CHILD HEALTH
Item
- Title
- CHILD HEALTH
- extracted text
-
dH-
Future Health Systems
Innovations for equity
FHS India
Research Brief
October 2013
are the children of the
Indian Sundarbans?
Findings from the first Sundarbans Health Watch
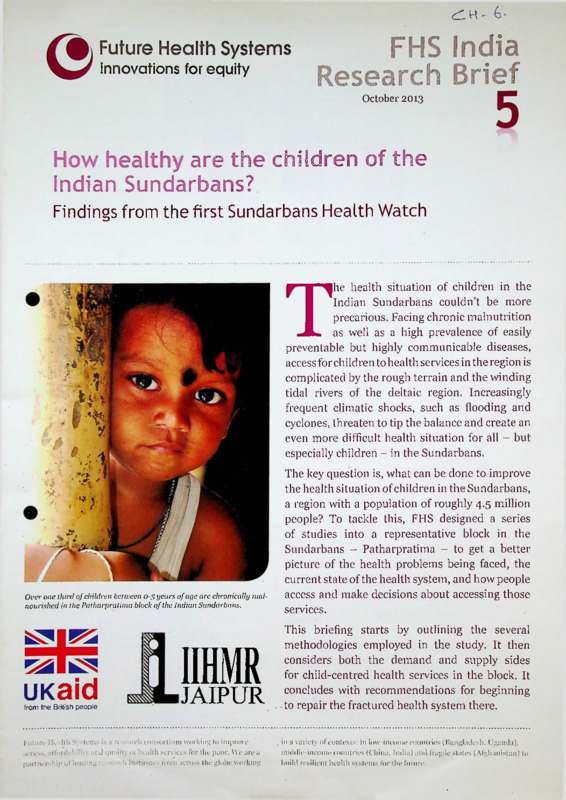
he health situation of children in the
Indian Sundarbans couldn’t be more
precarious. Facing chronic malnutrition
as well as a high prevalence of easily
preventable but highly communicable diseases,
access for children to health services in the region is
complicated by the rough terrain and the winding
tidal rivers of the deltaic region. Increasingly
frequent climatic shocks, such as flooding and
cyclones, threaten to tip the balance and create an
even more difficult health situation for all - but
especially children - in the Sundarbans.
T
Over one third of children between 0-5 years of age are chronically mal
nourished in the Patharpratima block of the Indian Sundarbans.
The key question is, what can be done to improve
the health situation of children in the Sundarbans,
a region with a population of roughly 4.5 million
people? To tackle this, FHS designed a series
of studies into a representative block in the
Sundarbans - Patharpratima - to get a better
picture of the health problems being faced, the
current state of the health system, and how people
access and make decisions about accessing those
services.
IIHMR
JAIPUR
This briefing starts by outlining the several
methodologies employed in the study. It then
considers both the demand and supply sides
for child-centred health sendees in the block. It
concludes with recommendations for beginning
to repair the fractured health system there.
Future Health S'.stems i - i research consortium working to improve
access. affotdabi:it> and cpnility <>f health .services for the poor. We are a
partnership of leading research institutes from across the globe, working
in a variety of contexts: in low-income countries (Bangladesh, Uganda),
middle-income countries (China, India) and fragile stales (Afghanistan) to
build resilient health systems for the future.
uKaid
from the British people
Table 1: Nutritional status of children (0-5 years) (N = 1332)
Percentage of undernourished children
Stunted
Total
Sex
Wasted
Underweight
<-2SD
<-3SD
< -2 SD
<-3SD
C-2.SD
35
11-7
12.9
25.2
8.6
38.6
12
37-6
11.6
12.5
10.7
Male
35-5
Female
10.5
25.3
8-3
8.9
39-6
11
7-6
10
37-5
40.2
25.2
<-3SD
Location
Deltaic
35
32.9
Non-deltaic
38.5
12.8
23-9
27.2
Age
0-12 months
18.3
4-9
21.7
6.5
18.9
5-9
13-24 months
41.3
45-8
37.6
15-1
17
33-2
13-5
27-3
8.5
10.4
■48.9
8.9
16.1
13-5
16.4
3<>-9
9
5-8
49
44.2
9.8
37-5
25-36 months
37-60 months
Self-perceived
poverty*
Poor
Less poor
43-8
33.6
10.9
25
25.3
13.9
15-5
14-4
11.6
earth and thatch houses
(kucc/ia), which provide
little protection against
climatic shocks. Many of
the families surveyed were
farmers (64%), while a small
number (5%) collected
items from the forest.
There were two areas of
disease burden for the
children of the Sundarbans:
under-nutrition, and acute
communicable diseases.
Nutrition
Over one third of children
between 0-5 years of age are
chronically malnourished.
Poor: those who reported to have no full square meal every day or any day during the last seven days,
(i.e. stunted or wasted), with’
Less poor: those who reported to have a full square meal every day during the last seven days
that rate nearly doubling for
girls between the ages of 1-3
Methodology
years old (Table 1). Rates of acute under-nutrition (i.e.
Four parallel surveys were conducted in 30 randomly
low weight for age) are similar, with 39% of children
selected villages in the Patharpratima block of South
between 0-5 years old underweight.
24 Parganas district in spring 2012. Of tire roughly
Children in the 1-3-years-old age range are suffering
331,000 in the block, around 12% are children aged
most, with nearly half of those stunted, as compared
0-5. The block was selected because it reflects a mix of
to 18% of children under 1 year old. Surprisingly, rates
deltaic and non-deltaic habitations as well as a mix of
of
under-nutrition are lower in the deltaic regions ethnicities - with scheduled castes, scheduled tribes,
perhaps because they have been more supported by
and religious minorities comprising almost 40% of
non-governmental organisations (NGOs). The weight
the population. It is also one of six blocks of 19 in the
of
the mother was a strong predictor of child under
Indian Sundarbans identified as most vulnerable to
nutrition,
which is worrying given that mothers with
climatic shocks (IIHMR, 2010).
a body-mass index (BMI) below 18.5 comprised a
Surveys conducted include: A household survey
little over a third of sampled households.
covering about 1200 households selected through a
two-stage stratified sampling; An exit interview of 253
Figure 1: Distribution of cases of underoutpatients in selected government facilities and Rural
five
moribity based on reported symp
Medical Practitioner (RMP) clinics; In-depth interviews
toms
(N= 1030)
with selected RMPs; and In-depth interviews with
facility-in-charge of government health and nutrition
A
15%
care facilities. The studies were supplemented with: a
mapping of formal and informal health care providers;
a rapid ethnographic study in two villages; and several
case studies on RMPs and their clients.
The demand side: Health
status of Sundarbans’ children
The study collected basic health information of 1503
children six years old and under from across the block.
Families in the deltaic regions faced significantly higher
economic and climatic difficulties. A large majority
(80%) of households in the block lived in rudimentary
Disease prevalence and incidence
1 he vicious cycle of under-nutrition and morbidity',
especially for children, is well established. And this
block of the Sundarbans is no different. About twothirds of the children sampled had suffered from at
least one ailment in the last thirty days.
The most common diseases reported for children by
their mothers (see Figure 1) were acute respiratory
infections (ARIs) and gastro-intestinal disorders
(GIDs). This is consistent with confirmed diagnoses
of hospitalisations of children during the same period.
This represents a worse situation than the rest of the
district (which sits outside of the Sundarbans) and the
state of West Bengal. The proportion of children in the
block who had at least one fever during the two weeks
prior to the survey was almost ten percentage points
higher than the state or the district averages (DLHS3). The incidence of diarrhoea was also considerably
higher in the block compared to the state average
from DLHS-3, even though the survey was carried out
in a relatively low-prevalence season (April- May).
There was also significant reporting of cases of skin
diseases and rashes (5%). This may be related to the
increasing salinity of the tidal streams, as reported in
the Bangladeshi Sundarbans (CCC, 2009).
The supply side: Health
services in the Sundarbans
.
Figure 2: Mapping of health services in
Patharpratima
p
Pi nuryi tej*-'i C«®«
ttnxylleaBlCcHIO
Wt *
s>
A
AWW, ASHA) is also obvious (Figure 3) - about
28% of the required staff were not available at the
time of the survey. The Indrapur PHC, located in the
southernmost deltaic gram panchayat of the block,
was running without a doctor at the time of the survey.
Beyond staffing, the quality' of care in the facilities
was highly dependent on infrastructure (e.g.
consistent electricity supply and number of beds).
