SCHOOL CARE CONFERENCE-PROTEIN CALORIE MALNUTRITION
Item
- Title
- SCHOOL CARE CONFERENCE-PROTEIN CALORIE MALNUTRITION
- extracted text
-
-Ijl-i^S
S
rM£6
Ca^o^cv-I-
4,
fg'Lo^
a
St. John’s Medical College Hospital, Bangalore-560 034
' J OJaU
‘
THE JOHN Me CORMACK HEALTH CENTRE
WardJ^.Z!u^._5...ekj£;v<?xtQuXw^
-ft Date_.i...........
■■ ■>
- Ah Al A
~ A l{i
Unit &
MRD. No.
.^Ur- g
(A
+■
" g)+ s’Name
f. ,
J^- /
J
<-
y>’
I
................
Q-^
2- ~ 2
l' ^
(^rv
19,
ending
A
r
O'6>'
c 'tp
A
Condition
4^
I
.$e
Oyv<^-teb4
— rt-^"
7v/
Midnight to Mkinight
^±J
.
^C
kxg-t<j ‘-Co.
!/2.‘-■.jU
~
(3
*F
‘E
€
T3
co
cu
Remarks
<D
Q
—4&U&
■
|VJ j ox**'"''—
I lAzJt
> (J
~
1 ©<<-4.7
-•'
e-v
<?-
.-s-y
C-U ft
• 9
Jhj.c,
OU
_
a
<<- &z>--aJ'-(‘^VtdMZCLuLC'j
t e bUM.K£ OX,
j^te^vrs-
h[ I o
f s/24_tx
v S I jZ-^. I /
— /\Z /Q Z).
» t
f'
<-> r- v
c^e c
p.
l£p
^-i--t-
Sr-^rt-H r r^uv j coJ
•f^Lcu..^
c
k^CLc
-S
A- c ^(l/t? 4.r/ crvjpo.^c^y?
(. L c..^ v i,~
(2^
s
”/
r-7-<J c ixl
<
cor z^. 2. £l<5
.
!<?
Ct
D/C
T —Sc-cuf' 4
ci
—
c 'c. . „
-2
ft
/c-^g
4
/te
e oc <2-L
4
C-C^uxytx .
asi'^
z run/' e
&
C>
LxC
- '§■ j c_t C?~X2>
t IaT
A tv_<o—0
crv^ .
A>'
6 2.
p>PoJ-i? Cc 0 ?.
v vcUL,?" z
<2
- Zfc ^suJ)
^<oO ( Ma c -vo
rf ..^0.1^-,
Aj C_-c La_a_oc_x_ !■, l
Ai
/
H/ - ■>
7^
/D/
1 '•
H
ee
C
H'-t
2 ,
cJLF;
•.^'^c><i
/
•^/
*
87^ t --
< Lc- £
\ ^cxL-4 <^>^> c p
03-003
NOTE : PLEASE ENTER THE TOTAL NUMBER OF PATIENTS AT THE BOTTOM AND SIGN.
(fL l < I C' -• r
AC’- <-3
tv V lk_'^C.
John’s Medical College Hospital,
Bangalore-560 034
THE JOHN Me CORMACK HEALTH CENTRE
Ward
.•••••
r^-i'/vaux
Q<LG.eA^> "
cjLl>~qP
do
Unit &
MRD. No.
V^<CLM&C^XA
C<£
Midnight to Midnight
/2:
4p(^AJ2^g
gLZXxOQ.Jo.
"CL
CD
O)
3v
/3/ 2..
Name
p.
C
Date.
•• •«••«••
•• «r«
rfodLs^
6Xpg Q
/\J
•••«••••
1 ,
O—
E
<
JZ
o
S2
Q
•4» -(P-*-
J2_^£ p
jz.
■w
CU
'UG^2t5ondition
CD
end i ng.19....
piCc.^ _______
S
-C
cu
CD
Q
Remarks
Lor - <5 • ?
RL - /i.2. 2 '■% ( ’^OgC- -
/ (
i
p 04 die
^Co^-V
O-J-. CP^Jr\
^deirtix.
- i >-»->
/ ~>o er*
ey> t
t HP
. bu^->^~
fir/2 ls^
"
Z-oa.-s
( S t-VX^ l C - VL'
ftr -
Pl O
SsA
1^
P.tZp 6
bi /<t>L
r
<L
? cic^. M—
aJ<bl'’
Z-LV<f <•'
v C$1
5^^
Qj’Tc^-C
eX><
<S>bi_S2_-£X-i
,
. V_4^..c <2
-
y
zV/^73
t
' <7
/
/'ITvCy
ck_^
‘ft
/Ue
^dlc/rx^-, ., £'fe-CJ ,
m id
f d
ZTT\ V Cd ^CxC-JCsSi-P
cJU.
> e ^Xc2<S>.
C^v_c g>_2 -CO-C
x-y
Ly
■
-
A [(o
N
^'L^-O
/-(C
-j—
A 2-
gotT’
< -a-x_cr ,4.
<?
2 ’ '
2^-
cStt/v-
_AkC
f
/,. <C-U^/ -€
9-
(2 C.
2 ^ncJ P
03-003
NOTE : PLEASE ENTER THE TOTAL NUMBER OF PATIENTS AT THE BOTTOM AND SIGN.
Vp' *1
0 c
St. Jhon’s Medical College Hospital, Bangalore-560 034
THE JOHN Me CORMACK HEALTH CENTRE
Midnight to Midnight
Date.
Ward
19
ending
■o
0
U)
Unit &
MRD. No.
co
Condition
Name
-C
o
<n
b
-a
o
*->
E
-o
<
m H
IT) <
M«
x:
ro
<D
O
£
Remarks
to
,
/ s, '
-• S^>X> i
“i—* Cc_c*JU vxX-X •-? Q
JT
i
th
►w.A'
c. JO
KT J
, scCU
9
rl
^Xjojz.
x/J
p>»J cP-’2’—b
t
£
y d.JL^Jl
L ‘t Q
I
L.^
^L-Jcuv
^/<-C
»M (l Z(■■
/
M PP 4
A,
TL^
• L'-
|-U|< ip-:$) 1^^-J
<?L
C5>n
P
U\
03-003
NOTE :
ra
(O.
G.
i/v.—L'-*-y.'
P/c&l'eXjL&A
GJU v—■£
(2
/3h^o
^-v>r
?
k
CPs{;L*> — tf.skxp-F
:l
(-£?-£? C?(L 1 •(_
XvJ'-c> v<J
O'ufeoy c
/'iorVLci
^1.
— C<C,
i i
0^2. a
A!
NJ fl b>
PLEASE ENTER THE TOTAL NUMBER OF PATIENTS AT THE BOTTOM AND SIGN.
St. Jhon’s Medical College Hospital, Bangalore-560 034
THE JOHN Me CORMACK HEALTH CENTRE
Ward
Date
Midnight to Midnight
ending
•u
Unit &
MRD. No.
O)
Name
Condition
co
o
OT
O
19
•o
•5
E
■O
<
co
<D
Q
03-003
NOTE: PLEASE ENTER THE TOTAL NUMBER OF PATIENTS AT THE BOTTOM AND SIGN.
Remarks
C/.<^b^)b<cj2Ztroo r.
d
-
j'cxtK^xj ^a^^e.
7g ,
N/?b -
i <eXvy? -^Q
2^
^kx^cJ,
.
, Mppi. £^-<-Q_ >-«dcJ_43f
C^d-r-tA^L^s
.
i)a t13
£ g ,_£)
(AZ^
<2^
5 e-rJ
D e c_
SsJllz.^ -
\ v^<^-5
<2-^
— 3 i-v-1
G2j^>l
C C Ou5 ‘Z_-
MiSf'O^L
• P c /z-X
—
- i&h f^v
(\
2
. g>,
f
—
J^-Q-P' •i—
p)f
/-iz'i
uTTc.aJ^'
P
c? B^ i-C^
fTT
cA^JbiJ-Dyv? C=L>^
TR
CS2
S
2* ^Wzrtif
c
i_!'
t^CTcjQ,
O-TSTLiLL'
f
/1~\^~)
A LL-^
.Z_£>
fo
€
/-
r
-r
z
P ~7 7 ,■ 4- 2^S
A 4 £ /M> "
f:
K
a/o
/O S
o
■g’. 2 c'-t3 /<i-^'T>D
c^^c-
Z,
I A i-------- 6^^
^r<x>( au
CLex-U-H.
/ izO e^/'fe^e A
' K; PA d-b-<^P
gtd 'PP^3')'
<F><aZq^-y^_^ ._
7xj i\- -Cs ,
—
—
-
r
<—(
>C^O^^<2^laJ'' ' —
f/i-S
/s/'
-J ''t-^
/■
CAO3H.
Pa)
^c.Oj^JL^
c^_o —
Wepi-^Lpp^
e. .t ic
___
/
, Am_a b-i
9
cot^c C’-O AZ/
/ A/ P P
a>~
I gjl
ru
n
■
jZ-x-xzx-)
X
A| 2t^o<--A
|2£Le>A
.h^ Q-o-K-7A
■3. z
X5 dpG o
< /g’Z? ,
/■
\p [Ll''
v u-°- c'
c.
QP
p^A>
^>-c
jczj ^'')^> ’<-1—
/^uz^
_ ■=gxp
PPp L-
/S’/'
7J)
^-Asrcs^1
i I'-'l ,
^£>u2l v<-p /4 .cc
^3||
?
^l>
^'C-i. '-^
.
Aps-c^ri^d^Q^
^.L &"
cjx-v-i
T
/?
t2^-<2p>
■
t
A
Co
1 c> '
UD>-AI2_
. jgUo^J ' c-c^-PgkZ-G
.S^Ci llP jAw-a-,
f
c_jry’ ro
k0
A
* Aj
,S’ A-O^^p
ftsGa
C-ZXj-^
—
,A
c’-^c c-
z-M2 Q-
bTX
T's
/ ^lo. S 1^'<J2_.
>29/<
-
i\&S^-'>- u
/2 p i' +~
22 l 2-
-^2 c?^
.1
1
<
Pf o
~ 1 r£p r;cl
s
|U-6<^r ■
Hk
vSH
1
- /s7^ - *
d
IO I
/ /t 1^
o
«2ch - 10 I0/ 2?^/o?b
/
\
♦
I
.
-I
■•• <«. . ■ .X • -rW
iT’f it'. 'IWiiiiif j
1
T/j
\j.'
-
. f—] co^j^v /2_C3--vr-) ,
7
A^cA.'~-a
—-----7
y>j
’^Ly'
pc <_
a
/ o - /
d
r
i ' ^ ■ Sc?
t^lfl^ r Z
y
'
xLo tA.
5?^tw£e‘
c llJt^ Ca>C^
^Jk.
‘
3l.
mcx^
Klj
LK -4o,_z5 '
•CI-^<jLg.LC|
--t—
G^M->n'-1>-]
A
I
J
v~> no u-< la-^
n
3-
CL-
7°-
vJ
1.1-
J_li
o
e
iC
z-sCO^A’- V—
"
lr=>
lA~
^^?/Gc
l
e^p&c ^CsvcdAi^
v \2
/V_JC22
A. «;7L c f
.zvc-tn -p c A - CJ^W
O-^XT T g
L
«^_r<j2-^—
c
r.
q^J'SlC’
r
’
.
pr
Oa^Xasx^
/ ^Jb-—i -Xs CLicJ''j2o.V'
f cj.Ctx^ts
Kl(I~ &-i Q^y
flL' <ZVX'
z
rS*^oj!-f ®K-Xf ^?A vrJ
^6>- XAtfS' —
/2S -
I p_>u-oi S €*^ ^-L>J.exLg -p
M X,
.
