
Table 1: Cause ol death and pattern of care seeking
No. ol children, by place of first consultation *
Total
Median days to
first consullation"
1Health centre
Outpatient
clinic
*
Ollier
No
information
No
consultation
No information on
care seeking
*
7(3-22)
2 (2-4 5)
13 (56.5)
4 (17 4)
4 (17.4)
2 (8.6)
0 (0.0)
0 (0.0)
23
4 (3-25)
10(5-30)
8 (2-20)
7 (2-30)
30 (25-60)
2(1 5)
3(1-5)
3 (2-5)
1 5 (0-15)
14 5 (1-46)
10 (31.3)
9 (56.3)
3 (50.0)
4(11.4)
8 (66.7)
10 (30.3)
7 (43.8)
3(50)
11 (34.3)
2(16.7)
7(21 1)
0 (0.0)
0 (0.0)
4 (11.4)
1 (8.3)
1 (3.0)
0 (0.0)
0 (O.O)
2 (5.7)
0 (0.0)
4(12 1)
0 (0.0)
0 (0 0)
4 (11.4)
0 (0.0)
1 (3.1)
0 (0.0)
0 (0.0)
9 (25.7)
1 (8-3)
33
16
6
35
12
47
38
16
5
8
11
125
' Figures in parentheses are the 25fh-75lh percentiles.
*
• Figures in parentheses are percentages.
' Mother and child health clinic or regional hospitals in the interior
* Malnutrition (n - 5). measles (n ~ 8), congenital diseases (n
0). sudden death (n - 3). unknown (n >- 11)
Total
H igh m ortality d e sp ite g o o d c a re -se e k in g b eh av io u r in G u in e a -B issa u
Acute
diarrhoea
Fever
Pneumonia
Malaria
*
Other
Chronic
diarrhoea
Median duration
ol Illness (days)"
M. Sodemann et al.
at home after being discharged from hospital. No
information on the location of death was available
for seven children
Time to consultation
To determine whether mothers delayed consultation
in fatal cases, we performed a nested case-control
study It was possible to match a surviving control for
93 cases Equal delay occurred in 9 of the matched
pairs. In 35 matched pairs, the case exhibited the
longest delay and in 49, the control. Cases were more
likely to have a shorter delay than controls, with an
odds ratio of 0.70 (95% CI; 0.50-0.99).
First consultation and hospitalization
Tne place of first consultation according to cause of
death is shown in Table 1. The median lime from
onset of symptoms to first consultation was inde
pendent of child’s age. ethnic group, mother's educa
tion. socioeconomic status, and cause of death.
Of the 47 children first seeking care at a health
centre, only 23 (49%) were admitted to hospital and.
of these. 20 only after the mother sought consulta
tion more than once Of the 38 children first seeking
care at the outpatient clinic al the paediatric ward. 22
(58%) were admitted to hospital. Immediate hospi
talization was more likely among children presenting
at the outpatient clinic first than for children present
ing at the health centre (risk ratio = 5.0. 95% CI:
2.0-12.5). Children taken to a health centre survived
longer (median. 8 days: 25—75th percentile: 2-24
days) following first consultation than children ini
tially taken to the paediatric ward (median. 2 days:
25—75th percentile- 0-8 days. P = 0.01). No differ
ence in survival time after first consultation was
found between children hospitalized immediately
(n = 18) and others (n = 20: P = 0.8). After control
ling for mother’s education, socioeconomic status.
and child’s age, there were no differences in place of
first contact with the health system. However, chil
dren with diarrhoea were more likely to contact a
health centre first. Of those children surviving at
least 2 days from first consultation without hospitali
zation. 39 (84.8%) later reattended a health facility.
Hospitalization: reasons for refusal
or discharge
Of the 114 deaths for which we have information.
103 children (90.3%) presented at hospital one or
more limes during their terminal illness. Of these.
10 children died on the way to hospital and 10 while
waiting for treatment in the outpatient clinic (Table
2). Of the remaining S3 children. 56 (67.4%) were
admitted either at the first visit (n = 22) or at a
subsequent visit; of those admitted. 18 children died
the day of admission. For the 61 children not admit
ted at first consultation. 15 of the mothers stated thev
were turned away from the outpatient clinic havin®
been informed that their child should be hospital
*
ized, but that there were insufficient beds. Refusal of
admission did not depend on mother’s education.
socioeconomic status, or child’s age (P = 0.9).
Elapsed time since disease onset (>14 days) in
creased the risk of refusal (risk ratio. 2.4; 95% Cl;
0.9-6.6).
Of the 56 children admitted to hospitaler)
(41.7%) were discharged before death, with thej >•
of discharge being independent of socioeconoifiic
status (P = 0.44) and child’s age (P = 0.35). Of these.
9 children were discharged as "cured". 10 as "im
proved” or "recuperating’. 1 was discharged by
the mother, and 2 had no status information at
discharge.
Case histories
Six representative case histories depicting the man
agement problems of severe childhood illness in the
study area are shown m Table 3.
Discussion
Despite a high percentage of children with fatal ill
ness obtaining treatment from a health professional.
infant mortality in the study suburban area of
Guinea-Bissau has continued to be hiah: (1987-90.
94 per 1000:1992-93.91 per 1000). The proportion of
children who later die after presenting for consulta
tion both at health centres and hospitals has in
creased significantly since our previous mortality
survey (5).
Among physicians and other health care work
ers in developing countries, a common explanaMpy
for high childhood mortality is that, as mothers s '
believed to be incapable of caring for a severely il
child, children are brought to care too late. More
over. they do not recognize severe symptoms an
may seek traditional care first. However, the present
study indicates that mothers sought care sooner m
cases of fatal illness than in other cases.
Conceivably, seriously ill children would have
better chance of survival if they were treated at tn
outpatient paediatric ward than at a health centreThe ratio of mothers choosing a health centre as>si
of first consultation to mothers choosing the paedia ric ward was the same, regardless of mother s educa
lion, socioeconomic status, child’s age. and einni
group. Moreover, the chance of being admitted im
2oa
WHO Suhei-n OMS
Vol 75 ’997
Who Bulletin QMS Vol "5 1997
Table 2: Place of first consultation and subsequent care seeking
Hospitalized:
Not hospitalized:
Died white wailing
lor consultation of
outpatient clinic
Total not
hospitalized
No information
on place of
death
Total
23(11)
22 (6)
2(t)
19(H)
7 (6)
2(1)
2
3
0
3
6
1
24
16
3
__
—
—
47
38
5
—
11
Directly
Total
hospitalized
*
Health centre
Outpatient clinic
Mothor-and child
health clinic
Hospital or health
clinic in the interior
No information
on place
No consultation
No information
on consultations
3
18
0
20
4
2
Total
Place
1
4
5(2)
3 (2)
3
0
6
—
—
4 (3)
__
__
—
1
—.
—
——
—
—
—
6
4
2
—
8
4
—
—
7
8
11
22
30
56 (23)
41 (20)
10
10
62
7
125
• Figures in parentheses are number of children subsequently discharged who died outside hospital
*■ Figures in parentheses are number of children dying al home alter one or moro reconciliations.
5
H igh m ortality d e sp ite g o o d c a re -se e k in g b eh av io u r in G u in ea-B issau
Died at
*
home
Died on the way
Io outpatient
clinic
Alter one or
more reconsullations
M. Sodemann at al.
Table 3. Typical case histories
s months at age presems at health centre with diarrhoea
fodwownp aher 2 days cl illness; given oral ;Bh^,a“nn”
and sent home, next cay mother see« care tor chrld al anomer
health centre, aher 2 more days, mother presents chid at
outpatient paediamc clinic where me cMd is given oral
rehydration salts and sent home: 20 days later child dies without
receiving additional care
Boy * months of age. presents at outpatient paediatnc clime
with diarrhoea and vomiting after 2 days of illness; given oral
rehydration salts and sent home: 3 days later mother seeks
care tor child at outpatient paediatnc dime- child given oral
rehyoration salts ano sent home: 10 days later, child collapses
at home and mother lakes child to outpatient paediatnc clinic.
child is sent home wilhout treatment and d>es same day
Boy W montns o! aoe. presents at outpatient paediatric clinic
with hign fever afieM day of illness: given medication and sent
home (mother told not enough hospital beds): child suffers
generalized seizures at home, and next day mother returns to
outpatient paediatric dinic with child comatose; after waiting 2
hours, child sent to laboratory for tests and dies without
receiving aoditional care.
Boy. 9 montns of age hospitalized twice within 2 months for
high fever ana multiple boils: eacn time dischargee as ‘cured’
2 weeks after last disenarge child dies at home witn fever and
convulsions.
Giri. 7 months of age. presents a: mother-and-cnifd health
clinic with hign lever ano chills after 2 days of illness: giver.
chloroquine and paracetamol and sen: home, same day child
worsens, and mother seeks care at ouioatient paediatnc clinic:
cnild dies before receiving additional care.
Boy. 12 montns of age. ©resents at healtn centre with fever.
vomiting, and constipation after 1 week of illness child given
lemon juce and sent home, after no improvement, mother see«s
care same day at outpatient paediatnc dinic; child admitted:
ane' waiting more than t hour for a blood samoie. and then
waiting for tne fatner to buy the necessary drugs (wnicn were
not in stock at hospital), child dies witnout receiving additional
care
mediately io the paediatric ward of the hospital was
remarkably lower for children presenting initially at
a health centre than for children presenting initially
at the outpatient paediatnc ward. It is therefore pos
sible that health centres retard needed hospitaliza
tion. As health centers were visited more frequently
than in our previous mortality survey, this could
have serious implications.