The BPHC in Madhavnagar is the apex health care
unit in the block. Serving 331,000 across 17 islands, it
is chronically over-subscribed, forcing a substantial
portion of sick children to travel out of the block for
treatment.
This section details the availability of health services
in the Patharpratima in both the public and non-state
sectors. Figure 2 shows their geographic distribution.
Most services are sought from and provided by the
non-state sector in the block. A lack of infrastructure
is a major reason for this. Those living in the deltaic
regions of the block would need to walk, take boats
and buses to reach the nearest public facilities, a
journey that can be prohibitively expensive.
Overall, the survey indicated that, while preventative
measures were mostly sufficient, curative services
for children were lacking.
Public sector services
————
Figure 3: Availability of health workforce
and facilities in Patharpratima block
(actual compared to IPH Standards)
The public health care system in the block delivers
preventive and curative services at multiple levels
and through outreach workers such as Auxiliary
Nurse and Midwives (ANM), Accredited Social
Health Activists (ASHA), and Anganwadi Workers
(AWW). Facilities range from sub-centres (SCs),
to primary health centres (PHCs), and block-level
primary health centres (BPHC).
■■■■MBH9UHMSB
The SCs in the block are the only facility type adequate
in number, based on the Indian Public Health Standard
(IPHS). The shortage of frontline workers (ANM,
■MM
50% gap (missing
174 AWW)
25% gap (missing 33
ANM)
73% gap (missing 8
PHCs)
Parallel services
With the gap in public senices, a number of parallel senices
have sprung up in the block, comprised of both informally
trained rural medical practitioners (RMPs) and NGOs.
Priority issues to address in the
Sundarbans health system
1.
Rural Medical Practitioners (RMPs)
The mapping found 376 RMPs in the block, about one for
every 900 people - many more than the one trained doctor.
This helps explain why RMPs were the first port of call for
child health services for over 85% of people in the block.
RMPs don't tend to have formal training, but over 60%
indicated some past experience working with qualified
professionals. This has led to questions on quality7 of care
given by these providers. The survey found that, for example,
35% of the child patients were given medicines with no
physical examination (compared to 13-16% in of public
facilities). Previous studies have indicated good knowledge
by RMPs of modern medicines and their purposes, but their
ability7 to properly diagnose and the incentives to rationally
prescribe these drugs is lacking. They often over-prescribe
antibiotics and steroids, which can provide short-term relief
but not a long-term cure.
Malnutrition and curative care: While coverage
of antenatal care and immunisation are comparatively
strong in the Sundarbans, there is an urgent need to
address malnutrition and curative care for common
ARIs and GIDs for children. This is particularly true for
children aged between 1-3 years olds to support them
through the critical first 1000 days.
2. Infrastructure gaps: Within the public health system,
infrastructure does not currently meet Indian Public
Health Standards. Where facilities do exist, they do not
have consistent electricity access, which is particularly
problematic for cold storage of medicines and vaccines.
Outside of the health system, access to care is challenging
owing to a lack of transportation infrastructure. Projects,
such as private-public partnerships, that address these
gaps should be prioritised.
3.
to climatic shocks like flooding and cyclones. More
projects that work to build resilience in the health
system to these changes are required. Existing projects,
such as one installing flood-resistant toilets that stop
the spread of disease, are strong starting points. These
projects should make use of local innovative knowledge
and include strong community7 participation.
Non-government Organisations (NGOs)
There are many NGOs operating in the Sundarbans, but few
work exclusively on health. NGO initiatives can be broadly
classified as: (1) Public-Private Partnerships (PPP), based
on a contractual agreement between the state government
and select NGOs, and (2) donor-assisted initiatives, where
an NGO implements a specific project. Two important
examples in the first category include: (a) mobile health
clinics (MHC), and (b) community-based delivery7 centres
(CDC). For the latter, a good example is Terre des Homines’
Special Nutrition Units (SNU). Across both categories, the
uptake of NGO services is far below the estimated need.
1.
Disaster risk management and climate chanat,
adaptation: The Sundarbans is particularly vulnera™
4.
Integrate parallel health sector: Integrating
parallel services into the health system, either directly
(e.g. through formal referral mechanisms) or indirectly
(e.g. through involving parallel service providers in
decision-making processes) is critical - as are projects
that improve the quality of care given by informal
providers (e.g. through training and franchising).
Climate Change Cell (2009) Climate change and health impacts in Bangladesh. Dhaka, Bangladesh: Climate Change Cell,
Department of Environment, MoEF. Retrieved from: http://bit.ly/13jYtJM
2.
UPS (2010). District-Level Household and Facility Survey (DLHS-3), 2007-08: India. Mumbai, India: UPS.
3.
IIHMR (2010) Health care in the Sundarbans (India): Challenges and plan for a better future. Kolkata, India: Future Health
Systems. Retrieved from: http://bit.ly/FHSind
4.
IIHMR (2012) How Healthy are the Children of the Indian Sundarbans? Sundarbans Health Watch, Series 1. Kolkata, India:
Future Health Systems. Retrieved from: http://bit.ly/16ri3Ra
JOHNS HOPKINS
BLOOMBERG
O
icddr,b
SCHOOL - PUBLIC HEALTH
|(j IIHMR
W
JlfcJAlPUR
This briefing was prepared by Barun Kanjilal, Jeff Knezovich and Shibaji Bose and is based on research from
the The Sundarbans Health Watch Report, Series: 1, which was compiled by the the entire FH$ India team.
This document has been funded by the UK Government. However, the views expressed herein are those of
the authors and do not necessarily reflect those of the UK Government or the partners in the Future Health
Systems research consortium.
Future Health Systems
® @ | This work is licensed under a Creative Commons Attribution-Noncommercial 3.0 Unported
E: fhs@jhsph.edu
T: ©futurehealthsys
immiwJ License. 2013.
W: www.futurehealthsystems.org
Legislative. Administrative Measures taken by Government for Children
Legislative Measures :
( inclusive of measures undertaken by State Governments)
I. The Andhra Pradesh Primary Education Act. 1961.
2. The Assam Elementary Education Act, 1962.
3. The Assam Students and Juvenile Smoking Act. 1923.
4. The Apprentices Act, 1961.
5. The Beedi and Cigar Workers (Conditions of Employment) Act, 1966.
6 The Bengal Juvenile Smoking Act, 1919
7 Tlie Constitution of India
S The Children (Pledging of Labour) Act, 1933.
9. The Child Labour (Prohibition and Regulation ) Act, 1986
10. The Code of Criminal Procedure. 1973.
11. The Citizenship Act, 1955.
12. The Delhi Primary Education Act. I960.
13. The Employment of Children Act. 1938.
14. The Factories Act, 1948.
15. The Hindu Marriage Act, 1955.
16 The Hindu Adoptions and Maintenance Act, 1956.
17. Tlie Hindu Minority and Guardianship Act, 1956
18 Tlie Himachal Pradesh Compulsory' Education Act. 1961
19. Tlie Indian Majority' Act, 1875
20. The Indian Penal Code, 1860.
21 Tlie Infant Milk Substitutes Feeding Bottles and Infant Foods Act. 1992.
22. Tlie Immoral Traffic (Prevention ) Act, 1956.
23. The Juvenile Justice Act, 1986.
24. Tie J and K Juvenile Smoking Act, 1986
25. Tlie Karnataka Compulsory Primary Education Act, 1961.
26. Tlie Karnataka Prevention of Juvenile Smoking Act, 1911
27. Tlie Mines Act. 1952
28. The Merchant Shipping Act, 1958
29. Tlie Motor Transport Workers Act, 1981.
30. Tlie Maharashtra Vaccination Act, 1964.
31 Tlie Maharashtra Regulation of Use of Pre-natal Diagnostic Techniques Act, 1990.
32. The Madhya Pradesh Vaccination Act, 1968
33. Tlie Madhya Pradesh Primary Education Act. 1961.
34 Tlie Marriage Law (Amendment) Act, 1981.
35. Tlie Plantations Labour Act, 1951
36. The Punjab Primary Education Act. 1960
37. Tlie Punjab Vaccination Act. 1953.
38. Tlie Probation of Offenders Act. 1958.
39. Tlie Rajasthan Primary Education Act. 1964
40 Tlie Rajasthan Prevention of Juvenile Smoking Act, 1950
41. Tlie Rajasthan Vaccination Act, 1957
42 Tlie Registration of Births and Deaths Act, 1969
43. Tlie Special Marriage Act. 1956.
15
Administrative Measures :
I Balwadi Nutrition Programme.