/V
iAX>.
Z^-AD f^r'
O-
/
Zi-S
Tv
I
i ? PPc
S^u^kP T
- fo-£^ye
"1/
7 0^ —
>
z r/o
;
^7 QU/Ca—C'-J
x°
Cc> I
X?C
->_4 Lxj_<-i_£
V<J
Z^vz^' C,
,LUzV c ^LJ1_O-P Q. Of
J LcJ) /
p
-la-a, Q_
i Q
n s? V;
'^252b '^O.x= ->
f?! <
-V V<4^
I^ToL^O -<^ ^A
2 - ? / l^/1^).
.
■'
“Sj
(M-o
-
■-GL.
fO ^J.1^
7J ^4X3.
G^O X^f
Vz IypY
A
, o
2o2 £
’/-) c; f i'
>-
CS)
J
i
hl. Na - 64t?O.
^4
2. D Li Lt °l
s J-rte^H
^'T ■ tjca-La-a^-A
q - s -1 'S h d
(2cx^<2t^- ’
*—A C-J?
to
— H/°
L
■4- C»CL_G>«^
S’C
- 0*2 £>
r K'^ Mfc ~k^soc
7
z
&-A5O
C,
S •> ^-
I
"
z ^/le
.
^A^VV-A-OC.
c."
LAa
/kXLA^
<^2£^t
r z cA15 c_
V ^7^
^.rt'
b~<-£^
.
d? Q <
(
<;1aL-W
•eC>-
2 c. - 2 r//?P f-
^<eAc—^P/
^U^VceJ
C-£V\
^■n I' '■J
>/o^z C'O-CJ z
^4Vs
C^eA~!
^e—
$
■2. )2
—
1^^
r^^i>
g - /2- c^U H’'>^n; ■^- -f~ F
( 3
SiO
-k' g^IslA^ -
X •AP~^ *
^4 '(rH
S
z
?‘P^3^
v^u <5>vni
|
dI
.
Qcfi-^ *T
14?
M A
vc.>JLV-
!?s=»-^ *2^o 5o >
/ 4^^
<r?X-0^
z1
As? -f^l
i
tM2 vl c.-^
/\J r iM f | A
)
^jdiwuJlD
/X) o
-O
c-,
<^-0- - /V_JQLA_K-X-*->
\ c.
f.
(i
f^J fQ-fi
y\ -j
ST. JOHN'S MEDICAL COLLEGE, BANGALORE
Class
Semester
Subject
Examination
Date
_
____________ _ ___________
5r 3
fcU^frvnc^
bo
Hi
H
2
Ji^L, 2 I
Dog).
— -2 S'11 /SO
old
CU\
'
Dept, of Community Medicine
________ _____ St. John's Medical College
B?nr>lor*-560 034.
Roll No.
Q.Ju^jXcu=t’
JUsJ '
-La^-q „
Y
•fr-
Oe»^4>G- I
-
O-J ^<=»r O_
JLq~^
2c. CL^-
XJ £ lb .
■
pfl
l/vOQ_&-&-» CVK-^-C-v-
rXu*j cxjs-^1-*
uSoo-pc*' uJ3?1q>P
I5ta Q
?P^
_ - •2^\ <
~
o
j
r^j^} j L.S'2
. Sgc's,
M
C->^A e t
2^/r -
Sx^crU M/ L^JO
—•
?P^L-
—Hkjv-O
pjoXe, vj<2^-LoxAb t c^CO—CxJ^ j
IM XST
o-
jnPA y
C<x^
*
/
/
Gw) h
: 2-
MEDICO SOCIAL CASiS ■70RK IN A HOSPITAL SET UP
Dr S.V. Rama Rao MBBS DPH MPH*
INTRODUCTION
A child is admitted to the Hospital suffering from Pneumonitis,
Hookworm infestation, anaemia and malnutrition. The Physician treats
the child with sulpha or antibiotic, gives anti hookworm treatment,
anaemia is treated with iron and reinforce its diet with let us say
powdered milk. The child is cured of the conditions and discharged. File
is closed. Six months later the child is seen again in out patients of
the hospital - this time with a reinfestation of hookworm, advanced
malnutrition and anaemia. This means that the malady in the child is
deeper. I^. is not sufficient to treat the disease. Mere treatment cannot
give permanent relief to the suffering child. The sick child has to be
considered in totality and not merely as a person. Sickness is not
due to a single etiolo>d.cal factor. There are multiple factors. The
clinician assesses the sick person by his examination in the hospital
set up. For a total diagnosis of the condition and complete treatment
he needs more information about the individual in his home and his
community because they have a bearing on his sickness. Information on
the physical, social and biological environment, economic status,
education, customs, habits, occupation, religion and a host of other
factors which build up his background. This means that the Clinician
should have full information on the medico social factors outside the
hospital. The Medical Social Worker (MSW) acts as a liaison between
the individual family and community and supplies the information by
making use of special techniques. The MSW will discover the adverse
factors which is particularly responsible for the Social Pathology
of the disease. When once this is identified diagnosis and treatment
could be taken care of to the best advantage of the sick by the
Physician.
k
Medical Social Work is a form of social service adjunct to
the personal service which the physician gives to his patients. It is
the art of helping patients who have social problems in sickness.
It is the work entrusted to a qualified and trlined social case
worker in a hospital or community set up. It is concerned with the
personal problems connected with illness that trouble the individual
patient and may hamper his recovery. MSW is a member of a team.
HISTORICAL BACKGROUND
Western countries - Englands Appointment of ’Enquiry Officers’
in 1876 who were the fore-runners of ’Almoners’ - These Enquiry Officers
main task was to enquire about ths patient’s means. First Lady Almoner
was appointed in 1895 at Royal Free Hospital.
1894. New York Presbityrean Hospital appointed
U.S.A.
a paid Social Worker. It was, however, Dr Richard Cabot who started
the Medical Social Work in the modern sense in the O.P.D. of Massachusettes
General Hospital in 1905.
In the beginning, hospital and medical profession were
averse to accept the new idea of Medical Social Work. But gradually
the advantages were realised. The report of the hospital standardization
(1929) of the American College of Surgeons greatly stimulated the
development and acceptance of the concept of Medical Social Service
in Hospitals.
p.t.o.«2
*ST JOHN’S MEDICAL COLLEGE, BANGALORE
:2:
INDIA: began her Medical Social Work more than 5 decades
ago in a few hospitals starting with Tuberculosis Clinic and Maternity
services. It was specifically mentioned in the Bhore Committee Report
(1946) and a trained medical social worker was first appointed in the
J.J. Hospital of Bombay in 1946. Since then MSUs are being employed
all over the country in hospitals, special departments, rehabilitation
centres, medical colleges etc.
NSBD FOR MBDICAL SOCIAL S^RVICij
The rapid social changes, demands from patients and
complex situations have given rise to problems which were not encountered
previously.
Eg: Economic difficulties
Unemployment
Over crowded living
Mental stress and strain
Domestic disharmony (strained inter, intra and
extra familial relations)
Increase of delinquency and me- ital disorders
Rush in hospitals and dispensaries
AIMS OF MEDICAL SOCIAL SJRVI.CB
1. To collect and provide information for arriving at
a correct diagnosis, eg. Illegitimate pregnancy,
self-inflicted injury, starvation, social conditions,
psychological and emotional states
2. Development of Medico Social piogrammes within the
medical institution
5. Participation in the development of social and health
programmes in the community to meet the demands of the
hospital
4. MSW to assist hospital authorities in formulating the
policies
5. Participation in teaching and research programmes of
the hospitai/community
M S D I C 0-S 0 C I A L
W 0 R K U R
-social case worker in a medical setting-
Medical Social work cannot bo carried out in isolation,
and closer the contact and mutual understanding between medical and
nursing staff and MSW, the better the results will be.
WORK — concerned with the personal problems connected with illness
that trouble the individual pitient and may hamper his
recovery. His/her functions is first and foremost to help
in the treatment of patient. His/her duties vary with the
type of hospital clinic or health organisation. But basically
the duties can be categorised into thiee fields:
1. Medical Social Work - connected with the doctor’s
investigation and treatment of patient’s illness
2. Teaching, Research or policy as it affects the welfare
of patients within the hospital or organization
:3:
5. Cooperation with other agencies both state and voluntary
connected with social aspects of d dicine, health & welfare
services.
MEDICO SOCI/Ju ^TOBK.
Directly concerns the patient’s treatment and after-care.
This will be the day-to-day work for most of the MSWs. Two important
aspects (a) Nature of work; and (b) Responsibility as a member of
the medical team.
(a) Nature of woik
i. Soci'il investigation and enquiry
ii. Social treatment
iii. After-care
(i) Social Investigation; Social erquiry is only eno of
many investigations which are
needed. Entails study of the social end personal
background of the pitient’s illness and consultation
with the doctor over those fac-ors which may be
relevant to diagnosis or treat1, ent
Overcrowding
Bad housing
Irregular working hours
Financial difficulties
Anxieties
Personal maladjustment
The MSWs report may influence is also suggest social
treatment. When detailed enquiry of investigations
are necessary, information may bo obtained not only
from the patient but also through other social agencies,
from relatives, from employees or other sources.
When social enquiry has been completed, social treatment
can be carried out. Enquiry and treatment are sometimes
both on a small scale. For example - How can an
amputated patient discharged from hospital with no
convenient bus service -attend hospital for subsequent
treatment from a remote village?
Social enquiry is concerned with alternative means
of transport-”! bullock cart comes every Friday for
for market day” J’A toddy loir;, is running daily”
(ii) Social Treatment: For some p. tients an explanation
is enough to relieve anxiety nd to ensure that
their needs arc fully undorstcod at house or at work.
For others sometimes simple? sometimes costly or
those difficult to secure may be necessery.
For yet others help needed may be on a more personal
level - here MSN must first g.-An confidence of the
patient, must use ill profossional skills md experience
in helping him to overcome scie difficulty in his
personal life or to make some social adjustment
without which he cannot fully respond to treatment*
Broadly speaking aim of all social treatment is
rehabilitation - assist in re-establishing the
patient in normal life - help him to deal with those
factors at home or at work which might lead a
4
:4:
recurrence of his illness. This ma r involve contacts
with industry or employer. Help neadedi. by the patient
is of various nature. Eg. special diet help in the home,
rest in a convalascent home, recre iticn, vocational
training, change of employment, frigidly contact. The
MSWs help will be needed in making the various contacts.
Social treatment is directed at re loving obstacles to
medical treatment or admission to hospital, smoothing out
other difficulties which arise during the course of an
illness, solving long term problems which remain when the
acute stage of illness is past, and adjusting.the social
environment so as to avoid where possible the particular
conditions most likely to cause relapse.
a Transport problem as one
b Not having money for bus'fare is another
(c) Patient may not be able to wait at out-patient
for a long time
(d) Difficulties vith employers may have to be smoothed out patient cannot take time off to come to hospital for
treatment
(e) How and where can special treatment be obtained?
(f) Mother wibi an advanced illness needing hospitalization
asserts that she can never leave her home leaving
husband and children (MSV to look out and arrange for
help at home during absence of mother)
(g) An agriculturist acutely ill in hospital was worried
about an underground pipe in "he field which may be
broken while ploughing - MSW rent instructions
Immediately.