Apart from five children dying suddenly at
home or on the way to their first consultation, onlv
five children were not presented for consultation
at hospital, which is a marked decrease from our
previous survey. However, it is significant that so
few fatally ill children were admitted to hospital.
even from among those who first presented at the
outpatient paediatric ward In many cases, the reason
was a shortage of beds. There were nine terminally
ill children attended by a paediatrician at the out
patient clinic 48 hours prior to death without beine
admitted. The risk of refusal of admission after
consultation at the outpatient paed.atnc ward was
higher if svmptoms had a duration of more than 14
davs. indicating that chronic illness was less likely to
be'seen as requiring hospitalization. This is signifi
cant as the two most common chronic illnesses, per
sistent diarrhoea and malnutrition, both have a very
*
high mortality (<?)• Since children not returning for a
second consultation died rapidly (median survival.
1 dav) mothers’ lack of knowledge does not explain
why" children were not hospitalized. Children not
hospitalized after a first visit to the outpatient paedi
atric clinic died as rapidly as those who were: it is
therefore unlikely that refusal of admission was
based exclusively on clinical criteria. Hospitalization
was not influenced by socioeconomic status, mother’s education, child's age. or ethnic group. How
ever. verbal autopsies suggested that hospitalization
was obtained more easily if a mother knew a staff
member in the outpatient clinic.
A considerable proportion of children died
wailing for consultation at the outpatient clinic or
laboratory. Some of these deaths could probably
have been avoided by means of a revision of clinic
procedures and by training health personnel to
recognize children requiring immediate care.
A major problem is the high proponion of chil
dren dying at home after discharge from hospital. In
light of discharge status this could not have been
caused by mothers fleeing the hospital with dying
children. No sociocultural factors were related to
risk of discharge, suggesting that inadequate recog
nition by medical staff of the potential consequences
of illness or nosocomial infections may have been
responsible. If so. this problem has been aggravated
since our previous mortality survey, since a larger
proportion of hospitalized children later die at home.
The number of beds in the paediatric ward remained
constant between the two surveys. Hence, demand
for limited bed space may have contributed to some
premature discharges. Hospital beds can be occu
pied for long periods of time by chronically ill
children suffering from malnutrition, persistent diarrhoea. complications resulting from cerebral malaria. or tetanus. A clearer distinction between acute
and long-term illness in terms of management and
the need for care, as well as a more strict set of rules
for admission and discharge could potentially lower
demand for bed space.
The present mortality survey consists of case
histories with a fatal outcome. Since medical con
sultations for terminally ill children represent only a
small fraction of all consultations for sick children.
this survey may be biased as an evaluation of the
adequacy of health system procedures. However.
t e present study does point to a number of specific
problems in case management. Previous studies ana-
210
WHO Bulletin OMS Vol 75 199?
High mortality despite good care-seeking behaviour in Guinea-Bissau
lysing care-seeking behaviour have focused particu
larly on traditional beliefs and practices that prevent
mothers from seeking proper medical care (5. 6. 9)
However, our experience suggests that it may be
equally important to examine the quality of the
medical care provided. This is supported by a Mexi
can study using verbal autopsies in a similar way. In
an area where no household was farther than 30
minutes from a health facility. 60% of the deaths in
children occurred at home and 80% of these children
had received qualified medical care within 3 days of
death (4).
A For dealing with problems associated with
Merely ill children WHO/UNICEF recommends
‘'integrated management of the sick child", which
combines the principles learnt over the past 15 years
in disease-specific health programmes into a unified
approach to managing childhood illness (J3). This
initiative focuses on improvements in health-worker
performance and changing family behaviour in rela
tion to sick children. Training courses for the inpa
tient case management of sick children have also
been developed.
The present analysis clearly supports the need
for such initiatives. Surveys analysing fatal cases can
be a valuable tool, and can serve as a cost-effective
means for health care workers to identify areas for
improvements in the case management of severe!} ill
children. Improving the management of such chil
dren may be as important for decreasing childhood
mortality as vaccination and antenatal care pro
grammes have been, especially in countries with
poorly educated and badly paid health care workers.
Inadequate supplies, physical facilities, and equip
ment may also contribute to the persistence of high
childhood mortality in Bissau. Such constraints em
phasize improved health system management as a
means of better using available resources.
A key step in improving case management
should be the establishment of an effective triage
'Kstem that singles out seriously ill children as soon
□ thes come Co a health facility and ensures that
appropriate action is taken. More formal criteria for
admission, referral, and discharge are also needed.
accompanied by clinical and system-management
training of staff. Finally, measures should be taken to
assure the quality of services provided by health care
workers, e.g. by medical audit or the use of epide
miological methods such as those used here. These
findings could be extended to the health services of
other developing countries: however, important dif
ferences may exist depending on available resources.
personnel, and payment systems. Hence, additional
studies investigating the case management of severe
illness at the primary health care and hospital levels
in other countries are warranted.
WHO Bulletin QMS. Vo> 75 199*
Acknowledgements
We are indebted to Angelina Da Silva and Queba Djana
for assistance during interviews and identification of
mothers. This study was supported by the Science and
Technology for Development Programme of the European
Community (contract No. TS3-CT92-0060) and by the
Danish Council for Development Research (grant No.
104.DAN8/535).
Resume
Une mortalite elevee malgre la
recherche de solns appropries: resultats
d’une enquete communautaire sur les
deces d’enfants en Guinee-Bissau
Bien que de nombreuses etudes aient fait 6tat d'un
declin significatif de la mortalite infantile a la suite
d'ameliorations generales des soins de same primaires, la vaccination et les soins prenatals ne
peuvent supprimer a eux seuls la surmortalite infan
tile dans les pays en developpement. Une prise
en charge plus efficace des enfants gravement
maiades est done necessaire. Hares sont les
etudes qui ont ete faites dans les pays en developpemem sur la recherche de soins appropries
comme moyen d'ameliorer la prise en charge des
enfants gravement maiades. La presente enquete
sur la demande de soins avant le deces a ete
conduite pour analyser le probleme de la mortalite
infantile en fonction de (‘attitude de la mere. II
s agissait de recueillir des antecedents medicaux
individuels en vue d'ameliorer la prise en charge
des cas dans le cadre de programmes de soins de
same primaires et ainsi. de reduire la mortalite in
fantile dans les pays en developpement.
La demande de soins par les meres de 125
enfants decedes entre 1 et 30 mois a ete etudiee au
moyen d'autopsies verbales dans une zone urbame
de Guinee-Bissau. Tous les habitants sont a morns
de 3km d'un centre de same. Au total, 93% des
enfants avaient 6te regus dans un centre de sante
ou un hopital dans les deux semaines ayant pre
cede leur deces. Notre precedente enquete, sur
la periode 1987—1990, avait montre que 78% des
meres des enfants ddeedes les avaient montres en
consultation; toutefois, malgre cette augmentation
de la demande de soins, la mortalite infantile n'a
pas baisse. Si I'on compare le temps ecoule entre
('apparition de la maladie et la premiere consultation
pour les enfants decedes et des temoins survivants
apparies. il apparait que cet intervalle avail ete plus
court pour les enfants qui sont decedes que pour
ceux qui ont survecu (odds ratio = 0,7; intervalle de
211
M. Sodemann et al.
confiance a 95% = 0,5-0,99). Sur les 125 enfants
qui etaient en phase terminale, 56 ont ete hospitalises Vmgt sont decectes lors du transport a I'hopital
ou en attendant d'etre vus en consultation dans
un dtspensaire. Faute de lits disponibles, 15 meres
se sont vu refuser I'hospitalisation de leur enfant.
Sur les enfants hospitalises. 42% ont ete declares
en meilleure same ou gueris et renvoyes chez eux
dans les 30 jours ayant precede leur deces. Ces
resultats montrent qu'il est necessaire d'ameliorer
les criteres d'hospitalisation, la reconnaissance
des symptomes des maladies graves et les cri
teres de sortie et de mettre en oeuvre des systemes d’assurance de la qualite des services de
sante.
La solution preconisee par I’OMS et I'UNICEF
pour le traiiement des enfants gravement malades
est la “prise en charge integtee de I’enfant malade"
qui associe les principes acquis depuis 15 ans
dans le cadre de programmes de lutte contre des
maladies determinees en une approche uniforme et
coherente de la prise en charge des maladies de
I’enfance. La presente etude montre tres clairement
que de telles initiatives sont necessaires. Les
enquetes sur les cas models peuvent etre un instru
ment precieux et fournir aux agents de sante un
moyen d'un bon rapport cout/efficacite de deter
miner les domaines dans lesquels des ameliora
tions doivent etre apportees a la prise en charge
des enfants gravement malades.
References
1.
Greenwood BM et al. Evaluation of a primary health
care programme in the Gambia. II. Its impact on mor
tality and morbidity in young children. Journal of tropi
cal medicine and hygiene. 1990, 93. 87-97
2.
Pison G et al. Rapid decline in child mortality in a rural
area of Senegal. Internationaljournal of epidemiolooy
1993,22:72-80.
Z’
3.
4.
Another audit. Lancet, 1988,1: 450-451
Gutierrez G et al. Study of the disease-health
seeking-death process: another use of the verbal
autopsy. International journal of epidemiology 1904
23: 427-428.
5.
Sutrisna B et al. Care-seeking for fatal illness in
young children in Indramayu. West Java, Indonesia
Lancet, 1993, 342: 787-789.
6.
Snow RW et al. Factors influencing admission to
hospital during terminal childhood illnesses in Kenya.
International journal of epidemiology, 1994,23:101^
1019.
7 De Francisco A et al. Comparison of mortality be
tween villages with and without Pnmary Health Care
workers in Upper River Division. The Gambia. Journal
of tropical medicine and hygiene. 1994, 97: 69-74.
8. Molbak K et al. Persistent and acute diarrhoea as the
leading causes of child mortality in urban GuineaBissau. Transactions of the Royal Society of Tropical
Medicine and Hygiene. 1992. 86. 21&-220
9 Shamebo D et al. The Butajira rural health project in
Ethiopia: mortality pattern of the under fives. Journal
of tropical pediatrics, 1991, 37- 254-261
10.