2. Early Childhood Education Programme.
3. Creches and Day Care Centres Service Programme.
4. Integrated Child Development Service.
5. Integrated Education for Disabled Children Programme.
6. Special Nutrition Programme.
7. Wheat Based Nutrition Programme
S Non Formal Education exclusively for Girls.
0. Child Survival and Safe Motherhood
10. Universal Immunisation Programme
11 National Policy Resolution for Children, 1474
12. National Plan of Action for Children
13. National Plan of Action for Girl Child 1901-2000 AD
4
Management of
Infantile Colic
Persistent crying is common in babies in the
early months of life1 and parents usually worry.
Almost one-third of normal infants are said to
cry for more th'an three hours a day in their first
three months. In most no underlying cause is
evident and their discomfort is attributed to
colic ('infantile colic-, ‘evening colic' or '3
month colic’) in which the baby has paroxysmal
episodes of inconsolable crying associated with
drawing up the legs, sometimes with abdominal
distension and passing wind.
CAUSES
It is generally assumed that the symptoms
originate in the gut but their cause remains a
mystery2.
Disturbance of digestion : Babies with colic
seem to produce excessive flatus and may
produce abnormal amounts of colonic gas. In
one study of 122 healthy newborn infants
given a feed of lactose containing human or
formula milk3, those with colic produced more
hydrogen in their breath than those without,
suggesting that colonic carbohydrate
fermentation differed in colicky children.
However, a second study found no difference
in breath hydrogen levels between colicky and
non-colicky infants".
If lactose fermentation does contribute then
colic might improve if the child's diet were
made lactose-free by giving either soya based.
or casein hydrolysate, milk. A double-blind
cross-over trial compared the effect of a soya
formula for a week with a standard formula
milk. In 11 of 19 infants with colic, symptoms
were less on soya milk and then relapsed when
challenged with a standard cow’s milk formula5.
In a second controlled trial babies were fed
casein hydroly; te<for four days, alternating
with cow’s milk. Children i/nproved on the first
change to casein hydrolysate, but the effect of
changing formula diminished with time and the
groups no longer differed by the third change
of formula. The effect was difficult to reproduce
Dr.in
Doctor
I 27
and marked day-to-day variations occurred
independently of the type of formula used6. A
third study compared soya milk with hydrolysed
casein in 60 infants with infantile colic. Thirtytwo of the children who had been identified as
having symptoms unchanged or worse on soya
milk were improved on hydrolysed casein.
Eleven of these children reacted to cow’s milk
at 6 months of age with symptoms including
diarrhoea, vomiting and ra ' es as well as
colic7.
Intestinal spasm : is another suggested cause
for colic. A prospective study from Sweden
found that infants who latter developed colic
were likely to have higher levels c! ■ aot'.lin (a
prokinetic gut hormone) than the controls in
cord blood and in later blood samples, but the
results overlapped8.
Psychological factors : Distressed infants
almost inevitably heighten parental anxiety
and although family tension may exacerbate
the problem, it seems an unlikely primary
cause of colic12.
MANAGEMENT
Infantile colic is a transient self-limiting
condition in an otherwise healthy and thriving
child. Parents seeking help to relieve the child’s
obvious distress are often given a bewildering
array of advice9.
Parental support : Once colic has been
diagnosed, it is important to reassure the family
that the baby is normal, that the condition is
common and that it gradually resolves. Some
babies appear to benefit by being carried
around10, others by being put in their cots.
Regular contact, support and reassurance may
be all that is necessary.
Dietary manipulation : For bottle-fed infants it
is tempting to change the baby's milk to a
lactose-free form 5-6. For breast fed children the
mother could try a diet without cow’s milk".
These changes are only worth trying where the
child is particularly fretful. When they are
effective substantial improvement occurs within
a we’ek. If the child is helped it is important to
tell the parents that the child's symptoms were
not due to an ‘allergy’ and that this improvement
does not presage a lifelong milk ‘allergy’
problem12.
51
Drug treatment : Various mixtures are sold to less severe14. A Sw. lish study compared the
the public ('gripe mixtures’, 'colic drops' etc.) effects of activated dimethicone with a matching
These mixtures contain sodium bicarbonate placebo in 27 infants in a double-blind cross
with other ingredients such as dill oil, caraway over study, for a week, with a five day 'wash
oil and tincture of ginger; they no longer contain out’ period. The babies were given dimethicone
alcohol. Two over-the-counter preparations. 28 mg before each feed. The parents kept 24Dentinox colic drops (DDD Ltd.) and Infacol hour records of behaviour and were interviewed
(Pharmax), contain activated dimethicone at home with periods of observation on two
(simethicone), Infacol is the only prescribable occasions. Two-thirds of the infants improved
drug specifically licensed for infantile colic.
during the treatment period in both the
Activated dimethicone is non-toxic and not dimethicone and placebo groups15.
absorbed. It is said to act by altering the
surface tension of mucus so allowing entrapped
gas bubbles to coalesce and be more easily
released by mouth or anus. Dimethicone can
relieve symptoms of indigestion in adults1-1.
A British study compared dimethicone 20 mg
four times a day with pla> ..bo in 26 infants.
Eleven of these infants with troublesome night
crying received a double dose (40 mg) in the
evening. Each treatment was given for a week
in random order and the parents kept diary
cards. By the fourth day in the dimethicone
group the episodes of crying were fewer and
CONCLUSION
Infantile .colic is a common, transient, self
limiting problem which distresses babies and
worries parents. Reassurance of the parents
may suffice, but should be coupled with advice
on careful attention to the child’s preferred
posture. If these fail it may be worth trying a
diet without cow’s milk for the breast feeding
mother or a lactose-free milk feed for the bottle
fed child. Perhaps a short course of activated
dimethicone might also be tried.
Reprinted from Drug and Therapeutics Bulletin Vol. 30,
Ho. 4, 1992. Reference will be supplied on request DDD
|/n our connlig activated dimethicone is auallable as DIMOL SUSPENSION (Wallace) containing
200 mg of the drug/5 nil — DDD]
Do You Know ?
Your subscribers’ code (S. Code) number which is mentioned in the address-label of each issue
of DDD. Please quote the number while requesting for a replacement copy and enquiries about
subscriptions, etc. It helps to respond promptly. Communications without S. Code number
result in inevitable delay.
Components of S. Code include —
State code : (eg. AP/MS/KTA/TN, etc.)
Serial number of the subscriber of each state.
Tenure of subscription : 9292 (annual), 9295 (four years), LIF (life), etc.
Please note your S. Code number. It is important
52
Drug Disease Doctor
27
Have your child weighed at the AW centre regularly
012 3 4
5 6 7 8 9 10 11 12 13 1<l 15 16 17 18 19 2021 2223 24 25 2627 28 29 30 31 32 33 34 3536
Growth lixjicaiorsi
Good
[Growth Chart]
12
.
Normal
Gradel
(mild)
I4X)
Grade II
(moderate)
Dangerous
Grade III
(severe)
A
9
(very severe)
Very donoeroijs
o'
&
$
8
§‘
e
13.0
125
3
w B
6
A
a
&
^Normal
tii
Weight in Kilograms
I
125
A
105
9
s
11
f8l
13-5
ioa
'Grade 1
£
s
;Grade;[ll
0--0 ■.y
<?
9 cd
s&
8 s
il!]p
y
:he.vi and itrri>:
during high favor and
take the child to the
health center
Diarrhoea
<? Breastfeed more afterc
•> Give extra fluids!
*.•> Give OHS)
<> Continue to give
ncinral diet 0
if hose motions do rot
step, take iha child to
tlvj iviaith center
+ Care During Illness +
If the child has rapid
and-1 or difficult
breaihir?g. lake the child
!o the health center
r?
tt?
(7o, moi^dc
^*41
«»o^
xrrff^os, «^Xujdt-H ’
, 5’4 j
AS!>\d &(»?
-^^CH^G
UTPf (S/^)~
^EB^nfri) e2)U
p corn d<js Good
UP) ^fegT
MEA9^s/cFmt^
fof\ child a pt eK
PooG Hd>ith%'
Q
^UUxt^U" (pcjx)H
w?