(h; A boy worried about his examination passing, which
decided his career was anxious.. MSV arranged for his
attendance at theory examination.
(i) Financial trouble for treatment - MSW showed
resources - Provident Fund or Life Insurance
etc.
For problems of this kind,MSW can keep a record of all
organizations and institutions which will support cases
of this type with financial aid aid help deserving cases by
using her good offices.
Emergency service includes finding accommodation for the
relative of severity ill patients>
Minor services : Advice about puzzling hospital procedure,
reassurance when some technical ts-ra has been misunderstood,
help in cashing salaries or pension, small by themselves
but gives peace of mind to the patient.
Long terra problems - resulting from illness or injury
require the longest, most intensive and most imaginative
treatment. For these, the normal way of life has been
checked or facing alteration. Some have to face disability
for many months or years or even life long.
eg. Mechanic who has lost his ri: ht hand;
Youth whose heart is permane~tly damaged due to
rheumatic fever;
House wife with failing eye sight;
Officer with head injury - less of speech
5
:5:
An MSW has .to use all her skills and expertise to overcome
and achieve to the fullest possible extent - independence
and functional ability and gainful vocation.
Methods of Social Treatment
More has been said about WHAT MSTfedo for patients than about
HOW they do it. General outline is furnished.
Before social treatment is instituted, need for it must be
discovered and this point needs emphasis, self-evident
through it may appear. Sooner the problem is dealt with,
better the result. Social problems are so closely linked up
with medical matters. It is often from the doctors that
initial request for treatment should come. The MSWs work
fluctuates strikingly both in quantity and kind according
to the interest taken by medical staff. Without medical
cooperation, the MSW can achieve very little. Often the
staff nurses discover the difficulties of the patients which
need MSWs help. They also contribute much for the success of
MSWs work.
When once the need is ascertained, the first step of MSW is
to consult doctors and find out the diagnosis and prognosis.
What treatment will be required and in what way the patient’ s
every day life will be affected.
Final responsibility for the form which her help will take must
be accepted by the MSW herself but she/he has to secure the
knowledge and approval of the medical staff before taking
ac ti on.
Her help should not overlap with help of other agencies and
she has to keep those agencies fully informed. MS1/ is only
one member of a team. Correct medical information when necessary
should be given.
A case of ’manipulation’ was mistaken for ’amputation*. Enquiries
about medic.il condition in general mus ; be referred bach to the
medical staff. When patients and relatives have been told as
much about the illness as the medical staff consider it advisable,
the MSW can proceed with her task of helping.
Patients are often slow to grasp the practical application
of medical recommendations to their daily life and interpreting
this to them is an important part of medical social work.
(iii) After-care; The MSW will keep in touch directly or indirectly
through some social agency with those patients still attending
the out-patients who need help over a long period to ensure
that the value of treatment is not lost.
Patients who cannot hope to return to cheir former activities
need help or advice in accepting or overcoming their limitations
in order to live their lives as fully as possible (cancer penis,
histerectomy after delivery etc)
Responsibility as a member of the medical team: Medico social
work is a te tm work and MSW is a member of the team. It is
necessary that MSW should have frequent consultation with
medical -•and nursing staff. Relevant social history (major
social problems with which the MSW has to de xl are commonly
those connected with poverty, loss of income through sickness,
with employment, with practical difficulties of domestic
care of patient or family with housing,'personal disturbances
and social maladjustments) should be readily accessible
to the medical staff.
.,o.6
:6:
What is the responsibility and role of the NSW in the out patient
set up of a hospital? Let us follow a patient who presents
himself at the Registration Counter of the Out Patient Department.
Registration
Doctor
__
Notes down complaint
I
subjective signs, symptoms, history of illness9 previous
treatment taken if any,
Examines and coraes to a
subjective
„ Elicits
further history.
tentative diagnosis
signs and symptoms for confirmation
Writes down
i
investigations to be undertaken and sends patient to
laboratory, X-ray or other diagnostic Centre
Patient
investigated
Comes back with results of laboratory
investigation
Doctor
Reviews the reports
Confirmation of diagnosis-- -- prescribes and advises
. (treatment and management)
Patient leaves '■he hospital.
The doctor may need the help of the MS ' at any of these
stages in the flow chart of the patient in the out patient
depending upon the type of dis ase.
]jjg:- (a) Person suffering from tuberculosis has taken treatment
previously. The doctor needs to know what treatment
was given, for how long and why ’the patient gave up
and came here? Any financial difficulty?
(b) Person suffering from malnutrition - What is the
usual diet at home? Wat are the cooking and
culinary practices? How much is spent on food and
what type of food is generally used? etc.
(c) A patient is afraid of lab investigation because
blood is being taken for testing. Patient needs
education
(d) Patient suffering from helminthiasis needs education
on personal hygiene etc.
II. TEACHING, RESEARCH AND COOP'CUTION WITH C fHER AGENCIES
(i) Teaching: Teaching of social implications of illness to
medical students and nurses in training as well as
to groups of social workers and others concerned with
health services - MS.W is not necessarily a good teacher.
Those who can teach should be given the opportunity to teach.
At least one member should be a person who can teach. He/she
should be given the special responsibility of teaching and
be given time and opdortunity for study and preparation of
case material involved.
(ii) Research: Where medical staff are engaged in special
clinical research, MS'/ should be asked to share in planning
that part of enquiry dealing with social factors. In the
field of social medicine NSW has a positive contribution
to make. There is a new demand on their knowledge and
experience.
7
:7:
Policy as it affects the welfare of the patients: The knowledge
of the pxtient’s point of view which the MSN possesses enables
her to contribute in policy making of hospital services.
III. COOPERATION WITH OTHSR vlG.JNCIJS
MSWs work for individual patients brings her into close touch with
other social service and other health organizations - local and
national statutory and voluntary. Those contacts broaden the
horizon and increases her exposure to various types of experience
of patient’s needs - helps to plan better or modify the existing
ones. Involves in attending committees and conferences. Contacts
help in closer cooperation with hospital.
ORGANIZATION OF THE MSW’s DEPARTMENT
ADMINISTRATIVE DUTIES
MSW is a professional worker
This should be borne in mind
He/she should be allotted only such administrative duties as
relate directly to her function as a MSN (clerical work, work
on assessment of income of patients, visits for administrative
purposes, substituting the MSV when Dietetician, Clerk, store Keeper
etc are on leave). Such duties will not only imp ;de the Medico
Social Work but gives a false conception of medico social work to
others. Medico Social Work and service is their primary7 function.
Any other type of work if entrusted bring -bout frustration,
dissatisfaction in job and finally inefficiency.
Staff; Conditions vary so consicerabl; thau no uniform scale of
adequate staffing can be laid down but in acute general and teaching
hospitals one MSV for 75 beds is suggested. In TB Hospitals one for
200 beds and in hospital for chronic sick one for 300 bods.
Accommodation: Office of MSW should be placed near to the Doctor’s
consulting room and should allow privacy for interviews. Typists
should not work in the same office as the MSW. There should be
adequate space for files. Extra room may be required for teaching.
The assessment of the MSN in the discharge of his/her duties
must be left to persons who know how to assess the job responsibi
lities of a NSW.
Many suggestions for the future co ld be made but one tiling is
certain. The MSN whatever the details of his/her work may be?
must concern herself before all else with the welfare of the
patient. Results of her work are not easil3^ measured, but she
has it in her power vitally to affect the lives of other people.
The future of the profession depends in the last resort upon the
quality and inspiration of the people who are attracted into it.
$
$
‘hl ■
1
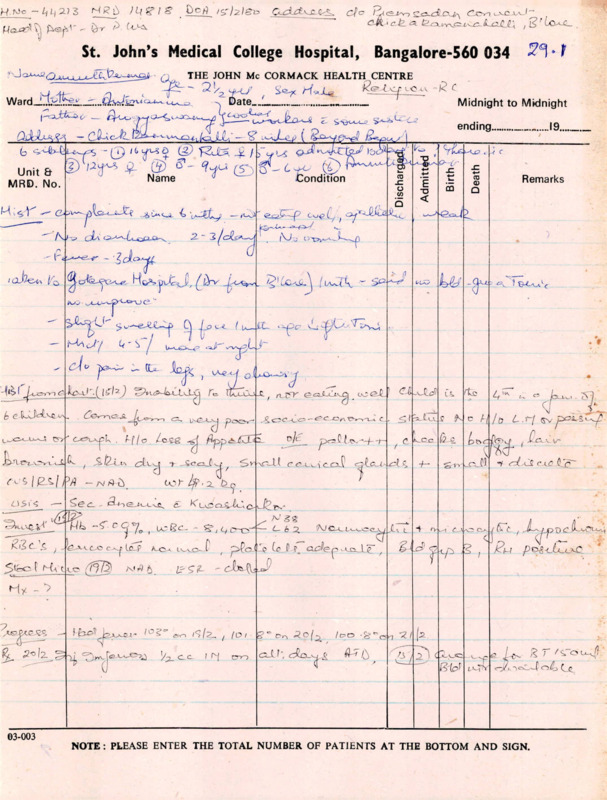
Case Study of a Marasmic Child in Rural Punjab
Gyn hzi *3
By
D.N.Kakar* , Ph.D; M.P.H.
Introduction:
Protein-calorie malnutrition is perhaps the most wide
spread and the most important pediatric problem in develonine:
countries. Many authorities believe that it is directly or
indirectly responsible for the high infant and childhood
mortality m these countries. It particularly strikes the
high risk groups^such as the children^ pregnant women and
old people. Children as well as pregnant and lactating mothers
have higher nutrient demands and if these are not met, inci
pient iorms 01 malnutrition develop and the individual catches
infection more easily. The synergism between malnutrition and
infection attacks the individual consequently diminishing his
chances of survival. High child mortality, especially in the
age group 6 months to 3 years, seems to be mostly attributable
to this synergism, notti biological and cultural factors in
fluence malnutrition. The cultural factors differ from place
to place but in general traditional feeding practices after
weaning do no c ensure the child enough proteins or even a
reasonable share in calories. Sometimes, the weaning is so
abrupt that it leads to psychological trc'iUma.’fea.
The Nutrition Project of the Johns Hopkins university1 s
Department of International Health is making a special study
relationship between malnutrition and infections among
Gn?'"’c'"ren ^'^cr three years of age in a selected group of
villages in Ludhiana District of Punjab. During the course
oi our study which involved a weekly morbidity survey of all
children under three years of ago, we found that marasmus,
locallyknown as Sokan was the main clinical syndrome of
malnutrition in those villages. Nutritional marasmus is a
lorm of severe protein-calorie malnutrition usually occurr
ing m the first throe years of life.
The present case study relates to a scheduled caste
Ramdasia girl, whose family situation end beliefs about
etiology and therapy of marasmus have been studied in
considerable details. In order to highlight some important
points, certain socio-cultural aspects of the case ere brief
ly presented here.-
* Dr.Kakar is working as an Anthropologist at the Rural
Health Research Centre j Narangual.