Mirza NM et al. Mortality patterns in a rural Kenyan
community East African medical journal, 1990. 67:
823-829.
11.
Alonso PL et al. A malaria control trial using
insecticide-treated bed nets and targeted chemopro
phylaxis in a rural area of The Gambia, West Afnca. 2.
Mortality and morbidity from malaria in the study area.
Transactions of the Royal Society of Tropical Medi
cine and Hygiene. 1993, 87(suppl. 2): 13-17.
12.
Kirkwood BR. Essentials of medical statistics.
Oxford, Blackwell Scientific Publications. 1988:179—
183.
13.
World Health Organization, Division of Diarrhoeal
and Acute Respiratory Disease Control. Integrated
management of the sick child. Bulletin of the World
Health Organization, 1995, 73 • 735-740.
MEMORAM BUM
to:
subject:
from:
Health Authorities end
Community Health Councils
Fluoridation of Water
Professor John Lenihan
Issued by The Fluoridation Society Ltd
63 Wimpole Street
London W1M 8AL
June 1984
This Memorandum has been prepared by Emeritus Professor John Lenihan,
who until recently was the Professor of Clinical Physics at the University of
Glasgow and the Director of the Department of Clinical Physics and
Bio-Engineering, West of Scotland Health Boards.
He directs this Memorandum to all those who need to make a decision about
the fluoridation of water supplies and warns them against accepting the spurious
evidence of the anti-fluoridation lobby.
C)
Issued by The Fluoridation Society Ltd
63 Wimpole Street
London W1M 8AL
First. I want to say something about poison - about a material which we are
obliged to take into our bodies every day, whether we like it or not. This
material, which has not been approved by the Committee on the Safety of
Medicines, is made of substances which cause painful illness leading to agonizing
death. I am speaking, of course, of sodium chloride - common salt, the salt that
we sprinkle in our soup. This substance is added by manufacturers, and without
consultation, to a great variety of foods and drinks. It is composed of two most
horrible poisons - sodium and chlorine. A tiny quantity of sodium, if taken into
the body, produces severe and painful burns. Chlorine is the original poison gas.
These two elements are present in almost all of our food. You may think that
there is something absurd here - and so there is. Every substance essential for
human life can also act as a poison - water, oxygen, calcium, phosphorus, and
many more. The idea that some substances are always wholesome and others
always poisonous is a favourite war cry of ‘pure-water' enthusiasts - but it has no
foundation in medicine, science or common sense.
Each generation seems to reproduce a particular mould of people who resist
the most obvious advances in public health. In an earlier generation they
resisted vaccinations, they resisted the chlorination of water and they resisted
the pasteurization of milk. Their modern-day prototypes resist the fluoridation
of drinking water with the same venom and enthusiasm. At all times these
protestors constitute a small proportion of the population, but they compensate
bv indulging in hysterical and wild verbosity. The inferiority of their arguments
causes them to quote bogus experiments, falsified evidence and palpable
untruths. They hope to win their battle by generating fear rather than by
reasoned argument. The danger is that by this method they do influence some
minds not in possession of the true facts, and in this respect they have achieved
some success by delaying the progress of fluoridation in the UK. They have also
caused more teeth to decay than need have, thereby increasing suffering and
adding to the ever-increasing costs of the NHS.
The anti-fluoridation lobby thought that in their pack of cards they had an
unbeatable Ace - this was the fluoridation-cancer scare. In their gambling game
they thought that if they played this Ace frequently and with skill they could kill
fluoridation once and for all. And this is what they attempted. Those who
introduced the rogue Ace were two Americans respectively called Dr Burk and
Dr Yiamouyannis but their evidence has not been published in any reputable
scientific journal - not surprisingly, because their report is riddled with
elementary errors. They compared cancer death rates in a number of American
cities, some with fluoridated water and some without. The death rates were
higher in the selected cities where fluoride was added to the water. Therefore,
they said, fluoride causes cancer. The cancer death rate in Glasgow is higher
than in East Kilbride. The consumption of beer per person is higher in Glasgow
than in East Kilbride. But if I told you. on this evidence, that beer causes
cancer, you would think that I was talking nonsense - and you would be right.
The death rate is higher in Glasgow because the average age of the population is
3
higher. Burk and Yiamouyannis ignored the elementary precaution of
correcting their death rates for age. sex and colour. When the corrections are
made it is seen that fluoride has no effect at all on the cancer death rate. This
same conclusion has been reached by similar studies in Britain and in hundreds
of communities all over the world. The non-association of fluoridation and
cancer has been established by the US National Cancer Institute (1972), the
Royal College of Physicians (1976). The Royal Statistical Society (1977), The
International Agency for Research on Cancer (1982). and the Institute of
Cancer Research: Royal Cancer Hospital. London (1982). Of course, what Drs
Burk and Yiamouyannis are really telling us is that people live longer in towns
where the fluoride content of the water has been brought to the correct level.
But if people live longer, more of them will die of cancer, simply because cancer
is mainly a disease of old age; more than half of those who die of cancer are over
sixty-five.
When challenged to answer these criticisms. Burk and Yiamouyannis put up a
smokescreen, claiming that their latest report answers all the criticisms - or that
they have a secret method of analysing the results (unknown to the rest of the
world) which gives support to their theories. Sometimes their friends claim (as
one of them did on Radio Scotland a little while ago) that the critics (including
Sir Richard Doll, the world’s foremost authority on cancer statistics) are now
convinced by the arguments of Burk and Yiamouyannis. This is either a slip of
the tongue or a barefaced lie.
In the Strathclyde fluoridation case Burk and Yiamouyannis attempted to win
the game by playing this particular Ace card but they had no success. The judge,
Lord Jauncey. in his report said, I found Dr Burk’s evidence on this question of
cancer deaths to be vague and unimpressive.’ And of his partner, the judge
commented. 'Dr Yiamouyannis displayed great ingenuity and a very fertile mind
during his evidence . . . but I was driven to the conclusion that he not
infrequently allowed his hostility to fluoridation to obscure his scientific
judgement.’ In this final denouncement one can be absolutely sure that this
manufactured ’Ace’ card is completely bogus.
The whole of this saga typifies the totally spurious approach of the
anti-fluoride lobby in its accusation that fluoridation causes other diseases. The
Pure Water Association circulates stories about work in Holland suggesting that
fluoride causes instant asthma, skin rashes, and in fact all kinds of allergies. The
doctor who made these claims refuses to give any scientific evidence for them
and they have not been verified anywhere else in the world. If fluoride at one
part per million causes so much trouble it is strange that no complaints have
come from the millions of people who drink tea or bathe in sea water, since both
of these liquids contain one part per million of fluoride ... or perhaps it is not
so strange, since the whole story is utter rubbish.
On the other hand the benefits of adjusting the fluoride level in water to the
correct value of one part per million cannot be disputed, except by the mentally
blind. The water supply in Birmingham has been fluoridated since 1964 and the
4
benefits have been spectacular. The number of children attending clinics for the
relief of toothache has dropped from over 10,000 in 1965 to under 2000 in 1977.
The number of children given general anaesthetics for the removal of teeth - a
procedure with some danger - has dropped from 18,398 to 3851 - a reduction of
78 per cent. In Wolverhampton (not fluoridated), during the same period, the
number of general anaesthetics actually increased by 30 percent. In Birmingham
last year sixty-two children were supplied with false teeth - representing one in
3500 of the school population. In Wolverhampton the corresponding figure was
one in 280 of the school population - twelve times higher. Students at the Dental
Hospital in Birmingham will soon have to go to other places to gain experience
of tooth decay.
The benefits of fluoridation are not confined to children. They continue into
adult life, so that natural teeth last longer. Attempts to belittle the benefits of
fluoridation are often made by people who don't know - and don’t want to know
- how fluoride works. It is not a magic remedy for tooth decay fully established.
To obtain the benefit, fluoride must be taken from the time that teeth are being
formed - very early in life for the milk teeth and a little later for the permanent
teeth. The benefits are not the same at all ages because the teeth most liable to
decay don't all appear at once. So it is easy to take one figure out of a table of
results and read a wrong conclusion.
But of course the anti-fluoride movement contains many people quite willing
to resort to this kind of manoeuvre to obtain the answer that they want. Indeed
it is a movement with some very odd people. In recent times Health Authorities
and Boards have been bombarded with propaganda coming directly or indirectly
from the National Health Foundation in California. This organization is well
known for its efforts to promote bogus remedies for cancer and for other
activities which have violated the law - and been suitably punished in the courts.
This sort of opposition is not new. Every major advance intended to improve
the public health - food hygiene, anaesthetics, vaccination - has been achieved
only in the face of ferocious opposition and hysterical abuse. The people who
suffer while the argument goes on are not the people who do the arguing. It is
the young, the poor and the under-privileged who suffer most.
It is sometimes suggested that fluoride should be given in other forms - in
school milk, table salt, toothpaste, or tablets. But none of these methods would
be effective. Protection by fluoride must begin at birth - not at the age of
starting school - if children’s teeth are to be saved. Babies and young children
don't take much salt - and not all of them use much toothpaste, or can be
persuaded to take a fluoride tablet every day from birth to fifteen. In a recent
project in England, parents of 3500 children were invited to take part; 759
children started the scheme but after nine months only seventy-nine were still
taking the tablets.
It is also said that even something so beneficial as fluoride should not be
added to drinking water because that is mass medication. But there is already a
lot of mass medication. Many substances are already added to water - chlorine.
5
to make it fit to drink. No doubt we
copper sulphate, alum, and a lot more
could each take untreated water and boil it, chlorinate it and generally purify it
for ourselves - but we don't. There are times when individual freedom must give
way to the greater need of the community. That's why we have a Parliament and local councils. It is sometimes claimed that fluoridation of water supplies is
illegal.