U KUJU
EARLY CHILD DEVELOPMENT AND THE BRAIN -
THE BASE FOR HEALTH, LEARNING AND BEHAVIOUR
J. F. Mustard - World Bank, April 10, 2000
I will first review the evidence concerning the relationship between the early
years of life and health, learning, and behaviour throughout the life cycle from a
historical perspective. I will then review evidence from biological studies, cross-
sectional studies, longitudinal studies, randomized trials of early child initiatives
to support early child development, observational studies, and animal studies.
The weight of all this evidence is compatible with the importance of the early
years in establishing a base for competence and coping skills throughout the life
cycle.
Slide 1
One of the striking changes in Western countries has been the effect of the
Industrial Revolution on the health of populations in Western countries. This
slide from Fogel's work shows the decline in mortality in France following the
start of the Industrial Revolution. Both he and Thomas McKeown, among
others, have tried to assess what caused this remarkable decline in mortality.
Slide 2
1
McKeown concluded that direct public health measures accounted for about
25% of the reduction in mortality rate and, by exclusion, the rest was largely
related to improved nutrition resulting from the gradual improvement in
prosperity resulting from the Industrial Revolution. His conclusion was
controversial, but Fogel, in a broader assessment of Western countries, also
concluded that better nutrition was the main factor and he also found that as the
mean heights of populations improved so did life expectancy improve. Since
nutrition during early childhood (including in utero) has a major effect on adult
height, he reasoned that conditions during early childhood affected the risks for
health problems in adult life. There were obviously other changes besides
improved nutrition that affected early child development during this period such
as family size. But the historical evidence shows a relationship between
economic growth and health that is not due to health care or more conventional
public health.
Slide 3
Being an economic historian, Fogel also concluded that a large part of the
economic growth during the Industrial Revolution was a consequence of the
better quality of the population. He estimated that this might account for as
much as 50% of the economic growth in the United Kingdom. The historical
evidence shows a clear relationship between economic prosperity and the
2
health and well-being of populations and the effect of the quality of the
population on economic growth.
An unresolved question from the historical evidence is how early life affects
health and well being in later life is, what biological pathways are involved and
how do the conditions of early child development affect these pathways?
Slide 4
The importance of these questions for all societies is set out in the recent report
to the British government on inequalities in health. The Acheson report reviewed
the evidence and concluded, as this slide shows, that conditions of early
childhood had a major effect on the mental and physical health problems of
adult life in developed countries. They also found that health care was of limited
importance in changing the inequalities in health. Early life experience
appeared to be an important contributor to inequalities in health in adult life.
Slide 5
In terms of the biological pathways that are involved: our increasing
understanding of organ development in the early years and how the brain as a
master control organ affects all aspects of body function through pathways that
affect the endocrine system, the immune system, and mental processes is
3
providing clues about what is going on. One has to suspect that brain
development in early childhood is a factor influencing health, learning and
behaviour throughout the life cycle. 1 would now like to briefly review this and
related evidence.
Slide 6
I will review the evidence from five different approaches to the study of early life
and its effects on competence and coping skills and health throughout the life
cycle. These areas are:
1. Biological
Neuroscience
Neuroendocrinology
Neuroimmunology
2. Animal studies
3. Cross-sectional and longitudinal studies of human
development
4. Randomized trials of interventions to improve early child
development
5. Observational studies
-
4
a
BIOLOGICAL STUDIES
Slide 7
This slide is a summary of some aspects of the control or regulatory function of
the brain. It does not show the sympathetic nervous system pathway which is
important. For this presentation, I will focus on the Hypophysis - Pituitary -
Adrenal Gland axis. We now have some evidence about its development in
early life and its effects on brain function and other important pathways such as
the immune system, sometimes referred to as the neuro - immunology pathway
or psycho neuro immunology pathway, PNI. Basically, sensory stimuli to the
brain from internal body systems and the external world in early life affects the
control pathways that determine sterol production from the adrenal gland. The
sterol levels and their duration in the blood affect all body systems and organs
including the brain. The brain regulates sterol levels in the blood through the
hippocampus hypophysis interaction. Settings in the brain for the balance
between the response of the HF A axis to stimuli and circulating levels of sterols
are set during the early period f brain development in animals. Thus, we have
evidence that shows one aspec of early brain development which through the
response to sensory stimuli influ :oes a wide range of functions such as the
brain, immune system, and the ct diovascuiar system throughout life.
5
Slide 8
Since our response to the world in which we live is driven by how our sensing
pathways work and how the different parts of the brain respond to these stimuli,
the development of these pathways in respect to the sites in the brain that
process the signals has become of considerable interest. The neurons in the
different parts of the brain develop their function in relation to the quality of the
sensory stimuli they receive during early life. The work on vision has shown that
there is a critical period during the early stages of development, when the brain
is most sensitive to the wiring and sculpting of the neurons in the occipital cortex
of the brain which receives and processes the signals from the eye. Despite
some different interpretations of this work, one of the neuroscientists whose
work is in this field summarizes the effects of total deprivation of signals from
both eyes in early life on the development of normal vision. We now know that
this relationship holds for other sensory pathways such as sound and touch. We
know relatively less about the development of neural pathways to other parts of
the brain that affect our responses to stimuli such as arousal, emotions,
behaviour, and aspects of cognition. It would appear that there are also periods
during development when similar processes (development of other neural
pathways) are occurring in respect to other functions of the brain and some of
these will occur, at least in part, after the development of the sensing pathways.
6
J
It seams that different parts of the brain have different periods for development
and some functions develop at a later period than the sensor/ systems.
ANIMAL STUDIES
Slide 9
Although we resist attempts to apply knowledge from animal biological
experiments to the development and function of our brain, we should always
keep in mind that much of the understanding of human physiology and disease
and its treatment comes from animal studies. Some reservation about the
relevance of animal studies to humans is sensible, but to ignore this information
is a mistake, partly because you can only begin to understand certain biological
systems through animal studies. Fortunately, mammals have neurons in their
heads that are similar to those in our heads (we have more of them) and they
have sensing systems and HPA sterol systems similar to our own. Finally, they
are the only approach available to examine early brain development and the
effects throughout the life cycle. None of us live long enough to study human
life cycles by direct observation. There is substantial data from studies in mice,
rats, and monkeys.
7
Slide 10
The rat data shows a number of interesting observations that relate
developmental neurobiology to function. This slide summarizes some of the
benefits to rat pups given an early rat pup development centre with the
involvement of the mother. In contrast to rat pups not given a centre for "play
based learning", these animals as adults had more neurons, more connections
(outcome of brain wiring and sculpting), and performed better in tests of rat
competence as adults. We also know from other studies that rat pups that are
intensively licked by their mothers in early life, set control points in the
hippocampus for the HPA axis that provides a balanced response to stimuli
(lower sterol levels to stressful stimuli). Again, these animals have improved
wiring and sculpting of the neurons in their head and sustain their coping skills in
adult life much better than rat pups that are not licked as intensively by their
mothers. So much for rats. Let me now briefly turn to the work with non human
primates which involves a number of groups. In this presentation, I will
specifically refer to the work of Steve Suomi and his colleagues at NIH in
Bethesda.
Slide 11
This slide summarizes some of the effects of poor "mothering" during the first 6
months of life on young Rhesus monkeys.
8
1. They show increased anxiety and depression as adults (behaviour).
2. They show excessive alcohol consumption if given access to alcohol.
3. They show impulse aggression and violent behaviour.
4. Females tend to be poor mothers.
5. Predisposed to high circulating sterol levels during development.
Slide 12
This slide summarizes some of the biological changes in poorly nurtured
Rhesus monkey infants.
1. High sterol levels to mild stress (stimulation).
2. Chronic deficits in serotonin metabolism.
3. Disrupted circadian rhythms for sterols.
Slide 13
This slide shows the effect of good nurturant mothers on the development of
genetically high risk Rhesus monkey infants.
1. Precocious in their exploratory patterns.
2. Females become very nurturant mothers.
9
*
3. Rise to top of social group dominance hierarchy.
4. Robust immune response.
These animal studies support the argument that early life influences brain
development and cognition, behaviour, and biological pathways that affect
health in later life. I will now turn to evidence from human studies.
HUMAN STUDIES
Slide 14
In the presentation of the material it will be important to be comfortable with the
concepts of gradients when health and measures of cognition and behaviour are
plotted against socioeconomic status (SES). SES is a composite index of
measurement like income, occupation, education. I would emphasize two
important points from the studies in the developed world. The gradients tend to
be linear, meaning there is no poverty threshold, that the cause of the gradients
is not genetic, and the association with socioeconomic status does not imply
direct causality. The other point, as we go through this material it will become
obvious that in countries like Canada, the greatest number of children in
difficulty are in the middle class. The challenge is to try and understand the
pathways by which socioeconomic factors affect development, health, learning,
and behaviour. I will argue that our improved understanding of biological
10
pathways, that I have briefly introduced you to, are important in determining
causality.