-:2si
Name' of the girl;
Age;
Sinder Xaur
32 months
Mother’s Fertility History
Mother married
First child (F)
Second "
(M)
Third child (F)
Fourth "
(M)
Fifth child (F)
Sixth child (F)
Seventh "
(F)
Eighth
Ninth
n
it
(F)
(M)
at the age of 15
-do18 (died)
-do20
-do26
-do27
-do28
-do30
-do33 (Sinder Kaur)
died
-do36 (died)
-do38
S^nd?r Kaur cojne from a poor family, her father had
crculosis and was an alcoholic and had been out of regular
t •
Ior
last live years. Casual labour never fetched
him more than Rs.50.00 a month - an amount inadequate to meet
the growing demands of his family. F
‘
Being
on alcoholic with"
considerable leisure-time? he spent a major nart of^h-fq
-- ---- > ear
nings on drinking country liquor. Continuing deterioration
in
beGame tho frequent source of bickerings
tn Ji
wilicb caused considerable irritation and anno Jnco
violdVoJbfS-0;f
Sindor Kaur's mother did not7"
in the Ji Jj
Pressures and horself went to work
m the fields collecting loddcr for the cattle and occasion-llv
S
^“5^- Hot oldest son, at l^tooT^117
teao?oo
oo- month® “b k°“ 5°-° Povor
hOUSO
whloh ‘i!'-rned hi”
the familv ?inJ; k n,a^S° J
V-strickon state of
biic icmily,
binder
Kaur
inevitably
deorivnd
r>r Jon.
cessary
parental
care
and
affection.remained
She ofSn
JSaJJ
in tho house for tho major part of tho dry without a Jr th
inadequately clothed end exposed to fliosf Ho- neglectJ’s
?X:fo±f8nogicct
±tS°tnS
1°^°
uo lomnlc infants.
uuug
0?“ X'l Si-
ago ofH6ryoJsSt
rJ djd °f '’Soka"
at the
-p y
9 Singer Kaur too wns considered c "Sokn” child
thfn
rav“-ana%S2)fQm-Qly
and
In order to
»;
a:.
-;3s-
,
Lij-C
Syana" happened to be the grond-f^-1-hr.T.
S,
took^’ wh0»w?s considered spiritSally more°powSful sPHgltual
took n both !?t5\h t®-Mlere,a
^1OSQ child had died
’took
" ;nV
citer the disposal of dead body, or had taken a
bath at a place where
& menstruating woman had just finished
taking a bath? corr , r’ 1o contacted
tne "Parchavan" of a woman
haying a "Soka" child in hc/lap."
.
While performing "Hath Ilola", he spelled out a powerful > "Mantra",
verbal formul
and then drew certain lines on the ground with his sickle
dipped in water and ashes, j-hon he told the mother that
this was a <case of~ spirit-intrusion
where the malignant
O- p- head child had entered into her body, and this
happened when the child (contacted
' '
“"Parchavan". The failure
of „ the4.4. "Syana"
.-r ato relieve the child of "Parch
- a......van
.„i" influence
wao attributed to the greater strength cl
of
the
malignant
spirit, for which a much more powerful spiritual healer
—_
TVClS
required.
,, .fiivcn oy frustration and sorrow,
sorrow, c,
and
because
of
eno worsening economic co
nH'>
condition
of the family the mother
finally loft the child to
to her own fate in a state of nogloct
and hopelessness.
------
— --■
k>AJUG>-X kJUi.
She v_.._
was^admitted to the Harangwal Health Centro and
the details of treatment
-j are given in the Appendix.
The Sequence of Bvcnts (First Stage)
1. The Lady Health Visitor was the first to r eport the
case to the Project Doctor.
The cz.sc
..
wh
case was
then
referred to the Project Officer
who took special interest
to »9
vs-as SEtEra i?v^iis“Jor Ka”
members of shaorVaV^drmhvr0inn)J^»hrhpO'Ia8h1' mot a‘L1
parents . They SsJItEt
gr?"d
ox the locality and the Sarpaneh tPawh^at' chin”) 1
°
-:4s4. The Anthropologist collected general information on
the Ramdasias, on Sindor Kaur's family situation and on beliefs
about the etiology, diagnosis and therapy of the predominant
diseases among the children, with special roforonco to marasmus.
5. After having a detailed discussion with the family
members, the Project Officer and the Anthropologist succeeded
in persuading the parents of Sindor Kaur to get her admitted
to the Health Centre at Narangwal*
6 • Tho most important factor in her hospitalization was
that her father was primarily interested in his own treatment.
Ho agreed to bo hospitalised with his daughter, Both of them
were hospitalised at the same time and they wore promised
complete treatment.
7.
Centre.
Free treatment was provided to both at the Health
8. As a result of hospitalization- , there x^as considerable improvement in their health, especially in Binder Kaur's
health.
9. Sindor Kaur continued to got the nutritional supple
ment from the Lady Health Visitor and her father was being
given the injections.
10. Improvement in the health of the child had a good
impact on the community and reportedly some other people also
approached the Lady Health Visitor for similar treatment.
(Second Stage)
11. However, after she attained the age of three years,
she was excluded from the study. As long as she remained a
'study child', she showed signs of improvement. Meanwhile,
another daughter was born to her mother, seven months after
Binder Kaur's discharge from tho hospital. Owing to deterio
rating economic situation of the family, this child too was
not looked after properly. Their father continued drinking
and mother had to work in the fields.
12. Thus Sindor Kaur again became marasmic and started
having fever. This time no medical treatment was provided
as it was not demanded.
Outcome;
The result was that Binder died of marasmus. After her
death, hor family was again contacted. It was evident from
interview with her parents that’ they continued believing in
-: 5: c‘;usation of marasmus because Binder Kaur had
was
Th“ainth
Discussion:
nf q-i t7hUST-ul'le 31)070 c?-se Clearly indicates
that the
death
indicates, that
the death
of Binder Kaur was Multi-causotional. Inability
’ ’ •of Project
'the study
______' j
his habit of drinking
butea to her neglect ultimately resulting into her deathf
—-X—
lDNK;jg»
50 copies
Sth Mar'72
APPENDIX
AksALa.SA£ecord, from Naran;:wal Health Centre
Cinder Kaur
Date of Birth: 2.7.1966
on1^3?/1!^ 0Ktbg1ir\Was
File No.601955
into Narangwal Health Centre
Sa? £»les‘ltiple a"a11
Dietary History -Diet consisted of breast milk9 water and
sips of tea.
Family History - Father suffered from pulmonary tuberculosis
shd was admitted into Narangwal Health Centre
with the Chilo, under the cure of Dr .Ian Lawson,
bmear and culture positive for A.F.B. (601954).
Other siblings- 1st female child died of marasmus at 6 years of age.
4 others healthy.
Mother healthy.
Findings;
0/E- Markedly emaciated
Weight 4.6 kg.
Marasmic
Pallor
Pulse 75 per minute
Angular stoniatitis
Bilateral cervical lymphadenopathy
bmall skin abrasions of both sides of neck & right eor
No oedema
°
Pyoderma over the skin
Heart- Systolic murmur in all areas
Ghost- Bronchial breathing right infrascapular area.Few crepitations.
Abd - NAD
Provisional diagnosis- Pulmonary tuberculosis with lymphadenopathy
and marasmus.
Investigations
Blood
Hb
ESR
VffiC
P
L
M
S
16.11.68
12g
lOmni
9200/
cnm
58%
35%
6%
1^
22.11.68
8.5 g (Project Technician)
12.12.68
10.6 g
36%
6%
5%
fSg.68
(
10250/
cum
53%
Incroasoci Hilar shadow with incro.asod lung field
markings.
9•12.68
Sarno
Montoux
1 • 10?000 Negative
Treatment; Streptomycin
vial 00
Px.S
1 gm TDS
INH
50 mg BO
Becadex
B-complex
Betnesal eye ointment
Discharged
12.12.68 - with advice to follow the above treatment.
- weight /.0 kg (gain of 2.4 kg in 4 weeks)
Follov up
Hoao
.S?a?ontil?UGd streptomycin, INH, Pas and vitamins. She
was advised to discontinue PAS and streptomycin on 6.2.69. She
but ^sit^LSllv 3 q£nit£ aJ- h0n0, She still
stilltZnnot\l^
cannot walk
o”
period.
'DNKijg*
60 copies
8th Mar'72
ogt'i’«d
nisgpo^osc!1!?s^7i3g"o?iijt
eo by Sothor unSo^supogiXon
episode of illness recorded during this
T
■
CASB STUDY - URCHIN
Name: Shrinath
Age: 14 years
Occupation: Channawalla
Native Place; Ghoda Raha, a small village in Uttar Pradesh.
PARENTS:
Down in his Native Place. Father works as a waiter in a
Toddy Shop. He has 3 sisters,, young, jobless sitting at home,
5 brothers two of which <are schooling in a government Free School
and 5 are jobless, mother jobless sitting at home.
MIGRATION:
Came to Bombay in 1974.
WHY?
Because his father sent him as there were no job opportunities in U-.P.
FIRST EXPERIENCE:
When he first came down to Bombay he did not know what he
was going to do; he felt if he got a chance he would run away
and go home. He felt rather frustrated. Thinking of his parents
and brothers and.sisters ho decided to stay on and.then found a
small business like selling channa and groundnuts.
On seeing the beautiful places of Bombay he:was quite fas
cinated and thought it was the best place ho ever saw.
HOME IN BOMBAY:
He stays in Thana in a small thatched hut shared with 5 other
ooys who are in the same business. Its a- thatched hut, with a
cowdung splashed flooring and walls. He pays a rert of Rs.10/a month.
i
HEALTH FACILITIES:
Nil.
He doos not have enough water to bathe daily.
MEADS:
Ho has 2 meals a dayJ •) one at 12 in the noon and one at 12
midnight, both prepared by himsallf.
EDUCATION:
He has passed his 5th class in the Govt. Free School but
he was forced to leave because he had to help his father to
support the house as none of the others were old enough to work.
SALARY:
Rs.3 to Rs.5 a day.
SENDS MONEY HOME:
Yes.
Rs. JO/-.
Aftor 3 or
mon-hhA whnn ho hn« gnhhorod about
.. .2
*
2
RELIGION:
He was rather quizzy; he finally said that he -worshipped
Santoshi Ma.
MISCELLANEOUS:
_'_2 j cause he felt that they
He was scared of political parties
and when a Riot broke
would stop him from his business, axxM.
------- out ne got
scared because he thought they would break his hut down and he
would be homeless.
He finally said that he would work to the best of his ability
ancl open up a small
and then manage tb gather some money, go back and
shop in his Native place.
THE PROCESS OF URBANISATION
To highlight the qco-political conditions operating in the process
of urbanisation, let us follow a hypothetical person 'Ramu .
RAMU IS AN INDIAN,
A TYPICAL INDIAN
WITH INCOME LESS
THAN RS.20/- P.M.
250 million earn
less than Rs.23/
20/- p.m.t ('61 prices)
Rs.50/- p.m. ('71 prices)
RAMU WAS A VILLAGER
A LANDLESS LABOURER
More than 220 million people living below
the poverty line are rural landless labourers
In 60-61 - 52 per cent C of the rural people
67-68 - 70 per cent < lived below the
[poverty line
IN '51, 1RAMU VJAS
A SMALL FARMER
In 1951 9 out of a 100 Indians
42 were small farmers
9 tenants
15 landless labourers
1 landlord
20 non-agri, workers
6 in commerce
2 in transport
7 in services & Miscellaneous
In 1951 13 per cent were agricultural
labourers
1961 16.71
cent
1971 25.76 Per cent
NOV/ RAMU HAS BEEN
WITH A SMALL
PIECE OF LAND TO
STAY
Distribution of land
1 percent own 16% of the land
T he t op
5 percent - 40%
- 56%
10
II
- 4 % of the land
the lower50
II
- no land at all
bottom
20
...3
■ RAMU NEEDS CREDIT
THE BANK?