You may think, as you weigh the evidence, that the merchants of fear are
quite right - that there is indeed a gigantic conspiracy involving the Royal
College of Physicians, the DHSS. the World Health Organization, and every
reputable body that has reported on the problem - that all of these people are
eager to poison themselves and their children. Or you may agree that fluoride is
simple, safe, cheap, and effective . . . that it has been tested more thoroughly
than any other measure to improve public health - not only in communities all
over the world but for thousands of years in nature's laboratory. You may prefer
the evidence and experience of our own reputable experts on cancer and on
general health including dental health rather than that of imported scaremongers
and carpetbaggers.
In conclusion, the petitioners in the legal enquiries held in Eire and in
Scotland had every financial and physical opportunity to bring evidence of the
dangers and inefficacy of fluoridation, in the form of both documentation and
witnesses. Independently both Mr Justice Kenny in Eire and Lord Jauncey in
Scotland dismissed the pleas of the petitioners and declared fluoridation to be
both safe and effective. Whereas Lord Jauncey ruled on a fine legal point that
fluoridation was not legal in Scotland, HM Government have stated their
intention to clarify the law for the whole of the UK. When this happens there
can be no logical reason for any further delay in introducing this well-proven
dental
health
measure
and
sounding
the death
knell
of the anti-fluoride
movement.
If you vote in favour of fluoridation
you will have the admiration and
gratitude of the vast majority of your people and of their children for all time to
come.
6
pisS- It
AN
OPTIMISTIC HORIZON
IN
EPILEPSY
Published by :
INDIAN EPILEPSY ASSOCIATION
(Bangalore Chapter)
No. 1, Old Veterinary Hospital Road
Basavanagudi, BANGALORE - 560 004
Courtesy :
HINDUSTAN CIBA-GEIGY LIMITED
Pharmaceuticals Division
14, J. Tata Road,
BOMBAY - 400 020
AN OPTIMISTIC HORIZON IN
EPILEPSY
Published by:
Indian Epilepsy Association (Banglore Chapter)
No.1, Old Veterinary Hospital Road
Basavanagudi, Bangalore - 560 004
Courtesy:
Hindustan CIBA - GEIGY Limited
Pharmaceuticals Division
14, J. Tata Road, Bombay - 400 020
Foreward
The Indian Epilepsy Association Bangalore
Chapter is very active in patient education and this
booklet is one such venture.
The advances that have taken place in the
diagnosis and treatment of seizures have
made
epilepsy a well controllable disorder, with the promise of
a good and normal life for the patients. Information and
knowledge regarding seizures is essential for patients
and relatives so that fear, ignorance and anxiety may be
expelled.
a
To achieve this goal, Prof. Dr. K.S. Mani,
renowned neurologist and an international expert in
Epilepsy has written a simple and informative book on
seizures which will be most useful. A study of this short
booklet will no doubt benefit a large number of people
with seizures and encourage them to lead a normal life.
(Sd/-)
Prof. Dr. B. Ramamurthi
Madras - 600 004
Immediate Past President
February 2,1995
Indian Epilepsy Association
AN OPTIMISTIC HORIZON IN EPILEPSY
General
Epilepsy is a common condition affecting 0.5 to 1 % of the general
population. No race, caste, community or gender is exempt, but it is
probably a poverty-related illness affecting more often the people in
the lower socio-economic strata of society. Its prevalence in certain
parts of the world like some areas of Africa, Central and South
America is very high. It is not caused by devils or evil spirits (fig 1). It
0
is often a result of a scar in the brain - a legacy of difficult delivery, child
hood infections, head injury or in the elderly, diffuse blood vessel
disease. Less common causes includebrain tumours. In certain parts
of the world, especially India and Central and South America, worm
infestation of the brain as in cysticercosis (fig. 2) and others are
common causes. However, it must be stressed that in a vast majority
of instances the cause is not known, at least during life or even if
known does not alter the total management of the problem.
Seizure Types
Epilepsy is like fever and consists of several types of attacks or
seizures. The common type called generalized tonic-clonic seizure
(GTCS) or grandmal or major seizure is well known and consists of a
sudden cry, fall - if erect - unconsciousness, stiffness and jerking of
limbs with eye balls rolled upwards. Froth, tongue bite, passage of
urine or injury are common, but not constant. The patients often go
to sleep and on waking up have severe headache, vomits, soreness
in muscles or tiredness.
Some patients experience a warning signal seconds or minutes
before an attack. This may be in the form of jerking of fingers, toes,
mouth, or eyes on one side or in the form of simple or elaborate
subjective feeling or experience, not obvious to others. These tend to
recur and have a constancy of pattern for that individual. These are
called Simple Partial Seizures (SPS) and last 1-2 minutes during
which the patient is fully alert. In another type called Complex Partial
Seizure (CPS) the patients have a partial disturbance ratherthan total
loss of consciousness. They have a vacant stare, champ the mouth,
smack the lips, or move the hands and legs in a bizarre, strange
2
k
Fig: 1
3
fashion - automatism. Response to questions are either absent or if
present incomplete or inappropriate. They are not aware of the
content of an attack. These last from 1/2 to 2 minutes followed
sometimes by sleep, tiredness or mild headache. SPS or CPS can
remain as such or as is much more common evolve into a GTCS.
SPS
----------------- >
CPS
GTCS
The latter can also arise straightaway without a preceding SPS
or CPS-primary GTCS.
>
GTCS-primary or secondary is the most
common seizure type (80%). Mixed seizure types are often seen in
those with brain damage. Repetitive lapses of consciousness lasting
5-15 seconds (absence seizures) or jerking of the limbs lasting 1 or
2 seconds only but on a background of full consciousness (myoclonic
seizures) are relatively uncommon.
DIAGNOSIS
Epilepsy can be diagnosed only by an accurate description of the
attack and nothing else.
Hence an eye witness account is very
essential. Failure to observe this simple rule results in overdiagnosis
of this condition. 15% of cases diagnosed as epilepsy do not suffer
from it I
EEG is of help in confirming the diagnosis of epilepsy - but only
in about 30% in the tropics - and also its type. In our set up, in nearly
two thirds the first EEG is unhelpful in the diagnosis of epilepsy.
Likewise in developing countries routine estimation of serum levels of
anti-epileptic drugs (AEDs) in a reliable laboratory is a luxury which
most - not all - patients can very well do without. CTor MRI scan are
of help not in the diagnosis of epilepsy but in determining the presence
of underlying structural disease. It should be emphasized that these
investigations cannot and should not be discarded but used intelli
gently with realization of their limitations, cost, reliability and ready
availability. They cannot and should not replace an adequate history,
follow-up evaluation and a practical common sense approach.
4
'
MANAGEMENT
The concept that epilepsy is a chronic recurrent disorder requir
ing life long medication is nolongertrue. We know today that in avast
majority of subjects, the attacks can be controlled, if not cured, by early
treatment with Anti Epileptic Drugs (AEDs). There are certain rules of
the game which must be followed scrupu lously. Drug treatment is not
for few days or weeks only but years - at least 2-5 years. Not a single
dose must be missed and it should be taken at the correct time (fig 3).
TAKE TABLETS AT THE CORRECT TIME
WITHOUT FAIL
Fig: 3
The drug prescribed depends on the seizure type.
In the most
common type of seizure-GTCS-Phenobarbitone (PB), Phenytoin
(PHT), Carbamazepine (CBZ), or Sodium Valproate (VPA) are equally
effective as far as seizure control is concerned. This is a point of
practical importance in rural epilepsy control program in developing
countries as confirmed by several studies in India, Pakistan, Kenya,
Tanzania, Turkey, and Ecuador (in South America). Sedative side
5
effects or restlessness do occur with PB but not in all cases nor are
they considered disturbing in every community and socio-cultural
milieu. We must learn to individualize and not generalize. VPAisthe
drug of choice in absence/myoclonic seizures-fortunately not com
mon. Every parent/patient must learn to recognize his/her seizure
type(s) and maintain an accurate diary of not only the attacks but also
their types. If properly utilized this can help the doctor to identify the
correct drug and dosage for that individual.
There is no fixed dosefor AEDs. Thedrug should always be given
as monotherapy (single drug).
Polytherapy (more than one drug)
more often than not is unnecessary, less effective, more expensive
and potentially more toxic. The dosage of the drug chosen has to be
stepped up gradually till side effects occur or seizures come under
control. In the event of the former, slow replacement by another AED
is necessary and the entire process repeated. This exercise may take
weeks, months or even years, requiring patience from the doctor and
the relatives. The limited value of serum AED level estimations has
already been referred to. It is worth emphasizing that PB or PHT can
often be given once daily, while CBZor VPA need to be given atleast
in two or three doses per day.
One question frequently asked is why a patient should have an
attack at a particular time even if drugs are being taken. This may be
from missed dose ortime, change of brand, use of drugs beyond their
date of expiry (never buy drugs loose), fever, vomits, diarrhea, use of
other drugs which interfere with the blood level of the AED or poor/
inadequate sleep. However, in most cases the cause remains un
known.
First Aid
A single tonic clonic seizure - the shaking or convulsive phase
lasts hardly 1 -2 minutes, though the subject may be unconscious for
longer periods. It does not call for any first aid measure. Do not insert
any object intothemouth, hold the patient, turn the neckorbodyduring
a seizure or pour fluids down the throat. These are all potentially
dangerous first aid measures.
Leave the patient severely alone
(fig.4). This maxim also applies to children who often develop
6
seizures during fever. However, if the convulsive phase lasts beyong
10 minutes by the clock, if consciousness is not regained in 1 -2 hours,
or if there are recurrent (more than 3) GTCS, the patient must betaken
to the nearest doctor. Rectal or oral diazepam (calmpose) - solution
meant for injection -1/2 to 2 ml - is a first aid measure at home, but
should not be resorted to for single seizure for the simple reason it is
unnecessary. Moreover tolerance to the drug tends to develop ren
dering it useless during a future emergency.