Slide 15
This slide shows the gradient in health at age 33 for the children bom in the UK
in March 1958 in relation to social class at birth. Social class 1 and 2 are the top
of the social economic structure and social class 5 is the bottom of the social
structure. Self-rated health at this stage in life is known to be a good predictor
of chronic physical and mental health problems in later life. The psychological
distress measure is related to subsequent mental health problems. Obviously,
circumstances after birth affect outcomes at age 33. Power and Hertzman have
split this into latency and pathway effects and show the importance of the
latency effects. Barker has shown the latency effect on health in adult life of
poor pregnancies.
Slide 16
This slide shows for the 1958 birth cohort that there is a gradient in educational
qualification by social class, reading by parents, and stability of families as
reflected by separation of parents by divorce. The key point is we are beginning
to see that the gradients in health and education show a similar relationship to
social class at birth and that one of the factors that may be influencing this is
11
parental support. Obviously reading has a large effect on the development of
verbal skills in early life and also appears to affect other pathways in brain
development. We now know from this and other longitudinal studies that about
one third of females brought up in dysfunctional families in the first years of life
will show signs of depression in their thirties.
INTERVENTION STUDIES
Slide 17
There are a number of intervention studies that initiatives that enhance early
child development, enhance outcomes at later stages of development.
The first of these is the Grantham-McGregor study in Jamaica about the
benefits of early child development initiatives on the development of
stunted children at birth in relation to a control group. The study group
was randomized into 4 groups: no enhanced support; improved nutrition;
enhanced nurturing or stimulation; and a group given both improved
nutrition and stimulation. Over the two year period, the group given no
support showed poor development; the groups given either improved
nutrition or stimulation improved about equally, and the group given both,
equaled the control group at two years. This study shows the value of
both nutrition and stimulation on development in the early years.
Obviously, good water and nutrition are important in early child
12
development. Unfortunately, we do not know whether this inten/ention
had long-term effects.
«•
Slide 18
The Carolina or Abecedarian project shows an effect of an early child
development initiative in a poor African-American population. The children
were randomized into two groups: one, an early child development
program starting shortly after birth continuing until the children entered
school; and the other, a control group not given the program. This study
showed gains in cognition (including IQ), in education performance, and
behaviour, still manifest at age 21. The effect on IQ is of interest since a
recent review of this subject concluded that the circumstances of the first
year of life affect IQ.
Slide 19
The well known High Scope Study has provided evidence from a
randomized study of an early child development initiative starting at age
three and continuing until the children entered the school system at age
six. At ages 18 to 20, the children given support showed better school
performance and fewer behaviour problems. This slide summarizes the
gains of the intervention group at age 27. In this assessment, we are
13
beginning to see the effects on mental health - fewer women in the
intervention group were in programs for "educable mental impairment".
This study did not have a sustained effect on IQ, perhaps because the
program was started after the first years.
Slide 20
We do know, however, that programs designed to enhance skills in
mathematics around ages 4 to 5, have an effect. This shows the results of
work by Case and colleagues to improve performance in mathematics
through an initiative called Right Start (the cognitive weight of numbers).
Children in a poor socioeconomic neighborhood were randomized into an
intervention group and a control group. The children given the special
preschool intervention program, at age 9 surpassed in the school system,
children in a middle class school.
Slide 21
Studies of early child development programs in other parts of the world
are beginning to show similar effects. This slide summarizes the results
from an examination of early child development programs in Brazil. The
results are compatible with the studies I have just reviewed.
14
OBSERVATIONAL STUDIES
Slide 22
Observational studies show the benefits of good support in the early years
of life . One of the most recent, concerns the adoption into British
Columbia families of Romanian orphanage children shortly after birth with
those adopted after many months or years from these orphanages with
very poor environments for early childhood development. The children
adopted after a longer period in the orphanage appear to be similar in
development to Canadian bom children in middle class families and show
significant behavioral problems and lower IQ’s than the children adopted
early. Megan Gunnar, who studies the HPA axis in children, has found
that the children adopted late have significantly higher sterol levels. If you
remember the animal experiments, the early years have a major effect on
the control of the sterol pathway which, among other things, affects brain
development.
Slide 23
Megan Gunnar in reviewing the stress sterol pathway and early childhood
came to the conclusion that caregivers and parents have a very powerful
effect on the development of this pathway in early life.
15
Slide 24
An important observational study was carried out by the Stanford
economist, Vic Fuchs, who looked at the relationship between an index of
early child development at the time children enter the school system and
the performance of children in grade eight math. Each of the points on
this slide represents a US state. The early child index was called
readiness to learn. Clearly, the states with the best measure of early child
development do best in mathematics. Fuchs concluded that if you wish to
substantially improve mathematics outcomes, investment in the preschool
is probably equally important to the investment in schools.
Slide 25
This summarizes what we now know about early brain development and a
variety of functions in terms of sensitive or critical periods. One of the
questions often asked, is it all over after the first few years. The answer is
no, but you probably do not establish the same base for brain function
later on that you can establish in the early years. You can, in Emmy
Werner’s phrase “overcome the odds”, later on but it is difficult.
16
Slide 26
It seems likely that the steepness of SES gradients in literacy and
mathematics found among countries and within countries reflect, at least
in part, the quality of early child development. This slide shows the
gradient for youth literacy against parents’ education among a number of
countries. The high performing countries have a very flat gradient and
these are countries that do have good early child development programs.
Theoretically, all countries should be able to establish high performance,
less steep gradients. Doug Willms will say more about this tomorrow.
Slide 27
We have some interesting observations from within Canada. This material
is from a report prepared by the Reference Group for the Ontario
government’s Minister for Children, our chair for this session, Margaret
Marland. The report’s title was "Reversing the Real Brain Drain".
Slide 28
We were able to secure a preschool measure of early child development
on a proper sample of all Ontario's children. This slide shows what we
found for verbal skills. The vertical axis is percentage of children below
the standard (% with low receptive vocabulary) and the horizontal scale is
17
a socioeconomic measure. Again, we have a gradient which is linear. A
larger number of children at the poor end of the SES scale on the left are
in difficulty, but close to 10% at the high end of the SES scale (on the
right) are not doing well. This also shows that Canada’s wealthiest
province is not doing as well as the rest of Canada where the gradient is
curvilinear. This assessment of verbal skills correlates with later
measures of development including literacy performance.
Slide 29
Thus, it is not surprising that the gradient of youth literacy for Ontario is
steeper than for the three Prairie provinces and Quebec. Obviously, if
Ontario is to improve literacy, it will have to do something about early child
development for all social classes.
Slide 30
The recommendation we gave to the Minister was to establish, in
partnership with communities, involving the public and private sector, early
child development and parenting centres sensitive to early child and brain
development. You will note from this chart that we would like these
centres to begin their support before the child is bom because of the
importance of the in utero period.
18
Slide 31
Our minister is here because she understands the importance of this for
her own community and understands the enormous importance for the
developing world. Her goal is to give the early years of human
development (tier 1) the same importance as the later years. The plan
she is developing to introduce in the province of Ontario is a direct steal
from the World Bank’s work and I close with Mary Young’s comments in
your 1996 report. This is relevant to all societies, rich and poor.
“Because learning begins at birth, and even before, the starting point for
involving families in early child development programs must be as early as
possible ... Knowledge and understanding of programs is no longer the
constraint facing early child development. Rather, transforming this
knowledge into action is the major limiting factor in implementing early
child development programs and requires the combined support of
governments, non-govemment organizations, the private sector and the
media. The challenge to care for society’s youngest members is not just a
challenge for a single country or continent; it is a challenge for the entire
world community.”
19
cv\- G •
MEETING EMOTIONAL NEEDS OF CHILDREN
What Parents can do?
DOCTORS are often asked what constitutes good emotional health
of a child. This is a difficult question to answer. Teachers
and parents know much more about them. To get over such
problems, the responsibility lied not with the doctors alone;
it rests more with those who are the custodians of child *s
emotional and physical development, viz., the parents and to
some extent the teachers.
Building the faculties and personality of a child is more
of parents’ responsibility. But the job is not simple. Whild
some parents say, "be strict", others think "let the child have
his way". And to-make matters worse a newspaper or a magazine
advocates a third line of action.