HE DOES NOT GET
IT.
Only 30 percent of the rural credit comes
from Cooperative credit, Nationalised Banks
etc. In
- 20 percent of agricultural
loan was supposed to be alotted to small and
economically weak farmers.
173-174 - 30 percent
<7/1—175 « 40
”
Actually in l73-,74
6 out of 24 Coop, banks gave 20 percent
9 out of 24 Coop, less than
5 percent
3 out of 24 Coop, less than 5-10 percent.
SO HE GETS IT
FROM THE MONEY
LENDER.
70 percent of rural credit was unaccounted
for by money lenders, many at an interest
of greater than 300 percent p.a.
RAMU LOOKS FOR
A JOB.
Out of a rural population of 436 million,
151.5 million (34 percent) are agricultural
labourers.
IT IS DTFEICULT
In ’50, 331 million were unemployed/under
employed
’70 4.06?
’/I 5-1
BE GETS A JOB.
WAGES: RS.2 A DAY
Minimum Wages Act
BUT HE IS STILL UN
EMPLOYED FOR A
MAJOR PART OF THE
YEAR.
Labourers are required in the field only
during ploughing, sowing and harvesting.
HE DOES NOT FIND
EMPLOYMENT IN
GOVERNMENT
PROGRAMMES.
A 50 crore Govt. prog, to benefit a 1000
persons in each district at 12.5 lakhs each
totally affecting only
million rural
une mpl oy e d/ unde r -e mpl oy e d.
IN ’71, ’72, ’73.
RAMU WORKS ON A
GOVT. RELIEF PRO
GRAMME - METAL
BREAKING.
In ’71, ’72, f73, Maharashtra was hit by 3
years of continuous drought. Massive Govt,
relief projects were not enough to relieve
the people.
The cattle die 9 the men starve...
A RELATIVE OE HIS
IS DOING FINE IN
BOMBAY AND CALLS
HIM TO THE CITY
TO FIND A JOB.
Sample percentage of workers of rural origin
in Bombay according to relatives working
in mills
66.6 percent
Close relatives
16
percent
Relations
17.2 percent
Villagers
No relations/villagers
1.2 percent
Rs.3/- per day
. ..4
4
SO RAMU migrates
In 1941 - 51 1 million people migrated, to
Bombay.
In 1951 - 61 % million people migrated
In 1961 - 71 X million people migrated
HE MEETS PEOPLE
1941 - %
51 - %
61 - %
71 - %
& MORE PEOPLE
1951 - 71 total urban pop. incr. by 250%
in 4 cities
400%
Delhi
706%
& TOO MANY PEOPLE
In 1961 Population density, in Calcutta-28,759
’C’ ward, Bombay 1,74,187
PEOPLE EROM TOWNS
In 1941, 35 % of class 1 city migrants came
from small towns
In 61 - 42- percent
In 72 - 52.4 percent.
HE LOOKS EOR
A JOB
Before 1st 5 yn plan 55 lakhs unemployed
fi
I!
n
End of 1st
53
ii
it
II
End of 2nd
71
n
II
11
End of 5rd ■
96
n
n
End of 4th
176
SOT® OF HIS COM-,
PANIONS. ARE ■
’PUSHED BACK1 TO
THE VILLAGES 6
In India
SO, RAMU IS A CITY
MAN, AN URBAN
WORKER
108.8 million urban people in India
52.2 million (50%) blue collared
28.6
(20%) white collared
RAMU GOES IN
SEARCH OF A
HOME
Annual deficit in housing in India 1 million
In 1961 deficit of houses 6.58 crores
71
8.57
ofurban population was 15.9
ofurban population was 17*5(5*4% in)
of urban population was 18.0( .7% in)
ofurban population was 19•9( *9% in)
8.2% of non migrants unemployed
migrants
.6.4%
In Bombay 7*1%
non migrants
migrants
4.5%
!
To provide these houses the Maharashtra
Gojvt. would have to spend Rs.50,000 crores.
IN THE CITY
10 % have to live in one room tenements.
1 % have to live in skyscrapers
IN THE SLUMS’
There are already slum demolishing proce
edings in 5 wards in Bombay.
19,750 families are alloted place in Dharavi
24,650 in Deonar
Each^family has been alloted 15 sq. mts.
and have to build a soMd structure costing
Rs.2,500 - 50Q0.
Even with a 80 percent loan - they must
have about 600/-.
...5
5
Imagine a family earning Rs.3/- to 5 a day
repaying a loan of Rs.2500 - 3000.
They will never more, as all families will
not get place and in some of these allotted
places there already exist large slums.
ON THE PAVEMENT
3 out of 5 pavement dwellers live with
the sky above their heads.
The other two in ’dilapidated set-ups’.
RAMU COMMUTES
FROM HIS SLUM
TO TOWN
40 percent of the total employed in Bombay
are concentrated in Fort area, a radius of
2 kms. where the density is 1,75,000.
This area has only 30 percent access to
other parts of the city.
The BEST has 1318 buses, of which more
than 50 percent have completed their
life span.
This provides 2.5 million journeys as
compared to the 4.6 million undertaken
by people.
RAMU IS A CASUAL
LABOURER IN A
FACTORY. WAGES
RS. 5-50 PER DAY.
The DD Mills in Bombay pays Rs.3-50 a day
for unskilled workers.
Only 1 out of 25 workers is permanent.
RAMU JOINS A
UNION.
Union of DD units is affiliated to the
Mazdoor Mills Sabha.
RAMU GOES ON
STRIKE.
300 workers go on strike on Sept. S^th *75.
Union comes to terms with the management.
The workers are dissatisfied. They join
the other union affiliated to INTUC.
The strike is on. Everything is peaceful
On Nov. 25th the workers are attacked by
some high goondas. Seven workers are
seriously injured. Many arrested.
o
NO WORK, NO INCOME, DRINKING, GAMBLING, LOAN?
DIE IF YOU WISH 9 YOU MISGUIDED COMMON MAN!
A. CASE STUDY?
(\ Tale of mnyfolded Exploitation
This story was told to us by a. farmer from Madurai District in
Tamil Nadu,
The farmer was operating a power-sprayer $ this was his job. But
he was not the owner of the sprayer? it was owned by one of the big
inlandlords who in his turn hired it to other farmers. The lease in
cluded the workerr
The man with the sprayer carried on his back told?
-I’m only doing this job because I need the money. IHow can a
man survive without work? I get on an average 5 Rupees a day, and
more during the. busy season when I’m payed on piece-rate, I know
it is a very dangerous job — but that’s, why I have to do it and
that’s why the owner himself refuses to. I have no choice - I must
take any job I can get.
-I have to carry th© sprayer• and the tanks directly on my back.
I have no cover on my body, My
f, brothers also worked with sprayers.
I know
I will
They are dead now§ they died because, of the spray.
....
e
Dust
to
be
alive
a
little.
die soon alsoj th0se sprayes kill a man* Z—
‘
longer I go to the Doctor every day and he gives me injections,, He
has told me nqV to eat food that is fat, not
i — to have cooking-oil
for example.7I don’t know exactly why he tcld me thia, but it had
something; Vo do with the poison in the spray.Some days I have to
spendzz12 Rupees, on medicines alone, because of this work that I do.
Ey'ferybody knows that it’s dangerous, but what can a poor man do?
I have to bring rice to my family’
-The. owner is leasing the sprayer to any farmer who wants his
fields coated. My work is. included in the lease the farmers, pay to
" ~Rupee• for each tank that I manage to
the owner. They have to pay 1
a
In
the
busy
season,
when
I’m paid at piece-rate, I can manaspray
to
30
tanks
during
one
day
of work. I get 25 paise for each
ge up
so
a
good
day
can
give
me
7.50
Rupees. But^the owner t^eatank,
the 75 paise. balance for each tank, so he
I gets 22.50 Rupees for my
work during the same day. The more I work , the more he gets.
_
■
II
_ . .— _
J. A I
-I only wish that this rich man who had money enough to buy the
sprayer which costs 1,000 Rupees, that he could also buy a uniform
for me. They are available in the markat? they cost only 150 Rupees.
That is nothing for him. It is. told even that you Ijava to
this uniform to be protected from the dangerous things in the spray,
but I cannot afford this, protection, f.nd the owner doesn t care he is not spraying those- things himself anyway...
EEV
780427
HAMID, THE BHOBIE.
rarely took Casual Leave and if he did, he replaced himself wi
a family member so the work did not suffer. He came to the
notice of the hospital management only during the monsoon
season when, due to la.k of washing and drying facilities
in the laundry shed and the small inventory of linen m
circulation, he could not keep up with the demand lor clean
dry linen.
This hospital was called _i
a 200 bed general hospital by the
The Medical Superintendent talked of
president of the society.
175 beds and the Business Manager in
in his reports listed 160.
The hospital
hospital was
women’’s and children’s hospital
The
was founded
founded as
as a
a women
Sa missionary shortly after the turn of the century and no one
missionary shortly after the tby a missio ry
recorded just how and when a conscious
could remember nor is
d'e^sion was made to expand the facilities to admit male patients.
For years the hospital was considered to be one of the bes
in tL area, and funds were available, not only through the
™L2ion, but also by contribution from abroad channelled
through individuals. The hospital had been ’’turned over t
the indigenous church, and subsidy was decreasing by Rs.5,000/
per year as per the Church plan. By Veceuber 1/73,
outside help had been reduced from Rs.50,000/- to 30,000/-
The organisational structure under which this hospital operated '
was typical of a number of church hospitals m India. First y,
the church Executive Council was to decide onpoMedical
and the selection of the three "appointees' ,
Superintendent, the Nursing Superintendent and the bursar in
each of 4 church hospitals. Secondly, there was a Medical
Board which nude recomendations to the Exec^1^
-•
regarding salary scales and financial requests and veryt often
ratified or rejected minor deMSions which were made by the
for all these
local hospital committee. It was not uncommon
bodies to spend much of their time on agenda itemsj such as
retaining a laboratory technician who was no longer wanted
in a certain hospital.
asso,iptiras h.a been
.irStowX’IS’lv'd, the
Depending on the personality of t
resented
position of Director was informally decided but resent
by the other two persons in charge.
In this hospital, there was a Nurses fining School with
its own Director
of Education
Director of
Education who
who controlled the budget i
ITS own uixe
atudents, of course, were trained m the
the school, The students,
Most’of the class IV workers
wards and OH) of the hospital,
by the Nursing Superincluding the dhobies were supervised
s
intendent (Service)
All tb. X-OT,
1.1
directly to the Medical Superintendent. The oitice
ground personnel were supervised by the Bursar.
2
-:2 s-
In January 1974j the Hospital Committee sent a request to the
Medical Board for permission to increase the salaries of all
employees. Increases ranged from Rs.75/— per month for the
medical staff to Rs.5/- per month for class IV workers.
Because salary scales were uniform in all 4 church hospitals
the Medical Board set up a special committee to stu^y the
proposals which were to be submitted at the next quarterly
Board Meeting. No decision was made at the April Board
Meeting.
The Hospital sent a request to the July Medical Board meeting
seeking permission to give an ad hoc increase of Rs.2/- per
month to the Class IV workers, effective July 1, 1974- This
request was approved by the Medical Board and sent on to
the Executive Council for final sanction. The overall
salary request was not finalized however.