RESULTS
Provided the rules of the game are followed - correct diagnosis,
proper identification of the seizure type, institution of the appropriate
drug as monotherapy (single drug) and strict 100% drug compliance
(not 99% I) - GTCS which are potentially harmful to life or limb can be
controlled fully - (100%) - in about 70% of all patients.
Half the
remainder will have their attacks reduced by more than 50%.
In general, the outlook for full control of seizures tends to become
less with each of the following parameters - presence of overt brain
damage, often in the form of mental retardation (hardly in 15% of all
epilepsies); CPS as the seizure type; poor drug compliance (irregular
drug intake); unnecessary polytherapy (monotherapy will do in most
cases); choice of wrong drug; failure to control the attacks early (gen
erally life time total of GTCS should not eceed 30-50, when control
7
Fig: 5
becomes progressively more difficult) and poor life style compliance,
especially with regard to adequancy and regularity of sleep (fig. 5).
In general, drug treatment can be withdrawn slowly over a period
of 1-1 1/2 years if the patient is totally seizure free for 2-5 years and
has no overt brain damage, though there are certain exceptions.
Relapses occur in about 20% of all epilepsies, generally during the
reduction phase or within one year of total cessation of AEDs.
LIFE STYLE
80% of patients with epilepsy have no mental or neurological
handicap. The patients are normal except for the few minutes during
a seizure which may be once an year or even daily - the latter an
extermely uncommon event. These patients can study (fig. 6), play
("let the children fall, break their bones which can mend, but don't
break their hearts" - Jeavons), work (fig. 7), eat what they like (the so
called tonics are a total waste of money) .They can marry (fig 8), have
children, breast feed the infant (fig. 9) and have full participation in
recreational and social activities including sports. (Jonty Rhodes the
South African T est Cricketer is a legendary living example). They can
cycle (fig. 10). Till the attacks come under control, they should avoid
cooking near an open fire when they are alone (fig. 11). It may also
be prudent not to lock the door while bathing (fig 12) or go near a tank
or an open well without a wall (fig. 13). Otherwise they can lead a
8
9
10
Fig: 12
Fig: 13
Fig: 14
11
perfectly normal life like anyone else, except that they should have
regular hours of sleep (about 7 hours a day)-beware of travel by night
bus (fig 14) - and keep off driving or swimming for 1 -2 years after the
last attack. Tobacco or moderate (social) intake of alcohol - 2 x 60 ml
of whisky twice a week - are not taboo from the point of view of
epilepsy, though there may be far weightier reasons to avoid them
totally.
PREGNANCY
Women with epilepsy can have children like anyone else. AEDs
should not be reduced or stopped during pregnancy which can make
epilepsy worse in athird, improve in anotherthird and have no effect
in the balance. Repeated seizures during pregnancy can result in
abortion or miscarriage.
AEDs do have harmful effects on the
developing child, but this tends to occur within the first 6 - 8 weeks of
pregnancy, when the lady is often not even aware of it. This very low
potential to cause developmental defects should not be blown out of
proportion. There are other equally important causes. Morethan95%
of pregnancies exposed to AEDs result in normal bouncing babies.
PREVENTION
The prevalence of epilepsy can be reduced by better primary
maternal and child welfare measures including universal immuniza
tion. Sri Lanka, parts of India, China and Cuba are classic examples.
So also are compulsory wearing of crash helmet by drivers and pillion
riders of 2-wheelers and better environmental hygiene and sanitation
to reduce the scourge of cysticercosis (infestation from contaminated
vegetables, consumption of imperfectly cooked 'measly' pork and
failure to wash the hands thoroughly with soap and water after toilet).
CHRONIC EPILEPSY
Chronic epilepsy can be reduced by early treatment of the illness
by monotherapy even with simple, inexpensive drugs rather than
allow the epilepsy to become chronic by irregular drug intake,
unnecessary polytherapy and choice of the wrong drug. The habit of
12
giving an additional dose by mouth for a single recurrence or change
of dose, drugs or doctors for every recurrence deserves to be
condemned. We will run out of drugs in no time, though not doctors!
Effective peripheral decentralized management of epilepsy with a
single drug at the rural level is the key towards prevention of chronic
epilepsy in developing countries and can be effectively merged with
other disease control programs like malaria, leprosy, tuberculosis
etc., to make it cost effective.
What of the 15 to 20% of patients who unfortunately have chronic
or drug resistant epilepsy
?
The term chronic or drug resistant
epilepsy should be reserved only for those who have not responded
to monotherapy with PB, PHT, CBZ or VPA in adequate dosage or
careful polytherapy with two drugs.
NEVER DRUGS/SURGERY
Newer drugs like Vigabatrin, Lamotrigine or Gabapentin have
been introduced into the market in Western countries, mostly as add
on-treatment for years, if not life. They are used mainly in CPS and
Lamotrigine also in Lennox-Gastaut Syndrome.
The latter is an
intractable type of epilepsy in children with brain damage
characterised by mental retardation, restlessness and mixed-seizure
types including myoclonic jerks and GTCS. Results in CPS show in
general full control in 10 -15%, and more than 50% control in an
additional 40 -45%. Surgery for epilepsy, especially in intractable
complex partial seizures has yet to be placed on a firm footing in
developing countries.
It should be stressed that AEDs must be
continued for at least 3-5 years after surgery and relapses occu r in 1020% of patients.
TEN COMMANDMENTS
These are as under:
1.
Epilepsy is an eminently controllable problem.
2.
3.
Epilepsy is NOT a mental illness.
If you witness an attack, note the details. An accurate descrip
tion prevents wrong diagnoses. First aid is rarely needed.
4.
Early treatment is the secret of success.
13
5.
The drugs prescribed have to be taken regularly.
6.
The duration of treatment in general is 2 to 5 years after the last
7.
attack.
-Restrictions forpersons with epilepsy are very few; ensure ade
8.
Patients can study, work and enjoy life.
9.
10.
Women with epilepsy can marry and bear children.
Treat problems as you would in asthma, headache, diabetes.
quate sleep.
Do not overprotect nor ostracize.
CONCLUSION
To conclude epilepsy is not a dreadful disease as made out to be.
It can be fully controlled in about 70 - 80% and totally cured in 50% of
patients by early and proper treatment even with simple, inexpensive
drugs. Children and adults can lead a perfectly normal life. The key
to success is not drugs alone but attempt on the part of the physician
to explain about the disease, drugs and their pros and cons to the
patients / relatives. Patient education, often a neglected aspect can
be achieved through pamphlets, booklets, discussions, television
programs and lay Epilepsy Associations. After all patients / relatives
have a right to know about their illness, don't they I
14
DIABETES
Health Committee
Lok Vidnyan Sanghatana, Maharashtra
What is diabetes? Why does it occur?
When sugar in our blood can not be utilised adequately by the cells
in the body, the level of blood sugar increases beyond the normal
limit and this is diabetes. In diabetes, not only does the sugar in
blood increase but the metabolism of carbohydrates, proteins and fats
gets disturbed and a complex disease process sets in.
The food we eat ultimately gets converted in our body into a sugar
called glucose. This glucose provides the energy required for the
body functions. A hormone called "insulin" is essential for the
utilisation of the glucose by the cells. Insulin is produced by some
special cells in the organ called "pancreas". In diabetes, this
insulin is either not produced in adequate quantities or does not act
properly, due to which the cells cannot utilise the glucose for
energy. Instead, sugar keeps accumulating in the blood.. This results
in an increased level of glucose in blood, but the cells are starved
of glucose.
•
There is no one single reason as to why insulin is not produced or
utilised properly. To some extent diabetes is hereditary. However,
obesity, lack of exercise and improper food habits are known to
interfere in the action of insulin. This is seen from the fact that
Indians settled abroad with affluent, sedentary, Western lifestyle
show a higher prevalence of diabetes.
What are the ill effects of diabetes?
If the level of sugar in blood increases beyond normal limits, it has
several ill effects. The fine blood vessels called "capillaries" get
damaged due to high blood sugar. This may cause blindness due to
bleeding from the capillaries in the retina of the eye. Diabetes
increases the chances of cataract or glaucoma (increase in the
pressure in the eye-ball).
Diabetes also affects the capillaries in the kidneys, heart, skin or
nerves. It also increases the proportion of fatty substances in the
blood which in turn leads to a condition called arteriosclerosis
(hardening of blood vessels called the arteries). A fatty substance
called cholesterol gets deposited on the inner lining of the arteries
and thus increasing the resistance to the flow of blood through the
arteries. This causes high blood pressure and thereby cause heart
attack.
&
1
Increased blood sugar increases the chances of infection as the sugar
itself is a good nutrient medium for the infectious agents to grow.
Therefore, the chances of fungal infection of external genital
organs, or of urine infection or T.B. are more in diabetic persons.
The prevalence of impotence in diabetic men is higher. In diabetic
women, if the disease is not kept under check during pregnancy, the
chances of still birth or of a deformed foetus are more. In fact a
diabetic women should attain a good control on diabetes before she
conceives.
When should diabetes be suspected?
Diabetes usually occurs after the age of 30 or 40 years. There is the
other, more severe form of diabetes in which the production of
insulin is grossly reduced. This can happen in childhood or in young
age also. In this juvenile diabetes, the patient becomes weak,
despite eating frequently. The person remains ever hungry because
despite having lot of sugar in the blood, the body cells cannot
utilise it (i.e. they remain starved). The muscles and fats in the
body get broken down into sugar in an attempt to provide sugar to the
cells. However, it is of no use due to lack of insulin. This break
down of muscles, fat causes loss in weight, tiredness ?nd excess
sugar gets filtered down into the urine. The sugar also absorbs more
water from the blood into the urine. This results in frequent
urination and persistent thirst. If this is not attended to, the
young diabetic falls seriously ill and may develop coma.