To tell the truth, no parent needs to carry in his hand
a reference book on child development which will help him
what to expect of a particular child at a particular age in a
particular situation. Nevertheless, it does help parents to
know something about the child they are dealing with.
Guidance helps
Children learn by parents ’ repeated guidance and help.
Parents must learn to handle unacceptable behaviour until
children can grow up sufficiently to behave the way their parents
would like them to do.
Apparently abnormal traits commonly observed in children
below five years of age are: restlessness and excitability,
(2() day-dreaming, laziness, lack of concentration; (3) general
anxiety, timidity, and shyness; (4) specific fears, seeing horrid
faces, (5) poor bladder control, bed wetting, (6) nervous habits,
nail biting, (7) cruelty, aggression, outbursts of anger,
(8) speech difficulty, (9) food fads, (10) temper tantrum,
(11) frequent crying, babyish behaviour, (12) lying and stealing,
(13) headache, stomach pain and constipation, (14) disobedience,
and (15) obsession.
While such traits should not go unnoticed; they need not
cause alarm. Such signs are not necessarily signs of neurosis
and maladjustment. Most of the children do have minor forms of
obsessive compulsions. Many cannot resist counting shops while
passing through market side. Yet all such children would not
necessarily become neurotics. Certain traits like thumb-sucking
and nail-biting are regarded as reflections of frustrations in
suckling. Deprivation of breast-feeds or sudden weaning are
causation for deviant behaviour.
. . .2
2
Abnormalities; Apassinq phase_
Apparent abnormalities in children are a passing phase.
Symptoms of emotional disturbances fade out gradually with
growing age in majority of children. Younger children showing
such symptoms have more changes of recovery from emotional upsets
than older children with similar troubles. Speech difficulties
disappear slowly. Anti-social behaviour like stealing,
cruelty and aggression pass off quickly, whereas specific fears
like seeing horrid faced are transitory. Lack of power of
concentration and day-dreaming seems to be resistant to change.
Fundamental needs
Why deviant or abnormal behaviour? The answer is simple.
Every child has fundamental needs both organic and emotional.
The former are for living and growing while the latter are for
developing and maturing. Some of the most important emotional
needs are; (1) love and affection, (2) security, (3) recognition,
(4) Friendship and company, (5) acceptance and belonging,
(6) achievement and success.
A child's first need is parents' love. This has no
substitute. The child needs to know that he is wanted and there
are people who care about him. In school, he wants that the
teacher and other pupils like him.
Feeling of security develops in the child a sense of
personal adequacy to meet different situations and problems while
insecurity tends to generate tension and anxiety. It is through
love, success and belonging at home and school that a child
gradually develops an inner security that enables him to cope with
newer challenges that confront him as he grows.
Each child has a desire to be recognized, admired and taught.
similarly, every child desires to experience certain amount of
success in areas which to him are important. A child likes company.
In school situation, group membership becomes important to the child
He wants to belong to one group or another and make friends. Hjs
desire for belonging becomes stronger at adolescence and he wants
to learn how to get along with others.
All these fundamental needs and their adequate fulfilment are
essential for the emotional health of the child. Failure to meeit
meet these needs in the right way creates behavioural problems.
A child who receives too much recognition may become self-centred.
On the other hand a child who is denied recognition may become
discouraged end develop feelings of inferiority.
.. ..3
3
A child who is adored and over-protected may be spoiled and have
difficulty in getting along with other pople, while a child who
is deprived of love and affection may feel unwanted, lonely,
defensive and unhappy. Therefore, it is essential that the
fundamental needs of a child are fulfilled, without making him
overprotected. Only this way can he be expected to blossom
into a promising adult with the dapacity to face the challenges
of life.
Source: SWASTH HIND - November 1980.
Puguc weAtry PeRSPKTW, tra^it/o/vac sy£TEMi & iffliw
Aivd major j>ireAses~~o^ cuiFbhoo^
CARS:
/ <y>^ecU-bt> g
wi-CCwtcttG
CC-
. C-tvvef
cH-b
tt^y ^zVAA/Vctve>viz
(■vC-tyttli z
-
z h>'uytL’'Vvi^c.xtu'Ac'
> jr > t^tv-cnvpvvtj '
d,-t£W,$c-
c^UW^utiSvVxtvdi?
c^Ltly wo--v b€kie<y,/xL-
CO^iFcw^b v-U:.
^yryAO a\-v vriyvuc
-
A^-EAjTC.Av-tuu^ c7>' Wtriy UyWwp^
^v£e'k.Jx>
c?7-
S/i-<?c'i/‘-'u'l-i-n-b'i S■txyi'VvvvCu’ ^vS/viy
N v ) !^u N /'V i c i\; r
/kvli
0'^-'
A-
^c/Mts
cy^vtj 60vU''Cvtv<n'V
^i'veb'Vvy-vnx’byv-o^x-
o^- ^Csv/i-ie'- F
IKz
^'^-v^uzu
C>~^
w
vu v v
LV-'^ee
^vyo V"C vlz-S
L-Viy (?'b?Cc''i<^4
vV<Uv6 4,-J P-'ACyA'b fV^-wt &VC
jtvvWbt
IvtCtbui
llZXCvvvirvt
/^ui-tdAby
7^vc 'i^UViXtfcL ^vvctyry c^ Cc dC^^tae.. Zi Co^icL&bC^t.Av AbCjphyviCs
^ACV^vvCvl^ p^^p'C^.^ ■
//vC- l>VC-L c'k'VUvuy^v vvJ An-l'y ^C'tco->iz C^,
C'LvVt C vvv-titfo-v^vvdvvt^bl-
pd'tC'vFt'^d^'tcci^Fcnv
/uvv
co<3 O'H/CJAS
kA 4jv d'^Lct^C
t\,^ou:Le'^ p/Ovw tTvZ'yt vyt'
fyi/CvC'^tbAvLwtc6A/Z b'bvvttt
lUj
^izLg, ci'^cvL^j &s 4zpv ^yy'Tyb (7uni% y
fcyMzbv-tLc/ii/v^LvvuL ,ys /\^C^C\C(A., C‘V /ve,C6’l'C v(./
c
{p-v d,££<-U\ &vx,&/\,&g.
j^'V^yy, ctAj'V'LJ
py\C'\i Z/UvtyffTP
,A
l£- tvA»W ^t>T/ ^ZLOC-^b'tyV'lj^S
TtyXtz •t'Vvycy foe CU^'&'VW'prfc&vLct ,Fv tii<y0^
T'lZay <bvb 'H'lX^Wzbuyi
^-yc^ xrz(, fcy>k>/b4.c'fe ^^voy^yC
E-ZV
by-
^pzc-LpCC' po C i'cC'Cie-vi (£-£ 4'kvfVvx
^L/jSvi.'fG,
€>Os tt-xx^ CQ,t^b,CC^Cx'7yoCV\/b
4w
pe-voceC cp,
bfWvc€-v£
4,L^kWi/v>^' CL^i/v\JC<>
tc^oipi bp pocowpi'
t
<^v\^cL
cvvvd. ^tA-cpp^^bc'
£ i/kvvS'(Z ^lJ-€^Vj€-
Lft'CC't.' bb. poi^&vvlb Sc/p4jclde.^
C\A/v-ib LwvvCb' ^bCStXb'i-CCb\A .
IbxCviOvbc&y-i
/<'Vt~vkWLj
/^(■^bo'CC b^CCcoL'/
■‘I'^l^Oj
iX.C-CCO^p'CCs.^b b^p-
l/vC\^,oL.' cb^pec-b 6Wt(<-{ cbC'S>^b<.'l-Cip
fo.egw L ■bx^A-
72tcw cvtc
^ci' bb^Cce
6'^
pozv-^v^c^cryv
^Vo/tfbvku
pkTJUV^-'kkt‘'^^'?
j>K^Va-Ci
blu i,c ^V vC
tz/’k'H" ^-iZv^- ^Ci/ihy
Lcv^ti (%fc l/V4vvC'U- po,cvcovtbi,^ p'V^c.bbce'i e\oxx^/vj /?€- ^oppb'C^bf
(CbCp^ciCv^
tA,p^
Ctoo tv^Uzuvs-^l-L Cv\sS/b<yvtj.
/.