In October 1974, bbe Executive Council approved the Rs.2/ad hoc increase' with the proviso that it be made effective
October 1, 1974, and that this ad hoc allowance of Rs.2/be deducted from any wages increase in the future. The
hospital started paying the Rs.2/- in October 1974\
TTjjj fifteen months after the initial request
Finally in April
1975
the Executive Council approved a Rs. 5/- increase for the
Class IV workers, but it was to be effective January 1, 1975(See Exhibit 2 for summary of dates).
The workers were quite happy that they were going to get a
Rs.5/“ per month increment. Hamid, the Chief Dhobie, immediately
borrowed money to buy two new tyres and tubes for his bicycle.
However, the peon who learned about the increase from the pay
roll clerk and who told his fellow class IV workers,.
did
not know that the increase was effective January 1, 1975
and not retroactive from October 1, 1974 as expected. Further
more, no one was informed that the Rs.2/- ad hoc amount
was to be deducted from the increase and they were to get
only Rs.$/- more starting January. However, the office’
peon did inform his co-workders that the doctors received
Rs.IOO/- per montji increase.
On April 50 when the workers received their pay it included
the January to March increase (Rs.5 x 5) less the ad hoc
allowance already paid (Rs. 5 x 2) for the same period.
The Bursar was out of station and the payroll clerk took
no responsibility for explaining the reasoning behind the
difference in their expectations and what was actually
realised. 'There were a number of angry exchanges. The
Medical Superintendent was unaware of the problem, and in
any case was very busy in the operating room all day.
The Bursar returned a few days later and when approached by
three employees: Hamid, the gateman, and the gardener, about
the small pay package, promptly told them that the policy was
fair. Furthermore, the hospital did not have a lot of money
and in any case this was a church decision and he could not
do anything, about it. He also tdld them, "Do not be so
foolish. I should have deducted the Rs. 2/- per month which
you got from October to December. If you continue to make
trouble, 1 will do that also.”
5
J sThe dhobie, Hamid was more persistent than the others and
tried a number of times to explain to, the.Bursar, Medical
" and Nursing Superintendents that he had borrowed money in
anticipation of a Rs.5/- per month increase. The response
by all the three officials was that he should be careful
as "they were not satisfied with his work 2nd he did not
have to worry about the increment as they were looking
for another dhobie to replace him.
In the next few days, Hamid was seldom in the dhobie shed
but was seen talking to small groups. The gate was not
opened on time at the beginning of visiting hours. On one
occasion, an emergency patient was taken to another hospital
because the gatecnh could not be found'. The work suffered.
Some ward Ayahs refused to empty the bed-pans. The linen
returned from the dhobie still dirty and an increase in
torn sheets was noticed. The officers were not very cout
cerned as they considered that replacing of the dhobie
would remove the only troublemaker. However, when several
previous applicants for the dhobie job were approached,
they all refused to accept an appointment although better
terns were offered. The hospital officers could not under
stand why the old faithful workers were so sullen and
difficult to get along with. The Business Manager drew
up a list of what he considered over-age workers, but
he could not establish their age as there were no personnel
records.
Approximately J weeks later, a notice was sent to the Hospital
Superintendent by the local Labour Officer that a hospital
union, to represent the 4 church hospitals had been registered
with the Government. The hospital authorities were summoned
to a meeting to discuss the union demands which were enclosed.
The newly recognized union had as president an influential
lawyer ’and local political leader.
The Medical Superintendent became angry and told the Bursar
in front of the office staff, ’’These Class IV Workers are
a terrible lot and show no. gratitude at all. From now on,
we will stick to hospital policy. No free treatment will
be given to the members of the workers’ families. Just
last week, we sent that gardener’s sister to a specialist
at the medical college hospital and we paid the transport
ation expenses. We will not do that again for any of them,
and especially that Hamid.”
$
The Bursar replied, ”1 agree that Hamid is behind this mess.
But we don’t have to worry about these foolish demands. When
the Labour Officer sees our large, accumulated financial
deficit he will reject their demands immediately.”
Exhibit: 1
EXECUTIVE COUNCIL
MELICAL BOARD
HOSPITAL 1
MANAGEMENT !
COMMITTEE (
| HOSPITAL
I HOSPITAL
I IvlANAGEMENT
J COMMUTE
i COMMITTEE
I
I
HOSPITAL
A
HOSPITAL |
j
I
N.S.
I
1
I MANAGEI'ffiNT I
B
I
HOSPITAL
MANAGEMENT
COMMITTEE
*
I
I
I HOSPITAL
C
M;S,
BURSAR
X-Ray Tech.
Lab. Tech.
Pharm.
!
Office Staff
grounds____
personnel
HOSPITAL
D
_i__
I
Ast
N’sing S
N’sing Edun.
Class TV's Students.
(Dhobis)
Ast
Exhibit ? 2
Hamid the Bhobie.
Summary of Medical Board and Executive Council meetings.
January
1974
Hospital Committee sends request to the
Medical Board Medical Board sets up a
"Salaries Review” committee.
April
1974
Medical Board takes no action.
July
1974
Hospital Committee requests an ad hoc
increase to be effective July 1, 1974
Medical Board recommends the Rs.2/ad hoc increase and submits to
Executive Council for sanction.
October
1974
Executive Council sanctions the ad hoc
Rs.2/- effective October 1 - This
ad hoc allowance to be deducted from
any future increase in the salary
scale. Hospital pays the ad hoc
starting October 1, 1974
April
1975
Executive Council approves a Rs.5/increase for Class IV and Rs.lOO/for the medical staff - new salary
scales to be effective from the
entire new salary scale was approved
ranging from Rs.5/- lor Class IV
up to Rs.100/- for Medical Staff,
to be effective from January 1, 1975»
/
; 7
: Xkg.iHNA D’iWi-uid'rH wT&’k OH' VINCENT D’BAXdfiSEJi
: 37 Tears
r'arrlad :I>FB3 I960
CHILDHEN: FOUR
f. Annie 13 June 61
2.3o nno 31 April 63
j.Dolla 8 Nov 64
4. Jeru 5 Feb 66
)
Now in Boarding
Schools.
HUSBANDS POSITION : Is an Employee of English
in
----- -—the 'Sr®ction
Erection Department that neads
needs absence fwm
from
home for long periods. Usually Project work. No
stable place of stay. Sick leave In^opa of cure
of wife now amounts to 3 months due to and this
week end « If not reporting back for duty - i-?®®
■ , Effect - Destitution of Husband,
of employment.
Wife & Children.
PRENT URSENT NEED t Institution/Hospltal ttet will
11
In present state and also affect a cure, as
it is not humanly possible for Husband to take «lfe
along with him and look after in her present condit
ion as well as attend to his duties. Being In
Erection Department also not sure where he will be
posted on reporting for duty.
CASK HTSTOgf s
POSTED TO KANPUR - JAN 68 - CONDITION : O.K.
EVLNT> BACK TO TARENTAL HOME : MAR 68 • Husband not able
'
to work for 6 months due to sickness.
Wifes Condition - Hands shaky.
SEP 68
Husband posted to Bombay. Left Vlfe under
care for 1 Year 4 Uths, during which she us&3 to
starve 4 to 5 days
with mottw.
Condition further deteriorated, -ulsc suspicious
hn?hand running after some other woman at Bombay.
Wrote letters to this effect.
JAN 70 Husband took wife and youngest child (Plaelnf.°^sr
3 children in Boarding sbhools) to Bombay, since
accomodation was not available at Bombay
ing with a newly married couple (Relation) sharing
a flat. Ton king after household. Cooking etc done
by relation as wife unable to do anythin®. Then
Wife was taken to Bombay, delation said that _<lfe
condition was deteriorated because she was loft in
Husbands Parental Hone and Wife was madea much or
by them. Treatment started in Happy atmosphere.
Ailment diagonised as Berry Berry. Tonics, Inject
ions and Vitamin Tablets given. Responded to
Treatment and state of shakiness left colletely
within 3 months and condition stabalized, and was
bodily normal.
.
Since Husband’s job at Bombay was of a nature in
/which
!
- 2 -
which he left home at 6am and returned at 11 pm
Wife was advised to have Breakfasttluaoh &
Dinner with Relation and not w it for him, which
was being done.
j
1PRIL 70
One day on Husbands return borne at 11 he noticed
Wife’s lints going bads: to old condition (shaking).
On asking wife, what hed happened, ther was no reply.
On questioning Halation, husband was told that she
is not sating. Further cpeatloning revealed that
Wife had starved for pest 4 days#
REASON : A bey was engaged fcr alternate wajfting of
clothes of the tw f•^ilise. one day the Relation
told ?Jffs . Ibdsy I an not giving Clothes, you give
the clothoe. Wife Replied : Today is not xy day.
You give it. In short none gave.
Th© next day
both gave the clothes and. the Relation told the boy
KAt to wash Wife’s household clothes, but only hers.
'Hite led to her attitude of Starvation for 4 days,
and continued to be adasiant even after Husbands
requests to oat. On sewing condition of VFife,
hueband took wife next day to ths Doctor. 3© got
an appointment with Dr.I Ulla Hon.Psyohiatrist Nair Hospital - Bombay. He had a sitting. He gave
some tablets. The Tablets were given on that day
(Sth day since starvation) and th© following day
at about 5 jan she told husband, she was hungry. Said
that she w ld only est on condition that Husband
cooks the food and not her Relation. Husband started
to ocok th© food from that day onwards for wife and
Pay Treatment was carried on as an Out Patient
(13 APR 70-3 NOV 70). The relationship between
Relation and Wife became ntrained and constant fault
finding by Relation culminating In being aeke
constantly asked to shift. Shift of abode took place
on obtaining one in Bombay (JULY 70) •
18
70 to g FOV 70
HAIR IX'.TIT T-
TRSATSEFT t Heuroais check up
Skull RX Ray
Blood Tests.
Sli.^it shocks was given on th® Taspls every other
day for 1 i week. Since no taprovwent was found
a Total of 16 RCTs war® ^iven and Drugs Bakasine,
Paeltone end largactil administered.
During this period Mfe found to be uxpacting one two mcntha . DSC wa« per omeA since wife found to
be unfit to look after self.
jAast ggycgg^mar sgTOHs - Krpa* bdy to
.ucetiono asked to "-"fa at sitting
PST : ’Aho is doing the cooking ?
Wife: Points out to husband.
/Pgy.
- 3 -
Psy : Who is doing the Marketing ?
Wife: Again points to Husband.
Psy : Dont you find that your husband is pulled down
in health ? Shouldnt you do the cooking or
should he diverse you ?
Wife: Replies No.
Psy : Should ho keep another woman to look after you
and himself?
Wifei Replies No.
Psy : Are you going to do the cooking ?
Wife*. Question is ignored, lust turns her head away
and does iibt answer.
Husband asks the Psychiatrist why she has not answered
this question.
Pay : SOHIZOPHDRNIA - They believe that they are
living in a make believe world of their own
in which they west expect everyone to help
them but they wont help themselves. NO
Improvement . Carry on Treatment.
Hearing these v.'ords Husband □topped treatment.
CONDITION OP WIFE jgTEH TREATMENT ;
bould walk on road, dlimb steps v/S.'-tiii assistance,
and in the house. Boil milk, wash utensils, go
to Toilet, wash face and Brush teeth (Husband
doii^j the cooking).
EVENTS :
DEC 71
Christmas Season - Anonths leax’e taken by husband.
Children brought by well wisher to home (Bombay)
for holidey from Madras. Wife does not like love
and attention of husband shared between her and
children. Becomes self centred.