The symptoms of diabetes in older age may often be relatively minor
or even absent. These patients have frequent hunger and thirst,
frequent urination and tiredness as in juvenile diabetes but in a
milder form. The patient has to get up at night for urination.
Delayed healing of wounds, tendency to develop pus, itching due to
fungal infection, dimness of vision, feeling of tingling, numbness in
hands and feet, impotency in men and unsuccessful pregnancy in
women.... all these symptoms can be due to diabetes. If close blood
relatives are/were diabetic, one should be more suspicious about
these symptoms. However, absence of these symptoms does not
necessarily mean absence of diabetes. Nearly 50% of diabetics do not
show these symptoms. Diabetes can be diagnosed with certainty only
through blood test. Therefore after the age of forty years, blood
sugar should be tested at least once in five years.
How is diabetes diagnosed?
As mentioned above, diabetes can be correctly diagnosed only by blood
sugar test. Test for only urine sugar does not give a certain
diagnosis. This is because in some cases urine may show sugar with
the blood sugar being normal or in some case blood sugar may be high
but sugar may be absent in urine.
2
The blood sugar is to be examined after the person remains without .
food, drink (except water) for 10-12 hours. This is called as the
"fasting" sugar. If it is more than 140 mg per ido ml of blood it
means the person has diabetes. However, if it is less than 140 mg it
does not necessarily indicate absence of diabetes. Therefore in such
persons, a test called post-glucose blood sugar is done. In this test
the person is asked to take 75 gram glucose in water after fasting
for 10-12 hours. The patient is advised not to take anything except
water, not to smoke or to exert for two hours after taking glucose.
Exactly after 2 hours another blood sample is taken to test the blood
sugar level. If the person has diabetes then the blood sugar level
would be more than 200 mg/100 ml of blood two hours after the glucose
meal. Some time instead of giving glucose, the patient is asked to
have normal food and the blood is tested two hours after. The test
performed by giving glucose is more reliable for correct diagnosis
because we are giving measured guantity of glucose. If the sugar
level is found to be 115 to 140 mg in fasting sample or between 140
and 200 mg in the sample after glucose/food the diagnosis of impaired
glucose tolerance or diabetes in the offing is made. Under such
circumstances further testing or freguent testing or testing after
controlling diet and doing exercises may be done on the advise of the
doctor.
Besides blood sugar what other tests are required?
If diabetes is confirmed by blood-sugar test a thorough physical
examination of the patient including weight, blood pressure,
examination of the heart, blood vessels, nervous system, retina is
carried out because diabetes can affect these systems. Any problem of
kidney function can be detected by simple urine examination. If any
problem is detected in this urine-examination, further test can be
done to know its extent and severity. Urine sugar is also tested.
Although, test for blood sugar is must for the diagnosis of diabetes,
once it is diagnosed urine can be tested every week at home by the
patient himself/herself to get a rough idea as to whether the disease
is under control or not.
Initially the urine is also tested for the presence of substances
called "ketones". The presence of ketones indicates that the persons
is suffering from severe diabetes. This calls for immediate
treatment. Once diabetes is detected tests for blood fats (lipids)
and electrocardiogram of the heart are also done. Diabetes is known
to induce abnormal changes in blood-fat and in the ECG. These tests
are therefore helpful to decide the line of treatment.
3
TREATMENT OR DIABETES
Health Committee
Lok Vidnyan Sanohatana, Maharashtra
Whet is the treatment for diabetes? Can it be cured?
Diabetes can not be completely cured and once acquired it stays for
life. However, with appropriate exercise, diet control and drugs it
can be kept under check. Mild diabetes can be kept under control
without taking medicines with the help of proper diet and exercise
alone. In addition to diet control and exercise, some patients have
to take antidiabetic drugs. In some, only tablets are needed, but in
some patients, insulin injection is to be taken daily.
Piet• Indian, especially Maharashtrian traditional balanced diet is
mainly based on cereals and pulses. There is no qualitative change
required in this diet for a diabetic person. One has to avoid
sugar/sugar meats consume only very limited quantities of oil,
butter, ghee, etc., take only limited quantities of food to maintain
weight within prescribed limits. The approximate formula for
prescribed limit of weight is - height in cms minus one hundred =
weight in kg. If your weight is more than this limit, with the help
of following simple guidelines change your diet to reduce weight.
To reduce 1 kg weight in a month through dieting, one will have to
reduce 7200 calories from diet (about 240 calories per day). One
hundred calories are provided by the following food items and
accordingly the calories can be controlled by appropriate reduction
in consumption. Cooked rice - .1 cup - 30 grams of dry rice); one
chapati of 6" diameter (made out of 30 grams of wheat); one sada
dosa; two idlis; two slices of bread; one cup (katori) liquid dal (in
the form of sambar, amti, etc.); one egg; one banana; 2.5 spoons of
butter, 2 spoons of oil or ghee.
The following can be consumed in liberal quantities as they have low
calories e.g. carrot, cucumber, onion, tomato, lavaki (dudhi bhopla),
radish, clear vegetable soup, etc.
The following should be taken only in moderate quantities: (The
calories contained in the oil used for cooking have not been taken
into account, oil should be used to the minimum). Vegetables like
cabbage, cauliflower, ladies finger, brinjal, etc. Fruits such as
papaya, sweet lime, oranges, figs, etc. Fluids such as butter milk
and milk without cream, tea without sugar, fish, lean chicken, etc.
The following should be taken in very small quantities: potato, sweet
potato, yam, sago, green peas, guava, banana, mango, custard apple,
etc.
1
The following should fee avoided as far as possible: Sugar, gud or
jaggery, honey, sweets, ice-cream, jams, pastries, cream, ghee,
butter, fried foods, oily pickles, groundnuts, almonds, cashew. They
are calorie-rich substances.
Alcohol also has calories like sugar. It should be avoided. This is
particularly so when the diabetes is severe and not under control or
when other complications are present. Eat a little at a time, four
times a day so that the sugar level in blood does not rise suddenly.
Use only limited guantity of oil for cooking. Daily 20 grams of oil
per head i.e. about 0.6 kg per head per month is the limit. Other
fats particularly animal fats such as ghee, butter should be avoided
as they are much more likely to increase cholesterol in diabetics.
Home made ghee may be used but it should be restricted (only one tea
spoon in a day - 10 grams).
Diabetes may also result in other problems relating to heart and
kidneys. If this happens, this would need further diet modification
(salt restriction, etc), which should be done under appropriate
medical advice. There is a general misconception that diabetic should
not eat rice. As a matter of fact rice has less calories as compared
to chapati or roti (weight for weight). However, since rice has less
fibre content its digestion is quicker which may cause a spike in
blood sugar after the meal. There is no harm in eating limited amount
of rice, as part of a balanced meal.
Exercise: Exercise reduces the amount of insulin required to control
blood sugar. With the help of proper diet and exercises it is
possible for some diabetics either to avoid use of drugs altogether
or reduce its dose. Therefore diabetics must do some light exercises.
Many diabetics are overweight and exercise helps to reduce it.
Walking is the simplest and the safest exercise. One should walk
briskly for at least half hour to stay fit, and for longer time to
reduce weight. To reduce 1 kg in a month one has to burn 7200
calories through exercise. Keeping in mind the need to reduce weight
to the desired level within 3-6 months, the diet and. exercises have
to be planned.
Types of activities and calorie consumption per minute: Cleaning
household utensils, mopping, gardening, painting - 2 to 5 cal; works
like masonary - 4 to 5 cal; brisk walk, climbing stairs, cycling,
tennis, carpentry - 5 to 10 cal.
In fact exercises are of three types and the exercise programme
preferably should include all the three. Please refer to the separate
booklet by the Health Committee on this subject. Diabetics should
consult doctor before starting these exercises, and also observe the
following precautions.
0
2
A patient taking insulin should eat 25 to 30 gms of carbohydrates
(half a banana or guava or half cup milk) before exercise. Otherwise
exercise may induce sudden drop in sugar level causing giddiness. If
the person also has hypertension or heart ailment, only such
exercises which can be easily tolerated should be done in
consultation with the doctor. However there is no need to consult a
specialist if one chooses only brisk walk as exercise. If there is a
problem in the retina of the eye, exercises which include jerky
movements and lifting of weights should be avoided since they may
trigger bursting of already weakened capillaries. Exercise causes
quicker absorption of insulin injected on arm or thigh. If the time
of exercise coincides with that of the injection, the injection may
be taken under the skin on the abdomen.
Medicines: The prescribed medicines should be taken at the right time
in correct dosages and should not be changed without medical advice.
Diabetes cannot be cured and therefore diet control should always be
properly observed. In some cases insulin is needed only for temporary
reasons such as during stress like pregnancy or during illness. Once
the stress is over, insulin can be replaced with tablets.
Diabetes may cause symptoms such as tingling and numbness or burning
or pains in hands and feet. Sometimes 'B' vitamin is prescribed to
treat these symptoms but its utility has not yet been scientifically
proved. However, due control on the blood sugar can reduce these
problems in some patients.
How to know whether diabetes is under control or not?
Symptoms of diabetes recede as diabetes is controlled. The true
indication of control of diabetes is level of blood sugar which to
some extent can be gauged by testing urine sugar. Urine sugar can be
tested at home. Its utility for a particular patient is determined by
the doctor depending upon factors like the severity of diabetes and
patient's attitude.
If the patient does not have to take insulin it is good to test the
blood and urine sugar every month (however, if the patient cannot
afford it, then at least every three months) to know whether diabetes
is under control. If the patient is on insulin then more frequent
testing for blood-sugar is required depending upon the severity of
the disease.
The usual blood sugar test indicates whether the sugar has increased
beyond normal limits on that particular day. A test called
'Glycosylated Hemoglobin' shows the control on blood sugar during the
preceding 3 months. Since this test is more expensive costing about
Rs. 150 to 200, doctors do not advice it to all the diabetics.