The
Lc VI 6V\,O ;
l^w^bCii, Po^0'vwc~[/u)'>2^ — ^vv^uvcjU^L Cb £
(rVCS fc. Cop AsVVXpO/frVbl'pj
C-L u-'
C^'i'U
CxZ&'Ct/bi 6-Vw<X> (ppv<^-CuCp Op
fri A^v(;;(zLV-<.<CkVk'l/h (Xox^c C'C'VWVWkkVkCK 6^ ,
lb 'to 'tt-VklzS ^Vkt,'
./Cc/CCkvCj G\> bCo<>\/o\opp pW p frypLcC^coo /[✓vv't-o ^O'fvvtbb ■ykw<<vn/i^
^ybZ/vC-tCtcX zl/t<'vbt-i>2^V|/C^, ^4z//_,
2 • ^pecbpCc' P'vc bec^oyt
-
44 ^j^zv^vL/tL'^v
C'O'V'vvi^i/i/^v^TAiZv'C C^i/S-c t fVkvvV jX’wvj^ws^ •J'yur^^^c'-xz.f tu A/wIcocc^b'
UCoC' 0<SVw/2-e4
o'
'v<uS£'V2-C
&/ P^'ve>y^^^
c\2&c<m-c-
uv> 4'i/vv<Z'tv€- 'Huvh/.
7H-to Ltw-b
fycpb&Ltcxb Cv (^pLOZ&J^ <Z')Cb&wt ,£v\s
/•£/pV^ V (j-pL-r
boj&v&v^thcn'L-
b^c <^C$^c^kl- .bo c\s co-x^v^wv^c^lc &yxc
la& cta^c^e p-vvccac /izw (X^tov fc>
•icdzvvoC^ic, av\,cL f (^)
a'vwpCCc<sx-aoxs to-'
yvvs^owt ^>'Z/D'Covt^<<fL (sVisa^csetpj .
byAV^b^iScCxx '. do (Sv p-^Lx'iy^vfs- ffy' aa^cj
^c-yvsd/i^\zyxccs cv^ cCwacfrlLcj act-i^av^ce-d. cslxs-enod:^. zP^^iy
y..
.Z^Xz^tX^iXvfcj
cCcU^it'C
.-^CCC^-ix-xi/i^z
civ<c^kL6 py^CciS^CC
yix^.CC’-VvvpCcZ^ k^'v^iixrLc-CX^C
ajj po,awfcc->x
X^VU^LA tz
C&s-o £tA.A>v4v^£/i_ e
as
(.
O}'yv\ Lyb-^j^i/ CAA^cb
"
Ca> ■ o-vc^yiAAi^atC, asAL-
Scc-tZlC/ Cd^LOixlScC'i^^C a^xci. LVaSLlZCy^iC
tv<?uv T/vOtzi/-)
<2-V
ZU>" /^(^Ltvu-I^izuz:/-
acb(jz-
pp
t
(s^ox.dL
b^-(d/]^b^(StApp-c^L
bj
^2>zlca/'<
^e^CVVC'L-^i/My) p/v^/v e^vAx?"
TAv fzC £W\y
&TX, XXx-CUX'Xz^X/LZcL-
.
L^tx^c &p py^ty^cbac'i'X'S'a
^T/iz^ tJC-v-Sx4? 6cz-L
P/izvt'-.'^t/vy
IV.J/.O.
©M
p ziZ4/ Oia/Izu (X7/V
H/tA-
ZZ4-U^
kV • H ,0 ,
cte-zf .-iaa^z
(Xzaa^l/
4] ett^x-ofziAx^
0(Z 4Aztrtr
W
G'W
(A/S.
Sd/idm
CA/Wtt •€^VV|'I^AZV/a/C^'V
^WxzL' (7^ S^v'LY^tA>Tzi_/ AAizu-^^
tc
iAz^vO'vV' .^W'UHz ^^aaZzU4xAm?vv
CY
, /•vA^CliZz'^'
ex^icaUy /\jlca$-nixed.
'{/xC^cti’^^>i-\C^L
^.C, /XC-l
IAaZZCvO^L /yWhC-fv^0>x£-A<
A^rLie^vC ^)Uvw>U^m/ A
■
COVVlzvCvv€.S C-^ U\Xz C'V>CvL^ J
/
(AZ
0\S
li T
STc-fi/C>A/(;OS
. I »(r
^J->tt/iAA,4
C^CA/S/t?,
2waac\awv\jaaJz
Itfc-O-
<
(Al
6V<
P\/>
Vv^vASzIaz I'Vvte- j"(.
,
izO<^ eTvuj/W
ivC-AvS€ t£ /Wv 'WiZ-SY'
?/2<'v4-izKc-Vbt;vL
(7\y >V^4Aa/^C^AAv// A04/VVVvi96v (5^
OVJ<AA/Lc'd^>(i^
i~.
j^'Y' P^y^A/vy
....
'
A/xa.
^AVtOU'/-
t&
J
i - .y
p^cMdvce^
(A/ta-C
t
'^oyiAA.^^cscX,
-yy^dZceiJ.
Aw
r
j .
jA/L<V't>4Az \/VzCzO^TVV''VS-<
-€ A(X , Xv^cli-UAz .
[\(AV\^\^C\
>Haaazl<o zha
(H-
Nc>'v^t'\ -- CAtzA ^wXAAz.
'7/xc
Aj'^Aucm^X
Sz6<%Z^z
z^MZM/bys o>ve^/
i/iVvCcn-M
po-tvcy
bL
--■ ' TZxZz COViAziyt^ ^VAZ (A> ^WZjO ■^Ac’C^C,
(To wiyD.^vA>AAA^ 0^ yt)/vvv*d5otf>
)IA^O\/&cL^/ 1/ti'xjA/l'VV
/\^
^tAcLcUx^,
--------
hl^-yi'y^CoL Cj
‘^b<Z-€Ci'cU ti
/0\A)
ajl(/\
’C^LCtoi^
/U’mt’iZ' A/9VW (/VUv^lA<>v£/vfe d,t> C'fc-'U?..
(I
J ,
„
„
J ,
,
tAX/VX/vcXx^^C' /l/w ^y/vvv'A/t^
yy<^vi (^' ^jp^^vvtvCCS^zixyS1
(^Cvv
O/^^C^C(ricr>^ vi .
.VlzAX^vC'i/kvC (
^lvve-€/lx
Th&},C- O^yjU I OS C&'LOC/^O^ (^ .S/Vx.cLv^&v^L'^i
f\/<M^^ (TV\^^C (ivizCvzxZ-
(2\,
fcv&w z?lC/l'vv<<''tziZ4
K
2/(yvtviy
{ I
'
{%W^ jj/vCC, f
^xCMzv^t^t'Ty{z/ 0^0 ^vtJu-vKv^1/
. 0 0f
(%'VK?C (7VW^Z>/xS ,AZ-Ot>^^>V1/fvC'T^
t'^iv-vC/4'V' '14 /V14cy<2^>1rl4z<'7
■vL/vlu C'xjtalC'K s^-c'-tct^ ,
7^1^ /Tiz>
"^‘Utz.
4A/X tv^AAA tr-oxc /WX It-YZz CaJTJzvL^ CU
FchaA. VWvitx'c'W ^LoiXtCvS
/c€<X7mm Av-vct
ttvx6
to
o^ocU^
CtXLcUo^
Cc^
ot a,
Otxtd.
\AA^cte^
JPXfVv’P-CvpZZL, ^Vxzc JvvvCU/CW dwc to
IVtbObhzvvv^ Cowg-b>
^A&X/ltcp,
7.00,000 pc/uWeO^AAyCvd: <X0Sa.iXyL0t2ci
(Xeeu ti pfr'Xo, Uv4<{e AiXzvtb K6a^>-vvz;i,t&v^ /qfM<tvWbe.x Pvv^6<>tv<?vv^ (X<aXv^
2- 'fo 3 OVVlXCl/<?->v PVWtAzAx -fVV-<>-< ,
0
I/\/3j&X Uvl
•VW^CuiLv’Lto-A--
K £/Lb bi^Vw^
LA/lCfcF
6^^&(nXLX\XA^y ..
byXvO ct-QC- i^^C-■X Wb <X^C 8^
,^46 C^vtTWv
:.. -I" AT. ., ,n
i-txa/v Ctvvi-C,
fc>
-T^aZA^UaA^ LU/^Cs
V '9 MiZ. 46
<y,6zVU ^Q/v
lOOO
tX^tOiS .
to uwicer^ "
&L
l\AM's; (XXLcUo^
OvQ' ItWvtfl lHC/lXl
tCuz
k/O^ibU
btwiX
ftCCZlA, aaa
4/T/v
o~p ciXl t£u> Le-c-dtdd cXdXd- ctcWJvS
cLcatt^ bccwb
,
A <7'a n. . CrMzlzw.fcJ
C'.