Before 15 days of children due for departure to Madras,
Husband mentioned to wife that he would have to book
tickets for self and children for Madras - going back
to school, and wanted her to remain with friends for a
period of 4 days. She didnt like the idea of her being
left at friends place and husband leaving for Madras
with children. Husband left home at 10 am for booking
tickets, on return at 6.30 pm the children on the
top 3rd floor were shouting ’Daddy we are hungry’. As
husband walc'ed up half way he heard his children scream
’Mummy is Burnt’. On hearing this and rushing into
the room found a Dekshi of Boiling Water spilt on the
floor and wife was saying ’Viney, Hot water has fallen
on me' . she rubbed her face and skin peeled off. The
Doctor down stairs was immediately informed. He
instructed that he was coming but in the meantime all
ber clothes be removed and oil applied. The Doctor
came immediately but Wife was smiling. He prescribed
some ointment and aid in case she complained of pain
he was to be informed, Wife did not complain of pain
and no injections given. Ointment procured same night
^and
I
\
M 4 *
next
and applied, The face was swllen shM day and
ey®s were closed and it was feared that eyesl^xt
affected. On the 3rd day, swelling subsided and.
Viiie could see* Scabs formed within 13 days and
as busbani was packing bags to take ^at4«a wife
to friends house for le ving her there, sh®
screamed out ”1 will not go* and scratched scabs
on her face and started howling like a manias*
Blood wes streami^* Hands had to be bound at
th® back for fear of further injury. Husband told
her that he would only release her hands providing
she promised that she will never hurt harself* She
promise?©, and waa realeased. Had calmed down. Next
day husband took wife along with children to friends
place. After laving wife with friends, left for
kafiras with 4 children. On return from Madras after
4 days bls friend told him that wife had not given
anj' trouble. She was taken back home*
*
JAN 71
Hueband tr^nsfare© to U^jain & other places* Takes
Kite along. Condition - As before, eat,drlik, wash
face, brush teeth, go to toilet (except Bathe)
without aid. Develops extrmo suspicion. If Husband
speaks to anyose - would oompleSn that he is
discussing her faults*
OCT 72
Husband
17 307 72
■Vife admitted as Tn Patient *t T J Hospital Donbay
baak to HomoTjr
KOT e
VJeotrnnarcosis and jruF.a.
. 22 FEN 73
nisoharged frota Hospital sayint- nothin^ mdh san be
done. Garry on "&reatmSit as Out Patient and advised
to administer Omgs
Tab askazina 10 mr 1 a day
2 PaoiMae 2 sag i
”
• LergactilBO sc 1 * **
Above 4rw^ given for 2 months*
Condition waa muoa detarior&tecl on disaaargG Iron
Hospital. Wife passing Urine & 3tools in Bod aad
could nob w tlk oa han own*
eas nourished and gob Mok health* Could manage
to go on o*n to toilet et©. but did not like otnar®
coa^uny.
EVWTS t
NOV 73
Husband, traasi'ered to Bihar. 3®y before leaving.
Husband obtained 1'©k?i Doctor Sedatives vhioh should
be given, only one per night. One was given on the
night before departure and Bottle left on Dining
Table,
J*ter giving he Bath and bringing her to
the dining table, Husband had fried an e&g and gl
/to
- 5 -
to Wife and as ha had turned to fry another,
something made him turn around and he saw
that she had emptied the Whole Bottle of 24
tablets into her mouth. Nbrmally when she
eats she keeps food for a little while In her
cheek. He put his finger in and drew out all
the tablets from her mouth and found that 4 had
been swallowed. Ths Doctor was immediately
brought and a bad situation averted. WhenW
Wife was asked shy she did this. There was no
reply. Same evening left for Bihar with Wife.
Since the climate was very cold at Bihar in
Nov - Jan, Exercises like walking outside home
was curtailed. Wife’s movements became alightly
worse.
STENTS ;
Husband transfsxad ta Bombay.
APRIL 74
Husband found Afternoon meals left untouched.
On return from 'worlc 7 pm and would only ea
eat on Husband telling bar to do so. Seeing
this condition. Husband got worried and got
her admitted in Govt Mental Hospital - Kilpauk.
j KIIPAUK (Mfe admitted)
S3 JUL 74
GOVT SBITTAL HOSPITAL
MAR
78
Husband transferad to Madras.
5 MAY
76
WIFE DI CHARGED FROM HOgPITA^ Husband told that
Wife has to be taken home and looked after. Condition
deteriorated to present condition. Husband took
leave for 40 days and took wife out of Hospital.
Massaged and exercised found slight improvament but
could not extend leave.
EVENTS ;
JUMK
78
Jfusband trausferad to Mysore.
Husband left for work sited with wife. But looking
after wife in present Condition and working led to
Mental and Physioal strain & breakdown leading to
collapse at work. Applied end was granted sick leave
Went to Angamall with Wife on Sick leeve on assurance
and hope of Complete cure of Wife as Priest in Gharge
of liar Ignatius Mental Hospital - Ans anal i was ««44
endowed with miraculous power of curing such oases.
88 AUG 78
Klfe admitted in M I M HOSPITAL
Unfortunately Priest met Cer Accident 3 or 4 days
Before arrival and Husband kept wife at Hospital
personally attending on her in hope that the Friost
would be able to attend on Wife on getting well.
But hopes all dashed to the ground as Priest Is stll
in a critical state. Husband’s Sick leave has now
eome to an end having availed all types of leave
w 6 w
and Ms to report in 10 Ssy« time or lose Me Job.
Farther wrteeMone l«?>essiMe.
11 NOV TO
wife gTSCHAHO^P. yRQg K I. /- 3Cf?IT -L
;ru
In. •Wile hoar of pesp^ratton r we Mg tbef- oelp be
-axM’vm 1r aowptin? Wife la present state, where
necessary oare and treatment towards her reeovory,
so that :?»vsba3d esn report In tine and ho?A on to
his exployrsoBt with poop? of wind *©« n •wmseletion
that wife <« In reapnwsible henfle*
}
‘•^JT l.J 9»y-?'?r?th BCf>th*r? ©f
arSflre^s t-
Sct. E<T D*T?eff'>roth
Bawl section
----Mr yeree statlcr. 7»leMlli <*>«•*
Hospital Toto west 5?. 0«
Bwjolere -15
(5 Nov
f
5
A Or* I
a
Fron tha
i) History of the complaints
ii) socioeconomic history
iii) Physical examination
iv) Clinical Investigation -
we can come to & diagnosis of 5
1) it-liiatrlUohstProtein-calorie type) - precipitated
initially by Massies and in the last few months by
j
acute gastroenteritis. associated with a) Anemia
b) ascarias/s
c) Upper despiratory infection
d) Urinary Iract infection
-.9
Complicated further by the socioeconomic factors ofs
1) Poverty- a general term which includes poor
housing, congested environ®ant, poor w^ter Supsly
and latrine facilities and inadequate nutrition.
2) lllegltimcyi and
.-'.IkT.lX.aLViu
3) Luck cf Psychosocial utirauli
necessary for normal
davalopaant.
1’fae diagnosis is has ad oxu
1.
a of onset
2. Dietary history
3. Clinical findings of i) Child's Height and wSight are far below standard,
il) rn/sic.l and mental development is retarded,
iii) deneralised odema bat mainly of lower limbs.
iv) Changes in skin,and fluky paint dermatosis and hair,
v) uiver enlargement.
4. Low Ho and serum protein levels.
t»ince this As a xex social case conference 1 will not
go into the discussion of a differential diagnosis
suffice to say that pathological conditions lise -
1) Chronic dysentery or Malabsorption syndrome,
ii) abdominal tuberculosis
iii> Gueliac disease
... 5 /
/
5
iv) Fibrocystic disease of the pancreas
v) ankylostomiasis
vi) hephritis can also produce similar signs and
ayaptoas.
«lso ixi evary c*se of apparent malnutrition
these can be associated aggravating or jrecipitating
factors.
a
small note may be made about tho skin manifestation
in this care.
Though like infantile pellagra it is
mainly on the exposal parts of tha body it was not
diagnosed as pellagra baca Isa s
il the lesions are not photosensitive
ii) they appeared in the ward as the odema cleared.
hext 1 must discuss the most important aspect of this
case and that is the question of management.
For
purposes of convenience I shall divide aanagamant
into two sub divisions:
I - hospital management
II- Follow up qara. It must be understood that
though they taay appear to be two different entities
altogether they are closely related and either one
without the other would be incomplete and bound to
result in therapeutic failure.
The Principles of hospital careX are:
1; resuscitation
2) Dietary therapy
3) anti-infective therapy.
1) !resuscitation - is of utmost importance especially
in the first M -48 hours after admission since most
of these cases dome in with ij Dehydration, ii) Electrolyte imbalance,
ill) ^cid-base disturbances, iv) i-evere anemia.
Dehydration is corrected by oral and or intravenous
fluids, blood transfusions are given if the iib is
less than 3 gms.
acidosis is corrected by admlnist-
ration sodium oic^ruonate
solution 4ml/kgm hypo-
... 7 /
llypoglywiia by oral or Tv glnecmu and electrolyte iabiMeii by adainict retina
of K a>l Mg eupplemttt* 4*5 i^rA'ya end 2*3 »
2.
1> the next
respectively.
and the seat isportMt step •
Pati*Bt is started on flueoae eelint zm! | atr. Mik feMo wMs?h ero gradually
IncrcR®^ to full st length Mik f«ide<
aa saon bb a»*weiato<
a irMfc
iiarrboM ie contreile^ ©olid fw&a are started with speeial atreoB ra th*lr
protein content 9 vi twain and iron aupplesrnt;© mss^t else W ctartef ■ ’'imltanaov^
5*
Malnutrition if* noet often associated with
one or iwr* of the following • ?B. aalarla, n®l«iinthiaBf Giardia@lst
An^loMwUsio, reaTlmta^and urinary traot infections.
Infee ti m&
Mcauae
of their aarke^ debilitatin' effaet on already aalMwlOhed childrea nuat be
diagnosed early aad actively aad adequately tr-ated.e
All these priaeipiea wem fello^l in thio caao doting the present
hoopltaliMtion*
1.
la thia caf?e Xv fluids
not started beeause :-
1. Patient was tolerating ©Tel fields ve.ry wall>
!!• iahe bar: ceaaralisee oadMa*
rowwr ^00 eas of whole blw^ irmwfuftioa were plv^n.
baslx was given for the
oadewt *mt with poor results probably b*eau.fMo the eau®c? of the odoma
primarily r.ypoproteifcieitia»
With proper hydration the !’b which was 9.4 unbelievably high and probably due
to hamo-con^ntratioa ease down to lt« actual figure of 4.8 gne.
2. The patient was given y atr. and then faU rtwngth nilk till the
diarrhoea auboided
soon started on a solid diet sfhi^h at present consiate of
!• 3 largfc clMeeii of silk ^ally (750 cc’s)
ii. 1
ill. Meat curry twice a day • ©ixed with "PF (a produce of CFT I eontainlng
high protein groandnut flow and Bengal gran).
iv. Ricet Bread
¥• 1 lantaiaa and ®wet Ilia® l/e®ch daily
Ti» Protein biaoulta
In additicm aha was started on a atandard
11 vitamin syrup and Iron syrup
(Tonoferron)
For the angular atcwaatltia a Ht< 3 Complex ®yr?jp
^•»od reeulte.
added in addition with
Anti^infeeiive Thsaanv l- ?h® diarrhoea wan controlled with proper diet
< dose of anthelminthic syrup ^a© given for
and F.ixtum T^ianuth kaolin*
rounclworas.