3
However, if the doctor suspects that the patient does not take the
necessary precautions related to diet, exercise and medicines, this
test becomes quite necessary.
In the initial stages of the treatment when there is a need to reduce
weight, the patient should keep a note of his/her weight every 15
days for a few months and if the progress is satisfactory, a monthly
check-up of weight is enough.
Once in a year it is necessary to do a general physical check up and
examination of eyes, urine, blood cholesterol and other lipids, ECG
as diabetes increases the possibility of certain problems in the
eyes, kidneys, and the heart. These diseases are symptomless in the
initial stages and hence they aggravate silently. These tests are
therefore needed to detect these diseases at an early stage. This is
more so for certain retinal problems which otherwise could cause
blindness. This blindness can be prevented by timely check up and
treatment of the disorder at an early stage.
What other care is required?
Any increase or recurrence of symptoms of diabetes should be reported
to the doctor and be properly treated. Any infection should also not
be ignored and a prompt, proper treatment for that infection is a
must, as any infection can quickly become serious in a diabetic
person.
Specific time table for for food and medicines should be strictly
observed. An excess dose of insulin or a powerful oral drug in
relation to diet may cause a sudden drop in the level of blood sugar.
If this happens, the patient may get profuse sweating, giddiness,
uneasiness and even unconsciousness. In this situation 4-5 spoonful
of sugar should be taken. A patient on insulin or oral anti-diabetic
drugs should carry a small plastic packet of sugar (about 5 spoonful)
in his/her packet. Patients taking insulin should carry an identity
card with a drug chart indicating the drug used and dosages.
Diabetics should avoid all forms of tobacco as it increases risk of
heart diseases. They should avoid walking barefoot, should cut their
nails properly and do proper early dressing for all kinds of injuries
including small cuts as diabetics are more prone to get their wounds
infected fast and develop a septic.
There is no scientific proof that diabetes is either cured or
controlled with non-allopathic drugs (e.g. Ayurvedic or Homeopathic).
However those who use these drugs on account of their faith in that
system of medicine, should periodically keep a check on blood and
urine sugar levels to avoid any possible threat to life.
4
V
Thus in brief proper care in the form of diet, exercise and
medication can keep diabetes under control. This depends more on the
patients themselves and the doctor's role is mainly of a guide.
Can diabetes be prevented?
Although diabetes is hereditary, at least to some extent it depends
upon one's life style. Lack of exercise, excessive consumption of
oily and rich foods, mental tension help to cause diabetes. This
should be avoided. Persons who have history of diabetes amongst close
blood relatives should be more careful about life style.
There is evidence that in children pancreas may get affected due to
malnutrition. This can reduce insulin production resulting in
diabetes. The high prevalence of malnourishment in India needs to be
overcome. This will also help in reducing the prevalence of diabetes
in India.
5
&
ISSN 0377-4910
1
CHANGING PARADIGMS OF INFECTIOUS DISEASES IN DEVELOPING COUNTRIES
New Paradigms of Infectious Diseases
Microbes and man liave been engaged in a continuing
hattie for ascendancy on this planet. In India whatever
successes had been achieved on the public liealth front were
largely in'the field of infectious diseases. Small-pox is an
excellent example. To this will soon be added elimination of
polio, guineawomi disease, tetanus in the newborn and
leprosy. Despite these successes, the microbial front remains
disturbing and is a cause of anxiety. Thirty new diseases
have appeared on our planet in the past 20 years. Infectious
diseaseS~T5ntinue ,to be die leading cause of death. What
diseases were thought to have been conquered or nearlyebnquered, have now staged a comeback. Examples are
plague, malaria and kala-azar. Diseases such as tuberculosisthought to .be controllable tiirough available teclrnologies
and for which elaborate national plans of control were
developed decades ago, still exist and are getting worse.
What has proved to be a new and deadly disease of mankind
tlirouglrout die world and despite its early recognition soon
after its introduction into India in 1985-86, HIV infection in
India is rising inexorably and there is a sense of despair.
Diseases such as dengue and cholera which are endemic in
Indiawithperiodic outbreaks from time to time, have now
assumed more virulent characteristics. These examples rep
resent a formidable array of emerging and re-emetging
infectious diseases and a new paradigm of infectious dis
eases is now in evidence due to a multiplicity of factors.
Recognition of these paradigms and the factors contributing
to them is essential for developing effective control
programmes. The increasing plienomenon of drug resistance
is a part of die paradigm.
Amongst die factors influencing die new paradigms of
infectious diseases, diere is die age-old factor of poor dying
conditions wliich in many areas liave worsened for certain
sections of die community, often in spite of growing overall
economic prosperity.
Otfier factors include die unintended effects on ecology,
at bodi macro and micro levels, rcsultihg“irpm human ac
tivities under die overall rubric of “development”. These
developmental activities include:
(i) Dams and irrigation projects which arc necessary
and bring about prosperity may also tend to create ecological
conditions, if not foreseen, conducive for re-emergence of
old diseases, especially vector-borne diseases.
(ii) Industrialisation and energy-producing initiatives
wliich are necessary for economic growtii but also lead to
environmental degradation widi health consequences.
(iii) Changes in land use patterns and human encroach
ments of forest areas, a common phenomenon today, expos
ing human populations to infections witii wliich they liave
had no previous encounter.
(iv) Unplanned urbanisation and expessive population
growtii creating optimal conditions for die entry and spread
Division pf Publication & Information, .1,CMR, New Delhi - I10' 029 <'
of infectious diseases in congested squatter settlements. The
essential problem here is the breakdown of infrastructure
and services in slum areas creating conditions conducive to
the resurgence ofdiseases once brought under control. Urban
f health is a matter of overwhelming urgency without much
time left to correct tire prevailing deficiencies and hazards.
(v) Growing trade, tourism and trucking accompanying
increased international travel leading to greater intermin
gling of people today tlian ever before creating conditions for
tl*e spread of infectious diseases. Tlie speed of transmission
of infections increased enormously as mankind transited
” from sailing ships to jet planes.
The changes in climatic conditions now reveal signifi
cant health effects. Atmospheric pollution, deforestation and
ozone depletion play a key role in global wanning. Tliis in
tum, would lead to higher surface water evaporation rates
with greater rainfall and heavier monsoons in key areas of
tlie planet. This would alter everything from migration of
birds, habitat ranges of insect vectors of disease and tlie
availability of arable land for agriculture. Dengue and
malaria transmitting vectors arc sensitive to rainfall and
ambient temperatures. As a result of global warming, malaria may spread further up tlie foothills of the Himalayas.
Tlie lesson of macro-ecology is that all life forms -and
chemical systems are closely linked in complex ways'. It
would appear that current and anticipated changes in local
and global ecologies would favour some' microbes and their
insect vectors.
In place of tlie Cold. War there are now multiple local
wars and conflicts which along with natural disasters, such
as famines and floods, lead to mass movement of people
internally witliin countries and across borders. Tlie living
conditions of the refugees provide a fertile ground for infec
tious diseases.
Changes in human lifestyles and behaviour including
sexual behaviour and food habits are another potent factor
in the changing paradigms of infectious diseases. Lastly, tlie
i /continuing inadequacy in tlie quality and outreach of health
|( Services is an important factor compounding tlie situation.
The challenges presented by die New Paradigms of
Infectious Diseases can be conveyed by tlie following four
diseases.
Dengue
Dengue, by tlie 14th of October 1996, liad caused 126
reported deaths and 2,545 cases of presumed dengue fever
complex admitted to public liospitals giving a mortality rate
2
of 5 per cent. Wliile tliis corresponds to tlie average rate Of
mortality in other parts of die world, Uierc may be scope for
it to be. reduced further by improved case management
tlirough early recognition of haemorrhagic manifestations
and shock, prompt and efficient replacement of lost plasma
through fluids and electrolytes, plasma/plasma expanders
and platelets as indicated. Blood transfusion will be needed
if there is internal bleeding. The modem regimen of treat
ment of Dengue Haemorrhagic Fever (DHF) and Dengue
Shock Syndrome (DSS) was evolved by Tliai physicians,
some years back and now forms tlie basis of WHO recom
mendations2. This regimen lias been shown to reduce die
mortality rate to 2.0 per cent or less.
Dengue had been known to be endemic for over two
centuries in India and for the most part had been running a
benign self-limited course. All die four known serotypes of
die dengue virus are now known to be in circulation. Tlie
disease has lately clianged its course manifesting itself in a
proportion of cases in a severe form of tlie disease, DHF/
DSS. Tliis new letlial manifestation of an old benign disease
broke out in Manila in flic Pliilippincs for tlie first time in
1953; then attacked Bangkok in Thailand in 1958; Havana,
Cuba experienced die worst DHF known to mankind in
1981. DHF had been raging in our immediate neighbour
Myanmar since 1970. Cambodia had seen a severe outbreak
of DHF last year. In Manila, dengue occurred each year after
tlie rains. Seasonal and cyclical epidemic pattemof dengue
with DHF/DSS in a proportion of cases is a recent pheno
menon developing in India and Sri Lanka in tlie same manner
as happened in the Philippines, Thailand and Indonesia. In
odicr words, there has been a westward movement of tliis
new paradigm into India, Pakistan, Sri Lanka and Maldives
in flic 1980s and early 90s in which Dengue 3 (DEN-3) had
been tlx: predominant serotype. Tlie history of Indian dengue
illustrates the well known transition from a paradigm of
small outbreaks to a paradigm of major outbreaks with
DHF/DSSW
Tlie new dengue disease paradigm has now secured a
firm foothold in India. The paradigm is manifesting itself
extensively in Latin America and tlie Caribbean since last
year. Its emergence as a major health problem has been most
dramatic in tlie American region. Tliis region had an excel
lent record oferadicating Aedes aegypti in the 1950s and 60s
as a part of tlie Yellow Fever Control Programme, but with
the discontinuation of this Programme from tlie 1970s,
Aedes returned, and flic worst ever outbreaks of dengue arc
now raging there. Tliis shows tliat even a year’s slackening
of vector control measures could bring back outbreaks of
vector-bome diseases. Similarly, relaxation of immunisation
can result in re-emergence of disease as in the Russian
Federation and the former USSR with respect to diphtheria.