4—r Zf
^C'AA-l-VX, K\ ^Ltt'lAA L-CVWVl/VC'Ci z
P>C
OAaX.
■'■*»v■A,<^L(^CI
- / /C a*z»^X,
J_ . /^MccXM-kb
tio / C l~fA/\A i /5fylzl
/A
f ^t/VV'W-JVUWlzvu^KU, >
- Ihctj
zv<2vvv/c£-c/l
3Zf^ ^VU<
ztca^
A/V-va-CT^, /3j tO“WvUA<CA XjsXLX .vuv'CUz- rf,<Z(x/sutw^ O^Vf^Z/v &X
i?S7 </l35M^s.
D
^oc> <a/-t^ encrypted &6j. Po-tzo oce^Aj tdapj . '/^ a^v^Lcd./uvic^ cd db’X c/x&AXoXc
S' be/v Lviz^^avlA- /uvv (6/viz€e4/
CA/uVq/vuvc?. A> TA^^/t^vCbUy zuaXzz 6-^ Sb pC^ 100,000.
S
O '2'’
. ’Avwp to S^(/c^l>caa otxO'^cd' 'tXtfX
AwtwiZV
wvvUZc-vu /iAa/A^wCs X'OOcL
d/OOcL (81 <V>jLQVbC'dcCb.L
nzpC'vlxzt 4>AzJvitbvvt^ nJ
Cp
ode 2^000,
77-tZz I ^8 i
'Kczul^ So, coo COMA
ctnJ'pO&vdjCpj AAA, €/}
AAA/tztz 1~) O &\s
/\AJTyC> zvCVv
/i-XO ^/p<?Vvv4Xz.cZ,
X/l-C^V
C<%'MzX£zi
Pvc>^
(7-7. 'VVvCO1
O'V-6'V S'5
V ofc^
t
!L^UJaAC,
OAZL
I
fjAX>JA^wvm£.
6^ Q>.C-(s]. i/^C,vvuZ zX^ffVlW/k
b CPvOC-iZi C\^ \a^C^ |/(Vi£A&(>v O — ^O^o)
44aV'A,WvU i'tvtzCuii y A/e<?-T^x6CbC /3-C-6>- <4 Sfo/Cjl tb O/dp^ toO-(oOyb
77-VzS
i-V-Ctt^VLCx^
^VU^Z-VCvutCi-cS u:
CC'w/ACc-tvuvn, .
<JLt^6vwv0z^ (2-'C^vLzii'U7z><:C tdA-^MX44zLc$Z< z 'Twoiz; So ^^ci/vvxi^xXx
bPT
CkkiTVVVv^'b
P^p^<\4v'<ZA z PiJA.C'KAUi C^w£ VgjTTUWVtzS 4X
CovvR^vuvcivdx^te^l avu ^cv^yjc /\z.t'Cc^0m4 C<^2^tCuz
.<vv aa^v^<%wCs tv^tVv
■'KZvl/vO
VvVV4O^Ltt4>tlZ-^_
c^trx-y c</p^
6>X tvvCtv
S-e-bTA'VAZ^ .
Pvo-wv ^tvo
L&wZz twr> (
lyi^o
C<7vvte^K^ek OJ
p>^c^e^bLc,y^ cd^
a^t
<4
cd^o,
#lz^ ’'A^ewP^ c^'^cv^.
4zvv 'kw^vv^
K^xt^vs\
c^tev^w Xx
b*
Kuuwi
Ia)^
Zoc^C (^(Wu^.
e^od^L
I^v X-VuJ
COwb'Zr , fa&dCfcdY^aJt ‘yy^Q.-dZcoL p'VACztixz^ (%vi4t
^4/^v/^en
Kc^Lttj CM/\^cL C^xZCcL S/W>i/c.m^L,
(Tctv M^vte^tZAZcit C%y>p/W<;u>^
b^&vvvs^L-is^i 'to .iaw/Tvcv^
Gt-vc
c^lv Lcv-tM. <^i
b(V34.-t>
bp
C'C&wtLy
4
^xz/jAzA-dzibL ^x&wM'O (rv^b<
htMx
A (J-i-
,(zU^ew <?1
j/UiJuM-S
Aw
'VVvvvCvlA>L
i(
e
f . Y
(^Ivv-tX-piX-tTvlj
'
y
^dU^^Lc,i^JL --- to
tU/x qzW^Ufc^ (^
• _
*'_
f
tr < *4
t'xyCOtk'X;tio-vcG\JU
fro
b/^i^cL
-^tw txj^Ldx (^ ‘
^v’wkz^
'? OvxtxA
zV<-» /rrlt — . _ .
•KL-. /
.<* z *
An
o-C^Cx. ,
/AvLz?
/XZ^z^^-evvt? t?e^ C\/v\.
t/A^^<7t<A>(Zz ^(AzOzv fzbtTVV^lZz kV\XC’t^O^VU> ^zVOl/t^bz tAXH> ir^
l( ^V<^/"<i/yKz
llv^ ce^vx
<7Vw iWty^n^ 7bouv< .<7 z4~
r’/bA/vtX'ii .A
/*\ tr.,.
J______ .
C_
„
S
(J
rlO'OCi/L'C
■Wv^5 fadL PmJMi
/Jw fcr*>Vb’-t>VV(tLc7>1z^
C^xC
txti/i 6t
t-VMzLC/v C-’VAX-
t-owa^U
11Ai'l'OlJ^tl^lC^ 'Vt-OW
CrvU^S,
■Clx
\aKM~(KS
fez^- vv Cz^vZ’Jzt€AAz4^/-(J
<AX
C--vdt/i ''JC\> bzTizvtcAZ z 6^ M-
£?UwkjX4^ C,n-vvHztzU2.l^
MzvCtt! CO-^Z S^stewv.
AA^^vxt
A/) t ddccJU ptviAz^tv^^
pc^(: z/uvv<^z^>evv(jt^w^^
ZVCiUv^ (^ ^o^xc^clA^t 1 (%H^VVC<!zVU>Z ^Uve^0p">VU4zvkc^(/C^Co^vlZz
/uv\f-e^zp<%lv<7->b
PLv^(/O S^OpPy/xCtid- f
C^i/\X^I>Uix^L
VVM/^VVU^ia/Lvi
py1' /^Mzvwvc
O\^CAJ^yvyx^
I© tcolce. C\>
PwplLes LtCfrUp
/yk.<v^fcj ^a.-vc- tigteoC beLruT j-t'
tvc^^-vl'c^vKcC £^Uwu
,M<?V)O'V (d.'vSXiViZI zlzuv
tb -Cpcplc^v^
Ci-wL^i-t-vi'tTz'L,
cn~TeCdi ves
/j
Io
(?vv lA-tg,(/Vyj£V)zvi/^
ColiDoto (A/{/<^X'L^pLc
(W vvcv> - (/X'tLc-^'otCv^ £m.s>L'E-vi/n
Aviztcitve<?^ 'Ywe-rb-LcloC^-
-h^oc-v CAixizjXc c^-
vv^ovt^Litx^
Ltvii YIXX ^'C-Ykv^'tic^^ _C>VO tt\jybzTUVto c^^-
2
d%4(7lzi po.oyv^crtvC’Y)^
'vtv(>n/
tcCto:^ f oCwti
CiAvCvt^Ct.^
'To IA/\AslLc/\£. tbViA^c'C tt-xO C
ut iaZtt'L ext Co-)x
&wv^'ixn/vvvvC-vit A/\A/ fXxZa^' S
Id /Cc'Ic-o^^Ba,,z
DEPii\)nioiv.s
CX^C\A 6
pok
cp .sn^y
OP WL'bHWb:.____
jv\/\tfc^
.C'Ve.-vvCK&S
C\ . PyJs^^Lx^Qy'.
f/l/VYWVC L'WV^
C- - Dx^vir^ ^./v?
t/C .
Vx^?j?^x
, iPksoiM ie^,
dbi-&z.a,'i&£.
Mw -
kplo pat
inc
£y s Tipfin £ 6P '
pppp
- Media
 RF_CH_7.3_SUDHA.pdf
RF_CH_7.3_SUDHA.pdf
Position: 3497 (3 views)