(PiperaBine 15 al.)
The upper respirator^ infection ^nd hand infection was treetod with
Procaine penicillin injection® and
phadrias nasal drops* And for the urinary
tract infection sulphas started (aulfatriad | tab/^th hrly).
by
vith this tr^ataent th® patient ^ade a clinical lupravemat shown aw
1* Marked reduction in odesa*
LOSS
ii* Initial
of weight ive to
of odeeia fluid sind then a gradual
increase related to s protein intake.
ill* Increase In Bb - to 9 ipso.
iv* Clearing up of urinary tract infection as shown by a clear urine
micro examination*
▼• Healing of angular stoaatlti®.
Thi® brings us to the min question in todays social ease conference i*e*
’low
is such & cane followed up after discharge frcm hospital or how doe® one present
the recurrence of the above clinical stoxy by tackling the socto*^oon<M3ic factors
involved*
^9 all realise by now that if "arina after mking adequate clinical
iraprovessat 1® Bent hose to the sbao conditions de cribed in detail by Kuapar -
she if* bom’ to return within a matter of few weeke with sms other infections
and the exacerbation ©f the previous system of ®almitrltioB*
If thie were to
happen thafcone in bound to question as to what has Men the une of the prsaent
treataent in th® hospital*
▼
c.<A
In our hospital orl^ntid. nodical education this is a
question worthwhile asking befor* we discharge mny of our other patient® with
similar bnekgro’-md.
For '4ariapi!s ease to be completely tackled the eeeond
subdivision of ' anagee^nt iae Follow up car» is very important and nust consist
of the fol’owiag
1* Regular weekly or fortnightly cheek up of the patient to detect.
i* continued improvement in c^^arnl health
ii* early signs of infection •» which should be adequately treated*
2* -hsckup of ether aoeMre of he family especially the three other children
for malnutrition
licet scabies and other infecti n® always a soelated with
ruch ©ocio-eoonoMc circumstances. These should be treated not only to improve
the general health of the family but also to prevent ’rarina fros getting
reinfected or developing i one new inrection.
5. ^dueailcflt of the particular seerwr of tbo family in thia ease the ^ran<!—
©o'.her — in sound nutrition in relation to their economic ntetu^ arid environment
They ahos-h* be asked to intro-luce &roiMdmta9 pulses, ra^t end ^reen
v^g’etahles isort of which will not MMmNMmrlly strain the family tad<at«
An egg a day would be ideal but my not always be practical. WT fefhlct is only
Rs. 160/kgm (monthly need of a child) cm be introduced with good result
y Groundnut
1/ liengal gram
4.
^afcUlto
t- This is an important aspect and can be tackled in each
indlvidml cam V close eoop«mtion
the Pediatricianst Medical ntudent»9
Medical social workers and Local voluntary or
social welfare ei$enci<wu
These would include i-
1* Fra** troataent of -arina and her family by th® hoapital (sdiich in already
beiafc done)
2. In thia particular cam since the Mld-'m are illegitiswite they could be
admitted into one of the well ron famftllat homes or orphanages in the city
bo that : !• we eoild lesmn th® harden on the grandparents*
lie ensure them (the chil ren) of n better fnturoe
3. With the help of ouw social workers to s*
1. find employment for Carina’s unemployed uncle who is a
melanic so timt the family incon® could be increased.
11. Rehabilitate th® epileptic aunt in aom harmless profession
or in an institution for such canes.
ill. Had her mother been here it would have Men necessary to
rehabilitate her in one of th® local inetltutlcns for
wo’wi no that
a. she could again restart a normal life
be po sibly - Iv® the children the ^jh
Illegitimate the aaterml love that the
so urgently require.
iv. Arrange to send the -otiw children to school so that they do
not by the force of eirciaMitanGes beoam future delinquents.
4. They al way© welcome effort mde by individual studeate, doctor® and
institution to try and help the faaily temporarily or permanently
through monetary aid, clothes and other necessities of life. hough
thia may be called charity, this can beclaef ified in tale cam under
the teportant term of *?ledleal Social Work1*.
I
5> While considering th*
a very Important quMtloe nriae®
and Wat is *^'hat are the clmnc^a of Marina and probably th^ other
children having permanent cental ^nd physical retartetioB ainee thay
did not eat valuable proteins so necessary for nonaal dewlonraent in
the mo^t active periods of growth* • I an not in a position to answer
thia ercept^I would like to read a eaall paragraph fro© a Cdwmary of
conference on the pr ♦v^ntion of Malnutrition in Freechool children*
Mid in Washinftott ■-'■•C in 1964 under the auspices of the National
Research Counoll*
*Prepehool nsslnvtrltion pemaratly impairs physical growth and
prcbatly causes irreversible aent&l and emotional ds»a<e« It is &
serious deterrent to progr os in developing: eountrieoj
it weakens
tM produotive capacities of adults Buffering from irreparable
daaaeec incurred in ohildliooda •Farther knovledfe io needed*
before such far reaching statements can be fully accepted * But
even if only partly true they show the <rnt importance of this
question of long tem ill sffocuu
»
H&l
v
CauS
buClaL
CuHFSHaRGS
29th JA»MKX 1972
PHUT^IN GziUihlri MLSUBOTIOK
Presented t>y»
Kumar
halani
Discussion:
Dr. Ravi
Narayan
Chairman
i
Dr. KeKe 68TB,
Professor of Pediatrics.
■
v
-
y
•
-
-
.
.
•
-,
■
-
I
)
z
*
SOCIO-ECONOMIC CASE CONFERENCE
Dlacusrion held on 29th Jan. ’72
Details of the case are as follows
:-HISTORY
Partigularg of the Patient sName
MARINA
Age
Sex
3 years
Female
Religion
Roman Catholic
C/o. Mrs. W. Smith
4th Cross,
Hutchin’s Road Extn.
Address
k
Hosp. No. 60364
M.R.D. No. 19415
Admitted on 23rd Dec. *71
Door No. 6,
BANGALORE - 5.
PRESENTING COMPLAINTS
Failure to gain weight —-----y
Loose motions with bloodABUCOus —
Swelling o£ face and limbs ———•
1 year
2 months
Passing scanty urine
5 weeks
h/o Present
1 month
---------
Complaints
Patient was quite alright till 2 months ago when she developed loose motions
4-5 times a day with blood and mucous. She was treated with Streptomycin and
sulphaguanid in©• Following this patient continued to have diarrhoea but no
blood and mucous. The stoools were brownish in colour watery, large in amount and
foul smelling. A few days later patient developed swelling of the face, upper and
lower limbs. The swelling increased progressively and soon became associated with
scanty micturition.
Systemic Review revealed H/O
No
H/O
H/O
passing roundworms orally and in stools
failure to gain weight since a year
fever, cough, throat or joint pains or abdominal pain
The patient is a 4th para full term normal delivery. Birth weight could not
be ascertained. The milestones were within normal limits but since the illness
the patient has become tooweak to either sit up or walk without help. She was
immunizsd against small pox but no BCG, triple vaccine or polio vaccine were
given. She was breast fed till the 10th month after which she was started on part
of the family diet, which consisted of coffee, rice and curry.
She hastan attack of measles when 1^ years old.
Famifor cum Socio Economic History
1. The patient is an illegitimate child who was left with her grandparents by the
mother when she was 10 months old. Her mother has 4 illegitimate children
of which the 1st and 3rd are also staying with the grandmother. The 2nd
child died of starvation.
2. Her grandmother aged 63 years is the head of the household,
members are
rv? o
The other family
o-xjcl
...2
I
2
a. An uncle aged 22 years
b. An unmarried aunt aged 27 years, ( an epileptic since childhood)
c. Another uncle aged 13 years and
d. A cousin aged 7 years.
The occupations and incomes of the persons in the family are as follows
1. Grandfather - Retd, watchward getting a pension of Hs. 40/- p.m.
2. Grandmother - Works in a School and gets a salary of Rs. 60/- p.m.
3. The 13 year old boy who works for a family gets Rs. 5/- p.m.
4. The other uncle and aunt are both unemployed and therefore in addition to the
3 children are dependents of the family.
Marina’s mother is at present working in a Convent in Tripura (Assam ) and
does not send any money for the upbringing of the children.
The total income therefore is Rs. 105/- p.m. of which Rs. 25.- p.m. goes
for rent.
Educational Status of Family J—
1. Grandfather
- 5th Std.
i
2. Grandmother
- Middle school
- Trained Automobile mechanic
3. Hncle
- Has done few years oF schooling
4. Aunt
5. None of the children are going or have gone to School.
Housing s—
xhe family stays in a house consisting of 2 bed rooms about 6* x 6*
and a smaller kitchen. They use a common bathroom , shared by 8 families.
Ventilation and lighting ar? sub standard.
Kitchen :
They use firewood as fuel.
Water supply :
is from a private tape for which they pay Rs. 5/-
-Nutrition
The family cooks once a day. The meal consists of rice and vegetable curry.
In addition they have coffee 3—4 times a day. They eat beef once a week.
Eggs, milk and fish do not form part of their diet due to the factor of cost.
Health of the Family raec.bers s —
Grandfather is fit.
Grandmother suffers from Angina.
Aunt is an epiletic.
All children are undernourished.
II
PHYSICAL EXAMINATION
The patient Is a girl of build and nutrn. far below average
Afebrile
Normal deci/butus.
Ht.
lit.
Wt.
- 74.5 cms.
(29.25 ins.)
- 7 kgs.
Since the patient is a case of malnutrition, the physical examination may be
subdivided into 2 iBuhgroupe.
...3
5
1. Nutritional Assessment from foct^rnal Slaw
The Hair is thin, brown, lacks lustre and is easily pluckible.
The Pace shows diffuse depigmentation. There is scaling of skin and rhinitis.
The eyes demonstrate a pale conjunctiva but there are no#* Bitots spots.
There is angular scarring of the lips indicating a healed angular stomatitis.
The tongue is smooth and pale.
There is tartar present over the teeth, The f'ums are not spongy and there
is no bleeding.
Neither the thyroid nor the parotid glands are enlarged.
The skin is brown and scaly and there is flaky paint dermatosis.
Skin over vulva shows a vulval dermatosis.
The nails are pale, flattened and widened.
The subcutaneous tissue demonstrates peripherialoedema with loss of
subcutaneous fat in nearly all parts of the body.
Biceps girth - 4"
Thigh girth * 6.5”
There is marked muscular wasting but there is no frontal or parietal
bossing. The f/ontanelles are fused.
There is swelling of the right index finger (foil, trauma)
2. Internal System Surrey J-
The gastrointestinal system reveals a just palpable liver and fluid thrill.
The Nervous System is clinically normal.
C.V.S. - P.R. 120/min. No cardiac enlargement. There Is a short systolic
murmur in the apical region. 3.P, 120/?0 m.m. Hg.
The R.Sf is clinically clear.
A CLINICAL DIAGflCSIS 0? PROTEIN CALORIE MALNUTRITION WAS MADE
AND ROUTINE AND PERTAINING INVESTIGATIONS WERE CARRIED OUT,
- Media
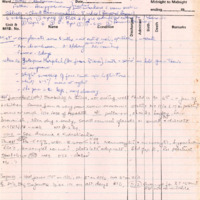 RF_COM_H_29_SUDHA.pdf
RF_COM_H_29_SUDHA.pdf
Position: 2093 (9 views)