Aedes is a very efficient epidemic vector of both dengue and
yellow fever3-*. Tire virus type responsible for the current
outbreak in Delhi lias not yet been identified but work in this
area is going on.
Hie reasons for this dramatic emergence in India and
around the globe of dengue/DHF as a major public health
problem, as already indicated, are many:Qneffective mos
quito control programme, major demographic changes-the
most important being uncontrolled urbanisation, excessive
population growth and urban decay cliaracterised by sub
standard housing and inadequate water and waste disposal
system. Increased travel by airplanes produces constant
exchange of dengue viruses.
Tliere is a crisis approach to public health in our coun
try, public health activities being largely punctuated from
crisis to crisis. What is needed are sustained programmes for
the prevention of epidemic transmission. Surveillance sys
tems are inadequate as the Tecluiical Advisory Committee’s
(TAC) Report on Plague demonstrated. Mosquito densities
in relation to rainfall and ambient temperatures ate not
available and early detection and reporting systems are
inadequate/ No dengue vaccine is available although a
quadrivalent attenuated live vaccine representing all four
serotypes has been developed in Thailand and is in advanced
stages of trial! This vaccine appears to be safe and effective
but it will probably be another 5 years before an effective
dengue vaccine will be available for public use. Prospects
for reversing the recent trends in dengue/DHF do not look
bright in Delhi and early breakthroughs may not happen.
And yet, there is no cause for despair.
In response to die recommendation of die TAC on
Plague, a National Apical Advisory Committee for Disease
Control through Surveillance and Response lias been estab
lished by the Government. Treatment regimens liave been
developed with respect to dengue2, control of die disease is
possible dirough efficient management of die disease and
dirough a double-pronged attack on mosquito vectors,
namely, insecticide spraying by Government action and
elimination of mosquito breeding by family and community
action to reduce sources of larval breeding. The latter strat
egy is particularly important, especially in die long run and
one would like to see social mobilisation efforts in much
greater evidence.
The most effective means of.dengue vector control is
environmental management dirough physical transforma
tion of largely man-made vector habitats, widiin and around
human dwellings. Education and community participation in
planning, execution and evaluation of diesc control measures
is die critical factor. Commonsense approach is needed.
Aerial spray is often used, where extensive areas must be
treated in a short period, but spectacular results may not be
expected as die Aedes rests indoors. The approach must be
complemented with larvicidal application in and around
homes where containers cannot be emptied or covered. The
most effective way to control Aedes is larvicidal source
reduction by eliminating clean water holding containers tiiat
serve as larval habitats
*.
The 1981 Aedes eradication cam
paign in Cuba depended upon reduction of larval habitats
in artificial and natural containers of water, intense public
education, and biological and chemical control methods. The
Tanzanian campaign consisted of source reduction, educa
tion and clean-up campaigns. Dengue control is an area
where Science and Society meet. There is considerable
expertise on tliis aspect within the ICMR in India which must.
be mobilised.
Pro-active, laboratory-based surveillance systems that
can provide early warning of an impending dengue epidemic
must be developed. An encouraging development is the Thai
dengue vaccine which could be available in the next few
years. Another possibility is the use of genetically engi
neered mosquitoes which cannot transmit the disease.
Malaria
After the initial successes India is now unable to get (lie
upper hand in malaria control and ever the past decade or
so tire number of malaria cases has remained unchanged with
tire addition of increase in falciparum malaria. The issue .
today is that malaria has now entered new ecological niches5.
Tire problem is essentially due to man-made environmental
alteration which provides excellent opportunities for the :
mosquito vector to breed. The new paradigm of malaria
consists of new eco-types such as irrigation malaria, urban
malaria, development project malaria, migration malaria
and border malaria5. These eco-types are in addition to the
already existing eco-type of rural malaria in rain-fed areas.
Environment degradation is conducive to the sustenance of
malaria. Epidemics are increasingly common such as that
currently in Mewat, Haryana. The revised malaria strategy
consists of early diagnosis and prompt treatment and focuses
on local transmission dynamics and control based on
selective and sustainable technologies. But tliere is a wide
gulf between the fine experimental projects involving source
reduction through biotechnological methods and their exten
sion into nation-wide malaria control programmes.
3
Malaria was one of tlx: first infectious diseases to be
treated successfully with the drug, quinine, extracted from
the bark of tire cinclrona tree. The latest and highly effective
anti-malarial compound is alyo derived from plantsArtemisla annua L.-for chloroquine resistant malaria. Forty
per cent of the world’s population is still at risk and is
yearning for a vaccine, cheap and effective. There is not
much private investment in malarial research throughout the
world and most of the work is done under Government
sponsored and cirarity auspices. Drug resistance is a real
problem and hence the different strains in different geo
graphic areas may require different drugs. It is disappointing
that the antimalaria vaccine developed by Dr. Manuel
Patarroyo, has now been shown to be not effective. Tlrcre
were initial successes with this vaccine, but only partially to
tlx; extent of 31-34 per cent protection but more recent
studies in tlx: Gambia and Thailand confinn the failure of
the vaccine. Tlx; Patarroyo vaccine is a harbinger of better
vaccines to come based on multi-stage antigens.
Cholera
A completely new strain of cholera vibrio had emerged
in India in 1992 in Madras. It has been cliristcncd Vibrio
cholerae 0139 Bengal, with pandemic potential. It produces
a clinical picture of severe disease, dehydration and
hyponatraemia similar to classical clwlcra but is susceptible
to some antibiotics. It lias spread througliout Lidia and went
to Bangladesh in 1993 and then on to South West China,
Thailand and other par ts of South-East Asia. What happens
To tlie Vibrio in between the outbreaks is not known and some
scientists had postulated tliat the Vibrio is dormant between
outbreaks in the Hilsa fish in tlxi Hooglily. No confirmatory
evidence had been forthcoming for this hypothesis but algal
blooms have been found to be responsible for tlie spread of
El tor cholera to Latin America in 1991, a continent that had
not experienced cholera over tlx: last 100 years. Algal
blooms where cholera organisms reside, are, in effect, “giant
floating gene pools” in which antibiotic resistance, virulent
genes and plasmids move about freely between viruses and
bacteria, hi tlie paradigms tliat are being discussed, marine
eco-systems influencing human health should fiixi an impor
tant place. It would appear tliat current and artificial clianges
in global ecologies favour microbes and their insect vectors.
Tuberculosis
With tlie increase in tlie incidence of AIDS, tuberculosis
is becoming worse. The efficacy of BCG vaccine in prevent
ing tuberculosis remains variable depending upongeograpliical and epidemiological factors. A better vaccine tlian BCG
is needed although tlie disease is still treatable with'existing
4
.
technologies just as HIV/AIDS is preventable. India has not
derived maximum benefits from the results of research at the
Tuberculosis Research Centre in Chennai with respect to
multi-drug and domiciliary therapy, though it is now pro
posed to use short course multi-drug therapy against tuber
culosis throughout the country. Case management with such
a therapy, case finding with liigh quality bacteriological
examination, improved programme management and dircctly-obscrvcd treatment can lead to a virtual cessation of
transmission of tuberculosis in the general population even
under adverse conditions.
DNA Vaccines
Multi-drug resistance is rapidly advancing in India and
gradually assuming serious proportions. New drugs and new
vaccines are needed to fight tuberculosis effectively. It is
noteworthy tliat mice injected with plasmid DNA- encoding
a single mycobacterial antigen (65 kDa) developed immu
nity against subsequent challenge widi tlie tubercle bacillus.
It seems likely tliat a DNA vaccine against tuberculosis
might replace tlie BCG. In animal models of several infec
tious diseases, DNA vaccines seem to be broadly applicable
for conferring protective immunity to a number of infectious
pathogens. Tlicy seem not to need replicating-vectors and
adjuvants and seem to be practical and safe. Eventually, a
cocktail vaccine, DNA plasmid-based may be needed encod
ing for a number of mycobacterial antigens to gciKiratc
complete and lasting protection against tuberculosis.
DNA vacciixa; may help man to be one step ahead of
microbial pathogens which are eiflier staging a comeback or
evolving into nwre virulent organisms. Surely, tlie biological
front is never static. To foresee is to govern.
References
I.
Garrett, L. The Coming Plague. Farrar, Straus and Giroax, New
York, p 557, 1994.
2.
World Health Organization: Dengue Haemorrhagic Fever: Diag
nosis, Treatment and Control, Second edition. In Press, 1996.
3.
Gubler, D. J. and Clark, G. G. Denguc/Dengue Haemorrhagic
Fever. Tlie emergence of a Global Health Problem. Emerg Infect
Dis, I (2): 55, 1995.
4.
Gubler, D. J. Denguc/Dengue Haemonliagic Fever, Personal
communication, 1996.
5.
Shannil. V. P. Malaria and its control in India, In: Global Meet
on Parasitic Diseases'. Abstracts & Scientific Programme, Ma
laria Research Centre, Delhi. p 2, 1996.
Tlie write-up is based on tlie Second Dr. B.R. Ambedkar Cen
tenary Award (1993-94) Oration of the ICMR delivered by
Dr. V. Ranialingaswami, National Research Professor, All India
Institute of Medical Sciences, New Delhi, on October 15,1996
at New Delhi.
- Media
 RF_DIS_1_A_SUDHA.pdf
RF_DIS_1_A_SUDHA.pdf
Position: 1537 (13 views)